User login
Caring for LGBTQ+ Patients with IBD
Cases
Patient 1: 55-year-old cis-male, who identifies as gay, has ulcerative colitis that has been refractory to multiple biologic therapies. His provider recommends a total proctocolectomy with ileal pouch anal anastomosis (TPC with IPAA), but the patient has questions regarding sexual function following surgery. Specifically, he is wondering when, or if, he can resume receptive anal intercourse. How would you counsel him?
Patient 2: 25-year-old, trans-female, status-post vaginoplasty with use of sigmoid colon and with well-controlled ulcerative colitis, presents with vaginal discharge, weight loss, and rectal bleeding. How do you explain what has happened to her? During your discussion, she also asks you why her chart continues to use her “dead name.” How do you respond?
Patient 3: 32-year-old, cis-female, G2P2, who identifies as a lesbian, has active ulcerative colitis. She wants to discuss medical or surgical therapy and future pregnancies. How would you counsel her?
Many gastroenterologists would likely know how to address patient 3’s concerns, but the concerns of patients 1 and 2 often go unaddressed or dismissed. Numerous studies and surveys have been conducted on patients with inflammatory bowel disease (IBD), but the focus of these studies has always been through a heteronormative cisgender lens. The focus of many studies is on fertility or sexual health and function in cisgender, heteronormative individuals.1-3 In the last few years, however, there has been increasing awareness of the health disparities, stigma, and discrimination that sexual and gender minorities (SGM) experience.4-6 For the purposes of this discussion, individuals within the lesbian, gay, bisexual, transgender, queer/questioning, intersex, and asexual (LGBTQIA+) community will be referred to as SGM. We recognize that even this exhaustive listing above does not acknowledge the full spectrum of diversity within the SGM community.
Clinical Care/Competency for SGM with IBD is Lacking
Almost 10% of the US population identifies as some form of SGM, and that number can be higher within the younger generations.4 SGM patients tend to delay or avoid seeking health care due to concern for provider mistreatment or lack of regard for their individual concerns. Additionally, there are several gaps in clinical knowledge about caring for SGM individuals. Little is known regarding the incidence or prevalence of IBD in SGM populations, but it is perceived to be similar to cisgender heterosexual individuals. Furthermore, as Newman et al. highlighted in their systematic review published in May 2023, there is a lack of guidance regarding sexual activity in the setting of IBD in SGM individuals.5 There is also a significant lack of knowledge on the impact of gender-affirming care on the natural history and treatments of IBD in transgender and gender non-conforming (TGNC) individuals. This can impact providers’ comfort and competence in caring for TGNC individuals.

Another important point to make is that the SGM community still faces discrimination due to sexual orientation or gender identity to this day, which impacts the quality and delivery of their care.7 Culturally-competent care should include care that is free from stigma, implicit and explicit biases, and discrimination. In 2011, an Institute of Medicine report documented, among other issues, provider discomfort in delivering care to SGM patients.8 While SGM individuals prefer a provider who acknowledges their sexual orientation and gender identity and treats them with the dignity and respect they deserve, many SGM individuals share valid concerns regarding their safety, which impact their desire to disclose their identity to health care providers.9 This certainly can have an impact on the quality of care they receive, including important health maintenance milestones and cancer screenings.10
An internal survey at our institution of providers (nurses, physician assistants, surgeons, and physicians) found that among 85 responders, 70% have cared for SGM who have undergone TPC with ileal pouch anal anastomosis (IPAA). Of these, 75% did not ask about sexual orientation or practices before pouch formation (though almost all of them agreed it would be important to ask). A total of 55% were comfortable in discussing SGM-related concerns; 53% did not feel comfortable discussing sexual orientation or practices; and in particular when it came to anoreceptive intercourse (ARI), 73% did not feel confident discussing recommendations.11
All of these issues highlight the importance of developing curricula that focus on reducing implicit and explicit biases towards SGM individuals and increasing the competence of providers to take care of SGM individuals in a safe space.

Additionally, it further justifies the need for ethical research that focuses on the needs of SGM individuals to guide evidence-based approaches to care. Given the implicit and explicit heterosexism and transphobia in society and many health care systems, Rainbows in Gastro was formed as an advocacy group for SGM patients, trainees, and staff in gastroenterology and hepatology.4
Research in SGM and IBD is lacking
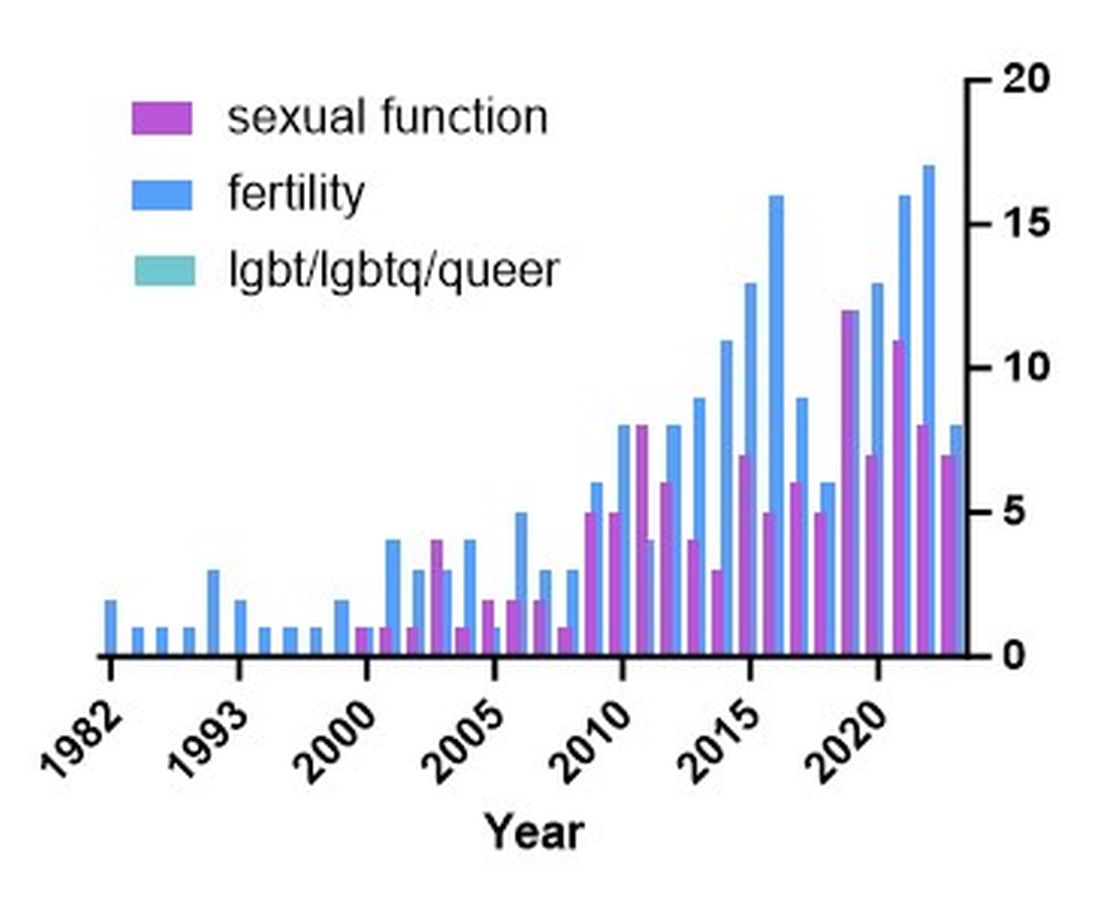
There are additional needs for research in IBD and how it pertains to the needs of SGM individuals. Figure 1 highlights the lack of PubMed results for the search terms “IBD + LGBT,” “IBD + LGBTQ,” or “IBD + queer.” In contrast, the search terms “IBD + fertility” and “IBD + sexual dysfunction” generate many results. Even a systemic review conducted by Newman et al. of multiple databases in 2022 found only seven articles that demonstrated appropriately performed studies on SGM patients with IBD.5 This highlights the significant dearth of research in the realm of SGM health in IBD.
Newman and colleagues have recently published research considerations for SGM individuals. They highlighted the need to include understanding the “unique combination of psychosocial, biomedical, and legal experiences” that results in different needs and outcomes. There were several areas identified, including minority stress, which comes from existence of being SGM, especially as transgender individuals face increasing legal challenges in a variety of settings, not just healthcare.6 In a retrospective chart review investigating social determinants of health in SGM-IBD populations,12 36% of patients reported some level of social isolation, and almost 50% reported some level of stress. A total of 40% of them self-reported some perceived level of risk with respect to employment, and 17% reported depression. Given that this was a chart review and not a strict questionnaire, this study was certainly limited, and we would hypothesize that these numbers are therefore underestimating the true proportion of SGM-IBD patients who deal with employment concerns, social isolation, or psychological distress.
What Next? Back to the Patients
Circling back to our patients from the introduction, how would you counsel each of them? In patient 1’s case, we would inform him that pelvic surgery can increase the risk for sexual dysfunction, such as erectile dysfunction. He additionally would be advised during a staged TPC with IPAA, he may experience issues with body image. However, should he desire to participate in receptive anal intercourse after completion of his surgeries, the general recommendation would be to wait at least 6 months and with proven remission. It should further be noted that these are not formalized recommendations, only highlighting the need for more research and consensus on standards of care for SGM patients. He should finally be told that because he has ulcerative colitis, removal of the colon does not remove the risk for future intestinal involvement such as possible pouchitis.
In patient 2’s case, she is likely experiencing diversion vaginitis related to use of her colon for her neo-vagina. She should undergo colonoscopy and vaginoscopy in addition to standard work-up for her known ulcerative colitis.13 Management should be done in a multidisciplinary approach between the IBD provider, gynecologist, and gender-affirming provider. The electronic medical record should be updated to reflect the patient’s preferred name, pronouns, and gender identity, and her medical records, including automated clinical reports, should be updated accordingly.
As for patient 3, she would be counseled according to well-documented guidelines on pregnancy and IBD, including risks of medications (such as Jak inhibitors or methotrexate) versus the risk of uncontrolled IBD during pregnancy.1
Regardless of a patient’s gender identity or sexual orientation, patient-centered, culturally competent, and sensitive care should be provided. At Mayo Clinic in Rochester, we started one of the first Pride in IBD Clinics, which focuses on the care of SGM individuals with IBD. Our focus is to address the needs of patients who belong to the SGM community in a wholistic approach within a safe space (https://www.youtube.com/watch?v=pYa_zYaCA6M; https://www.mayoclinic.org/departments-centers/inflammatory-bowel-disease-clinic/overview/ovc-20357763). Our process of developing the clinic included training all staff on proper communication and cultural sensitivity for the SGM community.
Furthermore, providing welcoming and affirming signs of inclusivity for SGM individuals at the provider’s office — including but not limited to rainbow progressive flags, gender-neutral bathroom signs, or pronoun pins on provider identification badges (see Figure 2) — are usually appreciated by patients. Ensuring that patient education materials do not assume gender (for example, using the term “parents” rather than “mother and father”) and using gender neutral terms on intake forms is very important. Inclusive communication includes providers introducing themselves by preferred name and pronouns, asking the patients to introduce themselves, and welcoming them to share their pronouns. These simple actions can provide an atmosphere of safety for SGM patients, which would serve to enhance the quality of care we can provide for them.
For Resources and Further Reading: CDC,14 the Fenway Institute’s National LGBTQIA+ Health Education Center,15 and US Department of Health and Human Services.16
Dr. Chiang and Dr. Chedid are both in the Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, Minnesota. Dr. Chedid is also with the Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, Mayo Clinic. Neither of the authors have any relevant conflicts of interest. They are on X, formerly Twitter: @dr_davidchiang , @VictorChedidMD .
CITATIONS
1. Mahadevan U et al. Inflammatory bowel disease in pregnancy clinical care pathway: A report from the American Gastroenterological Association IBD Parenthood Project Working Group. Gastroenterology. 2019;156:1508-24.
2. Pires F et al. A survey on the impact of IBD in sexual health: Into intimacy. Medicine (Baltimore). 2022;101:e32279.
3. Mules TC et al. The impact of disease activity on sexual and erectile dysfunction in patients with inflammatory bowel disease. Inflamm Bowel Dis. 2023;29:1244-54.
4. Duong N et al. Overcoming disparities for sexual and gender minority patients and providers in gastroenterology and hepatology: Introduction to Rainbows in Gastro. Lancet Gastroenterol Hepatol. 2023;8:299-301.
5. Newman KL et al. A systematic review of inflammatory bowel disease epidemiology and health outcomes in sexual and gender minority individuals. Gastroenterology. 2023;164:866-71.
6. Newman KL et al. Research considerations in Digestive and liver disease in transgender and gender-diverse populations. Gastroenterology. 2023;165:523-28 e1.
7. Velez C et al. Digestive health in sexual and gender minority populations. Am J Gastroenterol. 2022;117:865-75.
8. Medicine Io. Washington (DC): The National Academies Press, 2011.
9. Austin EL. Sexual orientation disclosure to health care providers among urban and non-urban southern lesbians. Women Health. 2013;53:41-55.
10. Oladeru OT et al. Breast and cervical cancer screening disparities in transgender people. Am J Clin Oncol. 2022;45:116-21.
11. Vinsard DG et al. Healthcare providers’ perspectives on anoreceptive intercourse in sexual and gender minorities with ileal pouch anal anastomosis. Digestive Disease Week (DDW). Chicago, IL, 2023.
12. Ghusn W et al. Social determinants of health in LGBTQIA+ patients with inflammatory bowel disease. American College of Gastroenterology (ACG). Charlotte, NC, 2022.
13. Grasman ME et al. Neovaginal sparing in a transgender woman with ulcerative colitis. Clin Gastroenterol Hepatol. 2016;14:e73-4.
14. Prevention CfDCa. Lesbian, Gay, Bisexual, and Transgender Health — https://www.cdc.gov/lgbthealth/index.htm.
15. Institute TF. National LGBTQIA+ Health Education Center — https://www.lgbtqiahealtheducation.org/.
16. Services UDoHaH. LGBTQI+ Resources — https://www.hhs.gov/programs/topic-sites/lgbtqi/resources/index.html.
Cases
Patient 1: 55-year-old cis-male, who identifies as gay, has ulcerative colitis that has been refractory to multiple biologic therapies. His provider recommends a total proctocolectomy with ileal pouch anal anastomosis (TPC with IPAA), but the patient has questions regarding sexual function following surgery. Specifically, he is wondering when, or if, he can resume receptive anal intercourse. How would you counsel him?
Patient 2: 25-year-old, trans-female, status-post vaginoplasty with use of sigmoid colon and with well-controlled ulcerative colitis, presents with vaginal discharge, weight loss, and rectal bleeding. How do you explain what has happened to her? During your discussion, she also asks you why her chart continues to use her “dead name.” How do you respond?
Patient 3: 32-year-old, cis-female, G2P2, who identifies as a lesbian, has active ulcerative colitis. She wants to discuss medical or surgical therapy and future pregnancies. How would you counsel her?
Many gastroenterologists would likely know how to address patient 3’s concerns, but the concerns of patients 1 and 2 often go unaddressed or dismissed. Numerous studies and surveys have been conducted on patients with inflammatory bowel disease (IBD), but the focus of these studies has always been through a heteronormative cisgender lens. The focus of many studies is on fertility or sexual health and function in cisgender, heteronormative individuals.1-3 In the last few years, however, there has been increasing awareness of the health disparities, stigma, and discrimination that sexual and gender minorities (SGM) experience.4-6 For the purposes of this discussion, individuals within the lesbian, gay, bisexual, transgender, queer/questioning, intersex, and asexual (LGBTQIA+) community will be referred to as SGM. We recognize that even this exhaustive listing above does not acknowledge the full spectrum of diversity within the SGM community.
Clinical Care/Competency for SGM with IBD is Lacking
Almost 10% of the US population identifies as some form of SGM, and that number can be higher within the younger generations.4 SGM patients tend to delay or avoid seeking health care due to concern for provider mistreatment or lack of regard for their individual concerns. Additionally, there are several gaps in clinical knowledge about caring for SGM individuals. Little is known regarding the incidence or prevalence of IBD in SGM populations, but it is perceived to be similar to cisgender heterosexual individuals. Furthermore, as Newman et al. highlighted in their systematic review published in May 2023, there is a lack of guidance regarding sexual activity in the setting of IBD in SGM individuals.5 There is also a significant lack of knowledge on the impact of gender-affirming care on the natural history and treatments of IBD in transgender and gender non-conforming (TGNC) individuals. This can impact providers’ comfort and competence in caring for TGNC individuals.
Another important point to make is that the SGM community still faces discrimination due to sexual orientation or gender identity to this day, which impacts the quality and delivery of their care.7 Culturally-competent care should include care that is free from stigma, implicit and explicit biases, and discrimination. In 2011, an Institute of Medicine report documented, among other issues, provider discomfort in delivering care to SGM patients.8 While SGM individuals prefer a provider who acknowledges their sexual orientation and gender identity and treats them with the dignity and respect they deserve, many SGM individuals share valid concerns regarding their safety, which impact their desire to disclose their identity to health care providers.9 This certainly can have an impact on the quality of care they receive, including important health maintenance milestones and cancer screenings.10
An internal survey at our institution of providers (nurses, physician assistants, surgeons, and physicians) found that among 85 responders, 70% have cared for SGM who have undergone TPC with ileal pouch anal anastomosis (IPAA). Of these, 75% did not ask about sexual orientation or practices before pouch formation (though almost all of them agreed it would be important to ask). A total of 55% were comfortable in discussing SGM-related concerns; 53% did not feel comfortable discussing sexual orientation or practices; and in particular when it came to anoreceptive intercourse (ARI), 73% did not feel confident discussing recommendations.11
All of these issues highlight the importance of developing curricula that focus on reducing implicit and explicit biases towards SGM individuals and increasing the competence of providers to take care of SGM individuals in a safe space.
Additionally, it further justifies the need for ethical research that focuses on the needs of SGM individuals to guide evidence-based approaches to care. Given the implicit and explicit heterosexism and transphobia in society and many health care systems, Rainbows in Gastro was formed as an advocacy group for SGM patients, trainees, and staff in gastroenterology and hepatology.4
Research in SGM and IBD is lacking
There are additional needs for research in IBD and how it pertains to the needs of SGM individuals. Figure 1 highlights the lack of PubMed results for the search terms “IBD + LGBT,” “IBD + LGBTQ,” or “IBD + queer.” In contrast, the search terms “IBD + fertility” and “IBD + sexual dysfunction” generate many results. Even a systemic review conducted by Newman et al. of multiple databases in 2022 found only seven articles that demonstrated appropriately performed studies on SGM patients with IBD.5 This highlights the significant dearth of research in the realm of SGM health in IBD.
Newman and colleagues have recently published research considerations for SGM individuals. They highlighted the need to include understanding the “unique combination of psychosocial, biomedical, and legal experiences” that results in different needs and outcomes. There were several areas identified, including minority stress, which comes from existence of being SGM, especially as transgender individuals face increasing legal challenges in a variety of settings, not just healthcare.6 In a retrospective chart review investigating social determinants of health in SGM-IBD populations,12 36% of patients reported some level of social isolation, and almost 50% reported some level of stress. A total of 40% of them self-reported some perceived level of risk with respect to employment, and 17% reported depression. Given that this was a chart review and not a strict questionnaire, this study was certainly limited, and we would hypothesize that these numbers are therefore underestimating the true proportion of SGM-IBD patients who deal with employment concerns, social isolation, or psychological distress.
What Next? Back to the Patients
Circling back to our patients from the introduction, how would you counsel each of them? In patient 1’s case, we would inform him that pelvic surgery can increase the risk for sexual dysfunction, such as erectile dysfunction. He additionally would be advised during a staged TPC with IPAA, he may experience issues with body image. However, should he desire to participate in receptive anal intercourse after completion of his surgeries, the general recommendation would be to wait at least 6 months and with proven remission. It should further be noted that these are not formalized recommendations, only highlighting the need for more research and consensus on standards of care for SGM patients. He should finally be told that because he has ulcerative colitis, removal of the colon does not remove the risk for future intestinal involvement such as possible pouchitis.
In patient 2’s case, she is likely experiencing diversion vaginitis related to use of her colon for her neo-vagina. She should undergo colonoscopy and vaginoscopy in addition to standard work-up for her known ulcerative colitis.13 Management should be done in a multidisciplinary approach between the IBD provider, gynecologist, and gender-affirming provider. The electronic medical record should be updated to reflect the patient’s preferred name, pronouns, and gender identity, and her medical records, including automated clinical reports, should be updated accordingly.
As for patient 3, she would be counseled according to well-documented guidelines on pregnancy and IBD, including risks of medications (such as Jak inhibitors or methotrexate) versus the risk of uncontrolled IBD during pregnancy.1
Regardless of a patient’s gender identity or sexual orientation, patient-centered, culturally competent, and sensitive care should be provided. At Mayo Clinic in Rochester, we started one of the first Pride in IBD Clinics, which focuses on the care of SGM individuals with IBD. Our focus is to address the needs of patients who belong to the SGM community in a wholistic approach within a safe space (https://www.youtube.com/watch?v=pYa_zYaCA6M; https://www.mayoclinic.org/departments-centers/inflammatory-bowel-disease-clinic/overview/ovc-20357763). Our process of developing the clinic included training all staff on proper communication and cultural sensitivity for the SGM community.
Furthermore, providing welcoming and affirming signs of inclusivity for SGM individuals at the provider’s office — including but not limited to rainbow progressive flags, gender-neutral bathroom signs, or pronoun pins on provider identification badges (see Figure 2) — are usually appreciated by patients. Ensuring that patient education materials do not assume gender (for example, using the term “parents” rather than “mother and father”) and using gender neutral terms on intake forms is very important. Inclusive communication includes providers introducing themselves by preferred name and pronouns, asking the patients to introduce themselves, and welcoming them to share their pronouns. These simple actions can provide an atmosphere of safety for SGM patients, which would serve to enhance the quality of care we can provide for them.
For Resources and Further Reading: CDC,14 the Fenway Institute’s National LGBTQIA+ Health Education Center,15 and US Department of Health and Human Services.16
Dr. Chiang and Dr. Chedid are both in the Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, Minnesota. Dr. Chedid is also with the Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, Mayo Clinic. Neither of the authors have any relevant conflicts of interest. They are on X, formerly Twitter: @dr_davidchiang , @VictorChedidMD .
CITATIONS
1. Mahadevan U et al. Inflammatory bowel disease in pregnancy clinical care pathway: A report from the American Gastroenterological Association IBD Parenthood Project Working Group. Gastroenterology. 2019;156:1508-24.
2. Pires F et al. A survey on the impact of IBD in sexual health: Into intimacy. Medicine (Baltimore). 2022;101:e32279.
3. Mules TC et al. The impact of disease activity on sexual and erectile dysfunction in patients with inflammatory bowel disease. Inflamm Bowel Dis. 2023;29:1244-54.
4. Duong N et al. Overcoming disparities for sexual and gender minority patients and providers in gastroenterology and hepatology: Introduction to Rainbows in Gastro. Lancet Gastroenterol Hepatol. 2023;8:299-301.
5. Newman KL et al. A systematic review of inflammatory bowel disease epidemiology and health outcomes in sexual and gender minority individuals. Gastroenterology. 2023;164:866-71.
6. Newman KL et al. Research considerations in Digestive and liver disease in transgender and gender-diverse populations. Gastroenterology. 2023;165:523-28 e1.
7. Velez C et al. Digestive health in sexual and gender minority populations. Am J Gastroenterol. 2022;117:865-75.
8. Medicine Io. Washington (DC): The National Academies Press, 2011.
9. Austin EL. Sexual orientation disclosure to health care providers among urban and non-urban southern lesbians. Women Health. 2013;53:41-55.
10. Oladeru OT et al. Breast and cervical cancer screening disparities in transgender people. Am J Clin Oncol. 2022;45:116-21.
11. Vinsard DG et al. Healthcare providers’ perspectives on anoreceptive intercourse in sexual and gender minorities with ileal pouch anal anastomosis. Digestive Disease Week (DDW). Chicago, IL, 2023.
12. Ghusn W et al. Social determinants of health in LGBTQIA+ patients with inflammatory bowel disease. American College of Gastroenterology (ACG). Charlotte, NC, 2022.
13. Grasman ME et al. Neovaginal sparing in a transgender woman with ulcerative colitis. Clin Gastroenterol Hepatol. 2016;14:e73-4.
14. Prevention CfDCa. Lesbian, Gay, Bisexual, and Transgender Health — https://www.cdc.gov/lgbthealth/index.htm.
15. Institute TF. National LGBTQIA+ Health Education Center — https://www.lgbtqiahealtheducation.org/.
16. Services UDoHaH. LGBTQI+ Resources — https://www.hhs.gov/programs/topic-sites/lgbtqi/resources/index.html.
Cases
Patient 1: 55-year-old cis-male, who identifies as gay, has ulcerative colitis that has been refractory to multiple biologic therapies. His provider recommends a total proctocolectomy with ileal pouch anal anastomosis (TPC with IPAA), but the patient has questions regarding sexual function following surgery. Specifically, he is wondering when, or if, he can resume receptive anal intercourse. How would you counsel him?
Patient 2: 25-year-old, trans-female, status-post vaginoplasty with use of sigmoid colon and with well-controlled ulcerative colitis, presents with vaginal discharge, weight loss, and rectal bleeding. How do you explain what has happened to her? During your discussion, she also asks you why her chart continues to use her “dead name.” How do you respond?
Patient 3: 32-year-old, cis-female, G2P2, who identifies as a lesbian, has active ulcerative colitis. She wants to discuss medical or surgical therapy and future pregnancies. How would you counsel her?
Many gastroenterologists would likely know how to address patient 3’s concerns, but the concerns of patients 1 and 2 often go unaddressed or dismissed. Numerous studies and surveys have been conducted on patients with inflammatory bowel disease (IBD), but the focus of these studies has always been through a heteronormative cisgender lens. The focus of many studies is on fertility or sexual health and function in cisgender, heteronormative individuals.1-3 In the last few years, however, there has been increasing awareness of the health disparities, stigma, and discrimination that sexual and gender minorities (SGM) experience.4-6 For the purposes of this discussion, individuals within the lesbian, gay, bisexual, transgender, queer/questioning, intersex, and asexual (LGBTQIA+) community will be referred to as SGM. We recognize that even this exhaustive listing above does not acknowledge the full spectrum of diversity within the SGM community.
Clinical Care/Competency for SGM with IBD is Lacking
Almost 10% of the US population identifies as some form of SGM, and that number can be higher within the younger generations.4 SGM patients tend to delay or avoid seeking health care due to concern for provider mistreatment or lack of regard for their individual concerns. Additionally, there are several gaps in clinical knowledge about caring for SGM individuals. Little is known regarding the incidence or prevalence of IBD in SGM populations, but it is perceived to be similar to cisgender heterosexual individuals. Furthermore, as Newman et al. highlighted in their systematic review published in May 2023, there is a lack of guidance regarding sexual activity in the setting of IBD in SGM individuals.5 There is also a significant lack of knowledge on the impact of gender-affirming care on the natural history and treatments of IBD in transgender and gender non-conforming (TGNC) individuals. This can impact providers’ comfort and competence in caring for TGNC individuals.
Another important point to make is that the SGM community still faces discrimination due to sexual orientation or gender identity to this day, which impacts the quality and delivery of their care.7 Culturally-competent care should include care that is free from stigma, implicit and explicit biases, and discrimination. In 2011, an Institute of Medicine report documented, among other issues, provider discomfort in delivering care to SGM patients.8 While SGM individuals prefer a provider who acknowledges their sexual orientation and gender identity and treats them with the dignity and respect they deserve, many SGM individuals share valid concerns regarding their safety, which impact their desire to disclose their identity to health care providers.9 This certainly can have an impact on the quality of care they receive, including important health maintenance milestones and cancer screenings.10
An internal survey at our institution of providers (nurses, physician assistants, surgeons, and physicians) found that among 85 responders, 70% have cared for SGM who have undergone TPC with ileal pouch anal anastomosis (IPAA). Of these, 75% did not ask about sexual orientation or practices before pouch formation (though almost all of them agreed it would be important to ask). A total of 55% were comfortable in discussing SGM-related concerns; 53% did not feel comfortable discussing sexual orientation or practices; and in particular when it came to anoreceptive intercourse (ARI), 73% did not feel confident discussing recommendations.11
All of these issues highlight the importance of developing curricula that focus on reducing implicit and explicit biases towards SGM individuals and increasing the competence of providers to take care of SGM individuals in a safe space.
Additionally, it further justifies the need for ethical research that focuses on the needs of SGM individuals to guide evidence-based approaches to care. Given the implicit and explicit heterosexism and transphobia in society and many health care systems, Rainbows in Gastro was formed as an advocacy group for SGM patients, trainees, and staff in gastroenterology and hepatology.4
Research in SGM and IBD is lacking
There are additional needs for research in IBD and how it pertains to the needs of SGM individuals. Figure 1 highlights the lack of PubMed results for the search terms “IBD + LGBT,” “IBD + LGBTQ,” or “IBD + queer.” In contrast, the search terms “IBD + fertility” and “IBD + sexual dysfunction” generate many results. Even a systemic review conducted by Newman et al. of multiple databases in 2022 found only seven articles that demonstrated appropriately performed studies on SGM patients with IBD.5 This highlights the significant dearth of research in the realm of SGM health in IBD.
Newman and colleagues have recently published research considerations for SGM individuals. They highlighted the need to include understanding the “unique combination of psychosocial, biomedical, and legal experiences” that results in different needs and outcomes. There were several areas identified, including minority stress, which comes from existence of being SGM, especially as transgender individuals face increasing legal challenges in a variety of settings, not just healthcare.6 In a retrospective chart review investigating social determinants of health in SGM-IBD populations,12 36% of patients reported some level of social isolation, and almost 50% reported some level of stress. A total of 40% of them self-reported some perceived level of risk with respect to employment, and 17% reported depression. Given that this was a chart review and not a strict questionnaire, this study was certainly limited, and we would hypothesize that these numbers are therefore underestimating the true proportion of SGM-IBD patients who deal with employment concerns, social isolation, or psychological distress.
What Next? Back to the Patients
Circling back to our patients from the introduction, how would you counsel each of them? In patient 1’s case, we would inform him that pelvic surgery can increase the risk for sexual dysfunction, such as erectile dysfunction. He additionally would be advised during a staged TPC with IPAA, he may experience issues with body image. However, should he desire to participate in receptive anal intercourse after completion of his surgeries, the general recommendation would be to wait at least 6 months and with proven remission. It should further be noted that these are not formalized recommendations, only highlighting the need for more research and consensus on standards of care for SGM patients. He should finally be told that because he has ulcerative colitis, removal of the colon does not remove the risk for future intestinal involvement such as possible pouchitis.
In patient 2’s case, she is likely experiencing diversion vaginitis related to use of her colon for her neo-vagina. She should undergo colonoscopy and vaginoscopy in addition to standard work-up for her known ulcerative colitis.13 Management should be done in a multidisciplinary approach between the IBD provider, gynecologist, and gender-affirming provider. The electronic medical record should be updated to reflect the patient’s preferred name, pronouns, and gender identity, and her medical records, including automated clinical reports, should be updated accordingly.
As for patient 3, she would be counseled according to well-documented guidelines on pregnancy and IBD, including risks of medications (such as Jak inhibitors or methotrexate) versus the risk of uncontrolled IBD during pregnancy.1
Regardless of a patient’s gender identity or sexual orientation, patient-centered, culturally competent, and sensitive care should be provided. At Mayo Clinic in Rochester, we started one of the first Pride in IBD Clinics, which focuses on the care of SGM individuals with IBD. Our focus is to address the needs of patients who belong to the SGM community in a wholistic approach within a safe space (https://www.youtube.com/watch?v=pYa_zYaCA6M; https://www.mayoclinic.org/departments-centers/inflammatory-bowel-disease-clinic/overview/ovc-20357763). Our process of developing the clinic included training all staff on proper communication and cultural sensitivity for the SGM community.
Furthermore, providing welcoming and affirming signs of inclusivity for SGM individuals at the provider’s office — including but not limited to rainbow progressive flags, gender-neutral bathroom signs, or pronoun pins on provider identification badges (see Figure 2) — are usually appreciated by patients. Ensuring that patient education materials do not assume gender (for example, using the term “parents” rather than “mother and father”) and using gender neutral terms on intake forms is very important. Inclusive communication includes providers introducing themselves by preferred name and pronouns, asking the patients to introduce themselves, and welcoming them to share their pronouns. These simple actions can provide an atmosphere of safety for SGM patients, which would serve to enhance the quality of care we can provide for them.
For Resources and Further Reading: CDC,14 the Fenway Institute’s National LGBTQIA+ Health Education Center,15 and US Department of Health and Human Services.16
Dr. Chiang and Dr. Chedid are both in the Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, Minnesota. Dr. Chedid is also with the Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, Mayo Clinic. Neither of the authors have any relevant conflicts of interest. They are on X, formerly Twitter: @dr_davidchiang , @VictorChedidMD .
CITATIONS
1. Mahadevan U et al. Inflammatory bowel disease in pregnancy clinical care pathway: A report from the American Gastroenterological Association IBD Parenthood Project Working Group. Gastroenterology. 2019;156:1508-24.
2. Pires F et al. A survey on the impact of IBD in sexual health: Into intimacy. Medicine (Baltimore). 2022;101:e32279.
3. Mules TC et al. The impact of disease activity on sexual and erectile dysfunction in patients with inflammatory bowel disease. Inflamm Bowel Dis. 2023;29:1244-54.
4. Duong N et al. Overcoming disparities for sexual and gender minority patients and providers in gastroenterology and hepatology: Introduction to Rainbows in Gastro. Lancet Gastroenterol Hepatol. 2023;8:299-301.
5. Newman KL et al. A systematic review of inflammatory bowel disease epidemiology and health outcomes in sexual and gender minority individuals. Gastroenterology. 2023;164:866-71.
6. Newman KL et al. Research considerations in Digestive and liver disease in transgender and gender-diverse populations. Gastroenterology. 2023;165:523-28 e1.
7. Velez C et al. Digestive health in sexual and gender minority populations. Am J Gastroenterol. 2022;117:865-75.
8. Medicine Io. Washington (DC): The National Academies Press, 2011.
9. Austin EL. Sexual orientation disclosure to health care providers among urban and non-urban southern lesbians. Women Health. 2013;53:41-55.
10. Oladeru OT et al. Breast and cervical cancer screening disparities in transgender people. Am J Clin Oncol. 2022;45:116-21.
11. Vinsard DG et al. Healthcare providers’ perspectives on anoreceptive intercourse in sexual and gender minorities with ileal pouch anal anastomosis. Digestive Disease Week (DDW). Chicago, IL, 2023.
12. Ghusn W et al. Social determinants of health in LGBTQIA+ patients with inflammatory bowel disease. American College of Gastroenterology (ACG). Charlotte, NC, 2022.
13. Grasman ME et al. Neovaginal sparing in a transgender woman with ulcerative colitis. Clin Gastroenterol Hepatol. 2016;14:e73-4.
14. Prevention CfDCa. Lesbian, Gay, Bisexual, and Transgender Health — https://www.cdc.gov/lgbthealth/index.htm.
15. Institute TF. National LGBTQIA+ Health Education Center — https://www.lgbtqiahealtheducation.org/.
16. Services UDoHaH. LGBTQI+ Resources — https://www.hhs.gov/programs/topic-sites/lgbtqi/resources/index.html.
‘We Will Rock You’ Into Real-time Diabetes Control
, reveals a series of experiments.
The research was published in The Lancet Diabetes & Endocrinology.
After developing a cell line in which music-sensitive calcium channels triggered the release of insulin-containing vesicles, the researchers conducted a series of studies identifying the optimal frequency, pitch, and volume of sounds for triggering release.
After settling on low-bass heavy popular music, they tested their system on mice with type 1 diabetes that had the insulin-releasing cells implanted in their abdomen. Applying the music directly at 60 dB led to near wild-type levels of insulin in the blood within 15 minutes.
“With only 4 hours required for a full refill, [the system] can provide several therapeutic doses a day,” says Martin Fussenegger, PhD, professor of biotechnology and bioengineering, Department of Biosystems Science and Engineering, ETH Zurich, Basel, Switzerland, and colleagues.
“This would match the typical needs of people with type 2 diabetes consuming three meals a day, and for whom administration of prandial insulin is an established treatment option, as they do not have capability for early postprandial insulin secretion from preformed insulin.”
As the system requires nothing more than portable battery-powered commercially available loudspeakers, the multiple daily dosing of biopharmaceuticals becomes “straightforward in the absence of medical infrastructure or staff, simply by having the patient listen to the prescribed music.”
It therefore “could be an interesting option for cell-based therapies, especially where the need for frequent dosing raises compliance issues.”
It is a “very exciting piece of work, no doubt,” said Anandwardhan A. Hardikar, PhD, group leader, Diabetes and Islet Biology Group, Translational Health Research Institute, Western Sydney University, Penrith NSW, Australia.
He pointed out that the concept of using music to drive gene expression “is something we’ve known for the last 20 years,” but bringing the different strands of research together to generate cells that can be implanted into mice is “an amazing idea.”
Dr. Hardikar, who was not involved in the study, said, however, the publication of the study as a correspondence “does not allow for a lot of the detail that I would have expected as an academic,” and consequently some questions remain.
The most important is whether the music itself is required to trigger the insulin release, as opposed simply to sounds in general.
Is Music or Sound the “Trigger?”
Music is “frequency, it’s the amplitude of the waveform, and it’s the duration for which those waveforms are present,” he noted, but the same profile can be achieved by cutting up and editing the melody so it becomes a jumble of sounds.
For Dr. Hardikar, the “best control” for the study would be to have no music as well as the edited song, with “bits of pieces” played randomly so “it sounds like it’s the same frequency and amplitude.”
Then it would be clear whether the effect is owing to the “noise, or we have to appreciate the melody.”
The other outstanding question is whether the results “can directly translate to larger animals,” such as humans, Dr. Hardikar said.
The authors point out that when translated into mechanical vibrations in the middle ear, the acoustic waves of music activate mechanosensitive ion channels, a form of trigger that is seen across the animal kingdom.
They go on to highlight that while gene switches have been developed for use in next-generation cell-based therapies for a range of conditions, small-molecular trigger compounds face a number of challenges and may cause adverse effects.
With “traceless triggers” such as light, ultrasound, magnetic fields, radio waves, electricity, and heat also facing issues, there is a “need for new switching modalities.”
The researchers therefore developed a music-inducible cellular control (MUSIC) system, which leverages the known intracellular calcium surge in response to music, via calcium-permeable mechanosensitive channels, to drive the release of biopharmaceuticals from vesicles.
They then generated MUSIC-controlled insulin-releasing cell lines, finding that, using a customized box containing off-the-shelf loudspeakers, they could induce channel activation and insulin release with 60 dB at 50 Hz, which is “within the safe range for the human ear.”
Further experiments revealed that insulin release was greatest at 50-100 Hz, and higher than that seen with potassium chloride, the “gold-standard” depolarization control for calcium channels.
The researchers then showed that with optimal stimulation at 50 Hz and 60 dB, channel activation and subsequent insulin release required at least 3 seconds of continuous music, “which might protect the cellular device from inadvertent activation during everyday activities.”
Next, they examined the impact of different musical genres on insulin release, finding that low-bass heavy popular music and movie soundtracks induced maximum release, while the responses were more diverse to classical and guitar-based music.
Specifically, “We Will Rock You,” by the British rock band Queen, induced the release of 70% of available insulin within 5 minutes and 100% within 15 minutes. This, the team notes, is “similar to the dynamics of glucose-triggered insulin release by human pancreatic islets.”
Exposing the cells to a second music session at different intervals revealed that full insulin refill was achieved within 4 hours, which “would be appropriate to attenuate glycemic excursions associated with typical dietary habits.”
Finally, the researchers tested the system in vivo, constructing a box with two off-the-shelf loudspeakers that focuses acoustic waves, via deflectors, onto the abdomens of mice with type 1 diabetes.
Exposing the mice, which had been implanted with microencapsulated MUSIC cells in the peritoneum, to low-bass acoustic waves at 60 dB (50 m/s2) for 15 minutes allowed them to achieve near wild-type levels of insulin in the blood and restored normoglycemia.
Moreover, “Queen’s song ‘We Will Rock You’ generated sufficient insulin to rapidly attenuate postprandial glycemic excursions during glucose tolerance tests,” the team says.
In contrast, animals without implants, or those that had implants but did not have music immersion, remained severely hyperglycemic, they add.
They also note that the effect was seen only when the sound waves “directly impinge on the skin just above the implantation site” for at least 15 minutes, with no increase in insulin release observed with commercially available headphones or ear plugs, such as Apple AirPods, or with loud environmental noises.
Consequently, “therapeutic MUSIC sessions would still be compatible with listening to other types of music or listening to all types of music via headphones,” the researchers write, and are “compatible with standard drug administration schemes.”
The study was supported by a European Research Council advanced grant and in part by the Swiss National Science Foundation NCCR Molecular Systems Engineering. One author acknowledges the support of the Chinese Scholarship Council.
No relevant financial relationships were declared.
A version of this article appeared on Medscape.com.
, reveals a series of experiments.
The research was published in The Lancet Diabetes & Endocrinology.
After developing a cell line in which music-sensitive calcium channels triggered the release of insulin-containing vesicles, the researchers conducted a series of studies identifying the optimal frequency, pitch, and volume of sounds for triggering release.
After settling on low-bass heavy popular music, they tested their system on mice with type 1 diabetes that had the insulin-releasing cells implanted in their abdomen. Applying the music directly at 60 dB led to near wild-type levels of insulin in the blood within 15 minutes.
“With only 4 hours required for a full refill, [the system] can provide several therapeutic doses a day,” says Martin Fussenegger, PhD, professor of biotechnology and bioengineering, Department of Biosystems Science and Engineering, ETH Zurich, Basel, Switzerland, and colleagues.
“This would match the typical needs of people with type 2 diabetes consuming three meals a day, and for whom administration of prandial insulin is an established treatment option, as they do not have capability for early postprandial insulin secretion from preformed insulin.”
As the system requires nothing more than portable battery-powered commercially available loudspeakers, the multiple daily dosing of biopharmaceuticals becomes “straightforward in the absence of medical infrastructure or staff, simply by having the patient listen to the prescribed music.”
It therefore “could be an interesting option for cell-based therapies, especially where the need for frequent dosing raises compliance issues.”
It is a “very exciting piece of work, no doubt,” said Anandwardhan A. Hardikar, PhD, group leader, Diabetes and Islet Biology Group, Translational Health Research Institute, Western Sydney University, Penrith NSW, Australia.
He pointed out that the concept of using music to drive gene expression “is something we’ve known for the last 20 years,” but bringing the different strands of research together to generate cells that can be implanted into mice is “an amazing idea.”
Dr. Hardikar, who was not involved in the study, said, however, the publication of the study as a correspondence “does not allow for a lot of the detail that I would have expected as an academic,” and consequently some questions remain.
The most important is whether the music itself is required to trigger the insulin release, as opposed simply to sounds in general.
Is Music or Sound the “Trigger?”
Music is “frequency, it’s the amplitude of the waveform, and it’s the duration for which those waveforms are present,” he noted, but the same profile can be achieved by cutting up and editing the melody so it becomes a jumble of sounds.
For Dr. Hardikar, the “best control” for the study would be to have no music as well as the edited song, with “bits of pieces” played randomly so “it sounds like it’s the same frequency and amplitude.”
Then it would be clear whether the effect is owing to the “noise, or we have to appreciate the melody.”
The other outstanding question is whether the results “can directly translate to larger animals,” such as humans, Dr. Hardikar said.
The authors point out that when translated into mechanical vibrations in the middle ear, the acoustic waves of music activate mechanosensitive ion channels, a form of trigger that is seen across the animal kingdom.
They go on to highlight that while gene switches have been developed for use in next-generation cell-based therapies for a range of conditions, small-molecular trigger compounds face a number of challenges and may cause adverse effects.
With “traceless triggers” such as light, ultrasound, magnetic fields, radio waves, electricity, and heat also facing issues, there is a “need for new switching modalities.”
The researchers therefore developed a music-inducible cellular control (MUSIC) system, which leverages the known intracellular calcium surge in response to music, via calcium-permeable mechanosensitive channels, to drive the release of biopharmaceuticals from vesicles.
They then generated MUSIC-controlled insulin-releasing cell lines, finding that, using a customized box containing off-the-shelf loudspeakers, they could induce channel activation and insulin release with 60 dB at 50 Hz, which is “within the safe range for the human ear.”
Further experiments revealed that insulin release was greatest at 50-100 Hz, and higher than that seen with potassium chloride, the “gold-standard” depolarization control for calcium channels.
The researchers then showed that with optimal stimulation at 50 Hz and 60 dB, channel activation and subsequent insulin release required at least 3 seconds of continuous music, “which might protect the cellular device from inadvertent activation during everyday activities.”
Next, they examined the impact of different musical genres on insulin release, finding that low-bass heavy popular music and movie soundtracks induced maximum release, while the responses were more diverse to classical and guitar-based music.
Specifically, “We Will Rock You,” by the British rock band Queen, induced the release of 70% of available insulin within 5 minutes and 100% within 15 minutes. This, the team notes, is “similar to the dynamics of glucose-triggered insulin release by human pancreatic islets.”
Exposing the cells to a second music session at different intervals revealed that full insulin refill was achieved within 4 hours, which “would be appropriate to attenuate glycemic excursions associated with typical dietary habits.”
Finally, the researchers tested the system in vivo, constructing a box with two off-the-shelf loudspeakers that focuses acoustic waves, via deflectors, onto the abdomens of mice with type 1 diabetes.
Exposing the mice, which had been implanted with microencapsulated MUSIC cells in the peritoneum, to low-bass acoustic waves at 60 dB (50 m/s2) for 15 minutes allowed them to achieve near wild-type levels of insulin in the blood and restored normoglycemia.
Moreover, “Queen’s song ‘We Will Rock You’ generated sufficient insulin to rapidly attenuate postprandial glycemic excursions during glucose tolerance tests,” the team says.
In contrast, animals without implants, or those that had implants but did not have music immersion, remained severely hyperglycemic, they add.
They also note that the effect was seen only when the sound waves “directly impinge on the skin just above the implantation site” for at least 15 minutes, with no increase in insulin release observed with commercially available headphones or ear plugs, such as Apple AirPods, or with loud environmental noises.
Consequently, “therapeutic MUSIC sessions would still be compatible with listening to other types of music or listening to all types of music via headphones,” the researchers write, and are “compatible with standard drug administration schemes.”
The study was supported by a European Research Council advanced grant and in part by the Swiss National Science Foundation NCCR Molecular Systems Engineering. One author acknowledges the support of the Chinese Scholarship Council.
No relevant financial relationships were declared.
A version of this article appeared on Medscape.com.
, reveals a series of experiments.
The research was published in The Lancet Diabetes & Endocrinology.
After developing a cell line in which music-sensitive calcium channels triggered the release of insulin-containing vesicles, the researchers conducted a series of studies identifying the optimal frequency, pitch, and volume of sounds for triggering release.
After settling on low-bass heavy popular music, they tested their system on mice with type 1 diabetes that had the insulin-releasing cells implanted in their abdomen. Applying the music directly at 60 dB led to near wild-type levels of insulin in the blood within 15 minutes.
“With only 4 hours required for a full refill, [the system] can provide several therapeutic doses a day,” says Martin Fussenegger, PhD, professor of biotechnology and bioengineering, Department of Biosystems Science and Engineering, ETH Zurich, Basel, Switzerland, and colleagues.
“This would match the typical needs of people with type 2 diabetes consuming three meals a day, and for whom administration of prandial insulin is an established treatment option, as they do not have capability for early postprandial insulin secretion from preformed insulin.”
As the system requires nothing more than portable battery-powered commercially available loudspeakers, the multiple daily dosing of biopharmaceuticals becomes “straightforward in the absence of medical infrastructure or staff, simply by having the patient listen to the prescribed music.”
It therefore “could be an interesting option for cell-based therapies, especially where the need for frequent dosing raises compliance issues.”
It is a “very exciting piece of work, no doubt,” said Anandwardhan A. Hardikar, PhD, group leader, Diabetes and Islet Biology Group, Translational Health Research Institute, Western Sydney University, Penrith NSW, Australia.
He pointed out that the concept of using music to drive gene expression “is something we’ve known for the last 20 years,” but bringing the different strands of research together to generate cells that can be implanted into mice is “an amazing idea.”
Dr. Hardikar, who was not involved in the study, said, however, the publication of the study as a correspondence “does not allow for a lot of the detail that I would have expected as an academic,” and consequently some questions remain.
The most important is whether the music itself is required to trigger the insulin release, as opposed simply to sounds in general.
Is Music or Sound the “Trigger?”
Music is “frequency, it’s the amplitude of the waveform, and it’s the duration for which those waveforms are present,” he noted, but the same profile can be achieved by cutting up and editing the melody so it becomes a jumble of sounds.
For Dr. Hardikar, the “best control” for the study would be to have no music as well as the edited song, with “bits of pieces” played randomly so “it sounds like it’s the same frequency and amplitude.”
Then it would be clear whether the effect is owing to the “noise, or we have to appreciate the melody.”
The other outstanding question is whether the results “can directly translate to larger animals,” such as humans, Dr. Hardikar said.
The authors point out that when translated into mechanical vibrations in the middle ear, the acoustic waves of music activate mechanosensitive ion channels, a form of trigger that is seen across the animal kingdom.
They go on to highlight that while gene switches have been developed for use in next-generation cell-based therapies for a range of conditions, small-molecular trigger compounds face a number of challenges and may cause adverse effects.
With “traceless triggers” such as light, ultrasound, magnetic fields, radio waves, electricity, and heat also facing issues, there is a “need for new switching modalities.”
The researchers therefore developed a music-inducible cellular control (MUSIC) system, which leverages the known intracellular calcium surge in response to music, via calcium-permeable mechanosensitive channels, to drive the release of biopharmaceuticals from vesicles.
They then generated MUSIC-controlled insulin-releasing cell lines, finding that, using a customized box containing off-the-shelf loudspeakers, they could induce channel activation and insulin release with 60 dB at 50 Hz, which is “within the safe range for the human ear.”
Further experiments revealed that insulin release was greatest at 50-100 Hz, and higher than that seen with potassium chloride, the “gold-standard” depolarization control for calcium channels.
The researchers then showed that with optimal stimulation at 50 Hz and 60 dB, channel activation and subsequent insulin release required at least 3 seconds of continuous music, “which might protect the cellular device from inadvertent activation during everyday activities.”
Next, they examined the impact of different musical genres on insulin release, finding that low-bass heavy popular music and movie soundtracks induced maximum release, while the responses were more diverse to classical and guitar-based music.
Specifically, “We Will Rock You,” by the British rock band Queen, induced the release of 70% of available insulin within 5 minutes and 100% within 15 minutes. This, the team notes, is “similar to the dynamics of glucose-triggered insulin release by human pancreatic islets.”
Exposing the cells to a second music session at different intervals revealed that full insulin refill was achieved within 4 hours, which “would be appropriate to attenuate glycemic excursions associated with typical dietary habits.”
Finally, the researchers tested the system in vivo, constructing a box with two off-the-shelf loudspeakers that focuses acoustic waves, via deflectors, onto the abdomens of mice with type 1 diabetes.
Exposing the mice, which had been implanted with microencapsulated MUSIC cells in the peritoneum, to low-bass acoustic waves at 60 dB (50 m/s2) for 15 minutes allowed them to achieve near wild-type levels of insulin in the blood and restored normoglycemia.
Moreover, “Queen’s song ‘We Will Rock You’ generated sufficient insulin to rapidly attenuate postprandial glycemic excursions during glucose tolerance tests,” the team says.
In contrast, animals without implants, or those that had implants but did not have music immersion, remained severely hyperglycemic, they add.
They also note that the effect was seen only when the sound waves “directly impinge on the skin just above the implantation site” for at least 15 minutes, with no increase in insulin release observed with commercially available headphones or ear plugs, such as Apple AirPods, or with loud environmental noises.
Consequently, “therapeutic MUSIC sessions would still be compatible with listening to other types of music or listening to all types of music via headphones,” the researchers write, and are “compatible with standard drug administration schemes.”
The study was supported by a European Research Council advanced grant and in part by the Swiss National Science Foundation NCCR Molecular Systems Engineering. One author acknowledges the support of the Chinese Scholarship Council.
No relevant financial relationships were declared.
A version of this article appeared on Medscape.com.
FROM THE LANCET DIABETES & ENDOCRINOLOGY
What causes obesity? More science points to the brain
For much of his life, 32-year-old Michael Smith had a war going on in his head.
After a big meal, he knew he should be full. But an inexplicable hunger would drive him to pick up the fork again.
Cravings for fried chicken or gummy bears overwhelmed him, fueling late-night DoorDash orders that — despite their bounty of fat and sugar — never satisfied him.
He recalls waking up on the couch, half-eaten takeout in his lap, feeling sluggish and out of control.
“It was like I was food drunk,” recalls Smith, who lives in Boston. “I had a moment I looked at myself in the mirror. I was around 380 pounds, and I said, ‘OK, something has got to give.’ “
Smith is among the 42% of U.S. adults living with obesity, a misunderstood and stubbornly hard-to-manage condition that doctors have only recently begun to call a disease. Its root causes have been debated for decades, with studies suggesting everything from genes to lifestyle to a shifting food supply loaded with carbohydrates and ultra-processed foods. Solutions have long targeted self-discipline and a simple “eat less, move more” strategy with remarkably grim results.
Those who successfully slim down tend to gain back 50% of that weight within 2 years, and 80% within 5 years. Meanwhile, the obesity epidemic marches on.
But a new frontier of brain-based therapies — from GLP-1 agonist drugs thought to act on reward and appetite centers to deep brain stimulation aimed at resetting neural circuits — has kindled hope among patients like Smith and the doctors who treat them. The treatments, and theories behind them, are not without controversy. They’re expensive, have side effects, and, critics contend, pull focus from diet and exercise.
But most agree that in the battle against obesity, one crucial organ has been overlooked.
“Obesity, in almost all circumstances, is most likely a disorder of the brain,” said Casey Halpern, MD, associate professor of neurosurgery at the University of Pennsylvania. “What these individuals need is not simply more willpower, but the therapeutic equivalent of an electrician that can make right these connections inside their brain.”
A Break in the Machine
Throughout the day, the machine that is our brain is constantly humming in the background, taking in subtle signals from our gut, hormones, and environment to determine when we’re hungry, how food makes us feel, and whether we are taking in enough energy, or expending too much, to survive.
said Kevin Hall, PhD, an obesity researcher with the National Institute of Diabetes and Digestive and Kidney Diseases. “I liken it to holding your breath. I can do that for a period of time, and I have some conscious control. But eventually, physiology wins out.”
Mounting evidence suggests that in people with obesity, something in the machine is broken.
One seminal 2001 study in The Lancet suggested that, like people addicted to cocaine or alcohol, they lack receptors to the feel-good brain chemical dopamine and overeat in pursuit of the pleasure they lack.
A recent study, not yet published, from Dr. Hall’s lab drew a slightly different conclusion, suggesting that people with obesity actually have too much dopamine, filling up those receptors so the pleasure spike from eating doesn’t feel like much.
“It’s kind of like trying to shout in a noisy room. You’re going to have to shout louder to have the same effect,” said Dr. Hall.
Gut-brain pathways that tell us we’re full may also be impaired.
In another study, Yale researchers tube-fed 500 calories of sugar or fat directly into the stomachs of 28 lean people and 30 people with obesity. Then they observed brain activity using functional magnetic resonance imaging (fMRI).
In lean people, about 30 regions of the brain quieted after the meal, including parts of the striatum (associated with cravings).
In those with obesity, the brain barely responded at all.
“In my clinic, patients will often say ‘I just finished my dinner, but it doesn’t feel like it,’” said senior author Mireille Serlie, MD, PhD, an obesity researcher at the Yale School of Medicine. “It may be that this nutrient-sensing interaction between the gut and the brain is less pronounced or comes too late for them after the meal.”
Dr. Halpern recently identified a brain circuit linking a memory center (hippocampus) to an appetite control region (hypothalamus). In people with obesity and binge eating disorder, the circuit appears jammed. This may cause them to, in a sense, forget they just ate.
“Some of their eating episodes are almost dissociative — they’re not realizing how much they are eating and can’t keep track of it,” he said.
Another brain system works to maintain longer-term homeostasis — or weight stability. Like a set thermostat, it kicks on to trigger hunger and fatigue when it senses we’re low on fat.
The hormone leptin, found in fat cells, sends signals to the hypothalamus to let it know how much energy we have on board.
“If leptin levels go up, it signals the brain that you have too much fat and you should eat less to return to the starting point,” said Rockefeller University geneticist Jeffrey Friedman, MD, PhD, who discovered the hormone in 1994. “If you have too little fat and leptin is low, that will stimulate appetite to return you to the starting point.”
In people with obesity, he said, the thermostat — or set point the body seeks to maintain — is too high.
All this raises a crucial question: How do these circuits and pathways malfunction in the first place?
What Breaks the Brain?
Genes, scientists agree, play a role.
Studies show that genetics underlie as much as 75% of people’s differences in body mass index (BMI), with certain gene combinations raising obesity risk in particular environments.
While hundreds of genes are believed to have a small effect, about a dozen single genes are thought to have a large effect. (Notably, most influence brain function.) For instance, about 6% of people with severe obesity since childhood have mutations in a gene called MC4R (melanocortin 4 receptor), which influences leptin signaling.
Still, genetics alone cannot account for the explosion in obesity in the U.S. over the last 50 years, says epidemiologist Deirdre Tobias, ScD, assistant professor of medicine at Harvard Medical School.
At the population level, “our genes don’t change that much in less than a generation,” she said.
But our food supply has.
Ultra-processed foods — those containing hydrogenated oils, high-fructose corn syrup, flavoring agents, emulsifiers, and other manufactured ingredients — now make up about 60% of the food supply.
“The evidence is fairly consistent indicating that there’s something about these foods that is possibly causing obesity,” said Tobias.
In one telling 2019 study, Dr. Hall and his colleagues brought 20 men and women into a study center to live for a month and tightly controlled their food intake and activity. One group was provided with meals with 80% of calories from ultra-processed food. The other was given meals with no processed food.
The three daily meals provided had the same calories, sugars, fats, fiber, and carbohydrates, and people were told to eat as much as they wanted.
Those on the ultra-processed diet ate about 500 calories more per day, ate faster, and gained weight. Those on the unprocessed diet lost weight.
“This is a stark example of how, when you can change the food environment, you cause really remarkable changes in food intake without people even being aware that they are overeating,” said Dr. Hall.
Just what it is about these relatively novel foods that may trigger overeating is unclear. It could be the crunch, the lack of water content, the engineered balance of sugar/salt/fat, their easy-to-devour texture, or something else.
Some research suggests that the foods may interfere with gut-brain signaling that tells the brain you’re full.
“Evidence is amassing that the nutritional content of processed foods is not accurately conveyed to the brain,” Dana M. Small, PhD, a neuroscientist at Yale, wrote in a recent perspective paper in Science.
Even more concerning: Some animal studies suggest processed foods reprogram the brain to dislike healthy foods.
And once these brain changes are made, they are hard to reverse.
“The problem is, our brain is not wired for this,” said Dr. Halpern. “We are not evolved to eat the food we are eating, so our brain adapts, but it adapts in a negative way that puts us at risk.”
That’s why changing the food environment via public policy must be part of the solution in combating obesity, Dr. Tobias said.
A New Era of Brain-Based Solutions
In the spring of 2021, after years of trying and failing to lose weight via the “move more, eat less” model, Michael Smith began to take a medication called Vyvanse. The drug was approved in 2008 for attention deficit hyperactivity disorder, but since it also influences levels of the hormones dopamine and norepinephrine to reduce cravings, it is now frequently prescribed for binge eating disorder.
“That was pretty much how I got rid of my first 60 to 70 pounds,” Smith said.
A few months later, after he hit a plateau, he had surgery to shrink the size of his stomach — a decision he now second-guesses.
While it kept him from overeating for a time, the fried chicken and gummy bear cravings returned a few months later.
His doctor, Fatima Cody Stanford, MD, put him on a second medication: semaglutide, or Wegovy, the weekly shot approved for weight loss in 2021. It works, in part, by mimicking glucagon-like peptide-1 (GLP-1), a key gut hormone that lets your brain know you are full.
The weight began to fall off again.
Smith’s success story is just one of many that Dr. Stanford, an obesity medicine doctor-scientist at Harvard, has heard in her office in recent years.
“I do not believe these drugs are a panacea,” she said. “There are nonresponders, and those are the patients I take off the medication. But for the high-responders, and there are many of them, they are telling me, ‘Oh my gosh. For the first time in my life, I am not constantly thinking about eating. My life has changed.’”
A Multi-Pronged Approach
Dr. Halpern, at Penn, has also been hearing success stories.
In recent years, he has placed permanent electrodes in the brains of three people with grade III, or severe, obesity and binge eating disorder.
All had tried exercise, dieting, support groups, medication, and weight loss surgery to no avail.
The electrodes modulate an area in the center of the brain called the nucleus accumbens, which in mice studies has been shown to reduce cravings when stimulated.
Thus far, all three are seeing promising results.
“It’s not like I don’t think about food at all,” one of them, Robyn Baldwin, told The New York Times. “But I’m no longer a craving person.”
Dr. Halpern is now extending the trial to more patients and hopes to ultimately include other areas of the brain, including those that involve memory.
He imagines a day when people with severe obesity, who have failed conventional treatments, can walk into a clinic and have their brain circuits assessed to see which ones may be misfiring.
Many might find relief with noninvasive brain stimulation, like transcranial magnetic stimulation (already in use for depression). Others might need a more extreme approach, like the deep brain stimulation, or DBS, therapy Dr. Halpern used.
“Obviously, DBS is hard to scale, so it would have to be reserved for the most severe patients,” he said.
Still, not everyone believes brain-based drugs and surgeries are the answer.
David Ludwig, MD, PhD, a professor of nutrition at the Harvard School of Public Health, played a key role in the discovery of GLP-1 and acknowledges that “of course” the brain influences body composition. But to him, explaining obesity as a disease of the brain oversimplifies it, discounting metabolic factors such as a tendency to store too much fat.
He noted that it’s hard to get drug companies, or any agencies, to fund large clinical trials on simple things like low-carbohydrate diets or exercise programs.
“We need all the tools we can get in the battle against the obesity epidemic, and new technologies are worth exploring,” he said. “However, the success of these drugs should not lead us to deprioritize diet and lifestyle interventions.”
Dr. Stanford, who has received consulting fees from Wegovy, believes the future of treatment lies in a multi-pronged approach, with surgery, medication, and lifestyle changes coalescing in a lasting, but fragile, remission.
“Unfortunately, there is no cure for obesity,” said Dr. Stanford, whose patients often have setbacks and must try new strategies. “There are treatments that work for a while, but they are constantly pushing up against this origin in the brain.”
Smith says understanding this has been a big part of his success.
He is now a leaner and healthier 5-foot-6 and 204 pounds. In addition to taking his medication, he walks to work, goes to the gym twice a week, limits his portions, and tries to reframe the way he thinks about food, viewing it as fuel rather than an indulgence.
Sometimes, when he looks in the mirror, he is reminded of his 380-pound self, and it scares him. He doesn’t want to go back there. He’s confident now that he won’t have to.
“There is this misconception out there that you just need to put the fork down, but I’m learning it’s more complicated than that,” he said. “I intend to treat this as the illness that it is and do what I need to combat it so I’m able to keep this new reality I have built for myself.”
A version of this article appeared on WebMD.com .
For much of his life, 32-year-old Michael Smith had a war going on in his head.
After a big meal, he knew he should be full. But an inexplicable hunger would drive him to pick up the fork again.
Cravings for fried chicken or gummy bears overwhelmed him, fueling late-night DoorDash orders that — despite their bounty of fat and sugar — never satisfied him.
He recalls waking up on the couch, half-eaten takeout in his lap, feeling sluggish and out of control.
“It was like I was food drunk,” recalls Smith, who lives in Boston. “I had a moment I looked at myself in the mirror. I was around 380 pounds, and I said, ‘OK, something has got to give.’ “
Smith is among the 42% of U.S. adults living with obesity, a misunderstood and stubbornly hard-to-manage condition that doctors have only recently begun to call a disease. Its root causes have been debated for decades, with studies suggesting everything from genes to lifestyle to a shifting food supply loaded with carbohydrates and ultra-processed foods. Solutions have long targeted self-discipline and a simple “eat less, move more” strategy with remarkably grim results.
Those who successfully slim down tend to gain back 50% of that weight within 2 years, and 80% within 5 years. Meanwhile, the obesity epidemic marches on.
But a new frontier of brain-based therapies — from GLP-1 agonist drugs thought to act on reward and appetite centers to deep brain stimulation aimed at resetting neural circuits — has kindled hope among patients like Smith and the doctors who treat them. The treatments, and theories behind them, are not without controversy. They’re expensive, have side effects, and, critics contend, pull focus from diet and exercise.
But most agree that in the battle against obesity, one crucial organ has been overlooked.
“Obesity, in almost all circumstances, is most likely a disorder of the brain,” said Casey Halpern, MD, associate professor of neurosurgery at the University of Pennsylvania. “What these individuals need is not simply more willpower, but the therapeutic equivalent of an electrician that can make right these connections inside their brain.”
A Break in the Machine
Throughout the day, the machine that is our brain is constantly humming in the background, taking in subtle signals from our gut, hormones, and environment to determine when we’re hungry, how food makes us feel, and whether we are taking in enough energy, or expending too much, to survive.
said Kevin Hall, PhD, an obesity researcher with the National Institute of Diabetes and Digestive and Kidney Diseases. “I liken it to holding your breath. I can do that for a period of time, and I have some conscious control. But eventually, physiology wins out.”
Mounting evidence suggests that in people with obesity, something in the machine is broken.
One seminal 2001 study in The Lancet suggested that, like people addicted to cocaine or alcohol, they lack receptors to the feel-good brain chemical dopamine and overeat in pursuit of the pleasure they lack.
A recent study, not yet published, from Dr. Hall’s lab drew a slightly different conclusion, suggesting that people with obesity actually have too much dopamine, filling up those receptors so the pleasure spike from eating doesn’t feel like much.
“It’s kind of like trying to shout in a noisy room. You’re going to have to shout louder to have the same effect,” said Dr. Hall.
Gut-brain pathways that tell us we’re full may also be impaired.
In another study, Yale researchers tube-fed 500 calories of sugar or fat directly into the stomachs of 28 lean people and 30 people with obesity. Then they observed brain activity using functional magnetic resonance imaging (fMRI).
In lean people, about 30 regions of the brain quieted after the meal, including parts of the striatum (associated with cravings).
In those with obesity, the brain barely responded at all.
“In my clinic, patients will often say ‘I just finished my dinner, but it doesn’t feel like it,’” said senior author Mireille Serlie, MD, PhD, an obesity researcher at the Yale School of Medicine. “It may be that this nutrient-sensing interaction between the gut and the brain is less pronounced or comes too late for them after the meal.”
Dr. Halpern recently identified a brain circuit linking a memory center (hippocampus) to an appetite control region (hypothalamus). In people with obesity and binge eating disorder, the circuit appears jammed. This may cause them to, in a sense, forget they just ate.
“Some of their eating episodes are almost dissociative — they’re not realizing how much they are eating and can’t keep track of it,” he said.
Another brain system works to maintain longer-term homeostasis — or weight stability. Like a set thermostat, it kicks on to trigger hunger and fatigue when it senses we’re low on fat.
The hormone leptin, found in fat cells, sends signals to the hypothalamus to let it know how much energy we have on board.
“If leptin levels go up, it signals the brain that you have too much fat and you should eat less to return to the starting point,” said Rockefeller University geneticist Jeffrey Friedman, MD, PhD, who discovered the hormone in 1994. “If you have too little fat and leptin is low, that will stimulate appetite to return you to the starting point.”
In people with obesity, he said, the thermostat — or set point the body seeks to maintain — is too high.
All this raises a crucial question: How do these circuits and pathways malfunction in the first place?
What Breaks the Brain?
Genes, scientists agree, play a role.
Studies show that genetics underlie as much as 75% of people’s differences in body mass index (BMI), with certain gene combinations raising obesity risk in particular environments.
While hundreds of genes are believed to have a small effect, about a dozen single genes are thought to have a large effect. (Notably, most influence brain function.) For instance, about 6% of people with severe obesity since childhood have mutations in a gene called MC4R (melanocortin 4 receptor), which influences leptin signaling.
Still, genetics alone cannot account for the explosion in obesity in the U.S. over the last 50 years, says epidemiologist Deirdre Tobias, ScD, assistant professor of medicine at Harvard Medical School.
At the population level, “our genes don’t change that much in less than a generation,” she said.
But our food supply has.
Ultra-processed foods — those containing hydrogenated oils, high-fructose corn syrup, flavoring agents, emulsifiers, and other manufactured ingredients — now make up about 60% of the food supply.
“The evidence is fairly consistent indicating that there’s something about these foods that is possibly causing obesity,” said Tobias.
In one telling 2019 study, Dr. Hall and his colleagues brought 20 men and women into a study center to live for a month and tightly controlled their food intake and activity. One group was provided with meals with 80% of calories from ultra-processed food. The other was given meals with no processed food.
The three daily meals provided had the same calories, sugars, fats, fiber, and carbohydrates, and people were told to eat as much as they wanted.
Those on the ultra-processed diet ate about 500 calories more per day, ate faster, and gained weight. Those on the unprocessed diet lost weight.
“This is a stark example of how, when you can change the food environment, you cause really remarkable changes in food intake without people even being aware that they are overeating,” said Dr. Hall.
Just what it is about these relatively novel foods that may trigger overeating is unclear. It could be the crunch, the lack of water content, the engineered balance of sugar/salt/fat, their easy-to-devour texture, or something else.
Some research suggests that the foods may interfere with gut-brain signaling that tells the brain you’re full.
“Evidence is amassing that the nutritional content of processed foods is not accurately conveyed to the brain,” Dana M. Small, PhD, a neuroscientist at Yale, wrote in a recent perspective paper in Science.
Even more concerning: Some animal studies suggest processed foods reprogram the brain to dislike healthy foods.
And once these brain changes are made, they are hard to reverse.
“The problem is, our brain is not wired for this,” said Dr. Halpern. “We are not evolved to eat the food we are eating, so our brain adapts, but it adapts in a negative way that puts us at risk.”
That’s why changing the food environment via public policy must be part of the solution in combating obesity, Dr. Tobias said.
A New Era of Brain-Based Solutions
In the spring of 2021, after years of trying and failing to lose weight via the “move more, eat less” model, Michael Smith began to take a medication called Vyvanse. The drug was approved in 2008 for attention deficit hyperactivity disorder, but since it also influences levels of the hormones dopamine and norepinephrine to reduce cravings, it is now frequently prescribed for binge eating disorder.
“That was pretty much how I got rid of my first 60 to 70 pounds,” Smith said.
A few months later, after he hit a plateau, he had surgery to shrink the size of his stomach — a decision he now second-guesses.
While it kept him from overeating for a time, the fried chicken and gummy bear cravings returned a few months later.
His doctor, Fatima Cody Stanford, MD, put him on a second medication: semaglutide, or Wegovy, the weekly shot approved for weight loss in 2021. It works, in part, by mimicking glucagon-like peptide-1 (GLP-1), a key gut hormone that lets your brain know you are full.
The weight began to fall off again.
Smith’s success story is just one of many that Dr. Stanford, an obesity medicine doctor-scientist at Harvard, has heard in her office in recent years.
“I do not believe these drugs are a panacea,” she said. “There are nonresponders, and those are the patients I take off the medication. But for the high-responders, and there are many of them, they are telling me, ‘Oh my gosh. For the first time in my life, I am not constantly thinking about eating. My life has changed.’”
A Multi-Pronged Approach
Dr. Halpern, at Penn, has also been hearing success stories.
In recent years, he has placed permanent electrodes in the brains of three people with grade III, or severe, obesity and binge eating disorder.
All had tried exercise, dieting, support groups, medication, and weight loss surgery to no avail.
The electrodes modulate an area in the center of the brain called the nucleus accumbens, which in mice studies has been shown to reduce cravings when stimulated.
Thus far, all three are seeing promising results.
“It’s not like I don’t think about food at all,” one of them, Robyn Baldwin, told The New York Times. “But I’m no longer a craving person.”
Dr. Halpern is now extending the trial to more patients and hopes to ultimately include other areas of the brain, including those that involve memory.
He imagines a day when people with severe obesity, who have failed conventional treatments, can walk into a clinic and have their brain circuits assessed to see which ones may be misfiring.
Many might find relief with noninvasive brain stimulation, like transcranial magnetic stimulation (already in use for depression). Others might need a more extreme approach, like the deep brain stimulation, or DBS, therapy Dr. Halpern used.
“Obviously, DBS is hard to scale, so it would have to be reserved for the most severe patients,” he said.
Still, not everyone believes brain-based drugs and surgeries are the answer.
David Ludwig, MD, PhD, a professor of nutrition at the Harvard School of Public Health, played a key role in the discovery of GLP-1 and acknowledges that “of course” the brain influences body composition. But to him, explaining obesity as a disease of the brain oversimplifies it, discounting metabolic factors such as a tendency to store too much fat.
He noted that it’s hard to get drug companies, or any agencies, to fund large clinical trials on simple things like low-carbohydrate diets or exercise programs.
“We need all the tools we can get in the battle against the obesity epidemic, and new technologies are worth exploring,” he said. “However, the success of these drugs should not lead us to deprioritize diet and lifestyle interventions.”
Dr. Stanford, who has received consulting fees from Wegovy, believes the future of treatment lies in a multi-pronged approach, with surgery, medication, and lifestyle changes coalescing in a lasting, but fragile, remission.
“Unfortunately, there is no cure for obesity,” said Dr. Stanford, whose patients often have setbacks and must try new strategies. “There are treatments that work for a while, but they are constantly pushing up against this origin in the brain.”
Smith says understanding this has been a big part of his success.
He is now a leaner and healthier 5-foot-6 and 204 pounds. In addition to taking his medication, he walks to work, goes to the gym twice a week, limits his portions, and tries to reframe the way he thinks about food, viewing it as fuel rather than an indulgence.
Sometimes, when he looks in the mirror, he is reminded of his 380-pound self, and it scares him. He doesn’t want to go back there. He’s confident now that he won’t have to.
“There is this misconception out there that you just need to put the fork down, but I’m learning it’s more complicated than that,” he said. “I intend to treat this as the illness that it is and do what I need to combat it so I’m able to keep this new reality I have built for myself.”
A version of this article appeared on WebMD.com .
For much of his life, 32-year-old Michael Smith had a war going on in his head.
After a big meal, he knew he should be full. But an inexplicable hunger would drive him to pick up the fork again.
Cravings for fried chicken or gummy bears overwhelmed him, fueling late-night DoorDash orders that — despite their bounty of fat and sugar — never satisfied him.
He recalls waking up on the couch, half-eaten takeout in his lap, feeling sluggish and out of control.
“It was like I was food drunk,” recalls Smith, who lives in Boston. “I had a moment I looked at myself in the mirror. I was around 380 pounds, and I said, ‘OK, something has got to give.’ “
Smith is among the 42% of U.S. adults living with obesity, a misunderstood and stubbornly hard-to-manage condition that doctors have only recently begun to call a disease. Its root causes have been debated for decades, with studies suggesting everything from genes to lifestyle to a shifting food supply loaded with carbohydrates and ultra-processed foods. Solutions have long targeted self-discipline and a simple “eat less, move more” strategy with remarkably grim results.
Those who successfully slim down tend to gain back 50% of that weight within 2 years, and 80% within 5 years. Meanwhile, the obesity epidemic marches on.
But a new frontier of brain-based therapies — from GLP-1 agonist drugs thought to act on reward and appetite centers to deep brain stimulation aimed at resetting neural circuits — has kindled hope among patients like Smith and the doctors who treat them. The treatments, and theories behind them, are not without controversy. They’re expensive, have side effects, and, critics contend, pull focus from diet and exercise.
But most agree that in the battle against obesity, one crucial organ has been overlooked.
“Obesity, in almost all circumstances, is most likely a disorder of the brain,” said Casey Halpern, MD, associate professor of neurosurgery at the University of Pennsylvania. “What these individuals need is not simply more willpower, but the therapeutic equivalent of an electrician that can make right these connections inside their brain.”
A Break in the Machine
Throughout the day, the machine that is our brain is constantly humming in the background, taking in subtle signals from our gut, hormones, and environment to determine when we’re hungry, how food makes us feel, and whether we are taking in enough energy, or expending too much, to survive.
said Kevin Hall, PhD, an obesity researcher with the National Institute of Diabetes and Digestive and Kidney Diseases. “I liken it to holding your breath. I can do that for a period of time, and I have some conscious control. But eventually, physiology wins out.”
Mounting evidence suggests that in people with obesity, something in the machine is broken.
One seminal 2001 study in The Lancet suggested that, like people addicted to cocaine or alcohol, they lack receptors to the feel-good brain chemical dopamine and overeat in pursuit of the pleasure they lack.
A recent study, not yet published, from Dr. Hall’s lab drew a slightly different conclusion, suggesting that people with obesity actually have too much dopamine, filling up those receptors so the pleasure spike from eating doesn’t feel like much.
“It’s kind of like trying to shout in a noisy room. You’re going to have to shout louder to have the same effect,” said Dr. Hall.
Gut-brain pathways that tell us we’re full may also be impaired.
In another study, Yale researchers tube-fed 500 calories of sugar or fat directly into the stomachs of 28 lean people and 30 people with obesity. Then they observed brain activity using functional magnetic resonance imaging (fMRI).
In lean people, about 30 regions of the brain quieted after the meal, including parts of the striatum (associated with cravings).
In those with obesity, the brain barely responded at all.
“In my clinic, patients will often say ‘I just finished my dinner, but it doesn’t feel like it,’” said senior author Mireille Serlie, MD, PhD, an obesity researcher at the Yale School of Medicine. “It may be that this nutrient-sensing interaction between the gut and the brain is less pronounced or comes too late for them after the meal.”
Dr. Halpern recently identified a brain circuit linking a memory center (hippocampus) to an appetite control region (hypothalamus). In people with obesity and binge eating disorder, the circuit appears jammed. This may cause them to, in a sense, forget they just ate.
“Some of their eating episodes are almost dissociative — they’re not realizing how much they are eating and can’t keep track of it,” he said.
Another brain system works to maintain longer-term homeostasis — or weight stability. Like a set thermostat, it kicks on to trigger hunger and fatigue when it senses we’re low on fat.
The hormone leptin, found in fat cells, sends signals to the hypothalamus to let it know how much energy we have on board.
“If leptin levels go up, it signals the brain that you have too much fat and you should eat less to return to the starting point,” said Rockefeller University geneticist Jeffrey Friedman, MD, PhD, who discovered the hormone in 1994. “If you have too little fat and leptin is low, that will stimulate appetite to return you to the starting point.”
In people with obesity, he said, the thermostat — or set point the body seeks to maintain — is too high.
All this raises a crucial question: How do these circuits and pathways malfunction in the first place?
What Breaks the Brain?
Genes, scientists agree, play a role.
Studies show that genetics underlie as much as 75% of people’s differences in body mass index (BMI), with certain gene combinations raising obesity risk in particular environments.
While hundreds of genes are believed to have a small effect, about a dozen single genes are thought to have a large effect. (Notably, most influence brain function.) For instance, about 6% of people with severe obesity since childhood have mutations in a gene called MC4R (melanocortin 4 receptor), which influences leptin signaling.
Still, genetics alone cannot account for the explosion in obesity in the U.S. over the last 50 years, says epidemiologist Deirdre Tobias, ScD, assistant professor of medicine at Harvard Medical School.
At the population level, “our genes don’t change that much in less than a generation,” she said.
But our food supply has.
Ultra-processed foods — those containing hydrogenated oils, high-fructose corn syrup, flavoring agents, emulsifiers, and other manufactured ingredients — now make up about 60% of the food supply.
“The evidence is fairly consistent indicating that there’s something about these foods that is possibly causing obesity,” said Tobias.
In one telling 2019 study, Dr. Hall and his colleagues brought 20 men and women into a study center to live for a month and tightly controlled their food intake and activity. One group was provided with meals with 80% of calories from ultra-processed food. The other was given meals with no processed food.
The three daily meals provided had the same calories, sugars, fats, fiber, and carbohydrates, and people were told to eat as much as they wanted.
Those on the ultra-processed diet ate about 500 calories more per day, ate faster, and gained weight. Those on the unprocessed diet lost weight.
“This is a stark example of how, when you can change the food environment, you cause really remarkable changes in food intake without people even being aware that they are overeating,” said Dr. Hall.
Just what it is about these relatively novel foods that may trigger overeating is unclear. It could be the crunch, the lack of water content, the engineered balance of sugar/salt/fat, their easy-to-devour texture, or something else.
Some research suggests that the foods may interfere with gut-brain signaling that tells the brain you’re full.
“Evidence is amassing that the nutritional content of processed foods is not accurately conveyed to the brain,” Dana M. Small, PhD, a neuroscientist at Yale, wrote in a recent perspective paper in Science.
Even more concerning: Some animal studies suggest processed foods reprogram the brain to dislike healthy foods.
And once these brain changes are made, they are hard to reverse.
“The problem is, our brain is not wired for this,” said Dr. Halpern. “We are not evolved to eat the food we are eating, so our brain adapts, but it adapts in a negative way that puts us at risk.”
That’s why changing the food environment via public policy must be part of the solution in combating obesity, Dr. Tobias said.
A New Era of Brain-Based Solutions
In the spring of 2021, after years of trying and failing to lose weight via the “move more, eat less” model, Michael Smith began to take a medication called Vyvanse. The drug was approved in 2008 for attention deficit hyperactivity disorder, but since it also influences levels of the hormones dopamine and norepinephrine to reduce cravings, it is now frequently prescribed for binge eating disorder.
“That was pretty much how I got rid of my first 60 to 70 pounds,” Smith said.
A few months later, after he hit a plateau, he had surgery to shrink the size of his stomach — a decision he now second-guesses.
While it kept him from overeating for a time, the fried chicken and gummy bear cravings returned a few months later.
His doctor, Fatima Cody Stanford, MD, put him on a second medication: semaglutide, or Wegovy, the weekly shot approved for weight loss in 2021. It works, in part, by mimicking glucagon-like peptide-1 (GLP-1), a key gut hormone that lets your brain know you are full.
The weight began to fall off again.
Smith’s success story is just one of many that Dr. Stanford, an obesity medicine doctor-scientist at Harvard, has heard in her office in recent years.
“I do not believe these drugs are a panacea,” she said. “There are nonresponders, and those are the patients I take off the medication. But for the high-responders, and there are many of them, they are telling me, ‘Oh my gosh. For the first time in my life, I am not constantly thinking about eating. My life has changed.’”
A Multi-Pronged Approach
Dr. Halpern, at Penn, has also been hearing success stories.
In recent years, he has placed permanent electrodes in the brains of three people with grade III, or severe, obesity and binge eating disorder.
All had tried exercise, dieting, support groups, medication, and weight loss surgery to no avail.
The electrodes modulate an area in the center of the brain called the nucleus accumbens, which in mice studies has been shown to reduce cravings when stimulated.
Thus far, all three are seeing promising results.
“It’s not like I don’t think about food at all,” one of them, Robyn Baldwin, told The New York Times. “But I’m no longer a craving person.”
Dr. Halpern is now extending the trial to more patients and hopes to ultimately include other areas of the brain, including those that involve memory.
He imagines a day when people with severe obesity, who have failed conventional treatments, can walk into a clinic and have their brain circuits assessed to see which ones may be misfiring.
Many might find relief with noninvasive brain stimulation, like transcranial magnetic stimulation (already in use for depression). Others might need a more extreme approach, like the deep brain stimulation, or DBS, therapy Dr. Halpern used.
“Obviously, DBS is hard to scale, so it would have to be reserved for the most severe patients,” he said.
Still, not everyone believes brain-based drugs and surgeries are the answer.
David Ludwig, MD, PhD, a professor of nutrition at the Harvard School of Public Health, played a key role in the discovery of GLP-1 and acknowledges that “of course” the brain influences body composition. But to him, explaining obesity as a disease of the brain oversimplifies it, discounting metabolic factors such as a tendency to store too much fat.
He noted that it’s hard to get drug companies, or any agencies, to fund large clinical trials on simple things like low-carbohydrate diets or exercise programs.
“We need all the tools we can get in the battle against the obesity epidemic, and new technologies are worth exploring,” he said. “However, the success of these drugs should not lead us to deprioritize diet and lifestyle interventions.”
Dr. Stanford, who has received consulting fees from Wegovy, believes the future of treatment lies in a multi-pronged approach, with surgery, medication, and lifestyle changes coalescing in a lasting, but fragile, remission.
“Unfortunately, there is no cure for obesity,” said Dr. Stanford, whose patients often have setbacks and must try new strategies. “There are treatments that work for a while, but they are constantly pushing up against this origin in the brain.”
Smith says understanding this has been a big part of his success.
He is now a leaner and healthier 5-foot-6 and 204 pounds. In addition to taking his medication, he walks to work, goes to the gym twice a week, limits his portions, and tries to reframe the way he thinks about food, viewing it as fuel rather than an indulgence.
Sometimes, when he looks in the mirror, he is reminded of his 380-pound self, and it scares him. He doesn’t want to go back there. He’s confident now that he won’t have to.
“There is this misconception out there that you just need to put the fork down, but I’m learning it’s more complicated than that,” he said. “I intend to treat this as the illness that it is and do what I need to combat it so I’m able to keep this new reality I have built for myself.”
A version of this article appeared on WebMD.com .
Early evidence supports psilocybin for bipolar depression
, a small, nonrandomized clinical trial shows. However, the investigators and other outside experts warn these results should not be overinterpreted.
Three weeks after receiving psilocybin and psychotherapy, all 15 participants’ depression scores dropped by an average of 24 points. Twelve met criteria for response and 11 for remission.
This benefit lasted until the 12-week mark, with 12 participants (80%) meeting criteria for both response and remission. There were no reports of mixed or manic symptoms, psychotic symptoms, or suicidal ideation.
Given the study’s small, open-label design, the findings should be interpreted cautiously, but the investigators say the results are promising.
“The results we saw from this trial are encouraging and further support the clinical study of psychedelics in patients with treatment-resistant bipolar II,” lead investigator Scott T. Aaronson, MD, chief science officer of the Institute for Advanced Diagnostics and Therapeutics at Sheppard Pratt Health System in Baltimore, Maryland, remarked in a press release. “One participant compared the transformation she experienced to taking a deep breath after breathing through a straw for years.”
The findings were published online on December 6, 2023, in JAMA Psychiatry.
Underserved Population
Previous studies show that psilocybin is effective in reducing the symptoms of treatment-resistant depression, major depressive disorder, and anorexia nervosa, most with only mild to moderate adverse effects.
Individuals with bipolar disorder (BPD) have been excluded from psilocybin studies in the last two decades. Investigators attribute this to anecdotal evidence that psychedelics may result in manic episodes in patients with BPD, even though empirical evidence of those effects is limited.
This study included 15 participants (9 female; mean age, 37.8 years) with BDII who had experienced an episode for more than 3 months and failed at least two medications within the current episode.
Participants stopped all psychotropic medications at least 2 weeks prior to the trial and received 25 mg of synthetic COMP360 psilocybin in a controlled setting. Psychotherapy included three sessions before dosing, one during the 8-hour dosing day, and three integration sessions posttreatment.
Depression was measured with the Montgomery Ǻsberg Depression Rating Scale (MADRS) at six points during the 12-week study.
By week 3, all 15 participants had lower MADRS scores, with a mean decrease of 24 points (P < .001). Twelve participants met the response criteria of ≥ 50% reduction in MADRS scores, and 11 met the criteria for remission of a MADRS score of ≤ 10 (both P < .001).
MADRS scores at each posttreatment time point were significantly lower than they were at baseline and the improvement persisted at 12 weeks.
Participants were also monitored for mania and suicidality at various time points during the study, and no significant changes were found from baseline.
“As a first open-label foray into this underserved and treatment-resistant population, care should be taken not to overinterpret the findings,” the authors note, adding that the findings may not apply to patients with BDI or BDII in a mixed or hypomanic phase of their illness.
No Definitive Conclusion
In an accompanying editorial, David B. Yaden, PhD, Johns Hopkins University School of Medicine, Baltimore, Maryland, and colleagues write that the findings are “tantalizingly suggestive,” but ultimately say nothing definitive about the efficacy of psilocybin for BDII.
“The danger is that some individuals will see the large (yet uncontrolled) effect size and believe that a new treatment of bipolar II has been discovered that is substantially better than all other treatments, while neglecting to mention the lack of control condition and substantial psychosocial support included in the study,” Dr. Yaden and colleagues wrote.
They also cautioned that due to the study’s limitations, which include its small sample size and lack of a control group, “it is imperative that the large effect size before to after the study is not overinterpreted.”
However, Dr. Yaden and colleagues also characterized the safety data as “compelling,” noting the safety profile could affect exclusion criteria in future studies involving people with BPD.
“The results of the present study provide preliminary evidence that perhaps those with bipolar II can be safely included in study samples without undue risk of triggering hypomanic episodes,” they wrote. “It also suggests re-evaluation of the need to exclude individuals with mere family history of bipolar II, which several studies do.”
The study was funded by COMPASS Pathways, who provided the study drug. Dr. Aaronson reported grants and nonfinancial support (supply of drug) from COMPASS Pathways during the conduct of the study and personal fees from LivaNova, Neuronetics, Genomind, and Sage Therapeutics outside the submitted work. Other disclosures are noted in the original article.
A version of this article appeared on Medscape.com.
, a small, nonrandomized clinical trial shows. However, the investigators and other outside experts warn these results should not be overinterpreted.
Three weeks after receiving psilocybin and psychotherapy, all 15 participants’ depression scores dropped by an average of 24 points. Twelve met criteria for response and 11 for remission.
This benefit lasted until the 12-week mark, with 12 participants (80%) meeting criteria for both response and remission. There were no reports of mixed or manic symptoms, psychotic symptoms, or suicidal ideation.
Given the study’s small, open-label design, the findings should be interpreted cautiously, but the investigators say the results are promising.
“The results we saw from this trial are encouraging and further support the clinical study of psychedelics in patients with treatment-resistant bipolar II,” lead investigator Scott T. Aaronson, MD, chief science officer of the Institute for Advanced Diagnostics and Therapeutics at Sheppard Pratt Health System in Baltimore, Maryland, remarked in a press release. “One participant compared the transformation she experienced to taking a deep breath after breathing through a straw for years.”
The findings were published online on December 6, 2023, in JAMA Psychiatry.
Underserved Population
Previous studies show that psilocybin is effective in reducing the symptoms of treatment-resistant depression, major depressive disorder, and anorexia nervosa, most with only mild to moderate adverse effects.
Individuals with bipolar disorder (BPD) have been excluded from psilocybin studies in the last two decades. Investigators attribute this to anecdotal evidence that psychedelics may result in manic episodes in patients with BPD, even though empirical evidence of those effects is limited.
This study included 15 participants (9 female; mean age, 37.8 years) with BDII who had experienced an episode for more than 3 months and failed at least two medications within the current episode.
Participants stopped all psychotropic medications at least 2 weeks prior to the trial and received 25 mg of synthetic COMP360 psilocybin in a controlled setting. Psychotherapy included three sessions before dosing, one during the 8-hour dosing day, and three integration sessions posttreatment.
Depression was measured with the Montgomery Ǻsberg Depression Rating Scale (MADRS) at six points during the 12-week study.
By week 3, all 15 participants had lower MADRS scores, with a mean decrease of 24 points (P < .001). Twelve participants met the response criteria of ≥ 50% reduction in MADRS scores, and 11 met the criteria for remission of a MADRS score of ≤ 10 (both P < .001).
MADRS scores at each posttreatment time point were significantly lower than they were at baseline and the improvement persisted at 12 weeks.
Participants were also monitored for mania and suicidality at various time points during the study, and no significant changes were found from baseline.
“As a first open-label foray into this underserved and treatment-resistant population, care should be taken not to overinterpret the findings,” the authors note, adding that the findings may not apply to patients with BDI or BDII in a mixed or hypomanic phase of their illness.
No Definitive Conclusion
In an accompanying editorial, David B. Yaden, PhD, Johns Hopkins University School of Medicine, Baltimore, Maryland, and colleagues write that the findings are “tantalizingly suggestive,” but ultimately say nothing definitive about the efficacy of psilocybin for BDII.
“The danger is that some individuals will see the large (yet uncontrolled) effect size and believe that a new treatment of bipolar II has been discovered that is substantially better than all other treatments, while neglecting to mention the lack of control condition and substantial psychosocial support included in the study,” Dr. Yaden and colleagues wrote.
They also cautioned that due to the study’s limitations, which include its small sample size and lack of a control group, “it is imperative that the large effect size before to after the study is not overinterpreted.”
However, Dr. Yaden and colleagues also characterized the safety data as “compelling,” noting the safety profile could affect exclusion criteria in future studies involving people with BPD.
“The results of the present study provide preliminary evidence that perhaps those with bipolar II can be safely included in study samples without undue risk of triggering hypomanic episodes,” they wrote. “It also suggests re-evaluation of the need to exclude individuals with mere family history of bipolar II, which several studies do.”
The study was funded by COMPASS Pathways, who provided the study drug. Dr. Aaronson reported grants and nonfinancial support (supply of drug) from COMPASS Pathways during the conduct of the study and personal fees from LivaNova, Neuronetics, Genomind, and Sage Therapeutics outside the submitted work. Other disclosures are noted in the original article.
A version of this article appeared on Medscape.com.
, a small, nonrandomized clinical trial shows. However, the investigators and other outside experts warn these results should not be overinterpreted.
Three weeks after receiving psilocybin and psychotherapy, all 15 participants’ depression scores dropped by an average of 24 points. Twelve met criteria for response and 11 for remission.
This benefit lasted until the 12-week mark, with 12 participants (80%) meeting criteria for both response and remission. There were no reports of mixed or manic symptoms, psychotic symptoms, or suicidal ideation.
Given the study’s small, open-label design, the findings should be interpreted cautiously, but the investigators say the results are promising.
“The results we saw from this trial are encouraging and further support the clinical study of psychedelics in patients with treatment-resistant bipolar II,” lead investigator Scott T. Aaronson, MD, chief science officer of the Institute for Advanced Diagnostics and Therapeutics at Sheppard Pratt Health System in Baltimore, Maryland, remarked in a press release. “One participant compared the transformation she experienced to taking a deep breath after breathing through a straw for years.”
The findings were published online on December 6, 2023, in JAMA Psychiatry.
Underserved Population
Previous studies show that psilocybin is effective in reducing the symptoms of treatment-resistant depression, major depressive disorder, and anorexia nervosa, most with only mild to moderate adverse effects.
Individuals with bipolar disorder (BPD) have been excluded from psilocybin studies in the last two decades. Investigators attribute this to anecdotal evidence that psychedelics may result in manic episodes in patients with BPD, even though empirical evidence of those effects is limited.
This study included 15 participants (9 female; mean age, 37.8 years) with BDII who had experienced an episode for more than 3 months and failed at least two medications within the current episode.
Participants stopped all psychotropic medications at least 2 weeks prior to the trial and received 25 mg of synthetic COMP360 psilocybin in a controlled setting. Psychotherapy included three sessions before dosing, one during the 8-hour dosing day, and three integration sessions posttreatment.
Depression was measured with the Montgomery Ǻsberg Depression Rating Scale (MADRS) at six points during the 12-week study.
By week 3, all 15 participants had lower MADRS scores, with a mean decrease of 24 points (P < .001). Twelve participants met the response criteria of ≥ 50% reduction in MADRS scores, and 11 met the criteria for remission of a MADRS score of ≤ 10 (both P < .001).
MADRS scores at each posttreatment time point were significantly lower than they were at baseline and the improvement persisted at 12 weeks.
Participants were also monitored for mania and suicidality at various time points during the study, and no significant changes were found from baseline.
“As a first open-label foray into this underserved and treatment-resistant population, care should be taken not to overinterpret the findings,” the authors note, adding that the findings may not apply to patients with BDI or BDII in a mixed or hypomanic phase of their illness.
No Definitive Conclusion
In an accompanying editorial, David B. Yaden, PhD, Johns Hopkins University School of Medicine, Baltimore, Maryland, and colleagues write that the findings are “tantalizingly suggestive,” but ultimately say nothing definitive about the efficacy of psilocybin for BDII.
“The danger is that some individuals will see the large (yet uncontrolled) effect size and believe that a new treatment of bipolar II has been discovered that is substantially better than all other treatments, while neglecting to mention the lack of control condition and substantial psychosocial support included in the study,” Dr. Yaden and colleagues wrote.
They also cautioned that due to the study’s limitations, which include its small sample size and lack of a control group, “it is imperative that the large effect size before to after the study is not overinterpreted.”
However, Dr. Yaden and colleagues also characterized the safety data as “compelling,” noting the safety profile could affect exclusion criteria in future studies involving people with BPD.
“The results of the present study provide preliminary evidence that perhaps those with bipolar II can be safely included in study samples without undue risk of triggering hypomanic episodes,” they wrote. “It also suggests re-evaluation of the need to exclude individuals with mere family history of bipolar II, which several studies do.”
The study was funded by COMPASS Pathways, who provided the study drug. Dr. Aaronson reported grants and nonfinancial support (supply of drug) from COMPASS Pathways during the conduct of the study and personal fees from LivaNova, Neuronetics, Genomind, and Sage Therapeutics outside the submitted work. Other disclosures are noted in the original article.
A version of this article appeared on Medscape.com.
FROM JAMA PSYCHIATRY
FDA approves implant for glaucoma
The iDose TR (Glaukos Corp) is inserted into a corneal incision on the temple side of the eye. Pivotal phase 3 clinical trials showed the treatment resulted in sustained reductions in IOP for 3 months ranging from 6.6 to 8.4 mm Hg, comparable to reductions with topical timolol 0.5% drops used twice daily. Normal IOP is 10-21 mm Hg, and glaucoma treatments are designed to reduce high IOP into the normal range.
Glaukos Corp said that it intends a commercial launch of the implant early in 2024, with a wholesale cost of $13,950 per implant.
Travoprost is a prostaglandin analog that has been long used as a topical formulation for lowering IOP in OAG and OHT. Timolol is a topical beta-blocker widely used for the same indications.
iDose TR comes in a preloaded handheld injector designed to deliver the implant into the sclera of the eye. The implant seats in the junction of the iris, sclera, and cornea.
In two phase 3 clinical trials, 81% of patients who received the iDose TR did not require supplemental drops to reduce IOP after 12 months compared with 95% of those who receive timolol alone.
The phase 3 trials included 1150 participants across 89 clinical sites. Both trials, GC-010 and GC-012, met the primary endpoints through 3 months and demonstrated a favorable tolerability and safety profile through 12 months, according to results that John Berdahl, MD, a researcher with Vance Thompson Vision in Sioux Falls, South Dakota, and an investigator for Glaukos, presented in May at the annual meeting of the American Society of Cataract and Refractive Surgery.
Based on these outcomes, the FDA concluded in the prescribing information that iDose TR demonstrated noninferiority to topical timolol in reduction of IOP during the first 3 months of treatment. The agency also noted that use of iDose TR did not demonstrate noninferiority over the next 9 months.
In the controlled studies, the most common ocular adverse reactions reported in 2% to 6% of patients who received iDose TR were increases in IOP , iritis, dry eye, and defects of the visual field, most of which were said to be mild and transient in nature.
A version of this article appeared on Medscape.com.
The iDose TR (Glaukos Corp) is inserted into a corneal incision on the temple side of the eye. Pivotal phase 3 clinical trials showed the treatment resulted in sustained reductions in IOP for 3 months ranging from 6.6 to 8.4 mm Hg, comparable to reductions with topical timolol 0.5% drops used twice daily. Normal IOP is 10-21 mm Hg, and glaucoma treatments are designed to reduce high IOP into the normal range.
Glaukos Corp said that it intends a commercial launch of the implant early in 2024, with a wholesale cost of $13,950 per implant.
Travoprost is a prostaglandin analog that has been long used as a topical formulation for lowering IOP in OAG and OHT. Timolol is a topical beta-blocker widely used for the same indications.
iDose TR comes in a preloaded handheld injector designed to deliver the implant into the sclera of the eye. The implant seats in the junction of the iris, sclera, and cornea.
In two phase 3 clinical trials, 81% of patients who received the iDose TR did not require supplemental drops to reduce IOP after 12 months compared with 95% of those who receive timolol alone.
The phase 3 trials included 1150 participants across 89 clinical sites. Both trials, GC-010 and GC-012, met the primary endpoints through 3 months and demonstrated a favorable tolerability and safety profile through 12 months, according to results that John Berdahl, MD, a researcher with Vance Thompson Vision in Sioux Falls, South Dakota, and an investigator for Glaukos, presented in May at the annual meeting of the American Society of Cataract and Refractive Surgery.
Based on these outcomes, the FDA concluded in the prescribing information that iDose TR demonstrated noninferiority to topical timolol in reduction of IOP during the first 3 months of treatment. The agency also noted that use of iDose TR did not demonstrate noninferiority over the next 9 months.
In the controlled studies, the most common ocular adverse reactions reported in 2% to 6% of patients who received iDose TR were increases in IOP , iritis, dry eye, and defects of the visual field, most of which were said to be mild and transient in nature.
A version of this article appeared on Medscape.com.
The iDose TR (Glaukos Corp) is inserted into a corneal incision on the temple side of the eye. Pivotal phase 3 clinical trials showed the treatment resulted in sustained reductions in IOP for 3 months ranging from 6.6 to 8.4 mm Hg, comparable to reductions with topical timolol 0.5% drops used twice daily. Normal IOP is 10-21 mm Hg, and glaucoma treatments are designed to reduce high IOP into the normal range.
Glaukos Corp said that it intends a commercial launch of the implant early in 2024, with a wholesale cost of $13,950 per implant.
Travoprost is a prostaglandin analog that has been long used as a topical formulation for lowering IOP in OAG and OHT. Timolol is a topical beta-blocker widely used for the same indications.
iDose TR comes in a preloaded handheld injector designed to deliver the implant into the sclera of the eye. The implant seats in the junction of the iris, sclera, and cornea.
In two phase 3 clinical trials, 81% of patients who received the iDose TR did not require supplemental drops to reduce IOP after 12 months compared with 95% of those who receive timolol alone.
The phase 3 trials included 1150 participants across 89 clinical sites. Both trials, GC-010 and GC-012, met the primary endpoints through 3 months and demonstrated a favorable tolerability and safety profile through 12 months, according to results that John Berdahl, MD, a researcher with Vance Thompson Vision in Sioux Falls, South Dakota, and an investigator for Glaukos, presented in May at the annual meeting of the American Society of Cataract and Refractive Surgery.
Based on these outcomes, the FDA concluded in the prescribing information that iDose TR demonstrated noninferiority to topical timolol in reduction of IOP during the first 3 months of treatment. The agency also noted that use of iDose TR did not demonstrate noninferiority over the next 9 months.
In the controlled studies, the most common ocular adverse reactions reported in 2% to 6% of patients who received iDose TR were increases in IOP , iritis, dry eye, and defects of the visual field, most of which were said to be mild and transient in nature.
A version of this article appeared on Medscape.com.
Catheter-directed strategy improves pulmonary artery occlusion
Use of pharmacomechanical catheter-directory thrombolysis significantly reduced the number of pulmonary artery branches with total or subtotal occlusions in patients with acute pulmonary embolism, based on data from more than 100 individuals.
Reduced distal vascular volume is a significant predictor of 30-day and 90-day mortality in acute pulmonary embolism (PE) patients, and pulmonary obstruction is often the cause, wrote Riyaz Bashir, MD, of Temple University, Philadelphia, Pennsylvania, and colleagues.
, the researchers said.
“The recently published RESCUE (Recombinant tPA by Endovascular Administration for the Treatment of Submassive PE Using CDT for the Reduction of Thrombus Burden) trial showed a 35.9% reduction in PA obstruction using the Refined Modified Miller Index (RMMI), the largest reduction of all published catheter studies with core lab measurement, with similar doses of tissue plasminogen activator (tPA),” the researchers wrote.
The Bashir endovascular catheter was designed to maximize thrombus reduction via a pharmacomechanical infusion. The catheter features an expandable basket of 6 nitinol-reinforced infusion limbs.
“There are three crucial goals that we want to accomplish in patients who have a severe pulmonary embolism,” Dr. Bashir said in an interview. “Those include, in the order of importance, survival, recovery of right ventricular function, and resolution of blocked pulmonary arteries; both segmental and proximal pulmonary arteries,” he said.
Most previous studies have focused on the first two goals, but they still need to evaluate the resolution of PA blockages carefully, said Dr. Bashir. “In our clinical practice, we have seen a large number of patients who develop debilitating shortness of breath from these blockages. We decided to carefully evaluate these blockages before and after pharmacomechanical catheter-directed thrombolysis with the Bashir endovascular catheter using the core lab data from the RESCUE study,” he said.
In the current study published in JACC: Advances), the researchers used baseline and 48-hour posttreatment contrast-enhanced chest computed tomography angiography of adult PE patients with right ventricular dilatation.
The study population included 107 adults with acute intermediate-risk PE who were treated with pharmacomechanical catheter-directory thrombolysis (PM-CDT) at 18 sites in the United States. Of these, 98 had intermediate high-risk PE with elevated troponin and/or brain-type natriuretic peptide (BNP) levels and 102 had bilateral PE.
The primary endpoint was the change in the number of segmental and proximal PA branches with total or subtotal occlusions (defined as > 65%) after 48 hours compared to baseline. Occlusions were assessed using McNemar’s test.
Patients with bilateral PE received two Bashir catheters; those with unilateral PE received one catheter each.
Each patient received a pulse spray of 2 mg of recombinant tPA (r-tPA) into each lung, followed by 5 mg of r-tPA over 5 hours; the total dose was 7 mg of r-tPA for patients with unilateral PEs and 14 mg for those with bilateral PEs, the researchers said. The median times for catheter placement and total procedure were 15 minutes and 54 minutes, respectively.
The number of segmental PA branches with total or subtotal occlusions decreased significantly, from 40.5% at baseline to 11.7% at 48 hours, and proximal PA branch total or subtotal occlusions decreased significantly, from 28.7% at baseline to 11.0% at 48 hours (P < 0.0001 for both).
The magnitude of the reductions in both total and subtotal occlusions of segmental arteries was significantly correlated with the extent of right ventricle recovery (measured by the reduction in right ventricular/left ventricular ratio) with a correlation coefficient of 0.287 (P = .0026); however, this correlation was not observed in the proximal PA arteries (correlation coefficient 0.132, P = .173).
One major bleeding event occurred within 72 hours in a patient who also experienced a device-related left common iliac vein thrombosis while not taking anticoagulation medication, and one death unrelated to PE occurred within 30 days.
“The two findings that surprised me include, first, a more than 70% reduction in total and subtotal occlusions in the segmental arteries with such a low dose of r-tPA and, second, the resolution of the blockages was seen not only in the arteries where the device was placed but also at remote sites away from the location of the catheter,” Dr. Bashir told this news organization.
The findings were limited by several factors including the lack of long-term clinical follow-up outcomes data and lack of comparison groups who underwent other treatments.
However, “This study implies that we now have a safe therapy for these patients that improves survival and right ventricular recovery in addition to dramatically improving blocked pulmonary arteries,” Dr. Bashir said.
As for additional research, “we need all the current and future prospective pulmonary embolism studies to include an assessment of pulmonary artery blockage resolution as an essential endpoint,” he said.
Catheter Expands Treatment Options
The current study, a subgroup analysis of the RESCUE trial, was one of the first to examine the impact of catheter-directed lysis on distal occlusions, study coauthor Parth M. Rali, MD, said in an interview.
To this point, literature has been limited to evaluation for proximal disease, said Dr. Rali, director of thoracic surgery and medicine and part of the Pulmonary Embolism Response Team at Temple University Hospital, Philadelphia.
Dr. Rali said he was encouraged to see confirmation that the BEC catheter, because of its design, works in patients with proximal or distal occlusive disease.
In clinical practice, “the catheter provides an additional option for care in patients with multiple distal occlusive disease when a systemic tissue plasminogen activator (tPA), may put patient at high bleeding risk,” Dr. Rali said.
Looking ahead, a prospective, observational multicenter study would be useful to validate the findings from the post hoc analysis of the current study, he noted.
The study was sponsored by the National Heart, Lung, and Blood Institute, Commonwealth of Pennsylvania, and Thrombolex Inc., a medical device company developing interventional catheter-based therapies for the rapid and effective treatment of acute venous thromboembolic disorders. Dr. Bashir is a cofounder and has an equity interest in Thrombolex Inc. Dr. Rali disclosed serving as a consultant for Thrombolex, Inari Medical, Viz AI, and ThinkSono.
Use of pharmacomechanical catheter-directory thrombolysis significantly reduced the number of pulmonary artery branches with total or subtotal occlusions in patients with acute pulmonary embolism, based on data from more than 100 individuals.
Reduced distal vascular volume is a significant predictor of 30-day and 90-day mortality in acute pulmonary embolism (PE) patients, and pulmonary obstruction is often the cause, wrote Riyaz Bashir, MD, of Temple University, Philadelphia, Pennsylvania, and colleagues.
, the researchers said.
“The recently published RESCUE (Recombinant tPA by Endovascular Administration for the Treatment of Submassive PE Using CDT for the Reduction of Thrombus Burden) trial showed a 35.9% reduction in PA obstruction using the Refined Modified Miller Index (RMMI), the largest reduction of all published catheter studies with core lab measurement, with similar doses of tissue plasminogen activator (tPA),” the researchers wrote.
The Bashir endovascular catheter was designed to maximize thrombus reduction via a pharmacomechanical infusion. The catheter features an expandable basket of 6 nitinol-reinforced infusion limbs.
“There are three crucial goals that we want to accomplish in patients who have a severe pulmonary embolism,” Dr. Bashir said in an interview. “Those include, in the order of importance, survival, recovery of right ventricular function, and resolution of blocked pulmonary arteries; both segmental and proximal pulmonary arteries,” he said.
Most previous studies have focused on the first two goals, but they still need to evaluate the resolution of PA blockages carefully, said Dr. Bashir. “In our clinical practice, we have seen a large number of patients who develop debilitating shortness of breath from these blockages. We decided to carefully evaluate these blockages before and after pharmacomechanical catheter-directed thrombolysis with the Bashir endovascular catheter using the core lab data from the RESCUE study,” he said.
In the current study published in JACC: Advances), the researchers used baseline and 48-hour posttreatment contrast-enhanced chest computed tomography angiography of adult PE patients with right ventricular dilatation.
The study population included 107 adults with acute intermediate-risk PE who were treated with pharmacomechanical catheter-directory thrombolysis (PM-CDT) at 18 sites in the United States. Of these, 98 had intermediate high-risk PE with elevated troponin and/or brain-type natriuretic peptide (BNP) levels and 102 had bilateral PE.
The primary endpoint was the change in the number of segmental and proximal PA branches with total or subtotal occlusions (defined as > 65%) after 48 hours compared to baseline. Occlusions were assessed using McNemar’s test.
Patients with bilateral PE received two Bashir catheters; those with unilateral PE received one catheter each.
Each patient received a pulse spray of 2 mg of recombinant tPA (r-tPA) into each lung, followed by 5 mg of r-tPA over 5 hours; the total dose was 7 mg of r-tPA for patients with unilateral PEs and 14 mg for those with bilateral PEs, the researchers said. The median times for catheter placement and total procedure were 15 minutes and 54 minutes, respectively.
The number of segmental PA branches with total or subtotal occlusions decreased significantly, from 40.5% at baseline to 11.7% at 48 hours, and proximal PA branch total or subtotal occlusions decreased significantly, from 28.7% at baseline to 11.0% at 48 hours (P < 0.0001 for both).
The magnitude of the reductions in both total and subtotal occlusions of segmental arteries was significantly correlated with the extent of right ventricle recovery (measured by the reduction in right ventricular/left ventricular ratio) with a correlation coefficient of 0.287 (P = .0026); however, this correlation was not observed in the proximal PA arteries (correlation coefficient 0.132, P = .173).
One major bleeding event occurred within 72 hours in a patient who also experienced a device-related left common iliac vein thrombosis while not taking anticoagulation medication, and one death unrelated to PE occurred within 30 days.
“The two findings that surprised me include, first, a more than 70% reduction in total and subtotal occlusions in the segmental arteries with such a low dose of r-tPA and, second, the resolution of the blockages was seen not only in the arteries where the device was placed but also at remote sites away from the location of the catheter,” Dr. Bashir told this news organization.
The findings were limited by several factors including the lack of long-term clinical follow-up outcomes data and lack of comparison groups who underwent other treatments.
However, “This study implies that we now have a safe therapy for these patients that improves survival and right ventricular recovery in addition to dramatically improving blocked pulmonary arteries,” Dr. Bashir said.
As for additional research, “we need all the current and future prospective pulmonary embolism studies to include an assessment of pulmonary artery blockage resolution as an essential endpoint,” he said.
Catheter Expands Treatment Options
The current study, a subgroup analysis of the RESCUE trial, was one of the first to examine the impact of catheter-directed lysis on distal occlusions, study coauthor Parth M. Rali, MD, said in an interview.
To this point, literature has been limited to evaluation for proximal disease, said Dr. Rali, director of thoracic surgery and medicine and part of the Pulmonary Embolism Response Team at Temple University Hospital, Philadelphia.
Dr. Rali said he was encouraged to see confirmation that the BEC catheter, because of its design, works in patients with proximal or distal occlusive disease.
In clinical practice, “the catheter provides an additional option for care in patients with multiple distal occlusive disease when a systemic tissue plasminogen activator (tPA), may put patient at high bleeding risk,” Dr. Rali said.
Looking ahead, a prospective, observational multicenter study would be useful to validate the findings from the post hoc analysis of the current study, he noted.
The study was sponsored by the National Heart, Lung, and Blood Institute, Commonwealth of Pennsylvania, and Thrombolex Inc., a medical device company developing interventional catheter-based therapies for the rapid and effective treatment of acute venous thromboembolic disorders. Dr. Bashir is a cofounder and has an equity interest in Thrombolex Inc. Dr. Rali disclosed serving as a consultant for Thrombolex, Inari Medical, Viz AI, and ThinkSono.
Use of pharmacomechanical catheter-directory thrombolysis significantly reduced the number of pulmonary artery branches with total or subtotal occlusions in patients with acute pulmonary embolism, based on data from more than 100 individuals.
Reduced distal vascular volume is a significant predictor of 30-day and 90-day mortality in acute pulmonary embolism (PE) patients, and pulmonary obstruction is often the cause, wrote Riyaz Bashir, MD, of Temple University, Philadelphia, Pennsylvania, and colleagues.
, the researchers said.
“The recently published RESCUE (Recombinant tPA by Endovascular Administration for the Treatment of Submassive PE Using CDT for the Reduction of Thrombus Burden) trial showed a 35.9% reduction in PA obstruction using the Refined Modified Miller Index (RMMI), the largest reduction of all published catheter studies with core lab measurement, with similar doses of tissue plasminogen activator (tPA),” the researchers wrote.
The Bashir endovascular catheter was designed to maximize thrombus reduction via a pharmacomechanical infusion. The catheter features an expandable basket of 6 nitinol-reinforced infusion limbs.
“There are three crucial goals that we want to accomplish in patients who have a severe pulmonary embolism,” Dr. Bashir said in an interview. “Those include, in the order of importance, survival, recovery of right ventricular function, and resolution of blocked pulmonary arteries; both segmental and proximal pulmonary arteries,” he said.
Most previous studies have focused on the first two goals, but they still need to evaluate the resolution of PA blockages carefully, said Dr. Bashir. “In our clinical practice, we have seen a large number of patients who develop debilitating shortness of breath from these blockages. We decided to carefully evaluate these blockages before and after pharmacomechanical catheter-directed thrombolysis with the Bashir endovascular catheter using the core lab data from the RESCUE study,” he said.
In the current study published in JACC: Advances), the researchers used baseline and 48-hour posttreatment contrast-enhanced chest computed tomography angiography of adult PE patients with right ventricular dilatation.
The study population included 107 adults with acute intermediate-risk PE who were treated with pharmacomechanical catheter-directory thrombolysis (PM-CDT) at 18 sites in the United States. Of these, 98 had intermediate high-risk PE with elevated troponin and/or brain-type natriuretic peptide (BNP) levels and 102 had bilateral PE.
The primary endpoint was the change in the number of segmental and proximal PA branches with total or subtotal occlusions (defined as > 65%) after 48 hours compared to baseline. Occlusions were assessed using McNemar’s test.
Patients with bilateral PE received two Bashir catheters; those with unilateral PE received one catheter each.
Each patient received a pulse spray of 2 mg of recombinant tPA (r-tPA) into each lung, followed by 5 mg of r-tPA over 5 hours; the total dose was 7 mg of r-tPA for patients with unilateral PEs and 14 mg for those with bilateral PEs, the researchers said. The median times for catheter placement and total procedure were 15 minutes and 54 minutes, respectively.
The number of segmental PA branches with total or subtotal occlusions decreased significantly, from 40.5% at baseline to 11.7% at 48 hours, and proximal PA branch total or subtotal occlusions decreased significantly, from 28.7% at baseline to 11.0% at 48 hours (P < 0.0001 for both).
The magnitude of the reductions in both total and subtotal occlusions of segmental arteries was significantly correlated with the extent of right ventricle recovery (measured by the reduction in right ventricular/left ventricular ratio) with a correlation coefficient of 0.287 (P = .0026); however, this correlation was not observed in the proximal PA arteries (correlation coefficient 0.132, P = .173).
One major bleeding event occurred within 72 hours in a patient who also experienced a device-related left common iliac vein thrombosis while not taking anticoagulation medication, and one death unrelated to PE occurred within 30 days.
“The two findings that surprised me include, first, a more than 70% reduction in total and subtotal occlusions in the segmental arteries with such a low dose of r-tPA and, second, the resolution of the blockages was seen not only in the arteries where the device was placed but also at remote sites away from the location of the catheter,” Dr. Bashir told this news organization.
The findings were limited by several factors including the lack of long-term clinical follow-up outcomes data and lack of comparison groups who underwent other treatments.
However, “This study implies that we now have a safe therapy for these patients that improves survival and right ventricular recovery in addition to dramatically improving blocked pulmonary arteries,” Dr. Bashir said.
As for additional research, “we need all the current and future prospective pulmonary embolism studies to include an assessment of pulmonary artery blockage resolution as an essential endpoint,” he said.
Catheter Expands Treatment Options
The current study, a subgroup analysis of the RESCUE trial, was one of the first to examine the impact of catheter-directed lysis on distal occlusions, study coauthor Parth M. Rali, MD, said in an interview.
To this point, literature has been limited to evaluation for proximal disease, said Dr. Rali, director of thoracic surgery and medicine and part of the Pulmonary Embolism Response Team at Temple University Hospital, Philadelphia.
Dr. Rali said he was encouraged to see confirmation that the BEC catheter, because of its design, works in patients with proximal or distal occlusive disease.
In clinical practice, “the catheter provides an additional option for care in patients with multiple distal occlusive disease when a systemic tissue plasminogen activator (tPA), may put patient at high bleeding risk,” Dr. Rali said.
Looking ahead, a prospective, observational multicenter study would be useful to validate the findings from the post hoc analysis of the current study, he noted.
The study was sponsored by the National Heart, Lung, and Blood Institute, Commonwealth of Pennsylvania, and Thrombolex Inc., a medical device company developing interventional catheter-based therapies for the rapid and effective treatment of acute venous thromboembolic disorders. Dr. Bashir is a cofounder and has an equity interest in Thrombolex Inc. Dr. Rali disclosed serving as a consultant for Thrombolex, Inari Medical, Viz AI, and ThinkSono.
FROM JACC: ADVANCES
Sometimes well-intended mental health treatment hurts
We love psychiatry. We love the idea that someone can come to receive care from a physician to alleviate psychological suffering.
Some people experience such severe anguish that they are unable to relate to others. Some are so despondent that they are unable to make decisions. Some are so distressed that their thoughts become inconsistent with reality. We want all those people, and many more, to have access to effective psychiatric care. However, there are reasonable expectations that one should be able to have that a treatment will help, and that appropriate informed consent is given.
One recent article reminded us of this in a particularly poignant way.

The study in question is a recent publication looking at the universal use of psychotherapy for teenagers.1 At face value, we would have certainly considered this to be a benevolent and well-meaning intervention. Anyone who has been a teenager or has talked to one, is aware of the emotional instability punctuated by episodes of intense anxiety or irritability. It is age appropriate for a teenager to question and explore their identity. Teenagers are notoriously impulsive with a deep desire for validating interpersonal relationships. One could continue to list the symptoms of borderline personality disorder (BPD) and find a lot of similarity with the condition of transitioning from a child to an adult.
It is thus common sense to consider applying the most established therapy for BPD, dialectical behavioral therapy (DBT), to teenagers. The basics of DBT would seem to be helpful to anyone but appear particularly appropriate to this population. Mindfulness, the practice of paying attention to your present experience, allows one to realize that they are trapped in past or hypothetical future moments. Emotional regulation provides the tools that offer a frame for our feelings and involves recognizing feelings and understanding what they mean. Interpersonal work allows one to recognize and adapt to the feelings of others, while learning how to have a healthy voice with others. Distress tolerance is the exercise of learning to experience and contain our feelings.
The study looked at about 1,000 young adolescents, around 13 years old across high schools in Sydney, Australia: 598 adolescents were allocated to the intervention, and 566 to the control. The intervention consisted of eight weekly sessions of DBT lasting about 50 minutes. The results were “contrary to predictions.” Participants who received DBT “reported significantly increased total difficulties,” and “significant increases in depression and anxiety.” The effects were worse in males yet significant in both genders. The study concludes with “a reminder that present enthusiasm for universal dissemination of short-term DBT-based group skills training within schools, specifically in early adolescence, is ahead of the research evidence.”

We can’t help but wonder why the outcomes of the study were this way; here are some ideas:
• Society has natural ways of developing interpersonal skills, emotional regulation, and the ability to appreciate the present. Interpersonal skills are consistently fostered and tested in schools. Navigating high school parties, the process of organizing them, and getting invited to them requires significant social dexterity. Rejection from romantic interest, alienation from peers, rewards for accomplishment, and acceptance by other peers are some of the daily emotional obstacles that teenagers face. Being constantly taught by older individuals and scolded by parents is its own course in mindfulness. Those are few of the many natural processes of interpersonal growth that formalized therapy may impede.
• The universal discussion of psychological terms and psychiatric symptoms may not only destigmatize mental illness, but also normalize and possibly even promote it. While punishing or stigmatizing a child for having mental illness is obviously unacceptable and cruel, we do wonder if the compulsory psychotherapy may provide negative effects. Psychotherapies, especially manualized ones, were developed to alleviate mental suffering. It seems possible that this format normalizes pathology.
In 1961, Erving Goffman described the concept of sane people appearing insane in an asylum as “mortification.” In 2023, we have much improved, but have we done something to internalize patterns of suffering and alienation rather than dispel them? They are given forms that explain what the feeling of depression is when they may have never considered it. They are given tools to handle distress, when distress may not be present.
• Many human beings live on a fairly tight rope of suppression and the less adaptive repression. Suppression is the defense mechanism by which individuals make an effort to put distressing thoughts out of conscious awareness. After a difficult breakup a teenager may ask some friends to go out and watch a movie, making efforts to put negative feelings out of conscious awareness until there is an opportunity to cope adaptively with those stressors.
Repression is the defense mechanism by which individuals make an effort to prevent distressing thoughts from entering conscious awareness in the first place. After a difficult breakup a teenager acts like nothing happened. While not particularly adaptive, many people live with significant repression and without particular anguish. It is possible that uncovering all of those repressed and suppressed feelings through the exploratory work of therapy may destabilize individuals from their tight rope.
• A less problematic explanation could also be what was previously referred to as therapeutic regression. In psychoanalytic theory, patients are generally thought to have a compromise formation, a psychological strategy used to reconcile conflicting drives. The compromise formation is the way a patient balances their desires against moral expectations and the realities of the external world. In therapy, that compromise formation can be challenged, leading to therapeutic regression.
By uncovering and confronting deeply rooted feelings, a patient may find that their symptoms temporarily intensify. This may not be a problem, but a necessary step to growth in some patients. It is possible that a program longer than 8 weeks would have overcome a temporary worsening in outcome measures.

While it’s easy to highlight the darker moments in psychiatric history, psychiatry has grown into a field which offers well-accepted and uncontroversially promoted forms of treatment. This is evolution, exemplified by the mere consideration of the universal use of psychotherapy for teenagers. But this raises important questions about the potential unintended consequences of normalizing and formalizing therapy. It prompted us to reflect on whether psychiatric treatment is always the best solution and if it might, at times, impede natural processes of growth and coping.
In this context, the study on universal DBT-based group skills training for teenagers challenged our assumptions. The unexpected outcomes suggest that societal and educational systems may naturally foster many of the skills that formalized therapy seeks to provide, and may do so with greater efficacy than that which prescriptive psychiatric treatments have to offer. Moreover, the universal discussion of psychiatric symptoms may not only destigmatize mental illness but also normalize it, potentially leading to unnecessary pathology.
Finally, the study prompted us to consider the fine balance that people find themselves in, questioning whether we should be so certain that our interventions can always provide a better outcome than an individual’s current coping mechanisms. These findings serve as a valuable reminder that our enthusiasm for widespread psychiatric interventions should be tempered by rigorous research and a nuanced understanding of human psychology and development.
This study could be an example of the grandiose stance psychiatry has at times taken of late, suggesting the field has an intervention for all that ails you and can serve as a corrective to society’s maladaptive deviations. Rising rates of mental illness in the community are not interpreted as a failing of the field of psychiatry, but as evidence that we need more psychiatrists. Acts of gun violence, ever increasing rates suicides, and even political disagreements are met with the idea that if only we had more mental health capacity, this could be avoided.
Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. He has no conflicts of interest. Dr. ZoBell is a fourth-year senior resident at UCSD Psychiatry Residency Program. She is currently serving as the program’s Chief Resident at the VA San Diego on the inpatient psychiatric unit. Dr. ZoBell is interested in outpatient and emergency psychiatry as well as psychotherapy. Dr. Lehman is a professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He has no conflicts of interest.
Reference
1. Harvey, LJ, et al. Investigating the efficacy of a Dialectical behaviour therapy-based universal intervention on adolescent social and emotional well-being outcomes. Behav Res Ther. 2023 Oct. doi: 10.1016/j.brat.2023.104408.
We love psychiatry. We love the idea that someone can come to receive care from a physician to alleviate psychological suffering.
Some people experience such severe anguish that they are unable to relate to others. Some are so despondent that they are unable to make decisions. Some are so distressed that their thoughts become inconsistent with reality. We want all those people, and many more, to have access to effective psychiatric care. However, there are reasonable expectations that one should be able to have that a treatment will help, and that appropriate informed consent is given.
One recent article reminded us of this in a particularly poignant way.
The study in question is a recent publication looking at the universal use of psychotherapy for teenagers.1 At face value, we would have certainly considered this to be a benevolent and well-meaning intervention. Anyone who has been a teenager or has talked to one, is aware of the emotional instability punctuated by episodes of intense anxiety or irritability. It is age appropriate for a teenager to question and explore their identity. Teenagers are notoriously impulsive with a deep desire for validating interpersonal relationships. One could continue to list the symptoms of borderline personality disorder (BPD) and find a lot of similarity with the condition of transitioning from a child to an adult.
It is thus common sense to consider applying the most established therapy for BPD, dialectical behavioral therapy (DBT), to teenagers. The basics of DBT would seem to be helpful to anyone but appear particularly appropriate to this population. Mindfulness, the practice of paying attention to your present experience, allows one to realize that they are trapped in past or hypothetical future moments. Emotional regulation provides the tools that offer a frame for our feelings and involves recognizing feelings and understanding what they mean. Interpersonal work allows one to recognize and adapt to the feelings of others, while learning how to have a healthy voice with others. Distress tolerance is the exercise of learning to experience and contain our feelings.
The study looked at about 1,000 young adolescents, around 13 years old across high schools in Sydney, Australia: 598 adolescents were allocated to the intervention, and 566 to the control. The intervention consisted of eight weekly sessions of DBT lasting about 50 minutes. The results were “contrary to predictions.” Participants who received DBT “reported significantly increased total difficulties,” and “significant increases in depression and anxiety.” The effects were worse in males yet significant in both genders. The study concludes with “a reminder that present enthusiasm for universal dissemination of short-term DBT-based group skills training within schools, specifically in early adolescence, is ahead of the research evidence.”
We can’t help but wonder why the outcomes of the study were this way; here are some ideas:
• Society has natural ways of developing interpersonal skills, emotional regulation, and the ability to appreciate the present. Interpersonal skills are consistently fostered and tested in schools. Navigating high school parties, the process of organizing them, and getting invited to them requires significant social dexterity. Rejection from romantic interest, alienation from peers, rewards for accomplishment, and acceptance by other peers are some of the daily emotional obstacles that teenagers face. Being constantly taught by older individuals and scolded by parents is its own course in mindfulness. Those are few of the many natural processes of interpersonal growth that formalized therapy may impede.
• The universal discussion of psychological terms and psychiatric symptoms may not only destigmatize mental illness, but also normalize and possibly even promote it. While punishing or stigmatizing a child for having mental illness is obviously unacceptable and cruel, we do wonder if the compulsory psychotherapy may provide negative effects. Psychotherapies, especially manualized ones, were developed to alleviate mental suffering. It seems possible that this format normalizes pathology.
In 1961, Erving Goffman described the concept of sane people appearing insane in an asylum as “mortification.” In 2023, we have much improved, but have we done something to internalize patterns of suffering and alienation rather than dispel them? They are given forms that explain what the feeling of depression is when they may have never considered it. They are given tools to handle distress, when distress may not be present.
• Many human beings live on a fairly tight rope of suppression and the less adaptive repression. Suppression is the defense mechanism by which individuals make an effort to put distressing thoughts out of conscious awareness. After a difficult breakup a teenager may ask some friends to go out and watch a movie, making efforts to put negative feelings out of conscious awareness until there is an opportunity to cope adaptively with those stressors.
Repression is the defense mechanism by which individuals make an effort to prevent distressing thoughts from entering conscious awareness in the first place. After a difficult breakup a teenager acts like nothing happened. While not particularly adaptive, many people live with significant repression and without particular anguish. It is possible that uncovering all of those repressed and suppressed feelings through the exploratory work of therapy may destabilize individuals from their tight rope.
• A less problematic explanation could also be what was previously referred to as therapeutic regression. In psychoanalytic theory, patients are generally thought to have a compromise formation, a psychological strategy used to reconcile conflicting drives. The compromise formation is the way a patient balances their desires against moral expectations and the realities of the external world. In therapy, that compromise formation can be challenged, leading to therapeutic regression.
By uncovering and confronting deeply rooted feelings, a patient may find that their symptoms temporarily intensify. This may not be a problem, but a necessary step to growth in some patients. It is possible that a program longer than 8 weeks would have overcome a temporary worsening in outcome measures.
While it’s easy to highlight the darker moments in psychiatric history, psychiatry has grown into a field which offers well-accepted and uncontroversially promoted forms of treatment. This is evolution, exemplified by the mere consideration of the universal use of psychotherapy for teenagers. But this raises important questions about the potential unintended consequences of normalizing and formalizing therapy. It prompted us to reflect on whether psychiatric treatment is always the best solution and if it might, at times, impede natural processes of growth and coping.
In this context, the study on universal DBT-based group skills training for teenagers challenged our assumptions. The unexpected outcomes suggest that societal and educational systems may naturally foster many of the skills that formalized therapy seeks to provide, and may do so with greater efficacy than that which prescriptive psychiatric treatments have to offer. Moreover, the universal discussion of psychiatric symptoms may not only destigmatize mental illness but also normalize it, potentially leading to unnecessary pathology.
Finally, the study prompted us to consider the fine balance that people find themselves in, questioning whether we should be so certain that our interventions can always provide a better outcome than an individual’s current coping mechanisms. These findings serve as a valuable reminder that our enthusiasm for widespread psychiatric interventions should be tempered by rigorous research and a nuanced understanding of human psychology and development.
This study could be an example of the grandiose stance psychiatry has at times taken of late, suggesting the field has an intervention for all that ails you and can serve as a corrective to society’s maladaptive deviations. Rising rates of mental illness in the community are not interpreted as a failing of the field of psychiatry, but as evidence that we need more psychiatrists. Acts of gun violence, ever increasing rates suicides, and even political disagreements are met with the idea that if only we had more mental health capacity, this could be avoided.
Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. He has no conflicts of interest. Dr. ZoBell is a fourth-year senior resident at UCSD Psychiatry Residency Program. She is currently serving as the program’s Chief Resident at the VA San Diego on the inpatient psychiatric unit. Dr. ZoBell is interested in outpatient and emergency psychiatry as well as psychotherapy. Dr. Lehman is a professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He has no conflicts of interest.
Reference
1. Harvey, LJ, et al. Investigating the efficacy of a Dialectical behaviour therapy-based universal intervention on adolescent social and emotional well-being outcomes. Behav Res Ther. 2023 Oct. doi: 10.1016/j.brat.2023.104408.
We love psychiatry. We love the idea that someone can come to receive care from a physician to alleviate psychological suffering.
Some people experience such severe anguish that they are unable to relate to others. Some are so despondent that they are unable to make decisions. Some are so distressed that their thoughts become inconsistent with reality. We want all those people, and many more, to have access to effective psychiatric care. However, there are reasonable expectations that one should be able to have that a treatment will help, and that appropriate informed consent is given.
One recent article reminded us of this in a particularly poignant way.
The study in question is a recent publication looking at the universal use of psychotherapy for teenagers.1 At face value, we would have certainly considered this to be a benevolent and well-meaning intervention. Anyone who has been a teenager or has talked to one, is aware of the emotional instability punctuated by episodes of intense anxiety or irritability. It is age appropriate for a teenager to question and explore their identity. Teenagers are notoriously impulsive with a deep desire for validating interpersonal relationships. One could continue to list the symptoms of borderline personality disorder (BPD) and find a lot of similarity with the condition of transitioning from a child to an adult.
It is thus common sense to consider applying the most established therapy for BPD, dialectical behavioral therapy (DBT), to teenagers. The basics of DBT would seem to be helpful to anyone but appear particularly appropriate to this population. Mindfulness, the practice of paying attention to your present experience, allows one to realize that they are trapped in past or hypothetical future moments. Emotional regulation provides the tools that offer a frame for our feelings and involves recognizing feelings and understanding what they mean. Interpersonal work allows one to recognize and adapt to the feelings of others, while learning how to have a healthy voice with others. Distress tolerance is the exercise of learning to experience and contain our feelings.
The study looked at about 1,000 young adolescents, around 13 years old across high schools in Sydney, Australia: 598 adolescents were allocated to the intervention, and 566 to the control. The intervention consisted of eight weekly sessions of DBT lasting about 50 minutes. The results were “contrary to predictions.” Participants who received DBT “reported significantly increased total difficulties,” and “significant increases in depression and anxiety.” The effects were worse in males yet significant in both genders. The study concludes with “a reminder that present enthusiasm for universal dissemination of short-term DBT-based group skills training within schools, specifically in early adolescence, is ahead of the research evidence.”
We can’t help but wonder why the outcomes of the study were this way; here are some ideas:
• Society has natural ways of developing interpersonal skills, emotional regulation, and the ability to appreciate the present. Interpersonal skills are consistently fostered and tested in schools. Navigating high school parties, the process of organizing them, and getting invited to them requires significant social dexterity. Rejection from romantic interest, alienation from peers, rewards for accomplishment, and acceptance by other peers are some of the daily emotional obstacles that teenagers face. Being constantly taught by older individuals and scolded by parents is its own course in mindfulness. Those are few of the many natural processes of interpersonal growth that formalized therapy may impede.
• The universal discussion of psychological terms and psychiatric symptoms may not only destigmatize mental illness, but also normalize and possibly even promote it. While punishing or stigmatizing a child for having mental illness is obviously unacceptable and cruel, we do wonder if the compulsory psychotherapy may provide negative effects. Psychotherapies, especially manualized ones, were developed to alleviate mental suffering. It seems possible that this format normalizes pathology.
In 1961, Erving Goffman described the concept of sane people appearing insane in an asylum as “mortification.” In 2023, we have much improved, but have we done something to internalize patterns of suffering and alienation rather than dispel them? They are given forms that explain what the feeling of depression is when they may have never considered it. They are given tools to handle distress, when distress may not be present.
• Many human beings live on a fairly tight rope of suppression and the less adaptive repression. Suppression is the defense mechanism by which individuals make an effort to put distressing thoughts out of conscious awareness. After a difficult breakup a teenager may ask some friends to go out and watch a movie, making efforts to put negative feelings out of conscious awareness until there is an opportunity to cope adaptively with those stressors.
Repression is the defense mechanism by which individuals make an effort to prevent distressing thoughts from entering conscious awareness in the first place. After a difficult breakup a teenager acts like nothing happened. While not particularly adaptive, many people live with significant repression and without particular anguish. It is possible that uncovering all of those repressed and suppressed feelings through the exploratory work of therapy may destabilize individuals from their tight rope.
• A less problematic explanation could also be what was previously referred to as therapeutic regression. In psychoanalytic theory, patients are generally thought to have a compromise formation, a psychological strategy used to reconcile conflicting drives. The compromise formation is the way a patient balances their desires against moral expectations and the realities of the external world. In therapy, that compromise formation can be challenged, leading to therapeutic regression.
By uncovering and confronting deeply rooted feelings, a patient may find that their symptoms temporarily intensify. This may not be a problem, but a necessary step to growth in some patients. It is possible that a program longer than 8 weeks would have overcome a temporary worsening in outcome measures.
While it’s easy to highlight the darker moments in psychiatric history, psychiatry has grown into a field which offers well-accepted and uncontroversially promoted forms of treatment. This is evolution, exemplified by the mere consideration of the universal use of psychotherapy for teenagers. But this raises important questions about the potential unintended consequences of normalizing and formalizing therapy. It prompted us to reflect on whether psychiatric treatment is always the best solution and if it might, at times, impede natural processes of growth and coping.
In this context, the study on universal DBT-based group skills training for teenagers challenged our assumptions. The unexpected outcomes suggest that societal and educational systems may naturally foster many of the skills that formalized therapy seeks to provide, and may do so with greater efficacy than that which prescriptive psychiatric treatments have to offer. Moreover, the universal discussion of psychiatric symptoms may not only destigmatize mental illness but also normalize it, potentially leading to unnecessary pathology.
Finally, the study prompted us to consider the fine balance that people find themselves in, questioning whether we should be so certain that our interventions can always provide a better outcome than an individual’s current coping mechanisms. These findings serve as a valuable reminder that our enthusiasm for widespread psychiatric interventions should be tempered by rigorous research and a nuanced understanding of human psychology and development.
This study could be an example of the grandiose stance psychiatry has at times taken of late, suggesting the field has an intervention for all that ails you and can serve as a corrective to society’s maladaptive deviations. Rising rates of mental illness in the community are not interpreted as a failing of the field of psychiatry, but as evidence that we need more psychiatrists. Acts of gun violence, ever increasing rates suicides, and even political disagreements are met with the idea that if only we had more mental health capacity, this could be avoided.
Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. He has no conflicts of interest. Dr. ZoBell is a fourth-year senior resident at UCSD Psychiatry Residency Program. She is currently serving as the program’s Chief Resident at the VA San Diego on the inpatient psychiatric unit. Dr. ZoBell is interested in outpatient and emergency psychiatry as well as psychotherapy. Dr. Lehman is a professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He has no conflicts of interest.
Reference
1. Harvey, LJ, et al. Investigating the efficacy of a Dialectical behaviour therapy-based universal intervention on adolescent social and emotional well-being outcomes. Behav Res Ther. 2023 Oct. doi: 10.1016/j.brat.2023.104408.
A 55-year-old female presented a with few years' history of pruritic plaques on her shins and wrists
. Lesions may have a covering of scale. HLP commonly affects middle aged men and women. Lesions are most commonly located bilaterally on the shins and ankles and can be painful or pruritic. The differential diagnosis for the condition includes lichen simplex chronicus, connective tissue disease, and other skin disorders that cause hyperkeratosis. This wide differential makes histopathological analysis a useful tool in confirming the diagnosis of HLP.
A definitive diagnosis can be made via skin biopsy. Histopathology reveals hyperkeratosis, acanthosis, and a band-like lymphocytic infiltrate in the dermis. An eosinophilic infiltrate may be present. Other common features include saw tooth rete ridges and Civatte bodies, which are apoptotic keratinocytes. The lymphocytic infiltrate may indicate an autoimmune etiology in which the body’s immune system erroneously attacks itself. However, the exact cause is not known and genetic and environmental factors may play a role.
The treatment of HLP includes symptomatic management and control of inflammation. Topical steroids can be prescribed to manage the inflammation and associated pruritus, and emollient creams and moisturizers are helpful in controlling the dryness. Oral steroids, immunosuppressant medications, or retinoids may be necessary in more severe cases. In addition, psoralen plus ultraviolet A (PUVA) light therapy has been found to be beneficial in some cases. Squamous cell carcinoma may arise in lesions.

This case and photo were submitted by Lucas Shapiro, BS, of Nova Southeastern University College of Osteopathic Medicine, Fort Lauderdale, Florida, and Donna Bilu Martin, MD; Premier Dermatology, MD, Aventura, Florida. The column was edited by Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
Arnold DL, Krishnamurthy K. Lichen Planus. [Updated 2023 Jun 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526126/
Jaime TJ et al. An Bras Dermatol. 2011 Jul-Aug;86(4 Suppl 1):S96-9.
Mirchandani S et al. Med Pharm Rep. 2020 Apr;93(2):210-2. .
Whittington CP et al. Arch Pathol Lab Med. 2023 Jun 19. doi: 10.5858/arpa.2022-0515-RA.
. Lesions may have a covering of scale. HLP commonly affects middle aged men and women. Lesions are most commonly located bilaterally on the shins and ankles and can be painful or pruritic. The differential diagnosis for the condition includes lichen simplex chronicus, connective tissue disease, and other skin disorders that cause hyperkeratosis. This wide differential makes histopathological analysis a useful tool in confirming the diagnosis of HLP.
A definitive diagnosis can be made via skin biopsy. Histopathology reveals hyperkeratosis, acanthosis, and a band-like lymphocytic infiltrate in the dermis. An eosinophilic infiltrate may be present. Other common features include saw tooth rete ridges and Civatte bodies, which are apoptotic keratinocytes. The lymphocytic infiltrate may indicate an autoimmune etiology in which the body’s immune system erroneously attacks itself. However, the exact cause is not known and genetic and environmental factors may play a role.
The treatment of HLP includes symptomatic management and control of inflammation. Topical steroids can be prescribed to manage the inflammation and associated pruritus, and emollient creams and moisturizers are helpful in controlling the dryness. Oral steroids, immunosuppressant medications, or retinoids may be necessary in more severe cases. In addition, psoralen plus ultraviolet A (PUVA) light therapy has been found to be beneficial in some cases. Squamous cell carcinoma may arise in lesions.
This case and photo were submitted by Lucas Shapiro, BS, of Nova Southeastern University College of Osteopathic Medicine, Fort Lauderdale, Florida, and Donna Bilu Martin, MD; Premier Dermatology, MD, Aventura, Florida. The column was edited by Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
Arnold DL, Krishnamurthy K. Lichen Planus. [Updated 2023 Jun 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526126/
Jaime TJ et al. An Bras Dermatol. 2011 Jul-Aug;86(4 Suppl 1):S96-9.
Mirchandani S et al. Med Pharm Rep. 2020 Apr;93(2):210-2. .
Whittington CP et al. Arch Pathol Lab Med. 2023 Jun 19. doi: 10.5858/arpa.2022-0515-RA.
. Lesions may have a covering of scale. HLP commonly affects middle aged men and women. Lesions are most commonly located bilaterally on the shins and ankles and can be painful or pruritic. The differential diagnosis for the condition includes lichen simplex chronicus, connective tissue disease, and other skin disorders that cause hyperkeratosis. This wide differential makes histopathological analysis a useful tool in confirming the diagnosis of HLP.
A definitive diagnosis can be made via skin biopsy. Histopathology reveals hyperkeratosis, acanthosis, and a band-like lymphocytic infiltrate in the dermis. An eosinophilic infiltrate may be present. Other common features include saw tooth rete ridges and Civatte bodies, which are apoptotic keratinocytes. The lymphocytic infiltrate may indicate an autoimmune etiology in which the body’s immune system erroneously attacks itself. However, the exact cause is not known and genetic and environmental factors may play a role.
The treatment of HLP includes symptomatic management and control of inflammation. Topical steroids can be prescribed to manage the inflammation and associated pruritus, and emollient creams and moisturizers are helpful in controlling the dryness. Oral steroids, immunosuppressant medications, or retinoids may be necessary in more severe cases. In addition, psoralen plus ultraviolet A (PUVA) light therapy has been found to be beneficial in some cases. Squamous cell carcinoma may arise in lesions.
This case and photo were submitted by Lucas Shapiro, BS, of Nova Southeastern University College of Osteopathic Medicine, Fort Lauderdale, Florida, and Donna Bilu Martin, MD; Premier Dermatology, MD, Aventura, Florida. The column was edited by Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
Arnold DL, Krishnamurthy K. Lichen Planus. [Updated 2023 Jun 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526126/
Jaime TJ et al. An Bras Dermatol. 2011 Jul-Aug;86(4 Suppl 1):S96-9.
Mirchandani S et al. Med Pharm Rep. 2020 Apr;93(2):210-2. .
Whittington CP et al. Arch Pathol Lab Med. 2023 Jun 19. doi: 10.5858/arpa.2022-0515-RA.

Light therapy a beacon of hope for Alzheimer’s?
TOPLINE:
Light therapy leads to significant improvement in several sleep measures and helps alleviate depression and agitation in patients with Alzheimer’s disease (AD), a meta-analysis of 15 high-quality trials shows.
METHODOLOGY:
- This meta-analysis included 15 randomized controlled trials involving 598 patients with mild to moderate AD.
- The included trials were written in English, published between 2005 and 2022, and performed in seven countries. A fixed-effects model was used for data analysis.
TAKEAWAY:
- Light therapy significantly improved sleep efficiency (mean difference [MD], −2.42; P < .00001), increased interdaily stability (MD, −0.04; P < .00001), and reduced intradaily variability (MD, −0.04; P < .00001), indicating better sleep quality.
- Light therapy reduced agitation (MD, −3.97; P < .00001), depression (MD, −2.55; P < .00001), and caregiver burden (MD, −3.57; P < .00001).
- Light therapy also had a significant advantage over usual care in reducing the severity of psychobehavioral symptoms as assessed by the Neuropsychiatric Inventory (MD, −3.07; P < .00001).
- Light therapy had no statistically significant effect on improving cognitive function as measured by the Mini-Mental State Examination.
IN PRACTICE:
“These findings, combined with its low side-effects, suggest the role of light therapy as a promising treatment for AD. Although light therapy has fewer side effects than pharmacological treatment, adverse behavioral outcomes in patients due to bright light exposure should be considered,” the authors wrote.
SOURCE:
The study by Lili Zang and colleagues from Weifang Medical University School of Nursing, Shandong Province, China, was published online on December 6, 2023, in PLOS One.
LIMITATIONS:
The types and degrees of dementia in the included studies were inconsistent, potentially affecting the outcome indicators. Some articles did not clearly describe their randomization and allocation concealment methods, indicating possible bias in these studies.
DISCLOSURES:
The study was supported by the Natural Science Foundation of Shandong Province, China. The authors declared no competing interests.
Megan Brooks has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
TOPLINE:
Light therapy leads to significant improvement in several sleep measures and helps alleviate depression and agitation in patients with Alzheimer’s disease (AD), a meta-analysis of 15 high-quality trials shows.
METHODOLOGY:
- This meta-analysis included 15 randomized controlled trials involving 598 patients with mild to moderate AD.
- The included trials were written in English, published between 2005 and 2022, and performed in seven countries. A fixed-effects model was used for data analysis.
TAKEAWAY:
- Light therapy significantly improved sleep efficiency (mean difference [MD], −2.42; P < .00001), increased interdaily stability (MD, −0.04; P < .00001), and reduced intradaily variability (MD, −0.04; P < .00001), indicating better sleep quality.
- Light therapy reduced agitation (MD, −3.97; P < .00001), depression (MD, −2.55; P < .00001), and caregiver burden (MD, −3.57; P < .00001).
- Light therapy also had a significant advantage over usual care in reducing the severity of psychobehavioral symptoms as assessed by the Neuropsychiatric Inventory (MD, −3.07; P < .00001).
- Light therapy had no statistically significant effect on improving cognitive function as measured by the Mini-Mental State Examination.
IN PRACTICE:
“These findings, combined with its low side-effects, suggest the role of light therapy as a promising treatment for AD. Although light therapy has fewer side effects than pharmacological treatment, adverse behavioral outcomes in patients due to bright light exposure should be considered,” the authors wrote.
SOURCE:
The study by Lili Zang and colleagues from Weifang Medical University School of Nursing, Shandong Province, China, was published online on December 6, 2023, in PLOS One.
LIMITATIONS:
The types and degrees of dementia in the included studies were inconsistent, potentially affecting the outcome indicators. Some articles did not clearly describe their randomization and allocation concealment methods, indicating possible bias in these studies.
DISCLOSURES:
The study was supported by the Natural Science Foundation of Shandong Province, China. The authors declared no competing interests.
Megan Brooks has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
TOPLINE:
Light therapy leads to significant improvement in several sleep measures and helps alleviate depression and agitation in patients with Alzheimer’s disease (AD), a meta-analysis of 15 high-quality trials shows.
METHODOLOGY:
- This meta-analysis included 15 randomized controlled trials involving 598 patients with mild to moderate AD.
- The included trials were written in English, published between 2005 and 2022, and performed in seven countries. A fixed-effects model was used for data analysis.
TAKEAWAY:
- Light therapy significantly improved sleep efficiency (mean difference [MD], −2.42; P < .00001), increased interdaily stability (MD, −0.04; P < .00001), and reduced intradaily variability (MD, −0.04; P < .00001), indicating better sleep quality.
- Light therapy reduced agitation (MD, −3.97; P < .00001), depression (MD, −2.55; P < .00001), and caregiver burden (MD, −3.57; P < .00001).
- Light therapy also had a significant advantage over usual care in reducing the severity of psychobehavioral symptoms as assessed by the Neuropsychiatric Inventory (MD, −3.07; P < .00001).
- Light therapy had no statistically significant effect on improving cognitive function as measured by the Mini-Mental State Examination.
IN PRACTICE:
“These findings, combined with its low side-effects, suggest the role of light therapy as a promising treatment for AD. Although light therapy has fewer side effects than pharmacological treatment, adverse behavioral outcomes in patients due to bright light exposure should be considered,” the authors wrote.
SOURCE:
The study by Lili Zang and colleagues from Weifang Medical University School of Nursing, Shandong Province, China, was published online on December 6, 2023, in PLOS One.
LIMITATIONS:
The types and degrees of dementia in the included studies were inconsistent, potentially affecting the outcome indicators. Some articles did not clearly describe their randomization and allocation concealment methods, indicating possible bias in these studies.
DISCLOSURES:
The study was supported by the Natural Science Foundation of Shandong Province, China. The authors declared no competing interests.
Megan Brooks has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Screening for alcohol use disorder cuts hospital readmission
Actively drinking patients who undergo screening, a brief intervention, and referral to treatment (SBIRT) for alcohol use disorder during hospital admission for alcohol-related conditions have fewer 30- and 90-day readmissions for alcohol-related liver disease, a new study suggests.
Nevertheless, SBIRT was administered to only 51.7% of patients admitted for alcohol-associated hepatitis (AAH) and 23.7% of patients admitted for decompensated alcohol-related cirrhosis (DARLC).
“Not only did conducting SBIRT with patients admitted for AAH reduce 30-day and 90-day liver-related readmissions, but even just being offered SBIRT reduced readmissions, too,” study author Dennis Wang, MD, of the adult gastroenterology residency program at McMaster University in Hamilton, Ontario, told this news organization. “The exact reason for this effect is unclear, but one can speculate that offering SBIRT to AAH patients may trigger them to consider abstaining from alcohol.”
By contrast, receiving or being offered SBIRT had no effect on readmissions for patients with DARLC.
The findings were published online on November 30 in the Journal of the Canadian Association of Gastroenterology.
Readmissions Significantly Reduced
The researchers retrospectively reviewed the electronic medical records of patients with AAH or DARLC who were admitted to Hamilton Health Sciences hospitals in Ontario from January 2017 to December 2021. Eligible patients were aged ≥ 18 years and actively drinking.
The study’s primary outcomes were the proportion of admissions in which SBIRT was conducted and the association between conducting SBIRT and 30- and 90-day readmissions for recurrent AAH or DARLC.
There were 120 admissions for AAH, representing 95 patients, 95 index admissions, 18 patients with 30-day readmissions, and 26 patients with 90-day readmissions. The sum of the index AAH admissions and 90-day readmissions was greater than the total number of AAH admissions because readmissions where patients were no longer actively drinking alcohol were included.
There were 177 admissions for DARLC, representing 132 patients, 132 index admissions, 13 30-day readmissions, and 31 90-day readmissions.
The mean age of patients admitted with AAH (47.7 years) was significantly lower than that of patients admitted with DARLC (58.2 years). Fewer men were admitted with AAH (59.2%) than with DARLC (73.4%).
There was no significant difference between AAH admissions and DARLC admissions in hospital length of stay, Model for End-Stage Liver Disease on admission, same-admission mortality, and 30- or 90-day readmissions.
SBIRT was conducted in 62 of 120 AAH admissions (51.7%) and 42 of 177 DARLC admissions (23.7%), mainly by social workers and addiction counselors and occasionally by physicians alone.
“Sometimes patients with AAH or DARLC can become so ill that they cannot participate in SBIRT,” noted Dr. Wang. “In addition, there may not be enough health care providers, resources, or time available to conduct high-quality SBIRT with all patients admitted to hospital.”
For patients with AAH, SBIRT was associated with significantly reduced 30-day (odds ratio [OR], 0.098) and 90-day (OR, 0.166) likelihood of readmission for recurrent AAH. However, there was no association with readmissions for patients with DARLC.
Liver Scarring Persists
“We suspect that DARLC patients do not see the same improvement in liver-related readmissions after receiving SBIRT because the liver scarring typically persists even with alcohol abstinence, and this scarring causes further decompensations,” said Dr. Wang.
“Physicians, social workers, addiction counselors, and other allied health providers should collaborate to conduct SBIRT for all actively drinking patients admitted for AAH or DARLC,” wrote the authors.
The researchers acknowledged that their study was limited by its inclusion of data from only a single center. The admissions for AAH and DARLC had a higher proportion of male patients than female patients, thus limiting the generalizability of the findings. In addition, there was a lack of data on ethnicity and socioeconomic status, which could affect readmissions.
Dr. Wang advises clinicians to “seek out and connect with other healthcare providers in their local and regional community, such as addiction counselors or psychologists, to build a robust referral network for patients wanting to reduce their alcohol use.”
In addition, “providers should become comfortable with asking patients nonjudgmentally about alcohol use, as this builds the initial rapport that lays the foundation for ongoing care,” he said. “Every interaction with a patient is a new opportunity to guide interested patients towards alcohol cessation.”
Multidisciplinary Team Essential
Commenting on the findings, Meena B. Bansal, MD, professor of medicine and director of translational research in liver diseases at the Icahn School of Medicine at Mount Sinai in New York, said that they reflect clinical experience in US hospitals. “Physicians are so busy handling the acute medical situation posed by the admission that while they do certainly tell the patient they should stop drinking, full discussion, intervention, and linkage to outpatient programs is often led by the social worker,” she said. Dr. Bansal was not involved in the study.
“Many alcohol use disorder therapies are not tested in extremely ill patients, and thus, pharmacotherapy is often reserved for outpatient management, when patients are more clinically stable,” she said. Yet, as mentioned by the authors, a recent study “showed that 71% of providers never prescribed pharmacotherapy for alcohol use disorder, with the most common reason being low comfort with the medications. We need to increase education around pharmacotherapy for alcohol use disorder to increase the comfort level of practicing gastroenterologists and hepatologists.”
Furthermore, she said, clinicians need to intervene and provide guidance to patients “wherever and whenever they touch our system, whether that be in the inpatient or outpatient setting, [and] provide SBIRT during inpatient admissions but then follow patients longitudinally in a multidisciplinary team to achieve long-term results.”
The study was conducted without external funding. Dr. Wang had no relevant conflicts to disclose. A coauthor acts as a consultant, clinical trial investigator, speaker, and member of the advisory board for AbbVie, Gilead, Intercept, and Novo Nordisk. He also acts as a speaker and member of the advisory board for Eisai and Lupin and as a clinical trial investigator for Madrigal.
A version of this article appeared on Medscape.com.
Actively drinking patients who undergo screening, a brief intervention, and referral to treatment (SBIRT) for alcohol use disorder during hospital admission for alcohol-related conditions have fewer 30- and 90-day readmissions for alcohol-related liver disease, a new study suggests.
Nevertheless, SBIRT was administered to only 51.7% of patients admitted for alcohol-associated hepatitis (AAH) and 23.7% of patients admitted for decompensated alcohol-related cirrhosis (DARLC).
“Not only did conducting SBIRT with patients admitted for AAH reduce 30-day and 90-day liver-related readmissions, but even just being offered SBIRT reduced readmissions, too,” study author Dennis Wang, MD, of the adult gastroenterology residency program at McMaster University in Hamilton, Ontario, told this news organization. “The exact reason for this effect is unclear, but one can speculate that offering SBIRT to AAH patients may trigger them to consider abstaining from alcohol.”
By contrast, receiving or being offered SBIRT had no effect on readmissions for patients with DARLC.
The findings were published online on November 30 in the Journal of the Canadian Association of Gastroenterology.
Readmissions Significantly Reduced
The researchers retrospectively reviewed the electronic medical records of patients with AAH or DARLC who were admitted to Hamilton Health Sciences hospitals in Ontario from January 2017 to December 2021. Eligible patients were aged ≥ 18 years and actively drinking.
The study’s primary outcomes were the proportion of admissions in which SBIRT was conducted and the association between conducting SBIRT and 30- and 90-day readmissions for recurrent AAH or DARLC.
There were 120 admissions for AAH, representing 95 patients, 95 index admissions, 18 patients with 30-day readmissions, and 26 patients with 90-day readmissions. The sum of the index AAH admissions and 90-day readmissions was greater than the total number of AAH admissions because readmissions where patients were no longer actively drinking alcohol were included.
There were 177 admissions for DARLC, representing 132 patients, 132 index admissions, 13 30-day readmissions, and 31 90-day readmissions.
The mean age of patients admitted with AAH (47.7 years) was significantly lower than that of patients admitted with DARLC (58.2 years). Fewer men were admitted with AAH (59.2%) than with DARLC (73.4%).
There was no significant difference between AAH admissions and DARLC admissions in hospital length of stay, Model for End-Stage Liver Disease on admission, same-admission mortality, and 30- or 90-day readmissions.
SBIRT was conducted in 62 of 120 AAH admissions (51.7%) and 42 of 177 DARLC admissions (23.7%), mainly by social workers and addiction counselors and occasionally by physicians alone.
“Sometimes patients with AAH or DARLC can become so ill that they cannot participate in SBIRT,” noted Dr. Wang. “In addition, there may not be enough health care providers, resources, or time available to conduct high-quality SBIRT with all patients admitted to hospital.”
For patients with AAH, SBIRT was associated with significantly reduced 30-day (odds ratio [OR], 0.098) and 90-day (OR, 0.166) likelihood of readmission for recurrent AAH. However, there was no association with readmissions for patients with DARLC.
Liver Scarring Persists
“We suspect that DARLC patients do not see the same improvement in liver-related readmissions after receiving SBIRT because the liver scarring typically persists even with alcohol abstinence, and this scarring causes further decompensations,” said Dr. Wang.
“Physicians, social workers, addiction counselors, and other allied health providers should collaborate to conduct SBIRT for all actively drinking patients admitted for AAH or DARLC,” wrote the authors.
The researchers acknowledged that their study was limited by its inclusion of data from only a single center. The admissions for AAH and DARLC had a higher proportion of male patients than female patients, thus limiting the generalizability of the findings. In addition, there was a lack of data on ethnicity and socioeconomic status, which could affect readmissions.
Dr. Wang advises clinicians to “seek out and connect with other healthcare providers in their local and regional community, such as addiction counselors or psychologists, to build a robust referral network for patients wanting to reduce their alcohol use.”
In addition, “providers should become comfortable with asking patients nonjudgmentally about alcohol use, as this builds the initial rapport that lays the foundation for ongoing care,” he said. “Every interaction with a patient is a new opportunity to guide interested patients towards alcohol cessation.”
Multidisciplinary Team Essential
Commenting on the findings, Meena B. Bansal, MD, professor of medicine and director of translational research in liver diseases at the Icahn School of Medicine at Mount Sinai in New York, said that they reflect clinical experience in US hospitals. “Physicians are so busy handling the acute medical situation posed by the admission that while they do certainly tell the patient they should stop drinking, full discussion, intervention, and linkage to outpatient programs is often led by the social worker,” she said. Dr. Bansal was not involved in the study.
“Many alcohol use disorder therapies are not tested in extremely ill patients, and thus, pharmacotherapy is often reserved for outpatient management, when patients are more clinically stable,” she said. Yet, as mentioned by the authors, a recent study “showed that 71% of providers never prescribed pharmacotherapy for alcohol use disorder, with the most common reason being low comfort with the medications. We need to increase education around pharmacotherapy for alcohol use disorder to increase the comfort level of practicing gastroenterologists and hepatologists.”
Furthermore, she said, clinicians need to intervene and provide guidance to patients “wherever and whenever they touch our system, whether that be in the inpatient or outpatient setting, [and] provide SBIRT during inpatient admissions but then follow patients longitudinally in a multidisciplinary team to achieve long-term results.”
The study was conducted without external funding. Dr. Wang had no relevant conflicts to disclose. A coauthor acts as a consultant, clinical trial investigator, speaker, and member of the advisory board for AbbVie, Gilead, Intercept, and Novo Nordisk. He also acts as a speaker and member of the advisory board for Eisai and Lupin and as a clinical trial investigator for Madrigal.
A version of this article appeared on Medscape.com.
Actively drinking patients who undergo screening, a brief intervention, and referral to treatment (SBIRT) for alcohol use disorder during hospital admission for alcohol-related conditions have fewer 30- and 90-day readmissions for alcohol-related liver disease, a new study suggests.
Nevertheless, SBIRT was administered to only 51.7% of patients admitted for alcohol-associated hepatitis (AAH) and 23.7% of patients admitted for decompensated alcohol-related cirrhosis (DARLC).
“Not only did conducting SBIRT with patients admitted for AAH reduce 30-day and 90-day liver-related readmissions, but even just being offered SBIRT reduced readmissions, too,” study author Dennis Wang, MD, of the adult gastroenterology residency program at McMaster University in Hamilton, Ontario, told this news organization. “The exact reason for this effect is unclear, but one can speculate that offering SBIRT to AAH patients may trigger them to consider abstaining from alcohol.”
By contrast, receiving or being offered SBIRT had no effect on readmissions for patients with DARLC.
The findings were published online on November 30 in the Journal of the Canadian Association of Gastroenterology.
Readmissions Significantly Reduced
The researchers retrospectively reviewed the electronic medical records of patients with AAH or DARLC who were admitted to Hamilton Health Sciences hospitals in Ontario from January 2017 to December 2021. Eligible patients were aged ≥ 18 years and actively drinking.
The study’s primary outcomes were the proportion of admissions in which SBIRT was conducted and the association between conducting SBIRT and 30- and 90-day readmissions for recurrent AAH or DARLC.
There were 120 admissions for AAH, representing 95 patients, 95 index admissions, 18 patients with 30-day readmissions, and 26 patients with 90-day readmissions. The sum of the index AAH admissions and 90-day readmissions was greater than the total number of AAH admissions because readmissions where patients were no longer actively drinking alcohol were included.
There were 177 admissions for DARLC, representing 132 patients, 132 index admissions, 13 30-day readmissions, and 31 90-day readmissions.
The mean age of patients admitted with AAH (47.7 years) was significantly lower than that of patients admitted with DARLC (58.2 years). Fewer men were admitted with AAH (59.2%) than with DARLC (73.4%).
There was no significant difference between AAH admissions and DARLC admissions in hospital length of stay, Model for End-Stage Liver Disease on admission, same-admission mortality, and 30- or 90-day readmissions.
SBIRT was conducted in 62 of 120 AAH admissions (51.7%) and 42 of 177 DARLC admissions (23.7%), mainly by social workers and addiction counselors and occasionally by physicians alone.
“Sometimes patients with AAH or DARLC can become so ill that they cannot participate in SBIRT,” noted Dr. Wang. “In addition, there may not be enough health care providers, resources, or time available to conduct high-quality SBIRT with all patients admitted to hospital.”
For patients with AAH, SBIRT was associated with significantly reduced 30-day (odds ratio [OR], 0.098) and 90-day (OR, 0.166) likelihood of readmission for recurrent AAH. However, there was no association with readmissions for patients with DARLC.
Liver Scarring Persists
“We suspect that DARLC patients do not see the same improvement in liver-related readmissions after receiving SBIRT because the liver scarring typically persists even with alcohol abstinence, and this scarring causes further decompensations,” said Dr. Wang.
“Physicians, social workers, addiction counselors, and other allied health providers should collaborate to conduct SBIRT for all actively drinking patients admitted for AAH or DARLC,” wrote the authors.
The researchers acknowledged that their study was limited by its inclusion of data from only a single center. The admissions for AAH and DARLC had a higher proportion of male patients than female patients, thus limiting the generalizability of the findings. In addition, there was a lack of data on ethnicity and socioeconomic status, which could affect readmissions.
Dr. Wang advises clinicians to “seek out and connect with other healthcare providers in their local and regional community, such as addiction counselors or psychologists, to build a robust referral network for patients wanting to reduce their alcohol use.”
In addition, “providers should become comfortable with asking patients nonjudgmentally about alcohol use, as this builds the initial rapport that lays the foundation for ongoing care,” he said. “Every interaction with a patient is a new opportunity to guide interested patients towards alcohol cessation.”
Multidisciplinary Team Essential
Commenting on the findings, Meena B. Bansal, MD, professor of medicine and director of translational research in liver diseases at the Icahn School of Medicine at Mount Sinai in New York, said that they reflect clinical experience in US hospitals. “Physicians are so busy handling the acute medical situation posed by the admission that while they do certainly tell the patient they should stop drinking, full discussion, intervention, and linkage to outpatient programs is often led by the social worker,” she said. Dr. Bansal was not involved in the study.
“Many alcohol use disorder therapies are not tested in extremely ill patients, and thus, pharmacotherapy is often reserved for outpatient management, when patients are more clinically stable,” she said. Yet, as mentioned by the authors, a recent study “showed that 71% of providers never prescribed pharmacotherapy for alcohol use disorder, with the most common reason being low comfort with the medications. We need to increase education around pharmacotherapy for alcohol use disorder to increase the comfort level of practicing gastroenterologists and hepatologists.”
Furthermore, she said, clinicians need to intervene and provide guidance to patients “wherever and whenever they touch our system, whether that be in the inpatient or outpatient setting, [and] provide SBIRT during inpatient admissions but then follow patients longitudinally in a multidisciplinary team to achieve long-term results.”
The study was conducted without external funding. Dr. Wang had no relevant conflicts to disclose. A coauthor acts as a consultant, clinical trial investigator, speaker, and member of the advisory board for AbbVie, Gilead, Intercept, and Novo Nordisk. He also acts as a speaker and member of the advisory board for Eisai and Lupin and as a clinical trial investigator for Madrigal.
A version of this article appeared on Medscape.com.