User login
This month in the journal CHEST®
Giants In Chest Medicine
Professor Emeritus Elizabeth F. Juniper, MCSP, MSc
By Dr. P. M. O’Byrne
Original Research
A Population-Based Cohort Study on the Drug-Specific Effect of Statins on Sepsis Outcome. 
A Multicenter Randomized Trial of a Checklist for Endotracheal Intubation of Critically Ill Adults.
By Dr. D. R. Janz, et al.
Determinants of Unintentional Leaks During CPAP Treatment in OSA.
By Dr. M. Lebret, et al.
Evidence-Based Medicine
Screening for Lung Cancer: CHEST Guideline and Expert Panel Report.
By Dr. P. J. Mazzone, et al.
Treating Cough Due to Non-CF and CF Bronchiectasis With Nonpharmacological Airway Clearance: CHEST Expert Panel Report.
By Dr. A. T. Hill, et al.
Giants In Chest Medicine
Professor Emeritus Elizabeth F. Juniper, MCSP, MSc
By Dr. P. M. O’Byrne
Original Research
A Population-Based Cohort Study on the Drug-Specific Effect of Statins on Sepsis Outcome.
A Multicenter Randomized Trial of a Checklist for Endotracheal Intubation of Critically Ill Adults.
By Dr. D. R. Janz, et al.
Determinants of Unintentional Leaks During CPAP Treatment in OSA.
By Dr. M. Lebret, et al.
Evidence-Based Medicine
Screening for Lung Cancer: CHEST Guideline and Expert Panel Report.
By Dr. P. J. Mazzone, et al.
Treating Cough Due to Non-CF and CF Bronchiectasis With Nonpharmacological Airway Clearance: CHEST Expert Panel Report.
By Dr. A. T. Hill, et al.
Giants In Chest Medicine
Professor Emeritus Elizabeth F. Juniper, MCSP, MSc
By Dr. P. M. O’Byrne
Original Research
A Population-Based Cohort Study on the Drug-Specific Effect of Statins on Sepsis Outcome.
A Multicenter Randomized Trial of a Checklist for Endotracheal Intubation of Critically Ill Adults.
By Dr. D. R. Janz, et al.
Determinants of Unintentional Leaks During CPAP Treatment in OSA.
By Dr. M. Lebret, et al.
Evidence-Based Medicine
Screening for Lung Cancer: CHEST Guideline and Expert Panel Report.
By Dr. P. J. Mazzone, et al.
Treating Cough Due to Non-CF and CF Bronchiectasis With Nonpharmacological Airway Clearance: CHEST Expert Panel Report.
By Dr. A. T. Hill, et al.
SAVE LIVES: Clean your hands
The World Health Organization (WHO) has announced its annual SAVE LIVES: Clean Your Hands 2018 campaign (Saito, et al. J Hosp Infect. 2018;98[4]:321), designating May 5, 2018, as world hand hygiene day.
Health-care-associated infections are a major patient safety problem. Unfortunately, their spread is common in hospitals and ICUs around the globe. The vehicle for these infections, including multidrug-resistant organisms, is frequently the contaminated hands of health-care workers. Health-care-acquired infections, as any other infection, can lead to sepsis and death. Infections acquired in the ICU are especially deadly, with mortalities that can be as high as 80%. Proper hand hygiene, despite being simple and inexpensive, is the single most important means of reducing the prevalence of hospital-acquired infections and the spread of antimicrobial resistance.
We have known about the significance of hand washing since the early 19th century. More recent data show that hand washing can reduce the overall prevalence of hospital-acquired infections and the cross-transmission of multidrug-resistant organisms. It is estimated that we can prevent 15% to 30% of these infections with adequate hand washing alone.
Despite the clear benefit and the understanding of the importance of hand washing, compliance with this simple intervention is only about 50%. Health-care workers tend to overestimate these rates, self-reporting a compliance of 75%. Even the latter number represents a lot of missed opportunities, and we must do something about it.
A multifaceted approach that combines education with written material, reminders, and continued feedback on performance can have an important effect on hand washing compliance and rates of hospital-acquired infections.
Sepsis is the single most important cause of death in hospitals in the United States. The campaign (http://www.who.int/infection-prevention/campaigns/clean-hands/en/), sponsored by the World Health Organization, should serve as a reminder to all health-care workers about the importance of adequate hand washing and as an opportunity to improve our compliance moving forward.
Despite the progress made, there is still a lot of room for improvement. We can have an impact on the number of deaths from sepsis by preventing them to occur in the first place. Wash your hands and do it well, it does not cost us anything.
Remember: It is in our hands – prevent sepsis and save lives!
Shruti Gadre, MD
Steering Committee Member, Critical Care NetWork
Angel Coz, MD, FCCP
Chair, Critical Care NetWork
The World Health Organization (WHO) has announced its annual SAVE LIVES: Clean Your Hands 2018 campaign (Saito, et al. J Hosp Infect. 2018;98[4]:321), designating May 5, 2018, as world hand hygiene day.
Health-care-associated infections are a major patient safety problem. Unfortunately, their spread is common in hospitals and ICUs around the globe. The vehicle for these infections, including multidrug-resistant organisms, is frequently the contaminated hands of health-care workers. Health-care-acquired infections, as any other infection, can lead to sepsis and death. Infections acquired in the ICU are especially deadly, with mortalities that can be as high as 80%. Proper hand hygiene, despite being simple and inexpensive, is the single most important means of reducing the prevalence of hospital-acquired infections and the spread of antimicrobial resistance.
We have known about the significance of hand washing since the early 19th century. More recent data show that hand washing can reduce the overall prevalence of hospital-acquired infections and the cross-transmission of multidrug-resistant organisms. It is estimated that we can prevent 15% to 30% of these infections with adequate hand washing alone.
Despite the clear benefit and the understanding of the importance of hand washing, compliance with this simple intervention is only about 50%. Health-care workers tend to overestimate these rates, self-reporting a compliance of 75%. Even the latter number represents a lot of missed opportunities, and we must do something about it.
A multifaceted approach that combines education with written material, reminders, and continued feedback on performance can have an important effect on hand washing compliance and rates of hospital-acquired infections.
Sepsis is the single most important cause of death in hospitals in the United States. The campaign (http://www.who.int/infection-prevention/campaigns/clean-hands/en/), sponsored by the World Health Organization, should serve as a reminder to all health-care workers about the importance of adequate hand washing and as an opportunity to improve our compliance moving forward.
Despite the progress made, there is still a lot of room for improvement. We can have an impact on the number of deaths from sepsis by preventing them to occur in the first place. Wash your hands and do it well, it does not cost us anything.
Remember: It is in our hands – prevent sepsis and save lives!
Shruti Gadre, MD
Steering Committee Member, Critical Care NetWork
Angel Coz, MD, FCCP
Chair, Critical Care NetWork
The World Health Organization (WHO) has announced its annual SAVE LIVES: Clean Your Hands 2018 campaign (Saito, et al. J Hosp Infect. 2018;98[4]:321), designating May 5, 2018, as world hand hygiene day.
Health-care-associated infections are a major patient safety problem. Unfortunately, their spread is common in hospitals and ICUs around the globe. The vehicle for these infections, including multidrug-resistant organisms, is frequently the contaminated hands of health-care workers. Health-care-acquired infections, as any other infection, can lead to sepsis and death. Infections acquired in the ICU are especially deadly, with mortalities that can be as high as 80%. Proper hand hygiene, despite being simple and inexpensive, is the single most important means of reducing the prevalence of hospital-acquired infections and the spread of antimicrobial resistance.
We have known about the significance of hand washing since the early 19th century. More recent data show that hand washing can reduce the overall prevalence of hospital-acquired infections and the cross-transmission of multidrug-resistant organisms. It is estimated that we can prevent 15% to 30% of these infections with adequate hand washing alone.
Despite the clear benefit and the understanding of the importance of hand washing, compliance with this simple intervention is only about 50%. Health-care workers tend to overestimate these rates, self-reporting a compliance of 75%. Even the latter number represents a lot of missed opportunities, and we must do something about it.
A multifaceted approach that combines education with written material, reminders, and continued feedback on performance can have an important effect on hand washing compliance and rates of hospital-acquired infections.
Sepsis is the single most important cause of death in hospitals in the United States. The campaign (http://www.who.int/infection-prevention/campaigns/clean-hands/en/), sponsored by the World Health Organization, should serve as a reminder to all health-care workers about the importance of adequate hand washing and as an opportunity to improve our compliance moving forward.
Despite the progress made, there is still a lot of room for improvement. We can have an impact on the number of deaths from sepsis by preventing them to occur in the first place. Wash your hands and do it well, it does not cost us anything.
Remember: It is in our hands – prevent sepsis and save lives!
Shruti Gadre, MD
Steering Committee Member, Critical Care NetWork
Angel Coz, MD, FCCP
Chair, Critical Care NetWork
AMA Insights
As many who read CHEST® Physician may know, we have a nucleus of dedicated volunteers who give unselfishly of their time and talent to represent our members in the area of “regulatory advocacy” and “policy advocacy” in the areas of pulmonary, critical care, and sleep medicine. It is our goal to recognize and support this valuable group of individuals who represent us in the space of coding and reimbursement, RUC activities, relationships with organizations like the ACP and the AMA, as well as our sister societies, such as ATS, SCCM, NAMDRC, CCNA, APSR, ALAT, and ERS, among others.
One of our goals, in addition to recognizing this group, is to identify and mentor the next generation of representatives. A great example of this mentorship is reflected in our involvement with the AMA. Dr. Bob McCaffree has represented CHEST for 22 years and is now mentoring Dr. Raj Desai who will be assuming this role of AMA Delegate this year. Special thanks to Dr. McCaffree for his unselfish service in this capacity and for his mentorship of Dr. Desai. I hope that you enjoy this and future CHEST® Physician articles summarizing and reflecting on the activities pertinent to CHEST at the AMA.
John Studdard, MD, FCCP
CHEST President
Collaborating with societies: CHEST and AMA
While the American Medical Association (AMA) is the oldest and largest national medical association, many physicians, both members and nonmembers, have limited understanding of the policies, processes, and strategic foci of the AMA. It is our goal to inform our membership about the workings of the AMA and how those interact with the goals of CHEST and our members. We hope to do this by publishing periodic articles in CHEST® Physician. One of the authors (DRM) has been the CHEST delegate to the AMA for more than 20 years, and the other (NRD) is CHEST’s new delegate.

- Create thriving physician practices.
- Create the medical school of the future.
- Improve health outcomes.
We will expand on these in future articles.
The AMA is both an individual member organization and a federation of geographic, ie, county and state, societies and specialty societies, as well as the uniformed services and the VA. It is this federation that comprises the House of Delegates (HOD or House), which is the principle policy-making body of the AMA. The number of delegates from each member organization (now numbering more than 170 organizations) depends on the number of individual AMA members among that organization’s members. Due to recent bylaws changes, CHEST now has two delegates. The HOD meets twice per year to establish policy on health, medical, professional, and governance matters, as well as the principles within which the AMA’s business activities are conducted.

Most member societies meet in caucuses or Section Councils prior to the voting in the House to discuss the pending business. The Specialty and Service Society (SSS) is the largest caucus in the AMA’s House of Delegates. The SSS meets twice annually in conjunction with the Interim and Annual Meetings of the HOD. There are two categories of groups in the SSS: those societies that have seats in the HOD and those seeking admission to the house.
SSS groups in the HOD include:
- 119 national medical specialties
- 2 professional interest medical associations
- 5 military service groups
An association must first be represented in the SSS for 3 years and meet the required number of AMA members before it is eligible to seek admission to the HOD.
The American College of Chest Physicians (CHEST) is an active member of the SSS but also joins with other societies of similar interests in the Section Council on Chest and Allergic Diseases. This caucus includes the ATS, SCCM, ASSM, and several allergy societies. Through the HOD, the SSS, and the Section Council, CHEST can partner with the AMA and other societies, such as ATS, to support each other’s resolutions or important regulatory issues.
In summary, the AMA plays an important role in many areas of interest to our members. And, it can be a useful forum for connecting with societies with similar interests in directing advocacy and setting policy. We plan to continue this update in future issues of CHEST® Physician.
References
1. https://www.ama-assn.org/content/ama-house-delegates Accessed: January 28, 2018
2. https://www.ama-assn.org/practice-management/ama-steps-forward-practice-improvement-strategies Accessed: January 28, 2018
As many who read CHEST® Physician may know, we have a nucleus of dedicated volunteers who give unselfishly of their time and talent to represent our members in the area of “regulatory advocacy” and “policy advocacy” in the areas of pulmonary, critical care, and sleep medicine. It is our goal to recognize and support this valuable group of individuals who represent us in the space of coding and reimbursement, RUC activities, relationships with organizations like the ACP and the AMA, as well as our sister societies, such as ATS, SCCM, NAMDRC, CCNA, APSR, ALAT, and ERS, among others.
One of our goals, in addition to recognizing this group, is to identify and mentor the next generation of representatives. A great example of this mentorship is reflected in our involvement with the AMA. Dr. Bob McCaffree has represented CHEST for 22 years and is now mentoring Dr. Raj Desai who will be assuming this role of AMA Delegate this year. Special thanks to Dr. McCaffree for his unselfish service in this capacity and for his mentorship of Dr. Desai. I hope that you enjoy this and future CHEST® Physician articles summarizing and reflecting on the activities pertinent to CHEST at the AMA.
John Studdard, MD, FCCP
CHEST President
Collaborating with societies: CHEST and AMA
While the American Medical Association (AMA) is the oldest and largest national medical association, many physicians, both members and nonmembers, have limited understanding of the policies, processes, and strategic foci of the AMA. It is our goal to inform our membership about the workings of the AMA and how those interact with the goals of CHEST and our members. We hope to do this by publishing periodic articles in CHEST® Physician. One of the authors (DRM) has been the CHEST delegate to the AMA for more than 20 years, and the other (NRD) is CHEST’s new delegate.
- Create thriving physician practices.
- Create the medical school of the future.
- Improve health outcomes.
We will expand on these in future articles.
The AMA is both an individual member organization and a federation of geographic, ie, county and state, societies and specialty societies, as well as the uniformed services and the VA. It is this federation that comprises the House of Delegates (HOD or House), which is the principle policy-making body of the AMA. The number of delegates from each member organization (now numbering more than 170 organizations) depends on the number of individual AMA members among that organization’s members. Due to recent bylaws changes, CHEST now has two delegates. The HOD meets twice per year to establish policy on health, medical, professional, and governance matters, as well as the principles within which the AMA’s business activities are conducted.
Most member societies meet in caucuses or Section Councils prior to the voting in the House to discuss the pending business. The Specialty and Service Society (SSS) is the largest caucus in the AMA’s House of Delegates. The SSS meets twice annually in conjunction with the Interim and Annual Meetings of the HOD. There are two categories of groups in the SSS: those societies that have seats in the HOD and those seeking admission to the house.
SSS groups in the HOD include:
- 119 national medical specialties
- 2 professional interest medical associations
- 5 military service groups
An association must first be represented in the SSS for 3 years and meet the required number of AMA members before it is eligible to seek admission to the HOD.
The American College of Chest Physicians (CHEST) is an active member of the SSS but also joins with other societies of similar interests in the Section Council on Chest and Allergic Diseases. This caucus includes the ATS, SCCM, ASSM, and several allergy societies. Through the HOD, the SSS, and the Section Council, CHEST can partner with the AMA and other societies, such as ATS, to support each other’s resolutions or important regulatory issues.
In summary, the AMA plays an important role in many areas of interest to our members. And, it can be a useful forum for connecting with societies with similar interests in directing advocacy and setting policy. We plan to continue this update in future issues of CHEST® Physician.
References
1. https://www.ama-assn.org/content/ama-house-delegates Accessed: January 28, 2018
2. https://www.ama-assn.org/practice-management/ama-steps-forward-practice-improvement-strategies Accessed: January 28, 2018
As many who read CHEST® Physician may know, we have a nucleus of dedicated volunteers who give unselfishly of their time and talent to represent our members in the area of “regulatory advocacy” and “policy advocacy” in the areas of pulmonary, critical care, and sleep medicine. It is our goal to recognize and support this valuable group of individuals who represent us in the space of coding and reimbursement, RUC activities, relationships with organizations like the ACP and the AMA, as well as our sister societies, such as ATS, SCCM, NAMDRC, CCNA, APSR, ALAT, and ERS, among others.
One of our goals, in addition to recognizing this group, is to identify and mentor the next generation of representatives. A great example of this mentorship is reflected in our involvement with the AMA. Dr. Bob McCaffree has represented CHEST for 22 years and is now mentoring Dr. Raj Desai who will be assuming this role of AMA Delegate this year. Special thanks to Dr. McCaffree for his unselfish service in this capacity and for his mentorship of Dr. Desai. I hope that you enjoy this and future CHEST® Physician articles summarizing and reflecting on the activities pertinent to CHEST at the AMA.
John Studdard, MD, FCCP
CHEST President
Collaborating with societies: CHEST and AMA
While the American Medical Association (AMA) is the oldest and largest national medical association, many physicians, both members and nonmembers, have limited understanding of the policies, processes, and strategic foci of the AMA. It is our goal to inform our membership about the workings of the AMA and how those interact with the goals of CHEST and our members. We hope to do this by publishing periodic articles in CHEST® Physician. One of the authors (DRM) has been the CHEST delegate to the AMA for more than 20 years, and the other (NRD) is CHEST’s new delegate.
- Create thriving physician practices.
- Create the medical school of the future.
- Improve health outcomes.
We will expand on these in future articles.
The AMA is both an individual member organization and a federation of geographic, ie, county and state, societies and specialty societies, as well as the uniformed services and the VA. It is this federation that comprises the House of Delegates (HOD or House), which is the principle policy-making body of the AMA. The number of delegates from each member organization (now numbering more than 170 organizations) depends on the number of individual AMA members among that organization’s members. Due to recent bylaws changes, CHEST now has two delegates. The HOD meets twice per year to establish policy on health, medical, professional, and governance matters, as well as the principles within which the AMA’s business activities are conducted.
Most member societies meet in caucuses or Section Councils prior to the voting in the House to discuss the pending business. The Specialty and Service Society (SSS) is the largest caucus in the AMA’s House of Delegates. The SSS meets twice annually in conjunction with the Interim and Annual Meetings of the HOD. There are two categories of groups in the SSS: those societies that have seats in the HOD and those seeking admission to the house.
SSS groups in the HOD include:
- 119 national medical specialties
- 2 professional interest medical associations
- 5 military service groups
An association must first be represented in the SSS for 3 years and meet the required number of AMA members before it is eligible to seek admission to the HOD.
The American College of Chest Physicians (CHEST) is an active member of the SSS but also joins with other societies of similar interests in the Section Council on Chest and Allergic Diseases. This caucus includes the ATS, SCCM, ASSM, and several allergy societies. Through the HOD, the SSS, and the Section Council, CHEST can partner with the AMA and other societies, such as ATS, to support each other’s resolutions or important regulatory issues.
In summary, the AMA plays an important role in many areas of interest to our members. And, it can be a useful forum for connecting with societies with similar interests in directing advocacy and setting policy. We plan to continue this update in future issues of CHEST® Physician.
References
1. https://www.ama-assn.org/content/ama-house-delegates Accessed: January 28, 2018
2. https://www.ama-assn.org/practice-management/ama-steps-forward-practice-improvement-strategies Accessed: January 28, 2018
Zika virus: Sexual contact risk may be limited to short window
Shedding of infectious Zika virus in the semen of symptomatic infected men appears to be uncommon and limited to the first few weeks after onset of illness, according to results of a recent prospective study.
Out of all semen samples with detectable Zika virus RNA, the only ones with infectious virus were those that had been obtained within 30 days of illness onset, study authors reported in the New England Journal of Medicine.
Sexual transmission of Zika virus, first documented in 2011, has now been reported in at least 13 countries, Dr. Mead and his colleagues wrote.
Usually, the cases have involved transmission from a symptomatic man to a woman, they added.
Previously, some investigators had proposed that sexual transmission of Zika virus could pose a greater risk of fetal infection than could mosquito-borne transmission, Dr. Mead and colleagues noted in their report. “If so, the interruption of sexual transmission could play a critical role in preventing the serious complications that have been associated with fetal infection,” they wrote.
To investigate further, Dr. Mead and his colleagues conducted a prospective study of men with symptomatic Zika virus infection. They collected 1,327 semen samples from 184 men and 1,038 urine samples from 183 men, according to the report.
They obtained specimens twice monthly for 6 months. Samples were tested for Zika RNA using real-time reverse transcriptase polymerase chain reaction assay and for infectious Zika virus using Vero cell culture and plaque assay.
Investigators detected Zika virus RNA in the semen of 60 men (33%), including semen samples from 22 of the 36 men (61%) tested within 30 days after illness onset, investigators said in the report.
While Zika virus RNA shedding decreased considerably in the 3 months after illness onset, it did continue for 281 days in one man, they noted.
Men who were older and those who ejaculated less frequently were more likely to have prolonged RNA shedding in semen, results of multivariable analysis showed.
Infectious Zika virus was isolated from just 3 out of the 78 semen samples with detectable Zika virus RNA that were tested by culture, investigators said. Notably, all 3 of the cases were among the 19 of those samples obtained within 30 days of illness onset, they reported.
Detection of Zika virus RNA in urine was rare, occurring in only 7 men (4%), possibly because of the timing of the first specimen collection, according to investigators. They said previous studies suggest a rapid decline in Zika virus shedding in urine during the first few weeks after onset of illness.
Important questions remain regarding sexual transmission of Zika virus, such as whether maternal infection through sex poses similar risks to the fetus as compared with maternal infection via mosquito bite, Dr. Mead and his coauthors said in the report.
“A better understanding of these issues is needed to guide the development of effective prevention strategies,” they wrote.
The study was supported by the Centers for Disease Control and Prevention. Dr. Mead and his coauthors reported they had no disclosures related to the study.
SOURCE: Mead PS et al. N Engl J Med. 2018;378(15):1377-85.
This study illustrates the apparent shortcomings of current virus-detection standards in terms of their relevance to public health, according to Heinz Feldmann, MD.
Approximately 4% of Zika virus RNA-positive semen samples were infectious, according to the report, and of those infectious samples, all were obtained within 30 days of the onset of illness. “This finding suggests that there is a short period during which Zika virus–infected men might transmit this virus through sexual contact,” Dr. Feldmann wrote in an editorial.
Current practice in some areas is to test semen samples sequentially until two or more consecutive negative results are obtained; however, that approach is controversial, according to Dr. Feldmann, because the person could be shedding the virus intermittently because of the potential for virus latency and reactivation.
“This also raises the question of whether modern molecular approaches are properly positioned to detect virus latency rather than persistence,” he said in his editorial. The goal, he added, should be to determine infectivity, which is probably best assessed by means of viral isolation – which is believed to be less sensitive than molecular detection.
“Thus, the diagnostic situation is far more complicated than it seems,” he noted.
However, he added, these diagnostic scenarios may be less applicable for public health entities, which have “quickly” disseminated recommendations for safer sex to prevent Zika virus spread and the potentially devastating consequences of fetal infection.
“These recommendations leverage the best data available and have been implemented, but ought to be updated as new data emerge,” Dr. Feldmann wrote.
Dr. Feldmann is with the National Institute of Allergy and Infectious Diseases, National Institutes of Health, and Rocky Mountain Laboratories, Hamilton, Mont. These comments are derived from his editorial N Engl J Med 2018;378:1377-85 . Dr. Feldmann reported that he had nothing to disclose related to the editorial.
This study illustrates the apparent shortcomings of current virus-detection standards in terms of their relevance to public health, according to Heinz Feldmann, MD.
Approximately 4% of Zika virus RNA-positive semen samples were infectious, according to the report, and of those infectious samples, all were obtained within 30 days of the onset of illness. “This finding suggests that there is a short period during which Zika virus–infected men might transmit this virus through sexual contact,” Dr. Feldmann wrote in an editorial.
Current practice in some areas is to test semen samples sequentially until two or more consecutive negative results are obtained; however, that approach is controversial, according to Dr. Feldmann, because the person could be shedding the virus intermittently because of the potential for virus latency and reactivation.
“This also raises the question of whether modern molecular approaches are properly positioned to detect virus latency rather than persistence,” he said in his editorial. The goal, he added, should be to determine infectivity, which is probably best assessed by means of viral isolation – which is believed to be less sensitive than molecular detection.
“Thus, the diagnostic situation is far more complicated than it seems,” he noted.
However, he added, these diagnostic scenarios may be less applicable for public health entities, which have “quickly” disseminated recommendations for safer sex to prevent Zika virus spread and the potentially devastating consequences of fetal infection.
“These recommendations leverage the best data available and have been implemented, but ought to be updated as new data emerge,” Dr. Feldmann wrote.
Dr. Feldmann is with the National Institute of Allergy and Infectious Diseases, National Institutes of Health, and Rocky Mountain Laboratories, Hamilton, Mont. These comments are derived from his editorial N Engl J Med 2018;378:1377-85 . Dr. Feldmann reported that he had nothing to disclose related to the editorial.
This study illustrates the apparent shortcomings of current virus-detection standards in terms of their relevance to public health, according to Heinz Feldmann, MD.
Approximately 4% of Zika virus RNA-positive semen samples were infectious, according to the report, and of those infectious samples, all were obtained within 30 days of the onset of illness. “This finding suggests that there is a short period during which Zika virus–infected men might transmit this virus through sexual contact,” Dr. Feldmann wrote in an editorial.
Current practice in some areas is to test semen samples sequentially until two or more consecutive negative results are obtained; however, that approach is controversial, according to Dr. Feldmann, because the person could be shedding the virus intermittently because of the potential for virus latency and reactivation.
“This also raises the question of whether modern molecular approaches are properly positioned to detect virus latency rather than persistence,” he said in his editorial. The goal, he added, should be to determine infectivity, which is probably best assessed by means of viral isolation – which is believed to be less sensitive than molecular detection.
“Thus, the diagnostic situation is far more complicated than it seems,” he noted.
However, he added, these diagnostic scenarios may be less applicable for public health entities, which have “quickly” disseminated recommendations for safer sex to prevent Zika virus spread and the potentially devastating consequences of fetal infection.
“These recommendations leverage the best data available and have been implemented, but ought to be updated as new data emerge,” Dr. Feldmann wrote.
Dr. Feldmann is with the National Institute of Allergy and Infectious Diseases, National Institutes of Health, and Rocky Mountain Laboratories, Hamilton, Mont. These comments are derived from his editorial N Engl J Med 2018;378:1377-85 . Dr. Feldmann reported that he had nothing to disclose related to the editorial.
Shedding of infectious Zika virus in the semen of symptomatic infected men appears to be uncommon and limited to the first few weeks after onset of illness, according to results of a recent prospective study.
Out of all semen samples with detectable Zika virus RNA, the only ones with infectious virus were those that had been obtained within 30 days of illness onset, study authors reported in the New England Journal of Medicine.
Sexual transmission of Zika virus, first documented in 2011, has now been reported in at least 13 countries, Dr. Mead and his colleagues wrote.
Usually, the cases have involved transmission from a symptomatic man to a woman, they added.
Previously, some investigators had proposed that sexual transmission of Zika virus could pose a greater risk of fetal infection than could mosquito-borne transmission, Dr. Mead and colleagues noted in their report. “If so, the interruption of sexual transmission could play a critical role in preventing the serious complications that have been associated with fetal infection,” they wrote.
To investigate further, Dr. Mead and his colleagues conducted a prospective study of men with symptomatic Zika virus infection. They collected 1,327 semen samples from 184 men and 1,038 urine samples from 183 men, according to the report.
They obtained specimens twice monthly for 6 months. Samples were tested for Zika RNA using real-time reverse transcriptase polymerase chain reaction assay and for infectious Zika virus using Vero cell culture and plaque assay.
Investigators detected Zika virus RNA in the semen of 60 men (33%), including semen samples from 22 of the 36 men (61%) tested within 30 days after illness onset, investigators said in the report.
While Zika virus RNA shedding decreased considerably in the 3 months after illness onset, it did continue for 281 days in one man, they noted.
Men who were older and those who ejaculated less frequently were more likely to have prolonged RNA shedding in semen, results of multivariable analysis showed.
Infectious Zika virus was isolated from just 3 out of the 78 semen samples with detectable Zika virus RNA that were tested by culture, investigators said. Notably, all 3 of the cases were among the 19 of those samples obtained within 30 days of illness onset, they reported.
Detection of Zika virus RNA in urine was rare, occurring in only 7 men (4%), possibly because of the timing of the first specimen collection, according to investigators. They said previous studies suggest a rapid decline in Zika virus shedding in urine during the first few weeks after onset of illness.
Important questions remain regarding sexual transmission of Zika virus, such as whether maternal infection through sex poses similar risks to the fetus as compared with maternal infection via mosquito bite, Dr. Mead and his coauthors said in the report.
“A better understanding of these issues is needed to guide the development of effective prevention strategies,” they wrote.
The study was supported by the Centers for Disease Control and Prevention. Dr. Mead and his coauthors reported they had no disclosures related to the study.
SOURCE: Mead PS et al. N Engl J Med. 2018;378(15):1377-85.
Shedding of infectious Zika virus in the semen of symptomatic infected men appears to be uncommon and limited to the first few weeks after onset of illness, according to results of a recent prospective study.
Out of all semen samples with detectable Zika virus RNA, the only ones with infectious virus were those that had been obtained within 30 days of illness onset, study authors reported in the New England Journal of Medicine.
Sexual transmission of Zika virus, first documented in 2011, has now been reported in at least 13 countries, Dr. Mead and his colleagues wrote.
Usually, the cases have involved transmission from a symptomatic man to a woman, they added.
Previously, some investigators had proposed that sexual transmission of Zika virus could pose a greater risk of fetal infection than could mosquito-borne transmission, Dr. Mead and colleagues noted in their report. “If so, the interruption of sexual transmission could play a critical role in preventing the serious complications that have been associated with fetal infection,” they wrote.
To investigate further, Dr. Mead and his colleagues conducted a prospective study of men with symptomatic Zika virus infection. They collected 1,327 semen samples from 184 men and 1,038 urine samples from 183 men, according to the report.
They obtained specimens twice monthly for 6 months. Samples were tested for Zika RNA using real-time reverse transcriptase polymerase chain reaction assay and for infectious Zika virus using Vero cell culture and plaque assay.
Investigators detected Zika virus RNA in the semen of 60 men (33%), including semen samples from 22 of the 36 men (61%) tested within 30 days after illness onset, investigators said in the report.
While Zika virus RNA shedding decreased considerably in the 3 months after illness onset, it did continue for 281 days in one man, they noted.
Men who were older and those who ejaculated less frequently were more likely to have prolonged RNA shedding in semen, results of multivariable analysis showed.
Infectious Zika virus was isolated from just 3 out of the 78 semen samples with detectable Zika virus RNA that were tested by culture, investigators said. Notably, all 3 of the cases were among the 19 of those samples obtained within 30 days of illness onset, they reported.
Detection of Zika virus RNA in urine was rare, occurring in only 7 men (4%), possibly because of the timing of the first specimen collection, according to investigators. They said previous studies suggest a rapid decline in Zika virus shedding in urine during the first few weeks after onset of illness.
Important questions remain regarding sexual transmission of Zika virus, such as whether maternal infection through sex poses similar risks to the fetus as compared with maternal infection via mosquito bite, Dr. Mead and his coauthors said in the report.
“A better understanding of these issues is needed to guide the development of effective prevention strategies,” they wrote.
The study was supported by the Centers for Disease Control and Prevention. Dr. Mead and his coauthors reported they had no disclosures related to the study.
SOURCE: Mead PS et al. N Engl J Med. 2018;378(15):1377-85.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: While Zika virus RNA is common and may persist for months in the semen of symptomatic infected men, shedding of infectious virus appears to be much less common and limited to the first few weeks after onset of illness.
Major finding: Out of 78 semen samples with detectable Zika virus RNA, 3 had infectious virus, and all 3 were obtained within 30 days of illness onset.
Study details: A prospective study of 1,327 semen samples from 184 men with symptomatic Zika virus infection.
Disclosures: The study was supported by the Centers for Disease Control and Prevention. Study authors reported they had nothing to disclose relative to the study.
Source: Mead PS et al. N Engl J Med. 2018 Apr 12;378(15):1377-85.
New genetic subtypes could facilitate precision medicine in DLBCL
Four genetic subtypes of diffuse large B-cell lymphoma (DLBCL) showed multiple distinct mutations, gene expression signatures, and treatment responses, researchers reported.
The findings “may provide a conceptual edifice on which to develop precision therapies for these aggressive cancers,” Roland Schmitz, PhD, and his associates wrote in the New England Journal of Medicine.
Other DLBCL studies have focused on individual mutations, but therapeutic response probably hinges on “constellations of genetic aberrations,” wrote Dr. Schmitz of the National Cancer Institute and his associates.
Therefore, they used exome and transcriptome sequencing, deep amplicon resequencing of 372 genes, and DNA copy-number analysis to analyze 572 fresh-frozen DLBCL biopsy specimens, nearly all of which were treatment-naïve.
This multiplatform approach yielded four genetic subtypes: MCD, so named for its co-occurring MYD88L265P and CD79B mutations; BN2, which has BCL6 fusions and NOTCH2 mutations; N1, which has NOTCH1 mutations; and EZB, which has EZH2 mutations and BCL2 translocations. Most MCD and N1 specimens were activated B-cell–like (ABC) tumors, EZB specimens were primarily germinal-center B-cell–like (GCB) tumors, and BN2 specimens included ABC, GCB, and unclassified cases.
A closer look at 119 previously untreated patients linked genetic subtypes with significant differences in progression-free survival (P less than .0001) and overall survival (P = .0002) following R-CHOP or CHOP-like chemotherapy.
The BN2 and EZB subtypes “[had] much more favorable outcomes than the MCD and N1 subtypes,” Dr. Schmitz and his associates said. “Analysis of genetic pathways suggested that MCD and BN2 DLBCLs rely on ‘chronic active’ B-cell receptor signaling that is amenable to therapeutic inhibition.”
Genetically subtyping DLBCL could help guide patients into appropriate clinical trials, the investigators wrote. For example, patients with the N1 subtype might be candidates for immune checkpoint inhibitor therapy, given N1’s prominent T-cell gene expression and poor response to R-CHOP.
Funders included the National Institutes of Health, the National Cancer Institute, the Dr. Mildred Scheel Stiftung fur Krebsforschung (Deutsche Krebshilfe), the Washington University in St. Louis, and the Kay Kendall Leukaemia Fund. Dr. Schmitz disclosed research funding from Dr. Mildred Scheel Stiftung fur Krebsforschung (Deutsche Krebshilfe).
SOURCE: Schmitz et al. New Eng J Med. 2018 Apr 11. doi: 10.1056/NEJMoa1801445.
Four genetic subtypes of diffuse large B-cell lymphoma (DLBCL) showed multiple distinct mutations, gene expression signatures, and treatment responses, researchers reported.
The findings “may provide a conceptual edifice on which to develop precision therapies for these aggressive cancers,” Roland Schmitz, PhD, and his associates wrote in the New England Journal of Medicine.
Other DLBCL studies have focused on individual mutations, but therapeutic response probably hinges on “constellations of genetic aberrations,” wrote Dr. Schmitz of the National Cancer Institute and his associates.
Therefore, they used exome and transcriptome sequencing, deep amplicon resequencing of 372 genes, and DNA copy-number analysis to analyze 572 fresh-frozen DLBCL biopsy specimens, nearly all of which were treatment-naïve.
This multiplatform approach yielded four genetic subtypes: MCD, so named for its co-occurring MYD88L265P and CD79B mutations; BN2, which has BCL6 fusions and NOTCH2 mutations; N1, which has NOTCH1 mutations; and EZB, which has EZH2 mutations and BCL2 translocations. Most MCD and N1 specimens were activated B-cell–like (ABC) tumors, EZB specimens were primarily germinal-center B-cell–like (GCB) tumors, and BN2 specimens included ABC, GCB, and unclassified cases.
A closer look at 119 previously untreated patients linked genetic subtypes with significant differences in progression-free survival (P less than .0001) and overall survival (P = .0002) following R-CHOP or CHOP-like chemotherapy.
The BN2 and EZB subtypes “[had] much more favorable outcomes than the MCD and N1 subtypes,” Dr. Schmitz and his associates said. “Analysis of genetic pathways suggested that MCD and BN2 DLBCLs rely on ‘chronic active’ B-cell receptor signaling that is amenable to therapeutic inhibition.”
Genetically subtyping DLBCL could help guide patients into appropriate clinical trials, the investigators wrote. For example, patients with the N1 subtype might be candidates for immune checkpoint inhibitor therapy, given N1’s prominent T-cell gene expression and poor response to R-CHOP.
Funders included the National Institutes of Health, the National Cancer Institute, the Dr. Mildred Scheel Stiftung fur Krebsforschung (Deutsche Krebshilfe), the Washington University in St. Louis, and the Kay Kendall Leukaemia Fund. Dr. Schmitz disclosed research funding from Dr. Mildred Scheel Stiftung fur Krebsforschung (Deutsche Krebshilfe).
SOURCE: Schmitz et al. New Eng J Med. 2018 Apr 11. doi: 10.1056/NEJMoa1801445.
Four genetic subtypes of diffuse large B-cell lymphoma (DLBCL) showed multiple distinct mutations, gene expression signatures, and treatment responses, researchers reported.
The findings “may provide a conceptual edifice on which to develop precision therapies for these aggressive cancers,” Roland Schmitz, PhD, and his associates wrote in the New England Journal of Medicine.
Other DLBCL studies have focused on individual mutations, but therapeutic response probably hinges on “constellations of genetic aberrations,” wrote Dr. Schmitz of the National Cancer Institute and his associates.
Therefore, they used exome and transcriptome sequencing, deep amplicon resequencing of 372 genes, and DNA copy-number analysis to analyze 572 fresh-frozen DLBCL biopsy specimens, nearly all of which were treatment-naïve.
This multiplatform approach yielded four genetic subtypes: MCD, so named for its co-occurring MYD88L265P and CD79B mutations; BN2, which has BCL6 fusions and NOTCH2 mutations; N1, which has NOTCH1 mutations; and EZB, which has EZH2 mutations and BCL2 translocations. Most MCD and N1 specimens were activated B-cell–like (ABC) tumors, EZB specimens were primarily germinal-center B-cell–like (GCB) tumors, and BN2 specimens included ABC, GCB, and unclassified cases.
A closer look at 119 previously untreated patients linked genetic subtypes with significant differences in progression-free survival (P less than .0001) and overall survival (P = .0002) following R-CHOP or CHOP-like chemotherapy.
The BN2 and EZB subtypes “[had] much more favorable outcomes than the MCD and N1 subtypes,” Dr. Schmitz and his associates said. “Analysis of genetic pathways suggested that MCD and BN2 DLBCLs rely on ‘chronic active’ B-cell receptor signaling that is amenable to therapeutic inhibition.”
Genetically subtyping DLBCL could help guide patients into appropriate clinical trials, the investigators wrote. For example, patients with the N1 subtype might be candidates for immune checkpoint inhibitor therapy, given N1’s prominent T-cell gene expression and poor response to R-CHOP.
Funders included the National Institutes of Health, the National Cancer Institute, the Dr. Mildred Scheel Stiftung fur Krebsforschung (Deutsche Krebshilfe), the Washington University in St. Louis, and the Kay Kendall Leukaemia Fund. Dr. Schmitz disclosed research funding from Dr. Mildred Scheel Stiftung fur Krebsforschung (Deutsche Krebshilfe).
SOURCE: Schmitz et al. New Eng J Med. 2018 Apr 11. doi: 10.1056/NEJMoa1801445.
FROM NEJM
Key clinical point: Multiplatform analyses identified four new genetic subtypes of DLBCL.
Major finding: The subtypes were distinguishable based on multiple genetic aberrations, phenotypes, and treatment responses.
Study details: Study of 574 DLBCL samples using exome and transcriptome sequencing, array-based DNA copy-number analysis, and targeted amplicon resequencing of 372 genes.
Disclosures: Funders included the National Institutes of Health, the National Cancer Institute, the Dr. Mildred Scheel Stiftung fur Krebsforschung (Deutsche Krebshilfe), the Washington University in St. Louis, and the Kay Kendall Leukaemia Fund. Dr. Schmitz disclosed research funding from Dr. Mildred Scheel Stiftung fur Krebsforschung (Deutsche Krebshilfe).
Source: Schmitz et al. New Eng J Med. 2018 Apr 11. doi: 10.1056/NEJMoa1801445.
Palliative care screening, sleep devices, novel biologics
Palliative and end-of-life care
Nurse-driven palliative care screening
Palliative care (PC) aims to improve quality of life for patients with a life-threatening illness, providing holistic patient-centered support along the continuum of the disease process. Although frequently implemented in critical care settings, integrating PC in the neuro ICU has been difficult to adopt in practice due to the uncertainty in prognostication of definitive outcomes and practice culture beliefs such as the self-fulfilling prophecy (Frontera, et al. Crit Care Med. 2015;43[9]:1964; Rubin, et al. Curr Opin Crit Care. 2017;23[2]:134; Knies, et al. Semin Neurol. 2016;36[6]:631).
At our institution, a nursing education project was conducted to pilot nurse-driven PC screenings on admission to the neuro ICU. The project evaluated nurse comfort and knowledge with identifying and recommending PC consults. Pre- and post-intervention surveys revealed that education and introduction of a PC screening tool significantly increased nurse comfort and knowledge of PC eligibility.

PC in the neuro ICU can exist to contribute to successful outcomes in patient and family care. Within neurocritical care, incorporating PC is essential to provide extra support to patients and families (Frontera, et al. 2015).
For these reasons and data from the project, nurse-driven screening may encourage appropriate early PC consults. Patient-centered care is the ultimate goal in the management of our patients. Nurse-driven PC screening can help bring various unmet PC needs to the health-care team for opportunities that might not have been met or otherwise assessed. Consider implementing nurse-driven PC screening protocols at your institution to aid in collaborative and proactive interdisciplinary care.
Danielle McCamey, ACNP
Steering Committee Member
Sleep medicine
Diagnostics, devices, and sleep
The past several months have been busy for the Sleep Medicine NetWork. We have been working to represent the interests of our membership and our patients in many arenas.
Devices coded as E0464, defined as life support mechanical ventilators used with mask-based ventilation in the home are being more frequently used. According to the Office of the Inspector General (OIG), there has been an 89-fold increase in billing for E0464 ventilators for Medicare and its beneficiaries between 2009 and 2015, increasing from $3.8M to $340M. In response, the Agency for Healthcare Research and Quality (AHRQ) requested a response to specific questions related to these devices.

In 2018, the CHEST Sleep Medicine NetWork will be participating in a Federal Drug Association-sponsored workshop entitled “Study Design Considerations for Devices including Digital Health Technologies for Sleep-Disordered Breathing (SDB) in Adults,” along with other national organizations and leaders in our field. This workshop will address available technologies for the diagnosis, monitoring, and treatment of SDB, as well as trends for digital health technologies and clinical trial design considerations.
Finally, the Sleep Medicine NetWork has wasted no time after a successful CHEST 2017 in Toronto in planning for the next annual meeting in San Antonio. We are excited to present an exciting curriculum in Sleep Medicine at CHEST 2018, so stay tuned.
Aneesa M. Das, MD, FCCP
NetWork Chair
Occupational and environmental health
Post-deployment lung disease
Since the early 1990s, ongoing military deployments to Southwest Asia remain a unique challenge from a pulmonary symptomology and diagnostic perspective.
Various airborne hazards in the deployment environment include geologic dusts, burn pit smoke, vehicle emissions, and industrial air pollution. Exposures can give rise to both acute respiratory symptoms and, in some instances, chronic lung disease. Currently, data are limited on whether inhalation of airborne particulate matter by military personnel is linked to increases in pulmonary diseases (Morris MJ, et al. US Army Med Dep J. 2016:173).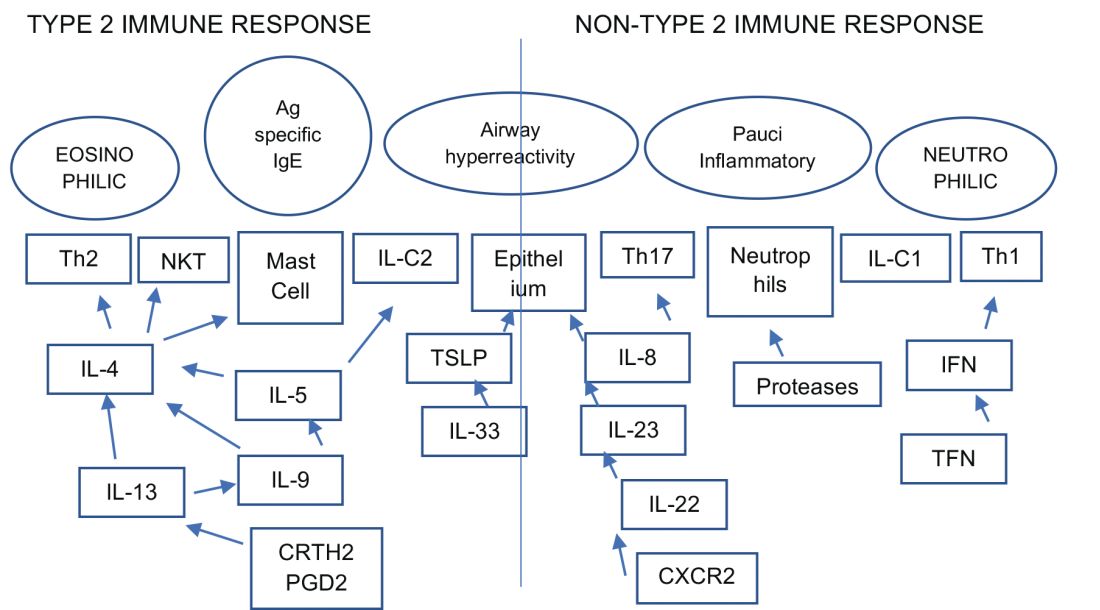
Ongoing research by the Veterans Affairs continues to enroll post-deployed personnel in an Airborne Hazard and Burn Pit Registry. Past approaches in evaluation of deployed individuals ranged from common tests such as spirometry, HRCT scanning, full PFTs, bronchoprovocation challenges, and, in some instances, lung biopsies (Krefft SD, et al. Fed Pract. 2015;32[6]:32). More novel evaluations of postdeployment dyspnea include impulse oscillometry, exhaled nitric oxide, bronchoscopy, and cardiopulmonary exercise testing (Huprikar, et al. Chest. 2016;150[4]:S934A).
Members of the CHEST Occupational and Environmental Health NetWork are currently updating comprehensive approaches to evaluate military personnel with chronic respiratory symptoms from deployments. Continued emphasis, however, should be placed on diagnosing and treating common diseases such as asthma, exercise-induced bronchospasm, GERD, and upper airway disorders.
Pedro F. Lucero, MD, FCCP
Steering Committee Member
Clinical pulmonary medicine
Biologics – Birth of a new era of precision management in asthma
An estimated 10% to 20% of patients with severe uncontrolled asthma do not respond to maximal best standard treatments, leading to substantial health-care costs. A paradigm shift is now underway in our approach to the care of these patients with the emergence of novel biologics targeting the complex and interconnected inflammatory pathways in asthma that result in a diverse profile of asthma endotypes and phenotypes (Fig 1).
Current FDA-approved biologics primarily target patients with a T2 high phenotype (Table1).
Dupilumab binds to the alpha unit of the IL-4 receptor and blocks both IL-4 and IL-13. It shows potential efficacy in patients with T2 high asthma with or without eosinophilia but has not yet received FDA approval.
Multiple newer biologics are currently in development (Table 2).
Pulmonologists need to get familiar with the logistics of administration of these novel agents. The two common methods of administering biologics are (1) buy and bill – where the provider buys the drug directly from the distributor; and (2) assignment of benefits (typically administered by a Pharmacy Benefit Manager) - specific dose of the medication is shipped to the physician’s office and physician only bills for the administration. CPT and J codes are shown in Table 1.
Shyamsunder Subramanian, MD, FCCP
Steering Committee Member
Palliative and end-of-life care
Nurse-driven palliative care screening
Palliative care (PC) aims to improve quality of life for patients with a life-threatening illness, providing holistic patient-centered support along the continuum of the disease process. Although frequently implemented in critical care settings, integrating PC in the neuro ICU has been difficult to adopt in practice due to the uncertainty in prognostication of definitive outcomes and practice culture beliefs such as the self-fulfilling prophecy (Frontera, et al. Crit Care Med. 2015;43[9]:1964; Rubin, et al. Curr Opin Crit Care. 2017;23[2]:134; Knies, et al. Semin Neurol. 2016;36[6]:631).
At our institution, a nursing education project was conducted to pilot nurse-driven PC screenings on admission to the neuro ICU. The project evaluated nurse comfort and knowledge with identifying and recommending PC consults. Pre- and post-intervention surveys revealed that education and introduction of a PC screening tool significantly increased nurse comfort and knowledge of PC eligibility.
PC in the neuro ICU can exist to contribute to successful outcomes in patient and family care. Within neurocritical care, incorporating PC is essential to provide extra support to patients and families (Frontera, et al. 2015).
For these reasons and data from the project, nurse-driven screening may encourage appropriate early PC consults. Patient-centered care is the ultimate goal in the management of our patients. Nurse-driven PC screening can help bring various unmet PC needs to the health-care team for opportunities that might not have been met or otherwise assessed. Consider implementing nurse-driven PC screening protocols at your institution to aid in collaborative and proactive interdisciplinary care.
Danielle McCamey, ACNP
Steering Committee Member
Sleep medicine
Diagnostics, devices, and sleep
The past several months have been busy for the Sleep Medicine NetWork. We have been working to represent the interests of our membership and our patients in many arenas.
Devices coded as E0464, defined as life support mechanical ventilators used with mask-based ventilation in the home are being more frequently used. According to the Office of the Inspector General (OIG), there has been an 89-fold increase in billing for E0464 ventilators for Medicare and its beneficiaries between 2009 and 2015, increasing from $3.8M to $340M. In response, the Agency for Healthcare Research and Quality (AHRQ) requested a response to specific questions related to these devices.
In 2018, the CHEST Sleep Medicine NetWork will be participating in a Federal Drug Association-sponsored workshop entitled “Study Design Considerations for Devices including Digital Health Technologies for Sleep-Disordered Breathing (SDB) in Adults,” along with other national organizations and leaders in our field. This workshop will address available technologies for the diagnosis, monitoring, and treatment of SDB, as well as trends for digital health technologies and clinical trial design considerations.
Finally, the Sleep Medicine NetWork has wasted no time after a successful CHEST 2017 in Toronto in planning for the next annual meeting in San Antonio. We are excited to present an exciting curriculum in Sleep Medicine at CHEST 2018, so stay tuned.
Aneesa M. Das, MD, FCCP
NetWork Chair
Occupational and environmental health
Post-deployment lung disease
Since the early 1990s, ongoing military deployments to Southwest Asia remain a unique challenge from a pulmonary symptomology and diagnostic perspective.
Various airborne hazards in the deployment environment include geologic dusts, burn pit smoke, vehicle emissions, and industrial air pollution. Exposures can give rise to both acute respiratory symptoms and, in some instances, chronic lung disease. Currently, data are limited on whether inhalation of airborne particulate matter by military personnel is linked to increases in pulmonary diseases (Morris MJ, et al. US Army Med Dep J. 2016:173).
Ongoing research by the Veterans Affairs continues to enroll post-deployed personnel in an Airborne Hazard and Burn Pit Registry. Past approaches in evaluation of deployed individuals ranged from common tests such as spirometry, HRCT scanning, full PFTs, bronchoprovocation challenges, and, in some instances, lung biopsies (Krefft SD, et al. Fed Pract. 2015;32[6]:32). More novel evaluations of postdeployment dyspnea include impulse oscillometry, exhaled nitric oxide, bronchoscopy, and cardiopulmonary exercise testing (Huprikar, et al. Chest. 2016;150[4]:S934A).
Members of the CHEST Occupational and Environmental Health NetWork are currently updating comprehensive approaches to evaluate military personnel with chronic respiratory symptoms from deployments. Continued emphasis, however, should be placed on diagnosing and treating common diseases such as asthma, exercise-induced bronchospasm, GERD, and upper airway disorders.
Pedro F. Lucero, MD, FCCP
Steering Committee Member
Clinical pulmonary medicine
Biologics – Birth of a new era of precision management in asthma
An estimated 10% to 20% of patients with severe uncontrolled asthma do not respond to maximal best standard treatments, leading to substantial health-care costs. A paradigm shift is now underway in our approach to the care of these patients with the emergence of novel biologics targeting the complex and interconnected inflammatory pathways in asthma that result in a diverse profile of asthma endotypes and phenotypes (Fig 1).
Current FDA-approved biologics primarily target patients with a T2 high phenotype (Table1).
Dupilumab binds to the alpha unit of the IL-4 receptor and blocks both IL-4 and IL-13. It shows potential efficacy in patients with T2 high asthma with or without eosinophilia but has not yet received FDA approval.
Multiple newer biologics are currently in development (Table 2).
Pulmonologists need to get familiar with the logistics of administration of these novel agents. The two common methods of administering biologics are (1) buy and bill – where the provider buys the drug directly from the distributor; and (2) assignment of benefits (typically administered by a Pharmacy Benefit Manager) - specific dose of the medication is shipped to the physician’s office and physician only bills for the administration. CPT and J codes are shown in Table 1.
Shyamsunder Subramanian, MD, FCCP
Steering Committee Member
Palliative and end-of-life care
Nurse-driven palliative care screening
Palliative care (PC) aims to improve quality of life for patients with a life-threatening illness, providing holistic patient-centered support along the continuum of the disease process. Although frequently implemented in critical care settings, integrating PC in the neuro ICU has been difficult to adopt in practice due to the uncertainty in prognostication of definitive outcomes and practice culture beliefs such as the self-fulfilling prophecy (Frontera, et al. Crit Care Med. 2015;43[9]:1964; Rubin, et al. Curr Opin Crit Care. 2017;23[2]:134; Knies, et al. Semin Neurol. 2016;36[6]:631).
At our institution, a nursing education project was conducted to pilot nurse-driven PC screenings on admission to the neuro ICU. The project evaluated nurse comfort and knowledge with identifying and recommending PC consults. Pre- and post-intervention surveys revealed that education and introduction of a PC screening tool significantly increased nurse comfort and knowledge of PC eligibility.
PC in the neuro ICU can exist to contribute to successful outcomes in patient and family care. Within neurocritical care, incorporating PC is essential to provide extra support to patients and families (Frontera, et al. 2015).
For these reasons and data from the project, nurse-driven screening may encourage appropriate early PC consults. Patient-centered care is the ultimate goal in the management of our patients. Nurse-driven PC screening can help bring various unmet PC needs to the health-care team for opportunities that might not have been met or otherwise assessed. Consider implementing nurse-driven PC screening protocols at your institution to aid in collaborative and proactive interdisciplinary care.
Danielle McCamey, ACNP
Steering Committee Member
Sleep medicine
Diagnostics, devices, and sleep
The past several months have been busy for the Sleep Medicine NetWork. We have been working to represent the interests of our membership and our patients in many arenas.
Devices coded as E0464, defined as life support mechanical ventilators used with mask-based ventilation in the home are being more frequently used. According to the Office of the Inspector General (OIG), there has been an 89-fold increase in billing for E0464 ventilators for Medicare and its beneficiaries between 2009 and 2015, increasing from $3.8M to $340M. In response, the Agency for Healthcare Research and Quality (AHRQ) requested a response to specific questions related to these devices.
In 2018, the CHEST Sleep Medicine NetWork will be participating in a Federal Drug Association-sponsored workshop entitled “Study Design Considerations for Devices including Digital Health Technologies for Sleep-Disordered Breathing (SDB) in Adults,” along with other national organizations and leaders in our field. This workshop will address available technologies for the diagnosis, monitoring, and treatment of SDB, as well as trends for digital health technologies and clinical trial design considerations.
Finally, the Sleep Medicine NetWork has wasted no time after a successful CHEST 2017 in Toronto in planning for the next annual meeting in San Antonio. We are excited to present an exciting curriculum in Sleep Medicine at CHEST 2018, so stay tuned.
Aneesa M. Das, MD, FCCP
NetWork Chair
Occupational and environmental health
Post-deployment lung disease
Since the early 1990s, ongoing military deployments to Southwest Asia remain a unique challenge from a pulmonary symptomology and diagnostic perspective.
Various airborne hazards in the deployment environment include geologic dusts, burn pit smoke, vehicle emissions, and industrial air pollution. Exposures can give rise to both acute respiratory symptoms and, in some instances, chronic lung disease. Currently, data are limited on whether inhalation of airborne particulate matter by military personnel is linked to increases in pulmonary diseases (Morris MJ, et al. US Army Med Dep J. 2016:173).
Ongoing research by the Veterans Affairs continues to enroll post-deployed personnel in an Airborne Hazard and Burn Pit Registry. Past approaches in evaluation of deployed individuals ranged from common tests such as spirometry, HRCT scanning, full PFTs, bronchoprovocation challenges, and, in some instances, lung biopsies (Krefft SD, et al. Fed Pract. 2015;32[6]:32). More novel evaluations of postdeployment dyspnea include impulse oscillometry, exhaled nitric oxide, bronchoscopy, and cardiopulmonary exercise testing (Huprikar, et al. Chest. 2016;150[4]:S934A).
Members of the CHEST Occupational and Environmental Health NetWork are currently updating comprehensive approaches to evaluate military personnel with chronic respiratory symptoms from deployments. Continued emphasis, however, should be placed on diagnosing and treating common diseases such as asthma, exercise-induced bronchospasm, GERD, and upper airway disorders.
Pedro F. Lucero, MD, FCCP
Steering Committee Member
Clinical pulmonary medicine
Biologics – Birth of a new era of precision management in asthma
An estimated 10% to 20% of patients with severe uncontrolled asthma do not respond to maximal best standard treatments, leading to substantial health-care costs. A paradigm shift is now underway in our approach to the care of these patients with the emergence of novel biologics targeting the complex and interconnected inflammatory pathways in asthma that result in a diverse profile of asthma endotypes and phenotypes (Fig 1).
Current FDA-approved biologics primarily target patients with a T2 high phenotype (Table1).
Dupilumab binds to the alpha unit of the IL-4 receptor and blocks both IL-4 and IL-13. It shows potential efficacy in patients with T2 high asthma with or without eosinophilia but has not yet received FDA approval.
Multiple newer biologics are currently in development (Table 2).
Pulmonologists need to get familiar with the logistics of administration of these novel agents. The two common methods of administering biologics are (1) buy and bill – where the provider buys the drug directly from the distributor; and (2) assignment of benefits (typically administered by a Pharmacy Benefit Manager) - specific dose of the medication is shipped to the physician’s office and physician only bills for the administration. CPT and J codes are shown in Table 1.
Shyamsunder Subramanian, MD, FCCP
Steering Committee Member
Transgender women on HT have lower bone density, more fat mass than men
CHICAGO – according to findings from a recent Brazilian study.
“Lumbar spine density was lower than in reference men but similar to that of reference women,” said Tayane Muniz Fighera, MD, speaking at the annual meeting of the Endocrine Society.
Lower lumbar spine density in transgender women was associated with lower appendicular lean mass and higher total fat mass, with correlation coefficients of 0.327 and 0.334, respectively (P = .0001 for both).
Dr. Fighera and her colleagues looked at the independent contribution of age, estradiol level, appendicular lean mass, and fat mass to bone mineral density (BMD) in the transgender patients, using linear regression analysis. Total fat mass and appendicular lean mass were both independent predictors of bone mineral density (P = .001 and P = .022, respectively). For femur BMD, age, and total fat mass were predictors (P = .001 and P = .000, respectively).
The study aimed to assess bone mineral density as well as other aspects of body composition within a cohort of transgender women initiating hormone therapy in order to determine how estrogen therapy affected BMD and assess the prevalence of low bone mass among this population.
The hypothesis, said Dr. Fighera, was that hormone therapy for transgender women might decrease muscle mass and increase fat mass, “leading to less bone surface strain and smaller bone size over time,” said Dr. Fighera, of the Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil.
Previous work has shown conflicting results, she said. “While some studies report that estrogen therapy is able to increase bone mass, others have observed no difference in BMD” despite the use of hormone therapy. The studies showing an association between estrogen therapy and decreased bone mass were those that followed patients for longer periods of time – 2 years or longer, she said.
Dr. Fighera explained that in Brazil, individuals with gender dysphoria have free access to hormone therapy and gender-affirming surgery through the public health service.
A total of 142 transgender women enrolled in the study, conducted at outpatient endocrine clinics for transgender people in Porto Alegre, Brazil. The clinics’ standardized hormone therapy protocol used daily estradiol valerate 1-4 mg, daily conjugated equine estrogen 0.625-2.5 mg, or daily transdermal 17 beta estradiol 0.5-2 mg. The estrogen therapy was accompanied by either spironolactone 50-150 mg per day, or cyproterone acetate 50-100 mg per day.
For comparison, the investigators enrolled 22 men and 17 women aged 18-40 years. All participants received a dual-energy x-ray absorptiometry (DXA) scan 3 months after those in the transgender arm began hormone therapy, and a second scan at 12 months. For the first year, participants were seen for clinical evaluation and lab studies every 3 months; they were seen every 6 months thereafter.
Although ranges were wide, estradiol levels in transgender women were, on average, approximately intermediate between the female and male control values. Total testosterone for transgender women was an average 1.17 nmol/L, closer to female (0.79 nmol/L) than male (16.39 nmol/L) values.
In a subgroup of 46 participants, Dr. Fighera and her colleagues also examined change over time for transgender women who remained on hormone therapy. Though they did find that appendicular lean mass declined and total fat mass increased from baseline, these changes in body composition were not associated with significant decreases in any BMD measurement when the DXA scan was repeated at 31 months.
Participants’ mean age was 33.7 years, and the mean BMI was 25.4 kg/m2. One-third of participants had already undergone gender-affirming surgery , and most (86.6%) had some previous exposure to hormone therapy. Almost all (96%) of study participants were white.
At 18%, “the prevalence of low bone mass for age was fairly high in this sample of [transgender women] from southern Brazil,” said Dr. Fighera. She called for more work to track change over time in hormone therapy–related bone loss for transgender women. “Until then, monitoring of bone mass should be considered in this population; nonpharmacological lifestyle-related strategies for preventing bone loss may benefit transgender women” who receive long-term hormone therapy, she said.
None of the study authors had disclosures to report.
SOURCE: Fighera T et al. ENDO 2018, Abstract OR 25-5.
CHICAGO – according to findings from a recent Brazilian study.
“Lumbar spine density was lower than in reference men but similar to that of reference women,” said Tayane Muniz Fighera, MD, speaking at the annual meeting of the Endocrine Society.
Lower lumbar spine density in transgender women was associated with lower appendicular lean mass and higher total fat mass, with correlation coefficients of 0.327 and 0.334, respectively (P = .0001 for both).
Dr. Fighera and her colleagues looked at the independent contribution of age, estradiol level, appendicular lean mass, and fat mass to bone mineral density (BMD) in the transgender patients, using linear regression analysis. Total fat mass and appendicular lean mass were both independent predictors of bone mineral density (P = .001 and P = .022, respectively). For femur BMD, age, and total fat mass were predictors (P = .001 and P = .000, respectively).
The study aimed to assess bone mineral density as well as other aspects of body composition within a cohort of transgender women initiating hormone therapy in order to determine how estrogen therapy affected BMD and assess the prevalence of low bone mass among this population.
The hypothesis, said Dr. Fighera, was that hormone therapy for transgender women might decrease muscle mass and increase fat mass, “leading to less bone surface strain and smaller bone size over time,” said Dr. Fighera, of the Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil.
Previous work has shown conflicting results, she said. “While some studies report that estrogen therapy is able to increase bone mass, others have observed no difference in BMD” despite the use of hormone therapy. The studies showing an association between estrogen therapy and decreased bone mass were those that followed patients for longer periods of time – 2 years or longer, she said.
Dr. Fighera explained that in Brazil, individuals with gender dysphoria have free access to hormone therapy and gender-affirming surgery through the public health service.
A total of 142 transgender women enrolled in the study, conducted at outpatient endocrine clinics for transgender people in Porto Alegre, Brazil. The clinics’ standardized hormone therapy protocol used daily estradiol valerate 1-4 mg, daily conjugated equine estrogen 0.625-2.5 mg, or daily transdermal 17 beta estradiol 0.5-2 mg. The estrogen therapy was accompanied by either spironolactone 50-150 mg per day, or cyproterone acetate 50-100 mg per day.
For comparison, the investigators enrolled 22 men and 17 women aged 18-40 years. All participants received a dual-energy x-ray absorptiometry (DXA) scan 3 months after those in the transgender arm began hormone therapy, and a second scan at 12 months. For the first year, participants were seen for clinical evaluation and lab studies every 3 months; they were seen every 6 months thereafter.
Although ranges were wide, estradiol levels in transgender women were, on average, approximately intermediate between the female and male control values. Total testosterone for transgender women was an average 1.17 nmol/L, closer to female (0.79 nmol/L) than male (16.39 nmol/L) values.
In a subgroup of 46 participants, Dr. Fighera and her colleagues also examined change over time for transgender women who remained on hormone therapy. Though they did find that appendicular lean mass declined and total fat mass increased from baseline, these changes in body composition were not associated with significant decreases in any BMD measurement when the DXA scan was repeated at 31 months.
Participants’ mean age was 33.7 years, and the mean BMI was 25.4 kg/m2. One-third of participants had already undergone gender-affirming surgery , and most (86.6%) had some previous exposure to hormone therapy. Almost all (96%) of study participants were white.
At 18%, “the prevalence of low bone mass for age was fairly high in this sample of [transgender women] from southern Brazil,” said Dr. Fighera. She called for more work to track change over time in hormone therapy–related bone loss for transgender women. “Until then, monitoring of bone mass should be considered in this population; nonpharmacological lifestyle-related strategies for preventing bone loss may benefit transgender women” who receive long-term hormone therapy, she said.
None of the study authors had disclosures to report.
SOURCE: Fighera T et al. ENDO 2018, Abstract OR 25-5.
CHICAGO – according to findings from a recent Brazilian study.
“Lumbar spine density was lower than in reference men but similar to that of reference women,” said Tayane Muniz Fighera, MD, speaking at the annual meeting of the Endocrine Society.
Lower lumbar spine density in transgender women was associated with lower appendicular lean mass and higher total fat mass, with correlation coefficients of 0.327 and 0.334, respectively (P = .0001 for both).
Dr. Fighera and her colleagues looked at the independent contribution of age, estradiol level, appendicular lean mass, and fat mass to bone mineral density (BMD) in the transgender patients, using linear regression analysis. Total fat mass and appendicular lean mass were both independent predictors of bone mineral density (P = .001 and P = .022, respectively). For femur BMD, age, and total fat mass were predictors (P = .001 and P = .000, respectively).
The study aimed to assess bone mineral density as well as other aspects of body composition within a cohort of transgender women initiating hormone therapy in order to determine how estrogen therapy affected BMD and assess the prevalence of low bone mass among this population.
The hypothesis, said Dr. Fighera, was that hormone therapy for transgender women might decrease muscle mass and increase fat mass, “leading to less bone surface strain and smaller bone size over time,” said Dr. Fighera, of the Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil.
Previous work has shown conflicting results, she said. “While some studies report that estrogen therapy is able to increase bone mass, others have observed no difference in BMD” despite the use of hormone therapy. The studies showing an association between estrogen therapy and decreased bone mass were those that followed patients for longer periods of time – 2 years or longer, she said.
Dr. Fighera explained that in Brazil, individuals with gender dysphoria have free access to hormone therapy and gender-affirming surgery through the public health service.
A total of 142 transgender women enrolled in the study, conducted at outpatient endocrine clinics for transgender people in Porto Alegre, Brazil. The clinics’ standardized hormone therapy protocol used daily estradiol valerate 1-4 mg, daily conjugated equine estrogen 0.625-2.5 mg, or daily transdermal 17 beta estradiol 0.5-2 mg. The estrogen therapy was accompanied by either spironolactone 50-150 mg per day, or cyproterone acetate 50-100 mg per day.
For comparison, the investigators enrolled 22 men and 17 women aged 18-40 years. All participants received a dual-energy x-ray absorptiometry (DXA) scan 3 months after those in the transgender arm began hormone therapy, and a second scan at 12 months. For the first year, participants were seen for clinical evaluation and lab studies every 3 months; they were seen every 6 months thereafter.
Although ranges were wide, estradiol levels in transgender women were, on average, approximately intermediate between the female and male control values. Total testosterone for transgender women was an average 1.17 nmol/L, closer to female (0.79 nmol/L) than male (16.39 nmol/L) values.
In a subgroup of 46 participants, Dr. Fighera and her colleagues also examined change over time for transgender women who remained on hormone therapy. Though they did find that appendicular lean mass declined and total fat mass increased from baseline, these changes in body composition were not associated with significant decreases in any BMD measurement when the DXA scan was repeated at 31 months.
Participants’ mean age was 33.7 years, and the mean BMI was 25.4 kg/m2. One-third of participants had already undergone gender-affirming surgery , and most (86.6%) had some previous exposure to hormone therapy. Almost all (96%) of study participants were white.
At 18%, “the prevalence of low bone mass for age was fairly high in this sample of [transgender women] from southern Brazil,” said Dr. Fighera. She called for more work to track change over time in hormone therapy–related bone loss for transgender women. “Until then, monitoring of bone mass should be considered in this population; nonpharmacological lifestyle-related strategies for preventing bone loss may benefit transgender women” who receive long-term hormone therapy, she said.
None of the study authors had disclosures to report.
SOURCE: Fighera T et al. ENDO 2018, Abstract OR 25-5.
REPORTING FROM ENDO 2018
Key clinical point: Transgender women on hormone therapy have bone mass more similar to women than men.
Major finding: Lower lumbar spine density was associated with higher total fat mass (P = .001).
Study details: Study of 142 transgender women receiving hormone therapy, tracked over time and compared with 22 men and 17 women for reference.
Disclosures: The study was sponsored by the Brazilian government. The authors reported that they have no conflicts of interest.
Source: Fighera T et al. ENDO 2018, Abstract OR 25-5.
FDA approves marketing for retinal imaging device that uses artificial intelligence
The Food and Drug Administration has permitted the marketing of IDx-DR, a retinal imaging device that uses artificial intelligence (AI) to detect greater than a mild level of diabetic retinopathy in adult patients with diabetes. It also is the first authorized device that provides a screening tool without the need of an eye care specialist, making it ideal for health care providers who do not specialize in eye care.
“Early detection of retinopathy is an important part of managing care for the millions of people with diabetes, yet many patients with diabetes are not adequately screened for diabetic retinopathy.” About 50% of people with diabetes do not have the recommended annual retinopathy screening exam, Malvina Eydelman, MD, director of the division of ophthalmic, and ear, nose, and throat devices at the FDA’s Center for Devices and Radiological Health noted in a press release.

The software behind IDx-DR utilizes an artificial intelligence program to analyze retinal images captured by a retinal camera, the Topcon NW400. After one or more images are taken, they are uploaded to a Cloud server, on which IDx-DR software is installed, where they can be analyzed using an algorithm. In cases in which the images are of sufficient quality, the software provides the doctor with one of two results: “More than mild diabetic retinopathy detected: refer to an eye care professional” or “Negative for more than mild diabetic retinopathy; rescreen in 12 months.”
If a positive result is detected, patients should see an eye care specialist for further diagnostic evaluation and treatment as soon as possible.
The FDA reviewed data obtained from a clinical study prior to approving IDx-DR for marketing. The study looked at retinal images from 900 patients at 10 primary care sites. The aim of the study was to determine how often IDx-DR was correct in identifying mild diabetic retinopathy. The device was accurate nearly 90% of the time, correctly identifying mild diabetic retinopathy 87.4% of the time. It was also able to identify correctly patients who did not have mild diabetic retinopathy 89.5% of the time.
IDx-DR was approved via the FDA’s De Novo premarket review pathway, which offers a way to approve novel, low to moderate risk devices for which there are no similar devices previously approved. It also was granted a Breakthrough Device designation, because of its effectiveness in treating or diagnosing a irreversibly debilitating disease or condition.
Michael Abramoff, MD, PhD, and founder and president of IDx, said in an interview: “The FDA’s authorization to market IDx-DR is a historic moment that will launch a transformation in the way U.S. health care is delivered. Autonomous AI systems have massive potential to improve health care productivity, lower health care costs, and improve accessibility and quality. As the first of its kind to be authorized for commercialization, IDx-DR provides a roadmap for the safe and responsible use of AI in medicine.”
IDx-DR is intended to identify mild diabetic retinopathy and should not be used to detect rapidly progressive cases of diabetic retinopathy, particularly in pregnant women in which the disease can progress quickly. Patients with a history of laser treatment, surgery, or injections in the eye and other types of retinopathy, including radiation retinopathy, should not use IDx-DR.
For more information on other uses of AI in the treatment of diabetic disorders, click here.
The Food and Drug Administration has permitted the marketing of IDx-DR, a retinal imaging device that uses artificial intelligence (AI) to detect greater than a mild level of diabetic retinopathy in adult patients with diabetes. It also is the first authorized device that provides a screening tool without the need of an eye care specialist, making it ideal for health care providers who do not specialize in eye care.
“Early detection of retinopathy is an important part of managing care for the millions of people with diabetes, yet many patients with diabetes are not adequately screened for diabetic retinopathy.” About 50% of people with diabetes do not have the recommended annual retinopathy screening exam, Malvina Eydelman, MD, director of the division of ophthalmic, and ear, nose, and throat devices at the FDA’s Center for Devices and Radiological Health noted in a press release.
The software behind IDx-DR utilizes an artificial intelligence program to analyze retinal images captured by a retinal camera, the Topcon NW400. After one or more images are taken, they are uploaded to a Cloud server, on which IDx-DR software is installed, where they can be analyzed using an algorithm. In cases in which the images are of sufficient quality, the software provides the doctor with one of two results: “More than mild diabetic retinopathy detected: refer to an eye care professional” or “Negative for more than mild diabetic retinopathy; rescreen in 12 months.”
If a positive result is detected, patients should see an eye care specialist for further diagnostic evaluation and treatment as soon as possible.
The FDA reviewed data obtained from a clinical study prior to approving IDx-DR for marketing. The study looked at retinal images from 900 patients at 10 primary care sites. The aim of the study was to determine how often IDx-DR was correct in identifying mild diabetic retinopathy. The device was accurate nearly 90% of the time, correctly identifying mild diabetic retinopathy 87.4% of the time. It was also able to identify correctly patients who did not have mild diabetic retinopathy 89.5% of the time.
IDx-DR was approved via the FDA’s De Novo premarket review pathway, which offers a way to approve novel, low to moderate risk devices for which there are no similar devices previously approved. It also was granted a Breakthrough Device designation, because of its effectiveness in treating or diagnosing a irreversibly debilitating disease or condition.
Michael Abramoff, MD, PhD, and founder and president of IDx, said in an interview: “The FDA’s authorization to market IDx-DR is a historic moment that will launch a transformation in the way U.S. health care is delivered. Autonomous AI systems have massive potential to improve health care productivity, lower health care costs, and improve accessibility and quality. As the first of its kind to be authorized for commercialization, IDx-DR provides a roadmap for the safe and responsible use of AI in medicine.”
IDx-DR is intended to identify mild diabetic retinopathy and should not be used to detect rapidly progressive cases of diabetic retinopathy, particularly in pregnant women in which the disease can progress quickly. Patients with a history of laser treatment, surgery, or injections in the eye and other types of retinopathy, including radiation retinopathy, should not use IDx-DR.
For more information on other uses of AI in the treatment of diabetic disorders, click here.
The Food and Drug Administration has permitted the marketing of IDx-DR, a retinal imaging device that uses artificial intelligence (AI) to detect greater than a mild level of diabetic retinopathy in adult patients with diabetes. It also is the first authorized device that provides a screening tool without the need of an eye care specialist, making it ideal for health care providers who do not specialize in eye care.
“Early detection of retinopathy is an important part of managing care for the millions of people with diabetes, yet many patients with diabetes are not adequately screened for diabetic retinopathy.” About 50% of people with diabetes do not have the recommended annual retinopathy screening exam, Malvina Eydelman, MD, director of the division of ophthalmic, and ear, nose, and throat devices at the FDA’s Center for Devices and Radiological Health noted in a press release.
The software behind IDx-DR utilizes an artificial intelligence program to analyze retinal images captured by a retinal camera, the Topcon NW400. After one or more images are taken, they are uploaded to a Cloud server, on which IDx-DR software is installed, where they can be analyzed using an algorithm. In cases in which the images are of sufficient quality, the software provides the doctor with one of two results: “More than mild diabetic retinopathy detected: refer to an eye care professional” or “Negative for more than mild diabetic retinopathy; rescreen in 12 months.”
If a positive result is detected, patients should see an eye care specialist for further diagnostic evaluation and treatment as soon as possible.
The FDA reviewed data obtained from a clinical study prior to approving IDx-DR for marketing. The study looked at retinal images from 900 patients at 10 primary care sites. The aim of the study was to determine how often IDx-DR was correct in identifying mild diabetic retinopathy. The device was accurate nearly 90% of the time, correctly identifying mild diabetic retinopathy 87.4% of the time. It was also able to identify correctly patients who did not have mild diabetic retinopathy 89.5% of the time.
IDx-DR was approved via the FDA’s De Novo premarket review pathway, which offers a way to approve novel, low to moderate risk devices for which there are no similar devices previously approved. It also was granted a Breakthrough Device designation, because of its effectiveness in treating or diagnosing a irreversibly debilitating disease or condition.
Michael Abramoff, MD, PhD, and founder and president of IDx, said in an interview: “The FDA’s authorization to market IDx-DR is a historic moment that will launch a transformation in the way U.S. health care is delivered. Autonomous AI systems have massive potential to improve health care productivity, lower health care costs, and improve accessibility and quality. As the first of its kind to be authorized for commercialization, IDx-DR provides a roadmap for the safe and responsible use of AI in medicine.”
IDx-DR is intended to identify mild diabetic retinopathy and should not be used to detect rapidly progressive cases of diabetic retinopathy, particularly in pregnant women in which the disease can progress quickly. Patients with a history of laser treatment, surgery, or injections in the eye and other types of retinopathy, including radiation retinopathy, should not use IDx-DR.
For more information on other uses of AI in the treatment of diabetic disorders, click here.
Make the Diagnosis - May 2018
Generally, school-aged children are most often affected. Infections are more likely in late winter and early spring. The virus is spread via respiratory secretions, blood products, and transmission from mother to fetus. The cutaneous findings occur about 10 days after exposure to the virus. By that time, the risk of being contagious is low.

Healthy individuals have no sequelae from fifth disease and require no treatment. However, in patients with hemoglobinopathies, such as sickle cell disease, an aplastic crisis can be triggered. In patients with deficient immune systems, parvovirus B19 may cause infection and anemia, requiring hospitalization. Pregnant women exposed to parvovirus B19 are at risk for hydrops fetalis and rarely, fetal malformations or fetal demise. Other uncommon associations include hepatitis, vasculitides, and neurologic disease.

Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit a case for possible publication, send an email to [email protected]. This case and photo were submitted by Dr. Bilu Martin.
Generally, school-aged children are most often affected. Infections are more likely in late winter and early spring. The virus is spread via respiratory secretions, blood products, and transmission from mother to fetus. The cutaneous findings occur about 10 days after exposure to the virus. By that time, the risk of being contagious is low.
Healthy individuals have no sequelae from fifth disease and require no treatment. However, in patients with hemoglobinopathies, such as sickle cell disease, an aplastic crisis can be triggered. In patients with deficient immune systems, parvovirus B19 may cause infection and anemia, requiring hospitalization. Pregnant women exposed to parvovirus B19 are at risk for hydrops fetalis and rarely, fetal malformations or fetal demise. Other uncommon associations include hepatitis, vasculitides, and neurologic disease.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit a case for possible publication, send an email to [email protected]. This case and photo were submitted by Dr. Bilu Martin.
Generally, school-aged children are most often affected. Infections are more likely in late winter and early spring. The virus is spread via respiratory secretions, blood products, and transmission from mother to fetus. The cutaneous findings occur about 10 days after exposure to the virus. By that time, the risk of being contagious is low.
Healthy individuals have no sequelae from fifth disease and require no treatment. However, in patients with hemoglobinopathies, such as sickle cell disease, an aplastic crisis can be triggered. In patients with deficient immune systems, parvovirus B19 may cause infection and anemia, requiring hospitalization. Pregnant women exposed to parvovirus B19 are at risk for hydrops fetalis and rarely, fetal malformations or fetal demise. Other uncommon associations include hepatitis, vasculitides, and neurologic disease.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit a case for possible publication, send an email to [email protected]. This case and photo were submitted by Dr. Bilu Martin.
Residual single-site ovarian cancer surpasses multisite outcomes
NEW ORLEANS – When complete resection of advanced-stage, epithelial ovarian cancer is not possible, surgical resection that leaves a small volume of residual tumor at a single site produces significantly better outcomes than leaving minimal residual cancer at multiple sites, according to a review of 510 patients at two U.S. centers.

“In the past, we separated these patients based on whether they had a complete resection, R0 disease, or had 1 cm or less of residual disease” regardless of the number of sites with this small amount of residual tumor. The third category was patients with more than 1 cm of residual tumor at one or more sites, explained Dr. Manning-Geist in an interview. “What we did was break down the patients with 1 cm or less of residual tumor into those with one site or multiple sites. This is the first reported study to use number of sites” as a clinical characteristic for analysis in this context.
The message from the findings is that, while the goal of debulking surgery in patients with advanced epithelial ovarian cancer is complete tumor resection, if that can’t be achieved, the next goal is to leave residual tumor at just a single site, she concluded. A question that remains is whether primary debulking surgery is preferable to neoadjuvant treatment followed by interval debulking surgery. In the results Dr. Manning-Geist presented, patients who underwent primary debulking had better outcomes than those with neoadjuvant therapy followed by interval debulking, but these two subgroups also had different clinical characteristics.
The study used data from 510 patients with stage IIIC or IV epithelial ovarian cancer treated at either Brigham and Women’s or Massachusetts General Hospital during 2010-2015. The study cohort included 240 patients who underwent primary debulking surgery and 270 who first received neoadjuvant chemotherapy and then underwent interval debulking surgery. The patients who received neoadjuvant therapy were, on average, older (65 years vs. 63 years), had a higher prevalence of stage IV disease (44% vs. 16%), and had a higher prevalence of tumors with serous histology (93% vs. 77%), compared with patients who underwent primary debulking.
Complete tumor resections occurred in 39% of the primary debulking patients and in 64% of those who received neoadjuvant therapy; residual disease of 1 cm or less at one site occurred in 17% and 13%, respectively; minimal residual disease at multiple sites remained in 28% and 17% respectively; and the remaining patients had residual disease of more than 1 cm in at least one site, 16% and 6% respectively.
For this analysis, Dr. Manning-Geist and her associates considered residual disease at any of seven possible sites: diaphragm, upper abdomen, bowel mesentary, bowel serosa, abdominal peritoneum, pelvis, and nodal. Even if multiple individual metastases remained within one of these sites after surgery, it was categorized as a single site of residual disease.
Among patients who underwent primary debulking surgery, progression-free survival persisted for a median of 23 months among patients with full resection, 19 months in patients with a single site with minimal residual disease, 13 months among those with multiple sites of residual disease, and 10 months in patients with more than 1 cm of residual tumor. Median overall survival in these four subgroups was not yet reached, 64 months, 50 months, and 49 months, respectively.
Among patients who received neoadjuvant chemotherapy and then underwent interval debulking surgery, median durations of progression-free survival were 14 months, 12 months, 10 months, and 6 months, respectively. Median overall survival rates were 58 months, 37 months, 26 months, and 33 months, respectively. Within each of these four analyses, the differences in both survival and progression-free survival across the four subgroups was statistically significant, with a P less than .001 for each analysis.
In multivariate analyses, among patients who underwent primary debulking surgery, the significant linkages with worsening progression-free and overall survival were age, cancer stage, and amount and site number of residual disease. Among patients who received neoadjuvant chemotherapy followed by interval debulking residual disease diameter and site number of residual tumor was the only significant determinant for both progression-free and overall survival, Dr. Manning-Geist reported.
Dr. Manning-Geist had no disclosures.
SOURCE: Manning-Geist B et al. SGO 2018, Abstract 43.
NEW ORLEANS – When complete resection of advanced-stage, epithelial ovarian cancer is not possible, surgical resection that leaves a small volume of residual tumor at a single site produces significantly better outcomes than leaving minimal residual cancer at multiple sites, according to a review of 510 patients at two U.S. centers.
“In the past, we separated these patients based on whether they had a complete resection, R0 disease, or had 1 cm or less of residual disease” regardless of the number of sites with this small amount of residual tumor. The third category was patients with more than 1 cm of residual tumor at one or more sites, explained Dr. Manning-Geist in an interview. “What we did was break down the patients with 1 cm or less of residual tumor into those with one site or multiple sites. This is the first reported study to use number of sites” as a clinical characteristic for analysis in this context.
The message from the findings is that, while the goal of debulking surgery in patients with advanced epithelial ovarian cancer is complete tumor resection, if that can’t be achieved, the next goal is to leave residual tumor at just a single site, she concluded. A question that remains is whether primary debulking surgery is preferable to neoadjuvant treatment followed by interval debulking surgery. In the results Dr. Manning-Geist presented, patients who underwent primary debulking had better outcomes than those with neoadjuvant therapy followed by interval debulking, but these two subgroups also had different clinical characteristics.
The study used data from 510 patients with stage IIIC or IV epithelial ovarian cancer treated at either Brigham and Women’s or Massachusetts General Hospital during 2010-2015. The study cohort included 240 patients who underwent primary debulking surgery and 270 who first received neoadjuvant chemotherapy and then underwent interval debulking surgery. The patients who received neoadjuvant therapy were, on average, older (65 years vs. 63 years), had a higher prevalence of stage IV disease (44% vs. 16%), and had a higher prevalence of tumors with serous histology (93% vs. 77%), compared with patients who underwent primary debulking.
Complete tumor resections occurred in 39% of the primary debulking patients and in 64% of those who received neoadjuvant therapy; residual disease of 1 cm or less at one site occurred in 17% and 13%, respectively; minimal residual disease at multiple sites remained in 28% and 17% respectively; and the remaining patients had residual disease of more than 1 cm in at least one site, 16% and 6% respectively.
For this analysis, Dr. Manning-Geist and her associates considered residual disease at any of seven possible sites: diaphragm, upper abdomen, bowel mesentary, bowel serosa, abdominal peritoneum, pelvis, and nodal. Even if multiple individual metastases remained within one of these sites after surgery, it was categorized as a single site of residual disease.
Among patients who underwent primary debulking surgery, progression-free survival persisted for a median of 23 months among patients with full resection, 19 months in patients with a single site with minimal residual disease, 13 months among those with multiple sites of residual disease, and 10 months in patients with more than 1 cm of residual tumor. Median overall survival in these four subgroups was not yet reached, 64 months, 50 months, and 49 months, respectively.
Among patients who received neoadjuvant chemotherapy and then underwent interval debulking surgery, median durations of progression-free survival were 14 months, 12 months, 10 months, and 6 months, respectively. Median overall survival rates were 58 months, 37 months, 26 months, and 33 months, respectively. Within each of these four analyses, the differences in both survival and progression-free survival across the four subgroups was statistically significant, with a P less than .001 for each analysis.
In multivariate analyses, among patients who underwent primary debulking surgery, the significant linkages with worsening progression-free and overall survival were age, cancer stage, and amount and site number of residual disease. Among patients who received neoadjuvant chemotherapy followed by interval debulking residual disease diameter and site number of residual tumor was the only significant determinant for both progression-free and overall survival, Dr. Manning-Geist reported.
Dr. Manning-Geist had no disclosures.
SOURCE: Manning-Geist B et al. SGO 2018, Abstract 43.
NEW ORLEANS – When complete resection of advanced-stage, epithelial ovarian cancer is not possible, surgical resection that leaves a small volume of residual tumor at a single site produces significantly better outcomes than leaving minimal residual cancer at multiple sites, according to a review of 510 patients at two U.S. centers.
“In the past, we separated these patients based on whether they had a complete resection, R0 disease, or had 1 cm or less of residual disease” regardless of the number of sites with this small amount of residual tumor. The third category was patients with more than 1 cm of residual tumor at one or more sites, explained Dr. Manning-Geist in an interview. “What we did was break down the patients with 1 cm or less of residual tumor into those with one site or multiple sites. This is the first reported study to use number of sites” as a clinical characteristic for analysis in this context.
The message from the findings is that, while the goal of debulking surgery in patients with advanced epithelial ovarian cancer is complete tumor resection, if that can’t be achieved, the next goal is to leave residual tumor at just a single site, she concluded. A question that remains is whether primary debulking surgery is preferable to neoadjuvant treatment followed by interval debulking surgery. In the results Dr. Manning-Geist presented, patients who underwent primary debulking had better outcomes than those with neoadjuvant therapy followed by interval debulking, but these two subgroups also had different clinical characteristics.
The study used data from 510 patients with stage IIIC or IV epithelial ovarian cancer treated at either Brigham and Women’s or Massachusetts General Hospital during 2010-2015. The study cohort included 240 patients who underwent primary debulking surgery and 270 who first received neoadjuvant chemotherapy and then underwent interval debulking surgery. The patients who received neoadjuvant therapy were, on average, older (65 years vs. 63 years), had a higher prevalence of stage IV disease (44% vs. 16%), and had a higher prevalence of tumors with serous histology (93% vs. 77%), compared with patients who underwent primary debulking.
Complete tumor resections occurred in 39% of the primary debulking patients and in 64% of those who received neoadjuvant therapy; residual disease of 1 cm or less at one site occurred in 17% and 13%, respectively; minimal residual disease at multiple sites remained in 28% and 17% respectively; and the remaining patients had residual disease of more than 1 cm in at least one site, 16% and 6% respectively.
For this analysis, Dr. Manning-Geist and her associates considered residual disease at any of seven possible sites: diaphragm, upper abdomen, bowel mesentary, bowel serosa, abdominal peritoneum, pelvis, and nodal. Even if multiple individual metastases remained within one of these sites after surgery, it was categorized as a single site of residual disease.
Among patients who underwent primary debulking surgery, progression-free survival persisted for a median of 23 months among patients with full resection, 19 months in patients with a single site with minimal residual disease, 13 months among those with multiple sites of residual disease, and 10 months in patients with more than 1 cm of residual tumor. Median overall survival in these four subgroups was not yet reached, 64 months, 50 months, and 49 months, respectively.
Among patients who received neoadjuvant chemotherapy and then underwent interval debulking surgery, median durations of progression-free survival were 14 months, 12 months, 10 months, and 6 months, respectively. Median overall survival rates were 58 months, 37 months, 26 months, and 33 months, respectively. Within each of these four analyses, the differences in both survival and progression-free survival across the four subgroups was statistically significant, with a P less than .001 for each analysis.
In multivariate analyses, among patients who underwent primary debulking surgery, the significant linkages with worsening progression-free and overall survival were age, cancer stage, and amount and site number of residual disease. Among patients who received neoadjuvant chemotherapy followed by interval debulking residual disease diameter and site number of residual tumor was the only significant determinant for both progression-free and overall survival, Dr. Manning-Geist reported.
Dr. Manning-Geist had no disclosures.
SOURCE: Manning-Geist B et al. SGO 2018, Abstract 43.
REPORTING FROM SGO 2018
Key clinical point:
Major finding: Median overall survival after primary debulking was 64 months with single-site residual disease and 50 months with multisite disease.
Study details: Retrospective review of 510 patients from two U.S. centers.
Disclosures: Dr. Manning-Geist had no disclosures.
Source: Manning-Geist BL et al. SGO 2018, Abstract 43.