User login
A call for innovation: Dr. Robert Wachter to discuss evolution of HM at closing plenary
As has become tradition, Robert Wachter, MD, MHM, of the University of California, San Francisco, will close the conference today and will focus on the broader changes that must happen as the role of the hospitalist continues to evolve.
“I am going to talk about the changes in the world of hospital care and the importance of the field to innovate,” Dr. Wachter said. “To me, there are gravitational forces in the health care world that are making … patients who are in hospitals sicker than they were before. More and more patients are going to be cared for in outpatient settings and at home. We are going start to ... see things like sensors and telemedicine to enable more care outside of the hospital.”

Dr. Wachter said hospital medicine must evolve and mature to continue to prove that hospitalists are indispensable staff members within the hospital.
“That was why the field became the fastest-growing profession in medical history. We can’t sit on our laurels. We have to continue to innovate,” he said. “Even as the system changes around us, I am confident that we will innovate. My talk will be a pep talk and will include reflections on how the world of health care is changing and what those changes will mean to hospitalists.”
Dr. Wachter noted that the trend of steering patients who are less sick to the outpatient setting, as well as other economic factors, would change the nature of hospitalist practice.
“It will be more acuity, more intensity, more complex relationships with your own hospital and often with partner hospitals,” he said. “More of the work will be digitally enabled than it would have been 5 or 10 years ago.”
Integration of data and technology innovation will be a key to better serving this sicker population, Dr. Wachter predicted. We need “to take much fuller advantage than we have so far of the fact that we are all dealing with digital records, and the decision support, the data analytics, the artificial intelligence that we get from our computer systems is pretty puny,” he said. “That is partly why physicians don’t love their computers so much. They spend huge amounts of time entering data into computers and don’t get much useful information out of it.”
Dr. Wachter also warned that too much data could have negative effects on the delivery of care.
“One of the challenges we face is continuing to stay alert, not turn our brains off, and become increasingly dependent on the computer to give us information,” he said. “How do we avoid the challenges we’ve already seen from things like alert and alarm fatigue as the computer becomes more robust as an information source? There is always the risk our computers are going to overwhelm us with too much information, and we are going to fall asleep at the switch. Or when the computer says something that really is not right for a patient, we will not be thinking clearly enough to catch it.”
Despite the looming challenges and industry consolidations that are expected, Dr. Wachter doesn’t believe there will be any shortage of demand for hospitalists.
“I think, in most circumstances, [hospitalists are a protected] profession given the complexity, the high variations, and the dependence that it still has on seeing the patient, talking to the patient, and having discussions with multiple consultants,” he said. “It’s a pretty hard thing to replace with technology. Overall, the job situation is pretty bright.”
As has become tradition, Robert Wachter, MD, MHM, of the University of California, San Francisco, will close the conference today and will focus on the broader changes that must happen as the role of the hospitalist continues to evolve.
“I am going to talk about the changes in the world of hospital care and the importance of the field to innovate,” Dr. Wachter said. “To me, there are gravitational forces in the health care world that are making … patients who are in hospitals sicker than they were before. More and more patients are going to be cared for in outpatient settings and at home. We are going start to ... see things like sensors and telemedicine to enable more care outside of the hospital.”
Dr. Wachter said hospital medicine must evolve and mature to continue to prove that hospitalists are indispensable staff members within the hospital.
“That was why the field became the fastest-growing profession in medical history. We can’t sit on our laurels. We have to continue to innovate,” he said. “Even as the system changes around us, I am confident that we will innovate. My talk will be a pep talk and will include reflections on how the world of health care is changing and what those changes will mean to hospitalists.”
Dr. Wachter noted that the trend of steering patients who are less sick to the outpatient setting, as well as other economic factors, would change the nature of hospitalist practice.
“It will be more acuity, more intensity, more complex relationships with your own hospital and often with partner hospitals,” he said. “More of the work will be digitally enabled than it would have been 5 or 10 years ago.”
Integration of data and technology innovation will be a key to better serving this sicker population, Dr. Wachter predicted. We need “to take much fuller advantage than we have so far of the fact that we are all dealing with digital records, and the decision support, the data analytics, the artificial intelligence that we get from our computer systems is pretty puny,” he said. “That is partly why physicians don’t love their computers so much. They spend huge amounts of time entering data into computers and don’t get much useful information out of it.”
Dr. Wachter also warned that too much data could have negative effects on the delivery of care.
“One of the challenges we face is continuing to stay alert, not turn our brains off, and become increasingly dependent on the computer to give us information,” he said. “How do we avoid the challenges we’ve already seen from things like alert and alarm fatigue as the computer becomes more robust as an information source? There is always the risk our computers are going to overwhelm us with too much information, and we are going to fall asleep at the switch. Or when the computer says something that really is not right for a patient, we will not be thinking clearly enough to catch it.”
Despite the looming challenges and industry consolidations that are expected, Dr. Wachter doesn’t believe there will be any shortage of demand for hospitalists.
“I think, in most circumstances, [hospitalists are a protected] profession given the complexity, the high variations, and the dependence that it still has on seeing the patient, talking to the patient, and having discussions with multiple consultants,” he said. “It’s a pretty hard thing to replace with technology. Overall, the job situation is pretty bright.”
As has become tradition, Robert Wachter, MD, MHM, of the University of California, San Francisco, will close the conference today and will focus on the broader changes that must happen as the role of the hospitalist continues to evolve.
“I am going to talk about the changes in the world of hospital care and the importance of the field to innovate,” Dr. Wachter said. “To me, there are gravitational forces in the health care world that are making … patients who are in hospitals sicker than they were before. More and more patients are going to be cared for in outpatient settings and at home. We are going start to ... see things like sensors and telemedicine to enable more care outside of the hospital.”
Dr. Wachter said hospital medicine must evolve and mature to continue to prove that hospitalists are indispensable staff members within the hospital.
“That was why the field became the fastest-growing profession in medical history. We can’t sit on our laurels. We have to continue to innovate,” he said. “Even as the system changes around us, I am confident that we will innovate. My talk will be a pep talk and will include reflections on how the world of health care is changing and what those changes will mean to hospitalists.”
Dr. Wachter noted that the trend of steering patients who are less sick to the outpatient setting, as well as other economic factors, would change the nature of hospitalist practice.
“It will be more acuity, more intensity, more complex relationships with your own hospital and often with partner hospitals,” he said. “More of the work will be digitally enabled than it would have been 5 or 10 years ago.”
Integration of data and technology innovation will be a key to better serving this sicker population, Dr. Wachter predicted. We need “to take much fuller advantage than we have so far of the fact that we are all dealing with digital records, and the decision support, the data analytics, the artificial intelligence that we get from our computer systems is pretty puny,” he said. “That is partly why physicians don’t love their computers so much. They spend huge amounts of time entering data into computers and don’t get much useful information out of it.”
Dr. Wachter also warned that too much data could have negative effects on the delivery of care.
“One of the challenges we face is continuing to stay alert, not turn our brains off, and become increasingly dependent on the computer to give us information,” he said. “How do we avoid the challenges we’ve already seen from things like alert and alarm fatigue as the computer becomes more robust as an information source? There is always the risk our computers are going to overwhelm us with too much information, and we are going to fall asleep at the switch. Or when the computer says something that really is not right for a patient, we will not be thinking clearly enough to catch it.”
Despite the looming challenges and industry consolidations that are expected, Dr. Wachter doesn’t believe there will be any shortage of demand for hospitalists.
“I think, in most circumstances, [hospitalists are a protected] profession given the complexity, the high variations, and the dependence that it still has on seeing the patient, talking to the patient, and having discussions with multiple consultants,” he said. “It’s a pretty hard thing to replace with technology. Overall, the job situation is pretty bright.”
Learn to employ cultural humility
Many health care providers are guilty of having implicit or unconscious biases against patients, which can negatively affect the care they give. “Once providers come to this realization, they can make a conscious effort to neutralize these biases from manifesting throughout a practice,” said Aziz Ansari, DO, SFHM, associate chief medical officer, Clinical Optimization and Revenue Integrity, and associate professor of medicine, Loyola University Medical Center, Maywood, Ill., who will present today’s session “Winning Hearts and Minds at the Bedside: Battling Unconscious Bias Through Cultural Humility.”

By practicing cultural humility, hospitalists can gain trust from patients and their families, whom they do not know in their everyday practice. This encourages providers to be humble, ascertain what is important to the patient, and learn from every patient encounter.
The session will begin with a case study involving bias, followed by a self-reflection exercise. To determine whether you may be biased against some patient groups, Dr. Ansari recommends taking the online implicit association test at Implicit.harvard.edu.
As a palliative care specialist, Dr. Ansari has repeatedly faced situations in which a lack of cultural humility caused patients or their family member to foster mistrust toward a provider. Consequently, patients and family members may choose aggressive measures that providers might consider futile.
Dr. Ansari also will define what implicit or unconscious biases entail in greater detail. The discussion will then circle back to the original case and reveal how providers can improve their mindset when facing difficult situations by employing a tool called “The 5 Rs of Cultural Humility,” which include reflection, respect, regard, relevance, and resiliency.
Dr. Ansari spearheaded the development of the 5 Rs tool when he chaired the Cultural Humility Workgroup of SHM’s Practice Management Committee. “The goal is to use the tool to attain cultural humility and transform a potentially negative encounter into a gratifying one,” he said.
At a minimum, attendees should take time during the session to reflect on their own thoughts and biases. “This introspection can bring to light practices that providers may have been unaware of and, ultimately, can change their behaviors so every patient and their family feels that they are being seen and heard,” Dr. Ansari said. “In today’s current climate it is more important than ever for providers to self-reflect on their attitudes and perceptions because an increasing number of groups in our diverse society are feeling more marginalized.”
Winning Hearts and Minds at the Bedside: Battling Unconscious Bias Through Cultural Humility
Wednesday, 9:10-9:50 a.m.
Crystal Ballroom G2/C-F
Many health care providers are guilty of having implicit or unconscious biases against patients, which can negatively affect the care they give. “Once providers come to this realization, they can make a conscious effort to neutralize these biases from manifesting throughout a practice,” said Aziz Ansari, DO, SFHM, associate chief medical officer, Clinical Optimization and Revenue Integrity, and associate professor of medicine, Loyola University Medical Center, Maywood, Ill., who will present today’s session “Winning Hearts and Minds at the Bedside: Battling Unconscious Bias Through Cultural Humility.”
By practicing cultural humility, hospitalists can gain trust from patients and their families, whom they do not know in their everyday practice. This encourages providers to be humble, ascertain what is important to the patient, and learn from every patient encounter.
The session will begin with a case study involving bias, followed by a self-reflection exercise. To determine whether you may be biased against some patient groups, Dr. Ansari recommends taking the online implicit association test at Implicit.harvard.edu.
As a palliative care specialist, Dr. Ansari has repeatedly faced situations in which a lack of cultural humility caused patients or their family member to foster mistrust toward a provider. Consequently, patients and family members may choose aggressive measures that providers might consider futile.
Dr. Ansari also will define what implicit or unconscious biases entail in greater detail. The discussion will then circle back to the original case and reveal how providers can improve their mindset when facing difficult situations by employing a tool called “The 5 Rs of Cultural Humility,” which include reflection, respect, regard, relevance, and resiliency.
Dr. Ansari spearheaded the development of the 5 Rs tool when he chaired the Cultural Humility Workgroup of SHM’s Practice Management Committee. “The goal is to use the tool to attain cultural humility and transform a potentially negative encounter into a gratifying one,” he said.
At a minimum, attendees should take time during the session to reflect on their own thoughts and biases. “This introspection can bring to light practices that providers may have been unaware of and, ultimately, can change their behaviors so every patient and their family feels that they are being seen and heard,” Dr. Ansari said. “In today’s current climate it is more important than ever for providers to self-reflect on their attitudes and perceptions because an increasing number of groups in our diverse society are feeling more marginalized.”
Winning Hearts and Minds at the Bedside: Battling Unconscious Bias Through Cultural Humility
Wednesday, 9:10-9:50 a.m.
Crystal Ballroom G2/C-F
Many health care providers are guilty of having implicit or unconscious biases against patients, which can negatively affect the care they give. “Once providers come to this realization, they can make a conscious effort to neutralize these biases from manifesting throughout a practice,” said Aziz Ansari, DO, SFHM, associate chief medical officer, Clinical Optimization and Revenue Integrity, and associate professor of medicine, Loyola University Medical Center, Maywood, Ill., who will present today’s session “Winning Hearts and Minds at the Bedside: Battling Unconscious Bias Through Cultural Humility.”
By practicing cultural humility, hospitalists can gain trust from patients and their families, whom they do not know in their everyday practice. This encourages providers to be humble, ascertain what is important to the patient, and learn from every patient encounter.
The session will begin with a case study involving bias, followed by a self-reflection exercise. To determine whether you may be biased against some patient groups, Dr. Ansari recommends taking the online implicit association test at Implicit.harvard.edu.
As a palliative care specialist, Dr. Ansari has repeatedly faced situations in which a lack of cultural humility caused patients or their family member to foster mistrust toward a provider. Consequently, patients and family members may choose aggressive measures that providers might consider futile.
Dr. Ansari also will define what implicit or unconscious biases entail in greater detail. The discussion will then circle back to the original case and reveal how providers can improve their mindset when facing difficult situations by employing a tool called “The 5 Rs of Cultural Humility,” which include reflection, respect, regard, relevance, and resiliency.
Dr. Ansari spearheaded the development of the 5 Rs tool when he chaired the Cultural Humility Workgroup of SHM’s Practice Management Committee. “The goal is to use the tool to attain cultural humility and transform a potentially negative encounter into a gratifying one,” he said.
At a minimum, attendees should take time during the session to reflect on their own thoughts and biases. “This introspection can bring to light practices that providers may have been unaware of and, ultimately, can change their behaviors so every patient and their family feels that they are being seen and heard,” Dr. Ansari said. “In today’s current climate it is more important than ever for providers to self-reflect on their attitudes and perceptions because an increasing number of groups in our diverse society are feeling more marginalized.”
Winning Hearts and Minds at the Bedside: Battling Unconscious Bias Through Cultural Humility
Wednesday, 9:10-9:50 a.m.
Crystal Ballroom G2/C-F
Session to cover expanding HM scope of practice to pre- and posthospitalization care
As the field of hospital medicine continues to grow, it is experiencing more requests for assistance with pre- and posthospital care. These increasing demands will be the focus of today’s session “Addressing the Expanding Scope of Practice in Hospital Medicine.”
“As hospital medicine continues to advance, we are being asked to help hospitals and health care systems with challenges that extend beyond the hospital,” presenter Nick Fitterman, MD, SFHM, vice chair of hospital medicine of Northwell Health in Long Island, N.Y., explained in an interview. “Sometimes, this is a natural extension of hospital medicine; other times, it may reflect gaps in primary care or the health care system in general. Hospital medicine can be supportive, but our course must be deliberate and not extend beyond our scope of practice.

“The health care system is facing a variety of challenges, which, in turn, make an impact on hospital medicine,” stated Dr. Fitterman. “Factors that result in increased demands on the field include lack of access to posthospitalization care, high-acuity patients in subacute rehabilitation, rising health care costs, and value-based payments that include ‘bundles’ of care stretching beyond hospitalization. Finally, the nation has a population that’s aging,” he continued, “thanks to the ‘silver tsunami’ of baby boomers.”
The session will include presentations by leaders in the fields of post-acute clinics and hospitals at home. Lauren Doctoroff, MD, FHM, of Beth Israel Deaconess Medical Center in Boston will discuss post-acute care clinics; David Levine, MD, of Brigham and Women’s Hospital and Harvard Medical School, both in Boston, will cover some hospital-at-home developments; and Efren Manjarrez, MD, SFHM, of the University of Miami Health System will speak about preoperative care. Dr. Fitterman will provide examples of the expanded scope of practice issues that can arise in a large health care system.
“There are a finite number of beds in any given hospital and extending our reach into pre- or posthospitalization care is an avenue to expand our book of business, cultivate new skills, and engage patients and colleagues in new settings,” Dr. Fitterman explained. “Done with a clear vision and plan and within our scope of practice, this can be quite rewarding. Executed only to meet a demand but without proper resources, this can pose a new challenge and become frustrating.”
“HM18 participants who attend the session will receive some insights into what works and what doesn’t work regarding extrahospital care for hospital medicine,” continued Dr. Fitterman. “And we hope it will help hospital medicine practitioners and groups as they determine where to focus their efforts.”
When asked about an overall take-home message for the session, Dr. Fitterman stated, “We hospital medicine professionals must be wary of accepting every challenge posed to us to solve. This session should provide those in attendance with tools that will assist in their decision making.”
Addressing the Expanding Scope of Practice in Hospital Medicine
Wednesday, 7:30-8:30 a.m.
Grand Ballroom 7B
As the field of hospital medicine continues to grow, it is experiencing more requests for assistance with pre- and posthospital care. These increasing demands will be the focus of today’s session “Addressing the Expanding Scope of Practice in Hospital Medicine.”
“As hospital medicine continues to advance, we are being asked to help hospitals and health care systems with challenges that extend beyond the hospital,” presenter Nick Fitterman, MD, SFHM, vice chair of hospital medicine of Northwell Health in Long Island, N.Y., explained in an interview. “Sometimes, this is a natural extension of hospital medicine; other times, it may reflect gaps in primary care or the health care system in general. Hospital medicine can be supportive, but our course must be deliberate and not extend beyond our scope of practice.
“The health care system is facing a variety of challenges, which, in turn, make an impact on hospital medicine,” stated Dr. Fitterman. “Factors that result in increased demands on the field include lack of access to posthospitalization care, high-acuity patients in subacute rehabilitation, rising health care costs, and value-based payments that include ‘bundles’ of care stretching beyond hospitalization. Finally, the nation has a population that’s aging,” he continued, “thanks to the ‘silver tsunami’ of baby boomers.”
The session will include presentations by leaders in the fields of post-acute clinics and hospitals at home. Lauren Doctoroff, MD, FHM, of Beth Israel Deaconess Medical Center in Boston will discuss post-acute care clinics; David Levine, MD, of Brigham and Women’s Hospital and Harvard Medical School, both in Boston, will cover some hospital-at-home developments; and Efren Manjarrez, MD, SFHM, of the University of Miami Health System will speak about preoperative care. Dr. Fitterman will provide examples of the expanded scope of practice issues that can arise in a large health care system.
“There are a finite number of beds in any given hospital and extending our reach into pre- or posthospitalization care is an avenue to expand our book of business, cultivate new skills, and engage patients and colleagues in new settings,” Dr. Fitterman explained. “Done with a clear vision and plan and within our scope of practice, this can be quite rewarding. Executed only to meet a demand but without proper resources, this can pose a new challenge and become frustrating.”
“HM18 participants who attend the session will receive some insights into what works and what doesn’t work regarding extrahospital care for hospital medicine,” continued Dr. Fitterman. “And we hope it will help hospital medicine practitioners and groups as they determine where to focus their efforts.”
When asked about an overall take-home message for the session, Dr. Fitterman stated, “We hospital medicine professionals must be wary of accepting every challenge posed to us to solve. This session should provide those in attendance with tools that will assist in their decision making.”
Addressing the Expanding Scope of Practice in Hospital Medicine
Wednesday, 7:30-8:30 a.m.
Grand Ballroom 7B
As the field of hospital medicine continues to grow, it is experiencing more requests for assistance with pre- and posthospital care. These increasing demands will be the focus of today’s session “Addressing the Expanding Scope of Practice in Hospital Medicine.”
“As hospital medicine continues to advance, we are being asked to help hospitals and health care systems with challenges that extend beyond the hospital,” presenter Nick Fitterman, MD, SFHM, vice chair of hospital medicine of Northwell Health in Long Island, N.Y., explained in an interview. “Sometimes, this is a natural extension of hospital medicine; other times, it may reflect gaps in primary care or the health care system in general. Hospital medicine can be supportive, but our course must be deliberate and not extend beyond our scope of practice.
“The health care system is facing a variety of challenges, which, in turn, make an impact on hospital medicine,” stated Dr. Fitterman. “Factors that result in increased demands on the field include lack of access to posthospitalization care, high-acuity patients in subacute rehabilitation, rising health care costs, and value-based payments that include ‘bundles’ of care stretching beyond hospitalization. Finally, the nation has a population that’s aging,” he continued, “thanks to the ‘silver tsunami’ of baby boomers.”
The session will include presentations by leaders in the fields of post-acute clinics and hospitals at home. Lauren Doctoroff, MD, FHM, of Beth Israel Deaconess Medical Center in Boston will discuss post-acute care clinics; David Levine, MD, of Brigham and Women’s Hospital and Harvard Medical School, both in Boston, will cover some hospital-at-home developments; and Efren Manjarrez, MD, SFHM, of the University of Miami Health System will speak about preoperative care. Dr. Fitterman will provide examples of the expanded scope of practice issues that can arise in a large health care system.
“There are a finite number of beds in any given hospital and extending our reach into pre- or posthospitalization care is an avenue to expand our book of business, cultivate new skills, and engage patients and colleagues in new settings,” Dr. Fitterman explained. “Done with a clear vision and plan and within our scope of practice, this can be quite rewarding. Executed only to meet a demand but without proper resources, this can pose a new challenge and become frustrating.”
“HM18 participants who attend the session will receive some insights into what works and what doesn’t work regarding extrahospital care for hospital medicine,” continued Dr. Fitterman. “And we hope it will help hospital medicine practitioners and groups as they determine where to focus their efforts.”
When asked about an overall take-home message for the session, Dr. Fitterman stated, “We hospital medicine professionals must be wary of accepting every challenge posed to us to solve. This session should provide those in attendance with tools that will assist in their decision making.”
Addressing the Expanding Scope of Practice in Hospital Medicine
Wednesday, 7:30-8:30 a.m.
Grand Ballroom 7B
Welcome to Day 3 at HM18
What an amazing 3 days! As we spoke on the first day, delivering higher value of care has been a highlight of this annual conference. With thought-provoking sessions from Kate Goodrich, MD, MHS, on payment reform; Eric Howell, MD, on “Value is NOT a 4-Letter Word”; and Lenny Feldman, MD, SFHM, on “Things We Do for No Reason,” hospital medicine’s focus on value is clear. I hope you also had the chance to attend the sessions on clinical topics of medicine, education, and practice management.

The final day of the conference is no exception when it comes to topics with impact. Starting off at 7:30 a.m., there is a diverse group of sessions on clinical medicine for adults and pediatrics, including “Peter Pan Grows Up: How to Care for Your Patients with Chronic Pediatric Conditions,” topics in health policy, how to advance in academic medicine with a focus on writing a winning abstract, and applying what you have learned at HM18 back home.
This day also offers sessions on advancement with topics for mid-career hospitalists and those aspiring to leadership roles. Promotion in academic medicine also will be addressed.
You can further strengthen your presentation skills in sessions that will teach you how to create valuable teaching points on the fly and deliver memorable lectures and talks. Other sessions will enhance your skills in emotional intelligence.
As always, we are extremely fortunate to wrap up the day with Bob Wachter, MD, MHM, who is sure to deliver a thought-provoking and entertaining presentation entitled “Hospitalists as Drivers of Innovation and System Change: Are We Doing Enough?”
As you wrap up your final day, I wish you a safe journey back home. Please continue your engagement with the Society through chapter meetings in your area, signing up for committees and interest groups, and dropping us a line – we look forward to continuing to work for you in the coming year.
Dr. Afsar is the incoming president of the Society of Hospital Medicine and the chief ambulatory officer & CMO for ACOs at UC Irvine Health in Orange, Calif.
What an amazing 3 days! As we spoke on the first day, delivering higher value of care has been a highlight of this annual conference. With thought-provoking sessions from Kate Goodrich, MD, MHS, on payment reform; Eric Howell, MD, on “Value is NOT a 4-Letter Word”; and Lenny Feldman, MD, SFHM, on “Things We Do for No Reason,” hospital medicine’s focus on value is clear. I hope you also had the chance to attend the sessions on clinical topics of medicine, education, and practice management.
The final day of the conference is no exception when it comes to topics with impact. Starting off at 7:30 a.m., there is a diverse group of sessions on clinical medicine for adults and pediatrics, including “Peter Pan Grows Up: How to Care for Your Patients with Chronic Pediatric Conditions,” topics in health policy, how to advance in academic medicine with a focus on writing a winning abstract, and applying what you have learned at HM18 back home.
This day also offers sessions on advancement with topics for mid-career hospitalists and those aspiring to leadership roles. Promotion in academic medicine also will be addressed.
You can further strengthen your presentation skills in sessions that will teach you how to create valuable teaching points on the fly and deliver memorable lectures and talks. Other sessions will enhance your skills in emotional intelligence.
As always, we are extremely fortunate to wrap up the day with Bob Wachter, MD, MHM, who is sure to deliver a thought-provoking and entertaining presentation entitled “Hospitalists as Drivers of Innovation and System Change: Are We Doing Enough?”
As you wrap up your final day, I wish you a safe journey back home. Please continue your engagement with the Society through chapter meetings in your area, signing up for committees and interest groups, and dropping us a line – we look forward to continuing to work for you in the coming year.
Dr. Afsar is the incoming president of the Society of Hospital Medicine and the chief ambulatory officer & CMO for ACOs at UC Irvine Health in Orange, Calif.
What an amazing 3 days! As we spoke on the first day, delivering higher value of care has been a highlight of this annual conference. With thought-provoking sessions from Kate Goodrich, MD, MHS, on payment reform; Eric Howell, MD, on “Value is NOT a 4-Letter Word”; and Lenny Feldman, MD, SFHM, on “Things We Do for No Reason,” hospital medicine’s focus on value is clear. I hope you also had the chance to attend the sessions on clinical topics of medicine, education, and practice management.
The final day of the conference is no exception when it comes to topics with impact. Starting off at 7:30 a.m., there is a diverse group of sessions on clinical medicine for adults and pediatrics, including “Peter Pan Grows Up: How to Care for Your Patients with Chronic Pediatric Conditions,” topics in health policy, how to advance in academic medicine with a focus on writing a winning abstract, and applying what you have learned at HM18 back home.
This day also offers sessions on advancement with topics for mid-career hospitalists and those aspiring to leadership roles. Promotion in academic medicine also will be addressed.
You can further strengthen your presentation skills in sessions that will teach you how to create valuable teaching points on the fly and deliver memorable lectures and talks. Other sessions will enhance your skills in emotional intelligence.
As always, we are extremely fortunate to wrap up the day with Bob Wachter, MD, MHM, who is sure to deliver a thought-provoking and entertaining presentation entitled “Hospitalists as Drivers of Innovation and System Change: Are We Doing Enough?”
As you wrap up your final day, I wish you a safe journey back home. Please continue your engagement with the Society through chapter meetings in your area, signing up for committees and interest groups, and dropping us a line – we look forward to continuing to work for you in the coming year.
Dr. Afsar is the incoming president of the Society of Hospital Medicine and the chief ambulatory officer & CMO for ACOs at UC Irvine Health in Orange, Calif.
Gene variants linked to survival after HSCT

New research has revealed a link between rare gene variants and survival after hematopoietic stem cell transplant (HSCT).
Researchers performed exome sequencing in nearly 2500 HSCT recipients and their matched, unrelated donors.
The sequencing revealed several gene variants—in both donors and recipients—that were significantly associated with overall survival (OS), transplant-related mortality (TRM), and disease-related mortality (DRM) after HSCT.
Qianqian Zhu, PhD, of Roswell Park Comprehensive Cancer Center in Buffalo, New York, and her colleagues described these findings in Blood.
The team performed exome sequencing—using the Illumina HumanExome BeadChip—in patients who participated in the DISCOVeRY-BMT study.
This included 2473 HSCT recipients who had acute myeloid leukemia, acute lymphoblastic leukemia, or myelodysplastic syndromes. It also included 2221 donors who were a 10/10 human leukocyte antigen match for each recipient.
The researchers looked at genetic variants in donors and recipients and assessed the variants’ associations with OS, TRM, and DRM.
Variants in recipients
Analyses revealed an increased risk of TRM when there was a mismatch between donors and recipients for a variant in TEX38—rs200092801. The increased risk was even more pronounced when either the recipient or the donor was female.
Among the recipients mismatched with their donors at rs200092801, every female recipient and every recipient with a female donor died from TRM. In comparison, 44% of the male recipients with male donors died from TRM.
The researchers said the rs200092801 variant may prompt the production of a mutant peptide that can be presented by MHC-I molecules to immune cells to trigger downstream immune response and TRM.
Dr Zhu and her colleagues also identified variants that appeared to have a positive impact on TRM and OS.
Recipients who had any of 6 variants in the gene OR51D1 had a decreased risk of TRM and improved OS.
The variants (rs138224979, rs148606808, rs141786655, rs61745314, rs200394876, and rs149135276) were not associated with DRM, so the researchers concluded that the improvement in OS was driven by protection against TRM.
Donor variants linked to OS
Donors had variants in 4 genes—ALPP, EMID1, SLC44A5, and LRP1—that were associated with OS but not TRM or DRM.
The 3 variants identified in ALPP (rs144454460, rs140078460, and rs142493383) were associated with improved OS.
And the 2 variants in SLC44A5 (rs143004355 and rs149696907) were associated with worse OS.
There were 2 variants in EMID1. One was associated with improved OS (rs34772704), and the other was associated with decreased OS (rs139996840).
And there were 27 variants in LRP1. Some had a positive association with OS, and others had a negative association.
Donor variants linked to TRM and DRM
Six variants in the HHAT gene were associated with TRM. Five of the variants appeared to have a protective effect against TRM (rs145455128, rs146916002, rs61744143, rs149597734, and rs145943928). For the other variant (rs141591165), the apparent effect was inconsistent between patient cohorts.
There were 3 variants in LYZL4 associated with DRM. Two were associated with an increased risk of DRM (rs147770623 and rs76947105), and 1 appeared to have a protective effect (rs181886204).
Six variants in NT5E appeared to have a protective effect against DRM (rs200250022, rs200369370, rs41271617, rs200648774, rs144719925, and rs145505137).
The researchers said the variants in NT5E probably reduce the enzyme activity of the gene. This supports preclinical findings showing that targeted blockade of NT5E can slow tumor growth.
“We have just started to uncover the biological relevance of these new and unexpected genes to a patient’s survival after [HSCT],” Dr Zhu said.
“Our findings shed light on new areas that were not considered before, but we need to further replicate and test our findings. We’re hoping that additional studies of this type will continue to discover novel genes leading to improved outcomes for patients.”
New research has revealed a link between rare gene variants and survival after hematopoietic stem cell transplant (HSCT).
Researchers performed exome sequencing in nearly 2500 HSCT recipients and their matched, unrelated donors.
The sequencing revealed several gene variants—in both donors and recipients—that were significantly associated with overall survival (OS), transplant-related mortality (TRM), and disease-related mortality (DRM) after HSCT.
Qianqian Zhu, PhD, of Roswell Park Comprehensive Cancer Center in Buffalo, New York, and her colleagues described these findings in Blood.
The team performed exome sequencing—using the Illumina HumanExome BeadChip—in patients who participated in the DISCOVeRY-BMT study.
This included 2473 HSCT recipients who had acute myeloid leukemia, acute lymphoblastic leukemia, or myelodysplastic syndromes. It also included 2221 donors who were a 10/10 human leukocyte antigen match for each recipient.
The researchers looked at genetic variants in donors and recipients and assessed the variants’ associations with OS, TRM, and DRM.
Variants in recipients
Analyses revealed an increased risk of TRM when there was a mismatch between donors and recipients for a variant in TEX38—rs200092801. The increased risk was even more pronounced when either the recipient or the donor was female.
Among the recipients mismatched with their donors at rs200092801, every female recipient and every recipient with a female donor died from TRM. In comparison, 44% of the male recipients with male donors died from TRM.
The researchers said the rs200092801 variant may prompt the production of a mutant peptide that can be presented by MHC-I molecules to immune cells to trigger downstream immune response and TRM.
Dr Zhu and her colleagues also identified variants that appeared to have a positive impact on TRM and OS.
Recipients who had any of 6 variants in the gene OR51D1 had a decreased risk of TRM and improved OS.
The variants (rs138224979, rs148606808, rs141786655, rs61745314, rs200394876, and rs149135276) were not associated with DRM, so the researchers concluded that the improvement in OS was driven by protection against TRM.
Donor variants linked to OS
Donors had variants in 4 genes—ALPP, EMID1, SLC44A5, and LRP1—that were associated with OS but not TRM or DRM.
The 3 variants identified in ALPP (rs144454460, rs140078460, and rs142493383) were associated with improved OS.
And the 2 variants in SLC44A5 (rs143004355 and rs149696907) were associated with worse OS.
There were 2 variants in EMID1. One was associated with improved OS (rs34772704), and the other was associated with decreased OS (rs139996840).
And there were 27 variants in LRP1. Some had a positive association with OS, and others had a negative association.
Donor variants linked to TRM and DRM
Six variants in the HHAT gene were associated with TRM. Five of the variants appeared to have a protective effect against TRM (rs145455128, rs146916002, rs61744143, rs149597734, and rs145943928). For the other variant (rs141591165), the apparent effect was inconsistent between patient cohorts.
There were 3 variants in LYZL4 associated with DRM. Two were associated with an increased risk of DRM (rs147770623 and rs76947105), and 1 appeared to have a protective effect (rs181886204).
Six variants in NT5E appeared to have a protective effect against DRM (rs200250022, rs200369370, rs41271617, rs200648774, rs144719925, and rs145505137).
The researchers said the variants in NT5E probably reduce the enzyme activity of the gene. This supports preclinical findings showing that targeted blockade of NT5E can slow tumor growth.
“We have just started to uncover the biological relevance of these new and unexpected genes to a patient’s survival after [HSCT],” Dr Zhu said.
“Our findings shed light on new areas that were not considered before, but we need to further replicate and test our findings. We’re hoping that additional studies of this type will continue to discover novel genes leading to improved outcomes for patients.”
New research has revealed a link between rare gene variants and survival after hematopoietic stem cell transplant (HSCT).
Researchers performed exome sequencing in nearly 2500 HSCT recipients and their matched, unrelated donors.
The sequencing revealed several gene variants—in both donors and recipients—that were significantly associated with overall survival (OS), transplant-related mortality (TRM), and disease-related mortality (DRM) after HSCT.
Qianqian Zhu, PhD, of Roswell Park Comprehensive Cancer Center in Buffalo, New York, and her colleagues described these findings in Blood.
The team performed exome sequencing—using the Illumina HumanExome BeadChip—in patients who participated in the DISCOVeRY-BMT study.
This included 2473 HSCT recipients who had acute myeloid leukemia, acute lymphoblastic leukemia, or myelodysplastic syndromes. It also included 2221 donors who were a 10/10 human leukocyte antigen match for each recipient.
The researchers looked at genetic variants in donors and recipients and assessed the variants’ associations with OS, TRM, and DRM.
Variants in recipients
Analyses revealed an increased risk of TRM when there was a mismatch between donors and recipients for a variant in TEX38—rs200092801. The increased risk was even more pronounced when either the recipient or the donor was female.
Among the recipients mismatched with their donors at rs200092801, every female recipient and every recipient with a female donor died from TRM. In comparison, 44% of the male recipients with male donors died from TRM.
The researchers said the rs200092801 variant may prompt the production of a mutant peptide that can be presented by MHC-I molecules to immune cells to trigger downstream immune response and TRM.
Dr Zhu and her colleagues also identified variants that appeared to have a positive impact on TRM and OS.
Recipients who had any of 6 variants in the gene OR51D1 had a decreased risk of TRM and improved OS.
The variants (rs138224979, rs148606808, rs141786655, rs61745314, rs200394876, and rs149135276) were not associated with DRM, so the researchers concluded that the improvement in OS was driven by protection against TRM.
Donor variants linked to OS
Donors had variants in 4 genes—ALPP, EMID1, SLC44A5, and LRP1—that were associated with OS but not TRM or DRM.
The 3 variants identified in ALPP (rs144454460, rs140078460, and rs142493383) were associated with improved OS.
And the 2 variants in SLC44A5 (rs143004355 and rs149696907) were associated with worse OS.
There were 2 variants in EMID1. One was associated with improved OS (rs34772704), and the other was associated with decreased OS (rs139996840).
And there were 27 variants in LRP1. Some had a positive association with OS, and others had a negative association.
Donor variants linked to TRM and DRM
Six variants in the HHAT gene were associated with TRM. Five of the variants appeared to have a protective effect against TRM (rs145455128, rs146916002, rs61744143, rs149597734, and rs145943928). For the other variant (rs141591165), the apparent effect was inconsistent between patient cohorts.
There were 3 variants in LYZL4 associated with DRM. Two were associated with an increased risk of DRM (rs147770623 and rs76947105), and 1 appeared to have a protective effect (rs181886204).
Six variants in NT5E appeared to have a protective effect against DRM (rs200250022, rs200369370, rs41271617, rs200648774, rs144719925, and rs145505137).
The researchers said the variants in NT5E probably reduce the enzyme activity of the gene. This supports preclinical findings showing that targeted blockade of NT5E can slow tumor growth.
“We have just started to uncover the biological relevance of these new and unexpected genes to a patient’s survival after [HSCT],” Dr Zhu said.
“Our findings shed light on new areas that were not considered before, but we need to further replicate and test our findings. We’re hoping that additional studies of this type will continue to discover novel genes leading to improved outcomes for patients.”
Tazemetostat exhibits antitumor activity in phase 1 trial

The EZH2 inhibitor tazemetostat demonstrated a “favorable safety profile and antitumor activity” in a phase 1 study, according to researchers.
The drug produced responses in 8 of 21 patients with relapsed/refractory B-cell non-Hodgkin lymphoma (NHL), including 3 complete responses (CRs).
The maximum tolerated dose of tazemetostat was not reached, and there were no fatal adverse events (AEs) related to treatment.
Grade 3/4 treatment-related AEs included thrombocytopenia, neutropenia, hepatocellular injury, and hypertension.
Antoine Italiano, MD, PhD, of Institut Bergonié in Bordeaux, France, and his colleagues reported these results in The Lancet Oncology. The trial was sponsored by Epizyme and Eisai.
The study enrolled 64 patients—43 with solid tumors and 21 with B-cell NHL. The following characteristics and dosing information pertain only to the patients with NHL.
Thirteen patients had diffuse large B-cell lymphoma (DLBCL), 7 had follicular lymphoma (FL), and 1 had marginal zone lymphoma (MZL).
The patients’ median age was 62 (range, 53-70), and 71% were male. They had an ECOG performance status of 0 (62%) or 1 (38%).
Most patients had received at least 3 prior therapies—38% had 3, 14% had 4, and 33% had 5 or more prior therapies. Forty-eight percent had prior hematopoietic stem cell transplant.
The patients received escalating doses of tazemetostat twice daily—100 mg (n=1), 200 mg (n=2), 400 mg (n=1), 800 mg (n=8), and 1600 mg (n=4).
The remaining 5 patients were enrolled in a substudy to evaluate food effect. These patients received a single 200 mg dose on day -8 and day -1, with or without food, followed by 400 mg twice daily starting on day 1. Specific results on the food effects were not included in the paper.
Safety
In the entire study cohort, there was 1 dose-limiting toxicity—grade 4 thrombocytopenia—at the 1600 mg dose. The maximum tolerated dose of tazemetostat was not reached, but the researchers decided upon 800 mg twice daily as the recommended phase 2 dose.
Overall, 77% (n=49) of patients had treatment-related AEs. Grade 3/4 treatment-related AEs included thrombocytopenia (4%, n=2), neutropenia (4%, n=2), hepatocellular injury (2%, n=1), and hypertension (2%, n=1).
Serious treatment-related AEs were neutropenia in 1 patient (800 mg group) and anemia and thrombocytopenia in another patient (1600 mg group).
Seven patients (11%) had fatal AEs, but none were considered treatment-related. They included general physical health deterioration (1 at 200 mg, 1 at 1600 mg, and 2 at 400 mg), respiratory distress (2 at 400 mg), and septic shock (1 at 1600 mg).
Efficacy
Eight of the 21 NHL patients responded to treatment. Three patients had a CR—1 with DLBCL and 2 with FL. Of the 5 partial responders, 3 had DLBCL, 1 had FL, and 1 had MZL.
The median time to first response was 3.5 months, and the median duration of response was 12.4 months.
The 3 complete responders remained on tazemetostat beyond 27.6 months (FL patient), 28.8 months (FL patient), and 33.6 months (DLBCL patient).
Two of the 43 patients with solid tumors responded to tazemetostat—1 with a CR and 1 with a partial response.
The complete responder had an INI1-negative malignant rhabdoid tumor, and the partial responder had a SMARCA4-negative malignant rhabdoid tumor of the ovary.
“Today’s publication in The Lancet Oncology reports the safety and tolerability endpoints for tazemetostat in this study, which enabled further evaluation of EZH2 inhibition in INI1- and SMARCA4-negative solid tumors and NHL,” Dr Italiano said. “I’m also encouraged by the preliminary antitumor activity observed in this study.”
The EZH2 inhibitor tazemetostat demonstrated a “favorable safety profile and antitumor activity” in a phase 1 study, according to researchers.
The drug produced responses in 8 of 21 patients with relapsed/refractory B-cell non-Hodgkin lymphoma (NHL), including 3 complete responses (CRs).
The maximum tolerated dose of tazemetostat was not reached, and there were no fatal adverse events (AEs) related to treatment.
Grade 3/4 treatment-related AEs included thrombocytopenia, neutropenia, hepatocellular injury, and hypertension.
Antoine Italiano, MD, PhD, of Institut Bergonié in Bordeaux, France, and his colleagues reported these results in The Lancet Oncology. The trial was sponsored by Epizyme and Eisai.
The study enrolled 64 patients—43 with solid tumors and 21 with B-cell NHL. The following characteristics and dosing information pertain only to the patients with NHL.
Thirteen patients had diffuse large B-cell lymphoma (DLBCL), 7 had follicular lymphoma (FL), and 1 had marginal zone lymphoma (MZL).
The patients’ median age was 62 (range, 53-70), and 71% were male. They had an ECOG performance status of 0 (62%) or 1 (38%).
Most patients had received at least 3 prior therapies—38% had 3, 14% had 4, and 33% had 5 or more prior therapies. Forty-eight percent had prior hematopoietic stem cell transplant.
The patients received escalating doses of tazemetostat twice daily—100 mg (n=1), 200 mg (n=2), 400 mg (n=1), 800 mg (n=8), and 1600 mg (n=4).
The remaining 5 patients were enrolled in a substudy to evaluate food effect. These patients received a single 200 mg dose on day -8 and day -1, with or without food, followed by 400 mg twice daily starting on day 1. Specific results on the food effects were not included in the paper.
Safety
In the entire study cohort, there was 1 dose-limiting toxicity—grade 4 thrombocytopenia—at the 1600 mg dose. The maximum tolerated dose of tazemetostat was not reached, but the researchers decided upon 800 mg twice daily as the recommended phase 2 dose.
Overall, 77% (n=49) of patients had treatment-related AEs. Grade 3/4 treatment-related AEs included thrombocytopenia (4%, n=2), neutropenia (4%, n=2), hepatocellular injury (2%, n=1), and hypertension (2%, n=1).
Serious treatment-related AEs were neutropenia in 1 patient (800 mg group) and anemia and thrombocytopenia in another patient (1600 mg group).
Seven patients (11%) had fatal AEs, but none were considered treatment-related. They included general physical health deterioration (1 at 200 mg, 1 at 1600 mg, and 2 at 400 mg), respiratory distress (2 at 400 mg), and septic shock (1 at 1600 mg).
Efficacy
Eight of the 21 NHL patients responded to treatment. Three patients had a CR—1 with DLBCL and 2 with FL. Of the 5 partial responders, 3 had DLBCL, 1 had FL, and 1 had MZL.
The median time to first response was 3.5 months, and the median duration of response was 12.4 months.
The 3 complete responders remained on tazemetostat beyond 27.6 months (FL patient), 28.8 months (FL patient), and 33.6 months (DLBCL patient).
Two of the 43 patients with solid tumors responded to tazemetostat—1 with a CR and 1 with a partial response.
The complete responder had an INI1-negative malignant rhabdoid tumor, and the partial responder had a SMARCA4-negative malignant rhabdoid tumor of the ovary.
“Today’s publication in The Lancet Oncology reports the safety and tolerability endpoints for tazemetostat in this study, which enabled further evaluation of EZH2 inhibition in INI1- and SMARCA4-negative solid tumors and NHL,” Dr Italiano said. “I’m also encouraged by the preliminary antitumor activity observed in this study.”
The EZH2 inhibitor tazemetostat demonstrated a “favorable safety profile and antitumor activity” in a phase 1 study, according to researchers.
The drug produced responses in 8 of 21 patients with relapsed/refractory B-cell non-Hodgkin lymphoma (NHL), including 3 complete responses (CRs).
The maximum tolerated dose of tazemetostat was not reached, and there were no fatal adverse events (AEs) related to treatment.
Grade 3/4 treatment-related AEs included thrombocytopenia, neutropenia, hepatocellular injury, and hypertension.
Antoine Italiano, MD, PhD, of Institut Bergonié in Bordeaux, France, and his colleagues reported these results in The Lancet Oncology. The trial was sponsored by Epizyme and Eisai.
The study enrolled 64 patients—43 with solid tumors and 21 with B-cell NHL. The following characteristics and dosing information pertain only to the patients with NHL.
Thirteen patients had diffuse large B-cell lymphoma (DLBCL), 7 had follicular lymphoma (FL), and 1 had marginal zone lymphoma (MZL).
The patients’ median age was 62 (range, 53-70), and 71% were male. They had an ECOG performance status of 0 (62%) or 1 (38%).
Most patients had received at least 3 prior therapies—38% had 3, 14% had 4, and 33% had 5 or more prior therapies. Forty-eight percent had prior hematopoietic stem cell transplant.
The patients received escalating doses of tazemetostat twice daily—100 mg (n=1), 200 mg (n=2), 400 mg (n=1), 800 mg (n=8), and 1600 mg (n=4).
The remaining 5 patients were enrolled in a substudy to evaluate food effect. These patients received a single 200 mg dose on day -8 and day -1, with or without food, followed by 400 mg twice daily starting on day 1. Specific results on the food effects were not included in the paper.
Safety
In the entire study cohort, there was 1 dose-limiting toxicity—grade 4 thrombocytopenia—at the 1600 mg dose. The maximum tolerated dose of tazemetostat was not reached, but the researchers decided upon 800 mg twice daily as the recommended phase 2 dose.
Overall, 77% (n=49) of patients had treatment-related AEs. Grade 3/4 treatment-related AEs included thrombocytopenia (4%, n=2), neutropenia (4%, n=2), hepatocellular injury (2%, n=1), and hypertension (2%, n=1).
Serious treatment-related AEs were neutropenia in 1 patient (800 mg group) and anemia and thrombocytopenia in another patient (1600 mg group).
Seven patients (11%) had fatal AEs, but none were considered treatment-related. They included general physical health deterioration (1 at 200 mg, 1 at 1600 mg, and 2 at 400 mg), respiratory distress (2 at 400 mg), and septic shock (1 at 1600 mg).
Efficacy
Eight of the 21 NHL patients responded to treatment. Three patients had a CR—1 with DLBCL and 2 with FL. Of the 5 partial responders, 3 had DLBCL, 1 had FL, and 1 had MZL.
The median time to first response was 3.5 months, and the median duration of response was 12.4 months.
The 3 complete responders remained on tazemetostat beyond 27.6 months (FL patient), 28.8 months (FL patient), and 33.6 months (DLBCL patient).
Two of the 43 patients with solid tumors responded to tazemetostat—1 with a CR and 1 with a partial response.
The complete responder had an INI1-negative malignant rhabdoid tumor, and the partial responder had a SMARCA4-negative malignant rhabdoid tumor of the ovary.
“Today’s publication in The Lancet Oncology reports the safety and tolerability endpoints for tazemetostat in this study, which enabled further evaluation of EZH2 inhibition in INI1- and SMARCA4-negative solid tumors and NHL,” Dr Italiano said. “I’m also encouraged by the preliminary antitumor activity observed in this study.”
Selinexor receives fast track designation for MM

The US Food and Drug Administration (FDA) has granted fast track designation to selinexor for the treatment of patients with penta-refractory multiple myeloma (MM).
The patients must have received at least 3 prior lines of therapy that included an alkylating agent, a glucocorticoid, bortezomib, carfilzomib, lenalidomide, pomalidomide, and daratumumab.
In addition, the patients must have disease that is refractory to at least 1 proteasome inhibitor, at least 1 immunomodulatory agent, glucocorticoids, daratumumab, and the patients’ most recent therapy.
“The designation of fast track for selinexor represents important recognition by the FDA of the potential of this anticancer agent to address the significant unmet need in the treatment of patients with penta-refractory myeloma that has continued to progress despite available therapies,” said Sharon Shacham, PhD, founder, president, and chief scientific officer of Karyopharm Therapeutics Inc., the company developing selinexor.
The FDA’s fast track drug development program is designed to expedite clinical development and submission of new drug applications for medicines with the potential to treat serious or life-threatening conditions and address unmet medical needs.
Fast track designation facilitates frequent interactions with the FDA review team, including meetings to discuss all aspects of development to support a drug’s approval, and also provides the opportunity to submit sections of a new drug application on a rolling basis as data become available.
About selinexor
Selinexor (formerly KPT-330) is a first-in-class, oral selective inhibitor of nuclear export compound.
Selinexor functions by binding with and inhibiting the nuclear export protein XPO1 (also called CRM1), leading to the accumulation of tumor suppressor proteins in the cell nucleus. This reinitiates and amplifies their tumor suppressor function and is believed to lead to apoptosis in cancer cells while largely sparing normal cells.
Selinexor is currently being evaluated in several clinical trials across multiple cancer indications.
In the phase 2 STORM trial, researchers are testing selinexor in combination with low-dose dexamethasone for patients with penta-refractory MM. Karyopharm Therapeutics plans to report top-line data from this study at the end of this month.
Trials of selinexor were placed on partial clinical hold in mid-March last year due to a lack of information about serious adverse events. However, the hold was lifted for trials of patients with hematologic malignancies at the end of that same month.
The US Food and Drug Administration (FDA) has granted fast track designation to selinexor for the treatment of patients with penta-refractory multiple myeloma (MM).
The patients must have received at least 3 prior lines of therapy that included an alkylating agent, a glucocorticoid, bortezomib, carfilzomib, lenalidomide, pomalidomide, and daratumumab.
In addition, the patients must have disease that is refractory to at least 1 proteasome inhibitor, at least 1 immunomodulatory agent, glucocorticoids, daratumumab, and the patients’ most recent therapy.
“The designation of fast track for selinexor represents important recognition by the FDA of the potential of this anticancer agent to address the significant unmet need in the treatment of patients with penta-refractory myeloma that has continued to progress despite available therapies,” said Sharon Shacham, PhD, founder, president, and chief scientific officer of Karyopharm Therapeutics Inc., the company developing selinexor.
The FDA’s fast track drug development program is designed to expedite clinical development and submission of new drug applications for medicines with the potential to treat serious or life-threatening conditions and address unmet medical needs.
Fast track designation facilitates frequent interactions with the FDA review team, including meetings to discuss all aspects of development to support a drug’s approval, and also provides the opportunity to submit sections of a new drug application on a rolling basis as data become available.
About selinexor
Selinexor (formerly KPT-330) is a first-in-class, oral selective inhibitor of nuclear export compound.
Selinexor functions by binding with and inhibiting the nuclear export protein XPO1 (also called CRM1), leading to the accumulation of tumor suppressor proteins in the cell nucleus. This reinitiates and amplifies their tumor suppressor function and is believed to lead to apoptosis in cancer cells while largely sparing normal cells.
Selinexor is currently being evaluated in several clinical trials across multiple cancer indications.
In the phase 2 STORM trial, researchers are testing selinexor in combination with low-dose dexamethasone for patients with penta-refractory MM. Karyopharm Therapeutics plans to report top-line data from this study at the end of this month.
Trials of selinexor were placed on partial clinical hold in mid-March last year due to a lack of information about serious adverse events. However, the hold was lifted for trials of patients with hematologic malignancies at the end of that same month.
The US Food and Drug Administration (FDA) has granted fast track designation to selinexor for the treatment of patients with penta-refractory multiple myeloma (MM).
The patients must have received at least 3 prior lines of therapy that included an alkylating agent, a glucocorticoid, bortezomib, carfilzomib, lenalidomide, pomalidomide, and daratumumab.
In addition, the patients must have disease that is refractory to at least 1 proteasome inhibitor, at least 1 immunomodulatory agent, glucocorticoids, daratumumab, and the patients’ most recent therapy.
“The designation of fast track for selinexor represents important recognition by the FDA of the potential of this anticancer agent to address the significant unmet need in the treatment of patients with penta-refractory myeloma that has continued to progress despite available therapies,” said Sharon Shacham, PhD, founder, president, and chief scientific officer of Karyopharm Therapeutics Inc., the company developing selinexor.
The FDA’s fast track drug development program is designed to expedite clinical development and submission of new drug applications for medicines with the potential to treat serious or life-threatening conditions and address unmet medical needs.
Fast track designation facilitates frequent interactions with the FDA review team, including meetings to discuss all aspects of development to support a drug’s approval, and also provides the opportunity to submit sections of a new drug application on a rolling basis as data become available.
About selinexor
Selinexor (formerly KPT-330) is a first-in-class, oral selective inhibitor of nuclear export compound.
Selinexor functions by binding with and inhibiting the nuclear export protein XPO1 (also called CRM1), leading to the accumulation of tumor suppressor proteins in the cell nucleus. This reinitiates and amplifies their tumor suppressor function and is believed to lead to apoptosis in cancer cells while largely sparing normal cells.
Selinexor is currently being evaluated in several clinical trials across multiple cancer indications.
In the phase 2 STORM trial, researchers are testing selinexor in combination with low-dose dexamethasone for patients with penta-refractory MM. Karyopharm Therapeutics plans to report top-line data from this study at the end of this month.
Trials of selinexor were placed on partial clinical hold in mid-March last year due to a lack of information about serious adverse events. However, the hold was lifted for trials of patients with hematologic malignancies at the end of that same month.
Caffeine for apnea of prematurity found safe, effective at 11 years
Caffeine for apnea of prematurity was neurobehaviorally safe and significantly improved fine motor coordination, visuomotor integration, visual perception, and visuospatial organization at 11-year follow-up, according to the results of a double-blind, randomized, controlled trial.
“There was little evidence for differences between the caffeine and placebo groups on tests of general intelligence, attention, executive function, and behavior. This highlights the long-term safety and efficacy of caffeine therapy for apnea of prematurity in very-low-birth-weight neonates,” wrote Ines M. Mürner-Lavanchy, PhD, of Monash University, Clayton, Australia, and her associates. The Caffeine for Apnea of Prematurity (CAP) trial, the first to assess long-term neurobehavioral outcomes of neonatal caffeine therapy, was published online April 11 in Pediatrics.
Neonatal caffeine therapy significantly lowered the risk of death before 18 months, cerebral palsy, cognitive delay, severe hearing loss, and bilateral blindness, as has been reported (N Engl J Med. 2007;357:1893-902). By 5 years, caffeine no longer showed significant benefits, apart from improved motor performance, Dr. Mürner-Lavanchy and her associates noted.
At 11 years, available data from 870 patients showed generally similar neurobehavioral outcomes between groups, although the caffeine group scored higher on most scales. The most apparent benefits included visuomotor integration (mean difference from placebo, 1.8; 95% confidence interval, 0.0-3.7; P less than .05), visual perception (2.0; 95% CI, 0.3-3.8; P = .02), fine motor coordination (2.9; 95% CI, 0.7-5.1; P = .01), and Rey Complex Figure copy accuracy, a measure of visuospatial organization (1.2; 95% CI, 0.4-2.0; P = .003).
Eleven-year follow-up data were missing for 22% of patients, but their birth characteristics and childhood outcomes resembled those of patients with available data, the investigators said. “Therefore, we are confident that the outcomes of the whole cohort are reflected in the present results with sufficient accuracy.”
The Canadian Institutes of Health Research provided funding. The investigators reported having no relevant conflicts of interest.
SOURCE: Mürner-Lavanchy IM et al. Pediatrics. 2018 Apr 11. doi: 10.1542/peds.2017-4047.
Caffeine for apnea of prematurity was neurobehaviorally safe and significantly improved fine motor coordination, visuomotor integration, visual perception, and visuospatial organization at 11-year follow-up, according to the results of a double-blind, randomized, controlled trial.
“There was little evidence for differences between the caffeine and placebo groups on tests of general intelligence, attention, executive function, and behavior. This highlights the long-term safety and efficacy of caffeine therapy for apnea of prematurity in very-low-birth-weight neonates,” wrote Ines M. Mürner-Lavanchy, PhD, of Monash University, Clayton, Australia, and her associates. The Caffeine for Apnea of Prematurity (CAP) trial, the first to assess long-term neurobehavioral outcomes of neonatal caffeine therapy, was published online April 11 in Pediatrics.
Neonatal caffeine therapy significantly lowered the risk of death before 18 months, cerebral palsy, cognitive delay, severe hearing loss, and bilateral blindness, as has been reported (N Engl J Med. 2007;357:1893-902). By 5 years, caffeine no longer showed significant benefits, apart from improved motor performance, Dr. Mürner-Lavanchy and her associates noted.
At 11 years, available data from 870 patients showed generally similar neurobehavioral outcomes between groups, although the caffeine group scored higher on most scales. The most apparent benefits included visuomotor integration (mean difference from placebo, 1.8; 95% confidence interval, 0.0-3.7; P less than .05), visual perception (2.0; 95% CI, 0.3-3.8; P = .02), fine motor coordination (2.9; 95% CI, 0.7-5.1; P = .01), and Rey Complex Figure copy accuracy, a measure of visuospatial organization (1.2; 95% CI, 0.4-2.0; P = .003).
Eleven-year follow-up data were missing for 22% of patients, but their birth characteristics and childhood outcomes resembled those of patients with available data, the investigators said. “Therefore, we are confident that the outcomes of the whole cohort are reflected in the present results with sufficient accuracy.”
The Canadian Institutes of Health Research provided funding. The investigators reported having no relevant conflicts of interest.
SOURCE: Mürner-Lavanchy IM et al. Pediatrics. 2018 Apr 11. doi: 10.1542/peds.2017-4047.
Caffeine for apnea of prematurity was neurobehaviorally safe and significantly improved fine motor coordination, visuomotor integration, visual perception, and visuospatial organization at 11-year follow-up, according to the results of a double-blind, randomized, controlled trial.
“There was little evidence for differences between the caffeine and placebo groups on tests of general intelligence, attention, executive function, and behavior. This highlights the long-term safety and efficacy of caffeine therapy for apnea of prematurity in very-low-birth-weight neonates,” wrote Ines M. Mürner-Lavanchy, PhD, of Monash University, Clayton, Australia, and her associates. The Caffeine for Apnea of Prematurity (CAP) trial, the first to assess long-term neurobehavioral outcomes of neonatal caffeine therapy, was published online April 11 in Pediatrics.
Neonatal caffeine therapy significantly lowered the risk of death before 18 months, cerebral palsy, cognitive delay, severe hearing loss, and bilateral blindness, as has been reported (N Engl J Med. 2007;357:1893-902). By 5 years, caffeine no longer showed significant benefits, apart from improved motor performance, Dr. Mürner-Lavanchy and her associates noted.
At 11 years, available data from 870 patients showed generally similar neurobehavioral outcomes between groups, although the caffeine group scored higher on most scales. The most apparent benefits included visuomotor integration (mean difference from placebo, 1.8; 95% confidence interval, 0.0-3.7; P less than .05), visual perception (2.0; 95% CI, 0.3-3.8; P = .02), fine motor coordination (2.9; 95% CI, 0.7-5.1; P = .01), and Rey Complex Figure copy accuracy, a measure of visuospatial organization (1.2; 95% CI, 0.4-2.0; P = .003).
Eleven-year follow-up data were missing for 22% of patients, but their birth characteristics and childhood outcomes resembled those of patients with available data, the investigators said. “Therefore, we are confident that the outcomes of the whole cohort are reflected in the present results with sufficient accuracy.”
The Canadian Institutes of Health Research provided funding. The investigators reported having no relevant conflicts of interest.
SOURCE: Mürner-Lavanchy IM et al. Pediatrics. 2018 Apr 11. doi: 10.1542/peds.2017-4047.
FROM PEDIATRICS
Key clinical point:
Major finding: At 11 years, the caffeine group outperformed the placebo group on measures of fine motor coordination (P = .01), visuomotor integration (P less than .05), visual perception (P = .02), and visuospatial organization (P = .003).
Study details: The Caffeine for Apnea of Prematurity (CAP) trial, a double-blind, multicenter, randomized, placebo-controlled trial of 870 very-low-birth-weight infants (500-1,250 g).
Disclosures: The Canadian Institutes of Health Research provided funding. The investigators reported having no relevant conflicts of interest.
Source: Pediatrics. 2018 Apr 11. doi: 10.1542/peds.2017-4047.
This Evaluation Is a Heart-stopper
ANSWER
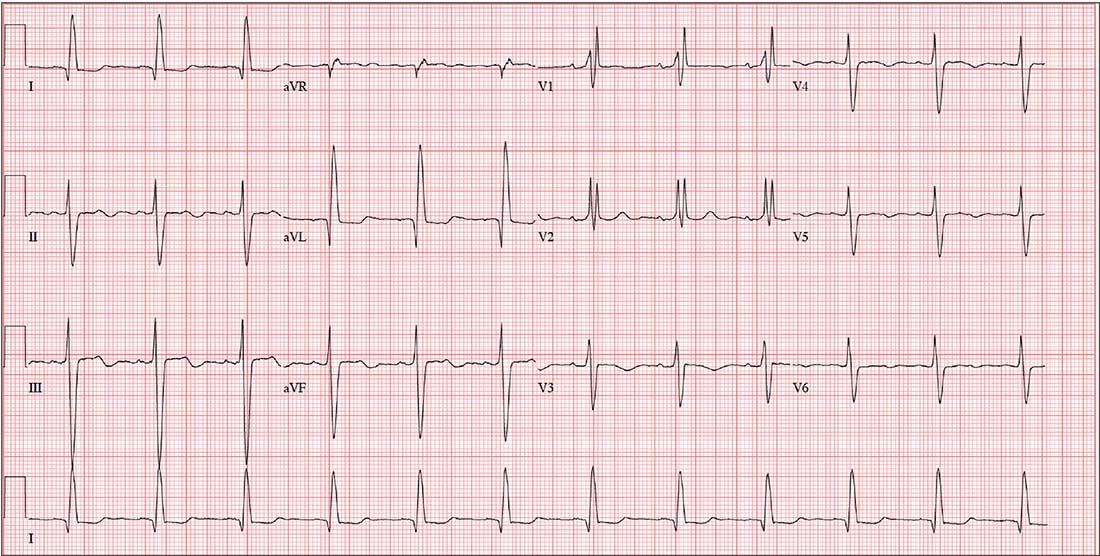
The correct interpretation includes normal sinus rhythm with left-axis deviation, a right bundle branch block (RBBB), and a left anterior fascicular block (LAFB).
Normal sinus rhythm is evidenced by a P for every QRS and a QRS for every P, with a consistent PR interval and a rate between 60 and 100 beats/min.
A left-axis deviation is indicated by an R-wave axis of –48°, which is less than the upper limit of normal (–30°).
Criteria for an RBBB include a QRS duration ≥ 120 ms with an RSR’ complex in lead V1. A terminal broad S wave in lead I, often seen with RBBB, is not evident in this ECG.
Finally, the criteria for LAFB include S waves > R waves in leads I, II, and aVF, which are well illustrated in this ECG. The combination of an RBBB and an LAFB is consistent with bifascicular block and places the patient at increased risk for complete heart block
ANSWER
The correct interpretation includes normal sinus rhythm with left-axis deviation, a right bundle branch block (RBBB), and a left anterior fascicular block (LAFB).
Normal sinus rhythm is evidenced by a P for every QRS and a QRS for every P, with a consistent PR interval and a rate between 60 and 100 beats/min.
A left-axis deviation is indicated by an R-wave axis of –48°, which is less than the upper limit of normal (–30°).
Criteria for an RBBB include a QRS duration ≥ 120 ms with an RSR’ complex in lead V1. A terminal broad S wave in lead I, often seen with RBBB, is not evident in this ECG.
Finally, the criteria for LAFB include S waves > R waves in leads I, II, and aVF, which are well illustrated in this ECG. The combination of an RBBB and an LAFB is consistent with bifascicular block and places the patient at increased risk for complete heart block
ANSWER
The correct interpretation includes normal sinus rhythm with left-axis deviation, a right bundle branch block (RBBB), and a left anterior fascicular block (LAFB).
Normal sinus rhythm is evidenced by a P for every QRS and a QRS for every P, with a consistent PR interval and a rate between 60 and 100 beats/min.
A left-axis deviation is indicated by an R-wave axis of –48°, which is less than the upper limit of normal (–30°).
Criteria for an RBBB include a QRS duration ≥ 120 ms with an RSR’ complex in lead V1. A terminal broad S wave in lead I, often seen with RBBB, is not evident in this ECG.
Finally, the criteria for LAFB include S waves > R waves in leads I, II, and aVF, which are well illustrated in this ECG. The combination of an RBBB and an LAFB is consistent with bifascicular block and places the patient at increased risk for complete heart block
A 79-year-old man with a history of aortic stenosis presents for preoperative evaluation for aortic valve replacement versus transcatheter aortic valve placement. Over the past three months, he has developed worsening shortness of breath, dyspnea on exertion, chest tightness, and lightheadedness, but no frank syncope. One month ago, he was hospitalized for heart failure, which improved with IV diuresis.
An echocardiogram performed one week ago showed an aortic valve area of 0.5 cm, with a peak velocity of 5.4 m/s and a mean gradient of 64 mm Hg. The left ventricular function was normal, with an ejection fraction of 72%. The pulmonary artery pressure measured 40 mm Hg. Other findings included mild-to-moderate mitral and tricuspid valve regurgitation.
Cardiac history is also positive for coronary artery disease, with a recent coronary angiogram showing 60% stenosis in the proximal left anterior descending artery and 80% stenosis of the mid-portion of the right coronary artery.
Medical history is positive for hypertension, type 2 diabetes, and osteoarthritis. Surgical history includes bilateral knee replacements. Current medications include aspirin, furosemide, metformin, atorvastatin, and metoprolol. The patient is allergic to sulfa-containing medications.
Social history reveals that he is a retired police officer who is married and has three adult children. He does not smoke, enjoys an occasional beer, and denies recreational drug use. Family history is notable for coronary artery disease, hypertension, and diabetes.
Review of systems reveals no additional complaints. It is noted that he wears hearing aids and glasses.
Vital signs include a blood pressure of 110/64 mm Hg; pulse, 70 beats/min; and respiratory rate, 14 breaths/min-1. O2 saturation is 96% on room air. His weight is 214 lb and his height, 74 in.
On physical exam, you find a congenial but inquisitive male in no distress, with jugular venous distention at 8 cm, clear lung fields, and a regular heart rate and rhythm. There is a grade 3/6 systolic ejection murmur at the right upper sternal border but no extra heart sounds or rubs. The abdomen is soft and nontender. Peripheral pulses are 2+ bilaterally without femoral bruits, and surgical scars are present over both knees. There is trace pitting edema bilaterally in the lower extremities. The neurologic exam is intact, without focal signs.
An ECG, obtained as part of his preoperative workup, reveals a ventricular rate of 71 beats/min; PR interval, 152 ms; QRS duration, 142 ms; QT/QTc interval, 476/517 ms; P axis, 76°; R axis, –48°; and T axis, 161°. What is your interpretation?

Video: SHM provides resources and community for practice administrators
ORLANDO – In a video interview, Ms. Tiffani Panek, SFHM, CLHM, who is the division manager of administration at the Johns Hopkins Bayview Medical Center, Baltimore, discussed the scope of SHM resources available for practice administrators.
She details how there are “an incredible number of resources for practice administrators that are available from SHM,” and she recommends the SHM website’s practice administrator’s page, with helpful links, including to their mentorship program. She describes how, just this year, “we are launching a podcast series called ‘The Leadership Launchpad Essentials.’ ”
In addition: “We [also] have our own HMX [Hospital Medicine Exchange] community, and I would say of any resource the practice administrator should access on a regular basis, that would be the one.” That’s the place that practice managers can go to network with their community, according to Ms. Panek.
ORLANDO – In a video interview, Ms. Tiffani Panek, SFHM, CLHM, who is the division manager of administration at the Johns Hopkins Bayview Medical Center, Baltimore, discussed the scope of SHM resources available for practice administrators.
She details how there are “an incredible number of resources for practice administrators that are available from SHM,” and she recommends the SHM website’s practice administrator’s page, with helpful links, including to their mentorship program. She describes how, just this year, “we are launching a podcast series called ‘The Leadership Launchpad Essentials.’ ”
In addition: “We [also] have our own HMX [Hospital Medicine Exchange] community, and I would say of any resource the practice administrator should access on a regular basis, that would be the one.” That’s the place that practice managers can go to network with their community, according to Ms. Panek.
ORLANDO – In a video interview, Ms. Tiffani Panek, SFHM, CLHM, who is the division manager of administration at the Johns Hopkins Bayview Medical Center, Baltimore, discussed the scope of SHM resources available for practice administrators.
She details how there are “an incredible number of resources for practice administrators that are available from SHM,” and she recommends the SHM website’s practice administrator’s page, with helpful links, including to their mentorship program. She describes how, just this year, “we are launching a podcast series called ‘The Leadership Launchpad Essentials.’ ”
In addition: “We [also] have our own HMX [Hospital Medicine Exchange] community, and I would say of any resource the practice administrator should access on a regular basis, that would be the one.” That’s the place that practice managers can go to network with their community, according to Ms. Panek.
REPORTING FROM HM18
