User login
Patient Views of Discharge and a Novel e-Tool to Improve Transition from the Hospital
From the Mayo Clinic, Rochester, MN.
Abstract
- Objective: To elicit patient perceptions of a computer tablet (“e-Board”) used to display information relevant to hospital discharge and to gather patients’ expectations and perceptions regarding hospital discharge.
- Methods: Adult patients discharged from 1 of 3 medical-surgical, noncardiac monitored units of a 1265-bed, academic, tertiary care hospital were interviewed during patient focus groups. Reviewer pairs performed qualitative analysis of focus group transcripts and identified key themes, which were grouped into categories.
- Results: Patients felt a novel e-Board could help with the discharge process. They identified coordination of discharge, communication about discharge, ramifications of unexpected admissions, and interpersonal interactions during admission as the most significant issues around discharge.
- Conclusions: Focus groups elicit actionable information from patients about hospital discharge. Using this information, e-tools may help to design a patient-centered discharge process.
Key words: hospitals; patient satisfaction; focus groups; acute inpatient care.
Transition from the hospital to home represents a critical time for patients after acute illness, and support of patients and their care partners can help decrease consequences of poor care transitions, such as readmissions [1]. Focused discharge planning may improve outcomes and increase patient satisfaction [2], which is a key metric in hospital value-based purchasing programs, which tie Hospital Consumer Assessment of Healthcare Providers and Services (HCAHPS) survey scores to reimbursement. Although patient experience surveys explore several categories of patient satisfaction, HCAHPS may not reveal readily actionable opportunities that would allow clinicians to improve patient experience. Conducting focus groups and interviews can help discern patients’ perceptions and provide patient-centered opportunities to improve hospital discharge processes. Recent studies using these methodologies have revealed patients’ perceptions of barriers to inter-professional collaboration during discharge [3] and their desires and expectations of, as well as suggestions for improvement of, hospitalization [4].
Care transition bundles have been developed to facilitate the process of transitioning home [1,5], but none include e-health tools to help facilitate the discharge process. A study group leveraged available software at our institution to create a bedside “e-Board,” addressing opportunities that surfaced during previous patient focus groups regarding our institution’s discharge process. The software tools were loaded onto a tablet computer (Apple iPad; Cupertino, CA) and included displays of the patient’s physician and nurse, with estimated time of team bedside rounds; day and time of anticipated discharge; display of discharge medications; and a screening tool, I-MOVE, to assess mobility prior to return to independent living [6].
We conducted focus groups to gather patients’ insights for incorporation into a bedside e-health tool for discharge and into our hospital’s current discharge process. The primary objective of the current study was to elicit patient and family perceptions of a bedside e-Board, created to display information regarding discharge. Our secondary objective was to learn about patient expectations and perceptions regarding the hospital discharge process.
Methods
Setting
The study setting was 3 medical-surgical, non-cardiac monitored units of a 1265-bed, academic, tertiary care hospital in Rochester, MN. The study was considered a minimal risk study by the center’s institutional review board.
Participants
Patients aged 18 years or older discharged from 1 of the 3 study units during 2012–2013 were eligible to participate. Patients were excluded if they were not discharged home or to assisted living, were clinic employees, retirees or dependents of clinic employees, were hospitalized longer than 6 months prior to study entry, lived further than 60 miles from the town of Rochester, could not travel, or did not sign research consent.
There were 975 patients who met inclusion criteria. The institution’s survey research center randomly selected 300 eligible patients and contacted them by letter after discharge. The letter was followed up with a telephone call and verbal consent was obtained if the patient expressed interest in participation. Of the 17 patients who gave consent, 12 patients participated in focus group interviews.
E-Board Development
Prior focus group discussions facilitated by our institution’s marketing department (Mr. Kent Seltman, personal communication) explored patients’ perceptions of the discharge process from the institution’s primary hospital. The opportunities for improvement that surfaced during these focus groups included identifying the date of discharge, communication about the time of discharge, and discharging the patient at the identified time, not several hours later. The study group leveraged software available at our institution to create a bedside e-Board that could possibly mitigate these issues by improving communication about discharge. The software tools were loaded onto a tablet computer for patients to use as a resource during their admission. These tools included:
- A photo display of the patient’s nurse and physician, with estimated time of bedside rounds
- A display of the day and time of anticipated discharge. Providing anticipated day and time of discharge has been found to be an achievable goal for internal medicine and surgical services [7].
- A medication display, named the “Durable Display at Discharge,” previously found to improve patient understanding of prescribed medications [8]
- A display of a mobility tool, I-MOVE, designed to screen for debility that could prevent patients’ return to independent living [6].
Focus Groups
Facilitated interviews were conducted on 2 consecutive days in March 2014. Participants were divided into a focus group of 5 to 6 participants if they were functionally independent, or dyads of patient and care partner if they were functionally dependent. Interviews were both video- and audiotaped.
A trained facilitator led 1.5-hour sessions with each focus group. The sessions began with introductions and guidelines by which the focus groups were conducted, including explanations of the video and audio recording equipment, and a request for participants to speak one person at a time to facilitate recording. Discussions were carried out in 2 parts, guided by a facilitator script ( available from the authors). First, participants were asked to share their experiences regarding planning for discharge and the information they received leading up to their planned day and time of hospital discharge. Second, participants were shown a prototype of the e-Board. Participants were asked to reflect as to whether they had received similar information when they had been hospitalized, whether that information was helpful or useful, what information they did not receive that would have been helpful, how information was given, and whether information displayed via an e-Board would be better or worse than the ways they received information while in the hospital.
Data Analysis
Three teams, each comprised of 2 reviewers, met to analyze the video and audio recordings of each focus group. Unfortunately, the video files from the dyad interviews were not recoverable after the recorded sessions, and thus those groups were excluded from the study. Reviewers met prior to analyzing the focus group video and audio recordings to review the qualitative analysis protocol developed by the research team [9] (protocol available froom the authors). The teams then independently reviewed the video recordings and transcripts of the focus groups. The reviewer teams observed the focus group recordings and identified (1) themes regarding perceptions of the bedside e-Board and (2) experiences and perceptions around discharge. The protocol helped reviewer teams create a classification structure by identifying the key themes, which were then combined to create categories. The reviewer teams then compared their classification structures and by incorporating the most frequently identified categories, built a relational model of discharge perceptions.
Results
Eleven patients participated in 2 focus groups, one group of 5 patients and the other of 6 patients. Patient participants included 6 females and 5 males ranging in age from 22 to 84 years. 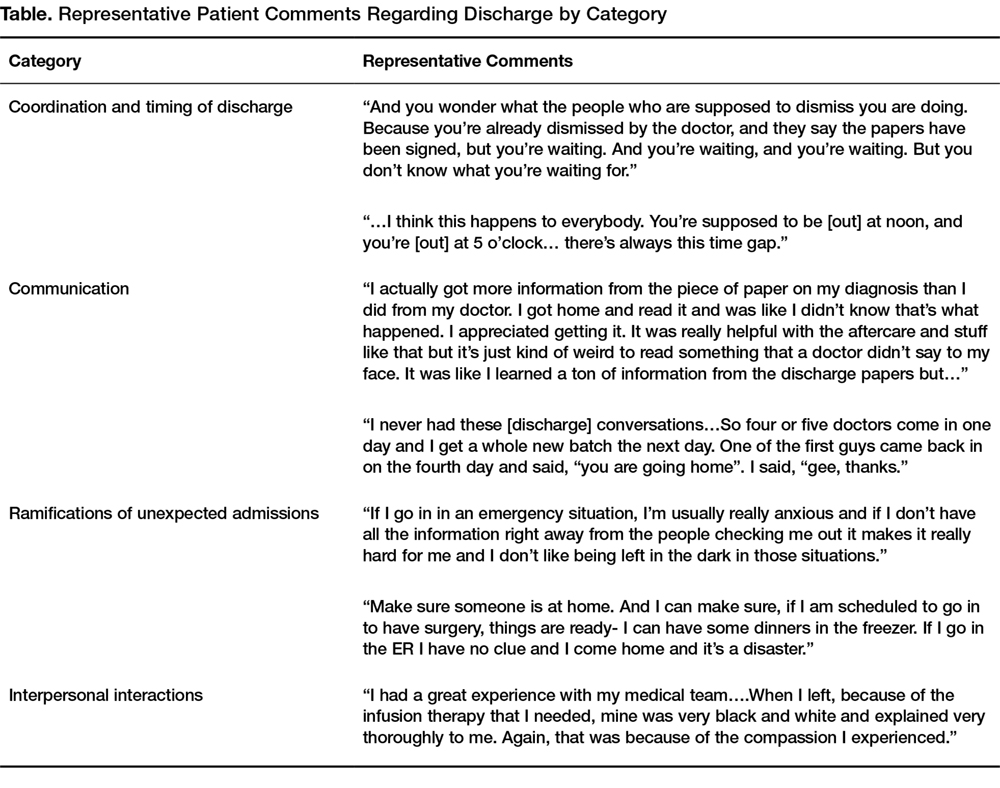
Using the qualitative analysis protocol, review teams grouped key themes from the focus group discussions about discharge into 4 categories. The categories, with themes listed below and representative patient comments in the Table, were
- Coordination and timing of discharge
- Giving patients the opportunity to prepare for discussion with clinician teams
- Communicating the specific time of discharge
- Internal collaboration of inter-professional teams
- Preparing for transition out of the hospital
2. Communication
- Patient inclusion in care discussions
- Discharge summary delay and/or completeness
- Education at the time of discharge
3. Ramifications of the unexpected and unknown
- Increased stress and frustration due to inability to plan, fear of the unknown, and lack of information
4. Interpersonal interactions
- Both favorable and unfavorable interactions caused an emotional response that impacts perceptions of hospitalization and discharge
The reviewers also analyzed patients’ comments regarding the bedside e-Board. The medication display (“Durable Display at Discharge,” Figure 1) was universally considered to be the most relevant and best-liked of the 4 elements tested. The visual display of medications and their purpose were commonly referenced as the most positive aspects of the display, and patients and caregivers were readily able to generate multiple potential uses for the display. Several mentioned that the information on the medication display were so desirable and necessary that if not supplied by the hospital, they hand-crafted such reminder displays at home. 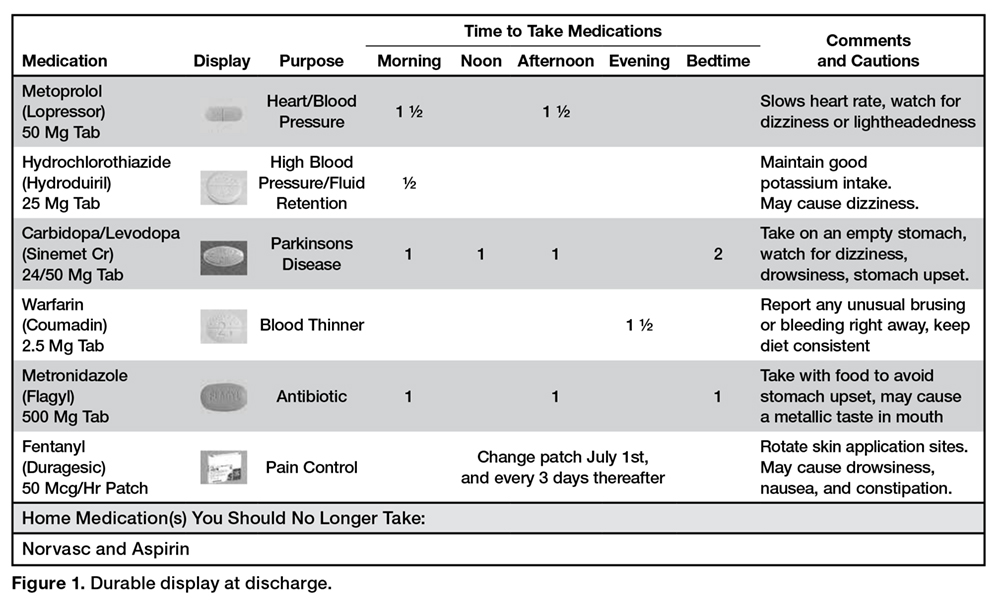
The display of the care team and rounding time was perceived as helpful in allowing patients and family members to coordinate schedules with family members or care partners who may wish to be present during rounds. Patients also favorably reviewed the discharge day and time display, although multiple comments were made that this information is only helpful if it is accurate. Discussion around discharge time evoked the most emotions of topics discussed and patients expressed frustration with the inaccuracy of discharge time communicated to them on the day of discharge. Elaborating on this sentiment, a patient specified, “I prefer they don’t tell me a time at all until they know for sure”, and another shared that, “there is only going to be frustration with that if you say 4 pm and it ends up being 7 pm.”
It was difficult for patients to see how the I-MOVE assessment (Figure 2) would apply to their discharge planning. They perceived I-MOVE as a tool for clinicians. One exception was a patient who had on a previous admission undergone heart surgery. She explained to the other patients that in such debilitated conditions, mobility independence assessments were important and commonly done. 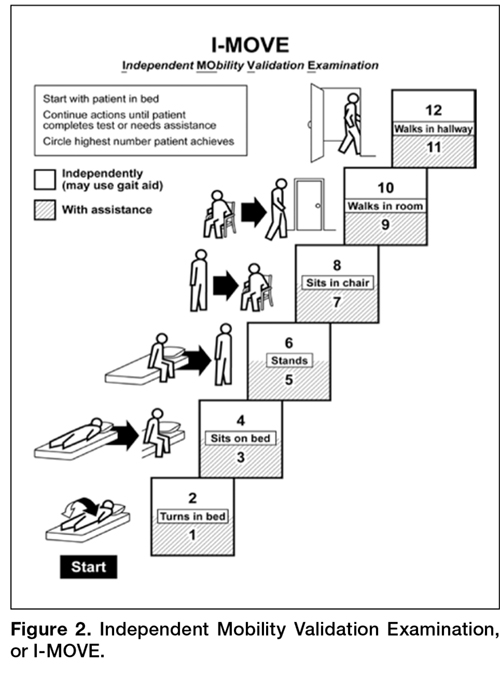
Patients voiced some skepticism and concerns regarding the e-Board, including expense, privacy, security, and cleanliness. One patient observed the tablet was “more current than a printed piece of paper. It’s more up to date.” Other patients, however, questioned the process required to update information and wondered how much electronic displays added compared to the dry-erase board already in each patient’s room with which they were more familiar. They also voiced concern that the tablet would replace face-to-face interactions with their care teams. A patient shared that, “if we don’t have the conversation and we just get it through this, then I would hate that…you want to be able to give your input.”
Discussion
In this study, we used available software to create a bedside e-Board that addressed opportunities for patient-centered improvement in our institution’s discharge process. Patients felt that 3 of 4 software tools on the tablet could enhance the discharge experience. Additionally, we explored patients’ expectations and perceptions of our hospital discharge process.
Key information to inform our current discharge process was divulged by our patients during focus groups. Patients conveyed that the only time that matters to them is the time they get to walk out the door of the hospital, and that general statements (eg, “You’ll probably be going home today.”) create anxiety and dissatisfaction. Since family and care partners need to manage hospital discharge in combination with regular activities of daily life (eg, work schedules, child care), un-communicated changes to the discharge time are very difficult to accommodate and should be discussed in advance. Further, acknowledging the disruption of hospital admission to patients’, their families’, and care partners’ daily lives, as well as being mindful of the impact of interpersonal interactions with patients, remind clinicians of the impact hospitalization has on patients.
Focus group discussions revealed that an ideal patient-centered discharge process would include active patient participation, clear communication regarding the discharge process, especially changes in the specific discharge date and time, and education regarding discharge summary instructions. Further, patients voiced that the unexpected nature of admissions can be very disruptive to patients’ lives and that interpersonal interactions during admission cause emotional responses in patients that influence their perceptions of hospitalization.
Comments regarding poor coordination and communication of internal processes, opportunities to improve collaboration within and across care teams, and need to improve communication with patients regarding timing of discharge and plan of care are consistent with recent studies that used focus groups to explore patient perceptions and expectations around discharge [3,4]. The ramifications of unexpected admissions and the emotional responses patients expressed regarding interpersonal interactions during admission have not been reported by others conducting patient focus groups.
The unexpected nature of many admissions, and the uncertainty of the day-to-day activities during hospitalization, caused patients anxiety and stress. These emotions perhaps heightened their response and memories of both favorable and unfavorable interpersonal interactions. These memories left lasting impressions on patients and care teams may help alleviate anxiety and stress by providing consistency and routine such as rounding at the same time daily, and communicating this time with patients. In this regard, the e-Board was helpful in communicating the patients’ care team and their planned rounding time.
Regarding the ability of e-tools to facilitate information sharing and planning for discharge, patients felt that the display of medications would have been most beneficial when thinking about post-discharge care. They perceived a display of discharge date and time estimate display as very useful to coordinate the activities around physically leaving the hospital, but based on their experiences did not find anticipated discharge times to be believable.
Patients’ perceptions of the tool were assessed after a recent hospitalization, and our data would have been strengthened had patients and their care partners used the e-Board during the actual admission. On the other hand, post-discharge, patients had time to reflect on opportunities for improving their recent admission and had insight into gaps in their discharge that the tool could potentially fill. Because we were unable to access video recordings from our dyad groups, which led us to exclude these participants, we lost care partners’ perceptions of the e-Board and discharge process. Care partners likely have different perceptions of discharge processes compared to patients, and their insight would have augmented our findings.
Several patients observed that the e-Board presented much of the same information that was filled out by care teams on the in-room dry erase boards and questioned whether the tablet was needed. These observations provide future opportunity for studies comparing display of discharge information on in-room dry-erase boards to an electronic tablet display. E-tools have shown some benefit when used for patient self-monitoring [10], to increase patient engagement [11,12], or to improve patient education [12]. Computer tablets may be most useful when used in these manners, compared to information display.
Focus groups provide patient-provided information that is readily actionable, and this work presents patient insight into discharge processes elicited through focus groups. Patients discussed their perceptions of an e-tool that might address patient-identified opportunities to improve the discharge process. Future work in this area will explore e-tools, and how best to leverage their functionality to design a patient-centered discharge process.
Acknowledgments: Our thanks to Mr. Thomas J. (Tripp) Welch for the original suggestion of this study design, and to Ms. Heidi Miller and Ms. Lizann Williams for their invaluable contributions to this work. A special thanks to our exceptional colleagues of the Mayo Clinic Department of Medicine Clinical Research Office Clinical Trials Unit for their efforts in executing this study, and to the study participants who participated in this research, without whom this project would not have been possible.
Corresponding author: Deanne Kashiwagi, MD, MS, 200 First Street SW, Rochester, MN 55902, [email protected].
Financial disclosures: None.
1. Coleman EA, Parry C, Chalmers S, et al. The care transitions intervention: results of a randomized controlled trial. Arch Intern Med 2006;166:1822–8.
2. Goncalves-Bradley DC, Lannin NA, Clemson LM, et al. Discharge planning from hospital. Cochrane Database Syst Rev 2016;1:CD000313.
3. Pinelli V, Stuckey HL, Gonzalo JD. Exploring challenges in the patient’s discharge process from the internal medicine service: A qualitative study of patients’ and providers’ perceptions. J Interprof Care 2017:1–9.
4. Neeman, N, Quinn K, Shoeb M, et al. Postdischarge focus groups to improve the hospital experience. Am J Med Qual 2013;28:536–8.
5. Jack, BW, Chetty VK, Anthony D, et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med 2009;150:178–87.
6. Manning, DM, Keller AS, Frank DL. Home alone: assessing mobility independence before discharge. J Hosp Med 2009;4:252–4.
7. Manning, DM, Tammel KJ, Blegen RN, et al. In-room display of day and time patient is anticipated to leave hospital: a “discharge appointment.” J Hosp Med 2007;2:13–6.
8. Manning, DM, O’Meara JG, Williams AR, et al. 3D: a tool for medication discharge education. Qual Saf Health Care 2007;16:71–6.
9. Vaismoradi M, Turunen H, Bondas T. Content analysis and thematic analysis: implications for conducting a qualitative descriptive study. Nurs Health Sci 2013;15:398–405.
10. Kampmeijer, R, Pavlova M, Tambor M, et al. The use of e-health and m-health tools in health promotion and primary prevention among older adults: a systematic literature review. BMC Health Serv Res 2016;16 Suppl 5:290.
11. Vawdrey, DK, Wilcox LG, Collins SA, et al. A tablet computer application for patients to participate in their hospital care. AMIA Annu Symp Proc 2011:1428–35.
12. Greysen, SR, Khanna RR, Jacolbia R, et al. Tablet computers for hospitalized patients: a pilot study to improve inpatient engagement. J Hosp Med 2014;9:396–9.
From the Mayo Clinic, Rochester, MN.
Abstract
- Objective: To elicit patient perceptions of a computer tablet (“e-Board”) used to display information relevant to hospital discharge and to gather patients’ expectations and perceptions regarding hospital discharge.
- Methods: Adult patients discharged from 1 of 3 medical-surgical, noncardiac monitored units of a 1265-bed, academic, tertiary care hospital were interviewed during patient focus groups. Reviewer pairs performed qualitative analysis of focus group transcripts and identified key themes, which were grouped into categories.
- Results: Patients felt a novel e-Board could help with the discharge process. They identified coordination of discharge, communication about discharge, ramifications of unexpected admissions, and interpersonal interactions during admission as the most significant issues around discharge.
- Conclusions: Focus groups elicit actionable information from patients about hospital discharge. Using this information, e-tools may help to design a patient-centered discharge process.
Key words: hospitals; patient satisfaction; focus groups; acute inpatient care.
Transition from the hospital to home represents a critical time for patients after acute illness, and support of patients and their care partners can help decrease consequences of poor care transitions, such as readmissions [1]. Focused discharge planning may improve outcomes and increase patient satisfaction [2], which is a key metric in hospital value-based purchasing programs, which tie Hospital Consumer Assessment of Healthcare Providers and Services (HCAHPS) survey scores to reimbursement. Although patient experience surveys explore several categories of patient satisfaction, HCAHPS may not reveal readily actionable opportunities that would allow clinicians to improve patient experience. Conducting focus groups and interviews can help discern patients’ perceptions and provide patient-centered opportunities to improve hospital discharge processes. Recent studies using these methodologies have revealed patients’ perceptions of barriers to inter-professional collaboration during discharge [3] and their desires and expectations of, as well as suggestions for improvement of, hospitalization [4].
Care transition bundles have been developed to facilitate the process of transitioning home [1,5], but none include e-health tools to help facilitate the discharge process. A study group leveraged available software at our institution to create a bedside “e-Board,” addressing opportunities that surfaced during previous patient focus groups regarding our institution’s discharge process. The software tools were loaded onto a tablet computer (Apple iPad; Cupertino, CA) and included displays of the patient’s physician and nurse, with estimated time of team bedside rounds; day and time of anticipated discharge; display of discharge medications; and a screening tool, I-MOVE, to assess mobility prior to return to independent living [6].
We conducted focus groups to gather patients’ insights for incorporation into a bedside e-health tool for discharge and into our hospital’s current discharge process. The primary objective of the current study was to elicit patient and family perceptions of a bedside e-Board, created to display information regarding discharge. Our secondary objective was to learn about patient expectations and perceptions regarding the hospital discharge process.
Methods
Setting
The study setting was 3 medical-surgical, non-cardiac monitored units of a 1265-bed, academic, tertiary care hospital in Rochester, MN. The study was considered a minimal risk study by the center’s institutional review board.
Participants
Patients aged 18 years or older discharged from 1 of the 3 study units during 2012–2013 were eligible to participate. Patients were excluded if they were not discharged home or to assisted living, were clinic employees, retirees or dependents of clinic employees, were hospitalized longer than 6 months prior to study entry, lived further than 60 miles from the town of Rochester, could not travel, or did not sign research consent.
There were 975 patients who met inclusion criteria. The institution’s survey research center randomly selected 300 eligible patients and contacted them by letter after discharge. The letter was followed up with a telephone call and verbal consent was obtained if the patient expressed interest in participation. Of the 17 patients who gave consent, 12 patients participated in focus group interviews.
E-Board Development
Prior focus group discussions facilitated by our institution’s marketing department (Mr. Kent Seltman, personal communication) explored patients’ perceptions of the discharge process from the institution’s primary hospital. The opportunities for improvement that surfaced during these focus groups included identifying the date of discharge, communication about the time of discharge, and discharging the patient at the identified time, not several hours later. The study group leveraged software available at our institution to create a bedside e-Board that could possibly mitigate these issues by improving communication about discharge. The software tools were loaded onto a tablet computer for patients to use as a resource during their admission. These tools included:
- A photo display of the patient’s nurse and physician, with estimated time of bedside rounds
- A display of the day and time of anticipated discharge. Providing anticipated day and time of discharge has been found to be an achievable goal for internal medicine and surgical services [7].
- A medication display, named the “Durable Display at Discharge,” previously found to improve patient understanding of prescribed medications [8]
- A display of a mobility tool, I-MOVE, designed to screen for debility that could prevent patients’ return to independent living [6].
Focus Groups
Facilitated interviews were conducted on 2 consecutive days in March 2014. Participants were divided into a focus group of 5 to 6 participants if they were functionally independent, or dyads of patient and care partner if they were functionally dependent. Interviews were both video- and audiotaped.
A trained facilitator led 1.5-hour sessions with each focus group. The sessions began with introductions and guidelines by which the focus groups were conducted, including explanations of the video and audio recording equipment, and a request for participants to speak one person at a time to facilitate recording. Discussions were carried out in 2 parts, guided by a facilitator script ( available from the authors). First, participants were asked to share their experiences regarding planning for discharge and the information they received leading up to their planned day and time of hospital discharge. Second, participants were shown a prototype of the e-Board. Participants were asked to reflect as to whether they had received similar information when they had been hospitalized, whether that information was helpful or useful, what information they did not receive that would have been helpful, how information was given, and whether information displayed via an e-Board would be better or worse than the ways they received information while in the hospital.
Data Analysis
Three teams, each comprised of 2 reviewers, met to analyze the video and audio recordings of each focus group. Unfortunately, the video files from the dyad interviews were not recoverable after the recorded sessions, and thus those groups were excluded from the study. Reviewers met prior to analyzing the focus group video and audio recordings to review the qualitative analysis protocol developed by the research team [9] (protocol available froom the authors). The teams then independently reviewed the video recordings and transcripts of the focus groups. The reviewer teams observed the focus group recordings and identified (1) themes regarding perceptions of the bedside e-Board and (2) experiences and perceptions around discharge. The protocol helped reviewer teams create a classification structure by identifying the key themes, which were then combined to create categories. The reviewer teams then compared their classification structures and by incorporating the most frequently identified categories, built a relational model of discharge perceptions.
Results
Eleven patients participated in 2 focus groups, one group of 5 patients and the other of 6 patients. Patient participants included 6 females and 5 males ranging in age from 22 to 84 years.
Using the qualitative analysis protocol, review teams grouped key themes from the focus group discussions about discharge into 4 categories. The categories, with themes listed below and representative patient comments in the Table, were
- Coordination and timing of discharge
- Giving patients the opportunity to prepare for discussion with clinician teams
- Communicating the specific time of discharge
- Internal collaboration of inter-professional teams
- Preparing for transition out of the hospital
2. Communication
- Patient inclusion in care discussions
- Discharge summary delay and/or completeness
- Education at the time of discharge
3. Ramifications of the unexpected and unknown
- Increased stress and frustration due to inability to plan, fear of the unknown, and lack of information
4. Interpersonal interactions
- Both favorable and unfavorable interactions caused an emotional response that impacts perceptions of hospitalization and discharge
The reviewers also analyzed patients’ comments regarding the bedside e-Board. The medication display (“Durable Display at Discharge,” Figure 1) was universally considered to be the most relevant and best-liked of the 4 elements tested. The visual display of medications and their purpose were commonly referenced as the most positive aspects of the display, and patients and caregivers were readily able to generate multiple potential uses for the display. Several mentioned that the information on the medication display were so desirable and necessary that if not supplied by the hospital, they hand-crafted such reminder displays at home.
The display of the care team and rounding time was perceived as helpful in allowing patients and family members to coordinate schedules with family members or care partners who may wish to be present during rounds. Patients also favorably reviewed the discharge day and time display, although multiple comments were made that this information is only helpful if it is accurate. Discussion around discharge time evoked the most emotions of topics discussed and patients expressed frustration with the inaccuracy of discharge time communicated to them on the day of discharge. Elaborating on this sentiment, a patient specified, “I prefer they don’t tell me a time at all until they know for sure”, and another shared that, “there is only going to be frustration with that if you say 4 pm and it ends up being 7 pm.”
It was difficult for patients to see how the I-MOVE assessment (Figure 2) would apply to their discharge planning. They perceived I-MOVE as a tool for clinicians. One exception was a patient who had on a previous admission undergone heart surgery. She explained to the other patients that in such debilitated conditions, mobility independence assessments were important and commonly done.
Patients voiced some skepticism and concerns regarding the e-Board, including expense, privacy, security, and cleanliness. One patient observed the tablet was “more current than a printed piece of paper. It’s more up to date.” Other patients, however, questioned the process required to update information and wondered how much electronic displays added compared to the dry-erase board already in each patient’s room with which they were more familiar. They also voiced concern that the tablet would replace face-to-face interactions with their care teams. A patient shared that, “if we don’t have the conversation and we just get it through this, then I would hate that…you want to be able to give your input.”
Discussion
In this study, we used available software to create a bedside e-Board that addressed opportunities for patient-centered improvement in our institution’s discharge process. Patients felt that 3 of 4 software tools on the tablet could enhance the discharge experience. Additionally, we explored patients’ expectations and perceptions of our hospital discharge process.
Key information to inform our current discharge process was divulged by our patients during focus groups. Patients conveyed that the only time that matters to them is the time they get to walk out the door of the hospital, and that general statements (eg, “You’ll probably be going home today.”) create anxiety and dissatisfaction. Since family and care partners need to manage hospital discharge in combination with regular activities of daily life (eg, work schedules, child care), un-communicated changes to the discharge time are very difficult to accommodate and should be discussed in advance. Further, acknowledging the disruption of hospital admission to patients’, their families’, and care partners’ daily lives, as well as being mindful of the impact of interpersonal interactions with patients, remind clinicians of the impact hospitalization has on patients.
Focus group discussions revealed that an ideal patient-centered discharge process would include active patient participation, clear communication regarding the discharge process, especially changes in the specific discharge date and time, and education regarding discharge summary instructions. Further, patients voiced that the unexpected nature of admissions can be very disruptive to patients’ lives and that interpersonal interactions during admission cause emotional responses in patients that influence their perceptions of hospitalization.
Comments regarding poor coordination and communication of internal processes, opportunities to improve collaboration within and across care teams, and need to improve communication with patients regarding timing of discharge and plan of care are consistent with recent studies that used focus groups to explore patient perceptions and expectations around discharge [3,4]. The ramifications of unexpected admissions and the emotional responses patients expressed regarding interpersonal interactions during admission have not been reported by others conducting patient focus groups.
The unexpected nature of many admissions, and the uncertainty of the day-to-day activities during hospitalization, caused patients anxiety and stress. These emotions perhaps heightened their response and memories of both favorable and unfavorable interpersonal interactions. These memories left lasting impressions on patients and care teams may help alleviate anxiety and stress by providing consistency and routine such as rounding at the same time daily, and communicating this time with patients. In this regard, the e-Board was helpful in communicating the patients’ care team and their planned rounding time.
Regarding the ability of e-tools to facilitate information sharing and planning for discharge, patients felt that the display of medications would have been most beneficial when thinking about post-discharge care. They perceived a display of discharge date and time estimate display as very useful to coordinate the activities around physically leaving the hospital, but based on their experiences did not find anticipated discharge times to be believable.
Patients’ perceptions of the tool were assessed after a recent hospitalization, and our data would have been strengthened had patients and their care partners used the e-Board during the actual admission. On the other hand, post-discharge, patients had time to reflect on opportunities for improving their recent admission and had insight into gaps in their discharge that the tool could potentially fill. Because we were unable to access video recordings from our dyad groups, which led us to exclude these participants, we lost care partners’ perceptions of the e-Board and discharge process. Care partners likely have different perceptions of discharge processes compared to patients, and their insight would have augmented our findings.
Several patients observed that the e-Board presented much of the same information that was filled out by care teams on the in-room dry erase boards and questioned whether the tablet was needed. These observations provide future opportunity for studies comparing display of discharge information on in-room dry-erase boards to an electronic tablet display. E-tools have shown some benefit when used for patient self-monitoring [10], to increase patient engagement [11,12], or to improve patient education [12]. Computer tablets may be most useful when used in these manners, compared to information display.
Focus groups provide patient-provided information that is readily actionable, and this work presents patient insight into discharge processes elicited through focus groups. Patients discussed their perceptions of an e-tool that might address patient-identified opportunities to improve the discharge process. Future work in this area will explore e-tools, and how best to leverage their functionality to design a patient-centered discharge process.
Acknowledgments: Our thanks to Mr. Thomas J. (Tripp) Welch for the original suggestion of this study design, and to Ms. Heidi Miller and Ms. Lizann Williams for their invaluable contributions to this work. A special thanks to our exceptional colleagues of the Mayo Clinic Department of Medicine Clinical Research Office Clinical Trials Unit for their efforts in executing this study, and to the study participants who participated in this research, without whom this project would not have been possible.
Corresponding author: Deanne Kashiwagi, MD, MS, 200 First Street SW, Rochester, MN 55902, [email protected].
Financial disclosures: None.
From the Mayo Clinic, Rochester, MN.
Abstract
- Objective: To elicit patient perceptions of a computer tablet (“e-Board”) used to display information relevant to hospital discharge and to gather patients’ expectations and perceptions regarding hospital discharge.
- Methods: Adult patients discharged from 1 of 3 medical-surgical, noncardiac monitored units of a 1265-bed, academic, tertiary care hospital were interviewed during patient focus groups. Reviewer pairs performed qualitative analysis of focus group transcripts and identified key themes, which were grouped into categories.
- Results: Patients felt a novel e-Board could help with the discharge process. They identified coordination of discharge, communication about discharge, ramifications of unexpected admissions, and interpersonal interactions during admission as the most significant issues around discharge.
- Conclusions: Focus groups elicit actionable information from patients about hospital discharge. Using this information, e-tools may help to design a patient-centered discharge process.
Key words: hospitals; patient satisfaction; focus groups; acute inpatient care.
Transition from the hospital to home represents a critical time for patients after acute illness, and support of patients and their care partners can help decrease consequences of poor care transitions, such as readmissions [1]. Focused discharge planning may improve outcomes and increase patient satisfaction [2], which is a key metric in hospital value-based purchasing programs, which tie Hospital Consumer Assessment of Healthcare Providers and Services (HCAHPS) survey scores to reimbursement. Although patient experience surveys explore several categories of patient satisfaction, HCAHPS may not reveal readily actionable opportunities that would allow clinicians to improve patient experience. Conducting focus groups and interviews can help discern patients’ perceptions and provide patient-centered opportunities to improve hospital discharge processes. Recent studies using these methodologies have revealed patients’ perceptions of barriers to inter-professional collaboration during discharge [3] and their desires and expectations of, as well as suggestions for improvement of, hospitalization [4].
Care transition bundles have been developed to facilitate the process of transitioning home [1,5], but none include e-health tools to help facilitate the discharge process. A study group leveraged available software at our institution to create a bedside “e-Board,” addressing opportunities that surfaced during previous patient focus groups regarding our institution’s discharge process. The software tools were loaded onto a tablet computer (Apple iPad; Cupertino, CA) and included displays of the patient’s physician and nurse, with estimated time of team bedside rounds; day and time of anticipated discharge; display of discharge medications; and a screening tool, I-MOVE, to assess mobility prior to return to independent living [6].
We conducted focus groups to gather patients’ insights for incorporation into a bedside e-health tool for discharge and into our hospital’s current discharge process. The primary objective of the current study was to elicit patient and family perceptions of a bedside e-Board, created to display information regarding discharge. Our secondary objective was to learn about patient expectations and perceptions regarding the hospital discharge process.
Methods
Setting
The study setting was 3 medical-surgical, non-cardiac monitored units of a 1265-bed, academic, tertiary care hospital in Rochester, MN. The study was considered a minimal risk study by the center’s institutional review board.
Participants
Patients aged 18 years or older discharged from 1 of the 3 study units during 2012–2013 were eligible to participate. Patients were excluded if they were not discharged home or to assisted living, were clinic employees, retirees or dependents of clinic employees, were hospitalized longer than 6 months prior to study entry, lived further than 60 miles from the town of Rochester, could not travel, or did not sign research consent.
There were 975 patients who met inclusion criteria. The institution’s survey research center randomly selected 300 eligible patients and contacted them by letter after discharge. The letter was followed up with a telephone call and verbal consent was obtained if the patient expressed interest in participation. Of the 17 patients who gave consent, 12 patients participated in focus group interviews.
E-Board Development
Prior focus group discussions facilitated by our institution’s marketing department (Mr. Kent Seltman, personal communication) explored patients’ perceptions of the discharge process from the institution’s primary hospital. The opportunities for improvement that surfaced during these focus groups included identifying the date of discharge, communication about the time of discharge, and discharging the patient at the identified time, not several hours later. The study group leveraged software available at our institution to create a bedside e-Board that could possibly mitigate these issues by improving communication about discharge. The software tools were loaded onto a tablet computer for patients to use as a resource during their admission. These tools included:
- A photo display of the patient’s nurse and physician, with estimated time of bedside rounds
- A display of the day and time of anticipated discharge. Providing anticipated day and time of discharge has been found to be an achievable goal for internal medicine and surgical services [7].
- A medication display, named the “Durable Display at Discharge,” previously found to improve patient understanding of prescribed medications [8]
- A display of a mobility tool, I-MOVE, designed to screen for debility that could prevent patients’ return to independent living [6].
Focus Groups
Facilitated interviews were conducted on 2 consecutive days in March 2014. Participants were divided into a focus group of 5 to 6 participants if they were functionally independent, or dyads of patient and care partner if they were functionally dependent. Interviews were both video- and audiotaped.
A trained facilitator led 1.5-hour sessions with each focus group. The sessions began with introductions and guidelines by which the focus groups were conducted, including explanations of the video and audio recording equipment, and a request for participants to speak one person at a time to facilitate recording. Discussions were carried out in 2 parts, guided by a facilitator script ( available from the authors). First, participants were asked to share their experiences regarding planning for discharge and the information they received leading up to their planned day and time of hospital discharge. Second, participants were shown a prototype of the e-Board. Participants were asked to reflect as to whether they had received similar information when they had been hospitalized, whether that information was helpful or useful, what information they did not receive that would have been helpful, how information was given, and whether information displayed via an e-Board would be better or worse than the ways they received information while in the hospital.
Data Analysis
Three teams, each comprised of 2 reviewers, met to analyze the video and audio recordings of each focus group. Unfortunately, the video files from the dyad interviews were not recoverable after the recorded sessions, and thus those groups were excluded from the study. Reviewers met prior to analyzing the focus group video and audio recordings to review the qualitative analysis protocol developed by the research team [9] (protocol available froom the authors). The teams then independently reviewed the video recordings and transcripts of the focus groups. The reviewer teams observed the focus group recordings and identified (1) themes regarding perceptions of the bedside e-Board and (2) experiences and perceptions around discharge. The protocol helped reviewer teams create a classification structure by identifying the key themes, which were then combined to create categories. The reviewer teams then compared their classification structures and by incorporating the most frequently identified categories, built a relational model of discharge perceptions.
Results
Eleven patients participated in 2 focus groups, one group of 5 patients and the other of 6 patients. Patient participants included 6 females and 5 males ranging in age from 22 to 84 years.
Using the qualitative analysis protocol, review teams grouped key themes from the focus group discussions about discharge into 4 categories. The categories, with themes listed below and representative patient comments in the Table, were
- Coordination and timing of discharge
- Giving patients the opportunity to prepare for discussion with clinician teams
- Communicating the specific time of discharge
- Internal collaboration of inter-professional teams
- Preparing for transition out of the hospital
2. Communication
- Patient inclusion in care discussions
- Discharge summary delay and/or completeness
- Education at the time of discharge
3. Ramifications of the unexpected and unknown
- Increased stress and frustration due to inability to plan, fear of the unknown, and lack of information
4. Interpersonal interactions
- Both favorable and unfavorable interactions caused an emotional response that impacts perceptions of hospitalization and discharge
The reviewers also analyzed patients’ comments regarding the bedside e-Board. The medication display (“Durable Display at Discharge,” Figure 1) was universally considered to be the most relevant and best-liked of the 4 elements tested. The visual display of medications and their purpose were commonly referenced as the most positive aspects of the display, and patients and caregivers were readily able to generate multiple potential uses for the display. Several mentioned that the information on the medication display were so desirable and necessary that if not supplied by the hospital, they hand-crafted such reminder displays at home.
The display of the care team and rounding time was perceived as helpful in allowing patients and family members to coordinate schedules with family members or care partners who may wish to be present during rounds. Patients also favorably reviewed the discharge day and time display, although multiple comments were made that this information is only helpful if it is accurate. Discussion around discharge time evoked the most emotions of topics discussed and patients expressed frustration with the inaccuracy of discharge time communicated to them on the day of discharge. Elaborating on this sentiment, a patient specified, “I prefer they don’t tell me a time at all until they know for sure”, and another shared that, “there is only going to be frustration with that if you say 4 pm and it ends up being 7 pm.”
It was difficult for patients to see how the I-MOVE assessment (Figure 2) would apply to their discharge planning. They perceived I-MOVE as a tool for clinicians. One exception was a patient who had on a previous admission undergone heart surgery. She explained to the other patients that in such debilitated conditions, mobility independence assessments were important and commonly done.
Patients voiced some skepticism and concerns regarding the e-Board, including expense, privacy, security, and cleanliness. One patient observed the tablet was “more current than a printed piece of paper. It’s more up to date.” Other patients, however, questioned the process required to update information and wondered how much electronic displays added compared to the dry-erase board already in each patient’s room with which they were more familiar. They also voiced concern that the tablet would replace face-to-face interactions with their care teams. A patient shared that, “if we don’t have the conversation and we just get it through this, then I would hate that…you want to be able to give your input.”
Discussion
In this study, we used available software to create a bedside e-Board that addressed opportunities for patient-centered improvement in our institution’s discharge process. Patients felt that 3 of 4 software tools on the tablet could enhance the discharge experience. Additionally, we explored patients’ expectations and perceptions of our hospital discharge process.
Key information to inform our current discharge process was divulged by our patients during focus groups. Patients conveyed that the only time that matters to them is the time they get to walk out the door of the hospital, and that general statements (eg, “You’ll probably be going home today.”) create anxiety and dissatisfaction. Since family and care partners need to manage hospital discharge in combination with regular activities of daily life (eg, work schedules, child care), un-communicated changes to the discharge time are very difficult to accommodate and should be discussed in advance. Further, acknowledging the disruption of hospital admission to patients’, their families’, and care partners’ daily lives, as well as being mindful of the impact of interpersonal interactions with patients, remind clinicians of the impact hospitalization has on patients.
Focus group discussions revealed that an ideal patient-centered discharge process would include active patient participation, clear communication regarding the discharge process, especially changes in the specific discharge date and time, and education regarding discharge summary instructions. Further, patients voiced that the unexpected nature of admissions can be very disruptive to patients’ lives and that interpersonal interactions during admission cause emotional responses in patients that influence their perceptions of hospitalization.
Comments regarding poor coordination and communication of internal processes, opportunities to improve collaboration within and across care teams, and need to improve communication with patients regarding timing of discharge and plan of care are consistent with recent studies that used focus groups to explore patient perceptions and expectations around discharge [3,4]. The ramifications of unexpected admissions and the emotional responses patients expressed regarding interpersonal interactions during admission have not been reported by others conducting patient focus groups.
The unexpected nature of many admissions, and the uncertainty of the day-to-day activities during hospitalization, caused patients anxiety and stress. These emotions perhaps heightened their response and memories of both favorable and unfavorable interpersonal interactions. These memories left lasting impressions on patients and care teams may help alleviate anxiety and stress by providing consistency and routine such as rounding at the same time daily, and communicating this time with patients. In this regard, the e-Board was helpful in communicating the patients’ care team and their planned rounding time.
Regarding the ability of e-tools to facilitate information sharing and planning for discharge, patients felt that the display of medications would have been most beneficial when thinking about post-discharge care. They perceived a display of discharge date and time estimate display as very useful to coordinate the activities around physically leaving the hospital, but based on their experiences did not find anticipated discharge times to be believable.
Patients’ perceptions of the tool were assessed after a recent hospitalization, and our data would have been strengthened had patients and their care partners used the e-Board during the actual admission. On the other hand, post-discharge, patients had time to reflect on opportunities for improving their recent admission and had insight into gaps in their discharge that the tool could potentially fill. Because we were unable to access video recordings from our dyad groups, which led us to exclude these participants, we lost care partners’ perceptions of the e-Board and discharge process. Care partners likely have different perceptions of discharge processes compared to patients, and their insight would have augmented our findings.
Several patients observed that the e-Board presented much of the same information that was filled out by care teams on the in-room dry erase boards and questioned whether the tablet was needed. These observations provide future opportunity for studies comparing display of discharge information on in-room dry-erase boards to an electronic tablet display. E-tools have shown some benefit when used for patient self-monitoring [10], to increase patient engagement [11,12], or to improve patient education [12]. Computer tablets may be most useful when used in these manners, compared to information display.
Focus groups provide patient-provided information that is readily actionable, and this work presents patient insight into discharge processes elicited through focus groups. Patients discussed their perceptions of an e-tool that might address patient-identified opportunities to improve the discharge process. Future work in this area will explore e-tools, and how best to leverage their functionality to design a patient-centered discharge process.
Acknowledgments: Our thanks to Mr. Thomas J. (Tripp) Welch for the original suggestion of this study design, and to Ms. Heidi Miller and Ms. Lizann Williams for their invaluable contributions to this work. A special thanks to our exceptional colleagues of the Mayo Clinic Department of Medicine Clinical Research Office Clinical Trials Unit for their efforts in executing this study, and to the study participants who participated in this research, without whom this project would not have been possible.
Corresponding author: Deanne Kashiwagi, MD, MS, 200 First Street SW, Rochester, MN 55902, [email protected].
Financial disclosures: None.
1. Coleman EA, Parry C, Chalmers S, et al. The care transitions intervention: results of a randomized controlled trial. Arch Intern Med 2006;166:1822–8.
2. Goncalves-Bradley DC, Lannin NA, Clemson LM, et al. Discharge planning from hospital. Cochrane Database Syst Rev 2016;1:CD000313.
3. Pinelli V, Stuckey HL, Gonzalo JD. Exploring challenges in the patient’s discharge process from the internal medicine service: A qualitative study of patients’ and providers’ perceptions. J Interprof Care 2017:1–9.
4. Neeman, N, Quinn K, Shoeb M, et al. Postdischarge focus groups to improve the hospital experience. Am J Med Qual 2013;28:536–8.
5. Jack, BW, Chetty VK, Anthony D, et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med 2009;150:178–87.
6. Manning, DM, Keller AS, Frank DL. Home alone: assessing mobility independence before discharge. J Hosp Med 2009;4:252–4.
7. Manning, DM, Tammel KJ, Blegen RN, et al. In-room display of day and time patient is anticipated to leave hospital: a “discharge appointment.” J Hosp Med 2007;2:13–6.
8. Manning, DM, O’Meara JG, Williams AR, et al. 3D: a tool for medication discharge education. Qual Saf Health Care 2007;16:71–6.
9. Vaismoradi M, Turunen H, Bondas T. Content analysis and thematic analysis: implications for conducting a qualitative descriptive study. Nurs Health Sci 2013;15:398–405.
10. Kampmeijer, R, Pavlova M, Tambor M, et al. The use of e-health and m-health tools in health promotion and primary prevention among older adults: a systematic literature review. BMC Health Serv Res 2016;16 Suppl 5:290.
11. Vawdrey, DK, Wilcox LG, Collins SA, et al. A tablet computer application for patients to participate in their hospital care. AMIA Annu Symp Proc 2011:1428–35.
12. Greysen, SR, Khanna RR, Jacolbia R, et al. Tablet computers for hospitalized patients: a pilot study to improve inpatient engagement. J Hosp Med 2014;9:396–9.
1. Coleman EA, Parry C, Chalmers S, et al. The care transitions intervention: results of a randomized controlled trial. Arch Intern Med 2006;166:1822–8.
2. Goncalves-Bradley DC, Lannin NA, Clemson LM, et al. Discharge planning from hospital. Cochrane Database Syst Rev 2016;1:CD000313.
3. Pinelli V, Stuckey HL, Gonzalo JD. Exploring challenges in the patient’s discharge process from the internal medicine service: A qualitative study of patients’ and providers’ perceptions. J Interprof Care 2017:1–9.
4. Neeman, N, Quinn K, Shoeb M, et al. Postdischarge focus groups to improve the hospital experience. Am J Med Qual 2013;28:536–8.
5. Jack, BW, Chetty VK, Anthony D, et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med 2009;150:178–87.
6. Manning, DM, Keller AS, Frank DL. Home alone: assessing mobility independence before discharge. J Hosp Med 2009;4:252–4.
7. Manning, DM, Tammel KJ, Blegen RN, et al. In-room display of day and time patient is anticipated to leave hospital: a “discharge appointment.” J Hosp Med 2007;2:13–6.
8. Manning, DM, O’Meara JG, Williams AR, et al. 3D: a tool for medication discharge education. Qual Saf Health Care 2007;16:71–6.
9. Vaismoradi M, Turunen H, Bondas T. Content analysis and thematic analysis: implications for conducting a qualitative descriptive study. Nurs Health Sci 2013;15:398–405.
10. Kampmeijer, R, Pavlova M, Tambor M, et al. The use of e-health and m-health tools in health promotion and primary prevention among older adults: a systematic literature review. BMC Health Serv Res 2016;16 Suppl 5:290.
11. Vawdrey, DK, Wilcox LG, Collins SA, et al. A tablet computer application for patients to participate in their hospital care. AMIA Annu Symp Proc 2011:1428–35.
12. Greysen, SR, Khanna RR, Jacolbia R, et al. Tablet computers for hospitalized patients: a pilot study to improve inpatient engagement. J Hosp Med 2014;9:396–9.
Endobronchial Valves for Severe Emphysema
Study Overview
Objective. To evaluate the efficacy and safety of Zephyr endobronchial valves (EBVs) in patients with heterogeneous emphysema and absence of collateral ventilation.
Design. Multicenter, randomized, nonblinded clinical trial.
Setting and participants. This study was conducted at 17 sites across Europe between 2014 and 2016. Patients with severe emphysema who were ex-smokers and ≥ 40 years old were recruited. Key inclusion criteria were post-bronchodilator FEV1 between 15%–45% predicted despite optimal medical management, total lung capacity greater than 100% predicted, residual volume ≥ 180% predicted, and a 6-minute walk distance of between 150 and 450 meters. Heterogenous emphysema was defined as a greater than 10% difference in destruction score between target and ipsilateral lobes as measured by high-resolution CT. All eligible patients underwent Chartis pulmonary assessment (Pulmonx, Redwood City, CA) assessment to determine the presence of collateral ventilation between the target and adjacent lobes, and patients with collateral ventilation were excluded.
Intervention. Patients were randomized 2:1 to either EBV plus standard of care (intervention) or standard of care alone (control) by blocked design and concealed envelopes. The EBV group underwent immediate placement of Zephyr EBVs with the intention of complete lobar occlusion.
Main outcome measures. The primary outcome at 3 months post-procedure was the percentage of subjects with FEV1 improvement from baseline of 12% or greater. Changes in FEV1, residual volume, 6-minute walk distance, St. George’s Respiratory Questionnaire score and modified Medical Research Council score were assessed at 3 and 6 months and target lobe volume reduction on chest CT at 3 months.
Main results. 97 subjects were randomized to the intervention (n = 65) or control group (n = 32). At 3 months, 55.4% of intervention and 6.5% of control subjects had an FEV1 improvement of 12% or more (P < 0.001). Improvements were maintained at 6 months: intervention, 56.3%, versus control, 3.2% (P < 0.001), with a mean ± SD change in FEV1% at 6 months of 20.7 ± 29.6% and –8.6 ± 13.0%, respectively. A total of 89.8% of intervention subjects had target lobe volume reduction greater than or equal to 350 mL (mean, 1.09 ± 0.62 L; P < 0.001). The differences in outcomes between the intervention and control groups were statistically significant, with the following measured differences: residual volume, –700 m; 6-minute walk distance, +78.7 m; St. George’s Respiratory Questionnaire score, –6.5 points; modified Medical Research Council dyspnea score, –0.6 points; and BODE (body mass index, airflow obstruction, dyspnea, and exercise capacity) index, –1.8 points (all P < 0.05). Pneumothorax was the most common adverse event, occurring in 19 of 65 (29.2%) of intervention subjects.
Conclusion. Endobronchial valve treatment in hyperinflated patients with heterogeneous emphysema without collateral ventilation resulted in clinically meaningful benefits in lung function, dyspnea, exercise tolerance and quality of life, with an acceptable safety profile.
Commentary
Patients with severe emphysema are difficult to manage. Optimal medical management is required to maintain their lung function and quality of life, with combination bronchodilators (long-acting beta 2 agonists, long-acting anticholinergics, and inhaled corticosteroids), roflumilast (selective phosphodiesterase-4 inhibitors), oral corticosteroids or macrolide antibiotics when indicated, long-term oxygen, and noninvasive ventilator support. Palliative team care consultation and support, adequate nutritional support, influenza and pneumococcal vaccination, and pulmonary rehabilitation/graded exercise training are important aspects of emphysema treatment [1].
To help patients with severe emphysema who experience further decline despite intensive medical management, a lung volume reduction strategy was devised. In 2003, the NETT trial was conducted [2]. In this study, lung volume reduction surgery was performed in 608 patients, who were followed for 29 months. This study revealed a lack of survival benefit with significant immediate postoperative mortality and complication rate. Despite this disappointing result, a subgroup of patients (upper-lobe predominant disease and low baseline exercise capacity) had a statistically significant mortality benefit from surgery.
Since then, many have sought to determine a less invasive method of lung volume reduction. So far, one-way endobronchial valves, self-activating coils, and targeted destruction and remodeling of emphysematous lung with vapor or sealant methods have been studied. Several studies have examined the efficacy and safety of coils, with reasonable improvement of 6-minute walk distance and FEV1; however, complications including death, pneumothorax and pneumonia were noted. Vapor ablation (STEP-UP trial) [3] and lung sealant [4] were also attempted in order to achieve lung volume reduction, but increased infection was problematic. The 2017 GOLD guidelines suggested lung volume reduction by endobronchial one-way valve or lung coils as interventional bronchoscopic options for lung volume reduction [1].
Two types of endobronchial valves have been introduced to date: the intra bronchial valve, developed by Olympus, and the Zephyr valve by Pulmonx. Endobronchial valves are deployed to the bronchi via bronchoscopic guidance, and limit airflow to the portions of the lung distal to the valve while allowing mucus and air movement in the proximal direction. The VENT study, the largest endobronchial valve trial using the Zephyr valve, was published in 2010 [5]. This study demonstrated the efficacy of endobronchial valve treatment, especially in patients with heterogeneous emphysema and complete interlobar fissures as opposed to homogeneous emphysema and incomplete interlobar fissures. Subsequent studies demonstrated the importance of absence of collateral ventilation, measured by the Chartis system, when considering endobronchial valves [6].
The current study by Kemp et al is the first multicenter randomized endobronchial valve trial conducted in Europe. The study was able to demonstrate remarkable improvement in FEV1 (mean 140 mL decrease vs 90 mL increase) and 6-minute walk distance (mean +36.2 meter vs –42.5 meter) after endobronchial valve treatment in severe emphysema patients. The amount of volume reduction was reaching up to 2 liters. Patients in the control group were given the opportunity to receive endobronchial valve after the 6 months study follow-up period and 30 out of 32 patients opted for the endobronchial valve treatment. The authors concluded that the endobronchial valve therapy resulted in clinically meaningful benefits in lung function, dyspnea, exercise tolerance and quality of life with an acceptable safety profile.
It is notable that the authors included only selected patients, limited to those with presence of heterogeneous emphysema, absence of collateral ventilation, low risk of COPD exacerbation or infection, and patients who were likely able to tolerate pneumothorax. Despite this, 13 patients developed pneumothorax and death occurred in 1 patient, leading to a significantly longer average length of hospital stay in the treatment group. Although this rate of complications is not higher than prior endobronchial valve studies, it is important to note when broadly applying the outcomes of this study to patient care. Lack of long-term follow-up and the nonblinded study design also limit the strength of this study.
Applications for Clinical Practice
Many patients suffer from emphysema. Among them, severe emphysema is the most difficult to manage. It is important to incorporate optimal medical management including bronchodilators, palliative care, oxygen therapy, pulmonary rehabilitation and non-invasive ventilation options. When patients with severe emphysema continue to decline or seek further improvement in their care, and when they meet the specific criteria for lung volume reduction, endobronchial valve therapy should be considered an option and physicians should refer them to appropriate centers. However, the risk of complications, such as pneumothorax, still remains high.
—Minkyung Kwon, MD, Pulmonary and Critical Care Medicine, Mayo Clinic Florida, Jacksonville, FL, and Joel Roberson, MD, Department of Radiology, William Beaumont Hospital, Royal Oak, MI
1. The Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2017.
2. Weinmann GG, Chiang YP, Sheingold S. The National Emphysema Treatment Trial (NETT): a study in agency collaboration. Proc Am Thorac Soc 2008;5:381–4.
3. Herth FJ, Valipour A, Shah PL, et al. Segmental volume reduction using thermal vapour ablation in patients with severe emphysema: 6-month results of the multicentre, parallel-group, open-label, randomised controlled STEP-UP trial. Lancet Respir Med 2016;4:185–93.
4. Come CE, Kramer MR, Dransfield MT, et al. A randomised trial of lung sealant versus medical therapy for advanced emphysema. Eur Respir J 2015;46:651–62.
5. Sciurba FC, Ernst A, Herth FJ, et al. A randomized study of endobronchial valves for advanced emphysema. N Engl J Med 2010;363:1233–44.
6. Klooster K, ten Hacken NH, Hartman JE, et al. Endobronchial valves for emphysema without interlobar collateral ventilation. N Engl J Med 2015;373:2325–35.
Study Overview
Objective. To evaluate the efficacy and safety of Zephyr endobronchial valves (EBVs) in patients with heterogeneous emphysema and absence of collateral ventilation.
Design. Multicenter, randomized, nonblinded clinical trial.
Setting and participants. This study was conducted at 17 sites across Europe between 2014 and 2016. Patients with severe emphysema who were ex-smokers and ≥ 40 years old were recruited. Key inclusion criteria were post-bronchodilator FEV1 between 15%–45% predicted despite optimal medical management, total lung capacity greater than 100% predicted, residual volume ≥ 180% predicted, and a 6-minute walk distance of between 150 and 450 meters. Heterogenous emphysema was defined as a greater than 10% difference in destruction score between target and ipsilateral lobes as measured by high-resolution CT. All eligible patients underwent Chartis pulmonary assessment (Pulmonx, Redwood City, CA) assessment to determine the presence of collateral ventilation between the target and adjacent lobes, and patients with collateral ventilation were excluded.
Intervention. Patients were randomized 2:1 to either EBV plus standard of care (intervention) or standard of care alone (control) by blocked design and concealed envelopes. The EBV group underwent immediate placement of Zephyr EBVs with the intention of complete lobar occlusion.
Main outcome measures. The primary outcome at 3 months post-procedure was the percentage of subjects with FEV1 improvement from baseline of 12% or greater. Changes in FEV1, residual volume, 6-minute walk distance, St. George’s Respiratory Questionnaire score and modified Medical Research Council score were assessed at 3 and 6 months and target lobe volume reduction on chest CT at 3 months.
Main results. 97 subjects were randomized to the intervention (n = 65) or control group (n = 32). At 3 months, 55.4% of intervention and 6.5% of control subjects had an FEV1 improvement of 12% or more (P < 0.001). Improvements were maintained at 6 months: intervention, 56.3%, versus control, 3.2% (P < 0.001), with a mean ± SD change in FEV1% at 6 months of 20.7 ± 29.6% and –8.6 ± 13.0%, respectively. A total of 89.8% of intervention subjects had target lobe volume reduction greater than or equal to 350 mL (mean, 1.09 ± 0.62 L; P < 0.001). The differences in outcomes between the intervention and control groups were statistically significant, with the following measured differences: residual volume, –700 m; 6-minute walk distance, +78.7 m; St. George’s Respiratory Questionnaire score, –6.5 points; modified Medical Research Council dyspnea score, –0.6 points; and BODE (body mass index, airflow obstruction, dyspnea, and exercise capacity) index, –1.8 points (all P < 0.05). Pneumothorax was the most common adverse event, occurring in 19 of 65 (29.2%) of intervention subjects.
Conclusion. Endobronchial valve treatment in hyperinflated patients with heterogeneous emphysema without collateral ventilation resulted in clinically meaningful benefits in lung function, dyspnea, exercise tolerance and quality of life, with an acceptable safety profile.
Commentary
Patients with severe emphysema are difficult to manage. Optimal medical management is required to maintain their lung function and quality of life, with combination bronchodilators (long-acting beta 2 agonists, long-acting anticholinergics, and inhaled corticosteroids), roflumilast (selective phosphodiesterase-4 inhibitors), oral corticosteroids or macrolide antibiotics when indicated, long-term oxygen, and noninvasive ventilator support. Palliative team care consultation and support, adequate nutritional support, influenza and pneumococcal vaccination, and pulmonary rehabilitation/graded exercise training are important aspects of emphysema treatment [1].
To help patients with severe emphysema who experience further decline despite intensive medical management, a lung volume reduction strategy was devised. In 2003, the NETT trial was conducted [2]. In this study, lung volume reduction surgery was performed in 608 patients, who were followed for 29 months. This study revealed a lack of survival benefit with significant immediate postoperative mortality and complication rate. Despite this disappointing result, a subgroup of patients (upper-lobe predominant disease and low baseline exercise capacity) had a statistically significant mortality benefit from surgery.
Since then, many have sought to determine a less invasive method of lung volume reduction. So far, one-way endobronchial valves, self-activating coils, and targeted destruction and remodeling of emphysematous lung with vapor or sealant methods have been studied. Several studies have examined the efficacy and safety of coils, with reasonable improvement of 6-minute walk distance and FEV1; however, complications including death, pneumothorax and pneumonia were noted. Vapor ablation (STEP-UP trial) [3] and lung sealant [4] were also attempted in order to achieve lung volume reduction, but increased infection was problematic. The 2017 GOLD guidelines suggested lung volume reduction by endobronchial one-way valve or lung coils as interventional bronchoscopic options for lung volume reduction [1].
Two types of endobronchial valves have been introduced to date: the intra bronchial valve, developed by Olympus, and the Zephyr valve by Pulmonx. Endobronchial valves are deployed to the bronchi via bronchoscopic guidance, and limit airflow to the portions of the lung distal to the valve while allowing mucus and air movement in the proximal direction. The VENT study, the largest endobronchial valve trial using the Zephyr valve, was published in 2010 [5]. This study demonstrated the efficacy of endobronchial valve treatment, especially in patients with heterogeneous emphysema and complete interlobar fissures as opposed to homogeneous emphysema and incomplete interlobar fissures. Subsequent studies demonstrated the importance of absence of collateral ventilation, measured by the Chartis system, when considering endobronchial valves [6].
The current study by Kemp et al is the first multicenter randomized endobronchial valve trial conducted in Europe. The study was able to demonstrate remarkable improvement in FEV1 (mean 140 mL decrease vs 90 mL increase) and 6-minute walk distance (mean +36.2 meter vs –42.5 meter) after endobronchial valve treatment in severe emphysema patients. The amount of volume reduction was reaching up to 2 liters. Patients in the control group were given the opportunity to receive endobronchial valve after the 6 months study follow-up period and 30 out of 32 patients opted for the endobronchial valve treatment. The authors concluded that the endobronchial valve therapy resulted in clinically meaningful benefits in lung function, dyspnea, exercise tolerance and quality of life with an acceptable safety profile.
It is notable that the authors included only selected patients, limited to those with presence of heterogeneous emphysema, absence of collateral ventilation, low risk of COPD exacerbation or infection, and patients who were likely able to tolerate pneumothorax. Despite this, 13 patients developed pneumothorax and death occurred in 1 patient, leading to a significantly longer average length of hospital stay in the treatment group. Although this rate of complications is not higher than prior endobronchial valve studies, it is important to note when broadly applying the outcomes of this study to patient care. Lack of long-term follow-up and the nonblinded study design also limit the strength of this study.
Applications for Clinical Practice
Many patients suffer from emphysema. Among them, severe emphysema is the most difficult to manage. It is important to incorporate optimal medical management including bronchodilators, palliative care, oxygen therapy, pulmonary rehabilitation and non-invasive ventilation options. When patients with severe emphysema continue to decline or seek further improvement in their care, and when they meet the specific criteria for lung volume reduction, endobronchial valve therapy should be considered an option and physicians should refer them to appropriate centers. However, the risk of complications, such as pneumothorax, still remains high.
—Minkyung Kwon, MD, Pulmonary and Critical Care Medicine, Mayo Clinic Florida, Jacksonville, FL, and Joel Roberson, MD, Department of Radiology, William Beaumont Hospital, Royal Oak, MI
Study Overview
Objective. To evaluate the efficacy and safety of Zephyr endobronchial valves (EBVs) in patients with heterogeneous emphysema and absence of collateral ventilation.
Design. Multicenter, randomized, nonblinded clinical trial.
Setting and participants. This study was conducted at 17 sites across Europe between 2014 and 2016. Patients with severe emphysema who were ex-smokers and ≥ 40 years old were recruited. Key inclusion criteria were post-bronchodilator FEV1 between 15%–45% predicted despite optimal medical management, total lung capacity greater than 100% predicted, residual volume ≥ 180% predicted, and a 6-minute walk distance of between 150 and 450 meters. Heterogenous emphysema was defined as a greater than 10% difference in destruction score between target and ipsilateral lobes as measured by high-resolution CT. All eligible patients underwent Chartis pulmonary assessment (Pulmonx, Redwood City, CA) assessment to determine the presence of collateral ventilation between the target and adjacent lobes, and patients with collateral ventilation were excluded.
Intervention. Patients were randomized 2:1 to either EBV plus standard of care (intervention) or standard of care alone (control) by blocked design and concealed envelopes. The EBV group underwent immediate placement of Zephyr EBVs with the intention of complete lobar occlusion.
Main outcome measures. The primary outcome at 3 months post-procedure was the percentage of subjects with FEV1 improvement from baseline of 12% or greater. Changes in FEV1, residual volume, 6-minute walk distance, St. George’s Respiratory Questionnaire score and modified Medical Research Council score were assessed at 3 and 6 months and target lobe volume reduction on chest CT at 3 months.
Main results. 97 subjects were randomized to the intervention (n = 65) or control group (n = 32). At 3 months, 55.4% of intervention and 6.5% of control subjects had an FEV1 improvement of 12% or more (P < 0.001). Improvements were maintained at 6 months: intervention, 56.3%, versus control, 3.2% (P < 0.001), with a mean ± SD change in FEV1% at 6 months of 20.7 ± 29.6% and –8.6 ± 13.0%, respectively. A total of 89.8% of intervention subjects had target lobe volume reduction greater than or equal to 350 mL (mean, 1.09 ± 0.62 L; P < 0.001). The differences in outcomes between the intervention and control groups were statistically significant, with the following measured differences: residual volume, –700 m; 6-minute walk distance, +78.7 m; St. George’s Respiratory Questionnaire score, –6.5 points; modified Medical Research Council dyspnea score, –0.6 points; and BODE (body mass index, airflow obstruction, dyspnea, and exercise capacity) index, –1.8 points (all P < 0.05). Pneumothorax was the most common adverse event, occurring in 19 of 65 (29.2%) of intervention subjects.
Conclusion. Endobronchial valve treatment in hyperinflated patients with heterogeneous emphysema without collateral ventilation resulted in clinically meaningful benefits in lung function, dyspnea, exercise tolerance and quality of life, with an acceptable safety profile.
Commentary
Patients with severe emphysema are difficult to manage. Optimal medical management is required to maintain their lung function and quality of life, with combination bronchodilators (long-acting beta 2 agonists, long-acting anticholinergics, and inhaled corticosteroids), roflumilast (selective phosphodiesterase-4 inhibitors), oral corticosteroids or macrolide antibiotics when indicated, long-term oxygen, and noninvasive ventilator support. Palliative team care consultation and support, adequate nutritional support, influenza and pneumococcal vaccination, and pulmonary rehabilitation/graded exercise training are important aspects of emphysema treatment [1].
To help patients with severe emphysema who experience further decline despite intensive medical management, a lung volume reduction strategy was devised. In 2003, the NETT trial was conducted [2]. In this study, lung volume reduction surgery was performed in 608 patients, who were followed for 29 months. This study revealed a lack of survival benefit with significant immediate postoperative mortality and complication rate. Despite this disappointing result, a subgroup of patients (upper-lobe predominant disease and low baseline exercise capacity) had a statistically significant mortality benefit from surgery.
Since then, many have sought to determine a less invasive method of lung volume reduction. So far, one-way endobronchial valves, self-activating coils, and targeted destruction and remodeling of emphysematous lung with vapor or sealant methods have been studied. Several studies have examined the efficacy and safety of coils, with reasonable improvement of 6-minute walk distance and FEV1; however, complications including death, pneumothorax and pneumonia were noted. Vapor ablation (STEP-UP trial) [3] and lung sealant [4] were also attempted in order to achieve lung volume reduction, but increased infection was problematic. The 2017 GOLD guidelines suggested lung volume reduction by endobronchial one-way valve or lung coils as interventional bronchoscopic options for lung volume reduction [1].
Two types of endobronchial valves have been introduced to date: the intra bronchial valve, developed by Olympus, and the Zephyr valve by Pulmonx. Endobronchial valves are deployed to the bronchi via bronchoscopic guidance, and limit airflow to the portions of the lung distal to the valve while allowing mucus and air movement in the proximal direction. The VENT study, the largest endobronchial valve trial using the Zephyr valve, was published in 2010 [5]. This study demonstrated the efficacy of endobronchial valve treatment, especially in patients with heterogeneous emphysema and complete interlobar fissures as opposed to homogeneous emphysema and incomplete interlobar fissures. Subsequent studies demonstrated the importance of absence of collateral ventilation, measured by the Chartis system, when considering endobronchial valves [6].
The current study by Kemp et al is the first multicenter randomized endobronchial valve trial conducted in Europe. The study was able to demonstrate remarkable improvement in FEV1 (mean 140 mL decrease vs 90 mL increase) and 6-minute walk distance (mean +36.2 meter vs –42.5 meter) after endobronchial valve treatment in severe emphysema patients. The amount of volume reduction was reaching up to 2 liters. Patients in the control group were given the opportunity to receive endobronchial valve after the 6 months study follow-up period and 30 out of 32 patients opted for the endobronchial valve treatment. The authors concluded that the endobronchial valve therapy resulted in clinically meaningful benefits in lung function, dyspnea, exercise tolerance and quality of life with an acceptable safety profile.
It is notable that the authors included only selected patients, limited to those with presence of heterogeneous emphysema, absence of collateral ventilation, low risk of COPD exacerbation or infection, and patients who were likely able to tolerate pneumothorax. Despite this, 13 patients developed pneumothorax and death occurred in 1 patient, leading to a significantly longer average length of hospital stay in the treatment group. Although this rate of complications is not higher than prior endobronchial valve studies, it is important to note when broadly applying the outcomes of this study to patient care. Lack of long-term follow-up and the nonblinded study design also limit the strength of this study.
Applications for Clinical Practice
Many patients suffer from emphysema. Among them, severe emphysema is the most difficult to manage. It is important to incorporate optimal medical management including bronchodilators, palliative care, oxygen therapy, pulmonary rehabilitation and non-invasive ventilation options. When patients with severe emphysema continue to decline or seek further improvement in their care, and when they meet the specific criteria for lung volume reduction, endobronchial valve therapy should be considered an option and physicians should refer them to appropriate centers. However, the risk of complications, such as pneumothorax, still remains high.
—Minkyung Kwon, MD, Pulmonary and Critical Care Medicine, Mayo Clinic Florida, Jacksonville, FL, and Joel Roberson, MD, Department of Radiology, William Beaumont Hospital, Royal Oak, MI
1. The Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2017.
2. Weinmann GG, Chiang YP, Sheingold S. The National Emphysema Treatment Trial (NETT): a study in agency collaboration. Proc Am Thorac Soc 2008;5:381–4.
3. Herth FJ, Valipour A, Shah PL, et al. Segmental volume reduction using thermal vapour ablation in patients with severe emphysema: 6-month results of the multicentre, parallel-group, open-label, randomised controlled STEP-UP trial. Lancet Respir Med 2016;4:185–93.
4. Come CE, Kramer MR, Dransfield MT, et al. A randomised trial of lung sealant versus medical therapy for advanced emphysema. Eur Respir J 2015;46:651–62.
5. Sciurba FC, Ernst A, Herth FJ, et al. A randomized study of endobronchial valves for advanced emphysema. N Engl J Med 2010;363:1233–44.
6. Klooster K, ten Hacken NH, Hartman JE, et al. Endobronchial valves for emphysema without interlobar collateral ventilation. N Engl J Med 2015;373:2325–35.
1. The Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2017.
2. Weinmann GG, Chiang YP, Sheingold S. The National Emphysema Treatment Trial (NETT): a study in agency collaboration. Proc Am Thorac Soc 2008;5:381–4.
3. Herth FJ, Valipour A, Shah PL, et al. Segmental volume reduction using thermal vapour ablation in patients with severe emphysema: 6-month results of the multicentre, parallel-group, open-label, randomised controlled STEP-UP trial. Lancet Respir Med 2016;4:185–93.
4. Come CE, Kramer MR, Dransfield MT, et al. A randomised trial of lung sealant versus medical therapy for advanced emphysema. Eur Respir J 2015;46:651–62.
5. Sciurba FC, Ernst A, Herth FJ, et al. A randomized study of endobronchial valves for advanced emphysema. N Engl J Med 2010;363:1233–44.
6. Klooster K, ten Hacken NH, Hartman JE, et al. Endobronchial valves for emphysema without interlobar collateral ventilation. N Engl J Med 2015;373:2325–35.
Management of Community-Acquired Pneumonia in Adults
From the University of North Dakota School of Medicine & Health Sciences, Fargo, ND.
Abstract
- Objective: To review the management of community-acquired pneumonia (CAP) in adults.
- Methods: Review of the literature.
- Results: Approximately 4 to 5 million cases of CAP are diagnosed in the United States annually, accounting for significant morbidity and mortality. While numerous studies have previously shown pneumococcus to be the most common causative pathogen, the 2015 EPIC study found that in nearly two-thirds of patients with CAP who required hospitalization, no pathogen was detected. Symptoms and signs of respiratory tract infection are useful in helping to diagnose pneumonia; however, they are less sensitive than chest imaging studies. Laboratory tests used in diagnosing pneumonia include sputum Gram stain and culture, blood culture, urinary antigen, polymerase chain reaction, and biologic markers. In empiric treatment of CAP, both the typical and atypical pathogens should be targeted. Influenza vaccine and pneumococcal polysaccharide and conjugate vaccines should be administered as recommended by the CDC to reduce risk of CAP.
- Conclusion: CAP is a common illness with high rates of morbidity and mortality. Treatment is for the most part empirical; diagnostic testing can be used to identify the causative organism and guide pathogen-specific therapy.
Key words: community-acquired pneumonia; adults; management; vaccines.
Despite advances in medical science, pneumonia remains a major cause of morbidity and mortality. In 2014, 50,620 patients in the United States died from the disease [1]. Pneumonia can be classified as community-acquired, hospital-acquired, or ventilator-associated. Another category, healthcare-associated pneumonia, was included in an earlier American Thoracic Society (ATS) and Infectious Diseases Society of America (IDSA) guideline but was removed from the 2016 guideline because there was no clear evidence that patients diagnosed with healthcare-associated pneumonia were at higher risk for harboring multidrug-resistant pathogens [2]. In this article, we review the epidemiology, microbiology, predisposing factors, diagnosis, treatment, and prevention of community-acquired pneumonia (CAP).
Definition and Epidemiology
CAP is defined as an acute infection of the lungs that develops in patients who have not been hospitalized recently and have not had regular exposure to the health care system [3]. A previously ambulatory patient who is diagnosed with pneumonia within 48 hours after admission also meets the criteria for CAP. Approximately 4 to 5 million cases of CAP are diagnosed in the United States annually [4]. About 25% of CAP patients require hospitalization, and about 5% to 10% of these patients are admitted to the intensive care unit (ICU) [5]. In-hospital mortality is considerable (~10% in population-based studies) [6] and 30-day mortality was found to be as high as 23% in a review by File and Marrie [7]. CAP also confers a high risk of long-term morbidity and mortality compared with the general population who have never had CAP, irrespective of age [8].
Causative Organisms
Numerous microorganisms can cause CAP. Common causes and less common causes are delineated in Table 1. 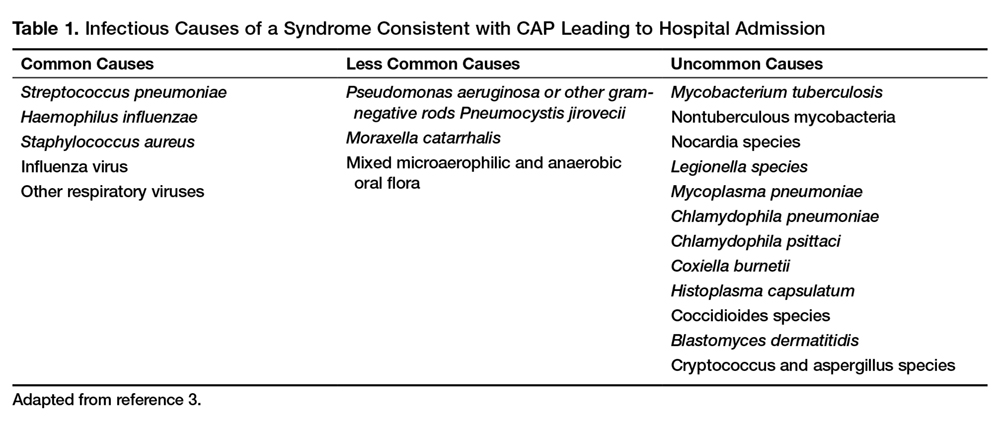
Predisposing Factors
Most people diagnosed with CAP have one or more predisposing factors [12,13] (Table 2). 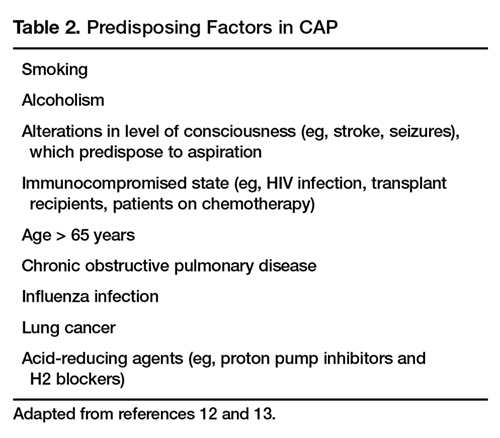
Clinical Signs and Symptoms
Symptoms of CAP include fever, chills, rigors, fatigue, anorexia, diaphoresis, dyspnea, cough (with or without sputum production), and pleuritic chest pain. There is no individual symptom or cluster of symptoms that can absolutely differentiate pneumonia from other acute respiratory diseases, including upper and lower respiratory infections. However, if a patient presents with the constellation of symptoms of fever ≥ 1000F (37.80C), productive cough, and tachycardia, it is more suggestive of pneumonia [14]. Abnormal vital signs include fever, hypothermia, tachypnea, tachycardia, and oxygen desaturation. Auscultation of the chest reveals crackles or other adventitious breath sounds. Elderly patients with pneumonia report a significantly lower number of both respiratory and nonrespiratory symptoms compared with younger patients. Clinicians should be aware of this phenomenon so it does not lead to delayed diagnosis and treatment [15].
Imaging Evaluation
The presence of a pulmonary consolidation or an infiltrate on chest radiograph is required to diagnose CAP, and a chest radiograph should be obtained when CAP is suspected [16]. It should be noted that there is no pattern of radiographic abnormalities reliable enough to differentiate infectious pneumonia from noninfectious causes [17].
There are case reports and case series demonstrating false-negative plain chest radiographs existing in dehydrated patients [18] or in neutropenic state. However, animal studies have shown that dogs challenged with pneumococcus showed abnormal pulmonary shadow, suggestive of pneumonia, regardless of hydration status [19]. There is also no reliable scientific evidence to support the notion that severe neutropenia can cause false-negative radiographs because of the inability to develop an acute inflammatory reaction in the lungs [20].
A chest CT scan is more sensitive than a plain chest radiograph in detecting pneumonia. Therefore, a chest CT should be performed in a patient with negative plain chest radiograph when pneumonia is still highly suspected [21]. A chest CT scan is also more sensitive in detecting cavitation, adenopathy, interstitial disease and empyema. It also has the advantage of better defining anatomical changes than plain films [22].
Because improvement of pulmonary opacities in patients with CAP lags behind clinical improvement, repeating chest imaging studies is not recommended in patients who demonstrate clinical improvement. Sometimes clearing of pulmonary infiltrate or consolidation can take 6 weeks or longer [23].
Laboratory Evaluation
Generally the etiologic agent of CAP cannot be determined solely on the basis of clinical signs and symptoms or imaging studies. Although routine microbiological testing for patients suspicious for CAP is not necessary for empirical treatment, by determining the etiologic agent of the pneumonia, a clinician will be able to narrow the antibiotics from a broad-spectrum empirical regimen to specific pathogen-directed therapy. Determination of certain etiologic agents causing the pneumonia can have important public health implications (eg, Mycobacterium tuberculosis and influenza virus) [24].
Sputum Gram Stain and Culture
Sputum Gram stain is an inexpensive test that may identify pathogens that cause CAP (eg, S. pneumonia and Haemophilus influenzae). A quality specimen is required. A sputum sample must contain > 25 neutrophils and < 10 squamous epithelial cells/low power field on Gram stain to be considered suitable for culture.
The sensitivity and specificity of sputum Gram stain and culture are highly variable in different clinical settings (eg, outpatient setting, nursing home, ICU). Reed et al’s meta-analysis of patients diagnosed with CAP in the United States showed the sensitivity and specificity of sputum Gram stain (compared with sputum culture) ranged from 15% to 100% and 11% to 100%, respectively [24]. In cases of proven bacteremic pneumococcal pneumonia, positive cultures from sputum samples were positive less than 50% of the time [25].
For patients who cannot provide sputum samples or are intubated, a deep-suction aspirate or bronchoalveolar lavage through a bronchoscopic procedure might be necessary to obtain pulmonary secretion for Gram stain and culture. Besides bacterial culture, sputum samples can also be sent for fungal and mycobacterial cultures and acid-fast stain if deemed clinically necessary.
Blood Culture
Because the positivity rate of blood culture in patients who are suspected to have pneumonia but not exposed to antimicrobial agents is disappointingly low (5%–14%), blood cultures are no longer recommended in patients hospitalized for CAP. Another reason for not recommending blood culture is positive culture rarely leads to changes in antibiotic regimen in patients without underlying diseases [26]. However, high-risk patients, including patients with severe CAP or in immunocompromised patients (eg, patients with neutropenia, asplenia or complement deficiencies) should have a blood culture done [24].
A multinational study published in 2008 examined 125 patients with pneumococcal bacteremic CAP versus 1847 patients with non-bacteremic CAP [27]. Analysis of the data demonstrated no association of pneumococcal bacteremic CAP and time to clinical stability, length of hospital stay, all-cause mortality or CAP-related mortality. The authors concluded that pneumococcal bacteremia does not increase the risk of poor outcomes in patients with CAP compared to non-bacteremic patients, and the presence of pneumococcal bacteremia should not deter de-escalation of therapy in clinically stable patients.
Urinary Antigen Tests
Urinary antigen tests may assist clinicians in narrowing antibiotic therapy when test results are positive. There are 2 U.S. Food and Drug Administration–approved tests available to clinicians for detecting pneumococcal and Legionella antigen in urine. The test for Legionella pneumophila detects disease due to serogroup 1 only, which accounts for 80% of community-acquired Legionnaires disease. The sensitivity and specificity of the Legionella urine antigen test are 90% and 99%, respectively. The pneumococcal urine antigen test is less sensitive and specific than the Legionella urine antigen test (sensitivity 80% and specificity > 90%) [28,29].
Advantages of the urinary antigen tests are that they are easily performed, results are available in less than an hour if done in-house, and results are not affected by prior exposure to antibiotics. However, the tests do not meet Clinical Laboratory Improvements Amendments criteria for waiver and must be performed by a technician in the laboratory.
Polymerase Chain Reaction
There are several FDA-approved polymerase chain reaction (PCR) tests commercially available to assist clinicians in diagnosing pneumonia. PCR test of nasopharyngeal swabs for diagnosing influenza have become standard in many medical U.S. facilities. The great advantage of using PCR to diagnose influenza is its high sensitivity and specificity and rapid turnaround time. PCR can also be used to detect Legionella species, S. pneumonia, Mycoplasma pneumoniae, Chlamydophila pneumonia and mycobacterial species [24].
One limitation of using PCR tests on respiratory specimens is that specimens can be contaminated with oral or upper airway flora, so the results must be interpreted with caution, bearing in mind that some of the pathogens isolated may be colonizers of the oral or upper airway flora [30].
Biologic Markers
Two biologic markers—procalcitonin and C-reactive protein (CRP)—can be used in conjunction with history, physical examination, laboratory tests and imaging studies to assist in the diagnosis and treatment of CAP [24]. Procalcitonin is a peptide precursor of the hormone calcitonin that is released by parenchymal cells into the bloodstream resulting in increased serum level in patients with bacterial infections. In contrast, there is no remarkable proclacitonin level increase with viral or noninfectious inflammation. The reference value of procalcitonin in the blood of an adult individual without infection or inflammation is < 0.15 ng/mL. In the blood, procalcitonin has a half-life of 25 to 30 hours. The quantitative immunoluminometric method (LUMI test, Brahms PCT, Berlin, Germany ) is the preferred test to use because of its high sensitivity [31].
A 2012 Cochrane meta-analysis that involved 4221 patients with acute respiratory infections (with half of the patients diagnosed with CAP) from 14 prospective trials found the use of procalcitonin test for antibiotic use significantly decreased median antibiotic exposure from 8 to 4 days without an increase in treatment failure, mortality rates in any clinical setting (eg, outpatient clinic, emergency room), or length of hospitalization [32]. A prospective study conducted in France on 100 ICU patients showed that increased procalcitonin from day 1 to day 3 has a poor prognosis factor for severe CAP whereas decreasing procalcitonin levels is associated with a favorable outcome [33].
CRP is an acute phase protein produced by the liver. CRP level in the blood increases in response to acute infection or inflammation. Use of CRP in assisting diagnosis and guiding treatment of CAP is more limited in part due to its poor specificity. A prospective study conducted on 168 consecutive patients presented with cough showed that a CRP > 40 mg/L had a sensitivity and specificity of 70% and 90%, respectively [34].
T reatment
Site of Care Decision
For patients with CAP, the clinician must decide whether the patient will be treated in an outpatient or inpatient setting, and for those in the inpatient setting, whether they can safely be treated on the general medical ward or should be the ICU. Two common scoring systems that can be used to aid the clinician in determining severity of the infection and guiding site-of-care decisions are the Pneumonia Severity Index (PSI) and CURB-65 scores.
The PSI score uses 20 different parameters, including comorbidities, laboratory parameters and radiographic findings to stratify patients into 5 mortality risk classes [35]. On the basis of associated mortality rates, it has been suggested that risk class I and II patients should be treated as outpatients, risk class III patients should be treated in an observation unit or with a short hospitalization, and risk class IV and V patients should be treated as inpatients [35].
The CURB-65 method of risk stratification is based on 5 clinical parameters: confusion, urea level, respiratory rate, systolic blood pressure and age ≥ 65 (Table 3) [36]. 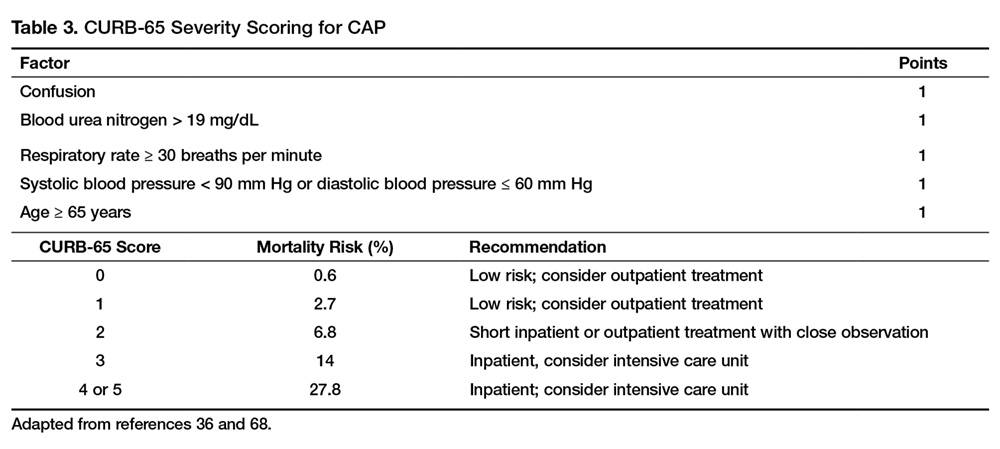
Patients with CURB-65 scores of 4 or 5 are considered to have severe pneumonia and admission to the ICU should be considered. Aside from the CURB-65 score, anyone requiring vasopressor support or mechanical ventilation merits admission to the ICU [16]. IDSA/ATS guidelines also recommend the use of “minor criteria” for making ICU admission decisions; these include respiratory rate ≥ 30 breaths / minute, PaO2 fraction ≤ 250, multilobar infiltrates, confusion, blood urea nitrogen ≥ 20 mg/dL, leukopenia, thrombocytopenia, hypothermia and hypotension [16]. These factors are associated with increased mortality due to CAP and admission to an ICU is indicated if 3 of the minor criteria for severe CAP are present.
Similar to CURB-65, another clinical calculator that can be used for assessing severity of CAP is SMART-COP [39]. This scoring system uses 8 weighted criteria to predict which patients will require intensive respiratory or vasopressor support. SMART-COP has a sensitivity of 79% and specificity 64% in predicting ICU admission, whereas CURB-65 had a pooled sensitivity of 57.2% and specificity of 77.2% [40].
Antibiotic Therapy
Antibiotics are the mainstay of treatment for CAP, with the majority of patients with CAP treated empirically taking into account the site of care, likely pathogen, and antimicrobial resistance issues. Patients with pneumonia who are treated as outpatients usually respond well to empiric antibiotic treatment and a causative pathogen is not usually sought. Patients who are hospitalized for treatment of CAP usually receive empiric antibiotic on admission. Once the etiology has been determined by microbiologic or serologic means, antimicrobial therapy should be adjusted accordingly. As noted previously, a CDC study found that the burden of viral etiologies was higher than previously thought, with rhinovirus and influenza accounting for 15% of cases and S. pneumoniae for only 5% [9]. This study highlighted the fact that despite advances in molecular techniques, most patients with pneumonia have no pathogen identified [9]. Given the lack of discernable pathogens in the majority of cases, unless a nonbacterial etiology is found patients should continue to be treated with antibiotics.
Outpatients without comorbidities or risk factors for drug-resistant S. pneumoniae (Table 4) 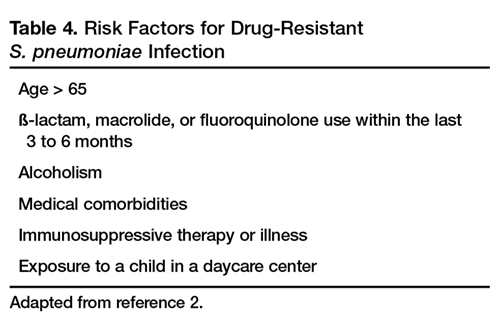
As previously mentioned, antibiotic therapy is typically empiric; neither clinical features nor radiographic features are sufficient to include or exclude infectious etiologies. Epidemiologic risk factors should be considered and, in certain cases, expanded antimicrobial coverage to include those entities; for example, treatment of anaerobes in the setting of lung abscess and antipseudomonal antibiotics for patients with bronchiectasis.
Of concern in the treatment of CAP is the increased prevalence of antimicrobial resistance among S. pneumoniae. The IDSA guidelines report that drug-resistant S. pneumoniae is more common in persons aged < 2 or > 65 years, and those with ß-lactam therapy within the previous 3 months, alcoholism, medical comorbidities, immunosuppressive illness or therapy, or exposure to a child who attends a day care center [16].
S. aureus should be considered during influenza outbreaks, with either vancomycin or linezolid being the recommended agents in the setting of methicillin-resistant S. aureus (MRSA). In a study comparing vancomycin versus linezolid for nosocomial pneumonia, the all-cause 60-day mortality was similar for both agents [41]. Datpomycin is another agent used against MRSA; however, its use in the setting of pneumonia is not indicated as daptomycin binds to surfactant, yielding it ineffective in the treatment of pneumonia [42]. Ceftaroline is a newer cephalosporin with activity against MRSA; its role in treatment of community-acquired MRSA pneumonia has not been fully elucidated, but it appears to be a useful agent for this indication [43,44]. 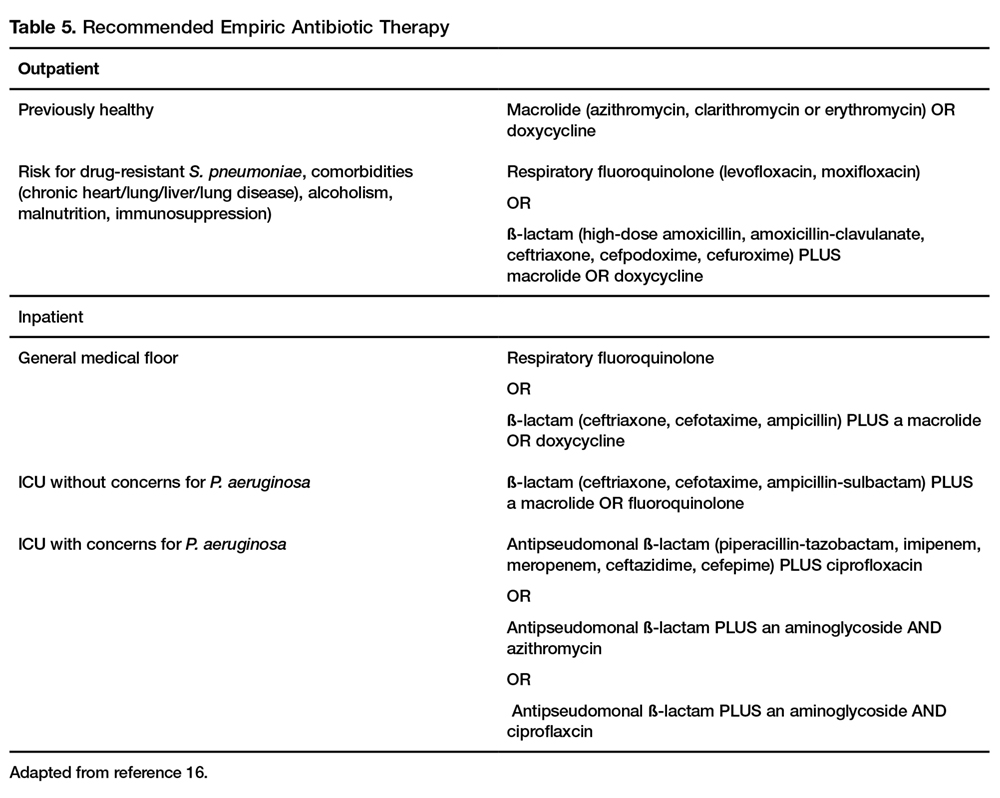
A summary of recommended empiric antibiotic therapy is presented in Table 5.
Antibiotic Therapy for Selected Pathogens
S. pneumoniae
Patients with pneumococcal pneumonia who have penicillin-susceptible strains can be treated with intravenous penicillin (2 or 3 million units every 4 hours) or ceftriaxone. Once a patient meets criteria of stability, they can then be transitioned to oral penicillin, amoxicillin, or clarithromycin. Those with strains with reduced susceptibility can still be treated with penicillin but at a higher dose (4 million units IV every 4 hours) or a third-generation cephalosporin. Those whose pneumococcal pneumonia is complicated by bacteremia will benefit from dual therapy if severely ill, requiring ICU monitoring. Those not severely ill can be treated with monotherapy [46].
S. aureus
S. aureus is more commonly associated with hospital-acquired pneumonia but may also be seen during the influenza season and in those with severe necrotizing CAP. Both linezolid and vancomycin can be used to treat MRSA CAP. As noted above, ceftaroline has activity against MRSA and is approved for treatment of CAP, but is not approved by the FDA for MRSA CAP treatment. Similarly, tigecycline is approved for CAP and has activity against MRSA, but is not approved for MRSA CAP. Moreover, the FDA has warned of increased risk of death with tigecycline and has a black box warning to that effect [47].
Legionella
Treatment of legionellosis can be achieved with tetracyclines, macrolides, or fluoroquinolones. For nonimmunosuppressed patients with mild pneumonia, any of the listed antibiotics is considered appropriate. However, patients with severe infection or those with immunosuppression should be treated with either levofloxacin or azithromycin for 7 to 10 days [48].
C. pneumoniae
As with other atypical organisms, C. pneumoniae can be treated with doxycycline, a macrolide, or respiratory fluoroquinolones. However, length of therapy varies by regimen used; whereas treating with doxycycline 100 mg twice daily generally requires 14–21 days, moxifloxacin 400 mg daily only requires 10 days [49].
M. pneumoniae
As with C. pneumoniae, length of therapy of M. pneumoniae varies by antimicrobial used. Shortest courses are seen with the use of macrolides for 5 days, whereas 14 days is considered standard for doxycycline or a respiratory fluoroquinolone [50]. It should be noted that there has been increasingly documented resistance to macrolides, with known resistance of 8.2% in the United States [51].
Duration of Treatment
Most patients with CAP respond within 72 hours to appropriate therapy. IDSA/ATS guidelines recommend that patients be treated for a minimum of 5 days, and before discontinuing antibiotics patients should be afebrile a minimum of 48-72 hours and be clinically stable (Table 6) [16]. 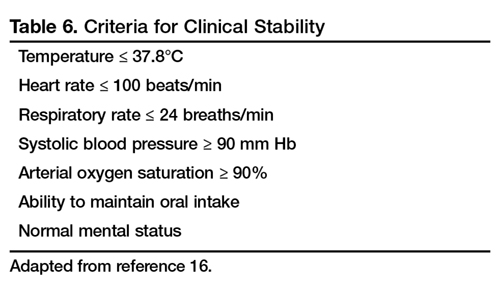
Hospitalized patients do not need to be monitored for an additional day once they have reached clinical stability (Table 6), are able to maintain oral intake, and have normal mentation, provided that other comorbidities are stable and social needs have been met [16]. Patients discharged from the hospital with instability have higher risk of readmission or death [55].
Transition to Oral Therapy
IDSA/ATS guidelines [16] recommend that patients should be transitioned from IV to oral antibiotics when they are improving clinically, have stable vital signs, and are able to ingest food/fluids and medications.
Management of Nonresponders
Although the majority of patients respond to antibiotics within 72 hours, treatment failure occurs in up to 15% of patients [45]. Nonresponding pneumonia is generally seen in 2 patterns: worsening of clinical status despite empiric antibiotics OR delay in achieving clinical stability as defined in Table 5 after 72 hours of treatment [13]. Risk factors associated with nonresponding pneumonia [56] are:
- Radiographic: multilobar infiltrates, pleural effusion, cavitation
- Bacteriologic: MRSA, gram-negative or Legionella pneumonia
- Severity index: PSI > 90
- Pharmacologic: incorrect antibiotic choice based on susceptibility
Patients with acute deterioration of clinical status will prompt transfer to a higher level of care and may require mechanical ventilator support. In those with delay in achieving clinical stability, question centers on whether the same antibiotics can be continued while doing further radiographic/microbiologic workup and/or changing antibiotics.
History should be reviewed with particular attention to exposures, travel history, and microbiologic and radiographic data. Clinicians should recall that viral causes account for up to 20% of pneumonias and there are also noninfectious causes that can mimic pyogenic infections [57]. If adequate initial cultures were not obtained, they should be obtained; however, care must be taken in reviewing new sets of cultures while on antibiotics as they may reveal colonization selected out by antibiotics and not a true pathogen. If repeat evaluation is unrevealing, then further evaluation with CT scan and bronchoscopy with bronchoalveolar lavage and biopsy is warranted. CT scans can show pleural effusions, bronchial obstructions or pattern suggestive of cryptogenic pneumonia. A bronchoscopy might yield a microbiologic diagnosis and with biopsy can also evaluate for noninfectious causes.
As with other infections, if escalation of antibiotics is undertaken, clinicians should be mindful to ensure that efforts are being made to elucidate the reason for nonresponse. To simply broaden antimicrobial therapy without attempts at establishing a microbiologic or radiographic cause for nonresponse may lead to inappropriate treatment recurrence of infection. Aside from patients who have bacteremic pneumococcal pneumonia in an ICU setting, there are no published reports pointing to superiority of combination antibiotics [46].
Other Treatment
Because of the inflammatory response associated with pneumonia, several agents have been evaluated as adjunctive treatment of pneumonia to decrease this inflammatory state; namely, steroids, macrolide antibiotics and statins. To date, only the use of steroids (methylprednisolone 0.5 mg/kg every 12 hours for 5 days) in those with severe CAP and high initial anti-inflammatory response (CRP > 150) was shown to decrease treatment failure, decreased risk of ARDS, possibly reduce length of stay, duration of intravenous antibiotics and clinical stability, without effect on mortality or adverse side effects [58,59].
Other adjunctive methods have not been found to have significant impact [16].
Prevention of Pneumonia
Prevention of pneumococcal pneumonia is twofold: prevention of infection caused by S. pneumoniae and prevention of influenza infection. As influenza infection is a risk factor for bacterial infection, specifically with S. pneumoniae, influenza vaccination can prevent bacterial pneumonia [60]. In their most recent recommendations, the CDC continues to recommend routine influenza vaccination for all persons aged greater than 6 months, unless otherwise contraindicated [61].
There are 2 vaccines for prevention of pneumococcal disease: the pneumococcal polysaccharide vaccine (PPSV23) and a conjugate vaccine (PCV13). Following vaccination with PPSV23, 80% of adults develop antibodies against at least 18 of the 23 serotypes [62]. Despite this response, PPSV23 is reported to be protective against invasive pneumococcal infection; yet there is no consensus regarding PPSV23 leading to decreased rates of pneumonia [63]. On the other hand, PCV13 vaccination was associated with prevention of both invasive disease and community-acquired pneumonia in adults 65 years or older [64]. The CDC recommends that all children aged 2 or under receive PCV13, whereas those aged 65 or older should receive PCV13 followed by a dose of PPSV23 [65]. The dose of PPSV23 should be given ≥1 year following the dose of PCV13 [66].Persons < 65 years of age with immunocompromising and certain other conditions should also receive vaccination [67] (Table 7). Full details, many scenarios, and timing of vaccinations can be found at www.cdc.gov/vaccines/schedules/downloads/adult/adult-schedule.pdf. 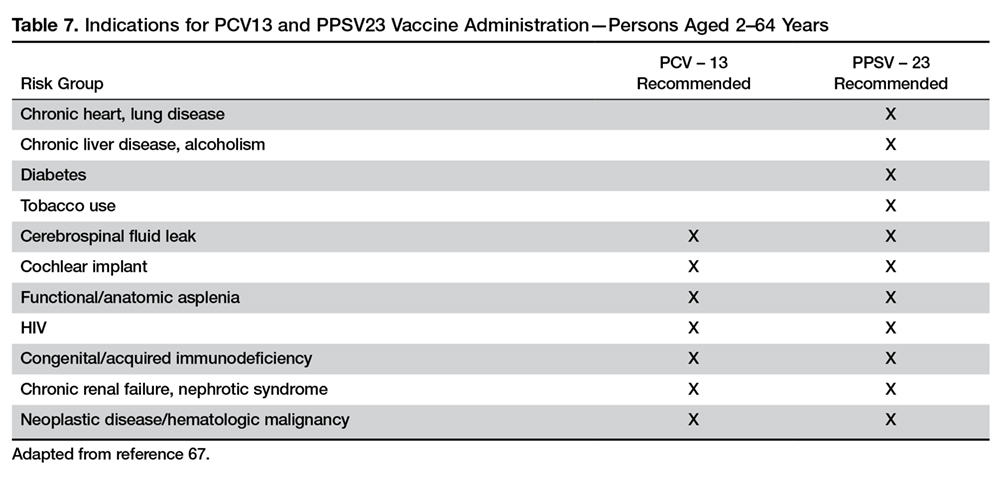
Cigarette smoking increases the risk of respiratory infections as evidenced by smokers accounting for almost half of all patients with invasive pneumococcal disease [11]. As this is a modifiable risk factor it should be a goal of a comprehensive approach towards prevention of pneumonia.
Summary
CAP remains a leading cause of hospitalization and death in the 21st century. Traditionally, pneumococcus has been considered the major pathogen causing CAP; however, the 2015 EPIC study found that in only 5% of patients diagnosed with CAP was S. pneumoniae detected. Despite the new findings, it is still recommended that empiric treatment for CAP target common typical bacteria (pneumococcus, H. influenzae, Moraxella catarrhalis) and atypical bacteria (M. pneumonia, C. pneumoniae, L. pneumophila).
Because diagnosing pneumonia through history and clinical examination is less than 50% sensitive, a chest imaging study (a plain chest radiograph or a chest CT scan) is usually required to make the diagnosis. Laboratory tests, such as sputum Gram stain/culture, blood culture, urinary antigen tests, PCR test, procalcitonin, and CRP are important adjunctive diagnostic modalities to assist in the diagnosis and management of CAP. However, no single test is sensitive and specific enough to be a stand-alone test. They should be used in conjunction with history, physical examination, and imaging studies. Because vaccination (PPSV23, PCV13, and influenza vaccine) remains the most effective tool in preventing the development of CAP, clinicians, should strive for 100% vaccination rates in appropriate persons.
Corresponding author: Tze Shein Lo, MD, University of North Dakota, 1919 Elm Street, Fargo, ND 58102, [email protected].
Financial disclosures: None.
Author contributions: drafting of article, PM, TSL; critical revision of the article, PM, TSL.
1. Centers for Disease Control and Prevention. National Center for Health Statistics. FastStats - Pneumonia. Accessed 6 Oct 2016 at www.cdc.gov/nchs/fastats/pneumonia.htm.
2. Kalil AC, Metersky ML, Klompas M, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis 2016;63:e61-e111.
3. Musher DM, Thorner AR. Community-acquired pneumonia. N Engl J Med 2014;371:1619–28.
4. Mandell LA. Epidemiology and etiology of community-acquired pneumonia. Infect Dis
5. Hoare Z, Lim WS. Pneumonia: update on diagnosis and management. BMJ 2006;332:1077–9.
6. Johnstone J, Marrie TJ, Eurich DT, Majumdar SR. Effect of pneumococcal vaccination in hospitalized adults with community-acquired pneumonia. Arch Intern Med 2007;167:1938–43
7. File TM Jr, Marrie TJ. Burden of community-acquired pneumonia in North American adults. Postgrad Med 2010;122:130–41.
8. Eurich DT, Marrie TJ, Minhas-Sandhu JK, Majumdar SR. Ten-year mortality after community-acquired pneumonia. a prospective cohort. Am J Respir Crit Care Med 2015;192:597-604.
9. Jain S, Self WH, Wunderink RG, et al. Community-acquired pneumonia requiring hospitalization among U.S. adults. N Engl J Med 2015;373:415–27.
10. Griffin MR, Zhu Y, Moore MR, et al. U.S. hospitalizations for pneumonia after a decade of pneumococcal vaccination. N Engl J Med 2013;369:155–63.
11. Nuorti JP, Butler JC, Farley MM, et al. Cigarette smoking and invasive pneumococcal disease. Active Bacterial Core Surveillance Team. N Engl J Med 2000;342:681–9.
12. Almirall J, Serra-Prat M, Bolíbar I, BalassoV. Risk factors for community-acquired pneumonia in adults: a systemic review of observational studies. Respiration 2017;94:299–311.
13. Janoff EM.Streptococcus pneumonia. In: Bennett JE, Dolin R, Blaser MJ, editors. Mandell, Douglas and Bennett’s principles and practice of infectioius diseases. 8th ed. Philadelphia: Sauders; 2015: 2310–27.
14. Diehr P, Wood RW, Bushyhead J, et al. Prediction of pneumonia in outpatients with acute cough--a statistical approach. J Chronic Dis 1984;37:215–25.
15. Metlay JP, Schulz R, Li YH, et al. Influence of age on symptoms at presentation in patients with community-acquired pneumonia. Arch Intern Med 1997;157:1453–9.
16. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007;44 Suppl 2:S27–72.
17. Jartti A, Rauvala E, Kauma H, et al. Chest imaging findings in hospitalized patients with H1N1 influenza. Acta Radiol 2011;52:297–304.
18. Basi SK, Marrie TJ, Huang JQ, Majumdar SR. Patients admitted to hospital with suspected pneumonia and normal chest radiographs: epidemiology, microbiology, and outcomes. Am J Med 2004;117:305–11.
19. Caldwell A, Glauser FL, Smith WR, et al. The effects of dehydration on the radiologic and pathologic appearance of experimental canine segmental pneumonia. Am Rev Respir Dis 1975;112:651–6.
20. Bartlett JG. Pneumonia. In: Barlett JG, editor. Management of respiratory tract infections. Philadelphia: Lippincott, Williams & Wilkins; 2001: 1–122.
21. Claessens YE, Debray MP, Tubach F, et al. Early chest computed tomography scan to assist diagnosis and guide treatment decision for suspected community-acquired pneumonia. Am J Respir Crit Care Med 2015;192:974–82.
22. Wheeler JH, Fishman EK. Computed tomography in the management of chest infections: current status. Clin Infect Dis 1996;23:232–40.
23. Chesnutt MP. Pulmonary disorders. In: Papadakis MM, editor. Current medical diagnosis and treatment. New York: McGraw-Hill; 2016: 242–320.
24. Mandell LW. Pneumonia. In: Kasper DF, editor. Harrison’s infectious diseases. 1st ed. New York: McGraw-Hill; 2010: 188–201.
25. Reed WW, Byrd GS, Gates RH Jr, et al. Sputum gram’s stain in community-acquired pneumococcal pneumonia. A meta-analysis. West J Med 1996;165:197–204.
26. Chalasani NP, Valdecanas MA, Gopal AK, et al. Clinical utility of blood cultures in adult patients with community-acquired pneumonia without defined underlying risks. Chest 1995;108:932–6.
27. Bordon J, Peyrani P, Brock GN, et al. The presence of pneumococcal bacteremia does not influence clinical outcomes in patients with community-acquired pneumonia: results from the Community-Acquired Pneumonia Organization (CAPO) International Cohort study. Chest 2008;133:618–24.
28. Helbig JH, Uldum SA, Bernander S, et al. Clinical utility of urinary antigen detection for diagnosis of community-acquired, travel-associated, and nosocomial legionnaires’ disease. J Clin Microbiol 2003;41:838–40.
29. Smith MD, Derrington P, Evans R, et al. Rapid diagnosis of bacteremic pneumococcal infections in adults by using the Binax NOW Streptococcus pneumoniae urinary antigen test: a prospective, controlled clinical evaluation. J Clin Microbiol 2003;41:2810–3.
30. Johansson N, Kalin M, Tiveljung-Lindell A, et al. Etiology of community-acquired pneumonia: increased microbiological yield with new diagnostic methods. Clin Infect Dis 2010;50:202–9.
31. Gilbert DN. Procalcitonin as a biomarker in respiratory tract infection. Clin Infect Dis 2011;52 Suppl 4:S346–50.
32. Schuetz P, Muller B, Christ-Crain M, et al. Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Cochrane Database Syst Rev 2012;(9):CD007498.
33. Boussekey N, Leroy O, Alfandari S, et al. Procalcitonin kinetics in the prognosis of severe community-acquired pneumonia. Intensive Care Med 2006;32:469–72.
34. Flanders SA, Stein J, Shochat G, et al. Performance of a bedside C-reactive protein test in the diagnosis of community-acquired pneumonia in adults with acute cough. Am J Med 2004;116:529–35.
35. Fine MJ, et al A prediction rule to identify low-risk patients with community-acquired pneumonia.N Engl J Med.1997;336:243-50.
36. Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax 2003;58:377–82.
37. Arnold FW, Ramirez JA, McDonald LC, Xia EL. Hospitalization for community-acquired pneumonia: the pneumonia severity index vs clinical judgment. Chest 2003;124:121–4.
38. Aujesky D, McCausland JB, Whittle J, et al. Reasons why emergency department providers do not rely on the pneumonia severity index to determine the initial site of treatment for patients with pneumonia. Clin Infect Dis 2009;49:e100–8.
39. Charles PG, Wolfe R, Whitby M, et al. SMART-COP: a tool for predicting the need for intensive respiratory or vasopressor support in community-acquired pneumonia. Clin Infect Dis 2008;47:375–84.
40. Marti C, Garin N, Grosgurin O, et al. Prediction of severe community-acquired pneumonia: a systematic review and meta-analysis. Crit Care 2012;16:R141.
41. Wunderink RG, Niederman MS, Kollef MH, et al. Linezolid in methicillin-resistant Staphylococcus aureus nosocomial pneumonia: a randomized, controlled study. Clin Infect Dis 2012;54:621–9.
42. Silverman JA, Mortin LI, Vanpraagh AD, et al. Inhibition of daptomycin by pulmonary surfactant: in vitro modeling and clinical impact. J Infect Dis 2005;191:2149–52.
43. El Hajj MS, Turgeon RD, Wilby KJ. Ceftaroline fosamil for community-acquired pneumonia and skin and skin structure infections: a systematic review. Int J Clin Pharm 2017 Jan 5.
44. Taboada M, Melnick D, Iaconis JP, et al. Ceftaroline fosamil versus ceftriaxone for the treatment of community-acquired pneumonia: individual patient data meta-analysis of randomized controlled trials. J Antimicrob Chemother 2016;71:862–70.
45. Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the infectious diseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children: executive summary. Clin Infect Dis 2011;52:285–92.
46. Baddour LM, Yu VL, Klugman KP, et al. Combination antibiotic therapy lowers mortality among severely ill patients with pneumococcal bacteremia. Am J Respir Crit Care Med 2004;170:440–4.
47. FDA Drug Safety Communication: FDA warns of increased risk of death with IV antibacterial Tygacil (tigecycline) and approves new boxed warning [Internet]. 15 Jan 2016. Available at www.fda.gov/Drugs/DrugSafety/ucm369580.htm.
48. Edelstein PR, CR. Legionnaires’ Disease and Pontiac Fever. In: Kasper DF, editor. Harrison’s infectious diseases. 1st ed. New York: McGraw-Hill; 2010: 2633.
49. Hammerschlag MR, Kohlhoff SA, Gaydos, CA. Chlamydia pneumoniae. In: Kasper DF, editor. Harrison’s infectious diseases. 1st ed. New York: McGraw-Hill; 2010: 2174.
50. Holzman RS, MS. Mycoplasma pneumoniae and Atypical Pneumonia. In: Kasper DF, editor. Harrison’s infectious diseases. 1st ed. New York: McGraw-Hill; 2010: 2183.
51. Yamada M, Buller R, Bledsoe S, Storch GA. Rising rates of macrolide-resistant Mycoplasma pneumoniae in the central United States. Pediatr Infect Dis J 2012;31:409–10.
52. Yi SH, Hatfield KM, Baggs J, et al. Duration of antibiotic use among adults with uncomplicated community-acquired pneumonia requiring hospitalization in the United States. Clin Infect Dis 2017 Nov 6.
53. Hayashi Y, Paterson DL. Strategies for reduction in duration of antibiotic use in hospitalized patients. Clin Infect Dis 2011;52:1232–40.
54. Akram AR, Chalmers JD, Taylor JK, et al. An evaluation of clinical stability criteria to predict hospital course in community-acquired pneumonia. Clin Microbiol Infect 2013;19:1174–80.
55. Halm EA, Fine MJ, Kapoor WN, et al. Instability on hospital discharge and the risk of adverse outcomes in patients with pneumonia. Arch Intern Med 2002;162:1278–84.
56. Roson B, Carratala J, Fernandez-Sabe N, et al. Causes and factors associated with early failure in hospitalized patients with community-acquired pneumonia. Arch Intern Med 2004;164:502–8.
57. El-Solh AA, Pietrantoni C, Bhat A, et al. Microbiology of severe aspiration pneumonia in institutionalized elderly. Am J Respir Crit Care Med 2003;167:1650–4.
58. Wan YD, Sun TW, Liu ZQ, et al. Efficacy and safety of corticosteroids for community-acquired pneumonia: a systematic review and meta-analysis. Chest 2016;149:209–19.
59. Torres A, Sibila O, Ferrer M, et al. Effect of corticosteroids on treatment failure among hospitalized patients with severe community-acquired pneumonia and high inflammatory response: a randomized clinical trial. JAMA 2015;313:677–86.
60. McCullers JA. Insights into the interaction between influenza virus and pneumococcus. Clin Microbiol Rev 2006;19:571–82.
61. Grohskopf LA, Sokolow LZ, Broder KR, et al. Prevention and control of seasonal influenza with vaccines. MMWR Recomm Rep 2016;65:1–54.
62. Rubins JB, Alter M, Loch J, Janoff EN. Determination of antibody responses of elderly adults to all 23 capsular polysaccharides after pneumococcal vaccination. Infect Immun 1999;67:5979–84.
63. Centers for Disease Control. Vaccines and preventable diseases [Internet]. 22 Nov 2016. Available at www.cdc.gov/vaccines/vpd/pneumo/hcp/about-vaccine.html.
64. Bonten MJ, Huijts SM, Bolkenbaas M, et al. Polysaccharide conjugate vaccine against pneumococcal pneumonia in adults. N Engl J Med 2015;372:1114–25.
65. Centers for Disease Control. Recommended adult immunization schedule -- United States -- 2016 [Internet]. 2016. Available at www.cdc.gov/vaccines/schedules/downloads/adult/adult-schedule.pdf.
66. Kobayashi M, Bennett NM, Gierke R, et al. Intervals between PCV13 and PPSV23 vaccines: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep 2015;64:944–7.
67. Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine for adults with immunocompromising conditions: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep 2012;61:816–9.
68. Aujesky D, Auble TE, Yealy DM, et al. Prospective comparison of three validated prediction rules for prognosis in community-acquired pneumonia. Am J Med 2005;118:384–92.
From the University of North Dakota School of Medicine & Health Sciences, Fargo, ND.
Abstract
- Objective: To review the management of community-acquired pneumonia (CAP) in adults.
- Methods: Review of the literature.
- Results: Approximately 4 to 5 million cases of CAP are diagnosed in the United States annually, accounting for significant morbidity and mortality. While numerous studies have previously shown pneumococcus to be the most common causative pathogen, the 2015 EPIC study found that in nearly two-thirds of patients with CAP who required hospitalization, no pathogen was detected. Symptoms and signs of respiratory tract infection are useful in helping to diagnose pneumonia; however, they are less sensitive than chest imaging studies. Laboratory tests used in diagnosing pneumonia include sputum Gram stain and culture, blood culture, urinary antigen, polymerase chain reaction, and biologic markers. In empiric treatment of CAP, both the typical and atypical pathogens should be targeted. Influenza vaccine and pneumococcal polysaccharide and conjugate vaccines should be administered as recommended by the CDC to reduce risk of CAP.
- Conclusion: CAP is a common illness with high rates of morbidity and mortality. Treatment is for the most part empirical; diagnostic testing can be used to identify the causative organism and guide pathogen-specific therapy.
Key words: community-acquired pneumonia; adults; management; vaccines.
Despite advances in medical science, pneumonia remains a major cause of morbidity and mortality. In 2014, 50,620 patients in the United States died from the disease [1]. Pneumonia can be classified as community-acquired, hospital-acquired, or ventilator-associated. Another category, healthcare-associated pneumonia, was included in an earlier American Thoracic Society (ATS) and Infectious Diseases Society of America (IDSA) guideline but was removed from the 2016 guideline because there was no clear evidence that patients diagnosed with healthcare-associated pneumonia were at higher risk for harboring multidrug-resistant pathogens [2]. In this article, we review the epidemiology, microbiology, predisposing factors, diagnosis, treatment, and prevention of community-acquired pneumonia (CAP).
Definition and Epidemiology
CAP is defined as an acute infection of the lungs that develops in patients who have not been hospitalized recently and have not had regular exposure to the health care system [3]. A previously ambulatory patient who is diagnosed with pneumonia within 48 hours after admission also meets the criteria for CAP. Approximately 4 to 5 million cases of CAP are diagnosed in the United States annually [4]. About 25% of CAP patients require hospitalization, and about 5% to 10% of these patients are admitted to the intensive care unit (ICU) [5]. In-hospital mortality is considerable (~10% in population-based studies) [6] and 30-day mortality was found to be as high as 23% in a review by File and Marrie [7]. CAP also confers a high risk of long-term morbidity and mortality compared with the general population who have never had CAP, irrespective of age [8].
Causative Organisms
Numerous microorganisms can cause CAP. Common causes and less common causes are delineated in Table 1.
Predisposing Factors
Most people diagnosed with CAP have one or more predisposing factors [12,13] (Table 2).
Clinical Signs and Symptoms
Symptoms of CAP include fever, chills, rigors, fatigue, anorexia, diaphoresis, dyspnea, cough (with or without sputum production), and pleuritic chest pain. There is no individual symptom or cluster of symptoms that can absolutely differentiate pneumonia from other acute respiratory diseases, including upper and lower respiratory infections. However, if a patient presents with the constellation of symptoms of fever ≥ 1000F (37.80C), productive cough, and tachycardia, it is more suggestive of pneumonia [14]. Abnormal vital signs include fever, hypothermia, tachypnea, tachycardia, and oxygen desaturation. Auscultation of the chest reveals crackles or other adventitious breath sounds. Elderly patients with pneumonia report a significantly lower number of both respiratory and nonrespiratory symptoms compared with younger patients. Clinicians should be aware of this phenomenon so it does not lead to delayed diagnosis and treatment [15].
Imaging Evaluation
The presence of a pulmonary consolidation or an infiltrate on chest radiograph is required to diagnose CAP, and a chest radiograph should be obtained when CAP is suspected [16]. It should be noted that there is no pattern of radiographic abnormalities reliable enough to differentiate infectious pneumonia from noninfectious causes [17].
There are case reports and case series demonstrating false-negative plain chest radiographs existing in dehydrated patients [18] or in neutropenic state. However, animal studies have shown that dogs challenged with pneumococcus showed abnormal pulmonary shadow, suggestive of pneumonia, regardless of hydration status [19]. There is also no reliable scientific evidence to support the notion that severe neutropenia can cause false-negative radiographs because of the inability to develop an acute inflammatory reaction in the lungs [20].
A chest CT scan is more sensitive than a plain chest radiograph in detecting pneumonia. Therefore, a chest CT should be performed in a patient with negative plain chest radiograph when pneumonia is still highly suspected [21]. A chest CT scan is also more sensitive in detecting cavitation, adenopathy, interstitial disease and empyema. It also has the advantage of better defining anatomical changes than plain films [22].
Because improvement of pulmonary opacities in patients with CAP lags behind clinical improvement, repeating chest imaging studies is not recommended in patients who demonstrate clinical improvement. Sometimes clearing of pulmonary infiltrate or consolidation can take 6 weeks or longer [23].
Laboratory Evaluation
Generally the etiologic agent of CAP cannot be determined solely on the basis of clinical signs and symptoms or imaging studies. Although routine microbiological testing for patients suspicious for CAP is not necessary for empirical treatment, by determining the etiologic agent of the pneumonia, a clinician will be able to narrow the antibiotics from a broad-spectrum empirical regimen to specific pathogen-directed therapy. Determination of certain etiologic agents causing the pneumonia can have important public health implications (eg, Mycobacterium tuberculosis and influenza virus) [24].
Sputum Gram Stain and Culture
Sputum Gram stain is an inexpensive test that may identify pathogens that cause CAP (eg, S. pneumonia and Haemophilus influenzae). A quality specimen is required. A sputum sample must contain > 25 neutrophils and < 10 squamous epithelial cells/low power field on Gram stain to be considered suitable for culture.
The sensitivity and specificity of sputum Gram stain and culture are highly variable in different clinical settings (eg, outpatient setting, nursing home, ICU). Reed et al’s meta-analysis of patients diagnosed with CAP in the United States showed the sensitivity and specificity of sputum Gram stain (compared with sputum culture) ranged from 15% to 100% and 11% to 100%, respectively [24]. In cases of proven bacteremic pneumococcal pneumonia, positive cultures from sputum samples were positive less than 50% of the time [25].
For patients who cannot provide sputum samples or are intubated, a deep-suction aspirate or bronchoalveolar lavage through a bronchoscopic procedure might be necessary to obtain pulmonary secretion for Gram stain and culture. Besides bacterial culture, sputum samples can also be sent for fungal and mycobacterial cultures and acid-fast stain if deemed clinically necessary.
Blood Culture
Because the positivity rate of blood culture in patients who are suspected to have pneumonia but not exposed to antimicrobial agents is disappointingly low (5%–14%), blood cultures are no longer recommended in patients hospitalized for CAP. Another reason for not recommending blood culture is positive culture rarely leads to changes in antibiotic regimen in patients without underlying diseases [26]. However, high-risk patients, including patients with severe CAP or in immunocompromised patients (eg, patients with neutropenia, asplenia or complement deficiencies) should have a blood culture done [24].
A multinational study published in 2008 examined 125 patients with pneumococcal bacteremic CAP versus 1847 patients with non-bacteremic CAP [27]. Analysis of the data demonstrated no association of pneumococcal bacteremic CAP and time to clinical stability, length of hospital stay, all-cause mortality or CAP-related mortality. The authors concluded that pneumococcal bacteremia does not increase the risk of poor outcomes in patients with CAP compared to non-bacteremic patients, and the presence of pneumococcal bacteremia should not deter de-escalation of therapy in clinically stable patients.
Urinary Antigen Tests
Urinary antigen tests may assist clinicians in narrowing antibiotic therapy when test results are positive. There are 2 U.S. Food and Drug Administration–approved tests available to clinicians for detecting pneumococcal and Legionella antigen in urine. The test for Legionella pneumophila detects disease due to serogroup 1 only, which accounts for 80% of community-acquired Legionnaires disease. The sensitivity and specificity of the Legionella urine antigen test are 90% and 99%, respectively. The pneumococcal urine antigen test is less sensitive and specific than the Legionella urine antigen test (sensitivity 80% and specificity > 90%) [28,29].
Advantages of the urinary antigen tests are that they are easily performed, results are available in less than an hour if done in-house, and results are not affected by prior exposure to antibiotics. However, the tests do not meet Clinical Laboratory Improvements Amendments criteria for waiver and must be performed by a technician in the laboratory.
Polymerase Chain Reaction
There are several FDA-approved polymerase chain reaction (PCR) tests commercially available to assist clinicians in diagnosing pneumonia. PCR test of nasopharyngeal swabs for diagnosing influenza have become standard in many medical U.S. facilities. The great advantage of using PCR to diagnose influenza is its high sensitivity and specificity and rapid turnaround time. PCR can also be used to detect Legionella species, S. pneumonia, Mycoplasma pneumoniae, Chlamydophila pneumonia and mycobacterial species [24].
One limitation of using PCR tests on respiratory specimens is that specimens can be contaminated with oral or upper airway flora, so the results must be interpreted with caution, bearing in mind that some of the pathogens isolated may be colonizers of the oral or upper airway flora [30].
Biologic Markers
Two biologic markers—procalcitonin and C-reactive protein (CRP)—can be used in conjunction with history, physical examination, laboratory tests and imaging studies to assist in the diagnosis and treatment of CAP [24]. Procalcitonin is a peptide precursor of the hormone calcitonin that is released by parenchymal cells into the bloodstream resulting in increased serum level in patients with bacterial infections. In contrast, there is no remarkable proclacitonin level increase with viral or noninfectious inflammation. The reference value of procalcitonin in the blood of an adult individual without infection or inflammation is < 0.15 ng/mL. In the blood, procalcitonin has a half-life of 25 to 30 hours. The quantitative immunoluminometric method (LUMI test, Brahms PCT, Berlin, Germany ) is the preferred test to use because of its high sensitivity [31].
A 2012 Cochrane meta-analysis that involved 4221 patients with acute respiratory infections (with half of the patients diagnosed with CAP) from 14 prospective trials found the use of procalcitonin test for antibiotic use significantly decreased median antibiotic exposure from 8 to 4 days without an increase in treatment failure, mortality rates in any clinical setting (eg, outpatient clinic, emergency room), or length of hospitalization [32]. A prospective study conducted in France on 100 ICU patients showed that increased procalcitonin from day 1 to day 3 has a poor prognosis factor for severe CAP whereas decreasing procalcitonin levels is associated with a favorable outcome [33].
CRP is an acute phase protein produced by the liver. CRP level in the blood increases in response to acute infection or inflammation. Use of CRP in assisting diagnosis and guiding treatment of CAP is more limited in part due to its poor specificity. A prospective study conducted on 168 consecutive patients presented with cough showed that a CRP > 40 mg/L had a sensitivity and specificity of 70% and 90%, respectively [34].
T reatment
Site of Care Decision
For patients with CAP, the clinician must decide whether the patient will be treated in an outpatient or inpatient setting, and for those in the inpatient setting, whether they can safely be treated on the general medical ward or should be the ICU. Two common scoring systems that can be used to aid the clinician in determining severity of the infection and guiding site-of-care decisions are the Pneumonia Severity Index (PSI) and CURB-65 scores.
The PSI score uses 20 different parameters, including comorbidities, laboratory parameters and radiographic findings to stratify patients into 5 mortality risk classes [35]. On the basis of associated mortality rates, it has been suggested that risk class I and II patients should be treated as outpatients, risk class III patients should be treated in an observation unit or with a short hospitalization, and risk class IV and V patients should be treated as inpatients [35].
The CURB-65 method of risk stratification is based on 5 clinical parameters: confusion, urea level, respiratory rate, systolic blood pressure and age ≥ 65 (Table 3) [36].
Patients with CURB-65 scores of 4 or 5 are considered to have severe pneumonia and admission to the ICU should be considered. Aside from the CURB-65 score, anyone requiring vasopressor support or mechanical ventilation merits admission to the ICU [16]. IDSA/ATS guidelines also recommend the use of “minor criteria” for making ICU admission decisions; these include respiratory rate ≥ 30 breaths / minute, PaO2 fraction ≤ 250, multilobar infiltrates, confusion, blood urea nitrogen ≥ 20 mg/dL, leukopenia, thrombocytopenia, hypothermia and hypotension [16]. These factors are associated with increased mortality due to CAP and admission to an ICU is indicated if 3 of the minor criteria for severe CAP are present.
Similar to CURB-65, another clinical calculator that can be used for assessing severity of CAP is SMART-COP [39]. This scoring system uses 8 weighted criteria to predict which patients will require intensive respiratory or vasopressor support. SMART-COP has a sensitivity of 79% and specificity 64% in predicting ICU admission, whereas CURB-65 had a pooled sensitivity of 57.2% and specificity of 77.2% [40].
Antibiotic Therapy
Antibiotics are the mainstay of treatment for CAP, with the majority of patients with CAP treated empirically taking into account the site of care, likely pathogen, and antimicrobial resistance issues. Patients with pneumonia who are treated as outpatients usually respond well to empiric antibiotic treatment and a causative pathogen is not usually sought. Patients who are hospitalized for treatment of CAP usually receive empiric antibiotic on admission. Once the etiology has been determined by microbiologic or serologic means, antimicrobial therapy should be adjusted accordingly. As noted previously, a CDC study found that the burden of viral etiologies was higher than previously thought, with rhinovirus and influenza accounting for 15% of cases and S. pneumoniae for only 5% [9]. This study highlighted the fact that despite advances in molecular techniques, most patients with pneumonia have no pathogen identified [9]. Given the lack of discernable pathogens in the majority of cases, unless a nonbacterial etiology is found patients should continue to be treated with antibiotics.
Outpatients without comorbidities or risk factors for drug-resistant S. pneumoniae (Table 4)
As previously mentioned, antibiotic therapy is typically empiric; neither clinical features nor radiographic features are sufficient to include or exclude infectious etiologies. Epidemiologic risk factors should be considered and, in certain cases, expanded antimicrobial coverage to include those entities; for example, treatment of anaerobes in the setting of lung abscess and antipseudomonal antibiotics for patients with bronchiectasis.
Of concern in the treatment of CAP is the increased prevalence of antimicrobial resistance among S. pneumoniae. The IDSA guidelines report that drug-resistant S. pneumoniae is more common in persons aged < 2 or > 65 years, and those with ß-lactam therapy within the previous 3 months, alcoholism, medical comorbidities, immunosuppressive illness or therapy, or exposure to a child who attends a day care center [16].
S. aureus should be considered during influenza outbreaks, with either vancomycin or linezolid being the recommended agents in the setting of methicillin-resistant S. aureus (MRSA). In a study comparing vancomycin versus linezolid for nosocomial pneumonia, the all-cause 60-day mortality was similar for both agents [41]. Datpomycin is another agent used against MRSA; however, its use in the setting of pneumonia is not indicated as daptomycin binds to surfactant, yielding it ineffective in the treatment of pneumonia [42]. Ceftaroline is a newer cephalosporin with activity against MRSA; its role in treatment of community-acquired MRSA pneumonia has not been fully elucidated, but it appears to be a useful agent for this indication [43,44].
A summary of recommended empiric antibiotic therapy is presented in Table 5.
Antibiotic Therapy for Selected Pathogens
S. pneumoniae
Patients with pneumococcal pneumonia who have penicillin-susceptible strains can be treated with intravenous penicillin (2 or 3 million units every 4 hours) or ceftriaxone. Once a patient meets criteria of stability, they can then be transitioned to oral penicillin, amoxicillin, or clarithromycin. Those with strains with reduced susceptibility can still be treated with penicillin but at a higher dose (4 million units IV every 4 hours) or a third-generation cephalosporin. Those whose pneumococcal pneumonia is complicated by bacteremia will benefit from dual therapy if severely ill, requiring ICU monitoring. Those not severely ill can be treated with monotherapy [46].
S. aureus
S. aureus is more commonly associated with hospital-acquired pneumonia but may also be seen during the influenza season and in those with severe necrotizing CAP. Both linezolid and vancomycin can be used to treat MRSA CAP. As noted above, ceftaroline has activity against MRSA and is approved for treatment of CAP, but is not approved by the FDA for MRSA CAP treatment. Similarly, tigecycline is approved for CAP and has activity against MRSA, but is not approved for MRSA CAP. Moreover, the FDA has warned of increased risk of death with tigecycline and has a black box warning to that effect [47].
Legionella
Treatment of legionellosis can be achieved with tetracyclines, macrolides, or fluoroquinolones. For nonimmunosuppressed patients with mild pneumonia, any of the listed antibiotics is considered appropriate. However, patients with severe infection or those with immunosuppression should be treated with either levofloxacin or azithromycin for 7 to 10 days [48].
C. pneumoniae
As with other atypical organisms, C. pneumoniae can be treated with doxycycline, a macrolide, or respiratory fluoroquinolones. However, length of therapy varies by regimen used; whereas treating with doxycycline 100 mg twice daily generally requires 14–21 days, moxifloxacin 400 mg daily only requires 10 days [49].
M. pneumoniae
As with C. pneumoniae, length of therapy of M. pneumoniae varies by antimicrobial used. Shortest courses are seen with the use of macrolides for 5 days, whereas 14 days is considered standard for doxycycline or a respiratory fluoroquinolone [50]. It should be noted that there has been increasingly documented resistance to macrolides, with known resistance of 8.2% in the United States [51].
Duration of Treatment
Most patients with CAP respond within 72 hours to appropriate therapy. IDSA/ATS guidelines recommend that patients be treated for a minimum of 5 days, and before discontinuing antibiotics patients should be afebrile a minimum of 48-72 hours and be clinically stable (Table 6) [16].
Hospitalized patients do not need to be monitored for an additional day once they have reached clinical stability (Table 6), are able to maintain oral intake, and have normal mentation, provided that other comorbidities are stable and social needs have been met [16]. Patients discharged from the hospital with instability have higher risk of readmission or death [55].
Transition to Oral Therapy
IDSA/ATS guidelines [16] recommend that patients should be transitioned from IV to oral antibiotics when they are improving clinically, have stable vital signs, and are able to ingest food/fluids and medications.
Management of Nonresponders
Although the majority of patients respond to antibiotics within 72 hours, treatment failure occurs in up to 15% of patients [45]. Nonresponding pneumonia is generally seen in 2 patterns: worsening of clinical status despite empiric antibiotics OR delay in achieving clinical stability as defined in Table 5 after 72 hours of treatment [13]. Risk factors associated with nonresponding pneumonia [56] are:
- Radiographic: multilobar infiltrates, pleural effusion, cavitation
- Bacteriologic: MRSA, gram-negative or Legionella pneumonia
- Severity index: PSI > 90
- Pharmacologic: incorrect antibiotic choice based on susceptibility
Patients with acute deterioration of clinical status will prompt transfer to a higher level of care and may require mechanical ventilator support. In those with delay in achieving clinical stability, question centers on whether the same antibiotics can be continued while doing further radiographic/microbiologic workup and/or changing antibiotics.
History should be reviewed with particular attention to exposures, travel history, and microbiologic and radiographic data. Clinicians should recall that viral causes account for up to 20% of pneumonias and there are also noninfectious causes that can mimic pyogenic infections [57]. If adequate initial cultures were not obtained, they should be obtained; however, care must be taken in reviewing new sets of cultures while on antibiotics as they may reveal colonization selected out by antibiotics and not a true pathogen. If repeat evaluation is unrevealing, then further evaluation with CT scan and bronchoscopy with bronchoalveolar lavage and biopsy is warranted. CT scans can show pleural effusions, bronchial obstructions or pattern suggestive of cryptogenic pneumonia. A bronchoscopy might yield a microbiologic diagnosis and with biopsy can also evaluate for noninfectious causes.
As with other infections, if escalation of antibiotics is undertaken, clinicians should be mindful to ensure that efforts are being made to elucidate the reason for nonresponse. To simply broaden antimicrobial therapy without attempts at establishing a microbiologic or radiographic cause for nonresponse may lead to inappropriate treatment recurrence of infection. Aside from patients who have bacteremic pneumococcal pneumonia in an ICU setting, there are no published reports pointing to superiority of combination antibiotics [46].
Other Treatment
Because of the inflammatory response associated with pneumonia, several agents have been evaluated as adjunctive treatment of pneumonia to decrease this inflammatory state; namely, steroids, macrolide antibiotics and statins. To date, only the use of steroids (methylprednisolone 0.5 mg/kg every 12 hours for 5 days) in those with severe CAP and high initial anti-inflammatory response (CRP > 150) was shown to decrease treatment failure, decreased risk of ARDS, possibly reduce length of stay, duration of intravenous antibiotics and clinical stability, without effect on mortality or adverse side effects [58,59].
Other adjunctive methods have not been found to have significant impact [16].
Prevention of Pneumonia
Prevention of pneumococcal pneumonia is twofold: prevention of infection caused by S. pneumoniae and prevention of influenza infection. As influenza infection is a risk factor for bacterial infection, specifically with S. pneumoniae, influenza vaccination can prevent bacterial pneumonia [60]. In their most recent recommendations, the CDC continues to recommend routine influenza vaccination for all persons aged greater than 6 months, unless otherwise contraindicated [61].
There are 2 vaccines for prevention of pneumococcal disease: the pneumococcal polysaccharide vaccine (PPSV23) and a conjugate vaccine (PCV13). Following vaccination with PPSV23, 80% of adults develop antibodies against at least 18 of the 23 serotypes [62]. Despite this response, PPSV23 is reported to be protective against invasive pneumococcal infection; yet there is no consensus regarding PPSV23 leading to decreased rates of pneumonia [63]. On the other hand, PCV13 vaccination was associated with prevention of both invasive disease and community-acquired pneumonia in adults 65 years or older [64]. The CDC recommends that all children aged 2 or under receive PCV13, whereas those aged 65 or older should receive PCV13 followed by a dose of PPSV23 [65]. The dose of PPSV23 should be given ≥1 year following the dose of PCV13 [66].Persons < 65 years of age with immunocompromising and certain other conditions should also receive vaccination [67] (Table 7). Full details, many scenarios, and timing of vaccinations can be found at www.cdc.gov/vaccines/schedules/downloads/adult/adult-schedule.pdf.
Cigarette smoking increases the risk of respiratory infections as evidenced by smokers accounting for almost half of all patients with invasive pneumococcal disease [11]. As this is a modifiable risk factor it should be a goal of a comprehensive approach towards prevention of pneumonia.
Summary
CAP remains a leading cause of hospitalization and death in the 21st century. Traditionally, pneumococcus has been considered the major pathogen causing CAP; however, the 2015 EPIC study found that in only 5% of patients diagnosed with CAP was S. pneumoniae detected. Despite the new findings, it is still recommended that empiric treatment for CAP target common typical bacteria (pneumococcus, H. influenzae, Moraxella catarrhalis) and atypical bacteria (M. pneumonia, C. pneumoniae, L. pneumophila).
Because diagnosing pneumonia through history and clinical examination is less than 50% sensitive, a chest imaging study (a plain chest radiograph or a chest CT scan) is usually required to make the diagnosis. Laboratory tests, such as sputum Gram stain/culture, blood culture, urinary antigen tests, PCR test, procalcitonin, and CRP are important adjunctive diagnostic modalities to assist in the diagnosis and management of CAP. However, no single test is sensitive and specific enough to be a stand-alone test. They should be used in conjunction with history, physical examination, and imaging studies. Because vaccination (PPSV23, PCV13, and influenza vaccine) remains the most effective tool in preventing the development of CAP, clinicians, should strive for 100% vaccination rates in appropriate persons.
Corresponding author: Tze Shein Lo, MD, University of North Dakota, 1919 Elm Street, Fargo, ND 58102, [email protected].
Financial disclosures: None.
Author contributions: drafting of article, PM, TSL; critical revision of the article, PM, TSL.
From the University of North Dakota School of Medicine & Health Sciences, Fargo, ND.
Abstract
- Objective: To review the management of community-acquired pneumonia (CAP) in adults.
- Methods: Review of the literature.
- Results: Approximately 4 to 5 million cases of CAP are diagnosed in the United States annually, accounting for significant morbidity and mortality. While numerous studies have previously shown pneumococcus to be the most common causative pathogen, the 2015 EPIC study found that in nearly two-thirds of patients with CAP who required hospitalization, no pathogen was detected. Symptoms and signs of respiratory tract infection are useful in helping to diagnose pneumonia; however, they are less sensitive than chest imaging studies. Laboratory tests used in diagnosing pneumonia include sputum Gram stain and culture, blood culture, urinary antigen, polymerase chain reaction, and biologic markers. In empiric treatment of CAP, both the typical and atypical pathogens should be targeted. Influenza vaccine and pneumococcal polysaccharide and conjugate vaccines should be administered as recommended by the CDC to reduce risk of CAP.
- Conclusion: CAP is a common illness with high rates of morbidity and mortality. Treatment is for the most part empirical; diagnostic testing can be used to identify the causative organism and guide pathogen-specific therapy.
Key words: community-acquired pneumonia; adults; management; vaccines.
Despite advances in medical science, pneumonia remains a major cause of morbidity and mortality. In 2014, 50,620 patients in the United States died from the disease [1]. Pneumonia can be classified as community-acquired, hospital-acquired, or ventilator-associated. Another category, healthcare-associated pneumonia, was included in an earlier American Thoracic Society (ATS) and Infectious Diseases Society of America (IDSA) guideline but was removed from the 2016 guideline because there was no clear evidence that patients diagnosed with healthcare-associated pneumonia were at higher risk for harboring multidrug-resistant pathogens [2]. In this article, we review the epidemiology, microbiology, predisposing factors, diagnosis, treatment, and prevention of community-acquired pneumonia (CAP).
Definition and Epidemiology
CAP is defined as an acute infection of the lungs that develops in patients who have not been hospitalized recently and have not had regular exposure to the health care system [3]. A previously ambulatory patient who is diagnosed with pneumonia within 48 hours after admission also meets the criteria for CAP. Approximately 4 to 5 million cases of CAP are diagnosed in the United States annually [4]. About 25% of CAP patients require hospitalization, and about 5% to 10% of these patients are admitted to the intensive care unit (ICU) [5]. In-hospital mortality is considerable (~10% in population-based studies) [6] and 30-day mortality was found to be as high as 23% in a review by File and Marrie [7]. CAP also confers a high risk of long-term morbidity and mortality compared with the general population who have never had CAP, irrespective of age [8].
Causative Organisms
Numerous microorganisms can cause CAP. Common causes and less common causes are delineated in Table 1.
Predisposing Factors
Most people diagnosed with CAP have one or more predisposing factors [12,13] (Table 2).
Clinical Signs and Symptoms
Symptoms of CAP include fever, chills, rigors, fatigue, anorexia, diaphoresis, dyspnea, cough (with or without sputum production), and pleuritic chest pain. There is no individual symptom or cluster of symptoms that can absolutely differentiate pneumonia from other acute respiratory diseases, including upper and lower respiratory infections. However, if a patient presents with the constellation of symptoms of fever ≥ 1000F (37.80C), productive cough, and tachycardia, it is more suggestive of pneumonia [14]. Abnormal vital signs include fever, hypothermia, tachypnea, tachycardia, and oxygen desaturation. Auscultation of the chest reveals crackles or other adventitious breath sounds. Elderly patients with pneumonia report a significantly lower number of both respiratory and nonrespiratory symptoms compared with younger patients. Clinicians should be aware of this phenomenon so it does not lead to delayed diagnosis and treatment [15].
Imaging Evaluation
The presence of a pulmonary consolidation or an infiltrate on chest radiograph is required to diagnose CAP, and a chest radiograph should be obtained when CAP is suspected [16]. It should be noted that there is no pattern of radiographic abnormalities reliable enough to differentiate infectious pneumonia from noninfectious causes [17].
There are case reports and case series demonstrating false-negative plain chest radiographs existing in dehydrated patients [18] or in neutropenic state. However, animal studies have shown that dogs challenged with pneumococcus showed abnormal pulmonary shadow, suggestive of pneumonia, regardless of hydration status [19]. There is also no reliable scientific evidence to support the notion that severe neutropenia can cause false-negative radiographs because of the inability to develop an acute inflammatory reaction in the lungs [20].
A chest CT scan is more sensitive than a plain chest radiograph in detecting pneumonia. Therefore, a chest CT should be performed in a patient with negative plain chest radiograph when pneumonia is still highly suspected [21]. A chest CT scan is also more sensitive in detecting cavitation, adenopathy, interstitial disease and empyema. It also has the advantage of better defining anatomical changes than plain films [22].
Because improvement of pulmonary opacities in patients with CAP lags behind clinical improvement, repeating chest imaging studies is not recommended in patients who demonstrate clinical improvement. Sometimes clearing of pulmonary infiltrate or consolidation can take 6 weeks or longer [23].
Laboratory Evaluation
Generally the etiologic agent of CAP cannot be determined solely on the basis of clinical signs and symptoms or imaging studies. Although routine microbiological testing for patients suspicious for CAP is not necessary for empirical treatment, by determining the etiologic agent of the pneumonia, a clinician will be able to narrow the antibiotics from a broad-spectrum empirical regimen to specific pathogen-directed therapy. Determination of certain etiologic agents causing the pneumonia can have important public health implications (eg, Mycobacterium tuberculosis and influenza virus) [24].
Sputum Gram Stain and Culture
Sputum Gram stain is an inexpensive test that may identify pathogens that cause CAP (eg, S. pneumonia and Haemophilus influenzae). A quality specimen is required. A sputum sample must contain > 25 neutrophils and < 10 squamous epithelial cells/low power field on Gram stain to be considered suitable for culture.
The sensitivity and specificity of sputum Gram stain and culture are highly variable in different clinical settings (eg, outpatient setting, nursing home, ICU). Reed et al’s meta-analysis of patients diagnosed with CAP in the United States showed the sensitivity and specificity of sputum Gram stain (compared with sputum culture) ranged from 15% to 100% and 11% to 100%, respectively [24]. In cases of proven bacteremic pneumococcal pneumonia, positive cultures from sputum samples were positive less than 50% of the time [25].
For patients who cannot provide sputum samples or are intubated, a deep-suction aspirate or bronchoalveolar lavage through a bronchoscopic procedure might be necessary to obtain pulmonary secretion for Gram stain and culture. Besides bacterial culture, sputum samples can also be sent for fungal and mycobacterial cultures and acid-fast stain if deemed clinically necessary.
Blood Culture
Because the positivity rate of blood culture in patients who are suspected to have pneumonia but not exposed to antimicrobial agents is disappointingly low (5%–14%), blood cultures are no longer recommended in patients hospitalized for CAP. Another reason for not recommending blood culture is positive culture rarely leads to changes in antibiotic regimen in patients without underlying diseases [26]. However, high-risk patients, including patients with severe CAP or in immunocompromised patients (eg, patients with neutropenia, asplenia or complement deficiencies) should have a blood culture done [24].
A multinational study published in 2008 examined 125 patients with pneumococcal bacteremic CAP versus 1847 patients with non-bacteremic CAP [27]. Analysis of the data demonstrated no association of pneumococcal bacteremic CAP and time to clinical stability, length of hospital stay, all-cause mortality or CAP-related mortality. The authors concluded that pneumococcal bacteremia does not increase the risk of poor outcomes in patients with CAP compared to non-bacteremic patients, and the presence of pneumococcal bacteremia should not deter de-escalation of therapy in clinically stable patients.
Urinary Antigen Tests
Urinary antigen tests may assist clinicians in narrowing antibiotic therapy when test results are positive. There are 2 U.S. Food and Drug Administration–approved tests available to clinicians for detecting pneumococcal and Legionella antigen in urine. The test for Legionella pneumophila detects disease due to serogroup 1 only, which accounts for 80% of community-acquired Legionnaires disease. The sensitivity and specificity of the Legionella urine antigen test are 90% and 99%, respectively. The pneumococcal urine antigen test is less sensitive and specific than the Legionella urine antigen test (sensitivity 80% and specificity > 90%) [28,29].
Advantages of the urinary antigen tests are that they are easily performed, results are available in less than an hour if done in-house, and results are not affected by prior exposure to antibiotics. However, the tests do not meet Clinical Laboratory Improvements Amendments criteria for waiver and must be performed by a technician in the laboratory.
Polymerase Chain Reaction
There are several FDA-approved polymerase chain reaction (PCR) tests commercially available to assist clinicians in diagnosing pneumonia. PCR test of nasopharyngeal swabs for diagnosing influenza have become standard in many medical U.S. facilities. The great advantage of using PCR to diagnose influenza is its high sensitivity and specificity and rapid turnaround time. PCR can also be used to detect Legionella species, S. pneumonia, Mycoplasma pneumoniae, Chlamydophila pneumonia and mycobacterial species [24].
One limitation of using PCR tests on respiratory specimens is that specimens can be contaminated with oral or upper airway flora, so the results must be interpreted with caution, bearing in mind that some of the pathogens isolated may be colonizers of the oral or upper airway flora [30].
Biologic Markers
Two biologic markers—procalcitonin and C-reactive protein (CRP)—can be used in conjunction with history, physical examination, laboratory tests and imaging studies to assist in the diagnosis and treatment of CAP [24]. Procalcitonin is a peptide precursor of the hormone calcitonin that is released by parenchymal cells into the bloodstream resulting in increased serum level in patients with bacterial infections. In contrast, there is no remarkable proclacitonin level increase with viral or noninfectious inflammation. The reference value of procalcitonin in the blood of an adult individual without infection or inflammation is < 0.15 ng/mL. In the blood, procalcitonin has a half-life of 25 to 30 hours. The quantitative immunoluminometric method (LUMI test, Brahms PCT, Berlin, Germany ) is the preferred test to use because of its high sensitivity [31].
A 2012 Cochrane meta-analysis that involved 4221 patients with acute respiratory infections (with half of the patients diagnosed with CAP) from 14 prospective trials found the use of procalcitonin test for antibiotic use significantly decreased median antibiotic exposure from 8 to 4 days without an increase in treatment failure, mortality rates in any clinical setting (eg, outpatient clinic, emergency room), or length of hospitalization [32]. A prospective study conducted in France on 100 ICU patients showed that increased procalcitonin from day 1 to day 3 has a poor prognosis factor for severe CAP whereas decreasing procalcitonin levels is associated with a favorable outcome [33].
CRP is an acute phase protein produced by the liver. CRP level in the blood increases in response to acute infection or inflammation. Use of CRP in assisting diagnosis and guiding treatment of CAP is more limited in part due to its poor specificity. A prospective study conducted on 168 consecutive patients presented with cough showed that a CRP > 40 mg/L had a sensitivity and specificity of 70% and 90%, respectively [34].
T reatment
Site of Care Decision
For patients with CAP, the clinician must decide whether the patient will be treated in an outpatient or inpatient setting, and for those in the inpatient setting, whether they can safely be treated on the general medical ward or should be the ICU. Two common scoring systems that can be used to aid the clinician in determining severity of the infection and guiding site-of-care decisions are the Pneumonia Severity Index (PSI) and CURB-65 scores.
The PSI score uses 20 different parameters, including comorbidities, laboratory parameters and radiographic findings to stratify patients into 5 mortality risk classes [35]. On the basis of associated mortality rates, it has been suggested that risk class I and II patients should be treated as outpatients, risk class III patients should be treated in an observation unit or with a short hospitalization, and risk class IV and V patients should be treated as inpatients [35].
The CURB-65 method of risk stratification is based on 5 clinical parameters: confusion, urea level, respiratory rate, systolic blood pressure and age ≥ 65 (Table 3) [36].
Patients with CURB-65 scores of 4 or 5 are considered to have severe pneumonia and admission to the ICU should be considered. Aside from the CURB-65 score, anyone requiring vasopressor support or mechanical ventilation merits admission to the ICU [16]. IDSA/ATS guidelines also recommend the use of “minor criteria” for making ICU admission decisions; these include respiratory rate ≥ 30 breaths / minute, PaO2 fraction ≤ 250, multilobar infiltrates, confusion, blood urea nitrogen ≥ 20 mg/dL, leukopenia, thrombocytopenia, hypothermia and hypotension [16]. These factors are associated with increased mortality due to CAP and admission to an ICU is indicated if 3 of the minor criteria for severe CAP are present.
Similar to CURB-65, another clinical calculator that can be used for assessing severity of CAP is SMART-COP [39]. This scoring system uses 8 weighted criteria to predict which patients will require intensive respiratory or vasopressor support. SMART-COP has a sensitivity of 79% and specificity 64% in predicting ICU admission, whereas CURB-65 had a pooled sensitivity of 57.2% and specificity of 77.2% [40].
Antibiotic Therapy
Antibiotics are the mainstay of treatment for CAP, with the majority of patients with CAP treated empirically taking into account the site of care, likely pathogen, and antimicrobial resistance issues. Patients with pneumonia who are treated as outpatients usually respond well to empiric antibiotic treatment and a causative pathogen is not usually sought. Patients who are hospitalized for treatment of CAP usually receive empiric antibiotic on admission. Once the etiology has been determined by microbiologic or serologic means, antimicrobial therapy should be adjusted accordingly. As noted previously, a CDC study found that the burden of viral etiologies was higher than previously thought, with rhinovirus and influenza accounting for 15% of cases and S. pneumoniae for only 5% [9]. This study highlighted the fact that despite advances in molecular techniques, most patients with pneumonia have no pathogen identified [9]. Given the lack of discernable pathogens in the majority of cases, unless a nonbacterial etiology is found patients should continue to be treated with antibiotics.
Outpatients without comorbidities or risk factors for drug-resistant S. pneumoniae (Table 4)
As previously mentioned, antibiotic therapy is typically empiric; neither clinical features nor radiographic features are sufficient to include or exclude infectious etiologies. Epidemiologic risk factors should be considered and, in certain cases, expanded antimicrobial coverage to include those entities; for example, treatment of anaerobes in the setting of lung abscess and antipseudomonal antibiotics for patients with bronchiectasis.
Of concern in the treatment of CAP is the increased prevalence of antimicrobial resistance among S. pneumoniae. The IDSA guidelines report that drug-resistant S. pneumoniae is more common in persons aged < 2 or > 65 years, and those with ß-lactam therapy within the previous 3 months, alcoholism, medical comorbidities, immunosuppressive illness or therapy, or exposure to a child who attends a day care center [16].
S. aureus should be considered during influenza outbreaks, with either vancomycin or linezolid being the recommended agents in the setting of methicillin-resistant S. aureus (MRSA). In a study comparing vancomycin versus linezolid for nosocomial pneumonia, the all-cause 60-day mortality was similar for both agents [41]. Datpomycin is another agent used against MRSA; however, its use in the setting of pneumonia is not indicated as daptomycin binds to surfactant, yielding it ineffective in the treatment of pneumonia [42]. Ceftaroline is a newer cephalosporin with activity against MRSA; its role in treatment of community-acquired MRSA pneumonia has not been fully elucidated, but it appears to be a useful agent for this indication [43,44].
A summary of recommended empiric antibiotic therapy is presented in Table 5.
Antibiotic Therapy for Selected Pathogens
S. pneumoniae
Patients with pneumococcal pneumonia who have penicillin-susceptible strains can be treated with intravenous penicillin (2 or 3 million units every 4 hours) or ceftriaxone. Once a patient meets criteria of stability, they can then be transitioned to oral penicillin, amoxicillin, or clarithromycin. Those with strains with reduced susceptibility can still be treated with penicillin but at a higher dose (4 million units IV every 4 hours) or a third-generation cephalosporin. Those whose pneumococcal pneumonia is complicated by bacteremia will benefit from dual therapy if severely ill, requiring ICU monitoring. Those not severely ill can be treated with monotherapy [46].
S. aureus
S. aureus is more commonly associated with hospital-acquired pneumonia but may also be seen during the influenza season and in those with severe necrotizing CAP. Both linezolid and vancomycin can be used to treat MRSA CAP. As noted above, ceftaroline has activity against MRSA and is approved for treatment of CAP, but is not approved by the FDA for MRSA CAP treatment. Similarly, tigecycline is approved for CAP and has activity against MRSA, but is not approved for MRSA CAP. Moreover, the FDA has warned of increased risk of death with tigecycline and has a black box warning to that effect [47].
Legionella
Treatment of legionellosis can be achieved with tetracyclines, macrolides, or fluoroquinolones. For nonimmunosuppressed patients with mild pneumonia, any of the listed antibiotics is considered appropriate. However, patients with severe infection or those with immunosuppression should be treated with either levofloxacin or azithromycin for 7 to 10 days [48].
C. pneumoniae
As with other atypical organisms, C. pneumoniae can be treated with doxycycline, a macrolide, or respiratory fluoroquinolones. However, length of therapy varies by regimen used; whereas treating with doxycycline 100 mg twice daily generally requires 14–21 days, moxifloxacin 400 mg daily only requires 10 days [49].
M. pneumoniae
As with C. pneumoniae, length of therapy of M. pneumoniae varies by antimicrobial used. Shortest courses are seen with the use of macrolides for 5 days, whereas 14 days is considered standard for doxycycline or a respiratory fluoroquinolone [50]. It should be noted that there has been increasingly documented resistance to macrolides, with known resistance of 8.2% in the United States [51].
Duration of Treatment
Most patients with CAP respond within 72 hours to appropriate therapy. IDSA/ATS guidelines recommend that patients be treated for a minimum of 5 days, and before discontinuing antibiotics patients should be afebrile a minimum of 48-72 hours and be clinically stable (Table 6) [16].
Hospitalized patients do not need to be monitored for an additional day once they have reached clinical stability (Table 6), are able to maintain oral intake, and have normal mentation, provided that other comorbidities are stable and social needs have been met [16]. Patients discharged from the hospital with instability have higher risk of readmission or death [55].
Transition to Oral Therapy
IDSA/ATS guidelines [16] recommend that patients should be transitioned from IV to oral antibiotics when they are improving clinically, have stable vital signs, and are able to ingest food/fluids and medications.
Management of Nonresponders
Although the majority of patients respond to antibiotics within 72 hours, treatment failure occurs in up to 15% of patients [45]. Nonresponding pneumonia is generally seen in 2 patterns: worsening of clinical status despite empiric antibiotics OR delay in achieving clinical stability as defined in Table 5 after 72 hours of treatment [13]. Risk factors associated with nonresponding pneumonia [56] are:
- Radiographic: multilobar infiltrates, pleural effusion, cavitation
- Bacteriologic: MRSA, gram-negative or Legionella pneumonia
- Severity index: PSI > 90
- Pharmacologic: incorrect antibiotic choice based on susceptibility
Patients with acute deterioration of clinical status will prompt transfer to a higher level of care and may require mechanical ventilator support. In those with delay in achieving clinical stability, question centers on whether the same antibiotics can be continued while doing further radiographic/microbiologic workup and/or changing antibiotics.
History should be reviewed with particular attention to exposures, travel history, and microbiologic and radiographic data. Clinicians should recall that viral causes account for up to 20% of pneumonias and there are also noninfectious causes that can mimic pyogenic infections [57]. If adequate initial cultures were not obtained, they should be obtained; however, care must be taken in reviewing new sets of cultures while on antibiotics as they may reveal colonization selected out by antibiotics and not a true pathogen. If repeat evaluation is unrevealing, then further evaluation with CT scan and bronchoscopy with bronchoalveolar lavage and biopsy is warranted. CT scans can show pleural effusions, bronchial obstructions or pattern suggestive of cryptogenic pneumonia. A bronchoscopy might yield a microbiologic diagnosis and with biopsy can also evaluate for noninfectious causes.
As with other infections, if escalation of antibiotics is undertaken, clinicians should be mindful to ensure that efforts are being made to elucidate the reason for nonresponse. To simply broaden antimicrobial therapy without attempts at establishing a microbiologic or radiographic cause for nonresponse may lead to inappropriate treatment recurrence of infection. Aside from patients who have bacteremic pneumococcal pneumonia in an ICU setting, there are no published reports pointing to superiority of combination antibiotics [46].
Other Treatment
Because of the inflammatory response associated with pneumonia, several agents have been evaluated as adjunctive treatment of pneumonia to decrease this inflammatory state; namely, steroids, macrolide antibiotics and statins. To date, only the use of steroids (methylprednisolone 0.5 mg/kg every 12 hours for 5 days) in those with severe CAP and high initial anti-inflammatory response (CRP > 150) was shown to decrease treatment failure, decreased risk of ARDS, possibly reduce length of stay, duration of intravenous antibiotics and clinical stability, without effect on mortality or adverse side effects [58,59].
Other adjunctive methods have not been found to have significant impact [16].
Prevention of Pneumonia
Prevention of pneumococcal pneumonia is twofold: prevention of infection caused by S. pneumoniae and prevention of influenza infection. As influenza infection is a risk factor for bacterial infection, specifically with S. pneumoniae, influenza vaccination can prevent bacterial pneumonia [60]. In their most recent recommendations, the CDC continues to recommend routine influenza vaccination for all persons aged greater than 6 months, unless otherwise contraindicated [61].
There are 2 vaccines for prevention of pneumococcal disease: the pneumococcal polysaccharide vaccine (PPSV23) and a conjugate vaccine (PCV13). Following vaccination with PPSV23, 80% of adults develop antibodies against at least 18 of the 23 serotypes [62]. Despite this response, PPSV23 is reported to be protective against invasive pneumococcal infection; yet there is no consensus regarding PPSV23 leading to decreased rates of pneumonia [63]. On the other hand, PCV13 vaccination was associated with prevention of both invasive disease and community-acquired pneumonia in adults 65 years or older [64]. The CDC recommends that all children aged 2 or under receive PCV13, whereas those aged 65 or older should receive PCV13 followed by a dose of PPSV23 [65]. The dose of PPSV23 should be given ≥1 year following the dose of PCV13 [66].Persons < 65 years of age with immunocompromising and certain other conditions should also receive vaccination [67] (Table 7). Full details, many scenarios, and timing of vaccinations can be found at www.cdc.gov/vaccines/schedules/downloads/adult/adult-schedule.pdf.
Cigarette smoking increases the risk of respiratory infections as evidenced by smokers accounting for almost half of all patients with invasive pneumococcal disease [11]. As this is a modifiable risk factor it should be a goal of a comprehensive approach towards prevention of pneumonia.
Summary
CAP remains a leading cause of hospitalization and death in the 21st century. Traditionally, pneumococcus has been considered the major pathogen causing CAP; however, the 2015 EPIC study found that in only 5% of patients diagnosed with CAP was S. pneumoniae detected. Despite the new findings, it is still recommended that empiric treatment for CAP target common typical bacteria (pneumococcus, H. influenzae, Moraxella catarrhalis) and atypical bacteria (M. pneumonia, C. pneumoniae, L. pneumophila).
Because diagnosing pneumonia through history and clinical examination is less than 50% sensitive, a chest imaging study (a plain chest radiograph or a chest CT scan) is usually required to make the diagnosis. Laboratory tests, such as sputum Gram stain/culture, blood culture, urinary antigen tests, PCR test, procalcitonin, and CRP are important adjunctive diagnostic modalities to assist in the diagnosis and management of CAP. However, no single test is sensitive and specific enough to be a stand-alone test. They should be used in conjunction with history, physical examination, and imaging studies. Because vaccination (PPSV23, PCV13, and influenza vaccine) remains the most effective tool in preventing the development of CAP, clinicians, should strive for 100% vaccination rates in appropriate persons.
Corresponding author: Tze Shein Lo, MD, University of North Dakota, 1919 Elm Street, Fargo, ND 58102, [email protected].
Financial disclosures: None.
Author contributions: drafting of article, PM, TSL; critical revision of the article, PM, TSL.
1. Centers for Disease Control and Prevention. National Center for Health Statistics. FastStats - Pneumonia. Accessed 6 Oct 2016 at www.cdc.gov/nchs/fastats/pneumonia.htm.
2. Kalil AC, Metersky ML, Klompas M, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis 2016;63:e61-e111.
3. Musher DM, Thorner AR. Community-acquired pneumonia. N Engl J Med 2014;371:1619–28.
4. Mandell LA. Epidemiology and etiology of community-acquired pneumonia. Infect Dis
5. Hoare Z, Lim WS. Pneumonia: update on diagnosis and management. BMJ 2006;332:1077–9.
6. Johnstone J, Marrie TJ, Eurich DT, Majumdar SR. Effect of pneumococcal vaccination in hospitalized adults with community-acquired pneumonia. Arch Intern Med 2007;167:1938–43
7. File TM Jr, Marrie TJ. Burden of community-acquired pneumonia in North American adults. Postgrad Med 2010;122:130–41.
8. Eurich DT, Marrie TJ, Minhas-Sandhu JK, Majumdar SR. Ten-year mortality after community-acquired pneumonia. a prospective cohort. Am J Respir Crit Care Med 2015;192:597-604.
9. Jain S, Self WH, Wunderink RG, et al. Community-acquired pneumonia requiring hospitalization among U.S. adults. N Engl J Med 2015;373:415–27.
10. Griffin MR, Zhu Y, Moore MR, et al. U.S. hospitalizations for pneumonia after a decade of pneumococcal vaccination. N Engl J Med 2013;369:155–63.
11. Nuorti JP, Butler JC, Farley MM, et al. Cigarette smoking and invasive pneumococcal disease. Active Bacterial Core Surveillance Team. N Engl J Med 2000;342:681–9.
12. Almirall J, Serra-Prat M, Bolíbar I, BalassoV. Risk factors for community-acquired pneumonia in adults: a systemic review of observational studies. Respiration 2017;94:299–311.
13. Janoff EM.Streptococcus pneumonia. In: Bennett JE, Dolin R, Blaser MJ, editors. Mandell, Douglas and Bennett’s principles and practice of infectioius diseases. 8th ed. Philadelphia: Sauders; 2015: 2310–27.
14. Diehr P, Wood RW, Bushyhead J, et al. Prediction of pneumonia in outpatients with acute cough--a statistical approach. J Chronic Dis 1984;37:215–25.
15. Metlay JP, Schulz R, Li YH, et al. Influence of age on symptoms at presentation in patients with community-acquired pneumonia. Arch Intern Med 1997;157:1453–9.
16. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007;44 Suppl 2:S27–72.
17. Jartti A, Rauvala E, Kauma H, et al. Chest imaging findings in hospitalized patients with H1N1 influenza. Acta Radiol 2011;52:297–304.
18. Basi SK, Marrie TJ, Huang JQ, Majumdar SR. Patients admitted to hospital with suspected pneumonia and normal chest radiographs: epidemiology, microbiology, and outcomes. Am J Med 2004;117:305–11.
19. Caldwell A, Glauser FL, Smith WR, et al. The effects of dehydration on the radiologic and pathologic appearance of experimental canine segmental pneumonia. Am Rev Respir Dis 1975;112:651–6.
20. Bartlett JG. Pneumonia. In: Barlett JG, editor. Management of respiratory tract infections. Philadelphia: Lippincott, Williams & Wilkins; 2001: 1–122.
21. Claessens YE, Debray MP, Tubach F, et al. Early chest computed tomography scan to assist diagnosis and guide treatment decision for suspected community-acquired pneumonia. Am J Respir Crit Care Med 2015;192:974–82.
22. Wheeler JH, Fishman EK. Computed tomography in the management of chest infections: current status. Clin Infect Dis 1996;23:232–40.
23. Chesnutt MP. Pulmonary disorders. In: Papadakis MM, editor. Current medical diagnosis and treatment. New York: McGraw-Hill; 2016: 242–320.
24. Mandell LW. Pneumonia. In: Kasper DF, editor. Harrison’s infectious diseases. 1st ed. New York: McGraw-Hill; 2010: 188–201.
25. Reed WW, Byrd GS, Gates RH Jr, et al. Sputum gram’s stain in community-acquired pneumococcal pneumonia. A meta-analysis. West J Med 1996;165:197–204.
26. Chalasani NP, Valdecanas MA, Gopal AK, et al. Clinical utility of blood cultures in adult patients with community-acquired pneumonia without defined underlying risks. Chest 1995;108:932–6.
27. Bordon J, Peyrani P, Brock GN, et al. The presence of pneumococcal bacteremia does not influence clinical outcomes in patients with community-acquired pneumonia: results from the Community-Acquired Pneumonia Organization (CAPO) International Cohort study. Chest 2008;133:618–24.
28. Helbig JH, Uldum SA, Bernander S, et al. Clinical utility of urinary antigen detection for diagnosis of community-acquired, travel-associated, and nosocomial legionnaires’ disease. J Clin Microbiol 2003;41:838–40.
29. Smith MD, Derrington P, Evans R, et al. Rapid diagnosis of bacteremic pneumococcal infections in adults by using the Binax NOW Streptococcus pneumoniae urinary antigen test: a prospective, controlled clinical evaluation. J Clin Microbiol 2003;41:2810–3.
30. Johansson N, Kalin M, Tiveljung-Lindell A, et al. Etiology of community-acquired pneumonia: increased microbiological yield with new diagnostic methods. Clin Infect Dis 2010;50:202–9.
31. Gilbert DN. Procalcitonin as a biomarker in respiratory tract infection. Clin Infect Dis 2011;52 Suppl 4:S346–50.
32. Schuetz P, Muller B, Christ-Crain M, et al. Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Cochrane Database Syst Rev 2012;(9):CD007498.
33. Boussekey N, Leroy O, Alfandari S, et al. Procalcitonin kinetics in the prognosis of severe community-acquired pneumonia. Intensive Care Med 2006;32:469–72.
34. Flanders SA, Stein J, Shochat G, et al. Performance of a bedside C-reactive protein test in the diagnosis of community-acquired pneumonia in adults with acute cough. Am J Med 2004;116:529–35.
35. Fine MJ, et al A prediction rule to identify low-risk patients with community-acquired pneumonia.N Engl J Med.1997;336:243-50.
36. Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax 2003;58:377–82.
37. Arnold FW, Ramirez JA, McDonald LC, Xia EL. Hospitalization for community-acquired pneumonia: the pneumonia severity index vs clinical judgment. Chest 2003;124:121–4.
38. Aujesky D, McCausland JB, Whittle J, et al. Reasons why emergency department providers do not rely on the pneumonia severity index to determine the initial site of treatment for patients with pneumonia. Clin Infect Dis 2009;49:e100–8.
39. Charles PG, Wolfe R, Whitby M, et al. SMART-COP: a tool for predicting the need for intensive respiratory or vasopressor support in community-acquired pneumonia. Clin Infect Dis 2008;47:375–84.
40. Marti C, Garin N, Grosgurin O, et al. Prediction of severe community-acquired pneumonia: a systematic review and meta-analysis. Crit Care 2012;16:R141.
41. Wunderink RG, Niederman MS, Kollef MH, et al. Linezolid in methicillin-resistant Staphylococcus aureus nosocomial pneumonia: a randomized, controlled study. Clin Infect Dis 2012;54:621–9.
42. Silverman JA, Mortin LI, Vanpraagh AD, et al. Inhibition of daptomycin by pulmonary surfactant: in vitro modeling and clinical impact. J Infect Dis 2005;191:2149–52.
43. El Hajj MS, Turgeon RD, Wilby KJ. Ceftaroline fosamil for community-acquired pneumonia and skin and skin structure infections: a systematic review. Int J Clin Pharm 2017 Jan 5.
44. Taboada M, Melnick D, Iaconis JP, et al. Ceftaroline fosamil versus ceftriaxone for the treatment of community-acquired pneumonia: individual patient data meta-analysis of randomized controlled trials. J Antimicrob Chemother 2016;71:862–70.
45. Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the infectious diseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children: executive summary. Clin Infect Dis 2011;52:285–92.
46. Baddour LM, Yu VL, Klugman KP, et al. Combination antibiotic therapy lowers mortality among severely ill patients with pneumococcal bacteremia. Am J Respir Crit Care Med 2004;170:440–4.
47. FDA Drug Safety Communication: FDA warns of increased risk of death with IV antibacterial Tygacil (tigecycline) and approves new boxed warning [Internet]. 15 Jan 2016. Available at www.fda.gov/Drugs/DrugSafety/ucm369580.htm.
48. Edelstein PR, CR. Legionnaires’ Disease and Pontiac Fever. In: Kasper DF, editor. Harrison’s infectious diseases. 1st ed. New York: McGraw-Hill; 2010: 2633.
49. Hammerschlag MR, Kohlhoff SA, Gaydos, CA. Chlamydia pneumoniae. In: Kasper DF, editor. Harrison’s infectious diseases. 1st ed. New York: McGraw-Hill; 2010: 2174.
50. Holzman RS, MS. Mycoplasma pneumoniae and Atypical Pneumonia. In: Kasper DF, editor. Harrison’s infectious diseases. 1st ed. New York: McGraw-Hill; 2010: 2183.
51. Yamada M, Buller R, Bledsoe S, Storch GA. Rising rates of macrolide-resistant Mycoplasma pneumoniae in the central United States. Pediatr Infect Dis J 2012;31:409–10.
52. Yi SH, Hatfield KM, Baggs J, et al. Duration of antibiotic use among adults with uncomplicated community-acquired pneumonia requiring hospitalization in the United States. Clin Infect Dis 2017 Nov 6.
53. Hayashi Y, Paterson DL. Strategies for reduction in duration of antibiotic use in hospitalized patients. Clin Infect Dis 2011;52:1232–40.
54. Akram AR, Chalmers JD, Taylor JK, et al. An evaluation of clinical stability criteria to predict hospital course in community-acquired pneumonia. Clin Microbiol Infect 2013;19:1174–80.
55. Halm EA, Fine MJ, Kapoor WN, et al. Instability on hospital discharge and the risk of adverse outcomes in patients with pneumonia. Arch Intern Med 2002;162:1278–84.
56. Roson B, Carratala J, Fernandez-Sabe N, et al. Causes and factors associated with early failure in hospitalized patients with community-acquired pneumonia. Arch Intern Med 2004;164:502–8.
57. El-Solh AA, Pietrantoni C, Bhat A, et al. Microbiology of severe aspiration pneumonia in institutionalized elderly. Am J Respir Crit Care Med 2003;167:1650–4.
58. Wan YD, Sun TW, Liu ZQ, et al. Efficacy and safety of corticosteroids for community-acquired pneumonia: a systematic review and meta-analysis. Chest 2016;149:209–19.
59. Torres A, Sibila O, Ferrer M, et al. Effect of corticosteroids on treatment failure among hospitalized patients with severe community-acquired pneumonia and high inflammatory response: a randomized clinical trial. JAMA 2015;313:677–86.
60. McCullers JA. Insights into the interaction between influenza virus and pneumococcus. Clin Microbiol Rev 2006;19:571–82.
61. Grohskopf LA, Sokolow LZ, Broder KR, et al. Prevention and control of seasonal influenza with vaccines. MMWR Recomm Rep 2016;65:1–54.
62. Rubins JB, Alter M, Loch J, Janoff EN. Determination of antibody responses of elderly adults to all 23 capsular polysaccharides after pneumococcal vaccination. Infect Immun 1999;67:5979–84.
63. Centers for Disease Control. Vaccines and preventable diseases [Internet]. 22 Nov 2016. Available at www.cdc.gov/vaccines/vpd/pneumo/hcp/about-vaccine.html.
64. Bonten MJ, Huijts SM, Bolkenbaas M, et al. Polysaccharide conjugate vaccine against pneumococcal pneumonia in adults. N Engl J Med 2015;372:1114–25.
65. Centers for Disease Control. Recommended adult immunization schedule -- United States -- 2016 [Internet]. 2016. Available at www.cdc.gov/vaccines/schedules/downloads/adult/adult-schedule.pdf.
66. Kobayashi M, Bennett NM, Gierke R, et al. Intervals between PCV13 and PPSV23 vaccines: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep 2015;64:944–7.
67. Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine for adults with immunocompromising conditions: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep 2012;61:816–9.
68. Aujesky D, Auble TE, Yealy DM, et al. Prospective comparison of three validated prediction rules for prognosis in community-acquired pneumonia. Am J Med 2005;118:384–92.
1. Centers for Disease Control and Prevention. National Center for Health Statistics. FastStats - Pneumonia. Accessed 6 Oct 2016 at www.cdc.gov/nchs/fastats/pneumonia.htm.
2. Kalil AC, Metersky ML, Klompas M, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis 2016;63:e61-e111.
3. Musher DM, Thorner AR. Community-acquired pneumonia. N Engl J Med 2014;371:1619–28.
4. Mandell LA. Epidemiology and etiology of community-acquired pneumonia. Infect Dis
5. Hoare Z, Lim WS. Pneumonia: update on diagnosis and management. BMJ 2006;332:1077–9.
6. Johnstone J, Marrie TJ, Eurich DT, Majumdar SR. Effect of pneumococcal vaccination in hospitalized adults with community-acquired pneumonia. Arch Intern Med 2007;167:1938–43
7. File TM Jr, Marrie TJ. Burden of community-acquired pneumonia in North American adults. Postgrad Med 2010;122:130–41.
8. Eurich DT, Marrie TJ, Minhas-Sandhu JK, Majumdar SR. Ten-year mortality after community-acquired pneumonia. a prospective cohort. Am J Respir Crit Care Med 2015;192:597-604.
9. Jain S, Self WH, Wunderink RG, et al. Community-acquired pneumonia requiring hospitalization among U.S. adults. N Engl J Med 2015;373:415–27.
10. Griffin MR, Zhu Y, Moore MR, et al. U.S. hospitalizations for pneumonia after a decade of pneumococcal vaccination. N Engl J Med 2013;369:155–63.
11. Nuorti JP, Butler JC, Farley MM, et al. Cigarette smoking and invasive pneumococcal disease. Active Bacterial Core Surveillance Team. N Engl J Med 2000;342:681–9.
12. Almirall J, Serra-Prat M, Bolíbar I, BalassoV. Risk factors for community-acquired pneumonia in adults: a systemic review of observational studies. Respiration 2017;94:299–311.
13. Janoff EM.Streptococcus pneumonia. In: Bennett JE, Dolin R, Blaser MJ, editors. Mandell, Douglas and Bennett’s principles and practice of infectioius diseases. 8th ed. Philadelphia: Sauders; 2015: 2310–27.
14. Diehr P, Wood RW, Bushyhead J, et al. Prediction of pneumonia in outpatients with acute cough--a statistical approach. J Chronic Dis 1984;37:215–25.
15. Metlay JP, Schulz R, Li YH, et al. Influence of age on symptoms at presentation in patients with community-acquired pneumonia. Arch Intern Med 1997;157:1453–9.
16. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007;44 Suppl 2:S27–72.
17. Jartti A, Rauvala E, Kauma H, et al. Chest imaging findings in hospitalized patients with H1N1 influenza. Acta Radiol 2011;52:297–304.
18. Basi SK, Marrie TJ, Huang JQ, Majumdar SR. Patients admitted to hospital with suspected pneumonia and normal chest radiographs: epidemiology, microbiology, and outcomes. Am J Med 2004;117:305–11.
19. Caldwell A, Glauser FL, Smith WR, et al. The effects of dehydration on the radiologic and pathologic appearance of experimental canine segmental pneumonia. Am Rev Respir Dis 1975;112:651–6.
20. Bartlett JG. Pneumonia. In: Barlett JG, editor. Management of respiratory tract infections. Philadelphia: Lippincott, Williams & Wilkins; 2001: 1–122.
21. Claessens YE, Debray MP, Tubach F, et al. Early chest computed tomography scan to assist diagnosis and guide treatment decision for suspected community-acquired pneumonia. Am J Respir Crit Care Med 2015;192:974–82.
22. Wheeler JH, Fishman EK. Computed tomography in the management of chest infections: current status. Clin Infect Dis 1996;23:232–40.
23. Chesnutt MP. Pulmonary disorders. In: Papadakis MM, editor. Current medical diagnosis and treatment. New York: McGraw-Hill; 2016: 242–320.
24. Mandell LW. Pneumonia. In: Kasper DF, editor. Harrison’s infectious diseases. 1st ed. New York: McGraw-Hill; 2010: 188–201.
25. Reed WW, Byrd GS, Gates RH Jr, et al. Sputum gram’s stain in community-acquired pneumococcal pneumonia. A meta-analysis. West J Med 1996;165:197–204.
26. Chalasani NP, Valdecanas MA, Gopal AK, et al. Clinical utility of blood cultures in adult patients with community-acquired pneumonia without defined underlying risks. Chest 1995;108:932–6.
27. Bordon J, Peyrani P, Brock GN, et al. The presence of pneumococcal bacteremia does not influence clinical outcomes in patients with community-acquired pneumonia: results from the Community-Acquired Pneumonia Organization (CAPO) International Cohort study. Chest 2008;133:618–24.
28. Helbig JH, Uldum SA, Bernander S, et al. Clinical utility of urinary antigen detection for diagnosis of community-acquired, travel-associated, and nosocomial legionnaires’ disease. J Clin Microbiol 2003;41:838–40.
29. Smith MD, Derrington P, Evans R, et al. Rapid diagnosis of bacteremic pneumococcal infections in adults by using the Binax NOW Streptococcus pneumoniae urinary antigen test: a prospective, controlled clinical evaluation. J Clin Microbiol 2003;41:2810–3.
30. Johansson N, Kalin M, Tiveljung-Lindell A, et al. Etiology of community-acquired pneumonia: increased microbiological yield with new diagnostic methods. Clin Infect Dis 2010;50:202–9.
31. Gilbert DN. Procalcitonin as a biomarker in respiratory tract infection. Clin Infect Dis 2011;52 Suppl 4:S346–50.
32. Schuetz P, Muller B, Christ-Crain M, et al. Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Cochrane Database Syst Rev 2012;(9):CD007498.
33. Boussekey N, Leroy O, Alfandari S, et al. Procalcitonin kinetics in the prognosis of severe community-acquired pneumonia. Intensive Care Med 2006;32:469–72.
34. Flanders SA, Stein J, Shochat G, et al. Performance of a bedside C-reactive protein test in the diagnosis of community-acquired pneumonia in adults with acute cough. Am J Med 2004;116:529–35.
35. Fine MJ, et al A prediction rule to identify low-risk patients with community-acquired pneumonia.N Engl J Med.1997;336:243-50.
36. Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax 2003;58:377–82.
37. Arnold FW, Ramirez JA, McDonald LC, Xia EL. Hospitalization for community-acquired pneumonia: the pneumonia severity index vs clinical judgment. Chest 2003;124:121–4.
38. Aujesky D, McCausland JB, Whittle J, et al. Reasons why emergency department providers do not rely on the pneumonia severity index to determine the initial site of treatment for patients with pneumonia. Clin Infect Dis 2009;49:e100–8.
39. Charles PG, Wolfe R, Whitby M, et al. SMART-COP: a tool for predicting the need for intensive respiratory or vasopressor support in community-acquired pneumonia. Clin Infect Dis 2008;47:375–84.
40. Marti C, Garin N, Grosgurin O, et al. Prediction of severe community-acquired pneumonia: a systematic review and meta-analysis. Crit Care 2012;16:R141.
41. Wunderink RG, Niederman MS, Kollef MH, et al. Linezolid in methicillin-resistant Staphylococcus aureus nosocomial pneumonia: a randomized, controlled study. Clin Infect Dis 2012;54:621–9.
42. Silverman JA, Mortin LI, Vanpraagh AD, et al. Inhibition of daptomycin by pulmonary surfactant: in vitro modeling and clinical impact. J Infect Dis 2005;191:2149–52.
43. El Hajj MS, Turgeon RD, Wilby KJ. Ceftaroline fosamil for community-acquired pneumonia and skin and skin structure infections: a systematic review. Int J Clin Pharm 2017 Jan 5.
44. Taboada M, Melnick D, Iaconis JP, et al. Ceftaroline fosamil versus ceftriaxone for the treatment of community-acquired pneumonia: individual patient data meta-analysis of randomized controlled trials. J Antimicrob Chemother 2016;71:862–70.
45. Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the infectious diseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children: executive summary. Clin Infect Dis 2011;52:285–92.
46. Baddour LM, Yu VL, Klugman KP, et al. Combination antibiotic therapy lowers mortality among severely ill patients with pneumococcal bacteremia. Am J Respir Crit Care Med 2004;170:440–4.
47. FDA Drug Safety Communication: FDA warns of increased risk of death with IV antibacterial Tygacil (tigecycline) and approves new boxed warning [Internet]. 15 Jan 2016. Available at www.fda.gov/Drugs/DrugSafety/ucm369580.htm.
48. Edelstein PR, CR. Legionnaires’ Disease and Pontiac Fever. In: Kasper DF, editor. Harrison’s infectious diseases. 1st ed. New York: McGraw-Hill; 2010: 2633.
49. Hammerschlag MR, Kohlhoff SA, Gaydos, CA. Chlamydia pneumoniae. In: Kasper DF, editor. Harrison’s infectious diseases. 1st ed. New York: McGraw-Hill; 2010: 2174.
50. Holzman RS, MS. Mycoplasma pneumoniae and Atypical Pneumonia. In: Kasper DF, editor. Harrison’s infectious diseases. 1st ed. New York: McGraw-Hill; 2010: 2183.
51. Yamada M, Buller R, Bledsoe S, Storch GA. Rising rates of macrolide-resistant Mycoplasma pneumoniae in the central United States. Pediatr Infect Dis J 2012;31:409–10.
52. Yi SH, Hatfield KM, Baggs J, et al. Duration of antibiotic use among adults with uncomplicated community-acquired pneumonia requiring hospitalization in the United States. Clin Infect Dis 2017 Nov 6.
53. Hayashi Y, Paterson DL. Strategies for reduction in duration of antibiotic use in hospitalized patients. Clin Infect Dis 2011;52:1232–40.
54. Akram AR, Chalmers JD, Taylor JK, et al. An evaluation of clinical stability criteria to predict hospital course in community-acquired pneumonia. Clin Microbiol Infect 2013;19:1174–80.
55. Halm EA, Fine MJ, Kapoor WN, et al. Instability on hospital discharge and the risk of adverse outcomes in patients with pneumonia. Arch Intern Med 2002;162:1278–84.
56. Roson B, Carratala J, Fernandez-Sabe N, et al. Causes and factors associated with early failure in hospitalized patients with community-acquired pneumonia. Arch Intern Med 2004;164:502–8.
57. El-Solh AA, Pietrantoni C, Bhat A, et al. Microbiology of severe aspiration pneumonia in institutionalized elderly. Am J Respir Crit Care Med 2003;167:1650–4.
58. Wan YD, Sun TW, Liu ZQ, et al. Efficacy and safety of corticosteroids for community-acquired pneumonia: a systematic review and meta-analysis. Chest 2016;149:209–19.
59. Torres A, Sibila O, Ferrer M, et al. Effect of corticosteroids on treatment failure among hospitalized patients with severe community-acquired pneumonia and high inflammatory response: a randomized clinical trial. JAMA 2015;313:677–86.
60. McCullers JA. Insights into the interaction between influenza virus and pneumococcus. Clin Microbiol Rev 2006;19:571–82.
61. Grohskopf LA, Sokolow LZ, Broder KR, et al. Prevention and control of seasonal influenza with vaccines. MMWR Recomm Rep 2016;65:1–54.
62. Rubins JB, Alter M, Loch J, Janoff EN. Determination of antibody responses of elderly adults to all 23 capsular polysaccharides after pneumococcal vaccination. Infect Immun 1999;67:5979–84.
63. Centers for Disease Control. Vaccines and preventable diseases [Internet]. 22 Nov 2016. Available at www.cdc.gov/vaccines/vpd/pneumo/hcp/about-vaccine.html.
64. Bonten MJ, Huijts SM, Bolkenbaas M, et al. Polysaccharide conjugate vaccine against pneumococcal pneumonia in adults. N Engl J Med 2015;372:1114–25.
65. Centers for Disease Control. Recommended adult immunization schedule -- United States -- 2016 [Internet]. 2016. Available at www.cdc.gov/vaccines/schedules/downloads/adult/adult-schedule.pdf.
66. Kobayashi M, Bennett NM, Gierke R, et al. Intervals between PCV13 and PPSV23 vaccines: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep 2015;64:944–7.
67. Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine for adults with immunocompromising conditions: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep 2012;61:816–9.
68. Aujesky D, Auble TE, Yealy DM, et al. Prospective comparison of three validated prediction rules for prognosis in community-acquired pneumonia. Am J Med 2005;118:384–92.
Brentuximab Vedotin with Chemotherapy Improves Progression-Free Survival in Advanced-Stage Hodgkin’s Lymphoma
Study Overview
Objective. To compare the efficacy of brentuximab vedotin, doxorubicin, vinblastine, and dacarbazine (A+AVD) with that of doxorubicin, bleomycin, vinblastine, and dacarbazine (ABVD) in patients with stage III or IV classic Hodgkin’s lymphoma.
Design. The ECHELON-1 trial, an international, openlabel, randomized phase 3 trial.
Setting and participants. In this multicenter international trial, a total of 1334 patients underwent randomization from November 2012 through January
2016. Eligible patients were 18 years of age older and had newly diagnosed and histologically proven classic Hodgkin’s lymphoma, Ann Arbor stage III or IV. Patients were eligible only if they had not received prior systemic chemotherapy or radiotherapy. All patients were required to have an ECOG performance status of ≤ 2 and adequate hematologic parameters (hemoglobin ≥ 8, ANC ≥ 1500, and platelet count ≥ 75,000). Patients with nodular lymphocyte predominant Hodgkin’s lymphoma, pre-existing peripheral sensory neuropathy, or known cerebral or meningeal disease were excluded.
Intervention. Patients were randomized in a 1:1 fashion to receive A+AVD (brentuximab vedotin 1.2 mg/kg, doxorubicin 25 mg/m2, vinblastine 6 mg/m2 and dacarbazine 375 mg/m2) or ABVD (doxorubicin 25 mg/m2, bleomycin 10 units/m2, vinblastine 6 mg/m2 and dacarbazine 375 mg/m2) IV on days 1 and 15 of each 28-day cycle for up to 6 cycles. A PET scan was done at the end of the second cycle (PET2) and if this showed increased uptake at any site or uptake at a new site of disease (Deauville score 5) patients could be switched to an alternative frontline therapy at the treating physician’s discretion.
Main outcome measures. The primary endpoint of this study was modified progression-free survival (mPFS), defined as time to disease progression, death, or modified progression (noncomplete response after completion of frontline therapy—Deauville score 3, 4, or 5 on PET). Modified progression was incorporated as an endpoint in order to assess the effectiveness of frontline therapy. A secondary endpoint of the study was overall survival (OS).
Results. The baseline characteristics were well balanced between the treatment arms. 58% of the patients were male and 64% had stage IV disease. The median age was 36 years and 9% in each group were over the age of 65. After a median follow-up of 24.9 months, the independently assessed 2-year mPFS was 82.1% and 77.2% in the A+AVD and ABVD groups, respectively (hazard ratio [HR] 0.77; 95% confidence interval [CI] 0.6–0.98). The 2-year mPFS rate according to investigator assessment was 81% and 74.4% in the A+AVD and ABVD groups, respectively. Modified progression (failure to achieve a complete response after completion of frontline therapy resulting in treatment with subsequent therapy) occurred in 9 and 22 patients in the
A+AVD and ABVD groups, respectively. A pre-specified subgroup analysis showed that patients from North America, male patients, patients with involvement of more than 1 extranodal site, patients with a high IPSS score (4–7), patients < 60 years old and those with stage IV disease appeared to benefit more from A+AVD. The rate of PET2 negativity was 89% with A+AVD and 86% with ABVD. The 2-year overall survival was 96.6% in the A+AVD group and 94.9% in the ABVD group (HR 0.72; 95% CI 0.44–1.17). Fewer patients in the A+AVD group received subsequent cancer-directed therapy.
Neutropenia was more commonly reported in the A+AVD group (58% vs. 45%). Moreover, febrile neutropenia was reported in 19% and 8% of patients in the A+AVD and ABVD groups, respectively. Discontinuation rates in either arm for febrile neutropenia was ≤ 1%. The rate of infections was 55% in the A+AVD group and 50% in the ABVD group (grade 3 or higher: 18% and 10%, respectively). After review of the rates of febrile neutropenia, the safety monitoring committee recommended that primary prophylaxis with granulocyte colony-stimulating factor (G-CSF) be used for patients who were yet to be enrolled. The rate of febrile neutropenia in the 83 patients in the A+AVD group who received primary prophylaxis was lower than those who did not (11% vs. 18%). Peripheral neuropathy occurred in 67% of patients in the A+AVD group and 42% in the ABVD group (grade 3 or higher: 11% vs 2%, respectively). Neuropathy lead to discontinuation of a study drug in 10% of patients in the A+AVD group. 67% of patients with peripheral neuropathy in the A+AVD group had resolution or improvement by one grade of their neuropathy at the time of last follow up. Pulmonary toxicity was reported in 2% of patients in the A+AVD group and 7% of the ABVD group (grade 3 or higher: < 1% vs. 3%, respectively). During treatment, 9 deaths were reported in the A+AVD group and 13 deaths in the ABVD group. Of the deaths in the ABVD group, 11 were associated with pulmonary toxicity.
Conclusion. A+AVD had superior efficacy to ABVD in the treatment of patients with advanced-stage Hodgkin’s lymphoma.
Commentary
Hodgkin’s lymphoma (HL) accounts for approximately 10% of all lymphomas in the world annually [1]. While outcomes with frontline therapy for patients with HL have dramatically improved with ABVD, up to 30% of patients have either refractory disease or relapse after initial therapy [2,3]. One particular area of concern in the current treatment of HL with ABVD is the associated pulmonary toxicity of bleomycin. Pulmonary toxicity from bleomycin occurs in approximately 20%–30% of patients and can lead to long-term morbidity [4,5]. In addition, approximately 15% or more of HL patients are elderly and may have co-existing pulmonary disease. In the previously published E2496 trial, the risk of bleomycin lung toxicity in the elderly was 24% [3]. Although the risk of clinically relevant lung toxicity remains low, there is considerable concern about this amongst clinicians. Recent data has challenged the benefit of bleomycin as a component of ABVD. For example, Johnson and colleagues have shown that in patients with a negtive PET scan after 2 cycles of ABVD, the omission of bleomycin (ie, continuation of AVD) resulted in only a 1.6% reduction in 3-year progression-free survival with a decrease in pulmonary toxicity [6].
Recently, there have been notable advances in the treatment of patients with relapsed or refractory HL, including the incorporation of the PD-1 inhibitor
nivolumab as well as the immunotoxin conjugated CD30 monoclonal antibody brentuximab vedotin (BV). Given the activity of such agents in relapsed and refractory patients, there has been much enthusiasm about incorporation of such agents into the frontline setting. In the current ECHELON-1 trial, Connors and colleagues present the results of a randomized phase 3 trial comparing ABVD, the current standard of care, to A+AVD, which replaces bleomycin with BV. The trial used a primary endpoint of modified progression-free survival, where a noncomplete response and after primary therapy and subsequent treatment with anticancer therapy was considered disease progression. Notably, this trial did meet its primary endpoint of improved
modified PFS, with a 4.9% lower risk of progression, death, or noncomplete response and subsequent need for treatment at 2 years. Overall survival was not significantly different at the time of analysis.
There are some noteworthy findings in addition to this. First, A+AVD was associated with a higher risk of febrile neutropenia and infectious complications; however, following the incorporation of G-CSF prophylaxis this risk was lowered. The pulmonary toxicity was lower in the A+AVD group (2% vs. 7%). A+AVD was associated with an increased risk of peripheral neuropathy, which appeared to improve or resolve following discontinuation of therapy. The neuropathy was mainly low grade with only 11% being grade 3 or higher. Although it remains early and follow-up short, A+AVD did appear to have superior efficacy with a decrease in the risk of pulmonary toxicity in this study. It is worth noting that the risk of neurotoxicity was higher, albeit reversible with drug discontinuation. Given these results, A+AVD warrants consideration as frontline therapy in newly diagnosed patients with advanced stage classic Hodgkin’s lymphoma.
Applications for Clinical Practice
The results of this trial suggest that A+AVD with G-CSF support compares favorably to ABVD and may represent an acceptable first-line treatment strategy, particularly for patients at higher risk for pulmonary toxicity, although follow-up remains short at this time.
—Daniel Isaac, DO, MS
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin 2017;67:7–30.
2. Canellos GP, Anderson JR, Propert KJ, et al. Chemotherapy of advanced Hodgkin’s disease with MOPP, ABVD, or MOPP alternating with ABVD. N Engl J Med 1992;327:1478–84.
3. Gordon LI, Hong F, Fisher RI, et al. Randomized phase III trial of ABVD versus Stanford V with or without radiation therapy in locally extensive and advanced-stage Hodgkin lymphoma: An intergroup study coordinated by the Eastern Cooperative Oncology Group (E2496). J Clin Oncol 2013;31:684–91.
4. Martin WG, Ristow KM, Habermann TM, et al. Bleomycin pulmonary toxicity has a negative impact on the outcome of patients with Hodgkin’s lymphoma. J Clin Oncol 2005;23:7614–20.
5. Hoskin PJ, Lowry L, Horwich A, et al. Randomized comparison of the Stanford V regimen and ABVD in the treatment of advanced Hodgkin’s lymphoma: United Kingdom National Cancer Research Institute Lymphoma Group Study ISRCTN 64141244. J Clin Oncol 2009;27:5390–6.
6. Johnson P, Federico M, Kirkwood A, et al. Adapted treatment guided by interim PET-CT scan in advanced Hodgkin’s lymphoma. N Engl J Med 2016;374:2419–29.
Study Overview
Objective. To compare the efficacy of brentuximab vedotin, doxorubicin, vinblastine, and dacarbazine (A+AVD) with that of doxorubicin, bleomycin, vinblastine, and dacarbazine (ABVD) in patients with stage III or IV classic Hodgkin’s lymphoma.
Design. The ECHELON-1 trial, an international, openlabel, randomized phase 3 trial.
Setting and participants. In this multicenter international trial, a total of 1334 patients underwent randomization from November 2012 through January
2016. Eligible patients were 18 years of age older and had newly diagnosed and histologically proven classic Hodgkin’s lymphoma, Ann Arbor stage III or IV. Patients were eligible only if they had not received prior systemic chemotherapy or radiotherapy. All patients were required to have an ECOG performance status of ≤ 2 and adequate hematologic parameters (hemoglobin ≥ 8, ANC ≥ 1500, and platelet count ≥ 75,000). Patients with nodular lymphocyte predominant Hodgkin’s lymphoma, pre-existing peripheral sensory neuropathy, or known cerebral or meningeal disease were excluded.
Intervention. Patients were randomized in a 1:1 fashion to receive A+AVD (brentuximab vedotin 1.2 mg/kg, doxorubicin 25 mg/m2, vinblastine 6 mg/m2 and dacarbazine 375 mg/m2) or ABVD (doxorubicin 25 mg/m2, bleomycin 10 units/m2, vinblastine 6 mg/m2 and dacarbazine 375 mg/m2) IV on days 1 and 15 of each 28-day cycle for up to 6 cycles. A PET scan was done at the end of the second cycle (PET2) and if this showed increased uptake at any site or uptake at a new site of disease (Deauville score 5) patients could be switched to an alternative frontline therapy at the treating physician’s discretion.
Main outcome measures. The primary endpoint of this study was modified progression-free survival (mPFS), defined as time to disease progression, death, or modified progression (noncomplete response after completion of frontline therapy—Deauville score 3, 4, or 5 on PET). Modified progression was incorporated as an endpoint in order to assess the effectiveness of frontline therapy. A secondary endpoint of the study was overall survival (OS).
Results. The baseline characteristics were well balanced between the treatment arms. 58% of the patients were male and 64% had stage IV disease. The median age was 36 years and 9% in each group were over the age of 65. After a median follow-up of 24.9 months, the independently assessed 2-year mPFS was 82.1% and 77.2% in the A+AVD and ABVD groups, respectively (hazard ratio [HR] 0.77; 95% confidence interval [CI] 0.6–0.98). The 2-year mPFS rate according to investigator assessment was 81% and 74.4% in the A+AVD and ABVD groups, respectively. Modified progression (failure to achieve a complete response after completion of frontline therapy resulting in treatment with subsequent therapy) occurred in 9 and 22 patients in the
A+AVD and ABVD groups, respectively. A pre-specified subgroup analysis showed that patients from North America, male patients, patients with involvement of more than 1 extranodal site, patients with a high IPSS score (4–7), patients < 60 years old and those with stage IV disease appeared to benefit more from A+AVD. The rate of PET2 negativity was 89% with A+AVD and 86% with ABVD. The 2-year overall survival was 96.6% in the A+AVD group and 94.9% in the ABVD group (HR 0.72; 95% CI 0.44–1.17). Fewer patients in the A+AVD group received subsequent cancer-directed therapy.
Neutropenia was more commonly reported in the A+AVD group (58% vs. 45%). Moreover, febrile neutropenia was reported in 19% and 8% of patients in the A+AVD and ABVD groups, respectively. Discontinuation rates in either arm for febrile neutropenia was ≤ 1%. The rate of infections was 55% in the A+AVD group and 50% in the ABVD group (grade 3 or higher: 18% and 10%, respectively). After review of the rates of febrile neutropenia, the safety monitoring committee recommended that primary prophylaxis with granulocyte colony-stimulating factor (G-CSF) be used for patients who were yet to be enrolled. The rate of febrile neutropenia in the 83 patients in the A+AVD group who received primary prophylaxis was lower than those who did not (11% vs. 18%). Peripheral neuropathy occurred in 67% of patients in the A+AVD group and 42% in the ABVD group (grade 3 or higher: 11% vs 2%, respectively). Neuropathy lead to discontinuation of a study drug in 10% of patients in the A+AVD group. 67% of patients with peripheral neuropathy in the A+AVD group had resolution or improvement by one grade of their neuropathy at the time of last follow up. Pulmonary toxicity was reported in 2% of patients in the A+AVD group and 7% of the ABVD group (grade 3 or higher: < 1% vs. 3%, respectively). During treatment, 9 deaths were reported in the A+AVD group and 13 deaths in the ABVD group. Of the deaths in the ABVD group, 11 were associated with pulmonary toxicity.
Conclusion. A+AVD had superior efficacy to ABVD in the treatment of patients with advanced-stage Hodgkin’s lymphoma.
Commentary
Hodgkin’s lymphoma (HL) accounts for approximately 10% of all lymphomas in the world annually [1]. While outcomes with frontline therapy for patients with HL have dramatically improved with ABVD, up to 30% of patients have either refractory disease or relapse after initial therapy [2,3]. One particular area of concern in the current treatment of HL with ABVD is the associated pulmonary toxicity of bleomycin. Pulmonary toxicity from bleomycin occurs in approximately 20%–30% of patients and can lead to long-term morbidity [4,5]. In addition, approximately 15% or more of HL patients are elderly and may have co-existing pulmonary disease. In the previously published E2496 trial, the risk of bleomycin lung toxicity in the elderly was 24% [3]. Although the risk of clinically relevant lung toxicity remains low, there is considerable concern about this amongst clinicians. Recent data has challenged the benefit of bleomycin as a component of ABVD. For example, Johnson and colleagues have shown that in patients with a negtive PET scan after 2 cycles of ABVD, the omission of bleomycin (ie, continuation of AVD) resulted in only a 1.6% reduction in 3-year progression-free survival with a decrease in pulmonary toxicity [6].
Recently, there have been notable advances in the treatment of patients with relapsed or refractory HL, including the incorporation of the PD-1 inhibitor
nivolumab as well as the immunotoxin conjugated CD30 monoclonal antibody brentuximab vedotin (BV). Given the activity of such agents in relapsed and refractory patients, there has been much enthusiasm about incorporation of such agents into the frontline setting. In the current ECHELON-1 trial, Connors and colleagues present the results of a randomized phase 3 trial comparing ABVD, the current standard of care, to A+AVD, which replaces bleomycin with BV. The trial used a primary endpoint of modified progression-free survival, where a noncomplete response and after primary therapy and subsequent treatment with anticancer therapy was considered disease progression. Notably, this trial did meet its primary endpoint of improved
modified PFS, with a 4.9% lower risk of progression, death, or noncomplete response and subsequent need for treatment at 2 years. Overall survival was not significantly different at the time of analysis.
There are some noteworthy findings in addition to this. First, A+AVD was associated with a higher risk of febrile neutropenia and infectious complications; however, following the incorporation of G-CSF prophylaxis this risk was lowered. The pulmonary toxicity was lower in the A+AVD group (2% vs. 7%). A+AVD was associated with an increased risk of peripheral neuropathy, which appeared to improve or resolve following discontinuation of therapy. The neuropathy was mainly low grade with only 11% being grade 3 or higher. Although it remains early and follow-up short, A+AVD did appear to have superior efficacy with a decrease in the risk of pulmonary toxicity in this study. It is worth noting that the risk of neurotoxicity was higher, albeit reversible with drug discontinuation. Given these results, A+AVD warrants consideration as frontline therapy in newly diagnosed patients with advanced stage classic Hodgkin’s lymphoma.
Applications for Clinical Practice
The results of this trial suggest that A+AVD with G-CSF support compares favorably to ABVD and may represent an acceptable first-line treatment strategy, particularly for patients at higher risk for pulmonary toxicity, although follow-up remains short at this time.
—Daniel Isaac, DO, MS
Study Overview
Objective. To compare the efficacy of brentuximab vedotin, doxorubicin, vinblastine, and dacarbazine (A+AVD) with that of doxorubicin, bleomycin, vinblastine, and dacarbazine (ABVD) in patients with stage III or IV classic Hodgkin’s lymphoma.
Design. The ECHELON-1 trial, an international, openlabel, randomized phase 3 trial.
Setting and participants. In this multicenter international trial, a total of 1334 patients underwent randomization from November 2012 through January
2016. Eligible patients were 18 years of age older and had newly diagnosed and histologically proven classic Hodgkin’s lymphoma, Ann Arbor stage III or IV. Patients were eligible only if they had not received prior systemic chemotherapy or radiotherapy. All patients were required to have an ECOG performance status of ≤ 2 and adequate hematologic parameters (hemoglobin ≥ 8, ANC ≥ 1500, and platelet count ≥ 75,000). Patients with nodular lymphocyte predominant Hodgkin’s lymphoma, pre-existing peripheral sensory neuropathy, or known cerebral or meningeal disease were excluded.
Intervention. Patients were randomized in a 1:1 fashion to receive A+AVD (brentuximab vedotin 1.2 mg/kg, doxorubicin 25 mg/m2, vinblastine 6 mg/m2 and dacarbazine 375 mg/m2) or ABVD (doxorubicin 25 mg/m2, bleomycin 10 units/m2, vinblastine 6 mg/m2 and dacarbazine 375 mg/m2) IV on days 1 and 15 of each 28-day cycle for up to 6 cycles. A PET scan was done at the end of the second cycle (PET2) and if this showed increased uptake at any site or uptake at a new site of disease (Deauville score 5) patients could be switched to an alternative frontline therapy at the treating physician’s discretion.
Main outcome measures. The primary endpoint of this study was modified progression-free survival (mPFS), defined as time to disease progression, death, or modified progression (noncomplete response after completion of frontline therapy—Deauville score 3, 4, or 5 on PET). Modified progression was incorporated as an endpoint in order to assess the effectiveness of frontline therapy. A secondary endpoint of the study was overall survival (OS).
Results. The baseline characteristics were well balanced between the treatment arms. 58% of the patients were male and 64% had stage IV disease. The median age was 36 years and 9% in each group were over the age of 65. After a median follow-up of 24.9 months, the independently assessed 2-year mPFS was 82.1% and 77.2% in the A+AVD and ABVD groups, respectively (hazard ratio [HR] 0.77; 95% confidence interval [CI] 0.6–0.98). The 2-year mPFS rate according to investigator assessment was 81% and 74.4% in the A+AVD and ABVD groups, respectively. Modified progression (failure to achieve a complete response after completion of frontline therapy resulting in treatment with subsequent therapy) occurred in 9 and 22 patients in the
A+AVD and ABVD groups, respectively. A pre-specified subgroup analysis showed that patients from North America, male patients, patients with involvement of more than 1 extranodal site, patients with a high IPSS score (4–7), patients < 60 years old and those with stage IV disease appeared to benefit more from A+AVD. The rate of PET2 negativity was 89% with A+AVD and 86% with ABVD. The 2-year overall survival was 96.6% in the A+AVD group and 94.9% in the ABVD group (HR 0.72; 95% CI 0.44–1.17). Fewer patients in the A+AVD group received subsequent cancer-directed therapy.
Neutropenia was more commonly reported in the A+AVD group (58% vs. 45%). Moreover, febrile neutropenia was reported in 19% and 8% of patients in the A+AVD and ABVD groups, respectively. Discontinuation rates in either arm for febrile neutropenia was ≤ 1%. The rate of infections was 55% in the A+AVD group and 50% in the ABVD group (grade 3 or higher: 18% and 10%, respectively). After review of the rates of febrile neutropenia, the safety monitoring committee recommended that primary prophylaxis with granulocyte colony-stimulating factor (G-CSF) be used for patients who were yet to be enrolled. The rate of febrile neutropenia in the 83 patients in the A+AVD group who received primary prophylaxis was lower than those who did not (11% vs. 18%). Peripheral neuropathy occurred in 67% of patients in the A+AVD group and 42% in the ABVD group (grade 3 or higher: 11% vs 2%, respectively). Neuropathy lead to discontinuation of a study drug in 10% of patients in the A+AVD group. 67% of patients with peripheral neuropathy in the A+AVD group had resolution or improvement by one grade of their neuropathy at the time of last follow up. Pulmonary toxicity was reported in 2% of patients in the A+AVD group and 7% of the ABVD group (grade 3 or higher: < 1% vs. 3%, respectively). During treatment, 9 deaths were reported in the A+AVD group and 13 deaths in the ABVD group. Of the deaths in the ABVD group, 11 were associated with pulmonary toxicity.
Conclusion. A+AVD had superior efficacy to ABVD in the treatment of patients with advanced-stage Hodgkin’s lymphoma.
Commentary
Hodgkin’s lymphoma (HL) accounts for approximately 10% of all lymphomas in the world annually [1]. While outcomes with frontline therapy for patients with HL have dramatically improved with ABVD, up to 30% of patients have either refractory disease or relapse after initial therapy [2,3]. One particular area of concern in the current treatment of HL with ABVD is the associated pulmonary toxicity of bleomycin. Pulmonary toxicity from bleomycin occurs in approximately 20%–30% of patients and can lead to long-term morbidity [4,5]. In addition, approximately 15% or more of HL patients are elderly and may have co-existing pulmonary disease. In the previously published E2496 trial, the risk of bleomycin lung toxicity in the elderly was 24% [3]. Although the risk of clinically relevant lung toxicity remains low, there is considerable concern about this amongst clinicians. Recent data has challenged the benefit of bleomycin as a component of ABVD. For example, Johnson and colleagues have shown that in patients with a negtive PET scan after 2 cycles of ABVD, the omission of bleomycin (ie, continuation of AVD) resulted in only a 1.6% reduction in 3-year progression-free survival with a decrease in pulmonary toxicity [6].
Recently, there have been notable advances in the treatment of patients with relapsed or refractory HL, including the incorporation of the PD-1 inhibitor
nivolumab as well as the immunotoxin conjugated CD30 monoclonal antibody brentuximab vedotin (BV). Given the activity of such agents in relapsed and refractory patients, there has been much enthusiasm about incorporation of such agents into the frontline setting. In the current ECHELON-1 trial, Connors and colleagues present the results of a randomized phase 3 trial comparing ABVD, the current standard of care, to A+AVD, which replaces bleomycin with BV. The trial used a primary endpoint of modified progression-free survival, where a noncomplete response and after primary therapy and subsequent treatment with anticancer therapy was considered disease progression. Notably, this trial did meet its primary endpoint of improved
modified PFS, with a 4.9% lower risk of progression, death, or noncomplete response and subsequent need for treatment at 2 years. Overall survival was not significantly different at the time of analysis.
There are some noteworthy findings in addition to this. First, A+AVD was associated with a higher risk of febrile neutropenia and infectious complications; however, following the incorporation of G-CSF prophylaxis this risk was lowered. The pulmonary toxicity was lower in the A+AVD group (2% vs. 7%). A+AVD was associated with an increased risk of peripheral neuropathy, which appeared to improve or resolve following discontinuation of therapy. The neuropathy was mainly low grade with only 11% being grade 3 or higher. Although it remains early and follow-up short, A+AVD did appear to have superior efficacy with a decrease in the risk of pulmonary toxicity in this study. It is worth noting that the risk of neurotoxicity was higher, albeit reversible with drug discontinuation. Given these results, A+AVD warrants consideration as frontline therapy in newly diagnosed patients with advanced stage classic Hodgkin’s lymphoma.
Applications for Clinical Practice
The results of this trial suggest that A+AVD with G-CSF support compares favorably to ABVD and may represent an acceptable first-line treatment strategy, particularly for patients at higher risk for pulmonary toxicity, although follow-up remains short at this time.
—Daniel Isaac, DO, MS
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin 2017;67:7–30.
2. Canellos GP, Anderson JR, Propert KJ, et al. Chemotherapy of advanced Hodgkin’s disease with MOPP, ABVD, or MOPP alternating with ABVD. N Engl J Med 1992;327:1478–84.
3. Gordon LI, Hong F, Fisher RI, et al. Randomized phase III trial of ABVD versus Stanford V with or without radiation therapy in locally extensive and advanced-stage Hodgkin lymphoma: An intergroup study coordinated by the Eastern Cooperative Oncology Group (E2496). J Clin Oncol 2013;31:684–91.
4. Martin WG, Ristow KM, Habermann TM, et al. Bleomycin pulmonary toxicity has a negative impact on the outcome of patients with Hodgkin’s lymphoma. J Clin Oncol 2005;23:7614–20.
5. Hoskin PJ, Lowry L, Horwich A, et al. Randomized comparison of the Stanford V regimen and ABVD in the treatment of advanced Hodgkin’s lymphoma: United Kingdom National Cancer Research Institute Lymphoma Group Study ISRCTN 64141244. J Clin Oncol 2009;27:5390–6.
6. Johnson P, Federico M, Kirkwood A, et al. Adapted treatment guided by interim PET-CT scan in advanced Hodgkin’s lymphoma. N Engl J Med 2016;374:2419–29.
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin 2017;67:7–30.
2. Canellos GP, Anderson JR, Propert KJ, et al. Chemotherapy of advanced Hodgkin’s disease with MOPP, ABVD, or MOPP alternating with ABVD. N Engl J Med 1992;327:1478–84.
3. Gordon LI, Hong F, Fisher RI, et al. Randomized phase III trial of ABVD versus Stanford V with or without radiation therapy in locally extensive and advanced-stage Hodgkin lymphoma: An intergroup study coordinated by the Eastern Cooperative Oncology Group (E2496). J Clin Oncol 2013;31:684–91.
4. Martin WG, Ristow KM, Habermann TM, et al. Bleomycin pulmonary toxicity has a negative impact on the outcome of patients with Hodgkin’s lymphoma. J Clin Oncol 2005;23:7614–20.
5. Hoskin PJ, Lowry L, Horwich A, et al. Randomized comparison of the Stanford V regimen and ABVD in the treatment of advanced Hodgkin’s lymphoma: United Kingdom National Cancer Research Institute Lymphoma Group Study ISRCTN 64141244. J Clin Oncol 2009;27:5390–6.
6. Johnson P, Federico M, Kirkwood A, et al. Adapted treatment guided by interim PET-CT scan in advanced Hodgkin’s lymphoma. N Engl J Med 2016;374:2419–29.
Self-Reported Cognitive Impairment Is Rising
More people are reporting cognitive impairment, according to CDC researchers. Overall, the rate of self-reported cognitive impairment rose from 5.7% in 1997 to 6.7% in 2015. Among non-Hispanic white respondents, the rate went from 5.2% to 6.1%. The researchers found no significant trends in cognitive impairment among non-Hispanic black, Native American, Hispanic, or Asian respondents.
Respondents to the National Health Survey were asked whether any family member was “limited in any way because of difficulty remembering or because of experiencing periods of confusion.” The rate of cognitive impairment increased with age in all 5 racial/ethnic groups. The rate was lowest among non-Hispanic white respondents until the 1943-1947 birth cohort. The data are “interesting,” the researchers say, because other recent studies that used data from cognitive tests and clinical assessments found a declining trend in dementia in the U.S. Direct comparisons among studies is inappropriate, however, they note, because of different study designs. Their own findings “might suggest that awareness of cognitive impairment has improved in the United States, especially in recent years,” in part due to heightened public attention to Alzheimer disease.
More public education may be needed to promote awareness, the researchers say, especially among the minority groups. Minorities had lower rates of self-reporting, perhaps because of different cultural beliefs about disease and aging, or because they are less likely to seek treatment for depression, which can contribute to cognitive decline.
More people are reporting cognitive impairment, according to CDC researchers. Overall, the rate of self-reported cognitive impairment rose from 5.7% in 1997 to 6.7% in 2015. Among non-Hispanic white respondents, the rate went from 5.2% to 6.1%. The researchers found no significant trends in cognitive impairment among non-Hispanic black, Native American, Hispanic, or Asian respondents.
Respondents to the National Health Survey were asked whether any family member was “limited in any way because of difficulty remembering or because of experiencing periods of confusion.” The rate of cognitive impairment increased with age in all 5 racial/ethnic groups. The rate was lowest among non-Hispanic white respondents until the 1943-1947 birth cohort. The data are “interesting,” the researchers say, because other recent studies that used data from cognitive tests and clinical assessments found a declining trend in dementia in the U.S. Direct comparisons among studies is inappropriate, however, they note, because of different study designs. Their own findings “might suggest that awareness of cognitive impairment has improved in the United States, especially in recent years,” in part due to heightened public attention to Alzheimer disease.
More public education may be needed to promote awareness, the researchers say, especially among the minority groups. Minorities had lower rates of self-reporting, perhaps because of different cultural beliefs about disease and aging, or because they are less likely to seek treatment for depression, which can contribute to cognitive decline.
More people are reporting cognitive impairment, according to CDC researchers. Overall, the rate of self-reported cognitive impairment rose from 5.7% in 1997 to 6.7% in 2015. Among non-Hispanic white respondents, the rate went from 5.2% to 6.1%. The researchers found no significant trends in cognitive impairment among non-Hispanic black, Native American, Hispanic, or Asian respondents.
Respondents to the National Health Survey were asked whether any family member was “limited in any way because of difficulty remembering or because of experiencing periods of confusion.” The rate of cognitive impairment increased with age in all 5 racial/ethnic groups. The rate was lowest among non-Hispanic white respondents until the 1943-1947 birth cohort. The data are “interesting,” the researchers say, because other recent studies that used data from cognitive tests and clinical assessments found a declining trend in dementia in the U.S. Direct comparisons among studies is inappropriate, however, they note, because of different study designs. Their own findings “might suggest that awareness of cognitive impairment has improved in the United States, especially in recent years,” in part due to heightened public attention to Alzheimer disease.
More public education may be needed to promote awareness, the researchers say, especially among the minority groups. Minorities had lower rates of self-reporting, perhaps because of different cultural beliefs about disease and aging, or because they are less likely to seek treatment for depression, which can contribute to cognitive decline.
Avoiding Inappropriate Medication Prescription in Older Intensive Care Survivors
From the Division of Allergy, Pulmonary, and Critical Care Medicine, Department of Medicine, Vanderbilt University Medical Center, Nashville, TN (Dr. Marra), Division of Anesthesiology Critical Care Medicine, Vanderbilt University Medical Center, Nashville, TN (Dr. Hayhurst, Dr. Hughes, Dr. Pandharipande), Department of Clinical and Experimental Science, University of Brescia, Brescia, Italy (Dr. Marengoni), School of Medicine and Surgery,
University of Milano-Bicocca, Milan, Italy (Dr. Bellelli), and Rehabilitation and Aged Care Unit Hospital Ancelle, Cremona, Italy (Dr. Morandi).
Abstract
- Objective: To present an overview of the phenomenon of inappropriate medication prescription in older critically ill patients and examine possible strategies of intervention.
- Methods: Review of the literature.
- Results: Polypharmacy and inappropriate prescribing of medications in older persons may lead to a significant risk of adverse drug-related events and mortality. The intensive care unit (ICU) is often the place where potentially inappropriate medications (PIMs) are first prescribed. Common PIMs at ICU discharge are antipsychotics, benzodiazepines, opioids, anticholinergic medications, antidepressants, and drugs causing orthostatic hypotension. Different classes of medications, typically intended for short-term use, are sometimes inappropriately continued after discharge from the hospital. At admission, potential risk factors for PIM are multiple morbidities, polypharmacy, frailty and cognitive decline; at discharge, a high number of pre-admission PIMs, discharge to a location other than home, discharge from a surgical service, longer length of ICU and hospital stay, and mechanical ventilation. Inappropriate prescribing in older patients can be detected through either the use of explicit criteria, drug utilization reviews, and multidisciplinary teams, including a geriatrician and/or the involvement of a clinical pharmacist.
- Conclusion: Use of PIMs may be common in critical patients, both on admission and at discharge from ICU. Therapeutic reconciliation is recommended at every transition of care (eg, at hospital or ICU admission and discharge) in order to improve appropriateness of prescription.
Key words: elderly; intensive care unit; inappropriate medications; antipsychotics.
Since older persons are often affected by multiple chronic diseases and are prescribed several medications, the quality and safety of prescribing these medications has become a global health care issue [1–4]. Polypharmacy and inappropriate prescribing of medications among the elderly is receiving significant attention in the medical literature [5,6]. Inappropriate medications in the elderly can lead to falls, cognitive impairment and delirium, poorer health status, and higher mortality [7–10]. Medications are considered potentially inappropriate when (a) the risks of treatment outweigh the benefits [11], (b) they are prescribed for periods longer than clinically indicated or without any clear indication, (c) they are not prescribed when indicated [12], and (d) they are likely to interact with other drugs and diseases. Medications included in this category are often referred to as potentially inappropriate medications (PIMs), as in some situations their use is justified; however, if the risk of harm from the drug is judged to outweigh the potential clinical benefit after an individual patient’s clinical circumstances are considered, these drugs are considered “actually inappropriate medications” (AIMs) [6].
Advancing age is associated with substantial pharmacokinetic and pharmacodynamics changes, such as altered distribution volumes and altered permeability of the blood-brain barrier, impaired liver metabolism and renal capacity, up- and down-regulation of target receptors, transmitters, and signaling pathways changes, impaired homeostasis, and increased risk of adverse drug reactions (ADRs) that lead to increased mortality and morbidity and higher health care costs [2,11,13–19]. Studies show that ADRs cause approximately 5% of hospital admissions in the general population, but the percentage rises to 10% in older persons [20].
Avoiding PIMs represents a strategy aimed at reducing drug-related mortality and morbidity. This article provides an overview of the phenomenon of inappropriate medication prescription in older critically ill patients and examines available strategies of intervention.
Inappropriate Medications at ICU Discharge
Though PIMs and AIMs may be identified at the time of hospital discharge, the intensive care unit (ICU) is often the place where these medications are first prescribed [21]. Acute hospitalization may increase PIM prescribing because of newly prescribed medications, the presence of multiple prescribers, inadequate medication reconciliation, and a lack of care coordination among inpatient providers or in the transition back to outpatient care [22)].
A known complication of critical illness and ICU stay is a significant increase in psychological symptoms, sleep cycle alterations, delirium, and cognitive impairment, which may be associated with increased prescription of specific PIMs, such as antipsychotics or benzodiazepines [6,23,24]. Despite the lack of reliable evidence supporting their use in the ICU, antipsychotic agents are used routinely in ICU patients [25] to treat a variety of conditions, such as substance withdrawal, agitation not responding to other therapies, or delirium. Results from a multicenter study of 164,996 hospitalizations across 71 academic medical centers in the US showed that 1 out of 10 ICU patients received an antipsychotic during their hospital stay [25]. Jasiak et al estimated that one-third of patients initiated on an atypical antipsychotic therapy for ICU delirium received a hospital discharge prescription for these medications, with a potential annual outpatient medication cost of approximately $2255 per patient [26].
One potential consequence of antipsychotic use in the ICU is their continuation after the transition to other clinical settings, including discharge from the hospital [27] (Table 1). 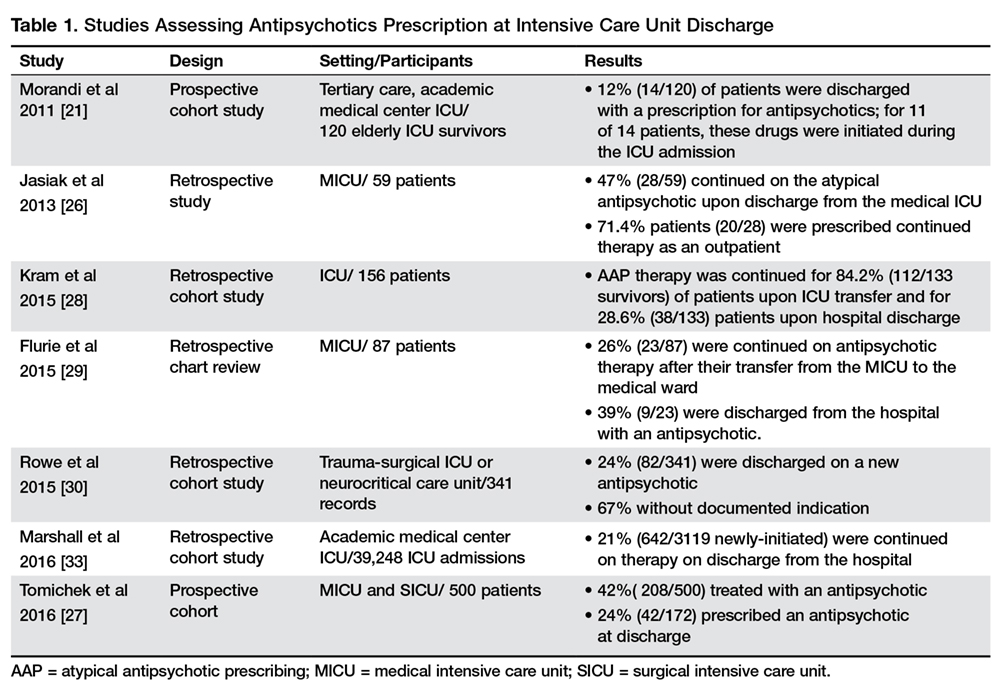
When examining the specific factors that may contribute to a patient being discharged on an antipsychotic, authors found that the specific antipsychotic used correlated with risk of continuation [27,30], with atypical antipsychotics having a greater likelihood of being continued than haloperidol [27,30]. Possible explanation for these results could be that physicians perceive less long-term risk from atypical agents, so may be more likely to continue them on discharge [30]. However, such an approach is not always safe. Indeed, although atypical antipsychotic agents tend to cause less tardive dyskinesia, they are known to be associated with similar rates of other adverse events compared with typical agents and have been linked to an increased risk of sudden cardiac death and pneumonia in the elderly [31,32].
Other factors independently associated with being discharged on a new antipsychotic medication were the severity of the acute illness as measured with the Acute Physiology and Chronic Health Evaluation II score at ICU admission (odds ratio [OR] 1 [95% confidence interval {CI}, 1.0–1.1]) and days treated with benzodiazepines (OR 1.1 [95% CI, 1.0–1.14]) [30]. Conversely, perhaps due to different practice patterns, Tomichek et al did not find an association between benzodiazepines administration and antipsychotic prescription at discharge in post hoc analyses [27].
Another possible reason for antipsychotic continuation may reside in the indication chosen [33]. Antipsychotic agents have sedative properties and they might be used to optimize sleep during hospitalization, despite the lack of evidence to support this indication [34]. Other factors potentially contributing to continuation of antipsychotics may include persistent delirium and agitation, newly diagnosed psychiatric illness, and difficulties experienced by physicians in deprescribing [35] with improper/incomplete medication reconciliation [33].
The continuation of antipsychotic therapy increased 30-day readmission rates in patients compared to those who had therapy stopped before discharge [33]. In addition to the well-described cardiac effects (prolonged QT interval), neuroleptic malignant syndrome and extrapyramidal symptoms may also occur, and longer-term use can predispose patients to metabolic disturbances, falls, and increase the risk of death in elderly patients with dementia [31].
Benzodiazepines and sedative hypnotics are commonly used to treat insomnia and agitation in older adults despite significant risk. Benzodiazepine administration was found to be an independent risk factor for a daily transition to delirium [36,37]. Pandharipande et al reported that every unit dose of lorazepam was associated with a higher risk for daily transition to delirium (OR 1.2, 95% CI 1.1–1.4, P = 0.003) [36] in critically ill patients. A more recent analysis found for every 5 mg of midazolam administered to a patient who is awake and without delirium, there is a 4% chance that this patient will develop delirium the next ICU day [37].
Given that the risk for benzodiazepine-associated delirium is dose-dependent, clinicians should use strategies known to reduce the daily number of benzodiazepines administered that often includes the use of a sedative associated with less delirium occurrence, such as dexmedetomidine or propofol [38]. Evidence has shown that long-term use of benzodiazepines has little benefit with many risks, including an increased susceptibility to spontaneous bacterial infection [39,40] and mortality in the setting of infection [41]. Nakafero et al showed that exposure to benzodiazepines was associated with increased occurrence of both influenza-like-illness–related pneumonia and mortality. Benzodiazepine use was associated also with increased occurrence of asthma exacerbation and with increased all-cause mortality during a median follow-up of 2 years in a cohort of asthmatic patients [42] as well with an increased risk of pneumonia and long-term mortality in patients with a prior diagnosis of community- acquired pneumonia [40]. Long-term use of benzodiazepines is also associated with increased risk of falls [43–45], cognitive impairment [46–48] and disability [49,50].
Other common types of PIMs at ICU discharge were opioids, anticholinergic medications, antidepressants, and drugs causing orthostatic hypotension [6]. Of the anticholinergic AIMs, H2 blockers (61%) and promethazine (15%) were the most common [6]. Only 16% of opioids, 23% of antidepressants, and 10% of drugs causing orthostatic hypotension were found to be actually inappropriate after the patient’s circumstances were considered (eg, postoperative pain control, a new diagnosis of major depressive disorder) [6].
Inappropriate Medications at Hospital Discharge
Medications typically intended for short-term use during acute illness are sometimes continued after discharge without documented indication [51]. Poudel et al found that in 206 patients 70 years of age and older discharged to residential aged care facilities from acute care, at least 1 PIM was identified in 112 (54.4%) patients on admission and 102 (49.5%) patients on discharge [11]. Commonly prescribed PIM categories, at both admission and discharge, were central nervous system, cardiovascular, gastrointestinal, and respiratory drugs and analgesics [6,11,52,53]. Of all medications prescribed at admission (1728), 10.8% were PIMs, and at discharge, of 1759 medications, 9.6% were PIMs. Of the total 187 PIMs on admission, 56 (30%) were stopped, and 131 (70%) were continued; 32 new PIMs were introduced [11].
Morandi et al in 2011 conducted a prospective cohort study including 120 patients age ≥ 60 who were discharged after receiving care in a medical, surgical, or cardiovascular ICU for shock or respiratory failure. The percentage of patients prescribed at least 1 PIM increased from 66% at pre-admission to 85% at discharge. The number of patients with 0 PIMs dropped from 34% at preadmission to 14% at discharge, and the number of patients with 3 or more PIMS increased from 16% at preadmission to 37% at discharge. While it is possible that these drugs may be appropriate when started during an acute illness in the ICU (eg, stress ulcer prophylaxis with H2-antagonists in mechanically ventilated patients), most should have been discontinued at ICU and/or hospital discharge [21].
Inappropriate prescriptions of proton pump inhibitors (PPIs) in hospital and primary care have been widely reported [54,55]. In a study conducted by Ahrens et al in 31 primary care practices, for 58% (263/506) of patients discharged from 35 hospitals with a PPI recommendation in hospital discharge letters, an appropriate indication was missing. In 57% of these cases general practitioners followed this recommendation and continued the prescription for more than 1 month [54]. The strongest factor associated with appropriate and inappropriate continuation of PPI after discharge was PPI prescription prior to hospitalization [54]. Although PPIs are safe, they can cause adverse effects. PPI intake has been found to have a significant association with risk of community-acquired pneumonia [56,57], hip fractures [58], Clostridium difficile-associated diarrhea [55,61,62], and to reduce the therapeutic effects of bisphosphonates [59] and low-dose aspirin [60].
Unintentional medication continuation is not a problem isolated to a single drug class or disease [63]. Scales et al evaluated rates of and risk factors for potentially unintentional medication continuation following hospitalization in a population of elderly patients (≥ 66 years) [51]. They created distinct cohorts by identifying seniors not previously receiving four classes of medications typically used to treat or prevent complications of acute illness: antipsychotic medications; gastric acid suppressants (ie, histamine-2 blockers and proton pump inhibitors); benzodiazepines; and inhaled bronchodilators and steroids [51]. Prescription without documented indication occurred across all medication classes, from 12,209 patients (1.4 %) for antipsychotic medications to 34,140 patients (6.1 %) for gastric acid suppressants [51].
Several potential risk factors were considered. The relationship between multimorbidity and polypharmacy is well described in the literature, and several studies have identified a positive association between the number of drugs and the use of PIMs [64–66]. Conversely, Poudel et al did not find any association between polypharmacy and PIM use [11]. Associations were found between the use of PIMs, frailty status, and cognitive decline of patients at admission and at discharge [11], while no association was observed with age, gender, in-hospital falls, delirium, and functional decline [11,67]. Other potential risk factors of a high number of PIMs at discharge were a high number of pre-admission PIMs, discharge to a location other than home, and discharge from a surgical service [1,6,68,69]. Length of ICU stay and mechanical ventilation had a positive influence on the number of PIMs used by acutely ill older patients [11,63,69]. In the study of Scales et al, the greatest absolute risk factor across all medication groups was longer hospitalization. The increased OR for medication continuation after a hospitalization lasting more than 7 days ranged from 2.03 (95% CI 1.94–2.11) for respiratory inhalers to 6.35 (95% CI 5.91–6.82) for antipsychotic medications [51].
Inappropriate Medications: Where and How to Intervene?
Early detection of PIMs may prevent adverse drug events and improve geriatric care in older adults [13,70]. PIM prevalence can often be a useful indicator of prescribing quality [2]. Appropriate interventions and an improved quality of prescribed medications require appropriate assessment tools to decrease the number of patients discharged on these medications [71,72]. Medication reconciliation is the process of avoiding inadvertent inconsistencies within a patient’s drug regimen, which can occur during transitions in different setting of care [73]. A multidisciplinary team should be involved in the medication reconciliation at each care transition to reevaluate medications use according to the clinical conditions, cognitive/functional status and the coexistence of geriatric syndromes (eg, dementia, malnutrition, delirium, urinary incontinence, frailty) (Figure).
Criteria for the Evaluation of Inappropriate Medications Prescription
Explicit criteria derived from expert reports or published reviews are available (Table 2).

Beers criteria PIMs have been found to be associated with poor health outcomes, including confusion, falls, and mortality [7,75,78]. The STOPP (Screening Tool of Older Person’s potentially inappropriate Prescriptions) and START (Screening Tool to Alert doctors to the Right Treatment) are evidence-based sets of criteria that were developed in Ireland and updated in October 2014, including some of the new criteria for direct oral anticoagulants, drugs affecting or affected by renal system and anti-muscarinic/anticholinergic agents [79]. 
Several other sets of criteria have been published to identify PIMs, such as the FORTA (Fit for the Aged) and the PRISCUS [86] criteria. FORTA allows a disease-related evaluation revealing over-treatment and under-treatment, and medications are graded as follows: A, indispensable drug, clear-cut benefit in terms of efficacy/safety ratio proven in elderly patients for a given indication; B, drugs with proven or obvious efficacy in the elderly, but limited extent of effect or safety concerns; C, drugs with questionable efficacy/safety profiles in the elderly which should be avoided or omitted in the presence of too many drugs or side effects; D, avoid in the elderly, omit first, refer also to negative listings. Negative lists such as PRISCUS, which provide an explicit listing of drugs, independent of the diagnosis, are easy to use. On the other hand, constant updates are needed, and such lists carry the risk of an assumption that drugs not listed would be appropriate in every case [87]. Both sets of criteria have in common that they refer to long-term medication and drugs frequently used during the inpatient stay, such as antibiotics, are hardly taken into account [87].
The Medication Appropriateness Index measures overall prescribing quality through 10 separate but interrelated domains [8]. Three components are used to detect PIMs: indication, effectiveness, and duplication. However, it does not give any precise guidance in relation to specific medicines and therefore has limited application for objectively defining PIMs.
Another prescribing quality assessment tool is the Inappropriate Prescribing in the Elderly Tool (IPET), which consists of a list of the 14 most prevalent prescription errors identified from an extensive list of inappropriate prescription instances drawn up by an expert Canadian Consensus Panel [88,89].
Another approach to assess the appropriateness of drugs prescribed for older people is the use of Drug Utilization Reviews (DURs) [16]. DURs use consensus opinion by drug therapy experts to define standards or explicit criteria for a single drug, class of drugs, or group of drugs [16]. DURs typically use retrospective information from large, nonclinical administrative databases to identify problems such as dosage range, duration, therapeutic duplication, and drug interactions [90, 91]. Monane et al [92] evaluated a program designed to decrease the use of PIMs among the elderly through a computerized online DUR database. Computer alerts triggered telephone calls to physicians by pharmacists to discuss a potential problem and any therapeutic substitution options. From a total of 43,007 telepharmacy calls generated by the alerts, they were able to reach 19,368 physicians regarding 24,266 alerts (56%). The rate of change to a more appropriate therapeutic agent was 24% (5860), but ranged from 40% for long half-life benzodiazepines to 2% to 7% for drugs that theoretically were contraindicated by patients’ self-reported history [92].
Computerized Support Systems to Reduce Inappropriate Prescribing in the Elderly
Other potential solutions for reducing inappropriate medications may include continuing medical education, electronic medical records surveillance, routine clinical evaluation, and/or improved hand-off communication between discharging and accepting providers. Incorporating this assessment of medication appropriateness into the medication reconciliation process when patients are discharged or transferred out of the ICU has the potential to enhance patient safety [21,93]. A randomized controlled trial conducted by Raebel et al [94] reported the effectiveness of a computerized pharmacy alert system plus collaboration between health care professionals for decreasing potentially inappropriate medication dispensing in elderly patients. Another study showed that computer-based access to complete drug profiles and alerts about potential prescribing problems reduced the occurrence of potentially inappropriate prescriptions [95]. A summary of these studies is shown in Table 3. 
Interdisciplinary Teams to Reduce Inappropriate Prescribing in the Elderly
Some studies evaluated the effect of multidisciplinary teamwork in improving inappropriate medication prescribing in the elderly (Table 4). 

Pharmacists in hospitals can play a significant role in the initiation of changes to patient’s therapy and management [11] (Table 5).
Mattison et al recently emphasized that studies of PIMs should determine scenarios in which it is appropriate to prescribe PIMs, moving beyond simply labeling some medications as “potentially inappropriate,” since some PIMs are appropriately prescribed in specific clinical situations [109]. Morandi et al showed that the positive predictive value (PPV) depends on the drug type. Thus, when developing a screening system, one cannot be concerned only with high negative predictive value (NPV), one must consider PPV as well [6]. Screening tools that include medication classes with low PPV will generate false positive “flags” or warnings, which could lead to misguided clinical decisions [6]. The fact that many PIMs are not AIMs also reveals the value of using a multidisciplinary team to identify AIMs from lists of PIMs generated when discharge medication lists are screened [6,110]. Thus, a multidisciplinary team is needed to consider the clinical context to distinguish PIMs from AIMs [6]. Of course, such a team is not available in some settings; when resources are limited, knowledge of which PIMs are most likely AIMs (ie, have high PPVs) could guide the development of computer-based decision support systems or other surveillance approaches that are efficient in that particular setting [6].
Approaches for optimizing prescribing in this population mainly depend on patient needs and comorbidities and most available data are derived from randomized controlled trials involving a single drug. Such trials do not take into account the confounding effects of multiple comorbidities and patient preferences. Therefore, approaches for optimizing prescription management that are available for and validated in younger patients are not applicable to elderly subjects [3,111].
Conclusion
Clinicians should seek to identify and discontinue AIMs at 3 important transitions during a critically ill elderly patient’s hospital course: at the time of hospital or ICU admission; at ICU discharge; and at hospital discharge. The patient’s clinical situation should be reviewed at every transition points, ideally by a multidisciplinary team of clinicians, to judge the appropriateness of each PIM [6]. After the hospital discharge, patient’s medications should be then reviewed by a multidisciplinary team and/or by the primary care physician according to the final discharge destination (ie, home, nursing home, rehabilitation) by using any of the validated tools. Regardless of the approach, it is clear that standardized care processes, including enhanced clinical decision support, are necessary to ensure that physicians do not continue exposing our patients to unnecessary medications and harm after discharge.
Corresponding author: Alessandro Morandi, MD, MPH, [email protected].
Funding/support: Dr. Pandiharipande is supported by National Institutes of Health HL111111 (Bethesda, MD) and by the VA Clinical Science Research and Development Service (Washington, DC) and the National Institutes of Health AG027472 and AG035117 (Bethesda, MD).
Financial disclosures: Dr. Pratik Pandharipande has received a research grant from Hospira Inc in collaboration with the NIH.
1. Lang PO, Hasso Y, Drame M, et al. Potentially inappropriate prescribing including under-use amongst older patients with cognitive or psychiatric co-morbidities. Age Ageing 2010;39:373–81.
2. Spinewine A, Schmader KE, Barber N, et al. Appropriate prescribing in elderly people: how well can it be measured and optimised? Lancet 2007;370:173–84.
3. Lang PO, Vogt-Ferrier N, Hasso Y, et al. Interdisciplinary geriatric and psychiatric care reduces potentially inappropriate prescribing in the hospital: interventional study in 150 acutely ill elderly patients with mental and somatic comorbid conditions. J Am Med Dir Assoc 2012;13:406 e1–7.
4. Cecile M, Seux V, Pauly V, et al. [Adverse drug events in hospitalized elderly patients in a geriatric medicine unit: study of prevalence and risk factors]. Rev Med Interne 2009;30:393–400.
5. Tosato M, Landi F, Martone AM, et al. Potentially inappropriate drug use among hospitalised older adults: results from the CRIME study. Age Ageing 2014;43:767–73.
6. Morandi A, Vasilevskis E, Pandharipande PP, et al. Inappropriate medication prescriptions in elderly adults surviving an intensive care unit hospitalization. J Am Geriatr Soc 2013;61:1128–34.
7. Fick DM, Mion LC, Beers MH, Waller JL. Health outcomes associated with potentially inappropriate medication use in older adults. Res Nurs Health 2008;31:42–51.
8. Hanlon JT, Schmader KE, Samsa GP, et al. A method for assessing drug therapy appropriateness. J Clin Epidemiol 1992;45:1045–51.
9. Lau DT, Kasper JD, Potter DEB, et al. Hospitalization and death associated with potentially inappropriate medication prescriptions among elderly nursing home residents. Arch Intern Med 2005;165:68–74.
10. Wright RM, Roumani YF, Boudreau R, et al. Effect of central nervous system medication use on decline in cognition in community-dwelling older adults: findings from the Health, Aging and Body Composition Study. J Am Geriatr Soc 2009;57:243–50.
11. Poudel A, Peel NM, Nissen L, et al. Potentially inappropriate prescribing in older patients discharged from acute care hospitals to residential aged care facilities. Ann Pharmacother 2014;48:1425–33.
12. Wahab MS, Nyfort-Hansen K, Kowalski SR. Inappropriate prescribing in hospitalised Australian elderly as determined by the STOPP criteria. Int J Clin Pharm 2012;34:855–62.
13. O’Mahony D, Gallagher PF. Inappropriate prescribing in the older population: need for new criteria. Age Ageing 2008;37:138–41.
14. Mangoni AA, Jansen PA, Jackson SH. Under-representation of older adults in pharmacokinetic and pharmacodynamic studies: a solvable problem? Exp Rev Clin Pharmacol 2013;6:35–9.
15. Klotz U. The elderly--a challenge for appropriate drug treatment. Eur J Clin Pharmacol 2008;64225–6.
16. Hanlon JT, Schmader KE, Ruby CM, Weinberger M. Suboptimal prescribing in older inpatients and outpatients. J Am Geriatr Soc 2001;49:200–9.
17. Hubbard RE, O’Mahony MS, Woodhouse KW. Medication prescribing in frail older people. Eur J Clin Pharmacol 2013;69:319–26.
18. American Geriatrics Society Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2012;60:616–31.
19. Page RL, Ruscin JM. The risk of adverse drug events and hospital-related morbidity and mortality among older adults with potentially inappropriate medication use. Am J Geriatr Pharmacother 2006;4:297–305.
20. Pirmohamed M, James S, Meakin S, et al. Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients. BMJ 2004;329:15–9.
21. Morandi A, Vasilevskis EE, Pandharipande PP, et al. Inappropriate medications in elderly ICU survivors: where to intervene? Arch Intern Med 2011;171:1032–4.
22. Page RL 2nd, Linnebur SA, Bryant LL, Ruscin JM. Inappropriate prescribing in the hospitalized elderly patient: defining the problem, evaluation tools, and possible solutions. Clin Interv Aging 2010;5:75–87.
23. Pandharipande PP, Girard TD, Jackson JC, et al. Long-term cognitive impairment after critical illness. N Engl J Med 2013;369:1306–16.
24. Ehlenbach WJ, Hough CL, Crane PK, et al. Association between acute care and critical illness hospitalization and cognitive function in older adults. JAMA 2010;303:763–70.
25. Swan JT, Fitousis K, Hall JB, et al. Antipsychotic use and diagnosis of delirium in the intensive care unit. Crit Care 2012;16:R84.
26. Jasiak KD, Middleton EA, Camamo JM, et al. Evaluation of discontinuation of atypical antipsychotics prescribed for ICU delirium. J Pharm Pract 2013;26:253–6.
27. Tomichek JE, Stollings JL, Pandharipande PP, et al. Antipsychotic prescribing patterns during and after critical illness: a prospective cohort study. Crit Care 2016;20:378.
28. Kram BL, Kram SJ, Brooks KR. Implications of atypical antipsychotic prescribing in the intensive care unit. J Crit Care 2015;30:814–8.
29. Flurie RW, Gonzales JP, Tata AL, et al. Hospital delirium treatment: Continuation of antipsychotic therapy from the intensive care unit to discharge. Am J Health Syst Pharm 2015;72(23 Suppl 3):S133–9.
30. Rowe AS, Hamilton LA, Curtis RA, et al. Risk factors for discharge on a new antipsychotic medication after admission to an intensive care unit. J Crit Care 2015;30:1283–6.
31. Ray WA, Chung CP, Murray KT, et al. Atypical antipsychotic drugs and the risk of sudden cardiac death. N Engl J Med 2009;360:225–35.
32. Wang PS, Schneeweiss S, Avorn J, et al. Risk of death in elderly users of conventional vs. atypical antipsychotic medications. N Engl J Med 2005;353:2335–41.
33. Marshall J, Herzig SJ, Howell MD, et al. Antipsychotic utilization in the intensive care unit and in transitions of care. J Crit Care 2016;33:119–24.
34. NIH State-of-the-science conference statement on manifestations and management of chronic insomnia in adults. NIH Consens State Sci Statements 2005;22:1–30.
35. Farrell B, Tsang C, Raman-Wilms L, et a;. What are priorities for deprescribing for elderly patients? Capturing the voice of practitioners: a modified delphi process. PLoS One 2015;10:e0122246.
36. Pandharipande P, Shintani A, Peterson J, et al. Lorazepam is an independent risk factor for transitioning to delirium in intensive care unit patients. Anesthesiology 2006;104:21–6.
37. Zaal IJ, Devlin JW, Hazelbag M, et al. Benzodiazepine-associated delirium in critically ill adults. Intensive Care Med 2015;41:2130–7.
38. Barr J, Fraser GL, Puntillo K, et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med 2013;41:263–306.
39. Riker RR, Shehabi Y, Bokesch PM, et al. Dexmedetomidine vs midazolam for sedation of critically ill patients: a randomized trial. JAMA 2009;301:489–99.
40. Obiora E, Hubbard R, Sanders RD, Myles PR. The impact of benzodiazepines on occurrence of pneumonia and mortality from pneumonia: a nested case-control and survival analysis in a population-based cohort. Thorax 2013;68:163–70.
41. Sanders RD, Godlee A, Fujimori T, et al. Benzodiazepine augmented gamma-amino-butyric acid signaling increases mortality from pneumonia in mice. Crit Care Med 2013;41:1627–36.
42. Nakafero G, Sanders RD, Nguyen-Van-Tam JS, Myles PR. Association between benzodiazepine use and exacerbations and mortality in patients with asthma: a matched case-control and survival analysis using the United Kingdom Clinical Practice Research Datalink. Pharmacoepidemiol Drug Saf 2015;24:793–802.
43. Hartikainen S, Lonnroos E, Louhivuori K. Medication as a risk factor for falls: critical systematic review. J Gerontol A Biol Sci Med Sci 2007;62:1172–81.
44. Pierfitte C, Macouillard G, Thicoipe M, et al. Benzodiazepines and hip fractures in elderly people: case-control study. BMJ 2001;322:704–8.
45. Landi F, Onder G, Cesari M, et al. Psychotropic medications and risk for falls among community-dwelling frail older people: an observational study. J Gerontol A Biol Sci Med Sci 2005;60:622–6.
46. Hanlon JT, Horner RD, Schmader KE, et al. Benzodiazepine use and cognitive function among community-dwelling elderly. Clin Pharmacol Ther 1998;64:684–92.
47. Greenblatt DJ, Harmatz JS, Shapiro L, et al. Sensitivity to triazolam in the elderly. N Engl J Med 1991;324:1691–8.
48. Bertz RJ, Kroboth PD, Kroboth FJ, et al. Alprazolam in young and elderly men: sensitivity and tolerance to psychomotor, sedative and memory effects. J Pharmacol Exp Ther 1997;281:1317–29.
49. Gray SL, LaCroix AZ, Blough D, et al. Is the use of benzodiazepines associated with incident disability? J Am Geriatr Soc 2002;50:1012–8.
50. Gray SL, LaCroix AZ, Hanlon JT, et al. Benzodiazepine use and physical disability in community-dwelling older adults. J Am Geriatr Soc 2006;54:224–30.
51. Scales DC, Fischer HD, Li P, et al. Unintentional continuation of medications intended for acute illness after hospital discharge: a population-based cohort study. J Gen Intern Med 2016;31:196–202.
52. Hamilton H, Gallagher P, Ryan C, et al. Potentially inappropriate medications defined by STOPP criteria and the risk of adverse drug events in older hospitalized patients. Arch Intern Med 2011;171:1013–9.
53. Hanlon JT, Artz MB, Pieper CF, et al. Inappropriate medication use among frail elderly inpatients. Ann Pharmacother 2004;38:9–14.
54. Ahrens D, Behrens G, Himmel W, et al. Appropriateness of proton pump inhibitor recommendations at hospital discharge and continuation in primary care. Int J Clin Pract 2012;66:767–73.
55. McDonald EG, Milligan J, Frenette C, Lee TC. Continuous proton pump inhibitor therapy and the associated risk of recurrent Clostridium difficile infection. JAMA Intern Med 2015;175:784–91.
56. Gulmez SE, Holm A, Frederiksen H, et al. Use of proton pump inhibitors and the risk of community-acquired pneumonia: a population-based case-control study. Arch Intern Med 2007;167:950–5.
57. Laheij RJ, Sturkenboom MC, Hassing RJ, et al. Risk of community-acquired pneumonia and use of gastric acid-suppressive drugs. JAMA 2004;292:1955–60.
58. Yang YX, Lewis JD, Epstein S, Metz DC. Long-term proton pump inhibitor therapy and risk of hip fracture. JAMA 2006;296:2947–53.
59. Abrahamsen B, Eiken P, Eastell R. Proton pump inhibitor use and the antifracture efficacy of alendronate. Arch Intern Med 2011;171:998–1004.
60. Charlot M, Grove EL, Hansen PR, et al. Proton pump inhibitor use and risk of adverse cardiovascular events in aspirin treated patients with first time myocardial infarction: nationwide propensity score matched study. BMJ 2011;342:d2690.
61. Dial S, Delaney JA, Barkun AN, Suissa S. Use of gastric acid-suppressive agents and the risk of community-acquired Clostridium difficile-associated disease. JAMA 2005;294:2989–95.
62. Leonard J, Marshall JK, Moayyedi P. Systematic review of the risk of enteric infection in patients taking acid suppression. Am J Gastroenterol 2007;102:2047–56; quiz 57.
63. Pavlov A, Muravyev R, Amoateng-Adjepong Y, Manthous CA. Inappropriate discharge on bronchodilators and acid-blocking medications after ICU admission: importance of medication reconciliation. Respir Care 2014;59:1524–9.
64. Baldoni Ade O, Ayres LR, Martinez EZ, et al. Factors associated with potentially inappropriate medications use by the elderly according to Beers criteria 2003 and 2012. Int J Clin Pharm 2014;36:316–24.
65. Gallagher PF, Barry PJ, Ryan C, et al. Inappropriate prescribing in an acutely ill population of elderly patients as determined by Beers’ Criteria. Age Ageing 2008;37:96–101.
66. Montastruc F, Duguet C, Rousseau V, et al. Potentially inappropriate medications and adverse drug reactions in the elderly: a study in a PharmacoVigilance database. Eur J Clin Pharmacol 2014;70:1123–7.
67. Ruggiero C, Dell’Aquila G, Gasperini B, et al. Potentially inappropriate drug prescriptions and risk of hospitalization among older, Italian, nursing home residents: the ULISSE project. Drugs Aging 2010;27:747–58.
68. Onder G, Landi F, Cesari M, et al. Inappropriate medication use among hospitalized older adults in Italy: results from the Italian Group of Pharmacoepidemiology in the Elderly. Eur J Clin Pharmacol 2003;59:157–62.
69. Harugeri A, Joseph J, Parthasarathi G, et al. Potentially inappropriate medication use in elderly patients: A study of prevalence and predictors in two teaching hospitals. J Postgrad Med 2010;56:186–91.
70. Garfinkel D, Mangin D. Feasibility study of a systematic approach for discontinuation of multiple medications in older adults: addressing polypharmacy. Arch Intern Med 2010;170:1648–54.
71. Dimitrow MS, Airaksinen MS, Kivela SL, et al. Comparison of prescribing criteria to evaluate the appropriateness of drug treatment in individuals aged 65 and older: a systematic review. J Am Geriatr Soc 2011;59:1521–30.
72. Levy HB, Marcus EL, Christen C. Beyond the beers criteria: A comparative overview of explicit criteria. Ann Pharmacother 2010;44:1968–75.
73. Marengoni A, Nobili A, Onder G. Best practices for drug prescribing in older adults: a call for action. Drugs Aging 2015;32:887–90.
74. Poudel A, Hubbard RE, Nissen L, Mitchell C. Frailty: a key indicator to minimize inappropriate medication in older people. QJM 2013;106:969–75.
75. American Geriatrics Society Beers Criteria Update Expert Panel. American Geriatrics Society 2015 updated Beers criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2015;63:2227–46.
76. Beers MH, Ouslander JG, Rollingher I, et al. Explicit criteria for determining inappropriate medication use in nursing home residents. UCLA Division of Geriatric Medicine. Arch Intern Med 1991;151:1825–32.
77. Blanco-Reina E, Ariza-Zafra G, Ocana-Riola R, Leon-Ortiz M. 2012 American Geriatrics Society Beers criteria: enhanced applicability for detecting potentially inappropriate medications in European older adults? A comparison with the Screening Tool of Older Person’s Potentially Inappropriate Prescriptions. J Am Geriatr Soc 2014;62:1217–23.
78. Stockl KM, Le L, Zhang S, Harada AS. Clinical and economic outcomes associated with potentially inappropriate prescribing in the elderly. Am J Manag Care 2010;16:e1–10.
79. Hill-Taylor B, Sketris I, Hayden J, et al. Application of the STOPP/START criteria: a systematic review of the prevalence of potentially inappropriate prescribing in older adults, and evidence of clinical, humanistic and economic impact. J Clin Pharm Ther 2013;38:360–72.
80. Barry PJ, Gallagher P, Ryan C, O’Mahony D. START (screening tool to alert doctors to the right treatment)--an evidence-based screening tool to detect prescribing omissions in elderly patients. Age Ageing 2007;36:632–8.
81. Gallagher P, Ryan C, Byrne S, Kennedy J, O’Mahony D. STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Ther 2008;46:72–83.
82. Haag JD, Davis AZ, Hoel RW, et al. Impact of pharmacist-provided medication therapy management on healthcare quality and utilization in recently discharged elderly patients. Am Health Drug Benefits 2016;9:259–68.
83. Gillespie U, Alassaad A, Hammarlund-Udenaes M, et al. Effects of pharmacists’ interventions on appropriateness of prescribing and evaluation of the instruments’ (MAI, STOPP and STARTs’) ability to predict hospitalization--analyses from a randomized controlled trial. PLoS One 2013;8:e62401.
84. Petrarca AM, Lengel AJ, Mangan MN. Inappropriate medication use in the elderly. Consult Pharm 2012;27:583–6.
85. Lavan AH, Gallagher P, Parsons C, O’Mahony D. STOPPFrail (Screening Tool of Older Persons Prescriptions in Frail adults with limited life expectancy): consensus validation. Age Ageing 2017;46:600–7.
86. Holt S, Schmiedl S, Thurmann PA. Potentially inappropriate medications in the elderly: the PRISCUS list. Dtsch Arztebl Int 2010;107:543–51.
87. Wickop B, Harterich S, Sommer C, et al. Potentially inappropriate medication use in multimorbid elderly inpatients: differences between the FORTA, PRISCUS and STOPP ratings. Drugs Real World Outcome 2016;3:317–25.
88. Naugler CT, Brymer C, Stolee P, Arcese ZA. Development and validation of an improving prescribing in the elderly tool. Can J Clin Pharmacol 2000;7:103–7.
89. Barry PJ, O’Keefe N, O’Connor KA, O’Mahony D. Inappropriate prescribing in the elderly: a comparison of the Beers criteria and the improved prescribing in the elderly tool (IPET) in acutely ill elderly hospitalized patients. J Clin Pharm Ther 2006;31:617–26.
90. Knapp DA. Development of criteria for drug utilization review. Clin Pharmacol Ther 1991;50(5 Pt 2):600–2.
91. Lipton HL, Bird JA. Drug utilization review in ambulatory settings: state of the science and directions for outcomes research. Med Care 1993;31:1069–82.
92. Monane M, Matthias DM, Nagle BA, Kelly MA. Improving prescribing patterns for the elderly through an online drug utilization review intervention: a system linking the physician, pharmacist, and computer. JAMA 1998;280:1249–52.
93. Kaur S, Mitchell G, Vitetta L, Roberts MS. Interventions that can reduce inappropriate prescribing in the elderly: a systematic review. Drugs Aging 2009;26:1013–28.
94. Raebel MA, Charles J, Dugan J, et al. Randomized trial to improve prescribing safety in ambulatory elderly patients. J Am Geriatr Soc 2007;55:977–85.
95. Tamblyn R, Huang A, Perreault R, et al. The medical office of the 21st century (MOXXI): effectiveness of computerized decision-making support in reducing inappropriate prescribing in primary care. CMAJ 2003;169:549–56.
96. Dalleur O, Boland B, Losseau C, et al. Reduction of potentially inappropriate medications using the STOPP criteria in frail older inpatients: a randomised controlled study. Drugs Aging 2014;31:291–8.
97. Schmader KE, Hanlon JT, Pieper CF, et al. Effects of geriatric evaluation and management on adverse drug reactions and suboptimal prescribing in the frail elderly. Am J Med 2004;116:394–401.
98. Crotty M, Halbert J, Rowett D, et al. An outreach geriatric medication advisory service in residential aged care: a randomised controlled trial of case conferencing. Age Ageing 2004;33:612–7.
99. Allard J, Hebert R, Rioux M, et al. Efficacy of a clinical medication review on the number of potentially inappropriate prescriptions prescribed for community-dwelling elderly people. CMAJ 2001;164:1291–6.
100. Spinewine A, Swine C, Dhillon S, et al. Effect of a collaborative approach on the quality of prescribing for geriatric inpatients: a randomized, controlled trial. J Am Geriatr Soc 2007;55:658–65.
101. Elliott RA, Woodward MC, Oborne CA. Improving benzodiazepine prescribing for elderly hospital inpatients using audit and multidisciplinary feedback. Intern Med J 2001;31:529–35.
102. Saltvedt I, Spigset O, Ruths S, et al. Patterns of drug prescription in a geriatric evaluation and management unit as compared with the general medical wards: a randomised study. Eur J Clin Pharmacol 2005;61:921–8.
103. Hanlon JT, Weinberger M, Samsa GP, et al. A randomized, controlled trial of a clinical pharmacist intervention to improve inappropriate prescribing in elderly outpatients with polypharmacy. Am J Med 1996;100:428–37.
104. Lipton HL, Bero LA, Bird JA, McPhee SJ. The impact of clinical pharmacists’ consultations on physicians’ geriatric drug prescribing. A randomized controlled trial. Med Care 1992;30:646–58.
105. Krska J, Cromarty JA, Arris F, et al. Pharmacist-led medication review in patients over 65: a randomized, controlled trial in primary care. Age Ageing 2001;30:205–11.
106. Brown BK, Earnhart J. Pharmacists and their effectiveness in ensuring the appropriateness of the chronic medication regimens of geriatric inpatients. Consult Pharm 2004;19:432–6.
107. Belfield KD, Kuyumjian AG, Teran R, et al. Impact of a collaborative strategy to reduce the inappropriate use of acid suppressive therapy in non-intensive care unit patients. Ann Pharmacother 2017;51:577–83.
108. Crotty M, Rowett D, Spurling L, et al. Does the addition of a pharmacist transition coordinator improve evidence-based medication management and health outcomes in older adults moving from the hospital to a long-term care facility? Results of a randomized, controlled trial. Am J Geriatr Pharmacother 2004;2:257–64.
109. Mattison MLP, Afonso KA, Ngo LH, Mukamal KJ. Preventing potentially inappropriate medication use in hospitalized older patients with a computerized provider order entry warning system. Arch Intern Med 2010;170:1331–6.
110. Kaboli PJ, Hoth AB, McClimon BJ, Schnipper JL. Clinical pharmacists and inpatient medical care: a systematic review. Arch Intern Med 2006;166:955–64.
111. Tinetti ME, Bogardus ST Jr, Agostini JV. Potential pitfalls of disease-specific guidelines for patients with multiple conditions. N Engl J Med 2004;351:2870–4.
112. Gokula M, Holmes HM. Tools to reduce polypharmacy. Clin Geriatr Med 2012;28:323–41.
From the Division of Allergy, Pulmonary, and Critical Care Medicine, Department of Medicine, Vanderbilt University Medical Center, Nashville, TN (Dr. Marra), Division of Anesthesiology Critical Care Medicine, Vanderbilt University Medical Center, Nashville, TN (Dr. Hayhurst, Dr. Hughes, Dr. Pandharipande), Department of Clinical and Experimental Science, University of Brescia, Brescia, Italy (Dr. Marengoni), School of Medicine and Surgery,
University of Milano-Bicocca, Milan, Italy (Dr. Bellelli), and Rehabilitation and Aged Care Unit Hospital Ancelle, Cremona, Italy (Dr. Morandi).
Abstract
- Objective: To present an overview of the phenomenon of inappropriate medication prescription in older critically ill patients and examine possible strategies of intervention.
- Methods: Review of the literature.
- Results: Polypharmacy and inappropriate prescribing of medications in older persons may lead to a significant risk of adverse drug-related events and mortality. The intensive care unit (ICU) is often the place where potentially inappropriate medications (PIMs) are first prescribed. Common PIMs at ICU discharge are antipsychotics, benzodiazepines, opioids, anticholinergic medications, antidepressants, and drugs causing orthostatic hypotension. Different classes of medications, typically intended for short-term use, are sometimes inappropriately continued after discharge from the hospital. At admission, potential risk factors for PIM are multiple morbidities, polypharmacy, frailty and cognitive decline; at discharge, a high number of pre-admission PIMs, discharge to a location other than home, discharge from a surgical service, longer length of ICU and hospital stay, and mechanical ventilation. Inappropriate prescribing in older patients can be detected through either the use of explicit criteria, drug utilization reviews, and multidisciplinary teams, including a geriatrician and/or the involvement of a clinical pharmacist.
- Conclusion: Use of PIMs may be common in critical patients, both on admission and at discharge from ICU. Therapeutic reconciliation is recommended at every transition of care (eg, at hospital or ICU admission and discharge) in order to improve appropriateness of prescription.
Key words: elderly; intensive care unit; inappropriate medications; antipsychotics.
Since older persons are often affected by multiple chronic diseases and are prescribed several medications, the quality and safety of prescribing these medications has become a global health care issue [1–4]. Polypharmacy and inappropriate prescribing of medications among the elderly is receiving significant attention in the medical literature [5,6]. Inappropriate medications in the elderly can lead to falls, cognitive impairment and delirium, poorer health status, and higher mortality [7–10]. Medications are considered potentially inappropriate when (a) the risks of treatment outweigh the benefits [11], (b) they are prescribed for periods longer than clinically indicated or without any clear indication, (c) they are not prescribed when indicated [12], and (d) they are likely to interact with other drugs and diseases. Medications included in this category are often referred to as potentially inappropriate medications (PIMs), as in some situations their use is justified; however, if the risk of harm from the drug is judged to outweigh the potential clinical benefit after an individual patient’s clinical circumstances are considered, these drugs are considered “actually inappropriate medications” (AIMs) [6].
Advancing age is associated with substantial pharmacokinetic and pharmacodynamics changes, such as altered distribution volumes and altered permeability of the blood-brain barrier, impaired liver metabolism and renal capacity, up- and down-regulation of target receptors, transmitters, and signaling pathways changes, impaired homeostasis, and increased risk of adverse drug reactions (ADRs) that lead to increased mortality and morbidity and higher health care costs [2,11,13–19]. Studies show that ADRs cause approximately 5% of hospital admissions in the general population, but the percentage rises to 10% in older persons [20].
Avoiding PIMs represents a strategy aimed at reducing drug-related mortality and morbidity. This article provides an overview of the phenomenon of inappropriate medication prescription in older critically ill patients and examines available strategies of intervention.
Inappropriate Medications at ICU Discharge
Though PIMs and AIMs may be identified at the time of hospital discharge, the intensive care unit (ICU) is often the place where these medications are first prescribed [21]. Acute hospitalization may increase PIM prescribing because of newly prescribed medications, the presence of multiple prescribers, inadequate medication reconciliation, and a lack of care coordination among inpatient providers or in the transition back to outpatient care [22)].
A known complication of critical illness and ICU stay is a significant increase in psychological symptoms, sleep cycle alterations, delirium, and cognitive impairment, which may be associated with increased prescription of specific PIMs, such as antipsychotics or benzodiazepines [6,23,24]. Despite the lack of reliable evidence supporting their use in the ICU, antipsychotic agents are used routinely in ICU patients [25] to treat a variety of conditions, such as substance withdrawal, agitation not responding to other therapies, or delirium. Results from a multicenter study of 164,996 hospitalizations across 71 academic medical centers in the US showed that 1 out of 10 ICU patients received an antipsychotic during their hospital stay [25]. Jasiak et al estimated that one-third of patients initiated on an atypical antipsychotic therapy for ICU delirium received a hospital discharge prescription for these medications, with a potential annual outpatient medication cost of approximately $2255 per patient [26].
One potential consequence of antipsychotic use in the ICU is their continuation after the transition to other clinical settings, including discharge from the hospital [27] (Table 1).
When examining the specific factors that may contribute to a patient being discharged on an antipsychotic, authors found that the specific antipsychotic used correlated with risk of continuation [27,30], with atypical antipsychotics having a greater likelihood of being continued than haloperidol [27,30]. Possible explanation for these results could be that physicians perceive less long-term risk from atypical agents, so may be more likely to continue them on discharge [30]. However, such an approach is not always safe. Indeed, although atypical antipsychotic agents tend to cause less tardive dyskinesia, they are known to be associated with similar rates of other adverse events compared with typical agents and have been linked to an increased risk of sudden cardiac death and pneumonia in the elderly [31,32].
Other factors independently associated with being discharged on a new antipsychotic medication were the severity of the acute illness as measured with the Acute Physiology and Chronic Health Evaluation II score at ICU admission (odds ratio [OR] 1 [95% confidence interval {CI}, 1.0–1.1]) and days treated with benzodiazepines (OR 1.1 [95% CI, 1.0–1.14]) [30]. Conversely, perhaps due to different practice patterns, Tomichek et al did not find an association between benzodiazepines administration and antipsychotic prescription at discharge in post hoc analyses [27].
Another possible reason for antipsychotic continuation may reside in the indication chosen [33]. Antipsychotic agents have sedative properties and they might be used to optimize sleep during hospitalization, despite the lack of evidence to support this indication [34]. Other factors potentially contributing to continuation of antipsychotics may include persistent delirium and agitation, newly diagnosed psychiatric illness, and difficulties experienced by physicians in deprescribing [35] with improper/incomplete medication reconciliation [33].
The continuation of antipsychotic therapy increased 30-day readmission rates in patients compared to those who had therapy stopped before discharge [33]. In addition to the well-described cardiac effects (prolonged QT interval), neuroleptic malignant syndrome and extrapyramidal symptoms may also occur, and longer-term use can predispose patients to metabolic disturbances, falls, and increase the risk of death in elderly patients with dementia [31].
Benzodiazepines and sedative hypnotics are commonly used to treat insomnia and agitation in older adults despite significant risk. Benzodiazepine administration was found to be an independent risk factor for a daily transition to delirium [36,37]. Pandharipande et al reported that every unit dose of lorazepam was associated with a higher risk for daily transition to delirium (OR 1.2, 95% CI 1.1–1.4, P = 0.003) [36] in critically ill patients. A more recent analysis found for every 5 mg of midazolam administered to a patient who is awake and without delirium, there is a 4% chance that this patient will develop delirium the next ICU day [37].
Given that the risk for benzodiazepine-associated delirium is dose-dependent, clinicians should use strategies known to reduce the daily number of benzodiazepines administered that often includes the use of a sedative associated with less delirium occurrence, such as dexmedetomidine or propofol [38]. Evidence has shown that long-term use of benzodiazepines has little benefit with many risks, including an increased susceptibility to spontaneous bacterial infection [39,40] and mortality in the setting of infection [41]. Nakafero et al showed that exposure to benzodiazepines was associated with increased occurrence of both influenza-like-illness–related pneumonia and mortality. Benzodiazepine use was associated also with increased occurrence of asthma exacerbation and with increased all-cause mortality during a median follow-up of 2 years in a cohort of asthmatic patients [42] as well with an increased risk of pneumonia and long-term mortality in patients with a prior diagnosis of community- acquired pneumonia [40]. Long-term use of benzodiazepines is also associated with increased risk of falls [43–45], cognitive impairment [46–48] and disability [49,50].
Other common types of PIMs at ICU discharge were opioids, anticholinergic medications, antidepressants, and drugs causing orthostatic hypotension [6]. Of the anticholinergic AIMs, H2 blockers (61%) and promethazine (15%) were the most common [6]. Only 16% of opioids, 23% of antidepressants, and 10% of drugs causing orthostatic hypotension were found to be actually inappropriate after the patient’s circumstances were considered (eg, postoperative pain control, a new diagnosis of major depressive disorder) [6].
Inappropriate Medications at Hospital Discharge
Medications typically intended for short-term use during acute illness are sometimes continued after discharge without documented indication [51]. Poudel et al found that in 206 patients 70 years of age and older discharged to residential aged care facilities from acute care, at least 1 PIM was identified in 112 (54.4%) patients on admission and 102 (49.5%) patients on discharge [11]. Commonly prescribed PIM categories, at both admission and discharge, were central nervous system, cardiovascular, gastrointestinal, and respiratory drugs and analgesics [6,11,52,53]. Of all medications prescribed at admission (1728), 10.8% were PIMs, and at discharge, of 1759 medications, 9.6% were PIMs. Of the total 187 PIMs on admission, 56 (30%) were stopped, and 131 (70%) were continued; 32 new PIMs were introduced [11].
Morandi et al in 2011 conducted a prospective cohort study including 120 patients age ≥ 60 who were discharged after receiving care in a medical, surgical, or cardiovascular ICU for shock or respiratory failure. The percentage of patients prescribed at least 1 PIM increased from 66% at pre-admission to 85% at discharge. The number of patients with 0 PIMs dropped from 34% at preadmission to 14% at discharge, and the number of patients with 3 or more PIMS increased from 16% at preadmission to 37% at discharge. While it is possible that these drugs may be appropriate when started during an acute illness in the ICU (eg, stress ulcer prophylaxis with H2-antagonists in mechanically ventilated patients), most should have been discontinued at ICU and/or hospital discharge [21].
Inappropriate prescriptions of proton pump inhibitors (PPIs) in hospital and primary care have been widely reported [54,55]. In a study conducted by Ahrens et al in 31 primary care practices, for 58% (263/506) of patients discharged from 35 hospitals with a PPI recommendation in hospital discharge letters, an appropriate indication was missing. In 57% of these cases general practitioners followed this recommendation and continued the prescription for more than 1 month [54]. The strongest factor associated with appropriate and inappropriate continuation of PPI after discharge was PPI prescription prior to hospitalization [54]. Although PPIs are safe, they can cause adverse effects. PPI intake has been found to have a significant association with risk of community-acquired pneumonia [56,57], hip fractures [58], Clostridium difficile-associated diarrhea [55,61,62], and to reduce the therapeutic effects of bisphosphonates [59] and low-dose aspirin [60].
Unintentional medication continuation is not a problem isolated to a single drug class or disease [63]. Scales et al evaluated rates of and risk factors for potentially unintentional medication continuation following hospitalization in a population of elderly patients (≥ 66 years) [51]. They created distinct cohorts by identifying seniors not previously receiving four classes of medications typically used to treat or prevent complications of acute illness: antipsychotic medications; gastric acid suppressants (ie, histamine-2 blockers and proton pump inhibitors); benzodiazepines; and inhaled bronchodilators and steroids [51]. Prescription without documented indication occurred across all medication classes, from 12,209 patients (1.4 %) for antipsychotic medications to 34,140 patients (6.1 %) for gastric acid suppressants [51].
Several potential risk factors were considered. The relationship between multimorbidity and polypharmacy is well described in the literature, and several studies have identified a positive association between the number of drugs and the use of PIMs [64–66]. Conversely, Poudel et al did not find any association between polypharmacy and PIM use [11]. Associations were found between the use of PIMs, frailty status, and cognitive decline of patients at admission and at discharge [11], while no association was observed with age, gender, in-hospital falls, delirium, and functional decline [11,67]. Other potential risk factors of a high number of PIMs at discharge were a high number of pre-admission PIMs, discharge to a location other than home, and discharge from a surgical service [1,6,68,69]. Length of ICU stay and mechanical ventilation had a positive influence on the number of PIMs used by acutely ill older patients [11,63,69]. In the study of Scales et al, the greatest absolute risk factor across all medication groups was longer hospitalization. The increased OR for medication continuation after a hospitalization lasting more than 7 days ranged from 2.03 (95% CI 1.94–2.11) for respiratory inhalers to 6.35 (95% CI 5.91–6.82) for antipsychotic medications [51].
Inappropriate Medications: Where and How to Intervene?
Early detection of PIMs may prevent adverse drug events and improve geriatric care in older adults [13,70]. PIM prevalence can often be a useful indicator of prescribing quality [2]. Appropriate interventions and an improved quality of prescribed medications require appropriate assessment tools to decrease the number of patients discharged on these medications [71,72]. Medication reconciliation is the process of avoiding inadvertent inconsistencies within a patient’s drug regimen, which can occur during transitions in different setting of care [73]. A multidisciplinary team should be involved in the medication reconciliation at each care transition to reevaluate medications use according to the clinical conditions, cognitive/functional status and the coexistence of geriatric syndromes (eg, dementia, malnutrition, delirium, urinary incontinence, frailty) (Figure).
Criteria for the Evaluation of Inappropriate Medications Prescription
Explicit criteria derived from expert reports or published reviews are available (Table 2).
Beers criteria PIMs have been found to be associated with poor health outcomes, including confusion, falls, and mortality [7,75,78]. The STOPP (Screening Tool of Older Person’s potentially inappropriate Prescriptions) and START (Screening Tool to Alert doctors to the Right Treatment) are evidence-based sets of criteria that were developed in Ireland and updated in October 2014, including some of the new criteria for direct oral anticoagulants, drugs affecting or affected by renal system and anti-muscarinic/anticholinergic agents [79].
Several other sets of criteria have been published to identify PIMs, such as the FORTA (Fit for the Aged) and the PRISCUS [86] criteria. FORTA allows a disease-related evaluation revealing over-treatment and under-treatment, and medications are graded as follows: A, indispensable drug, clear-cut benefit in terms of efficacy/safety ratio proven in elderly patients for a given indication; B, drugs with proven or obvious efficacy in the elderly, but limited extent of effect or safety concerns; C, drugs with questionable efficacy/safety profiles in the elderly which should be avoided or omitted in the presence of too many drugs or side effects; D, avoid in the elderly, omit first, refer also to negative listings. Negative lists such as PRISCUS, which provide an explicit listing of drugs, independent of the diagnosis, are easy to use. On the other hand, constant updates are needed, and such lists carry the risk of an assumption that drugs not listed would be appropriate in every case [87]. Both sets of criteria have in common that they refer to long-term medication and drugs frequently used during the inpatient stay, such as antibiotics, are hardly taken into account [87].
The Medication Appropriateness Index measures overall prescribing quality through 10 separate but interrelated domains [8]. Three components are used to detect PIMs: indication, effectiveness, and duplication. However, it does not give any precise guidance in relation to specific medicines and therefore has limited application for objectively defining PIMs.
Another prescribing quality assessment tool is the Inappropriate Prescribing in the Elderly Tool (IPET), which consists of a list of the 14 most prevalent prescription errors identified from an extensive list of inappropriate prescription instances drawn up by an expert Canadian Consensus Panel [88,89].
Another approach to assess the appropriateness of drugs prescribed for older people is the use of Drug Utilization Reviews (DURs) [16]. DURs use consensus opinion by drug therapy experts to define standards or explicit criteria for a single drug, class of drugs, or group of drugs [16]. DURs typically use retrospective information from large, nonclinical administrative databases to identify problems such as dosage range, duration, therapeutic duplication, and drug interactions [90, 91]. Monane et al [92] evaluated a program designed to decrease the use of PIMs among the elderly through a computerized online DUR database. Computer alerts triggered telephone calls to physicians by pharmacists to discuss a potential problem and any therapeutic substitution options. From a total of 43,007 telepharmacy calls generated by the alerts, they were able to reach 19,368 physicians regarding 24,266 alerts (56%). The rate of change to a more appropriate therapeutic agent was 24% (5860), but ranged from 40% for long half-life benzodiazepines to 2% to 7% for drugs that theoretically were contraindicated by patients’ self-reported history [92].
Computerized Support Systems to Reduce Inappropriate Prescribing in the Elderly
Other potential solutions for reducing inappropriate medications may include continuing medical education, electronic medical records surveillance, routine clinical evaluation, and/or improved hand-off communication between discharging and accepting providers. Incorporating this assessment of medication appropriateness into the medication reconciliation process when patients are discharged or transferred out of the ICU has the potential to enhance patient safety [21,93]. A randomized controlled trial conducted by Raebel et al [94] reported the effectiveness of a computerized pharmacy alert system plus collaboration between health care professionals for decreasing potentially inappropriate medication dispensing in elderly patients. Another study showed that computer-based access to complete drug profiles and alerts about potential prescribing problems reduced the occurrence of potentially inappropriate prescriptions [95]. A summary of these studies is shown in Table 3.
Interdisciplinary Teams to Reduce Inappropriate Prescribing in the Elderly
Some studies evaluated the effect of multidisciplinary teamwork in improving inappropriate medication prescribing in the elderly (Table 4).
Pharmacists in hospitals can play a significant role in the initiation of changes to patient’s therapy and management [11] (Table 5).
Mattison et al recently emphasized that studies of PIMs should determine scenarios in which it is appropriate to prescribe PIMs, moving beyond simply labeling some medications as “potentially inappropriate,” since some PIMs are appropriately prescribed in specific clinical situations [109]. Morandi et al showed that the positive predictive value (PPV) depends on the drug type. Thus, when developing a screening system, one cannot be concerned only with high negative predictive value (NPV), one must consider PPV as well [6]. Screening tools that include medication classes with low PPV will generate false positive “flags” or warnings, which could lead to misguided clinical decisions [6]. The fact that many PIMs are not AIMs also reveals the value of using a multidisciplinary team to identify AIMs from lists of PIMs generated when discharge medication lists are screened [6,110]. Thus, a multidisciplinary team is needed to consider the clinical context to distinguish PIMs from AIMs [6]. Of course, such a team is not available in some settings; when resources are limited, knowledge of which PIMs are most likely AIMs (ie, have high PPVs) could guide the development of computer-based decision support systems or other surveillance approaches that are efficient in that particular setting [6].
Approaches for optimizing prescribing in this population mainly depend on patient needs and comorbidities and most available data are derived from randomized controlled trials involving a single drug. Such trials do not take into account the confounding effects of multiple comorbidities and patient preferences. Therefore, approaches for optimizing prescription management that are available for and validated in younger patients are not applicable to elderly subjects [3,111].
Conclusion
Clinicians should seek to identify and discontinue AIMs at 3 important transitions during a critically ill elderly patient’s hospital course: at the time of hospital or ICU admission; at ICU discharge; and at hospital discharge. The patient’s clinical situation should be reviewed at every transition points, ideally by a multidisciplinary team of clinicians, to judge the appropriateness of each PIM [6]. After the hospital discharge, patient’s medications should be then reviewed by a multidisciplinary team and/or by the primary care physician according to the final discharge destination (ie, home, nursing home, rehabilitation) by using any of the validated tools. Regardless of the approach, it is clear that standardized care processes, including enhanced clinical decision support, are necessary to ensure that physicians do not continue exposing our patients to unnecessary medications and harm after discharge.
Corresponding author: Alessandro Morandi, MD, MPH, [email protected].
Funding/support: Dr. Pandiharipande is supported by National Institutes of Health HL111111 (Bethesda, MD) and by the VA Clinical Science Research and Development Service (Washington, DC) and the National Institutes of Health AG027472 and AG035117 (Bethesda, MD).
Financial disclosures: Dr. Pratik Pandharipande has received a research grant from Hospira Inc in collaboration with the NIH.
From the Division of Allergy, Pulmonary, and Critical Care Medicine, Department of Medicine, Vanderbilt University Medical Center, Nashville, TN (Dr. Marra), Division of Anesthesiology Critical Care Medicine, Vanderbilt University Medical Center, Nashville, TN (Dr. Hayhurst, Dr. Hughes, Dr. Pandharipande), Department of Clinical and Experimental Science, University of Brescia, Brescia, Italy (Dr. Marengoni), School of Medicine and Surgery,
University of Milano-Bicocca, Milan, Italy (Dr. Bellelli), and Rehabilitation and Aged Care Unit Hospital Ancelle, Cremona, Italy (Dr. Morandi).
Abstract
- Objective: To present an overview of the phenomenon of inappropriate medication prescription in older critically ill patients and examine possible strategies of intervention.
- Methods: Review of the literature.
- Results: Polypharmacy and inappropriate prescribing of medications in older persons may lead to a significant risk of adverse drug-related events and mortality. The intensive care unit (ICU) is often the place where potentially inappropriate medications (PIMs) are first prescribed. Common PIMs at ICU discharge are antipsychotics, benzodiazepines, opioids, anticholinergic medications, antidepressants, and drugs causing orthostatic hypotension. Different classes of medications, typically intended for short-term use, are sometimes inappropriately continued after discharge from the hospital. At admission, potential risk factors for PIM are multiple morbidities, polypharmacy, frailty and cognitive decline; at discharge, a high number of pre-admission PIMs, discharge to a location other than home, discharge from a surgical service, longer length of ICU and hospital stay, and mechanical ventilation. Inappropriate prescribing in older patients can be detected through either the use of explicit criteria, drug utilization reviews, and multidisciplinary teams, including a geriatrician and/or the involvement of a clinical pharmacist.
- Conclusion: Use of PIMs may be common in critical patients, both on admission and at discharge from ICU. Therapeutic reconciliation is recommended at every transition of care (eg, at hospital or ICU admission and discharge) in order to improve appropriateness of prescription.
Key words: elderly; intensive care unit; inappropriate medications; antipsychotics.
Since older persons are often affected by multiple chronic diseases and are prescribed several medications, the quality and safety of prescribing these medications has become a global health care issue [1–4]. Polypharmacy and inappropriate prescribing of medications among the elderly is receiving significant attention in the medical literature [5,6]. Inappropriate medications in the elderly can lead to falls, cognitive impairment and delirium, poorer health status, and higher mortality [7–10]. Medications are considered potentially inappropriate when (a) the risks of treatment outweigh the benefits [11], (b) they are prescribed for periods longer than clinically indicated or without any clear indication, (c) they are not prescribed when indicated [12], and (d) they are likely to interact with other drugs and diseases. Medications included in this category are often referred to as potentially inappropriate medications (PIMs), as in some situations their use is justified; however, if the risk of harm from the drug is judged to outweigh the potential clinical benefit after an individual patient’s clinical circumstances are considered, these drugs are considered “actually inappropriate medications” (AIMs) [6].
Advancing age is associated with substantial pharmacokinetic and pharmacodynamics changes, such as altered distribution volumes and altered permeability of the blood-brain barrier, impaired liver metabolism and renal capacity, up- and down-regulation of target receptors, transmitters, and signaling pathways changes, impaired homeostasis, and increased risk of adverse drug reactions (ADRs) that lead to increased mortality and morbidity and higher health care costs [2,11,13–19]. Studies show that ADRs cause approximately 5% of hospital admissions in the general population, but the percentage rises to 10% in older persons [20].
Avoiding PIMs represents a strategy aimed at reducing drug-related mortality and morbidity. This article provides an overview of the phenomenon of inappropriate medication prescription in older critically ill patients and examines available strategies of intervention.
Inappropriate Medications at ICU Discharge
Though PIMs and AIMs may be identified at the time of hospital discharge, the intensive care unit (ICU) is often the place where these medications are first prescribed [21]. Acute hospitalization may increase PIM prescribing because of newly prescribed medications, the presence of multiple prescribers, inadequate medication reconciliation, and a lack of care coordination among inpatient providers or in the transition back to outpatient care [22)].
A known complication of critical illness and ICU stay is a significant increase in psychological symptoms, sleep cycle alterations, delirium, and cognitive impairment, which may be associated with increased prescription of specific PIMs, such as antipsychotics or benzodiazepines [6,23,24]. Despite the lack of reliable evidence supporting their use in the ICU, antipsychotic agents are used routinely in ICU patients [25] to treat a variety of conditions, such as substance withdrawal, agitation not responding to other therapies, or delirium. Results from a multicenter study of 164,996 hospitalizations across 71 academic medical centers in the US showed that 1 out of 10 ICU patients received an antipsychotic during their hospital stay [25]. Jasiak et al estimated that one-third of patients initiated on an atypical antipsychotic therapy for ICU delirium received a hospital discharge prescription for these medications, with a potential annual outpatient medication cost of approximately $2255 per patient [26].
One potential consequence of antipsychotic use in the ICU is their continuation after the transition to other clinical settings, including discharge from the hospital [27] (Table 1).
When examining the specific factors that may contribute to a patient being discharged on an antipsychotic, authors found that the specific antipsychotic used correlated with risk of continuation [27,30], with atypical antipsychotics having a greater likelihood of being continued than haloperidol [27,30]. Possible explanation for these results could be that physicians perceive less long-term risk from atypical agents, so may be more likely to continue them on discharge [30]. However, such an approach is not always safe. Indeed, although atypical antipsychotic agents tend to cause less tardive dyskinesia, they are known to be associated with similar rates of other adverse events compared with typical agents and have been linked to an increased risk of sudden cardiac death and pneumonia in the elderly [31,32].
Other factors independently associated with being discharged on a new antipsychotic medication were the severity of the acute illness as measured with the Acute Physiology and Chronic Health Evaluation II score at ICU admission (odds ratio [OR] 1 [95% confidence interval {CI}, 1.0–1.1]) and days treated with benzodiazepines (OR 1.1 [95% CI, 1.0–1.14]) [30]. Conversely, perhaps due to different practice patterns, Tomichek et al did not find an association between benzodiazepines administration and antipsychotic prescription at discharge in post hoc analyses [27].
Another possible reason for antipsychotic continuation may reside in the indication chosen [33]. Antipsychotic agents have sedative properties and they might be used to optimize sleep during hospitalization, despite the lack of evidence to support this indication [34]. Other factors potentially contributing to continuation of antipsychotics may include persistent delirium and agitation, newly diagnosed psychiatric illness, and difficulties experienced by physicians in deprescribing [35] with improper/incomplete medication reconciliation [33].
The continuation of antipsychotic therapy increased 30-day readmission rates in patients compared to those who had therapy stopped before discharge [33]. In addition to the well-described cardiac effects (prolonged QT interval), neuroleptic malignant syndrome and extrapyramidal symptoms may also occur, and longer-term use can predispose patients to metabolic disturbances, falls, and increase the risk of death in elderly patients with dementia [31].
Benzodiazepines and sedative hypnotics are commonly used to treat insomnia and agitation in older adults despite significant risk. Benzodiazepine administration was found to be an independent risk factor for a daily transition to delirium [36,37]. Pandharipande et al reported that every unit dose of lorazepam was associated with a higher risk for daily transition to delirium (OR 1.2, 95% CI 1.1–1.4, P = 0.003) [36] in critically ill patients. A more recent analysis found for every 5 mg of midazolam administered to a patient who is awake and without delirium, there is a 4% chance that this patient will develop delirium the next ICU day [37].
Given that the risk for benzodiazepine-associated delirium is dose-dependent, clinicians should use strategies known to reduce the daily number of benzodiazepines administered that often includes the use of a sedative associated with less delirium occurrence, such as dexmedetomidine or propofol [38]. Evidence has shown that long-term use of benzodiazepines has little benefit with many risks, including an increased susceptibility to spontaneous bacterial infection [39,40] and mortality in the setting of infection [41]. Nakafero et al showed that exposure to benzodiazepines was associated with increased occurrence of both influenza-like-illness–related pneumonia and mortality. Benzodiazepine use was associated also with increased occurrence of asthma exacerbation and with increased all-cause mortality during a median follow-up of 2 years in a cohort of asthmatic patients [42] as well with an increased risk of pneumonia and long-term mortality in patients with a prior diagnosis of community- acquired pneumonia [40]. Long-term use of benzodiazepines is also associated with increased risk of falls [43–45], cognitive impairment [46–48] and disability [49,50].
Other common types of PIMs at ICU discharge were opioids, anticholinergic medications, antidepressants, and drugs causing orthostatic hypotension [6]. Of the anticholinergic AIMs, H2 blockers (61%) and promethazine (15%) were the most common [6]. Only 16% of opioids, 23% of antidepressants, and 10% of drugs causing orthostatic hypotension were found to be actually inappropriate after the patient’s circumstances were considered (eg, postoperative pain control, a new diagnosis of major depressive disorder) [6].
Inappropriate Medications at Hospital Discharge
Medications typically intended for short-term use during acute illness are sometimes continued after discharge without documented indication [51]. Poudel et al found that in 206 patients 70 years of age and older discharged to residential aged care facilities from acute care, at least 1 PIM was identified in 112 (54.4%) patients on admission and 102 (49.5%) patients on discharge [11]. Commonly prescribed PIM categories, at both admission and discharge, were central nervous system, cardiovascular, gastrointestinal, and respiratory drugs and analgesics [6,11,52,53]. Of all medications prescribed at admission (1728), 10.8% were PIMs, and at discharge, of 1759 medications, 9.6% were PIMs. Of the total 187 PIMs on admission, 56 (30%) were stopped, and 131 (70%) were continued; 32 new PIMs were introduced [11].
Morandi et al in 2011 conducted a prospective cohort study including 120 patients age ≥ 60 who were discharged after receiving care in a medical, surgical, or cardiovascular ICU for shock or respiratory failure. The percentage of patients prescribed at least 1 PIM increased from 66% at pre-admission to 85% at discharge. The number of patients with 0 PIMs dropped from 34% at preadmission to 14% at discharge, and the number of patients with 3 or more PIMS increased from 16% at preadmission to 37% at discharge. While it is possible that these drugs may be appropriate when started during an acute illness in the ICU (eg, stress ulcer prophylaxis with H2-antagonists in mechanically ventilated patients), most should have been discontinued at ICU and/or hospital discharge [21].
Inappropriate prescriptions of proton pump inhibitors (PPIs) in hospital and primary care have been widely reported [54,55]. In a study conducted by Ahrens et al in 31 primary care practices, for 58% (263/506) of patients discharged from 35 hospitals with a PPI recommendation in hospital discharge letters, an appropriate indication was missing. In 57% of these cases general practitioners followed this recommendation and continued the prescription for more than 1 month [54]. The strongest factor associated with appropriate and inappropriate continuation of PPI after discharge was PPI prescription prior to hospitalization [54]. Although PPIs are safe, they can cause adverse effects. PPI intake has been found to have a significant association with risk of community-acquired pneumonia [56,57], hip fractures [58], Clostridium difficile-associated diarrhea [55,61,62], and to reduce the therapeutic effects of bisphosphonates [59] and low-dose aspirin [60].
Unintentional medication continuation is not a problem isolated to a single drug class or disease [63]. Scales et al evaluated rates of and risk factors for potentially unintentional medication continuation following hospitalization in a population of elderly patients (≥ 66 years) [51]. They created distinct cohorts by identifying seniors not previously receiving four classes of medications typically used to treat or prevent complications of acute illness: antipsychotic medications; gastric acid suppressants (ie, histamine-2 blockers and proton pump inhibitors); benzodiazepines; and inhaled bronchodilators and steroids [51]. Prescription without documented indication occurred across all medication classes, from 12,209 patients (1.4 %) for antipsychotic medications to 34,140 patients (6.1 %) for gastric acid suppressants [51].
Several potential risk factors were considered. The relationship between multimorbidity and polypharmacy is well described in the literature, and several studies have identified a positive association between the number of drugs and the use of PIMs [64–66]. Conversely, Poudel et al did not find any association between polypharmacy and PIM use [11]. Associations were found between the use of PIMs, frailty status, and cognitive decline of patients at admission and at discharge [11], while no association was observed with age, gender, in-hospital falls, delirium, and functional decline [11,67]. Other potential risk factors of a high number of PIMs at discharge were a high number of pre-admission PIMs, discharge to a location other than home, and discharge from a surgical service [1,6,68,69]. Length of ICU stay and mechanical ventilation had a positive influence on the number of PIMs used by acutely ill older patients [11,63,69]. In the study of Scales et al, the greatest absolute risk factor across all medication groups was longer hospitalization. The increased OR for medication continuation after a hospitalization lasting more than 7 days ranged from 2.03 (95% CI 1.94–2.11) for respiratory inhalers to 6.35 (95% CI 5.91–6.82) for antipsychotic medications [51].
Inappropriate Medications: Where and How to Intervene?
Early detection of PIMs may prevent adverse drug events and improve geriatric care in older adults [13,70]. PIM prevalence can often be a useful indicator of prescribing quality [2]. Appropriate interventions and an improved quality of prescribed medications require appropriate assessment tools to decrease the number of patients discharged on these medications [71,72]. Medication reconciliation is the process of avoiding inadvertent inconsistencies within a patient’s drug regimen, which can occur during transitions in different setting of care [73]. A multidisciplinary team should be involved in the medication reconciliation at each care transition to reevaluate medications use according to the clinical conditions, cognitive/functional status and the coexistence of geriatric syndromes (eg, dementia, malnutrition, delirium, urinary incontinence, frailty) (Figure).
Criteria for the Evaluation of Inappropriate Medications Prescription
Explicit criteria derived from expert reports or published reviews are available (Table 2).
Beers criteria PIMs have been found to be associated with poor health outcomes, including confusion, falls, and mortality [7,75,78]. The STOPP (Screening Tool of Older Person’s potentially inappropriate Prescriptions) and START (Screening Tool to Alert doctors to the Right Treatment) are evidence-based sets of criteria that were developed in Ireland and updated in October 2014, including some of the new criteria for direct oral anticoagulants, drugs affecting or affected by renal system and anti-muscarinic/anticholinergic agents [79].
Several other sets of criteria have been published to identify PIMs, such as the FORTA (Fit for the Aged) and the PRISCUS [86] criteria. FORTA allows a disease-related evaluation revealing over-treatment and under-treatment, and medications are graded as follows: A, indispensable drug, clear-cut benefit in terms of efficacy/safety ratio proven in elderly patients for a given indication; B, drugs with proven or obvious efficacy in the elderly, but limited extent of effect or safety concerns; C, drugs with questionable efficacy/safety profiles in the elderly which should be avoided or omitted in the presence of too many drugs or side effects; D, avoid in the elderly, omit first, refer also to negative listings. Negative lists such as PRISCUS, which provide an explicit listing of drugs, independent of the diagnosis, are easy to use. On the other hand, constant updates are needed, and such lists carry the risk of an assumption that drugs not listed would be appropriate in every case [87]. Both sets of criteria have in common that they refer to long-term medication and drugs frequently used during the inpatient stay, such as antibiotics, are hardly taken into account [87].
The Medication Appropriateness Index measures overall prescribing quality through 10 separate but interrelated domains [8]. Three components are used to detect PIMs: indication, effectiveness, and duplication. However, it does not give any precise guidance in relation to specific medicines and therefore has limited application for objectively defining PIMs.
Another prescribing quality assessment tool is the Inappropriate Prescribing in the Elderly Tool (IPET), which consists of a list of the 14 most prevalent prescription errors identified from an extensive list of inappropriate prescription instances drawn up by an expert Canadian Consensus Panel [88,89].
Another approach to assess the appropriateness of drugs prescribed for older people is the use of Drug Utilization Reviews (DURs) [16]. DURs use consensus opinion by drug therapy experts to define standards or explicit criteria for a single drug, class of drugs, or group of drugs [16]. DURs typically use retrospective information from large, nonclinical administrative databases to identify problems such as dosage range, duration, therapeutic duplication, and drug interactions [90, 91]. Monane et al [92] evaluated a program designed to decrease the use of PIMs among the elderly through a computerized online DUR database. Computer alerts triggered telephone calls to physicians by pharmacists to discuss a potential problem and any therapeutic substitution options. From a total of 43,007 telepharmacy calls generated by the alerts, they were able to reach 19,368 physicians regarding 24,266 alerts (56%). The rate of change to a more appropriate therapeutic agent was 24% (5860), but ranged from 40% for long half-life benzodiazepines to 2% to 7% for drugs that theoretically were contraindicated by patients’ self-reported history [92].
Computerized Support Systems to Reduce Inappropriate Prescribing in the Elderly
Other potential solutions for reducing inappropriate medications may include continuing medical education, electronic medical records surveillance, routine clinical evaluation, and/or improved hand-off communication between discharging and accepting providers. Incorporating this assessment of medication appropriateness into the medication reconciliation process when patients are discharged or transferred out of the ICU has the potential to enhance patient safety [21,93]. A randomized controlled trial conducted by Raebel et al [94] reported the effectiveness of a computerized pharmacy alert system plus collaboration between health care professionals for decreasing potentially inappropriate medication dispensing in elderly patients. Another study showed that computer-based access to complete drug profiles and alerts about potential prescribing problems reduced the occurrence of potentially inappropriate prescriptions [95]. A summary of these studies is shown in Table 3.
Interdisciplinary Teams to Reduce Inappropriate Prescribing in the Elderly
Some studies evaluated the effect of multidisciplinary teamwork in improving inappropriate medication prescribing in the elderly (Table 4).
Pharmacists in hospitals can play a significant role in the initiation of changes to patient’s therapy and management [11] (Table 5).
Mattison et al recently emphasized that studies of PIMs should determine scenarios in which it is appropriate to prescribe PIMs, moving beyond simply labeling some medications as “potentially inappropriate,” since some PIMs are appropriately prescribed in specific clinical situations [109]. Morandi et al showed that the positive predictive value (PPV) depends on the drug type. Thus, when developing a screening system, one cannot be concerned only with high negative predictive value (NPV), one must consider PPV as well [6]. Screening tools that include medication classes with low PPV will generate false positive “flags” or warnings, which could lead to misguided clinical decisions [6]. The fact that many PIMs are not AIMs also reveals the value of using a multidisciplinary team to identify AIMs from lists of PIMs generated when discharge medication lists are screened [6,110]. Thus, a multidisciplinary team is needed to consider the clinical context to distinguish PIMs from AIMs [6]. Of course, such a team is not available in some settings; when resources are limited, knowledge of which PIMs are most likely AIMs (ie, have high PPVs) could guide the development of computer-based decision support systems or other surveillance approaches that are efficient in that particular setting [6].
Approaches for optimizing prescribing in this population mainly depend on patient needs and comorbidities and most available data are derived from randomized controlled trials involving a single drug. Such trials do not take into account the confounding effects of multiple comorbidities and patient preferences. Therefore, approaches for optimizing prescription management that are available for and validated in younger patients are not applicable to elderly subjects [3,111].
Conclusion
Clinicians should seek to identify and discontinue AIMs at 3 important transitions during a critically ill elderly patient’s hospital course: at the time of hospital or ICU admission; at ICU discharge; and at hospital discharge. The patient’s clinical situation should be reviewed at every transition points, ideally by a multidisciplinary team of clinicians, to judge the appropriateness of each PIM [6]. After the hospital discharge, patient’s medications should be then reviewed by a multidisciplinary team and/or by the primary care physician according to the final discharge destination (ie, home, nursing home, rehabilitation) by using any of the validated tools. Regardless of the approach, it is clear that standardized care processes, including enhanced clinical decision support, are necessary to ensure that physicians do not continue exposing our patients to unnecessary medications and harm after discharge.
Corresponding author: Alessandro Morandi, MD, MPH, [email protected].
Funding/support: Dr. Pandiharipande is supported by National Institutes of Health HL111111 (Bethesda, MD) and by the VA Clinical Science Research and Development Service (Washington, DC) and the National Institutes of Health AG027472 and AG035117 (Bethesda, MD).
Financial disclosures: Dr. Pratik Pandharipande has received a research grant from Hospira Inc in collaboration with the NIH.
1. Lang PO, Hasso Y, Drame M, et al. Potentially inappropriate prescribing including under-use amongst older patients with cognitive or psychiatric co-morbidities. Age Ageing 2010;39:373–81.
2. Spinewine A, Schmader KE, Barber N, et al. Appropriate prescribing in elderly people: how well can it be measured and optimised? Lancet 2007;370:173–84.
3. Lang PO, Vogt-Ferrier N, Hasso Y, et al. Interdisciplinary geriatric and psychiatric care reduces potentially inappropriate prescribing in the hospital: interventional study in 150 acutely ill elderly patients with mental and somatic comorbid conditions. J Am Med Dir Assoc 2012;13:406 e1–7.
4. Cecile M, Seux V, Pauly V, et al. [Adverse drug events in hospitalized elderly patients in a geriatric medicine unit: study of prevalence and risk factors]. Rev Med Interne 2009;30:393–400.
5. Tosato M, Landi F, Martone AM, et al. Potentially inappropriate drug use among hospitalised older adults: results from the CRIME study. Age Ageing 2014;43:767–73.
6. Morandi A, Vasilevskis E, Pandharipande PP, et al. Inappropriate medication prescriptions in elderly adults surviving an intensive care unit hospitalization. J Am Geriatr Soc 2013;61:1128–34.
7. Fick DM, Mion LC, Beers MH, Waller JL. Health outcomes associated with potentially inappropriate medication use in older adults. Res Nurs Health 2008;31:42–51.
8. Hanlon JT, Schmader KE, Samsa GP, et al. A method for assessing drug therapy appropriateness. J Clin Epidemiol 1992;45:1045–51.
9. Lau DT, Kasper JD, Potter DEB, et al. Hospitalization and death associated with potentially inappropriate medication prescriptions among elderly nursing home residents. Arch Intern Med 2005;165:68–74.
10. Wright RM, Roumani YF, Boudreau R, et al. Effect of central nervous system medication use on decline in cognition in community-dwelling older adults: findings from the Health, Aging and Body Composition Study. J Am Geriatr Soc 2009;57:243–50.
11. Poudel A, Peel NM, Nissen L, et al. Potentially inappropriate prescribing in older patients discharged from acute care hospitals to residential aged care facilities. Ann Pharmacother 2014;48:1425–33.
12. Wahab MS, Nyfort-Hansen K, Kowalski SR. Inappropriate prescribing in hospitalised Australian elderly as determined by the STOPP criteria. Int J Clin Pharm 2012;34:855–62.
13. O’Mahony D, Gallagher PF. Inappropriate prescribing in the older population: need for new criteria. Age Ageing 2008;37:138–41.
14. Mangoni AA, Jansen PA, Jackson SH. Under-representation of older adults in pharmacokinetic and pharmacodynamic studies: a solvable problem? Exp Rev Clin Pharmacol 2013;6:35–9.
15. Klotz U. The elderly--a challenge for appropriate drug treatment. Eur J Clin Pharmacol 2008;64225–6.
16. Hanlon JT, Schmader KE, Ruby CM, Weinberger M. Suboptimal prescribing in older inpatients and outpatients. J Am Geriatr Soc 2001;49:200–9.
17. Hubbard RE, O’Mahony MS, Woodhouse KW. Medication prescribing in frail older people. Eur J Clin Pharmacol 2013;69:319–26.
18. American Geriatrics Society Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2012;60:616–31.
19. Page RL, Ruscin JM. The risk of adverse drug events and hospital-related morbidity and mortality among older adults with potentially inappropriate medication use. Am J Geriatr Pharmacother 2006;4:297–305.
20. Pirmohamed M, James S, Meakin S, et al. Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients. BMJ 2004;329:15–9.
21. Morandi A, Vasilevskis EE, Pandharipande PP, et al. Inappropriate medications in elderly ICU survivors: where to intervene? Arch Intern Med 2011;171:1032–4.
22. Page RL 2nd, Linnebur SA, Bryant LL, Ruscin JM. Inappropriate prescribing in the hospitalized elderly patient: defining the problem, evaluation tools, and possible solutions. Clin Interv Aging 2010;5:75–87.
23. Pandharipande PP, Girard TD, Jackson JC, et al. Long-term cognitive impairment after critical illness. N Engl J Med 2013;369:1306–16.
24. Ehlenbach WJ, Hough CL, Crane PK, et al. Association between acute care and critical illness hospitalization and cognitive function in older adults. JAMA 2010;303:763–70.
25. Swan JT, Fitousis K, Hall JB, et al. Antipsychotic use and diagnosis of delirium in the intensive care unit. Crit Care 2012;16:R84.
26. Jasiak KD, Middleton EA, Camamo JM, et al. Evaluation of discontinuation of atypical antipsychotics prescribed for ICU delirium. J Pharm Pract 2013;26:253–6.
27. Tomichek JE, Stollings JL, Pandharipande PP, et al. Antipsychotic prescribing patterns during and after critical illness: a prospective cohort study. Crit Care 2016;20:378.
28. Kram BL, Kram SJ, Brooks KR. Implications of atypical antipsychotic prescribing in the intensive care unit. J Crit Care 2015;30:814–8.
29. Flurie RW, Gonzales JP, Tata AL, et al. Hospital delirium treatment: Continuation of antipsychotic therapy from the intensive care unit to discharge. Am J Health Syst Pharm 2015;72(23 Suppl 3):S133–9.
30. Rowe AS, Hamilton LA, Curtis RA, et al. Risk factors for discharge on a new antipsychotic medication after admission to an intensive care unit. J Crit Care 2015;30:1283–6.
31. Ray WA, Chung CP, Murray KT, et al. Atypical antipsychotic drugs and the risk of sudden cardiac death. N Engl J Med 2009;360:225–35.
32. Wang PS, Schneeweiss S, Avorn J, et al. Risk of death in elderly users of conventional vs. atypical antipsychotic medications. N Engl J Med 2005;353:2335–41.
33. Marshall J, Herzig SJ, Howell MD, et al. Antipsychotic utilization in the intensive care unit and in transitions of care. J Crit Care 2016;33:119–24.
34. NIH State-of-the-science conference statement on manifestations and management of chronic insomnia in adults. NIH Consens State Sci Statements 2005;22:1–30.
35. Farrell B, Tsang C, Raman-Wilms L, et a;. What are priorities for deprescribing for elderly patients? Capturing the voice of practitioners: a modified delphi process. PLoS One 2015;10:e0122246.
36. Pandharipande P, Shintani A, Peterson J, et al. Lorazepam is an independent risk factor for transitioning to delirium in intensive care unit patients. Anesthesiology 2006;104:21–6.
37. Zaal IJ, Devlin JW, Hazelbag M, et al. Benzodiazepine-associated delirium in critically ill adults. Intensive Care Med 2015;41:2130–7.
38. Barr J, Fraser GL, Puntillo K, et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med 2013;41:263–306.
39. Riker RR, Shehabi Y, Bokesch PM, et al. Dexmedetomidine vs midazolam for sedation of critically ill patients: a randomized trial. JAMA 2009;301:489–99.
40. Obiora E, Hubbard R, Sanders RD, Myles PR. The impact of benzodiazepines on occurrence of pneumonia and mortality from pneumonia: a nested case-control and survival analysis in a population-based cohort. Thorax 2013;68:163–70.
41. Sanders RD, Godlee A, Fujimori T, et al. Benzodiazepine augmented gamma-amino-butyric acid signaling increases mortality from pneumonia in mice. Crit Care Med 2013;41:1627–36.
42. Nakafero G, Sanders RD, Nguyen-Van-Tam JS, Myles PR. Association between benzodiazepine use and exacerbations and mortality in patients with asthma: a matched case-control and survival analysis using the United Kingdom Clinical Practice Research Datalink. Pharmacoepidemiol Drug Saf 2015;24:793–802.
43. Hartikainen S, Lonnroos E, Louhivuori K. Medication as a risk factor for falls: critical systematic review. J Gerontol A Biol Sci Med Sci 2007;62:1172–81.
44. Pierfitte C, Macouillard G, Thicoipe M, et al. Benzodiazepines and hip fractures in elderly people: case-control study. BMJ 2001;322:704–8.
45. Landi F, Onder G, Cesari M, et al. Psychotropic medications and risk for falls among community-dwelling frail older people: an observational study. J Gerontol A Biol Sci Med Sci 2005;60:622–6.
46. Hanlon JT, Horner RD, Schmader KE, et al. Benzodiazepine use and cognitive function among community-dwelling elderly. Clin Pharmacol Ther 1998;64:684–92.
47. Greenblatt DJ, Harmatz JS, Shapiro L, et al. Sensitivity to triazolam in the elderly. N Engl J Med 1991;324:1691–8.
48. Bertz RJ, Kroboth PD, Kroboth FJ, et al. Alprazolam in young and elderly men: sensitivity and tolerance to psychomotor, sedative and memory effects. J Pharmacol Exp Ther 1997;281:1317–29.
49. Gray SL, LaCroix AZ, Blough D, et al. Is the use of benzodiazepines associated with incident disability? J Am Geriatr Soc 2002;50:1012–8.
50. Gray SL, LaCroix AZ, Hanlon JT, et al. Benzodiazepine use and physical disability in community-dwelling older adults. J Am Geriatr Soc 2006;54:224–30.
51. Scales DC, Fischer HD, Li P, et al. Unintentional continuation of medications intended for acute illness after hospital discharge: a population-based cohort study. J Gen Intern Med 2016;31:196–202.
52. Hamilton H, Gallagher P, Ryan C, et al. Potentially inappropriate medications defined by STOPP criteria and the risk of adverse drug events in older hospitalized patients. Arch Intern Med 2011;171:1013–9.
53. Hanlon JT, Artz MB, Pieper CF, et al. Inappropriate medication use among frail elderly inpatients. Ann Pharmacother 2004;38:9–14.
54. Ahrens D, Behrens G, Himmel W, et al. Appropriateness of proton pump inhibitor recommendations at hospital discharge and continuation in primary care. Int J Clin Pract 2012;66:767–73.
55. McDonald EG, Milligan J, Frenette C, Lee TC. Continuous proton pump inhibitor therapy and the associated risk of recurrent Clostridium difficile infection. JAMA Intern Med 2015;175:784–91.
56. Gulmez SE, Holm A, Frederiksen H, et al. Use of proton pump inhibitors and the risk of community-acquired pneumonia: a population-based case-control study. Arch Intern Med 2007;167:950–5.
57. Laheij RJ, Sturkenboom MC, Hassing RJ, et al. Risk of community-acquired pneumonia and use of gastric acid-suppressive drugs. JAMA 2004;292:1955–60.
58. Yang YX, Lewis JD, Epstein S, Metz DC. Long-term proton pump inhibitor therapy and risk of hip fracture. JAMA 2006;296:2947–53.
59. Abrahamsen B, Eiken P, Eastell R. Proton pump inhibitor use and the antifracture efficacy of alendronate. Arch Intern Med 2011;171:998–1004.
60. Charlot M, Grove EL, Hansen PR, et al. Proton pump inhibitor use and risk of adverse cardiovascular events in aspirin treated patients with first time myocardial infarction: nationwide propensity score matched study. BMJ 2011;342:d2690.
61. Dial S, Delaney JA, Barkun AN, Suissa S. Use of gastric acid-suppressive agents and the risk of community-acquired Clostridium difficile-associated disease. JAMA 2005;294:2989–95.
62. Leonard J, Marshall JK, Moayyedi P. Systematic review of the risk of enteric infection in patients taking acid suppression. Am J Gastroenterol 2007;102:2047–56; quiz 57.
63. Pavlov A, Muravyev R, Amoateng-Adjepong Y, Manthous CA. Inappropriate discharge on bronchodilators and acid-blocking medications after ICU admission: importance of medication reconciliation. Respir Care 2014;59:1524–9.
64. Baldoni Ade O, Ayres LR, Martinez EZ, et al. Factors associated with potentially inappropriate medications use by the elderly according to Beers criteria 2003 and 2012. Int J Clin Pharm 2014;36:316–24.
65. Gallagher PF, Barry PJ, Ryan C, et al. Inappropriate prescribing in an acutely ill population of elderly patients as determined by Beers’ Criteria. Age Ageing 2008;37:96–101.
66. Montastruc F, Duguet C, Rousseau V, et al. Potentially inappropriate medications and adverse drug reactions in the elderly: a study in a PharmacoVigilance database. Eur J Clin Pharmacol 2014;70:1123–7.
67. Ruggiero C, Dell’Aquila G, Gasperini B, et al. Potentially inappropriate drug prescriptions and risk of hospitalization among older, Italian, nursing home residents: the ULISSE project. Drugs Aging 2010;27:747–58.
68. Onder G, Landi F, Cesari M, et al. Inappropriate medication use among hospitalized older adults in Italy: results from the Italian Group of Pharmacoepidemiology in the Elderly. Eur J Clin Pharmacol 2003;59:157–62.
69. Harugeri A, Joseph J, Parthasarathi G, et al. Potentially inappropriate medication use in elderly patients: A study of prevalence and predictors in two teaching hospitals. J Postgrad Med 2010;56:186–91.
70. Garfinkel D, Mangin D. Feasibility study of a systematic approach for discontinuation of multiple medications in older adults: addressing polypharmacy. Arch Intern Med 2010;170:1648–54.
71. Dimitrow MS, Airaksinen MS, Kivela SL, et al. Comparison of prescribing criteria to evaluate the appropriateness of drug treatment in individuals aged 65 and older: a systematic review. J Am Geriatr Soc 2011;59:1521–30.
72. Levy HB, Marcus EL, Christen C. Beyond the beers criteria: A comparative overview of explicit criteria. Ann Pharmacother 2010;44:1968–75.
73. Marengoni A, Nobili A, Onder G. Best practices for drug prescribing in older adults: a call for action. Drugs Aging 2015;32:887–90.
74. Poudel A, Hubbard RE, Nissen L, Mitchell C. Frailty: a key indicator to minimize inappropriate medication in older people. QJM 2013;106:969–75.
75. American Geriatrics Society Beers Criteria Update Expert Panel. American Geriatrics Society 2015 updated Beers criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2015;63:2227–46.
76. Beers MH, Ouslander JG, Rollingher I, et al. Explicit criteria for determining inappropriate medication use in nursing home residents. UCLA Division of Geriatric Medicine. Arch Intern Med 1991;151:1825–32.
77. Blanco-Reina E, Ariza-Zafra G, Ocana-Riola R, Leon-Ortiz M. 2012 American Geriatrics Society Beers criteria: enhanced applicability for detecting potentially inappropriate medications in European older adults? A comparison with the Screening Tool of Older Person’s Potentially Inappropriate Prescriptions. J Am Geriatr Soc 2014;62:1217–23.
78. Stockl KM, Le L, Zhang S, Harada AS. Clinical and economic outcomes associated with potentially inappropriate prescribing in the elderly. Am J Manag Care 2010;16:e1–10.
79. Hill-Taylor B, Sketris I, Hayden J, et al. Application of the STOPP/START criteria: a systematic review of the prevalence of potentially inappropriate prescribing in older adults, and evidence of clinical, humanistic and economic impact. J Clin Pharm Ther 2013;38:360–72.
80. Barry PJ, Gallagher P, Ryan C, O’Mahony D. START (screening tool to alert doctors to the right treatment)--an evidence-based screening tool to detect prescribing omissions in elderly patients. Age Ageing 2007;36:632–8.
81. Gallagher P, Ryan C, Byrne S, Kennedy J, O’Mahony D. STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Ther 2008;46:72–83.
82. Haag JD, Davis AZ, Hoel RW, et al. Impact of pharmacist-provided medication therapy management on healthcare quality and utilization in recently discharged elderly patients. Am Health Drug Benefits 2016;9:259–68.
83. Gillespie U, Alassaad A, Hammarlund-Udenaes M, et al. Effects of pharmacists’ interventions on appropriateness of prescribing and evaluation of the instruments’ (MAI, STOPP and STARTs’) ability to predict hospitalization--analyses from a randomized controlled trial. PLoS One 2013;8:e62401.
84. Petrarca AM, Lengel AJ, Mangan MN. Inappropriate medication use in the elderly. Consult Pharm 2012;27:583–6.
85. Lavan AH, Gallagher P, Parsons C, O’Mahony D. STOPPFrail (Screening Tool of Older Persons Prescriptions in Frail adults with limited life expectancy): consensus validation. Age Ageing 2017;46:600–7.
86. Holt S, Schmiedl S, Thurmann PA. Potentially inappropriate medications in the elderly: the PRISCUS list. Dtsch Arztebl Int 2010;107:543–51.
87. Wickop B, Harterich S, Sommer C, et al. Potentially inappropriate medication use in multimorbid elderly inpatients: differences between the FORTA, PRISCUS and STOPP ratings. Drugs Real World Outcome 2016;3:317–25.
88. Naugler CT, Brymer C, Stolee P, Arcese ZA. Development and validation of an improving prescribing in the elderly tool. Can J Clin Pharmacol 2000;7:103–7.
89. Barry PJ, O’Keefe N, O’Connor KA, O’Mahony D. Inappropriate prescribing in the elderly: a comparison of the Beers criteria and the improved prescribing in the elderly tool (IPET) in acutely ill elderly hospitalized patients. J Clin Pharm Ther 2006;31:617–26.
90. Knapp DA. Development of criteria for drug utilization review. Clin Pharmacol Ther 1991;50(5 Pt 2):600–2.
91. Lipton HL, Bird JA. Drug utilization review in ambulatory settings: state of the science and directions for outcomes research. Med Care 1993;31:1069–82.
92. Monane M, Matthias DM, Nagle BA, Kelly MA. Improving prescribing patterns for the elderly through an online drug utilization review intervention: a system linking the physician, pharmacist, and computer. JAMA 1998;280:1249–52.
93. Kaur S, Mitchell G, Vitetta L, Roberts MS. Interventions that can reduce inappropriate prescribing in the elderly: a systematic review. Drugs Aging 2009;26:1013–28.
94. Raebel MA, Charles J, Dugan J, et al. Randomized trial to improve prescribing safety in ambulatory elderly patients. J Am Geriatr Soc 2007;55:977–85.
95. Tamblyn R, Huang A, Perreault R, et al. The medical office of the 21st century (MOXXI): effectiveness of computerized decision-making support in reducing inappropriate prescribing in primary care. CMAJ 2003;169:549–56.
96. Dalleur O, Boland B, Losseau C, et al. Reduction of potentially inappropriate medications using the STOPP criteria in frail older inpatients: a randomised controlled study. Drugs Aging 2014;31:291–8.
97. Schmader KE, Hanlon JT, Pieper CF, et al. Effects of geriatric evaluation and management on adverse drug reactions and suboptimal prescribing in the frail elderly. Am J Med 2004;116:394–401.
98. Crotty M, Halbert J, Rowett D, et al. An outreach geriatric medication advisory service in residential aged care: a randomised controlled trial of case conferencing. Age Ageing 2004;33:612–7.
99. Allard J, Hebert R, Rioux M, et al. Efficacy of a clinical medication review on the number of potentially inappropriate prescriptions prescribed for community-dwelling elderly people. CMAJ 2001;164:1291–6.
100. Spinewine A, Swine C, Dhillon S, et al. Effect of a collaborative approach on the quality of prescribing for geriatric inpatients: a randomized, controlled trial. J Am Geriatr Soc 2007;55:658–65.
101. Elliott RA, Woodward MC, Oborne CA. Improving benzodiazepine prescribing for elderly hospital inpatients using audit and multidisciplinary feedback. Intern Med J 2001;31:529–35.
102. Saltvedt I, Spigset O, Ruths S, et al. Patterns of drug prescription in a geriatric evaluation and management unit as compared with the general medical wards: a randomised study. Eur J Clin Pharmacol 2005;61:921–8.
103. Hanlon JT, Weinberger M, Samsa GP, et al. A randomized, controlled trial of a clinical pharmacist intervention to improve inappropriate prescribing in elderly outpatients with polypharmacy. Am J Med 1996;100:428–37.
104. Lipton HL, Bero LA, Bird JA, McPhee SJ. The impact of clinical pharmacists’ consultations on physicians’ geriatric drug prescribing. A randomized controlled trial. Med Care 1992;30:646–58.
105. Krska J, Cromarty JA, Arris F, et al. Pharmacist-led medication review in patients over 65: a randomized, controlled trial in primary care. Age Ageing 2001;30:205–11.
106. Brown BK, Earnhart J. Pharmacists and their effectiveness in ensuring the appropriateness of the chronic medication regimens of geriatric inpatients. Consult Pharm 2004;19:432–6.
107. Belfield KD, Kuyumjian AG, Teran R, et al. Impact of a collaborative strategy to reduce the inappropriate use of acid suppressive therapy in non-intensive care unit patients. Ann Pharmacother 2017;51:577–83.
108. Crotty M, Rowett D, Spurling L, et al. Does the addition of a pharmacist transition coordinator improve evidence-based medication management and health outcomes in older adults moving from the hospital to a long-term care facility? Results of a randomized, controlled trial. Am J Geriatr Pharmacother 2004;2:257–64.
109. Mattison MLP, Afonso KA, Ngo LH, Mukamal KJ. Preventing potentially inappropriate medication use in hospitalized older patients with a computerized provider order entry warning system. Arch Intern Med 2010;170:1331–6.
110. Kaboli PJ, Hoth AB, McClimon BJ, Schnipper JL. Clinical pharmacists and inpatient medical care: a systematic review. Arch Intern Med 2006;166:955–64.
111. Tinetti ME, Bogardus ST Jr, Agostini JV. Potential pitfalls of disease-specific guidelines for patients with multiple conditions. N Engl J Med 2004;351:2870–4.
112. Gokula M, Holmes HM. Tools to reduce polypharmacy. Clin Geriatr Med 2012;28:323–41.
1. Lang PO, Hasso Y, Drame M, et al. Potentially inappropriate prescribing including under-use amongst older patients with cognitive or psychiatric co-morbidities. Age Ageing 2010;39:373–81.
2. Spinewine A, Schmader KE, Barber N, et al. Appropriate prescribing in elderly people: how well can it be measured and optimised? Lancet 2007;370:173–84.
3. Lang PO, Vogt-Ferrier N, Hasso Y, et al. Interdisciplinary geriatric and psychiatric care reduces potentially inappropriate prescribing in the hospital: interventional study in 150 acutely ill elderly patients with mental and somatic comorbid conditions. J Am Med Dir Assoc 2012;13:406 e1–7.
4. Cecile M, Seux V, Pauly V, et al. [Adverse drug events in hospitalized elderly patients in a geriatric medicine unit: study of prevalence and risk factors]. Rev Med Interne 2009;30:393–400.
5. Tosato M, Landi F, Martone AM, et al. Potentially inappropriate drug use among hospitalised older adults: results from the CRIME study. Age Ageing 2014;43:767–73.
6. Morandi A, Vasilevskis E, Pandharipande PP, et al. Inappropriate medication prescriptions in elderly adults surviving an intensive care unit hospitalization. J Am Geriatr Soc 2013;61:1128–34.
7. Fick DM, Mion LC, Beers MH, Waller JL. Health outcomes associated with potentially inappropriate medication use in older adults. Res Nurs Health 2008;31:42–51.
8. Hanlon JT, Schmader KE, Samsa GP, et al. A method for assessing drug therapy appropriateness. J Clin Epidemiol 1992;45:1045–51.
9. Lau DT, Kasper JD, Potter DEB, et al. Hospitalization and death associated with potentially inappropriate medication prescriptions among elderly nursing home residents. Arch Intern Med 2005;165:68–74.
10. Wright RM, Roumani YF, Boudreau R, et al. Effect of central nervous system medication use on decline in cognition in community-dwelling older adults: findings from the Health, Aging and Body Composition Study. J Am Geriatr Soc 2009;57:243–50.
11. Poudel A, Peel NM, Nissen L, et al. Potentially inappropriate prescribing in older patients discharged from acute care hospitals to residential aged care facilities. Ann Pharmacother 2014;48:1425–33.
12. Wahab MS, Nyfort-Hansen K, Kowalski SR. Inappropriate prescribing in hospitalised Australian elderly as determined by the STOPP criteria. Int J Clin Pharm 2012;34:855–62.
13. O’Mahony D, Gallagher PF. Inappropriate prescribing in the older population: need for new criteria. Age Ageing 2008;37:138–41.
14. Mangoni AA, Jansen PA, Jackson SH. Under-representation of older adults in pharmacokinetic and pharmacodynamic studies: a solvable problem? Exp Rev Clin Pharmacol 2013;6:35–9.
15. Klotz U. The elderly--a challenge for appropriate drug treatment. Eur J Clin Pharmacol 2008;64225–6.
16. Hanlon JT, Schmader KE, Ruby CM, Weinberger M. Suboptimal prescribing in older inpatients and outpatients. J Am Geriatr Soc 2001;49:200–9.
17. Hubbard RE, O’Mahony MS, Woodhouse KW. Medication prescribing in frail older people. Eur J Clin Pharmacol 2013;69:319–26.
18. American Geriatrics Society Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2012;60:616–31.
19. Page RL, Ruscin JM. The risk of adverse drug events and hospital-related morbidity and mortality among older adults with potentially inappropriate medication use. Am J Geriatr Pharmacother 2006;4:297–305.
20. Pirmohamed M, James S, Meakin S, et al. Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients. BMJ 2004;329:15–9.
21. Morandi A, Vasilevskis EE, Pandharipande PP, et al. Inappropriate medications in elderly ICU survivors: where to intervene? Arch Intern Med 2011;171:1032–4.
22. Page RL 2nd, Linnebur SA, Bryant LL, Ruscin JM. Inappropriate prescribing in the hospitalized elderly patient: defining the problem, evaluation tools, and possible solutions. Clin Interv Aging 2010;5:75–87.
23. Pandharipande PP, Girard TD, Jackson JC, et al. Long-term cognitive impairment after critical illness. N Engl J Med 2013;369:1306–16.
24. Ehlenbach WJ, Hough CL, Crane PK, et al. Association between acute care and critical illness hospitalization and cognitive function in older adults. JAMA 2010;303:763–70.
25. Swan JT, Fitousis K, Hall JB, et al. Antipsychotic use and diagnosis of delirium in the intensive care unit. Crit Care 2012;16:R84.
26. Jasiak KD, Middleton EA, Camamo JM, et al. Evaluation of discontinuation of atypical antipsychotics prescribed for ICU delirium. J Pharm Pract 2013;26:253–6.
27. Tomichek JE, Stollings JL, Pandharipande PP, et al. Antipsychotic prescribing patterns during and after critical illness: a prospective cohort study. Crit Care 2016;20:378.
28. Kram BL, Kram SJ, Brooks KR. Implications of atypical antipsychotic prescribing in the intensive care unit. J Crit Care 2015;30:814–8.
29. Flurie RW, Gonzales JP, Tata AL, et al. Hospital delirium treatment: Continuation of antipsychotic therapy from the intensive care unit to discharge. Am J Health Syst Pharm 2015;72(23 Suppl 3):S133–9.
30. Rowe AS, Hamilton LA, Curtis RA, et al. Risk factors for discharge on a new antipsychotic medication after admission to an intensive care unit. J Crit Care 2015;30:1283–6.
31. Ray WA, Chung CP, Murray KT, et al. Atypical antipsychotic drugs and the risk of sudden cardiac death. N Engl J Med 2009;360:225–35.
32. Wang PS, Schneeweiss S, Avorn J, et al. Risk of death in elderly users of conventional vs. atypical antipsychotic medications. N Engl J Med 2005;353:2335–41.
33. Marshall J, Herzig SJ, Howell MD, et al. Antipsychotic utilization in the intensive care unit and in transitions of care. J Crit Care 2016;33:119–24.
34. NIH State-of-the-science conference statement on manifestations and management of chronic insomnia in adults. NIH Consens State Sci Statements 2005;22:1–30.
35. Farrell B, Tsang C, Raman-Wilms L, et a;. What are priorities for deprescribing for elderly patients? Capturing the voice of practitioners: a modified delphi process. PLoS One 2015;10:e0122246.
36. Pandharipande P, Shintani A, Peterson J, et al. Lorazepam is an independent risk factor for transitioning to delirium in intensive care unit patients. Anesthesiology 2006;104:21–6.
37. Zaal IJ, Devlin JW, Hazelbag M, et al. Benzodiazepine-associated delirium in critically ill adults. Intensive Care Med 2015;41:2130–7.
38. Barr J, Fraser GL, Puntillo K, et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med 2013;41:263–306.
39. Riker RR, Shehabi Y, Bokesch PM, et al. Dexmedetomidine vs midazolam for sedation of critically ill patients: a randomized trial. JAMA 2009;301:489–99.
40. Obiora E, Hubbard R, Sanders RD, Myles PR. The impact of benzodiazepines on occurrence of pneumonia and mortality from pneumonia: a nested case-control and survival analysis in a population-based cohort. Thorax 2013;68:163–70.
41. Sanders RD, Godlee A, Fujimori T, et al. Benzodiazepine augmented gamma-amino-butyric acid signaling increases mortality from pneumonia in mice. Crit Care Med 2013;41:1627–36.
42. Nakafero G, Sanders RD, Nguyen-Van-Tam JS, Myles PR. Association between benzodiazepine use and exacerbations and mortality in patients with asthma: a matched case-control and survival analysis using the United Kingdom Clinical Practice Research Datalink. Pharmacoepidemiol Drug Saf 2015;24:793–802.
43. Hartikainen S, Lonnroos E, Louhivuori K. Medication as a risk factor for falls: critical systematic review. J Gerontol A Biol Sci Med Sci 2007;62:1172–81.
44. Pierfitte C, Macouillard G, Thicoipe M, et al. Benzodiazepines and hip fractures in elderly people: case-control study. BMJ 2001;322:704–8.
45. Landi F, Onder G, Cesari M, et al. Psychotropic medications and risk for falls among community-dwelling frail older people: an observational study. J Gerontol A Biol Sci Med Sci 2005;60:622–6.
46. Hanlon JT, Horner RD, Schmader KE, et al. Benzodiazepine use and cognitive function among community-dwelling elderly. Clin Pharmacol Ther 1998;64:684–92.
47. Greenblatt DJ, Harmatz JS, Shapiro L, et al. Sensitivity to triazolam in the elderly. N Engl J Med 1991;324:1691–8.
48. Bertz RJ, Kroboth PD, Kroboth FJ, et al. Alprazolam in young and elderly men: sensitivity and tolerance to psychomotor, sedative and memory effects. J Pharmacol Exp Ther 1997;281:1317–29.
49. Gray SL, LaCroix AZ, Blough D, et al. Is the use of benzodiazepines associated with incident disability? J Am Geriatr Soc 2002;50:1012–8.
50. Gray SL, LaCroix AZ, Hanlon JT, et al. Benzodiazepine use and physical disability in community-dwelling older adults. J Am Geriatr Soc 2006;54:224–30.
51. Scales DC, Fischer HD, Li P, et al. Unintentional continuation of medications intended for acute illness after hospital discharge: a population-based cohort study. J Gen Intern Med 2016;31:196–202.
52. Hamilton H, Gallagher P, Ryan C, et al. Potentially inappropriate medications defined by STOPP criteria and the risk of adverse drug events in older hospitalized patients. Arch Intern Med 2011;171:1013–9.
53. Hanlon JT, Artz MB, Pieper CF, et al. Inappropriate medication use among frail elderly inpatients. Ann Pharmacother 2004;38:9–14.
54. Ahrens D, Behrens G, Himmel W, et al. Appropriateness of proton pump inhibitor recommendations at hospital discharge and continuation in primary care. Int J Clin Pract 2012;66:767–73.
55. McDonald EG, Milligan J, Frenette C, Lee TC. Continuous proton pump inhibitor therapy and the associated risk of recurrent Clostridium difficile infection. JAMA Intern Med 2015;175:784–91.
56. Gulmez SE, Holm A, Frederiksen H, et al. Use of proton pump inhibitors and the risk of community-acquired pneumonia: a population-based case-control study. Arch Intern Med 2007;167:950–5.
57. Laheij RJ, Sturkenboom MC, Hassing RJ, et al. Risk of community-acquired pneumonia and use of gastric acid-suppressive drugs. JAMA 2004;292:1955–60.
58. Yang YX, Lewis JD, Epstein S, Metz DC. Long-term proton pump inhibitor therapy and risk of hip fracture. JAMA 2006;296:2947–53.
59. Abrahamsen B, Eiken P, Eastell R. Proton pump inhibitor use and the antifracture efficacy of alendronate. Arch Intern Med 2011;171:998–1004.
60. Charlot M, Grove EL, Hansen PR, et al. Proton pump inhibitor use and risk of adverse cardiovascular events in aspirin treated patients with first time myocardial infarction: nationwide propensity score matched study. BMJ 2011;342:d2690.
61. Dial S, Delaney JA, Barkun AN, Suissa S. Use of gastric acid-suppressive agents and the risk of community-acquired Clostridium difficile-associated disease. JAMA 2005;294:2989–95.
62. Leonard J, Marshall JK, Moayyedi P. Systematic review of the risk of enteric infection in patients taking acid suppression. Am J Gastroenterol 2007;102:2047–56; quiz 57.
63. Pavlov A, Muravyev R, Amoateng-Adjepong Y, Manthous CA. Inappropriate discharge on bronchodilators and acid-blocking medications after ICU admission: importance of medication reconciliation. Respir Care 2014;59:1524–9.
64. Baldoni Ade O, Ayres LR, Martinez EZ, et al. Factors associated with potentially inappropriate medications use by the elderly according to Beers criteria 2003 and 2012. Int J Clin Pharm 2014;36:316–24.
65. Gallagher PF, Barry PJ, Ryan C, et al. Inappropriate prescribing in an acutely ill population of elderly patients as determined by Beers’ Criteria. Age Ageing 2008;37:96–101.
66. Montastruc F, Duguet C, Rousseau V, et al. Potentially inappropriate medications and adverse drug reactions in the elderly: a study in a PharmacoVigilance database. Eur J Clin Pharmacol 2014;70:1123–7.
67. Ruggiero C, Dell’Aquila G, Gasperini B, et al. Potentially inappropriate drug prescriptions and risk of hospitalization among older, Italian, nursing home residents: the ULISSE project. Drugs Aging 2010;27:747–58.
68. Onder G, Landi F, Cesari M, et al. Inappropriate medication use among hospitalized older adults in Italy: results from the Italian Group of Pharmacoepidemiology in the Elderly. Eur J Clin Pharmacol 2003;59:157–62.
69. Harugeri A, Joseph J, Parthasarathi G, et al. Potentially inappropriate medication use in elderly patients: A study of prevalence and predictors in two teaching hospitals. J Postgrad Med 2010;56:186–91.
70. Garfinkel D, Mangin D. Feasibility study of a systematic approach for discontinuation of multiple medications in older adults: addressing polypharmacy. Arch Intern Med 2010;170:1648–54.
71. Dimitrow MS, Airaksinen MS, Kivela SL, et al. Comparison of prescribing criteria to evaluate the appropriateness of drug treatment in individuals aged 65 and older: a systematic review. J Am Geriatr Soc 2011;59:1521–30.
72. Levy HB, Marcus EL, Christen C. Beyond the beers criteria: A comparative overview of explicit criteria. Ann Pharmacother 2010;44:1968–75.
73. Marengoni A, Nobili A, Onder G. Best practices for drug prescribing in older adults: a call for action. Drugs Aging 2015;32:887–90.
74. Poudel A, Hubbard RE, Nissen L, Mitchell C. Frailty: a key indicator to minimize inappropriate medication in older people. QJM 2013;106:969–75.
75. American Geriatrics Society Beers Criteria Update Expert Panel. American Geriatrics Society 2015 updated Beers criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2015;63:2227–46.
76. Beers MH, Ouslander JG, Rollingher I, et al. Explicit criteria for determining inappropriate medication use in nursing home residents. UCLA Division of Geriatric Medicine. Arch Intern Med 1991;151:1825–32.
77. Blanco-Reina E, Ariza-Zafra G, Ocana-Riola R, Leon-Ortiz M. 2012 American Geriatrics Society Beers criteria: enhanced applicability for detecting potentially inappropriate medications in European older adults? A comparison with the Screening Tool of Older Person’s Potentially Inappropriate Prescriptions. J Am Geriatr Soc 2014;62:1217–23.
78. Stockl KM, Le L, Zhang S, Harada AS. Clinical and economic outcomes associated with potentially inappropriate prescribing in the elderly. Am J Manag Care 2010;16:e1–10.
79. Hill-Taylor B, Sketris I, Hayden J, et al. Application of the STOPP/START criteria: a systematic review of the prevalence of potentially inappropriate prescribing in older adults, and evidence of clinical, humanistic and economic impact. J Clin Pharm Ther 2013;38:360–72.
80. Barry PJ, Gallagher P, Ryan C, O’Mahony D. START (screening tool to alert doctors to the right treatment)--an evidence-based screening tool to detect prescribing omissions in elderly patients. Age Ageing 2007;36:632–8.
81. Gallagher P, Ryan C, Byrne S, Kennedy J, O’Mahony D. STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Ther 2008;46:72–83.
82. Haag JD, Davis AZ, Hoel RW, et al. Impact of pharmacist-provided medication therapy management on healthcare quality and utilization in recently discharged elderly patients. Am Health Drug Benefits 2016;9:259–68.
83. Gillespie U, Alassaad A, Hammarlund-Udenaes M, et al. Effects of pharmacists’ interventions on appropriateness of prescribing and evaluation of the instruments’ (MAI, STOPP and STARTs’) ability to predict hospitalization--analyses from a randomized controlled trial. PLoS One 2013;8:e62401.
84. Petrarca AM, Lengel AJ, Mangan MN. Inappropriate medication use in the elderly. Consult Pharm 2012;27:583–6.
85. Lavan AH, Gallagher P, Parsons C, O’Mahony D. STOPPFrail (Screening Tool of Older Persons Prescriptions in Frail adults with limited life expectancy): consensus validation. Age Ageing 2017;46:600–7.
86. Holt S, Schmiedl S, Thurmann PA. Potentially inappropriate medications in the elderly: the PRISCUS list. Dtsch Arztebl Int 2010;107:543–51.
87. Wickop B, Harterich S, Sommer C, et al. Potentially inappropriate medication use in multimorbid elderly inpatients: differences between the FORTA, PRISCUS and STOPP ratings. Drugs Real World Outcome 2016;3:317–25.
88. Naugler CT, Brymer C, Stolee P, Arcese ZA. Development and validation of an improving prescribing in the elderly tool. Can J Clin Pharmacol 2000;7:103–7.
89. Barry PJ, O’Keefe N, O’Connor KA, O’Mahony D. Inappropriate prescribing in the elderly: a comparison of the Beers criteria and the improved prescribing in the elderly tool (IPET) in acutely ill elderly hospitalized patients. J Clin Pharm Ther 2006;31:617–26.
90. Knapp DA. Development of criteria for drug utilization review. Clin Pharmacol Ther 1991;50(5 Pt 2):600–2.
91. Lipton HL, Bird JA. Drug utilization review in ambulatory settings: state of the science and directions for outcomes research. Med Care 1993;31:1069–82.
92. Monane M, Matthias DM, Nagle BA, Kelly MA. Improving prescribing patterns for the elderly through an online drug utilization review intervention: a system linking the physician, pharmacist, and computer. JAMA 1998;280:1249–52.
93. Kaur S, Mitchell G, Vitetta L, Roberts MS. Interventions that can reduce inappropriate prescribing in the elderly: a systematic review. Drugs Aging 2009;26:1013–28.
94. Raebel MA, Charles J, Dugan J, et al. Randomized trial to improve prescribing safety in ambulatory elderly patients. J Am Geriatr Soc 2007;55:977–85.
95. Tamblyn R, Huang A, Perreault R, et al. The medical office of the 21st century (MOXXI): effectiveness of computerized decision-making support in reducing inappropriate prescribing in primary care. CMAJ 2003;169:549–56.
96. Dalleur O, Boland B, Losseau C, et al. Reduction of potentially inappropriate medications using the STOPP criteria in frail older inpatients: a randomised controlled study. Drugs Aging 2014;31:291–8.
97. Schmader KE, Hanlon JT, Pieper CF, et al. Effects of geriatric evaluation and management on adverse drug reactions and suboptimal prescribing in the frail elderly. Am J Med 2004;116:394–401.
98. Crotty M, Halbert J, Rowett D, et al. An outreach geriatric medication advisory service in residential aged care: a randomised controlled trial of case conferencing. Age Ageing 2004;33:612–7.
99. Allard J, Hebert R, Rioux M, et al. Efficacy of a clinical medication review on the number of potentially inappropriate prescriptions prescribed for community-dwelling elderly people. CMAJ 2001;164:1291–6.
100. Spinewine A, Swine C, Dhillon S, et al. Effect of a collaborative approach on the quality of prescribing for geriatric inpatients: a randomized, controlled trial. J Am Geriatr Soc 2007;55:658–65.
101. Elliott RA, Woodward MC, Oborne CA. Improving benzodiazepine prescribing for elderly hospital inpatients using audit and multidisciplinary feedback. Intern Med J 2001;31:529–35.
102. Saltvedt I, Spigset O, Ruths S, et al. Patterns of drug prescription in a geriatric evaluation and management unit as compared with the general medical wards: a randomised study. Eur J Clin Pharmacol 2005;61:921–8.
103. Hanlon JT, Weinberger M, Samsa GP, et al. A randomized, controlled trial of a clinical pharmacist intervention to improve inappropriate prescribing in elderly outpatients with polypharmacy. Am J Med 1996;100:428–37.
104. Lipton HL, Bero LA, Bird JA, McPhee SJ. The impact of clinical pharmacists’ consultations on physicians’ geriatric drug prescribing. A randomized controlled trial. Med Care 1992;30:646–58.
105. Krska J, Cromarty JA, Arris F, et al. Pharmacist-led medication review in patients over 65: a randomized, controlled trial in primary care. Age Ageing 2001;30:205–11.
106. Brown BK, Earnhart J. Pharmacists and their effectiveness in ensuring the appropriateness of the chronic medication regimens of geriatric inpatients. Consult Pharm 2004;19:432–6.
107. Belfield KD, Kuyumjian AG, Teran R, et al. Impact of a collaborative strategy to reduce the inappropriate use of acid suppressive therapy in non-intensive care unit patients. Ann Pharmacother 2017;51:577–83.
108. Crotty M, Rowett D, Spurling L, et al. Does the addition of a pharmacist transition coordinator improve evidence-based medication management and health outcomes in older adults moving from the hospital to a long-term care facility? Results of a randomized, controlled trial. Am J Geriatr Pharmacother 2004;2:257–64.
109. Mattison MLP, Afonso KA, Ngo LH, Mukamal KJ. Preventing potentially inappropriate medication use in hospitalized older patients with a computerized provider order entry warning system. Arch Intern Med 2010;170:1331–6.
110. Kaboli PJ, Hoth AB, McClimon BJ, Schnipper JL. Clinical pharmacists and inpatient medical care: a systematic review. Arch Intern Med 2006;166:955–64.
111. Tinetti ME, Bogardus ST Jr, Agostini JV. Potential pitfalls of disease-specific guidelines for patients with multiple conditions. N Engl J Med 2004;351:2870–4.
112. Gokula M, Holmes HM. Tools to reduce polypharmacy. Clin Geriatr Med 2012;28:323–41.
FDG PET can’t replace BM biopsy, study suggests

LA JOLLA, CA—Fluorodeoxyglucose positron emission tomography (FDG PET) cannot replace bone marrow (BM) biopsy in T-cell lymphomas, according to a speaker at the 10th Annual T-cell Lymphoma Forum.
Researchers found that FDG PET results did not exactly correlate with BM biopsy results relating to tumor involvement in patients with T-cell lymphomas.
However, results from FDG PET were found to be an independent prognostic factor for progression-free survival (PFS) and overall survival (OS).
Youngil Koh, MD, of Seoul National University Hospital in Seoul, South Korea, presented this research in a poster and oral presentation at this year’s T-cell Lymphoma Forum.
He and his colleagues set out to investigate the clinical value of FDG PET for evaluating BM tumor involvement and prognosis in T-cell lymphoma patients.
The team analyzed 109 patients who underwent staging with FDG PET and BM biopsy. Most patients had extranodal natural killer/T-cell lymphoma, nasal type (NKTCL, n=46), or angioimmunoblastic T-cell lymphoma (AITL, n=41).
Patients also had peripheral T-cell lymphoma not otherwise specified (n=12), anaplastic large-cell lymphoma (n=4), enteropathy-associated T-cell lymphoma (n=4), and subcutaneous panniculitis-like T-cell lymphoma (n=2).
Most patients (87.2%) received chemotherapy as first-line treatment. Fifty percent were CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisolone) or CHOP-like regimens, 48.1% were IMEP (ifosphamide, methotrexate, etoposide, and prednisolone) or IMEP-like regimens, and 1.9% were “other” regimens.
Other first-line treatments included radiotherapy followed by chemotherapy (10.1%), excision (0.9%), and no treatment (1.8%).
The patients’ median OS was 60.03 months, and the median PFS was 15.7 months.
BM involvement
The researchers analyzed PET BM uptake both visually and quantitatively using the marrow-to-liver ratio (MLR), and they compared these results to BM biopsy results.
According to BM biopsy, 35.8% of patients had tumor involvement.
By visual analysis, the sensitivity of PET for diagnosing positive BM biopsy was 58.5%, and the specificity was 77.9%. By MLR, the sensitivity was 64.1%, and the specificity was 72.9%.
The diagnostic performance of PET for BM involvement was not different across the lymphoma subtypes, Dr Koh said.
Prognosis
“Although FDG PET did not correlate very well with bone marrow biopsy, it had prognostic value, especially MLR,” Dr Koh noted. “And most importantly, in bone marrow biopsy-negative patients, it [MLR] had prognostic value.”
MLR was a significant prognostic factor for PFS (P=0.005) and OS (P<0.001). The same was true for BM biopsy (P=0.009 for PFS and P<0.001 for OS), while visual PET analysis was a significant prognostic factor for OS (P=0.015) but not PFS (P=0.476).
In patients negative by BM biopsy, MLR was a significant prognostic factor for PFS (P=0.001) and OS (P=0.005).
Dr Koh and his colleagues also analyzed the prognostic value of PET and BM biopsy specifically in patients with NKTCL and AITL.
In AITL patients, BM biopsy was a significant prognostic factor for OS (P=0.002) but not PFS (P=0.246). Visual PET analysis was not significant for PFS (P=0.910) or OS (P=0.581), and neither was MLR (P=0.053 for PFS and P=0.156 for OS).
In patients with NKTCL, BM biopsy was a significant prognostic factor for PFS (P=0.008) and OS (P<0.001). Visual PET analysis was not significant for PFS (P=0.469) or OS (P=0.092). And MLR was significant for PFS (P=0.004) and OS (P=0.012).
“Bone marrow findings of FDG PET are an independent prognostic factor in these tumors,” Dr Koh said, “suggesting the biologic relevance of FDG PET findings for aggressiveness or covert bone marrow involvement of tumor cells.” ![]()
LA JOLLA, CA—Fluorodeoxyglucose positron emission tomography (FDG PET) cannot replace bone marrow (BM) biopsy in T-cell lymphomas, according to a speaker at the 10th Annual T-cell Lymphoma Forum.
Researchers found that FDG PET results did not exactly correlate with BM biopsy results relating to tumor involvement in patients with T-cell lymphomas.
However, results from FDG PET were found to be an independent prognostic factor for progression-free survival (PFS) and overall survival (OS).
Youngil Koh, MD, of Seoul National University Hospital in Seoul, South Korea, presented this research in a poster and oral presentation at this year’s T-cell Lymphoma Forum.
He and his colleagues set out to investigate the clinical value of FDG PET for evaluating BM tumor involvement and prognosis in T-cell lymphoma patients.
The team analyzed 109 patients who underwent staging with FDG PET and BM biopsy. Most patients had extranodal natural killer/T-cell lymphoma, nasal type (NKTCL, n=46), or angioimmunoblastic T-cell lymphoma (AITL, n=41).
Patients also had peripheral T-cell lymphoma not otherwise specified (n=12), anaplastic large-cell lymphoma (n=4), enteropathy-associated T-cell lymphoma (n=4), and subcutaneous panniculitis-like T-cell lymphoma (n=2).
Most patients (87.2%) received chemotherapy as first-line treatment. Fifty percent were CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisolone) or CHOP-like regimens, 48.1% were IMEP (ifosphamide, methotrexate, etoposide, and prednisolone) or IMEP-like regimens, and 1.9% were “other” regimens.
Other first-line treatments included radiotherapy followed by chemotherapy (10.1%), excision (0.9%), and no treatment (1.8%).
The patients’ median OS was 60.03 months, and the median PFS was 15.7 months.
BM involvement
The researchers analyzed PET BM uptake both visually and quantitatively using the marrow-to-liver ratio (MLR), and they compared these results to BM biopsy results.
According to BM biopsy, 35.8% of patients had tumor involvement.
By visual analysis, the sensitivity of PET for diagnosing positive BM biopsy was 58.5%, and the specificity was 77.9%. By MLR, the sensitivity was 64.1%, and the specificity was 72.9%.
The diagnostic performance of PET for BM involvement was not different across the lymphoma subtypes, Dr Koh said.
Prognosis
“Although FDG PET did not correlate very well with bone marrow biopsy, it had prognostic value, especially MLR,” Dr Koh noted. “And most importantly, in bone marrow biopsy-negative patients, it [MLR] had prognostic value.”
MLR was a significant prognostic factor for PFS (P=0.005) and OS (P<0.001). The same was true for BM biopsy (P=0.009 for PFS and P<0.001 for OS), while visual PET analysis was a significant prognostic factor for OS (P=0.015) but not PFS (P=0.476).
In patients negative by BM biopsy, MLR was a significant prognostic factor for PFS (P=0.001) and OS (P=0.005).
Dr Koh and his colleagues also analyzed the prognostic value of PET and BM biopsy specifically in patients with NKTCL and AITL.
In AITL patients, BM biopsy was a significant prognostic factor for OS (P=0.002) but not PFS (P=0.246). Visual PET analysis was not significant for PFS (P=0.910) or OS (P=0.581), and neither was MLR (P=0.053 for PFS and P=0.156 for OS).
In patients with NKTCL, BM biopsy was a significant prognostic factor for PFS (P=0.008) and OS (P<0.001). Visual PET analysis was not significant for PFS (P=0.469) or OS (P=0.092). And MLR was significant for PFS (P=0.004) and OS (P=0.012).
“Bone marrow findings of FDG PET are an independent prognostic factor in these tumors,” Dr Koh said, “suggesting the biologic relevance of FDG PET findings for aggressiveness or covert bone marrow involvement of tumor cells.” ![]()
LA JOLLA, CA—Fluorodeoxyglucose positron emission tomography (FDG PET) cannot replace bone marrow (BM) biopsy in T-cell lymphomas, according to a speaker at the 10th Annual T-cell Lymphoma Forum.
Researchers found that FDG PET results did not exactly correlate with BM biopsy results relating to tumor involvement in patients with T-cell lymphomas.
However, results from FDG PET were found to be an independent prognostic factor for progression-free survival (PFS) and overall survival (OS).
Youngil Koh, MD, of Seoul National University Hospital in Seoul, South Korea, presented this research in a poster and oral presentation at this year’s T-cell Lymphoma Forum.
He and his colleagues set out to investigate the clinical value of FDG PET for evaluating BM tumor involvement and prognosis in T-cell lymphoma patients.
The team analyzed 109 patients who underwent staging with FDG PET and BM biopsy. Most patients had extranodal natural killer/T-cell lymphoma, nasal type (NKTCL, n=46), or angioimmunoblastic T-cell lymphoma (AITL, n=41).
Patients also had peripheral T-cell lymphoma not otherwise specified (n=12), anaplastic large-cell lymphoma (n=4), enteropathy-associated T-cell lymphoma (n=4), and subcutaneous panniculitis-like T-cell lymphoma (n=2).
Most patients (87.2%) received chemotherapy as first-line treatment. Fifty percent were CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisolone) or CHOP-like regimens, 48.1% were IMEP (ifosphamide, methotrexate, etoposide, and prednisolone) or IMEP-like regimens, and 1.9% were “other” regimens.
Other first-line treatments included radiotherapy followed by chemotherapy (10.1%), excision (0.9%), and no treatment (1.8%).
The patients’ median OS was 60.03 months, and the median PFS was 15.7 months.
BM involvement
The researchers analyzed PET BM uptake both visually and quantitatively using the marrow-to-liver ratio (MLR), and they compared these results to BM biopsy results.
According to BM biopsy, 35.8% of patients had tumor involvement.
By visual analysis, the sensitivity of PET for diagnosing positive BM biopsy was 58.5%, and the specificity was 77.9%. By MLR, the sensitivity was 64.1%, and the specificity was 72.9%.
The diagnostic performance of PET for BM involvement was not different across the lymphoma subtypes, Dr Koh said.
Prognosis
“Although FDG PET did not correlate very well with bone marrow biopsy, it had prognostic value, especially MLR,” Dr Koh noted. “And most importantly, in bone marrow biopsy-negative patients, it [MLR] had prognostic value.”
MLR was a significant prognostic factor for PFS (P=0.005) and OS (P<0.001). The same was true for BM biopsy (P=0.009 for PFS and P<0.001 for OS), while visual PET analysis was a significant prognostic factor for OS (P=0.015) but not PFS (P=0.476).
In patients negative by BM biopsy, MLR was a significant prognostic factor for PFS (P=0.001) and OS (P=0.005).
Dr Koh and his colleagues also analyzed the prognostic value of PET and BM biopsy specifically in patients with NKTCL and AITL.
In AITL patients, BM biopsy was a significant prognostic factor for OS (P=0.002) but not PFS (P=0.246). Visual PET analysis was not significant for PFS (P=0.910) or OS (P=0.581), and neither was MLR (P=0.053 for PFS and P=0.156 for OS).
In patients with NKTCL, BM biopsy was a significant prognostic factor for PFS (P=0.008) and OS (P<0.001). Visual PET analysis was not significant for PFS (P=0.469) or OS (P=0.092). And MLR was significant for PFS (P=0.004) and OS (P=0.012).
“Bone marrow findings of FDG PET are an independent prognostic factor in these tumors,” Dr Koh said, “suggesting the biologic relevance of FDG PET findings for aggressiveness or covert bone marrow involvement of tumor cells.” ![]()
Inhibitor provides clinical improvement in MF

LA JOLLA, CA—Results of a phase 1 trial suggest MRG-106 can provide clinical improvement in patients with mycosis fungoides (MF), whether the drug is given alone or in conjunction with other therapies.
MRG-106 is an inhibitor of microRNA-155, which is upregulated in MF.
In this ongoing trial, 90% of patients who received MRG-106 have experienced an improvement in mSWAT score, and 59% of patients who received the drug for at least 1 month had a partial response.
The most common adverse events (AEs) attributed to MRG-106 were neutropenia, injection site pain, and fatigue.
Christiane Querfeld, MD, PhD, of the City of Hope in Duarte, California, presented these results at the 10th Annual T-cell Lymphoma Forum. The research is sponsored by miRagen Therapeutics, Inc., the company developing MRG-106.
The trial has enrolled 36 MF patients, 69% of whom are male. Their median age at enrollment was 63 (range, 21-85).
Patients had received a median of 4 prior systemic therapies (range, 1-13) and a median of 3 prior skin-directed therapies (range, 1-8).
At baseline, patients had a median mSWAT score of 43 (range, 2-180). The modified Severity Weighted Assessment Tool (mSWAT) measures the severity of skin disease over a patient’s body.
Part A
In part A of the study, 6 patients received MRG-106 via intralesional injection. A 75 mg dose of the drug was found to be well-tolerated, producing generally minor injection site reactions.
In addition, intralesional injection of MRG-106 produced improvements in CAILS score. The Composite Assessment of Index Lesion Severity (CAILS) score is obtained by adding the severity score of erythema, scaling, plaque elevation, and surface area for up to 5 index lesions.
Part B
In part B, 30 patients received MRG-106 via subcutaneous (SQ) injection, intravenous (IV) infusion, or IV bolus injection.
Patients who received SQ injection or IV infusion received doses of 300 mg, 600 mg, or 900 mg. Those who received an IV bolus only received the 300 mg dose.
Twenty-nine of the 30 patients in part B were evaluable for efficacy. Twenty-six of these patients—90%—had an improvement in mSWAT score from baseline.
“Twenty-six patients had at least stable disease to partial response,” Dr Querfeld noted. “No complete responses yet, but we’re close.”
Twelve patients were still receiving MRG-106 at last follow-up.
Ten of the 17 patients (59%) who had received MRG-106 for more than 1 month had at least a 50% improvement in mSWAT score, or a partial response. Once this was achieved, responses were durable.
One patient was still in response at roughly 470 days of follow-up.
Concomitant therapies
Dr Querfeld and her colleagues looked at patient outcomes in the context of concomitant therapies as well. They analyzed data from 26 patients who had received at least 6 doses of MRG-106.
Half of these patients were receiving MRG-106 alone, and the other half were receiving concomitant therapies, including bexarotene (n=7), interferon-alfa (n=2), methotrexate (n=1), vorinostat (n=1), and “other” treatments (n=2). Patients had been receiving these therapies for anywhere from 4 months to 45 months.
Outcomes were similar in the monotherapy and combination treatment groups. Seven patients in each group had at least a 50% improvement in mSWAT score.
Dosing and administration
“It appears the infusion is superior to the subcutaneous administration,” Dr Querfeld said.
She noted that durable partial responses have been achieved at all dose levels, but the 300 mg and 600 mg IV infusions had the best efficacy and tolerability profiles.
With the 300 mg IV bolus, fewer patients remained on treatment for more than 1 cycle, as compared to the other dosing cohorts. Dr Querfeld said this may be a result of lower total exposure or tolerability due to higher plasma Cmax.
She also noted that patients who received MRG-106 SQ at 600 mg or higher had a higher incidence of injection site reactions.
Safety
AEs of any grade that were attributed to MRG-106 include neutropenia (16%), injection site pain (16%), fatigue (14%), nausea (5%), pruritus (5%), and headache (5%).
Grade 3/4 AEs attributed to MRG-106 were neutropenia (5%) and pruritus (5%).
There were no serious AEs attributed to MRG-106, but there were 2 dose-limiting toxicities. One was a grade 3 tumor flare in a patient receiving the 300 mg IV bolus.
The other dose-limiting toxicity was grade 3 worsening pruritus and possible tumor flare, which occurred twice in 1 patient—with the 900 mg SQ dose and with the 300 mg IV infusion.
The 300 mg IV infusion is the anticipated phase 2 dose. ![]()
LA JOLLA, CA—Results of a phase 1 trial suggest MRG-106 can provide clinical improvement in patients with mycosis fungoides (MF), whether the drug is given alone or in conjunction with other therapies.
MRG-106 is an inhibitor of microRNA-155, which is upregulated in MF.
In this ongoing trial, 90% of patients who received MRG-106 have experienced an improvement in mSWAT score, and 59% of patients who received the drug for at least 1 month had a partial response.
The most common adverse events (AEs) attributed to MRG-106 were neutropenia, injection site pain, and fatigue.
Christiane Querfeld, MD, PhD, of the City of Hope in Duarte, California, presented these results at the 10th Annual T-cell Lymphoma Forum. The research is sponsored by miRagen Therapeutics, Inc., the company developing MRG-106.
The trial has enrolled 36 MF patients, 69% of whom are male. Their median age at enrollment was 63 (range, 21-85).
Patients had received a median of 4 prior systemic therapies (range, 1-13) and a median of 3 prior skin-directed therapies (range, 1-8).
At baseline, patients had a median mSWAT score of 43 (range, 2-180). The modified Severity Weighted Assessment Tool (mSWAT) measures the severity of skin disease over a patient’s body.
Part A
In part A of the study, 6 patients received MRG-106 via intralesional injection. A 75 mg dose of the drug was found to be well-tolerated, producing generally minor injection site reactions.
In addition, intralesional injection of MRG-106 produced improvements in CAILS score. The Composite Assessment of Index Lesion Severity (CAILS) score is obtained by adding the severity score of erythema, scaling, plaque elevation, and surface area for up to 5 index lesions.
Part B
In part B, 30 patients received MRG-106 via subcutaneous (SQ) injection, intravenous (IV) infusion, or IV bolus injection.
Patients who received SQ injection or IV infusion received doses of 300 mg, 600 mg, or 900 mg. Those who received an IV bolus only received the 300 mg dose.
Twenty-nine of the 30 patients in part B were evaluable for efficacy. Twenty-six of these patients—90%—had an improvement in mSWAT score from baseline.
“Twenty-six patients had at least stable disease to partial response,” Dr Querfeld noted. “No complete responses yet, but we’re close.”
Twelve patients were still receiving MRG-106 at last follow-up.
Ten of the 17 patients (59%) who had received MRG-106 for more than 1 month had at least a 50% improvement in mSWAT score, or a partial response. Once this was achieved, responses were durable.
One patient was still in response at roughly 470 days of follow-up.
Concomitant therapies
Dr Querfeld and her colleagues looked at patient outcomes in the context of concomitant therapies as well. They analyzed data from 26 patients who had received at least 6 doses of MRG-106.
Half of these patients were receiving MRG-106 alone, and the other half were receiving concomitant therapies, including bexarotene (n=7), interferon-alfa (n=2), methotrexate (n=1), vorinostat (n=1), and “other” treatments (n=2). Patients had been receiving these therapies for anywhere from 4 months to 45 months.
Outcomes were similar in the monotherapy and combination treatment groups. Seven patients in each group had at least a 50% improvement in mSWAT score.
Dosing and administration
“It appears the infusion is superior to the subcutaneous administration,” Dr Querfeld said.
She noted that durable partial responses have been achieved at all dose levels, but the 300 mg and 600 mg IV infusions had the best efficacy and tolerability profiles.
With the 300 mg IV bolus, fewer patients remained on treatment for more than 1 cycle, as compared to the other dosing cohorts. Dr Querfeld said this may be a result of lower total exposure or tolerability due to higher plasma Cmax.
She also noted that patients who received MRG-106 SQ at 600 mg or higher had a higher incidence of injection site reactions.
Safety
AEs of any grade that were attributed to MRG-106 include neutropenia (16%), injection site pain (16%), fatigue (14%), nausea (5%), pruritus (5%), and headache (5%).
Grade 3/4 AEs attributed to MRG-106 were neutropenia (5%) and pruritus (5%).
There were no serious AEs attributed to MRG-106, but there were 2 dose-limiting toxicities. One was a grade 3 tumor flare in a patient receiving the 300 mg IV bolus.
The other dose-limiting toxicity was grade 3 worsening pruritus and possible tumor flare, which occurred twice in 1 patient—with the 900 mg SQ dose and with the 300 mg IV infusion.
The 300 mg IV infusion is the anticipated phase 2 dose. ![]()
LA JOLLA, CA—Results of a phase 1 trial suggest MRG-106 can provide clinical improvement in patients with mycosis fungoides (MF), whether the drug is given alone or in conjunction with other therapies.
MRG-106 is an inhibitor of microRNA-155, which is upregulated in MF.
In this ongoing trial, 90% of patients who received MRG-106 have experienced an improvement in mSWAT score, and 59% of patients who received the drug for at least 1 month had a partial response.
The most common adverse events (AEs) attributed to MRG-106 were neutropenia, injection site pain, and fatigue.
Christiane Querfeld, MD, PhD, of the City of Hope in Duarte, California, presented these results at the 10th Annual T-cell Lymphoma Forum. The research is sponsored by miRagen Therapeutics, Inc., the company developing MRG-106.
The trial has enrolled 36 MF patients, 69% of whom are male. Their median age at enrollment was 63 (range, 21-85).
Patients had received a median of 4 prior systemic therapies (range, 1-13) and a median of 3 prior skin-directed therapies (range, 1-8).
At baseline, patients had a median mSWAT score of 43 (range, 2-180). The modified Severity Weighted Assessment Tool (mSWAT) measures the severity of skin disease over a patient’s body.
Part A
In part A of the study, 6 patients received MRG-106 via intralesional injection. A 75 mg dose of the drug was found to be well-tolerated, producing generally minor injection site reactions.
In addition, intralesional injection of MRG-106 produced improvements in CAILS score. The Composite Assessment of Index Lesion Severity (CAILS) score is obtained by adding the severity score of erythema, scaling, plaque elevation, and surface area for up to 5 index lesions.
Part B
In part B, 30 patients received MRG-106 via subcutaneous (SQ) injection, intravenous (IV) infusion, or IV bolus injection.
Patients who received SQ injection or IV infusion received doses of 300 mg, 600 mg, or 900 mg. Those who received an IV bolus only received the 300 mg dose.
Twenty-nine of the 30 patients in part B were evaluable for efficacy. Twenty-six of these patients—90%—had an improvement in mSWAT score from baseline.
“Twenty-six patients had at least stable disease to partial response,” Dr Querfeld noted. “No complete responses yet, but we’re close.”
Twelve patients were still receiving MRG-106 at last follow-up.
Ten of the 17 patients (59%) who had received MRG-106 for more than 1 month had at least a 50% improvement in mSWAT score, or a partial response. Once this was achieved, responses were durable.
One patient was still in response at roughly 470 days of follow-up.
Concomitant therapies
Dr Querfeld and her colleagues looked at patient outcomes in the context of concomitant therapies as well. They analyzed data from 26 patients who had received at least 6 doses of MRG-106.
Half of these patients were receiving MRG-106 alone, and the other half were receiving concomitant therapies, including bexarotene (n=7), interferon-alfa (n=2), methotrexate (n=1), vorinostat (n=1), and “other” treatments (n=2). Patients had been receiving these therapies for anywhere from 4 months to 45 months.
Outcomes were similar in the monotherapy and combination treatment groups. Seven patients in each group had at least a 50% improvement in mSWAT score.
Dosing and administration
“It appears the infusion is superior to the subcutaneous administration,” Dr Querfeld said.
She noted that durable partial responses have been achieved at all dose levels, but the 300 mg and 600 mg IV infusions had the best efficacy and tolerability profiles.
With the 300 mg IV bolus, fewer patients remained on treatment for more than 1 cycle, as compared to the other dosing cohorts. Dr Querfeld said this may be a result of lower total exposure or tolerability due to higher plasma Cmax.
She also noted that patients who received MRG-106 SQ at 600 mg or higher had a higher incidence of injection site reactions.
Safety
AEs of any grade that were attributed to MRG-106 include neutropenia (16%), injection site pain (16%), fatigue (14%), nausea (5%), pruritus (5%), and headache (5%).
Grade 3/4 AEs attributed to MRG-106 were neutropenia (5%) and pruritus (5%).
There were no serious AEs attributed to MRG-106, but there were 2 dose-limiting toxicities. One was a grade 3 tumor flare in a patient receiving the 300 mg IV bolus.
The other dose-limiting toxicity was grade 3 worsening pruritus and possible tumor flare, which occurred twice in 1 patient—with the 900 mg SQ dose and with the 300 mg IV infusion.
The 300 mg IV infusion is the anticipated phase 2 dose. ![]()
Drugs appear comparable for delaying SREs in MM
In a phase 3 trial, denosumab proved non-inferior to zoledronic acid for delaying skeletal-related events (SREs) in patients with multiple myeloma (MM).
The median time to first on-study SRE was 23 months in the denosumab arm and 24 months in the zoledronic acid arm.
There were fewer renal adverse events (AEs) but more hypocalcemia AEs in the denosumab arm.
“Until recently, treatment options for the prevention of skeletal-related events in multiple myeloma were limited to bisphosphonates, which are cleared through the kidneys and can be associated with increased renal impairment,” said Noopur Raje, MD, of Massachusetts General Hospital Cancer Center in Boston.
“Denosumab, which is not cleared through the kidneys, provides a new treatment option for the prevention of skeletal-related events in patients with multiple myeloma.”
Dr Raje and her colleagues conducted this phase 3 trial of denosumab and reported the results in The Lancet Oncology. The trial was sponsored by Amgen, the company developing denosumab.
Denosumab is the first fully human monoclonal antibody that binds to and neutralizes RANK ligand—a protein essential for the formation, function, and survival of osteoclasts—thereby inhibiting osteoclast-mediated bone destruction.
In this trial, researchers compared denosumab to zoledronic acid for the prevention of SREs in adults with newly diagnosed MM and bone disease.
The team randomized 1718 patients to receive subcutaneous denosumab at 120 mg and intravenous placebo every 4 weeks (n=859) or intravenous zoledronic acid at 4 mg (adjusted for renal function at baseline) and subcutaneous placebo every 4 weeks (n=859). All patients also received investigators’ choice of first-line MM therapy.
Skeletal surveys using conventional radiography were obtained every 12 to 24 weeks per protocol. The primary endpoint of the study was non-inferiority of denosumab to zoledronic acid for time to first on-study SRE (pathologic fracture, radiation to bone, surgery to bone, or spinal cord compression).
The primary endpoint was met. The median time to first on-study SRE was 22.8 months for patients in the denosumab arm and 24 months for those in the zoledronic acid arm (hazard ratio [HR]=0.98; 95% confidence interval [CI]: 0.85-1.14; P non-inferiority=0.010).
Approximately 60% of all first SREs occurred within the first 3 months, and 81% occurred within the first 6 months.
Overall survival, a secondary endpoint, was similar between the denosumab and zoledronic acid arms (HR=0.90; 95% CI: 0.70-1.16; P=0.41).
There were fewer renal treatment-emergent AEs in the denosumab arm than the zoledronic acid arm—10% and 17%, respectively. There were more hypocalcemia AEs in the denosumab arm than the zoledronic acid arm—17% and 12%, respectively.
The incidence of osteonecrosis of the jaw was 4% in the denosumab arm and 3% in the zoledronic acid arm.
The most common grade 3 or higher treatment-emergent AEs (in the denosumab and zoledronic acid arms, respectively) were neutropenia (15% in both arms), thrombocytopenia (14% and 12%), anemia (12% and 10%), febrile neutropenia (11% and 10%), and pneumonia (8% in both arms).
The most common serious AE was pneumonia (8% in both arms).
Treatment-emergent AEs led to study drug discontinuation in 13% of patients in the denosumab arm and 12% in the zoledronic acid arm.
One patient in the zoledronic acid arm died of cardiac arrest that was deemed treatment-related. No other deaths were considered treatment-related. ![]()
In a phase 3 trial, denosumab proved non-inferior to zoledronic acid for delaying skeletal-related events (SREs) in patients with multiple myeloma (MM).
The median time to first on-study SRE was 23 months in the denosumab arm and 24 months in the zoledronic acid arm.
There were fewer renal adverse events (AEs) but more hypocalcemia AEs in the denosumab arm.
“Until recently, treatment options for the prevention of skeletal-related events in multiple myeloma were limited to bisphosphonates, which are cleared through the kidneys and can be associated with increased renal impairment,” said Noopur Raje, MD, of Massachusetts General Hospital Cancer Center in Boston.
“Denosumab, which is not cleared through the kidneys, provides a new treatment option for the prevention of skeletal-related events in patients with multiple myeloma.”
Dr Raje and her colleagues conducted this phase 3 trial of denosumab and reported the results in The Lancet Oncology. The trial was sponsored by Amgen, the company developing denosumab.
Denosumab is the first fully human monoclonal antibody that binds to and neutralizes RANK ligand—a protein essential for the formation, function, and survival of osteoclasts—thereby inhibiting osteoclast-mediated bone destruction.
In this trial, researchers compared denosumab to zoledronic acid for the prevention of SREs in adults with newly diagnosed MM and bone disease.
The team randomized 1718 patients to receive subcutaneous denosumab at 120 mg and intravenous placebo every 4 weeks (n=859) or intravenous zoledronic acid at 4 mg (adjusted for renal function at baseline) and subcutaneous placebo every 4 weeks (n=859). All patients also received investigators’ choice of first-line MM therapy.
Skeletal surveys using conventional radiography were obtained every 12 to 24 weeks per protocol. The primary endpoint of the study was non-inferiority of denosumab to zoledronic acid for time to first on-study SRE (pathologic fracture, radiation to bone, surgery to bone, or spinal cord compression).
The primary endpoint was met. The median time to first on-study SRE was 22.8 months for patients in the denosumab arm and 24 months for those in the zoledronic acid arm (hazard ratio [HR]=0.98; 95% confidence interval [CI]: 0.85-1.14; P non-inferiority=0.010).
Approximately 60% of all first SREs occurred within the first 3 months, and 81% occurred within the first 6 months.
Overall survival, a secondary endpoint, was similar between the denosumab and zoledronic acid arms (HR=0.90; 95% CI: 0.70-1.16; P=0.41).
There were fewer renal treatment-emergent AEs in the denosumab arm than the zoledronic acid arm—10% and 17%, respectively. There were more hypocalcemia AEs in the denosumab arm than the zoledronic acid arm—17% and 12%, respectively.
The incidence of osteonecrosis of the jaw was 4% in the denosumab arm and 3% in the zoledronic acid arm.
The most common grade 3 or higher treatment-emergent AEs (in the denosumab and zoledronic acid arms, respectively) were neutropenia (15% in both arms), thrombocytopenia (14% and 12%), anemia (12% and 10%), febrile neutropenia (11% and 10%), and pneumonia (8% in both arms).
The most common serious AE was pneumonia (8% in both arms).
Treatment-emergent AEs led to study drug discontinuation in 13% of patients in the denosumab arm and 12% in the zoledronic acid arm.
One patient in the zoledronic acid arm died of cardiac arrest that was deemed treatment-related. No other deaths were considered treatment-related. ![]()
In a phase 3 trial, denosumab proved non-inferior to zoledronic acid for delaying skeletal-related events (SREs) in patients with multiple myeloma (MM).
The median time to first on-study SRE was 23 months in the denosumab arm and 24 months in the zoledronic acid arm.
There were fewer renal adverse events (AEs) but more hypocalcemia AEs in the denosumab arm.
“Until recently, treatment options for the prevention of skeletal-related events in multiple myeloma were limited to bisphosphonates, which are cleared through the kidneys and can be associated with increased renal impairment,” said Noopur Raje, MD, of Massachusetts General Hospital Cancer Center in Boston.
“Denosumab, which is not cleared through the kidneys, provides a new treatment option for the prevention of skeletal-related events in patients with multiple myeloma.”
Dr Raje and her colleagues conducted this phase 3 trial of denosumab and reported the results in The Lancet Oncology. The trial was sponsored by Amgen, the company developing denosumab.
Denosumab is the first fully human monoclonal antibody that binds to and neutralizes RANK ligand—a protein essential for the formation, function, and survival of osteoclasts—thereby inhibiting osteoclast-mediated bone destruction.
In this trial, researchers compared denosumab to zoledronic acid for the prevention of SREs in adults with newly diagnosed MM and bone disease.
The team randomized 1718 patients to receive subcutaneous denosumab at 120 mg and intravenous placebo every 4 weeks (n=859) or intravenous zoledronic acid at 4 mg (adjusted for renal function at baseline) and subcutaneous placebo every 4 weeks (n=859). All patients also received investigators’ choice of first-line MM therapy.
Skeletal surveys using conventional radiography were obtained every 12 to 24 weeks per protocol. The primary endpoint of the study was non-inferiority of denosumab to zoledronic acid for time to first on-study SRE (pathologic fracture, radiation to bone, surgery to bone, or spinal cord compression).
The primary endpoint was met. The median time to first on-study SRE was 22.8 months for patients in the denosumab arm and 24 months for those in the zoledronic acid arm (hazard ratio [HR]=0.98; 95% confidence interval [CI]: 0.85-1.14; P non-inferiority=0.010).
Approximately 60% of all first SREs occurred within the first 3 months, and 81% occurred within the first 6 months.
Overall survival, a secondary endpoint, was similar between the denosumab and zoledronic acid arms (HR=0.90; 95% CI: 0.70-1.16; P=0.41).
There were fewer renal treatment-emergent AEs in the denosumab arm than the zoledronic acid arm—10% and 17%, respectively. There were more hypocalcemia AEs in the denosumab arm than the zoledronic acid arm—17% and 12%, respectively.
The incidence of osteonecrosis of the jaw was 4% in the denosumab arm and 3% in the zoledronic acid arm.
The most common grade 3 or higher treatment-emergent AEs (in the denosumab and zoledronic acid arms, respectively) were neutropenia (15% in both arms), thrombocytopenia (14% and 12%), anemia (12% and 10%), febrile neutropenia (11% and 10%), and pneumonia (8% in both arms).
The most common serious AE was pneumonia (8% in both arms).
Treatment-emergent AEs led to study drug discontinuation in 13% of patients in the denosumab arm and 12% in the zoledronic acid arm.
One patient in the zoledronic acid arm died of cardiac arrest that was deemed treatment-related. No other deaths were considered treatment-related. ![]()
Tamsulosin for Patients With Ureteral Stones?
A 54-year-old man presents to the emergency department (ED) with acute-onset left flank pain that radiates to the groin. CT of the abdomen/pelvis without contrast reveals a 7-mm distal ureteral stone. He is deemed an appropriate candidate for outpatient management. In addition to pain medications, should you prescribe tamsulosin?
According to the most recent National Health and Nutrition Examination Survey, the population prevalence of kidney stones is 8.8%, with a self-reported prevalence of 10.6% in men and 7.1% in women.2 Most ureteral stones can be treated in the outpatient setting with oral hydration, antiemetics, and pain control with NSAIDs as firstline treatment and opioids as a second-line option.3
In addition, α-blockers are used for medical expulsive therapy (MET). In fact, the European Association of Urology guideline on urolithiasis states that MET may accelerate passage of ureteral stones.3
Recently, however, uncertainty has surrounded the effectiveness of the α-blocker tamsulosin. Two systematic reviews (limited by heterogeneity because some of the studies lacked a placebo control and blinding) concluded that α-blockers increased stone passage within one to six weeks when compared with placebo or no additional therapy.4,5 However, a recent large, multicenter RCT revealed no difference between tamsulosin and nifedipine, or either one compared with placebo, at decreasing the need for further treatment to achieve stone passage within four weeks.6
STUDY SUMMARY
Results broken down by stone size
This meta-analysis, comprising eight double-blind RCTs, examined the effect of oral tamsulosin (0.4 mg/d; average course, 28 d) on distal ureteral stone passage in adult patients (N = 1,384).1 A subgroup analysis comparing stone size (< 5 mm and 5-10 mm) was also conducted to determine whether size modified the effect of tamsulosin.
The eight selected studies were published between 2009 and 2015; the trials were conducted in multiple countries, in ED and outpatient urology settings. The main outcome measure was the risk difference (RD) in stone passage between the tamsulosin group and placebo group after follow-up imaging at three weeks with CT or plain film radiographs.
Tamsulosin helps some, but not all. The pooled risk for stone passage was higher in the tamsulosin group than in the placebo group (85% vs 66%; RD, 17%), but significant heterogeneity existed across the trials (I2, 80.2%). Subgroup analysis by stone size (< 5 mm vs 5-10 mm) revealed that, compared to placebo, tamsulosin was beneficial for larger stones (6 trials, N = 514; RD, 22%; number needed to treat, 5) but not for smaller stones (4 trials, N = 533; RD, –0.3%). The 5-to-10–mm subgroup had a less heterogeneous population of studies than did the < 5-mm subgroup (I2, 33% and 0% respectively).
In terms of adverse events, tamsulosin did not increase the risk for dizziness (RD, 0.2%) or postural hypotension (RD, 0.1%), compared with placebo.
WHAT’S NEW
Increased passage of larger stones
This meta-analysis included only double-blind RCTs; prior meta-analyses did not. Also, this review included the SUSPEND (Spontaneous Urinary Stone Passage Enabled by Drugs) trial, an RCT discussed in a previous PURL (Clinician Reviews. 2016;26[4]:20,44), which recommended against the use of α-blockers tamsulosin and nifedipine for ureteral stones measuring < 10 mm.6,7
But the subgroup analysis in this review went one step further by examining passage rates by stone size (< 5 mm vs 5-10 mm) and revealing that passage of larger stones increased with tamsulosin use. The different results based on stone size may explain the recent uncertainty as to whether tamsulosin improves the rate of stone passage.
CAVEATS
What about proximal or XL stones?
Only distal stones were included in seven of the eight trials in this analysis. Thus, this meta-analysis was unable to determine the effect on more proximal stones. Also, it’s unclear if the drug provides any benefit with stones > 10 mm in size.
CHALLENGES TO IMPLEMENTATION
None worth mentioning
We see no challenges to implementation of this recommendation.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2018. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice (2018; 67[1]:37-38).
1. Wang RC, Smith-Bindman R, Whitaker E, et al. Effect of tamsulosin on stone passage for ureteral stones: a systematic review and meta-analysis. Ann Emerg Med. 2017;69(3):353-361.
2. Scales CD Jr, Smith AC, Hanley JM, et al. Prevalence of kidney stones in the United States. Eur Urol. 2012;62(1): 160-165.
3. Türk C, Petrik A, Sarica K, et al. EAU guidelines on diagnosis and conservative management of urolithiasis. Eur Urol. 2016;69(3):468-474.
4. Hollingsworth JM, Canales BK, Rogers MAM, et al. Alpha blockers for treatment of ureteric stones: systematic review and meta-analysis. BMJ. 2016;355:i6112.
5. Campschroer T, Zhu Y, Duijvesz D, et al. Alpha-blockers as medical expulsive therapy for ureteral stones. Cochrane Database Syst Rev. 2014:CD008509.
6. Pickard R, Starr K, MacLennan G, et al. Medical expulsion therapy in adults with ureteric colic: a multicentre, randomized, placebo-controlled trial. Lancet. 2015; 386(9991):341-349.
7. Slattengren AH, Prasad S, Jarrett JB. Kidney stones? It’s time to rethink those meds. J Fam Pract. 2016;65(2): 118-120.
A 54-year-old man presents to the emergency department (ED) with acute-onset left flank pain that radiates to the groin. CT of the abdomen/pelvis without contrast reveals a 7-mm distal ureteral stone. He is deemed an appropriate candidate for outpatient management. In addition to pain medications, should you prescribe tamsulosin?
According to the most recent National Health and Nutrition Examination Survey, the population prevalence of kidney stones is 8.8%, with a self-reported prevalence of 10.6% in men and 7.1% in women.2 Most ureteral stones can be treated in the outpatient setting with oral hydration, antiemetics, and pain control with NSAIDs as firstline treatment and opioids as a second-line option.3
In addition, α-blockers are used for medical expulsive therapy (MET). In fact, the European Association of Urology guideline on urolithiasis states that MET may accelerate passage of ureteral stones.3
Recently, however, uncertainty has surrounded the effectiveness of the α-blocker tamsulosin. Two systematic reviews (limited by heterogeneity because some of the studies lacked a placebo control and blinding) concluded that α-blockers increased stone passage within one to six weeks when compared with placebo or no additional therapy.4,5 However, a recent large, multicenter RCT revealed no difference between tamsulosin and nifedipine, or either one compared with placebo, at decreasing the need for further treatment to achieve stone passage within four weeks.6
STUDY SUMMARY
Results broken down by stone size
This meta-analysis, comprising eight double-blind RCTs, examined the effect of oral tamsulosin (0.4 mg/d; average course, 28 d) on distal ureteral stone passage in adult patients (N = 1,384).1 A subgroup analysis comparing stone size (< 5 mm and 5-10 mm) was also conducted to determine whether size modified the effect of tamsulosin.
The eight selected studies were published between 2009 and 2015; the trials were conducted in multiple countries, in ED and outpatient urology settings. The main outcome measure was the risk difference (RD) in stone passage between the tamsulosin group and placebo group after follow-up imaging at three weeks with CT or plain film radiographs.
Tamsulosin helps some, but not all. The pooled risk for stone passage was higher in the tamsulosin group than in the placebo group (85% vs 66%; RD, 17%), but significant heterogeneity existed across the trials (I2, 80.2%). Subgroup analysis by stone size (< 5 mm vs 5-10 mm) revealed that, compared to placebo, tamsulosin was beneficial for larger stones (6 trials, N = 514; RD, 22%; number needed to treat, 5) but not for smaller stones (4 trials, N = 533; RD, –0.3%). The 5-to-10–mm subgroup had a less heterogeneous population of studies than did the < 5-mm subgroup (I2, 33% and 0% respectively).
In terms of adverse events, tamsulosin did not increase the risk for dizziness (RD, 0.2%) or postural hypotension (RD, 0.1%), compared with placebo.
WHAT’S NEW
Increased passage of larger stones
This meta-analysis included only double-blind RCTs; prior meta-analyses did not. Also, this review included the SUSPEND (Spontaneous Urinary Stone Passage Enabled by Drugs) trial, an RCT discussed in a previous PURL (Clinician Reviews. 2016;26[4]:20,44), which recommended against the use of α-blockers tamsulosin and nifedipine for ureteral stones measuring < 10 mm.6,7
But the subgroup analysis in this review went one step further by examining passage rates by stone size (< 5 mm vs 5-10 mm) and revealing that passage of larger stones increased with tamsulosin use. The different results based on stone size may explain the recent uncertainty as to whether tamsulosin improves the rate of stone passage.
CAVEATS
What about proximal or XL stones?
Only distal stones were included in seven of the eight trials in this analysis. Thus, this meta-analysis was unable to determine the effect on more proximal stones. Also, it’s unclear if the drug provides any benefit with stones > 10 mm in size.
CHALLENGES TO IMPLEMENTATION
None worth mentioning
We see no challenges to implementation of this recommendation.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2018. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice (2018; 67[1]:37-38).
A 54-year-old man presents to the emergency department (ED) with acute-onset left flank pain that radiates to the groin. CT of the abdomen/pelvis without contrast reveals a 7-mm distal ureteral stone. He is deemed an appropriate candidate for outpatient management. In addition to pain medications, should you prescribe tamsulosin?
According to the most recent National Health and Nutrition Examination Survey, the population prevalence of kidney stones is 8.8%, with a self-reported prevalence of 10.6% in men and 7.1% in women.2 Most ureteral stones can be treated in the outpatient setting with oral hydration, antiemetics, and pain control with NSAIDs as firstline treatment and opioids as a second-line option.3
In addition, α-blockers are used for medical expulsive therapy (MET). In fact, the European Association of Urology guideline on urolithiasis states that MET may accelerate passage of ureteral stones.3
Recently, however, uncertainty has surrounded the effectiveness of the α-blocker tamsulosin. Two systematic reviews (limited by heterogeneity because some of the studies lacked a placebo control and blinding) concluded that α-blockers increased stone passage within one to six weeks when compared with placebo or no additional therapy.4,5 However, a recent large, multicenter RCT revealed no difference between tamsulosin and nifedipine, or either one compared with placebo, at decreasing the need for further treatment to achieve stone passage within four weeks.6
STUDY SUMMARY
Results broken down by stone size
This meta-analysis, comprising eight double-blind RCTs, examined the effect of oral tamsulosin (0.4 mg/d; average course, 28 d) on distal ureteral stone passage in adult patients (N = 1,384).1 A subgroup analysis comparing stone size (< 5 mm and 5-10 mm) was also conducted to determine whether size modified the effect of tamsulosin.
The eight selected studies were published between 2009 and 2015; the trials were conducted in multiple countries, in ED and outpatient urology settings. The main outcome measure was the risk difference (RD) in stone passage between the tamsulosin group and placebo group after follow-up imaging at three weeks with CT or plain film radiographs.
Tamsulosin helps some, but not all. The pooled risk for stone passage was higher in the tamsulosin group than in the placebo group (85% vs 66%; RD, 17%), but significant heterogeneity existed across the trials (I2, 80.2%). Subgroup analysis by stone size (< 5 mm vs 5-10 mm) revealed that, compared to placebo, tamsulosin was beneficial for larger stones (6 trials, N = 514; RD, 22%; number needed to treat, 5) but not for smaller stones (4 trials, N = 533; RD, –0.3%). The 5-to-10–mm subgroup had a less heterogeneous population of studies than did the < 5-mm subgroup (I2, 33% and 0% respectively).
In terms of adverse events, tamsulosin did not increase the risk for dizziness (RD, 0.2%) or postural hypotension (RD, 0.1%), compared with placebo.
WHAT’S NEW
Increased passage of larger stones
This meta-analysis included only double-blind RCTs; prior meta-analyses did not. Also, this review included the SUSPEND (Spontaneous Urinary Stone Passage Enabled by Drugs) trial, an RCT discussed in a previous PURL (Clinician Reviews. 2016;26[4]:20,44), which recommended against the use of α-blockers tamsulosin and nifedipine for ureteral stones measuring < 10 mm.6,7
But the subgroup analysis in this review went one step further by examining passage rates by stone size (< 5 mm vs 5-10 mm) and revealing that passage of larger stones increased with tamsulosin use. The different results based on stone size may explain the recent uncertainty as to whether tamsulosin improves the rate of stone passage.
CAVEATS
What about proximal or XL stones?
Only distal stones were included in seven of the eight trials in this analysis. Thus, this meta-analysis was unable to determine the effect on more proximal stones. Also, it’s unclear if the drug provides any benefit with stones > 10 mm in size.
CHALLENGES TO IMPLEMENTATION
None worth mentioning
We see no challenges to implementation of this recommendation.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2018. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice (2018; 67[1]:37-38).
1. Wang RC, Smith-Bindman R, Whitaker E, et al. Effect of tamsulosin on stone passage for ureteral stones: a systematic review and meta-analysis. Ann Emerg Med. 2017;69(3):353-361.
2. Scales CD Jr, Smith AC, Hanley JM, et al. Prevalence of kidney stones in the United States. Eur Urol. 2012;62(1): 160-165.
3. Türk C, Petrik A, Sarica K, et al. EAU guidelines on diagnosis and conservative management of urolithiasis. Eur Urol. 2016;69(3):468-474.
4. Hollingsworth JM, Canales BK, Rogers MAM, et al. Alpha blockers for treatment of ureteric stones: systematic review and meta-analysis. BMJ. 2016;355:i6112.
5. Campschroer T, Zhu Y, Duijvesz D, et al. Alpha-blockers as medical expulsive therapy for ureteral stones. Cochrane Database Syst Rev. 2014:CD008509.
6. Pickard R, Starr K, MacLennan G, et al. Medical expulsion therapy in adults with ureteric colic: a multicentre, randomized, placebo-controlled trial. Lancet. 2015; 386(9991):341-349.
7. Slattengren AH, Prasad S, Jarrett JB. Kidney stones? It’s time to rethink those meds. J Fam Pract. 2016;65(2): 118-120.
1. Wang RC, Smith-Bindman R, Whitaker E, et al. Effect of tamsulosin on stone passage for ureteral stones: a systematic review and meta-analysis. Ann Emerg Med. 2017;69(3):353-361.
2. Scales CD Jr, Smith AC, Hanley JM, et al. Prevalence of kidney stones in the United States. Eur Urol. 2012;62(1): 160-165.
3. Türk C, Petrik A, Sarica K, et al. EAU guidelines on diagnosis and conservative management of urolithiasis. Eur Urol. 2016;69(3):468-474.
4. Hollingsworth JM, Canales BK, Rogers MAM, et al. Alpha blockers for treatment of ureteric stones: systematic review and meta-analysis. BMJ. 2016;355:i6112.
5. Campschroer T, Zhu Y, Duijvesz D, et al. Alpha-blockers as medical expulsive therapy for ureteral stones. Cochrane Database Syst Rev. 2014:CD008509.
6. Pickard R, Starr K, MacLennan G, et al. Medical expulsion therapy in adults with ureteric colic: a multicentre, randomized, placebo-controlled trial. Lancet. 2015; 386(9991):341-349.
7. Slattengren AH, Prasad S, Jarrett JB. Kidney stones? It’s time to rethink those meds. J Fam Pract. 2016;65(2): 118-120.
