User login
Status asthmaticus risk upped fourfold with IV labetalol for preeclampsia
DALLAS – A maternal death occurred at Columbia University Medical Center after a patient with asthma was given intravenous labetalol, prompting a study that found an elevated risk of status asthmaticus associated with intravenous (IV) labetalol administration but not with the uterotonic carboprost.
“Overall, 71.4% of status asthmaticus cases occurred among women receiving IV labetalol,” said Whitney A. Booker, MD, speaking about the findings at the meeting sponsored by the Society for Maternal-Fetal Medicine.

The risk of status asthmaticus didn’t reach statistical significance when women with asthma who experienced postpartum hemorrhage were given carboprost, compared with other uterotonics (3.1 vs. 1.0 per 1,000 patients; P = .56).
“Some regularly used medications in obstetrics can trigger bronchospasm,” said Dr. Booker; the American College of Obstetricians and Gynecologists lists both carboprost and labetalol as contraindicated for use in patients with asthma because of the potential for bronchospasm with each medication.
However, she said, data on the actual risk of bronchospasm when these medications are used in obstetric patients is limited.
The retrospective cohort study constructed by Dr. Booker and her colleagues at Columbia University Medical Center’s department of obstetrics and gynecology tapped 10 years’ worth of data from a large inpatient drug utilization database.
Dr. Booker, a maternal-fetal medicine fellow, said that patients were included if they were admitted for delivery and had a diagnosis of preeclampsia or postpartum hemorrhage. Of the 5.7 million hospitalizations from 2006 to 2015, 2.5% were for postpartum hemorrhage, and 4.2% for preeclampsia.
Of the patients with hemorrhage, 5,633 had a prior history of asthma, as did 12,486 of the patients with preeclampsia. In both groups, a little more than a third of patients were younger than 25 years, and about a quarter were black. Half were on Medicaid, and most were in urban areas and cared for in a teaching hospital.
The first outcome that Dr. Booker and her colleagues looked at was how practice patterns for postpartum hemorrhage varied according to whether patients had asthma; to do so, they looked at receipt of carboprost, misoprostol, and methylergonovine. A similar analysis was performed for the second outcome addressing patients with preeclampsia, in which investigators examined the use of both IV and oral labetalol, hydralazine, and nifedipine. For this and the hemorrhage outcome, the investigators performed multivariable analysis, with receipt of carboprost and IV labetalol as the outcomes of interest.
Finally, the investigators assessed the risk of status asthmaticus by comparing receipt of either carboprost (for postpartum hemorrhage) or IV labetalol (for preeclampsia) with receipt of the other medications to treat these conditions.
They found that overall, 11.4% of patients with asthma and 18% of patients without asthma received carboprost to treat postpartum hemorrhage, which makes for an adjusted risk model of 0.68 (95% confidence interval, 0.62-0.74) for receipt of carboprost for patients with asthma versus those without.
However, the pattern was different for IV labetalol: 18.5% of patients with asthma and preeclampsia received labetalol, compared with 16.7% of those without asthma. After statistical adjustment, patients with asthma had a risk ratio of 0.93 (95% CI, 0.90-0.97) for receiving IV labetalol for preeclampsia.
The analysis showed that pregnant patients with asthma were less likely to be given carboprost than labetalol, although the actual risk of status asthmaticus was higher when patients with asthma received labetalol than when they received carboprost.
“Given similar theoretical risks, obstetric providers currently administer carboprost differently than labetalol. ... Obstetricians should proceed with caution prior to giving labetalol to patients with underlying asthma,” said Dr. Booker.
During the discussion after the presentation, one attendee suggested that a next step might be to examine claims databases in conjunction with the findings of Dr. Booker’s current work in order to see whether there’s an association between asthma medication prescription fills – a surrogate for disease severity – and the risk of bronchospasm. Dr. Booker agreed that this might be a promising line of inquiry.
Dr. Booker and her colleagues reported that they had no conflicts of interest. The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
SOURCE: Booker W et al. Am J Obstet Gynecol. 2018 Jan;218:S51.
I teach my residents and fellows the “rule of thirds”: One-third of asthma patients get worse during pregnancy; one-third get better; one-third stay the same.” Asthma during pregnancy remains a challenging problem, with physicians striving to treat two complicated patients (mother and child) safely and effectively. We learn now that the use of labetalol, a beta-blocker, to treat preeclampsia in pregnant asthma patients may be associated with an increased incidence of status asthmaticus. Until we learn more about these occurrences, we should use great caution in treating pregnant asthma patients with labetalol and other beta-blockers

I teach my residents and fellows the “rule of thirds”: One-third of asthma patients get worse during pregnancy; one-third get better; one-third stay the same.” Asthma during pregnancy remains a challenging problem, with physicians striving to treat two complicated patients (mother and child) safely and effectively. We learn now that the use of labetalol, a beta-blocker, to treat preeclampsia in pregnant asthma patients may be associated with an increased incidence of status asthmaticus. Until we learn more about these occurrences, we should use great caution in treating pregnant asthma patients with labetalol and other beta-blockers
I teach my residents and fellows the “rule of thirds”: One-third of asthma patients get worse during pregnancy; one-third get better; one-third stay the same.” Asthma during pregnancy remains a challenging problem, with physicians striving to treat two complicated patients (mother and child) safely and effectively. We learn now that the use of labetalol, a beta-blocker, to treat preeclampsia in pregnant asthma patients may be associated with an increased incidence of status asthmaticus. Until we learn more about these occurrences, we should use great caution in treating pregnant asthma patients with labetalol and other beta-blockers
DALLAS – A maternal death occurred at Columbia University Medical Center after a patient with asthma was given intravenous labetalol, prompting a study that found an elevated risk of status asthmaticus associated with intravenous (IV) labetalol administration but not with the uterotonic carboprost.
“Overall, 71.4% of status asthmaticus cases occurred among women receiving IV labetalol,” said Whitney A. Booker, MD, speaking about the findings at the meeting sponsored by the Society for Maternal-Fetal Medicine.
The risk of status asthmaticus didn’t reach statistical significance when women with asthma who experienced postpartum hemorrhage were given carboprost, compared with other uterotonics (3.1 vs. 1.0 per 1,000 patients; P = .56).
“Some regularly used medications in obstetrics can trigger bronchospasm,” said Dr. Booker; the American College of Obstetricians and Gynecologists lists both carboprost and labetalol as contraindicated for use in patients with asthma because of the potential for bronchospasm with each medication.
However, she said, data on the actual risk of bronchospasm when these medications are used in obstetric patients is limited.
The retrospective cohort study constructed by Dr. Booker and her colleagues at Columbia University Medical Center’s department of obstetrics and gynecology tapped 10 years’ worth of data from a large inpatient drug utilization database.
Dr. Booker, a maternal-fetal medicine fellow, said that patients were included if they were admitted for delivery and had a diagnosis of preeclampsia or postpartum hemorrhage. Of the 5.7 million hospitalizations from 2006 to 2015, 2.5% were for postpartum hemorrhage, and 4.2% for preeclampsia.
Of the patients with hemorrhage, 5,633 had a prior history of asthma, as did 12,486 of the patients with preeclampsia. In both groups, a little more than a third of patients were younger than 25 years, and about a quarter were black. Half were on Medicaid, and most were in urban areas and cared for in a teaching hospital.
The first outcome that Dr. Booker and her colleagues looked at was how practice patterns for postpartum hemorrhage varied according to whether patients had asthma; to do so, they looked at receipt of carboprost, misoprostol, and methylergonovine. A similar analysis was performed for the second outcome addressing patients with preeclampsia, in which investigators examined the use of both IV and oral labetalol, hydralazine, and nifedipine. For this and the hemorrhage outcome, the investigators performed multivariable analysis, with receipt of carboprost and IV labetalol as the outcomes of interest.
Finally, the investigators assessed the risk of status asthmaticus by comparing receipt of either carboprost (for postpartum hemorrhage) or IV labetalol (for preeclampsia) with receipt of the other medications to treat these conditions.
They found that overall, 11.4% of patients with asthma and 18% of patients without asthma received carboprost to treat postpartum hemorrhage, which makes for an adjusted risk model of 0.68 (95% confidence interval, 0.62-0.74) for receipt of carboprost for patients with asthma versus those without.
However, the pattern was different for IV labetalol: 18.5% of patients with asthma and preeclampsia received labetalol, compared with 16.7% of those without asthma. After statistical adjustment, patients with asthma had a risk ratio of 0.93 (95% CI, 0.90-0.97) for receiving IV labetalol for preeclampsia.
The analysis showed that pregnant patients with asthma were less likely to be given carboprost than labetalol, although the actual risk of status asthmaticus was higher when patients with asthma received labetalol than when they received carboprost.
“Given similar theoretical risks, obstetric providers currently administer carboprost differently than labetalol. ... Obstetricians should proceed with caution prior to giving labetalol to patients with underlying asthma,” said Dr. Booker.
During the discussion after the presentation, one attendee suggested that a next step might be to examine claims databases in conjunction with the findings of Dr. Booker’s current work in order to see whether there’s an association between asthma medication prescription fills – a surrogate for disease severity – and the risk of bronchospasm. Dr. Booker agreed that this might be a promising line of inquiry.
Dr. Booker and her colleagues reported that they had no conflicts of interest. The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
SOURCE: Booker W et al. Am J Obstet Gynecol. 2018 Jan;218:S51.
DALLAS – A maternal death occurred at Columbia University Medical Center after a patient with asthma was given intravenous labetalol, prompting a study that found an elevated risk of status asthmaticus associated with intravenous (IV) labetalol administration but not with the uterotonic carboprost.
“Overall, 71.4% of status asthmaticus cases occurred among women receiving IV labetalol,” said Whitney A. Booker, MD, speaking about the findings at the meeting sponsored by the Society for Maternal-Fetal Medicine.
The risk of status asthmaticus didn’t reach statistical significance when women with asthma who experienced postpartum hemorrhage were given carboprost, compared with other uterotonics (3.1 vs. 1.0 per 1,000 patients; P = .56).
“Some regularly used medications in obstetrics can trigger bronchospasm,” said Dr. Booker; the American College of Obstetricians and Gynecologists lists both carboprost and labetalol as contraindicated for use in patients with asthma because of the potential for bronchospasm with each medication.
However, she said, data on the actual risk of bronchospasm when these medications are used in obstetric patients is limited.
The retrospective cohort study constructed by Dr. Booker and her colleagues at Columbia University Medical Center’s department of obstetrics and gynecology tapped 10 years’ worth of data from a large inpatient drug utilization database.
Dr. Booker, a maternal-fetal medicine fellow, said that patients were included if they were admitted for delivery and had a diagnosis of preeclampsia or postpartum hemorrhage. Of the 5.7 million hospitalizations from 2006 to 2015, 2.5% were for postpartum hemorrhage, and 4.2% for preeclampsia.
Of the patients with hemorrhage, 5,633 had a prior history of asthma, as did 12,486 of the patients with preeclampsia. In both groups, a little more than a third of patients were younger than 25 years, and about a quarter were black. Half were on Medicaid, and most were in urban areas and cared for in a teaching hospital.
The first outcome that Dr. Booker and her colleagues looked at was how practice patterns for postpartum hemorrhage varied according to whether patients had asthma; to do so, they looked at receipt of carboprost, misoprostol, and methylergonovine. A similar analysis was performed for the second outcome addressing patients with preeclampsia, in which investigators examined the use of both IV and oral labetalol, hydralazine, and nifedipine. For this and the hemorrhage outcome, the investigators performed multivariable analysis, with receipt of carboprost and IV labetalol as the outcomes of interest.
Finally, the investigators assessed the risk of status asthmaticus by comparing receipt of either carboprost (for postpartum hemorrhage) or IV labetalol (for preeclampsia) with receipt of the other medications to treat these conditions.
They found that overall, 11.4% of patients with asthma and 18% of patients without asthma received carboprost to treat postpartum hemorrhage, which makes for an adjusted risk model of 0.68 (95% confidence interval, 0.62-0.74) for receipt of carboprost for patients with asthma versus those without.
However, the pattern was different for IV labetalol: 18.5% of patients with asthma and preeclampsia received labetalol, compared with 16.7% of those without asthma. After statistical adjustment, patients with asthma had a risk ratio of 0.93 (95% CI, 0.90-0.97) for receiving IV labetalol for preeclampsia.
The analysis showed that pregnant patients with asthma were less likely to be given carboprost than labetalol, although the actual risk of status asthmaticus was higher when patients with asthma received labetalol than when they received carboprost.
“Given similar theoretical risks, obstetric providers currently administer carboprost differently than labetalol. ... Obstetricians should proceed with caution prior to giving labetalol to patients with underlying asthma,” said Dr. Booker.
During the discussion after the presentation, one attendee suggested that a next step might be to examine claims databases in conjunction with the findings of Dr. Booker’s current work in order to see whether there’s an association between asthma medication prescription fills – a surrogate for disease severity – and the risk of bronchospasm. Dr. Booker agreed that this might be a promising line of inquiry.
Dr. Booker and her colleagues reported that they had no conflicts of interest. The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
SOURCE: Booker W et al. Am J Obstet Gynecol. 2018 Jan;218:S51.
REPORTING FROM THE PREGNANCY MEETING
Key clinical point: IV labetalol receipt meant a fourfold increase in risk of status asthmaticus for women with preeclampsia and asthma.
Major finding: Status asthmaticus occurred in 6.5 per 1,000 patients given IV labetalol, and 1.7 per 1,000 given a different antihypertensive.
Study details: Retrospective review of 10 years’ data from a national inpatient database, which gathered data on 18,149 women with asthma and either preeclampsia or postpartum hemorrhage.
Disclosures: The study was sponsored by the Eunice Kennedy Shriver National Institute of Child Health and Human Development. The study authors had no conflicts of interest.
Source: Booker W et al. Am J Obstet Gynecol. 2018 Jan;218:S51.
Study: Half of doctors sued by age 55
By age 55, nearly half of physicians have been sued for malpractice, with general surgeons and obstetricians-gynecologists facing the highest lawsuit risks, according to data from the America Medical Association.
Investigators with the AMA surveyed 3,500 postresidency physicians who were not employed by the federal government. Findings show that the probability of getting sued increases with age, and that male doctors are more likely to be sued than female physicians. For example, only 8% of doctors under 40 have been sued, compared to nearly half of physicians over age 54, the study found. In addition, nearly 40% of male physicians have been sued over the course of their careers, compared with 23% of female doctors.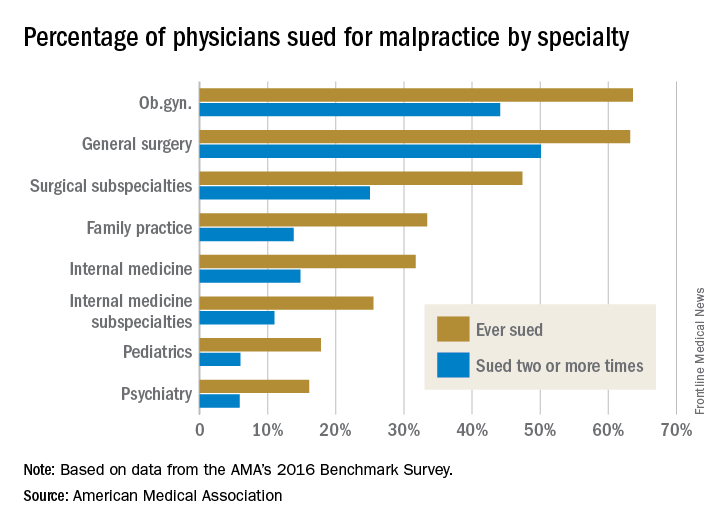
Employed physicians were no more or less likely than were physician-owners to have been sued. In addition, while solo practitioners had more claims filed against them than did doctors in single-specialty groups, the estimate was not statistically significant.
In a second report, an analysis showed the average expense incurred during a medical liability claim is $54,165 – a 65% increase since 2006. For the study, the AMA analyzed data from PIAA, a trade association for the medical professional liability insurance industry, and evaluated payments, expenses, and claim disposition within a sample of 90,473 medical liability claims that closed between 2006 and 2015.

Only 7% of claims were decided by a trial verdict with the vast majority (88%) won by the defendant health care provider. In about 25% of claims, a payment was paid to the plaintiff. The average indemnity payment to a plaintiff was $365,503 and the median payment was $200,000.
The new research paints a bleak picture of physicians’ experiences with medical liability claims and the associated cost burdens on the health system, AMA President David O. Barbe, MD, said in a statement.
“Even though the vast majority of claims are dropped, dismissed, or withdrawn, the heavy cost associated with a litigious climate takes a significant financial toll on our health care system when the nation is working to reduce unnecessary health care costs,” Dr. Barbe said.
By age 55, nearly half of physicians have been sued for malpractice, with general surgeons and obstetricians-gynecologists facing the highest lawsuit risks, according to data from the America Medical Association.
Investigators with the AMA surveyed 3,500 postresidency physicians who were not employed by the federal government. Findings show that the probability of getting sued increases with age, and that male doctors are more likely to be sued than female physicians. For example, only 8% of doctors under 40 have been sued, compared to nearly half of physicians over age 54, the study found. In addition, nearly 40% of male physicians have been sued over the course of their careers, compared with 23% of female doctors.
Employed physicians were no more or less likely than were physician-owners to have been sued. In addition, while solo practitioners had more claims filed against them than did doctors in single-specialty groups, the estimate was not statistically significant.
In a second report, an analysis showed the average expense incurred during a medical liability claim is $54,165 – a 65% increase since 2006. For the study, the AMA analyzed data from PIAA, a trade association for the medical professional liability insurance industry, and evaluated payments, expenses, and claim disposition within a sample of 90,473 medical liability claims that closed between 2006 and 2015.
Only 7% of claims were decided by a trial verdict with the vast majority (88%) won by the defendant health care provider. In about 25% of claims, a payment was paid to the plaintiff. The average indemnity payment to a plaintiff was $365,503 and the median payment was $200,000.
The new research paints a bleak picture of physicians’ experiences with medical liability claims and the associated cost burdens on the health system, AMA President David O. Barbe, MD, said in a statement.
“Even though the vast majority of claims are dropped, dismissed, or withdrawn, the heavy cost associated with a litigious climate takes a significant financial toll on our health care system when the nation is working to reduce unnecessary health care costs,” Dr. Barbe said.
By age 55, nearly half of physicians have been sued for malpractice, with general surgeons and obstetricians-gynecologists facing the highest lawsuit risks, according to data from the America Medical Association.
Investigators with the AMA surveyed 3,500 postresidency physicians who were not employed by the federal government. Findings show that the probability of getting sued increases with age, and that male doctors are more likely to be sued than female physicians. For example, only 8% of doctors under 40 have been sued, compared to nearly half of physicians over age 54, the study found. In addition, nearly 40% of male physicians have been sued over the course of their careers, compared with 23% of female doctors.
Employed physicians were no more or less likely than were physician-owners to have been sued. In addition, while solo practitioners had more claims filed against them than did doctors in single-specialty groups, the estimate was not statistically significant.
In a second report, an analysis showed the average expense incurred during a medical liability claim is $54,165 – a 65% increase since 2006. For the study, the AMA analyzed data from PIAA, a trade association for the medical professional liability insurance industry, and evaluated payments, expenses, and claim disposition within a sample of 90,473 medical liability claims that closed between 2006 and 2015.
Only 7% of claims were decided by a trial verdict with the vast majority (88%) won by the defendant health care provider. In about 25% of claims, a payment was paid to the plaintiff. The average indemnity payment to a plaintiff was $365,503 and the median payment was $200,000.
The new research paints a bleak picture of physicians’ experiences with medical liability claims and the associated cost burdens on the health system, AMA President David O. Barbe, MD, said in a statement.
“Even though the vast majority of claims are dropped, dismissed, or withdrawn, the heavy cost associated with a litigious climate takes a significant financial toll on our health care system when the nation is working to reduce unnecessary health care costs,” Dr. Barbe said.
Classifying Headache Types from Children’s Drawings
Diplopia, commonly known as double vision, was depicted in a significantly higher percentage of drawings by children (aged 6-18 years) with pseudotumor cerebri than drawings by children with migraine, a recent study found. In all other respects, headache drawings by both groups of children were similar. In this study, children attending university hospital pediatric neurology clinics were asked to draw a picture of how their headache feels. Headache drawings of 21 children (16 females) with pseudotumor were compared with those of 518 children with migraine. Researchers found:
- Pseudotumor drawings depicted a variety of symptoms including pounding pain (n=11), pressure-like pain (n=3), photophobia (n=3), dizziness (n=1), and recumbency (n=1).
- Severe pain indicators included hammers, bombs, an anvil, and vise grip.
- Positive visual phenomena included scintillations, scotomata, or blurring (n=8).
- Negative visual phenomena included field defects (n=2).
Pseudotumor drawings were similar to migraine drawings except that 6 of 21 pseudotumor drawings (28.6%) depicted diplopia, whereas only 3 of 518 migraine drawings (0.6%) depicted diplopia.
Evidence of diplopia in children's headache drawings helps to differentiate pseudotumor cerebri from migraine. 2018;79:40-44. Pediatr Neurol. doi:10.1016/j.pediatrneurol.2017.10.020.
Diplopia, commonly known as double vision, was depicted in a significantly higher percentage of drawings by children (aged 6-18 years) with pseudotumor cerebri than drawings by children with migraine, a recent study found. In all other respects, headache drawings by both groups of children were similar. In this study, children attending university hospital pediatric neurology clinics were asked to draw a picture of how their headache feels. Headache drawings of 21 children (16 females) with pseudotumor were compared with those of 518 children with migraine. Researchers found:
- Pseudotumor drawings depicted a variety of symptoms including pounding pain (n=11), pressure-like pain (n=3), photophobia (n=3), dizziness (n=1), and recumbency (n=1).
- Severe pain indicators included hammers, bombs, an anvil, and vise grip.
- Positive visual phenomena included scintillations, scotomata, or blurring (n=8).
- Negative visual phenomena included field defects (n=2).
Pseudotumor drawings were similar to migraine drawings except that 6 of 21 pseudotumor drawings (28.6%) depicted diplopia, whereas only 3 of 518 migraine drawings (0.6%) depicted diplopia.
Evidence of diplopia in children's headache drawings helps to differentiate pseudotumor cerebri from migraine. 2018;79:40-44. Pediatr Neurol. doi:10.1016/j.pediatrneurol.2017.10.020.
Diplopia, commonly known as double vision, was depicted in a significantly higher percentage of drawings by children (aged 6-18 years) with pseudotumor cerebri than drawings by children with migraine, a recent study found. In all other respects, headache drawings by both groups of children were similar. In this study, children attending university hospital pediatric neurology clinics were asked to draw a picture of how their headache feels. Headache drawings of 21 children (16 females) with pseudotumor were compared with those of 518 children with migraine. Researchers found:
- Pseudotumor drawings depicted a variety of symptoms including pounding pain (n=11), pressure-like pain (n=3), photophobia (n=3), dizziness (n=1), and recumbency (n=1).
- Severe pain indicators included hammers, bombs, an anvil, and vise grip.
- Positive visual phenomena included scintillations, scotomata, or blurring (n=8).
- Negative visual phenomena included field defects (n=2).
Pseudotumor drawings were similar to migraine drawings except that 6 of 21 pseudotumor drawings (28.6%) depicted diplopia, whereas only 3 of 518 migraine drawings (0.6%) depicted diplopia.
Evidence of diplopia in children's headache drawings helps to differentiate pseudotumor cerebri from migraine. 2018;79:40-44. Pediatr Neurol. doi:10.1016/j.pediatrneurol.2017.10.020.
Levetiracetam increased time between seizures for infants with epilepsy
, a multicenter, prospective, observational study has shown.
“Our findings suggest that levetiracetam has superior effectiveness compared with phenobarbital as initial monotherapy for nonsyndromic epilepsy in infants,” wrote Zachary Grinspan, MD, director of the pediatric epilepsy program at Cornell University, New York, and his colleagues. “We estimate that for every 100 infants with epilepsy treated with levetiracetam instead of phenobarbital, 44 infants would be free from monotherapy failure instead of 16.”
To evaluate the effectiveness of levetiracetam vs. phenobarbital, Dr. Grinspan and his colleagues developed the Early Life Epilepsy Study, a multicenter, prospective, observational investigation of 155 children with nonsyndromic epilepsy. Patient information for this study was obtained from medical records and was collected from March 1, 2012, through April 30, 2015. All of the patients in the study were observed in the first 3 years of life.
Of the 155 children included in the analysis for this study, 117 were treated with levetiracetam and 38 with phenobarbital. There were some differences between the groups. Children treated with levetiracetam were, on average, 2 months older at seizure onset than were those in the phenobarbital group (5.2 months vs. 3.0 months; P less than .001). Infants treated with levetiracetam also tended to begin treatment further from the time of their first seizure and exhibited less developmental delay at the time of epilepsy diagnosis. There were some other differences of possible clinical importance (developmental structural brain abnormalities, head circumference) that did not reach statistical significance.
Freedom from monotherapy failure was greater in the levetiracetam group (47 [40.2%] vs. 6 [15.8%]; P = .01; odds ratio, 3.6; 95% confidence interval, 1.5-10). Overall, the researchers concluded that levetiracetam was superior to phenobarbital for nonsyndromic epilepsy in pediatric patients (OR, 4.2; 95% CI, 1.1-16; number needed to treat, 3.5 [95% CI, 1.7-60]).
Outcome information was missing for more infants treated with levetiracetam than for those treated with phenobarbital, which could have skewed the analyses, Dr. Grinspan and his associates said. The nature of nonsyndromic epilepsy also makes it difficult to study because of the intricate genetic interactions that can influence the disorder.
Although this study provides information that could potentially benefit infantile epilepsy patients, the investigators said that more work must be done on the topic.
“A prospective clinical trial is needed. Levetiracetam and phenobarbital are both commonly used for infantile-onset epilepsy, indicating community equipoise regarding their relative effectiveness,” they wrote. “However, the effect size in our analysis was surprisingly large (number needed to treat, 3.5), suggesting that a change in practice could meaningfully improve outcomes.”
The investigators reported receiving grants and fees and consulting with a range of institutions, and the complete list can be found on the JAMA Pediatrics website. This study was funded by the Pediatric Epilepsy Research Foundation.
SOURCE: Grinspan Z et al. JAMA Pediatr. 2018 Feb 12. doi: 10.1001/jamapediatrics.2017.5211.
, a multicenter, prospective, observational study has shown.
“Our findings suggest that levetiracetam has superior effectiveness compared with phenobarbital as initial monotherapy for nonsyndromic epilepsy in infants,” wrote Zachary Grinspan, MD, director of the pediatric epilepsy program at Cornell University, New York, and his colleagues. “We estimate that for every 100 infants with epilepsy treated with levetiracetam instead of phenobarbital, 44 infants would be free from monotherapy failure instead of 16.”
To evaluate the effectiveness of levetiracetam vs. phenobarbital, Dr. Grinspan and his colleagues developed the Early Life Epilepsy Study, a multicenter, prospective, observational investigation of 155 children with nonsyndromic epilepsy. Patient information for this study was obtained from medical records and was collected from March 1, 2012, through April 30, 2015. All of the patients in the study were observed in the first 3 years of life.
Of the 155 children included in the analysis for this study, 117 were treated with levetiracetam and 38 with phenobarbital. There were some differences between the groups. Children treated with levetiracetam were, on average, 2 months older at seizure onset than were those in the phenobarbital group (5.2 months vs. 3.0 months; P less than .001). Infants treated with levetiracetam also tended to begin treatment further from the time of their first seizure and exhibited less developmental delay at the time of epilepsy diagnosis. There were some other differences of possible clinical importance (developmental structural brain abnormalities, head circumference) that did not reach statistical significance.
Freedom from monotherapy failure was greater in the levetiracetam group (47 [40.2%] vs. 6 [15.8%]; P = .01; odds ratio, 3.6; 95% confidence interval, 1.5-10). Overall, the researchers concluded that levetiracetam was superior to phenobarbital for nonsyndromic epilepsy in pediatric patients (OR, 4.2; 95% CI, 1.1-16; number needed to treat, 3.5 [95% CI, 1.7-60]).
Outcome information was missing for more infants treated with levetiracetam than for those treated with phenobarbital, which could have skewed the analyses, Dr. Grinspan and his associates said. The nature of nonsyndromic epilepsy also makes it difficult to study because of the intricate genetic interactions that can influence the disorder.
Although this study provides information that could potentially benefit infantile epilepsy patients, the investigators said that more work must be done on the topic.
“A prospective clinical trial is needed. Levetiracetam and phenobarbital are both commonly used for infantile-onset epilepsy, indicating community equipoise regarding their relative effectiveness,” they wrote. “However, the effect size in our analysis was surprisingly large (number needed to treat, 3.5), suggesting that a change in practice could meaningfully improve outcomes.”
The investigators reported receiving grants and fees and consulting with a range of institutions, and the complete list can be found on the JAMA Pediatrics website. This study was funded by the Pediatric Epilepsy Research Foundation.
SOURCE: Grinspan Z et al. JAMA Pediatr. 2018 Feb 12. doi: 10.1001/jamapediatrics.2017.5211.
, a multicenter, prospective, observational study has shown.
“Our findings suggest that levetiracetam has superior effectiveness compared with phenobarbital as initial monotherapy for nonsyndromic epilepsy in infants,” wrote Zachary Grinspan, MD, director of the pediatric epilepsy program at Cornell University, New York, and his colleagues. “We estimate that for every 100 infants with epilepsy treated with levetiracetam instead of phenobarbital, 44 infants would be free from monotherapy failure instead of 16.”
To evaluate the effectiveness of levetiracetam vs. phenobarbital, Dr. Grinspan and his colleagues developed the Early Life Epilepsy Study, a multicenter, prospective, observational investigation of 155 children with nonsyndromic epilepsy. Patient information for this study was obtained from medical records and was collected from March 1, 2012, through April 30, 2015. All of the patients in the study were observed in the first 3 years of life.
Of the 155 children included in the analysis for this study, 117 were treated with levetiracetam and 38 with phenobarbital. There were some differences between the groups. Children treated with levetiracetam were, on average, 2 months older at seizure onset than were those in the phenobarbital group (5.2 months vs. 3.0 months; P less than .001). Infants treated with levetiracetam also tended to begin treatment further from the time of their first seizure and exhibited less developmental delay at the time of epilepsy diagnosis. There were some other differences of possible clinical importance (developmental structural brain abnormalities, head circumference) that did not reach statistical significance.
Freedom from monotherapy failure was greater in the levetiracetam group (47 [40.2%] vs. 6 [15.8%]; P = .01; odds ratio, 3.6; 95% confidence interval, 1.5-10). Overall, the researchers concluded that levetiracetam was superior to phenobarbital for nonsyndromic epilepsy in pediatric patients (OR, 4.2; 95% CI, 1.1-16; number needed to treat, 3.5 [95% CI, 1.7-60]).
Outcome information was missing for more infants treated with levetiracetam than for those treated with phenobarbital, which could have skewed the analyses, Dr. Grinspan and his associates said. The nature of nonsyndromic epilepsy also makes it difficult to study because of the intricate genetic interactions that can influence the disorder.
Although this study provides information that could potentially benefit infantile epilepsy patients, the investigators said that more work must be done on the topic.
“A prospective clinical trial is needed. Levetiracetam and phenobarbital are both commonly used for infantile-onset epilepsy, indicating community equipoise regarding their relative effectiveness,” they wrote. “However, the effect size in our analysis was surprisingly large (number needed to treat, 3.5), suggesting that a change in practice could meaningfully improve outcomes.”
The investigators reported receiving grants and fees and consulting with a range of institutions, and the complete list can be found on the JAMA Pediatrics website. This study was funded by the Pediatric Epilepsy Research Foundation.
SOURCE: Grinspan Z et al. JAMA Pediatr. 2018 Feb 12. doi: 10.1001/jamapediatrics.2017.5211.
FROM JAMA PEDIATRICS
Key clinical point: Levetiracetam gave infants with nonsyndromic epilepsy greater freedom from seizure.
Major finding: Freedom from monotherapy failure was greater with levetiracetam than with phenobarbital (40.2% vs. 15.8%).
Study details: A multicenter, prospective, observational study of 155 children with nonsyndromic epilepsy.
Disclosures: The investigators reported receiving grants and fees and consulting with a range of institutions, and the complete list can be found on the JAMA Pediatrics website. This study was funded by the Pediatric Epilepsy Research Foundation.
Source: Grinspan Z et al. JAMA Pediatr. 2018 Feb 12. doi: 10.1001/jamapediatrics.2017.5211.
Rivaroxaban versus warfarin in mild acute ischemic stroke secondary to atrial fibrillation
Clinical question: Is rivaroxaban as effective and safe as warfarin immediately following minor acute ischemic stroke from atrial fibrillation?
Background: There is uncertainty regarding the best approach to anticoagulation acutely after ischemic stroke secondary to atrial fibrillation. To reduce the risk of intracranial hemorrhage, many physicians start aspirin immediately and delay initiating warfarin until days to weeks later. With their more predictable and rapid anticoagulant effect with potentially lower risk of intracranial hemorrhage, direct oral anticoagulants such as rivaroxaban are an attractive possible alternative to warfarin in the acute setting. 
Study design: Multicenter, randomized, open-label superiority trial with blinded outcome assessment.
Setting: Fourteen academic hospitals in South Korea.
Synopsis: One hundred eighty-three patients with mild acute (within 5 days) ischemic stroke secondary to nonvalvular atrial fibrillation were randomized to immediately initiate either rivaroxaban or warfarin. The primary outcome (composite of new ischemic lesion or new intracranial hemorrhage on MRI at 4 weeks) occurred at similar frequency between groups (49.5% versus 54.5%, P = .49). Rates of adverse events were comparable in each group. Median hospitalization length was shorter in those randomized to rivaroxaban (4.0 versus 6.0 days, P less than .001). Limitations include a radiographic primary outcome that captured many asymptomatic lesions, homogenous study population, and lack of a delayed anticoagulation group.
Bottom line: In patients with mild acute stroke from nonvalvular atrial fibrillation, rivaroxaban and warfarin demonstrated comparable efficacy and safety. More study is needed to determine the optimal anticoagulation strategy in acute stroke.
Citation: Hong K-S et al. Rivaroxaban vs. warfarin sodium in the ultra-early period after atrial fibrillation-related mild ischemic stroke: A randomized clinical trial. JAMA Neurol. 2017; 74(10):1206-15.
Dr. Kanjee is a hospitalist, Beth Israel Deaconess Medical Center, and instructor in medicine, Harvard Medical School, Boston.
Clinical question: Is rivaroxaban as effective and safe as warfarin immediately following minor acute ischemic stroke from atrial fibrillation?
Background: There is uncertainty regarding the best approach to anticoagulation acutely after ischemic stroke secondary to atrial fibrillation. To reduce the risk of intracranial hemorrhage, many physicians start aspirin immediately and delay initiating warfarin until days to weeks later. With their more predictable and rapid anticoagulant effect with potentially lower risk of intracranial hemorrhage, direct oral anticoagulants such as rivaroxaban are an attractive possible alternative to warfarin in the acute setting.
Study design: Multicenter, randomized, open-label superiority trial with blinded outcome assessment.
Setting: Fourteen academic hospitals in South Korea.
Synopsis: One hundred eighty-three patients with mild acute (within 5 days) ischemic stroke secondary to nonvalvular atrial fibrillation were randomized to immediately initiate either rivaroxaban or warfarin. The primary outcome (composite of new ischemic lesion or new intracranial hemorrhage on MRI at 4 weeks) occurred at similar frequency between groups (49.5% versus 54.5%, P = .49). Rates of adverse events were comparable in each group. Median hospitalization length was shorter in those randomized to rivaroxaban (4.0 versus 6.0 days, P less than .001). Limitations include a radiographic primary outcome that captured many asymptomatic lesions, homogenous study population, and lack of a delayed anticoagulation group.
Bottom line: In patients with mild acute stroke from nonvalvular atrial fibrillation, rivaroxaban and warfarin demonstrated comparable efficacy and safety. More study is needed to determine the optimal anticoagulation strategy in acute stroke.
Citation: Hong K-S et al. Rivaroxaban vs. warfarin sodium in the ultra-early period after atrial fibrillation-related mild ischemic stroke: A randomized clinical trial. JAMA Neurol. 2017; 74(10):1206-15.
Dr. Kanjee is a hospitalist, Beth Israel Deaconess Medical Center, and instructor in medicine, Harvard Medical School, Boston.
Clinical question: Is rivaroxaban as effective and safe as warfarin immediately following minor acute ischemic stroke from atrial fibrillation?
Background: There is uncertainty regarding the best approach to anticoagulation acutely after ischemic stroke secondary to atrial fibrillation. To reduce the risk of intracranial hemorrhage, many physicians start aspirin immediately and delay initiating warfarin until days to weeks later. With their more predictable and rapid anticoagulant effect with potentially lower risk of intracranial hemorrhage, direct oral anticoagulants such as rivaroxaban are an attractive possible alternative to warfarin in the acute setting.
Study design: Multicenter, randomized, open-label superiority trial with blinded outcome assessment.
Setting: Fourteen academic hospitals in South Korea.
Synopsis: One hundred eighty-three patients with mild acute (within 5 days) ischemic stroke secondary to nonvalvular atrial fibrillation were randomized to immediately initiate either rivaroxaban or warfarin. The primary outcome (composite of new ischemic lesion or new intracranial hemorrhage on MRI at 4 weeks) occurred at similar frequency between groups (49.5% versus 54.5%, P = .49). Rates of adverse events were comparable in each group. Median hospitalization length was shorter in those randomized to rivaroxaban (4.0 versus 6.0 days, P less than .001). Limitations include a radiographic primary outcome that captured many asymptomatic lesions, homogenous study population, and lack of a delayed anticoagulation group.
Bottom line: In patients with mild acute stroke from nonvalvular atrial fibrillation, rivaroxaban and warfarin demonstrated comparable efficacy and safety. More study is needed to determine the optimal anticoagulation strategy in acute stroke.
Citation: Hong K-S et al. Rivaroxaban vs. warfarin sodium in the ultra-early period after atrial fibrillation-related mild ischemic stroke: A randomized clinical trial. JAMA Neurol. 2017; 74(10):1206-15.
Dr. Kanjee is a hospitalist, Beth Israel Deaconess Medical Center, and instructor in medicine, Harvard Medical School, Boston.
Webinar on Medicare Reimbursement is Thursday; Still Time to Avoid ’17 Penalties
The SVS Patient Safety Organization and the SVS Quality and Performance Measures Committee (QPMC) will hold a webinar at 8 p.m. Eastern Standard Time, Thursday, Feb. 15. It will help unravel the new Quality Payment Program (QPP) under Medicare, including what surgeons still can do for 2017 to avoid reimbursement penalties. Learn more here and register here.
The SVS Patient Safety Organization and the SVS Quality and Performance Measures Committee (QPMC) will hold a webinar at 8 p.m. Eastern Standard Time, Thursday, Feb. 15. It will help unravel the new Quality Payment Program (QPP) under Medicare, including what surgeons still can do for 2017 to avoid reimbursement penalties. Learn more here and register here.
The SVS Patient Safety Organization and the SVS Quality and Performance Measures Committee (QPMC) will hold a webinar at 8 p.m. Eastern Standard Time, Thursday, Feb. 15. It will help unravel the new Quality Payment Program (QPP) under Medicare, including what surgeons still can do for 2017 to avoid reimbursement penalties. Learn more here and register here.
Rheumatologists target prior authorization, Stark Law as barriers to competition
Onerous prior authorization rules, Stark Law, and other issues are creating barriers to health care choice and competition, the American College of Rheumatology recently told the Department of Health & Human Services.
The agency recently issued an informal request for information seeking “input from the public on the extent to which existing state and federal laws, regulations, guidance, requirements, and policies limit choice and competition across all health care markets, and the identification of actions that states or the federal government could take to support the development and operations of a health care system that provides high-quality care at affordable prices for the American people.”
“We believe this is a waste of valuable resources that results in delays in care and does not add value to health care delivery,” the ACR said in its Jan. 25 reply to the request for information. The ACR offered a series of recommendations to make the use of prior authorization by the Centers for Medicare & Medicaid Services more efficient.
Among the requested changes are:
• CMS should require all Medicare Advantage and Part D prescription drug plans to publicly disclose in a searchable electronic format to both patients and physicians all drugs and medical services that are subject to coverage restrictions (prior authorization, step therapy, formulary restrictions, quantity limits), and provide this information to vendors to be displayed in electronic health records.
• CMS should ensure that all utilization management requirements are based on accurate and up-to-date, publicly available clinical criteria and never cost alone.
• CMS should ensure that any “peer-to-peer” reviews utilize physicians from the same specialty/subspecialty as the ordering physician.
• CMS should restrict prior authorization requirements to “outlier” providers whose prescribing or ordering patterns differ significantly from their peers after adjusting for patient mix.
• CMS should not allow Part B services to be subject to prior authorization requirements because this would increase physician time spent on administrative tasks and reduce availability for patient care.
In addition, the ACR expressed concern about the consolidated pharmacy benefit managers market, noting that two PBMs cover more than 170 million Americans, and urged the HHS to “consider policies that require PBMs to be more transparent about their payment practices, including transparency around the true cost of prescription drugs.”
In the area of the Stark Law, the ACR called for the HHS to waive the prohibitions “for physicians seeking to develop and operate alternative payment models (APMs) as was provided to accountable care organizations in the Affordable Care Act. We also recommend removing the ‘volume or value’ prohibition in Stark policy so that physician practices can incentivize physicians to abide by best practices and succeed in new value-based alternative payment models.”
The ACR asked the CMS not to alter policy on assigning unique J-codes to biosimilars, as the unique codes allow for better monitoring of effectiveness and ensure adequate pharmacovigilance.
The physician organization also called for the removal of antitrust exemptions to insurance companies to give “the federal government the ability to intervene in places where insurance monopolies exist or develop.”
One request made – the removal of Part B drug payments from being adjusted by scoring in the Merit-based Incentive Payment System in the Quality Payment Program created by MACRA – was addressed in legislation passed by Congress and signed into law Feb. 9 by President Trump that provided short-term funding for the government and funding and other policy changes in the health care space, among other issues.
Onerous prior authorization rules, Stark Law, and other issues are creating barriers to health care choice and competition, the American College of Rheumatology recently told the Department of Health & Human Services.
The agency recently issued an informal request for information seeking “input from the public on the extent to which existing state and federal laws, regulations, guidance, requirements, and policies limit choice and competition across all health care markets, and the identification of actions that states or the federal government could take to support the development and operations of a health care system that provides high-quality care at affordable prices for the American people.”
“We believe this is a waste of valuable resources that results in delays in care and does not add value to health care delivery,” the ACR said in its Jan. 25 reply to the request for information. The ACR offered a series of recommendations to make the use of prior authorization by the Centers for Medicare & Medicaid Services more efficient.
Among the requested changes are:
• CMS should require all Medicare Advantage and Part D prescription drug plans to publicly disclose in a searchable electronic format to both patients and physicians all drugs and medical services that are subject to coverage restrictions (prior authorization, step therapy, formulary restrictions, quantity limits), and provide this information to vendors to be displayed in electronic health records.
• CMS should ensure that all utilization management requirements are based on accurate and up-to-date, publicly available clinical criteria and never cost alone.
• CMS should ensure that any “peer-to-peer” reviews utilize physicians from the same specialty/subspecialty as the ordering physician.
• CMS should restrict prior authorization requirements to “outlier” providers whose prescribing or ordering patterns differ significantly from their peers after adjusting for patient mix.
• CMS should not allow Part B services to be subject to prior authorization requirements because this would increase physician time spent on administrative tasks and reduce availability for patient care.
In addition, the ACR expressed concern about the consolidated pharmacy benefit managers market, noting that two PBMs cover more than 170 million Americans, and urged the HHS to “consider policies that require PBMs to be more transparent about their payment practices, including transparency around the true cost of prescription drugs.”
In the area of the Stark Law, the ACR called for the HHS to waive the prohibitions “for physicians seeking to develop and operate alternative payment models (APMs) as was provided to accountable care organizations in the Affordable Care Act. We also recommend removing the ‘volume or value’ prohibition in Stark policy so that physician practices can incentivize physicians to abide by best practices and succeed in new value-based alternative payment models.”
The ACR asked the CMS not to alter policy on assigning unique J-codes to biosimilars, as the unique codes allow for better monitoring of effectiveness and ensure adequate pharmacovigilance.
The physician organization also called for the removal of antitrust exemptions to insurance companies to give “the federal government the ability to intervene in places where insurance monopolies exist or develop.”
One request made – the removal of Part B drug payments from being adjusted by scoring in the Merit-based Incentive Payment System in the Quality Payment Program created by MACRA – was addressed in legislation passed by Congress and signed into law Feb. 9 by President Trump that provided short-term funding for the government and funding and other policy changes in the health care space, among other issues.
Onerous prior authorization rules, Stark Law, and other issues are creating barriers to health care choice and competition, the American College of Rheumatology recently told the Department of Health & Human Services.
The agency recently issued an informal request for information seeking “input from the public on the extent to which existing state and federal laws, regulations, guidance, requirements, and policies limit choice and competition across all health care markets, and the identification of actions that states or the federal government could take to support the development and operations of a health care system that provides high-quality care at affordable prices for the American people.”
“We believe this is a waste of valuable resources that results in delays in care and does not add value to health care delivery,” the ACR said in its Jan. 25 reply to the request for information. The ACR offered a series of recommendations to make the use of prior authorization by the Centers for Medicare & Medicaid Services more efficient.
Among the requested changes are:
• CMS should require all Medicare Advantage and Part D prescription drug plans to publicly disclose in a searchable electronic format to both patients and physicians all drugs and medical services that are subject to coverage restrictions (prior authorization, step therapy, formulary restrictions, quantity limits), and provide this information to vendors to be displayed in electronic health records.
• CMS should ensure that all utilization management requirements are based on accurate and up-to-date, publicly available clinical criteria and never cost alone.
• CMS should ensure that any “peer-to-peer” reviews utilize physicians from the same specialty/subspecialty as the ordering physician.
• CMS should restrict prior authorization requirements to “outlier” providers whose prescribing or ordering patterns differ significantly from their peers after adjusting for patient mix.
• CMS should not allow Part B services to be subject to prior authorization requirements because this would increase physician time spent on administrative tasks and reduce availability for patient care.
In addition, the ACR expressed concern about the consolidated pharmacy benefit managers market, noting that two PBMs cover more than 170 million Americans, and urged the HHS to “consider policies that require PBMs to be more transparent about their payment practices, including transparency around the true cost of prescription drugs.”
In the area of the Stark Law, the ACR called for the HHS to waive the prohibitions “for physicians seeking to develop and operate alternative payment models (APMs) as was provided to accountable care organizations in the Affordable Care Act. We also recommend removing the ‘volume or value’ prohibition in Stark policy so that physician practices can incentivize physicians to abide by best practices and succeed in new value-based alternative payment models.”
The ACR asked the CMS not to alter policy on assigning unique J-codes to biosimilars, as the unique codes allow for better monitoring of effectiveness and ensure adequate pharmacovigilance.
The physician organization also called for the removal of antitrust exemptions to insurance companies to give “the federal government the ability to intervene in places where insurance monopolies exist or develop.”
One request made – the removal of Part B drug payments from being adjusted by scoring in the Merit-based Incentive Payment System in the Quality Payment Program created by MACRA – was addressed in legislation passed by Congress and signed into law Feb. 9 by President Trump that provided short-term funding for the government and funding and other policy changes in the health care space, among other issues.
It takes a missile to focus your mind
I was one of about 600 dermatologists sitting in a lecture hall during a meeting in Maui when our muted smartphones suddenly started howling in unison. A text message popped up stating, “BALLISTIC MISSILE THREAT INBOUND TO HAWAII. SEEK IMMEDIATE SHELTER. THIS IS NOT A DRILL.” We all assumed a nuclear weapon from North Korea was headed our way.
The lecture was interrupted. The confused and concerned attendees milled around. The immediate response was largely “this can’t be real.” Meanwhile, the text alarm went off again transmitting the same message. The hotel intercom repeated the message and warned us to get inside the ballroom.

Among the attendees was David Cohen, trained in disaster preparedness. He ran up to his room, filled his bathtub, and put his mattress against the glass window. Richard Winkelman went down to the beach where he could at least witness what was about to annihilate him. Dirk Elston speculated the missile’s target was Kauai, where nuclear weapons are siloed. My wife was confident that the missiles would be intercepted, similar to the way they are under the Israeli missile defense system, and shot down before they hit any target.
And so, we mostly waited. The 30 minutes of largely silent confusion gave me a unique opportunity for self-reflection. I realized that many of my issues are petty and that I am insignificant in the scheme of things. I have never felt so helpless in my life. My mind entered a sort of fugue state, and I looked back on my life and realized it had been a darn good ride. I thought about my teenage children. I realized I had many, many things to be grateful for. I felt a huge burden lift off my shoulders and felt like I was floating about an inch above the floor. As I stared into nothingness, I internally reprioritized objectives. I was ready to die.
Then, just as suddenly and unpredictably as it arrived, the alert was called off. The imminent attack was no more than the mistaken push of a button.
But the event remains a defining moment for me. All the small battles that make up a life and career will continue, but I can no longer take them as seriously, and I will now take more time to reflect. I think I will get closer to God. I will try to be a better man, a better father, and a better citizen. It changed me, I think for the better.
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Write to him at [email protected].
I was one of about 600 dermatologists sitting in a lecture hall during a meeting in Maui when our muted smartphones suddenly started howling in unison. A text message popped up stating, “BALLISTIC MISSILE THREAT INBOUND TO HAWAII. SEEK IMMEDIATE SHELTER. THIS IS NOT A DRILL.” We all assumed a nuclear weapon from North Korea was headed our way.
The lecture was interrupted. The confused and concerned attendees milled around. The immediate response was largely “this can’t be real.” Meanwhile, the text alarm went off again transmitting the same message. The hotel intercom repeated the message and warned us to get inside the ballroom.
Among the attendees was David Cohen, trained in disaster preparedness. He ran up to his room, filled his bathtub, and put his mattress against the glass window. Richard Winkelman went down to the beach where he could at least witness what was about to annihilate him. Dirk Elston speculated the missile’s target was Kauai, where nuclear weapons are siloed. My wife was confident that the missiles would be intercepted, similar to the way they are under the Israeli missile defense system, and shot down before they hit any target.
And so, we mostly waited. The 30 minutes of largely silent confusion gave me a unique opportunity for self-reflection. I realized that many of my issues are petty and that I am insignificant in the scheme of things. I have never felt so helpless in my life. My mind entered a sort of fugue state, and I looked back on my life and realized it had been a darn good ride. I thought about my teenage children. I realized I had many, many things to be grateful for. I felt a huge burden lift off my shoulders and felt like I was floating about an inch above the floor. As I stared into nothingness, I internally reprioritized objectives. I was ready to die.
Then, just as suddenly and unpredictably as it arrived, the alert was called off. The imminent attack was no more than the mistaken push of a button.
But the event remains a defining moment for me. All the small battles that make up a life and career will continue, but I can no longer take them as seriously, and I will now take more time to reflect. I think I will get closer to God. I will try to be a better man, a better father, and a better citizen. It changed me, I think for the better.
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Write to him at [email protected].
I was one of about 600 dermatologists sitting in a lecture hall during a meeting in Maui when our muted smartphones suddenly started howling in unison. A text message popped up stating, “BALLISTIC MISSILE THREAT INBOUND TO HAWAII. SEEK IMMEDIATE SHELTER. THIS IS NOT A DRILL.” We all assumed a nuclear weapon from North Korea was headed our way.
The lecture was interrupted. The confused and concerned attendees milled around. The immediate response was largely “this can’t be real.” Meanwhile, the text alarm went off again transmitting the same message. The hotel intercom repeated the message and warned us to get inside the ballroom.
Among the attendees was David Cohen, trained in disaster preparedness. He ran up to his room, filled his bathtub, and put his mattress against the glass window. Richard Winkelman went down to the beach where he could at least witness what was about to annihilate him. Dirk Elston speculated the missile’s target was Kauai, where nuclear weapons are siloed. My wife was confident that the missiles would be intercepted, similar to the way they are under the Israeli missile defense system, and shot down before they hit any target.
And so, we mostly waited. The 30 minutes of largely silent confusion gave me a unique opportunity for self-reflection. I realized that many of my issues are petty and that I am insignificant in the scheme of things. I have never felt so helpless in my life. My mind entered a sort of fugue state, and I looked back on my life and realized it had been a darn good ride. I thought about my teenage children. I realized I had many, many things to be grateful for. I felt a huge burden lift off my shoulders and felt like I was floating about an inch above the floor. As I stared into nothingness, I internally reprioritized objectives. I was ready to die.
Then, just as suddenly and unpredictably as it arrived, the alert was called off. The imminent attack was no more than the mistaken push of a button.
But the event remains a defining moment for me. All the small battles that make up a life and career will continue, but I can no longer take them as seriously, and I will now take more time to reflect. I think I will get closer to God. I will try to be a better man, a better father, and a better citizen. It changed me, I think for the better.
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Write to him at [email protected].
Choosing noninvasive tightening treatments wisely
We all have one priority with all of our facial rejuvenation patients: Having happy, satisfied patients. With this in mind, I find I am torn by the armamentarium of noninvasive tightening devices to choose from. What are the critical factors in choosing a platform for your practice? Most practices look at pain, downtime, cost, and the number of treatments necessary to reach the expected outcome.

The treatment options are varied and include radio-frequency, ultrasound, and fractional resurfacing. There are numerous devices on the market that deliver energy into the dermis thereby causing collagen contraction and neocollagenesis. In my experience, the more “invasive” procedures or surgical tissue-tightening procedures provide the most reliable and immediate results. The radio-frequency and ultrasound devices that are “noninvasive” have little down-time, but multiple treatments are often needed and have inconsistent outcomes.
The technology for noninvasive modalities has improved over the last decade, but there are still no longterm clinical data, and results are highly varied. The difference in protocols and outcomes depends on proper patient selection, method of energy delivery, and sequential treatments.

We believe the optimal way to utilize these devices is as a combination approach with other procedures to optimize skin tightening and improvement in tone and texture. Tissue-tightening devices should be used with fractional ablative or nonablative resurfacing, fillers, and toxins. Often, we recommend starting with fillers and resurfacing treatments first to get the immediate “wow” factor and achieve immediate patient satisfaction. If patients want to then add skin tightening, this can be useful as an adjunct treatment and can even be used as a maintenance approach once per year. Actinic damage is also highly predictive of the degree of tissue laxity. Treating both the dermis and epidermis together delivers more immediate results. Using a fractional resurfacing device provides tissue tightening, improved skin color, decreased discoloration, and a reduction in the number of brown spots and freckles. Patients usually only need one to two treatments, there is minimal downtime, and satisfaction is very high.

In my practice, I choose fractional resurfacing treatments first. If patients want additional tissue tightening, radio-frequency is used as an adjunct treatment. This keeps costs lower, patients happier, and results more attainable.
When choosing devices for my practice, I follow a simple mantra: highest satisfaction per patient dollar spent. Happy patients build trust and integrity for the provider and practice. Don’t just buy a device because others are using it, and don’t just recommend a device because you have it.
Dr. Lily Talakoub and Dr. Naissan Wesley are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They have no relevant disclosures.
We all have one priority with all of our facial rejuvenation patients: Having happy, satisfied patients. With this in mind, I find I am torn by the armamentarium of noninvasive tightening devices to choose from. What are the critical factors in choosing a platform for your practice? Most practices look at pain, downtime, cost, and the number of treatments necessary to reach the expected outcome.
The treatment options are varied and include radio-frequency, ultrasound, and fractional resurfacing. There are numerous devices on the market that deliver energy into the dermis thereby causing collagen contraction and neocollagenesis. In my experience, the more “invasive” procedures or surgical tissue-tightening procedures provide the most reliable and immediate results. The radio-frequency and ultrasound devices that are “noninvasive” have little down-time, but multiple treatments are often needed and have inconsistent outcomes.
The technology for noninvasive modalities has improved over the last decade, but there are still no longterm clinical data, and results are highly varied. The difference in protocols and outcomes depends on proper patient selection, method of energy delivery, and sequential treatments.
We believe the optimal way to utilize these devices is as a combination approach with other procedures to optimize skin tightening and improvement in tone and texture. Tissue-tightening devices should be used with fractional ablative or nonablative resurfacing, fillers, and toxins. Often, we recommend starting with fillers and resurfacing treatments first to get the immediate “wow” factor and achieve immediate patient satisfaction. If patients want to then add skin tightening, this can be useful as an adjunct treatment and can even be used as a maintenance approach once per year. Actinic damage is also highly predictive of the degree of tissue laxity. Treating both the dermis and epidermis together delivers more immediate results. Using a fractional resurfacing device provides tissue tightening, improved skin color, decreased discoloration, and a reduction in the number of brown spots and freckles. Patients usually only need one to two treatments, there is minimal downtime, and satisfaction is very high.
In my practice, I choose fractional resurfacing treatments first. If patients want additional tissue tightening, radio-frequency is used as an adjunct treatment. This keeps costs lower, patients happier, and results more attainable.
When choosing devices for my practice, I follow a simple mantra: highest satisfaction per patient dollar spent. Happy patients build trust and integrity for the provider and practice. Don’t just buy a device because others are using it, and don’t just recommend a device because you have it.
Dr. Lily Talakoub and Dr. Naissan Wesley are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They have no relevant disclosures.
We all have one priority with all of our facial rejuvenation patients: Having happy, satisfied patients. With this in mind, I find I am torn by the armamentarium of noninvasive tightening devices to choose from. What are the critical factors in choosing a platform for your practice? Most practices look at pain, downtime, cost, and the number of treatments necessary to reach the expected outcome.
The treatment options are varied and include radio-frequency, ultrasound, and fractional resurfacing. There are numerous devices on the market that deliver energy into the dermis thereby causing collagen contraction and neocollagenesis. In my experience, the more “invasive” procedures or surgical tissue-tightening procedures provide the most reliable and immediate results. The radio-frequency and ultrasound devices that are “noninvasive” have little down-time, but multiple treatments are often needed and have inconsistent outcomes.
The technology for noninvasive modalities has improved over the last decade, but there are still no longterm clinical data, and results are highly varied. The difference in protocols and outcomes depends on proper patient selection, method of energy delivery, and sequential treatments.
We believe the optimal way to utilize these devices is as a combination approach with other procedures to optimize skin tightening and improvement in tone and texture. Tissue-tightening devices should be used with fractional ablative or nonablative resurfacing, fillers, and toxins. Often, we recommend starting with fillers and resurfacing treatments first to get the immediate “wow” factor and achieve immediate patient satisfaction. If patients want to then add skin tightening, this can be useful as an adjunct treatment and can even be used as a maintenance approach once per year. Actinic damage is also highly predictive of the degree of tissue laxity. Treating both the dermis and epidermis together delivers more immediate results. Using a fractional resurfacing device provides tissue tightening, improved skin color, decreased discoloration, and a reduction in the number of brown spots and freckles. Patients usually only need one to two treatments, there is minimal downtime, and satisfaction is very high.
In my practice, I choose fractional resurfacing treatments first. If patients want additional tissue tightening, radio-frequency is used as an adjunct treatment. This keeps costs lower, patients happier, and results more attainable.
When choosing devices for my practice, I follow a simple mantra: highest satisfaction per patient dollar spent. Happy patients build trust and integrity for the provider and practice. Don’t just buy a device because others are using it, and don’t just recommend a device because you have it.
Dr. Lily Talakoub and Dr. Naissan Wesley are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They have no relevant disclosures.
MDedge Daily News: The P word and the flu
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Is it time to use the P word about influenza? Your Medicare Part B drug pay earns a reprieve, a pregnancy-friendly psoriasis biologic is coming, and it’s good news, bad news for melanoma.
Listen to the MDedge Daily News podcast for all the details on today’s top news.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Is it time to use the P word about influenza? Your Medicare Part B drug pay earns a reprieve, a pregnancy-friendly psoriasis biologic is coming, and it’s good news, bad news for melanoma.
Listen to the MDedge Daily News podcast for all the details on today’s top news.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Is it time to use the P word about influenza? Your Medicare Part B drug pay earns a reprieve, a pregnancy-friendly psoriasis biologic is coming, and it’s good news, bad news for melanoma.
Listen to the MDedge Daily News podcast for all the details on today’s top news.
