User login
A mismatched haplotype may improve outcomes in second BMT
Undergoing a second allogeneic bone or marrow transplant (BMT) is a feasible strategy for patients who have relapsed after their first transplantation, according to findings reported in Biology of Blood and Marrow Transplantation.
Specifically, there may be an advantage to selecting a donor with a new mismatched haplotype after a failed HLA-matched allograft. Among patients who had a second graft transplanted that did not harbor a new mismatched haplotype, median survival was 552 days (95% CI, 376-2,950+). But median survival was not reached in the cohort whose allograft contained a new mismatched haplotype (hazard ratio, 0.36; 95% confidence interval, 0.14-0.9; P = .02).
“In the case of a failed HLA-matched transplantation, when haplotype loss would not be favored through selective pressure and thus would not provide a mechanism of relapse, switching to a different haploidentical donor may be beneficial by increasing major histocompatibility mismatch,” Philip H. Imus, MD, of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, and colleagues wrote.
For this retrospective review, the researchers examined 40 consecutive patients who underwent a second BMT for a relapsed hematologic malignancy at a single institution between 2005 and 2014. In all, 21 patients had their first allograft from a haploidentical donor, with 14 of these patients receiving a second haploidentical transplant (8 from a donor sharing the same shared haplotype as the first donor and 6 from a second donor sharing the other haplotype).
The other 19 patients received their first allograft from a fully matched donor, with 14 patients receiving a haploidentical allograft at the second transplantation and 5 receiving a second matched allograft. Overall, a total of 20 patients had a second allograft with a new mismatched haplotype.
The median overall survival for the six patients who were retransplantated with an HLA-haploidentical donor sharing the different haplotype from the first haploidentical donor had not been reached, compared with 502 days (95% CI, 317-2,950+) for the eight patients with a second haplo allograft that shared the same haplotype (HR, 0.37; 95% CI, 0.08 to 1.7; P = .16).
The median event free survival was also superior among those retransplanted with a new mismatched haplotype (not reached vs. 401 days; HR, .50; 95% CI, .22-1.14, P = .09).
A higher risk of mortality was observed in patients who had relapsed within 6 months of their first transplantation (HR, 2.49; 95% CI, 1.0-6.2; P = .07), as well as in those who had progressive or refractory disease prior to their second alloBMT (HR, 2.56; 95% CI, 1.03-6.25; P = .06).
“For patients who relapse more than 6 months after a BMT and who achieve remission with salvage therapy, results are very encouraging,” the researchers wrote. “Although a randomized trial to study selecting donors with a new mismatched haplotype may be impractical, larger numbers should provide additional information on the effectiveness of such an approach.”
The researchers reported having no financial disclosures.
SOURCE: Imus P et al. Biol Blood Marrow Transplant. 2017;23:1887-94.
Undergoing a second allogeneic bone or marrow transplant (BMT) is a feasible strategy for patients who have relapsed after their first transplantation, according to findings reported in Biology of Blood and Marrow Transplantation.
Specifically, there may be an advantage to selecting a donor with a new mismatched haplotype after a failed HLA-matched allograft. Among patients who had a second graft transplanted that did not harbor a new mismatched haplotype, median survival was 552 days (95% CI, 376-2,950+). But median survival was not reached in the cohort whose allograft contained a new mismatched haplotype (hazard ratio, 0.36; 95% confidence interval, 0.14-0.9; P = .02).
“In the case of a failed HLA-matched transplantation, when haplotype loss would not be favored through selective pressure and thus would not provide a mechanism of relapse, switching to a different haploidentical donor may be beneficial by increasing major histocompatibility mismatch,” Philip H. Imus, MD, of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, and colleagues wrote.
For this retrospective review, the researchers examined 40 consecutive patients who underwent a second BMT for a relapsed hematologic malignancy at a single institution between 2005 and 2014. In all, 21 patients had their first allograft from a haploidentical donor, with 14 of these patients receiving a second haploidentical transplant (8 from a donor sharing the same shared haplotype as the first donor and 6 from a second donor sharing the other haplotype).
The other 19 patients received their first allograft from a fully matched donor, with 14 patients receiving a haploidentical allograft at the second transplantation and 5 receiving a second matched allograft. Overall, a total of 20 patients had a second allograft with a new mismatched haplotype.
The median overall survival for the six patients who were retransplantated with an HLA-haploidentical donor sharing the different haplotype from the first haploidentical donor had not been reached, compared with 502 days (95% CI, 317-2,950+) for the eight patients with a second haplo allograft that shared the same haplotype (HR, 0.37; 95% CI, 0.08 to 1.7; P = .16).
The median event free survival was also superior among those retransplanted with a new mismatched haplotype (not reached vs. 401 days; HR, .50; 95% CI, .22-1.14, P = .09).
A higher risk of mortality was observed in patients who had relapsed within 6 months of their first transplantation (HR, 2.49; 95% CI, 1.0-6.2; P = .07), as well as in those who had progressive or refractory disease prior to their second alloBMT (HR, 2.56; 95% CI, 1.03-6.25; P = .06).
“For patients who relapse more than 6 months after a BMT and who achieve remission with salvage therapy, results are very encouraging,” the researchers wrote. “Although a randomized trial to study selecting donors with a new mismatched haplotype may be impractical, larger numbers should provide additional information on the effectiveness of such an approach.”
The researchers reported having no financial disclosures.
SOURCE: Imus P et al. Biol Blood Marrow Transplant. 2017;23:1887-94.
Undergoing a second allogeneic bone or marrow transplant (BMT) is a feasible strategy for patients who have relapsed after their first transplantation, according to findings reported in Biology of Blood and Marrow Transplantation.
Specifically, there may be an advantage to selecting a donor with a new mismatched haplotype after a failed HLA-matched allograft. Among patients who had a second graft transplanted that did not harbor a new mismatched haplotype, median survival was 552 days (95% CI, 376-2,950+). But median survival was not reached in the cohort whose allograft contained a new mismatched haplotype (hazard ratio, 0.36; 95% confidence interval, 0.14-0.9; P = .02).
“In the case of a failed HLA-matched transplantation, when haplotype loss would not be favored through selective pressure and thus would not provide a mechanism of relapse, switching to a different haploidentical donor may be beneficial by increasing major histocompatibility mismatch,” Philip H. Imus, MD, of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, and colleagues wrote.
For this retrospective review, the researchers examined 40 consecutive patients who underwent a second BMT for a relapsed hematologic malignancy at a single institution between 2005 and 2014. In all, 21 patients had their first allograft from a haploidentical donor, with 14 of these patients receiving a second haploidentical transplant (8 from a donor sharing the same shared haplotype as the first donor and 6 from a second donor sharing the other haplotype).
The other 19 patients received their first allograft from a fully matched donor, with 14 patients receiving a haploidentical allograft at the second transplantation and 5 receiving a second matched allograft. Overall, a total of 20 patients had a second allograft with a new mismatched haplotype.
The median overall survival for the six patients who were retransplantated with an HLA-haploidentical donor sharing the different haplotype from the first haploidentical donor had not been reached, compared with 502 days (95% CI, 317-2,950+) for the eight patients with a second haplo allograft that shared the same haplotype (HR, 0.37; 95% CI, 0.08 to 1.7; P = .16).
The median event free survival was also superior among those retransplanted with a new mismatched haplotype (not reached vs. 401 days; HR, .50; 95% CI, .22-1.14, P = .09).
A higher risk of mortality was observed in patients who had relapsed within 6 months of their first transplantation (HR, 2.49; 95% CI, 1.0-6.2; P = .07), as well as in those who had progressive or refractory disease prior to their second alloBMT (HR, 2.56; 95% CI, 1.03-6.25; P = .06).
“For patients who relapse more than 6 months after a BMT and who achieve remission with salvage therapy, results are very encouraging,” the researchers wrote. “Although a randomized trial to study selecting donors with a new mismatched haplotype may be impractical, larger numbers should provide additional information on the effectiveness of such an approach.”
The researchers reported having no financial disclosures.
SOURCE: Imus P et al. Biol Blood Marrow Transplant. 2017;23:1887-94.
FROM BIOLOGY OF BLOOD AND MARROW TRANSPLANTATION
Key clinical point:
Major finding: Median survival was 552 days (95% CI, 376-2,950+) for those without a new mismatched haplotype vs. not being reached for patients with a new mismatched haplotype on second transplant (HR, 0.36; 95% CI, 0.14-0.9; P = .02).
Study details: Retrospective review in a single institution that included 40 patients who underwent a second BMT between 2005 and 2014.
Disclosures: The researchers reported having no financial disclosures.
Source: Imus P et al. Biol Blood Marrow Transplant. 2017;23:1887-94.
Acne evaluations using photos with digital tool comparable to in-person exams
Dermatologist evaluation of photographs of acne taken by patients using a telemedicine and mobile data collection tool produced similar Investigator’s Global Assessment (IGA) findings and lesion counts, compared with traditional in-person examinations, in a pilot study sponsored by the tool’s manufacturer.
, the Network Oriented Research Assistant (NORA), Hannah Singer, a medical student at Columbia University, New York, and her coinvestigators concluded. The study was published online Dec. 20 in JAMA Dermatology.
To determine the effectiveness of the tool, investigators compared in-person evaluations of acne patients with digital evaluations in 60 patients in one dermatology practice. The “intraclass correlation coefficient (ICC)” was used to compare the in-person exam and the digital photo assessments of the IGA score and acne lesion counts; ICC scores ranged from 0 to 1, with 0 indicating no agreement and 1 indicating perfect agreement.
Study participants, who were aged 12-54 years (mean age 23 years) were trained to use NORA on an iPhone 6 and were instructed to take five photographs of different facial regions: the forehead, chin, right cheek, left cheek, and the whole face. The evaluation of patient-photographed acne and the in-person evaluation were separated by 1 week.
The ICC for IGA scores was 0.75, and the ICC for total lesion count was 0.81. Inflammatory lesion count and noninflammatory lesion count both had an ICC score of 0.72, while cyst count had the highest ICC score of 0.82. The ICC results demonstrated “strong agreement” between assessment scores from in-person examinations and the patient-taken digital photos, the authors wrote.
The study had several limitations, including the small patient sample size and limited geographic area, and although there was a 1- to 2-week gap between the digital and in-person evaluations, there may have been recall bias because the same physicians conducted both evaluations, they added.
Future studies should collect data from multiple centers, with a longer follow-up, and cost analysis and patient-reported measures, the researchers wrote.
The NORA technology platform is currently being evaluated in studies of patients with diagnoses including atopic dermatitis, pemphigus vulgaris, and liver disease. “Use of the NORA platform in telemedicine-based clinical trials will allow for increased access, a broader diversity of patients, and improved adherence among participants in trials for acne vulgaris and other therapeutic areas,” the researchers noted.
The study was sponsored by Science 37, a mobile technology and clinical trial company that developed NORA, the software used in this study. Other than Ms. Singer, who had no disclosures, the remaining 10 authors are Science 37 employees and have stock options in the company.
SOURCE: M. Singer, JAMA Dermatol 2017 Dec 20; doi:10.1001/jamadermatol.2017.5141.
Dermatologist evaluation of photographs of acne taken by patients using a telemedicine and mobile data collection tool produced similar Investigator’s Global Assessment (IGA) findings and lesion counts, compared with traditional in-person examinations, in a pilot study sponsored by the tool’s manufacturer.
, the Network Oriented Research Assistant (NORA), Hannah Singer, a medical student at Columbia University, New York, and her coinvestigators concluded. The study was published online Dec. 20 in JAMA Dermatology.
To determine the effectiveness of the tool, investigators compared in-person evaluations of acne patients with digital evaluations in 60 patients in one dermatology practice. The “intraclass correlation coefficient (ICC)” was used to compare the in-person exam and the digital photo assessments of the IGA score and acne lesion counts; ICC scores ranged from 0 to 1, with 0 indicating no agreement and 1 indicating perfect agreement.
Study participants, who were aged 12-54 years (mean age 23 years) were trained to use NORA on an iPhone 6 and were instructed to take five photographs of different facial regions: the forehead, chin, right cheek, left cheek, and the whole face. The evaluation of patient-photographed acne and the in-person evaluation were separated by 1 week.
The ICC for IGA scores was 0.75, and the ICC for total lesion count was 0.81. Inflammatory lesion count and noninflammatory lesion count both had an ICC score of 0.72, while cyst count had the highest ICC score of 0.82. The ICC results demonstrated “strong agreement” between assessment scores from in-person examinations and the patient-taken digital photos, the authors wrote.
The study had several limitations, including the small patient sample size and limited geographic area, and although there was a 1- to 2-week gap between the digital and in-person evaluations, there may have been recall bias because the same physicians conducted both evaluations, they added.
Future studies should collect data from multiple centers, with a longer follow-up, and cost analysis and patient-reported measures, the researchers wrote.
The NORA technology platform is currently being evaluated in studies of patients with diagnoses including atopic dermatitis, pemphigus vulgaris, and liver disease. “Use of the NORA platform in telemedicine-based clinical trials will allow for increased access, a broader diversity of patients, and improved adherence among participants in trials for acne vulgaris and other therapeutic areas,” the researchers noted.
The study was sponsored by Science 37, a mobile technology and clinical trial company that developed NORA, the software used in this study. Other than Ms. Singer, who had no disclosures, the remaining 10 authors are Science 37 employees and have stock options in the company.
SOURCE: M. Singer, JAMA Dermatol 2017 Dec 20; doi:10.1001/jamadermatol.2017.5141.
Dermatologist evaluation of photographs of acne taken by patients using a telemedicine and mobile data collection tool produced similar Investigator’s Global Assessment (IGA) findings and lesion counts, compared with traditional in-person examinations, in a pilot study sponsored by the tool’s manufacturer.
, the Network Oriented Research Assistant (NORA), Hannah Singer, a medical student at Columbia University, New York, and her coinvestigators concluded. The study was published online Dec. 20 in JAMA Dermatology.
To determine the effectiveness of the tool, investigators compared in-person evaluations of acne patients with digital evaluations in 60 patients in one dermatology practice. The “intraclass correlation coefficient (ICC)” was used to compare the in-person exam and the digital photo assessments of the IGA score and acne lesion counts; ICC scores ranged from 0 to 1, with 0 indicating no agreement and 1 indicating perfect agreement.
Study participants, who were aged 12-54 years (mean age 23 years) were trained to use NORA on an iPhone 6 and were instructed to take five photographs of different facial regions: the forehead, chin, right cheek, left cheek, and the whole face. The evaluation of patient-photographed acne and the in-person evaluation were separated by 1 week.
The ICC for IGA scores was 0.75, and the ICC for total lesion count was 0.81. Inflammatory lesion count and noninflammatory lesion count both had an ICC score of 0.72, while cyst count had the highest ICC score of 0.82. The ICC results demonstrated “strong agreement” between assessment scores from in-person examinations and the patient-taken digital photos, the authors wrote.
The study had several limitations, including the small patient sample size and limited geographic area, and although there was a 1- to 2-week gap between the digital and in-person evaluations, there may have been recall bias because the same physicians conducted both evaluations, they added.
Future studies should collect data from multiple centers, with a longer follow-up, and cost analysis and patient-reported measures, the researchers wrote.
The NORA technology platform is currently being evaluated in studies of patients with diagnoses including atopic dermatitis, pemphigus vulgaris, and liver disease. “Use of the NORA platform in telemedicine-based clinical trials will allow for increased access, a broader diversity of patients, and improved adherence among participants in trials for acne vulgaris and other therapeutic areas,” the researchers noted.
The study was sponsored by Science 37, a mobile technology and clinical trial company that developed NORA, the software used in this study. Other than Ms. Singer, who had no disclosures, the remaining 10 authors are Science 37 employees and have stock options in the company.
SOURCE: M. Singer, JAMA Dermatol 2017 Dec 20; doi:10.1001/jamadermatol.2017.5141.
FROM JAMA DERMATOLOGY
Key clinical point: In-person evaluations and digital evaluations of self-photographed acne produced comparable results.
Major finding: There was “strong agreement” in the Investigator’s Global Assessment scores and acne lesion counts between assessments of digital photos and in-person exams.
Study details: A pilot study of 60 acne patients at a dermatology office compared assessments with digital photos and in-person exams.
Disclosures: The study was sponsored by Science 37, a mobile technology and clinical trial company that developed NORA, the software used in this study. Other than the lead author, who had no disclosures, the 10 remaining authors are Science 37 employees and have stock options in the company.
Source: M Singer, JAMA Dermatol. 2017 Dec 20; doi: 10.1001/jamadermatol.2017.5141.
Study: Test carcinoembryonic antigen in colon cancer after surgery
A new study challenges the practice of measuring carcinoembryonic antigen (CEA) in patients with colon cancer prior to surgery, as is currently recommended by some guidelines. Researchers found that the levels do have predictive value about risk of recurrence when tested after surgery, but they challenge its use before.
“Consistent with the literature, our data show that postoperative CEA is more informative than preoperative CEA,” the study authors wrote. “Emphasis should be placed on postoperative CEA, and in the setting of modern high-quality imaging, we question the utility of measuring preoperative CEA.”
The study, which was published online in JAMA Oncology, noted that testing for CEA – a colorectal cancer tumor marker – had more value prior to the current era of imaging because it could indicate the need to widen a search for metastases.
“In the era of high-quality computed tomography (CT), the utility of measuring preoperative CEA is less obvious because an elevated preoperative CEA with a normal CT scan does not preclude surgery with curative intent,” wrote Tsuyoshi Konishi, MD, of Memorial Sloan-Kettering Cancer Center in New York and his coauthors.
CEA levels can return to normal after colon cancer surgery – but not always. According to the study, the National Comprehensive Cancer Network, the American Society of Clinical Oncology, and the European Group on Tumor Markers recommend its measurement prior to surgery in patients with nonmetastatic cancer.
For the new study, the authors sought to understand the predictive value of various CEA levels both before and after surgery.
The researchers retrospectively tracked 1,027 patients at a single center with stage I-III colon cancer (50.4% male; median age, 64 years). (Another 221 patients had been removed because of exclusion criteria, such as recent malignancy treatment and preoperative chemotherapy or radiation treatment.)
Nearly 70% of the 1,027 patients had normal preoperative CEA levels, and the rest had elevated levels.
Of the 312 patients with elevated preoperative CEA levels, 113 were lost to follow-up postoperative CEA tests. In the remaining patients, CEA levels returned to normal in 71%.
Patients were followed for a median of 38 months; 10.3% had recurrences, and 4.6% died. The 3-year recurrence-free survival rate was 88.4%.
Researchers found that those with normal preoperative CEA levels were more likely to reach recurrence-free survival at 3 years (89.7%) than were those who had elevated preoperative CEA levels (82.3%; P = .05). The higher level wasn’t much different than the recurrence-free survival level in those whose CEA levels had normalized after the operation (87.9%; P = .86).
Those with elevated CEA levels after surgery had a lower likelihood of reaching recurrence-free survival at 3 years (74.5%) than did those who had normal postoperative CEA levels (89.4%).
The study also linked abnormal postoperative CEA levels to shorter recurrence-free survival (hazard ratio, 2.0; 95% confidence interval, 1.1-3.5). Normalized postoperative CEA levels, however, were not linked to shorter recurrence-free survival (HR, 0.77; 95% CI, 0.45-1.30).
The researchers noted that they didn’t control for factors such as smoking (which increases CEA levels) and disease like gastritis and diabetes, which can produce misleading CEA levels. “Rather, this study is pragmatic,” the researchers wrote, “and represents what is likely to be seen in real-world colorectal cancer care.”
Moving forward, the researchers wrote, “patients with elevated postoperative CEA tend to experience recurrence early, which might justify a risk-adjusted and individualized surveillance strategy.”
The study authors report no relevant disclosures. The National Institutes of Health/National Cancer Institute funded the study in part.
SOURCE: Konishi T et al. JAMA Oncol. 2017. doi: 10.1001/jamaoncol.2017.4420.
Multiple organizations recommend that patients with nonmetastatic colorectal cancer undergo carcinoembryonic antigen (CEA) measurement prior to surgery, and there’s talk that it should be added to the staging system of the American Joint Committee on Cancer.
This new study, however, provides a challenge to the use of preoperative CEA tests in this population. As the researchers report, patients with normalized CEA levels postsurgery – even those with abnormal levels before surgery – were more likely to reach recurrence-free survival for 3 years.
The findings spotlight the value of real-world evidence and real-world data rather than statistics gathered during a controlled clinical trial.
There are limitations to this study, such as generalizability (it was performed at a single center), loss of patients to CEA follow-up postsurgery, and timing (the study period began a decade ago).
Still, the findings, once confirmed, could change clinical practice, and they point to the potential use of CEA as a biomarker early-warning sign that a tumor may recur.
Rebecca Anne Miksad, MD, MPH, is with Harvard Medical School in Boston (leave of absence from 2017 to 2018) and Neal J. Meropol, MD, is with Case Western Reserve University in Cleveland. They disclose employment by Flatiron Health. These comments are taken from their editorial accompanying the study by Konishi et al. in JAMA Oncology, doi:10.1001/jamaoncol.2017.4420.
Multiple organizations recommend that patients with nonmetastatic colorectal cancer undergo carcinoembryonic antigen (CEA) measurement prior to surgery, and there’s talk that it should be added to the staging system of the American Joint Committee on Cancer.
This new study, however, provides a challenge to the use of preoperative CEA tests in this population. As the researchers report, patients with normalized CEA levels postsurgery – even those with abnormal levels before surgery – were more likely to reach recurrence-free survival for 3 years.
The findings spotlight the value of real-world evidence and real-world data rather than statistics gathered during a controlled clinical trial.
There are limitations to this study, such as generalizability (it was performed at a single center), loss of patients to CEA follow-up postsurgery, and timing (the study period began a decade ago).
Still, the findings, once confirmed, could change clinical practice, and they point to the potential use of CEA as a biomarker early-warning sign that a tumor may recur.
Rebecca Anne Miksad, MD, MPH, is with Harvard Medical School in Boston (leave of absence from 2017 to 2018) and Neal J. Meropol, MD, is with Case Western Reserve University in Cleveland. They disclose employment by Flatiron Health. These comments are taken from their editorial accompanying the study by Konishi et al. in JAMA Oncology, doi:10.1001/jamaoncol.2017.4420.
Multiple organizations recommend that patients with nonmetastatic colorectal cancer undergo carcinoembryonic antigen (CEA) measurement prior to surgery, and there’s talk that it should be added to the staging system of the American Joint Committee on Cancer.
This new study, however, provides a challenge to the use of preoperative CEA tests in this population. As the researchers report, patients with normalized CEA levels postsurgery – even those with abnormal levels before surgery – were more likely to reach recurrence-free survival for 3 years.
The findings spotlight the value of real-world evidence and real-world data rather than statistics gathered during a controlled clinical trial.
There are limitations to this study, such as generalizability (it was performed at a single center), loss of patients to CEA follow-up postsurgery, and timing (the study period began a decade ago).
Still, the findings, once confirmed, could change clinical practice, and they point to the potential use of CEA as a biomarker early-warning sign that a tumor may recur.
Rebecca Anne Miksad, MD, MPH, is with Harvard Medical School in Boston (leave of absence from 2017 to 2018) and Neal J. Meropol, MD, is with Case Western Reserve University in Cleveland. They disclose employment by Flatiron Health. These comments are taken from their editorial accompanying the study by Konishi et al. in JAMA Oncology, doi:10.1001/jamaoncol.2017.4420.
A new study challenges the practice of measuring carcinoembryonic antigen (CEA) in patients with colon cancer prior to surgery, as is currently recommended by some guidelines. Researchers found that the levels do have predictive value about risk of recurrence when tested after surgery, but they challenge its use before.
“Consistent with the literature, our data show that postoperative CEA is more informative than preoperative CEA,” the study authors wrote. “Emphasis should be placed on postoperative CEA, and in the setting of modern high-quality imaging, we question the utility of measuring preoperative CEA.”
The study, which was published online in JAMA Oncology, noted that testing for CEA – a colorectal cancer tumor marker – had more value prior to the current era of imaging because it could indicate the need to widen a search for metastases.
“In the era of high-quality computed tomography (CT), the utility of measuring preoperative CEA is less obvious because an elevated preoperative CEA with a normal CT scan does not preclude surgery with curative intent,” wrote Tsuyoshi Konishi, MD, of Memorial Sloan-Kettering Cancer Center in New York and his coauthors.
CEA levels can return to normal after colon cancer surgery – but not always. According to the study, the National Comprehensive Cancer Network, the American Society of Clinical Oncology, and the European Group on Tumor Markers recommend its measurement prior to surgery in patients with nonmetastatic cancer.
For the new study, the authors sought to understand the predictive value of various CEA levels both before and after surgery.
The researchers retrospectively tracked 1,027 patients at a single center with stage I-III colon cancer (50.4% male; median age, 64 years). (Another 221 patients had been removed because of exclusion criteria, such as recent malignancy treatment and preoperative chemotherapy or radiation treatment.)
Nearly 70% of the 1,027 patients had normal preoperative CEA levels, and the rest had elevated levels.
Of the 312 patients with elevated preoperative CEA levels, 113 were lost to follow-up postoperative CEA tests. In the remaining patients, CEA levels returned to normal in 71%.
Patients were followed for a median of 38 months; 10.3% had recurrences, and 4.6% died. The 3-year recurrence-free survival rate was 88.4%.
Researchers found that those with normal preoperative CEA levels were more likely to reach recurrence-free survival at 3 years (89.7%) than were those who had elevated preoperative CEA levels (82.3%; P = .05). The higher level wasn’t much different than the recurrence-free survival level in those whose CEA levels had normalized after the operation (87.9%; P = .86).
Those with elevated CEA levels after surgery had a lower likelihood of reaching recurrence-free survival at 3 years (74.5%) than did those who had normal postoperative CEA levels (89.4%).
The study also linked abnormal postoperative CEA levels to shorter recurrence-free survival (hazard ratio, 2.0; 95% confidence interval, 1.1-3.5). Normalized postoperative CEA levels, however, were not linked to shorter recurrence-free survival (HR, 0.77; 95% CI, 0.45-1.30).
The researchers noted that they didn’t control for factors such as smoking (which increases CEA levels) and disease like gastritis and diabetes, which can produce misleading CEA levels. “Rather, this study is pragmatic,” the researchers wrote, “and represents what is likely to be seen in real-world colorectal cancer care.”
Moving forward, the researchers wrote, “patients with elevated postoperative CEA tend to experience recurrence early, which might justify a risk-adjusted and individualized surveillance strategy.”
The study authors report no relevant disclosures. The National Institutes of Health/National Cancer Institute funded the study in part.
SOURCE: Konishi T et al. JAMA Oncol. 2017. doi: 10.1001/jamaoncol.2017.4420.
A new study challenges the practice of measuring carcinoembryonic antigen (CEA) in patients with colon cancer prior to surgery, as is currently recommended by some guidelines. Researchers found that the levels do have predictive value about risk of recurrence when tested after surgery, but they challenge its use before.
“Consistent with the literature, our data show that postoperative CEA is more informative than preoperative CEA,” the study authors wrote. “Emphasis should be placed on postoperative CEA, and in the setting of modern high-quality imaging, we question the utility of measuring preoperative CEA.”
The study, which was published online in JAMA Oncology, noted that testing for CEA – a colorectal cancer tumor marker – had more value prior to the current era of imaging because it could indicate the need to widen a search for metastases.
“In the era of high-quality computed tomography (CT), the utility of measuring preoperative CEA is less obvious because an elevated preoperative CEA with a normal CT scan does not preclude surgery with curative intent,” wrote Tsuyoshi Konishi, MD, of Memorial Sloan-Kettering Cancer Center in New York and his coauthors.
CEA levels can return to normal after colon cancer surgery – but not always. According to the study, the National Comprehensive Cancer Network, the American Society of Clinical Oncology, and the European Group on Tumor Markers recommend its measurement prior to surgery in patients with nonmetastatic cancer.
For the new study, the authors sought to understand the predictive value of various CEA levels both before and after surgery.
The researchers retrospectively tracked 1,027 patients at a single center with stage I-III colon cancer (50.4% male; median age, 64 years). (Another 221 patients had been removed because of exclusion criteria, such as recent malignancy treatment and preoperative chemotherapy or radiation treatment.)
Nearly 70% of the 1,027 patients had normal preoperative CEA levels, and the rest had elevated levels.
Of the 312 patients with elevated preoperative CEA levels, 113 were lost to follow-up postoperative CEA tests. In the remaining patients, CEA levels returned to normal in 71%.
Patients were followed for a median of 38 months; 10.3% had recurrences, and 4.6% died. The 3-year recurrence-free survival rate was 88.4%.
Researchers found that those with normal preoperative CEA levels were more likely to reach recurrence-free survival at 3 years (89.7%) than were those who had elevated preoperative CEA levels (82.3%; P = .05). The higher level wasn’t much different than the recurrence-free survival level in those whose CEA levels had normalized after the operation (87.9%; P = .86).
Those with elevated CEA levels after surgery had a lower likelihood of reaching recurrence-free survival at 3 years (74.5%) than did those who had normal postoperative CEA levels (89.4%).
The study also linked abnormal postoperative CEA levels to shorter recurrence-free survival (hazard ratio, 2.0; 95% confidence interval, 1.1-3.5). Normalized postoperative CEA levels, however, were not linked to shorter recurrence-free survival (HR, 0.77; 95% CI, 0.45-1.30).
The researchers noted that they didn’t control for factors such as smoking (which increases CEA levels) and disease like gastritis and diabetes, which can produce misleading CEA levels. “Rather, this study is pragmatic,” the researchers wrote, “and represents what is likely to be seen in real-world colorectal cancer care.”
Moving forward, the researchers wrote, “patients with elevated postoperative CEA tend to experience recurrence early, which might justify a risk-adjusted and individualized surveillance strategy.”
The study authors report no relevant disclosures. The National Institutes of Health/National Cancer Institute funded the study in part.
SOURCE: Konishi T et al. JAMA Oncol. 2017. doi: 10.1001/jamaoncol.2017.4420.
FROM JAMA ONCOLOGY
Key clinical point: Measurement of CEA levels in patients with colon cancer appears to have value postoperatively but not preoperatively.
Major finding: Patients with abnormal postoperative CEA levels were less likely to reach 3-year recurrence-free survival than were those with normal levels (74.5% vs. 89.4%).
Study details: Retrospective, single-center study of 1,027 patients with stage I-III colon cancer (50.4% male; median age, 64 years).
Disclosures: The study authors report no relevant disclosures. The National Institutes of Health/National Cancer Institute funded the study in part.
Source: Konishi T et al. JAMA Oncol. 2017. doi: 10.1001/jamaoncol.2017.4420.
Online education program linked to less anxiety, medication use in colonoscopies
An online education program appeared to dampen anxiety levels in colonoscopy patients and even seemed to reduce the burden of the procedure in terms of time and medication used, a study showed.
“The program was very well received and generally improved patient’s anxiety,” said lead author Siddhartha Parker, MD, a gastroenterologist at Dartmouth-Hitchcock Medical Center, Lebanon, N.H. “Only 4% of patients described feeling more anxious after watching the program whereas 58% felt less anxious.”

“Patients who are afraid or anxious may require more sedation, experience more pain, and, most importantly, may be less likely to have a procedure done,” he said. “Some patients don’t schedule at all, while others may schedule and then cancel last minute or no-show an appointment, which has its own implications and costs to the health care system.”
In terms of anxiety prevention, he said, “primarily we rely on nurses and doctors to discuss the need for screening and provide reassurance about low risks and real benefits.”
For the current study, published in the Journal of Clinical Gastroenterology, researchers tested a Web-based colonoscopy education program from a company called Emmi Solutions.
The program is designed to provide details about the colonoscopy process. “It covers what to expect before, during, and after the procedure including possible findings (e.g., polyps),” Dr. Parker said. “It also covers risks and benefits with some tips on recovery after the procedure. I think having some dedicated time to understand the procedure is most helpful. It is rare that a patient gets 15-20 minutes to review any topic with their doctor, and the Emmi program has the added benefit of visual cues.”
The researchers recruited and randomly assigned 51 patients to a control group and 52 patients to the intervention. All were scheduled to undergo colonoscopies within at least 2 weeks.
The groups were similar: Most patients were white (100% of the control group, 89% of the intervention group), and most were female; the average age was 48 years The intervention group had more education, at 69% with college degrees vs. 43% in the control group (P = .01).
Patients in the control group received usual colonoscopy education materials, while those in the intervention group were also directed to the education website.
All participants took a survey immediately before their procedures and received a $10 gift card as reimbursement for their participation.
Researchers found that patients in the intervention group scored higher than did those in the control group on questions about colonoscopy knowledge (82% of questions correct vs. 74%, P less than .001).
Also, the education website may have convinced its viewers to worry less about the procedure and more about its ultimate findings. Compared with the control group, those in the intervention group were more likely to say they were most concerned about the findings (38.5% vs. 21.6%) and less likely to say they were more concerned about both the findings and the procedure (38.5% vs. 56.9%). Roughly 20% of those in both groups said they were most concerned about the procedure.
“Some patients report being more concerned about findings, e.g., cancer, before the program but more anxious about complications after the program,” Dr. Parker said. “I think that is a reasonable outcome as asymptomatic patients should have very little concern about findings, given the goal is to find and remove polyps.”
Researchers also tracked the use of sedatives during the procedure. Those in the intervention group required less midazolam (Versed) (average dose of 3.66 mg vs. 4.46 mg, P = .004). They also required less fentanyl (164 mcg vs. 186 mcg), but this finding was not statistically significant (P = .063).
“There was also a trend, not quite statistically significant, to improved prep quality,” Dr. Parker said. (In the intervention vs. the control group, 96% vs. 88% of subjects were rated as good or excellent in terms of prep quality, P = .27).
“This is important because a poor or inadequate prep leads to a need for a repeat procedure to ensure adequate screening,” he said. “If prep quality improves, that means fewer unnecessary repeated procedures.”
The researchers reported study limitations such as multiple endoscopists and sedation nurses and the variation in education levels of the participants.
The cost of the interactive program was not available.
According to Dr. Parker, Dartmouth-Hitchcock Medical Center now offers the education program to all colonoscopy patients, and a modified version is available for those undergoing upper endoscopies.
“Not all patients have adequate computer resources, and some patients simply choose not to watch,” he said. “But my impression is that those who watched the program are more relaxed during the informed consent process. However, we are not actively tracking outcomes such as procedure time or medication usage.”
No more studies of the program are planned at the institution, he said.
One of the study authors is an employee of Emmi Solutions, which provided the program for free for use in the study. The other authors reported no relevant disclosures. No study funding was reported.
SOURCE: Parker S et al. J Clin Gastroenterol. doi: 10.1097/MCG.0000000000000958
An online education program appeared to dampen anxiety levels in colonoscopy patients and even seemed to reduce the burden of the procedure in terms of time and medication used, a study showed.
“The program was very well received and generally improved patient’s anxiety,” said lead author Siddhartha Parker, MD, a gastroenterologist at Dartmouth-Hitchcock Medical Center, Lebanon, N.H. “Only 4% of patients described feeling more anxious after watching the program whereas 58% felt less anxious.”
“Patients who are afraid or anxious may require more sedation, experience more pain, and, most importantly, may be less likely to have a procedure done,” he said. “Some patients don’t schedule at all, while others may schedule and then cancel last minute or no-show an appointment, which has its own implications and costs to the health care system.”
In terms of anxiety prevention, he said, “primarily we rely on nurses and doctors to discuss the need for screening and provide reassurance about low risks and real benefits.”
For the current study, published in the Journal of Clinical Gastroenterology, researchers tested a Web-based colonoscopy education program from a company called Emmi Solutions.
The program is designed to provide details about the colonoscopy process. “It covers what to expect before, during, and after the procedure including possible findings (e.g., polyps),” Dr. Parker said. “It also covers risks and benefits with some tips on recovery after the procedure. I think having some dedicated time to understand the procedure is most helpful. It is rare that a patient gets 15-20 minutes to review any topic with their doctor, and the Emmi program has the added benefit of visual cues.”
The researchers recruited and randomly assigned 51 patients to a control group and 52 patients to the intervention. All were scheduled to undergo colonoscopies within at least 2 weeks.
The groups were similar: Most patients were white (100% of the control group, 89% of the intervention group), and most were female; the average age was 48 years The intervention group had more education, at 69% with college degrees vs. 43% in the control group (P = .01).
Patients in the control group received usual colonoscopy education materials, while those in the intervention group were also directed to the education website.
All participants took a survey immediately before their procedures and received a $10 gift card as reimbursement for their participation.
Researchers found that patients in the intervention group scored higher than did those in the control group on questions about colonoscopy knowledge (82% of questions correct vs. 74%, P less than .001).
Also, the education website may have convinced its viewers to worry less about the procedure and more about its ultimate findings. Compared with the control group, those in the intervention group were more likely to say they were most concerned about the findings (38.5% vs. 21.6%) and less likely to say they were more concerned about both the findings and the procedure (38.5% vs. 56.9%). Roughly 20% of those in both groups said they were most concerned about the procedure.
“Some patients report being more concerned about findings, e.g., cancer, before the program but more anxious about complications after the program,” Dr. Parker said. “I think that is a reasonable outcome as asymptomatic patients should have very little concern about findings, given the goal is to find and remove polyps.”
Researchers also tracked the use of sedatives during the procedure. Those in the intervention group required less midazolam (Versed) (average dose of 3.66 mg vs. 4.46 mg, P = .004). They also required less fentanyl (164 mcg vs. 186 mcg), but this finding was not statistically significant (P = .063).
“There was also a trend, not quite statistically significant, to improved prep quality,” Dr. Parker said. (In the intervention vs. the control group, 96% vs. 88% of subjects were rated as good or excellent in terms of prep quality, P = .27).
“This is important because a poor or inadequate prep leads to a need for a repeat procedure to ensure adequate screening,” he said. “If prep quality improves, that means fewer unnecessary repeated procedures.”
The researchers reported study limitations such as multiple endoscopists and sedation nurses and the variation in education levels of the participants.
The cost of the interactive program was not available.
According to Dr. Parker, Dartmouth-Hitchcock Medical Center now offers the education program to all colonoscopy patients, and a modified version is available for those undergoing upper endoscopies.
“Not all patients have adequate computer resources, and some patients simply choose not to watch,” he said. “But my impression is that those who watched the program are more relaxed during the informed consent process. However, we are not actively tracking outcomes such as procedure time or medication usage.”
No more studies of the program are planned at the institution, he said.
One of the study authors is an employee of Emmi Solutions, which provided the program for free for use in the study. The other authors reported no relevant disclosures. No study funding was reported.
SOURCE: Parker S et al. J Clin Gastroenterol. doi: 10.1097/MCG.0000000000000958
An online education program appeared to dampen anxiety levels in colonoscopy patients and even seemed to reduce the burden of the procedure in terms of time and medication used, a study showed.
“The program was very well received and generally improved patient’s anxiety,” said lead author Siddhartha Parker, MD, a gastroenterologist at Dartmouth-Hitchcock Medical Center, Lebanon, N.H. “Only 4% of patients described feeling more anxious after watching the program whereas 58% felt less anxious.”
“Patients who are afraid or anxious may require more sedation, experience more pain, and, most importantly, may be less likely to have a procedure done,” he said. “Some patients don’t schedule at all, while others may schedule and then cancel last minute or no-show an appointment, which has its own implications and costs to the health care system.”
In terms of anxiety prevention, he said, “primarily we rely on nurses and doctors to discuss the need for screening and provide reassurance about low risks and real benefits.”
For the current study, published in the Journal of Clinical Gastroenterology, researchers tested a Web-based colonoscopy education program from a company called Emmi Solutions.
The program is designed to provide details about the colonoscopy process. “It covers what to expect before, during, and after the procedure including possible findings (e.g., polyps),” Dr. Parker said. “It also covers risks and benefits with some tips on recovery after the procedure. I think having some dedicated time to understand the procedure is most helpful. It is rare that a patient gets 15-20 minutes to review any topic with their doctor, and the Emmi program has the added benefit of visual cues.”
The researchers recruited and randomly assigned 51 patients to a control group and 52 patients to the intervention. All were scheduled to undergo colonoscopies within at least 2 weeks.
The groups were similar: Most patients were white (100% of the control group, 89% of the intervention group), and most were female; the average age was 48 years The intervention group had more education, at 69% with college degrees vs. 43% in the control group (P = .01).
Patients in the control group received usual colonoscopy education materials, while those in the intervention group were also directed to the education website.
All participants took a survey immediately before their procedures and received a $10 gift card as reimbursement for their participation.
Researchers found that patients in the intervention group scored higher than did those in the control group on questions about colonoscopy knowledge (82% of questions correct vs. 74%, P less than .001).
Also, the education website may have convinced its viewers to worry less about the procedure and more about its ultimate findings. Compared with the control group, those in the intervention group were more likely to say they were most concerned about the findings (38.5% vs. 21.6%) and less likely to say they were more concerned about both the findings and the procedure (38.5% vs. 56.9%). Roughly 20% of those in both groups said they were most concerned about the procedure.
“Some patients report being more concerned about findings, e.g., cancer, before the program but more anxious about complications after the program,” Dr. Parker said. “I think that is a reasonable outcome as asymptomatic patients should have very little concern about findings, given the goal is to find and remove polyps.”
Researchers also tracked the use of sedatives during the procedure. Those in the intervention group required less midazolam (Versed) (average dose of 3.66 mg vs. 4.46 mg, P = .004). They also required less fentanyl (164 mcg vs. 186 mcg), but this finding was not statistically significant (P = .063).
“There was also a trend, not quite statistically significant, to improved prep quality,” Dr. Parker said. (In the intervention vs. the control group, 96% vs. 88% of subjects were rated as good or excellent in terms of prep quality, P = .27).
“This is important because a poor or inadequate prep leads to a need for a repeat procedure to ensure adequate screening,” he said. “If prep quality improves, that means fewer unnecessary repeated procedures.”
The researchers reported study limitations such as multiple endoscopists and sedation nurses and the variation in education levels of the participants.
The cost of the interactive program was not available.
According to Dr. Parker, Dartmouth-Hitchcock Medical Center now offers the education program to all colonoscopy patients, and a modified version is available for those undergoing upper endoscopies.
“Not all patients have adequate computer resources, and some patients simply choose not to watch,” he said. “But my impression is that those who watched the program are more relaxed during the informed consent process. However, we are not actively tracking outcomes such as procedure time or medication usage.”
No more studies of the program are planned at the institution, he said.
One of the study authors is an employee of Emmi Solutions, which provided the program for free for use in the study. The other authors reported no relevant disclosures. No study funding was reported.
SOURCE: Parker S et al. J Clin Gastroenterol. doi: 10.1097/MCG.0000000000000958
FROM THE JOURNAL OF CLINICAL GASTROENTEROLOGY
Key clinical point:
Major finding: Among program users, 58% reported being less anxious and required less midazolam during their procedures (average dose of 3.66 mg vs. 4.46 mg, P = .004).
Study details: A randomized, prospective study of 51 patients (control group) and 52 patients assigned to visit a website for a multimedia education program prior to colonoscopy.
Disclosures: One study author is an employee of the company that provided the program for free. The other study authors reported no relevant disclosures. No study funding was reported.
Source: Parker S et al. J Clin Gastroenterology. doi: 10.1097/MCG.0000000000000958.
Watchman device PREVAILs for stroke prevention
DENVER – Left atrial appendage closure using the Watchman device is as effective as warfarin in preventing strokes in patients with atrial fibrillation, but the strokes in Watchman recipients are 55% less likely to be disabling, according to a meta-analysis of 5-year outcomes in the PREVAIL and PROTECT AF randomized trials.
The device therapy showed additional advantages over warfarin: significantly reduced risks of mortality, non–procedure-related major bleeding, and hemorrhagic stroke, Saibal Kar, MD, reported in presenting the results of the meta-analysis at the Transcatheter Cardiovascular Therapeutics annual educational meeting.

“We have prevailed,” he declared, referring to device safety concerns that arose early on and have since been laid to rest.
The patient-level meta-analysis of 5-year outcomes included 1,114 patients with atrial fibrillation who were randomized 2:1 to the Watchman device or warfarin, with 4,343 patient-years of follow-up. This was a fairly high–stroke risk population, with CHA2DS2-VASc scores in the 3.6-3.9 range, and 40% of patients aged 75 years or more. At baseline, 23% of subjects had a history of stroke or transient ischemic attack.
At 5 years’ follow-up, the composite endpoint of all stroke or systemic embolism was the same in the two study arms. However, the rate of hemorrhagic stroke was 80% lower in the Watchman group, the risk of disabling or fatal stroke was reduced by 55%, the rate of cardiovascular or unexplained death was 41% lower, all-cause mortality was reduced by 27%, and postprocedure major bleeding was 52% less frequent in the device therapy group. All of these differences achieved statistical significance, the cardiologist reported at the meeting sponsored by the Cardiovascular Research Foundation.
On the downside, the rate of ischemic stroke trended higher in the Watchman group, although the 71% increase in relative risk didn’t achieve statistical significance (P = .08). Dr. Kar asserted that this unhappy trend was a statistical fluke resulting from a low number of events and an implausibly low ischemic stroke rate of 0.73% per year in the warfarin group.
“This is the lowest rate of ischemic stroke in any study of warfarin. In fact, if this was the ischemic stroke rate in any of the NOAC [novel oral anticoagulant] studies, none of those drugs would actually have been approved. Why did we get such an implausibly low ischemic stroke rate? It’s a function of lower numbers and larger confidence intervals,” he said.
Gregg W. Stone, MD, who moderated the discussion panel at the late-breaking clinical trial session, advised Dr. Kar to be less defensive about the ischemic stroke findings.
“I think we have to be a little less apologetic for the great outcomes in the warfarin arm in PREVAIL. We do these randomized trials, and we get what we get,” said Dr. Stone, professor of medicine at Columbia University in New York.
Stephen G. Ellis, MD, said he was particularly impressed with the reduced rate of disabling stroke in the Watchman group.
“Severity of stroke is important. I hadn’t seen that data before,” commented Dr. Ellis, professor of medicine and director of the cardiac catheterization laboratory at the Cleveland Clinic. “The overall message, I think, is that for the patients who would have been candidates to be enrolled in these trials, the device seems to be quite worthwhile. I take note of the overall benefit in terms of cardiovascular death and all-cause death.”
Robert J. Sommer, MD, said that in patients with high CHA2DS2-VASc scores and previous bleeding on oral anticoagulants, the new data show that the Watchman “is a no-brainer. The patients all want it, the physicians all want it. It’s a very easy decision to make.”
“But you get into other groups who may potentially be interested in the device – particularly the younger patients who are very active and don’t want to be on anticoagulation – I think the ischemic stroke rate in the device arm trending to be higher is a problem for them. And it’s certainly going to be a problem for their physicians. But as we go on, I think with further studies we’ll see expanded indications. Patients with CAD who potentially would need triple therapy – that’s a nice population to study in this area. We’ll also be seeing data on other devices that may have different ischemic stroke rates,” said Dr. Sommer, director of invasive adult congenital heart disease at Columbia University Medical Center.
“I find this data extraordinarily helpful as I think about my conversations with patients about stroke prevention,” said Brian K. Whisenant, MD, medical director of structural heart disease at the Intermountain Medical Center Heart Institute in Salt Lake City.
“I tell them we think of oral anticoagulants as first-line therapy based on a stroke rate of 1% per year or less in most datasets. The data for the Watchman device has been very consistent in that we have a stroke rate that’s a little bit higher, at 1.3%-1.8% per year. And we have extensive data for predicting the stroke rate in the absence of oral anticoagulation: In most of our patients, that rate is in excess of 5% per year. So while the Watchman device may not provide the absolute reduction in ischemic stroke rate that oral anticoagulants do, a stroke rate of less than 2% is a whole lot better than no therapy for many of these patients,” the cardiologist said.
Martin B. Leon, MD, opined that the ischemic stroke data cannot be explained away. But he added that the totality of the meta-analysis data gives him confidence that this is the appropriate treatment in these patients.
“It does leave open the question of whether we can do better with ischemic strokes. Some people are suggesting that maybe adjunctive pharmacotherapy – perhaps a low-dose NOAC – may be a reasonable option in some patients to get even better results. That’s something I believe is open for discussion,” said Dr. Leon, professor of medicine at Columbia University and director of the Center for Interventional Vascular Therapy at New York-Presbyterian/Columbia University Medical Center, New York.
Dr. Stone summed up: “There’s uniformity among the panel that there may be a slightly lower ischemic stroke rate with oral anticoagulation, and the NOACs probably provide some additional benefit, with an additional 50% reduction in hemorrhagic stroke, compared to warfarin. But that being said, I believe that left atrial appendage closure with the Watchman is the viable and now clearly safe approach for patients with any sort of contraindication or strong desire to avoid oral anticoagulation.”
The PREVAIL and PROTECT AF trials and meta-analysis were sponsored by Boston Scientific. Dr. Kar reported receiving research grants from and serving as a consultant to that company as well as Abbott Vascular.
Simultaneously with Dr. Kar’s presentation at TCT 2017, the findings were published online in the Journal of the American College of Cardiology.
SOURCE: Reddy VY et al. TCT 2017; J Am Coll Cardiol. 2017 Nov 4. pii:S0735-1097(17)41187-9. doi: 10.1016/j.jacc.2017.10.021.
DENVER – Left atrial appendage closure using the Watchman device is as effective as warfarin in preventing strokes in patients with atrial fibrillation, but the strokes in Watchman recipients are 55% less likely to be disabling, according to a meta-analysis of 5-year outcomes in the PREVAIL and PROTECT AF randomized trials.
The device therapy showed additional advantages over warfarin: significantly reduced risks of mortality, non–procedure-related major bleeding, and hemorrhagic stroke, Saibal Kar, MD, reported in presenting the results of the meta-analysis at the Transcatheter Cardiovascular Therapeutics annual educational meeting.
“We have prevailed,” he declared, referring to device safety concerns that arose early on and have since been laid to rest.
The patient-level meta-analysis of 5-year outcomes included 1,114 patients with atrial fibrillation who were randomized 2:1 to the Watchman device or warfarin, with 4,343 patient-years of follow-up. This was a fairly high–stroke risk population, with CHA2DS2-VASc scores in the 3.6-3.9 range, and 40% of patients aged 75 years or more. At baseline, 23% of subjects had a history of stroke or transient ischemic attack.
At 5 years’ follow-up, the composite endpoint of all stroke or systemic embolism was the same in the two study arms. However, the rate of hemorrhagic stroke was 80% lower in the Watchman group, the risk of disabling or fatal stroke was reduced by 55%, the rate of cardiovascular or unexplained death was 41% lower, all-cause mortality was reduced by 27%, and postprocedure major bleeding was 52% less frequent in the device therapy group. All of these differences achieved statistical significance, the cardiologist reported at the meeting sponsored by the Cardiovascular Research Foundation.
On the downside, the rate of ischemic stroke trended higher in the Watchman group, although the 71% increase in relative risk didn’t achieve statistical significance (P = .08). Dr. Kar asserted that this unhappy trend was a statistical fluke resulting from a low number of events and an implausibly low ischemic stroke rate of 0.73% per year in the warfarin group.
“This is the lowest rate of ischemic stroke in any study of warfarin. In fact, if this was the ischemic stroke rate in any of the NOAC [novel oral anticoagulant] studies, none of those drugs would actually have been approved. Why did we get such an implausibly low ischemic stroke rate? It’s a function of lower numbers and larger confidence intervals,” he said.
Gregg W. Stone, MD, who moderated the discussion panel at the late-breaking clinical trial session, advised Dr. Kar to be less defensive about the ischemic stroke findings.
“I think we have to be a little less apologetic for the great outcomes in the warfarin arm in PREVAIL. We do these randomized trials, and we get what we get,” said Dr. Stone, professor of medicine at Columbia University in New York.
Stephen G. Ellis, MD, said he was particularly impressed with the reduced rate of disabling stroke in the Watchman group.
“Severity of stroke is important. I hadn’t seen that data before,” commented Dr. Ellis, professor of medicine and director of the cardiac catheterization laboratory at the Cleveland Clinic. “The overall message, I think, is that for the patients who would have been candidates to be enrolled in these trials, the device seems to be quite worthwhile. I take note of the overall benefit in terms of cardiovascular death and all-cause death.”
Robert J. Sommer, MD, said that in patients with high CHA2DS2-VASc scores and previous bleeding on oral anticoagulants, the new data show that the Watchman “is a no-brainer. The patients all want it, the physicians all want it. It’s a very easy decision to make.”
“But you get into other groups who may potentially be interested in the device – particularly the younger patients who are very active and don’t want to be on anticoagulation – I think the ischemic stroke rate in the device arm trending to be higher is a problem for them. And it’s certainly going to be a problem for their physicians. But as we go on, I think with further studies we’ll see expanded indications. Patients with CAD who potentially would need triple therapy – that’s a nice population to study in this area. We’ll also be seeing data on other devices that may have different ischemic stroke rates,” said Dr. Sommer, director of invasive adult congenital heart disease at Columbia University Medical Center.
“I find this data extraordinarily helpful as I think about my conversations with patients about stroke prevention,” said Brian K. Whisenant, MD, medical director of structural heart disease at the Intermountain Medical Center Heart Institute in Salt Lake City.
“I tell them we think of oral anticoagulants as first-line therapy based on a stroke rate of 1% per year or less in most datasets. The data for the Watchman device has been very consistent in that we have a stroke rate that’s a little bit higher, at 1.3%-1.8% per year. And we have extensive data for predicting the stroke rate in the absence of oral anticoagulation: In most of our patients, that rate is in excess of 5% per year. So while the Watchman device may not provide the absolute reduction in ischemic stroke rate that oral anticoagulants do, a stroke rate of less than 2% is a whole lot better than no therapy for many of these patients,” the cardiologist said.
Martin B. Leon, MD, opined that the ischemic stroke data cannot be explained away. But he added that the totality of the meta-analysis data gives him confidence that this is the appropriate treatment in these patients.
“It does leave open the question of whether we can do better with ischemic strokes. Some people are suggesting that maybe adjunctive pharmacotherapy – perhaps a low-dose NOAC – may be a reasonable option in some patients to get even better results. That’s something I believe is open for discussion,” said Dr. Leon, professor of medicine at Columbia University and director of the Center for Interventional Vascular Therapy at New York-Presbyterian/Columbia University Medical Center, New York.
Dr. Stone summed up: “There’s uniformity among the panel that there may be a slightly lower ischemic stroke rate with oral anticoagulation, and the NOACs probably provide some additional benefit, with an additional 50% reduction in hemorrhagic stroke, compared to warfarin. But that being said, I believe that left atrial appendage closure with the Watchman is the viable and now clearly safe approach for patients with any sort of contraindication or strong desire to avoid oral anticoagulation.”
The PREVAIL and PROTECT AF trials and meta-analysis were sponsored by Boston Scientific. Dr. Kar reported receiving research grants from and serving as a consultant to that company as well as Abbott Vascular.
Simultaneously with Dr. Kar’s presentation at TCT 2017, the findings were published online in the Journal of the American College of Cardiology.
SOURCE: Reddy VY et al. TCT 2017; J Am Coll Cardiol. 2017 Nov 4. pii:S0735-1097(17)41187-9. doi: 10.1016/j.jacc.2017.10.021.
DENVER – Left atrial appendage closure using the Watchman device is as effective as warfarin in preventing strokes in patients with atrial fibrillation, but the strokes in Watchman recipients are 55% less likely to be disabling, according to a meta-analysis of 5-year outcomes in the PREVAIL and PROTECT AF randomized trials.
The device therapy showed additional advantages over warfarin: significantly reduced risks of mortality, non–procedure-related major bleeding, and hemorrhagic stroke, Saibal Kar, MD, reported in presenting the results of the meta-analysis at the Transcatheter Cardiovascular Therapeutics annual educational meeting.
“We have prevailed,” he declared, referring to device safety concerns that arose early on and have since been laid to rest.
The patient-level meta-analysis of 5-year outcomes included 1,114 patients with atrial fibrillation who were randomized 2:1 to the Watchman device or warfarin, with 4,343 patient-years of follow-up. This was a fairly high–stroke risk population, with CHA2DS2-VASc scores in the 3.6-3.9 range, and 40% of patients aged 75 years or more. At baseline, 23% of subjects had a history of stroke or transient ischemic attack.
At 5 years’ follow-up, the composite endpoint of all stroke or systemic embolism was the same in the two study arms. However, the rate of hemorrhagic stroke was 80% lower in the Watchman group, the risk of disabling or fatal stroke was reduced by 55%, the rate of cardiovascular or unexplained death was 41% lower, all-cause mortality was reduced by 27%, and postprocedure major bleeding was 52% less frequent in the device therapy group. All of these differences achieved statistical significance, the cardiologist reported at the meeting sponsored by the Cardiovascular Research Foundation.
On the downside, the rate of ischemic stroke trended higher in the Watchman group, although the 71% increase in relative risk didn’t achieve statistical significance (P = .08). Dr. Kar asserted that this unhappy trend was a statistical fluke resulting from a low number of events and an implausibly low ischemic stroke rate of 0.73% per year in the warfarin group.
“This is the lowest rate of ischemic stroke in any study of warfarin. In fact, if this was the ischemic stroke rate in any of the NOAC [novel oral anticoagulant] studies, none of those drugs would actually have been approved. Why did we get such an implausibly low ischemic stroke rate? It’s a function of lower numbers and larger confidence intervals,” he said.
Gregg W. Stone, MD, who moderated the discussion panel at the late-breaking clinical trial session, advised Dr. Kar to be less defensive about the ischemic stroke findings.
“I think we have to be a little less apologetic for the great outcomes in the warfarin arm in PREVAIL. We do these randomized trials, and we get what we get,” said Dr. Stone, professor of medicine at Columbia University in New York.
Stephen G. Ellis, MD, said he was particularly impressed with the reduced rate of disabling stroke in the Watchman group.
“Severity of stroke is important. I hadn’t seen that data before,” commented Dr. Ellis, professor of medicine and director of the cardiac catheterization laboratory at the Cleveland Clinic. “The overall message, I think, is that for the patients who would have been candidates to be enrolled in these trials, the device seems to be quite worthwhile. I take note of the overall benefit in terms of cardiovascular death and all-cause death.”
Robert J. Sommer, MD, said that in patients with high CHA2DS2-VASc scores and previous bleeding on oral anticoagulants, the new data show that the Watchman “is a no-brainer. The patients all want it, the physicians all want it. It’s a very easy decision to make.”
“But you get into other groups who may potentially be interested in the device – particularly the younger patients who are very active and don’t want to be on anticoagulation – I think the ischemic stroke rate in the device arm trending to be higher is a problem for them. And it’s certainly going to be a problem for their physicians. But as we go on, I think with further studies we’ll see expanded indications. Patients with CAD who potentially would need triple therapy – that’s a nice population to study in this area. We’ll also be seeing data on other devices that may have different ischemic stroke rates,” said Dr. Sommer, director of invasive adult congenital heart disease at Columbia University Medical Center.
“I find this data extraordinarily helpful as I think about my conversations with patients about stroke prevention,” said Brian K. Whisenant, MD, medical director of structural heart disease at the Intermountain Medical Center Heart Institute in Salt Lake City.
“I tell them we think of oral anticoagulants as first-line therapy based on a stroke rate of 1% per year or less in most datasets. The data for the Watchman device has been very consistent in that we have a stroke rate that’s a little bit higher, at 1.3%-1.8% per year. And we have extensive data for predicting the stroke rate in the absence of oral anticoagulation: In most of our patients, that rate is in excess of 5% per year. So while the Watchman device may not provide the absolute reduction in ischemic stroke rate that oral anticoagulants do, a stroke rate of less than 2% is a whole lot better than no therapy for many of these patients,” the cardiologist said.
Martin B. Leon, MD, opined that the ischemic stroke data cannot be explained away. But he added that the totality of the meta-analysis data gives him confidence that this is the appropriate treatment in these patients.
“It does leave open the question of whether we can do better with ischemic strokes. Some people are suggesting that maybe adjunctive pharmacotherapy – perhaps a low-dose NOAC – may be a reasonable option in some patients to get even better results. That’s something I believe is open for discussion,” said Dr. Leon, professor of medicine at Columbia University and director of the Center for Interventional Vascular Therapy at New York-Presbyterian/Columbia University Medical Center, New York.
Dr. Stone summed up: “There’s uniformity among the panel that there may be a slightly lower ischemic stroke rate with oral anticoagulation, and the NOACs probably provide some additional benefit, with an additional 50% reduction in hemorrhagic stroke, compared to warfarin. But that being said, I believe that left atrial appendage closure with the Watchman is the viable and now clearly safe approach for patients with any sort of contraindication or strong desire to avoid oral anticoagulation.”
The PREVAIL and PROTECT AF trials and meta-analysis were sponsored by Boston Scientific. Dr. Kar reported receiving research grants from and serving as a consultant to that company as well as Abbott Vascular.
Simultaneously with Dr. Kar’s presentation at TCT 2017, the findings were published online in the Journal of the American College of Cardiology.
SOURCE: Reddy VY et al. TCT 2017; J Am Coll Cardiol. 2017 Nov 4. pii:S0735-1097(17)41187-9. doi: 10.1016/j.jacc.2017.10.021.
REPORTING FROM TCT 2017
Key clinical point:
Major finding: All-cause mortality was reduced by 27% in patients randomized to left atrial appendage closure with the Watchman device, compared with those assigned to warfarin.
Study details: This patient-level meta-analysis included 5-year follow-up data on 1,114 patients with atrial fibrillation at increased stroke risk who were randomized 2:1 to the Watchman device or warfarin.
Disclosures: The study presenter reported receiving research grants from and serving as a consultant to study sponsor Boston Scientific.

Mutations linked to checkpoint inhibitor response in RCC
in a derivation and validation study involving a total of 98 patients.
This finding “has important implications as a molecular tool for considering immunotherapy responsiveness” in patients with ccRCC and possibly patients with other cancer types, wrote Eliezer M. Van Allen, MD, of Dana Farber Cancer Institute in Boston and coauthors.
The derivation cohort included 35 patients with metastatic ccRCC treated with nivolumab in a prospective clinical trial. Genome sequencing of pretreatment tumor specimens showed that improved survival after treatment was significantly linked with truncating mutations in a gene, PBRM1, that codes for a protein in the SWI/SNF chromatin-remodeling complex. Patients in the derivation cohort who had these mutations were nearly 13-fold more likely to have clinical benefit from treatment, compared with those without these mutations.
The validation study included specimens and treatment-outcome results from 63 patients with metastatic ccRCC treated with either nivolumab or a different checkpoint inhibitor, such as atezolizumab (Tecentriq). In the validation study, PBRM1 mutations linked with a sixfold higher rate of clinical benefit from treatment.
The researchers noted that the types of mutations they identified as likely involved occur in more than 20% of all cancer types. Results from mouse studies have suggested that tumor cells with these types of mutations are more sensitive to T cell–mediated cytotoxicity, an observation that “lends a mechanistic basis” to the observed findings.
The study received funding in part from Bristol-Myers Squibb, the company that markets nivolumab (Obdivo). Several researchers involved in this study have received honoraria and research support from Bristol-Myers Squibb and from several other drug companies.
[email protected]
On Twitter @mitchelzoler
SOURCE: Miao D et al. Science. 2018 Jan 4. doi: 10.1126/science.aan5951
in a derivation and validation study involving a total of 98 patients.
This finding “has important implications as a molecular tool for considering immunotherapy responsiveness” in patients with ccRCC and possibly patients with other cancer types, wrote Eliezer M. Van Allen, MD, of Dana Farber Cancer Institute in Boston and coauthors.
The derivation cohort included 35 patients with metastatic ccRCC treated with nivolumab in a prospective clinical trial. Genome sequencing of pretreatment tumor specimens showed that improved survival after treatment was significantly linked with truncating mutations in a gene, PBRM1, that codes for a protein in the SWI/SNF chromatin-remodeling complex. Patients in the derivation cohort who had these mutations were nearly 13-fold more likely to have clinical benefit from treatment, compared with those without these mutations.
The validation study included specimens and treatment-outcome results from 63 patients with metastatic ccRCC treated with either nivolumab or a different checkpoint inhibitor, such as atezolizumab (Tecentriq). In the validation study, PBRM1 mutations linked with a sixfold higher rate of clinical benefit from treatment.
The researchers noted that the types of mutations they identified as likely involved occur in more than 20% of all cancer types. Results from mouse studies have suggested that tumor cells with these types of mutations are more sensitive to T cell–mediated cytotoxicity, an observation that “lends a mechanistic basis” to the observed findings.
The study received funding in part from Bristol-Myers Squibb, the company that markets nivolumab (Obdivo). Several researchers involved in this study have received honoraria and research support from Bristol-Myers Squibb and from several other drug companies.
[email protected]
On Twitter @mitchelzoler
SOURCE: Miao D et al. Science. 2018 Jan 4. doi: 10.1126/science.aan5951
in a derivation and validation study involving a total of 98 patients.
This finding “has important implications as a molecular tool for considering immunotherapy responsiveness” in patients with ccRCC and possibly patients with other cancer types, wrote Eliezer M. Van Allen, MD, of Dana Farber Cancer Institute in Boston and coauthors.
The derivation cohort included 35 patients with metastatic ccRCC treated with nivolumab in a prospective clinical trial. Genome sequencing of pretreatment tumor specimens showed that improved survival after treatment was significantly linked with truncating mutations in a gene, PBRM1, that codes for a protein in the SWI/SNF chromatin-remodeling complex. Patients in the derivation cohort who had these mutations were nearly 13-fold more likely to have clinical benefit from treatment, compared with those without these mutations.
The validation study included specimens and treatment-outcome results from 63 patients with metastatic ccRCC treated with either nivolumab or a different checkpoint inhibitor, such as atezolizumab (Tecentriq). In the validation study, PBRM1 mutations linked with a sixfold higher rate of clinical benefit from treatment.
The researchers noted that the types of mutations they identified as likely involved occur in more than 20% of all cancer types. Results from mouse studies have suggested that tumor cells with these types of mutations are more sensitive to T cell–mediated cytotoxicity, an observation that “lends a mechanistic basis” to the observed findings.
The study received funding in part from Bristol-Myers Squibb, the company that markets nivolumab (Obdivo). Several researchers involved in this study have received honoraria and research support from Bristol-Myers Squibb and from several other drug companies.
[email protected]
On Twitter @mitchelzoler
SOURCE: Miao D et al. Science. 2018 Jan 4. doi: 10.1126/science.aan5951
FROM SCIENCE
Key clinical point: Mutations in PBRM1 linked with better survival after immune checkpoint inhibitor therapy.
Major finding: Patients with a PBRM1 mutation were 6- to 13-fold more likely to have clinical benefit from checkpoint inhibitor treatment.
Study details: Derivation and validation studies that included 98 total patients with metastatic clear cell renal cell carcinoma.
Disclosures: The study received funding in part from Bristol-Myers Squibb, the company that markets nivolumab (Obdivo). Several researchers involved in this study have received honoraria and research support from Bristol-Myers Squibb and from several other drug companies.
Source: Miao D et al. Science. 2018 Jan 4. doi: 10.1126/science.aan5951.
See for yourself
About 800 million radiology exams were performed in this country in the past year, and they generated approximately 60 billion images, according to an article published in 2017 in the Wall Street Journal (“No need for radiologists to be negative on AI,” by Greg Ip, Nov. 24, 2017). How many of those millions of radiology studies did you order? And how many of the scores of images you requested did you see with your own two eyes? In fact, how many of the radiologists’ reports that were sent to you did you read in their entirety? How often did you just skip over the radiologist’s CYA disclaimers and simply read the final summary, “exam negative”?

I enjoy the challenge of interpreting x-ray images. In fact, I toyed with becoming a pediatric radiologist, but that career path would have meant settling in or near a large city, a compromise my wife and I were unwilling to make. I hoped to continue my habit of looking at all my patients’ x-rays, but because my practice was not in or near the hospital, I reluctantly had to bend my rules and admit I didn’t see every image I had ordered. But, I did read every report in its entirety. In one case, an offhand comment buried in the middle of the radiologist’s report referring to the “residual barium from a previous study” caught my eye, because I knew the patient hadn’t had a previous contrast study. Unfortunately, the neuroblastoma that the radiologist had missed initially, and I had seen the next day, never responded to treatment.
Toward the end of my career, digital imagery allowed me to view my patients’ x-rays without having to leave my desk, which got me closer to my goal of seeing all my patients’ studies. However, the advent of computerized axial tomography and magnetic resonance imaging meant that an increasing number of studies pushed my anatomic knowledge beyond its limits.
I suspect that many of you benefited from the if-you-order-it-look-at-it mantra during your training. How many of you have continued to follow the dictum? With the advent of digitized imagery, there is really little excuse for not taking a minute or 2 to pull up your patients’ images on your desktop. One could argue that looking inside your patient is part of a complete exam. Forcing yourself to take that extra step and look at the study may nudge you into thinking twice about whether you really needed the information the imaging study might add to the diagnostic process. Was your click to order the study just a reflex subliminally related to the fear of a lawsuit? Was it important enough to deserve a firsthand look?
At the very least, being able to say, “I’ve looked at your x-rays myself, and they look fine” may be more comforting to your patient than a third-hand relay of a “negative reading” performed by someone whom they have likely never met.

Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
About 800 million radiology exams were performed in this country in the past year, and they generated approximately 60 billion images, according to an article published in 2017 in the Wall Street Journal (“No need for radiologists to be negative on AI,” by Greg Ip, Nov. 24, 2017). How many of those millions of radiology studies did you order? And how many of the scores of images you requested did you see with your own two eyes? In fact, how many of the radiologists’ reports that were sent to you did you read in their entirety? How often did you just skip over the radiologist’s CYA disclaimers and simply read the final summary, “exam negative”?
I enjoy the challenge of interpreting x-ray images. In fact, I toyed with becoming a pediatric radiologist, but that career path would have meant settling in or near a large city, a compromise my wife and I were unwilling to make. I hoped to continue my habit of looking at all my patients’ x-rays, but because my practice was not in or near the hospital, I reluctantly had to bend my rules and admit I didn’t see every image I had ordered. But, I did read every report in its entirety. In one case, an offhand comment buried in the middle of the radiologist’s report referring to the “residual barium from a previous study” caught my eye, because I knew the patient hadn’t had a previous contrast study. Unfortunately, the neuroblastoma that the radiologist had missed initially, and I had seen the next day, never responded to treatment.
Toward the end of my career, digital imagery allowed me to view my patients’ x-rays without having to leave my desk, which got me closer to my goal of seeing all my patients’ studies. However, the advent of computerized axial tomography and magnetic resonance imaging meant that an increasing number of studies pushed my anatomic knowledge beyond its limits.
I suspect that many of you benefited from the if-you-order-it-look-at-it mantra during your training. How many of you have continued to follow the dictum? With the advent of digitized imagery, there is really little excuse for not taking a minute or 2 to pull up your patients’ images on your desktop. One could argue that looking inside your patient is part of a complete exam. Forcing yourself to take that extra step and look at the study may nudge you into thinking twice about whether you really needed the information the imaging study might add to the diagnostic process. Was your click to order the study just a reflex subliminally related to the fear of a lawsuit? Was it important enough to deserve a firsthand look?
At the very least, being able to say, “I’ve looked at your x-rays myself, and they look fine” may be more comforting to your patient than a third-hand relay of a “negative reading” performed by someone whom they have likely never met.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
About 800 million radiology exams were performed in this country in the past year, and they generated approximately 60 billion images, according to an article published in 2017 in the Wall Street Journal (“No need for radiologists to be negative on AI,” by Greg Ip, Nov. 24, 2017). How many of those millions of radiology studies did you order? And how many of the scores of images you requested did you see with your own two eyes? In fact, how many of the radiologists’ reports that were sent to you did you read in their entirety? How often did you just skip over the radiologist’s CYA disclaimers and simply read the final summary, “exam negative”?
I enjoy the challenge of interpreting x-ray images. In fact, I toyed with becoming a pediatric radiologist, but that career path would have meant settling in or near a large city, a compromise my wife and I were unwilling to make. I hoped to continue my habit of looking at all my patients’ x-rays, but because my practice was not in or near the hospital, I reluctantly had to bend my rules and admit I didn’t see every image I had ordered. But, I did read every report in its entirety. In one case, an offhand comment buried in the middle of the radiologist’s report referring to the “residual barium from a previous study” caught my eye, because I knew the patient hadn’t had a previous contrast study. Unfortunately, the neuroblastoma that the radiologist had missed initially, and I had seen the next day, never responded to treatment.
Toward the end of my career, digital imagery allowed me to view my patients’ x-rays without having to leave my desk, which got me closer to my goal of seeing all my patients’ studies. However, the advent of computerized axial tomography and magnetic resonance imaging meant that an increasing number of studies pushed my anatomic knowledge beyond its limits.
I suspect that many of you benefited from the if-you-order-it-look-at-it mantra during your training. How many of you have continued to follow the dictum? With the advent of digitized imagery, there is really little excuse for not taking a minute or 2 to pull up your patients’ images on your desktop. One could argue that looking inside your patient is part of a complete exam. Forcing yourself to take that extra step and look at the study may nudge you into thinking twice about whether you really needed the information the imaging study might add to the diagnostic process. Was your click to order the study just a reflex subliminally related to the fear of a lawsuit? Was it important enough to deserve a firsthand look?
At the very least, being able to say, “I’ve looked at your x-rays myself, and they look fine” may be more comforting to your patient than a third-hand relay of a “negative reading” performed by someone whom they have likely never met.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
DNA sequencing could help identify relapse risk in treated AML
ATLANTA – Clinicians may be able to get a jump on identifying risk factors for relapse among adults with acute myeloid leukemia (AML) in first complete remission through the use of next-generation DNA sequencing, investigators reported.
Among 430 adults with AML with somatic driver mutations persistent in bone marrow during morphological complete remission (CR) following induction therapy, the presence of minimal residual disease (MRD) bearing specific disease-related mutations on next-generation sequencing (NGS) was significantly associated with both the cumulative incidence of relapse and with overall survival. Tim Grob, MD, of Erasmus University Medical Center in Rotterdam, the Netherlands, reported the findings during a late-breaking abstract session at the annual meeting of the American Society of Hematology.

By excluding three common AML mutations in genes commonly associated with clonal hematopoiesis – DNMT3A, TET2, and ASXL1 (collectively, DTA) – Dr. Grob and his colleagues at centers in the Netherlands, Belgium, and Switzerland were able to demonstrate that non-DTA mutations present in the marrow of patients in CR are highly predictive for relapse within 5 years and for worse overall survival.
They also showed that mutations associated with clonal hematopoiesis (the presence of small, preleukemic clones) in CR is not significantly associated with risk of relapse.
More than 80% of patients with AML are able to have a CR after induction therapy, but a significant proportion of patients will also experience relapse. Investigators have yet to nail down which leukemia-specific mutations that linger in patients with CR may be responsible for subsequent relapses, Dr. Grob said.
To get a better handle on which residual mutations may signal the need for extra vigilance or additional therapy in patients in CR after two cycles of induction therapy, the investigators used targeted next-generation (high-throughput) sequencing at the time of diagnosis and first CR in 430 patients enrolled in joint Dutch/Swiss clinical trials. The median patient age was 51.
The investigators screened marrow samples using a commercially available gene panel (Illumina) covering 54 genes that are commonly mutated in myeloid malignancies.
They divided the patients into a training cohort (283 patients) and a validation set (147) for confirmation of results.
About half of all patients in the training cohort (51.4%) had persistent mutations in bone marrow that occurred with highly variable variant allele frequencies. The most common mutations were in the DTA group with the most frequently mutated gene being DNMT3A (78.7% variant allele frequency), followed by TET2 (54.2%) and ASXL1 (51.6%).
Mutations in DTA genes in this cohort were not associated with the incidence of relapse at any variant allele frequency cut-off point used, which indicated that these mutations represented a stage of clonal hematopoiesis rather than early relapse signals.
However, among patients who had persistent DTA mutations, there was significant correlation with a risk for relapse when they also had persistence of any other non-DTA mutations. The cumulative 5-year incidence of relapse in patients with both persistent DTA and non-DTA mutations was 76.4%, compared with 39.4% for those without other, non-DTA mutations (P = .002).
Also in the training cohort, persistent non-DTA mutations (NGS MRD) were found to be highly associated with the risk of relapse with a subdistribution hazard ratio (SHR) of 1.85 (P = .001). In the validation set the effect was even stronger, with an SHR or 2.81 (P less than .001).
When data from the training and validation cohort were combined, the 5-year cumulative incidence of relapse was 58.3% for non-DTA mutation, vs. 33.9% (P less than .001).
NGS MRD was also predictive of overall survival, with a hazard ratio in the training cohort of 1.64 (P = .012) and an HR in the validation cohort of 3.08 (P less than .001).
In multivariable analysis of all 430 patients, adjusted for age, white blood cell count, 2017 European LeukemiaNet risk category, and number of induction cycles need to achieve CR, NGS MRD was an independent prognostic factor for both relapse (SHR 1.89, P less than .001) and overall survival (HR 1.64 P = .003).
When the investigators conducted a sensitivity analysis with time-dependent correction for allogeneic stem cell transplantation, they found that NGS MRD was still significantly prognostic for both relapse and survival.
The study was supported by the Dutch Cancer Society, the Haemato-Oncology Foundation for Adults in the Netherlands, the Swiss Group for Clinical Cancer Research, and The Netherlands Organization for Health Research and Development. Dr. Grob reported having no relevant disclosures.
SOURCE: Jongen-Lavrencic M et al. ASH 2017 Abstract LBA 5.
ATLANTA – Clinicians may be able to get a jump on identifying risk factors for relapse among adults with acute myeloid leukemia (AML) in first complete remission through the use of next-generation DNA sequencing, investigators reported.
Among 430 adults with AML with somatic driver mutations persistent in bone marrow during morphological complete remission (CR) following induction therapy, the presence of minimal residual disease (MRD) bearing specific disease-related mutations on next-generation sequencing (NGS) was significantly associated with both the cumulative incidence of relapse and with overall survival. Tim Grob, MD, of Erasmus University Medical Center in Rotterdam, the Netherlands, reported the findings during a late-breaking abstract session at the annual meeting of the American Society of Hematology.
By excluding three common AML mutations in genes commonly associated with clonal hematopoiesis – DNMT3A, TET2, and ASXL1 (collectively, DTA) – Dr. Grob and his colleagues at centers in the Netherlands, Belgium, and Switzerland were able to demonstrate that non-DTA mutations present in the marrow of patients in CR are highly predictive for relapse within 5 years and for worse overall survival.
They also showed that mutations associated with clonal hematopoiesis (the presence of small, preleukemic clones) in CR is not significantly associated with risk of relapse.
More than 80% of patients with AML are able to have a CR after induction therapy, but a significant proportion of patients will also experience relapse. Investigators have yet to nail down which leukemia-specific mutations that linger in patients with CR may be responsible for subsequent relapses, Dr. Grob said.
To get a better handle on which residual mutations may signal the need for extra vigilance or additional therapy in patients in CR after two cycles of induction therapy, the investigators used targeted next-generation (high-throughput) sequencing at the time of diagnosis and first CR in 430 patients enrolled in joint Dutch/Swiss clinical trials. The median patient age was 51.
The investigators screened marrow samples using a commercially available gene panel (Illumina) covering 54 genes that are commonly mutated in myeloid malignancies.
They divided the patients into a training cohort (283 patients) and a validation set (147) for confirmation of results.
About half of all patients in the training cohort (51.4%) had persistent mutations in bone marrow that occurred with highly variable variant allele frequencies. The most common mutations were in the DTA group with the most frequently mutated gene being DNMT3A (78.7% variant allele frequency), followed by TET2 (54.2%) and ASXL1 (51.6%).
Mutations in DTA genes in this cohort were not associated with the incidence of relapse at any variant allele frequency cut-off point used, which indicated that these mutations represented a stage of clonal hematopoiesis rather than early relapse signals.
However, among patients who had persistent DTA mutations, there was significant correlation with a risk for relapse when they also had persistence of any other non-DTA mutations. The cumulative 5-year incidence of relapse in patients with both persistent DTA and non-DTA mutations was 76.4%, compared with 39.4% for those without other, non-DTA mutations (P = .002).
Also in the training cohort, persistent non-DTA mutations (NGS MRD) were found to be highly associated with the risk of relapse with a subdistribution hazard ratio (SHR) of 1.85 (P = .001). In the validation set the effect was even stronger, with an SHR or 2.81 (P less than .001).
When data from the training and validation cohort were combined, the 5-year cumulative incidence of relapse was 58.3% for non-DTA mutation, vs. 33.9% (P less than .001).
NGS MRD was also predictive of overall survival, with a hazard ratio in the training cohort of 1.64 (P = .012) and an HR in the validation cohort of 3.08 (P less than .001).
In multivariable analysis of all 430 patients, adjusted for age, white blood cell count, 2017 European LeukemiaNet risk category, and number of induction cycles need to achieve CR, NGS MRD was an independent prognostic factor for both relapse (SHR 1.89, P less than .001) and overall survival (HR 1.64 P = .003).
When the investigators conducted a sensitivity analysis with time-dependent correction for allogeneic stem cell transplantation, they found that NGS MRD was still significantly prognostic for both relapse and survival.
The study was supported by the Dutch Cancer Society, the Haemato-Oncology Foundation for Adults in the Netherlands, the Swiss Group for Clinical Cancer Research, and The Netherlands Organization for Health Research and Development. Dr. Grob reported having no relevant disclosures.
SOURCE: Jongen-Lavrencic M et al. ASH 2017 Abstract LBA 5.
ATLANTA – Clinicians may be able to get a jump on identifying risk factors for relapse among adults with acute myeloid leukemia (AML) in first complete remission through the use of next-generation DNA sequencing, investigators reported.
Among 430 adults with AML with somatic driver mutations persistent in bone marrow during morphological complete remission (CR) following induction therapy, the presence of minimal residual disease (MRD) bearing specific disease-related mutations on next-generation sequencing (NGS) was significantly associated with both the cumulative incidence of relapse and with overall survival. Tim Grob, MD, of Erasmus University Medical Center in Rotterdam, the Netherlands, reported the findings during a late-breaking abstract session at the annual meeting of the American Society of Hematology.
By excluding three common AML mutations in genes commonly associated with clonal hematopoiesis – DNMT3A, TET2, and ASXL1 (collectively, DTA) – Dr. Grob and his colleagues at centers in the Netherlands, Belgium, and Switzerland were able to demonstrate that non-DTA mutations present in the marrow of patients in CR are highly predictive for relapse within 5 years and for worse overall survival.
They also showed that mutations associated with clonal hematopoiesis (the presence of small, preleukemic clones) in CR is not significantly associated with risk of relapse.
More than 80% of patients with AML are able to have a CR after induction therapy, but a significant proportion of patients will also experience relapse. Investigators have yet to nail down which leukemia-specific mutations that linger in patients with CR may be responsible for subsequent relapses, Dr. Grob said.
To get a better handle on which residual mutations may signal the need for extra vigilance or additional therapy in patients in CR after two cycles of induction therapy, the investigators used targeted next-generation (high-throughput) sequencing at the time of diagnosis and first CR in 430 patients enrolled in joint Dutch/Swiss clinical trials. The median patient age was 51.
The investigators screened marrow samples using a commercially available gene panel (Illumina) covering 54 genes that are commonly mutated in myeloid malignancies.
They divided the patients into a training cohort (283 patients) and a validation set (147) for confirmation of results.
About half of all patients in the training cohort (51.4%) had persistent mutations in bone marrow that occurred with highly variable variant allele frequencies. The most common mutations were in the DTA group with the most frequently mutated gene being DNMT3A (78.7% variant allele frequency), followed by TET2 (54.2%) and ASXL1 (51.6%).
Mutations in DTA genes in this cohort were not associated with the incidence of relapse at any variant allele frequency cut-off point used, which indicated that these mutations represented a stage of clonal hematopoiesis rather than early relapse signals.
However, among patients who had persistent DTA mutations, there was significant correlation with a risk for relapse when they also had persistence of any other non-DTA mutations. The cumulative 5-year incidence of relapse in patients with both persistent DTA and non-DTA mutations was 76.4%, compared with 39.4% for those without other, non-DTA mutations (P = .002).
Also in the training cohort, persistent non-DTA mutations (NGS MRD) were found to be highly associated with the risk of relapse with a subdistribution hazard ratio (SHR) of 1.85 (P = .001). In the validation set the effect was even stronger, with an SHR or 2.81 (P less than .001).
When data from the training and validation cohort were combined, the 5-year cumulative incidence of relapse was 58.3% for non-DTA mutation, vs. 33.9% (P less than .001).
NGS MRD was also predictive of overall survival, with a hazard ratio in the training cohort of 1.64 (P = .012) and an HR in the validation cohort of 3.08 (P less than .001).
In multivariable analysis of all 430 patients, adjusted for age, white blood cell count, 2017 European LeukemiaNet risk category, and number of induction cycles need to achieve CR, NGS MRD was an independent prognostic factor for both relapse (SHR 1.89, P less than .001) and overall survival (HR 1.64 P = .003).
When the investigators conducted a sensitivity analysis with time-dependent correction for allogeneic stem cell transplantation, they found that NGS MRD was still significantly prognostic for both relapse and survival.
The study was supported by the Dutch Cancer Society, the Haemato-Oncology Foundation for Adults in the Netherlands, the Swiss Group for Clinical Cancer Research, and The Netherlands Organization for Health Research and Development. Dr. Grob reported having no relevant disclosures.
SOURCE: Jongen-Lavrencic M et al. ASH 2017 Abstract LBA 5.
REPORTING FROM ASH 2017
Key clinical point:
Major finding: The presence of any non-DTA mutation after CR was an independent prognostic factor for relapse (SHR 1.89) and overall survival (HR 1.64).
Study details: Prospective analysis of bone marrow samples from 430 patients with AML at diagnosis and in first complete remission.
Disclosures: The study was supported by the Dutch Cancer Society, the Haemato-Oncology Foundation for Adults in the Netherlands, the Swiss Group for Clinical Cancer Research, and The Netherlands Organization for Health Research and Development. Dr. Grob reported having no relevant disclosures.
Source: Jongen-Lavrencic M et al. ASH 2017 Abstract LBA 5.
How to manage a patient presenting with syncope
Case
A 38-year-old construction worker without significant medical history presents following witnessed syncope at her job, after standing for at least 2 hours on a particularly warm day. She reported an episode of syncope under similar circumstances 2 months prior. With each episode, she experienced “tunneling” of peripheral vision, then loss of consciousness without palpitations or incontinence. Her physical exam, vital signs (including orthostatic blood pressures), labs, and ECG were unremarkable.
Brief overview

The American College of Cardiology, American Heart Association, and Heart Rhythm Society guidelines define syncope as “a symptom that presents with an abrupt, transient, complete loss of consciousness, associated with inability to maintain postural tone, with rapid and spontaneous recovery” with cerebral hypoperfusion as the presumed mechanism.1 Furthermore, “there should not be clinical features of other nonsyncope causes of loss of consciousness, such as seizure, antecedent head trauma, or apparent loss of consciousness (that is, pseudosyncope).”1
A careful history revolving around the patient’s behavior prior to, during, and following the event, a thorough past medical history, and a review of current medications are essential. Potential obstacles in obtaining details of the event include lack of witnesses, patient’s inability to recall the experience, and inaccurate description of convulsive syncope as a “seizure” by bystanders.2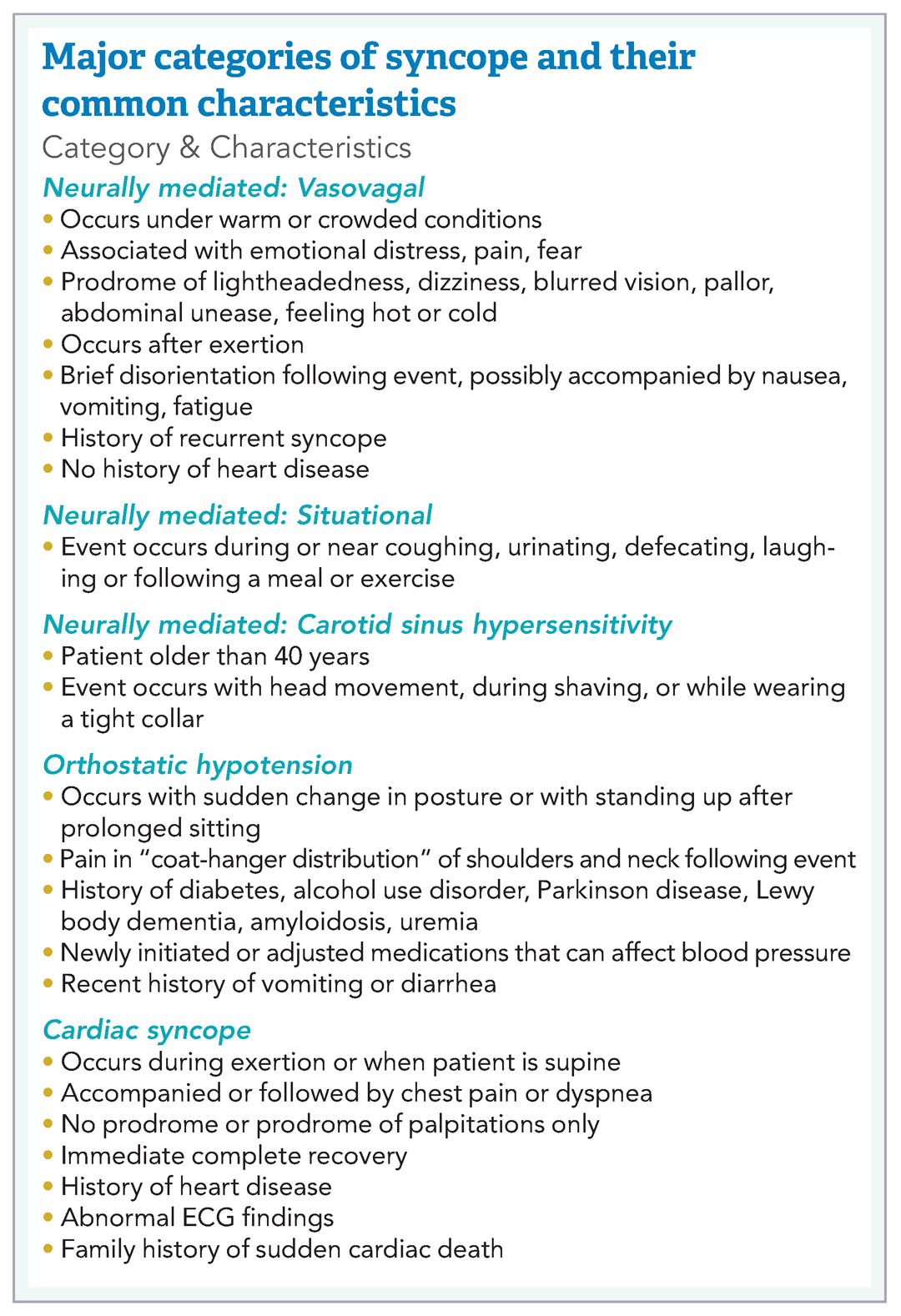
Overview of data
Obtaining a detailed history is crucial to understanding both the etiology of the syncopal event and determining which patients are at high risk for adverse outcomes. The etiology of syncope can be determined by history alone in 26% of patients younger than 65 years.3 Data on the prevalence of syncope by cause varies widely. As a general rule, in younger patients, especially those under 40 years of age, neurally mediated syncope is most common. As patients age, orthostatic hypotension and cardiac causes (including arrhythmias and structural diseases) occur more frequently, though neurally mediated syncope is still the most common.

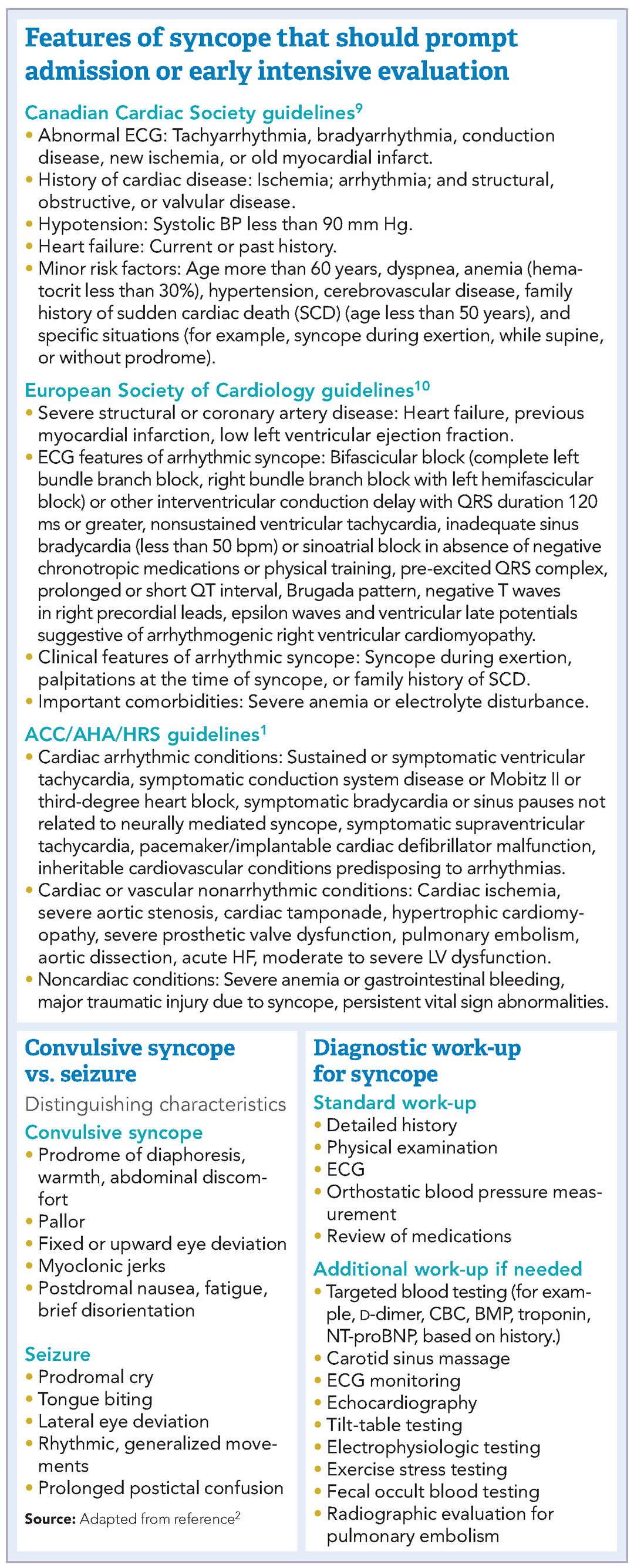
Many of these predictors, however, would raise the clinical suspicion of most hospitalists for adverse outcomes in their hospitalized patients independent of the presence or absence of syncope. In fact, a meta-analysis has concluded that “None of the evaluated prediction tools (SFSR, EGSYS) performed better than clinical judgment in identifying serious outcomes during emergency department stay, and at 10 and 30 days after syncope.”6
Once the patient is hospitalized, further evaluation should be based on a careful history and physical examination. Standard evaluation also includes careful review of medications, an ECG to exclude findings suggestive of arrhythmias as well as structural or coronary artery disease, and orthostatic blood pressure measurements.1 Additional tests should be considered as deemed appropriate. For example, in patients over 40 years of age without history of carotid artery disease or stroke and in whom no carotid artery bruit is appreciated, a carotid sinus massage may be considered. The correct technique is to massage the sinus on the right then left, each for 5 seconds in both supine and standing positions with continuous heart rate and frequent blood pressure monitoring. Reproduction of syncope, especially concurrent with a cardiac pause of greater than 3 seconds and a systolic blood pressure drop of greater than 50 mmHg, is considered a positive test. Tilt-table testing should be considered in those for whom neurally mediated syncope is suspected but not confirmed, or in patients who might benefit from further elucidation of their prodromal symptoms.

Of note, a study recently published in the New England Journal of Medicine suggests that the prevalence of PE in patients (median age, 80 years) presenting with a first episode of syncope was 17%, a rate that is substantially higher than historically presumed.8 Although the prevalence of PE was highest among patients presenting with syncope of unclear origin (25%), nearly 13% of patients with other explanations for syncope also had PE.
Application of data
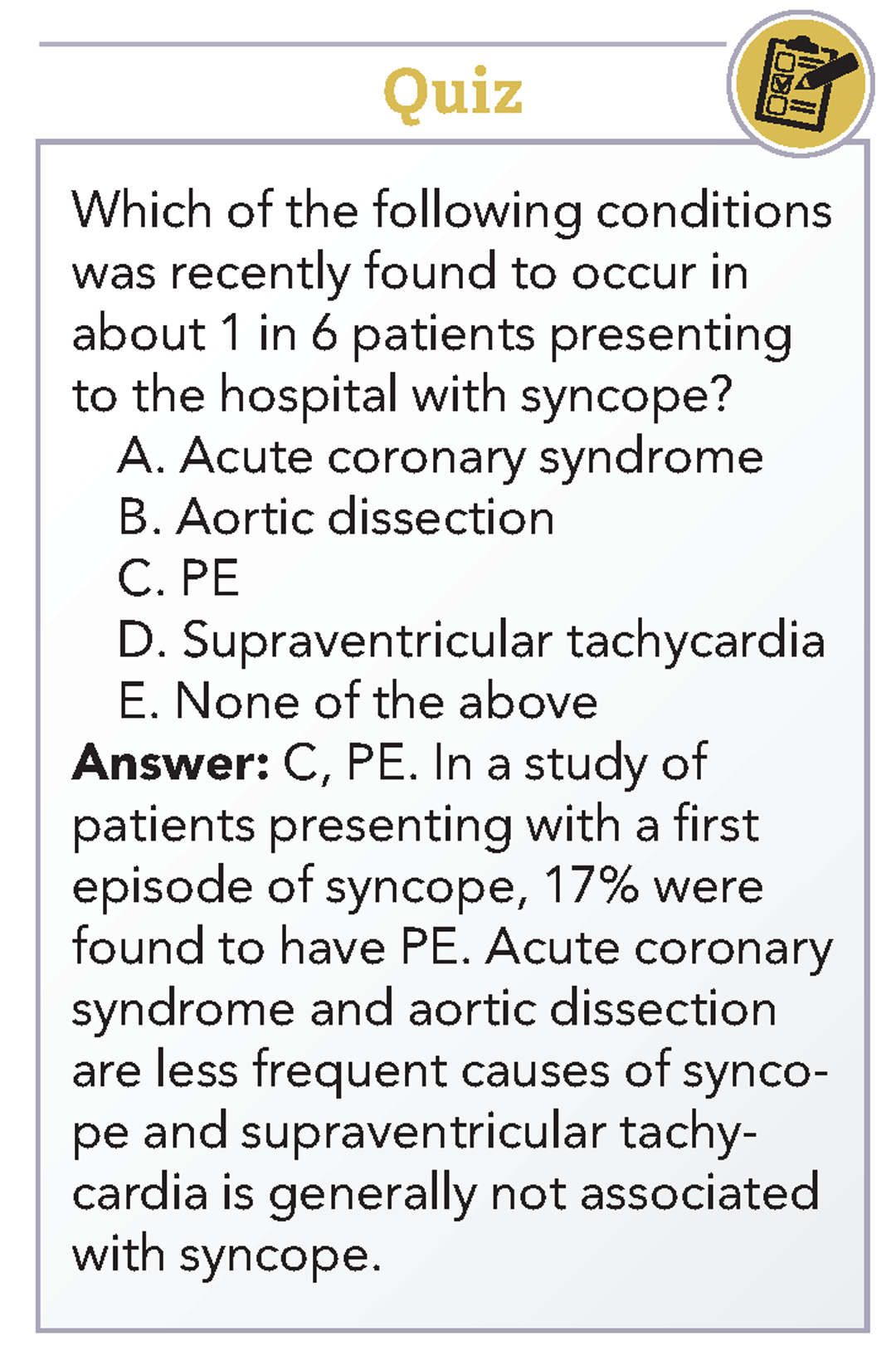
Bottom Line
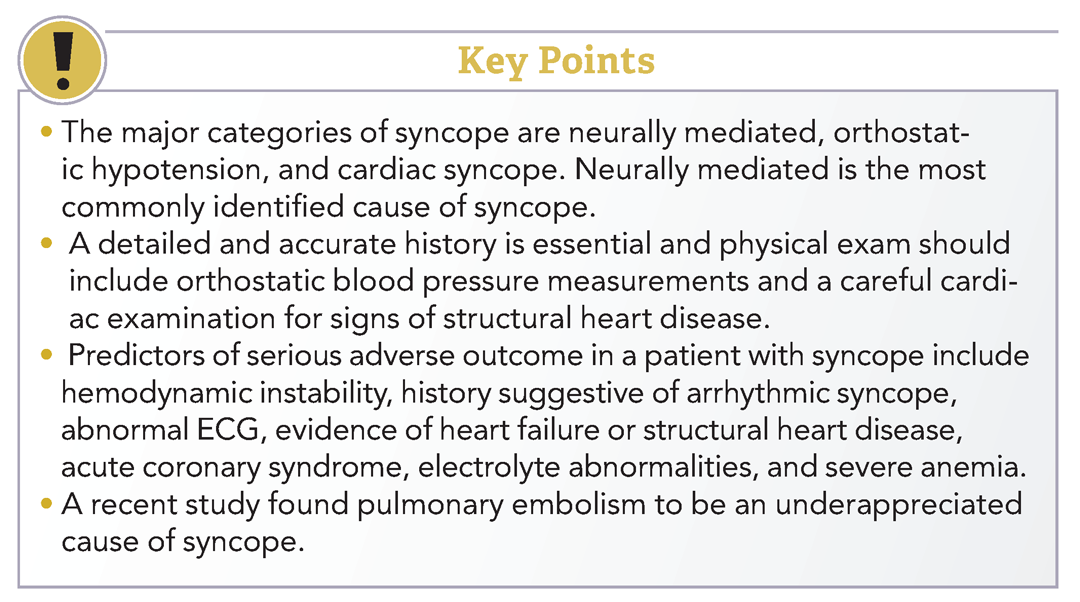
Dr. Roberts, Dr. Krason, and Dr. Manian are hospitalists at Massachusetts General Hospital in Boston.
References
1. Shen W-K et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope. J Am Coll Cardiol. 2017 Aug 1;70(5):e39-e110.
2. Sheldon R. How to differentiate syncope from seizure. Cardiol Clin. 2015 Aug;33(3):377-85.
3. Del Rosso A et al. Relation of clinical presentation of syncope to the age of patients. Am J Cardiol. 2005 Nov 15;96(10):1431-5.
4. Blanc JJ. Syncope: Definition, epidemiology, and classification. Cardiol Clin. 2015 Aug;33(3):341-5.
5. Matthews IG et al. Syncope in the older person. Cardiol Clin. 2015 Aug;33(3):411-21.
6. Costantino G et al. Syncope risk stratification tools vs clinical judgment: An individual patient data meta-analysis. Am J Med. 2014 Nov;127(11):1126.e13-25.
7. Chiu DT et al. Are echocardiography, telemetry, ambulatory electrocardiography monitoring, and cardiac enzymes in emergency department patients presenting with syncope useful tests? A preliminary investigation. J Emerg Med. 2014;47:113-8.
8. Prandoni P et al. Prevalence of pulmonary embolism among patients hospitalized for syncope. N Engl J Med. 2016 Oct;375(20):1524-31.
9. Sheldon RS et al. Standardized approaches to the investigation of syncope: Canadian Cardiovascular Society position paper. Can J Cardiol. 2011 Mar-Apr;27(2):246-253.
10. Moya A et al. Guidelines for the diagnosis and management of syncope (version 2009): the Task Force for the Diagnosis and Management of Syncope of the European Society of Cardiology (ESC). Eur Heart J. 2009 Nov;30(21):2631-71.
Additional reading
1. Brignole M, Hamdan MH. New concepts in the assessment of syncope. J Am Coll Cardiol. 2012 May; 59(18):1583-91.
2. Rosanio S et al. Syncope in adults: systematic review and proposal of a diagnostic and therapeutic algorithm. Int J Cardiol. 2013 Jan;162(3):149-57.
Case
A 38-year-old construction worker without significant medical history presents following witnessed syncope at her job, after standing for at least 2 hours on a particularly warm day. She reported an episode of syncope under similar circumstances 2 months prior. With each episode, she experienced “tunneling” of peripheral vision, then loss of consciousness without palpitations or incontinence. Her physical exam, vital signs (including orthostatic blood pressures), labs, and ECG were unremarkable.
Brief overview
The American College of Cardiology, American Heart Association, and Heart Rhythm Society guidelines define syncope as “a symptom that presents with an abrupt, transient, complete loss of consciousness, associated with inability to maintain postural tone, with rapid and spontaneous recovery” with cerebral hypoperfusion as the presumed mechanism.1 Furthermore, “there should not be clinical features of other nonsyncope causes of loss of consciousness, such as seizure, antecedent head trauma, or apparent loss of consciousness (that is, pseudosyncope).”1
A careful history revolving around the patient’s behavior prior to, during, and following the event, a thorough past medical history, and a review of current medications are essential. Potential obstacles in obtaining details of the event include lack of witnesses, patient’s inability to recall the experience, and inaccurate description of convulsive syncope as a “seizure” by bystanders.2
Overview of data
Obtaining a detailed history is crucial to understanding both the etiology of the syncopal event and determining which patients are at high risk for adverse outcomes. The etiology of syncope can be determined by history alone in 26% of patients younger than 65 years.3 Data on the prevalence of syncope by cause varies widely. As a general rule, in younger patients, especially those under 40 years of age, neurally mediated syncope is most common. As patients age, orthostatic hypotension and cardiac causes (including arrhythmias and structural diseases) occur more frequently, though neurally mediated syncope is still the most common.
Many of these predictors, however, would raise the clinical suspicion of most hospitalists for adverse outcomes in their hospitalized patients independent of the presence or absence of syncope. In fact, a meta-analysis has concluded that “None of the evaluated prediction tools (SFSR, EGSYS) performed better than clinical judgment in identifying serious outcomes during emergency department stay, and at 10 and 30 days after syncope.”6
Once the patient is hospitalized, further evaluation should be based on a careful history and physical examination. Standard evaluation also includes careful review of medications, an ECG to exclude findings suggestive of arrhythmias as well as structural or coronary artery disease, and orthostatic blood pressure measurements.1 Additional tests should be considered as deemed appropriate. For example, in patients over 40 years of age without history of carotid artery disease or stroke and in whom no carotid artery bruit is appreciated, a carotid sinus massage may be considered. The correct technique is to massage the sinus on the right then left, each for 5 seconds in both supine and standing positions with continuous heart rate and frequent blood pressure monitoring. Reproduction of syncope, especially concurrent with a cardiac pause of greater than 3 seconds and a systolic blood pressure drop of greater than 50 mmHg, is considered a positive test. Tilt-table testing should be considered in those for whom neurally mediated syncope is suspected but not confirmed, or in patients who might benefit from further elucidation of their prodromal symptoms.
Of note, a study recently published in the New England Journal of Medicine suggests that the prevalence of PE in patients (median age, 80 years) presenting with a first episode of syncope was 17%, a rate that is substantially higher than historically presumed.8 Although the prevalence of PE was highest among patients presenting with syncope of unclear origin (25%), nearly 13% of patients with other explanations for syncope also had PE.
Application of data
Bottom Line
Dr. Roberts, Dr. Krason, and Dr. Manian are hospitalists at Massachusetts General Hospital in Boston.
References
1. Shen W-K et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope. J Am Coll Cardiol. 2017 Aug 1;70(5):e39-e110.
2. Sheldon R. How to differentiate syncope from seizure. Cardiol Clin. 2015 Aug;33(3):377-85.
3. Del Rosso A et al. Relation of clinical presentation of syncope to the age of patients. Am J Cardiol. 2005 Nov 15;96(10):1431-5.
4. Blanc JJ. Syncope: Definition, epidemiology, and classification. Cardiol Clin. 2015 Aug;33(3):341-5.
5. Matthews IG et al. Syncope in the older person. Cardiol Clin. 2015 Aug;33(3):411-21.
6. Costantino G et al. Syncope risk stratification tools vs clinical judgment: An individual patient data meta-analysis. Am J Med. 2014 Nov;127(11):1126.e13-25.
7. Chiu DT et al. Are echocardiography, telemetry, ambulatory electrocardiography monitoring, and cardiac enzymes in emergency department patients presenting with syncope useful tests? A preliminary investigation. J Emerg Med. 2014;47:113-8.
8. Prandoni P et al. Prevalence of pulmonary embolism among patients hospitalized for syncope. N Engl J Med. 2016 Oct;375(20):1524-31.
9. Sheldon RS et al. Standardized approaches to the investigation of syncope: Canadian Cardiovascular Society position paper. Can J Cardiol. 2011 Mar-Apr;27(2):246-253.
10. Moya A et al. Guidelines for the diagnosis and management of syncope (version 2009): the Task Force for the Diagnosis and Management of Syncope of the European Society of Cardiology (ESC). Eur Heart J. 2009 Nov;30(21):2631-71.
Additional reading
1. Brignole M, Hamdan MH. New concepts in the assessment of syncope. J Am Coll Cardiol. 2012 May; 59(18):1583-91.
2. Rosanio S et al. Syncope in adults: systematic review and proposal of a diagnostic and therapeutic algorithm. Int J Cardiol. 2013 Jan;162(3):149-57.
Case
A 38-year-old construction worker without significant medical history presents following witnessed syncope at her job, after standing for at least 2 hours on a particularly warm day. She reported an episode of syncope under similar circumstances 2 months prior. With each episode, she experienced “tunneling” of peripheral vision, then loss of consciousness without palpitations or incontinence. Her physical exam, vital signs (including orthostatic blood pressures), labs, and ECG were unremarkable.
Brief overview
The American College of Cardiology, American Heart Association, and Heart Rhythm Society guidelines define syncope as “a symptom that presents with an abrupt, transient, complete loss of consciousness, associated with inability to maintain postural tone, with rapid and spontaneous recovery” with cerebral hypoperfusion as the presumed mechanism.1 Furthermore, “there should not be clinical features of other nonsyncope causes of loss of consciousness, such as seizure, antecedent head trauma, or apparent loss of consciousness (that is, pseudosyncope).”1
A careful history revolving around the patient’s behavior prior to, during, and following the event, a thorough past medical history, and a review of current medications are essential. Potential obstacles in obtaining details of the event include lack of witnesses, patient’s inability to recall the experience, and inaccurate description of convulsive syncope as a “seizure” by bystanders.2
Overview of data
Obtaining a detailed history is crucial to understanding both the etiology of the syncopal event and determining which patients are at high risk for adverse outcomes. The etiology of syncope can be determined by history alone in 26% of patients younger than 65 years.3 Data on the prevalence of syncope by cause varies widely. As a general rule, in younger patients, especially those under 40 years of age, neurally mediated syncope is most common. As patients age, orthostatic hypotension and cardiac causes (including arrhythmias and structural diseases) occur more frequently, though neurally mediated syncope is still the most common.
Many of these predictors, however, would raise the clinical suspicion of most hospitalists for adverse outcomes in their hospitalized patients independent of the presence or absence of syncope. In fact, a meta-analysis has concluded that “None of the evaluated prediction tools (SFSR, EGSYS) performed better than clinical judgment in identifying serious outcomes during emergency department stay, and at 10 and 30 days after syncope.”6
Once the patient is hospitalized, further evaluation should be based on a careful history and physical examination. Standard evaluation also includes careful review of medications, an ECG to exclude findings suggestive of arrhythmias as well as structural or coronary artery disease, and orthostatic blood pressure measurements.1 Additional tests should be considered as deemed appropriate. For example, in patients over 40 years of age without history of carotid artery disease or stroke and in whom no carotid artery bruit is appreciated, a carotid sinus massage may be considered. The correct technique is to massage the sinus on the right then left, each for 5 seconds in both supine and standing positions with continuous heart rate and frequent blood pressure monitoring. Reproduction of syncope, especially concurrent with a cardiac pause of greater than 3 seconds and a systolic blood pressure drop of greater than 50 mmHg, is considered a positive test. Tilt-table testing should be considered in those for whom neurally mediated syncope is suspected but not confirmed, or in patients who might benefit from further elucidation of their prodromal symptoms.
Of note, a study recently published in the New England Journal of Medicine suggests that the prevalence of PE in patients (median age, 80 years) presenting with a first episode of syncope was 17%, a rate that is substantially higher than historically presumed.8 Although the prevalence of PE was highest among patients presenting with syncope of unclear origin (25%), nearly 13% of patients with other explanations for syncope also had PE.
Application of data
Bottom Line
Dr. Roberts, Dr. Krason, and Dr. Manian are hospitalists at Massachusetts General Hospital in Boston.
References
1. Shen W-K et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope. J Am Coll Cardiol. 2017 Aug 1;70(5):e39-e110.
2. Sheldon R. How to differentiate syncope from seizure. Cardiol Clin. 2015 Aug;33(3):377-85.
3. Del Rosso A et al. Relation of clinical presentation of syncope to the age of patients. Am J Cardiol. 2005 Nov 15;96(10):1431-5.
4. Blanc JJ. Syncope: Definition, epidemiology, and classification. Cardiol Clin. 2015 Aug;33(3):341-5.
5. Matthews IG et al. Syncope in the older person. Cardiol Clin. 2015 Aug;33(3):411-21.
6. Costantino G et al. Syncope risk stratification tools vs clinical judgment: An individual patient data meta-analysis. Am J Med. 2014 Nov;127(11):1126.e13-25.
7. Chiu DT et al. Are echocardiography, telemetry, ambulatory electrocardiography monitoring, and cardiac enzymes in emergency department patients presenting with syncope useful tests? A preliminary investigation. J Emerg Med. 2014;47:113-8.
8. Prandoni P et al. Prevalence of pulmonary embolism among patients hospitalized for syncope. N Engl J Med. 2016 Oct;375(20):1524-31.
9. Sheldon RS et al. Standardized approaches to the investigation of syncope: Canadian Cardiovascular Society position paper. Can J Cardiol. 2011 Mar-Apr;27(2):246-253.
10. Moya A et al. Guidelines for the diagnosis and management of syncope (version 2009): the Task Force for the Diagnosis and Management of Syncope of the European Society of Cardiology (ESC). Eur Heart J. 2009 Nov;30(21):2631-71.
Additional reading
1. Brignole M, Hamdan MH. New concepts in the assessment of syncope. J Am Coll Cardiol. 2012 May; 59(18):1583-91.
2. Rosanio S et al. Syncope in adults: systematic review and proposal of a diagnostic and therapeutic algorithm. Int J Cardiol. 2013 Jan;162(3):149-57.
Risks identified for drug-resistant bacteremia in cirrhosis
In patients hospitalized with cirrhosis, biliary cirrhosis, recent health care exposure, nonwhite race, and cultures taken more than 48 hours after admission all independently predicted that bacteremia would be caused by multidrug-resistant organisms (MDROs), according to a medical record review at CHI St. Luke’s Medical Center, an 850-bed tertiary care center in Houston.
“These variables along with severity of infection and liver disease may help clinicians identify patients who will benefit most from broader-spectrum empiric antimicrobial therapy,” wrote the investigators, led by Jennifer Addo Smith, PharmD, of St. Luke’s, in the Journal of Clinical Gastroenterology.
But local epidemiology remains important. “Although a gram-positive agent (e.g., vancomycin) and a carbapenem-sparing gram-negative agent (e.g., ceftriaxone, cefepime) are reasonable empiric agents at our center, other centers with different resistance patterns may warrant different empiric therapy. Given the low prevalence of VRE [vancomycin-resistant Enterococcus] in this study ... and E. faecium in other studies (4%-7%), an empiric agent active against VRE does not seem to be routinely required,” they said.
The team looked into the issue because there hasn’t been much investigation in the United States of the role of multidrug resistant organisms in bacteremia among patients hospitalized with cirrhosis.
Thirty patients in the study had bacteremia caused by MDROs while 60 had bacteremia from non-MDROs, giving a 33% prevalence of MDRO bacteremia, which was consistent with previous, mostly European studies.
Enterobacteriaceae (43%), Staphylococcus aureus (18%), Streptococcus spp. (11%), Enterococcus spp. (10%), and nonfermenting gram-negative bacilli (6%) were the main causes of bacteremia overall.
Among the 30 MDRO cases, methicillin-resistant S. aureus was isolated in seven (23%); methicillin-resistant coagulase-negative Staphylococci in four (13%); fluoroquinolone-resistant Enterobacteriaceae in nine (30%); extended spectrum beta-lactamase–producing Enterobacteriaceae in three (10%), and VRE in two (7%). No carbapenemase-producing gram-negative bacteria were identified.
The predictors of MDRO bacteremia emerged on multivariate analysis and included biliary cirrhosis (adjusted odds ratio, 11.75; 95% confidence interval, 2.08-66.32); recent health care exposure (aOR, 9.81; 95% CI, 2.15-44.88); blood cultures obtained 48 hours after hospital admission (aOR, 6.02; 95% CI, 1.70-21.40) and nonwhite race (aOR , 3.35; 95% CI, 1.19-9.38).
Blood cultures past 48 hours and recent health care exposure – generally hospitalization within the past 90 days – were likely surrogates for nosocomial infection.
The link with biliary cirrhosis is unclear. “Compared with other cirrhotic patients, perhaps patients with PBC [primary biliary cholangitis] have had more cumulative antimicrobial exposure because of [their] higher risk for UTIs [urinary tract infections] and therefore are at increased risk for MDROs,” they wrote.
The median age in the study was 59 years. Half of the patients were white; 46% were women. Hepatitis C was the most common cause of cirrhosis, followed by alcohol.
MDRO was defined in the study as bacteria not susceptible to at least one antibiotic in at least three antimicrobial categories; 90 cirrhosis patients without bacteremia served as controls.
The funding source was not reported. Dr. Addo Smith had no disclosures.
SOURCE: Smith JA et al. J Clin Gastroenterol. 2017 Nov 23. doi: 10.1097/MCG.0000000000000964.
*This story was updated on 1/10/2018.
In patients hospitalized with cirrhosis, biliary cirrhosis, recent health care exposure, nonwhite race, and cultures taken more than 48 hours after admission all independently predicted that bacteremia would be caused by multidrug-resistant organisms (MDROs), according to a medical record review at CHI St. Luke’s Medical Center, an 850-bed tertiary care center in Houston.
“These variables along with severity of infection and liver disease may help clinicians identify patients who will benefit most from broader-spectrum empiric antimicrobial therapy,” wrote the investigators, led by Jennifer Addo Smith, PharmD, of St. Luke’s, in the Journal of Clinical Gastroenterology.
But local epidemiology remains important. “Although a gram-positive agent (e.g., vancomycin) and a carbapenem-sparing gram-negative agent (e.g., ceftriaxone, cefepime) are reasonable empiric agents at our center, other centers with different resistance patterns may warrant different empiric therapy. Given the low prevalence of VRE [vancomycin-resistant Enterococcus] in this study ... and E. faecium in other studies (4%-7%), an empiric agent active against VRE does not seem to be routinely required,” they said.
The team looked into the issue because there hasn’t been much investigation in the United States of the role of multidrug resistant organisms in bacteremia among patients hospitalized with cirrhosis.
Thirty patients in the study had bacteremia caused by MDROs while 60 had bacteremia from non-MDROs, giving a 33% prevalence of MDRO bacteremia, which was consistent with previous, mostly European studies.
Enterobacteriaceae (43%), Staphylococcus aureus (18%), Streptococcus spp. (11%), Enterococcus spp. (10%), and nonfermenting gram-negative bacilli (6%) were the main causes of bacteremia overall.
Among the 30 MDRO cases, methicillin-resistant S. aureus was isolated in seven (23%); methicillin-resistant coagulase-negative Staphylococci in four (13%); fluoroquinolone-resistant Enterobacteriaceae in nine (30%); extended spectrum beta-lactamase–producing Enterobacteriaceae in three (10%), and VRE in two (7%). No carbapenemase-producing gram-negative bacteria were identified.
The predictors of MDRO bacteremia emerged on multivariate analysis and included biliary cirrhosis (adjusted odds ratio, 11.75; 95% confidence interval, 2.08-66.32); recent health care exposure (aOR, 9.81; 95% CI, 2.15-44.88); blood cultures obtained 48 hours after hospital admission (aOR, 6.02; 95% CI, 1.70-21.40) and nonwhite race (aOR , 3.35; 95% CI, 1.19-9.38).
Blood cultures past 48 hours and recent health care exposure – generally hospitalization within the past 90 days – were likely surrogates for nosocomial infection.
The link with biliary cirrhosis is unclear. “Compared with other cirrhotic patients, perhaps patients with PBC [primary biliary cholangitis] have had more cumulative antimicrobial exposure because of [their] higher risk for UTIs [urinary tract infections] and therefore are at increased risk for MDROs,” they wrote.
The median age in the study was 59 years. Half of the patients were white; 46% were women. Hepatitis C was the most common cause of cirrhosis, followed by alcohol.
MDRO was defined in the study as bacteria not susceptible to at least one antibiotic in at least three antimicrobial categories; 90 cirrhosis patients without bacteremia served as controls.
The funding source was not reported. Dr. Addo Smith had no disclosures.
SOURCE: Smith JA et al. J Clin Gastroenterol. 2017 Nov 23. doi: 10.1097/MCG.0000000000000964.
*This story was updated on 1/10/2018.
In patients hospitalized with cirrhosis, biliary cirrhosis, recent health care exposure, nonwhite race, and cultures taken more than 48 hours after admission all independently predicted that bacteremia would be caused by multidrug-resistant organisms (MDROs), according to a medical record review at CHI St. Luke’s Medical Center, an 850-bed tertiary care center in Houston.
“These variables along with severity of infection and liver disease may help clinicians identify patients who will benefit most from broader-spectrum empiric antimicrobial therapy,” wrote the investigators, led by Jennifer Addo Smith, PharmD, of St. Luke’s, in the Journal of Clinical Gastroenterology.
But local epidemiology remains important. “Although a gram-positive agent (e.g., vancomycin) and a carbapenem-sparing gram-negative agent (e.g., ceftriaxone, cefepime) are reasonable empiric agents at our center, other centers with different resistance patterns may warrant different empiric therapy. Given the low prevalence of VRE [vancomycin-resistant Enterococcus] in this study ... and E. faecium in other studies (4%-7%), an empiric agent active against VRE does not seem to be routinely required,” they said.
The team looked into the issue because there hasn’t been much investigation in the United States of the role of multidrug resistant organisms in bacteremia among patients hospitalized with cirrhosis.
Thirty patients in the study had bacteremia caused by MDROs while 60 had bacteremia from non-MDROs, giving a 33% prevalence of MDRO bacteremia, which was consistent with previous, mostly European studies.
Enterobacteriaceae (43%), Staphylococcus aureus (18%), Streptococcus spp. (11%), Enterococcus spp. (10%), and nonfermenting gram-negative bacilli (6%) were the main causes of bacteremia overall.
Among the 30 MDRO cases, methicillin-resistant S. aureus was isolated in seven (23%); methicillin-resistant coagulase-negative Staphylococci in four (13%); fluoroquinolone-resistant Enterobacteriaceae in nine (30%); extended spectrum beta-lactamase–producing Enterobacteriaceae in three (10%), and VRE in two (7%). No carbapenemase-producing gram-negative bacteria were identified.
The predictors of MDRO bacteremia emerged on multivariate analysis and included biliary cirrhosis (adjusted odds ratio, 11.75; 95% confidence interval, 2.08-66.32); recent health care exposure (aOR, 9.81; 95% CI, 2.15-44.88); blood cultures obtained 48 hours after hospital admission (aOR, 6.02; 95% CI, 1.70-21.40) and nonwhite race (aOR , 3.35; 95% CI, 1.19-9.38).
Blood cultures past 48 hours and recent health care exposure – generally hospitalization within the past 90 days – were likely surrogates for nosocomial infection.
The link with biliary cirrhosis is unclear. “Compared with other cirrhotic patients, perhaps patients with PBC [primary biliary cholangitis] have had more cumulative antimicrobial exposure because of [their] higher risk for UTIs [urinary tract infections] and therefore are at increased risk for MDROs,” they wrote.
The median age in the study was 59 years. Half of the patients were white; 46% were women. Hepatitis C was the most common cause of cirrhosis, followed by alcohol.
MDRO was defined in the study as bacteria not susceptible to at least one antibiotic in at least three antimicrobial categories; 90 cirrhosis patients without bacteremia served as controls.
The funding source was not reported. Dr. Addo Smith had no disclosures.
SOURCE: Smith JA et al. J Clin Gastroenterol. 2017 Nov 23. doi: 10.1097/MCG.0000000000000964.
*This story was updated on 1/10/2018.
FROM THE JOURNAL OF CLINICAL GASTROENTEROLOGY
Key clinical point: In patients hospitalized with cirrhosis, nonwhite race, biliary involvement, recent health care exposure, and cultures taken more than 48 hours after hospital admission all independently predicted that bacteremia would be caused by multidrug-resistant organisms.
Major finding: The predictors of multidrug-resistant organism bacteremia emerged on multivariate analysis and included biliary cirrhosis (aOR 11.75; 95% CI, 2.08-66.32); recent health care exposure (aOR 9.81; 95% CI, 2.15-44.88); and blood cultures obtained 48 hours after hospital admission (aOR 6.02; 95% CI, 1.70-21.40).
Study details: Review of 90 cirrhotic patients with bacteremia, plus 90 controls.
Disclosures: The lead investigator had no disclosures.
Source: Smith JA et al. J Clin Gastroenterol. 2017 Nov 23. doi: 10.1097/MCG.0000000000000964.