User login
Fentanyl analogues an increasing factor in opioid deaths
Fentanyl analogues were involved in 14% of opioid overdose deaths in the second half of 2016, according to an analysis of 10 states reporting to the Enhanced State Opioid Overdose Surveillance program.
“Illicitly manufactured fentanyl is a key factor driving opioid overdose deaths and … fentanyl analogues [such as carfentanil, furanylfentanyl, and acetylfentanyl] are increasingly contributing to a complex illicit opioid market with significant public health implications,” investigators said in a report from the Centers for Disease Control and Prevention (MMWR 2017 Oct 27;66[early release]:1-6).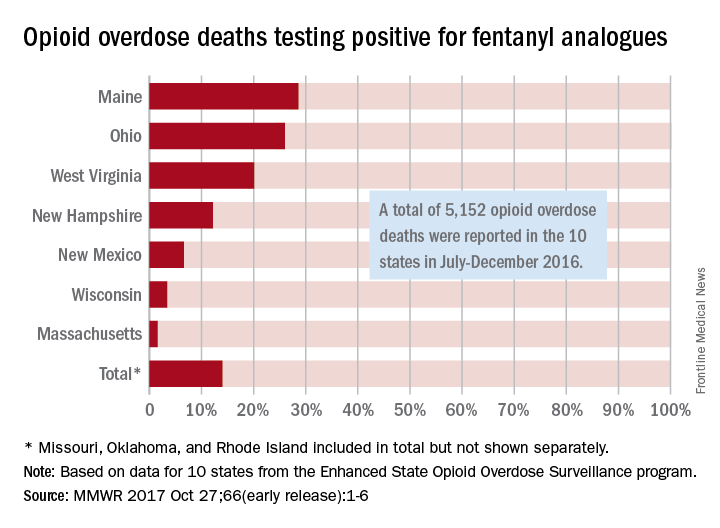
The overall rate of 14% represents 720 of the 5,152 total opioid deaths occurring in 10 states over the 6-month study period, they noted.
Of the 10 states in the analysis, Maine had the largest proportion (28.6%) of opioid overdose deaths involving fentanyl analogues, with Ohio second at 26% and West Virginia third at 20.1%. Ohio had the largest overall number of analogue-involved overdose deaths, however, at 531 during July-December 2016. At 1.6%, Massachusetts had the lowest rate of fentanyl analogue–involved deaths among the seven states for which separate figures were given, the published data show. (Three states – Missouri [22 counties], Oklahoma, and Rhode Island – were grouped together and had a combined rate of 1%.)
More than half of the overdose deaths involving fentanyl or a fentanyl analogue also involved heroin, cocaine, or methamphetamine, which means that almost half of the deaths “did not test positive for other illicit opioids, suggesting that fentanyl and fentanyl analogues might be emerging as unique illicit products,” the investigators wrote, adding that the fentanyl analogue situation “might mirror the rapidly rising trajectory of fentanyl overdose deaths that began in 2013 and become a major factor in opioid overdose deaths.”
Fentanyl analogues were involved in 14% of opioid overdose deaths in the second half of 2016, according to an analysis of 10 states reporting to the Enhanced State Opioid Overdose Surveillance program.
“Illicitly manufactured fentanyl is a key factor driving opioid overdose deaths and … fentanyl analogues [such as carfentanil, furanylfentanyl, and acetylfentanyl] are increasingly contributing to a complex illicit opioid market with significant public health implications,” investigators said in a report from the Centers for Disease Control and Prevention (MMWR 2017 Oct 27;66[early release]:1-6).
The overall rate of 14% represents 720 of the 5,152 total opioid deaths occurring in 10 states over the 6-month study period, they noted.
Of the 10 states in the analysis, Maine had the largest proportion (28.6%) of opioid overdose deaths involving fentanyl analogues, with Ohio second at 26% and West Virginia third at 20.1%. Ohio had the largest overall number of analogue-involved overdose deaths, however, at 531 during July-December 2016. At 1.6%, Massachusetts had the lowest rate of fentanyl analogue–involved deaths among the seven states for which separate figures were given, the published data show. (Three states – Missouri [22 counties], Oklahoma, and Rhode Island – were grouped together and had a combined rate of 1%.)
More than half of the overdose deaths involving fentanyl or a fentanyl analogue also involved heroin, cocaine, or methamphetamine, which means that almost half of the deaths “did not test positive for other illicit opioids, suggesting that fentanyl and fentanyl analogues might be emerging as unique illicit products,” the investigators wrote, adding that the fentanyl analogue situation “might mirror the rapidly rising trajectory of fentanyl overdose deaths that began in 2013 and become a major factor in opioid overdose deaths.”
Fentanyl analogues were involved in 14% of opioid overdose deaths in the second half of 2016, according to an analysis of 10 states reporting to the Enhanced State Opioid Overdose Surveillance program.
“Illicitly manufactured fentanyl is a key factor driving opioid overdose deaths and … fentanyl analogues [such as carfentanil, furanylfentanyl, and acetylfentanyl] are increasingly contributing to a complex illicit opioid market with significant public health implications,” investigators said in a report from the Centers for Disease Control and Prevention (MMWR 2017 Oct 27;66[early release]:1-6).
The overall rate of 14% represents 720 of the 5,152 total opioid deaths occurring in 10 states over the 6-month study period, they noted.
Of the 10 states in the analysis, Maine had the largest proportion (28.6%) of opioid overdose deaths involving fentanyl analogues, with Ohio second at 26% and West Virginia third at 20.1%. Ohio had the largest overall number of analogue-involved overdose deaths, however, at 531 during July-December 2016. At 1.6%, Massachusetts had the lowest rate of fentanyl analogue–involved deaths among the seven states for which separate figures were given, the published data show. (Three states – Missouri [22 counties], Oklahoma, and Rhode Island – were grouped together and had a combined rate of 1%.)
More than half of the overdose deaths involving fentanyl or a fentanyl analogue also involved heroin, cocaine, or methamphetamine, which means that almost half of the deaths “did not test positive for other illicit opioids, suggesting that fentanyl and fentanyl analogues might be emerging as unique illicit products,” the investigators wrote, adding that the fentanyl analogue situation “might mirror the rapidly rising trajectory of fentanyl overdose deaths that began in 2013 and become a major factor in opioid overdose deaths.”
FROM MMWR
Are Two Antithrombotic Agents Better Than Three?
Dual antithrombotic therapy with dabigatran and a P2Y12 inhibitor (eg, clopidogrel or ticagrelor) is associated with a lower risk of bleeding, compared with standard triple antithrombotic therapy, after percutaneous coronary intervention (PCI) for patients with atrial fibrillation, according to research published online ahead of print August 27 in the New England Journal of Medicine. Dual therapy also is noninferior to triple therapy regarding the risk of thromboembolic events.
“Patients who received two anticlotting medications—including one of a newer class of drug—had fewer bleeding events without being more at risk for a stroke or other cardiac events,” said Christopher P. Cannon, MD, Professor of Medicine at Harvard Medical School and a cardiovascular medicine specialist at Brigham and Women’s Hospital in Boston, and colleagues.

Standard triple antithrombotic therapy (ie, warfarin plus two antiplatelet agents) has been associated with a high risk of bleeding, thus prompting researchers to seek a better approach to treatment. One emerging therapy omits aspirin from the standard regimen and uses a single P2Y12 inhibitor in combination with an oral anticoagulant. A moderate-sized trial found that this form of dual-therapy lowered the risk of bleeding, compared with standard triple therapy. Another trial supported standard triple therapy for a shorter duration. Finally, a recent trial found that the risk of bleeding was lower with a regimen of reduced-dose rivaroxaban plus a P2Y12 inhibitor than with standard triple therapy.
Dual Therapy Versus Triple Therapy
To compare two regimens of dual antithrombotic therapy that include dabigatran with a regimen of triple antithrombotic therapy that includes warfarin, Dr. Cannon and colleagues conducted the RE-DUAL PCI trial. Eligible participants were 18 or older, had nonvalvular atrial fibrillation, and had successfully undergone PCI with a bare-metal or drug-eluting stent within the previous 120 hours. Patients with bioprosthetic or mechanical heart valves, severe renal insufficiency, or other major coexisting conditions were excluded.
All patients in the United States and nonelderly patients in other countries were randomized 1:1:1 to receive triple therapy with warfarin plus a PSY12 inhibitor and aspirin for one to three months, or to receive dual therapy with dabigatran (110 mg or 150 mg twice daily) plus a P2Y12 inhibitor and no aspirin. Outside the US, elderly patients (ie, 70 or older in Japan and 80 or older elsewhere) were randomized 1:1 to receive 110 mg of dual therapy or triple therapy.
The primary end point was the first major or clinically relevant nonmajor bleeding event. A major secondary end point was the composite of thromboembolic events (ie, myocardial infarction, stroke, or systemic embolism), death, or unplanned revascularization. Other secondary end points included a composite of thromboembolic events or death, as well as the individual thromboembolic events and definite stent thrombosis.
No Significant Difference in Serious Adverse Events Between Groups
Between July 21, 2014, and October 31, 2016, 2,725 participants underwent randomization at 414 sites in 41 countries. The mean age of participants was 70.8. The mean duration of treatment with the trial anticoagulant was 12.3 months, and the mean duration of follow-up was 14 months. Six patients were lost to follow-up. Most patients received clopidogrel as their P2Y12 inhibitor, and 12% received ticagrelor.
The incidence of the primary end point was 15.4% in the 110-mg dual-therapy group, compared with 26.9% in the triple-therapy group, and 20.2% in the 150-mg dual-therapy group, compared with 25.7% in the corresponding triple-therapy group. The incidence of the composite efficacy end point was 13.7% in both dual-therapy groups combined, compared with 13.4% in the triple-therapy group.
Researchers found no significant difference between groups in the rate of serious adverse events. Fatal serious adverse events occurred during treatment in 38 patients in the 100-mg dual-therapy group, 24 patients in the 150-mg dual-therapy group, and 41 patients in the triple-therapy group.
“We now have new information to help select the right treatment for individual patients,” said Dr. Cannon. “With respect to the results for both the bleeding and thromboembolic-event end points, we may only speculate on the relative contributions of the omission of aspirin and the type of oral anticoagulant in the dual-therapy groups and the triple-therapy group. A trial conducted with a formal two-by-two factorial design would be able to discern these contributions, and one such trial is ongoing.”
One limitation of this trial was that researchers enrolled a smaller number of patients than initially planned. The power of the trial to examine efficacy according to dabigatran dose consequently was limited, said the authors.
This study was supported by Boehringer Ingelheim.
—Erica Tricarico
Suggested Reading
Cannon CP, Bhatt DL, Oldgren J, et al. Dual antithrombotic therapy with dabigatran after PCI in atrial fibrillation. N Engl J Med. 2017 Aug 27 [Epub ahead of print].
Dual antithrombotic therapy with dabigatran and a P2Y12 inhibitor (eg, clopidogrel or ticagrelor) is associated with a lower risk of bleeding, compared with standard triple antithrombotic therapy, after percutaneous coronary intervention (PCI) for patients with atrial fibrillation, according to research published online ahead of print August 27 in the New England Journal of Medicine. Dual therapy also is noninferior to triple therapy regarding the risk of thromboembolic events.
“Patients who received two anticlotting medications—including one of a newer class of drug—had fewer bleeding events without being more at risk for a stroke or other cardiac events,” said Christopher P. Cannon, MD, Professor of Medicine at Harvard Medical School and a cardiovascular medicine specialist at Brigham and Women’s Hospital in Boston, and colleagues.
Standard triple antithrombotic therapy (ie, warfarin plus two antiplatelet agents) has been associated with a high risk of bleeding, thus prompting researchers to seek a better approach to treatment. One emerging therapy omits aspirin from the standard regimen and uses a single P2Y12 inhibitor in combination with an oral anticoagulant. A moderate-sized trial found that this form of dual-therapy lowered the risk of bleeding, compared with standard triple therapy. Another trial supported standard triple therapy for a shorter duration. Finally, a recent trial found that the risk of bleeding was lower with a regimen of reduced-dose rivaroxaban plus a P2Y12 inhibitor than with standard triple therapy.
Dual Therapy Versus Triple Therapy
To compare two regimens of dual antithrombotic therapy that include dabigatran with a regimen of triple antithrombotic therapy that includes warfarin, Dr. Cannon and colleagues conducted the RE-DUAL PCI trial. Eligible participants were 18 or older, had nonvalvular atrial fibrillation, and had successfully undergone PCI with a bare-metal or drug-eluting stent within the previous 120 hours. Patients with bioprosthetic or mechanical heart valves, severe renal insufficiency, or other major coexisting conditions were excluded.
All patients in the United States and nonelderly patients in other countries were randomized 1:1:1 to receive triple therapy with warfarin plus a PSY12 inhibitor and aspirin for one to three months, or to receive dual therapy with dabigatran (110 mg or 150 mg twice daily) plus a P2Y12 inhibitor and no aspirin. Outside the US, elderly patients (ie, 70 or older in Japan and 80 or older elsewhere) were randomized 1:1 to receive 110 mg of dual therapy or triple therapy.
The primary end point was the first major or clinically relevant nonmajor bleeding event. A major secondary end point was the composite of thromboembolic events (ie, myocardial infarction, stroke, or systemic embolism), death, or unplanned revascularization. Other secondary end points included a composite of thromboembolic events or death, as well as the individual thromboembolic events and definite stent thrombosis.
No Significant Difference in Serious Adverse Events Between Groups
Between July 21, 2014, and October 31, 2016, 2,725 participants underwent randomization at 414 sites in 41 countries. The mean age of participants was 70.8. The mean duration of treatment with the trial anticoagulant was 12.3 months, and the mean duration of follow-up was 14 months. Six patients were lost to follow-up. Most patients received clopidogrel as their P2Y12 inhibitor, and 12% received ticagrelor.
The incidence of the primary end point was 15.4% in the 110-mg dual-therapy group, compared with 26.9% in the triple-therapy group, and 20.2% in the 150-mg dual-therapy group, compared with 25.7% in the corresponding triple-therapy group. The incidence of the composite efficacy end point was 13.7% in both dual-therapy groups combined, compared with 13.4% in the triple-therapy group.
Researchers found no significant difference between groups in the rate of serious adverse events. Fatal serious adverse events occurred during treatment in 38 patients in the 100-mg dual-therapy group, 24 patients in the 150-mg dual-therapy group, and 41 patients in the triple-therapy group.
“We now have new information to help select the right treatment for individual patients,” said Dr. Cannon. “With respect to the results for both the bleeding and thromboembolic-event end points, we may only speculate on the relative contributions of the omission of aspirin and the type of oral anticoagulant in the dual-therapy groups and the triple-therapy group. A trial conducted with a formal two-by-two factorial design would be able to discern these contributions, and one such trial is ongoing.”
One limitation of this trial was that researchers enrolled a smaller number of patients than initially planned. The power of the trial to examine efficacy according to dabigatran dose consequently was limited, said the authors.
This study was supported by Boehringer Ingelheim.
—Erica Tricarico
Suggested Reading
Cannon CP, Bhatt DL, Oldgren J, et al. Dual antithrombotic therapy with dabigatran after PCI in atrial fibrillation. N Engl J Med. 2017 Aug 27 [Epub ahead of print].
Dual antithrombotic therapy with dabigatran and a P2Y12 inhibitor (eg, clopidogrel or ticagrelor) is associated with a lower risk of bleeding, compared with standard triple antithrombotic therapy, after percutaneous coronary intervention (PCI) for patients with atrial fibrillation, according to research published online ahead of print August 27 in the New England Journal of Medicine. Dual therapy also is noninferior to triple therapy regarding the risk of thromboembolic events.
“Patients who received two anticlotting medications—including one of a newer class of drug—had fewer bleeding events without being more at risk for a stroke or other cardiac events,” said Christopher P. Cannon, MD, Professor of Medicine at Harvard Medical School and a cardiovascular medicine specialist at Brigham and Women’s Hospital in Boston, and colleagues.
Standard triple antithrombotic therapy (ie, warfarin plus two antiplatelet agents) has been associated with a high risk of bleeding, thus prompting researchers to seek a better approach to treatment. One emerging therapy omits aspirin from the standard regimen and uses a single P2Y12 inhibitor in combination with an oral anticoagulant. A moderate-sized trial found that this form of dual-therapy lowered the risk of bleeding, compared with standard triple therapy. Another trial supported standard triple therapy for a shorter duration. Finally, a recent trial found that the risk of bleeding was lower with a regimen of reduced-dose rivaroxaban plus a P2Y12 inhibitor than with standard triple therapy.
Dual Therapy Versus Triple Therapy
To compare two regimens of dual antithrombotic therapy that include dabigatran with a regimen of triple antithrombotic therapy that includes warfarin, Dr. Cannon and colleagues conducted the RE-DUAL PCI trial. Eligible participants were 18 or older, had nonvalvular atrial fibrillation, and had successfully undergone PCI with a bare-metal or drug-eluting stent within the previous 120 hours. Patients with bioprosthetic or mechanical heart valves, severe renal insufficiency, or other major coexisting conditions were excluded.
All patients in the United States and nonelderly patients in other countries were randomized 1:1:1 to receive triple therapy with warfarin plus a PSY12 inhibitor and aspirin for one to three months, or to receive dual therapy with dabigatran (110 mg or 150 mg twice daily) plus a P2Y12 inhibitor and no aspirin. Outside the US, elderly patients (ie, 70 or older in Japan and 80 or older elsewhere) were randomized 1:1 to receive 110 mg of dual therapy or triple therapy.
The primary end point was the first major or clinically relevant nonmajor bleeding event. A major secondary end point was the composite of thromboembolic events (ie, myocardial infarction, stroke, or systemic embolism), death, or unplanned revascularization. Other secondary end points included a composite of thromboembolic events or death, as well as the individual thromboembolic events and definite stent thrombosis.
No Significant Difference in Serious Adverse Events Between Groups
Between July 21, 2014, and October 31, 2016, 2,725 participants underwent randomization at 414 sites in 41 countries. The mean age of participants was 70.8. The mean duration of treatment with the trial anticoagulant was 12.3 months, and the mean duration of follow-up was 14 months. Six patients were lost to follow-up. Most patients received clopidogrel as their P2Y12 inhibitor, and 12% received ticagrelor.
The incidence of the primary end point was 15.4% in the 110-mg dual-therapy group, compared with 26.9% in the triple-therapy group, and 20.2% in the 150-mg dual-therapy group, compared with 25.7% in the corresponding triple-therapy group. The incidence of the composite efficacy end point was 13.7% in both dual-therapy groups combined, compared with 13.4% in the triple-therapy group.
Researchers found no significant difference between groups in the rate of serious adverse events. Fatal serious adverse events occurred during treatment in 38 patients in the 100-mg dual-therapy group, 24 patients in the 150-mg dual-therapy group, and 41 patients in the triple-therapy group.
“We now have new information to help select the right treatment for individual patients,” said Dr. Cannon. “With respect to the results for both the bleeding and thromboembolic-event end points, we may only speculate on the relative contributions of the omission of aspirin and the type of oral anticoagulant in the dual-therapy groups and the triple-therapy group. A trial conducted with a formal two-by-two factorial design would be able to discern these contributions, and one such trial is ongoing.”
One limitation of this trial was that researchers enrolled a smaller number of patients than initially planned. The power of the trial to examine efficacy according to dabigatran dose consequently was limited, said the authors.
This study was supported by Boehringer Ingelheim.
—Erica Tricarico
Suggested Reading
Cannon CP, Bhatt DL, Oldgren J, et al. Dual antithrombotic therapy with dabigatran after PCI in atrial fibrillation. N Engl J Med. 2017 Aug 27 [Epub ahead of print].
Loss of Functional Connectivity May Cause Hallucinations in Parkinson’s Disease
Visual hallucinations in Parkinson’s disease may arise from a global loss of network efficiency in the brain that disturbs visual attention and visual processing, according to research published online ahead of print September 27 in Radiology. A specific pattern of brain disconnection on fMRI may therefore help predict the development of visual hallucinations in patients with Parkinson’s disease.

An imperfect understanding of the pathophysiology behind visual hallucinations in Parkinson’s disease has hindered the development of effective treatments. Previous fMRI studies of these symptoms focused on task-based imaging, but visual hallucinations are associated with the development of cognitive decline, which could have influenced participants’ ability to perform specific tasks in the imager.
Dagmar H. Hepp, MD, of the Department of Neurology at VU University Medical Center in Amsterdam, and colleagues retrospectively examined resting-state fMRI data for 55 patients with Parkinson’s disease and 15 healthy controls who participated in a prospective cohort study. Of the participants with Parkinson’s disease, 15 had visual hallucinations. Dr. Hepp’s team calculated functional connectivity between 47 brain regions of interest. They compared whole-brain and region-specific means of connectivity using a general linear model with false discovery rate control for multiple comparisons.
In eight regions in the occipital lobe and paracentral area, functional connectivity was lower in all patients with Parkinson’s disease, compared with controls. Compared with controls, patients with Parkinson’s disease and visual hallucinations—but not patients with Parkinson’s disease without visual hallucinations—had nine brain regions with reduced functional connectivity. These regions were in the frontal cortex (ie, the superior frontal gyrus), temporal cortex (eg, the superior temporal gyrus), rolandic operculum, occipital cortex, and striatum. Connectivity of the superior temporal gyrus was correlated with orientation, attention, praxis, perception, and intraextra dimensional set shifting. Loss of functional connectivity of the rolandic operculum correlated with lower cognitive test scores in the subdomains of praxis and perception.
The superior frontal gyrus contributes to the allocation and maintenance of visuospatial attention and inhibitory control. This region also may allow an individual to reflect on sensory experience and judge its possible significance in relation to the self. Investigators believe that the superior temporal gyrus influences visual attention and controls the dorsal and ventral visual streams. Disconnection of frontal and temporal areas may impair the discrimination of external perceptions from internally generated information.
“Our findings argue against the notion that a single specific functional brain region or network is the neural substrate of visual hallucinations in Parkinson’s disease, but rather supply further evidence for a more global loss of network efficiency, which could drive disturbed attentional and visual processing and thereby lead to visual hallucinations in Parkinson’s disease,” the authors concluded.
—Erik Greb
Suggested Reading
Hepp DH, Foncke EMJ, Olde Dubbelink KTE, et al. Loss of functional connectivity in patients with Parkinson disease and visual hallucinations. Radiology. 2017 Sep 27 [Epub ahead of print].
Visual hallucinations in Parkinson’s disease may arise from a global loss of network efficiency in the brain that disturbs visual attention and visual processing, according to research published online ahead of print September 27 in Radiology. A specific pattern of brain disconnection on fMRI may therefore help predict the development of visual hallucinations in patients with Parkinson’s disease.
An imperfect understanding of the pathophysiology behind visual hallucinations in Parkinson’s disease has hindered the development of effective treatments. Previous fMRI studies of these symptoms focused on task-based imaging, but visual hallucinations are associated with the development of cognitive decline, which could have influenced participants’ ability to perform specific tasks in the imager.
Dagmar H. Hepp, MD, of the Department of Neurology at VU University Medical Center in Amsterdam, and colleagues retrospectively examined resting-state fMRI data for 55 patients with Parkinson’s disease and 15 healthy controls who participated in a prospective cohort study. Of the participants with Parkinson’s disease, 15 had visual hallucinations. Dr. Hepp’s team calculated functional connectivity between 47 brain regions of interest. They compared whole-brain and region-specific means of connectivity using a general linear model with false discovery rate control for multiple comparisons.
In eight regions in the occipital lobe and paracentral area, functional connectivity was lower in all patients with Parkinson’s disease, compared with controls. Compared with controls, patients with Parkinson’s disease and visual hallucinations—but not patients with Parkinson’s disease without visual hallucinations—had nine brain regions with reduced functional connectivity. These regions were in the frontal cortex (ie, the superior frontal gyrus), temporal cortex (eg, the superior temporal gyrus), rolandic operculum, occipital cortex, and striatum. Connectivity of the superior temporal gyrus was correlated with orientation, attention, praxis, perception, and intraextra dimensional set shifting. Loss of functional connectivity of the rolandic operculum correlated with lower cognitive test scores in the subdomains of praxis and perception.
The superior frontal gyrus contributes to the allocation and maintenance of visuospatial attention and inhibitory control. This region also may allow an individual to reflect on sensory experience and judge its possible significance in relation to the self. Investigators believe that the superior temporal gyrus influences visual attention and controls the dorsal and ventral visual streams. Disconnection of frontal and temporal areas may impair the discrimination of external perceptions from internally generated information.
“Our findings argue against the notion that a single specific functional brain region or network is the neural substrate of visual hallucinations in Parkinson’s disease, but rather supply further evidence for a more global loss of network efficiency, which could drive disturbed attentional and visual processing and thereby lead to visual hallucinations in Parkinson’s disease,” the authors concluded.
—Erik Greb
Suggested Reading
Hepp DH, Foncke EMJ, Olde Dubbelink KTE, et al. Loss of functional connectivity in patients with Parkinson disease and visual hallucinations. Radiology. 2017 Sep 27 [Epub ahead of print].
Visual hallucinations in Parkinson’s disease may arise from a global loss of network efficiency in the brain that disturbs visual attention and visual processing, according to research published online ahead of print September 27 in Radiology. A specific pattern of brain disconnection on fMRI may therefore help predict the development of visual hallucinations in patients with Parkinson’s disease.
An imperfect understanding of the pathophysiology behind visual hallucinations in Parkinson’s disease has hindered the development of effective treatments. Previous fMRI studies of these symptoms focused on task-based imaging, but visual hallucinations are associated with the development of cognitive decline, which could have influenced participants’ ability to perform specific tasks in the imager.
Dagmar H. Hepp, MD, of the Department of Neurology at VU University Medical Center in Amsterdam, and colleagues retrospectively examined resting-state fMRI data for 55 patients with Parkinson’s disease and 15 healthy controls who participated in a prospective cohort study. Of the participants with Parkinson’s disease, 15 had visual hallucinations. Dr. Hepp’s team calculated functional connectivity between 47 brain regions of interest. They compared whole-brain and region-specific means of connectivity using a general linear model with false discovery rate control for multiple comparisons.
In eight regions in the occipital lobe and paracentral area, functional connectivity was lower in all patients with Parkinson’s disease, compared with controls. Compared with controls, patients with Parkinson’s disease and visual hallucinations—but not patients with Parkinson’s disease without visual hallucinations—had nine brain regions with reduced functional connectivity. These regions were in the frontal cortex (ie, the superior frontal gyrus), temporal cortex (eg, the superior temporal gyrus), rolandic operculum, occipital cortex, and striatum. Connectivity of the superior temporal gyrus was correlated with orientation, attention, praxis, perception, and intraextra dimensional set shifting. Loss of functional connectivity of the rolandic operculum correlated with lower cognitive test scores in the subdomains of praxis and perception.
The superior frontal gyrus contributes to the allocation and maintenance of visuospatial attention and inhibitory control. This region also may allow an individual to reflect on sensory experience and judge its possible significance in relation to the self. Investigators believe that the superior temporal gyrus influences visual attention and controls the dorsal and ventral visual streams. Disconnection of frontal and temporal areas may impair the discrimination of external perceptions from internally generated information.
“Our findings argue against the notion that a single specific functional brain region or network is the neural substrate of visual hallucinations in Parkinson’s disease, but rather supply further evidence for a more global loss of network efficiency, which could drive disturbed attentional and visual processing and thereby lead to visual hallucinations in Parkinson’s disease,” the authors concluded.
—Erik Greb
Suggested Reading
Hepp DH, Foncke EMJ, Olde Dubbelink KTE, et al. Loss of functional connectivity in patients with Parkinson disease and visual hallucinations. Radiology. 2017 Sep 27 [Epub ahead of print].
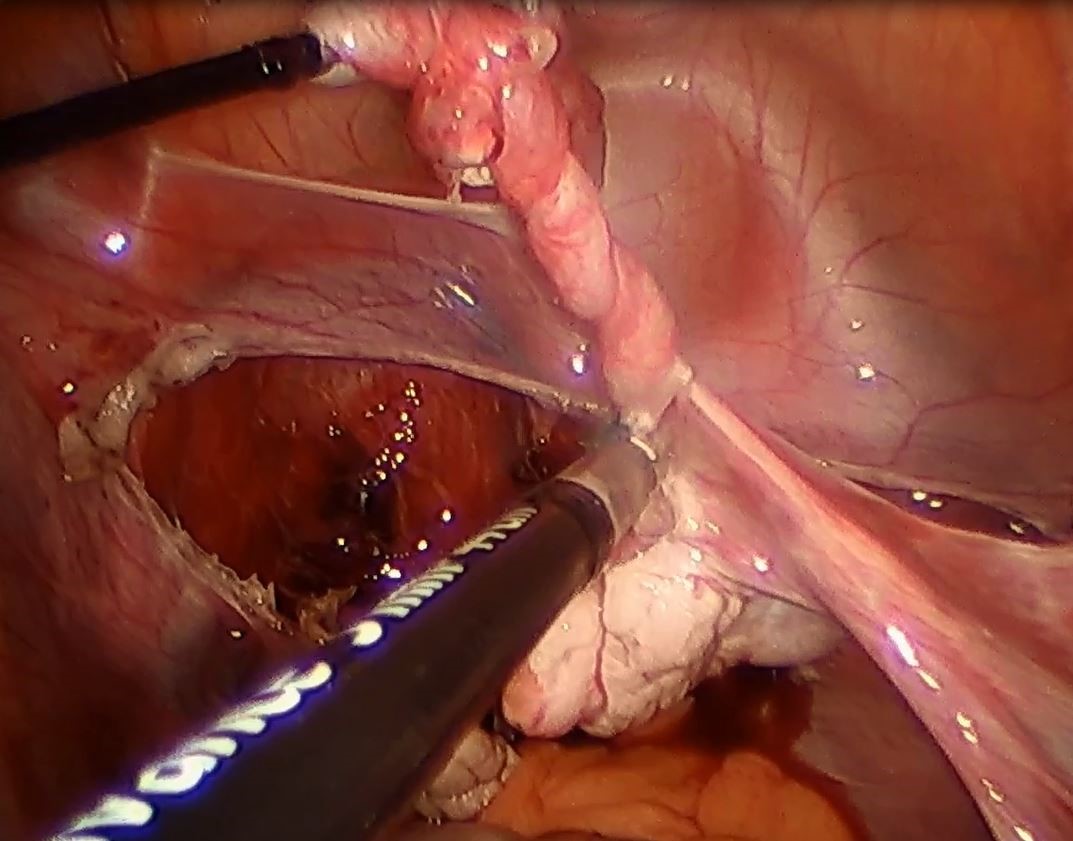
Strategies to overcome the loss of port placement triangulation

Visit the Society of Gynecologic Surgeons online: sgsonline.org
Additional videos from SGS are available here, including these recent offerings:
Visit the Society of Gynecologic Surgeons online: sgsonline.org
Additional videos from SGS are available here, including these recent offerings:
Visit the Society of Gynecologic Surgeons online: sgsonline.org
Additional videos from SGS are available here, including these recent offerings:
This video is brought to you by![]()
Clinical Challenges - November 2017 What's your diagnosis?
The diagnosis
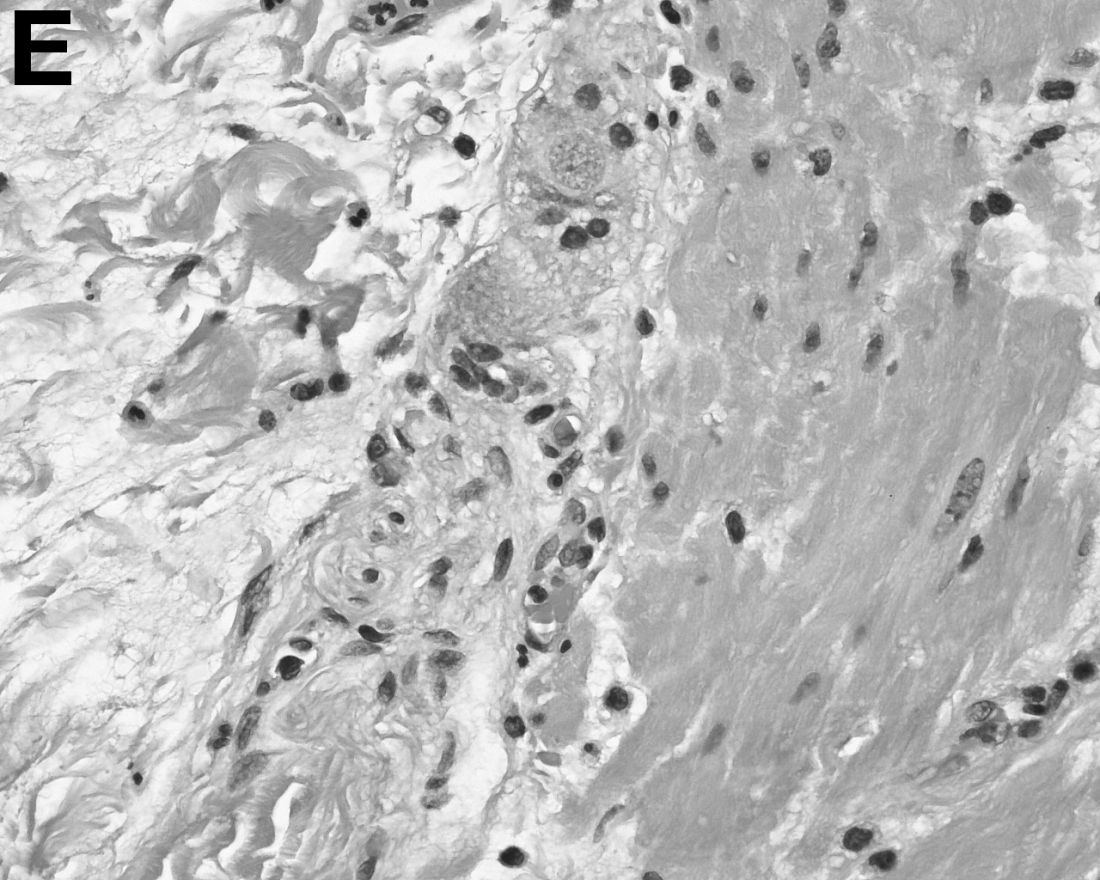
Answer: Hepatic foregut duplication cyst and concurrent acute gangrenous cholecystitis


References
1. Imamoglu K.H., Walt, A.J. Duplication of the duodenum extending into liver. Am J Surg. 1977;133:628-32.
2. Seidman J.D., Yale-Loehr A.J., Beaver B., et al. Alimentary duplication presenting as an hepatic cyst in a neonate. Am J Surg Pathol. 1991;15:695-8.
3. Vick D.J., Goodman Z.D., Deavers M.T., et al. Ciliated hepatic foregut cyst: A study of six cases and review of the literature. Am J Surg Pathol. 1999;23:671-7.
The diagnosis
Answer: Hepatic foregut duplication cyst and concurrent acute gangrenous cholecystitis
References
1. Imamoglu K.H., Walt, A.J. Duplication of the duodenum extending into liver. Am J Surg. 1977;133:628-32.
2. Seidman J.D., Yale-Loehr A.J., Beaver B., et al. Alimentary duplication presenting as an hepatic cyst in a neonate. Am J Surg Pathol. 1991;15:695-8.
3. Vick D.J., Goodman Z.D., Deavers M.T., et al. Ciliated hepatic foregut cyst: A study of six cases and review of the literature. Am J Surg Pathol. 1999;23:671-7.
The diagnosis
Answer: Hepatic foregut duplication cyst and concurrent acute gangrenous cholecystitis
References
1. Imamoglu K.H., Walt, A.J. Duplication of the duodenum extending into liver. Am J Surg. 1977;133:628-32.
2. Seidman J.D., Yale-Loehr A.J., Beaver B., et al. Alimentary duplication presenting as an hepatic cyst in a neonate. Am J Surg Pathol. 1991;15:695-8.
3. Vick D.J., Goodman Z.D., Deavers M.T., et al. Ciliated hepatic foregut cyst: A study of six cases and review of the literature. Am J Surg Pathol. 1999;23:671-7.
By Ryan Law, MD, Thomas C. Smyrk, and Stephen C. Hauser. Published previously in Gastroenterology (2013;144[3]:508, 658).
A 43-year-old woman presented with progressively worsening right upper-quadrant abdominal pain. The episodic pain occurred after high-fat meals and lasted from minutes to hours with accompanying nausea. Her previous medical history was notable for endometriosis. She denied other constitutional symptoms. Physical examination revealed no hepatosplenomegaly, jaundice, right upper-quadrant mass, or stigmata of chronic liver disease.
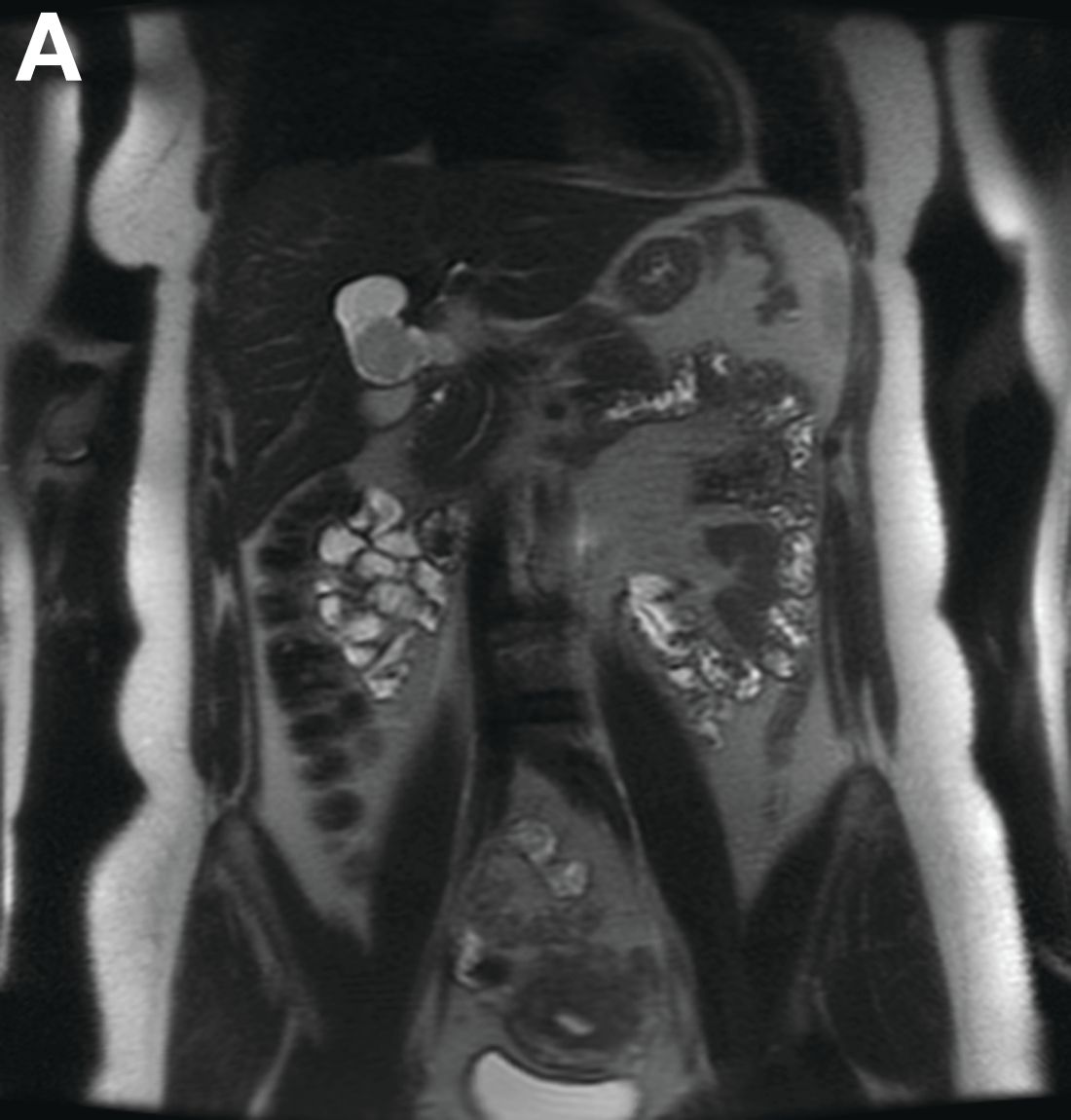
Initial laboratory evaluation yielded normal white blood cell count and liver chemistries. Ultrasonography, computed tomography, and magnetic resonance imaging of the abdomen all demonstrated a 2.0 × 4.1 × 3.9-cm, nonenhancing, elongated, cystic mass located superior to the gallbladder within the porta hepatis, with possible communication at the bile duct confluence and abutment of the right portal vein (Figure A). No definitive findings of acute cholecystitis were present.
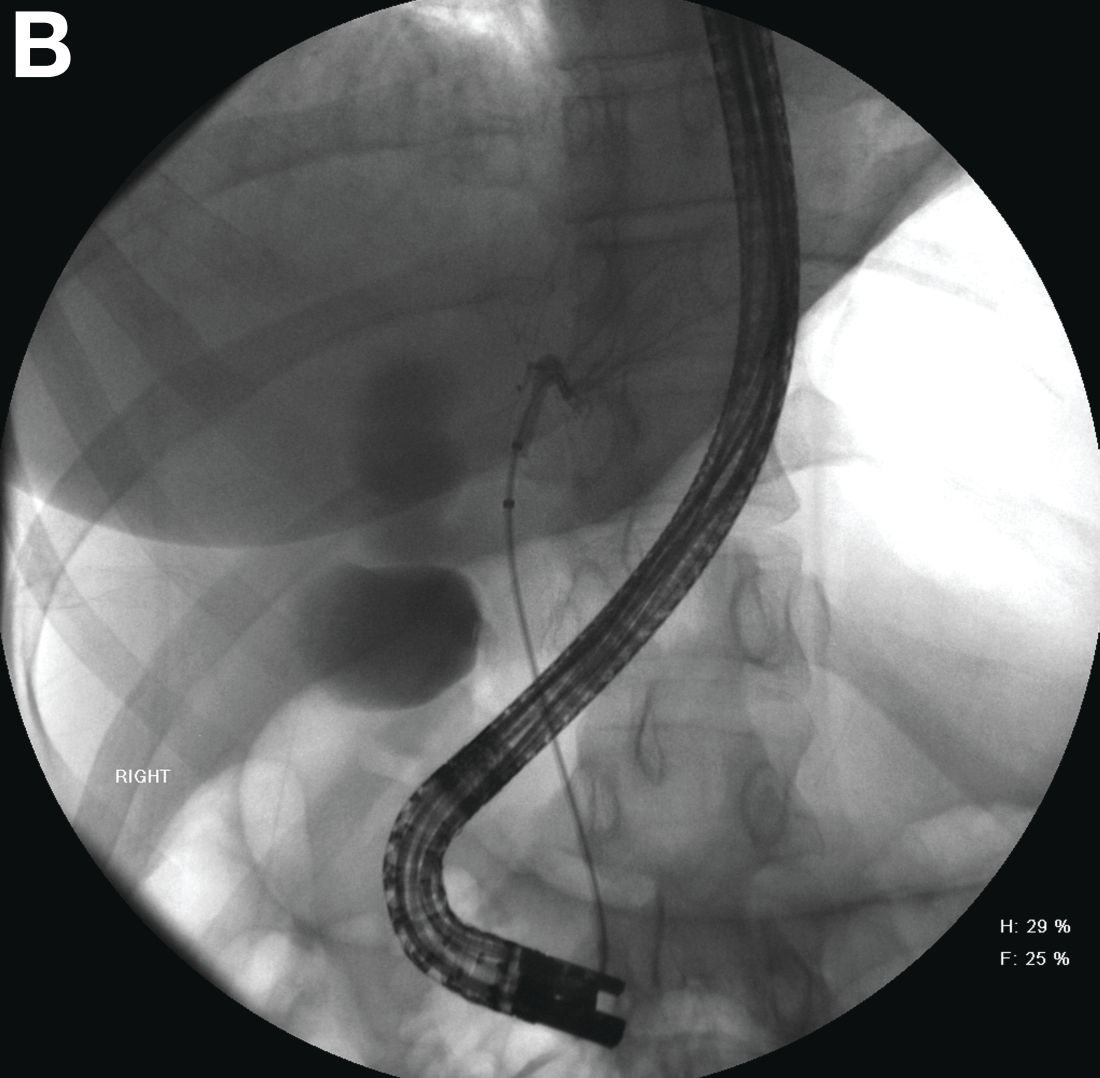
Endoscopic retrograde cholangiopancreatography with endoscopic ultrasonography was performed to further delineate the anatomy of the lesion. On endoscopic ultrasonography, the structure in question seemed to be embedded in the hepatic parenchyma with partial extension beyond the liver edge. Adherent debris was noted within the cystic structure. No lymphadenopathy was present. Cholangiography demonstrated filling of the lesion from a central right intrahepatic duct (Figure B). Attempts at cannulation of the cyst were unsuccessful.
The patient subsequently developed abnormal liver chemistries with continued right upper-quadrant pain. She was referred to an experienced hepatobiliary surgeon and underwent operative intervention. What is the diagnosis and how would you treat this patient?
Smell Test May Identify Increased Risk of Parkinson’s Disease
A smell test may identify people at increased risk of incident Parkinson’s disease as many as 10 years before diagnosis, according to research published in the October 3 issue of Neurology. The association between poor olfaction and incident Parkinson’s disease may be stronger among men than among women, and among whites than among blacks, and this possibility requires further investigation, said the authors.

“Earlier studies had shown prediction of Parkinson’s disease about four to five years after the smell test was taken,” said Honglei Chen, MD, PhD, Professor of Epidemiology and Biostatistics at the Michigan State University College of Human Medicine in East Lansing. “Our study shows that this test may be able to inform the risk much earlier than that.”
A Prospective Study of the Elderly
Dr. Chen and colleagues examined data for 1,510 white participants and 952 black participants in the Health, Aging, and Body Composition study. During clinical examinations in 1999 and 2000, the participants underwent the Brief Smell Identification Test (BSIT). The researchers followed the population until the date of Parkinson’s disease diagnosis, death, last contact, or August 31, 2012, whichever came first. Parkinson’s disease was diagnosed retrospectively using several data sources. Dr. Chen and colleagues used multivariable Cox models to estimate hazard ratios for Parkinson’s disease.
Participants’ mean age was 76. About 49% of participants were male, and approximately 39% of the population was black. During a mean follow-up duration of 9.8 years, the researchers identified 42 incident cases of Parkinson’s disease, including 30 white participants and 12 black participants.
Patients in the lowest tertile of BSIT scores (ie, those with the worst olfaction) were older and more likely to be male, black, and current smokers, compared with participants in the highest tertile of BSIT scores. Participants in the lowest BSIT tertile also were less likely to report education beyond high school or optimal health.
Olfaction Predicted Parkinson’s Disease
Overall, poor olfaction was associated with a higher risk of Parkinson’s disease. Compared with the highest BSIT tertile, the hazard ratio for Parkinson’s disease was 1.3 for the middle tertile and 4.8 for the lowest tertile. The association between olfaction and Parkinson’s disease was stronger among whites than among blacks, and stronger among men than among women.
Furthermore, the association between olfaction and Parkinson’s disease was significant for the first five years of follow-up, as well as for the period of follow-up after five years. In lagged analyses that excluded the first years of follow-up, the association remained similarly strong for the first six years of follow-up (hazard ratio, 4.1–5.0), after which point the hazard ratio decreased to 2.9.
“Previous studies have shown that black people are more likely to have a poor sense of smell than whites, and yet may be less likely to develop Parkinson’s disease,” said Dr. Chen. “We found no statistical significance for a link between poor sense of smell and Parkinson’s disease in blacks, but that may have been due to the small sample size. More research is needed to further investigate a possible link.”
Several Factors Could Explain Hyposmia
“The observation that black participants have higher prevalence of hyposmia yet lower incidence of Parkinson’s disease needs further clarification to determine whether this observation is simply methodologic … or if there is a true biologic explanation,” said Gene L. Bowman, ND, MPH, Adjunct Assistant Professor of Neurology at Oregon Health and Science University in Portland, in an accompanying editorial.
One of the study’s limitations is that other factors besides neurodegeneration could explain hyposmia. The cause of the olfactory dysfunction observed in the study could be a subject for further research. “More granularity on the specific aspects of the smell tests that are impaired (eg, detection, identification, intensity) would help time-constrained clinicians focus on the most relevant tests,” Dr. Bowman concluded.
—Erik Greb
Suggested Reading
Bowman GL. Biomarkers for early detection of Parkinson disease: a scent of consistency with olfactory dysfunction. Neurology. 2017;89(14):1432-1434.
Chen H, Shrestha S, Huang X, et al. Olfaction and incident Parkinson disease in US white and black older adults. Neurology. 2017
A smell test may identify people at increased risk of incident Parkinson’s disease as many as 10 years before diagnosis, according to research published in the October 3 issue of Neurology. The association between poor olfaction and incident Parkinson’s disease may be stronger among men than among women, and among whites than among blacks, and this possibility requires further investigation, said the authors.
“Earlier studies had shown prediction of Parkinson’s disease about four to five years after the smell test was taken,” said Honglei Chen, MD, PhD, Professor of Epidemiology and Biostatistics at the Michigan State University College of Human Medicine in East Lansing. “Our study shows that this test may be able to inform the risk much earlier than that.”
A Prospective Study of the Elderly
Dr. Chen and colleagues examined data for 1,510 white participants and 952 black participants in the Health, Aging, and Body Composition study. During clinical examinations in 1999 and 2000, the participants underwent the Brief Smell Identification Test (BSIT). The researchers followed the population until the date of Parkinson’s disease diagnosis, death, last contact, or August 31, 2012, whichever came first. Parkinson’s disease was diagnosed retrospectively using several data sources. Dr. Chen and colleagues used multivariable Cox models to estimate hazard ratios for Parkinson’s disease.
Participants’ mean age was 76. About 49% of participants were male, and approximately 39% of the population was black. During a mean follow-up duration of 9.8 years, the researchers identified 42 incident cases of Parkinson’s disease, including 30 white participants and 12 black participants.
Patients in the lowest tertile of BSIT scores (ie, those with the worst olfaction) were older and more likely to be male, black, and current smokers, compared with participants in the highest tertile of BSIT scores. Participants in the lowest BSIT tertile also were less likely to report education beyond high school or optimal health.
Olfaction Predicted Parkinson’s Disease
Overall, poor olfaction was associated with a higher risk of Parkinson’s disease. Compared with the highest BSIT tertile, the hazard ratio for Parkinson’s disease was 1.3 for the middle tertile and 4.8 for the lowest tertile. The association between olfaction and Parkinson’s disease was stronger among whites than among blacks, and stronger among men than among women.
Furthermore, the association between olfaction and Parkinson’s disease was significant for the first five years of follow-up, as well as for the period of follow-up after five years. In lagged analyses that excluded the first years of follow-up, the association remained similarly strong for the first six years of follow-up (hazard ratio, 4.1–5.0), after which point the hazard ratio decreased to 2.9.
“Previous studies have shown that black people are more likely to have a poor sense of smell than whites, and yet may be less likely to develop Parkinson’s disease,” said Dr. Chen. “We found no statistical significance for a link between poor sense of smell and Parkinson’s disease in blacks, but that may have been due to the small sample size. More research is needed to further investigate a possible link.”
Several Factors Could Explain Hyposmia
“The observation that black participants have higher prevalence of hyposmia yet lower incidence of Parkinson’s disease needs further clarification to determine whether this observation is simply methodologic … or if there is a true biologic explanation,” said Gene L. Bowman, ND, MPH, Adjunct Assistant Professor of Neurology at Oregon Health and Science University in Portland, in an accompanying editorial.
One of the study’s limitations is that other factors besides neurodegeneration could explain hyposmia. The cause of the olfactory dysfunction observed in the study could be a subject for further research. “More granularity on the specific aspects of the smell tests that are impaired (eg, detection, identification, intensity) would help time-constrained clinicians focus on the most relevant tests,” Dr. Bowman concluded.
—Erik Greb
Suggested Reading
Bowman GL. Biomarkers for early detection of Parkinson disease: a scent of consistency with olfactory dysfunction. Neurology. 2017;89(14):1432-1434.
Chen H, Shrestha S, Huang X, et al. Olfaction and incident Parkinson disease in US white and black older adults. Neurology. 2017
A smell test may identify people at increased risk of incident Parkinson’s disease as many as 10 years before diagnosis, according to research published in the October 3 issue of Neurology. The association between poor olfaction and incident Parkinson’s disease may be stronger among men than among women, and among whites than among blacks, and this possibility requires further investigation, said the authors.
“Earlier studies had shown prediction of Parkinson’s disease about four to five years after the smell test was taken,” said Honglei Chen, MD, PhD, Professor of Epidemiology and Biostatistics at the Michigan State University College of Human Medicine in East Lansing. “Our study shows that this test may be able to inform the risk much earlier than that.”
A Prospective Study of the Elderly
Dr. Chen and colleagues examined data for 1,510 white participants and 952 black participants in the Health, Aging, and Body Composition study. During clinical examinations in 1999 and 2000, the participants underwent the Brief Smell Identification Test (BSIT). The researchers followed the population until the date of Parkinson’s disease diagnosis, death, last contact, or August 31, 2012, whichever came first. Parkinson’s disease was diagnosed retrospectively using several data sources. Dr. Chen and colleagues used multivariable Cox models to estimate hazard ratios for Parkinson’s disease.
Participants’ mean age was 76. About 49% of participants were male, and approximately 39% of the population was black. During a mean follow-up duration of 9.8 years, the researchers identified 42 incident cases of Parkinson’s disease, including 30 white participants and 12 black participants.
Patients in the lowest tertile of BSIT scores (ie, those with the worst olfaction) were older and more likely to be male, black, and current smokers, compared with participants in the highest tertile of BSIT scores. Participants in the lowest BSIT tertile also were less likely to report education beyond high school or optimal health.
Olfaction Predicted Parkinson’s Disease
Overall, poor olfaction was associated with a higher risk of Parkinson’s disease. Compared with the highest BSIT tertile, the hazard ratio for Parkinson’s disease was 1.3 for the middle tertile and 4.8 for the lowest tertile. The association between olfaction and Parkinson’s disease was stronger among whites than among blacks, and stronger among men than among women.
Furthermore, the association between olfaction and Parkinson’s disease was significant for the first five years of follow-up, as well as for the period of follow-up after five years. In lagged analyses that excluded the first years of follow-up, the association remained similarly strong for the first six years of follow-up (hazard ratio, 4.1–5.0), after which point the hazard ratio decreased to 2.9.
“Previous studies have shown that black people are more likely to have a poor sense of smell than whites, and yet may be less likely to develop Parkinson’s disease,” said Dr. Chen. “We found no statistical significance for a link between poor sense of smell and Parkinson’s disease in blacks, but that may have been due to the small sample size. More research is needed to further investigate a possible link.”
Several Factors Could Explain Hyposmia
“The observation that black participants have higher prevalence of hyposmia yet lower incidence of Parkinson’s disease needs further clarification to determine whether this observation is simply methodologic … or if there is a true biologic explanation,” said Gene L. Bowman, ND, MPH, Adjunct Assistant Professor of Neurology at Oregon Health and Science University in Portland, in an accompanying editorial.
One of the study’s limitations is that other factors besides neurodegeneration could explain hyposmia. The cause of the olfactory dysfunction observed in the study could be a subject for further research. “More granularity on the specific aspects of the smell tests that are impaired (eg, detection, identification, intensity) would help time-constrained clinicians focus on the most relevant tests,” Dr. Bowman concluded.
—Erik Greb
Suggested Reading
Bowman GL. Biomarkers for early detection of Parkinson disease: a scent of consistency with olfactory dysfunction. Neurology. 2017;89(14):1432-1434.
Chen H, Shrestha S, Huang X, et al. Olfaction and incident Parkinson disease in US white and black older adults. Neurology. 2017
Endoscopic therapy effective for early cancer in Barrett’s esophagus
ORLANDO – Endoscopic therapy is as effective in Barrett’s esophagus patients with early cancer as in those with high-grade dysplasia, according to findings from an international multicenter consortium.
The findings suggest that invasive surgery may be avoidable in many Barrett’s esophagus patients with early cancer, Rajesh Krishnamoorthi, MD, of Virginia Mason Medical Center, Seattle, reported at the World Congress of Gastroenterology at ACG 2017.

Further, after adjustment for age, sex, and Barrett’s esophagus length, there was no statistical difference in the CE-IM rate (hazard ratio, 1.15) or CE-D rate (HR, 1.21) between the two groups.
The rates of recurrent intestinal metaplasia (Re-IM) in the groups were also statistically similar at 43.9% and 34.7%, respectively, said Dr. Krishnamoorthi, whose work received a 2017 Esophagus Category Award at the meeting.
Endoscopic therapy is the treatment of choice for Barrett’s esophagus patients with high-grade dysplasia, and is also used in some cases as a noninvasive alternative to surgery in Barrett’s esophagus patients with intramucosal cancer. However, data comparing outcomes of endoscopic therapy for these two conditions are lacking.
For the current study, all subjects from the EET database of patients from 10 centers in the United States, Europe, and Australia with either intramucosal cancer or high-grade dysplasia who underwent endoscopic therapy since April 2012 were reviewed. The patients were treated with endoscopic mucosal resection if visible lesions were noted, and/or with mucosal ablation for the flat Barrett’s esophagus. Those who underwent at least four esophagogastroduodenoscopies with endoscopic therapy were included.
The median age of the patients was 66 years, 84% were men, and median Barrett’s esophagus segment length was 6 cm. Baseline characteristics did not differ between the groups, Dr. Krishnamoorthi noted.
Although limited by the relatively small number of patients in each study group, by the exclusion of patients who were lost to follow-up, and by the observational nature of the study, the findings could have implications for treatment selection in some patients with Barrett’s esophagus and early cancer.
“In this large well-defined cohort of Barrett’s patients, effectiveness of endoscopic therapy in intramucosal cancer is comparable to that of high-grade dysplasia. Consideration of endoscopic therapy in Barrett’s patients with early cancer could reduce the need for invasive surgery,” he concluded.
During a discussion period, however, it was pointed out that the centers involved in this study are “centers with a lot of expertise in this,” and that the generalizability of the findings to gastroenterology practices is something that should be looked at, especially considering that the diagnosis of intramucosal cancer “may not be uniformly accurate across the spectrum of gastroenterology practices.”
“I completely agree with that,” Dr. Krishnamoorthi said, adding that the diagnosis must be confirmed by a pathologist, and that the procedure should be performed by an endoscopist with extensive experience.
Dr. Krishnamoorthi reported having no disclosures.
ORLANDO – Endoscopic therapy is as effective in Barrett’s esophagus patients with early cancer as in those with high-grade dysplasia, according to findings from an international multicenter consortium.
The findings suggest that invasive surgery may be avoidable in many Barrett’s esophagus patients with early cancer, Rajesh Krishnamoorthi, MD, of Virginia Mason Medical Center, Seattle, reported at the World Congress of Gastroenterology at ACG 2017.
Further, after adjustment for age, sex, and Barrett’s esophagus length, there was no statistical difference in the CE-IM rate (hazard ratio, 1.15) or CE-D rate (HR, 1.21) between the two groups.
The rates of recurrent intestinal metaplasia (Re-IM) in the groups were also statistically similar at 43.9% and 34.7%, respectively, said Dr. Krishnamoorthi, whose work received a 2017 Esophagus Category Award at the meeting.
Endoscopic therapy is the treatment of choice for Barrett’s esophagus patients with high-grade dysplasia, and is also used in some cases as a noninvasive alternative to surgery in Barrett’s esophagus patients with intramucosal cancer. However, data comparing outcomes of endoscopic therapy for these two conditions are lacking.
For the current study, all subjects from the EET database of patients from 10 centers in the United States, Europe, and Australia with either intramucosal cancer or high-grade dysplasia who underwent endoscopic therapy since April 2012 were reviewed. The patients were treated with endoscopic mucosal resection if visible lesions were noted, and/or with mucosal ablation for the flat Barrett’s esophagus. Those who underwent at least four esophagogastroduodenoscopies with endoscopic therapy were included.
The median age of the patients was 66 years, 84% were men, and median Barrett’s esophagus segment length was 6 cm. Baseline characteristics did not differ between the groups, Dr. Krishnamoorthi noted.
Although limited by the relatively small number of patients in each study group, by the exclusion of patients who were lost to follow-up, and by the observational nature of the study, the findings could have implications for treatment selection in some patients with Barrett’s esophagus and early cancer.
“In this large well-defined cohort of Barrett’s patients, effectiveness of endoscopic therapy in intramucosal cancer is comparable to that of high-grade dysplasia. Consideration of endoscopic therapy in Barrett’s patients with early cancer could reduce the need for invasive surgery,” he concluded.
During a discussion period, however, it was pointed out that the centers involved in this study are “centers with a lot of expertise in this,” and that the generalizability of the findings to gastroenterology practices is something that should be looked at, especially considering that the diagnosis of intramucosal cancer “may not be uniformly accurate across the spectrum of gastroenterology practices.”
“I completely agree with that,” Dr. Krishnamoorthi said, adding that the diagnosis must be confirmed by a pathologist, and that the procedure should be performed by an endoscopist with extensive experience.
Dr. Krishnamoorthi reported having no disclosures.
ORLANDO – Endoscopic therapy is as effective in Barrett’s esophagus patients with early cancer as in those with high-grade dysplasia, according to findings from an international multicenter consortium.
The findings suggest that invasive surgery may be avoidable in many Barrett’s esophagus patients with early cancer, Rajesh Krishnamoorthi, MD, of Virginia Mason Medical Center, Seattle, reported at the World Congress of Gastroenterology at ACG 2017.
Further, after adjustment for age, sex, and Barrett’s esophagus length, there was no statistical difference in the CE-IM rate (hazard ratio, 1.15) or CE-D rate (HR, 1.21) between the two groups.
The rates of recurrent intestinal metaplasia (Re-IM) in the groups were also statistically similar at 43.9% and 34.7%, respectively, said Dr. Krishnamoorthi, whose work received a 2017 Esophagus Category Award at the meeting.
Endoscopic therapy is the treatment of choice for Barrett’s esophagus patients with high-grade dysplasia, and is also used in some cases as a noninvasive alternative to surgery in Barrett’s esophagus patients with intramucosal cancer. However, data comparing outcomes of endoscopic therapy for these two conditions are lacking.
For the current study, all subjects from the EET database of patients from 10 centers in the United States, Europe, and Australia with either intramucosal cancer or high-grade dysplasia who underwent endoscopic therapy since April 2012 were reviewed. The patients were treated with endoscopic mucosal resection if visible lesions were noted, and/or with mucosal ablation for the flat Barrett’s esophagus. Those who underwent at least four esophagogastroduodenoscopies with endoscopic therapy were included.
The median age of the patients was 66 years, 84% were men, and median Barrett’s esophagus segment length was 6 cm. Baseline characteristics did not differ between the groups, Dr. Krishnamoorthi noted.
Although limited by the relatively small number of patients in each study group, by the exclusion of patients who were lost to follow-up, and by the observational nature of the study, the findings could have implications for treatment selection in some patients with Barrett’s esophagus and early cancer.
“In this large well-defined cohort of Barrett’s patients, effectiveness of endoscopic therapy in intramucosal cancer is comparable to that of high-grade dysplasia. Consideration of endoscopic therapy in Barrett’s patients with early cancer could reduce the need for invasive surgery,” he concluded.
During a discussion period, however, it was pointed out that the centers involved in this study are “centers with a lot of expertise in this,” and that the generalizability of the findings to gastroenterology practices is something that should be looked at, especially considering that the diagnosis of intramucosal cancer “may not be uniformly accurate across the spectrum of gastroenterology practices.”
“I completely agree with that,” Dr. Krishnamoorthi said, adding that the diagnosis must be confirmed by a pathologist, and that the procedure should be performed by an endoscopist with extensive experience.
Dr. Krishnamoorthi reported having no disclosures.
AT THE 13th WORLD CONGRESS OF GASTROENTEROLOGY
Key clinical point:
Major finding: Outcomes did not differ significantly between Barrett’s esophagus patients with early cancer and those with high-grade dysplasia (hazard ratios for CE-IM and CE-D, respectively: 1.15, and 1.21).
Data source: Study of 276 patients from a prospective database.
Disclosures: Dr. Krishnamoorthi reported having no disclosures.
Quick Byte: Telemental health visits on the rise
Telemental health visits are on the rise.

In 2014, there were 5.3 and 11.8 telemental health visits per 100 rural beneficiaries with any mental illness or serious mental illness, respectively.
Reference
Mehrotra A, Huskamp HA, Souza J, et al. Rapid growth in mental health telemedicine use among rural Medicare beneficiaries, wide variation across states. Health Aff. 2017 May 1;36(5):909-17. Accessed May 24, 2017.
Telemental health visits are on the rise.
In 2014, there were 5.3 and 11.8 telemental health visits per 100 rural beneficiaries with any mental illness or serious mental illness, respectively.
Reference
Mehrotra A, Huskamp HA, Souza J, et al. Rapid growth in mental health telemedicine use among rural Medicare beneficiaries, wide variation across states. Health Aff. 2017 May 1;36(5):909-17. Accessed May 24, 2017.
Telemental health visits are on the rise.
In 2014, there were 5.3 and 11.8 telemental health visits per 100 rural beneficiaries with any mental illness or serious mental illness, respectively.
Reference
Mehrotra A, Huskamp HA, Souza J, et al. Rapid growth in mental health telemedicine use among rural Medicare beneficiaries, wide variation across states. Health Aff. 2017 May 1;36(5):909-17. Accessed May 24, 2017.

Guidelines are not cookbooks
For many years I have counseled medical students and residents that half of what I was taught in medical school has since been proven obsolete or frankly wrong. I counsel them that I have no reason to believe that I am any better than my professors were. So I wish them luck sorting out what is true. Earlier in my career, that warning was mild hyperbole, but not anymore.
Upper respiratory infections (URIs) are the most common reason for an office visit during the winter. Bronchiolitis is the most frequent diagnosis for a winter admission of an infant to a community hospital. Pediatricians have nuanced assessments and many options when treating these diseases. Best practices have changed frequently over the past 3 decades, mostly by eliminating previously espoused treatments as ineffective. In infants and young children, those obsolete treatments include decongestants and cough suppressants for young children with common colds, inhaled beta-agonists and steroids for infants with bronchiolitis, and antibiotics for simple otitis media in older children. In other words, most of what I was originally taught.
There is a discontinuity between guidelines that forbid routine steroids and beta-agonists for bronchiolitis in infants, and guidelines that strongly prescribe steroids, metered dose inhalers, and asthma action plans for all discharged wheezers over age 2 years. When I worked as a hospitalist in the pulmonology department, I frequently diagnosed asthma under age 1 year. As a general pediatric hospitalist, one winter I twice ran afoul of a hospital quality metric that benchmarked 100% compliance with providing steroids, inhaled corticosteroids, and asthma action plans on discharge for all wheezers over age 2. Fortunately for both me and the quality team working on that quality dashboard, my thorough documentation of why I didn’t think a particular wheezer had asthma was detailed enough to satisfy peer review.
Historically, medical knowledge has been dependent upon these types of observation which then are taught to the next generation of physicians and, if confirmed repeatedly, become memes with some degree of reliability. An all-too-typical Cochrane library entry may challenge these memes by looking at 200 articles, finding 20 relevant studies, selecting only 2 underpowered studies as meeting their randomized controlled trial criteria, and then concluding that there is “insufficient evidence” to prove the treatment works. But absence of proof is not proof of absence. Twenty five years after coining the phrase “evidence-based medicine,” our medical knowledge base has not been purified.

In medicine, absolute certainty isn’t possible. Using 95% confidence intervals for a research paper does not even mean it is 95% likely to be right. So part of (which is tainted with confirmation bias.) It is a very imperfect art.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
For many years I have counseled medical students and residents that half of what I was taught in medical school has since been proven obsolete or frankly wrong. I counsel them that I have no reason to believe that I am any better than my professors were. So I wish them luck sorting out what is true. Earlier in my career, that warning was mild hyperbole, but not anymore.
Upper respiratory infections (URIs) are the most common reason for an office visit during the winter. Bronchiolitis is the most frequent diagnosis for a winter admission of an infant to a community hospital. Pediatricians have nuanced assessments and many options when treating these diseases. Best practices have changed frequently over the past 3 decades, mostly by eliminating previously espoused treatments as ineffective. In infants and young children, those obsolete treatments include decongestants and cough suppressants for young children with common colds, inhaled beta-agonists and steroids for infants with bronchiolitis, and antibiotics for simple otitis media in older children. In other words, most of what I was originally taught.
There is a discontinuity between guidelines that forbid routine steroids and beta-agonists for bronchiolitis in infants, and guidelines that strongly prescribe steroids, metered dose inhalers, and asthma action plans for all discharged wheezers over age 2 years. When I worked as a hospitalist in the pulmonology department, I frequently diagnosed asthma under age 1 year. As a general pediatric hospitalist, one winter I twice ran afoul of a hospital quality metric that benchmarked 100% compliance with providing steroids, inhaled corticosteroids, and asthma action plans on discharge for all wheezers over age 2. Fortunately for both me and the quality team working on that quality dashboard, my thorough documentation of why I didn’t think a particular wheezer had asthma was detailed enough to satisfy peer review.
Historically, medical knowledge has been dependent upon these types of observation which then are taught to the next generation of physicians and, if confirmed repeatedly, become memes with some degree of reliability. An all-too-typical Cochrane library entry may challenge these memes by looking at 200 articles, finding 20 relevant studies, selecting only 2 underpowered studies as meeting their randomized controlled trial criteria, and then concluding that there is “insufficient evidence” to prove the treatment works. But absence of proof is not proof of absence. Twenty five years after coining the phrase “evidence-based medicine,” our medical knowledge base has not been purified.
In medicine, absolute certainty isn’t possible. Using 95% confidence intervals for a research paper does not even mean it is 95% likely to be right. So part of (which is tainted with confirmation bias.) It is a very imperfect art.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
For many years I have counseled medical students and residents that half of what I was taught in medical school has since been proven obsolete or frankly wrong. I counsel them that I have no reason to believe that I am any better than my professors were. So I wish them luck sorting out what is true. Earlier in my career, that warning was mild hyperbole, but not anymore.
Upper respiratory infections (URIs) are the most common reason for an office visit during the winter. Bronchiolitis is the most frequent diagnosis for a winter admission of an infant to a community hospital. Pediatricians have nuanced assessments and many options when treating these diseases. Best practices have changed frequently over the past 3 decades, mostly by eliminating previously espoused treatments as ineffective. In infants and young children, those obsolete treatments include decongestants and cough suppressants for young children with common colds, inhaled beta-agonists and steroids for infants with bronchiolitis, and antibiotics for simple otitis media in older children. In other words, most of what I was originally taught.
There is a discontinuity between guidelines that forbid routine steroids and beta-agonists for bronchiolitis in infants, and guidelines that strongly prescribe steroids, metered dose inhalers, and asthma action plans for all discharged wheezers over age 2 years. When I worked as a hospitalist in the pulmonology department, I frequently diagnosed asthma under age 1 year. As a general pediatric hospitalist, one winter I twice ran afoul of a hospital quality metric that benchmarked 100% compliance with providing steroids, inhaled corticosteroids, and asthma action plans on discharge for all wheezers over age 2. Fortunately for both me and the quality team working on that quality dashboard, my thorough documentation of why I didn’t think a particular wheezer had asthma was detailed enough to satisfy peer review.
Historically, medical knowledge has been dependent upon these types of observation which then are taught to the next generation of physicians and, if confirmed repeatedly, become memes with some degree of reliability. An all-too-typical Cochrane library entry may challenge these memes by looking at 200 articles, finding 20 relevant studies, selecting only 2 underpowered studies as meeting their randomized controlled trial criteria, and then concluding that there is “insufficient evidence” to prove the treatment works. But absence of proof is not proof of absence. Twenty five years after coining the phrase “evidence-based medicine,” our medical knowledge base has not been purified.
In medicine, absolute certainty isn’t possible. Using 95% confidence intervals for a research paper does not even mean it is 95% likely to be right. So part of (which is tainted with confirmation bias.) It is a very imperfect art.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
“Great debates” at ACR 2017 address biosimilar switching, new curricular milestones
Two “Great Debates” at this year’s annual meeting of the American College of Rheumatology in San Diego will center on important, but completely separate, issues in rheumatology: whether it is safe to switch to a biosimilar and the relevance of curricular milestones in rheumatology training.
At 2:30 p.m. on Sunday, Nov. 5, a session titled “Biosimilars ... To Switch or Not to Switch? That Is the Question“ will pit Jonathan Kay, MD, against Roy Fleischmann, MD, to try to sway the audience to their point of view in the face of a small evidence base about the consequences of switching.
Dr. Kay, the Timothy S. and Elaine L. Peterson Chair in Rheumatology and professor of medicine at the University of Massachusetts, Worcester, where he directs clinical research in the division of rheumatology, will discuss and defend the usefulness of biosimilars for rheumatoid arthritis in his presentation, “The Data Supports That It Is Safe, Effective and Cost-Effective to Switch to a Biosimilar.” He has been greatly involved in clinical research on the development of biosimilars to treat rheumatic diseases in recent years.
In his presentation, “The Data Is Not Convincing. One Study Cannot Be Generalized to All Indications, and Some Studies Suggest That It Is Not Safe, Not Effective and Not Cost-Effective to Switch All Patients (YET) to a Biosimilar,” Dr. Fleischmann will discuss and defend the position that biosimilars are not yet well-enough researched to confidently allow switching. Dr. Fleischmann is clinical professor in the department of internal medicine at the University of Texas Southwestern Medical Center, Dallas.
At 7:30 a.m. on Monday, Nov. 6, two clinician-educators will advocate for opposing opinions in “The Great (Educational) Debate: Milestones: Meaningful vs. Millstone.” The debate will focus on the relative merits of the Accreditation Council for Graduate Medical Education’s Next Accreditation System, which in 2013 led to a paradigm shift in how training programs approach curriculum development, and how both trainees and their programs are assessed.
Calvin Brown, MD, professor of medicine in the division of rheumatology and director of the rheumatology training program at Northwestern University, Chicago, will describe the reported and perceived benefits of the milestones, while Simon Helfgott, MD, of Brigham and Women’s Hospital, Boston, will summarize the arguments that underlie the call for radical change in the milestones system of evaluation
Two “Great Debates” at this year’s annual meeting of the American College of Rheumatology in San Diego will center on important, but completely separate, issues in rheumatology: whether it is safe to switch to a biosimilar and the relevance of curricular milestones in rheumatology training.
At 2:30 p.m. on Sunday, Nov. 5, a session titled “Biosimilars ... To Switch or Not to Switch? That Is the Question“ will pit Jonathan Kay, MD, against Roy Fleischmann, MD, to try to sway the audience to their point of view in the face of a small evidence base about the consequences of switching.
Dr. Kay, the Timothy S. and Elaine L. Peterson Chair in Rheumatology and professor of medicine at the University of Massachusetts, Worcester, where he directs clinical research in the division of rheumatology, will discuss and defend the usefulness of biosimilars for rheumatoid arthritis in his presentation, “The Data Supports That It Is Safe, Effective and Cost-Effective to Switch to a Biosimilar.” He has been greatly involved in clinical research on the development of biosimilars to treat rheumatic diseases in recent years.
In his presentation, “The Data Is Not Convincing. One Study Cannot Be Generalized to All Indications, and Some Studies Suggest That It Is Not Safe, Not Effective and Not Cost-Effective to Switch All Patients (YET) to a Biosimilar,” Dr. Fleischmann will discuss and defend the position that biosimilars are not yet well-enough researched to confidently allow switching. Dr. Fleischmann is clinical professor in the department of internal medicine at the University of Texas Southwestern Medical Center, Dallas.
At 7:30 a.m. on Monday, Nov. 6, two clinician-educators will advocate for opposing opinions in “The Great (Educational) Debate: Milestones: Meaningful vs. Millstone.” The debate will focus on the relative merits of the Accreditation Council for Graduate Medical Education’s Next Accreditation System, which in 2013 led to a paradigm shift in how training programs approach curriculum development, and how both trainees and their programs are assessed.
Calvin Brown, MD, professor of medicine in the division of rheumatology and director of the rheumatology training program at Northwestern University, Chicago, will describe the reported and perceived benefits of the milestones, while Simon Helfgott, MD, of Brigham and Women’s Hospital, Boston, will summarize the arguments that underlie the call for radical change in the milestones system of evaluation
Two “Great Debates” at this year’s annual meeting of the American College of Rheumatology in San Diego will center on important, but completely separate, issues in rheumatology: whether it is safe to switch to a biosimilar and the relevance of curricular milestones in rheumatology training.
At 2:30 p.m. on Sunday, Nov. 5, a session titled “Biosimilars ... To Switch or Not to Switch? That Is the Question“ will pit Jonathan Kay, MD, against Roy Fleischmann, MD, to try to sway the audience to their point of view in the face of a small evidence base about the consequences of switching.
Dr. Kay, the Timothy S. and Elaine L. Peterson Chair in Rheumatology and professor of medicine at the University of Massachusetts, Worcester, where he directs clinical research in the division of rheumatology, will discuss and defend the usefulness of biosimilars for rheumatoid arthritis in his presentation, “The Data Supports That It Is Safe, Effective and Cost-Effective to Switch to a Biosimilar.” He has been greatly involved in clinical research on the development of biosimilars to treat rheumatic diseases in recent years.
In his presentation, “The Data Is Not Convincing. One Study Cannot Be Generalized to All Indications, and Some Studies Suggest That It Is Not Safe, Not Effective and Not Cost-Effective to Switch All Patients (YET) to a Biosimilar,” Dr. Fleischmann will discuss and defend the position that biosimilars are not yet well-enough researched to confidently allow switching. Dr. Fleischmann is clinical professor in the department of internal medicine at the University of Texas Southwestern Medical Center, Dallas.
At 7:30 a.m. on Monday, Nov. 6, two clinician-educators will advocate for opposing opinions in “The Great (Educational) Debate: Milestones: Meaningful vs. Millstone.” The debate will focus on the relative merits of the Accreditation Council for Graduate Medical Education’s Next Accreditation System, which in 2013 led to a paradigm shift in how training programs approach curriculum development, and how both trainees and their programs are assessed.
Calvin Brown, MD, professor of medicine in the division of rheumatology and director of the rheumatology training program at Northwestern University, Chicago, will describe the reported and perceived benefits of the milestones, while Simon Helfgott, MD, of Brigham and Women’s Hospital, Boston, will summarize the arguments that underlie the call for radical change in the milestones system of evaluation
FROM ACR 2017