User login
Management of adults with syncope
Syncope is characterized by sudden transient loss of consciousness due to cerebral hypoperfusion and is typically associated with an inability to maintain postural tone. There are many different causes and clinical presentations of syncope and the incidence varies depending on the population. Estimated lifetime prevalence rates are as high as 41% for a single episode of syncope, with recurrent syncope occurring in 13.5% of the general population. Incidence follows a trimodal distribution with peaks at age 20, 60, and 80 years for both men and women. The National Hospital Ambulatory Medical Care Survey reported 6.7 million episodes of syncope in the emergency department, which is where most patients with syncope initially present. However, patients may also present to the primary care outpatient setting, and providers should be equipped for initial evaluation and management.
Previous and current treatment guidelines
Although there have been general reviews published by general and specialty societies, there were no comprehensive guidelines on the evaluation and management of syncope until recently. The 2017 guideline from the American College of Cardiology, American Heart Association, and Heart Rhythm Society is intended to provide guidance on evaluation and management of syncope, specifically in the context of different clinical settings, specific causes, or selected circumstances.1
What primary care providers should know
A detailed history and physical exam should be performed in all patients with syncope. Useful details include the setting in which syncope occurs, prodromal symptoms, witness reports, postevent symptoms, comorbidities, medication use, past medical history, and family history. The physical exam should include orthostatic vital signs, cardiac exam, neurologic exam, and any other relevant systems. A resting 12-lead ECG in the initial evaluation is recommended to detect underlying arrhythmia or structural heart disease (Class I recommendation – strong).
There are many different causes of syncope (see Table 1). Vasovagal syncope, a form of reflex syncope mediated by the vasovagal reflex, is the most common cause of syncope and a frequent reason for emergency department visits. There is often a prodrome of diaphoresis, warmth, nausea, and/or pallor, often followed by fatigue. The diagnosis can be made by the history, physical exam, and eyewitness observation.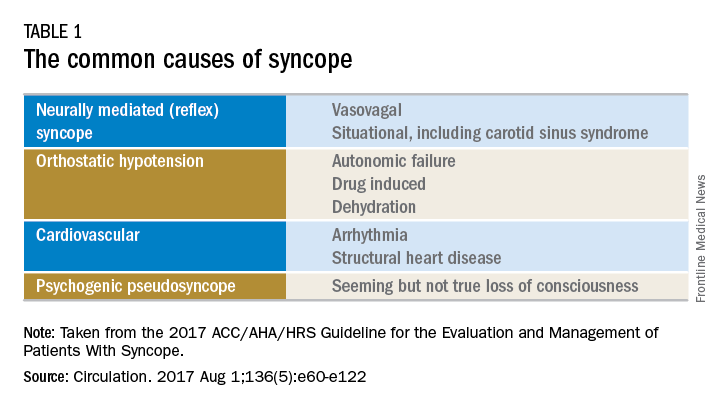
Once the initial evaluation is complete, further evaluation and management depends on the presence of risk factors presented in Table 2. Outpatient management is reasonable for patients with presumptive reflex-mediated syncope when there is an absence of serious medical conditions such as cardiac disease or comorbid neurologic disease. While hospital-based evaluation has not been shown to improve outcomes in patients with a low risk profile, hospital-based evaluation and treatment are recommended for patients presenting with syncope who have a serious medical condition potentially relevant to the cause of syncope.2 Serious medical conditions that require hospital management include arrhythmia, cardiac ischemia, severe aortic stenosis, hypertrophic cardiomyopathy, aortic dissection, acute heart failure, severe anemia, or major traumatic injury. Finally, patients with intermediate risk may benefit from an observational protocol in the emergency department.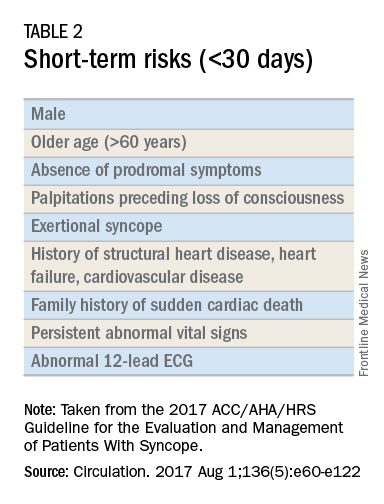
Routine and comprehensive laboratory testing is not useful in syncope work-up (Class III recommendation – no benefit). Routine cardiac imaging is not recommended unless a cardiac etiology is suspected and routine neurological imaging and EEG are not recommended in the absence of focal neurologic findings. Additional work-up may be indicated if initial evaluation suggests a more specific etiology. If the initial evaluation suggests neurogenic orthostatic hypotension but the diagnosis is not clear, then referral for an autonomic evaluation is reasonable. If reflex syncope is suspected, tilt-table testing may be helpful to confirm the diagnosis. Lastly, if a cardiovascular etiology is suspected, it is recommended that the patient have cardiac monitoring in the acute care setting. In this later group, stress testing, transthoracic echocardiogram, electrophysiology study, and/or MRI or CT may be useful. Electrophysiologic testing is reasonable in patients with suspected arrhythmia as the etiology for syncope (Class IIa recommendation – moderate strength). The guideline provides a convenient summary algorithm to approach the initial and subsequent evaluations for syncope based on the initial evaluation and presenting symptoms.

Special populations
There are specific considerations for certain populations. In the pediatric population, the vast majority of syncopal episodes are reflex syncope but breath-holding spells should also be considered. In the geriatric population, particularly individuals older than 75 years, the incidence of syncope is high, the differential diagnosis is broad, and the diagnosis may be imprecise given amnesia, falls, lack of witnesses, and polypharmacy. In this group, morbidity is high because of multimorbidity and frailty. A careful history and physical exam with orthostatic vital signs is important, as is a multidisciplinary approach with geriatric consultation when needed.

Summary
Syncope is a common clinical syndrome often presenting to the emergency department or primary care setting. There are many causes, the most common being vasovagal syncope. In the initial evaluation, providers should perform a detailed history and physical exam, check orthostatic signs and perform a 12-lead ECG. Patients can be evaluated and managed safely in the outpatient setting in the absence of risk factors. Routine comprehensive laboratory testing and cardiac imaging are often not needed. For patients with defined risk factors, a more detailed evaluation in the hospital is recommended.
Dr. Li is a second-year resident in the family medicine residency program in the department of family and community medicine at the Sidney Kimmel Medical College at Thomas Jefferson University, Philadelphia. Dr. Mills is assistant residency program director and assistant professor in the departments of family and community medicine and physiology at the Sidney Kimmel Medical College. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health.
References
1. Shen W, Sheldon RS, Benditt DG, et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope. Circulation. 2017 Aug 1;136(5):e60-e122. doi: 10.1161/CIR.0000000000000499. Epub 2017 Mar 9.
2. Soteriades ES, Evans JC, Larson MG, et al. Incidence and prognosis of syncope. N Engl J Med. 2002;347(12):878-85.
Syncope is characterized by sudden transient loss of consciousness due to cerebral hypoperfusion and is typically associated with an inability to maintain postural tone. There are many different causes and clinical presentations of syncope and the incidence varies depending on the population. Estimated lifetime prevalence rates are as high as 41% for a single episode of syncope, with recurrent syncope occurring in 13.5% of the general population. Incidence follows a trimodal distribution with peaks at age 20, 60, and 80 years for both men and women. The National Hospital Ambulatory Medical Care Survey reported 6.7 million episodes of syncope in the emergency department, which is where most patients with syncope initially present. However, patients may also present to the primary care outpatient setting, and providers should be equipped for initial evaluation and management.
Previous and current treatment guidelines
Although there have been general reviews published by general and specialty societies, there were no comprehensive guidelines on the evaluation and management of syncope until recently. The 2017 guideline from the American College of Cardiology, American Heart Association, and Heart Rhythm Society is intended to provide guidance on evaluation and management of syncope, specifically in the context of different clinical settings, specific causes, or selected circumstances.1
What primary care providers should know
A detailed history and physical exam should be performed in all patients with syncope. Useful details include the setting in which syncope occurs, prodromal symptoms, witness reports, postevent symptoms, comorbidities, medication use, past medical history, and family history. The physical exam should include orthostatic vital signs, cardiac exam, neurologic exam, and any other relevant systems. A resting 12-lead ECG in the initial evaluation is recommended to detect underlying arrhythmia or structural heart disease (Class I recommendation – strong).
There are many different causes of syncope (see Table 1). Vasovagal syncope, a form of reflex syncope mediated by the vasovagal reflex, is the most common cause of syncope and a frequent reason for emergency department visits. There is often a prodrome of diaphoresis, warmth, nausea, and/or pallor, often followed by fatigue. The diagnosis can be made by the history, physical exam, and eyewitness observation.
Once the initial evaluation is complete, further evaluation and management depends on the presence of risk factors presented in Table 2. Outpatient management is reasonable for patients with presumptive reflex-mediated syncope when there is an absence of serious medical conditions such as cardiac disease or comorbid neurologic disease. While hospital-based evaluation has not been shown to improve outcomes in patients with a low risk profile, hospital-based evaluation and treatment are recommended for patients presenting with syncope who have a serious medical condition potentially relevant to the cause of syncope.2 Serious medical conditions that require hospital management include arrhythmia, cardiac ischemia, severe aortic stenosis, hypertrophic cardiomyopathy, aortic dissection, acute heart failure, severe anemia, or major traumatic injury. Finally, patients with intermediate risk may benefit from an observational protocol in the emergency department.
Routine and comprehensive laboratory testing is not useful in syncope work-up (Class III recommendation – no benefit). Routine cardiac imaging is not recommended unless a cardiac etiology is suspected and routine neurological imaging and EEG are not recommended in the absence of focal neurologic findings. Additional work-up may be indicated if initial evaluation suggests a more specific etiology. If the initial evaluation suggests neurogenic orthostatic hypotension but the diagnosis is not clear, then referral for an autonomic evaluation is reasonable. If reflex syncope is suspected, tilt-table testing may be helpful to confirm the diagnosis. Lastly, if a cardiovascular etiology is suspected, it is recommended that the patient have cardiac monitoring in the acute care setting. In this later group, stress testing, transthoracic echocardiogram, electrophysiology study, and/or MRI or CT may be useful. Electrophysiologic testing is reasonable in patients with suspected arrhythmia as the etiology for syncope (Class IIa recommendation – moderate strength). The guideline provides a convenient summary algorithm to approach the initial and subsequent evaluations for syncope based on the initial evaluation and presenting symptoms.
Special populations
There are specific considerations for certain populations. In the pediatric population, the vast majority of syncopal episodes are reflex syncope but breath-holding spells should also be considered. In the geriatric population, particularly individuals older than 75 years, the incidence of syncope is high, the differential diagnosis is broad, and the diagnosis may be imprecise given amnesia, falls, lack of witnesses, and polypharmacy. In this group, morbidity is high because of multimorbidity and frailty. A careful history and physical exam with orthostatic vital signs is important, as is a multidisciplinary approach with geriatric consultation when needed.
Summary
Syncope is a common clinical syndrome often presenting to the emergency department or primary care setting. There are many causes, the most common being vasovagal syncope. In the initial evaluation, providers should perform a detailed history and physical exam, check orthostatic signs and perform a 12-lead ECG. Patients can be evaluated and managed safely in the outpatient setting in the absence of risk factors. Routine comprehensive laboratory testing and cardiac imaging are often not needed. For patients with defined risk factors, a more detailed evaluation in the hospital is recommended.
Dr. Li is a second-year resident in the family medicine residency program in the department of family and community medicine at the Sidney Kimmel Medical College at Thomas Jefferson University, Philadelphia. Dr. Mills is assistant residency program director and assistant professor in the departments of family and community medicine and physiology at the Sidney Kimmel Medical College. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health.
References
1. Shen W, Sheldon RS, Benditt DG, et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope. Circulation. 2017 Aug 1;136(5):e60-e122. doi: 10.1161/CIR.0000000000000499. Epub 2017 Mar 9.
2. Soteriades ES, Evans JC, Larson MG, et al. Incidence and prognosis of syncope. N Engl J Med. 2002;347(12):878-85.
Syncope is characterized by sudden transient loss of consciousness due to cerebral hypoperfusion and is typically associated with an inability to maintain postural tone. There are many different causes and clinical presentations of syncope and the incidence varies depending on the population. Estimated lifetime prevalence rates are as high as 41% for a single episode of syncope, with recurrent syncope occurring in 13.5% of the general population. Incidence follows a trimodal distribution with peaks at age 20, 60, and 80 years for both men and women. The National Hospital Ambulatory Medical Care Survey reported 6.7 million episodes of syncope in the emergency department, which is where most patients with syncope initially present. However, patients may also present to the primary care outpatient setting, and providers should be equipped for initial evaluation and management.
Previous and current treatment guidelines
Although there have been general reviews published by general and specialty societies, there were no comprehensive guidelines on the evaluation and management of syncope until recently. The 2017 guideline from the American College of Cardiology, American Heart Association, and Heart Rhythm Society is intended to provide guidance on evaluation and management of syncope, specifically in the context of different clinical settings, specific causes, or selected circumstances.1
What primary care providers should know
A detailed history and physical exam should be performed in all patients with syncope. Useful details include the setting in which syncope occurs, prodromal symptoms, witness reports, postevent symptoms, comorbidities, medication use, past medical history, and family history. The physical exam should include orthostatic vital signs, cardiac exam, neurologic exam, and any other relevant systems. A resting 12-lead ECG in the initial evaluation is recommended to detect underlying arrhythmia or structural heart disease (Class I recommendation – strong).
There are many different causes of syncope (see Table 1). Vasovagal syncope, a form of reflex syncope mediated by the vasovagal reflex, is the most common cause of syncope and a frequent reason for emergency department visits. There is often a prodrome of diaphoresis, warmth, nausea, and/or pallor, often followed by fatigue. The diagnosis can be made by the history, physical exam, and eyewitness observation.
Once the initial evaluation is complete, further evaluation and management depends on the presence of risk factors presented in Table 2. Outpatient management is reasonable for patients with presumptive reflex-mediated syncope when there is an absence of serious medical conditions such as cardiac disease or comorbid neurologic disease. While hospital-based evaluation has not been shown to improve outcomes in patients with a low risk profile, hospital-based evaluation and treatment are recommended for patients presenting with syncope who have a serious medical condition potentially relevant to the cause of syncope.2 Serious medical conditions that require hospital management include arrhythmia, cardiac ischemia, severe aortic stenosis, hypertrophic cardiomyopathy, aortic dissection, acute heart failure, severe anemia, or major traumatic injury. Finally, patients with intermediate risk may benefit from an observational protocol in the emergency department.
Routine and comprehensive laboratory testing is not useful in syncope work-up (Class III recommendation – no benefit). Routine cardiac imaging is not recommended unless a cardiac etiology is suspected and routine neurological imaging and EEG are not recommended in the absence of focal neurologic findings. Additional work-up may be indicated if initial evaluation suggests a more specific etiology. If the initial evaluation suggests neurogenic orthostatic hypotension but the diagnosis is not clear, then referral for an autonomic evaluation is reasonable. If reflex syncope is suspected, tilt-table testing may be helpful to confirm the diagnosis. Lastly, if a cardiovascular etiology is suspected, it is recommended that the patient have cardiac monitoring in the acute care setting. In this later group, stress testing, transthoracic echocardiogram, electrophysiology study, and/or MRI or CT may be useful. Electrophysiologic testing is reasonable in patients with suspected arrhythmia as the etiology for syncope (Class IIa recommendation – moderate strength). The guideline provides a convenient summary algorithm to approach the initial and subsequent evaluations for syncope based on the initial evaluation and presenting symptoms.
Special populations
There are specific considerations for certain populations. In the pediatric population, the vast majority of syncopal episodes are reflex syncope but breath-holding spells should also be considered. In the geriatric population, particularly individuals older than 75 years, the incidence of syncope is high, the differential diagnosis is broad, and the diagnosis may be imprecise given amnesia, falls, lack of witnesses, and polypharmacy. In this group, morbidity is high because of multimorbidity and frailty. A careful history and physical exam with orthostatic vital signs is important, as is a multidisciplinary approach with geriatric consultation when needed.
Summary
Syncope is a common clinical syndrome often presenting to the emergency department or primary care setting. There are many causes, the most common being vasovagal syncope. In the initial evaluation, providers should perform a detailed history and physical exam, check orthostatic signs and perform a 12-lead ECG. Patients can be evaluated and managed safely in the outpatient setting in the absence of risk factors. Routine comprehensive laboratory testing and cardiac imaging are often not needed. For patients with defined risk factors, a more detailed evaluation in the hospital is recommended.
Dr. Li is a second-year resident in the family medicine residency program in the department of family and community medicine at the Sidney Kimmel Medical College at Thomas Jefferson University, Philadelphia. Dr. Mills is assistant residency program director and assistant professor in the departments of family and community medicine and physiology at the Sidney Kimmel Medical College. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health.
References
1. Shen W, Sheldon RS, Benditt DG, et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope. Circulation. 2017 Aug 1;136(5):e60-e122. doi: 10.1161/CIR.0000000000000499. Epub 2017 Mar 9.
2. Soteriades ES, Evans JC, Larson MG, et al. Incidence and prognosis of syncope. N Engl J Med. 2002;347(12):878-85.
Unskilled and unaware
In 1999, two psychologists, David Dunning and his student Justin Kruger, published a paper that demonstrated people who are really bad at something tend to believe that they are really good (J Pers Soc Psychol. 1999;77:1121-34). They also posited that most competent people underestimate their abilities while the rest of us overestimate them, and the worse we are, the more we overestimate our capabilities. In essence, they postulate that one needs a degree of skill in performing an activity in order to assess one's aptitude. In other words, it’s impossible to tell if you are bad at something if you’re too bad to know that you’re bad.

No, I’m not writing another diatribe about cardiologists (although this surely applies to some!). Rather this is a semi-apology to the vascular fellow who I featured in my last editorial, wherein I bemoaned that the endo-revolution resulted in some younger surgeons lacking open skills. That young man is an example of a highly competent trainee who probably underestimates his abilities to perform complex open procedures. In fact, an honest self-evaluation of my own clinical experience has made me realize that there is a corollary to newly minted vascular surgeons having limited open experience … rather, that some older surgeons, well versed in open surgery, may be inexperienced in some complex endo-procedures. The implications for the practice of vascular surgery are significant and warrant discussion. Perhaps my personal experience in learning endovascular methods will be revealing.
I performed my vascular fellowship at Montefiore with Frank Veith, MD, in 1980. At the time, Dr. Veith was a principal investigator in a multicenter, randomized trial to evaluate whether PTFE could be an acceptable substitute for saphenous vein in infra-inguinal bypass. As his fellow, I gained an enormous experience in these procedures. I stayed on in academic vascular surgery for another 6years honing my techniques in other forms of open surgery. In 1986 I moved to Sarasota, Fla., to start a private practice. Here, vascular surgery was performed by general surgeons who, although competent in the vascular procedures of that time, treated most infrapopliteal disease with an amputation. My calling card was my ability to do a distal bypass. What an anachronism! Of course, I still do a fair number of tibial bypasses, but femoropopliteal bypass is almost ready for the museum. The reason is that the tidal force of the endo-tsunami had just begun to wash up on the sunny beaches of Sarasota.
While at Montefiore I had witnessed the beginning of the endovascular wave. I realized that if I didn’t learn this new technology, I might well have become a surgical dinosaur. Accordingly, soon after arriving in Sarasota, I left town to spend a week with a pioneering radiologist who allowed me to observe his team’s early experience with aortic endografts. I left my practice a second time to visit with a very busy invasive cardiologist where I had hands-on experience with balloon angioplasty and early Palmaz stents. On my return, I cautiously started performing diagnostic arteriograms in the operating room using early C-arms. Eventually, my partner, David Showalter, MD, and I convinced the hospital to outfit a room as a semi “hybrid” suite, a fixed sliding X-ray table coupled with the most advanced C-arm of the time. Over the objections of local radiologists and cardiologists, we ultimately obtained privileges to perform our endo cases in their radiology suites and cath labs. This allowed us to expand our endovascular experience, first by improving our proficiency as diagnostic arteriographers, then by advancing our angioplasty and, ultimately, stent techniques. In the interim, however, endovascular technology had flourished with the introduction of TEVAR, FEVAR, chimneys and snorkels, rotor-rooters, lasers, drills, drug-eluting balloons and stents, radial and tibial access. Unfortunately, I must not have read Dale Carnegie’s book on how to win friends and influence people since by then I had alienated some of the general surgeons and all the radiologists and cardiologists. Accordingly, we had to train ourselves on these new devices and indications. Fortunately, training programs were by then producing endo-competent vascular surgeons and we were able to incorporate, and learn from, two of these younger surgeons, Michael Lepore, MD, and Deepak Nair, MD, who had joined our practice.
I suspect that many vascular surgeons who trained in the early eighties, and perhaps even nineties, were similarly self-taught. In fact, I suggest that some program directors, who now teach endovascular procedures, also had to learn on the job. This does not imply that we are all less skilled. Rather, that our generation of vascular surgeons come to the endo table with prejudices that favor open surgery and which may prevent us from fully embracing new technologies. Further, the host of new equipment alternatives makes it almost impossible to gain a global experience unless one has an extensive clinical practice or works within a large group or academic program. Thus, if we are not exposed to these devices and are not aware of their pluses and minuses, we might not be as good at them as we think we are.
An even more unfortunate repercussion of the endo-tsunami drowning open skills of young surgeons is that it may be having a similar effect on their more senior colleagues. Surgeons over the age of 50 are now in the majority and most have appropriately embraced endovascular procedures. However, in so doing their open volume falls and their expertise in this segment of their practice must diminish. I realize that there are many surgeons of my generation who are masters of all techniques, and I applaud their resilience. However, some may need to acknowledge that they may be just a little less proficient in the operating room. Accordingly, we need to be careful not to cast too many stones at our junior colleagues.
So, there are young vascular surgeons who may have lesser open skills, older surgeons who may have lesser endo skills, and some senior surgeons who may not be totally expert at either skill. I propose that it is now up to those of you, in the middle of your careers, to make sure that you keep up with changing paradigms, never lose your hard-earned skills, teach the new graduates all you can and, even more importantly, always remain aware of your inadequacies.
Russell Samson, MD, is a physician in the practice of Sarasota Vascular Specialists and clinical professor of surgery, Florida State University, Tallahassee. He is also the medical editor of Vascular Specialist.
In 1999, two psychologists, David Dunning and his student Justin Kruger, published a paper that demonstrated people who are really bad at something tend to believe that they are really good (J Pers Soc Psychol. 1999;77:1121-34). They also posited that most competent people underestimate their abilities while the rest of us overestimate them, and the worse we are, the more we overestimate our capabilities. In essence, they postulate that one needs a degree of skill in performing an activity in order to assess one's aptitude. In other words, it’s impossible to tell if you are bad at something if you’re too bad to know that you’re bad.
No, I’m not writing another diatribe about cardiologists (although this surely applies to some!). Rather this is a semi-apology to the vascular fellow who I featured in my last editorial, wherein I bemoaned that the endo-revolution resulted in some younger surgeons lacking open skills. That young man is an example of a highly competent trainee who probably underestimates his abilities to perform complex open procedures. In fact, an honest self-evaluation of my own clinical experience has made me realize that there is a corollary to newly minted vascular surgeons having limited open experience … rather, that some older surgeons, well versed in open surgery, may be inexperienced in some complex endo-procedures. The implications for the practice of vascular surgery are significant and warrant discussion. Perhaps my personal experience in learning endovascular methods will be revealing.
I performed my vascular fellowship at Montefiore with Frank Veith, MD, in 1980. At the time, Dr. Veith was a principal investigator in a multicenter, randomized trial to evaluate whether PTFE could be an acceptable substitute for saphenous vein in infra-inguinal bypass. As his fellow, I gained an enormous experience in these procedures. I stayed on in academic vascular surgery for another 6years honing my techniques in other forms of open surgery. In 1986 I moved to Sarasota, Fla., to start a private practice. Here, vascular surgery was performed by general surgeons who, although competent in the vascular procedures of that time, treated most infrapopliteal disease with an amputation. My calling card was my ability to do a distal bypass. What an anachronism! Of course, I still do a fair number of tibial bypasses, but femoropopliteal bypass is almost ready for the museum. The reason is that the tidal force of the endo-tsunami had just begun to wash up on the sunny beaches of Sarasota.
While at Montefiore I had witnessed the beginning of the endovascular wave. I realized that if I didn’t learn this new technology, I might well have become a surgical dinosaur. Accordingly, soon after arriving in Sarasota, I left town to spend a week with a pioneering radiologist who allowed me to observe his team’s early experience with aortic endografts. I left my practice a second time to visit with a very busy invasive cardiologist where I had hands-on experience with balloon angioplasty and early Palmaz stents. On my return, I cautiously started performing diagnostic arteriograms in the operating room using early C-arms. Eventually, my partner, David Showalter, MD, and I convinced the hospital to outfit a room as a semi “hybrid” suite, a fixed sliding X-ray table coupled with the most advanced C-arm of the time. Over the objections of local radiologists and cardiologists, we ultimately obtained privileges to perform our endo cases in their radiology suites and cath labs. This allowed us to expand our endovascular experience, first by improving our proficiency as diagnostic arteriographers, then by advancing our angioplasty and, ultimately, stent techniques. In the interim, however, endovascular technology had flourished with the introduction of TEVAR, FEVAR, chimneys and snorkels, rotor-rooters, lasers, drills, drug-eluting balloons and stents, radial and tibial access. Unfortunately, I must not have read Dale Carnegie’s book on how to win friends and influence people since by then I had alienated some of the general surgeons and all the radiologists and cardiologists. Accordingly, we had to train ourselves on these new devices and indications. Fortunately, training programs were by then producing endo-competent vascular surgeons and we were able to incorporate, and learn from, two of these younger surgeons, Michael Lepore, MD, and Deepak Nair, MD, who had joined our practice.
I suspect that many vascular surgeons who trained in the early eighties, and perhaps even nineties, were similarly self-taught. In fact, I suggest that some program directors, who now teach endovascular procedures, also had to learn on the job. This does not imply that we are all less skilled. Rather, that our generation of vascular surgeons come to the endo table with prejudices that favor open surgery and which may prevent us from fully embracing new technologies. Further, the host of new equipment alternatives makes it almost impossible to gain a global experience unless one has an extensive clinical practice or works within a large group or academic program. Thus, if we are not exposed to these devices and are not aware of their pluses and minuses, we might not be as good at them as we think we are.
An even more unfortunate repercussion of the endo-tsunami drowning open skills of young surgeons is that it may be having a similar effect on their more senior colleagues. Surgeons over the age of 50 are now in the majority and most have appropriately embraced endovascular procedures. However, in so doing their open volume falls and their expertise in this segment of their practice must diminish. I realize that there are many surgeons of my generation who are masters of all techniques, and I applaud their resilience. However, some may need to acknowledge that they may be just a little less proficient in the operating room. Accordingly, we need to be careful not to cast too many stones at our junior colleagues.
So, there are young vascular surgeons who may have lesser open skills, older surgeons who may have lesser endo skills, and some senior surgeons who may not be totally expert at either skill. I propose that it is now up to those of you, in the middle of your careers, to make sure that you keep up with changing paradigms, never lose your hard-earned skills, teach the new graduates all you can and, even more importantly, always remain aware of your inadequacies.
Russell Samson, MD, is a physician in the practice of Sarasota Vascular Specialists and clinical professor of surgery, Florida State University, Tallahassee. He is also the medical editor of Vascular Specialist.
In 1999, two psychologists, David Dunning and his student Justin Kruger, published a paper that demonstrated people who are really bad at something tend to believe that they are really good (J Pers Soc Psychol. 1999;77:1121-34). They also posited that most competent people underestimate their abilities while the rest of us overestimate them, and the worse we are, the more we overestimate our capabilities. In essence, they postulate that one needs a degree of skill in performing an activity in order to assess one's aptitude. In other words, it’s impossible to tell if you are bad at something if you’re too bad to know that you’re bad.
No, I’m not writing another diatribe about cardiologists (although this surely applies to some!). Rather this is a semi-apology to the vascular fellow who I featured in my last editorial, wherein I bemoaned that the endo-revolution resulted in some younger surgeons lacking open skills. That young man is an example of a highly competent trainee who probably underestimates his abilities to perform complex open procedures. In fact, an honest self-evaluation of my own clinical experience has made me realize that there is a corollary to newly minted vascular surgeons having limited open experience … rather, that some older surgeons, well versed in open surgery, may be inexperienced in some complex endo-procedures. The implications for the practice of vascular surgery are significant and warrant discussion. Perhaps my personal experience in learning endovascular methods will be revealing.
I performed my vascular fellowship at Montefiore with Frank Veith, MD, in 1980. At the time, Dr. Veith was a principal investigator in a multicenter, randomized trial to evaluate whether PTFE could be an acceptable substitute for saphenous vein in infra-inguinal bypass. As his fellow, I gained an enormous experience in these procedures. I stayed on in academic vascular surgery for another 6years honing my techniques in other forms of open surgery. In 1986 I moved to Sarasota, Fla., to start a private practice. Here, vascular surgery was performed by general surgeons who, although competent in the vascular procedures of that time, treated most infrapopliteal disease with an amputation. My calling card was my ability to do a distal bypass. What an anachronism! Of course, I still do a fair number of tibial bypasses, but femoropopliteal bypass is almost ready for the museum. The reason is that the tidal force of the endo-tsunami had just begun to wash up on the sunny beaches of Sarasota.
While at Montefiore I had witnessed the beginning of the endovascular wave. I realized that if I didn’t learn this new technology, I might well have become a surgical dinosaur. Accordingly, soon after arriving in Sarasota, I left town to spend a week with a pioneering radiologist who allowed me to observe his team’s early experience with aortic endografts. I left my practice a second time to visit with a very busy invasive cardiologist where I had hands-on experience with balloon angioplasty and early Palmaz stents. On my return, I cautiously started performing diagnostic arteriograms in the operating room using early C-arms. Eventually, my partner, David Showalter, MD, and I convinced the hospital to outfit a room as a semi “hybrid” suite, a fixed sliding X-ray table coupled with the most advanced C-arm of the time. Over the objections of local radiologists and cardiologists, we ultimately obtained privileges to perform our endo cases in their radiology suites and cath labs. This allowed us to expand our endovascular experience, first by improving our proficiency as diagnostic arteriographers, then by advancing our angioplasty and, ultimately, stent techniques. In the interim, however, endovascular technology had flourished with the introduction of TEVAR, FEVAR, chimneys and snorkels, rotor-rooters, lasers, drills, drug-eluting balloons and stents, radial and tibial access. Unfortunately, I must not have read Dale Carnegie’s book on how to win friends and influence people since by then I had alienated some of the general surgeons and all the radiologists and cardiologists. Accordingly, we had to train ourselves on these new devices and indications. Fortunately, training programs were by then producing endo-competent vascular surgeons and we were able to incorporate, and learn from, two of these younger surgeons, Michael Lepore, MD, and Deepak Nair, MD, who had joined our practice.
I suspect that many vascular surgeons who trained in the early eighties, and perhaps even nineties, were similarly self-taught. In fact, I suggest that some program directors, who now teach endovascular procedures, also had to learn on the job. This does not imply that we are all less skilled. Rather, that our generation of vascular surgeons come to the endo table with prejudices that favor open surgery and which may prevent us from fully embracing new technologies. Further, the host of new equipment alternatives makes it almost impossible to gain a global experience unless one has an extensive clinical practice or works within a large group or academic program. Thus, if we are not exposed to these devices and are not aware of their pluses and minuses, we might not be as good at them as we think we are.
An even more unfortunate repercussion of the endo-tsunami drowning open skills of young surgeons is that it may be having a similar effect on their more senior colleagues. Surgeons over the age of 50 are now in the majority and most have appropriately embraced endovascular procedures. However, in so doing their open volume falls and their expertise in this segment of their practice must diminish. I realize that there are many surgeons of my generation who are masters of all techniques, and I applaud their resilience. However, some may need to acknowledge that they may be just a little less proficient in the operating room. Accordingly, we need to be careful not to cast too many stones at our junior colleagues.
So, there are young vascular surgeons who may have lesser open skills, older surgeons who may have lesser endo skills, and some senior surgeons who may not be totally expert at either skill. I propose that it is now up to those of you, in the middle of your careers, to make sure that you keep up with changing paradigms, never lose your hard-earned skills, teach the new graduates all you can and, even more importantly, always remain aware of your inadequacies.
Russell Samson, MD, is a physician in the practice of Sarasota Vascular Specialists and clinical professor of surgery, Florida State University, Tallahassee. He is also the medical editor of Vascular Specialist.
Never too old
What are the age parameters for your practice? I suspect that at one end of the spectrum, you feel that a child is never too young to come to your practice. In fact you may even go out of your way to encourage expectant mothers to make a get-acquainted visit before they deliver because you know that a face-to-face encounter is very likely to make your job easier for the next decade or two.
On the other hand, I suspect that you have set an upper age limit above which you suggest that your patients transition to a physician whose practice is focused on adult care. Is this limit stated as a number – 18? 19? 21? Or are you so uncomfortable with the challenges of adolescent medicine that you urge the teenagers in your practice to find another medical home?
In my practice, I had a very simple and seldom-enforced upper age limit. A patient who was still a student, not even a full-time student, was welcome to keep coming to see me. This made us very popular with college students who knew that we would be there for them when they came home between semesters with a sore throat or needed a refill for their anxiety medicine. No long waits to see a customer-unfriendly internist. Of course, this meant that it was not unusual for me to see patients who were working on their master’s degree or just a few months short of their doctoral dissertation.
One of our exam rooms had large plywood cutouts of the number 1-10 on the walls, but otherwise I avoided large murals of jungle figures or cartoon characters. A checked shirt and a muted wine-red knit tie were about as wild and crazy as my professional wardrobe ever got. I never really bought into the notion that I could put a nervous young child at ease by dressing like a clown. In my experience, it was the personality and warmth radiating from the caregiver that set the tone of the visit, not what he or she was wearing.

Recently, the American Academy of Pediatrics published a recommendation discouraging pediatricians from setting upper age limits for their patients (Pediatrics. 2017;140[3]:e20172151). As someone who practiced most of his career with a very lenient age limit policy, I think this is an excellent and long overdue recommendation.
Patients in their older teens and early twenties seldom present with problems that are beyond our professional competency. Furthermore, one cannot underestimate the value that comes from the years of continuity we can fall back on, particularly for those patients with chronic and multiorgan system disease. But most of all, the chance to spend a few quiet minutes having an adult conversation and catching up with someone you have known since infancy can be a pleasant oasis in an otherwise hectic day spent seeing unappreciative, inarticulate infants and whining toddlers.
[polldaddy:{"method":"iframe","type":"survey","src":"//newspolls2017.polldaddy.com/s/never-too-old?iframe=1"}]
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
What are the age parameters for your practice? I suspect that at one end of the spectrum, you feel that a child is never too young to come to your practice. In fact you may even go out of your way to encourage expectant mothers to make a get-acquainted visit before they deliver because you know that a face-to-face encounter is very likely to make your job easier for the next decade or two.
On the other hand, I suspect that you have set an upper age limit above which you suggest that your patients transition to a physician whose practice is focused on adult care. Is this limit stated as a number – 18? 19? 21? Or are you so uncomfortable with the challenges of adolescent medicine that you urge the teenagers in your practice to find another medical home?
In my practice, I had a very simple and seldom-enforced upper age limit. A patient who was still a student, not even a full-time student, was welcome to keep coming to see me. This made us very popular with college students who knew that we would be there for them when they came home between semesters with a sore throat or needed a refill for their anxiety medicine. No long waits to see a customer-unfriendly internist. Of course, this meant that it was not unusual for me to see patients who were working on their master’s degree or just a few months short of their doctoral dissertation.
One of our exam rooms had large plywood cutouts of the number 1-10 on the walls, but otherwise I avoided large murals of jungle figures or cartoon characters. A checked shirt and a muted wine-red knit tie were about as wild and crazy as my professional wardrobe ever got. I never really bought into the notion that I could put a nervous young child at ease by dressing like a clown. In my experience, it was the personality and warmth radiating from the caregiver that set the tone of the visit, not what he or she was wearing.
Recently, the American Academy of Pediatrics published a recommendation discouraging pediatricians from setting upper age limits for their patients (Pediatrics. 2017;140[3]:e20172151). As someone who practiced most of his career with a very lenient age limit policy, I think this is an excellent and long overdue recommendation.
Patients in their older teens and early twenties seldom present with problems that are beyond our professional competency. Furthermore, one cannot underestimate the value that comes from the years of continuity we can fall back on, particularly for those patients with chronic and multiorgan system disease. But most of all, the chance to spend a few quiet minutes having an adult conversation and catching up with someone you have known since infancy can be a pleasant oasis in an otherwise hectic day spent seeing unappreciative, inarticulate infants and whining toddlers.
[polldaddy:{"method":"iframe","type":"survey","src":"//newspolls2017.polldaddy.com/s/never-too-old?iframe=1"}]
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
What are the age parameters for your practice? I suspect that at one end of the spectrum, you feel that a child is never too young to come to your practice. In fact you may even go out of your way to encourage expectant mothers to make a get-acquainted visit before they deliver because you know that a face-to-face encounter is very likely to make your job easier for the next decade or two.
On the other hand, I suspect that you have set an upper age limit above which you suggest that your patients transition to a physician whose practice is focused on adult care. Is this limit stated as a number – 18? 19? 21? Or are you so uncomfortable with the challenges of adolescent medicine that you urge the teenagers in your practice to find another medical home?
In my practice, I had a very simple and seldom-enforced upper age limit. A patient who was still a student, not even a full-time student, was welcome to keep coming to see me. This made us very popular with college students who knew that we would be there for them when they came home between semesters with a sore throat or needed a refill for their anxiety medicine. No long waits to see a customer-unfriendly internist. Of course, this meant that it was not unusual for me to see patients who were working on their master’s degree or just a few months short of their doctoral dissertation.
One of our exam rooms had large plywood cutouts of the number 1-10 on the walls, but otherwise I avoided large murals of jungle figures or cartoon characters. A checked shirt and a muted wine-red knit tie were about as wild and crazy as my professional wardrobe ever got. I never really bought into the notion that I could put a nervous young child at ease by dressing like a clown. In my experience, it was the personality and warmth radiating from the caregiver that set the tone of the visit, not what he or she was wearing.
Recently, the American Academy of Pediatrics published a recommendation discouraging pediatricians from setting upper age limits for their patients (Pediatrics. 2017;140[3]:e20172151). As someone who practiced most of his career with a very lenient age limit policy, I think this is an excellent and long overdue recommendation.
Patients in their older teens and early twenties seldom present with problems that are beyond our professional competency. Furthermore, one cannot underestimate the value that comes from the years of continuity we can fall back on, particularly for those patients with chronic and multiorgan system disease. But most of all, the chance to spend a few quiet minutes having an adult conversation and catching up with someone you have known since infancy can be a pleasant oasis in an otherwise hectic day spent seeing unappreciative, inarticulate infants and whining toddlers.
[polldaddy:{"method":"iframe","type":"survey","src":"//newspolls2017.polldaddy.com/s/never-too-old?iframe=1"}]
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”

FDA approves Vabomere for complicated UTI in adults
The Food and Drug Administration has approved Vabomere (meropenem and vaborbactam) for adults with complicated urinary tract infection (cUTI), including pyelonephritis caused by susceptible Enterobacteriaceae, the agency has announced.
The approval was based on results of the TANGO 1 trial, a phase 3, multicenter, double-blind study of 545 adult patients with cUTI. Overall, 98.4% of patients treated with Vabomere saw improvement in symptoms and negative urine culture tests by the end of intravenous treatment, compared with 94.3% of those treated with piperacillin/tazobactam (95% confidence interval, 0.3%-8.8%). Improvement continued in about 77% of patients treated with Vabomere who had resolved symptoms 7 days after completing treatment, compared with about 73% of those who were treated with piperacillin/tazobactam, the FDA said Aug. 29 in a press release.
Headache, infusion site reactions, and diarrhea were common adverse effects of Vabomere. The drug also has been associated with allergic reactions and seizures, so it should not be administered to patients with a history of anaphylaxis.
“Vabomere represents a significant new advancement in addressing [Klebsiella pneumoniae carbapenemase]-producing Enterobacteriaceae, for which there are currently limited treatment options,” Clive A. Meanwell, MD, PhD, chief executive officer of The Medicines Company, said in the statement.
Rempex Pharmaceuticals, a Medicines Company unit, received the approval. The Medicines Company said the drug is expected to be available before the end of the year.
The Food and Drug Administration has approved Vabomere (meropenem and vaborbactam) for adults with complicated urinary tract infection (cUTI), including pyelonephritis caused by susceptible Enterobacteriaceae, the agency has announced.
The approval was based on results of the TANGO 1 trial, a phase 3, multicenter, double-blind study of 545 adult patients with cUTI. Overall, 98.4% of patients treated with Vabomere saw improvement in symptoms and negative urine culture tests by the end of intravenous treatment, compared with 94.3% of those treated with piperacillin/tazobactam (95% confidence interval, 0.3%-8.8%). Improvement continued in about 77% of patients treated with Vabomere who had resolved symptoms 7 days after completing treatment, compared with about 73% of those who were treated with piperacillin/tazobactam, the FDA said Aug. 29 in a press release.
Headache, infusion site reactions, and diarrhea were common adverse effects of Vabomere. The drug also has been associated with allergic reactions and seizures, so it should not be administered to patients with a history of anaphylaxis.
“Vabomere represents a significant new advancement in addressing [Klebsiella pneumoniae carbapenemase]-producing Enterobacteriaceae, for which there are currently limited treatment options,” Clive A. Meanwell, MD, PhD, chief executive officer of The Medicines Company, said in the statement.
Rempex Pharmaceuticals, a Medicines Company unit, received the approval. The Medicines Company said the drug is expected to be available before the end of the year.
The Food and Drug Administration has approved Vabomere (meropenem and vaborbactam) for adults with complicated urinary tract infection (cUTI), including pyelonephritis caused by susceptible Enterobacteriaceae, the agency has announced.
The approval was based on results of the TANGO 1 trial, a phase 3, multicenter, double-blind study of 545 adult patients with cUTI. Overall, 98.4% of patients treated with Vabomere saw improvement in symptoms and negative urine culture tests by the end of intravenous treatment, compared with 94.3% of those treated with piperacillin/tazobactam (95% confidence interval, 0.3%-8.8%). Improvement continued in about 77% of patients treated with Vabomere who had resolved symptoms 7 days after completing treatment, compared with about 73% of those who were treated with piperacillin/tazobactam, the FDA said Aug. 29 in a press release.
Headache, infusion site reactions, and diarrhea were common adverse effects of Vabomere. The drug also has been associated with allergic reactions and seizures, so it should not be administered to patients with a history of anaphylaxis.
“Vabomere represents a significant new advancement in addressing [Klebsiella pneumoniae carbapenemase]-producing Enterobacteriaceae, for which there are currently limited treatment options,” Clive A. Meanwell, MD, PhD, chief executive officer of The Medicines Company, said in the statement.
Rempex Pharmaceuticals, a Medicines Company unit, received the approval. The Medicines Company said the drug is expected to be available before the end of the year.
Learn All About Coding
Learn all about coding and reimbursement, from the essentials to modifiers to future initiatives at the SVS Coding and Reimbursement Workshop, Oct. 13-14, in Chicago.
Hours are 1 to 5 p.m. Friday, Oct. 13, and 7:30 a.m. to 4:15 p.m. Saturday, Oct. 14. An optional E&M workshop (separate fee applies) will be held from 9 a.m. to noon Friday, Oct. 13.
Friday topics are: coding and reimbursement essentials, global surgical packages, getting paid the first time when applying surgical modifiers and the Medicare rule on non-physician practitioner billing.
Saturday topics include an overview of Current Procedural Terminology, coding for open surgical reconstruction; catheterization, angiography, angioplasty and stenting: cerebrovascular, brachiocephalic, visceral and renal; lower-extremity endovascular arterial intervention; open and endovascular treatments for venous insufficiency and IVC filters; aneurysm repair coding, fenestrated endovascular repair of the visceral and infrarenal aorta coding, hemodialysis access and wound care coding; vascular lab coding and information on MACRA, MIPS and APMs.
Also on the agenda is future SVS CPT coding initiatives.
Cost is: $880 for an SVS member or staff, $955 for a non-member and $250 for residents and trainees.
Cost for the optional workshop if $100 for an SVS member or staff, $215 for a non-member and $50 for residents and trainees.
Instructors are Teri Romano, RN, MBA, CPC, CMDP; Sean P. Roddy, MD; Robert M. Zwolak, MD, PhD; and Sunita D. Srivastava, MD.
Learn all about coding and reimbursement, from the essentials to modifiers to future initiatives at the SVS Coding and Reimbursement Workshop, Oct. 13-14, in Chicago.
Hours are 1 to 5 p.m. Friday, Oct. 13, and 7:30 a.m. to 4:15 p.m. Saturday, Oct. 14. An optional E&M workshop (separate fee applies) will be held from 9 a.m. to noon Friday, Oct. 13.
Friday topics are: coding and reimbursement essentials, global surgical packages, getting paid the first time when applying surgical modifiers and the Medicare rule on non-physician practitioner billing.
Saturday topics include an overview of Current Procedural Terminology, coding for open surgical reconstruction; catheterization, angiography, angioplasty and stenting: cerebrovascular, brachiocephalic, visceral and renal; lower-extremity endovascular arterial intervention; open and endovascular treatments for venous insufficiency and IVC filters; aneurysm repair coding, fenestrated endovascular repair of the visceral and infrarenal aorta coding, hemodialysis access and wound care coding; vascular lab coding and information on MACRA, MIPS and APMs.
Also on the agenda is future SVS CPT coding initiatives.
Cost is: $880 for an SVS member or staff, $955 for a non-member and $250 for residents and trainees.
Cost for the optional workshop if $100 for an SVS member or staff, $215 for a non-member and $50 for residents and trainees.
Instructors are Teri Romano, RN, MBA, CPC, CMDP; Sean P. Roddy, MD; Robert M. Zwolak, MD, PhD; and Sunita D. Srivastava, MD.
Learn all about coding and reimbursement, from the essentials to modifiers to future initiatives at the SVS Coding and Reimbursement Workshop, Oct. 13-14, in Chicago.
Hours are 1 to 5 p.m. Friday, Oct. 13, and 7:30 a.m. to 4:15 p.m. Saturday, Oct. 14. An optional E&M workshop (separate fee applies) will be held from 9 a.m. to noon Friday, Oct. 13.
Friday topics are: coding and reimbursement essentials, global surgical packages, getting paid the first time when applying surgical modifiers and the Medicare rule on non-physician practitioner billing.
Saturday topics include an overview of Current Procedural Terminology, coding for open surgical reconstruction; catheterization, angiography, angioplasty and stenting: cerebrovascular, brachiocephalic, visceral and renal; lower-extremity endovascular arterial intervention; open and endovascular treatments for venous insufficiency and IVC filters; aneurysm repair coding, fenestrated endovascular repair of the visceral and infrarenal aorta coding, hemodialysis access and wound care coding; vascular lab coding and information on MACRA, MIPS and APMs.
Also on the agenda is future SVS CPT coding initiatives.
Cost is: $880 for an SVS member or staff, $955 for a non-member and $250 for residents and trainees.
Cost for the optional workshop if $100 for an SVS member or staff, $215 for a non-member and $50 for residents and trainees.
Instructors are Teri Romano, RN, MBA, CPC, CMDP; Sean P. Roddy, MD; Robert M. Zwolak, MD, PhD; and Sunita D. Srivastava, MD.
Appreciates treatment options for recurrent BV
“EFFECTIVE TREATMENT OF RECURRENT BACTERIAL VAGINOSIS”
ROBERT L. BARBIERI, MD (EDITORIAL; JULY 2017)
Appreciates treatment options for recurrent BV
I thank Dr. Barbieri for his editorial on effective treatment of recurrent bacterial vaginosis (BV). I practice only outpatient gynecology, and recurrent BV is the most frustrating condition I have to deal with. Now I have 3 treatment options in my armamentarium for taking care of patients. I clipped the article pages from OBG
I have a related question: I see trichomonal vaginitis rarely, maybe 1 to 2 cases in a year. What do you think the reason is?
Vimal Goyle, MD
New York, New York
Beyond BV: Candidiasis and diabetes medications
Thank you for addressing the recurrent BV problem. After many years of throwing antibiotics at this problem I have been underwhelmed. Patients do not want to keep chasing their tails between BV and yeast. I have been suggesting that patients place plain yogurt containing Lactobacillus in a tampon applicator and apply it to the vagina weekly at night, after the original “overgrowth” has been treated, to return the “good bacteria” to the vagina. This avoids overuse of antibiotics (an impending epidemic of resistant organisms), boric acid (a dangerous pill to have around toddlers), and the expense that comes with multiple visits and multiple courses of antibiotics. I believe that in Canada a vaginal ovule with vitamin C and probiotics is available (something to ponder).
Another problem is recurrent yeast infections. We are seeing that many new diabetes medications are increasing the clearance of glucose and are causing severe and intractable Candida vulvovaginitis. In addition, I would like to know the best topical treatments and skin care for yeast in the folds of the panniculus in the morbidly obese. Unfortunately, these patients often have poor or no insurance and therefore cannot afford the cost of many effective remedies.
John Lewis, MD
Bedford, Massachusetts
Another treatment protocol for BV
For recurrent BV, I treat with standard metronidazole 500 mg orally twice daily for 7 days, then immediately start boric acid suppositories for 3 days in a row followed by 1 weekly for 6 weeks, and that usually takes care of it. However, a few caveats: I instruct patients to keep a supply of boric acid suppositories on hand, and if they start to experience symptoms again, to repeat the 3-day, then weekly-for-6 weeks regimen, so essentially they can manage a recurrence themselves.
For patients who come in thinking they have a recurrent yeast infection or BV, which was initially treated elsewhere, I culture for Mycoplasma and Ureaplasma. I often find that one of those organisms is responsible for the infection, requiring completely different treatment.
I also frequently check the vaginal pH, because patients like to see a visual on what I am talking about.
Rebecca Levy-Gantt, DO
Napa, California
Clindamycin appears superior for BV recurrence prevention
In my practice for the past number of years I have been treating BV with clindamycin vaginal cream instead of metronidazole. I have found that the number of women returning with recurrent BV has dropped dramatically. Furthermore, since switching medications, I cannot recall the last time someone required a maintenance dosing regimen. Although anecdotal, the difference between metronidazole and clindamycin treatment seems striking to me.
Daniel N. Sacks, MD
West Palm Beach, Florida
Uses BV regimens in stepwise fashion
To answer Dr. Barbieri’s instant poll question, my preference for treating BV is to start off with Regimen 1 (metronidazole treatment followed by twice weekly vaginal metronidazole for 6 months), as described in his editorial. If problem reports resolve but recur at a later date, then I use Regimen 2 (metronidazole treatment plus 21 days of boric acid vaginal capsules followed by twice weekly vaginal metronidazole for 6 months). I am aware of Regimen 3 (single-dose oral metronidazole plus fluconazole followed by once-monthly metronidazole and fluconazole) but rarely use it.
Carole W. Campbell, DNP, CNM
Gadsden, Alabama
- Gaydos CA, Beqaj S, Schwebke JR, et al. Clinical validation of a test for the diagnosis of vaginitis. Obstet Gynecol. 2017;130(1):181–189.
- Oduyebo OO, Anorlu RI, Ogunsola FL. The effects of antimicrobial therapy on bacterial vaginosis in non-pregnant women. Cochrane Database Syst Rev. 2009;(3):CD006055.
“EFFECTIVE TREATMENT OF RECURRENT BACTERIAL VAGINOSIS”
ROBERT L. BARBIERI, MD (EDITORIAL; JULY 2017)
Appreciates treatment options for recurrent BV
I thank Dr. Barbieri for his editorial on effective treatment of recurrent bacterial vaginosis (BV). I practice only outpatient gynecology, and recurrent BV is the most frustrating condition I have to deal with. Now I have 3 treatment options in my armamentarium for taking care of patients. I clipped the article pages from OBG
I have a related question: I see trichomonal vaginitis rarely, maybe 1 to 2 cases in a year. What do you think the reason is?
Vimal Goyle, MD
New York, New York
Beyond BV: Candidiasis and diabetes medications
Thank you for addressing the recurrent BV problem. After many years of throwing antibiotics at this problem I have been underwhelmed. Patients do not want to keep chasing their tails between BV and yeast. I have been suggesting that patients place plain yogurt containing Lactobacillus in a tampon applicator and apply it to the vagina weekly at night, after the original “overgrowth” has been treated, to return the “good bacteria” to the vagina. This avoids overuse of antibiotics (an impending epidemic of resistant organisms), boric acid (a dangerous pill to have around toddlers), and the expense that comes with multiple visits and multiple courses of antibiotics. I believe that in Canada a vaginal ovule with vitamin C and probiotics is available (something to ponder).
Another problem is recurrent yeast infections. We are seeing that many new diabetes medications are increasing the clearance of glucose and are causing severe and intractable Candida vulvovaginitis. In addition, I would like to know the best topical treatments and skin care for yeast in the folds of the panniculus in the morbidly obese. Unfortunately, these patients often have poor or no insurance and therefore cannot afford the cost of many effective remedies.
John Lewis, MD
Bedford, Massachusetts
Another treatment protocol for BV
For recurrent BV, I treat with standard metronidazole 500 mg orally twice daily for 7 days, then immediately start boric acid suppositories for 3 days in a row followed by 1 weekly for 6 weeks, and that usually takes care of it. However, a few caveats: I instruct patients to keep a supply of boric acid suppositories on hand, and if they start to experience symptoms again, to repeat the 3-day, then weekly-for-6 weeks regimen, so essentially they can manage a recurrence themselves.
For patients who come in thinking they have a recurrent yeast infection or BV, which was initially treated elsewhere, I culture for Mycoplasma and Ureaplasma. I often find that one of those organisms is responsible for the infection, requiring completely different treatment.
I also frequently check the vaginal pH, because patients like to see a visual on what I am talking about.
Rebecca Levy-Gantt, DO
Napa, California
Clindamycin appears superior for BV recurrence prevention
In my practice for the past number of years I have been treating BV with clindamycin vaginal cream instead of metronidazole. I have found that the number of women returning with recurrent BV has dropped dramatically. Furthermore, since switching medications, I cannot recall the last time someone required a maintenance dosing regimen. Although anecdotal, the difference between metronidazole and clindamycin treatment seems striking to me.
Daniel N. Sacks, MD
West Palm Beach, Florida
Uses BV regimens in stepwise fashion
To answer Dr. Barbieri’s instant poll question, my preference for treating BV is to start off with Regimen 1 (metronidazole treatment followed by twice weekly vaginal metronidazole for 6 months), as described in his editorial. If problem reports resolve but recur at a later date, then I use Regimen 2 (metronidazole treatment plus 21 days of boric acid vaginal capsules followed by twice weekly vaginal metronidazole for 6 months). I am aware of Regimen 3 (single-dose oral metronidazole plus fluconazole followed by once-monthly metronidazole and fluconazole) but rarely use it.
Carole W. Campbell, DNP, CNM
Gadsden, Alabama
“EFFECTIVE TREATMENT OF RECURRENT BACTERIAL VAGINOSIS”
ROBERT L. BARBIERI, MD (EDITORIAL; JULY 2017)
Appreciates treatment options for recurrent BV
I thank Dr. Barbieri for his editorial on effective treatment of recurrent bacterial vaginosis (BV). I practice only outpatient gynecology, and recurrent BV is the most frustrating condition I have to deal with. Now I have 3 treatment options in my armamentarium for taking care of patients. I clipped the article pages from OBG
I have a related question: I see trichomonal vaginitis rarely, maybe 1 to 2 cases in a year. What do you think the reason is?
Vimal Goyle, MD
New York, New York
Beyond BV: Candidiasis and diabetes medications
Thank you for addressing the recurrent BV problem. After many years of throwing antibiotics at this problem I have been underwhelmed. Patients do not want to keep chasing their tails between BV and yeast. I have been suggesting that patients place plain yogurt containing Lactobacillus in a tampon applicator and apply it to the vagina weekly at night, after the original “overgrowth” has been treated, to return the “good bacteria” to the vagina. This avoids overuse of antibiotics (an impending epidemic of resistant organisms), boric acid (a dangerous pill to have around toddlers), and the expense that comes with multiple visits and multiple courses of antibiotics. I believe that in Canada a vaginal ovule with vitamin C and probiotics is available (something to ponder).
Another problem is recurrent yeast infections. We are seeing that many new diabetes medications are increasing the clearance of glucose and are causing severe and intractable Candida vulvovaginitis. In addition, I would like to know the best topical treatments and skin care for yeast in the folds of the panniculus in the morbidly obese. Unfortunately, these patients often have poor or no insurance and therefore cannot afford the cost of many effective remedies.
John Lewis, MD
Bedford, Massachusetts
Another treatment protocol for BV
For recurrent BV, I treat with standard metronidazole 500 mg orally twice daily for 7 days, then immediately start boric acid suppositories for 3 days in a row followed by 1 weekly for 6 weeks, and that usually takes care of it. However, a few caveats: I instruct patients to keep a supply of boric acid suppositories on hand, and if they start to experience symptoms again, to repeat the 3-day, then weekly-for-6 weeks regimen, so essentially they can manage a recurrence themselves.
For patients who come in thinking they have a recurrent yeast infection or BV, which was initially treated elsewhere, I culture for Mycoplasma and Ureaplasma. I often find that one of those organisms is responsible for the infection, requiring completely different treatment.
I also frequently check the vaginal pH, because patients like to see a visual on what I am talking about.
Rebecca Levy-Gantt, DO
Napa, California
Clindamycin appears superior for BV recurrence prevention
In my practice for the past number of years I have been treating BV with clindamycin vaginal cream instead of metronidazole. I have found that the number of women returning with recurrent BV has dropped dramatically. Furthermore, since switching medications, I cannot recall the last time someone required a maintenance dosing regimen. Although anecdotal, the difference between metronidazole and clindamycin treatment seems striking to me.
Daniel N. Sacks, MD
West Palm Beach, Florida
Uses BV regimens in stepwise fashion
To answer Dr. Barbieri’s instant poll question, my preference for treating BV is to start off with Regimen 1 (metronidazole treatment followed by twice weekly vaginal metronidazole for 6 months), as described in his editorial. If problem reports resolve but recur at a later date, then I use Regimen 2 (metronidazole treatment plus 21 days of boric acid vaginal capsules followed by twice weekly vaginal metronidazole for 6 months). I am aware of Regimen 3 (single-dose oral metronidazole plus fluconazole followed by once-monthly metronidazole and fluconazole) but rarely use it.
Carole W. Campbell, DNP, CNM
Gadsden, Alabama
- Gaydos CA, Beqaj S, Schwebke JR, et al. Clinical validation of a test for the diagnosis of vaginitis. Obstet Gynecol. 2017;130(1):181–189.
- Oduyebo OO, Anorlu RI, Ogunsola FL. The effects of antimicrobial therapy on bacterial vaginosis in non-pregnant women. Cochrane Database Syst Rev. 2009;(3):CD006055.
- Gaydos CA, Beqaj S, Schwebke JR, et al. Clinical validation of a test for the diagnosis of vaginitis. Obstet Gynecol. 2017;130(1):181–189.
- Oduyebo OO, Anorlu RI, Ogunsola FL. The effects of antimicrobial therapy on bacterial vaginosis in non-pregnant women. Cochrane Database Syst Rev. 2009;(3):CD006055.

Calls for respect for transgender patients
“CARING FOR THE TRANSGENDER PATIENT: THE ROLE OF THE GYNECOLOGIST”
CECILE A. UNGER, MD, MPH (JUNE 2017)
Calls for respect for transgender patients
We must keep in mind that transgender males are still sexually anatomically female, with all of the medical needs of any other female. Transgender is merely a social construct. We must treat them with kindness and respect.
Laurence Burns, DO
Grand Rapids, Michigan
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
“CARING FOR THE TRANSGENDER PATIENT: THE ROLE OF THE GYNECOLOGIST”
CECILE A. UNGER, MD, MPH (JUNE 2017)
Calls for respect for transgender patients
We must keep in mind that transgender males are still sexually anatomically female, with all of the medical needs of any other female. Transgender is merely a social construct. We must treat them with kindness and respect.
Laurence Burns, DO
Grand Rapids, Michigan
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
“CARING FOR THE TRANSGENDER PATIENT: THE ROLE OF THE GYNECOLOGIST”
CECILE A. UNGER, MD, MPH (JUNE 2017)
Calls for respect for transgender patients
We must keep in mind that transgender males are still sexually anatomically female, with all of the medical needs of any other female. Transgender is merely a social construct. We must treat them with kindness and respect.
Laurence Burns, DO
Grand Rapids, Michigan
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
What’s in a name?
The quest for earlier diagnosis and treatment of polycystic ovarian syndrome may be branding too many young women with an unnecessary – and emotionally burdensome – tag, experts fear.
There’s little doubt that the classic phenotypes of PCOS, driven by androgen excess, can impair fertility and increase the long-term risks of cardiovascular complications and type 2 diabetes mellitus. But the recent expansion of those phenotypes to include categories that are not androgen driven has vastly increased the number of diagnosable cases, especially in teens. Recent analyses suggest that up to 21% of teenage girls now could potentially fit one of the phenotypes – a considerable increase from the 4%-6% prevalence associated with the original National Institutes of Health criteria of 20 years ago.
Some of these newly established phenotypes include signs and symptoms that may be driven by genetics or lifestyle instead of hormones, like hirsutism, acne, and obesity. Other problems may resolve spontaneously as a girl matures or loses weight, leaving her with a perfectly normal physiology, but a lifelong PCOS label.
Tessa Copp, a PhD student at the University of Sydney, is particularly interested in this issue. She and her mentor, psychologist Jesse Janssen, PhD, also of the university, recently published their analysis of the potential harms of these ever-proliferating PCOS diagnostic categories (BMJ. 2017;358:j3694).

“Women with a diagnosis of PCOS tend to have higher rates of depression and anxiety, a negative body image, and reduced relationship and sexual satisfaction,” Ms. Copp said in an interview. “But it’s unclear if those are because of the condition or the impact of getting a diagnosis associated with infertility and poor long-term health outcomes.”
“This label can induce fear and anxiety about the future. And young women may feel pressured to make altered life decisions about their future fertility at times when they may not be prepared to do so.”
Evolving diagnostic criteria
Three sets of diagnostic criteria have been proposed over the past 3 decades, said Ricardo Azziz, MD, chief officer of academic health and hospital affairs for the State University of New York system, and a renowned expert on PCOS. Dr. Azziz has had a hand in constructing several of the current diagnostic criteria.
In the 1990s, the key diagnostic features of PCOS were clinical or biochemical hyperandrogenism and chronic oligoanovulation. But in 2003, members of the European Society for Human Reproduction and Embryology and the American Society for Reproductive Medicine met in Rotterdam, the Netherlands, to review the data and refine these criteria. For the first time, ultrasound entered the picture; polycystic ovarian morphology became part of the diagnostic criteria.
A diagnosis using the new Rotterdam criteria required two of three characteristics: hyperandrogenicity, chronic ovulatory dysfunction, and polycystic ovarian morphology. These changes substantially expanded the number of diagnosable patients, Dr. Azziz said in an interview. Many have since criticized the inclusion of polycystic ovaries, because they are often present in women who don’t have any other PCOS symptom, especially younger women.
In 2006, the Androgen Excess & PCOS Society took a crack at the issue. They conducted a large data review and concluded that PCOS diagnosis should be based on the presence of clinical or biochemical hyperandrogenism in combination with ovarian dysfunction, thus taking the ovaries completely out of the picture.
This definition, however, resulted in some confusion in clinical practice, Dr. Azziz said. So in 2012, the National Institutes of Health gathered an international panel of PCOS experts, who reviewed the pros and cons of the diagnostic system. The panel endorsed the broader Rotterdam criteria, which included ovarian morphology, but issued a detailed description of four phenotypes. These are now the ones most often used in clinical practice:
• A. Hyperandrogenicity (clinical or biochemical) with ovarian dysfunction and polycystic ovarian morphology
• B. Hyperandrogenicity plus ovarian dysfunction
• C. Hyperandrogenicity plus polycystic ovarian morphology
• D. Ovarian dysfunction plus polycystic ovarian morphology
When is PCOS not PCOS?
Although Dr. Azziz has been a leader in this effort to impose diagnostic order, he also gets the system’s potential problems, especially when it comes to teenagers.
“I have been involved in each of these successive expansions, I understand the concern of people who worry that we are getting further away from classic PCOS, especially by adding phenotypes with normal ovulation. Are these actually the same disorder? Do they imply the same risks? Using the Rotterdam criteria does capture the greatest number of patients, but we have to be very careful of these phenotypes.”
Phenotypes A and B have accrued the most long-term data and clearly carry associated long-term cardiovascular and metabolic risks. For these women, Dr. Azziz said, early diagnosis leads to early treatment and a jump start on modifying those risks.
The picture is much different for phenotypes C and D. “As we get more data, it becomes increasingly clear that types C and D don’t behave in the same way or carry the same risks.”
Part of the problem is that some of the secondary definitions of signs and symptoms are themselves not well defined and don’t account for other possible etiologies, said Lubna Pal, MD, another PCOS expert. Hirsutism and acne are good examples. “What about the young woman who is overweight, and complains about acne and being hairy? You might think of these as PCOS symptoms, but in her history, find out that her mother or sisters also have a lot of hair and had acne. How do you treat that information then?”
None of the classic signs and symptoms of PCOS have been validated in teens, said Dr. Pal, director of the Polycystic Ovary Syndrome (PCOS) Program at the Yale Reproductive Endocrinology center, New Haven, Conn. There are no validated cutoffs for abnormal androgen in teen females, and no one really knows whether the adult values are meaningful in younger women.
Nor is there an age-specific cut-off for “polycystic-appearing ovaries,” Ms. Copp said. “Right now, the Rotterdam criteria define this as 12 or more follicles on ultrasound, but that was based on the ultrasound technology available at the time – and that count might be normal in early adulthood.” She noted that in 2014, an expert panel recommended increasing the threshold to more than 24 follicles per ovary, in accordance with findings using advanced imaging techniques. This recommendation has not been adopted.
Some classic symptoms, like menstrual irregularity, acne, and high body weight, can also be part of a transitory developmental phase as a girl moves through puberty into a more adult physiology. Others, like insulin resistance, can resolve if the patient loses weight, Dr. Pal said. So are those things really indicators of a true PCOS state?
These questions all need to be answered, said Ms. Copp. In the meantime, young women are being tagged as having a chronic disorder that might not be there, or if it is, might spontaneously resolve.

“There are at least three studies in different populations that have found that the prevalence of PCOS falls rapidly after 25 years of age,” she said. “So these signs and symptoms of PCOS might really be transitory for many.”
Women with “true,” androgen-driven PCOS benefit from early identification, treatment, and metabolic and cardiovascular risk management. But everyone interviewed for this article agreed that a PCOS label for every young woman who is overweight, hirsute, acne-prone, and irregular in her periods, is inappropriate and potentially harmful. All three mentioned that while a diagnostic label may bring an element of relief – as in “I finally know what’s going on” - it carries attendant anxiety about a future with an incurable disorder which may not even impart much long-term risk, or even daily bother. There is also a risk of potentially unnecessary medical screenings and interventions, Ms. Copp noted.
Treat the syndrome – or the patient?
A better way to proceed, Dr. Pal suggested, is to drop the labels and embrace the patient’s experience.
“I ask them, ‘What is your bother?’ Is it the irregular periods? The acne? The hair? The weight? It may be that a more mature woman wants to start a family, and that is the issue we address. Or for younger women, it may be the other issues, and for them, that should be our primary concern.”
Dr. Azziz agreed.
“We need to confirm the diagnosis, and then confirm any related disorders, and make sure our patients are healthy in other ways. PCOS alone is not so much a concern. We simply cannot treat all our patients the same. Instead, we need to get very clear with them about their own objectives. Are they trying to lose weight or get pregnant? We are talking about basic personalized medicine here, not labeling just for the sake of giving something a name.”
Ms. Copp’s thoughts were in the same vein as well.
“Do all these women really need to be ‘diagnosed,’ or can we monitor their symptoms and treat what is bothersome without a label? A diagnostic label doesn’t change the treatment, especially for young women whose PCOS symptoms might be transient and not require treatment at all.”
None of those interviewed for this article had any relevant financial disclosures.
[email protected]
On Twitter @Alz_Gal
The quest for earlier diagnosis and treatment of polycystic ovarian syndrome may be branding too many young women with an unnecessary – and emotionally burdensome – tag, experts fear.
There’s little doubt that the classic phenotypes of PCOS, driven by androgen excess, can impair fertility and increase the long-term risks of cardiovascular complications and type 2 diabetes mellitus. But the recent expansion of those phenotypes to include categories that are not androgen driven has vastly increased the number of diagnosable cases, especially in teens. Recent analyses suggest that up to 21% of teenage girls now could potentially fit one of the phenotypes – a considerable increase from the 4%-6% prevalence associated with the original National Institutes of Health criteria of 20 years ago.
Some of these newly established phenotypes include signs and symptoms that may be driven by genetics or lifestyle instead of hormones, like hirsutism, acne, and obesity. Other problems may resolve spontaneously as a girl matures or loses weight, leaving her with a perfectly normal physiology, but a lifelong PCOS label.
Tessa Copp, a PhD student at the University of Sydney, is particularly interested in this issue. She and her mentor, psychologist Jesse Janssen, PhD, also of the university, recently published their analysis of the potential harms of these ever-proliferating PCOS diagnostic categories (BMJ. 2017;358:j3694).
“Women with a diagnosis of PCOS tend to have higher rates of depression and anxiety, a negative body image, and reduced relationship and sexual satisfaction,” Ms. Copp said in an interview. “But it’s unclear if those are because of the condition or the impact of getting a diagnosis associated with infertility and poor long-term health outcomes.”
“This label can induce fear and anxiety about the future. And young women may feel pressured to make altered life decisions about their future fertility at times when they may not be prepared to do so.”
Evolving diagnostic criteria
Three sets of diagnostic criteria have been proposed over the past 3 decades, said Ricardo Azziz, MD, chief officer of academic health and hospital affairs for the State University of New York system, and a renowned expert on PCOS. Dr. Azziz has had a hand in constructing several of the current diagnostic criteria.
In the 1990s, the key diagnostic features of PCOS were clinical or biochemical hyperandrogenism and chronic oligoanovulation. But in 2003, members of the European Society for Human Reproduction and Embryology and the American Society for Reproductive Medicine met in Rotterdam, the Netherlands, to review the data and refine these criteria. For the first time, ultrasound entered the picture; polycystic ovarian morphology became part of the diagnostic criteria.
A diagnosis using the new Rotterdam criteria required two of three characteristics: hyperandrogenicity, chronic ovulatory dysfunction, and polycystic ovarian morphology. These changes substantially expanded the number of diagnosable patients, Dr. Azziz said in an interview. Many have since criticized the inclusion of polycystic ovaries, because they are often present in women who don’t have any other PCOS symptom, especially younger women.
In 2006, the Androgen Excess & PCOS Society took a crack at the issue. They conducted a large data review and concluded that PCOS diagnosis should be based on the presence of clinical or biochemical hyperandrogenism in combination with ovarian dysfunction, thus taking the ovaries completely out of the picture.
This definition, however, resulted in some confusion in clinical practice, Dr. Azziz said. So in 2012, the National Institutes of Health gathered an international panel of PCOS experts, who reviewed the pros and cons of the diagnostic system. The panel endorsed the broader Rotterdam criteria, which included ovarian morphology, but issued a detailed description of four phenotypes. These are now the ones most often used in clinical practice:
• A. Hyperandrogenicity (clinical or biochemical) with ovarian dysfunction and polycystic ovarian morphology
• B. Hyperandrogenicity plus ovarian dysfunction
• C. Hyperandrogenicity plus polycystic ovarian morphology
• D. Ovarian dysfunction plus polycystic ovarian morphology
When is PCOS not PCOS?
Although Dr. Azziz has been a leader in this effort to impose diagnostic order, he also gets the system’s potential problems, especially when it comes to teenagers.
“I have been involved in each of these successive expansions, I understand the concern of people who worry that we are getting further away from classic PCOS, especially by adding phenotypes with normal ovulation. Are these actually the same disorder? Do they imply the same risks? Using the Rotterdam criteria does capture the greatest number of patients, but we have to be very careful of these phenotypes.”
Phenotypes A and B have accrued the most long-term data and clearly carry associated long-term cardiovascular and metabolic risks. For these women, Dr. Azziz said, early diagnosis leads to early treatment and a jump start on modifying those risks.
The picture is much different for phenotypes C and D. “As we get more data, it becomes increasingly clear that types C and D don’t behave in the same way or carry the same risks.”
Part of the problem is that some of the secondary definitions of signs and symptoms are themselves not well defined and don’t account for other possible etiologies, said Lubna Pal, MD, another PCOS expert. Hirsutism and acne are good examples. “What about the young woman who is overweight, and complains about acne and being hairy? You might think of these as PCOS symptoms, but in her history, find out that her mother or sisters also have a lot of hair and had acne. How do you treat that information then?”
None of the classic signs and symptoms of PCOS have been validated in teens, said Dr. Pal, director of the Polycystic Ovary Syndrome (PCOS) Program at the Yale Reproductive Endocrinology center, New Haven, Conn. There are no validated cutoffs for abnormal androgen in teen females, and no one really knows whether the adult values are meaningful in younger women.
Nor is there an age-specific cut-off for “polycystic-appearing ovaries,” Ms. Copp said. “Right now, the Rotterdam criteria define this as 12 or more follicles on ultrasound, but that was based on the ultrasound technology available at the time – and that count might be normal in early adulthood.” She noted that in 2014, an expert panel recommended increasing the threshold to more than 24 follicles per ovary, in accordance with findings using advanced imaging techniques. This recommendation has not been adopted.
Some classic symptoms, like menstrual irregularity, acne, and high body weight, can also be part of a transitory developmental phase as a girl moves through puberty into a more adult physiology. Others, like insulin resistance, can resolve if the patient loses weight, Dr. Pal said. So are those things really indicators of a true PCOS state?
These questions all need to be answered, said Ms. Copp. In the meantime, young women are being tagged as having a chronic disorder that might not be there, or if it is, might spontaneously resolve.
“There are at least three studies in different populations that have found that the prevalence of PCOS falls rapidly after 25 years of age,” she said. “So these signs and symptoms of PCOS might really be transitory for many.”
Women with “true,” androgen-driven PCOS benefit from early identification, treatment, and metabolic and cardiovascular risk management. But everyone interviewed for this article agreed that a PCOS label for every young woman who is overweight, hirsute, acne-prone, and irregular in her periods, is inappropriate and potentially harmful. All three mentioned that while a diagnostic label may bring an element of relief – as in “I finally know what’s going on” - it carries attendant anxiety about a future with an incurable disorder which may not even impart much long-term risk, or even daily bother. There is also a risk of potentially unnecessary medical screenings and interventions, Ms. Copp noted.
Treat the syndrome – or the patient?
A better way to proceed, Dr. Pal suggested, is to drop the labels and embrace the patient’s experience.
“I ask them, ‘What is your bother?’ Is it the irregular periods? The acne? The hair? The weight? It may be that a more mature woman wants to start a family, and that is the issue we address. Or for younger women, it may be the other issues, and for them, that should be our primary concern.”
Dr. Azziz agreed.
“We need to confirm the diagnosis, and then confirm any related disorders, and make sure our patients are healthy in other ways. PCOS alone is not so much a concern. We simply cannot treat all our patients the same. Instead, we need to get very clear with them about their own objectives. Are they trying to lose weight or get pregnant? We are talking about basic personalized medicine here, not labeling just for the sake of giving something a name.”
Ms. Copp’s thoughts were in the same vein as well.
“Do all these women really need to be ‘diagnosed,’ or can we monitor their symptoms and treat what is bothersome without a label? A diagnostic label doesn’t change the treatment, especially for young women whose PCOS symptoms might be transient and not require treatment at all.”
None of those interviewed for this article had any relevant financial disclosures.
[email protected]
On Twitter @Alz_Gal
The quest for earlier diagnosis and treatment of polycystic ovarian syndrome may be branding too many young women with an unnecessary – and emotionally burdensome – tag, experts fear.
There’s little doubt that the classic phenotypes of PCOS, driven by androgen excess, can impair fertility and increase the long-term risks of cardiovascular complications and type 2 diabetes mellitus. But the recent expansion of those phenotypes to include categories that are not androgen driven has vastly increased the number of diagnosable cases, especially in teens. Recent analyses suggest that up to 21% of teenage girls now could potentially fit one of the phenotypes – a considerable increase from the 4%-6% prevalence associated with the original National Institutes of Health criteria of 20 years ago.
Some of these newly established phenotypes include signs and symptoms that may be driven by genetics or lifestyle instead of hormones, like hirsutism, acne, and obesity. Other problems may resolve spontaneously as a girl matures or loses weight, leaving her with a perfectly normal physiology, but a lifelong PCOS label.
Tessa Copp, a PhD student at the University of Sydney, is particularly interested in this issue. She and her mentor, psychologist Jesse Janssen, PhD, also of the university, recently published their analysis of the potential harms of these ever-proliferating PCOS diagnostic categories (BMJ. 2017;358:j3694).
“Women with a diagnosis of PCOS tend to have higher rates of depression and anxiety, a negative body image, and reduced relationship and sexual satisfaction,” Ms. Copp said in an interview. “But it’s unclear if those are because of the condition or the impact of getting a diagnosis associated with infertility and poor long-term health outcomes.”
“This label can induce fear and anxiety about the future. And young women may feel pressured to make altered life decisions about their future fertility at times when they may not be prepared to do so.”
Evolving diagnostic criteria
Three sets of diagnostic criteria have been proposed over the past 3 decades, said Ricardo Azziz, MD, chief officer of academic health and hospital affairs for the State University of New York system, and a renowned expert on PCOS. Dr. Azziz has had a hand in constructing several of the current diagnostic criteria.
In the 1990s, the key diagnostic features of PCOS were clinical or biochemical hyperandrogenism and chronic oligoanovulation. But in 2003, members of the European Society for Human Reproduction and Embryology and the American Society for Reproductive Medicine met in Rotterdam, the Netherlands, to review the data and refine these criteria. For the first time, ultrasound entered the picture; polycystic ovarian morphology became part of the diagnostic criteria.
A diagnosis using the new Rotterdam criteria required two of three characteristics: hyperandrogenicity, chronic ovulatory dysfunction, and polycystic ovarian morphology. These changes substantially expanded the number of diagnosable patients, Dr. Azziz said in an interview. Many have since criticized the inclusion of polycystic ovaries, because they are often present in women who don’t have any other PCOS symptom, especially younger women.
In 2006, the Androgen Excess & PCOS Society took a crack at the issue. They conducted a large data review and concluded that PCOS diagnosis should be based on the presence of clinical or biochemical hyperandrogenism in combination with ovarian dysfunction, thus taking the ovaries completely out of the picture.
This definition, however, resulted in some confusion in clinical practice, Dr. Azziz said. So in 2012, the National Institutes of Health gathered an international panel of PCOS experts, who reviewed the pros and cons of the diagnostic system. The panel endorsed the broader Rotterdam criteria, which included ovarian morphology, but issued a detailed description of four phenotypes. These are now the ones most often used in clinical practice:
• A. Hyperandrogenicity (clinical or biochemical) with ovarian dysfunction and polycystic ovarian morphology
• B. Hyperandrogenicity plus ovarian dysfunction
• C. Hyperandrogenicity plus polycystic ovarian morphology
• D. Ovarian dysfunction plus polycystic ovarian morphology
When is PCOS not PCOS?
Although Dr. Azziz has been a leader in this effort to impose diagnostic order, he also gets the system’s potential problems, especially when it comes to teenagers.
“I have been involved in each of these successive expansions, I understand the concern of people who worry that we are getting further away from classic PCOS, especially by adding phenotypes with normal ovulation. Are these actually the same disorder? Do they imply the same risks? Using the Rotterdam criteria does capture the greatest number of patients, but we have to be very careful of these phenotypes.”
Phenotypes A and B have accrued the most long-term data and clearly carry associated long-term cardiovascular and metabolic risks. For these women, Dr. Azziz said, early diagnosis leads to early treatment and a jump start on modifying those risks.
The picture is much different for phenotypes C and D. “As we get more data, it becomes increasingly clear that types C and D don’t behave in the same way or carry the same risks.”
Part of the problem is that some of the secondary definitions of signs and symptoms are themselves not well defined and don’t account for other possible etiologies, said Lubna Pal, MD, another PCOS expert. Hirsutism and acne are good examples. “What about the young woman who is overweight, and complains about acne and being hairy? You might think of these as PCOS symptoms, but in her history, find out that her mother or sisters also have a lot of hair and had acne. How do you treat that information then?”
None of the classic signs and symptoms of PCOS have been validated in teens, said Dr. Pal, director of the Polycystic Ovary Syndrome (PCOS) Program at the Yale Reproductive Endocrinology center, New Haven, Conn. There are no validated cutoffs for abnormal androgen in teen females, and no one really knows whether the adult values are meaningful in younger women.
Nor is there an age-specific cut-off for “polycystic-appearing ovaries,” Ms. Copp said. “Right now, the Rotterdam criteria define this as 12 or more follicles on ultrasound, but that was based on the ultrasound technology available at the time – and that count might be normal in early adulthood.” She noted that in 2014, an expert panel recommended increasing the threshold to more than 24 follicles per ovary, in accordance with findings using advanced imaging techniques. This recommendation has not been adopted.
Some classic symptoms, like menstrual irregularity, acne, and high body weight, can also be part of a transitory developmental phase as a girl moves through puberty into a more adult physiology. Others, like insulin resistance, can resolve if the patient loses weight, Dr. Pal said. So are those things really indicators of a true PCOS state?
These questions all need to be answered, said Ms. Copp. In the meantime, young women are being tagged as having a chronic disorder that might not be there, or if it is, might spontaneously resolve.
“There are at least three studies in different populations that have found that the prevalence of PCOS falls rapidly after 25 years of age,” she said. “So these signs and symptoms of PCOS might really be transitory for many.”
Women with “true,” androgen-driven PCOS benefit from early identification, treatment, and metabolic and cardiovascular risk management. But everyone interviewed for this article agreed that a PCOS label for every young woman who is overweight, hirsute, acne-prone, and irregular in her periods, is inappropriate and potentially harmful. All three mentioned that while a diagnostic label may bring an element of relief – as in “I finally know what’s going on” - it carries attendant anxiety about a future with an incurable disorder which may not even impart much long-term risk, or even daily bother. There is also a risk of potentially unnecessary medical screenings and interventions, Ms. Copp noted.
Treat the syndrome – or the patient?
A better way to proceed, Dr. Pal suggested, is to drop the labels and embrace the patient’s experience.
“I ask them, ‘What is your bother?’ Is it the irregular periods? The acne? The hair? The weight? It may be that a more mature woman wants to start a family, and that is the issue we address. Or for younger women, it may be the other issues, and for them, that should be our primary concern.”
Dr. Azziz agreed.
“We need to confirm the diagnosis, and then confirm any related disorders, and make sure our patients are healthy in other ways. PCOS alone is not so much a concern. We simply cannot treat all our patients the same. Instead, we need to get very clear with them about their own objectives. Are they trying to lose weight or get pregnant? We are talking about basic personalized medicine here, not labeling just for the sake of giving something a name.”
Ms. Copp’s thoughts were in the same vein as well.
“Do all these women really need to be ‘diagnosed,’ or can we monitor their symptoms and treat what is bothersome without a label? A diagnostic label doesn’t change the treatment, especially for young women whose PCOS symptoms might be transient and not require treatment at all.”
None of those interviewed for this article had any relevant financial disclosures.
[email protected]
On Twitter @Alz_Gal
FDA grants breakthrough status to epidermolysis bullosa gene therapy
The U.S. Food and Drug Administration has granted breakthrough therapy status to Abeona Therapeutics’s EB-101 gene therapy program for patients with recessive dystrophic epidermolysis bullosa, according to a company statement.
The breakthrough therapy designation will expedite the phase 3 trial, intended to start in 2018, and the approval process and make this therapy available to patients who have few or no other treatment options for this serious and painful condition.
The experimental treatment “utilizes a patient’s own cells and genetically engineer[s] them to produce the correct version of collagen, which helps hold skin on to the body, thereby reducing the number of painful blisters caused by injury and improving wound healing,” Timothy J. Miller, PhD, CEO and president of Abeona, said in a statement. “We are grateful that the FDA has recognized the promising clinical data from the EB-101 program with Breakthrough Therapy designation.”
The U.S. Food and Drug Administration has granted breakthrough therapy status to Abeona Therapeutics’s EB-101 gene therapy program for patients with recessive dystrophic epidermolysis bullosa, according to a company statement.
The breakthrough therapy designation will expedite the phase 3 trial, intended to start in 2018, and the approval process and make this therapy available to patients who have few or no other treatment options for this serious and painful condition.
The experimental treatment “utilizes a patient’s own cells and genetically engineer[s] them to produce the correct version of collagen, which helps hold skin on to the body, thereby reducing the number of painful blisters caused by injury and improving wound healing,” Timothy J. Miller, PhD, CEO and president of Abeona, said in a statement. “We are grateful that the FDA has recognized the promising clinical data from the EB-101 program with Breakthrough Therapy designation.”
The U.S. Food and Drug Administration has granted breakthrough therapy status to Abeona Therapeutics’s EB-101 gene therapy program for patients with recessive dystrophic epidermolysis bullosa, according to a company statement.
The breakthrough therapy designation will expedite the phase 3 trial, intended to start in 2018, and the approval process and make this therapy available to patients who have few or no other treatment options for this serious and painful condition.
The experimental treatment “utilizes a patient’s own cells and genetically engineer[s] them to produce the correct version of collagen, which helps hold skin on to the body, thereby reducing the number of painful blisters caused by injury and improving wound healing,” Timothy J. Miller, PhD, CEO and president of Abeona, said in a statement. “We are grateful that the FDA has recognized the promising clinical data from the EB-101 program with Breakthrough Therapy designation.”
Genes May Hold the Key to Immunotherapy Resistance
Why do some tumors not respond to immunotherapy? Why do some respond at first and then develop resistance? A National Institutes of Health (NIH) study holds some clues to the answer. Using patient samples from The Cancer Genome Atlas, the researchers found > 100 genes that may help T cells destroy tumors.
Related: Which Acute Myeloid Leukemia Patients Are Good Immunotherapy Candidates?
The researchers used CRISPR, a gene-editing technology that stops the expression of individual genes in cancer cells. By first “knocking out” every known protein-encoding gene in the human genome and then testing the ability of modified melanoma cells to respond to T cells, they identified “candidate” genes.
A number of the genes identified by the CRISPR screen were associated with cytolytic activity. One, APLNR, which produces a protein called the apelin receptor, had been “suspected to contribute” to cancer development—now, the NIH researchers say, they have the first indication of a role in response to T cells. In some patients who were resistant to immunotherapies, the apelin receptor protein was nonfunctional, indicating that the loss of that protein could limit the response to immunotherapy.
Related: First Cancer Treatment Based on Biomarkers Is Approved
“Many more genes than we originally expected play a vital role in dictating the success of cancer immunotherapies,” said Shashank Patel, PhD, first author of the study. Their “gene list” could serve as a blueprint to study the emergence of tumor resistance, the researchers say, and lead to more effective treatments.
Source:
NCI study identifies essential genes for cancer immunotherapy [news release] Bethesda, Maryland: National Institutes of Health; August 7, 2017. https://www.nih.gov/news-events/news-releases/nci-study-identifies-essential-genes-cancer-immunotherapy. Accessed August 29, 2017.
Why do some tumors not respond to immunotherapy? Why do some respond at first and then develop resistance? A National Institutes of Health (NIH) study holds some clues to the answer. Using patient samples from The Cancer Genome Atlas, the researchers found > 100 genes that may help T cells destroy tumors.
Related: Which Acute Myeloid Leukemia Patients Are Good Immunotherapy Candidates?
The researchers used CRISPR, a gene-editing technology that stops the expression of individual genes in cancer cells. By first “knocking out” every known protein-encoding gene in the human genome and then testing the ability of modified melanoma cells to respond to T cells, they identified “candidate” genes.
A number of the genes identified by the CRISPR screen were associated with cytolytic activity. One, APLNR, which produces a protein called the apelin receptor, had been “suspected to contribute” to cancer development—now, the NIH researchers say, they have the first indication of a role in response to T cells. In some patients who were resistant to immunotherapies, the apelin receptor protein was nonfunctional, indicating that the loss of that protein could limit the response to immunotherapy.
Related: First Cancer Treatment Based on Biomarkers Is Approved
“Many more genes than we originally expected play a vital role in dictating the success of cancer immunotherapies,” said Shashank Patel, PhD, first author of the study. Their “gene list” could serve as a blueprint to study the emergence of tumor resistance, the researchers say, and lead to more effective treatments.
Source:
NCI study identifies essential genes for cancer immunotherapy [news release] Bethesda, Maryland: National Institutes of Health; August 7, 2017. https://www.nih.gov/news-events/news-releases/nci-study-identifies-essential-genes-cancer-immunotherapy. Accessed August 29, 2017.
Why do some tumors not respond to immunotherapy? Why do some respond at first and then develop resistance? A National Institutes of Health (NIH) study holds some clues to the answer. Using patient samples from The Cancer Genome Atlas, the researchers found > 100 genes that may help T cells destroy tumors.
Related: Which Acute Myeloid Leukemia Patients Are Good Immunotherapy Candidates?
The researchers used CRISPR, a gene-editing technology that stops the expression of individual genes in cancer cells. By first “knocking out” every known protein-encoding gene in the human genome and then testing the ability of modified melanoma cells to respond to T cells, they identified “candidate” genes.
A number of the genes identified by the CRISPR screen were associated with cytolytic activity. One, APLNR, which produces a protein called the apelin receptor, had been “suspected to contribute” to cancer development—now, the NIH researchers say, they have the first indication of a role in response to T cells. In some patients who were resistant to immunotherapies, the apelin receptor protein was nonfunctional, indicating that the loss of that protein could limit the response to immunotherapy.
Related: First Cancer Treatment Based on Biomarkers Is Approved
“Many more genes than we originally expected play a vital role in dictating the success of cancer immunotherapies,” said Shashank Patel, PhD, first author of the study. Their “gene list” could serve as a blueprint to study the emergence of tumor resistance, the researchers say, and lead to more effective treatments.
Source:
NCI study identifies essential genes for cancer immunotherapy [news release] Bethesda, Maryland: National Institutes of Health; August 7, 2017. https://www.nih.gov/news-events/news-releases/nci-study-identifies-essential-genes-cancer-immunotherapy. Accessed August 29, 2017.