User login
Zika outbreak forces better history taking, tracking
ANNAPOLIS, MD. – The definition of taking a thorough travel history has expanded with the spread of Zika.
Physicians “need to focus not only on patients’ travel histories, but also the travel histories and future travel plans of our patients’ sexual partners,” Ilona T. Goldfarb, a perinatologist at Massachusetts General Hospital, Boston, said in an interview. “We cannot rely on our patients to just [offer] that they’ve been in the Caribbean. We have to ask them diligently, and at every visit.”

Dr. Goldfarb added that immigration is a risk for Zika exposure, and may be a barrier to accurate history taking. In these cases, travel history will need to be performed in the patient’s spoken language to ensure accuracy, Dr. Goldfarb said. To track and communicate Zika information, Dr. Goldfarb and her colleagues have developed a three-part response based on their experience with previous infectious disease emergencies:
1. Communication. The practice is in regular communication with the Centers for Disease Control and Prevention and the state public health department to ensure they are up to date on all guidelines.
2. Education. Dr. Goldfarb and her practice colleagues routinely brief each other and patients on any new information, including recommended testing and guidelines, as well as travel warnings.
3. Tracking. Clinicians use a tracking worksheet for every patient screened for potential Zika exposure, allowing them to prospectively and retrospectively review patients. This has already proven useful, Dr. Goldfarb said, when the CDC changed its guidance around testing of asymptomatic patients.
In a presentation at the annual scientific meeting of the Infectious Diseases Society for Obstetrics and Gynecology, Dr. Goldfarb presented the data that she and her colleagues have collected so far on patients with Zika exposure.
As of Aug. 10, 2016, the practice had screened 142 women for Zika virus exposure since January 2016. More than 80% of the exposure came from travel to Zika-endemic areas. There have been few cases of exposure reported through sex, but Dr. Goldfarb said she thinks this type of exposure has been underreported because the link between infection and sex was not known until more recently.
Of the patients screened, 87% were appropriate candidates for Zika virus serum testing under CDC guidelines. There have been four positive serum tests for Zika exposure in Dr. Goldfarb’s patients so far.
In the one live birth, the newborn showed no visible signs of abnormalities. Testing revealed Zika virus RNA in the placenta, but not in the cord blood. The other three pregnancies were either terminated or associated with miscarriages. Again, Zika was detected in the placentas, but not in the fetuses.
Testing protocols have been a moving target since the outbreak began, according to Dr. Goldfarb. Some patients who call or are screened for possible exposure “are not actually eligible for testing because of the time frame or location of travel.”
To make sure that appropriate testing is being performed, Dr. Goldfarb advised designating an in-practice “Zika expert.” In her own practice, Dr. Goldfarb and one other colleague handle all Zika screening and inquiries from patients and colleagues. “This has greatly improved our efficiency and the experience for the patients,” she said in an interview.
The Massachusetts Department of Public Health is piloting a program with Dr. Goldfarb’s practice to determine if using the “designated expert” approach will improve laboratory wait times, compared with the standard protocol of having clinicians obtain approval from a state epidemiologist before sending patient serum samples for testing.
It has taken from 2 to 68 days to receive test results from the state lab, although a period of 17 days is typical, Dr. Goldfarb reported. The process has improved since last March when state health officials ramped up their capacity, she said.
As of Aug. 10, Dr. Goldfarb’s practice has performed 107 ultrasounds for patients with suspected Zika virus, averaging 3 per patient. Across all ultrasounds, there were three abnormalities, including one case of bilateral ventriculomegaly. Earlier in that pregnancy, the patient had tested negative for Zika on real-time reverse transcription polymerase chain reaction testing, which simultaneously screens for dengue, chikungunya, and Zika. Serum testing was also negative for Zika in the two other pregnancies with fetal abnormalities.
Dr. Goldfarb said she couldn’t quantify how much time is being spent on Zika screening and counseling since that is not being tracked, but she estimated that her practice takes between three and five calls or questions per day regarding the virus.
On Twitter @whitneymcknight
ANNAPOLIS, MD. – The definition of taking a thorough travel history has expanded with the spread of Zika.
Physicians “need to focus not only on patients’ travel histories, but also the travel histories and future travel plans of our patients’ sexual partners,” Ilona T. Goldfarb, a perinatologist at Massachusetts General Hospital, Boston, said in an interview. “We cannot rely on our patients to just [offer] that they’ve been in the Caribbean. We have to ask them diligently, and at every visit.”
Dr. Goldfarb added that immigration is a risk for Zika exposure, and may be a barrier to accurate history taking. In these cases, travel history will need to be performed in the patient’s spoken language to ensure accuracy, Dr. Goldfarb said. To track and communicate Zika information, Dr. Goldfarb and her colleagues have developed a three-part response based on their experience with previous infectious disease emergencies:
1. Communication. The practice is in regular communication with the Centers for Disease Control and Prevention and the state public health department to ensure they are up to date on all guidelines.
2. Education. Dr. Goldfarb and her practice colleagues routinely brief each other and patients on any new information, including recommended testing and guidelines, as well as travel warnings.
3. Tracking. Clinicians use a tracking worksheet for every patient screened for potential Zika exposure, allowing them to prospectively and retrospectively review patients. This has already proven useful, Dr. Goldfarb said, when the CDC changed its guidance around testing of asymptomatic patients.
In a presentation at the annual scientific meeting of the Infectious Diseases Society for Obstetrics and Gynecology, Dr. Goldfarb presented the data that she and her colleagues have collected so far on patients with Zika exposure.
As of Aug. 10, 2016, the practice had screened 142 women for Zika virus exposure since January 2016. More than 80% of the exposure came from travel to Zika-endemic areas. There have been few cases of exposure reported through sex, but Dr. Goldfarb said she thinks this type of exposure has been underreported because the link between infection and sex was not known until more recently.
Of the patients screened, 87% were appropriate candidates for Zika virus serum testing under CDC guidelines. There have been four positive serum tests for Zika exposure in Dr. Goldfarb’s patients so far.
In the one live birth, the newborn showed no visible signs of abnormalities. Testing revealed Zika virus RNA in the placenta, but not in the cord blood. The other three pregnancies were either terminated or associated with miscarriages. Again, Zika was detected in the placentas, but not in the fetuses.
Testing protocols have been a moving target since the outbreak began, according to Dr. Goldfarb. Some patients who call or are screened for possible exposure “are not actually eligible for testing because of the time frame or location of travel.”
To make sure that appropriate testing is being performed, Dr. Goldfarb advised designating an in-practice “Zika expert.” In her own practice, Dr. Goldfarb and one other colleague handle all Zika screening and inquiries from patients and colleagues. “This has greatly improved our efficiency and the experience for the patients,” she said in an interview.
The Massachusetts Department of Public Health is piloting a program with Dr. Goldfarb’s practice to determine if using the “designated expert” approach will improve laboratory wait times, compared with the standard protocol of having clinicians obtain approval from a state epidemiologist before sending patient serum samples for testing.
It has taken from 2 to 68 days to receive test results from the state lab, although a period of 17 days is typical, Dr. Goldfarb reported. The process has improved since last March when state health officials ramped up their capacity, she said.
As of Aug. 10, Dr. Goldfarb’s practice has performed 107 ultrasounds for patients with suspected Zika virus, averaging 3 per patient. Across all ultrasounds, there were three abnormalities, including one case of bilateral ventriculomegaly. Earlier in that pregnancy, the patient had tested negative for Zika on real-time reverse transcription polymerase chain reaction testing, which simultaneously screens for dengue, chikungunya, and Zika. Serum testing was also negative for Zika in the two other pregnancies with fetal abnormalities.
Dr. Goldfarb said she couldn’t quantify how much time is being spent on Zika screening and counseling since that is not being tracked, but she estimated that her practice takes between three and five calls or questions per day regarding the virus.
On Twitter @whitneymcknight
ANNAPOLIS, MD. – The definition of taking a thorough travel history has expanded with the spread of Zika.
Physicians “need to focus not only on patients’ travel histories, but also the travel histories and future travel plans of our patients’ sexual partners,” Ilona T. Goldfarb, a perinatologist at Massachusetts General Hospital, Boston, said in an interview. “We cannot rely on our patients to just [offer] that they’ve been in the Caribbean. We have to ask them diligently, and at every visit.”
Dr. Goldfarb added that immigration is a risk for Zika exposure, and may be a barrier to accurate history taking. In these cases, travel history will need to be performed in the patient’s spoken language to ensure accuracy, Dr. Goldfarb said. To track and communicate Zika information, Dr. Goldfarb and her colleagues have developed a three-part response based on their experience with previous infectious disease emergencies:
1. Communication. The practice is in regular communication with the Centers for Disease Control and Prevention and the state public health department to ensure they are up to date on all guidelines.
2. Education. Dr. Goldfarb and her practice colleagues routinely brief each other and patients on any new information, including recommended testing and guidelines, as well as travel warnings.
3. Tracking. Clinicians use a tracking worksheet for every patient screened for potential Zika exposure, allowing them to prospectively and retrospectively review patients. This has already proven useful, Dr. Goldfarb said, when the CDC changed its guidance around testing of asymptomatic patients.
In a presentation at the annual scientific meeting of the Infectious Diseases Society for Obstetrics and Gynecology, Dr. Goldfarb presented the data that she and her colleagues have collected so far on patients with Zika exposure.
As of Aug. 10, 2016, the practice had screened 142 women for Zika virus exposure since January 2016. More than 80% of the exposure came from travel to Zika-endemic areas. There have been few cases of exposure reported through sex, but Dr. Goldfarb said she thinks this type of exposure has been underreported because the link between infection and sex was not known until more recently.
Of the patients screened, 87% were appropriate candidates for Zika virus serum testing under CDC guidelines. There have been four positive serum tests for Zika exposure in Dr. Goldfarb’s patients so far.
In the one live birth, the newborn showed no visible signs of abnormalities. Testing revealed Zika virus RNA in the placenta, but not in the cord blood. The other three pregnancies were either terminated or associated with miscarriages. Again, Zika was detected in the placentas, but not in the fetuses.
Testing protocols have been a moving target since the outbreak began, according to Dr. Goldfarb. Some patients who call or are screened for possible exposure “are not actually eligible for testing because of the time frame or location of travel.”
To make sure that appropriate testing is being performed, Dr. Goldfarb advised designating an in-practice “Zika expert.” In her own practice, Dr. Goldfarb and one other colleague handle all Zika screening and inquiries from patients and colleagues. “This has greatly improved our efficiency and the experience for the patients,” she said in an interview.
The Massachusetts Department of Public Health is piloting a program with Dr. Goldfarb’s practice to determine if using the “designated expert” approach will improve laboratory wait times, compared with the standard protocol of having clinicians obtain approval from a state epidemiologist before sending patient serum samples for testing.
It has taken from 2 to 68 days to receive test results from the state lab, although a period of 17 days is typical, Dr. Goldfarb reported. The process has improved since last March when state health officials ramped up their capacity, she said.
As of Aug. 10, Dr. Goldfarb’s practice has performed 107 ultrasounds for patients with suspected Zika virus, averaging 3 per patient. Across all ultrasounds, there were three abnormalities, including one case of bilateral ventriculomegaly. Earlier in that pregnancy, the patient had tested negative for Zika on real-time reverse transcription polymerase chain reaction testing, which simultaneously screens for dengue, chikungunya, and Zika. Serum testing was also negative for Zika in the two other pregnancies with fetal abnormalities.
Dr. Goldfarb said she couldn’t quantify how much time is being spent on Zika screening and counseling since that is not being tracked, but she estimated that her practice takes between three and five calls or questions per day regarding the virus.
On Twitter @whitneymcknight
EXPERT ANALYSIS FROM IDSOG

Request for Applications for JVS Editorial Positions
The editors of the Journal of Vascular Surgery Publications are seeking nominations, including self-nominations, for multiple editorial positions. All applicants must be active or senior members of the Society for Vascular Surgery. Prior service on the JVS editorial board is preferred. An annual financial stipend is provided for these editorial roles.
More information about each of the positions listed below can be found in this online document.
Assistant editor of abstracts and book reviews. This editor selects non-JVS abstracts and writes short commentaries for those abstracts for publication in the JVS and JVS-VL. This editor will also write and solicit book reviews.
Assistant editor of social media and press releases. This position requires writing short press release articles for the JVS Journals and drafting Facebook, Twitter and LinkedIn posts to promote JVS content.
Assistant editor of reviews for the Journal of Vascular Surgery. The assistant editor solicits review articles and manages the peer-review process for systematic reviews, meta-analyses, and evidence summaries.
Associate basic science editor for the JVS and the JVSVL. This associate editor manages the peer-review process and makes the final decision on manuscript publication for about 200 basic science submissions a year.
Associate editor of the Journal of Vascular Surgery. The JVS associate editor manages the peer-review process of about 600 submissions a year, recommending a final decision to the editors regarding the publication of a submission.
If you would like to apply for one of these editorial positions, please send your name and a brief summary of your qualifications Jessica McEwan, JVS managing editor at: [email protected]. The deadline for applications is Oct. 1, 2016.
The editors of the Journal of Vascular Surgery Publications are seeking nominations, including self-nominations, for multiple editorial positions. All applicants must be active or senior members of the Society for Vascular Surgery. Prior service on the JVS editorial board is preferred. An annual financial stipend is provided for these editorial roles.
More information about each of the positions listed below can be found in this online document.
Assistant editor of abstracts and book reviews. This editor selects non-JVS abstracts and writes short commentaries for those abstracts for publication in the JVS and JVS-VL. This editor will also write and solicit book reviews.
Assistant editor of social media and press releases. This position requires writing short press release articles for the JVS Journals and drafting Facebook, Twitter and LinkedIn posts to promote JVS content.
Assistant editor of reviews for the Journal of Vascular Surgery. The assistant editor solicits review articles and manages the peer-review process for systematic reviews, meta-analyses, and evidence summaries.
Associate basic science editor for the JVS and the JVSVL. This associate editor manages the peer-review process and makes the final decision on manuscript publication for about 200 basic science submissions a year.
Associate editor of the Journal of Vascular Surgery. The JVS associate editor manages the peer-review process of about 600 submissions a year, recommending a final decision to the editors regarding the publication of a submission.
If you would like to apply for one of these editorial positions, please send your name and a brief summary of your qualifications Jessica McEwan, JVS managing editor at: [email protected]. The deadline for applications is Oct. 1, 2016.
The editors of the Journal of Vascular Surgery Publications are seeking nominations, including self-nominations, for multiple editorial positions. All applicants must be active or senior members of the Society for Vascular Surgery. Prior service on the JVS editorial board is preferred. An annual financial stipend is provided for these editorial roles.
More information about each of the positions listed below can be found in this online document.
Assistant editor of abstracts and book reviews. This editor selects non-JVS abstracts and writes short commentaries for those abstracts for publication in the JVS and JVS-VL. This editor will also write and solicit book reviews.
Assistant editor of social media and press releases. This position requires writing short press release articles for the JVS Journals and drafting Facebook, Twitter and LinkedIn posts to promote JVS content.
Assistant editor of reviews for the Journal of Vascular Surgery. The assistant editor solicits review articles and manages the peer-review process for systematic reviews, meta-analyses, and evidence summaries.
Associate basic science editor for the JVS and the JVSVL. This associate editor manages the peer-review process and makes the final decision on manuscript publication for about 200 basic science submissions a year.
Associate editor of the Journal of Vascular Surgery. The JVS associate editor manages the peer-review process of about 600 submissions a year, recommending a final decision to the editors regarding the publication of a submission.
If you would like to apply for one of these editorial positions, please send your name and a brief summary of your qualifications Jessica McEwan, JVS managing editor at: [email protected]. The deadline for applications is Oct. 1, 2016.

Submit Proposals for VAM 2017
All SVS members may submit proposals for invited sessions for the 2017 Vascular Annual Meeting, set for May 31 to June 3 (plenaries and exhibits are June 1 to 3) in San Diego, Calif.
Previously, the process was open only to SVS committees; planners opened the process to all members this year, with any and all ideas for sessions to be reviewed for further development.
Invited sessions include postgraduate courses, breakfast and concurrent sessions and workshops. Initial submissions are due Sept. 16. Learn more here.
All SVS members may submit proposals for invited sessions for the 2017 Vascular Annual Meeting, set for May 31 to June 3 (plenaries and exhibits are June 1 to 3) in San Diego, Calif.
Previously, the process was open only to SVS committees; planners opened the process to all members this year, with any and all ideas for sessions to be reviewed for further development.
Invited sessions include postgraduate courses, breakfast and concurrent sessions and workshops. Initial submissions are due Sept. 16. Learn more here.
All SVS members may submit proposals for invited sessions for the 2017 Vascular Annual Meeting, set for May 31 to June 3 (plenaries and exhibits are June 1 to 3) in San Diego, Calif.
Previously, the process was open only to SVS committees; planners opened the process to all members this year, with any and all ideas for sessions to be reviewed for further development.
Invited sessions include postgraduate courses, breakfast and concurrent sessions and workshops. Initial submissions are due Sept. 16. Learn more here.

VIDEO: PCSK9 inhibitor can nearly replace need for apheresis in HeFH
ROME – Treating patients with heterozygous familial hypercholesterolemia (HeFH) with PCSK9 inhibitors can reduce their need for lipoprotein apheresis and its associated costs, Patrick M. Moriarty, MD, said in a video interview at the annual congress of the European Society of Cardiology.
In the randomized, phase III ODYSSEY ESCAPE trial, HeFH patients who underwent weekly apheresis were treated with either alirocumab, a proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor, or placebo. At the end of the study, the alirocumab-treated patients had a 75% greater reduction in need for apheresis, compared with those on placebo – a statistically significant difference.
With a price tag of $50,000-$75,000 a year for lipoprotein apheresis, compared with the roughly $12,000 cost for a PCSK9 inhibitor, this represents a significant savings for patients with HeFH, which occurs in roughly 1 in 200 people worldwide, Dr. Moriarty of the University of Kansas, Kansas City, told reporter Bruce Jancin.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ROME – Treating patients with heterozygous familial hypercholesterolemia (HeFH) with PCSK9 inhibitors can reduce their need for lipoprotein apheresis and its associated costs, Patrick M. Moriarty, MD, said in a video interview at the annual congress of the European Society of Cardiology.
In the randomized, phase III ODYSSEY ESCAPE trial, HeFH patients who underwent weekly apheresis were treated with either alirocumab, a proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor, or placebo. At the end of the study, the alirocumab-treated patients had a 75% greater reduction in need for apheresis, compared with those on placebo – a statistically significant difference.
With a price tag of $50,000-$75,000 a year for lipoprotein apheresis, compared with the roughly $12,000 cost for a PCSK9 inhibitor, this represents a significant savings for patients with HeFH, which occurs in roughly 1 in 200 people worldwide, Dr. Moriarty of the University of Kansas, Kansas City, told reporter Bruce Jancin.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ROME – Treating patients with heterozygous familial hypercholesterolemia (HeFH) with PCSK9 inhibitors can reduce their need for lipoprotein apheresis and its associated costs, Patrick M. Moriarty, MD, said in a video interview at the annual congress of the European Society of Cardiology.
In the randomized, phase III ODYSSEY ESCAPE trial, HeFH patients who underwent weekly apheresis were treated with either alirocumab, a proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor, or placebo. At the end of the study, the alirocumab-treated patients had a 75% greater reduction in need for apheresis, compared with those on placebo – a statistically significant difference.
With a price tag of $50,000-$75,000 a year for lipoprotein apheresis, compared with the roughly $12,000 cost for a PCSK9 inhibitor, this represents a significant savings for patients with HeFH, which occurs in roughly 1 in 200 people worldwide, Dr. Moriarty of the University of Kansas, Kansas City, told reporter Bruce Jancin.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE ESC CONGRESS 2016

First TOS Reporting Standards Published
SVS members now have access to the first-ever reporting standards for Thoracic Outlet Syndrome, published in the September issue (online) at the Journal of Vascular Surgery. Drs. Karl Illig and Audra Duncan led the TOS Reporting Standards Writing Group, which worked for three years to create the reporting standards. The group hopes that with unified data collection, practice guidelines can follow in five to 10 years.
Access the reporting standards here.
SVS members now have access to the first-ever reporting standards for Thoracic Outlet Syndrome, published in the September issue (online) at the Journal of Vascular Surgery. Drs. Karl Illig and Audra Duncan led the TOS Reporting Standards Writing Group, which worked for three years to create the reporting standards. The group hopes that with unified data collection, practice guidelines can follow in five to 10 years.
Access the reporting standards here.
SVS members now have access to the first-ever reporting standards for Thoracic Outlet Syndrome, published in the September issue (online) at the Journal of Vascular Surgery. Drs. Karl Illig and Audra Duncan led the TOS Reporting Standards Writing Group, which worked for three years to create the reporting standards. The group hopes that with unified data collection, practice guidelines can follow in five to 10 years.
Access the reporting standards here.

Review Course Recordings Available
Just in time for the September recertification exam! Recordings of the 2015 Comprehensive Vascular Review Course are available for purchase.
The 2015 intensive two-day course was led by vascular surgeons with extensive expertise in their respective fields. The recordings include didactic lectures and review of essential VESAP questions.
The recordings also provide a comprehensive update in all areas of vascular surgery. No CME credit is available.
Purchase the recordings here.
Just in time for the September recertification exam! Recordings of the 2015 Comprehensive Vascular Review Course are available for purchase.
The 2015 intensive two-day course was led by vascular surgeons with extensive expertise in their respective fields. The recordings include didactic lectures and review of essential VESAP questions.
The recordings also provide a comprehensive update in all areas of vascular surgery. No CME credit is available.
Purchase the recordings here.
Just in time for the September recertification exam! Recordings of the 2015 Comprehensive Vascular Review Course are available for purchase.
The 2015 intensive two-day course was led by vascular surgeons with extensive expertise in their respective fields. The recordings include didactic lectures and review of essential VESAP questions.
The recordings also provide a comprehensive update in all areas of vascular surgery. No CME credit is available.
Purchase the recordings here.

Psoriasis cardiovascular risk parallels type 2 diabetes
Psoriasis increased the measures of coronary artery calcium at a level similar to that seen in type 2 diabetes mellitus, independent of cardiovascular disease risk factors, based on data from a trio of cross-sectional studies including 387 adults. .
“Psoriasis and type 2 diabetes share similar cardiovascular risk profiles, which may predispose patients to developing coronary atherosclerosis at a relatively young age,” wrote Bobbak Mansouri, MD, of Baylor University Medical Center in Dallas and his associates (JAMA Dermatol. 2016. [doi: 10.1001/jamadermatol.2016.2907]).

The researchers compared coronary artery calcium (CAC) levels in patients with psoriasis, patients with type 2 diabetes, and healthy controls. CAC has become an accepted measure of atherosclerosis and “the cornerstone for screening the risk of future cardiac events and improving cardiovascular risk stratification beyond traditional risk factors, especially in higher-risk groups,” according to the investigators. The average age of the patients was 52 years, 50% were female, and at least 92% were white.
The researchers used a hierarchical Tobit regression analysis to determine the association between disease and CAC level, as measured by the Agatston score. After controlling for confounding variables, including cardiovascular risk factors (low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, fasting blood glucose, systolic blood pressure, and tobacco use), the association with CAC was similar in psoriasis patients and type 2 diabetes patients (Tobit regression ratio [TRR], 0.89 and 0.79, respectively).
In a logistic multivariate regression analysis, patients with either psoriasis or type 2 diabetes were approximately twice as likely to have evidence of CAC as were healthy controls (odds ratio, 2.35 and 2.18, respectively), and psoriasis remained independently associated with the presence of CAC.
“When we added use of systemic or biological therapy to the models, the TRR and OR increased; however, these analyses were exploratory,” wrote Dr. Mansouri and his associates.
The study was limited by factors including the cross-sectional design and lack of diversity in the patient population, the investigators noted. However, the results suggest that “CAC assessment may be considered in patients with psoriasis who have two or more traditional cardiovascular risk factors given the high prevalence of CAC observed in this study,” they said.
Dr. Mansouri disclosed serving on an advisory board and receiving an honorarium from Celgene, maker of the psoriasis drug apremilast (Otezl). Study coauthors disclosed financial relationships with multiple pharmaceutical companies.
Psoriasis increased the measures of coronary artery calcium at a level similar to that seen in type 2 diabetes mellitus, independent of cardiovascular disease risk factors, based on data from a trio of cross-sectional studies including 387 adults. .
“Psoriasis and type 2 diabetes share similar cardiovascular risk profiles, which may predispose patients to developing coronary atherosclerosis at a relatively young age,” wrote Bobbak Mansouri, MD, of Baylor University Medical Center in Dallas and his associates (JAMA Dermatol. 2016. [doi: 10.1001/jamadermatol.2016.2907]).
The researchers compared coronary artery calcium (CAC) levels in patients with psoriasis, patients with type 2 diabetes, and healthy controls. CAC has become an accepted measure of atherosclerosis and “the cornerstone for screening the risk of future cardiac events and improving cardiovascular risk stratification beyond traditional risk factors, especially in higher-risk groups,” according to the investigators. The average age of the patients was 52 years, 50% were female, and at least 92% were white.
The researchers used a hierarchical Tobit regression analysis to determine the association between disease and CAC level, as measured by the Agatston score. After controlling for confounding variables, including cardiovascular risk factors (low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, fasting blood glucose, systolic blood pressure, and tobacco use), the association with CAC was similar in psoriasis patients and type 2 diabetes patients (Tobit regression ratio [TRR], 0.89 and 0.79, respectively).
In a logistic multivariate regression analysis, patients with either psoriasis or type 2 diabetes were approximately twice as likely to have evidence of CAC as were healthy controls (odds ratio, 2.35 and 2.18, respectively), and psoriasis remained independently associated with the presence of CAC.
“When we added use of systemic or biological therapy to the models, the TRR and OR increased; however, these analyses were exploratory,” wrote Dr. Mansouri and his associates.
The study was limited by factors including the cross-sectional design and lack of diversity in the patient population, the investigators noted. However, the results suggest that “CAC assessment may be considered in patients with psoriasis who have two or more traditional cardiovascular risk factors given the high prevalence of CAC observed in this study,” they said.
Dr. Mansouri disclosed serving on an advisory board and receiving an honorarium from Celgene, maker of the psoriasis drug apremilast (Otezl). Study coauthors disclosed financial relationships with multiple pharmaceutical companies.
Psoriasis increased the measures of coronary artery calcium at a level similar to that seen in type 2 diabetes mellitus, independent of cardiovascular disease risk factors, based on data from a trio of cross-sectional studies including 387 adults. .
“Psoriasis and type 2 diabetes share similar cardiovascular risk profiles, which may predispose patients to developing coronary atherosclerosis at a relatively young age,” wrote Bobbak Mansouri, MD, of Baylor University Medical Center in Dallas and his associates (JAMA Dermatol. 2016. [doi: 10.1001/jamadermatol.2016.2907]).
The researchers compared coronary artery calcium (CAC) levels in patients with psoriasis, patients with type 2 diabetes, and healthy controls. CAC has become an accepted measure of atherosclerosis and “the cornerstone for screening the risk of future cardiac events and improving cardiovascular risk stratification beyond traditional risk factors, especially in higher-risk groups,” according to the investigators. The average age of the patients was 52 years, 50% were female, and at least 92% were white.
The researchers used a hierarchical Tobit regression analysis to determine the association between disease and CAC level, as measured by the Agatston score. After controlling for confounding variables, including cardiovascular risk factors (low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, fasting blood glucose, systolic blood pressure, and tobacco use), the association with CAC was similar in psoriasis patients and type 2 diabetes patients (Tobit regression ratio [TRR], 0.89 and 0.79, respectively).
In a logistic multivariate regression analysis, patients with either psoriasis or type 2 diabetes were approximately twice as likely to have evidence of CAC as were healthy controls (odds ratio, 2.35 and 2.18, respectively), and psoriasis remained independently associated with the presence of CAC.
“When we added use of systemic or biological therapy to the models, the TRR and OR increased; however, these analyses were exploratory,” wrote Dr. Mansouri and his associates.
The study was limited by factors including the cross-sectional design and lack of diversity in the patient population, the investigators noted. However, the results suggest that “CAC assessment may be considered in patients with psoriasis who have two or more traditional cardiovascular risk factors given the high prevalence of CAC observed in this study,” they said.
Dr. Mansouri disclosed serving on an advisory board and receiving an honorarium from Celgene, maker of the psoriasis drug apremilast (Otezl). Study coauthors disclosed financial relationships with multiple pharmaceutical companies.
FROM JAMA DERMATOLOGY
Key clinical point: Psoriasis patients have increased coronary artery calcium levels similar to those seen in type 2 diabetes patients, suggesting subclinical atherosclerosis.
Major finding: Psoriasis patients were more than twice as likely (odds ratio, 2.35) to have evidence of coronary artery calcium, compared with healthy controls.
Data source: A set of three single-center, cross-sectional studies totaling 387 adults and including individuals with psoriasis or type 2 diabetes, and healthy controls.
Disclosures: Dr. Mansouri disclosed serving on an advisory board and receiving an honorarium from Celgene, maker of the psoriasis drug apremilast (Otezl). Study coauthors disclosed financial relationships with multiple pharmaceutical companies.
Cycling accounts for the most sports-related ED visits
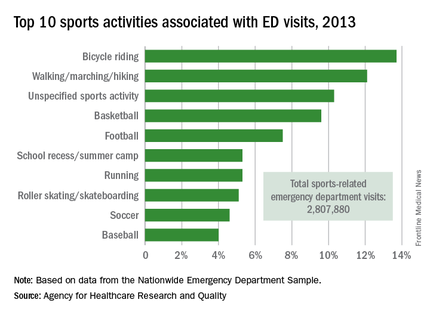
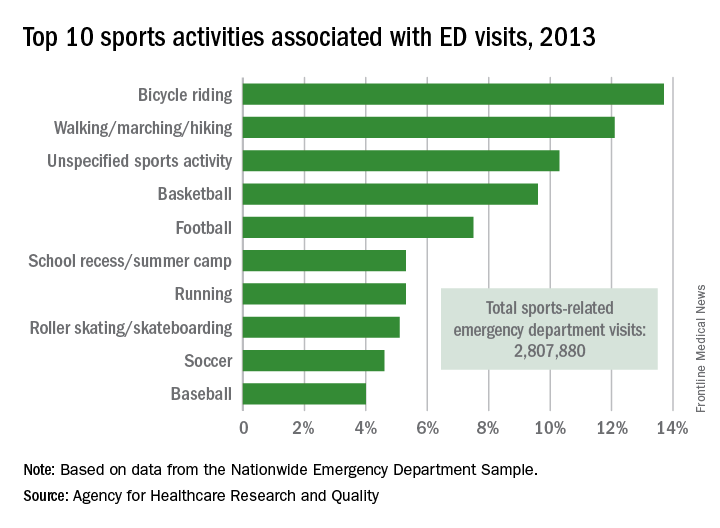
Bicycle riding results in more visits to the emergency department than any other sports activity, according to the Agency for Healthcare Research and Quality.
In 2013, cycling accounted for 13.7% of the 2.8 million ED visits in which the patient was discharged. Walking/marching/hiking was next with 12.1% of ED visits, while unspecified sports activities were third with 10.3% of visits. Team sports took the next two spots: basketball accounted for 9.6% of visits and football accounted for 7.5%, the AHRQ reported.
Among those under age 18 years, who accounted for over 1.5 million ED visits (54.7%) in 2013, football was associated with the most visits for boys (16.4%) and school recess/summer camp led to the most visits (12.8%) for girls. Bicycle riding was the leading reason for males aged 18-44 (16%) and 45-64 (34.9%), while walking/marching/hiking was the leading reason for females aged 18-44 (25.6%) and 45-64 years (49%). For those older than 65 years, walking/marching/hiking was the most common reason for ED visits among both men (54.3%) and women (79.7%), according to data from the Nationwide Emergency Department Sample.
The most common injuries in 2013 for sports-related ED visits (discharged) were sprains (24%), fractures (21%), and superficial injuries (18%). Among the top 10 injury-producing sports activities, cycling had the highest rate of superficial injuries at 26%, school recess/summer camp had the highest fracture rate (42%), and basketball led with a sprain rate of 40%, the AHRQ said.
Bicycle riding results in more visits to the emergency department than any other sports activity, according to the Agency for Healthcare Research and Quality.
In 2013, cycling accounted for 13.7% of the 2.8 million ED visits in which the patient was discharged. Walking/marching/hiking was next with 12.1% of ED visits, while unspecified sports activities were third with 10.3% of visits. Team sports took the next two spots: basketball accounted for 9.6% of visits and football accounted for 7.5%, the AHRQ reported.
Among those under age 18 years, who accounted for over 1.5 million ED visits (54.7%) in 2013, football was associated with the most visits for boys (16.4%) and school recess/summer camp led to the most visits (12.8%) for girls. Bicycle riding was the leading reason for males aged 18-44 (16%) and 45-64 (34.9%), while walking/marching/hiking was the leading reason for females aged 18-44 (25.6%) and 45-64 years (49%). For those older than 65 years, walking/marching/hiking was the most common reason for ED visits among both men (54.3%) and women (79.7%), according to data from the Nationwide Emergency Department Sample.
The most common injuries in 2013 for sports-related ED visits (discharged) were sprains (24%), fractures (21%), and superficial injuries (18%). Among the top 10 injury-producing sports activities, cycling had the highest rate of superficial injuries at 26%, school recess/summer camp had the highest fracture rate (42%), and basketball led with a sprain rate of 40%, the AHRQ said.
Bicycle riding results in more visits to the emergency department than any other sports activity, according to the Agency for Healthcare Research and Quality.
In 2013, cycling accounted for 13.7% of the 2.8 million ED visits in which the patient was discharged. Walking/marching/hiking was next with 12.1% of ED visits, while unspecified sports activities were third with 10.3% of visits. Team sports took the next two spots: basketball accounted for 9.6% of visits and football accounted for 7.5%, the AHRQ reported.
Among those under age 18 years, who accounted for over 1.5 million ED visits (54.7%) in 2013, football was associated with the most visits for boys (16.4%) and school recess/summer camp led to the most visits (12.8%) for girls. Bicycle riding was the leading reason for males aged 18-44 (16%) and 45-64 (34.9%), while walking/marching/hiking was the leading reason for females aged 18-44 (25.6%) and 45-64 years (49%). For those older than 65 years, walking/marching/hiking was the most common reason for ED visits among both men (54.3%) and women (79.7%), according to data from the Nationwide Emergency Department Sample.
The most common injuries in 2013 for sports-related ED visits (discharged) were sprains (24%), fractures (21%), and superficial injuries (18%). Among the top 10 injury-producing sports activities, cycling had the highest rate of superficial injuries at 26%, school recess/summer camp had the highest fracture rate (42%), and basketball led with a sprain rate of 40%, the AHRQ said.
Vaccine refusals and pediatrician dismissals increasing
More parents have been refusing vaccines in recent years than a decade ago, according to surveys of pediatricians by the American Academy of Pediatrics published in Pediatrics Aug. 29.
“In a busy practice, vaccine refusals and delays occur daily (if not multiple times per day),” wrote Catherine Hough-Telford, MD, of the University of Alabama at Birmingham and her colleagues (Pediatrics. 2016 Aug. 29. doi: 10.1542/peds.2016-2127).

“From the perspective of the pediatricians, parents who delay vaccines may do so because of concern for their child’s discomfort and concern about immune system burden, whereas vaccine refusers are more likely to believe that vaccines are unnecessary,” the authors wrote. “Pediatricians report that they continue to provide education to vaccine-refusing and delaying parents at high rates.”
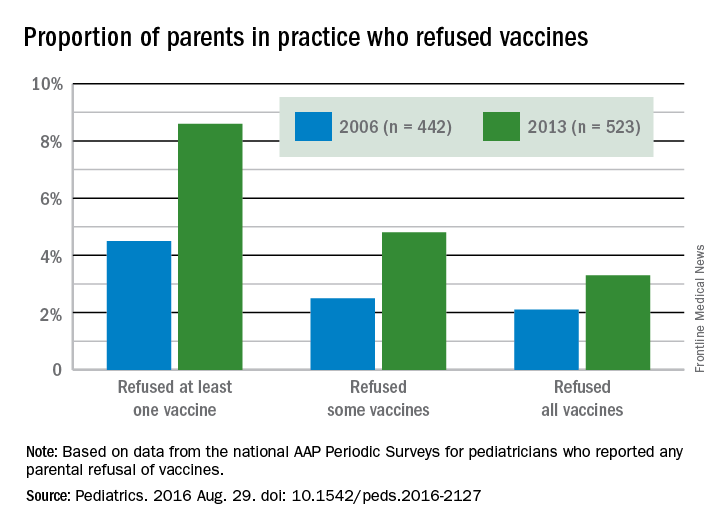
Dr. Hough-Telford’s team compared the national AAP Periodic Surveys of 2006 and 2013 that dealt exclusively with immunizations to learn how currently practicing pediatricians perceived three issues related to vaccination: the prevalence of vaccine refusals and delays, why parents refuse or delay vaccines, and the decision of doctors to dismiss families who refuse to vaccinate.
The researchers excluded pediatricians who did not routinely administer vaccines or otherwise adhere to the Centers for Disease Control and Prevention–recommended immunization schedule for their patients. The 2006 survey had a response rate of 52.6% and included 629 final respondents; the 2013 survey had a response rate of 52.7% and included 627 respondents.
The proportion of pediatricians reporting parental refusals in their practice increased from 74.5% in 2006 to 87% in 2013 (odds ratio, 2.29; P less than .001). These pediatricians estimated in 2013 that 8.6% of their patients refused at least one vaccine, compared with 4.5% in 2006. Similarly, 2.5% of parents refused some vaccines in 2006, the physicians reported, compared with 4.8% in 2013. Those refusing all vaccines increased from 2.1% in 2006 to 3.3% in 2013.
A perceived 73.1% of parents refused vaccines in 2013 because they regarded them as unnecessary, the pediatricians reported, compared with 63.4% in 2006. But parental concern over autism and/or thimerosal dropped from 74.2% of vaccine-refusing parents in 2006 to 64.3% in 2013. Further, the parents refusing vaccines because of safety/side effects concerns dropped from 73.7% in 2006 to 66.6% in 2013, and those worried about their children receiving too many shots more than halved from 42.1% in 2006 to 17% in 2013. Concern among parents about their baby being too small to receive vaccines also dropped.

Physicians estimated that 7.3% of their parents wanted to delay one vaccine, 7.1% wanted to delay multiple vaccines, and 4.3% wanted to delay all vaccines. Urban, inner-city pediatricians were less likely to have parents requesting delays than were parents in other areas, but requests for vaccine delays were geographically similar across different U.S. regions. Only the 2013 survey included questions on delaying vaccines.
Pediatricians reported that 75% of their patients wanted to delay vaccines to reduce discomfort to their child, and 72.5% wanted to delay because they perceived too many vaccines would overburden their child’s immune system.
The percentage of pediatricians who always dismiss patients who continue to refuse vaccines increased from 6.1% in 2006 to 11.7% in 2013; they cited a lack of trust between physician and patient as a major reason (87.4% in 2006; 79.9% in 2013). Further, 80.5% of pediatricians reported in 2013 (the only year asked) that they dismissed vaccine-refusing patients out of concern for their other patients.
Despite no notable geographic differences in dismissals in 2006, the 2013 survey revealed that pediatricians in the West had three to four times greater odds of dismissing patients than those in the Midwest and South. Suburban pediatricians had three times greater odds of dismissing patients than did urban physicians.
The research was funded by the AAP and the CDC Childhood Immunization Support Program. Dr. Kimberlin was a site principal investigator for two multisite studies conducted by GlaxoSmithKline and Gilead.
More parents have been refusing vaccines in recent years than a decade ago, according to surveys of pediatricians by the American Academy of Pediatrics published in Pediatrics Aug. 29.
“In a busy practice, vaccine refusals and delays occur daily (if not multiple times per day),” wrote Catherine Hough-Telford, MD, of the University of Alabama at Birmingham and her colleagues (Pediatrics. 2016 Aug. 29. doi: 10.1542/peds.2016-2127).
“From the perspective of the pediatricians, parents who delay vaccines may do so because of concern for their child’s discomfort and concern about immune system burden, whereas vaccine refusers are more likely to believe that vaccines are unnecessary,” the authors wrote. “Pediatricians report that they continue to provide education to vaccine-refusing and delaying parents at high rates.”
Dr. Hough-Telford’s team compared the national AAP Periodic Surveys of 2006 and 2013 that dealt exclusively with immunizations to learn how currently practicing pediatricians perceived three issues related to vaccination: the prevalence of vaccine refusals and delays, why parents refuse or delay vaccines, and the decision of doctors to dismiss families who refuse to vaccinate.
The researchers excluded pediatricians who did not routinely administer vaccines or otherwise adhere to the Centers for Disease Control and Prevention–recommended immunization schedule for their patients. The 2006 survey had a response rate of 52.6% and included 629 final respondents; the 2013 survey had a response rate of 52.7% and included 627 respondents.
The proportion of pediatricians reporting parental refusals in their practice increased from 74.5% in 2006 to 87% in 2013 (odds ratio, 2.29; P less than .001). These pediatricians estimated in 2013 that 8.6% of their patients refused at least one vaccine, compared with 4.5% in 2006. Similarly, 2.5% of parents refused some vaccines in 2006, the physicians reported, compared with 4.8% in 2013. Those refusing all vaccines increased from 2.1% in 2006 to 3.3% in 2013.
A perceived 73.1% of parents refused vaccines in 2013 because they regarded them as unnecessary, the pediatricians reported, compared with 63.4% in 2006. But parental concern over autism and/or thimerosal dropped from 74.2% of vaccine-refusing parents in 2006 to 64.3% in 2013. Further, the parents refusing vaccines because of safety/side effects concerns dropped from 73.7% in 2006 to 66.6% in 2013, and those worried about their children receiving too many shots more than halved from 42.1% in 2006 to 17% in 2013. Concern among parents about their baby being too small to receive vaccines also dropped.
Physicians estimated that 7.3% of their parents wanted to delay one vaccine, 7.1% wanted to delay multiple vaccines, and 4.3% wanted to delay all vaccines. Urban, inner-city pediatricians were less likely to have parents requesting delays than were parents in other areas, but requests for vaccine delays were geographically similar across different U.S. regions. Only the 2013 survey included questions on delaying vaccines.
Pediatricians reported that 75% of their patients wanted to delay vaccines to reduce discomfort to their child, and 72.5% wanted to delay because they perceived too many vaccines would overburden their child’s immune system.
The percentage of pediatricians who always dismiss patients who continue to refuse vaccines increased from 6.1% in 2006 to 11.7% in 2013; they cited a lack of trust between physician and patient as a major reason (87.4% in 2006; 79.9% in 2013). Further, 80.5% of pediatricians reported in 2013 (the only year asked) that they dismissed vaccine-refusing patients out of concern for their other patients.
Despite no notable geographic differences in dismissals in 2006, the 2013 survey revealed that pediatricians in the West had three to four times greater odds of dismissing patients than those in the Midwest and South. Suburban pediatricians had three times greater odds of dismissing patients than did urban physicians.
The research was funded by the AAP and the CDC Childhood Immunization Support Program. Dr. Kimberlin was a site principal investigator for two multisite studies conducted by GlaxoSmithKline and Gilead.
More parents have been refusing vaccines in recent years than a decade ago, according to surveys of pediatricians by the American Academy of Pediatrics published in Pediatrics Aug. 29.
“In a busy practice, vaccine refusals and delays occur daily (if not multiple times per day),” wrote Catherine Hough-Telford, MD, of the University of Alabama at Birmingham and her colleagues (Pediatrics. 2016 Aug. 29. doi: 10.1542/peds.2016-2127).
“From the perspective of the pediatricians, parents who delay vaccines may do so because of concern for their child’s discomfort and concern about immune system burden, whereas vaccine refusers are more likely to believe that vaccines are unnecessary,” the authors wrote. “Pediatricians report that they continue to provide education to vaccine-refusing and delaying parents at high rates.”
Dr. Hough-Telford’s team compared the national AAP Periodic Surveys of 2006 and 2013 that dealt exclusively with immunizations to learn how currently practicing pediatricians perceived three issues related to vaccination: the prevalence of vaccine refusals and delays, why parents refuse or delay vaccines, and the decision of doctors to dismiss families who refuse to vaccinate.
The researchers excluded pediatricians who did not routinely administer vaccines or otherwise adhere to the Centers for Disease Control and Prevention–recommended immunization schedule for their patients. The 2006 survey had a response rate of 52.6% and included 629 final respondents; the 2013 survey had a response rate of 52.7% and included 627 respondents.
The proportion of pediatricians reporting parental refusals in their practice increased from 74.5% in 2006 to 87% in 2013 (odds ratio, 2.29; P less than .001). These pediatricians estimated in 2013 that 8.6% of their patients refused at least one vaccine, compared with 4.5% in 2006. Similarly, 2.5% of parents refused some vaccines in 2006, the physicians reported, compared with 4.8% in 2013. Those refusing all vaccines increased from 2.1% in 2006 to 3.3% in 2013.
A perceived 73.1% of parents refused vaccines in 2013 because they regarded them as unnecessary, the pediatricians reported, compared with 63.4% in 2006. But parental concern over autism and/or thimerosal dropped from 74.2% of vaccine-refusing parents in 2006 to 64.3% in 2013. Further, the parents refusing vaccines because of safety/side effects concerns dropped from 73.7% in 2006 to 66.6% in 2013, and those worried about their children receiving too many shots more than halved from 42.1% in 2006 to 17% in 2013. Concern among parents about their baby being too small to receive vaccines also dropped.
Physicians estimated that 7.3% of their parents wanted to delay one vaccine, 7.1% wanted to delay multiple vaccines, and 4.3% wanted to delay all vaccines. Urban, inner-city pediatricians were less likely to have parents requesting delays than were parents in other areas, but requests for vaccine delays were geographically similar across different U.S. regions. Only the 2013 survey included questions on delaying vaccines.
Pediatricians reported that 75% of their patients wanted to delay vaccines to reduce discomfort to their child, and 72.5% wanted to delay because they perceived too many vaccines would overburden their child’s immune system.
The percentage of pediatricians who always dismiss patients who continue to refuse vaccines increased from 6.1% in 2006 to 11.7% in 2013; they cited a lack of trust between physician and patient as a major reason (87.4% in 2006; 79.9% in 2013). Further, 80.5% of pediatricians reported in 2013 (the only year asked) that they dismissed vaccine-refusing patients out of concern for their other patients.
Despite no notable geographic differences in dismissals in 2006, the 2013 survey revealed that pediatricians in the West had three to four times greater odds of dismissing patients than those in the Midwest and South. Suburban pediatricians had three times greater odds of dismissing patients than did urban physicians.
The research was funded by the AAP and the CDC Childhood Immunization Support Program. Dr. Kimberlin was a site principal investigator for two multisite studies conducted by GlaxoSmithKline and Gilead.
FROM PEDIATRICS
Key clinical point: More parents have been refusing vaccines, and more pediatricians have been dismissing vaccine-refusing patients, since 2006.
Major finding: 11.7% of pediatricians reported dismissing patients for refusing vaccines in 2013, compared with 6.1% in 2006, and 8.6% of parents refused at least one vaccine in 2013, compared with 4.5% in 2006.
Data source: The findings are based on surveys of practicing members of the American Academy of Pediatrics, with 629 pediatricians in 2006 and 627 pediatricians in 2013.
Disclosures: The research was funded by the AAP and the Centers for Disease Control and Prevention Childhood Immunization Support Program. Dr. Kimberlin was a site principal investigator for two multisite studies conducted by GlaxoSmithKline and Gilead.
Navigating the obstacle course of diagnosing, managing pediatric hypertension
The clinical context of high blood pressure shifts abruptly when a person comes of age.
In adults 18 years old and up it’s fairly simple. Blood pressure above 140/90 mm Hg is generally a clear problem, less than 130/85 is probably okay for now, and in between is something to monitor. When pressure stays above 140/90 mm Hg despite lifestyle interventions it’s time to start treatment with any of several antihypertensive drug options that mostly have well-documented safety and efficacy track records in adults and widely agreed-on benefits that outweigh risks.
For pediatric practice, children and adolescents 3-17 years old, dealing with high blood pressure is much more an obstacle course of complex diagnostic criteria, challenges in pressure measurement, and seemingly inconsistent recommendations. Pediatric hypertension also often brings clinicians up against the child and adolescent obesity epidemic, which has made pediatric hypertension more common than ever.
Against this backdrop, a panel assembled by the American Academy of Pediatrics is revising the 2004 The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents, the reigning standard for pediatric blood pressure assessment and hypertension management and now more than a decade old. With new guidance from the AAP expected in the second half of 2017, best-practice approaches to pediatric hypertension are in flux and need updating just when the disorder is more prevalent than it’s ever been.
Diagnosing pediatric hypertension falls short
This shifting landscape and increasing burden of pediatric hypertension comes at a time when primary-care pediatricians and family practice physicians are failing to perform fully comprehensive blood pressure monitoring of their pediatric patients. Current practice recommendations from the National Heart Lung and Blood Institute (in the form of the 2004 Fourth Report), and from American Heart Association (most recently reiterated in a scientific statement in August 2016) call measuring blood pressure levels at every patient encounter starting at 3 years old, the approach also endorsed by the American Academy of Pediatrics.
But that’s often not done. “Results from plenty of studies show that we are not doing a great job” identifying children and adolescents with hypertension, said Tammy M. Brady, MD, a pediatric nephrologist at Johns Hopkins Medical Center in Baltimore.

One piece of evidence she cited was a study of more than 93,000 U.S. ambulatory pediatric visits during 2000-2009 in data collected by the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey, and sampling that represented an average 142 million ambulatory visits each year by 3-18 year olds. The data showed blood pressure screening occurred during 35% of ambulatory visits, 67% of preventive visits, and during 84% of preventive visits for a child or adolescent who was overweight or obese (Pediatrics. 2012 October;130[4]:604-10).
While the numbers showed good practice with a reasonably high level of routine blood pressure measurement in overweight and obese patients, they also suggest that perhaps a third of all U.S. children and adolescents don’t have their blood pressure checked at least once a year. Statistical analyses from this study showed that blood pressure measurement was about twice as likely in children diagnosed as overweight or obese than normal-weight patients, and that blood pressure measurement was 2.6-fold more common in adolescents 13-18 years old compared with children 3-7 years old.
In a second, recent study of 29,000 2-17 years old seen at Children’s Hospital of Chicago, 3% had at least three elevated blood pressure measurements in their hospital record, but in this subset of patients at high risk of having hypertension 21% were actually identified in their medical record as having high blood pressure.
Dr. Brady pointed out that while many of the children and adolescents in this study with three or more high blood pressure readings may not actually have hypertension, defined as a sustained elevation of blood pressure, they are all at risk for development of hypertension and should be targeted for prevention.
“We do a bad job identifying when blood pressure is high,” Dr. Brady said in an interview. She cited a study she recently ran that examined the impact that EMR alerts could have on this diagnostic challenge. She reviewed records for 1,305 patient encounters done before or after institution of a EMR alert that warmed clinicians when a patient’s blood pressure measurement fell above the normal range. The results showed that for these patients, 3-21 years old, the rate of recognition of a high pressure measurement increased from 13% before the alert system started to 42% with the alert system in place (Clin Ped. 2015 June;54[7]:667-75). “That meant more than half the patients with high blood pressure measurements were still going unrecognized”, even with an EMR alert, Dr. Brady said.
“The U.S. clinical community falls way short” of adequately following blood pressure levels in children and adolescents, agreed Julia Steinberger, MD, professor and director of pediatric cardiology at the University of Minnesota in Minneapolis. She chalks this up to several factors: time-pressured clinicians who may let blood pressure slide when other aspects of a visit require more attention and the index of suspicion for elevated blood pressure is low, insufficient education to the primary-care community on how to proceed once an elevated blood pressure reading is made, the difficulty of measuring blood pressure in young or uncooperative patients, and lack of size-appropriate equipment.

Once a single high pressure is recorded, ideal follow-up means measuring and finding elevated blood pressures again on at least two subsequent visits, followed by even more confirmation with home monitoring or 24-hour ambulatory blood pressure monitoring (ABPM), now considered the gold standard for both diagnosing and following pediatric patients with hypertension, especially if they receive antihypertensive medications. In 2014, a scientific statement from the American Heart Association said routine APBM was indicated to confirm the diagnosis of hypertension in a patient with high casual blood pressure measurements. Not many primary-care physicians have ready access to or experience using and interpreting ABPM.
Other reasons for low diagnostic rates include therapeutic inertia, and the sheer complexity and time of identifying what is a high blood pressure reading, at least until automated calculation of high levels by EMRs became possible. “With a paper analysis you need to look at two different charts” and factor in the patient’s sex, age, and height to determine if a pressure reading is high or not for a particular patient. “Diagnosis has been a problem, especially in busy practice,” noted Dr. Brady. “I think we are addressing that with the EMR and pop-up alerts.”
Streamlining the diagnostic process
“We have a complex way to diagnose hypertension in kids,” admitted Bonita Falkner, MD, who chaired the Fourth Report panel that produced the complicated diagnostic process still used today. “It’s complex and tedious to calculate. There have been a number of reports of missed hypertension because of the complexity of the tables,” said Dr. Falkner, professor and director of hypertension and obesity research at Thomas Jefferson University in Philadelphia. “Because it’s so burdensome to diagnose the detection rate of hypertension is not as accurate as it should be. Hopefully this will be improved with the new guidelines. We plan to make them simpler, easier to use and more streamlined,” she said in an interview.
“One of the challenges is how to make high blood pressure identification simpler and more straightforward. Without question there are children and adolescents with persistently high blood pressures who fall through the cracks,” said Stephen R. Daniels, MD, professor and chairman of pediatrics at the University of Colorado in Aurora. “Recognizing hypertension in adults is much simpler, with a single set of values. The AAP is in the process of developing new guidelines and one goal is to make blood pressure measurement and recognition of hypertension as simple as possible. There is a tension between simplicity and precision. Finding the right balance will be the trick.”
Dr. Falkner highlighted two other new aspects the revised pediatric hypertension recommendations will address. The panel appears to be on track to recalculate the reference blood pressure tables to eliminate the contribution of overweight and obese children and adolescents. Because high blood pressure is defined statistically--pressures at or above the 95th percentile for a child’s sex, age and height--inclusion of overweight and obese children and adolescents in the databases that produced the original tables skewed the 95th percentile thresholds higher than they would be for those who are at normal-weights. “It will make the reference numbers somewhat lower, but not dramatically lower,” Dr. Falkner said.
When the 2004 Fourth Report was written and the calculation tables created “it was early in the obesity epidemic and we were not as tuned into it as a problem” for hypertension,” said Dr. Daniels, also a member of the Fourth Report panel.
Another new aspect will likely be highlighting the role of overweight in addition to obesity as a hypertension risk factor. “In 2004, obesity was a concern but overweight was considered just a risk factor for obesity. Now if a child is overweight we know they are also at increased risk for having high blood pressure,” said Dr. Falkner. “We’ve been trying to get an update of the Fourth Report going for some time; a lot has happened since 2004.”
The Preventive Services Task Force effect
One notable recent development in the field of pediatric hypertension was the 2013 statement by the U.S. Preventive Services Task Force that reinforced a similar conclusion the group had reached a decade before, in 2003. In 2013, the USPSTF said that following a review of the evidence “the USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for primary hypertension in asymptomatic children and adolescents to prevent subsequent cardiovascular disease in childhood or adulthood. (I statement)” (Pediatrics. 2013 Nov;132[5]:907-14).
The USPSTF’s 2013 reassertion of this position triggered several strong reactions from pediatric hypertension specialists, who critiqued the Task Force’s analysis as being overly restrictive. Among those weighing with comments that highlighted the flaws in the Task Force’s reasoning were Dr. Falkner, Dr. Brady, and Dr. Steinberger. Earlier in 2013, before the Task Force statement, Dr. Daniels wrote a commentary with similar arguments in favor of routine blood pressure measurements in response to a published assessment of pediatric blood pressure screening that largely presaged what the USPSTF said.
In brief, the USPSTF analysis “was flawed by an overly-narrow selection of evidence,” Dr. Steinberger said recently. “Short-term and observational studies were not considered. We think that in the absence of perfect data the practitioner must use common sense when superior evidence does not exist. The question of whether hypertension in adults can be prevented or modified by early intervention will never be answered unless we continue to measure blood pressure in children.”
“One of the problems with the USPSTF statement was the questions they addressed: Is blood pressure in children and adolescents clearly associated with hard cardiovascular disease outcomes in adults? That is a very tough question to answer. It would need studies that are 30, 40 years in duration, and is almost unanswerable,” said Dr. Daniels in an interview. “I think the USPSTF paid less attention to the fact that clearly a certain percentage of children and adolescents with hypertension already have developed left ventricular hypertrophy, increased carotid intimal-medial thickness and vascular stiffness. This shows that higher blood pressure in the short term is having several adverse effects on the cardiovascular system. If you insist on seeing a connection between pediatric blood pressure and adult outcomes there will always be insufficient evidence.”
Although, as Dr. Steinberger pointed out, the International Childhood Cardiovascular Cohort Consortium has been putting together long-term follow-up data from seven observational cohorts established in several different world regions. Collectively these seven cohorts include more than 340,000 people who have now been followed for about 40 years. This analysis may soon yield more definitive insight into the long-term consequences of childhood hypertension, Dr. Steinberger said.
Another relevant issue is that prevention of adult cardiovascular disease “is not why children are screened for hypertension, or at least not the primary reason,” Dr. Falkner said. “They are screened to find high blood pressure with an underlying cause, like coarctation of the aorta, which is only picked up by first noting a high blood pressure. Several other cardiovascular and renal disorders that can exist in childhood can also cause high blood pressure and measuring blood pressure is the only way to find them. It would be a tragedy to miss coarctation of the aorta by not measuring blood pressure.”
The family practice position
Despite rejection of the USPSTF analysis by many pediatric hypertension specialists, the USPSTF position has been officially embraced by the family practice community. The American Academy of Family Practice has adopted the USPSTF position as its own, although family practice physicians are also quick to point out that the USPSTF conclusion does not say that pediatric blood pressures should not be measured.
“An I level from the USPSTF doesn’t mean that screening is harmful or shouldn’t be done, just that more research is needed to fully evaluate if blood pressure screening in childhood has long-term health impacts,” said Margaret A. Riley, MD, a family practice physician at the University of Michigan in Ann Arbor with an interest in pediatric hypertension.
“I think the I rating has had little impact on practice. Measuring blood pressure is a routine and standard part of office practice. If the USPSTF had given blood pressure screening a D rating, causing more harm than good, that would be different. In my practice I screen blood pressure at every visit or at least once a year,” Dr. Riley said in an interview.
That’s the same approach taken by Wanda D. Filer, MD, a family practice physician in York, Pa. and president of the American Academy of Family Physicians. “This does not mean you don’t screen blood pressure, and it doesn’t mean you should screen. It says that data are not there either way. In my office we check everyone age 3 and up, and I think a lot of family practice physicians do that routinely.

“Most of us screen blood pressure, but the AAFP approach is to always look at the evidence. The AAFP stand is not opposite to other organizations [that have endorsed routine blood pressure measurements]. They take a stronger position in favor of screening than we do, but we don’t say do not screen. Other societies have relied on less direct evidence or expert opinion. Our approach is to see proof of benefit,” Dr. Filer said in an interview.
“I imagine most family practice physicians measure blood pressure in children aged 3 or older,” she added. “I work in a Federally-qualified health center, and we have a very diverse population. We routinely measure blood pressures because the patients are so diverse. Other family practice practices may come to a different decision. You need to look at your practice and your work flow and decide whether it is an appropriate use of time.
“I do it because I’m convinced there is a possibility of benefit from screening,” Dr. Filer said. “I am also convinced that the evidence is not there [to prove benefits]. But I won’t wait for the evidence to do this in my practice. For the mix of patients I see it is important to screen blood pressures, but I am comfortable if a family practice physician with a different patient population says that high blood pressure yields are not there; they never see them.”
Overweight and obesity raise a red flag
If there is one subgroup of the pediatric population that most everyone agrees needs close attention to blood pressure it’s the overweight or obese child or teenager. “Primary hypertension in children and adolescents is largely associated with obesity,” said Dr. Falkner. Study findings also suggest that obese children and teens with hypertension are much more likely to have or develop left ventricular hypertrophy than normal-weight patients with elevated blood pressures.
The consequences are two fold: First, it suggests that even if the entire pediatric population fails to get their blood pressures checked regularly diligent attention to blood pressure is a must for overweight and obese children and adolescents, many experts agree. “A child who is overweight as well as obese requires attention to their blood pressure. That is emerging as a guideline,” Dr. Falkner said.
Second, a growing number of U.S. clinical programs are geared to addressing hypertension in the overweight or obese pediatric patient using an aggressive and multidisciplinary treatment approach.
For example, a clinic devoted to the overweight or obese child or teen with hypertension, the ReNEW (Reversing the Negative Cardiovascular Effects of Weight) program, opened at Johns Hopkins Medical Center in February 2015.
“We were seeing a lot of obesity-related hypertension without an underlying secondary cause. And in a study we ran the only thing that could predict left ventricular hypertrophy in children with hypertension was body mass index,” said Dr. Brady, medical director for ReNEW. “This motivated me to try to find a better way to treat obesity and hypertension; the only real treatment for hypertension in obese patients is to treat the obesity.”
During its first year, the ReNEW program enrolled 35 patients 5-22 years old. “We assess them for any secondary cause of hypertension,” Dr. Brady said. “We do an echocardiography examination and assess left ventricular hypertrophy and the need for blood pressure reducing medications. We do interventions for weight loss, diet, exercise, a musculoskeletal assessment, psychiatric assessment and other comorbidity interventions such as for sleep apnea. We start blood pressure reducing drugs when appropriate.”
The average body mass index among the first 35 patients was 38 kg/m2, with an average 31 kg/m2 in kids 5-10 years old and 43 kg/m2 in those 18-21 years old. Fifty percent had obstructive sleep apnea, 33% had anxiety or depression, and about 25%-33% had diabetes. “These kids are at a really great risk for a cardiac event in early adulthood. They are probably one of the most vulnerable populations we see,” she said.
A major lesson she’s learned from the ReNEW experience so far is the spectrum of comorbidities that can affect these patients and the importance of behavioral change for the entire family to produce favorable changes in the patient. “Depression and anxiety are big factors that can affect a family’s success with weight loss. Many kids also have underlying orthopedic issues. There remains a lot of confusion about diet. We try to offer families a one-stop shop, a multidisciplinary clinic that can thoroughly address the patient’s full range of cardiovascular-disease risk factors.
“I’ve been how shocked by how complex these patients are. When there is a significant overweight or obesity problem the only way to succeed is to involve the whole family. And don’t forget about the role of mental health. That is a significant part of overweight and obesity,” Many of the psychiatric disorders that overweight and obese children and teenagers show results from learned family behaviors, Dr. Brady said.
Another U.S. clinic specifically targeted at obese children and adolescents also sees many patients with hypertension at the University of Minnesota, a program begun in about 2010 that now has treated more than 1,000 patients including “hundreds” with comorbid hypertension, as well as similar numbers with comorbid hyperlipidemia and comorbid diabetes , said Dr. Steinberger.
“There are very few of these programs in the U.S.; it is not widely available. The cardiovascular health promotion effort should include this approach because for the primary care physician there is insufficient time or expertise to do these evaluations and treatments. You need a group of clinicians with the needed expertise,” she said. “Our multidisciplinary approach to treating comorbidities like hypertension, dyslipidemia and elevated glucose uses specialists for each of these areas as well as dieticians, social workers, and other specialists.
“In general, when the primary care physician does not have the resources to further evaluate and treat overweight or obesity they should be able to refer the patient to a program like this. It is never too soon to refer and treat. To treat overweight you need to involve the whole family. Most children do not ‘grow out’ of overweight or obesity. The overweight or obese child will generally grow up to be the overweight or obese adult,” Dr. Steinberger said.
Targeting the greatest hypertension risk
The growing trend to focus multidisciplinary resources on hypertension in the overweight or obese pediatric patient may exemplify part of a new era of targeted attention for pediatric blood pressure screening.
“We have a hard time measuring blood pressure in kids, we know the importance of obesity [in causing hypertension] and we also know that first-line management for most hypertensive patients is non-drug, lifestyle interventions. Therefore, is it possible that a greater good can be achieved by addressing lifestyle and all the health issues that would reduce the risk for hypertension, such as making sure all children engage in more movement and exercise and get off devices rather than medicalizing the problem” with frequent blood pressure measurement, wondered Howard Trachtman, MD, a pediatric nephrologist at New York University.

“Routinely screening blood pressure in every child and adolescent is very burdensome and carries the potential cost of inconvenience and mislabeling errors. Could clinicians focus on the children and adolescents who really are at risk of high blood pressure? Can we use the EMR and alerts to make sure that repeated measures of blood pressure are done only when needed, after we identify who is at greatest risk?
“We need to become more precise in defining who is it in the age range of 8-17 years old who needs to be regularly screened for high blood pressure so we can focus our resources on these people and better avoid mislabeling and causing anxiety” for the many children and adolescents who have a very low risk for having hypertension, said Dr. Trachtman. He said that he is currently collaborating on a study that is examining whether data contained in a patient’s EMR can help in improving blood pressure assessment.
“We need to keep an open mind about who might have hypertension, but there are good data that it tracks with waist circumference, hypertriglyceridemia, and insulin resistance. The more of these you have the greater your risk. This is the kind of productive research I’m talking about, to determine whether you can be more thoughtful in identifying who is at risk of high blood pressure and who needs more systematic screening. Targeting blood pressure screening to overweight or obese kids is a step toward trying to be more methodical. The USPSTF statement should be a spur to pediatric nephrologists to make our case for blood pressure screening more cogently and to collect better data so that when we speak about this it is not based on speculation or extrapolation but on data,” Dr. Trachtman said.
“There are no arguments against optimizing health and reducing risk factors in all children, but that is not an acceptable rationale for not measuring blood pressure and attending to elevated levels in children,” responded Dr. Falkner. Dr Trachtman’s proposal to reduce health risks in all children “is a public health issue whereas the issue of detecting and managing hypertension in childhood is a clinical issue” faced by physicians as they see individual patients, she said.
Many pediatric hypertension specialists may not warm to a screening proposition that retreats from the notion that every child and teen 3 years old and up should have their blood pressure checked at least annually. But many of those specialists also realize that what’s now done has a lot of problems and that a more user-friendly approach is needed. As an expert panel works to produce a revision to the Fourth Report next year (which will not be the Fifth Report as the update is now outside the NHLBI purview), changes in how pediatric hypertension will be approached in the future seem likely.
Dr. Brady, Dr. Steinberger, Dr. Falkner, Dr. Daniels, Dr. Riley, Dr. Filer, and Dr. Trachtman had no disclosures.
On Twitter @mitchelzoler
The clinical context of high blood pressure shifts abruptly when a person comes of age.
In adults 18 years old and up it’s fairly simple. Blood pressure above 140/90 mm Hg is generally a clear problem, less than 130/85 is probably okay for now, and in between is something to monitor. When pressure stays above 140/90 mm Hg despite lifestyle interventions it’s time to start treatment with any of several antihypertensive drug options that mostly have well-documented safety and efficacy track records in adults and widely agreed-on benefits that outweigh risks.
For pediatric practice, children and adolescents 3-17 years old, dealing with high blood pressure is much more an obstacle course of complex diagnostic criteria, challenges in pressure measurement, and seemingly inconsistent recommendations. Pediatric hypertension also often brings clinicians up against the child and adolescent obesity epidemic, which has made pediatric hypertension more common than ever.
Against this backdrop, a panel assembled by the American Academy of Pediatrics is revising the 2004 The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents, the reigning standard for pediatric blood pressure assessment and hypertension management and now more than a decade old. With new guidance from the AAP expected in the second half of 2017, best-practice approaches to pediatric hypertension are in flux and need updating just when the disorder is more prevalent than it’s ever been.
Diagnosing pediatric hypertension falls short
This shifting landscape and increasing burden of pediatric hypertension comes at a time when primary-care pediatricians and family practice physicians are failing to perform fully comprehensive blood pressure monitoring of their pediatric patients. Current practice recommendations from the National Heart Lung and Blood Institute (in the form of the 2004 Fourth Report), and from American Heart Association (most recently reiterated in a scientific statement in August 2016) call measuring blood pressure levels at every patient encounter starting at 3 years old, the approach also endorsed by the American Academy of Pediatrics.
But that’s often not done. “Results from plenty of studies show that we are not doing a great job” identifying children and adolescents with hypertension, said Tammy M. Brady, MD, a pediatric nephrologist at Johns Hopkins Medical Center in Baltimore.
One piece of evidence she cited was a study of more than 93,000 U.S. ambulatory pediatric visits during 2000-2009 in data collected by the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey, and sampling that represented an average 142 million ambulatory visits each year by 3-18 year olds. The data showed blood pressure screening occurred during 35% of ambulatory visits, 67% of preventive visits, and during 84% of preventive visits for a child or adolescent who was overweight or obese (Pediatrics. 2012 October;130[4]:604-10).
While the numbers showed good practice with a reasonably high level of routine blood pressure measurement in overweight and obese patients, they also suggest that perhaps a third of all U.S. children and adolescents don’t have their blood pressure checked at least once a year. Statistical analyses from this study showed that blood pressure measurement was about twice as likely in children diagnosed as overweight or obese than normal-weight patients, and that blood pressure measurement was 2.6-fold more common in adolescents 13-18 years old compared with children 3-7 years old.
In a second, recent study of 29,000 2-17 years old seen at Children’s Hospital of Chicago, 3% had at least three elevated blood pressure measurements in their hospital record, but in this subset of patients at high risk of having hypertension 21% were actually identified in their medical record as having high blood pressure.
Dr. Brady pointed out that while many of the children and adolescents in this study with three or more high blood pressure readings may not actually have hypertension, defined as a sustained elevation of blood pressure, they are all at risk for development of hypertension and should be targeted for prevention.
“We do a bad job identifying when blood pressure is high,” Dr. Brady said in an interview. She cited a study she recently ran that examined the impact that EMR alerts could have on this diagnostic challenge. She reviewed records for 1,305 patient encounters done before or after institution of a EMR alert that warmed clinicians when a patient’s blood pressure measurement fell above the normal range. The results showed that for these patients, 3-21 years old, the rate of recognition of a high pressure measurement increased from 13% before the alert system started to 42% with the alert system in place (Clin Ped. 2015 June;54[7]:667-75). “That meant more than half the patients with high blood pressure measurements were still going unrecognized”, even with an EMR alert, Dr. Brady said.
“The U.S. clinical community falls way short” of adequately following blood pressure levels in children and adolescents, agreed Julia Steinberger, MD, professor and director of pediatric cardiology at the University of Minnesota in Minneapolis. She chalks this up to several factors: time-pressured clinicians who may let blood pressure slide when other aspects of a visit require more attention and the index of suspicion for elevated blood pressure is low, insufficient education to the primary-care community on how to proceed once an elevated blood pressure reading is made, the difficulty of measuring blood pressure in young or uncooperative patients, and lack of size-appropriate equipment.
Once a single high pressure is recorded, ideal follow-up means measuring and finding elevated blood pressures again on at least two subsequent visits, followed by even more confirmation with home monitoring or 24-hour ambulatory blood pressure monitoring (ABPM), now considered the gold standard for both diagnosing and following pediatric patients with hypertension, especially if they receive antihypertensive medications. In 2014, a scientific statement from the American Heart Association said routine APBM was indicated to confirm the diagnosis of hypertension in a patient with high casual blood pressure measurements. Not many primary-care physicians have ready access to or experience using and interpreting ABPM.
Other reasons for low diagnostic rates include therapeutic inertia, and the sheer complexity and time of identifying what is a high blood pressure reading, at least until automated calculation of high levels by EMRs became possible. “With a paper analysis you need to look at two different charts” and factor in the patient’s sex, age, and height to determine if a pressure reading is high or not for a particular patient. “Diagnosis has been a problem, especially in busy practice,” noted Dr. Brady. “I think we are addressing that with the EMR and pop-up alerts.”
Streamlining the diagnostic process
“We have a complex way to diagnose hypertension in kids,” admitted Bonita Falkner, MD, who chaired the Fourth Report panel that produced the complicated diagnostic process still used today. “It’s complex and tedious to calculate. There have been a number of reports of missed hypertension because of the complexity of the tables,” said Dr. Falkner, professor and director of hypertension and obesity research at Thomas Jefferson University in Philadelphia. “Because it’s so burdensome to diagnose the detection rate of hypertension is not as accurate as it should be. Hopefully this will be improved with the new guidelines. We plan to make them simpler, easier to use and more streamlined,” she said in an interview.
“One of the challenges is how to make high blood pressure identification simpler and more straightforward. Without question there are children and adolescents with persistently high blood pressures who fall through the cracks,” said Stephen R. Daniels, MD, professor and chairman of pediatrics at the University of Colorado in Aurora. “Recognizing hypertension in adults is much simpler, with a single set of values. The AAP is in the process of developing new guidelines and one goal is to make blood pressure measurement and recognition of hypertension as simple as possible. There is a tension between simplicity and precision. Finding the right balance will be the trick.”
Dr. Falkner highlighted two other new aspects the revised pediatric hypertension recommendations will address. The panel appears to be on track to recalculate the reference blood pressure tables to eliminate the contribution of overweight and obese children and adolescents. Because high blood pressure is defined statistically--pressures at or above the 95th percentile for a child’s sex, age and height--inclusion of overweight and obese children and adolescents in the databases that produced the original tables skewed the 95th percentile thresholds higher than they would be for those who are at normal-weights. “It will make the reference numbers somewhat lower, but not dramatically lower,” Dr. Falkner said.
When the 2004 Fourth Report was written and the calculation tables created “it was early in the obesity epidemic and we were not as tuned into it as a problem” for hypertension,” said Dr. Daniels, also a member of the Fourth Report panel.
Another new aspect will likely be highlighting the role of overweight in addition to obesity as a hypertension risk factor. “In 2004, obesity was a concern but overweight was considered just a risk factor for obesity. Now if a child is overweight we know they are also at increased risk for having high blood pressure,” said Dr. Falkner. “We’ve been trying to get an update of the Fourth Report going for some time; a lot has happened since 2004.”
The Preventive Services Task Force effect
One notable recent development in the field of pediatric hypertension was the 2013 statement by the U.S. Preventive Services Task Force that reinforced a similar conclusion the group had reached a decade before, in 2003. In 2013, the USPSTF said that following a review of the evidence “the USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for primary hypertension in asymptomatic children and adolescents to prevent subsequent cardiovascular disease in childhood or adulthood. (I statement)” (Pediatrics. 2013 Nov;132[5]:907-14).
The USPSTF’s 2013 reassertion of this position triggered several strong reactions from pediatric hypertension specialists, who critiqued the Task Force’s analysis as being overly restrictive. Among those weighing with comments that highlighted the flaws in the Task Force’s reasoning were Dr. Falkner, Dr. Brady, and Dr. Steinberger. Earlier in 2013, before the Task Force statement, Dr. Daniels wrote a commentary with similar arguments in favor of routine blood pressure measurements in response to a published assessment of pediatric blood pressure screening that largely presaged what the USPSTF said.
In brief, the USPSTF analysis “was flawed by an overly-narrow selection of evidence,” Dr. Steinberger said recently. “Short-term and observational studies were not considered. We think that in the absence of perfect data the practitioner must use common sense when superior evidence does not exist. The question of whether hypertension in adults can be prevented or modified by early intervention will never be answered unless we continue to measure blood pressure in children.”
“One of the problems with the USPSTF statement was the questions they addressed: Is blood pressure in children and adolescents clearly associated with hard cardiovascular disease outcomes in adults? That is a very tough question to answer. It would need studies that are 30, 40 years in duration, and is almost unanswerable,” said Dr. Daniels in an interview. “I think the USPSTF paid less attention to the fact that clearly a certain percentage of children and adolescents with hypertension already have developed left ventricular hypertrophy, increased carotid intimal-medial thickness and vascular stiffness. This shows that higher blood pressure in the short term is having several adverse effects on the cardiovascular system. If you insist on seeing a connection between pediatric blood pressure and adult outcomes there will always be insufficient evidence.”
Although, as Dr. Steinberger pointed out, the International Childhood Cardiovascular Cohort Consortium has been putting together long-term follow-up data from seven observational cohorts established in several different world regions. Collectively these seven cohorts include more than 340,000 people who have now been followed for about 40 years. This analysis may soon yield more definitive insight into the long-term consequences of childhood hypertension, Dr. Steinberger said.
Another relevant issue is that prevention of adult cardiovascular disease “is not why children are screened for hypertension, or at least not the primary reason,” Dr. Falkner said. “They are screened to find high blood pressure with an underlying cause, like coarctation of the aorta, which is only picked up by first noting a high blood pressure. Several other cardiovascular and renal disorders that can exist in childhood can also cause high blood pressure and measuring blood pressure is the only way to find them. It would be a tragedy to miss coarctation of the aorta by not measuring blood pressure.”
The family practice position
Despite rejection of the USPSTF analysis by many pediatric hypertension specialists, the USPSTF position has been officially embraced by the family practice community. The American Academy of Family Practice has adopted the USPSTF position as its own, although family practice physicians are also quick to point out that the USPSTF conclusion does not say that pediatric blood pressures should not be measured.
“An I level from the USPSTF doesn’t mean that screening is harmful or shouldn’t be done, just that more research is needed to fully evaluate if blood pressure screening in childhood has long-term health impacts,” said Margaret A. Riley, MD, a family practice physician at the University of Michigan in Ann Arbor with an interest in pediatric hypertension.
“I think the I rating has had little impact on practice. Measuring blood pressure is a routine and standard part of office practice. If the USPSTF had given blood pressure screening a D rating, causing more harm than good, that would be different. In my practice I screen blood pressure at every visit or at least once a year,” Dr. Riley said in an interview.
That’s the same approach taken by Wanda D. Filer, MD, a family practice physician in York, Pa. and president of the American Academy of Family Physicians. “This does not mean you don’t screen blood pressure, and it doesn’t mean you should screen. It says that data are not there either way. In my office we check everyone age 3 and up, and I think a lot of family practice physicians do that routinely.
“Most of us screen blood pressure, but the AAFP approach is to always look at the evidence. The AAFP stand is not opposite to other organizations [that have endorsed routine blood pressure measurements]. They take a stronger position in favor of screening than we do, but we don’t say do not screen. Other societies have relied on less direct evidence or expert opinion. Our approach is to see proof of benefit,” Dr. Filer said in an interview.
“I imagine most family practice physicians measure blood pressure in children aged 3 or older,” she added. “I work in a Federally-qualified health center, and we have a very diverse population. We routinely measure blood pressures because the patients are so diverse. Other family practice practices may come to a different decision. You need to look at your practice and your work flow and decide whether it is an appropriate use of time.
“I do it because I’m convinced there is a possibility of benefit from screening,” Dr. Filer said. “I am also convinced that the evidence is not there [to prove benefits]. But I won’t wait for the evidence to do this in my practice. For the mix of patients I see it is important to screen blood pressures, but I am comfortable if a family practice physician with a different patient population says that high blood pressure yields are not there; they never see them.”
Overweight and obesity raise a red flag
If there is one subgroup of the pediatric population that most everyone agrees needs close attention to blood pressure it’s the overweight or obese child or teenager. “Primary hypertension in children and adolescents is largely associated with obesity,” said Dr. Falkner. Study findings also suggest that obese children and teens with hypertension are much more likely to have or develop left ventricular hypertrophy than normal-weight patients with elevated blood pressures.
The consequences are two fold: First, it suggests that even if the entire pediatric population fails to get their blood pressures checked regularly diligent attention to blood pressure is a must for overweight and obese children and adolescents, many experts agree. “A child who is overweight as well as obese requires attention to their blood pressure. That is emerging as a guideline,” Dr. Falkner said.
Second, a growing number of U.S. clinical programs are geared to addressing hypertension in the overweight or obese pediatric patient using an aggressive and multidisciplinary treatment approach.
For example, a clinic devoted to the overweight or obese child or teen with hypertension, the ReNEW (Reversing the Negative Cardiovascular Effects of Weight) program, opened at Johns Hopkins Medical Center in February 2015.
“We were seeing a lot of obesity-related hypertension without an underlying secondary cause. And in a study we ran the only thing that could predict left ventricular hypertrophy in children with hypertension was body mass index,” said Dr. Brady, medical director for ReNEW. “This motivated me to try to find a better way to treat obesity and hypertension; the only real treatment for hypertension in obese patients is to treat the obesity.”
During its first year, the ReNEW program enrolled 35 patients 5-22 years old. “We assess them for any secondary cause of hypertension,” Dr. Brady said. “We do an echocardiography examination and assess left ventricular hypertrophy and the need for blood pressure reducing medications. We do interventions for weight loss, diet, exercise, a musculoskeletal assessment, psychiatric assessment and other comorbidity interventions such as for sleep apnea. We start blood pressure reducing drugs when appropriate.”
The average body mass index among the first 35 patients was 38 kg/m2, with an average 31 kg/m2 in kids 5-10 years old and 43 kg/m2 in those 18-21 years old. Fifty percent had obstructive sleep apnea, 33% had anxiety or depression, and about 25%-33% had diabetes. “These kids are at a really great risk for a cardiac event in early adulthood. They are probably one of the most vulnerable populations we see,” she said.
A major lesson she’s learned from the ReNEW experience so far is the spectrum of comorbidities that can affect these patients and the importance of behavioral change for the entire family to produce favorable changes in the patient. “Depression and anxiety are big factors that can affect a family’s success with weight loss. Many kids also have underlying orthopedic issues. There remains a lot of confusion about diet. We try to offer families a one-stop shop, a multidisciplinary clinic that can thoroughly address the patient’s full range of cardiovascular-disease risk factors.
“I’ve been how shocked by how complex these patients are. When there is a significant overweight or obesity problem the only way to succeed is to involve the whole family. And don’t forget about the role of mental health. That is a significant part of overweight and obesity,” Many of the psychiatric disorders that overweight and obese children and teenagers show results from learned family behaviors, Dr. Brady said.
Another U.S. clinic specifically targeted at obese children and adolescents also sees many patients with hypertension at the University of Minnesota, a program begun in about 2010 that now has treated more than 1,000 patients including “hundreds” with comorbid hypertension, as well as similar numbers with comorbid hyperlipidemia and comorbid diabetes , said Dr. Steinberger.
“There are very few of these programs in the U.S.; it is not widely available. The cardiovascular health promotion effort should include this approach because for the primary care physician there is insufficient time or expertise to do these evaluations and treatments. You need a group of clinicians with the needed expertise,” she said. “Our multidisciplinary approach to treating comorbidities like hypertension, dyslipidemia and elevated glucose uses specialists for each of these areas as well as dieticians, social workers, and other specialists.
“In general, when the primary care physician does not have the resources to further evaluate and treat overweight or obesity they should be able to refer the patient to a program like this. It is never too soon to refer and treat. To treat overweight you need to involve the whole family. Most children do not ‘grow out’ of overweight or obesity. The overweight or obese child will generally grow up to be the overweight or obese adult,” Dr. Steinberger said.
Targeting the greatest hypertension risk
The growing trend to focus multidisciplinary resources on hypertension in the overweight or obese pediatric patient may exemplify part of a new era of targeted attention for pediatric blood pressure screening.
“We have a hard time measuring blood pressure in kids, we know the importance of obesity [in causing hypertension] and we also know that first-line management for most hypertensive patients is non-drug, lifestyle interventions. Therefore, is it possible that a greater good can be achieved by addressing lifestyle and all the health issues that would reduce the risk for hypertension, such as making sure all children engage in more movement and exercise and get off devices rather than medicalizing the problem” with frequent blood pressure measurement, wondered Howard Trachtman, MD, a pediatric nephrologist at New York University.
“Routinely screening blood pressure in every child and adolescent is very burdensome and carries the potential cost of inconvenience and mislabeling errors. Could clinicians focus on the children and adolescents who really are at risk of high blood pressure? Can we use the EMR and alerts to make sure that repeated measures of blood pressure are done only when needed, after we identify who is at greatest risk?
“We need to become more precise in defining who is it in the age range of 8-17 years old who needs to be regularly screened for high blood pressure so we can focus our resources on these people and better avoid mislabeling and causing anxiety” for the many children and adolescents who have a very low risk for having hypertension, said Dr. Trachtman. He said that he is currently collaborating on a study that is examining whether data contained in a patient’s EMR can help in improving blood pressure assessment.
“We need to keep an open mind about who might have hypertension, but there are good data that it tracks with waist circumference, hypertriglyceridemia, and insulin resistance. The more of these you have the greater your risk. This is the kind of productive research I’m talking about, to determine whether you can be more thoughtful in identifying who is at risk of high blood pressure and who needs more systematic screening. Targeting blood pressure screening to overweight or obese kids is a step toward trying to be more methodical. The USPSTF statement should be a spur to pediatric nephrologists to make our case for blood pressure screening more cogently and to collect better data so that when we speak about this it is not based on speculation or extrapolation but on data,” Dr. Trachtman said.
“There are no arguments against optimizing health and reducing risk factors in all children, but that is not an acceptable rationale for not measuring blood pressure and attending to elevated levels in children,” responded Dr. Falkner. Dr Trachtman’s proposal to reduce health risks in all children “is a public health issue whereas the issue of detecting and managing hypertension in childhood is a clinical issue” faced by physicians as they see individual patients, she said.
Many pediatric hypertension specialists may not warm to a screening proposition that retreats from the notion that every child and teen 3 years old and up should have their blood pressure checked at least annually. But many of those specialists also realize that what’s now done has a lot of problems and that a more user-friendly approach is needed. As an expert panel works to produce a revision to the Fourth Report next year (which will not be the Fifth Report as the update is now outside the NHLBI purview), changes in how pediatric hypertension will be approached in the future seem likely.
Dr. Brady, Dr. Steinberger, Dr. Falkner, Dr. Daniels, Dr. Riley, Dr. Filer, and Dr. Trachtman had no disclosures.
On Twitter @mitchelzoler
The clinical context of high blood pressure shifts abruptly when a person comes of age.
In adults 18 years old and up it’s fairly simple. Blood pressure above 140/90 mm Hg is generally a clear problem, less than 130/85 is probably okay for now, and in between is something to monitor. When pressure stays above 140/90 mm Hg despite lifestyle interventions it’s time to start treatment with any of several antihypertensive drug options that mostly have well-documented safety and efficacy track records in adults and widely agreed-on benefits that outweigh risks.
For pediatric practice, children and adolescents 3-17 years old, dealing with high blood pressure is much more an obstacle course of complex diagnostic criteria, challenges in pressure measurement, and seemingly inconsistent recommendations. Pediatric hypertension also often brings clinicians up against the child and adolescent obesity epidemic, which has made pediatric hypertension more common than ever.
Against this backdrop, a panel assembled by the American Academy of Pediatrics is revising the 2004 The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents, the reigning standard for pediatric blood pressure assessment and hypertension management and now more than a decade old. With new guidance from the AAP expected in the second half of 2017, best-practice approaches to pediatric hypertension are in flux and need updating just when the disorder is more prevalent than it’s ever been.
Diagnosing pediatric hypertension falls short
This shifting landscape and increasing burden of pediatric hypertension comes at a time when primary-care pediatricians and family practice physicians are failing to perform fully comprehensive blood pressure monitoring of their pediatric patients. Current practice recommendations from the National Heart Lung and Blood Institute (in the form of the 2004 Fourth Report), and from American Heart Association (most recently reiterated in a scientific statement in August 2016) call measuring blood pressure levels at every patient encounter starting at 3 years old, the approach also endorsed by the American Academy of Pediatrics.
But that’s often not done. “Results from plenty of studies show that we are not doing a great job” identifying children and adolescents with hypertension, said Tammy M. Brady, MD, a pediatric nephrologist at Johns Hopkins Medical Center in Baltimore.
One piece of evidence she cited was a study of more than 93,000 U.S. ambulatory pediatric visits during 2000-2009 in data collected by the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey, and sampling that represented an average 142 million ambulatory visits each year by 3-18 year olds. The data showed blood pressure screening occurred during 35% of ambulatory visits, 67% of preventive visits, and during 84% of preventive visits for a child or adolescent who was overweight or obese (Pediatrics. 2012 October;130[4]:604-10).
While the numbers showed good practice with a reasonably high level of routine blood pressure measurement in overweight and obese patients, they also suggest that perhaps a third of all U.S. children and adolescents don’t have their blood pressure checked at least once a year. Statistical analyses from this study showed that blood pressure measurement was about twice as likely in children diagnosed as overweight or obese than normal-weight patients, and that blood pressure measurement was 2.6-fold more common in adolescents 13-18 years old compared with children 3-7 years old.
In a second, recent study of 29,000 2-17 years old seen at Children’s Hospital of Chicago, 3% had at least three elevated blood pressure measurements in their hospital record, but in this subset of patients at high risk of having hypertension 21% were actually identified in their medical record as having high blood pressure.
Dr. Brady pointed out that while many of the children and adolescents in this study with three or more high blood pressure readings may not actually have hypertension, defined as a sustained elevation of blood pressure, they are all at risk for development of hypertension and should be targeted for prevention.
“We do a bad job identifying when blood pressure is high,” Dr. Brady said in an interview. She cited a study she recently ran that examined the impact that EMR alerts could have on this diagnostic challenge. She reviewed records for 1,305 patient encounters done before or after institution of a EMR alert that warmed clinicians when a patient’s blood pressure measurement fell above the normal range. The results showed that for these patients, 3-21 years old, the rate of recognition of a high pressure measurement increased from 13% before the alert system started to 42% with the alert system in place (Clin Ped. 2015 June;54[7]:667-75). “That meant more than half the patients with high blood pressure measurements were still going unrecognized”, even with an EMR alert, Dr. Brady said.
“The U.S. clinical community falls way short” of adequately following blood pressure levels in children and adolescents, agreed Julia Steinberger, MD, professor and director of pediatric cardiology at the University of Minnesota in Minneapolis. She chalks this up to several factors: time-pressured clinicians who may let blood pressure slide when other aspects of a visit require more attention and the index of suspicion for elevated blood pressure is low, insufficient education to the primary-care community on how to proceed once an elevated blood pressure reading is made, the difficulty of measuring blood pressure in young or uncooperative patients, and lack of size-appropriate equipment.
Once a single high pressure is recorded, ideal follow-up means measuring and finding elevated blood pressures again on at least two subsequent visits, followed by even more confirmation with home monitoring or 24-hour ambulatory blood pressure monitoring (ABPM), now considered the gold standard for both diagnosing and following pediatric patients with hypertension, especially if they receive antihypertensive medications. In 2014, a scientific statement from the American Heart Association said routine APBM was indicated to confirm the diagnosis of hypertension in a patient with high casual blood pressure measurements. Not many primary-care physicians have ready access to or experience using and interpreting ABPM.
Other reasons for low diagnostic rates include therapeutic inertia, and the sheer complexity and time of identifying what is a high blood pressure reading, at least until automated calculation of high levels by EMRs became possible. “With a paper analysis you need to look at two different charts” and factor in the patient’s sex, age, and height to determine if a pressure reading is high or not for a particular patient. “Diagnosis has been a problem, especially in busy practice,” noted Dr. Brady. “I think we are addressing that with the EMR and pop-up alerts.”
Streamlining the diagnostic process
“We have a complex way to diagnose hypertension in kids,” admitted Bonita Falkner, MD, who chaired the Fourth Report panel that produced the complicated diagnostic process still used today. “It’s complex and tedious to calculate. There have been a number of reports of missed hypertension because of the complexity of the tables,” said Dr. Falkner, professor and director of hypertension and obesity research at Thomas Jefferson University in Philadelphia. “Because it’s so burdensome to diagnose the detection rate of hypertension is not as accurate as it should be. Hopefully this will be improved with the new guidelines. We plan to make them simpler, easier to use and more streamlined,” she said in an interview.
“One of the challenges is how to make high blood pressure identification simpler and more straightforward. Without question there are children and adolescents with persistently high blood pressures who fall through the cracks,” said Stephen R. Daniels, MD, professor and chairman of pediatrics at the University of Colorado in Aurora. “Recognizing hypertension in adults is much simpler, with a single set of values. The AAP is in the process of developing new guidelines and one goal is to make blood pressure measurement and recognition of hypertension as simple as possible. There is a tension between simplicity and precision. Finding the right balance will be the trick.”
Dr. Falkner highlighted two other new aspects the revised pediatric hypertension recommendations will address. The panel appears to be on track to recalculate the reference blood pressure tables to eliminate the contribution of overweight and obese children and adolescents. Because high blood pressure is defined statistically--pressures at or above the 95th percentile for a child’s sex, age and height--inclusion of overweight and obese children and adolescents in the databases that produced the original tables skewed the 95th percentile thresholds higher than they would be for those who are at normal-weights. “It will make the reference numbers somewhat lower, but not dramatically lower,” Dr. Falkner said.
When the 2004 Fourth Report was written and the calculation tables created “it was early in the obesity epidemic and we were not as tuned into it as a problem” for hypertension,” said Dr. Daniels, also a member of the Fourth Report panel.
Another new aspect will likely be highlighting the role of overweight in addition to obesity as a hypertension risk factor. “In 2004, obesity was a concern but overweight was considered just a risk factor for obesity. Now if a child is overweight we know they are also at increased risk for having high blood pressure,” said Dr. Falkner. “We’ve been trying to get an update of the Fourth Report going for some time; a lot has happened since 2004.”
The Preventive Services Task Force effect
One notable recent development in the field of pediatric hypertension was the 2013 statement by the U.S. Preventive Services Task Force that reinforced a similar conclusion the group had reached a decade before, in 2003. In 2013, the USPSTF said that following a review of the evidence “the USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for primary hypertension in asymptomatic children and adolescents to prevent subsequent cardiovascular disease in childhood or adulthood. (I statement)” (Pediatrics. 2013 Nov;132[5]:907-14).
The USPSTF’s 2013 reassertion of this position triggered several strong reactions from pediatric hypertension specialists, who critiqued the Task Force’s analysis as being overly restrictive. Among those weighing with comments that highlighted the flaws in the Task Force’s reasoning were Dr. Falkner, Dr. Brady, and Dr. Steinberger. Earlier in 2013, before the Task Force statement, Dr. Daniels wrote a commentary with similar arguments in favor of routine blood pressure measurements in response to a published assessment of pediatric blood pressure screening that largely presaged what the USPSTF said.
In brief, the USPSTF analysis “was flawed by an overly-narrow selection of evidence,” Dr. Steinberger said recently. “Short-term and observational studies were not considered. We think that in the absence of perfect data the practitioner must use common sense when superior evidence does not exist. The question of whether hypertension in adults can be prevented or modified by early intervention will never be answered unless we continue to measure blood pressure in children.”
“One of the problems with the USPSTF statement was the questions they addressed: Is blood pressure in children and adolescents clearly associated with hard cardiovascular disease outcomes in adults? That is a very tough question to answer. It would need studies that are 30, 40 years in duration, and is almost unanswerable,” said Dr. Daniels in an interview. “I think the USPSTF paid less attention to the fact that clearly a certain percentage of children and adolescents with hypertension already have developed left ventricular hypertrophy, increased carotid intimal-medial thickness and vascular stiffness. This shows that higher blood pressure in the short term is having several adverse effects on the cardiovascular system. If you insist on seeing a connection between pediatric blood pressure and adult outcomes there will always be insufficient evidence.”
Although, as Dr. Steinberger pointed out, the International Childhood Cardiovascular Cohort Consortium has been putting together long-term follow-up data from seven observational cohorts established in several different world regions. Collectively these seven cohorts include more than 340,000 people who have now been followed for about 40 years. This analysis may soon yield more definitive insight into the long-term consequences of childhood hypertension, Dr. Steinberger said.
Another relevant issue is that prevention of adult cardiovascular disease “is not why children are screened for hypertension, or at least not the primary reason,” Dr. Falkner said. “They are screened to find high blood pressure with an underlying cause, like coarctation of the aorta, which is only picked up by first noting a high blood pressure. Several other cardiovascular and renal disorders that can exist in childhood can also cause high blood pressure and measuring blood pressure is the only way to find them. It would be a tragedy to miss coarctation of the aorta by not measuring blood pressure.”
The family practice position
Despite rejection of the USPSTF analysis by many pediatric hypertension specialists, the USPSTF position has been officially embraced by the family practice community. The American Academy of Family Practice has adopted the USPSTF position as its own, although family practice physicians are also quick to point out that the USPSTF conclusion does not say that pediatric blood pressures should not be measured.
“An I level from the USPSTF doesn’t mean that screening is harmful or shouldn’t be done, just that more research is needed to fully evaluate if blood pressure screening in childhood has long-term health impacts,” said Margaret A. Riley, MD, a family practice physician at the University of Michigan in Ann Arbor with an interest in pediatric hypertension.
“I think the I rating has had little impact on practice. Measuring blood pressure is a routine and standard part of office practice. If the USPSTF had given blood pressure screening a D rating, causing more harm than good, that would be different. In my practice I screen blood pressure at every visit or at least once a year,” Dr. Riley said in an interview.
That’s the same approach taken by Wanda D. Filer, MD, a family practice physician in York, Pa. and president of the American Academy of Family Physicians. “This does not mean you don’t screen blood pressure, and it doesn’t mean you should screen. It says that data are not there either way. In my office we check everyone age 3 and up, and I think a lot of family practice physicians do that routinely.
“Most of us screen blood pressure, but the AAFP approach is to always look at the evidence. The AAFP stand is not opposite to other organizations [that have endorsed routine blood pressure measurements]. They take a stronger position in favor of screening than we do, but we don’t say do not screen. Other societies have relied on less direct evidence or expert opinion. Our approach is to see proof of benefit,” Dr. Filer said in an interview.
“I imagine most family practice physicians measure blood pressure in children aged 3 or older,” she added. “I work in a Federally-qualified health center, and we have a very diverse population. We routinely measure blood pressures because the patients are so diverse. Other family practice practices may come to a different decision. You need to look at your practice and your work flow and decide whether it is an appropriate use of time.
“I do it because I’m convinced there is a possibility of benefit from screening,” Dr. Filer said. “I am also convinced that the evidence is not there [to prove benefits]. But I won’t wait for the evidence to do this in my practice. For the mix of patients I see it is important to screen blood pressures, but I am comfortable if a family practice physician with a different patient population says that high blood pressure yields are not there; they never see them.”
Overweight and obesity raise a red flag
If there is one subgroup of the pediatric population that most everyone agrees needs close attention to blood pressure it’s the overweight or obese child or teenager. “Primary hypertension in children and adolescents is largely associated with obesity,” said Dr. Falkner. Study findings also suggest that obese children and teens with hypertension are much more likely to have or develop left ventricular hypertrophy than normal-weight patients with elevated blood pressures.
The consequences are two fold: First, it suggests that even if the entire pediatric population fails to get their blood pressures checked regularly diligent attention to blood pressure is a must for overweight and obese children and adolescents, many experts agree. “A child who is overweight as well as obese requires attention to their blood pressure. That is emerging as a guideline,” Dr. Falkner said.
Second, a growing number of U.S. clinical programs are geared to addressing hypertension in the overweight or obese pediatric patient using an aggressive and multidisciplinary treatment approach.
For example, a clinic devoted to the overweight or obese child or teen with hypertension, the ReNEW (Reversing the Negative Cardiovascular Effects of Weight) program, opened at Johns Hopkins Medical Center in February 2015.
“We were seeing a lot of obesity-related hypertension without an underlying secondary cause. And in a study we ran the only thing that could predict left ventricular hypertrophy in children with hypertension was body mass index,” said Dr. Brady, medical director for ReNEW. “This motivated me to try to find a better way to treat obesity and hypertension; the only real treatment for hypertension in obese patients is to treat the obesity.”
During its first year, the ReNEW program enrolled 35 patients 5-22 years old. “We assess them for any secondary cause of hypertension,” Dr. Brady said. “We do an echocardiography examination and assess left ventricular hypertrophy and the need for blood pressure reducing medications. We do interventions for weight loss, diet, exercise, a musculoskeletal assessment, psychiatric assessment and other comorbidity interventions such as for sleep apnea. We start blood pressure reducing drugs when appropriate.”
The average body mass index among the first 35 patients was 38 kg/m2, with an average 31 kg/m2 in kids 5-10 years old and 43 kg/m2 in those 18-21 years old. Fifty percent had obstructive sleep apnea, 33% had anxiety or depression, and about 25%-33% had diabetes. “These kids are at a really great risk for a cardiac event in early adulthood. They are probably one of the most vulnerable populations we see,” she said.
A major lesson she’s learned from the ReNEW experience so far is the spectrum of comorbidities that can affect these patients and the importance of behavioral change for the entire family to produce favorable changes in the patient. “Depression and anxiety are big factors that can affect a family’s success with weight loss. Many kids also have underlying orthopedic issues. There remains a lot of confusion about diet. We try to offer families a one-stop shop, a multidisciplinary clinic that can thoroughly address the patient’s full range of cardiovascular-disease risk factors.
“I’ve been how shocked by how complex these patients are. When there is a significant overweight or obesity problem the only way to succeed is to involve the whole family. And don’t forget about the role of mental health. That is a significant part of overweight and obesity,” Many of the psychiatric disorders that overweight and obese children and teenagers show results from learned family behaviors, Dr. Brady said.
Another U.S. clinic specifically targeted at obese children and adolescents also sees many patients with hypertension at the University of Minnesota, a program begun in about 2010 that now has treated more than 1,000 patients including “hundreds” with comorbid hypertension, as well as similar numbers with comorbid hyperlipidemia and comorbid diabetes , said Dr. Steinberger.
“There are very few of these programs in the U.S.; it is not widely available. The cardiovascular health promotion effort should include this approach because for the primary care physician there is insufficient time or expertise to do these evaluations and treatments. You need a group of clinicians with the needed expertise,” she said. “Our multidisciplinary approach to treating comorbidities like hypertension, dyslipidemia and elevated glucose uses specialists for each of these areas as well as dieticians, social workers, and other specialists.
“In general, when the primary care physician does not have the resources to further evaluate and treat overweight or obesity they should be able to refer the patient to a program like this. It is never too soon to refer and treat. To treat overweight you need to involve the whole family. Most children do not ‘grow out’ of overweight or obesity. The overweight or obese child will generally grow up to be the overweight or obese adult,” Dr. Steinberger said.
Targeting the greatest hypertension risk
The growing trend to focus multidisciplinary resources on hypertension in the overweight or obese pediatric patient may exemplify part of a new era of targeted attention for pediatric blood pressure screening.
“We have a hard time measuring blood pressure in kids, we know the importance of obesity [in causing hypertension] and we also know that first-line management for most hypertensive patients is non-drug, lifestyle interventions. Therefore, is it possible that a greater good can be achieved by addressing lifestyle and all the health issues that would reduce the risk for hypertension, such as making sure all children engage in more movement and exercise and get off devices rather than medicalizing the problem” with frequent blood pressure measurement, wondered Howard Trachtman, MD, a pediatric nephrologist at New York University.
“Routinely screening blood pressure in every child and adolescent is very burdensome and carries the potential cost of inconvenience and mislabeling errors. Could clinicians focus on the children and adolescents who really are at risk of high blood pressure? Can we use the EMR and alerts to make sure that repeated measures of blood pressure are done only when needed, after we identify who is at greatest risk?
“We need to become more precise in defining who is it in the age range of 8-17 years old who needs to be regularly screened for high blood pressure so we can focus our resources on these people and better avoid mislabeling and causing anxiety” for the many children and adolescents who have a very low risk for having hypertension, said Dr. Trachtman. He said that he is currently collaborating on a study that is examining whether data contained in a patient’s EMR can help in improving blood pressure assessment.
“We need to keep an open mind about who might have hypertension, but there are good data that it tracks with waist circumference, hypertriglyceridemia, and insulin resistance. The more of these you have the greater your risk. This is the kind of productive research I’m talking about, to determine whether you can be more thoughtful in identifying who is at risk of high blood pressure and who needs more systematic screening. Targeting blood pressure screening to overweight or obese kids is a step toward trying to be more methodical. The USPSTF statement should be a spur to pediatric nephrologists to make our case for blood pressure screening more cogently and to collect better data so that when we speak about this it is not based on speculation or extrapolation but on data,” Dr. Trachtman said.
“There are no arguments against optimizing health and reducing risk factors in all children, but that is not an acceptable rationale for not measuring blood pressure and attending to elevated levels in children,” responded Dr. Falkner. Dr Trachtman’s proposal to reduce health risks in all children “is a public health issue whereas the issue of detecting and managing hypertension in childhood is a clinical issue” faced by physicians as they see individual patients, she said.
Many pediatric hypertension specialists may not warm to a screening proposition that retreats from the notion that every child and teen 3 years old and up should have their blood pressure checked at least annually. But many of those specialists also realize that what’s now done has a lot of problems and that a more user-friendly approach is needed. As an expert panel works to produce a revision to the Fourth Report next year (which will not be the Fifth Report as the update is now outside the NHLBI purview), changes in how pediatric hypertension will be approached in the future seem likely.
Dr. Brady, Dr. Steinberger, Dr. Falkner, Dr. Daniels, Dr. Riley, Dr. Filer, and Dr. Trachtman had no disclosures.
On Twitter @mitchelzoler
