User login
Effects of IV iron treatment with ferumoxytol on health-related quality of life of patients with iron deficiency anemia
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Rate of abnormal vaginal bleeding and contraception counseling in women undergoing chemotherapy
Background Reproductive-age women who are undergoing cancer treatment are at risk for heavy menstrual bleeding, unintended pregnancy, and have a contraindication to estrogen-containing products. The incidence of vaginal bleeding and contraception use is not known.
Objective To describe clinical practices regarding menstrual suppression, estimate the incidence of vaginal bleeding complaints, and investigate contraceptive counseling and provision in women undergoing chemotherapy.
Methods We performed a chart review using ICD-9 codes to identify women aged 14-40 years who received chemotherapy at our institution during July 2008-June 2013. Electronic medical records were examined for menstrual suppression therapy, contraception counseling, and abnormal vaginal bleeding.
Results We identified 137 women for this study. 24 (18%) received prophylactic menstrual suppression counseling, of whom 17 (71%) initiated treatment, primarily with combined oral contraceptives, all prescribed by hematologist-oncologists. During the first 6 months of chemotherapy, 36 women (26%) complained of abnormal vaginal bleeding, including 10 women who were on prophylactic treatment. 19 women noted moderate to severe bleeding. 11 (12%) women received contraceptive counseling before chemotherapy, all from hematologist-oncologists; 86 women (63%) initiated chemotherapy without a documented contraceptive method.
Limitations Data were generated from billing codes, so all eligible women may not have been included.
Conclusions Reproductive-age women undergoing chemotherapy may not receive adequate contraception and menstrual suppression counseling. We encourage consulting gynecologists, especially family planning specialists, at the time of cancer diagnosis to support women with decisions about menstrual suppression and contraception.
Funding/sponsorship Society of Family Planning, National Center for Advancing Translational Sciences, National Institutes of Health, Lillian Mae Rapp Research Endowment
Click on the PDF icon at the top of this introduction to read the full article.
Background Reproductive-age women who are undergoing cancer treatment are at risk for heavy menstrual bleeding, unintended pregnancy, and have a contraindication to estrogen-containing products. The incidence of vaginal bleeding and contraception use is not known.
Objective To describe clinical practices regarding menstrual suppression, estimate the incidence of vaginal bleeding complaints, and investigate contraceptive counseling and provision in women undergoing chemotherapy.
Methods We performed a chart review using ICD-9 codes to identify women aged 14-40 years who received chemotherapy at our institution during July 2008-June 2013. Electronic medical records were examined for menstrual suppression therapy, contraception counseling, and abnormal vaginal bleeding.
Results We identified 137 women for this study. 24 (18%) received prophylactic menstrual suppression counseling, of whom 17 (71%) initiated treatment, primarily with combined oral contraceptives, all prescribed by hematologist-oncologists. During the first 6 months of chemotherapy, 36 women (26%) complained of abnormal vaginal bleeding, including 10 women who were on prophylactic treatment. 19 women noted moderate to severe bleeding. 11 (12%) women received contraceptive counseling before chemotherapy, all from hematologist-oncologists; 86 women (63%) initiated chemotherapy without a documented contraceptive method.
Limitations Data were generated from billing codes, so all eligible women may not have been included.
Conclusions Reproductive-age women undergoing chemotherapy may not receive adequate contraception and menstrual suppression counseling. We encourage consulting gynecologists, especially family planning specialists, at the time of cancer diagnosis to support women with decisions about menstrual suppression and contraception.
Funding/sponsorship Society of Family Planning, National Center for Advancing Translational Sciences, National Institutes of Health, Lillian Mae Rapp Research Endowment
Click on the PDF icon at the top of this introduction to read the full article.
Background Reproductive-age women who are undergoing cancer treatment are at risk for heavy menstrual bleeding, unintended pregnancy, and have a contraindication to estrogen-containing products. The incidence of vaginal bleeding and contraception use is not known.
Objective To describe clinical practices regarding menstrual suppression, estimate the incidence of vaginal bleeding complaints, and investigate contraceptive counseling and provision in women undergoing chemotherapy.
Methods We performed a chart review using ICD-9 codes to identify women aged 14-40 years who received chemotherapy at our institution during July 2008-June 2013. Electronic medical records were examined for menstrual suppression therapy, contraception counseling, and abnormal vaginal bleeding.
Results We identified 137 women for this study. 24 (18%) received prophylactic menstrual suppression counseling, of whom 17 (71%) initiated treatment, primarily with combined oral contraceptives, all prescribed by hematologist-oncologists. During the first 6 months of chemotherapy, 36 women (26%) complained of abnormal vaginal bleeding, including 10 women who were on prophylactic treatment. 19 women noted moderate to severe bleeding. 11 (12%) women received contraceptive counseling before chemotherapy, all from hematologist-oncologists; 86 women (63%) initiated chemotherapy without a documented contraceptive method.
Limitations Data were generated from billing codes, so all eligible women may not have been included.
Conclusions Reproductive-age women undergoing chemotherapy may not receive adequate contraception and menstrual suppression counseling. We encourage consulting gynecologists, especially family planning specialists, at the time of cancer diagnosis to support women with decisions about menstrual suppression and contraception.
Funding/sponsorship Society of Family Planning, National Center for Advancing Translational Sciences, National Institutes of Health, Lillian Mae Rapp Research Endowment
Click on the PDF icon at the top of this introduction to read the full article.
Elotuzumab and ixazomib join the therapeutic arsenal for multiple myeloma
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Rotavirus vaccine again linked to small increase in risk of intussusception hospitalization
The first dose of rotavirus vaccine was again linked to a small, short-term increase in the risk of hospitalization for intussusception, but the benefits of the vaccine exceed this risk, according to a report.
In absolute numbers, there were an estimated 7 to 26 more intussusception cases per year among U.S. children aged 8-11 weeks during the postvaccine era, compared with the prevaccine era, said Jacqueline E. Tate, PhD, of the National Center for Immunization and Respiratory Diseases, Centers for Disease Control and Prevention, Atlanta, and her associates.

The increased risk did not extend to older children, which “is consistent with other U.S. studies,” the investigators said. “[Given] the magnitude of the declines in rotavirus disease compared with the small increased risk of intussusception, the public health benefits of rotavirus vaccination far exceed the increased risk of intussusception.”
Human rotavirus vaccines have been linked to rare events of intussusception since at least 1999, when Rotashield was withdrawn from the market for this reason. The next two rotavirus vaccines to receive Food and Drug Administration approval, RotaTeq and Rotarix, were not linked to intussusception in large trials or early postmarketing studies, but were estimated to cause 1-5 excess cases of intussusception per 100,000 population in more recent studies. Furthermore, a prior analysis of U.S. hospital discharge data found a small increase in the risk of intussusception hospitalization among 8- to 11-week-olds between 2007 to 2009, compared with baseline data from the prevaccine era, the investigators noted (Pediatrics. 2016 Aug 24. doi: 10.1542/peds.2016-1082).
To build on that analysis, they calculated rates of intussusception between 2000 and 2013 overall and among recommended age windows for rotavirus vaccination, which are 6-14 weeks for the first dose, 15-24 weeks for the second dose, and 25-34 weeks for the third dose. For consistency, they also looked at hospitalization rates among children aged 8-11 weeks.
The investigators identified 15,231 intussusception hospitalizations among children under 1 year of age during the study from 2000-2013. There were no overall trends in intussusception hospitalizations for all children under 1 year of age or subgroups of children aged 15-24 weeks or 25-34 weeks. Among children aged 8-11 weeks, intussusception hospitalization rates did rise significantly during the postvaccine era, compared with the prevaccine era for all years except 2011 and 2013. Excluding those two years, annual rates of intussusception hospitalizations among 8- to 11-week-olds were 46%-101% higher (16.7 to 22.9 hospitalizations per 100,000 population) during the postvaccine era than during the prevaccine era (11.4 hospitalizations per 100,000 population).
These results are “consistent with other U.S. studies that have been able to associate an increased risk of intussusception in the first week after the first dose of vaccine,” the researchers concluded. The advent of rotavirus vaccination prevented more than 176,000 hospitalizations, 242,000 emergency department visits, and 1.1 million outpatient visits from 2007 to 2011 (JAMA. 2015;313(22):2282-4), they noted.
The investigators reported no external funding sources and had no disclosures.
The first dose of rotavirus vaccine was again linked to a small, short-term increase in the risk of hospitalization for intussusception, but the benefits of the vaccine exceed this risk, according to a report.
In absolute numbers, there were an estimated 7 to 26 more intussusception cases per year among U.S. children aged 8-11 weeks during the postvaccine era, compared with the prevaccine era, said Jacqueline E. Tate, PhD, of the National Center for Immunization and Respiratory Diseases, Centers for Disease Control and Prevention, Atlanta, and her associates.
The increased risk did not extend to older children, which “is consistent with other U.S. studies,” the investigators said. “[Given] the magnitude of the declines in rotavirus disease compared with the small increased risk of intussusception, the public health benefits of rotavirus vaccination far exceed the increased risk of intussusception.”
Human rotavirus vaccines have been linked to rare events of intussusception since at least 1999, when Rotashield was withdrawn from the market for this reason. The next two rotavirus vaccines to receive Food and Drug Administration approval, RotaTeq and Rotarix, were not linked to intussusception in large trials or early postmarketing studies, but were estimated to cause 1-5 excess cases of intussusception per 100,000 population in more recent studies. Furthermore, a prior analysis of U.S. hospital discharge data found a small increase in the risk of intussusception hospitalization among 8- to 11-week-olds between 2007 to 2009, compared with baseline data from the prevaccine era, the investigators noted (Pediatrics. 2016 Aug 24. doi: 10.1542/peds.2016-1082).
To build on that analysis, they calculated rates of intussusception between 2000 and 2013 overall and among recommended age windows for rotavirus vaccination, which are 6-14 weeks for the first dose, 15-24 weeks for the second dose, and 25-34 weeks for the third dose. For consistency, they also looked at hospitalization rates among children aged 8-11 weeks.
The investigators identified 15,231 intussusception hospitalizations among children under 1 year of age during the study from 2000-2013. There were no overall trends in intussusception hospitalizations for all children under 1 year of age or subgroups of children aged 15-24 weeks or 25-34 weeks. Among children aged 8-11 weeks, intussusception hospitalization rates did rise significantly during the postvaccine era, compared with the prevaccine era for all years except 2011 and 2013. Excluding those two years, annual rates of intussusception hospitalizations among 8- to 11-week-olds were 46%-101% higher (16.7 to 22.9 hospitalizations per 100,000 population) during the postvaccine era than during the prevaccine era (11.4 hospitalizations per 100,000 population).
These results are “consistent with other U.S. studies that have been able to associate an increased risk of intussusception in the first week after the first dose of vaccine,” the researchers concluded. The advent of rotavirus vaccination prevented more than 176,000 hospitalizations, 242,000 emergency department visits, and 1.1 million outpatient visits from 2007 to 2011 (JAMA. 2015;313(22):2282-4), they noted.
The investigators reported no external funding sources and had no disclosures.
The first dose of rotavirus vaccine was again linked to a small, short-term increase in the risk of hospitalization for intussusception, but the benefits of the vaccine exceed this risk, according to a report.
In absolute numbers, there were an estimated 7 to 26 more intussusception cases per year among U.S. children aged 8-11 weeks during the postvaccine era, compared with the prevaccine era, said Jacqueline E. Tate, PhD, of the National Center for Immunization and Respiratory Diseases, Centers for Disease Control and Prevention, Atlanta, and her associates.
The increased risk did not extend to older children, which “is consistent with other U.S. studies,” the investigators said. “[Given] the magnitude of the declines in rotavirus disease compared with the small increased risk of intussusception, the public health benefits of rotavirus vaccination far exceed the increased risk of intussusception.”
Human rotavirus vaccines have been linked to rare events of intussusception since at least 1999, when Rotashield was withdrawn from the market for this reason. The next two rotavirus vaccines to receive Food and Drug Administration approval, RotaTeq and Rotarix, were not linked to intussusception in large trials or early postmarketing studies, but were estimated to cause 1-5 excess cases of intussusception per 100,000 population in more recent studies. Furthermore, a prior analysis of U.S. hospital discharge data found a small increase in the risk of intussusception hospitalization among 8- to 11-week-olds between 2007 to 2009, compared with baseline data from the prevaccine era, the investigators noted (Pediatrics. 2016 Aug 24. doi: 10.1542/peds.2016-1082).
To build on that analysis, they calculated rates of intussusception between 2000 and 2013 overall and among recommended age windows for rotavirus vaccination, which are 6-14 weeks for the first dose, 15-24 weeks for the second dose, and 25-34 weeks for the third dose. For consistency, they also looked at hospitalization rates among children aged 8-11 weeks.
The investigators identified 15,231 intussusception hospitalizations among children under 1 year of age during the study from 2000-2013. There were no overall trends in intussusception hospitalizations for all children under 1 year of age or subgroups of children aged 15-24 weeks or 25-34 weeks. Among children aged 8-11 weeks, intussusception hospitalization rates did rise significantly during the postvaccine era, compared with the prevaccine era for all years except 2011 and 2013. Excluding those two years, annual rates of intussusception hospitalizations among 8- to 11-week-olds were 46%-101% higher (16.7 to 22.9 hospitalizations per 100,000 population) during the postvaccine era than during the prevaccine era (11.4 hospitalizations per 100,000 population).
These results are “consistent with other U.S. studies that have been able to associate an increased risk of intussusception in the first week after the first dose of vaccine,” the researchers concluded. The advent of rotavirus vaccination prevented more than 176,000 hospitalizations, 242,000 emergency department visits, and 1.1 million outpatient visits from 2007 to 2011 (JAMA. 2015;313(22):2282-4), they noted.
The investigators reported no external funding sources and had no disclosures.
FROM PEDIATRICS
Key clinical point: The first dose of rotavirus vaccination is associated with a slight increase in risk of hospitalization for intussusception.
Major finding: Among 8-week-old infants to 11-week-old infants, rates of intussusception hospitalizations were significantly (46% to 101%) higher than in the prevaccine era for all postvaccine years except 2011 and 2013.
Data source: An analysis of hospitalization data from 2000 through 2013 from the State Inpatient Database, which covers 26 U.S. states.
Disclosures: The investigators had no external funding sources and no disclosures.

Loss of autonomy
At the summer meetings of the American Academy of Dermatology, AAD President Abel Torres screened a video of members responding to the question, “What keeps you up at night?” A recurring refrain in many of their responses was, “loss of autonomy.”
Many physicians feel they are losing autonomy. No doubt they are right. But physicians are not alone in their loss.
A young academic friend of mine had a similar lament. “Some assistant dean sent me an email ordering me to grade my students in a way that made no sense,” he said. “I challenged him to explain why. He answered that my school was following the guidelines of some organization I’d never heard of.”

“Academics used to be autonomous,” he said. “No more.”
Another professor friend decided to retire. “Forty years in the department,” he said, “10 as chair. Now a junior administrator tells me that I have to spend more hours on campus, even though I don’t have anything useful to do when I’m there. She said there are new rules for more academic efficiency.”
New administrators. Guidelines. Efficiency. Experienced hands dropping out or retiring out of frustration. Any of these sound familiar?
Teachers also complain to me about their loss of autonomy. “I used to be able to use judgment,” said one. “I knew what worked for a specific student. Now I just teach to the standardized test.
“For every one of my 23 kindergartners, I spent 1 hour filling out an iPad questionnaire on reading readiness. I’ve had it.”
“What will you do instead?” I asked him.
“Something with dogs,” he said.
And so it goes. Accountants and attorneys complain about heavy reporting regulations, with new ones added each year. Judges in Wisconsin make sentencing decisions using proprietary algorithms that no one outside the company that sells the algorithms has validated. Financial advisers have clients sign boilerplate statements documenting that they accept a certain level of risk. These clients may or may not understand what “level of risk” really implies, but either way they must sign a form, and the form must be filed. If you didn’t document it, you didn’t do it. If you documented it, you did it, even though you may not have really done anything meaningful.
An internist told me how things are in her new dispensation.
“They allow 15 minutes for a physical,” she said, “which is not enough anyway. But I also have to check off boxes for the EMR that add nothing to patient care. Last year we had to start asking about gender status. ‘What was your gender assignment at birth?’ ‘What is it now?’ We have to ask that every year – and click the box that says we did it.
“Several docs in our group retired. Another bunch went concierge. They couldn’t deal with it anymore.”
Metrics. Algorithms. Higher authorities who tell professionals what to do, how to do it, how to record it, business quants with scant understanding of what professionals actually profess. All so familiar and tiresome. It’s everywhere, and it’s bigger than any of us.
Loss of autonomy by professionals across the board reflects a changed understanding by society at large of what quality service is and how it should be judged. Numbers are in. Personal judgment – in our case, clinical judgment – is out. Since judgment can’t be measured, it cannot be trusted.
To a certain extent, autonomy is an illusion. We can do what we want as long as powers larger than we are – natural, social, political – let us do it. Those powers may lie dormant for a while, but they’re always there, and always have been. When they wake up and change the rules of the game, everyone has to adapt. New burdens in the practice of medicine are just one instance of a much broader trend.
Our professional organizations know this well. They are hard at work giving the authorities, government, and insurance administrators what they demand: data showing that what we do is useful, in the quantitative terms the authorities will accept.
To the extent that they succeed, we will be able to do some of what we want to do. Young people entering the medical field will expect nothing more. Some of their older colleagues will be satisfied that they are autonomous enough. The rest will have to find something else to do.
Dr. Rockoff practices dermatology in Brookline, Mass. He is on the clinical faculty at Tufts University School of Medicine, Boston, and has taught senior medical students and other trainees for 30 years.
At the summer meetings of the American Academy of Dermatology, AAD President Abel Torres screened a video of members responding to the question, “What keeps you up at night?” A recurring refrain in many of their responses was, “loss of autonomy.”
Many physicians feel they are losing autonomy. No doubt they are right. But physicians are not alone in their loss.
A young academic friend of mine had a similar lament. “Some assistant dean sent me an email ordering me to grade my students in a way that made no sense,” he said. “I challenged him to explain why. He answered that my school was following the guidelines of some organization I’d never heard of.”
“Academics used to be autonomous,” he said. “No more.”
Another professor friend decided to retire. “Forty years in the department,” he said, “10 as chair. Now a junior administrator tells me that I have to spend more hours on campus, even though I don’t have anything useful to do when I’m there. She said there are new rules for more academic efficiency.”
New administrators. Guidelines. Efficiency. Experienced hands dropping out or retiring out of frustration. Any of these sound familiar?
Teachers also complain to me about their loss of autonomy. “I used to be able to use judgment,” said one. “I knew what worked for a specific student. Now I just teach to the standardized test.
“For every one of my 23 kindergartners, I spent 1 hour filling out an iPad questionnaire on reading readiness. I’ve had it.”
“What will you do instead?” I asked him.
“Something with dogs,” he said.
And so it goes. Accountants and attorneys complain about heavy reporting regulations, with new ones added each year. Judges in Wisconsin make sentencing decisions using proprietary algorithms that no one outside the company that sells the algorithms has validated. Financial advisers have clients sign boilerplate statements documenting that they accept a certain level of risk. These clients may or may not understand what “level of risk” really implies, but either way they must sign a form, and the form must be filed. If you didn’t document it, you didn’t do it. If you documented it, you did it, even though you may not have really done anything meaningful.
An internist told me how things are in her new dispensation.
“They allow 15 minutes for a physical,” she said, “which is not enough anyway. But I also have to check off boxes for the EMR that add nothing to patient care. Last year we had to start asking about gender status. ‘What was your gender assignment at birth?’ ‘What is it now?’ We have to ask that every year – and click the box that says we did it.
“Several docs in our group retired. Another bunch went concierge. They couldn’t deal with it anymore.”
Metrics. Algorithms. Higher authorities who tell professionals what to do, how to do it, how to record it, business quants with scant understanding of what professionals actually profess. All so familiar and tiresome. It’s everywhere, and it’s bigger than any of us.
Loss of autonomy by professionals across the board reflects a changed understanding by society at large of what quality service is and how it should be judged. Numbers are in. Personal judgment – in our case, clinical judgment – is out. Since judgment can’t be measured, it cannot be trusted.
To a certain extent, autonomy is an illusion. We can do what we want as long as powers larger than we are – natural, social, political – let us do it. Those powers may lie dormant for a while, but they’re always there, and always have been. When they wake up and change the rules of the game, everyone has to adapt. New burdens in the practice of medicine are just one instance of a much broader trend.
Our professional organizations know this well. They are hard at work giving the authorities, government, and insurance administrators what they demand: data showing that what we do is useful, in the quantitative terms the authorities will accept.
To the extent that they succeed, we will be able to do some of what we want to do. Young people entering the medical field will expect nothing more. Some of their older colleagues will be satisfied that they are autonomous enough. The rest will have to find something else to do.
Dr. Rockoff practices dermatology in Brookline, Mass. He is on the clinical faculty at Tufts University School of Medicine, Boston, and has taught senior medical students and other trainees for 30 years.
At the summer meetings of the American Academy of Dermatology, AAD President Abel Torres screened a video of members responding to the question, “What keeps you up at night?” A recurring refrain in many of their responses was, “loss of autonomy.”
Many physicians feel they are losing autonomy. No doubt they are right. But physicians are not alone in their loss.
A young academic friend of mine had a similar lament. “Some assistant dean sent me an email ordering me to grade my students in a way that made no sense,” he said. “I challenged him to explain why. He answered that my school was following the guidelines of some organization I’d never heard of.”
“Academics used to be autonomous,” he said. “No more.”
Another professor friend decided to retire. “Forty years in the department,” he said, “10 as chair. Now a junior administrator tells me that I have to spend more hours on campus, even though I don’t have anything useful to do when I’m there. She said there are new rules for more academic efficiency.”
New administrators. Guidelines. Efficiency. Experienced hands dropping out or retiring out of frustration. Any of these sound familiar?
Teachers also complain to me about their loss of autonomy. “I used to be able to use judgment,” said one. “I knew what worked for a specific student. Now I just teach to the standardized test.
“For every one of my 23 kindergartners, I spent 1 hour filling out an iPad questionnaire on reading readiness. I’ve had it.”
“What will you do instead?” I asked him.
“Something with dogs,” he said.
And so it goes. Accountants and attorneys complain about heavy reporting regulations, with new ones added each year. Judges in Wisconsin make sentencing decisions using proprietary algorithms that no one outside the company that sells the algorithms has validated. Financial advisers have clients sign boilerplate statements documenting that they accept a certain level of risk. These clients may or may not understand what “level of risk” really implies, but either way they must sign a form, and the form must be filed. If you didn’t document it, you didn’t do it. If you documented it, you did it, even though you may not have really done anything meaningful.
An internist told me how things are in her new dispensation.
“They allow 15 minutes for a physical,” she said, “which is not enough anyway. But I also have to check off boxes for the EMR that add nothing to patient care. Last year we had to start asking about gender status. ‘What was your gender assignment at birth?’ ‘What is it now?’ We have to ask that every year – and click the box that says we did it.
“Several docs in our group retired. Another bunch went concierge. They couldn’t deal with it anymore.”
Metrics. Algorithms. Higher authorities who tell professionals what to do, how to do it, how to record it, business quants with scant understanding of what professionals actually profess. All so familiar and tiresome. It’s everywhere, and it’s bigger than any of us.
Loss of autonomy by professionals across the board reflects a changed understanding by society at large of what quality service is and how it should be judged. Numbers are in. Personal judgment – in our case, clinical judgment – is out. Since judgment can’t be measured, it cannot be trusted.
To a certain extent, autonomy is an illusion. We can do what we want as long as powers larger than we are – natural, social, political – let us do it. Those powers may lie dormant for a while, but they’re always there, and always have been. When they wake up and change the rules of the game, everyone has to adapt. New burdens in the practice of medicine are just one instance of a much broader trend.
Our professional organizations know this well. They are hard at work giving the authorities, government, and insurance administrators what they demand: data showing that what we do is useful, in the quantitative terms the authorities will accept.
To the extent that they succeed, we will be able to do some of what we want to do. Young people entering the medical field will expect nothing more. Some of their older colleagues will be satisfied that they are autonomous enough. The rest will have to find something else to do.
Dr. Rockoff practices dermatology in Brookline, Mass. He is on the clinical faculty at Tufts University School of Medicine, Boston, and has taught senior medical students and other trainees for 30 years.

Uridine triacetate provides antidote for 5-fluorouracil overdose and toxicity
Fluorouracil or 5-fluorouracil (5-FU) is an effective cytotoxic drug that is incorporated into various chemotherapeutic regimens for the treatment of numerous tumor types, but its clinical utility is limited by its narrow therapeutic index and the risk of overdose and serious toxic effects. Until recently, these outcomes were managed with supportive care, but the approval of uridine triacetate provides an antidote to reverse 5-FU-associated toxicity, to prevent death and potentially allow some patients to resume chemotherapy.
Click on the PDF icon at the top of this introduction to read the full article.
Fluorouracil or 5-fluorouracil (5-FU) is an effective cytotoxic drug that is incorporated into various chemotherapeutic regimens for the treatment of numerous tumor types, but its clinical utility is limited by its narrow therapeutic index and the risk of overdose and serious toxic effects. Until recently, these outcomes were managed with supportive care, but the approval of uridine triacetate provides an antidote to reverse 5-FU-associated toxicity, to prevent death and potentially allow some patients to resume chemotherapy.
Click on the PDF icon at the top of this introduction to read the full article.
Fluorouracil or 5-fluorouracil (5-FU) is an effective cytotoxic drug that is incorporated into various chemotherapeutic regimens for the treatment of numerous tumor types, but its clinical utility is limited by its narrow therapeutic index and the risk of overdose and serious toxic effects. Until recently, these outcomes were managed with supportive care, but the approval of uridine triacetate provides an antidote to reverse 5-FU-associated toxicity, to prevent death and potentially allow some patients to resume chemotherapy.
Click on the PDF icon at the top of this introduction to read the full article.
Sterilization rates decline for women despite coverage
Fewer women aged 20-44 years are using sterilization as their primary method of contraception, despite no-cost coverage of the procedure under the Affordable Care Act.
Sterilization rates in 2011-2013 for women in this age group was 25%, down from 27% in 2002, according to a new report from the Kaiser Family Foundation. Rates declined across income groups, dropping from 41% in 2002 to 37% in 2011-2013 for women whose incomes were up to 149% of the federal poverty level (FPL). For women with incomes within 150%-299% of the FPL, the rate declined from 33% to 28%, and for those at 300% or more of the FPL, the rate declined from 20% to 18%, according to the report.

While expanded coverage under the ACA may, in the long run, lead to greater use of sterilization by women, “it remains to be seen whether the growing availability of [long-acting reversible contraception] will offset this as IUDs and implants serve as semi-permanent substitutes for sterilization,” the Kaiser researchers wrote.
From 2011 to 2013, about 5% of men aged 15-44 years reported undergoing a vasectomy, according to Kaiser. The ACA does not require health plans to cover sterilization for men, but two states – Vermont and Maryland – have passed laws requiring coverage within their borders in the future.
Male sterilization rates increased with age (1% of those aged 15-34 years, compared with 13% of those aged 35-44 years), income (3% for those below 200% of the FPL, 5% for those 200%-399%, and 10% for those above 400%), and education (3% of those with up to a high school diploma/GED, 5% of those with some college, and 13% of those with at least a 4-year college degree). Comparative changes in male sterilization rates were not provided.
Fewer women aged 20-44 years are using sterilization as their primary method of contraception, despite no-cost coverage of the procedure under the Affordable Care Act.
Sterilization rates in 2011-2013 for women in this age group was 25%, down from 27% in 2002, according to a new report from the Kaiser Family Foundation. Rates declined across income groups, dropping from 41% in 2002 to 37% in 2011-2013 for women whose incomes were up to 149% of the federal poverty level (FPL). For women with incomes within 150%-299% of the FPL, the rate declined from 33% to 28%, and for those at 300% or more of the FPL, the rate declined from 20% to 18%, according to the report.
While expanded coverage under the ACA may, in the long run, lead to greater use of sterilization by women, “it remains to be seen whether the growing availability of [long-acting reversible contraception] will offset this as IUDs and implants serve as semi-permanent substitutes for sterilization,” the Kaiser researchers wrote.
From 2011 to 2013, about 5% of men aged 15-44 years reported undergoing a vasectomy, according to Kaiser. The ACA does not require health plans to cover sterilization for men, but two states – Vermont and Maryland – have passed laws requiring coverage within their borders in the future.
Male sterilization rates increased with age (1% of those aged 15-34 years, compared with 13% of those aged 35-44 years), income (3% for those below 200% of the FPL, 5% for those 200%-399%, and 10% for those above 400%), and education (3% of those with up to a high school diploma/GED, 5% of those with some college, and 13% of those with at least a 4-year college degree). Comparative changes in male sterilization rates were not provided.
Fewer women aged 20-44 years are using sterilization as their primary method of contraception, despite no-cost coverage of the procedure under the Affordable Care Act.
Sterilization rates in 2011-2013 for women in this age group was 25%, down from 27% in 2002, according to a new report from the Kaiser Family Foundation. Rates declined across income groups, dropping from 41% in 2002 to 37% in 2011-2013 for women whose incomes were up to 149% of the federal poverty level (FPL). For women with incomes within 150%-299% of the FPL, the rate declined from 33% to 28%, and for those at 300% or more of the FPL, the rate declined from 20% to 18%, according to the report.
While expanded coverage under the ACA may, in the long run, lead to greater use of sterilization by women, “it remains to be seen whether the growing availability of [long-acting reversible contraception] will offset this as IUDs and implants serve as semi-permanent substitutes for sterilization,” the Kaiser researchers wrote.
From 2011 to 2013, about 5% of men aged 15-44 years reported undergoing a vasectomy, according to Kaiser. The ACA does not require health plans to cover sterilization for men, but two states – Vermont and Maryland – have passed laws requiring coverage within their borders in the future.
Male sterilization rates increased with age (1% of those aged 15-34 years, compared with 13% of those aged 35-44 years), income (3% for those below 200% of the FPL, 5% for those 200%-399%, and 10% for those above 400%), and education (3% of those with up to a high school diploma/GED, 5% of those with some college, and 13% of those with at least a 4-year college degree). Comparative changes in male sterilization rates were not provided.

It’s health care … but not as we know it
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Expert shares new insights on the pathophysiology of rosacea
NEWPORT BEACH, CALIF. – In the clinical opinion of Richard L. Gallo, MD, PhD, current nomenclature for the diagnosis of rosacea could use a makeover.
“Currently, we’re still operating with an almost 20-year-old set of diagnostic subtypes of rosacea,” Dr. Gallo said at the annual meeting of the Pacific Dermatologic Association. He plans to participate in consensus meeting of experts who will convene this fall in an effort to update and modify these diagnostic criteria.

According to current nomenclature, subtype 1 is erythematotelangiectatic rosacea characterized by facial redness; subtype 2 is papulopustular, marked by bumps and pimples; subtype 3 is phymatous, characterized by enlargement of the nose, and subtype 4 is ocular, marked by eye irritation. Dr. Gallo pointed out that it’s rare to see just one of these subtypes in rosacea patients, with the exception of the erythematotelangiectatic rosacea (ETR). “There is a large population with ETR alone,” he said.” Most patients with the papulopustular subtype have aspects of ETR. There is a mix of subtypes of rosacea and we clearly need to modify our diagnostic criteria.”
Secondary rosacea features may include burning or stinging, plaque, dry appearance and scale, edema, ocular manifestations, peripheral location, and phymatous changes. Work by several researchers in recent years has shed light on the pathophysiology of rosacea. “We’re learning that there are many aspects to this disease that both trigger it and result in progression of the disease,” said Dr. Gallo, professor and chair of the department of dermatology at the University of California, San Diego. “It seems to have biological triggers that exist both in the environment and initiate from internal sources. We’re understanding more about the nature of those, at least specific molecules externally from microbes and so forth. Internally we understand more about the unique inflammatory signals.”
For example, he and other researchers began to look at the innate immune system patients with rosacea and identified LL37, a multifunction peptide that plays a role in a number of skin diseases, as something that can promote inflammation (Nat Med. 2007;13[8]:975-80). “It also promotes the vascular changes [that occur with the disease],” Dr. Gallo said. “We’re now learning how a dysregulation of enzymes in the skin contributes to making too much of these types of peptides. Therefore, treatment approaches that might modify enzymatic activity become useful.” Researchers have also discovered that some of the innate recognition molecules like toll-like receptor 2 (TLR2) are overexpressed in rosacea patients. “Similarly, in terms of the vascular signals, a number of labs are identifying some of the newer vascular transmitters that seem to be uniquely elevated in rosacea, so there’s great reason to be optimistic that given the increased specificity and understanding of what uniquely makes this disease happen, we’ll be able to target it in a safe way.”
A number of published studies have supported these notions, including an analysis of 275 twin pairs (JAMA Dermatol. 2015;151[11]:1213-9). The researchers found that compared with fraternal twins, identical twins had a higher association of National Rosacea Society scores (P = .04), “supporting the concept that there are fundamental genetic factors that are influencing disease,” Dr. Gallo said. Environmental factors found to be associated with rosacea include lifetime UV exposure, smoking, obesity, and alcohol use.
In an assessment of the genetic basis of rosacea by genome-wide association study, researchers identified one confirmed single-nucleotide polymorphism that could be associated with rosacea (J Invest Dermatol. 2015;135[6]:1548-55). It was located in an intergenic region between HLA-DRA and BTNL2, “which is consistent with the overall concept that there is perhaps a genetic abnormality that is leading to increased amino modulation of difficulties,” Dr. Gallo said. For another recent study, researchers analyzed 14 randomized or case control trials involving rosacea patients (Int J Med Sci. 2015;12[5]:387-96). They concluded that vasculature, chronic inflammatory responses, environmental triggers, food and chemicals ingested, and microorganisms either alone or in combination are responsible for rosacea.
Dr. Gallo went on to highlight findings from several studies that link rosacea to an increased risk for certain comorbidities. One, a nationwide case-control study from Taiwan that comprised 35,553 rosacea patients, found that the disease was significantly associated with a risk of certain cardiovascular comorbidities (J Acad Dermatol. 2015;73:249-54). These included dyslipidemia (OR 1.41), coronary artery disease (OR 1.35), and hypertension (OR 1.17). A separate analysis, based 93,314 participants in the Nurse’s Health Study, found that rosacea was significantly associated with a risk of coronary artery disease (OR 2.2). The researchers also observed that comorbidities seemed to increase with duration of the disease (Clin Gastroenterol Hepatol. 2016;14[2]:220-5). Another smaller case-control study of 65 patients and 65 controls found an increased risk with rosacea for coronary artery disease, hyperlipidemia, hypertension, and gastroesophageal reflux disease (J Am Acad Dermatol. 2015;73[4]:604-8).
A recent analysis of 75,088 participants in the Nurses’ Health Study found that women with rosacea faced an increased risk of thyroid cancer (HR 1.59) and basal cell carcinoma (HR 1.50; Br J Cancer 2015;113[3]:520-3). Rosacea may also impact one’s risk for developing certain neurological conditions. One study found an increased risk for dementia (HR 1.42) and Alzheimer’s disease (HR 1.92; Ann Neurol. 2016;79:921-8), while another found an increased risk for Parkinson’s disease (an adjusted incident ratio of 1.71 in patients with rosacea, compared with the referent population; JAMA Neurol. 2016;73[5]:529-34).
As for therapy, a recent Cochrane systematic review found strong evidence supporting benefits of several therapies over placebo, including metronidazole, azelaic acid, brimonidine, tetracycline, doxycycline 40 mg, ivermectin, and isotretinoin (Br J Dermatol. 2015;173[3]:651-2). A separate, 7-year retrospective study of 275 adults with rosacea published online in The Journal of Dermatology on Oct. 28, 2015, found that patients with the PPR subtype had a better overall prognosis, compared with their counterparts with the other subtypes. Overall, the median time to complete remission was 56 months. Complete remission was achieved in 46% of those with PPR subtype, compared with 19% of those with mixed subtype and 11% of those with ETR subtype.
Dr. Gallo disclosed that he has received research grants from the National Institutes of Health, Allergan, L’Oreal, Colgate-Palmolive, Regeneron, GSK, Galderma, and Bayer. He is a consultant for Allergan, Colgate-Palmolive, Sente, Matrisys, Dermata, Alnylam, Abbvie, Roche, and Promius.
NEWPORT BEACH, CALIF. – In the clinical opinion of Richard L. Gallo, MD, PhD, current nomenclature for the diagnosis of rosacea could use a makeover.
“Currently, we’re still operating with an almost 20-year-old set of diagnostic subtypes of rosacea,” Dr. Gallo said at the annual meeting of the Pacific Dermatologic Association. He plans to participate in consensus meeting of experts who will convene this fall in an effort to update and modify these diagnostic criteria.
According to current nomenclature, subtype 1 is erythematotelangiectatic rosacea characterized by facial redness; subtype 2 is papulopustular, marked by bumps and pimples; subtype 3 is phymatous, characterized by enlargement of the nose, and subtype 4 is ocular, marked by eye irritation. Dr. Gallo pointed out that it’s rare to see just one of these subtypes in rosacea patients, with the exception of the erythematotelangiectatic rosacea (ETR). “There is a large population with ETR alone,” he said.” Most patients with the papulopustular subtype have aspects of ETR. There is a mix of subtypes of rosacea and we clearly need to modify our diagnostic criteria.”
Secondary rosacea features may include burning or stinging, plaque, dry appearance and scale, edema, ocular manifestations, peripheral location, and phymatous changes. Work by several researchers in recent years has shed light on the pathophysiology of rosacea. “We’re learning that there are many aspects to this disease that both trigger it and result in progression of the disease,” said Dr. Gallo, professor and chair of the department of dermatology at the University of California, San Diego. “It seems to have biological triggers that exist both in the environment and initiate from internal sources. We’re understanding more about the nature of those, at least specific molecules externally from microbes and so forth. Internally we understand more about the unique inflammatory signals.”
For example, he and other researchers began to look at the innate immune system patients with rosacea and identified LL37, a multifunction peptide that plays a role in a number of skin diseases, as something that can promote inflammation (Nat Med. 2007;13[8]:975-80). “It also promotes the vascular changes [that occur with the disease],” Dr. Gallo said. “We’re now learning how a dysregulation of enzymes in the skin contributes to making too much of these types of peptides. Therefore, treatment approaches that might modify enzymatic activity become useful.” Researchers have also discovered that some of the innate recognition molecules like toll-like receptor 2 (TLR2) are overexpressed in rosacea patients. “Similarly, in terms of the vascular signals, a number of labs are identifying some of the newer vascular transmitters that seem to be uniquely elevated in rosacea, so there’s great reason to be optimistic that given the increased specificity and understanding of what uniquely makes this disease happen, we’ll be able to target it in a safe way.”
A number of published studies have supported these notions, including an analysis of 275 twin pairs (JAMA Dermatol. 2015;151[11]:1213-9). The researchers found that compared with fraternal twins, identical twins had a higher association of National Rosacea Society scores (P = .04), “supporting the concept that there are fundamental genetic factors that are influencing disease,” Dr. Gallo said. Environmental factors found to be associated with rosacea include lifetime UV exposure, smoking, obesity, and alcohol use.
In an assessment of the genetic basis of rosacea by genome-wide association study, researchers identified one confirmed single-nucleotide polymorphism that could be associated with rosacea (J Invest Dermatol. 2015;135[6]:1548-55). It was located in an intergenic region between HLA-DRA and BTNL2, “which is consistent with the overall concept that there is perhaps a genetic abnormality that is leading to increased amino modulation of difficulties,” Dr. Gallo said. For another recent study, researchers analyzed 14 randomized or case control trials involving rosacea patients (Int J Med Sci. 2015;12[5]:387-96). They concluded that vasculature, chronic inflammatory responses, environmental triggers, food and chemicals ingested, and microorganisms either alone or in combination are responsible for rosacea.
Dr. Gallo went on to highlight findings from several studies that link rosacea to an increased risk for certain comorbidities. One, a nationwide case-control study from Taiwan that comprised 35,553 rosacea patients, found that the disease was significantly associated with a risk of certain cardiovascular comorbidities (J Acad Dermatol. 2015;73:249-54). These included dyslipidemia (OR 1.41), coronary artery disease (OR 1.35), and hypertension (OR 1.17). A separate analysis, based 93,314 participants in the Nurse’s Health Study, found that rosacea was significantly associated with a risk of coronary artery disease (OR 2.2). The researchers also observed that comorbidities seemed to increase with duration of the disease (Clin Gastroenterol Hepatol. 2016;14[2]:220-5). Another smaller case-control study of 65 patients and 65 controls found an increased risk with rosacea for coronary artery disease, hyperlipidemia, hypertension, and gastroesophageal reflux disease (J Am Acad Dermatol. 2015;73[4]:604-8).
A recent analysis of 75,088 participants in the Nurses’ Health Study found that women with rosacea faced an increased risk of thyroid cancer (HR 1.59) and basal cell carcinoma (HR 1.50; Br J Cancer 2015;113[3]:520-3). Rosacea may also impact one’s risk for developing certain neurological conditions. One study found an increased risk for dementia (HR 1.42) and Alzheimer’s disease (HR 1.92; Ann Neurol. 2016;79:921-8), while another found an increased risk for Parkinson’s disease (an adjusted incident ratio of 1.71 in patients with rosacea, compared with the referent population; JAMA Neurol. 2016;73[5]:529-34).
As for therapy, a recent Cochrane systematic review found strong evidence supporting benefits of several therapies over placebo, including metronidazole, azelaic acid, brimonidine, tetracycline, doxycycline 40 mg, ivermectin, and isotretinoin (Br J Dermatol. 2015;173[3]:651-2). A separate, 7-year retrospective study of 275 adults with rosacea published online in The Journal of Dermatology on Oct. 28, 2015, found that patients with the PPR subtype had a better overall prognosis, compared with their counterparts with the other subtypes. Overall, the median time to complete remission was 56 months. Complete remission was achieved in 46% of those with PPR subtype, compared with 19% of those with mixed subtype and 11% of those with ETR subtype.
Dr. Gallo disclosed that he has received research grants from the National Institutes of Health, Allergan, L’Oreal, Colgate-Palmolive, Regeneron, GSK, Galderma, and Bayer. He is a consultant for Allergan, Colgate-Palmolive, Sente, Matrisys, Dermata, Alnylam, Abbvie, Roche, and Promius.
NEWPORT BEACH, CALIF. – In the clinical opinion of Richard L. Gallo, MD, PhD, current nomenclature for the diagnosis of rosacea could use a makeover.
“Currently, we’re still operating with an almost 20-year-old set of diagnostic subtypes of rosacea,” Dr. Gallo said at the annual meeting of the Pacific Dermatologic Association. He plans to participate in consensus meeting of experts who will convene this fall in an effort to update and modify these diagnostic criteria.
According to current nomenclature, subtype 1 is erythematotelangiectatic rosacea characterized by facial redness; subtype 2 is papulopustular, marked by bumps and pimples; subtype 3 is phymatous, characterized by enlargement of the nose, and subtype 4 is ocular, marked by eye irritation. Dr. Gallo pointed out that it’s rare to see just one of these subtypes in rosacea patients, with the exception of the erythematotelangiectatic rosacea (ETR). “There is a large population with ETR alone,” he said.” Most patients with the papulopustular subtype have aspects of ETR. There is a mix of subtypes of rosacea and we clearly need to modify our diagnostic criteria.”
Secondary rosacea features may include burning or stinging, plaque, dry appearance and scale, edema, ocular manifestations, peripheral location, and phymatous changes. Work by several researchers in recent years has shed light on the pathophysiology of rosacea. “We’re learning that there are many aspects to this disease that both trigger it and result in progression of the disease,” said Dr. Gallo, professor and chair of the department of dermatology at the University of California, San Diego. “It seems to have biological triggers that exist both in the environment and initiate from internal sources. We’re understanding more about the nature of those, at least specific molecules externally from microbes and so forth. Internally we understand more about the unique inflammatory signals.”
For example, he and other researchers began to look at the innate immune system patients with rosacea and identified LL37, a multifunction peptide that plays a role in a number of skin diseases, as something that can promote inflammation (Nat Med. 2007;13[8]:975-80). “It also promotes the vascular changes [that occur with the disease],” Dr. Gallo said. “We’re now learning how a dysregulation of enzymes in the skin contributes to making too much of these types of peptides. Therefore, treatment approaches that might modify enzymatic activity become useful.” Researchers have also discovered that some of the innate recognition molecules like toll-like receptor 2 (TLR2) are overexpressed in rosacea patients. “Similarly, in terms of the vascular signals, a number of labs are identifying some of the newer vascular transmitters that seem to be uniquely elevated in rosacea, so there’s great reason to be optimistic that given the increased specificity and understanding of what uniquely makes this disease happen, we’ll be able to target it in a safe way.”
A number of published studies have supported these notions, including an analysis of 275 twin pairs (JAMA Dermatol. 2015;151[11]:1213-9). The researchers found that compared with fraternal twins, identical twins had a higher association of National Rosacea Society scores (P = .04), “supporting the concept that there are fundamental genetic factors that are influencing disease,” Dr. Gallo said. Environmental factors found to be associated with rosacea include lifetime UV exposure, smoking, obesity, and alcohol use.
In an assessment of the genetic basis of rosacea by genome-wide association study, researchers identified one confirmed single-nucleotide polymorphism that could be associated with rosacea (J Invest Dermatol. 2015;135[6]:1548-55). It was located in an intergenic region between HLA-DRA and BTNL2, “which is consistent with the overall concept that there is perhaps a genetic abnormality that is leading to increased amino modulation of difficulties,” Dr. Gallo said. For another recent study, researchers analyzed 14 randomized or case control trials involving rosacea patients (Int J Med Sci. 2015;12[5]:387-96). They concluded that vasculature, chronic inflammatory responses, environmental triggers, food and chemicals ingested, and microorganisms either alone or in combination are responsible for rosacea.
Dr. Gallo went on to highlight findings from several studies that link rosacea to an increased risk for certain comorbidities. One, a nationwide case-control study from Taiwan that comprised 35,553 rosacea patients, found that the disease was significantly associated with a risk of certain cardiovascular comorbidities (J Acad Dermatol. 2015;73:249-54). These included dyslipidemia (OR 1.41), coronary artery disease (OR 1.35), and hypertension (OR 1.17). A separate analysis, based 93,314 participants in the Nurse’s Health Study, found that rosacea was significantly associated with a risk of coronary artery disease (OR 2.2). The researchers also observed that comorbidities seemed to increase with duration of the disease (Clin Gastroenterol Hepatol. 2016;14[2]:220-5). Another smaller case-control study of 65 patients and 65 controls found an increased risk with rosacea for coronary artery disease, hyperlipidemia, hypertension, and gastroesophageal reflux disease (J Am Acad Dermatol. 2015;73[4]:604-8).
A recent analysis of 75,088 participants in the Nurses’ Health Study found that women with rosacea faced an increased risk of thyroid cancer (HR 1.59) and basal cell carcinoma (HR 1.50; Br J Cancer 2015;113[3]:520-3). Rosacea may also impact one’s risk for developing certain neurological conditions. One study found an increased risk for dementia (HR 1.42) and Alzheimer’s disease (HR 1.92; Ann Neurol. 2016;79:921-8), while another found an increased risk for Parkinson’s disease (an adjusted incident ratio of 1.71 in patients with rosacea, compared with the referent population; JAMA Neurol. 2016;73[5]:529-34).
As for therapy, a recent Cochrane systematic review found strong evidence supporting benefits of several therapies over placebo, including metronidazole, azelaic acid, brimonidine, tetracycline, doxycycline 40 mg, ivermectin, and isotretinoin (Br J Dermatol. 2015;173[3]:651-2). A separate, 7-year retrospective study of 275 adults with rosacea published online in The Journal of Dermatology on Oct. 28, 2015, found that patients with the PPR subtype had a better overall prognosis, compared with their counterparts with the other subtypes. Overall, the median time to complete remission was 56 months. Complete remission was achieved in 46% of those with PPR subtype, compared with 19% of those with mixed subtype and 11% of those with ETR subtype.
Dr. Gallo disclosed that he has received research grants from the National Institutes of Health, Allergan, L’Oreal, Colgate-Palmolive, Regeneron, GSK, Galderma, and Bayer. He is a consultant for Allergan, Colgate-Palmolive, Sente, Matrisys, Dermata, Alnylam, Abbvie, Roche, and Promius.
EXPERT ANALYSIS AT PDA 2016

Anastrozole-Induced Subacute Cutaneous Lupus Erythematosus
Drug-induced subacute cutaneous lupus erythematosus (DI-SCLE) was first described in 1985 in 5 patients who had been taking hydrochlorothiazide.1 The skin lesions in these patients were identical to those seen in idiopathic subacute cutaneous lupus erythematosus (SCLE) and were accompanied by the same autoantibodies (anti-Ro/Sjögren syndrome antigen A [SS-A] and anti-La/Sjögren syndrome antigen B [SS-B]) and HLA type (HLA-DR2/DR3) that are known to be associated with idiopathic SCLE. The skin lesions of SCLE in these 5 patients resolved spontaneously after discontinuing hydrochlorothiazide; however, anti-Ro/SS-A antibodies persisted in all except 1 patient.1 Over the last decade, an increasing number of drugs from different classes have been implicated to be associated with DI-SCLE. Since the concept of DI-SCLE was introduced, it has been reported to look identical to idiopathic SCLE, both clinically and histopathologically; however, one report suggested that the 2 entities can be distinguished based on clinical variations.2 In general, patients with DI-SCLE develop the same anti-Ro antibodies as seen in idiopathic SCLE. In addition, although the rash in DI-SCLE typically resolves with withdrawal of the offending drug, the antibodies tend to persist. Herein, we report a case of a patient being treated with an aromatase inhibitor who presented with clinical, serologic, and histopathologic evidence of DI-SCLE.
Case Report
A 69-year-old woman diagnosed with breast cancer 4 years prior to her presentation to dermatology initially underwent a lumpectomy and radiation treatment. She was subsequently started on anastrozole 2 years later. After 16 months of treatment with anastrozole, she developed an erythematous scaly rash on sun-exposed areas of the skin. The patient was seen by an outside dermatologist who treated her for a patient-perceived drug rash based on biopsy results that simply demonstrated interface dermatitis. She was treated with both topical and oral steroids with little improvement and therefore presented to our office approximately 6 months after starting treatment seeking a second opinion.
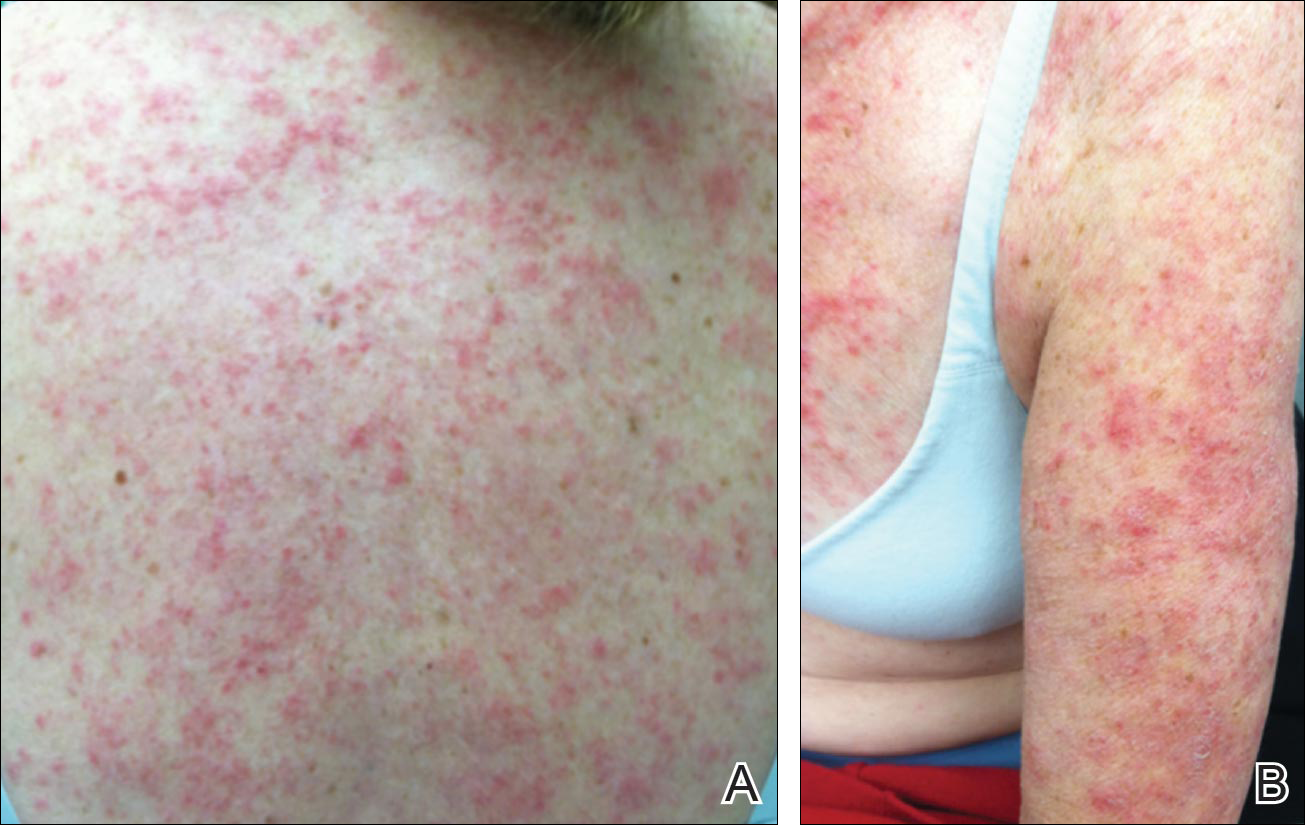
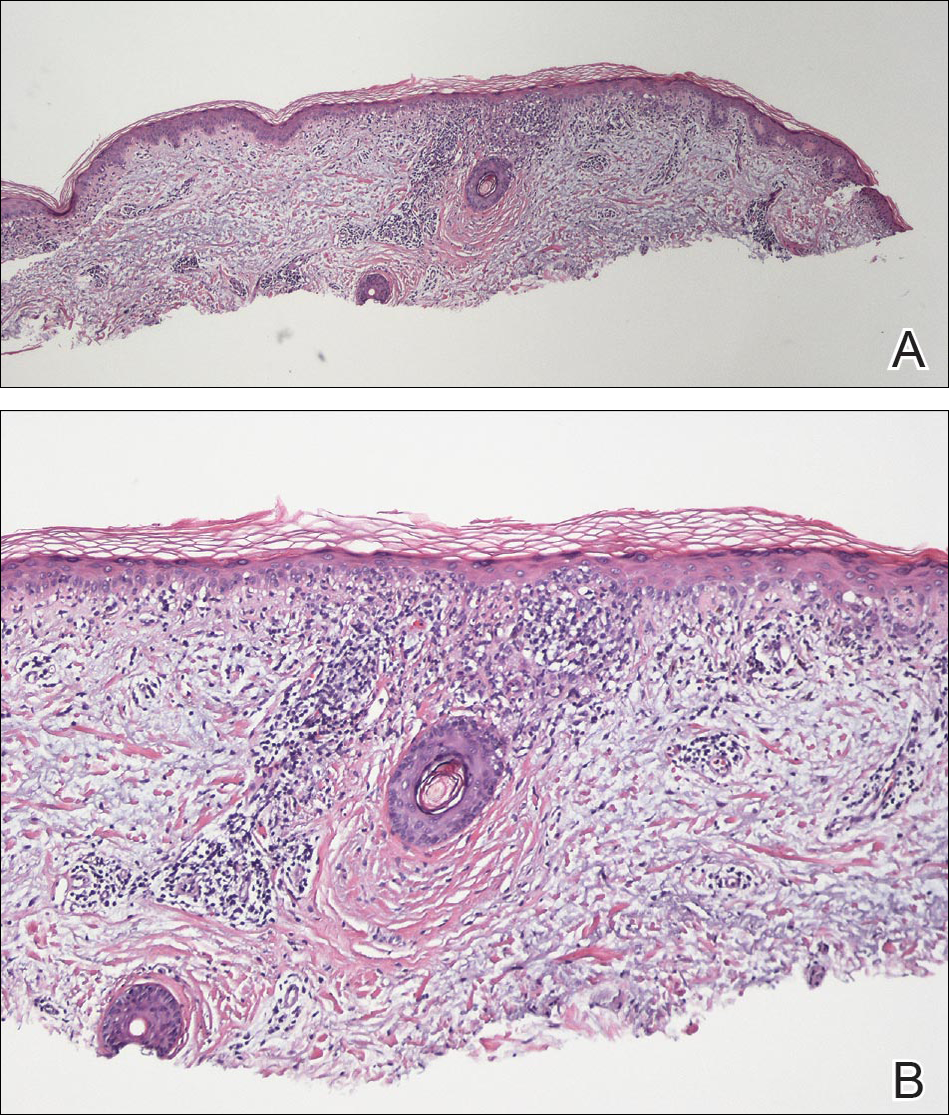
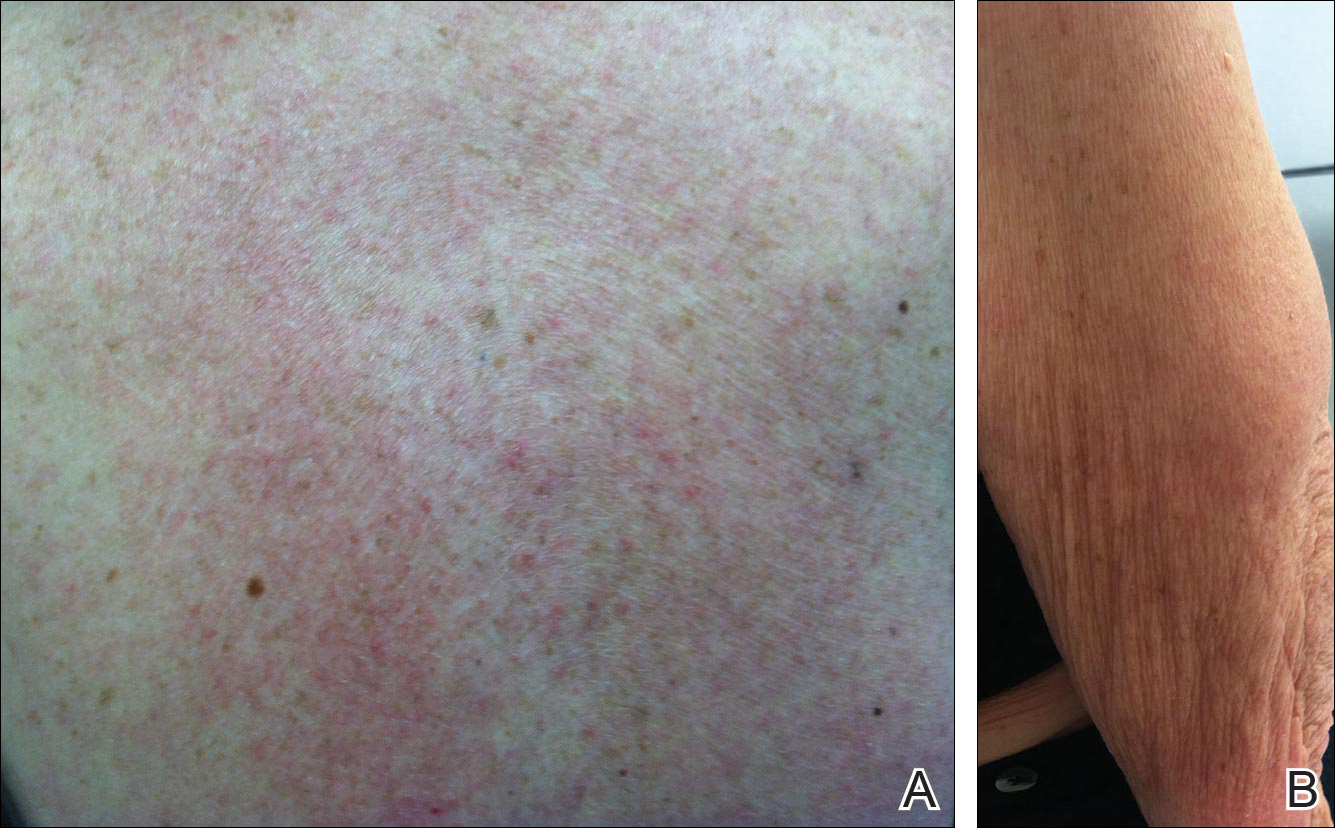
Physical examination revealed numerous erythematous scaly papules and plaques in a photodistributed pattern on the chest, back, legs, and arms (Figure 1). On further questioning, the patient noted that the rash became worse when she was at the beach or playing tennis outside as well as under indoor lights. A repeat biopsy was performed, revealing interface and perivascular dermatitis with an infiltrate composed of lymphocytes, histiocytes, and scattered pigment-laden macrophages (Figure 2). Given the appearance and distribution of the rash as well as the clinical scenario, drug-induced lupus was suspected. Anastrozole was the only medication being taken. Laboratory evaluation was performed and was negative for antinuclear antibodies, antihistone antibodies, and anti-La/SS-B antibodies but was positive for anti-Ro/SS-A antibodies (>8.0 U [reference range, <1.0 U]). Based on these findings, anastrozole-induced SCLE was the most likely explanation for this presentation. The patient was started on a sun-protective regimen (ie, wide-brimmed hat, daily sunscreen) and anastrozole was discontinued by her oncologist; the combination led to moderate improvement in symptoms. One week later, oral hydroxychloroquine 200 mg twice daily was started, which led to notable improvement (Figure 3). The patient was seen for 2 additional follow-up visits, each time with sustained resolution of the rash. The hydroxychloroquine was then stopped at her last visit 3 months after diagnosis. The patient was subsequently lost to follow-up.
Comment
Presentation of SCLE
Subacute cutaneous lupus erythematosus is a form of lupus erythematosus characterized by nonscarring, annular, scaly, erythematous plaques that occur on sun-exposed skin. The lesions are classically distributed on the upper back, chest, dorsal arms, and lateral neck but also can be found in other locations.3,4 Subacute cutaneous lupus erythematosus may be idiopathic; may occur in patients with systemic lupus erythematosus, Sjögren syndrome, or deficiency of the second component of complement (C2d); or may be drug induced.5 On histology SCLE presents as a lichenoid tissue reaction with focal vacuolization of the epidermal basal layer and perivascular lymphocytic infiltrate. On direct immunofluorescence, both idiopathic and drug-induced SCLE present with granular deposition of IgM, IgG, and C3 in a bandlike array at the dermoepidermal junction and circulating anti-Ro/SS-A antibodies. Therefore, histopathologically and immunologically, DI-SCLE is indistinguishable from idiopathic cases.6
Differential Diagnosis
It was previously thought that the clinical presentation of DI-SCLE and idiopathic SCLE were indistinguishable; however, Marzano et al2 described remarkable differences in the cutaneous manifestations of the 2 diseases. Drug-induced SCLE lesions are more widespread, occur more frequently on the legs, and may be bullous or erythema multiforme–like versus the idiopathic lesions, which tend to be more concentrated on the upper body and classically present as scaly erythematous plaques. Additionally, malar rash and vasculitic lesions, such as purpura and necrotic-ulcerative lesions, are seen more often in DI-SCLE.
Drug-induced systemic lupus erythematosus (DI-SLE) is a lupuslike syndrome that can be differentiated from DI-SCLE by virtue of its clinical and serological presentation. It differs from DI-SCLE in that DI-SLE typically does not present with skin symptoms; rather, systemic symptoms such as fever, weight loss, arthralgia, polyarthritis, pericarditis, and pleuritis are more commonly seen. Additionally, it has been associated with antihistone antibodies.4 More than 80 drugs have been reported to cause DI-SLE, including procainamide, hydralazine, and quinidine.7
To be classified as either DI-SCLE or DI-SLE, symptoms need to present after administration of the triggering drug and must resolve after the drug is discontinued.7 The drugs most commonly associated with DI-SCLE are thiazides, calcium channel blockers, tumor necrosis factor α inhibitors, angiotensin-converting enzyme inhibitors, and terbinafine, with few cases citing anastrozole as the inciting agent.4,6,8,9 The incubation period for DI-SCLE varies substantially. Thiazide diuretics and calcium channel blockers typically have the longest incubation period, ranging from 6 months to 5 years for thiazides,1,6,10,11 while calcium channel blockers have an average incubation period of 3 years.12 Drug-induced SCLE associated with antifungals, however, usually is much more rapid in onset; the incubation period on average is 5 weeks for terbinafine and 2 weeks for griseofulvin.13-15
Antiestrogen Drugs and SCLE
Anastrozole, the inciting agent in our case, is a third-generation, selective, nonsteroidal, aromatase inhibitor with no progestogenic, androgenic, or estrogenic activity. Anastrozole, when taken at its recommended dosage of 1 mg daily, will suppress estradiol. It is used as an adjuvant treatment of estrogen-sensitive breast cancer in postmenopausal women. In contrast to a prior case of DI-SCLE secondary to anastrozole in which the incubation period was approximately 1 month,8 our patient had an incubation period of approximately 16 months. Tamoxifen, another antiestrogen drug, also has been associated with DI-SCLE.9 In cases of tamoxifen-induced SCLE, the incubation period was several years, which is more similar to our patient. Although these drugs do not have the same mechanism of action, they both have antiestrogen properties.9 A systemic review of DI-SCLE reported that incubation periods between drug exposure and appearance of DI-SCLE varied greatly and were drug class dependent. It is possible that reactions associated with antiestrogen medications have a delayed presentation; however, given there are limited cases of anastrozole-induced DI-SCLE, we cannot make a clear statement on incubation periods.6
Reports of DI-SCLE caused by antiestrogen drugs are particularly interesting because sex hormones in relation to lupus disease activity have been the subject of debate for decades. Women are considerably more likely to develop autoimmune diseases than men, suggesting that steroid hormones, especially estrogen and progesterone, influence the immune system.16 Estrogen actions are proinflammatory, while the actions of progesterone, androgens, and glucocorticoids are anti-inflammatory.17 Studies in women with lupus revealed an increased rate of mild- to moderate-intensity disease flares associated with estrogen-containing hormone replace-ment therapy.18-20
Over the years, several antiestrogen therapies have been used in murine models, which showed remarkable clinical improvement in the course of SLE. The precise mechanisms involved in disease immunomodulation by these therapies have not been elucidated.21-23 It is thought that estrogen plays a role in the synthesis and expression of Ro antigens on the surface of keratinocytes, increasing the fixation of anti-Ro antibodies in keratinocytes and provoking the appearance of a cutaneous eruption in patients with a susceptible HLA profile.6
Conclusion
We report a rare case of SCLE induced by anastrozole use. Cases such as ours and others that implicate antiestrogen drugs in association with DI-SCLE are particularly noteworthy, considering many studies are looking at the potential usefulness of antiestrogen therapy in the treatment of SLE. Further research on this relationship is warranted.
- Reed B, Huff J, Jones S, et al. Subacute cutaneous lupus erythematosus associated with hydrochlorothiazide therapy. Ann Intern Med. 1985;103:49-51.
- Marzano A, Lazzari R, Polloni I, et al. Drug-induced subacute cutaneous lupus erythematosus: evidence for differences from its idiopathic counterpart. Br J Dermatol. 2011;165:335-341.
- Bonsmann G, Schiller M, Luger T, et al. Terbinafine-induced subacute cutaneous lupus erythematosus. J Am Acad Dermatol. 2001;44:925-931.
- Callen J. Review: drug induced subacute cutaneous lupus erythematosus. Lupus. 2010;19:1107-1111.
- Lin J, Callen JP. Subacute cutaneous lupus erythematosus (SCLE). Medscape website. http://emedicine.medscape.com/article/1065657-overview. Updated March 7, 2016. Accessed April 29, 2016.
- Lowe GC, Henderson CL, Grau RH, et al. A systematic review of drug-induced subacute cutaneous lupus erythematosus. Br J Dermatol. 2011;164:465-472.
- Vedove C, Giglio M, Schena D, et al. Drug-induced lupus erythematosus. Arch Dermatol Res. 2009;301:99-105.
- Trancart M, Cavailhes A, Balme B, et al. Anastrozole-induced subacute cutaneous lupus erythematosus [published online December 6, 2007]. Br J Dermatol. 2008;158:628-629.
- Fumal I, Danchin A, Cosserat F, et al. Subacute cutaneous lupus erythematosus associated with tamoxifen therapy: two cases. Dermatology. 2005;210:251-252.
- Brown C, Deng J. Thiazide diuretics induce cutaneous lupus-like adverse reaction. J Toxicol Clin Toxicol. 1995;33:729-733.
- Sontheimer R. Subacute cutaneous lupus erythematosus: 25-year evolution of a prototypic subset (subphenotype) of lupus erythematosus defined by characteristic cutaneous, pathological, immunological, and genetic findings. Autoimmun Rev. 2005;4:253-263.
- Crowson A, Magro C. Subacute cutaneous lupus erythematosus arising in the setting of calcium channel blocker therapy. Hum Pathol. 1997;28:67-73.
- Lorentz K, Booken N, Goerdt S, et al. Subacute cutaneous lupus erythematosus induced by terbinafine: case report and review of literature. J Dtsch Dermatol Ges. 2008;6:823-837.
- Kasperkiewicz M, Anemüller W, Angelova-Fischer I, et al. Subacute cutaneous lupus erythematosus associated with terbinafine. Clin Exp Dermatol. 2009;34:403-404.
- Miyagawa S, Okuchi T, Shiomi Y, et al. Subacute cutaneous lupus erythematosus lesions precipitated by griseofulvin. J Am Acad Dermatol. 1989;21:343-346.
- Inman RD. Immunologic sex differences and the female predominance in systemic lupus erythematosus. Arthritis Rheum. 1978;21:849-854.
- Cutolo M, Wilder RL. Different roles of androgens and estrogens in the susceptibility to autoimmune rheumatic diseases. Rheum Dis Clin North Am. 2000;26:825-839.
- Petri M. Sex hormones and systemic lupus erythematosus. Lupus. 2008;17:412-415.
- Lateef A, Petri M. Hormone replacement and contraceptive therapy in autoimmune diseases [published online January 18, 2012]. J Autoimmun. 2012;38:J170-J176.
- Buyon JP, Petri M, Kim MY, et al. The effect of combined estrogen and progesterone hormone replacement therapy on disease activity in systemic lupus erythematosus: a randomized trial. Ann Intern Med. 2005;142:954-962.
- Wu W, Suen J, Lin B, et al. Tamoxifen alleviates disease severity and decreases double negative T cells in autoimmune MRL-lpr/lpr mice. Immunology. 2000;100:110-118.
- Dayan M, Zinger H, Kalush F, et al. The beneficial effects of treatment with tamoxifen and anti-oestradiol antibody on experimental systemic lupus erythematosus are associated with cytokine modulations. Immunology. 1997;90:101-108.
- Sthoeger Z, Zinger H, Mozes E. Beneficial effects of the anti-oestrogen tamoxifen on systemic lupus erythematosus of (NZBxNZW)F1 female mice are associated with specific reduction of IgG3 autoantibodies. Ann Rheum Dis. 2003;62:341-346.
Drug-induced subacute cutaneous lupus erythematosus (DI-SCLE) was first described in 1985 in 5 patients who had been taking hydrochlorothiazide.1 The skin lesions in these patients were identical to those seen in idiopathic subacute cutaneous lupus erythematosus (SCLE) and were accompanied by the same autoantibodies (anti-Ro/Sjögren syndrome antigen A [SS-A] and anti-La/Sjögren syndrome antigen B [SS-B]) and HLA type (HLA-DR2/DR3) that are known to be associated with idiopathic SCLE. The skin lesions of SCLE in these 5 patients resolved spontaneously after discontinuing hydrochlorothiazide; however, anti-Ro/SS-A antibodies persisted in all except 1 patient.1 Over the last decade, an increasing number of drugs from different classes have been implicated to be associated with DI-SCLE. Since the concept of DI-SCLE was introduced, it has been reported to look identical to idiopathic SCLE, both clinically and histopathologically; however, one report suggested that the 2 entities can be distinguished based on clinical variations.2 In general, patients with DI-SCLE develop the same anti-Ro antibodies as seen in idiopathic SCLE. In addition, although the rash in DI-SCLE typically resolves with withdrawal of the offending drug, the antibodies tend to persist. Herein, we report a case of a patient being treated with an aromatase inhibitor who presented with clinical, serologic, and histopathologic evidence of DI-SCLE.
Case Report
A 69-year-old woman diagnosed with breast cancer 4 years prior to her presentation to dermatology initially underwent a lumpectomy and radiation treatment. She was subsequently started on anastrozole 2 years later. After 16 months of treatment with anastrozole, she developed an erythematous scaly rash on sun-exposed areas of the skin. The patient was seen by an outside dermatologist who treated her for a patient-perceived drug rash based on biopsy results that simply demonstrated interface dermatitis. She was treated with both topical and oral steroids with little improvement and therefore presented to our office approximately 6 months after starting treatment seeking a second opinion.
Physical examination revealed numerous erythematous scaly papules and plaques in a photodistributed pattern on the chest, back, legs, and arms (Figure 1). On further questioning, the patient noted that the rash became worse when she was at the beach or playing tennis outside as well as under indoor lights. A repeat biopsy was performed, revealing interface and perivascular dermatitis with an infiltrate composed of lymphocytes, histiocytes, and scattered pigment-laden macrophages (Figure 2). Given the appearance and distribution of the rash as well as the clinical scenario, drug-induced lupus was suspected. Anastrozole was the only medication being taken. Laboratory evaluation was performed and was negative for antinuclear antibodies, antihistone antibodies, and anti-La/SS-B antibodies but was positive for anti-Ro/SS-A antibodies (>8.0 U [reference range, <1.0 U]). Based on these findings, anastrozole-induced SCLE was the most likely explanation for this presentation. The patient was started on a sun-protective regimen (ie, wide-brimmed hat, daily sunscreen) and anastrozole was discontinued by her oncologist; the combination led to moderate improvement in symptoms. One week later, oral hydroxychloroquine 200 mg twice daily was started, which led to notable improvement (Figure 3). The patient was seen for 2 additional follow-up visits, each time with sustained resolution of the rash. The hydroxychloroquine was then stopped at her last visit 3 months after diagnosis. The patient was subsequently lost to follow-up.
Comment
Presentation of SCLE
Subacute cutaneous lupus erythematosus is a form of lupus erythematosus characterized by nonscarring, annular, scaly, erythematous plaques that occur on sun-exposed skin. The lesions are classically distributed on the upper back, chest, dorsal arms, and lateral neck but also can be found in other locations.3,4 Subacute cutaneous lupus erythematosus may be idiopathic; may occur in patients with systemic lupus erythematosus, Sjögren syndrome, or deficiency of the second component of complement (C2d); or may be drug induced.5 On histology SCLE presents as a lichenoid tissue reaction with focal vacuolization of the epidermal basal layer and perivascular lymphocytic infiltrate. On direct immunofluorescence, both idiopathic and drug-induced SCLE present with granular deposition of IgM, IgG, and C3 in a bandlike array at the dermoepidermal junction and circulating anti-Ro/SS-A antibodies. Therefore, histopathologically and immunologically, DI-SCLE is indistinguishable from idiopathic cases.6
Differential Diagnosis
It was previously thought that the clinical presentation of DI-SCLE and idiopathic SCLE were indistinguishable; however, Marzano et al2 described remarkable differences in the cutaneous manifestations of the 2 diseases. Drug-induced SCLE lesions are more widespread, occur more frequently on the legs, and may be bullous or erythema multiforme–like versus the idiopathic lesions, which tend to be more concentrated on the upper body and classically present as scaly erythematous plaques. Additionally, malar rash and vasculitic lesions, such as purpura and necrotic-ulcerative lesions, are seen more often in DI-SCLE.
Drug-induced systemic lupus erythematosus (DI-SLE) is a lupuslike syndrome that can be differentiated from DI-SCLE by virtue of its clinical and serological presentation. It differs from DI-SCLE in that DI-SLE typically does not present with skin symptoms; rather, systemic symptoms such as fever, weight loss, arthralgia, polyarthritis, pericarditis, and pleuritis are more commonly seen. Additionally, it has been associated with antihistone antibodies.4 More than 80 drugs have been reported to cause DI-SLE, including procainamide, hydralazine, and quinidine.7
To be classified as either DI-SCLE or DI-SLE, symptoms need to present after administration of the triggering drug and must resolve after the drug is discontinued.7 The drugs most commonly associated with DI-SCLE are thiazides, calcium channel blockers, tumor necrosis factor α inhibitors, angiotensin-converting enzyme inhibitors, and terbinafine, with few cases citing anastrozole as the inciting agent.4,6,8,9 The incubation period for DI-SCLE varies substantially. Thiazide diuretics and calcium channel blockers typically have the longest incubation period, ranging from 6 months to 5 years for thiazides,1,6,10,11 while calcium channel blockers have an average incubation period of 3 years.12 Drug-induced SCLE associated with antifungals, however, usually is much more rapid in onset; the incubation period on average is 5 weeks for terbinafine and 2 weeks for griseofulvin.13-15
Antiestrogen Drugs and SCLE
Anastrozole, the inciting agent in our case, is a third-generation, selective, nonsteroidal, aromatase inhibitor with no progestogenic, androgenic, or estrogenic activity. Anastrozole, when taken at its recommended dosage of 1 mg daily, will suppress estradiol. It is used as an adjuvant treatment of estrogen-sensitive breast cancer in postmenopausal women. In contrast to a prior case of DI-SCLE secondary to anastrozole in which the incubation period was approximately 1 month,8 our patient had an incubation period of approximately 16 months. Tamoxifen, another antiestrogen drug, also has been associated with DI-SCLE.9 In cases of tamoxifen-induced SCLE, the incubation period was several years, which is more similar to our patient. Although these drugs do not have the same mechanism of action, they both have antiestrogen properties.9 A systemic review of DI-SCLE reported that incubation periods between drug exposure and appearance of DI-SCLE varied greatly and were drug class dependent. It is possible that reactions associated with antiestrogen medications have a delayed presentation; however, given there are limited cases of anastrozole-induced DI-SCLE, we cannot make a clear statement on incubation periods.6
Reports of DI-SCLE caused by antiestrogen drugs are particularly interesting because sex hormones in relation to lupus disease activity have been the subject of debate for decades. Women are considerably more likely to develop autoimmune diseases than men, suggesting that steroid hormones, especially estrogen and progesterone, influence the immune system.16 Estrogen actions are proinflammatory, while the actions of progesterone, androgens, and glucocorticoids are anti-inflammatory.17 Studies in women with lupus revealed an increased rate of mild- to moderate-intensity disease flares associated with estrogen-containing hormone replace-ment therapy.18-20
Over the years, several antiestrogen therapies have been used in murine models, which showed remarkable clinical improvement in the course of SLE. The precise mechanisms involved in disease immunomodulation by these therapies have not been elucidated.21-23 It is thought that estrogen plays a role in the synthesis and expression of Ro antigens on the surface of keratinocytes, increasing the fixation of anti-Ro antibodies in keratinocytes and provoking the appearance of a cutaneous eruption in patients with a susceptible HLA profile.6
Conclusion
We report a rare case of SCLE induced by anastrozole use. Cases such as ours and others that implicate antiestrogen drugs in association with DI-SCLE are particularly noteworthy, considering many studies are looking at the potential usefulness of antiestrogen therapy in the treatment of SLE. Further research on this relationship is warranted.
Drug-induced subacute cutaneous lupus erythematosus (DI-SCLE) was first described in 1985 in 5 patients who had been taking hydrochlorothiazide.1 The skin lesions in these patients were identical to those seen in idiopathic subacute cutaneous lupus erythematosus (SCLE) and were accompanied by the same autoantibodies (anti-Ro/Sjögren syndrome antigen A [SS-A] and anti-La/Sjögren syndrome antigen B [SS-B]) and HLA type (HLA-DR2/DR3) that are known to be associated with idiopathic SCLE. The skin lesions of SCLE in these 5 patients resolved spontaneously after discontinuing hydrochlorothiazide; however, anti-Ro/SS-A antibodies persisted in all except 1 patient.1 Over the last decade, an increasing number of drugs from different classes have been implicated to be associated with DI-SCLE. Since the concept of DI-SCLE was introduced, it has been reported to look identical to idiopathic SCLE, both clinically and histopathologically; however, one report suggested that the 2 entities can be distinguished based on clinical variations.2 In general, patients with DI-SCLE develop the same anti-Ro antibodies as seen in idiopathic SCLE. In addition, although the rash in DI-SCLE typically resolves with withdrawal of the offending drug, the antibodies tend to persist. Herein, we report a case of a patient being treated with an aromatase inhibitor who presented with clinical, serologic, and histopathologic evidence of DI-SCLE.
Case Report
A 69-year-old woman diagnosed with breast cancer 4 years prior to her presentation to dermatology initially underwent a lumpectomy and radiation treatment. She was subsequently started on anastrozole 2 years later. After 16 months of treatment with anastrozole, she developed an erythematous scaly rash on sun-exposed areas of the skin. The patient was seen by an outside dermatologist who treated her for a patient-perceived drug rash based on biopsy results that simply demonstrated interface dermatitis. She was treated with both topical and oral steroids with little improvement and therefore presented to our office approximately 6 months after starting treatment seeking a second opinion.
Physical examination revealed numerous erythematous scaly papules and plaques in a photodistributed pattern on the chest, back, legs, and arms (Figure 1). On further questioning, the patient noted that the rash became worse when she was at the beach or playing tennis outside as well as under indoor lights. A repeat biopsy was performed, revealing interface and perivascular dermatitis with an infiltrate composed of lymphocytes, histiocytes, and scattered pigment-laden macrophages (Figure 2). Given the appearance and distribution of the rash as well as the clinical scenario, drug-induced lupus was suspected. Anastrozole was the only medication being taken. Laboratory evaluation was performed and was negative for antinuclear antibodies, antihistone antibodies, and anti-La/SS-B antibodies but was positive for anti-Ro/SS-A antibodies (>8.0 U [reference range, <1.0 U]). Based on these findings, anastrozole-induced SCLE was the most likely explanation for this presentation. The patient was started on a sun-protective regimen (ie, wide-brimmed hat, daily sunscreen) and anastrozole was discontinued by her oncologist; the combination led to moderate improvement in symptoms. One week later, oral hydroxychloroquine 200 mg twice daily was started, which led to notable improvement (Figure 3). The patient was seen for 2 additional follow-up visits, each time with sustained resolution of the rash. The hydroxychloroquine was then stopped at her last visit 3 months after diagnosis. The patient was subsequently lost to follow-up.
Comment
Presentation of SCLE
Subacute cutaneous lupus erythematosus is a form of lupus erythematosus characterized by nonscarring, annular, scaly, erythematous plaques that occur on sun-exposed skin. The lesions are classically distributed on the upper back, chest, dorsal arms, and lateral neck but also can be found in other locations.3,4 Subacute cutaneous lupus erythematosus may be idiopathic; may occur in patients with systemic lupus erythematosus, Sjögren syndrome, or deficiency of the second component of complement (C2d); or may be drug induced.5 On histology SCLE presents as a lichenoid tissue reaction with focal vacuolization of the epidermal basal layer and perivascular lymphocytic infiltrate. On direct immunofluorescence, both idiopathic and drug-induced SCLE present with granular deposition of IgM, IgG, and C3 in a bandlike array at the dermoepidermal junction and circulating anti-Ro/SS-A antibodies. Therefore, histopathologically and immunologically, DI-SCLE is indistinguishable from idiopathic cases.6
Differential Diagnosis
It was previously thought that the clinical presentation of DI-SCLE and idiopathic SCLE were indistinguishable; however, Marzano et al2 described remarkable differences in the cutaneous manifestations of the 2 diseases. Drug-induced SCLE lesions are more widespread, occur more frequently on the legs, and may be bullous or erythema multiforme–like versus the idiopathic lesions, which tend to be more concentrated on the upper body and classically present as scaly erythematous plaques. Additionally, malar rash and vasculitic lesions, such as purpura and necrotic-ulcerative lesions, are seen more often in DI-SCLE.
Drug-induced systemic lupus erythematosus (DI-SLE) is a lupuslike syndrome that can be differentiated from DI-SCLE by virtue of its clinical and serological presentation. It differs from DI-SCLE in that DI-SLE typically does not present with skin symptoms; rather, systemic symptoms such as fever, weight loss, arthralgia, polyarthritis, pericarditis, and pleuritis are more commonly seen. Additionally, it has been associated with antihistone antibodies.4 More than 80 drugs have been reported to cause DI-SLE, including procainamide, hydralazine, and quinidine.7
To be classified as either DI-SCLE or DI-SLE, symptoms need to present after administration of the triggering drug and must resolve after the drug is discontinued.7 The drugs most commonly associated with DI-SCLE are thiazides, calcium channel blockers, tumor necrosis factor α inhibitors, angiotensin-converting enzyme inhibitors, and terbinafine, with few cases citing anastrozole as the inciting agent.4,6,8,9 The incubation period for DI-SCLE varies substantially. Thiazide diuretics and calcium channel blockers typically have the longest incubation period, ranging from 6 months to 5 years for thiazides,1,6,10,11 while calcium channel blockers have an average incubation period of 3 years.12 Drug-induced SCLE associated with antifungals, however, usually is much more rapid in onset; the incubation period on average is 5 weeks for terbinafine and 2 weeks for griseofulvin.13-15
Antiestrogen Drugs and SCLE
Anastrozole, the inciting agent in our case, is a third-generation, selective, nonsteroidal, aromatase inhibitor with no progestogenic, androgenic, or estrogenic activity. Anastrozole, when taken at its recommended dosage of 1 mg daily, will suppress estradiol. It is used as an adjuvant treatment of estrogen-sensitive breast cancer in postmenopausal women. In contrast to a prior case of DI-SCLE secondary to anastrozole in which the incubation period was approximately 1 month,8 our patient had an incubation period of approximately 16 months. Tamoxifen, another antiestrogen drug, also has been associated with DI-SCLE.9 In cases of tamoxifen-induced SCLE, the incubation period was several years, which is more similar to our patient. Although these drugs do not have the same mechanism of action, they both have antiestrogen properties.9 A systemic review of DI-SCLE reported that incubation periods between drug exposure and appearance of DI-SCLE varied greatly and were drug class dependent. It is possible that reactions associated with antiestrogen medications have a delayed presentation; however, given there are limited cases of anastrozole-induced DI-SCLE, we cannot make a clear statement on incubation periods.6
Reports of DI-SCLE caused by antiestrogen drugs are particularly interesting because sex hormones in relation to lupus disease activity have been the subject of debate for decades. Women are considerably more likely to develop autoimmune diseases than men, suggesting that steroid hormones, especially estrogen and progesterone, influence the immune system.16 Estrogen actions are proinflammatory, while the actions of progesterone, androgens, and glucocorticoids are anti-inflammatory.17 Studies in women with lupus revealed an increased rate of mild- to moderate-intensity disease flares associated with estrogen-containing hormone replace-ment therapy.18-20
Over the years, several antiestrogen therapies have been used in murine models, which showed remarkable clinical improvement in the course of SLE. The precise mechanisms involved in disease immunomodulation by these therapies have not been elucidated.21-23 It is thought that estrogen plays a role in the synthesis and expression of Ro antigens on the surface of keratinocytes, increasing the fixation of anti-Ro antibodies in keratinocytes and provoking the appearance of a cutaneous eruption in patients with a susceptible HLA profile.6
Conclusion
We report a rare case of SCLE induced by anastrozole use. Cases such as ours and others that implicate antiestrogen drugs in association with DI-SCLE are particularly noteworthy, considering many studies are looking at the potential usefulness of antiestrogen therapy in the treatment of SLE. Further research on this relationship is warranted.
- Reed B, Huff J, Jones S, et al. Subacute cutaneous lupus erythematosus associated with hydrochlorothiazide therapy. Ann Intern Med. 1985;103:49-51.
- Marzano A, Lazzari R, Polloni I, et al. Drug-induced subacute cutaneous lupus erythematosus: evidence for differences from its idiopathic counterpart. Br J Dermatol. 2011;165:335-341.
- Bonsmann G, Schiller M, Luger T, et al. Terbinafine-induced subacute cutaneous lupus erythematosus. J Am Acad Dermatol. 2001;44:925-931.
- Callen J. Review: drug induced subacute cutaneous lupus erythematosus. Lupus. 2010;19:1107-1111.
- Lin J, Callen JP. Subacute cutaneous lupus erythematosus (SCLE). Medscape website. http://emedicine.medscape.com/article/1065657-overview. Updated March 7, 2016. Accessed April 29, 2016.
- Lowe GC, Henderson CL, Grau RH, et al. A systematic review of drug-induced subacute cutaneous lupus erythematosus. Br J Dermatol. 2011;164:465-472.
- Vedove C, Giglio M, Schena D, et al. Drug-induced lupus erythematosus. Arch Dermatol Res. 2009;301:99-105.
- Trancart M, Cavailhes A, Balme B, et al. Anastrozole-induced subacute cutaneous lupus erythematosus [published online December 6, 2007]. Br J Dermatol. 2008;158:628-629.
- Fumal I, Danchin A, Cosserat F, et al. Subacute cutaneous lupus erythematosus associated with tamoxifen therapy: two cases. Dermatology. 2005;210:251-252.
- Brown C, Deng J. Thiazide diuretics induce cutaneous lupus-like adverse reaction. J Toxicol Clin Toxicol. 1995;33:729-733.
- Sontheimer R. Subacute cutaneous lupus erythematosus: 25-year evolution of a prototypic subset (subphenotype) of lupus erythematosus defined by characteristic cutaneous, pathological, immunological, and genetic findings. Autoimmun Rev. 2005;4:253-263.
- Crowson A, Magro C. Subacute cutaneous lupus erythematosus arising in the setting of calcium channel blocker therapy. Hum Pathol. 1997;28:67-73.
- Lorentz K, Booken N, Goerdt S, et al. Subacute cutaneous lupus erythematosus induced by terbinafine: case report and review of literature. J Dtsch Dermatol Ges. 2008;6:823-837.
- Kasperkiewicz M, Anemüller W, Angelova-Fischer I, et al. Subacute cutaneous lupus erythematosus associated with terbinafine. Clin Exp Dermatol. 2009;34:403-404.
- Miyagawa S, Okuchi T, Shiomi Y, et al. Subacute cutaneous lupus erythematosus lesions precipitated by griseofulvin. J Am Acad Dermatol. 1989;21:343-346.
- Inman RD. Immunologic sex differences and the female predominance in systemic lupus erythematosus. Arthritis Rheum. 1978;21:849-854.
- Cutolo M, Wilder RL. Different roles of androgens and estrogens in the susceptibility to autoimmune rheumatic diseases. Rheum Dis Clin North Am. 2000;26:825-839.
- Petri M. Sex hormones and systemic lupus erythematosus. Lupus. 2008;17:412-415.
- Lateef A, Petri M. Hormone replacement and contraceptive therapy in autoimmune diseases [published online January 18, 2012]. J Autoimmun. 2012;38:J170-J176.
- Buyon JP, Petri M, Kim MY, et al. The effect of combined estrogen and progesterone hormone replacement therapy on disease activity in systemic lupus erythematosus: a randomized trial. Ann Intern Med. 2005;142:954-962.
- Wu W, Suen J, Lin B, et al. Tamoxifen alleviates disease severity and decreases double negative T cells in autoimmune MRL-lpr/lpr mice. Immunology. 2000;100:110-118.
- Dayan M, Zinger H, Kalush F, et al. The beneficial effects of treatment with tamoxifen and anti-oestradiol antibody on experimental systemic lupus erythematosus are associated with cytokine modulations. Immunology. 1997;90:101-108.
- Sthoeger Z, Zinger H, Mozes E. Beneficial effects of the anti-oestrogen tamoxifen on systemic lupus erythematosus of (NZBxNZW)F1 female mice are associated with specific reduction of IgG3 autoantibodies. Ann Rheum Dis. 2003;62:341-346.
- Reed B, Huff J, Jones S, et al. Subacute cutaneous lupus erythematosus associated with hydrochlorothiazide therapy. Ann Intern Med. 1985;103:49-51.
- Marzano A, Lazzari R, Polloni I, et al. Drug-induced subacute cutaneous lupus erythematosus: evidence for differences from its idiopathic counterpart. Br J Dermatol. 2011;165:335-341.
- Bonsmann G, Schiller M, Luger T, et al. Terbinafine-induced subacute cutaneous lupus erythematosus. J Am Acad Dermatol. 2001;44:925-931.
- Callen J. Review: drug induced subacute cutaneous lupus erythematosus. Lupus. 2010;19:1107-1111.
- Lin J, Callen JP. Subacute cutaneous lupus erythematosus (SCLE). Medscape website. http://emedicine.medscape.com/article/1065657-overview. Updated March 7, 2016. Accessed April 29, 2016.
- Lowe GC, Henderson CL, Grau RH, et al. A systematic review of drug-induced subacute cutaneous lupus erythematosus. Br J Dermatol. 2011;164:465-472.
- Vedove C, Giglio M, Schena D, et al. Drug-induced lupus erythematosus. Arch Dermatol Res. 2009;301:99-105.
- Trancart M, Cavailhes A, Balme B, et al. Anastrozole-induced subacute cutaneous lupus erythematosus [published online December 6, 2007]. Br J Dermatol. 2008;158:628-629.
- Fumal I, Danchin A, Cosserat F, et al. Subacute cutaneous lupus erythematosus associated with tamoxifen therapy: two cases. Dermatology. 2005;210:251-252.
- Brown C, Deng J. Thiazide diuretics induce cutaneous lupus-like adverse reaction. J Toxicol Clin Toxicol. 1995;33:729-733.
- Sontheimer R. Subacute cutaneous lupus erythematosus: 25-year evolution of a prototypic subset (subphenotype) of lupus erythematosus defined by characteristic cutaneous, pathological, immunological, and genetic findings. Autoimmun Rev. 2005;4:253-263.
- Crowson A, Magro C. Subacute cutaneous lupus erythematosus arising in the setting of calcium channel blocker therapy. Hum Pathol. 1997;28:67-73.
- Lorentz K, Booken N, Goerdt S, et al. Subacute cutaneous lupus erythematosus induced by terbinafine: case report and review of literature. J Dtsch Dermatol Ges. 2008;6:823-837.
- Kasperkiewicz M, Anemüller W, Angelova-Fischer I, et al. Subacute cutaneous lupus erythematosus associated with terbinafine. Clin Exp Dermatol. 2009;34:403-404.
- Miyagawa S, Okuchi T, Shiomi Y, et al. Subacute cutaneous lupus erythematosus lesions precipitated by griseofulvin. J Am Acad Dermatol. 1989;21:343-346.
- Inman RD. Immunologic sex differences and the female predominance in systemic lupus erythematosus. Arthritis Rheum. 1978;21:849-854.
- Cutolo M, Wilder RL. Different roles of androgens and estrogens in the susceptibility to autoimmune rheumatic diseases. Rheum Dis Clin North Am. 2000;26:825-839.
- Petri M. Sex hormones and systemic lupus erythematosus. Lupus. 2008;17:412-415.
- Lateef A, Petri M. Hormone replacement and contraceptive therapy in autoimmune diseases [published online January 18, 2012]. J Autoimmun. 2012;38:J170-J176.
- Buyon JP, Petri M, Kim MY, et al. The effect of combined estrogen and progesterone hormone replacement therapy on disease activity in systemic lupus erythematosus: a randomized trial. Ann Intern Med. 2005;142:954-962.
- Wu W, Suen J, Lin B, et al. Tamoxifen alleviates disease severity and decreases double negative T cells in autoimmune MRL-lpr/lpr mice. Immunology. 2000;100:110-118.
- Dayan M, Zinger H, Kalush F, et al. The beneficial effects of treatment with tamoxifen and anti-oestradiol antibody on experimental systemic lupus erythematosus are associated with cytokine modulations. Immunology. 1997;90:101-108.
- Sthoeger Z, Zinger H, Mozes E. Beneficial effects of the anti-oestrogen tamoxifen on systemic lupus erythematosus of (NZBxNZW)F1 female mice are associated with specific reduction of IgG3 autoantibodies. Ann Rheum Dis. 2003;62:341-346.
Practice Points
- There are numerous cases of drug-induced subacute cutaneous lupus erythematosus (DI-SCLE) published in the literature; however, there are limited reports with anastrozole implicated as the causative agent.
- Cases of DI-SCLE are clinically and histologically indistinguishable from idiopathic cases. It is important to recognize and withdraw the offending agent.
