User login
European Commission’s Proposed Criteria for Endocrine Disruptors Trigger Multiple Concerns
The European Commission has proposed regulatory criteria on endocrine-disrupting chemicals that are too strict and so fall short of protecting the public, as they were intended to do, experts contend.
Endocrine-disrupting chemicals cost Europe billions in health care costs each year (Andrology. 2016 Jul;4[4]:565-72).
Published in June, the criteria would require proof that chemicals harm human endocrine health to define them as endocrine-disrupting chemicals (EDCs) – even if data from animal and in vitro studies already suggest so. “Because health effects can take years or even generations to become apparent, this proposal will not protect public health,” the Endocrine Society noted in a sharp formal critique.
Endocrine-disrupting chemicals mimic or block hormones central to brain development, reproduction, metabolism, growth, and other key physiologic processes. The European Union is the largest single economy to regulate EDCs specifically, which more than 1,300 studies have linked to health problems such as infertility, diabetes, obesity, hormone-related cancers, and neurological disorders, the Endocrine Society concluded in a 2015 scientific statement.
Exposure to even low doses of EDCs such as bisphenol A (BPA) can cause adverse effects. But to fulfill the regulatory definition of the European Commission, EDCs would have to meet an even greater burden of proof than carcinogens – a backward step that “defeats the purpose of the regulations – to shield the public from EDCs that pose a threat to human health,” Rémy Slama, PhD, a member of the Society’s European Union Endocrine-Disrupting Chemicals Task Force, stated in an Endocrine Society news release. Of particular concern is the proposal that EDCs must have a single known “mode of action,” which “represents a fundamental misunderstanding of how endocrine signaling works by connecting different organ systems within the body,” said Dr. Slama, senior investigator at Inserm (the National Institute of Health and Medical Research) in Paris.

Deborah M. Kurrasch, PhD, assistant professor and principal investigator at the University of Calgary (Alta.), agreed. The “mode of action” criterion misses the point that EDCs are “messy” compounds that target various proteins and elicit a range of potential cellular responses based on dose, target tissue, and age, she said in an interview. An EDC may lack a single mode of action, or its mode of action may be far harder to pinpoint than its effects on processes such as reproduction, sleep, mood, and growth, she added. “In my opinion, an endocrine-disrupting chemical is one that disrupts the endocrine system. Despite some internal dialogue, the name for this broad and diverse group of chemicals is, and likely will remain, EDCs because the name so accurately describes their one unifying effect – they all perturb normal endocrine function.”
Ultimately, enacting such tight criteria would tie the hands of regulators with regard to newly recognized and even some well-studied EDCs, “despite evidence that they affect endocrine signaling, because their mode of action is not yet known,” Dr. Kurrasch said.
Experts also noted that the EC criteria would keep regulatory bodies from ranking chemicals based on the strength of evidence that they disrupt endocrine function. Instead, the Endocrine Society advocates for a tiered ranking system based on available data. “As the European Parliament and member countries consider whether to implement the European Commission’s criteria, the Society will continue to advocate for criteria that reflect the state of the science,” the organization emphasized.
Dr. Kurrasch is a member of the Endocrine Society and had no other disclosures.
The European Commission has proposed regulatory criteria on endocrine-disrupting chemicals that are too strict and so fall short of protecting the public, as they were intended to do, experts contend.
Endocrine-disrupting chemicals cost Europe billions in health care costs each year (Andrology. 2016 Jul;4[4]:565-72).
Published in June, the criteria would require proof that chemicals harm human endocrine health to define them as endocrine-disrupting chemicals (EDCs) – even if data from animal and in vitro studies already suggest so. “Because health effects can take years or even generations to become apparent, this proposal will not protect public health,” the Endocrine Society noted in a sharp formal critique.
Endocrine-disrupting chemicals mimic or block hormones central to brain development, reproduction, metabolism, growth, and other key physiologic processes. The European Union is the largest single economy to regulate EDCs specifically, which more than 1,300 studies have linked to health problems such as infertility, diabetes, obesity, hormone-related cancers, and neurological disorders, the Endocrine Society concluded in a 2015 scientific statement.
Exposure to even low doses of EDCs such as bisphenol A (BPA) can cause adverse effects. But to fulfill the regulatory definition of the European Commission, EDCs would have to meet an even greater burden of proof than carcinogens – a backward step that “defeats the purpose of the regulations – to shield the public from EDCs that pose a threat to human health,” Rémy Slama, PhD, a member of the Society’s European Union Endocrine-Disrupting Chemicals Task Force, stated in an Endocrine Society news release. Of particular concern is the proposal that EDCs must have a single known “mode of action,” which “represents a fundamental misunderstanding of how endocrine signaling works by connecting different organ systems within the body,” said Dr. Slama, senior investigator at Inserm (the National Institute of Health and Medical Research) in Paris.
Deborah M. Kurrasch, PhD, assistant professor and principal investigator at the University of Calgary (Alta.), agreed. The “mode of action” criterion misses the point that EDCs are “messy” compounds that target various proteins and elicit a range of potential cellular responses based on dose, target tissue, and age, she said in an interview. An EDC may lack a single mode of action, or its mode of action may be far harder to pinpoint than its effects on processes such as reproduction, sleep, mood, and growth, she added. “In my opinion, an endocrine-disrupting chemical is one that disrupts the endocrine system. Despite some internal dialogue, the name for this broad and diverse group of chemicals is, and likely will remain, EDCs because the name so accurately describes their one unifying effect – they all perturb normal endocrine function.”
Ultimately, enacting such tight criteria would tie the hands of regulators with regard to newly recognized and even some well-studied EDCs, “despite evidence that they affect endocrine signaling, because their mode of action is not yet known,” Dr. Kurrasch said.
Experts also noted that the EC criteria would keep regulatory bodies from ranking chemicals based on the strength of evidence that they disrupt endocrine function. Instead, the Endocrine Society advocates for a tiered ranking system based on available data. “As the European Parliament and member countries consider whether to implement the European Commission’s criteria, the Society will continue to advocate for criteria that reflect the state of the science,” the organization emphasized.
Dr. Kurrasch is a member of the Endocrine Society and had no other disclosures.
The European Commission has proposed regulatory criteria on endocrine-disrupting chemicals that are too strict and so fall short of protecting the public, as they were intended to do, experts contend.
Endocrine-disrupting chemicals cost Europe billions in health care costs each year (Andrology. 2016 Jul;4[4]:565-72).
Published in June, the criteria would require proof that chemicals harm human endocrine health to define them as endocrine-disrupting chemicals (EDCs) – even if data from animal and in vitro studies already suggest so. “Because health effects can take years or even generations to become apparent, this proposal will not protect public health,” the Endocrine Society noted in a sharp formal critique.
Endocrine-disrupting chemicals mimic or block hormones central to brain development, reproduction, metabolism, growth, and other key physiologic processes. The European Union is the largest single economy to regulate EDCs specifically, which more than 1,300 studies have linked to health problems such as infertility, diabetes, obesity, hormone-related cancers, and neurological disorders, the Endocrine Society concluded in a 2015 scientific statement.
Exposure to even low doses of EDCs such as bisphenol A (BPA) can cause adverse effects. But to fulfill the regulatory definition of the European Commission, EDCs would have to meet an even greater burden of proof than carcinogens – a backward step that “defeats the purpose of the regulations – to shield the public from EDCs that pose a threat to human health,” Rémy Slama, PhD, a member of the Society’s European Union Endocrine-Disrupting Chemicals Task Force, stated in an Endocrine Society news release. Of particular concern is the proposal that EDCs must have a single known “mode of action,” which “represents a fundamental misunderstanding of how endocrine signaling works by connecting different organ systems within the body,” said Dr. Slama, senior investigator at Inserm (the National Institute of Health and Medical Research) in Paris.
Deborah M. Kurrasch, PhD, assistant professor and principal investigator at the University of Calgary (Alta.), agreed. The “mode of action” criterion misses the point that EDCs are “messy” compounds that target various proteins and elicit a range of potential cellular responses based on dose, target tissue, and age, she said in an interview. An EDC may lack a single mode of action, or its mode of action may be far harder to pinpoint than its effects on processes such as reproduction, sleep, mood, and growth, she added. “In my opinion, an endocrine-disrupting chemical is one that disrupts the endocrine system. Despite some internal dialogue, the name for this broad and diverse group of chemicals is, and likely will remain, EDCs because the name so accurately describes their one unifying effect – they all perturb normal endocrine function.”
Ultimately, enacting such tight criteria would tie the hands of regulators with regard to newly recognized and even some well-studied EDCs, “despite evidence that they affect endocrine signaling, because their mode of action is not yet known,” Dr. Kurrasch said.
Experts also noted that the EC criteria would keep regulatory bodies from ranking chemicals based on the strength of evidence that they disrupt endocrine function. Instead, the Endocrine Society advocates for a tiered ranking system based on available data. “As the European Parliament and member countries consider whether to implement the European Commission’s criteria, the Society will continue to advocate for criteria that reflect the state of the science,” the organization emphasized.
Dr. Kurrasch is a member of the Endocrine Society and had no other disclosures.

European Commission’s proposed criteria for endocrine disruptors trigger multiple concerns
The European Commission has proposed regulatory criteria on endocrine-disrupting chemicals that are too strict and so fall short of protecting the public, as they were intended to do, experts contend.
Endocrine-disrupting chemicals cost Europe billions in health care costs each year (Andrology. 2016 Jul;4[4]:565-72).
Published in June, the criteria would require proof that chemicals harm human endocrine health to define them as endocrine-disrupting chemicals (EDCs) – even if data from animal and in vitro studies already suggest so. “Because health effects can take years or even generations to become apparent, this proposal will not protect public health,” the Endocrine Society noted in a sharp formal critique.
Endocrine-disrupting chemicals mimic or block hormones central to brain development, reproduction, metabolism, growth, and other key physiologic processes. The European Union is the largest single economy to regulate EDCs specifically, which more than 1,300 studies have linked to health problems such as infertility, diabetes, obesity, hormone-related cancers, and neurological disorders, the Endocrine Society concluded in a 2015 scientific statement.
Exposure to even low doses of EDCs such as bisphenol A (BPA) can cause adverse effects. But to fulfill the regulatory definition of the European Commission, EDCs would have to meet an even greater burden of proof than carcinogens – a backward step that “defeats the purpose of the regulations – to shield the public from EDCs that pose a threat to human health,” Rémy Slama, PhD, a member of the Society’s European Union Endocrine-Disrupting Chemicals Task Force, stated in an Endocrine Society news release. Of particular concern is the proposal that EDCs must have a single known “mode of action,” which “represents a fundamental misunderstanding of how endocrine signaling works by connecting different organ systems within the body,” said Dr. Slama, senior investigator at Inserm (the National Institute of Health and Medical Research) in Paris.

Deborah M. Kurrasch, PhD, assistant professor and principal investigator at the University of Calgary (Alta.), agreed. The “mode of action” criterion misses the point that EDCs are “messy” compounds that target various proteins and elicit a range of potential cellular responses based on dose, target tissue, and age, she said in an interview. An EDC may lack a single mode of action, or its mode of action may be far harder to pinpoint than its effects on processes such as reproduction, sleep, mood, and growth, she added. “In my opinion, an endocrine-disrupting chemical is one that disrupts the endocrine system. Despite some internal dialogue, the name for this broad and diverse group of chemicals is, and likely will remain, EDCs because the name so accurately describes their one unifying effect – they all perturb normal endocrine function.”
Ultimately, enacting such tight criteria would tie the hands of regulators with regard to newly recognized and even some well-studied EDCs, “despite evidence that they affect endocrine signaling, because their mode of action is not yet known,” Dr. Kurrasch said.
Experts also noted that the EC criteria would keep regulatory bodies from ranking chemicals based on the strength of evidence that they disrupt endocrine function. Instead, the Endocrine Society advocates for a tiered ranking system based on available data. “As the European Parliament and member countries consider whether to implement the European Commission’s criteria, the Society will continue to advocate for criteria that reflect the state of the science,” the organization emphasized.
Dr. Kurrasch is a member of the Endocrine Society and had no other disclosures.
The European Commission has proposed regulatory criteria on endocrine-disrupting chemicals that are too strict and so fall short of protecting the public, as they were intended to do, experts contend.
Endocrine-disrupting chemicals cost Europe billions in health care costs each year (Andrology. 2016 Jul;4[4]:565-72).
Published in June, the criteria would require proof that chemicals harm human endocrine health to define them as endocrine-disrupting chemicals (EDCs) – even if data from animal and in vitro studies already suggest so. “Because health effects can take years or even generations to become apparent, this proposal will not protect public health,” the Endocrine Society noted in a sharp formal critique.
Endocrine-disrupting chemicals mimic or block hormones central to brain development, reproduction, metabolism, growth, and other key physiologic processes. The European Union is the largest single economy to regulate EDCs specifically, which more than 1,300 studies have linked to health problems such as infertility, diabetes, obesity, hormone-related cancers, and neurological disorders, the Endocrine Society concluded in a 2015 scientific statement.
Exposure to even low doses of EDCs such as bisphenol A (BPA) can cause adverse effects. But to fulfill the regulatory definition of the European Commission, EDCs would have to meet an even greater burden of proof than carcinogens – a backward step that “defeats the purpose of the regulations – to shield the public from EDCs that pose a threat to human health,” Rémy Slama, PhD, a member of the Society’s European Union Endocrine-Disrupting Chemicals Task Force, stated in an Endocrine Society news release. Of particular concern is the proposal that EDCs must have a single known “mode of action,” which “represents a fundamental misunderstanding of how endocrine signaling works by connecting different organ systems within the body,” said Dr. Slama, senior investigator at Inserm (the National Institute of Health and Medical Research) in Paris.
Deborah M. Kurrasch, PhD, assistant professor and principal investigator at the University of Calgary (Alta.), agreed. The “mode of action” criterion misses the point that EDCs are “messy” compounds that target various proteins and elicit a range of potential cellular responses based on dose, target tissue, and age, she said in an interview. An EDC may lack a single mode of action, or its mode of action may be far harder to pinpoint than its effects on processes such as reproduction, sleep, mood, and growth, she added. “In my opinion, an endocrine-disrupting chemical is one that disrupts the endocrine system. Despite some internal dialogue, the name for this broad and diverse group of chemicals is, and likely will remain, EDCs because the name so accurately describes their one unifying effect – they all perturb normal endocrine function.”
Ultimately, enacting such tight criteria would tie the hands of regulators with regard to newly recognized and even some well-studied EDCs, “despite evidence that they affect endocrine signaling, because their mode of action is not yet known,” Dr. Kurrasch said.
Experts also noted that the EC criteria would keep regulatory bodies from ranking chemicals based on the strength of evidence that they disrupt endocrine function. Instead, the Endocrine Society advocates for a tiered ranking system based on available data. “As the European Parliament and member countries consider whether to implement the European Commission’s criteria, the Society will continue to advocate for criteria that reflect the state of the science,” the organization emphasized.
Dr. Kurrasch is a member of the Endocrine Society and had no other disclosures.
The European Commission has proposed regulatory criteria on endocrine-disrupting chemicals that are too strict and so fall short of protecting the public, as they were intended to do, experts contend.
Endocrine-disrupting chemicals cost Europe billions in health care costs each year (Andrology. 2016 Jul;4[4]:565-72).
Published in June, the criteria would require proof that chemicals harm human endocrine health to define them as endocrine-disrupting chemicals (EDCs) – even if data from animal and in vitro studies already suggest so. “Because health effects can take years or even generations to become apparent, this proposal will not protect public health,” the Endocrine Society noted in a sharp formal critique.
Endocrine-disrupting chemicals mimic or block hormones central to brain development, reproduction, metabolism, growth, and other key physiologic processes. The European Union is the largest single economy to regulate EDCs specifically, which more than 1,300 studies have linked to health problems such as infertility, diabetes, obesity, hormone-related cancers, and neurological disorders, the Endocrine Society concluded in a 2015 scientific statement.
Exposure to even low doses of EDCs such as bisphenol A (BPA) can cause adverse effects. But to fulfill the regulatory definition of the European Commission, EDCs would have to meet an even greater burden of proof than carcinogens – a backward step that “defeats the purpose of the regulations – to shield the public from EDCs that pose a threat to human health,” Rémy Slama, PhD, a member of the Society’s European Union Endocrine-Disrupting Chemicals Task Force, stated in an Endocrine Society news release. Of particular concern is the proposal that EDCs must have a single known “mode of action,” which “represents a fundamental misunderstanding of how endocrine signaling works by connecting different organ systems within the body,” said Dr. Slama, senior investigator at Inserm (the National Institute of Health and Medical Research) in Paris.
Deborah M. Kurrasch, PhD, assistant professor and principal investigator at the University of Calgary (Alta.), agreed. The “mode of action” criterion misses the point that EDCs are “messy” compounds that target various proteins and elicit a range of potential cellular responses based on dose, target tissue, and age, she said in an interview. An EDC may lack a single mode of action, or its mode of action may be far harder to pinpoint than its effects on processes such as reproduction, sleep, mood, and growth, she added. “In my opinion, an endocrine-disrupting chemical is one that disrupts the endocrine system. Despite some internal dialogue, the name for this broad and diverse group of chemicals is, and likely will remain, EDCs because the name so accurately describes their one unifying effect – they all perturb normal endocrine function.”
Ultimately, enacting such tight criteria would tie the hands of regulators with regard to newly recognized and even some well-studied EDCs, “despite evidence that they affect endocrine signaling, because their mode of action is not yet known,” Dr. Kurrasch said.
Experts also noted that the EC criteria would keep regulatory bodies from ranking chemicals based on the strength of evidence that they disrupt endocrine function. Instead, the Endocrine Society advocates for a tiered ranking system based on available data. “As the European Parliament and member countries consider whether to implement the European Commission’s criteria, the Society will continue to advocate for criteria that reflect the state of the science,” the organization emphasized.
Dr. Kurrasch is a member of the Endocrine Society and had no other disclosures.

Obstetrics Moonshots: 50 years of discoveries
In 1961 before Congress, and in 1962 at Rice University, Houston, President John F. Kennedy called on America to land a man on the moon and bring him back safely, and to look beyond the moon as well, and pursue an ambitious space exploration program. He challenged the country to think and act boldly, telling Americans in his speech at Rice that “we choose to go the moon in this decade and do the other things, not because they are easy, but because they are hard.”
When Neil Armstrong and Buzz Aldrin set foot on the moon in 1969 – even before President Kennedy’s 10-year deadline had arrived – the country’s primary moonshot was realized. The President had inspired the nation, teams of engineers and others had collectively met daunting technological challenges, and space consequently was more open to us than ever before.
In looking at the field of obstetrics and how far it has come in the past 50 years, since the 1960s, it is similarly astonishing and inspiring to reflect on what extraordinary advances we have made. Who would have thought that the fetus would become such a visible and intimate patient – one who, like the mother, can be interrogated, monitored, and sometimes treated before birth? Who would have thought we would be utilizing genomic studies in a now well-established field of prenatal diagnosis, or that fetal therapy would become a field in and of itself?
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Our specialty has advanced through a series of moonshots that have been inspired and driven by technological advancement and by our continually bold goals and vision for the health and well-being of women and their offspring. We have taken on ambitious challenges, achieved many goals, and embraced advancements in practice only to then set new targets that previously were unimaginable.
Yet just as our country’s space exploration program has faced disappointments, so has our field. It is sobering, for instance, that we have made only incremental improvements in prematurity and infant mortality, and that the age-old maternal problem of preeclampsia is still with us. We also face new challenges, such as the rising rate of maternal obesity and diabetes, which threaten both maternal and fetal health.
President Kennedy spoke of having “examined where we are strong, and where we are not.” Such self-reflection and assessment is a critical underpinning of advancement in fields across all of science, medicine, and health care, and in our specialty, it is a process that has driven ambitious new research efforts to improve fetal and maternal health.
A step back to more in-depth fundamental research on the biomolecular mechanisms of premature labor and diabetes-associated birth defects, for instance, as well as new efforts to approach fetal surgery less invasively, are positioning us to both conquer our disappointments and achieve ambitious new moonshots.
The fetus as our patient
Fifty years ago, in 1966, a seminal paper in the Lancet reported that amniotic fluid cells could be cultured and were suitable for karyotyping (1[7434]:383-5). The tapping and examination of amniotic fluid had been reported on sporadically for many decades, for various clinical purposes, but by and large the fetal compartment was not invaded or directly examined. The fetus was instead the hopeful beneficiary of pregnancy care that focused on the mother. Fetal outcome was clouded in mystery, known only at birth.
With the Lancet report, prenatal detection of chromosomal disorders began to feel achievable, and the 1960s marked the beginning of a journey first through invasive methods of prenatal diagnosis and then through increasingly non-invasive approaches.
In 1970, just several years after the report on chromosome analysis of amniotic-fluid cells, another landmark paper in the New England Journal of Medicine described 162 amniocenteses performed between the 13th and 18th weeks of gestation and the detection of 10 cases of Down syndrome, as well as a few other cases of metabolic and other disorders (282[11]:596-9). This report provided an impetus for broader use of the procedure to detect neural tube defects, Down syndrome, and other abnormalities.
The adoption of amniocentesis for prenatal diagnosis still took some time, however. The procedure was used primarily early on to determine fetal lung maturity, and to predict the ability of the fetus to survive after delivery.
At the time, it was widely praised as an advanced method for evaluating the fetus. Yet, looking back, the early years of the procedure seem primitive. The procedure was done late in pregnancy and it was performed blindly, with the puncture site located either with external palpation of the uterus or with the assistance of static ultrasound. Patients who had scans would usually visit the radiologist, who would mark on the patient’s abdomen a suggested location for needle insertion. Upon the patient’s return, the obstetrician would then insert a needle into that spot, blindly and likely after the fetus had moved.
The development and adoption of real-time ultrasound was a revolutionary achievement. Ultrasound-guided amniocentesis was first described in 1972, 14 years after Ian Donald’s seminal paper introducing obstetric ultrasound was published in the Lancet (1958 Jun 7;1[7032]:1188-95).
As real-time ultrasound made its way into practice, it marked the true realization of a moonshot for obstetrics.
Not only could we simultaneously visualize the needle tip and place the needle safety, but we could see the real-time movement of the fetus, its activity, and the surrounding pockets of fluid. It was like looking up into the sky and seeing the stars for the first time. We could see fetal arrhythmia – not only hear it. With this window into the fetal compartment, we could visualize the fetal bowel migrating into the chest cavity due to a hole (hernia) in the diaphragm. We could visualize other malformations as well.
Chorionic villus sampling (CVS) was technically more difficult and took longer to evolve. For years, through the early 1980s, it was performed only at select centers throughout the country. Patients traveled for the procedure and faced relatively significant risks of complications.
By the end of the 1980s, however, with successive improvements in equipment and technique (including development of a transabdominal approach in addition to transvaginal) the procedure was deemed safe, effective, and acceptable for routine use. Fetoscopy, pioneered by John Hobbins, MD, and his colleagues at Yale University, New Haven, Conn., had also advanced and was being used to diagnose sickle cell anemia, Tay-Sachs disease, congenital fetal skin diseases, and other disorders.
With these advances and with our newfound ability to obtain and analyze a tissue sample earlier in pregnancy – even before a woman shared the news of her pregnancy, in some cases – it seemed that we had achieved our goals and may have even reached past the moon.
Yet there were other moonshots being pursued, including initiatives to make prenatal diagnosis less invasive. The discovery in 1997 of cell-free fetal DNA in maternal plasma and serum, for instance, was a pivotal development that opened the door for noninvasive prenatal testing.
This, and other advances in areas from biochemistry to ultrasound to genomic analysis, led to an array of prenatal diagnostic tools that today enable women and their physicians to assess the genetic, chromosomal, and biophysical aspects of their fetus considerably before the time of viability, and from both the maternal side and directly in the fetal compartment.
First-trimester screening is a current option, and we now have the ability to more selectively perform amniocentesis and CVS based on probability testing, and not solely on maternal age. Ultrasound technology now encompasses color Doppler, 3D and 4D imaging, and other techniques that can be used to assess the placenta, various structures inside the brain, and the heart, as well as blood flow through the ductus venosus.
Parents have called for and welcomed having the option of assessing the fetus in greater detail, and of having either assurance when anomalies are excluded or the opportunity to plan and make decisions when anomalies are detected.
Fetal surgery has been a natural extension of our unprecedented access to the fetus. Our ability to visualize malformations and their evolution led to animal studies that advanced our interest in arresting, correcting, or reversing fetal anomalies through in-utero interventions. In 1981, surgeons performed the first human open fetal surgery to correct congenital hydronephrosis.
Today, we can employ endoscopic laser ablation or laser coagulation to treat severe twin-to-twin syndrome, for instance, as well as other surgical techniques to repair defects such as congenital diaphragmatic hernia, lower urinary tract obstruction, and myelomeningocele. Such advances were unimaginable decades ago.
Old foes and new threats
Despite these advances in diagnosis and care, obstetrics faces unrealized moonshots – lingering challenges that, 50 years ago, we would have predicted would have been solved. Who would have thought that we would still have as high an infant mortality rate as we do, and that we would not be further along in solving the problem of prematurity? Our progress has been only incremental.
Fifty years ago, we lacked an understanding of the basic biology of preterm labor. Prematurity was viewed simply as term labor occurring too early, and many efforts were made over the years to halt the premature labor process through the use of various drugs and other therapeutics, with variable and minimally impactful levels of success.
In the last 25 years, and especially in the last decade, we have made greater efforts to better understand the biology of premature labor – to elucidate how and why it occurs – and we have come to understand that premature labor is very different physiologically from term labor.
Thanks to the work at the Perinatology Research Branch of the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), led by Roberto Romero, MD, attention has consequently shifted toward prediction, identification of women at highest risk, and prevention of the onset of premature labor among those deemed to be at highest risk.
Cervical length in the mid-trimester is now a well-verified predictor of preterm birth, and vaginal progesterone has been shown to benefit women without other known risk factors who are diagnosed with a shortened cervical length.
We have consequently seen the preterm birth rate decline a bit. In 2013, the last year for which we have complete data, the preterm birth rate dropped to 11.4%, down from a high of 12.8% in 2006, according to the Centers for Disease Control and Prevention.
Infant mortality similarly remains unacceptably high, due largely to the high preterm birth rate and to our failure to significantly alter the prevalence of birth defects. In 2010, according to the CDC, the infant mortality rate in the U.S. was 6.1 deaths per 1,000 live births (compared with 6.87 in 2005), and the United States ranked 26th in infant mortality among countries belonging to the Organisation for Economic Co-operation and Development, despite the fact that we spend a significant portion of our gross domestic product (17.5% in 2014) on health care.
Birth defects have taken over as a leading cause of infant mortality after early newborn life, and while we’ve made some advancements in understanding and diagnosing them, the majority of causes of birth defects are still unknown.
On the maternal side of obstetrical care, our progress has similarly been more modest than we have hoped for. Preeclampsia remains a problem, for instance. Despite decades of research into its pathogenesis, our advancements have been only incremental, and the condition – particularly its severe form – continues to be a vexing and high-risk problem.
Added to such age-old foes, moreover, are the growing threats of maternal obesity and diabetes, two closely related and often chronic conditions that affect not only the health of the mother but the in-utero environment and the health of the fetus. Today, more than one-third of all adults in the U.S., and 34% of women aged 20-39 years, are obese, and almost 10% of the U.S. population has diabetes.
Both conditions are on the rise, and obstetrics is confronting an epidemic of “diabesity” that would not necessarily have been predicted 50 years ago. It is particularly alarming given our growing knowledge of how obesity can be programmed in-utero and essentially passed on from generation to generation, of how diabetes can negatively affect perinatal outcomes, and of how the two conditions can have an additive effect on fetal complications.
Achieving new moonshots
Concerted efforts in the past several decades to step back and try to understand the basic biology and physiology of term labor and of premature labor have better positioned our specialty to achieve the moonshot of significantly reducing the incidence of preterm birth.
Establishment in the mid-1980s of the NICHD’s Perinatology Research Branch was a major development in this regard, helping to build and direct research efforts, including basic laboratory science, toward questions about what triggers and propagates labor. There has been notable progress in the past decade, in particular, and our specialty is now on the right path toward development of therapeutic interventions for preventing prematurity.
Additionally, the NICHD’s recently launched Human Placenta Project is building upon the branch-sponsored animal and cell culture model systems of the placenta to allow researchers, for the first time, to monitor human placental health in real time. By more fully understanding the role of the placenta in health and disease, we will be able to better evaluate pregnancy risks and improve pregnancy outcomes.
We also are learning through research in the University of Maryland Birth Defects Research Laboratory, which I am privileged to direct, and at other facilities, that maternal hyperglycemia is a teratogen, creating insults that can trigger a series of developmental fetal defects. By studying the biomolecular mechanisms of hyperglycemia-induced birth defects and developing “molecular maps,” we expect to be able to develop strategies for preventing or mitigating the development of such anomalies. I hope and expect that these future advancements, combined with reductions in prematurity, will significantly impact the infant mortality rate.
Fetal therapy and surgery will also continue to advance, with a much more minimally invasive approach taken in the next 50 years to addressing the fetal condition without putting the mother at increased risk. Just as surgery in other fields has moved from open laparotomy to minimally invasive techniques, I believe we will develop endoscopic or laparoscopic means of correcting the various problems in-utero, such as the repair of neural tube defects and diaphragmatic hernias. It already appears likely that a fetoscopic approach to treating myelomeningocele can reduce maternal morbidity while achieving infant neurological outcomes that are at least as good as outcomes achieved with open fetal surgery.
We’re in a much different position than we were 50 years ago in that we have two patients – the mother and the fetus – with whom we can closely work. We also have a relatively new and urgent obligation to place our attention not only on women’s reproductive health, but on the general gynecologic state. Ob.gyns. often are the only primary care physicians whom women see for routine care, and the quality of our attention to their weight and their diabetes risk factors will have far-reaching consequences, both for them and for their offspring.
As we have since the 1960s, we will continue to set new moonshots and meet new challenges, working with each other and with our patients to evaluate where we are strong and where we must improve. We will persistently harness the power of technology, choosing to do the things that “are hard,” while stepping back as needed to ask and address fundamental questions.
As a result, I can envision the next 50 years as a revolutionary time period for obstetrics – a time in which current problems and disorders are abated or eliminated through a combination of genomics, microbiomics, and other technological advances. Someday in the future, we will look back on some of our many achievements and marvel at how we have transformed the unimaginable to reality.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at [email protected].
Select advances through the years
1960s
1965: Siemens Corp. introduces first real-time ultrasound scanner.
1966: Lancet paper reports that amniotic fluid cells can be cultured and karyotyped.
1970s
1970: New England Journal of Medicine paper describes mid-trimester amniocenteses and detection of Down syndrome cases.
1972: Ultrasound-guided amniocentesis first described.
1973: Fetoscopy introduced.
1980s
1981: First human open fetal surgery to correct congenital hydronephrosis.
Early 1980s: Chorionic villus sampling introduced at select centers.
1985: Color Doppler incorporated into ultrasound.
1990s
1990: Embryoscopy first described.
Mid-1990s: 3D/4D ultrasound begins to assume major role in ob.gyn. imaging.1997: Discovery of cell-free fetal DNA in maternal plasma.
2000s
2003: MOMS (Management of Myelomeningocele Study) was launched.
2010s
2012: The American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine support cell-free DNA screening for women at increased risk of fetal aneuploidy.
2013: Preterm birth rate drops to 11.4%
2014: Diabetes incidence marks a 4-fold increase since 1980.
In 1961 before Congress, and in 1962 at Rice University, Houston, President John F. Kennedy called on America to land a man on the moon and bring him back safely, and to look beyond the moon as well, and pursue an ambitious space exploration program. He challenged the country to think and act boldly, telling Americans in his speech at Rice that “we choose to go the moon in this decade and do the other things, not because they are easy, but because they are hard.”
When Neil Armstrong and Buzz Aldrin set foot on the moon in 1969 – even before President Kennedy’s 10-year deadline had arrived – the country’s primary moonshot was realized. The President had inspired the nation, teams of engineers and others had collectively met daunting technological challenges, and space consequently was more open to us than ever before.
In looking at the field of obstetrics and how far it has come in the past 50 years, since the 1960s, it is similarly astonishing and inspiring to reflect on what extraordinary advances we have made. Who would have thought that the fetus would become such a visible and intimate patient – one who, like the mother, can be interrogated, monitored, and sometimes treated before birth? Who would have thought we would be utilizing genomic studies in a now well-established field of prenatal diagnosis, or that fetal therapy would become a field in and of itself?
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Our specialty has advanced through a series of moonshots that have been inspired and driven by technological advancement and by our continually bold goals and vision for the health and well-being of women and their offspring. We have taken on ambitious challenges, achieved many goals, and embraced advancements in practice only to then set new targets that previously were unimaginable.
Yet just as our country’s space exploration program has faced disappointments, so has our field. It is sobering, for instance, that we have made only incremental improvements in prematurity and infant mortality, and that the age-old maternal problem of preeclampsia is still with us. We also face new challenges, such as the rising rate of maternal obesity and diabetes, which threaten both maternal and fetal health.
President Kennedy spoke of having “examined where we are strong, and where we are not.” Such self-reflection and assessment is a critical underpinning of advancement in fields across all of science, medicine, and health care, and in our specialty, it is a process that has driven ambitious new research efforts to improve fetal and maternal health.
A step back to more in-depth fundamental research on the biomolecular mechanisms of premature labor and diabetes-associated birth defects, for instance, as well as new efforts to approach fetal surgery less invasively, are positioning us to both conquer our disappointments and achieve ambitious new moonshots.
The fetus as our patient
Fifty years ago, in 1966, a seminal paper in the Lancet reported that amniotic fluid cells could be cultured and were suitable for karyotyping (1[7434]:383-5). The tapping and examination of amniotic fluid had been reported on sporadically for many decades, for various clinical purposes, but by and large the fetal compartment was not invaded or directly examined. The fetus was instead the hopeful beneficiary of pregnancy care that focused on the mother. Fetal outcome was clouded in mystery, known only at birth.
With the Lancet report, prenatal detection of chromosomal disorders began to feel achievable, and the 1960s marked the beginning of a journey first through invasive methods of prenatal diagnosis and then through increasingly non-invasive approaches.
In 1970, just several years after the report on chromosome analysis of amniotic-fluid cells, another landmark paper in the New England Journal of Medicine described 162 amniocenteses performed between the 13th and 18th weeks of gestation and the detection of 10 cases of Down syndrome, as well as a few other cases of metabolic and other disorders (282[11]:596-9). This report provided an impetus for broader use of the procedure to detect neural tube defects, Down syndrome, and other abnormalities.
The adoption of amniocentesis for prenatal diagnosis still took some time, however. The procedure was used primarily early on to determine fetal lung maturity, and to predict the ability of the fetus to survive after delivery.
At the time, it was widely praised as an advanced method for evaluating the fetus. Yet, looking back, the early years of the procedure seem primitive. The procedure was done late in pregnancy and it was performed blindly, with the puncture site located either with external palpation of the uterus or with the assistance of static ultrasound. Patients who had scans would usually visit the radiologist, who would mark on the patient’s abdomen a suggested location for needle insertion. Upon the patient’s return, the obstetrician would then insert a needle into that spot, blindly and likely after the fetus had moved.
The development and adoption of real-time ultrasound was a revolutionary achievement. Ultrasound-guided amniocentesis was first described in 1972, 14 years after Ian Donald’s seminal paper introducing obstetric ultrasound was published in the Lancet (1958 Jun 7;1[7032]:1188-95).
As real-time ultrasound made its way into practice, it marked the true realization of a moonshot for obstetrics.
Not only could we simultaneously visualize the needle tip and place the needle safety, but we could see the real-time movement of the fetus, its activity, and the surrounding pockets of fluid. It was like looking up into the sky and seeing the stars for the first time. We could see fetal arrhythmia – not only hear it. With this window into the fetal compartment, we could visualize the fetal bowel migrating into the chest cavity due to a hole (hernia) in the diaphragm. We could visualize other malformations as well.
Chorionic villus sampling (CVS) was technically more difficult and took longer to evolve. For years, through the early 1980s, it was performed only at select centers throughout the country. Patients traveled for the procedure and faced relatively significant risks of complications.
By the end of the 1980s, however, with successive improvements in equipment and technique (including development of a transabdominal approach in addition to transvaginal) the procedure was deemed safe, effective, and acceptable for routine use. Fetoscopy, pioneered by John Hobbins, MD, and his colleagues at Yale University, New Haven, Conn., had also advanced and was being used to diagnose sickle cell anemia, Tay-Sachs disease, congenital fetal skin diseases, and other disorders.
With these advances and with our newfound ability to obtain and analyze a tissue sample earlier in pregnancy – even before a woman shared the news of her pregnancy, in some cases – it seemed that we had achieved our goals and may have even reached past the moon.
Yet there were other moonshots being pursued, including initiatives to make prenatal diagnosis less invasive. The discovery in 1997 of cell-free fetal DNA in maternal plasma and serum, for instance, was a pivotal development that opened the door for noninvasive prenatal testing.
This, and other advances in areas from biochemistry to ultrasound to genomic analysis, led to an array of prenatal diagnostic tools that today enable women and their physicians to assess the genetic, chromosomal, and biophysical aspects of their fetus considerably before the time of viability, and from both the maternal side and directly in the fetal compartment.
First-trimester screening is a current option, and we now have the ability to more selectively perform amniocentesis and CVS based on probability testing, and not solely on maternal age. Ultrasound technology now encompasses color Doppler, 3D and 4D imaging, and other techniques that can be used to assess the placenta, various structures inside the brain, and the heart, as well as blood flow through the ductus venosus.
Parents have called for and welcomed having the option of assessing the fetus in greater detail, and of having either assurance when anomalies are excluded or the opportunity to plan and make decisions when anomalies are detected.
Fetal surgery has been a natural extension of our unprecedented access to the fetus. Our ability to visualize malformations and their evolution led to animal studies that advanced our interest in arresting, correcting, or reversing fetal anomalies through in-utero interventions. In 1981, surgeons performed the first human open fetal surgery to correct congenital hydronephrosis.
Today, we can employ endoscopic laser ablation or laser coagulation to treat severe twin-to-twin syndrome, for instance, as well as other surgical techniques to repair defects such as congenital diaphragmatic hernia, lower urinary tract obstruction, and myelomeningocele. Such advances were unimaginable decades ago.
Old foes and new threats
Despite these advances in diagnosis and care, obstetrics faces unrealized moonshots – lingering challenges that, 50 years ago, we would have predicted would have been solved. Who would have thought that we would still have as high an infant mortality rate as we do, and that we would not be further along in solving the problem of prematurity? Our progress has been only incremental.
Fifty years ago, we lacked an understanding of the basic biology of preterm labor. Prematurity was viewed simply as term labor occurring too early, and many efforts were made over the years to halt the premature labor process through the use of various drugs and other therapeutics, with variable and minimally impactful levels of success.
In the last 25 years, and especially in the last decade, we have made greater efforts to better understand the biology of premature labor – to elucidate how and why it occurs – and we have come to understand that premature labor is very different physiologically from term labor.
Thanks to the work at the Perinatology Research Branch of the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), led by Roberto Romero, MD, attention has consequently shifted toward prediction, identification of women at highest risk, and prevention of the onset of premature labor among those deemed to be at highest risk.
Cervical length in the mid-trimester is now a well-verified predictor of preterm birth, and vaginal progesterone has been shown to benefit women without other known risk factors who are diagnosed with a shortened cervical length.
We have consequently seen the preterm birth rate decline a bit. In 2013, the last year for which we have complete data, the preterm birth rate dropped to 11.4%, down from a high of 12.8% in 2006, according to the Centers for Disease Control and Prevention.
Infant mortality similarly remains unacceptably high, due largely to the high preterm birth rate and to our failure to significantly alter the prevalence of birth defects. In 2010, according to the CDC, the infant mortality rate in the U.S. was 6.1 deaths per 1,000 live births (compared with 6.87 in 2005), and the United States ranked 26th in infant mortality among countries belonging to the Organisation for Economic Co-operation and Development, despite the fact that we spend a significant portion of our gross domestic product (17.5% in 2014) on health care.
Birth defects have taken over as a leading cause of infant mortality after early newborn life, and while we’ve made some advancements in understanding and diagnosing them, the majority of causes of birth defects are still unknown.
On the maternal side of obstetrical care, our progress has similarly been more modest than we have hoped for. Preeclampsia remains a problem, for instance. Despite decades of research into its pathogenesis, our advancements have been only incremental, and the condition – particularly its severe form – continues to be a vexing and high-risk problem.
Added to such age-old foes, moreover, are the growing threats of maternal obesity and diabetes, two closely related and often chronic conditions that affect not only the health of the mother but the in-utero environment and the health of the fetus. Today, more than one-third of all adults in the U.S., and 34% of women aged 20-39 years, are obese, and almost 10% of the U.S. population has diabetes.
Both conditions are on the rise, and obstetrics is confronting an epidemic of “diabesity” that would not necessarily have been predicted 50 years ago. It is particularly alarming given our growing knowledge of how obesity can be programmed in-utero and essentially passed on from generation to generation, of how diabetes can negatively affect perinatal outcomes, and of how the two conditions can have an additive effect on fetal complications.
Achieving new moonshots
Concerted efforts in the past several decades to step back and try to understand the basic biology and physiology of term labor and of premature labor have better positioned our specialty to achieve the moonshot of significantly reducing the incidence of preterm birth.
Establishment in the mid-1980s of the NICHD’s Perinatology Research Branch was a major development in this regard, helping to build and direct research efforts, including basic laboratory science, toward questions about what triggers and propagates labor. There has been notable progress in the past decade, in particular, and our specialty is now on the right path toward development of therapeutic interventions for preventing prematurity.
Additionally, the NICHD’s recently launched Human Placenta Project is building upon the branch-sponsored animal and cell culture model systems of the placenta to allow researchers, for the first time, to monitor human placental health in real time. By more fully understanding the role of the placenta in health and disease, we will be able to better evaluate pregnancy risks and improve pregnancy outcomes.
We also are learning through research in the University of Maryland Birth Defects Research Laboratory, which I am privileged to direct, and at other facilities, that maternal hyperglycemia is a teratogen, creating insults that can trigger a series of developmental fetal defects. By studying the biomolecular mechanisms of hyperglycemia-induced birth defects and developing “molecular maps,” we expect to be able to develop strategies for preventing or mitigating the development of such anomalies. I hope and expect that these future advancements, combined with reductions in prematurity, will significantly impact the infant mortality rate.
Fetal therapy and surgery will also continue to advance, with a much more minimally invasive approach taken in the next 50 years to addressing the fetal condition without putting the mother at increased risk. Just as surgery in other fields has moved from open laparotomy to minimally invasive techniques, I believe we will develop endoscopic or laparoscopic means of correcting the various problems in-utero, such as the repair of neural tube defects and diaphragmatic hernias. It already appears likely that a fetoscopic approach to treating myelomeningocele can reduce maternal morbidity while achieving infant neurological outcomes that are at least as good as outcomes achieved with open fetal surgery.
We’re in a much different position than we were 50 years ago in that we have two patients – the mother and the fetus – with whom we can closely work. We also have a relatively new and urgent obligation to place our attention not only on women’s reproductive health, but on the general gynecologic state. Ob.gyns. often are the only primary care physicians whom women see for routine care, and the quality of our attention to their weight and their diabetes risk factors will have far-reaching consequences, both for them and for their offspring.
As we have since the 1960s, we will continue to set new moonshots and meet new challenges, working with each other and with our patients to evaluate where we are strong and where we must improve. We will persistently harness the power of technology, choosing to do the things that “are hard,” while stepping back as needed to ask and address fundamental questions.
As a result, I can envision the next 50 years as a revolutionary time period for obstetrics – a time in which current problems and disorders are abated or eliminated through a combination of genomics, microbiomics, and other technological advances. Someday in the future, we will look back on some of our many achievements and marvel at how we have transformed the unimaginable to reality.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at [email protected].
Select advances through the years
1960s
1965: Siemens Corp. introduces first real-time ultrasound scanner.
1966: Lancet paper reports that amniotic fluid cells can be cultured and karyotyped.
1970s
1970: New England Journal of Medicine paper describes mid-trimester amniocenteses and detection of Down syndrome cases.
1972: Ultrasound-guided amniocentesis first described.
1973: Fetoscopy introduced.
1980s
1981: First human open fetal surgery to correct congenital hydronephrosis.
Early 1980s: Chorionic villus sampling introduced at select centers.
1985: Color Doppler incorporated into ultrasound.
1990s
1990: Embryoscopy first described.
Mid-1990s: 3D/4D ultrasound begins to assume major role in ob.gyn. imaging.1997: Discovery of cell-free fetal DNA in maternal plasma.
2000s
2003: MOMS (Management of Myelomeningocele Study) was launched.
2010s
2012: The American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine support cell-free DNA screening for women at increased risk of fetal aneuploidy.
2013: Preterm birth rate drops to 11.4%
2014: Diabetes incidence marks a 4-fold increase since 1980.
In 1961 before Congress, and in 1962 at Rice University, Houston, President John F. Kennedy called on America to land a man on the moon and bring him back safely, and to look beyond the moon as well, and pursue an ambitious space exploration program. He challenged the country to think and act boldly, telling Americans in his speech at Rice that “we choose to go the moon in this decade and do the other things, not because they are easy, but because they are hard.”
When Neil Armstrong and Buzz Aldrin set foot on the moon in 1969 – even before President Kennedy’s 10-year deadline had arrived – the country’s primary moonshot was realized. The President had inspired the nation, teams of engineers and others had collectively met daunting technological challenges, and space consequently was more open to us than ever before.
In looking at the field of obstetrics and how far it has come in the past 50 years, since the 1960s, it is similarly astonishing and inspiring to reflect on what extraordinary advances we have made. Who would have thought that the fetus would become such a visible and intimate patient – one who, like the mother, can be interrogated, monitored, and sometimes treated before birth? Who would have thought we would be utilizing genomic studies in a now well-established field of prenatal diagnosis, or that fetal therapy would become a field in and of itself?
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Our specialty has advanced through a series of moonshots that have been inspired and driven by technological advancement and by our continually bold goals and vision for the health and well-being of women and their offspring. We have taken on ambitious challenges, achieved many goals, and embraced advancements in practice only to then set new targets that previously were unimaginable.
Yet just as our country’s space exploration program has faced disappointments, so has our field. It is sobering, for instance, that we have made only incremental improvements in prematurity and infant mortality, and that the age-old maternal problem of preeclampsia is still with us. We also face new challenges, such as the rising rate of maternal obesity and diabetes, which threaten both maternal and fetal health.
President Kennedy spoke of having “examined where we are strong, and where we are not.” Such self-reflection and assessment is a critical underpinning of advancement in fields across all of science, medicine, and health care, and in our specialty, it is a process that has driven ambitious new research efforts to improve fetal and maternal health.
A step back to more in-depth fundamental research on the biomolecular mechanisms of premature labor and diabetes-associated birth defects, for instance, as well as new efforts to approach fetal surgery less invasively, are positioning us to both conquer our disappointments and achieve ambitious new moonshots.
The fetus as our patient
Fifty years ago, in 1966, a seminal paper in the Lancet reported that amniotic fluid cells could be cultured and were suitable for karyotyping (1[7434]:383-5). The tapping and examination of amniotic fluid had been reported on sporadically for many decades, for various clinical purposes, but by and large the fetal compartment was not invaded or directly examined. The fetus was instead the hopeful beneficiary of pregnancy care that focused on the mother. Fetal outcome was clouded in mystery, known only at birth.
With the Lancet report, prenatal detection of chromosomal disorders began to feel achievable, and the 1960s marked the beginning of a journey first through invasive methods of prenatal diagnosis and then through increasingly non-invasive approaches.
In 1970, just several years after the report on chromosome analysis of amniotic-fluid cells, another landmark paper in the New England Journal of Medicine described 162 amniocenteses performed between the 13th and 18th weeks of gestation and the detection of 10 cases of Down syndrome, as well as a few other cases of metabolic and other disorders (282[11]:596-9). This report provided an impetus for broader use of the procedure to detect neural tube defects, Down syndrome, and other abnormalities.
The adoption of amniocentesis for prenatal diagnosis still took some time, however. The procedure was used primarily early on to determine fetal lung maturity, and to predict the ability of the fetus to survive after delivery.
At the time, it was widely praised as an advanced method for evaluating the fetus. Yet, looking back, the early years of the procedure seem primitive. The procedure was done late in pregnancy and it was performed blindly, with the puncture site located either with external palpation of the uterus or with the assistance of static ultrasound. Patients who had scans would usually visit the radiologist, who would mark on the patient’s abdomen a suggested location for needle insertion. Upon the patient’s return, the obstetrician would then insert a needle into that spot, blindly and likely after the fetus had moved.
The development and adoption of real-time ultrasound was a revolutionary achievement. Ultrasound-guided amniocentesis was first described in 1972, 14 years after Ian Donald’s seminal paper introducing obstetric ultrasound was published in the Lancet (1958 Jun 7;1[7032]:1188-95).
As real-time ultrasound made its way into practice, it marked the true realization of a moonshot for obstetrics.
Not only could we simultaneously visualize the needle tip and place the needle safety, but we could see the real-time movement of the fetus, its activity, and the surrounding pockets of fluid. It was like looking up into the sky and seeing the stars for the first time. We could see fetal arrhythmia – not only hear it. With this window into the fetal compartment, we could visualize the fetal bowel migrating into the chest cavity due to a hole (hernia) in the diaphragm. We could visualize other malformations as well.
Chorionic villus sampling (CVS) was technically more difficult and took longer to evolve. For years, through the early 1980s, it was performed only at select centers throughout the country. Patients traveled for the procedure and faced relatively significant risks of complications.
By the end of the 1980s, however, with successive improvements in equipment and technique (including development of a transabdominal approach in addition to transvaginal) the procedure was deemed safe, effective, and acceptable for routine use. Fetoscopy, pioneered by John Hobbins, MD, and his colleagues at Yale University, New Haven, Conn., had also advanced and was being used to diagnose sickle cell anemia, Tay-Sachs disease, congenital fetal skin diseases, and other disorders.
With these advances and with our newfound ability to obtain and analyze a tissue sample earlier in pregnancy – even before a woman shared the news of her pregnancy, in some cases – it seemed that we had achieved our goals and may have even reached past the moon.
Yet there were other moonshots being pursued, including initiatives to make prenatal diagnosis less invasive. The discovery in 1997 of cell-free fetal DNA in maternal plasma and serum, for instance, was a pivotal development that opened the door for noninvasive prenatal testing.
This, and other advances in areas from biochemistry to ultrasound to genomic analysis, led to an array of prenatal diagnostic tools that today enable women and their physicians to assess the genetic, chromosomal, and biophysical aspects of their fetus considerably before the time of viability, and from both the maternal side and directly in the fetal compartment.
First-trimester screening is a current option, and we now have the ability to more selectively perform amniocentesis and CVS based on probability testing, and not solely on maternal age. Ultrasound technology now encompasses color Doppler, 3D and 4D imaging, and other techniques that can be used to assess the placenta, various structures inside the brain, and the heart, as well as blood flow through the ductus venosus.
Parents have called for and welcomed having the option of assessing the fetus in greater detail, and of having either assurance when anomalies are excluded or the opportunity to plan and make decisions when anomalies are detected.
Fetal surgery has been a natural extension of our unprecedented access to the fetus. Our ability to visualize malformations and their evolution led to animal studies that advanced our interest in arresting, correcting, or reversing fetal anomalies through in-utero interventions. In 1981, surgeons performed the first human open fetal surgery to correct congenital hydronephrosis.
Today, we can employ endoscopic laser ablation or laser coagulation to treat severe twin-to-twin syndrome, for instance, as well as other surgical techniques to repair defects such as congenital diaphragmatic hernia, lower urinary tract obstruction, and myelomeningocele. Such advances were unimaginable decades ago.
Old foes and new threats
Despite these advances in diagnosis and care, obstetrics faces unrealized moonshots – lingering challenges that, 50 years ago, we would have predicted would have been solved. Who would have thought that we would still have as high an infant mortality rate as we do, and that we would not be further along in solving the problem of prematurity? Our progress has been only incremental.
Fifty years ago, we lacked an understanding of the basic biology of preterm labor. Prematurity was viewed simply as term labor occurring too early, and many efforts were made over the years to halt the premature labor process through the use of various drugs and other therapeutics, with variable and minimally impactful levels of success.
In the last 25 years, and especially in the last decade, we have made greater efforts to better understand the biology of premature labor – to elucidate how and why it occurs – and we have come to understand that premature labor is very different physiologically from term labor.
Thanks to the work at the Perinatology Research Branch of the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), led by Roberto Romero, MD, attention has consequently shifted toward prediction, identification of women at highest risk, and prevention of the onset of premature labor among those deemed to be at highest risk.
Cervical length in the mid-trimester is now a well-verified predictor of preterm birth, and vaginal progesterone has been shown to benefit women without other known risk factors who are diagnosed with a shortened cervical length.
We have consequently seen the preterm birth rate decline a bit. In 2013, the last year for which we have complete data, the preterm birth rate dropped to 11.4%, down from a high of 12.8% in 2006, according to the Centers for Disease Control and Prevention.
Infant mortality similarly remains unacceptably high, due largely to the high preterm birth rate and to our failure to significantly alter the prevalence of birth defects. In 2010, according to the CDC, the infant mortality rate in the U.S. was 6.1 deaths per 1,000 live births (compared with 6.87 in 2005), and the United States ranked 26th in infant mortality among countries belonging to the Organisation for Economic Co-operation and Development, despite the fact that we spend a significant portion of our gross domestic product (17.5% in 2014) on health care.
Birth defects have taken over as a leading cause of infant mortality after early newborn life, and while we’ve made some advancements in understanding and diagnosing them, the majority of causes of birth defects are still unknown.
On the maternal side of obstetrical care, our progress has similarly been more modest than we have hoped for. Preeclampsia remains a problem, for instance. Despite decades of research into its pathogenesis, our advancements have been only incremental, and the condition – particularly its severe form – continues to be a vexing and high-risk problem.
Added to such age-old foes, moreover, are the growing threats of maternal obesity and diabetes, two closely related and often chronic conditions that affect not only the health of the mother but the in-utero environment and the health of the fetus. Today, more than one-third of all adults in the U.S., and 34% of women aged 20-39 years, are obese, and almost 10% of the U.S. population has diabetes.
Both conditions are on the rise, and obstetrics is confronting an epidemic of “diabesity” that would not necessarily have been predicted 50 years ago. It is particularly alarming given our growing knowledge of how obesity can be programmed in-utero and essentially passed on from generation to generation, of how diabetes can negatively affect perinatal outcomes, and of how the two conditions can have an additive effect on fetal complications.
Achieving new moonshots
Concerted efforts in the past several decades to step back and try to understand the basic biology and physiology of term labor and of premature labor have better positioned our specialty to achieve the moonshot of significantly reducing the incidence of preterm birth.
Establishment in the mid-1980s of the NICHD’s Perinatology Research Branch was a major development in this regard, helping to build and direct research efforts, including basic laboratory science, toward questions about what triggers and propagates labor. There has been notable progress in the past decade, in particular, and our specialty is now on the right path toward development of therapeutic interventions for preventing prematurity.
Additionally, the NICHD’s recently launched Human Placenta Project is building upon the branch-sponsored animal and cell culture model systems of the placenta to allow researchers, for the first time, to monitor human placental health in real time. By more fully understanding the role of the placenta in health and disease, we will be able to better evaluate pregnancy risks and improve pregnancy outcomes.
We also are learning through research in the University of Maryland Birth Defects Research Laboratory, which I am privileged to direct, and at other facilities, that maternal hyperglycemia is a teratogen, creating insults that can trigger a series of developmental fetal defects. By studying the biomolecular mechanisms of hyperglycemia-induced birth defects and developing “molecular maps,” we expect to be able to develop strategies for preventing or mitigating the development of such anomalies. I hope and expect that these future advancements, combined with reductions in prematurity, will significantly impact the infant mortality rate.
Fetal therapy and surgery will also continue to advance, with a much more minimally invasive approach taken in the next 50 years to addressing the fetal condition without putting the mother at increased risk. Just as surgery in other fields has moved from open laparotomy to minimally invasive techniques, I believe we will develop endoscopic or laparoscopic means of correcting the various problems in-utero, such as the repair of neural tube defects and diaphragmatic hernias. It already appears likely that a fetoscopic approach to treating myelomeningocele can reduce maternal morbidity while achieving infant neurological outcomes that are at least as good as outcomes achieved with open fetal surgery.
We’re in a much different position than we were 50 years ago in that we have two patients – the mother and the fetus – with whom we can closely work. We also have a relatively new and urgent obligation to place our attention not only on women’s reproductive health, but on the general gynecologic state. Ob.gyns. often are the only primary care physicians whom women see for routine care, and the quality of our attention to their weight and their diabetes risk factors will have far-reaching consequences, both for them and for their offspring.
As we have since the 1960s, we will continue to set new moonshots and meet new challenges, working with each other and with our patients to evaluate where we are strong and where we must improve. We will persistently harness the power of technology, choosing to do the things that “are hard,” while stepping back as needed to ask and address fundamental questions.
As a result, I can envision the next 50 years as a revolutionary time period for obstetrics – a time in which current problems and disorders are abated or eliminated through a combination of genomics, microbiomics, and other technological advances. Someday in the future, we will look back on some of our many achievements and marvel at how we have transformed the unimaginable to reality.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at [email protected].
Select advances through the years
1960s
1965: Siemens Corp. introduces first real-time ultrasound scanner.
1966: Lancet paper reports that amniotic fluid cells can be cultured and karyotyped.
1970s
1970: New England Journal of Medicine paper describes mid-trimester amniocenteses and detection of Down syndrome cases.
1972: Ultrasound-guided amniocentesis first described.
1973: Fetoscopy introduced.
1980s
1981: First human open fetal surgery to correct congenital hydronephrosis.
Early 1980s: Chorionic villus sampling introduced at select centers.
1985: Color Doppler incorporated into ultrasound.
1990s
1990: Embryoscopy first described.
Mid-1990s: 3D/4D ultrasound begins to assume major role in ob.gyn. imaging.1997: Discovery of cell-free fetal DNA in maternal plasma.
2000s
2003: MOMS (Management of Myelomeningocele Study) was launched.
2010s
2012: The American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine support cell-free DNA screening for women at increased risk of fetal aneuploidy.
2013: Preterm birth rate drops to 11.4%
2014: Diabetes incidence marks a 4-fold increase since 1980.
Study aims to better understand readmissions in pediatric surgery
SAN DIEGO – Readmission rates and the underlying reasons for them vary between medical specialties following surgery in children, a study of national data suggests.
“Hospital readmission is a very hot topic, particularly in light of the Affordable Care Act,” Afif N. Kulaylat, MD, said at the American College of Surgeons/National Surgical Quality Improvement Program National Conference. “Beyond economic costs there are very tangible costs to patients that we must consider. Readmissions have been associated with significant morbidity for patients. They often herald or implicate a postoperative complication. There are also indirect costs to patients and families such as time off from school or work.”

Dr. Kulaylat, of the division of pediatric surgery at Penn State Children’s Hospital, Hershey, Penn., presented findings from a retrospective analysis of NSQIP Pediatric (NSQIP-P), an ongoing collaboration between the ACS and the American Pediatric Surgical Association to improve the care of young patients. The researchers evaluated NSQIP-P data from 2013 and 2014 and focused on unplanned readmission within 30 days, including reasons for readmission based on NSQIP-P readmission categories and ICD-9 readmission codes as categorized by the AHRQ Clinical Classification Software. Multivariate logistic regression was used to evaluate factors associated with unplanned readmission.
Dr. Kulaylat reported results from a cohort of 129,849 patients cared for by 64 NSQIP-P participating hospitals. Among these, the all-cause readmission rate was 4.7%. After excluding patients with planned readmissions, the unplanned readmission rate was found to be 3.9%. From this cohort, 28% required reoperation within 30 days, and the median time from discharge to unplanned readmission was 8 days, with an interquartile range between 3 and 14 days.
Among the procedures captured in NSQIP-P, neurosurgery accounted for the highest readmission rate (10.8%), followed by general/thoracic surgery (5.2%), urology (2.6%), ENT (2%), orthopedic (1.9%), and plastic and reconstructive surgery (1.3%). The most common reason for readmission was surgical site infection at 23%, followed by GI complications such as ileus, obstruction, and constipation (17%); pulmonary-related complications (9%); device-related complications including shunt malfunction (8%); neurologic (7%); pain (6%); other medical diseases (6%); sepsis (5%); electrolytes/dehydration (5%); and urinary tract infection (UTI, 3%). It is estimated that at least two-thirds of unplanned readmissions (63%) were directly related to surgery. “These reasons for readmission and their frequency closely parallel what is seen in adults, with the exception of bleeding complications, which were rare in children compared to adults,” Dr. Kulaylat said.
The top five CPT codes associated with readmissions were laparoscopic appendectomy, laparoscopic gastrostomy tube placement, and three additional codes related to placement and replacement/revision of ventricular shunts/catheters.
Reasons for readmission varied among specialties. For example, among general and thoracic surgery, surgical-site infections (SSI) and GI-related issues dominated, while in neurosurgery SSI and device issues dominated. In urology, UTIs were the most frequent, while ENT had a greater proportion of pulmonary complications. Certain patient variables were also associated with an increased risk of hospital readmission, including comorbidities related to GI, CNS, renal, and immunosuppression and nutrition (P less than .001 for all). The strongest association was the occurrence of a postoperative complication, namely a post-discharge complication.
“The granularity of NSQIP-P can continue to be refined to help predict who is likely to get readmitted or if specific follow-up strategies might identify those headed to readmission,” remarked Robert E. Cilley, MD, a senior author and surgeon-in-chief at Penn State Children’s Hospital. Dr. Kulaylat acknowledged certain limitations of the study, including its retrospective design, the potential for data entry/data interpretation error, and that the researchers were unable to adjust for clustering at the hospital level. Directions of future research include a plan to study readmissions and predictive factors at the procedural level, establish risk-adjusted specialty/procedural-specific benchmarks for readmission rates, and refine the accuracy and reliability of the readmission data. “With these NSQIP-P data there is substantial opportunity for quality improvement as we strive to improve the care of children everywhere,” Dr. Kulaylat said. He reported having no relevant disclosures.
SAN DIEGO – Readmission rates and the underlying reasons for them vary between medical specialties following surgery in children, a study of national data suggests.
“Hospital readmission is a very hot topic, particularly in light of the Affordable Care Act,” Afif N. Kulaylat, MD, said at the American College of Surgeons/National Surgical Quality Improvement Program National Conference. “Beyond economic costs there are very tangible costs to patients that we must consider. Readmissions have been associated with significant morbidity for patients. They often herald or implicate a postoperative complication. There are also indirect costs to patients and families such as time off from school or work.”
Dr. Kulaylat, of the division of pediatric surgery at Penn State Children’s Hospital, Hershey, Penn., presented findings from a retrospective analysis of NSQIP Pediatric (NSQIP-P), an ongoing collaboration between the ACS and the American Pediatric Surgical Association to improve the care of young patients. The researchers evaluated NSQIP-P data from 2013 and 2014 and focused on unplanned readmission within 30 days, including reasons for readmission based on NSQIP-P readmission categories and ICD-9 readmission codes as categorized by the AHRQ Clinical Classification Software. Multivariate logistic regression was used to evaluate factors associated with unplanned readmission.
Dr. Kulaylat reported results from a cohort of 129,849 patients cared for by 64 NSQIP-P participating hospitals. Among these, the all-cause readmission rate was 4.7%. After excluding patients with planned readmissions, the unplanned readmission rate was found to be 3.9%. From this cohort, 28% required reoperation within 30 days, and the median time from discharge to unplanned readmission was 8 days, with an interquartile range between 3 and 14 days.
Among the procedures captured in NSQIP-P, neurosurgery accounted for the highest readmission rate (10.8%), followed by general/thoracic surgery (5.2%), urology (2.6%), ENT (2%), orthopedic (1.9%), and plastic and reconstructive surgery (1.3%). The most common reason for readmission was surgical site infection at 23%, followed by GI complications such as ileus, obstruction, and constipation (17%); pulmonary-related complications (9%); device-related complications including shunt malfunction (8%); neurologic (7%); pain (6%); other medical diseases (6%); sepsis (5%); electrolytes/dehydration (5%); and urinary tract infection (UTI, 3%). It is estimated that at least two-thirds of unplanned readmissions (63%) were directly related to surgery. “These reasons for readmission and their frequency closely parallel what is seen in adults, with the exception of bleeding complications, which were rare in children compared to adults,” Dr. Kulaylat said.
The top five CPT codes associated with readmissions were laparoscopic appendectomy, laparoscopic gastrostomy tube placement, and three additional codes related to placement and replacement/revision of ventricular shunts/catheters.
Reasons for readmission varied among specialties. For example, among general and thoracic surgery, surgical-site infections (SSI) and GI-related issues dominated, while in neurosurgery SSI and device issues dominated. In urology, UTIs were the most frequent, while ENT had a greater proportion of pulmonary complications. Certain patient variables were also associated with an increased risk of hospital readmission, including comorbidities related to GI, CNS, renal, and immunosuppression and nutrition (P less than .001 for all). The strongest association was the occurrence of a postoperative complication, namely a post-discharge complication.
“The granularity of NSQIP-P can continue to be refined to help predict who is likely to get readmitted or if specific follow-up strategies might identify those headed to readmission,” remarked Robert E. Cilley, MD, a senior author and surgeon-in-chief at Penn State Children’s Hospital. Dr. Kulaylat acknowledged certain limitations of the study, including its retrospective design, the potential for data entry/data interpretation error, and that the researchers were unable to adjust for clustering at the hospital level. Directions of future research include a plan to study readmissions and predictive factors at the procedural level, establish risk-adjusted specialty/procedural-specific benchmarks for readmission rates, and refine the accuracy and reliability of the readmission data. “With these NSQIP-P data there is substantial opportunity for quality improvement as we strive to improve the care of children everywhere,” Dr. Kulaylat said. He reported having no relevant disclosures.
SAN DIEGO – Readmission rates and the underlying reasons for them vary between medical specialties following surgery in children, a study of national data suggests.
“Hospital readmission is a very hot topic, particularly in light of the Affordable Care Act,” Afif N. Kulaylat, MD, said at the American College of Surgeons/National Surgical Quality Improvement Program National Conference. “Beyond economic costs there are very tangible costs to patients that we must consider. Readmissions have been associated with significant morbidity for patients. They often herald or implicate a postoperative complication. There are also indirect costs to patients and families such as time off from school or work.”
Dr. Kulaylat, of the division of pediatric surgery at Penn State Children’s Hospital, Hershey, Penn., presented findings from a retrospective analysis of NSQIP Pediatric (NSQIP-P), an ongoing collaboration between the ACS and the American Pediatric Surgical Association to improve the care of young patients. The researchers evaluated NSQIP-P data from 2013 and 2014 and focused on unplanned readmission within 30 days, including reasons for readmission based on NSQIP-P readmission categories and ICD-9 readmission codes as categorized by the AHRQ Clinical Classification Software. Multivariate logistic regression was used to evaluate factors associated with unplanned readmission.
Dr. Kulaylat reported results from a cohort of 129,849 patients cared for by 64 NSQIP-P participating hospitals. Among these, the all-cause readmission rate was 4.7%. After excluding patients with planned readmissions, the unplanned readmission rate was found to be 3.9%. From this cohort, 28% required reoperation within 30 days, and the median time from discharge to unplanned readmission was 8 days, with an interquartile range between 3 and 14 days.
Among the procedures captured in NSQIP-P, neurosurgery accounted for the highest readmission rate (10.8%), followed by general/thoracic surgery (5.2%), urology (2.6%), ENT (2%), orthopedic (1.9%), and plastic and reconstructive surgery (1.3%). The most common reason for readmission was surgical site infection at 23%, followed by GI complications such as ileus, obstruction, and constipation (17%); pulmonary-related complications (9%); device-related complications including shunt malfunction (8%); neurologic (7%); pain (6%); other medical diseases (6%); sepsis (5%); electrolytes/dehydration (5%); and urinary tract infection (UTI, 3%). It is estimated that at least two-thirds of unplanned readmissions (63%) were directly related to surgery. “These reasons for readmission and their frequency closely parallel what is seen in adults, with the exception of bleeding complications, which were rare in children compared to adults,” Dr. Kulaylat said.
The top five CPT codes associated with readmissions were laparoscopic appendectomy, laparoscopic gastrostomy tube placement, and three additional codes related to placement and replacement/revision of ventricular shunts/catheters.
Reasons for readmission varied among specialties. For example, among general and thoracic surgery, surgical-site infections (SSI) and GI-related issues dominated, while in neurosurgery SSI and device issues dominated. In urology, UTIs were the most frequent, while ENT had a greater proportion of pulmonary complications. Certain patient variables were also associated with an increased risk of hospital readmission, including comorbidities related to GI, CNS, renal, and immunosuppression and nutrition (P less than .001 for all). The strongest association was the occurrence of a postoperative complication, namely a post-discharge complication.
“The granularity of NSQIP-P can continue to be refined to help predict who is likely to get readmitted or if specific follow-up strategies might identify those headed to readmission,” remarked Robert E. Cilley, MD, a senior author and surgeon-in-chief at Penn State Children’s Hospital. Dr. Kulaylat acknowledged certain limitations of the study, including its retrospective design, the potential for data entry/data interpretation error, and that the researchers were unable to adjust for clustering at the hospital level. Directions of future research include a plan to study readmissions and predictive factors at the procedural level, establish risk-adjusted specialty/procedural-specific benchmarks for readmission rates, and refine the accuracy and reliability of the readmission data. “With these NSQIP-P data there is substantial opportunity for quality improvement as we strive to improve the care of children everywhere,” Dr. Kulaylat said. He reported having no relevant disclosures.
AT THE ACS NSQIP NATIONAL CONFERENCE
Key clinical point: Readmission rates following pediatric surgery vary between medical specialties.
Major finding: Among the procedures captured in ACS NSQIP Pediatric (NSQIP-P), neurosurgery accounted for the highest readmission rate (10.8%), followed by general/thoracic surgery (5.2%), urology (2.6%), ENT (2%), orthopedic (1.9%), and plastic and reconstructive surgery (1.3%).
Data source: An analysis of 129,849 pediatric patients cared for by 64 NSQIP-P participating hospitals.
Disclosures: Dr. Kulaylat reported having no financial disclosures.

How Should a Hospitalized Patient with Newly Diagnosed Cirrhosis Be Evaluated and Managed?
The Case
A 50-year-old man with no known medical history presents with two months of increasing abdominal distension. Exam is notable for scleral icterus, telangiectasias on the upper chest, abdominal distention with a positive fluid wave, and bilateral pitting lower-extremity edema. An abdominal ultrasound shows large ascites and a nodular liver consistent with cirrhosis. How should this patient with newly diagnosed cirrhosis be evaluated and managed?
Background
Cirrhosis is a leading cause of death among people ages 25–64 and associated with a mortality rate of 11.5 per 100,000 people.1 In 2010, 101,000 people were discharged from the hospital with chronic liver disease and cirrhosis as the first-listed diagnosis.2 Given the myriad etiologies and the asymptomatic nature of many of these conditions, hospitalists frequently encounter patients presenting with advanced disease.
Evaluation

The gold standard for diagnosis is liver biopsy, although this is now usually reserved for atypical cases or where the etiology of cirrhosis is unclear. Alcohol and viral hepatitis (B and C) are the most common causes of chronic liver disease, with nonalcoholic steatohepatitis (NASH) increasing in prevalence. Other less common etiologies and characteristic test findings are listed in Figure 2.

Recently, the Centers for Disease Control and Prevention (CDC) recommended that adults born between 1945 and 1965 receive one-time testing for hepatitis C virus (HCV) infection, regardless of other risk factors, given the higher prevalence in this birth cohort and the introduction of newer oral treatments that achieve sustained virologic response.3
Management
The three classic complications of cirrhosis that will typically prompt inpatient admission are volume overload/ascites, gastrointestinal variceal bleeding, and hepatic encephalopathy.
Volume overload/ascites. Ascites is the most common major complication of cirrhosis, with roughly 50% of patients with asymptomatic cirrhosis developing ascites within 10 years.4 Ascites development portends a poor prognosis, with a mortality of 15% within one year and 44% within five years of diagnosis.4 Patients presenting with new-onset ascites should have a diagnostic paracentesis performed to determine the etiology and evaluate for infection.
Ascitic fluid should be sent for an albumin level and a cell count with differential. A serum-ascites albumin gradient (SAAG) of greater than or equal to 1.1 g/dL is consistent with portal hypertension and cirrhosis, while values less than 1.1 g/dL suggest a non-cirrhotic cause, such as infection or malignancy. Due to the high prevalence of spontaneous bacterial peritonitis (SBP) in hospitalized patients, fluid should also be immediately inoculated in aerobic and anaerobic culture bottles at the bedside, as this has been shown to improve the yield compared to inoculation of culture bottles in the laboratory. Other testing (such as cytology for the evaluation of malignancy) should only be performed if there is significant concern for a particular disease since the vast majority of cases are secondary to uncomplicated cirrhosis.4
In patients with a large amount of ascites and related symptoms (eg, abdominal pain, shortness of breath), therapeutic paracentesis should be performed. Although there is controversy over the need for routine albumin administration, guidelines currently recommend the infusion of 6–8 g of albumin per liter of ascites removed for paracentesis volumes of greater than 4–5 liters.4
No data support the routine administration of fresh frozen plasma (FFP) or platelets prior to paracentesis. Although significant complications of paracentesis (including bowel perforation and hemorrhage) may occur, these are exceedingly rare. Ultrasonography can be used to decrease risks and identify suitable pockets of fluid to tap, even when fluid is not obvious on physical exam alone.5
For patients with significant edema or ascites that is due to portal hypertension (SAAG >1.1 g/dL), the first-line therapy is sodium restriction to less than 2,000 mg/day. Consulting a nutritionist may be beneficial for patient education.
For patients with significant natriuresis (>78 mmol daily urine sodium excretion), dietary restriction alone can manage fluid retention. Most patients (85%–90%), however, require diuretics to increase sodium output. Single-agent spironolactone is more efficacious than single-agent furosemide, but diuresis is improved when both agents are used.4 A dosing regimen of once-daily 40 mg furosemide and 100 mg spironolactone is the recommended starting regimen to promote diuresis while maintaining normokalemia. Due to the long half-life of spironolactone, the dose can be increased every three to five days if needed for diuresis.4
Gastroesophageal variceal bleeding. Approximately 50% of patients with cirrhosis have gastroesophageal varices as a consequence of portal hypertension, with prevalence increasing in those with more severe disease.6 As many patients with cirrhosis have advanced disease at the time of diagnosis, it is recommended that patients be referred for endoscopic screening when diagnosed.6 Nonselective beta-blockers decrease the risk of bleeding in patients with known varices but should not be initiated empirically in all patients with cirrhosis given significant side effects, including worsening of ascites.
There is increasing evidence that there is a “window” period for beta-blocker use in cirrhosis with the window opening after the diagnosis of varices and the window closing at advanced stages of disease (marked by an episode of spontaneous bacterial peritonitis, refractory ascites, or hepatorenal syndrome, for example).7
Hepatic encephalopathy. Hepatic encephalopathy (HE) is another complication of portal hypertension and is seen in 10%–14% of patients at the time of cirrhosis diagnosis.8 Overt HE is estimated to occur in 30%–40% of patients with cirrhosis at some point during their disease course, and more subtle forms (minimal or covert HE) are seen in up to 80%.8 HE can cause numerous neurologic and psychiatric issues including personality changes, poor memory, sleep-wake disturbances, and alterations in consciousness.
In patients with an episode of encephalopathy, precipitating factors should be evaluated. Typical precipitants include infections, bleeding, electrolyte disorders, and constipation. Ammonia levels are frequently drawn as part of the evaluation of hepatic encephalopathy, but elevated levels do not significantly change diagnostic probabilities or add prognostic information.8 A low ammonia level, on the other hand, may be useful in lowering the probability of hepatic encephalopathy in a patient with altered mental status of unknown etiology.8
Routine primary prophylaxis of HE in all patients with cirrhosis is not currently recommended. Treatment is only recommended in patients with overt HE, with secondary prophylaxis administered following an episode due to the high risk for recurrence.
Other Issues
VTE prophylaxis. Although patients with cirrhosis are often presumed to be “auto-anticoagulated” due to an elevated international normalized ratio (INR), they experience thrombotic complications during hospitalization at the same rate or higher than patients with other chronic illnesses.9 Unfortunately, studies examining venous thromboembolism (VTE) prophylaxis in hospitalized patients have generally excluded cirrhotics. Therefore, risks/benefits of prophylaxis need to be considered on an individual basis, taking into account the presence of varices (if known), platelet count, and other VTE risk factors.
Drugs to avoid. As detailed above, nonselective beta-blockers should be avoided when outside the “window” period of benefit. Patients with cirrhosis should be counseled to avoid nonsteroidal anti-inflammatory drugs (NSAIDs) due to an increased risk of bleeding and renal dysfunction. ACE inhibitors (ACE-Is) and angiotensin-receptor blockers (ARBs) can also precipitate renal dysfunction and should generally be avoided unless strongly indicated for another diagnosis.
There is conflicting evidence with regard to whether the use of proton-pump inhibitors (PPIs) in cirrhotics increases the risk of SBP.10,11 Nevertheless, it is prudent to reevaluate the need for PPIs in patients with cirrhosis to determine where a true indication exists.
Post-hospitalization care. Patients with a new diagnosis of cirrhosis require screening for esophageal varices and hepatocellular carcinoma (HCC), with frequency of subsequent testing based on initial results. They should also be immunized against hepatitis A (HAV) and hepatitis B (HBV), if not already immune. Specific treatments are available for many causes of cirrhosis, including new antiviral agents against hepatitis C (HCV), and liver transplantation is an option for select patients. Given the complexity of subsequent diagnostic and treatment options, patients with new cirrhosis should be referred to a gastroenterologist or hepatologist, if possible.
Back to the Case
The patient is hospitalized, and a large-volume paracentesis is performed. Four liters are removed without the administration of albumin. Ascitic fluid analysis reveals a SAAG of greater than 1.1 g/dL and a polymorphonuclear cell count of 50 cell/mm3, suggesting ascites due to portal hypertension and ruling out infection. Nutrition is consulted and educates the patient on a restricted-sodium diet. Furosemide is started at 40 mg daily; spironolactone is started at 100 mg daily. Initial workup and serologies demonstrate active HCV infection (HCV RNA positive), with immunity to HBV due to vaccination. HAV vaccination is administered given lack of seropositivity. The patient is screened for alcohol and found not to drink alcohol. By the time of discharge, the patient is experiencing daily 0.5 kg weight loss due to diuretics and has stable renal function. The patient is referred to outpatient gastroenterology for gastroesophageal variceal screening and consideration of HCV treatment and/or liver transplantation.
Bottom Line
Workup and management of cirrhosis should focus on revealing the underlying etiology, managing complications, and discharging patients with a comprehensive follow-up plan. TH
Dr. Sehgal and Dr. Hanson are hospitalists in the division of hospital medicine at the University of Texas Health Science Center at San Antonio and the South Texas Veterans Health Care System.
References
- Heron M. Deaths: leading causes for 2012. Natl Vital Stat Rep. 2015;64(10):1-93.
- Chronic liver disease and cirrhosis. Centers for Disease Control and Prevention website. Accessed March 17, 2016.
- Smith BD, Morgan RL, Beckett GA, Falck-Ytter Y, Holtzman D, Ward JW. Hepatitis C virus testing of persons born during 1945-1965: recommendations from the Centers for Disease Control and Prevention. Ann Intern Med. 2012;157(11):817-822. doi:10.7326/0003-4819-157-9-201211060-00529.
- Runyon BA, AASLD. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline management of adult patients with ascites due to cirrhosis 2012. Hepatology. 2013;57(4):1651-1653. doi:10.1002/hep.26359.
- Udell JA, Wang CS, Tinmouth J, et al. Does this patient with liver disease have cirrhosis? JAMA. 2012;307(8):832-842. doi:10.1001/jama.2012.186.
- Garcia-Tsao G, Sanyal AJ, Grace ND, Carey W, Practice Guidelines Committee of the American Association for the Study of Liver Diseases, Practice Parameters Committee of the American College of Gastroenterology. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology. 2007;46(3):922-938. doi:10.1002/hep.21907.
- Mandorfer M, Bota S, Schwabl P, et al. Nonselective β blockers increase risk for hepatorenal syndrome and death in patients with cirrhosis and spontaneous bacterial peritonitis. Gastroenterology. 2014;146(7):1680-90.e1. doi:10.1053/j.gastro.2014.03.005.
- Vilstrup H, Amodio P, Bajaj J, et al. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology. 2014;60(2):715-735. doi:10.1002/hep.27210.
- Khoury T, Ayman AR, Cohen J, Daher S, Shmuel C, Mizrahi M. The complex role of anticoagulation in cirrhosis: an updated review of where we are and where we are going. Digestion. 2016;93(2):149-159. doi:10.1159/000442877.
- Terg R, Casciato P, Garbe C, et al. Proton pump inhibitor therapy does not increase the incidence of spontaneous bacterial peritonitis in cirrhosis: a multicenter prospective study. J Hepatol. 2015;62(5):1056-1060. doi:10.1016/j.jhep.2014.11.036.
- Deshpande A, Pasupuleti V, Thota P, et al. Acid-suppressive therapy is associated with spontaneous bacterial peritonitis in cirrhotic patients: a meta-analysis. J Gastroenterol Hepatol. 2013;28(2):235-242. doi:10.1111/jgh.12065.
Key Points
- Cirrhosis has many etiologies, and new diagnoses require further investigation as to the underlying etiology.
- Initial management should focus on evaluation and treatment of complications, including ascites, esophageal varices, and hepatic encephalopathy.
- A diagnostic paracentesis, salt restriction, and a nutrition consult are the initial therapies for ascites although most patients will also require diuretics to increase sodium excretion.
- Once stabilized, the cirrhotic patient will require specialty care for possible liver biopsy (if etiology remains unclear), treatment (eg, HCV antivirals), and/or referral for liver transplantation.
The Case
A 50-year-old man with no known medical history presents with two months of increasing abdominal distension. Exam is notable for scleral icterus, telangiectasias on the upper chest, abdominal distention with a positive fluid wave, and bilateral pitting lower-extremity edema. An abdominal ultrasound shows large ascites and a nodular liver consistent with cirrhosis. How should this patient with newly diagnosed cirrhosis be evaluated and managed?
Background
Cirrhosis is a leading cause of death among people ages 25–64 and associated with a mortality rate of 11.5 per 100,000 people.1 In 2010, 101,000 people were discharged from the hospital with chronic liver disease and cirrhosis as the first-listed diagnosis.2 Given the myriad etiologies and the asymptomatic nature of many of these conditions, hospitalists frequently encounter patients presenting with advanced disease.
Evaluation
The gold standard for diagnosis is liver biopsy, although this is now usually reserved for atypical cases or where the etiology of cirrhosis is unclear. Alcohol and viral hepatitis (B and C) are the most common causes of chronic liver disease, with nonalcoholic steatohepatitis (NASH) increasing in prevalence. Other less common etiologies and characteristic test findings are listed in Figure 2.
Recently, the Centers for Disease Control and Prevention (CDC) recommended that adults born between 1945 and 1965 receive one-time testing for hepatitis C virus (HCV) infection, regardless of other risk factors, given the higher prevalence in this birth cohort and the introduction of newer oral treatments that achieve sustained virologic response.3
Management
The three classic complications of cirrhosis that will typically prompt inpatient admission are volume overload/ascites, gastrointestinal variceal bleeding, and hepatic encephalopathy.
Volume overload/ascites. Ascites is the most common major complication of cirrhosis, with roughly 50% of patients with asymptomatic cirrhosis developing ascites within 10 years.4 Ascites development portends a poor prognosis, with a mortality of 15% within one year and 44% within five years of diagnosis.4 Patients presenting with new-onset ascites should have a diagnostic paracentesis performed to determine the etiology and evaluate for infection.
Ascitic fluid should be sent for an albumin level and a cell count with differential. A serum-ascites albumin gradient (SAAG) of greater than or equal to 1.1 g/dL is consistent with portal hypertension and cirrhosis, while values less than 1.1 g/dL suggest a non-cirrhotic cause, such as infection or malignancy. Due to the high prevalence of spontaneous bacterial peritonitis (SBP) in hospitalized patients, fluid should also be immediately inoculated in aerobic and anaerobic culture bottles at the bedside, as this has been shown to improve the yield compared to inoculation of culture bottles in the laboratory. Other testing (such as cytology for the evaluation of malignancy) should only be performed if there is significant concern for a particular disease since the vast majority of cases are secondary to uncomplicated cirrhosis.4
In patients with a large amount of ascites and related symptoms (eg, abdominal pain, shortness of breath), therapeutic paracentesis should be performed. Although there is controversy over the need for routine albumin administration, guidelines currently recommend the infusion of 6–8 g of albumin per liter of ascites removed for paracentesis volumes of greater than 4–5 liters.4
No data support the routine administration of fresh frozen plasma (FFP) or platelets prior to paracentesis. Although significant complications of paracentesis (including bowel perforation and hemorrhage) may occur, these are exceedingly rare. Ultrasonography can be used to decrease risks and identify suitable pockets of fluid to tap, even when fluid is not obvious on physical exam alone.5
For patients with significant edema or ascites that is due to portal hypertension (SAAG >1.1 g/dL), the first-line therapy is sodium restriction to less than 2,000 mg/day. Consulting a nutritionist may be beneficial for patient education.
For patients with significant natriuresis (>78 mmol daily urine sodium excretion), dietary restriction alone can manage fluid retention. Most patients (85%–90%), however, require diuretics to increase sodium output. Single-agent spironolactone is more efficacious than single-agent furosemide, but diuresis is improved when both agents are used.4 A dosing regimen of once-daily 40 mg furosemide and 100 mg spironolactone is the recommended starting regimen to promote diuresis while maintaining normokalemia. Due to the long half-life of spironolactone, the dose can be increased every three to five days if needed for diuresis.4
Gastroesophageal variceal bleeding. Approximately 50% of patients with cirrhosis have gastroesophageal varices as a consequence of portal hypertension, with prevalence increasing in those with more severe disease.6 As many patients with cirrhosis have advanced disease at the time of diagnosis, it is recommended that patients be referred for endoscopic screening when diagnosed.6 Nonselective beta-blockers decrease the risk of bleeding in patients with known varices but should not be initiated empirically in all patients with cirrhosis given significant side effects, including worsening of ascites.
There is increasing evidence that there is a “window” period for beta-blocker use in cirrhosis with the window opening after the diagnosis of varices and the window closing at advanced stages of disease (marked by an episode of spontaneous bacterial peritonitis, refractory ascites, or hepatorenal syndrome, for example).7
Hepatic encephalopathy. Hepatic encephalopathy (HE) is another complication of portal hypertension and is seen in 10%–14% of patients at the time of cirrhosis diagnosis.8 Overt HE is estimated to occur in 30%–40% of patients with cirrhosis at some point during their disease course, and more subtle forms (minimal or covert HE) are seen in up to 80%.8 HE can cause numerous neurologic and psychiatric issues including personality changes, poor memory, sleep-wake disturbances, and alterations in consciousness.
In patients with an episode of encephalopathy, precipitating factors should be evaluated. Typical precipitants include infections, bleeding, electrolyte disorders, and constipation. Ammonia levels are frequently drawn as part of the evaluation of hepatic encephalopathy, but elevated levels do not significantly change diagnostic probabilities or add prognostic information.8 A low ammonia level, on the other hand, may be useful in lowering the probability of hepatic encephalopathy in a patient with altered mental status of unknown etiology.8
Routine primary prophylaxis of HE in all patients with cirrhosis is not currently recommended. Treatment is only recommended in patients with overt HE, with secondary prophylaxis administered following an episode due to the high risk for recurrence.
Other Issues
VTE prophylaxis. Although patients with cirrhosis are often presumed to be “auto-anticoagulated” due to an elevated international normalized ratio (INR), they experience thrombotic complications during hospitalization at the same rate or higher than patients with other chronic illnesses.9 Unfortunately, studies examining venous thromboembolism (VTE) prophylaxis in hospitalized patients have generally excluded cirrhotics. Therefore, risks/benefits of prophylaxis need to be considered on an individual basis, taking into account the presence of varices (if known), platelet count, and other VTE risk factors.
Drugs to avoid. As detailed above, nonselective beta-blockers should be avoided when outside the “window” period of benefit. Patients with cirrhosis should be counseled to avoid nonsteroidal anti-inflammatory drugs (NSAIDs) due to an increased risk of bleeding and renal dysfunction. ACE inhibitors (ACE-Is) and angiotensin-receptor blockers (ARBs) can also precipitate renal dysfunction and should generally be avoided unless strongly indicated for another diagnosis.
There is conflicting evidence with regard to whether the use of proton-pump inhibitors (PPIs) in cirrhotics increases the risk of SBP.10,11 Nevertheless, it is prudent to reevaluate the need for PPIs in patients with cirrhosis to determine where a true indication exists.
Post-hospitalization care. Patients with a new diagnosis of cirrhosis require screening for esophageal varices and hepatocellular carcinoma (HCC), with frequency of subsequent testing based on initial results. They should also be immunized against hepatitis A (HAV) and hepatitis B (HBV), if not already immune. Specific treatments are available for many causes of cirrhosis, including new antiviral agents against hepatitis C (HCV), and liver transplantation is an option for select patients. Given the complexity of subsequent diagnostic and treatment options, patients with new cirrhosis should be referred to a gastroenterologist or hepatologist, if possible.
Back to the Case
The patient is hospitalized, and a large-volume paracentesis is performed. Four liters are removed without the administration of albumin. Ascitic fluid analysis reveals a SAAG of greater than 1.1 g/dL and a polymorphonuclear cell count of 50 cell/mm3, suggesting ascites due to portal hypertension and ruling out infection. Nutrition is consulted and educates the patient on a restricted-sodium diet. Furosemide is started at 40 mg daily; spironolactone is started at 100 mg daily. Initial workup and serologies demonstrate active HCV infection (HCV RNA positive), with immunity to HBV due to vaccination. HAV vaccination is administered given lack of seropositivity. The patient is screened for alcohol and found not to drink alcohol. By the time of discharge, the patient is experiencing daily 0.5 kg weight loss due to diuretics and has stable renal function. The patient is referred to outpatient gastroenterology for gastroesophageal variceal screening and consideration of HCV treatment and/or liver transplantation.
Bottom Line
Workup and management of cirrhosis should focus on revealing the underlying etiology, managing complications, and discharging patients with a comprehensive follow-up plan. TH
Dr. Sehgal and Dr. Hanson are hospitalists in the division of hospital medicine at the University of Texas Health Science Center at San Antonio and the South Texas Veterans Health Care System.
References
- Heron M. Deaths: leading causes for 2012. Natl Vital Stat Rep. 2015;64(10):1-93.
- Chronic liver disease and cirrhosis. Centers for Disease Control and Prevention website. Accessed March 17, 2016.
- Smith BD, Morgan RL, Beckett GA, Falck-Ytter Y, Holtzman D, Ward JW. Hepatitis C virus testing of persons born during 1945-1965: recommendations from the Centers for Disease Control and Prevention. Ann Intern Med. 2012;157(11):817-822. doi:10.7326/0003-4819-157-9-201211060-00529.
- Runyon BA, AASLD. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline management of adult patients with ascites due to cirrhosis 2012. Hepatology. 2013;57(4):1651-1653. doi:10.1002/hep.26359.
- Udell JA, Wang CS, Tinmouth J, et al. Does this patient with liver disease have cirrhosis? JAMA. 2012;307(8):832-842. doi:10.1001/jama.2012.186.
- Garcia-Tsao G, Sanyal AJ, Grace ND, Carey W, Practice Guidelines Committee of the American Association for the Study of Liver Diseases, Practice Parameters Committee of the American College of Gastroenterology. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology. 2007;46(3):922-938. doi:10.1002/hep.21907.
- Mandorfer M, Bota S, Schwabl P, et al. Nonselective β blockers increase risk for hepatorenal syndrome and death in patients with cirrhosis and spontaneous bacterial peritonitis. Gastroenterology. 2014;146(7):1680-90.e1. doi:10.1053/j.gastro.2014.03.005.
- Vilstrup H, Amodio P, Bajaj J, et al. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology. 2014;60(2):715-735. doi:10.1002/hep.27210.
- Khoury T, Ayman AR, Cohen J, Daher S, Shmuel C, Mizrahi M. The complex role of anticoagulation in cirrhosis: an updated review of where we are and where we are going. Digestion. 2016;93(2):149-159. doi:10.1159/000442877.
- Terg R, Casciato P, Garbe C, et al. Proton pump inhibitor therapy does not increase the incidence of spontaneous bacterial peritonitis in cirrhosis: a multicenter prospective study. J Hepatol. 2015;62(5):1056-1060. doi:10.1016/j.jhep.2014.11.036.
- Deshpande A, Pasupuleti V, Thota P, et al. Acid-suppressive therapy is associated with spontaneous bacterial peritonitis in cirrhotic patients: a meta-analysis. J Gastroenterol Hepatol. 2013;28(2):235-242. doi:10.1111/jgh.12065.
Key Points
- Cirrhosis has many etiologies, and new diagnoses require further investigation as to the underlying etiology.
- Initial management should focus on evaluation and treatment of complications, including ascites, esophageal varices, and hepatic encephalopathy.
- A diagnostic paracentesis, salt restriction, and a nutrition consult are the initial therapies for ascites although most patients will also require diuretics to increase sodium excretion.
- Once stabilized, the cirrhotic patient will require specialty care for possible liver biopsy (if etiology remains unclear), treatment (eg, HCV antivirals), and/or referral for liver transplantation.
The Case
A 50-year-old man with no known medical history presents with two months of increasing abdominal distension. Exam is notable for scleral icterus, telangiectasias on the upper chest, abdominal distention with a positive fluid wave, and bilateral pitting lower-extremity edema. An abdominal ultrasound shows large ascites and a nodular liver consistent with cirrhosis. How should this patient with newly diagnosed cirrhosis be evaluated and managed?
Background
Cirrhosis is a leading cause of death among people ages 25–64 and associated with a mortality rate of 11.5 per 100,000 people.1 In 2010, 101,000 people were discharged from the hospital with chronic liver disease and cirrhosis as the first-listed diagnosis.2 Given the myriad etiologies and the asymptomatic nature of many of these conditions, hospitalists frequently encounter patients presenting with advanced disease.
Evaluation
The gold standard for diagnosis is liver biopsy, although this is now usually reserved for atypical cases or where the etiology of cirrhosis is unclear. Alcohol and viral hepatitis (B and C) are the most common causes of chronic liver disease, with nonalcoholic steatohepatitis (NASH) increasing in prevalence. Other less common etiologies and characteristic test findings are listed in Figure 2.
Recently, the Centers for Disease Control and Prevention (CDC) recommended that adults born between 1945 and 1965 receive one-time testing for hepatitis C virus (HCV) infection, regardless of other risk factors, given the higher prevalence in this birth cohort and the introduction of newer oral treatments that achieve sustained virologic response.3
Management
The three classic complications of cirrhosis that will typically prompt inpatient admission are volume overload/ascites, gastrointestinal variceal bleeding, and hepatic encephalopathy.
Volume overload/ascites. Ascites is the most common major complication of cirrhosis, with roughly 50% of patients with asymptomatic cirrhosis developing ascites within 10 years.4 Ascites development portends a poor prognosis, with a mortality of 15% within one year and 44% within five years of diagnosis.4 Patients presenting with new-onset ascites should have a diagnostic paracentesis performed to determine the etiology and evaluate for infection.
Ascitic fluid should be sent for an albumin level and a cell count with differential. A serum-ascites albumin gradient (SAAG) of greater than or equal to 1.1 g/dL is consistent with portal hypertension and cirrhosis, while values less than 1.1 g/dL suggest a non-cirrhotic cause, such as infection or malignancy. Due to the high prevalence of spontaneous bacterial peritonitis (SBP) in hospitalized patients, fluid should also be immediately inoculated in aerobic and anaerobic culture bottles at the bedside, as this has been shown to improve the yield compared to inoculation of culture bottles in the laboratory. Other testing (such as cytology for the evaluation of malignancy) should only be performed if there is significant concern for a particular disease since the vast majority of cases are secondary to uncomplicated cirrhosis.4
In patients with a large amount of ascites and related symptoms (eg, abdominal pain, shortness of breath), therapeutic paracentesis should be performed. Although there is controversy over the need for routine albumin administration, guidelines currently recommend the infusion of 6–8 g of albumin per liter of ascites removed for paracentesis volumes of greater than 4–5 liters.4
No data support the routine administration of fresh frozen plasma (FFP) or platelets prior to paracentesis. Although significant complications of paracentesis (including bowel perforation and hemorrhage) may occur, these are exceedingly rare. Ultrasonography can be used to decrease risks and identify suitable pockets of fluid to tap, even when fluid is not obvious on physical exam alone.5
For patients with significant edema or ascites that is due to portal hypertension (SAAG >1.1 g/dL), the first-line therapy is sodium restriction to less than 2,000 mg/day. Consulting a nutritionist may be beneficial for patient education.
For patients with significant natriuresis (>78 mmol daily urine sodium excretion), dietary restriction alone can manage fluid retention. Most patients (85%–90%), however, require diuretics to increase sodium output. Single-agent spironolactone is more efficacious than single-agent furosemide, but diuresis is improved when both agents are used.4 A dosing regimen of once-daily 40 mg furosemide and 100 mg spironolactone is the recommended starting regimen to promote diuresis while maintaining normokalemia. Due to the long half-life of spironolactone, the dose can be increased every three to five days if needed for diuresis.4
Gastroesophageal variceal bleeding. Approximately 50% of patients with cirrhosis have gastroesophageal varices as a consequence of portal hypertension, with prevalence increasing in those with more severe disease.6 As many patients with cirrhosis have advanced disease at the time of diagnosis, it is recommended that patients be referred for endoscopic screening when diagnosed.6 Nonselective beta-blockers decrease the risk of bleeding in patients with known varices but should not be initiated empirically in all patients with cirrhosis given significant side effects, including worsening of ascites.
There is increasing evidence that there is a “window” period for beta-blocker use in cirrhosis with the window opening after the diagnosis of varices and the window closing at advanced stages of disease (marked by an episode of spontaneous bacterial peritonitis, refractory ascites, or hepatorenal syndrome, for example).7
Hepatic encephalopathy. Hepatic encephalopathy (HE) is another complication of portal hypertension and is seen in 10%–14% of patients at the time of cirrhosis diagnosis.8 Overt HE is estimated to occur in 30%–40% of patients with cirrhosis at some point during their disease course, and more subtle forms (minimal or covert HE) are seen in up to 80%.8 HE can cause numerous neurologic and psychiatric issues including personality changes, poor memory, sleep-wake disturbances, and alterations in consciousness.
In patients with an episode of encephalopathy, precipitating factors should be evaluated. Typical precipitants include infections, bleeding, electrolyte disorders, and constipation. Ammonia levels are frequently drawn as part of the evaluation of hepatic encephalopathy, but elevated levels do not significantly change diagnostic probabilities or add prognostic information.8 A low ammonia level, on the other hand, may be useful in lowering the probability of hepatic encephalopathy in a patient with altered mental status of unknown etiology.8
Routine primary prophylaxis of HE in all patients with cirrhosis is not currently recommended. Treatment is only recommended in patients with overt HE, with secondary prophylaxis administered following an episode due to the high risk for recurrence.
Other Issues
VTE prophylaxis. Although patients with cirrhosis are often presumed to be “auto-anticoagulated” due to an elevated international normalized ratio (INR), they experience thrombotic complications during hospitalization at the same rate or higher than patients with other chronic illnesses.9 Unfortunately, studies examining venous thromboembolism (VTE) prophylaxis in hospitalized patients have generally excluded cirrhotics. Therefore, risks/benefits of prophylaxis need to be considered on an individual basis, taking into account the presence of varices (if known), platelet count, and other VTE risk factors.
Drugs to avoid. As detailed above, nonselective beta-blockers should be avoided when outside the “window” period of benefit. Patients with cirrhosis should be counseled to avoid nonsteroidal anti-inflammatory drugs (NSAIDs) due to an increased risk of bleeding and renal dysfunction. ACE inhibitors (ACE-Is) and angiotensin-receptor blockers (ARBs) can also precipitate renal dysfunction and should generally be avoided unless strongly indicated for another diagnosis.
There is conflicting evidence with regard to whether the use of proton-pump inhibitors (PPIs) in cirrhotics increases the risk of SBP.10,11 Nevertheless, it is prudent to reevaluate the need for PPIs in patients with cirrhosis to determine where a true indication exists.
Post-hospitalization care. Patients with a new diagnosis of cirrhosis require screening for esophageal varices and hepatocellular carcinoma (HCC), with frequency of subsequent testing based on initial results. They should also be immunized against hepatitis A (HAV) and hepatitis B (HBV), if not already immune. Specific treatments are available for many causes of cirrhosis, including new antiviral agents against hepatitis C (HCV), and liver transplantation is an option for select patients. Given the complexity of subsequent diagnostic and treatment options, patients with new cirrhosis should be referred to a gastroenterologist or hepatologist, if possible.
Back to the Case
The patient is hospitalized, and a large-volume paracentesis is performed. Four liters are removed without the administration of albumin. Ascitic fluid analysis reveals a SAAG of greater than 1.1 g/dL and a polymorphonuclear cell count of 50 cell/mm3, suggesting ascites due to portal hypertension and ruling out infection. Nutrition is consulted and educates the patient on a restricted-sodium diet. Furosemide is started at 40 mg daily; spironolactone is started at 100 mg daily. Initial workup and serologies demonstrate active HCV infection (HCV RNA positive), with immunity to HBV due to vaccination. HAV vaccination is administered given lack of seropositivity. The patient is screened for alcohol and found not to drink alcohol. By the time of discharge, the patient is experiencing daily 0.5 kg weight loss due to diuretics and has stable renal function. The patient is referred to outpatient gastroenterology for gastroesophageal variceal screening and consideration of HCV treatment and/or liver transplantation.
Bottom Line
Workup and management of cirrhosis should focus on revealing the underlying etiology, managing complications, and discharging patients with a comprehensive follow-up plan. TH
Dr. Sehgal and Dr. Hanson are hospitalists in the division of hospital medicine at the University of Texas Health Science Center at San Antonio and the South Texas Veterans Health Care System.
References
- Heron M. Deaths: leading causes for 2012. Natl Vital Stat Rep. 2015;64(10):1-93.
- Chronic liver disease and cirrhosis. Centers for Disease Control and Prevention website. Accessed March 17, 2016.
- Smith BD, Morgan RL, Beckett GA, Falck-Ytter Y, Holtzman D, Ward JW. Hepatitis C virus testing of persons born during 1945-1965: recommendations from the Centers for Disease Control and Prevention. Ann Intern Med. 2012;157(11):817-822. doi:10.7326/0003-4819-157-9-201211060-00529.
- Runyon BA, AASLD. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline management of adult patients with ascites due to cirrhosis 2012. Hepatology. 2013;57(4):1651-1653. doi:10.1002/hep.26359.
- Udell JA, Wang CS, Tinmouth J, et al. Does this patient with liver disease have cirrhosis? JAMA. 2012;307(8):832-842. doi:10.1001/jama.2012.186.
- Garcia-Tsao G, Sanyal AJ, Grace ND, Carey W, Practice Guidelines Committee of the American Association for the Study of Liver Diseases, Practice Parameters Committee of the American College of Gastroenterology. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology. 2007;46(3):922-938. doi:10.1002/hep.21907.
- Mandorfer M, Bota S, Schwabl P, et al. Nonselective β blockers increase risk for hepatorenal syndrome and death in patients with cirrhosis and spontaneous bacterial peritonitis. Gastroenterology. 2014;146(7):1680-90.e1. doi:10.1053/j.gastro.2014.03.005.
- Vilstrup H, Amodio P, Bajaj J, et al. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology. 2014;60(2):715-735. doi:10.1002/hep.27210.
- Khoury T, Ayman AR, Cohen J, Daher S, Shmuel C, Mizrahi M. The complex role of anticoagulation in cirrhosis: an updated review of where we are and where we are going. Digestion. 2016;93(2):149-159. doi:10.1159/000442877.
- Terg R, Casciato P, Garbe C, et al. Proton pump inhibitor therapy does not increase the incidence of spontaneous bacterial peritonitis in cirrhosis: a multicenter prospective study. J Hepatol. 2015;62(5):1056-1060. doi:10.1016/j.jhep.2014.11.036.
- Deshpande A, Pasupuleti V, Thota P, et al. Acid-suppressive therapy is associated with spontaneous bacterial peritonitis in cirrhotic patients: a meta-analysis. J Gastroenterol Hepatol. 2013;28(2):235-242. doi:10.1111/jgh.12065.
Key Points
- Cirrhosis has many etiologies, and new diagnoses require further investigation as to the underlying etiology.
- Initial management should focus on evaluation and treatment of complications, including ascites, esophageal varices, and hepatic encephalopathy.
- A diagnostic paracentesis, salt restriction, and a nutrition consult are the initial therapies for ascites although most patients will also require diuretics to increase sodium excretion.
- Once stabilized, the cirrhotic patient will require specialty care for possible liver biopsy (if etiology remains unclear), treatment (eg, HCV antivirals), and/or referral for liver transplantation.
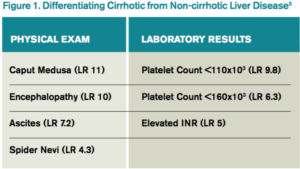
Antibody prevents migration of lymphoma cells

Preclinical research suggests a novel antibody can inhibit the migration of lymphoma cells and stop the cells from proliferating.
“Since they cannot survive in the blood for long, [lymphoma] cells are compelled to find a more accommodating environment—such as the lymphatic system—where they can proliferate,” explained Thomas Matthes, MD, of the University of Geneva in Switzerland.
“We decided to focus on this Achilles’ heel by containing them in the blood so as to prevent any resulting harm.”
Dr Matthes and his colleagues described this approach in the Journal of Leukocyte Biology.
The team noted that the inner wall of blood vessels is formed by a layer of endothelial cells that act as a barrier, which prevents the blood cells from leaving the circulation.
Yet, some lymphoma cells are equipped with a surface marker, the JAM-C protein, that is also present on the surface of endothelial cells. JAM-C’s presence on the surface of lymphoma cells facilitates their migration through the vessel walls between adjacent endothelial cells.
To block the effect of this protein, Dr Matthes and his colleagues developed an antibody targeting JAM-C.
This antibody, H225, was designed to bind solely to JAM-C. In doing so, H225 was able to prevent lymphoma cells from migrating out of the blood vessels.
In fact, H225 decreased the transit of lymphoma cells into the organs of the lymphatic system by over 50%.
“This is not its only effect,” Dr Matthes noted. “H225 also significantly limited cell proliferation, even when tumor cells had already settled in the lymphatic system. In our mice, we observed the nearly complete disappearance of already present tumor cells in the organs.”
Specifically, H225 reduced tumor growth of JAM-C+ mantle cell lymphoma cells in the bone marrow, spleen, liver, and lymph nodes.
The researchers believe this work has laid the foundation for a new therapeutic strategy against lymphoma. The team is now focusing its efforts on the quest for an efficient treatment that could be offered to patients. ![]()
Preclinical research suggests a novel antibody can inhibit the migration of lymphoma cells and stop the cells from proliferating.
“Since they cannot survive in the blood for long, [lymphoma] cells are compelled to find a more accommodating environment—such as the lymphatic system—where they can proliferate,” explained Thomas Matthes, MD, of the University of Geneva in Switzerland.
“We decided to focus on this Achilles’ heel by containing them in the blood so as to prevent any resulting harm.”
Dr Matthes and his colleagues described this approach in the Journal of Leukocyte Biology.
The team noted that the inner wall of blood vessels is formed by a layer of endothelial cells that act as a barrier, which prevents the blood cells from leaving the circulation.
Yet, some lymphoma cells are equipped with a surface marker, the JAM-C protein, that is also present on the surface of endothelial cells. JAM-C’s presence on the surface of lymphoma cells facilitates their migration through the vessel walls between adjacent endothelial cells.
To block the effect of this protein, Dr Matthes and his colleagues developed an antibody targeting JAM-C.
This antibody, H225, was designed to bind solely to JAM-C. In doing so, H225 was able to prevent lymphoma cells from migrating out of the blood vessels.
In fact, H225 decreased the transit of lymphoma cells into the organs of the lymphatic system by over 50%.
“This is not its only effect,” Dr Matthes noted. “H225 also significantly limited cell proliferation, even when tumor cells had already settled in the lymphatic system. In our mice, we observed the nearly complete disappearance of already present tumor cells in the organs.”
Specifically, H225 reduced tumor growth of JAM-C+ mantle cell lymphoma cells in the bone marrow, spleen, liver, and lymph nodes.
The researchers believe this work has laid the foundation for a new therapeutic strategy against lymphoma. The team is now focusing its efforts on the quest for an efficient treatment that could be offered to patients. ![]()
Preclinical research suggests a novel antibody can inhibit the migration of lymphoma cells and stop the cells from proliferating.
“Since they cannot survive in the blood for long, [lymphoma] cells are compelled to find a more accommodating environment—such as the lymphatic system—where they can proliferate,” explained Thomas Matthes, MD, of the University of Geneva in Switzerland.
“We decided to focus on this Achilles’ heel by containing them in the blood so as to prevent any resulting harm.”
Dr Matthes and his colleagues described this approach in the Journal of Leukocyte Biology.
The team noted that the inner wall of blood vessels is formed by a layer of endothelial cells that act as a barrier, which prevents the blood cells from leaving the circulation.
Yet, some lymphoma cells are equipped with a surface marker, the JAM-C protein, that is also present on the surface of endothelial cells. JAM-C’s presence on the surface of lymphoma cells facilitates their migration through the vessel walls between adjacent endothelial cells.
To block the effect of this protein, Dr Matthes and his colleagues developed an antibody targeting JAM-C.
This antibody, H225, was designed to bind solely to JAM-C. In doing so, H225 was able to prevent lymphoma cells from migrating out of the blood vessels.
In fact, H225 decreased the transit of lymphoma cells into the organs of the lymphatic system by over 50%.
“This is not its only effect,” Dr Matthes noted. “H225 also significantly limited cell proliferation, even when tumor cells had already settled in the lymphatic system. In our mice, we observed the nearly complete disappearance of already present tumor cells in the organs.”
Specifically, H225 reduced tumor growth of JAM-C+ mantle cell lymphoma cells in the bone marrow, spleen, liver, and lymph nodes.
The researchers believe this work has laid the foundation for a new therapeutic strategy against lymphoma. The team is now focusing its efforts on the quest for an efficient treatment that could be offered to patients. ![]()
Teva launches generic imatinib tablets in US

Photo by Steven Harbour
Teva Pharmaceutical Industries Ltd. has announced the US launch of imatinib mesylate, the generic equivalent of Novartis’s Gleevec®, in 100 mg and 400 mg tablets.
In the US, imatinib is approved to treat newly diagnosed Philadelphia-chromosome-positive (Ph+) chronic myeloid leukemia in chronic phase, blast crisis, and accelerated phase, as well as Ph+
chronic myeloid leukemia in chronic phase after failure of interferon-alpha therapy.
Imatinib is also approved to treat adults with relapsed or refractory Ph+ acute lymphoblastic leukemia, adults with myelodysplastic syndromes or myeloproliferative neoplasms associated with platelet-derived growth factor receptor gene re-arrangements, and adults with aggressive systemic mastocytosis without the D816V c-Kit mutation or with unknown c-Kit mutational status.
In addition, imatinib is approved to treat adults with hypereosinophilic syndrome and/or chronic eosinophilic leukemia (regardless of whether they have the FIP1L1-PDGFRα fusion kinase) and adults with unresectable, recurrent, and/or metastatic dermatofibrosarcoma protuberans.
Finally, the drug is approved as an adjuvant treatment following complete gross resection of Kit (CD117)-positive gastrointestinal stromal tumors in adults.
For more details on imatinib, see the full prescribing information. ![]()
Photo by Steven Harbour
Teva Pharmaceutical Industries Ltd. has announced the US launch of imatinib mesylate, the generic equivalent of Novartis’s Gleevec®, in 100 mg and 400 mg tablets.
In the US, imatinib is approved to treat newly diagnosed Philadelphia-chromosome-positive (Ph+) chronic myeloid leukemia in chronic phase, blast crisis, and accelerated phase, as well as Ph+
chronic myeloid leukemia in chronic phase after failure of interferon-alpha therapy.
Imatinib is also approved to treat adults with relapsed or refractory Ph+ acute lymphoblastic leukemia, adults with myelodysplastic syndromes or myeloproliferative neoplasms associated with platelet-derived growth factor receptor gene re-arrangements, and adults with aggressive systemic mastocytosis without the D816V c-Kit mutation or with unknown c-Kit mutational status.
In addition, imatinib is approved to treat adults with hypereosinophilic syndrome and/or chronic eosinophilic leukemia (regardless of whether they have the FIP1L1-PDGFRα fusion kinase) and adults with unresectable, recurrent, and/or metastatic dermatofibrosarcoma protuberans.
Finally, the drug is approved as an adjuvant treatment following complete gross resection of Kit (CD117)-positive gastrointestinal stromal tumors in adults.
For more details on imatinib, see the full prescribing information. ![]()
Photo by Steven Harbour
Teva Pharmaceutical Industries Ltd. has announced the US launch of imatinib mesylate, the generic equivalent of Novartis’s Gleevec®, in 100 mg and 400 mg tablets.
In the US, imatinib is approved to treat newly diagnosed Philadelphia-chromosome-positive (Ph+) chronic myeloid leukemia in chronic phase, blast crisis, and accelerated phase, as well as Ph+
chronic myeloid leukemia in chronic phase after failure of interferon-alpha therapy.
Imatinib is also approved to treat adults with relapsed or refractory Ph+ acute lymphoblastic leukemia, adults with myelodysplastic syndromes or myeloproliferative neoplasms associated with platelet-derived growth factor receptor gene re-arrangements, and adults with aggressive systemic mastocytosis without the D816V c-Kit mutation or with unknown c-Kit mutational status.
In addition, imatinib is approved to treat adults with hypereosinophilic syndrome and/or chronic eosinophilic leukemia (regardless of whether they have the FIP1L1-PDGFRα fusion kinase) and adults with unresectable, recurrent, and/or metastatic dermatofibrosarcoma protuberans.
Finally, the drug is approved as an adjuvant treatment following complete gross resection of Kit (CD117)-positive gastrointestinal stromal tumors in adults.
For more details on imatinib, see the full prescribing information. ![]()
Extended pneumococcal vaccination schedule boosts early immunity for preemies
A randomized clinical trial evaluating three dosing strategies for 13-valent pneumococcal vaccine (PCV13) in preterm infants found that more widely spaced priming vaccinations resulted in higher immunoglobulin G (IgG) during the first 12 months of life, but reduced the immune response seen after the 12-month booster was given.
After the primary schedule, the percent of infants lacking seroprotection for more than one half of the serotypes in the PCV13 formulation was 25% on a reduced two-dose schedule, 12% on an accelerated schedule, and 3% on an extended schedule (P less than .001).
Conversely, “A reduced priming schedule of PCV13 resulted in higher post-booster IgG concentrations but lower post-primary concentrations,” wrote Alison Kent, MBChB, and her coinvestigators in the PUNS (Prems Under New Schedule) Study Group (Pediatrics. 2016;138[3]:e20153945).
“Infants who received the extended schedule had lower fold increases in concentrations after booster vaccination than the other groups,” wrote Dr. Kent of the Pediatric Infectious Diseases Research Group and Vaccine Institute, St. George’s, University of London, and her collaborators. Participants receiving the extended schedule had lower geometric mean concentrations (GMCs) of antibodies than did those on the reduced schedule for nine serotypes and those on the accelerated schedule for four serotypes.
The study enrolled 210 premature infants in a phase IV, controlled, open-label trial at 12 sites in the United Kingdom. Infants of less than 35 weeks gestation, and between 7 and 12 weeks of age, were randomly assigned to receive PCV13 on one of three schedules. The reduced schedule gave two priming doses at 2 and 4 months of age; the accelerated schedule gave the doses at 2, 3, and 4 months of age; and the extended schedule gave doses at 2, 4, and 6 months of age. All infants received a booster vaccination at 12 or 13 months of age, and all received a standard suite of childhood immunizations for other diseases. The entire study was completed by 194 patients.
Serotype-specific IgG concentrations were obtained pre-vaccination, 1 month after the primary vaccination, and before and 1 month after the booster vaccination was given. IgG levels were reported for each PCV serotype; “there was considerable variation between serotypes,” ranging from 0.16 ng/mL for serotype 6b on the reduced schedule to 8.49 ng/mL for serotype 14 on the extended schedule, the investigators said.
Dr. Kent and her collaborators also used logistic regression analysis to explore how the vaccine’s effectiveness was affected by a number of factors. These included gestational length, the receipt of blood transfusions or pre- or post-natal steroids, BCG vaccination, early postvaccination acetaminophen, and the presence of chronic lung disease.
Later gestation was associated with increased seroprotection for four serotypes at 2 months of age, and with an increase in post-primary vaccination IgG concentrations for three others (P-values ranging from P less than .001 to P = .021).
No other factors were associated with protective IgG levels at any point, except that receipt of prenatal steroids had a negative association with seroprotection for several serotypes. “At no time points were antenatal steroids associated with higher antibody concentrations,” wrote the investigators.
Most studies of immunogenicity of infant vaccination schedules have been completed using term infants, with limited knowledge about efficacy in preterm infants. Previous work had shown that preterm infants had lower IgG concentrations after the primary and booster vaccinations for eight serotypes of PCV, compared with term infants. “The lower immunogenicity ... is concerning because premature infants are also less likely to benefit from the protective maternal antibodies transferred during late pregnancy,” Dr. Kent and her coauthors wrote.
The lower booster immunogenicity after the extended schedule is an effect that has been previously observed with other vaccinations and may be related to the formation of immune complexes with previously existing antibodies with the vaccine antigen, said Dr. Kent and her coauthors. The variation in immunogenicity timing for the various priming schedules, they said, will be helpful for those caring for preterm infants, enabling them “to consider this finding in the context of their own immunization programs and epidemiologic situations.”
The study was funded by Pfizer as an investigator-led study, without Pfizer’s input on the conduct of the trial, analysis of data, interpretation of results, or the preparation of this manuscript. Pfizer manufactures Prevnar 13.
On Twitter @karioakes
The needs of varying populations, the prevalence of various serotypes, and other local epidemiologic and economic factors all influence vaccination schedules. For PCV, the present study showed how widely seroprotection varied between serotypes and between different priming schedules.
Invasive pneumococcal disease (IPD) can be devastating in the vulnerable preterm population, as can pneumococcal pneumonia. Though the current vaccination schedule recommendations in the United States takes into account age-related changes in the immune system, truly optimized vaccine delivery for all populations, including this vulnerable one, is still more a goal than a reality.
However, each of the schedules examined in this study have been studied in areas where they are in clinical use, and all are generally protective of IPD. The timing of other vaccinations, as well as economic and logistic realities, will also affect vaccination schedules, and must be taken into account.
The findings of this study show that no one schedule is best for all populations, and also highlight why those making vaccine policy around the globe will continue to arrive at varying answers when considering the needs of their populations.
Mark H. Sawyer, MD, is a professor of pediatrics at the University of California, San Diego. Mobeen Rathore, MD, is director of the University of Florida Center for HIV/AIDS Research, Education and Service. They had no conflicts of interest to declare. Their remarks are drawn from a companion commentary in Pediatrics (Pediatrics. 2016;138[3]:e20160975).
The needs of varying populations, the prevalence of various serotypes, and other local epidemiologic and economic factors all influence vaccination schedules. For PCV, the present study showed how widely seroprotection varied between serotypes and between different priming schedules.
Invasive pneumococcal disease (IPD) can be devastating in the vulnerable preterm population, as can pneumococcal pneumonia. Though the current vaccination schedule recommendations in the United States takes into account age-related changes in the immune system, truly optimized vaccine delivery for all populations, including this vulnerable one, is still more a goal than a reality.
However, each of the schedules examined in this study have been studied in areas where they are in clinical use, and all are generally protective of IPD. The timing of other vaccinations, as well as economic and logistic realities, will also affect vaccination schedules, and must be taken into account.
The findings of this study show that no one schedule is best for all populations, and also highlight why those making vaccine policy around the globe will continue to arrive at varying answers when considering the needs of their populations.
Mark H. Sawyer, MD, is a professor of pediatrics at the University of California, San Diego. Mobeen Rathore, MD, is director of the University of Florida Center for HIV/AIDS Research, Education and Service. They had no conflicts of interest to declare. Their remarks are drawn from a companion commentary in Pediatrics (Pediatrics. 2016;138[3]:e20160975).
The needs of varying populations, the prevalence of various serotypes, and other local epidemiologic and economic factors all influence vaccination schedules. For PCV, the present study showed how widely seroprotection varied between serotypes and between different priming schedules.
Invasive pneumococcal disease (IPD) can be devastating in the vulnerable preterm population, as can pneumococcal pneumonia. Though the current vaccination schedule recommendations in the United States takes into account age-related changes in the immune system, truly optimized vaccine delivery for all populations, including this vulnerable one, is still more a goal than a reality.
However, each of the schedules examined in this study have been studied in areas where they are in clinical use, and all are generally protective of IPD. The timing of other vaccinations, as well as economic and logistic realities, will also affect vaccination schedules, and must be taken into account.
The findings of this study show that no one schedule is best for all populations, and also highlight why those making vaccine policy around the globe will continue to arrive at varying answers when considering the needs of their populations.
Mark H. Sawyer, MD, is a professor of pediatrics at the University of California, San Diego. Mobeen Rathore, MD, is director of the University of Florida Center for HIV/AIDS Research, Education and Service. They had no conflicts of interest to declare. Their remarks are drawn from a companion commentary in Pediatrics (Pediatrics. 2016;138[3]:e20160975).
A randomized clinical trial evaluating three dosing strategies for 13-valent pneumococcal vaccine (PCV13) in preterm infants found that more widely spaced priming vaccinations resulted in higher immunoglobulin G (IgG) during the first 12 months of life, but reduced the immune response seen after the 12-month booster was given.
After the primary schedule, the percent of infants lacking seroprotection for more than one half of the serotypes in the PCV13 formulation was 25% on a reduced two-dose schedule, 12% on an accelerated schedule, and 3% on an extended schedule (P less than .001).
Conversely, “A reduced priming schedule of PCV13 resulted in higher post-booster IgG concentrations but lower post-primary concentrations,” wrote Alison Kent, MBChB, and her coinvestigators in the PUNS (Prems Under New Schedule) Study Group (Pediatrics. 2016;138[3]:e20153945).
“Infants who received the extended schedule had lower fold increases in concentrations after booster vaccination than the other groups,” wrote Dr. Kent of the Pediatric Infectious Diseases Research Group and Vaccine Institute, St. George’s, University of London, and her collaborators. Participants receiving the extended schedule had lower geometric mean concentrations (GMCs) of antibodies than did those on the reduced schedule for nine serotypes and those on the accelerated schedule for four serotypes.
The study enrolled 210 premature infants in a phase IV, controlled, open-label trial at 12 sites in the United Kingdom. Infants of less than 35 weeks gestation, and between 7 and 12 weeks of age, were randomly assigned to receive PCV13 on one of three schedules. The reduced schedule gave two priming doses at 2 and 4 months of age; the accelerated schedule gave the doses at 2, 3, and 4 months of age; and the extended schedule gave doses at 2, 4, and 6 months of age. All infants received a booster vaccination at 12 or 13 months of age, and all received a standard suite of childhood immunizations for other diseases. The entire study was completed by 194 patients.
Serotype-specific IgG concentrations were obtained pre-vaccination, 1 month after the primary vaccination, and before and 1 month after the booster vaccination was given. IgG levels were reported for each PCV serotype; “there was considerable variation between serotypes,” ranging from 0.16 ng/mL for serotype 6b on the reduced schedule to 8.49 ng/mL for serotype 14 on the extended schedule, the investigators said.
Dr. Kent and her collaborators also used logistic regression analysis to explore how the vaccine’s effectiveness was affected by a number of factors. These included gestational length, the receipt of blood transfusions or pre- or post-natal steroids, BCG vaccination, early postvaccination acetaminophen, and the presence of chronic lung disease.
Later gestation was associated with increased seroprotection for four serotypes at 2 months of age, and with an increase in post-primary vaccination IgG concentrations for three others (P-values ranging from P less than .001 to P = .021).
No other factors were associated with protective IgG levels at any point, except that receipt of prenatal steroids had a negative association with seroprotection for several serotypes. “At no time points were antenatal steroids associated with higher antibody concentrations,” wrote the investigators.
Most studies of immunogenicity of infant vaccination schedules have been completed using term infants, with limited knowledge about efficacy in preterm infants. Previous work had shown that preterm infants had lower IgG concentrations after the primary and booster vaccinations for eight serotypes of PCV, compared with term infants. “The lower immunogenicity ... is concerning because premature infants are also less likely to benefit from the protective maternal antibodies transferred during late pregnancy,” Dr. Kent and her coauthors wrote.
The lower booster immunogenicity after the extended schedule is an effect that has been previously observed with other vaccinations and may be related to the formation of immune complexes with previously existing antibodies with the vaccine antigen, said Dr. Kent and her coauthors. The variation in immunogenicity timing for the various priming schedules, they said, will be helpful for those caring for preterm infants, enabling them “to consider this finding in the context of their own immunization programs and epidemiologic situations.”
The study was funded by Pfizer as an investigator-led study, without Pfizer’s input on the conduct of the trial, analysis of data, interpretation of results, or the preparation of this manuscript. Pfizer manufactures Prevnar 13.
On Twitter @karioakes
A randomized clinical trial evaluating three dosing strategies for 13-valent pneumococcal vaccine (PCV13) in preterm infants found that more widely spaced priming vaccinations resulted in higher immunoglobulin G (IgG) during the first 12 months of life, but reduced the immune response seen after the 12-month booster was given.
After the primary schedule, the percent of infants lacking seroprotection for more than one half of the serotypes in the PCV13 formulation was 25% on a reduced two-dose schedule, 12% on an accelerated schedule, and 3% on an extended schedule (P less than .001).
Conversely, “A reduced priming schedule of PCV13 resulted in higher post-booster IgG concentrations but lower post-primary concentrations,” wrote Alison Kent, MBChB, and her coinvestigators in the PUNS (Prems Under New Schedule) Study Group (Pediatrics. 2016;138[3]:e20153945).
“Infants who received the extended schedule had lower fold increases in concentrations after booster vaccination than the other groups,” wrote Dr. Kent of the Pediatric Infectious Diseases Research Group and Vaccine Institute, St. George’s, University of London, and her collaborators. Participants receiving the extended schedule had lower geometric mean concentrations (GMCs) of antibodies than did those on the reduced schedule for nine serotypes and those on the accelerated schedule for four serotypes.
The study enrolled 210 premature infants in a phase IV, controlled, open-label trial at 12 sites in the United Kingdom. Infants of less than 35 weeks gestation, and between 7 and 12 weeks of age, were randomly assigned to receive PCV13 on one of three schedules. The reduced schedule gave two priming doses at 2 and 4 months of age; the accelerated schedule gave the doses at 2, 3, and 4 months of age; and the extended schedule gave doses at 2, 4, and 6 months of age. All infants received a booster vaccination at 12 or 13 months of age, and all received a standard suite of childhood immunizations for other diseases. The entire study was completed by 194 patients.
Serotype-specific IgG concentrations were obtained pre-vaccination, 1 month after the primary vaccination, and before and 1 month after the booster vaccination was given. IgG levels were reported for each PCV serotype; “there was considerable variation between serotypes,” ranging from 0.16 ng/mL for serotype 6b on the reduced schedule to 8.49 ng/mL for serotype 14 on the extended schedule, the investigators said.
Dr. Kent and her collaborators also used logistic regression analysis to explore how the vaccine’s effectiveness was affected by a number of factors. These included gestational length, the receipt of blood transfusions or pre- or post-natal steroids, BCG vaccination, early postvaccination acetaminophen, and the presence of chronic lung disease.
Later gestation was associated with increased seroprotection for four serotypes at 2 months of age, and with an increase in post-primary vaccination IgG concentrations for three others (P-values ranging from P less than .001 to P = .021).
No other factors were associated with protective IgG levels at any point, except that receipt of prenatal steroids had a negative association with seroprotection for several serotypes. “At no time points were antenatal steroids associated with higher antibody concentrations,” wrote the investigators.
Most studies of immunogenicity of infant vaccination schedules have been completed using term infants, with limited knowledge about efficacy in preterm infants. Previous work had shown that preterm infants had lower IgG concentrations after the primary and booster vaccinations for eight serotypes of PCV, compared with term infants. “The lower immunogenicity ... is concerning because premature infants are also less likely to benefit from the protective maternal antibodies transferred during late pregnancy,” Dr. Kent and her coauthors wrote.
The lower booster immunogenicity after the extended schedule is an effect that has been previously observed with other vaccinations and may be related to the formation of immune complexes with previously existing antibodies with the vaccine antigen, said Dr. Kent and her coauthors. The variation in immunogenicity timing for the various priming schedules, they said, will be helpful for those caring for preterm infants, enabling them “to consider this finding in the context of their own immunization programs and epidemiologic situations.”
The study was funded by Pfizer as an investigator-led study, without Pfizer’s input on the conduct of the trial, analysis of data, interpretation of results, or the preparation of this manuscript. Pfizer manufactures Prevnar 13.
On Twitter @karioakes
FROM PEDIATRICS
Key clinical point: More widely-spaced pneumococcal vaccinations boosted early immunity but reduced the effectiveness of a 12-month booster in preterm infants.
Major finding: Of preterm infants on an extended pneumococcal conjugate vaccine (PCV13) schedule, just 3% lacked seroprotection for over half of the serotypes.
Data source: Randomized, placebo-controlled, open-label study of 210 preterm infants receiving PCV13vaccination on one of three dosing schedules.
Disclosures: The study was funded by Pfizer as an investigator-led study, without Pfizer’s input on the conduct of the trial, analysis of data, interpretation of results, or the preparation of this manuscript. Pfizer manufactures Prevnar 13.
Hemophilia may not be protective against CVD
ORLANDO – Conventional wisdom holds that persons with hemophilia are at lower risk for death from cardiovascular events than the general population, but there are conflicting data from studies attempting to confirm or refute this notion.
In a prospective, multicenter European study of more than 500 patients with hemophilia, the predicted cardiovascular disease (CVD) event rate was less than half of what was expected, reported Paul R. van der Valk, MD, from University Medical Center in Utrecht, the Netherlands, and colleagues.
In patients with hemophilia, “the leading cause of death seems to be malignancy related and intracranial hemorrhage. Atrial fibrillation is quite common,” they wrote in a scientific poster presented at the World Federation of Hemophilia World Congress.
But a second study of 100 patients with hemophilia showed that the bleeding disorder did not appear to offer protection against cardiovascular or thrombotic adverse events, Beatriz Delgado, MD, and colleagues at the Centro Hospitalar São João in Porto, Portugal, also presented in a poster session.
Risk scores considered
The prospective study by Dr. van der Valk and colleagues was designed to assess the incidence of CVD in patients with hemophilia in the Netherlands and the United Kingdom, compared with the general population. They used the QRISK2 cardiovascular risk score (2011 version). This instrument is used to calculate risk of CVD events in adults from 30 to 84 with no history of CVD or statin use.
Among 557 patients with a calculable QRISK2 score at 2 years of follow-up, there were four CVD events, including two cases of ischemic heart disease, one ischemic stroke, and one intracranial hemorrhage. The median 2-year QRISK2 score was 1.7%, and the 10-year risk was 9.0%, which translated in to an expected 9.5 CVD events during 2 years of follow-up.
Among the additional 104 patients who could not have a QRISK2 score calculated because of age over 84, statin use, or history of CVD, there were four CVD events: ischemic heart disease, transient ischemic attack/carotid artery stenosis, myocardial infarction, and intracranial hemorrhage.
Other CVD events occurring in both groups included atrial fibrillation in eight patients, other arrhythmia in three, and, in one patient each, aortic valve pathology, pericarditis, and carotid artery plaque.
Portuguese experience
Dr, Delgado and colleagues noted that although hemophilia has traditionally been regarded as protective against ischemic heart disease or thrombotic events, modern management “has prolonged life expectancy of people with hemophilia and consequently, an associated increase in incidence and prevalence of conditions that affect the general older population, such as cardiovascular disease and hypertension, are expected.”
They conducted a retrospective analysis of 100 adults (69 with hemophilia A, and 31 with hemophilia B) treated at their center. Overall, 29 patients had severe hemophilia A, 20 moderate hemophilia A, and 20 mild hemophilia A. Among patients with hemophilia B, 11 had severe, 15 moderate, and 5 mild disease.
Two patients (one with moderate and one with severe hemophilia) had angina episodes with coronary artery disease and underwent multiple coronary bypass grafts. The patient with severe disease had a disabling ischemic stroke during recovery from bypass surgery, and the patient with moderate hemophilia had an acute myocardial infarction prior to bypass surgery.
Two other patients had transient ischemic strokes from which they recovered without disability.
The main cardiovascular risk factors identified in this population were hypertension, diabetes mellitus, heavy smoking, obesity, and dyslipidemia. All patients were screened for prothrombotic risk, and all patients had negative test results.
“Hemophilia does not seem to have a protective effect against thrombotic/cardiovascular events, mainly in [patients with] coronary artery disease,” the investigators wrote.
Endothelial function

In a study presented in an oral abstract session, Shannon Jackson, MD, of the University of British Columbia in Vancouver found that men with hemophilia appear to have better macrovascular endothelial function but worse microvascular endothelial function than did men with normal clotting parameters.
“Based on endothelial function, contemporary hemophilia cohorts may have a different profile of cardiovascular risk than healthy controls,” she said.
Although they do not have an obvious mechanistic explanation for the differences in microvascular function among patients with hemophilia vs. healthy controls, there is evidence to show that microvascular function is predictive of cardiovascular events independent of other risk factors in otherwise healthy people. Their findings indicate that further study of the association between endothelial function, cardiovascular risk factors, and atherosclerosis among patients with hemophilia is warranted, she said.
Dr. van der Valk and colleagues and Dr. Delgado and colleagues did not disclose funding or conflicts of interest. The study by Dr. Jackson and colleagues was supported by the Canadian Hemophilia Society and Pfizer. She disclosed honoraria for speaking engagements for Biogen, Baxalta, and Pfizer and for participating in scientific advisory boards for Bayer, Pfizer, Baxalta, CLS Behring, and Novo Nordisk.
ORLANDO – Conventional wisdom holds that persons with hemophilia are at lower risk for death from cardiovascular events than the general population, but there are conflicting data from studies attempting to confirm or refute this notion.
In a prospective, multicenter European study of more than 500 patients with hemophilia, the predicted cardiovascular disease (CVD) event rate was less than half of what was expected, reported Paul R. van der Valk, MD, from University Medical Center in Utrecht, the Netherlands, and colleagues.
In patients with hemophilia, “the leading cause of death seems to be malignancy related and intracranial hemorrhage. Atrial fibrillation is quite common,” they wrote in a scientific poster presented at the World Federation of Hemophilia World Congress.
But a second study of 100 patients with hemophilia showed that the bleeding disorder did not appear to offer protection against cardiovascular or thrombotic adverse events, Beatriz Delgado, MD, and colleagues at the Centro Hospitalar São João in Porto, Portugal, also presented in a poster session.
Risk scores considered
The prospective study by Dr. van der Valk and colleagues was designed to assess the incidence of CVD in patients with hemophilia in the Netherlands and the United Kingdom, compared with the general population. They used the QRISK2 cardiovascular risk score (2011 version). This instrument is used to calculate risk of CVD events in adults from 30 to 84 with no history of CVD or statin use.
Among 557 patients with a calculable QRISK2 score at 2 years of follow-up, there were four CVD events, including two cases of ischemic heart disease, one ischemic stroke, and one intracranial hemorrhage. The median 2-year QRISK2 score was 1.7%, and the 10-year risk was 9.0%, which translated in to an expected 9.5 CVD events during 2 years of follow-up.
Among the additional 104 patients who could not have a QRISK2 score calculated because of age over 84, statin use, or history of CVD, there were four CVD events: ischemic heart disease, transient ischemic attack/carotid artery stenosis, myocardial infarction, and intracranial hemorrhage.
Other CVD events occurring in both groups included atrial fibrillation in eight patients, other arrhythmia in three, and, in one patient each, aortic valve pathology, pericarditis, and carotid artery plaque.
Portuguese experience
Dr, Delgado and colleagues noted that although hemophilia has traditionally been regarded as protective against ischemic heart disease or thrombotic events, modern management “has prolonged life expectancy of people with hemophilia and consequently, an associated increase in incidence and prevalence of conditions that affect the general older population, such as cardiovascular disease and hypertension, are expected.”
They conducted a retrospective analysis of 100 adults (69 with hemophilia A, and 31 with hemophilia B) treated at their center. Overall, 29 patients had severe hemophilia A, 20 moderate hemophilia A, and 20 mild hemophilia A. Among patients with hemophilia B, 11 had severe, 15 moderate, and 5 mild disease.
Two patients (one with moderate and one with severe hemophilia) had angina episodes with coronary artery disease and underwent multiple coronary bypass grafts. The patient with severe disease had a disabling ischemic stroke during recovery from bypass surgery, and the patient with moderate hemophilia had an acute myocardial infarction prior to bypass surgery.
Two other patients had transient ischemic strokes from which they recovered without disability.
The main cardiovascular risk factors identified in this population were hypertension, diabetes mellitus, heavy smoking, obesity, and dyslipidemia. All patients were screened for prothrombotic risk, and all patients had negative test results.
“Hemophilia does not seem to have a protective effect against thrombotic/cardiovascular events, mainly in [patients with] coronary artery disease,” the investigators wrote.
Endothelial function
In a study presented in an oral abstract session, Shannon Jackson, MD, of the University of British Columbia in Vancouver found that men with hemophilia appear to have better macrovascular endothelial function but worse microvascular endothelial function than did men with normal clotting parameters.
“Based on endothelial function, contemporary hemophilia cohorts may have a different profile of cardiovascular risk than healthy controls,” she said.
Although they do not have an obvious mechanistic explanation for the differences in microvascular function among patients with hemophilia vs. healthy controls, there is evidence to show that microvascular function is predictive of cardiovascular events independent of other risk factors in otherwise healthy people. Their findings indicate that further study of the association between endothelial function, cardiovascular risk factors, and atherosclerosis among patients with hemophilia is warranted, she said.
Dr. van der Valk and colleagues and Dr. Delgado and colleagues did not disclose funding or conflicts of interest. The study by Dr. Jackson and colleagues was supported by the Canadian Hemophilia Society and Pfizer. She disclosed honoraria for speaking engagements for Biogen, Baxalta, and Pfizer and for participating in scientific advisory boards for Bayer, Pfizer, Baxalta, CLS Behring, and Novo Nordisk.
ORLANDO – Conventional wisdom holds that persons with hemophilia are at lower risk for death from cardiovascular events than the general population, but there are conflicting data from studies attempting to confirm or refute this notion.
In a prospective, multicenter European study of more than 500 patients with hemophilia, the predicted cardiovascular disease (CVD) event rate was less than half of what was expected, reported Paul R. van der Valk, MD, from University Medical Center in Utrecht, the Netherlands, and colleagues.
In patients with hemophilia, “the leading cause of death seems to be malignancy related and intracranial hemorrhage. Atrial fibrillation is quite common,” they wrote in a scientific poster presented at the World Federation of Hemophilia World Congress.
But a second study of 100 patients with hemophilia showed that the bleeding disorder did not appear to offer protection against cardiovascular or thrombotic adverse events, Beatriz Delgado, MD, and colleagues at the Centro Hospitalar São João in Porto, Portugal, also presented in a poster session.
Risk scores considered
The prospective study by Dr. van der Valk and colleagues was designed to assess the incidence of CVD in patients with hemophilia in the Netherlands and the United Kingdom, compared with the general population. They used the QRISK2 cardiovascular risk score (2011 version). This instrument is used to calculate risk of CVD events in adults from 30 to 84 with no history of CVD or statin use.
Among 557 patients with a calculable QRISK2 score at 2 years of follow-up, there were four CVD events, including two cases of ischemic heart disease, one ischemic stroke, and one intracranial hemorrhage. The median 2-year QRISK2 score was 1.7%, and the 10-year risk was 9.0%, which translated in to an expected 9.5 CVD events during 2 years of follow-up.
Among the additional 104 patients who could not have a QRISK2 score calculated because of age over 84, statin use, or history of CVD, there were four CVD events: ischemic heart disease, transient ischemic attack/carotid artery stenosis, myocardial infarction, and intracranial hemorrhage.
Other CVD events occurring in both groups included atrial fibrillation in eight patients, other arrhythmia in three, and, in one patient each, aortic valve pathology, pericarditis, and carotid artery plaque.
Portuguese experience
Dr, Delgado and colleagues noted that although hemophilia has traditionally been regarded as protective against ischemic heart disease or thrombotic events, modern management “has prolonged life expectancy of people with hemophilia and consequently, an associated increase in incidence and prevalence of conditions that affect the general older population, such as cardiovascular disease and hypertension, are expected.”
They conducted a retrospective analysis of 100 adults (69 with hemophilia A, and 31 with hemophilia B) treated at their center. Overall, 29 patients had severe hemophilia A, 20 moderate hemophilia A, and 20 mild hemophilia A. Among patients with hemophilia B, 11 had severe, 15 moderate, and 5 mild disease.
Two patients (one with moderate and one with severe hemophilia) had angina episodes with coronary artery disease and underwent multiple coronary bypass grafts. The patient with severe disease had a disabling ischemic stroke during recovery from bypass surgery, and the patient with moderate hemophilia had an acute myocardial infarction prior to bypass surgery.
Two other patients had transient ischemic strokes from which they recovered without disability.
The main cardiovascular risk factors identified in this population were hypertension, diabetes mellitus, heavy smoking, obesity, and dyslipidemia. All patients were screened for prothrombotic risk, and all patients had negative test results.
“Hemophilia does not seem to have a protective effect against thrombotic/cardiovascular events, mainly in [patients with] coronary artery disease,” the investigators wrote.
Endothelial function
In a study presented in an oral abstract session, Shannon Jackson, MD, of the University of British Columbia in Vancouver found that men with hemophilia appear to have better macrovascular endothelial function but worse microvascular endothelial function than did men with normal clotting parameters.
“Based on endothelial function, contemporary hemophilia cohorts may have a different profile of cardiovascular risk than healthy controls,” she said.
Although they do not have an obvious mechanistic explanation for the differences in microvascular function among patients with hemophilia vs. healthy controls, there is evidence to show that microvascular function is predictive of cardiovascular events independent of other risk factors in otherwise healthy people. Their findings indicate that further study of the association between endothelial function, cardiovascular risk factors, and atherosclerosis among patients with hemophilia is warranted, she said.
Dr. van der Valk and colleagues and Dr. Delgado and colleagues did not disclose funding or conflicts of interest. The study by Dr. Jackson and colleagues was supported by the Canadian Hemophilia Society and Pfizer. She disclosed honoraria for speaking engagements for Biogen, Baxalta, and Pfizer and for participating in scientific advisory boards for Bayer, Pfizer, Baxalta, CLS Behring, and Novo Nordisk.
At WFH 2016 World Congress
Key clinical point: Hemophilia has traditionally been considered protective against CVD but data presented at the World Federation of Hemophilia World Congress show conflicting results.Major finding: The CVD event rate in one study was lower than predicted by risk scores, but a separate study showed a higher rate of events. A third study suggests that men with hemophilia have worse microvascular endothelial function than men without bleeding disorders.
Data source: Two prospective and one retrospective study of CVD in patients with hemophilia.
Disclosures: Dr. van der Valk and colleagues and Dr. Delgado and colleagues did not disclose funding or conflicts of interest. The study by Dr. Jackson and colleagues was supported by the Canadian Hemophilia Society and Pfizer. She disclosed honoraria for speaking engagements for Biogen, Baxalta, and Pfizer and for participating in scientific advisory boards for Bayer, Pfizer, Baxalta, CLS Behring, and Novo Nordisk.

Age, not infusion frequency, affects hemophilia prophylaxis adherence
ORLANDO – The frequency of prophylactic clotting factor infusions does not appear to adversely affect adherence to hemophilia therapy in children, but age seems to play a role in compliance to prescribed regimens, investigators in two separate studies report.
A study of pediatric patients with moderate to severe hemophilia A or B on bleeding prophylaxis showed no significant differences in adherence between patients receiving two clotting factor infusions per week and those receiving three or four per week, reported Karen Strike, a physiotherapist at McMaster Children’s Hospital in Hamilton, Ont., and colleagues.

“This study demonstrates that our patients have a very high degree of adherence, and it doesn’t appear to be related to infusion frequency,” she said in an interview at a scientific poster session at the World Federation of Hemophilia World Congress.
Although their sample size was small – just 23 patients – the median levels of adherence were high for both twice-weekly infusers (99.5%) and 3-4 times per week infusers (96%; P = .053).
Ms. Strike acknowledges that the borderline P value could be due to the small sample size instead of a lack of association. Additionally, because the patients are managed by a regional hemophilia treatment center, they tend to be more engaged and more likely to cooperate with clinician instructions, she said.
“Basically, patients are either going to do what’s prescribed or they’re not. What that actual prescription is doesn’t seem to matter. If they prescribe you twice a week or they prescribe me every other day, you’re going to be adherent to twice a week or you’re not.
The investigators have expanded their study to include adult patients on primary prophylaxis and to look at additional co-variates that might have an effect on adherence, including interactions with a health care team, geographical distance from a hemophilia treatment center, joint health status, and infusion delivery method (peripheral vs. port).
Age may be a factor
In a separate study, German investigators report that adherence appears to vary by age.
Wolfgang Miesbach, MD, from Goethe University Hospital in Frankfurt, Germany, and colleagues asked all members of the German hemophilia patient organization with moderate or severe hemophilia to fill out the VERITAS-PRO (Validated Hemophilia Regimen Treatment Adherence Scale-Prophylaxis) questionnaire and compared scores across age groups.
Data were available on a total of 364 patients. The investigators found that among 131 children from birth to age 19, adherence to prescribed regimens was 100%. In contrast, the adherence rate among 189 adults aged 20-59 was 88.1%. After age 59, adherence rates began to improve as those 60 and older (44 patients) reported 93.9% adherence.
“Within the patients aged 20+, care by a hemophilia center was the only significant indicator for better adherence. The tendency of better adherence of patients aged greater than 60 compared to patients 20-59 may be explained by the significant association of the occurrence of pain with increasing age although a significant influence of pain on the adherence levels could not be demonstrated,” the investigators wrote.
Their findings point the way to possible interventions to facilitate adherence to prophylaxis among patients with hemophilia, they wrote.
Both studies were internally funded. The authors reported no relevant disclosures.
ORLANDO – The frequency of prophylactic clotting factor infusions does not appear to adversely affect adherence to hemophilia therapy in children, but age seems to play a role in compliance to prescribed regimens, investigators in two separate studies report.
A study of pediatric patients with moderate to severe hemophilia A or B on bleeding prophylaxis showed no significant differences in adherence between patients receiving two clotting factor infusions per week and those receiving three or four per week, reported Karen Strike, a physiotherapist at McMaster Children’s Hospital in Hamilton, Ont., and colleagues.
“This study demonstrates that our patients have a very high degree of adherence, and it doesn’t appear to be related to infusion frequency,” she said in an interview at a scientific poster session at the World Federation of Hemophilia World Congress.
Although their sample size was small – just 23 patients – the median levels of adherence were high for both twice-weekly infusers (99.5%) and 3-4 times per week infusers (96%; P = .053).
Ms. Strike acknowledges that the borderline P value could be due to the small sample size instead of a lack of association. Additionally, because the patients are managed by a regional hemophilia treatment center, they tend to be more engaged and more likely to cooperate with clinician instructions, she said.
“Basically, patients are either going to do what’s prescribed or they’re not. What that actual prescription is doesn’t seem to matter. If they prescribe you twice a week or they prescribe me every other day, you’re going to be adherent to twice a week or you’re not.
The investigators have expanded their study to include adult patients on primary prophylaxis and to look at additional co-variates that might have an effect on adherence, including interactions with a health care team, geographical distance from a hemophilia treatment center, joint health status, and infusion delivery method (peripheral vs. port).
Age may be a factor
In a separate study, German investigators report that adherence appears to vary by age.
Wolfgang Miesbach, MD, from Goethe University Hospital in Frankfurt, Germany, and colleagues asked all members of the German hemophilia patient organization with moderate or severe hemophilia to fill out the VERITAS-PRO (Validated Hemophilia Regimen Treatment Adherence Scale-Prophylaxis) questionnaire and compared scores across age groups.
Data were available on a total of 364 patients. The investigators found that among 131 children from birth to age 19, adherence to prescribed regimens was 100%. In contrast, the adherence rate among 189 adults aged 20-59 was 88.1%. After age 59, adherence rates began to improve as those 60 and older (44 patients) reported 93.9% adherence.
“Within the patients aged 20+, care by a hemophilia center was the only significant indicator for better adherence. The tendency of better adherence of patients aged greater than 60 compared to patients 20-59 may be explained by the significant association of the occurrence of pain with increasing age although a significant influence of pain on the adherence levels could not be demonstrated,” the investigators wrote.
Their findings point the way to possible interventions to facilitate adherence to prophylaxis among patients with hemophilia, they wrote.
Both studies were internally funded. The authors reported no relevant disclosures.
ORLANDO – The frequency of prophylactic clotting factor infusions does not appear to adversely affect adherence to hemophilia therapy in children, but age seems to play a role in compliance to prescribed regimens, investigators in two separate studies report.
A study of pediatric patients with moderate to severe hemophilia A or B on bleeding prophylaxis showed no significant differences in adherence between patients receiving two clotting factor infusions per week and those receiving three or four per week, reported Karen Strike, a physiotherapist at McMaster Children’s Hospital in Hamilton, Ont., and colleagues.
“This study demonstrates that our patients have a very high degree of adherence, and it doesn’t appear to be related to infusion frequency,” she said in an interview at a scientific poster session at the World Federation of Hemophilia World Congress.
Although their sample size was small – just 23 patients – the median levels of adherence were high for both twice-weekly infusers (99.5%) and 3-4 times per week infusers (96%; P = .053).
Ms. Strike acknowledges that the borderline P value could be due to the small sample size instead of a lack of association. Additionally, because the patients are managed by a regional hemophilia treatment center, they tend to be more engaged and more likely to cooperate with clinician instructions, she said.
“Basically, patients are either going to do what’s prescribed or they’re not. What that actual prescription is doesn’t seem to matter. If they prescribe you twice a week or they prescribe me every other day, you’re going to be adherent to twice a week or you’re not.
The investigators have expanded their study to include adult patients on primary prophylaxis and to look at additional co-variates that might have an effect on adherence, including interactions with a health care team, geographical distance from a hemophilia treatment center, joint health status, and infusion delivery method (peripheral vs. port).
Age may be a factor
In a separate study, German investigators report that adherence appears to vary by age.
Wolfgang Miesbach, MD, from Goethe University Hospital in Frankfurt, Germany, and colleagues asked all members of the German hemophilia patient organization with moderate or severe hemophilia to fill out the VERITAS-PRO (Validated Hemophilia Regimen Treatment Adherence Scale-Prophylaxis) questionnaire and compared scores across age groups.
Data were available on a total of 364 patients. The investigators found that among 131 children from birth to age 19, adherence to prescribed regimens was 100%. In contrast, the adherence rate among 189 adults aged 20-59 was 88.1%. After age 59, adherence rates began to improve as those 60 and older (44 patients) reported 93.9% adherence.
“Within the patients aged 20+, care by a hemophilia center was the only significant indicator for better adherence. The tendency of better adherence of patients aged greater than 60 compared to patients 20-59 may be explained by the significant association of the occurrence of pain with increasing age although a significant influence of pain on the adherence levels could not be demonstrated,” the investigators wrote.
Their findings point the way to possible interventions to facilitate adherence to prophylaxis among patients with hemophilia, they wrote.
Both studies were internally funded. The authors reported no relevant disclosures.
AT WFH 2016 WORLD CONGRESS
Key clinical point: Adherence to hemophilia prophylaxis regimens may be influenced by age but not frequency of infusions.
Major finding: Infusion frequency did not make a difference in adherence rates, but young and middle-aged adults reported lower adherence than did children or seniors.
Data source: A study of 23 pediatric hemophilia patients in Canada, and a separate study of 364 children and adults with moderate to severe hemophilia in Germany.
Disclosures: Both studies were internally funded. The authors reported no relevant disclosures.
