User login
Families in Psychiatry: Parental alienation and shared delusional disorders
Disturbances in family emotional involvement are best understood at the extremes. At one end, there is extreme cutoff in the controversial diagnosis of parental alienation. At the other end is the extreme enmeshment in shared delusional disorders. What are the mechanisms that allow these conditions to develop? Helping families understand these mechanisms can help them change the trajectory of the family, by moving toward the middle, toward appropriate family emotional involvement.
How does enmeshment begin?
Good parents want to instill good morals, values, and behaviors in their children. Good parents want to teach their children to be good citizens, have good manners, and to treat others with respect. However, sometimes parents desire something more from their children; they want their children to continue a family business, be part of their religious organization, or to be “just like us.” Parental influence is easier when communities are isolated. When shared family beliefs are pervasive and impede the individuation of thoughts, feelings, and behaviors, these families are considered enmeshed and undifferentiated. Enmeshed families are more susceptible to indoctrination. Indoctrination is easier when there is a high level of emotional involvement, meaning that children are kept close, and differentiation and individuation are discouraged.
Using a child for one’s own needs is exploitative;however, many parents might not understand how their own unconscious psychological needs affect their children. This is seen clearly when children are rejected because they are “different.” For example, some parents have stated that a lesbian, gay, bisexual, and transgender sexual orientation is “against their religion,” and demand that their child conform to the family beliefs and norms. In these cases, the adolescent or young adult has to decide whether to leave the family, conform to its beliefs, or hide his or her identity.
Enmeshment
Emotional overinvolvement in undifferentiated enmeshed families is central to the diagnosis of shared delusional disorder. One example of a shared delusion is delusional parasitosis. This is a rare delusional disorder where the patient is convinced of being infested with worms, insects, parasites, or bacteria while no objective evidence exists to support this belief. Somatic delusions are shared with one or more members of a family in 5%-15% of cases (J. Behav. Health 2014;3:200-2).
Salvador Minuchin, Ph.D., and his colleagues outlined the impact of enmeshment in families where a child has an eating disorder. They described children so overprotected that there was a virtual moat around the family system, blocking out the world. Interpersonal differentiation in an enmeshed family system was poor, with identity fusion between parent and child. In this dynamic, the child is unable to establish a clear identity apart from the parent. Orthorexia, a term coined in 1997 by Dr. Steven Bratman, is defined as an obsession with “healthy or righteous eating.” The obsession with healthy foods can be structured within family habits. When enmeshment and family isolation are present, orthorexia can show up as a folie à famille (Heru, personal experience).
More exotic examples are known by the French terms folie à deux and folie à famille. Dr. Ernest-Charles Lasegue (Ann. Med. Psychol. 1877;18:321) was the first person to describe folie à deux. He stated that the inducer created the delusions from his/her psychosis and imposed them upon a “passive” individual; the induced subject was not truly psychotic but instead “absurdly credulous.” Several varieties are described. Folie imposée is the one we typically think of, where the naive individual has a resolution of symptoms when removed from the dominant person. Folie simultanée is where simultaneous and identical psychoses occur in two predisposed people who have had a long and intimate association with each other. There is usually no dominant partner, and separation does not alleviate the symptomatology. Folie communiquée involves the transfer of psychotic delusions after a long period of resistance by the passive partner. The recipient of the delusions subsequently develops his own delusions, independent of the primary subject’s, and these persist following separation.
Folie induite, a variant of folie communiquée, is diagnosed when new delusions are added to old ones under the influence of another deluded patient. The secondary person enriches the newly acquired delusions. Another method of classification is based on the number of individuals involved: folie à trois (three), folie à quatre (four), folie à cinq (five), and, as mentioned earlier, folie àfamille.
What is the mechanism for enmeshment? Several predisposing factors can occur: social isolation, the presence of a naive or “absurdly credulous” person, and in the case of relatives, a shared genetic predisposition. It is most common for the dominant person to drive the belief that is then accepted by dependent family members. In the case of children, there is also identification with a parent and a lack of drive for separation.
Role of alienation
At the opposite end of the spectrum is alienation, most publicly described in the disputed diagnosis of parental alienation syndrome (PAS) (The Parental Alienation Syndrome, 2nd ed., Cresskill, N.J.:Creative Therapeutics Inc., 1998). PAS sometimes arises in the context of child-custody disputes. The primary manifestation is the child’s unjustified denigration of one parent. According to Dr. William Bernet and Amy J.L. Baker, Ph.D., PAS features “abnormal, maladaptive behavior (refusal to have a relationship with a loving parent) that is driven by an abnormal mental state (the false belief that the rejected parent is evil, dangerous, or unworthy of love)” (J. Am. Acad. Psychiatry Law 2013;41:98-104). There is considered to be brainwashing of the child by one parent against the other parent in order to gain leverage in a court of law.
What is the mechanism in alienation? Enmeshment and overidentification of the child with the favored custodial parent is common. The child depends on this adult for his survival. The process of divorce can increase enmeshment with the custodial parent. The parent might reinforce the enmeshment by instilling fear of the “other” parent. The belief that the “other parent” is “bad” is transmitted through conscious and unconscious mechanisms.
The conscious mechanism is direct expression of anger toward the alienated parent. The anger might be motivated by rejection or as revenge for rejection with a desire to punish. The unconscious mechanisms include projective identification. In this situation, anger is seen as being embodied within the “other.” The projecting parent who continues to “hate” keeps the children tied to her out of projected fear of the “other.” The parent who uses projection is likely to have a primitive character structure. The child of the narcissistic custodial parent then acts out the shame and rage at the failure of the marriage.
These domestic tragedies have been around since the beginning of time. In Greek mythology, Medea, having been abandoned by Jason, took her revenge by murdering her two children. “Hell hath no fury like a woman scorned” is a paraphrase from William Congreve’s The Mourning Bride (1697).
What does the DSM-5 say?
Are these disorders and syndromes “real” psychiatric illnesses? The DSM-5 no longer separates delusional disorder from shared delusional disorder. If criteria are met for delusional disorder, that diagnosis is made. If the diagnosis cannot be made but shared beliefs are present, the diagnosis “other specified schizophrenia spectrum and other psychotic disorder” is used.
Those who advocated for inclusion of PAS cited the benefits that follow from a legitimate diagnosis such as legitimatizing problems that family therapists and psychotherapists encounter, allowing insurance coverage, and stimulating research. However, PAS was rejected as not having a good enough scientific basis.
Managing affective involvement
How does the psychiatrist manage families where emotional involvement is extreme? Psychiatrists first need to decide whether the family is capable of making changes and is willing to work on structural change within the family. If not, we can help patients remove themselves from destructive family situations. If the patient in your office wants to leave the family system or minimize the impact of the family system, individual psychotherapy that identifies the impact of family dysfunction, such as cognitive-behavioral therapy, can be used as a type of deprogramming. Exit strategies also can be discussed.
Al-Anon, for example, clarifies the influence of the family system on family members’ well-being by asking several questions, including:
Do you tell lies to cover up for someone else’s drinking?
Do you feel that if they cared about you, they would stop drinking to please you?
Do you make threats, such as, “If you don’t stop drinking, I’ll leave you?”
Are you afraid to upset someone for fear it will set off a drinking bout?
Have you considered calling the police for help in fear of abuse?
Do you feel like a failure because you can’t control the drinking?
Do you think that if they stopped drinking, your other problems would be solved?
If you think there is capacity for family change, the following strategies are helpful:
1. Education about appropriate differentiation
According to Dr. Murray Bowen, one of the main tasks of individuation is finding the right level of differentiation from parents. At one end of the differentiation spectrum is emotional fusion, and at the other end is emotional cutoff (disconnection between family members or refusal to engage with certain family members) (see “Family Evaluation,” New York: W.W. Norton & Co., 1988).
When family enmeshment is present, we can educate the family about individuation. In this way, the family develops a greater intellectual understanding of how they function, compared to their cultural norm. The family may benefit from creating a genogram that clarifies patterns of emotional involvement in their family of origin. Look for intergenerational patterns, and discuss how emotional differentiation occurred in prior generations. Teach the family about the emotional tasks of differentiation.
2. If there is alienation, parse out the reasons
Clarify conscious mechanisms that force the child to reject the other parent. Help the parent understand the consequences for the child in having no access to the other parent. Again, using a genogram helps identify intergenerational patterns, such as emotional cutoffs. Explore the reason for prior family emotional cutoffs. Identify typical patterns in the family for managing anger and conflicts.
In cases of divorce of the custodial parent, look at how anger is managed and stages of grief. Look for the presence of narcissistic injury. Discuss what a good divorce is and the healthiest way for the child to grow up. Help the parent manage and process her own affect without contaminating the child. It is not the role of the child to be the parental caregiver.
Help the child see that there was a loving relationship in the past and that new family goals can be created. The child also might experience anger and grief, and it is important to educate the child about how to manage those feelings appropriately rather than using blame and alienation. Help the child be empowered by positive ideals rather than negative emotions.
Psychiatrists often avoid working with these families, and perceive them as stuck and unable to change. This might be true for some families but certainly not all. Many families find themselves in situations that they do not understand and with problems they need help resolving. Educating and working with families who are stuck and who ask for and want change can change the life trajectory of many people.
Dr. Heru is with the department of psychiatry at the University of Colorado Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013).
Disturbances in family emotional involvement are best understood at the extremes. At one end, there is extreme cutoff in the controversial diagnosis of parental alienation. At the other end is the extreme enmeshment in shared delusional disorders. What are the mechanisms that allow these conditions to develop? Helping families understand these mechanisms can help them change the trajectory of the family, by moving toward the middle, toward appropriate family emotional involvement.
How does enmeshment begin?
Good parents want to instill good morals, values, and behaviors in their children. Good parents want to teach their children to be good citizens, have good manners, and to treat others with respect. However, sometimes parents desire something more from their children; they want their children to continue a family business, be part of their religious organization, or to be “just like us.” Parental influence is easier when communities are isolated. When shared family beliefs are pervasive and impede the individuation of thoughts, feelings, and behaviors, these families are considered enmeshed and undifferentiated. Enmeshed families are more susceptible to indoctrination. Indoctrination is easier when there is a high level of emotional involvement, meaning that children are kept close, and differentiation and individuation are discouraged.
Using a child for one’s own needs is exploitative;however, many parents might not understand how their own unconscious psychological needs affect their children. This is seen clearly when children are rejected because they are “different.” For example, some parents have stated that a lesbian, gay, bisexual, and transgender sexual orientation is “against their religion,” and demand that their child conform to the family beliefs and norms. In these cases, the adolescent or young adult has to decide whether to leave the family, conform to its beliefs, or hide his or her identity.
Enmeshment
Emotional overinvolvement in undifferentiated enmeshed families is central to the diagnosis of shared delusional disorder. One example of a shared delusion is delusional parasitosis. This is a rare delusional disorder where the patient is convinced of being infested with worms, insects, parasites, or bacteria while no objective evidence exists to support this belief. Somatic delusions are shared with one or more members of a family in 5%-15% of cases (J. Behav. Health 2014;3:200-2).
Salvador Minuchin, Ph.D., and his colleagues outlined the impact of enmeshment in families where a child has an eating disorder. They described children so overprotected that there was a virtual moat around the family system, blocking out the world. Interpersonal differentiation in an enmeshed family system was poor, with identity fusion between parent and child. In this dynamic, the child is unable to establish a clear identity apart from the parent. Orthorexia, a term coined in 1997 by Dr. Steven Bratman, is defined as an obsession with “healthy or righteous eating.” The obsession with healthy foods can be structured within family habits. When enmeshment and family isolation are present, orthorexia can show up as a folie à famille (Heru, personal experience).
More exotic examples are known by the French terms folie à deux and folie à famille. Dr. Ernest-Charles Lasegue (Ann. Med. Psychol. 1877;18:321) was the first person to describe folie à deux. He stated that the inducer created the delusions from his/her psychosis and imposed them upon a “passive” individual; the induced subject was not truly psychotic but instead “absurdly credulous.” Several varieties are described. Folie imposée is the one we typically think of, where the naive individual has a resolution of symptoms when removed from the dominant person. Folie simultanée is where simultaneous and identical psychoses occur in two predisposed people who have had a long and intimate association with each other. There is usually no dominant partner, and separation does not alleviate the symptomatology. Folie communiquée involves the transfer of psychotic delusions after a long period of resistance by the passive partner. The recipient of the delusions subsequently develops his own delusions, independent of the primary subject’s, and these persist following separation.
Folie induite, a variant of folie communiquée, is diagnosed when new delusions are added to old ones under the influence of another deluded patient. The secondary person enriches the newly acquired delusions. Another method of classification is based on the number of individuals involved: folie à trois (three), folie à quatre (four), folie à cinq (five), and, as mentioned earlier, folie àfamille.
What is the mechanism for enmeshment? Several predisposing factors can occur: social isolation, the presence of a naive or “absurdly credulous” person, and in the case of relatives, a shared genetic predisposition. It is most common for the dominant person to drive the belief that is then accepted by dependent family members. In the case of children, there is also identification with a parent and a lack of drive for separation.
Role of alienation
At the opposite end of the spectrum is alienation, most publicly described in the disputed diagnosis of parental alienation syndrome (PAS) (The Parental Alienation Syndrome, 2nd ed., Cresskill, N.J.:Creative Therapeutics Inc., 1998). PAS sometimes arises in the context of child-custody disputes. The primary manifestation is the child’s unjustified denigration of one parent. According to Dr. William Bernet and Amy J.L. Baker, Ph.D., PAS features “abnormal, maladaptive behavior (refusal to have a relationship with a loving parent) that is driven by an abnormal mental state (the false belief that the rejected parent is evil, dangerous, or unworthy of love)” (J. Am. Acad. Psychiatry Law 2013;41:98-104). There is considered to be brainwashing of the child by one parent against the other parent in order to gain leverage in a court of law.
What is the mechanism in alienation? Enmeshment and overidentification of the child with the favored custodial parent is common. The child depends on this adult for his survival. The process of divorce can increase enmeshment with the custodial parent. The parent might reinforce the enmeshment by instilling fear of the “other” parent. The belief that the “other parent” is “bad” is transmitted through conscious and unconscious mechanisms.
The conscious mechanism is direct expression of anger toward the alienated parent. The anger might be motivated by rejection or as revenge for rejection with a desire to punish. The unconscious mechanisms include projective identification. In this situation, anger is seen as being embodied within the “other.” The projecting parent who continues to “hate” keeps the children tied to her out of projected fear of the “other.” The parent who uses projection is likely to have a primitive character structure. The child of the narcissistic custodial parent then acts out the shame and rage at the failure of the marriage.
These domestic tragedies have been around since the beginning of time. In Greek mythology, Medea, having been abandoned by Jason, took her revenge by murdering her two children. “Hell hath no fury like a woman scorned” is a paraphrase from William Congreve’s The Mourning Bride (1697).
What does the DSM-5 say?
Are these disorders and syndromes “real” psychiatric illnesses? The DSM-5 no longer separates delusional disorder from shared delusional disorder. If criteria are met for delusional disorder, that diagnosis is made. If the diagnosis cannot be made but shared beliefs are present, the diagnosis “other specified schizophrenia spectrum and other psychotic disorder” is used.
Those who advocated for inclusion of PAS cited the benefits that follow from a legitimate diagnosis such as legitimatizing problems that family therapists and psychotherapists encounter, allowing insurance coverage, and stimulating research. However, PAS was rejected as not having a good enough scientific basis.
Managing affective involvement
How does the psychiatrist manage families where emotional involvement is extreme? Psychiatrists first need to decide whether the family is capable of making changes and is willing to work on structural change within the family. If not, we can help patients remove themselves from destructive family situations. If the patient in your office wants to leave the family system or minimize the impact of the family system, individual psychotherapy that identifies the impact of family dysfunction, such as cognitive-behavioral therapy, can be used as a type of deprogramming. Exit strategies also can be discussed.
Al-Anon, for example, clarifies the influence of the family system on family members’ well-being by asking several questions, including:
Do you tell lies to cover up for someone else’s drinking?
Do you feel that if they cared about you, they would stop drinking to please you?
Do you make threats, such as, “If you don’t stop drinking, I’ll leave you?”
Are you afraid to upset someone for fear it will set off a drinking bout?
Have you considered calling the police for help in fear of abuse?
Do you feel like a failure because you can’t control the drinking?
Do you think that if they stopped drinking, your other problems would be solved?
If you think there is capacity for family change, the following strategies are helpful:
1. Education about appropriate differentiation
According to Dr. Murray Bowen, one of the main tasks of individuation is finding the right level of differentiation from parents. At one end of the differentiation spectrum is emotional fusion, and at the other end is emotional cutoff (disconnection between family members or refusal to engage with certain family members) (see “Family Evaluation,” New York: W.W. Norton & Co., 1988).
When family enmeshment is present, we can educate the family about individuation. In this way, the family develops a greater intellectual understanding of how they function, compared to their cultural norm. The family may benefit from creating a genogram that clarifies patterns of emotional involvement in their family of origin. Look for intergenerational patterns, and discuss how emotional differentiation occurred in prior generations. Teach the family about the emotional tasks of differentiation.
2. If there is alienation, parse out the reasons
Clarify conscious mechanisms that force the child to reject the other parent. Help the parent understand the consequences for the child in having no access to the other parent. Again, using a genogram helps identify intergenerational patterns, such as emotional cutoffs. Explore the reason for prior family emotional cutoffs. Identify typical patterns in the family for managing anger and conflicts.
In cases of divorce of the custodial parent, look at how anger is managed and stages of grief. Look for the presence of narcissistic injury. Discuss what a good divorce is and the healthiest way for the child to grow up. Help the parent manage and process her own affect without contaminating the child. It is not the role of the child to be the parental caregiver.
Help the child see that there was a loving relationship in the past and that new family goals can be created. The child also might experience anger and grief, and it is important to educate the child about how to manage those feelings appropriately rather than using blame and alienation. Help the child be empowered by positive ideals rather than negative emotions.
Psychiatrists often avoid working with these families, and perceive them as stuck and unable to change. This might be true for some families but certainly not all. Many families find themselves in situations that they do not understand and with problems they need help resolving. Educating and working with families who are stuck and who ask for and want change can change the life trajectory of many people.
Dr. Heru is with the department of psychiatry at the University of Colorado Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013).
Disturbances in family emotional involvement are best understood at the extremes. At one end, there is extreme cutoff in the controversial diagnosis of parental alienation. At the other end is the extreme enmeshment in shared delusional disorders. What are the mechanisms that allow these conditions to develop? Helping families understand these mechanisms can help them change the trajectory of the family, by moving toward the middle, toward appropriate family emotional involvement.
How does enmeshment begin?
Good parents want to instill good morals, values, and behaviors in their children. Good parents want to teach their children to be good citizens, have good manners, and to treat others with respect. However, sometimes parents desire something more from their children; they want their children to continue a family business, be part of their religious organization, or to be “just like us.” Parental influence is easier when communities are isolated. When shared family beliefs are pervasive and impede the individuation of thoughts, feelings, and behaviors, these families are considered enmeshed and undifferentiated. Enmeshed families are more susceptible to indoctrination. Indoctrination is easier when there is a high level of emotional involvement, meaning that children are kept close, and differentiation and individuation are discouraged.
Using a child for one’s own needs is exploitative;however, many parents might not understand how their own unconscious psychological needs affect their children. This is seen clearly when children are rejected because they are “different.” For example, some parents have stated that a lesbian, gay, bisexual, and transgender sexual orientation is “against their religion,” and demand that their child conform to the family beliefs and norms. In these cases, the adolescent or young adult has to decide whether to leave the family, conform to its beliefs, or hide his or her identity.
Enmeshment
Emotional overinvolvement in undifferentiated enmeshed families is central to the diagnosis of shared delusional disorder. One example of a shared delusion is delusional parasitosis. This is a rare delusional disorder where the patient is convinced of being infested with worms, insects, parasites, or bacteria while no objective evidence exists to support this belief. Somatic delusions are shared with one or more members of a family in 5%-15% of cases (J. Behav. Health 2014;3:200-2).
Salvador Minuchin, Ph.D., and his colleagues outlined the impact of enmeshment in families where a child has an eating disorder. They described children so overprotected that there was a virtual moat around the family system, blocking out the world. Interpersonal differentiation in an enmeshed family system was poor, with identity fusion between parent and child. In this dynamic, the child is unable to establish a clear identity apart from the parent. Orthorexia, a term coined in 1997 by Dr. Steven Bratman, is defined as an obsession with “healthy or righteous eating.” The obsession with healthy foods can be structured within family habits. When enmeshment and family isolation are present, orthorexia can show up as a folie à famille (Heru, personal experience).
More exotic examples are known by the French terms folie à deux and folie à famille. Dr. Ernest-Charles Lasegue (Ann. Med. Psychol. 1877;18:321) was the first person to describe folie à deux. He stated that the inducer created the delusions from his/her psychosis and imposed them upon a “passive” individual; the induced subject was not truly psychotic but instead “absurdly credulous.” Several varieties are described. Folie imposée is the one we typically think of, where the naive individual has a resolution of symptoms when removed from the dominant person. Folie simultanée is where simultaneous and identical psychoses occur in two predisposed people who have had a long and intimate association with each other. There is usually no dominant partner, and separation does not alleviate the symptomatology. Folie communiquée involves the transfer of psychotic delusions after a long period of resistance by the passive partner. The recipient of the delusions subsequently develops his own delusions, independent of the primary subject’s, and these persist following separation.
Folie induite, a variant of folie communiquée, is diagnosed when new delusions are added to old ones under the influence of another deluded patient. The secondary person enriches the newly acquired delusions. Another method of classification is based on the number of individuals involved: folie à trois (three), folie à quatre (four), folie à cinq (five), and, as mentioned earlier, folie àfamille.
What is the mechanism for enmeshment? Several predisposing factors can occur: social isolation, the presence of a naive or “absurdly credulous” person, and in the case of relatives, a shared genetic predisposition. It is most common for the dominant person to drive the belief that is then accepted by dependent family members. In the case of children, there is also identification with a parent and a lack of drive for separation.
Role of alienation
At the opposite end of the spectrum is alienation, most publicly described in the disputed diagnosis of parental alienation syndrome (PAS) (The Parental Alienation Syndrome, 2nd ed., Cresskill, N.J.:Creative Therapeutics Inc., 1998). PAS sometimes arises in the context of child-custody disputes. The primary manifestation is the child’s unjustified denigration of one parent. According to Dr. William Bernet and Amy J.L. Baker, Ph.D., PAS features “abnormal, maladaptive behavior (refusal to have a relationship with a loving parent) that is driven by an abnormal mental state (the false belief that the rejected parent is evil, dangerous, or unworthy of love)” (J. Am. Acad. Psychiatry Law 2013;41:98-104). There is considered to be brainwashing of the child by one parent against the other parent in order to gain leverage in a court of law.
What is the mechanism in alienation? Enmeshment and overidentification of the child with the favored custodial parent is common. The child depends on this adult for his survival. The process of divorce can increase enmeshment with the custodial parent. The parent might reinforce the enmeshment by instilling fear of the “other” parent. The belief that the “other parent” is “bad” is transmitted through conscious and unconscious mechanisms.
The conscious mechanism is direct expression of anger toward the alienated parent. The anger might be motivated by rejection or as revenge for rejection with a desire to punish. The unconscious mechanisms include projective identification. In this situation, anger is seen as being embodied within the “other.” The projecting parent who continues to “hate” keeps the children tied to her out of projected fear of the “other.” The parent who uses projection is likely to have a primitive character structure. The child of the narcissistic custodial parent then acts out the shame and rage at the failure of the marriage.
These domestic tragedies have been around since the beginning of time. In Greek mythology, Medea, having been abandoned by Jason, took her revenge by murdering her two children. “Hell hath no fury like a woman scorned” is a paraphrase from William Congreve’s The Mourning Bride (1697).
What does the DSM-5 say?
Are these disorders and syndromes “real” psychiatric illnesses? The DSM-5 no longer separates delusional disorder from shared delusional disorder. If criteria are met for delusional disorder, that diagnosis is made. If the diagnosis cannot be made but shared beliefs are present, the diagnosis “other specified schizophrenia spectrum and other psychotic disorder” is used.
Those who advocated for inclusion of PAS cited the benefits that follow from a legitimate diagnosis such as legitimatizing problems that family therapists and psychotherapists encounter, allowing insurance coverage, and stimulating research. However, PAS was rejected as not having a good enough scientific basis.
Managing affective involvement
How does the psychiatrist manage families where emotional involvement is extreme? Psychiatrists first need to decide whether the family is capable of making changes and is willing to work on structural change within the family. If not, we can help patients remove themselves from destructive family situations. If the patient in your office wants to leave the family system or minimize the impact of the family system, individual psychotherapy that identifies the impact of family dysfunction, such as cognitive-behavioral therapy, can be used as a type of deprogramming. Exit strategies also can be discussed.
Al-Anon, for example, clarifies the influence of the family system on family members’ well-being by asking several questions, including:
Do you tell lies to cover up for someone else’s drinking?
Do you feel that if they cared about you, they would stop drinking to please you?
Do you make threats, such as, “If you don’t stop drinking, I’ll leave you?”
Are you afraid to upset someone for fear it will set off a drinking bout?
Have you considered calling the police for help in fear of abuse?
Do you feel like a failure because you can’t control the drinking?
Do you think that if they stopped drinking, your other problems would be solved?
If you think there is capacity for family change, the following strategies are helpful:
1. Education about appropriate differentiation
According to Dr. Murray Bowen, one of the main tasks of individuation is finding the right level of differentiation from parents. At one end of the differentiation spectrum is emotional fusion, and at the other end is emotional cutoff (disconnection between family members or refusal to engage with certain family members) (see “Family Evaluation,” New York: W.W. Norton & Co., 1988).
When family enmeshment is present, we can educate the family about individuation. In this way, the family develops a greater intellectual understanding of how they function, compared to their cultural norm. The family may benefit from creating a genogram that clarifies patterns of emotional involvement in their family of origin. Look for intergenerational patterns, and discuss how emotional differentiation occurred in prior generations. Teach the family about the emotional tasks of differentiation.
2. If there is alienation, parse out the reasons
Clarify conscious mechanisms that force the child to reject the other parent. Help the parent understand the consequences for the child in having no access to the other parent. Again, using a genogram helps identify intergenerational patterns, such as emotional cutoffs. Explore the reason for prior family emotional cutoffs. Identify typical patterns in the family for managing anger and conflicts.
In cases of divorce of the custodial parent, look at how anger is managed and stages of grief. Look for the presence of narcissistic injury. Discuss what a good divorce is and the healthiest way for the child to grow up. Help the parent manage and process her own affect without contaminating the child. It is not the role of the child to be the parental caregiver.
Help the child see that there was a loving relationship in the past and that new family goals can be created. The child also might experience anger and grief, and it is important to educate the child about how to manage those feelings appropriately rather than using blame and alienation. Help the child be empowered by positive ideals rather than negative emotions.
Psychiatrists often avoid working with these families, and perceive them as stuck and unable to change. This might be true for some families but certainly not all. Many families find themselves in situations that they do not understand and with problems they need help resolving. Educating and working with families who are stuck and who ask for and want change can change the life trajectory of many people.
Dr. Heru is with the department of psychiatry at the University of Colorado Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013).

More than 75% with sickle cell crises don’t get hydroxyurea
More than 75% of adults with sickle cell anemia who have frequent pain crises fail to receive hydroxyurea therapy as strongly recommended in National Heart, Lung, and Blood Institute clinical guidelines, according to a Research Letter to the Editor published online April 28 in JAMA.
Despite proven benefits in decreasing pain crises, hospitalizations, blood transfusions, and possibly mortality, hydroxyurea, a “safe and inexpensive drug,” is thought to be underused. To document the actual use of the drug when indicated, investigators analyzed information in a nationwide insurance claims database covering nearly 27 million patients per year. They focused on the records of 570 adults hospitalized or treated in an emergency department for a sickle cell pain crisis at least three times during a 1-year period, said Dr. Nicolas Stettler of the Lewin Group, a health care consulting firm in Falls Church, Va., and his associates.
Only 15.1% of these patients received hydroxyurea within 3 months of their third crisis, only 18.2% received the agent within 6 months, and only 22.7% received it within 12 months. These figures likely represent a conservative estimate of the hydroxyurea treatment gap, since the study didn’t include the large uninsured and publicly insured populations who have more limited access to health care, Dr. Stettler and his associates noted (JAMA 2015;313:1671-2).
Several barriers to this treatment have been identified in previous research, including fear of adverse events, lack of clinician training, and failure to use shared decision making. “To address this gap, it may be necessary to enhance patient outreach and clinician training and develop health care quality measures aimed at increasing the use of hydroxyurea for all patients who would benefit,” they added.
More than 75% of adults with sickle cell anemia who have frequent pain crises fail to receive hydroxyurea therapy as strongly recommended in National Heart, Lung, and Blood Institute clinical guidelines, according to a Research Letter to the Editor published online April 28 in JAMA.
Despite proven benefits in decreasing pain crises, hospitalizations, blood transfusions, and possibly mortality, hydroxyurea, a “safe and inexpensive drug,” is thought to be underused. To document the actual use of the drug when indicated, investigators analyzed information in a nationwide insurance claims database covering nearly 27 million patients per year. They focused on the records of 570 adults hospitalized or treated in an emergency department for a sickle cell pain crisis at least three times during a 1-year period, said Dr. Nicolas Stettler of the Lewin Group, a health care consulting firm in Falls Church, Va., and his associates.
Only 15.1% of these patients received hydroxyurea within 3 months of their third crisis, only 18.2% received the agent within 6 months, and only 22.7% received it within 12 months. These figures likely represent a conservative estimate of the hydroxyurea treatment gap, since the study didn’t include the large uninsured and publicly insured populations who have more limited access to health care, Dr. Stettler and his associates noted (JAMA 2015;313:1671-2).
Several barriers to this treatment have been identified in previous research, including fear of adverse events, lack of clinician training, and failure to use shared decision making. “To address this gap, it may be necessary to enhance patient outreach and clinician training and develop health care quality measures aimed at increasing the use of hydroxyurea for all patients who would benefit,” they added.
More than 75% of adults with sickle cell anemia who have frequent pain crises fail to receive hydroxyurea therapy as strongly recommended in National Heart, Lung, and Blood Institute clinical guidelines, according to a Research Letter to the Editor published online April 28 in JAMA.
Despite proven benefits in decreasing pain crises, hospitalizations, blood transfusions, and possibly mortality, hydroxyurea, a “safe and inexpensive drug,” is thought to be underused. To document the actual use of the drug when indicated, investigators analyzed information in a nationwide insurance claims database covering nearly 27 million patients per year. They focused on the records of 570 adults hospitalized or treated in an emergency department for a sickle cell pain crisis at least three times during a 1-year period, said Dr. Nicolas Stettler of the Lewin Group, a health care consulting firm in Falls Church, Va., and his associates.
Only 15.1% of these patients received hydroxyurea within 3 months of their third crisis, only 18.2% received the agent within 6 months, and only 22.7% received it within 12 months. These figures likely represent a conservative estimate of the hydroxyurea treatment gap, since the study didn’t include the large uninsured and publicly insured populations who have more limited access to health care, Dr. Stettler and his associates noted (JAMA 2015;313:1671-2).
Several barriers to this treatment have been identified in previous research, including fear of adverse events, lack of clinician training, and failure to use shared decision making. “To address this gap, it may be necessary to enhance patient outreach and clinician training and develop health care quality measures aimed at increasing the use of hydroxyurea for all patients who would benefit,” they added.
FROM JAMA
Key clinical point: More than 75% of adults with sickle cell anemia who have frequent pain crises fail to get hydroxyurea therapy as recommended.
Major finding: Only 15.1% of adults with sickle cell anemia received hydroxyurea within 3 months of their third pain crisis, only 18.2% received the agent within 6 months, and only 22.7% received it within 12 months.
Data source: An analysis of information in a large nationwide insurance claims database involving 570 adults with frequent hospitalizations for sickle cell pain crises.
Disclosures: This study was funded by the Lewin Group, a health care consulting firm. Dr. Stettler and his associates reported having no relevant financial disclosures.
Phone Counseling Bolsters Recovery and Reduces Pain Following Spinal Surgery
Participating in a short series of phone conversations with trained counselors can substantially boost recovery and reduce pain in patients after spinal surgery, according to a study published online ahead of print March 28 in Archives of Physical Medicine and Rehabilitation.
The phone calls were designed to enhance standard pre- and post-operative care by reinforcing the value of continuing with physical therapy and back-strengthening exercise regimens.
“Phone counseling appears to be an easy, low-cost strategy that yields meaningful results by improving patient engagement in physical therapy and at-home exercise programs that are so vital for their recovery,” said lead study author Richard Skolasky Jr., ScD, Associate Professor of Orthopedic Surgery at the Johns Hopkins University School of Medicine in Baltimore.

The study included 122 patients ages 46 to 72, who underwent surgery at Johns Hopkins University between 2009 and 2012 to correct spinal stenosis. Each patient was assigned either home exercise programs or physical therapy to help accelerate their recovery time. About half of the patients also received a series of phone counseling sessions from a trained spinal surgery counselor to discuss the importance of exercise in their recovery. The first and most detailed phone session took place a few weeks before the patients had their surgeries. Two follow-up sessions occurred at 6 weeks and at 3 months after the operation was performed.
The study found that patients who received phone calls participated in physical therapy and home exercise at higher rates, and had less pain and less disability 6 months after their surgery, compared with the standard-approach group. Six months after surgery, 74% of patients who received phone counseling experienced significant improvements on standard measures of physical functioning and self-reported measures of pain, compared with 41% of people who did not receive phone calls.
“Modern orthopedic science has made great strides in surgical techniques to correct spinal deformities and achieved significant progress in developing physical therapies that boost the benefits of surgery, but we have not been all that good at motivating and engaging patients to partake in such post-surgical recovery programs,” said co-investigator Stephen Wegener, PhD, Associate Professor of Physical Medicine and Rehabilitation at Johns Hopkins University.
“The findings of our research suggest we may have found a way to add that missing ingredient that draws patients to be more active participants in their physical rehabilitation and recovery,” stated Dr. Wegener.
Suggested Reading
Skolasky RL, Maggard AM, Li D, et al. Health behavior change counseling in surgery for degenerative lumbar spinal stenosis. part I: improvement in rehabilitation engagement and functional outcomes. Arch Phys Med Rehabil. 2015 Mar 28 [Epub ahead of print].
Participating in a short series of phone conversations with trained counselors can substantially boost recovery and reduce pain in patients after spinal surgery, according to a study published online ahead of print March 28 in Archives of Physical Medicine and Rehabilitation.
The phone calls were designed to enhance standard pre- and post-operative care by reinforcing the value of continuing with physical therapy and back-strengthening exercise regimens.
“Phone counseling appears to be an easy, low-cost strategy that yields meaningful results by improving patient engagement in physical therapy and at-home exercise programs that are so vital for their recovery,” said lead study author Richard Skolasky Jr., ScD, Associate Professor of Orthopedic Surgery at the Johns Hopkins University School of Medicine in Baltimore.
The study included 122 patients ages 46 to 72, who underwent surgery at Johns Hopkins University between 2009 and 2012 to correct spinal stenosis. Each patient was assigned either home exercise programs or physical therapy to help accelerate their recovery time. About half of the patients also received a series of phone counseling sessions from a trained spinal surgery counselor to discuss the importance of exercise in their recovery. The first and most detailed phone session took place a few weeks before the patients had their surgeries. Two follow-up sessions occurred at 6 weeks and at 3 months after the operation was performed.
The study found that patients who received phone calls participated in physical therapy and home exercise at higher rates, and had less pain and less disability 6 months after their surgery, compared with the standard-approach group. Six months after surgery, 74% of patients who received phone counseling experienced significant improvements on standard measures of physical functioning and self-reported measures of pain, compared with 41% of people who did not receive phone calls.
“Modern orthopedic science has made great strides in surgical techniques to correct spinal deformities and achieved significant progress in developing physical therapies that boost the benefits of surgery, but we have not been all that good at motivating and engaging patients to partake in such post-surgical recovery programs,” said co-investigator Stephen Wegener, PhD, Associate Professor of Physical Medicine and Rehabilitation at Johns Hopkins University.
“The findings of our research suggest we may have found a way to add that missing ingredient that draws patients to be more active participants in their physical rehabilitation and recovery,” stated Dr. Wegener.
Participating in a short series of phone conversations with trained counselors can substantially boost recovery and reduce pain in patients after spinal surgery, according to a study published online ahead of print March 28 in Archives of Physical Medicine and Rehabilitation.
The phone calls were designed to enhance standard pre- and post-operative care by reinforcing the value of continuing with physical therapy and back-strengthening exercise regimens.
“Phone counseling appears to be an easy, low-cost strategy that yields meaningful results by improving patient engagement in physical therapy and at-home exercise programs that are so vital for their recovery,” said lead study author Richard Skolasky Jr., ScD, Associate Professor of Orthopedic Surgery at the Johns Hopkins University School of Medicine in Baltimore.
The study included 122 patients ages 46 to 72, who underwent surgery at Johns Hopkins University between 2009 and 2012 to correct spinal stenosis. Each patient was assigned either home exercise programs or physical therapy to help accelerate their recovery time. About half of the patients also received a series of phone counseling sessions from a trained spinal surgery counselor to discuss the importance of exercise in their recovery. The first and most detailed phone session took place a few weeks before the patients had their surgeries. Two follow-up sessions occurred at 6 weeks and at 3 months after the operation was performed.
The study found that patients who received phone calls participated in physical therapy and home exercise at higher rates, and had less pain and less disability 6 months after their surgery, compared with the standard-approach group. Six months after surgery, 74% of patients who received phone counseling experienced significant improvements on standard measures of physical functioning and self-reported measures of pain, compared with 41% of people who did not receive phone calls.
“Modern orthopedic science has made great strides in surgical techniques to correct spinal deformities and achieved significant progress in developing physical therapies that boost the benefits of surgery, but we have not been all that good at motivating and engaging patients to partake in such post-surgical recovery programs,” said co-investigator Stephen Wegener, PhD, Associate Professor of Physical Medicine and Rehabilitation at Johns Hopkins University.
“The findings of our research suggest we may have found a way to add that missing ingredient that draws patients to be more active participants in their physical rehabilitation and recovery,” stated Dr. Wegener.
Suggested Reading
Skolasky RL, Maggard AM, Li D, et al. Health behavior change counseling in surgery for degenerative lumbar spinal stenosis. part I: improvement in rehabilitation engagement and functional outcomes. Arch Phys Med Rehabil. 2015 Mar 28 [Epub ahead of print].
Suggested Reading
Skolasky RL, Maggard AM, Li D, et al. Health behavior change counseling in surgery for degenerative lumbar spinal stenosis. part I: improvement in rehabilitation engagement and functional outcomes. Arch Phys Med Rehabil. 2015 Mar 28 [Epub ahead of print].

Molecule increases TRAIL expression to fight NHL

Convention Center, site of the
AACR Annual Meeting 2015
PHILADELPHIA—When current treatment approaches failed to save a young patient with non-Hodgkin lymphoma (NHL), a researcher from The Children’s Hospital of Philadelphia was driven to investigate new therapeutic options.
The investigation led the researcher, Mala Talekar, MBBS, to ONC201 (formerly TIC10), a small molecule that induces apoptosis by increasing surface expression of tumor necrosis factor-related apoptosis-inducing ligand (TRAIL).
Preclinical experiments showed that ONC201 is active against NHL as a single agent, and it synergizes with chemotherapeutic drugs that are already used to treat NHL.
Dr Talekar and her colleagues described these experiments in a poster presented at the AACR Annual Meeting 2015 (abstract 5387). Some of the investigators involved in this research are employed by Oncoceutics, Inc., the company developing ONC201.
A researcher’s inspiration
“When I was doing my fellowship training, I had a teenage boy who had a rare form of non-Hodgkin’s lymphoma,” Dr Talekar explained. “He did not survive, despite receiving multiple treatments that are available for pediatric non-Hodgkin’s lymphoma.”
The boy’s death inspired Dr Talekar to seek new and better approaches to treat NHL. A search of the medical literature unearthed several articles detailing a TRAIL-based approach to treating lymphoma. So she decided to further investigate the effects of TRAIL in NHL.
“I first tried TRAIL in one lymphoma cell line,” she said. “And even though it did kill the cancer cells, it did not really give a satisfactory response.”
So Dr Talekar turned to the TRAIL agonist antibodies lexatumumab and mapatumumab, introducing each of them to human lymphoma cells. Although the antibodies caused more cell death than TRAIL itself, the response was still not satisfactory, she said.
“Fortunately for me, while I was working in the lab, one of the postdocs, Joshua Allen, discovered a new molecule called TRAIL-inducing compound 10, or TIC10,” Dr Talekar said. “So I tried TIC10—it is now called ONC201—and it gave a beautiful dose-response curve, causing complete cell death of the lymphoma cells.”
Dr Talekar was “very inspired” by this result and decided to test ONC201 in 8 different NHL cell lines—4 Burkitt lymphoma (Daudi, Raji, Ramos, and BJAB), 1 anaplastic large-cell lymphoma (Karpas299), and 3 mantle cell lymphoma (UPN2, Granta, and NCEB) cell lines.
“I found a beautiful dose-response curve,” Dr Talekar said, “suggesting that this molecule works in micromolar concentrations across all of the lymphoma cell lines.”
Elucidating the mechanism
Dr Talekar then set out to determine exactly how ONC201 causes cell death in NHL. Flow cytometry revealed that, as the dose of ONC201 increases, cell death increases, as does sub-G1 DNA content. This suggests the drug is causing cell death by apoptosis.
Next, Dr Talekar introduced ONC201 to NHL cell lines along with a pan-caspase inhibitor. She found the inhibitor blocked ONC201-induced apoptosis, which suggests ONC201 works via the caspase-mediated apoptotic pathway.
“The initial mechanism of action proposed for ONC201 was dual inactivation of two kinases, Akt and ERK,” Dr Talekar noted. “The dual inactivation causes dephosphorylation of Foxo3a. This causes its translocation to the nucleus and downstream upregulation of TRAIL, and, therefore, increased surface TRAIL expression. And we know increases in surface TRAIL cause cell death by apoptosis.”
With this in mind, Dr Talekar looked for increases in surface TRIAL after she incubated lymphoma cells with ONC201. She observed a dose-dependent increase in surface TRAIL and a linear correlation between the increase in TRAIL and apoptosis.
Then, she introduced ONC201 and a TRAIL-sequestering antibody, RIK-2, to lymphoma cells. RIK-2 inhibited apoptosis, which suggests ONC201 works as an anti-apoptotic agent via the TRAIL pathway.
Further testing
As a final step, Dr Talekar tested ONC201 in combination with chemotherapy drugs that are already used to treat pediatric NHL. She observed at least an additive effect, and sometimes a synergistic effect, between the drugs. The best responses occurred when she combined ONC201 with cytarabine, bortezomib, or doxorubicin.
Now, Dr Talekar is working on testing ONC201 in combination with cytarabine in a xenograft model of Burkitt lymphoma.
She noted that other in vivo research has suggested ONC201 has a “very benign safety profile.” In another poster presented at AACR 2015 (abstract 4479), researchers reported results indicating that ONC201 is safe.
“They have tested it in mice and dogs and found that, at 10-fold the therapeutic dose, you don’t see much toxicity at all,” Dr Talekar said.
ONC201 is also being tested in a phase 1 study of adults with advanced solid tumors. Phase 1 studies of the drug in relapsed or refractory NHL and relapsed or refractory acute leukemias and high-risk myelodysplastic syndromes are not yet recruiting patients. ![]()
Convention Center, site of the
AACR Annual Meeting 2015
PHILADELPHIA—When current treatment approaches failed to save a young patient with non-Hodgkin lymphoma (NHL), a researcher from The Children’s Hospital of Philadelphia was driven to investigate new therapeutic options.
The investigation led the researcher, Mala Talekar, MBBS, to ONC201 (formerly TIC10), a small molecule that induces apoptosis by increasing surface expression of tumor necrosis factor-related apoptosis-inducing ligand (TRAIL).
Preclinical experiments showed that ONC201 is active against NHL as a single agent, and it synergizes with chemotherapeutic drugs that are already used to treat NHL.
Dr Talekar and her colleagues described these experiments in a poster presented at the AACR Annual Meeting 2015 (abstract 5387). Some of the investigators involved in this research are employed by Oncoceutics, Inc., the company developing ONC201.
A researcher’s inspiration
“When I was doing my fellowship training, I had a teenage boy who had a rare form of non-Hodgkin’s lymphoma,” Dr Talekar explained. “He did not survive, despite receiving multiple treatments that are available for pediatric non-Hodgkin’s lymphoma.”
The boy’s death inspired Dr Talekar to seek new and better approaches to treat NHL. A search of the medical literature unearthed several articles detailing a TRAIL-based approach to treating lymphoma. So she decided to further investigate the effects of TRAIL in NHL.
“I first tried TRAIL in one lymphoma cell line,” she said. “And even though it did kill the cancer cells, it did not really give a satisfactory response.”
So Dr Talekar turned to the TRAIL agonist antibodies lexatumumab and mapatumumab, introducing each of them to human lymphoma cells. Although the antibodies caused more cell death than TRAIL itself, the response was still not satisfactory, she said.
“Fortunately for me, while I was working in the lab, one of the postdocs, Joshua Allen, discovered a new molecule called TRAIL-inducing compound 10, or TIC10,” Dr Talekar said. “So I tried TIC10—it is now called ONC201—and it gave a beautiful dose-response curve, causing complete cell death of the lymphoma cells.”
Dr Talekar was “very inspired” by this result and decided to test ONC201 in 8 different NHL cell lines—4 Burkitt lymphoma (Daudi, Raji, Ramos, and BJAB), 1 anaplastic large-cell lymphoma (Karpas299), and 3 mantle cell lymphoma (UPN2, Granta, and NCEB) cell lines.
“I found a beautiful dose-response curve,” Dr Talekar said, “suggesting that this molecule works in micromolar concentrations across all of the lymphoma cell lines.”
Elucidating the mechanism
Dr Talekar then set out to determine exactly how ONC201 causes cell death in NHL. Flow cytometry revealed that, as the dose of ONC201 increases, cell death increases, as does sub-G1 DNA content. This suggests the drug is causing cell death by apoptosis.
Next, Dr Talekar introduced ONC201 to NHL cell lines along with a pan-caspase inhibitor. She found the inhibitor blocked ONC201-induced apoptosis, which suggests ONC201 works via the caspase-mediated apoptotic pathway.
“The initial mechanism of action proposed for ONC201 was dual inactivation of two kinases, Akt and ERK,” Dr Talekar noted. “The dual inactivation causes dephosphorylation of Foxo3a. This causes its translocation to the nucleus and downstream upregulation of TRAIL, and, therefore, increased surface TRAIL expression. And we know increases in surface TRAIL cause cell death by apoptosis.”
With this in mind, Dr Talekar looked for increases in surface TRIAL after she incubated lymphoma cells with ONC201. She observed a dose-dependent increase in surface TRAIL and a linear correlation between the increase in TRAIL and apoptosis.
Then, she introduced ONC201 and a TRAIL-sequestering antibody, RIK-2, to lymphoma cells. RIK-2 inhibited apoptosis, which suggests ONC201 works as an anti-apoptotic agent via the TRAIL pathway.
Further testing
As a final step, Dr Talekar tested ONC201 in combination with chemotherapy drugs that are already used to treat pediatric NHL. She observed at least an additive effect, and sometimes a synergistic effect, between the drugs. The best responses occurred when she combined ONC201 with cytarabine, bortezomib, or doxorubicin.
Now, Dr Talekar is working on testing ONC201 in combination with cytarabine in a xenograft model of Burkitt lymphoma.
She noted that other in vivo research has suggested ONC201 has a “very benign safety profile.” In another poster presented at AACR 2015 (abstract 4479), researchers reported results indicating that ONC201 is safe.
“They have tested it in mice and dogs and found that, at 10-fold the therapeutic dose, you don’t see much toxicity at all,” Dr Talekar said.
ONC201 is also being tested in a phase 1 study of adults with advanced solid tumors. Phase 1 studies of the drug in relapsed or refractory NHL and relapsed or refractory acute leukemias and high-risk myelodysplastic syndromes are not yet recruiting patients. ![]()
Convention Center, site of the
AACR Annual Meeting 2015
PHILADELPHIA—When current treatment approaches failed to save a young patient with non-Hodgkin lymphoma (NHL), a researcher from The Children’s Hospital of Philadelphia was driven to investigate new therapeutic options.
The investigation led the researcher, Mala Talekar, MBBS, to ONC201 (formerly TIC10), a small molecule that induces apoptosis by increasing surface expression of tumor necrosis factor-related apoptosis-inducing ligand (TRAIL).
Preclinical experiments showed that ONC201 is active against NHL as a single agent, and it synergizes with chemotherapeutic drugs that are already used to treat NHL.
Dr Talekar and her colleagues described these experiments in a poster presented at the AACR Annual Meeting 2015 (abstract 5387). Some of the investigators involved in this research are employed by Oncoceutics, Inc., the company developing ONC201.
A researcher’s inspiration
“When I was doing my fellowship training, I had a teenage boy who had a rare form of non-Hodgkin’s lymphoma,” Dr Talekar explained. “He did not survive, despite receiving multiple treatments that are available for pediatric non-Hodgkin’s lymphoma.”
The boy’s death inspired Dr Talekar to seek new and better approaches to treat NHL. A search of the medical literature unearthed several articles detailing a TRAIL-based approach to treating lymphoma. So she decided to further investigate the effects of TRAIL in NHL.
“I first tried TRAIL in one lymphoma cell line,” she said. “And even though it did kill the cancer cells, it did not really give a satisfactory response.”
So Dr Talekar turned to the TRAIL agonist antibodies lexatumumab and mapatumumab, introducing each of them to human lymphoma cells. Although the antibodies caused more cell death than TRAIL itself, the response was still not satisfactory, she said.
“Fortunately for me, while I was working in the lab, one of the postdocs, Joshua Allen, discovered a new molecule called TRAIL-inducing compound 10, or TIC10,” Dr Talekar said. “So I tried TIC10—it is now called ONC201—and it gave a beautiful dose-response curve, causing complete cell death of the lymphoma cells.”
Dr Talekar was “very inspired” by this result and decided to test ONC201 in 8 different NHL cell lines—4 Burkitt lymphoma (Daudi, Raji, Ramos, and BJAB), 1 anaplastic large-cell lymphoma (Karpas299), and 3 mantle cell lymphoma (UPN2, Granta, and NCEB) cell lines.
“I found a beautiful dose-response curve,” Dr Talekar said, “suggesting that this molecule works in micromolar concentrations across all of the lymphoma cell lines.”
Elucidating the mechanism
Dr Talekar then set out to determine exactly how ONC201 causes cell death in NHL. Flow cytometry revealed that, as the dose of ONC201 increases, cell death increases, as does sub-G1 DNA content. This suggests the drug is causing cell death by apoptosis.
Next, Dr Talekar introduced ONC201 to NHL cell lines along with a pan-caspase inhibitor. She found the inhibitor blocked ONC201-induced apoptosis, which suggests ONC201 works via the caspase-mediated apoptotic pathway.
“The initial mechanism of action proposed for ONC201 was dual inactivation of two kinases, Akt and ERK,” Dr Talekar noted. “The dual inactivation causes dephosphorylation of Foxo3a. This causes its translocation to the nucleus and downstream upregulation of TRAIL, and, therefore, increased surface TRAIL expression. And we know increases in surface TRAIL cause cell death by apoptosis.”
With this in mind, Dr Talekar looked for increases in surface TRIAL after she incubated lymphoma cells with ONC201. She observed a dose-dependent increase in surface TRAIL and a linear correlation between the increase in TRAIL and apoptosis.
Then, she introduced ONC201 and a TRAIL-sequestering antibody, RIK-2, to lymphoma cells. RIK-2 inhibited apoptosis, which suggests ONC201 works as an anti-apoptotic agent via the TRAIL pathway.
Further testing
As a final step, Dr Talekar tested ONC201 in combination with chemotherapy drugs that are already used to treat pediatric NHL. She observed at least an additive effect, and sometimes a synergistic effect, between the drugs. The best responses occurred when she combined ONC201 with cytarabine, bortezomib, or doxorubicin.
Now, Dr Talekar is working on testing ONC201 in combination with cytarabine in a xenograft model of Burkitt lymphoma.
She noted that other in vivo research has suggested ONC201 has a “very benign safety profile.” In another poster presented at AACR 2015 (abstract 4479), researchers reported results indicating that ONC201 is safe.
“They have tested it in mice and dogs and found that, at 10-fold the therapeutic dose, you don’t see much toxicity at all,” Dr Talekar said.
ONC201 is also being tested in a phase 1 study of adults with advanced solid tumors. Phase 1 studies of the drug in relapsed or refractory NHL and relapsed or refractory acute leukemias and high-risk myelodysplastic syndromes are not yet recruiting patients. ![]()
Study sheds new light on decitabine
Image by Christoph Bock
A new study helps explain how the anticancer drug decitabine reverses cell damage and has revealed a potential biomarker that could indicate a
patient’s cancer stage and response to treatment.
Investigators found that decitabine combats some of cancer’s effects by taking the place of the nucleotide cytosine at specific locations on a replicating DNA strand.
In mimicking cytosine, the drug helps “tame” cancerous cells by turning on tumor suppressors and turning off oncogenes.
The investigators also found that decitabine causes an unexpected boost in the amount of a molecule known as 5-hydroxymethylcytosine (5hmC). Because many types of cancer cause 5hmC levels to plummet, an uptick in 5hmC could be a sign that cancer treatments are working.
“We think that the expression of 5hmC could be used as a biomarker to define the stage or the aggressiveness of cancer and to possibly indicate the effectiveness of cancer treatment,” said Joseph Irudayaraj, PhD, of Purdue University in West Lafayette, Indiana. “This could help us monitor the clinical success of patients receiving decitabine.”
Dr Irudayaraj and his colleagues reported these findings in Nature Scientific Reports.
Decitabine, one of the first epigenetic drugs, helps reverse the altered methylation patterns in cancerous cells, but its precise mode of action has not been clear.
Using a combination of models, Dr Irudayaraj and his colleagues showed that decitabine is taking the place of cytosine at strategic positions on replicating strands of DNA in cancer cells.
When an enzyme tries to add a methyl group to silence decitabine, the drug traps it in place, preventing methylation. This triggers another group of enzymes to transform a methylated cytosine on the parent DNA strand into 5hmC, a molecule whose biological function is not yet known.
The investigators confirmed the increase in 5hmC levels in decitabine-treated leukemia cells.
To better explain the team’s findings, Basudev Chowdhury, PhD, also of Purdue University, likened decitabine to a text editor that restores meaning to a garbled sentence and compared conventional chemotherapy to a delete button.
“Think of nucleotides as the alphabet with which our cells compose messages,” he said. “Epigenetics helps translate those messages into actions such as the production of proteins. But cancer can jumble the messages, making them nonsensical. Decitabine helps revise the messages so they can be understood.” ![]()
Image by Christoph Bock
A new study helps explain how the anticancer drug decitabine reverses cell damage and has revealed a potential biomarker that could indicate a
patient’s cancer stage and response to treatment.
Investigators found that decitabine combats some of cancer’s effects by taking the place of the nucleotide cytosine at specific locations on a replicating DNA strand.
In mimicking cytosine, the drug helps “tame” cancerous cells by turning on tumor suppressors and turning off oncogenes.
The investigators also found that decitabine causes an unexpected boost in the amount of a molecule known as 5-hydroxymethylcytosine (5hmC). Because many types of cancer cause 5hmC levels to plummet, an uptick in 5hmC could be a sign that cancer treatments are working.
“We think that the expression of 5hmC could be used as a biomarker to define the stage or the aggressiveness of cancer and to possibly indicate the effectiveness of cancer treatment,” said Joseph Irudayaraj, PhD, of Purdue University in West Lafayette, Indiana. “This could help us monitor the clinical success of patients receiving decitabine.”
Dr Irudayaraj and his colleagues reported these findings in Nature Scientific Reports.
Decitabine, one of the first epigenetic drugs, helps reverse the altered methylation patterns in cancerous cells, but its precise mode of action has not been clear.
Using a combination of models, Dr Irudayaraj and his colleagues showed that decitabine is taking the place of cytosine at strategic positions on replicating strands of DNA in cancer cells.
When an enzyme tries to add a methyl group to silence decitabine, the drug traps it in place, preventing methylation. This triggers another group of enzymes to transform a methylated cytosine on the parent DNA strand into 5hmC, a molecule whose biological function is not yet known.
The investigators confirmed the increase in 5hmC levels in decitabine-treated leukemia cells.
To better explain the team’s findings, Basudev Chowdhury, PhD, also of Purdue University, likened decitabine to a text editor that restores meaning to a garbled sentence and compared conventional chemotherapy to a delete button.
“Think of nucleotides as the alphabet with which our cells compose messages,” he said. “Epigenetics helps translate those messages into actions such as the production of proteins. But cancer can jumble the messages, making them nonsensical. Decitabine helps revise the messages so they can be understood.” ![]()
Image by Christoph Bock
A new study helps explain how the anticancer drug decitabine reverses cell damage and has revealed a potential biomarker that could indicate a
patient’s cancer stage and response to treatment.
Investigators found that decitabine combats some of cancer’s effects by taking the place of the nucleotide cytosine at specific locations on a replicating DNA strand.
In mimicking cytosine, the drug helps “tame” cancerous cells by turning on tumor suppressors and turning off oncogenes.
The investigators also found that decitabine causes an unexpected boost in the amount of a molecule known as 5-hydroxymethylcytosine (5hmC). Because many types of cancer cause 5hmC levels to plummet, an uptick in 5hmC could be a sign that cancer treatments are working.
“We think that the expression of 5hmC could be used as a biomarker to define the stage or the aggressiveness of cancer and to possibly indicate the effectiveness of cancer treatment,” said Joseph Irudayaraj, PhD, of Purdue University in West Lafayette, Indiana. “This could help us monitor the clinical success of patients receiving decitabine.”
Dr Irudayaraj and his colleagues reported these findings in Nature Scientific Reports.
Decitabine, one of the first epigenetic drugs, helps reverse the altered methylation patterns in cancerous cells, but its precise mode of action has not been clear.
Using a combination of models, Dr Irudayaraj and his colleagues showed that decitabine is taking the place of cytosine at strategic positions on replicating strands of DNA in cancer cells.
When an enzyme tries to add a methyl group to silence decitabine, the drug traps it in place, preventing methylation. This triggers another group of enzymes to transform a methylated cytosine on the parent DNA strand into 5hmC, a molecule whose biological function is not yet known.
The investigators confirmed the increase in 5hmC levels in decitabine-treated leukemia cells.
To better explain the team’s findings, Basudev Chowdhury, PhD, also of Purdue University, likened decitabine to a text editor that restores meaning to a garbled sentence and compared conventional chemotherapy to a delete button.
“Think of nucleotides as the alphabet with which our cells compose messages,” he said. “Epigenetics helps translate those messages into actions such as the production of proteins. But cancer can jumble the messages, making them nonsensical. Decitabine helps revise the messages so they can be understood.” ![]()
HL survivors have long-term risk of cardiovascular disease

Photo by Rhoda Baer
Survivors of Hodgkin lymphoma (HL) have an increased risk of developing cardiovascular diseases throughout their lives, according to a study published in JAMA Internal Medicine.
Previous research suggested that HL treatment is associated with an increased risk of cardiovascular diseases.
However, those studies did not determine how long the increased risk persists or pinpoint the risk factors for various cardiovascular diseases.
So Flora E. van Leeuwen, PhD, of the Netherlands Cancer Institute in Amsterdam, and her colleagues decided to investigate.
The team examined the risk for cardiovascular disease in HL survivors up to 40 years after they received treatment and compared that with the risk for cardiovascular disease in the general population. The researchers also studied treatment-related risk factors.
The study included 2524 Dutch patients who were diagnosed with HL when they were younger than 51 years of age. The patients’ median age was 27.3 years.
The patients were treated from 1965 through 1995 and had survived for at least 5 years after diagnosis. In all, 2052 patients (81.3%) had received mediastinal radiotherapy, and 773 (30.6%) had received chemotherapy containing an anthracycline.
At a median of 20.3 years of follow-up, there were 1713 cardiovascular events in 797 patients (31.6%), and 410 of those patients (51.4%) had experienced 2 events or more.
The most frequently occurring cardiovascular disease was coronary heart disease (CHD), with 401 patients developing it as their first event. This was followed by valvular heart disease (VHD, 374 events) and heart failure (HF, 140 events).
HL survivors had a 3.2-fold increased risk of developing CHD and a 6.8-fold increased risk of developing HF compared to the general population.
HL survivors who had been treated before age 25 had a 4.6-fold to 7.5-fold increased risk of CHD and a 10.9-fold to 40.5-fold increased risk of HF, depending on the age they ultimately attained.
HL survivors treated at 35 to 50 years of age had a 2.0-fold to 2.3-fold increased risk of CHD and a 3.1-fold to 5.2-fold increased risk of HF, depending on their attained age.
The risks of CHD and HF remained significantly increased beyond 35 years after HL treatment. The standardized incidence ratios were 3.9 and 5.8, respectively.
The median times between HL treatment and first cardiovascular disease events were 18 years for CHD, 24 years for VHD, and 19 years for HF.
The cumulative risk of any type of cardiovascular disease was 50% at 40 years after HL diagnosis. For patients who were treated for HL before they were 25, the cumulative risk of developing a cardiovascular disease at 60 years of age or older was 20% for CHD, 31% for VHD, and 11% for HF.
The study also suggested that mediastinal radiotherapy increased the risk of CHD, VHD, and HF. But anthracycline-containing chemotherapy only increased the risk of VHD and HF.
Dr van Leeuwen and her colleagues concluded that both physicians and patients should be aware that HL survivors have a persistently increased risk of developing cardiovascular diseases throughout their lives. The team also believes the results of their study may direct guidelines for follow-up in HL survivors.
A commentary related to this research is available in JAMA Internal Medicine as well. ![]()
Photo by Rhoda Baer
Survivors of Hodgkin lymphoma (HL) have an increased risk of developing cardiovascular diseases throughout their lives, according to a study published in JAMA Internal Medicine.
Previous research suggested that HL treatment is associated with an increased risk of cardiovascular diseases.
However, those studies did not determine how long the increased risk persists or pinpoint the risk factors for various cardiovascular diseases.
So Flora E. van Leeuwen, PhD, of the Netherlands Cancer Institute in Amsterdam, and her colleagues decided to investigate.
The team examined the risk for cardiovascular disease in HL survivors up to 40 years after they received treatment and compared that with the risk for cardiovascular disease in the general population. The researchers also studied treatment-related risk factors.
The study included 2524 Dutch patients who were diagnosed with HL when they were younger than 51 years of age. The patients’ median age was 27.3 years.
The patients were treated from 1965 through 1995 and had survived for at least 5 years after diagnosis. In all, 2052 patients (81.3%) had received mediastinal radiotherapy, and 773 (30.6%) had received chemotherapy containing an anthracycline.
At a median of 20.3 years of follow-up, there were 1713 cardiovascular events in 797 patients (31.6%), and 410 of those patients (51.4%) had experienced 2 events or more.
The most frequently occurring cardiovascular disease was coronary heart disease (CHD), with 401 patients developing it as their first event. This was followed by valvular heart disease (VHD, 374 events) and heart failure (HF, 140 events).
HL survivors had a 3.2-fold increased risk of developing CHD and a 6.8-fold increased risk of developing HF compared to the general population.
HL survivors who had been treated before age 25 had a 4.6-fold to 7.5-fold increased risk of CHD and a 10.9-fold to 40.5-fold increased risk of HF, depending on the age they ultimately attained.
HL survivors treated at 35 to 50 years of age had a 2.0-fold to 2.3-fold increased risk of CHD and a 3.1-fold to 5.2-fold increased risk of HF, depending on their attained age.
The risks of CHD and HF remained significantly increased beyond 35 years after HL treatment. The standardized incidence ratios were 3.9 and 5.8, respectively.
The median times between HL treatment and first cardiovascular disease events were 18 years for CHD, 24 years for VHD, and 19 years for HF.
The cumulative risk of any type of cardiovascular disease was 50% at 40 years after HL diagnosis. For patients who were treated for HL before they were 25, the cumulative risk of developing a cardiovascular disease at 60 years of age or older was 20% for CHD, 31% for VHD, and 11% for HF.
The study also suggested that mediastinal radiotherapy increased the risk of CHD, VHD, and HF. But anthracycline-containing chemotherapy only increased the risk of VHD and HF.
Dr van Leeuwen and her colleagues concluded that both physicians and patients should be aware that HL survivors have a persistently increased risk of developing cardiovascular diseases throughout their lives. The team also believes the results of their study may direct guidelines for follow-up in HL survivors.
A commentary related to this research is available in JAMA Internal Medicine as well. ![]()
Photo by Rhoda Baer
Survivors of Hodgkin lymphoma (HL) have an increased risk of developing cardiovascular diseases throughout their lives, according to a study published in JAMA Internal Medicine.
Previous research suggested that HL treatment is associated with an increased risk of cardiovascular diseases.
However, those studies did not determine how long the increased risk persists or pinpoint the risk factors for various cardiovascular diseases.
So Flora E. van Leeuwen, PhD, of the Netherlands Cancer Institute in Amsterdam, and her colleagues decided to investigate.
The team examined the risk for cardiovascular disease in HL survivors up to 40 years after they received treatment and compared that with the risk for cardiovascular disease in the general population. The researchers also studied treatment-related risk factors.
The study included 2524 Dutch patients who were diagnosed with HL when they were younger than 51 years of age. The patients’ median age was 27.3 years.
The patients were treated from 1965 through 1995 and had survived for at least 5 years after diagnosis. In all, 2052 patients (81.3%) had received mediastinal radiotherapy, and 773 (30.6%) had received chemotherapy containing an anthracycline.
At a median of 20.3 years of follow-up, there were 1713 cardiovascular events in 797 patients (31.6%), and 410 of those patients (51.4%) had experienced 2 events or more.
The most frequently occurring cardiovascular disease was coronary heart disease (CHD), with 401 patients developing it as their first event. This was followed by valvular heart disease (VHD, 374 events) and heart failure (HF, 140 events).
HL survivors had a 3.2-fold increased risk of developing CHD and a 6.8-fold increased risk of developing HF compared to the general population.
HL survivors who had been treated before age 25 had a 4.6-fold to 7.5-fold increased risk of CHD and a 10.9-fold to 40.5-fold increased risk of HF, depending on the age they ultimately attained.
HL survivors treated at 35 to 50 years of age had a 2.0-fold to 2.3-fold increased risk of CHD and a 3.1-fold to 5.2-fold increased risk of HF, depending on their attained age.
The risks of CHD and HF remained significantly increased beyond 35 years after HL treatment. The standardized incidence ratios were 3.9 and 5.8, respectively.
The median times between HL treatment and first cardiovascular disease events were 18 years for CHD, 24 years for VHD, and 19 years for HF.
The cumulative risk of any type of cardiovascular disease was 50% at 40 years after HL diagnosis. For patients who were treated for HL before they were 25, the cumulative risk of developing a cardiovascular disease at 60 years of age or older was 20% for CHD, 31% for VHD, and 11% for HF.
The study also suggested that mediastinal radiotherapy increased the risk of CHD, VHD, and HF. But anthracycline-containing chemotherapy only increased the risk of VHD and HF.
Dr van Leeuwen and her colleagues concluded that both physicians and patients should be aware that HL survivors have a persistently increased risk of developing cardiovascular diseases throughout their lives. The team also believes the results of their study may direct guidelines for follow-up in HL survivors.
A commentary related to this research is available in JAMA Internal Medicine as well. ![]()
MM drug met accelerated approval requirements

Photo courtesy of the CDC
Celgene Corporation has fulfilled the requirements for accelerated approval of pomalidomide (Pomalyst) in the US, based on results from the phase 3 MM-003 trial.
The trial showed that pomalidomide in combination with dexamethasone can improve survival in patients with relapsed or refractory multiple
myeloma (MM).
A drug can be granted accelerated approval in the US based on a surrogate endpoint thought to predict clinical benefit.
To retain approval from the US Food and Drug Administration (FDA), the drug must demonstrate an actual clinical benefit.
In 2013, the FDA granted pomalidomide accelerated approval for use in combination with dexamethasone to treat MM patients who have received at least 2 prior therapies, including lenalidomide and a proteasome inhibitor, and have demonstrated disease progression on or within 60 days of completing their last therapy.
The FDA’s approval was based on results from a phase 2 trial known as MM-002. The trial showed that pomalidomide plus dexamethasone can improve the overall response rate in relapsed/refractory MM patients when compared to pomalidomide alone.
About 29% of patients in the pomalidomide-dexamethasone arm achieved a partial response or better, compared to about 7% of patients in the pomalidomide-alone arm.
Now, results of the MM-003 trial have shown that pomalidomide plus low-dose dexamethasone can improve progression-free survival and overall survival in relapsed/refractory MM patients, when compared to high-dose dexamethasone alone.
The median progression-free survival was 3.6 months in the pomalidomide-dexamethasone arm and 1.8 months in the dexamethasone arm (P<0.001). And the median overall survival was 12.4 months and 8 months, respectively (P=0.009).
These outcomes suggest pomalidomide, in combination with dexamethasone, provides a clinical benefit for previously treated MM patients, which fulfills the requirements for accelerated approval. So the drug’s label has been updated to reflect his change.
For more details on pomalidomide, see the full prescribing information. ![]()
Photo courtesy of the CDC
Celgene Corporation has fulfilled the requirements for accelerated approval of pomalidomide (Pomalyst) in the US, based on results from the phase 3 MM-003 trial.
The trial showed that pomalidomide in combination with dexamethasone can improve survival in patients with relapsed or refractory multiple
myeloma (MM).
A drug can be granted accelerated approval in the US based on a surrogate endpoint thought to predict clinical benefit.
To retain approval from the US Food and Drug Administration (FDA), the drug must demonstrate an actual clinical benefit.
In 2013, the FDA granted pomalidomide accelerated approval for use in combination with dexamethasone to treat MM patients who have received at least 2 prior therapies, including lenalidomide and a proteasome inhibitor, and have demonstrated disease progression on or within 60 days of completing their last therapy.
The FDA’s approval was based on results from a phase 2 trial known as MM-002. The trial showed that pomalidomide plus dexamethasone can improve the overall response rate in relapsed/refractory MM patients when compared to pomalidomide alone.
About 29% of patients in the pomalidomide-dexamethasone arm achieved a partial response or better, compared to about 7% of patients in the pomalidomide-alone arm.
Now, results of the MM-003 trial have shown that pomalidomide plus low-dose dexamethasone can improve progression-free survival and overall survival in relapsed/refractory MM patients, when compared to high-dose dexamethasone alone.
The median progression-free survival was 3.6 months in the pomalidomide-dexamethasone arm and 1.8 months in the dexamethasone arm (P<0.001). And the median overall survival was 12.4 months and 8 months, respectively (P=0.009).
These outcomes suggest pomalidomide, in combination with dexamethasone, provides a clinical benefit for previously treated MM patients, which fulfills the requirements for accelerated approval. So the drug’s label has been updated to reflect his change.
For more details on pomalidomide, see the full prescribing information. ![]()
Photo courtesy of the CDC
Celgene Corporation has fulfilled the requirements for accelerated approval of pomalidomide (Pomalyst) in the US, based on results from the phase 3 MM-003 trial.
The trial showed that pomalidomide in combination with dexamethasone can improve survival in patients with relapsed or refractory multiple
myeloma (MM).
A drug can be granted accelerated approval in the US based on a surrogate endpoint thought to predict clinical benefit.
To retain approval from the US Food and Drug Administration (FDA), the drug must demonstrate an actual clinical benefit.
In 2013, the FDA granted pomalidomide accelerated approval for use in combination with dexamethasone to treat MM patients who have received at least 2 prior therapies, including lenalidomide and a proteasome inhibitor, and have demonstrated disease progression on or within 60 days of completing their last therapy.
The FDA’s approval was based on results from a phase 2 trial known as MM-002. The trial showed that pomalidomide plus dexamethasone can improve the overall response rate in relapsed/refractory MM patients when compared to pomalidomide alone.
About 29% of patients in the pomalidomide-dexamethasone arm achieved a partial response or better, compared to about 7% of patients in the pomalidomide-alone arm.
Now, results of the MM-003 trial have shown that pomalidomide plus low-dose dexamethasone can improve progression-free survival and overall survival in relapsed/refractory MM patients, when compared to high-dose dexamethasone alone.
The median progression-free survival was 3.6 months in the pomalidomide-dexamethasone arm and 1.8 months in the dexamethasone arm (P<0.001). And the median overall survival was 12.4 months and 8 months, respectively (P=0.009).
These outcomes suggest pomalidomide, in combination with dexamethasone, provides a clinical benefit for previously treated MM patients, which fulfills the requirements for accelerated approval. So the drug’s label has been updated to reflect his change.
For more details on pomalidomide, see the full prescribing information. ![]()
TCS Among Children with Pneumonia
National guidelines for the management of childhood pneumonia highlight the need for the development of objective outcome measures to inform clinical decision making, establish benchmarks of care, and compare treatments and interventions.[1] Time to clinical stability (TCS) is a measure reported in adult pneumonia studies that incorporates vital signs, ability to eat, and mental status to objectively assess readiness for discharge.[2, 3, 4] TCS has not been validated among children as it has in adults,[5, 6, 7, 8] although such measures could prove useful for assessing discharge readiness with applications in both clinical and research settings. The objective of our study was to test the performance of pediatric TCS measures among children hospitalized with pneumonia.
METHODS
Study Population
We studied children hospitalized with community‐acquired pneumonia at Monroe Carell Jr. Children's Hospital at Vanderbilt between January 6, 2010 and May 9, 2011. Study children were enrolled as part of the Centers for Disease Control & Prevention (CDC) Etiology of Pneumonia in the Community (EPIC) study, a prospective, population‐based study of community‐acquired pneumonia hospitalizations. Detailed enrollment criteria for the EPIC study were reported previously.[9] Institutional review boards at Vanderbilt University and the CDC approved this study. Informed consent was obtained from enrolled families.
Data Elements and Study Definitions
Baseline data, including demographics, illness history, comorbidities, and clinical outcomes (eg, length of stay [LOS], intensive care admission), were systematically and prospectively collected. Additionally, data for 4 physiologic parameters, including temperature, heart rate, respiratory rate, and use of supplemental oxygen were obtained from the electronic medical record. These parameters were measured at least every 6 hours from admission through discharge as part of routine care. Readmissions within 7 calendar days of discharge were also obtained from the electronic medical record.
Stability for each parameter was defined as follows: normal temperature (36.037.9C), normal respiratory and heart rates in accordance with Pediatric Advanced Life Support age‐based values (see Supporting Table 1 in the online version of this article),[10] and no administration of supplemental oxygen. If the last recorded value for a given parameter was abnormal, that parameter was considered unstable at discharge. Otherwise, the time and date of the last abnormal value for each parameter was subtracted from admission time and date to determine TCS for that parameter in hours.
To determine overall stability, we evaluated 4 combination TCS measures, each incorporating 2 individual parameters. All combinations included respiratory rate and need for supplemental oxygen, as these parameters are the most explicit clinical indicators of pneumonia. Stability for each combination measure was defined as normalization of all included measures.
Clinical Outcomes for the Combined TCS Measures
The 4 combined TCS measures were compared against clinical outcomes including hospital LOS (measured in hours) and an ordinal severity scale. The ordinal scale categorized children into 3 mutually exclusive groups as follows: nonsevere (hospitalization without need for intensive care or empyema requiring drainage), severe (intensive care admission without invasive mechanical ventilation or vasopressor support and no empyema requiring drainage), and very severe (invasive mechanical ventilation, vasopressor support, or empyema requiring drainage).
Statistical Analysis
Categorical and continuous variables were summarized using frequencies and percentages and median and interquartile range (IQR) values, respectively. Analyses were stratified by age (2 years, 24 years, 517 years). We also plotted summary statistics for the combined measures and LOS, and computed the median absolute difference between these measures for each level of the ordinal severity scale. Analyses were conducted using Stata 13 (StataCorp, College Station, TX).
RESULTS
Study Population
Among 336 children enrolled in the EPIC study at Vanderbilt during the study period, 334 (99.4%) with complete data were included. Median age was 33 months (IQR, 1480). Median LOS was 56.4 hours (IQR, 41.591.7). There were 249 (74.5%) children classified as nonsevere, 39 (11.7) as severe, and 46 (13.8) as very severe (for age‐based characteristics see Supporting Table 2 in the online version of this article). Overall, 12 (3.6%) children were readmitted within 7 days of discharge.
Individual Stability Parameters
Overall, 323 (96.7%) children had 1 parameter abnormal on admission. Respiratory rate (81.4%) was the most common abnormal parameter, followed by abnormal temperature (71.4%), use of supplemental oxygen (63.8%), and abnormal heart rate (54.4%). Overall, use of supplemental oxygen had the longest TCS, followed by respiratory rate (Table 1). In comparison, heart rate and temperature stabilized relatively quickly.
| Parameter | 2 Years, n=130 | 24 Years, n=90 | 517 Years, n=101 | |||
|---|---|---|---|---|---|---|
| No. (%)* | Median (IQR) TCS, h | No. (%) | Median (IQR) TCS, h | No. (%) | Median (IQR) TCS, h | |
| ||||||
| Respiratory rate | 97 (74.6) | 38.6 (18.768.9) | 63 (70.0) | 31.6 (9.561.9) | 63 (62.4) | 24.3 (10.859.2) |
| Oxygen | 90 (69.2) | 39.5 (19.273.6) | 58 (64.4) | 44.2 (2477.6) | 61 (60.4) | 38.3 (1870.6) |
| Heart rate | 21 (16.2) | 4.5 (0.318.4) | 73 (81.1) | 21.8 (5.751.9) | 62 (61.4) | 18 (5.842.2) |
| Temperature | 101 (77.7) | 14.5 (4.545.3) | 61 (67.8) | 18.4 (2.842.8) | 62 (61.4) | 10.6 (0.834) |
Seventy children (21.0%) had 1 parameter abnormal at discharge, including abnormal respiratory rate in 13.7%, heart rate in 7.0%, and temperature in 3.3%. One child (0.3%) was discharged with supplemental oxygen. Ten children (3.0%) had 2 parameters abnormal at discharge. There was no difference in 7‐day readmissions for children with 1 parameter abnormal at discharge (1.4%) compared to those with no abnormal parameters at discharge (4.4%, P=0.253).
Combination TCS Measures
Within each age group, the percentage of children achieving stability was relatively consistent across the 4 combined TCS measures (Table 2); however, more children were considered unstable at discharge (and fewer classified as stable on admission) as the number of included parameters increased. More children 5 years of age reached stability (range, 80.0%85.6%) compared to children 5 years of age (range, 68.3%72.3%). We also noted increasing median TCS with increasing disease severity (Figure 1, P0.01) (see Supporting Fig. 1AC in the online version of this article); TCS was only slightly shorter than LOS across all 3 levels of the severity scale.
| TCS Measures | 2 Years, n=130 | 24 Years, n=90 | 517 Years, n=101 | P Value | |||
|---|---|---|---|---|---|---|---|
| No. (%)* | Median (IQR) TCS, h | No. (%) | Median (IQR) TCS, h | No. (%) | Median (IQR) TCS, h | ||
| |||||||
| RR+O2 | 108 (83.1) | 40.5 (20.175.0) | 72 (80.0) | 39.6 (15.679.2) | 69 (68.3) | 30.4 (14.759.2) | 0.08 |
| RR+O2+HR | 109 (83.8) | 40.2 (19.573.9) | 73 (81.1) | 35.9 (15.977.6) | 68 (67.3) | 29.8 (17.256.6) | 0.11 |
| RR+O2+T | 110 (84.6) | 40.5 (20.770.1) | 77 (85.6) | 39.1 (18.477.6) | 73 (72.3) | 28.2 (14.744.7) | 0.03 |
| RR+O2+HR+T | 110 (84.6) | 40.5 (20.770.1) | 72 (80.0) | 39.7 (20.177.5) | 71 (70.3) | 29.2 (18.254) | 0.05 |
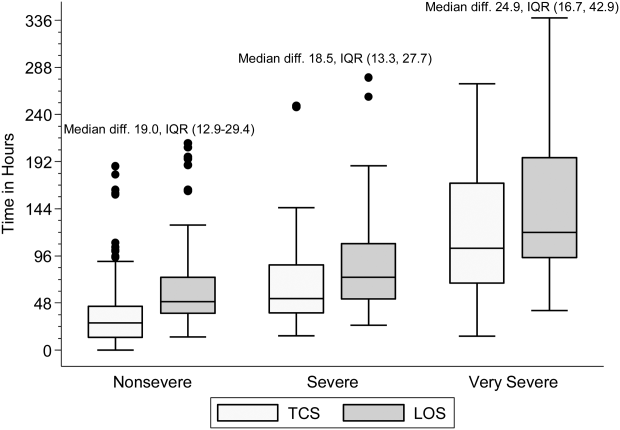
DISCUSSION
Our study demonstrates that longitudinal TCS measures consisting of routinely collected physiologic parameters may be useful for objectively assessing disease recovery and clinical readiness for discharge among children hospitalized with pneumonia. A simple TCS measure incorporating respiratory rate and oxygen requirement performed similarly to the more complex combinations and classified fewer children as unstable at discharge. However, we also note several challenges that deserve additional study prior to the application of a pediatric TCS measure in clinical and research settings.
Vital signs and supplemental oxygen use are used clinically to assess disease severity and response to therapy among children with acute respiratory illness. Because these objective parameters are routinely collected among hospitalized children, the systematization of these data could inform clinical decision making around hospital discharge. Similar to early warning scores used to detect impending clinical deterioration,[11] TCS measures, by signaling normalization of stability parameters in a consistent and objective manner, could serve as an early signal of readiness for discharge. However, maximizing the clinical utility of TCS would require embedding the process within the electronic health record, a tool that could also have implications for the Centers for Medicare and Medicaid Services' meaningful use regulations.[12]
TCS could also serve as an outcome measure in research and quality efforts. Increased disease severity was associated with longer TCS for the 4 combined measures; TCS also demonstrated strong agreement with LOS. Furthermore, TCS minimizes the influence of factors unrelated to disease that may impact LOS (eg, frequency of hospital rounds, transportation difficulties, or social impediments to discharge), an advantage when studying outcomes for research and quality benchmarking.
The percentage of children reaching stability and the median TCS for the combined measures demonstrated little variation within each age group, likely because respiratory rate and need for supplemental oxygen, 2 of the parameters with the longest individual time to stability, were also included in each of the combination measures. This suggests that less‐complex measures incorporating only respiratory rate and need for supplemental oxygen may be sufficient to assess clinical stability, particularly because these parameters are objectively measured and possess a direct physiological link to pneumonia. In contrast, the other parameters may be more often influenced by factors unrelated to disease severity.
Our study also highlights several shortcomings of the pediatric TCS measures. Despite use of published, age‐based reference values,[13] we noted wide variation in the achievement of stability across individual parameters, especially for children 5 years old. Overall, 21% of children had 1 abnormal parameter at discharge. Even the simplest combined measure classified 13.4% of children as unstable at discharge. Discharge with unstable parameters was not associated with 7‐day readmission, although our study was underpowered to detect small differences. Additional study is therefore needed to evaluate less restrictive cutoff values on calculated TCS and the impact of hospital discharge prior to reaching stability. In particular, relaxing the upper limit for normal respiratory rate in adolescents (16 breaths per minute) to more closely approximate the adult TCS parameter (24 breaths per minute) should be explored. Refinement and standardization of age‐based vital sign reference values specific to hospitalized children may also improve the performance of these measures.[14]
Several limitations deserve discussion. TCS parameters and readmission data were abstracted retrospectively from a single institution, and our findings may not be generalizable. Although clinical staff routinely measured these data, measurement variation likely exists. Nevertheless, such variation is likely systematic, limiting the impact of potential misclassification. TCS was calculated based on the last abnormal value for each parameter; prior fluctuations between normal and abnormal periods of stability were not captured. We were unable to assess room air oxygen saturations. Instead, supplemental oxygen use served as a surrogate for hypoxia. At our institution, oxygen therapy is provided for children with pneumonia to maintain oxygen saturations of 90% to 92%. We did not assess work of breathing (a marker of severe pneumonia) or ability to eat (a component of adult TCS measures). We initially considered the evaluation of intravenous fluids as a proxy for ability to eat (addition of this parameter to the 4 parameter TCS resulted in a modest increase in median time to stability, data not shown); however, we felt the lack of institutional policy and subjective nature of this parameter detracted from our study's objectives. Finally, we were not able to determine clinical readiness for discharge beyond the measurement of vital sign parameters. Therefore, prospective evaluation of the proposed pediatric TCS measures in broader populations will be important to build upon our findings, refine stability parameters, and test the utility of new parameters (eg, ability to eat, work of breathing) prior to use in clinical settings.
Our study provides an initial evaluation of TCS measures for assessing severity and recovery among children hospitalized with pneumonia. Similar to adults, such validated TCS measures may ultimately prove useful for improving the quality of both clinical care and research, although additional study to more clearly define stability criteria is needed prior to implementation.
Disclosures
This work was supported by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health under Award Number K23AI104779 to Dr. Williams. The EPIC study was supported by the Influenza Division in the National Center for Immunizations and Respiratory Diseases at the Centers for Disease Control and Prevention through cooperative agreements with each study site and was based on a competitive research funding opportunity. The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention or the National Institutes of Health. Dr. Grijalva serves as a consultant to Glaxo‐Smith‐Kline and Pfizer outside of the scope of this article. Dr. Edwards is supported through grants from Novartis for the conduction of a Group B strep vaccine study and serves as the Chair of the Data Safety and Monitoring Data Committee for Influenza Study outside the scope of this article. Dr. Self reports grants from CareFusion, BioMerieux, Affinium Pharmaceuticals, Astute Medical, Crucell Holland BV, BRAHMS GmbH, Pfizer, Rapid Pathogen Screening, Venaxis, BioAegis Inc., Sphingotec GmbH, and Cempra Pharmaceuticals; personal fees from BioFire Diagnostics and Venaxis, Inc; and patent 13/632,874 (Sterile Blood Culture Collection System) pending; all outside the scope of this article.
- Healthcare Cost and Utilization Project. Available at: http://www.ahrq.gov/research/data/hcup/index.html. Accessed February 1, 2014.
- , , , et al. Time to clinical stability in patients hospitalized with community‐acquired pneumonia: implications for practice guidelines. JAMA. 1998;279:1452–1457.
- , , , et al.; Neumofail Group. Reaching stability in community‐acquired pneumonia: the effects of the severity of disease, treatment, and the characteristics of patients. Clin Infect Dis. 2004;39:1783–1790.
- , , , et al.; Community‐Acquired Pneumonia Organization. The pneumonia severity index predicts time to clinical stability in patients with community‐acquired pneumonia. Int J Tuberc Lung Dis. 2006;10:739–743.
- , , , , . Efficacy of corticosteroids in community‐acquired pneumonia: a randomized double‐blinded clinical trial. Am J Respir Crit Care Med. 2010;181:975–982.
- , , , et al. Early administration of antibiotics does not shorten time to clinical stability in patients with moderate‐to‐severe community‐acquired pneumonia. Chest 2003;124:1798–1804.
- , , , . A comparison between time to clinical stability in community‐acquired aspiration pneumonia and community‐acquired pneumonia. Intern Emerg Med. 2014;9:143–150.
- , , , et al.; Community‐Acquired Pneumonia Organization (CAPO) Investigators. A worldwide perspective of atypical pathogens in community‐acquired pneumonia. Am J Respir Crit Care Med. 2007;175:1086–1093.
- , , , et al.; CDC EPIC Study Team. Community‐acquired pneumonia requiring hospitalization among U.S. children. N Engl J Med. 2015;372:835–845.
- American Heart Association. 2005 American Heart Association (AHA) guidelines for cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) of pediatric and neonatal patients: pediatric basic life support. Pediatrics. 2006;117:e989–e1004.
- , , . Development and initial validation of the Bedside Paediatric Early Warning System score. Crit Care. 2009;13:R135.
- Centers for Medicare and Medicaid Services. Regulations and guidance. EHR incentive programs. Available at: http://www.cms.gov/Regulations‐and‐Guidance/Legislation/EHRIncentivePrograms/index.html. Accessed February 20, 2015
- , , , , , . Development of heart and respiratory rate percentile curves for hospitalized children. Pediatrics. 2013;131:e1150–e1157.
- , , , et al. Length of stay after reaching clinical stability drives hospital costs associated with adult community‐acquired pneumonia. Scand J Infect Dis. 2013;45:219–226.
National guidelines for the management of childhood pneumonia highlight the need for the development of objective outcome measures to inform clinical decision making, establish benchmarks of care, and compare treatments and interventions.[1] Time to clinical stability (TCS) is a measure reported in adult pneumonia studies that incorporates vital signs, ability to eat, and mental status to objectively assess readiness for discharge.[2, 3, 4] TCS has not been validated among children as it has in adults,[5, 6, 7, 8] although such measures could prove useful for assessing discharge readiness with applications in both clinical and research settings. The objective of our study was to test the performance of pediatric TCS measures among children hospitalized with pneumonia.
METHODS
Study Population
We studied children hospitalized with community‐acquired pneumonia at Monroe Carell Jr. Children's Hospital at Vanderbilt between January 6, 2010 and May 9, 2011. Study children were enrolled as part of the Centers for Disease Control & Prevention (CDC) Etiology of Pneumonia in the Community (EPIC) study, a prospective, population‐based study of community‐acquired pneumonia hospitalizations. Detailed enrollment criteria for the EPIC study were reported previously.[9] Institutional review boards at Vanderbilt University and the CDC approved this study. Informed consent was obtained from enrolled families.
Data Elements and Study Definitions
Baseline data, including demographics, illness history, comorbidities, and clinical outcomes (eg, length of stay [LOS], intensive care admission), were systematically and prospectively collected. Additionally, data for 4 physiologic parameters, including temperature, heart rate, respiratory rate, and use of supplemental oxygen were obtained from the electronic medical record. These parameters were measured at least every 6 hours from admission through discharge as part of routine care. Readmissions within 7 calendar days of discharge were also obtained from the electronic medical record.
Stability for each parameter was defined as follows: normal temperature (36.037.9C), normal respiratory and heart rates in accordance with Pediatric Advanced Life Support age‐based values (see Supporting Table 1 in the online version of this article),[10] and no administration of supplemental oxygen. If the last recorded value for a given parameter was abnormal, that parameter was considered unstable at discharge. Otherwise, the time and date of the last abnormal value for each parameter was subtracted from admission time and date to determine TCS for that parameter in hours.
To determine overall stability, we evaluated 4 combination TCS measures, each incorporating 2 individual parameters. All combinations included respiratory rate and need for supplemental oxygen, as these parameters are the most explicit clinical indicators of pneumonia. Stability for each combination measure was defined as normalization of all included measures.
Clinical Outcomes for the Combined TCS Measures
The 4 combined TCS measures were compared against clinical outcomes including hospital LOS (measured in hours) and an ordinal severity scale. The ordinal scale categorized children into 3 mutually exclusive groups as follows: nonsevere (hospitalization without need for intensive care or empyema requiring drainage), severe (intensive care admission without invasive mechanical ventilation or vasopressor support and no empyema requiring drainage), and very severe (invasive mechanical ventilation, vasopressor support, or empyema requiring drainage).
Statistical Analysis
Categorical and continuous variables were summarized using frequencies and percentages and median and interquartile range (IQR) values, respectively. Analyses were stratified by age (2 years, 24 years, 517 years). We also plotted summary statistics for the combined measures and LOS, and computed the median absolute difference between these measures for each level of the ordinal severity scale. Analyses were conducted using Stata 13 (StataCorp, College Station, TX).
RESULTS
Study Population
Among 336 children enrolled in the EPIC study at Vanderbilt during the study period, 334 (99.4%) with complete data were included. Median age was 33 months (IQR, 1480). Median LOS was 56.4 hours (IQR, 41.591.7). There were 249 (74.5%) children classified as nonsevere, 39 (11.7) as severe, and 46 (13.8) as very severe (for age‐based characteristics see Supporting Table 2 in the online version of this article). Overall, 12 (3.6%) children were readmitted within 7 days of discharge.
Individual Stability Parameters
Overall, 323 (96.7%) children had 1 parameter abnormal on admission. Respiratory rate (81.4%) was the most common abnormal parameter, followed by abnormal temperature (71.4%), use of supplemental oxygen (63.8%), and abnormal heart rate (54.4%). Overall, use of supplemental oxygen had the longest TCS, followed by respiratory rate (Table 1). In comparison, heart rate and temperature stabilized relatively quickly.
| Parameter | 2 Years, n=130 | 24 Years, n=90 | 517 Years, n=101 | |||
|---|---|---|---|---|---|---|
| No. (%)* | Median (IQR) TCS, h | No. (%) | Median (IQR) TCS, h | No. (%) | Median (IQR) TCS, h | |
| ||||||
| Respiratory rate | 97 (74.6) | 38.6 (18.768.9) | 63 (70.0) | 31.6 (9.561.9) | 63 (62.4) | 24.3 (10.859.2) |
| Oxygen | 90 (69.2) | 39.5 (19.273.6) | 58 (64.4) | 44.2 (2477.6) | 61 (60.4) | 38.3 (1870.6) |
| Heart rate | 21 (16.2) | 4.5 (0.318.4) | 73 (81.1) | 21.8 (5.751.9) | 62 (61.4) | 18 (5.842.2) |
| Temperature | 101 (77.7) | 14.5 (4.545.3) | 61 (67.8) | 18.4 (2.842.8) | 62 (61.4) | 10.6 (0.834) |
Seventy children (21.0%) had 1 parameter abnormal at discharge, including abnormal respiratory rate in 13.7%, heart rate in 7.0%, and temperature in 3.3%. One child (0.3%) was discharged with supplemental oxygen. Ten children (3.0%) had 2 parameters abnormal at discharge. There was no difference in 7‐day readmissions for children with 1 parameter abnormal at discharge (1.4%) compared to those with no abnormal parameters at discharge (4.4%, P=0.253).
Combination TCS Measures
Within each age group, the percentage of children achieving stability was relatively consistent across the 4 combined TCS measures (Table 2); however, more children were considered unstable at discharge (and fewer classified as stable on admission) as the number of included parameters increased. More children 5 years of age reached stability (range, 80.0%85.6%) compared to children 5 years of age (range, 68.3%72.3%). We also noted increasing median TCS with increasing disease severity (Figure 1, P0.01) (see Supporting Fig. 1AC in the online version of this article); TCS was only slightly shorter than LOS across all 3 levels of the severity scale.
| TCS Measures | 2 Years, n=130 | 24 Years, n=90 | 517 Years, n=101 | P Value | |||
|---|---|---|---|---|---|---|---|
| No. (%)* | Median (IQR) TCS, h | No. (%) | Median (IQR) TCS, h | No. (%) | Median (IQR) TCS, h | ||
| |||||||
| RR+O2 | 108 (83.1) | 40.5 (20.175.0) | 72 (80.0) | 39.6 (15.679.2) | 69 (68.3) | 30.4 (14.759.2) | 0.08 |
| RR+O2+HR | 109 (83.8) | 40.2 (19.573.9) | 73 (81.1) | 35.9 (15.977.6) | 68 (67.3) | 29.8 (17.256.6) | 0.11 |
| RR+O2+T | 110 (84.6) | 40.5 (20.770.1) | 77 (85.6) | 39.1 (18.477.6) | 73 (72.3) | 28.2 (14.744.7) | 0.03 |
| RR+O2+HR+T | 110 (84.6) | 40.5 (20.770.1) | 72 (80.0) | 39.7 (20.177.5) | 71 (70.3) | 29.2 (18.254) | 0.05 |
DISCUSSION
Our study demonstrates that longitudinal TCS measures consisting of routinely collected physiologic parameters may be useful for objectively assessing disease recovery and clinical readiness for discharge among children hospitalized with pneumonia. A simple TCS measure incorporating respiratory rate and oxygen requirement performed similarly to the more complex combinations and classified fewer children as unstable at discharge. However, we also note several challenges that deserve additional study prior to the application of a pediatric TCS measure in clinical and research settings.
Vital signs and supplemental oxygen use are used clinically to assess disease severity and response to therapy among children with acute respiratory illness. Because these objective parameters are routinely collected among hospitalized children, the systematization of these data could inform clinical decision making around hospital discharge. Similar to early warning scores used to detect impending clinical deterioration,[11] TCS measures, by signaling normalization of stability parameters in a consistent and objective manner, could serve as an early signal of readiness for discharge. However, maximizing the clinical utility of TCS would require embedding the process within the electronic health record, a tool that could also have implications for the Centers for Medicare and Medicaid Services' meaningful use regulations.[12]
TCS could also serve as an outcome measure in research and quality efforts. Increased disease severity was associated with longer TCS for the 4 combined measures; TCS also demonstrated strong agreement with LOS. Furthermore, TCS minimizes the influence of factors unrelated to disease that may impact LOS (eg, frequency of hospital rounds, transportation difficulties, or social impediments to discharge), an advantage when studying outcomes for research and quality benchmarking.
The percentage of children reaching stability and the median TCS for the combined measures demonstrated little variation within each age group, likely because respiratory rate and need for supplemental oxygen, 2 of the parameters with the longest individual time to stability, were also included in each of the combination measures. This suggests that less‐complex measures incorporating only respiratory rate and need for supplemental oxygen may be sufficient to assess clinical stability, particularly because these parameters are objectively measured and possess a direct physiological link to pneumonia. In contrast, the other parameters may be more often influenced by factors unrelated to disease severity.
Our study also highlights several shortcomings of the pediatric TCS measures. Despite use of published, age‐based reference values,[13] we noted wide variation in the achievement of stability across individual parameters, especially for children 5 years old. Overall, 21% of children had 1 abnormal parameter at discharge. Even the simplest combined measure classified 13.4% of children as unstable at discharge. Discharge with unstable parameters was not associated with 7‐day readmission, although our study was underpowered to detect small differences. Additional study is therefore needed to evaluate less restrictive cutoff values on calculated TCS and the impact of hospital discharge prior to reaching stability. In particular, relaxing the upper limit for normal respiratory rate in adolescents (16 breaths per minute) to more closely approximate the adult TCS parameter (24 breaths per minute) should be explored. Refinement and standardization of age‐based vital sign reference values specific to hospitalized children may also improve the performance of these measures.[14]
Several limitations deserve discussion. TCS parameters and readmission data were abstracted retrospectively from a single institution, and our findings may not be generalizable. Although clinical staff routinely measured these data, measurement variation likely exists. Nevertheless, such variation is likely systematic, limiting the impact of potential misclassification. TCS was calculated based on the last abnormal value for each parameter; prior fluctuations between normal and abnormal periods of stability were not captured. We were unable to assess room air oxygen saturations. Instead, supplemental oxygen use served as a surrogate for hypoxia. At our institution, oxygen therapy is provided for children with pneumonia to maintain oxygen saturations of 90% to 92%. We did not assess work of breathing (a marker of severe pneumonia) or ability to eat (a component of adult TCS measures). We initially considered the evaluation of intravenous fluids as a proxy for ability to eat (addition of this parameter to the 4 parameter TCS resulted in a modest increase in median time to stability, data not shown); however, we felt the lack of institutional policy and subjective nature of this parameter detracted from our study's objectives. Finally, we were not able to determine clinical readiness for discharge beyond the measurement of vital sign parameters. Therefore, prospective evaluation of the proposed pediatric TCS measures in broader populations will be important to build upon our findings, refine stability parameters, and test the utility of new parameters (eg, ability to eat, work of breathing) prior to use in clinical settings.
Our study provides an initial evaluation of TCS measures for assessing severity and recovery among children hospitalized with pneumonia. Similar to adults, such validated TCS measures may ultimately prove useful for improving the quality of both clinical care and research, although additional study to more clearly define stability criteria is needed prior to implementation.
Disclosures
This work was supported by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health under Award Number K23AI104779 to Dr. Williams. The EPIC study was supported by the Influenza Division in the National Center for Immunizations and Respiratory Diseases at the Centers for Disease Control and Prevention through cooperative agreements with each study site and was based on a competitive research funding opportunity. The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention or the National Institutes of Health. Dr. Grijalva serves as a consultant to Glaxo‐Smith‐Kline and Pfizer outside of the scope of this article. Dr. Edwards is supported through grants from Novartis for the conduction of a Group B strep vaccine study and serves as the Chair of the Data Safety and Monitoring Data Committee for Influenza Study outside the scope of this article. Dr. Self reports grants from CareFusion, BioMerieux, Affinium Pharmaceuticals, Astute Medical, Crucell Holland BV, BRAHMS GmbH, Pfizer, Rapid Pathogen Screening, Venaxis, BioAegis Inc., Sphingotec GmbH, and Cempra Pharmaceuticals; personal fees from BioFire Diagnostics and Venaxis, Inc; and patent 13/632,874 (Sterile Blood Culture Collection System) pending; all outside the scope of this article.
National guidelines for the management of childhood pneumonia highlight the need for the development of objective outcome measures to inform clinical decision making, establish benchmarks of care, and compare treatments and interventions.[1] Time to clinical stability (TCS) is a measure reported in adult pneumonia studies that incorporates vital signs, ability to eat, and mental status to objectively assess readiness for discharge.[2, 3, 4] TCS has not been validated among children as it has in adults,[5, 6, 7, 8] although such measures could prove useful for assessing discharge readiness with applications in both clinical and research settings. The objective of our study was to test the performance of pediatric TCS measures among children hospitalized with pneumonia.
METHODS
Study Population
We studied children hospitalized with community‐acquired pneumonia at Monroe Carell Jr. Children's Hospital at Vanderbilt between January 6, 2010 and May 9, 2011. Study children were enrolled as part of the Centers for Disease Control & Prevention (CDC) Etiology of Pneumonia in the Community (EPIC) study, a prospective, population‐based study of community‐acquired pneumonia hospitalizations. Detailed enrollment criteria for the EPIC study were reported previously.[9] Institutional review boards at Vanderbilt University and the CDC approved this study. Informed consent was obtained from enrolled families.
Data Elements and Study Definitions
Baseline data, including demographics, illness history, comorbidities, and clinical outcomes (eg, length of stay [LOS], intensive care admission), were systematically and prospectively collected. Additionally, data for 4 physiologic parameters, including temperature, heart rate, respiratory rate, and use of supplemental oxygen were obtained from the electronic medical record. These parameters were measured at least every 6 hours from admission through discharge as part of routine care. Readmissions within 7 calendar days of discharge were also obtained from the electronic medical record.
Stability for each parameter was defined as follows: normal temperature (36.037.9C), normal respiratory and heart rates in accordance with Pediatric Advanced Life Support age‐based values (see Supporting Table 1 in the online version of this article),[10] and no administration of supplemental oxygen. If the last recorded value for a given parameter was abnormal, that parameter was considered unstable at discharge. Otherwise, the time and date of the last abnormal value for each parameter was subtracted from admission time and date to determine TCS for that parameter in hours.
To determine overall stability, we evaluated 4 combination TCS measures, each incorporating 2 individual parameters. All combinations included respiratory rate and need for supplemental oxygen, as these parameters are the most explicit clinical indicators of pneumonia. Stability for each combination measure was defined as normalization of all included measures.
Clinical Outcomes for the Combined TCS Measures
The 4 combined TCS measures were compared against clinical outcomes including hospital LOS (measured in hours) and an ordinal severity scale. The ordinal scale categorized children into 3 mutually exclusive groups as follows: nonsevere (hospitalization without need for intensive care or empyema requiring drainage), severe (intensive care admission without invasive mechanical ventilation or vasopressor support and no empyema requiring drainage), and very severe (invasive mechanical ventilation, vasopressor support, or empyema requiring drainage).
Statistical Analysis
Categorical and continuous variables were summarized using frequencies and percentages and median and interquartile range (IQR) values, respectively. Analyses were stratified by age (2 years, 24 years, 517 years). We also plotted summary statistics for the combined measures and LOS, and computed the median absolute difference between these measures for each level of the ordinal severity scale. Analyses were conducted using Stata 13 (StataCorp, College Station, TX).
RESULTS
Study Population
Among 336 children enrolled in the EPIC study at Vanderbilt during the study period, 334 (99.4%) with complete data were included. Median age was 33 months (IQR, 1480). Median LOS was 56.4 hours (IQR, 41.591.7). There were 249 (74.5%) children classified as nonsevere, 39 (11.7) as severe, and 46 (13.8) as very severe (for age‐based characteristics see Supporting Table 2 in the online version of this article). Overall, 12 (3.6%) children were readmitted within 7 days of discharge.
Individual Stability Parameters
Overall, 323 (96.7%) children had 1 parameter abnormal on admission. Respiratory rate (81.4%) was the most common abnormal parameter, followed by abnormal temperature (71.4%), use of supplemental oxygen (63.8%), and abnormal heart rate (54.4%). Overall, use of supplemental oxygen had the longest TCS, followed by respiratory rate (Table 1). In comparison, heart rate and temperature stabilized relatively quickly.
| Parameter | 2 Years, n=130 | 24 Years, n=90 | 517 Years, n=101 | |||
|---|---|---|---|---|---|---|
| No. (%)* | Median (IQR) TCS, h | No. (%) | Median (IQR) TCS, h | No. (%) | Median (IQR) TCS, h | |
| ||||||
| Respiratory rate | 97 (74.6) | 38.6 (18.768.9) | 63 (70.0) | 31.6 (9.561.9) | 63 (62.4) | 24.3 (10.859.2) |
| Oxygen | 90 (69.2) | 39.5 (19.273.6) | 58 (64.4) | 44.2 (2477.6) | 61 (60.4) | 38.3 (1870.6) |
| Heart rate | 21 (16.2) | 4.5 (0.318.4) | 73 (81.1) | 21.8 (5.751.9) | 62 (61.4) | 18 (5.842.2) |
| Temperature | 101 (77.7) | 14.5 (4.545.3) | 61 (67.8) | 18.4 (2.842.8) | 62 (61.4) | 10.6 (0.834) |
Seventy children (21.0%) had 1 parameter abnormal at discharge, including abnormal respiratory rate in 13.7%, heart rate in 7.0%, and temperature in 3.3%. One child (0.3%) was discharged with supplemental oxygen. Ten children (3.0%) had 2 parameters abnormal at discharge. There was no difference in 7‐day readmissions for children with 1 parameter abnormal at discharge (1.4%) compared to those with no abnormal parameters at discharge (4.4%, P=0.253).
Combination TCS Measures
Within each age group, the percentage of children achieving stability was relatively consistent across the 4 combined TCS measures (Table 2); however, more children were considered unstable at discharge (and fewer classified as stable on admission) as the number of included parameters increased. More children 5 years of age reached stability (range, 80.0%85.6%) compared to children 5 years of age (range, 68.3%72.3%). We also noted increasing median TCS with increasing disease severity (Figure 1, P0.01) (see Supporting Fig. 1AC in the online version of this article); TCS was only slightly shorter than LOS across all 3 levels of the severity scale.
| TCS Measures | 2 Years, n=130 | 24 Years, n=90 | 517 Years, n=101 | P Value | |||
|---|---|---|---|---|---|---|---|
| No. (%)* | Median (IQR) TCS, h | No. (%) | Median (IQR) TCS, h | No. (%) | Median (IQR) TCS, h | ||
| |||||||
| RR+O2 | 108 (83.1) | 40.5 (20.175.0) | 72 (80.0) | 39.6 (15.679.2) | 69 (68.3) | 30.4 (14.759.2) | 0.08 |
| RR+O2+HR | 109 (83.8) | 40.2 (19.573.9) | 73 (81.1) | 35.9 (15.977.6) | 68 (67.3) | 29.8 (17.256.6) | 0.11 |
| RR+O2+T | 110 (84.6) | 40.5 (20.770.1) | 77 (85.6) | 39.1 (18.477.6) | 73 (72.3) | 28.2 (14.744.7) | 0.03 |
| RR+O2+HR+T | 110 (84.6) | 40.5 (20.770.1) | 72 (80.0) | 39.7 (20.177.5) | 71 (70.3) | 29.2 (18.254) | 0.05 |
DISCUSSION
Our study demonstrates that longitudinal TCS measures consisting of routinely collected physiologic parameters may be useful for objectively assessing disease recovery and clinical readiness for discharge among children hospitalized with pneumonia. A simple TCS measure incorporating respiratory rate and oxygen requirement performed similarly to the more complex combinations and classified fewer children as unstable at discharge. However, we also note several challenges that deserve additional study prior to the application of a pediatric TCS measure in clinical and research settings.
Vital signs and supplemental oxygen use are used clinically to assess disease severity and response to therapy among children with acute respiratory illness. Because these objective parameters are routinely collected among hospitalized children, the systematization of these data could inform clinical decision making around hospital discharge. Similar to early warning scores used to detect impending clinical deterioration,[11] TCS measures, by signaling normalization of stability parameters in a consistent and objective manner, could serve as an early signal of readiness for discharge. However, maximizing the clinical utility of TCS would require embedding the process within the electronic health record, a tool that could also have implications for the Centers for Medicare and Medicaid Services' meaningful use regulations.[12]
TCS could also serve as an outcome measure in research and quality efforts. Increased disease severity was associated with longer TCS for the 4 combined measures; TCS also demonstrated strong agreement with LOS. Furthermore, TCS minimizes the influence of factors unrelated to disease that may impact LOS (eg, frequency of hospital rounds, transportation difficulties, or social impediments to discharge), an advantage when studying outcomes for research and quality benchmarking.
The percentage of children reaching stability and the median TCS for the combined measures demonstrated little variation within each age group, likely because respiratory rate and need for supplemental oxygen, 2 of the parameters with the longest individual time to stability, were also included in each of the combination measures. This suggests that less‐complex measures incorporating only respiratory rate and need for supplemental oxygen may be sufficient to assess clinical stability, particularly because these parameters are objectively measured and possess a direct physiological link to pneumonia. In contrast, the other parameters may be more often influenced by factors unrelated to disease severity.
Our study also highlights several shortcomings of the pediatric TCS measures. Despite use of published, age‐based reference values,[13] we noted wide variation in the achievement of stability across individual parameters, especially for children 5 years old. Overall, 21% of children had 1 abnormal parameter at discharge. Even the simplest combined measure classified 13.4% of children as unstable at discharge. Discharge with unstable parameters was not associated with 7‐day readmission, although our study was underpowered to detect small differences. Additional study is therefore needed to evaluate less restrictive cutoff values on calculated TCS and the impact of hospital discharge prior to reaching stability. In particular, relaxing the upper limit for normal respiratory rate in adolescents (16 breaths per minute) to more closely approximate the adult TCS parameter (24 breaths per minute) should be explored. Refinement and standardization of age‐based vital sign reference values specific to hospitalized children may also improve the performance of these measures.[14]
Several limitations deserve discussion. TCS parameters and readmission data were abstracted retrospectively from a single institution, and our findings may not be generalizable. Although clinical staff routinely measured these data, measurement variation likely exists. Nevertheless, such variation is likely systematic, limiting the impact of potential misclassification. TCS was calculated based on the last abnormal value for each parameter; prior fluctuations between normal and abnormal periods of stability were not captured. We were unable to assess room air oxygen saturations. Instead, supplemental oxygen use served as a surrogate for hypoxia. At our institution, oxygen therapy is provided for children with pneumonia to maintain oxygen saturations of 90% to 92%. We did not assess work of breathing (a marker of severe pneumonia) or ability to eat (a component of adult TCS measures). We initially considered the evaluation of intravenous fluids as a proxy for ability to eat (addition of this parameter to the 4 parameter TCS resulted in a modest increase in median time to stability, data not shown); however, we felt the lack of institutional policy and subjective nature of this parameter detracted from our study's objectives. Finally, we were not able to determine clinical readiness for discharge beyond the measurement of vital sign parameters. Therefore, prospective evaluation of the proposed pediatric TCS measures in broader populations will be important to build upon our findings, refine stability parameters, and test the utility of new parameters (eg, ability to eat, work of breathing) prior to use in clinical settings.
Our study provides an initial evaluation of TCS measures for assessing severity and recovery among children hospitalized with pneumonia. Similar to adults, such validated TCS measures may ultimately prove useful for improving the quality of both clinical care and research, although additional study to more clearly define stability criteria is needed prior to implementation.
Disclosures
This work was supported by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health under Award Number K23AI104779 to Dr. Williams. The EPIC study was supported by the Influenza Division in the National Center for Immunizations and Respiratory Diseases at the Centers for Disease Control and Prevention through cooperative agreements with each study site and was based on a competitive research funding opportunity. The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention or the National Institutes of Health. Dr. Grijalva serves as a consultant to Glaxo‐Smith‐Kline and Pfizer outside of the scope of this article. Dr. Edwards is supported through grants from Novartis for the conduction of a Group B strep vaccine study and serves as the Chair of the Data Safety and Monitoring Data Committee for Influenza Study outside the scope of this article. Dr. Self reports grants from CareFusion, BioMerieux, Affinium Pharmaceuticals, Astute Medical, Crucell Holland BV, BRAHMS GmbH, Pfizer, Rapid Pathogen Screening, Venaxis, BioAegis Inc., Sphingotec GmbH, and Cempra Pharmaceuticals; personal fees from BioFire Diagnostics and Venaxis, Inc; and patent 13/632,874 (Sterile Blood Culture Collection System) pending; all outside the scope of this article.
- Healthcare Cost and Utilization Project. Available at: http://www.ahrq.gov/research/data/hcup/index.html. Accessed February 1, 2014.
- , , , et al. Time to clinical stability in patients hospitalized with community‐acquired pneumonia: implications for practice guidelines. JAMA. 1998;279:1452–1457.
- , , , et al.; Neumofail Group. Reaching stability in community‐acquired pneumonia: the effects of the severity of disease, treatment, and the characteristics of patients. Clin Infect Dis. 2004;39:1783–1790.
- , , , et al.; Community‐Acquired Pneumonia Organization. The pneumonia severity index predicts time to clinical stability in patients with community‐acquired pneumonia. Int J Tuberc Lung Dis. 2006;10:739–743.
- , , , , . Efficacy of corticosteroids in community‐acquired pneumonia: a randomized double‐blinded clinical trial. Am J Respir Crit Care Med. 2010;181:975–982.
- , , , et al. Early administration of antibiotics does not shorten time to clinical stability in patients with moderate‐to‐severe community‐acquired pneumonia. Chest 2003;124:1798–1804.
- , , , . A comparison between time to clinical stability in community‐acquired aspiration pneumonia and community‐acquired pneumonia. Intern Emerg Med. 2014;9:143–150.
- , , , et al.; Community‐Acquired Pneumonia Organization (CAPO) Investigators. A worldwide perspective of atypical pathogens in community‐acquired pneumonia. Am J Respir Crit Care Med. 2007;175:1086–1093.
- , , , et al.; CDC EPIC Study Team. Community‐acquired pneumonia requiring hospitalization among U.S. children. N Engl J Med. 2015;372:835–845.
- American Heart Association. 2005 American Heart Association (AHA) guidelines for cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) of pediatric and neonatal patients: pediatric basic life support. Pediatrics. 2006;117:e989–e1004.
- , , . Development and initial validation of the Bedside Paediatric Early Warning System score. Crit Care. 2009;13:R135.
- Centers for Medicare and Medicaid Services. Regulations and guidance. EHR incentive programs. Available at: http://www.cms.gov/Regulations‐and‐Guidance/Legislation/EHRIncentivePrograms/index.html. Accessed February 20, 2015
- , , , , , . Development of heart and respiratory rate percentile curves for hospitalized children. Pediatrics. 2013;131:e1150–e1157.
- , , , et al. Length of stay after reaching clinical stability drives hospital costs associated with adult community‐acquired pneumonia. Scand J Infect Dis. 2013;45:219–226.
- Healthcare Cost and Utilization Project. Available at: http://www.ahrq.gov/research/data/hcup/index.html. Accessed February 1, 2014.
- , , , et al. Time to clinical stability in patients hospitalized with community‐acquired pneumonia: implications for practice guidelines. JAMA. 1998;279:1452–1457.
- , , , et al.; Neumofail Group. Reaching stability in community‐acquired pneumonia: the effects of the severity of disease, treatment, and the characteristics of patients. Clin Infect Dis. 2004;39:1783–1790.
- , , , et al.; Community‐Acquired Pneumonia Organization. The pneumonia severity index predicts time to clinical stability in patients with community‐acquired pneumonia. Int J Tuberc Lung Dis. 2006;10:739–743.
- , , , , . Efficacy of corticosteroids in community‐acquired pneumonia: a randomized double‐blinded clinical trial. Am J Respir Crit Care Med. 2010;181:975–982.
- , , , et al. Early administration of antibiotics does not shorten time to clinical stability in patients with moderate‐to‐severe community‐acquired pneumonia. Chest 2003;124:1798–1804.
- , , , . A comparison between time to clinical stability in community‐acquired aspiration pneumonia and community‐acquired pneumonia. Intern Emerg Med. 2014;9:143–150.
- , , , et al.; Community‐Acquired Pneumonia Organization (CAPO) Investigators. A worldwide perspective of atypical pathogens in community‐acquired pneumonia. Am J Respir Crit Care Med. 2007;175:1086–1093.
- , , , et al.; CDC EPIC Study Team. Community‐acquired pneumonia requiring hospitalization among U.S. children. N Engl J Med. 2015;372:835–845.
- American Heart Association. 2005 American Heart Association (AHA) guidelines for cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) of pediatric and neonatal patients: pediatric basic life support. Pediatrics. 2006;117:e989–e1004.
- , , . Development and initial validation of the Bedside Paediatric Early Warning System score. Crit Care. 2009;13:R135.
- Centers for Medicare and Medicaid Services. Regulations and guidance. EHR incentive programs. Available at: http://www.cms.gov/Regulations‐and‐Guidance/Legislation/EHRIncentivePrograms/index.html. Accessed February 20, 2015
- , , , , , . Development of heart and respiratory rate percentile curves for hospitalized children. Pediatrics. 2013;131:e1150–e1157.
- , , , et al. Length of stay after reaching clinical stability drives hospital costs associated with adult community‐acquired pneumonia. Scand J Infect Dis. 2013;45:219–226.
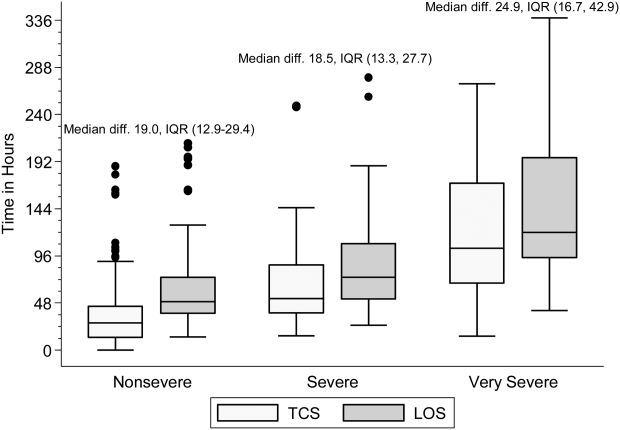
Drug can prevent bleeding in kids with hemophilia A
A recombinant factor VIII Fc fusion protein (rFVIIIFc/efmoroctocog alfa, Eloctate/Elocta) can prevent and control bleeding in previously treated children with severe hemophilia A, results of the phase 3 KIDS A-LONG study suggest.
Children who were previously receiving factor VIII prophylaxis saw their median annualized bleeding rate (ABR) decrease with rFVIIIFc, and close to half of the children on this study did not have any bleeding episodes while they were receiving rFVIIIFc.
None of the patients developed inhibitors to rFVIIIFc. And researchers said adverse events on this trial were typical of a pediatric hemophilia population.
The team reported these results in the Journal of Thrombosis and Haemostasis. The trial was sponsored by Biogen Idec and Sobi, the companies developing rFVIIIFc.
The study included 71 boys younger than 12 years of age who had severe hemophilia A. The patients had at least 50 prior exposure days to factor VIII and no history of factor VIII inhibitors.
The children were set to receive twice-weekly prophylactic infusions of rFVIIIFc, 25 IU/kg on day 1 and 50 IU/kg on day 4, but the researchers made adjustments to dosing as needed.
The median average weekly rFVIIIFc prophylactic dose was 88.11 IU kg. About 90% of the patients were on twice-weekly dosing at the end of the study. Seventy-four percent of patients were able to reduce their dosing frequency with rFVIIIFc compared to factor VIII prophylaxis.
About 46% of patients did not have any bleeding events on study. The median ABR was 1.96 overall and 0 for spontaneous and traumatic bleeding episodes, as well as for spontaneous joint bleeding episodes.
Among patients who were previously receiving factor VIII prophylaxis, their median ABR decreased with rFVIIIFc. For children younger than 6 years of age, the median ABR fell from 1.50 to 0. For children ages 6 through 11, the median ABR fell from 2.50 to 2.01.
About 86% of patients had at least one adverse event while on rFVIIIFc, but none of them discontinued treatment as a result.
Two non-serious events (myalgia and erythematous rash) were considered related to rFVIIIFc. And 5 patients experienced 7 serious adverse events that were not related to treatment. ![]()
A recombinant factor VIII Fc fusion protein (rFVIIIFc/efmoroctocog alfa, Eloctate/Elocta) can prevent and control bleeding in previously treated children with severe hemophilia A, results of the phase 3 KIDS A-LONG study suggest.
Children who were previously receiving factor VIII prophylaxis saw their median annualized bleeding rate (ABR) decrease with rFVIIIFc, and close to half of the children on this study did not have any bleeding episodes while they were receiving rFVIIIFc.
None of the patients developed inhibitors to rFVIIIFc. And researchers said adverse events on this trial were typical of a pediatric hemophilia population.
The team reported these results in the Journal of Thrombosis and Haemostasis. The trial was sponsored by Biogen Idec and Sobi, the companies developing rFVIIIFc.
The study included 71 boys younger than 12 years of age who had severe hemophilia A. The patients had at least 50 prior exposure days to factor VIII and no history of factor VIII inhibitors.
The children were set to receive twice-weekly prophylactic infusions of rFVIIIFc, 25 IU/kg on day 1 and 50 IU/kg on day 4, but the researchers made adjustments to dosing as needed.
The median average weekly rFVIIIFc prophylactic dose was 88.11 IU kg. About 90% of the patients were on twice-weekly dosing at the end of the study. Seventy-four percent of patients were able to reduce their dosing frequency with rFVIIIFc compared to factor VIII prophylaxis.
About 46% of patients did not have any bleeding events on study. The median ABR was 1.96 overall and 0 for spontaneous and traumatic bleeding episodes, as well as for spontaneous joint bleeding episodes.
Among patients who were previously receiving factor VIII prophylaxis, their median ABR decreased with rFVIIIFc. For children younger than 6 years of age, the median ABR fell from 1.50 to 0. For children ages 6 through 11, the median ABR fell from 2.50 to 2.01.
About 86% of patients had at least one adverse event while on rFVIIIFc, but none of them discontinued treatment as a result.
Two non-serious events (myalgia and erythematous rash) were considered related to rFVIIIFc. And 5 patients experienced 7 serious adverse events that were not related to treatment. ![]()
A recombinant factor VIII Fc fusion protein (rFVIIIFc/efmoroctocog alfa, Eloctate/Elocta) can prevent and control bleeding in previously treated children with severe hemophilia A, results of the phase 3 KIDS A-LONG study suggest.
Children who were previously receiving factor VIII prophylaxis saw their median annualized bleeding rate (ABR) decrease with rFVIIIFc, and close to half of the children on this study did not have any bleeding episodes while they were receiving rFVIIIFc.
None of the patients developed inhibitors to rFVIIIFc. And researchers said adverse events on this trial were typical of a pediatric hemophilia population.
The team reported these results in the Journal of Thrombosis and Haemostasis. The trial was sponsored by Biogen Idec and Sobi, the companies developing rFVIIIFc.
The study included 71 boys younger than 12 years of age who had severe hemophilia A. The patients had at least 50 prior exposure days to factor VIII and no history of factor VIII inhibitors.
The children were set to receive twice-weekly prophylactic infusions of rFVIIIFc, 25 IU/kg on day 1 and 50 IU/kg on day 4, but the researchers made adjustments to dosing as needed.
The median average weekly rFVIIIFc prophylactic dose was 88.11 IU kg. About 90% of the patients were on twice-weekly dosing at the end of the study. Seventy-four percent of patients were able to reduce their dosing frequency with rFVIIIFc compared to factor VIII prophylaxis.
About 46% of patients did not have any bleeding events on study. The median ABR was 1.96 overall and 0 for spontaneous and traumatic bleeding episodes, as well as for spontaneous joint bleeding episodes.
Among patients who were previously receiving factor VIII prophylaxis, their median ABR decreased with rFVIIIFc. For children younger than 6 years of age, the median ABR fell from 1.50 to 0. For children ages 6 through 11, the median ABR fell from 2.50 to 2.01.
About 86% of patients had at least one adverse event while on rFVIIIFc, but none of them discontinued treatment as a result.
Two non-serious events (myalgia and erythematous rash) were considered related to rFVIIIFc. And 5 patients experienced 7 serious adverse events that were not related to treatment. ![]()
Chemotherapy drugs recalled in US

Photo by Bill Branson
The pharmaceutical company Mylan is conducting a US-wide recall of several injectable chemotherapy drugs.
Testing of retention samples revealed foreign particulate matter in lots of gemcitabine, carboplatin, methotrexate, and cytarabine. So Mylan issued a
recall of these lots to the hospital/user level.
To date, Mylan has not received any reports of adverse events related to this recall. However, administering injectables that contain foreign particulates can have severe consequences.
Intrathecal administration could result in a life-threatening adverse event or permanent impairment of a body function. Intravenous administration has the potential to damage and/or obstruct blood vessels, which could induce emboli, particularly in the lungs. Intravenous injection can also result in local inflammation, phlebitis, allergic response, and/or embolization in the body and infection.
Intra-arterial administration could result in damage to blood vessels in the distal extremities or organs. And intramuscular administration could result in foreign-body inflammatory response, with local pain, swelling, and possible long-term granuloma formation.
Recall details
The following drugs are included in this recall:
- Gemcitabine for Injection, USP 200 mg; 10 mL; NDC number: 67457-464-20; Lot number: 7801396; Expiration date: 08/2016
- Gemcitabine for Injection, USP 200 mg; 10 mL; NDC number: 67457-464-20; Lot number: 7801401; Expiration date: 08/2016
- Gemcitabine for Injection, USP 200 mg; 10 mL; NDC number: 0069-3857-10; Lot number: 7801089; Expiration date: 07/2015
- Gemcitabine for Injection, USP 2 g; 100 mL; NDC number: 67457-463-02; Lot number: 7801222; Expiration date: 03/2016
- Gemcitabine for Injection, USP 1 g; 50 mL; NDC number: 67457-462-01; Lot number: 7801273; Expiration date: 05/2016
- Carboplatin Injection 10 mg/mL; 100 mL; NDC number: 67457-493-46; Lot number: 7801312; Expiration date: 06/2015
- Methotrexate Injection, USP 25 mg/mL; 2 mL (5 x 2 mL); NDC number: 0069-0146-02; Lot number: 7801082; Expiration date: 07/2015
- Cytarabine Injection 20 mg/mL; 5 mL (10 x 5mL); NDC number: 0069-0152-02; Lot number: 7801050; Expiration date: 05/2015.
Gemcitabine for Injection, USP 200 mg is an intravenously administered product indicated for the treatment of ovarian cancer, breast cancer, non-small cell lung cancer, and pancreatic cancer. These lots were distributed in the US between February 18, 2014, and December 19, 2014, and were manufactured and packaged by Agila Onco Therapies Limited, a Mylan company. Lot 7801089 is packaged with a Pfizer Injectable label.
Carboplatin Injection 10 mg/mL is an intravenously administered product indicated for the treatment of advanced ovarian carcinoma. The lot was distributed in the US between August 11, 2014, and October 7, 2014, and was packaged by Agila Onco Therapies Limited, a Mylan company, with a Mylan Institutional label.
Methotrexate Injection, USP 25 mg/mL can be administered intramuscularly, intravenously, intra-arterially, or intrathecally and is indicated for certain neoplastic diseases, severe psoriasis, and adult rheumatoid arthritis. The lot was distributed in the US between January 16, 2014, and March 25, 2014, and was packaged by Agila Onco Therapies Limited, a Mylan company, with a Pfizer Injectables label.
Cytarabine Injection can be administered intravenously or intrathecally and in combination with other approved anticancer drugs. Cytarabine is indicated for remission induction in acute non-lymphocytic leukemia in adults and pediatric patients. The lot was distributed in the US between May 02, 2014, and July 24, 2014, and was manufactured and packaged by Agila Onco Therapies Limited, a Mylan company located in Bangalore, India, and is packaged with a Pfizer Injectables label.
Mylan is notifying its distributors and customers by letter and is arranging for the return of all recalled products. Distributors, retailers, hospitals, clinics, and physicians with the recalled products should stop using them and return them to the place of purchase.
Consumers with questions regarding this recall can contact Mylan Customer Relations at 1-800-796-9526 or [email protected], Monday through Friday from 8 am to 5 pm EST.
Consumers should contact their physicians or healthcare providers if they have experienced any problems that may be related to using these drugs.
Adverse reactions or quality problems related to the use of these product may be reported to the US Food and Drug Administration’s MedWatch Adverse Event Reporting Program. ![]()
Photo by Bill Branson
The pharmaceutical company Mylan is conducting a US-wide recall of several injectable chemotherapy drugs.
Testing of retention samples revealed foreign particulate matter in lots of gemcitabine, carboplatin, methotrexate, and cytarabine. So Mylan issued a
recall of these lots to the hospital/user level.
To date, Mylan has not received any reports of adverse events related to this recall. However, administering injectables that contain foreign particulates can have severe consequences.
Intrathecal administration could result in a life-threatening adverse event or permanent impairment of a body function. Intravenous administration has the potential to damage and/or obstruct blood vessels, which could induce emboli, particularly in the lungs. Intravenous injection can also result in local inflammation, phlebitis, allergic response, and/or embolization in the body and infection.
Intra-arterial administration could result in damage to blood vessels in the distal extremities or organs. And intramuscular administration could result in foreign-body inflammatory response, with local pain, swelling, and possible long-term granuloma formation.
Recall details
The following drugs are included in this recall:
- Gemcitabine for Injection, USP 200 mg; 10 mL; NDC number: 67457-464-20; Lot number: 7801396; Expiration date: 08/2016
- Gemcitabine for Injection, USP 200 mg; 10 mL; NDC number: 67457-464-20; Lot number: 7801401; Expiration date: 08/2016
- Gemcitabine for Injection, USP 200 mg; 10 mL; NDC number: 0069-3857-10; Lot number: 7801089; Expiration date: 07/2015
- Gemcitabine for Injection, USP 2 g; 100 mL; NDC number: 67457-463-02; Lot number: 7801222; Expiration date: 03/2016
- Gemcitabine for Injection, USP 1 g; 50 mL; NDC number: 67457-462-01; Lot number: 7801273; Expiration date: 05/2016
- Carboplatin Injection 10 mg/mL; 100 mL; NDC number: 67457-493-46; Lot number: 7801312; Expiration date: 06/2015
- Methotrexate Injection, USP 25 mg/mL; 2 mL (5 x 2 mL); NDC number: 0069-0146-02; Lot number: 7801082; Expiration date: 07/2015
- Cytarabine Injection 20 mg/mL; 5 mL (10 x 5mL); NDC number: 0069-0152-02; Lot number: 7801050; Expiration date: 05/2015.
Gemcitabine for Injection, USP 200 mg is an intravenously administered product indicated for the treatment of ovarian cancer, breast cancer, non-small cell lung cancer, and pancreatic cancer. These lots were distributed in the US between February 18, 2014, and December 19, 2014, and were manufactured and packaged by Agila Onco Therapies Limited, a Mylan company. Lot 7801089 is packaged with a Pfizer Injectable label.
Carboplatin Injection 10 mg/mL is an intravenously administered product indicated for the treatment of advanced ovarian carcinoma. The lot was distributed in the US between August 11, 2014, and October 7, 2014, and was packaged by Agila Onco Therapies Limited, a Mylan company, with a Mylan Institutional label.
Methotrexate Injection, USP 25 mg/mL can be administered intramuscularly, intravenously, intra-arterially, or intrathecally and is indicated for certain neoplastic diseases, severe psoriasis, and adult rheumatoid arthritis. The lot was distributed in the US between January 16, 2014, and March 25, 2014, and was packaged by Agila Onco Therapies Limited, a Mylan company, with a Pfizer Injectables label.
Cytarabine Injection can be administered intravenously or intrathecally and in combination with other approved anticancer drugs. Cytarabine is indicated for remission induction in acute non-lymphocytic leukemia in adults and pediatric patients. The lot was distributed in the US between May 02, 2014, and July 24, 2014, and was manufactured and packaged by Agila Onco Therapies Limited, a Mylan company located in Bangalore, India, and is packaged with a Pfizer Injectables label.
Mylan is notifying its distributors and customers by letter and is arranging for the return of all recalled products. Distributors, retailers, hospitals, clinics, and physicians with the recalled products should stop using them and return them to the place of purchase.
Consumers with questions regarding this recall can contact Mylan Customer Relations at 1-800-796-9526 or [email protected], Monday through Friday from 8 am to 5 pm EST.
Consumers should contact their physicians or healthcare providers if they have experienced any problems that may be related to using these drugs.
Adverse reactions or quality problems related to the use of these product may be reported to the US Food and Drug Administration’s MedWatch Adverse Event Reporting Program. ![]()
Photo by Bill Branson
The pharmaceutical company Mylan is conducting a US-wide recall of several injectable chemotherapy drugs.
Testing of retention samples revealed foreign particulate matter in lots of gemcitabine, carboplatin, methotrexate, and cytarabine. So Mylan issued a
recall of these lots to the hospital/user level.
To date, Mylan has not received any reports of adverse events related to this recall. However, administering injectables that contain foreign particulates can have severe consequences.
Intrathecal administration could result in a life-threatening adverse event or permanent impairment of a body function. Intravenous administration has the potential to damage and/or obstruct blood vessels, which could induce emboli, particularly in the lungs. Intravenous injection can also result in local inflammation, phlebitis, allergic response, and/or embolization in the body and infection.
Intra-arterial administration could result in damage to blood vessels in the distal extremities or organs. And intramuscular administration could result in foreign-body inflammatory response, with local pain, swelling, and possible long-term granuloma formation.
Recall details
The following drugs are included in this recall:
- Gemcitabine for Injection, USP 200 mg; 10 mL; NDC number: 67457-464-20; Lot number: 7801396; Expiration date: 08/2016
- Gemcitabine for Injection, USP 200 mg; 10 mL; NDC number: 67457-464-20; Lot number: 7801401; Expiration date: 08/2016
- Gemcitabine for Injection, USP 200 mg; 10 mL; NDC number: 0069-3857-10; Lot number: 7801089; Expiration date: 07/2015
- Gemcitabine for Injection, USP 2 g; 100 mL; NDC number: 67457-463-02; Lot number: 7801222; Expiration date: 03/2016
- Gemcitabine for Injection, USP 1 g; 50 mL; NDC number: 67457-462-01; Lot number: 7801273; Expiration date: 05/2016
- Carboplatin Injection 10 mg/mL; 100 mL; NDC number: 67457-493-46; Lot number: 7801312; Expiration date: 06/2015
- Methotrexate Injection, USP 25 mg/mL; 2 mL (5 x 2 mL); NDC number: 0069-0146-02; Lot number: 7801082; Expiration date: 07/2015
- Cytarabine Injection 20 mg/mL; 5 mL (10 x 5mL); NDC number: 0069-0152-02; Lot number: 7801050; Expiration date: 05/2015.
Gemcitabine for Injection, USP 200 mg is an intravenously administered product indicated for the treatment of ovarian cancer, breast cancer, non-small cell lung cancer, and pancreatic cancer. These lots were distributed in the US between February 18, 2014, and December 19, 2014, and were manufactured and packaged by Agila Onco Therapies Limited, a Mylan company. Lot 7801089 is packaged with a Pfizer Injectable label.
Carboplatin Injection 10 mg/mL is an intravenously administered product indicated for the treatment of advanced ovarian carcinoma. The lot was distributed in the US between August 11, 2014, and October 7, 2014, and was packaged by Agila Onco Therapies Limited, a Mylan company, with a Mylan Institutional label.
Methotrexate Injection, USP 25 mg/mL can be administered intramuscularly, intravenously, intra-arterially, or intrathecally and is indicated for certain neoplastic diseases, severe psoriasis, and adult rheumatoid arthritis. The lot was distributed in the US between January 16, 2014, and March 25, 2014, and was packaged by Agila Onco Therapies Limited, a Mylan company, with a Pfizer Injectables label.
Cytarabine Injection can be administered intravenously or intrathecally and in combination with other approved anticancer drugs. Cytarabine is indicated for remission induction in acute non-lymphocytic leukemia in adults and pediatric patients. The lot was distributed in the US between May 02, 2014, and July 24, 2014, and was manufactured and packaged by Agila Onco Therapies Limited, a Mylan company located in Bangalore, India, and is packaged with a Pfizer Injectables label.
Mylan is notifying its distributors and customers by letter and is arranging for the return of all recalled products. Distributors, retailers, hospitals, clinics, and physicians with the recalled products should stop using them and return them to the place of purchase.
Consumers with questions regarding this recall can contact Mylan Customer Relations at 1-800-796-9526 or [email protected], Monday through Friday from 8 am to 5 pm EST.
Consumers should contact their physicians or healthcare providers if they have experienced any problems that may be related to using these drugs.
Adverse reactions or quality problems related to the use of these product may be reported to the US Food and Drug Administration’s MedWatch Adverse Event Reporting Program. ![]()