Surveillance of circulating tumor DNA (ctDNA) can help predict relapse in most patients with diffuse large B-cell lymphoma before there is clinical evidence of the disease, according to a study published in The Lancet Oncology.
Investigators analyzed ctDNA using the clonoSEQ minimal residual disease (MRD) test and found they could predict relapse with a positive predictive value (PPV) of 88% and a negative predictive value (NPV) of 98%.
The test detected relapse a median of 3.5 months quicker than computed tomography (CT) scans.
“Patients with DLBCL with low amounts of disease at relapse have better survival than those with more disease, which is the rationale for surveillance CT scans,” said study author Wyndham Wilson, MD, PhD, of the National Cancer Institute in Bethesda, Maryland.
“Because the ctDNA test detects disease at a molecular level, it detects microscopic disease, which cannot be detected by CT scans, and may improve patient survival. Furthermore, ctDNA is non-invasive and can be employed as frequently needed, unlike surveillance CT scans, which expose patients to radiation and intravenous contrast.”
For this study, Dr Wilson and his colleagues evaluated 126 DLBCL patients who had participated in clinical trials from May 1993 to June 2013 and were followed for a median of 11 years post-treatment.
Surveillance monitoring
To investigate whether ctDNA monitoring could overcome the limitations of standard imaging techniques, the researchers compared serial ctDNA samples to CT scans taken at the same time post-treatment in patients who had achieved complete remission. This was known as “surveillance monitoring.”
The investigators performed surveillance monitoring of ctDNA in 107 patients who achieved complete remission.
The hazard ratio for clinical disease progression was 228 for patients who had detectable ctDNA during surveillance, when compared to patients with undetectable ctDNA (P<0.0001).
Surveillance ctDNA had a PPV of 88.2% and an NPV of 97.8%. And it revealed the risk of recurrence at a median of 3.5 months (range, 0-200 months) before there was evidence of clinical disease.
Interim monitoring
The researchers also analyzed whether the presence of ctDNA at the beginning of the third cycle of treatment predicted relapse, regardless of whether patients achieved complete remission by the end of treatment. This was known as “interim monitoring.”
Of the 108 patients included in the interim monitoring analysis, ctDNA was detected in 24 patients, 15 of whom eventually relapsed. Only 17 of the 84 patients with undetectable interim ctDNA relapsed.
Five years after the interim serum samples were taken, 80.2% of the patients who were negative for ctDNA were relapse-free, as were 41.7% of patients who were positive for ctDNA (P<0.0001).
Detectable interim ctDNA had a PPV of 62.5% and an NPV of 79.8%.
Fourteen of the 15 patients with detectable ctDNA who relapsed did so within 6 months of the end of treatment, as did 7 of the 17 patients without interim ctDNA.
Based on these results, the investigators concluded that surveillance monitoring of ctDNA identifies DLBCL patients at risk of disease recurrence before clinical evidence of disease in most patients, and interim monitoring of ctDNA is a promising biomarker to identify patients at high risk of treatment failure.
This research was funded by Adaptive Biotechnologies, the company developing the clonoSEQ MRD test, as well as the National Cancer Institute.
Surveillance of circulating tumor DNA (ctDNA) can help predict relapse in most patients with diffuse large B-cell lymphoma before there is clinical evidence of the disease, according to a study published in The Lancet Oncology.
Investigators analyzed ctDNA using the clonoSEQ minimal residual disease (MRD) test and found they could predict relapse with a positive predictive value (PPV) of 88% and a negative predictive value (NPV) of 98%.
The test detected relapse a median of 3.5 months quicker than computed tomography (CT) scans.
“Patients with DLBCL with low amounts of disease at relapse have better survival than those with more disease, which is the rationale for surveillance CT scans,” said study author Wyndham Wilson, MD, PhD, of the National Cancer Institute in Bethesda, Maryland.
“Because the ctDNA test detects disease at a molecular level, it detects microscopic disease, which cannot be detected by CT scans, and may improve patient survival. Furthermore, ctDNA is non-invasive and can be employed as frequently needed, unlike surveillance CT scans, which expose patients to radiation and intravenous contrast.”
For this study, Dr Wilson and his colleagues evaluated 126 DLBCL patients who had participated in clinical trials from May 1993 to June 2013 and were followed for a median of 11 years post-treatment.
Surveillance monitoring
To investigate whether ctDNA monitoring could overcome the limitations of standard imaging techniques, the researchers compared serial ctDNA samples to CT scans taken at the same time post-treatment in patients who had achieved complete remission. This was known as “surveillance monitoring.”
The investigators performed surveillance monitoring of ctDNA in 107 patients who achieved complete remission.
The hazard ratio for clinical disease progression was 228 for patients who had detectable ctDNA during surveillance, when compared to patients with undetectable ctDNA (P<0.0001).
Surveillance ctDNA had a PPV of 88.2% and an NPV of 97.8%. And it revealed the risk of recurrence at a median of 3.5 months (range, 0-200 months) before there was evidence of clinical disease.
Interim monitoring
The researchers also analyzed whether the presence of ctDNA at the beginning of the third cycle of treatment predicted relapse, regardless of whether patients achieved complete remission by the end of treatment. This was known as “interim monitoring.”
Of the 108 patients included in the interim monitoring analysis, ctDNA was detected in 24 patients, 15 of whom eventually relapsed. Only 17 of the 84 patients with undetectable interim ctDNA relapsed.
Five years after the interim serum samples were taken, 80.2% of the patients who were negative for ctDNA were relapse-free, as were 41.7% of patients who were positive for ctDNA (P<0.0001).
Detectable interim ctDNA had a PPV of 62.5% and an NPV of 79.8%.
Fourteen of the 15 patients with detectable ctDNA who relapsed did so within 6 months of the end of treatment, as did 7 of the 17 patients without interim ctDNA.
Based on these results, the investigators concluded that surveillance monitoring of ctDNA identifies DLBCL patients at risk of disease recurrence before clinical evidence of disease in most patients, and interim monitoring of ctDNA is a promising biomarker to identify patients at high risk of treatment failure.
This research was funded by Adaptive Biotechnologies, the company developing the clonoSEQ MRD test, as well as the National Cancer Institute.
Wyndham Wilson, MD, PhD
Photo by Larry Young
Surveillance of circulating tumor DNA (ctDNA) can help predict relapse in most patients with diffuse large B-cell lymphoma before there is clinical evidence of the disease, according to a study published in The Lancet Oncology.
Investigators analyzed ctDNA using the clonoSEQ minimal residual disease (MRD) test and found they could predict relapse with a positive predictive value (PPV) of 88% and a negative predictive value (NPV) of 98%.
The test detected relapse a median of 3.5 months quicker than computed tomography (CT) scans.
“Patients with DLBCL with low amounts of disease at relapse have better survival than those with more disease, which is the rationale for surveillance CT scans,” said study author Wyndham Wilson, MD, PhD, of the National Cancer Institute in Bethesda, Maryland.
“Because the ctDNA test detects disease at a molecular level, it detects microscopic disease, which cannot be detected by CT scans, and may improve patient survival. Furthermore, ctDNA is non-invasive and can be employed as frequently needed, unlike surveillance CT scans, which expose patients to radiation and intravenous contrast.”
For this study, Dr Wilson and his colleagues evaluated 126 DLBCL patients who had participated in clinical trials from May 1993 to June 2013 and were followed for a median of 11 years post-treatment.
Surveillance monitoring
To investigate whether ctDNA monitoring could overcome the limitations of standard imaging techniques, the researchers compared serial ctDNA samples to CT scans taken at the same time post-treatment in patients who had achieved complete remission. This was known as “surveillance monitoring.”
The investigators performed surveillance monitoring of ctDNA in 107 patients who achieved complete remission.
The hazard ratio for clinical disease progression was 228 for patients who had detectable ctDNA during surveillance, when compared to patients with undetectable ctDNA (P<0.0001).
Surveillance ctDNA had a PPV of 88.2% and an NPV of 97.8%. And it revealed the risk of recurrence at a median of 3.5 months (range, 0-200 months) before there was evidence of clinical disease.
Interim monitoring
The researchers also analyzed whether the presence of ctDNA at the beginning of the third cycle of treatment predicted relapse, regardless of whether patients achieved complete remission by the end of treatment. This was known as “interim monitoring.”
Of the 108 patients included in the interim monitoring analysis, ctDNA was detected in 24 patients, 15 of whom eventually relapsed. Only 17 of the 84 patients with undetectable interim ctDNA relapsed.
Five years after the interim serum samples were taken, 80.2% of the patients who were negative for ctDNA were relapse-free, as were 41.7% of patients who were positive for ctDNA (P<0.0001).
Detectable interim ctDNA had a PPV of 62.5% and an NPV of 79.8%.
Fourteen of the 15 patients with detectable ctDNA who relapsed did so within 6 months of the end of treatment, as did 7 of the 17 patients without interim ctDNA.
Based on these results, the investigators concluded that surveillance monitoring of ctDNA identifies DLBCL patients at risk of disease recurrence before clinical evidence of disease in most patients, and interim monitoring of ctDNA is a promising biomarker to identify patients at high risk of treatment failure.
This research was funded by Adaptive Biotechnologies, the company developing the clonoSEQ MRD test, as well as the National Cancer Institute.
New discoveries concerning a well-known tumor suppressor protein could help advance the diagnosis and treatment of chronic myeloid leukemia (CML), according to researchers.
They found that levels of the protein, BRCA1, are significantly decreased in advanced phases of CML, the expression of BCR-ABL1 correlates with decreased levels of BRCA1, and this downregulation of BRCA1 is caused by the inhibition of BRCA1 messenger RNA (mRNA) translation.
These discoveries explain the mechanism that supports CML development and uncover its weakness, the investigators said. They reported their findings in Cell Cycle.
“Our data demonstrated that BRCA1 synthesis is diminished in [the] advanced stage[s] of CML,” said study author Paulina Podszywałow-Bartnicka, PhD, of the Nencki Institute in Warsaw, Poland.
“The gene coding for BRCA1 protein is not mutated. However, BRCA1 mRNA, which is necessary for the protein production, is aggregated and stored in protein complexes [and], thus, not available for the protein synthesis.”
To gain more insight into this phenomenon, the investigators looked at 2 mRNA-binding proteins, HuR and TIAR. They found that BCR-ABL1 promoted cytosolic localization of TIAR and HuR, the proteins’ binding to BRCA1 mRNA, and formation of the TIAR-HuR complex.
The researchers also found that HuR positively regulated BRCA1 mRNA stability and translation, while TIAR negatively regulated BRCA1 translation.
TIAR-dependent downregulation of BRCA1 was a result of endoplasmic reticulum stress, which is activated in BCR-ABL1 expressing cells. And experiments showed that silencing TIAR in CML cells elevated BRCA1 levels.
This suggests that TIAR-mediated repression of BRCA1 mRNA translation is responsible for the downregulation of BRCA1 observed in BCR-ABL1-positive leukemia cells.
The investigators said this research indicates that BRCA1 deficiency, which supports CML, can be also used as a weapon against the disease.
“When a cell has damaged one signaling pathway or one gene, it may function properly due to alternative pathways . . . ,” explained study author Tomasz Skorski, MD, PhD, of Temple University School of Medicine in Philadelphia, Pennsylvania.
“Only when this alternative pathway is inhibited [do cells] lose the ability to survive. As we know that one of the [DNA double-strand break] repair pathways which depend on BRCA1 is blocked in leukemia cells, we can try to find the alternative, parallel pathway and inhibit it as well.”
This will induce apoptosis via synthetic lethality, but only in leukemia cells, because healthy cells still have functional BRCA1-dependent signaling. Dr Skorski noted that therapies based on BRCA1 deficiency are currently under investigation in clinical trials.
New discoveries concerning a well-known tumor suppressor protein could help advance the diagnosis and treatment of chronic myeloid leukemia (CML), according to researchers.
They found that levels of the protein, BRCA1, are significantly decreased in advanced phases of CML, the expression of BCR-ABL1 correlates with decreased levels of BRCA1, and this downregulation of BRCA1 is caused by the inhibition of BRCA1 messenger RNA (mRNA) translation.
These discoveries explain the mechanism that supports CML development and uncover its weakness, the investigators said. They reported their findings in Cell Cycle.
“Our data demonstrated that BRCA1 synthesis is diminished in [the] advanced stage[s] of CML,” said study author Paulina Podszywałow-Bartnicka, PhD, of the Nencki Institute in Warsaw, Poland.
“The gene coding for BRCA1 protein is not mutated. However, BRCA1 mRNA, which is necessary for the protein production, is aggregated and stored in protein complexes [and], thus, not available for the protein synthesis.”
To gain more insight into this phenomenon, the investigators looked at 2 mRNA-binding proteins, HuR and TIAR. They found that BCR-ABL1 promoted cytosolic localization of TIAR and HuR, the proteins’ binding to BRCA1 mRNA, and formation of the TIAR-HuR complex.
The researchers also found that HuR positively regulated BRCA1 mRNA stability and translation, while TIAR negatively regulated BRCA1 translation.
TIAR-dependent downregulation of BRCA1 was a result of endoplasmic reticulum stress, which is activated in BCR-ABL1 expressing cells. And experiments showed that silencing TIAR in CML cells elevated BRCA1 levels.
This suggests that TIAR-mediated repression of BRCA1 mRNA translation is responsible for the downregulation of BRCA1 observed in BCR-ABL1-positive leukemia cells.
The investigators said this research indicates that BRCA1 deficiency, which supports CML, can be also used as a weapon against the disease.
“When a cell has damaged one signaling pathway or one gene, it may function properly due to alternative pathways . . . ,” explained study author Tomasz Skorski, MD, PhD, of Temple University School of Medicine in Philadelphia, Pennsylvania.
“Only when this alternative pathway is inhibited [do cells] lose the ability to survive. As we know that one of the [DNA double-strand break] repair pathways which depend on BRCA1 is blocked in leukemia cells, we can try to find the alternative, parallel pathway and inhibit it as well.”
This will induce apoptosis via synthetic lethality, but only in leukemia cells, because healthy cells still have functional BRCA1-dependent signaling. Dr Skorski noted that therapies based on BRCA1 deficiency are currently under investigation in clinical trials.
Micrograph showing CML
Image courtesy of UCSD
New discoveries concerning a well-known tumor suppressor protein could help advance the diagnosis and treatment of chronic myeloid leukemia (CML), according to researchers.
They found that levels of the protein, BRCA1, are significantly decreased in advanced phases of CML, the expression of BCR-ABL1 correlates with decreased levels of BRCA1, and this downregulation of BRCA1 is caused by the inhibition of BRCA1 messenger RNA (mRNA) translation.
These discoveries explain the mechanism that supports CML development and uncover its weakness, the investigators said. They reported their findings in Cell Cycle.
“Our data demonstrated that BRCA1 synthesis is diminished in [the] advanced stage[s] of CML,” said study author Paulina Podszywałow-Bartnicka, PhD, of the Nencki Institute in Warsaw, Poland.
“The gene coding for BRCA1 protein is not mutated. However, BRCA1 mRNA, which is necessary for the protein production, is aggregated and stored in protein complexes [and], thus, not available for the protein synthesis.”
To gain more insight into this phenomenon, the investigators looked at 2 mRNA-binding proteins, HuR and TIAR. They found that BCR-ABL1 promoted cytosolic localization of TIAR and HuR, the proteins’ binding to BRCA1 mRNA, and formation of the TIAR-HuR complex.
The researchers also found that HuR positively regulated BRCA1 mRNA stability and translation, while TIAR negatively regulated BRCA1 translation.
TIAR-dependent downregulation of BRCA1 was a result of endoplasmic reticulum stress, which is activated in BCR-ABL1 expressing cells. And experiments showed that silencing TIAR in CML cells elevated BRCA1 levels.
This suggests that TIAR-mediated repression of BRCA1 mRNA translation is responsible for the downregulation of BRCA1 observed in BCR-ABL1-positive leukemia cells.
The investigators said this research indicates that BRCA1 deficiency, which supports CML, can be also used as a weapon against the disease.
“When a cell has damaged one signaling pathway or one gene, it may function properly due to alternative pathways . . . ,” explained study author Tomasz Skorski, MD, PhD, of Temple University School of Medicine in Philadelphia, Pennsylvania.
“Only when this alternative pathway is inhibited [do cells] lose the ability to survive. As we know that one of the [DNA double-strand break] repair pathways which depend on BRCA1 is blocked in leukemia cells, we can try to find the alternative, parallel pathway and inhibit it as well.”
This will induce apoptosis via synthetic lethality, but only in leukemia cells, because healthy cells still have functional BRCA1-dependent signaling. Dr Skorski noted that therapies based on BRCA1 deficiency are currently under investigation in clinical trials.
The US Food and Drug Administration (FDA) has granted orphan drug designation for IMO-8400, an antagonist of the endosomal toll-like receptors (TLRs) 7, 8, and 9, for the treatment of diffuse large B-cell lymphoma (DLBCL).
The FDA grants orphan designation to drugs intended to treat conditions that affect fewer than 200,000 people in the US.
The designation will provide Idera Pharmaceuticals, the company developing IMO-8400, with certain incentives. These include eligibility for federal grants, research and development tax credits, and a 7-year period of marketing exclusivity if the product is approved.
Relevant research
Preclinical research published in Leukemia showed that the MYD88 L265P oncogenic mutation is an independent prognostic factor in DLBCL. In DLBCL patients with this mutation, TLR signaling is over-activated, which enables tumor cell survival and proliferation.
Data presented at the 2014 AACR Annual Meeting showed that IMO-8400 inhibited the survival and proliferation of DLBCL cells and Waldenstrom’s macroglobulinemia (WM) cells harboring the MYD88 L265P mutation.
A phase 1 trial of IMO-8400 presented at the 2013 FOCIS Annual Meeting showed the drug was active and well-tolerated in 42 healthy subjects. IMO-8400 was given at single and multiple escalating doses up to 0.6 mg/kg for 4 weeks. The drug inhibited immune responses mediated by TLRs 7, 8, and 9.
Idera Pharmaceuticals is currently conducting a phase 1/2 trial of IMO-8400 in patients with relapsed or refractory DLBCL who harbor the MYD88 L265P mutation. The protocol includes 3 dose-escalation cohorts in which IMO-8400 is administered subcutaneously.
Idera is also pursuing clinical development of IMO-8400 in WM. The FDA recently granted the drug orphan designation to treat WM.
The US Food and Drug Administration (FDA) has granted orphan drug designation for IMO-8400, an antagonist of the endosomal toll-like receptors (TLRs) 7, 8, and 9, for the treatment of diffuse large B-cell lymphoma (DLBCL).
The FDA grants orphan designation to drugs intended to treat conditions that affect fewer than 200,000 people in the US.
The designation will provide Idera Pharmaceuticals, the company developing IMO-8400, with certain incentives. These include eligibility for federal grants, research and development tax credits, and a 7-year period of marketing exclusivity if the product is approved.
Relevant research
Preclinical research published in Leukemia showed that the MYD88 L265P oncogenic mutation is an independent prognostic factor in DLBCL. In DLBCL patients with this mutation, TLR signaling is over-activated, which enables tumor cell survival and proliferation.
Data presented at the 2014 AACR Annual Meeting showed that IMO-8400 inhibited the survival and proliferation of DLBCL cells and Waldenstrom’s macroglobulinemia (WM) cells harboring the MYD88 L265P mutation.
A phase 1 trial of IMO-8400 presented at the 2013 FOCIS Annual Meeting showed the drug was active and well-tolerated in 42 healthy subjects. IMO-8400 was given at single and multiple escalating doses up to 0.6 mg/kg for 4 weeks. The drug inhibited immune responses mediated by TLRs 7, 8, and 9.
Idera Pharmaceuticals is currently conducting a phase 1/2 trial of IMO-8400 in patients with relapsed or refractory DLBCL who harbor the MYD88 L265P mutation. The protocol includes 3 dose-escalation cohorts in which IMO-8400 is administered subcutaneously.
Idera is also pursuing clinical development of IMO-8400 in WM. The FDA recently granted the drug orphan designation to treat WM.
Micrograph showing DLBCL
The US Food and Drug Administration (FDA) has granted orphan drug designation for IMO-8400, an antagonist of the endosomal toll-like receptors (TLRs) 7, 8, and 9, for the treatment of diffuse large B-cell lymphoma (DLBCL).
The FDA grants orphan designation to drugs intended to treat conditions that affect fewer than 200,000 people in the US.
The designation will provide Idera Pharmaceuticals, the company developing IMO-8400, with certain incentives. These include eligibility for federal grants, research and development tax credits, and a 7-year period of marketing exclusivity if the product is approved.
Relevant research
Preclinical research published in Leukemia showed that the MYD88 L265P oncogenic mutation is an independent prognostic factor in DLBCL. In DLBCL patients with this mutation, TLR signaling is over-activated, which enables tumor cell survival and proliferation.
Data presented at the 2014 AACR Annual Meeting showed that IMO-8400 inhibited the survival and proliferation of DLBCL cells and Waldenstrom’s macroglobulinemia (WM) cells harboring the MYD88 L265P mutation.
A phase 1 trial of IMO-8400 presented at the 2013 FOCIS Annual Meeting showed the drug was active and well-tolerated in 42 healthy subjects. IMO-8400 was given at single and multiple escalating doses up to 0.6 mg/kg for 4 weeks. The drug inhibited immune responses mediated by TLRs 7, 8, and 9.
Idera Pharmaceuticals is currently conducting a phase 1/2 trial of IMO-8400 in patients with relapsed or refractory DLBCL who harbor the MYD88 L265P mutation. The protocol includes 3 dose-escalation cohorts in which IMO-8400 is administered subcutaneously.
Idera is also pursuing clinical development of IMO-8400 in WM. The FDA recently granted the drug orphan designation to treat WM.
New research suggests the prevalence of childhood cancer survivors in the US has increased, and the majority of pediatric patients who have survived 5
or more years beyond cancer diagnosis may have at least one chronic health condition.
About 70% of the childhood cancer survivors studied were estimated to have a mild or moderate chronic condition, and nearly a third were estimated to have a severe, disabling, or life-threatening chronic condition.
“Our study findings highlight that a singular focus on curing cancer yields an incomplete picture of childhood cancer survivorship,” said study author Siobhan M. Phillips, PhD, of Northwestern University Feinberg School of Medicine in Chicago, Illinois.
“The burden of chronic conditions in this population is profound, both in occurrence and severity. Efforts to understand how to effectively decrease morbidity burden and incorporate effective care coordination and rehabilitation models to optimize longevity and well-being in this population should be a priority.”
The researchers analyzed data on cancer incidence and survival for children who were diagnosed with cancer between 0 and 19 years of age. The data had been recorded between 1975 and 2011 in 9 different US Surveillance, Epidemiology, and End Results (SEER) registries.
The team also used data from the Childhood Cancer Survivor Study (CCSS) cohort, which had information on a range of potential adverse and late effects of cancer treatment from more than 14,000 long-term survivors of childhood cancers who were treated at 26 cancer centers across the US and Canada.
The investigators first obtained estimates of the probability of each measure of morbidity from CCSS and then multiplied these estimates by the relevant number of survivors in the US estimated from the SEER data.
The researchers estimated the number of childhood cancer survivors in the US to be 388,501, which is an increase of 59,849 from the previous estimate made in 2005 by a team from the National Cancer Institute.
Of these patients, about 84% had survived 5 or more years post-diagnosis, and about 45% had survived for 20 years or more.
About 70% of the survivors were estimated to have a mild or moderate chronic condition (grade 1-2), and about 32% were estimated to have a severe, disabling, or life-threatening chronic condition (grade 3-4).
An estimated 35% of the survivors, ages 20 to 49, had neurocognitive dysfunction. About 13% to 17% of survivors in this age group had self-reported functional impairment, activity limitations, impaired mental health, pain, or anxiety/fear.
“We know that many of these morbidities are at least somewhat modifiable in the general population,” Dr Phillips noted. “However, we don’t know if typical population guidelines for preventive behaviors apply to [childhood cancer survivors].”
“We need to develop a better understanding of the multilevel factors—including, but not limited to, physical activity, diet, and treatment characteristics—which influence childhood cancer survivors’ susceptibility to these morbidities in order to effectively prevent and delay their onset.”
New research suggests the prevalence of childhood cancer survivors in the US has increased, and the majority of pediatric patients who have survived 5
or more years beyond cancer diagnosis may have at least one chronic health condition.
About 70% of the childhood cancer survivors studied were estimated to have a mild or moderate chronic condition, and nearly a third were estimated to have a severe, disabling, or life-threatening chronic condition.
“Our study findings highlight that a singular focus on curing cancer yields an incomplete picture of childhood cancer survivorship,” said study author Siobhan M. Phillips, PhD, of Northwestern University Feinberg School of Medicine in Chicago, Illinois.
“The burden of chronic conditions in this population is profound, both in occurrence and severity. Efforts to understand how to effectively decrease morbidity burden and incorporate effective care coordination and rehabilitation models to optimize longevity and well-being in this population should be a priority.”
The researchers analyzed data on cancer incidence and survival for children who were diagnosed with cancer between 0 and 19 years of age. The data had been recorded between 1975 and 2011 in 9 different US Surveillance, Epidemiology, and End Results (SEER) registries.
The team also used data from the Childhood Cancer Survivor Study (CCSS) cohort, which had information on a range of potential adverse and late effects of cancer treatment from more than 14,000 long-term survivors of childhood cancers who were treated at 26 cancer centers across the US and Canada.
The investigators first obtained estimates of the probability of each measure of morbidity from CCSS and then multiplied these estimates by the relevant number of survivors in the US estimated from the SEER data.
The researchers estimated the number of childhood cancer survivors in the US to be 388,501, which is an increase of 59,849 from the previous estimate made in 2005 by a team from the National Cancer Institute.
Of these patients, about 84% had survived 5 or more years post-diagnosis, and about 45% had survived for 20 years or more.
About 70% of the survivors were estimated to have a mild or moderate chronic condition (grade 1-2), and about 32% were estimated to have a severe, disabling, or life-threatening chronic condition (grade 3-4).
An estimated 35% of the survivors, ages 20 to 49, had neurocognitive dysfunction. About 13% to 17% of survivors in this age group had self-reported functional impairment, activity limitations, impaired mental health, pain, or anxiety/fear.
“We know that many of these morbidities are at least somewhat modifiable in the general population,” Dr Phillips noted. “However, we don’t know if typical population guidelines for preventive behaviors apply to [childhood cancer survivors].”
“We need to develop a better understanding of the multilevel factors—including, but not limited to, physical activity, diet, and treatment characteristics—which influence childhood cancer survivors’ susceptibility to these morbidities in order to effectively prevent and delay their onset.”
Doctor examining a child
Photo by Logan Tuttle
New research suggests the prevalence of childhood cancer survivors in the US has increased, and the majority of pediatric patients who have survived 5
or more years beyond cancer diagnosis may have at least one chronic health condition.
About 70% of the childhood cancer survivors studied were estimated to have a mild or moderate chronic condition, and nearly a third were estimated to have a severe, disabling, or life-threatening chronic condition.
“Our study findings highlight that a singular focus on curing cancer yields an incomplete picture of childhood cancer survivorship,” said study author Siobhan M. Phillips, PhD, of Northwestern University Feinberg School of Medicine in Chicago, Illinois.
“The burden of chronic conditions in this population is profound, both in occurrence and severity. Efforts to understand how to effectively decrease morbidity burden and incorporate effective care coordination and rehabilitation models to optimize longevity and well-being in this population should be a priority.”
The researchers analyzed data on cancer incidence and survival for children who were diagnosed with cancer between 0 and 19 years of age. The data had been recorded between 1975 and 2011 in 9 different US Surveillance, Epidemiology, and End Results (SEER) registries.
The team also used data from the Childhood Cancer Survivor Study (CCSS) cohort, which had information on a range of potential adverse and late effects of cancer treatment from more than 14,000 long-term survivors of childhood cancers who were treated at 26 cancer centers across the US and Canada.
The investigators first obtained estimates of the probability of each measure of morbidity from CCSS and then multiplied these estimates by the relevant number of survivors in the US estimated from the SEER data.
The researchers estimated the number of childhood cancer survivors in the US to be 388,501, which is an increase of 59,849 from the previous estimate made in 2005 by a team from the National Cancer Institute.
Of these patients, about 84% had survived 5 or more years post-diagnosis, and about 45% had survived for 20 years or more.
About 70% of the survivors were estimated to have a mild or moderate chronic condition (grade 1-2), and about 32% were estimated to have a severe, disabling, or life-threatening chronic condition (grade 3-4).
An estimated 35% of the survivors, ages 20 to 49, had neurocognitive dysfunction. About 13% to 17% of survivors in this age group had self-reported functional impairment, activity limitations, impaired mental health, pain, or anxiety/fear.
“We know that many of these morbidities are at least somewhat modifiable in the general population,” Dr Phillips noted. “However, we don’t know if typical population guidelines for preventive behaviors apply to [childhood cancer survivors].”
“We need to develop a better understanding of the multilevel factors—including, but not limited to, physical activity, diet, and treatment characteristics—which influence childhood cancer survivors’ susceptibility to these morbidities in order to effectively prevent and delay their onset.”
Hand hygiene is a proven and guideline‐recommended safety practice, although clinicians and particularly physicians are unreliable at performing it.[1] Like hands, stethoscopes can carry pathogens from patient to patient. In 1 study, stethoscopes were as likely to be contaminated after use with methicillin‐resistant Staphylococcus aureuspositive patients as the provider's hands.[2] Furthermore, like hands, stethoscopes can be effectively decolonized with alcohol.[3, 4] However, although hand hygiene rates have been extensively studied,[1] and hand hygiene has been linked to reductions in nosocomial infection,[5] stethoscope hygiene is less well studied and emphasized less by guidelines.[6] Several surveys have documented low self‐reported compliance with stethoscope hygiene.[7, 8, 9, 10] Of 150 healthcare workers, 48% reported stethoscope hygiene between daily and weekly, 37% did stethoscope hygiene monthly, and 7% did stethoscope hygiene annually or never.[8] Of 1401 doctors asked about their stethoscope hygiene beliefs and practices, 76% believed that stethoscopes could transmit infection, but only 24% reported cleaning their scopes regularly.[9] Moreover, of 308 students, 22% had never done stethoscope hygiene, and 4% did it consistently.[10] However, we were unable to find any data on observed rates of stethoscope hygiene. Thus, we observed student and trainee physician stethoscope hygiene performance during hospital medicine rotations as part of the baseline data‐collection phase of a quality‐improvement effort linked to hand hygiene efforts.
METHODS
Attending hospitalists (I.H.J., B.M., and A.A.) and 1 graduate assistant (J.W.) at 3 sites observed stethoscope hygiene opportunities over an 11‐month period. Stethoscope hygiene was counted as performed if a patient‐specific stethoscope was used in an isolation room, or if any type of cleaning (alcohol gel, alcohol wipe, or cleansing cloth) was performed on a stethoscope carried out of the room. Observers also recorded whether stethoscope hygiene opportunities occurred in isolation rooms or nonisolation rooms, and noted if stethoscope hygiene was obviously triggered by an attending's stethoscope hygiene behavior (eg, a trainee asked an attending why he performed stethoscope hygiene, then performed it him or herself). Trainees were not aware that their stethoscope hygiene behaviors were being recorded.
RESULTS
We observed 352 opportunities for stethoscope hygiene, in which doctors or students used stethoscope hygiene in 58 encounters (16%). Twenty of the 58 stethoscope hygiene events occurred only after a trainee observed an attending physician perform stethoscope hygiene. Eliminating stethoscope hygiene events that were triggered by attending physicians, stethoscope hygiene was performed in 38 of 332 opportunities (11%). There was a significant difference between the rate of stethoscope hygiene performed in isolation versus nonisolation rooms: 24/29 (82.7%) versus 14 of 303 (4.6%) (P0.001 by Pearson 2 statistic). In isolation room stethoscope hygiene, in which the type of hygiene was recorded, 18 of 20 (90%) involved use of an isolation stethoscope, and 2 of 20 (10%) involved cleaning of a personal stethoscope.
DISCUSSION
Stethoscope hygiene is rarely performed by trainees. Stethoscope hygiene performance depends on the isolation status of the patient, with more than 80% performance in isolated patients and 5% in nonisolated patients.
Although little is known about the rate of infection related to stethoscopes, colonization of stethoscopes with nosocomial bacteria is well described.[2] Transmission of pathogens from patient to patient by stethoscopes could undermine the benefits of hand hygiene programs, as patients are commonly exposed to unclean stethoscopes.
Our observations are limited by several factors. We used a convenience sample of general medicine trainee behavior at academic medical centers; the behavior of attending physicians, ancillary staff, and nonacademic physicians may be different. Moreover, attending behavior may have prompted more episodes of stethoscope hygiene performance than we recorded, because we only noted when stethoscope hygiene was clearly related to attending behavior. The very low rate of stethoscope hygiene after contact with nonisolation patients represents a current and potentially serious safety threat. Future research might be able to quantify the risk associated with uncleaned stethoscopes or demonstrate the effectiveness of stethoscope hygiene programs. The effect of modeling on hand hygiene and stethoscope hygiene[10, 11] and on stethoscope hygiene in our data suggests a method for improving stethoscope hygiene.
World Health Organization. WHO Guidelines on Hand Hygiene in HealthCare. Global Patient Safety Challenge 2005‐2006: Clean Care Is Safer Care. Geneva, Switzerland: WHO Press; 2009.
Longtin Y, Schneider A, Tschopp C, et al. Contamination of stethoscopes and physicians' hands after a physical examination. Mayo Clin Proc. 2014;89:291–299.
Bernard L, Kereveur A, Durand D, et al. Bacterial contamination of hospital physicians’ stethoscopes. Infect Control Hosp Epidemiol. 1999;20:626–628.
Schroeder A, Schroeder MA, D'Amico F.What's growing on your stethoscope? (and what you can do about it). J Fam Pract. 2009;58(8):404–409.
Pittet D, Hugonnet S, Harbarth S, et al. Effectiveness of a hospital wide program aimed at improving compliance with hand hygiene. Lancet. 2000;356:1307–1312.
Bearman G, Bryant K, Leekha S, et al. Healthcare personnel attire in non‐operating‐room settings. Infect Control Hosp Epidemiol. 2014;35:107–121.
Breathnach AS, Jenkins DR, Pedler SJ.Stethoscopes as possible vectors of infection by staphylococci. BMJ. 1992;305:1573–1574.
Jones JS, Hoerle D, Riekse R.Stethoscopes: a potential vector of infection?Ann Emerg Med.1995;26:296–299.
Muniz J, Sethi RK, Zaghi J, Ziniel SI, Sandora TJ.Predictors of stethoscope disinfection among pediatric health care providers. Am J Infect Control.2012;40:922–925.
Saunders C, Hryhorskyj L, Skinner J.Factors influencing stethoscope cleanliness among clinical medical students. J Hosp Infect.2013;84(3):242–244.
Jumaa PA.Hand hygiene: simple and complex. Int J Infect Dis.2005;9:3–14.
Hand hygiene is a proven and guideline‐recommended safety practice, although clinicians and particularly physicians are unreliable at performing it.[1] Like hands, stethoscopes can carry pathogens from patient to patient. In 1 study, stethoscopes were as likely to be contaminated after use with methicillin‐resistant Staphylococcus aureuspositive patients as the provider's hands.[2] Furthermore, like hands, stethoscopes can be effectively decolonized with alcohol.[3, 4] However, although hand hygiene rates have been extensively studied,[1] and hand hygiene has been linked to reductions in nosocomial infection,[5] stethoscope hygiene is less well studied and emphasized less by guidelines.[6] Several surveys have documented low self‐reported compliance with stethoscope hygiene.[7, 8, 9, 10] Of 150 healthcare workers, 48% reported stethoscope hygiene between daily and weekly, 37% did stethoscope hygiene monthly, and 7% did stethoscope hygiene annually or never.[8] Of 1401 doctors asked about their stethoscope hygiene beliefs and practices, 76% believed that stethoscopes could transmit infection, but only 24% reported cleaning their scopes regularly.[9] Moreover, of 308 students, 22% had never done stethoscope hygiene, and 4% did it consistently.[10] However, we were unable to find any data on observed rates of stethoscope hygiene. Thus, we observed student and trainee physician stethoscope hygiene performance during hospital medicine rotations as part of the baseline data‐collection phase of a quality‐improvement effort linked to hand hygiene efforts.
METHODS
Attending hospitalists (I.H.J., B.M., and A.A.) and 1 graduate assistant (J.W.) at 3 sites observed stethoscope hygiene opportunities over an 11‐month period. Stethoscope hygiene was counted as performed if a patient‐specific stethoscope was used in an isolation room, or if any type of cleaning (alcohol gel, alcohol wipe, or cleansing cloth) was performed on a stethoscope carried out of the room. Observers also recorded whether stethoscope hygiene opportunities occurred in isolation rooms or nonisolation rooms, and noted if stethoscope hygiene was obviously triggered by an attending's stethoscope hygiene behavior (eg, a trainee asked an attending why he performed stethoscope hygiene, then performed it him or herself). Trainees were not aware that their stethoscope hygiene behaviors were being recorded.
RESULTS
We observed 352 opportunities for stethoscope hygiene, in which doctors or students used stethoscope hygiene in 58 encounters (16%). Twenty of the 58 stethoscope hygiene events occurred only after a trainee observed an attending physician perform stethoscope hygiene. Eliminating stethoscope hygiene events that were triggered by attending physicians, stethoscope hygiene was performed in 38 of 332 opportunities (11%). There was a significant difference between the rate of stethoscope hygiene performed in isolation versus nonisolation rooms: 24/29 (82.7%) versus 14 of 303 (4.6%) (P0.001 by Pearson 2 statistic). In isolation room stethoscope hygiene, in which the type of hygiene was recorded, 18 of 20 (90%) involved use of an isolation stethoscope, and 2 of 20 (10%) involved cleaning of a personal stethoscope.
DISCUSSION
Stethoscope hygiene is rarely performed by trainees. Stethoscope hygiene performance depends on the isolation status of the patient, with more than 80% performance in isolated patients and 5% in nonisolated patients.
Although little is known about the rate of infection related to stethoscopes, colonization of stethoscopes with nosocomial bacteria is well described.[2] Transmission of pathogens from patient to patient by stethoscopes could undermine the benefits of hand hygiene programs, as patients are commonly exposed to unclean stethoscopes.
Our observations are limited by several factors. We used a convenience sample of general medicine trainee behavior at academic medical centers; the behavior of attending physicians, ancillary staff, and nonacademic physicians may be different. Moreover, attending behavior may have prompted more episodes of stethoscope hygiene performance than we recorded, because we only noted when stethoscope hygiene was clearly related to attending behavior. The very low rate of stethoscope hygiene after contact with nonisolation patients represents a current and potentially serious safety threat. Future research might be able to quantify the risk associated with uncleaned stethoscopes or demonstrate the effectiveness of stethoscope hygiene programs. The effect of modeling on hand hygiene and stethoscope hygiene[10, 11] and on stethoscope hygiene in our data suggests a method for improving stethoscope hygiene.
Disclosure
Nothing to report.
Hand hygiene is a proven and guideline‐recommended safety practice, although clinicians and particularly physicians are unreliable at performing it.[1] Like hands, stethoscopes can carry pathogens from patient to patient. In 1 study, stethoscopes were as likely to be contaminated after use with methicillin‐resistant Staphylococcus aureuspositive patients as the provider's hands.[2] Furthermore, like hands, stethoscopes can be effectively decolonized with alcohol.[3, 4] However, although hand hygiene rates have been extensively studied,[1] and hand hygiene has been linked to reductions in nosocomial infection,[5] stethoscope hygiene is less well studied and emphasized less by guidelines.[6] Several surveys have documented low self‐reported compliance with stethoscope hygiene.[7, 8, 9, 10] Of 150 healthcare workers, 48% reported stethoscope hygiene between daily and weekly, 37% did stethoscope hygiene monthly, and 7% did stethoscope hygiene annually or never.[8] Of 1401 doctors asked about their stethoscope hygiene beliefs and practices, 76% believed that stethoscopes could transmit infection, but only 24% reported cleaning their scopes regularly.[9] Moreover, of 308 students, 22% had never done stethoscope hygiene, and 4% did it consistently.[10] However, we were unable to find any data on observed rates of stethoscope hygiene. Thus, we observed student and trainee physician stethoscope hygiene performance during hospital medicine rotations as part of the baseline data‐collection phase of a quality‐improvement effort linked to hand hygiene efforts.
METHODS
Attending hospitalists (I.H.J., B.M., and A.A.) and 1 graduate assistant (J.W.) at 3 sites observed stethoscope hygiene opportunities over an 11‐month period. Stethoscope hygiene was counted as performed if a patient‐specific stethoscope was used in an isolation room, or if any type of cleaning (alcohol gel, alcohol wipe, or cleansing cloth) was performed on a stethoscope carried out of the room. Observers also recorded whether stethoscope hygiene opportunities occurred in isolation rooms or nonisolation rooms, and noted if stethoscope hygiene was obviously triggered by an attending's stethoscope hygiene behavior (eg, a trainee asked an attending why he performed stethoscope hygiene, then performed it him or herself). Trainees were not aware that their stethoscope hygiene behaviors were being recorded.
RESULTS
We observed 352 opportunities for stethoscope hygiene, in which doctors or students used stethoscope hygiene in 58 encounters (16%). Twenty of the 58 stethoscope hygiene events occurred only after a trainee observed an attending physician perform stethoscope hygiene. Eliminating stethoscope hygiene events that were triggered by attending physicians, stethoscope hygiene was performed in 38 of 332 opportunities (11%). There was a significant difference between the rate of stethoscope hygiene performed in isolation versus nonisolation rooms: 24/29 (82.7%) versus 14 of 303 (4.6%) (P0.001 by Pearson 2 statistic). In isolation room stethoscope hygiene, in which the type of hygiene was recorded, 18 of 20 (90%) involved use of an isolation stethoscope, and 2 of 20 (10%) involved cleaning of a personal stethoscope.
DISCUSSION
Stethoscope hygiene is rarely performed by trainees. Stethoscope hygiene performance depends on the isolation status of the patient, with more than 80% performance in isolated patients and 5% in nonisolated patients.
Although little is known about the rate of infection related to stethoscopes, colonization of stethoscopes with nosocomial bacteria is well described.[2] Transmission of pathogens from patient to patient by stethoscopes could undermine the benefits of hand hygiene programs, as patients are commonly exposed to unclean stethoscopes.
Our observations are limited by several factors. We used a convenience sample of general medicine trainee behavior at academic medical centers; the behavior of attending physicians, ancillary staff, and nonacademic physicians may be different. Moreover, attending behavior may have prompted more episodes of stethoscope hygiene performance than we recorded, because we only noted when stethoscope hygiene was clearly related to attending behavior. The very low rate of stethoscope hygiene after contact with nonisolation patients represents a current and potentially serious safety threat. Future research might be able to quantify the risk associated with uncleaned stethoscopes or demonstrate the effectiveness of stethoscope hygiene programs. The effect of modeling on hand hygiene and stethoscope hygiene[10, 11] and on stethoscope hygiene in our data suggests a method for improving stethoscope hygiene.
Disclosure
Nothing to report.
References
World Health Organization. WHO Guidelines on Hand Hygiene in HealthCare. Global Patient Safety Challenge 2005‐2006: Clean Care Is Safer Care. Geneva, Switzerland: WHO Press; 2009.
Longtin Y, Schneider A, Tschopp C, et al. Contamination of stethoscopes and physicians' hands after a physical examination. Mayo Clin Proc. 2014;89:291–299.
Bernard L, Kereveur A, Durand D, et al. Bacterial contamination of hospital physicians’ stethoscopes. Infect Control Hosp Epidemiol. 1999;20:626–628.
Schroeder A, Schroeder MA, D'Amico F.What's growing on your stethoscope? (and what you can do about it). J Fam Pract. 2009;58(8):404–409.
Pittet D, Hugonnet S, Harbarth S, et al. Effectiveness of a hospital wide program aimed at improving compliance with hand hygiene. Lancet. 2000;356:1307–1312.
Bearman G, Bryant K, Leekha S, et al. Healthcare personnel attire in non‐operating‐room settings. Infect Control Hosp Epidemiol. 2014;35:107–121.
Breathnach AS, Jenkins DR, Pedler SJ.Stethoscopes as possible vectors of infection by staphylococci. BMJ. 1992;305:1573–1574.
Jones JS, Hoerle D, Riekse R.Stethoscopes: a potential vector of infection?Ann Emerg Med.1995;26:296–299.
Muniz J, Sethi RK, Zaghi J, Ziniel SI, Sandora TJ.Predictors of stethoscope disinfection among pediatric health care providers. Am J Infect Control.2012;40:922–925.
Saunders C, Hryhorskyj L, Skinner J.Factors influencing stethoscope cleanliness among clinical medical students. J Hosp Infect.2013;84(3):242–244.
Jumaa PA.Hand hygiene: simple and complex. Int J Infect Dis.2005;9:3–14.
References
World Health Organization. WHO Guidelines on Hand Hygiene in HealthCare. Global Patient Safety Challenge 2005‐2006: Clean Care Is Safer Care. Geneva, Switzerland: WHO Press; 2009.
Longtin Y, Schneider A, Tschopp C, et al. Contamination of stethoscopes and physicians' hands after a physical examination. Mayo Clin Proc. 2014;89:291–299.
Bernard L, Kereveur A, Durand D, et al. Bacterial contamination of hospital physicians’ stethoscopes. Infect Control Hosp Epidemiol. 1999;20:626–628.
Schroeder A, Schroeder MA, D'Amico F.What's growing on your stethoscope? (and what you can do about it). J Fam Pract. 2009;58(8):404–409.
Pittet D, Hugonnet S, Harbarth S, et al. Effectiveness of a hospital wide program aimed at improving compliance with hand hygiene. Lancet. 2000;356:1307–1312.
Bearman G, Bryant K, Leekha S, et al. Healthcare personnel attire in non‐operating‐room settings. Infect Control Hosp Epidemiol. 2014;35:107–121.
Breathnach AS, Jenkins DR, Pedler SJ.Stethoscopes as possible vectors of infection by staphylococci. BMJ. 1992;305:1573–1574.
Jones JS, Hoerle D, Riekse R.Stethoscopes: a potential vector of infection?Ann Emerg Med.1995;26:296–299.
Muniz J, Sethi RK, Zaghi J, Ziniel SI, Sandora TJ.Predictors of stethoscope disinfection among pediatric health care providers. Am J Infect Control.2012;40:922–925.
Saunders C, Hryhorskyj L, Skinner J.Factors influencing stethoscope cleanliness among clinical medical students. J Hosp Infect.2013;84(3):242–244.
Jumaa PA.Hand hygiene: simple and complex. Int J Infect Dis.2005;9:3–14.
Address for correspondence and reprint requests: Ian Harold Jenkins, MD, Department of Medicine, University of California, San Diego, San Diego, CA 92103; E‐mail: [email protected]
Content Gating
Gated (full article locked unless allowed per User)
I read with great interest the article by McAlister and colleagues[1] on weekend versus weekday discharge outcomes.
The authors addressed length of stay (LOS) as a potential confounder in their inquiry. They ran regressions with and without LOS as a control and stated their results did not change; the findings imply LOS did not rest in the causal pathway between calendar day of discharge and outcomes.
I would like to highlight a recent article in which the authors found the reverse. Bartel et al.[2] applied a clever instrumental analysischoosing admission day (Sunday and Monday vs Tuesday through Saturday) as the instrumentto determine outcomes based on LOS. The investigators also ran a number of convincing falsification tests to verify their study design. They found an inverse association between greater length of hospital stay and readmissions and mortality.
Although Bartel et al. used a narrower spectrum of diagnoses and analyzed Medicare beneficiaries only, the results illuminate the difficulty in understanding the relationship between time in house and the day of discharge. If LOS influences mortality and readmission rates, overlooking its effect may obscure physician efforts to reduce LOS, for the laudatory goal of lessening return hospital trips and death.
The book on LOS impact remains open. We must remain uncertain of the interplay between days in house, mortality, readmission, and the weekend effect until further studies can elucidate how these variables interact.
References
McAlister FA, Youngson E, Padwal RS, Majumdar SR. Similar outcomes among general medicine patients discharged on weekends. J Hosp Med. 2015;10(2):69–74.
Bartel AP, Chan CW, Kim S‐H. Should hospitals keep their patients longer? The role of inpatient and outpatient care in reducing readmissions. NBER working paper no. 20499. National Bureau of Economic Research website. Available at: http://www.nber.org/papers/w20499. Published September 2014. Accessed December 26, 2014.
I read with great interest the article by McAlister and colleagues[1] on weekend versus weekday discharge outcomes.
The authors addressed length of stay (LOS) as a potential confounder in their inquiry. They ran regressions with and without LOS as a control and stated their results did not change; the findings imply LOS did not rest in the causal pathway between calendar day of discharge and outcomes.
I would like to highlight a recent article in which the authors found the reverse. Bartel et al.[2] applied a clever instrumental analysischoosing admission day (Sunday and Monday vs Tuesday through Saturday) as the instrumentto determine outcomes based on LOS. The investigators also ran a number of convincing falsification tests to verify their study design. They found an inverse association between greater length of hospital stay and readmissions and mortality.
Although Bartel et al. used a narrower spectrum of diagnoses and analyzed Medicare beneficiaries only, the results illuminate the difficulty in understanding the relationship between time in house and the day of discharge. If LOS influences mortality and readmission rates, overlooking its effect may obscure physician efforts to reduce LOS, for the laudatory goal of lessening return hospital trips and death.
The book on LOS impact remains open. We must remain uncertain of the interplay between days in house, mortality, readmission, and the weekend effect until further studies can elucidate how these variables interact.
I read with great interest the article by McAlister and colleagues[1] on weekend versus weekday discharge outcomes.
The authors addressed length of stay (LOS) as a potential confounder in their inquiry. They ran regressions with and without LOS as a control and stated their results did not change; the findings imply LOS did not rest in the causal pathway between calendar day of discharge and outcomes.
I would like to highlight a recent article in which the authors found the reverse. Bartel et al.[2] applied a clever instrumental analysischoosing admission day (Sunday and Monday vs Tuesday through Saturday) as the instrumentto determine outcomes based on LOS. The investigators also ran a number of convincing falsification tests to verify their study design. They found an inverse association between greater length of hospital stay and readmissions and mortality.
Although Bartel et al. used a narrower spectrum of diagnoses and analyzed Medicare beneficiaries only, the results illuminate the difficulty in understanding the relationship between time in house and the day of discharge. If LOS influences mortality and readmission rates, overlooking its effect may obscure physician efforts to reduce LOS, for the laudatory goal of lessening return hospital trips and death.
The book on LOS impact remains open. We must remain uncertain of the interplay between days in house, mortality, readmission, and the weekend effect until further studies can elucidate how these variables interact.
References
McAlister FA, Youngson E, Padwal RS, Majumdar SR. Similar outcomes among general medicine patients discharged on weekends. J Hosp Med. 2015;10(2):69–74.
Bartel AP, Chan CW, Kim S‐H. Should hospitals keep their patients longer? The role of inpatient and outpatient care in reducing readmissions. NBER working paper no. 20499. National Bureau of Economic Research website. Available at: http://www.nber.org/papers/w20499. Published September 2014. Accessed December 26, 2014.
References
McAlister FA, Youngson E, Padwal RS, Majumdar SR. Similar outcomes among general medicine patients discharged on weekends. J Hosp Med. 2015;10(2):69–74.
Bartel AP, Chan CW, Kim S‐H. Should hospitals keep their patients longer? The role of inpatient and outpatient care in reducing readmissions. NBER working paper no. 20499. National Bureau of Economic Research website. Available at: http://www.nber.org/papers/w20499. Published September 2014. Accessed December 26, 2014.
HM15 presenters: Verity Schaye, Michael Janjigian, Frank Volpicelli, Susan Hunt.
Performing a physical exam is the standard of care for evaluating patients. It has been shown to have higher diagnostic utility than many technology based tests. The physical exam is the Gold Standard for dermatological and mental status assessment for which technological tests are not readily available. The tradition “laying on of hands” has important benefits for the physician patient relationship.
The teaching of physical exam skills is increasingly problematic. Barriers include attending time, comfort and skill level as well as challenges of patient comfort and potential isolation issues.
The Peyton Model provides a better means of teaching physical exam skills than the traditional “See one, do one, teach one” model. The Peyton Model has four steps:
Demonstration. The teacher performs the exam at normal speed without commentary.
Deconstruction. The teacher performs the exam while describing the steps.
Comprehension. The teacher performs the exam while the learner describes the steps.
Performance. The learner performs the exam while also describing the steps.
This approach can be abbreviated for more advanced learners with the middle two steps being combined to a discussion between the teacher and learner to highlight any differences or changes in technique. TH
HM15 presenters: Verity Schaye, Michael Janjigian, Frank Volpicelli, Susan Hunt.
Performing a physical exam is the standard of care for evaluating patients. It has been shown to have higher diagnostic utility than many technology based tests. The physical exam is the Gold Standard for dermatological and mental status assessment for which technological tests are not readily available. The tradition “laying on of hands” has important benefits for the physician patient relationship.
The teaching of physical exam skills is increasingly problematic. Barriers include attending time, comfort and skill level as well as challenges of patient comfort and potential isolation issues.
The Peyton Model provides a better means of teaching physical exam skills than the traditional “See one, do one, teach one” model. The Peyton Model has four steps:
Demonstration. The teacher performs the exam at normal speed without commentary.
Deconstruction. The teacher performs the exam while describing the steps.
Comprehension. The teacher performs the exam while the learner describes the steps.
Performance. The learner performs the exam while also describing the steps.
This approach can be abbreviated for more advanced learners with the middle two steps being combined to a discussion between the teacher and learner to highlight any differences or changes in technique. TH
HM15 presenters: Verity Schaye, Michael Janjigian, Frank Volpicelli, Susan Hunt.
Performing a physical exam is the standard of care for evaluating patients. It has been shown to have higher diagnostic utility than many technology based tests. The physical exam is the Gold Standard for dermatological and mental status assessment for which technological tests are not readily available. The tradition “laying on of hands” has important benefits for the physician patient relationship.
The teaching of physical exam skills is increasingly problematic. Barriers include attending time, comfort and skill level as well as challenges of patient comfort and potential isolation issues.
The Peyton Model provides a better means of teaching physical exam skills than the traditional “See one, do one, teach one” model. The Peyton Model has four steps:
Demonstration. The teacher performs the exam at normal speed without commentary.
Deconstruction. The teacher performs the exam while describing the steps.
Comprehension. The teacher performs the exam while the learner describes the steps.
Performance. The learner performs the exam while also describing the steps.
This approach can be abbreviated for more advanced learners with the middle two steps being combined to a discussion between the teacher and learner to highlight any differences or changes in technique. TH
Kathleen Finn, MD, FHM and Jeffrey Greenwald, MD, SFHM engaged the audience with their playful banter while reviewing medical literature of clinical significance for the hospitalist in Update in Hospital Medicine. The studies presented were high-quality, practical and addressed questions that arise in our day-to-day practice. A wide variety of topics were addressed and key points are summarized below.
Key takeaways
In the PARADIGM-HF study, Angiotensin Receptor Blocker (ARB) + Neprilysin Inhibitor decreased cardiovascular mortality and reduced CHF hospitalization by 20% when compared to Enalapril alone in heart failure patients. The combination drug is an alternative choice to ACE inhibitors. FDA approval is forthcoming.
Is the risk of contrast-induced nephrotoxicity really as great as we have come to believe? Review of propensity matched studies suggests that AKI, 30 day need for emergent hemodi
alysis and death are unrelated to contrast. If CT with contrast makes a difference to the patient, consider using it if GFR>30 ml/min.
SAGES trial and Project Recovery developed a delirium screening method in hospitalized patients. The CAM (Confusion Assessment Method) scoring system assesses delirium severity in elderly patients (70+). Hospital and post-hospital outcomes in delirious vs. non-delirious patients showed that the more severe the delirium, the longer the patient stayed in the hospital. Further, the rate of new SNF placement and 90 day mortality was higher in the delirious group. The CAM score correlates with prognosis in medical patients. Addressing long-term goals of care in this patient population may be warranted.
A randomized placebo-controlled trail looked at the preventive effects of Ramelteon (melatonin receptor agonist) on delirium. Ramelteon 8mg was given to patients at 9pm for 7 days (or d/c). Although this was a small and short study, Ramelteon appears to reduce incident delirium in medical and non-intubated ICU patients.
The HELP randomized clinical trial compared Lactulose vs. Polyethylene Glycol (PEG) electrolyte solution for treatment of overt hepatic encephalopathy. Patients received either PEG (4L in 4 hours) or Lactulose (20-30g 3+doses/24hrs). Primary outcome was an improvement in HESA (Hepatic Encephalopathy Scoring Algorithm ) score by 1 at 24 hours. HESA score improved and patients had a shorter length of stay in the PEG group. In addition, patients requested PEG at discharge because it tasted better.
A retrospective study looked at Nonselective beta blockers (NSBB) in patients with Spontaneous Bacterial Peritonitis (SBP). It suggests that the use of NSBB after SBP onset increases the risk of AKI, Hepatorenal Syndrome and mortality by 58%. NSBB appear beneficial before SBP onset suggesting that as cirrhosis becomes more severe, NSBB may not be effective.
A retrospective cohort trial (Michigan Hospital Medicine Safety Consortium) assessed hospital performance of VTE prophylaxis. The rate of clinically evident, confirmed VTE was measured. There was no difference in VTE occurrence during hospitalization, 90 day VTE rates and PE vs. DVT rates. No clear benefit was evident from VTE prophylaxis for medical patients. This could indicate the need to risk stratify patients’ VTE risk.
Direct oral anticoagulants (DOACs) were compared with Vitamin K antagonists (VKA) for treatment of acute VTE in a meta-analysis reviewed by the speakers. Death, safety and bleeding were assessed. DOACs seem to work as well as VKAs for VTE. They also had a better safety profile. In cancer patients, DOACs vs. LMWH study is still needed. In patients with atrial fibrillation (AF), DOACs prevent AF-associated strokes better than VKAs. They also reduce hemorrhagic stroke and intracranial hemorrhage.
In the elderly (75 or older) patient, DOACs are as safe as VKAs and LMWH for AF and VTE treatment.
Randomized control trails compared once weekly Dalbavancin or single-dose Oritavancin vs. daily conventional therapy for acute bacterial skin infections (cellulitis, major abscess, wound infection, 75cm² erythema). Outcomes measured were cessation of spread of erythema and no fever X3 readings in 48-72 hours. Dalbavancin once weekly was non-inferior to Vancomycin in safety profile and outcome measures. Direct cost of Dalbavancin was higher although patients on this drug had shorter length of stays which is cost effective. FDA approved for skin infections.
The presence of family during CPR decreased PTSD, anxiety and depression symptoms in family members. Outcomes were similar when participants were assesses at 90 days and 1 year. While this study was conducted in an out of hospital setting, it may be worthwhile to assess if it is applicable to patients who code in the hospital.
Kathleen Finn, MD, FHM and Jeffrey Greenwald, MD, SFHM engaged the audience with their playful banter while reviewing medical literature of clinical significance for the hospitalist in Update in Hospital Medicine. The studies presented were high-quality, practical and addressed questions that arise in our day-to-day practice. A wide variety of topics were addressed and key points are summarized below.
Key takeaways
In the PARADIGM-HF study, Angiotensin Receptor Blocker (ARB) + Neprilysin Inhibitor decreased cardiovascular mortality and reduced CHF hospitalization by 20% when compared to Enalapril alone in heart failure patients. The combination drug is an alternative choice to ACE inhibitors. FDA approval is forthcoming.
Is the risk of contrast-induced nephrotoxicity really as great as we have come to believe? Review of propensity matched studies suggests that AKI, 30 day need for emergent hemodi
alysis and death are unrelated to contrast. If CT with contrast makes a difference to the patient, consider using it if GFR>30 ml/min.
SAGES trial and Project Recovery developed a delirium screening method in hospitalized patients. The CAM (Confusion Assessment Method) scoring system assesses delirium severity in elderly patients (70+). Hospital and post-hospital outcomes in delirious vs. non-delirious patients showed that the more severe the delirium, the longer the patient stayed in the hospital. Further, the rate of new SNF placement and 90 day mortality was higher in the delirious group. The CAM score correlates with prognosis in medical patients. Addressing long-term goals of care in this patient population may be warranted.
A randomized placebo-controlled trail looked at the preventive effects of Ramelteon (melatonin receptor agonist) on delirium. Ramelteon 8mg was given to patients at 9pm for 7 days (or d/c). Although this was a small and short study, Ramelteon appears to reduce incident delirium in medical and non-intubated ICU patients.
The HELP randomized clinical trial compared Lactulose vs. Polyethylene Glycol (PEG) electrolyte solution for treatment of overt hepatic encephalopathy. Patients received either PEG (4L in 4 hours) or Lactulose (20-30g 3+doses/24hrs). Primary outcome was an improvement in HESA (Hepatic Encephalopathy Scoring Algorithm ) score by 1 at 24 hours. HESA score improved and patients had a shorter length of stay in the PEG group. In addition, patients requested PEG at discharge because it tasted better.
A retrospective study looked at Nonselective beta blockers (NSBB) in patients with Spontaneous Bacterial Peritonitis (SBP). It suggests that the use of NSBB after SBP onset increases the risk of AKI, Hepatorenal Syndrome and mortality by 58%. NSBB appear beneficial before SBP onset suggesting that as cirrhosis becomes more severe, NSBB may not be effective.
A retrospective cohort trial (Michigan Hospital Medicine Safety Consortium) assessed hospital performance of VTE prophylaxis. The rate of clinically evident, confirmed VTE was measured. There was no difference in VTE occurrence during hospitalization, 90 day VTE rates and PE vs. DVT rates. No clear benefit was evident from VTE prophylaxis for medical patients. This could indicate the need to risk stratify patients’ VTE risk.
Direct oral anticoagulants (DOACs) were compared with Vitamin K antagonists (VKA) for treatment of acute VTE in a meta-analysis reviewed by the speakers. Death, safety and bleeding were assessed. DOACs seem to work as well as VKAs for VTE. They also had a better safety profile. In cancer patients, DOACs vs. LMWH study is still needed. In patients with atrial fibrillation (AF), DOACs prevent AF-associated strokes better than VKAs. They also reduce hemorrhagic stroke and intracranial hemorrhage.
In the elderly (75 or older) patient, DOACs are as safe as VKAs and LMWH for AF and VTE treatment.
Randomized control trails compared once weekly Dalbavancin or single-dose Oritavancin vs. daily conventional therapy for acute bacterial skin infections (cellulitis, major abscess, wound infection, 75cm² erythema). Outcomes measured were cessation of spread of erythema and no fever X3 readings in 48-72 hours. Dalbavancin once weekly was non-inferior to Vancomycin in safety profile and outcome measures. Direct cost of Dalbavancin was higher although patients on this drug had shorter length of stays which is cost effective. FDA approved for skin infections.
The presence of family during CPR decreased PTSD, anxiety and depression symptoms in family members. Outcomes were similar when participants were assesses at 90 days and 1 year. While this study was conducted in an out of hospital setting, it may be worthwhile to assess if it is applicable to patients who code in the hospital.
Kathleen Finn, MD, FHM and Jeffrey Greenwald, MD, SFHM engaged the audience with their playful banter while reviewing medical literature of clinical significance for the hospitalist in Update in Hospital Medicine. The studies presented were high-quality, practical and addressed questions that arise in our day-to-day practice. A wide variety of topics were addressed and key points are summarized below.
Key takeaways
In the PARADIGM-HF study, Angiotensin Receptor Blocker (ARB) + Neprilysin Inhibitor decreased cardiovascular mortality and reduced CHF hospitalization by 20% when compared to Enalapril alone in heart failure patients. The combination drug is an alternative choice to ACE inhibitors. FDA approval is forthcoming.
Is the risk of contrast-induced nephrotoxicity really as great as we have come to believe? Review of propensity matched studies suggests that AKI, 30 day need for emergent hemodi
alysis and death are unrelated to contrast. If CT with contrast makes a difference to the patient, consider using it if GFR>30 ml/min.
SAGES trial and Project Recovery developed a delirium screening method in hospitalized patients. The CAM (Confusion Assessment Method) scoring system assesses delirium severity in elderly patients (70+). Hospital and post-hospital outcomes in delirious vs. non-delirious patients showed that the more severe the delirium, the longer the patient stayed in the hospital. Further, the rate of new SNF placement and 90 day mortality was higher in the delirious group. The CAM score correlates with prognosis in medical patients. Addressing long-term goals of care in this patient population may be warranted.
A randomized placebo-controlled trail looked at the preventive effects of Ramelteon (melatonin receptor agonist) on delirium. Ramelteon 8mg was given to patients at 9pm for 7 days (or d/c). Although this was a small and short study, Ramelteon appears to reduce incident delirium in medical and non-intubated ICU patients.
The HELP randomized clinical trial compared Lactulose vs. Polyethylene Glycol (PEG) electrolyte solution for treatment of overt hepatic encephalopathy. Patients received either PEG (4L in 4 hours) or Lactulose (20-30g 3+doses/24hrs). Primary outcome was an improvement in HESA (Hepatic Encephalopathy Scoring Algorithm ) score by 1 at 24 hours. HESA score improved and patients had a shorter length of stay in the PEG group. In addition, patients requested PEG at discharge because it tasted better.
A retrospective study looked at Nonselective beta blockers (NSBB) in patients with Spontaneous Bacterial Peritonitis (SBP). It suggests that the use of NSBB after SBP onset increases the risk of AKI, Hepatorenal Syndrome and mortality by 58%. NSBB appear beneficial before SBP onset suggesting that as cirrhosis becomes more severe, NSBB may not be effective.
A retrospective cohort trial (Michigan Hospital Medicine Safety Consortium) assessed hospital performance of VTE prophylaxis. The rate of clinically evident, confirmed VTE was measured. There was no difference in VTE occurrence during hospitalization, 90 day VTE rates and PE vs. DVT rates. No clear benefit was evident from VTE prophylaxis for medical patients. This could indicate the need to risk stratify patients’ VTE risk.
Direct oral anticoagulants (DOACs) were compared with Vitamin K antagonists (VKA) for treatment of acute VTE in a meta-analysis reviewed by the speakers. Death, safety and bleeding were assessed. DOACs seem to work as well as VKAs for VTE. They also had a better safety profile. In cancer patients, DOACs vs. LMWH study is still needed. In patients with atrial fibrillation (AF), DOACs prevent AF-associated strokes better than VKAs. They also reduce hemorrhagic stroke and intracranial hemorrhage.
In the elderly (75 or older) patient, DOACs are as safe as VKAs and LMWH for AF and VTE treatment.
Randomized control trails compared once weekly Dalbavancin or single-dose Oritavancin vs. daily conventional therapy for acute bacterial skin infections (cellulitis, major abscess, wound infection, 75cm² erythema). Outcomes measured were cessation of spread of erythema and no fever X3 readings in 48-72 hours. Dalbavancin once weekly was non-inferior to Vancomycin in safety profile and outcome measures. Direct cost of Dalbavancin was higher although patients on this drug had shorter length of stays which is cost effective. FDA approved for skin infections.
The presence of family during CPR decreased PTSD, anxiety and depression symptoms in family members. Outcomes were similar when participants were assesses at 90 days and 1 year. While this study was conducted in an out of hospital setting, it may be worthwhile to assess if it is applicable to patients who code in the hospital.
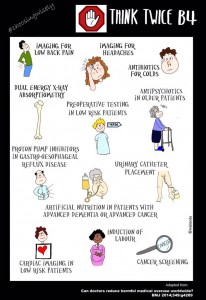
John Bulger, DO, MBA reviewed the components of the Choosing Wisely campaign and SHM’s recommendations in an era where providing high value cost-conscious care is key to optimizing the health of our patients. Choosing Wisely is an initiative of the ABIM foundation to foster communication between physicians and patients about common tests and procedures that may fail to provide value or enhance patient outcomes. It’s a partnership with 70-plus medical societies including an innovative partnership with Consumer Reports. SHM’s evidence-based recommendations are:
Don’t leave urinary catheters in place for convenience or monitoring of output for non-critically ill patients.
Don’t prescribe stress ulcer prophylaxis to hospitalized patients unless they are at high risk for GI complications.
Avoid transfusion of PRBC for arbitrary hemoglobin in the absence of CAD, CHF or CVA.
Don’t order continuous telemetry monitoring outside of the ICU without a protocol.
Don’t perform repetitive CBC and chemistry testing in a clinically stable patient.
Dr. Bulger highlighted that the Choosing Wisely campaign is designed to encourage conversations to
improve patient care. While cost-conscious care is a natural by-product of this effort, the primary focus when these guidelines were developed was to provide better healthcare for our patients. This year, SHM’s Choosing Wisely Case Competition has triggered the application of the above recommendations in institutions across the country. A summary of these efforts will be published in the near future to assist fellow hospitalists with their efforts to minimize waste and improve care in their own institutions. Look for the Hospitalist Guide to Choosing Wisely which is expected to be published in spring 2015. Choosing Wisely has now become a world-wide effort with Canada, Europe and Brazil implementing similar recommendations to improve healthcare.
Dr.Bulger concluded that while tradition is hard to change, it is of paramount importance to think differently to find innovative solutions to common problems in healthcare. Join the conversation using #ChoosingWisely or #LessIsMore on twitter.
Key Takeaways
Choosing Wisely is an ABIM campaign developed to address and promote conversations about common tests and procedures that are of low-value.
SHM’s recommendations were implemented in institutions with positive results as evidenced by the Choosing Wisely case competition at #HospMed15.
Look for a summary of these efforts to be published in the spring of 2015.
Use these guidelines to educate, provoke dialogue and achieve optimal patient outcomes in your institution.
John Bulger, DO, MBA reviewed the components of the Choosing Wisely campaign and SHM’s recommendations in an era where providing high value cost-conscious care is key to optimizing the health of our patients. Choosing Wisely is an initiative of the ABIM foundation to foster communication between physicians and patients about common tests and procedures that may fail to provide value or enhance patient outcomes. It’s a partnership with 70-plus medical societies including an innovative partnership with Consumer Reports. SHM’s evidence-based recommendations are:
Don’t leave urinary catheters in place for convenience or monitoring of output for non-critically ill patients.
Don’t prescribe stress ulcer prophylaxis to hospitalized patients unless they are at high risk for GI complications.
Avoid transfusion of PRBC for arbitrary hemoglobin in the absence of CAD, CHF or CVA.
Don’t order continuous telemetry monitoring outside of the ICU without a protocol.
Don’t perform repetitive CBC and chemistry testing in a clinically stable patient.
Dr. Bulger highlighted that the Choosing Wisely campaign is designed to encourage conversations to
improve patient care. While cost-conscious care is a natural by-product of this effort, the primary focus when these guidelines were developed was to provide better healthcare for our patients. This year, SHM’s Choosing Wisely Case Competition has triggered the application of the above recommendations in institutions across the country. A summary of these efforts will be published in the near future to assist fellow hospitalists with their efforts to minimize waste and improve care in their own institutions. Look for the Hospitalist Guide to Choosing Wisely which is expected to be published in spring 2015. Choosing Wisely has now become a world-wide effort with Canada, Europe and Brazil implementing similar recommendations to improve healthcare.
Dr.Bulger concluded that while tradition is hard to change, it is of paramount importance to think differently to find innovative solutions to common problems in healthcare. Join the conversation using #ChoosingWisely or #LessIsMore on twitter.
Key Takeaways
Choosing Wisely is an ABIM campaign developed to address and promote conversations about common tests and procedures that are of low-value.
SHM’s recommendations were implemented in institutions with positive results as evidenced by the Choosing Wisely case competition at #HospMed15.
Look for a summary of these efforts to be published in the spring of 2015.
Use these guidelines to educate, provoke dialogue and achieve optimal patient outcomes in your institution.
John Bulger, DO, MBA reviewed the components of the Choosing Wisely campaign and SHM’s recommendations in an era where providing high value cost-conscious care is key to optimizing the health of our patients. Choosing Wisely is an initiative of the ABIM foundation to foster communication between physicians and patients about common tests and procedures that may fail to provide value or enhance patient outcomes. It’s a partnership with 70-plus medical societies including an innovative partnership with Consumer Reports. SHM’s evidence-based recommendations are:
Don’t leave urinary catheters in place for convenience or monitoring of output for non-critically ill patients.
Don’t prescribe stress ulcer prophylaxis to hospitalized patients unless they are at high risk for GI complications.
Avoid transfusion of PRBC for arbitrary hemoglobin in the absence of CAD, CHF or CVA.
Don’t order continuous telemetry monitoring outside of the ICU without a protocol.
Don’t perform repetitive CBC and chemistry testing in a clinically stable patient.
Dr. Bulger highlighted that the Choosing Wisely campaign is designed to encourage conversations to
improve patient care. While cost-conscious care is a natural by-product of this effort, the primary focus when these guidelines were developed was to provide better healthcare for our patients. This year, SHM’s Choosing Wisely Case Competition has triggered the application of the above recommendations in institutions across the country. A summary of these efforts will be published in the near future to assist fellow hospitalists with their efforts to minimize waste and improve care in their own institutions. Look for the Hospitalist Guide to Choosing Wisely which is expected to be published in spring 2015. Choosing Wisely has now become a world-wide effort with Canada, Europe and Brazil implementing similar recommendations to improve healthcare.
Dr.Bulger concluded that while tradition is hard to change, it is of paramount importance to think differently to find innovative solutions to common problems in healthcare. Join the conversation using #ChoosingWisely or #LessIsMore on twitter.
Key Takeaways
Choosing Wisely is an ABIM campaign developed to address and promote conversations about common tests and procedures that are of low-value.
SHM’s recommendations were implemented in institutions with positive results as evidenced by the Choosing Wisely case competition at #HospMed15.
Look for a summary of these efforts to be published in the spring of 2015.
Use these guidelines to educate, provoke dialogue and achieve optimal patient outcomes in your institution.