User login
Effect of Hospitalist Discontinuity on AE
Although definitions vary, continuity of care can be thought of as the patient's experience of a continuous caring relationship with an identified healthcare professional.[1] Research in ambulatory settings has found that patients who see their primary care physician for a higher proportion of office visits have higher patient satisfaction, better hypertensive control, lower risk of hospitalization, and fewer emergency department visits.[2, 3, 4, 5] Continuity with a single hospital‐based physician is difficult to achieve because of the need to provide care 24 hours a day, 7 days a week. Key clinical information may be lost during physician‐to‐physician handoffs (eg, at admission, at the end of rotations on service) during hospitalization. Our research group recently found that lower hospital physician continuity was associated with modestly increased hospital costs, but also a trend toward lower readmissions.[6] We speculated that physicians newly taking over patient care from colleagues reassess diagnoses and treatment plans. This reassessment may identify errors missed by the previous hospital physician. Thus, discontinuity may theoretically help or hinder the provision of safe hospital care.
We sought to examine the relationship between hospital physician continuity and the incidence of adverse events (AEs). We combined data from 2 previously published studies by our research group; one investigated the relationship between hospital physician continuity and costs and 30‐day readmissions, the other assessed the impact of unit‐based interventions on AEs.[6, 7]
METHODS
Setting and Study Design
This retrospective, observational study was conducted at Northwestern Memorial Hospital, an 876‐bed tertiary care teaching hospital in Chicago, Illinois, and was approved by the institutional review board of Northwestern University. Subjects included patients admitted to an adult nonteaching hospitalist service between March 1, 2009 and December 31, 2011. Hospitalists on this service worked without resident physicians in rotations usually lasting 7 consecutive days beginning on Mondays and ending on Sundays. Hospitalists were allowed to switch portions of their schedule with one another, creating the possibility that certain rotations may have been slightly shorter or longer than 7 days. Hospitalists gave verbal sign‐out via telephone to the hospitalist taking over their service on the afternoon of the last day of their rotation. These handoffs customarily involved both hospitalists viewing the electronic health record during the discussion but were not standardized. Night hospitalists performed admissions and cross‐coverage each night from 7 pm to 7 am. Night hospitalists printed history and physicals for day hospitalists, but typically did not give verbal sign‐out on new admissions.
Acquisition of Study Population Data
We identified all patients admitted to the nonteaching hospitalist service using the Northwestern Medicine Enterprise Data Warehouse (EDW), an integrated repository of all clinical and research data sources on the campus. We excluded patients admitted under observation status, those initially admitted to other services (eg, intensive care, general surgery), those discharged from other services, and those cared for by advanced practice providers (ie, nurse practitioners and physician assistants).
Predictor Variables
We identified physicians completing the primary service history and physicals (H&P) and progress notes throughout patients' hospitalizations to calculate 2 measures of continuity: the Number of Physicians Index (NPI), and the Usual Provider of Continuity (UPC) Index.[8, 9] The NPI represented the total number of unique hospitalists completing H&Ps and/or progress notes for a patient. The UPC was calculated as the largest number of notes signed by a single hospitalist divided by the total number of hospitalist notes for a patient. For example, if Dr. John Smith wrote notes on the first 4 days of a patient's hospital stay, and Dr. Mary Jones wrote notes on the following 2 days (total stay=6 days), the NPI would be 2 and the UPC would be 0.67. Therefore, higher NPI and lower UPC designate lower continuity. Significant events occurring during the nighttime were documented in separate notes titled cross‐cover notes. These cross‐cover notes were not included in the calculation of NPI or UPC. In the rare event that 2 or more progress notes were written on the same day, we selected the one used for billing to calculate UPC and NPI.
Outcome Variables
We used AE data from a study we conducted to assess the impact of unit‐based interventions to improve teamwork and patient safety, the methods of which have been previously described.[7] Briefly, we used a 2‐stage medical record review similar to that performed in prior studies.[10, 11, 12, 13] In the first stage, we identified potential AEs using automated queries of the Northwestern Medicine EDW. These queries were based on screening criteria used in the Harvard Medical Practice Study and the Institute for Healthcare Improvement (IHI) Global Trigger Tool.[12, 13] Examples of queries included abnormal laboratory values (eg, international normalized ratio [INR] >6 after hospital day 2 and excluding patients with INR >4 on day 1), administration of rescue medications (eg, naloxone), certain types of incident reports (eg, pressure ulcer), International Classification of Diseases, Ninth Revision (ICD‐9) codes indicating hospital‐acquired conditions (eg, venous thromboembolism), and text searches of progress notes and discharge summaries using natural language processing.[14] Prior research by our group confirmed these automated screens identify a similar number of AEs as manual medical record screening.[14] For each patient with 1 or more potential AE, a research nurse performed a medical record abstraction and created a description of each potential AE.
In the second stage, 2 physician researchers independently reviewed each potential AE in a blinded fashion to determine whether or not an AE was present. An AE was defined as injury due to medical management rather than the natural history of the illness,[15] and included injuries that prolonged the hospital stay or produced disability as well as those resulting in transient disability or abnormal lab values.[16] After independent review, physician reviewers discussed discrepancies in their ratings to achieve consensus.
We tested the reliability of medical record abstractions in our prior study by conducting duplicate abstractions and consensus ratings for a randomly selected sample of 294 patients.[7] The inter‐rater reliability was good for determining the presence of AEs (=0.63).
Statistical Analyses
We calculated descriptive statistics for patient characteristics. Primary discharge diagnosis ICD‐9 codes were categorized using the Healthcare Cost and Utilization Project Clinical Classification Software.[17] We created multivariable logistic regression models with the independent variable being the measure of continuity (NPI or UPC) and the dependent variable being experiencing 1 or more AEs. Covariates included patient age, sex, race, payer, night admission, weekend admission, intensive care unit stay, Medicare Severity Diagnosis Related Group (MS‐DRG) weight, and total number of Elixhauser comorbidities.[18] The length of stay (LOS) was also included as a covariate, as longer LOS increases the probability of discontinuity and may increase the risk for AEs. Because MS‐DRG weight and LOS were highly correlated, we created several models; the first including both as continuous variables, the second including both categorized into quartiles, and a third excluding MS‐DRG weight and including LOS as a continuous variable. Our prior study assessing the impact of unit‐based interventions did not show a statistically significant difference in the pre‐ versus postintervention period, thus we did not include study period as a covariate.
RESULTS
Patient Characteristics
Our analyses included data from 474 hospitalizations. Patient characteristics are shown in Table 1. Patients were a mean 51.118.8 years of age, hospitalized for a mean 3.43.1 days, included 241 (50.8%) women, and 233 (49.2%) persons of nonwhite race. The mean and standard deviation of NPI and UPC were 2.51.0 and 0.60.2. Overall, 47 patients (9.9%) experienced 55 total AEs. AEs included 31 adverse drug events, 6 falls, 5 procedural injuries, 4 manifestations of poor glycemic control, 3 hospital‐acquired infections, 2 episodes of acute renal failure, 1 episode of delirium, 1 pressure ulcer, and 2 categorized as other.
| Characteristic | Value |
|---|---|
| |
| Mean age (SD), y | 55.1 (18.8) |
| Mean length of stay (SD), d | 3.4 (3.1) |
| Women, n (%) | 241 (50.8) |
| Nonwhite race, n (%) | 233 (49.2) |
| Payer, n (%) | |
| Private | 180 (38) |
| Medicare | 165 (34.8) |
| Medicaid | 47 (9.9) |
| Self‐pay/other | 82 (17.3) |
| Night admission, n (%) | 245 (51.7) |
| Weekend admission, n (%) | 135 (28.5) |
| Intensive care unit stay, n (%) | 18 (3.8) |
| Diagnosis, n (%) | |
| Diseases of the circulatory system | 95 (20.0) |
| Diseases of the digestive system | 65 (13.7) |
| Diseases of the respiratory system | 49 (10.3) |
| Injury and poisoning | 41 (8.7) |
| Diseases of the skin and soft tissue | 31 (6.5) |
| Symptoms, signs, and ill‐defined conditions and factors influencing health status | 28 (5.9) |
| Endocrine, nutritional, and metabolic diseases and immunity disorders | 25 (5.3) |
| Diseases of the genitourinary system | 24 (5.1) |
| Diseases of the musculoskeletal system and connective tissue | 23 (4.9) |
| Diseases of the nervous system | 23 (4.9) |
| Other | 70 (14.8) |
| Mean no. of Elixhauser comorbidities (SD) | 2.3 (1.7) |
| Mean MS‐DRG weight (SD) | 1.0 (1.0) |
| Mean NPI (SD) | 2.5 (1.0) |
| Mean UPC (SD) | 0.6 (0.2) |
Association Between Continuity and Adverse Events
In unadjusted models, each 1‐unit increase in the NPI (ie, less continuity) was significantly associated with the incidence of 1 or more AEs (odds ratio [OR]=1.75; P<0.001). However, UPC was not associated with incidence of AEs (OR=1.03; P=0.68) (Table 2). Across all adjusted models, neither NPI nor UPC was significantly associated with the incidence of AEs. The direction of the effect of discontinuity on AEs was inconsistent across models. Though all 3 adjusted models using NPI as the independent variable showed a trend toward increased odds of experiencing 1 or more AE with discontinuity, 2 of the 3 models using UPC showed trends in the opposite direction.
| NPI OR (95% CI)* | P Value | UPC OR (95% CI)* | P Value | ||
|---|---|---|---|---|---|
| |||||
| Unadjusted model | 1.75 (1.332.29) | <0.0001 | 1.03 (0.89‐1.21) | 0.68 | |
| Adjusted models | |||||
| Model 1 | MS‐DRG and LOS continuous | 1.16 (0.781.72) | 0.47 | 0.96 (0.791.14) | 0.60 |
| Model 2 | MS‐DRG and LOS in quartiles | 1.38 (0.981.94) | 0.07 | 1.05 (0.881.26) | 0.59 |
| Model 3 | MS‐DRG dropped, LOS continuous | 1.14 (0.771.70) | 0.51 | 0.95 (0.791.14) | 0.56 |
DISCUSSION
We found that hospitalist physician continuity was not associated with the incidence of AEs. Our findings are somewhat surprising because of the high value placed on continuity of care and patient safety concerns related to handoffs. Key clinical information may be lost when patient care is transitioned to a new hospitalist shortly after admission (eg, from a night hospitalist) or at the end of a rotation. Thus, it is logical to assume that discontinuity inherently increases the risk for harm. On the other hand, a physician newly taking over patient care from another may not be anchored to the initial diagnosis and treatment plan established by the first. This second look could potentially prevent missed/delayed diagnoses and optimize the plan of care.[19] These countervailing forces may explain our findings.
Several other potential explanations for our findings should be considered. First, the quality of handoffs may have been sufficient to overcome the potential for information loss. We feel this is unlikely given that little attention had been dedicated to improving the quality of patient handoffs among hospitalists in our institution. Notably, though a number of studies have evaluated resident physician handoffs, most of the work has focused on night coverage, and little is known about the quality of attending handoffs.[20] Second, access to a fully integrated electronic health record may have assisted hospitalists in complementing information received during handoffs. For example, a hospitalist about to start his or her rotation may have remotely accessed and reviewed patient medical records prior to receiving the phone handoff from the outgoing hospitalist. Third, other efforts to improve patient safety may have reduced the overall risk and provided some resilience in the system. Unit‐based interventions, including structured interdisciplinary rounds and nurse‐physician coleadership, improved teamwork climate and reduced AEs in the study hospital over time.[7]
Another factor to consider relates to the fact that hospital care is provided by teams of clinicians (eg, nurses, specialist physicians, therapists, social workers). Hospital teams are often large and have dynamic team membership. Similar to hospitalists, nurses, physician specialists, and other team members handoff care throughout the course of a patient's hospital stay. Yet, discontinuity for each professional type may occur at different times and frequencies. For example, a patient may be handed off from one hospitalist to another, yet the care continues with the same cardiologist or nurse. Future research should better characterize hospital team complexity (eg, size, relationships among members) and dynamics (eg, continuity for various professional types) and the impact of these factors on patient outcomes.
Our findings are important because hospitalist physician discontinuity is common during hospital stays. Hospital medicine groups vary in their staffing and scheduling models. Policies related to admission distribution and rotation length (consecutive days worked) systematically impact physician continuity. Few studies have evaluated the effect on continuity on hospitalized patient outcomes, and no prior research, to our knowledge, has explored the association of continuity on measures of patient safety.[6, 21, 22] Though our study might suggest that staffing models have little impact on patient safety, as previously mentioned, other team factors may influence patient outcomes.
Our study has several limitations. First, we assessed the impact of continuity on AEs in a single site. Although the 7 days on/7 days off model is the most common scheduling pattern used by adult hospital medicine groups,[23] staffing models and patient safety practices vary across hospitals, potentially limiting the generalizability of our study. Second, continuity can be defined and measured in a variety of ways. We used 2 different measures of physician continuity. As previously mentioned, assessing continuity of other clinicians may allow for a more complete understanding of the potential problems related to fragmentation of care. Third, this study excluded patients who experienced care transitions from other hospitals or other units within the hospital. Patients transferred from other hospitals are often complex, severely ill, and may be at higher risk for loss of key clinical information. Fourth, we used automated screens of an EDW to identify potential AEs. Although our prior research found that this method identified a similar number of AEs as manual medical record review screening, there was poor agreement between the 2 methods. Unfortunately, there is no gold standard to identify AEs. The EDW‐facilitated method allowed us to feasibly screen a larger number of charts, increasing statistical power, and minimized any potential bias that might occur during a manual review to identify potential AEs. Finally, we used data available from 2 prior studies and may have been underpowered to detect a significant association between continuity and AEs due to the relatively low percentage of patients experiencing an AE. In a post hoc power calculation, we estimated that we had 70% power to detect a 33% change in the proportion of patients with 1 or more AE for each 1‐unit increase in NPI, and 80% power to detect a 20% change for each 0.1‐unit decrease in UPC.
CONCLUSION
In conclusion, we found that hospitalist physician continuity was not associated with the incidence of AEs. We speculate that hospitalist continuity is only 1 of many team factors that may influence patient safety, and that prior efforts within our institution may have reduced our ability to detect an association. Future research should better characterize hospital team complexity and dynamics and the impact of these factors on patient outcomes.
Disclosures
This project was supported by a grant from the Agency for Healthcare Research and Quality and an Excellence in Academic Medicine Award, administered by Northwestern Memorial Hospital. The authors report no conflicts of interest.
- , , . What is “continuity of care”? J Health Serv Res Policy. 2006;11:248–250.
- , . Interpersonal continuity of care and care outcomes: a critical review. Ann Fam Med. 2005;3:159–166.
- , , , . The association between continuity of care and outcomes: a systematic and critical review. J Eval Clin Pract. 2010;16:947–956.
- , . Interpersonal continuity of care and patient satisfaction: a critical review. Ann Fam Med. 2004;2:445–451.
- , , , . Continuity of care in a family practice residency program. Impact on physician satisfaction. J Fam Pract. 1990;31:69–73.
- , , , et al. The impact of hospitalist discontinuity on hospital cost, readmissions, and patient satisfaction. J Gen Intern Med. 2014;29:1004–1008.
- , , , et al. Implementation of unit‐based interventions to improve teamwork and patient safety on a medical service [published online ahead of print June 11, 2014]. Am J Med Qual. doi: 10.1177/1062860614538093.
- . Measuring provider continuity in ambulatory care: an assessment of alternative approaches. Med Care. 1979;17:551–565.
- . Defining and measuring interpersonal continuity of care. Ann Fam Med. 2003;1:134–143.
- U.S. Department of Health and Human Services. Agency for Healthcare Research and Quality. Adverse events in hospitals: national incidence among medical beneficiaries. Available at: http://psnet.ahrq.gov/resource.aspx?resourceID=19811. Published November 2010. Accessed on December 15, 2014.
- , , , et al. “Global trigger tool” shows that adverse events in hospitals may be ten times greater than previously measured. Health Aff (Millwood). 2011;30:581–589.
- , , , et al. A study of medical injury and medical malpractice. N Engl J Med. 1989;321:480–484.
- , , , et al. Incidence and types of adverse events and negligent care in Utah and Colorado. Med Care. 2000;38:261–271.
- , , , et al. Comparison of traditional trigger tool to data warehouse based screening for identifying hospital adverse events. BMJ Qual Saf. 2013;22:130–138.
- , , , et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. N Engl J Med. 1991;324:370–376.
- , , . Safety of patients isolated for infection control. JAMA. 2003;290:1899–1905.
- HCUP Clinical Classification Software. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp. Accessed on December 15, 2014.
- , , , . Comorbidity measures for use with administrative data. Med Care. 1998;36:8–27.
- . Does continuity of care matter? No: discontinuity can improve patient care. West J Med. 2001;175:5.
- , , , , , . Hospitalist handoffs: a systematic review and task force recommendations. J Hosp Med. 2009;4:433–440.
- , , , , . The impact of fragmentation of hospitalist care on length of stay. J Hosp Med. 2010;5:335–338.
- , , . The Creating Incentives and Continuity Leading to Efficiency staffing model: a quality improvement initiative in hospital medicine. Mayo Clin Proc. 2012;87:364–371.
- Society of Hospital Medicine. 2014 state of hospital medicine report. Philadelphia, PA: Society of Hospital Medicine; 2014.
Although definitions vary, continuity of care can be thought of as the patient's experience of a continuous caring relationship with an identified healthcare professional.[1] Research in ambulatory settings has found that patients who see their primary care physician for a higher proportion of office visits have higher patient satisfaction, better hypertensive control, lower risk of hospitalization, and fewer emergency department visits.[2, 3, 4, 5] Continuity with a single hospital‐based physician is difficult to achieve because of the need to provide care 24 hours a day, 7 days a week. Key clinical information may be lost during physician‐to‐physician handoffs (eg, at admission, at the end of rotations on service) during hospitalization. Our research group recently found that lower hospital physician continuity was associated with modestly increased hospital costs, but also a trend toward lower readmissions.[6] We speculated that physicians newly taking over patient care from colleagues reassess diagnoses and treatment plans. This reassessment may identify errors missed by the previous hospital physician. Thus, discontinuity may theoretically help or hinder the provision of safe hospital care.
We sought to examine the relationship between hospital physician continuity and the incidence of adverse events (AEs). We combined data from 2 previously published studies by our research group; one investigated the relationship between hospital physician continuity and costs and 30‐day readmissions, the other assessed the impact of unit‐based interventions on AEs.[6, 7]
METHODS
Setting and Study Design
This retrospective, observational study was conducted at Northwestern Memorial Hospital, an 876‐bed tertiary care teaching hospital in Chicago, Illinois, and was approved by the institutional review board of Northwestern University. Subjects included patients admitted to an adult nonteaching hospitalist service between March 1, 2009 and December 31, 2011. Hospitalists on this service worked without resident physicians in rotations usually lasting 7 consecutive days beginning on Mondays and ending on Sundays. Hospitalists were allowed to switch portions of their schedule with one another, creating the possibility that certain rotations may have been slightly shorter or longer than 7 days. Hospitalists gave verbal sign‐out via telephone to the hospitalist taking over their service on the afternoon of the last day of their rotation. These handoffs customarily involved both hospitalists viewing the electronic health record during the discussion but were not standardized. Night hospitalists performed admissions and cross‐coverage each night from 7 pm to 7 am. Night hospitalists printed history and physicals for day hospitalists, but typically did not give verbal sign‐out on new admissions.
Acquisition of Study Population Data
We identified all patients admitted to the nonteaching hospitalist service using the Northwestern Medicine Enterprise Data Warehouse (EDW), an integrated repository of all clinical and research data sources on the campus. We excluded patients admitted under observation status, those initially admitted to other services (eg, intensive care, general surgery), those discharged from other services, and those cared for by advanced practice providers (ie, nurse practitioners and physician assistants).
Predictor Variables
We identified physicians completing the primary service history and physicals (H&P) and progress notes throughout patients' hospitalizations to calculate 2 measures of continuity: the Number of Physicians Index (NPI), and the Usual Provider of Continuity (UPC) Index.[8, 9] The NPI represented the total number of unique hospitalists completing H&Ps and/or progress notes for a patient. The UPC was calculated as the largest number of notes signed by a single hospitalist divided by the total number of hospitalist notes for a patient. For example, if Dr. John Smith wrote notes on the first 4 days of a patient's hospital stay, and Dr. Mary Jones wrote notes on the following 2 days (total stay=6 days), the NPI would be 2 and the UPC would be 0.67. Therefore, higher NPI and lower UPC designate lower continuity. Significant events occurring during the nighttime were documented in separate notes titled cross‐cover notes. These cross‐cover notes were not included in the calculation of NPI or UPC. In the rare event that 2 or more progress notes were written on the same day, we selected the one used for billing to calculate UPC and NPI.
Outcome Variables
We used AE data from a study we conducted to assess the impact of unit‐based interventions to improve teamwork and patient safety, the methods of which have been previously described.[7] Briefly, we used a 2‐stage medical record review similar to that performed in prior studies.[10, 11, 12, 13] In the first stage, we identified potential AEs using automated queries of the Northwestern Medicine EDW. These queries were based on screening criteria used in the Harvard Medical Practice Study and the Institute for Healthcare Improvement (IHI) Global Trigger Tool.[12, 13] Examples of queries included abnormal laboratory values (eg, international normalized ratio [INR] >6 after hospital day 2 and excluding patients with INR >4 on day 1), administration of rescue medications (eg, naloxone), certain types of incident reports (eg, pressure ulcer), International Classification of Diseases, Ninth Revision (ICD‐9) codes indicating hospital‐acquired conditions (eg, venous thromboembolism), and text searches of progress notes and discharge summaries using natural language processing.[14] Prior research by our group confirmed these automated screens identify a similar number of AEs as manual medical record screening.[14] For each patient with 1 or more potential AE, a research nurse performed a medical record abstraction and created a description of each potential AE.
In the second stage, 2 physician researchers independently reviewed each potential AE in a blinded fashion to determine whether or not an AE was present. An AE was defined as injury due to medical management rather than the natural history of the illness,[15] and included injuries that prolonged the hospital stay or produced disability as well as those resulting in transient disability or abnormal lab values.[16] After independent review, physician reviewers discussed discrepancies in their ratings to achieve consensus.
We tested the reliability of medical record abstractions in our prior study by conducting duplicate abstractions and consensus ratings for a randomly selected sample of 294 patients.[7] The inter‐rater reliability was good for determining the presence of AEs (=0.63).
Statistical Analyses
We calculated descriptive statistics for patient characteristics. Primary discharge diagnosis ICD‐9 codes were categorized using the Healthcare Cost and Utilization Project Clinical Classification Software.[17] We created multivariable logistic regression models with the independent variable being the measure of continuity (NPI or UPC) and the dependent variable being experiencing 1 or more AEs. Covariates included patient age, sex, race, payer, night admission, weekend admission, intensive care unit stay, Medicare Severity Diagnosis Related Group (MS‐DRG) weight, and total number of Elixhauser comorbidities.[18] The length of stay (LOS) was also included as a covariate, as longer LOS increases the probability of discontinuity and may increase the risk for AEs. Because MS‐DRG weight and LOS were highly correlated, we created several models; the first including both as continuous variables, the second including both categorized into quartiles, and a third excluding MS‐DRG weight and including LOS as a continuous variable. Our prior study assessing the impact of unit‐based interventions did not show a statistically significant difference in the pre‐ versus postintervention period, thus we did not include study period as a covariate.
RESULTS
Patient Characteristics
Our analyses included data from 474 hospitalizations. Patient characteristics are shown in Table 1. Patients were a mean 51.118.8 years of age, hospitalized for a mean 3.43.1 days, included 241 (50.8%) women, and 233 (49.2%) persons of nonwhite race. The mean and standard deviation of NPI and UPC were 2.51.0 and 0.60.2. Overall, 47 patients (9.9%) experienced 55 total AEs. AEs included 31 adverse drug events, 6 falls, 5 procedural injuries, 4 manifestations of poor glycemic control, 3 hospital‐acquired infections, 2 episodes of acute renal failure, 1 episode of delirium, 1 pressure ulcer, and 2 categorized as other.
| Characteristic | Value |
|---|---|
| |
| Mean age (SD), y | 55.1 (18.8) |
| Mean length of stay (SD), d | 3.4 (3.1) |
| Women, n (%) | 241 (50.8) |
| Nonwhite race, n (%) | 233 (49.2) |
| Payer, n (%) | |
| Private | 180 (38) |
| Medicare | 165 (34.8) |
| Medicaid | 47 (9.9) |
| Self‐pay/other | 82 (17.3) |
| Night admission, n (%) | 245 (51.7) |
| Weekend admission, n (%) | 135 (28.5) |
| Intensive care unit stay, n (%) | 18 (3.8) |
| Diagnosis, n (%) | |
| Diseases of the circulatory system | 95 (20.0) |
| Diseases of the digestive system | 65 (13.7) |
| Diseases of the respiratory system | 49 (10.3) |
| Injury and poisoning | 41 (8.7) |
| Diseases of the skin and soft tissue | 31 (6.5) |
| Symptoms, signs, and ill‐defined conditions and factors influencing health status | 28 (5.9) |
| Endocrine, nutritional, and metabolic diseases and immunity disorders | 25 (5.3) |
| Diseases of the genitourinary system | 24 (5.1) |
| Diseases of the musculoskeletal system and connective tissue | 23 (4.9) |
| Diseases of the nervous system | 23 (4.9) |
| Other | 70 (14.8) |
| Mean no. of Elixhauser comorbidities (SD) | 2.3 (1.7) |
| Mean MS‐DRG weight (SD) | 1.0 (1.0) |
| Mean NPI (SD) | 2.5 (1.0) |
| Mean UPC (SD) | 0.6 (0.2) |
Association Between Continuity and Adverse Events
In unadjusted models, each 1‐unit increase in the NPI (ie, less continuity) was significantly associated with the incidence of 1 or more AEs (odds ratio [OR]=1.75; P<0.001). However, UPC was not associated with incidence of AEs (OR=1.03; P=0.68) (Table 2). Across all adjusted models, neither NPI nor UPC was significantly associated with the incidence of AEs. The direction of the effect of discontinuity on AEs was inconsistent across models. Though all 3 adjusted models using NPI as the independent variable showed a trend toward increased odds of experiencing 1 or more AE with discontinuity, 2 of the 3 models using UPC showed trends in the opposite direction.
| NPI OR (95% CI)* | P Value | UPC OR (95% CI)* | P Value | ||
|---|---|---|---|---|---|
| |||||
| Unadjusted model | 1.75 (1.332.29) | <0.0001 | 1.03 (0.89‐1.21) | 0.68 | |
| Adjusted models | |||||
| Model 1 | MS‐DRG and LOS continuous | 1.16 (0.781.72) | 0.47 | 0.96 (0.791.14) | 0.60 |
| Model 2 | MS‐DRG and LOS in quartiles | 1.38 (0.981.94) | 0.07 | 1.05 (0.881.26) | 0.59 |
| Model 3 | MS‐DRG dropped, LOS continuous | 1.14 (0.771.70) | 0.51 | 0.95 (0.791.14) | 0.56 |
DISCUSSION
We found that hospitalist physician continuity was not associated with the incidence of AEs. Our findings are somewhat surprising because of the high value placed on continuity of care and patient safety concerns related to handoffs. Key clinical information may be lost when patient care is transitioned to a new hospitalist shortly after admission (eg, from a night hospitalist) or at the end of a rotation. Thus, it is logical to assume that discontinuity inherently increases the risk for harm. On the other hand, a physician newly taking over patient care from another may not be anchored to the initial diagnosis and treatment plan established by the first. This second look could potentially prevent missed/delayed diagnoses and optimize the plan of care.[19] These countervailing forces may explain our findings.
Several other potential explanations for our findings should be considered. First, the quality of handoffs may have been sufficient to overcome the potential for information loss. We feel this is unlikely given that little attention had been dedicated to improving the quality of patient handoffs among hospitalists in our institution. Notably, though a number of studies have evaluated resident physician handoffs, most of the work has focused on night coverage, and little is known about the quality of attending handoffs.[20] Second, access to a fully integrated electronic health record may have assisted hospitalists in complementing information received during handoffs. For example, a hospitalist about to start his or her rotation may have remotely accessed and reviewed patient medical records prior to receiving the phone handoff from the outgoing hospitalist. Third, other efforts to improve patient safety may have reduced the overall risk and provided some resilience in the system. Unit‐based interventions, including structured interdisciplinary rounds and nurse‐physician coleadership, improved teamwork climate and reduced AEs in the study hospital over time.[7]
Another factor to consider relates to the fact that hospital care is provided by teams of clinicians (eg, nurses, specialist physicians, therapists, social workers). Hospital teams are often large and have dynamic team membership. Similar to hospitalists, nurses, physician specialists, and other team members handoff care throughout the course of a patient's hospital stay. Yet, discontinuity for each professional type may occur at different times and frequencies. For example, a patient may be handed off from one hospitalist to another, yet the care continues with the same cardiologist or nurse. Future research should better characterize hospital team complexity (eg, size, relationships among members) and dynamics (eg, continuity for various professional types) and the impact of these factors on patient outcomes.
Our findings are important because hospitalist physician discontinuity is common during hospital stays. Hospital medicine groups vary in their staffing and scheduling models. Policies related to admission distribution and rotation length (consecutive days worked) systematically impact physician continuity. Few studies have evaluated the effect on continuity on hospitalized patient outcomes, and no prior research, to our knowledge, has explored the association of continuity on measures of patient safety.[6, 21, 22] Though our study might suggest that staffing models have little impact on patient safety, as previously mentioned, other team factors may influence patient outcomes.
Our study has several limitations. First, we assessed the impact of continuity on AEs in a single site. Although the 7 days on/7 days off model is the most common scheduling pattern used by adult hospital medicine groups,[23] staffing models and patient safety practices vary across hospitals, potentially limiting the generalizability of our study. Second, continuity can be defined and measured in a variety of ways. We used 2 different measures of physician continuity. As previously mentioned, assessing continuity of other clinicians may allow for a more complete understanding of the potential problems related to fragmentation of care. Third, this study excluded patients who experienced care transitions from other hospitals or other units within the hospital. Patients transferred from other hospitals are often complex, severely ill, and may be at higher risk for loss of key clinical information. Fourth, we used automated screens of an EDW to identify potential AEs. Although our prior research found that this method identified a similar number of AEs as manual medical record review screening, there was poor agreement between the 2 methods. Unfortunately, there is no gold standard to identify AEs. The EDW‐facilitated method allowed us to feasibly screen a larger number of charts, increasing statistical power, and minimized any potential bias that might occur during a manual review to identify potential AEs. Finally, we used data available from 2 prior studies and may have been underpowered to detect a significant association between continuity and AEs due to the relatively low percentage of patients experiencing an AE. In a post hoc power calculation, we estimated that we had 70% power to detect a 33% change in the proportion of patients with 1 or more AE for each 1‐unit increase in NPI, and 80% power to detect a 20% change for each 0.1‐unit decrease in UPC.
CONCLUSION
In conclusion, we found that hospitalist physician continuity was not associated with the incidence of AEs. We speculate that hospitalist continuity is only 1 of many team factors that may influence patient safety, and that prior efforts within our institution may have reduced our ability to detect an association. Future research should better characterize hospital team complexity and dynamics and the impact of these factors on patient outcomes.
Disclosures
This project was supported by a grant from the Agency for Healthcare Research and Quality and an Excellence in Academic Medicine Award, administered by Northwestern Memorial Hospital. The authors report no conflicts of interest.
Although definitions vary, continuity of care can be thought of as the patient's experience of a continuous caring relationship with an identified healthcare professional.[1] Research in ambulatory settings has found that patients who see their primary care physician for a higher proportion of office visits have higher patient satisfaction, better hypertensive control, lower risk of hospitalization, and fewer emergency department visits.[2, 3, 4, 5] Continuity with a single hospital‐based physician is difficult to achieve because of the need to provide care 24 hours a day, 7 days a week. Key clinical information may be lost during physician‐to‐physician handoffs (eg, at admission, at the end of rotations on service) during hospitalization. Our research group recently found that lower hospital physician continuity was associated with modestly increased hospital costs, but also a trend toward lower readmissions.[6] We speculated that physicians newly taking over patient care from colleagues reassess diagnoses and treatment plans. This reassessment may identify errors missed by the previous hospital physician. Thus, discontinuity may theoretically help or hinder the provision of safe hospital care.
We sought to examine the relationship between hospital physician continuity and the incidence of adverse events (AEs). We combined data from 2 previously published studies by our research group; one investigated the relationship between hospital physician continuity and costs and 30‐day readmissions, the other assessed the impact of unit‐based interventions on AEs.[6, 7]
METHODS
Setting and Study Design
This retrospective, observational study was conducted at Northwestern Memorial Hospital, an 876‐bed tertiary care teaching hospital in Chicago, Illinois, and was approved by the institutional review board of Northwestern University. Subjects included patients admitted to an adult nonteaching hospitalist service between March 1, 2009 and December 31, 2011. Hospitalists on this service worked without resident physicians in rotations usually lasting 7 consecutive days beginning on Mondays and ending on Sundays. Hospitalists were allowed to switch portions of their schedule with one another, creating the possibility that certain rotations may have been slightly shorter or longer than 7 days. Hospitalists gave verbal sign‐out via telephone to the hospitalist taking over their service on the afternoon of the last day of their rotation. These handoffs customarily involved both hospitalists viewing the electronic health record during the discussion but were not standardized. Night hospitalists performed admissions and cross‐coverage each night from 7 pm to 7 am. Night hospitalists printed history and physicals for day hospitalists, but typically did not give verbal sign‐out on new admissions.
Acquisition of Study Population Data
We identified all patients admitted to the nonteaching hospitalist service using the Northwestern Medicine Enterprise Data Warehouse (EDW), an integrated repository of all clinical and research data sources on the campus. We excluded patients admitted under observation status, those initially admitted to other services (eg, intensive care, general surgery), those discharged from other services, and those cared for by advanced practice providers (ie, nurse practitioners and physician assistants).
Predictor Variables
We identified physicians completing the primary service history and physicals (H&P) and progress notes throughout patients' hospitalizations to calculate 2 measures of continuity: the Number of Physicians Index (NPI), and the Usual Provider of Continuity (UPC) Index.[8, 9] The NPI represented the total number of unique hospitalists completing H&Ps and/or progress notes for a patient. The UPC was calculated as the largest number of notes signed by a single hospitalist divided by the total number of hospitalist notes for a patient. For example, if Dr. John Smith wrote notes on the first 4 days of a patient's hospital stay, and Dr. Mary Jones wrote notes on the following 2 days (total stay=6 days), the NPI would be 2 and the UPC would be 0.67. Therefore, higher NPI and lower UPC designate lower continuity. Significant events occurring during the nighttime were documented in separate notes titled cross‐cover notes. These cross‐cover notes were not included in the calculation of NPI or UPC. In the rare event that 2 or more progress notes were written on the same day, we selected the one used for billing to calculate UPC and NPI.
Outcome Variables
We used AE data from a study we conducted to assess the impact of unit‐based interventions to improve teamwork and patient safety, the methods of which have been previously described.[7] Briefly, we used a 2‐stage medical record review similar to that performed in prior studies.[10, 11, 12, 13] In the first stage, we identified potential AEs using automated queries of the Northwestern Medicine EDW. These queries were based on screening criteria used in the Harvard Medical Practice Study and the Institute for Healthcare Improvement (IHI) Global Trigger Tool.[12, 13] Examples of queries included abnormal laboratory values (eg, international normalized ratio [INR] >6 after hospital day 2 and excluding patients with INR >4 on day 1), administration of rescue medications (eg, naloxone), certain types of incident reports (eg, pressure ulcer), International Classification of Diseases, Ninth Revision (ICD‐9) codes indicating hospital‐acquired conditions (eg, venous thromboembolism), and text searches of progress notes and discharge summaries using natural language processing.[14] Prior research by our group confirmed these automated screens identify a similar number of AEs as manual medical record screening.[14] For each patient with 1 or more potential AE, a research nurse performed a medical record abstraction and created a description of each potential AE.
In the second stage, 2 physician researchers independently reviewed each potential AE in a blinded fashion to determine whether or not an AE was present. An AE was defined as injury due to medical management rather than the natural history of the illness,[15] and included injuries that prolonged the hospital stay or produced disability as well as those resulting in transient disability or abnormal lab values.[16] After independent review, physician reviewers discussed discrepancies in their ratings to achieve consensus.
We tested the reliability of medical record abstractions in our prior study by conducting duplicate abstractions and consensus ratings for a randomly selected sample of 294 patients.[7] The inter‐rater reliability was good for determining the presence of AEs (=0.63).
Statistical Analyses
We calculated descriptive statistics for patient characteristics. Primary discharge diagnosis ICD‐9 codes were categorized using the Healthcare Cost and Utilization Project Clinical Classification Software.[17] We created multivariable logistic regression models with the independent variable being the measure of continuity (NPI or UPC) and the dependent variable being experiencing 1 or more AEs. Covariates included patient age, sex, race, payer, night admission, weekend admission, intensive care unit stay, Medicare Severity Diagnosis Related Group (MS‐DRG) weight, and total number of Elixhauser comorbidities.[18] The length of stay (LOS) was also included as a covariate, as longer LOS increases the probability of discontinuity and may increase the risk for AEs. Because MS‐DRG weight and LOS were highly correlated, we created several models; the first including both as continuous variables, the second including both categorized into quartiles, and a third excluding MS‐DRG weight and including LOS as a continuous variable. Our prior study assessing the impact of unit‐based interventions did not show a statistically significant difference in the pre‐ versus postintervention period, thus we did not include study period as a covariate.
RESULTS
Patient Characteristics
Our analyses included data from 474 hospitalizations. Patient characteristics are shown in Table 1. Patients were a mean 51.118.8 years of age, hospitalized for a mean 3.43.1 days, included 241 (50.8%) women, and 233 (49.2%) persons of nonwhite race. The mean and standard deviation of NPI and UPC were 2.51.0 and 0.60.2. Overall, 47 patients (9.9%) experienced 55 total AEs. AEs included 31 adverse drug events, 6 falls, 5 procedural injuries, 4 manifestations of poor glycemic control, 3 hospital‐acquired infections, 2 episodes of acute renal failure, 1 episode of delirium, 1 pressure ulcer, and 2 categorized as other.
| Characteristic | Value |
|---|---|
| |
| Mean age (SD), y | 55.1 (18.8) |
| Mean length of stay (SD), d | 3.4 (3.1) |
| Women, n (%) | 241 (50.8) |
| Nonwhite race, n (%) | 233 (49.2) |
| Payer, n (%) | |
| Private | 180 (38) |
| Medicare | 165 (34.8) |
| Medicaid | 47 (9.9) |
| Self‐pay/other | 82 (17.3) |
| Night admission, n (%) | 245 (51.7) |
| Weekend admission, n (%) | 135 (28.5) |
| Intensive care unit stay, n (%) | 18 (3.8) |
| Diagnosis, n (%) | |
| Diseases of the circulatory system | 95 (20.0) |
| Diseases of the digestive system | 65 (13.7) |
| Diseases of the respiratory system | 49 (10.3) |
| Injury and poisoning | 41 (8.7) |
| Diseases of the skin and soft tissue | 31 (6.5) |
| Symptoms, signs, and ill‐defined conditions and factors influencing health status | 28 (5.9) |
| Endocrine, nutritional, and metabolic diseases and immunity disorders | 25 (5.3) |
| Diseases of the genitourinary system | 24 (5.1) |
| Diseases of the musculoskeletal system and connective tissue | 23 (4.9) |
| Diseases of the nervous system | 23 (4.9) |
| Other | 70 (14.8) |
| Mean no. of Elixhauser comorbidities (SD) | 2.3 (1.7) |
| Mean MS‐DRG weight (SD) | 1.0 (1.0) |
| Mean NPI (SD) | 2.5 (1.0) |
| Mean UPC (SD) | 0.6 (0.2) |
Association Between Continuity and Adverse Events
In unadjusted models, each 1‐unit increase in the NPI (ie, less continuity) was significantly associated with the incidence of 1 or more AEs (odds ratio [OR]=1.75; P<0.001). However, UPC was not associated with incidence of AEs (OR=1.03; P=0.68) (Table 2). Across all adjusted models, neither NPI nor UPC was significantly associated with the incidence of AEs. The direction of the effect of discontinuity on AEs was inconsistent across models. Though all 3 adjusted models using NPI as the independent variable showed a trend toward increased odds of experiencing 1 or more AE with discontinuity, 2 of the 3 models using UPC showed trends in the opposite direction.
| NPI OR (95% CI)* | P Value | UPC OR (95% CI)* | P Value | ||
|---|---|---|---|---|---|
| |||||
| Unadjusted model | 1.75 (1.332.29) | <0.0001 | 1.03 (0.89‐1.21) | 0.68 | |
| Adjusted models | |||||
| Model 1 | MS‐DRG and LOS continuous | 1.16 (0.781.72) | 0.47 | 0.96 (0.791.14) | 0.60 |
| Model 2 | MS‐DRG and LOS in quartiles | 1.38 (0.981.94) | 0.07 | 1.05 (0.881.26) | 0.59 |
| Model 3 | MS‐DRG dropped, LOS continuous | 1.14 (0.771.70) | 0.51 | 0.95 (0.791.14) | 0.56 |
DISCUSSION
We found that hospitalist physician continuity was not associated with the incidence of AEs. Our findings are somewhat surprising because of the high value placed on continuity of care and patient safety concerns related to handoffs. Key clinical information may be lost when patient care is transitioned to a new hospitalist shortly after admission (eg, from a night hospitalist) or at the end of a rotation. Thus, it is logical to assume that discontinuity inherently increases the risk for harm. On the other hand, a physician newly taking over patient care from another may not be anchored to the initial diagnosis and treatment plan established by the first. This second look could potentially prevent missed/delayed diagnoses and optimize the plan of care.[19] These countervailing forces may explain our findings.
Several other potential explanations for our findings should be considered. First, the quality of handoffs may have been sufficient to overcome the potential for information loss. We feel this is unlikely given that little attention had been dedicated to improving the quality of patient handoffs among hospitalists in our institution. Notably, though a number of studies have evaluated resident physician handoffs, most of the work has focused on night coverage, and little is known about the quality of attending handoffs.[20] Second, access to a fully integrated electronic health record may have assisted hospitalists in complementing information received during handoffs. For example, a hospitalist about to start his or her rotation may have remotely accessed and reviewed patient medical records prior to receiving the phone handoff from the outgoing hospitalist. Third, other efforts to improve patient safety may have reduced the overall risk and provided some resilience in the system. Unit‐based interventions, including structured interdisciplinary rounds and nurse‐physician coleadership, improved teamwork climate and reduced AEs in the study hospital over time.[7]
Another factor to consider relates to the fact that hospital care is provided by teams of clinicians (eg, nurses, specialist physicians, therapists, social workers). Hospital teams are often large and have dynamic team membership. Similar to hospitalists, nurses, physician specialists, and other team members handoff care throughout the course of a patient's hospital stay. Yet, discontinuity for each professional type may occur at different times and frequencies. For example, a patient may be handed off from one hospitalist to another, yet the care continues with the same cardiologist or nurse. Future research should better characterize hospital team complexity (eg, size, relationships among members) and dynamics (eg, continuity for various professional types) and the impact of these factors on patient outcomes.
Our findings are important because hospitalist physician discontinuity is common during hospital stays. Hospital medicine groups vary in their staffing and scheduling models. Policies related to admission distribution and rotation length (consecutive days worked) systematically impact physician continuity. Few studies have evaluated the effect on continuity on hospitalized patient outcomes, and no prior research, to our knowledge, has explored the association of continuity on measures of patient safety.[6, 21, 22] Though our study might suggest that staffing models have little impact on patient safety, as previously mentioned, other team factors may influence patient outcomes.
Our study has several limitations. First, we assessed the impact of continuity on AEs in a single site. Although the 7 days on/7 days off model is the most common scheduling pattern used by adult hospital medicine groups,[23] staffing models and patient safety practices vary across hospitals, potentially limiting the generalizability of our study. Second, continuity can be defined and measured in a variety of ways. We used 2 different measures of physician continuity. As previously mentioned, assessing continuity of other clinicians may allow for a more complete understanding of the potential problems related to fragmentation of care. Third, this study excluded patients who experienced care transitions from other hospitals or other units within the hospital. Patients transferred from other hospitals are often complex, severely ill, and may be at higher risk for loss of key clinical information. Fourth, we used automated screens of an EDW to identify potential AEs. Although our prior research found that this method identified a similar number of AEs as manual medical record review screening, there was poor agreement between the 2 methods. Unfortunately, there is no gold standard to identify AEs. The EDW‐facilitated method allowed us to feasibly screen a larger number of charts, increasing statistical power, and minimized any potential bias that might occur during a manual review to identify potential AEs. Finally, we used data available from 2 prior studies and may have been underpowered to detect a significant association between continuity and AEs due to the relatively low percentage of patients experiencing an AE. In a post hoc power calculation, we estimated that we had 70% power to detect a 33% change in the proportion of patients with 1 or more AE for each 1‐unit increase in NPI, and 80% power to detect a 20% change for each 0.1‐unit decrease in UPC.
CONCLUSION
In conclusion, we found that hospitalist physician continuity was not associated with the incidence of AEs. We speculate that hospitalist continuity is only 1 of many team factors that may influence patient safety, and that prior efforts within our institution may have reduced our ability to detect an association. Future research should better characterize hospital team complexity and dynamics and the impact of these factors on patient outcomes.
Disclosures
This project was supported by a grant from the Agency for Healthcare Research and Quality and an Excellence in Academic Medicine Award, administered by Northwestern Memorial Hospital. The authors report no conflicts of interest.
- , , . What is “continuity of care”? J Health Serv Res Policy. 2006;11:248–250.
- , . Interpersonal continuity of care and care outcomes: a critical review. Ann Fam Med. 2005;3:159–166.
- , , , . The association between continuity of care and outcomes: a systematic and critical review. J Eval Clin Pract. 2010;16:947–956.
- , . Interpersonal continuity of care and patient satisfaction: a critical review. Ann Fam Med. 2004;2:445–451.
- , , , . Continuity of care in a family practice residency program. Impact on physician satisfaction. J Fam Pract. 1990;31:69–73.
- , , , et al. The impact of hospitalist discontinuity on hospital cost, readmissions, and patient satisfaction. J Gen Intern Med. 2014;29:1004–1008.
- , , , et al. Implementation of unit‐based interventions to improve teamwork and patient safety on a medical service [published online ahead of print June 11, 2014]. Am J Med Qual. doi: 10.1177/1062860614538093.
- . Measuring provider continuity in ambulatory care: an assessment of alternative approaches. Med Care. 1979;17:551–565.
- . Defining and measuring interpersonal continuity of care. Ann Fam Med. 2003;1:134–143.
- U.S. Department of Health and Human Services. Agency for Healthcare Research and Quality. Adverse events in hospitals: national incidence among medical beneficiaries. Available at: http://psnet.ahrq.gov/resource.aspx?resourceID=19811. Published November 2010. Accessed on December 15, 2014.
- , , , et al. “Global trigger tool” shows that adverse events in hospitals may be ten times greater than previously measured. Health Aff (Millwood). 2011;30:581–589.
- , , , et al. A study of medical injury and medical malpractice. N Engl J Med. 1989;321:480–484.
- , , , et al. Incidence and types of adverse events and negligent care in Utah and Colorado. Med Care. 2000;38:261–271.
- , , , et al. Comparison of traditional trigger tool to data warehouse based screening for identifying hospital adverse events. BMJ Qual Saf. 2013;22:130–138.
- , , , et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. N Engl J Med. 1991;324:370–376.
- , , . Safety of patients isolated for infection control. JAMA. 2003;290:1899–1905.
- HCUP Clinical Classification Software. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp. Accessed on December 15, 2014.
- , , , . Comorbidity measures for use with administrative data. Med Care. 1998;36:8–27.
- . Does continuity of care matter? No: discontinuity can improve patient care. West J Med. 2001;175:5.
- , , , , , . Hospitalist handoffs: a systematic review and task force recommendations. J Hosp Med. 2009;4:433–440.
- , , , , . The impact of fragmentation of hospitalist care on length of stay. J Hosp Med. 2010;5:335–338.
- , , . The Creating Incentives and Continuity Leading to Efficiency staffing model: a quality improvement initiative in hospital medicine. Mayo Clin Proc. 2012;87:364–371.
- Society of Hospital Medicine. 2014 state of hospital medicine report. Philadelphia, PA: Society of Hospital Medicine; 2014.
- , , . What is “continuity of care”? J Health Serv Res Policy. 2006;11:248–250.
- , . Interpersonal continuity of care and care outcomes: a critical review. Ann Fam Med. 2005;3:159–166.
- , , , . The association between continuity of care and outcomes: a systematic and critical review. J Eval Clin Pract. 2010;16:947–956.
- , . Interpersonal continuity of care and patient satisfaction: a critical review. Ann Fam Med. 2004;2:445–451.
- , , , . Continuity of care in a family practice residency program. Impact on physician satisfaction. J Fam Pract. 1990;31:69–73.
- , , , et al. The impact of hospitalist discontinuity on hospital cost, readmissions, and patient satisfaction. J Gen Intern Med. 2014;29:1004–1008.
- , , , et al. Implementation of unit‐based interventions to improve teamwork and patient safety on a medical service [published online ahead of print June 11, 2014]. Am J Med Qual. doi: 10.1177/1062860614538093.
- . Measuring provider continuity in ambulatory care: an assessment of alternative approaches. Med Care. 1979;17:551–565.
- . Defining and measuring interpersonal continuity of care. Ann Fam Med. 2003;1:134–143.
- U.S. Department of Health and Human Services. Agency for Healthcare Research and Quality. Adverse events in hospitals: national incidence among medical beneficiaries. Available at: http://psnet.ahrq.gov/resource.aspx?resourceID=19811. Published November 2010. Accessed on December 15, 2014.
- , , , et al. “Global trigger tool” shows that adverse events in hospitals may be ten times greater than previously measured. Health Aff (Millwood). 2011;30:581–589.
- , , , et al. A study of medical injury and medical malpractice. N Engl J Med. 1989;321:480–484.
- , , , et al. Incidence and types of adverse events and negligent care in Utah and Colorado. Med Care. 2000;38:261–271.
- , , , et al. Comparison of traditional trigger tool to data warehouse based screening for identifying hospital adverse events. BMJ Qual Saf. 2013;22:130–138.
- , , , et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. N Engl J Med. 1991;324:370–376.
- , , . Safety of patients isolated for infection control. JAMA. 2003;290:1899–1905.
- HCUP Clinical Classification Software. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp. Accessed on December 15, 2014.
- , , , . Comorbidity measures for use with administrative data. Med Care. 1998;36:8–27.
- . Does continuity of care matter? No: discontinuity can improve patient care. West J Med. 2001;175:5.
- , , , , , . Hospitalist handoffs: a systematic review and task force recommendations. J Hosp Med. 2009;4:433–440.
- , , , , . The impact of fragmentation of hospitalist care on length of stay. J Hosp Med. 2010;5:335–338.
- , , . The Creating Incentives and Continuity Leading to Efficiency staffing model: a quality improvement initiative in hospital medicine. Mayo Clin Proc. 2012;87:364–371.
- Society of Hospital Medicine. 2014 state of hospital medicine report. Philadelphia, PA: Society of Hospital Medicine; 2014.
© 2014 Society of Hospital Medicine
Office-Based Rapid Prototyping in Orthopedic Surgery: A Novel Planning Technique and Review of the Literature
Three-dimensional (3-D) printing is a rapidly evolving technology with both medical and nonmedical applications.1,2 Rapid prototyping involves creating a physical model of human tissue from a 3-D computer-generated rendering.3 The method relies on export of Digital Imaging and Communications in Medicine (DICOM)–based computed tomography (CT) or magnetic resonance imaging (MRI) data into standard triangular language (STL) format. Reducing CT or MRI slice thickness increases resolution of the final model.2 Five types of rapid prototyping exist: STL, selective laser sintering, fused deposition modeling, multijet modeling, and 3-D printing.
Most implant manufacturers can produce a 3-D model based on surgeon-provided DICOM images. The ability to produce anatomical models in an office-based setting is a more recent development. Three-dimensional modeling may allow for more accurate and extensive preoperative planning than radiographic examination alone does, and may even allow surgeons to perform procedures as part of preoperative preparation. This can allow for early recognition of unanticipated intraoperative problems or of the need for special techniques and implants that would not have been otherwise available, all of which may ultimately reduce operative time.
The breadth of applications for office-based 3-D prototyping is not well described in the orthopedic surgery literature. In this article, we describe 7 cases of complex orthopedic disorders that were surgically treated after preoperative planning in which use of a 3-D printer allowed for “mock” surgery before the actual procedures. In 3 of the cases, the models were made by the implant manufacturers. Working with these models prompted us to buy a 3-D printer (Fortus 250; Stratasys, Eden Prairie, Minnesota) for in-office use. In the other 4 cases, we used this printer to create our own models. As indicated in the manufacturer’s literature, the printer uses fused deposition modeling, which builds a model layer by layer by heating thermoplastic material to a semi-liquid state and extruding it according to computer-controlled pathways.
We present preoperative images, preoperative 3-D modeling, and intraoperative and postoperative images along with brief case descriptions (Table). The patients provided written informed consent for print and electronic publication of these case reports.
Case Reports
Case 1
A 28-year-old woman with a history of spondyloepiphyseal dysplasia presented to our clinic with bilateral hip pain. About 8 years earlier, she had undergone bilateral proximal and distal femoral osteotomies. Her function had initially improved, but over the 2 to 3 years before presentation she began having more pain and stiffness with activity. At time of initial evaluation, she was able to walk only 1 to 2 blocks and had difficulty getting in and out of a car and up out of a seated position.
On physical examination, the patient was 3 feet 10 inches tall and weighed 77 pounds. She ambulated with decreased stance phase on both lower extremities and had developed a significant amount of increased forward pelvic inclination and increased lumbar lordosis. Both hips and thighs had multiple healed scars from prior surgeries and pin tracts. Range of motion (ROM) on both sides was restricted to 85° of flexion, 10° of internal rotation, 15° of external rotation, and 15° of abduction.
Plain radiographs showed advanced degenerative joint disease (DJD) of both hips with dysplastic acetabuli and evidence of healed osteotomies (Figure 1). Femoral deformities, noted bilaterally, consisted of marked valgus proximally and varus distally. Preoperative CT was used to create a 3-D model of the pelvis and femur. The model was created by the same implant manufacturer that produced the final components (Depuy, Warsaw, Indiana). Corrective femoral osteotomy was performed on the model to allow for design and use of a custom implant, while the modeled pelvis confirmed the ability to reproduce the normal hip center with a 44-mm conventional hemispherical socket.
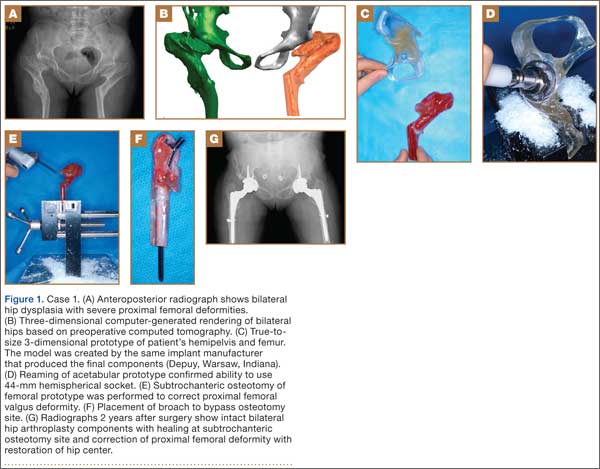
After surgery, the patient was able to ambulate without a limp and return to work. Her hip ROM was pain-free passively and actively with flexion to 100°, internal rotation to 35°, external rotation to 20°, and abduction to 30°.
Case 2
A 48-year-old woman with a history of Crowe IV hip dysplasia presented to our clinic with a chronically dislocated right total hip arthroplasty (THA) (Figure 2). Her initial THA was revised 1 year later because of acetabular component failure. Two years later, she was diagnosed with a deep periprosthetic infection, which was ultimately treated with 2-stage reimplantation. She subsequently dislocated and underwent re-revision of the S-ROM body and stem (DePuy Synthes, Warsaw, Indiana). At a visit after that revision, she was noted to be chronically dislocated, and was sent to our clinic for further management.
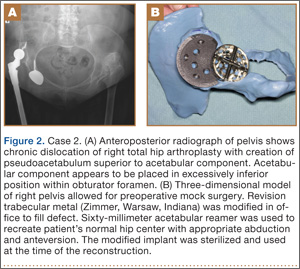
Preoperative radiographs showed a right uncemented THA with the femoral head dislocated toward the false acetabulum, retained hardware, and an old ununited trochanteric fragment. Both the femoral and acetabular components appeared well-fixed, though the acetabular component was positioned inferior, toward the obturator foramen.
Preoperative CT with metal artifact subtraction was used to create a 3-D model of the residual bony pelvis. The model was made by an implant manufacturer (Zimmer, Warsaw, Indiana). The shape of the superior defect was amenable to reconstruction using a modified revision trabecular metal socket. The pelvic model was reamed to accept a conventional hemispherical socket. The defect was reamed to accept a modified revision trabecular metal socket. The real implant was fashioned before surgery and was sterilized to avoid the need for intraoperative modification. Use of the preoperative model significantly reduced the time that would have been needed to modify the implant during actual surgery.
The patient’s right THA was revised. At time of surgery, the modified revision trabecular metal acetabular component was noted to seat appropriately in the superior defect. The true acetabulum was reestablished, and a hemispherical socket was placed with multiple screws. The 2 components were then unitized using cement in the same manner as would be done with an off-the-shelf augment.
Case 3
A 57-year-old man presented with a 10-year history of right knee pain. About 30 years before presentation at our clinic, he was treated for an open right tibia fracture sustained in a motorcycle accident. He had been treated nonsurgically, with injections, but they failed to provide sustained relief.
Preoperative radiographs showed severe advanced DJD in conjunction with an extra-articular posttraumatic varus tibial shaft deformity (Figure 3). An implant manufacturer (Zimmer) used a CT scan to create a model of the deformity. The resultant center of rotation angle was calculated using preoperative images and conventional techniques for deformity correction, and a lateral closing-wedge osteotomy was performed on the CT-based model. The initial attempt at deformity correction was slightly excessive, and the amount of resected bone slightly thicker than the calculated wedge, resulting in a valgus deformity. This error was noted, and the decision was made to recut a new model with a slight amount of residual varus that could be corrected during the final knee arthroplasty procedure.
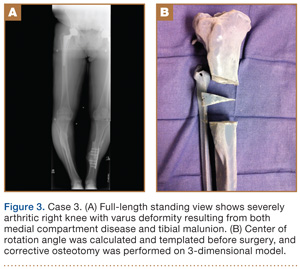
Corrective osteotomy was performed with a lateral plate. Six months later, the patient had no residual pain, and CT confirmed union at the osteotomy site and a slight amount of residual varus. The patient then underwent routine total knee arthroplasty (TKA) using an abbreviated keel to avoid the need for removal of the previously placed hardware. The varus deformity was completely corrected.
Case 4
A 73-year-old man had a history of shoulder pain dating back to his childhood. Despite treatment with nonsteroidal anti-inflammatory drugs, physical therapy, and injections, his debilitating pain persisted. Physical examination revealed limited ROM and an intact rotator cuff.
Plain radiographs showed severe DJD of the glenohumeral joint (Figure 4). Severe erosions of the glenoid were noted, prompting further workup with CT, which showed significant bone loss, particularly along the posterior margin of the glenoid. We used our 3-D printer to create a model of the scapula from CT images. The model was then reamed in the usual fashion to accept a 3-pegged glenoid component. On placement of a trial implant, a large deficiency was seen posteriorly. We thought the size and location of the defect made it amenable to grafting using the patient’s humeral head.
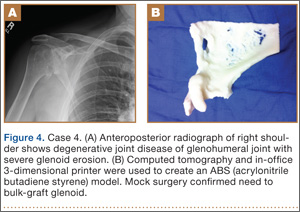
The patient elected to undergo right total shoulder arthroplasty. During the procedure, the glenoid defect was found to be identical to what was encountered with the model before surgery. A portion of the patient’s humeral head was then fashioned to fit the defect, and was secured with three 2.7-mm screws, after provisional fixation using 2.0-mm Kirschner wires. The screws were countersunk, and the graft was contoured by hand to match the previous reaming. A 3-pegged 52-mm glenoid component was then cemented into position with excellent stability.
Case 5
A 64-year-old man presented to our clinic with left hip pain 40 years after THA. The original procedure was performed for resolved proximal femoral osteomyelitis. Plain radiographs showed a loose cemented McKee-Farrar hip arthroplasty (Figure 5). Because of the elevated position of the acetabular component relative to the native hip center, CT was used to determine the amount of femoral bone loss.
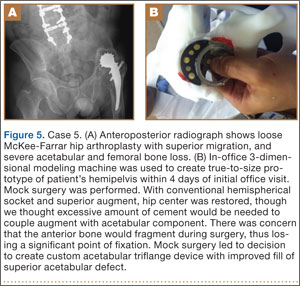
We used our 3-D printer to create a model and tried to recreate the native hip center with conventional off-the-shelf implants. A 50-mm hemispherical socket trial was placed in the appropriate location, along with a trabecular metal augment trial to provide extended coverage over the superolateral portion of the socket. Noted between the socket and the augment was a large gap; a substantial amount of cement would have been needed to unitize the construct. We thought a custom acetabular component would avoid the need for cement. In addition, given the patient’s small stature, the conventional acetabular component would allow a head only 32 mm in diameter. With a custom implant, the head could be enlarged to 36 mm, providing improved ROM and stability.
The patient underwent revision left hip arthroplasty using a custom acetabular component. A 3-D model available at time of surgery was used to aid implant placement.
Case 6
A 23-year-old man with multiple hereditary exostoses presented to our clinic with a painful mass in the left calf. Plain radiographs showed extensive osteochondromatosis involving the left proximal tibiofibular joint (Figure 6). The exostosis extended posteromedially, displacing the arterial trifurcation. MRI showed a small cartilage cap without evidence of malignant transformation.
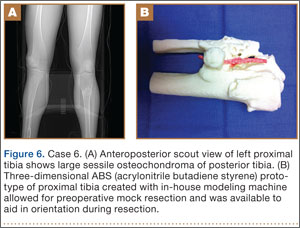
CT angiogram allowed the vasculature to be modeled along with the deformity. A 3-D model was fabricated. The model included the entire proximal tibiofibular joint, as well as the anterior tibial, peroneal, and posterior tibial arteries. Cautious intralesional resection was recommended because of the proximity to all 3 vessels.
The patient underwent tumor resection through a longitudinal posterior approach. The interval between the medial and lateral heads of the gastrocnemius muscles was developed to expose the underlying soleus muscle. The soleus was split longitudinally from its hiatus to the inferior portion of the exostosis. This allowed for identification of the trifurcation and the tibial nerve, which were protected. Osteotomes were used to resect the mass at its base, the edges were carefully trimmed, and bone wax was placed over the defect. Anterior and lateral to this mass was another large mass (under the soleus muscle), which was also transected using an osteotome. The gastrocnemius and soleus muscles were then reflected off the fibula in order to remove 2 other exostoses, beneath the neck and head of the fibula.
Case 7
A 71-year-old man with a history of idiopathic lymphedema and peripheral neuropathy presented to our clinic with a left cavovarus foot deformity and a history of recurrent neuropathic foot ulcers (Figure 7). Physical examination revealed a callus over the lateral aspect of the base of the fifth metatarsal. Preoperative radiograph showed evidence of prior triple arthrodesis with a cavovarus foot deformity. CT scan was used to create a 3-D model of the foot. The model was then used to identify an appropriate location for lateral midtarsal and calcaneal closing-wedge osteotomies.
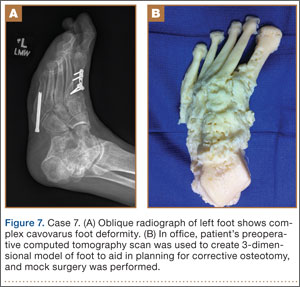
The patient underwent midfoot and hindfoot surgical correction. At surgery, the lateral closing-wedge osteotomies were performed according to the preoperative model. Radiographs 1 year after surgery showed correction of the forefoot varus.
Discussion
Three-dimensional printing for medical applications of anatomical modeling is not a new concept.1,3,4 Its use has been reported for a variety of applications in orthopedic surgery, including the printing of porous and metallic surfaces5 and bone-tissue engineering.6-9 Rapid prototyping for medical application was first reported in 1990 when a CT-based model was used to create a cranial bone.10 Reports of using the technique are becoming more widespread, particularly in the dental and maxillofacial literature, which includes reports on a variety of applications, including patient-specific drill guides, splints, and implants.11-14 The ability to perform mock surgery in advance of an actual procedure provides an invaluable opportunity to anticipate potential intraoperative problems, reduce operative time, and improve the accuracy of reconstruction.
Office-based rapid prototyping that uses an in-house 3-D printer is a novel application of this technology. It allows for creation of a patient-specific model for preoperative planning purposes. We are unaware of any other reports demonstrating the breadth and utility of office-based rapid prototyping in orthopedic surgery. For general reference, a printer similar to ours requires an initial investment of $52,000 to $56,000. This cost generally covers the printer, printer base cabinet, installation, training, and printer software (different from the 3-D modeling software), plus a 1-year warranty. A service agreement costs about $4000 annually. Printer and model supply expenses depend on the material used for the model (eg, ABS [acrylonitrile butadiene styrene]) and on the size and complexity of the 3-D models created. Average time to generate an appropriately formatted 3-D printing file is about 1 hour, though times can vary largely, according to amount of metal artifact subtraction necessary and the experience of the software user. For the rare, extremely complex deformities that require a significant amount of metal artifact subtraction, file preparation times can exceed 3 or 4 hours. We think these preparation times will decrease as communication between radiology file export format and modeling software ultimately allows for metal artifact subtraction images to function within the modeling software environment. Once an appropriately formatted file has been created, typical printing times vary according to the size of the to-be-modeled bone. For a hemipelvis, printing time is 30 to 40 hours; printing that is started on a Friday afternoon will be complete by Monday morning.
There are few reports of rapid prototyping in orthopedic surgery. In 2003, Minns and colleagues15 used a 3-D model in the planning of a tibial resection for TKA. They found the model to be accurate at time of surgery, resulting in appropriate tibial coverage by a conventional meniscal-bearing implant. Munjal and colleagues16 reported on 10 complex failed hip arthroplasty cases in which patients had revision surgery after preoperative planning using 3-D modeling techniques. The authors found that, in 8 of the 10 cases, conventional classification systems of bone loss were inaccurate in comparison with the prototype. Four cases required reconstruction with a custom triflange when conventional implants were not deemed reasonable based on the pelvic model. Tam and colleagues17 reported using a 3-D prototype as an aid in surgical planning for resection of a scapular osteochondroma in a 6-year-old patient. They found the rapid prototype to be useful at time of resection—similar to what we found with 1 patient (case 6). Adding contrast media to our patient’s scan allowed for 3-D visualization of the lesion and the encased vasculature. Fu and colleagues18 reported using a patient-specific drill template to insert anterior transpedicular screws. They constructed 24 prototypes of a formalin-preserved cervical vertebra to create a patient-specific biocompatible drill template for use in correcting multilevel cervical instability. They found the technique to be highly reproducible and accurate. Zein and colleagues19 used a rapid prototype of 3 consecutive human livers to preoperatively identify the vascular and biliary tract anatomy. They reported a high degree of accuracy—mean dimensional errors of less than 4 mm for the entire model and 1.3 mm for the vascular diameter.
The models created by implant manufacturers in this series were used to perform “mock” surgery before the actual procedures. Working with these models prompted us to buy our own 3-D printer. The learning curve can be steep, but commercially available 3-D printers allow for prompt in-office production of high-quality realistic prototypes at relatively low per-case cost (Figure 8). Three-dimensional modeling allows surgeons to assess the accuracy of their original surgical plans and, if necessary, correct them before surgery. Although computer-aided design models are useful, the ability to “perform surgery preoperatively” adds another element to surgeons’ understanding of the potential issues that may arise. Also, an in-office printer can help improve surgeons’ understanding and control over the process by which images are translated from radiographic file to 3-D model. Disadvantages of an in-office system include start-up and maintenance costs, office space requirements, and a significant learning curve for software and hardware applications. In addition, creation of 3-D models requires close interaction with radiologists who can provide appropriately formatted DICOM images, as metal artifact subtraction can be challenging. We think that, as image formatting and software capabilities are continually refined, this technology will become an invaluable part of multiple subspecialties across orthopedic surgery, with potentially infinite clinical, educational, and research applications.

1. McGurk M, Amis AA, Potamianos P, Goodger NM. Rapid prototyping techniques for anatomical modelling in medicine. Ann R Coll Surg Engl. 1997;79(3):169-174.
2. Webb PA. A review of rapid prototyping (RP) techniques in the medical and biomedical sector. J Med Eng Technol. 2000;24(4):149-153.
3. Esses SJ, Berman P, Bloom AI, Sosna J. Clinical applications of physical 3D models derived from MDCT data and created by rapid prototyping. AJR Am J Roentgenol. 2011;196(6):W683-W688.
4. Torres K, Staśkiewicz G, Śnieżyński M, Drop A, Maciejewski R. Application of rapid prototyping techniques for modelling of anatomical structures in medical training and education. Folia Morphol. 2011;70(1):1-4.
5. Melican MC, Zimmerman MC, Dhillon MS, Ponnambalam AR, Curodeau A, Parsons JR. Three-dimensional printing and porous metallic surfaces: a new orthopedic application. J Biomed Mater Res. 2001;55(2):194-202.
6. Butscher A, Bohner M, Hofmann S, Gauckler L, Müller R. Structural and material approaches to bone tissue engineering in powder-based three-dimensional printing. Acta Biomater. 2011;7(3):907-920.
7. Ciocca L, De Crescenzio F, Fantini M, Scotti R. CAD/CAM and rapid prototyped scaffold construction for bone regenerative medicine and surgical transfer of virtual planning: a pilot study. Comput Med Imaging Graph. 2009;33(1):58-62.
8. Leukers B, Gülkan H, Irsen SH, et al. Hydroxyapatite scaffolds for bone tissue engineering made by 3D printing. J Mater Sci Mater Med. 2005;16(12):1121-1124.
9. Seitz H, Rieder W, Irsen S, Leukers B, Tille C. Three-dimensional printing of porous ceramic scaffolds for bone tissue engineering. J Biomed Mater Res B Appl Biomater. 2005;74(2):782-788.
10. Mankovich NJ, Cheeseman AM, Stoker NG. The display of three-dimensional anatomy with stereolithographic models. J Digit Imaging. 1990;3(3):200-203.
11. Flügge TV, Nelson K, Schmelzeisen R, Metzger MC. Three-dimensional plotting and printing of an implant drilling guide: simplifying guided implant surgery. J Oral Maxillofac Surg. 2013;71(8):1340-1346.
12. Goiato MC, Santos MR, Pesqueira AA, Moreno A, dos Santos DM, Haddad MF. Prototyping for surgical and prosthetic treatment. J Craniofac Surg. 2011;22(3):914-917.
13. Metzger MC, Hohlweg-Majert B, Schwarz U, Teschner M, Hammer B, Schmelzeisen R. Manufacturing splints for orthognathic surgery using a three-dimensional printer. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105(2):e1-e7.
14. Robiony M, Salvo I, Costa F, et al. Virtual reality surgical planning for maxillofacial distraction osteogenesis: the role of reverse engineering rapid prototyping and cooperative work. J Oral Maxillofac Surg. 2007;65(6):1198-1208.
15. Minns RJ, Bibb R, Banks R, Sutton RA. The use of a reconstructed three-dimensional solid model from CT to aid the surgical management of a total knee arthroplasty: a case study. Med Eng Phys. 2003;25(6):523-526.
16. Munjal S, Leopold SS, Kornreich D, Shott S, Finn HA. CT-generated 3-dimensional models for complex acetabular reconstruction. J Arthroplasty. 2000;15(5):644-653.
17. Tam MD, Laycock SD, Bell D, Chojnowski A. 3-D printout of a DICOM file to aid surgical planning in a 6 year old patient with a large scapular osteochondroma complicating congenital diaphyseal aclasia. J Radiol Case Rep. 2012;6(1):31-37.
18. Fu M, Lin L, Kong X, et al. Construction and accuracy assessment of patient-specific biocompatible drill template for cervical anterior transpedicular screw (ATPS) insertion: an in vitro study. PLoS One. 2013;8(1):e53580.
19. Zein NN, Hanouneh IA, Bishop PD, et al. Three-dimensional print of a liver for preoperative planning in living donor liver transplantation. Liver Transpl. 2013;19(12):1304-1310.
Three-dimensional (3-D) printing is a rapidly evolving technology with both medical and nonmedical applications.1,2 Rapid prototyping involves creating a physical model of human tissue from a 3-D computer-generated rendering.3 The method relies on export of Digital Imaging and Communications in Medicine (DICOM)–based computed tomography (CT) or magnetic resonance imaging (MRI) data into standard triangular language (STL) format. Reducing CT or MRI slice thickness increases resolution of the final model.2 Five types of rapid prototyping exist: STL, selective laser sintering, fused deposition modeling, multijet modeling, and 3-D printing.
Most implant manufacturers can produce a 3-D model based on surgeon-provided DICOM images. The ability to produce anatomical models in an office-based setting is a more recent development. Three-dimensional modeling may allow for more accurate and extensive preoperative planning than radiographic examination alone does, and may even allow surgeons to perform procedures as part of preoperative preparation. This can allow for early recognition of unanticipated intraoperative problems or of the need for special techniques and implants that would not have been otherwise available, all of which may ultimately reduce operative time.
The breadth of applications for office-based 3-D prototyping is not well described in the orthopedic surgery literature. In this article, we describe 7 cases of complex orthopedic disorders that were surgically treated after preoperative planning in which use of a 3-D printer allowed for “mock” surgery before the actual procedures. In 3 of the cases, the models were made by the implant manufacturers. Working with these models prompted us to buy a 3-D printer (Fortus 250; Stratasys, Eden Prairie, Minnesota) for in-office use. In the other 4 cases, we used this printer to create our own models. As indicated in the manufacturer’s literature, the printer uses fused deposition modeling, which builds a model layer by layer by heating thermoplastic material to a semi-liquid state and extruding it according to computer-controlled pathways.
We present preoperative images, preoperative 3-D modeling, and intraoperative and postoperative images along with brief case descriptions (Table). The patients provided written informed consent for print and electronic publication of these case reports.
Case Reports
Case 1
A 28-year-old woman with a history of spondyloepiphyseal dysplasia presented to our clinic with bilateral hip pain. About 8 years earlier, she had undergone bilateral proximal and distal femoral osteotomies. Her function had initially improved, but over the 2 to 3 years before presentation she began having more pain and stiffness with activity. At time of initial evaluation, she was able to walk only 1 to 2 blocks and had difficulty getting in and out of a car and up out of a seated position.
On physical examination, the patient was 3 feet 10 inches tall and weighed 77 pounds. She ambulated with decreased stance phase on both lower extremities and had developed a significant amount of increased forward pelvic inclination and increased lumbar lordosis. Both hips and thighs had multiple healed scars from prior surgeries and pin tracts. Range of motion (ROM) on both sides was restricted to 85° of flexion, 10° of internal rotation, 15° of external rotation, and 15° of abduction.
Plain radiographs showed advanced degenerative joint disease (DJD) of both hips with dysplastic acetabuli and evidence of healed osteotomies (Figure 1). Femoral deformities, noted bilaterally, consisted of marked valgus proximally and varus distally. Preoperative CT was used to create a 3-D model of the pelvis and femur. The model was created by the same implant manufacturer that produced the final components (Depuy, Warsaw, Indiana). Corrective femoral osteotomy was performed on the model to allow for design and use of a custom implant, while the modeled pelvis confirmed the ability to reproduce the normal hip center with a 44-mm conventional hemispherical socket.
After surgery, the patient was able to ambulate without a limp and return to work. Her hip ROM was pain-free passively and actively with flexion to 100°, internal rotation to 35°, external rotation to 20°, and abduction to 30°.
Case 2
A 48-year-old woman with a history of Crowe IV hip dysplasia presented to our clinic with a chronically dislocated right total hip arthroplasty (THA) (Figure 2). Her initial THA was revised 1 year later because of acetabular component failure. Two years later, she was diagnosed with a deep periprosthetic infection, which was ultimately treated with 2-stage reimplantation. She subsequently dislocated and underwent re-revision of the S-ROM body and stem (DePuy Synthes, Warsaw, Indiana). At a visit after that revision, she was noted to be chronically dislocated, and was sent to our clinic for further management.
Preoperative radiographs showed a right uncemented THA with the femoral head dislocated toward the false acetabulum, retained hardware, and an old ununited trochanteric fragment. Both the femoral and acetabular components appeared well-fixed, though the acetabular component was positioned inferior, toward the obturator foramen.
Preoperative CT with metal artifact subtraction was used to create a 3-D model of the residual bony pelvis. The model was made by an implant manufacturer (Zimmer, Warsaw, Indiana). The shape of the superior defect was amenable to reconstruction using a modified revision trabecular metal socket. The pelvic model was reamed to accept a conventional hemispherical socket. The defect was reamed to accept a modified revision trabecular metal socket. The real implant was fashioned before surgery and was sterilized to avoid the need for intraoperative modification. Use of the preoperative model significantly reduced the time that would have been needed to modify the implant during actual surgery.
The patient’s right THA was revised. At time of surgery, the modified revision trabecular metal acetabular component was noted to seat appropriately in the superior defect. The true acetabulum was reestablished, and a hemispherical socket was placed with multiple screws. The 2 components were then unitized using cement in the same manner as would be done with an off-the-shelf augment.
Case 3
A 57-year-old man presented with a 10-year history of right knee pain. About 30 years before presentation at our clinic, he was treated for an open right tibia fracture sustained in a motorcycle accident. He had been treated nonsurgically, with injections, but they failed to provide sustained relief.
Preoperative radiographs showed severe advanced DJD in conjunction with an extra-articular posttraumatic varus tibial shaft deformity (Figure 3). An implant manufacturer (Zimmer) used a CT scan to create a model of the deformity. The resultant center of rotation angle was calculated using preoperative images and conventional techniques for deformity correction, and a lateral closing-wedge osteotomy was performed on the CT-based model. The initial attempt at deformity correction was slightly excessive, and the amount of resected bone slightly thicker than the calculated wedge, resulting in a valgus deformity. This error was noted, and the decision was made to recut a new model with a slight amount of residual varus that could be corrected during the final knee arthroplasty procedure.
Corrective osteotomy was performed with a lateral plate. Six months later, the patient had no residual pain, and CT confirmed union at the osteotomy site and a slight amount of residual varus. The patient then underwent routine total knee arthroplasty (TKA) using an abbreviated keel to avoid the need for removal of the previously placed hardware. The varus deformity was completely corrected.
Case 4
A 73-year-old man had a history of shoulder pain dating back to his childhood. Despite treatment with nonsteroidal anti-inflammatory drugs, physical therapy, and injections, his debilitating pain persisted. Physical examination revealed limited ROM and an intact rotator cuff.
Plain radiographs showed severe DJD of the glenohumeral joint (Figure 4). Severe erosions of the glenoid were noted, prompting further workup with CT, which showed significant bone loss, particularly along the posterior margin of the glenoid. We used our 3-D printer to create a model of the scapula from CT images. The model was then reamed in the usual fashion to accept a 3-pegged glenoid component. On placement of a trial implant, a large deficiency was seen posteriorly. We thought the size and location of the defect made it amenable to grafting using the patient’s humeral head.
The patient elected to undergo right total shoulder arthroplasty. During the procedure, the glenoid defect was found to be identical to what was encountered with the model before surgery. A portion of the patient’s humeral head was then fashioned to fit the defect, and was secured with three 2.7-mm screws, after provisional fixation using 2.0-mm Kirschner wires. The screws were countersunk, and the graft was contoured by hand to match the previous reaming. A 3-pegged 52-mm glenoid component was then cemented into position with excellent stability.
Case 5
A 64-year-old man presented to our clinic with left hip pain 40 years after THA. The original procedure was performed for resolved proximal femoral osteomyelitis. Plain radiographs showed a loose cemented McKee-Farrar hip arthroplasty (Figure 5). Because of the elevated position of the acetabular component relative to the native hip center, CT was used to determine the amount of femoral bone loss.
We used our 3-D printer to create a model and tried to recreate the native hip center with conventional off-the-shelf implants. A 50-mm hemispherical socket trial was placed in the appropriate location, along with a trabecular metal augment trial to provide extended coverage over the superolateral portion of the socket. Noted between the socket and the augment was a large gap; a substantial amount of cement would have been needed to unitize the construct. We thought a custom acetabular component would avoid the need for cement. In addition, given the patient’s small stature, the conventional acetabular component would allow a head only 32 mm in diameter. With a custom implant, the head could be enlarged to 36 mm, providing improved ROM and stability.
The patient underwent revision left hip arthroplasty using a custom acetabular component. A 3-D model available at time of surgery was used to aid implant placement.
Case 6
A 23-year-old man with multiple hereditary exostoses presented to our clinic with a painful mass in the left calf. Plain radiographs showed extensive osteochondromatosis involving the left proximal tibiofibular joint (Figure 6). The exostosis extended posteromedially, displacing the arterial trifurcation. MRI showed a small cartilage cap without evidence of malignant transformation.
CT angiogram allowed the vasculature to be modeled along with the deformity. A 3-D model was fabricated. The model included the entire proximal tibiofibular joint, as well as the anterior tibial, peroneal, and posterior tibial arteries. Cautious intralesional resection was recommended because of the proximity to all 3 vessels.
The patient underwent tumor resection through a longitudinal posterior approach. The interval between the medial and lateral heads of the gastrocnemius muscles was developed to expose the underlying soleus muscle. The soleus was split longitudinally from its hiatus to the inferior portion of the exostosis. This allowed for identification of the trifurcation and the tibial nerve, which were protected. Osteotomes were used to resect the mass at its base, the edges were carefully trimmed, and bone wax was placed over the defect. Anterior and lateral to this mass was another large mass (under the soleus muscle), which was also transected using an osteotome. The gastrocnemius and soleus muscles were then reflected off the fibula in order to remove 2 other exostoses, beneath the neck and head of the fibula.
Case 7
A 71-year-old man with a history of idiopathic lymphedema and peripheral neuropathy presented to our clinic with a left cavovarus foot deformity and a history of recurrent neuropathic foot ulcers (Figure 7). Physical examination revealed a callus over the lateral aspect of the base of the fifth metatarsal. Preoperative radiograph showed evidence of prior triple arthrodesis with a cavovarus foot deformity. CT scan was used to create a 3-D model of the foot. The model was then used to identify an appropriate location for lateral midtarsal and calcaneal closing-wedge osteotomies.
The patient underwent midfoot and hindfoot surgical correction. At surgery, the lateral closing-wedge osteotomies were performed according to the preoperative model. Radiographs 1 year after surgery showed correction of the forefoot varus.
Discussion
Three-dimensional printing for medical applications of anatomical modeling is not a new concept.1,3,4 Its use has been reported for a variety of applications in orthopedic surgery, including the printing of porous and metallic surfaces5 and bone-tissue engineering.6-9 Rapid prototyping for medical application was first reported in 1990 when a CT-based model was used to create a cranial bone.10 Reports of using the technique are becoming more widespread, particularly in the dental and maxillofacial literature, which includes reports on a variety of applications, including patient-specific drill guides, splints, and implants.11-14 The ability to perform mock surgery in advance of an actual procedure provides an invaluable opportunity to anticipate potential intraoperative problems, reduce operative time, and improve the accuracy of reconstruction.
Office-based rapid prototyping that uses an in-house 3-D printer is a novel application of this technology. It allows for creation of a patient-specific model for preoperative planning purposes. We are unaware of any other reports demonstrating the breadth and utility of office-based rapid prototyping in orthopedic surgery. For general reference, a printer similar to ours requires an initial investment of $52,000 to $56,000. This cost generally covers the printer, printer base cabinet, installation, training, and printer software (different from the 3-D modeling software), plus a 1-year warranty. A service agreement costs about $4000 annually. Printer and model supply expenses depend on the material used for the model (eg, ABS [acrylonitrile butadiene styrene]) and on the size and complexity of the 3-D models created. Average time to generate an appropriately formatted 3-D printing file is about 1 hour, though times can vary largely, according to amount of metal artifact subtraction necessary and the experience of the software user. For the rare, extremely complex deformities that require a significant amount of metal artifact subtraction, file preparation times can exceed 3 or 4 hours. We think these preparation times will decrease as communication between radiology file export format and modeling software ultimately allows for metal artifact subtraction images to function within the modeling software environment. Once an appropriately formatted file has been created, typical printing times vary according to the size of the to-be-modeled bone. For a hemipelvis, printing time is 30 to 40 hours; printing that is started on a Friday afternoon will be complete by Monday morning.
There are few reports of rapid prototyping in orthopedic surgery. In 2003, Minns and colleagues15 used a 3-D model in the planning of a tibial resection for TKA. They found the model to be accurate at time of surgery, resulting in appropriate tibial coverage by a conventional meniscal-bearing implant. Munjal and colleagues16 reported on 10 complex failed hip arthroplasty cases in which patients had revision surgery after preoperative planning using 3-D modeling techniques. The authors found that, in 8 of the 10 cases, conventional classification systems of bone loss were inaccurate in comparison with the prototype. Four cases required reconstruction with a custom triflange when conventional implants were not deemed reasonable based on the pelvic model. Tam and colleagues17 reported using a 3-D prototype as an aid in surgical planning for resection of a scapular osteochondroma in a 6-year-old patient. They found the rapid prototype to be useful at time of resection—similar to what we found with 1 patient (case 6). Adding contrast media to our patient’s scan allowed for 3-D visualization of the lesion and the encased vasculature. Fu and colleagues18 reported using a patient-specific drill template to insert anterior transpedicular screws. They constructed 24 prototypes of a formalin-preserved cervical vertebra to create a patient-specific biocompatible drill template for use in correcting multilevel cervical instability. They found the technique to be highly reproducible and accurate. Zein and colleagues19 used a rapid prototype of 3 consecutive human livers to preoperatively identify the vascular and biliary tract anatomy. They reported a high degree of accuracy—mean dimensional errors of less than 4 mm for the entire model and 1.3 mm for the vascular diameter.
The models created by implant manufacturers in this series were used to perform “mock” surgery before the actual procedures. Working with these models prompted us to buy our own 3-D printer. The learning curve can be steep, but commercially available 3-D printers allow for prompt in-office production of high-quality realistic prototypes at relatively low per-case cost (Figure 8). Three-dimensional modeling allows surgeons to assess the accuracy of their original surgical plans and, if necessary, correct them before surgery. Although computer-aided design models are useful, the ability to “perform surgery preoperatively” adds another element to surgeons’ understanding of the potential issues that may arise. Also, an in-office printer can help improve surgeons’ understanding and control over the process by which images are translated from radiographic file to 3-D model. Disadvantages of an in-office system include start-up and maintenance costs, office space requirements, and a significant learning curve for software and hardware applications. In addition, creation of 3-D models requires close interaction with radiologists who can provide appropriately formatted DICOM images, as metal artifact subtraction can be challenging. We think that, as image formatting and software capabilities are continually refined, this technology will become an invaluable part of multiple subspecialties across orthopedic surgery, with potentially infinite clinical, educational, and research applications.
Three-dimensional (3-D) printing is a rapidly evolving technology with both medical and nonmedical applications.1,2 Rapid prototyping involves creating a physical model of human tissue from a 3-D computer-generated rendering.3 The method relies on export of Digital Imaging and Communications in Medicine (DICOM)–based computed tomography (CT) or magnetic resonance imaging (MRI) data into standard triangular language (STL) format. Reducing CT or MRI slice thickness increases resolution of the final model.2 Five types of rapid prototyping exist: STL, selective laser sintering, fused deposition modeling, multijet modeling, and 3-D printing.
Most implant manufacturers can produce a 3-D model based on surgeon-provided DICOM images. The ability to produce anatomical models in an office-based setting is a more recent development. Three-dimensional modeling may allow for more accurate and extensive preoperative planning than radiographic examination alone does, and may even allow surgeons to perform procedures as part of preoperative preparation. This can allow for early recognition of unanticipated intraoperative problems or of the need for special techniques and implants that would not have been otherwise available, all of which may ultimately reduce operative time.
The breadth of applications for office-based 3-D prototyping is not well described in the orthopedic surgery literature. In this article, we describe 7 cases of complex orthopedic disorders that were surgically treated after preoperative planning in which use of a 3-D printer allowed for “mock” surgery before the actual procedures. In 3 of the cases, the models were made by the implant manufacturers. Working with these models prompted us to buy a 3-D printer (Fortus 250; Stratasys, Eden Prairie, Minnesota) for in-office use. In the other 4 cases, we used this printer to create our own models. As indicated in the manufacturer’s literature, the printer uses fused deposition modeling, which builds a model layer by layer by heating thermoplastic material to a semi-liquid state and extruding it according to computer-controlled pathways.
We present preoperative images, preoperative 3-D modeling, and intraoperative and postoperative images along with brief case descriptions (Table). The patients provided written informed consent for print and electronic publication of these case reports.
Case Reports
Case 1
A 28-year-old woman with a history of spondyloepiphyseal dysplasia presented to our clinic with bilateral hip pain. About 8 years earlier, she had undergone bilateral proximal and distal femoral osteotomies. Her function had initially improved, but over the 2 to 3 years before presentation she began having more pain and stiffness with activity. At time of initial evaluation, she was able to walk only 1 to 2 blocks and had difficulty getting in and out of a car and up out of a seated position.
On physical examination, the patient was 3 feet 10 inches tall and weighed 77 pounds. She ambulated with decreased stance phase on both lower extremities and had developed a significant amount of increased forward pelvic inclination and increased lumbar lordosis. Both hips and thighs had multiple healed scars from prior surgeries and pin tracts. Range of motion (ROM) on both sides was restricted to 85° of flexion, 10° of internal rotation, 15° of external rotation, and 15° of abduction.
Plain radiographs showed advanced degenerative joint disease (DJD) of both hips with dysplastic acetabuli and evidence of healed osteotomies (Figure 1). Femoral deformities, noted bilaterally, consisted of marked valgus proximally and varus distally. Preoperative CT was used to create a 3-D model of the pelvis and femur. The model was created by the same implant manufacturer that produced the final components (Depuy, Warsaw, Indiana). Corrective femoral osteotomy was performed on the model to allow for design and use of a custom implant, while the modeled pelvis confirmed the ability to reproduce the normal hip center with a 44-mm conventional hemispherical socket.
After surgery, the patient was able to ambulate without a limp and return to work. Her hip ROM was pain-free passively and actively with flexion to 100°, internal rotation to 35°, external rotation to 20°, and abduction to 30°.
Case 2
A 48-year-old woman with a history of Crowe IV hip dysplasia presented to our clinic with a chronically dislocated right total hip arthroplasty (THA) (Figure 2). Her initial THA was revised 1 year later because of acetabular component failure. Two years later, she was diagnosed with a deep periprosthetic infection, which was ultimately treated with 2-stage reimplantation. She subsequently dislocated and underwent re-revision of the S-ROM body and stem (DePuy Synthes, Warsaw, Indiana). At a visit after that revision, she was noted to be chronically dislocated, and was sent to our clinic for further management.
Preoperative radiographs showed a right uncemented THA with the femoral head dislocated toward the false acetabulum, retained hardware, and an old ununited trochanteric fragment. Both the femoral and acetabular components appeared well-fixed, though the acetabular component was positioned inferior, toward the obturator foramen.
Preoperative CT with metal artifact subtraction was used to create a 3-D model of the residual bony pelvis. The model was made by an implant manufacturer (Zimmer, Warsaw, Indiana). The shape of the superior defect was amenable to reconstruction using a modified revision trabecular metal socket. The pelvic model was reamed to accept a conventional hemispherical socket. The defect was reamed to accept a modified revision trabecular metal socket. The real implant was fashioned before surgery and was sterilized to avoid the need for intraoperative modification. Use of the preoperative model significantly reduced the time that would have been needed to modify the implant during actual surgery.
The patient’s right THA was revised. At time of surgery, the modified revision trabecular metal acetabular component was noted to seat appropriately in the superior defect. The true acetabulum was reestablished, and a hemispherical socket was placed with multiple screws. The 2 components were then unitized using cement in the same manner as would be done with an off-the-shelf augment.
Case 3
A 57-year-old man presented with a 10-year history of right knee pain. About 30 years before presentation at our clinic, he was treated for an open right tibia fracture sustained in a motorcycle accident. He had been treated nonsurgically, with injections, but they failed to provide sustained relief.
Preoperative radiographs showed severe advanced DJD in conjunction with an extra-articular posttraumatic varus tibial shaft deformity (Figure 3). An implant manufacturer (Zimmer) used a CT scan to create a model of the deformity. The resultant center of rotation angle was calculated using preoperative images and conventional techniques for deformity correction, and a lateral closing-wedge osteotomy was performed on the CT-based model. The initial attempt at deformity correction was slightly excessive, and the amount of resected bone slightly thicker than the calculated wedge, resulting in a valgus deformity. This error was noted, and the decision was made to recut a new model with a slight amount of residual varus that could be corrected during the final knee arthroplasty procedure.
Corrective osteotomy was performed with a lateral plate. Six months later, the patient had no residual pain, and CT confirmed union at the osteotomy site and a slight amount of residual varus. The patient then underwent routine total knee arthroplasty (TKA) using an abbreviated keel to avoid the need for removal of the previously placed hardware. The varus deformity was completely corrected.
Case 4
A 73-year-old man had a history of shoulder pain dating back to his childhood. Despite treatment with nonsteroidal anti-inflammatory drugs, physical therapy, and injections, his debilitating pain persisted. Physical examination revealed limited ROM and an intact rotator cuff.
Plain radiographs showed severe DJD of the glenohumeral joint (Figure 4). Severe erosions of the glenoid were noted, prompting further workup with CT, which showed significant bone loss, particularly along the posterior margin of the glenoid. We used our 3-D printer to create a model of the scapula from CT images. The model was then reamed in the usual fashion to accept a 3-pegged glenoid component. On placement of a trial implant, a large deficiency was seen posteriorly. We thought the size and location of the defect made it amenable to grafting using the patient’s humeral head.
The patient elected to undergo right total shoulder arthroplasty. During the procedure, the glenoid defect was found to be identical to what was encountered with the model before surgery. A portion of the patient’s humeral head was then fashioned to fit the defect, and was secured with three 2.7-mm screws, after provisional fixation using 2.0-mm Kirschner wires. The screws were countersunk, and the graft was contoured by hand to match the previous reaming. A 3-pegged 52-mm glenoid component was then cemented into position with excellent stability.
Case 5
A 64-year-old man presented to our clinic with left hip pain 40 years after THA. The original procedure was performed for resolved proximal femoral osteomyelitis. Plain radiographs showed a loose cemented McKee-Farrar hip arthroplasty (Figure 5). Because of the elevated position of the acetabular component relative to the native hip center, CT was used to determine the amount of femoral bone loss.
We used our 3-D printer to create a model and tried to recreate the native hip center with conventional off-the-shelf implants. A 50-mm hemispherical socket trial was placed in the appropriate location, along with a trabecular metal augment trial to provide extended coverage over the superolateral portion of the socket. Noted between the socket and the augment was a large gap; a substantial amount of cement would have been needed to unitize the construct. We thought a custom acetabular component would avoid the need for cement. In addition, given the patient’s small stature, the conventional acetabular component would allow a head only 32 mm in diameter. With a custom implant, the head could be enlarged to 36 mm, providing improved ROM and stability.
The patient underwent revision left hip arthroplasty using a custom acetabular component. A 3-D model available at time of surgery was used to aid implant placement.
Case 6
A 23-year-old man with multiple hereditary exostoses presented to our clinic with a painful mass in the left calf. Plain radiographs showed extensive osteochondromatosis involving the left proximal tibiofibular joint (Figure 6). The exostosis extended posteromedially, displacing the arterial trifurcation. MRI showed a small cartilage cap without evidence of malignant transformation.
CT angiogram allowed the vasculature to be modeled along with the deformity. A 3-D model was fabricated. The model included the entire proximal tibiofibular joint, as well as the anterior tibial, peroneal, and posterior tibial arteries. Cautious intralesional resection was recommended because of the proximity to all 3 vessels.
The patient underwent tumor resection through a longitudinal posterior approach. The interval between the medial and lateral heads of the gastrocnemius muscles was developed to expose the underlying soleus muscle. The soleus was split longitudinally from its hiatus to the inferior portion of the exostosis. This allowed for identification of the trifurcation and the tibial nerve, which were protected. Osteotomes were used to resect the mass at its base, the edges were carefully trimmed, and bone wax was placed over the defect. Anterior and lateral to this mass was another large mass (under the soleus muscle), which was also transected using an osteotome. The gastrocnemius and soleus muscles were then reflected off the fibula in order to remove 2 other exostoses, beneath the neck and head of the fibula.
Case 7
A 71-year-old man with a history of idiopathic lymphedema and peripheral neuropathy presented to our clinic with a left cavovarus foot deformity and a history of recurrent neuropathic foot ulcers (Figure 7). Physical examination revealed a callus over the lateral aspect of the base of the fifth metatarsal. Preoperative radiograph showed evidence of prior triple arthrodesis with a cavovarus foot deformity. CT scan was used to create a 3-D model of the foot. The model was then used to identify an appropriate location for lateral midtarsal and calcaneal closing-wedge osteotomies.
The patient underwent midfoot and hindfoot surgical correction. At surgery, the lateral closing-wedge osteotomies were performed according to the preoperative model. Radiographs 1 year after surgery showed correction of the forefoot varus.
Discussion
Three-dimensional printing for medical applications of anatomical modeling is not a new concept.1,3,4 Its use has been reported for a variety of applications in orthopedic surgery, including the printing of porous and metallic surfaces5 and bone-tissue engineering.6-9 Rapid prototyping for medical application was first reported in 1990 when a CT-based model was used to create a cranial bone.10 Reports of using the technique are becoming more widespread, particularly in the dental and maxillofacial literature, which includes reports on a variety of applications, including patient-specific drill guides, splints, and implants.11-14 The ability to perform mock surgery in advance of an actual procedure provides an invaluable opportunity to anticipate potential intraoperative problems, reduce operative time, and improve the accuracy of reconstruction.
Office-based rapid prototyping that uses an in-house 3-D printer is a novel application of this technology. It allows for creation of a patient-specific model for preoperative planning purposes. We are unaware of any other reports demonstrating the breadth and utility of office-based rapid prototyping in orthopedic surgery. For general reference, a printer similar to ours requires an initial investment of $52,000 to $56,000. This cost generally covers the printer, printer base cabinet, installation, training, and printer software (different from the 3-D modeling software), plus a 1-year warranty. A service agreement costs about $4000 annually. Printer and model supply expenses depend on the material used for the model (eg, ABS [acrylonitrile butadiene styrene]) and on the size and complexity of the 3-D models created. Average time to generate an appropriately formatted 3-D printing file is about 1 hour, though times can vary largely, according to amount of metal artifact subtraction necessary and the experience of the software user. For the rare, extremely complex deformities that require a significant amount of metal artifact subtraction, file preparation times can exceed 3 or 4 hours. We think these preparation times will decrease as communication between radiology file export format and modeling software ultimately allows for metal artifact subtraction images to function within the modeling software environment. Once an appropriately formatted file has been created, typical printing times vary according to the size of the to-be-modeled bone. For a hemipelvis, printing time is 30 to 40 hours; printing that is started on a Friday afternoon will be complete by Monday morning.
There are few reports of rapid prototyping in orthopedic surgery. In 2003, Minns and colleagues15 used a 3-D model in the planning of a tibial resection for TKA. They found the model to be accurate at time of surgery, resulting in appropriate tibial coverage by a conventional meniscal-bearing implant. Munjal and colleagues16 reported on 10 complex failed hip arthroplasty cases in which patients had revision surgery after preoperative planning using 3-D modeling techniques. The authors found that, in 8 of the 10 cases, conventional classification systems of bone loss were inaccurate in comparison with the prototype. Four cases required reconstruction with a custom triflange when conventional implants were not deemed reasonable based on the pelvic model. Tam and colleagues17 reported using a 3-D prototype as an aid in surgical planning for resection of a scapular osteochondroma in a 6-year-old patient. They found the rapid prototype to be useful at time of resection—similar to what we found with 1 patient (case 6). Adding contrast media to our patient’s scan allowed for 3-D visualization of the lesion and the encased vasculature. Fu and colleagues18 reported using a patient-specific drill template to insert anterior transpedicular screws. They constructed 24 prototypes of a formalin-preserved cervical vertebra to create a patient-specific biocompatible drill template for use in correcting multilevel cervical instability. They found the technique to be highly reproducible and accurate. Zein and colleagues19 used a rapid prototype of 3 consecutive human livers to preoperatively identify the vascular and biliary tract anatomy. They reported a high degree of accuracy—mean dimensional errors of less than 4 mm for the entire model and 1.3 mm for the vascular diameter.
The models created by implant manufacturers in this series were used to perform “mock” surgery before the actual procedures. Working with these models prompted us to buy our own 3-D printer. The learning curve can be steep, but commercially available 3-D printers allow for prompt in-office production of high-quality realistic prototypes at relatively low per-case cost (Figure 8). Three-dimensional modeling allows surgeons to assess the accuracy of their original surgical plans and, if necessary, correct them before surgery. Although computer-aided design models are useful, the ability to “perform surgery preoperatively” adds another element to surgeons’ understanding of the potential issues that may arise. Also, an in-office printer can help improve surgeons’ understanding and control over the process by which images are translated from radiographic file to 3-D model. Disadvantages of an in-office system include start-up and maintenance costs, office space requirements, and a significant learning curve for software and hardware applications. In addition, creation of 3-D models requires close interaction with radiologists who can provide appropriately formatted DICOM images, as metal artifact subtraction can be challenging. We think that, as image formatting and software capabilities are continually refined, this technology will become an invaluable part of multiple subspecialties across orthopedic surgery, with potentially infinite clinical, educational, and research applications.
1. McGurk M, Amis AA, Potamianos P, Goodger NM. Rapid prototyping techniques for anatomical modelling in medicine. Ann R Coll Surg Engl. 1997;79(3):169-174.
2. Webb PA. A review of rapid prototyping (RP) techniques in the medical and biomedical sector. J Med Eng Technol. 2000;24(4):149-153.
3. Esses SJ, Berman P, Bloom AI, Sosna J. Clinical applications of physical 3D models derived from MDCT data and created by rapid prototyping. AJR Am J Roentgenol. 2011;196(6):W683-W688.
4. Torres K, Staśkiewicz G, Śnieżyński M, Drop A, Maciejewski R. Application of rapid prototyping techniques for modelling of anatomical structures in medical training and education. Folia Morphol. 2011;70(1):1-4.
5. Melican MC, Zimmerman MC, Dhillon MS, Ponnambalam AR, Curodeau A, Parsons JR. Three-dimensional printing and porous metallic surfaces: a new orthopedic application. J Biomed Mater Res. 2001;55(2):194-202.
6. Butscher A, Bohner M, Hofmann S, Gauckler L, Müller R. Structural and material approaches to bone tissue engineering in powder-based three-dimensional printing. Acta Biomater. 2011;7(3):907-920.
7. Ciocca L, De Crescenzio F, Fantini M, Scotti R. CAD/CAM and rapid prototyped scaffold construction for bone regenerative medicine and surgical transfer of virtual planning: a pilot study. Comput Med Imaging Graph. 2009;33(1):58-62.
8. Leukers B, Gülkan H, Irsen SH, et al. Hydroxyapatite scaffolds for bone tissue engineering made by 3D printing. J Mater Sci Mater Med. 2005;16(12):1121-1124.
9. Seitz H, Rieder W, Irsen S, Leukers B, Tille C. Three-dimensional printing of porous ceramic scaffolds for bone tissue engineering. J Biomed Mater Res B Appl Biomater. 2005;74(2):782-788.
10. Mankovich NJ, Cheeseman AM, Stoker NG. The display of three-dimensional anatomy with stereolithographic models. J Digit Imaging. 1990;3(3):200-203.
11. Flügge TV, Nelson K, Schmelzeisen R, Metzger MC. Three-dimensional plotting and printing of an implant drilling guide: simplifying guided implant surgery. J Oral Maxillofac Surg. 2013;71(8):1340-1346.
12. Goiato MC, Santos MR, Pesqueira AA, Moreno A, dos Santos DM, Haddad MF. Prototyping for surgical and prosthetic treatment. J Craniofac Surg. 2011;22(3):914-917.
13. Metzger MC, Hohlweg-Majert B, Schwarz U, Teschner M, Hammer B, Schmelzeisen R. Manufacturing splints for orthognathic surgery using a three-dimensional printer. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105(2):e1-e7.
14. Robiony M, Salvo I, Costa F, et al. Virtual reality surgical planning for maxillofacial distraction osteogenesis: the role of reverse engineering rapid prototyping and cooperative work. J Oral Maxillofac Surg. 2007;65(6):1198-1208.
15. Minns RJ, Bibb R, Banks R, Sutton RA. The use of a reconstructed three-dimensional solid model from CT to aid the surgical management of a total knee arthroplasty: a case study. Med Eng Phys. 2003;25(6):523-526.
16. Munjal S, Leopold SS, Kornreich D, Shott S, Finn HA. CT-generated 3-dimensional models for complex acetabular reconstruction. J Arthroplasty. 2000;15(5):644-653.
17. Tam MD, Laycock SD, Bell D, Chojnowski A. 3-D printout of a DICOM file to aid surgical planning in a 6 year old patient with a large scapular osteochondroma complicating congenital diaphyseal aclasia. J Radiol Case Rep. 2012;6(1):31-37.
18. Fu M, Lin L, Kong X, et al. Construction and accuracy assessment of patient-specific biocompatible drill template for cervical anterior transpedicular screw (ATPS) insertion: an in vitro study. PLoS One. 2013;8(1):e53580.
19. Zein NN, Hanouneh IA, Bishop PD, et al. Three-dimensional print of a liver for preoperative planning in living donor liver transplantation. Liver Transpl. 2013;19(12):1304-1310.
1. McGurk M, Amis AA, Potamianos P, Goodger NM. Rapid prototyping techniques for anatomical modelling in medicine. Ann R Coll Surg Engl. 1997;79(3):169-174.
2. Webb PA. A review of rapid prototyping (RP) techniques in the medical and biomedical sector. J Med Eng Technol. 2000;24(4):149-153.
3. Esses SJ, Berman P, Bloom AI, Sosna J. Clinical applications of physical 3D models derived from MDCT data and created by rapid prototyping. AJR Am J Roentgenol. 2011;196(6):W683-W688.
4. Torres K, Staśkiewicz G, Śnieżyński M, Drop A, Maciejewski R. Application of rapid prototyping techniques for modelling of anatomical structures in medical training and education. Folia Morphol. 2011;70(1):1-4.
5. Melican MC, Zimmerman MC, Dhillon MS, Ponnambalam AR, Curodeau A, Parsons JR. Three-dimensional printing and porous metallic surfaces: a new orthopedic application. J Biomed Mater Res. 2001;55(2):194-202.
6. Butscher A, Bohner M, Hofmann S, Gauckler L, Müller R. Structural and material approaches to bone tissue engineering in powder-based three-dimensional printing. Acta Biomater. 2011;7(3):907-920.
7. Ciocca L, De Crescenzio F, Fantini M, Scotti R. CAD/CAM and rapid prototyped scaffold construction for bone regenerative medicine and surgical transfer of virtual planning: a pilot study. Comput Med Imaging Graph. 2009;33(1):58-62.
8. Leukers B, Gülkan H, Irsen SH, et al. Hydroxyapatite scaffolds for bone tissue engineering made by 3D printing. J Mater Sci Mater Med. 2005;16(12):1121-1124.
9. Seitz H, Rieder W, Irsen S, Leukers B, Tille C. Three-dimensional printing of porous ceramic scaffolds for bone tissue engineering. J Biomed Mater Res B Appl Biomater. 2005;74(2):782-788.
10. Mankovich NJ, Cheeseman AM, Stoker NG. The display of three-dimensional anatomy with stereolithographic models. J Digit Imaging. 1990;3(3):200-203.
11. Flügge TV, Nelson K, Schmelzeisen R, Metzger MC. Three-dimensional plotting and printing of an implant drilling guide: simplifying guided implant surgery. J Oral Maxillofac Surg. 2013;71(8):1340-1346.
12. Goiato MC, Santos MR, Pesqueira AA, Moreno A, dos Santos DM, Haddad MF. Prototyping for surgical and prosthetic treatment. J Craniofac Surg. 2011;22(3):914-917.
13. Metzger MC, Hohlweg-Majert B, Schwarz U, Teschner M, Hammer B, Schmelzeisen R. Manufacturing splints for orthognathic surgery using a three-dimensional printer. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105(2):e1-e7.
14. Robiony M, Salvo I, Costa F, et al. Virtual reality surgical planning for maxillofacial distraction osteogenesis: the role of reverse engineering rapid prototyping and cooperative work. J Oral Maxillofac Surg. 2007;65(6):1198-1208.
15. Minns RJ, Bibb R, Banks R, Sutton RA. The use of a reconstructed three-dimensional solid model from CT to aid the surgical management of a total knee arthroplasty: a case study. Med Eng Phys. 2003;25(6):523-526.
16. Munjal S, Leopold SS, Kornreich D, Shott S, Finn HA. CT-generated 3-dimensional models for complex acetabular reconstruction. J Arthroplasty. 2000;15(5):644-653.
17. Tam MD, Laycock SD, Bell D, Chojnowski A. 3-D printout of a DICOM file to aid surgical planning in a 6 year old patient with a large scapular osteochondroma complicating congenital diaphyseal aclasia. J Radiol Case Rep. 2012;6(1):31-37.
18. Fu M, Lin L, Kong X, et al. Construction and accuracy assessment of patient-specific biocompatible drill template for cervical anterior transpedicular screw (ATPS) insertion: an in vitro study. PLoS One. 2013;8(1):e53580.
19. Zein NN, Hanouneh IA, Bishop PD, et al. Three-dimensional print of a liver for preoperative planning in living donor liver transplantation. Liver Transpl. 2013;19(12):1304-1310.

Synovial Fistula After Tension Band Plating for Genu Valgum Correction
Children often present to orthopedic surgeons with angular deformities about the knee. Temporary hemiepiphysiodesis, which is a frequently performed procedure to address such deformities, is safe and reversible. Specifically, tension band plating has become one of the most commonly performed techniques, especially given its low complication rates and minimally invasive nature.1-4 Complications reported with this method include mechanical hardware failure,5 implant migration,4 and recurvatum.3
We present an unreported complication of a synovial fistula formation after the removal of a tension band plate in a child who had achieved appropriate correction of her genu valgum. The patient and her family provided written informed consent for print and electronic publication of this case report.
Case Report
An 11-year-old girl presented to the pediatric orthopedics clinic with concern for genu valgum of the right lower extremity. She underwent a right proximal tibia medial hemiepiphysiodesis via tension band plating technique. Her clinic visit 4 weeks after surgery showed well-healed incisions and no signs of infection. She achieved appropriate correction and underwent hardware removal approximately 6 months after her initial surgery.
One month after hardware removal, the patient began to notice increased swelling and erythema around her incision site with associated pain. No fluid or drainage was seen at that time. She underwent irrigation and débridement shortly thereafter, and the wound was left open for wet-to-dry dressing changes (Figure 1). Intraoperative cultures were negative, but the patient received empiric antibiotic therapy. She continued to have difficulty with wound healing for the next month and was referred to plastic surgery. She underwent repeat irrigation and débridement, followed by coverage with a split-thickness skin graft by the plastic surgery service. Intraoperative cultures were again negative. During both irrigation and débridement procedures, care was taken to remain superficial and not violate the knee capsule.

At her 2-week postoperative check, the bolster covering the split thickness skin graft was removed, which revealed a 2×2-mm area of clear erosion near the central portion of her wound with synovial fluid drainage (Figure 2). Because of concern for a synovial fistula, magnetic resonance imaging (MRI) of the right knee was obtained, which confirmed the synovial fistula (Figures 3A, 3B). The coronal cut on MRI clearly showed the fistula with synovial fluid tracking into the epiphyseal screw tract through the breached capsule and to the level of the skin. She was immobilized in a long leg cast with the knee in extension for 6 weeks. Upon return, her fistula had closed, and she has not had any more wound issues.

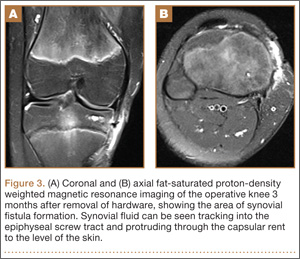
Discussion
To our knowledge, this is the first report of a synovial fistula after temporary hemiepiphysiodesis performed via tension band plating. Capsular knee anatomy may explain the etiology of the synovial fistula after hardware removal. The medial knee capsule composition and attachment sites have been extensively studied.6 In contrast to other joints, such as the shoulder, elbow, ankle, and hip, the metaphysis of the knee lies outside the capsule because the capsule inserts proximal at the level of the physis.7 During tension band plating, the epiphyseal screw breaches the capsule but serves as a plug while in place, which prevents the formation of a synovial fistula. When the screw is removed, the capsular rent spontaneously closes in almost all cases. However, the opportunity exists for a synovial fistula to form while the capsule heals, as evidenced by the current case. Such an issue does not apply to the metaphyseal screw because it is inserted outside the capsule.
Although it is possible that the synovial fistula was inadvertently created during one of the irrigation and débridement procedures, this is very unlikely. The surgeons who performed these washout procedures are knowledgeable and familiar with knee anatomy. Both irrigation and débridement procedures were superficial, and care was taken not to violate the knee capsule.
A synovial fistula after knee surgery is rare. Larsen8 described the fistula as a phenomenon that develops when excessive synovial fluid forces its way through a synovial incision with knee flexion and muscle contraction. Such a complication is most routinely described after knee arthroscopy. Proffer and colleagues9 reported an incidence of 6.1 per 1000 after knee arthroscopies. The average number of days until fistula diagnosis was 6 days (range, 3-10 days). All fistulae were treated with immobilization and closed after an average of 9 days (range, 7-14 days). There were no associated infections, although prophylactic antibiotics were given. A national survey found that knee fistulae accounted for only 3.2% of all complications of knee arthroscopy.10
The treatment for a synovial fistula is largely nonoperative. Most will resolve with a brief period of immobilization, which allows the fistula to close.9-10 Literature addressing fistulae that fail to heal with nonoperative treatment is limited. Excision and direct closure of the fistula, especially when chronic, often proves futile and leads to a high recurrence rate.11 An alternative but more extensive treatment involves excision and coverage with a myofascial flap.12
Complications reported after tension band plating are uncommon. Two studies reported no complications regarding the use of the tension band plate.1-2 Burghardt and colleagues,5 in reporting the results of a multicenter survey, found that 15% of surgeons who had used tension band plating had seen a total of 65 cases of mechanical failure. In all cases, the screws, not the plate, failed. Another study reported implant migration in 1 patient but attributed the complication to a technical error from placing the distal screw too close to the physis.4 A third study documented that 2 patients developed clinically significant recurvatum, most likely because of anterior placement of the plate.3 It is important to identify a synovial fistula postoperatively because it provides a direct route for pathogens from the external environment to enter the intra-articular space and the opportunity for a septic joint to develop. Infection should always be ruled out and, if present, appropriately treated.
Conclusion
Physicians performing tension band plating in the knee should be aware of the possible complication of a synovial fistula, which has traditionally been reported only in relation to knee arthroscopy. Given the proposed etiology of the synovial fistula, we recommend a brief period of immobilization of 3 to 5 days after tension band plate removal, allowing the capsular rent to heal and minimizing the risk of a synovial fistula.
1. Burghardt RD, Herzenberg JE, Standard SC, Paley D. Temporary hemiepiphyseal arrest using a screw and plate device to treat knee and ankle deformities in children: a preliminary report. J Child Orthop. 2008;2(3):187-197.
2. Boero S, Michelis MB, Riganti S. Use of the eight-plate for angular correction of knee deformities due to idiopathic and pathologic physis: initiating treatment according to etiology. J Child Orthop. 2011;5(3):209-216.
3. Guzman H, Yaszay B, Scott VP, Bastrom TP, Mubarak SJ. Early experience with medial femoral tension band plating in idiopathic genu valgum. J Child Orthop. 2011;5(1):11-17.
4. Ballal MS, Bruce CE, Nayagam S. Correcting genu varum and genu valgum in children by guided growth: temporary hemiepiphysiodesis using tension band plates. J Bone Joint Surg Br. 2010; 92(2):273-276.
5. Burghardt RD, Specht SC, Herzenberg JE. Mechanical failures of eight-plate guided growth system for temporary hemiepiphysiodesis. J Pediatr Orthop. 2010;30(6):594-597.
6. LaPrade RF, Engebretsen AH, Ly TV, Johansen S, Wentorf FA, Engebretsen L. The anatomy of the medial part of the knee. J Bone Joint Surg Am. 2007;89(9):2000-2010.
7. Montgomery CO, Siegel E, Blasier RD, Suva LJ. Concurrent septic arthritis and osteomyelitis in children. J Pediatr Orthop. 2013;33(4):464-467.
8. Larsen RL. Synovial sinus. In: Epps CH Jr, ed. Complications in Orthopaedic Surgery. 2nd ed. Philadelphia, PA: JB Lippincott; 1978:5-11.
9. Proffer DS, Drez D Jr, Daus GP. Synovial fistula of the knee: a complication of arthroscopy. Arthroscopy. 1991;7(1):98-100.
10. Committee on Complications of Arthroscopy Association of North America. Complications of arthroscopy and arthroscopic surgery: results of a national survey. Arthroscopy. 1985;1(4):214-220.
11. Yiannakopoulos CK. Diagnosis and treatment of postarthroscopic synovial knee fistulae: a report of four cases and review of the literature. J Knee Surg. 2007;20(1):34-38.
12. Méndez-Fernández MA. Treatment of chronic recurrent fistulae with myofascial flaps. Br J Plast Surg. 1993;46(4):303-306.
Children often present to orthopedic surgeons with angular deformities about the knee. Temporary hemiepiphysiodesis, which is a frequently performed procedure to address such deformities, is safe and reversible. Specifically, tension band plating has become one of the most commonly performed techniques, especially given its low complication rates and minimally invasive nature.1-4 Complications reported with this method include mechanical hardware failure,5 implant migration,4 and recurvatum.3
We present an unreported complication of a synovial fistula formation after the removal of a tension band plate in a child who had achieved appropriate correction of her genu valgum. The patient and her family provided written informed consent for print and electronic publication of this case report.
Case Report
An 11-year-old girl presented to the pediatric orthopedics clinic with concern for genu valgum of the right lower extremity. She underwent a right proximal tibia medial hemiepiphysiodesis via tension band plating technique. Her clinic visit 4 weeks after surgery showed well-healed incisions and no signs of infection. She achieved appropriate correction and underwent hardware removal approximately 6 months after her initial surgery.
One month after hardware removal, the patient began to notice increased swelling and erythema around her incision site with associated pain. No fluid or drainage was seen at that time. She underwent irrigation and débridement shortly thereafter, and the wound was left open for wet-to-dry dressing changes (Figure 1). Intraoperative cultures were negative, but the patient received empiric antibiotic therapy. She continued to have difficulty with wound healing for the next month and was referred to plastic surgery. She underwent repeat irrigation and débridement, followed by coverage with a split-thickness skin graft by the plastic surgery service. Intraoperative cultures were again negative. During both irrigation and débridement procedures, care was taken to remain superficial and not violate the knee capsule.
At her 2-week postoperative check, the bolster covering the split thickness skin graft was removed, which revealed a 2×2-mm area of clear erosion near the central portion of her wound with synovial fluid drainage (Figure 2). Because of concern for a synovial fistula, magnetic resonance imaging (MRI) of the right knee was obtained, which confirmed the synovial fistula (Figures 3A, 3B). The coronal cut on MRI clearly showed the fistula with synovial fluid tracking into the epiphyseal screw tract through the breached capsule and to the level of the skin. She was immobilized in a long leg cast with the knee in extension for 6 weeks. Upon return, her fistula had closed, and she has not had any more wound issues.
Discussion
To our knowledge, this is the first report of a synovial fistula after temporary hemiepiphysiodesis performed via tension band plating. Capsular knee anatomy may explain the etiology of the synovial fistula after hardware removal. The medial knee capsule composition and attachment sites have been extensively studied.6 In contrast to other joints, such as the shoulder, elbow, ankle, and hip, the metaphysis of the knee lies outside the capsule because the capsule inserts proximal at the level of the physis.7 During tension band plating, the epiphyseal screw breaches the capsule but serves as a plug while in place, which prevents the formation of a synovial fistula. When the screw is removed, the capsular rent spontaneously closes in almost all cases. However, the opportunity exists for a synovial fistula to form while the capsule heals, as evidenced by the current case. Such an issue does not apply to the metaphyseal screw because it is inserted outside the capsule.
Although it is possible that the synovial fistula was inadvertently created during one of the irrigation and débridement procedures, this is very unlikely. The surgeons who performed these washout procedures are knowledgeable and familiar with knee anatomy. Both irrigation and débridement procedures were superficial, and care was taken not to violate the knee capsule.
A synovial fistula after knee surgery is rare. Larsen8 described the fistula as a phenomenon that develops when excessive synovial fluid forces its way through a synovial incision with knee flexion and muscle contraction. Such a complication is most routinely described after knee arthroscopy. Proffer and colleagues9 reported an incidence of 6.1 per 1000 after knee arthroscopies. The average number of days until fistula diagnosis was 6 days (range, 3-10 days). All fistulae were treated with immobilization and closed after an average of 9 days (range, 7-14 days). There were no associated infections, although prophylactic antibiotics were given. A national survey found that knee fistulae accounted for only 3.2% of all complications of knee arthroscopy.10
The treatment for a synovial fistula is largely nonoperative. Most will resolve with a brief period of immobilization, which allows the fistula to close.9-10 Literature addressing fistulae that fail to heal with nonoperative treatment is limited. Excision and direct closure of the fistula, especially when chronic, often proves futile and leads to a high recurrence rate.11 An alternative but more extensive treatment involves excision and coverage with a myofascial flap.12
Complications reported after tension band plating are uncommon. Two studies reported no complications regarding the use of the tension band plate.1-2 Burghardt and colleagues,5 in reporting the results of a multicenter survey, found that 15% of surgeons who had used tension band plating had seen a total of 65 cases of mechanical failure. In all cases, the screws, not the plate, failed. Another study reported implant migration in 1 patient but attributed the complication to a technical error from placing the distal screw too close to the physis.4 A third study documented that 2 patients developed clinically significant recurvatum, most likely because of anterior placement of the plate.3 It is important to identify a synovial fistula postoperatively because it provides a direct route for pathogens from the external environment to enter the intra-articular space and the opportunity for a septic joint to develop. Infection should always be ruled out and, if present, appropriately treated.
Conclusion
Physicians performing tension band plating in the knee should be aware of the possible complication of a synovial fistula, which has traditionally been reported only in relation to knee arthroscopy. Given the proposed etiology of the synovial fistula, we recommend a brief period of immobilization of 3 to 5 days after tension band plate removal, allowing the capsular rent to heal and minimizing the risk of a synovial fistula.
Children often present to orthopedic surgeons with angular deformities about the knee. Temporary hemiepiphysiodesis, which is a frequently performed procedure to address such deformities, is safe and reversible. Specifically, tension band plating has become one of the most commonly performed techniques, especially given its low complication rates and minimally invasive nature.1-4 Complications reported with this method include mechanical hardware failure,5 implant migration,4 and recurvatum.3
We present an unreported complication of a synovial fistula formation after the removal of a tension band plate in a child who had achieved appropriate correction of her genu valgum. The patient and her family provided written informed consent for print and electronic publication of this case report.
Case Report
An 11-year-old girl presented to the pediatric orthopedics clinic with concern for genu valgum of the right lower extremity. She underwent a right proximal tibia medial hemiepiphysiodesis via tension band plating technique. Her clinic visit 4 weeks after surgery showed well-healed incisions and no signs of infection. She achieved appropriate correction and underwent hardware removal approximately 6 months after her initial surgery.
One month after hardware removal, the patient began to notice increased swelling and erythema around her incision site with associated pain. No fluid or drainage was seen at that time. She underwent irrigation and débridement shortly thereafter, and the wound was left open for wet-to-dry dressing changes (Figure 1). Intraoperative cultures were negative, but the patient received empiric antibiotic therapy. She continued to have difficulty with wound healing for the next month and was referred to plastic surgery. She underwent repeat irrigation and débridement, followed by coverage with a split-thickness skin graft by the plastic surgery service. Intraoperative cultures were again negative. During both irrigation and débridement procedures, care was taken to remain superficial and not violate the knee capsule.
At her 2-week postoperative check, the bolster covering the split thickness skin graft was removed, which revealed a 2×2-mm area of clear erosion near the central portion of her wound with synovial fluid drainage (Figure 2). Because of concern for a synovial fistula, magnetic resonance imaging (MRI) of the right knee was obtained, which confirmed the synovial fistula (Figures 3A, 3B). The coronal cut on MRI clearly showed the fistula with synovial fluid tracking into the epiphyseal screw tract through the breached capsule and to the level of the skin. She was immobilized in a long leg cast with the knee in extension for 6 weeks. Upon return, her fistula had closed, and she has not had any more wound issues.
Discussion
To our knowledge, this is the first report of a synovial fistula after temporary hemiepiphysiodesis performed via tension band plating. Capsular knee anatomy may explain the etiology of the synovial fistula after hardware removal. The medial knee capsule composition and attachment sites have been extensively studied.6 In contrast to other joints, such as the shoulder, elbow, ankle, and hip, the metaphysis of the knee lies outside the capsule because the capsule inserts proximal at the level of the physis.7 During tension band plating, the epiphyseal screw breaches the capsule but serves as a plug while in place, which prevents the formation of a synovial fistula. When the screw is removed, the capsular rent spontaneously closes in almost all cases. However, the opportunity exists for a synovial fistula to form while the capsule heals, as evidenced by the current case. Such an issue does not apply to the metaphyseal screw because it is inserted outside the capsule.
Although it is possible that the synovial fistula was inadvertently created during one of the irrigation and débridement procedures, this is very unlikely. The surgeons who performed these washout procedures are knowledgeable and familiar with knee anatomy. Both irrigation and débridement procedures were superficial, and care was taken not to violate the knee capsule.
A synovial fistula after knee surgery is rare. Larsen8 described the fistula as a phenomenon that develops when excessive synovial fluid forces its way through a synovial incision with knee flexion and muscle contraction. Such a complication is most routinely described after knee arthroscopy. Proffer and colleagues9 reported an incidence of 6.1 per 1000 after knee arthroscopies. The average number of days until fistula diagnosis was 6 days (range, 3-10 days). All fistulae were treated with immobilization and closed after an average of 9 days (range, 7-14 days). There were no associated infections, although prophylactic antibiotics were given. A national survey found that knee fistulae accounted for only 3.2% of all complications of knee arthroscopy.10
The treatment for a synovial fistula is largely nonoperative. Most will resolve with a brief period of immobilization, which allows the fistula to close.9-10 Literature addressing fistulae that fail to heal with nonoperative treatment is limited. Excision and direct closure of the fistula, especially when chronic, often proves futile and leads to a high recurrence rate.11 An alternative but more extensive treatment involves excision and coverage with a myofascial flap.12
Complications reported after tension band plating are uncommon. Two studies reported no complications regarding the use of the tension band plate.1-2 Burghardt and colleagues,5 in reporting the results of a multicenter survey, found that 15% of surgeons who had used tension band plating had seen a total of 65 cases of mechanical failure. In all cases, the screws, not the plate, failed. Another study reported implant migration in 1 patient but attributed the complication to a technical error from placing the distal screw too close to the physis.4 A third study documented that 2 patients developed clinically significant recurvatum, most likely because of anterior placement of the plate.3 It is important to identify a synovial fistula postoperatively because it provides a direct route for pathogens from the external environment to enter the intra-articular space and the opportunity for a septic joint to develop. Infection should always be ruled out and, if present, appropriately treated.
Conclusion
Physicians performing tension band plating in the knee should be aware of the possible complication of a synovial fistula, which has traditionally been reported only in relation to knee arthroscopy. Given the proposed etiology of the synovial fistula, we recommend a brief period of immobilization of 3 to 5 days after tension band plate removal, allowing the capsular rent to heal and minimizing the risk of a synovial fistula.
1. Burghardt RD, Herzenberg JE, Standard SC, Paley D. Temporary hemiepiphyseal arrest using a screw and plate device to treat knee and ankle deformities in children: a preliminary report. J Child Orthop. 2008;2(3):187-197.
2. Boero S, Michelis MB, Riganti S. Use of the eight-plate for angular correction of knee deformities due to idiopathic and pathologic physis: initiating treatment according to etiology. J Child Orthop. 2011;5(3):209-216.
3. Guzman H, Yaszay B, Scott VP, Bastrom TP, Mubarak SJ. Early experience with medial femoral tension band plating in idiopathic genu valgum. J Child Orthop. 2011;5(1):11-17.
4. Ballal MS, Bruce CE, Nayagam S. Correcting genu varum and genu valgum in children by guided growth: temporary hemiepiphysiodesis using tension band plates. J Bone Joint Surg Br. 2010; 92(2):273-276.
5. Burghardt RD, Specht SC, Herzenberg JE. Mechanical failures of eight-plate guided growth system for temporary hemiepiphysiodesis. J Pediatr Orthop. 2010;30(6):594-597.
6. LaPrade RF, Engebretsen AH, Ly TV, Johansen S, Wentorf FA, Engebretsen L. The anatomy of the medial part of the knee. J Bone Joint Surg Am. 2007;89(9):2000-2010.
7. Montgomery CO, Siegel E, Blasier RD, Suva LJ. Concurrent septic arthritis and osteomyelitis in children. J Pediatr Orthop. 2013;33(4):464-467.
8. Larsen RL. Synovial sinus. In: Epps CH Jr, ed. Complications in Orthopaedic Surgery. 2nd ed. Philadelphia, PA: JB Lippincott; 1978:5-11.
9. Proffer DS, Drez D Jr, Daus GP. Synovial fistula of the knee: a complication of arthroscopy. Arthroscopy. 1991;7(1):98-100.
10. Committee on Complications of Arthroscopy Association of North America. Complications of arthroscopy and arthroscopic surgery: results of a national survey. Arthroscopy. 1985;1(4):214-220.
11. Yiannakopoulos CK. Diagnosis and treatment of postarthroscopic synovial knee fistulae: a report of four cases and review of the literature. J Knee Surg. 2007;20(1):34-38.
12. Méndez-Fernández MA. Treatment of chronic recurrent fistulae with myofascial flaps. Br J Plast Surg. 1993;46(4):303-306.
1. Burghardt RD, Herzenberg JE, Standard SC, Paley D. Temporary hemiepiphyseal arrest using a screw and plate device to treat knee and ankle deformities in children: a preliminary report. J Child Orthop. 2008;2(3):187-197.
2. Boero S, Michelis MB, Riganti S. Use of the eight-plate for angular correction of knee deformities due to idiopathic and pathologic physis: initiating treatment according to etiology. J Child Orthop. 2011;5(3):209-216.
3. Guzman H, Yaszay B, Scott VP, Bastrom TP, Mubarak SJ. Early experience with medial femoral tension band plating in idiopathic genu valgum. J Child Orthop. 2011;5(1):11-17.
4. Ballal MS, Bruce CE, Nayagam S. Correcting genu varum and genu valgum in children by guided growth: temporary hemiepiphysiodesis using tension band plates. J Bone Joint Surg Br. 2010; 92(2):273-276.
5. Burghardt RD, Specht SC, Herzenberg JE. Mechanical failures of eight-plate guided growth system for temporary hemiepiphysiodesis. J Pediatr Orthop. 2010;30(6):594-597.
6. LaPrade RF, Engebretsen AH, Ly TV, Johansen S, Wentorf FA, Engebretsen L. The anatomy of the medial part of the knee. J Bone Joint Surg Am. 2007;89(9):2000-2010.
7. Montgomery CO, Siegel E, Blasier RD, Suva LJ. Concurrent septic arthritis and osteomyelitis in children. J Pediatr Orthop. 2013;33(4):464-467.
8. Larsen RL. Synovial sinus. In: Epps CH Jr, ed. Complications in Orthopaedic Surgery. 2nd ed. Philadelphia, PA: JB Lippincott; 1978:5-11.
9. Proffer DS, Drez D Jr, Daus GP. Synovial fistula of the knee: a complication of arthroscopy. Arthroscopy. 1991;7(1):98-100.
10. Committee on Complications of Arthroscopy Association of North America. Complications of arthroscopy and arthroscopic surgery: results of a national survey. Arthroscopy. 1985;1(4):214-220.
11. Yiannakopoulos CK. Diagnosis and treatment of postarthroscopic synovial knee fistulae: a report of four cases and review of the literature. J Knee Surg. 2007;20(1):34-38.
12. Méndez-Fernández MA. Treatment of chronic recurrent fistulae with myofascial flaps. Br J Plast Surg. 1993;46(4):303-306.

Health-Related Quality-of-Life Scores, Spine-Related Symptoms, and Reoperations in Young Adults 7 to 17 Years After Surgical Treatment of Adolescent Idiopathic Scoliosis
The goal of surgical treatment of adolescent idiopathic scoliosis (AIS) is to prevent disability associated with curve progression.1 Early studies tended to focus on radiographic measures, such as curve correction and sagittal balance, rather than on improvements in quality of life (QOL).2-5 Although studies have reported on QOL in patients treated surgically for scoliosis,6-11 these studies were largely limited by small sample size and inclusion of patients with congenital and neuromuscular scoliosis,9 lack of a generic measure of QOL,6,7 or lack of surgical treatment of patients in the cohort.10
We conducted a study to determine disease-specific and general health-related QOL (HR-QOL) in young adults who underwent surgical correction of their spinal deformity during adolescence and to evaluate associated complications and reoperations.
Materials and Methods
After obtaining institutional review board approval, we queried the surgical database of a large metropolitan tertiary referral center for consecutive patients who had undergone spine deformity correction between the ages of 10 and 17 years (January 1993–December 2003). Hospital and medical records were retrospectively reviewed to confirm the diagnosis of AIS. Patients with congenital, neuromuscular, juvenile, or infantile scoliosis were excluded. Patients with intraspinal pathology (eg, tethered cord, syringomyelia), developmental delay, chromosomal abnormality, or congenital heart disease were also excluded. Patients were contacted by mail or telephone, and the Scoliosis Research Society–22R (SRS-22R)12-15 and the Short Form–12 (SF-12)16 were administered. Standard demographic and surgical data were also collected.
The SRS-22R is a scoliosis-specific HR-QOL questionnaire with 22 items, 5 domains (pain, activity, appearance, mental, satisfaction), and a total score.12-15 Each domain score ranges from 1 to 5 (higher scores indicating better outcomes). The SRS-22R is the outcome instrument most widely used to measure HR-QOL changes in patients with scoliosis, and it is available in several languages.17-26
The SF-12, a 12-item self-administered short-form health status survey developed in the Medical Outcomes Study, measures patient-based health status. Two composite scores can be calculated: physical composite summary (PCS) and mental composite summary (MCS).16 Using norm-based scoring, all domain scales have a mean (SD) of 50 (10) based on the general 1998 US population. Thus, scores under 50 fall below the general population mean.
In addition, patients were surveyed to determine the incidence of spine-related symptoms and complaints, including activity limitations, rib prominence, waistline asymmetry, back pain, limited range of motion (ROM), shortness of breath, wound/scar problems, lung disease/asthma, heart disease, high blood pressure, and arthritis. Data regarding postoperative treatment regimens of physical therapy, narcotic pain medication, spinal/epidural injections, and nonsteroidal anti-inflammatory drug (NSAID) use were collected. Patients were also queried regarding their current working status and smoking status.
Standard demographic and surgical data were collected from hospital and office charts and radiographs. Data collected included history of bracing, age at index surgery, number of levels fused, surgical approach (anterior, posterior, combined), postoperative complications (eg, ileus, wound infection, anemia, pneumonia), and immediate preoperative and final postoperative radiographic measures. Data on need for subsequent revision surgery and indications for revision surgery were also collected.
Preoperative and latest follow-up radiographs were measured to determine curve magnitude, sagittal and coronal balance, and percentage curve correction. Coronal balance was defined as the distance between a plumb line drawn vertically from the spinous process of C7 and the central sacral line on full-length posteroanterior radiographs. Sagittal balance was defined as the distance of a plumb line drawn vertically from the center of the body of C7 and the posterosuperior endplate of S1.27
Regression analysis was performed to identify factors predictive of SRS-22R total scores. Factors included in the analysis were sex, age at surgery, Lenke type, surgery type (anterior, posterior, anteroposterior), number of levels fused, lowest instrumented vertebra, perioperative complications, percentage curve correction, postoperative coronal and sagittal balance, smoking status, and need for revision surgery. Although age and sex were considered variables outside the surgeon’s control, they were included in the model, as previous studies have shown that SRS scores varied by age and sex both in adolescents28 and adults.29 Significance was set at P < .01. All data analysis was performed with IBM SPSS Version 19.0 (Somers, New York).
Results
Of the 384 postoperative patients identified for study inclusion, 134 (35%) completed surveys. Sixteen patients with nonidiopathic scoliosis were excluded, leaving 118 available for analysis. Of the remaining patients, 248 (64%) could not be contacted because of a change in address or phone number. Two patients (1%) were unwilling to complete survey requests. There was no statistically significant difference in demographics between patients with and without follow-up data available. Demographics are summarized in Table 1. There were 109 females (92%). Mean (SD) age at surgery was 14.1 (1.9) years. Only 37 (31%) were braced before surgery. Table 2 summarizes the radiographic data. Mean (SD) major Cobb angle was 49.7° (7.8°). Eighty-five patients (72%) underwent posterior fusion with instrumentation using hooks only; another 16 (14%) had anterior-only surgery, and another 17 (14%) had combined anterior-posterior surgery. A mean of 7.8 levels were fused. Index surgery data and lowest instrumented vertebra distribution are summarized in Table 3. Mean (SD) percentage curve correction was 48.9% (8.4%).
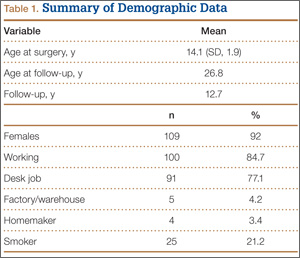
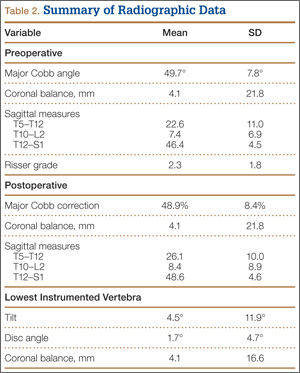
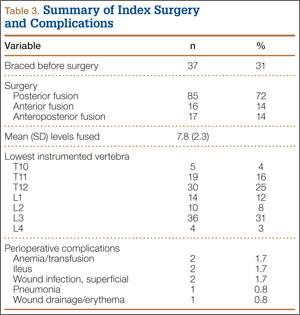
Seven patients had a total of 8 perioperative complications: anemia requiring transfusion (2), ileus necessitating nasogastric tube insertion (2), superficial wound infection treated with oral antibiotics and local wound care (2), wound drainage and erythema (1), and pneumonia (1). Mean (SD) length of clinical and radiographic follow-up was 57.9 (36.3) months.
Table 4 summarizes the long-term complications. Of the 38 patients with long-term complications, 14 required reoperation. The indications were disc herniation (2 patients), painful instrumentation (7), crankshaft phenomenon (1), nonunion (1), and adjacent-level degeneration (3). Both disc herniations were at L5–S1, several segments below the distal extent of the fusion. Of the 7 patients who had painful instrumentation removed, 6 had the entire construct removed, and 1 had the proximal half of a rod taken out. The 3 patients with adjacent-level degeneration had stenosis at the distal end of the construct—at L5–S1 (2 patients) or L2–L3 (1 patient).
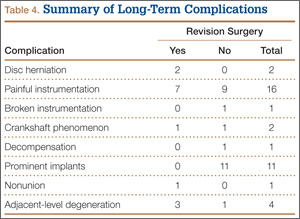
Mean (SD) time between surgery and completion of the surveys/questionnaires was 12.7 (3.2) years (range, 10-18 years). Mean age of respondents was 26.8 years. Twenty-five respondents (21%) were smokers. Mean (SD) outcome scores were 50.9 (9.4) for SF-12 PCS and 49.4 (10.2) for SF-12 MCS. Eighteen patients (15%) had SF-12 PCS scores 1 SD below normal, and 15 (13%) had SF-12 MCS scores 1 SD below normal. Mean (SD) SRS-22R Total score was 4.0 (0.7). Means, standard deviations, and distribution of SRS domain scores are summarized in Table 5. Of the variables, only current smoking (P < .001) was predictive of SRS-22R Total scores, accounting for 20% of their variability (Table 6).
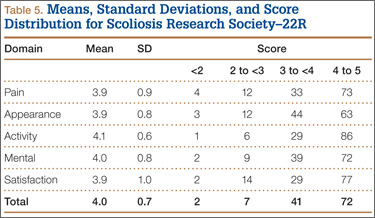
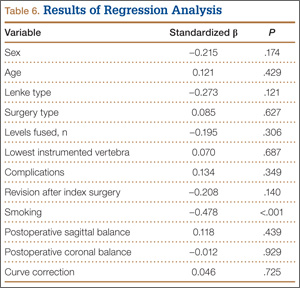
One hundred patients (85%) had jobs, mostly desk jobs. The postoperative limitations most commonly reported are summarized in Table 7. These included at least intermittent back pain in 90 patients (76%), limited ROM in 52 (44%), and activity limitations in 54 (46%). Less common limitations were waistline imbalance in 41 (35%), rib prominence in 28 (24%), wound/scar problems in 18 (15%), and shortness of breath in 18 (15%). Other related medical problems were lung disease/asthma in 11 (9%), osteoarthritis/degenerative arthritis in 11 (9%), heart disease in 3 (3%), and high blood pressure in 2 (2%).
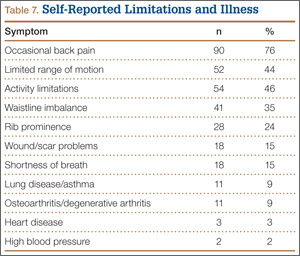
A minority of patients also participated in postoperative treatment regimens. The most common treatment was regular use of NSAIDs (25 patients, 21%). Other treatments were physical therapy (14, 12%), narcotic pain medication use (5, 4%), and epidural steroid injections (5, 4%). Table 8 summarizes the postoperative treatments used by patients with scoliosis.
Discussion
A major concern about prophylactic interventions for diseases is that the treatment will harm the patient. This is especially true for major spine surgery performed on adolescents with minimal symptoms. Although the incidence of perioperative complications in children undergoing corrective spinal surgery for AIS has been reported,30-32 the effect of the surgery on the disease-specific HR-QOL outcomes of these individuals as young adults has not been previously studied. Over the past few decades, a paradigm shift in understanding health and disability has occurred, with increased emphasis being placed on HR-QOL outcomes measures and understanding disability as relating to a measureable impact of the functioning of an individual after a change in health or environment. This change was substantiated when the World Health Organization endorsed the International Classification of Functioning, Disability and Health.33 In light of this shift, we present the disease-specific and general HR-QOL outcomes of young adults who had undergone surgical correction for spinal deformity during adolescence, as well as their associated complications and reoperations, in an attempt to identify targets for improvement.
Our patient-reported outcomes demonstrated a high incidence of occasional back pain, activity-related complaints, and limited ROM. Comparison of our cohort’s SRS-22R outcomes with previously published normative values for the unaffected adolescent population28,34 suggests worse scores for the disease-specific SRS-22R domains of pain and appearance. In 2012, Daubs and colleagues34 reported that normative scores on various SRS-22 domains were statistically lower with age (scores decreased from age 10 to age 19 years). Both Verma and colleagues28 and Daubs and colleagues34 reported lower scores for females than for males. Therefore, it is unclear whether the differences observed in our cohort may be accounted for by the larger proportion of females compared with the normative data.
General health scores on the SF-12 were similar to the population norm (mean [SD]) of 50 (10) referenced by Ware and colleagues.16 These findings suggest that, though pain and appearance may be statistically lower in our cohort—as measured with the SRS-22R—the cohort’s spine-related symptoms do not seem to lower its general health. Eighty-five percent of the patients were working at the time of the survey, further supporting a relatively normal level of overall function. In a retrospective review by Takayama and colleagues,9 similar results were found with regard to working after AIS fusion surgery. Of 32 patients treated surgically for scoliosis, at a mean of 21.1 years after the index fusion 27 (84.4%) were or had been engaged in various occupations without marked difficulty.
Our results in a cohort of patients with segmental instrumentation using hooks are similar to results in other studies of long-term HR-QOL measures in patients with AIS and Harrington rod instrumentation. Danielsson and Nachemson35 evaluated patients with surgically treated AIS with at least 20-year follow-up and reported that, in their surgical cohort with a mean age of 39.7 years, mean SF-36 PCS score was 50.9, and mean SF-36 MCS score was 50.2. In a recent study of patients with AIS and Harrington rod instrumentation, those of a mean age of 32.3 years had a mean score of 50.9 for both SF-36 PCS and SF-36 MCS.36
Regression analysis identified only smoking as a predictor of SRS-22R Total scores. This finding, that smokers have a lower health state, is expected even in the general population.37 Interestingly, bracing before surgery, Lenke type, surgery type, number of levels fused, lowest instrumented vertebra, incidence of perioperative complications, percentage curve correction, postoperative sagittal and coronal balance, and need for revision surgery did not influence HR-QOL measures in this cohort.
Our cohort’s incidence of occasional back pain was 76% (90/118 patients). Other reports have had similar findings. In 2012, Bas and colleagues38 studied self-reported pain in 126 consecutive patients with scoliosis and instrumented fusion. In their cohort, “most participants reported ‘no pain’ (38.5%) or ‘mild pain’ (30.8%) and 72.1% of participants reported a current work/school activity level of 100% normal.” Also in 2012, Rushton and Grevitt39 reported on a review and statistical analysis of the literature on HR-QOL in adolescents with untreated AIS and in unaffected adolescents. Their goal was to identify whether there were any differences in HR-QOL and, if so, whether they were clinically relevant. The authors concluded that pain and self-image tended to be statistically lower among cohorts with AIS but that only self-image was consistently different clinically between untreated patients with AIS and their unaffected peers.
Cosmetic complaints, though less common than functional concerns, affected a substantial percentage of our cohort. Waistline imbalance complaints were more common than rib prominence or scar-related complaints. The validity of patient-reported waistline imbalance is not known but may contribute to the SRS-22R outcomes in this cohort, particularly with regard to appearance scores. Respiratory symptoms, particularly those related to shortness of breath, were reported by 15% of patients. Respiratory symptoms may be in part secondary to underlying lung disease; smoking was reported by 21% of patients and asthma by 9%.
Few additional postoperative treatments were reported by patients. The most common treatment was regular use of NSAIDs (21%), followed by postoperative physical therapy (12%). Opiate medication use and spinal injections were rare—consistent with results reported by Danielsson and Nachemson35 in 2003.
Implant-related complaints, including painful instrumentation (13%) and implant prominence (9%), were some of the most common complaints in our study group. Although not all symptomatic instrumentation required surgical revision, 7 (50%) of the 14 additional spine surgeries were related to painful and/or prominent posterior instrumentation. Additional spine surgery was reported in 11.9% of our patients. Other indications for reoperation were disc herniation, crankshaft phenomenon, nonunion, and adjacent-level degeneration. Our rate of revision surgery is supported by the literature. In 2009, Luhmann and colleagues40 reported that 41 (3.9%) of 1057 primary spine fusions for idiopathic scoliosis required reoperation; the indications included infection (16/1057, 1.5%), pseudarthrosis (12, 1.1%), and painful/prominent implant (7, 0.7%). Richards and colleagues41 similarly reported on 1046 patients who underwent fusion for AIS. Of these patients, 135 underwent 172 repeat surgical interventions (12.9% reoperation rate), with 29 (21.5%) of the 135 undergoing 2 or more separate procedures. The most common reasons for reoperation were infection, symptomatic implant, and pseudarthrosis. The authors concluded that repeat surgeries were relatively common after the initial surgical procedures. Having a clearer understanding of instrumentation-related complaints and reoperations may lead to improvement in this surgeon-controlled variable.
There are limitations to this study. The data regarding clinical courses were collected by retrospective chart review, which has known limitations. To offset this, we collected prospective outcome data with use of the SF-12, the SRS-22R, and a spine-related complaints questionnaire. No control group was available for comparison of outcomes in our cohort. We used the SF-12 and previously published normative values for the SRS-22R for comparison with population norms. Such comparisons have inherent limitations, as the groups vary by sex and mean age; our cohort was primarily female and more than a decade older than the controls.
Only 35% of the patients who met the inclusion criteria had complete data that could be included in our analysis. Although there was no statistically significant difference in demographics between patients with and without follow-up data available, this low response rate could have introduced selection bias. Ideally, patients should have been seen in clinic, standing radiographs should have been taken, and pulmonary function tests should have been performed. However, these patients were asymptomatic, and ethical and insurance issues prevented those actions. Thus, any radiographic changes occurring over the intervening years, from the last clinic visit to completion of the surveys, were not documented. This situation may or may not have limited our findings, as other authors have found low correlation between radiographic outcomes and clinical outcome measures.13,14,19,36 During the period when these surgeries were performed, segmental spine instrumentation with hooks was the standard of care for deformity correction in AIS; therefore, all posterior instrumentations were done with hook-only segmental fixation. Current pedicle screw–based techniques that allow for additional correction of the deformity may provide different outcomes in the future.
We think that, despite the inherent limitations of this study, our data will be useful in the treatment of AIS. Our results suggest that postoperative spinal complaints are common and that, compared with an unaffected adolescent population, patients with AIS score significantly lower on pain and appearance domains of outcomes testing at a mean of 12.7 years after index fusion. Nevertheless, the outcomes do not seem to be of sufficient severity to affect general health and QOL as measured by outcomes testing.
Spinal deformity correction is performed to prevent impaired pulmonary function and spine-related disability later in life.42,43 Thus, longer-term studies, involving patients in their fifth and sixth decades of life, are needed to determine whether patients with AIS will have QOL outcomes, pulmonary function, and spine-related problems similar to those in the general population. In this cohort of young adults, smoking status was the only predictor of HR-QOL measures, and spinal deformity correction did not lead to decreased HR-QOL.
1. Tsutsui S, Pawelek J, Bastrom T, et al. Dissecting the effects of spinal fusion and deformity magnitude on quality of life in patients with adolescent idiopathic scoliosis. Spine. 2009;34(18):E653-E658.
2. Bonnett C, Brown JC, Cross B, Barron R. Posterior spinal fusion with Harrington rod instrumentation in 100 consecutive patients. Contemp Orthop. 1980;2:396-399.
3. Harrington PR, Dixon JR. An eleven year clinical investigation of Harrington instrument. Clin Orthop. 1973;(93):113-130.
4. Mielke CH, Lonstein JE, Denis F, Vandenbrink K, Winter RB. Surgical treatment of adolescent idiopathic scoliosis. A comparative analysis. J Bone Joint Surg Am. 1989;71(8):1170-1177.
5. Moskowitz A, Moe JH, Winter RB, Binner H. Long-term follow-up of scoliosis fusion. J Bone Joint Surg Am. 1980;62(3):529-554.
6. Akazawa T, Minami S, Kotani T, Nemoto T, Koshi T, Takahashi K. Health-related quality of life and low back pain of patients surgically treated for scoliosis after 21 years or more of follow-up: comparison among non-idiopathic scoliosis, idiopathic scoliosis, and healthy subjects. Spine. 2012;37(22):1899-1903.
7. Akazawa T, Minami S, Kotani T, Nemoto T, Koshi T, Takahashi K. Long-term clinical outcomes of surgery for adolescent idiopathic scoliosis 21 to 41 years later. Spine. 2012;37(5):402-405.
8. Pehrsson K, Bake B, Larsson S, Nachemson A. Lung function in adult idiopathic scoliosis: a 20 year follow up. Thorax. 1991;46(7):474-478.
9. Takayama K, Nakamura H, Matsuda H. Quality of life in patients treated surgically for scoliosis: longer than sixteen-year follow-up. Spine. 2009;34(20):2179-2184.
10. Weinstein SL, Dolan LA, Cheng JC, Danielsson A, Morcuende JA. Adolescent idiopathic scoliosis. Lancet. 2008;371(9623):1527-1537.
11. Westrick ER, Ward WT. Adolescent idiopathic scoliosis: 5-year to 20-year evidence-based surgical results. J Pediatr Orthop. 2011;31(1 suppl):S61-S68.
12. Asher MA, Lai SM, Glattes RC, Burton DC, Alanay A, Bago J. Refinement of the SRS-22 health-related quality of life questionnaire Function domain. Spine. 2006;31(5):593-597.
13. Asher M, Min Lai S, Burton D, Manna B. Scoliosis Research Society–22 patient questionnaire: responsiveness to change associated with surgical treatment. Spine. 2003;28(1):70-73.
14. Asher M, Min Lai S, Burton D, Manna B. The reliability and concurrent validity of the Scoliosis Research Society–22 patient questionnaire for idiopathic scoliosis. Spine. 2003;28(1):63-69.
15. Asher M, Min Lai S, Burton D, Manna B. Discrimination validity of the Scoliosis Research Society–22 patient questionnaire: relationship to idiopathic scoliosis curve pattern and curve size. Spine. 2003;28(1):74-78.
16. Ware J Jr, Kosinski M, Keller SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220-233.
17. Alanay A, Cil A, Berk H, et al. Reliability and validity of adapted Turkish version of Scoliosis Research Society–22 (SRS-22) questionnaire. Spine. 2005;30(21):2464-2468.
18. Beauséjour M, Joncas J, Goulet L, et al. Reliability and validity of adapted French Canadian version of Scoliosis Research Society outcomes questionnaire (SRS-22) in Quebec. Spine. 2009;34(6):623-628.
19. Climent JM, Bago J, Ey A, Perez-Grueso FJ, Izquierdo E. Validity of the Spanish version of the Scoliosis Research Society–22 (SRS-22) patient questionnaire. Spine. 2005;30(6):705-709.
20. Glowacki M, Misterska E, Laurentowska M, Mankowski P. Polish adaptation of Scoliosis Research Society–22 questionnaire. Spine. 2009;34(10):1060-1065.
21. Hashimoto H, Sase T, Arai Y, Maruyama T, Isobe K, Shouno Y. Validation of a Japanese version of the Scoliosis Research Society–22 patient questionnaire among idiopathic scoliosis patients in Japan. Spine. 2007;32(4):E141-E146.
22. Li M, Wang CF, Gu SX, et al. Adapted simplified Chinese (mainland) version of Scoliosis Research Society–22 questionnaire. Spine. 2009;34(12):1321-1324.
23. Monticone M, Carabalona R, Negrini S. Reliability of the Scoliosis Research Society–22 patient questionnaire (Italian version) in mild adolescent vertebral deformities. Eura Medicophys. 2004;40(3):191-197.
24. Niemeyer T, Schubert C, Halm HF, Herberts T, Leichtle C, Gesicki M. Validity and reliability of an adapted German version of Scoliosis Research Society–22 questionnaire. Spine. 2009;34(8):818-821.
25. Lai SM, Asher M, Burton D. Estimating SRS-22 quality of life measures with SF-36: application in idiopathic scoliosis. Spine. 2006;31(4):473-478.
26. Glattes RC, Burton DC, Lai SM, Frasier E, Asher MA. The reliability and concurrent validity of the Scoliosis Research Society–22R patient questionnaire compared with the Child Health Questionnaire–CF87 patient questionnaire for adolescent spinal deformity. Spine. 2007;32(16):1778-1784.
27. Blanke KM, Kuklo TR, Lenke LG, et al. Adolescent idiopathic scoliosis. In O’Brien MF, Kuklo TR, Blanke KM, Lenke LG, eds. Spinal Deformity Study Group Radiographic Measurement Manual. Memphis, TN: Medtronic; 2004.
28. Verma K, Lonner B, Hoashi JS, et al. Demographic factors affect Scoliosis Research Society–22 performance in healthy adolescents: a comparative baseline for adolescents with idiopathic scoliosis. Spine. 2010;35(24):2134-2139.
29. Baldus C, Bridwell KH, Harrast J, et al. Age-gender matched comparison of SRS instrument scores between adult deformity and normal adults: are all SRS domains disease specific? Spine. 2008;33(20):2214-2218.
30. Brown CA, Lenke LG, Bridwell KH, Geideman WM, Hasan SA, Blanke K. Complication of pediatric thoracolumbar and lumbar pedicle screws. Spine. 1998;23(14):1566-1571.
31. Coe JD, Arlet V, Donaldson W, et al. Complications in spinal fusion for adolescent idiopathic scoliosis in the new millennium. A report of the Scoliosis Research Society Morbidity and Mortality Committee. Spine. 2006;31(3):345-349.
32. Fu KM, Smith JS, Polly DW, et al. Scoliosis Research Society Morbidity and Mortality Committee. Morbidity and mortality associated with spinal surgery in children: a review of the Scoliosis Research Society morbidity and mortality database. J Neurosurg Pediatr. 2011;7(1):37-41.
33. World Health Organization. International Classification of Functioning, Disability and Health: ICF Short Version. Geneva, Switzerland: World Health Organization; 2001.
34. Daubs M, Lawrence B, Hung M, et al. Scoliosis Research Society–22 results in 3,052 healthy adolescents age ten to 19 years. Abstract presented at: 47th Annual Meeting and Course of the Scoliosis Research Society; September 5-8, 2012; Chicago, IL. Abstract 72.
35. Danielsson AL, Nachemson AL. Back pain and function 23 years after fusion for adolescent idiopathic scoliosis: a case–control study—part II. Spine. 2003;28(18):E373-E383.
36. Götze C, Liljenqvist UR, Slomka A, Götze HG, Steinbeck J. Quality of life and back pain: outcome 16.7 years after Harrington instrumentation. Spine. 2002;27(13):1456-1463.
37. Quercioli C, Messina G, Barbini E, Carriero G, Fanì M, Nante N. Importance of sociodemographic and morbidity aspects in measuring health-related quality of life: performances of three tools: comparison of three questionnaire scores. Eur J Health Econ. 2009;10(4):389-397.
38. Bas T, Franco N, Bas P, Bas JL. Pain and disability following fusion for idiopathic adolescent scoliosis: prevalence and associated factors. Evid Based Spine Care J. 2012;3(2):17-24.
39. Rushton PR, Grevitt MP. Comparison of untreated adolescent idiopathic scoliosis with normal controls: a review and statistical analysis of the literature. Spine. 2013;38(9):778-785.
40. Luhmann SJ, Lenke LG, Bridwell KH, Schootman M. Revision surgery after primary spine fusion for idiopathic scoliosis. Spine. 2009;34(20):2191-2197.
41. Richards BS, Hasley BP, Casey VF. Repeat surgical interventions following “definitive” instrumentation and fusion for idiopathic scoliosis. Spine. 2006;31(26):3018-3026.
42. Bjure J, Grimby G, Kasalický J, Lindh M, Nachemson A. Respiratory impairment and airway closure in patients with untreated idiopathic scoliosis. Thorax. 1970;25(4):451-456.
43. Haefeli M, Elfering A, Kilian R, Min K, Boos N. Nonoperative treatment for adolescent idiopathic scoliosis: a 10- to 60-year follow-up with special reference to health-related quality of life. Spine. 2006;31(3):355-366.
The goal of surgical treatment of adolescent idiopathic scoliosis (AIS) is to prevent disability associated with curve progression.1 Early studies tended to focus on radiographic measures, such as curve correction and sagittal balance, rather than on improvements in quality of life (QOL).2-5 Although studies have reported on QOL in patients treated surgically for scoliosis,6-11 these studies were largely limited by small sample size and inclusion of patients with congenital and neuromuscular scoliosis,9 lack of a generic measure of QOL,6,7 or lack of surgical treatment of patients in the cohort.10
We conducted a study to determine disease-specific and general health-related QOL (HR-QOL) in young adults who underwent surgical correction of their spinal deformity during adolescence and to evaluate associated complications and reoperations.
Materials and Methods
After obtaining institutional review board approval, we queried the surgical database of a large metropolitan tertiary referral center for consecutive patients who had undergone spine deformity correction between the ages of 10 and 17 years (January 1993–December 2003). Hospital and medical records were retrospectively reviewed to confirm the diagnosis of AIS. Patients with congenital, neuromuscular, juvenile, or infantile scoliosis were excluded. Patients with intraspinal pathology (eg, tethered cord, syringomyelia), developmental delay, chromosomal abnormality, or congenital heart disease were also excluded. Patients were contacted by mail or telephone, and the Scoliosis Research Society–22R (SRS-22R)12-15 and the Short Form–12 (SF-12)16 were administered. Standard demographic and surgical data were also collected.
The SRS-22R is a scoliosis-specific HR-QOL questionnaire with 22 items, 5 domains (pain, activity, appearance, mental, satisfaction), and a total score.12-15 Each domain score ranges from 1 to 5 (higher scores indicating better outcomes). The SRS-22R is the outcome instrument most widely used to measure HR-QOL changes in patients with scoliosis, and it is available in several languages.17-26
The SF-12, a 12-item self-administered short-form health status survey developed in the Medical Outcomes Study, measures patient-based health status. Two composite scores can be calculated: physical composite summary (PCS) and mental composite summary (MCS).16 Using norm-based scoring, all domain scales have a mean (SD) of 50 (10) based on the general 1998 US population. Thus, scores under 50 fall below the general population mean.
In addition, patients were surveyed to determine the incidence of spine-related symptoms and complaints, including activity limitations, rib prominence, waistline asymmetry, back pain, limited range of motion (ROM), shortness of breath, wound/scar problems, lung disease/asthma, heart disease, high blood pressure, and arthritis. Data regarding postoperative treatment regimens of physical therapy, narcotic pain medication, spinal/epidural injections, and nonsteroidal anti-inflammatory drug (NSAID) use were collected. Patients were also queried regarding their current working status and smoking status.
Standard demographic and surgical data were collected from hospital and office charts and radiographs. Data collected included history of bracing, age at index surgery, number of levels fused, surgical approach (anterior, posterior, combined), postoperative complications (eg, ileus, wound infection, anemia, pneumonia), and immediate preoperative and final postoperative radiographic measures. Data on need for subsequent revision surgery and indications for revision surgery were also collected.
Preoperative and latest follow-up radiographs were measured to determine curve magnitude, sagittal and coronal balance, and percentage curve correction. Coronal balance was defined as the distance between a plumb line drawn vertically from the spinous process of C7 and the central sacral line on full-length posteroanterior radiographs. Sagittal balance was defined as the distance of a plumb line drawn vertically from the center of the body of C7 and the posterosuperior endplate of S1.27
Regression analysis was performed to identify factors predictive of SRS-22R total scores. Factors included in the analysis were sex, age at surgery, Lenke type, surgery type (anterior, posterior, anteroposterior), number of levels fused, lowest instrumented vertebra, perioperative complications, percentage curve correction, postoperative coronal and sagittal balance, smoking status, and need for revision surgery. Although age and sex were considered variables outside the surgeon’s control, they were included in the model, as previous studies have shown that SRS scores varied by age and sex both in adolescents28 and adults.29 Significance was set at P < .01. All data analysis was performed with IBM SPSS Version 19.0 (Somers, New York).
Results
Of the 384 postoperative patients identified for study inclusion, 134 (35%) completed surveys. Sixteen patients with nonidiopathic scoliosis were excluded, leaving 118 available for analysis. Of the remaining patients, 248 (64%) could not be contacted because of a change in address or phone number. Two patients (1%) were unwilling to complete survey requests. There was no statistically significant difference in demographics between patients with and without follow-up data available. Demographics are summarized in Table 1. There were 109 females (92%). Mean (SD) age at surgery was 14.1 (1.9) years. Only 37 (31%) were braced before surgery. Table 2 summarizes the radiographic data. Mean (SD) major Cobb angle was 49.7° (7.8°). Eighty-five patients (72%) underwent posterior fusion with instrumentation using hooks only; another 16 (14%) had anterior-only surgery, and another 17 (14%) had combined anterior-posterior surgery. A mean of 7.8 levels were fused. Index surgery data and lowest instrumented vertebra distribution are summarized in Table 3. Mean (SD) percentage curve correction was 48.9% (8.4%).
Seven patients had a total of 8 perioperative complications: anemia requiring transfusion (2), ileus necessitating nasogastric tube insertion (2), superficial wound infection treated with oral antibiotics and local wound care (2), wound drainage and erythema (1), and pneumonia (1). Mean (SD) length of clinical and radiographic follow-up was 57.9 (36.3) months.
Table 4 summarizes the long-term complications. Of the 38 patients with long-term complications, 14 required reoperation. The indications were disc herniation (2 patients), painful instrumentation (7), crankshaft phenomenon (1), nonunion (1), and adjacent-level degeneration (3). Both disc herniations were at L5–S1, several segments below the distal extent of the fusion. Of the 7 patients who had painful instrumentation removed, 6 had the entire construct removed, and 1 had the proximal half of a rod taken out. The 3 patients with adjacent-level degeneration had stenosis at the distal end of the construct—at L5–S1 (2 patients) or L2–L3 (1 patient).
Mean (SD) time between surgery and completion of the surveys/questionnaires was 12.7 (3.2) years (range, 10-18 years). Mean age of respondents was 26.8 years. Twenty-five respondents (21%) were smokers. Mean (SD) outcome scores were 50.9 (9.4) for SF-12 PCS and 49.4 (10.2) for SF-12 MCS. Eighteen patients (15%) had SF-12 PCS scores 1 SD below normal, and 15 (13%) had SF-12 MCS scores 1 SD below normal. Mean (SD) SRS-22R Total score was 4.0 (0.7). Means, standard deviations, and distribution of SRS domain scores are summarized in Table 5. Of the variables, only current smoking (P < .001) was predictive of SRS-22R Total scores, accounting for 20% of their variability (Table 6).
One hundred patients (85%) had jobs, mostly desk jobs. The postoperative limitations most commonly reported are summarized in Table 7. These included at least intermittent back pain in 90 patients (76%), limited ROM in 52 (44%), and activity limitations in 54 (46%). Less common limitations were waistline imbalance in 41 (35%), rib prominence in 28 (24%), wound/scar problems in 18 (15%), and shortness of breath in 18 (15%). Other related medical problems were lung disease/asthma in 11 (9%), osteoarthritis/degenerative arthritis in 11 (9%), heart disease in 3 (3%), and high blood pressure in 2 (2%).
A minority of patients also participated in postoperative treatment regimens. The most common treatment was regular use of NSAIDs (25 patients, 21%). Other treatments were physical therapy (14, 12%), narcotic pain medication use (5, 4%), and epidural steroid injections (5, 4%). Table 8 summarizes the postoperative treatments used by patients with scoliosis.
Discussion
A major concern about prophylactic interventions for diseases is that the treatment will harm the patient. This is especially true for major spine surgery performed on adolescents with minimal symptoms. Although the incidence of perioperative complications in children undergoing corrective spinal surgery for AIS has been reported,30-32 the effect of the surgery on the disease-specific HR-QOL outcomes of these individuals as young adults has not been previously studied. Over the past few decades, a paradigm shift in understanding health and disability has occurred, with increased emphasis being placed on HR-QOL outcomes measures and understanding disability as relating to a measureable impact of the functioning of an individual after a change in health or environment. This change was substantiated when the World Health Organization endorsed the International Classification of Functioning, Disability and Health.33 In light of this shift, we present the disease-specific and general HR-QOL outcomes of young adults who had undergone surgical correction for spinal deformity during adolescence, as well as their associated complications and reoperations, in an attempt to identify targets for improvement.
Our patient-reported outcomes demonstrated a high incidence of occasional back pain, activity-related complaints, and limited ROM. Comparison of our cohort’s SRS-22R outcomes with previously published normative values for the unaffected adolescent population28,34 suggests worse scores for the disease-specific SRS-22R domains of pain and appearance. In 2012, Daubs and colleagues34 reported that normative scores on various SRS-22 domains were statistically lower with age (scores decreased from age 10 to age 19 years). Both Verma and colleagues28 and Daubs and colleagues34 reported lower scores for females than for males. Therefore, it is unclear whether the differences observed in our cohort may be accounted for by the larger proportion of females compared with the normative data.
General health scores on the SF-12 were similar to the population norm (mean [SD]) of 50 (10) referenced by Ware and colleagues.16 These findings suggest that, though pain and appearance may be statistically lower in our cohort—as measured with the SRS-22R—the cohort’s spine-related symptoms do not seem to lower its general health. Eighty-five percent of the patients were working at the time of the survey, further supporting a relatively normal level of overall function. In a retrospective review by Takayama and colleagues,9 similar results were found with regard to working after AIS fusion surgery. Of 32 patients treated surgically for scoliosis, at a mean of 21.1 years after the index fusion 27 (84.4%) were or had been engaged in various occupations without marked difficulty.
Our results in a cohort of patients with segmental instrumentation using hooks are similar to results in other studies of long-term HR-QOL measures in patients with AIS and Harrington rod instrumentation. Danielsson and Nachemson35 evaluated patients with surgically treated AIS with at least 20-year follow-up and reported that, in their surgical cohort with a mean age of 39.7 years, mean SF-36 PCS score was 50.9, and mean SF-36 MCS score was 50.2. In a recent study of patients with AIS and Harrington rod instrumentation, those of a mean age of 32.3 years had a mean score of 50.9 for both SF-36 PCS and SF-36 MCS.36
Regression analysis identified only smoking as a predictor of SRS-22R Total scores. This finding, that smokers have a lower health state, is expected even in the general population.37 Interestingly, bracing before surgery, Lenke type, surgery type, number of levels fused, lowest instrumented vertebra, incidence of perioperative complications, percentage curve correction, postoperative sagittal and coronal balance, and need for revision surgery did not influence HR-QOL measures in this cohort.
Our cohort’s incidence of occasional back pain was 76% (90/118 patients). Other reports have had similar findings. In 2012, Bas and colleagues38 studied self-reported pain in 126 consecutive patients with scoliosis and instrumented fusion. In their cohort, “most participants reported ‘no pain’ (38.5%) or ‘mild pain’ (30.8%) and 72.1% of participants reported a current work/school activity level of 100% normal.” Also in 2012, Rushton and Grevitt39 reported on a review and statistical analysis of the literature on HR-QOL in adolescents with untreated AIS and in unaffected adolescents. Their goal was to identify whether there were any differences in HR-QOL and, if so, whether they were clinically relevant. The authors concluded that pain and self-image tended to be statistically lower among cohorts with AIS but that only self-image was consistently different clinically between untreated patients with AIS and their unaffected peers.
Cosmetic complaints, though less common than functional concerns, affected a substantial percentage of our cohort. Waistline imbalance complaints were more common than rib prominence or scar-related complaints. The validity of patient-reported waistline imbalance is not known but may contribute to the SRS-22R outcomes in this cohort, particularly with regard to appearance scores. Respiratory symptoms, particularly those related to shortness of breath, were reported by 15% of patients. Respiratory symptoms may be in part secondary to underlying lung disease; smoking was reported by 21% of patients and asthma by 9%.
Few additional postoperative treatments were reported by patients. The most common treatment was regular use of NSAIDs (21%), followed by postoperative physical therapy (12%). Opiate medication use and spinal injections were rare—consistent with results reported by Danielsson and Nachemson35 in 2003.
Implant-related complaints, including painful instrumentation (13%) and implant prominence (9%), were some of the most common complaints in our study group. Although not all symptomatic instrumentation required surgical revision, 7 (50%) of the 14 additional spine surgeries were related to painful and/or prominent posterior instrumentation. Additional spine surgery was reported in 11.9% of our patients. Other indications for reoperation were disc herniation, crankshaft phenomenon, nonunion, and adjacent-level degeneration. Our rate of revision surgery is supported by the literature. In 2009, Luhmann and colleagues40 reported that 41 (3.9%) of 1057 primary spine fusions for idiopathic scoliosis required reoperation; the indications included infection (16/1057, 1.5%), pseudarthrosis (12, 1.1%), and painful/prominent implant (7, 0.7%). Richards and colleagues41 similarly reported on 1046 patients who underwent fusion for AIS. Of these patients, 135 underwent 172 repeat surgical interventions (12.9% reoperation rate), with 29 (21.5%) of the 135 undergoing 2 or more separate procedures. The most common reasons for reoperation were infection, symptomatic implant, and pseudarthrosis. The authors concluded that repeat surgeries were relatively common after the initial surgical procedures. Having a clearer understanding of instrumentation-related complaints and reoperations may lead to improvement in this surgeon-controlled variable.
There are limitations to this study. The data regarding clinical courses were collected by retrospective chart review, which has known limitations. To offset this, we collected prospective outcome data with use of the SF-12, the SRS-22R, and a spine-related complaints questionnaire. No control group was available for comparison of outcomes in our cohort. We used the SF-12 and previously published normative values for the SRS-22R for comparison with population norms. Such comparisons have inherent limitations, as the groups vary by sex and mean age; our cohort was primarily female and more than a decade older than the controls.
Only 35% of the patients who met the inclusion criteria had complete data that could be included in our analysis. Although there was no statistically significant difference in demographics between patients with and without follow-up data available, this low response rate could have introduced selection bias. Ideally, patients should have been seen in clinic, standing radiographs should have been taken, and pulmonary function tests should have been performed. However, these patients were asymptomatic, and ethical and insurance issues prevented those actions. Thus, any radiographic changes occurring over the intervening years, from the last clinic visit to completion of the surveys, were not documented. This situation may or may not have limited our findings, as other authors have found low correlation between radiographic outcomes and clinical outcome measures.13,14,19,36 During the period when these surgeries were performed, segmental spine instrumentation with hooks was the standard of care for deformity correction in AIS; therefore, all posterior instrumentations were done with hook-only segmental fixation. Current pedicle screw–based techniques that allow for additional correction of the deformity may provide different outcomes in the future.
We think that, despite the inherent limitations of this study, our data will be useful in the treatment of AIS. Our results suggest that postoperative spinal complaints are common and that, compared with an unaffected adolescent population, patients with AIS score significantly lower on pain and appearance domains of outcomes testing at a mean of 12.7 years after index fusion. Nevertheless, the outcomes do not seem to be of sufficient severity to affect general health and QOL as measured by outcomes testing.
Spinal deformity correction is performed to prevent impaired pulmonary function and spine-related disability later in life.42,43 Thus, longer-term studies, involving patients in their fifth and sixth decades of life, are needed to determine whether patients with AIS will have QOL outcomes, pulmonary function, and spine-related problems similar to those in the general population. In this cohort of young adults, smoking status was the only predictor of HR-QOL measures, and spinal deformity correction did not lead to decreased HR-QOL.
The goal of surgical treatment of adolescent idiopathic scoliosis (AIS) is to prevent disability associated with curve progression.1 Early studies tended to focus on radiographic measures, such as curve correction and sagittal balance, rather than on improvements in quality of life (QOL).2-5 Although studies have reported on QOL in patients treated surgically for scoliosis,6-11 these studies were largely limited by small sample size and inclusion of patients with congenital and neuromuscular scoliosis,9 lack of a generic measure of QOL,6,7 or lack of surgical treatment of patients in the cohort.10
We conducted a study to determine disease-specific and general health-related QOL (HR-QOL) in young adults who underwent surgical correction of their spinal deformity during adolescence and to evaluate associated complications and reoperations.
Materials and Methods
After obtaining institutional review board approval, we queried the surgical database of a large metropolitan tertiary referral center for consecutive patients who had undergone spine deformity correction between the ages of 10 and 17 years (January 1993–December 2003). Hospital and medical records were retrospectively reviewed to confirm the diagnosis of AIS. Patients with congenital, neuromuscular, juvenile, or infantile scoliosis were excluded. Patients with intraspinal pathology (eg, tethered cord, syringomyelia), developmental delay, chromosomal abnormality, or congenital heart disease were also excluded. Patients were contacted by mail or telephone, and the Scoliosis Research Society–22R (SRS-22R)12-15 and the Short Form–12 (SF-12)16 were administered. Standard demographic and surgical data were also collected.
The SRS-22R is a scoliosis-specific HR-QOL questionnaire with 22 items, 5 domains (pain, activity, appearance, mental, satisfaction), and a total score.12-15 Each domain score ranges from 1 to 5 (higher scores indicating better outcomes). The SRS-22R is the outcome instrument most widely used to measure HR-QOL changes in patients with scoliosis, and it is available in several languages.17-26
The SF-12, a 12-item self-administered short-form health status survey developed in the Medical Outcomes Study, measures patient-based health status. Two composite scores can be calculated: physical composite summary (PCS) and mental composite summary (MCS).16 Using norm-based scoring, all domain scales have a mean (SD) of 50 (10) based on the general 1998 US population. Thus, scores under 50 fall below the general population mean.
In addition, patients were surveyed to determine the incidence of spine-related symptoms and complaints, including activity limitations, rib prominence, waistline asymmetry, back pain, limited range of motion (ROM), shortness of breath, wound/scar problems, lung disease/asthma, heart disease, high blood pressure, and arthritis. Data regarding postoperative treatment regimens of physical therapy, narcotic pain medication, spinal/epidural injections, and nonsteroidal anti-inflammatory drug (NSAID) use were collected. Patients were also queried regarding their current working status and smoking status.
Standard demographic and surgical data were collected from hospital and office charts and radiographs. Data collected included history of bracing, age at index surgery, number of levels fused, surgical approach (anterior, posterior, combined), postoperative complications (eg, ileus, wound infection, anemia, pneumonia), and immediate preoperative and final postoperative radiographic measures. Data on need for subsequent revision surgery and indications for revision surgery were also collected.
Preoperative and latest follow-up radiographs were measured to determine curve magnitude, sagittal and coronal balance, and percentage curve correction. Coronal balance was defined as the distance between a plumb line drawn vertically from the spinous process of C7 and the central sacral line on full-length posteroanterior radiographs. Sagittal balance was defined as the distance of a plumb line drawn vertically from the center of the body of C7 and the posterosuperior endplate of S1.27
Regression analysis was performed to identify factors predictive of SRS-22R total scores. Factors included in the analysis were sex, age at surgery, Lenke type, surgery type (anterior, posterior, anteroposterior), number of levels fused, lowest instrumented vertebra, perioperative complications, percentage curve correction, postoperative coronal and sagittal balance, smoking status, and need for revision surgery. Although age and sex were considered variables outside the surgeon’s control, they were included in the model, as previous studies have shown that SRS scores varied by age and sex both in adolescents28 and adults.29 Significance was set at P < .01. All data analysis was performed with IBM SPSS Version 19.0 (Somers, New York).
Results
Of the 384 postoperative patients identified for study inclusion, 134 (35%) completed surveys. Sixteen patients with nonidiopathic scoliosis were excluded, leaving 118 available for analysis. Of the remaining patients, 248 (64%) could not be contacted because of a change in address or phone number. Two patients (1%) were unwilling to complete survey requests. There was no statistically significant difference in demographics between patients with and without follow-up data available. Demographics are summarized in Table 1. There were 109 females (92%). Mean (SD) age at surgery was 14.1 (1.9) years. Only 37 (31%) were braced before surgery. Table 2 summarizes the radiographic data. Mean (SD) major Cobb angle was 49.7° (7.8°). Eighty-five patients (72%) underwent posterior fusion with instrumentation using hooks only; another 16 (14%) had anterior-only surgery, and another 17 (14%) had combined anterior-posterior surgery. A mean of 7.8 levels were fused. Index surgery data and lowest instrumented vertebra distribution are summarized in Table 3. Mean (SD) percentage curve correction was 48.9% (8.4%).
Seven patients had a total of 8 perioperative complications: anemia requiring transfusion (2), ileus necessitating nasogastric tube insertion (2), superficial wound infection treated with oral antibiotics and local wound care (2), wound drainage and erythema (1), and pneumonia (1). Mean (SD) length of clinical and radiographic follow-up was 57.9 (36.3) months.
Table 4 summarizes the long-term complications. Of the 38 patients with long-term complications, 14 required reoperation. The indications were disc herniation (2 patients), painful instrumentation (7), crankshaft phenomenon (1), nonunion (1), and adjacent-level degeneration (3). Both disc herniations were at L5–S1, several segments below the distal extent of the fusion. Of the 7 patients who had painful instrumentation removed, 6 had the entire construct removed, and 1 had the proximal half of a rod taken out. The 3 patients with adjacent-level degeneration had stenosis at the distal end of the construct—at L5–S1 (2 patients) or L2–L3 (1 patient).
Mean (SD) time between surgery and completion of the surveys/questionnaires was 12.7 (3.2) years (range, 10-18 years). Mean age of respondents was 26.8 years. Twenty-five respondents (21%) were smokers. Mean (SD) outcome scores were 50.9 (9.4) for SF-12 PCS and 49.4 (10.2) for SF-12 MCS. Eighteen patients (15%) had SF-12 PCS scores 1 SD below normal, and 15 (13%) had SF-12 MCS scores 1 SD below normal. Mean (SD) SRS-22R Total score was 4.0 (0.7). Means, standard deviations, and distribution of SRS domain scores are summarized in Table 5. Of the variables, only current smoking (P < .001) was predictive of SRS-22R Total scores, accounting for 20% of their variability (Table 6).
One hundred patients (85%) had jobs, mostly desk jobs. The postoperative limitations most commonly reported are summarized in Table 7. These included at least intermittent back pain in 90 patients (76%), limited ROM in 52 (44%), and activity limitations in 54 (46%). Less common limitations were waistline imbalance in 41 (35%), rib prominence in 28 (24%), wound/scar problems in 18 (15%), and shortness of breath in 18 (15%). Other related medical problems were lung disease/asthma in 11 (9%), osteoarthritis/degenerative arthritis in 11 (9%), heart disease in 3 (3%), and high blood pressure in 2 (2%).
A minority of patients also participated in postoperative treatment regimens. The most common treatment was regular use of NSAIDs (25 patients, 21%). Other treatments were physical therapy (14, 12%), narcotic pain medication use (5, 4%), and epidural steroid injections (5, 4%). Table 8 summarizes the postoperative treatments used by patients with scoliosis.
Discussion
A major concern about prophylactic interventions for diseases is that the treatment will harm the patient. This is especially true for major spine surgery performed on adolescents with minimal symptoms. Although the incidence of perioperative complications in children undergoing corrective spinal surgery for AIS has been reported,30-32 the effect of the surgery on the disease-specific HR-QOL outcomes of these individuals as young adults has not been previously studied. Over the past few decades, a paradigm shift in understanding health and disability has occurred, with increased emphasis being placed on HR-QOL outcomes measures and understanding disability as relating to a measureable impact of the functioning of an individual after a change in health or environment. This change was substantiated when the World Health Organization endorsed the International Classification of Functioning, Disability and Health.33 In light of this shift, we present the disease-specific and general HR-QOL outcomes of young adults who had undergone surgical correction for spinal deformity during adolescence, as well as their associated complications and reoperations, in an attempt to identify targets for improvement.
Our patient-reported outcomes demonstrated a high incidence of occasional back pain, activity-related complaints, and limited ROM. Comparison of our cohort’s SRS-22R outcomes with previously published normative values for the unaffected adolescent population28,34 suggests worse scores for the disease-specific SRS-22R domains of pain and appearance. In 2012, Daubs and colleagues34 reported that normative scores on various SRS-22 domains were statistically lower with age (scores decreased from age 10 to age 19 years). Both Verma and colleagues28 and Daubs and colleagues34 reported lower scores for females than for males. Therefore, it is unclear whether the differences observed in our cohort may be accounted for by the larger proportion of females compared with the normative data.
General health scores on the SF-12 were similar to the population norm (mean [SD]) of 50 (10) referenced by Ware and colleagues.16 These findings suggest that, though pain and appearance may be statistically lower in our cohort—as measured with the SRS-22R—the cohort’s spine-related symptoms do not seem to lower its general health. Eighty-five percent of the patients were working at the time of the survey, further supporting a relatively normal level of overall function. In a retrospective review by Takayama and colleagues,9 similar results were found with regard to working after AIS fusion surgery. Of 32 patients treated surgically for scoliosis, at a mean of 21.1 years after the index fusion 27 (84.4%) were or had been engaged in various occupations without marked difficulty.
Our results in a cohort of patients with segmental instrumentation using hooks are similar to results in other studies of long-term HR-QOL measures in patients with AIS and Harrington rod instrumentation. Danielsson and Nachemson35 evaluated patients with surgically treated AIS with at least 20-year follow-up and reported that, in their surgical cohort with a mean age of 39.7 years, mean SF-36 PCS score was 50.9, and mean SF-36 MCS score was 50.2. In a recent study of patients with AIS and Harrington rod instrumentation, those of a mean age of 32.3 years had a mean score of 50.9 for both SF-36 PCS and SF-36 MCS.36
Regression analysis identified only smoking as a predictor of SRS-22R Total scores. This finding, that smokers have a lower health state, is expected even in the general population.37 Interestingly, bracing before surgery, Lenke type, surgery type, number of levels fused, lowest instrumented vertebra, incidence of perioperative complications, percentage curve correction, postoperative sagittal and coronal balance, and need for revision surgery did not influence HR-QOL measures in this cohort.
Our cohort’s incidence of occasional back pain was 76% (90/118 patients). Other reports have had similar findings. In 2012, Bas and colleagues38 studied self-reported pain in 126 consecutive patients with scoliosis and instrumented fusion. In their cohort, “most participants reported ‘no pain’ (38.5%) or ‘mild pain’ (30.8%) and 72.1% of participants reported a current work/school activity level of 100% normal.” Also in 2012, Rushton and Grevitt39 reported on a review and statistical analysis of the literature on HR-QOL in adolescents with untreated AIS and in unaffected adolescents. Their goal was to identify whether there were any differences in HR-QOL and, if so, whether they were clinically relevant. The authors concluded that pain and self-image tended to be statistically lower among cohorts with AIS but that only self-image was consistently different clinically between untreated patients with AIS and their unaffected peers.
Cosmetic complaints, though less common than functional concerns, affected a substantial percentage of our cohort. Waistline imbalance complaints were more common than rib prominence or scar-related complaints. The validity of patient-reported waistline imbalance is not known but may contribute to the SRS-22R outcomes in this cohort, particularly with regard to appearance scores. Respiratory symptoms, particularly those related to shortness of breath, were reported by 15% of patients. Respiratory symptoms may be in part secondary to underlying lung disease; smoking was reported by 21% of patients and asthma by 9%.
Few additional postoperative treatments were reported by patients. The most common treatment was regular use of NSAIDs (21%), followed by postoperative physical therapy (12%). Opiate medication use and spinal injections were rare—consistent with results reported by Danielsson and Nachemson35 in 2003.
Implant-related complaints, including painful instrumentation (13%) and implant prominence (9%), were some of the most common complaints in our study group. Although not all symptomatic instrumentation required surgical revision, 7 (50%) of the 14 additional spine surgeries were related to painful and/or prominent posterior instrumentation. Additional spine surgery was reported in 11.9% of our patients. Other indications for reoperation were disc herniation, crankshaft phenomenon, nonunion, and adjacent-level degeneration. Our rate of revision surgery is supported by the literature. In 2009, Luhmann and colleagues40 reported that 41 (3.9%) of 1057 primary spine fusions for idiopathic scoliosis required reoperation; the indications included infection (16/1057, 1.5%), pseudarthrosis (12, 1.1%), and painful/prominent implant (7, 0.7%). Richards and colleagues41 similarly reported on 1046 patients who underwent fusion for AIS. Of these patients, 135 underwent 172 repeat surgical interventions (12.9% reoperation rate), with 29 (21.5%) of the 135 undergoing 2 or more separate procedures. The most common reasons for reoperation were infection, symptomatic implant, and pseudarthrosis. The authors concluded that repeat surgeries were relatively common after the initial surgical procedures. Having a clearer understanding of instrumentation-related complaints and reoperations may lead to improvement in this surgeon-controlled variable.
There are limitations to this study. The data regarding clinical courses were collected by retrospective chart review, which has known limitations. To offset this, we collected prospective outcome data with use of the SF-12, the SRS-22R, and a spine-related complaints questionnaire. No control group was available for comparison of outcomes in our cohort. We used the SF-12 and previously published normative values for the SRS-22R for comparison with population norms. Such comparisons have inherent limitations, as the groups vary by sex and mean age; our cohort was primarily female and more than a decade older than the controls.
Only 35% of the patients who met the inclusion criteria had complete data that could be included in our analysis. Although there was no statistically significant difference in demographics between patients with and without follow-up data available, this low response rate could have introduced selection bias. Ideally, patients should have been seen in clinic, standing radiographs should have been taken, and pulmonary function tests should have been performed. However, these patients were asymptomatic, and ethical and insurance issues prevented those actions. Thus, any radiographic changes occurring over the intervening years, from the last clinic visit to completion of the surveys, were not documented. This situation may or may not have limited our findings, as other authors have found low correlation between radiographic outcomes and clinical outcome measures.13,14,19,36 During the period when these surgeries were performed, segmental spine instrumentation with hooks was the standard of care for deformity correction in AIS; therefore, all posterior instrumentations were done with hook-only segmental fixation. Current pedicle screw–based techniques that allow for additional correction of the deformity may provide different outcomes in the future.
We think that, despite the inherent limitations of this study, our data will be useful in the treatment of AIS. Our results suggest that postoperative spinal complaints are common and that, compared with an unaffected adolescent population, patients with AIS score significantly lower on pain and appearance domains of outcomes testing at a mean of 12.7 years after index fusion. Nevertheless, the outcomes do not seem to be of sufficient severity to affect general health and QOL as measured by outcomes testing.
Spinal deformity correction is performed to prevent impaired pulmonary function and spine-related disability later in life.42,43 Thus, longer-term studies, involving patients in their fifth and sixth decades of life, are needed to determine whether patients with AIS will have QOL outcomes, pulmonary function, and spine-related problems similar to those in the general population. In this cohort of young adults, smoking status was the only predictor of HR-QOL measures, and spinal deformity correction did not lead to decreased HR-QOL.
1. Tsutsui S, Pawelek J, Bastrom T, et al. Dissecting the effects of spinal fusion and deformity magnitude on quality of life in patients with adolescent idiopathic scoliosis. Spine. 2009;34(18):E653-E658.
2. Bonnett C, Brown JC, Cross B, Barron R. Posterior spinal fusion with Harrington rod instrumentation in 100 consecutive patients. Contemp Orthop. 1980;2:396-399.
3. Harrington PR, Dixon JR. An eleven year clinical investigation of Harrington instrument. Clin Orthop. 1973;(93):113-130.
4. Mielke CH, Lonstein JE, Denis F, Vandenbrink K, Winter RB. Surgical treatment of adolescent idiopathic scoliosis. A comparative analysis. J Bone Joint Surg Am. 1989;71(8):1170-1177.
5. Moskowitz A, Moe JH, Winter RB, Binner H. Long-term follow-up of scoliosis fusion. J Bone Joint Surg Am. 1980;62(3):529-554.
6. Akazawa T, Minami S, Kotani T, Nemoto T, Koshi T, Takahashi K. Health-related quality of life and low back pain of patients surgically treated for scoliosis after 21 years or more of follow-up: comparison among non-idiopathic scoliosis, idiopathic scoliosis, and healthy subjects. Spine. 2012;37(22):1899-1903.
7. Akazawa T, Minami S, Kotani T, Nemoto T, Koshi T, Takahashi K. Long-term clinical outcomes of surgery for adolescent idiopathic scoliosis 21 to 41 years later. Spine. 2012;37(5):402-405.
8. Pehrsson K, Bake B, Larsson S, Nachemson A. Lung function in adult idiopathic scoliosis: a 20 year follow up. Thorax. 1991;46(7):474-478.
9. Takayama K, Nakamura H, Matsuda H. Quality of life in patients treated surgically for scoliosis: longer than sixteen-year follow-up. Spine. 2009;34(20):2179-2184.
10. Weinstein SL, Dolan LA, Cheng JC, Danielsson A, Morcuende JA. Adolescent idiopathic scoliosis. Lancet. 2008;371(9623):1527-1537.
11. Westrick ER, Ward WT. Adolescent idiopathic scoliosis: 5-year to 20-year evidence-based surgical results. J Pediatr Orthop. 2011;31(1 suppl):S61-S68.
12. Asher MA, Lai SM, Glattes RC, Burton DC, Alanay A, Bago J. Refinement of the SRS-22 health-related quality of life questionnaire Function domain. Spine. 2006;31(5):593-597.
13. Asher M, Min Lai S, Burton D, Manna B. Scoliosis Research Society–22 patient questionnaire: responsiveness to change associated with surgical treatment. Spine. 2003;28(1):70-73.
14. Asher M, Min Lai S, Burton D, Manna B. The reliability and concurrent validity of the Scoliosis Research Society–22 patient questionnaire for idiopathic scoliosis. Spine. 2003;28(1):63-69.
15. Asher M, Min Lai S, Burton D, Manna B. Discrimination validity of the Scoliosis Research Society–22 patient questionnaire: relationship to idiopathic scoliosis curve pattern and curve size. Spine. 2003;28(1):74-78.
16. Ware J Jr, Kosinski M, Keller SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220-233.
17. Alanay A, Cil A, Berk H, et al. Reliability and validity of adapted Turkish version of Scoliosis Research Society–22 (SRS-22) questionnaire. Spine. 2005;30(21):2464-2468.
18. Beauséjour M, Joncas J, Goulet L, et al. Reliability and validity of adapted French Canadian version of Scoliosis Research Society outcomes questionnaire (SRS-22) in Quebec. Spine. 2009;34(6):623-628.
19. Climent JM, Bago J, Ey A, Perez-Grueso FJ, Izquierdo E. Validity of the Spanish version of the Scoliosis Research Society–22 (SRS-22) patient questionnaire. Spine. 2005;30(6):705-709.
20. Glowacki M, Misterska E, Laurentowska M, Mankowski P. Polish adaptation of Scoliosis Research Society–22 questionnaire. Spine. 2009;34(10):1060-1065.
21. Hashimoto H, Sase T, Arai Y, Maruyama T, Isobe K, Shouno Y. Validation of a Japanese version of the Scoliosis Research Society–22 patient questionnaire among idiopathic scoliosis patients in Japan. Spine. 2007;32(4):E141-E146.
22. Li M, Wang CF, Gu SX, et al. Adapted simplified Chinese (mainland) version of Scoliosis Research Society–22 questionnaire. Spine. 2009;34(12):1321-1324.
23. Monticone M, Carabalona R, Negrini S. Reliability of the Scoliosis Research Society–22 patient questionnaire (Italian version) in mild adolescent vertebral deformities. Eura Medicophys. 2004;40(3):191-197.
24. Niemeyer T, Schubert C, Halm HF, Herberts T, Leichtle C, Gesicki M. Validity and reliability of an adapted German version of Scoliosis Research Society–22 questionnaire. Spine. 2009;34(8):818-821.
25. Lai SM, Asher M, Burton D. Estimating SRS-22 quality of life measures with SF-36: application in idiopathic scoliosis. Spine. 2006;31(4):473-478.
26. Glattes RC, Burton DC, Lai SM, Frasier E, Asher MA. The reliability and concurrent validity of the Scoliosis Research Society–22R patient questionnaire compared with the Child Health Questionnaire–CF87 patient questionnaire for adolescent spinal deformity. Spine. 2007;32(16):1778-1784.
27. Blanke KM, Kuklo TR, Lenke LG, et al. Adolescent idiopathic scoliosis. In O’Brien MF, Kuklo TR, Blanke KM, Lenke LG, eds. Spinal Deformity Study Group Radiographic Measurement Manual. Memphis, TN: Medtronic; 2004.
28. Verma K, Lonner B, Hoashi JS, et al. Demographic factors affect Scoliosis Research Society–22 performance in healthy adolescents: a comparative baseline for adolescents with idiopathic scoliosis. Spine. 2010;35(24):2134-2139.
29. Baldus C, Bridwell KH, Harrast J, et al. Age-gender matched comparison of SRS instrument scores between adult deformity and normal adults: are all SRS domains disease specific? Spine. 2008;33(20):2214-2218.
30. Brown CA, Lenke LG, Bridwell KH, Geideman WM, Hasan SA, Blanke K. Complication of pediatric thoracolumbar and lumbar pedicle screws. Spine. 1998;23(14):1566-1571.
31. Coe JD, Arlet V, Donaldson W, et al. Complications in spinal fusion for adolescent idiopathic scoliosis in the new millennium. A report of the Scoliosis Research Society Morbidity and Mortality Committee. Spine. 2006;31(3):345-349.
32. Fu KM, Smith JS, Polly DW, et al. Scoliosis Research Society Morbidity and Mortality Committee. Morbidity and mortality associated with spinal surgery in children: a review of the Scoliosis Research Society morbidity and mortality database. J Neurosurg Pediatr. 2011;7(1):37-41.
33. World Health Organization. International Classification of Functioning, Disability and Health: ICF Short Version. Geneva, Switzerland: World Health Organization; 2001.
34. Daubs M, Lawrence B, Hung M, et al. Scoliosis Research Society–22 results in 3,052 healthy adolescents age ten to 19 years. Abstract presented at: 47th Annual Meeting and Course of the Scoliosis Research Society; September 5-8, 2012; Chicago, IL. Abstract 72.
35. Danielsson AL, Nachemson AL. Back pain and function 23 years after fusion for adolescent idiopathic scoliosis: a case–control study—part II. Spine. 2003;28(18):E373-E383.
36. Götze C, Liljenqvist UR, Slomka A, Götze HG, Steinbeck J. Quality of life and back pain: outcome 16.7 years after Harrington instrumentation. Spine. 2002;27(13):1456-1463.
37. Quercioli C, Messina G, Barbini E, Carriero G, Fanì M, Nante N. Importance of sociodemographic and morbidity aspects in measuring health-related quality of life: performances of three tools: comparison of three questionnaire scores. Eur J Health Econ. 2009;10(4):389-397.
38. Bas T, Franco N, Bas P, Bas JL. Pain and disability following fusion for idiopathic adolescent scoliosis: prevalence and associated factors. Evid Based Spine Care J. 2012;3(2):17-24.
39. Rushton PR, Grevitt MP. Comparison of untreated adolescent idiopathic scoliosis with normal controls: a review and statistical analysis of the literature. Spine. 2013;38(9):778-785.
40. Luhmann SJ, Lenke LG, Bridwell KH, Schootman M. Revision surgery after primary spine fusion for idiopathic scoliosis. Spine. 2009;34(20):2191-2197.
41. Richards BS, Hasley BP, Casey VF. Repeat surgical interventions following “definitive” instrumentation and fusion for idiopathic scoliosis. Spine. 2006;31(26):3018-3026.
42. Bjure J, Grimby G, Kasalický J, Lindh M, Nachemson A. Respiratory impairment and airway closure in patients with untreated idiopathic scoliosis. Thorax. 1970;25(4):451-456.
43. Haefeli M, Elfering A, Kilian R, Min K, Boos N. Nonoperative treatment for adolescent idiopathic scoliosis: a 10- to 60-year follow-up with special reference to health-related quality of life. Spine. 2006;31(3):355-366.
1. Tsutsui S, Pawelek J, Bastrom T, et al. Dissecting the effects of spinal fusion and deformity magnitude on quality of life in patients with adolescent idiopathic scoliosis. Spine. 2009;34(18):E653-E658.
2. Bonnett C, Brown JC, Cross B, Barron R. Posterior spinal fusion with Harrington rod instrumentation in 100 consecutive patients. Contemp Orthop. 1980;2:396-399.
3. Harrington PR, Dixon JR. An eleven year clinical investigation of Harrington instrument. Clin Orthop. 1973;(93):113-130.
4. Mielke CH, Lonstein JE, Denis F, Vandenbrink K, Winter RB. Surgical treatment of adolescent idiopathic scoliosis. A comparative analysis. J Bone Joint Surg Am. 1989;71(8):1170-1177.
5. Moskowitz A, Moe JH, Winter RB, Binner H. Long-term follow-up of scoliosis fusion. J Bone Joint Surg Am. 1980;62(3):529-554.
6. Akazawa T, Minami S, Kotani T, Nemoto T, Koshi T, Takahashi K. Health-related quality of life and low back pain of patients surgically treated for scoliosis after 21 years or more of follow-up: comparison among non-idiopathic scoliosis, idiopathic scoliosis, and healthy subjects. Spine. 2012;37(22):1899-1903.
7. Akazawa T, Minami S, Kotani T, Nemoto T, Koshi T, Takahashi K. Long-term clinical outcomes of surgery for adolescent idiopathic scoliosis 21 to 41 years later. Spine. 2012;37(5):402-405.
8. Pehrsson K, Bake B, Larsson S, Nachemson A. Lung function in adult idiopathic scoliosis: a 20 year follow up. Thorax. 1991;46(7):474-478.
9. Takayama K, Nakamura H, Matsuda H. Quality of life in patients treated surgically for scoliosis: longer than sixteen-year follow-up. Spine. 2009;34(20):2179-2184.
10. Weinstein SL, Dolan LA, Cheng JC, Danielsson A, Morcuende JA. Adolescent idiopathic scoliosis. Lancet. 2008;371(9623):1527-1537.
11. Westrick ER, Ward WT. Adolescent idiopathic scoliosis: 5-year to 20-year evidence-based surgical results. J Pediatr Orthop. 2011;31(1 suppl):S61-S68.
12. Asher MA, Lai SM, Glattes RC, Burton DC, Alanay A, Bago J. Refinement of the SRS-22 health-related quality of life questionnaire Function domain. Spine. 2006;31(5):593-597.
13. Asher M, Min Lai S, Burton D, Manna B. Scoliosis Research Society–22 patient questionnaire: responsiveness to change associated with surgical treatment. Spine. 2003;28(1):70-73.
14. Asher M, Min Lai S, Burton D, Manna B. The reliability and concurrent validity of the Scoliosis Research Society–22 patient questionnaire for idiopathic scoliosis. Spine. 2003;28(1):63-69.
15. Asher M, Min Lai S, Burton D, Manna B. Discrimination validity of the Scoliosis Research Society–22 patient questionnaire: relationship to idiopathic scoliosis curve pattern and curve size. Spine. 2003;28(1):74-78.
16. Ware J Jr, Kosinski M, Keller SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220-233.
17. Alanay A, Cil A, Berk H, et al. Reliability and validity of adapted Turkish version of Scoliosis Research Society–22 (SRS-22) questionnaire. Spine. 2005;30(21):2464-2468.
18. Beauséjour M, Joncas J, Goulet L, et al. Reliability and validity of adapted French Canadian version of Scoliosis Research Society outcomes questionnaire (SRS-22) in Quebec. Spine. 2009;34(6):623-628.
19. Climent JM, Bago J, Ey A, Perez-Grueso FJ, Izquierdo E. Validity of the Spanish version of the Scoliosis Research Society–22 (SRS-22) patient questionnaire. Spine. 2005;30(6):705-709.
20. Glowacki M, Misterska E, Laurentowska M, Mankowski P. Polish adaptation of Scoliosis Research Society–22 questionnaire. Spine. 2009;34(10):1060-1065.
21. Hashimoto H, Sase T, Arai Y, Maruyama T, Isobe K, Shouno Y. Validation of a Japanese version of the Scoliosis Research Society–22 patient questionnaire among idiopathic scoliosis patients in Japan. Spine. 2007;32(4):E141-E146.
22. Li M, Wang CF, Gu SX, et al. Adapted simplified Chinese (mainland) version of Scoliosis Research Society–22 questionnaire. Spine. 2009;34(12):1321-1324.
23. Monticone M, Carabalona R, Negrini S. Reliability of the Scoliosis Research Society–22 patient questionnaire (Italian version) in mild adolescent vertebral deformities. Eura Medicophys. 2004;40(3):191-197.
24. Niemeyer T, Schubert C, Halm HF, Herberts T, Leichtle C, Gesicki M. Validity and reliability of an adapted German version of Scoliosis Research Society–22 questionnaire. Spine. 2009;34(8):818-821.
25. Lai SM, Asher M, Burton D. Estimating SRS-22 quality of life measures with SF-36: application in idiopathic scoliosis. Spine. 2006;31(4):473-478.
26. Glattes RC, Burton DC, Lai SM, Frasier E, Asher MA. The reliability and concurrent validity of the Scoliosis Research Society–22R patient questionnaire compared with the Child Health Questionnaire–CF87 patient questionnaire for adolescent spinal deformity. Spine. 2007;32(16):1778-1784.
27. Blanke KM, Kuklo TR, Lenke LG, et al. Adolescent idiopathic scoliosis. In O’Brien MF, Kuklo TR, Blanke KM, Lenke LG, eds. Spinal Deformity Study Group Radiographic Measurement Manual. Memphis, TN: Medtronic; 2004.
28. Verma K, Lonner B, Hoashi JS, et al. Demographic factors affect Scoliosis Research Society–22 performance in healthy adolescents: a comparative baseline for adolescents with idiopathic scoliosis. Spine. 2010;35(24):2134-2139.
29. Baldus C, Bridwell KH, Harrast J, et al. Age-gender matched comparison of SRS instrument scores between adult deformity and normal adults: are all SRS domains disease specific? Spine. 2008;33(20):2214-2218.
30. Brown CA, Lenke LG, Bridwell KH, Geideman WM, Hasan SA, Blanke K. Complication of pediatric thoracolumbar and lumbar pedicle screws. Spine. 1998;23(14):1566-1571.
31. Coe JD, Arlet V, Donaldson W, et al. Complications in spinal fusion for adolescent idiopathic scoliosis in the new millennium. A report of the Scoliosis Research Society Morbidity and Mortality Committee. Spine. 2006;31(3):345-349.
32. Fu KM, Smith JS, Polly DW, et al. Scoliosis Research Society Morbidity and Mortality Committee. Morbidity and mortality associated with spinal surgery in children: a review of the Scoliosis Research Society morbidity and mortality database. J Neurosurg Pediatr. 2011;7(1):37-41.
33. World Health Organization. International Classification of Functioning, Disability and Health: ICF Short Version. Geneva, Switzerland: World Health Organization; 2001.
34. Daubs M, Lawrence B, Hung M, et al. Scoliosis Research Society–22 results in 3,052 healthy adolescents age ten to 19 years. Abstract presented at: 47th Annual Meeting and Course of the Scoliosis Research Society; September 5-8, 2012; Chicago, IL. Abstract 72.
35. Danielsson AL, Nachemson AL. Back pain and function 23 years after fusion for adolescent idiopathic scoliosis: a case–control study—part II. Spine. 2003;28(18):E373-E383.
36. Götze C, Liljenqvist UR, Slomka A, Götze HG, Steinbeck J. Quality of life and back pain: outcome 16.7 years after Harrington instrumentation. Spine. 2002;27(13):1456-1463.
37. Quercioli C, Messina G, Barbini E, Carriero G, Fanì M, Nante N. Importance of sociodemographic and morbidity aspects in measuring health-related quality of life: performances of three tools: comparison of three questionnaire scores. Eur J Health Econ. 2009;10(4):389-397.
38. Bas T, Franco N, Bas P, Bas JL. Pain and disability following fusion for idiopathic adolescent scoliosis: prevalence and associated factors. Evid Based Spine Care J. 2012;3(2):17-24.
39. Rushton PR, Grevitt MP. Comparison of untreated adolescent idiopathic scoliosis with normal controls: a review and statistical analysis of the literature. Spine. 2013;38(9):778-785.
40. Luhmann SJ, Lenke LG, Bridwell KH, Schootman M. Revision surgery after primary spine fusion for idiopathic scoliosis. Spine. 2009;34(20):2191-2197.
41. Richards BS, Hasley BP, Casey VF. Repeat surgical interventions following “definitive” instrumentation and fusion for idiopathic scoliosis. Spine. 2006;31(26):3018-3026.
42. Bjure J, Grimby G, Kasalický J, Lindh M, Nachemson A. Respiratory impairment and airway closure in patients with untreated idiopathic scoliosis. Thorax. 1970;25(4):451-456.
43. Haefeli M, Elfering A, Kilian R, Min K, Boos N. Nonoperative treatment for adolescent idiopathic scoliosis: a 10- to 60-year follow-up with special reference to health-related quality of life. Spine. 2006;31(3):355-366.
2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society
Recommendations
Each recommendation has been mapped from the NHLBI grading format to the American College of Cardiology/American Heart Association Class of Recommendation/Level of Evidence (ACC/AHA COR/LOE) construct and is expressed in both formats. Because of the inherent differences in grading systems and the clinical questions driving the recommendations, alignment between the NHLBI and ACC/AHA formats is in some cases imperfect. Definitions for the NHLBI strength of recommendation (A-E, N) and quality of evidence (High, Moderate, Low) and the ACC/AHA levels of the evidence (LOE: A-C) and classes of recommendations (COR: I-III) are provided at the end of the "Major Recommendations" field.
Summary of Recommendations for Obesity
Identifying Patients Who Need to Lose Weight (Body Mass Index [BMI] and Waist Circumference)
1a. Measure height and weight and calculate BMI at annual visits or more frequently. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: I; ACC/AHA LOE: C
1b. Use the current cutpoints for overweight (BMI 25.0–29.9 kg/m2) and obesity (BMI ≥30 kg/m2) to identify adults who may be at elevated risk of cardiovascular disease (CVD) and the current cutpoints for obesity (BMI ≥30 kg/m2) to identify adults who may be at elevated risk of mortality from all causes. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: B
1c. Advise overweight and obese adults that the greater the BMI, the greater the risk of CVD, type 2 diabetes, and all-cause mortality. NHLBI Grade: A (Strong) ACC/AHA COR: I; ACC/AHA LOE: B
1d. Measure waist circumference at annual visits or more frequently in overweight and obese adults. Advise adults that the greater the waist circumference, the greater the risk of CVD, type 2 diabetes, and all-cause mortality. The cutpoints currently in common use (from either National Institutes of Health [NIH]/NHLBI or World Health Organization/International Diabetes Federation [WHO/IDF]) may continue to be used to identify patients who may be at increased risk until further evidence becomes available. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B
Matching Treatment Benefits with Risk Profiles (Reduction in Body Weight Effect on Risk Factors for CVD, Events, Morbidity and Mortality)
2. Counsel overweight and obese adults with cardiovascular risk factors (high blood pressure [BP], hyperlipidemia, and hyperglycemia) that lifestyle changes that produce even modest, sustained weight loss of 3% to 5% produce clinically meaningful health benefits, and greater weight losses produce greater benefits NHLBI Grade: A (Strong) ACC/AHA COR: I; ACC/AHA LOE: A.
a. Sustained weight loss of 3% to 5% is likely to result in clinically meaningful reductions in triglycerides, blood glucose, hemoglobin A1c, and the risk of developing type 2 diabetes.
b. Greater amounts of weight loss will reduce BP, improve low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C), and reduce the need for medications to control BP, blood glucose, and lipids as well as further reduce triglycerides and blood glucose.
Diets for Weight Loss (Dietary Strategies for Weight Loss)
3a. Prescribe a diet to achieve reduced calorie intake for obese or overweight individuals who would benefit from weight loss, as part of a comprehensive lifestyle intervention. Any one of the following methods can be used to reduce food and calorie intake: NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
a. Prescribe 1,200–1,500 kcal/d for women and 1,500–1,800 kcal/d for men (kilocalorie levels are usually adjusted for the individual's body weight)
b. Prescribe a 500-kcal/d or 750-kcal/d energy deficit or
c. Prescribe one of the evidence-based diets that restricts certain food types (such as high-carbohydrate foods, low-fiber foods, or high-fat foods) in order to create an energy deficit by reduced food intake.
3b. Prescribe a calorie-restricted diet for obese and overweight individuals who would benefit from weight loss, based on the patient's preferences and health status, and preferably refer to a nutrition professional* for counseling. A variety of dietary approaches can produce weight loss in overweight and obese adults, as presented in critical question (CQ) 3, evidence statement (ES) 2. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
Lifestyle Intervention and Counseling (Comprehensive Lifestyle Intervention)
4a. Advise overweight and obese individuals who would benefit from weight loss to participate for ≥6 months in a comprehensive lifestyle program that assists participants in adhering to a lower-calorie diet and in increasing physical activity through the use of behavioral strategies. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
4b. Prescribe on-site, high-intensity (i.e., ≥14 sessions in 6 mo) comprehensive weight loss interventions provided in individual or group sessions by a trained interventionist.† NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
4c. Electronically-delivered weight loss programs (including by telephone) that include personalized feedback from a trained interventionist† can be prescribed for weight loss but may result in smaller weight loss than face-to-face interventions. NHLBI Grade: B (Moderate); ACC/AHA COR: IIa; ACC/AHA LOE: A
4d. Some commercial-based programs that provide a comprehensive lifestyle intervention can be prescribed as an option for weight loss, provided there is peer-reviewed published evidence of their safety and efficacy. NHLBI Grade: B (Moderate); ACC/AHA COR: IIa; ACC/AHA LOE: A
4e. Use a very-low-calorie diet (defined as <800 kcal/d) only in limited circumstances and only when provided by trained practitioners in a medical care setting where medical monitoring and high-intensity lifestyle intervention can be provided. Medical supervision is required because of the rapid rate of weight loss and potential for health complications. NHLBI Grade: A (Strong); ACC/AHA COR: IIa‡ ACC/AHA LOE: A
4f. Advise overweight and obese individuals who have lost weight to participate long term (≥1 year) in a comprehensive weight loss maintenance program. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
4g. For weight loss maintenance, prescribe face-to-face or telephone-delivered weight loss maintenance programs that provide regular contact (monthly or more frequently) with a trained interventionist† who helps participants engage in high levels of physical activity (i.e., 200–300 min/wk), monitor body weight regularly (i.e., weekly or more frequently), and consume a reduced-calorie diet (needed to maintain lower body weight). NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
Selecting Patients for Bariatric Surgical Treatment for Obesity (Bariatric Surgical Treatment for Obesity)
5a. Advise adults with a BMI ≥40 kg/m2 or BMI ≥35 kg/m2 with obesity-related comorbid conditions who are motivated to lose weight and who have not responded to behavioral treatment with or without pharmacotherapy with sufficient weight loss to achieve targeted health outcome goals that bariatric surgery may be an appropriate option to improve health and offer referral to an experienced bariatric surgeon for consultation and evaluation. NHLBI Grade: A (Strong); ACC/AHA COR: IIa§; ACC/AHA LOE: A
5b. For individuals with a BMI <35 kg/m2, there is insufficient evidence to recommend for or against undergoing bariatric surgical procedures. NHLBI Grade: N (No Recommendation)
5c. Advise patients that choice of a specific bariatric surgical procedure may be affected by patient factors, including age, severity of obesity/BMI, obesity-related comorbid conditions, other operative risk factors, risk of short- and long-term complications, behavioral and psychosocial factors, and patient tolerance for risk, as well as provider factors (surgeon and facility). NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIb; ACC/AHA LOE: C
*Nutrition professional: In the studies that form the evidence base for this recommendation, a registered dietitian usually delivered the dietary guidance; in most cases, the intervention was delivered in university nutrition departments or in hospital medical care settings where access to nutrition professionals was available.
†Trained interventionist: In the studies reviewed, trained interventionists included mostly health professionals (e.g., registered dietitians, psychologists, exercise specialists, health counselors, or professionals in training) who adhered to formal protocols in weight management. In a few cases, lay persons were used as trained interventionists; they received instruction in weight management protocols (designed by health professionals) in programs that have been validated in high-quality trials published in peer-reviewed journals.
‡There is strong evidence that if a provider is going to use a very-low-calorie diet, it should be done with high levels of monitoring by experienced personnel; that does not mean that practitioners should prescribe very-low-calorie diets. Because of concern that an ACC/AHA Class I recommendation would be interpreted to mean that the patients should go on a very-low-calorie diet, it was the consensus of the Expert Panel that this maps more closely to an ACC/AHA Class IIa recommendation.
§There is strong evidence that the benefits of surgery outweigh the risks for some patients. These patients can be offered a referral to discuss surgery as an option. This does not mean that all patients who meet the criteria should have surgery. This decision-making process is quite complex and is best performed by experts. The ACC/AHA criterion for a Class I recommendation states that the treatment/procedure should be performed/administered. This recommendation as stated does not meet the criterion that the treatment should be performed. Thus, the ACC/AHA classification criteria do not directly map to the NHLBI grade assigned by the Expert Panel.
Definitions:
NHLBI Grading of the Strength of Recommendations
| Grade | Strength of Recommendation* |
|---|---|
| A | Strong recommendation There is high certainty based on evidence that the net benefit† is substantial. |
| B | Moderate recommendation There is moderate certainty based on evidence that the net benefit is moderate to substantial, or there is high certainty that the net benefit is moderate. |
| C | Weak recommendation There is at least moderate certainty based on evidence that there is a small net benefit. |
| D | Recommendation against There is at least moderate certainty based on evidence that there is no net benefit or that risks/harms outweigh benefits. |
| E | Expert opinion ("There is insufficient evidence or evidence is unclear or conflicting, but this is what the Work Group recommends.") Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, unclear evidence, or conflicting evidence, but the Work Group thought it was important to provide clinical guidance and make a recommendation. Further research is recommended in this area. |
| N | No recommendation for or against ("There is insufficient evidence or evidence is unclear or conflicting.") Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, unclear evidence, or conflicting evidence, and the Work Group thought no recommendation should be made. Further research is recommended in this area. |
*In most cases, the strength of the recommendation should be closely aligned with the quality of the evidence; however, under some circumstances, there may be valid reasons for making recommendations that are not closely aligned with the quality of the evidence (e.g., strong recommendation when the evidence quality is moderate, such as smoking cessation to reduce cardiovascular disease [CVD] risk or ordering an electrocardiogram [ECG] as part of the initial diagnostic work-up for a patient presenting with possible myocardial infarction [MI]). Those situations should be limited and the rationale explained clearly by the Work Group.
†Net benefit is defined as benefits minus risks/harms of the service/intervention.
NHLBI Quality Rating of the Strength of Evidence
| Type of Evidence | Quality Rating* |
|---|---|
| High |
| Moderate |
| Low |
*In some cases, other evidence, such as large all-or-none case series (e.g., jumping from airplanes or tall structures), can represent high- or moderate-quality evidence. In such cases, the rationale for the evidence rating exception should be explained by the Work Group and clearly justified.
†"Well-designed, well-executed" refers to studies that directly address the question; use adequate randomization, blinding, and allocation concealment; are adequately powered; use intention-to-treat analyses; and have high follow-up rates.
‡Limitations include concerns with the design and execution of a study that result in decreased confidence in the true estimate of the effect. Examples of such limitations include but are not limited to: inadequate randomization, lack of blinding of study participants or outcome assessors, inadequate power, outcomes of interest that are not prespecified for the primary outcomes, low follow-up rates, and findings based on subgroup analyses. Whether the limitations are considered minor or major is based on the number and severity of flaws in design or execution. Rules for determining whether the limitations are considered minor or major and how they will affect rating of the individual studies will be developed collaboratively with the methodology team.
§Nonrandomized controlled studies refer to intervention studies where assignment to intervention and comparison groups is not random (e.g., quasi-experimental study design).
¶Observational studies include prospective and retrospective cohort, case-control, and cross-sectional studies.
Applying Classification of Recommendations and Level of Evidence
| Size of Treatment Effect | |||||||
|---|---|---|---|---|---|---|---|
| CLASS I Benefit >>> Risk Procedure/Treatment SHOULD be performed/ administered | CLASS IIa Benefit >> Risk Additional studies with focused objectives needed IT IS REASONABLE to perform procedure/administer treatment | CLASS IIb Benefit ≥ Risk Additional studies with broad objectives needed; additional registry data would be helpful Procedure/Treatment MAY BE CONSIDERED | CLASS III No Benefit or Class III Harm | ||||
| Procedure/Test | Treatment | ||||||
| COR III: No Benefit | Not helpful | No proven benefit | |||||
| COR III: Harm | Excess cost without benefit or harmful | Harmful to patients | |||||
| Estimate of Certainty (Precision) of Treatment Effect | LEVEL A Multiple populations evaluated* Data derived from multiple randomized clinical trials or meta-analyses |
|
|
|
| ||
| LEVEL B Limited populations evaluated* Data derived from a single randomized trial or nonrandomized studies |
|
|
|
| |||
| LEVEL C Very limited populations evaluated* Only consensus opinion of experts, case studies, or standard of care |
|
|
|
| |||
A recommendation with Level of Evidence B or C does not imply the recommendation is weak. Many important clinical questions addressed in the guidelines do not lend themselves to clinical trials. Even when randomized trials are unavailable, there may be a very clear clinical consensus that a particular test or therapy is useful or effective.
*Data available from clinical trials or registries about the usefulness/efficacy in different subpopulations, such as sex, age, history of diabetes, history of prior myocardial infarction, history of heart failure, and prior aspirin use.
†For comparative-effectiveness recommendations (Class I and IIa; Level of Evidence A and B only), studies that support the use of comparator verbs should involve direct comparisons of the treatments or strategies being evaluated.
Recommendations
Each recommendation has been mapped from the NHLBI grading format to the American College of Cardiology/American Heart Association Class of Recommendation/Level of Evidence (ACC/AHA COR/LOE) construct and is expressed in both formats. Because of the inherent differences in grading systems and the clinical questions driving the recommendations, alignment between the NHLBI and ACC/AHA formats is in some cases imperfect. Definitions for the NHLBI strength of recommendation (A-E, N) and quality of evidence (High, Moderate, Low) and the ACC/AHA levels of the evidence (LOE: A-C) and classes of recommendations (COR: I-III) are provided at the end of the "Major Recommendations" field.
Summary of Recommendations for Obesity
Identifying Patients Who Need to Lose Weight (Body Mass Index [BMI] and Waist Circumference)
1a. Measure height and weight and calculate BMI at annual visits or more frequently. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: I; ACC/AHA LOE: C
1b. Use the current cutpoints for overweight (BMI 25.0–29.9 kg/m2) and obesity (BMI ≥30 kg/m2) to identify adults who may be at elevated risk of cardiovascular disease (CVD) and the current cutpoints for obesity (BMI ≥30 kg/m2) to identify adults who may be at elevated risk of mortality from all causes. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: B
1c. Advise overweight and obese adults that the greater the BMI, the greater the risk of CVD, type 2 diabetes, and all-cause mortality. NHLBI Grade: A (Strong) ACC/AHA COR: I; ACC/AHA LOE: B
1d. Measure waist circumference at annual visits or more frequently in overweight and obese adults. Advise adults that the greater the waist circumference, the greater the risk of CVD, type 2 diabetes, and all-cause mortality. The cutpoints currently in common use (from either National Institutes of Health [NIH]/NHLBI or World Health Organization/International Diabetes Federation [WHO/IDF]) may continue to be used to identify patients who may be at increased risk until further evidence becomes available. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B
Matching Treatment Benefits with Risk Profiles (Reduction in Body Weight Effect on Risk Factors for CVD, Events, Morbidity and Mortality)
2. Counsel overweight and obese adults with cardiovascular risk factors (high blood pressure [BP], hyperlipidemia, and hyperglycemia) that lifestyle changes that produce even modest, sustained weight loss of 3% to 5% produce clinically meaningful health benefits, and greater weight losses produce greater benefits NHLBI Grade: A (Strong) ACC/AHA COR: I; ACC/AHA LOE: A.
a. Sustained weight loss of 3% to 5% is likely to result in clinically meaningful reductions in triglycerides, blood glucose, hemoglobin A1c, and the risk of developing type 2 diabetes.
b. Greater amounts of weight loss will reduce BP, improve low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C), and reduce the need for medications to control BP, blood glucose, and lipids as well as further reduce triglycerides and blood glucose.
Diets for Weight Loss (Dietary Strategies for Weight Loss)
3a. Prescribe a diet to achieve reduced calorie intake for obese or overweight individuals who would benefit from weight loss, as part of a comprehensive lifestyle intervention. Any one of the following methods can be used to reduce food and calorie intake: NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
a. Prescribe 1,200–1,500 kcal/d for women and 1,500–1,800 kcal/d for men (kilocalorie levels are usually adjusted for the individual's body weight)
b. Prescribe a 500-kcal/d or 750-kcal/d energy deficit or
c. Prescribe one of the evidence-based diets that restricts certain food types (such as high-carbohydrate foods, low-fiber foods, or high-fat foods) in order to create an energy deficit by reduced food intake.
3b. Prescribe a calorie-restricted diet for obese and overweight individuals who would benefit from weight loss, based on the patient's preferences and health status, and preferably refer to a nutrition professional* for counseling. A variety of dietary approaches can produce weight loss in overweight and obese adults, as presented in critical question (CQ) 3, evidence statement (ES) 2. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
Lifestyle Intervention and Counseling (Comprehensive Lifestyle Intervention)
4a. Advise overweight and obese individuals who would benefit from weight loss to participate for ≥6 months in a comprehensive lifestyle program that assists participants in adhering to a lower-calorie diet and in increasing physical activity through the use of behavioral strategies. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
4b. Prescribe on-site, high-intensity (i.e., ≥14 sessions in 6 mo) comprehensive weight loss interventions provided in individual or group sessions by a trained interventionist.† NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
4c. Electronically-delivered weight loss programs (including by telephone) that include personalized feedback from a trained interventionist† can be prescribed for weight loss but may result in smaller weight loss than face-to-face interventions. NHLBI Grade: B (Moderate); ACC/AHA COR: IIa; ACC/AHA LOE: A
4d. Some commercial-based programs that provide a comprehensive lifestyle intervention can be prescribed as an option for weight loss, provided there is peer-reviewed published evidence of their safety and efficacy. NHLBI Grade: B (Moderate); ACC/AHA COR: IIa; ACC/AHA LOE: A
4e. Use a very-low-calorie diet (defined as <800 kcal/d) only in limited circumstances and only when provided by trained practitioners in a medical care setting where medical monitoring and high-intensity lifestyle intervention can be provided. Medical supervision is required because of the rapid rate of weight loss and potential for health complications. NHLBI Grade: A (Strong); ACC/AHA COR: IIa‡ ACC/AHA LOE: A
4f. Advise overweight and obese individuals who have lost weight to participate long term (≥1 year) in a comprehensive weight loss maintenance program. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
4g. For weight loss maintenance, prescribe face-to-face or telephone-delivered weight loss maintenance programs that provide regular contact (monthly or more frequently) with a trained interventionist† who helps participants engage in high levels of physical activity (i.e., 200–300 min/wk), monitor body weight regularly (i.e., weekly or more frequently), and consume a reduced-calorie diet (needed to maintain lower body weight). NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
Selecting Patients for Bariatric Surgical Treatment for Obesity (Bariatric Surgical Treatment for Obesity)
5a. Advise adults with a BMI ≥40 kg/m2 or BMI ≥35 kg/m2 with obesity-related comorbid conditions who are motivated to lose weight and who have not responded to behavioral treatment with or without pharmacotherapy with sufficient weight loss to achieve targeted health outcome goals that bariatric surgery may be an appropriate option to improve health and offer referral to an experienced bariatric surgeon for consultation and evaluation. NHLBI Grade: A (Strong); ACC/AHA COR: IIa§; ACC/AHA LOE: A
5b. For individuals with a BMI <35 kg/m2, there is insufficient evidence to recommend for or against undergoing bariatric surgical procedures. NHLBI Grade: N (No Recommendation)
5c. Advise patients that choice of a specific bariatric surgical procedure may be affected by patient factors, including age, severity of obesity/BMI, obesity-related comorbid conditions, other operative risk factors, risk of short- and long-term complications, behavioral and psychosocial factors, and patient tolerance for risk, as well as provider factors (surgeon and facility). NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIb; ACC/AHA LOE: C
*Nutrition professional: In the studies that form the evidence base for this recommendation, a registered dietitian usually delivered the dietary guidance; in most cases, the intervention was delivered in university nutrition departments or in hospital medical care settings where access to nutrition professionals was available.
†Trained interventionist: In the studies reviewed, trained interventionists included mostly health professionals (e.g., registered dietitians, psychologists, exercise specialists, health counselors, or professionals in training) who adhered to formal protocols in weight management. In a few cases, lay persons were used as trained interventionists; they received instruction in weight management protocols (designed by health professionals) in programs that have been validated in high-quality trials published in peer-reviewed journals.
‡There is strong evidence that if a provider is going to use a very-low-calorie diet, it should be done with high levels of monitoring by experienced personnel; that does not mean that practitioners should prescribe very-low-calorie diets. Because of concern that an ACC/AHA Class I recommendation would be interpreted to mean that the patients should go on a very-low-calorie diet, it was the consensus of the Expert Panel that this maps more closely to an ACC/AHA Class IIa recommendation.
§There is strong evidence that the benefits of surgery outweigh the risks for some patients. These patients can be offered a referral to discuss surgery as an option. This does not mean that all patients who meet the criteria should have surgery. This decision-making process is quite complex and is best performed by experts. The ACC/AHA criterion for a Class I recommendation states that the treatment/procedure should be performed/administered. This recommendation as stated does not meet the criterion that the treatment should be performed. Thus, the ACC/AHA classification criteria do not directly map to the NHLBI grade assigned by the Expert Panel.
Definitions:
NHLBI Grading of the Strength of Recommendations
| Grade | Strength of Recommendation* |
|---|---|
| A | Strong recommendation There is high certainty based on evidence that the net benefit† is substantial. |
| B | Moderate recommendation There is moderate certainty based on evidence that the net benefit is moderate to substantial, or there is high certainty that the net benefit is moderate. |
| C | Weak recommendation There is at least moderate certainty based on evidence that there is a small net benefit. |
| D | Recommendation against There is at least moderate certainty based on evidence that there is no net benefit or that risks/harms outweigh benefits. |
| E | Expert opinion ("There is insufficient evidence or evidence is unclear or conflicting, but this is what the Work Group recommends.") Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, unclear evidence, or conflicting evidence, but the Work Group thought it was important to provide clinical guidance and make a recommendation. Further research is recommended in this area. |
| N | No recommendation for or against ("There is insufficient evidence or evidence is unclear or conflicting.") Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, unclear evidence, or conflicting evidence, and the Work Group thought no recommendation should be made. Further research is recommended in this area. |
*In most cases, the strength of the recommendation should be closely aligned with the quality of the evidence; however, under some circumstances, there may be valid reasons for making recommendations that are not closely aligned with the quality of the evidence (e.g., strong recommendation when the evidence quality is moderate, such as smoking cessation to reduce cardiovascular disease [CVD] risk or ordering an electrocardiogram [ECG] as part of the initial diagnostic work-up for a patient presenting with possible myocardial infarction [MI]). Those situations should be limited and the rationale explained clearly by the Work Group.
†Net benefit is defined as benefits minus risks/harms of the service/intervention.
NHLBI Quality Rating of the Strength of Evidence
| Type of Evidence | Quality Rating* |
|---|---|
| High |
| Moderate |
| Low |
*In some cases, other evidence, such as large all-or-none case series (e.g., jumping from airplanes or tall structures), can represent high- or moderate-quality evidence. In such cases, the rationale for the evidence rating exception should be explained by the Work Group and clearly justified.
†"Well-designed, well-executed" refers to studies that directly address the question; use adequate randomization, blinding, and allocation concealment; are adequately powered; use intention-to-treat analyses; and have high follow-up rates.
‡Limitations include concerns with the design and execution of a study that result in decreased confidence in the true estimate of the effect. Examples of such limitations include but are not limited to: inadequate randomization, lack of blinding of study participants or outcome assessors, inadequate power, outcomes of interest that are not prespecified for the primary outcomes, low follow-up rates, and findings based on subgroup analyses. Whether the limitations are considered minor or major is based on the number and severity of flaws in design or execution. Rules for determining whether the limitations are considered minor or major and how they will affect rating of the individual studies will be developed collaboratively with the methodology team.
§Nonrandomized controlled studies refer to intervention studies where assignment to intervention and comparison groups is not random (e.g., quasi-experimental study design).
¶Observational studies include prospective and retrospective cohort, case-control, and cross-sectional studies.
Applying Classification of Recommendations and Level of Evidence
| Size of Treatment Effect | |||||||
|---|---|---|---|---|---|---|---|
| CLASS I Benefit >>> Risk Procedure/Treatment SHOULD be performed/ administered | CLASS IIa Benefit >> Risk Additional studies with focused objectives needed IT IS REASONABLE to perform procedure/administer treatment | CLASS IIb Benefit ≥ Risk Additional studies with broad objectives needed; additional registry data would be helpful Procedure/Treatment MAY BE CONSIDERED | CLASS III No Benefit or Class III Harm | ||||
| Procedure/Test | Treatment | ||||||
| COR III: No Benefit | Not helpful | No proven benefit | |||||
| COR III: Harm | Excess cost without benefit or harmful | Harmful to patients | |||||
| Estimate of Certainty (Precision) of Treatment Effect | LEVEL A Multiple populations evaluated* Data derived from multiple randomized clinical trials or meta-analyses |
|
|
|
| ||
| LEVEL B Limited populations evaluated* Data derived from a single randomized trial or nonrandomized studies |
|
|
|
| |||
| LEVEL C Very limited populations evaluated* Only consensus opinion of experts, case studies, or standard of care |
|
|
|
| |||
A recommendation with Level of Evidence B or C does not imply the recommendation is weak. Many important clinical questions addressed in the guidelines do not lend themselves to clinical trials. Even when randomized trials are unavailable, there may be a very clear clinical consensus that a particular test or therapy is useful or effective.
*Data available from clinical trials or registries about the usefulness/efficacy in different subpopulations, such as sex, age, history of diabetes, history of prior myocardial infarction, history of heart failure, and prior aspirin use.
†For comparative-effectiveness recommendations (Class I and IIa; Level of Evidence A and B only), studies that support the use of comparator verbs should involve direct comparisons of the treatments or strategies being evaluated.
Recommendations
Each recommendation has been mapped from the NHLBI grading format to the American College of Cardiology/American Heart Association Class of Recommendation/Level of Evidence (ACC/AHA COR/LOE) construct and is expressed in both formats. Because of the inherent differences in grading systems and the clinical questions driving the recommendations, alignment between the NHLBI and ACC/AHA formats is in some cases imperfect. Definitions for the NHLBI strength of recommendation (A-E, N) and quality of evidence (High, Moderate, Low) and the ACC/AHA levels of the evidence (LOE: A-C) and classes of recommendations (COR: I-III) are provided at the end of the "Major Recommendations" field.
Summary of Recommendations for Obesity
Identifying Patients Who Need to Lose Weight (Body Mass Index [BMI] and Waist Circumference)
1a. Measure height and weight and calculate BMI at annual visits or more frequently. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: I; ACC/AHA LOE: C
1b. Use the current cutpoints for overweight (BMI 25.0–29.9 kg/m2) and obesity (BMI ≥30 kg/m2) to identify adults who may be at elevated risk of cardiovascular disease (CVD) and the current cutpoints for obesity (BMI ≥30 kg/m2) to identify adults who may be at elevated risk of mortality from all causes. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: B
1c. Advise overweight and obese adults that the greater the BMI, the greater the risk of CVD, type 2 diabetes, and all-cause mortality. NHLBI Grade: A (Strong) ACC/AHA COR: I; ACC/AHA LOE: B
1d. Measure waist circumference at annual visits or more frequently in overweight and obese adults. Advise adults that the greater the waist circumference, the greater the risk of CVD, type 2 diabetes, and all-cause mortality. The cutpoints currently in common use (from either National Institutes of Health [NIH]/NHLBI or World Health Organization/International Diabetes Federation [WHO/IDF]) may continue to be used to identify patients who may be at increased risk until further evidence becomes available. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B
Matching Treatment Benefits with Risk Profiles (Reduction in Body Weight Effect on Risk Factors for CVD, Events, Morbidity and Mortality)
2. Counsel overweight and obese adults with cardiovascular risk factors (high blood pressure [BP], hyperlipidemia, and hyperglycemia) that lifestyle changes that produce even modest, sustained weight loss of 3% to 5% produce clinically meaningful health benefits, and greater weight losses produce greater benefits NHLBI Grade: A (Strong) ACC/AHA COR: I; ACC/AHA LOE: A.
a. Sustained weight loss of 3% to 5% is likely to result in clinically meaningful reductions in triglycerides, blood glucose, hemoglobin A1c, and the risk of developing type 2 diabetes.
b. Greater amounts of weight loss will reduce BP, improve low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C), and reduce the need for medications to control BP, blood glucose, and lipids as well as further reduce triglycerides and blood glucose.
Diets for Weight Loss (Dietary Strategies for Weight Loss)
3a. Prescribe a diet to achieve reduced calorie intake for obese or overweight individuals who would benefit from weight loss, as part of a comprehensive lifestyle intervention. Any one of the following methods can be used to reduce food and calorie intake: NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
a. Prescribe 1,200–1,500 kcal/d for women and 1,500–1,800 kcal/d for men (kilocalorie levels are usually adjusted for the individual's body weight)
b. Prescribe a 500-kcal/d or 750-kcal/d energy deficit or
c. Prescribe one of the evidence-based diets that restricts certain food types (such as high-carbohydrate foods, low-fiber foods, or high-fat foods) in order to create an energy deficit by reduced food intake.
3b. Prescribe a calorie-restricted diet for obese and overweight individuals who would benefit from weight loss, based on the patient's preferences and health status, and preferably refer to a nutrition professional* for counseling. A variety of dietary approaches can produce weight loss in overweight and obese adults, as presented in critical question (CQ) 3, evidence statement (ES) 2. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
Lifestyle Intervention and Counseling (Comprehensive Lifestyle Intervention)
4a. Advise overweight and obese individuals who would benefit from weight loss to participate for ≥6 months in a comprehensive lifestyle program that assists participants in adhering to a lower-calorie diet and in increasing physical activity through the use of behavioral strategies. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
4b. Prescribe on-site, high-intensity (i.e., ≥14 sessions in 6 mo) comprehensive weight loss interventions provided in individual or group sessions by a trained interventionist.† NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
4c. Electronically-delivered weight loss programs (including by telephone) that include personalized feedback from a trained interventionist† can be prescribed for weight loss but may result in smaller weight loss than face-to-face interventions. NHLBI Grade: B (Moderate); ACC/AHA COR: IIa; ACC/AHA LOE: A
4d. Some commercial-based programs that provide a comprehensive lifestyle intervention can be prescribed as an option for weight loss, provided there is peer-reviewed published evidence of their safety and efficacy. NHLBI Grade: B (Moderate); ACC/AHA COR: IIa; ACC/AHA LOE: A
4e. Use a very-low-calorie diet (defined as <800 kcal/d) only in limited circumstances and only when provided by trained practitioners in a medical care setting where medical monitoring and high-intensity lifestyle intervention can be provided. Medical supervision is required because of the rapid rate of weight loss and potential for health complications. NHLBI Grade: A (Strong); ACC/AHA COR: IIa‡ ACC/AHA LOE: A
4f. Advise overweight and obese individuals who have lost weight to participate long term (≥1 year) in a comprehensive weight loss maintenance program. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
4g. For weight loss maintenance, prescribe face-to-face or telephone-delivered weight loss maintenance programs that provide regular contact (monthly or more frequently) with a trained interventionist† who helps participants engage in high levels of physical activity (i.e., 200–300 min/wk), monitor body weight regularly (i.e., weekly or more frequently), and consume a reduced-calorie diet (needed to maintain lower body weight). NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
Selecting Patients for Bariatric Surgical Treatment for Obesity (Bariatric Surgical Treatment for Obesity)
5a. Advise adults with a BMI ≥40 kg/m2 or BMI ≥35 kg/m2 with obesity-related comorbid conditions who are motivated to lose weight and who have not responded to behavioral treatment with or without pharmacotherapy with sufficient weight loss to achieve targeted health outcome goals that bariatric surgery may be an appropriate option to improve health and offer referral to an experienced bariatric surgeon for consultation and evaluation. NHLBI Grade: A (Strong); ACC/AHA COR: IIa§; ACC/AHA LOE: A
5b. For individuals with a BMI <35 kg/m2, there is insufficient evidence to recommend for or against undergoing bariatric surgical procedures. NHLBI Grade: N (No Recommendation)
5c. Advise patients that choice of a specific bariatric surgical procedure may be affected by patient factors, including age, severity of obesity/BMI, obesity-related comorbid conditions, other operative risk factors, risk of short- and long-term complications, behavioral and psychosocial factors, and patient tolerance for risk, as well as provider factors (surgeon and facility). NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIb; ACC/AHA LOE: C
*Nutrition professional: In the studies that form the evidence base for this recommendation, a registered dietitian usually delivered the dietary guidance; in most cases, the intervention was delivered in university nutrition departments or in hospital medical care settings where access to nutrition professionals was available.
†Trained interventionist: In the studies reviewed, trained interventionists included mostly health professionals (e.g., registered dietitians, psychologists, exercise specialists, health counselors, or professionals in training) who adhered to formal protocols in weight management. In a few cases, lay persons were used as trained interventionists; they received instruction in weight management protocols (designed by health professionals) in programs that have been validated in high-quality trials published in peer-reviewed journals.
‡There is strong evidence that if a provider is going to use a very-low-calorie diet, it should be done with high levels of monitoring by experienced personnel; that does not mean that practitioners should prescribe very-low-calorie diets. Because of concern that an ACC/AHA Class I recommendation would be interpreted to mean that the patients should go on a very-low-calorie diet, it was the consensus of the Expert Panel that this maps more closely to an ACC/AHA Class IIa recommendation.
§There is strong evidence that the benefits of surgery outweigh the risks for some patients. These patients can be offered a referral to discuss surgery as an option. This does not mean that all patients who meet the criteria should have surgery. This decision-making process is quite complex and is best performed by experts. The ACC/AHA criterion for a Class I recommendation states that the treatment/procedure should be performed/administered. This recommendation as stated does not meet the criterion that the treatment should be performed. Thus, the ACC/AHA classification criteria do not directly map to the NHLBI grade assigned by the Expert Panel.
Definitions:
NHLBI Grading of the Strength of Recommendations
| Grade | Strength of Recommendation* |
|---|---|
| A | Strong recommendation There is high certainty based on evidence that the net benefit† is substantial. |
| B | Moderate recommendation There is moderate certainty based on evidence that the net benefit is moderate to substantial, or there is high certainty that the net benefit is moderate. |
| C | Weak recommendation There is at least moderate certainty based on evidence that there is a small net benefit. |
| D | Recommendation against There is at least moderate certainty based on evidence that there is no net benefit or that risks/harms outweigh benefits. |
| E | Expert opinion ("There is insufficient evidence or evidence is unclear or conflicting, but this is what the Work Group recommends.") Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, unclear evidence, or conflicting evidence, but the Work Group thought it was important to provide clinical guidance and make a recommendation. Further research is recommended in this area. |
| N | No recommendation for or against ("There is insufficient evidence or evidence is unclear or conflicting.") Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, unclear evidence, or conflicting evidence, and the Work Group thought no recommendation should be made. Further research is recommended in this area. |
*In most cases, the strength of the recommendation should be closely aligned with the quality of the evidence; however, under some circumstances, there may be valid reasons for making recommendations that are not closely aligned with the quality of the evidence (e.g., strong recommendation when the evidence quality is moderate, such as smoking cessation to reduce cardiovascular disease [CVD] risk or ordering an electrocardiogram [ECG] as part of the initial diagnostic work-up for a patient presenting with possible myocardial infarction [MI]). Those situations should be limited and the rationale explained clearly by the Work Group.
†Net benefit is defined as benefits minus risks/harms of the service/intervention.
NHLBI Quality Rating of the Strength of Evidence
| Type of Evidence | Quality Rating* |
|---|---|
| High |
| Moderate |
| Low |
*In some cases, other evidence, such as large all-or-none case series (e.g., jumping from airplanes or tall structures), can represent high- or moderate-quality evidence. In such cases, the rationale for the evidence rating exception should be explained by the Work Group and clearly justified.
†"Well-designed, well-executed" refers to studies that directly address the question; use adequate randomization, blinding, and allocation concealment; are adequately powered; use intention-to-treat analyses; and have high follow-up rates.
‡Limitations include concerns with the design and execution of a study that result in decreased confidence in the true estimate of the effect. Examples of such limitations include but are not limited to: inadequate randomization, lack of blinding of study participants or outcome assessors, inadequate power, outcomes of interest that are not prespecified for the primary outcomes, low follow-up rates, and findings based on subgroup analyses. Whether the limitations are considered minor or major is based on the number and severity of flaws in design or execution. Rules for determining whether the limitations are considered minor or major and how they will affect rating of the individual studies will be developed collaboratively with the methodology team.
§Nonrandomized controlled studies refer to intervention studies where assignment to intervention and comparison groups is not random (e.g., quasi-experimental study design).
¶Observational studies include prospective and retrospective cohort, case-control, and cross-sectional studies.
Applying Classification of Recommendations and Level of Evidence
| Size of Treatment Effect | |||||||
|---|---|---|---|---|---|---|---|
| CLASS I Benefit >>> Risk Procedure/Treatment SHOULD be performed/ administered | CLASS IIa Benefit >> Risk Additional studies with focused objectives needed IT IS REASONABLE to perform procedure/administer treatment | CLASS IIb Benefit ≥ Risk Additional studies with broad objectives needed; additional registry data would be helpful Procedure/Treatment MAY BE CONSIDERED | CLASS III No Benefit or Class III Harm | ||||
| Procedure/Test | Treatment | ||||||
| COR III: No Benefit | Not helpful | No proven benefit | |||||
| COR III: Harm | Excess cost without benefit or harmful | Harmful to patients | |||||
| Estimate of Certainty (Precision) of Treatment Effect | LEVEL A Multiple populations evaluated* Data derived from multiple randomized clinical trials or meta-analyses |
|
|
|
| ||
| LEVEL B Limited populations evaluated* Data derived from a single randomized trial or nonrandomized studies |
|
|
|
| |||
| LEVEL C Very limited populations evaluated* Only consensus opinion of experts, case studies, or standard of care |
|
|
|
| |||
A recommendation with Level of Evidence B or C does not imply the recommendation is weak. Many important clinical questions addressed in the guidelines do not lend themselves to clinical trials. Even when randomized trials are unavailable, there may be a very clear clinical consensus that a particular test or therapy is useful or effective.
*Data available from clinical trials or registries about the usefulness/efficacy in different subpopulations, such as sex, age, history of diabetes, history of prior myocardial infarction, history of heart failure, and prior aspirin use.
†For comparative-effectiveness recommendations (Class I and IIa; Level of Evidence A and B only), studies that support the use of comparator verbs should involve direct comparisons of the treatments or strategies being evaluated.
OBJECTIVE: To develop clinical practice guidelines for management of overweight and obesity in adults.
Guidelines are copyright © 2014 American College of Cardiology/American Heart Association/Obesity Society. All rights reserved. The summary is provided by the Agency for Healthcare Research and Quality.
2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines
Recommendations
Each recommendation has been mapped from the NHLBI grading format to the American College of Cardiology/American Heart Association Class of Recommendation/Level of Evidence (ACC/AHA COR/LOE) construct and is expressed in both formats. Because of the inherent differences in grading systems and the clinical questions driving the recommendations, alignment between the NHLBI and ACC/AHA formats is in some cases imperfect. Definitions for the NHLBI strength of recommendation (A-E, N) and quality of evidence (High, Moderate, Low) and the ACC/AHA levels of the evidence (LOE: A-C) and classes of recommendations (COR: I-III) are provided at the end of the "Major Recommendations" field.
Summary of Recommendations for Lifestyle Management
Diet
Low-density lipoprotein cholesterol (LDL-C): Advise adults who would benefit from LDL-C lowering* to:
- Consume a dietary pattern that emphasizes intake of vegetables, fruits, and whole grains; includes low-fat dairy products, poultry, fish, legumes, nontropical vegetable oils, and nuts; and limits intake of sweets, sugar-sweetened beverages, and red meats. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
- Adapt this dietary pattern to appropriate calorie requirements, personal and cultural food preferences, and nutrition therapy for other medical conditions (including diabetes).
- Achieve this pattern by following plans such as the Dietary Approaches to Stop Hypertension (DASH) dietary pattern, the U.S. Department of Agriculture (USDA) Food Pattern, or the AHA Diet.
- Aim for a dietary pattern that achieves 5% to 6% of calories from saturated fat. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
- Reduce percent of calories from saturated fat. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
- Reduce percent of calories from trans fat. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
Blood pressure (BP): Advise adults who would benefit from BP lowering to:
- Consume a dietary pattern that emphasizes intake of vegetables, fruits, and whole grains; includes low-fat dairy products, poultry, fish, legumes, nontropical vegetable oils, and nuts; and limits intake of sweets, sugar-sweetened beverages, and red meats. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
- Adapt this dietary pattern to appropriate calorie requirements, personal and cultural food preferences, and nutrition therapy for other medical conditions (including diabetes).
- Achieve this pattern by following plans such as the DASH dietary pattern, the USDA Food Pattern, or the AHA Diet.
- Lower sodium intake. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
- a. Consume no more than 2,400 mg of sodium/d; b. Further reduction of sodium intake to 1,500 mg/d can result in even greater reduction in BP; and c. Even without achieving these goals, reducing sodium intake by at least 1,000 mg/d lowers BP. NHLBI Grade: B (Moderate); ACC/AHA COR: IIa; ACC/AHA LOE: B
- Combine the DASH dietary pattern with lower sodium intake. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
Physical Activity
Lipids
- In general, advise adults to engage in aerobic physical activity to reduce LDL-C and non-high-density lipoprotein cholesterol (non–HDL-C): 3–4 sessions per week, lasting on average 40 minutes per session, and involving moderate- to vigorous-intensity physical activity. NHLBI Grade: B (Moderate); ACC/AHA COR: IIa; ACC/AHA LOE: A
BP
- In general, advise adults to engage in aerobic physical activity to lower BP: 3 to 4 sessions per week, lasting on average 40 minutes per session, and involving moderate- to vigorous-intensity physical activity. NHLBI Grade: B (Moderate); ACC/AHA COR: IIa; ACC/AHA LOE: A
*Refer to the NGC summary 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines.
See Tables 7-10, 13, 15, and 16 in the original guideline document for additional diet and physical activity guidelines and resources.
Definitions:
NHLBI Grading of the Strength of Recommendations
| Grade | Strength of Recommendation* |
|---|---|
| A | Strong recommendation There is high certainty based on evidence that the net benefit† is substantial. |
| B | Moderate recommendation There is moderate certainty based on evidence that the net benefit is moderate to substantial, or there is high certainty that the net benefit is moderate. |
| C | Weak recommendation There is at least moderate certainty based on evidence that there is a small net benefit. |
| D | Recommendation against There is at least moderate certainty based on evidence that there is no net benefit or that risks/harms outweigh benefits. |
| E | Expert opinion ("There is insufficient evidence or evidence is unclear or conflicting, but this is what the Work Group recommends.") Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, unclear evidence, or conflicting evidence, but the Work Group thought it was important to provide clinical guidance and make a recommendation. Further research is recommended in this area. |
| N | No recommendation for or against ("There is insufficient evidence or evidence is unclear or conflicting.") Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, unclear evidence, or conflicting evidence, and the Work Group thought no recommendation should be made. Further research is recommended in this area. |
*In most cases, the strength of the recommendation should be closely aligned with the quality of the evidence; however, under some circumstances, there may be valid reasons for making recommendations that are not closely aligned with the quality of the evidence (e.g., strong recommendation when the evidence quality is moderate, such as smoking cessation to reduce cardiovascular disease [CVD] risk or ordering an electrocardiogram [ECG] as part of the initial diagnostic work-up for a patient presenting with possible myocardial infarction [MI]). Those situations should be limited and the rationale explained clearly by the Work Group.
†Net benefit is defined as benefits minus risks/harms of the service/intervention.
NHLBI Quality Rating of the Strength of Evidence
| Type of Evidence | Quality Rating* |
|---|---|
| High |
| Moderate |
| Low |
*In some cases, other evidence, such as large all-or-none case series (e.g., jumping from airplanes or tall structures), can represent high- or moderate-quality evidence. In such cases, the rationale for the evidence rating exception should be explained by the Work Group and clearly justified.
†"Well-designed, well-executed" refers to studies that directly address the question; use adequate randomization, blinding, and allocation concealment; are adequately powered; use intention-to-treat analyses; and have high follow-up rates.
‡Limitations include concerns with the design and execution of a study that result in decreased confidence in the true estimate of the effect. Examples of such limitations include but are not limited to: inadequate randomization, lack of blinding of study participants or outcome assessors, inadequate power, outcomes of interest that are not prespecified for the primary outcomes, low follow-up rates, and findings based on subgroup analyses. Whether the limitations are considered minor or major is based on the number and severity of flaws in design or execution. Rules for determining whether the limitations are considered minor or major and how they will affect rating of the individual studies will be developed collaboratively with the methodology team.
§Nonrandomized controlled studies refer to intervention studies where assignment to intervention and comparison groups is not random (e.g., quasi-experimental study design).
¶Observational studies include prospective and retrospective cohort, case-control, and cross-sectional studies.
Applying Classification of Recommendations and Level of Evidence
| Size of Treatment Effect | |||||||
|---|---|---|---|---|---|---|---|
| CLASS I Benefit >>> Risk Procedure/Treatment SHOULD be performed/ administered | CLASS IIa Benefit >> Risk Additional studies with focused objectives needed IT IS REASONABLE to perform procedure/administer treatment | CLASS IIb Benefit ≥ Risk Additional studies with broad objectives needed; additional registry data would be helpful Procedure/Treatment MAY BE CONSIDERED | CLASS III No Benefit or Class III Harm | ||||
| Procedure/Test | Treatment | ||||||
| COR III: No Benefit | Not helpful | No proven benefit | |||||
| COR III: Harm | Excess cost without benefit or harmful | Harmful to patients | |||||
| Estimate of Certainty (Precision) of Treatment Effect | LEVEL A Multiple populations evaluated* Data derived from multiple randomized clinical trials or meta-analyses |
|
|
|
| ||
| LEVEL B Limited populations evaluated* Data derived from a single randomized trial or nonrandomized studies |
|
|
|
| |||
| LEVEL C Very limited populations evaluated* Only consensus opinion of experts, case studies, or standard of care |
|
|
|
| |||
A recommendation with Level of Evidence B or C does not imply the recommendation is weak. Many important clinical questions addressed in the guidelines do not lend themselves to clinical trials. Even when randomized trials are unavailable, there may be a very clear clinical consensus that a particular test or therapy is useful or effective.
*Data available from clinical trials or registries about the usefulness/efficacy in different subpopulations, such as sex, age, history of diabetes, history of prior myocardial infarction, history of heart failure, and prior aspirin use.
†For comparative-effectiveness recommendations (Class I and IIa; Level of Evidence A and B only), studies that support the use of comparator verbs should involve direct comparisons of the treatments or strategies being evaluated.
Recommendations
Each recommendation has been mapped from the NHLBI grading format to the American College of Cardiology/American Heart Association Class of Recommendation/Level of Evidence (ACC/AHA COR/LOE) construct and is expressed in both formats. Because of the inherent differences in grading systems and the clinical questions driving the recommendations, alignment between the NHLBI and ACC/AHA formats is in some cases imperfect. Definitions for the NHLBI strength of recommendation (A-E, N) and quality of evidence (High, Moderate, Low) and the ACC/AHA levels of the evidence (LOE: A-C) and classes of recommendations (COR: I-III) are provided at the end of the "Major Recommendations" field.
Summary of Recommendations for Lifestyle Management
Diet
Low-density lipoprotein cholesterol (LDL-C): Advise adults who would benefit from LDL-C lowering* to:
- Consume a dietary pattern that emphasizes intake of vegetables, fruits, and whole grains; includes low-fat dairy products, poultry, fish, legumes, nontropical vegetable oils, and nuts; and limits intake of sweets, sugar-sweetened beverages, and red meats. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
- Adapt this dietary pattern to appropriate calorie requirements, personal and cultural food preferences, and nutrition therapy for other medical conditions (including diabetes).
- Achieve this pattern by following plans such as the Dietary Approaches to Stop Hypertension (DASH) dietary pattern, the U.S. Department of Agriculture (USDA) Food Pattern, or the AHA Diet.
- Aim for a dietary pattern that achieves 5% to 6% of calories from saturated fat. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
- Reduce percent of calories from saturated fat. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
- Reduce percent of calories from trans fat. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
Blood pressure (BP): Advise adults who would benefit from BP lowering to:
- Consume a dietary pattern that emphasizes intake of vegetables, fruits, and whole grains; includes low-fat dairy products, poultry, fish, legumes, nontropical vegetable oils, and nuts; and limits intake of sweets, sugar-sweetened beverages, and red meats. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
- Adapt this dietary pattern to appropriate calorie requirements, personal and cultural food preferences, and nutrition therapy for other medical conditions (including diabetes).
- Achieve this pattern by following plans such as the DASH dietary pattern, the USDA Food Pattern, or the AHA Diet.
- Lower sodium intake. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
- a. Consume no more than 2,400 mg of sodium/d; b. Further reduction of sodium intake to 1,500 mg/d can result in even greater reduction in BP; and c. Even without achieving these goals, reducing sodium intake by at least 1,000 mg/d lowers BP. NHLBI Grade: B (Moderate); ACC/AHA COR: IIa; ACC/AHA LOE: B
- Combine the DASH dietary pattern with lower sodium intake. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
Physical Activity
Lipids
- In general, advise adults to engage in aerobic physical activity to reduce LDL-C and non-high-density lipoprotein cholesterol (non–HDL-C): 3–4 sessions per week, lasting on average 40 minutes per session, and involving moderate- to vigorous-intensity physical activity. NHLBI Grade: B (Moderate); ACC/AHA COR: IIa; ACC/AHA LOE: A
BP
- In general, advise adults to engage in aerobic physical activity to lower BP: 3 to 4 sessions per week, lasting on average 40 minutes per session, and involving moderate- to vigorous-intensity physical activity. NHLBI Grade: B (Moderate); ACC/AHA COR: IIa; ACC/AHA LOE: A
*Refer to the NGC summary 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines.
See Tables 7-10, 13, 15, and 16 in the original guideline document for additional diet and physical activity guidelines and resources.
Definitions:
NHLBI Grading of the Strength of Recommendations
| Grade | Strength of Recommendation* |
|---|---|
| A | Strong recommendation There is high certainty based on evidence that the net benefit† is substantial. |
| B | Moderate recommendation There is moderate certainty based on evidence that the net benefit is moderate to substantial, or there is high certainty that the net benefit is moderate. |
| C | Weak recommendation There is at least moderate certainty based on evidence that there is a small net benefit. |
| D | Recommendation against There is at least moderate certainty based on evidence that there is no net benefit or that risks/harms outweigh benefits. |
| E | Expert opinion ("There is insufficient evidence or evidence is unclear or conflicting, but this is what the Work Group recommends.") Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, unclear evidence, or conflicting evidence, but the Work Group thought it was important to provide clinical guidance and make a recommendation. Further research is recommended in this area. |
| N | No recommendation for or against ("There is insufficient evidence or evidence is unclear or conflicting.") Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, unclear evidence, or conflicting evidence, and the Work Group thought no recommendation should be made. Further research is recommended in this area. |
*In most cases, the strength of the recommendation should be closely aligned with the quality of the evidence; however, under some circumstances, there may be valid reasons for making recommendations that are not closely aligned with the quality of the evidence (e.g., strong recommendation when the evidence quality is moderate, such as smoking cessation to reduce cardiovascular disease [CVD] risk or ordering an electrocardiogram [ECG] as part of the initial diagnostic work-up for a patient presenting with possible myocardial infarction [MI]). Those situations should be limited and the rationale explained clearly by the Work Group.
†Net benefit is defined as benefits minus risks/harms of the service/intervention.
NHLBI Quality Rating of the Strength of Evidence
| Type of Evidence | Quality Rating* |
|---|---|
| High |
| Moderate |
| Low |
*In some cases, other evidence, such as large all-or-none case series (e.g., jumping from airplanes or tall structures), can represent high- or moderate-quality evidence. In such cases, the rationale for the evidence rating exception should be explained by the Work Group and clearly justified.
†"Well-designed, well-executed" refers to studies that directly address the question; use adequate randomization, blinding, and allocation concealment; are adequately powered; use intention-to-treat analyses; and have high follow-up rates.
‡Limitations include concerns with the design and execution of a study that result in decreased confidence in the true estimate of the effect. Examples of such limitations include but are not limited to: inadequate randomization, lack of blinding of study participants or outcome assessors, inadequate power, outcomes of interest that are not prespecified for the primary outcomes, low follow-up rates, and findings based on subgroup analyses. Whether the limitations are considered minor or major is based on the number and severity of flaws in design or execution. Rules for determining whether the limitations are considered minor or major and how they will affect rating of the individual studies will be developed collaboratively with the methodology team.
§Nonrandomized controlled studies refer to intervention studies where assignment to intervention and comparison groups is not random (e.g., quasi-experimental study design).
¶Observational studies include prospective and retrospective cohort, case-control, and cross-sectional studies.
Applying Classification of Recommendations and Level of Evidence
| Size of Treatment Effect | |||||||
|---|---|---|---|---|---|---|---|
| CLASS I Benefit >>> Risk Procedure/Treatment SHOULD be performed/ administered | CLASS IIa Benefit >> Risk Additional studies with focused objectives needed IT IS REASONABLE to perform procedure/administer treatment | CLASS IIb Benefit ≥ Risk Additional studies with broad objectives needed; additional registry data would be helpful Procedure/Treatment MAY BE CONSIDERED | CLASS III No Benefit or Class III Harm | ||||
| Procedure/Test | Treatment | ||||||
| COR III: No Benefit | Not helpful | No proven benefit | |||||
| COR III: Harm | Excess cost without benefit or harmful | Harmful to patients | |||||
| Estimate of Certainty (Precision) of Treatment Effect | LEVEL A Multiple populations evaluated* Data derived from multiple randomized clinical trials or meta-analyses |
|
|
|
| ||
| LEVEL B Limited populations evaluated* Data derived from a single randomized trial or nonrandomized studies |
|
|
|
| |||
| LEVEL C Very limited populations evaluated* Only consensus opinion of experts, case studies, or standard of care |
|
|
|
| |||
A recommendation with Level of Evidence B or C does not imply the recommendation is weak. Many important clinical questions addressed in the guidelines do not lend themselves to clinical trials. Even when randomized trials are unavailable, there may be a very clear clinical consensus that a particular test or therapy is useful or effective.
*Data available from clinical trials or registries about the usefulness/efficacy in different subpopulations, such as sex, age, history of diabetes, history of prior myocardial infarction, history of heart failure, and prior aspirin use.
†For comparative-effectiveness recommendations (Class I and IIa; Level of Evidence A and B only), studies that support the use of comparator verbs should involve direct comparisons of the treatments or strategies being evaluated.
Recommendations
Each recommendation has been mapped from the NHLBI grading format to the American College of Cardiology/American Heart Association Class of Recommendation/Level of Evidence (ACC/AHA COR/LOE) construct and is expressed in both formats. Because of the inherent differences in grading systems and the clinical questions driving the recommendations, alignment between the NHLBI and ACC/AHA formats is in some cases imperfect. Definitions for the NHLBI strength of recommendation (A-E, N) and quality of evidence (High, Moderate, Low) and the ACC/AHA levels of the evidence (LOE: A-C) and classes of recommendations (COR: I-III) are provided at the end of the "Major Recommendations" field.
Summary of Recommendations for Lifestyle Management
Diet
Low-density lipoprotein cholesterol (LDL-C): Advise adults who would benefit from LDL-C lowering* to:
- Consume a dietary pattern that emphasizes intake of vegetables, fruits, and whole grains; includes low-fat dairy products, poultry, fish, legumes, nontropical vegetable oils, and nuts; and limits intake of sweets, sugar-sweetened beverages, and red meats. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
- Adapt this dietary pattern to appropriate calorie requirements, personal and cultural food preferences, and nutrition therapy for other medical conditions (including diabetes).
- Achieve this pattern by following plans such as the Dietary Approaches to Stop Hypertension (DASH) dietary pattern, the U.S. Department of Agriculture (USDA) Food Pattern, or the AHA Diet.
- Aim for a dietary pattern that achieves 5% to 6% of calories from saturated fat. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
- Reduce percent of calories from saturated fat. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
- Reduce percent of calories from trans fat. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
Blood pressure (BP): Advise adults who would benefit from BP lowering to:
- Consume a dietary pattern that emphasizes intake of vegetables, fruits, and whole grains; includes low-fat dairy products, poultry, fish, legumes, nontropical vegetable oils, and nuts; and limits intake of sweets, sugar-sweetened beverages, and red meats. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
- Adapt this dietary pattern to appropriate calorie requirements, personal and cultural food preferences, and nutrition therapy for other medical conditions (including diabetes).
- Achieve this pattern by following plans such as the DASH dietary pattern, the USDA Food Pattern, or the AHA Diet.
- Lower sodium intake. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
- a. Consume no more than 2,400 mg of sodium/d; b. Further reduction of sodium intake to 1,500 mg/d can result in even greater reduction in BP; and c. Even without achieving these goals, reducing sodium intake by at least 1,000 mg/d lowers BP. NHLBI Grade: B (Moderate); ACC/AHA COR: IIa; ACC/AHA LOE: B
- Combine the DASH dietary pattern with lower sodium intake. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
Physical Activity
Lipids
- In general, advise adults to engage in aerobic physical activity to reduce LDL-C and non-high-density lipoprotein cholesterol (non–HDL-C): 3–4 sessions per week, lasting on average 40 minutes per session, and involving moderate- to vigorous-intensity physical activity. NHLBI Grade: B (Moderate); ACC/AHA COR: IIa; ACC/AHA LOE: A
BP
- In general, advise adults to engage in aerobic physical activity to lower BP: 3 to 4 sessions per week, lasting on average 40 minutes per session, and involving moderate- to vigorous-intensity physical activity. NHLBI Grade: B (Moderate); ACC/AHA COR: IIa; ACC/AHA LOE: A
*Refer to the NGC summary 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines.
See Tables 7-10, 13, 15, and 16 in the original guideline document for additional diet and physical activity guidelines and resources.
Definitions:
NHLBI Grading of the Strength of Recommendations
| Grade | Strength of Recommendation* |
|---|---|
| A | Strong recommendation There is high certainty based on evidence that the net benefit† is substantial. |
| B | Moderate recommendation There is moderate certainty based on evidence that the net benefit is moderate to substantial, or there is high certainty that the net benefit is moderate. |
| C | Weak recommendation There is at least moderate certainty based on evidence that there is a small net benefit. |
| D | Recommendation against There is at least moderate certainty based on evidence that there is no net benefit or that risks/harms outweigh benefits. |
| E | Expert opinion ("There is insufficient evidence or evidence is unclear or conflicting, but this is what the Work Group recommends.") Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, unclear evidence, or conflicting evidence, but the Work Group thought it was important to provide clinical guidance and make a recommendation. Further research is recommended in this area. |
| N | No recommendation for or against ("There is insufficient evidence or evidence is unclear or conflicting.") Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, unclear evidence, or conflicting evidence, and the Work Group thought no recommendation should be made. Further research is recommended in this area. |
*In most cases, the strength of the recommendation should be closely aligned with the quality of the evidence; however, under some circumstances, there may be valid reasons for making recommendations that are not closely aligned with the quality of the evidence (e.g., strong recommendation when the evidence quality is moderate, such as smoking cessation to reduce cardiovascular disease [CVD] risk or ordering an electrocardiogram [ECG] as part of the initial diagnostic work-up for a patient presenting with possible myocardial infarction [MI]). Those situations should be limited and the rationale explained clearly by the Work Group.
†Net benefit is defined as benefits minus risks/harms of the service/intervention.
NHLBI Quality Rating of the Strength of Evidence
| Type of Evidence | Quality Rating* |
|---|---|
| High |
| Moderate |
| Low |
*In some cases, other evidence, such as large all-or-none case series (e.g., jumping from airplanes or tall structures), can represent high- or moderate-quality evidence. In such cases, the rationale for the evidence rating exception should be explained by the Work Group and clearly justified.
†"Well-designed, well-executed" refers to studies that directly address the question; use adequate randomization, blinding, and allocation concealment; are adequately powered; use intention-to-treat analyses; and have high follow-up rates.
‡Limitations include concerns with the design and execution of a study that result in decreased confidence in the true estimate of the effect. Examples of such limitations include but are not limited to: inadequate randomization, lack of blinding of study participants or outcome assessors, inadequate power, outcomes of interest that are not prespecified for the primary outcomes, low follow-up rates, and findings based on subgroup analyses. Whether the limitations are considered minor or major is based on the number and severity of flaws in design or execution. Rules for determining whether the limitations are considered minor or major and how they will affect rating of the individual studies will be developed collaboratively with the methodology team.
§Nonrandomized controlled studies refer to intervention studies where assignment to intervention and comparison groups is not random (e.g., quasi-experimental study design).
¶Observational studies include prospective and retrospective cohort, case-control, and cross-sectional studies.
Applying Classification of Recommendations and Level of Evidence
| Size of Treatment Effect | |||||||
|---|---|---|---|---|---|---|---|
| CLASS I Benefit >>> Risk Procedure/Treatment SHOULD be performed/ administered | CLASS IIa Benefit >> Risk Additional studies with focused objectives needed IT IS REASONABLE to perform procedure/administer treatment | CLASS IIb Benefit ≥ Risk Additional studies with broad objectives needed; additional registry data would be helpful Procedure/Treatment MAY BE CONSIDERED | CLASS III No Benefit or Class III Harm | ||||
| Procedure/Test | Treatment | ||||||
| COR III: No Benefit | Not helpful | No proven benefit | |||||
| COR III: Harm | Excess cost without benefit or harmful | Harmful to patients | |||||
| Estimate of Certainty (Precision) of Treatment Effect | LEVEL A Multiple populations evaluated* Data derived from multiple randomized clinical trials or meta-analyses |
|
|
|
| ||
| LEVEL B Limited populations evaluated* Data derived from a single randomized trial or nonrandomized studies |
|
|
|
| |||
| LEVEL C Very limited populations evaluated* Only consensus opinion of experts, case studies, or standard of care |
|
|
|
| |||
A recommendation with Level of Evidence B or C does not imply the recommendation is weak. Many important clinical questions addressed in the guidelines do not lend themselves to clinical trials. Even when randomized trials are unavailable, there may be a very clear clinical consensus that a particular test or therapy is useful or effective.
*Data available from clinical trials or registries about the usefulness/efficacy in different subpopulations, such as sex, age, history of diabetes, history of prior myocardial infarction, history of heart failure, and prior aspirin use.
†For comparative-effectiveness recommendations (Class I and IIa; Level of Evidence A and B only), studies that support the use of comparator verbs should involve direct comparisons of the treatments or strategies being evaluated.
OBJECTIVE: To evaluate evidence that particular dietary patterns, nutrient intake, and levels and types of physical activity can play a major role in cardiovascular disease (CVD) prevention and treatment through effects on modifiable CVD risk factors (i.e., blood pressure [BP] and lipids).
Guidelines are copyright © 2014 American College of Cardiology/American Heart Association. All rights reserved. The summary is provided by the Agency for Healthcare Research and Quality.
2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines.
Recommendations
Each recommendation has been mapped from the NHLBI grading format to the American College of Cardiology/American Heart Association Class of Recommendation/Level of Evidence (ACC/AHA COR/LOE) construct and is expressed in both formats. Because of the inherent differences in grading systems and the clinical questions driving the recommendations, alignment between the NHLBI and ACC/AHA formats is in some cases imperfect. Definitions for the NHLBI strength of recommendation (A-E, N) and quality of evidence (High, Moderate, Low) and the ACC/AHA levels of the evidence (LOE: A-C) and classes of recommendations (COR: I-III) are provided at the end of the "Major Recommendations" field.
What's New in the Guideline?
Focus on Atherosclerotic Cardiovascular Disease (ASCVD Risk) Reduction: 4 Statin Benefit Groups
1. This guideline is based on a comprehensive set of data from randomized control trials (RCTs) from which 4 statin benefit groups were identified that focus efforts to reduce ASCVD events in secondary and primary prevention.
2. This guideline identifies high-intensity and moderate-intensity statin therapy for use in secondary and primary prevention.
A New Perspective on Low-density Lipoprotein Cholesterol (LDL-C) and/or Non–High-density Lipoprotein Cholesterol (HDL-C) Treatment Goals
1. The Expert Panel was unable to find RCT evidence to support continued use of specific LDL-C or non–HDL-C treatment targets.
2. The appropriate intensity of statin therapy should be used to reduce ASCVD risk in those most likely to benefit.
3. Nonstatin therapies, as compared with statin therapy, do not provide acceptable ASCVD risk-reduction benefits relative to their potential for adverse effects in the routine prevention of ASCVD.
Global Risk Assessment for Primary Prevention
1. This guideline recommends use of the new Pooled Cohort Equations to estimate 10-year ASCVD risk in both white and black men and women.
2. By more accurately identifying higher-risk individuals for statin therapy, the guideline focuses statin therapy on those most likely to benefit.
3. It also indicates, on the basis of RCT data, those high-risk groups that might not benefit.
4. This guideline recommends a discussion between clinicians and patients before initiation of statin therapy.
Safety Recommendations
1. This guideline used RCTs to identify important safety considerations in individuals receiving treatment of blood cholesterol to reduce ASCVD risk.
2. Using RCTs to determine statin adverse effects facilitates understanding of the net benefit from statin therapy.
3. This guideline provides expert guidance on management of statin-associated adverse effects, including muscle symptoms.
Role of Biomarkers and Noninvasive Tests
1. Treatment decisions in selected individuals who are not included in the 4 statin benefit groups may be informed by other factors as recommended by the Risk Assessment Work Group and Blood Cholesterol Expert Panel.
Future Updates to the Blood Cholesterol Guideline
1. This is a comprehensive guideline for the evidence-based treatment of blood cholesterol to reduce ASCVD risk.
2. Future updates will build on this foundation to provide expert guidance on the management of complex lipid disorders and incorporate refinements in risk stratification based on critical review of emerging data.
3. RCTs comparing alternative treatment strategies are needed in order to inform future evidence-based guidelines for the optimum ASCVD risk-reduction approach.
Note: See Appendix 5 in the original guideline document for an expanded discussion of what's new in the guideline.
Recommendations for Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults—Statin Treatment
Treatment Targets
1. The Expert Panel makes no recommendations for or against specific LDL-C or non–HDL-C targets for the primary or secondary prevention of ASCVD. NHLBI Grade: N (No recommendation); ACC/AHA COR: n/a; ACC/AHA LOE: n/a
Secondary Prevention
1. High-intensity statin therapy should be initiated or continued as first-line therapy in women and men ≤75 years of age who have clinical ASCVD*, unless contraindicated. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
2. In individuals with clinical ASCVD* in whom high-intensity statin therapy would otherwise be used, when high-intensity statin therapy is contraindicated† or when characteristics predisposing to statin-associated adverse effects are present, moderate-intensity statin should be used as the second option if tolerated (see "Safety of Statins," below). NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
3. In individuals with clinical ASCVD >75 years of age, it is reasonable to evaluate the potential for ASCVD risk-reduction benefits and for adverse effects and drug–drug interactions and to consider patient preferences when initiating a moderate- or high-intensity statin. It is reasonable to continue statin therapy in those who are tolerating it. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B (Heart Protection Study Collaborative Group, 2002; Cholesterol Treatment Trialists' [CTT] Collaboration et al., 2010; Tikkanen et al., 2009; Holmes et al., 2006; Akushevich et al., 2012; Wolff, Starfield &, Anderson, 2002; Fried et al., "Effects," 2011; Robinson et al., 2007; Porock et al., 2005; Stineman et al., 2012; Schonberg et al., 2011; Fried et al., "Health outcome," 2011; Barry & Edgman-Levitan, 2012; Man-Son-Hing, Gage, & Montgomery, 2005; Fried et al., 2002; Ditto et al., 1996; Rosenfeld, Wenger, & Kagawa-Singer, 2000; Nease et al., 1995; Glynn et al., 2010; Shepherd et al., 2002; Trompet et al., 2010; Gray et al., 2011; LaCroix et al., 2008; Hippisley-Cox et al., 2005; Forman et al., 2011)
Primary Prevention in Individuals ≥21 Years of Age with LDL-C ≥190 mg/dL
1. Individuals with LDL-C ≥190 mg/dL or triglycerides ≥500 mg/dL should be evaluated for secondary causes of hyperlipidemia (see Table 6 in the original guideline document). NHLBI Grade: B (Moderate); ACC/AHA COR: I‡; ACC/AHA LOE: B (Berglund et al., 2012; Miller et al., 2011)
2. Adults ≥21 years of age with primary LDL-C ≥190 mg/dL should be treated with statin therapy (10-year ASCVD risk estimation is not required) NHLBI Grade: B (Moderate); ACC/AHA COR: I§; ACC/AHA LOE: B:
- Use high-intensity statin therapy unless contraindicated.
- For individuals unable to tolerate high-intensity statin therapy, use the maximum tolerated statin intensity.
3. For individuals ≥21 years of age with an untreated primary LDL-C ≥190 mg/dL, it is reasonable to intensify statin therapy to achieve at least a 50% LDL-C reduction. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B (CTT Collaboration et al., 2010; LaRosa et al., 2005; Pedersen et al., 2005; Cannon et al., 2004; Ridker et al, 2008; Baigent et al., 2005)
4. For individuals ≥21 years of age with an untreated primary LDL-C ≥190 mg/dL, after the maximum intensity of statin therapy has been achieved, addition of a nonstatin drug may be considered to further lower LDL-C. Evaluate the potential for ASCVD risk-reduction benefits, adverse effects, and drug–drug interactions, and consider patient preferences. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIb; ACC/AHA LOE: C (Thompson, Packard, & Stone, 2004)
Primary Prevention in Individuals with Diabetes and LDL-C 70–189 mg/dL
1. Moderate-intensity statin therapy should be initiated or continued for adults 40 to 75 years of age with diabetes. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
2. High-intensity statin therapy is reasonable for adults 40 to 75 years of age with diabetes with a ≥7.5% estimated 10-year ASCVD risk‖ unless contraindicated. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B (Ridker et al., 2008; Ridker et al., 2012)
3. In adults with diabetes, who are <40 years of age or >75 years of age, or with LDL <70 mg/dL, it is reasonable to evaluate the potential for ASCVD benefits and for adverse effects and drug–drug interactions and to consider patient preferences when deciding to initiate, continue, or intensify statin therapy. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (Roffi, Angiolillo, & Kappetein, 2011; Nathan et al., 2005; Rhodes et al., 2012; Paynter et al., 2011; Elley et al., 2010; Stevens et al., 2004; Bibbins-Domingo et al., 2007; Daniels et al., 2009; Jacob & Cho, 2010; Bainey & Jugdutt, 2009)
Primary Prevention in Individuals without Diabetes and with LDL-C 70–189 mg/dL
1. The Pooled Cohort Equations should be used to estimate 10-year ASCVD‖ risk for individuals with LDL-C 70–189 mg/dL without clinical ASCVD* to guide initiation of statin therapy for the primary prevention of ASCVD. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: I; ACC/AHA LOE: B (Goff et al., 2014)
2. Adults 40 to 75 years of age with LDL-C 70–189 mg/dL, without clinical ASCVD* or diabetes, and with an estimated 10-year ASCVD‖ risk ≥7.5% should be treated with moderate- to high-intensity statin therapy. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
3. It is reasonable to offer treatment with a moderate-intensity statin to adults 40 to 75 years of age, with LDL-C 70–189 mg/dL, without clinical ASCVD* or diabetes, and with an estimated 10-year ASCVD‖ risk of 5% to <7.5%. NHLBI Grade: C (Weak); ACC/AHA COR: IIa; ACC/AHA LOE: B
4. Before initiation of statin therapy for the primary prevention of ASCVD in adults with LDL-C 70–189 mg/dL without clinical ASCVD* or diabetes, it is reasonable for clinicians and patients to engage in a discussion that considers the potential for ASCVD risk-reduction benefits and for adverse effects and drug–drug interactions, as well as patient preferences for treatment. NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (Yu et al., 2013)
5. In adults with LDL-C <190 mg/dL who are not otherwise identified in a statin benefit group, or for whom after quantitative risk assessment a risk-based treatment decision is uncertain, additional factors¶ may be considered to inform treatment decision making. In these individuals, statin therapy for primary prevention may be considered after evaluation of the potential for ASCVD risk-reduction benefits, adverse effects, and drug–drug interactions and consider patient preferences. NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIb; ACC/AHA LOE: C (Goff et al., 2014; CTT Collaborators et al., 2012)
Heart Failure and Hemodialysis
1. The Expert Panel makes no recommendations regarding the initiation or discontinuation of statins in patients with NYHA class II–IV ischemic systolic heart failure or in patients on maintenance hemodialysis. NHBLI Grade: N (No Recommendation); ACC/AHA COR: n/a; ACC/AHA LOE: n/a
*Clinical ASCVD includes acute coronary syndromes, history of myocardial infarction (MI), stable or unstable angina, coronary or other arterial revascularization, stroke, transient ischaemic attack (TIA), or peripheral arterial disease presumed to be of atherosclerotic origin.
†Contraindications, warnings, and precautions are defined for each statin according to the manufacturer's prescribing information ("Lescol," 2012; "Pravachol," 2012; "Livalo," 2012; "Zocor," 2012; "Mevacor," 2012; "Lipitor," 2012; "Crestor," 2013).
‡Individuals with secondary causes of hyperlipidemia were excluded from RCTs reviewed. A triglyceride level ≥500 mg/dL was an exclusion criterion for almost all RCTs. Therefore, ruling out secondary causes is necessary to avoid inappropriate statin therapy.
§No RCTs included only individuals with LDL-C ≥190 mg/dL. However, many trials did include individuals with LDL-C ≥190 mg/dL, and all of these trials consistently demonstrated a reduction in ASCVD events. In addition, the Cholesterol Treatment Trialists meta-analyses have shown that each 39-mg/dL reduction in LDL-C with statin therapy reduced ASCVD events by 22%, and the relative reductions in ASCVD events were consistent across the range of LDL-C levels. Therefore, individuals with primary LDL-C ≥190 mg/dL should be treated with statin therapy.
ǁEstimated 10-year or "hard" ASCVD risk includes first occurrence of nonfatal MI, coronary heart disease death, and nonfatal and fatal stroke as used by the Risk Assessment Work Group in developing the Pooled Cohort Equations.
¶These factors may include primary LDL-C ≥160 mg/dL or other evidence of genetic hyperlipidemias; family history of premature ASCVD with onset <55 years of age in a first-degree male relative or <65 years of age in a first-degree female relative; high-sensitivity C-reactive protein ≥2 mg/L; coronary artery calcium (CAC) score ≥300 Agatston units or ≥75th percentile for age, sex, and ethnicity (for additional information, see http://www.mesa-nhlbi.org/CACReference.aspx ![]()
See Table 5 in the original guideline document for high-, moderate-, and low-intensity statin therapies used in the RCTs reviewed by the Expert Panel.
Statin Safety Recommendations
Safety
1. To maximize the safety of statins, selection of the appropriate statin and dose in men and nonpregnant/nonnursing women should be based on patient characteristics, level of ASCVD* risk, and potential for adverse effects. Moderate-intensity statin therapy should be used in individuals in whom high-intensity statin therapy would otherwise be recommended when characteristics predisposing them to statin-associated adverse effects are present. Characteristics predisposing individuals to statin adverse effects include but are not limited to: NHBLI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: B
- Multiple or serious comorbidities, including impaired renal or hepatic function
- History of previous statin intolerance or muscle disorders
- Unexplained alanine aminotransferase (ALT) elevations ≥3 times the upper limit of normal (ULN)
- Patient characteristics or concomitant use of drugs affecting statin metabolism
- Age >75 years
Additional characteristics that could modify the decision to use higher statin intensities might include but are not limited to:
- History of hemorrhagic stroke
- Asian ancestry
2a. Creatine kinase (CK) should not be routinely measured in individuals receiving statin therapy. NHBLI Grade: A (Strong); ACC/AHA COR: III: No Benefit; ACC/AHA LOE: A
2b. Baseline measurement of CK is reasonable for individuals believed to be at increased risk for adverse muscle events because of a personal or family history of statin intolerance or muscle disease, clinical presentation, or concomitant drug therapy that might increase the risk of myopathy. NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (Eckel, 2010)
2c. During statin therapy, it is reasonable to measure CK in individuals with muscle symptoms, including pain, tenderness, stiffness, cramping, weakness, or generalized fatigue. NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (Eckel, 2010)
3a. Baseline measurement of hepatic transaminase levels (ALT) should be performed before initiation of statin therapy. NHBLI Grade: B (Moderate); ACC/AHA COR: I†; ACC/AHA LOE: B
3b. During statin therapy, it is reasonable to measure hepatic function if symptoms suggesting hepatotoxicity arise (e.g., unusual fatigue or weakness, loss of appetite, abdominal pain, dark-colored urine, or yellowing of the skin or sclera). NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (U.S. Food and Drug Administration, 2012)
4. Decreasing the statin dose may be considered when 2 consecutive values of LDL-C levels are <40 mg/dL. NHBLI Grade: C (Weak); ACC/AHA COR: IIb; ACC/AHA LOE: C
5. It may be harmful to initiate simvastatin at 80 mg daily or increase the dose of simvastatin to 80 mg daily. NHBLI Grade: B (Moderate); ACC/AHA COR: III: Harm; ACC/AHA LOE: A ("Zocor," 2012; U.S. Food and Drug Administration, 2010)
6. Individuals receiving statin therapy should be evaluated for new-onset diabetes according to the current diabetes screening guidelines (American Diabetes Association, 2013). Those who develop diabetes during statin therapy should be encouraged to adhere to a heart-healthy dietary pattern, engage in physical activity, achieve and maintain a healthy body weight, cease tobacco use, and continue statin therapy to reduce their risk of ASCVD events. NHBLI Grade: B (Moderate); ACC/AHA COR: I‡; ACC/AHA LOE: B
7. For individuals taking any dose of statins, it is reasonable to use caution in individuals >75 years of age, as well as in individuals who are taking concomitant medications that alter drug metabolism, taking multiple drugs, or taking drugs for conditions that require complex medication regimens (e.g., those who have undergone solid organ transplantation or are receiving treatment for human immunodeficiency virus [HIV]). A review of the manufacturer's prescribing information may be useful before initiation of any cholesterol-lowering drug. NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (Heart Protection Study Collaborative Group, 2002; "Lescol," 2012; "Pravachol," 2012; "Livalo," 2012; "Zocor," 2012; "Mevacor," 2012; "Lipitor," 2012; "Crestor," 2013; U.S. Food and Drug Administration, 2012; Rawlins, 2008; Schwartz et al., 2001; Shepherd et al., 2006)
8. It is reasonable to evaluate and treat muscle symptoms, including pain, tenderness, stiffness, cramping, weakness, or fatigue, in statin-treated patients according to the following management algorithm: NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B (Taylor et al., 2011; Eckel, 2010; Baigent et al., 2010; Mills et al., 2008; Dale et al., 2007)
- To avoid unnecessary discontinuation of statins, obtain a history of prior or current muscle symptoms to establish a baseline before initiation of statin therapy.
- If unexplained severe muscle symptoms or fatigue develop during statin therapy, promptly discontinue the statin and address the possibility of rhabdomyolysis by evaluating CK and creatinine and performing urinalysis for myoglobinuria.
- If mild to moderate muscle symptoms develop during statin therapy:
- Discontinue the statin until the symptoms can be evaluated.
- Evaluate the patient for other conditions that might increase the risk for muscle symptoms (e.g., hypothyroidism, reduced renal or hepatic function, rheumatologic disorders such as polymyalgia rheumatica, steroid myopathy, vitamin D deficiency, or primary muscle diseases).
- If muscle symptoms resolve, and if no contraindication exists, give the patient the original or a lower dose of the same statin to establish a causal relationship between the muscle symptoms and statin therapy.
- If a causal relationship exists, discontinue the original statin. Once muscle symptoms resolve, use a low dose of a different statin.
- Once a low dose of a statin is tolerated, gradually increase the dose as tolerated.
- If, after 2 months without statin treatment, muscle symptoms or elevated CK levels do not resolve completely, consider other causes of muscle symptoms listed above.
- If persistent muscle symptoms are determined to arise from a condition unrelated to statin therapy, or if the predisposing condition has been treated, resume statin therapy at the original dose.
9. For individuals presenting with a confusional state or memory impairment while on statin therapy, it may be reasonable to evaluate the patient for nonstatin causes, such as exposure to other drugs, as well as for systemic and neuropsychiatric causes, in addition to the possibility of adverse effects associated with statin drug therapy. NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIb; ACC/AHA LOE: C (Shepherd et al., 2002; U.S. Food and Drug Administration, 2012; Collins et al., 2004; Roberts, 2009)
*Based on the presence of clinical ASCVD, diabetes, LDL-C ≥190 mg/dL, or level of estimated 10-year ASCVD risk.
†Individuals with elevated ALT levels (usually >1.5 or 2 times ULN) were excluded from RCT participation. Unexplained ALT ≥3 times ULN is a contraindication to statin therapy as listed in manufacturer's prescribing information.
‡Statin use is associated with a very modest excess risk of new-onset diabetes in RCTs and meta-analyses of RCTs (i.e., ∼0.1 excess cases per 100 individuals treated for 1 year with moderate-intensity statin therapy and ∼0.3 excess cases per 100 individuals treated for 1 year with high-intensity statin therapy. The increased risk of new-onset diabetes appears to be confined to those with risk factors for diabetes. These individuals are also at higher risk of ASCVD because of these risk factors. Therefore, if a statin-treated individual develops diabetes as detected by current diabetes screening guidelines, he or she should be counseled to adhere to a heart-healthy dietary pattern, engage in physical activity, achieve and maintain a healthy body weight, cease tobacco use, and continue statin therapy to reduce the risk of ASCVD events.
Nonstatin Safety Recommendations
Safety of Niacin
1. Baseline hepatic transaminases, fasting blood glucose or hemoglobin A1c, and uric acid should be obtained before initiation of niacin, and again during up-titration to a maintenance dose and every 6 months thereafter. NHLBI Grade: B (Moderate); ACC/AHA COR: I; ACC/AHA LOE: B
2. Niacin should not be used if:
- Hepatic transaminase elevations are higher than 2 to 3 times ULN. NHLBI Grade: A (Strong); ACC/AHA COR: III: Harm; ACC/AHA LOE: B
- Persistent severe cutaneous symptoms, persistent hyperglycemia, acute gout, or unexplained abdominal pain or gastrointestinal symptoms occur. NHLBI Grade: B (Moderate); ACC/AHA COR: III: Harm; ACC/AHA LOE: B
- New-onset atrial fibrillation or weight loss occurs. NHLBI Grade: C (Weak); ACC/AHA COR: III: Harm; ACC/AHA LOE: B
3. In individuals with adverse effects from niacin, the potential for ASCVD benefits and the potential for adverse effects should be reconsidered before reinitiation of niacin therapy. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: I; ACC/AHA LOE: B (AIM-HIGH Investigators et al., 2011; "Clofibrate and niacin in coronary heart disease," 1975; Guyton & Bays, 2007; Brown & Zhao, 2008; Grundy et al., 2002)
4. To reduce the frequency and severity of adverse cutaneous symptoms, it is reasonable to: NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (AIM-HIGH Investigators et al., 2011; "Clofibrate and niacin in coronary heart disease," 1975; Guyton & Bays, 2007; Brown & Zhao, 2008; Grundy et al., 2002)
- Start niacin at a low dose and titrate to a higher dose over a period of weeks as tolerated.
- Take niacin with food or premedicate with aspirin 325 mg 30 minutes before niacin dosing to alleviate flushing symptoms.
- If an extended-release preparation is used, increase the dose of extended-release niacin from 500 mg to a maximum of 2,000 mg/day over 4 to 8 weeks, with the dose of extended-release niacin increasing not more than weekly.
- If immediate-release niacin is chosen, start at a dose of 100 mg 3 times daily and up-titrate to 3 g/day, divided into 2 or 3 doses.
Safety of Bile Acid Sequestrants (BAS)
1. BAS should not be used in individuals with baseline fasting triglyceride levels ≥300 mg/dL or type III hyperlipoproteinemia, because severe triglyceride elevations might occur. (A fasting lipid panel should be obtained before BAS is initiated, 3 months after initiation, and every 6 to 12 months thereafter.) NHLBI Grade: C (Weak); ACC/AHA COR: III: Harm; ACC/AHA LOE: B
2. It is reasonable to use BAS with caution if baseline triglyceride levels are 250 to 299 mg/dL, and evaluate a fasting lipid panel in 4 to 6 weeks after initiation. Discontinue the BAS if triglycerides exceed 400 mg/dL. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (Crouse, 1987)
Safety of Cholesterol-Absorption Inhibitors
1. It is reasonable to obtain baseline hepatic transaminases before initiation of ezetimibe. When ezetimibe is coadministered with a statin, monitor transaminase levels as clinically indicated, and discontinue ezetimibe if persistent ALT elevations ≥3 times ULN occur. NHLBI Grade: C (Weak); ACC/AHA COR: IIa; ACC/AHA LOE: B
Safety of Fibrates
1. Gemfibrozil should not be initiated in patients on statin therapy because of an increased risk for muscle symptoms and rhabdomyolysis. NHLBI Grade: B (Moderate); ACC/AHA COR: III: Harm; ACC/AHA LOE: B
2. Fenofibrate may be considered concomitantly with a low- or moderate-intensity statin only if the benefits from ASCVD risk reduction or triglyceride lowering when triglycerides are ≥500 mg/dL are judged to outweigh the potential risk for adverse effects. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIb; ACC/AHA LOE: C (ACCORD Study Group et al., 2010)
3. Renal status should be evaluated before fenofibrate initiation, within 3 months after initiation, and every 6 months thereafter. Assess renal safety with both a serum creatinine level and an estimated glomerular filtration rate (eGFR) based on creatinine. NHLBI Grade: B (Moderate); ACC/AHA COR: I; ACC/AHA LOE: B
- Fenofibrate should not be used if moderate or severe renal impairment, defined as eGFR <30 mL/min per 1.73 m2, is present. ACC/AHA COR: III: Harm; ACC/AHA LOE: B
- If eGFR is between 30 and 59 mL/min per 1.73 m2, the dose of fenofibrate should not exceed 54 mg/day.*
- If, during follow-up, the eGFR decreases persistently to ≤30 mL/min per 1.73 m2, fenofibrate should be discontinued.
*Consult the manufacturer's prescribing information as there are several forms of fenofibrate available.
Safety of Omega-3 Fatty Acids
1. If eicosapentaenoic acid (EPA) and/or docosahexanoic acid (DHA) are used for the management of severe hypertriglyceridemia, defined as triglycerides ≥500 mg/dL, it is reasonable to evaluate the patient for gastrointestinal disturbances, skin changes, and bleeding. NHLBI Grade: C (Weak); ACC/AHA COR: IIa; ACC/AHA LOE: B
Recommendations for Monitoring, Optimizing, and Addressing Insufficient Response to Statin Therapy
Monitoring Statin Therapy
1. Adherence to medication and lifestyle, therapeutic response to statin therapy, and safety should be regularly assessed. This should also include a fasting lipid panel performed within 4–12 weeks after initiation or dose adjustment, and every 3–12 months thereafter. Other safety measurements should be measured as clinically indicated. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
Optimizing Statin Therapy
1. The maximum tolerated intensity of statin should be used in individuals for whom a high- or moderate-intensity statin is recommended but not tolerated. NHLBI Grade: B (Moderate); ACC/AHA COR: I*; ACC/AHA LOE: B
Insufficient Response to Statin Therapy
1. In individuals who have a less-than-anticipated therapeutic response or are intolerant of the recommended intensity of statin therapy, the following should be performed: NHLBI Grade A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
- Reinforce medication adherence.
- Reinforce adherence to intensive lifestyle changes.
- Exclude secondary causes of hyperlipidemia.
2. It is reasonable to use the following as indicators of anticipated therapeutic response to the recommended intensity of statin therapy. Focus is on the intensity of the statin therapy. As an aid to monitoring: NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B (LaRosa et al., 2005; Pedersen et al., 2005; Cannon et al., 2004; Amarenco et al., 2006; Thompson & HEART-UK LDL Apheresis Working Group, 2008; Schwertz & Badellino, 2008)
- High-intensity statin therapy† generally results in an average LDL-C reduction of ≥50% from the untreated baseline.
- Moderate-intensity statin therapy generally results in an average LDL-C reduction of 30% to <50% from the untreated baseline.
- LDL-C levels and percents reduction are to be used only to assess response to therapy and adherence. They are not to be used as performance standards.
3. In individuals at higher ASCVD risk receiving the maximum tolerated intensity of statin therapy who continue to have a less-than-anticipated therapeutic response, addition of nonstatin cholesterol-lowering drug(s) may be considered if the ASCVD risk-reduction benefits outweigh the potential for adverse effects. Higher-risk individuals include: NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIb: ACC/AHA LOE: C (AIM-HIGH Investigators et al., 2011; ACCORD Study Group et al., 2010; Rossebo et al., 2007; Sharp Collaborative Group, 2010; Yokoyama, Origasa, & JELIS Investigators, 2003)
- Individuals with clinical ASCVD‡ <75 years of age.
- Individuals with baseline LDL-C ≥190 mg/dL.
- Individuals 40 to 75 years of age with diabetes.
Preference should be given to nonstatin cholesterol-lowering drugs shown to reduce ASCVD events in RCTs.
4. In individuals who are candidates for statin treatment but are completely statin intolerant, it is reasonable to use nonstatin cholesterol-lowering drugs that have been shown to reduce ASCVD events in RCTs if the ASCVD risk-reduction benefits outweigh the potential for adverse effects. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B (Eckel, 2010; "Clofibrate and niacin in coronary heart disease," 1975; Frick et al., 1987; Lipid Research Clinics Program, 1984; "The Lipid Research Clinics Coronary Primary Prevention Trial results. II.," 1984; Rubins et al., 1999; Keech et al., 2005; HPS2-THRIVE Collaborative Group, 2013)
*Several RCTs found that low-intensity and low-moderate–intensity statin therapy reduced ASCVD events. In addition, the Cholesterol Treatment Trialists meta-analyses found that each 39-mg/dL reduction in LDL-C reduces ASCVD risk by 22%. Therefore, the Panel considered that submaximal statin therapy should be used to reduce ASCVD risk in those unable to tolerate moderate- or high-intensity statin therapy.
†In those already on a statin, in whom baseline LDL-C is unknown, an LDL-C level <100 mg/dL was observed in most individuals receiving high-intensity statin therapy.
‡Clinical ASCVD includes acute coronary syndromes, or a history of myocardial infarction, stable or unstable angina, coronary or other arterial revascularization, stroke, transient ischemic attack, or peripheral arterial disease presumed to be of atherosclerotic origin.
Definitions:
NHLBI Grading of the Strength of Recommendations
| Grade | Strength of Recommendation* |
|---|---|
| A | Strong recommendation There is high certainty based on evidence that the net benefit† is substantial. |
| B | Moderate recommendation There is moderate certainty based on evidence that the net benefit is moderate to substantial, or there is high certainty that the net benefit is moderate. |
| C | Weak recommendation There is at least moderate certainty based on evidence that there is a small net benefit. |
| D | Recommendation against There is at least moderate certainty based on evidence that there is no net benefit or that risks/harms outweigh benefits. |
| E | Expert opinion ("There is insufficient evidence or evidence is unclear or conflicting, but this is what the Work Group recommends.") Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, unclear evidence, or conflicting evidence, but the Work Group thought it was important to provide clinical guidance and make a recommendation. Further research is recommended in this area. |
| N | No recommendation for or against ("There is insufficient evidence or evidence is unclear or conflicting.") Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, unclear evidence, or conflicting evidence, and the Work Group thought no recommendation should be made. Further research is recommended in this area. |
*In most cases, the strength of the recommendation should be closely aligned with the quality of the evidence; however, under some circumstances, there may be valid reasons for making recommendations that are not closely aligned with the quality of the evidence (e.g., strong recommendation when the evidence quality is moderate, such as smoking cessation to reduce cardiovascular disease [CVD] risk or ordering an electrocardiogram [ECG] as part of the initial diagnostic work-up for a patient presenting with possible myocardial infarction [MI]). Those situations should be limited and the rationale explained clearly by the Work Group.
†Net benefit is defined as benefits minus risks/harms of the service/intervention.
NHLBI Quality Rating of the Strength of Evidence
| Type of Evidence | Quality Rating* |
|---|---|
| High |
| Moderate |
| Low |
*In some cases, other evidence, such as large all-or-none case series (e.g., jumping from airplanes or tall structures), can represent high- or moderate-quality evidence. In such cases, the rationale for the evidence rating exception should be explained by the Work Group and clearly justified.
†"Well-designed, well-executed" refers to studies that directly address the question; use adequate randomization, blinding, and allocation concealment; are adequately powered; use intention-to-treat analyses; and have high follow-up rates.
‡Limitations include concerns with the design and execution of a study that result in decreased confidence in the true estimate of the effect. Examples of such limitations include but are not limited to: inadequate randomization, lack of blinding of study participants or outcome assessors, inadequate power, outcomes of interest that are not prespecified for the primary outcomes, low follow-up rates, and findings based on subgroup analyses. Whether the limitations are considered minor or major is based on the number and severity of flaws in design or execution. Rules for determining whether the limitations are considered minor or major and how they will affect rating of the individual studies will be developed collaboratively with the methodology team.
§Nonrandomized controlled studies refer to intervention studies where assignment to intervention and comparison groups is not random (e.g., quasi-experimental study design).
¶Observational studies include prospective and retrospective cohort, case-control, and cross-sectional studies.
Applying Classification of Recommendations and Level of Evidence
| Size of Treatment Effect | |||||||
|---|---|---|---|---|---|---|---|
| CLASS I Benefit >>> Risk Procedure/Treatment SHOULD be performed/ administered | CLASS IIa Benefit >> Risk Additional studies with focused objectives needed IT IS REASONABLE to perform procedure/administer treatment | CLASS IIb Benefit ≥ Risk Additional studies with broad objectives needed; additional registry data would be helpful Procedure/Treatment MAY BE CONSIDERED | CLASS III No Benefit or Class III Harm | ||||
| Procedure/Test | Treatment | ||||||
| COR III: No Benefit | Not helpful | No proven benefit | |||||
| COR III: Harm | Excess cost without benefit or harmful | Harmful to patients | |||||
| Estimate of Certainty (Precision) of Treatment Effect | LEVEL A Multiple populations evaluated* Data derived from multiple randomized clinical trials or meta-analyses |
|
|
|
| ||
| LEVEL B Limited populations evaluated* Data derived from a single randomized trial or nonrandomized studies |
|
|
|
| |||
| LEVEL C Very limited populations evaluated* Only consensus opinion of experts, case studies, or standard of care |
|
|
|
| |||
A recommendation with Level of Evidence B or C does not imply that the recommendation is weak. Many important clinical questions addressed in the guidelines do not lend themselves to clinical trials. Although randomized trials are unavailable, there may be a very clear clinical consensus that a particular test or therapy is useful or effective.
*Data available from clinical trials or registries about the usefulness/efficacy in different subpopulations, such as sex, age, history of diabetes, history of prior myocardial infarction, history of heart failure, and prior aspirin use.
†For comparative-effectiveness recommendations (Class I and IIa; Level of Evidence A and B only), studies that support the use of comparator verbs should involve direct comparisons of the treatments or strategies being evaluated.
- Summary of Statin Initiation Recommendations for the Treatment of Blood Cholesterol to Reduce ASCVD Risk in Adults
- Initiating Statin Therapy in Individuals with Clinical ASCVD
- Initiating Statin Therapy in Individuals without Clinical ASCVD
- Statin Therapy: Monitoring Therapeutic Response and Adherence
Recommendations
Each recommendation has been mapped from the NHLBI grading format to the American College of Cardiology/American Heart Association Class of Recommendation/Level of Evidence (ACC/AHA COR/LOE) construct and is expressed in both formats. Because of the inherent differences in grading systems and the clinical questions driving the recommendations, alignment between the NHLBI and ACC/AHA formats is in some cases imperfect. Definitions for the NHLBI strength of recommendation (A-E, N) and quality of evidence (High, Moderate, Low) and the ACC/AHA levels of the evidence (LOE: A-C) and classes of recommendations (COR: I-III) are provided at the end of the "Major Recommendations" field.
What's New in the Guideline?
Focus on Atherosclerotic Cardiovascular Disease (ASCVD Risk) Reduction: 4 Statin Benefit Groups
1. This guideline is based on a comprehensive set of data from randomized control trials (RCTs) from which 4 statin benefit groups were identified that focus efforts to reduce ASCVD events in secondary and primary prevention.
2. This guideline identifies high-intensity and moderate-intensity statin therapy for use in secondary and primary prevention.
A New Perspective on Low-density Lipoprotein Cholesterol (LDL-C) and/or Non–High-density Lipoprotein Cholesterol (HDL-C) Treatment Goals
1. The Expert Panel was unable to find RCT evidence to support continued use of specific LDL-C or non–HDL-C treatment targets.
2. The appropriate intensity of statin therapy should be used to reduce ASCVD risk in those most likely to benefit.
3. Nonstatin therapies, as compared with statin therapy, do not provide acceptable ASCVD risk-reduction benefits relative to their potential for adverse effects in the routine prevention of ASCVD.
Global Risk Assessment for Primary Prevention
1. This guideline recommends use of the new Pooled Cohort Equations to estimate 10-year ASCVD risk in both white and black men and women.
2. By more accurately identifying higher-risk individuals for statin therapy, the guideline focuses statin therapy on those most likely to benefit.
3. It also indicates, on the basis of RCT data, those high-risk groups that might not benefit.
4. This guideline recommends a discussion between clinicians and patients before initiation of statin therapy.
Safety Recommendations
1. This guideline used RCTs to identify important safety considerations in individuals receiving treatment of blood cholesterol to reduce ASCVD risk.
2. Using RCTs to determine statin adverse effects facilitates understanding of the net benefit from statin therapy.
3. This guideline provides expert guidance on management of statin-associated adverse effects, including muscle symptoms.
Role of Biomarkers and Noninvasive Tests
1. Treatment decisions in selected individuals who are not included in the 4 statin benefit groups may be informed by other factors as recommended by the Risk Assessment Work Group and Blood Cholesterol Expert Panel.
Future Updates to the Blood Cholesterol Guideline
1. This is a comprehensive guideline for the evidence-based treatment of blood cholesterol to reduce ASCVD risk.
2. Future updates will build on this foundation to provide expert guidance on the management of complex lipid disorders and incorporate refinements in risk stratification based on critical review of emerging data.
3. RCTs comparing alternative treatment strategies are needed in order to inform future evidence-based guidelines for the optimum ASCVD risk-reduction approach.
Note: See Appendix 5 in the original guideline document for an expanded discussion of what's new in the guideline.
Recommendations for Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults—Statin Treatment
Treatment Targets
1. The Expert Panel makes no recommendations for or against specific LDL-C or non–HDL-C targets for the primary or secondary prevention of ASCVD. NHLBI Grade: N (No recommendation); ACC/AHA COR: n/a; ACC/AHA LOE: n/a
Secondary Prevention
1. High-intensity statin therapy should be initiated or continued as first-line therapy in women and men ≤75 years of age who have clinical ASCVD*, unless contraindicated. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
2. In individuals with clinical ASCVD* in whom high-intensity statin therapy would otherwise be used, when high-intensity statin therapy is contraindicated† or when characteristics predisposing to statin-associated adverse effects are present, moderate-intensity statin should be used as the second option if tolerated (see "Safety of Statins," below). NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
3. In individuals with clinical ASCVD >75 years of age, it is reasonable to evaluate the potential for ASCVD risk-reduction benefits and for adverse effects and drug–drug interactions and to consider patient preferences when initiating a moderate- or high-intensity statin. It is reasonable to continue statin therapy in those who are tolerating it. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B (Heart Protection Study Collaborative Group, 2002; Cholesterol Treatment Trialists' [CTT] Collaboration et al., 2010; Tikkanen et al., 2009; Holmes et al., 2006; Akushevich et al., 2012; Wolff, Starfield &, Anderson, 2002; Fried et al., "Effects," 2011; Robinson et al., 2007; Porock et al., 2005; Stineman et al., 2012; Schonberg et al., 2011; Fried et al., "Health outcome," 2011; Barry & Edgman-Levitan, 2012; Man-Son-Hing, Gage, & Montgomery, 2005; Fried et al., 2002; Ditto et al., 1996; Rosenfeld, Wenger, & Kagawa-Singer, 2000; Nease et al., 1995; Glynn et al., 2010; Shepherd et al., 2002; Trompet et al., 2010; Gray et al., 2011; LaCroix et al., 2008; Hippisley-Cox et al., 2005; Forman et al., 2011)
Primary Prevention in Individuals ≥21 Years of Age with LDL-C ≥190 mg/dL
1. Individuals with LDL-C ≥190 mg/dL or triglycerides ≥500 mg/dL should be evaluated for secondary causes of hyperlipidemia (see Table 6 in the original guideline document). NHLBI Grade: B (Moderate); ACC/AHA COR: I‡; ACC/AHA LOE: B (Berglund et al., 2012; Miller et al., 2011)
2. Adults ≥21 years of age with primary LDL-C ≥190 mg/dL should be treated with statin therapy (10-year ASCVD risk estimation is not required) NHLBI Grade: B (Moderate); ACC/AHA COR: I§; ACC/AHA LOE: B:
- Use high-intensity statin therapy unless contraindicated.
- For individuals unable to tolerate high-intensity statin therapy, use the maximum tolerated statin intensity.
3. For individuals ≥21 years of age with an untreated primary LDL-C ≥190 mg/dL, it is reasonable to intensify statin therapy to achieve at least a 50% LDL-C reduction. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B (CTT Collaboration et al., 2010; LaRosa et al., 2005; Pedersen et al., 2005; Cannon et al., 2004; Ridker et al, 2008; Baigent et al., 2005)
4. For individuals ≥21 years of age with an untreated primary LDL-C ≥190 mg/dL, after the maximum intensity of statin therapy has been achieved, addition of a nonstatin drug may be considered to further lower LDL-C. Evaluate the potential for ASCVD risk-reduction benefits, adverse effects, and drug–drug interactions, and consider patient preferences. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIb; ACC/AHA LOE: C (Thompson, Packard, & Stone, 2004)
Primary Prevention in Individuals with Diabetes and LDL-C 70–189 mg/dL
1. Moderate-intensity statin therapy should be initiated or continued for adults 40 to 75 years of age with diabetes. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
2. High-intensity statin therapy is reasonable for adults 40 to 75 years of age with diabetes with a ≥7.5% estimated 10-year ASCVD risk‖ unless contraindicated. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B (Ridker et al., 2008; Ridker et al., 2012)
3. In adults with diabetes, who are <40 years of age or >75 years of age, or with LDL <70 mg/dL, it is reasonable to evaluate the potential for ASCVD benefits and for adverse effects and drug–drug interactions and to consider patient preferences when deciding to initiate, continue, or intensify statin therapy. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (Roffi, Angiolillo, & Kappetein, 2011; Nathan et al., 2005; Rhodes et al., 2012; Paynter et al., 2011; Elley et al., 2010; Stevens et al., 2004; Bibbins-Domingo et al., 2007; Daniels et al., 2009; Jacob & Cho, 2010; Bainey & Jugdutt, 2009)
Primary Prevention in Individuals without Diabetes and with LDL-C 70–189 mg/dL
1. The Pooled Cohort Equations should be used to estimate 10-year ASCVD‖ risk for individuals with LDL-C 70–189 mg/dL without clinical ASCVD* to guide initiation of statin therapy for the primary prevention of ASCVD. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: I; ACC/AHA LOE: B (Goff et al., 2014)
2. Adults 40 to 75 years of age with LDL-C 70–189 mg/dL, without clinical ASCVD* or diabetes, and with an estimated 10-year ASCVD‖ risk ≥7.5% should be treated with moderate- to high-intensity statin therapy. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
3. It is reasonable to offer treatment with a moderate-intensity statin to adults 40 to 75 years of age, with LDL-C 70–189 mg/dL, without clinical ASCVD* or diabetes, and with an estimated 10-year ASCVD‖ risk of 5% to <7.5%. NHLBI Grade: C (Weak); ACC/AHA COR: IIa; ACC/AHA LOE: B
4. Before initiation of statin therapy for the primary prevention of ASCVD in adults with LDL-C 70–189 mg/dL without clinical ASCVD* or diabetes, it is reasonable for clinicians and patients to engage in a discussion that considers the potential for ASCVD risk-reduction benefits and for adverse effects and drug–drug interactions, as well as patient preferences for treatment. NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (Yu et al., 2013)
5. In adults with LDL-C <190 mg/dL who are not otherwise identified in a statin benefit group, or for whom after quantitative risk assessment a risk-based treatment decision is uncertain, additional factors¶ may be considered to inform treatment decision making. In these individuals, statin therapy for primary prevention may be considered after evaluation of the potential for ASCVD risk-reduction benefits, adverse effects, and drug–drug interactions and consider patient preferences. NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIb; ACC/AHA LOE: C (Goff et al., 2014; CTT Collaborators et al., 2012)
Heart Failure and Hemodialysis
1. The Expert Panel makes no recommendations regarding the initiation or discontinuation of statins in patients with NYHA class II–IV ischemic systolic heart failure or in patients on maintenance hemodialysis. NHBLI Grade: N (No Recommendation); ACC/AHA COR: n/a; ACC/AHA LOE: n/a
*Clinical ASCVD includes acute coronary syndromes, history of myocardial infarction (MI), stable or unstable angina, coronary or other arterial revascularization, stroke, transient ischaemic attack (TIA), or peripheral arterial disease presumed to be of atherosclerotic origin.
†Contraindications, warnings, and precautions are defined for each statin according to the manufacturer's prescribing information ("Lescol," 2012; "Pravachol," 2012; "Livalo," 2012; "Zocor," 2012; "Mevacor," 2012; "Lipitor," 2012; "Crestor," 2013).
‡Individuals with secondary causes of hyperlipidemia were excluded from RCTs reviewed. A triglyceride level ≥500 mg/dL was an exclusion criterion for almost all RCTs. Therefore, ruling out secondary causes is necessary to avoid inappropriate statin therapy.
§No RCTs included only individuals with LDL-C ≥190 mg/dL. However, many trials did include individuals with LDL-C ≥190 mg/dL, and all of these trials consistently demonstrated a reduction in ASCVD events. In addition, the Cholesterol Treatment Trialists meta-analyses have shown that each 39-mg/dL reduction in LDL-C with statin therapy reduced ASCVD events by 22%, and the relative reductions in ASCVD events were consistent across the range of LDL-C levels. Therefore, individuals with primary LDL-C ≥190 mg/dL should be treated with statin therapy.
ǁEstimated 10-year or "hard" ASCVD risk includes first occurrence of nonfatal MI, coronary heart disease death, and nonfatal and fatal stroke as used by the Risk Assessment Work Group in developing the Pooled Cohort Equations.
¶These factors may include primary LDL-C ≥160 mg/dL or other evidence of genetic hyperlipidemias; family history of premature ASCVD with onset <55 years of age in a first-degree male relative or <65 years of age in a first-degree female relative; high-sensitivity C-reactive protein ≥2 mg/L; coronary artery calcium (CAC) score ≥300 Agatston units or ≥75th percentile for age, sex, and ethnicity (for additional information, see http://www.mesa-nhlbi.org/CACReference.aspx ![]()
See Table 5 in the original guideline document for high-, moderate-, and low-intensity statin therapies used in the RCTs reviewed by the Expert Panel.
Statin Safety Recommendations
Safety
1. To maximize the safety of statins, selection of the appropriate statin and dose in men and nonpregnant/nonnursing women should be based on patient characteristics, level of ASCVD* risk, and potential for adverse effects. Moderate-intensity statin therapy should be used in individuals in whom high-intensity statin therapy would otherwise be recommended when characteristics predisposing them to statin-associated adverse effects are present. Characteristics predisposing individuals to statin adverse effects include but are not limited to: NHBLI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: B
- Multiple or serious comorbidities, including impaired renal or hepatic function
- History of previous statin intolerance or muscle disorders
- Unexplained alanine aminotransferase (ALT) elevations ≥3 times the upper limit of normal (ULN)
- Patient characteristics or concomitant use of drugs affecting statin metabolism
- Age >75 years
Additional characteristics that could modify the decision to use higher statin intensities might include but are not limited to:
- History of hemorrhagic stroke
- Asian ancestry
2a. Creatine kinase (CK) should not be routinely measured in individuals receiving statin therapy. NHBLI Grade: A (Strong); ACC/AHA COR: III: No Benefit; ACC/AHA LOE: A
2b. Baseline measurement of CK is reasonable for individuals believed to be at increased risk for adverse muscle events because of a personal or family history of statin intolerance or muscle disease, clinical presentation, or concomitant drug therapy that might increase the risk of myopathy. NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (Eckel, 2010)
2c. During statin therapy, it is reasonable to measure CK in individuals with muscle symptoms, including pain, tenderness, stiffness, cramping, weakness, or generalized fatigue. NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (Eckel, 2010)
3a. Baseline measurement of hepatic transaminase levels (ALT) should be performed before initiation of statin therapy. NHBLI Grade: B (Moderate); ACC/AHA COR: I†; ACC/AHA LOE: B
3b. During statin therapy, it is reasonable to measure hepatic function if symptoms suggesting hepatotoxicity arise (e.g., unusual fatigue or weakness, loss of appetite, abdominal pain, dark-colored urine, or yellowing of the skin or sclera). NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (U.S. Food and Drug Administration, 2012)
4. Decreasing the statin dose may be considered when 2 consecutive values of LDL-C levels are <40 mg/dL. NHBLI Grade: C (Weak); ACC/AHA COR: IIb; ACC/AHA LOE: C
5. It may be harmful to initiate simvastatin at 80 mg daily or increase the dose of simvastatin to 80 mg daily. NHBLI Grade: B (Moderate); ACC/AHA COR: III: Harm; ACC/AHA LOE: A ("Zocor," 2012; U.S. Food and Drug Administration, 2010)
6. Individuals receiving statin therapy should be evaluated for new-onset diabetes according to the current diabetes screening guidelines (American Diabetes Association, 2013). Those who develop diabetes during statin therapy should be encouraged to adhere to a heart-healthy dietary pattern, engage in physical activity, achieve and maintain a healthy body weight, cease tobacco use, and continue statin therapy to reduce their risk of ASCVD events. NHBLI Grade: B (Moderate); ACC/AHA COR: I‡; ACC/AHA LOE: B
7. For individuals taking any dose of statins, it is reasonable to use caution in individuals >75 years of age, as well as in individuals who are taking concomitant medications that alter drug metabolism, taking multiple drugs, or taking drugs for conditions that require complex medication regimens (e.g., those who have undergone solid organ transplantation or are receiving treatment for human immunodeficiency virus [HIV]). A review of the manufacturer's prescribing information may be useful before initiation of any cholesterol-lowering drug. NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (Heart Protection Study Collaborative Group, 2002; "Lescol," 2012; "Pravachol," 2012; "Livalo," 2012; "Zocor," 2012; "Mevacor," 2012; "Lipitor," 2012; "Crestor," 2013; U.S. Food and Drug Administration, 2012; Rawlins, 2008; Schwartz et al., 2001; Shepherd et al., 2006)
8. It is reasonable to evaluate and treat muscle symptoms, including pain, tenderness, stiffness, cramping, weakness, or fatigue, in statin-treated patients according to the following management algorithm: NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B (Taylor et al., 2011; Eckel, 2010; Baigent et al., 2010; Mills et al., 2008; Dale et al., 2007)
- To avoid unnecessary discontinuation of statins, obtain a history of prior or current muscle symptoms to establish a baseline before initiation of statin therapy.
- If unexplained severe muscle symptoms or fatigue develop during statin therapy, promptly discontinue the statin and address the possibility of rhabdomyolysis by evaluating CK and creatinine and performing urinalysis for myoglobinuria.
- If mild to moderate muscle symptoms develop during statin therapy:
- Discontinue the statin until the symptoms can be evaluated.
- Evaluate the patient for other conditions that might increase the risk for muscle symptoms (e.g., hypothyroidism, reduced renal or hepatic function, rheumatologic disorders such as polymyalgia rheumatica, steroid myopathy, vitamin D deficiency, or primary muscle diseases).
- If muscle symptoms resolve, and if no contraindication exists, give the patient the original or a lower dose of the same statin to establish a causal relationship between the muscle symptoms and statin therapy.
- If a causal relationship exists, discontinue the original statin. Once muscle symptoms resolve, use a low dose of a different statin.
- Once a low dose of a statin is tolerated, gradually increase the dose as tolerated.
- If, after 2 months without statin treatment, muscle symptoms or elevated CK levels do not resolve completely, consider other causes of muscle symptoms listed above.
- If persistent muscle symptoms are determined to arise from a condition unrelated to statin therapy, or if the predisposing condition has been treated, resume statin therapy at the original dose.
9. For individuals presenting with a confusional state or memory impairment while on statin therapy, it may be reasonable to evaluate the patient for nonstatin causes, such as exposure to other drugs, as well as for systemic and neuropsychiatric causes, in addition to the possibility of adverse effects associated with statin drug therapy. NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIb; ACC/AHA LOE: C (Shepherd et al., 2002; U.S. Food and Drug Administration, 2012; Collins et al., 2004; Roberts, 2009)
*Based on the presence of clinical ASCVD, diabetes, LDL-C ≥190 mg/dL, or level of estimated 10-year ASCVD risk.
†Individuals with elevated ALT levels (usually >1.5 or 2 times ULN) were excluded from RCT participation. Unexplained ALT ≥3 times ULN is a contraindication to statin therapy as listed in manufacturer's prescribing information.
‡Statin use is associated with a very modest excess risk of new-onset diabetes in RCTs and meta-analyses of RCTs (i.e., ∼0.1 excess cases per 100 individuals treated for 1 year with moderate-intensity statin therapy and ∼0.3 excess cases per 100 individuals treated for 1 year with high-intensity statin therapy. The increased risk of new-onset diabetes appears to be confined to those with risk factors for diabetes. These individuals are also at higher risk of ASCVD because of these risk factors. Therefore, if a statin-treated individual develops diabetes as detected by current diabetes screening guidelines, he or she should be counseled to adhere to a heart-healthy dietary pattern, engage in physical activity, achieve and maintain a healthy body weight, cease tobacco use, and continue statin therapy to reduce the risk of ASCVD events.
Nonstatin Safety Recommendations
Safety of Niacin
1. Baseline hepatic transaminases, fasting blood glucose or hemoglobin A1c, and uric acid should be obtained before initiation of niacin, and again during up-titration to a maintenance dose and every 6 months thereafter. NHLBI Grade: B (Moderate); ACC/AHA COR: I; ACC/AHA LOE: B
2. Niacin should not be used if:
- Hepatic transaminase elevations are higher than 2 to 3 times ULN. NHLBI Grade: A (Strong); ACC/AHA COR: III: Harm; ACC/AHA LOE: B
- Persistent severe cutaneous symptoms, persistent hyperglycemia, acute gout, or unexplained abdominal pain or gastrointestinal symptoms occur. NHLBI Grade: B (Moderate); ACC/AHA COR: III: Harm; ACC/AHA LOE: B
- New-onset atrial fibrillation or weight loss occurs. NHLBI Grade: C (Weak); ACC/AHA COR: III: Harm; ACC/AHA LOE: B
3. In individuals with adverse effects from niacin, the potential for ASCVD benefits and the potential for adverse effects should be reconsidered before reinitiation of niacin therapy. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: I; ACC/AHA LOE: B (AIM-HIGH Investigators et al., 2011; "Clofibrate and niacin in coronary heart disease," 1975; Guyton & Bays, 2007; Brown & Zhao, 2008; Grundy et al., 2002)
4. To reduce the frequency and severity of adverse cutaneous symptoms, it is reasonable to: NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (AIM-HIGH Investigators et al., 2011; "Clofibrate and niacin in coronary heart disease," 1975; Guyton & Bays, 2007; Brown & Zhao, 2008; Grundy et al., 2002)
- Start niacin at a low dose and titrate to a higher dose over a period of weeks as tolerated.
- Take niacin with food or premedicate with aspirin 325 mg 30 minutes before niacin dosing to alleviate flushing symptoms.
- If an extended-release preparation is used, increase the dose of extended-release niacin from 500 mg to a maximum of 2,000 mg/day over 4 to 8 weeks, with the dose of extended-release niacin increasing not more than weekly.
- If immediate-release niacin is chosen, start at a dose of 100 mg 3 times daily and up-titrate to 3 g/day, divided into 2 or 3 doses.
Safety of Bile Acid Sequestrants (BAS)
1. BAS should not be used in individuals with baseline fasting triglyceride levels ≥300 mg/dL or type III hyperlipoproteinemia, because severe triglyceride elevations might occur. (A fasting lipid panel should be obtained before BAS is initiated, 3 months after initiation, and every 6 to 12 months thereafter.) NHLBI Grade: C (Weak); ACC/AHA COR: III: Harm; ACC/AHA LOE: B
2. It is reasonable to use BAS with caution if baseline triglyceride levels are 250 to 299 mg/dL, and evaluate a fasting lipid panel in 4 to 6 weeks after initiation. Discontinue the BAS if triglycerides exceed 400 mg/dL. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (Crouse, 1987)
Safety of Cholesterol-Absorption Inhibitors
1. It is reasonable to obtain baseline hepatic transaminases before initiation of ezetimibe. When ezetimibe is coadministered with a statin, monitor transaminase levels as clinically indicated, and discontinue ezetimibe if persistent ALT elevations ≥3 times ULN occur. NHLBI Grade: C (Weak); ACC/AHA COR: IIa; ACC/AHA LOE: B
Safety of Fibrates
1. Gemfibrozil should not be initiated in patients on statin therapy because of an increased risk for muscle symptoms and rhabdomyolysis. NHLBI Grade: B (Moderate); ACC/AHA COR: III: Harm; ACC/AHA LOE: B
2. Fenofibrate may be considered concomitantly with a low- or moderate-intensity statin only if the benefits from ASCVD risk reduction or triglyceride lowering when triglycerides are ≥500 mg/dL are judged to outweigh the potential risk for adverse effects. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIb; ACC/AHA LOE: C (ACCORD Study Group et al., 2010)
3. Renal status should be evaluated before fenofibrate initiation, within 3 months after initiation, and every 6 months thereafter. Assess renal safety with both a serum creatinine level and an estimated glomerular filtration rate (eGFR) based on creatinine. NHLBI Grade: B (Moderate); ACC/AHA COR: I; ACC/AHA LOE: B
- Fenofibrate should not be used if moderate or severe renal impairment, defined as eGFR <30 mL/min per 1.73 m2, is present. ACC/AHA COR: III: Harm; ACC/AHA LOE: B
- If eGFR is between 30 and 59 mL/min per 1.73 m2, the dose of fenofibrate should not exceed 54 mg/day.*
- If, during follow-up, the eGFR decreases persistently to ≤30 mL/min per 1.73 m2, fenofibrate should be discontinued.
*Consult the manufacturer's prescribing information as there are several forms of fenofibrate available.
Safety of Omega-3 Fatty Acids
1. If eicosapentaenoic acid (EPA) and/or docosahexanoic acid (DHA) are used for the management of severe hypertriglyceridemia, defined as triglycerides ≥500 mg/dL, it is reasonable to evaluate the patient for gastrointestinal disturbances, skin changes, and bleeding. NHLBI Grade: C (Weak); ACC/AHA COR: IIa; ACC/AHA LOE: B
Recommendations for Monitoring, Optimizing, and Addressing Insufficient Response to Statin Therapy
Monitoring Statin Therapy
1. Adherence to medication and lifestyle, therapeutic response to statin therapy, and safety should be regularly assessed. This should also include a fasting lipid panel performed within 4–12 weeks after initiation or dose adjustment, and every 3–12 months thereafter. Other safety measurements should be measured as clinically indicated. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
Optimizing Statin Therapy
1. The maximum tolerated intensity of statin should be used in individuals for whom a high- or moderate-intensity statin is recommended but not tolerated. NHLBI Grade: B (Moderate); ACC/AHA COR: I*; ACC/AHA LOE: B
Insufficient Response to Statin Therapy
1. In individuals who have a less-than-anticipated therapeutic response or are intolerant of the recommended intensity of statin therapy, the following should be performed: NHLBI Grade A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
- Reinforce medication adherence.
- Reinforce adherence to intensive lifestyle changes.
- Exclude secondary causes of hyperlipidemia.
2. It is reasonable to use the following as indicators of anticipated therapeutic response to the recommended intensity of statin therapy. Focus is on the intensity of the statin therapy. As an aid to monitoring: NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B (LaRosa et al., 2005; Pedersen et al., 2005; Cannon et al., 2004; Amarenco et al., 2006; Thompson & HEART-UK LDL Apheresis Working Group, 2008; Schwertz & Badellino, 2008)
- High-intensity statin therapy† generally results in an average LDL-C reduction of ≥50% from the untreated baseline.
- Moderate-intensity statin therapy generally results in an average LDL-C reduction of 30% to <50% from the untreated baseline.
- LDL-C levels and percents reduction are to be used only to assess response to therapy and adherence. They are not to be used as performance standards.
3. In individuals at higher ASCVD risk receiving the maximum tolerated intensity of statin therapy who continue to have a less-than-anticipated therapeutic response, addition of nonstatin cholesterol-lowering drug(s) may be considered if the ASCVD risk-reduction benefits outweigh the potential for adverse effects. Higher-risk individuals include: NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIb: ACC/AHA LOE: C (AIM-HIGH Investigators et al., 2011; ACCORD Study Group et al., 2010; Rossebo et al., 2007; Sharp Collaborative Group, 2010; Yokoyama, Origasa, & JELIS Investigators, 2003)
- Individuals with clinical ASCVD‡ <75 years of age.
- Individuals with baseline LDL-C ≥190 mg/dL.
- Individuals 40 to 75 years of age with diabetes.
Preference should be given to nonstatin cholesterol-lowering drugs shown to reduce ASCVD events in RCTs.
4. In individuals who are candidates for statin treatment but are completely statin intolerant, it is reasonable to use nonstatin cholesterol-lowering drugs that have been shown to reduce ASCVD events in RCTs if the ASCVD risk-reduction benefits outweigh the potential for adverse effects. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B (Eckel, 2010; "Clofibrate and niacin in coronary heart disease," 1975; Frick et al., 1987; Lipid Research Clinics Program, 1984; "The Lipid Research Clinics Coronary Primary Prevention Trial results. II.," 1984; Rubins et al., 1999; Keech et al., 2005; HPS2-THRIVE Collaborative Group, 2013)
*Several RCTs found that low-intensity and low-moderate–intensity statin therapy reduced ASCVD events. In addition, the Cholesterol Treatment Trialists meta-analyses found that each 39-mg/dL reduction in LDL-C reduces ASCVD risk by 22%. Therefore, the Panel considered that submaximal statin therapy should be used to reduce ASCVD risk in those unable to tolerate moderate- or high-intensity statin therapy.
†In those already on a statin, in whom baseline LDL-C is unknown, an LDL-C level <100 mg/dL was observed in most individuals receiving high-intensity statin therapy.
‡Clinical ASCVD includes acute coronary syndromes, or a history of myocardial infarction, stable or unstable angina, coronary or other arterial revascularization, stroke, transient ischemic attack, or peripheral arterial disease presumed to be of atherosclerotic origin.
Definitions:
NHLBI Grading of the Strength of Recommendations
| Grade | Strength of Recommendation* |
|---|---|
| A | Strong recommendation There is high certainty based on evidence that the net benefit† is substantial. |
| B | Moderate recommendation There is moderate certainty based on evidence that the net benefit is moderate to substantial, or there is high certainty that the net benefit is moderate. |
| C | Weak recommendation There is at least moderate certainty based on evidence that there is a small net benefit. |
| D | Recommendation against There is at least moderate certainty based on evidence that there is no net benefit or that risks/harms outweigh benefits. |
| E | Expert opinion ("There is insufficient evidence or evidence is unclear or conflicting, but this is what the Work Group recommends.") Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, unclear evidence, or conflicting evidence, but the Work Group thought it was important to provide clinical guidance and make a recommendation. Further research is recommended in this area. |
| N | No recommendation for or against ("There is insufficient evidence or evidence is unclear or conflicting.") Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, unclear evidence, or conflicting evidence, and the Work Group thought no recommendation should be made. Further research is recommended in this area. |
*In most cases, the strength of the recommendation should be closely aligned with the quality of the evidence; however, under some circumstances, there may be valid reasons for making recommendations that are not closely aligned with the quality of the evidence (e.g., strong recommendation when the evidence quality is moderate, such as smoking cessation to reduce cardiovascular disease [CVD] risk or ordering an electrocardiogram [ECG] as part of the initial diagnostic work-up for a patient presenting with possible myocardial infarction [MI]). Those situations should be limited and the rationale explained clearly by the Work Group.
†Net benefit is defined as benefits minus risks/harms of the service/intervention.
NHLBI Quality Rating of the Strength of Evidence
| Type of Evidence | Quality Rating* |
|---|---|
| High |
| Moderate |
| Low |
*In some cases, other evidence, such as large all-or-none case series (e.g., jumping from airplanes or tall structures), can represent high- or moderate-quality evidence. In such cases, the rationale for the evidence rating exception should be explained by the Work Group and clearly justified.
†"Well-designed, well-executed" refers to studies that directly address the question; use adequate randomization, blinding, and allocation concealment; are adequately powered; use intention-to-treat analyses; and have high follow-up rates.
‡Limitations include concerns with the design and execution of a study that result in decreased confidence in the true estimate of the effect. Examples of such limitations include but are not limited to: inadequate randomization, lack of blinding of study participants or outcome assessors, inadequate power, outcomes of interest that are not prespecified for the primary outcomes, low follow-up rates, and findings based on subgroup analyses. Whether the limitations are considered minor or major is based on the number and severity of flaws in design or execution. Rules for determining whether the limitations are considered minor or major and how they will affect rating of the individual studies will be developed collaboratively with the methodology team.
§Nonrandomized controlled studies refer to intervention studies where assignment to intervention and comparison groups is not random (e.g., quasi-experimental study design).
¶Observational studies include prospective and retrospective cohort, case-control, and cross-sectional studies.
Applying Classification of Recommendations and Level of Evidence
| Size of Treatment Effect | |||||||
|---|---|---|---|---|---|---|---|
| CLASS I Benefit >>> Risk Procedure/Treatment SHOULD be performed/ administered | CLASS IIa Benefit >> Risk Additional studies with focused objectives needed IT IS REASONABLE to perform procedure/administer treatment | CLASS IIb Benefit ≥ Risk Additional studies with broad objectives needed; additional registry data would be helpful Procedure/Treatment MAY BE CONSIDERED | CLASS III No Benefit or Class III Harm | ||||
| Procedure/Test | Treatment | ||||||
| COR III: No Benefit | Not helpful | No proven benefit | |||||
| COR III: Harm | Excess cost without benefit or harmful | Harmful to patients | |||||
| Estimate of Certainty (Precision) of Treatment Effect | LEVEL A Multiple populations evaluated* Data derived from multiple randomized clinical trials or meta-analyses |
|
|
|
| ||
| LEVEL B Limited populations evaluated* Data derived from a single randomized trial or nonrandomized studies |
|
|
|
| |||
| LEVEL C Very limited populations evaluated* Only consensus opinion of experts, case studies, or standard of care |
|
|
|
| |||
A recommendation with Level of Evidence B or C does not imply that the recommendation is weak. Many important clinical questions addressed in the guidelines do not lend themselves to clinical trials. Although randomized trials are unavailable, there may be a very clear clinical consensus that a particular test or therapy is useful or effective.
*Data available from clinical trials or registries about the usefulness/efficacy in different subpopulations, such as sex, age, history of diabetes, history of prior myocardial infarction, history of heart failure, and prior aspirin use.
†For comparative-effectiveness recommendations (Class I and IIa; Level of Evidence A and B only), studies that support the use of comparator verbs should involve direct comparisons of the treatments or strategies being evaluated.
- Summary of Statin Initiation Recommendations for the Treatment of Blood Cholesterol to Reduce ASCVD Risk in Adults
- Initiating Statin Therapy in Individuals with Clinical ASCVD
- Initiating Statin Therapy in Individuals without Clinical ASCVD
- Statin Therapy: Monitoring Therapeutic Response and Adherence
Recommendations
Each recommendation has been mapped from the NHLBI grading format to the American College of Cardiology/American Heart Association Class of Recommendation/Level of Evidence (ACC/AHA COR/LOE) construct and is expressed in both formats. Because of the inherent differences in grading systems and the clinical questions driving the recommendations, alignment between the NHLBI and ACC/AHA formats is in some cases imperfect. Definitions for the NHLBI strength of recommendation (A-E, N) and quality of evidence (High, Moderate, Low) and the ACC/AHA levels of the evidence (LOE: A-C) and classes of recommendations (COR: I-III) are provided at the end of the "Major Recommendations" field.
What's New in the Guideline?
Focus on Atherosclerotic Cardiovascular Disease (ASCVD Risk) Reduction: 4 Statin Benefit Groups
1. This guideline is based on a comprehensive set of data from randomized control trials (RCTs) from which 4 statin benefit groups were identified that focus efforts to reduce ASCVD events in secondary and primary prevention.
2. This guideline identifies high-intensity and moderate-intensity statin therapy for use in secondary and primary prevention.
A New Perspective on Low-density Lipoprotein Cholesterol (LDL-C) and/or Non–High-density Lipoprotein Cholesterol (HDL-C) Treatment Goals
1. The Expert Panel was unable to find RCT evidence to support continued use of specific LDL-C or non–HDL-C treatment targets.
2. The appropriate intensity of statin therapy should be used to reduce ASCVD risk in those most likely to benefit.
3. Nonstatin therapies, as compared with statin therapy, do not provide acceptable ASCVD risk-reduction benefits relative to their potential for adverse effects in the routine prevention of ASCVD.
Global Risk Assessment for Primary Prevention
1. This guideline recommends use of the new Pooled Cohort Equations to estimate 10-year ASCVD risk in both white and black men and women.
2. By more accurately identifying higher-risk individuals for statin therapy, the guideline focuses statin therapy on those most likely to benefit.
3. It also indicates, on the basis of RCT data, those high-risk groups that might not benefit.
4. This guideline recommends a discussion between clinicians and patients before initiation of statin therapy.
Safety Recommendations
1. This guideline used RCTs to identify important safety considerations in individuals receiving treatment of blood cholesterol to reduce ASCVD risk.
2. Using RCTs to determine statin adverse effects facilitates understanding of the net benefit from statin therapy.
3. This guideline provides expert guidance on management of statin-associated adverse effects, including muscle symptoms.
Role of Biomarkers and Noninvasive Tests
1. Treatment decisions in selected individuals who are not included in the 4 statin benefit groups may be informed by other factors as recommended by the Risk Assessment Work Group and Blood Cholesterol Expert Panel.
Future Updates to the Blood Cholesterol Guideline
1. This is a comprehensive guideline for the evidence-based treatment of blood cholesterol to reduce ASCVD risk.
2. Future updates will build on this foundation to provide expert guidance on the management of complex lipid disorders and incorporate refinements in risk stratification based on critical review of emerging data.
3. RCTs comparing alternative treatment strategies are needed in order to inform future evidence-based guidelines for the optimum ASCVD risk-reduction approach.
Note: See Appendix 5 in the original guideline document for an expanded discussion of what's new in the guideline.
Recommendations for Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults—Statin Treatment
Treatment Targets
1. The Expert Panel makes no recommendations for or against specific LDL-C or non–HDL-C targets for the primary or secondary prevention of ASCVD. NHLBI Grade: N (No recommendation); ACC/AHA COR: n/a; ACC/AHA LOE: n/a
Secondary Prevention
1. High-intensity statin therapy should be initiated or continued as first-line therapy in women and men ≤75 years of age who have clinical ASCVD*, unless contraindicated. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
2. In individuals with clinical ASCVD* in whom high-intensity statin therapy would otherwise be used, when high-intensity statin therapy is contraindicated† or when characteristics predisposing to statin-associated adverse effects are present, moderate-intensity statin should be used as the second option if tolerated (see "Safety of Statins," below). NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
3. In individuals with clinical ASCVD >75 years of age, it is reasonable to evaluate the potential for ASCVD risk-reduction benefits and for adverse effects and drug–drug interactions and to consider patient preferences when initiating a moderate- or high-intensity statin. It is reasonable to continue statin therapy in those who are tolerating it. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B (Heart Protection Study Collaborative Group, 2002; Cholesterol Treatment Trialists' [CTT] Collaboration et al., 2010; Tikkanen et al., 2009; Holmes et al., 2006; Akushevich et al., 2012; Wolff, Starfield &, Anderson, 2002; Fried et al., "Effects," 2011; Robinson et al., 2007; Porock et al., 2005; Stineman et al., 2012; Schonberg et al., 2011; Fried et al., "Health outcome," 2011; Barry & Edgman-Levitan, 2012; Man-Son-Hing, Gage, & Montgomery, 2005; Fried et al., 2002; Ditto et al., 1996; Rosenfeld, Wenger, & Kagawa-Singer, 2000; Nease et al., 1995; Glynn et al., 2010; Shepherd et al., 2002; Trompet et al., 2010; Gray et al., 2011; LaCroix et al., 2008; Hippisley-Cox et al., 2005; Forman et al., 2011)
Primary Prevention in Individuals ≥21 Years of Age with LDL-C ≥190 mg/dL
1. Individuals with LDL-C ≥190 mg/dL or triglycerides ≥500 mg/dL should be evaluated for secondary causes of hyperlipidemia (see Table 6 in the original guideline document). NHLBI Grade: B (Moderate); ACC/AHA COR: I‡; ACC/AHA LOE: B (Berglund et al., 2012; Miller et al., 2011)
2. Adults ≥21 years of age with primary LDL-C ≥190 mg/dL should be treated with statin therapy (10-year ASCVD risk estimation is not required) NHLBI Grade: B (Moderate); ACC/AHA COR: I§; ACC/AHA LOE: B:
- Use high-intensity statin therapy unless contraindicated.
- For individuals unable to tolerate high-intensity statin therapy, use the maximum tolerated statin intensity.
3. For individuals ≥21 years of age with an untreated primary LDL-C ≥190 mg/dL, it is reasonable to intensify statin therapy to achieve at least a 50% LDL-C reduction. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B (CTT Collaboration et al., 2010; LaRosa et al., 2005; Pedersen et al., 2005; Cannon et al., 2004; Ridker et al, 2008; Baigent et al., 2005)
4. For individuals ≥21 years of age with an untreated primary LDL-C ≥190 mg/dL, after the maximum intensity of statin therapy has been achieved, addition of a nonstatin drug may be considered to further lower LDL-C. Evaluate the potential for ASCVD risk-reduction benefits, adverse effects, and drug–drug interactions, and consider patient preferences. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIb; ACC/AHA LOE: C (Thompson, Packard, & Stone, 2004)
Primary Prevention in Individuals with Diabetes and LDL-C 70–189 mg/dL
1. Moderate-intensity statin therapy should be initiated or continued for adults 40 to 75 years of age with diabetes. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
2. High-intensity statin therapy is reasonable for adults 40 to 75 years of age with diabetes with a ≥7.5% estimated 10-year ASCVD risk‖ unless contraindicated. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B (Ridker et al., 2008; Ridker et al., 2012)
3. In adults with diabetes, who are <40 years of age or >75 years of age, or with LDL <70 mg/dL, it is reasonable to evaluate the potential for ASCVD benefits and for adverse effects and drug–drug interactions and to consider patient preferences when deciding to initiate, continue, or intensify statin therapy. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (Roffi, Angiolillo, & Kappetein, 2011; Nathan et al., 2005; Rhodes et al., 2012; Paynter et al., 2011; Elley et al., 2010; Stevens et al., 2004; Bibbins-Domingo et al., 2007; Daniels et al., 2009; Jacob & Cho, 2010; Bainey & Jugdutt, 2009)
Primary Prevention in Individuals without Diabetes and with LDL-C 70–189 mg/dL
1. The Pooled Cohort Equations should be used to estimate 10-year ASCVD‖ risk for individuals with LDL-C 70–189 mg/dL without clinical ASCVD* to guide initiation of statin therapy for the primary prevention of ASCVD. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: I; ACC/AHA LOE: B (Goff et al., 2014)
2. Adults 40 to 75 years of age with LDL-C 70–189 mg/dL, without clinical ASCVD* or diabetes, and with an estimated 10-year ASCVD‖ risk ≥7.5% should be treated with moderate- to high-intensity statin therapy. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
3. It is reasonable to offer treatment with a moderate-intensity statin to adults 40 to 75 years of age, with LDL-C 70–189 mg/dL, without clinical ASCVD* or diabetes, and with an estimated 10-year ASCVD‖ risk of 5% to <7.5%. NHLBI Grade: C (Weak); ACC/AHA COR: IIa; ACC/AHA LOE: B
4. Before initiation of statin therapy for the primary prevention of ASCVD in adults with LDL-C 70–189 mg/dL without clinical ASCVD* or diabetes, it is reasonable for clinicians and patients to engage in a discussion that considers the potential for ASCVD risk-reduction benefits and for adverse effects and drug–drug interactions, as well as patient preferences for treatment. NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (Yu et al., 2013)
5. In adults with LDL-C <190 mg/dL who are not otherwise identified in a statin benefit group, or for whom after quantitative risk assessment a risk-based treatment decision is uncertain, additional factors¶ may be considered to inform treatment decision making. In these individuals, statin therapy for primary prevention may be considered after evaluation of the potential for ASCVD risk-reduction benefits, adverse effects, and drug–drug interactions and consider patient preferences. NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIb; ACC/AHA LOE: C (Goff et al., 2014; CTT Collaborators et al., 2012)
Heart Failure and Hemodialysis
1. The Expert Panel makes no recommendations regarding the initiation or discontinuation of statins in patients with NYHA class II–IV ischemic systolic heart failure or in patients on maintenance hemodialysis. NHBLI Grade: N (No Recommendation); ACC/AHA COR: n/a; ACC/AHA LOE: n/a
*Clinical ASCVD includes acute coronary syndromes, history of myocardial infarction (MI), stable or unstable angina, coronary or other arterial revascularization, stroke, transient ischaemic attack (TIA), or peripheral arterial disease presumed to be of atherosclerotic origin.
†Contraindications, warnings, and precautions are defined for each statin according to the manufacturer's prescribing information ("Lescol," 2012; "Pravachol," 2012; "Livalo," 2012; "Zocor," 2012; "Mevacor," 2012; "Lipitor," 2012; "Crestor," 2013).
‡Individuals with secondary causes of hyperlipidemia were excluded from RCTs reviewed. A triglyceride level ≥500 mg/dL was an exclusion criterion for almost all RCTs. Therefore, ruling out secondary causes is necessary to avoid inappropriate statin therapy.
§No RCTs included only individuals with LDL-C ≥190 mg/dL. However, many trials did include individuals with LDL-C ≥190 mg/dL, and all of these trials consistently demonstrated a reduction in ASCVD events. In addition, the Cholesterol Treatment Trialists meta-analyses have shown that each 39-mg/dL reduction in LDL-C with statin therapy reduced ASCVD events by 22%, and the relative reductions in ASCVD events were consistent across the range of LDL-C levels. Therefore, individuals with primary LDL-C ≥190 mg/dL should be treated with statin therapy.
ǁEstimated 10-year or "hard" ASCVD risk includes first occurrence of nonfatal MI, coronary heart disease death, and nonfatal and fatal stroke as used by the Risk Assessment Work Group in developing the Pooled Cohort Equations.
¶These factors may include primary LDL-C ≥160 mg/dL or other evidence of genetic hyperlipidemias; family history of premature ASCVD with onset <55 years of age in a first-degree male relative or <65 years of age in a first-degree female relative; high-sensitivity C-reactive protein ≥2 mg/L; coronary artery calcium (CAC) score ≥300 Agatston units or ≥75th percentile for age, sex, and ethnicity (for additional information, see http://www.mesa-nhlbi.org/CACReference.aspx ![]()
See Table 5 in the original guideline document for high-, moderate-, and low-intensity statin therapies used in the RCTs reviewed by the Expert Panel.
Statin Safety Recommendations
Safety
1. To maximize the safety of statins, selection of the appropriate statin and dose in men and nonpregnant/nonnursing women should be based on patient characteristics, level of ASCVD* risk, and potential for adverse effects. Moderate-intensity statin therapy should be used in individuals in whom high-intensity statin therapy would otherwise be recommended when characteristics predisposing them to statin-associated adverse effects are present. Characteristics predisposing individuals to statin adverse effects include but are not limited to: NHBLI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: B
- Multiple or serious comorbidities, including impaired renal or hepatic function
- History of previous statin intolerance or muscle disorders
- Unexplained alanine aminotransferase (ALT) elevations ≥3 times the upper limit of normal (ULN)
- Patient characteristics or concomitant use of drugs affecting statin metabolism
- Age >75 years
Additional characteristics that could modify the decision to use higher statin intensities might include but are not limited to:
- History of hemorrhagic stroke
- Asian ancestry
2a. Creatine kinase (CK) should not be routinely measured in individuals receiving statin therapy. NHBLI Grade: A (Strong); ACC/AHA COR: III: No Benefit; ACC/AHA LOE: A
2b. Baseline measurement of CK is reasonable for individuals believed to be at increased risk for adverse muscle events because of a personal or family history of statin intolerance or muscle disease, clinical presentation, or concomitant drug therapy that might increase the risk of myopathy. NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (Eckel, 2010)
2c. During statin therapy, it is reasonable to measure CK in individuals with muscle symptoms, including pain, tenderness, stiffness, cramping, weakness, or generalized fatigue. NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (Eckel, 2010)
3a. Baseline measurement of hepatic transaminase levels (ALT) should be performed before initiation of statin therapy. NHBLI Grade: B (Moderate); ACC/AHA COR: I†; ACC/AHA LOE: B
3b. During statin therapy, it is reasonable to measure hepatic function if symptoms suggesting hepatotoxicity arise (e.g., unusual fatigue or weakness, loss of appetite, abdominal pain, dark-colored urine, or yellowing of the skin or sclera). NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (U.S. Food and Drug Administration, 2012)
4. Decreasing the statin dose may be considered when 2 consecutive values of LDL-C levels are <40 mg/dL. NHBLI Grade: C (Weak); ACC/AHA COR: IIb; ACC/AHA LOE: C
5. It may be harmful to initiate simvastatin at 80 mg daily or increase the dose of simvastatin to 80 mg daily. NHBLI Grade: B (Moderate); ACC/AHA COR: III: Harm; ACC/AHA LOE: A ("Zocor," 2012; U.S. Food and Drug Administration, 2010)
6. Individuals receiving statin therapy should be evaluated for new-onset diabetes according to the current diabetes screening guidelines (American Diabetes Association, 2013). Those who develop diabetes during statin therapy should be encouraged to adhere to a heart-healthy dietary pattern, engage in physical activity, achieve and maintain a healthy body weight, cease tobacco use, and continue statin therapy to reduce their risk of ASCVD events. NHBLI Grade: B (Moderate); ACC/AHA COR: I‡; ACC/AHA LOE: B
7. For individuals taking any dose of statins, it is reasonable to use caution in individuals >75 years of age, as well as in individuals who are taking concomitant medications that alter drug metabolism, taking multiple drugs, or taking drugs for conditions that require complex medication regimens (e.g., those who have undergone solid organ transplantation or are receiving treatment for human immunodeficiency virus [HIV]). A review of the manufacturer's prescribing information may be useful before initiation of any cholesterol-lowering drug. NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (Heart Protection Study Collaborative Group, 2002; "Lescol," 2012; "Pravachol," 2012; "Livalo," 2012; "Zocor," 2012; "Mevacor," 2012; "Lipitor," 2012; "Crestor," 2013; U.S. Food and Drug Administration, 2012; Rawlins, 2008; Schwartz et al., 2001; Shepherd et al., 2006)
8. It is reasonable to evaluate and treat muscle symptoms, including pain, tenderness, stiffness, cramping, weakness, or fatigue, in statin-treated patients according to the following management algorithm: NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B (Taylor et al., 2011; Eckel, 2010; Baigent et al., 2010; Mills et al., 2008; Dale et al., 2007)
- To avoid unnecessary discontinuation of statins, obtain a history of prior or current muscle symptoms to establish a baseline before initiation of statin therapy.
- If unexplained severe muscle symptoms or fatigue develop during statin therapy, promptly discontinue the statin and address the possibility of rhabdomyolysis by evaluating CK and creatinine and performing urinalysis for myoglobinuria.
- If mild to moderate muscle symptoms develop during statin therapy:
- Discontinue the statin until the symptoms can be evaluated.
- Evaluate the patient for other conditions that might increase the risk for muscle symptoms (e.g., hypothyroidism, reduced renal or hepatic function, rheumatologic disorders such as polymyalgia rheumatica, steroid myopathy, vitamin D deficiency, or primary muscle diseases).
- If muscle symptoms resolve, and if no contraindication exists, give the patient the original or a lower dose of the same statin to establish a causal relationship between the muscle symptoms and statin therapy.
- If a causal relationship exists, discontinue the original statin. Once muscle symptoms resolve, use a low dose of a different statin.
- Once a low dose of a statin is tolerated, gradually increase the dose as tolerated.
- If, after 2 months without statin treatment, muscle symptoms or elevated CK levels do not resolve completely, consider other causes of muscle symptoms listed above.
- If persistent muscle symptoms are determined to arise from a condition unrelated to statin therapy, or if the predisposing condition has been treated, resume statin therapy at the original dose.
9. For individuals presenting with a confusional state or memory impairment while on statin therapy, it may be reasonable to evaluate the patient for nonstatin causes, such as exposure to other drugs, as well as for systemic and neuropsychiatric causes, in addition to the possibility of adverse effects associated with statin drug therapy. NHBLI Grade: E (Expert Opinion); ACC/AHA COR: IIb; ACC/AHA LOE: C (Shepherd et al., 2002; U.S. Food and Drug Administration, 2012; Collins et al., 2004; Roberts, 2009)
*Based on the presence of clinical ASCVD, diabetes, LDL-C ≥190 mg/dL, or level of estimated 10-year ASCVD risk.
†Individuals with elevated ALT levels (usually >1.5 or 2 times ULN) were excluded from RCT participation. Unexplained ALT ≥3 times ULN is a contraindication to statin therapy as listed in manufacturer's prescribing information.
‡Statin use is associated with a very modest excess risk of new-onset diabetes in RCTs and meta-analyses of RCTs (i.e., ∼0.1 excess cases per 100 individuals treated for 1 year with moderate-intensity statin therapy and ∼0.3 excess cases per 100 individuals treated for 1 year with high-intensity statin therapy. The increased risk of new-onset diabetes appears to be confined to those with risk factors for diabetes. These individuals are also at higher risk of ASCVD because of these risk factors. Therefore, if a statin-treated individual develops diabetes as detected by current diabetes screening guidelines, he or she should be counseled to adhere to a heart-healthy dietary pattern, engage in physical activity, achieve and maintain a healthy body weight, cease tobacco use, and continue statin therapy to reduce the risk of ASCVD events.
Nonstatin Safety Recommendations
Safety of Niacin
1. Baseline hepatic transaminases, fasting blood glucose or hemoglobin A1c, and uric acid should be obtained before initiation of niacin, and again during up-titration to a maintenance dose and every 6 months thereafter. NHLBI Grade: B (Moderate); ACC/AHA COR: I; ACC/AHA LOE: B
2. Niacin should not be used if:
- Hepatic transaminase elevations are higher than 2 to 3 times ULN. NHLBI Grade: A (Strong); ACC/AHA COR: III: Harm; ACC/AHA LOE: B
- Persistent severe cutaneous symptoms, persistent hyperglycemia, acute gout, or unexplained abdominal pain or gastrointestinal symptoms occur. NHLBI Grade: B (Moderate); ACC/AHA COR: III: Harm; ACC/AHA LOE: B
- New-onset atrial fibrillation or weight loss occurs. NHLBI Grade: C (Weak); ACC/AHA COR: III: Harm; ACC/AHA LOE: B
3. In individuals with adverse effects from niacin, the potential for ASCVD benefits and the potential for adverse effects should be reconsidered before reinitiation of niacin therapy. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: I; ACC/AHA LOE: B (AIM-HIGH Investigators et al., 2011; "Clofibrate and niacin in coronary heart disease," 1975; Guyton & Bays, 2007; Brown & Zhao, 2008; Grundy et al., 2002)
4. To reduce the frequency and severity of adverse cutaneous symptoms, it is reasonable to: NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (AIM-HIGH Investigators et al., 2011; "Clofibrate and niacin in coronary heart disease," 1975; Guyton & Bays, 2007; Brown & Zhao, 2008; Grundy et al., 2002)
- Start niacin at a low dose and titrate to a higher dose over a period of weeks as tolerated.
- Take niacin with food or premedicate with aspirin 325 mg 30 minutes before niacin dosing to alleviate flushing symptoms.
- If an extended-release preparation is used, increase the dose of extended-release niacin from 500 mg to a maximum of 2,000 mg/day over 4 to 8 weeks, with the dose of extended-release niacin increasing not more than weekly.
- If immediate-release niacin is chosen, start at a dose of 100 mg 3 times daily and up-titrate to 3 g/day, divided into 2 or 3 doses.
Safety of Bile Acid Sequestrants (BAS)
1. BAS should not be used in individuals with baseline fasting triglyceride levels ≥300 mg/dL or type III hyperlipoproteinemia, because severe triglyceride elevations might occur. (A fasting lipid panel should be obtained before BAS is initiated, 3 months after initiation, and every 6 to 12 months thereafter.) NHLBI Grade: C (Weak); ACC/AHA COR: III: Harm; ACC/AHA LOE: B
2. It is reasonable to use BAS with caution if baseline triglyceride levels are 250 to 299 mg/dL, and evaluate a fasting lipid panel in 4 to 6 weeks after initiation. Discontinue the BAS if triglycerides exceed 400 mg/dL. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: C (Crouse, 1987)
Safety of Cholesterol-Absorption Inhibitors
1. It is reasonable to obtain baseline hepatic transaminases before initiation of ezetimibe. When ezetimibe is coadministered with a statin, monitor transaminase levels as clinically indicated, and discontinue ezetimibe if persistent ALT elevations ≥3 times ULN occur. NHLBI Grade: C (Weak); ACC/AHA COR: IIa; ACC/AHA LOE: B
Safety of Fibrates
1. Gemfibrozil should not be initiated in patients on statin therapy because of an increased risk for muscle symptoms and rhabdomyolysis. NHLBI Grade: B (Moderate); ACC/AHA COR: III: Harm; ACC/AHA LOE: B
2. Fenofibrate may be considered concomitantly with a low- or moderate-intensity statin only if the benefits from ASCVD risk reduction or triglyceride lowering when triglycerides are ≥500 mg/dL are judged to outweigh the potential risk for adverse effects. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIb; ACC/AHA LOE: C (ACCORD Study Group et al., 2010)
3. Renal status should be evaluated before fenofibrate initiation, within 3 months after initiation, and every 6 months thereafter. Assess renal safety with both a serum creatinine level and an estimated glomerular filtration rate (eGFR) based on creatinine. NHLBI Grade: B (Moderate); ACC/AHA COR: I; ACC/AHA LOE: B
- Fenofibrate should not be used if moderate or severe renal impairment, defined as eGFR <30 mL/min per 1.73 m2, is present. ACC/AHA COR: III: Harm; ACC/AHA LOE: B
- If eGFR is between 30 and 59 mL/min per 1.73 m2, the dose of fenofibrate should not exceed 54 mg/day.*
- If, during follow-up, the eGFR decreases persistently to ≤30 mL/min per 1.73 m2, fenofibrate should be discontinued.
*Consult the manufacturer's prescribing information as there are several forms of fenofibrate available.
Safety of Omega-3 Fatty Acids
1. If eicosapentaenoic acid (EPA) and/or docosahexanoic acid (DHA) are used for the management of severe hypertriglyceridemia, defined as triglycerides ≥500 mg/dL, it is reasonable to evaluate the patient for gastrointestinal disturbances, skin changes, and bleeding. NHLBI Grade: C (Weak); ACC/AHA COR: IIa; ACC/AHA LOE: B
Recommendations for Monitoring, Optimizing, and Addressing Insufficient Response to Statin Therapy
Monitoring Statin Therapy
1. Adherence to medication and lifestyle, therapeutic response to statin therapy, and safety should be regularly assessed. This should also include a fasting lipid panel performed within 4–12 weeks after initiation or dose adjustment, and every 3–12 months thereafter. Other safety measurements should be measured as clinically indicated. NHLBI Grade: A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
Optimizing Statin Therapy
1. The maximum tolerated intensity of statin should be used in individuals for whom a high- or moderate-intensity statin is recommended but not tolerated. NHLBI Grade: B (Moderate); ACC/AHA COR: I*; ACC/AHA LOE: B
Insufficient Response to Statin Therapy
1. In individuals who have a less-than-anticipated therapeutic response or are intolerant of the recommended intensity of statin therapy, the following should be performed: NHLBI Grade A (Strong); ACC/AHA COR: I; ACC/AHA LOE: A
- Reinforce medication adherence.
- Reinforce adherence to intensive lifestyle changes.
- Exclude secondary causes of hyperlipidemia.
2. It is reasonable to use the following as indicators of anticipated therapeutic response to the recommended intensity of statin therapy. Focus is on the intensity of the statin therapy. As an aid to monitoring: NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B (LaRosa et al., 2005; Pedersen et al., 2005; Cannon et al., 2004; Amarenco et al., 2006; Thompson & HEART-UK LDL Apheresis Working Group, 2008; Schwertz & Badellino, 2008)
- High-intensity statin therapy† generally results in an average LDL-C reduction of ≥50% from the untreated baseline.
- Moderate-intensity statin therapy generally results in an average LDL-C reduction of 30% to <50% from the untreated baseline.
- LDL-C levels and percents reduction are to be used only to assess response to therapy and adherence. They are not to be used as performance standards.
3. In individuals at higher ASCVD risk receiving the maximum tolerated intensity of statin therapy who continue to have a less-than-anticipated therapeutic response, addition of nonstatin cholesterol-lowering drug(s) may be considered if the ASCVD risk-reduction benefits outweigh the potential for adverse effects. Higher-risk individuals include: NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIb: ACC/AHA LOE: C (AIM-HIGH Investigators et al., 2011; ACCORD Study Group et al., 2010; Rossebo et al., 2007; Sharp Collaborative Group, 2010; Yokoyama, Origasa, & JELIS Investigators, 2003)
- Individuals with clinical ASCVD‡ <75 years of age.
- Individuals with baseline LDL-C ≥190 mg/dL.
- Individuals 40 to 75 years of age with diabetes.
Preference should be given to nonstatin cholesterol-lowering drugs shown to reduce ASCVD events in RCTs.
4. In individuals who are candidates for statin treatment but are completely statin intolerant, it is reasonable to use nonstatin cholesterol-lowering drugs that have been shown to reduce ASCVD events in RCTs if the ASCVD risk-reduction benefits outweigh the potential for adverse effects. NHLBI Grade: E (Expert Opinion); ACC/AHA COR: IIa; ACC/AHA LOE: B (Eckel, 2010; "Clofibrate and niacin in coronary heart disease," 1975; Frick et al., 1987; Lipid Research Clinics Program, 1984; "The Lipid Research Clinics Coronary Primary Prevention Trial results. II.," 1984; Rubins et al., 1999; Keech et al., 2005; HPS2-THRIVE Collaborative Group, 2013)
*Several RCTs found that low-intensity and low-moderate–intensity statin therapy reduced ASCVD events. In addition, the Cholesterol Treatment Trialists meta-analyses found that each 39-mg/dL reduction in LDL-C reduces ASCVD risk by 22%. Therefore, the Panel considered that submaximal statin therapy should be used to reduce ASCVD risk in those unable to tolerate moderate- or high-intensity statin therapy.
†In those already on a statin, in whom baseline LDL-C is unknown, an LDL-C level <100 mg/dL was observed in most individuals receiving high-intensity statin therapy.
‡Clinical ASCVD includes acute coronary syndromes, or a history of myocardial infarction, stable or unstable angina, coronary or other arterial revascularization, stroke, transient ischemic attack, or peripheral arterial disease presumed to be of atherosclerotic origin.
Definitions:
NHLBI Grading of the Strength of Recommendations
| Grade | Strength of Recommendation* |
|---|---|
| A | Strong recommendation There is high certainty based on evidence that the net benefit† is substantial. |
| B | Moderate recommendation There is moderate certainty based on evidence that the net benefit is moderate to substantial, or there is high certainty that the net benefit is moderate. |
| C | Weak recommendation There is at least moderate certainty based on evidence that there is a small net benefit. |
| D | Recommendation against There is at least moderate certainty based on evidence that there is no net benefit or that risks/harms outweigh benefits. |
| E | Expert opinion ("There is insufficient evidence or evidence is unclear or conflicting, but this is what the Work Group recommends.") Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, unclear evidence, or conflicting evidence, but the Work Group thought it was important to provide clinical guidance and make a recommendation. Further research is recommended in this area. |
| N | No recommendation for or against ("There is insufficient evidence or evidence is unclear or conflicting.") Net benefit is unclear. Balance of benefits and harms cannot be determined because of no evidence, insufficient evidence, unclear evidence, or conflicting evidence, and the Work Group thought no recommendation should be made. Further research is recommended in this area. |
*In most cases, the strength of the recommendation should be closely aligned with the quality of the evidence; however, under some circumstances, there may be valid reasons for making recommendations that are not closely aligned with the quality of the evidence (e.g., strong recommendation when the evidence quality is moderate, such as smoking cessation to reduce cardiovascular disease [CVD] risk or ordering an electrocardiogram [ECG] as part of the initial diagnostic work-up for a patient presenting with possible myocardial infarction [MI]). Those situations should be limited and the rationale explained clearly by the Work Group.
†Net benefit is defined as benefits minus risks/harms of the service/intervention.
NHLBI Quality Rating of the Strength of Evidence
| Type of Evidence | Quality Rating* |
|---|---|
| High |
| Moderate |
| Low |
*In some cases, other evidence, such as large all-or-none case series (e.g., jumping from airplanes or tall structures), can represent high- or moderate-quality evidence. In such cases, the rationale for the evidence rating exception should be explained by the Work Group and clearly justified.
†"Well-designed, well-executed" refers to studies that directly address the question; use adequate randomization, blinding, and allocation concealment; are adequately powered; use intention-to-treat analyses; and have high follow-up rates.
‡Limitations include concerns with the design and execution of a study that result in decreased confidence in the true estimate of the effect. Examples of such limitations include but are not limited to: inadequate randomization, lack of blinding of study participants or outcome assessors, inadequate power, outcomes of interest that are not prespecified for the primary outcomes, low follow-up rates, and findings based on subgroup analyses. Whether the limitations are considered minor or major is based on the number and severity of flaws in design or execution. Rules for determining whether the limitations are considered minor or major and how they will affect rating of the individual studies will be developed collaboratively with the methodology team.
§Nonrandomized controlled studies refer to intervention studies where assignment to intervention and comparison groups is not random (e.g., quasi-experimental study design).
¶Observational studies include prospective and retrospective cohort, case-control, and cross-sectional studies.
Applying Classification of Recommendations and Level of Evidence
| Size of Treatment Effect | |||||||
|---|---|---|---|---|---|---|---|
| CLASS I Benefit >>> Risk Procedure/Treatment SHOULD be performed/ administered | CLASS IIa Benefit >> Risk Additional studies with focused objectives needed IT IS REASONABLE to perform procedure/administer treatment | CLASS IIb Benefit ≥ Risk Additional studies with broad objectives needed; additional registry data would be helpful Procedure/Treatment MAY BE CONSIDERED | CLASS III No Benefit or Class III Harm | ||||
| Procedure/Test | Treatment | ||||||
| COR III: No Benefit | Not helpful | No proven benefit | |||||
| COR III: Harm | Excess cost without benefit or harmful | Harmful to patients | |||||
| Estimate of Certainty (Precision) of Treatment Effect | LEVEL A Multiple populations evaluated* Data derived from multiple randomized clinical trials or meta-analyses |
|
|
|
| ||
| LEVEL B Limited populations evaluated* Data derived from a single randomized trial or nonrandomized studies |
|
|
|
| |||
| LEVEL C Very limited populations evaluated* Only consensus opinion of experts, case studies, or standard of care |
|
|
|
| |||
A recommendation with Level of Evidence B or C does not imply that the recommendation is weak. Many important clinical questions addressed in the guidelines do not lend themselves to clinical trials. Although randomized trials are unavailable, there may be a very clear clinical consensus that a particular test or therapy is useful or effective.
*Data available from clinical trials or registries about the usefulness/efficacy in different subpopulations, such as sex, age, history of diabetes, history of prior myocardial infarction, history of heart failure, and prior aspirin use.
†For comparative-effectiveness recommendations (Class I and IIa; Level of Evidence A and B only), studies that support the use of comparator verbs should involve direct comparisons of the treatments or strategies being evaluated.
- Summary of Statin Initiation Recommendations for the Treatment of Blood Cholesterol to Reduce ASCVD Risk in Adults
- Initiating Statin Therapy in Individuals with Clinical ASCVD
- Initiating Statin Therapy in Individuals without Clinical ASCVD
- Statin Therapy: Monitoring Therapeutic Response and Adherence
OBJECTIVE: To update the clinical practice recommendations for the treatment of blood cholesterol levels to reduce atherosclerotic cardiovascular disease (ASCVD) risk using data from randomized controlled trials (RCTs) and systematic reviews and meta-analyses of RCTs. To provide a strong, evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men
Guidelines are copyright © 2014 American College of Cardiology/American Heart Association. All rights reserved. The summary is provided by the Agency for Healthcare Research and Quality.
LMWH should replace warfarin, doc says
SAN FRANCISCO—Low-molecular-weight heparin (LMWH) should replace warfarin as thromboprophylaxis in cancer patients, according to a speaker at the 2014 ASH Annual Meeting.
Results of the phase 3 CATCH trial showed that long-term treatment with the LMWH tinzaparin was associated with a 35% lower risk of recurrent venous thromboembolism (VTE) when compared to warfarin, although the difference between the treatment arms was not statistically significant.
Patients who received tinzaparin did have a significantly lower risk of symptomatic deep vein thrombosis (DVT) and clinically relevant, non-major bleeding.
However, there was no difference between the treatment arms with regard to major bleeding or overall mortality.
Agnes Y.Y. Lee, MD, of the University of British Columbia and Vancouver Coastal Health in British Columbia, Canada, presented these results at ASH as LBA-2.*
“CATCH is the largest randomized trial studying treatment of cancer-associated thrombosis,” she said. “It provides confirmatory data for improved efficacy of low-molecular-weight heparin over warfarin.”
The trial included 900 cancer patients from 164 centers around the world. The mean patient age was 59 (range, 18-89), and 59% were female. The most common cancers were gynecologic, colorectal, upper gastrointestinal, and lung.
Patients were stratified by geographic region, tumor characteristics, and history of VTE. They were randomized to receive tinzaparin at 175 IU/kg once daily for 6 months (n=449) or initial tinzaparin at 175 IU/kg once daily for 5 to 10 days overlapped and followed by dose-adjusted warfarin for 6 months (n=451).
In all, 416 patients completed treatment with tinzaparin, and 401 completed warfarin treatment. The patients were followed up to 6 months or death, whichever came first.
Efficacy data
The primary efficacy outcome was recurrent VTE, which included symptomatic DVT and/or pulmonary embolism (PE), incidental proximal DVT and/or PE, and fatal PE.
The rate of recurrent VTE was 7.2% in the tinzaparin arm and 10.5% in the warfarin arm (hazard ratio [HR]=0.65, P=0.07). This represents a 35% reduction in recurrent VTE with the LMWH.
In the per-protocol analysis, the rates of recurrent VTE were 8.3% and 12.7%, respectively (HR=0.62), which translates to a 38% reduction in recurrent VTE with tinzaparin.
“Pre-specified efficacy analyses further showed that tinzaparin significantly reduced symptomatic, recurrent DVT by 52%,” Dr Lee noted. “There were very few symptomatic PEs, equal numbers of fatal PEs occurred in each arm, and there were only 2 incidental thrombotic events, both in the warfarin arm.”
Symptomatic, non-fatal DVT occurred in 12 patients (2.7%) in the tinzaparin arm and 24 (5.3%) in the warfarin arm (HR=0.48, P=0.04). Symptomatic, non-fatal PE occurred in 3 patients (0.7%) and 2 patients (0.4%), respectively. And fatal PE occurred in 17 patients (3.8%) in each arm (HR=0.96).
“We were clearly disappointed that our primary efficacy outcome did not achieve statistical significance,” Dr Lee said. “But our sample size was based on an estimated recurrent [VTE] rate of 12.6% in the warfarin group, and we only saw a 10% [sic] recurrence. So, basically, our study was slightly underpowered to achieve statistical significance.”
“I think that, given the symptomatic DVT results, as well as the per-protocol analysis, in additon to all the previous data on low-molecular-weight heparin, this is still very strong confirmatory data that low-molecular-weight heparin is more effective than warfarin therapy in treating cancer patients with thrombosis.”
Safety and mortality
The primary safety endpoint was major bleeding, which occurred in 2.9% of patients in the tinzaparin arm and 2.6% in the warfarin arm (HR=0.89).
The rate of clinically relevant, non-major bleeding was 11.1% and 16.2%, respectively (HR=0.69, P=0.03).
“Tinzaparin reduced the rate of clinically relevant, non-major bleeding by 31%,” Dr Lee noted.
On the other hand, there was no significant difference between the arms with regard to 180-day overall mortality, which was 34.2% in the tinzaparin arm and 32.3% in the warfarin arm (HR=1.08).
This research was sponsored by LEO Pharma, the company developing tinzaparin (Innohep). ![]()
*Information in the abstract differs from that presented at the meeting.
SAN FRANCISCO—Low-molecular-weight heparin (LMWH) should replace warfarin as thromboprophylaxis in cancer patients, according to a speaker at the 2014 ASH Annual Meeting.
Results of the phase 3 CATCH trial showed that long-term treatment with the LMWH tinzaparin was associated with a 35% lower risk of recurrent venous thromboembolism (VTE) when compared to warfarin, although the difference between the treatment arms was not statistically significant.
Patients who received tinzaparin did have a significantly lower risk of symptomatic deep vein thrombosis (DVT) and clinically relevant, non-major bleeding.
However, there was no difference between the treatment arms with regard to major bleeding or overall mortality.
Agnes Y.Y. Lee, MD, of the University of British Columbia and Vancouver Coastal Health in British Columbia, Canada, presented these results at ASH as LBA-2.*
“CATCH is the largest randomized trial studying treatment of cancer-associated thrombosis,” she said. “It provides confirmatory data for improved efficacy of low-molecular-weight heparin over warfarin.”
The trial included 900 cancer patients from 164 centers around the world. The mean patient age was 59 (range, 18-89), and 59% were female. The most common cancers were gynecologic, colorectal, upper gastrointestinal, and lung.
Patients were stratified by geographic region, tumor characteristics, and history of VTE. They were randomized to receive tinzaparin at 175 IU/kg once daily for 6 months (n=449) or initial tinzaparin at 175 IU/kg once daily for 5 to 10 days overlapped and followed by dose-adjusted warfarin for 6 months (n=451).
In all, 416 patients completed treatment with tinzaparin, and 401 completed warfarin treatment. The patients were followed up to 6 months or death, whichever came first.
Efficacy data
The primary efficacy outcome was recurrent VTE, which included symptomatic DVT and/or pulmonary embolism (PE), incidental proximal DVT and/or PE, and fatal PE.
The rate of recurrent VTE was 7.2% in the tinzaparin arm and 10.5% in the warfarin arm (hazard ratio [HR]=0.65, P=0.07). This represents a 35% reduction in recurrent VTE with the LMWH.
In the per-protocol analysis, the rates of recurrent VTE were 8.3% and 12.7%, respectively (HR=0.62), which translates to a 38% reduction in recurrent VTE with tinzaparin.
“Pre-specified efficacy analyses further showed that tinzaparin significantly reduced symptomatic, recurrent DVT by 52%,” Dr Lee noted. “There were very few symptomatic PEs, equal numbers of fatal PEs occurred in each arm, and there were only 2 incidental thrombotic events, both in the warfarin arm.”
Symptomatic, non-fatal DVT occurred in 12 patients (2.7%) in the tinzaparin arm and 24 (5.3%) in the warfarin arm (HR=0.48, P=0.04). Symptomatic, non-fatal PE occurred in 3 patients (0.7%) and 2 patients (0.4%), respectively. And fatal PE occurred in 17 patients (3.8%) in each arm (HR=0.96).
“We were clearly disappointed that our primary efficacy outcome did not achieve statistical significance,” Dr Lee said. “But our sample size was based on an estimated recurrent [VTE] rate of 12.6% in the warfarin group, and we only saw a 10% [sic] recurrence. So, basically, our study was slightly underpowered to achieve statistical significance.”
“I think that, given the symptomatic DVT results, as well as the per-protocol analysis, in additon to all the previous data on low-molecular-weight heparin, this is still very strong confirmatory data that low-molecular-weight heparin is more effective than warfarin therapy in treating cancer patients with thrombosis.”
Safety and mortality
The primary safety endpoint was major bleeding, which occurred in 2.9% of patients in the tinzaparin arm and 2.6% in the warfarin arm (HR=0.89).
The rate of clinically relevant, non-major bleeding was 11.1% and 16.2%, respectively (HR=0.69, P=0.03).
“Tinzaparin reduced the rate of clinically relevant, non-major bleeding by 31%,” Dr Lee noted.
On the other hand, there was no significant difference between the arms with regard to 180-day overall mortality, which was 34.2% in the tinzaparin arm and 32.3% in the warfarin arm (HR=1.08).
This research was sponsored by LEO Pharma, the company developing tinzaparin (Innohep). ![]()
*Information in the abstract differs from that presented at the meeting.
SAN FRANCISCO—Low-molecular-weight heparin (LMWH) should replace warfarin as thromboprophylaxis in cancer patients, according to a speaker at the 2014 ASH Annual Meeting.
Results of the phase 3 CATCH trial showed that long-term treatment with the LMWH tinzaparin was associated with a 35% lower risk of recurrent venous thromboembolism (VTE) when compared to warfarin, although the difference between the treatment arms was not statistically significant.
Patients who received tinzaparin did have a significantly lower risk of symptomatic deep vein thrombosis (DVT) and clinically relevant, non-major bleeding.
However, there was no difference between the treatment arms with regard to major bleeding or overall mortality.
Agnes Y.Y. Lee, MD, of the University of British Columbia and Vancouver Coastal Health in British Columbia, Canada, presented these results at ASH as LBA-2.*
“CATCH is the largest randomized trial studying treatment of cancer-associated thrombosis,” she said. “It provides confirmatory data for improved efficacy of low-molecular-weight heparin over warfarin.”
The trial included 900 cancer patients from 164 centers around the world. The mean patient age was 59 (range, 18-89), and 59% were female. The most common cancers were gynecologic, colorectal, upper gastrointestinal, and lung.
Patients were stratified by geographic region, tumor characteristics, and history of VTE. They were randomized to receive tinzaparin at 175 IU/kg once daily for 6 months (n=449) or initial tinzaparin at 175 IU/kg once daily for 5 to 10 days overlapped and followed by dose-adjusted warfarin for 6 months (n=451).
In all, 416 patients completed treatment with tinzaparin, and 401 completed warfarin treatment. The patients were followed up to 6 months or death, whichever came first.
Efficacy data
The primary efficacy outcome was recurrent VTE, which included symptomatic DVT and/or pulmonary embolism (PE), incidental proximal DVT and/or PE, and fatal PE.
The rate of recurrent VTE was 7.2% in the tinzaparin arm and 10.5% in the warfarin arm (hazard ratio [HR]=0.65, P=0.07). This represents a 35% reduction in recurrent VTE with the LMWH.
In the per-protocol analysis, the rates of recurrent VTE were 8.3% and 12.7%, respectively (HR=0.62), which translates to a 38% reduction in recurrent VTE with tinzaparin.
“Pre-specified efficacy analyses further showed that tinzaparin significantly reduced symptomatic, recurrent DVT by 52%,” Dr Lee noted. “There were very few symptomatic PEs, equal numbers of fatal PEs occurred in each arm, and there were only 2 incidental thrombotic events, both in the warfarin arm.”
Symptomatic, non-fatal DVT occurred in 12 patients (2.7%) in the tinzaparin arm and 24 (5.3%) in the warfarin arm (HR=0.48, P=0.04). Symptomatic, non-fatal PE occurred in 3 patients (0.7%) and 2 patients (0.4%), respectively. And fatal PE occurred in 17 patients (3.8%) in each arm (HR=0.96).
“We were clearly disappointed that our primary efficacy outcome did not achieve statistical significance,” Dr Lee said. “But our sample size was based on an estimated recurrent [VTE] rate of 12.6% in the warfarin group, and we only saw a 10% [sic] recurrence. So, basically, our study was slightly underpowered to achieve statistical significance.”
“I think that, given the symptomatic DVT results, as well as the per-protocol analysis, in additon to all the previous data on low-molecular-weight heparin, this is still very strong confirmatory data that low-molecular-weight heparin is more effective than warfarin therapy in treating cancer patients with thrombosis.”
Safety and mortality
The primary safety endpoint was major bleeding, which occurred in 2.9% of patients in the tinzaparin arm and 2.6% in the warfarin arm (HR=0.89).
The rate of clinically relevant, non-major bleeding was 11.1% and 16.2%, respectively (HR=0.69, P=0.03).
“Tinzaparin reduced the rate of clinically relevant, non-major bleeding by 31%,” Dr Lee noted.
On the other hand, there was no significant difference between the arms with regard to 180-day overall mortality, which was 34.2% in the tinzaparin arm and 32.3% in the warfarin arm (HR=1.08).
This research was sponsored by LEO Pharma, the company developing tinzaparin (Innohep). ![]()
*Information in the abstract differs from that presented at the meeting.
Study confirms IDH2 as therapeutic target in AML, MDS

in the Moscone Center
SAN FRANCISCO—The first-in-human study of AG-221 has confirmed IDH2 as a therapeutic target in acute myeloid leukemia (AML) and myelodysplastic syndromes (MDS), according to investigators.
From the first dose of therapy, the high plasma level observed in patients “translates into a drastic decrease in 2-HG,” said Eytan M. Stein, MD, of Memorial Sloan Kettering Cancer Center in New York.
Mutations in IDH1 and IDH2 result in the accumulation of the oncometabolite 2-HG. And high levels of 2-HG prompt epigenetic changes to the cell, resulting in impaired cellular differentiation.
“By cycle 1, day 15, at all dose levels, there was fantastic inhibition of 2-HG,” Dr Stein said. “Indeed, this drastic inhibition of 2-HG led to profound clinical benefit.”
He presented interim results of the phase 1 study of AG-221 at the 2014 ASH Annual Meeting (abstract 115).*
The investigators have treated 73 patients with advanced IDH2-mutation-positive hematologic malignancies since the study began in September 2013.
Patients were a median age of 67 years (range, 33-90), and 74% had IDH2 R140 mutations. Most had relapsed/refractory AML (n=55), and the rest had MDS (n=6), untreated AML (n=5), chronic myelomonocytic leukemia (n=5), and myeloid sarcoma (n=1).
Patients received AG-221 as a single agent orally, once or twice a day, continuously, in 28-day cycles. Four dose-expansion cohorts at 100 mg each day were added last October.
To date, the maximum tolerated dose has not been reached, with the highest cumulative daily dose being 300 mg. Investigators observed a single dose-limiting toxicity in 1 patient: grade 5 hypoxia with fungal pneumonia and septic shock.
As of the data cutoff on October 1, 2014, 38 patients were still on therapy, and 35 had discontinued. Five patients withdrew after achieving complete remission (CR) in order to pursue allogeneic transplant.
Dr Stein pointed out that although the median number of prior chemotherapy regimens for the entire cohort was 2, “all of the patients who went on study were predicted to have dismal outcomes with conventional therapy.”
Safety
The therapy was well tolerated, with the most common adverse events (AEs) overall being typical for patients with advanced AML: nausea (23%), pyrexia (19%), and diarrhea (17%).
The majority of serious AEs were disease-related and unrelated to the study drug, Dr Stein said. Thirteen patients experienced 21 serious AEs that were possibly or probably related to treatment.
Investigators observed treatment-related leukocytosis in 3 patients, “but we think that is a differentiating effect of the study drug,” Dr Stein said.
He also pointed out that there was no increase in AEs with increased dose of the drug.
Of the 11 deaths reported, 9 were unrelated to the drug, and 2—sepsis/hypoxia and atrial flutter—were possibly related. The 30-day and 60-day all-cause mortality rates were 4.1% and 13.7%, respectively.
Efficacy
Of the 45 patients who were treated for at least 1 cycle and were evaluable for efficacy, 15 achieved a CR (n=6) or a CR with incomplete blood count recovery. The overall response rate is 56% (25/45).
“Responses appear durable,” Dr Stein commented, “and 90% of responders have had a response duration of at least 3 months, with the earliest patients on study having had durable responses for over 6 months.”
Many of the durable responses are partial remissions, he noted.
Seventeen patients have stable disease, and many of these patients remain on study. Two patients had progressive disease.
“Patients with stable disease have remained on study for a similar amount of time as the responders,” Dr Stein said, “suggesting that, despite the lack of a formal partial remission, many patients are deriving clinical benefit from study treatment.”
This study was sponsored by Agios Pharmaceuticals Inc., the company developing AG-221 in collaboration with Celgene.
Previous results from this study were presented at the 2014 EHA Annual Congress. Based on those results, AG-221 received fast track designation from the US Food and Drug Administration. ![]()
*Data in the presentation were updated from the abstract.
in the Moscone Center
SAN FRANCISCO—The first-in-human study of AG-221 has confirmed IDH2 as a therapeutic target in acute myeloid leukemia (AML) and myelodysplastic syndromes (MDS), according to investigators.
From the first dose of therapy, the high plasma level observed in patients “translates into a drastic decrease in 2-HG,” said Eytan M. Stein, MD, of Memorial Sloan Kettering Cancer Center in New York.
Mutations in IDH1 and IDH2 result in the accumulation of the oncometabolite 2-HG. And high levels of 2-HG prompt epigenetic changes to the cell, resulting in impaired cellular differentiation.
“By cycle 1, day 15, at all dose levels, there was fantastic inhibition of 2-HG,” Dr Stein said. “Indeed, this drastic inhibition of 2-HG led to profound clinical benefit.”
He presented interim results of the phase 1 study of AG-221 at the 2014 ASH Annual Meeting (abstract 115).*
The investigators have treated 73 patients with advanced IDH2-mutation-positive hematologic malignancies since the study began in September 2013.
Patients were a median age of 67 years (range, 33-90), and 74% had IDH2 R140 mutations. Most had relapsed/refractory AML (n=55), and the rest had MDS (n=6), untreated AML (n=5), chronic myelomonocytic leukemia (n=5), and myeloid sarcoma (n=1).
Patients received AG-221 as a single agent orally, once or twice a day, continuously, in 28-day cycles. Four dose-expansion cohorts at 100 mg each day were added last October.
To date, the maximum tolerated dose has not been reached, with the highest cumulative daily dose being 300 mg. Investigators observed a single dose-limiting toxicity in 1 patient: grade 5 hypoxia with fungal pneumonia and septic shock.
As of the data cutoff on October 1, 2014, 38 patients were still on therapy, and 35 had discontinued. Five patients withdrew after achieving complete remission (CR) in order to pursue allogeneic transplant.
Dr Stein pointed out that although the median number of prior chemotherapy regimens for the entire cohort was 2, “all of the patients who went on study were predicted to have dismal outcomes with conventional therapy.”
Safety
The therapy was well tolerated, with the most common adverse events (AEs) overall being typical for patients with advanced AML: nausea (23%), pyrexia (19%), and diarrhea (17%).
The majority of serious AEs were disease-related and unrelated to the study drug, Dr Stein said. Thirteen patients experienced 21 serious AEs that were possibly or probably related to treatment.
Investigators observed treatment-related leukocytosis in 3 patients, “but we think that is a differentiating effect of the study drug,” Dr Stein said.
He also pointed out that there was no increase in AEs with increased dose of the drug.
Of the 11 deaths reported, 9 were unrelated to the drug, and 2—sepsis/hypoxia and atrial flutter—were possibly related. The 30-day and 60-day all-cause mortality rates were 4.1% and 13.7%, respectively.
Efficacy
Of the 45 patients who were treated for at least 1 cycle and were evaluable for efficacy, 15 achieved a CR (n=6) or a CR with incomplete blood count recovery. The overall response rate is 56% (25/45).
“Responses appear durable,” Dr Stein commented, “and 90% of responders have had a response duration of at least 3 months, with the earliest patients on study having had durable responses for over 6 months.”
Many of the durable responses are partial remissions, he noted.
Seventeen patients have stable disease, and many of these patients remain on study. Two patients had progressive disease.
“Patients with stable disease have remained on study for a similar amount of time as the responders,” Dr Stein said, “suggesting that, despite the lack of a formal partial remission, many patients are deriving clinical benefit from study treatment.”
This study was sponsored by Agios Pharmaceuticals Inc., the company developing AG-221 in collaboration with Celgene.
Previous results from this study were presented at the 2014 EHA Annual Congress. Based on those results, AG-221 received fast track designation from the US Food and Drug Administration. ![]()
*Data in the presentation were updated from the abstract.
in the Moscone Center
SAN FRANCISCO—The first-in-human study of AG-221 has confirmed IDH2 as a therapeutic target in acute myeloid leukemia (AML) and myelodysplastic syndromes (MDS), according to investigators.
From the first dose of therapy, the high plasma level observed in patients “translates into a drastic decrease in 2-HG,” said Eytan M. Stein, MD, of Memorial Sloan Kettering Cancer Center in New York.
Mutations in IDH1 and IDH2 result in the accumulation of the oncometabolite 2-HG. And high levels of 2-HG prompt epigenetic changes to the cell, resulting in impaired cellular differentiation.
“By cycle 1, day 15, at all dose levels, there was fantastic inhibition of 2-HG,” Dr Stein said. “Indeed, this drastic inhibition of 2-HG led to profound clinical benefit.”
He presented interim results of the phase 1 study of AG-221 at the 2014 ASH Annual Meeting (abstract 115).*
The investigators have treated 73 patients with advanced IDH2-mutation-positive hematologic malignancies since the study began in September 2013.
Patients were a median age of 67 years (range, 33-90), and 74% had IDH2 R140 mutations. Most had relapsed/refractory AML (n=55), and the rest had MDS (n=6), untreated AML (n=5), chronic myelomonocytic leukemia (n=5), and myeloid sarcoma (n=1).
Patients received AG-221 as a single agent orally, once or twice a day, continuously, in 28-day cycles. Four dose-expansion cohorts at 100 mg each day were added last October.
To date, the maximum tolerated dose has not been reached, with the highest cumulative daily dose being 300 mg. Investigators observed a single dose-limiting toxicity in 1 patient: grade 5 hypoxia with fungal pneumonia and septic shock.
As of the data cutoff on October 1, 2014, 38 patients were still on therapy, and 35 had discontinued. Five patients withdrew after achieving complete remission (CR) in order to pursue allogeneic transplant.
Dr Stein pointed out that although the median number of prior chemotherapy regimens for the entire cohort was 2, “all of the patients who went on study were predicted to have dismal outcomes with conventional therapy.”
Safety
The therapy was well tolerated, with the most common adverse events (AEs) overall being typical for patients with advanced AML: nausea (23%), pyrexia (19%), and diarrhea (17%).
The majority of serious AEs were disease-related and unrelated to the study drug, Dr Stein said. Thirteen patients experienced 21 serious AEs that were possibly or probably related to treatment.
Investigators observed treatment-related leukocytosis in 3 patients, “but we think that is a differentiating effect of the study drug,” Dr Stein said.
He also pointed out that there was no increase in AEs with increased dose of the drug.
Of the 11 deaths reported, 9 were unrelated to the drug, and 2—sepsis/hypoxia and atrial flutter—were possibly related. The 30-day and 60-day all-cause mortality rates were 4.1% and 13.7%, respectively.
Efficacy
Of the 45 patients who were treated for at least 1 cycle and were evaluable for efficacy, 15 achieved a CR (n=6) or a CR with incomplete blood count recovery. The overall response rate is 56% (25/45).
“Responses appear durable,” Dr Stein commented, “and 90% of responders have had a response duration of at least 3 months, with the earliest patients on study having had durable responses for over 6 months.”
Many of the durable responses are partial remissions, he noted.
Seventeen patients have stable disease, and many of these patients remain on study. Two patients had progressive disease.
“Patients with stable disease have remained on study for a similar amount of time as the responders,” Dr Stein said, “suggesting that, despite the lack of a formal partial remission, many patients are deriving clinical benefit from study treatment.”
This study was sponsored by Agios Pharmaceuticals Inc., the company developing AG-221 in collaboration with Celgene.
Previous results from this study were presented at the 2014 EHA Annual Congress. Based on those results, AG-221 received fast track designation from the US Food and Drug Administration. ![]()
*Data in the presentation were updated from the abstract.
Referring Smokers to Quitlines
Telephone-based programs to encourage and support quitting smoking—known as “quitlines”—have been established as effective both clinically and in the “real world.” However, quitlines rely on smokers calling in for them to work. Researchers from the Tobacco Cessation and Prevention Program and the Massachusetts Department of Public Health, both in Boston, say being referred to quitlines by their health care providers might help even more smokers quit.
The researchers collected data for 2,737 provider-referred and 530 self-referred smokers from the Massachusetts Smokers’ Helpline, which offers evidence-based proactive telephone counseling sessions, nicotine replacement therapy (NRT), and self-help materials. They then examined differences in demographics, service utilization, and quit outcomes. The primary outcome was quit status at the 6- to 8-month follow-up.
Twenty percent of provider-referred clients quit smoking; 26% of self-referred clients quit. Provider-referred smokers who used the quitline services had higher odds of quitting, compared with those who used methods not including a quitline. However, the provider-referral model was limited by lower enrollment, lower use, and poorer outcomes compared with self-referred services. Patients aged 18 to 34 years and those aged > 65 years had the best chances of quitting and staying smoke-free. Patients referred from private practices were more likely to quit than were those referred from a hospital.
Provider-referred smokers who read the self-help materials had 1.2 times the odds of quitting compared with those who didn’t. Using any amount of the 2-week supply of NRT doubled the odds of quitting. Clients who used a combination of counseling and NRT had the greatest success, with more than triple the chances of quitting, compared with clients who did neither.
Self-referred smokers also had good results, although not usually as quickly as provider-referred smokers, who saw significantly improved outcomes after 3 counseling sessions. It took 4 sessions for the self-referred smokers to see the same results.
Readiness to quit was an important predictor of success. Tobacco dependence also predicted quitting success. Clients in both groups who could wait > 30 minutes before smoking their first cigarette had better luck than did those who had to smoke immediately after waking.
The researchers suggest some ways to improve the provider-referred model. One is to offer more support for smokers from lower socioeconomic levels. According to other research, those smokers may need more treatment content and access to more intensive pharmacotherapy, the researchers say.
It might also help all quitline clients, they add, to minimize the wait time between referral and actual provision of service. Longer wait times can “increase the room for ambivalence for any smoker,” they note, “but may be especially detrimental for provider-referred smokers who are less ready to make a quit attempt.”
And what is the provider’s role in assessing patient readiness to quit and preparing patients for the quitline services? In reality, the researchers say, not all patients have received an evidence-based intervention or are ready to quit when they are enrolled. Moreover, many are lost in the callback process. Using 3 callback attempts, the Massachusetts quitline only reaches 40% of their potential quitters. Upping the callback rate to 5 attempts raises the reach slightly, to 50%. That shows the need, the researchers say, for better and more frequent provider training, outreach, feedback reporting, clinical champions on site, and systems support.
Source
Song G, Landau AS, Gorin TJ, Keithly L. Am J Prev Med. 2014;47(4):392-402.
doi: 10.1016/j.amepre.2014.05.043.
Telephone-based programs to encourage and support quitting smoking—known as “quitlines”—have been established as effective both clinically and in the “real world.” However, quitlines rely on smokers calling in for them to work. Researchers from the Tobacco Cessation and Prevention Program and the Massachusetts Department of Public Health, both in Boston, say being referred to quitlines by their health care providers might help even more smokers quit.
The researchers collected data for 2,737 provider-referred and 530 self-referred smokers from the Massachusetts Smokers’ Helpline, which offers evidence-based proactive telephone counseling sessions, nicotine replacement therapy (NRT), and self-help materials. They then examined differences in demographics, service utilization, and quit outcomes. The primary outcome was quit status at the 6- to 8-month follow-up.
Twenty percent of provider-referred clients quit smoking; 26% of self-referred clients quit. Provider-referred smokers who used the quitline services had higher odds of quitting, compared with those who used methods not including a quitline. However, the provider-referral model was limited by lower enrollment, lower use, and poorer outcomes compared with self-referred services. Patients aged 18 to 34 years and those aged > 65 years had the best chances of quitting and staying smoke-free. Patients referred from private practices were more likely to quit than were those referred from a hospital.
Provider-referred smokers who read the self-help materials had 1.2 times the odds of quitting compared with those who didn’t. Using any amount of the 2-week supply of NRT doubled the odds of quitting. Clients who used a combination of counseling and NRT had the greatest success, with more than triple the chances of quitting, compared with clients who did neither.
Self-referred smokers also had good results, although not usually as quickly as provider-referred smokers, who saw significantly improved outcomes after 3 counseling sessions. It took 4 sessions for the self-referred smokers to see the same results.
Readiness to quit was an important predictor of success. Tobacco dependence also predicted quitting success. Clients in both groups who could wait > 30 minutes before smoking their first cigarette had better luck than did those who had to smoke immediately after waking.
The researchers suggest some ways to improve the provider-referred model. One is to offer more support for smokers from lower socioeconomic levels. According to other research, those smokers may need more treatment content and access to more intensive pharmacotherapy, the researchers say.
It might also help all quitline clients, they add, to minimize the wait time between referral and actual provision of service. Longer wait times can “increase the room for ambivalence for any smoker,” they note, “but may be especially detrimental for provider-referred smokers who are less ready to make a quit attempt.”
And what is the provider’s role in assessing patient readiness to quit and preparing patients for the quitline services? In reality, the researchers say, not all patients have received an evidence-based intervention or are ready to quit when they are enrolled. Moreover, many are lost in the callback process. Using 3 callback attempts, the Massachusetts quitline only reaches 40% of their potential quitters. Upping the callback rate to 5 attempts raises the reach slightly, to 50%. That shows the need, the researchers say, for better and more frequent provider training, outreach, feedback reporting, clinical champions on site, and systems support.
Source
Song G, Landau AS, Gorin TJ, Keithly L. Am J Prev Med. 2014;47(4):392-402.
doi: 10.1016/j.amepre.2014.05.043.
Telephone-based programs to encourage and support quitting smoking—known as “quitlines”—have been established as effective both clinically and in the “real world.” However, quitlines rely on smokers calling in for them to work. Researchers from the Tobacco Cessation and Prevention Program and the Massachusetts Department of Public Health, both in Boston, say being referred to quitlines by their health care providers might help even more smokers quit.
The researchers collected data for 2,737 provider-referred and 530 self-referred smokers from the Massachusetts Smokers’ Helpline, which offers evidence-based proactive telephone counseling sessions, nicotine replacement therapy (NRT), and self-help materials. They then examined differences in demographics, service utilization, and quit outcomes. The primary outcome was quit status at the 6- to 8-month follow-up.
Twenty percent of provider-referred clients quit smoking; 26% of self-referred clients quit. Provider-referred smokers who used the quitline services had higher odds of quitting, compared with those who used methods not including a quitline. However, the provider-referral model was limited by lower enrollment, lower use, and poorer outcomes compared with self-referred services. Patients aged 18 to 34 years and those aged > 65 years had the best chances of quitting and staying smoke-free. Patients referred from private practices were more likely to quit than were those referred from a hospital.
Provider-referred smokers who read the self-help materials had 1.2 times the odds of quitting compared with those who didn’t. Using any amount of the 2-week supply of NRT doubled the odds of quitting. Clients who used a combination of counseling and NRT had the greatest success, with more than triple the chances of quitting, compared with clients who did neither.
Self-referred smokers also had good results, although not usually as quickly as provider-referred smokers, who saw significantly improved outcomes after 3 counseling sessions. It took 4 sessions for the self-referred smokers to see the same results.
Readiness to quit was an important predictor of success. Tobacco dependence also predicted quitting success. Clients in both groups who could wait > 30 minutes before smoking their first cigarette had better luck than did those who had to smoke immediately after waking.
The researchers suggest some ways to improve the provider-referred model. One is to offer more support for smokers from lower socioeconomic levels. According to other research, those smokers may need more treatment content and access to more intensive pharmacotherapy, the researchers say.
It might also help all quitline clients, they add, to minimize the wait time between referral and actual provision of service. Longer wait times can “increase the room for ambivalence for any smoker,” they note, “but may be especially detrimental for provider-referred smokers who are less ready to make a quit attempt.”
And what is the provider’s role in assessing patient readiness to quit and preparing patients for the quitline services? In reality, the researchers say, not all patients have received an evidence-based intervention or are ready to quit when they are enrolled. Moreover, many are lost in the callback process. Using 3 callback attempts, the Massachusetts quitline only reaches 40% of their potential quitters. Upping the callback rate to 5 attempts raises the reach slightly, to 50%. That shows the need, the researchers say, for better and more frequent provider training, outreach, feedback reporting, clinical champions on site, and systems support.
Source
Song G, Landau AS, Gorin TJ, Keithly L. Am J Prev Med. 2014;47(4):392-402.
doi: 10.1016/j.amepre.2014.05.043.