User login
CKT more important than del(17p) in CLL, group finds
SAN FRANCISCO—New research suggests complex metaphase karyotype (CKT) is a stronger predictor of inferior outcome than 17p deletion in patients with relapsed or refractory chronic lymphocytic leukemia (CLL) who are treated with the BTK inhibitor ibrutinib.
The study showed that CKT, defined as 3 or more distinct chromosomal abnormalities, was independently associated with inferior event-free survival (EFS) and overall survival (OS), but del(17p) was not.
According to investigators, this suggests that del(17p) patients without CKT could be managed with long-term ibrutinib and close monitoring, as these patients have similar outcomes as patients without del(17p).
However, patients with CKT will likely require treatment-intensification strategies after ibrutinib-based therapy.
“We believe that patients with a complex karyotype represent an ideal group in whom to study novel treatment approaches, including ibrutinib-based combination regimens and/or consolidated approaches after initial ibrutinib response,” said investigator Philip A. Thompson, MBBS, of the University of Texas MD Anderson Cancer Center in Houston.
Dr Thompson presented his group’s findings at the 2014 ASH Annual Meeting as abstract 22.* Investigators involved in this study received research funding or consultancy fees from Pharmacyclics, Inc., makers of ibrutinib.
Patient characteristics
Dr Thompson and his colleagues analyzed 100 patients with relapsed/refractory CLL who received treatment with ibrutinib-based regimens—50 with ibrutinib alone, 36 with ibrutinib and rituximab, and 14 with ibrutinib, rituximab, and bendamustine.
The median age was 65 (range, 35-83), patients received a median of 2 prior therapies (range, 1-12), and 19% were fludarabine-refractory. Sixty percent of patients had Rai stage III-IV disease, 52% had bulky adenopathy, 81% had unmutated IGHV, and 56% had β2-microglobulin ≥ 4.0 mg/L.
FISH was available for 94 patients, and metaphase analysis was available for 65 patients. Forty-two percent (27/65) of patients had CKT, 28% (26/94) had del(11q), and 48% (45/94) had del(17p).
Of the 45 patients who had del(17p), 23 also had CKT. And of the 49 patients who did not have del(17p), 4 had CKT.
Event-free survival
The median follow-up in surviving patients was 27 months (range, 11-48). Eight patients had planned allogeneic stem cell transplant and were censored for the EFS analysis.
“As has been shown previously, patients with 17p deletion by FISH did have inferior event-free survival,” Dr Thompson said. “And when we looked at those patients with complex metaphase karyotype, there was a highly significant inferior event-free survival in these patients, compared to those with complex karyotype.”
EFS was 78% in patients with neither del(17p) nor del(11q), 69% in patients with del(11q), and 60% in patients with del(17p) (P=0.014).
EFS was 82% in patients without CKT and 44% in those with CKT (P<0.0001). In patients with del(17p), EFS was 78% in those without CKT and 48% in those with CKT (P=0.047).
In patients without CKT, EFS was 79% in those without del(17p) or del(11q), 90% in those with del(11q), and 78% in those with del(17p) (P=0.516).
“Interestingly, when we looked at the events that occurred in those patients without complex karyotype, none were due to CLL progression or Richter’s transformation,” Dr Thompson said.
In multivariable analysis, CKT was significantly associated with EFS (P=0.011), but del(17p) was not (P=0.887).
Overall survival
There was no significant difference in OS according to the presence of del(17p) or del(11q). OS was 87% in patients with neither del(17p) nor del(11q), 81% in patients with del(11q), and 67% in patients with del(17p) (P=0.054).
However, there was a significant difference in OS for patients with and without CKT. OS was 82% in patients without CKT and 56% in patients with CKT (P=0.006).
Among patients without CKT, OS was 84% in those with neither del(17p) nor del(11q), 80% in those with del(11q), and 78% in those with del(17p) (P=0.52).
In multivariable analysis, OS was significantly associated with CKT (P=0.011) and fludarabine-refractory disease (P=0.004) but not del(17p) (P=0.981).
“So, in summary, complex karyotype appears to be a more important predictor of outcomes in patients with relapsed or refractory CLL treated with ibrutinib-based regimens than the presence of del(17p) by FISH,” Dr Thompson said.
“Patients without complex karyotype have a low rate of disease progression, including those who have del(17p). Most progressions during ibrutinib therapy occur late, beyond the 12-month time point, but survival is short after disease progression.” ![]()
*Information in the abstract differs from that presented at the meeting.
SAN FRANCISCO—New research suggests complex metaphase karyotype (CKT) is a stronger predictor of inferior outcome than 17p deletion in patients with relapsed or refractory chronic lymphocytic leukemia (CLL) who are treated with the BTK inhibitor ibrutinib.
The study showed that CKT, defined as 3 or more distinct chromosomal abnormalities, was independently associated with inferior event-free survival (EFS) and overall survival (OS), but del(17p) was not.
According to investigators, this suggests that del(17p) patients without CKT could be managed with long-term ibrutinib and close monitoring, as these patients have similar outcomes as patients without del(17p).
However, patients with CKT will likely require treatment-intensification strategies after ibrutinib-based therapy.
“We believe that patients with a complex karyotype represent an ideal group in whom to study novel treatment approaches, including ibrutinib-based combination regimens and/or consolidated approaches after initial ibrutinib response,” said investigator Philip A. Thompson, MBBS, of the University of Texas MD Anderson Cancer Center in Houston.
Dr Thompson presented his group’s findings at the 2014 ASH Annual Meeting as abstract 22.* Investigators involved in this study received research funding or consultancy fees from Pharmacyclics, Inc., makers of ibrutinib.
Patient characteristics
Dr Thompson and his colleagues analyzed 100 patients with relapsed/refractory CLL who received treatment with ibrutinib-based regimens—50 with ibrutinib alone, 36 with ibrutinib and rituximab, and 14 with ibrutinib, rituximab, and bendamustine.
The median age was 65 (range, 35-83), patients received a median of 2 prior therapies (range, 1-12), and 19% were fludarabine-refractory. Sixty percent of patients had Rai stage III-IV disease, 52% had bulky adenopathy, 81% had unmutated IGHV, and 56% had β2-microglobulin ≥ 4.0 mg/L.
FISH was available for 94 patients, and metaphase analysis was available for 65 patients. Forty-two percent (27/65) of patients had CKT, 28% (26/94) had del(11q), and 48% (45/94) had del(17p).
Of the 45 patients who had del(17p), 23 also had CKT. And of the 49 patients who did not have del(17p), 4 had CKT.
Event-free survival
The median follow-up in surviving patients was 27 months (range, 11-48). Eight patients had planned allogeneic stem cell transplant and were censored for the EFS analysis.
“As has been shown previously, patients with 17p deletion by FISH did have inferior event-free survival,” Dr Thompson said. “And when we looked at those patients with complex metaphase karyotype, there was a highly significant inferior event-free survival in these patients, compared to those with complex karyotype.”
EFS was 78% in patients with neither del(17p) nor del(11q), 69% in patients with del(11q), and 60% in patients with del(17p) (P=0.014).
EFS was 82% in patients without CKT and 44% in those with CKT (P<0.0001). In patients with del(17p), EFS was 78% in those without CKT and 48% in those with CKT (P=0.047).
In patients without CKT, EFS was 79% in those without del(17p) or del(11q), 90% in those with del(11q), and 78% in those with del(17p) (P=0.516).
“Interestingly, when we looked at the events that occurred in those patients without complex karyotype, none were due to CLL progression or Richter’s transformation,” Dr Thompson said.
In multivariable analysis, CKT was significantly associated with EFS (P=0.011), but del(17p) was not (P=0.887).
Overall survival
There was no significant difference in OS according to the presence of del(17p) or del(11q). OS was 87% in patients with neither del(17p) nor del(11q), 81% in patients with del(11q), and 67% in patients with del(17p) (P=0.054).
However, there was a significant difference in OS for patients with and without CKT. OS was 82% in patients without CKT and 56% in patients with CKT (P=0.006).
Among patients without CKT, OS was 84% in those with neither del(17p) nor del(11q), 80% in those with del(11q), and 78% in those with del(17p) (P=0.52).
In multivariable analysis, OS was significantly associated with CKT (P=0.011) and fludarabine-refractory disease (P=0.004) but not del(17p) (P=0.981).
“So, in summary, complex karyotype appears to be a more important predictor of outcomes in patients with relapsed or refractory CLL treated with ibrutinib-based regimens than the presence of del(17p) by FISH,” Dr Thompson said.
“Patients without complex karyotype have a low rate of disease progression, including those who have del(17p). Most progressions during ibrutinib therapy occur late, beyond the 12-month time point, but survival is short after disease progression.” ![]()
*Information in the abstract differs from that presented at the meeting.
SAN FRANCISCO—New research suggests complex metaphase karyotype (CKT) is a stronger predictor of inferior outcome than 17p deletion in patients with relapsed or refractory chronic lymphocytic leukemia (CLL) who are treated with the BTK inhibitor ibrutinib.
The study showed that CKT, defined as 3 or more distinct chromosomal abnormalities, was independently associated with inferior event-free survival (EFS) and overall survival (OS), but del(17p) was not.
According to investigators, this suggests that del(17p) patients without CKT could be managed with long-term ibrutinib and close monitoring, as these patients have similar outcomes as patients without del(17p).
However, patients with CKT will likely require treatment-intensification strategies after ibrutinib-based therapy.
“We believe that patients with a complex karyotype represent an ideal group in whom to study novel treatment approaches, including ibrutinib-based combination regimens and/or consolidated approaches after initial ibrutinib response,” said investigator Philip A. Thompson, MBBS, of the University of Texas MD Anderson Cancer Center in Houston.
Dr Thompson presented his group’s findings at the 2014 ASH Annual Meeting as abstract 22.* Investigators involved in this study received research funding or consultancy fees from Pharmacyclics, Inc., makers of ibrutinib.
Patient characteristics
Dr Thompson and his colleagues analyzed 100 patients with relapsed/refractory CLL who received treatment with ibrutinib-based regimens—50 with ibrutinib alone, 36 with ibrutinib and rituximab, and 14 with ibrutinib, rituximab, and bendamustine.
The median age was 65 (range, 35-83), patients received a median of 2 prior therapies (range, 1-12), and 19% were fludarabine-refractory. Sixty percent of patients had Rai stage III-IV disease, 52% had bulky adenopathy, 81% had unmutated IGHV, and 56% had β2-microglobulin ≥ 4.0 mg/L.
FISH was available for 94 patients, and metaphase analysis was available for 65 patients. Forty-two percent (27/65) of patients had CKT, 28% (26/94) had del(11q), and 48% (45/94) had del(17p).
Of the 45 patients who had del(17p), 23 also had CKT. And of the 49 patients who did not have del(17p), 4 had CKT.
Event-free survival
The median follow-up in surviving patients was 27 months (range, 11-48). Eight patients had planned allogeneic stem cell transplant and were censored for the EFS analysis.
“As has been shown previously, patients with 17p deletion by FISH did have inferior event-free survival,” Dr Thompson said. “And when we looked at those patients with complex metaphase karyotype, there was a highly significant inferior event-free survival in these patients, compared to those with complex karyotype.”
EFS was 78% in patients with neither del(17p) nor del(11q), 69% in patients with del(11q), and 60% in patients with del(17p) (P=0.014).
EFS was 82% in patients without CKT and 44% in those with CKT (P<0.0001). In patients with del(17p), EFS was 78% in those without CKT and 48% in those with CKT (P=0.047).
In patients without CKT, EFS was 79% in those without del(17p) or del(11q), 90% in those with del(11q), and 78% in those with del(17p) (P=0.516).
“Interestingly, when we looked at the events that occurred in those patients without complex karyotype, none were due to CLL progression or Richter’s transformation,” Dr Thompson said.
In multivariable analysis, CKT was significantly associated with EFS (P=0.011), but del(17p) was not (P=0.887).
Overall survival
There was no significant difference in OS according to the presence of del(17p) or del(11q). OS was 87% in patients with neither del(17p) nor del(11q), 81% in patients with del(11q), and 67% in patients with del(17p) (P=0.054).
However, there was a significant difference in OS for patients with and without CKT. OS was 82% in patients without CKT and 56% in patients with CKT (P=0.006).
Among patients without CKT, OS was 84% in those with neither del(17p) nor del(11q), 80% in those with del(11q), and 78% in those with del(17p) (P=0.52).
In multivariable analysis, OS was significantly associated with CKT (P=0.011) and fludarabine-refractory disease (P=0.004) but not del(17p) (P=0.981).
“So, in summary, complex karyotype appears to be a more important predictor of outcomes in patients with relapsed or refractory CLL treated with ibrutinib-based regimens than the presence of del(17p) by FISH,” Dr Thompson said.
“Patients without complex karyotype have a low rate of disease progression, including those who have del(17p). Most progressions during ibrutinib therapy occur late, beyond the 12-month time point, but survival is short after disease progression.” ![]()
*Information in the abstract differs from that presented at the meeting.
Long-Acting Insulin Analogs: Effects on Diabetic Retinopathy
Long-acting insulin analogs are designed to enhance glycemic control without excessively lowering blood glucose. But structural modifications of the insulin molecule can alter biological responses and binding characteristics with specific receptors; in short, they can potentially raise the risk of sight-threatening diabetic retinopathy (STDR), say researchers from Taipei City Hospital and National Taiwan University, both in Taiwan.
The researchers note that some clinical trials have reported that intensification of endogenous insulin might accelerate progression of pre-existing STDR. However, they add that some studies used cancer cell lines, and insulin was administered at supraphysiologic concentrations.
The researchers conducted a retrospective study to evaluate the effects of long-acting insulin analogs (glargine and/or detemir) with neutral protamine Hagedorn (NPH) insulin on the progression of STDR in 46,739 patients with type 2 diabetesmellitus (T2DM).
They found no changed risk of STDR with the long-acting insulin analogs, between either matched or unmatched cohorts. For instance, with a median follow-up of 483 days, they found 479 events with glargine initiators in 8,947 patients. There were 541 events in a median of 541 days’ follow-up for 8,947 patients in the NPH initiators group. The detemir group, with 411 days of follow-up, had 64 events.
Despite a “relatively short” observation period, the researchers say their findings agree with those of a previous open-label randomized study of patients with T2DM, which found treatment with insulin glargine over 5 years did not increase progression of STDR, compared with NPH insulin treatment.
Source
Lin JC, Shau WY, Lai MS. Clin Ther. 2014;36(9):1255-1268.
doi: 10.1016/j.clinthera.2014.06.031.3.
Long-acting insulin analogs are designed to enhance glycemic control without excessively lowering blood glucose. But structural modifications of the insulin molecule can alter biological responses and binding characteristics with specific receptors; in short, they can potentially raise the risk of sight-threatening diabetic retinopathy (STDR), say researchers from Taipei City Hospital and National Taiwan University, both in Taiwan.
The researchers note that some clinical trials have reported that intensification of endogenous insulin might accelerate progression of pre-existing STDR. However, they add that some studies used cancer cell lines, and insulin was administered at supraphysiologic concentrations.
The researchers conducted a retrospective study to evaluate the effects of long-acting insulin analogs (glargine and/or detemir) with neutral protamine Hagedorn (NPH) insulin on the progression of STDR in 46,739 patients with type 2 diabetesmellitus (T2DM).
They found no changed risk of STDR with the long-acting insulin analogs, between either matched or unmatched cohorts. For instance, with a median follow-up of 483 days, they found 479 events with glargine initiators in 8,947 patients. There were 541 events in a median of 541 days’ follow-up for 8,947 patients in the NPH initiators group. The detemir group, with 411 days of follow-up, had 64 events.
Despite a “relatively short” observation period, the researchers say their findings agree with those of a previous open-label randomized study of patients with T2DM, which found treatment with insulin glargine over 5 years did not increase progression of STDR, compared with NPH insulin treatment.
Source
Lin JC, Shau WY, Lai MS. Clin Ther. 2014;36(9):1255-1268.
doi: 10.1016/j.clinthera.2014.06.031.3.
Long-acting insulin analogs are designed to enhance glycemic control without excessively lowering blood glucose. But structural modifications of the insulin molecule can alter biological responses and binding characteristics with specific receptors; in short, they can potentially raise the risk of sight-threatening diabetic retinopathy (STDR), say researchers from Taipei City Hospital and National Taiwan University, both in Taiwan.
The researchers note that some clinical trials have reported that intensification of endogenous insulin might accelerate progression of pre-existing STDR. However, they add that some studies used cancer cell lines, and insulin was administered at supraphysiologic concentrations.
The researchers conducted a retrospective study to evaluate the effects of long-acting insulin analogs (glargine and/or detemir) with neutral protamine Hagedorn (NPH) insulin on the progression of STDR in 46,739 patients with type 2 diabetesmellitus (T2DM).
They found no changed risk of STDR with the long-acting insulin analogs, between either matched or unmatched cohorts. For instance, with a median follow-up of 483 days, they found 479 events with glargine initiators in 8,947 patients. There were 541 events in a median of 541 days’ follow-up for 8,947 patients in the NPH initiators group. The detemir group, with 411 days of follow-up, had 64 events.
Despite a “relatively short” observation period, the researchers say their findings agree with those of a previous open-label randomized study of patients with T2DM, which found treatment with insulin glargine over 5 years did not increase progression of STDR, compared with NPH insulin treatment.
Source
Lin JC, Shau WY, Lai MS. Clin Ther. 2014;36(9):1255-1268.
doi: 10.1016/j.clinthera.2014.06.031.3.
CHMP supports expanding use of lenalidomide in MM

The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) is recommending approval of continuous oral treatment with lenalidomide (Revlimid) in adults with previously untreated multiple myeloma (MM) who are ineligible for hematopoietic stem cell transplant (HSCT).
The European Commission, which generally follows the CHMP’s recommendations, is expected to make its final decision in about 2 months.
Lenalidomide is not currently approved to treat newly diagnosed MM in any country.
The drug is approved in the European Union (EU) for use in combination with dexamethasone to treat adults with MM who have received at least one prior therapy.
Lenalidomide is also approved in the EU to treat patients with transfusion-dependent anemia due to low- or intermediate-1-risk myelodysplastic syndromes associated with 5q deletion when other therapeutic options are insufficient or inadequate.
The CHMP’s recommendation to extend the use of lenalidomide to HSCT-ineligible patients with newly diagnosed MM was based on the results of 2 studies: MM-015 and MM-020, also known as FIRST.
The FIRST trial
In the phase 3 FIRST trial, researchers enrolled 1623 patients who were newly diagnosed with MM and not eligible for HSCT.
Patients were randomized to receive lenalidomide and dexamethasone (Rd) in 28-day cycles until disease progression (n=535), 18 cycles of lenalidomide and dexamethasone (Rd18) for 72 weeks (n=541), or melphalan, prednisone, and thalidomide (MPT) for 72 weeks (n=547).
Response rates were significantly better with continuous Rd (75%) and Rd18 (73%) than with MPT (62%, P<0.001 for both comparisons). Complete response rates were 15%, 14%, and 9%, respectively.
The median progression-free survival was 25.5 months with continuous Rd, 20.7 months with Rd18, and 21.2 months with MPT.
This resulted in a 28% reduction in the risk of progression or death for patients treated with continuous Rd compared with those treated with MPT (hazard ratio[HR]=0.72, P<0.001) and a 30% reduction compared with Rd18 (HR=0.70, P<0.001).
The pre-planned interim analysis of overall survival showed a 22% reduction in the risk of death for continuous Rd vs MPT (HR=0.78, P=0.02), but the difference did not cross the pre-specified superiority boundary (P<0.0096).
Adverse events reported in 20% or more of patients in the continuous Rd, Rd18, or MPT arms included diarrhea (45.5%, 38.5%, 16.5%), anemia (43.8%, 35.7%, 42.3%), neutropenia (35.0%, 33.0%, 60.6%), fatigue (32.5%, 32.8%, 28.5%), back pain (32.0%, 26.9%, 21.4%), insomnia (27.6%, 23.5%, 9.8%), asthenia (28.2%, 22.8%, 22.9%), rash (26.1%, 28.0%, 19.4%), decreased appetite (23.1%, 21.3%, 13.3%), cough (22.7%, 17.4%, 12.6%), pyrexia (21.4%, 18.9%, 14.0%), muscle spasms (20.5%, 18.9%, 11.3%) and abdominal pain (20.5%, 14.4%, 11.1%).
The incidence of invasive second primary malignancies was 3% in patients taking continuous Rd, 6% in patients taking Rd18, and 5% in those taking MPT. The overall incidence of solid tumors was identical in the continuous Rd and MPT arms (3%) and 5% in the Rd18 arm.
The MM-015 trial
In the phase 3 MM-015 study, researchers enrolled 459 patients who were 65 or older and newly diagnosed with MM. The team compared melphalan-prednisone-lenalidomide induction followed by lenalidomide maintenance (MPR-R) with melphalan-prednisone-lenalidomide (MPR) or melphalan-prednisone (MP) followed by placebo.
Patients who received MPR-R or MPR had significantly better response rates than patients who received MP, at 77%, 68%, and 50%, respectively (P<0.001 and P=0.002, respectively, for the comparison with MP).
And the median progression-free survival was significantly longer with MPR-R (31 months) than with MPR (14 months, HR=0.49, P<0.001) or MP (13 months, HR=0.40, P<0.001).
During induction, the most frequent adverse events were hematologic. Grade 4 neutropenia occurred in 35% of patients in the MPR-R arm, 32% in the MPR arm, and 8% in the MP arm. The 3-year rate of second primary malignancies was 7%, 7%, and 3%, respectively. ![]()
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) is recommending approval of continuous oral treatment with lenalidomide (Revlimid) in adults with previously untreated multiple myeloma (MM) who are ineligible for hematopoietic stem cell transplant (HSCT).
The European Commission, which generally follows the CHMP’s recommendations, is expected to make its final decision in about 2 months.
Lenalidomide is not currently approved to treat newly diagnosed MM in any country.
The drug is approved in the European Union (EU) for use in combination with dexamethasone to treat adults with MM who have received at least one prior therapy.
Lenalidomide is also approved in the EU to treat patients with transfusion-dependent anemia due to low- or intermediate-1-risk myelodysplastic syndromes associated with 5q deletion when other therapeutic options are insufficient or inadequate.
The CHMP’s recommendation to extend the use of lenalidomide to HSCT-ineligible patients with newly diagnosed MM was based on the results of 2 studies: MM-015 and MM-020, also known as FIRST.
The FIRST trial
In the phase 3 FIRST trial, researchers enrolled 1623 patients who were newly diagnosed with MM and not eligible for HSCT.
Patients were randomized to receive lenalidomide and dexamethasone (Rd) in 28-day cycles until disease progression (n=535), 18 cycles of lenalidomide and dexamethasone (Rd18) for 72 weeks (n=541), or melphalan, prednisone, and thalidomide (MPT) for 72 weeks (n=547).
Response rates were significantly better with continuous Rd (75%) and Rd18 (73%) than with MPT (62%, P<0.001 for both comparisons). Complete response rates were 15%, 14%, and 9%, respectively.
The median progression-free survival was 25.5 months with continuous Rd, 20.7 months with Rd18, and 21.2 months with MPT.
This resulted in a 28% reduction in the risk of progression or death for patients treated with continuous Rd compared with those treated with MPT (hazard ratio[HR]=0.72, P<0.001) and a 30% reduction compared with Rd18 (HR=0.70, P<0.001).
The pre-planned interim analysis of overall survival showed a 22% reduction in the risk of death for continuous Rd vs MPT (HR=0.78, P=0.02), but the difference did not cross the pre-specified superiority boundary (P<0.0096).
Adverse events reported in 20% or more of patients in the continuous Rd, Rd18, or MPT arms included diarrhea (45.5%, 38.5%, 16.5%), anemia (43.8%, 35.7%, 42.3%), neutropenia (35.0%, 33.0%, 60.6%), fatigue (32.5%, 32.8%, 28.5%), back pain (32.0%, 26.9%, 21.4%), insomnia (27.6%, 23.5%, 9.8%), asthenia (28.2%, 22.8%, 22.9%), rash (26.1%, 28.0%, 19.4%), decreased appetite (23.1%, 21.3%, 13.3%), cough (22.7%, 17.4%, 12.6%), pyrexia (21.4%, 18.9%, 14.0%), muscle spasms (20.5%, 18.9%, 11.3%) and abdominal pain (20.5%, 14.4%, 11.1%).
The incidence of invasive second primary malignancies was 3% in patients taking continuous Rd, 6% in patients taking Rd18, and 5% in those taking MPT. The overall incidence of solid tumors was identical in the continuous Rd and MPT arms (3%) and 5% in the Rd18 arm.
The MM-015 trial
In the phase 3 MM-015 study, researchers enrolled 459 patients who were 65 or older and newly diagnosed with MM. The team compared melphalan-prednisone-lenalidomide induction followed by lenalidomide maintenance (MPR-R) with melphalan-prednisone-lenalidomide (MPR) or melphalan-prednisone (MP) followed by placebo.
Patients who received MPR-R or MPR had significantly better response rates than patients who received MP, at 77%, 68%, and 50%, respectively (P<0.001 and P=0.002, respectively, for the comparison with MP).
And the median progression-free survival was significantly longer with MPR-R (31 months) than with MPR (14 months, HR=0.49, P<0.001) or MP (13 months, HR=0.40, P<0.001).
During induction, the most frequent adverse events were hematologic. Grade 4 neutropenia occurred in 35% of patients in the MPR-R arm, 32% in the MPR arm, and 8% in the MP arm. The 3-year rate of second primary malignancies was 7%, 7%, and 3%, respectively. ![]()
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) is recommending approval of continuous oral treatment with lenalidomide (Revlimid) in adults with previously untreated multiple myeloma (MM) who are ineligible for hematopoietic stem cell transplant (HSCT).
The European Commission, which generally follows the CHMP’s recommendations, is expected to make its final decision in about 2 months.
Lenalidomide is not currently approved to treat newly diagnosed MM in any country.
The drug is approved in the European Union (EU) for use in combination with dexamethasone to treat adults with MM who have received at least one prior therapy.
Lenalidomide is also approved in the EU to treat patients with transfusion-dependent anemia due to low- or intermediate-1-risk myelodysplastic syndromes associated with 5q deletion when other therapeutic options are insufficient or inadequate.
The CHMP’s recommendation to extend the use of lenalidomide to HSCT-ineligible patients with newly diagnosed MM was based on the results of 2 studies: MM-015 and MM-020, also known as FIRST.
The FIRST trial
In the phase 3 FIRST trial, researchers enrolled 1623 patients who were newly diagnosed with MM and not eligible for HSCT.
Patients were randomized to receive lenalidomide and dexamethasone (Rd) in 28-day cycles until disease progression (n=535), 18 cycles of lenalidomide and dexamethasone (Rd18) for 72 weeks (n=541), or melphalan, prednisone, and thalidomide (MPT) for 72 weeks (n=547).
Response rates were significantly better with continuous Rd (75%) and Rd18 (73%) than with MPT (62%, P<0.001 for both comparisons). Complete response rates were 15%, 14%, and 9%, respectively.
The median progression-free survival was 25.5 months with continuous Rd, 20.7 months with Rd18, and 21.2 months with MPT.
This resulted in a 28% reduction in the risk of progression or death for patients treated with continuous Rd compared with those treated with MPT (hazard ratio[HR]=0.72, P<0.001) and a 30% reduction compared with Rd18 (HR=0.70, P<0.001).
The pre-planned interim analysis of overall survival showed a 22% reduction in the risk of death for continuous Rd vs MPT (HR=0.78, P=0.02), but the difference did not cross the pre-specified superiority boundary (P<0.0096).
Adverse events reported in 20% or more of patients in the continuous Rd, Rd18, or MPT arms included diarrhea (45.5%, 38.5%, 16.5%), anemia (43.8%, 35.7%, 42.3%), neutropenia (35.0%, 33.0%, 60.6%), fatigue (32.5%, 32.8%, 28.5%), back pain (32.0%, 26.9%, 21.4%), insomnia (27.6%, 23.5%, 9.8%), asthenia (28.2%, 22.8%, 22.9%), rash (26.1%, 28.0%, 19.4%), decreased appetite (23.1%, 21.3%, 13.3%), cough (22.7%, 17.4%, 12.6%), pyrexia (21.4%, 18.9%, 14.0%), muscle spasms (20.5%, 18.9%, 11.3%) and abdominal pain (20.5%, 14.4%, 11.1%).
The incidence of invasive second primary malignancies was 3% in patients taking continuous Rd, 6% in patients taking Rd18, and 5% in those taking MPT. The overall incidence of solid tumors was identical in the continuous Rd and MPT arms (3%) and 5% in the Rd18 arm.
The MM-015 trial
In the phase 3 MM-015 study, researchers enrolled 459 patients who were 65 or older and newly diagnosed with MM. The team compared melphalan-prednisone-lenalidomide induction followed by lenalidomide maintenance (MPR-R) with melphalan-prednisone-lenalidomide (MPR) or melphalan-prednisone (MP) followed by placebo.
Patients who received MPR-R or MPR had significantly better response rates than patients who received MP, at 77%, 68%, and 50%, respectively (P<0.001 and P=0.002, respectively, for the comparison with MP).
And the median progression-free survival was significantly longer with MPR-R (31 months) than with MPR (14 months, HR=0.49, P<0.001) or MP (13 months, HR=0.40, P<0.001).
During induction, the most frequent adverse events were hematologic. Grade 4 neutropenia occurred in 35% of patients in the MPR-R arm, 32% in the MPR arm, and 8% in the MP arm. The 3-year rate of second primary malignancies was 7%, 7%, and 3%, respectively. ![]()
Bisphosphonates may protect against endometrial cancer
The use of nitrogenous bisphosphonates was associated with a nearly 50% reduction in the incidence of endometrial cancer among women in the PLCO, or Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial.
The endometrial cancer incidence rate among women in the study who reported ever using nitrogenous bisphosphonates was 8.7/10,000 person-years, compared with 17.7/10,000 person-years among those who reported never being exposed to nitrogenous bisphosphonates (rate ratio, 0.49), Sharon Hensley Alford, Ph.D., of the Henry Ford Health System, Detroit, and her colleagues reported online Dec. 22 in Cancer.

The effect was similar after adjustment for age, race, body mass index, smoking status, and use of hormone therapy (hazard ratio, 0.56). The effect was also similar for both type I and type II disease, although there were only nine cases of type II disease, so the finding did not reach statistical significance, the investigators reported (Cancer 2014 Dec. 22 [doi:10.1002/cncr.28952]).
PLCO study subjects included in the current analysis were 23,485 women aged 55-74 years at study entry between 1993 and 2001, who had no cancer diagnosed prior to year 5 of the study when they completed a supplemental questionnaire to assess bone medication use. The women were followed until last known contact, death, or endometrial cancer diagnosis.
The findings support those of preclinical studies demonstrating antitumor effects of bisphosphonates, and suggest that their use may protect against endometrial cancer, the investigators said.
“However, additional studies are needed that include other potential confounders and a larger sample so that type II endometrial cancer could be assessed more confidently,” they concluded, adding that a trial assessing for endometrial, breast, and colorectal cancer in postmenopausal women would be ideal.
The PLCO trial was funded by the National Institutes of Health. The authors reported having no relevant financial disclosures.
The use of nitrogenous bisphosphonates was associated with a nearly 50% reduction in the incidence of endometrial cancer among women in the PLCO, or Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial.
The endometrial cancer incidence rate among women in the study who reported ever using nitrogenous bisphosphonates was 8.7/10,000 person-years, compared with 17.7/10,000 person-years among those who reported never being exposed to nitrogenous bisphosphonates (rate ratio, 0.49), Sharon Hensley Alford, Ph.D., of the Henry Ford Health System, Detroit, and her colleagues reported online Dec. 22 in Cancer.
The effect was similar after adjustment for age, race, body mass index, smoking status, and use of hormone therapy (hazard ratio, 0.56). The effect was also similar for both type I and type II disease, although there were only nine cases of type II disease, so the finding did not reach statistical significance, the investigators reported (Cancer 2014 Dec. 22 [doi:10.1002/cncr.28952]).
PLCO study subjects included in the current analysis were 23,485 women aged 55-74 years at study entry between 1993 and 2001, who had no cancer diagnosed prior to year 5 of the study when they completed a supplemental questionnaire to assess bone medication use. The women were followed until last known contact, death, or endometrial cancer diagnosis.
The findings support those of preclinical studies demonstrating antitumor effects of bisphosphonates, and suggest that their use may protect against endometrial cancer, the investigators said.
“However, additional studies are needed that include other potential confounders and a larger sample so that type II endometrial cancer could be assessed more confidently,” they concluded, adding that a trial assessing for endometrial, breast, and colorectal cancer in postmenopausal women would be ideal.
The PLCO trial was funded by the National Institutes of Health. The authors reported having no relevant financial disclosures.
The use of nitrogenous bisphosphonates was associated with a nearly 50% reduction in the incidence of endometrial cancer among women in the PLCO, or Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial.
The endometrial cancer incidence rate among women in the study who reported ever using nitrogenous bisphosphonates was 8.7/10,000 person-years, compared with 17.7/10,000 person-years among those who reported never being exposed to nitrogenous bisphosphonates (rate ratio, 0.49), Sharon Hensley Alford, Ph.D., of the Henry Ford Health System, Detroit, and her colleagues reported online Dec. 22 in Cancer.
The effect was similar after adjustment for age, race, body mass index, smoking status, and use of hormone therapy (hazard ratio, 0.56). The effect was also similar for both type I and type II disease, although there were only nine cases of type II disease, so the finding did not reach statistical significance, the investigators reported (Cancer 2014 Dec. 22 [doi:10.1002/cncr.28952]).
PLCO study subjects included in the current analysis were 23,485 women aged 55-74 years at study entry between 1993 and 2001, who had no cancer diagnosed prior to year 5 of the study when they completed a supplemental questionnaire to assess bone medication use. The women were followed until last known contact, death, or endometrial cancer diagnosis.
The findings support those of preclinical studies demonstrating antitumor effects of bisphosphonates, and suggest that their use may protect against endometrial cancer, the investigators said.
“However, additional studies are needed that include other potential confounders and a larger sample so that type II endometrial cancer could be assessed more confidently,” they concluded, adding that a trial assessing for endometrial, breast, and colorectal cancer in postmenopausal women would be ideal.
The PLCO trial was funded by the National Institutes of Health. The authors reported having no relevant financial disclosures.
FROM CANCER
Key clinical point: Women with a history of bisphosphonate use had a reduced risk of developing endometrial cancer.
Major finding: The endometrial cancer incidence rate was 8.7 vs. 17.7/10,000 person-years for ever vs. never users of nitrogenous bisphosphonates (rate ratio, 0.49).
Data source: An analysis of data from 23,485 women from a randomized population-based trial.
Disclosures: The PLCO trial was funded by the National Institutes of Health. The authors reported having no financial disclosures.

A Decision Aid Did Not Improve Patient Empowerment for Setting and Achieving Diabetes Treatment Goals
Study Overview
Objective. To determine if a patient-oriented decision aid for prioritizing treatment goals in diabetes leads to changes in patient empowerment for setting and achieving goals and in treatment.
Design. Randomized controlled trial.
Setting and participants. Study participants were recruited from 18 general practices in the north of the Netherlands between April 2011 and August 2012. Participants were included if they had a diagnosis of type 2 diabetes and were managed in primary care. Participants were identified from the electronic medical record system and at least 40 patients were selected from each practice to be contacted for participation. Subjects were excluded if they had myocardial infarction in the preceding year, experienced a stroke, had heart failure, angina, or a terminal illness, or were more than 65 years of age when they received their diabetes diagnosis. Other exclusion criteria include dementia, cognitive deficits, blindness, or an inability to read Dutch. Eligibility criteria were confirmed with the health care provider from each practice. Practices that were included in the study had several features: (1) each had an electronic medical record system supporting structured care protocols; (2) most practices have a nurse practitioner or specialized assistant for diabetes care who carries out the quarterly diabetes checks and is trained to conduct physical examinations, risk assessments, patient education, and counseling; (3) all practices received training in motivational interviewing.
The decision aid format was either a computer screen or printed version, and presented as either a short version, showing treatment effects on myocardial infarction risk only, or as an extended version, including effects on additional outcomes (stroke, amputation, blindness, renal failure). Practices were randomly assigned to use the computer screen or printed version, stratified by practice size (< 2500 patients or > 2500 patients) and number of GPs (solo or several). Within each practice, consenting patients were randomized to receive the short version aid, the extended version, or to the control group.
Intervention. The decision aid presents individually tailored information on risks and treatment options for multiple risk factors. The aid focuses on shared goal setting and decision making, particularly with respect to the drug treatment of risk factors including hemoglobin A1c, systolic blood pressure, low density lipoprotein cholesterol, and smoking. The decision aid is designed to be used by patients before a regular check-up and discussed with their health care provider during a visit to help prioritize treatment that will maximize outcomes; the aid helps to summarize effects of the various treatment options. The patients were asked to come to the practice 15 minutes in advance to go through the information, either in print or on the computer; health care providers were expected to support patients to think about treatment goals and options. Patients in the control received care as usual.
Main outcome measures. The primary outcome measure was the empowerment of patients for setting and achieving goals, which was measured with the Diabetes Empowerment Scale (DES-III). Other outcome measures included changes in treatment, including intensification of drug treatment and treatment with ACE inhibitors.
Main results. A total of 344 patients were included in the study and were randomized to the intervention (n = 225) or usual care group (n = 119). Patients in the intervention group were comparable to usual care patients in terms of age, sex, and educational level. However, there were several differences between the 2 groups: intervention patients were more likely to have well-controlled HbA1c level at baseline and less likely to have well-controlled blood pressure at baseline. Among participants in the intervention group, only 46% reported to have received the basic elements of the intervention. The mean empowerment score increased 0.1 point on a 5-point scale in the intervention group, which was not different from the control group (mean adjusted difference, 0.039 points [95% confidence interval {CI}], −0.056 to 0.134). Lipid lowering medication treatment was intensified in 25% of intervention and 12% of control participants (odds ratio [OR], 2.5 [95% CI, 0.89–7.23]). Explorative analyses comparing printed version of the aid with control did find that lipid lowering medication treatment was more intensified although the confidence interval was wide (OR, 3.90 [95% CI, 1.29–11.80]). No other differences in treatment plan were observed.
Conclusions. The treatment decision aid for diabetes did not improve patient empowerment or substantially alter treatment plan when compared to usual care. However, this finding is limited by the uptake of use of the decision aid during the study period.
Commentary
Patient engagement through shared decision making is an important element in chronic disease management, particularly in diseases such as diabetes where there are a number of significant tasks, including monitoring and administration of medication, that are key to its successful management. The use of decision aids is an innovation that has demonstrated effects in improving patient understanding of disease, and has potential downstream effect in improving management and control of the disease [1]. However, the use of decision aids is not without limitations—patients with poorer health literacy, and perhaps lower socioeconomic status, may derive less clinical benefit [2], and in older adults cognitive and physical limitations may also limit their use.
This study found that the decision aid used in the study did not significantly improve patient empowerment or alter treatment plan. In comparison with previous studies on decision aids for diabetes [3,4], this study is notable that it did not find any significant clinical impact of the decision aid when compared with usual care. However, it is important to consider reasons that may explain its null finding. First, the study has a rather complicated design, with 4 different intervention groups. The study design attempts to differentiate intervention groups with differences in its delivery (computer screen vs. printed) and content (focused information on myocardial infarction risk outcome only vs. all outcomes). The rationale was that it could provide evidence to perhaps suggest the most effective decision aid, but the drawback is that it has the potential to weaken the power of the study, increasing the likelihood of a false-negative finding. Second, in contrast to other studies, this study also uses a different measurement as its primary outcome—a measurement of patient empowerment. Though an important concept to measure, it is less clear what the expected impact and what the level of clinical significance would be. Third, as noted by the investigators, the decision aid had limited uptake in the intervention group; this may be related to its design and format. The challenge in design of a decision aid is that it needs to be simple and easy to use, consume little time, yet be adequately informative with helpful information for patients. Finally, another unique feature of the study is that the control group was an active control group, in that the providers in the practices had significant training in motivational interviewing and communication, which may have made it more challenging to demonstrate impact in intervention group.
Applications for Clinical Practice
Decision aids remain a potentially important addition for patients in the management of chronic diseases such as diabetes. Most studies have demonstrated significant impact. Despite the limitations of the current study, it does point out that different formats of decision aid may have different effects on patient outcomes. For practices that are adopting decision aids for chronic disease management, they need to take into account the format, the information, and the burden of use of the decision aid. Further studies may help to elucidate how decision aids can be optimized for maximizing clinical impact.
—William Hung, MD, MPH
1. Stacey D, Légaré F, Col NF, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev 2014;1:CD001431.
2. Coylewright M, Branda M, Inselman JW, et al. Impact of sociodemographic patient characteristics on the efficacy of decision AIDS: a patient-level meta-analysis of 7 randomized trials. Circ Cardiovasc Qual Outcomes 2014;7:360–7.
3. Mathers N, Ng CJ, Campbell MJ, et al. Clinical effectiveness of a patient decision aid to improve decision quality and glycaemic control in people with diabetes making treatment choices: a cluster randomized controlled trial (PANDAs) in general practice. BMJ Open 2012;2:e001469.
4. Branda ME, LeBlanc A, Shah ND, et al. Shared decision making for patients with type 2 diabetes: a randomized trial in primary care. BMC Health Serv Res 2013;13:301.
Study Overview
Objective. To determine if a patient-oriented decision aid for prioritizing treatment goals in diabetes leads to changes in patient empowerment for setting and achieving goals and in treatment.
Design. Randomized controlled trial.
Setting and participants. Study participants were recruited from 18 general practices in the north of the Netherlands between April 2011 and August 2012. Participants were included if they had a diagnosis of type 2 diabetes and were managed in primary care. Participants were identified from the electronic medical record system and at least 40 patients were selected from each practice to be contacted for participation. Subjects were excluded if they had myocardial infarction in the preceding year, experienced a stroke, had heart failure, angina, or a terminal illness, or were more than 65 years of age when they received their diabetes diagnosis. Other exclusion criteria include dementia, cognitive deficits, blindness, or an inability to read Dutch. Eligibility criteria were confirmed with the health care provider from each practice. Practices that were included in the study had several features: (1) each had an electronic medical record system supporting structured care protocols; (2) most practices have a nurse practitioner or specialized assistant for diabetes care who carries out the quarterly diabetes checks and is trained to conduct physical examinations, risk assessments, patient education, and counseling; (3) all practices received training in motivational interviewing.
The decision aid format was either a computer screen or printed version, and presented as either a short version, showing treatment effects on myocardial infarction risk only, or as an extended version, including effects on additional outcomes (stroke, amputation, blindness, renal failure). Practices were randomly assigned to use the computer screen or printed version, stratified by practice size (< 2500 patients or > 2500 patients) and number of GPs (solo or several). Within each practice, consenting patients were randomized to receive the short version aid, the extended version, or to the control group.
Intervention. The decision aid presents individually tailored information on risks and treatment options for multiple risk factors. The aid focuses on shared goal setting and decision making, particularly with respect to the drug treatment of risk factors including hemoglobin A1c, systolic blood pressure, low density lipoprotein cholesterol, and smoking. The decision aid is designed to be used by patients before a regular check-up and discussed with their health care provider during a visit to help prioritize treatment that will maximize outcomes; the aid helps to summarize effects of the various treatment options. The patients were asked to come to the practice 15 minutes in advance to go through the information, either in print or on the computer; health care providers were expected to support patients to think about treatment goals and options. Patients in the control received care as usual.
Main outcome measures. The primary outcome measure was the empowerment of patients for setting and achieving goals, which was measured with the Diabetes Empowerment Scale (DES-III). Other outcome measures included changes in treatment, including intensification of drug treatment and treatment with ACE inhibitors.
Main results. A total of 344 patients were included in the study and were randomized to the intervention (n = 225) or usual care group (n = 119). Patients in the intervention group were comparable to usual care patients in terms of age, sex, and educational level. However, there were several differences between the 2 groups: intervention patients were more likely to have well-controlled HbA1c level at baseline and less likely to have well-controlled blood pressure at baseline. Among participants in the intervention group, only 46% reported to have received the basic elements of the intervention. The mean empowerment score increased 0.1 point on a 5-point scale in the intervention group, which was not different from the control group (mean adjusted difference, 0.039 points [95% confidence interval {CI}], −0.056 to 0.134). Lipid lowering medication treatment was intensified in 25% of intervention and 12% of control participants (odds ratio [OR], 2.5 [95% CI, 0.89–7.23]). Explorative analyses comparing printed version of the aid with control did find that lipid lowering medication treatment was more intensified although the confidence interval was wide (OR, 3.90 [95% CI, 1.29–11.80]). No other differences in treatment plan were observed.
Conclusions. The treatment decision aid for diabetes did not improve patient empowerment or substantially alter treatment plan when compared to usual care. However, this finding is limited by the uptake of use of the decision aid during the study period.
Commentary
Patient engagement through shared decision making is an important element in chronic disease management, particularly in diseases such as diabetes where there are a number of significant tasks, including monitoring and administration of medication, that are key to its successful management. The use of decision aids is an innovation that has demonstrated effects in improving patient understanding of disease, and has potential downstream effect in improving management and control of the disease [1]. However, the use of decision aids is not without limitations—patients with poorer health literacy, and perhaps lower socioeconomic status, may derive less clinical benefit [2], and in older adults cognitive and physical limitations may also limit their use.
This study found that the decision aid used in the study did not significantly improve patient empowerment or alter treatment plan. In comparison with previous studies on decision aids for diabetes [3,4], this study is notable that it did not find any significant clinical impact of the decision aid when compared with usual care. However, it is important to consider reasons that may explain its null finding. First, the study has a rather complicated design, with 4 different intervention groups. The study design attempts to differentiate intervention groups with differences in its delivery (computer screen vs. printed) and content (focused information on myocardial infarction risk outcome only vs. all outcomes). The rationale was that it could provide evidence to perhaps suggest the most effective decision aid, but the drawback is that it has the potential to weaken the power of the study, increasing the likelihood of a false-negative finding. Second, in contrast to other studies, this study also uses a different measurement as its primary outcome—a measurement of patient empowerment. Though an important concept to measure, it is less clear what the expected impact and what the level of clinical significance would be. Third, as noted by the investigators, the decision aid had limited uptake in the intervention group; this may be related to its design and format. The challenge in design of a decision aid is that it needs to be simple and easy to use, consume little time, yet be adequately informative with helpful information for patients. Finally, another unique feature of the study is that the control group was an active control group, in that the providers in the practices had significant training in motivational interviewing and communication, which may have made it more challenging to demonstrate impact in intervention group.
Applications for Clinical Practice
Decision aids remain a potentially important addition for patients in the management of chronic diseases such as diabetes. Most studies have demonstrated significant impact. Despite the limitations of the current study, it does point out that different formats of decision aid may have different effects on patient outcomes. For practices that are adopting decision aids for chronic disease management, they need to take into account the format, the information, and the burden of use of the decision aid. Further studies may help to elucidate how decision aids can be optimized for maximizing clinical impact.
—William Hung, MD, MPH
Study Overview
Objective. To determine if a patient-oriented decision aid for prioritizing treatment goals in diabetes leads to changes in patient empowerment for setting and achieving goals and in treatment.
Design. Randomized controlled trial.
Setting and participants. Study participants were recruited from 18 general practices in the north of the Netherlands between April 2011 and August 2012. Participants were included if they had a diagnosis of type 2 diabetes and were managed in primary care. Participants were identified from the electronic medical record system and at least 40 patients were selected from each practice to be contacted for participation. Subjects were excluded if they had myocardial infarction in the preceding year, experienced a stroke, had heart failure, angina, or a terminal illness, or were more than 65 years of age when they received their diabetes diagnosis. Other exclusion criteria include dementia, cognitive deficits, blindness, or an inability to read Dutch. Eligibility criteria were confirmed with the health care provider from each practice. Practices that were included in the study had several features: (1) each had an electronic medical record system supporting structured care protocols; (2) most practices have a nurse practitioner or specialized assistant for diabetes care who carries out the quarterly diabetes checks and is trained to conduct physical examinations, risk assessments, patient education, and counseling; (3) all practices received training in motivational interviewing.
The decision aid format was either a computer screen or printed version, and presented as either a short version, showing treatment effects on myocardial infarction risk only, or as an extended version, including effects on additional outcomes (stroke, amputation, blindness, renal failure). Practices were randomly assigned to use the computer screen or printed version, stratified by practice size (< 2500 patients or > 2500 patients) and number of GPs (solo or several). Within each practice, consenting patients were randomized to receive the short version aid, the extended version, or to the control group.
Intervention. The decision aid presents individually tailored information on risks and treatment options for multiple risk factors. The aid focuses on shared goal setting and decision making, particularly with respect to the drug treatment of risk factors including hemoglobin A1c, systolic blood pressure, low density lipoprotein cholesterol, and smoking. The decision aid is designed to be used by patients before a regular check-up and discussed with their health care provider during a visit to help prioritize treatment that will maximize outcomes; the aid helps to summarize effects of the various treatment options. The patients were asked to come to the practice 15 minutes in advance to go through the information, either in print or on the computer; health care providers were expected to support patients to think about treatment goals and options. Patients in the control received care as usual.
Main outcome measures. The primary outcome measure was the empowerment of patients for setting and achieving goals, which was measured with the Diabetes Empowerment Scale (DES-III). Other outcome measures included changes in treatment, including intensification of drug treatment and treatment with ACE inhibitors.
Main results. A total of 344 patients were included in the study and were randomized to the intervention (n = 225) or usual care group (n = 119). Patients in the intervention group were comparable to usual care patients in terms of age, sex, and educational level. However, there were several differences between the 2 groups: intervention patients were more likely to have well-controlled HbA1c level at baseline and less likely to have well-controlled blood pressure at baseline. Among participants in the intervention group, only 46% reported to have received the basic elements of the intervention. The mean empowerment score increased 0.1 point on a 5-point scale in the intervention group, which was not different from the control group (mean adjusted difference, 0.039 points [95% confidence interval {CI}], −0.056 to 0.134). Lipid lowering medication treatment was intensified in 25% of intervention and 12% of control participants (odds ratio [OR], 2.5 [95% CI, 0.89–7.23]). Explorative analyses comparing printed version of the aid with control did find that lipid lowering medication treatment was more intensified although the confidence interval was wide (OR, 3.90 [95% CI, 1.29–11.80]). No other differences in treatment plan were observed.
Conclusions. The treatment decision aid for diabetes did not improve patient empowerment or substantially alter treatment plan when compared to usual care. However, this finding is limited by the uptake of use of the decision aid during the study period.
Commentary
Patient engagement through shared decision making is an important element in chronic disease management, particularly in diseases such as diabetes where there are a number of significant tasks, including monitoring and administration of medication, that are key to its successful management. The use of decision aids is an innovation that has demonstrated effects in improving patient understanding of disease, and has potential downstream effect in improving management and control of the disease [1]. However, the use of decision aids is not without limitations—patients with poorer health literacy, and perhaps lower socioeconomic status, may derive less clinical benefit [2], and in older adults cognitive and physical limitations may also limit their use.
This study found that the decision aid used in the study did not significantly improve patient empowerment or alter treatment plan. In comparison with previous studies on decision aids for diabetes [3,4], this study is notable that it did not find any significant clinical impact of the decision aid when compared with usual care. However, it is important to consider reasons that may explain its null finding. First, the study has a rather complicated design, with 4 different intervention groups. The study design attempts to differentiate intervention groups with differences in its delivery (computer screen vs. printed) and content (focused information on myocardial infarction risk outcome only vs. all outcomes). The rationale was that it could provide evidence to perhaps suggest the most effective decision aid, but the drawback is that it has the potential to weaken the power of the study, increasing the likelihood of a false-negative finding. Second, in contrast to other studies, this study also uses a different measurement as its primary outcome—a measurement of patient empowerment. Though an important concept to measure, it is less clear what the expected impact and what the level of clinical significance would be. Third, as noted by the investigators, the decision aid had limited uptake in the intervention group; this may be related to its design and format. The challenge in design of a decision aid is that it needs to be simple and easy to use, consume little time, yet be adequately informative with helpful information for patients. Finally, another unique feature of the study is that the control group was an active control group, in that the providers in the practices had significant training in motivational interviewing and communication, which may have made it more challenging to demonstrate impact in intervention group.
Applications for Clinical Practice
Decision aids remain a potentially important addition for patients in the management of chronic diseases such as diabetes. Most studies have demonstrated significant impact. Despite the limitations of the current study, it does point out that different formats of decision aid may have different effects on patient outcomes. For practices that are adopting decision aids for chronic disease management, they need to take into account the format, the information, and the burden of use of the decision aid. Further studies may help to elucidate how decision aids can be optimized for maximizing clinical impact.
—William Hung, MD, MPH
1. Stacey D, Légaré F, Col NF, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev 2014;1:CD001431.
2. Coylewright M, Branda M, Inselman JW, et al. Impact of sociodemographic patient characteristics on the efficacy of decision AIDS: a patient-level meta-analysis of 7 randomized trials. Circ Cardiovasc Qual Outcomes 2014;7:360–7.
3. Mathers N, Ng CJ, Campbell MJ, et al. Clinical effectiveness of a patient decision aid to improve decision quality and glycaemic control in people with diabetes making treatment choices: a cluster randomized controlled trial (PANDAs) in general practice. BMJ Open 2012;2:e001469.
4. Branda ME, LeBlanc A, Shah ND, et al. Shared decision making for patients with type 2 diabetes: a randomized trial in primary care. BMC Health Serv Res 2013;13:301.
1. Stacey D, Légaré F, Col NF, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev 2014;1:CD001431.
2. Coylewright M, Branda M, Inselman JW, et al. Impact of sociodemographic patient characteristics on the efficacy of decision AIDS: a patient-level meta-analysis of 7 randomized trials. Circ Cardiovasc Qual Outcomes 2014;7:360–7.
3. Mathers N, Ng CJ, Campbell MJ, et al. Clinical effectiveness of a patient decision aid to improve decision quality and glycaemic control in people with diabetes making treatment choices: a cluster randomized controlled trial (PANDAs) in general practice. BMJ Open 2012;2:e001469.
4. Branda ME, LeBlanc A, Shah ND, et al. Shared decision making for patients with type 2 diabetes: a randomized trial in primary care. BMC Health Serv Res 2013;13:301.
Letting Our Patients “Fail Fast”: Early Non-Response to Lorcaserin May Be a Good Reason to Discontinue Medication
Study Overview
Objective. To examine whether an early response (or non-response) to lorcaserin therapy predicts ≥ 5% weight loss achieved at 1 year.
Study design. Secondary analysis of data collected in 3 placebo-controlled blinded randomized trials.
Setting and participants. This study relied upon data collected as part of 3 separate phase 3 clinical trials of lorcaserin, a weight loss drug and selective serotonin 2c (5-HT2c) agonist. The first study, “Behavioral Modification and Lorcaserin for Overweight and Obesity Management” (BLOOM; n = 3182) enrolled overweight (with at least 1 comorbidity) or obese (no comorbidity needed) adult patients (18–65 yr) without diabetes, to determine the safety and efficacy of lorcaserin. The second trial, “Behavioral Modification and Lorcaserin Second Study of Obesity Management” (BLOSSOM; n = 4008) enrolled a similar population as BLOOM. For both BLOOM and BLOSSOM, patients were randomly assigned to receive either lorcaserin (10 mg po bid) or placebo for a 1-year period, and all patients received advice and instruction in exercise goals (at least 30 min/day) and caloric intake (600 kcal less than recommended for weight maintenance for that individual) necessary to promote weight loss. The third trial, BLOOM-DM (n = 604) focused on overweight or obese diabetic patients, but otherwise was similar in methodology to BLOOM and BLOSSOM. All studies took place in multiple US academic and private medical centers and were funded by Arena Pharmaceuticals. For the current analysis, the investigators used data from these trials and classified participants as either “responders” or “non-responders” based on each participant’s early weight loss response to either lorcaserin or placebo.
Main outcome measures. The investigators used area under the curve for the receiver operating characteristic (AUC for ROC) analysis to determine whether an early weight loss response to lorcaserin or placebo predicted a patient’s longer-term (52-week) weight loss. Several steps were used to conduct these analyses.
First, the investigators needed to determine what amount of weight loss at which of several early time-points would qualify a participant as a “responder” to either drug or placebo. They compared weight lost at weeks 2, 4, 8 and 12, using AUC for ROC analysis to identify the appropriate “responder” or “non-responder” cut-points, and classified all participants with data points in these early weeks as such. Second, all of the early responder and non-responder participants with 52-week weight data were then classified as to whether or not they had achieved at least a 5% weight loss at the end of the study. AUC for ROC analysis was again used to determine whether this early categorization was predictive of final study response. In addition to looking at early response as predictive of final weight loss, the investigators also examined the response/non-response variable’s ability to predict other health outcomes, including changes in lipid levels, blood pressure, and, for type 2 diabetic participants, changes in glycemic control (fasting plasma glucose [FPG] and HgbA1c). Finally, the investigators examined the incidence of adverse events in the different groups as well.
Results. The investigators identified a 4.6% weight loss by week 12 on lorcaserin or placebo as the optimal cut-point for determining whether a participant was a “responder” or “non-responder” (“W12R” or “W12NR”). This cut-point had an AUC (95% CI) of 0.849 (0.828–0.870) for predicting ≥ 5% weight loss at 52 weeks, with a positive predictive value (PPV) of 0.855 and negative predictive value (NPV) of 0.740, thus optimizing specificity and sensitivity of the time/weight cut-point compared to those at weeks 2, 4, or 8. Given the need for practical clinical recommendations, however, the investigators used a cut-point of 5% weight loss by week 12 to determine response/non-response for the health outcome analyses. The breakdown of responders vs. non-responders was as follows: For the pooled BLOOM/BLOSSOM participants, there were 1251 lorcaserin-recipient responders and 1286 lorcaserin-recipient non-responders (about 40% of those randomized to lorcaserin were “responders”). Among placebo recipients, there were 541 early responders and 1852 non-responders (about 17% of those randomized to placebo were “responders”). For the diabetic BLOOM-DM participants, the ratios were similar although slightly less favorable, with only about 30% (n = 78) of lorcaserin patients classified W12 responders (139 non-responders), and 10% (n = 25) of placebo patients as W12 responders (192 non-responders).
The lorcaserin and placebo groups in BLOOM and BLOSSOM were similar to one another, with overall mean (SD) age of 43.8 (11.6) years for lorcaserin and 44.0 (11.4) years for placebo. The vast majority of participants in these 2 trials were female (81.7% in lorcaserin arms, 81.0% in placebo), and the majority were non-Hispanic white (67.6% in lorcaserin and 66.2% in placebo). The mean (SD) baseline body mass index (BMI, kg/m2) was 36.1 (4.3) for lorcaserin and 36.1 (4.2) for placebo. The BLOOM-DM participants were also similar in the lorcaserin and placebo arms, although they were older (mean age, 53.2 years lorcaserin, 52 years placebo), and more likely to be female (53.5% lorcaserin, 54.4% placebo). Otherwise, the BLOOM-DM participants were similar on reported demographic characteristics to those in the other 2 trials.
Importantly, however, for all 3 trials there were differences in demographic characteristics between those participants characterized as responders and those characterized as non-responders. Amongst the nondiabetic participants in the BLOOM and BLOSSOM studies, responders (to both lorcaserin and placebo) were more likely to be non-Hispanic white (as opposed to African American or Hispanic participants, who were more likely to be non-responders), and responders were older than non-responders. Interestingly, for the diabetics in the BLOOM-DM trial, the responder/non-responder differences were less pronounced, although the responders were still slightly more likely to be non-Hispanic white and older, particularly for placebo.
Among BLOOM and BLOSSOM participants who received lorcaserin, mean weight loss at 52 weeks was 10.8% among W12Rs and only 2.7% among W12NRs. A similar pattern was observed in the BLOOM and BLOSSOM placebo participants; W12Rs averaged 9.5% weight loss at 52 weeks, versus just 1.1% in W12NRs. Among diabetics receiving lorcaserin in the BLOOM-DM study, weight loss at 1 year was 9.1% in W12Rs versus 3.1% in W12NRs. Similarly, in placebo-recipients in BLOOM-DM, weight loss at 1 year was 7% for W12Rs and 1.3% for W12NRs. When the weight loss at 1 year was categorized in terms of whether or not participants achieved at least 5% or 10% weight loss, once again early responders to either lorcaserin or placebo had higher rates of achieving both thresholds. Namely, 85.5% of nondiabetic W12Rs had achieved or maintained 5% weight loss at week 52, while only 26% of the W12NRs ultimately did so. Seventy percent of diabetic W12Rs to lorcaserin had ≥ 5% weight loss at week 52 and 25.2% of W12NRs did. The pattern of prediction for achieving 10% weight loss at week 52 was even more pronounced, with, for example, 49.8% of nondiabetic W12Rs having lost at least 10% of their starting weight at 1 year, versus just 4.7% of W12NRs.
When cardiometabolic outcomes were examined, the differences between W12 lorcaserin responders and non-responders appeared to be somewhat attenuated. For example, among diabetic patients, W12 lorcaserin responders had a mean decrease of 1.2% in their A1c level by study end, compared to a nearly 1% decrease in W12NRs. For fasting plasma glucose, the improvement at week 52 was pronounced (about 30 mg/dL lower than baseline) and very similar in W12 responders and non-responders.
Among nondiabetics, average blood pressure lowering (SBP and DBP) at week 52 was greater among lorcaserin W12 responders (SBP dropped 4 mm Hg on average, DBP 3 mm Hg) than it was among non-responders (SBP and DBP dropped by about 1 mm Hg). Other than triglycerides, which decreased substantially among W12 responders (whether on placebo or lorcaserin), changes to lipid profile were relatively small for nondiabetics. Among diabetics, however, LDL and HDL both increased on average in all 4 groups (W12 responders/non-responders to placebo/lorcaserin) by week 52.
Common adverse events for lorcaserin-treated patients included headache (15%–17%), upper respiratory infections (9%–14%), nausea (8%–9%), and dizziness (8% among nondiabetics). Among diabetics, hypoglycemia occurred in 29.3% of those treated with lorcaserin (vs. 21% on placebo). Week 12 responders and non-responders appeared to have a similar adverse event profile, and, in general, adverse events were more common among lorcaserin than placebo participants.
Conclusion. The authors of this study concluded that a week-12 weight loss of ≥ 5% on lorcaserin was a strong predictor of achieving at least that same amount of weight loss, as well as improvements in some cardiometabolic parameters, at 1 year.
Commentary
In 2013, the American Medical Association officially recognized obesity as a disease. This shift in terminology, coupled with a movement towards reimbursing primary care providers for obesity-related interventions, has created a growing awareness among providers that better treatment options for this chronic condition are sorely needed. Just as we treat patients with hypertension and type 2 diabetes by titrating medications, discontinuing those that aren’t effective and continuing those that are, so should we approach the management of our patients with obesity. Although behavioral interventions centered around lifestyle changes (diet/exercise) remain first-line therapies for the treatment of obesity [1], many patients will seek additional tools, such as meal replacement, medication, or even bariatric surgery, to help achieve and maintain weight loss.
In the past 2 to 3 years, there has been a flurry of activity by the FDA to approve new medications for weight loss. In keeping with the view of obesity as a chronic condition, some of these medications, including lorcaserin and phentermine-topiramate ER, have even been approved for patient long-term use [2]. While the addition of new options to the weight loss toolkit is exciting, it may also be daunting for clinicians who have witnessed a bevy of weight loss drugs come on, and then off, the market over the years due to serious adverse events experienced by patients. For physicians and patients considering the use of a new weight loss medication, there is therefore a clear need to minimize risk for adverse effects related to the drug, while maximizing the patient’s chances of losing weight.
Growing evidence from trials of behavioral interventions as well as weight loss medications suggests that the individuals who will ultimately achieve weight loss success with a given intervention/medication, tend to indicate that success relatively early on in the course of therapy [3–5]. For clinicians, this fact is extremely useful, because it may allow the physician and patient to more rapidly make a decision to discontinue a likely ineffective option in favor of another that has not yet been tried, thus minimizing risks for adverse events while maximizing chances of weight loss outcomes.
In this paper, Smith and colleagues addressed this very important issue for one of the more recently FDA-approved medications, lorcaserin. This 5-HT2c agonist is a useful addition to the list of weight loss medications, as it has relatively few contraindications, other than that it cannot be used in pregnancy/lactation and should be avoided in those with a history of heart failure. However, lorcaserin is still relatively costly (eg, compared to phentermine) and, if it is going to be used for long-term weight loss/maintenance, the financial outlay faced by patients might be considerable. In addition to answering an important question, this paper also examined not only weight loss outcomes but also cardiometabolic impacts of the medication. Furthermore, the authors separately examined outcomes for diabetic and nondiabetic patients, as the risk/benefit ratio of remaining on this medication could be quite different between the 2 groups.
Importantly, the study represented a group of secondary analyses of data aggregated from several trials—trials that were not originally designed to answer this question. Although the majority of original trial participants did have data at weeks 12 and 52 (requirement for inclusion in this analysis), up to a quarter of patients in some groups were missing one or the other measure. Whether or not those analyzed represented a biased subsample, and therefore do not have generalizable results, cannot be ascertained.
In reviewing the outcomes achieved by early responders and non-responders, it was very interesting to note that so-called “responders” to placebo followed a nearly identical weight loss trajectory as those on lorcaserin. This fact should not be taken to indicate that lorcaserin is no different from placebo, as the overall chances of achieving weight loss were significantly greater among the lorcaserin participants. However, it is interesting that, for those placebo patients who clearly followed the recommended lifestyle changes, they did just as well as patients receiving active study drug. This underscores the need to educate patients and encourage them, first and foremost, to make a real effort to diet and exercise regardless of what other tools are employed to achieve weight loss.
Another issue to consider for this study is that there are clear differences in the racial/ethnic makeup of responders versus non-responders. This finding is not unexpected, as in many prior weight loss trials, particularly for behavioral interventions, African-American women have experienced less weight loss than their non-Hispanic white counterparts [6]. These differences were observed both for lorcaserin and placebo patients, raising a concern that the lifestyle intervention component of the study was not equally successful for minorities compared to the non-Hispanic white participants. More research is needed on behavioral interventions that work well in diverse populations.
One finding of interest is that among diabetic participants (BLOOM-DM), glycemic control parameters improved nearly equally between lorcaserin early responders and non-responders, despite the differences between those groups for year-end weight loss. The reasons for this are not clear but could merit further investigation.
Ultimately however, even among this large group of randomized trial participants, who were likely highly motivated, only about 40% of nondiabetics and 30% of diabetics were classified as week 12 responders to lorcaserin. That means that likely well over half of the real-world patients who initiate the drug may not achieve their desired weight loss goals with it. Given the cost of the medication, this must be considered before prescribing it, and it reinforces the importance of being willing to reassess a patient’s weight loss progress early and often so that the medication can be discontinued in favor of other therapies as needed.
Applications for Clinical Practice
For providers interested in prescribing lorcaserin to their patients, a clear plan should be made to have regular and early follow-up to assess the patient’s response to the medication. Patients should understand that if they are not responding to the medication within 3 months, or perhaps sooner if they are experiencing any negative side effects, their physician may elect to discontinue it. Importantly, they should only be given lorcaserin if they are also willing to undertake the behavioral changes necessary to promote weight loss, and it should be underscored that their chances of successful weight loss with or without the medication will be greatly enhanced by doing so.
—Kristina Lewis, MD, MPH
1. Jensen MD, Ryan DH, Apovian CM, et al. 2013 AHA/ACC/TOS Guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. J Am Coll Cardiol 2014;63(25 Pt B):2985–3023.
2. Hurt RT, Jithinraj EV, Ebbert JO. New pharmacological treatments for the management of obesity. Cur Gastroenterol Rep 2014;16.6:1–8.
3. Wadden TA, Foster GD, Wang J, et al. Clinical correlates of short- and long-term weight loss. Am J Clin Nutr 1992;56(Suppl 1):271S–274S.
4. Rissanen A, Lean M, Rossner S, et al. Predictive value of early weight loss in obesity management with orlistat: An evidence-based assessment of prescribing guidelines. Int J Obes Relat Metab Disord 2003;27:103–9.
5. O’Neil P, Foster G, Billes S, et al. Early weight loss with naltrexone SR/bupropion SR combination therapy for obesity predicts long-term weight loss (Abstract). Obesity 2009;17:S109.
6. Kumanyika SK, Whitt-Glover MC, Haire-Joshu D. What works for obesity prevention and treatment in black Americans? Research directions. Obes Rev 2014;15:204–12.
Study Overview
Objective. To examine whether an early response (or non-response) to lorcaserin therapy predicts ≥ 5% weight loss achieved at 1 year.
Study design. Secondary analysis of data collected in 3 placebo-controlled blinded randomized trials.
Setting and participants. This study relied upon data collected as part of 3 separate phase 3 clinical trials of lorcaserin, a weight loss drug and selective serotonin 2c (5-HT2c) agonist. The first study, “Behavioral Modification and Lorcaserin for Overweight and Obesity Management” (BLOOM; n = 3182) enrolled overweight (with at least 1 comorbidity) or obese (no comorbidity needed) adult patients (18–65 yr) without diabetes, to determine the safety and efficacy of lorcaserin. The second trial, “Behavioral Modification and Lorcaserin Second Study of Obesity Management” (BLOSSOM; n = 4008) enrolled a similar population as BLOOM. For both BLOOM and BLOSSOM, patients were randomly assigned to receive either lorcaserin (10 mg po bid) or placebo for a 1-year period, and all patients received advice and instruction in exercise goals (at least 30 min/day) and caloric intake (600 kcal less than recommended for weight maintenance for that individual) necessary to promote weight loss. The third trial, BLOOM-DM (n = 604) focused on overweight or obese diabetic patients, but otherwise was similar in methodology to BLOOM and BLOSSOM. All studies took place in multiple US academic and private medical centers and were funded by Arena Pharmaceuticals. For the current analysis, the investigators used data from these trials and classified participants as either “responders” or “non-responders” based on each participant’s early weight loss response to either lorcaserin or placebo.
Main outcome measures. The investigators used area under the curve for the receiver operating characteristic (AUC for ROC) analysis to determine whether an early weight loss response to lorcaserin or placebo predicted a patient’s longer-term (52-week) weight loss. Several steps were used to conduct these analyses.
First, the investigators needed to determine what amount of weight loss at which of several early time-points would qualify a participant as a “responder” to either drug or placebo. They compared weight lost at weeks 2, 4, 8 and 12, using AUC for ROC analysis to identify the appropriate “responder” or “non-responder” cut-points, and classified all participants with data points in these early weeks as such. Second, all of the early responder and non-responder participants with 52-week weight data were then classified as to whether or not they had achieved at least a 5% weight loss at the end of the study. AUC for ROC analysis was again used to determine whether this early categorization was predictive of final study response. In addition to looking at early response as predictive of final weight loss, the investigators also examined the response/non-response variable’s ability to predict other health outcomes, including changes in lipid levels, blood pressure, and, for type 2 diabetic participants, changes in glycemic control (fasting plasma glucose [FPG] and HgbA1c). Finally, the investigators examined the incidence of adverse events in the different groups as well.
Results. The investigators identified a 4.6% weight loss by week 12 on lorcaserin or placebo as the optimal cut-point for determining whether a participant was a “responder” or “non-responder” (“W12R” or “W12NR”). This cut-point had an AUC (95% CI) of 0.849 (0.828–0.870) for predicting ≥ 5% weight loss at 52 weeks, with a positive predictive value (PPV) of 0.855 and negative predictive value (NPV) of 0.740, thus optimizing specificity and sensitivity of the time/weight cut-point compared to those at weeks 2, 4, or 8. Given the need for practical clinical recommendations, however, the investigators used a cut-point of 5% weight loss by week 12 to determine response/non-response for the health outcome analyses. The breakdown of responders vs. non-responders was as follows: For the pooled BLOOM/BLOSSOM participants, there were 1251 lorcaserin-recipient responders and 1286 lorcaserin-recipient non-responders (about 40% of those randomized to lorcaserin were “responders”). Among placebo recipients, there were 541 early responders and 1852 non-responders (about 17% of those randomized to placebo were “responders”). For the diabetic BLOOM-DM participants, the ratios were similar although slightly less favorable, with only about 30% (n = 78) of lorcaserin patients classified W12 responders (139 non-responders), and 10% (n = 25) of placebo patients as W12 responders (192 non-responders).
The lorcaserin and placebo groups in BLOOM and BLOSSOM were similar to one another, with overall mean (SD) age of 43.8 (11.6) years for lorcaserin and 44.0 (11.4) years for placebo. The vast majority of participants in these 2 trials were female (81.7% in lorcaserin arms, 81.0% in placebo), and the majority were non-Hispanic white (67.6% in lorcaserin and 66.2% in placebo). The mean (SD) baseline body mass index (BMI, kg/m2) was 36.1 (4.3) for lorcaserin and 36.1 (4.2) for placebo. The BLOOM-DM participants were also similar in the lorcaserin and placebo arms, although they were older (mean age, 53.2 years lorcaserin, 52 years placebo), and more likely to be female (53.5% lorcaserin, 54.4% placebo). Otherwise, the BLOOM-DM participants were similar on reported demographic characteristics to those in the other 2 trials.
Importantly, however, for all 3 trials there were differences in demographic characteristics between those participants characterized as responders and those characterized as non-responders. Amongst the nondiabetic participants in the BLOOM and BLOSSOM studies, responders (to both lorcaserin and placebo) were more likely to be non-Hispanic white (as opposed to African American or Hispanic participants, who were more likely to be non-responders), and responders were older than non-responders. Interestingly, for the diabetics in the BLOOM-DM trial, the responder/non-responder differences were less pronounced, although the responders were still slightly more likely to be non-Hispanic white and older, particularly for placebo.
Among BLOOM and BLOSSOM participants who received lorcaserin, mean weight loss at 52 weeks was 10.8% among W12Rs and only 2.7% among W12NRs. A similar pattern was observed in the BLOOM and BLOSSOM placebo participants; W12Rs averaged 9.5% weight loss at 52 weeks, versus just 1.1% in W12NRs. Among diabetics receiving lorcaserin in the BLOOM-DM study, weight loss at 1 year was 9.1% in W12Rs versus 3.1% in W12NRs. Similarly, in placebo-recipients in BLOOM-DM, weight loss at 1 year was 7% for W12Rs and 1.3% for W12NRs. When the weight loss at 1 year was categorized in terms of whether or not participants achieved at least 5% or 10% weight loss, once again early responders to either lorcaserin or placebo had higher rates of achieving both thresholds. Namely, 85.5% of nondiabetic W12Rs had achieved or maintained 5% weight loss at week 52, while only 26% of the W12NRs ultimately did so. Seventy percent of diabetic W12Rs to lorcaserin had ≥ 5% weight loss at week 52 and 25.2% of W12NRs did. The pattern of prediction for achieving 10% weight loss at week 52 was even more pronounced, with, for example, 49.8% of nondiabetic W12Rs having lost at least 10% of their starting weight at 1 year, versus just 4.7% of W12NRs.
When cardiometabolic outcomes were examined, the differences between W12 lorcaserin responders and non-responders appeared to be somewhat attenuated. For example, among diabetic patients, W12 lorcaserin responders had a mean decrease of 1.2% in their A1c level by study end, compared to a nearly 1% decrease in W12NRs. For fasting plasma glucose, the improvement at week 52 was pronounced (about 30 mg/dL lower than baseline) and very similar in W12 responders and non-responders.
Among nondiabetics, average blood pressure lowering (SBP and DBP) at week 52 was greater among lorcaserin W12 responders (SBP dropped 4 mm Hg on average, DBP 3 mm Hg) than it was among non-responders (SBP and DBP dropped by about 1 mm Hg). Other than triglycerides, which decreased substantially among W12 responders (whether on placebo or lorcaserin), changes to lipid profile were relatively small for nondiabetics. Among diabetics, however, LDL and HDL both increased on average in all 4 groups (W12 responders/non-responders to placebo/lorcaserin) by week 52.
Common adverse events for lorcaserin-treated patients included headache (15%–17%), upper respiratory infections (9%–14%), nausea (8%–9%), and dizziness (8% among nondiabetics). Among diabetics, hypoglycemia occurred in 29.3% of those treated with lorcaserin (vs. 21% on placebo). Week 12 responders and non-responders appeared to have a similar adverse event profile, and, in general, adverse events were more common among lorcaserin than placebo participants.
Conclusion. The authors of this study concluded that a week-12 weight loss of ≥ 5% on lorcaserin was a strong predictor of achieving at least that same amount of weight loss, as well as improvements in some cardiometabolic parameters, at 1 year.
Commentary
In 2013, the American Medical Association officially recognized obesity as a disease. This shift in terminology, coupled with a movement towards reimbursing primary care providers for obesity-related interventions, has created a growing awareness among providers that better treatment options for this chronic condition are sorely needed. Just as we treat patients with hypertension and type 2 diabetes by titrating medications, discontinuing those that aren’t effective and continuing those that are, so should we approach the management of our patients with obesity. Although behavioral interventions centered around lifestyle changes (diet/exercise) remain first-line therapies for the treatment of obesity [1], many patients will seek additional tools, such as meal replacement, medication, or even bariatric surgery, to help achieve and maintain weight loss.
In the past 2 to 3 years, there has been a flurry of activity by the FDA to approve new medications for weight loss. In keeping with the view of obesity as a chronic condition, some of these medications, including lorcaserin and phentermine-topiramate ER, have even been approved for patient long-term use [2]. While the addition of new options to the weight loss toolkit is exciting, it may also be daunting for clinicians who have witnessed a bevy of weight loss drugs come on, and then off, the market over the years due to serious adverse events experienced by patients. For physicians and patients considering the use of a new weight loss medication, there is therefore a clear need to minimize risk for adverse effects related to the drug, while maximizing the patient’s chances of losing weight.
Growing evidence from trials of behavioral interventions as well as weight loss medications suggests that the individuals who will ultimately achieve weight loss success with a given intervention/medication, tend to indicate that success relatively early on in the course of therapy [3–5]. For clinicians, this fact is extremely useful, because it may allow the physician and patient to more rapidly make a decision to discontinue a likely ineffective option in favor of another that has not yet been tried, thus minimizing risks for adverse events while maximizing chances of weight loss outcomes.
In this paper, Smith and colleagues addressed this very important issue for one of the more recently FDA-approved medications, lorcaserin. This 5-HT2c agonist is a useful addition to the list of weight loss medications, as it has relatively few contraindications, other than that it cannot be used in pregnancy/lactation and should be avoided in those with a history of heart failure. However, lorcaserin is still relatively costly (eg, compared to phentermine) and, if it is going to be used for long-term weight loss/maintenance, the financial outlay faced by patients might be considerable. In addition to answering an important question, this paper also examined not only weight loss outcomes but also cardiometabolic impacts of the medication. Furthermore, the authors separately examined outcomes for diabetic and nondiabetic patients, as the risk/benefit ratio of remaining on this medication could be quite different between the 2 groups.
Importantly, the study represented a group of secondary analyses of data aggregated from several trials—trials that were not originally designed to answer this question. Although the majority of original trial participants did have data at weeks 12 and 52 (requirement for inclusion in this analysis), up to a quarter of patients in some groups were missing one or the other measure. Whether or not those analyzed represented a biased subsample, and therefore do not have generalizable results, cannot be ascertained.
In reviewing the outcomes achieved by early responders and non-responders, it was very interesting to note that so-called “responders” to placebo followed a nearly identical weight loss trajectory as those on lorcaserin. This fact should not be taken to indicate that lorcaserin is no different from placebo, as the overall chances of achieving weight loss were significantly greater among the lorcaserin participants. However, it is interesting that, for those placebo patients who clearly followed the recommended lifestyle changes, they did just as well as patients receiving active study drug. This underscores the need to educate patients and encourage them, first and foremost, to make a real effort to diet and exercise regardless of what other tools are employed to achieve weight loss.
Another issue to consider for this study is that there are clear differences in the racial/ethnic makeup of responders versus non-responders. This finding is not unexpected, as in many prior weight loss trials, particularly for behavioral interventions, African-American women have experienced less weight loss than their non-Hispanic white counterparts [6]. These differences were observed both for lorcaserin and placebo patients, raising a concern that the lifestyle intervention component of the study was not equally successful for minorities compared to the non-Hispanic white participants. More research is needed on behavioral interventions that work well in diverse populations.
One finding of interest is that among diabetic participants (BLOOM-DM), glycemic control parameters improved nearly equally between lorcaserin early responders and non-responders, despite the differences between those groups for year-end weight loss. The reasons for this are not clear but could merit further investigation.
Ultimately however, even among this large group of randomized trial participants, who were likely highly motivated, only about 40% of nondiabetics and 30% of diabetics were classified as week 12 responders to lorcaserin. That means that likely well over half of the real-world patients who initiate the drug may not achieve their desired weight loss goals with it. Given the cost of the medication, this must be considered before prescribing it, and it reinforces the importance of being willing to reassess a patient’s weight loss progress early and often so that the medication can be discontinued in favor of other therapies as needed.
Applications for Clinical Practice
For providers interested in prescribing lorcaserin to their patients, a clear plan should be made to have regular and early follow-up to assess the patient’s response to the medication. Patients should understand that if they are not responding to the medication within 3 months, or perhaps sooner if they are experiencing any negative side effects, their physician may elect to discontinue it. Importantly, they should only be given lorcaserin if they are also willing to undertake the behavioral changes necessary to promote weight loss, and it should be underscored that their chances of successful weight loss with or without the medication will be greatly enhanced by doing so.
—Kristina Lewis, MD, MPH
Study Overview
Objective. To examine whether an early response (or non-response) to lorcaserin therapy predicts ≥ 5% weight loss achieved at 1 year.
Study design. Secondary analysis of data collected in 3 placebo-controlled blinded randomized trials.
Setting and participants. This study relied upon data collected as part of 3 separate phase 3 clinical trials of lorcaserin, a weight loss drug and selective serotonin 2c (5-HT2c) agonist. The first study, “Behavioral Modification and Lorcaserin for Overweight and Obesity Management” (BLOOM; n = 3182) enrolled overweight (with at least 1 comorbidity) or obese (no comorbidity needed) adult patients (18–65 yr) without diabetes, to determine the safety and efficacy of lorcaserin. The second trial, “Behavioral Modification and Lorcaserin Second Study of Obesity Management” (BLOSSOM; n = 4008) enrolled a similar population as BLOOM. For both BLOOM and BLOSSOM, patients were randomly assigned to receive either lorcaserin (10 mg po bid) or placebo for a 1-year period, and all patients received advice and instruction in exercise goals (at least 30 min/day) and caloric intake (600 kcal less than recommended for weight maintenance for that individual) necessary to promote weight loss. The third trial, BLOOM-DM (n = 604) focused on overweight or obese diabetic patients, but otherwise was similar in methodology to BLOOM and BLOSSOM. All studies took place in multiple US academic and private medical centers and were funded by Arena Pharmaceuticals. For the current analysis, the investigators used data from these trials and classified participants as either “responders” or “non-responders” based on each participant’s early weight loss response to either lorcaserin or placebo.
Main outcome measures. The investigators used area under the curve for the receiver operating characteristic (AUC for ROC) analysis to determine whether an early weight loss response to lorcaserin or placebo predicted a patient’s longer-term (52-week) weight loss. Several steps were used to conduct these analyses.
First, the investigators needed to determine what amount of weight loss at which of several early time-points would qualify a participant as a “responder” to either drug or placebo. They compared weight lost at weeks 2, 4, 8 and 12, using AUC for ROC analysis to identify the appropriate “responder” or “non-responder” cut-points, and classified all participants with data points in these early weeks as such. Second, all of the early responder and non-responder participants with 52-week weight data were then classified as to whether or not they had achieved at least a 5% weight loss at the end of the study. AUC for ROC analysis was again used to determine whether this early categorization was predictive of final study response. In addition to looking at early response as predictive of final weight loss, the investigators also examined the response/non-response variable’s ability to predict other health outcomes, including changes in lipid levels, blood pressure, and, for type 2 diabetic participants, changes in glycemic control (fasting plasma glucose [FPG] and HgbA1c). Finally, the investigators examined the incidence of adverse events in the different groups as well.
Results. The investigators identified a 4.6% weight loss by week 12 on lorcaserin or placebo as the optimal cut-point for determining whether a participant was a “responder” or “non-responder” (“W12R” or “W12NR”). This cut-point had an AUC (95% CI) of 0.849 (0.828–0.870) for predicting ≥ 5% weight loss at 52 weeks, with a positive predictive value (PPV) of 0.855 and negative predictive value (NPV) of 0.740, thus optimizing specificity and sensitivity of the time/weight cut-point compared to those at weeks 2, 4, or 8. Given the need for practical clinical recommendations, however, the investigators used a cut-point of 5% weight loss by week 12 to determine response/non-response for the health outcome analyses. The breakdown of responders vs. non-responders was as follows: For the pooled BLOOM/BLOSSOM participants, there were 1251 lorcaserin-recipient responders and 1286 lorcaserin-recipient non-responders (about 40% of those randomized to lorcaserin were “responders”). Among placebo recipients, there were 541 early responders and 1852 non-responders (about 17% of those randomized to placebo were “responders”). For the diabetic BLOOM-DM participants, the ratios were similar although slightly less favorable, with only about 30% (n = 78) of lorcaserin patients classified W12 responders (139 non-responders), and 10% (n = 25) of placebo patients as W12 responders (192 non-responders).
The lorcaserin and placebo groups in BLOOM and BLOSSOM were similar to one another, with overall mean (SD) age of 43.8 (11.6) years for lorcaserin and 44.0 (11.4) years for placebo. The vast majority of participants in these 2 trials were female (81.7% in lorcaserin arms, 81.0% in placebo), and the majority were non-Hispanic white (67.6% in lorcaserin and 66.2% in placebo). The mean (SD) baseline body mass index (BMI, kg/m2) was 36.1 (4.3) for lorcaserin and 36.1 (4.2) for placebo. The BLOOM-DM participants were also similar in the lorcaserin and placebo arms, although they were older (mean age, 53.2 years lorcaserin, 52 years placebo), and more likely to be female (53.5% lorcaserin, 54.4% placebo). Otherwise, the BLOOM-DM participants were similar on reported demographic characteristics to those in the other 2 trials.
Importantly, however, for all 3 trials there were differences in demographic characteristics between those participants characterized as responders and those characterized as non-responders. Amongst the nondiabetic participants in the BLOOM and BLOSSOM studies, responders (to both lorcaserin and placebo) were more likely to be non-Hispanic white (as opposed to African American or Hispanic participants, who were more likely to be non-responders), and responders were older than non-responders. Interestingly, for the diabetics in the BLOOM-DM trial, the responder/non-responder differences were less pronounced, although the responders were still slightly more likely to be non-Hispanic white and older, particularly for placebo.
Among BLOOM and BLOSSOM participants who received lorcaserin, mean weight loss at 52 weeks was 10.8% among W12Rs and only 2.7% among W12NRs. A similar pattern was observed in the BLOOM and BLOSSOM placebo participants; W12Rs averaged 9.5% weight loss at 52 weeks, versus just 1.1% in W12NRs. Among diabetics receiving lorcaserin in the BLOOM-DM study, weight loss at 1 year was 9.1% in W12Rs versus 3.1% in W12NRs. Similarly, in placebo-recipients in BLOOM-DM, weight loss at 1 year was 7% for W12Rs and 1.3% for W12NRs. When the weight loss at 1 year was categorized in terms of whether or not participants achieved at least 5% or 10% weight loss, once again early responders to either lorcaserin or placebo had higher rates of achieving both thresholds. Namely, 85.5% of nondiabetic W12Rs had achieved or maintained 5% weight loss at week 52, while only 26% of the W12NRs ultimately did so. Seventy percent of diabetic W12Rs to lorcaserin had ≥ 5% weight loss at week 52 and 25.2% of W12NRs did. The pattern of prediction for achieving 10% weight loss at week 52 was even more pronounced, with, for example, 49.8% of nondiabetic W12Rs having lost at least 10% of their starting weight at 1 year, versus just 4.7% of W12NRs.
When cardiometabolic outcomes were examined, the differences between W12 lorcaserin responders and non-responders appeared to be somewhat attenuated. For example, among diabetic patients, W12 lorcaserin responders had a mean decrease of 1.2% in their A1c level by study end, compared to a nearly 1% decrease in W12NRs. For fasting plasma glucose, the improvement at week 52 was pronounced (about 30 mg/dL lower than baseline) and very similar in W12 responders and non-responders.
Among nondiabetics, average blood pressure lowering (SBP and DBP) at week 52 was greater among lorcaserin W12 responders (SBP dropped 4 mm Hg on average, DBP 3 mm Hg) than it was among non-responders (SBP and DBP dropped by about 1 mm Hg). Other than triglycerides, which decreased substantially among W12 responders (whether on placebo or lorcaserin), changes to lipid profile were relatively small for nondiabetics. Among diabetics, however, LDL and HDL both increased on average in all 4 groups (W12 responders/non-responders to placebo/lorcaserin) by week 52.
Common adverse events for lorcaserin-treated patients included headache (15%–17%), upper respiratory infections (9%–14%), nausea (8%–9%), and dizziness (8% among nondiabetics). Among diabetics, hypoglycemia occurred in 29.3% of those treated with lorcaserin (vs. 21% on placebo). Week 12 responders and non-responders appeared to have a similar adverse event profile, and, in general, adverse events were more common among lorcaserin than placebo participants.
Conclusion. The authors of this study concluded that a week-12 weight loss of ≥ 5% on lorcaserin was a strong predictor of achieving at least that same amount of weight loss, as well as improvements in some cardiometabolic parameters, at 1 year.
Commentary
In 2013, the American Medical Association officially recognized obesity as a disease. This shift in terminology, coupled with a movement towards reimbursing primary care providers for obesity-related interventions, has created a growing awareness among providers that better treatment options for this chronic condition are sorely needed. Just as we treat patients with hypertension and type 2 diabetes by titrating medications, discontinuing those that aren’t effective and continuing those that are, so should we approach the management of our patients with obesity. Although behavioral interventions centered around lifestyle changes (diet/exercise) remain first-line therapies for the treatment of obesity [1], many patients will seek additional tools, such as meal replacement, medication, or even bariatric surgery, to help achieve and maintain weight loss.
In the past 2 to 3 years, there has been a flurry of activity by the FDA to approve new medications for weight loss. In keeping with the view of obesity as a chronic condition, some of these medications, including lorcaserin and phentermine-topiramate ER, have even been approved for patient long-term use [2]. While the addition of new options to the weight loss toolkit is exciting, it may also be daunting for clinicians who have witnessed a bevy of weight loss drugs come on, and then off, the market over the years due to serious adverse events experienced by patients. For physicians and patients considering the use of a new weight loss medication, there is therefore a clear need to minimize risk for adverse effects related to the drug, while maximizing the patient’s chances of losing weight.
Growing evidence from trials of behavioral interventions as well as weight loss medications suggests that the individuals who will ultimately achieve weight loss success with a given intervention/medication, tend to indicate that success relatively early on in the course of therapy [3–5]. For clinicians, this fact is extremely useful, because it may allow the physician and patient to more rapidly make a decision to discontinue a likely ineffective option in favor of another that has not yet been tried, thus minimizing risks for adverse events while maximizing chances of weight loss outcomes.
In this paper, Smith and colleagues addressed this very important issue for one of the more recently FDA-approved medications, lorcaserin. This 5-HT2c agonist is a useful addition to the list of weight loss medications, as it has relatively few contraindications, other than that it cannot be used in pregnancy/lactation and should be avoided in those with a history of heart failure. However, lorcaserin is still relatively costly (eg, compared to phentermine) and, if it is going to be used for long-term weight loss/maintenance, the financial outlay faced by patients might be considerable. In addition to answering an important question, this paper also examined not only weight loss outcomes but also cardiometabolic impacts of the medication. Furthermore, the authors separately examined outcomes for diabetic and nondiabetic patients, as the risk/benefit ratio of remaining on this medication could be quite different between the 2 groups.
Importantly, the study represented a group of secondary analyses of data aggregated from several trials—trials that were not originally designed to answer this question. Although the majority of original trial participants did have data at weeks 12 and 52 (requirement for inclusion in this analysis), up to a quarter of patients in some groups were missing one or the other measure. Whether or not those analyzed represented a biased subsample, and therefore do not have generalizable results, cannot be ascertained.
In reviewing the outcomes achieved by early responders and non-responders, it was very interesting to note that so-called “responders” to placebo followed a nearly identical weight loss trajectory as those on lorcaserin. This fact should not be taken to indicate that lorcaserin is no different from placebo, as the overall chances of achieving weight loss were significantly greater among the lorcaserin participants. However, it is interesting that, for those placebo patients who clearly followed the recommended lifestyle changes, they did just as well as patients receiving active study drug. This underscores the need to educate patients and encourage them, first and foremost, to make a real effort to diet and exercise regardless of what other tools are employed to achieve weight loss.
Another issue to consider for this study is that there are clear differences in the racial/ethnic makeup of responders versus non-responders. This finding is not unexpected, as in many prior weight loss trials, particularly for behavioral interventions, African-American women have experienced less weight loss than their non-Hispanic white counterparts [6]. These differences were observed both for lorcaserin and placebo patients, raising a concern that the lifestyle intervention component of the study was not equally successful for minorities compared to the non-Hispanic white participants. More research is needed on behavioral interventions that work well in diverse populations.
One finding of interest is that among diabetic participants (BLOOM-DM), glycemic control parameters improved nearly equally between lorcaserin early responders and non-responders, despite the differences between those groups for year-end weight loss. The reasons for this are not clear but could merit further investigation.
Ultimately however, even among this large group of randomized trial participants, who were likely highly motivated, only about 40% of nondiabetics and 30% of diabetics were classified as week 12 responders to lorcaserin. That means that likely well over half of the real-world patients who initiate the drug may not achieve their desired weight loss goals with it. Given the cost of the medication, this must be considered before prescribing it, and it reinforces the importance of being willing to reassess a patient’s weight loss progress early and often so that the medication can be discontinued in favor of other therapies as needed.
Applications for Clinical Practice
For providers interested in prescribing lorcaserin to their patients, a clear plan should be made to have regular and early follow-up to assess the patient’s response to the medication. Patients should understand that if they are not responding to the medication within 3 months, or perhaps sooner if they are experiencing any negative side effects, their physician may elect to discontinue it. Importantly, they should only be given lorcaserin if they are also willing to undertake the behavioral changes necessary to promote weight loss, and it should be underscored that their chances of successful weight loss with or without the medication will be greatly enhanced by doing so.
—Kristina Lewis, MD, MPH
1. Jensen MD, Ryan DH, Apovian CM, et al. 2013 AHA/ACC/TOS Guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. J Am Coll Cardiol 2014;63(25 Pt B):2985–3023.
2. Hurt RT, Jithinraj EV, Ebbert JO. New pharmacological treatments for the management of obesity. Cur Gastroenterol Rep 2014;16.6:1–8.
3. Wadden TA, Foster GD, Wang J, et al. Clinical correlates of short- and long-term weight loss. Am J Clin Nutr 1992;56(Suppl 1):271S–274S.
4. Rissanen A, Lean M, Rossner S, et al. Predictive value of early weight loss in obesity management with orlistat: An evidence-based assessment of prescribing guidelines. Int J Obes Relat Metab Disord 2003;27:103–9.
5. O’Neil P, Foster G, Billes S, et al. Early weight loss with naltrexone SR/bupropion SR combination therapy for obesity predicts long-term weight loss (Abstract). Obesity 2009;17:S109.
6. Kumanyika SK, Whitt-Glover MC, Haire-Joshu D. What works for obesity prevention and treatment in black Americans? Research directions. Obes Rev 2014;15:204–12.
1. Jensen MD, Ryan DH, Apovian CM, et al. 2013 AHA/ACC/TOS Guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. J Am Coll Cardiol 2014;63(25 Pt B):2985–3023.
2. Hurt RT, Jithinraj EV, Ebbert JO. New pharmacological treatments for the management of obesity. Cur Gastroenterol Rep 2014;16.6:1–8.
3. Wadden TA, Foster GD, Wang J, et al. Clinical correlates of short- and long-term weight loss. Am J Clin Nutr 1992;56(Suppl 1):271S–274S.
4. Rissanen A, Lean M, Rossner S, et al. Predictive value of early weight loss in obesity management with orlistat: An evidence-based assessment of prescribing guidelines. Int J Obes Relat Metab Disord 2003;27:103–9.
5. O’Neil P, Foster G, Billes S, et al. Early weight loss with naltrexone SR/bupropion SR combination therapy for obesity predicts long-term weight loss (Abstract). Obesity 2009;17:S109.
6. Kumanyika SK, Whitt-Glover MC, Haire-Joshu D. What works for obesity prevention and treatment in black Americans? Research directions. Obes Rev 2014;15:204–12.
Auditory Rehabilitation Programs for Adults—Are They Effective?
Study Overview
Objective. To determine the effectiveness of adult auditory rehabilitation programs that focus on the use of communication strategies.
Design. Nonsystematic review of the literature.
Methods. The authors used the PubMed database to search for systematic reviews investigating the effectiveness of auditory training and auditory rehabilitation programs. Auditory training involves the patient participating in a program of training designed to enhance speech perception. Training is typically provided on a repeated basis over a number of sessions and involves practice with listening and recognition of speech-based material. Auditory rehabilitation programs can be delivered to groups or individuals and usually have a focus on supplementing information about hearing loss and hearing aids with advice and/or practice with communication strategies and the management of psychosocial aspects of hearing loss.
Main outcome measures. A variety of outcomes were measured in the individual studies.
Results. One systematic review of individual auditory training and 2 systematic reviews of group auditory rehabilitation were identified. Sweetow and Palmer [1] found that auditory training in which speech was broken down into its parts was associated with improvements in the perception of speech in the presence of background noise and better use of active listening strategies. With regard to rehabilitation programs, Hawkins [2] found evidence of short-term reduction in perceived hearing handicap but less evidence of effectiveness for other outcomes. A more recent review by Chisolm and Arnold [3] included only randomized studies that examined the effect of the program on social participation and quality of life. References for the included studies were given but the summary results of this review were not included in this paper.
Conclusion. The authors conclude that there is some evidence that auditory rehabilitation programs are associated with improvements in social participation and quality of life but they acknowledge that more evidence is required.
Commentary
Adult acquired hearing loss is a common long-term condition which in the majority of cases is not remediable by surgical or medical intervention. It is the second leading cause of years lived with a disability [4]. Intervention options for people with hearing loss include hearing aid fitting and/or participation in a rehabilitative program that might include information about hearing and communication and practice or experience with listening or communication tasks [5,6]. Poorly managed hearing loss is associated with negative consequences including depression and cognitive decline [7,8]. Identifying effective management options for hearing loss can reduce these consequences and improve quality of life. In the current paper, Cardemil et al review the evidence for the effectiveness of adult auditory rehabilitation. They note that hearing aids alone cannot ameliorate all of the difficulties caused by age-related hearing loss, where cognitive factors play a significant role. They provide a rationale for why communication-based training in auditory rehabilitation has been recommended as a substitute or supplement to hearing aid fitting. That is, such training addresses the cognitive and communication difficulties that exist in addition to the hearing loss.
This paper summarises the findings of 3 systematic reviews: one on individual auditory rehabilitation and 2 on group rehabilitation. There was heterogeneity among the programs and the methods used to assess their effectiveness were variable. The reviewers conclude that there appears to be some short-term benefit to auditory rehabilitation programs but effect sizes, where effects are seen, are small and more research is needed to establish the effectiveness of these programs.
A limitation of this review is that it was nonsystematic and did not critically appraise the quality of the included systematic reviews. One weakness of the systematic reviews presented is that they did not consider interactions between content and delivery of interventions and comparisons. Individual auditory rehabilitation and group rehabilitation are typically delivered over many sessions in contrast to control groups, which often receive “standard care” delivered over a single or limited number of sessions. Therefore, where an effect exists it is unclear whether the “active ingredient” contributing to the effect is the rehabilitative content delivered or the number of sessions over which it is provided. This is a possible confounding factor not acknowledged or discussed in these systematic reviews.
In addition, any discussion which seeks to assess effectiveness should define outcomes of interest or at least review the range of outcomes that have been studied and how they are relevant to the problem being addressed. There is a lack of consensus on what the important clinical outcomes are for hearing health care [9] and a dearth of research on longer-term outcomes; this could have been explored.
Applications for Clinical Practice
This summary of 3 systematic reviews highlights the need for further research in this area. Studies that measure long-term outcomes (1 year or more) and that are appropriately powered are needed. In addition, the possible interaction between different potentially active components of complex interventions must be acknowledged. Health care professionals and policy makers need to be aware of these factors when reviewing evidence and making decisions that impact on clinical practice.
—Fiona Barker, Department of Health Care Management and Policy, University of Surrey, Guildford, UK
1. Sweetow R, Palmer CV. Efficacy of individual auditory training in adults: a systematic review of the evidence. J Am Acad Audiol 2005;16:494–504.
2. Hawkins DB. Effectiveness of counseling-based adult group aural rehabilitation programs: a systematic review of the evidence. J Am Acad Audiol 2005;16:485–93.
3. Chisolm TH, Arnold M. Evidence about the effectiveness of aural rehabilitation programs for adults. In: Wong L, Hickson L, editors. Evidence-based practice in audiology. San Diego: Plural; 2012.
4. World Health Organisation. Facts about deafness. 2012. Accessed 6 Nov 2014 at www.who.int/pbd/deafness/facts/en/.
5. Laplante-Levesque A, Hickson L, Worrall L. Rehabilitation of older adults with hearing impairment: a critical review. J Aging Health 2010;22:143–53.
6. Pronk M, Kramer SE, Davis AC, Stephens D, Smith PA, Thodi C, et al. Interventions following hearing screening in adults: a systematic descriptive review. Int J Audiol 2011;50:594–609.
7. Lin FR. Hearing loss and cognition among older adults in the United States. J Gerontol A Biol Sci Med Sci 2011;66:1131–6.
8. Saito H, Nishiwaki Y, Michikawa T, et al. Hearing handicap predicts the development of depressive symptoms after 3 years in older community-dwelling Japanese. J Am Geriatr Soc 2010;58:93–7.
9. Humes LE, Krull V. Hearing aids for adults. In: Wong L, Hickson L, editors. Evidence-based practice in audiology. San Diego: Plural; 2012.
Study Overview
Objective. To determine the effectiveness of adult auditory rehabilitation programs that focus on the use of communication strategies.
Design. Nonsystematic review of the literature.
Methods. The authors used the PubMed database to search for systematic reviews investigating the effectiveness of auditory training and auditory rehabilitation programs. Auditory training involves the patient participating in a program of training designed to enhance speech perception. Training is typically provided on a repeated basis over a number of sessions and involves practice with listening and recognition of speech-based material. Auditory rehabilitation programs can be delivered to groups or individuals and usually have a focus on supplementing information about hearing loss and hearing aids with advice and/or practice with communication strategies and the management of psychosocial aspects of hearing loss.
Main outcome measures. A variety of outcomes were measured in the individual studies.
Results. One systematic review of individual auditory training and 2 systematic reviews of group auditory rehabilitation were identified. Sweetow and Palmer [1] found that auditory training in which speech was broken down into its parts was associated with improvements in the perception of speech in the presence of background noise and better use of active listening strategies. With regard to rehabilitation programs, Hawkins [2] found evidence of short-term reduction in perceived hearing handicap but less evidence of effectiveness for other outcomes. A more recent review by Chisolm and Arnold [3] included only randomized studies that examined the effect of the program on social participation and quality of life. References for the included studies were given but the summary results of this review were not included in this paper.
Conclusion. The authors conclude that there is some evidence that auditory rehabilitation programs are associated with improvements in social participation and quality of life but they acknowledge that more evidence is required.
Commentary
Adult acquired hearing loss is a common long-term condition which in the majority of cases is not remediable by surgical or medical intervention. It is the second leading cause of years lived with a disability [4]. Intervention options for people with hearing loss include hearing aid fitting and/or participation in a rehabilitative program that might include information about hearing and communication and practice or experience with listening or communication tasks [5,6]. Poorly managed hearing loss is associated with negative consequences including depression and cognitive decline [7,8]. Identifying effective management options for hearing loss can reduce these consequences and improve quality of life. In the current paper, Cardemil et al review the evidence for the effectiveness of adult auditory rehabilitation. They note that hearing aids alone cannot ameliorate all of the difficulties caused by age-related hearing loss, where cognitive factors play a significant role. They provide a rationale for why communication-based training in auditory rehabilitation has been recommended as a substitute or supplement to hearing aid fitting. That is, such training addresses the cognitive and communication difficulties that exist in addition to the hearing loss.
This paper summarises the findings of 3 systematic reviews: one on individual auditory rehabilitation and 2 on group rehabilitation. There was heterogeneity among the programs and the methods used to assess their effectiveness were variable. The reviewers conclude that there appears to be some short-term benefit to auditory rehabilitation programs but effect sizes, where effects are seen, are small and more research is needed to establish the effectiveness of these programs.
A limitation of this review is that it was nonsystematic and did not critically appraise the quality of the included systematic reviews. One weakness of the systematic reviews presented is that they did not consider interactions between content and delivery of interventions and comparisons. Individual auditory rehabilitation and group rehabilitation are typically delivered over many sessions in contrast to control groups, which often receive “standard care” delivered over a single or limited number of sessions. Therefore, where an effect exists it is unclear whether the “active ingredient” contributing to the effect is the rehabilitative content delivered or the number of sessions over which it is provided. This is a possible confounding factor not acknowledged or discussed in these systematic reviews.
In addition, any discussion which seeks to assess effectiveness should define outcomes of interest or at least review the range of outcomes that have been studied and how they are relevant to the problem being addressed. There is a lack of consensus on what the important clinical outcomes are for hearing health care [9] and a dearth of research on longer-term outcomes; this could have been explored.
Applications for Clinical Practice
This summary of 3 systematic reviews highlights the need for further research in this area. Studies that measure long-term outcomes (1 year or more) and that are appropriately powered are needed. In addition, the possible interaction between different potentially active components of complex interventions must be acknowledged. Health care professionals and policy makers need to be aware of these factors when reviewing evidence and making decisions that impact on clinical practice.
—Fiona Barker, Department of Health Care Management and Policy, University of Surrey, Guildford, UK
Study Overview
Objective. To determine the effectiveness of adult auditory rehabilitation programs that focus on the use of communication strategies.
Design. Nonsystematic review of the literature.
Methods. The authors used the PubMed database to search for systematic reviews investigating the effectiveness of auditory training and auditory rehabilitation programs. Auditory training involves the patient participating in a program of training designed to enhance speech perception. Training is typically provided on a repeated basis over a number of sessions and involves practice with listening and recognition of speech-based material. Auditory rehabilitation programs can be delivered to groups or individuals and usually have a focus on supplementing information about hearing loss and hearing aids with advice and/or practice with communication strategies and the management of psychosocial aspects of hearing loss.
Main outcome measures. A variety of outcomes were measured in the individual studies.
Results. One systematic review of individual auditory training and 2 systematic reviews of group auditory rehabilitation were identified. Sweetow and Palmer [1] found that auditory training in which speech was broken down into its parts was associated with improvements in the perception of speech in the presence of background noise and better use of active listening strategies. With regard to rehabilitation programs, Hawkins [2] found evidence of short-term reduction in perceived hearing handicap but less evidence of effectiveness for other outcomes. A more recent review by Chisolm and Arnold [3] included only randomized studies that examined the effect of the program on social participation and quality of life. References for the included studies were given but the summary results of this review were not included in this paper.
Conclusion. The authors conclude that there is some evidence that auditory rehabilitation programs are associated with improvements in social participation and quality of life but they acknowledge that more evidence is required.
Commentary
Adult acquired hearing loss is a common long-term condition which in the majority of cases is not remediable by surgical or medical intervention. It is the second leading cause of years lived with a disability [4]. Intervention options for people with hearing loss include hearing aid fitting and/or participation in a rehabilitative program that might include information about hearing and communication and practice or experience with listening or communication tasks [5,6]. Poorly managed hearing loss is associated with negative consequences including depression and cognitive decline [7,8]. Identifying effective management options for hearing loss can reduce these consequences and improve quality of life. In the current paper, Cardemil et al review the evidence for the effectiveness of adult auditory rehabilitation. They note that hearing aids alone cannot ameliorate all of the difficulties caused by age-related hearing loss, where cognitive factors play a significant role. They provide a rationale for why communication-based training in auditory rehabilitation has been recommended as a substitute or supplement to hearing aid fitting. That is, such training addresses the cognitive and communication difficulties that exist in addition to the hearing loss.
This paper summarises the findings of 3 systematic reviews: one on individual auditory rehabilitation and 2 on group rehabilitation. There was heterogeneity among the programs and the methods used to assess their effectiveness were variable. The reviewers conclude that there appears to be some short-term benefit to auditory rehabilitation programs but effect sizes, where effects are seen, are small and more research is needed to establish the effectiveness of these programs.
A limitation of this review is that it was nonsystematic and did not critically appraise the quality of the included systematic reviews. One weakness of the systematic reviews presented is that they did not consider interactions between content and delivery of interventions and comparisons. Individual auditory rehabilitation and group rehabilitation are typically delivered over many sessions in contrast to control groups, which often receive “standard care” delivered over a single or limited number of sessions. Therefore, where an effect exists it is unclear whether the “active ingredient” contributing to the effect is the rehabilitative content delivered or the number of sessions over which it is provided. This is a possible confounding factor not acknowledged or discussed in these systematic reviews.
In addition, any discussion which seeks to assess effectiveness should define outcomes of interest or at least review the range of outcomes that have been studied and how they are relevant to the problem being addressed. There is a lack of consensus on what the important clinical outcomes are for hearing health care [9] and a dearth of research on longer-term outcomes; this could have been explored.
Applications for Clinical Practice
This summary of 3 systematic reviews highlights the need for further research in this area. Studies that measure long-term outcomes (1 year or more) and that are appropriately powered are needed. In addition, the possible interaction between different potentially active components of complex interventions must be acknowledged. Health care professionals and policy makers need to be aware of these factors when reviewing evidence and making decisions that impact on clinical practice.
—Fiona Barker, Department of Health Care Management and Policy, University of Surrey, Guildford, UK
1. Sweetow R, Palmer CV. Efficacy of individual auditory training in adults: a systematic review of the evidence. J Am Acad Audiol 2005;16:494–504.
2. Hawkins DB. Effectiveness of counseling-based adult group aural rehabilitation programs: a systematic review of the evidence. J Am Acad Audiol 2005;16:485–93.
3. Chisolm TH, Arnold M. Evidence about the effectiveness of aural rehabilitation programs for adults. In: Wong L, Hickson L, editors. Evidence-based practice in audiology. San Diego: Plural; 2012.
4. World Health Organisation. Facts about deafness. 2012. Accessed 6 Nov 2014 at www.who.int/pbd/deafness/facts/en/.
5. Laplante-Levesque A, Hickson L, Worrall L. Rehabilitation of older adults with hearing impairment: a critical review. J Aging Health 2010;22:143–53.
6. Pronk M, Kramer SE, Davis AC, Stephens D, Smith PA, Thodi C, et al. Interventions following hearing screening in adults: a systematic descriptive review. Int J Audiol 2011;50:594–609.
7. Lin FR. Hearing loss and cognition among older adults in the United States. J Gerontol A Biol Sci Med Sci 2011;66:1131–6.
8. Saito H, Nishiwaki Y, Michikawa T, et al. Hearing handicap predicts the development of depressive symptoms after 3 years in older community-dwelling Japanese. J Am Geriatr Soc 2010;58:93–7.
9. Humes LE, Krull V. Hearing aids for adults. In: Wong L, Hickson L, editors. Evidence-based practice in audiology. San Diego: Plural; 2012.
1. Sweetow R, Palmer CV. Efficacy of individual auditory training in adults: a systematic review of the evidence. J Am Acad Audiol 2005;16:494–504.
2. Hawkins DB. Effectiveness of counseling-based adult group aural rehabilitation programs: a systematic review of the evidence. J Am Acad Audiol 2005;16:485–93.
3. Chisolm TH, Arnold M. Evidence about the effectiveness of aural rehabilitation programs for adults. In: Wong L, Hickson L, editors. Evidence-based practice in audiology. San Diego: Plural; 2012.
4. World Health Organisation. Facts about deafness. 2012. Accessed 6 Nov 2014 at www.who.int/pbd/deafness/facts/en/.
5. Laplante-Levesque A, Hickson L, Worrall L. Rehabilitation of older adults with hearing impairment: a critical review. J Aging Health 2010;22:143–53.
6. Pronk M, Kramer SE, Davis AC, Stephens D, Smith PA, Thodi C, et al. Interventions following hearing screening in adults: a systematic descriptive review. Int J Audiol 2011;50:594–609.
7. Lin FR. Hearing loss and cognition among older adults in the United States. J Gerontol A Biol Sci Med Sci 2011;66:1131–6.
8. Saito H, Nishiwaki Y, Michikawa T, et al. Hearing handicap predicts the development of depressive symptoms after 3 years in older community-dwelling Japanese. J Am Geriatr Soc 2010;58:93–7.
9. Humes LE, Krull V. Hearing aids for adults. In: Wong L, Hickson L, editors. Evidence-based practice in audiology. San Diego: Plural; 2012.
Integrating Lay Health Care Workers into the Primary Care Team
From Allina Health, Minneapolis, MN.
Abstract
- Objective: To describe a care model in which lay “care guides” are integrated into the primary care team to help patients with chronic disease and their providers achieve care goals.
- Methods: Care guides are individuals without formal medical training who receive brief training about chronic conditions and behavior change. General activities include educating and encouraging patients to take control of their illness, supporting medication and treatment adherence, and facilitating resolution of barriers to quality care.
- Results: The care guide model can improve care for some patients with chronic disease at low cost. In a randomized trial testing the intervention, patients with care guides achieved more goals than usual care patients at 1 year (odds ratio, 1.31; 95% confidence interval, 1.16–1.47; P < 0.001).
- Conclusion: Lay health care workers with relevant skills and training, located in clinic waiting rooms where they can meet patients and providers face-to-face, can help chronic disease patients and their providers improve the quality of care.
Improving the quality of care for chronic disease patients is an important goal for the US health care system. Almost half of American with chronic disease fail to receive evidence-based care [1–3]. Reasons for this include limited access to the health care delivery system [4,5] and payment systems that undervalue primary care and provide incentives for more but not necessarily better care [6]. Not only is there a need to improve the quality of care among chronic disease patients, but also to recognize the constraints faced by primary care providers (PCPs) and clinic staff in the current health care environment.
One approach for improving care for patients with chronic disease has been care coordination, or management by health care professionals such as nurses and certified medical assistants [7]. These care managers are usually located in primary care medical offices and have some face-to-face contact with both patients and providers in addition to telephone or electronic contact [7,8]. Care management provided by registered nurses can be effective but is expensive, and it is unclear where payment for these services will come from [7,9].
An alternative approach is employing lay health care workers. In the literature lay health care workers have been referred to as promotoras de salud, lay advisors or navigators, and peer coaches [10–12]. Some of these workers are employees while others are part-time volunteers [13,14]. Tasks assigned to these workers are often limited, such as improving access to cancer care [15], teaching self-help techniques [16–18], or goal-setting [19], and are usually focused on a specific disease or problem. Some of workers do have contact with nurses and doctors, but they tend not to work with the primary care team in the day-to-day provision of care [14].
To improve the quality and efficiency of chronic disease care, Allina Health, a large not-for-profit system of hospitals and clinics in Minnesota and western Wisconsin, hired lay “care guides” to help patients and providers achieve care goals and integrated them into the primary care team. In this article, we describe the care guide model we used and tested and discuss adoption considerations.
Role and Responsibilities of a Care Guide
Care guides are individuals without formal medical training whose general activities include:
- fostering a longitudinal relationship to encourage patients to take control of their chronic illness;
- educating patients about the considerable benefits of best practice treatment;
- communicating with patients, families and providers to keep the entire care team, including the PCP, focused on meeting care guidelines;
- supporting medication and treatment adherence;
- identifying and facilitating resolution of barriers to quality care;
- facilitating referrals to extended care team members and introducing patients to appropriate services or resources within the clinic, health system and/or community they live or work in.
How do care guides differ from other personnel used as care managers? Care guides can explain the value of meeting standard goals, but unlike nurses cannot answer clinical questions. Care guides and medical assistants have similar salaries but care guides have higher educational requirements, less clinical training, and no competing duties in clinic. Like community health workers, care guides are culturally similar to the patients they serve, but are located in the clinic. Care guides were recruited for specific traits and competencies: an outgoing personality, the ability to engage easily with people of different ages and backgrounds, and a second language where needed (eg, Spanish and Somali in the pilot study) [20].
Implementation Trial
![]()
The study recruited 2135 patients. Both groups had an increased percentage of goals met at the end of the 1-year study compared to baseline. Care guide patients met a larger percentage of possible care goals at 1 year than did usual care patients (odds ratio, 1.31; 95% confidence interval, 1.16–1.47; P < 0.001). Care guide patients reduced unmet goals by 30.1%, usual care patients by 12.6%. The difference in outcomes between the 2 groups was minimally affected by differences in the times of final measurement for each goal. The benefit of working with a care guide was not different across demographic categories of age, sex, race, language, insurance, or education. In this study, care guides helped a broad range of patients who were meeting many goals at baseline and who were cared for by providers already receiving regular quality-improvement feedback. Estimated cost was $286 per patient per year.
Development Process
At each clinic, the research team enlisted the help of a site-specific implementation team consisting of a provider champion and clinic leader (ie, the clinic manager, clinic supervisor, or business office supervisor) to customize the study implementation. After selecting the target patient population, chronic disease focus, and eligibility criteria, the research team solicited the help of providers, nurses, medical assistants, and other clinic support staff to develop care guide workflows and processes. Clinic providers and staff were involved early and often in the model planning process. The team gave thoughtful consideration to existing clinic work processes and personnel dynamics to help ensure that the care guide would be accepted and integrated into the clinic culture.
Concurrent with designing workflows for the interactions between care guides and providers, clinical staff, and patients, the research team worked with a variety of support departments at Allina Health System to ensure that the necessary tools were in place for care guides to do their work effectively. They collaborated with human resources to screen for care guide candidates with appropriate skills and personal attributes; information systems to create new tools and security access within the electronic health record; learning and development to organize resources and devise an appropriate training schedule; and marketing/communications to broadcast this new initiative on a system-wide level.
Once details of the model and workflows were established, the research team secured subject matter experts to build content for care guide training. The research team partnered with PCPs whose expertise was treating these chronic diseases as well as pharmacists, nutritionists, diabetes nurse educators, and behavioral health specialists available within the health system. These subject matter experts provided the training content as well as conducted the training. Training took place over 2 weeks and included basic training on the 3 chronic disease conditions, pharmacology, nutrition, and mental health issues, barriers to care, and behavioral change techniques.
Benefits
What were the key interactions leading to clinical improvements? What made the intervention successful? Care guides described using a variety of techniques to yield clinical improvements. With patients, care guides took time to explain the benefits of meeting goals in lay language, used their non-medical backgrounds to create an environment where patients felt at ease asking questions, called patients following office visits to ensure instructions were understood, and helped develop specific action plans. With providers and nurses, care guides gave reminders about unmet goals on the day of an appointment (when this information would be most useful) and supplied information such as “this patient reports difficulty affording medication” or “this patient seems ready to quit tobacco.” Care guides reinforced the effectiveness of longer-term care relationships; for example, most patients who quit tobacco did so between 9 and 12 months after enrollment in the care guide program. In after-study surveys, care guide patients reported significantly more positive perceptions of their care than usual care patients in constructs measuring social support, individualized care, help, reinforcement, and understanding of how to improve their health.
Care guides, using their relationships with providers, served as quality improvement advocates integrated into the daily process of providing primary care. This arrangement differed from the common practice of giving providers periodic feedback based on data gleaned from the electronic health record.
Moving the quality improvement process into the primary care office resolved many problems related to strictly electronic health record–based feedback. Each patient was considered individually. There was opportunity for conversations about care quality to occur face-to-face; members of the primary care team could discuss when to deviate from a care guideline. Strong relationships and a sense of teamwork increased workplace satisfaction [22]. In a post-study survey of 115 providers and nurses, 93% felt that care guides improved patient care and 94% felt that care guides were an effective use of resources.
Adoption Considerations
Adding a care guide into an existing clinic structure and culture requires planning and customization. In order to fully integrate this role into clinics and on care teams and achieve expected results, 6 steps are recommended:
- Program set-up through recruitment of the proper set of stakeholders to plan for implementation, including logistics, budget, etc.
- Defining details, such as the target patient population and eligibility criteria, how interactions will take place with patients, and the duration of the patient relationship.
- Clinic readiness and program development, including detailed clinic staff orientation and workflow development.
- Clinic-specific development of the care guide training, including enlisting the help of subject matter experts to develop content.
- A 2-week training of newly-hired care guides
- Defining the expectations and job responsibilities of the care guide and proper integration of care guides into care teams.
- Monitoring and evaluation – This is not the last step in the process but rather requires the ongoing work of the clinic staff, providers, and care guides to measure progress and outcomes.
Although transforming care teams in primary care clinics is no easy task, it is the foundation of the care guide model. The premise of the care guide role is simple and relatable, thereby making it transferrable to different patient populations and settings as well as attractive to different types of providers. The model is flexible, allowing room for adaptations while maintaining its focus on serving patients and families and reducing burden for providers and other clinic staff. The model is currently being adapted and used in different settings outside of traditional primary care, including urgent care and emergency departments, specialty services, and patient-centered medical homes, among others. In addition, care guides are being used across different patient populations, including high-risk patients in an accountable care organization, pediatric patients, and patients late in life, to name a few. Each adaptation may have population-specific goals and outcomes, but the core of the model remains focused on the Institute for Healthcare Improvement's triple aim: improving the patient experience of care, improving the health of populations, and reducing the per capita cost of health care.
For clinics and care providers interested in integrating care guides within their own clinic, a toolkit, eLearning modules, and evaluation templates, among other resources, are available at no cost through the Care Copilot Institute (www.carecopilotinstitute.org). The Institute was created to translate and disseminate the care guide research.
Conclusion
Lay health care workers with relevant skills and training, located in clinic waiting rooms where they can meet patients and providers face-to-face, can help chronic disease patients and their providers improve the quality of care. Because of its low cost, this model can be implemented in many settings, including small independent primary care offices, where much primary care in the US is still delivered [7,23–25].
Corresponding author: Kim Radel, MHA, Allina Health, Minneapolis, MN, [email protected].
Financial disclosures: Dr. Christianson disclosed that he received grant support from the Robina Foundation.
1. Banerjee D, Stafford R. Lack of improvement in outpatient management of congestive heart failure in the United States Arch Intern Med 2010;16:1–2.
2. Egan BM, Zhao Y, RN A. US trends in prevalence, awareness, treatment, and control of hypertension. JAMA 2010;303:2043–50.
3. McGlynn E, Asch S, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med 2003;348:2635–45.
4. Ghorob A, Bodenheimer T. Sharing the care to improve access to primary care. N Engl J Med 2012;366:1955–7.
5. Schroeder SA. Shattuck Lecture. We can do better - improving the health of the American people. N Engl J Med 2007;357:1221–8.
6. Bazinsky KR, Herrera L, Sharfstein JM. Toward innovative models of health care and financing: matchmaking in Maryland. JAMA 2012;307:1261–2.
7. Berry-Millett R, Bodenheimer TS. Care management of patients with complex health care needs. Synth Proj Res Synth Rep 2009;(19).
8. Peikes D, Chen A, Schore J, Brown R. Effects of care coordination on hospitalization, quality of care, and health care expenditures among Medicare beneficiaries: 15 randomized trials. JAMA 2009;301:603–18.
9. Ayanian JZ. The elusive quest for quality and cost savings in the Medicare program. JAMA 2009;301:668–70.
10. Babamoto KS, Sey KA, Camilleri AJ, et al. Improving diabetes care and health measures among hispanics using community health workers: results from a randomized controlled trial. Health Educ Behav 2009;36:113–26.
11. Brownstein JN, Hirsch GR, Rosenthal EL, Rush CH. Community health workers “101” for primary care providers and other stakeholders in health care systems. J Ambul Care Manage 2011;34:210–20.
12. Lewin S, Dick J, Pond P, et al. Lay health workers in primary and community health care. Cochrane Database Syst Rev 2005;(1):CD004015.
13. Doull M, O’Connor A, Welch V, et al. Peer support strategies for improving the health and well-being of individuals with chronic diseases. Cochrane Database Syst Rev 2004;(2):CD004774.
14. Witmer A, Seifer SD, Finocchio L, et al. Community health workers: integral members of the health care work force. Am J Public Health 1995;85(8 Pt 1):1055–8.
15. Steinberg ML, Fremont A, Khan DC, et al. Lay patient navigator program implementation for equal access to cancer care and clinical trials: essential steps and initial challenges. Cancer 2006;107:2669–77.
16. Fu D, Fu H, McGowan P, et al. Implementation and quantitative evaluation of chronic disease self-management programme in Shanghai, China: randomized controlled trial. Bull World Health Organ 2003;81:174–82.
17. Kennedy A, Reeves D, Bower P, et al. The effectiveness and cost effectiveness of a national lay-led self care support programme for patients with long-term conditions: a pragmatic randomised controlled trial. J Epidemiol Comm Health 2007;61:254–61.
18. Rhodes SD, Foley KL, Zometa CS, Bloom FR. Lay health advisor interventions among Hispanics/Latinos: a qualitative systematic review. Am J Prev Med 2007;33:418–27.
19. Heisler M, Spencer M, Forman J, et al. Participants’ assessments of the effects of a community health worker intervention on their diabetes self-management and interactions with healthcare providers. Am J Prev Med 2009;37(6 Suppl 1):S270–9.
20. Adair R, Christianson JB, Wholey DR, et al. Care guides: employing nonclinical laypersons to help primary care teams manage chronic disease. J Ambul Care Manage 2012;35:27–37.
21. Adair R, Wholey DR, Christianson JB, et al. Improving chronic disease care by adding laypersons to the primary care team: a parallel randomized trial. Ann Intern Med 2013;159:176–84.
22. Cassel CK, Jain S. Assessing individual physician performance: does measurement suppress motivation? JAMA 2012;307:2595–6.
23. Nocon RS, Sharma R, Birnberg JM, et al. Association between patient-centered medical home rating and operating cost at federally funded health centers. JAMA 2012;308:60–6.
24. Rittenhouse D, Casalino L. Small and medium-size physician practices use few patient-centered medical home processes. Health Aff 2011;30:1575–84.
25. Fifield J, Forrest DD, Martin-Peele M, et al. A randomized, controlled trial of implementing the patient-centered medical home model in solo and small practices. J Gen Intern Med 2012;28:770–7.
From Allina Health, Minneapolis, MN.
Abstract
- Objective: To describe a care model in which lay “care guides” are integrated into the primary care team to help patients with chronic disease and their providers achieve care goals.
- Methods: Care guides are individuals without formal medical training who receive brief training about chronic conditions and behavior change. General activities include educating and encouraging patients to take control of their illness, supporting medication and treatment adherence, and facilitating resolution of barriers to quality care.
- Results: The care guide model can improve care for some patients with chronic disease at low cost. In a randomized trial testing the intervention, patients with care guides achieved more goals than usual care patients at 1 year (odds ratio, 1.31; 95% confidence interval, 1.16–1.47; P < 0.001).
- Conclusion: Lay health care workers with relevant skills and training, located in clinic waiting rooms where they can meet patients and providers face-to-face, can help chronic disease patients and their providers improve the quality of care.
Improving the quality of care for chronic disease patients is an important goal for the US health care system. Almost half of American with chronic disease fail to receive evidence-based care [1–3]. Reasons for this include limited access to the health care delivery system [4,5] and payment systems that undervalue primary care and provide incentives for more but not necessarily better care [6]. Not only is there a need to improve the quality of care among chronic disease patients, but also to recognize the constraints faced by primary care providers (PCPs) and clinic staff in the current health care environment.
One approach for improving care for patients with chronic disease has been care coordination, or management by health care professionals such as nurses and certified medical assistants [7]. These care managers are usually located in primary care medical offices and have some face-to-face contact with both patients and providers in addition to telephone or electronic contact [7,8]. Care management provided by registered nurses can be effective but is expensive, and it is unclear where payment for these services will come from [7,9].
An alternative approach is employing lay health care workers. In the literature lay health care workers have been referred to as promotoras de salud, lay advisors or navigators, and peer coaches [10–12]. Some of these workers are employees while others are part-time volunteers [13,14]. Tasks assigned to these workers are often limited, such as improving access to cancer care [15], teaching self-help techniques [16–18], or goal-setting [19], and are usually focused on a specific disease or problem. Some of workers do have contact with nurses and doctors, but they tend not to work with the primary care team in the day-to-day provision of care [14].
To improve the quality and efficiency of chronic disease care, Allina Health, a large not-for-profit system of hospitals and clinics in Minnesota and western Wisconsin, hired lay “care guides” to help patients and providers achieve care goals and integrated them into the primary care team. In this article, we describe the care guide model we used and tested and discuss adoption considerations.
Role and Responsibilities of a Care Guide
Care guides are individuals without formal medical training whose general activities include:
- fostering a longitudinal relationship to encourage patients to take control of their chronic illness;
- educating patients about the considerable benefits of best practice treatment;
- communicating with patients, families and providers to keep the entire care team, including the PCP, focused on meeting care guidelines;
- supporting medication and treatment adherence;
- identifying and facilitating resolution of barriers to quality care;
- facilitating referrals to extended care team members and introducing patients to appropriate services or resources within the clinic, health system and/or community they live or work in.
How do care guides differ from other personnel used as care managers? Care guides can explain the value of meeting standard goals, but unlike nurses cannot answer clinical questions. Care guides and medical assistants have similar salaries but care guides have higher educational requirements, less clinical training, and no competing duties in clinic. Like community health workers, care guides are culturally similar to the patients they serve, but are located in the clinic. Care guides were recruited for specific traits and competencies: an outgoing personality, the ability to engage easily with people of different ages and backgrounds, and a second language where needed (eg, Spanish and Somali in the pilot study) [20].
Implementation Trial
![]()
The study recruited 2135 patients. Both groups had an increased percentage of goals met at the end of the 1-year study compared to baseline. Care guide patients met a larger percentage of possible care goals at 1 year than did usual care patients (odds ratio, 1.31; 95% confidence interval, 1.16–1.47; P < 0.001). Care guide patients reduced unmet goals by 30.1%, usual care patients by 12.6%. The difference in outcomes between the 2 groups was minimally affected by differences in the times of final measurement for each goal. The benefit of working with a care guide was not different across demographic categories of age, sex, race, language, insurance, or education. In this study, care guides helped a broad range of patients who were meeting many goals at baseline and who were cared for by providers already receiving regular quality-improvement feedback. Estimated cost was $286 per patient per year.
Development Process
At each clinic, the research team enlisted the help of a site-specific implementation team consisting of a provider champion and clinic leader (ie, the clinic manager, clinic supervisor, or business office supervisor) to customize the study implementation. After selecting the target patient population, chronic disease focus, and eligibility criteria, the research team solicited the help of providers, nurses, medical assistants, and other clinic support staff to develop care guide workflows and processes. Clinic providers and staff were involved early and often in the model planning process. The team gave thoughtful consideration to existing clinic work processes and personnel dynamics to help ensure that the care guide would be accepted and integrated into the clinic culture.
Concurrent with designing workflows for the interactions between care guides and providers, clinical staff, and patients, the research team worked with a variety of support departments at Allina Health System to ensure that the necessary tools were in place for care guides to do their work effectively. They collaborated with human resources to screen for care guide candidates with appropriate skills and personal attributes; information systems to create new tools and security access within the electronic health record; learning and development to organize resources and devise an appropriate training schedule; and marketing/communications to broadcast this new initiative on a system-wide level.
Once details of the model and workflows were established, the research team secured subject matter experts to build content for care guide training. The research team partnered with PCPs whose expertise was treating these chronic diseases as well as pharmacists, nutritionists, diabetes nurse educators, and behavioral health specialists available within the health system. These subject matter experts provided the training content as well as conducted the training. Training took place over 2 weeks and included basic training on the 3 chronic disease conditions, pharmacology, nutrition, and mental health issues, barriers to care, and behavioral change techniques.
Benefits
What were the key interactions leading to clinical improvements? What made the intervention successful? Care guides described using a variety of techniques to yield clinical improvements. With patients, care guides took time to explain the benefits of meeting goals in lay language, used their non-medical backgrounds to create an environment where patients felt at ease asking questions, called patients following office visits to ensure instructions were understood, and helped develop specific action plans. With providers and nurses, care guides gave reminders about unmet goals on the day of an appointment (when this information would be most useful) and supplied information such as “this patient reports difficulty affording medication” or “this patient seems ready to quit tobacco.” Care guides reinforced the effectiveness of longer-term care relationships; for example, most patients who quit tobacco did so between 9 and 12 months after enrollment in the care guide program. In after-study surveys, care guide patients reported significantly more positive perceptions of their care than usual care patients in constructs measuring social support, individualized care, help, reinforcement, and understanding of how to improve their health.
Care guides, using their relationships with providers, served as quality improvement advocates integrated into the daily process of providing primary care. This arrangement differed from the common practice of giving providers periodic feedback based on data gleaned from the electronic health record.
Moving the quality improvement process into the primary care office resolved many problems related to strictly electronic health record–based feedback. Each patient was considered individually. There was opportunity for conversations about care quality to occur face-to-face; members of the primary care team could discuss when to deviate from a care guideline. Strong relationships and a sense of teamwork increased workplace satisfaction [22]. In a post-study survey of 115 providers and nurses, 93% felt that care guides improved patient care and 94% felt that care guides were an effective use of resources.
Adoption Considerations
Adding a care guide into an existing clinic structure and culture requires planning and customization. In order to fully integrate this role into clinics and on care teams and achieve expected results, 6 steps are recommended:
- Program set-up through recruitment of the proper set of stakeholders to plan for implementation, including logistics, budget, etc.
- Defining details, such as the target patient population and eligibility criteria, how interactions will take place with patients, and the duration of the patient relationship.
- Clinic readiness and program development, including detailed clinic staff orientation and workflow development.
- Clinic-specific development of the care guide training, including enlisting the help of subject matter experts to develop content.
- A 2-week training of newly-hired care guides
- Defining the expectations and job responsibilities of the care guide and proper integration of care guides into care teams.
- Monitoring and evaluation – This is not the last step in the process but rather requires the ongoing work of the clinic staff, providers, and care guides to measure progress and outcomes.
Although transforming care teams in primary care clinics is no easy task, it is the foundation of the care guide model. The premise of the care guide role is simple and relatable, thereby making it transferrable to different patient populations and settings as well as attractive to different types of providers. The model is flexible, allowing room for adaptations while maintaining its focus on serving patients and families and reducing burden for providers and other clinic staff. The model is currently being adapted and used in different settings outside of traditional primary care, including urgent care and emergency departments, specialty services, and patient-centered medical homes, among others. In addition, care guides are being used across different patient populations, including high-risk patients in an accountable care organization, pediatric patients, and patients late in life, to name a few. Each adaptation may have population-specific goals and outcomes, but the core of the model remains focused on the Institute for Healthcare Improvement's triple aim: improving the patient experience of care, improving the health of populations, and reducing the per capita cost of health care.
For clinics and care providers interested in integrating care guides within their own clinic, a toolkit, eLearning modules, and evaluation templates, among other resources, are available at no cost through the Care Copilot Institute (www.carecopilotinstitute.org). The Institute was created to translate and disseminate the care guide research.
Conclusion
Lay health care workers with relevant skills and training, located in clinic waiting rooms where they can meet patients and providers face-to-face, can help chronic disease patients and their providers improve the quality of care. Because of its low cost, this model can be implemented in many settings, including small independent primary care offices, where much primary care in the US is still delivered [7,23–25].
Corresponding author: Kim Radel, MHA, Allina Health, Minneapolis, MN, [email protected].
Financial disclosures: Dr. Christianson disclosed that he received grant support from the Robina Foundation.
From Allina Health, Minneapolis, MN.
Abstract
- Objective: To describe a care model in which lay “care guides” are integrated into the primary care team to help patients with chronic disease and their providers achieve care goals.
- Methods: Care guides are individuals without formal medical training who receive brief training about chronic conditions and behavior change. General activities include educating and encouraging patients to take control of their illness, supporting medication and treatment adherence, and facilitating resolution of barriers to quality care.
- Results: The care guide model can improve care for some patients with chronic disease at low cost. In a randomized trial testing the intervention, patients with care guides achieved more goals than usual care patients at 1 year (odds ratio, 1.31; 95% confidence interval, 1.16–1.47; P < 0.001).
- Conclusion: Lay health care workers with relevant skills and training, located in clinic waiting rooms where they can meet patients and providers face-to-face, can help chronic disease patients and their providers improve the quality of care.
Improving the quality of care for chronic disease patients is an important goal for the US health care system. Almost half of American with chronic disease fail to receive evidence-based care [1–3]. Reasons for this include limited access to the health care delivery system [4,5] and payment systems that undervalue primary care and provide incentives for more but not necessarily better care [6]. Not only is there a need to improve the quality of care among chronic disease patients, but also to recognize the constraints faced by primary care providers (PCPs) and clinic staff in the current health care environment.
One approach for improving care for patients with chronic disease has been care coordination, or management by health care professionals such as nurses and certified medical assistants [7]. These care managers are usually located in primary care medical offices and have some face-to-face contact with both patients and providers in addition to telephone or electronic contact [7,8]. Care management provided by registered nurses can be effective but is expensive, and it is unclear where payment for these services will come from [7,9].
An alternative approach is employing lay health care workers. In the literature lay health care workers have been referred to as promotoras de salud, lay advisors or navigators, and peer coaches [10–12]. Some of these workers are employees while others are part-time volunteers [13,14]. Tasks assigned to these workers are often limited, such as improving access to cancer care [15], teaching self-help techniques [16–18], or goal-setting [19], and are usually focused on a specific disease or problem. Some of workers do have contact with nurses and doctors, but they tend not to work with the primary care team in the day-to-day provision of care [14].
To improve the quality and efficiency of chronic disease care, Allina Health, a large not-for-profit system of hospitals and clinics in Minnesota and western Wisconsin, hired lay “care guides” to help patients and providers achieve care goals and integrated them into the primary care team. In this article, we describe the care guide model we used and tested and discuss adoption considerations.
Role and Responsibilities of a Care Guide
Care guides are individuals without formal medical training whose general activities include:
- fostering a longitudinal relationship to encourage patients to take control of their chronic illness;
- educating patients about the considerable benefits of best practice treatment;
- communicating with patients, families and providers to keep the entire care team, including the PCP, focused on meeting care guidelines;
- supporting medication and treatment adherence;
- identifying and facilitating resolution of barriers to quality care;
- facilitating referrals to extended care team members and introducing patients to appropriate services or resources within the clinic, health system and/or community they live or work in.
How do care guides differ from other personnel used as care managers? Care guides can explain the value of meeting standard goals, but unlike nurses cannot answer clinical questions. Care guides and medical assistants have similar salaries but care guides have higher educational requirements, less clinical training, and no competing duties in clinic. Like community health workers, care guides are culturally similar to the patients they serve, but are located in the clinic. Care guides were recruited for specific traits and competencies: an outgoing personality, the ability to engage easily with people of different ages and backgrounds, and a second language where needed (eg, Spanish and Somali in the pilot study) [20].
Implementation Trial
![]()
The study recruited 2135 patients. Both groups had an increased percentage of goals met at the end of the 1-year study compared to baseline. Care guide patients met a larger percentage of possible care goals at 1 year than did usual care patients (odds ratio, 1.31; 95% confidence interval, 1.16–1.47; P < 0.001). Care guide patients reduced unmet goals by 30.1%, usual care patients by 12.6%. The difference in outcomes between the 2 groups was minimally affected by differences in the times of final measurement for each goal. The benefit of working with a care guide was not different across demographic categories of age, sex, race, language, insurance, or education. In this study, care guides helped a broad range of patients who were meeting many goals at baseline and who were cared for by providers already receiving regular quality-improvement feedback. Estimated cost was $286 per patient per year.
Development Process
At each clinic, the research team enlisted the help of a site-specific implementation team consisting of a provider champion and clinic leader (ie, the clinic manager, clinic supervisor, or business office supervisor) to customize the study implementation. After selecting the target patient population, chronic disease focus, and eligibility criteria, the research team solicited the help of providers, nurses, medical assistants, and other clinic support staff to develop care guide workflows and processes. Clinic providers and staff were involved early and often in the model planning process. The team gave thoughtful consideration to existing clinic work processes and personnel dynamics to help ensure that the care guide would be accepted and integrated into the clinic culture.
Concurrent with designing workflows for the interactions between care guides and providers, clinical staff, and patients, the research team worked with a variety of support departments at Allina Health System to ensure that the necessary tools were in place for care guides to do their work effectively. They collaborated with human resources to screen for care guide candidates with appropriate skills and personal attributes; information systems to create new tools and security access within the electronic health record; learning and development to organize resources and devise an appropriate training schedule; and marketing/communications to broadcast this new initiative on a system-wide level.
Once details of the model and workflows were established, the research team secured subject matter experts to build content for care guide training. The research team partnered with PCPs whose expertise was treating these chronic diseases as well as pharmacists, nutritionists, diabetes nurse educators, and behavioral health specialists available within the health system. These subject matter experts provided the training content as well as conducted the training. Training took place over 2 weeks and included basic training on the 3 chronic disease conditions, pharmacology, nutrition, and mental health issues, barriers to care, and behavioral change techniques.
Benefits
What were the key interactions leading to clinical improvements? What made the intervention successful? Care guides described using a variety of techniques to yield clinical improvements. With patients, care guides took time to explain the benefits of meeting goals in lay language, used their non-medical backgrounds to create an environment where patients felt at ease asking questions, called patients following office visits to ensure instructions were understood, and helped develop specific action plans. With providers and nurses, care guides gave reminders about unmet goals on the day of an appointment (when this information would be most useful) and supplied information such as “this patient reports difficulty affording medication” or “this patient seems ready to quit tobacco.” Care guides reinforced the effectiveness of longer-term care relationships; for example, most patients who quit tobacco did so between 9 and 12 months after enrollment in the care guide program. In after-study surveys, care guide patients reported significantly more positive perceptions of their care than usual care patients in constructs measuring social support, individualized care, help, reinforcement, and understanding of how to improve their health.
Care guides, using their relationships with providers, served as quality improvement advocates integrated into the daily process of providing primary care. This arrangement differed from the common practice of giving providers periodic feedback based on data gleaned from the electronic health record.
Moving the quality improvement process into the primary care office resolved many problems related to strictly electronic health record–based feedback. Each patient was considered individually. There was opportunity for conversations about care quality to occur face-to-face; members of the primary care team could discuss when to deviate from a care guideline. Strong relationships and a sense of teamwork increased workplace satisfaction [22]. In a post-study survey of 115 providers and nurses, 93% felt that care guides improved patient care and 94% felt that care guides were an effective use of resources.
Adoption Considerations
Adding a care guide into an existing clinic structure and culture requires planning and customization. In order to fully integrate this role into clinics and on care teams and achieve expected results, 6 steps are recommended:
- Program set-up through recruitment of the proper set of stakeholders to plan for implementation, including logistics, budget, etc.
- Defining details, such as the target patient population and eligibility criteria, how interactions will take place with patients, and the duration of the patient relationship.
- Clinic readiness and program development, including detailed clinic staff orientation and workflow development.
- Clinic-specific development of the care guide training, including enlisting the help of subject matter experts to develop content.
- A 2-week training of newly-hired care guides
- Defining the expectations and job responsibilities of the care guide and proper integration of care guides into care teams.
- Monitoring and evaluation – This is not the last step in the process but rather requires the ongoing work of the clinic staff, providers, and care guides to measure progress and outcomes.
Although transforming care teams in primary care clinics is no easy task, it is the foundation of the care guide model. The premise of the care guide role is simple and relatable, thereby making it transferrable to different patient populations and settings as well as attractive to different types of providers. The model is flexible, allowing room for adaptations while maintaining its focus on serving patients and families and reducing burden for providers and other clinic staff. The model is currently being adapted and used in different settings outside of traditional primary care, including urgent care and emergency departments, specialty services, and patient-centered medical homes, among others. In addition, care guides are being used across different patient populations, including high-risk patients in an accountable care organization, pediatric patients, and patients late in life, to name a few. Each adaptation may have population-specific goals and outcomes, but the core of the model remains focused on the Institute for Healthcare Improvement's triple aim: improving the patient experience of care, improving the health of populations, and reducing the per capita cost of health care.
For clinics and care providers interested in integrating care guides within their own clinic, a toolkit, eLearning modules, and evaluation templates, among other resources, are available at no cost through the Care Copilot Institute (www.carecopilotinstitute.org). The Institute was created to translate and disseminate the care guide research.
Conclusion
Lay health care workers with relevant skills and training, located in clinic waiting rooms where they can meet patients and providers face-to-face, can help chronic disease patients and their providers improve the quality of care. Because of its low cost, this model can be implemented in many settings, including small independent primary care offices, where much primary care in the US is still delivered [7,23–25].
Corresponding author: Kim Radel, MHA, Allina Health, Minneapolis, MN, [email protected].
Financial disclosures: Dr. Christianson disclosed that he received grant support from the Robina Foundation.
1. Banerjee D, Stafford R. Lack of improvement in outpatient management of congestive heart failure in the United States Arch Intern Med 2010;16:1–2.
2. Egan BM, Zhao Y, RN A. US trends in prevalence, awareness, treatment, and control of hypertension. JAMA 2010;303:2043–50.
3. McGlynn E, Asch S, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med 2003;348:2635–45.
4. Ghorob A, Bodenheimer T. Sharing the care to improve access to primary care. N Engl J Med 2012;366:1955–7.
5. Schroeder SA. Shattuck Lecture. We can do better - improving the health of the American people. N Engl J Med 2007;357:1221–8.
6. Bazinsky KR, Herrera L, Sharfstein JM. Toward innovative models of health care and financing: matchmaking in Maryland. JAMA 2012;307:1261–2.
7. Berry-Millett R, Bodenheimer TS. Care management of patients with complex health care needs. Synth Proj Res Synth Rep 2009;(19).
8. Peikes D, Chen A, Schore J, Brown R. Effects of care coordination on hospitalization, quality of care, and health care expenditures among Medicare beneficiaries: 15 randomized trials. JAMA 2009;301:603–18.
9. Ayanian JZ. The elusive quest for quality and cost savings in the Medicare program. JAMA 2009;301:668–70.
10. Babamoto KS, Sey KA, Camilleri AJ, et al. Improving diabetes care and health measures among hispanics using community health workers: results from a randomized controlled trial. Health Educ Behav 2009;36:113–26.
11. Brownstein JN, Hirsch GR, Rosenthal EL, Rush CH. Community health workers “101” for primary care providers and other stakeholders in health care systems. J Ambul Care Manage 2011;34:210–20.
12. Lewin S, Dick J, Pond P, et al. Lay health workers in primary and community health care. Cochrane Database Syst Rev 2005;(1):CD004015.
13. Doull M, O’Connor A, Welch V, et al. Peer support strategies for improving the health and well-being of individuals with chronic diseases. Cochrane Database Syst Rev 2004;(2):CD004774.
14. Witmer A, Seifer SD, Finocchio L, et al. Community health workers: integral members of the health care work force. Am J Public Health 1995;85(8 Pt 1):1055–8.
15. Steinberg ML, Fremont A, Khan DC, et al. Lay patient navigator program implementation for equal access to cancer care and clinical trials: essential steps and initial challenges. Cancer 2006;107:2669–77.
16. Fu D, Fu H, McGowan P, et al. Implementation and quantitative evaluation of chronic disease self-management programme in Shanghai, China: randomized controlled trial. Bull World Health Organ 2003;81:174–82.
17. Kennedy A, Reeves D, Bower P, et al. The effectiveness and cost effectiveness of a national lay-led self care support programme for patients with long-term conditions: a pragmatic randomised controlled trial. J Epidemiol Comm Health 2007;61:254–61.
18. Rhodes SD, Foley KL, Zometa CS, Bloom FR. Lay health advisor interventions among Hispanics/Latinos: a qualitative systematic review. Am J Prev Med 2007;33:418–27.
19. Heisler M, Spencer M, Forman J, et al. Participants’ assessments of the effects of a community health worker intervention on their diabetes self-management and interactions with healthcare providers. Am J Prev Med 2009;37(6 Suppl 1):S270–9.
20. Adair R, Christianson JB, Wholey DR, et al. Care guides: employing nonclinical laypersons to help primary care teams manage chronic disease. J Ambul Care Manage 2012;35:27–37.
21. Adair R, Wholey DR, Christianson JB, et al. Improving chronic disease care by adding laypersons to the primary care team: a parallel randomized trial. Ann Intern Med 2013;159:176–84.
22. Cassel CK, Jain S. Assessing individual physician performance: does measurement suppress motivation? JAMA 2012;307:2595–6.
23. Nocon RS, Sharma R, Birnberg JM, et al. Association between patient-centered medical home rating and operating cost at federally funded health centers. JAMA 2012;308:60–6.
24. Rittenhouse D, Casalino L. Small and medium-size physician practices use few patient-centered medical home processes. Health Aff 2011;30:1575–84.
25. Fifield J, Forrest DD, Martin-Peele M, et al. A randomized, controlled trial of implementing the patient-centered medical home model in solo and small practices. J Gen Intern Med 2012;28:770–7.
1. Banerjee D, Stafford R. Lack of improvement in outpatient management of congestive heart failure in the United States Arch Intern Med 2010;16:1–2.
2. Egan BM, Zhao Y, RN A. US trends in prevalence, awareness, treatment, and control of hypertension. JAMA 2010;303:2043–50.
3. McGlynn E, Asch S, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med 2003;348:2635–45.
4. Ghorob A, Bodenheimer T. Sharing the care to improve access to primary care. N Engl J Med 2012;366:1955–7.
5. Schroeder SA. Shattuck Lecture. We can do better - improving the health of the American people. N Engl J Med 2007;357:1221–8.
6. Bazinsky KR, Herrera L, Sharfstein JM. Toward innovative models of health care and financing: matchmaking in Maryland. JAMA 2012;307:1261–2.
7. Berry-Millett R, Bodenheimer TS. Care management of patients with complex health care needs. Synth Proj Res Synth Rep 2009;(19).
8. Peikes D, Chen A, Schore J, Brown R. Effects of care coordination on hospitalization, quality of care, and health care expenditures among Medicare beneficiaries: 15 randomized trials. JAMA 2009;301:603–18.
9. Ayanian JZ. The elusive quest for quality and cost savings in the Medicare program. JAMA 2009;301:668–70.
10. Babamoto KS, Sey KA, Camilleri AJ, et al. Improving diabetes care and health measures among hispanics using community health workers: results from a randomized controlled trial. Health Educ Behav 2009;36:113–26.
11. Brownstein JN, Hirsch GR, Rosenthal EL, Rush CH. Community health workers “101” for primary care providers and other stakeholders in health care systems. J Ambul Care Manage 2011;34:210–20.
12. Lewin S, Dick J, Pond P, et al. Lay health workers in primary and community health care. Cochrane Database Syst Rev 2005;(1):CD004015.
13. Doull M, O’Connor A, Welch V, et al. Peer support strategies for improving the health and well-being of individuals with chronic diseases. Cochrane Database Syst Rev 2004;(2):CD004774.
14. Witmer A, Seifer SD, Finocchio L, et al. Community health workers: integral members of the health care work force. Am J Public Health 1995;85(8 Pt 1):1055–8.
15. Steinberg ML, Fremont A, Khan DC, et al. Lay patient navigator program implementation for equal access to cancer care and clinical trials: essential steps and initial challenges. Cancer 2006;107:2669–77.
16. Fu D, Fu H, McGowan P, et al. Implementation and quantitative evaluation of chronic disease self-management programme in Shanghai, China: randomized controlled trial. Bull World Health Organ 2003;81:174–82.
17. Kennedy A, Reeves D, Bower P, et al. The effectiveness and cost effectiveness of a national lay-led self care support programme for patients with long-term conditions: a pragmatic randomised controlled trial. J Epidemiol Comm Health 2007;61:254–61.
18. Rhodes SD, Foley KL, Zometa CS, Bloom FR. Lay health advisor interventions among Hispanics/Latinos: a qualitative systematic review. Am J Prev Med 2007;33:418–27.
19. Heisler M, Spencer M, Forman J, et al. Participants’ assessments of the effects of a community health worker intervention on their diabetes self-management and interactions with healthcare providers. Am J Prev Med 2009;37(6 Suppl 1):S270–9.
20. Adair R, Christianson JB, Wholey DR, et al. Care guides: employing nonclinical laypersons to help primary care teams manage chronic disease. J Ambul Care Manage 2012;35:27–37.
21. Adair R, Wholey DR, Christianson JB, et al. Improving chronic disease care by adding laypersons to the primary care team: a parallel randomized trial. Ann Intern Med 2013;159:176–84.
22. Cassel CK, Jain S. Assessing individual physician performance: does measurement suppress motivation? JAMA 2012;307:2595–6.
23. Nocon RS, Sharma R, Birnberg JM, et al. Association between patient-centered medical home rating and operating cost at federally funded health centers. JAMA 2012;308:60–6.
24. Rittenhouse D, Casalino L. Small and medium-size physician practices use few patient-centered medical home processes. Health Aff 2011;30:1575–84.
25. Fifield J, Forrest DD, Martin-Peele M, et al. A randomized, controlled trial of implementing the patient-centered medical home model in solo and small practices. J Gen Intern Med 2012;28:770–7.
Team Approach for Improving Outcomes in a Culturally Diverse Patient Population
From the Samuel U. Rodgers Health Center, Kansas City, MO.
Abstract
- Objective: To describe the application of the Health Home model in a center that provides care for a culturally diverse patient population.
- Methods: The initiative serves 300 Medicaid beneficiaries, providing intense primary care and behavioral health services for patients with 2 or more chronic diseases. The program addresses multicultural issues and health literacy in addition to assessing patients’ physical and mental health issues and basic needs. It builds upon the patient-centered medical home model, employing a team-based, holistic approach that integrates a behavioral health component to encompass the needs of the whole person, including psychosocial requirements.
- Results: Implementation has led to improved clinical outcomes, including lower A1c levels in our diabetic patients and fewer emergency department visits and hospitalizations.
- Conclusion: The Health Home model has improved our ability to provide high quality, culturally competent health care to our diverse patient population.
Samuel U. Rodgers Health Center (SURHC) has a long and proud history in Kansas City. It was founded in 1967 and incorporated in 1968 as the fourth federally qualified health center in the United States and the first in Missouri. SURHC provides comprehensive primary and urgent care to persons of all ages in the areas of adult and senior medicine, obstetrics/gynecology, pediatric and adolescent health, behavioral health, and dental health services for our community’s most medically vulnerable families, regardless of their ability to pay or health insurance status.
SURHC has a New Americans program in partnership with the Jewish Vocational Immigration Intake Center, in which all newly arrived refugees come to SURHC to receive their physical health exam and be brought up to date with necessary vaccinations. A large proportion of SURHC’s patients are refugees from war-torn and famine-impacted countries, many of which lived in refugee camps with inconsistent access to health care. Some arrive feeling hopeless, fearful, and drained while others have been tortured, maimed, and/or raped. Given these extraordinary circumstances, many patients come to us without a clear understanding of their illness or what constitutes a healthy lifestyle, including diet and exercise, preventive health screenings, and immunizations. Assistance is often required for behavioral health issues associated with acculturation stress, migration, and resettlement in addition to medical care.
Our refugees come from culturally diverse populations and may have limited literacy rates, be impacted by race-related health disparities, and be non-English speaking. Twenty-nine percent of SURHC’s total patient population and 43% of our patient population at our primary downtown campus location are non-English speaking refugees and/or immigrants. Within our chronic disease population, 68% require interpreter services. The health center employs interpreters for English, Somali, Spanish, Arabic, Burmese, and Vietnamese, but for languages less commonly used in the clinic—such as Karen, Nepalese, and Swahili—phone language interpreter services are used.
One problem we identified while working with our unique patient population was the lack of appropriate educational materials. As a result, the “traditional” method of working with patients would not be effective, necessitating a new approach to meeting the needs of our patients if there was to be any impact on their health outcomes or quality of life or provision of cost savings to the health care system. We recognized the need to address multicultural issues involving health literacy levels in addition to assessing the patient’s physical and mental health issues and basic needs before confronting their chronic disease. The stress produced from these concerns was notably interfering with the patient’s ability to focus on their overall health. We describe our approach to addressing these issues in this article.
Approach to Care
SURHC has been successful in fully integrating behavioral health care with primary care as part of our participation in the Missouri Medicaid primary care Health Home (PCHH) initiative. Our PCHH participation began in 2012 and provides SURHC with the opportunity to benefit from a fully integrated model of care. The initiative serves 300 Missouri Medicaid beneficiaries, providing intense primary care and behavioral health services for patients with 2 or more chronic diseases. The patient centered medical home laid the foundation for PCHH, which relies on a team-based care approach. PCHH employs a holistic approach similar to the medical home model and includes behavioral health as part of the front-line interventions to manage physical and mental health issues, including the determinants of health factors that may be influencing the ability of the patient to adhere to the treatment plan and live a healthy life.
Working with multiple cultures involves developing a staff that is culturally competent. This includes education on the values and beliefs of different cultures which enhances staff’s ability to understand, communicate with, and create an effective learning experience for the patient. Evidence shows that understanding someone’s culture aids in developing trust between patient and team member. This relationship greatly contributes to successful results and the reaching of patient self-management goals.
Working with different cultures also necessitates a multidisciplinary team, comprising a care coordinator, behavioral health consultant, and an RN care manager. The multidisciplinary team works in coordination with the primary care provider, LPN, and medical assistant to address the physical, mental, and social needs of the patient.
The care coordinator maintains current insurance status on patients. Specific doctor-prescribed medical supplies go through the coordinator to be pre-certified through our Cyber Access (electronic health record). The coordinator completes our measures report for meaningful use. The care coordinator answers patient calls and schedules and redirects calls as needed. A newsletter is created and mailed out monthly to our patients.
The behavioral health consultant addresses the mental processes of the patient. An assessment may include an evaluation of the patient’s emotional and spiritual needs as well as possible behavioral modification. The behavioral health consultant also addresses smoking cessation, stress reduction, and exercising. Assessment of motivation and readiness is evaluated to assist the patient in setting goals for the self-management of chronic diseases. The behavioral health consultant and RN care manager work closely together by integrating the behavioral health with the primary medical care of the patient.
The RN care manager sees patients when they come in for appointments with their primary care provider (PCP). The RN uses this time to answer patient questions regarding chronic disease, to check if patients know which medications they are taking and why, and for following up on any previous chronic disease teaching or hospital visits they may have had. This team member also coordinates with other specialists and agencies outside of the clinic to assure the patient is followed up with.
Self-Management Support
The ultimate goal in educating a multicultural patient is to wean them from hands-on support provided by the multidisciplinary staff to be able to effectively self-manage their disease. With effective self-management, the patient understands his or her condition, how it affects the body, and can monitor the condition in order to make any necessary changes to stay healthy.
Health literacy plays a significant role in educating the patient about their chronic disease. It is important to measure each patient’s ability to read and write—not only in their native language, but in English as well. This assessment enabled the multidisciplinary team to create new methods of working distinctively with each individual to support their self-management.
One of the self-management techniques that has helped patients and staff track their progress is the use of wall calendars. Our practice provides a wall calendar for interested patients to help track daily fasting, blood glucose, blood pressure, medications taken, etc. The patient can track times they took their medications by using stickers to indicate if they have taken their morning, noon, or evening medications. Our practice supplies the patient with stickers of their choice to use. These wall calendars are helpful for providing daily and monthly accounts of self-management activitites and patients are encouraged to bring them to their appointments. Future appointments can be added to the calendar before the patient leaves the doctor’s office.
Having on-site, professionally certified interpreters greatly improves the education and learning-time for non-English speaking patients. These team members are crucial for their abilities to visually assess the patient’s understanding of teaching materials and interpreting if the patient is showing signs of confusion. The interpreter is also helpful in re-labeling prescription bottles in the patient’s language or with stickers to help them understand how to take the medication correctly. Interpreters have also helped in creating new patient information tools written in different languages for patients that are literate. We have also noted that patients appear more comfortable in the learning environment when a personal interpreter is present as opposed to a telecommunication service.
Scheduled appointment times are set for the patient to meet one-on-one with the nurse care manager or behavioral health consultant for education during which 1 or 2 main points relating to their chronic disease is discussed. This strategy, called “chunking,” breaks the content down into bite-sized segments, helping the patient to learn and retain the information presented. These sessions are good times to work on specifics of the individual’s lifestyle and history and allow time for the patient to ask questions. Most information on a chronic disease can be given in 2 to 4 sessions, with an hour allotted for each one. Follow-up can be done as needed for each patient.
Teaching patients how to read nutrition labels is another useful skill. This is helpful for patients that have diabetes, hypertension, and/or hyperlipidemia. Our staff has collected empty food containers, snack packages, and drink bottles of different ethnic foods. Patients are taught how to read the nutrition labels to help them make healthy choices; for instance, a patient with diabetes is taught to read the serving size and then assess the carbohydrate amount. When comparing foods of the same kind, patients then know to choose the one with less carbohydrates per serving for the healthiest choice. A patient with hypertension would look at serving size and sodium content whereas a patient with hyperlipidemia would learn to pay attention to the serving size, fats, and cholesterol amounts. Using actual food containers as props has been an eye-opening experience for many of patients and those that understand and follow instructions on how to read nutrition labels have higher success rates in their self-management.
To further encourage healthy eating, with the help of our international interpreters we took pictures of prepared foods from different countries. Each picture was then placed on a red, yellow, or green sheet of paper (the stop light method) based on the ingredients in the food depicted. When a patient comes for teaching, we have them go through the pictures and pull out the ones they recognize and consume. We then teach the patient that foods depicted on green paper may be consumed as much as desired, foods on the yellow paper should be limited in the quantity, and foods on the red sheets represent the unhealthiest choices. Time is spent teaching patients how they can make these red-sheet dishes in a healthier manner.
Outcomes
Although SURHC’s patient population faces many challenges in achieving and maintaining control over their health, we are having success in improving clinical outcomes resulting from the implementation of the PCHH model. For example, within a 6-month period, 80% of our patients with an A1c > 8% saw a reduction in their A1c level. In addition, we found emergency room visits and hospitalizations dropped from 332 in December 2012 to 176 in August 2013. This reflects a 53% decrease in visits, for a conservative estimate of over $327,600 in savings to the health care system.
Discussion
Our outcomes support the fact that interventions and one-on-one work with patients have been helpful. The PCHH model provides personal attention to the patient—such as individually-structured teaching plans to assist in setting and attaining goals—which makes patients more accountable for self-management of their health. The use of interpreters in the education process was key to successful goal management and outcomes as they provided the bridge for patients to learn how to set and reach their goals. This model also integrates a behavioral health component to encompass the needs of the whole person, including psychosocial requirements.
Health literacy is an important factor in working with our multicultural population. It is important to provide literate patients with information in their native tongue, which can help teach them more about their chronic disease. We found some helpful educational handouts online in different languages. We also have used our onsite interpreters to help us in creating new educational handouts. In addition, we developed videos that feature our health center’s personal interpreters providing information in 6 languages about “Medications” and “What do I need to bring to my appointment?” The medication video explains the importance of taking the prescribed medicine every day or as the provider orders, and how to refill medications. The other video explains the need to bring all medications, glucose or blood pressure readings, etc, to appointments. These multilingual videos play in the waiting room throughout the day. Seeing employees on the video helps draw the patients into listening and learning the information provided.
We found that we needed to address the basic needs of the patient before confronting their chronic disease. This process sometimes involved finding beds or providing food for the patient. Many had dental issues that needed to be addressed before we could work with them on their diabetic diet issues or other contributing chronic issues. If these needs are met, it can ameliorate stress, which can have negative effects on their health.
On review of current A1c findings, there was a decrease in the percentage of patients who showed improvement. This is reflective of the most challenging patients we continue to work with. Moving forward, as more refugees representing increasingly diverse cultures come to our clinic, greater understanding of cultural nuances remains a challenge. Additional work is necessary to produce and accumulate more diverse educational materials to meet the health literacy needs of each patient.
Samuel U. Rodgers Health Center has earned the trust of our diverse communities and we are confident and proud of our ability to provide high quality, culturally-competent health care to our diverse patient population.
Corresponding author: Robyn McCright, RN, 825 Euclid Ave., Kansas City, MO 64124, [email protected].
Financial disclosures: None.
From the Samuel U. Rodgers Health Center, Kansas City, MO.
Abstract
- Objective: To describe the application of the Health Home model in a center that provides care for a culturally diverse patient population.
- Methods: The initiative serves 300 Medicaid beneficiaries, providing intense primary care and behavioral health services for patients with 2 or more chronic diseases. The program addresses multicultural issues and health literacy in addition to assessing patients’ physical and mental health issues and basic needs. It builds upon the patient-centered medical home model, employing a team-based, holistic approach that integrates a behavioral health component to encompass the needs of the whole person, including psychosocial requirements.
- Results: Implementation has led to improved clinical outcomes, including lower A1c levels in our diabetic patients and fewer emergency department visits and hospitalizations.
- Conclusion: The Health Home model has improved our ability to provide high quality, culturally competent health care to our diverse patient population.
Samuel U. Rodgers Health Center (SURHC) has a long and proud history in Kansas City. It was founded in 1967 and incorporated in 1968 as the fourth federally qualified health center in the United States and the first in Missouri. SURHC provides comprehensive primary and urgent care to persons of all ages in the areas of adult and senior medicine, obstetrics/gynecology, pediatric and adolescent health, behavioral health, and dental health services for our community’s most medically vulnerable families, regardless of their ability to pay or health insurance status.
SURHC has a New Americans program in partnership with the Jewish Vocational Immigration Intake Center, in which all newly arrived refugees come to SURHC to receive their physical health exam and be brought up to date with necessary vaccinations. A large proportion of SURHC’s patients are refugees from war-torn and famine-impacted countries, many of which lived in refugee camps with inconsistent access to health care. Some arrive feeling hopeless, fearful, and drained while others have been tortured, maimed, and/or raped. Given these extraordinary circumstances, many patients come to us without a clear understanding of their illness or what constitutes a healthy lifestyle, including diet and exercise, preventive health screenings, and immunizations. Assistance is often required for behavioral health issues associated with acculturation stress, migration, and resettlement in addition to medical care.
Our refugees come from culturally diverse populations and may have limited literacy rates, be impacted by race-related health disparities, and be non-English speaking. Twenty-nine percent of SURHC’s total patient population and 43% of our patient population at our primary downtown campus location are non-English speaking refugees and/or immigrants. Within our chronic disease population, 68% require interpreter services. The health center employs interpreters for English, Somali, Spanish, Arabic, Burmese, and Vietnamese, but for languages less commonly used in the clinic—such as Karen, Nepalese, and Swahili—phone language interpreter services are used.
One problem we identified while working with our unique patient population was the lack of appropriate educational materials. As a result, the “traditional” method of working with patients would not be effective, necessitating a new approach to meeting the needs of our patients if there was to be any impact on their health outcomes or quality of life or provision of cost savings to the health care system. We recognized the need to address multicultural issues involving health literacy levels in addition to assessing the patient’s physical and mental health issues and basic needs before confronting their chronic disease. The stress produced from these concerns was notably interfering with the patient’s ability to focus on their overall health. We describe our approach to addressing these issues in this article.
Approach to Care
SURHC has been successful in fully integrating behavioral health care with primary care as part of our participation in the Missouri Medicaid primary care Health Home (PCHH) initiative. Our PCHH participation began in 2012 and provides SURHC with the opportunity to benefit from a fully integrated model of care. The initiative serves 300 Missouri Medicaid beneficiaries, providing intense primary care and behavioral health services for patients with 2 or more chronic diseases. The patient centered medical home laid the foundation for PCHH, which relies on a team-based care approach. PCHH employs a holistic approach similar to the medical home model and includes behavioral health as part of the front-line interventions to manage physical and mental health issues, including the determinants of health factors that may be influencing the ability of the patient to adhere to the treatment plan and live a healthy life.
Working with multiple cultures involves developing a staff that is culturally competent. This includes education on the values and beliefs of different cultures which enhances staff’s ability to understand, communicate with, and create an effective learning experience for the patient. Evidence shows that understanding someone’s culture aids in developing trust between patient and team member. This relationship greatly contributes to successful results and the reaching of patient self-management goals.
Working with different cultures also necessitates a multidisciplinary team, comprising a care coordinator, behavioral health consultant, and an RN care manager. The multidisciplinary team works in coordination with the primary care provider, LPN, and medical assistant to address the physical, mental, and social needs of the patient.
The care coordinator maintains current insurance status on patients. Specific doctor-prescribed medical supplies go through the coordinator to be pre-certified through our Cyber Access (electronic health record). The coordinator completes our measures report for meaningful use. The care coordinator answers patient calls and schedules and redirects calls as needed. A newsletter is created and mailed out monthly to our patients.
The behavioral health consultant addresses the mental processes of the patient. An assessment may include an evaluation of the patient’s emotional and spiritual needs as well as possible behavioral modification. The behavioral health consultant also addresses smoking cessation, stress reduction, and exercising. Assessment of motivation and readiness is evaluated to assist the patient in setting goals for the self-management of chronic diseases. The behavioral health consultant and RN care manager work closely together by integrating the behavioral health with the primary medical care of the patient.
The RN care manager sees patients when they come in for appointments with their primary care provider (PCP). The RN uses this time to answer patient questions regarding chronic disease, to check if patients know which medications they are taking and why, and for following up on any previous chronic disease teaching or hospital visits they may have had. This team member also coordinates with other specialists and agencies outside of the clinic to assure the patient is followed up with.
Self-Management Support
The ultimate goal in educating a multicultural patient is to wean them from hands-on support provided by the multidisciplinary staff to be able to effectively self-manage their disease. With effective self-management, the patient understands his or her condition, how it affects the body, and can monitor the condition in order to make any necessary changes to stay healthy.
Health literacy plays a significant role in educating the patient about their chronic disease. It is important to measure each patient’s ability to read and write—not only in their native language, but in English as well. This assessment enabled the multidisciplinary team to create new methods of working distinctively with each individual to support their self-management.
One of the self-management techniques that has helped patients and staff track their progress is the use of wall calendars. Our practice provides a wall calendar for interested patients to help track daily fasting, blood glucose, blood pressure, medications taken, etc. The patient can track times they took their medications by using stickers to indicate if they have taken their morning, noon, or evening medications. Our practice supplies the patient with stickers of their choice to use. These wall calendars are helpful for providing daily and monthly accounts of self-management activitites and patients are encouraged to bring them to their appointments. Future appointments can be added to the calendar before the patient leaves the doctor’s office.
Having on-site, professionally certified interpreters greatly improves the education and learning-time for non-English speaking patients. These team members are crucial for their abilities to visually assess the patient’s understanding of teaching materials and interpreting if the patient is showing signs of confusion. The interpreter is also helpful in re-labeling prescription bottles in the patient’s language or with stickers to help them understand how to take the medication correctly. Interpreters have also helped in creating new patient information tools written in different languages for patients that are literate. We have also noted that patients appear more comfortable in the learning environment when a personal interpreter is present as opposed to a telecommunication service.
Scheduled appointment times are set for the patient to meet one-on-one with the nurse care manager or behavioral health consultant for education during which 1 or 2 main points relating to their chronic disease is discussed. This strategy, called “chunking,” breaks the content down into bite-sized segments, helping the patient to learn and retain the information presented. These sessions are good times to work on specifics of the individual’s lifestyle and history and allow time for the patient to ask questions. Most information on a chronic disease can be given in 2 to 4 sessions, with an hour allotted for each one. Follow-up can be done as needed for each patient.
Teaching patients how to read nutrition labels is another useful skill. This is helpful for patients that have diabetes, hypertension, and/or hyperlipidemia. Our staff has collected empty food containers, snack packages, and drink bottles of different ethnic foods. Patients are taught how to read the nutrition labels to help them make healthy choices; for instance, a patient with diabetes is taught to read the serving size and then assess the carbohydrate amount. When comparing foods of the same kind, patients then know to choose the one with less carbohydrates per serving for the healthiest choice. A patient with hypertension would look at serving size and sodium content whereas a patient with hyperlipidemia would learn to pay attention to the serving size, fats, and cholesterol amounts. Using actual food containers as props has been an eye-opening experience for many of patients and those that understand and follow instructions on how to read nutrition labels have higher success rates in their self-management.
To further encourage healthy eating, with the help of our international interpreters we took pictures of prepared foods from different countries. Each picture was then placed on a red, yellow, or green sheet of paper (the stop light method) based on the ingredients in the food depicted. When a patient comes for teaching, we have them go through the pictures and pull out the ones they recognize and consume. We then teach the patient that foods depicted on green paper may be consumed as much as desired, foods on the yellow paper should be limited in the quantity, and foods on the red sheets represent the unhealthiest choices. Time is spent teaching patients how they can make these red-sheet dishes in a healthier manner.
Outcomes
Although SURHC’s patient population faces many challenges in achieving and maintaining control over their health, we are having success in improving clinical outcomes resulting from the implementation of the PCHH model. For example, within a 6-month period, 80% of our patients with an A1c > 8% saw a reduction in their A1c level. In addition, we found emergency room visits and hospitalizations dropped from 332 in December 2012 to 176 in August 2013. This reflects a 53% decrease in visits, for a conservative estimate of over $327,600 in savings to the health care system.
Discussion
Our outcomes support the fact that interventions and one-on-one work with patients have been helpful. The PCHH model provides personal attention to the patient—such as individually-structured teaching plans to assist in setting and attaining goals—which makes patients more accountable for self-management of their health. The use of interpreters in the education process was key to successful goal management and outcomes as they provided the bridge for patients to learn how to set and reach their goals. This model also integrates a behavioral health component to encompass the needs of the whole person, including psychosocial requirements.
Health literacy is an important factor in working with our multicultural population. It is important to provide literate patients with information in their native tongue, which can help teach them more about their chronic disease. We found some helpful educational handouts online in different languages. We also have used our onsite interpreters to help us in creating new educational handouts. In addition, we developed videos that feature our health center’s personal interpreters providing information in 6 languages about “Medications” and “What do I need to bring to my appointment?” The medication video explains the importance of taking the prescribed medicine every day or as the provider orders, and how to refill medications. The other video explains the need to bring all medications, glucose or blood pressure readings, etc, to appointments. These multilingual videos play in the waiting room throughout the day. Seeing employees on the video helps draw the patients into listening and learning the information provided.
We found that we needed to address the basic needs of the patient before confronting their chronic disease. This process sometimes involved finding beds or providing food for the patient. Many had dental issues that needed to be addressed before we could work with them on their diabetic diet issues or other contributing chronic issues. If these needs are met, it can ameliorate stress, which can have negative effects on their health.
On review of current A1c findings, there was a decrease in the percentage of patients who showed improvement. This is reflective of the most challenging patients we continue to work with. Moving forward, as more refugees representing increasingly diverse cultures come to our clinic, greater understanding of cultural nuances remains a challenge. Additional work is necessary to produce and accumulate more diverse educational materials to meet the health literacy needs of each patient.
Samuel U. Rodgers Health Center has earned the trust of our diverse communities and we are confident and proud of our ability to provide high quality, culturally-competent health care to our diverse patient population.
Corresponding author: Robyn McCright, RN, 825 Euclid Ave., Kansas City, MO 64124, [email protected].
Financial disclosures: None.
From the Samuel U. Rodgers Health Center, Kansas City, MO.
Abstract
- Objective: To describe the application of the Health Home model in a center that provides care for a culturally diverse patient population.
- Methods: The initiative serves 300 Medicaid beneficiaries, providing intense primary care and behavioral health services for patients with 2 or more chronic diseases. The program addresses multicultural issues and health literacy in addition to assessing patients’ physical and mental health issues and basic needs. It builds upon the patient-centered medical home model, employing a team-based, holistic approach that integrates a behavioral health component to encompass the needs of the whole person, including psychosocial requirements.
- Results: Implementation has led to improved clinical outcomes, including lower A1c levels in our diabetic patients and fewer emergency department visits and hospitalizations.
- Conclusion: The Health Home model has improved our ability to provide high quality, culturally competent health care to our diverse patient population.
Samuel U. Rodgers Health Center (SURHC) has a long and proud history in Kansas City. It was founded in 1967 and incorporated in 1968 as the fourth federally qualified health center in the United States and the first in Missouri. SURHC provides comprehensive primary and urgent care to persons of all ages in the areas of adult and senior medicine, obstetrics/gynecology, pediatric and adolescent health, behavioral health, and dental health services for our community’s most medically vulnerable families, regardless of their ability to pay or health insurance status.
SURHC has a New Americans program in partnership with the Jewish Vocational Immigration Intake Center, in which all newly arrived refugees come to SURHC to receive their physical health exam and be brought up to date with necessary vaccinations. A large proportion of SURHC’s patients are refugees from war-torn and famine-impacted countries, many of which lived in refugee camps with inconsistent access to health care. Some arrive feeling hopeless, fearful, and drained while others have been tortured, maimed, and/or raped. Given these extraordinary circumstances, many patients come to us without a clear understanding of their illness or what constitutes a healthy lifestyle, including diet and exercise, preventive health screenings, and immunizations. Assistance is often required for behavioral health issues associated with acculturation stress, migration, and resettlement in addition to medical care.
Our refugees come from culturally diverse populations and may have limited literacy rates, be impacted by race-related health disparities, and be non-English speaking. Twenty-nine percent of SURHC’s total patient population and 43% of our patient population at our primary downtown campus location are non-English speaking refugees and/or immigrants. Within our chronic disease population, 68% require interpreter services. The health center employs interpreters for English, Somali, Spanish, Arabic, Burmese, and Vietnamese, but for languages less commonly used in the clinic—such as Karen, Nepalese, and Swahili—phone language interpreter services are used.
One problem we identified while working with our unique patient population was the lack of appropriate educational materials. As a result, the “traditional” method of working with patients would not be effective, necessitating a new approach to meeting the needs of our patients if there was to be any impact on their health outcomes or quality of life or provision of cost savings to the health care system. We recognized the need to address multicultural issues involving health literacy levels in addition to assessing the patient’s physical and mental health issues and basic needs before confronting their chronic disease. The stress produced from these concerns was notably interfering with the patient’s ability to focus on their overall health. We describe our approach to addressing these issues in this article.
Approach to Care
SURHC has been successful in fully integrating behavioral health care with primary care as part of our participation in the Missouri Medicaid primary care Health Home (PCHH) initiative. Our PCHH participation began in 2012 and provides SURHC with the opportunity to benefit from a fully integrated model of care. The initiative serves 300 Missouri Medicaid beneficiaries, providing intense primary care and behavioral health services for patients with 2 or more chronic diseases. The patient centered medical home laid the foundation for PCHH, which relies on a team-based care approach. PCHH employs a holistic approach similar to the medical home model and includes behavioral health as part of the front-line interventions to manage physical and mental health issues, including the determinants of health factors that may be influencing the ability of the patient to adhere to the treatment plan and live a healthy life.
Working with multiple cultures involves developing a staff that is culturally competent. This includes education on the values and beliefs of different cultures which enhances staff’s ability to understand, communicate with, and create an effective learning experience for the patient. Evidence shows that understanding someone’s culture aids in developing trust between patient and team member. This relationship greatly contributes to successful results and the reaching of patient self-management goals.
Working with different cultures also necessitates a multidisciplinary team, comprising a care coordinator, behavioral health consultant, and an RN care manager. The multidisciplinary team works in coordination with the primary care provider, LPN, and medical assistant to address the physical, mental, and social needs of the patient.
The care coordinator maintains current insurance status on patients. Specific doctor-prescribed medical supplies go through the coordinator to be pre-certified through our Cyber Access (electronic health record). The coordinator completes our measures report for meaningful use. The care coordinator answers patient calls and schedules and redirects calls as needed. A newsletter is created and mailed out monthly to our patients.
The behavioral health consultant addresses the mental processes of the patient. An assessment may include an evaluation of the patient’s emotional and spiritual needs as well as possible behavioral modification. The behavioral health consultant also addresses smoking cessation, stress reduction, and exercising. Assessment of motivation and readiness is evaluated to assist the patient in setting goals for the self-management of chronic diseases. The behavioral health consultant and RN care manager work closely together by integrating the behavioral health with the primary medical care of the patient.
The RN care manager sees patients when they come in for appointments with their primary care provider (PCP). The RN uses this time to answer patient questions regarding chronic disease, to check if patients know which medications they are taking and why, and for following up on any previous chronic disease teaching or hospital visits they may have had. This team member also coordinates with other specialists and agencies outside of the clinic to assure the patient is followed up with.
Self-Management Support
The ultimate goal in educating a multicultural patient is to wean them from hands-on support provided by the multidisciplinary staff to be able to effectively self-manage their disease. With effective self-management, the patient understands his or her condition, how it affects the body, and can monitor the condition in order to make any necessary changes to stay healthy.
Health literacy plays a significant role in educating the patient about their chronic disease. It is important to measure each patient’s ability to read and write—not only in their native language, but in English as well. This assessment enabled the multidisciplinary team to create new methods of working distinctively with each individual to support their self-management.
One of the self-management techniques that has helped patients and staff track their progress is the use of wall calendars. Our practice provides a wall calendar for interested patients to help track daily fasting, blood glucose, blood pressure, medications taken, etc. The patient can track times they took their medications by using stickers to indicate if they have taken their morning, noon, or evening medications. Our practice supplies the patient with stickers of their choice to use. These wall calendars are helpful for providing daily and monthly accounts of self-management activitites and patients are encouraged to bring them to their appointments. Future appointments can be added to the calendar before the patient leaves the doctor’s office.
Having on-site, professionally certified interpreters greatly improves the education and learning-time for non-English speaking patients. These team members are crucial for their abilities to visually assess the patient’s understanding of teaching materials and interpreting if the patient is showing signs of confusion. The interpreter is also helpful in re-labeling prescription bottles in the patient’s language or with stickers to help them understand how to take the medication correctly. Interpreters have also helped in creating new patient information tools written in different languages for patients that are literate. We have also noted that patients appear more comfortable in the learning environment when a personal interpreter is present as opposed to a telecommunication service.
Scheduled appointment times are set for the patient to meet one-on-one with the nurse care manager or behavioral health consultant for education during which 1 or 2 main points relating to their chronic disease is discussed. This strategy, called “chunking,” breaks the content down into bite-sized segments, helping the patient to learn and retain the information presented. These sessions are good times to work on specifics of the individual’s lifestyle and history and allow time for the patient to ask questions. Most information on a chronic disease can be given in 2 to 4 sessions, with an hour allotted for each one. Follow-up can be done as needed for each patient.
Teaching patients how to read nutrition labels is another useful skill. This is helpful for patients that have diabetes, hypertension, and/or hyperlipidemia. Our staff has collected empty food containers, snack packages, and drink bottles of different ethnic foods. Patients are taught how to read the nutrition labels to help them make healthy choices; for instance, a patient with diabetes is taught to read the serving size and then assess the carbohydrate amount. When comparing foods of the same kind, patients then know to choose the one with less carbohydrates per serving for the healthiest choice. A patient with hypertension would look at serving size and sodium content whereas a patient with hyperlipidemia would learn to pay attention to the serving size, fats, and cholesterol amounts. Using actual food containers as props has been an eye-opening experience for many of patients and those that understand and follow instructions on how to read nutrition labels have higher success rates in their self-management.
To further encourage healthy eating, with the help of our international interpreters we took pictures of prepared foods from different countries. Each picture was then placed on a red, yellow, or green sheet of paper (the stop light method) based on the ingredients in the food depicted. When a patient comes for teaching, we have them go through the pictures and pull out the ones they recognize and consume. We then teach the patient that foods depicted on green paper may be consumed as much as desired, foods on the yellow paper should be limited in the quantity, and foods on the red sheets represent the unhealthiest choices. Time is spent teaching patients how they can make these red-sheet dishes in a healthier manner.
Outcomes
Although SURHC’s patient population faces many challenges in achieving and maintaining control over their health, we are having success in improving clinical outcomes resulting from the implementation of the PCHH model. For example, within a 6-month period, 80% of our patients with an A1c > 8% saw a reduction in their A1c level. In addition, we found emergency room visits and hospitalizations dropped from 332 in December 2012 to 176 in August 2013. This reflects a 53% decrease in visits, for a conservative estimate of over $327,600 in savings to the health care system.
Discussion
Our outcomes support the fact that interventions and one-on-one work with patients have been helpful. The PCHH model provides personal attention to the patient—such as individually-structured teaching plans to assist in setting and attaining goals—which makes patients more accountable for self-management of their health. The use of interpreters in the education process was key to successful goal management and outcomes as they provided the bridge for patients to learn how to set and reach their goals. This model also integrates a behavioral health component to encompass the needs of the whole person, including psychosocial requirements.
Health literacy is an important factor in working with our multicultural population. It is important to provide literate patients with information in their native tongue, which can help teach them more about their chronic disease. We found some helpful educational handouts online in different languages. We also have used our onsite interpreters to help us in creating new educational handouts. In addition, we developed videos that feature our health center’s personal interpreters providing information in 6 languages about “Medications” and “What do I need to bring to my appointment?” The medication video explains the importance of taking the prescribed medicine every day or as the provider orders, and how to refill medications. The other video explains the need to bring all medications, glucose or blood pressure readings, etc, to appointments. These multilingual videos play in the waiting room throughout the day. Seeing employees on the video helps draw the patients into listening and learning the information provided.
We found that we needed to address the basic needs of the patient before confronting their chronic disease. This process sometimes involved finding beds or providing food for the patient. Many had dental issues that needed to be addressed before we could work with them on their diabetic diet issues or other contributing chronic issues. If these needs are met, it can ameliorate stress, which can have negative effects on their health.
On review of current A1c findings, there was a decrease in the percentage of patients who showed improvement. This is reflective of the most challenging patients we continue to work with. Moving forward, as more refugees representing increasingly diverse cultures come to our clinic, greater understanding of cultural nuances remains a challenge. Additional work is necessary to produce and accumulate more diverse educational materials to meet the health literacy needs of each patient.
Samuel U. Rodgers Health Center has earned the trust of our diverse communities and we are confident and proud of our ability to provide high quality, culturally-competent health care to our diverse patient population.
Corresponding author: Robyn McCright, RN, 825 Euclid Ave., Kansas City, MO 64124, [email protected].
Financial disclosures: None.
Psychological Stress Interventions and Asthma: Therapeutic Considerations
From the Department of Medicine, The University of Mississippi Medical Center, Jackson, MS.
Abstract
- Objective: To review psychological stress interventions employed to improve asthma outcomes.
- Methods: Review of the literature.
- Results: In general, there are 2 approaches to managing stress in asthma patients—direct psychological interventions, and modalities where stress management is an indirect effect. The most direct approach involves mindfulness-based stress reduction, which has been shown to have a positive effect on asthma control. Cognitive behavioral therapy, biofeedback, music therapy, art therapy, and relaxation training also have been evaluated with varying results. Physical therapies, including yoga, chi gong, massage, reflexology, specific controlled breathing programs, and spinal manipulation have also been studied without consistent effectiveness demonstrated. Pharmacologic therapy for anxiety and depressive disorders has been shown to be associated with improvement in asthma symptoms and control.
- Conclusion: Although further research is needed to verify the beneficial role of specific stress intervention modalities for specific asthma populations, there is sufficient evidence of efficacy to validate the concept of stress management as a viable therapeutic approach for optimal asthma control.
The increasing levels of chronic psychological stress in the people’s everyday lives has been well recognized [1]. As technological advances continue to progress, the psychological and physical pressures associated with family- and work-role expectations, decreased free or “down” time, greater sleep deficits, increasing career-related pressures, social issues, and other factors have led to ever increasing levels of personal stress [2]. From an immune standpoint, these chronic stressors impact immune balance and may be at least partially responsible for the rise in incidence, prevalence, and severity of inflammatory diseases such as asthma [3]. As the factors responsible for increased levels of psychosocial stress in our society are not likely to decrease in the near future [4], the potential value of directed stress intervention therapies in the overall care plans for patients with asthma is an area of interest. Such stress management strategies must be evidence-based, pragmatic, and cost-effective. This review provides background, scientific and clinical rationale, and progress to date for various therapeutic approaches to stress management for asthma patients.
Asthma as Inflammatory Disease
Asthma is a breathlessness syndrome typically characterized by varying combinations of paroxysmal wheezing, cough, breathlessness, and chest tightness. The constellation of symptoms is often precipitated by exposure to volatile irritants, allergens, cold air, and exercise. Gastroesophageal reflux disease, respiratory viral infections, and pregnancy may also precipitate or worsen existing asthma [5,6]. Symptoms typically improve after appropriate asthma treatment.
While the role of IgE-mediated mechanisms in asthma has been questioned by some, studies have demonstrated the presence of IgE-mediated (“allergic”) mechanisms in most asthma cases [7]. Depending on the specific population, as many as 70% to 90% of asthma patients can be considered to have an allergic component to their asthma [8]. Such allergic sensitivities can be to seasonal pollens but even more commonly to perennial allergens such as dust mites, molds, cockroaches, and pet dander (especially cat) [9]. These associations have led to therapeutic approaches for many asthma patients based largely on those classically used for allergic rhinitis, including avoidance, environmental control, and even allergen immunotherapy [10]. Some of the newest and most promising pharmacotherapies for asthma are based on antagonism and/or prevention of the allergic cascade (production and activity of IgE) [11].
Psychological Stress and Asthma
Research regarding the relationships between asthma and chronic stress has been conducted in a variety of populations, using both cross-sectional and prospective designs [12,13]. It has been found that perceived stress negatively affects quality of life of patients with asthma and is associated with reduced medication compliance [14,15] and symptom perception [14,16]. Stress has been linked to both the onset of allergic asthma [17,18] and to enhanced skin test reactivity in response to allergens [19].Oh et al [12] suggested a dose-dependent relationship, with individuals who report increasingly higher levels of stress being more likely to report symptoms of asthma.
People with asthma who are exposed to various types of chronic stress tend to have worse severity and poorer control of their asthma symptoms [20,21]. Interventions to help manage stress in people with asthma are needed at the individual, family, and community levels; all levels are known to influence asthma and asthma morbidity [20,22].
If stress is associated with increased disease incidence and severity, then stress modulation could be expected to have beneficial effects. Advice to work fewer hours, get more sleep, and optimize relaxation can be unproductive and even frustrating to busy persons striving to meet all the demands of life. More realistic are interventions based upon helping people manage stress. Studies have reported benefit from stress management for a number of chronic diseases, including hypertension [23], obesity [24], diabetes [25], and HIV [26]. Given the associations noted above, stress intervention as a therapeutic modality for asthma management is a valid option that should be explored [27].
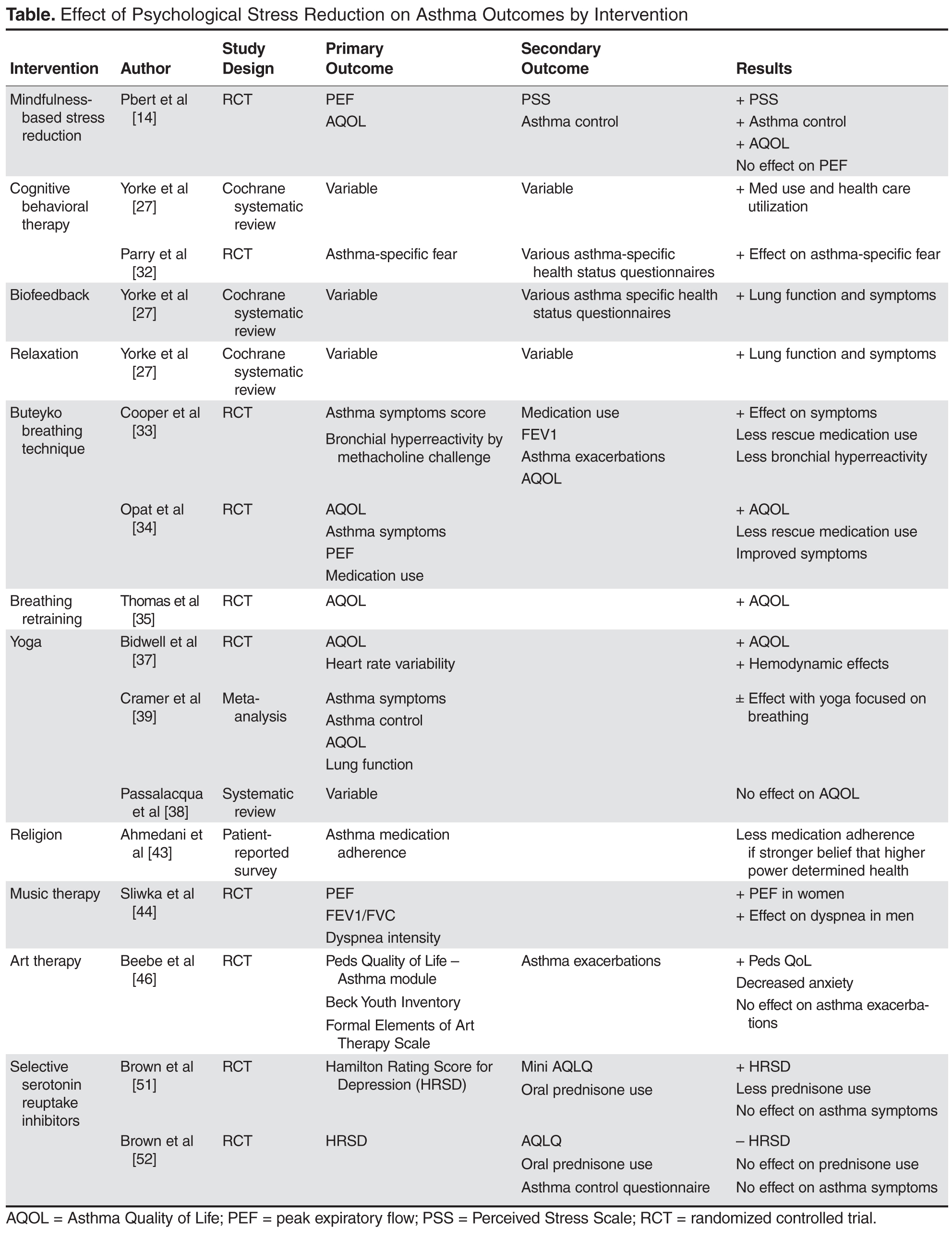
Psychologically Focused Interventions
Mindfulness-based stress reduction (MBSR) has been recognized as an important modality for treatment of many chronic diseases, including chronic pain [28], cardiovascular disease [29], type 2 diabetes mellitus [29], cancer [30], and fibromyalgia [28]. MBSR teaches patients to recognize disease symptoms and personal reactions to these symptoms, and to develop a nonreactive awareness of these elements [14]. It is an individual or group-based therapeutic approach that uses education, discussion, and various meditation techniques to reduce perceived general and disease-associated stress [14,31]. Pbert et al performed an RCT comparing a MBSR program with a traditional education program in adults with mild, moderate, or severe persistent asthma. The primary outcomes were centered on lung function as measured by peak expiratory flow (PEF) and quality of life using the Asthma Quality of Life Questionnaire (AQLQ). Secondary outcomes included changes in perceived stress as measured by the 10-question Perceived Stress Scale (PSS) and overall asthma control. At 12 months, results indicated that MBSR had positive effects on overall asthma control, with improvement in quality of life, a decrease in perceived stress, and a decrease in use of rescue therapies, but no significant effect on peak expiratory flow [14].
Various other psychological interventions have been studied as supplemental therapy to medications in the treatment of asthma. Yorke et al performed a systematic review of 14 RCTs evaluating various psychological interventions in asthma, including cognitive behavioral therapy (CBT), biofeedback, and various relaxation techniques [27]. Because there are no standardized outcomes measured across all studies, results are often conflicting. While CBT had a positive effect on asthma health care utilization, relaxation therapy had no significant effects; both did have positive effects on symptoms of depression and anxiety. Relaxation therapy had positive effects on relieving asthma symptoms such as cough and wheeze but CBT did not. Biofeedback and relaxation were the only interventions that had positive effect on improving lung function and decreasing medication usage [27].
In an RCT, Parry and colleagues evaluated the effects of CBT added to clinical care on asthma-specific fear when compared to standard clinical asthma care alone. They demonstrated a significant reduction in panic and fear related to asthma exacerbations using CBT [32].
Various other mind-body–based interventions, including meditation, yoga, and breathing techniques, have been evaluated as complementary asthma therapy. Several studies utilized the Buteyko breathing technique (BBT), which focuses on controlling breathing to restore normal levels of PaCo2 in order to improve tissue oxygenation and reduce bronchospasm. Cooper et al performed an RCT that evaluated asthma symptom scores and methacholine sensitivity (concentration of bronchial irritant causing decline in FEV1 > 20%) for the presence of bronchial hyperreactivity (BHR), a measure of asthma activity. The BBT group demonstrated a reduction in asthma symptoms and rescue inhaler use but no change in BHR [33]. Opat measured asthma QOL, asthma symptoms, rescue medication use, and lung function in patients who received instruction in BBT and patients in a sham control group. BBT was associated with improvement in asthma QOL and bronchodilator use but not in other outcome parameters [34]. Thomas et al demonstrated in an RCT involving asthma patients with symptoms of dysfunctional breathing that rebreathing-retraining physiotherapy improved asthma-related QOL compared with traditional nurse-provided education [35].
Physical Stress Management Interventions
Yoga, which involves various aspects of controlled breathing, stretching, and meditation techniques [36], aims to achieve synergy between the mind and body to produce a more relaxed psychophysiological state [37]. This popular modality is frequently used by patients, including those with asthma, for symptom control and disease management. Results from RCTs have varied in their reports of efficacy. The 2006 Allergic Rhinitis and Asthma (ARIA) work group performed a systematic review of 5 trials evaluating yoga and asthma. Though the quality of the trials varied greatly, the review demonstrated a possible benefit of yoga on asthma-related QOL but no other studied parameters [38]. QOL and hemodynamic improvement was also demonstrated in 1 RCT comparing yoga added to standard asthma therapy vs. standard therapy alone in female patients [37]. Cramer et al performed an extensive systematic review and meta-analysis of 14 RCTs evaluating the effects of yoga on all or some components of asthma-related QOL, asthma control, symptoms, and pulmonary function [39]. Though there may be some benefit of yoga breathing techniques on asthma-related QOL, the quality of these studies is very poor and reported results were highly variable. These limitations demonstrate the need for methodologically sound, standardized approaches to research in this field, which will be needed before definitive conclusions or treatment recommendations can be made [38,39].
Complementary and Alternative Medicine Interventions
Therapeutic massage, reflexology, spinal manipulation, and prayer are commonly used components of complementary medicine that are perceived by many to be helpful in asthma management [40,41]. However, the published data supporting these techniques is limited. In 2005, Hondras et al performed a Cochrane database review of RCTs evaluating manual therapy, including therapeutic massage, in asthma. Variations in measured outcomes, study design, and reporting made the evidence presented in the review difficult to interpret. Methodologically sound RCTs are needed before any inferences as to relative efficacy of these techniques can be drawn [42]. Since 2005, there have been no significant RCTs reported that would change this conclusion. Data on prayer, religious beliefs, and how these affect asthma and stress control are scarce. One nonrandomized patient reporting survey analysis to evaluate the presence of a high power in life and asthma medication adherence was reported by Ahmedani and colleagues. Results showed that overall medication adherence was low, particularly among those who believed a higher power was in control of their health [43].
Other relaxation methods for managing stress in asthma include music therapy [44] and art therapy [45,46]. Music therapy has had varying reported therapeutic success in other medical settings, such as cardiac rehabilitation [47] and prior to endoscopy [48]. Several studies have evaluated passive or active music therapy in various stages of asthma management with variable results reported. One RCT of patients admitted for asthma exacerbation evaluated the effectiveness of standard pulmonary rehabilitation for asthma with or without concomitant music therapy. Measured outcomes included lung function parameters (PEF and FEV1/FVC) and self-reported anxiety scales. There was a small improvement in PEF in women in the music therapy group. Secondary statistical analysis showed lung function improvements with music therapy only in the patients with mild asthma [44]. Art therapy, the opportunity to share feelings through the use of art materials and expressions, has been used effectively to reduce psychological distress in pediatric chronic disease. One RCT of 23 children examined the potential utility of art therapy in pediatric asthma management. While it did not affect number of exacerbations, art therapy dramatically improved quality of life in children with asthma by decreasing worry and anxiety. The effect persisted for at least 6 months after the intervention was completed [46].
Pharmacotherapy Interventions
Given that anxiety and depression are commonly reported in patients with asthma, particularly in severe and difficult to control disease [49], traditional pharmacologic treatment of anxiety and depression is often attempted. Both depression and anxiety in patients with asthma has been associated with poor asthma-related QOL, but depressive disorders were more commonly associated with poorer levels of asthma control [50]. The use of antidepressant medications, especially selective serotonin reuptake inhibitors (SSRIs), in this patient population has had varying success reported. One randomized placebo-controlled trial evaluated the use of citalopram in 90 adults with asthma and major depressive disorder. Not surprisingly, there was a positive effect on the primary outcome measuring depression using the Hamilton Rating Scale for Depression. Secondary outcome analysis also showed a decrease in oral corticosteroid use in the group treated with citalopram; however, no difference in asthma symptoms between groups was observed [51]. A similar but smaller RCT evaluated the use of escitalopram in major depression and severe asthma. The escitalopram group failed to show a statistical difference in depressive symptoms, asthma control, or oral prednisone use when compared with placebo [52].
The Future for Stress Management as a Fundamental Component of Asthma Care
Historically, avoidance of known triggers and use of pharmacologic maintenance and treatment modalities has been the cornerstone of asthma care. The recognition of excess psychological stress as a recognized trigger and treatment target is continuing to evolve in our therapeutic armamentarium. Our understanding of the effects of stress management in asthma patients provides clinical support for the neuroendocrine immune link between the bronchial inflammatory response characteristic in asthma and that of the human stress response. Understanding the relationships of psychological stress in asthma physiology, clinical morbidity, and therapeutic options is imperative, as the changing health care environment increasingly demands preventive, practical, cost-effective, evidence-based medicine. Some psychological stressors will no doubt be more difficult to address than others, but implementation of nonpharmacologic stress management paradigms should help improve effective asthma management across all patient demographics and should hopefully lead to decreased population health care costs, fewer days of work lost, and improved quality of life. Despite a clear molecular link between asthma, inflammation and stress and a clinical trend toward benefit, the heterogeneity of studies and poor quality evidence for each stress reduction modality make it difficult to draw any firm conclusions on the comparative efficacy of specific psychological interventions in asthma management programs. Mindfulness-based stress reduction has the highest quality evidence and shows the most promise thus far. Further research employing methodically sound RCTs that use standardized physiologic and nonphysiologic outcome measures is needed to elucidate the role for stress reduction interventions in routine clinical practice.
Corresponding author: Gailen D. Marshall Jr, MD, PhD, Div. of Clinical Immunology and Allergy, Dept. of Medicine, The University of Mississippi Medical Ctr., 2500 N. State St. N416 Jackson, MS 39216, [email protected].
Financial disclosures: None.
Author contributions: conception and design, CRP, AMW, GDM; drafting of article, CRP, AMW, GDM; critical revision of the article, CRP, AMW, GDM; administrative or technical support, GDM.
1. Kondo N. Socioeconomic disparities and health: impacts and pathways. J Epidemiol 2012;22:2–6.
2. Nakata A. Psychosocial job stress and immunity: a systematic review. Methods Mol Biol 2012;934:39–7.
3. Van Lieshout RJ, Macqueen GM. Relation between asthma and psychological distress: an old idea revisited. Chem Immunol Allergy 2012;98:1–13.
4. Marshall GD Jr. The adverse effects of psychological stress on immunoregulatory balance: applications to human inflammatory diseases. Immunol Allergy Clin North Am 2011;31:133–40.
5. Murphy VE, Gibson PG, Smith R, et al. Asthma during pregnancy: mechanisms and treatment implications. Eur Respir J 2005;25:1–750.
6. Harding SM. Acid reflux and asthma. Curr Opin Pulm Med 2003;9:42–5.
7. Umetsu DT, McIntire JJ, Akbari O, et al. Asthma: an epidemic of dysregulated immunity. Nat Immunol 2002;3:715–20.
8. Matricardi PM. Prevalence of atopy and asthma in eastern versus western Europe: why the difference? Ann Allergy Asthma Immunol 2001;87:24–7.
9. Murray CS, Woodcock A, Custovic A. The role of indoor allergen exposure in the development of sensitization and asthma. Curr Opin Allergy Clin Immunol 2001;1:407–12.
10. TePas EC, Umetsu DT. Immunotherapy of asthma and allergic diseases. Curr Opin Pediatr 2000;12:574–78.
11. Babu KS, Holgate ST. Newer therapies for asthma: a focus on anti-IgE. Indian J Chest Dis Allied Sci 2002;44:107–15.
12. Oh Y, Kim Y, Yoo S, et al. Association between stress and asthma symptoms: a population based study. Respirology 2004;9:363–8.
13. Sandberg S, Paton JY, Ahola S, et al. The role of acute and chronic stress in asthma attacks in children. Lancet 2000;356:982–7.
14. Pbert L, Madison JM, Druker S, et al. Effect of mindfulness training on asthma quality of life and lung function: a randomized controlled trial. Thorax 2012;67:769–76.
15. Wisnivesky JP, Lorenzo J, Feldman JM, et al. The relationship between perceived stress and morbidity among adult inner-city asthmatics. J Asthma 2010;47:100–4.
16. Janssens T, Verleden G, De Peuter S, et al. Inaccurate perception of asthma symptoms: a cognitive-affective framework and implications for asthma treatment. Clin Psychol Rev 2009;29:317–27.
17. Wright RJ, Cohen S, Carey V, et al. Parental stress as a predictor of wheezing in infancy: a prospective birth-cohort study. Am J Resp Crit Care Med 2002;165:358–65.
18. Wright RJ, Mitchell H, Visness CM, et al. Community violence and asthma morbidity in the Inner-City Asthma Study. Am J Public Health 2004;94:625–32.
19. Michel FB. Psychology of the allergic patient. Allergy 1994;49:28–30.
20. Yonas MA, Lange NE, Celedon JC. Psychosocial stress and asthma morbidity. Curr Opin Allergy Clin Immunol 2012;12:202–10.
21. Apter AJ, Garcia LA, Boyd RC, et al. Exposure to community violence is associated with asthma hospitalizations and emergency department visits. J Allergy Clin Immunol 2010;126:552–7.
22. Wright RJ. Epidemiology of stress and asthma: from constricting communities and fragile families to epigenetics. Immunol Allergy Clin North Am 2011;31:19–39.
23. Tyagi A, Cohen M. Yoga and hypertension: a systematic review. Altern Ther Health Med 2014;20:32-59.
24. Moore CJ, Cunningham SA. Social position, psychological stress, and obesity: a systematic review. J Acad Nutr Diet 2012;112:518–26.
25. Plack K, Herpertz S, Petrak F. Behavioral medicine interventions in diabetes. Curr Opin Psychiatry 2010;23:131–8.
26. Clucas C, Sibley E, Harding R, et al. A systematic review of interventions for anxiety in people with HIV. Psychol Health Med 2011;16:528–47.
27. Yorke J, Fleming SL, Shuldham C. Psychological interventions for adults with asthma: a systematic review. Respir Med 2007;101:1–14.
28. Merkes M. Mindfulness-based stress reduction for people with chronic diseases. Aust J Prim Health 2010;16:200–10.
29. Kopf S, Oikonomou D, Hartmann M. Effects of stress reduction on cardiovascular risk factors in type 2 diabetes patients with early kidney disease- results of a randomized controlled trial (HEIDIS). Exp Clin Endocrinol Diabetes 2014;122:341–9.
30. Musial F, Bussing A, Heusser P, et al. Mindfulness-based stress reduction for integrative cancer care- a summary of evidence. Forsch Komplementmed 2011;18:192–202.
31. Shigaki CL, Glass B, Schopp LH. Mindfulness-based stress reduction in medical settings. J Clin Psychl Med Settings 2006;13:209-16.
32. Parry GD, Cooper CL, Moore JM. Cognitive behavioural intervention for adults with anxiety complications of asthma: prospective randomized trial. Respir Med 2012;106;802–10.
33. Cooper S, Oborne J, Newton S, et al. Effect of two breathing exercises (Buteyko and pranayama) in asthma: a randomized controlled trial. Thorax 2003;58:674–9.
34. Opat AJ, Cohen MM, Bailey MJ, et al. A clinical trial of the Buteyko breathing technique in asthma as taught by a video. J Asthma 2000;37:557–64.
35. Thomas M, McKinley RK, Freeman E, et al. Breathing retraining for dysfunctional breathing in asthma: a randomized controlled trial. Thorax 2003;58:110–15.
36. Markham AW, Wilkinson JM. Complementary and alternative medicines (CAM) in the management of asthma: an examination of the evidence. J Asthma 2004;41:131–9.
37. Bidwell AM, Yazel B, Davin D, et al. Yoga training improves quality of life in women with asthma. J Altern Complement Med 2012;18:749–55.
38. Passalacqua G, Bousquet PJ, Carlsen KH, et al. ARIA update: I- Systematic review of complementary and alternative medicine for rhinitis and asthma. J Allergy Clin Immunol 2006;117:1054–62.
39. Cramer H, Posadzki P, Dobos G, et al. Yoga for asthma: a systematic review and meta-analysis. Ann Allergy Asthma Immunol 2014;112:503–10.
40. Slader CA, Reddel HK, Jenkins CR, et al. Complementary and alternative medicine use in asthma: who is using what? Respirology 2006;11:373–87.
41. Silvers WS, Bailey HK. Integrative approach to allergy and asthma using complementary and alternative medicine. Ann Allergy Asthma Immunol 2014;112;280-85.
42. Hondras MA, Linde K, Jones AP. Manual therapy for asthma. Cochrane Database Syst Rev 2005;(2):CD001002.
43. Ahmedani BK, Peterson EL, Wells KE, et al. Asthma medication adherence: the role of God and other health locus of control factors. Ann Allergy Asthma Immunol 2013;110:75–9.
44. Sliwka A, Nowobilski R, Polczyk R, et al. Mild asthmatics benefit from music therapy. J Asthma 2012;49:401–8.
45. Clarke SA, Calam R. The effectiveness of psychosocial interventions designed to improve health-related quality of life (HRQOL) amongst asthmatic children and their families: a systematic review. Qual Life Res 2012;21:747–64.
46. Beebe A, Gelfand EW, Bender B. A randomized trial to test the effectiveness of art therapy for children with asthma. J Allergy Clin Immunol 2010;126:262–6.
47. Metzger LK. Assessment of use of music by patients participating in cardiac rehabilitation. J Music Ther 2004;41:55–69.
48. El-Hassan H, McKeown K, Muller AF. Clinical trial: music reduces anxiety levels in patients attending for endoscopy. Aliment Pharmacol Ther 2009;30:718–24.
49. Thomas M, Bruton An, Moffatt M, et al. Asthma and psychological dysfunction. Prim Care Respir J 2011;20:250–6.
50. Lavoie KL, Bacon SL, Barone S, et al. What is worse for asthma control and quality of life: depressive disorders, anxiety disorders, or both? Chest 2006;130:1039–47.
51. Brown ES, Vigil L, Khan DA, et al. A randomized trial of citalopram versus placebo in outpatients with asthma and major depressive disorder: a proof of concept study. Biol Psychiatry 2005;58:865–70.
52. Brown ES, Howard C, Khan DA, et al. Escitalopram for severe asthma and major depressive disorder: a randomized, double-blind, placebo-controlled proof-of-concept study. Psychosomatics 2012;53:75–80.
From the Department of Medicine, The University of Mississippi Medical Center, Jackson, MS.
Abstract
- Objective: To review psychological stress interventions employed to improve asthma outcomes.
- Methods: Review of the literature.
- Results: In general, there are 2 approaches to managing stress in asthma patients—direct psychological interventions, and modalities where stress management is an indirect effect. The most direct approach involves mindfulness-based stress reduction, which has been shown to have a positive effect on asthma control. Cognitive behavioral therapy, biofeedback, music therapy, art therapy, and relaxation training also have been evaluated with varying results. Physical therapies, including yoga, chi gong, massage, reflexology, specific controlled breathing programs, and spinal manipulation have also been studied without consistent effectiveness demonstrated. Pharmacologic therapy for anxiety and depressive disorders has been shown to be associated with improvement in asthma symptoms and control.
- Conclusion: Although further research is needed to verify the beneficial role of specific stress intervention modalities for specific asthma populations, there is sufficient evidence of efficacy to validate the concept of stress management as a viable therapeutic approach for optimal asthma control.
The increasing levels of chronic psychological stress in the people’s everyday lives has been well recognized [1]. As technological advances continue to progress, the psychological and physical pressures associated with family- and work-role expectations, decreased free or “down” time, greater sleep deficits, increasing career-related pressures, social issues, and other factors have led to ever increasing levels of personal stress [2]. From an immune standpoint, these chronic stressors impact immune balance and may be at least partially responsible for the rise in incidence, prevalence, and severity of inflammatory diseases such as asthma [3]. As the factors responsible for increased levels of psychosocial stress in our society are not likely to decrease in the near future [4], the potential value of directed stress intervention therapies in the overall care plans for patients with asthma is an area of interest. Such stress management strategies must be evidence-based, pragmatic, and cost-effective. This review provides background, scientific and clinical rationale, and progress to date for various therapeutic approaches to stress management for asthma patients.
Asthma as Inflammatory Disease
Asthma is a breathlessness syndrome typically characterized by varying combinations of paroxysmal wheezing, cough, breathlessness, and chest tightness. The constellation of symptoms is often precipitated by exposure to volatile irritants, allergens, cold air, and exercise. Gastroesophageal reflux disease, respiratory viral infections, and pregnancy may also precipitate or worsen existing asthma [5,6]. Symptoms typically improve after appropriate asthma treatment.
While the role of IgE-mediated mechanisms in asthma has been questioned by some, studies have demonstrated the presence of IgE-mediated (“allergic”) mechanisms in most asthma cases [7]. Depending on the specific population, as many as 70% to 90% of asthma patients can be considered to have an allergic component to their asthma [8]. Such allergic sensitivities can be to seasonal pollens but even more commonly to perennial allergens such as dust mites, molds, cockroaches, and pet dander (especially cat) [9]. These associations have led to therapeutic approaches for many asthma patients based largely on those classically used for allergic rhinitis, including avoidance, environmental control, and even allergen immunotherapy [10]. Some of the newest and most promising pharmacotherapies for asthma are based on antagonism and/or prevention of the allergic cascade (production and activity of IgE) [11].
Psychological Stress and Asthma
Research regarding the relationships between asthma and chronic stress has been conducted in a variety of populations, using both cross-sectional and prospective designs [12,13]. It has been found that perceived stress negatively affects quality of life of patients with asthma and is associated with reduced medication compliance [14,15] and symptom perception [14,16]. Stress has been linked to both the onset of allergic asthma [17,18] and to enhanced skin test reactivity in response to allergens [19].Oh et al [12] suggested a dose-dependent relationship, with individuals who report increasingly higher levels of stress being more likely to report symptoms of asthma.
People with asthma who are exposed to various types of chronic stress tend to have worse severity and poorer control of their asthma symptoms [20,21]. Interventions to help manage stress in people with asthma are needed at the individual, family, and community levels; all levels are known to influence asthma and asthma morbidity [20,22].
If stress is associated with increased disease incidence and severity, then stress modulation could be expected to have beneficial effects. Advice to work fewer hours, get more sleep, and optimize relaxation can be unproductive and even frustrating to busy persons striving to meet all the demands of life. More realistic are interventions based upon helping people manage stress. Studies have reported benefit from stress management for a number of chronic diseases, including hypertension [23], obesity [24], diabetes [25], and HIV [26]. Given the associations noted above, stress intervention as a therapeutic modality for asthma management is a valid option that should be explored [27].
Psychologically Focused Interventions
Mindfulness-based stress reduction (MBSR) has been recognized as an important modality for treatment of many chronic diseases, including chronic pain [28], cardiovascular disease [29], type 2 diabetes mellitus [29], cancer [30], and fibromyalgia [28]. MBSR teaches patients to recognize disease symptoms and personal reactions to these symptoms, and to develop a nonreactive awareness of these elements [14]. It is an individual or group-based therapeutic approach that uses education, discussion, and various meditation techniques to reduce perceived general and disease-associated stress [14,31]. Pbert et al performed an RCT comparing a MBSR program with a traditional education program in adults with mild, moderate, or severe persistent asthma. The primary outcomes were centered on lung function as measured by peak expiratory flow (PEF) and quality of life using the Asthma Quality of Life Questionnaire (AQLQ). Secondary outcomes included changes in perceived stress as measured by the 10-question Perceived Stress Scale (PSS) and overall asthma control. At 12 months, results indicated that MBSR had positive effects on overall asthma control, with improvement in quality of life, a decrease in perceived stress, and a decrease in use of rescue therapies, but no significant effect on peak expiratory flow [14].
Various other psychological interventions have been studied as supplemental therapy to medications in the treatment of asthma. Yorke et al performed a systematic review of 14 RCTs evaluating various psychological interventions in asthma, including cognitive behavioral therapy (CBT), biofeedback, and various relaxation techniques [27]. Because there are no standardized outcomes measured across all studies, results are often conflicting. While CBT had a positive effect on asthma health care utilization, relaxation therapy had no significant effects; both did have positive effects on symptoms of depression and anxiety. Relaxation therapy had positive effects on relieving asthma symptoms such as cough and wheeze but CBT did not. Biofeedback and relaxation were the only interventions that had positive effect on improving lung function and decreasing medication usage [27].
In an RCT, Parry and colleagues evaluated the effects of CBT added to clinical care on asthma-specific fear when compared to standard clinical asthma care alone. They demonstrated a significant reduction in panic and fear related to asthma exacerbations using CBT [32].
Various other mind-body–based interventions, including meditation, yoga, and breathing techniques, have been evaluated as complementary asthma therapy. Several studies utilized the Buteyko breathing technique (BBT), which focuses on controlling breathing to restore normal levels of PaCo2 in order to improve tissue oxygenation and reduce bronchospasm. Cooper et al performed an RCT that evaluated asthma symptom scores and methacholine sensitivity (concentration of bronchial irritant causing decline in FEV1 > 20%) for the presence of bronchial hyperreactivity (BHR), a measure of asthma activity. The BBT group demonstrated a reduction in asthma symptoms and rescue inhaler use but no change in BHR [33]. Opat measured asthma QOL, asthma symptoms, rescue medication use, and lung function in patients who received instruction in BBT and patients in a sham control group. BBT was associated with improvement in asthma QOL and bronchodilator use but not in other outcome parameters [34]. Thomas et al demonstrated in an RCT involving asthma patients with symptoms of dysfunctional breathing that rebreathing-retraining physiotherapy improved asthma-related QOL compared with traditional nurse-provided education [35].
Physical Stress Management Interventions
Yoga, which involves various aspects of controlled breathing, stretching, and meditation techniques [36], aims to achieve synergy between the mind and body to produce a more relaxed psychophysiological state [37]. This popular modality is frequently used by patients, including those with asthma, for symptom control and disease management. Results from RCTs have varied in their reports of efficacy. The 2006 Allergic Rhinitis and Asthma (ARIA) work group performed a systematic review of 5 trials evaluating yoga and asthma. Though the quality of the trials varied greatly, the review demonstrated a possible benefit of yoga on asthma-related QOL but no other studied parameters [38]. QOL and hemodynamic improvement was also demonstrated in 1 RCT comparing yoga added to standard asthma therapy vs. standard therapy alone in female patients [37]. Cramer et al performed an extensive systematic review and meta-analysis of 14 RCTs evaluating the effects of yoga on all or some components of asthma-related QOL, asthma control, symptoms, and pulmonary function [39]. Though there may be some benefit of yoga breathing techniques on asthma-related QOL, the quality of these studies is very poor and reported results were highly variable. These limitations demonstrate the need for methodologically sound, standardized approaches to research in this field, which will be needed before definitive conclusions or treatment recommendations can be made [38,39].
Complementary and Alternative Medicine Interventions
Therapeutic massage, reflexology, spinal manipulation, and prayer are commonly used components of complementary medicine that are perceived by many to be helpful in asthma management [40,41]. However, the published data supporting these techniques is limited. In 2005, Hondras et al performed a Cochrane database review of RCTs evaluating manual therapy, including therapeutic massage, in asthma. Variations in measured outcomes, study design, and reporting made the evidence presented in the review difficult to interpret. Methodologically sound RCTs are needed before any inferences as to relative efficacy of these techniques can be drawn [42]. Since 2005, there have been no significant RCTs reported that would change this conclusion. Data on prayer, religious beliefs, and how these affect asthma and stress control are scarce. One nonrandomized patient reporting survey analysis to evaluate the presence of a high power in life and asthma medication adherence was reported by Ahmedani and colleagues. Results showed that overall medication adherence was low, particularly among those who believed a higher power was in control of their health [43].
Other relaxation methods for managing stress in asthma include music therapy [44] and art therapy [45,46]. Music therapy has had varying reported therapeutic success in other medical settings, such as cardiac rehabilitation [47] and prior to endoscopy [48]. Several studies have evaluated passive or active music therapy in various stages of asthma management with variable results reported. One RCT of patients admitted for asthma exacerbation evaluated the effectiveness of standard pulmonary rehabilitation for asthma with or without concomitant music therapy. Measured outcomes included lung function parameters (PEF and FEV1/FVC) and self-reported anxiety scales. There was a small improvement in PEF in women in the music therapy group. Secondary statistical analysis showed lung function improvements with music therapy only in the patients with mild asthma [44]. Art therapy, the opportunity to share feelings through the use of art materials and expressions, has been used effectively to reduce psychological distress in pediatric chronic disease. One RCT of 23 children examined the potential utility of art therapy in pediatric asthma management. While it did not affect number of exacerbations, art therapy dramatically improved quality of life in children with asthma by decreasing worry and anxiety. The effect persisted for at least 6 months after the intervention was completed [46].
Pharmacotherapy Interventions
Given that anxiety and depression are commonly reported in patients with asthma, particularly in severe and difficult to control disease [49], traditional pharmacologic treatment of anxiety and depression is often attempted. Both depression and anxiety in patients with asthma has been associated with poor asthma-related QOL, but depressive disorders were more commonly associated with poorer levels of asthma control [50]. The use of antidepressant medications, especially selective serotonin reuptake inhibitors (SSRIs), in this patient population has had varying success reported. One randomized placebo-controlled trial evaluated the use of citalopram in 90 adults with asthma and major depressive disorder. Not surprisingly, there was a positive effect on the primary outcome measuring depression using the Hamilton Rating Scale for Depression. Secondary outcome analysis also showed a decrease in oral corticosteroid use in the group treated with citalopram; however, no difference in asthma symptoms between groups was observed [51]. A similar but smaller RCT evaluated the use of escitalopram in major depression and severe asthma. The escitalopram group failed to show a statistical difference in depressive symptoms, asthma control, or oral prednisone use when compared with placebo [52].
The Future for Stress Management as a Fundamental Component of Asthma Care
Historically, avoidance of known triggers and use of pharmacologic maintenance and treatment modalities has been the cornerstone of asthma care. The recognition of excess psychological stress as a recognized trigger and treatment target is continuing to evolve in our therapeutic armamentarium. Our understanding of the effects of stress management in asthma patients provides clinical support for the neuroendocrine immune link between the bronchial inflammatory response characteristic in asthma and that of the human stress response. Understanding the relationships of psychological stress in asthma physiology, clinical morbidity, and therapeutic options is imperative, as the changing health care environment increasingly demands preventive, practical, cost-effective, evidence-based medicine. Some psychological stressors will no doubt be more difficult to address than others, but implementation of nonpharmacologic stress management paradigms should help improve effective asthma management across all patient demographics and should hopefully lead to decreased population health care costs, fewer days of work lost, and improved quality of life. Despite a clear molecular link between asthma, inflammation and stress and a clinical trend toward benefit, the heterogeneity of studies and poor quality evidence for each stress reduction modality make it difficult to draw any firm conclusions on the comparative efficacy of specific psychological interventions in asthma management programs. Mindfulness-based stress reduction has the highest quality evidence and shows the most promise thus far. Further research employing methodically sound RCTs that use standardized physiologic and nonphysiologic outcome measures is needed to elucidate the role for stress reduction interventions in routine clinical practice.
Corresponding author: Gailen D. Marshall Jr, MD, PhD, Div. of Clinical Immunology and Allergy, Dept. of Medicine, The University of Mississippi Medical Ctr., 2500 N. State St. N416 Jackson, MS 39216, [email protected].
Financial disclosures: None.
Author contributions: conception and design, CRP, AMW, GDM; drafting of article, CRP, AMW, GDM; critical revision of the article, CRP, AMW, GDM; administrative or technical support, GDM.
From the Department of Medicine, The University of Mississippi Medical Center, Jackson, MS.
Abstract
- Objective: To review psychological stress interventions employed to improve asthma outcomes.
- Methods: Review of the literature.
- Results: In general, there are 2 approaches to managing stress in asthma patients—direct psychological interventions, and modalities where stress management is an indirect effect. The most direct approach involves mindfulness-based stress reduction, which has been shown to have a positive effect on asthma control. Cognitive behavioral therapy, biofeedback, music therapy, art therapy, and relaxation training also have been evaluated with varying results. Physical therapies, including yoga, chi gong, massage, reflexology, specific controlled breathing programs, and spinal manipulation have also been studied without consistent effectiveness demonstrated. Pharmacologic therapy for anxiety and depressive disorders has been shown to be associated with improvement in asthma symptoms and control.
- Conclusion: Although further research is needed to verify the beneficial role of specific stress intervention modalities for specific asthma populations, there is sufficient evidence of efficacy to validate the concept of stress management as a viable therapeutic approach for optimal asthma control.
The increasing levels of chronic psychological stress in the people’s everyday lives has been well recognized [1]. As technological advances continue to progress, the psychological and physical pressures associated with family- and work-role expectations, decreased free or “down” time, greater sleep deficits, increasing career-related pressures, social issues, and other factors have led to ever increasing levels of personal stress [2]. From an immune standpoint, these chronic stressors impact immune balance and may be at least partially responsible for the rise in incidence, prevalence, and severity of inflammatory diseases such as asthma [3]. As the factors responsible for increased levels of psychosocial stress in our society are not likely to decrease in the near future [4], the potential value of directed stress intervention therapies in the overall care plans for patients with asthma is an area of interest. Such stress management strategies must be evidence-based, pragmatic, and cost-effective. This review provides background, scientific and clinical rationale, and progress to date for various therapeutic approaches to stress management for asthma patients.
Asthma as Inflammatory Disease
Asthma is a breathlessness syndrome typically characterized by varying combinations of paroxysmal wheezing, cough, breathlessness, and chest tightness. The constellation of symptoms is often precipitated by exposure to volatile irritants, allergens, cold air, and exercise. Gastroesophageal reflux disease, respiratory viral infections, and pregnancy may also precipitate or worsen existing asthma [5,6]. Symptoms typically improve after appropriate asthma treatment.
While the role of IgE-mediated mechanisms in asthma has been questioned by some, studies have demonstrated the presence of IgE-mediated (“allergic”) mechanisms in most asthma cases [7]. Depending on the specific population, as many as 70% to 90% of asthma patients can be considered to have an allergic component to their asthma [8]. Such allergic sensitivities can be to seasonal pollens but even more commonly to perennial allergens such as dust mites, molds, cockroaches, and pet dander (especially cat) [9]. These associations have led to therapeutic approaches for many asthma patients based largely on those classically used for allergic rhinitis, including avoidance, environmental control, and even allergen immunotherapy [10]. Some of the newest and most promising pharmacotherapies for asthma are based on antagonism and/or prevention of the allergic cascade (production and activity of IgE) [11].
Psychological Stress and Asthma
Research regarding the relationships between asthma and chronic stress has been conducted in a variety of populations, using both cross-sectional and prospective designs [12,13]. It has been found that perceived stress negatively affects quality of life of patients with asthma and is associated with reduced medication compliance [14,15] and symptom perception [14,16]. Stress has been linked to both the onset of allergic asthma [17,18] and to enhanced skin test reactivity in response to allergens [19].Oh et al [12] suggested a dose-dependent relationship, with individuals who report increasingly higher levels of stress being more likely to report symptoms of asthma.
People with asthma who are exposed to various types of chronic stress tend to have worse severity and poorer control of their asthma symptoms [20,21]. Interventions to help manage stress in people with asthma are needed at the individual, family, and community levels; all levels are known to influence asthma and asthma morbidity [20,22].
If stress is associated with increased disease incidence and severity, then stress modulation could be expected to have beneficial effects. Advice to work fewer hours, get more sleep, and optimize relaxation can be unproductive and even frustrating to busy persons striving to meet all the demands of life. More realistic are interventions based upon helping people manage stress. Studies have reported benefit from stress management for a number of chronic diseases, including hypertension [23], obesity [24], diabetes [25], and HIV [26]. Given the associations noted above, stress intervention as a therapeutic modality for asthma management is a valid option that should be explored [27].
Psychologically Focused Interventions
Mindfulness-based stress reduction (MBSR) has been recognized as an important modality for treatment of many chronic diseases, including chronic pain [28], cardiovascular disease [29], type 2 diabetes mellitus [29], cancer [30], and fibromyalgia [28]. MBSR teaches patients to recognize disease symptoms and personal reactions to these symptoms, and to develop a nonreactive awareness of these elements [14]. It is an individual or group-based therapeutic approach that uses education, discussion, and various meditation techniques to reduce perceived general and disease-associated stress [14,31]. Pbert et al performed an RCT comparing a MBSR program with a traditional education program in adults with mild, moderate, or severe persistent asthma. The primary outcomes were centered on lung function as measured by peak expiratory flow (PEF) and quality of life using the Asthma Quality of Life Questionnaire (AQLQ). Secondary outcomes included changes in perceived stress as measured by the 10-question Perceived Stress Scale (PSS) and overall asthma control. At 12 months, results indicated that MBSR had positive effects on overall asthma control, with improvement in quality of life, a decrease in perceived stress, and a decrease in use of rescue therapies, but no significant effect on peak expiratory flow [14].
Various other psychological interventions have been studied as supplemental therapy to medications in the treatment of asthma. Yorke et al performed a systematic review of 14 RCTs evaluating various psychological interventions in asthma, including cognitive behavioral therapy (CBT), biofeedback, and various relaxation techniques [27]. Because there are no standardized outcomes measured across all studies, results are often conflicting. While CBT had a positive effect on asthma health care utilization, relaxation therapy had no significant effects; both did have positive effects on symptoms of depression and anxiety. Relaxation therapy had positive effects on relieving asthma symptoms such as cough and wheeze but CBT did not. Biofeedback and relaxation were the only interventions that had positive effect on improving lung function and decreasing medication usage [27].
In an RCT, Parry and colleagues evaluated the effects of CBT added to clinical care on asthma-specific fear when compared to standard clinical asthma care alone. They demonstrated a significant reduction in panic and fear related to asthma exacerbations using CBT [32].
Various other mind-body–based interventions, including meditation, yoga, and breathing techniques, have been evaluated as complementary asthma therapy. Several studies utilized the Buteyko breathing technique (BBT), which focuses on controlling breathing to restore normal levels of PaCo2 in order to improve tissue oxygenation and reduce bronchospasm. Cooper et al performed an RCT that evaluated asthma symptom scores and methacholine sensitivity (concentration of bronchial irritant causing decline in FEV1 > 20%) for the presence of bronchial hyperreactivity (BHR), a measure of asthma activity. The BBT group demonstrated a reduction in asthma symptoms and rescue inhaler use but no change in BHR [33]. Opat measured asthma QOL, asthma symptoms, rescue medication use, and lung function in patients who received instruction in BBT and patients in a sham control group. BBT was associated with improvement in asthma QOL and bronchodilator use but not in other outcome parameters [34]. Thomas et al demonstrated in an RCT involving asthma patients with symptoms of dysfunctional breathing that rebreathing-retraining physiotherapy improved asthma-related QOL compared with traditional nurse-provided education [35].
Physical Stress Management Interventions
Yoga, which involves various aspects of controlled breathing, stretching, and meditation techniques [36], aims to achieve synergy between the mind and body to produce a more relaxed psychophysiological state [37]. This popular modality is frequently used by patients, including those with asthma, for symptom control and disease management. Results from RCTs have varied in their reports of efficacy. The 2006 Allergic Rhinitis and Asthma (ARIA) work group performed a systematic review of 5 trials evaluating yoga and asthma. Though the quality of the trials varied greatly, the review demonstrated a possible benefit of yoga on asthma-related QOL but no other studied parameters [38]. QOL and hemodynamic improvement was also demonstrated in 1 RCT comparing yoga added to standard asthma therapy vs. standard therapy alone in female patients [37]. Cramer et al performed an extensive systematic review and meta-analysis of 14 RCTs evaluating the effects of yoga on all or some components of asthma-related QOL, asthma control, symptoms, and pulmonary function [39]. Though there may be some benefit of yoga breathing techniques on asthma-related QOL, the quality of these studies is very poor and reported results were highly variable. These limitations demonstrate the need for methodologically sound, standardized approaches to research in this field, which will be needed before definitive conclusions or treatment recommendations can be made [38,39].
Complementary and Alternative Medicine Interventions
Therapeutic massage, reflexology, spinal manipulation, and prayer are commonly used components of complementary medicine that are perceived by many to be helpful in asthma management [40,41]. However, the published data supporting these techniques is limited. In 2005, Hondras et al performed a Cochrane database review of RCTs evaluating manual therapy, including therapeutic massage, in asthma. Variations in measured outcomes, study design, and reporting made the evidence presented in the review difficult to interpret. Methodologically sound RCTs are needed before any inferences as to relative efficacy of these techniques can be drawn [42]. Since 2005, there have been no significant RCTs reported that would change this conclusion. Data on prayer, religious beliefs, and how these affect asthma and stress control are scarce. One nonrandomized patient reporting survey analysis to evaluate the presence of a high power in life and asthma medication adherence was reported by Ahmedani and colleagues. Results showed that overall medication adherence was low, particularly among those who believed a higher power was in control of their health [43].
Other relaxation methods for managing stress in asthma include music therapy [44] and art therapy [45,46]. Music therapy has had varying reported therapeutic success in other medical settings, such as cardiac rehabilitation [47] and prior to endoscopy [48]. Several studies have evaluated passive or active music therapy in various stages of asthma management with variable results reported. One RCT of patients admitted for asthma exacerbation evaluated the effectiveness of standard pulmonary rehabilitation for asthma with or without concomitant music therapy. Measured outcomes included lung function parameters (PEF and FEV1/FVC) and self-reported anxiety scales. There was a small improvement in PEF in women in the music therapy group. Secondary statistical analysis showed lung function improvements with music therapy only in the patients with mild asthma [44]. Art therapy, the opportunity to share feelings through the use of art materials and expressions, has been used effectively to reduce psychological distress in pediatric chronic disease. One RCT of 23 children examined the potential utility of art therapy in pediatric asthma management. While it did not affect number of exacerbations, art therapy dramatically improved quality of life in children with asthma by decreasing worry and anxiety. The effect persisted for at least 6 months after the intervention was completed [46].
Pharmacotherapy Interventions
Given that anxiety and depression are commonly reported in patients with asthma, particularly in severe and difficult to control disease [49], traditional pharmacologic treatment of anxiety and depression is often attempted. Both depression and anxiety in patients with asthma has been associated with poor asthma-related QOL, but depressive disorders were more commonly associated with poorer levels of asthma control [50]. The use of antidepressant medications, especially selective serotonin reuptake inhibitors (SSRIs), in this patient population has had varying success reported. One randomized placebo-controlled trial evaluated the use of citalopram in 90 adults with asthma and major depressive disorder. Not surprisingly, there was a positive effect on the primary outcome measuring depression using the Hamilton Rating Scale for Depression. Secondary outcome analysis also showed a decrease in oral corticosteroid use in the group treated with citalopram; however, no difference in asthma symptoms between groups was observed [51]. A similar but smaller RCT evaluated the use of escitalopram in major depression and severe asthma. The escitalopram group failed to show a statistical difference in depressive symptoms, asthma control, or oral prednisone use when compared with placebo [52].
The Future for Stress Management as a Fundamental Component of Asthma Care
Historically, avoidance of known triggers and use of pharmacologic maintenance and treatment modalities has been the cornerstone of asthma care. The recognition of excess psychological stress as a recognized trigger and treatment target is continuing to evolve in our therapeutic armamentarium. Our understanding of the effects of stress management in asthma patients provides clinical support for the neuroendocrine immune link between the bronchial inflammatory response characteristic in asthma and that of the human stress response. Understanding the relationships of psychological stress in asthma physiology, clinical morbidity, and therapeutic options is imperative, as the changing health care environment increasingly demands preventive, practical, cost-effective, evidence-based medicine. Some psychological stressors will no doubt be more difficult to address than others, but implementation of nonpharmacologic stress management paradigms should help improve effective asthma management across all patient demographics and should hopefully lead to decreased population health care costs, fewer days of work lost, and improved quality of life. Despite a clear molecular link between asthma, inflammation and stress and a clinical trend toward benefit, the heterogeneity of studies and poor quality evidence for each stress reduction modality make it difficult to draw any firm conclusions on the comparative efficacy of specific psychological interventions in asthma management programs. Mindfulness-based stress reduction has the highest quality evidence and shows the most promise thus far. Further research employing methodically sound RCTs that use standardized physiologic and nonphysiologic outcome measures is needed to elucidate the role for stress reduction interventions in routine clinical practice.
Corresponding author: Gailen D. Marshall Jr, MD, PhD, Div. of Clinical Immunology and Allergy, Dept. of Medicine, The University of Mississippi Medical Ctr., 2500 N. State St. N416 Jackson, MS 39216, [email protected].
Financial disclosures: None.
Author contributions: conception and design, CRP, AMW, GDM; drafting of article, CRP, AMW, GDM; critical revision of the article, CRP, AMW, GDM; administrative or technical support, GDM.
1. Kondo N. Socioeconomic disparities and health: impacts and pathways. J Epidemiol 2012;22:2–6.
2. Nakata A. Psychosocial job stress and immunity: a systematic review. Methods Mol Biol 2012;934:39–7.
3. Van Lieshout RJ, Macqueen GM. Relation between asthma and psychological distress: an old idea revisited. Chem Immunol Allergy 2012;98:1–13.
4. Marshall GD Jr. The adverse effects of psychological stress on immunoregulatory balance: applications to human inflammatory diseases. Immunol Allergy Clin North Am 2011;31:133–40.
5. Murphy VE, Gibson PG, Smith R, et al. Asthma during pregnancy: mechanisms and treatment implications. Eur Respir J 2005;25:1–750.
6. Harding SM. Acid reflux and asthma. Curr Opin Pulm Med 2003;9:42–5.
7. Umetsu DT, McIntire JJ, Akbari O, et al. Asthma: an epidemic of dysregulated immunity. Nat Immunol 2002;3:715–20.
8. Matricardi PM. Prevalence of atopy and asthma in eastern versus western Europe: why the difference? Ann Allergy Asthma Immunol 2001;87:24–7.
9. Murray CS, Woodcock A, Custovic A. The role of indoor allergen exposure in the development of sensitization and asthma. Curr Opin Allergy Clin Immunol 2001;1:407–12.
10. TePas EC, Umetsu DT. Immunotherapy of asthma and allergic diseases. Curr Opin Pediatr 2000;12:574–78.
11. Babu KS, Holgate ST. Newer therapies for asthma: a focus on anti-IgE. Indian J Chest Dis Allied Sci 2002;44:107–15.
12. Oh Y, Kim Y, Yoo S, et al. Association between stress and asthma symptoms: a population based study. Respirology 2004;9:363–8.
13. Sandberg S, Paton JY, Ahola S, et al. The role of acute and chronic stress in asthma attacks in children. Lancet 2000;356:982–7.
14. Pbert L, Madison JM, Druker S, et al. Effect of mindfulness training on asthma quality of life and lung function: a randomized controlled trial. Thorax 2012;67:769–76.
15. Wisnivesky JP, Lorenzo J, Feldman JM, et al. The relationship between perceived stress and morbidity among adult inner-city asthmatics. J Asthma 2010;47:100–4.
16. Janssens T, Verleden G, De Peuter S, et al. Inaccurate perception of asthma symptoms: a cognitive-affective framework and implications for asthma treatment. Clin Psychol Rev 2009;29:317–27.
17. Wright RJ, Cohen S, Carey V, et al. Parental stress as a predictor of wheezing in infancy: a prospective birth-cohort study. Am J Resp Crit Care Med 2002;165:358–65.
18. Wright RJ, Mitchell H, Visness CM, et al. Community violence and asthma morbidity in the Inner-City Asthma Study. Am J Public Health 2004;94:625–32.
19. Michel FB. Psychology of the allergic patient. Allergy 1994;49:28–30.
20. Yonas MA, Lange NE, Celedon JC. Psychosocial stress and asthma morbidity. Curr Opin Allergy Clin Immunol 2012;12:202–10.
21. Apter AJ, Garcia LA, Boyd RC, et al. Exposure to community violence is associated with asthma hospitalizations and emergency department visits. J Allergy Clin Immunol 2010;126:552–7.
22. Wright RJ. Epidemiology of stress and asthma: from constricting communities and fragile families to epigenetics. Immunol Allergy Clin North Am 2011;31:19–39.
23. Tyagi A, Cohen M. Yoga and hypertension: a systematic review. Altern Ther Health Med 2014;20:32-59.
24. Moore CJ, Cunningham SA. Social position, psychological stress, and obesity: a systematic review. J Acad Nutr Diet 2012;112:518–26.
25. Plack K, Herpertz S, Petrak F. Behavioral medicine interventions in diabetes. Curr Opin Psychiatry 2010;23:131–8.
26. Clucas C, Sibley E, Harding R, et al. A systematic review of interventions for anxiety in people with HIV. Psychol Health Med 2011;16:528–47.
27. Yorke J, Fleming SL, Shuldham C. Psychological interventions for adults with asthma: a systematic review. Respir Med 2007;101:1–14.
28. Merkes M. Mindfulness-based stress reduction for people with chronic diseases. Aust J Prim Health 2010;16:200–10.
29. Kopf S, Oikonomou D, Hartmann M. Effects of stress reduction on cardiovascular risk factors in type 2 diabetes patients with early kidney disease- results of a randomized controlled trial (HEIDIS). Exp Clin Endocrinol Diabetes 2014;122:341–9.
30. Musial F, Bussing A, Heusser P, et al. Mindfulness-based stress reduction for integrative cancer care- a summary of evidence. Forsch Komplementmed 2011;18:192–202.
31. Shigaki CL, Glass B, Schopp LH. Mindfulness-based stress reduction in medical settings. J Clin Psychl Med Settings 2006;13:209-16.
32. Parry GD, Cooper CL, Moore JM. Cognitive behavioural intervention for adults with anxiety complications of asthma: prospective randomized trial. Respir Med 2012;106;802–10.
33. Cooper S, Oborne J, Newton S, et al. Effect of two breathing exercises (Buteyko and pranayama) in asthma: a randomized controlled trial. Thorax 2003;58:674–9.
34. Opat AJ, Cohen MM, Bailey MJ, et al. A clinical trial of the Buteyko breathing technique in asthma as taught by a video. J Asthma 2000;37:557–64.
35. Thomas M, McKinley RK, Freeman E, et al. Breathing retraining for dysfunctional breathing in asthma: a randomized controlled trial. Thorax 2003;58:110–15.
36. Markham AW, Wilkinson JM. Complementary and alternative medicines (CAM) in the management of asthma: an examination of the evidence. J Asthma 2004;41:131–9.
37. Bidwell AM, Yazel B, Davin D, et al. Yoga training improves quality of life in women with asthma. J Altern Complement Med 2012;18:749–55.
38. Passalacqua G, Bousquet PJ, Carlsen KH, et al. ARIA update: I- Systematic review of complementary and alternative medicine for rhinitis and asthma. J Allergy Clin Immunol 2006;117:1054–62.
39. Cramer H, Posadzki P, Dobos G, et al. Yoga for asthma: a systematic review and meta-analysis. Ann Allergy Asthma Immunol 2014;112:503–10.
40. Slader CA, Reddel HK, Jenkins CR, et al. Complementary and alternative medicine use in asthma: who is using what? Respirology 2006;11:373–87.
41. Silvers WS, Bailey HK. Integrative approach to allergy and asthma using complementary and alternative medicine. Ann Allergy Asthma Immunol 2014;112;280-85.
42. Hondras MA, Linde K, Jones AP. Manual therapy for asthma. Cochrane Database Syst Rev 2005;(2):CD001002.
43. Ahmedani BK, Peterson EL, Wells KE, et al. Asthma medication adherence: the role of God and other health locus of control factors. Ann Allergy Asthma Immunol 2013;110:75–9.
44. Sliwka A, Nowobilski R, Polczyk R, et al. Mild asthmatics benefit from music therapy. J Asthma 2012;49:401–8.
45. Clarke SA, Calam R. The effectiveness of psychosocial interventions designed to improve health-related quality of life (HRQOL) amongst asthmatic children and their families: a systematic review. Qual Life Res 2012;21:747–64.
46. Beebe A, Gelfand EW, Bender B. A randomized trial to test the effectiveness of art therapy for children with asthma. J Allergy Clin Immunol 2010;126:262–6.
47. Metzger LK. Assessment of use of music by patients participating in cardiac rehabilitation. J Music Ther 2004;41:55–69.
48. El-Hassan H, McKeown K, Muller AF. Clinical trial: music reduces anxiety levels in patients attending for endoscopy. Aliment Pharmacol Ther 2009;30:718–24.
49. Thomas M, Bruton An, Moffatt M, et al. Asthma and psychological dysfunction. Prim Care Respir J 2011;20:250–6.
50. Lavoie KL, Bacon SL, Barone S, et al. What is worse for asthma control and quality of life: depressive disorders, anxiety disorders, or both? Chest 2006;130:1039–47.
51. Brown ES, Vigil L, Khan DA, et al. A randomized trial of citalopram versus placebo in outpatients with asthma and major depressive disorder: a proof of concept study. Biol Psychiatry 2005;58:865–70.
52. Brown ES, Howard C, Khan DA, et al. Escitalopram for severe asthma and major depressive disorder: a randomized, double-blind, placebo-controlled proof-of-concept study. Psychosomatics 2012;53:75–80.
1. Kondo N. Socioeconomic disparities and health: impacts and pathways. J Epidemiol 2012;22:2–6.
2. Nakata A. Psychosocial job stress and immunity: a systematic review. Methods Mol Biol 2012;934:39–7.
3. Van Lieshout RJ, Macqueen GM. Relation between asthma and psychological distress: an old idea revisited. Chem Immunol Allergy 2012;98:1–13.
4. Marshall GD Jr. The adverse effects of psychological stress on immunoregulatory balance: applications to human inflammatory diseases. Immunol Allergy Clin North Am 2011;31:133–40.
5. Murphy VE, Gibson PG, Smith R, et al. Asthma during pregnancy: mechanisms and treatment implications. Eur Respir J 2005;25:1–750.
6. Harding SM. Acid reflux and asthma. Curr Opin Pulm Med 2003;9:42–5.
7. Umetsu DT, McIntire JJ, Akbari O, et al. Asthma: an epidemic of dysregulated immunity. Nat Immunol 2002;3:715–20.
8. Matricardi PM. Prevalence of atopy and asthma in eastern versus western Europe: why the difference? Ann Allergy Asthma Immunol 2001;87:24–7.
9. Murray CS, Woodcock A, Custovic A. The role of indoor allergen exposure in the development of sensitization and asthma. Curr Opin Allergy Clin Immunol 2001;1:407–12.
10. TePas EC, Umetsu DT. Immunotherapy of asthma and allergic diseases. Curr Opin Pediatr 2000;12:574–78.
11. Babu KS, Holgate ST. Newer therapies for asthma: a focus on anti-IgE. Indian J Chest Dis Allied Sci 2002;44:107–15.
12. Oh Y, Kim Y, Yoo S, et al. Association between stress and asthma symptoms: a population based study. Respirology 2004;9:363–8.
13. Sandberg S, Paton JY, Ahola S, et al. The role of acute and chronic stress in asthma attacks in children. Lancet 2000;356:982–7.
14. Pbert L, Madison JM, Druker S, et al. Effect of mindfulness training on asthma quality of life and lung function: a randomized controlled trial. Thorax 2012;67:769–76.
15. Wisnivesky JP, Lorenzo J, Feldman JM, et al. The relationship between perceived stress and morbidity among adult inner-city asthmatics. J Asthma 2010;47:100–4.
16. Janssens T, Verleden G, De Peuter S, et al. Inaccurate perception of asthma symptoms: a cognitive-affective framework and implications for asthma treatment. Clin Psychol Rev 2009;29:317–27.
17. Wright RJ, Cohen S, Carey V, et al. Parental stress as a predictor of wheezing in infancy: a prospective birth-cohort study. Am J Resp Crit Care Med 2002;165:358–65.
18. Wright RJ, Mitchell H, Visness CM, et al. Community violence and asthma morbidity in the Inner-City Asthma Study. Am J Public Health 2004;94:625–32.
19. Michel FB. Psychology of the allergic patient. Allergy 1994;49:28–30.
20. Yonas MA, Lange NE, Celedon JC. Psychosocial stress and asthma morbidity. Curr Opin Allergy Clin Immunol 2012;12:202–10.
21. Apter AJ, Garcia LA, Boyd RC, et al. Exposure to community violence is associated with asthma hospitalizations and emergency department visits. J Allergy Clin Immunol 2010;126:552–7.
22. Wright RJ. Epidemiology of stress and asthma: from constricting communities and fragile families to epigenetics. Immunol Allergy Clin North Am 2011;31:19–39.
23. Tyagi A, Cohen M. Yoga and hypertension: a systematic review. Altern Ther Health Med 2014;20:32-59.
24. Moore CJ, Cunningham SA. Social position, psychological stress, and obesity: a systematic review. J Acad Nutr Diet 2012;112:518–26.
25. Plack K, Herpertz S, Petrak F. Behavioral medicine interventions in diabetes. Curr Opin Psychiatry 2010;23:131–8.
26. Clucas C, Sibley E, Harding R, et al. A systematic review of interventions for anxiety in people with HIV. Psychol Health Med 2011;16:528–47.
27. Yorke J, Fleming SL, Shuldham C. Psychological interventions for adults with asthma: a systematic review. Respir Med 2007;101:1–14.
28. Merkes M. Mindfulness-based stress reduction for people with chronic diseases. Aust J Prim Health 2010;16:200–10.
29. Kopf S, Oikonomou D, Hartmann M. Effects of stress reduction on cardiovascular risk factors in type 2 diabetes patients with early kidney disease- results of a randomized controlled trial (HEIDIS). Exp Clin Endocrinol Diabetes 2014;122:341–9.
30. Musial F, Bussing A, Heusser P, et al. Mindfulness-based stress reduction for integrative cancer care- a summary of evidence. Forsch Komplementmed 2011;18:192–202.
31. Shigaki CL, Glass B, Schopp LH. Mindfulness-based stress reduction in medical settings. J Clin Psychl Med Settings 2006;13:209-16.
32. Parry GD, Cooper CL, Moore JM. Cognitive behavioural intervention for adults with anxiety complications of asthma: prospective randomized trial. Respir Med 2012;106;802–10.
33. Cooper S, Oborne J, Newton S, et al. Effect of two breathing exercises (Buteyko and pranayama) in asthma: a randomized controlled trial. Thorax 2003;58:674–9.
34. Opat AJ, Cohen MM, Bailey MJ, et al. A clinical trial of the Buteyko breathing technique in asthma as taught by a video. J Asthma 2000;37:557–64.
35. Thomas M, McKinley RK, Freeman E, et al. Breathing retraining for dysfunctional breathing in asthma: a randomized controlled trial. Thorax 2003;58:110–15.
36. Markham AW, Wilkinson JM. Complementary and alternative medicines (CAM) in the management of asthma: an examination of the evidence. J Asthma 2004;41:131–9.
37. Bidwell AM, Yazel B, Davin D, et al. Yoga training improves quality of life in women with asthma. J Altern Complement Med 2012;18:749–55.
38. Passalacqua G, Bousquet PJ, Carlsen KH, et al. ARIA update: I- Systematic review of complementary and alternative medicine for rhinitis and asthma. J Allergy Clin Immunol 2006;117:1054–62.
39. Cramer H, Posadzki P, Dobos G, et al. Yoga for asthma: a systematic review and meta-analysis. Ann Allergy Asthma Immunol 2014;112:503–10.
40. Slader CA, Reddel HK, Jenkins CR, et al. Complementary and alternative medicine use in asthma: who is using what? Respirology 2006;11:373–87.
41. Silvers WS, Bailey HK. Integrative approach to allergy and asthma using complementary and alternative medicine. Ann Allergy Asthma Immunol 2014;112;280-85.
42. Hondras MA, Linde K, Jones AP. Manual therapy for asthma. Cochrane Database Syst Rev 2005;(2):CD001002.
43. Ahmedani BK, Peterson EL, Wells KE, et al. Asthma medication adherence: the role of God and other health locus of control factors. Ann Allergy Asthma Immunol 2013;110:75–9.
44. Sliwka A, Nowobilski R, Polczyk R, et al. Mild asthmatics benefit from music therapy. J Asthma 2012;49:401–8.
45. Clarke SA, Calam R. The effectiveness of psychosocial interventions designed to improve health-related quality of life (HRQOL) amongst asthmatic children and their families: a systematic review. Qual Life Res 2012;21:747–64.
46. Beebe A, Gelfand EW, Bender B. A randomized trial to test the effectiveness of art therapy for children with asthma. J Allergy Clin Immunol 2010;126:262–6.
47. Metzger LK. Assessment of use of music by patients participating in cardiac rehabilitation. J Music Ther 2004;41:55–69.
48. El-Hassan H, McKeown K, Muller AF. Clinical trial: music reduces anxiety levels in patients attending for endoscopy. Aliment Pharmacol Ther 2009;30:718–24.
49. Thomas M, Bruton An, Moffatt M, et al. Asthma and psychological dysfunction. Prim Care Respir J 2011;20:250–6.
50. Lavoie KL, Bacon SL, Barone S, et al. What is worse for asthma control and quality of life: depressive disorders, anxiety disorders, or both? Chest 2006;130:1039–47.
51. Brown ES, Vigil L, Khan DA, et al. A randomized trial of citalopram versus placebo in outpatients with asthma and major depressive disorder: a proof of concept study. Biol Psychiatry 2005;58:865–70.
52. Brown ES, Howard C, Khan DA, et al. Escitalopram for severe asthma and major depressive disorder: a randomized, double-blind, placebo-controlled proof-of-concept study. Psychosomatics 2012;53:75–80.