User login
Why Hospitalists Should Focus on Patient-Care Basics


We all are too familiar with the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey, a standardized set of questions randomly deployed to recently discharged patients. More recently, hospitalists have noticed the introduction of the Clinician and Groups Consumer Assessment of Healthcare Providers and Systems (CG-CAHPS) survey, randomly deployed to recently evaluated ambulatory patients. HCAHPS has been publicly reported since 2008. CG-CAHPS will be in the near future. In addition to these, there are a variety of other types of CAHPS surveys, ranging from ambulatory surgery to patient-centered medical homes. For HCAHPS alone, there are more than 8,200 adult surveys completed every day from almost 4,000 different U.S. hospitals.1
In addition to these surveys being publicly reported and widely viewed online by patients, payors, and employers, the results now are tightly coupled to the reimbursement of hospitals and, in some cases, individual providers. As of October 2012, Medicare has relegated 30% of its hospital value-based purchasing (VBP) program to the results of hospitals’ HCAPHS survey results. For the foreseeable future, about one-third of the financial bonus—or penalty—of a hospital rests in the hands of how well our patients perceive their care. Many individual hospitals and practice groups have started coupling individual physicians’ compensation to their patients’ CAHPS scores. Within the (approximately) seven minutes it takes to complete the survey, our patients determine millions of dollars of physician and hospital reimbursement.1
With all of the financial and reputational emphasis on HCAHPS, it is vital that hospitalists understand what it is these surveys are actually measuring, and if they have any correlation with the quality of the care the patient receives. The questions currently address 11 different domains of hospital care:
- Communication with doctors;
- Communication with nurses;
- Responsiveness of hospital staff;
- Pain management;
- Communication about medicines;
- Discharge information;
- Cleanliness of hospital environment;
- Quietness of hospital environment;
- Transitions of care;
- Overall rating of the hospital; and
- Willingness to recommend the hospital.
As the domains of care are all very different, one can imagine a wide range of answers to the various questions; a patient can perceive that communication was excellent but the quietness and cleanliness was disgraceful. And, depending on what they consider the most important aspects of their stay, they therefore may rate their overall stay as excellent or disgraceful. Why? Because each of these rest in the eye of the beholder.
But to keep pace, hospitals and providers across the country have invested millions of hours dissecting the meaning of the results and trying to improve upon them. My hospital has struggled for years with the “cleanliness” question, trying to figure out what our patients are trying to tell us: that we need to sweep and mop more often, that hospital supplies are cluttering our patient rooms, that the trashcans are overflowing or within eyesight? When we ask focus groups, we often get all of the above—and then try to implement several solutions all at once.
The quietness question is much easier to interpret but certainly difficult to improve upon. We have implemented “yacker trackers,” “quiet time,” and soft-wheeled trash cans. And the results of the surveys take months to come back and get analyzed, so it is difficult to quickly know if your interventions are actually working. Given that so many hospitals and providers are back-flipping to “play to the test,” we really need some validation that care is truly improving based on this patient feedback.
A recent New York Times article calls to light a natural paradox in the medical field, in that patients who understand more about disease processes and medical information actually feel less, rather than more, informed. In other words, those who are actually the most well-informed may rate communication the lowest. The article also calls to light the natural paradox between providers being honest and providers being likable, especially considering they routinely have to deliver messages that patients do not want to hear:
- You need to quit smoking;
- Your weight is affecting your health; and
- Your disease is not curable.
Given these natural paradoxes, the article argues that it is difficult to reconcile why hospitals and providers should be held financially accountable for their patients’ perception of care, when that perception may not equate to “real” care quality.2
However, there is some evidence that patient satisfaction surveys may actually be good proxies for care quality. A large study found that hospitals with the highest quartile HCAHPS ratings also have about 2%-3% higher quality scores for acute MI, CHF, pneumonia, and surgery, compared to those in the lowest quartile. The highest scoring hospitals also have about 2%-3% lower readmission rates for acute MI, CHF, and pneumonia.3,4 And, similar to other quality metrics, there is evidence that the longer a hospital has been administering HCAHPS, the better are their scores. So maybe hospital systems and providers can improve not only the perception a patient has of the quality of the care they received, but improve the quality, as measured by the patient’s perception.
Although there are legitimate arguments on both sides as to whether a patient’s perception of care reflects “real” care quality, in the end these CAHPS surveys are, and have been publicly reported, and will be tightly coupled to reimbursement for hospitals and (likely) providers for the foreseeable future. So in the meantime, we should continue to focus on patient-centered care, take seriously any voiced concerns, and have a relentless pursuit of perfection for how patients perceive their care. Because in the end, you would do it for your family so we should do it for our patients.
References
- Centers for Medicare & Medicaid Services. Spring 2013 HCAHPS Executive Insight Letter. Available at: www.hcahpsonline.org/Executive_Insight. Accessed Aug. 15, 2013.
- Rosenbaum L. When doctors tell patients what they don’t want to hear. The New Yorker website. Available at: www.newyorker.com/online/blogs/elements/2013/07/when-doctors-tell-patients-what-they-dont-want-to-hear.html. Published July 23, 2013. Accessed Aug. 15, 2013.
- Jha AK, Orav EJ, Zheng J, Epstein AM. Patients' perception of hospital care in the US. New Eng J Med. 2008;359(18):1921-1931.
- Boulding W, Glickman SW, Manary MP, Schulman KA, Staelin R. Relationship between patient satisfaction with inpatient care and hospital readmission within 30 days. Am J Manag Care. 2011;17(1):41-48.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
We all are too familiar with the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey, a standardized set of questions randomly deployed to recently discharged patients. More recently, hospitalists have noticed the introduction of the Clinician and Groups Consumer Assessment of Healthcare Providers and Systems (CG-CAHPS) survey, randomly deployed to recently evaluated ambulatory patients. HCAHPS has been publicly reported since 2008. CG-CAHPS will be in the near future. In addition to these, there are a variety of other types of CAHPS surveys, ranging from ambulatory surgery to patient-centered medical homes. For HCAHPS alone, there are more than 8,200 adult surveys completed every day from almost 4,000 different U.S. hospitals.1
In addition to these surveys being publicly reported and widely viewed online by patients, payors, and employers, the results now are tightly coupled to the reimbursement of hospitals and, in some cases, individual providers. As of October 2012, Medicare has relegated 30% of its hospital value-based purchasing (VBP) program to the results of hospitals’ HCAPHS survey results. For the foreseeable future, about one-third of the financial bonus—or penalty—of a hospital rests in the hands of how well our patients perceive their care. Many individual hospitals and practice groups have started coupling individual physicians’ compensation to their patients’ CAHPS scores. Within the (approximately) seven minutes it takes to complete the survey, our patients determine millions of dollars of physician and hospital reimbursement.1
With all of the financial and reputational emphasis on HCAHPS, it is vital that hospitalists understand what it is these surveys are actually measuring, and if they have any correlation with the quality of the care the patient receives. The questions currently address 11 different domains of hospital care:
- Communication with doctors;
- Communication with nurses;
- Responsiveness of hospital staff;
- Pain management;
- Communication about medicines;
- Discharge information;
- Cleanliness of hospital environment;
- Quietness of hospital environment;
- Transitions of care;
- Overall rating of the hospital; and
- Willingness to recommend the hospital.
As the domains of care are all very different, one can imagine a wide range of answers to the various questions; a patient can perceive that communication was excellent but the quietness and cleanliness was disgraceful. And, depending on what they consider the most important aspects of their stay, they therefore may rate their overall stay as excellent or disgraceful. Why? Because each of these rest in the eye of the beholder.
But to keep pace, hospitals and providers across the country have invested millions of hours dissecting the meaning of the results and trying to improve upon them. My hospital has struggled for years with the “cleanliness” question, trying to figure out what our patients are trying to tell us: that we need to sweep and mop more often, that hospital supplies are cluttering our patient rooms, that the trashcans are overflowing or within eyesight? When we ask focus groups, we often get all of the above—and then try to implement several solutions all at once.
The quietness question is much easier to interpret but certainly difficult to improve upon. We have implemented “yacker trackers,” “quiet time,” and soft-wheeled trash cans. And the results of the surveys take months to come back and get analyzed, so it is difficult to quickly know if your interventions are actually working. Given that so many hospitals and providers are back-flipping to “play to the test,” we really need some validation that care is truly improving based on this patient feedback.
A recent New York Times article calls to light a natural paradox in the medical field, in that patients who understand more about disease processes and medical information actually feel less, rather than more, informed. In other words, those who are actually the most well-informed may rate communication the lowest. The article also calls to light the natural paradox between providers being honest and providers being likable, especially considering they routinely have to deliver messages that patients do not want to hear:
- You need to quit smoking;
- Your weight is affecting your health; and
- Your disease is not curable.
Given these natural paradoxes, the article argues that it is difficult to reconcile why hospitals and providers should be held financially accountable for their patients’ perception of care, when that perception may not equate to “real” care quality.2
However, there is some evidence that patient satisfaction surveys may actually be good proxies for care quality. A large study found that hospitals with the highest quartile HCAHPS ratings also have about 2%-3% higher quality scores for acute MI, CHF, pneumonia, and surgery, compared to those in the lowest quartile. The highest scoring hospitals also have about 2%-3% lower readmission rates for acute MI, CHF, and pneumonia.3,4 And, similar to other quality metrics, there is evidence that the longer a hospital has been administering HCAHPS, the better are their scores. So maybe hospital systems and providers can improve not only the perception a patient has of the quality of the care they received, but improve the quality, as measured by the patient’s perception.
Although there are legitimate arguments on both sides as to whether a patient’s perception of care reflects “real” care quality, in the end these CAHPS surveys are, and have been publicly reported, and will be tightly coupled to reimbursement for hospitals and (likely) providers for the foreseeable future. So in the meantime, we should continue to focus on patient-centered care, take seriously any voiced concerns, and have a relentless pursuit of perfection for how patients perceive their care. Because in the end, you would do it for your family so we should do it for our patients.
References
- Centers for Medicare & Medicaid Services. Spring 2013 HCAHPS Executive Insight Letter. Available at: www.hcahpsonline.org/Executive_Insight. Accessed Aug. 15, 2013.
- Rosenbaum L. When doctors tell patients what they don’t want to hear. The New Yorker website. Available at: www.newyorker.com/online/blogs/elements/2013/07/when-doctors-tell-patients-what-they-dont-want-to-hear.html. Published July 23, 2013. Accessed Aug. 15, 2013.
- Jha AK, Orav EJ, Zheng J, Epstein AM. Patients' perception of hospital care in the US. New Eng J Med. 2008;359(18):1921-1931.
- Boulding W, Glickman SW, Manary MP, Schulman KA, Staelin R. Relationship between patient satisfaction with inpatient care and hospital readmission within 30 days. Am J Manag Care. 2011;17(1):41-48.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
We all are too familiar with the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey, a standardized set of questions randomly deployed to recently discharged patients. More recently, hospitalists have noticed the introduction of the Clinician and Groups Consumer Assessment of Healthcare Providers and Systems (CG-CAHPS) survey, randomly deployed to recently evaluated ambulatory patients. HCAHPS has been publicly reported since 2008. CG-CAHPS will be in the near future. In addition to these, there are a variety of other types of CAHPS surveys, ranging from ambulatory surgery to patient-centered medical homes. For HCAHPS alone, there are more than 8,200 adult surveys completed every day from almost 4,000 different U.S. hospitals.1
In addition to these surveys being publicly reported and widely viewed online by patients, payors, and employers, the results now are tightly coupled to the reimbursement of hospitals and, in some cases, individual providers. As of October 2012, Medicare has relegated 30% of its hospital value-based purchasing (VBP) program to the results of hospitals’ HCAPHS survey results. For the foreseeable future, about one-third of the financial bonus—or penalty—of a hospital rests in the hands of how well our patients perceive their care. Many individual hospitals and practice groups have started coupling individual physicians’ compensation to their patients’ CAHPS scores. Within the (approximately) seven minutes it takes to complete the survey, our patients determine millions of dollars of physician and hospital reimbursement.1
With all of the financial and reputational emphasis on HCAHPS, it is vital that hospitalists understand what it is these surveys are actually measuring, and if they have any correlation with the quality of the care the patient receives. The questions currently address 11 different domains of hospital care:
- Communication with doctors;
- Communication with nurses;
- Responsiveness of hospital staff;
- Pain management;
- Communication about medicines;
- Discharge information;
- Cleanliness of hospital environment;
- Quietness of hospital environment;
- Transitions of care;
- Overall rating of the hospital; and
- Willingness to recommend the hospital.
As the domains of care are all very different, one can imagine a wide range of answers to the various questions; a patient can perceive that communication was excellent but the quietness and cleanliness was disgraceful. And, depending on what they consider the most important aspects of their stay, they therefore may rate their overall stay as excellent or disgraceful. Why? Because each of these rest in the eye of the beholder.
But to keep pace, hospitals and providers across the country have invested millions of hours dissecting the meaning of the results and trying to improve upon them. My hospital has struggled for years with the “cleanliness” question, trying to figure out what our patients are trying to tell us: that we need to sweep and mop more often, that hospital supplies are cluttering our patient rooms, that the trashcans are overflowing or within eyesight? When we ask focus groups, we often get all of the above—and then try to implement several solutions all at once.
The quietness question is much easier to interpret but certainly difficult to improve upon. We have implemented “yacker trackers,” “quiet time,” and soft-wheeled trash cans. And the results of the surveys take months to come back and get analyzed, so it is difficult to quickly know if your interventions are actually working. Given that so many hospitals and providers are back-flipping to “play to the test,” we really need some validation that care is truly improving based on this patient feedback.
A recent New York Times article calls to light a natural paradox in the medical field, in that patients who understand more about disease processes and medical information actually feel less, rather than more, informed. In other words, those who are actually the most well-informed may rate communication the lowest. The article also calls to light the natural paradox between providers being honest and providers being likable, especially considering they routinely have to deliver messages that patients do not want to hear:
- You need to quit smoking;
- Your weight is affecting your health; and
- Your disease is not curable.
Given these natural paradoxes, the article argues that it is difficult to reconcile why hospitals and providers should be held financially accountable for their patients’ perception of care, when that perception may not equate to “real” care quality.2
However, there is some evidence that patient satisfaction surveys may actually be good proxies for care quality. A large study found that hospitals with the highest quartile HCAHPS ratings also have about 2%-3% higher quality scores for acute MI, CHF, pneumonia, and surgery, compared to those in the lowest quartile. The highest scoring hospitals also have about 2%-3% lower readmission rates for acute MI, CHF, and pneumonia.3,4 And, similar to other quality metrics, there is evidence that the longer a hospital has been administering HCAHPS, the better are their scores. So maybe hospital systems and providers can improve not only the perception a patient has of the quality of the care they received, but improve the quality, as measured by the patient’s perception.
Although there are legitimate arguments on both sides as to whether a patient’s perception of care reflects “real” care quality, in the end these CAHPS surveys are, and have been publicly reported, and will be tightly coupled to reimbursement for hospitals and (likely) providers for the foreseeable future. So in the meantime, we should continue to focus on patient-centered care, take seriously any voiced concerns, and have a relentless pursuit of perfection for how patients perceive their care. Because in the end, you would do it for your family so we should do it for our patients.
References
- Centers for Medicare & Medicaid Services. Spring 2013 HCAHPS Executive Insight Letter. Available at: www.hcahpsonline.org/Executive_Insight. Accessed Aug. 15, 2013.
- Rosenbaum L. When doctors tell patients what they don’t want to hear. The New Yorker website. Available at: www.newyorker.com/online/blogs/elements/2013/07/when-doctors-tell-patients-what-they-dont-want-to-hear.html. Published July 23, 2013. Accessed Aug. 15, 2013.
- Jha AK, Orav EJ, Zheng J, Epstein AM. Patients' perception of hospital care in the US. New Eng J Med. 2008;359(18):1921-1931.
- Boulding W, Glickman SW, Manary MP, Schulman KA, Staelin R. Relationship between patient satisfaction with inpatient care and hospital readmission within 30 days. Am J Manag Care. 2011;17(1):41-48.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Hospitalists as Industrial Engineers

Wikipedia defines “industrial engineering” as a branch of engineering that deals with the optimization of complex processes or systems. It goes on to link industrial engineering to “operations” and use of quantitative methods to “specify, predict, and evaluate” results. Any hospitalist that’s been tapped to reduce length of stay, help manage readmissions, implement an electronic health record, or increase the quality of care likely can relate to that definition. It seems to me that hospitalists often are the de facto industrial engineers in many of our hospitals.
The hospitalist as an industrial engineer makes perfect sense. What other group of physicians, nurse practitioners, and physician assistants provide services in virtually any clinical venue, from ED to DC, from (occasionally) PACU to ICU, the wards, and even post-discharge? Hospitalists see it all, from the first few hours of life (pediatrics) to life’s last stages (palliative care) and all stages in between. As a parody to “there’s an app for that,” Dr. Mindy Kantsiper, a hospitalist in Columbia, Md., says if there’s something that needs to be fixed, “there’s a hospitalist for that.” We are the Swiss Army knives of the medical world.
Looking through the HMX “Practice Management” discussions on the SHM website (www.hospitalmedicine.com/xchange) confirms my belief. Topics are as varied as using RNs in hospitalist practices, medication reconciliation, billing, outpatient orders (!!) after discharge, and patient-centered care/patient satisfaction. And that was just the last two weeks!
Type “hospitalist” into PubMed, and the words that auto-populate are: model, care, quality, discharge, communication, program, and handoff—all words I think of as system-related issues. Oh, sure, there are clinical-related topics, too, of course, just like for the “organ-based” specialties. However, none of the common organ-based specialties had any words auto-populate in PubMed that could be deemed related to “industrial engineering.”
Engineer Training
Like all engineers, we de facto industrial engineers need tools and skills to be effective at in our new engineering role. While we may not need slide rules and calculus like a more traditional engineer, many of the new skills we will need as industrial engineers were not taught in medical school, and the tools were not readily available for us to use in our training.
Fortunately, there are a plethora of options for us budding, de facto industrial engineers. Here are the ones I believe you will need and where to get them:
Skill No. 1: Negotiation.
HM is a team sport, and teams bring interpersonal dynamics and tension and conflict. Effective negotiation skills can help hospitalists use conflict to spur team growth and development rather than team dysfunction.
Tools: SHM’s Leadership Academies have effective negotiation modules in each of the leveled courses. If you can’t spare the time, then books to read include “Getting to Yes” by Fisher and Ury, or “Renegotiating Health Care” by Leonard Marcus (he lectures at SHM’s leadership academies).
Skill No. 2: Data analytics.
All engineers, including industrial engineers, need to be able to evaluate. Whether it’s quality and safety, clinical operations, or financial improvement, if you don’t measure it, you can’t change it. Some of the data will be handed to you, and you need to know the strengths and weaknesses to best interpret it. Some data you will need to define and develop measurement systems for on your own, and even basic dashboard development requires understanding data.
Tools: Wow. There are a lot here, so I am only going to mention the highlights. You could get your MBA, or MPH, or even a PhD! You certainly could train to become a “true” diploma-carrying industrial engineer. And I know of a few insightful hospitals that employ them. A less in-depth, but cheaper and faster, option is to take specific courses related to your area of interest.
The SHM-AAIM Quality and Safety Educators Academy and SHM’s Leadership Academies are two great examples. Participating in a mentored project (i.e., Project BOOST) provides structure and an experienced mentor with a cadre of experts to back them up. Many institutions have courses on data analytics, basic finance, and quality improvement. The easiest, cheapest, and probably the most common is to find a mentor at your own institution. CFOs, CNOs, CQOs, and CMOs often are eager to partner with clinicians—and frequently are delighted to talk about their areas of expertise.
Skill No. 3: Leadership.
I don’t know many leaders who were born that way. Most learned through experience and continuous self-improvement. Understanding your personality traits, the traits of others (as an introvert, I still am trying to understand how extroverts work, especially my wife), and how to get all of those different personalities to work together as a team is an important component of any team-based engineering success.
Tools: I have found the books “From Good to Great” by Jim Collins and “Switch” by Chip and Dan Heath to be invaluable. I think another one of my recent reads, “Drive” by Daniel Pink, had important lessons, too. Formal courses, such as SHM’s Leadership Academies, QSEA, and those offered by the American Hospital Association, are designed to provide hospitalists with the leadership skills they need in a variety of hospital environments.
Skill No. 4: Thinking “system” instead of “individual.”
So many of us were trained that to make improvements, we just need to “be better,” to know more, try harder, and to work longer. Good industrial engineers design systems that make it easier for our doctors, healthcare providers, and patients to succeed. Of course, we need to be accountable, too, but supportive systems are a key component to successful individuals. The airline industry learned this long ago.
Tools: I really think “Switch” is an excellent read for those of us trying to help re-engineer our complex systems. It discusses how humans are both rational and emotional, and how our environment can help both sides succeed. Another helpful tool for me is asking “why” whenever someone says “if only they would do something differently for a better outcome…”
For example, “if only the hospitalists would discharge before 2 p.m.,” or “if only the ED didn’t clump their admissions,” or “if only the nurse didn’t call during rounds”—these are all classic systems problems, not people problems, and the solution isn’t to mandate 2 p.m. discharges, or stand up in a meeting finger pointing at the ED, or admonish a nurse for calling during rounds. The solution is to find out why these behaviors occur, then eliminate, change, or minimize the reasons.
Hospitalists don’t discharge by 2 p.m. often because they are waiting on tests; ED docs work in an environment that has highly variable workloads, coupled with dysfunctional systems that promote “batching” work patterns; and nurses may not be included in rounds but still need to be able to manage minute-to-minute patient-care needs. Sure, there are a few bad apples that need to be scolded, but I bet most of the issues at your hospital aren’t related to evildoers but good people who are often trapped in dysfunctional, antiquated systems and are just trying to do the best they can for their patients.
In Closing
I’d like to say thank you to all of the “de facto” industrial engineers out there. Keep up the critically important work of that most complex system—the hospital.
Dr. Howell is president of SHM, chief of the division of hospital medicine at Johns Hopkins Bayview in Baltimore, and spends a significant part of his time and research on hospital operations. Email questions or comments to [email protected].
Wikipedia defines “industrial engineering” as a branch of engineering that deals with the optimization of complex processes or systems. It goes on to link industrial engineering to “operations” and use of quantitative methods to “specify, predict, and evaluate” results. Any hospitalist that’s been tapped to reduce length of stay, help manage readmissions, implement an electronic health record, or increase the quality of care likely can relate to that definition. It seems to me that hospitalists often are the de facto industrial engineers in many of our hospitals.
The hospitalist as an industrial engineer makes perfect sense. What other group of physicians, nurse practitioners, and physician assistants provide services in virtually any clinical venue, from ED to DC, from (occasionally) PACU to ICU, the wards, and even post-discharge? Hospitalists see it all, from the first few hours of life (pediatrics) to life’s last stages (palliative care) and all stages in between. As a parody to “there’s an app for that,” Dr. Mindy Kantsiper, a hospitalist in Columbia, Md., says if there’s something that needs to be fixed, “there’s a hospitalist for that.” We are the Swiss Army knives of the medical world.
Looking through the HMX “Practice Management” discussions on the SHM website (www.hospitalmedicine.com/xchange) confirms my belief. Topics are as varied as using RNs in hospitalist practices, medication reconciliation, billing, outpatient orders (!!) after discharge, and patient-centered care/patient satisfaction. And that was just the last two weeks!
Type “hospitalist” into PubMed, and the words that auto-populate are: model, care, quality, discharge, communication, program, and handoff—all words I think of as system-related issues. Oh, sure, there are clinical-related topics, too, of course, just like for the “organ-based” specialties. However, none of the common organ-based specialties had any words auto-populate in PubMed that could be deemed related to “industrial engineering.”
Engineer Training
Like all engineers, we de facto industrial engineers need tools and skills to be effective at in our new engineering role. While we may not need slide rules and calculus like a more traditional engineer, many of the new skills we will need as industrial engineers were not taught in medical school, and the tools were not readily available for us to use in our training.
Fortunately, there are a plethora of options for us budding, de facto industrial engineers. Here are the ones I believe you will need and where to get them:
Skill No. 1: Negotiation.
HM is a team sport, and teams bring interpersonal dynamics and tension and conflict. Effective negotiation skills can help hospitalists use conflict to spur team growth and development rather than team dysfunction.
Tools: SHM’s Leadership Academies have effective negotiation modules in each of the leveled courses. If you can’t spare the time, then books to read include “Getting to Yes” by Fisher and Ury, or “Renegotiating Health Care” by Leonard Marcus (he lectures at SHM’s leadership academies).
Skill No. 2: Data analytics.
All engineers, including industrial engineers, need to be able to evaluate. Whether it’s quality and safety, clinical operations, or financial improvement, if you don’t measure it, you can’t change it. Some of the data will be handed to you, and you need to know the strengths and weaknesses to best interpret it. Some data you will need to define and develop measurement systems for on your own, and even basic dashboard development requires understanding data.
Tools: Wow. There are a lot here, so I am only going to mention the highlights. You could get your MBA, or MPH, or even a PhD! You certainly could train to become a “true” diploma-carrying industrial engineer. And I know of a few insightful hospitals that employ them. A less in-depth, but cheaper and faster, option is to take specific courses related to your area of interest.
The SHM-AAIM Quality and Safety Educators Academy and SHM’s Leadership Academies are two great examples. Participating in a mentored project (i.e., Project BOOST) provides structure and an experienced mentor with a cadre of experts to back them up. Many institutions have courses on data analytics, basic finance, and quality improvement. The easiest, cheapest, and probably the most common is to find a mentor at your own institution. CFOs, CNOs, CQOs, and CMOs often are eager to partner with clinicians—and frequently are delighted to talk about their areas of expertise.
Skill No. 3: Leadership.
I don’t know many leaders who were born that way. Most learned through experience and continuous self-improvement. Understanding your personality traits, the traits of others (as an introvert, I still am trying to understand how extroverts work, especially my wife), and how to get all of those different personalities to work together as a team is an important component of any team-based engineering success.
Tools: I have found the books “From Good to Great” by Jim Collins and “Switch” by Chip and Dan Heath to be invaluable. I think another one of my recent reads, “Drive” by Daniel Pink, had important lessons, too. Formal courses, such as SHM’s Leadership Academies, QSEA, and those offered by the American Hospital Association, are designed to provide hospitalists with the leadership skills they need in a variety of hospital environments.
Skill No. 4: Thinking “system” instead of “individual.”
So many of us were trained that to make improvements, we just need to “be better,” to know more, try harder, and to work longer. Good industrial engineers design systems that make it easier for our doctors, healthcare providers, and patients to succeed. Of course, we need to be accountable, too, but supportive systems are a key component to successful individuals. The airline industry learned this long ago.
Tools: I really think “Switch” is an excellent read for those of us trying to help re-engineer our complex systems. It discusses how humans are both rational and emotional, and how our environment can help both sides succeed. Another helpful tool for me is asking “why” whenever someone says “if only they would do something differently for a better outcome…”
For example, “if only the hospitalists would discharge before 2 p.m.,” or “if only the ED didn’t clump their admissions,” or “if only the nurse didn’t call during rounds”—these are all classic systems problems, not people problems, and the solution isn’t to mandate 2 p.m. discharges, or stand up in a meeting finger pointing at the ED, or admonish a nurse for calling during rounds. The solution is to find out why these behaviors occur, then eliminate, change, or minimize the reasons.
Hospitalists don’t discharge by 2 p.m. often because they are waiting on tests; ED docs work in an environment that has highly variable workloads, coupled with dysfunctional systems that promote “batching” work patterns; and nurses may not be included in rounds but still need to be able to manage minute-to-minute patient-care needs. Sure, there are a few bad apples that need to be scolded, but I bet most of the issues at your hospital aren’t related to evildoers but good people who are often trapped in dysfunctional, antiquated systems and are just trying to do the best they can for their patients.
In Closing
I’d like to say thank you to all of the “de facto” industrial engineers out there. Keep up the critically important work of that most complex system—the hospital.
Dr. Howell is president of SHM, chief of the division of hospital medicine at Johns Hopkins Bayview in Baltimore, and spends a significant part of his time and research on hospital operations. Email questions or comments to [email protected].
Wikipedia defines “industrial engineering” as a branch of engineering that deals with the optimization of complex processes or systems. It goes on to link industrial engineering to “operations” and use of quantitative methods to “specify, predict, and evaluate” results. Any hospitalist that’s been tapped to reduce length of stay, help manage readmissions, implement an electronic health record, or increase the quality of care likely can relate to that definition. It seems to me that hospitalists often are the de facto industrial engineers in many of our hospitals.
The hospitalist as an industrial engineer makes perfect sense. What other group of physicians, nurse practitioners, and physician assistants provide services in virtually any clinical venue, from ED to DC, from (occasionally) PACU to ICU, the wards, and even post-discharge? Hospitalists see it all, from the first few hours of life (pediatrics) to life’s last stages (palliative care) and all stages in between. As a parody to “there’s an app for that,” Dr. Mindy Kantsiper, a hospitalist in Columbia, Md., says if there’s something that needs to be fixed, “there’s a hospitalist for that.” We are the Swiss Army knives of the medical world.
Looking through the HMX “Practice Management” discussions on the SHM website (www.hospitalmedicine.com/xchange) confirms my belief. Topics are as varied as using RNs in hospitalist practices, medication reconciliation, billing, outpatient orders (!!) after discharge, and patient-centered care/patient satisfaction. And that was just the last two weeks!
Type “hospitalist” into PubMed, and the words that auto-populate are: model, care, quality, discharge, communication, program, and handoff—all words I think of as system-related issues. Oh, sure, there are clinical-related topics, too, of course, just like for the “organ-based” specialties. However, none of the common organ-based specialties had any words auto-populate in PubMed that could be deemed related to “industrial engineering.”
Engineer Training
Like all engineers, we de facto industrial engineers need tools and skills to be effective at in our new engineering role. While we may not need slide rules and calculus like a more traditional engineer, many of the new skills we will need as industrial engineers were not taught in medical school, and the tools were not readily available for us to use in our training.
Fortunately, there are a plethora of options for us budding, de facto industrial engineers. Here are the ones I believe you will need and where to get them:
Skill No. 1: Negotiation.
HM is a team sport, and teams bring interpersonal dynamics and tension and conflict. Effective negotiation skills can help hospitalists use conflict to spur team growth and development rather than team dysfunction.
Tools: SHM’s Leadership Academies have effective negotiation modules in each of the leveled courses. If you can’t spare the time, then books to read include “Getting to Yes” by Fisher and Ury, or “Renegotiating Health Care” by Leonard Marcus (he lectures at SHM’s leadership academies).
Skill No. 2: Data analytics.
All engineers, including industrial engineers, need to be able to evaluate. Whether it’s quality and safety, clinical operations, or financial improvement, if you don’t measure it, you can’t change it. Some of the data will be handed to you, and you need to know the strengths and weaknesses to best interpret it. Some data you will need to define and develop measurement systems for on your own, and even basic dashboard development requires understanding data.
Tools: Wow. There are a lot here, so I am only going to mention the highlights. You could get your MBA, or MPH, or even a PhD! You certainly could train to become a “true” diploma-carrying industrial engineer. And I know of a few insightful hospitals that employ them. A less in-depth, but cheaper and faster, option is to take specific courses related to your area of interest.
The SHM-AAIM Quality and Safety Educators Academy and SHM’s Leadership Academies are two great examples. Participating in a mentored project (i.e., Project BOOST) provides structure and an experienced mentor with a cadre of experts to back them up. Many institutions have courses on data analytics, basic finance, and quality improvement. The easiest, cheapest, and probably the most common is to find a mentor at your own institution. CFOs, CNOs, CQOs, and CMOs often are eager to partner with clinicians—and frequently are delighted to talk about their areas of expertise.
Skill No. 3: Leadership.
I don’t know many leaders who were born that way. Most learned through experience and continuous self-improvement. Understanding your personality traits, the traits of others (as an introvert, I still am trying to understand how extroverts work, especially my wife), and how to get all of those different personalities to work together as a team is an important component of any team-based engineering success.
Tools: I have found the books “From Good to Great” by Jim Collins and “Switch” by Chip and Dan Heath to be invaluable. I think another one of my recent reads, “Drive” by Daniel Pink, had important lessons, too. Formal courses, such as SHM’s Leadership Academies, QSEA, and those offered by the American Hospital Association, are designed to provide hospitalists with the leadership skills they need in a variety of hospital environments.
Skill No. 4: Thinking “system” instead of “individual.”
So many of us were trained that to make improvements, we just need to “be better,” to know more, try harder, and to work longer. Good industrial engineers design systems that make it easier for our doctors, healthcare providers, and patients to succeed. Of course, we need to be accountable, too, but supportive systems are a key component to successful individuals. The airline industry learned this long ago.
Tools: I really think “Switch” is an excellent read for those of us trying to help re-engineer our complex systems. It discusses how humans are both rational and emotional, and how our environment can help both sides succeed. Another helpful tool for me is asking “why” whenever someone says “if only they would do something differently for a better outcome…”
For example, “if only the hospitalists would discharge before 2 p.m.,” or “if only the ED didn’t clump their admissions,” or “if only the nurse didn’t call during rounds”—these are all classic systems problems, not people problems, and the solution isn’t to mandate 2 p.m. discharges, or stand up in a meeting finger pointing at the ED, or admonish a nurse for calling during rounds. The solution is to find out why these behaviors occur, then eliminate, change, or minimize the reasons.
Hospitalists don’t discharge by 2 p.m. often because they are waiting on tests; ED docs work in an environment that has highly variable workloads, coupled with dysfunctional systems that promote “batching” work patterns; and nurses may not be included in rounds but still need to be able to manage minute-to-minute patient-care needs. Sure, there are a few bad apples that need to be scolded, but I bet most of the issues at your hospital aren’t related to evildoers but good people who are often trapped in dysfunctional, antiquated systems and are just trying to do the best they can for their patients.
In Closing
I’d like to say thank you to all of the “de facto” industrial engineers out there. Keep up the critically important work of that most complex system—the hospital.
Dr. Howell is president of SHM, chief of the division of hospital medicine at Johns Hopkins Bayview in Baltimore, and spends a significant part of his time and research on hospital operations. Email questions or comments to [email protected].
New Rules for Value-Based Purchasing, Readmission Penalties, Admissions


The View from
![]()
Looking for more information to formulate a plan of attack? SHM offers a variety of HVBP resources to orient hospitalists and hospital leaders. The “What Every Hospitalist Should Know About Hospital Value-Based Purchasing” webinar and SHM’s free resource library (www.hospitalmedicine.org/hvbp) offer basic orientation on what to expect on pay-for-performance-related issues. The HVBP resource center also provides multiple case studies from various hospitals across the country, with success stories related to reducing readmissions, increasing evidence-based care focus, and enhancing performance on core measures.
In order to proactively address CMS’ new 30-day readmissions criteria for COPD, SHM’s COPD Resource Center (www.hospitalmedicine.org/copd) provides hospitalists with the most up-to-date guidelines, reviews, and peer-reviewed clinical trials that define evidence-based practice for the care of the COPD patient.
Hospitalists not only are under pressure to help improve hospital-level performance, but also will need to begin reporting physician-level measures. Beginning in 2015, CMS’s Physician Quality Reporting System (PQRS) will apply a penalty to all physicians who do not satisfactorily report data on quality measures for covered professional services.
The time to act is now. Reporting during the 2013 PQRS program year will be used to determine whether a 1.5% penalty applies in 2015. SHM has partnered with CECity to offer discounted access to PQRIwizard, a tool that facilitates PQRS reporting through SHM’s Learning Portal (www.shmlearningportal.org).
October is the beginning of a new year—in this case, fiscal-year 2014 for the Centers for Medicare & Medicaid Services (CMS). It’s a time when the new rules kick in. This month, we’ll look at some highlights, focusing on the new developments affecting your practice. Because you are held accountable for hospital-side performance on programs such as hospital value-based purchasing (HVBP) and the Readmissions Reduction Program, a working knowledge of the 2014 edition of the programs is crucial.
Close the Loop on HVBP
How will your hospital get paid under the 2014 version of HVBP? This past July, your hospital received a report outlining how its Medicare payments will be affected based on your hospital’s performance on process of care (heart failure, pneumonia, myocardial infarction, and surgery), patient experience (HCAHPS), and outcomes (30-day mortality for heart failure, pneumonia, and myocardial infarction).
Here are two hypothetical hospitals and how their performance in the program affects their 2014 payment. As background, in 2014, all hospitals have their base diagnosis related group (DRG) payments reduced by 1.25% for HVBP. They can earn back some, all, or an amount in excess of the 1.25% based on their performance. Payment is based on performance during the April 1 to Dec. 31, 2012, period. Under HVBP, CMS incentive payments occur at the level of individual patients, each of which is assigned a DRG.
Let’s look at two examples:
Hospital 1
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.48%.
- Net change in base DRG payment: +0.23%.
Hospital 2
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.08%.
- Net change in base DRG payment: -0.17%.
Hospital 1 performed relatively well, getting a bump of 0.23% in its base DRG rate. Hospital 2 did not perform so well, so it took a 0.17% hit on its base DRG rate.
In order to determine total dollars made or lost for your hospital, one multiplies the total number of eligible Medicare inpatients for 2014 times the base DRG payment times the percent change in base DRG payment. If Hospital 1 has 10,000 eligible patients in 2014 and a base DRG payment of $5,000, the value is 10,000 x $5,000 x 0.0023 (0.23%) = $115,000 gained. Hospital 2, with the same number of patients and base DRG payment, loses (10,000 x $5,000 x 0.0017 = $85,000).
Readmissions and Penalties
For 2014, CMS is adding 30-day readmissions for COPD to readmissions for heart failure, pneumonia, and myocardial infarction for its penalty program. CMS added COPD because it is the fourth-leading cause of readmissions, according to a recent Medicare Payment Advisory Commission report, and because there is wide variation in the rates (from 18% to 25%) of COPD hospital readmissions.
For 2014, CMS raises the ceiling on readmission penalties to a maximum of 2% of reimbursement for all of a hospital’s Medicare inpatients. (The maximum hit during the first round of readmission penalties, which began in October 2012, was 1%.) More than 2,200 U.S. hospitals will face some financial penalty for excess 30-day readmissions.
Disappointingly, CMS did not add a risk adjustment for socioeconomic status despite being under pressure to do so. There is growing evidence that these factors have a major impact on readmission rates.1,2
New Definition of an Admission
Amidst confusion from many and major blowback from beneficiaries saddled with large out-of-pocket expenses for observation stays and subsequent skilled-nursing-facility stays, CMS is clarifying the definition of an inpatient admission. The agency will define an admission as a hospital stay that spans at least two midnights. If a patient is in the hospital for a shorter period of time, CMS will deem the patient to be on observation status, unless medical record documentation supports a physician’s expectation “that the beneficiary would need care spanning at least two midnights” but unanticipated events led to a shorter stay.
Plan of Attack
For HVBP, make contact with your director of quality to understand your hospital’s performance and payment for 2014. If you have incentive compensation riding on HVBP, make sure you understand how your employer or contracted hospital is calculating the payout (because, for example, the performance period was in 2012!) and that your hospitalist group understands the payout calculation.
For COPD readmissions prevention, ensure patients have a home management plan; appropriate specialist follow-up and that they understand medication use, including inhalers and supplemental oxygen; and that you consider early referral for pulmonary rehabilitation for eligible patients.
For the new definition of inpatient admission, work with your hospital’s physician advisor and case management to ensure your group is getting appropriate guidance on documentation requirements. You are probably being held accountable for your hospital’s total number of observation hours, so remember to track these metrics following implementation of the new rule, as they (hopefully) should decrease. If they do, take some of the credit!
References
- Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675-681.
- Lindenauer PK, Lagu T, Rothberg MB, et al. Income inequality and 30 day outcomes after acute myocardial infarction, heart failure, and pneumonia: retrospective cohort study. BMJ. 2013;346:f521.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at [email protected].
The View from
![]()
Looking for more information to formulate a plan of attack? SHM offers a variety of HVBP resources to orient hospitalists and hospital leaders. The “What Every Hospitalist Should Know About Hospital Value-Based Purchasing” webinar and SHM’s free resource library (www.hospitalmedicine.org/hvbp) offer basic orientation on what to expect on pay-for-performance-related issues. The HVBP resource center also provides multiple case studies from various hospitals across the country, with success stories related to reducing readmissions, increasing evidence-based care focus, and enhancing performance on core measures.
In order to proactively address CMS’ new 30-day readmissions criteria for COPD, SHM’s COPD Resource Center (www.hospitalmedicine.org/copd) provides hospitalists with the most up-to-date guidelines, reviews, and peer-reviewed clinical trials that define evidence-based practice for the care of the COPD patient.
Hospitalists not only are under pressure to help improve hospital-level performance, but also will need to begin reporting physician-level measures. Beginning in 2015, CMS’s Physician Quality Reporting System (PQRS) will apply a penalty to all physicians who do not satisfactorily report data on quality measures for covered professional services.
The time to act is now. Reporting during the 2013 PQRS program year will be used to determine whether a 1.5% penalty applies in 2015. SHM has partnered with CECity to offer discounted access to PQRIwizard, a tool that facilitates PQRS reporting through SHM’s Learning Portal (www.shmlearningportal.org).
October is the beginning of a new year—in this case, fiscal-year 2014 for the Centers for Medicare & Medicaid Services (CMS). It’s a time when the new rules kick in. This month, we’ll look at some highlights, focusing on the new developments affecting your practice. Because you are held accountable for hospital-side performance on programs such as hospital value-based purchasing (HVBP) and the Readmissions Reduction Program, a working knowledge of the 2014 edition of the programs is crucial.
Close the Loop on HVBP
How will your hospital get paid under the 2014 version of HVBP? This past July, your hospital received a report outlining how its Medicare payments will be affected based on your hospital’s performance on process of care (heart failure, pneumonia, myocardial infarction, and surgery), patient experience (HCAHPS), and outcomes (30-day mortality for heart failure, pneumonia, and myocardial infarction).
Here are two hypothetical hospitals and how their performance in the program affects their 2014 payment. As background, in 2014, all hospitals have their base diagnosis related group (DRG) payments reduced by 1.25% for HVBP. They can earn back some, all, or an amount in excess of the 1.25% based on their performance. Payment is based on performance during the April 1 to Dec. 31, 2012, period. Under HVBP, CMS incentive payments occur at the level of individual patients, each of which is assigned a DRG.
Let’s look at two examples:
Hospital 1
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.48%.
- Net change in base DRG payment: +0.23%.
Hospital 2
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.08%.
- Net change in base DRG payment: -0.17%.
Hospital 1 performed relatively well, getting a bump of 0.23% in its base DRG rate. Hospital 2 did not perform so well, so it took a 0.17% hit on its base DRG rate.
In order to determine total dollars made or lost for your hospital, one multiplies the total number of eligible Medicare inpatients for 2014 times the base DRG payment times the percent change in base DRG payment. If Hospital 1 has 10,000 eligible patients in 2014 and a base DRG payment of $5,000, the value is 10,000 x $5,000 x 0.0023 (0.23%) = $115,000 gained. Hospital 2, with the same number of patients and base DRG payment, loses (10,000 x $5,000 x 0.0017 = $85,000).
Readmissions and Penalties
For 2014, CMS is adding 30-day readmissions for COPD to readmissions for heart failure, pneumonia, and myocardial infarction for its penalty program. CMS added COPD because it is the fourth-leading cause of readmissions, according to a recent Medicare Payment Advisory Commission report, and because there is wide variation in the rates (from 18% to 25%) of COPD hospital readmissions.
For 2014, CMS raises the ceiling on readmission penalties to a maximum of 2% of reimbursement for all of a hospital’s Medicare inpatients. (The maximum hit during the first round of readmission penalties, which began in October 2012, was 1%.) More than 2,200 U.S. hospitals will face some financial penalty for excess 30-day readmissions.
Disappointingly, CMS did not add a risk adjustment for socioeconomic status despite being under pressure to do so. There is growing evidence that these factors have a major impact on readmission rates.1,2
New Definition of an Admission
Amidst confusion from many and major blowback from beneficiaries saddled with large out-of-pocket expenses for observation stays and subsequent skilled-nursing-facility stays, CMS is clarifying the definition of an inpatient admission. The agency will define an admission as a hospital stay that spans at least two midnights. If a patient is in the hospital for a shorter period of time, CMS will deem the patient to be on observation status, unless medical record documentation supports a physician’s expectation “that the beneficiary would need care spanning at least two midnights” but unanticipated events led to a shorter stay.
Plan of Attack
For HVBP, make contact with your director of quality to understand your hospital’s performance and payment for 2014. If you have incentive compensation riding on HVBP, make sure you understand how your employer or contracted hospital is calculating the payout (because, for example, the performance period was in 2012!) and that your hospitalist group understands the payout calculation.
For COPD readmissions prevention, ensure patients have a home management plan; appropriate specialist follow-up and that they understand medication use, including inhalers and supplemental oxygen; and that you consider early referral for pulmonary rehabilitation for eligible patients.
For the new definition of inpatient admission, work with your hospital’s physician advisor and case management to ensure your group is getting appropriate guidance on documentation requirements. You are probably being held accountable for your hospital’s total number of observation hours, so remember to track these metrics following implementation of the new rule, as they (hopefully) should decrease. If they do, take some of the credit!
References
- Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675-681.
- Lindenauer PK, Lagu T, Rothberg MB, et al. Income inequality and 30 day outcomes after acute myocardial infarction, heart failure, and pneumonia: retrospective cohort study. BMJ. 2013;346:f521.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at [email protected].
The View from
![]()
Looking for more information to formulate a plan of attack? SHM offers a variety of HVBP resources to orient hospitalists and hospital leaders. The “What Every Hospitalist Should Know About Hospital Value-Based Purchasing” webinar and SHM’s free resource library (www.hospitalmedicine.org/hvbp) offer basic orientation on what to expect on pay-for-performance-related issues. The HVBP resource center also provides multiple case studies from various hospitals across the country, with success stories related to reducing readmissions, increasing evidence-based care focus, and enhancing performance on core measures.
In order to proactively address CMS’ new 30-day readmissions criteria for COPD, SHM’s COPD Resource Center (www.hospitalmedicine.org/copd) provides hospitalists with the most up-to-date guidelines, reviews, and peer-reviewed clinical trials that define evidence-based practice for the care of the COPD patient.
Hospitalists not only are under pressure to help improve hospital-level performance, but also will need to begin reporting physician-level measures. Beginning in 2015, CMS’s Physician Quality Reporting System (PQRS) will apply a penalty to all physicians who do not satisfactorily report data on quality measures for covered professional services.
The time to act is now. Reporting during the 2013 PQRS program year will be used to determine whether a 1.5% penalty applies in 2015. SHM has partnered with CECity to offer discounted access to PQRIwizard, a tool that facilitates PQRS reporting through SHM’s Learning Portal (www.shmlearningportal.org).
October is the beginning of a new year—in this case, fiscal-year 2014 for the Centers for Medicare & Medicaid Services (CMS). It’s a time when the new rules kick in. This month, we’ll look at some highlights, focusing on the new developments affecting your practice. Because you are held accountable for hospital-side performance on programs such as hospital value-based purchasing (HVBP) and the Readmissions Reduction Program, a working knowledge of the 2014 edition of the programs is crucial.
Close the Loop on HVBP
How will your hospital get paid under the 2014 version of HVBP? This past July, your hospital received a report outlining how its Medicare payments will be affected based on your hospital’s performance on process of care (heart failure, pneumonia, myocardial infarction, and surgery), patient experience (HCAHPS), and outcomes (30-day mortality for heart failure, pneumonia, and myocardial infarction).
Here are two hypothetical hospitals and how their performance in the program affects their 2014 payment. As background, in 2014, all hospitals have their base diagnosis related group (DRG) payments reduced by 1.25% for HVBP. They can earn back some, all, or an amount in excess of the 1.25% based on their performance. Payment is based on performance during the April 1 to Dec. 31, 2012, period. Under HVBP, CMS incentive payments occur at the level of individual patients, each of which is assigned a DRG.
Let’s look at two examples:
Hospital 1
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.48%.
- Net change in base DRG payment: +0.23%.
Hospital 2
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.08%.
- Net change in base DRG payment: -0.17%.
Hospital 1 performed relatively well, getting a bump of 0.23% in its base DRG rate. Hospital 2 did not perform so well, so it took a 0.17% hit on its base DRG rate.
In order to determine total dollars made or lost for your hospital, one multiplies the total number of eligible Medicare inpatients for 2014 times the base DRG payment times the percent change in base DRG payment. If Hospital 1 has 10,000 eligible patients in 2014 and a base DRG payment of $5,000, the value is 10,000 x $5,000 x 0.0023 (0.23%) = $115,000 gained. Hospital 2, with the same number of patients and base DRG payment, loses (10,000 x $5,000 x 0.0017 = $85,000).
Readmissions and Penalties
For 2014, CMS is adding 30-day readmissions for COPD to readmissions for heart failure, pneumonia, and myocardial infarction for its penalty program. CMS added COPD because it is the fourth-leading cause of readmissions, according to a recent Medicare Payment Advisory Commission report, and because there is wide variation in the rates (from 18% to 25%) of COPD hospital readmissions.
For 2014, CMS raises the ceiling on readmission penalties to a maximum of 2% of reimbursement for all of a hospital’s Medicare inpatients. (The maximum hit during the first round of readmission penalties, which began in October 2012, was 1%.) More than 2,200 U.S. hospitals will face some financial penalty for excess 30-day readmissions.
Disappointingly, CMS did not add a risk adjustment for socioeconomic status despite being under pressure to do so. There is growing evidence that these factors have a major impact on readmission rates.1,2
New Definition of an Admission
Amidst confusion from many and major blowback from beneficiaries saddled with large out-of-pocket expenses for observation stays and subsequent skilled-nursing-facility stays, CMS is clarifying the definition of an inpatient admission. The agency will define an admission as a hospital stay that spans at least two midnights. If a patient is in the hospital for a shorter period of time, CMS will deem the patient to be on observation status, unless medical record documentation supports a physician’s expectation “that the beneficiary would need care spanning at least two midnights” but unanticipated events led to a shorter stay.
Plan of Attack
For HVBP, make contact with your director of quality to understand your hospital’s performance and payment for 2014. If you have incentive compensation riding on HVBP, make sure you understand how your employer or contracted hospital is calculating the payout (because, for example, the performance period was in 2012!) and that your hospitalist group understands the payout calculation.
For COPD readmissions prevention, ensure patients have a home management plan; appropriate specialist follow-up and that they understand medication use, including inhalers and supplemental oxygen; and that you consider early referral for pulmonary rehabilitation for eligible patients.
For the new definition of inpatient admission, work with your hospital’s physician advisor and case management to ensure your group is getting appropriate guidance on documentation requirements. You are probably being held accountable for your hospital’s total number of observation hours, so remember to track these metrics following implementation of the new rule, as they (hopefully) should decrease. If they do, take some of the credit!
References
- Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675-681.
- Lindenauer PK, Lagu T, Rothberg MB, et al. Income inequality and 30 day outcomes after acute myocardial infarction, heart failure, and pneumonia: retrospective cohort study. BMJ. 2013;346:f521.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at [email protected].
Hospitalist James O’Callaghan Finds Career Satisfaction in Pediatric Medicine


It took a while for James J. O’Callaghan, MD, FAAP, FHM, to settle on a career path. First, he pursued the life of a chemical engineer. Then, in his third year at Rensselaer Polytechnic Institute in Troy, N.Y., he realized the kind of job he would be getting into was not quite for him. His then-girlfriend was a pre-med student, and it wasn’t long until he switched majors.
Hospital medicine drew his interest during residency, when he spent a monthlong rotation with a small group of physicians at a community hospital in Cleveland.
“Their days consisted of rounding on pediatric inpatients, examining normal newborns, completing pediatric consults in the ED, and performing minor procedures on the floor,” he says. “To me, it seemed the perfect job.”
Dr. O’Callaghan married an adult-medicine hospitalist and moved to Seattle, but he could not find a good fit in a hospitalist practice. He did private practice for two years, and in 2004, he landed a position in pediatric hospital medicine.
“I quickly changed career paths,” he says.
Dr. O’Callaghan is now a regional pediatric hospitalist at Evergreen Hospital in Kirkland, Wash., and a medical hospitalist at Seattle Children’s Hospital. He is a clinical assistant professor at the University of Washington and one of nine new Team Hospitalist members, The Hospitalist’s volunteer editorial advisory group.
As the section head for pediatrics at Evergreen, Dr. O’Callaghan spends most of his time seeing patients. However, he has in recent years developed a keen interest in quality improvement (QI). He’s the lead pediatric hospitalist on two clinical pathways at Seattle Children’s and has been an active member of SHM’s Hospital Quality and Patient Safety Committee since 2012.
“I want to continue to expand on this QI work,” he says, “with the goal of developing into a formal QI role at either, or both, hospitals.”
Question: What do you like most about working as a hospitalist?
Answer: I like the fact that the work I am doing as a hospitalist can have both an immediate impact on a single patient and a prolonged impact on multiple patients. I can admit a child with community-acquired pneumonia and, through my treatment, prevent serious sequelae from developing. However, I can also develop an evidenced-based, community-acquired pneumonia pathway and, potentially, affect the care of hundreds of children. There is immediate gratification in treating today’s patient and delayed gratification knowing that you are helping many of tomorrow’s patients.
Q: What do you dislike?
A: One of the hardest parts of a career in HM is trying to effect culture change. Hospital systems are typically large, complex organizations with their own culture. In order to successfully produce sustainable, long-term improvement, you must change this culture. You can perform a robust search of the literature to produce a brilliant clinical-care path, but unless you can affect behavior, your work and effort may not last. It can be frustrating to think you have the answer to a clinical problem only to see your effort fail because you could not change culture.
Q: What’s the biggest change you’ve seen in HM in your career?
A: In the early years, much of the conversation in HM was centered on the viability of a career in HM. Could one make a sustainable career in HM? Would hospitals and health systems continue to support physicians in HM? The biggest change I have seen is that we are no longer having those conversations. Now, the conversations are focused on determining which areas of medicine will be owned by HM: First it was QI work, then patient safety, and now resource utilization and cost containment. We are no longer spending time and energy worrying about the future of HM, but rather now our efforts are focused on the present work of HM. As a sustainable career, HM is here to stay.
Q: For group leaders, why is it important for you to continue seeing patients?
A: In my QI work, I have studied Lean thinking and methodology. Lean thinking teaches you that change and improvement do not come down from leadership, but rather develop up from front-line workers. Group leaders need to continue seeing patients to truly understand the processes and problems inherent in clinical work. Effective solutions must come from those actually doing the work, rather than from those managing the work from above.
Q: What does it mean to you to be elected a Fellow in Hospital Medicine?
A: It meant that I had committed fully to a career in hospital medicine. I use the FHM designation proudly in all my communications, as a signal to others of my commitment and dedication to hospital medicine. Someday, I hope to earn the designation of SFHM, as a validation and recognition of my contributions to the field of pediatric hospital medicine.
Q: When you aren’t working, what is important to you?
A: After family, it is important for me to maintain a healthy lifestyle and stay in shape. I am able to commute to Seattle Children’s Hospital by bicycle and I try to run two to three times a week. I squeeze in half-marathons and marathons, along with century [100 miles] and double-century bicycle rides each year.
Q: If you weren’t a doctor, what would you be doing right now?
A: I would love to be a stay-at-home father for my boys and also devote the time and energy into pursuing a career in trail running.
Q: What’s the best book you’ve read recently?
A: I recently read Jim Collins’ “Good to Great” as part of a management training course at Seattle Children’s Hospital. This easy-to-read, highly entertaining book clearly demonstrates the culture changes that need to occur for companies to move from good to great. As a field, hospital medicine, with its focus on QI work and patient safety, is now in the midst of trying to become “great.”
Q: How many Apple products (phones, iPods, tablets, iTunes, etc.) do you interface with in a given week?
A: As many as possible. My wife and I own two iPhones, two iPads, and a MacBook Air, which she thinks we share but, in actuality, is mine. We are hoping to purchase a Mac desktop, and then we will have fully given over to the dark side.
Richard Quinn is a freelance writer in New Jersey.
It took a while for James J. O’Callaghan, MD, FAAP, FHM, to settle on a career path. First, he pursued the life of a chemical engineer. Then, in his third year at Rensselaer Polytechnic Institute in Troy, N.Y., he realized the kind of job he would be getting into was not quite for him. His then-girlfriend was a pre-med student, and it wasn’t long until he switched majors.
Hospital medicine drew his interest during residency, when he spent a monthlong rotation with a small group of physicians at a community hospital in Cleveland.
“Their days consisted of rounding on pediatric inpatients, examining normal newborns, completing pediatric consults in the ED, and performing minor procedures on the floor,” he says. “To me, it seemed the perfect job.”
Dr. O’Callaghan married an adult-medicine hospitalist and moved to Seattle, but he could not find a good fit in a hospitalist practice. He did private practice for two years, and in 2004, he landed a position in pediatric hospital medicine.
“I quickly changed career paths,” he says.
Dr. O’Callaghan is now a regional pediatric hospitalist at Evergreen Hospital in Kirkland, Wash., and a medical hospitalist at Seattle Children’s Hospital. He is a clinical assistant professor at the University of Washington and one of nine new Team Hospitalist members, The Hospitalist’s volunteer editorial advisory group.
As the section head for pediatrics at Evergreen, Dr. O’Callaghan spends most of his time seeing patients. However, he has in recent years developed a keen interest in quality improvement (QI). He’s the lead pediatric hospitalist on two clinical pathways at Seattle Children’s and has been an active member of SHM’s Hospital Quality and Patient Safety Committee since 2012.
“I want to continue to expand on this QI work,” he says, “with the goal of developing into a formal QI role at either, or both, hospitals.”
Question: What do you like most about working as a hospitalist?
Answer: I like the fact that the work I am doing as a hospitalist can have both an immediate impact on a single patient and a prolonged impact on multiple patients. I can admit a child with community-acquired pneumonia and, through my treatment, prevent serious sequelae from developing. However, I can also develop an evidenced-based, community-acquired pneumonia pathway and, potentially, affect the care of hundreds of children. There is immediate gratification in treating today’s patient and delayed gratification knowing that you are helping many of tomorrow’s patients.
Q: What do you dislike?
A: One of the hardest parts of a career in HM is trying to effect culture change. Hospital systems are typically large, complex organizations with their own culture. In order to successfully produce sustainable, long-term improvement, you must change this culture. You can perform a robust search of the literature to produce a brilliant clinical-care path, but unless you can affect behavior, your work and effort may not last. It can be frustrating to think you have the answer to a clinical problem only to see your effort fail because you could not change culture.
Q: What’s the biggest change you’ve seen in HM in your career?
A: In the early years, much of the conversation in HM was centered on the viability of a career in HM. Could one make a sustainable career in HM? Would hospitals and health systems continue to support physicians in HM? The biggest change I have seen is that we are no longer having those conversations. Now, the conversations are focused on determining which areas of medicine will be owned by HM: First it was QI work, then patient safety, and now resource utilization and cost containment. We are no longer spending time and energy worrying about the future of HM, but rather now our efforts are focused on the present work of HM. As a sustainable career, HM is here to stay.
Q: For group leaders, why is it important for you to continue seeing patients?
A: In my QI work, I have studied Lean thinking and methodology. Lean thinking teaches you that change and improvement do not come down from leadership, but rather develop up from front-line workers. Group leaders need to continue seeing patients to truly understand the processes and problems inherent in clinical work. Effective solutions must come from those actually doing the work, rather than from those managing the work from above.
Q: What does it mean to you to be elected a Fellow in Hospital Medicine?
A: It meant that I had committed fully to a career in hospital medicine. I use the FHM designation proudly in all my communications, as a signal to others of my commitment and dedication to hospital medicine. Someday, I hope to earn the designation of SFHM, as a validation and recognition of my contributions to the field of pediatric hospital medicine.
Q: When you aren’t working, what is important to you?
A: After family, it is important for me to maintain a healthy lifestyle and stay in shape. I am able to commute to Seattle Children’s Hospital by bicycle and I try to run two to three times a week. I squeeze in half-marathons and marathons, along with century [100 miles] and double-century bicycle rides each year.
Q: If you weren’t a doctor, what would you be doing right now?
A: I would love to be a stay-at-home father for my boys and also devote the time and energy into pursuing a career in trail running.
Q: What’s the best book you’ve read recently?
A: I recently read Jim Collins’ “Good to Great” as part of a management training course at Seattle Children’s Hospital. This easy-to-read, highly entertaining book clearly demonstrates the culture changes that need to occur for companies to move from good to great. As a field, hospital medicine, with its focus on QI work and patient safety, is now in the midst of trying to become “great.”
Q: How many Apple products (phones, iPods, tablets, iTunes, etc.) do you interface with in a given week?
A: As many as possible. My wife and I own two iPhones, two iPads, and a MacBook Air, which she thinks we share but, in actuality, is mine. We are hoping to purchase a Mac desktop, and then we will have fully given over to the dark side.
Richard Quinn is a freelance writer in New Jersey.
It took a while for James J. O’Callaghan, MD, FAAP, FHM, to settle on a career path. First, he pursued the life of a chemical engineer. Then, in his third year at Rensselaer Polytechnic Institute in Troy, N.Y., he realized the kind of job he would be getting into was not quite for him. His then-girlfriend was a pre-med student, and it wasn’t long until he switched majors.
Hospital medicine drew his interest during residency, when he spent a monthlong rotation with a small group of physicians at a community hospital in Cleveland.
“Their days consisted of rounding on pediatric inpatients, examining normal newborns, completing pediatric consults in the ED, and performing minor procedures on the floor,” he says. “To me, it seemed the perfect job.”
Dr. O’Callaghan married an adult-medicine hospitalist and moved to Seattle, but he could not find a good fit in a hospitalist practice. He did private practice for two years, and in 2004, he landed a position in pediatric hospital medicine.
“I quickly changed career paths,” he says.
Dr. O’Callaghan is now a regional pediatric hospitalist at Evergreen Hospital in Kirkland, Wash., and a medical hospitalist at Seattle Children’s Hospital. He is a clinical assistant professor at the University of Washington and one of nine new Team Hospitalist members, The Hospitalist’s volunteer editorial advisory group.
As the section head for pediatrics at Evergreen, Dr. O’Callaghan spends most of his time seeing patients. However, he has in recent years developed a keen interest in quality improvement (QI). He’s the lead pediatric hospitalist on two clinical pathways at Seattle Children’s and has been an active member of SHM’s Hospital Quality and Patient Safety Committee since 2012.
“I want to continue to expand on this QI work,” he says, “with the goal of developing into a formal QI role at either, or both, hospitals.”
Question: What do you like most about working as a hospitalist?
Answer: I like the fact that the work I am doing as a hospitalist can have both an immediate impact on a single patient and a prolonged impact on multiple patients. I can admit a child with community-acquired pneumonia and, through my treatment, prevent serious sequelae from developing. However, I can also develop an evidenced-based, community-acquired pneumonia pathway and, potentially, affect the care of hundreds of children. There is immediate gratification in treating today’s patient and delayed gratification knowing that you are helping many of tomorrow’s patients.
Q: What do you dislike?
A: One of the hardest parts of a career in HM is trying to effect culture change. Hospital systems are typically large, complex organizations with their own culture. In order to successfully produce sustainable, long-term improvement, you must change this culture. You can perform a robust search of the literature to produce a brilliant clinical-care path, but unless you can affect behavior, your work and effort may not last. It can be frustrating to think you have the answer to a clinical problem only to see your effort fail because you could not change culture.
Q: What’s the biggest change you’ve seen in HM in your career?
A: In the early years, much of the conversation in HM was centered on the viability of a career in HM. Could one make a sustainable career in HM? Would hospitals and health systems continue to support physicians in HM? The biggest change I have seen is that we are no longer having those conversations. Now, the conversations are focused on determining which areas of medicine will be owned by HM: First it was QI work, then patient safety, and now resource utilization and cost containment. We are no longer spending time and energy worrying about the future of HM, but rather now our efforts are focused on the present work of HM. As a sustainable career, HM is here to stay.
Q: For group leaders, why is it important for you to continue seeing patients?
A: In my QI work, I have studied Lean thinking and methodology. Lean thinking teaches you that change and improvement do not come down from leadership, but rather develop up from front-line workers. Group leaders need to continue seeing patients to truly understand the processes and problems inherent in clinical work. Effective solutions must come from those actually doing the work, rather than from those managing the work from above.
Q: What does it mean to you to be elected a Fellow in Hospital Medicine?
A: It meant that I had committed fully to a career in hospital medicine. I use the FHM designation proudly in all my communications, as a signal to others of my commitment and dedication to hospital medicine. Someday, I hope to earn the designation of SFHM, as a validation and recognition of my contributions to the field of pediatric hospital medicine.
Q: When you aren’t working, what is important to you?
A: After family, it is important for me to maintain a healthy lifestyle and stay in shape. I am able to commute to Seattle Children’s Hospital by bicycle and I try to run two to three times a week. I squeeze in half-marathons and marathons, along with century [100 miles] and double-century bicycle rides each year.
Q: If you weren’t a doctor, what would you be doing right now?
A: I would love to be a stay-at-home father for my boys and also devote the time and energy into pursuing a career in trail running.
Q: What’s the best book you’ve read recently?
A: I recently read Jim Collins’ “Good to Great” as part of a management training course at Seattle Children’s Hospital. This easy-to-read, highly entertaining book clearly demonstrates the culture changes that need to occur for companies to move from good to great. As a field, hospital medicine, with its focus on QI work and patient safety, is now in the midst of trying to become “great.”
Q: How many Apple products (phones, iPods, tablets, iTunes, etc.) do you interface with in a given week?
A: As many as possible. My wife and I own two iPhones, two iPads, and a MacBook Air, which she thinks we share but, in actuality, is mine. We are hoping to purchase a Mac desktop, and then we will have fully given over to the dark side.
Richard Quinn is a freelance writer in New Jersey.
Society of Hospital Medicine’s MARQUIS Initiative Highlights Need For Improved Medication Reconciliation


–Jeffrey Schnipper, MD, MPH, FHM
What is the best possible medication history? How is it done? Who should do it? When should it be done during a patient’s journey in and out of the hospital? What medication discrepancies—and potential adverse drug events—are most likely?
Those are questions veteran hospitalist Jason Stein, MD, tried to answer during an HM13 breakout session on medication reconciliation at the Gaylord National Resort and Conference Center in National Harbor, Md.
“How do you know as the discharging provider if the medication list you’re looking at is gold or garbage?” said Dr. Stein, associate director for quality improvement (QI) at Emory University in Atlanta and a mentor for SHM’s Multi-Center Medication Reconciliation Quality Improvement Study (MARQUIS) quality-research initiative.
The concept of the “best possible medication history” (BPMH) originated with patient-safety expert Edward Etchells, MD, MSc, at Sunnybrook Health Sciences Centre in Toronto. The concept is outlined on a pocket reminder card for MARQUIS participants, explained co-presenter and principal investigator Jeffrey Schnipper MD, MPH, FHM, a hospitalist at Brigham & Women’s Hospital in Boston.
“Sometimes it’s impossible to know what the patient was or wasn’t taking, but it doesn’t mean you don’t do your best,” he said, adding that hospitalists should attempt to get at least one reliable, corroborating source of information for a patient’s medical history.
Sometimes it is necessary to speak to family members or the community pharmacy, Dr. Schnipper said, because many patients can’t remember all of the drugs they are taking. Trying to do medication reconciliation at the time of discharge when BPMH has not been done can lead to more work for the provider, medication errors, or rehospitalizations. Ideally, knowledge of what the patient was taking before admission, as well as the patient’s health literacy and adherence history, should be gathered and documented once, early, and well during the hospitalization by a trained provider, according to Dr. Schnipper.
An SHM survey, however, showed 50% to 70% percent of front-line providers have never received BPMH training, and 60% say they are not given the time.
“Not knowing means a diligent provider would need to take a BPMH at discharge, which is a waste,” Dr. Stein said. It would be nice to tell from the electronic health record whether a true BPMH had been taken for every hospitalized patient—or at least every high-risk patient—but this goal is not well-supported by current information technology, MARQUIS investigators said they have learned.
The MARQUIS program was launched in 2011 with a grant from the federal Agency for Healthcare Research and Quality. It began with a thorough review of the literature on medication reconciliation and the development of a toolkit of best practices. In 2012, six pilot sites were offered a menu of 11 MARQUIS medication-reconciliation interventions to choose from and help in implementing them from an SHM mentor, with expertise in both QI and medication safety.
Participating sites have mobilized high-level hospital leadership and utilize a local champion, usually a hospitalist, tools for assessing high-risk patients, medication-reconciliation assistants or counselors, and pharmacist involvement. Different sites have employed different professional staff to take medication histories.
Dr. Schnipper said he expects another round of MARQUIS-mentored implementation, probably in 2014, after data from the first round have been analyzed. The program is tracking such outcomes as the number of potentially harmful, unintentional medication discrepancies per patient at participating sites.
The MARQUIS toolkit is available on the SHM website at www.hospitalmedicine.org/marquis.
Larry Beresford is a freelance writer in San Francisco.
–Jeffrey Schnipper, MD, MPH, FHM
What is the best possible medication history? How is it done? Who should do it? When should it be done during a patient’s journey in and out of the hospital? What medication discrepancies—and potential adverse drug events—are most likely?
Those are questions veteran hospitalist Jason Stein, MD, tried to answer during an HM13 breakout session on medication reconciliation at the Gaylord National Resort and Conference Center in National Harbor, Md.
“How do you know as the discharging provider if the medication list you’re looking at is gold or garbage?” said Dr. Stein, associate director for quality improvement (QI) at Emory University in Atlanta and a mentor for SHM’s Multi-Center Medication Reconciliation Quality Improvement Study (MARQUIS) quality-research initiative.
The concept of the “best possible medication history” (BPMH) originated with patient-safety expert Edward Etchells, MD, MSc, at Sunnybrook Health Sciences Centre in Toronto. The concept is outlined on a pocket reminder card for MARQUIS participants, explained co-presenter and principal investigator Jeffrey Schnipper MD, MPH, FHM, a hospitalist at Brigham & Women’s Hospital in Boston.
“Sometimes it’s impossible to know what the patient was or wasn’t taking, but it doesn’t mean you don’t do your best,” he said, adding that hospitalists should attempt to get at least one reliable, corroborating source of information for a patient’s medical history.
Sometimes it is necessary to speak to family members or the community pharmacy, Dr. Schnipper said, because many patients can’t remember all of the drugs they are taking. Trying to do medication reconciliation at the time of discharge when BPMH has not been done can lead to more work for the provider, medication errors, or rehospitalizations. Ideally, knowledge of what the patient was taking before admission, as well as the patient’s health literacy and adherence history, should be gathered and documented once, early, and well during the hospitalization by a trained provider, according to Dr. Schnipper.
An SHM survey, however, showed 50% to 70% percent of front-line providers have never received BPMH training, and 60% say they are not given the time.
“Not knowing means a diligent provider would need to take a BPMH at discharge, which is a waste,” Dr. Stein said. It would be nice to tell from the electronic health record whether a true BPMH had been taken for every hospitalized patient—or at least every high-risk patient—but this goal is not well-supported by current information technology, MARQUIS investigators said they have learned.
The MARQUIS program was launched in 2011 with a grant from the federal Agency for Healthcare Research and Quality. It began with a thorough review of the literature on medication reconciliation and the development of a toolkit of best practices. In 2012, six pilot sites were offered a menu of 11 MARQUIS medication-reconciliation interventions to choose from and help in implementing them from an SHM mentor, with expertise in both QI and medication safety.
Participating sites have mobilized high-level hospital leadership and utilize a local champion, usually a hospitalist, tools for assessing high-risk patients, medication-reconciliation assistants or counselors, and pharmacist involvement. Different sites have employed different professional staff to take medication histories.
Dr. Schnipper said he expects another round of MARQUIS-mentored implementation, probably in 2014, after data from the first round have been analyzed. The program is tracking such outcomes as the number of potentially harmful, unintentional medication discrepancies per patient at participating sites.
The MARQUIS toolkit is available on the SHM website at www.hospitalmedicine.org/marquis.
Larry Beresford is a freelance writer in San Francisco.
–Jeffrey Schnipper, MD, MPH, FHM
What is the best possible medication history? How is it done? Who should do it? When should it be done during a patient’s journey in and out of the hospital? What medication discrepancies—and potential adverse drug events—are most likely?
Those are questions veteran hospitalist Jason Stein, MD, tried to answer during an HM13 breakout session on medication reconciliation at the Gaylord National Resort and Conference Center in National Harbor, Md.
“How do you know as the discharging provider if the medication list you’re looking at is gold or garbage?” said Dr. Stein, associate director for quality improvement (QI) at Emory University in Atlanta and a mentor for SHM’s Multi-Center Medication Reconciliation Quality Improvement Study (MARQUIS) quality-research initiative.
The concept of the “best possible medication history” (BPMH) originated with patient-safety expert Edward Etchells, MD, MSc, at Sunnybrook Health Sciences Centre in Toronto. The concept is outlined on a pocket reminder card for MARQUIS participants, explained co-presenter and principal investigator Jeffrey Schnipper MD, MPH, FHM, a hospitalist at Brigham & Women’s Hospital in Boston.
“Sometimes it’s impossible to know what the patient was or wasn’t taking, but it doesn’t mean you don’t do your best,” he said, adding that hospitalists should attempt to get at least one reliable, corroborating source of information for a patient’s medical history.
Sometimes it is necessary to speak to family members or the community pharmacy, Dr. Schnipper said, because many patients can’t remember all of the drugs they are taking. Trying to do medication reconciliation at the time of discharge when BPMH has not been done can lead to more work for the provider, medication errors, or rehospitalizations. Ideally, knowledge of what the patient was taking before admission, as well as the patient’s health literacy and adherence history, should be gathered and documented once, early, and well during the hospitalization by a trained provider, according to Dr. Schnipper.
An SHM survey, however, showed 50% to 70% percent of front-line providers have never received BPMH training, and 60% say they are not given the time.
“Not knowing means a diligent provider would need to take a BPMH at discharge, which is a waste,” Dr. Stein said. It would be nice to tell from the electronic health record whether a true BPMH had been taken for every hospitalized patient—or at least every high-risk patient—but this goal is not well-supported by current information technology, MARQUIS investigators said they have learned.
The MARQUIS program was launched in 2011 with a grant from the federal Agency for Healthcare Research and Quality. It began with a thorough review of the literature on medication reconciliation and the development of a toolkit of best practices. In 2012, six pilot sites were offered a menu of 11 MARQUIS medication-reconciliation interventions to choose from and help in implementing them from an SHM mentor, with expertise in both QI and medication safety.
Participating sites have mobilized high-level hospital leadership and utilize a local champion, usually a hospitalist, tools for assessing high-risk patients, medication-reconciliation assistants or counselors, and pharmacist involvement. Different sites have employed different professional staff to take medication histories.
Dr. Schnipper said he expects another round of MARQUIS-mentored implementation, probably in 2014, after data from the first round have been analyzed. The program is tracking such outcomes as the number of potentially harmful, unintentional medication discrepancies per patient at participating sites.
The MARQUIS toolkit is available on the SHM website at www.hospitalmedicine.org/marquis.
Larry Beresford is a freelance writer in San Francisco.
How To Avoid Medicare Denials for Critical-Care Billing

Are your critical-care claims at risk for denial or repayment upon review? Several payors have identified increased potential for critical-care reporting discrepancies, which has resulted in targeted prepayment reviews of this code.1 Some payors have implemented 100% review when critical care is reported in settings other than inpatient hospitals, outpatient hospitals, or emergency departments.2 To ensure a successful outcome, make sure the documentation meets the basic principles of the critical-care guidelines.
Defining Critical Illness/Injury
CPT and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g. central-nervous-system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).3 The provider’s time must be solely directed toward the critically ill patient. Highly complex decision-making and interventions of high intensity are required to prevent the patient’s inevitable decline if left untreated. Payment may be made for critical-care services provided in any reasonable location, as long as the care provided meets the definition of critical care. Critical-care services cannot be reported for a patient who is not critically ill but happens to be in a critical-care unit, or when a particular physician is only treating one of the patient’s conditions that is not considered the critical illness.4
Examples of patients who may not satisfy Medicare medical-necessity criteria, do not meet critical-care criteria, or who do not have a critical-care illness or injury and therefore are not eligible for critical-care payment:
- Patients admitted to a critical-care unit because no other hospital beds were available;
- Patients admitted to a critical-care unit for close nursing observation and/or frequent monitoring of vital signs (e.g. drug toxicity or overdose);
- Patients admitted to a critical-care unit because hospital rules require certain treatments (e.g. insulin infusions) to be administered in the critical-care unit; and
- Care of only a chronic illness in the absence of caring for a critical illness (e.g. daily management of a chronic ventilator patient; management of or care related to dialysis for an ESRD).
These circumstances would require using subsequent hospital care codes (99231-99233), initial hospital care codes (99221-99223), or hospital consultation codes (99251-99255) when applicable.3,5
Because critical-care time is a cumulative service, providers keep track of their total time throughout a single calendar day. For each date and encounter entry, the physician’s progress notes shall document the total time that critical-care services were provided (e.g. 45 minutes).4 Some payors impose the notation of “start-and-stop time” per encounter (e.g. 10 to 10:45 a.m.).
Code This Case
Consider the following scenario: A hospitalist admits a 75-year-old patient to the ICU with acute respiratory failure. He spends 45 minutes in critical-care time. The patient’s family arrives soon thereafter to discuss the patient’s condition with a second hospitalist. The discussion lasts an additional 20 minutes, and the decision regarding the patient’s DNR status is made.
Family meetings must take place at the bedside or on the patient’s unit/floor. The patient must participate, unless they are medically unable or clinically incompetent to participate. A notation in the chart should indicate the patient’s inability to participate and the reason. Meeting time can only involve obtaining a medical history and/or discussing treatment options or the limitations of treatment. The conversation must bear directly on patient management.5,6 Meetings that take place for family grief counseling (90846, 90847, 90849) are not included in critical-care time and cannot be billed separately.
Do not count time associated with periodic condition updates to the family or answering questions about the patient’s condition that are unrelated to decision-making.
Family discussions can take place via phone as long as the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.6
Critically ill patients often require the care of multiple providers.3 Payors implement code logic in their systems that allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical-care hours. Documentation must demonstrate that care is not duplicative of other specialists and does not overlap the same time period of any other physician reporting critical-care services.
Same-specialty physicians (two hospitalists from the same group practice) bill and are paid as one physician. The initial critical-care hour (99291) must be met by a single physician. Medically necessary critical-care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. Cumulative physician time should be reported under one provider number on a single invoice in order to prevent denials from billing 99292 independently (see “Critical-Care Services: Time Reminders,”).
When a physician and a nurse practitioner (NP) see a patient on the same calendar day, critical-care reporting is handled differently. A single unit of critical-care time cannot be split or shared between a physician and a qualified NP. One individual must meet the entire time requirement of the reported service code.
More specifically, the hospitalist must individually meet the criteria for the first critical-care hour before reporting 99291, and the NP must individually meet the criteria for an additional 30 minutes of critical care before reporting 99292. The same is true if the NP provided the initial hour while the hospitalist provided the additional critical-care time.
Payors who recognize NPs as independent billing providers (e.g. Medicare and Aetna) require a “split” invoice: an invoice for 99291 with the hospitalist NPI and an invoice for 99292 with the NP’s NPI.9 This ensures reimbursement-rate accuracy, as the physician receives 100% of the allowable rate while the NP receives 85%. If the 99292 invoice is denied due to the payor’s system edits disallowing separate invoicing of add-on codes, appeal with documentation by both the hospitalist and NP to identify the circumstances and reclaim payment.
Critical-Care Services: Time Reminders
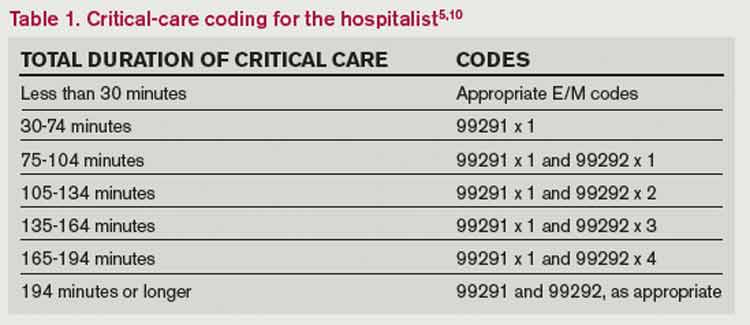
Two available codes:
99291: Critical care, evaluation and management of the critically ill or critically injured patient: first 30-74 minutes. It is reported only once per day, per physician or group member of the same specialty.
+99292: Critical care, evaluation and management of the critically ill or critically injured patient: each additional 30 minutes (list separately in addition to code for primary service). Categorized as an “add on” code, it must be reported on the same invoice as its “primary” code, 99291. Multiple units of code 99292 can be reported per day per physician/group (see Table 1).
Critical-care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient. Also count physician time associated with the performance and/or interpretation of labs, diagnostic studies, and procedures inherent to the provision of critical care:
- Cardiac output measurements (93561, 93562);
- Chest X-rays (71010, 71015, 71020);
- Pulse oximetry (94760, 94761, 94762);
- Blood gases and interpretation of data stored in computers (e.g. ECGs, blood pressures, hematologic data [99090]);
- Gastric intubation (43752, 91105);
- Temporary transcutaneous pacing (92953);
- Ventilation management (94002-94004, 94660, 94662); and
- Vascular access procedures (36000, 36410, 36415, 36591, 36600).5
Other separately billable services or procedures cannot be added to critical-care time. A notation in the medical record is highly recommended (e.g. “central-line insertion is not included as critical-care time”) for validation to prevent payor inquiries.
Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g. reviewing data or calling the family from the office) toward critical-care time. Activities on the floor/unit that do not directly contribute to patient care or management (e.g. review of literature, teaching rounds) cannot be counted toward critical-care time.
—Carol Pohlig
References
- Cahaba Government Benefit Administrators LLC. Widespread prepayment targeted review notification—CPT 99291. Cahaba Government Benefit Administrators LLC website. Available at: http://www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed May 4, 2013.
- First Coast Service Options Inc. Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options Inc. website. Available at: http://medicare.fcso.com/Medical_documentation/249650.asp. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12A. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12B. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12E. Centers for Medicare and Medicaid Services website. Available at http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 6, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012.
- Novitas Solutions Inc. Evaluation & management: service-specific coding instructions. Novitas Solutions Inc. website. Available at: http://www.novitas-solutions.com/em/coding.html. Accessed May 7, 2013.
- United Healthcare. Same day same service policy—adding edits. United Healthcare website. Available at: http://www.unitedhealthcareonline.com/ccmcontent/ ProviderII/ UHC/en-US/Assets/ProviderStaticFiles/ProviderStaticFilesPdf/News/Network_Bulletin_November _2012_Volume_52.pdf. Accessed May 7, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12I. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 10, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12G. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 4, 2013.
Are your critical-care claims at risk for denial or repayment upon review? Several payors have identified increased potential for critical-care reporting discrepancies, which has resulted in targeted prepayment reviews of this code.1 Some payors have implemented 100% review when critical care is reported in settings other than inpatient hospitals, outpatient hospitals, or emergency departments.2 To ensure a successful outcome, make sure the documentation meets the basic principles of the critical-care guidelines.
Defining Critical Illness/Injury
CPT and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g. central-nervous-system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).3 The provider’s time must be solely directed toward the critically ill patient. Highly complex decision-making and interventions of high intensity are required to prevent the patient’s inevitable decline if left untreated. Payment may be made for critical-care services provided in any reasonable location, as long as the care provided meets the definition of critical care. Critical-care services cannot be reported for a patient who is not critically ill but happens to be in a critical-care unit, or when a particular physician is only treating one of the patient’s conditions that is not considered the critical illness.4
Examples of patients who may not satisfy Medicare medical-necessity criteria, do not meet critical-care criteria, or who do not have a critical-care illness or injury and therefore are not eligible for critical-care payment:
- Patients admitted to a critical-care unit because no other hospital beds were available;
- Patients admitted to a critical-care unit for close nursing observation and/or frequent monitoring of vital signs (e.g. drug toxicity or overdose);
- Patients admitted to a critical-care unit because hospital rules require certain treatments (e.g. insulin infusions) to be administered in the critical-care unit; and
- Care of only a chronic illness in the absence of caring for a critical illness (e.g. daily management of a chronic ventilator patient; management of or care related to dialysis for an ESRD).
These circumstances would require using subsequent hospital care codes (99231-99233), initial hospital care codes (99221-99223), or hospital consultation codes (99251-99255) when applicable.3,5
Because critical-care time is a cumulative service, providers keep track of their total time throughout a single calendar day. For each date and encounter entry, the physician’s progress notes shall document the total time that critical-care services were provided (e.g. 45 minutes).4 Some payors impose the notation of “start-and-stop time” per encounter (e.g. 10 to 10:45 a.m.).
Code This Case
Consider the following scenario: A hospitalist admits a 75-year-old patient to the ICU with acute respiratory failure. He spends 45 minutes in critical-care time. The patient’s family arrives soon thereafter to discuss the patient’s condition with a second hospitalist. The discussion lasts an additional 20 minutes, and the decision regarding the patient’s DNR status is made.
Family meetings must take place at the bedside or on the patient’s unit/floor. The patient must participate, unless they are medically unable or clinically incompetent to participate. A notation in the chart should indicate the patient’s inability to participate and the reason. Meeting time can only involve obtaining a medical history and/or discussing treatment options or the limitations of treatment. The conversation must bear directly on patient management.5,6 Meetings that take place for family grief counseling (90846, 90847, 90849) are not included in critical-care time and cannot be billed separately.
Do not count time associated with periodic condition updates to the family or answering questions about the patient’s condition that are unrelated to decision-making.
Family discussions can take place via phone as long as the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.6
Critically ill patients often require the care of multiple providers.3 Payors implement code logic in their systems that allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical-care hours. Documentation must demonstrate that care is not duplicative of other specialists and does not overlap the same time period of any other physician reporting critical-care services.
Same-specialty physicians (two hospitalists from the same group practice) bill and are paid as one physician. The initial critical-care hour (99291) must be met by a single physician. Medically necessary critical-care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. Cumulative physician time should be reported under one provider number on a single invoice in order to prevent denials from billing 99292 independently (see “Critical-Care Services: Time Reminders,”).
When a physician and a nurse practitioner (NP) see a patient on the same calendar day, critical-care reporting is handled differently. A single unit of critical-care time cannot be split or shared between a physician and a qualified NP. One individual must meet the entire time requirement of the reported service code.
More specifically, the hospitalist must individually meet the criteria for the first critical-care hour before reporting 99291, and the NP must individually meet the criteria for an additional 30 minutes of critical care before reporting 99292. The same is true if the NP provided the initial hour while the hospitalist provided the additional critical-care time.
Payors who recognize NPs as independent billing providers (e.g. Medicare and Aetna) require a “split” invoice: an invoice for 99291 with the hospitalist NPI and an invoice for 99292 with the NP’s NPI.9 This ensures reimbursement-rate accuracy, as the physician receives 100% of the allowable rate while the NP receives 85%. If the 99292 invoice is denied due to the payor’s system edits disallowing separate invoicing of add-on codes, appeal with documentation by both the hospitalist and NP to identify the circumstances and reclaim payment.
Critical-Care Services: Time Reminders
Two available codes:
99291: Critical care, evaluation and management of the critically ill or critically injured patient: first 30-74 minutes. It is reported only once per day, per physician or group member of the same specialty.
+99292: Critical care, evaluation and management of the critically ill or critically injured patient: each additional 30 minutes (list separately in addition to code for primary service). Categorized as an “add on” code, it must be reported on the same invoice as its “primary” code, 99291. Multiple units of code 99292 can be reported per day per physician/group (see Table 1).
Critical-care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient. Also count physician time associated with the performance and/or interpretation of labs, diagnostic studies, and procedures inherent to the provision of critical care:
- Cardiac output measurements (93561, 93562);
- Chest X-rays (71010, 71015, 71020);
- Pulse oximetry (94760, 94761, 94762);
- Blood gases and interpretation of data stored in computers (e.g. ECGs, blood pressures, hematologic data [99090]);
- Gastric intubation (43752, 91105);
- Temporary transcutaneous pacing (92953);
- Ventilation management (94002-94004, 94660, 94662); and
- Vascular access procedures (36000, 36410, 36415, 36591, 36600).5
Other separately billable services or procedures cannot be added to critical-care time. A notation in the medical record is highly recommended (e.g. “central-line insertion is not included as critical-care time”) for validation to prevent payor inquiries.
Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g. reviewing data or calling the family from the office) toward critical-care time. Activities on the floor/unit that do not directly contribute to patient care or management (e.g. review of literature, teaching rounds) cannot be counted toward critical-care time.
—Carol Pohlig
References
- Cahaba Government Benefit Administrators LLC. Widespread prepayment targeted review notification—CPT 99291. Cahaba Government Benefit Administrators LLC website. Available at: http://www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed May 4, 2013.
- First Coast Service Options Inc. Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options Inc. website. Available at: http://medicare.fcso.com/Medical_documentation/249650.asp. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12A. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12B. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12E. Centers for Medicare and Medicaid Services website. Available at http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 6, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012.
- Novitas Solutions Inc. Evaluation & management: service-specific coding instructions. Novitas Solutions Inc. website. Available at: http://www.novitas-solutions.com/em/coding.html. Accessed May 7, 2013.
- United Healthcare. Same day same service policy—adding edits. United Healthcare website. Available at: http://www.unitedhealthcareonline.com/ccmcontent/ ProviderII/ UHC/en-US/Assets/ProviderStaticFiles/ProviderStaticFilesPdf/News/Network_Bulletin_November _2012_Volume_52.pdf. Accessed May 7, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12I. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 10, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12G. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 4, 2013.
Are your critical-care claims at risk for denial or repayment upon review? Several payors have identified increased potential for critical-care reporting discrepancies, which has resulted in targeted prepayment reviews of this code.1 Some payors have implemented 100% review when critical care is reported in settings other than inpatient hospitals, outpatient hospitals, or emergency departments.2 To ensure a successful outcome, make sure the documentation meets the basic principles of the critical-care guidelines.
Defining Critical Illness/Injury
CPT and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g. central-nervous-system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).3 The provider’s time must be solely directed toward the critically ill patient. Highly complex decision-making and interventions of high intensity are required to prevent the patient’s inevitable decline if left untreated. Payment may be made for critical-care services provided in any reasonable location, as long as the care provided meets the definition of critical care. Critical-care services cannot be reported for a patient who is not critically ill but happens to be in a critical-care unit, or when a particular physician is only treating one of the patient’s conditions that is not considered the critical illness.4
Examples of patients who may not satisfy Medicare medical-necessity criteria, do not meet critical-care criteria, or who do not have a critical-care illness or injury and therefore are not eligible for critical-care payment:
- Patients admitted to a critical-care unit because no other hospital beds were available;
- Patients admitted to a critical-care unit for close nursing observation and/or frequent monitoring of vital signs (e.g. drug toxicity or overdose);
- Patients admitted to a critical-care unit because hospital rules require certain treatments (e.g. insulin infusions) to be administered in the critical-care unit; and
- Care of only a chronic illness in the absence of caring for a critical illness (e.g. daily management of a chronic ventilator patient; management of or care related to dialysis for an ESRD).
These circumstances would require using subsequent hospital care codes (99231-99233), initial hospital care codes (99221-99223), or hospital consultation codes (99251-99255) when applicable.3,5
Because critical-care time is a cumulative service, providers keep track of their total time throughout a single calendar day. For each date and encounter entry, the physician’s progress notes shall document the total time that critical-care services were provided (e.g. 45 minutes).4 Some payors impose the notation of “start-and-stop time” per encounter (e.g. 10 to 10:45 a.m.).
Code This Case
Consider the following scenario: A hospitalist admits a 75-year-old patient to the ICU with acute respiratory failure. He spends 45 minutes in critical-care time. The patient’s family arrives soon thereafter to discuss the patient’s condition with a second hospitalist. The discussion lasts an additional 20 minutes, and the decision regarding the patient’s DNR status is made.
Family meetings must take place at the bedside or on the patient’s unit/floor. The patient must participate, unless they are medically unable or clinically incompetent to participate. A notation in the chart should indicate the patient’s inability to participate and the reason. Meeting time can only involve obtaining a medical history and/or discussing treatment options or the limitations of treatment. The conversation must bear directly on patient management.5,6 Meetings that take place for family grief counseling (90846, 90847, 90849) are not included in critical-care time and cannot be billed separately.
Do not count time associated with periodic condition updates to the family or answering questions about the patient’s condition that are unrelated to decision-making.
Family discussions can take place via phone as long as the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.6
Critically ill patients often require the care of multiple providers.3 Payors implement code logic in their systems that allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical-care hours. Documentation must demonstrate that care is not duplicative of other specialists and does not overlap the same time period of any other physician reporting critical-care services.
Same-specialty physicians (two hospitalists from the same group practice) bill and are paid as one physician. The initial critical-care hour (99291) must be met by a single physician. Medically necessary critical-care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. Cumulative physician time should be reported under one provider number on a single invoice in order to prevent denials from billing 99292 independently (see “Critical-Care Services: Time Reminders,”).
When a physician and a nurse practitioner (NP) see a patient on the same calendar day, critical-care reporting is handled differently. A single unit of critical-care time cannot be split or shared between a physician and a qualified NP. One individual must meet the entire time requirement of the reported service code.
More specifically, the hospitalist must individually meet the criteria for the first critical-care hour before reporting 99291, and the NP must individually meet the criteria for an additional 30 minutes of critical care before reporting 99292. The same is true if the NP provided the initial hour while the hospitalist provided the additional critical-care time.
Payors who recognize NPs as independent billing providers (e.g. Medicare and Aetna) require a “split” invoice: an invoice for 99291 with the hospitalist NPI and an invoice for 99292 with the NP’s NPI.9 This ensures reimbursement-rate accuracy, as the physician receives 100% of the allowable rate while the NP receives 85%. If the 99292 invoice is denied due to the payor’s system edits disallowing separate invoicing of add-on codes, appeal with documentation by both the hospitalist and NP to identify the circumstances and reclaim payment.
Critical-Care Services: Time Reminders
Two available codes:
99291: Critical care, evaluation and management of the critically ill or critically injured patient: first 30-74 minutes. It is reported only once per day, per physician or group member of the same specialty.
+99292: Critical care, evaluation and management of the critically ill or critically injured patient: each additional 30 minutes (list separately in addition to code for primary service). Categorized as an “add on” code, it must be reported on the same invoice as its “primary” code, 99291. Multiple units of code 99292 can be reported per day per physician/group (see Table 1).
Critical-care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient. Also count physician time associated with the performance and/or interpretation of labs, diagnostic studies, and procedures inherent to the provision of critical care:
- Cardiac output measurements (93561, 93562);
- Chest X-rays (71010, 71015, 71020);
- Pulse oximetry (94760, 94761, 94762);
- Blood gases and interpretation of data stored in computers (e.g. ECGs, blood pressures, hematologic data [99090]);
- Gastric intubation (43752, 91105);
- Temporary transcutaneous pacing (92953);
- Ventilation management (94002-94004, 94660, 94662); and
- Vascular access procedures (36000, 36410, 36415, 36591, 36600).5
Other separately billable services or procedures cannot be added to critical-care time. A notation in the medical record is highly recommended (e.g. “central-line insertion is not included as critical-care time”) for validation to prevent payor inquiries.
Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g. reviewing data or calling the family from the office) toward critical-care time. Activities on the floor/unit that do not directly contribute to patient care or management (e.g. review of literature, teaching rounds) cannot be counted toward critical-care time.
—Carol Pohlig
References
- Cahaba Government Benefit Administrators LLC. Widespread prepayment targeted review notification—CPT 99291. Cahaba Government Benefit Administrators LLC website. Available at: http://www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed May 4, 2013.
- First Coast Service Options Inc. Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options Inc. website. Available at: http://medicare.fcso.com/Medical_documentation/249650.asp. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12A. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12B. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12E. Centers for Medicare and Medicaid Services website. Available at http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 6, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012.
- Novitas Solutions Inc. Evaluation & management: service-specific coding instructions. Novitas Solutions Inc. website. Available at: http://www.novitas-solutions.com/em/coding.html. Accessed May 7, 2013.
- United Healthcare. Same day same service policy—adding edits. United Healthcare website. Available at: http://www.unitedhealthcareonline.com/ccmcontent/ ProviderII/ UHC/en-US/Assets/ProviderStaticFiles/ProviderStaticFilesPdf/News/Network_Bulletin_November _2012_Volume_52.pdf. Accessed May 7, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12I. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 10, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12G. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 4, 2013.
Feds Extend HIPAA Obligations, Violation Penalties
Key Takeaways for Hospitalist Groups

- Covered entities and business associates should review their business associate agreements and determine whether the agreements qualify for grandfathered status and, if needed, enter into new business-associate agreements.
- Covered entities and business associates will need to review their policies and procedures so that they can implement all necessary changes in a timely manner.
- Notices of Privacy Practices will need to be revised, and appropriate training should be provided to personnel of covered entities and business associates.
- Any vendor or business that performs functions for a covered entity or another business associate involving the use or disclosure of PHI should determine whether it is a “business associate” and, if so, what needs to be done in order to comply with the Final Rule.
On Jan. 17, 2013, the Office for Civil Rights (OCR) of the U.S. Department of Health and Human Services (HHS) issued an omnibus Final Rule implementing various provisions of the Health Information Technology for Economic and Clinical Health, or HITECH, Act. The Final Rule revises the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and the interim final Breach Notification Rule.
The HITECH Act, which took effect as part of the American Recovery and Reinvestment Act of 2009, expanded the obligations of covered entities and business associates to protect the confidentiality and security of protected health information (PHI).
Under HIPAA, “covered entities” may disclose PHI to “business associates,” and permit business associates to create and receive PHI on behalf of the covered entity, subject to the terms of a business-associate agreement between the parties. A “covered entity” is defined as a health plan, healthcare clearinghouse, or healthcare provider (e.g. physician practice or hospital) that transmits health information electronically. In general, the HIPAA regulations have traditionally defined a “business associate” as a person (other than a member of the covered entity’s workforce) or entity who, on behalf of a covered entity, performs a function or activity involving the use or disclosure of PHI, such as the performance of financial, legal, actuarial, accounting, consulting, data aggregation, management, administrative, or accreditation services to or for a covered entity.
Prior to the HITECH Act, business associates were contractually obligated to maintain the privacy and security of PHI but could not be sanctioned for failing to comply with HIPAA. The HITECH Act expands those obligations and exposure of business associates by:
- Applying many of the privacy and security standards to business associates;
- Subjecting business associates to the breach-notification requirements; and
- Imposing civil and criminal penalties on business associates for HIPAA violations.
In addition, the HITECH Act strengthened the penalties and enforcement mechanisms under HIPAA and required periodic audits to ensure that covered entities and business associates are compliant.
Expansion of Breach-Notification Requirements
The Final Rule expands the breach-notification obligations of covered entities and business associates by revising the definition of “breach” and the risk-assessment process for determining whether notification is required. A use or disclosure of unsecured PHI that is not permitted under the Privacy Rule is presumed to be a breach (and therefore requires notification to the individual, OCR, and possibly the media) unless the incident satisfies an exception, or the covered entity or business associate demonstrates a low probability that PHI has been compromised.1 This risk analysis is based on at least the following four factors:
- The nature and extent of the PHI, including the types of identifiers and the likelihood of re-identification;
- The unauthorized person who used or accessed the PHI;
- Whether the PHI was actually acquired or viewed; and
- The extent to which the risk is mitigated (e.g. by obtaining reliable assurances by a recipient of PHI that the information will be destroyed or will not be used or disclosed).
Expansion of Business-Associate Obligations
The Final Rule implements the HITECH Act’s expansion of business associates’ HIPAA obligations by applying the Privacy and Security Rules directly to business associates and by imposing civil and criminal penalties on business associates for HIPAA violations. It also extends obligations and potential penalties to subcontractors of business associates if a business associate delegates a function, activity, or service to the subcontractor, and the subcontractor creates, receives, maintains, or transmits PHI on behalf of the business associate. Any business associate that delegates a function involving the use or disclosure of PHI to a subcontractor will be required to enter into a business-associate agreement with the subcontractor.
Additional Provisions
The Final Rule addresses the following additional issues by:
- Requiring covered entities to modify their Notices of Privacy Practices;
- Allowing individuals to obtain a copy of PHI in an electronic format if the covered entity uses an electronic health record;
- Restricting marketing activities;
- Allowing covered entities to disclose relevant PHI of a deceased person to a family member, close friend, or other person designated by the deceased, unless the disclosure is inconsistent with the deceased person’s known prior expressed preference;
- Requiring covered entities to agree to an individual’s request to restrict disclosure of PHI to a health plan when the individual (or someone other than the health plan) pays for the healthcare item or service in full;
- Revising the definition of PHI to exclude information about a person who has been deceased for more than 50 years;
- Prohibiting the sale of PHI without authorization from the individual, and adding a requirement of authorization in order for a covered entity to receive remuneration for disclosing PHI;
- Clarifying OCR’s view that covered entities are allowed to send electronic PHI to individuals in unencrypted e-mails only after notifying the individual of the risk;
- Prohibiting health plans from using or disclosing genetic information for underwriting, as required by the Genetic Information Nondiscrimination Act of 2008 (GINA);
- Allowing disclosure of proof of immunization to schools if agreed by the parent, guardian, or individual;
- Permitting compound authorizations for clinical-research studies; and
- Revising the Enforcement Rule (which was previously revised in 2009 as an interim Final Rule), which:
- Requires the secretary of HHS to investigate a HIPAA complaint if a preliminary investigation indicates a possible violation due to willful neglect;
- Permits HHS to disclose PHI to other government agencies (including state attorneys general) for civil or criminal law-enforcement purposes; and
- Revises standards for determining the levels of civil money penalties.
Effective Date, Compliance Date
Although most provisions of the Final Rule became effective on March 26, many provisions impacting covered entities and business associates (including subcontractors) required compliance by Sept. 23. However, if certain conditions are met, the Final Rule allows additional time to revise business associate agreements to make them compliant. In particular, transition provisions will allow covered entities and business associates to continue to operate under existing business-associate agreements for up to one year beyond the compliance date (until Sept. 22, 2014) if the business-associate agreement:
- Is in writing;
- Is in place prior to Jan. 25, 2013 (the publication date of the Final Rule);
- Is compliant with the Privacy and Security Rules, in effect immediately prior to Jan. 25, 2013; and
- Is not modified or renewed.
This additional time for grandfathered business-associate agreements applies only to the written-documentation requirement. Covered entities, business associates and subcontractors will be required to comply with all other HIPAA requirements beginning on the compliance date, even if the business-associate agreement qualifies for grandfathered status
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Footnote
The exceptions relate to (i) unintentional, good-faith access, acquisition or use by members of the covered entity’s or business associate’s workforce, (ii) inadvertent disclosure limited to persons with authorized access and not resulting in further unpermitted use or disclosure, and (iii) good-faith belief that the unauthorized recipient would be unable to retain the PHI.
Key Takeaways for Hospitalist Groups
- Covered entities and business associates should review their business associate agreements and determine whether the agreements qualify for grandfathered status and, if needed, enter into new business-associate agreements.
- Covered entities and business associates will need to review their policies and procedures so that they can implement all necessary changes in a timely manner.
- Notices of Privacy Practices will need to be revised, and appropriate training should be provided to personnel of covered entities and business associates.
- Any vendor or business that performs functions for a covered entity or another business associate involving the use or disclosure of PHI should determine whether it is a “business associate” and, if so, what needs to be done in order to comply with the Final Rule.
On Jan. 17, 2013, the Office for Civil Rights (OCR) of the U.S. Department of Health and Human Services (HHS) issued an omnibus Final Rule implementing various provisions of the Health Information Technology for Economic and Clinical Health, or HITECH, Act. The Final Rule revises the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and the interim final Breach Notification Rule.
The HITECH Act, which took effect as part of the American Recovery and Reinvestment Act of 2009, expanded the obligations of covered entities and business associates to protect the confidentiality and security of protected health information (PHI).
Under HIPAA, “covered entities” may disclose PHI to “business associates,” and permit business associates to create and receive PHI on behalf of the covered entity, subject to the terms of a business-associate agreement between the parties. A “covered entity” is defined as a health plan, healthcare clearinghouse, or healthcare provider (e.g. physician practice or hospital) that transmits health information electronically. In general, the HIPAA regulations have traditionally defined a “business associate” as a person (other than a member of the covered entity’s workforce) or entity who, on behalf of a covered entity, performs a function or activity involving the use or disclosure of PHI, such as the performance of financial, legal, actuarial, accounting, consulting, data aggregation, management, administrative, or accreditation services to or for a covered entity.
Prior to the HITECH Act, business associates were contractually obligated to maintain the privacy and security of PHI but could not be sanctioned for failing to comply with HIPAA. The HITECH Act expands those obligations and exposure of business associates by:
- Applying many of the privacy and security standards to business associates;
- Subjecting business associates to the breach-notification requirements; and
- Imposing civil and criminal penalties on business associates for HIPAA violations.
In addition, the HITECH Act strengthened the penalties and enforcement mechanisms under HIPAA and required periodic audits to ensure that covered entities and business associates are compliant.
Expansion of Breach-Notification Requirements
The Final Rule expands the breach-notification obligations of covered entities and business associates by revising the definition of “breach” and the risk-assessment process for determining whether notification is required. A use or disclosure of unsecured PHI that is not permitted under the Privacy Rule is presumed to be a breach (and therefore requires notification to the individual, OCR, and possibly the media) unless the incident satisfies an exception, or the covered entity or business associate demonstrates a low probability that PHI has been compromised.1 This risk analysis is based on at least the following four factors:
- The nature and extent of the PHI, including the types of identifiers and the likelihood of re-identification;
- The unauthorized person who used or accessed the PHI;
- Whether the PHI was actually acquired or viewed; and
- The extent to which the risk is mitigated (e.g. by obtaining reliable assurances by a recipient of PHI that the information will be destroyed or will not be used or disclosed).
Expansion of Business-Associate Obligations
The Final Rule implements the HITECH Act’s expansion of business associates’ HIPAA obligations by applying the Privacy and Security Rules directly to business associates and by imposing civil and criminal penalties on business associates for HIPAA violations. It also extends obligations and potential penalties to subcontractors of business associates if a business associate delegates a function, activity, or service to the subcontractor, and the subcontractor creates, receives, maintains, or transmits PHI on behalf of the business associate. Any business associate that delegates a function involving the use or disclosure of PHI to a subcontractor will be required to enter into a business-associate agreement with the subcontractor.
Additional Provisions
The Final Rule addresses the following additional issues by:
- Requiring covered entities to modify their Notices of Privacy Practices;
- Allowing individuals to obtain a copy of PHI in an electronic format if the covered entity uses an electronic health record;
- Restricting marketing activities;
- Allowing covered entities to disclose relevant PHI of a deceased person to a family member, close friend, or other person designated by the deceased, unless the disclosure is inconsistent with the deceased person’s known prior expressed preference;
- Requiring covered entities to agree to an individual’s request to restrict disclosure of PHI to a health plan when the individual (or someone other than the health plan) pays for the healthcare item or service in full;
- Revising the definition of PHI to exclude information about a person who has been deceased for more than 50 years;
- Prohibiting the sale of PHI without authorization from the individual, and adding a requirement of authorization in order for a covered entity to receive remuneration for disclosing PHI;
- Clarifying OCR’s view that covered entities are allowed to send electronic PHI to individuals in unencrypted e-mails only after notifying the individual of the risk;
- Prohibiting health plans from using or disclosing genetic information for underwriting, as required by the Genetic Information Nondiscrimination Act of 2008 (GINA);
- Allowing disclosure of proof of immunization to schools if agreed by the parent, guardian, or individual;
- Permitting compound authorizations for clinical-research studies; and
- Revising the Enforcement Rule (which was previously revised in 2009 as an interim Final Rule), which:
- Requires the secretary of HHS to investigate a HIPAA complaint if a preliminary investigation indicates a possible violation due to willful neglect;
- Permits HHS to disclose PHI to other government agencies (including state attorneys general) for civil or criminal law-enforcement purposes; and
- Revises standards for determining the levels of civil money penalties.
Effective Date, Compliance Date
Although most provisions of the Final Rule became effective on March 26, many provisions impacting covered entities and business associates (including subcontractors) required compliance by Sept. 23. However, if certain conditions are met, the Final Rule allows additional time to revise business associate agreements to make them compliant. In particular, transition provisions will allow covered entities and business associates to continue to operate under existing business-associate agreements for up to one year beyond the compliance date (until Sept. 22, 2014) if the business-associate agreement:
- Is in writing;
- Is in place prior to Jan. 25, 2013 (the publication date of the Final Rule);
- Is compliant with the Privacy and Security Rules, in effect immediately prior to Jan. 25, 2013; and
- Is not modified or renewed.
This additional time for grandfathered business-associate agreements applies only to the written-documentation requirement. Covered entities, business associates and subcontractors will be required to comply with all other HIPAA requirements beginning on the compliance date, even if the business-associate agreement qualifies for grandfathered status
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Footnote
The exceptions relate to (i) unintentional, good-faith access, acquisition or use by members of the covered entity’s or business associate’s workforce, (ii) inadvertent disclosure limited to persons with authorized access and not resulting in further unpermitted use or disclosure, and (iii) good-faith belief that the unauthorized recipient would be unable to retain the PHI.
Key Takeaways for Hospitalist Groups
- Covered entities and business associates should review their business associate agreements and determine whether the agreements qualify for grandfathered status and, if needed, enter into new business-associate agreements.
- Covered entities and business associates will need to review their policies and procedures so that they can implement all necessary changes in a timely manner.
- Notices of Privacy Practices will need to be revised, and appropriate training should be provided to personnel of covered entities and business associates.
- Any vendor or business that performs functions for a covered entity or another business associate involving the use or disclosure of PHI should determine whether it is a “business associate” and, if so, what needs to be done in order to comply with the Final Rule.
On Jan. 17, 2013, the Office for Civil Rights (OCR) of the U.S. Department of Health and Human Services (HHS) issued an omnibus Final Rule implementing various provisions of the Health Information Technology for Economic and Clinical Health, or HITECH, Act. The Final Rule revises the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and the interim final Breach Notification Rule.
The HITECH Act, which took effect as part of the American Recovery and Reinvestment Act of 2009, expanded the obligations of covered entities and business associates to protect the confidentiality and security of protected health information (PHI).
Under HIPAA, “covered entities” may disclose PHI to “business associates,” and permit business associates to create and receive PHI on behalf of the covered entity, subject to the terms of a business-associate agreement between the parties. A “covered entity” is defined as a health plan, healthcare clearinghouse, or healthcare provider (e.g. physician practice or hospital) that transmits health information electronically. In general, the HIPAA regulations have traditionally defined a “business associate” as a person (other than a member of the covered entity’s workforce) or entity who, on behalf of a covered entity, performs a function or activity involving the use or disclosure of PHI, such as the performance of financial, legal, actuarial, accounting, consulting, data aggregation, management, administrative, or accreditation services to or for a covered entity.
Prior to the HITECH Act, business associates were contractually obligated to maintain the privacy and security of PHI but could not be sanctioned for failing to comply with HIPAA. The HITECH Act expands those obligations and exposure of business associates by:
- Applying many of the privacy and security standards to business associates;
- Subjecting business associates to the breach-notification requirements; and
- Imposing civil and criminal penalties on business associates for HIPAA violations.
In addition, the HITECH Act strengthened the penalties and enforcement mechanisms under HIPAA and required periodic audits to ensure that covered entities and business associates are compliant.
Expansion of Breach-Notification Requirements
The Final Rule expands the breach-notification obligations of covered entities and business associates by revising the definition of “breach” and the risk-assessment process for determining whether notification is required. A use or disclosure of unsecured PHI that is not permitted under the Privacy Rule is presumed to be a breach (and therefore requires notification to the individual, OCR, and possibly the media) unless the incident satisfies an exception, or the covered entity or business associate demonstrates a low probability that PHI has been compromised.1 This risk analysis is based on at least the following four factors:
- The nature and extent of the PHI, including the types of identifiers and the likelihood of re-identification;
- The unauthorized person who used or accessed the PHI;
- Whether the PHI was actually acquired or viewed; and
- The extent to which the risk is mitigated (e.g. by obtaining reliable assurances by a recipient of PHI that the information will be destroyed or will not be used or disclosed).
Expansion of Business-Associate Obligations
The Final Rule implements the HITECH Act’s expansion of business associates’ HIPAA obligations by applying the Privacy and Security Rules directly to business associates and by imposing civil and criminal penalties on business associates for HIPAA violations. It also extends obligations and potential penalties to subcontractors of business associates if a business associate delegates a function, activity, or service to the subcontractor, and the subcontractor creates, receives, maintains, or transmits PHI on behalf of the business associate. Any business associate that delegates a function involving the use or disclosure of PHI to a subcontractor will be required to enter into a business-associate agreement with the subcontractor.
Additional Provisions
The Final Rule addresses the following additional issues by:
- Requiring covered entities to modify their Notices of Privacy Practices;
- Allowing individuals to obtain a copy of PHI in an electronic format if the covered entity uses an electronic health record;
- Restricting marketing activities;
- Allowing covered entities to disclose relevant PHI of a deceased person to a family member, close friend, or other person designated by the deceased, unless the disclosure is inconsistent with the deceased person’s known prior expressed preference;
- Requiring covered entities to agree to an individual’s request to restrict disclosure of PHI to a health plan when the individual (or someone other than the health plan) pays for the healthcare item or service in full;
- Revising the definition of PHI to exclude information about a person who has been deceased for more than 50 years;
- Prohibiting the sale of PHI without authorization from the individual, and adding a requirement of authorization in order for a covered entity to receive remuneration for disclosing PHI;
- Clarifying OCR’s view that covered entities are allowed to send electronic PHI to individuals in unencrypted e-mails only after notifying the individual of the risk;
- Prohibiting health plans from using or disclosing genetic information for underwriting, as required by the Genetic Information Nondiscrimination Act of 2008 (GINA);
- Allowing disclosure of proof of immunization to schools if agreed by the parent, guardian, or individual;
- Permitting compound authorizations for clinical-research studies; and
- Revising the Enforcement Rule (which was previously revised in 2009 as an interim Final Rule), which:
- Requires the secretary of HHS to investigate a HIPAA complaint if a preliminary investigation indicates a possible violation due to willful neglect;
- Permits HHS to disclose PHI to other government agencies (including state attorneys general) for civil or criminal law-enforcement purposes; and
- Revises standards for determining the levels of civil money penalties.
Effective Date, Compliance Date
Although most provisions of the Final Rule became effective on March 26, many provisions impacting covered entities and business associates (including subcontractors) required compliance by Sept. 23. However, if certain conditions are met, the Final Rule allows additional time to revise business associate agreements to make them compliant. In particular, transition provisions will allow covered entities and business associates to continue to operate under existing business-associate agreements for up to one year beyond the compliance date (until Sept. 22, 2014) if the business-associate agreement:
- Is in writing;
- Is in place prior to Jan. 25, 2013 (the publication date of the Final Rule);
- Is compliant with the Privacy and Security Rules, in effect immediately prior to Jan. 25, 2013; and
- Is not modified or renewed.
This additional time for grandfathered business-associate agreements applies only to the written-documentation requirement. Covered entities, business associates and subcontractors will be required to comply with all other HIPAA requirements beginning on the compliance date, even if the business-associate agreement qualifies for grandfathered status
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Footnote
The exceptions relate to (i) unintentional, good-faith access, acquisition or use by members of the covered entity’s or business associate’s workforce, (ii) inadvertent disclosure limited to persons with authorized access and not resulting in further unpermitted use or disclosure, and (iii) good-faith belief that the unauthorized recipient would be unable to retain the PHI.
Pallative Care Programs Offered in 84% of U.S. Hospitals by 2014
The proportion of U.S. hospitals projected to offer palliative-care programs by 2014, according to the most recent survey of the industry by the Center to Advance Palliative Care.7 The report estimates a 67% increase in palliative-care services at hospitals of 50 or more beds. The highest concentration for hospital-based palliative care is in the Northeast regions, with the lowest percentage in the South region.
Larry Beresford is a freelance writer in San Francisco.
References
- Harrison J, Quinn K, Mourad M. Is anyone home? The association between being reached for a post-discharge telephone call and 30-day hospital readmission. Harrison J, Quinn K, Mourad M. Any questions? The relationship between responses to post-discharge call questions and 30-day hospital readmissions [abstracts]. Journal of Hospital Medicine, 2013, 8 Suppl 1.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Institute of Medicine website. Available at: http://www.iom.edu/~/media/Files/Report%20Files/2001/Crossing-the-Quality-Chasm/Quality%20Chasm%202001%20%20report%20brief.pdf. Accessed Sept. 9, 2013.
- Shlaes DM, Sahm D, Opiela C, Spellberg B. Commentary: the FDA reboot of antibiotic development. Antimicrob Agents Chemother. 29 Jul 2013 [Epub ahead of print].
- Alliance for Aging Research. HAIs growing problem, group says. Alliance for Aging Research website. Available at: http://www.agingresearch.org/content/article/detail/33504. Accessed Sept. 9, 2013.
- Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. 2013;368:2255-2265.
- Hospitals in Pursuit of Excellence. Eliminating catheter-associated urinary tract infections. Hospitals in Pursuit of Excellence website. Available at: http://www.hpoe.org/Reports-HPOE/eliminating_catheter_associated_urinary_tract_infection.pdf. Accessed Sept. 9, 2013.
- Center to Advance Palliative Care. Growth of palliative care in U.S. hospitals 2013 snapshot. Center to Advance Palliative Care website. Available at: http://www.capc.org/capc-growth-analysis-snapshot-2013.pdf. Accessed Sept. 9, 2013.
The proportion of U.S. hospitals projected to offer palliative-care programs by 2014, according to the most recent survey of the industry by the Center to Advance Palliative Care.7 The report estimates a 67% increase in palliative-care services at hospitals of 50 or more beds. The highest concentration for hospital-based palliative care is in the Northeast regions, with the lowest percentage in the South region.
Larry Beresford is a freelance writer in San Francisco.
References
- Harrison J, Quinn K, Mourad M. Is anyone home? The association between being reached for a post-discharge telephone call and 30-day hospital readmission. Harrison J, Quinn K, Mourad M. Any questions? The relationship between responses to post-discharge call questions and 30-day hospital readmissions [abstracts]. Journal of Hospital Medicine, 2013, 8 Suppl 1.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Institute of Medicine website. Available at: http://www.iom.edu/~/media/Files/Report%20Files/2001/Crossing-the-Quality-Chasm/Quality%20Chasm%202001%20%20report%20brief.pdf. Accessed Sept. 9, 2013.
- Shlaes DM, Sahm D, Opiela C, Spellberg B. Commentary: the FDA reboot of antibiotic development. Antimicrob Agents Chemother. 29 Jul 2013 [Epub ahead of print].
- Alliance for Aging Research. HAIs growing problem, group says. Alliance for Aging Research website. Available at: http://www.agingresearch.org/content/article/detail/33504. Accessed Sept. 9, 2013.
- Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. 2013;368:2255-2265.
- Hospitals in Pursuit of Excellence. Eliminating catheter-associated urinary tract infections. Hospitals in Pursuit of Excellence website. Available at: http://www.hpoe.org/Reports-HPOE/eliminating_catheter_associated_urinary_tract_infection.pdf. Accessed Sept. 9, 2013.
- Center to Advance Palliative Care. Growth of palliative care in U.S. hospitals 2013 snapshot. Center to Advance Palliative Care website. Available at: http://www.capc.org/capc-growth-analysis-snapshot-2013.pdf. Accessed Sept. 9, 2013.
The proportion of U.S. hospitals projected to offer palliative-care programs by 2014, according to the most recent survey of the industry by the Center to Advance Palliative Care.7 The report estimates a 67% increase in palliative-care services at hospitals of 50 or more beds. The highest concentration for hospital-based palliative care is in the Northeast regions, with the lowest percentage in the South region.
Larry Beresford is a freelance writer in San Francisco.
References
- Harrison J, Quinn K, Mourad M. Is anyone home? The association between being reached for a post-discharge telephone call and 30-day hospital readmission. Harrison J, Quinn K, Mourad M. Any questions? The relationship between responses to post-discharge call questions and 30-day hospital readmissions [abstracts]. Journal of Hospital Medicine, 2013, 8 Suppl 1.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Institute of Medicine website. Available at: http://www.iom.edu/~/media/Files/Report%20Files/2001/Crossing-the-Quality-Chasm/Quality%20Chasm%202001%20%20report%20brief.pdf. Accessed Sept. 9, 2013.
- Shlaes DM, Sahm D, Opiela C, Spellberg B. Commentary: the FDA reboot of antibiotic development. Antimicrob Agents Chemother. 29 Jul 2013 [Epub ahead of print].
- Alliance for Aging Research. HAIs growing problem, group says. Alliance for Aging Research website. Available at: http://www.agingresearch.org/content/article/detail/33504. Accessed Sept. 9, 2013.
- Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. 2013;368:2255-2265.
- Hospitals in Pursuit of Excellence. Eliminating catheter-associated urinary tract infections. Hospitals in Pursuit of Excellence website. Available at: http://www.hpoe.org/Reports-HPOE/eliminating_catheter_associated_urinary_tract_infection.pdf. Accessed Sept. 9, 2013.
- Center to Advance Palliative Care. Growth of palliative care in U.S. hospitals 2013 snapshot. Center to Advance Palliative Care website. Available at: http://www.capc.org/capc-growth-analysis-snapshot-2013.pdf. Accessed Sept. 9, 2013.
Little Resistance to Rising Hospital-Acquired Infections
Antibiotic resistance to hospital-acquired infections (HAIs) is rising at faster rates than predicted in 2008 by the Centers for Disease Control and Prevention (CDC), according to an analysis of privately gathered data reported in a recent commentary in Antimicrobial Agents and Chemotherapy, concluding that resistance is “at crisis levels.”3
Antibiotic-resistant microbes infect more than 2 million Americans each year and kill more than 100,000.
“We must act to find new weapons in the global battle against deadly superbugs,” particularly three common HAIs: acinetobacter, E. coli, and klebsiella, said co-author Brad Spellberg, MD, infectious-disease specialist at Harbor-UCLA Medical Center in Los Angeles.
A recent fact sheet from the Alliance for Aging Research notes that older patients, who represent 45% of HAIs annually, carry a higher burden of illness and less favorable outcomes than younger patients.4
Meanwhile, a study of the ICUs at 43 Hospital Corporation of America hospitals, published in the New England Journal of Medicine, provides support for treating all ICU patients with universal precautions for methicillin-resistant Staphylococcus aureus (MRSA).5 Washing all ICU patients with antibiotic soap and administering nasal antibiotics reduced all types of bloodstream infections by 44% and proved more effective than the common practice of screening patients for MRSA first, then treating those testing positive.
Another recent resource for HAIs is the “Eliminating Catheter-Associated Urinary Tract Infections” guide from the American Hospital Association’s Hospitals in Pursuit of Excellence unit.6 The booklet recommends an evidence-based, three-step action plan derived from AHA’s On the CUSP: Stop CAUTI project, and is available free on the AHA website. It has an accompanying webinar, which outlines the business case for eliminating catheter-associated urinary tract infections (CAUTIs) and the importance of hospital culture in achieving sustainability.
Larry Beresford is a freelance writer in San Francisco.
References
- Harrison J, Quinn K, Mourad M. Is anyone home? The association between being reached for a post-discharge telephone call and 30-day hospital readmission. Harrison J, Quinn K, Mourad M. Any questions? The relationship between responses to post-discharge call questions and 30-day hospital readmissions [abstracts]. Journal of Hospital Medicine, 2013, 8 Suppl 1.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Institute of Medicine website. Available at: http://www.iom.edu/~/media/Files/Report%20Files/2001/Crossing-the-Quality-Chasm/Quality%20Chasm%202001%20%20report%20brief.pdf. Accessed Sept. 9, 2013.
- Shlaes DM, Sahm D, Opiela C, Spellberg B. Commentary: the FDA reboot of antibiotic development. Antimicrob Agents Chemother. 29 Jul 2013 [Epub ahead of print].
- Alliance for Aging Research. HAIs growing problem, group says. Alliance for Aging Research website. Available at: http://www.agingresearch.org/content/article/detail/33504. Accessed Sept. 9, 2013.
- Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. 2013;368:2255-2265.
- Hospitals in Pursuit of Excellence. Eliminating catheter-associated urinary tract infections. Hospitals in Pursuit of Excellence website. Available at: http://www.hpoe.org/Reports-HPOE/eliminating_catheter_associated_urinary_tract_infection.pdf. Accessed Sept. 9, 2013.
- Center to Advance Palliative Care. Growth of palliative care in U.S. hospitals 2013 snapshot. Center to Advance Palliative Care website. Available at: http://www.capc.org/capc-growth-analysis-snapshot-2013.pdf. Accessed Sept. 9, 2013.
Antibiotic resistance to hospital-acquired infections (HAIs) is rising at faster rates than predicted in 2008 by the Centers for Disease Control and Prevention (CDC), according to an analysis of privately gathered data reported in a recent commentary in Antimicrobial Agents and Chemotherapy, concluding that resistance is “at crisis levels.”3
Antibiotic-resistant microbes infect more than 2 million Americans each year and kill more than 100,000.
“We must act to find new weapons in the global battle against deadly superbugs,” particularly three common HAIs: acinetobacter, E. coli, and klebsiella, said co-author Brad Spellberg, MD, infectious-disease specialist at Harbor-UCLA Medical Center in Los Angeles.
A recent fact sheet from the Alliance for Aging Research notes that older patients, who represent 45% of HAIs annually, carry a higher burden of illness and less favorable outcomes than younger patients.4
Meanwhile, a study of the ICUs at 43 Hospital Corporation of America hospitals, published in the New England Journal of Medicine, provides support for treating all ICU patients with universal precautions for methicillin-resistant Staphylococcus aureus (MRSA).5 Washing all ICU patients with antibiotic soap and administering nasal antibiotics reduced all types of bloodstream infections by 44% and proved more effective than the common practice of screening patients for MRSA first, then treating those testing positive.
Another recent resource for HAIs is the “Eliminating Catheter-Associated Urinary Tract Infections” guide from the American Hospital Association’s Hospitals in Pursuit of Excellence unit.6 The booklet recommends an evidence-based, three-step action plan derived from AHA’s On the CUSP: Stop CAUTI project, and is available free on the AHA website. It has an accompanying webinar, which outlines the business case for eliminating catheter-associated urinary tract infections (CAUTIs) and the importance of hospital culture in achieving sustainability.
Larry Beresford is a freelance writer in San Francisco.
References
- Harrison J, Quinn K, Mourad M. Is anyone home? The association between being reached for a post-discharge telephone call and 30-day hospital readmission. Harrison J, Quinn K, Mourad M. Any questions? The relationship between responses to post-discharge call questions and 30-day hospital readmissions [abstracts]. Journal of Hospital Medicine, 2013, 8 Suppl 1.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Institute of Medicine website. Available at: http://www.iom.edu/~/media/Files/Report%20Files/2001/Crossing-the-Quality-Chasm/Quality%20Chasm%202001%20%20report%20brief.pdf. Accessed Sept. 9, 2013.
- Shlaes DM, Sahm D, Opiela C, Spellberg B. Commentary: the FDA reboot of antibiotic development. Antimicrob Agents Chemother. 29 Jul 2013 [Epub ahead of print].
- Alliance for Aging Research. HAIs growing problem, group says. Alliance for Aging Research website. Available at: http://www.agingresearch.org/content/article/detail/33504. Accessed Sept. 9, 2013.
- Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. 2013;368:2255-2265.
- Hospitals in Pursuit of Excellence. Eliminating catheter-associated urinary tract infections. Hospitals in Pursuit of Excellence website. Available at: http://www.hpoe.org/Reports-HPOE/eliminating_catheter_associated_urinary_tract_infection.pdf. Accessed Sept. 9, 2013.
- Center to Advance Palliative Care. Growth of palliative care in U.S. hospitals 2013 snapshot. Center to Advance Palliative Care website. Available at: http://www.capc.org/capc-growth-analysis-snapshot-2013.pdf. Accessed Sept. 9, 2013.
Antibiotic resistance to hospital-acquired infections (HAIs) is rising at faster rates than predicted in 2008 by the Centers for Disease Control and Prevention (CDC), according to an analysis of privately gathered data reported in a recent commentary in Antimicrobial Agents and Chemotherapy, concluding that resistance is “at crisis levels.”3
Antibiotic-resistant microbes infect more than 2 million Americans each year and kill more than 100,000.
“We must act to find new weapons in the global battle against deadly superbugs,” particularly three common HAIs: acinetobacter, E. coli, and klebsiella, said co-author Brad Spellberg, MD, infectious-disease specialist at Harbor-UCLA Medical Center in Los Angeles.
A recent fact sheet from the Alliance for Aging Research notes that older patients, who represent 45% of HAIs annually, carry a higher burden of illness and less favorable outcomes than younger patients.4
Meanwhile, a study of the ICUs at 43 Hospital Corporation of America hospitals, published in the New England Journal of Medicine, provides support for treating all ICU patients with universal precautions for methicillin-resistant Staphylococcus aureus (MRSA).5 Washing all ICU patients with antibiotic soap and administering nasal antibiotics reduced all types of bloodstream infections by 44% and proved more effective than the common practice of screening patients for MRSA first, then treating those testing positive.
Another recent resource for HAIs is the “Eliminating Catheter-Associated Urinary Tract Infections” guide from the American Hospital Association’s Hospitals in Pursuit of Excellence unit.6 The booklet recommends an evidence-based, three-step action plan derived from AHA’s On the CUSP: Stop CAUTI project, and is available free on the AHA website. It has an accompanying webinar, which outlines the business case for eliminating catheter-associated urinary tract infections (CAUTIs) and the importance of hospital culture in achieving sustainability.
Larry Beresford is a freelance writer in San Francisco.
References
- Harrison J, Quinn K, Mourad M. Is anyone home? The association between being reached for a post-discharge telephone call and 30-day hospital readmission. Harrison J, Quinn K, Mourad M. Any questions? The relationship between responses to post-discharge call questions and 30-day hospital readmissions [abstracts]. Journal of Hospital Medicine, 2013, 8 Suppl 1.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Institute of Medicine website. Available at: http://www.iom.edu/~/media/Files/Report%20Files/2001/Crossing-the-Quality-Chasm/Quality%20Chasm%202001%20%20report%20brief.pdf. Accessed Sept. 9, 2013.
- Shlaes DM, Sahm D, Opiela C, Spellberg B. Commentary: the FDA reboot of antibiotic development. Antimicrob Agents Chemother. 29 Jul 2013 [Epub ahead of print].
- Alliance for Aging Research. HAIs growing problem, group says. Alliance for Aging Research website. Available at: http://www.agingresearch.org/content/article/detail/33504. Accessed Sept. 9, 2013.
- Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. 2013;368:2255-2265.
- Hospitals in Pursuit of Excellence. Eliminating catheter-associated urinary tract infections. Hospitals in Pursuit of Excellence website. Available at: http://www.hpoe.org/Reports-HPOE/eliminating_catheter_associated_urinary_tract_infection.pdf. Accessed Sept. 9, 2013.
- Center to Advance Palliative Care. Growth of palliative care in U.S. hospitals 2013 snapshot. Center to Advance Palliative Care website. Available at: http://www.capc.org/capc-growth-analysis-snapshot-2013.pdf. Accessed Sept. 9, 2013.
Boston Hospital Earns Quality Award
In July, four U.S. hospitals were recognized for their leadership and innovation in quality improvement (QI) and safety—as defined by the Institute of Medicine (IOM)—through the American Hospital Association’s McKesson Quest for Quality Prize.2 Beth Israel Deaconess Medical Center (BIDMC) in Boston was awarded the overall prize for its sustainable approach and hospitalwide commitment to pursuing IOM’s quality aims for safe, effective, efficient, timely, patient-centered, and equitable health care.
The award, presented since 2002, is supported by healthcare-services company McKesson Corp., based in San Francisco.
Key to BIDMC’s success is the clear message of its top leadership’s commitment to quality and a strong partnership with the medical community, says Kenneth Sands, MD, MPH, BIDMC’s senior vice president for healthcare quality. “That includes an official vote by the hospital’s board to adopt IOM’s definition of quality. And everyone here participates in the quality process,” he says.
Each year, the hospital holds a quality symposium featuring QI projects solicited from across the organization. This year’s poster contest recognized three winners, one from the finance department, one from an ICU, and a third from the hospital cafeteria (it tracked the percentage of days that fresh fish is offered as a healthy menu choice).
“To see these three winners standing together on the podium sends a powerful message,” Dr. Sands says. “These are not quality-improvement experts, but front-line staff.”
Another quality initiative involves a hospitalist leader trying to promote “conversation readiness” for a hospital staff’s ability to respond to patients’ expressed desires to complete advance directives, then make sure these documents get captured in the medical record.
Larry Beresford is a freelance writer in San Francisco.
References
- Harrison J, Quinn K, Mourad M. Is anyone home? The association between being reached for a post-discharge telephone call and 30-day hospital readmission. Harrison J, Quinn K, Mourad M. Any questions? The relationship between responses to post-discharge call questions and 30-day hospital readmissions [abstracts]. Journal of Hospital Medicine, 2013, 8 Suppl 1.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Institute of Medicine website. Available at: http://www.iom.edu/~/media/Files/Report%20Files/2001/Crossing-the-Quality-Chasm/Quality%20Chasm%202001%20%20report%20brief.pdf. Accessed Sept. 9, 2013.
- Shlaes DM, Sahm D, Opiela C, Spellberg B. Commentary: the FDA reboot of antibiotic development. Antimicrob Agents Chemother. 29 Jul 2013 [Epub ahead of print].
- Alliance for Aging Research. HAIs growing problem, group says. Alliance for Aging Research website. Available at: http://www.agingresearch.org/content/article/detail/33504. Accessed Sept. 9, 2013.
- Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. 2013;368:2255-2265.
- Hospitals in Pursuit of Excellence. Eliminating catheter-associated urinary tract infections. Hospitals in Pursuit of Excellence website. Available at: http://www.hpoe.org/Reports-HPOE/eliminating_catheter_associated_urinary_tract_infection.pdf. Accessed Sept. 9, 2013.
- Center to Advance Palliative Care. Growth of palliative care in U.S. hospitals 2013 snapshot. Center to Advance Palliative Care website. Available at: http://www.capc.org/capc-growth-analysis-snapshot-2013.pdf. Accessed Sept. 9, 2013.
In July, four U.S. hospitals were recognized for their leadership and innovation in quality improvement (QI) and safety—as defined by the Institute of Medicine (IOM)—through the American Hospital Association’s McKesson Quest for Quality Prize.2 Beth Israel Deaconess Medical Center (BIDMC) in Boston was awarded the overall prize for its sustainable approach and hospitalwide commitment to pursuing IOM’s quality aims for safe, effective, efficient, timely, patient-centered, and equitable health care.
The award, presented since 2002, is supported by healthcare-services company McKesson Corp., based in San Francisco.
Key to BIDMC’s success is the clear message of its top leadership’s commitment to quality and a strong partnership with the medical community, says Kenneth Sands, MD, MPH, BIDMC’s senior vice president for healthcare quality. “That includes an official vote by the hospital’s board to adopt IOM’s definition of quality. And everyone here participates in the quality process,” he says.
Each year, the hospital holds a quality symposium featuring QI projects solicited from across the organization. This year’s poster contest recognized three winners, one from the finance department, one from an ICU, and a third from the hospital cafeteria (it tracked the percentage of days that fresh fish is offered as a healthy menu choice).
“To see these three winners standing together on the podium sends a powerful message,” Dr. Sands says. “These are not quality-improvement experts, but front-line staff.”
Another quality initiative involves a hospitalist leader trying to promote “conversation readiness” for a hospital staff’s ability to respond to patients’ expressed desires to complete advance directives, then make sure these documents get captured in the medical record.
Larry Beresford is a freelance writer in San Francisco.
References
- Harrison J, Quinn K, Mourad M. Is anyone home? The association between being reached for a post-discharge telephone call and 30-day hospital readmission. Harrison J, Quinn K, Mourad M. Any questions? The relationship between responses to post-discharge call questions and 30-day hospital readmissions [abstracts]. Journal of Hospital Medicine, 2013, 8 Suppl 1.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Institute of Medicine website. Available at: http://www.iom.edu/~/media/Files/Report%20Files/2001/Crossing-the-Quality-Chasm/Quality%20Chasm%202001%20%20report%20brief.pdf. Accessed Sept. 9, 2013.
- Shlaes DM, Sahm D, Opiela C, Spellberg B. Commentary: the FDA reboot of antibiotic development. Antimicrob Agents Chemother. 29 Jul 2013 [Epub ahead of print].
- Alliance for Aging Research. HAIs growing problem, group says. Alliance for Aging Research website. Available at: http://www.agingresearch.org/content/article/detail/33504. Accessed Sept. 9, 2013.
- Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. 2013;368:2255-2265.
- Hospitals in Pursuit of Excellence. Eliminating catheter-associated urinary tract infections. Hospitals in Pursuit of Excellence website. Available at: http://www.hpoe.org/Reports-HPOE/eliminating_catheter_associated_urinary_tract_infection.pdf. Accessed Sept. 9, 2013.
- Center to Advance Palliative Care. Growth of palliative care in U.S. hospitals 2013 snapshot. Center to Advance Palliative Care website. Available at: http://www.capc.org/capc-growth-analysis-snapshot-2013.pdf. Accessed Sept. 9, 2013.
In July, four U.S. hospitals were recognized for their leadership and innovation in quality improvement (QI) and safety—as defined by the Institute of Medicine (IOM)—through the American Hospital Association’s McKesson Quest for Quality Prize.2 Beth Israel Deaconess Medical Center (BIDMC) in Boston was awarded the overall prize for its sustainable approach and hospitalwide commitment to pursuing IOM’s quality aims for safe, effective, efficient, timely, patient-centered, and equitable health care.
The award, presented since 2002, is supported by healthcare-services company McKesson Corp., based in San Francisco.
Key to BIDMC’s success is the clear message of its top leadership’s commitment to quality and a strong partnership with the medical community, says Kenneth Sands, MD, MPH, BIDMC’s senior vice president for healthcare quality. “That includes an official vote by the hospital’s board to adopt IOM’s definition of quality. And everyone here participates in the quality process,” he says.
Each year, the hospital holds a quality symposium featuring QI projects solicited from across the organization. This year’s poster contest recognized three winners, one from the finance department, one from an ICU, and a third from the hospital cafeteria (it tracked the percentage of days that fresh fish is offered as a healthy menu choice).
“To see these three winners standing together on the podium sends a powerful message,” Dr. Sands says. “These are not quality-improvement experts, but front-line staff.”
Another quality initiative involves a hospitalist leader trying to promote “conversation readiness” for a hospital staff’s ability to respond to patients’ expressed desires to complete advance directives, then make sure these documents get captured in the medical record.
Larry Beresford is a freelance writer in San Francisco.
References
- Harrison J, Quinn K, Mourad M. Is anyone home? The association between being reached for a post-discharge telephone call and 30-day hospital readmission. Harrison J, Quinn K, Mourad M. Any questions? The relationship between responses to post-discharge call questions and 30-day hospital readmissions [abstracts]. Journal of Hospital Medicine, 2013, 8 Suppl 1.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Institute of Medicine website. Available at: http://www.iom.edu/~/media/Files/Report%20Files/2001/Crossing-the-Quality-Chasm/Quality%20Chasm%202001%20%20report%20brief.pdf. Accessed Sept. 9, 2013.
- Shlaes DM, Sahm D, Opiela C, Spellberg B. Commentary: the FDA reboot of antibiotic development. Antimicrob Agents Chemother. 29 Jul 2013 [Epub ahead of print].
- Alliance for Aging Research. HAIs growing problem, group says. Alliance for Aging Research website. Available at: http://www.agingresearch.org/content/article/detail/33504. Accessed Sept. 9, 2013.
- Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. 2013;368:2255-2265.
- Hospitals in Pursuit of Excellence. Eliminating catheter-associated urinary tract infections. Hospitals in Pursuit of Excellence website. Available at: http://www.hpoe.org/Reports-HPOE/eliminating_catheter_associated_urinary_tract_infection.pdf. Accessed Sept. 9, 2013.
- Center to Advance Palliative Care. Growth of palliative care in U.S. hospitals 2013 snapshot. Center to Advance Palliative Care website. Available at: http://www.capc.org/capc-growth-analysis-snapshot-2013.pdf. Accessed Sept. 9, 2013.