User login
Fellow in Hospital Medicine Spotlight: Arvind Gupta, MD, FACP, FHM

Dr. Gupta is a hospitalist at Wellspan York Hospital in York, Pa. He is the former medical director of the hospitalist program at Holy Spirit Hospital in Camp Hill, Pa., and the former director of the department of medicine research at Lehigh Valley Hospital in Allentown, Pa. He is president and founder of the South Central Pennsylvania chapter of SHM.
Undergraduate education: Punjab University, India
Medical school: Ross University School of Medicine, Dominica
Notable: After spending 10 years as a director of microbiology at Vencor Hospital in Arlington, Va., Dr. Gupta began attending medical school when he was 36. Although he started his hospitalist career much later than most, he has made up the time through active participation at the hospitals in which he worked. He has been a part of the medical executive committee, the quality council, and the performance improvement committee,. He also chaired the credential committee. As a research specialist, he has taken part in 34 clinical trials. As a hospitalist, he focuses on providing efficient, safe, and cost-effective care for his patients.
FYI: Dr. Gupta’s favorite pastime is golf. He loves watching sports and movies with his family. He says one of his greatest achievements is having sons who attend Duke University and Cornell University.
Quotable: “Becoming an SHM fellow is a great honor and recognition. It means a lot for the new designation of the hospitalist.”
Dr. Gupta is a hospitalist at Wellspan York Hospital in York, Pa. He is the former medical director of the hospitalist program at Holy Spirit Hospital in Camp Hill, Pa., and the former director of the department of medicine research at Lehigh Valley Hospital in Allentown, Pa. He is president and founder of the South Central Pennsylvania chapter of SHM.
Undergraduate education: Punjab University, India
Medical school: Ross University School of Medicine, Dominica
Notable: After spending 10 years as a director of microbiology at Vencor Hospital in Arlington, Va., Dr. Gupta began attending medical school when he was 36. Although he started his hospitalist career much later than most, he has made up the time through active participation at the hospitals in which he worked. He has been a part of the medical executive committee, the quality council, and the performance improvement committee,. He also chaired the credential committee. As a research specialist, he has taken part in 34 clinical trials. As a hospitalist, he focuses on providing efficient, safe, and cost-effective care for his patients.
FYI: Dr. Gupta’s favorite pastime is golf. He loves watching sports and movies with his family. He says one of his greatest achievements is having sons who attend Duke University and Cornell University.
Quotable: “Becoming an SHM fellow is a great honor and recognition. It means a lot for the new designation of the hospitalist.”
Dr. Gupta is a hospitalist at Wellspan York Hospital in York, Pa. He is the former medical director of the hospitalist program at Holy Spirit Hospital in Camp Hill, Pa., and the former director of the department of medicine research at Lehigh Valley Hospital in Allentown, Pa. He is president and founder of the South Central Pennsylvania chapter of SHM.
Undergraduate education: Punjab University, India
Medical school: Ross University School of Medicine, Dominica
Notable: After spending 10 years as a director of microbiology at Vencor Hospital in Arlington, Va., Dr. Gupta began attending medical school when he was 36. Although he started his hospitalist career much later than most, he has made up the time through active participation at the hospitals in which he worked. He has been a part of the medical executive committee, the quality council, and the performance improvement committee,. He also chaired the credential committee. As a research specialist, he has taken part in 34 clinical trials. As a hospitalist, he focuses on providing efficient, safe, and cost-effective care for his patients.
FYI: Dr. Gupta’s favorite pastime is golf. He loves watching sports and movies with his family. He says one of his greatest achievements is having sons who attend Duke University and Cornell University.
Quotable: “Becoming an SHM fellow is a great honor and recognition. It means a lot for the new designation of the hospitalist.”
Larry Wellikson: Exceptional Hospitalists Bring Positive Change to Health Care Industry

Exceptional hospitalists





Even though hospital medicine and SHM are still relatively young, we can be very proud of what our specialty already has brought to changing our nation’s health care for the better. Many of these accomplishments, from winning the prestigious Eisenberg Award to our change leadership by SHM’s Center for Healthcare Innovation and Improvement at more 300 hospitals to the extraordinary growth of our specialty, have been well chronicled in The Hospitalist and elsewhere the last few years.
I wanted to use this month’s column to highlight the unique career directions of a few SHM members to shine a bright light on the influence hospitalists are making nationwide. Certainly, there are many more hospitalists beyond this group of five that I have selected, but this small cadre should serve as an example of the talent and reach of our specialty—with only more and greater things ahead to come in the future.
Chief Medical Officer of CMS
Pat Conway, MD, SFHM, is a pediatric hospitalist and the former chair of SHM’s Public Policy Committee. He left his pediatric academic practice to become a White House fellow, then returned to Cincinnati Children’s Hospital to serve as chief medical officer (CMO). When Don Berwick was in charge of the Centers for Medicare & Medicaid Services (CMS), he reached out to Pat and asked him to come to Washington to be part of Medicare’s senior team as the CMO for CMS. In this role, Pat has been a nationally recognized leader in performance improvement and patient safety, and he has been instrumental in bringing about evolutionary changes to the largest healthcare program in the world. Pat will be sharing his perspectives as a keynote speaker at HM13 (check out our 10-page HM13 preview starting on p. 45).
Resident Fellow at the American Enterprise Institute
Scott Gottlieb, MD, is a practicing hospitalist in New York City, but he is better known as a leading expert in healthcare policy, most recently acting as an advisor to presidential candidate Mitt Romney. From 2005 to 2007, Scott was a deputy commissioner at the FDA. He has worked as a senior advisor to the administrator at CMS, where he played an instrumental role in the implementation of the Medicare Drug Benefit in 2004.
Scott is best known for his frequent contributions to The Wall Street Journal, The New York Times, USA Today, and Forbes. He has held editorial positions at the British Medical Journal and the Journal of the American Medical Association, regularly appears as a guest commentator on CNBC, and is a frequent contributor to Politico.
At SHM, Scott has brought his national viewpoint to the Public Policy Committee. He proudly touts his experience as a practicing hospitalist as bringing a front-line reality to his national recognition and much-sought-after critical thinking about healthcare policy.
Chairman of the American Board of Internal Medicine
Bob Wachter, MD, MHM, was a thought leader in HM before our specialty even had a name, writing the initial peer-reviewed articles and coining the term “hospitalist.” Bob has built a pre-eminent hospitalist program at the University of California at San Francisco and helped influence and populate much of academic HM. His Wachter’s World blog (www.wachtersworld.com) is one of the most widely read medical blogs, reaching an audience well beyond our specialty.
Bob was one of the first presidents of SHM—back when we were known as NAIP, or the National Association of Inpatient Physicians—and set SHM on its strong growth and innovative direction that has made us the envy of other medical specialty societies. Last year, Modern Healthcare hailed Bob as the 14th most influential physician executive in the entire country.
On the ABIM board, Bob has represented the best of HM and brought our innovative spirit and our commitment to improvement, safety, and change leadership, culminating this year in the ABIM chairmanship. Bob will offer his unique insights into HM and the national healthcare agenda at HM13 (www.hospitalmedicine 2013.org).
CEO: Telemedicine for the ICU
Mary Jo Gorman, MD, MHM, is a hospitalist and intensivist who made her mark on HM as the chief medical officer (CMO) of IPC: The Hospitalist Company. As she offered her talents to SHM, she became chairman of SHM’s Public Policy Committee and eventually SHM president.
For the last few years, Mary Jo has been the CEO of ICUMedicine. In this role, she has been active around the country, bringing ICU competencies to many community hospitals by offering a telemedicine solution for critically ill patients. This unconventional approach to meeting a glaring need fits into Mary Jo’s career history of looking for new and different ways to bring better healthcare solutions to the front lines of patient care. Last year, Modern Healthcare recognized Mary Jo as one of the most influential female physician executives in the country.
CEO, Medical University of South Carolina (MUSC) Hospitals
After leaving Duke University, Pat Cawley, MD, MBA, MHM, started his career as a community-based hospitalist leader. After a number of leadership roles at SHM, Pat served as SHM president and was elected a Master in Hospital Medicine in 2012.
Pat initially was recruited to MUSC to build and manage their HM group. Soon he was tapped to be the CMO at MUSC. Earlier this year, Pat became the first hospitalist to be chosen to run a major academic medical center when he was promoted to CEO at MUSC.
In recent years, Pat has been a leading voice as the American Hospital Association looks to involve physician leaders. He is a rising star at AHA, helping to merge the cultures of hospital administrators and physicians to create the hospital of the future.
Hospitalists Contribute at the Highest Level
Obviously, I could go on and on, adding other hospitalists who are making unique and important contributions at the local and national level. It is interesting that at a time when many are still trying to get their heads around just what HM is, we already can recognize the immense talent that resides in hospitalist groups across the country. At a time when the U.S. healthcare system is being reshaped, hospitalists, such as those mentioned above and oh-so-many more, are already making large and small steps forward. We are helping to create a new healthcare enterprise, based on value, efficiency, effectiveness, and putting the patient first.
SHM wants to continue to be the place where the innovators and thought leaders of today and tomorrow can come together to multiply their efforts. The challenges are daunting, but the results can be rewarding, and the members of SHM are ready to bring our talents, energies, and commitments to do our part in this great American journey.
Exceptional hospitalists
Even though hospital medicine and SHM are still relatively young, we can be very proud of what our specialty already has brought to changing our nation’s health care for the better. Many of these accomplishments, from winning the prestigious Eisenberg Award to our change leadership by SHM’s Center for Healthcare Innovation and Improvement at more 300 hospitals to the extraordinary growth of our specialty, have been well chronicled in The Hospitalist and elsewhere the last few years.
I wanted to use this month’s column to highlight the unique career directions of a few SHM members to shine a bright light on the influence hospitalists are making nationwide. Certainly, there are many more hospitalists beyond this group of five that I have selected, but this small cadre should serve as an example of the talent and reach of our specialty—with only more and greater things ahead to come in the future.
Chief Medical Officer of CMS
Pat Conway, MD, SFHM, is a pediatric hospitalist and the former chair of SHM’s Public Policy Committee. He left his pediatric academic practice to become a White House fellow, then returned to Cincinnati Children’s Hospital to serve as chief medical officer (CMO). When Don Berwick was in charge of the Centers for Medicare & Medicaid Services (CMS), he reached out to Pat and asked him to come to Washington to be part of Medicare’s senior team as the CMO for CMS. In this role, Pat has been a nationally recognized leader in performance improvement and patient safety, and he has been instrumental in bringing about evolutionary changes to the largest healthcare program in the world. Pat will be sharing his perspectives as a keynote speaker at HM13 (check out our 10-page HM13 preview starting on p. 45).
Resident Fellow at the American Enterprise Institute
Scott Gottlieb, MD, is a practicing hospitalist in New York City, but he is better known as a leading expert in healthcare policy, most recently acting as an advisor to presidential candidate Mitt Romney. From 2005 to 2007, Scott was a deputy commissioner at the FDA. He has worked as a senior advisor to the administrator at CMS, where he played an instrumental role in the implementation of the Medicare Drug Benefit in 2004.
Scott is best known for his frequent contributions to The Wall Street Journal, The New York Times, USA Today, and Forbes. He has held editorial positions at the British Medical Journal and the Journal of the American Medical Association, regularly appears as a guest commentator on CNBC, and is a frequent contributor to Politico.
At SHM, Scott has brought his national viewpoint to the Public Policy Committee. He proudly touts his experience as a practicing hospitalist as bringing a front-line reality to his national recognition and much-sought-after critical thinking about healthcare policy.
Chairman of the American Board of Internal Medicine
Bob Wachter, MD, MHM, was a thought leader in HM before our specialty even had a name, writing the initial peer-reviewed articles and coining the term “hospitalist.” Bob has built a pre-eminent hospitalist program at the University of California at San Francisco and helped influence and populate much of academic HM. His Wachter’s World blog (www.wachtersworld.com) is one of the most widely read medical blogs, reaching an audience well beyond our specialty.
Bob was one of the first presidents of SHM—back when we were known as NAIP, or the National Association of Inpatient Physicians—and set SHM on its strong growth and innovative direction that has made us the envy of other medical specialty societies. Last year, Modern Healthcare hailed Bob as the 14th most influential physician executive in the entire country.
On the ABIM board, Bob has represented the best of HM and brought our innovative spirit and our commitment to improvement, safety, and change leadership, culminating this year in the ABIM chairmanship. Bob will offer his unique insights into HM and the national healthcare agenda at HM13 (www.hospitalmedicine 2013.org).
CEO: Telemedicine for the ICU
Mary Jo Gorman, MD, MHM, is a hospitalist and intensivist who made her mark on HM as the chief medical officer (CMO) of IPC: The Hospitalist Company. As she offered her talents to SHM, she became chairman of SHM’s Public Policy Committee and eventually SHM president.
For the last few years, Mary Jo has been the CEO of ICUMedicine. In this role, she has been active around the country, bringing ICU competencies to many community hospitals by offering a telemedicine solution for critically ill patients. This unconventional approach to meeting a glaring need fits into Mary Jo’s career history of looking for new and different ways to bring better healthcare solutions to the front lines of patient care. Last year, Modern Healthcare recognized Mary Jo as one of the most influential female physician executives in the country.
CEO, Medical University of South Carolina (MUSC) Hospitals
After leaving Duke University, Pat Cawley, MD, MBA, MHM, started his career as a community-based hospitalist leader. After a number of leadership roles at SHM, Pat served as SHM president and was elected a Master in Hospital Medicine in 2012.
Pat initially was recruited to MUSC to build and manage their HM group. Soon he was tapped to be the CMO at MUSC. Earlier this year, Pat became the first hospitalist to be chosen to run a major academic medical center when he was promoted to CEO at MUSC.
In recent years, Pat has been a leading voice as the American Hospital Association looks to involve physician leaders. He is a rising star at AHA, helping to merge the cultures of hospital administrators and physicians to create the hospital of the future.
Hospitalists Contribute at the Highest Level
Obviously, I could go on and on, adding other hospitalists who are making unique and important contributions at the local and national level. It is interesting that at a time when many are still trying to get their heads around just what HM is, we already can recognize the immense talent that resides in hospitalist groups across the country. At a time when the U.S. healthcare system is being reshaped, hospitalists, such as those mentioned above and oh-so-many more, are already making large and small steps forward. We are helping to create a new healthcare enterprise, based on value, efficiency, effectiveness, and putting the patient first.
SHM wants to continue to be the place where the innovators and thought leaders of today and tomorrow can come together to multiply their efforts. The challenges are daunting, but the results can be rewarding, and the members of SHM are ready to bring our talents, energies, and commitments to do our part in this great American journey.
Exceptional hospitalists
Even though hospital medicine and SHM are still relatively young, we can be very proud of what our specialty already has brought to changing our nation’s health care for the better. Many of these accomplishments, from winning the prestigious Eisenberg Award to our change leadership by SHM’s Center for Healthcare Innovation and Improvement at more 300 hospitals to the extraordinary growth of our specialty, have been well chronicled in The Hospitalist and elsewhere the last few years.
I wanted to use this month’s column to highlight the unique career directions of a few SHM members to shine a bright light on the influence hospitalists are making nationwide. Certainly, there are many more hospitalists beyond this group of five that I have selected, but this small cadre should serve as an example of the talent and reach of our specialty—with only more and greater things ahead to come in the future.
Chief Medical Officer of CMS
Pat Conway, MD, SFHM, is a pediatric hospitalist and the former chair of SHM’s Public Policy Committee. He left his pediatric academic practice to become a White House fellow, then returned to Cincinnati Children’s Hospital to serve as chief medical officer (CMO). When Don Berwick was in charge of the Centers for Medicare & Medicaid Services (CMS), he reached out to Pat and asked him to come to Washington to be part of Medicare’s senior team as the CMO for CMS. In this role, Pat has been a nationally recognized leader in performance improvement and patient safety, and he has been instrumental in bringing about evolutionary changes to the largest healthcare program in the world. Pat will be sharing his perspectives as a keynote speaker at HM13 (check out our 10-page HM13 preview starting on p. 45).
Resident Fellow at the American Enterprise Institute
Scott Gottlieb, MD, is a practicing hospitalist in New York City, but he is better known as a leading expert in healthcare policy, most recently acting as an advisor to presidential candidate Mitt Romney. From 2005 to 2007, Scott was a deputy commissioner at the FDA. He has worked as a senior advisor to the administrator at CMS, where he played an instrumental role in the implementation of the Medicare Drug Benefit in 2004.
Scott is best known for his frequent contributions to The Wall Street Journal, The New York Times, USA Today, and Forbes. He has held editorial positions at the British Medical Journal and the Journal of the American Medical Association, regularly appears as a guest commentator on CNBC, and is a frequent contributor to Politico.
At SHM, Scott has brought his national viewpoint to the Public Policy Committee. He proudly touts his experience as a practicing hospitalist as bringing a front-line reality to his national recognition and much-sought-after critical thinking about healthcare policy.
Chairman of the American Board of Internal Medicine
Bob Wachter, MD, MHM, was a thought leader in HM before our specialty even had a name, writing the initial peer-reviewed articles and coining the term “hospitalist.” Bob has built a pre-eminent hospitalist program at the University of California at San Francisco and helped influence and populate much of academic HM. His Wachter’s World blog (www.wachtersworld.com) is one of the most widely read medical blogs, reaching an audience well beyond our specialty.
Bob was one of the first presidents of SHM—back when we were known as NAIP, or the National Association of Inpatient Physicians—and set SHM on its strong growth and innovative direction that has made us the envy of other medical specialty societies. Last year, Modern Healthcare hailed Bob as the 14th most influential physician executive in the entire country.
On the ABIM board, Bob has represented the best of HM and brought our innovative spirit and our commitment to improvement, safety, and change leadership, culminating this year in the ABIM chairmanship. Bob will offer his unique insights into HM and the national healthcare agenda at HM13 (www.hospitalmedicine 2013.org).
CEO: Telemedicine for the ICU
Mary Jo Gorman, MD, MHM, is a hospitalist and intensivist who made her mark on HM as the chief medical officer (CMO) of IPC: The Hospitalist Company. As she offered her talents to SHM, she became chairman of SHM’s Public Policy Committee and eventually SHM president.
For the last few years, Mary Jo has been the CEO of ICUMedicine. In this role, she has been active around the country, bringing ICU competencies to many community hospitals by offering a telemedicine solution for critically ill patients. This unconventional approach to meeting a glaring need fits into Mary Jo’s career history of looking for new and different ways to bring better healthcare solutions to the front lines of patient care. Last year, Modern Healthcare recognized Mary Jo as one of the most influential female physician executives in the country.
CEO, Medical University of South Carolina (MUSC) Hospitals
After leaving Duke University, Pat Cawley, MD, MBA, MHM, started his career as a community-based hospitalist leader. After a number of leadership roles at SHM, Pat served as SHM president and was elected a Master in Hospital Medicine in 2012.
Pat initially was recruited to MUSC to build and manage their HM group. Soon he was tapped to be the CMO at MUSC. Earlier this year, Pat became the first hospitalist to be chosen to run a major academic medical center when he was promoted to CEO at MUSC.
In recent years, Pat has been a leading voice as the American Hospital Association looks to involve physician leaders. He is a rising star at AHA, helping to merge the cultures of hospital administrators and physicians to create the hospital of the future.
Hospitalists Contribute at the Highest Level
Obviously, I could go on and on, adding other hospitalists who are making unique and important contributions at the local and national level. It is interesting that at a time when many are still trying to get their heads around just what HM is, we already can recognize the immense talent that resides in hospitalist groups across the country. At a time when the U.S. healthcare system is being reshaped, hospitalists, such as those mentioned above and oh-so-many more, are already making large and small steps forward. We are helping to create a new healthcare enterprise, based on value, efficiency, effectiveness, and putting the patient first.
SHM wants to continue to be the place where the innovators and thought leaders of today and tomorrow can come together to multiply their efforts. The challenges are daunting, but the results can be rewarding, and the members of SHM are ready to bring our talents, energies, and commitments to do our part in this great American journey.
Win Whitcomb: Front-Line Hospitalists Fight Against Health Care-Associated Infections (HAIs)

2013 marks a turning point in the way hospitals are held accountable for the prevention of healthcare-associated infections (HAIs). It has been known for some time that HAIs are a serious cause of morbidity, with 1 in 20 hospital patients in the U.S. acquiring one. That represents 1.7 million Americans and accounts for about 100,000 lives lost each year. On a personal note, my father died of an HAI after surgery in 2000.
Now, with the Affordable Care Act coming into full swing, hospitals must get serious about preventing HAIs. This presents a major opportunity for hospitalists. There are three ways that hospitals will be affected:
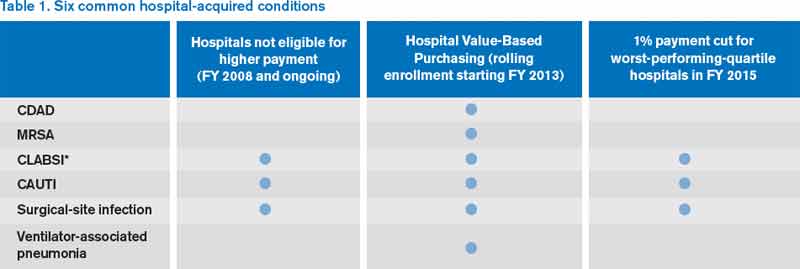
- Since 2008, hospitals have not been reimbursed at a higher rate for vascular catheter-associated infections, catheter-associated urinary tract infections (UTIs), or surgical-site infections when acquired in the hospital.
- Over the next few years, Medicare’s Hospital Value-Based Purchasing (HVBP) program will begin to pay hospitals more or less, depending on how they perform, on six HAIs.
- Beginning in October 2014, in a roll-up measure for hospital-acquired conditions (which include infections), the worst-performing quartile of U.S. hospitals will be penalized 1% of their Medicare inpatient payments (see Table 1, below).
There are six HAIs that will be increasingly tied to hospital reimbursement. Each can be partially or completely prevented based on sets of practices, or care bundles, that require teamwork both in the planning stages and at the bedside. And, of course, the single most important way to reduce the spread of HAIs is to clean your hands before and after each patient encounter.
Clostridium-Difficile-Associated Disease (CDAD)
It is likely that your hospital has some type of CDAD prevention program. Here are a few things to keep in mind for CDAD prevention:
- Avoid alcohol-based hand rubs, because they do not kill C. diff spores. Vigorous hand washing with soap and water is the best approach.
- Use clindamycin, fluoroquinolones, and third-generation cephalosporins judiciously, as their restriction has been associated with reduced rates of CDAD.
- Place patients with suspected or proven C. diff infection on contact precautions, including gloves and gowns.
Methicillin-Resistant Staphylococcus Aureus (MRSA)
This includes hospital-acquired MRSA bacteremia. This topic will be discussed in future columns. Approaches to prevention include hand hygiene, cohorting patients, effective environmental cleaning, and antibiotic stewardship.
Central-Line-Associated Bloodstream Infection (CLABSI)
Adherence to the central-line insertion bundle has been conclusively shown to prevent CLABSI. It will become a process measure for HVBP in the near future. Prevention measures include hand hygiene, maximal barrier precautions during insertion, skin antisepsis with chlorhexidine, avoidance of the femoral vein, and daily assessment for readiness to discontinue the central line (which should involve every hospitalist).
Catheter-Associated Urinary Tract Infection (CAUTI)
CAUTI has been mentioned frequently in this column, and for good reason: It is the most common HAI. Although the evidence supporting practices that prevent CAUTI is not as strong as for CLABSI, every institution should have a bundle of practices embedded in nurses’ and doctors’ workflow to prevent CAUTI (see “Quality Meets Finance,” January 2013, p. 31).
Surgical-Site Infection (SSI)
For the most part, SSI can be left to the surgeons and other operating room professionals. However, with increasing involvement of hospitalists in surgical cases, we must have an understanding of how SSIs are prevented. The World Health Organization surgical checklist (www.who.int/patientsafety/safesurgery) is a great starting point for any organization.
Ventilator-Associated Pneumonia (VAP)
For hospitalists who provide critical care, adherence to a VAP prevention bundle includes:
- Elevation of the head of the bed;
- Daily “sedation vacation” and readiness to extubate;
- Oral care with chlorhexidine; and
- Peptic ulcer disease and venous thromboembolism prophylaxis.
In 2009, the U.S. Department of Health and Human Services (HHS) launched an action plan to prevent HAIs. As part of this effort, the Agency for Health Research and Quality (AHRQ) created a comprehensive unit-based safety program (CUSP) aimed at preventing CLABSI and CAUTI. The effort also focuses on safety culture and teamwork. For those interested in participating, visit www.onthecuspstophai.org.
Another way to get involved is to work Partnership for Patients, a public-private partnership led by HHS (http://partnershipforpatients.cms.gov), if a team at your hospital is participating. The Partnership for Patients seeks to reduce harm, including HAIs, by 40% by the end of 2013 compared with a 2010 baseline.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at [email protected].
The View from The Center
As many of you know, SHM recently submitted five recommendations to the American Board of Internal Medicine Foundation’s Choosing Wisely campaign. This campaign encourages physicians and patients to have crucial conversations about appropriate utilization of tests and treatments. Seventeen specialty societies released lists in the second phase of the campaign. Many of the lists, including SHM’s, include recommendations that can help reduce hospital-acquired infections.
For example, one of SHM’s recommendations suggests not placing, or leaving in place, urinary catheters for any reason other than those indicated by the guidelines (e.g. bladder outlet obstruction, acute urinary retention, patient requires prolonged immobilization, to improve comfort for end of life, selected perioperative conditions). As Dr. Whitcomb indicates above, CAUTIs are low-hanging fruit when it comes to improving this condition—the guidelines are clear-cut, and relatively simple protocols can be put into place to prevent CAUTI.
Among the American Academy of Family Physicians and other society recommendations is avoidance of routine prescriptions of antibiotics for acute sinusitis or upper respiratory infections. Good antimicrobial stewardship policies are another approach to reduce or eliminate harmful antibiotic-resistant infections.
SHM will be offering multiple opportunities in the coming months to support your institution in Choosing Wisely. A daylong pre-course and two breakout sessions will be offered at HM13 (www.hospitalmedicine2013.org) addressing how you can implement the various recommendations. Additionally, publications are in the works describing the evidence base for SHM’s “avoid lists.” For resources, more information about SHM’s recommendations, and the latest Choosing Wisely developments, visit www.hospitalmedicine.org/choosingwisely.
2013 marks a turning point in the way hospitals are held accountable for the prevention of healthcare-associated infections (HAIs). It has been known for some time that HAIs are a serious cause of morbidity, with 1 in 20 hospital patients in the U.S. acquiring one. That represents 1.7 million Americans and accounts for about 100,000 lives lost each year. On a personal note, my father died of an HAI after surgery in 2000.
Now, with the Affordable Care Act coming into full swing, hospitals must get serious about preventing HAIs. This presents a major opportunity for hospitalists. There are three ways that hospitals will be affected:
- Since 2008, hospitals have not been reimbursed at a higher rate for vascular catheter-associated infections, catheter-associated urinary tract infections (UTIs), or surgical-site infections when acquired in the hospital.
- Over the next few years, Medicare’s Hospital Value-Based Purchasing (HVBP) program will begin to pay hospitals more or less, depending on how they perform, on six HAIs.
- Beginning in October 2014, in a roll-up measure for hospital-acquired conditions (which include infections), the worst-performing quartile of U.S. hospitals will be penalized 1% of their Medicare inpatient payments (see Table 1, below).
There are six HAIs that will be increasingly tied to hospital reimbursement. Each can be partially or completely prevented based on sets of practices, or care bundles, that require teamwork both in the planning stages and at the bedside. And, of course, the single most important way to reduce the spread of HAIs is to clean your hands before and after each patient encounter.
Clostridium-Difficile-Associated Disease (CDAD)
It is likely that your hospital has some type of CDAD prevention program. Here are a few things to keep in mind for CDAD prevention:
- Avoid alcohol-based hand rubs, because they do not kill C. diff spores. Vigorous hand washing with soap and water is the best approach.
- Use clindamycin, fluoroquinolones, and third-generation cephalosporins judiciously, as their restriction has been associated with reduced rates of CDAD.
- Place patients with suspected or proven C. diff infection on contact precautions, including gloves and gowns.
Methicillin-Resistant Staphylococcus Aureus (MRSA)
This includes hospital-acquired MRSA bacteremia. This topic will be discussed in future columns. Approaches to prevention include hand hygiene, cohorting patients, effective environmental cleaning, and antibiotic stewardship.
Central-Line-Associated Bloodstream Infection (CLABSI)
Adherence to the central-line insertion bundle has been conclusively shown to prevent CLABSI. It will become a process measure for HVBP in the near future. Prevention measures include hand hygiene, maximal barrier precautions during insertion, skin antisepsis with chlorhexidine, avoidance of the femoral vein, and daily assessment for readiness to discontinue the central line (which should involve every hospitalist).
Catheter-Associated Urinary Tract Infection (CAUTI)
CAUTI has been mentioned frequently in this column, and for good reason: It is the most common HAI. Although the evidence supporting practices that prevent CAUTI is not as strong as for CLABSI, every institution should have a bundle of practices embedded in nurses’ and doctors’ workflow to prevent CAUTI (see “Quality Meets Finance,” January 2013, p. 31).
Surgical-Site Infection (SSI)
For the most part, SSI can be left to the surgeons and other operating room professionals. However, with increasing involvement of hospitalists in surgical cases, we must have an understanding of how SSIs are prevented. The World Health Organization surgical checklist (www.who.int/patientsafety/safesurgery) is a great starting point for any organization.
Ventilator-Associated Pneumonia (VAP)
For hospitalists who provide critical care, adherence to a VAP prevention bundle includes:
- Elevation of the head of the bed;
- Daily “sedation vacation” and readiness to extubate;
- Oral care with chlorhexidine; and
- Peptic ulcer disease and venous thromboembolism prophylaxis.
In 2009, the U.S. Department of Health and Human Services (HHS) launched an action plan to prevent HAIs. As part of this effort, the Agency for Health Research and Quality (AHRQ) created a comprehensive unit-based safety program (CUSP) aimed at preventing CLABSI and CAUTI. The effort also focuses on safety culture and teamwork. For those interested in participating, visit www.onthecuspstophai.org.
Another way to get involved is to work Partnership for Patients, a public-private partnership led by HHS (http://partnershipforpatients.cms.gov), if a team at your hospital is participating. The Partnership for Patients seeks to reduce harm, including HAIs, by 40% by the end of 2013 compared with a 2010 baseline.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at [email protected].
The View from The Center
As many of you know, SHM recently submitted five recommendations to the American Board of Internal Medicine Foundation’s Choosing Wisely campaign. This campaign encourages physicians and patients to have crucial conversations about appropriate utilization of tests and treatments. Seventeen specialty societies released lists in the second phase of the campaign. Many of the lists, including SHM’s, include recommendations that can help reduce hospital-acquired infections.
For example, one of SHM’s recommendations suggests not placing, or leaving in place, urinary catheters for any reason other than those indicated by the guidelines (e.g. bladder outlet obstruction, acute urinary retention, patient requires prolonged immobilization, to improve comfort for end of life, selected perioperative conditions). As Dr. Whitcomb indicates above, CAUTIs are low-hanging fruit when it comes to improving this condition—the guidelines are clear-cut, and relatively simple protocols can be put into place to prevent CAUTI.
Among the American Academy of Family Physicians and other society recommendations is avoidance of routine prescriptions of antibiotics for acute sinusitis or upper respiratory infections. Good antimicrobial stewardship policies are another approach to reduce or eliminate harmful antibiotic-resistant infections.
SHM will be offering multiple opportunities in the coming months to support your institution in Choosing Wisely. A daylong pre-course and two breakout sessions will be offered at HM13 (www.hospitalmedicine2013.org) addressing how you can implement the various recommendations. Additionally, publications are in the works describing the evidence base for SHM’s “avoid lists.” For resources, more information about SHM’s recommendations, and the latest Choosing Wisely developments, visit www.hospitalmedicine.org/choosingwisely.
2013 marks a turning point in the way hospitals are held accountable for the prevention of healthcare-associated infections (HAIs). It has been known for some time that HAIs are a serious cause of morbidity, with 1 in 20 hospital patients in the U.S. acquiring one. That represents 1.7 million Americans and accounts for about 100,000 lives lost each year. On a personal note, my father died of an HAI after surgery in 2000.
Now, with the Affordable Care Act coming into full swing, hospitals must get serious about preventing HAIs. This presents a major opportunity for hospitalists. There are three ways that hospitals will be affected:
- Since 2008, hospitals have not been reimbursed at a higher rate for vascular catheter-associated infections, catheter-associated urinary tract infections (UTIs), or surgical-site infections when acquired in the hospital.
- Over the next few years, Medicare’s Hospital Value-Based Purchasing (HVBP) program will begin to pay hospitals more or less, depending on how they perform, on six HAIs.
- Beginning in October 2014, in a roll-up measure for hospital-acquired conditions (which include infections), the worst-performing quartile of U.S. hospitals will be penalized 1% of their Medicare inpatient payments (see Table 1, below).
There are six HAIs that will be increasingly tied to hospital reimbursement. Each can be partially or completely prevented based on sets of practices, or care bundles, that require teamwork both in the planning stages and at the bedside. And, of course, the single most important way to reduce the spread of HAIs is to clean your hands before and after each patient encounter.
Clostridium-Difficile-Associated Disease (CDAD)
It is likely that your hospital has some type of CDAD prevention program. Here are a few things to keep in mind for CDAD prevention:
- Avoid alcohol-based hand rubs, because they do not kill C. diff spores. Vigorous hand washing with soap and water is the best approach.
- Use clindamycin, fluoroquinolones, and third-generation cephalosporins judiciously, as their restriction has been associated with reduced rates of CDAD.
- Place patients with suspected or proven C. diff infection on contact precautions, including gloves and gowns.
Methicillin-Resistant Staphylococcus Aureus (MRSA)
This includes hospital-acquired MRSA bacteremia. This topic will be discussed in future columns. Approaches to prevention include hand hygiene, cohorting patients, effective environmental cleaning, and antibiotic stewardship.
Central-Line-Associated Bloodstream Infection (CLABSI)
Adherence to the central-line insertion bundle has been conclusively shown to prevent CLABSI. It will become a process measure for HVBP in the near future. Prevention measures include hand hygiene, maximal barrier precautions during insertion, skin antisepsis with chlorhexidine, avoidance of the femoral vein, and daily assessment for readiness to discontinue the central line (which should involve every hospitalist).
Catheter-Associated Urinary Tract Infection (CAUTI)
CAUTI has been mentioned frequently in this column, and for good reason: It is the most common HAI. Although the evidence supporting practices that prevent CAUTI is not as strong as for CLABSI, every institution should have a bundle of practices embedded in nurses’ and doctors’ workflow to prevent CAUTI (see “Quality Meets Finance,” January 2013, p. 31).
Surgical-Site Infection (SSI)
For the most part, SSI can be left to the surgeons and other operating room professionals. However, with increasing involvement of hospitalists in surgical cases, we must have an understanding of how SSIs are prevented. The World Health Organization surgical checklist (www.who.int/patientsafety/safesurgery) is a great starting point for any organization.
Ventilator-Associated Pneumonia (VAP)
For hospitalists who provide critical care, adherence to a VAP prevention bundle includes:
- Elevation of the head of the bed;
- Daily “sedation vacation” and readiness to extubate;
- Oral care with chlorhexidine; and
- Peptic ulcer disease and venous thromboembolism prophylaxis.
In 2009, the U.S. Department of Health and Human Services (HHS) launched an action plan to prevent HAIs. As part of this effort, the Agency for Health Research and Quality (AHRQ) created a comprehensive unit-based safety program (CUSP) aimed at preventing CLABSI and CAUTI. The effort also focuses on safety culture and teamwork. For those interested in participating, visit www.onthecuspstophai.org.
Another way to get involved is to work Partnership for Patients, a public-private partnership led by HHS (http://partnershipforpatients.cms.gov), if a team at your hospital is participating. The Partnership for Patients seeks to reduce harm, including HAIs, by 40% by the end of 2013 compared with a 2010 baseline.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at [email protected].
The View from The Center
As many of you know, SHM recently submitted five recommendations to the American Board of Internal Medicine Foundation’s Choosing Wisely campaign. This campaign encourages physicians and patients to have crucial conversations about appropriate utilization of tests and treatments. Seventeen specialty societies released lists in the second phase of the campaign. Many of the lists, including SHM’s, include recommendations that can help reduce hospital-acquired infections.
For example, one of SHM’s recommendations suggests not placing, or leaving in place, urinary catheters for any reason other than those indicated by the guidelines (e.g. bladder outlet obstruction, acute urinary retention, patient requires prolonged immobilization, to improve comfort for end of life, selected perioperative conditions). As Dr. Whitcomb indicates above, CAUTIs are low-hanging fruit when it comes to improving this condition—the guidelines are clear-cut, and relatively simple protocols can be put into place to prevent CAUTI.
Among the American Academy of Family Physicians and other society recommendations is avoidance of routine prescriptions of antibiotics for acute sinusitis or upper respiratory infections. Good antimicrobial stewardship policies are another approach to reduce or eliminate harmful antibiotic-resistant infections.
SHM will be offering multiple opportunities in the coming months to support your institution in Choosing Wisely. A daylong pre-course and two breakout sessions will be offered at HM13 (www.hospitalmedicine2013.org) addressing how you can implement the various recommendations. Additionally, publications are in the works describing the evidence base for SHM’s “avoid lists.” For resources, more information about SHM’s recommendations, and the latest Choosing Wisely developments, visit www.hospitalmedicine.org/choosingwisely.
John Nelson: Excessive Workload a Concern for Many Hospitalists

“Forty percent of physicians reported that their typical inpatient census exceeded safe levels at least monthly.”1
This quote is taken from an article by Henry Michtalik and colleagues that appeared at the end of January this year in JAMA Internal Medicine. In 2010 the authors conducted an on-line survey asking hospitalists their perceptions of their workload. Respondents indicated that with concerning frequency a high workload prevented them from adequately discussing with patients treatment options or answering questions, delay admitting or discharging patients until the next day or shift, or in some other way risk patient safety or the overall quality of their work.
This alarming finding matches my anecdotal experience working with many different hospitalist groups around the country. I think few hospitalists were surprised by the survey’s findings. Excess hospitalist workloads are indeed a problem in some settings, and those who bear them are typically not shy about speaking out.
The demand for hospitalists has exceeded the supply of doctors available to do the work throughout the history of the field. Under the weight of stunningly rapid growth in referral volume, from about 1995 to 2002, it was reasonably common for the original doctors in a hospitalist practice to become overwhelmed and leave for other work after a year or two, sometimes resulting in the collapse of the practice. Most practices are no longer in such a rapid-growth phase, but for many of them, staffing has not yet caught up with workload. The result can be chronic excess work, and even if daily patient volume is not seen as being unsafe, the number of days or shifts worked might be excessive and lead to fatigue and poor performance.
Other Workload Data
The respondents to the Michtalik survey reported that regardless of any assistance, “they could safely see 15 patients per shift, if their effort was 100% clinical.” What we don’t know is how long their shifts were, whether they included things like ICU coverage, and how many shifts they work consecutively or in a year.
SHM’s 2012 State of Hospital Medicine report, which is based on 2011 data, provides additional context. It shows that hospitalists serving adult patients report a median 2,092 billed encounters annually (mean 2,245, standard deviation 1,161). They spread this work over a median 185 shifts (“work periods”) annually (mean 192). While there are lots of methodological problems in manipulating those numbers further, 2,092 encounters divided by 185 shifts yields 11.3 encounters per shift. These numbers exclude academicians who typically spend significant time in activities other than direct patient care, and I’m intentionally ignoring such issues as the night-shift doctor, who typically has low productivity, bringing down the average per full-time doctor in a practice.
The numbers from both surveys are sort of fuzzy because they aren’t audited or verified, but the 2012 State of Hospital Medicine data suggest that typical workloads aren’t too high in most practices, yet 40% of respondents in the Michtalik survey said they were high enough—unreasonably high—to risk quality and safety at least once a month.
One way to reconcile these findings is to take into account the standard deviation in daily volume in a single practice of about 30% to 40% on above or below the mean. If a hospitalist averages 14 encounters each day shift, then he should expect that the daily number might vary between about eight and 20. The Michtalik survey responses were likely reflecting the shifts on the high end.
Perspective
I wonder what a survey of physician workload opinions in other specialties would show, or what a survey of workers across all segments of the U.S. workforce in and out of healthcare would show. Of course, many or most jobs outside of healthcare don’t risk another’s health or well-being as significantly as ours do, but it would still be instructive to know how people in general think about the work they do.
I suspect a significant number of people across many different jobs feel like too much work is expected of them, and they can point to the ways their performance suffers as a result. It is difficult to know what portion of those who report too much work is just complaining versus a thoughtful self-reflection of the determinants of their performance. Lots of hospitalists do face worrisome high workloads, but some would probably still complain even with a much lower workload.
What Can Be Done?
For those practices facing remarkably high patient volumes, the solution is to make sure you’re recruiting additional doctors, and/or NPs/PAs, as fast as you can. But a portion of these practices must first convince their employers that more staff is needed. Some practices face a real uphill battle in getting the required additional funding, and the place to start is with a careful analysis of your current workload—based on hard numbers from your practice, not just anecdotes and estimates.
Don’t forget that some hospitalists put themselves in the position of having to manage high daily patient volumes by choosing a schedule of relatively few worked days annually. For example, a group working a seven-on/seven-off schedule that also has 14 shifts of time off means that each doctor will work only 168.5 shifts annually. Compressing a year’s worth of work into only 168 shifts means that each shift will be busy, and many will involve patient volumes that exceed what is seen as safe.
It could make more sense to titrate that same work volume over more annual shifts so that the average shift is less busy. I would love to see the Michtalik data segregated by those who work many shifts annually versus those who work few shifts. It is possible that those working more shifts have reported excessive workloads less often.
SHM has a role in influencing hospitalist workloads and promotes dissemination of data and opinions about it. At HM13 next month in Washington, D.C., I am leading a session titled “Hospitalist Workload: Is 15 the Right Number?” Although it won’t provide the “right” workload for all hospitalists, it will offer worthwhile data and food for thought.
It is much more difficult to do studies of how workload influences performance than something like effects of sleep deprivation on performance, so we may never get clear answers. You could take some consolation in the fact that successive surveys have shown little change or even modest decreases in annual patient encounters. But then again, maybe that hasn’t helped with excess work since providing hospital care gets harder and more complex every year.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at [email protected].
Reference
“Forty percent of physicians reported that their typical inpatient census exceeded safe levels at least monthly.”1
This quote is taken from an article by Henry Michtalik and colleagues that appeared at the end of January this year in JAMA Internal Medicine. In 2010 the authors conducted an on-line survey asking hospitalists their perceptions of their workload. Respondents indicated that with concerning frequency a high workload prevented them from adequately discussing with patients treatment options or answering questions, delay admitting or discharging patients until the next day or shift, or in some other way risk patient safety or the overall quality of their work.
This alarming finding matches my anecdotal experience working with many different hospitalist groups around the country. I think few hospitalists were surprised by the survey’s findings. Excess hospitalist workloads are indeed a problem in some settings, and those who bear them are typically not shy about speaking out.
The demand for hospitalists has exceeded the supply of doctors available to do the work throughout the history of the field. Under the weight of stunningly rapid growth in referral volume, from about 1995 to 2002, it was reasonably common for the original doctors in a hospitalist practice to become overwhelmed and leave for other work after a year or two, sometimes resulting in the collapse of the practice. Most practices are no longer in such a rapid-growth phase, but for many of them, staffing has not yet caught up with workload. The result can be chronic excess work, and even if daily patient volume is not seen as being unsafe, the number of days or shifts worked might be excessive and lead to fatigue and poor performance.
Other Workload Data
The respondents to the Michtalik survey reported that regardless of any assistance, “they could safely see 15 patients per shift, if their effort was 100% clinical.” What we don’t know is how long their shifts were, whether they included things like ICU coverage, and how many shifts they work consecutively or in a year.
SHM’s 2012 State of Hospital Medicine report, which is based on 2011 data, provides additional context. It shows that hospitalists serving adult patients report a median 2,092 billed encounters annually (mean 2,245, standard deviation 1,161). They spread this work over a median 185 shifts (“work periods”) annually (mean 192). While there are lots of methodological problems in manipulating those numbers further, 2,092 encounters divided by 185 shifts yields 11.3 encounters per shift. These numbers exclude academicians who typically spend significant time in activities other than direct patient care, and I’m intentionally ignoring such issues as the night-shift doctor, who typically has low productivity, bringing down the average per full-time doctor in a practice.
The numbers from both surveys are sort of fuzzy because they aren’t audited or verified, but the 2012 State of Hospital Medicine data suggest that typical workloads aren’t too high in most practices, yet 40% of respondents in the Michtalik survey said they were high enough—unreasonably high—to risk quality and safety at least once a month.
One way to reconcile these findings is to take into account the standard deviation in daily volume in a single practice of about 30% to 40% on above or below the mean. If a hospitalist averages 14 encounters each day shift, then he should expect that the daily number might vary between about eight and 20. The Michtalik survey responses were likely reflecting the shifts on the high end.
Perspective
I wonder what a survey of physician workload opinions in other specialties would show, or what a survey of workers across all segments of the U.S. workforce in and out of healthcare would show. Of course, many or most jobs outside of healthcare don’t risk another’s health or well-being as significantly as ours do, but it would still be instructive to know how people in general think about the work they do.
I suspect a significant number of people across many different jobs feel like too much work is expected of them, and they can point to the ways their performance suffers as a result. It is difficult to know what portion of those who report too much work is just complaining versus a thoughtful self-reflection of the determinants of their performance. Lots of hospitalists do face worrisome high workloads, but some would probably still complain even with a much lower workload.
What Can Be Done?
For those practices facing remarkably high patient volumes, the solution is to make sure you’re recruiting additional doctors, and/or NPs/PAs, as fast as you can. But a portion of these practices must first convince their employers that more staff is needed. Some practices face a real uphill battle in getting the required additional funding, and the place to start is with a careful analysis of your current workload—based on hard numbers from your practice, not just anecdotes and estimates.
Don’t forget that some hospitalists put themselves in the position of having to manage high daily patient volumes by choosing a schedule of relatively few worked days annually. For example, a group working a seven-on/seven-off schedule that also has 14 shifts of time off means that each doctor will work only 168.5 shifts annually. Compressing a year’s worth of work into only 168 shifts means that each shift will be busy, and many will involve patient volumes that exceed what is seen as safe.
It could make more sense to titrate that same work volume over more annual shifts so that the average shift is less busy. I would love to see the Michtalik data segregated by those who work many shifts annually versus those who work few shifts. It is possible that those working more shifts have reported excessive workloads less often.
SHM has a role in influencing hospitalist workloads and promotes dissemination of data and opinions about it. At HM13 next month in Washington, D.C., I am leading a session titled “Hospitalist Workload: Is 15 the Right Number?” Although it won’t provide the “right” workload for all hospitalists, it will offer worthwhile data and food for thought.
It is much more difficult to do studies of how workload influences performance than something like effects of sleep deprivation on performance, so we may never get clear answers. You could take some consolation in the fact that successive surveys have shown little change or even modest decreases in annual patient encounters. But then again, maybe that hasn’t helped with excess work since providing hospital care gets harder and more complex every year.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at [email protected].
Reference
“Forty percent of physicians reported that their typical inpatient census exceeded safe levels at least monthly.”1
This quote is taken from an article by Henry Michtalik and colleagues that appeared at the end of January this year in JAMA Internal Medicine. In 2010 the authors conducted an on-line survey asking hospitalists their perceptions of their workload. Respondents indicated that with concerning frequency a high workload prevented them from adequately discussing with patients treatment options or answering questions, delay admitting or discharging patients until the next day or shift, or in some other way risk patient safety or the overall quality of their work.
This alarming finding matches my anecdotal experience working with many different hospitalist groups around the country. I think few hospitalists were surprised by the survey’s findings. Excess hospitalist workloads are indeed a problem in some settings, and those who bear them are typically not shy about speaking out.
The demand for hospitalists has exceeded the supply of doctors available to do the work throughout the history of the field. Under the weight of stunningly rapid growth in referral volume, from about 1995 to 2002, it was reasonably common for the original doctors in a hospitalist practice to become overwhelmed and leave for other work after a year or two, sometimes resulting in the collapse of the practice. Most practices are no longer in such a rapid-growth phase, but for many of them, staffing has not yet caught up with workload. The result can be chronic excess work, and even if daily patient volume is not seen as being unsafe, the number of days or shifts worked might be excessive and lead to fatigue and poor performance.
Other Workload Data
The respondents to the Michtalik survey reported that regardless of any assistance, “they could safely see 15 patients per shift, if their effort was 100% clinical.” What we don’t know is how long their shifts were, whether they included things like ICU coverage, and how many shifts they work consecutively or in a year.
SHM’s 2012 State of Hospital Medicine report, which is based on 2011 data, provides additional context. It shows that hospitalists serving adult patients report a median 2,092 billed encounters annually (mean 2,245, standard deviation 1,161). They spread this work over a median 185 shifts (“work periods”) annually (mean 192). While there are lots of methodological problems in manipulating those numbers further, 2,092 encounters divided by 185 shifts yields 11.3 encounters per shift. These numbers exclude academicians who typically spend significant time in activities other than direct patient care, and I’m intentionally ignoring such issues as the night-shift doctor, who typically has low productivity, bringing down the average per full-time doctor in a practice.
The numbers from both surveys are sort of fuzzy because they aren’t audited or verified, but the 2012 State of Hospital Medicine data suggest that typical workloads aren’t too high in most practices, yet 40% of respondents in the Michtalik survey said they were high enough—unreasonably high—to risk quality and safety at least once a month.
One way to reconcile these findings is to take into account the standard deviation in daily volume in a single practice of about 30% to 40% on above or below the mean. If a hospitalist averages 14 encounters each day shift, then he should expect that the daily number might vary between about eight and 20. The Michtalik survey responses were likely reflecting the shifts on the high end.
Perspective
I wonder what a survey of physician workload opinions in other specialties would show, or what a survey of workers across all segments of the U.S. workforce in and out of healthcare would show. Of course, many or most jobs outside of healthcare don’t risk another’s health or well-being as significantly as ours do, but it would still be instructive to know how people in general think about the work they do.
I suspect a significant number of people across many different jobs feel like too much work is expected of them, and they can point to the ways their performance suffers as a result. It is difficult to know what portion of those who report too much work is just complaining versus a thoughtful self-reflection of the determinants of their performance. Lots of hospitalists do face worrisome high workloads, but some would probably still complain even with a much lower workload.
What Can Be Done?
For those practices facing remarkably high patient volumes, the solution is to make sure you’re recruiting additional doctors, and/or NPs/PAs, as fast as you can. But a portion of these practices must first convince their employers that more staff is needed. Some practices face a real uphill battle in getting the required additional funding, and the place to start is with a careful analysis of your current workload—based on hard numbers from your practice, not just anecdotes and estimates.
Don’t forget that some hospitalists put themselves in the position of having to manage high daily patient volumes by choosing a schedule of relatively few worked days annually. For example, a group working a seven-on/seven-off schedule that also has 14 shifts of time off means that each doctor will work only 168.5 shifts annually. Compressing a year’s worth of work into only 168 shifts means that each shift will be busy, and many will involve patient volumes that exceed what is seen as safe.
It could make more sense to titrate that same work volume over more annual shifts so that the average shift is less busy. I would love to see the Michtalik data segregated by those who work many shifts annually versus those who work few shifts. It is possible that those working more shifts have reported excessive workloads less often.
SHM has a role in influencing hospitalist workloads and promotes dissemination of data and opinions about it. At HM13 next month in Washington, D.C., I am leading a session titled “Hospitalist Workload: Is 15 the Right Number?” Although it won’t provide the “right” workload for all hospitalists, it will offer worthwhile data and food for thought.
It is much more difficult to do studies of how workload influences performance than something like effects of sleep deprivation on performance, so we may never get clear answers. You could take some consolation in the fact that successive surveys have shown little change or even modest decreases in annual patient encounters. But then again, maybe that hasn’t helped with excess work since providing hospital care gets harder and more complex every year.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at [email protected].
Reference
Bob Wachter Puts Forward Spin on Patient Safety, Quality of Care at HM13

Most hospitalists have heard the adage “If you’ve seen one hospitalist group, you’ve seen one hospitalist group.” Another HM truism is “If you’ve seen one SHM annual meeting, then you’ve seen Bob Wachter, MD, MHM.”
Dr. Wachter, professor, chief of the division of hospital medicine, and chief of the medical service at the University of California at San Francisco Medical Center, is to HM conventions as warfarin is to anticoagulation. His keynote address is the finale to the yearly confab, and HM13’s version is scheduled for noon May 19 at the Gaylord National Harbor Resort & Convention Center in National Harbor, Md.
This year’s address is titled “Quality, Safety, and IT: A Decade of Successes, Failures, Surprises, and Epiphanies.” Dr. Wachter spoke recently with The Hospitalist about his annual tradition.
Question: With your interest in the intersection between healthcare and politics, to be back in D.C. has to be something enjoyable for you to write and talk about.
Answer: It’s a very interesting time in the life of healthcare, in that now that everybody knows that the [Affordable Care Act] is real and not going away, and we’re actually beginning to implement parts of it, you can kind of see what the future is going to look like, and everybody’s responding. And there are parts of that that are very exciting, because they’re forcing us to think about value in new ways. [And] there are parts of it that are somewhat frustrating.
Q: Does that give the hospitalist community the chance to ride herd on more global issues?
A: I think that’s the most optimistic interpretation—that we stick to our knitting, that we continue to be the leaders in improvement, and eventually all of the deals will be done, lawyers will be dismissed, and people will turn back to focusing on performance and say to us, “Thank goodness you’ve been doing this work, because now we realize that it’s not just about contracts; it’s about how we deliver care, and you’re the ones that have been leading the way.”
Q: What’s the most realistic interpretation?
A: This work gets less attention and less support than it needs. … I think we’re going to go through three to five years where we’re continuing to do the work. It’s really important—in many ways, it’s as important as growing—but as its importance is growing, the importance of other things that require more tending-to by the senior leadership is growing even faster. The risk is that there will be a disconnect.
Q: When you see the literature that suggests just how difficult the nuts and bolts implementation of reform is, what message do you want to get across to the people who are going to be listening, in terms of actually implementing all of this?
A: The message I don’t want to get across is “frustration, burnout, and it’s not worth it.” The endgame is worth it. The endgame is not even elective. We have to get to a place where we’re delivering higher-quality, safer, more satisfying care to patients at a lower cost. We’re in a unique position to deliver on that promise. … This is really tough stuff, and it takes time and it takes learning.
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Richard Quinn is a freelance writer in New Jersey.
Most hospitalists have heard the adage “If you’ve seen one hospitalist group, you’ve seen one hospitalist group.” Another HM truism is “If you’ve seen one SHM annual meeting, then you’ve seen Bob Wachter, MD, MHM.”
Dr. Wachter, professor, chief of the division of hospital medicine, and chief of the medical service at the University of California at San Francisco Medical Center, is to HM conventions as warfarin is to anticoagulation. His keynote address is the finale to the yearly confab, and HM13’s version is scheduled for noon May 19 at the Gaylord National Harbor Resort & Convention Center in National Harbor, Md.
This year’s address is titled “Quality, Safety, and IT: A Decade of Successes, Failures, Surprises, and Epiphanies.” Dr. Wachter spoke recently with The Hospitalist about his annual tradition.
Question: With your interest in the intersection between healthcare and politics, to be back in D.C. has to be something enjoyable for you to write and talk about.
Answer: It’s a very interesting time in the life of healthcare, in that now that everybody knows that the [Affordable Care Act] is real and not going away, and we’re actually beginning to implement parts of it, you can kind of see what the future is going to look like, and everybody’s responding. And there are parts of that that are very exciting, because they’re forcing us to think about value in new ways. [And] there are parts of it that are somewhat frustrating.
Q: Does that give the hospitalist community the chance to ride herd on more global issues?
A: I think that’s the most optimistic interpretation—that we stick to our knitting, that we continue to be the leaders in improvement, and eventually all of the deals will be done, lawyers will be dismissed, and people will turn back to focusing on performance and say to us, “Thank goodness you’ve been doing this work, because now we realize that it’s not just about contracts; it’s about how we deliver care, and you’re the ones that have been leading the way.”
Q: What’s the most realistic interpretation?
A: This work gets less attention and less support than it needs. … I think we’re going to go through three to five years where we’re continuing to do the work. It’s really important—in many ways, it’s as important as growing—but as its importance is growing, the importance of other things that require more tending-to by the senior leadership is growing even faster. The risk is that there will be a disconnect.
Q: When you see the literature that suggests just how difficult the nuts and bolts implementation of reform is, what message do you want to get across to the people who are going to be listening, in terms of actually implementing all of this?
A: The message I don’t want to get across is “frustration, burnout, and it’s not worth it.” The endgame is worth it. The endgame is not even elective. We have to get to a place where we’re delivering higher-quality, safer, more satisfying care to patients at a lower cost. We’re in a unique position to deliver on that promise. … This is really tough stuff, and it takes time and it takes learning.
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Richard Quinn is a freelance writer in New Jersey.
Most hospitalists have heard the adage “If you’ve seen one hospitalist group, you’ve seen one hospitalist group.” Another HM truism is “If you’ve seen one SHM annual meeting, then you’ve seen Bob Wachter, MD, MHM.”
Dr. Wachter, professor, chief of the division of hospital medicine, and chief of the medical service at the University of California at San Francisco Medical Center, is to HM conventions as warfarin is to anticoagulation. His keynote address is the finale to the yearly confab, and HM13’s version is scheduled for noon May 19 at the Gaylord National Harbor Resort & Convention Center in National Harbor, Md.
This year’s address is titled “Quality, Safety, and IT: A Decade of Successes, Failures, Surprises, and Epiphanies.” Dr. Wachter spoke recently with The Hospitalist about his annual tradition.
Question: With your interest in the intersection between healthcare and politics, to be back in D.C. has to be something enjoyable for you to write and talk about.
Answer: It’s a very interesting time in the life of healthcare, in that now that everybody knows that the [Affordable Care Act] is real and not going away, and we’re actually beginning to implement parts of it, you can kind of see what the future is going to look like, and everybody’s responding. And there are parts of that that are very exciting, because they’re forcing us to think about value in new ways. [And] there are parts of it that are somewhat frustrating.
Q: Does that give the hospitalist community the chance to ride herd on more global issues?
A: I think that’s the most optimistic interpretation—that we stick to our knitting, that we continue to be the leaders in improvement, and eventually all of the deals will be done, lawyers will be dismissed, and people will turn back to focusing on performance and say to us, “Thank goodness you’ve been doing this work, because now we realize that it’s not just about contracts; it’s about how we deliver care, and you’re the ones that have been leading the way.”
Q: What’s the most realistic interpretation?
A: This work gets less attention and less support than it needs. … I think we’re going to go through three to five years where we’re continuing to do the work. It’s really important—in many ways, it’s as important as growing—but as its importance is growing, the importance of other things that require more tending-to by the senior leadership is growing even faster. The risk is that there will be a disconnect.
Q: When you see the literature that suggests just how difficult the nuts and bolts implementation of reform is, what message do you want to get across to the people who are going to be listening, in terms of actually implementing all of this?
A: The message I don’t want to get across is “frustration, burnout, and it’s not worth it.” The endgame is worth it. The endgame is not even elective. We have to get to a place where we’re delivering higher-quality, safer, more satisfying care to patients at a lower cost. We’re in a unique position to deliver on that promise. … This is really tough stuff, and it takes time and it takes learning.
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Richard Quinn is a freelance writer in New Jersey.
UCLA Exec: Patient-Centered Approach Essential to Quality of Hospital Care

–David Feinberg, MD, MBA, president of UCLA Health System in Los Angeles
Patient satisfaction is a buzzword in HM circles, as compensation is increasingly tied to performance in keeping inpatients happy. David Feinberg, MD, MBA, president of UCLA Health System in Los Angeles, could be called a guru of patient satisfaction.
Just don’t tell him that.
“I hope I’m not seen as ‘patient satisfaction,’” he says. “I hope I’m seen as ‘patient centeredness.’ And patient satisfaction is a key piece of patient centeredness.”
Dr. Feinberg, who assumed his current role UCLA Health System in 2011, is a national voice for pushing a patient-centric model of care delivery. To wit, he will be one of the keynote speakers at HM13 next month at the Gaylord National Resort & Convention Center in National Harbor, Md. His address is fittingly titled “Healing Humankind One Patient at a Time.”
The Hospitalist spoke to Dr. Feinberg about his message to hospitalists.
Question: What do you think is the evolution of patient centeredness, as that becomes more of a focus for others?
Answer: Patient centeredness to me is the true north, and I think everything else that we’ve done that isn’t patient-centered has been a distraction. … It’s why we signed up to get into healthcare. It’s what we should be doing today and tonight, and it should guide our future tomorrow. It would be like me saying to the restaurateur, “How important is the food?”


Q: Is it something that hasn’t always been done?
A: It’s pathetic. You’re totally right. We’ve lost our way.
Q: If it’s so common-sense, how did we lose our way?
A: It really became, to me, the coin of the realm in medicine was how much the doctor made, how great their reputation was. It even got to the point of: You were a good doctor if your waiting room was packed. … I keep saying the waiting room should be for the doctors. The patient shouldn’t have to wait. You should be back in the exam room and the doctor should be waiting to see you. So we’ve got to completely change the paradigm. … It’s really the patient who’s at the top of the pyramid. And I just think we’ve lost that completely.
Q: How does a hospitalist engage quickly to ensure that they’re trying to accomplish patient centeredness and manage outcomes properly?
A: Hospitalists have a unique opportunity there, because everybody remembers when they got put in the hospital. It is a big deal when you’re hospitalized. Your family is in a vulnerable state, everybody is in a heightened sense of alertness and focus. Think about how important those four days are around education, around myths and demystifying, around beliefs and disbelief.
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Q: So what is the one thing you want hospitalists to take away from your address?
A: That they should join with all of us who want to heal humankind; that they are healers, above all.
Q: How do you translate “I want to be a healer” to the grind of daily work?
A: Well, I don’t think this is a grind. I think that when you’re in this healing profession, that you come here with a purpose. I think if we asked them to look at their personal statements of why they went into med school, every single one of them has something to do with, “I was sick as a kid, my grandmother got sick, I had had this doctor who was a role model, I like to help people, I was a volunteer and I met this patient.” Everyone says that. So this is different than trying to inspire the workers at Costco. These are people that, by definition, have gone and chosen this. We know they’re all smart. They could have all become investment bankers, they could have all become schoolteachers, but what they chose was to go into this field that’s about healing others, and that’s what I think we need to and what I would want them to do, is to get back in touch with themselves because I know it’s there. By definition, it’s there.
Q: Then why don’t more people just make that connection? What is the hurdle?
A: There are a lot of distractions. There are a lot of things coming your way. Worrying about your own life; doctors have lives at home. Worrying about the pressures of making a living. Some of this stuff is really, really hard. There are a million things going on. I believe, and I hope at UCLA, that we believe the strategy to make all of that stuff work is to get it right with the patient. And if you get it right with the patient, then all of that other stuff seems to fall into place and starts to make sense. The finances work out. The market share works out. The healthcare reform works out. I think it is the answer.
Richard Quinn is a freelance writer in New Jersey.
–David Feinberg, MD, MBA, president of UCLA Health System in Los Angeles
Patient satisfaction is a buzzword in HM circles, as compensation is increasingly tied to performance in keeping inpatients happy. David Feinberg, MD, MBA, president of UCLA Health System in Los Angeles, could be called a guru of patient satisfaction.
Just don’t tell him that.
“I hope I’m not seen as ‘patient satisfaction,’” he says. “I hope I’m seen as ‘patient centeredness.’ And patient satisfaction is a key piece of patient centeredness.”
Dr. Feinberg, who assumed his current role UCLA Health System in 2011, is a national voice for pushing a patient-centric model of care delivery. To wit, he will be one of the keynote speakers at HM13 next month at the Gaylord National Resort & Convention Center in National Harbor, Md. His address is fittingly titled “Healing Humankind One Patient at a Time.”
The Hospitalist spoke to Dr. Feinberg about his message to hospitalists.
Question: What do you think is the evolution of patient centeredness, as that becomes more of a focus for others?
Answer: Patient centeredness to me is the true north, and I think everything else that we’ve done that isn’t patient-centered has been a distraction. … It’s why we signed up to get into healthcare. It’s what we should be doing today and tonight, and it should guide our future tomorrow. It would be like me saying to the restaurateur, “How important is the food?”
Q: Is it something that hasn’t always been done?
A: It’s pathetic. You’re totally right. We’ve lost our way.
Q: If it’s so common-sense, how did we lose our way?
A: It really became, to me, the coin of the realm in medicine was how much the doctor made, how great their reputation was. It even got to the point of: You were a good doctor if your waiting room was packed. … I keep saying the waiting room should be for the doctors. The patient shouldn’t have to wait. You should be back in the exam room and the doctor should be waiting to see you. So we’ve got to completely change the paradigm. … It’s really the patient who’s at the top of the pyramid. And I just think we’ve lost that completely.
Q: How does a hospitalist engage quickly to ensure that they’re trying to accomplish patient centeredness and manage outcomes properly?
A: Hospitalists have a unique opportunity there, because everybody remembers when they got put in the hospital. It is a big deal when you’re hospitalized. Your family is in a vulnerable state, everybody is in a heightened sense of alertness and focus. Think about how important those four days are around education, around myths and demystifying, around beliefs and disbelief.
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Q: So what is the one thing you want hospitalists to take away from your address?
A: That they should join with all of us who want to heal humankind; that they are healers, above all.
Q: How do you translate “I want to be a healer” to the grind of daily work?
A: Well, I don’t think this is a grind. I think that when you’re in this healing profession, that you come here with a purpose. I think if we asked them to look at their personal statements of why they went into med school, every single one of them has something to do with, “I was sick as a kid, my grandmother got sick, I had had this doctor who was a role model, I like to help people, I was a volunteer and I met this patient.” Everyone says that. So this is different than trying to inspire the workers at Costco. These are people that, by definition, have gone and chosen this. We know they’re all smart. They could have all become investment bankers, they could have all become schoolteachers, but what they chose was to go into this field that’s about healing others, and that’s what I think we need to and what I would want them to do, is to get back in touch with themselves because I know it’s there. By definition, it’s there.
Q: Then why don’t more people just make that connection? What is the hurdle?
A: There are a lot of distractions. There are a lot of things coming your way. Worrying about your own life; doctors have lives at home. Worrying about the pressures of making a living. Some of this stuff is really, really hard. There are a million things going on. I believe, and I hope at UCLA, that we believe the strategy to make all of that stuff work is to get it right with the patient. And if you get it right with the patient, then all of that other stuff seems to fall into place and starts to make sense. The finances work out. The market share works out. The healthcare reform works out. I think it is the answer.
Richard Quinn is a freelance writer in New Jersey.
–David Feinberg, MD, MBA, president of UCLA Health System in Los Angeles
Patient satisfaction is a buzzword in HM circles, as compensation is increasingly tied to performance in keeping inpatients happy. David Feinberg, MD, MBA, president of UCLA Health System in Los Angeles, could be called a guru of patient satisfaction.
Just don’t tell him that.
“I hope I’m not seen as ‘patient satisfaction,’” he says. “I hope I’m seen as ‘patient centeredness.’ And patient satisfaction is a key piece of patient centeredness.”
Dr. Feinberg, who assumed his current role UCLA Health System in 2011, is a national voice for pushing a patient-centric model of care delivery. To wit, he will be one of the keynote speakers at HM13 next month at the Gaylord National Resort & Convention Center in National Harbor, Md. His address is fittingly titled “Healing Humankind One Patient at a Time.”
The Hospitalist spoke to Dr. Feinberg about his message to hospitalists.
Question: What do you think is the evolution of patient centeredness, as that becomes more of a focus for others?
Answer: Patient centeredness to me is the true north, and I think everything else that we’ve done that isn’t patient-centered has been a distraction. … It’s why we signed up to get into healthcare. It’s what we should be doing today and tonight, and it should guide our future tomorrow. It would be like me saying to the restaurateur, “How important is the food?”
Q: Is it something that hasn’t always been done?
A: It’s pathetic. You’re totally right. We’ve lost our way.
Q: If it’s so common-sense, how did we lose our way?
A: It really became, to me, the coin of the realm in medicine was how much the doctor made, how great their reputation was. It even got to the point of: You were a good doctor if your waiting room was packed. … I keep saying the waiting room should be for the doctors. The patient shouldn’t have to wait. You should be back in the exam room and the doctor should be waiting to see you. So we’ve got to completely change the paradigm. … It’s really the patient who’s at the top of the pyramid. And I just think we’ve lost that completely.
Q: How does a hospitalist engage quickly to ensure that they’re trying to accomplish patient centeredness and manage outcomes properly?
A: Hospitalists have a unique opportunity there, because everybody remembers when they got put in the hospital. It is a big deal when you’re hospitalized. Your family is in a vulnerable state, everybody is in a heightened sense of alertness and focus. Think about how important those four days are around education, around myths and demystifying, around beliefs and disbelief.
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Q: So what is the one thing you want hospitalists to take away from your address?
A: That they should join with all of us who want to heal humankind; that they are healers, above all.
Q: How do you translate “I want to be a healer” to the grind of daily work?
A: Well, I don’t think this is a grind. I think that when you’re in this healing profession, that you come here with a purpose. I think if we asked them to look at their personal statements of why they went into med school, every single one of them has something to do with, “I was sick as a kid, my grandmother got sick, I had had this doctor who was a role model, I like to help people, I was a volunteer and I met this patient.” Everyone says that. So this is different than trying to inspire the workers at Costco. These are people that, by definition, have gone and chosen this. We know they’re all smart. They could have all become investment bankers, they could have all become schoolteachers, but what they chose was to go into this field that’s about healing others, and that’s what I think we need to and what I would want them to do, is to get back in touch with themselves because I know it’s there. By definition, it’s there.
Q: Then why don’t more people just make that connection? What is the hurdle?
A: There are a lot of distractions. There are a lot of things coming your way. Worrying about your own life; doctors have lives at home. Worrying about the pressures of making a living. Some of this stuff is really, really hard. There are a million things going on. I believe, and I hope at UCLA, that we believe the strategy to make all of that stuff work is to get it right with the patient. And if you get it right with the patient, then all of that other stuff seems to fall into place and starts to make sense. The finances work out. The market share works out. The healthcare reform works out. I think it is the answer.
Richard Quinn is a freelance writer in New Jersey.
Medicare CMO Encourages Hospitalists to Become Experts in Managing Quality Patient Care

–Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer, Centers for Medicaid & Medicare Service
Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer of the Centers for Medicaid & Medicare Services (CMS), often says that physicians need to come to the proverbial table to tell CMS what they think is best. So it’s fitting that at HM13 at the Gaylord National Resort & Convention Center in National Harbor, Md., Dr. Conway will be a keynote speaker who can deliver his message of quality through teamwork to more than 2,500 hospitalists.
A pediatric hospitalist who also serves as director of the Office of Clinical Standards and Quality at the U.S. Department of Health and Human Services in Washington, D.C., Dr. Conway will paint a picture of what hospitalists can do to become the quality-improvement (QI) leaders healthcare needs in the coming years in a presentation titled “The Ideal Hospitalist in 2014 and Beyond: Active Change Agent.”
“Are hospitalists going to accept that challenge?” he asks. “I hope they are.”
This is the second year in a row that Dr. Conway will be a plenary speaker. Last year in San Diego, he told a packed room that CMS had to move from a “passive payor to an active facilitator and catalyst for quality improvement,” says Danielle Scheurer, MD, MSCR, SFHM, physician editor of The Hospitalist. Or, in his own words: “better health, better care, and lower cost.”
But many of the issues in his 2012 commentary were in flux. The Affordable Care Act (ACA), now moving through the slow process of implementation, was then still a law very much in doubt. It wasn’t until last summer that the law was upheld by a bitterly divided U.S. Supreme Court and it became clear much of the proposed reforms would move forward.
This year, he will urge hospitalists to step up their focus on patient-centered outcomes and stop questioning whether that should be the way the HM and other physicians should be judged.
“Given the changing context of payment, hospitalists are going to have to become true experts in managing the quality of care,” Dr. Conway says. “The days of you just graduating residency, seeing as many patients as you can, and you go home at the end of the day—that’s gone for hospital medicine.”
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Hospitalists can take charge of quality initiatives via involvement with accountable-care organizations (ACOs), health exchanges, and CMS’ value-based purchasing modifier (VBPM). In part, HM is perfectly positioned to assume leadership roles over the next few years because hospitalists already work across multiple departments.
“Hospital medicine is already ahead of a lot of specialties,” Dr. Conway says. “Hospital medicine physicians are already taking on much larger roles in their systems. I think you’re going to see an increasing trend.”
Richard Quinn is a freelance writer in New Jersey.
–Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer, Centers for Medicaid & Medicare Service
Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer of the Centers for Medicaid & Medicare Services (CMS), often says that physicians need to come to the proverbial table to tell CMS what they think is best. So it’s fitting that at HM13 at the Gaylord National Resort & Convention Center in National Harbor, Md., Dr. Conway will be a keynote speaker who can deliver his message of quality through teamwork to more than 2,500 hospitalists.
A pediatric hospitalist who also serves as director of the Office of Clinical Standards and Quality at the U.S. Department of Health and Human Services in Washington, D.C., Dr. Conway will paint a picture of what hospitalists can do to become the quality-improvement (QI) leaders healthcare needs in the coming years in a presentation titled “The Ideal Hospitalist in 2014 and Beyond: Active Change Agent.”
“Are hospitalists going to accept that challenge?” he asks. “I hope they are.”
This is the second year in a row that Dr. Conway will be a plenary speaker. Last year in San Diego, he told a packed room that CMS had to move from a “passive payor to an active facilitator and catalyst for quality improvement,” says Danielle Scheurer, MD, MSCR, SFHM, physician editor of The Hospitalist. Or, in his own words: “better health, better care, and lower cost.”
But many of the issues in his 2012 commentary were in flux. The Affordable Care Act (ACA), now moving through the slow process of implementation, was then still a law very much in doubt. It wasn’t until last summer that the law was upheld by a bitterly divided U.S. Supreme Court and it became clear much of the proposed reforms would move forward.
This year, he will urge hospitalists to step up their focus on patient-centered outcomes and stop questioning whether that should be the way the HM and other physicians should be judged.
“Given the changing context of payment, hospitalists are going to have to become true experts in managing the quality of care,” Dr. Conway says. “The days of you just graduating residency, seeing as many patients as you can, and you go home at the end of the day—that’s gone for hospital medicine.”
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Hospitalists can take charge of quality initiatives via involvement with accountable-care organizations (ACOs), health exchanges, and CMS’ value-based purchasing modifier (VBPM). In part, HM is perfectly positioned to assume leadership roles over the next few years because hospitalists already work across multiple departments.
“Hospital medicine is already ahead of a lot of specialties,” Dr. Conway says. “Hospital medicine physicians are already taking on much larger roles in their systems. I think you’re going to see an increasing trend.”
Richard Quinn is a freelance writer in New Jersey.
–Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer, Centers for Medicaid & Medicare Service
Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer of the Centers for Medicaid & Medicare Services (CMS), often says that physicians need to come to the proverbial table to tell CMS what they think is best. So it’s fitting that at HM13 at the Gaylord National Resort & Convention Center in National Harbor, Md., Dr. Conway will be a keynote speaker who can deliver his message of quality through teamwork to more than 2,500 hospitalists.
A pediatric hospitalist who also serves as director of the Office of Clinical Standards and Quality at the U.S. Department of Health and Human Services in Washington, D.C., Dr. Conway will paint a picture of what hospitalists can do to become the quality-improvement (QI) leaders healthcare needs in the coming years in a presentation titled “The Ideal Hospitalist in 2014 and Beyond: Active Change Agent.”
“Are hospitalists going to accept that challenge?” he asks. “I hope they are.”
This is the second year in a row that Dr. Conway will be a plenary speaker. Last year in San Diego, he told a packed room that CMS had to move from a “passive payor to an active facilitator and catalyst for quality improvement,” says Danielle Scheurer, MD, MSCR, SFHM, physician editor of The Hospitalist. Or, in his own words: “better health, better care, and lower cost.”
But many of the issues in his 2012 commentary were in flux. The Affordable Care Act (ACA), now moving through the slow process of implementation, was then still a law very much in doubt. It wasn’t until last summer that the law was upheld by a bitterly divided U.S. Supreme Court and it became clear much of the proposed reforms would move forward.
This year, he will urge hospitalists to step up their focus on patient-centered outcomes and stop questioning whether that should be the way the HM and other physicians should be judged.
“Given the changing context of payment, hospitalists are going to have to become true experts in managing the quality of care,” Dr. Conway says. “The days of you just graduating residency, seeing as many patients as you can, and you go home at the end of the day—that’s gone for hospital medicine.”
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Hospitalists can take charge of quality initiatives via involvement with accountable-care organizations (ACOs), health exchanges, and CMS’ value-based purchasing modifier (VBPM). In part, HM is perfectly positioned to assume leadership roles over the next few years because hospitalists already work across multiple departments.
“Hospital medicine is already ahead of a lot of specialties,” Dr. Conway says. “Hospital medicine physicians are already taking on much larger roles in their systems. I think you’re going to see an increasing trend.”
Richard Quinn is a freelance writer in New Jersey.
Educational, Networking Opportunities for Hospitalists Abound at HM13
Ask Dan Brotman, MD, FACP, SFHM, how to get the most out of the annual meeting of hospitalists and you’ll get a simple, one-word answer: Go.
“It sounds so trivial,” says Dr. Brotman, HM13 course director. “But there are a lot more hospitalists out there than we see at the meeting, and I think that [we should be] getting out the word that this is the best single opportunity that hospitalists have to network and learn about their field, not only content knowledge but also understanding where the field is going from thought leaders.”
The annual pilgrimage of hospitalists is expected to be larger than ever this year, with SHM expecting nearly 3,000 hospitalists to attend. Last year, roughly 2,700 hospitalists attended in San Diego.
But navigating a four-day maze of pre-courses, plenaries, and presentations can overwhelm even the most experienced attendee, much less a first-timer. And that’s before the annual rite that is the Research, Innovation, and Clinical Vignettes (RIV) poster competition and the Hospitalists on the Hill event that is particularly fitting this year as Capitol Hill happens to be just a few miles away.
So what’s the best advice to have the best meeting experience? Planning, planning, and a little more planning.
Ken Simone, DO, SFHM, principal of Hospitalist and Practice Solutions in Veazie, Maine, says the plethora of workshops, keynote speakers, and formalized educational offerings means attendees should “game plan” their schedule as much as possible.
“It behooves everyone to really study the offerings each day and each hour and plan their schedule accordingly,” says Dr. Simone, a Team Hospitalist member. “I typically create my schedule before I leave home for the conference.”
But don’t plan too much, he adds. Having a list of sessions to attend is important, but part of the meeting’s allure is the ability to mingle with clinical, administrative, and society leaders from around the country.
“Flexibility is the key,” he says. “Having something well planned doesn’t mean you can’t be flexible.”
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Dr. Brotman says meeting organizers take the same approach. While some topics are old favorites, SHM adds new offerings each year to adapt in real time to important trends. For example, he says, a new track this year focused on comanagement will appeal to hospitalists and subspecialists who take care of stroke patients, surgical patients, and pregnant women, among others.
The new track is in addition to the existing offerings: clinical, academic/research, rapid fire, pediatric, practice management, quality, and potpourri. The last item is in its second year and offers a break from the didactic and lecture approaches taken in nearly all of the annual meeting’s other breakout sessions. A particularly popular event is expected to be “History of Hospitals,” presented by hospitalist historian Jordan Messler, MD, SFHM.
There are two new pre-courses this year: “Bugs, Drugs and You: Infectious Disease Essentials for the Hospitalist” and “What Keeps You Awake at Night? Hot Topics in Hospitalist Practice Management.” Pre-course mainstays scheduled again this year include “ABIM Maintenance Certification,” “Medical Procedures for the Hospitalist,” and “Portable Ultrasounds for the Hospitalist.”
“As the society has gotten bigger, the meeting has gotten bigger in terms of its scope,” says Dr. Brotman, whose day job is director of the hospitalist program at Johns Hopkins Hospital in Baltimore. “So we have Friday, Saturday, and Sunday, plus the evening activities, plus the pre-courses. One of the adjustments that we’ve made over time is that we do recognize that with a larger constituency and a larger amount of topical information that we’d like to cover, the meeting does get longer. The hope is that people can commit close to a week toward advancing their knowledge; it’s well worth the time.”
Richard Quinn is a freelance writer in New Jersey.
Ask Dan Brotman, MD, FACP, SFHM, how to get the most out of the annual meeting of hospitalists and you’ll get a simple, one-word answer: Go.
“It sounds so trivial,” says Dr. Brotman, HM13 course director. “But there are a lot more hospitalists out there than we see at the meeting, and I think that [we should be] getting out the word that this is the best single opportunity that hospitalists have to network and learn about their field, not only content knowledge but also understanding where the field is going from thought leaders.”
The annual pilgrimage of hospitalists is expected to be larger than ever this year, with SHM expecting nearly 3,000 hospitalists to attend. Last year, roughly 2,700 hospitalists attended in San Diego.
But navigating a four-day maze of pre-courses, plenaries, and presentations can overwhelm even the most experienced attendee, much less a first-timer. And that’s before the annual rite that is the Research, Innovation, and Clinical Vignettes (RIV) poster competition and the Hospitalists on the Hill event that is particularly fitting this year as Capitol Hill happens to be just a few miles away.
So what’s the best advice to have the best meeting experience? Planning, planning, and a little more planning.
Ken Simone, DO, SFHM, principal of Hospitalist and Practice Solutions in Veazie, Maine, says the plethora of workshops, keynote speakers, and formalized educational offerings means attendees should “game plan” their schedule as much as possible.
“It behooves everyone to really study the offerings each day and each hour and plan their schedule accordingly,” says Dr. Simone, a Team Hospitalist member. “I typically create my schedule before I leave home for the conference.”
But don’t plan too much, he adds. Having a list of sessions to attend is important, but part of the meeting’s allure is the ability to mingle with clinical, administrative, and society leaders from around the country.
“Flexibility is the key,” he says. “Having something well planned doesn’t mean you can’t be flexible.”
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Dr. Brotman says meeting organizers take the same approach. While some topics are old favorites, SHM adds new offerings each year to adapt in real time to important trends. For example, he says, a new track this year focused on comanagement will appeal to hospitalists and subspecialists who take care of stroke patients, surgical patients, and pregnant women, among others.
The new track is in addition to the existing offerings: clinical, academic/research, rapid fire, pediatric, practice management, quality, and potpourri. The last item is in its second year and offers a break from the didactic and lecture approaches taken in nearly all of the annual meeting’s other breakout sessions. A particularly popular event is expected to be “History of Hospitals,” presented by hospitalist historian Jordan Messler, MD, SFHM.
There are two new pre-courses this year: “Bugs, Drugs and You: Infectious Disease Essentials for the Hospitalist” and “What Keeps You Awake at Night? Hot Topics in Hospitalist Practice Management.” Pre-course mainstays scheduled again this year include “ABIM Maintenance Certification,” “Medical Procedures for the Hospitalist,” and “Portable Ultrasounds for the Hospitalist.”
“As the society has gotten bigger, the meeting has gotten bigger in terms of its scope,” says Dr. Brotman, whose day job is director of the hospitalist program at Johns Hopkins Hospital in Baltimore. “So we have Friday, Saturday, and Sunday, plus the evening activities, plus the pre-courses. One of the adjustments that we’ve made over time is that we do recognize that with a larger constituency and a larger amount of topical information that we’d like to cover, the meeting does get longer. The hope is that people can commit close to a week toward advancing their knowledge; it’s well worth the time.”
Richard Quinn is a freelance writer in New Jersey.
Ask Dan Brotman, MD, FACP, SFHM, how to get the most out of the annual meeting of hospitalists and you’ll get a simple, one-word answer: Go.
“It sounds so trivial,” says Dr. Brotman, HM13 course director. “But there are a lot more hospitalists out there than we see at the meeting, and I think that [we should be] getting out the word that this is the best single opportunity that hospitalists have to network and learn about their field, not only content knowledge but also understanding where the field is going from thought leaders.”
The annual pilgrimage of hospitalists is expected to be larger than ever this year, with SHM expecting nearly 3,000 hospitalists to attend. Last year, roughly 2,700 hospitalists attended in San Diego.
But navigating a four-day maze of pre-courses, plenaries, and presentations can overwhelm even the most experienced attendee, much less a first-timer. And that’s before the annual rite that is the Research, Innovation, and Clinical Vignettes (RIV) poster competition and the Hospitalists on the Hill event that is particularly fitting this year as Capitol Hill happens to be just a few miles away.
So what’s the best advice to have the best meeting experience? Planning, planning, and a little more planning.
Ken Simone, DO, SFHM, principal of Hospitalist and Practice Solutions in Veazie, Maine, says the plethora of workshops, keynote speakers, and formalized educational offerings means attendees should “game plan” their schedule as much as possible.
“It behooves everyone to really study the offerings each day and each hour and plan their schedule accordingly,” says Dr. Simone, a Team Hospitalist member. “I typically create my schedule before I leave home for the conference.”
But don’t plan too much, he adds. Having a list of sessions to attend is important, but part of the meeting’s allure is the ability to mingle with clinical, administrative, and society leaders from around the country.
“Flexibility is the key,” he says. “Having something well planned doesn’t mean you can’t be flexible.”
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Dr. Brotman says meeting organizers take the same approach. While some topics are old favorites, SHM adds new offerings each year to adapt in real time to important trends. For example, he says, a new track this year focused on comanagement will appeal to hospitalists and subspecialists who take care of stroke patients, surgical patients, and pregnant women, among others.
The new track is in addition to the existing offerings: clinical, academic/research, rapid fire, pediatric, practice management, quality, and potpourri. The last item is in its second year and offers a break from the didactic and lecture approaches taken in nearly all of the annual meeting’s other breakout sessions. A particularly popular event is expected to be “History of Hospitals,” presented by hospitalist historian Jordan Messler, MD, SFHM.
There are two new pre-courses this year: “Bugs, Drugs and You: Infectious Disease Essentials for the Hospitalist” and “What Keeps You Awake at Night? Hot Topics in Hospitalist Practice Management.” Pre-course mainstays scheduled again this year include “ABIM Maintenance Certification,” “Medical Procedures for the Hospitalist,” and “Portable Ultrasounds for the Hospitalist.”
“As the society has gotten bigger, the meeting has gotten bigger in terms of its scope,” says Dr. Brotman, whose day job is director of the hospitalist program at Johns Hopkins Hospital in Baltimore. “So we have Friday, Saturday, and Sunday, plus the evening activities, plus the pre-courses. One of the adjustments that we’ve made over time is that we do recognize that with a larger constituency and a larger amount of topical information that we’d like to cover, the meeting does get longer. The hope is that people can commit close to a week toward advancing their knowledge; it’s well worth the time.”
Richard Quinn is a freelance writer in New Jersey.
Hospitalists Gear Up to Lobby Congress on Health Care Policy

Mangla Gulati, MD, FACP, FHM, an academic hospitalist and medical director of clinical effectiveness at University of Maryland Medical Center in Baltimore, had never been involved in a lobbying trip before the waning days of last year. But then, just as members of Congress were wrestling with potential Draconian cuts to Medicare reimbursements and a $10 million slash in Medicare funding for the National Quality Forum (NQF), Dr. Gulati found herself on a daylong trip with SHM government guru Laura Allendorf and an NQF representative to make a series of in-person appeals to politicians in Washington, D.C. “When you’re a practicing physician, even though you know there’s regulation and compliance and mandates, you really don’t understand how they come to fruition and what the thought process is,” says Dr. Gulati, secretary of SHM’s Maryland chapter. “It was really interesting to see the other side of that and how people up on the Hill make a lot of decisions based on the information that’s given to them.”
The Hill she’s referring to is none other than Capitol Hill, and Dr. Gulati is making a return just a few months after her visit. And this time, she’s bringing a few hundred hospitalists with her. Hospitalists on the Hill 2013 (www.hospitalmedicine 2013.org/advocacy) is the annual trek made by SHM leadership and rank-and-file members to lobby legislators and federal staffers “on the way policies affect your practice and your patients,” SHM says on its website. This year, the showing in Washington is expected to be among the best ever, as the lobbying trip is May 16, just before HM13’s full program kicks off at the Gaylord National Resort & Convention Center in National Harbor, Md.
The all-day affair kicks off in the morning, as participants will receive briefings from SHM Public Policy Committee Chair Ron Greeno, MD, FCCP, MHM, and Allendorf, SHM’s senior advisor for advocacy and government affairs. Then comes a two-hour training course from Advocacy Associates (http://advocacyassociates.com), a boutique communications firm that helps organizations, such as SHM, tailor their message to policymakers. After that, it’s a six-hour whirlwind of meetings with home-state legislators, career administrators, and aide-de-camps that one former participant described as “almost like speed-dial dating with congressmen and -women.” Lastly, participants regroup at day’s end for a debriefing.
“I think what’s different at SHM is we go to Washington with an agenda of how we can improve patient safety and quality outcomes,” says Patrick Torcson, MD, MMM, FACP, SFHM, chair of SHM’s Performance Measurement and Reporting Committee. “We’re not there about just protecting our turf and making sure that our reimbursement stays at a reasonable level. We’ve been very clear to offer innovations about care transitions and Project BOOST, and different things that can be done to improve things like quality and service for Medicare beneficiaries.”
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Dr. Torcson says congressional contacts he’s made in past years “always look forward to our visits, because we really do come with an attitude of how can we help fix a broken system.”
He counts several victories as fruit of the annual trip. First, he believes the trip has “clearly educated our politicians, congressional staffers, and CMS [the Centers for Medicare & Medicaid Services] that the predominant model of the way patients are taken care of in the hospital is by a hospitalist.”
Second, and more granularly, SHM really gets into the weeds. Take CMS’ Quality and Resource Use Report (QRUR), which is part of the rollout of its value-based purchasing modifier (VBPM). Dr. Torcson says SHM carefully reviewed the report to register its concerns about proper attribution, fair comparisons, relevant metrics, and other issues. In turn, CMS signaled its appreciation of SHM’s due diligence and has indicated a willingness to work with SHM to address its concerns.
CMS chief medical officer Patrick Conway, MD, MSc, FAAP, SFHM, sees it from both sides of the equation. A pediatric hospitalist by training, he has been on trips to push federal officials to promulgate rules that make the most sense for HM. But in his current job, he’s often the one being pushed—and he welcomes the visits.
“We’re trying to partner up with physicians,” he says.
Dr. Conway believes lobbying trips like SHM’s are critical to informing both politicians and professionals on what physicians need or want most.
“People often think, ‘How could it matter?’ Sure, some of it will be hits and misses. But you’ll hit some key points that resonate,” he says.
Hospitalist Rick Hilger, MD, SFHM, director of resident education and adjunct associate professor of medicine at the University of Minnesota Medical School in Minneapolis, learned that lesson last year during his first Hospitalists on the Hill. A first-time member of SHM’s Public Policy Committee, he met with the legislative assistants for U.S. Sens.
Al Franken (D-Minn.) and Amy Klobuchar (D-Minn.), as well as had a face-to-face meeting with U.S. Rep. Allyson Schwartz (D-Pa.). The latter has been a staunch advocate of Medicare payment reform, sponsoring several bills—with SHM’s support—to repeal the sustainable growth rate (SGR) formula.
“It’s an investment in time, and especially for the senators and congressmen and -women from your own state, it’s more about trying to develop a relationship,” Dr. Hilger says. “I’ve already exchanged emails with the aides that I met that day concerning other healthcare issues. … I’m not sure I can completely answer for the long-term impact, but it definitely feels better than doing nothing.”
How to Climb the Hill

SHM’s Hospitalists on the Hill event is May 16, the first day of HM13. Even if you can’t make it, these tips from SHM’s advocacy veterans are helpful when using SHM’s new Legislative Action Center (www.hospitalmedicine.org/advocacy).
- Don’t be afraid. Often, hospitalists think that lobbying efforts are only fruitful if done by industry leaders. SHM wants as many members involved as possible to strengthen its message. “Numbers are important,” Dr. Greeno says. “The more people we can get there to participate, the better. It just means the more people we can get in front of it.”
- Bring a point of view. “We all come to the table with different experiences, different thoughts on healthcare reform,” Dr. Hilger says. “So we try to come to a consensus for everyone. The worst thing you can do is to say nothing.”
- Be positive. Change doesn’t happen overnight, so take the long view on how valuable conversations with policy leaders can be and how they can further the progress started by the loudest voices in HM. “They’ve pushed the envelope,” Dr. Gulati says. “We need to keep pushing it, because if you don’t push, you can’t make change.”
Richard Quinn is a freelance writer in New Jersey.
Mangla Gulati, MD, FACP, FHM, an academic hospitalist and medical director of clinical effectiveness at University of Maryland Medical Center in Baltimore, had never been involved in a lobbying trip before the waning days of last year. But then, just as members of Congress were wrestling with potential Draconian cuts to Medicare reimbursements and a $10 million slash in Medicare funding for the National Quality Forum (NQF), Dr. Gulati found herself on a daylong trip with SHM government guru Laura Allendorf and an NQF representative to make a series of in-person appeals to politicians in Washington, D.C. “When you’re a practicing physician, even though you know there’s regulation and compliance and mandates, you really don’t understand how they come to fruition and what the thought process is,” says Dr. Gulati, secretary of SHM’s Maryland chapter. “It was really interesting to see the other side of that and how people up on the Hill make a lot of decisions based on the information that’s given to them.”
The Hill she’s referring to is none other than Capitol Hill, and Dr. Gulati is making a return just a few months after her visit. And this time, she’s bringing a few hundred hospitalists with her. Hospitalists on the Hill 2013 (www.hospitalmedicine 2013.org/advocacy) is the annual trek made by SHM leadership and rank-and-file members to lobby legislators and federal staffers “on the way policies affect your practice and your patients,” SHM says on its website. This year, the showing in Washington is expected to be among the best ever, as the lobbying trip is May 16, just before HM13’s full program kicks off at the Gaylord National Resort & Convention Center in National Harbor, Md.
The all-day affair kicks off in the morning, as participants will receive briefings from SHM Public Policy Committee Chair Ron Greeno, MD, FCCP, MHM, and Allendorf, SHM’s senior advisor for advocacy and government affairs. Then comes a two-hour training course from Advocacy Associates (http://advocacyassociates.com), a boutique communications firm that helps organizations, such as SHM, tailor their message to policymakers. After that, it’s a six-hour whirlwind of meetings with home-state legislators, career administrators, and aide-de-camps that one former participant described as “almost like speed-dial dating with congressmen and -women.” Lastly, participants regroup at day’s end for a debriefing.
“I think what’s different at SHM is we go to Washington with an agenda of how we can improve patient safety and quality outcomes,” says Patrick Torcson, MD, MMM, FACP, SFHM, chair of SHM’s Performance Measurement and Reporting Committee. “We’re not there about just protecting our turf and making sure that our reimbursement stays at a reasonable level. We’ve been very clear to offer innovations about care transitions and Project BOOST, and different things that can be done to improve things like quality and service for Medicare beneficiaries.”
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Dr. Torcson says congressional contacts he’s made in past years “always look forward to our visits, because we really do come with an attitude of how can we help fix a broken system.”
He counts several victories as fruit of the annual trip. First, he believes the trip has “clearly educated our politicians, congressional staffers, and CMS [the Centers for Medicare & Medicaid Services] that the predominant model of the way patients are taken care of in the hospital is by a hospitalist.”
Second, and more granularly, SHM really gets into the weeds. Take CMS’ Quality and Resource Use Report (QRUR), which is part of the rollout of its value-based purchasing modifier (VBPM). Dr. Torcson says SHM carefully reviewed the report to register its concerns about proper attribution, fair comparisons, relevant metrics, and other issues. In turn, CMS signaled its appreciation of SHM’s due diligence and has indicated a willingness to work with SHM to address its concerns.
CMS chief medical officer Patrick Conway, MD, MSc, FAAP, SFHM, sees it from both sides of the equation. A pediatric hospitalist by training, he has been on trips to push federal officials to promulgate rules that make the most sense for HM. But in his current job, he’s often the one being pushed—and he welcomes the visits.
“We’re trying to partner up with physicians,” he says.
Dr. Conway believes lobbying trips like SHM’s are critical to informing both politicians and professionals on what physicians need or want most.
“People often think, ‘How could it matter?’ Sure, some of it will be hits and misses. But you’ll hit some key points that resonate,” he says.
Hospitalist Rick Hilger, MD, SFHM, director of resident education and adjunct associate professor of medicine at the University of Minnesota Medical School in Minneapolis, learned that lesson last year during his first Hospitalists on the Hill. A first-time member of SHM’s Public Policy Committee, he met with the legislative assistants for U.S. Sens.
Al Franken (D-Minn.) and Amy Klobuchar (D-Minn.), as well as had a face-to-face meeting with U.S. Rep. Allyson Schwartz (D-Pa.). The latter has been a staunch advocate of Medicare payment reform, sponsoring several bills—with SHM’s support—to repeal the sustainable growth rate (SGR) formula.
“It’s an investment in time, and especially for the senators and congressmen and -women from your own state, it’s more about trying to develop a relationship,” Dr. Hilger says. “I’ve already exchanged emails with the aides that I met that day concerning other healthcare issues. … I’m not sure I can completely answer for the long-term impact, but it definitely feels better than doing nothing.”
How to Climb the Hill
SHM’s Hospitalists on the Hill event is May 16, the first day of HM13. Even if you can’t make it, these tips from SHM’s advocacy veterans are helpful when using SHM’s new Legislative Action Center (www.hospitalmedicine.org/advocacy).
- Don’t be afraid. Often, hospitalists think that lobbying efforts are only fruitful if done by industry leaders. SHM wants as many members involved as possible to strengthen its message. “Numbers are important,” Dr. Greeno says. “The more people we can get there to participate, the better. It just means the more people we can get in front of it.”
- Bring a point of view. “We all come to the table with different experiences, different thoughts on healthcare reform,” Dr. Hilger says. “So we try to come to a consensus for everyone. The worst thing you can do is to say nothing.”
- Be positive. Change doesn’t happen overnight, so take the long view on how valuable conversations with policy leaders can be and how they can further the progress started by the loudest voices in HM. “They’ve pushed the envelope,” Dr. Gulati says. “We need to keep pushing it, because if you don’t push, you can’t make change.”
Richard Quinn is a freelance writer in New Jersey.
Mangla Gulati, MD, FACP, FHM, an academic hospitalist and medical director of clinical effectiveness at University of Maryland Medical Center in Baltimore, had never been involved in a lobbying trip before the waning days of last year. But then, just as members of Congress were wrestling with potential Draconian cuts to Medicare reimbursements and a $10 million slash in Medicare funding for the National Quality Forum (NQF), Dr. Gulati found herself on a daylong trip with SHM government guru Laura Allendorf and an NQF representative to make a series of in-person appeals to politicians in Washington, D.C. “When you’re a practicing physician, even though you know there’s regulation and compliance and mandates, you really don’t understand how they come to fruition and what the thought process is,” says Dr. Gulati, secretary of SHM’s Maryland chapter. “It was really interesting to see the other side of that and how people up on the Hill make a lot of decisions based on the information that’s given to them.”
The Hill she’s referring to is none other than Capitol Hill, and Dr. Gulati is making a return just a few months after her visit. And this time, she’s bringing a few hundred hospitalists with her. Hospitalists on the Hill 2013 (www.hospitalmedicine 2013.org/advocacy) is the annual trek made by SHM leadership and rank-and-file members to lobby legislators and federal staffers “on the way policies affect your practice and your patients,” SHM says on its website. This year, the showing in Washington is expected to be among the best ever, as the lobbying trip is May 16, just before HM13’s full program kicks off at the Gaylord National Resort & Convention Center in National Harbor, Md.
The all-day affair kicks off in the morning, as participants will receive briefings from SHM Public Policy Committee Chair Ron Greeno, MD, FCCP, MHM, and Allendorf, SHM’s senior advisor for advocacy and government affairs. Then comes a two-hour training course from Advocacy Associates (http://advocacyassociates.com), a boutique communications firm that helps organizations, such as SHM, tailor their message to policymakers. After that, it’s a six-hour whirlwind of meetings with home-state legislators, career administrators, and aide-de-camps that one former participant described as “almost like speed-dial dating with congressmen and -women.” Lastly, participants regroup at day’s end for a debriefing.
“I think what’s different at SHM is we go to Washington with an agenda of how we can improve patient safety and quality outcomes,” says Patrick Torcson, MD, MMM, FACP, SFHM, chair of SHM’s Performance Measurement and Reporting Committee. “We’re not there about just protecting our turf and making sure that our reimbursement stays at a reasonable level. We’ve been very clear to offer innovations about care transitions and Project BOOST, and different things that can be done to improve things like quality and service for Medicare beneficiaries.”
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Dr. Torcson says congressional contacts he’s made in past years “always look forward to our visits, because we really do come with an attitude of how can we help fix a broken system.”
He counts several victories as fruit of the annual trip. First, he believes the trip has “clearly educated our politicians, congressional staffers, and CMS [the Centers for Medicare & Medicaid Services] that the predominant model of the way patients are taken care of in the hospital is by a hospitalist.”
Second, and more granularly, SHM really gets into the weeds. Take CMS’ Quality and Resource Use Report (QRUR), which is part of the rollout of its value-based purchasing modifier (VBPM). Dr. Torcson says SHM carefully reviewed the report to register its concerns about proper attribution, fair comparisons, relevant metrics, and other issues. In turn, CMS signaled its appreciation of SHM’s due diligence and has indicated a willingness to work with SHM to address its concerns.
CMS chief medical officer Patrick Conway, MD, MSc, FAAP, SFHM, sees it from both sides of the equation. A pediatric hospitalist by training, he has been on trips to push federal officials to promulgate rules that make the most sense for HM. But in his current job, he’s often the one being pushed—and he welcomes the visits.
“We’re trying to partner up with physicians,” he says.
Dr. Conway believes lobbying trips like SHM’s are critical to informing both politicians and professionals on what physicians need or want most.
“People often think, ‘How could it matter?’ Sure, some of it will be hits and misses. But you’ll hit some key points that resonate,” he says.
Hospitalist Rick Hilger, MD, SFHM, director of resident education and adjunct associate professor of medicine at the University of Minnesota Medical School in Minneapolis, learned that lesson last year during his first Hospitalists on the Hill. A first-time member of SHM’s Public Policy Committee, he met with the legislative assistants for U.S. Sens.
Al Franken (D-Minn.) and Amy Klobuchar (D-Minn.), as well as had a face-to-face meeting with U.S. Rep. Allyson Schwartz (D-Pa.). The latter has been a staunch advocate of Medicare payment reform, sponsoring several bills—with SHM’s support—to repeal the sustainable growth rate (SGR) formula.
“It’s an investment in time, and especially for the senators and congressmen and -women from your own state, it’s more about trying to develop a relationship,” Dr. Hilger says. “I’ve already exchanged emails with the aides that I met that day concerning other healthcare issues. … I’m not sure I can completely answer for the long-term impact, but it definitely feels better than doing nothing.”
How to Climb the Hill
SHM’s Hospitalists on the Hill event is May 16, the first day of HM13. Even if you can’t make it, these tips from SHM’s advocacy veterans are helpful when using SHM’s new Legislative Action Center (www.hospitalmedicine.org/advocacy).
- Don’t be afraid. Often, hospitalists think that lobbying efforts are only fruitful if done by industry leaders. SHM wants as many members involved as possible to strengthen its message. “Numbers are important,” Dr. Greeno says. “The more people we can get there to participate, the better. It just means the more people we can get in front of it.”
- Bring a point of view. “We all come to the table with different experiences, different thoughts on healthcare reform,” Dr. Hilger says. “So we try to come to a consensus for everyone. The worst thing you can do is to say nothing.”
- Be positive. Change doesn’t happen overnight, so take the long view on how valuable conversations with policy leaders can be and how they can further the progress started by the loudest voices in HM. “They’ve pushed the envelope,” Dr. Gulati says. “We need to keep pushing it, because if you don’t push, you can’t make change.”
Richard Quinn is a freelance writer in New Jersey.
Continuing Medical Education (CME) Courses for Hospitalists Thrive Online


Hospitalist Lenny Feldman, MD, FACP, FAAP, SFHM, of John Hopkins School of Medicine in Baltimore, is the proverbial study in contrasts. He is the longtime editor of SHM’s Consultative & Perioperative Medicine Essentials for Hospitalists, a free continuing medical education (CME) repository more commonly known as SHMConsults (www.shmconsults.com). But in February, he helped lead “Updates in Hospital Medicine 2013: Evidence-Based Reviews on the Management of Hospitalized Patients.” That program, arranged by Canadian education provider CMEatSea (www.cmeatsea.org) and held aboard a cruise ship in the eastern Caribbean, attracted some 60 hospitalists, nurse practitioners, and physician assistants interested in earning up to 14 credits.
On the one hand, Dr. Feldman is a pioneer of free virtual CME. On the other, he is an example of the big-ticket CME events that were much more commonplace five or 10 years ago.
“It’s tough,” Dr. Feldman says. “There’s no doubt that once you’ve built that virtual infrastructure, it allows many more people access to CME than if they have to come together. But with that said, particularly at a meeting like HM13, there’s so much more to it than just the CME. The networking is a huge part of that.”
This is the current state of CME, in which ever-tightening physician budgets plus a massive pullback of pharmaceutical industry support equals a landscape of fewer and fewer big-ticket events and more and more online offerings. The expense of large-scale offerings means that many physicians look for more than just the credits available when deciding which events to attend.
For many hospitalists, of course, SHM’s annual meeting remains the best opportunity of the year for CME. Accordingly, those credits are often cited as one of the biggest lures for many of the nearly 3,000 hospitalists who are expected to convene May 16-19 at the Gaylord National Resort & Convention Center in National Harbor, Md.
“You can always get CME credits locally by attending lectures at your own institution, but so often the content of these lectures is really not something that has been vetted and put forward by hospitalists,” says HM13 course director Daniel Brotman, MD, FACP, SFHM. “I think the people who attend this meeting know where the field is going, not only because of the content that’s offered, but because of who else is there. That’s different than going to an hourlong lecture by a cardiologist at your institution on atrial fibrillation.”

—Lenny Feldman, MD, FACP, FAAP, SFHM, John Hopkins School of Medicine, Baltimore
Pharma Pullback
CME budgets typically run $3,000 to $3,500 per physician, but can range from as low as $2,000 to as high as $5,000 annually, according to rough estimates from industry leaders. Opinions are mixed on whether those budgets have been significantly reduced over the past few years, but “they’re certainly not going up,” Dr. Feldman says.
What is falling year after year is the amount of money that the pharmaceutical industry is providing to support CME, says Daniel Guinee, executive vice president of educational firm ASiM of Somerville, N.J. The drug industry funded $1.2 billion of CME in 2007, according to the Accreditation Council for Continuing Medical Education (ACCME). That number dropped to $736 million in 2011, the latest year for which ACCME has statistics. Guinee says many expect the total for 2012 to be approximately $600 million, then level off.
Some applaud the drop-off in industry funding as a needed correction to ensure any potential bias is eliminated. To that end, the American Medical Association’s (AMA) Council on Ethical and Judicial Affairs in 2011 adopted a policy urging the avoidance of industry funding of CME when possible. But just 42% of physicians in one study said they were willing to pay higher fees to eliminate that funding source (Arch Intern Med. 2011;171(9):840-846).
Guinee attributes much of the drug industry’s pullback in funding to companies’ uncertainty over transparency and reporting required by ACCME, the FDA, and the U.S. Department of Health & Human Services (HHS).
“The companies want to use their money as they want to,” Guinee says. “Instead of putting the money out there … as way to support medical education, they’re saying, ‘You know what? We’ll just hang on to it and spend it in other ways.’”
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Dr. Feldman, whose SHMConsults project has been supported by the pharmaceutical industry for seven years, says it’s unclear where future funding will come from in order to support CME. But ACCME president and chief executive officer Murray Kopelow, MD, says that while commercial support—the industry term for pharmaceutical funding—has steadily fallen, “other income” rose 221% from 2006 to 2011 for ACCME-accredited providers and ACCME–recognized, state-accredited providers. ACCME says that income can include activity registration fees, government or nonprofit foundation grants, and allocations from accredited providers’ parent organizations.
“The balance of revenue has shifted,” Dr. Kopelow says.
Education When You Need It
Also shifting is the nature of CME delivery. Since 2007, the number of live Internet CME activities has risen 33%, while the number of journal CME activities has risen 13%, according to ACCME figures. The number of courses in which participants physically attend is virtually static.
SHM has embraced the virtual concept and is looking to add as many online learning opportunities as feasible, says Catharine Smith, SHM’s senior director for education. That includes updates to SHMConsults and the Hospital Quality and Patient Safety Online Academy (www.hospitalmedicine.org/hqps), as well as future offerings based on core competencies. Virtual CME allows hospitalists to meet CME requirements when it is convenient for them and allows providers to set up both live events and enduring materials, Smith says.
“More online CME opportunities from SHM’s Learning Portal is about bringing quality content to hospitalists,” Smith said in a statement. “This reflects SHM’s understanding of the professional needs of hospitalists.”
She added that measuring outcomes can be easier online, as data recording in that manner is easier than during a big meeting. Then again, it’s also difficult to gauge just how well a learned lesson is then incorporated into practice.
For all its advantages, online CME shouldn’t replace all face-to-face learning, Dr. Kopelow says.
“Physicians consult colleagues and reflect on what they have learned before integrating the new information into their practice for the benefit of patients,” he adds. “It is this process that accredited CME promotes and supports. Online CME supports this process, but it does not replace the total process of continuing professional development.”
Dr. Feldman says physicians will have to decide for themselves what works for them, particularly if reduced CME spending by the drug industry continues to crimp offerings.
“There’s going to be a huge sea change there in terms of folks needing to decide where they’re going to want to spend their CME money,” he adds. “Are they going to choose some of these easier-to-use, online CME offerings if they think that going to meetings is becoming prohibitively expensive? Only time is going to tell.”
CME in History

1847: The American Medical Association (AMA) is founded, and one of its first two committees is the Committee on Medical Education.
1901: The committee is recast as the Council on Medical Education, the name it still goes by.
1940s-’50s: The council’s eye is trained on postgraduate medical education (PGME), resulting in a 1955 report that found nearly one-third of 5,000 surveyed physicians reported they had participated in PGME in the preceding five years.
1968: AMA establishes the AMA Physician Recognition Award (PRA). The related credit system was developed to determine qualifications for the PRA.
1981: AMA and six other national organizations form the Accreditation Council for Continuing Medical Education (ACCME). The AMA only allows PRA credits to be designated and awarded by organizations accredited by the ACCME or by a state medical society recognized by the ACCME.
2011: AMA’s Council on Ethical and Judicial Affairs adopts a policy that urges avoiding industry funding of CME when possible to avoid potential bias issues.
Source: American Medical Association
Hospitalist Lenny Feldman, MD, FACP, FAAP, SFHM, of John Hopkins School of Medicine in Baltimore, is the proverbial study in contrasts. He is the longtime editor of SHM’s Consultative & Perioperative Medicine Essentials for Hospitalists, a free continuing medical education (CME) repository more commonly known as SHMConsults (www.shmconsults.com). But in February, he helped lead “Updates in Hospital Medicine 2013: Evidence-Based Reviews on the Management of Hospitalized Patients.” That program, arranged by Canadian education provider CMEatSea (www.cmeatsea.org) and held aboard a cruise ship in the eastern Caribbean, attracted some 60 hospitalists, nurse practitioners, and physician assistants interested in earning up to 14 credits.
On the one hand, Dr. Feldman is a pioneer of free virtual CME. On the other, he is an example of the big-ticket CME events that were much more commonplace five or 10 years ago.
“It’s tough,” Dr. Feldman says. “There’s no doubt that once you’ve built that virtual infrastructure, it allows many more people access to CME than if they have to come together. But with that said, particularly at a meeting like HM13, there’s so much more to it than just the CME. The networking is a huge part of that.”
This is the current state of CME, in which ever-tightening physician budgets plus a massive pullback of pharmaceutical industry support equals a landscape of fewer and fewer big-ticket events and more and more online offerings. The expense of large-scale offerings means that many physicians look for more than just the credits available when deciding which events to attend.
For many hospitalists, of course, SHM’s annual meeting remains the best opportunity of the year for CME. Accordingly, those credits are often cited as one of the biggest lures for many of the nearly 3,000 hospitalists who are expected to convene May 16-19 at the Gaylord National Resort & Convention Center in National Harbor, Md.
“You can always get CME credits locally by attending lectures at your own institution, but so often the content of these lectures is really not something that has been vetted and put forward by hospitalists,” says HM13 course director Daniel Brotman, MD, FACP, SFHM. “I think the people who attend this meeting know where the field is going, not only because of the content that’s offered, but because of who else is there. That’s different than going to an hourlong lecture by a cardiologist at your institution on atrial fibrillation.”
—Lenny Feldman, MD, FACP, FAAP, SFHM, John Hopkins School of Medicine, Baltimore
Pharma Pullback
CME budgets typically run $3,000 to $3,500 per physician, but can range from as low as $2,000 to as high as $5,000 annually, according to rough estimates from industry leaders. Opinions are mixed on whether those budgets have been significantly reduced over the past few years, but “they’re certainly not going up,” Dr. Feldman says.
What is falling year after year is the amount of money that the pharmaceutical industry is providing to support CME, says Daniel Guinee, executive vice president of educational firm ASiM of Somerville, N.J. The drug industry funded $1.2 billion of CME in 2007, according to the Accreditation Council for Continuing Medical Education (ACCME). That number dropped to $736 million in 2011, the latest year for which ACCME has statistics. Guinee says many expect the total for 2012 to be approximately $600 million, then level off.
Some applaud the drop-off in industry funding as a needed correction to ensure any potential bias is eliminated. To that end, the American Medical Association’s (AMA) Council on Ethical and Judicial Affairs in 2011 adopted a policy urging the avoidance of industry funding of CME when possible. But just 42% of physicians in one study said they were willing to pay higher fees to eliminate that funding source (Arch Intern Med. 2011;171(9):840-846).
Guinee attributes much of the drug industry’s pullback in funding to companies’ uncertainty over transparency and reporting required by ACCME, the FDA, and the U.S. Department of Health & Human Services (HHS).
“The companies want to use their money as they want to,” Guinee says. “Instead of putting the money out there … as way to support medical education, they’re saying, ‘You know what? We’ll just hang on to it and spend it in other ways.’”
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Dr. Feldman, whose SHMConsults project has been supported by the pharmaceutical industry for seven years, says it’s unclear where future funding will come from in order to support CME. But ACCME president and chief executive officer Murray Kopelow, MD, says that while commercial support—the industry term for pharmaceutical funding—has steadily fallen, “other income” rose 221% from 2006 to 2011 for ACCME-accredited providers and ACCME–recognized, state-accredited providers. ACCME says that income can include activity registration fees, government or nonprofit foundation grants, and allocations from accredited providers’ parent organizations.
“The balance of revenue has shifted,” Dr. Kopelow says.
Education When You Need It
Also shifting is the nature of CME delivery. Since 2007, the number of live Internet CME activities has risen 33%, while the number of journal CME activities has risen 13%, according to ACCME figures. The number of courses in which participants physically attend is virtually static.
SHM has embraced the virtual concept and is looking to add as many online learning opportunities as feasible, says Catharine Smith, SHM’s senior director for education. That includes updates to SHMConsults and the Hospital Quality and Patient Safety Online Academy (www.hospitalmedicine.org/hqps), as well as future offerings based on core competencies. Virtual CME allows hospitalists to meet CME requirements when it is convenient for them and allows providers to set up both live events and enduring materials, Smith says.
“More online CME opportunities from SHM’s Learning Portal is about bringing quality content to hospitalists,” Smith said in a statement. “This reflects SHM’s understanding of the professional needs of hospitalists.”
She added that measuring outcomes can be easier online, as data recording in that manner is easier than during a big meeting. Then again, it’s also difficult to gauge just how well a learned lesson is then incorporated into practice.
For all its advantages, online CME shouldn’t replace all face-to-face learning, Dr. Kopelow says.
“Physicians consult colleagues and reflect on what they have learned before integrating the new information into their practice for the benefit of patients,” he adds. “It is this process that accredited CME promotes and supports. Online CME supports this process, but it does not replace the total process of continuing professional development.”
Dr. Feldman says physicians will have to decide for themselves what works for them, particularly if reduced CME spending by the drug industry continues to crimp offerings.
“There’s going to be a huge sea change there in terms of folks needing to decide where they’re going to want to spend their CME money,” he adds. “Are they going to choose some of these easier-to-use, online CME offerings if they think that going to meetings is becoming prohibitively expensive? Only time is going to tell.”
CME in History
1847: The American Medical Association (AMA) is founded, and one of its first two committees is the Committee on Medical Education.
1901: The committee is recast as the Council on Medical Education, the name it still goes by.
1940s-’50s: The council’s eye is trained on postgraduate medical education (PGME), resulting in a 1955 report that found nearly one-third of 5,000 surveyed physicians reported they had participated in PGME in the preceding five years.
1968: AMA establishes the AMA Physician Recognition Award (PRA). The related credit system was developed to determine qualifications for the PRA.
1981: AMA and six other national organizations form the Accreditation Council for Continuing Medical Education (ACCME). The AMA only allows PRA credits to be designated and awarded by organizations accredited by the ACCME or by a state medical society recognized by the ACCME.
2011: AMA’s Council on Ethical and Judicial Affairs adopts a policy that urges avoiding industry funding of CME when possible to avoid potential bias issues.
Source: American Medical Association
Hospitalist Lenny Feldman, MD, FACP, FAAP, SFHM, of John Hopkins School of Medicine in Baltimore, is the proverbial study in contrasts. He is the longtime editor of SHM’s Consultative & Perioperative Medicine Essentials for Hospitalists, a free continuing medical education (CME) repository more commonly known as SHMConsults (www.shmconsults.com). But in February, he helped lead “Updates in Hospital Medicine 2013: Evidence-Based Reviews on the Management of Hospitalized Patients.” That program, arranged by Canadian education provider CMEatSea (www.cmeatsea.org) and held aboard a cruise ship in the eastern Caribbean, attracted some 60 hospitalists, nurse practitioners, and physician assistants interested in earning up to 14 credits.
On the one hand, Dr. Feldman is a pioneer of free virtual CME. On the other, he is an example of the big-ticket CME events that were much more commonplace five or 10 years ago.
“It’s tough,” Dr. Feldman says. “There’s no doubt that once you’ve built that virtual infrastructure, it allows many more people access to CME than if they have to come together. But with that said, particularly at a meeting like HM13, there’s so much more to it than just the CME. The networking is a huge part of that.”
This is the current state of CME, in which ever-tightening physician budgets plus a massive pullback of pharmaceutical industry support equals a landscape of fewer and fewer big-ticket events and more and more online offerings. The expense of large-scale offerings means that many physicians look for more than just the credits available when deciding which events to attend.
For many hospitalists, of course, SHM’s annual meeting remains the best opportunity of the year for CME. Accordingly, those credits are often cited as one of the biggest lures for many of the nearly 3,000 hospitalists who are expected to convene May 16-19 at the Gaylord National Resort & Convention Center in National Harbor, Md.
“You can always get CME credits locally by attending lectures at your own institution, but so often the content of these lectures is really not something that has been vetted and put forward by hospitalists,” says HM13 course director Daniel Brotman, MD, FACP, SFHM. “I think the people who attend this meeting know where the field is going, not only because of the content that’s offered, but because of who else is there. That’s different than going to an hourlong lecture by a cardiologist at your institution on atrial fibrillation.”
—Lenny Feldman, MD, FACP, FAAP, SFHM, John Hopkins School of Medicine, Baltimore
Pharma Pullback
CME budgets typically run $3,000 to $3,500 per physician, but can range from as low as $2,000 to as high as $5,000 annually, according to rough estimates from industry leaders. Opinions are mixed on whether those budgets have been significantly reduced over the past few years, but “they’re certainly not going up,” Dr. Feldman says.
What is falling year after year is the amount of money that the pharmaceutical industry is providing to support CME, says Daniel Guinee, executive vice president of educational firm ASiM of Somerville, N.J. The drug industry funded $1.2 billion of CME in 2007, according to the Accreditation Council for Continuing Medical Education (ACCME). That number dropped to $736 million in 2011, the latest year for which ACCME has statistics. Guinee says many expect the total for 2012 to be approximately $600 million, then level off.
Some applaud the drop-off in industry funding as a needed correction to ensure any potential bias is eliminated. To that end, the American Medical Association’s (AMA) Council on Ethical and Judicial Affairs in 2011 adopted a policy urging the avoidance of industry funding of CME when possible. But just 42% of physicians in one study said they were willing to pay higher fees to eliminate that funding source (Arch Intern Med. 2011;171(9):840-846).
Guinee attributes much of the drug industry’s pullback in funding to companies’ uncertainty over transparency and reporting required by ACCME, the FDA, and the U.S. Department of Health & Human Services (HHS).
“The companies want to use their money as they want to,” Guinee says. “Instead of putting the money out there … as way to support medical education, they’re saying, ‘You know what? We’ll just hang on to it and spend it in other ways.’”
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Dr. Feldman, whose SHMConsults project has been supported by the pharmaceutical industry for seven years, says it’s unclear where future funding will come from in order to support CME. But ACCME president and chief executive officer Murray Kopelow, MD, says that while commercial support—the industry term for pharmaceutical funding—has steadily fallen, “other income” rose 221% from 2006 to 2011 for ACCME-accredited providers and ACCME–recognized, state-accredited providers. ACCME says that income can include activity registration fees, government or nonprofit foundation grants, and allocations from accredited providers’ parent organizations.
“The balance of revenue has shifted,” Dr. Kopelow says.
Education When You Need It
Also shifting is the nature of CME delivery. Since 2007, the number of live Internet CME activities has risen 33%, while the number of journal CME activities has risen 13%, according to ACCME figures. The number of courses in which participants physically attend is virtually static.
SHM has embraced the virtual concept and is looking to add as many online learning opportunities as feasible, says Catharine Smith, SHM’s senior director for education. That includes updates to SHMConsults and the Hospital Quality and Patient Safety Online Academy (www.hospitalmedicine.org/hqps), as well as future offerings based on core competencies. Virtual CME allows hospitalists to meet CME requirements when it is convenient for them and allows providers to set up both live events and enduring materials, Smith says.
“More online CME opportunities from SHM’s Learning Portal is about bringing quality content to hospitalists,” Smith said in a statement. “This reflects SHM’s understanding of the professional needs of hospitalists.”
She added that measuring outcomes can be easier online, as data recording in that manner is easier than during a big meeting. Then again, it’s also difficult to gauge just how well a learned lesson is then incorporated into practice.
For all its advantages, online CME shouldn’t replace all face-to-face learning, Dr. Kopelow says.
“Physicians consult colleagues and reflect on what they have learned before integrating the new information into their practice for the benefit of patients,” he adds. “It is this process that accredited CME promotes and supports. Online CME supports this process, but it does not replace the total process of continuing professional development.”
Dr. Feldman says physicians will have to decide for themselves what works for them, particularly if reduced CME spending by the drug industry continues to crimp offerings.
“There’s going to be a huge sea change there in terms of folks needing to decide where they’re going to want to spend their CME money,” he adds. “Are they going to choose some of these easier-to-use, online CME offerings if they think that going to meetings is becoming prohibitively expensive? Only time is going to tell.”
CME in History
1847: The American Medical Association (AMA) is founded, and one of its first two committees is the Committee on Medical Education.
1901: The committee is recast as the Council on Medical Education, the name it still goes by.
1940s-’50s: The council’s eye is trained on postgraduate medical education (PGME), resulting in a 1955 report that found nearly one-third of 5,000 surveyed physicians reported they had participated in PGME in the preceding five years.
1968: AMA establishes the AMA Physician Recognition Award (PRA). The related credit system was developed to determine qualifications for the PRA.
1981: AMA and six other national organizations form the Accreditation Council for Continuing Medical Education (ACCME). The AMA only allows PRA credits to be designated and awarded by organizations accredited by the ACCME or by a state medical society recognized by the ACCME.
2011: AMA’s Council on Ethical and Judicial Affairs adopts a policy that urges avoiding industry funding of CME when possible to avoid potential bias issues.
Source: American Medical Association