User login
How Should a Patient with Cocaine-Associated Chest Pain be Treated?

Case
A 38-year-old man with a history of tobacco use presents to the emergency department complaining of constant substernal chest pain for three hours. His temperature is 37.7°C, his heart rate is 110 beats per minute, and his blood pressure is 155/95 mmHg. He appears anxious and diaphoretic but examination is otherwise unremarkable. He admits to cocaine use one hour before the onset of symptoms. What are the appropriate treatments for his condition?
Overview
Cocaine is the second-most-commonly used illicit drug in the U.S. and represents 31% of all ED visits related to substance abuse.1,2 According to recent survey results, 2.1 million people report recent cocaine use, and 1.6 million engage in cocaine abuse or dependence.2 Acute cardiopulmonary complaints are common in individuals who present to the ED after cocaine use, with chest pain being the most frequently reported symptom in 40%.3
Numerous etiologies for cocaine-associated chest pain (CACP) have been discovered, including musculoskeletal pain, pulmonary hypertension, cardiomyopathy, arrhythmias, and endocarditis.4 Only 0.5% of patients with aortic dissection over a four-year period had a recent history of cocaine use, making cocaine a rare cause of a rare condition.5 Cardiac chest pain remains the most frequent underlying etiology, resulting in the most common complication of myocardial infarction (MI) in up to 6% of patients.6,7
The ways in which cocaine use can cause myocardial ischemia and MI are multifactorial. A vigorous central sympathomimetic effect, coronary artery vasoconstriction, stimulation of platelets, and enhanced atherosclerosis all lead to a myocardial oxygen supply-demand imbalance.8 Other key interactions in the cardiovascular system are displayed in Figure 1. Understanding the role of these mechanisms in CACP is crucial to patient care.
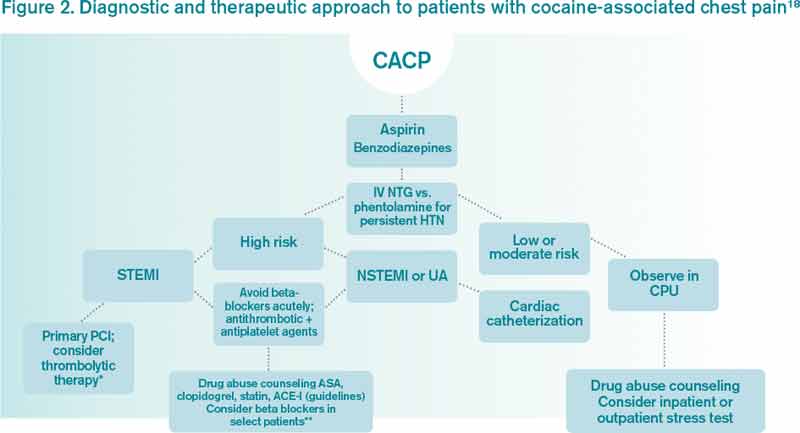
Clinician goals in the management of CACP are to rapidly and accurately exclude life-threatening etiologies; assess the need for urgent acute coronary syndrome (ACS) evaluation; risk-stratify patients and ensure appropriate disposition; normalize the toxic effects of cocaine; treat resultant organ damage; and prevent long-term complications. An algorithm detailing this approach is provided in Figure 2.

Review of the Data
Diagnostic evaluation. Given potential differences in treatment regimens, it is imperative to differentiate patients who present with CACP from those whose chest pain is not associated with cocaine either by direct questioning or by screening of urine for cocaine metabolites. Once the presence of cocaine has been confirmed, guideline-based evaluation for potential ACS with serial electrocardiograms (ECG), cardiac biomarkers, and close monitoring of cardiac rhythms and hemodynamics is largely similar to standard management of all patients presenting with chest pain, with a few caveats.
Interpretation of the ECG can be challenging in the setting of cocaine. Studies have shown “abnormal” ECGs in 56% to 84% of patients, with many representing early repolarization or left ventricular hypertrophy.9,10 Likewise, patients with MI are as likely to present with normal or nonspecific ECG findings as with ischemic findings.7,11 ECG interpretation to diagnose ischemia or infarction in patients with CACP yields a sensitivity of 36% and specificity of 90%.7
Creatine kinase (CK), CK-MB fraction, and myoglobin have low specificity for the diagnosis of ischemia, as cocaine can induce skeletal muscle injury and rhabdomyolysis.9,12 Cardiac troponins demonstrate a superior specificity compared to CK and CK-MB and are thus the preferred cardiac biomarkers in diagnosing cocaine-associated MI.12
Initial management and disposition. Patients at high risk for cardiovascular events are generally admitted to a monitored bed.13 Immediate reperfusion therapy with primary percutaneous coronary intervention is recommended in patients with ST-elevation MI (STEMI). Treatment with thrombolytic agents is associated with an increased risk of intracerebral hemorrhage and lacks documented efficacy in patients with CACP. Thrombolysis should therefore only be utilized if the diagnosis of STEMI is unequivocal and an experienced cardiac catheterization laboratory is unavailable.14,15
Patients with unstable angina (UA) or non-ST-elevation MI (NSTEMI) are at higher risk for further cardiac events in a similar manner to those with ACS unrelated to cocaine. These cases might benefit from early cardiac catheterization and revascularization.16 Because of the increased risk of stent thrombosis in cocaine-users, thought to be due to recidivism, a detailed risk-benefit analysis should be undertaken prior to the implantation of cardiac stents.
Other diagnostic tests, such as stress testing and myocardial imaging, have not shown significant accuracy in diagnosing MI in this setting; moreover, these patients are at low overall risk for cardiac events and mortality. Consequently, an extensive diagnostic evaluation might not be cost-effective.7,10,13,17 Patients who have CACP without MI have a very low frequency of delayed complications.3,17 As such, cost-effective evaluation strategies, such as nine- or 12-hour observation periods in a chest pain unit, are appropriate for many of these low- to moderate-risk patients.13 For all CACP patients, the most critical post-discharge interventions are cardiac risk modification and cocaine cessation.13
Normalizing the toxic effects of cocaine with medications.
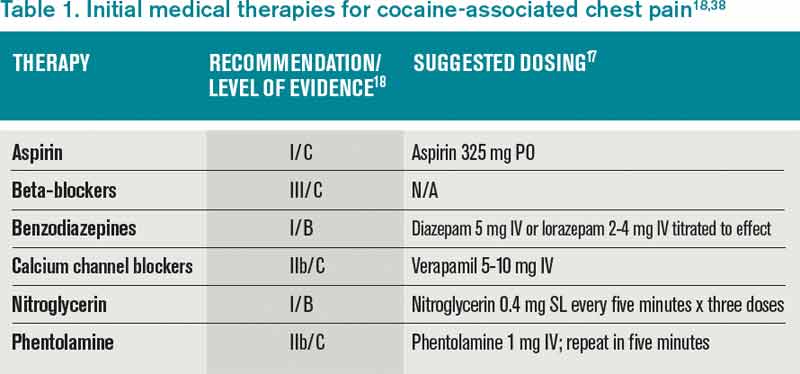
Aspirin: While no specific study has been performed in patients with CACP and aspirin, CACP guidelines, based on data supporting ACS guidelines for all patients, recommend administration of full-dose aspirin given its associated reduction in morbidity and mortality.18,19 Furthermore, given the platelet-stimulating effects of cocaine, using aspirin in this setting seems very reasonable.
Benzodiazepines: CACP guidelines support the use of benzodiazepines early in management to indirectly combat the agitation, hypertension, and tachycardia resulting from the stimulatory effects of cocaine.18,20 These recommendations are based on several animal and human studies that demonstrate significant reduction in heart rate and systemic arterial pressure with the use of these agents.21,22
Nitroglycerin: Cardiac catheterization studies have shown reversal of vasoconstriction with administration of nitroglycerin. One study demonstrated a benefit of the drug in 49% of participants.23 Additional investigation into the benefit of benzodiazepine and nitroglycerin combination therapy revealed mixed results. In one study, lorazepam plus nitroglycerin was found to be more efficacious than nitroglycerin alone.24 In another, however, use of diazepam in combination with nitroglycerin did not show benefit when evaluating pain relief, cardiac dynamics, and left ventricular function.25
Phentolamine: Phentolamine administration has been studied much less in the literature. This nonselective alpha-adrenergic antagonist exerts a dose-dependent reversal of cocaine’s vasoconstrictive properties in monkeys and humans.26,27 International guidelines for Emergency Cardiovascular Care recommend its use in treatment of cocaine-associated ACS;27 however, the AHA recommends it less strongly.18
Calcium channel blockers: Calcium channel blockers (CCBs) have not shown promise as first-line agents. While catheterization studies demonstrate the vasodilatory properties of verapamil, larger studies looking at all-cause mortality conclude that CCBs might worsen mortality rates,28 and animal studies indicate an increased risk of seizures.29 At this time, CCBs are recommended only if cardiac symptoms continue after both benzodiazepines and nitroglycerin are administered.18
The beta-blocker controversy: The use of beta-blockers in patients with CACP remains controversial given the theoretical risk of unopposed alpha-adrenergic activation. Coronary vasospasm, decreased myocardial oxygen delivery, and increased systemic vascular resistance can result from their use.30
Propranolol, a nonselective beta-blocker, was shown in catheterization studies to potentiate the coronary vasoconstriction of cocaine.31 Labetalol, a combined alpha/beta-blocker, reduced mean arterial pressure after cocaine administration during cardiac catheterization but did not reverse coronary vasoconstriction.32 This was attributed to the predominating beta greater than alpha blockade at doses administered. The selective beta-1 antagonists esmolol and metoprolol have shown no benefit in CACP.33 Carvedilol, a combined alpha/beta-blocker with both peripheral and central nervous system activity, has potential to attenuate both physiologic and behavioral response to cocaine, but it has not been well studied in this patient subset.34
The 2005 ACC/AHA STEMI guidelines recommended against beta-blockers in the setting of STEMI precipitated by cocaine use due to the potential of exacerbating coronary vasoconstriction.35 The 2007 ACC/AHA UA/NSTEMI guidelines stated that the use of a combined alpha/beta-blocker in patients with cocaine-induced ACS may be reasonable for patients with hypertension or tachycardia if pre-treated with a vasodilator.19 The 2008 ACC/AHA guidelines on the management of cocaine-related chest pain and MI recommended against the use of beta-blockers in the acute setting given the low incidence of cocaine-related MI and death.18
In a more recent study, Dattilo et al showed that beta-blockers administered to patients admitted with positive urine toxicology for cocaine significantly reduced MI and in-hospital mortality. Reduction of MI was of borderline significance in those admitted with a chief complaint of chest pain.36 Limitations of this study include unknown time of cocaine ingestion, lack of follow-up on discharge mortality, and a small sample size of 348 patients lacking statistical power.
Another retrospective cohort study examined patients admitted with chest pain and urine toxicology positive for cocaine and found that beta-blocker administration during hospitalization was not associated with increased incident mortality. Further, after a mean follow-up of 2.5 years, there was a statistically significant decrease in cardiovascular death.37 Drawbacks of this study included an older patient population, greater proportion of coronary artery disease, and higher follow-up of cardiovascular mortality rates than in previous studies, suggesting this subset might have received greater benefit from beta-blockers as a result of these characteristics.
The 2008 ACC/AHA guidelines instruct individualized consideration of the risk/benefit ratio for beta-blocker use in patients with CACP given the high rate of recidivism in cocaine abusers. The strongest indication is given to those with documented MI, left ventricular systolic dysfunction, or ventricular arrhythmias.18
It is important to note that these recommendations are based on cardiac catheterization laboratory studies, case reports, retrospective analyses, and animal experiments. No prospective controlled trials evaluating the role of beta-blockers in CACP and MI exist, and no trials regarding therapies to improve outcomes of patients sustaining a cocaine-associated MI have been reported.18
Back to the Case
This patient was experiencing cocaine-associated chest pain, which was confirmed with positive urine toxicology. Initial diagnostic workup with basic laboratory studies and cardiac biomarkers showed mild elevation in CK with troponin levels within normal limits. His ECG showed changes consistent with left ventricular hypertrophy. Chest radiograph was unremarkable.
He received aspirin, benzodiazepines, and nitroglycerin with normalization of vital signs, as well as subjective improvement in chest pain and anxiety. He was deemed to be at low risk for potential cardiac complications; thus, further cardiac testing was not pursued. Rather, he was admitted to an overnight observation unit with telemetry monitoring, where his chest pain did not recur.
He was seen in consultation with social work staff who arranged for drug abuse counseling after discharge. Given the uncertainty of relapse to cocaine use, as well as lack of known cardiac risk factors, he was not discharged on any new medications.
Bottom Line
The treatment of CACP includes normalizing the toxic systemic effects of the drug and minimizing the direct ischemic damage to the myocardium. Management varies slightly from traditional chest pain algorithms and includes benzodiazepines as well as antiplatelet agents and vasodilators to achieve this goal. Initial therapy with beta-blockers remains undefined and is largely discouraged in the acute setting. The role of beta-blockade upon discharge, however, can be beneficial in specific populations, especially those found to have underlying coronary disease.
Dr. Houchens and Dr. Czarnik are clinical instructors and Dr. Mack is a clinical lecturer at the University of Michigan Health System in Ann Arbor.
References
- Hughes A, Sathe N, Spagnola K. State Estimates of Substance Use from the 2005-2006 National Surveys on Drug Use and Health. DHHS Publication No. SMA 08-4311, NSDUH Series H-33. Rockville, MD: Substance Abuse and Mental Health Services Administration, Office of Applied Studies; 2008.
- Volkow ND. Cocaine: Abuse and Addiction. National Institute on Drug Abuse. Washington, DC: U.S. Department of Health and Human Services; 2009.
- Brody SL, Slovis CM, Wrenn KD. Cocaine-related medical problems: consecutive series of 233 patients. Am J Med. 1990;88:325-331.
- Levis JT, Garmel GM. Cocaine-associated chest pain. Emerg Med Clin North Am. 2005;23:1083-1103.
- Eagle KA, Isselbacher EM, DeSanctis RW. Cocaine-related aortic dissection in perspective. Circulation. 2002;105:1529-1530.
- Feldman JA, Fish SS, Beshansky JR, Griffith JL, Woolard RH, Selker HP. Acute cardiac ischemia in patients with cocaine-associated complaints: results of a multicenter trial. Ann Emerg Med. 2000;36:469-476.
- Hollander JE, Hoffman RS, Gennis P, et al. Prospective multicenter evaluation of cocaine associated chest pain. Cocaine Associated Chest Pain (COCHPA) Study Group. Acad Emerg Med. 1994;1:330-339.
- Schwartz BG, Rezkalla S, Kloner RA. Cardiovascular effects of cocaine. Circulation. 2010;122:2558-2569.
- Gitter MJ, Goldsmith SR, Dunbar DN, et al. Cocaine and chest pain: clinical features and outcomes of patients hospitalized to rule out myocardial infarction. Ann Intern Med. 1991;115:277-282.
- Amin M, Gabelman G, Karpel J, et al. Acute myocardial infarction and chest pain syndromes after cocaine use. Am J Cardiol. 1990;66:1434-1437.
- Tokarski GF, Paganussi P, Urbanski R, et al. An evaluation of cocaine-induced chest pain. Ann Emerg Med. 1990;19:1088-1092.
- Hollander JE, Levitt MA, Young GP, Briglia E, Wetli CV, Gawad Y. Effect of recent cocaine use on the specificity of cardiac markers for diagnosis of acute myocardial infarction. Am Heart J. 1998;135(2 Pt 1):245-252.
- Weber JE, Shofer FS, Larkin GL, Kalaria AS, Hollander JE. Validation of a brief observation period for patients with cocaine-associated chest pain. N Engl J Med. 2003;348:510-517.
- Hahn IH, Hoffman RS. Diagnosis and treatment of acute myocardial infarction: cocaine use and acute myocardial infarction. Emerg Med Clin North Am. 2001;19(2):1-18.
- Hoffman RS, Hollander JE. Evaluation of patients with chest pain after cocaine use. Crit Care Clin. 1997;13:809-828. Cannon CP, Weintraub WS, Demopoulos LA, et al.
- Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med. 2001;344:1879-1887.
- Hollander JE, Hoffman RS. Cocaine-induced myocardial infarction: an analysis and review of the literature. J Emerg Med. 1992;10:169-177.
- McCord J, Jneid H, Hollander JE, et al. Management of cocaine-associated chest pain and myocardial infarction: a scientific statement from the American Heart Association Acute Cardiac Care Committee of the Council on Clinical Cardiology. Circulation. 2008;117:1897-1907.
- Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol. 2007;50:E1-E157.
- Hollander JE. Management of cocaine-associated myocardial ischemia. N Engl J Med. 1995;333:1267-1272.
- Brubacher JR, Hoffman RS. Cocaine toxicity. Top Emerg Med. 1997;19(4):1-16.
- Catavas JD, Waters IW. Acute cocaine intoxication in the conscious dog: studies on the mechanism of lethality. J Pharmacol Exp Ther. 1981;217:350-356.
- Hollander JE, Hoffman RS, Gennis P, et al. Nitroglycerin in the treatment of cocaine associated chest pain—clinical safety and efficacy. J Toxicol Clin Toxicol. 1994;32(3): 243-256.
- Honderick T, Williams D, Seaberg D, Wears R. A prospective, randomized, controlled trial of benzodiazepines and nitroglycerin or nitroglycerin alone in the treatment of cocaine-associated acute coronary syndromes. Am J Emerg Med. 2003;21(1):39-42.
- Baumann BM, Perrone J, Hornig SE, Shofer FS, Hollander JE. Randomized, double-blind, placebo-controlled trial of diazepam, nitroglycerin, or both for treatment of patients with potential cocaine-associated acute coronary syndromes. Acad Emerg Med. 2000;7:878-885.
- Schindler CW, Tella SR, Goldberg SR. Adrenoceptor mechanisms in the cardiovascular effects of cocaine in conscious squirrel monkeys. Life Sci. 1992;51(9):653-660.
- Lange RA, Cigarroa RG, Yancy CW Jr., et al. Cocaine-induced coronary-artery vasoconstriction. N Engl J Med. 1989;321(23):1557-1562.
- Furberg CD, Psaty BM, Meyer JV. Nifedipine. Dose-related increase in mortality in patients with coronary heart disease. Circulation. 1995;92:1326-1331.
- Derlet RW, Albertson TE. Potentiation of cocaine toxicity with calcium channel blockers. Am J Emerg Med. 1989;7:464-468.
- Lange RA, Hillis LD. Cardiovascular complications of cocaine use. N Engl J Med. 2001;345:351-358.
- Lange RA, Cigarroa RG, Flores ED, et al. Potentiation of cocaine-induced coronary vasoconstriction by beta-adrenergic blockade. Ann Intern Med. 1990;112:897-903.
- Boehrer JD, Moliterno DJ, Willard JE, Hillis LD, Lange RA. Influence of labetalol on cocaine-induced coronary vasoconstriction in humans. Am J Med. 1993;94:608-610.
- Sand IC, Brody SL, Wrenn KD, Slovis CM. Experience with esmolol for the treatment of cocaine-associated cardiovascular complications. Am J Emerg Med. 1991;9:161-163.
- Sofuoglo M, Brown S, Babb DA, Pentel PR, Hatsukami DK. Carvedilol affects the physiological and behavioral response to smoked cocaine in humans. Drug Alcohol Depend. 2000;60:69-76.
- Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force of Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of patients with acute myocardial infarction). J Am Coll Cardiol. 2004;44:E1-E211.
- Dattilo PB, Hailpern SM, Fearon K, Sohal D, Nordin C. Beta-blockers are associated with reduced risk of myocardial infarction after cocaine use. Ann Emerg Med. 2008;51:117-125.
- Rangel C, Shu RG, Lazar LD, Vittinghoff E, Hsue PY, Marcus GM. Beta-blockers for chest pain associated with recent cocaine use. Arch Intern Med. 2010;170:874-879.
Case
A 38-year-old man with a history of tobacco use presents to the emergency department complaining of constant substernal chest pain for three hours. His temperature is 37.7°C, his heart rate is 110 beats per minute, and his blood pressure is 155/95 mmHg. He appears anxious and diaphoretic but examination is otherwise unremarkable. He admits to cocaine use one hour before the onset of symptoms. What are the appropriate treatments for his condition?
Overview
Cocaine is the second-most-commonly used illicit drug in the U.S. and represents 31% of all ED visits related to substance abuse.1,2 According to recent survey results, 2.1 million people report recent cocaine use, and 1.6 million engage in cocaine abuse or dependence.2 Acute cardiopulmonary complaints are common in individuals who present to the ED after cocaine use, with chest pain being the most frequently reported symptom in 40%.3
Numerous etiologies for cocaine-associated chest pain (CACP) have been discovered, including musculoskeletal pain, pulmonary hypertension, cardiomyopathy, arrhythmias, and endocarditis.4 Only 0.5% of patients with aortic dissection over a four-year period had a recent history of cocaine use, making cocaine a rare cause of a rare condition.5 Cardiac chest pain remains the most frequent underlying etiology, resulting in the most common complication of myocardial infarction (MI) in up to 6% of patients.6,7
The ways in which cocaine use can cause myocardial ischemia and MI are multifactorial. A vigorous central sympathomimetic effect, coronary artery vasoconstriction, stimulation of platelets, and enhanced atherosclerosis all lead to a myocardial oxygen supply-demand imbalance.8 Other key interactions in the cardiovascular system are displayed in Figure 1. Understanding the role of these mechanisms in CACP is crucial to patient care.
Clinician goals in the management of CACP are to rapidly and accurately exclude life-threatening etiologies; assess the need for urgent acute coronary syndrome (ACS) evaluation; risk-stratify patients and ensure appropriate disposition; normalize the toxic effects of cocaine; treat resultant organ damage; and prevent long-term complications. An algorithm detailing this approach is provided in Figure 2.
Review of the Data
Diagnostic evaluation. Given potential differences in treatment regimens, it is imperative to differentiate patients who present with CACP from those whose chest pain is not associated with cocaine either by direct questioning or by screening of urine for cocaine metabolites. Once the presence of cocaine has been confirmed, guideline-based evaluation for potential ACS with serial electrocardiograms (ECG), cardiac biomarkers, and close monitoring of cardiac rhythms and hemodynamics is largely similar to standard management of all patients presenting with chest pain, with a few caveats.
Interpretation of the ECG can be challenging in the setting of cocaine. Studies have shown “abnormal” ECGs in 56% to 84% of patients, with many representing early repolarization or left ventricular hypertrophy.9,10 Likewise, patients with MI are as likely to present with normal or nonspecific ECG findings as with ischemic findings.7,11 ECG interpretation to diagnose ischemia or infarction in patients with CACP yields a sensitivity of 36% and specificity of 90%.7
Creatine kinase (CK), CK-MB fraction, and myoglobin have low specificity for the diagnosis of ischemia, as cocaine can induce skeletal muscle injury and rhabdomyolysis.9,12 Cardiac troponins demonstrate a superior specificity compared to CK and CK-MB and are thus the preferred cardiac biomarkers in diagnosing cocaine-associated MI.12
Initial management and disposition. Patients at high risk for cardiovascular events are generally admitted to a monitored bed.13 Immediate reperfusion therapy with primary percutaneous coronary intervention is recommended in patients with ST-elevation MI (STEMI). Treatment with thrombolytic agents is associated with an increased risk of intracerebral hemorrhage and lacks documented efficacy in patients with CACP. Thrombolysis should therefore only be utilized if the diagnosis of STEMI is unequivocal and an experienced cardiac catheterization laboratory is unavailable.14,15
Patients with unstable angina (UA) or non-ST-elevation MI (NSTEMI) are at higher risk for further cardiac events in a similar manner to those with ACS unrelated to cocaine. These cases might benefit from early cardiac catheterization and revascularization.16 Because of the increased risk of stent thrombosis in cocaine-users, thought to be due to recidivism, a detailed risk-benefit analysis should be undertaken prior to the implantation of cardiac stents.
Other diagnostic tests, such as stress testing and myocardial imaging, have not shown significant accuracy in diagnosing MI in this setting; moreover, these patients are at low overall risk for cardiac events and mortality. Consequently, an extensive diagnostic evaluation might not be cost-effective.7,10,13,17 Patients who have CACP without MI have a very low frequency of delayed complications.3,17 As such, cost-effective evaluation strategies, such as nine- or 12-hour observation periods in a chest pain unit, are appropriate for many of these low- to moderate-risk patients.13 For all CACP patients, the most critical post-discharge interventions are cardiac risk modification and cocaine cessation.13
Normalizing the toxic effects of cocaine with medications.
Aspirin: While no specific study has been performed in patients with CACP and aspirin, CACP guidelines, based on data supporting ACS guidelines for all patients, recommend administration of full-dose aspirin given its associated reduction in morbidity and mortality.18,19 Furthermore, given the platelet-stimulating effects of cocaine, using aspirin in this setting seems very reasonable.
Benzodiazepines: CACP guidelines support the use of benzodiazepines early in management to indirectly combat the agitation, hypertension, and tachycardia resulting from the stimulatory effects of cocaine.18,20 These recommendations are based on several animal and human studies that demonstrate significant reduction in heart rate and systemic arterial pressure with the use of these agents.21,22
Nitroglycerin: Cardiac catheterization studies have shown reversal of vasoconstriction with administration of nitroglycerin. One study demonstrated a benefit of the drug in 49% of participants.23 Additional investigation into the benefit of benzodiazepine and nitroglycerin combination therapy revealed mixed results. In one study, lorazepam plus nitroglycerin was found to be more efficacious than nitroglycerin alone.24 In another, however, use of diazepam in combination with nitroglycerin did not show benefit when evaluating pain relief, cardiac dynamics, and left ventricular function.25
Phentolamine: Phentolamine administration has been studied much less in the literature. This nonselective alpha-adrenergic antagonist exerts a dose-dependent reversal of cocaine’s vasoconstrictive properties in monkeys and humans.26,27 International guidelines for Emergency Cardiovascular Care recommend its use in treatment of cocaine-associated ACS;27 however, the AHA recommends it less strongly.18
Calcium channel blockers: Calcium channel blockers (CCBs) have not shown promise as first-line agents. While catheterization studies demonstrate the vasodilatory properties of verapamil, larger studies looking at all-cause mortality conclude that CCBs might worsen mortality rates,28 and animal studies indicate an increased risk of seizures.29 At this time, CCBs are recommended only if cardiac symptoms continue after both benzodiazepines and nitroglycerin are administered.18
The beta-blocker controversy: The use of beta-blockers in patients with CACP remains controversial given the theoretical risk of unopposed alpha-adrenergic activation. Coronary vasospasm, decreased myocardial oxygen delivery, and increased systemic vascular resistance can result from their use.30
Propranolol, a nonselective beta-blocker, was shown in catheterization studies to potentiate the coronary vasoconstriction of cocaine.31 Labetalol, a combined alpha/beta-blocker, reduced mean arterial pressure after cocaine administration during cardiac catheterization but did not reverse coronary vasoconstriction.32 This was attributed to the predominating beta greater than alpha blockade at doses administered. The selective beta-1 antagonists esmolol and metoprolol have shown no benefit in CACP.33 Carvedilol, a combined alpha/beta-blocker with both peripheral and central nervous system activity, has potential to attenuate both physiologic and behavioral response to cocaine, but it has not been well studied in this patient subset.34
The 2005 ACC/AHA STEMI guidelines recommended against beta-blockers in the setting of STEMI precipitated by cocaine use due to the potential of exacerbating coronary vasoconstriction.35 The 2007 ACC/AHA UA/NSTEMI guidelines stated that the use of a combined alpha/beta-blocker in patients with cocaine-induced ACS may be reasonable for patients with hypertension or tachycardia if pre-treated with a vasodilator.19 The 2008 ACC/AHA guidelines on the management of cocaine-related chest pain and MI recommended against the use of beta-blockers in the acute setting given the low incidence of cocaine-related MI and death.18
In a more recent study, Dattilo et al showed that beta-blockers administered to patients admitted with positive urine toxicology for cocaine significantly reduced MI and in-hospital mortality. Reduction of MI was of borderline significance in those admitted with a chief complaint of chest pain.36 Limitations of this study include unknown time of cocaine ingestion, lack of follow-up on discharge mortality, and a small sample size of 348 patients lacking statistical power.
Another retrospective cohort study examined patients admitted with chest pain and urine toxicology positive for cocaine and found that beta-blocker administration during hospitalization was not associated with increased incident mortality. Further, after a mean follow-up of 2.5 years, there was a statistically significant decrease in cardiovascular death.37 Drawbacks of this study included an older patient population, greater proportion of coronary artery disease, and higher follow-up of cardiovascular mortality rates than in previous studies, suggesting this subset might have received greater benefit from beta-blockers as a result of these characteristics.
The 2008 ACC/AHA guidelines instruct individualized consideration of the risk/benefit ratio for beta-blocker use in patients with CACP given the high rate of recidivism in cocaine abusers. The strongest indication is given to those with documented MI, left ventricular systolic dysfunction, or ventricular arrhythmias.18
It is important to note that these recommendations are based on cardiac catheterization laboratory studies, case reports, retrospective analyses, and animal experiments. No prospective controlled trials evaluating the role of beta-blockers in CACP and MI exist, and no trials regarding therapies to improve outcomes of patients sustaining a cocaine-associated MI have been reported.18
Back to the Case
This patient was experiencing cocaine-associated chest pain, which was confirmed with positive urine toxicology. Initial diagnostic workup with basic laboratory studies and cardiac biomarkers showed mild elevation in CK with troponin levels within normal limits. His ECG showed changes consistent with left ventricular hypertrophy. Chest radiograph was unremarkable.
He received aspirin, benzodiazepines, and nitroglycerin with normalization of vital signs, as well as subjective improvement in chest pain and anxiety. He was deemed to be at low risk for potential cardiac complications; thus, further cardiac testing was not pursued. Rather, he was admitted to an overnight observation unit with telemetry monitoring, where his chest pain did not recur.
He was seen in consultation with social work staff who arranged for drug abuse counseling after discharge. Given the uncertainty of relapse to cocaine use, as well as lack of known cardiac risk factors, he was not discharged on any new medications.
Bottom Line
The treatment of CACP includes normalizing the toxic systemic effects of the drug and minimizing the direct ischemic damage to the myocardium. Management varies slightly from traditional chest pain algorithms and includes benzodiazepines as well as antiplatelet agents and vasodilators to achieve this goal. Initial therapy with beta-blockers remains undefined and is largely discouraged in the acute setting. The role of beta-blockade upon discharge, however, can be beneficial in specific populations, especially those found to have underlying coronary disease.
Dr. Houchens and Dr. Czarnik are clinical instructors and Dr. Mack is a clinical lecturer at the University of Michigan Health System in Ann Arbor.
References
- Hughes A, Sathe N, Spagnola K. State Estimates of Substance Use from the 2005-2006 National Surveys on Drug Use and Health. DHHS Publication No. SMA 08-4311, NSDUH Series H-33. Rockville, MD: Substance Abuse and Mental Health Services Administration, Office of Applied Studies; 2008.
- Volkow ND. Cocaine: Abuse and Addiction. National Institute on Drug Abuse. Washington, DC: U.S. Department of Health and Human Services; 2009.
- Brody SL, Slovis CM, Wrenn KD. Cocaine-related medical problems: consecutive series of 233 patients. Am J Med. 1990;88:325-331.
- Levis JT, Garmel GM. Cocaine-associated chest pain. Emerg Med Clin North Am. 2005;23:1083-1103.
- Eagle KA, Isselbacher EM, DeSanctis RW. Cocaine-related aortic dissection in perspective. Circulation. 2002;105:1529-1530.
- Feldman JA, Fish SS, Beshansky JR, Griffith JL, Woolard RH, Selker HP. Acute cardiac ischemia in patients with cocaine-associated complaints: results of a multicenter trial. Ann Emerg Med. 2000;36:469-476.
- Hollander JE, Hoffman RS, Gennis P, et al. Prospective multicenter evaluation of cocaine associated chest pain. Cocaine Associated Chest Pain (COCHPA) Study Group. Acad Emerg Med. 1994;1:330-339.
- Schwartz BG, Rezkalla S, Kloner RA. Cardiovascular effects of cocaine. Circulation. 2010;122:2558-2569.
- Gitter MJ, Goldsmith SR, Dunbar DN, et al. Cocaine and chest pain: clinical features and outcomes of patients hospitalized to rule out myocardial infarction. Ann Intern Med. 1991;115:277-282.
- Amin M, Gabelman G, Karpel J, et al. Acute myocardial infarction and chest pain syndromes after cocaine use. Am J Cardiol. 1990;66:1434-1437.
- Tokarski GF, Paganussi P, Urbanski R, et al. An evaluation of cocaine-induced chest pain. Ann Emerg Med. 1990;19:1088-1092.
- Hollander JE, Levitt MA, Young GP, Briglia E, Wetli CV, Gawad Y. Effect of recent cocaine use on the specificity of cardiac markers for diagnosis of acute myocardial infarction. Am Heart J. 1998;135(2 Pt 1):245-252.
- Weber JE, Shofer FS, Larkin GL, Kalaria AS, Hollander JE. Validation of a brief observation period for patients with cocaine-associated chest pain. N Engl J Med. 2003;348:510-517.
- Hahn IH, Hoffman RS. Diagnosis and treatment of acute myocardial infarction: cocaine use and acute myocardial infarction. Emerg Med Clin North Am. 2001;19(2):1-18.
- Hoffman RS, Hollander JE. Evaluation of patients with chest pain after cocaine use. Crit Care Clin. 1997;13:809-828. Cannon CP, Weintraub WS, Demopoulos LA, et al.
- Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med. 2001;344:1879-1887.
- Hollander JE, Hoffman RS. Cocaine-induced myocardial infarction: an analysis and review of the literature. J Emerg Med. 1992;10:169-177.
- McCord J, Jneid H, Hollander JE, et al. Management of cocaine-associated chest pain and myocardial infarction: a scientific statement from the American Heart Association Acute Cardiac Care Committee of the Council on Clinical Cardiology. Circulation. 2008;117:1897-1907.
- Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol. 2007;50:E1-E157.
- Hollander JE. Management of cocaine-associated myocardial ischemia. N Engl J Med. 1995;333:1267-1272.
- Brubacher JR, Hoffman RS. Cocaine toxicity. Top Emerg Med. 1997;19(4):1-16.
- Catavas JD, Waters IW. Acute cocaine intoxication in the conscious dog: studies on the mechanism of lethality. J Pharmacol Exp Ther. 1981;217:350-356.
- Hollander JE, Hoffman RS, Gennis P, et al. Nitroglycerin in the treatment of cocaine associated chest pain—clinical safety and efficacy. J Toxicol Clin Toxicol. 1994;32(3): 243-256.
- Honderick T, Williams D, Seaberg D, Wears R. A prospective, randomized, controlled trial of benzodiazepines and nitroglycerin or nitroglycerin alone in the treatment of cocaine-associated acute coronary syndromes. Am J Emerg Med. 2003;21(1):39-42.
- Baumann BM, Perrone J, Hornig SE, Shofer FS, Hollander JE. Randomized, double-blind, placebo-controlled trial of diazepam, nitroglycerin, or both for treatment of patients with potential cocaine-associated acute coronary syndromes. Acad Emerg Med. 2000;7:878-885.
- Schindler CW, Tella SR, Goldberg SR. Adrenoceptor mechanisms in the cardiovascular effects of cocaine in conscious squirrel monkeys. Life Sci. 1992;51(9):653-660.
- Lange RA, Cigarroa RG, Yancy CW Jr., et al. Cocaine-induced coronary-artery vasoconstriction. N Engl J Med. 1989;321(23):1557-1562.
- Furberg CD, Psaty BM, Meyer JV. Nifedipine. Dose-related increase in mortality in patients with coronary heart disease. Circulation. 1995;92:1326-1331.
- Derlet RW, Albertson TE. Potentiation of cocaine toxicity with calcium channel blockers. Am J Emerg Med. 1989;7:464-468.
- Lange RA, Hillis LD. Cardiovascular complications of cocaine use. N Engl J Med. 2001;345:351-358.
- Lange RA, Cigarroa RG, Flores ED, et al. Potentiation of cocaine-induced coronary vasoconstriction by beta-adrenergic blockade. Ann Intern Med. 1990;112:897-903.
- Boehrer JD, Moliterno DJ, Willard JE, Hillis LD, Lange RA. Influence of labetalol on cocaine-induced coronary vasoconstriction in humans. Am J Med. 1993;94:608-610.
- Sand IC, Brody SL, Wrenn KD, Slovis CM. Experience with esmolol for the treatment of cocaine-associated cardiovascular complications. Am J Emerg Med. 1991;9:161-163.
- Sofuoglo M, Brown S, Babb DA, Pentel PR, Hatsukami DK. Carvedilol affects the physiological and behavioral response to smoked cocaine in humans. Drug Alcohol Depend. 2000;60:69-76.
- Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force of Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of patients with acute myocardial infarction). J Am Coll Cardiol. 2004;44:E1-E211.
- Dattilo PB, Hailpern SM, Fearon K, Sohal D, Nordin C. Beta-blockers are associated with reduced risk of myocardial infarction after cocaine use. Ann Emerg Med. 2008;51:117-125.
- Rangel C, Shu RG, Lazar LD, Vittinghoff E, Hsue PY, Marcus GM. Beta-blockers for chest pain associated with recent cocaine use. Arch Intern Med. 2010;170:874-879.
Case
A 38-year-old man with a history of tobacco use presents to the emergency department complaining of constant substernal chest pain for three hours. His temperature is 37.7°C, his heart rate is 110 beats per minute, and his blood pressure is 155/95 mmHg. He appears anxious and diaphoretic but examination is otherwise unremarkable. He admits to cocaine use one hour before the onset of symptoms. What are the appropriate treatments for his condition?
Overview
Cocaine is the second-most-commonly used illicit drug in the U.S. and represents 31% of all ED visits related to substance abuse.1,2 According to recent survey results, 2.1 million people report recent cocaine use, and 1.6 million engage in cocaine abuse or dependence.2 Acute cardiopulmonary complaints are common in individuals who present to the ED after cocaine use, with chest pain being the most frequently reported symptom in 40%.3
Numerous etiologies for cocaine-associated chest pain (CACP) have been discovered, including musculoskeletal pain, pulmonary hypertension, cardiomyopathy, arrhythmias, and endocarditis.4 Only 0.5% of patients with aortic dissection over a four-year period had a recent history of cocaine use, making cocaine a rare cause of a rare condition.5 Cardiac chest pain remains the most frequent underlying etiology, resulting in the most common complication of myocardial infarction (MI) in up to 6% of patients.6,7
The ways in which cocaine use can cause myocardial ischemia and MI are multifactorial. A vigorous central sympathomimetic effect, coronary artery vasoconstriction, stimulation of platelets, and enhanced atherosclerosis all lead to a myocardial oxygen supply-demand imbalance.8 Other key interactions in the cardiovascular system are displayed in Figure 1. Understanding the role of these mechanisms in CACP is crucial to patient care.
Clinician goals in the management of CACP are to rapidly and accurately exclude life-threatening etiologies; assess the need for urgent acute coronary syndrome (ACS) evaluation; risk-stratify patients and ensure appropriate disposition; normalize the toxic effects of cocaine; treat resultant organ damage; and prevent long-term complications. An algorithm detailing this approach is provided in Figure 2.
Review of the Data
Diagnostic evaluation. Given potential differences in treatment regimens, it is imperative to differentiate patients who present with CACP from those whose chest pain is not associated with cocaine either by direct questioning or by screening of urine for cocaine metabolites. Once the presence of cocaine has been confirmed, guideline-based evaluation for potential ACS with serial electrocardiograms (ECG), cardiac biomarkers, and close monitoring of cardiac rhythms and hemodynamics is largely similar to standard management of all patients presenting with chest pain, with a few caveats.
Interpretation of the ECG can be challenging in the setting of cocaine. Studies have shown “abnormal” ECGs in 56% to 84% of patients, with many representing early repolarization or left ventricular hypertrophy.9,10 Likewise, patients with MI are as likely to present with normal or nonspecific ECG findings as with ischemic findings.7,11 ECG interpretation to diagnose ischemia or infarction in patients with CACP yields a sensitivity of 36% and specificity of 90%.7
Creatine kinase (CK), CK-MB fraction, and myoglobin have low specificity for the diagnosis of ischemia, as cocaine can induce skeletal muscle injury and rhabdomyolysis.9,12 Cardiac troponins demonstrate a superior specificity compared to CK and CK-MB and are thus the preferred cardiac biomarkers in diagnosing cocaine-associated MI.12
Initial management and disposition. Patients at high risk for cardiovascular events are generally admitted to a monitored bed.13 Immediate reperfusion therapy with primary percutaneous coronary intervention is recommended in patients with ST-elevation MI (STEMI). Treatment with thrombolytic agents is associated with an increased risk of intracerebral hemorrhage and lacks documented efficacy in patients with CACP. Thrombolysis should therefore only be utilized if the diagnosis of STEMI is unequivocal and an experienced cardiac catheterization laboratory is unavailable.14,15
Patients with unstable angina (UA) or non-ST-elevation MI (NSTEMI) are at higher risk for further cardiac events in a similar manner to those with ACS unrelated to cocaine. These cases might benefit from early cardiac catheterization and revascularization.16 Because of the increased risk of stent thrombosis in cocaine-users, thought to be due to recidivism, a detailed risk-benefit analysis should be undertaken prior to the implantation of cardiac stents.
Other diagnostic tests, such as stress testing and myocardial imaging, have not shown significant accuracy in diagnosing MI in this setting; moreover, these patients are at low overall risk for cardiac events and mortality. Consequently, an extensive diagnostic evaluation might not be cost-effective.7,10,13,17 Patients who have CACP without MI have a very low frequency of delayed complications.3,17 As such, cost-effective evaluation strategies, such as nine- or 12-hour observation periods in a chest pain unit, are appropriate for many of these low- to moderate-risk patients.13 For all CACP patients, the most critical post-discharge interventions are cardiac risk modification and cocaine cessation.13
Normalizing the toxic effects of cocaine with medications.
Aspirin: While no specific study has been performed in patients with CACP and aspirin, CACP guidelines, based on data supporting ACS guidelines for all patients, recommend administration of full-dose aspirin given its associated reduction in morbidity and mortality.18,19 Furthermore, given the platelet-stimulating effects of cocaine, using aspirin in this setting seems very reasonable.
Benzodiazepines: CACP guidelines support the use of benzodiazepines early in management to indirectly combat the agitation, hypertension, and tachycardia resulting from the stimulatory effects of cocaine.18,20 These recommendations are based on several animal and human studies that demonstrate significant reduction in heart rate and systemic arterial pressure with the use of these agents.21,22
Nitroglycerin: Cardiac catheterization studies have shown reversal of vasoconstriction with administration of nitroglycerin. One study demonstrated a benefit of the drug in 49% of participants.23 Additional investigation into the benefit of benzodiazepine and nitroglycerin combination therapy revealed mixed results. In one study, lorazepam plus nitroglycerin was found to be more efficacious than nitroglycerin alone.24 In another, however, use of diazepam in combination with nitroglycerin did not show benefit when evaluating pain relief, cardiac dynamics, and left ventricular function.25
Phentolamine: Phentolamine administration has been studied much less in the literature. This nonselective alpha-adrenergic antagonist exerts a dose-dependent reversal of cocaine’s vasoconstrictive properties in monkeys and humans.26,27 International guidelines for Emergency Cardiovascular Care recommend its use in treatment of cocaine-associated ACS;27 however, the AHA recommends it less strongly.18
Calcium channel blockers: Calcium channel blockers (CCBs) have not shown promise as first-line agents. While catheterization studies demonstrate the vasodilatory properties of verapamil, larger studies looking at all-cause mortality conclude that CCBs might worsen mortality rates,28 and animal studies indicate an increased risk of seizures.29 At this time, CCBs are recommended only if cardiac symptoms continue after both benzodiazepines and nitroglycerin are administered.18
The beta-blocker controversy: The use of beta-blockers in patients with CACP remains controversial given the theoretical risk of unopposed alpha-adrenergic activation. Coronary vasospasm, decreased myocardial oxygen delivery, and increased systemic vascular resistance can result from their use.30
Propranolol, a nonselective beta-blocker, was shown in catheterization studies to potentiate the coronary vasoconstriction of cocaine.31 Labetalol, a combined alpha/beta-blocker, reduced mean arterial pressure after cocaine administration during cardiac catheterization but did not reverse coronary vasoconstriction.32 This was attributed to the predominating beta greater than alpha blockade at doses administered. The selective beta-1 antagonists esmolol and metoprolol have shown no benefit in CACP.33 Carvedilol, a combined alpha/beta-blocker with both peripheral and central nervous system activity, has potential to attenuate both physiologic and behavioral response to cocaine, but it has not been well studied in this patient subset.34
The 2005 ACC/AHA STEMI guidelines recommended against beta-blockers in the setting of STEMI precipitated by cocaine use due to the potential of exacerbating coronary vasoconstriction.35 The 2007 ACC/AHA UA/NSTEMI guidelines stated that the use of a combined alpha/beta-blocker in patients with cocaine-induced ACS may be reasonable for patients with hypertension or tachycardia if pre-treated with a vasodilator.19 The 2008 ACC/AHA guidelines on the management of cocaine-related chest pain and MI recommended against the use of beta-blockers in the acute setting given the low incidence of cocaine-related MI and death.18
In a more recent study, Dattilo et al showed that beta-blockers administered to patients admitted with positive urine toxicology for cocaine significantly reduced MI and in-hospital mortality. Reduction of MI was of borderline significance in those admitted with a chief complaint of chest pain.36 Limitations of this study include unknown time of cocaine ingestion, lack of follow-up on discharge mortality, and a small sample size of 348 patients lacking statistical power.
Another retrospective cohort study examined patients admitted with chest pain and urine toxicology positive for cocaine and found that beta-blocker administration during hospitalization was not associated with increased incident mortality. Further, after a mean follow-up of 2.5 years, there was a statistically significant decrease in cardiovascular death.37 Drawbacks of this study included an older patient population, greater proportion of coronary artery disease, and higher follow-up of cardiovascular mortality rates than in previous studies, suggesting this subset might have received greater benefit from beta-blockers as a result of these characteristics.
The 2008 ACC/AHA guidelines instruct individualized consideration of the risk/benefit ratio for beta-blocker use in patients with CACP given the high rate of recidivism in cocaine abusers. The strongest indication is given to those with documented MI, left ventricular systolic dysfunction, or ventricular arrhythmias.18
It is important to note that these recommendations are based on cardiac catheterization laboratory studies, case reports, retrospective analyses, and animal experiments. No prospective controlled trials evaluating the role of beta-blockers in CACP and MI exist, and no trials regarding therapies to improve outcomes of patients sustaining a cocaine-associated MI have been reported.18
Back to the Case
This patient was experiencing cocaine-associated chest pain, which was confirmed with positive urine toxicology. Initial diagnostic workup with basic laboratory studies and cardiac biomarkers showed mild elevation in CK with troponin levels within normal limits. His ECG showed changes consistent with left ventricular hypertrophy. Chest radiograph was unremarkable.
He received aspirin, benzodiazepines, and nitroglycerin with normalization of vital signs, as well as subjective improvement in chest pain and anxiety. He was deemed to be at low risk for potential cardiac complications; thus, further cardiac testing was not pursued. Rather, he was admitted to an overnight observation unit with telemetry monitoring, where his chest pain did not recur.
He was seen in consultation with social work staff who arranged for drug abuse counseling after discharge. Given the uncertainty of relapse to cocaine use, as well as lack of known cardiac risk factors, he was not discharged on any new medications.
Bottom Line
The treatment of CACP includes normalizing the toxic systemic effects of the drug and minimizing the direct ischemic damage to the myocardium. Management varies slightly from traditional chest pain algorithms and includes benzodiazepines as well as antiplatelet agents and vasodilators to achieve this goal. Initial therapy with beta-blockers remains undefined and is largely discouraged in the acute setting. The role of beta-blockade upon discharge, however, can be beneficial in specific populations, especially those found to have underlying coronary disease.
Dr. Houchens and Dr. Czarnik are clinical instructors and Dr. Mack is a clinical lecturer at the University of Michigan Health System in Ann Arbor.
References
- Hughes A, Sathe N, Spagnola K. State Estimates of Substance Use from the 2005-2006 National Surveys on Drug Use and Health. DHHS Publication No. SMA 08-4311, NSDUH Series H-33. Rockville, MD: Substance Abuse and Mental Health Services Administration, Office of Applied Studies; 2008.
- Volkow ND. Cocaine: Abuse and Addiction. National Institute on Drug Abuse. Washington, DC: U.S. Department of Health and Human Services; 2009.
- Brody SL, Slovis CM, Wrenn KD. Cocaine-related medical problems: consecutive series of 233 patients. Am J Med. 1990;88:325-331.
- Levis JT, Garmel GM. Cocaine-associated chest pain. Emerg Med Clin North Am. 2005;23:1083-1103.
- Eagle KA, Isselbacher EM, DeSanctis RW. Cocaine-related aortic dissection in perspective. Circulation. 2002;105:1529-1530.
- Feldman JA, Fish SS, Beshansky JR, Griffith JL, Woolard RH, Selker HP. Acute cardiac ischemia in patients with cocaine-associated complaints: results of a multicenter trial. Ann Emerg Med. 2000;36:469-476.
- Hollander JE, Hoffman RS, Gennis P, et al. Prospective multicenter evaluation of cocaine associated chest pain. Cocaine Associated Chest Pain (COCHPA) Study Group. Acad Emerg Med. 1994;1:330-339.
- Schwartz BG, Rezkalla S, Kloner RA. Cardiovascular effects of cocaine. Circulation. 2010;122:2558-2569.
- Gitter MJ, Goldsmith SR, Dunbar DN, et al. Cocaine and chest pain: clinical features and outcomes of patients hospitalized to rule out myocardial infarction. Ann Intern Med. 1991;115:277-282.
- Amin M, Gabelman G, Karpel J, et al. Acute myocardial infarction and chest pain syndromes after cocaine use. Am J Cardiol. 1990;66:1434-1437.
- Tokarski GF, Paganussi P, Urbanski R, et al. An evaluation of cocaine-induced chest pain. Ann Emerg Med. 1990;19:1088-1092.
- Hollander JE, Levitt MA, Young GP, Briglia E, Wetli CV, Gawad Y. Effect of recent cocaine use on the specificity of cardiac markers for diagnosis of acute myocardial infarction. Am Heart J. 1998;135(2 Pt 1):245-252.
- Weber JE, Shofer FS, Larkin GL, Kalaria AS, Hollander JE. Validation of a brief observation period for patients with cocaine-associated chest pain. N Engl J Med. 2003;348:510-517.
- Hahn IH, Hoffman RS. Diagnosis and treatment of acute myocardial infarction: cocaine use and acute myocardial infarction. Emerg Med Clin North Am. 2001;19(2):1-18.
- Hoffman RS, Hollander JE. Evaluation of patients with chest pain after cocaine use. Crit Care Clin. 1997;13:809-828. Cannon CP, Weintraub WS, Demopoulos LA, et al.
- Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med. 2001;344:1879-1887.
- Hollander JE, Hoffman RS. Cocaine-induced myocardial infarction: an analysis and review of the literature. J Emerg Med. 1992;10:169-177.
- McCord J, Jneid H, Hollander JE, et al. Management of cocaine-associated chest pain and myocardial infarction: a scientific statement from the American Heart Association Acute Cardiac Care Committee of the Council on Clinical Cardiology. Circulation. 2008;117:1897-1907.
- Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol. 2007;50:E1-E157.
- Hollander JE. Management of cocaine-associated myocardial ischemia. N Engl J Med. 1995;333:1267-1272.
- Brubacher JR, Hoffman RS. Cocaine toxicity. Top Emerg Med. 1997;19(4):1-16.
- Catavas JD, Waters IW. Acute cocaine intoxication in the conscious dog: studies on the mechanism of lethality. J Pharmacol Exp Ther. 1981;217:350-356.
- Hollander JE, Hoffman RS, Gennis P, et al. Nitroglycerin in the treatment of cocaine associated chest pain—clinical safety and efficacy. J Toxicol Clin Toxicol. 1994;32(3): 243-256.
- Honderick T, Williams D, Seaberg D, Wears R. A prospective, randomized, controlled trial of benzodiazepines and nitroglycerin or nitroglycerin alone in the treatment of cocaine-associated acute coronary syndromes. Am J Emerg Med. 2003;21(1):39-42.
- Baumann BM, Perrone J, Hornig SE, Shofer FS, Hollander JE. Randomized, double-blind, placebo-controlled trial of diazepam, nitroglycerin, or both for treatment of patients with potential cocaine-associated acute coronary syndromes. Acad Emerg Med. 2000;7:878-885.
- Schindler CW, Tella SR, Goldberg SR. Adrenoceptor mechanisms in the cardiovascular effects of cocaine in conscious squirrel monkeys. Life Sci. 1992;51(9):653-660.
- Lange RA, Cigarroa RG, Yancy CW Jr., et al. Cocaine-induced coronary-artery vasoconstriction. N Engl J Med. 1989;321(23):1557-1562.
- Furberg CD, Psaty BM, Meyer JV. Nifedipine. Dose-related increase in mortality in patients with coronary heart disease. Circulation. 1995;92:1326-1331.
- Derlet RW, Albertson TE. Potentiation of cocaine toxicity with calcium channel blockers. Am J Emerg Med. 1989;7:464-468.
- Lange RA, Hillis LD. Cardiovascular complications of cocaine use. N Engl J Med. 2001;345:351-358.
- Lange RA, Cigarroa RG, Flores ED, et al. Potentiation of cocaine-induced coronary vasoconstriction by beta-adrenergic blockade. Ann Intern Med. 1990;112:897-903.
- Boehrer JD, Moliterno DJ, Willard JE, Hillis LD, Lange RA. Influence of labetalol on cocaine-induced coronary vasoconstriction in humans. Am J Med. 1993;94:608-610.
- Sand IC, Brody SL, Wrenn KD, Slovis CM. Experience with esmolol for the treatment of cocaine-associated cardiovascular complications. Am J Emerg Med. 1991;9:161-163.
- Sofuoglo M, Brown S, Babb DA, Pentel PR, Hatsukami DK. Carvedilol affects the physiological and behavioral response to smoked cocaine in humans. Drug Alcohol Depend. 2000;60:69-76.
- Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force of Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of patients with acute myocardial infarction). J Am Coll Cardiol. 2004;44:E1-E211.
- Dattilo PB, Hailpern SM, Fearon K, Sohal D, Nordin C. Beta-blockers are associated with reduced risk of myocardial infarction after cocaine use. Ann Emerg Med. 2008;51:117-125.
- Rangel C, Shu RG, Lazar LD, Vittinghoff E, Hsue PY, Marcus GM. Beta-blockers for chest pain associated with recent cocaine use. Arch Intern Med. 2010;170:874-879.
Hospitalists Encouraged to Embrace Medicare’s VBPM Program Now
Hospitalists have heard ad infinitum that, starting this year, providers in groups of 100 or more might be penalized in two years by the Centers for Medicare & Medicaid Services’ (CMS) value-based payment modifier (VBPM) program, which correlates the cost of services to the quality of those services. And while it is true VBPM won’t apply to individual providers until 2017, HM leaders say now is the time to lobby on what metrics should be considered to determine clinician quality.
“With the speed at which policy becomes reality, we need to start now,” says Gregory Seymann, MD, SFHM, chief of the division of hospital medicine at the University of California at San Diego School of Medicine. “The trick about the immediacy is that it appears that it’s four years away because 2017 is when it applies to everyone. That’s deceptive; they start measuring performance for 2017 in 2015. The immediacy is real for everyone.”
VBPM: The Next Step
VBPM is a separate program from, but overlaps with, the Physician Quality Reporting System (PQRS). In essence, PQRS was a pay-for-reporting system that rewarded compliant physicians a 0.5% incentive payment for total Medicare Part B Physician Fee Schedule (PFS) charges for covered services (which means the incentive covers all PFS payments, not just those applied to the services being reported). The landmark Affordable Care Act (ACA) has gone a step further: Nonparticipating physicians will lose 1.5% of allowable Medicare charges beginning in 2015. The reimbursement reduction increases to 2% in 2016.
Once a group is participating in PQRS, VBPM is the next step: a pay-for-quality system that will offers variable rewards for the most efficient providers and a 1% penalty for those groups that fail to participate. Because VBPM sets a two-year time lag between performance year and payment adjustment, the first adjustments in 2015 will be based on data gathered this year.
For the 2015 adjustment, CMS only is looking at results from groups of 100 or more eligible professionals—currently defined as physicians, practitioners, and therapists—under a lone tax identification number (TIN). Hospitalists in large groups or at large academic centers could be eligible, as billing for those physicians often is done in tandem with other specialties, says Dr. Seymann, a member of SHM’s Performance Measurement and Reporting Committee (PMRC). He recommends hospitalists check with administrators to learn if they are in such a group.
Payment adjustments for individual providers will begin in 2017 and likely will be based on a 2015 performance period. PMRC chair Patrick Torcson, MD, MMM, FACP, SFHM, says the time is now for SHM and providers to lobby for the right metrics to be used. Dr. Torcson’s first priority would be for Medicare to recognize HM as its own specialty, as current measures don’t correctly capture the activities on which most hospitalists focus.
“The performance measures that are available for hospitalists really are for general internal medicine and are just left over because we’re lumped in with the internists,” he says. “For example, there may be a heart failure measure or a pneumonia measure, and hospitalists treat a lot of heart failure and pneumonia, but the way that the measure is specified is that it has specifications that can only be reported in the outpatient setting. So the inpatient setting doesn’t allow for a hospitalist to be able to report.”
Suboptimal Measures
Dr. Seymann notes that tailoring measures to patient discharge and transitions of care could provide metrics that would better measure the quality of care provided by hospitalists. SHM and others have lobbied for such metrics, but CMS has not weighed in yet. Dr. Seymann adds CMS has asked for feedback on whether physicians should be allowed to align their reporting with the quality measures required for hospitals’ Inpatient Hospital Quality Reporting (IHQR) measures. SHM has supported the idea, as long as hospitalists aren’t required to report that way.
“Hospitalists can say, ‘If my hospital does well on these measures, that’s a reflection of my contribution as well, so we can count these measures for our value-based modifier,’” he says. “Those are promising pathways to more options for hospitalists.”
Dr. Torcson urges physicians to lobby their local federal officials and Medicare contacts to ensure that when all hospitalists are subject to the VBPM, the most accurate metrics available are used to gauge their quality of care delivery.
“Ideally, for a hospital medicine practice to be measured and have relevant outcomes, it would have to include performance measures that address things like transitions of care, medication reconciliation, patient safety, efficiency, and use of resources,” he says. “We’re really in the infancy of the methodology and performance measurement world of having relevant measures that do address those specific things. That’s on our hospitalist wish list.”
Richard Quinn is a freelance writer in New Jersey.
What Can I Do Now?

SHM has lobbied federal officials for changes to CMS’ Value-Based Payment Modifier Program, and will continue to do so. But here are tips individual providers can use now:
- Make sure your group is participating in PQRS. While that might sound commonplace, CMS data showed that in 2010, roughly 25% of eligible providers were participating in PQRS’ optional predecessor, the Physician Quality Reporting Initiative (PQRI).
- Find out how your workplace handles its billing. If your billing is submitted with other specialties and physicians from inside the institution, you might be in a group of 100 eligible providers. If so, your compliance with PQRS measures this year will determine your payment adjustment in 2015.
- Pay attention to Medicare’s QRUR. 2013 is the first year all physicians will receive the report, which was launched last year as a pilot program in just nine states. The reports essentially rank providers based on cost and quality of care, and can be skewed for hospitalists as the measures don’t necessarily take into account that hospitalists often care for the acutely ill. SHM has lobbied CMS to improve the reports so they are more accurate in relation to HM services, but the more examples SHM can provide, the more weight the argument will likely hold.
Hospitalists have heard ad infinitum that, starting this year, providers in groups of 100 or more might be penalized in two years by the Centers for Medicare & Medicaid Services’ (CMS) value-based payment modifier (VBPM) program, which correlates the cost of services to the quality of those services. And while it is true VBPM won’t apply to individual providers until 2017, HM leaders say now is the time to lobby on what metrics should be considered to determine clinician quality.
“With the speed at which policy becomes reality, we need to start now,” says Gregory Seymann, MD, SFHM, chief of the division of hospital medicine at the University of California at San Diego School of Medicine. “The trick about the immediacy is that it appears that it’s four years away because 2017 is when it applies to everyone. That’s deceptive; they start measuring performance for 2017 in 2015. The immediacy is real for everyone.”
VBPM: The Next Step
VBPM is a separate program from, but overlaps with, the Physician Quality Reporting System (PQRS). In essence, PQRS was a pay-for-reporting system that rewarded compliant physicians a 0.5% incentive payment for total Medicare Part B Physician Fee Schedule (PFS) charges for covered services (which means the incentive covers all PFS payments, not just those applied to the services being reported). The landmark Affordable Care Act (ACA) has gone a step further: Nonparticipating physicians will lose 1.5% of allowable Medicare charges beginning in 2015. The reimbursement reduction increases to 2% in 2016.
Once a group is participating in PQRS, VBPM is the next step: a pay-for-quality system that will offers variable rewards for the most efficient providers and a 1% penalty for those groups that fail to participate. Because VBPM sets a two-year time lag between performance year and payment adjustment, the first adjustments in 2015 will be based on data gathered this year.
For the 2015 adjustment, CMS only is looking at results from groups of 100 or more eligible professionals—currently defined as physicians, practitioners, and therapists—under a lone tax identification number (TIN). Hospitalists in large groups or at large academic centers could be eligible, as billing for those physicians often is done in tandem with other specialties, says Dr. Seymann, a member of SHM’s Performance Measurement and Reporting Committee (PMRC). He recommends hospitalists check with administrators to learn if they are in such a group.
Payment adjustments for individual providers will begin in 2017 and likely will be based on a 2015 performance period. PMRC chair Patrick Torcson, MD, MMM, FACP, SFHM, says the time is now for SHM and providers to lobby for the right metrics to be used. Dr. Torcson’s first priority would be for Medicare to recognize HM as its own specialty, as current measures don’t correctly capture the activities on which most hospitalists focus.
“The performance measures that are available for hospitalists really are for general internal medicine and are just left over because we’re lumped in with the internists,” he says. “For example, there may be a heart failure measure or a pneumonia measure, and hospitalists treat a lot of heart failure and pneumonia, but the way that the measure is specified is that it has specifications that can only be reported in the outpatient setting. So the inpatient setting doesn’t allow for a hospitalist to be able to report.”
Suboptimal Measures
Dr. Seymann notes that tailoring measures to patient discharge and transitions of care could provide metrics that would better measure the quality of care provided by hospitalists. SHM and others have lobbied for such metrics, but CMS has not weighed in yet. Dr. Seymann adds CMS has asked for feedback on whether physicians should be allowed to align their reporting with the quality measures required for hospitals’ Inpatient Hospital Quality Reporting (IHQR) measures. SHM has supported the idea, as long as hospitalists aren’t required to report that way.
“Hospitalists can say, ‘If my hospital does well on these measures, that’s a reflection of my contribution as well, so we can count these measures for our value-based modifier,’” he says. “Those are promising pathways to more options for hospitalists.”
Dr. Torcson urges physicians to lobby their local federal officials and Medicare contacts to ensure that when all hospitalists are subject to the VBPM, the most accurate metrics available are used to gauge their quality of care delivery.
“Ideally, for a hospital medicine practice to be measured and have relevant outcomes, it would have to include performance measures that address things like transitions of care, medication reconciliation, patient safety, efficiency, and use of resources,” he says. “We’re really in the infancy of the methodology and performance measurement world of having relevant measures that do address those specific things. That’s on our hospitalist wish list.”
Richard Quinn is a freelance writer in New Jersey.
What Can I Do Now?
SHM has lobbied federal officials for changes to CMS’ Value-Based Payment Modifier Program, and will continue to do so. But here are tips individual providers can use now:
- Make sure your group is participating in PQRS. While that might sound commonplace, CMS data showed that in 2010, roughly 25% of eligible providers were participating in PQRS’ optional predecessor, the Physician Quality Reporting Initiative (PQRI).
- Find out how your workplace handles its billing. If your billing is submitted with other specialties and physicians from inside the institution, you might be in a group of 100 eligible providers. If so, your compliance with PQRS measures this year will determine your payment adjustment in 2015.
- Pay attention to Medicare’s QRUR. 2013 is the first year all physicians will receive the report, which was launched last year as a pilot program in just nine states. The reports essentially rank providers based on cost and quality of care, and can be skewed for hospitalists as the measures don’t necessarily take into account that hospitalists often care for the acutely ill. SHM has lobbied CMS to improve the reports so they are more accurate in relation to HM services, but the more examples SHM can provide, the more weight the argument will likely hold.
Hospitalists have heard ad infinitum that, starting this year, providers in groups of 100 or more might be penalized in two years by the Centers for Medicare & Medicaid Services’ (CMS) value-based payment modifier (VBPM) program, which correlates the cost of services to the quality of those services. And while it is true VBPM won’t apply to individual providers until 2017, HM leaders say now is the time to lobby on what metrics should be considered to determine clinician quality.
“With the speed at which policy becomes reality, we need to start now,” says Gregory Seymann, MD, SFHM, chief of the division of hospital medicine at the University of California at San Diego School of Medicine. “The trick about the immediacy is that it appears that it’s four years away because 2017 is when it applies to everyone. That’s deceptive; they start measuring performance for 2017 in 2015. The immediacy is real for everyone.”
VBPM: The Next Step
VBPM is a separate program from, but overlaps with, the Physician Quality Reporting System (PQRS). In essence, PQRS was a pay-for-reporting system that rewarded compliant physicians a 0.5% incentive payment for total Medicare Part B Physician Fee Schedule (PFS) charges for covered services (which means the incentive covers all PFS payments, not just those applied to the services being reported). The landmark Affordable Care Act (ACA) has gone a step further: Nonparticipating physicians will lose 1.5% of allowable Medicare charges beginning in 2015. The reimbursement reduction increases to 2% in 2016.
Once a group is participating in PQRS, VBPM is the next step: a pay-for-quality system that will offers variable rewards for the most efficient providers and a 1% penalty for those groups that fail to participate. Because VBPM sets a two-year time lag between performance year and payment adjustment, the first adjustments in 2015 will be based on data gathered this year.
For the 2015 adjustment, CMS only is looking at results from groups of 100 or more eligible professionals—currently defined as physicians, practitioners, and therapists—under a lone tax identification number (TIN). Hospitalists in large groups or at large academic centers could be eligible, as billing for those physicians often is done in tandem with other specialties, says Dr. Seymann, a member of SHM’s Performance Measurement and Reporting Committee (PMRC). He recommends hospitalists check with administrators to learn if they are in such a group.
Payment adjustments for individual providers will begin in 2017 and likely will be based on a 2015 performance period. PMRC chair Patrick Torcson, MD, MMM, FACP, SFHM, says the time is now for SHM and providers to lobby for the right metrics to be used. Dr. Torcson’s first priority would be for Medicare to recognize HM as its own specialty, as current measures don’t correctly capture the activities on which most hospitalists focus.
“The performance measures that are available for hospitalists really are for general internal medicine and are just left over because we’re lumped in with the internists,” he says. “For example, there may be a heart failure measure or a pneumonia measure, and hospitalists treat a lot of heart failure and pneumonia, but the way that the measure is specified is that it has specifications that can only be reported in the outpatient setting. So the inpatient setting doesn’t allow for a hospitalist to be able to report.”
Suboptimal Measures
Dr. Seymann notes that tailoring measures to patient discharge and transitions of care could provide metrics that would better measure the quality of care provided by hospitalists. SHM and others have lobbied for such metrics, but CMS has not weighed in yet. Dr. Seymann adds CMS has asked for feedback on whether physicians should be allowed to align their reporting with the quality measures required for hospitals’ Inpatient Hospital Quality Reporting (IHQR) measures. SHM has supported the idea, as long as hospitalists aren’t required to report that way.
“Hospitalists can say, ‘If my hospital does well on these measures, that’s a reflection of my contribution as well, so we can count these measures for our value-based modifier,’” he says. “Those are promising pathways to more options for hospitalists.”
Dr. Torcson urges physicians to lobby their local federal officials and Medicare contacts to ensure that when all hospitalists are subject to the VBPM, the most accurate metrics available are used to gauge their quality of care delivery.
“Ideally, for a hospital medicine practice to be measured and have relevant outcomes, it would have to include performance measures that address things like transitions of care, medication reconciliation, patient safety, efficiency, and use of resources,” he says. “We’re really in the infancy of the methodology and performance measurement world of having relevant measures that do address those specific things. That’s on our hospitalist wish list.”
Richard Quinn is a freelance writer in New Jersey.
What Can I Do Now?
SHM has lobbied federal officials for changes to CMS’ Value-Based Payment Modifier Program, and will continue to do so. But here are tips individual providers can use now:
- Make sure your group is participating in PQRS. While that might sound commonplace, CMS data showed that in 2010, roughly 25% of eligible providers were participating in PQRS’ optional predecessor, the Physician Quality Reporting Initiative (PQRI).
- Find out how your workplace handles its billing. If your billing is submitted with other specialties and physicians from inside the institution, you might be in a group of 100 eligible providers. If so, your compliance with PQRS measures this year will determine your payment adjustment in 2015.
- Pay attention to Medicare’s QRUR. 2013 is the first year all physicians will receive the report, which was launched last year as a pilot program in just nine states. The reports essentially rank providers based on cost and quality of care, and can be skewed for hospitalists as the measures don’t necessarily take into account that hospitalists often care for the acutely ill. SHM has lobbied CMS to improve the reports so they are more accurate in relation to HM services, but the more examples SHM can provide, the more weight the argument will likely hold.
The Process of Selling a Hospitalist Group from Start to Finish
Whether your hospitalist group has five or 500 practitioners, you and your partners might be thinking about whether you want—or need—to enter into a merger or acquisition in the near future. For some hospitalist groups, mergers and acquisitions could be part of a growth strategy designed to increase geographic footprint, market penetration, or bargaining power. These types of transactions will allow larger groups to increase their competitiveness by being able to leverage investments in such items as information technology upgrades across a larger base of business.
For others, a desire to retire or an inability to either afford or justify certain capital investments needed to remain competitive might be leading some players to consider selling their hospitalist groups. Moreover, changes in the healthcare industry, coupled with the anticipation of tax increases, could factor into decisions to sell practices in the relatively near term.
While each transaction is unique, most tend to follow a similar process, incorporating a number of relatively standard phases that must be undertaken in order to complete a transaction. The transaction process typically takes between three and nine months, although preparations are often best begun in advance of the actual deal process.
Preliminary Matters
For hospitalist group owners and executives considering selling their practice, a number of preliminary matters should be addressed in preparation for a sale. First, potential sellers should carefully consider whether they really wish to enter into the sale process. The sale process is lengthy, time-consuming, and costly, and it is often stressful and demanding on the practice’s management. Thus, potential sellers should not undertake the process unless they are serious about selling and have a realistic expectation of what they will receive as the purchase price.
As part of the preparation, sellers should begin by assembling an experienced transaction team. Typically, the team includes key members of the practice’s management, as well as experienced healthcare mergers and acquisitions attorneys and accountants. These experienced professionals can be of great assistance in making sure that a transaction is executed on a timely basis and under terms appropriate for the specific transaction.
Another prudent step is undertaking a tax analysis to determine the implications of the sale on both the selling practice and its individual owners. This analysis should be performed as far in advance of a proposed transaction as possible, in order to allow time for adjustments to be made (if necessary) to limit the tax implications in advance of the sale. Sellers also will want to use this preparatory phase to make sure that the practice’s books and records are in good order in preparation for the buyer’s due diligence review, as well as to address any issues in order to make the practice more attractive to potential buyers. Some sellers might want to have an investment banker or other qualified professional provide a valuation appraisal of the practice to provide a realistic purchase price.
Finding a Buyer
As a seller begins the process to find a buyer, the seller must first consider the approach that it wants to take. Some larger groups are sold through auction-like processes in which a number of bidders are contacted and invited to participate. The advantage of this type of process is that it typically drives prices higher by introducing competition into the bidding process. On the other hand, this type of process has certain disadvantages, such as a longer time frame and increased risk of a breach of confidentiality.
For some sellers, a more targeted approach, with limited participants, might be more desirable. If a fair purchase price can be obtained without involving multiple potential buyers, the process can be completed faster and with less risk to the ongoing business operations.
The process of finding a buyer typically requires the seller to provide potential buyers with confidential information regarding the business so the interested parties can evaluate whether the selling group is even of interest and the amount that they will be willing to pay. However, the selling practice should only provide this confidential information after potential buyers have signed nondisclosure agreements.
Ultimately, the process will lead to the submission of specific proposals from interested parties. Typically, this results in the seller and the selected buyer entering into a letter of intent, a statement of key terms for the proposed transaction. Letters of intent are largely not binding and are subject to the satisfaction of conditions, such as the negotiation of definitive written agreements. Typically, in this phase of the process, the basic structure of the transaction, the purchase price, and the manner of payment are determined.
Due Diligence
In almost all sale transactions, the buyer will conduct a review and investigation of the seller’s business. The purpose of this review is to confirm the information previously provided by the seller and to allow the buyer to gain a thorough understanding of the business to determine whether it is truly willing to buy the business on the terms identified in the letter of intent. The buyer will want to confirm that it is not going to inherit any unexpected liabilities or problems, such as healthcare regulatory issues or lawsuits. To comply with the information requests from the buyer as it conducts its due diligence review, the seller will be required to assemble many documents and voluminous amounts of financial and other information. The burden of providing this information to the buyer will be substantial and could distract management from their day-to-day duties of running the practice.
Upon completion of the due diligence process, the buyer will either confirm that it is willing to move forward with the transaction “as is,” or, if the due diligence review reveals troubling information, the buyer can either demand changes to the transaction (such as a reduction of the purchase price) or be unwilling to proceed with the transaction altogether.
Negotiating Definitive Agreements
The parties will need to negotiate and agree on certain definitive written agreements, which will govern the transaction. First and foremost, this will include a purchase agreement, such as a stock purchase agreement or an asset purchase agreement. In addition, there may also be various ancillary agreements, such as noncompetition agreements between the buyer and the owners of the selling practice and new employment agreements for the sellers.
Typically, the negotiation of definitive agreements proceeds in parallel with the buyer’s due diligence review.
Closing
At the closing, both sides will sign numerous documents, including those necessary to transfer ownership of the purchased group to the buyer, as well as all ancillary agreements and other documents needed for the transaction. Once signatures have been obtained and exchanged between the parties, the transfer of title will occur and the buyer will tender the purchase price.
Post-Closing
Although the vast majority of the work associated with the transaction will terminate upon the completion of the closing, certain aspects of the sale will require some attention after the closing. For example, there may be purchase price adjustments based upon the final balance sheet or net working capital position of the seller’s business as of the closing date. Typically, these adjustments are addressed in the months following the closing. Also, if any indemnification claims are brought, the parties will need to address those claims and reach a resolution.
Merger and acquisition transactions are complex, time-consuming matters that require a great deal of effort on the part of all parties involved. An orderly process is essential for both buyers and sellers. Sellers will want to take steps to make sure that the transaction is completed in a timely manner while minimizing risk to the ongoing business operations. At the same time, buyers will want to make sure that the value that they are receiving from the seller’s business is commensurate with the purchase price and that the buyer’s goals for entering into the sale will truly be met post-closing.
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Whether your hospitalist group has five or 500 practitioners, you and your partners might be thinking about whether you want—or need—to enter into a merger or acquisition in the near future. For some hospitalist groups, mergers and acquisitions could be part of a growth strategy designed to increase geographic footprint, market penetration, or bargaining power. These types of transactions will allow larger groups to increase their competitiveness by being able to leverage investments in such items as information technology upgrades across a larger base of business.
For others, a desire to retire or an inability to either afford or justify certain capital investments needed to remain competitive might be leading some players to consider selling their hospitalist groups. Moreover, changes in the healthcare industry, coupled with the anticipation of tax increases, could factor into decisions to sell practices in the relatively near term.
While each transaction is unique, most tend to follow a similar process, incorporating a number of relatively standard phases that must be undertaken in order to complete a transaction. The transaction process typically takes between three and nine months, although preparations are often best begun in advance of the actual deal process.
Preliminary Matters
For hospitalist group owners and executives considering selling their practice, a number of preliminary matters should be addressed in preparation for a sale. First, potential sellers should carefully consider whether they really wish to enter into the sale process. The sale process is lengthy, time-consuming, and costly, and it is often stressful and demanding on the practice’s management. Thus, potential sellers should not undertake the process unless they are serious about selling and have a realistic expectation of what they will receive as the purchase price.
As part of the preparation, sellers should begin by assembling an experienced transaction team. Typically, the team includes key members of the practice’s management, as well as experienced healthcare mergers and acquisitions attorneys and accountants. These experienced professionals can be of great assistance in making sure that a transaction is executed on a timely basis and under terms appropriate for the specific transaction.
Another prudent step is undertaking a tax analysis to determine the implications of the sale on both the selling practice and its individual owners. This analysis should be performed as far in advance of a proposed transaction as possible, in order to allow time for adjustments to be made (if necessary) to limit the tax implications in advance of the sale. Sellers also will want to use this preparatory phase to make sure that the practice’s books and records are in good order in preparation for the buyer’s due diligence review, as well as to address any issues in order to make the practice more attractive to potential buyers. Some sellers might want to have an investment banker or other qualified professional provide a valuation appraisal of the practice to provide a realistic purchase price.
Finding a Buyer
As a seller begins the process to find a buyer, the seller must first consider the approach that it wants to take. Some larger groups are sold through auction-like processes in which a number of bidders are contacted and invited to participate. The advantage of this type of process is that it typically drives prices higher by introducing competition into the bidding process. On the other hand, this type of process has certain disadvantages, such as a longer time frame and increased risk of a breach of confidentiality.
For some sellers, a more targeted approach, with limited participants, might be more desirable. If a fair purchase price can be obtained without involving multiple potential buyers, the process can be completed faster and with less risk to the ongoing business operations.
The process of finding a buyer typically requires the seller to provide potential buyers with confidential information regarding the business so the interested parties can evaluate whether the selling group is even of interest and the amount that they will be willing to pay. However, the selling practice should only provide this confidential information after potential buyers have signed nondisclosure agreements.
Ultimately, the process will lead to the submission of specific proposals from interested parties. Typically, this results in the seller and the selected buyer entering into a letter of intent, a statement of key terms for the proposed transaction. Letters of intent are largely not binding and are subject to the satisfaction of conditions, such as the negotiation of definitive written agreements. Typically, in this phase of the process, the basic structure of the transaction, the purchase price, and the manner of payment are determined.
Due Diligence
In almost all sale transactions, the buyer will conduct a review and investigation of the seller’s business. The purpose of this review is to confirm the information previously provided by the seller and to allow the buyer to gain a thorough understanding of the business to determine whether it is truly willing to buy the business on the terms identified in the letter of intent. The buyer will want to confirm that it is not going to inherit any unexpected liabilities or problems, such as healthcare regulatory issues or lawsuits. To comply with the information requests from the buyer as it conducts its due diligence review, the seller will be required to assemble many documents and voluminous amounts of financial and other information. The burden of providing this information to the buyer will be substantial and could distract management from their day-to-day duties of running the practice.
Upon completion of the due diligence process, the buyer will either confirm that it is willing to move forward with the transaction “as is,” or, if the due diligence review reveals troubling information, the buyer can either demand changes to the transaction (such as a reduction of the purchase price) or be unwilling to proceed with the transaction altogether.
Negotiating Definitive Agreements
The parties will need to negotiate and agree on certain definitive written agreements, which will govern the transaction. First and foremost, this will include a purchase agreement, such as a stock purchase agreement or an asset purchase agreement. In addition, there may also be various ancillary agreements, such as noncompetition agreements between the buyer and the owners of the selling practice and new employment agreements for the sellers.
Typically, the negotiation of definitive agreements proceeds in parallel with the buyer’s due diligence review.
Closing
At the closing, both sides will sign numerous documents, including those necessary to transfer ownership of the purchased group to the buyer, as well as all ancillary agreements and other documents needed for the transaction. Once signatures have been obtained and exchanged between the parties, the transfer of title will occur and the buyer will tender the purchase price.
Post-Closing
Although the vast majority of the work associated with the transaction will terminate upon the completion of the closing, certain aspects of the sale will require some attention after the closing. For example, there may be purchase price adjustments based upon the final balance sheet or net working capital position of the seller’s business as of the closing date. Typically, these adjustments are addressed in the months following the closing. Also, if any indemnification claims are brought, the parties will need to address those claims and reach a resolution.
Merger and acquisition transactions are complex, time-consuming matters that require a great deal of effort on the part of all parties involved. An orderly process is essential for both buyers and sellers. Sellers will want to take steps to make sure that the transaction is completed in a timely manner while minimizing risk to the ongoing business operations. At the same time, buyers will want to make sure that the value that they are receiving from the seller’s business is commensurate with the purchase price and that the buyer’s goals for entering into the sale will truly be met post-closing.
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Whether your hospitalist group has five or 500 practitioners, you and your partners might be thinking about whether you want—or need—to enter into a merger or acquisition in the near future. For some hospitalist groups, mergers and acquisitions could be part of a growth strategy designed to increase geographic footprint, market penetration, or bargaining power. These types of transactions will allow larger groups to increase their competitiveness by being able to leverage investments in such items as information technology upgrades across a larger base of business.
For others, a desire to retire or an inability to either afford or justify certain capital investments needed to remain competitive might be leading some players to consider selling their hospitalist groups. Moreover, changes in the healthcare industry, coupled with the anticipation of tax increases, could factor into decisions to sell practices in the relatively near term.
While each transaction is unique, most tend to follow a similar process, incorporating a number of relatively standard phases that must be undertaken in order to complete a transaction. The transaction process typically takes between three and nine months, although preparations are often best begun in advance of the actual deal process.
Preliminary Matters
For hospitalist group owners and executives considering selling their practice, a number of preliminary matters should be addressed in preparation for a sale. First, potential sellers should carefully consider whether they really wish to enter into the sale process. The sale process is lengthy, time-consuming, and costly, and it is often stressful and demanding on the practice’s management. Thus, potential sellers should not undertake the process unless they are serious about selling and have a realistic expectation of what they will receive as the purchase price.
As part of the preparation, sellers should begin by assembling an experienced transaction team. Typically, the team includes key members of the practice’s management, as well as experienced healthcare mergers and acquisitions attorneys and accountants. These experienced professionals can be of great assistance in making sure that a transaction is executed on a timely basis and under terms appropriate for the specific transaction.
Another prudent step is undertaking a tax analysis to determine the implications of the sale on both the selling practice and its individual owners. This analysis should be performed as far in advance of a proposed transaction as possible, in order to allow time for adjustments to be made (if necessary) to limit the tax implications in advance of the sale. Sellers also will want to use this preparatory phase to make sure that the practice’s books and records are in good order in preparation for the buyer’s due diligence review, as well as to address any issues in order to make the practice more attractive to potential buyers. Some sellers might want to have an investment banker or other qualified professional provide a valuation appraisal of the practice to provide a realistic purchase price.
Finding a Buyer
As a seller begins the process to find a buyer, the seller must first consider the approach that it wants to take. Some larger groups are sold through auction-like processes in which a number of bidders are contacted and invited to participate. The advantage of this type of process is that it typically drives prices higher by introducing competition into the bidding process. On the other hand, this type of process has certain disadvantages, such as a longer time frame and increased risk of a breach of confidentiality.
For some sellers, a more targeted approach, with limited participants, might be more desirable. If a fair purchase price can be obtained without involving multiple potential buyers, the process can be completed faster and with less risk to the ongoing business operations.
The process of finding a buyer typically requires the seller to provide potential buyers with confidential information regarding the business so the interested parties can evaluate whether the selling group is even of interest and the amount that they will be willing to pay. However, the selling practice should only provide this confidential information after potential buyers have signed nondisclosure agreements.
Ultimately, the process will lead to the submission of specific proposals from interested parties. Typically, this results in the seller and the selected buyer entering into a letter of intent, a statement of key terms for the proposed transaction. Letters of intent are largely not binding and are subject to the satisfaction of conditions, such as the negotiation of definitive written agreements. Typically, in this phase of the process, the basic structure of the transaction, the purchase price, and the manner of payment are determined.
Due Diligence
In almost all sale transactions, the buyer will conduct a review and investigation of the seller’s business. The purpose of this review is to confirm the information previously provided by the seller and to allow the buyer to gain a thorough understanding of the business to determine whether it is truly willing to buy the business on the terms identified in the letter of intent. The buyer will want to confirm that it is not going to inherit any unexpected liabilities or problems, such as healthcare regulatory issues or lawsuits. To comply with the information requests from the buyer as it conducts its due diligence review, the seller will be required to assemble many documents and voluminous amounts of financial and other information. The burden of providing this information to the buyer will be substantial and could distract management from their day-to-day duties of running the practice.
Upon completion of the due diligence process, the buyer will either confirm that it is willing to move forward with the transaction “as is,” or, if the due diligence review reveals troubling information, the buyer can either demand changes to the transaction (such as a reduction of the purchase price) or be unwilling to proceed with the transaction altogether.
Negotiating Definitive Agreements
The parties will need to negotiate and agree on certain definitive written agreements, which will govern the transaction. First and foremost, this will include a purchase agreement, such as a stock purchase agreement or an asset purchase agreement. In addition, there may also be various ancillary agreements, such as noncompetition agreements between the buyer and the owners of the selling practice and new employment agreements for the sellers.
Typically, the negotiation of definitive agreements proceeds in parallel with the buyer’s due diligence review.
Closing
At the closing, both sides will sign numerous documents, including those necessary to transfer ownership of the purchased group to the buyer, as well as all ancillary agreements and other documents needed for the transaction. Once signatures have been obtained and exchanged between the parties, the transfer of title will occur and the buyer will tender the purchase price.
Post-Closing
Although the vast majority of the work associated with the transaction will terminate upon the completion of the closing, certain aspects of the sale will require some attention after the closing. For example, there may be purchase price adjustments based upon the final balance sheet or net working capital position of the seller’s business as of the closing date. Typically, these adjustments are addressed in the months following the closing. Also, if any indemnification claims are brought, the parties will need to address those claims and reach a resolution.
Merger and acquisition transactions are complex, time-consuming matters that require a great deal of effort on the part of all parties involved. An orderly process is essential for both buyers and sellers. Sellers will want to take steps to make sure that the transaction is completed in a timely manner while minimizing risk to the ongoing business operations. At the same time, buyers will want to make sure that the value that they are receiving from the seller’s business is commensurate with the purchase price and that the buyer’s goals for entering into the sale will truly be met post-closing.
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Clarifying the Role of Hospitalists Focused on Family Medicine in the ICU

Clarifying Family-Practice Hospitalists’ Value, Focused-Practice Opportunities
I am writing regarding the letter and your response in the January 2013 issue of The Hospitalist regarding hospitalists trained in family medicine and practice in critical-care units. I am the chair of the Family Medicine Committee for SHM, a practicing hospitalist, and an SHM member for over 10 years. There is an error in your reply, in that physicians who are board-certified through the American Board of Family Medicine (ABFM) are indeed eligible to take the examination for Recognition of Focused Practice in Hospital Medicine (RFPHM). This examination is administered by the American Board of Internal Medicine (ABIM), and is the same examination for all physicians, regardless of whether their residency was completed in family or internal medicine.
I am proud to be among the six family physicians who took and passed the first examination in October 2010. Through 2012, there have been 28 family physicians who have passed this exam, and attained RFPHM (verbal communication from ABFM). According to the ABIM website, there have been 267 total physicians who have taken the examination through 2011, which includes family-medicine-trained physicians. There are a number of Maintenance of Certification (MOC) modules offered through the ABIM that are available to hospitalists trained in family medicine.
A prior study showed that 66% of hospitalists trained in family medicine practice in critical-care units (McElrath et al). You are correct that there is no current pathway for HTFM to pursue a critical-care fellowship or attain board certification by the SCCM, as diplomats of the ABFM are excluded. However, there are many hospitalists trained in family medicine providing excellent care to patients in critical-care units. There are clearly not enough board certified intensivists to provide the care.
—Kevin Ahern, MD, SFHM, chief hospitalist, Sound Physicians, Urbana, Ohio
Dr. Hospitalist responds:
You are absolutely correct in your point of clarification regarding the Recognition of Focused Practice in Hospital Medicine from the ABFM. I was aware of this at the time of the article; however, in my efforts to outline the proposed path from RFPHM to ICU certification, I focused solely on the ABIM pathway without mentioning the additional recognition available to family-practice physicians. In no way was this meant to denigrate the efforts or contributions of family-practice physicians to HM and SHM, but I could have been much more clear on this point. Having hired and worked alongside family-practice hospitalists, I know just how valuable you are.
The overall picture is consistent with what you described in that there are “clearly not enough board-certified intensivists” to fully staff ICUs. However, it is evident that it will be an uphill battle to sanction an alternate pathway that lets any hospitalist gain certification as an ICU physician. Truth be told, there are fundamental differences in the amount of ICU exposure between internal-medicine and family-practice training programs. As a result, in the current proposal there is no overt discussion of the role for family-practice hospitalists in the ICU. I think that this will continue to remain a conscious omission for both political and practical reasons.
Clarifying Family-Practice Hospitalists’ Value, Focused-Practice Opportunities
I am writing regarding the letter and your response in the January 2013 issue of The Hospitalist regarding hospitalists trained in family medicine and practice in critical-care units. I am the chair of the Family Medicine Committee for SHM, a practicing hospitalist, and an SHM member for over 10 years. There is an error in your reply, in that physicians who are board-certified through the American Board of Family Medicine (ABFM) are indeed eligible to take the examination for Recognition of Focused Practice in Hospital Medicine (RFPHM). This examination is administered by the American Board of Internal Medicine (ABIM), and is the same examination for all physicians, regardless of whether their residency was completed in family or internal medicine.
I am proud to be among the six family physicians who took and passed the first examination in October 2010. Through 2012, there have been 28 family physicians who have passed this exam, and attained RFPHM (verbal communication from ABFM). According to the ABIM website, there have been 267 total physicians who have taken the examination through 2011, which includes family-medicine-trained physicians. There are a number of Maintenance of Certification (MOC) modules offered through the ABIM that are available to hospitalists trained in family medicine.
A prior study showed that 66% of hospitalists trained in family medicine practice in critical-care units (McElrath et al). You are correct that there is no current pathway for HTFM to pursue a critical-care fellowship or attain board certification by the SCCM, as diplomats of the ABFM are excluded. However, there are many hospitalists trained in family medicine providing excellent care to patients in critical-care units. There are clearly not enough board certified intensivists to provide the care.
—Kevin Ahern, MD, SFHM, chief hospitalist, Sound Physicians, Urbana, Ohio
Dr. Hospitalist responds:
You are absolutely correct in your point of clarification regarding the Recognition of Focused Practice in Hospital Medicine from the ABFM. I was aware of this at the time of the article; however, in my efforts to outline the proposed path from RFPHM to ICU certification, I focused solely on the ABIM pathway without mentioning the additional recognition available to family-practice physicians. In no way was this meant to denigrate the efforts or contributions of family-practice physicians to HM and SHM, but I could have been much more clear on this point. Having hired and worked alongside family-practice hospitalists, I know just how valuable you are.
The overall picture is consistent with what you described in that there are “clearly not enough board-certified intensivists” to fully staff ICUs. However, it is evident that it will be an uphill battle to sanction an alternate pathway that lets any hospitalist gain certification as an ICU physician. Truth be told, there are fundamental differences in the amount of ICU exposure between internal-medicine and family-practice training programs. As a result, in the current proposal there is no overt discussion of the role for family-practice hospitalists in the ICU. I think that this will continue to remain a conscious omission for both political and practical reasons.
Clarifying Family-Practice Hospitalists’ Value, Focused-Practice Opportunities
I am writing regarding the letter and your response in the January 2013 issue of The Hospitalist regarding hospitalists trained in family medicine and practice in critical-care units. I am the chair of the Family Medicine Committee for SHM, a practicing hospitalist, and an SHM member for over 10 years. There is an error in your reply, in that physicians who are board-certified through the American Board of Family Medicine (ABFM) are indeed eligible to take the examination for Recognition of Focused Practice in Hospital Medicine (RFPHM). This examination is administered by the American Board of Internal Medicine (ABIM), and is the same examination for all physicians, regardless of whether their residency was completed in family or internal medicine.
I am proud to be among the six family physicians who took and passed the first examination in October 2010. Through 2012, there have been 28 family physicians who have passed this exam, and attained RFPHM (verbal communication from ABFM). According to the ABIM website, there have been 267 total physicians who have taken the examination through 2011, which includes family-medicine-trained physicians. There are a number of Maintenance of Certification (MOC) modules offered through the ABIM that are available to hospitalists trained in family medicine.
A prior study showed that 66% of hospitalists trained in family medicine practice in critical-care units (McElrath et al). You are correct that there is no current pathway for HTFM to pursue a critical-care fellowship or attain board certification by the SCCM, as diplomats of the ABFM are excluded. However, there are many hospitalists trained in family medicine providing excellent care to patients in critical-care units. There are clearly not enough board certified intensivists to provide the care.
—Kevin Ahern, MD, SFHM, chief hospitalist, Sound Physicians, Urbana, Ohio
Dr. Hospitalist responds:
You are absolutely correct in your point of clarification regarding the Recognition of Focused Practice in Hospital Medicine from the ABFM. I was aware of this at the time of the article; however, in my efforts to outline the proposed path from RFPHM to ICU certification, I focused solely on the ABIM pathway without mentioning the additional recognition available to family-practice physicians. In no way was this meant to denigrate the efforts or contributions of family-practice physicians to HM and SHM, but I could have been much more clear on this point. Having hired and worked alongside family-practice hospitalists, I know just how valuable you are.
The overall picture is consistent with what you described in that there are “clearly not enough board-certified intensivists” to fully staff ICUs. However, it is evident that it will be an uphill battle to sanction an alternate pathway that lets any hospitalist gain certification as an ICU physician. Truth be told, there are fundamental differences in the amount of ICU exposure between internal-medicine and family-practice training programs. As a result, in the current proposal there is no overt discussion of the role for family-practice hospitalists in the ICU. I think that this will continue to remain a conscious omission for both political and practical reasons.
Record Number of Physicians Pass Hospice and Palliative Medicine Exam
Number of physicians who passed for the first time the most recent Hospice and Palliative Medicine (HPM) board-certifying exam given in October by the American Board of Internal Medicine (ABIM). This number, an 83% success rate, represents a major influx of mid-career physicians qualifying in HPM just ahead of the closure of an experiential pathway to HPM board certification. Starting in 2013, physicians must complete a full-time, yearlong fellowship in HPM in order to sit for its board exam. ABIM and nine other specialty societies are responsible for HPM board certification. The last experiential pathway exam for HPM, in osteopathy, will be in September.
Number of physicians who passed for the first time the most recent Hospice and Palliative Medicine (HPM) board-certifying exam given in October by the American Board of Internal Medicine (ABIM). This number, an 83% success rate, represents a major influx of mid-career physicians qualifying in HPM just ahead of the closure of an experiential pathway to HPM board certification. Starting in 2013, physicians must complete a full-time, yearlong fellowship in HPM in order to sit for its board exam. ABIM and nine other specialty societies are responsible for HPM board certification. The last experiential pathway exam for HPM, in osteopathy, will be in September.
Number of physicians who passed for the first time the most recent Hospice and Palliative Medicine (HPM) board-certifying exam given in October by the American Board of Internal Medicine (ABIM). This number, an 83% success rate, represents a major influx of mid-career physicians qualifying in HPM just ahead of the closure of an experiential pathway to HPM board certification. Starting in 2013, physicians must complete a full-time, yearlong fellowship in HPM in order to sit for its board exam. ABIM and nine other specialty societies are responsible for HPM board certification. The last experiential pathway exam for HPM, in osteopathy, will be in September.
VIDEO: Five Reasons You Should Attend Hospital Medicine 2013 in Washington, D.C.
Clinical Guidelines Updated for Surviving Sepsis in Hospitals
The Surviving Sepsis Campaign (www.survivingsepsis.org) has updated its best clinical practices for patients with severe sepsis or septic shock.6 Sixty-eight international experts worked to update the campaign’s 2008 guidelines. For example, the update includes a strong recommendation for the use of crystalloids (e.g. normal saline) as the initial fluid resuscitation for patients with severe sepsis.
The campaign, a collaboration of the Society of Critical Care Medicine and the European Society of Intensive Care Medicine, estimates 400,000 lives could be saved per year worldwide if 10,000 hospitals were committed to its recommendations and if even half of eligible patients were treated in conformance with the campaign’s quality bundles. The campaign also tries to develop strategies for improving the care of septic patients in settings where healthcare resources are limited.
Larry Beresford is a freelance writer in Oakland, Calif.
Reference
The Surviving Sepsis Campaign (www.survivingsepsis.org) has updated its best clinical practices for patients with severe sepsis or septic shock.6 Sixty-eight international experts worked to update the campaign’s 2008 guidelines. For example, the update includes a strong recommendation for the use of crystalloids (e.g. normal saline) as the initial fluid resuscitation for patients with severe sepsis.
The campaign, a collaboration of the Society of Critical Care Medicine and the European Society of Intensive Care Medicine, estimates 400,000 lives could be saved per year worldwide if 10,000 hospitals were committed to its recommendations and if even half of eligible patients were treated in conformance with the campaign’s quality bundles. The campaign also tries to develop strategies for improving the care of septic patients in settings where healthcare resources are limited.
Larry Beresford is a freelance writer in Oakland, Calif.
Reference
The Surviving Sepsis Campaign (www.survivingsepsis.org) has updated its best clinical practices for patients with severe sepsis or septic shock.6 Sixty-eight international experts worked to update the campaign’s 2008 guidelines. For example, the update includes a strong recommendation for the use of crystalloids (e.g. normal saline) as the initial fluid resuscitation for patients with severe sepsis.
The campaign, a collaboration of the Society of Critical Care Medicine and the European Society of Intensive Care Medicine, estimates 400,000 lives could be saved per year worldwide if 10,000 hospitals were committed to its recommendations and if even half of eligible patients were treated in conformance with the campaign’s quality bundles. The campaign also tries to develop strategies for improving the care of septic patients in settings where healthcare resources are limited.
Larry Beresford is a freelance writer in Oakland, Calif.
Reference
Robotic Vaporizers Reduce Hospital Bacterial Infections
Paired, robotlike devices that disperse a bleaching disinfectant into the air of hospital rooms, then detoxify the disinfecting chemical, were found to be highly effective at killing and preventing the spread of “superbug” bacteria, according to research from Johns Hopkins Hospital published in Clinical Infectious Diseases.5 Hydrogen peroxide vaporizers were first deployed in Singapore hospitals in 2002 during an outbreak of severe acute respiratory syndrome (SARS).
Almost half of a study group of 6,350 patients in and out of 180 hospital rooms over a two-and-a-half-year period received the enhanced cleaning technology, while the others received routine cleaning only. Manufactured by Bioquell Inc. of Horsham, Pa. (www.bioquell.com), each device is about the size of a washing machine. They were deployed in hospital rooms with sealed vents, dispersing a thin film of hydrogen peroxide across all exposed surfaces, equipment, floors, and walls. This approach reduced by 64% the number of patients who later became contaminated with any of the most common drug-resistant organisms, including methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci, Clostridium difficile, and Acinetobacter baumannii.
Spreading the bleaching vapor this way “represents a major technological advance in preventing the spread of dangerous bacteria inside hospital rooms,” says senior investigator Trish Perl, MD, MSc, professor of medicine and an infectious disease specialist at Johns Hopkins. The hospital announced in December that it would begin decontaminating isolation rooms with these devices as standard practice starting in January.
Reference
Paired, robotlike devices that disperse a bleaching disinfectant into the air of hospital rooms, then detoxify the disinfecting chemical, were found to be highly effective at killing and preventing the spread of “superbug” bacteria, according to research from Johns Hopkins Hospital published in Clinical Infectious Diseases.5 Hydrogen peroxide vaporizers were first deployed in Singapore hospitals in 2002 during an outbreak of severe acute respiratory syndrome (SARS).
Almost half of a study group of 6,350 patients in and out of 180 hospital rooms over a two-and-a-half-year period received the enhanced cleaning technology, while the others received routine cleaning only. Manufactured by Bioquell Inc. of Horsham, Pa. (www.bioquell.com), each device is about the size of a washing machine. They were deployed in hospital rooms with sealed vents, dispersing a thin film of hydrogen peroxide across all exposed surfaces, equipment, floors, and walls. This approach reduced by 64% the number of patients who later became contaminated with any of the most common drug-resistant organisms, including methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci, Clostridium difficile, and Acinetobacter baumannii.
Spreading the bleaching vapor this way “represents a major technological advance in preventing the spread of dangerous bacteria inside hospital rooms,” says senior investigator Trish Perl, MD, MSc, professor of medicine and an infectious disease specialist at Johns Hopkins. The hospital announced in December that it would begin decontaminating isolation rooms with these devices as standard practice starting in January.
Reference
Paired, robotlike devices that disperse a bleaching disinfectant into the air of hospital rooms, then detoxify the disinfecting chemical, were found to be highly effective at killing and preventing the spread of “superbug” bacteria, according to research from Johns Hopkins Hospital published in Clinical Infectious Diseases.5 Hydrogen peroxide vaporizers were first deployed in Singapore hospitals in 2002 during an outbreak of severe acute respiratory syndrome (SARS).
Almost half of a study group of 6,350 patients in and out of 180 hospital rooms over a two-and-a-half-year period received the enhanced cleaning technology, while the others received routine cleaning only. Manufactured by Bioquell Inc. of Horsham, Pa. (www.bioquell.com), each device is about the size of a washing machine. They were deployed in hospital rooms with sealed vents, dispersing a thin film of hydrogen peroxide across all exposed surfaces, equipment, floors, and walls. This approach reduced by 64% the number of patients who later became contaminated with any of the most common drug-resistant organisms, including methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci, Clostridium difficile, and Acinetobacter baumannii.
Spreading the bleaching vapor this way “represents a major technological advance in preventing the spread of dangerous bacteria inside hospital rooms,” says senior investigator Trish Perl, MD, MSc, professor of medicine and an infectious disease specialist at Johns Hopkins. The hospital announced in December that it would begin decontaminating isolation rooms with these devices as standard practice starting in January.
Reference
Digital Diagnostic Tools Unpopular with Patients, Study Finds
A recent study from the University of Missouri to explore how patients react to physicians’ use of computerized clinical decision support systems finds that these devices could leave patients feeling ignored and dissatisfied with their medical care, potentially increasing noncompliance with treatment while distracting physicians from the patient encounter.1
“Patients may be concerned that the decision aids reduce their face-to-face time with physicians,” says lead author Victoria Shaffer, PhD, assistant professor of health and psychological sciences at the University of Missouri. She recommends incorporating computerized systems as teaching tools to engage patients and help them understand their diagnoses and recommendations. “Anything physicians or nurses can do to humanize the process may make patients more comfortable,” she says.
The study presented participants with written descriptions of hypothetical physician-patient encounters, with the physician using unaided judgment, pursuing advice from a medical expert, or using computerized clinical decision support. Physicians using the latter were viewed as less capable, but participants also were less likely to assign those physicians responsibility for negative outcomes.
A concurrent study from Missouri, part of a $14 million project funded by the Centers for Medicare & Medicaid Services (CMS) to reduce avoidable rehospitalizations of nursing home residents, suggests that sophisticated information technology (IT) can lead to more robust and integrated communication strategies among clinical staff, as well as better-coordinated care.2 Nursing informatics expert Gregory Alexander found that nursing homes with IT used it to help make clinical decisions, electronically track patient care, and securely relay medical information.
References
- Shaffer VA, Probst CA, Merkle EC, Arkes HR, Mitchell AM. Why do patients derogate physicians who use a computer-based diagnostic support system? Med Decis Making. 2013;33(1):108-118.
- Alexander GL, Steege LM, Pasupathy KS, Wise K. Case studies of IT sophistication in nursing homes: a mixed method approach to examine communication strategies about pressure ulcer prevention practices. SciVerse website. Available at: http://www.sciencedirect.com/science/article/pii/S0169814112001229. Accessed March 10, 2013.
A recent study from the University of Missouri to explore how patients react to physicians’ use of computerized clinical decision support systems finds that these devices could leave patients feeling ignored and dissatisfied with their medical care, potentially increasing noncompliance with treatment while distracting physicians from the patient encounter.1
“Patients may be concerned that the decision aids reduce their face-to-face time with physicians,” says lead author Victoria Shaffer, PhD, assistant professor of health and psychological sciences at the University of Missouri. She recommends incorporating computerized systems as teaching tools to engage patients and help them understand their diagnoses and recommendations. “Anything physicians or nurses can do to humanize the process may make patients more comfortable,” she says.
The study presented participants with written descriptions of hypothetical physician-patient encounters, with the physician using unaided judgment, pursuing advice from a medical expert, or using computerized clinical decision support. Physicians using the latter were viewed as less capable, but participants also were less likely to assign those physicians responsibility for negative outcomes.
A concurrent study from Missouri, part of a $14 million project funded by the Centers for Medicare & Medicaid Services (CMS) to reduce avoidable rehospitalizations of nursing home residents, suggests that sophisticated information technology (IT) can lead to more robust and integrated communication strategies among clinical staff, as well as better-coordinated care.2 Nursing informatics expert Gregory Alexander found that nursing homes with IT used it to help make clinical decisions, electronically track patient care, and securely relay medical information.
References
- Shaffer VA, Probst CA, Merkle EC, Arkes HR, Mitchell AM. Why do patients derogate physicians who use a computer-based diagnostic support system? Med Decis Making. 2013;33(1):108-118.
- Alexander GL, Steege LM, Pasupathy KS, Wise K. Case studies of IT sophistication in nursing homes: a mixed method approach to examine communication strategies about pressure ulcer prevention practices. SciVerse website. Available at: http://www.sciencedirect.com/science/article/pii/S0169814112001229. Accessed March 10, 2013.
A recent study from the University of Missouri to explore how patients react to physicians’ use of computerized clinical decision support systems finds that these devices could leave patients feeling ignored and dissatisfied with their medical care, potentially increasing noncompliance with treatment while distracting physicians from the patient encounter.1
“Patients may be concerned that the decision aids reduce their face-to-face time with physicians,” says lead author Victoria Shaffer, PhD, assistant professor of health and psychological sciences at the University of Missouri. She recommends incorporating computerized systems as teaching tools to engage patients and help them understand their diagnoses and recommendations. “Anything physicians or nurses can do to humanize the process may make patients more comfortable,” she says.
The study presented participants with written descriptions of hypothetical physician-patient encounters, with the physician using unaided judgment, pursuing advice from a medical expert, or using computerized clinical decision support. Physicians using the latter were viewed as less capable, but participants also were less likely to assign those physicians responsibility for negative outcomes.
A concurrent study from Missouri, part of a $14 million project funded by the Centers for Medicare & Medicaid Services (CMS) to reduce avoidable rehospitalizations of nursing home residents, suggests that sophisticated information technology (IT) can lead to more robust and integrated communication strategies among clinical staff, as well as better-coordinated care.2 Nursing informatics expert Gregory Alexander found that nursing homes with IT used it to help make clinical decisions, electronically track patient care, and securely relay medical information.
References
- Shaffer VA, Probst CA, Merkle EC, Arkes HR, Mitchell AM. Why do patients derogate physicians who use a computer-based diagnostic support system? Med Decis Making. 2013;33(1):108-118.
- Alexander GL, Steege LM, Pasupathy KS, Wise K. Case studies of IT sophistication in nursing homes: a mixed method approach to examine communication strategies about pressure ulcer prevention practices. SciVerse website. Available at: http://www.sciencedirect.com/science/article/pii/S0169814112001229. Accessed March 10, 2013.
National Medicare Readmissions Study Identifies Little Progress
A new Dartmouth Atlas Project study of Medicare 30-day hospital readmissions found that rates essentially stayed the same (15.9% for medical discharges) between 2008 and 2010. But readmission rates varied widely across regions, with medical discharges at 18.1% in Bronx, N.Y., versus 11.4% in Ogden, Utah.
The report, The Revolving Door: A Report on U.S. Hospital Readmissions, also incorporates results from in-depth interviews with patients and providers.1 It sheds light on why so many patients (1 in 6 medical and 1 in 8 surgical discharges) end up back in the hospital so soon—and what hospitals, physicians, nurses, and others are doing to limit avoidable readmissions.
An online interactive map (available at www.rwjf.org) displays the Dartmouth data on 30-day readmissions by hospital referral region.
The research was supported and publicized by the Robert Wood Johnson Foundation of Princeton, N.J., which has a number of other efforts under way to address readmissions. Another recent study supported by the foundation’s Nurse Faculty Scholars Program found that increased nurse-to-patient staffing ratios and good working environments for nurses were associated with significantly reduced 30-day readmissions.2
The foundation recently named the five winners of its “Transitions to Better Care” video contest, in which hospitals and health systems submitted short films to highlight innovative local practices to improve care transitions before, during, and after discharge. Check out the winning videos by searching “contest” at rwjf.org.
References
- The Dartmouth Atlas of Health Care. The Revolving Door: A Report on U.S. Hospital Readmissions. The Dartmouth Atlas of Health Care website. Available at: http://www.dartmouthatlas.org/pages/readmissions2013. Accessed March 10, 2013.
- McHugh M, Ma C. Hospital nursing and 30-day readmissions among Medicare patients with heart failure, acute myocardial infarction, and pneumonia. Med Care. 2013;51(1):52-59.
A new Dartmouth Atlas Project study of Medicare 30-day hospital readmissions found that rates essentially stayed the same (15.9% for medical discharges) between 2008 and 2010. But readmission rates varied widely across regions, with medical discharges at 18.1% in Bronx, N.Y., versus 11.4% in Ogden, Utah.
The report, The Revolving Door: A Report on U.S. Hospital Readmissions, also incorporates results from in-depth interviews with patients and providers.1 It sheds light on why so many patients (1 in 6 medical and 1 in 8 surgical discharges) end up back in the hospital so soon—and what hospitals, physicians, nurses, and others are doing to limit avoidable readmissions.
An online interactive map (available at www.rwjf.org) displays the Dartmouth data on 30-day readmissions by hospital referral region.
The research was supported and publicized by the Robert Wood Johnson Foundation of Princeton, N.J., which has a number of other efforts under way to address readmissions. Another recent study supported by the foundation’s Nurse Faculty Scholars Program found that increased nurse-to-patient staffing ratios and good working environments for nurses were associated with significantly reduced 30-day readmissions.2
The foundation recently named the five winners of its “Transitions to Better Care” video contest, in which hospitals and health systems submitted short films to highlight innovative local practices to improve care transitions before, during, and after discharge. Check out the winning videos by searching “contest” at rwjf.org.
References
- The Dartmouth Atlas of Health Care. The Revolving Door: A Report on U.S. Hospital Readmissions. The Dartmouth Atlas of Health Care website. Available at: http://www.dartmouthatlas.org/pages/readmissions2013. Accessed March 10, 2013.
- McHugh M, Ma C. Hospital nursing and 30-day readmissions among Medicare patients with heart failure, acute myocardial infarction, and pneumonia. Med Care. 2013;51(1):52-59.
A new Dartmouth Atlas Project study of Medicare 30-day hospital readmissions found that rates essentially stayed the same (15.9% for medical discharges) between 2008 and 2010. But readmission rates varied widely across regions, with medical discharges at 18.1% in Bronx, N.Y., versus 11.4% in Ogden, Utah.
The report, The Revolving Door: A Report on U.S. Hospital Readmissions, also incorporates results from in-depth interviews with patients and providers.1 It sheds light on why so many patients (1 in 6 medical and 1 in 8 surgical discharges) end up back in the hospital so soon—and what hospitals, physicians, nurses, and others are doing to limit avoidable readmissions.
An online interactive map (available at www.rwjf.org) displays the Dartmouth data on 30-day readmissions by hospital referral region.
The research was supported and publicized by the Robert Wood Johnson Foundation of Princeton, N.J., which has a number of other efforts under way to address readmissions. Another recent study supported by the foundation’s Nurse Faculty Scholars Program found that increased nurse-to-patient staffing ratios and good working environments for nurses were associated with significantly reduced 30-day readmissions.2
The foundation recently named the five winners of its “Transitions to Better Care” video contest, in which hospitals and health systems submitted short films to highlight innovative local practices to improve care transitions before, during, and after discharge. Check out the winning videos by searching “contest” at rwjf.org.
References
- The Dartmouth Atlas of Health Care. The Revolving Door: A Report on U.S. Hospital Readmissions. The Dartmouth Atlas of Health Care website. Available at: http://www.dartmouthatlas.org/pages/readmissions2013. Accessed March 10, 2013.
- McHugh M, Ma C. Hospital nursing and 30-day readmissions among Medicare patients with heart failure, acute myocardial infarction, and pneumonia. Med Care. 2013;51(1):52-59.