User login
ONLINE EXCLUSIVE: HM is a perfect fit for a palliative care service
John Harney, COO at University of Colorado Hospital, moved west in 2008 after working at New York University Hospitals Center. The East Coast hospital had used a grant to establish a palliative-care program and witnessed immediate results.
“We truly believed it resulted in reductions in length of stay, as well as humanistic benefits,” Harney says. “When I came out to Colorado, I was pleasantly surprised at the breadth and depth of the programs here.”
Harney says he believes HM is a logical place to advance palliative care to the next level, as most HM groups already possess an in-house presence and commitment to efficient throughput. Hospital administrators will be concerned with consistency, routines, and protocols, he says, as well as the palliative-care service’s commitment to quality improvement. Those same administrators appreciate the need for program and salary support, although he advises palliative-care advocates to do their homework and develop a viable business plan.
“Hospital administrators will quickly figure out the math,” Harney says. “If you’re coming to speak to us, you need to have your numbers in order. You also need some monitoring in place.”
The initial salvo should include confirmation that HM group leaders have done their homework: surveyed their HM staff and discussed the idea with oncologists and other specialists. “It’s also helpful to have real champions in nursing and social work,” Harney says. “It’s never easy to get financial support for a new program, but if you have those ducks lined up, it goes better.”
John Harney, COO at University of Colorado Hospital, moved west in 2008 after working at New York University Hospitals Center. The East Coast hospital had used a grant to establish a palliative-care program and witnessed immediate results.
“We truly believed it resulted in reductions in length of stay, as well as humanistic benefits,” Harney says. “When I came out to Colorado, I was pleasantly surprised at the breadth and depth of the programs here.”
Harney says he believes HM is a logical place to advance palliative care to the next level, as most HM groups already possess an in-house presence and commitment to efficient throughput. Hospital administrators will be concerned with consistency, routines, and protocols, he says, as well as the palliative-care service’s commitment to quality improvement. Those same administrators appreciate the need for program and salary support, although he advises palliative-care advocates to do their homework and develop a viable business plan.
“Hospital administrators will quickly figure out the math,” Harney says. “If you’re coming to speak to us, you need to have your numbers in order. You also need some monitoring in place.”
The initial salvo should include confirmation that HM group leaders have done their homework: surveyed their HM staff and discussed the idea with oncologists and other specialists. “It’s also helpful to have real champions in nursing and social work,” Harney says. “It’s never easy to get financial support for a new program, but if you have those ducks lined up, it goes better.”
John Harney, COO at University of Colorado Hospital, moved west in 2008 after working at New York University Hospitals Center. The East Coast hospital had used a grant to establish a palliative-care program and witnessed immediate results.
“We truly believed it resulted in reductions in length of stay, as well as humanistic benefits,” Harney says. “When I came out to Colorado, I was pleasantly surprised at the breadth and depth of the programs here.”
Harney says he believes HM is a logical place to advance palliative care to the next level, as most HM groups already possess an in-house presence and commitment to efficient throughput. Hospital administrators will be concerned with consistency, routines, and protocols, he says, as well as the palliative-care service’s commitment to quality improvement. Those same administrators appreciate the need for program and salary support, although he advises palliative-care advocates to do their homework and develop a viable business plan.
“Hospital administrators will quickly figure out the math,” Harney says. “If you’re coming to speak to us, you need to have your numbers in order. You also need some monitoring in place.”
The initial salvo should include confirmation that HM group leaders have done their homework: surveyed their HM staff and discussed the idea with oncologists and other specialists. “It’s also helpful to have real champions in nursing and social work,” Harney says. “It’s never easy to get financial support for a new program, but if you have those ducks lined up, it goes better.”
ONLINE EXCLUSIVE: Early-Career Hospitalists Spark Growth in On-Site Night Coverage
They have grown up in an era of reality television and hyperbolic politics. They prefer news alerts and fantasy football on their handhelds to daily newspapers and leather-bound novels. They text, they text, they text.
The generation known as millennials—those who were born in the years 1982 to 1995—is a breed unto itself. Millennials have grown up in the information age, are adept with new technologies, and have been trained under the umbrella of duty-hour guidelines that protect both the patient and the physician.
So when you hire a millennial for your hospitalist group, you’d better be clear about your expectations. “Millennials are looking for jobs that provide flexibility—time with family, time with friends, time to do other things,” says Troy Ahlstrom, MD, FHM, CFO of Traverse City-based Hospitalists of Northern Michigan and a member of SHM’s Practice Analysis committee. “There is nothing wrong with that, except that the baby boomers look at millennials and say, ‘Gosh, you slugs don’t want to work.’ ”
Dr. Ahlstrom says the influx of millennials into HM in recent years has had a significant impact on group administration—namely, an increase in use of 24/7 on-site coverage. The State of Hospital Medicine: 2010 Report Based on 2009 Data shows 68% of hospitalist groups provide on-site coverage at night. SHM’s 2007-2008 survey data showed only 53% of HM groups provided on-site coverage at night; the 2005-2006 figure was 51%. (Although the 2010 report includes a small percentage of truly academic hospitalist groups and, therefore, probably pushes the on-site coverage a little higher than in past years, Dr. Ahlstrom says he expects the trend toward on-site coverage at night to continue in the near future.)
“Baby boomers are perfectly fine with the idea of working more. They grew up working those horrifically long shifts, 36 hours straight,” Dr. Ahlstrom says. “The millennials would rather have clearly defined shifts, with nocturnists around to work the nights. Or maybe they get to be the nocturnist and work the nights. That’s the trend with younger physicians: They are more interested in seeing that split, where the days and nights are clearly set off.”
Then again, not all physicians, young or old, are against the idea of working long hours. And plenty of well-seasoned physicians are more than happy to have a nocturnist around, “but not if it’s going to cost them a lot of money or productivity,” Dr. Ahlstrom says.
They have grown up in an era of reality television and hyperbolic politics. They prefer news alerts and fantasy football on their handhelds to daily newspapers and leather-bound novels. They text, they text, they text.
The generation known as millennials—those who were born in the years 1982 to 1995—is a breed unto itself. Millennials have grown up in the information age, are adept with new technologies, and have been trained under the umbrella of duty-hour guidelines that protect both the patient and the physician.
So when you hire a millennial for your hospitalist group, you’d better be clear about your expectations. “Millennials are looking for jobs that provide flexibility—time with family, time with friends, time to do other things,” says Troy Ahlstrom, MD, FHM, CFO of Traverse City-based Hospitalists of Northern Michigan and a member of SHM’s Practice Analysis committee. “There is nothing wrong with that, except that the baby boomers look at millennials and say, ‘Gosh, you slugs don’t want to work.’ ”
Dr. Ahlstrom says the influx of millennials into HM in recent years has had a significant impact on group administration—namely, an increase in use of 24/7 on-site coverage. The State of Hospital Medicine: 2010 Report Based on 2009 Data shows 68% of hospitalist groups provide on-site coverage at night. SHM’s 2007-2008 survey data showed only 53% of HM groups provided on-site coverage at night; the 2005-2006 figure was 51%. (Although the 2010 report includes a small percentage of truly academic hospitalist groups and, therefore, probably pushes the on-site coverage a little higher than in past years, Dr. Ahlstrom says he expects the trend toward on-site coverage at night to continue in the near future.)
“Baby boomers are perfectly fine with the idea of working more. They grew up working those horrifically long shifts, 36 hours straight,” Dr. Ahlstrom says. “The millennials would rather have clearly defined shifts, with nocturnists around to work the nights. Or maybe they get to be the nocturnist and work the nights. That’s the trend with younger physicians: They are more interested in seeing that split, where the days and nights are clearly set off.”
Then again, not all physicians, young or old, are against the idea of working long hours. And plenty of well-seasoned physicians are more than happy to have a nocturnist around, “but not if it’s going to cost them a lot of money or productivity,” Dr. Ahlstrom says.
They have grown up in an era of reality television and hyperbolic politics. They prefer news alerts and fantasy football on their handhelds to daily newspapers and leather-bound novels. They text, they text, they text.
The generation known as millennials—those who were born in the years 1982 to 1995—is a breed unto itself. Millennials have grown up in the information age, are adept with new technologies, and have been trained under the umbrella of duty-hour guidelines that protect both the patient and the physician.
So when you hire a millennial for your hospitalist group, you’d better be clear about your expectations. “Millennials are looking for jobs that provide flexibility—time with family, time with friends, time to do other things,” says Troy Ahlstrom, MD, FHM, CFO of Traverse City-based Hospitalists of Northern Michigan and a member of SHM’s Practice Analysis committee. “There is nothing wrong with that, except that the baby boomers look at millennials and say, ‘Gosh, you slugs don’t want to work.’ ”
Dr. Ahlstrom says the influx of millennials into HM in recent years has had a significant impact on group administration—namely, an increase in use of 24/7 on-site coverage. The State of Hospital Medicine: 2010 Report Based on 2009 Data shows 68% of hospitalist groups provide on-site coverage at night. SHM’s 2007-2008 survey data showed only 53% of HM groups provided on-site coverage at night; the 2005-2006 figure was 51%. (Although the 2010 report includes a small percentage of truly academic hospitalist groups and, therefore, probably pushes the on-site coverage a little higher than in past years, Dr. Ahlstrom says he expects the trend toward on-site coverage at night to continue in the near future.)
“Baby boomers are perfectly fine with the idea of working more. They grew up working those horrifically long shifts, 36 hours straight,” Dr. Ahlstrom says. “The millennials would rather have clearly defined shifts, with nocturnists around to work the nights. Or maybe they get to be the nocturnist and work the nights. That’s the trend with younger physicians: They are more interested in seeing that split, where the days and nights are clearly set off.”
Then again, not all physicians, young or old, are against the idea of working long hours. And plenty of well-seasoned physicians are more than happy to have a nocturnist around, “but not if it’s going to cost them a lot of money or productivity,” Dr. Ahlstrom says.
ONLINE EXCLUSIVE: Audio interview with MGMA systems analyst David Litzau
MGMA analyst David Litzau discusses the new compensation and productivity report, and gives advice on how best to use benchmarking data in your practice
MGMA analyst David Litzau discusses the new compensation and productivity report, and gives advice on how best to use benchmarking data in your practice
MGMA analyst David Litzau discusses the new compensation and productivity report, and gives advice on how best to use benchmarking data in your practice
Medical Tourism
David Dupray, a 60-year-old uninsured coffee shop owner from Bar Harbor, Maine, had been having left leg pain on ambulation for four years. His cardiologist recommended stent placement for left iliac artery stenosis. The estimated bill: approximately $35,000.
Unable to afford the procedure, Dupray began searching the Web for affordable medical care overseas. His physician suggested Thailand. Within days, Dupray had an appointment with a cardiologist halfway around the world—at Bumrungrad Hospital in Bangkok, Thailand. Dupray spent two days in the hotel-like hospital, had three stents placed in his leg arteries, and completed a cardiac stress test. The total bill: $18,000.
“I will never go to a hospital in the U.S.,” says Dupray, who represents a growing number of Americans searching for affordable healthcare in the global marketplace.
With rising U.S. healthcare costs and millions of Americans uninsured or underinsured, more American patients are seeking affordable, high-quality medical care abroad—known as “medical tourism.” In 2007, an estimated 750,000 Americans traveled abroad for medical care; the number is expected to increase to 6 million by the end of this year.1 On the flip side, only a little more than 400,000 nonresidents visited the U.S. in 2008 for the latest medical care.1 Globally, the medical tourism industry is estimated to grow into a $21 billion-a-year industry by 2012, with much of the growth expected from Western patients traveling overseas for affordable care.2
“As hospitalists, we have been seeing increasing numbers of patients going overseas for urgent and elective procedures, as it is a general perception the medical treatment overseas is less expensive,” says Joseph Ming Wah Li, MD, SFHM, director of hospital medicine at Beth Israel Deaconess Medical Center in Boston and SHM president-elect.
Physicians in U.S. hospitals encounter potential medical tourists all the time. Some are uninsured or underinsured. Some have insurance carriers that limit or exclude coverage for certain procedures and treatments. Even those with insurance sometimes struggle to pay deductibles, copays, and their costs after insurance has paid its part. Others are uncomfortable with the language barriers and cultural differences of U.S. hospitals and physicians.
Medical tourism also lures patients who are citizens of countries (e.g. Canada, the United Kingdom) that offer universal healthcare, Dr. Li says.3 For example, more expatriates from India and Malaysia are traveling to their native countries for medical care, as they receive affordable and quicker medical care while visiting family.
Hospitalists routinely care for patients requiring essential cardiac or orthopedic surgeries—conditions that are common in the medical tourism trade. With medical tourism growing in scope and popularity, it is essential that hospitalists are prepared to discuss with their patients the pros and cons of traveling for medical care. Hospitalists should be able to:
- Identify patients who might benefit from medical tourism;
- Know where and how to look for an accredited overseas facility; and
- Explain to patients the potential travel risks and complications, including insurance coverage and legal restrictions in destination countries.
A basic understanding of the industry and the issues can help guide your patients through medical decisions and help you care for those who have returned from a medical trip.
Big Menu, Discount Prices
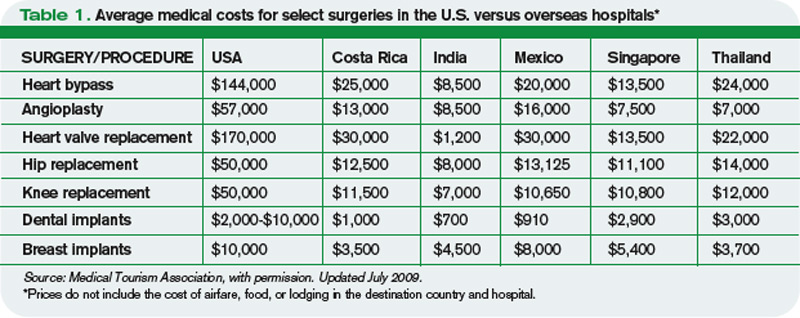
Medical tourism offers a wide range of medical services performed in hospitals on nearly every continent, with a wide range of costs for certain procedures (Table 1, p. 26). Most surgeries cost 50% to 90% less than the average cost of the same surgery at a U.S. hospital. Many in the medical tourism industry say these types of savings have brought once-unaffordable surgery within the reach of most Americans, regardless of insurance status. For example, cardiac bypass surgery on average costs $144,000 in the U.S.; it costs about $8,500 in India.
The reasons the costs are so much less at overseas hospitals, as compared with U.S. costs, are many:
- Lower wages for providers;
- Less expensive medical devices and pharmaceutical products;
- Less involvement by third-party payors; and
- Lower malpractice premiums.4
For example, the annual liability insurance premium for a surgeon in India is $4,000; the average cost of a New York City surgeon’s liability insurance premium is $100,000.5
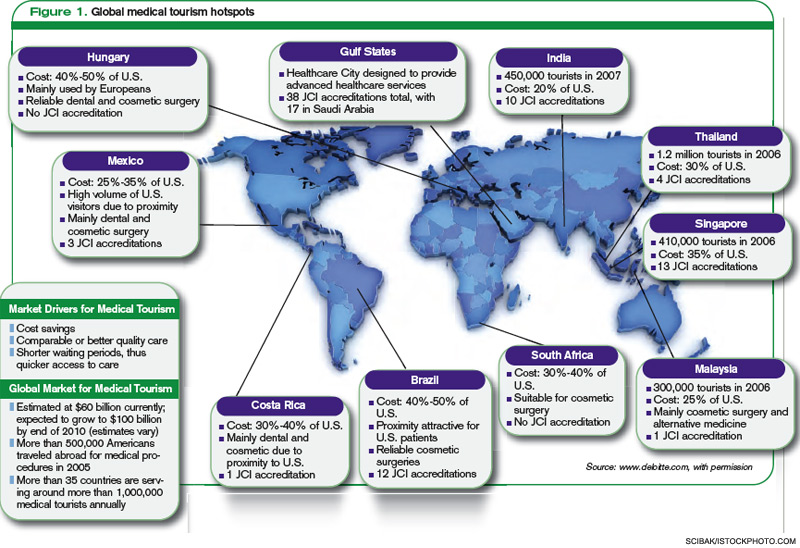
Brazil, Costa Rica, and Mexico are attractive destinations for cosmetic and dental surgeries; Singapore, Malaysia, Thailand, and India have emerged as hubs for cardiac and orthopedic surgeries (Table 1, above).6
The growth in medical tourism led the Joint Commission in 1999 to launch Joint Commission International (JCI), which ensures that offshore hospitals provide the highest-quality care to international patients (see “Ultra-Affordable Prices and No Decline in Quality of Care,” p. 28). JCI has accredited 120 overseas hospitals that meet these standards.
“Overseas hospitals are always keen in partnering with U.S. hospitals,” Dr. Li says. Collaborations, such as Johns Hopkins International Medical Center’s partnership with International Medical Clinic Singapore, and Partners Harvard Medical International’s affiliation with Wockhardt Hospitals in Mumbai, India, have helped facilitate the accreditation process and alleviate U.S. patient concerns.
Overseas hospitals not only offer greatly discounted rates than insurer-negotiated U.S. prices, but many of the international hospitals also report quality scores equal to or better than the average U.S. hospital’s.7
Before You Book a Trip …
How do patients find overseas facilities? It’s as easy as a click of the mouse.
“Our survey shows 75 percent of patients located offshore hospitals through the Internet,” says Renee-Marie Stephano, president of the Medical Tourism Association, a nonprofit group based in West Palm Beach, Fla., that was established in 2007 to promote education, transparency, and communication in the medical tourism community. Patients use overseas hospital websites, international medical coordinators, and medical tourism companies, such as PlanetHospital.com and MedRetreat.com, to find facilities and providers, and to coordinate medical travel.
“Medical tourism is currently unregulated,” Stephano says. “One of our goals is to certify medical tourism facilitators to create the best standard of practice.”
In 2007, the American Medical Association (AMA) published medical tourism guidelines to help healthcare entities engaged in overseas medical care.8 (Download a PDF of the guidelines at www.ama-assn.org/ama1/pub/upload/mm/31/medicaltourism.pdf.) The AMA suggests that:
- Medical care outside the U.S. should be voluntary, and patients should be informed of their legal rights and recourses before agreeing to travel outside the U.S.;
- Before traveling, local follow-up care should be arranged to ensure continuity of care;
- Patients should have access to physician licensing, facility accreditation, and outcomes data for both;
- Medical record transfers should follow HIPAA guidelines; and
- Patients should be informed of the potential risks of combining surgical procedures with long flights and vacation activities.
—Kenneth Mays, senior director, marketing and business development, Bumrungrad Hospital, Bangkok, Thailand
Patient Concerns
Hospitalists are highly focused on a patient’s quality of care; the same can be said of some overseas hospitals that attract large numbers of medical tourists. “I think the service and quality of care provided at our hospital compares favorably with the very best American hospitals,” says Kenneth Mays, senior director of hospital marketing and business development at Bumrungrad Hospital in Bangkok.
That might be so, but the growth of medical tourism also raises concerns stateside. With sleek websites making it easy for U.S. patients to schedule procedure vacations from their kitchen tables, many U.S. physician and watchdog groups worry about patient safety, privacy, liability, and continuity of care. Although most international hospitals and physicians provide outcomes data, rarely do the benchmarks compare directly with U.S. hospital quality and safety data.
“Quality comparisons are difficult, even within U.S. hospitals, as hospitals use different methodologies to collect data,” says Stephano. “Patients have to rely on JCI accreditation, surgeon experience, volume, and outcomes to decide.”
Recent studies echo the Medical Tourism Association’s claim: Increased cardiac surgery volume at Apollo Hospitals—an 8,500-bed healthcare system with 50 locations throughout India—and Narayana Hospital in Bommasandra, India, has lowered costs, with similar, or even lower, mortality rates compared with the average U.S. hospital.7,9 Other challenges like getting medical records exist even within U.S. hospitals, so emerging platforms like Google Health and Microsoft Vault, where medical records can be uploaded at the touch of a button, “will benefit patients and providers,” Dr. Li says.
The Medical Tourism Association envisions U.S.-based physicians offering follow-up care to medical tourism patients. “Currently, we encourage patients to follow up with their primary-care physician,” Stephano says.
Dr. Li says malpractice is always a concern when traveling overseas; however, he also notes the legal system in the U.S. is strong enough “to handle any medical malpractice.” That said, a patient who experiences a poor medical outcome as the result of overseas treatment might seek legal remedies, but the reality is that malpractice laws are either nonexistent or not well implemented in some destination countries. That makes malpractice claims on overseas procedures a dicey proposition.
“Patients receiving overseas treatment need to realize that they are agreeing to the jurisdiction of the destination country,” Stephano says. Other risks associated with extended travel include exposure to regional infectious diseases and poor infrastructure in the destination country, which could undermine the benefits of medical travel.
Cost-saving benefits have led some U.S. insurance companies to begin integrating overseas medical coverage. For example, Blue Cross Blue Shield of South Carolina offers incentives for patients willing to obtain medical care overseas at JCI-approved hospitals. BCBS then waives deductibles and copays, and several other insurers have launched similar pilot programs.10 “We will see more of these changes,” Stephano says, “to cut costs and remain competitive.”
Immediate Impact
In 2008, U.S. healthcare spending was $2.3 trillion.11 A 2005 Institute of Medicine report suggests that 30% to 40% of current U.S. healthcare expenditure is wasted.12 U.S. lawmakers, employers, hospitals, and consumers are scrambling to find ways to reduce healthcare costs and improve efficiency. Medical tourism seems to benefit a select few Americans, only lowering U.S. healthcare spending by 1% to 2%.12
Medical tourism revenue generated in destination countries currently is limited to the private sector, but that might change soon. Government funding for healthcare initiatives in such countries as India, Brazil, and Thailand is declining. Some entrepreneurial physicians and hospitals are looking to medical tourism to fill the funding gap.
Medical tourism likely will continue to grow; so too will the legal, quality, and insurance protections for patients. Efficient resource utilization might help reduce U.S. healthcare costs, and improved distribution of destination-country resources might help improve infrastructure and access to better healthcare for their own citizens.
With their leadership skills and expertise, hospitalists can play a major role in reducing healthcare costs.
However, what actual reforms healthcare legislation brings to medical tourism remain to be seen. TH
Dr. Thakkar is a hospitalist and assistant professor in the division of hospital medicine at Johns Hopkins University School of Medicine in Baltimore.
References
- Medical tourism: Consumers in search of value. Deloitte Consulting LLP website. Available at: www.deloitte.com/dtt/cda/doc/content/us%5Fchs%5FMedicalTourismStudy(1).pdf. Accessed Sept. 13, 2010.
- Pafford B. The third wave—medical tourism in the 21st century. South Med J. 2009;102(8):810-813.
- Kher U. Outsourcing your heart. Available at: http://proquest.umi.com/pqdweb?did=1041533291&Fmt=7&clientId=5241&RQT=309&VName=PQD. Accessed Sept. 13, 2010.
- Forgione DA, Smith PC. Medical tourism and its impact on the US health care system. J Health Care Finance. 2007;34(1):27-35.
- Lancaster J. Surgeries, side trips for “medical tourists.” The Washington Post website. Available at: www.washingtonpost.com/wp-dyn/articles/A497432004Oct20.html. Accessed Sept. 13, 2010.
- Horowitz MD, Rosensweig JA, Jones CA. Medical tourism: Globaliz-ation of the healthcare marketplace. MedGenMed. 2007;9(4):33.
- Milstein A, Smith M. Will the surgical world become flat? Health Aff (Millwood). 2007;26(1):137-141.
- New AMA guidelines on medical tourism. AMA website. Available at: www.ama-assn.org/ama1/pub/upload/mm/31/medicaltourism.pdf. Accessed March 26, 2010.
- Anand G. The Henry Ford of heart surgery. Wall Street Journal website. Available at: online.wsj.com/article/SB12587589288795811.html.
- Einhorn B. Outsourcing the patients. Business Week website. Available at: www.businessweek.com/magazine/content/08_12/b40760367 77780.htm. Accessed Sept. 13, 2010.
- . Hartman M, Martin A, Nuccio O, Catlin A, et al. Health spending growth at a historic low in 2008. Health Aff (Millwood). 2010;29(1): 147-155.
- Milstein A, Smith M. America’s new refugees—seeking affordable surgery offshore. N Engl J Med. 2006;355(16):1637-1640.
David Dupray, a 60-year-old uninsured coffee shop owner from Bar Harbor, Maine, had been having left leg pain on ambulation for four years. His cardiologist recommended stent placement for left iliac artery stenosis. The estimated bill: approximately $35,000.
Unable to afford the procedure, Dupray began searching the Web for affordable medical care overseas. His physician suggested Thailand. Within days, Dupray had an appointment with a cardiologist halfway around the world—at Bumrungrad Hospital in Bangkok, Thailand. Dupray spent two days in the hotel-like hospital, had three stents placed in his leg arteries, and completed a cardiac stress test. The total bill: $18,000.
“I will never go to a hospital in the U.S.,” says Dupray, who represents a growing number of Americans searching for affordable healthcare in the global marketplace.
With rising U.S. healthcare costs and millions of Americans uninsured or underinsured, more American patients are seeking affordable, high-quality medical care abroad—known as “medical tourism.” In 2007, an estimated 750,000 Americans traveled abroad for medical care; the number is expected to increase to 6 million by the end of this year.1 On the flip side, only a little more than 400,000 nonresidents visited the U.S. in 2008 for the latest medical care.1 Globally, the medical tourism industry is estimated to grow into a $21 billion-a-year industry by 2012, with much of the growth expected from Western patients traveling overseas for affordable care.2
“As hospitalists, we have been seeing increasing numbers of patients going overseas for urgent and elective procedures, as it is a general perception the medical treatment overseas is less expensive,” says Joseph Ming Wah Li, MD, SFHM, director of hospital medicine at Beth Israel Deaconess Medical Center in Boston and SHM president-elect.
Physicians in U.S. hospitals encounter potential medical tourists all the time. Some are uninsured or underinsured. Some have insurance carriers that limit or exclude coverage for certain procedures and treatments. Even those with insurance sometimes struggle to pay deductibles, copays, and their costs after insurance has paid its part. Others are uncomfortable with the language barriers and cultural differences of U.S. hospitals and physicians.
Medical tourism also lures patients who are citizens of countries (e.g. Canada, the United Kingdom) that offer universal healthcare, Dr. Li says.3 For example, more expatriates from India and Malaysia are traveling to their native countries for medical care, as they receive affordable and quicker medical care while visiting family.
Hospitalists routinely care for patients requiring essential cardiac or orthopedic surgeries—conditions that are common in the medical tourism trade. With medical tourism growing in scope and popularity, it is essential that hospitalists are prepared to discuss with their patients the pros and cons of traveling for medical care. Hospitalists should be able to:
- Identify patients who might benefit from medical tourism;
- Know where and how to look for an accredited overseas facility; and
- Explain to patients the potential travel risks and complications, including insurance coverage and legal restrictions in destination countries.
A basic understanding of the industry and the issues can help guide your patients through medical decisions and help you care for those who have returned from a medical trip.
Big Menu, Discount Prices
Medical tourism offers a wide range of medical services performed in hospitals on nearly every continent, with a wide range of costs for certain procedures (Table 1, p. 26). Most surgeries cost 50% to 90% less than the average cost of the same surgery at a U.S. hospital. Many in the medical tourism industry say these types of savings have brought once-unaffordable surgery within the reach of most Americans, regardless of insurance status. For example, cardiac bypass surgery on average costs $144,000 in the U.S.; it costs about $8,500 in India.
The reasons the costs are so much less at overseas hospitals, as compared with U.S. costs, are many:
- Lower wages for providers;
- Less expensive medical devices and pharmaceutical products;
- Less involvement by third-party payors; and
- Lower malpractice premiums.4
For example, the annual liability insurance premium for a surgeon in India is $4,000; the average cost of a New York City surgeon’s liability insurance premium is $100,000.5
Brazil, Costa Rica, and Mexico are attractive destinations for cosmetic and dental surgeries; Singapore, Malaysia, Thailand, and India have emerged as hubs for cardiac and orthopedic surgeries (Table 1, above).6
The growth in medical tourism led the Joint Commission in 1999 to launch Joint Commission International (JCI), which ensures that offshore hospitals provide the highest-quality care to international patients (see “Ultra-Affordable Prices and No Decline in Quality of Care,” p. 28). JCI has accredited 120 overseas hospitals that meet these standards.
“Overseas hospitals are always keen in partnering with U.S. hospitals,” Dr. Li says. Collaborations, such as Johns Hopkins International Medical Center’s partnership with International Medical Clinic Singapore, and Partners Harvard Medical International’s affiliation with Wockhardt Hospitals in Mumbai, India, have helped facilitate the accreditation process and alleviate U.S. patient concerns.
Overseas hospitals not only offer greatly discounted rates than insurer-negotiated U.S. prices, but many of the international hospitals also report quality scores equal to or better than the average U.S. hospital’s.7
Before You Book a Trip …
How do patients find overseas facilities? It’s as easy as a click of the mouse.
“Our survey shows 75 percent of patients located offshore hospitals through the Internet,” says Renee-Marie Stephano, president of the Medical Tourism Association, a nonprofit group based in West Palm Beach, Fla., that was established in 2007 to promote education, transparency, and communication in the medical tourism community. Patients use overseas hospital websites, international medical coordinators, and medical tourism companies, such as PlanetHospital.com and MedRetreat.com, to find facilities and providers, and to coordinate medical travel.
“Medical tourism is currently unregulated,” Stephano says. “One of our goals is to certify medical tourism facilitators to create the best standard of practice.”
In 2007, the American Medical Association (AMA) published medical tourism guidelines to help healthcare entities engaged in overseas medical care.8 (Download a PDF of the guidelines at www.ama-assn.org/ama1/pub/upload/mm/31/medicaltourism.pdf.) The AMA suggests that:
- Medical care outside the U.S. should be voluntary, and patients should be informed of their legal rights and recourses before agreeing to travel outside the U.S.;
- Before traveling, local follow-up care should be arranged to ensure continuity of care;
- Patients should have access to physician licensing, facility accreditation, and outcomes data for both;
- Medical record transfers should follow HIPAA guidelines; and
- Patients should be informed of the potential risks of combining surgical procedures with long flights and vacation activities.
—Kenneth Mays, senior director, marketing and business development, Bumrungrad Hospital, Bangkok, Thailand
Patient Concerns
Hospitalists are highly focused on a patient’s quality of care; the same can be said of some overseas hospitals that attract large numbers of medical tourists. “I think the service and quality of care provided at our hospital compares favorably with the very best American hospitals,” says Kenneth Mays, senior director of hospital marketing and business development at Bumrungrad Hospital in Bangkok.
That might be so, but the growth of medical tourism also raises concerns stateside. With sleek websites making it easy for U.S. patients to schedule procedure vacations from their kitchen tables, many U.S. physician and watchdog groups worry about patient safety, privacy, liability, and continuity of care. Although most international hospitals and physicians provide outcomes data, rarely do the benchmarks compare directly with U.S. hospital quality and safety data.
“Quality comparisons are difficult, even within U.S. hospitals, as hospitals use different methodologies to collect data,” says Stephano. “Patients have to rely on JCI accreditation, surgeon experience, volume, and outcomes to decide.”
Recent studies echo the Medical Tourism Association’s claim: Increased cardiac surgery volume at Apollo Hospitals—an 8,500-bed healthcare system with 50 locations throughout India—and Narayana Hospital in Bommasandra, India, has lowered costs, with similar, or even lower, mortality rates compared with the average U.S. hospital.7,9 Other challenges like getting medical records exist even within U.S. hospitals, so emerging platforms like Google Health and Microsoft Vault, where medical records can be uploaded at the touch of a button, “will benefit patients and providers,” Dr. Li says.
The Medical Tourism Association envisions U.S.-based physicians offering follow-up care to medical tourism patients. “Currently, we encourage patients to follow up with their primary-care physician,” Stephano says.
Dr. Li says malpractice is always a concern when traveling overseas; however, he also notes the legal system in the U.S. is strong enough “to handle any medical malpractice.” That said, a patient who experiences a poor medical outcome as the result of overseas treatment might seek legal remedies, but the reality is that malpractice laws are either nonexistent or not well implemented in some destination countries. That makes malpractice claims on overseas procedures a dicey proposition.
“Patients receiving overseas treatment need to realize that they are agreeing to the jurisdiction of the destination country,” Stephano says. Other risks associated with extended travel include exposure to regional infectious diseases and poor infrastructure in the destination country, which could undermine the benefits of medical travel.
Cost-saving benefits have led some U.S. insurance companies to begin integrating overseas medical coverage. For example, Blue Cross Blue Shield of South Carolina offers incentives for patients willing to obtain medical care overseas at JCI-approved hospitals. BCBS then waives deductibles and copays, and several other insurers have launched similar pilot programs.10 “We will see more of these changes,” Stephano says, “to cut costs and remain competitive.”
Immediate Impact
In 2008, U.S. healthcare spending was $2.3 trillion.11 A 2005 Institute of Medicine report suggests that 30% to 40% of current U.S. healthcare expenditure is wasted.12 U.S. lawmakers, employers, hospitals, and consumers are scrambling to find ways to reduce healthcare costs and improve efficiency. Medical tourism seems to benefit a select few Americans, only lowering U.S. healthcare spending by 1% to 2%.12
Medical tourism revenue generated in destination countries currently is limited to the private sector, but that might change soon. Government funding for healthcare initiatives in such countries as India, Brazil, and Thailand is declining. Some entrepreneurial physicians and hospitals are looking to medical tourism to fill the funding gap.
Medical tourism likely will continue to grow; so too will the legal, quality, and insurance protections for patients. Efficient resource utilization might help reduce U.S. healthcare costs, and improved distribution of destination-country resources might help improve infrastructure and access to better healthcare for their own citizens.
With their leadership skills and expertise, hospitalists can play a major role in reducing healthcare costs.
However, what actual reforms healthcare legislation brings to medical tourism remain to be seen. TH
Dr. Thakkar is a hospitalist and assistant professor in the division of hospital medicine at Johns Hopkins University School of Medicine in Baltimore.
References
- Medical tourism: Consumers in search of value. Deloitte Consulting LLP website. Available at: www.deloitte.com/dtt/cda/doc/content/us%5Fchs%5FMedicalTourismStudy(1).pdf. Accessed Sept. 13, 2010.
- Pafford B. The third wave—medical tourism in the 21st century. South Med J. 2009;102(8):810-813.
- Kher U. Outsourcing your heart. Available at: http://proquest.umi.com/pqdweb?did=1041533291&Fmt=7&clientId=5241&RQT=309&VName=PQD. Accessed Sept. 13, 2010.
- Forgione DA, Smith PC. Medical tourism and its impact on the US health care system. J Health Care Finance. 2007;34(1):27-35.
- Lancaster J. Surgeries, side trips for “medical tourists.” The Washington Post website. Available at: www.washingtonpost.com/wp-dyn/articles/A497432004Oct20.html. Accessed Sept. 13, 2010.
- Horowitz MD, Rosensweig JA, Jones CA. Medical tourism: Globaliz-ation of the healthcare marketplace. MedGenMed. 2007;9(4):33.
- Milstein A, Smith M. Will the surgical world become flat? Health Aff (Millwood). 2007;26(1):137-141.
- New AMA guidelines on medical tourism. AMA website. Available at: www.ama-assn.org/ama1/pub/upload/mm/31/medicaltourism.pdf. Accessed March 26, 2010.
- Anand G. The Henry Ford of heart surgery. Wall Street Journal website. Available at: online.wsj.com/article/SB12587589288795811.html.
- Einhorn B. Outsourcing the patients. Business Week website. Available at: www.businessweek.com/magazine/content/08_12/b40760367 77780.htm. Accessed Sept. 13, 2010.
- . Hartman M, Martin A, Nuccio O, Catlin A, et al. Health spending growth at a historic low in 2008. Health Aff (Millwood). 2010;29(1): 147-155.
- Milstein A, Smith M. America’s new refugees—seeking affordable surgery offshore. N Engl J Med. 2006;355(16):1637-1640.
David Dupray, a 60-year-old uninsured coffee shop owner from Bar Harbor, Maine, had been having left leg pain on ambulation for four years. His cardiologist recommended stent placement for left iliac artery stenosis. The estimated bill: approximately $35,000.
Unable to afford the procedure, Dupray began searching the Web for affordable medical care overseas. His physician suggested Thailand. Within days, Dupray had an appointment with a cardiologist halfway around the world—at Bumrungrad Hospital in Bangkok, Thailand. Dupray spent two days in the hotel-like hospital, had three stents placed in his leg arteries, and completed a cardiac stress test. The total bill: $18,000.
“I will never go to a hospital in the U.S.,” says Dupray, who represents a growing number of Americans searching for affordable healthcare in the global marketplace.
With rising U.S. healthcare costs and millions of Americans uninsured or underinsured, more American patients are seeking affordable, high-quality medical care abroad—known as “medical tourism.” In 2007, an estimated 750,000 Americans traveled abroad for medical care; the number is expected to increase to 6 million by the end of this year.1 On the flip side, only a little more than 400,000 nonresidents visited the U.S. in 2008 for the latest medical care.1 Globally, the medical tourism industry is estimated to grow into a $21 billion-a-year industry by 2012, with much of the growth expected from Western patients traveling overseas for affordable care.2
“As hospitalists, we have been seeing increasing numbers of patients going overseas for urgent and elective procedures, as it is a general perception the medical treatment overseas is less expensive,” says Joseph Ming Wah Li, MD, SFHM, director of hospital medicine at Beth Israel Deaconess Medical Center in Boston and SHM president-elect.
Physicians in U.S. hospitals encounter potential medical tourists all the time. Some are uninsured or underinsured. Some have insurance carriers that limit or exclude coverage for certain procedures and treatments. Even those with insurance sometimes struggle to pay deductibles, copays, and their costs after insurance has paid its part. Others are uncomfortable with the language barriers and cultural differences of U.S. hospitals and physicians.
Medical tourism also lures patients who are citizens of countries (e.g. Canada, the United Kingdom) that offer universal healthcare, Dr. Li says.3 For example, more expatriates from India and Malaysia are traveling to their native countries for medical care, as they receive affordable and quicker medical care while visiting family.
Hospitalists routinely care for patients requiring essential cardiac or orthopedic surgeries—conditions that are common in the medical tourism trade. With medical tourism growing in scope and popularity, it is essential that hospitalists are prepared to discuss with their patients the pros and cons of traveling for medical care. Hospitalists should be able to:
- Identify patients who might benefit from medical tourism;
- Know where and how to look for an accredited overseas facility; and
- Explain to patients the potential travel risks and complications, including insurance coverage and legal restrictions in destination countries.
A basic understanding of the industry and the issues can help guide your patients through medical decisions and help you care for those who have returned from a medical trip.
Big Menu, Discount Prices
Medical tourism offers a wide range of medical services performed in hospitals on nearly every continent, with a wide range of costs for certain procedures (Table 1, p. 26). Most surgeries cost 50% to 90% less than the average cost of the same surgery at a U.S. hospital. Many in the medical tourism industry say these types of savings have brought once-unaffordable surgery within the reach of most Americans, regardless of insurance status. For example, cardiac bypass surgery on average costs $144,000 in the U.S.; it costs about $8,500 in India.
The reasons the costs are so much less at overseas hospitals, as compared with U.S. costs, are many:
- Lower wages for providers;
- Less expensive medical devices and pharmaceutical products;
- Less involvement by third-party payors; and
- Lower malpractice premiums.4
For example, the annual liability insurance premium for a surgeon in India is $4,000; the average cost of a New York City surgeon’s liability insurance premium is $100,000.5
Brazil, Costa Rica, and Mexico are attractive destinations for cosmetic and dental surgeries; Singapore, Malaysia, Thailand, and India have emerged as hubs for cardiac and orthopedic surgeries (Table 1, above).6
The growth in medical tourism led the Joint Commission in 1999 to launch Joint Commission International (JCI), which ensures that offshore hospitals provide the highest-quality care to international patients (see “Ultra-Affordable Prices and No Decline in Quality of Care,” p. 28). JCI has accredited 120 overseas hospitals that meet these standards.
“Overseas hospitals are always keen in partnering with U.S. hospitals,” Dr. Li says. Collaborations, such as Johns Hopkins International Medical Center’s partnership with International Medical Clinic Singapore, and Partners Harvard Medical International’s affiliation with Wockhardt Hospitals in Mumbai, India, have helped facilitate the accreditation process and alleviate U.S. patient concerns.
Overseas hospitals not only offer greatly discounted rates than insurer-negotiated U.S. prices, but many of the international hospitals also report quality scores equal to or better than the average U.S. hospital’s.7
Before You Book a Trip …
How do patients find overseas facilities? It’s as easy as a click of the mouse.
“Our survey shows 75 percent of patients located offshore hospitals through the Internet,” says Renee-Marie Stephano, president of the Medical Tourism Association, a nonprofit group based in West Palm Beach, Fla., that was established in 2007 to promote education, transparency, and communication in the medical tourism community. Patients use overseas hospital websites, international medical coordinators, and medical tourism companies, such as PlanetHospital.com and MedRetreat.com, to find facilities and providers, and to coordinate medical travel.
“Medical tourism is currently unregulated,” Stephano says. “One of our goals is to certify medical tourism facilitators to create the best standard of practice.”
In 2007, the American Medical Association (AMA) published medical tourism guidelines to help healthcare entities engaged in overseas medical care.8 (Download a PDF of the guidelines at www.ama-assn.org/ama1/pub/upload/mm/31/medicaltourism.pdf.) The AMA suggests that:
- Medical care outside the U.S. should be voluntary, and patients should be informed of their legal rights and recourses before agreeing to travel outside the U.S.;
- Before traveling, local follow-up care should be arranged to ensure continuity of care;
- Patients should have access to physician licensing, facility accreditation, and outcomes data for both;
- Medical record transfers should follow HIPAA guidelines; and
- Patients should be informed of the potential risks of combining surgical procedures with long flights and vacation activities.
—Kenneth Mays, senior director, marketing and business development, Bumrungrad Hospital, Bangkok, Thailand
Patient Concerns
Hospitalists are highly focused on a patient’s quality of care; the same can be said of some overseas hospitals that attract large numbers of medical tourists. “I think the service and quality of care provided at our hospital compares favorably with the very best American hospitals,” says Kenneth Mays, senior director of hospital marketing and business development at Bumrungrad Hospital in Bangkok.
That might be so, but the growth of medical tourism also raises concerns stateside. With sleek websites making it easy for U.S. patients to schedule procedure vacations from their kitchen tables, many U.S. physician and watchdog groups worry about patient safety, privacy, liability, and continuity of care. Although most international hospitals and physicians provide outcomes data, rarely do the benchmarks compare directly with U.S. hospital quality and safety data.
“Quality comparisons are difficult, even within U.S. hospitals, as hospitals use different methodologies to collect data,” says Stephano. “Patients have to rely on JCI accreditation, surgeon experience, volume, and outcomes to decide.”
Recent studies echo the Medical Tourism Association’s claim: Increased cardiac surgery volume at Apollo Hospitals—an 8,500-bed healthcare system with 50 locations throughout India—and Narayana Hospital in Bommasandra, India, has lowered costs, with similar, or even lower, mortality rates compared with the average U.S. hospital.7,9 Other challenges like getting medical records exist even within U.S. hospitals, so emerging platforms like Google Health and Microsoft Vault, where medical records can be uploaded at the touch of a button, “will benefit patients and providers,” Dr. Li says.
The Medical Tourism Association envisions U.S.-based physicians offering follow-up care to medical tourism patients. “Currently, we encourage patients to follow up with their primary-care physician,” Stephano says.
Dr. Li says malpractice is always a concern when traveling overseas; however, he also notes the legal system in the U.S. is strong enough “to handle any medical malpractice.” That said, a patient who experiences a poor medical outcome as the result of overseas treatment might seek legal remedies, but the reality is that malpractice laws are either nonexistent or not well implemented in some destination countries. That makes malpractice claims on overseas procedures a dicey proposition.
“Patients receiving overseas treatment need to realize that they are agreeing to the jurisdiction of the destination country,” Stephano says. Other risks associated with extended travel include exposure to regional infectious diseases and poor infrastructure in the destination country, which could undermine the benefits of medical travel.
Cost-saving benefits have led some U.S. insurance companies to begin integrating overseas medical coverage. For example, Blue Cross Blue Shield of South Carolina offers incentives for patients willing to obtain medical care overseas at JCI-approved hospitals. BCBS then waives deductibles and copays, and several other insurers have launched similar pilot programs.10 “We will see more of these changes,” Stephano says, “to cut costs and remain competitive.”
Immediate Impact
In 2008, U.S. healthcare spending was $2.3 trillion.11 A 2005 Institute of Medicine report suggests that 30% to 40% of current U.S. healthcare expenditure is wasted.12 U.S. lawmakers, employers, hospitals, and consumers are scrambling to find ways to reduce healthcare costs and improve efficiency. Medical tourism seems to benefit a select few Americans, only lowering U.S. healthcare spending by 1% to 2%.12
Medical tourism revenue generated in destination countries currently is limited to the private sector, but that might change soon. Government funding for healthcare initiatives in such countries as India, Brazil, and Thailand is declining. Some entrepreneurial physicians and hospitals are looking to medical tourism to fill the funding gap.
Medical tourism likely will continue to grow; so too will the legal, quality, and insurance protections for patients. Efficient resource utilization might help reduce U.S. healthcare costs, and improved distribution of destination-country resources might help improve infrastructure and access to better healthcare for their own citizens.
With their leadership skills and expertise, hospitalists can play a major role in reducing healthcare costs.
However, what actual reforms healthcare legislation brings to medical tourism remain to be seen. TH
Dr. Thakkar is a hospitalist and assistant professor in the division of hospital medicine at Johns Hopkins University School of Medicine in Baltimore.
References
- Medical tourism: Consumers in search of value. Deloitte Consulting LLP website. Available at: www.deloitte.com/dtt/cda/doc/content/us%5Fchs%5FMedicalTourismStudy(1).pdf. Accessed Sept. 13, 2010.
- Pafford B. The third wave—medical tourism in the 21st century. South Med J. 2009;102(8):810-813.
- Kher U. Outsourcing your heart. Available at: http://proquest.umi.com/pqdweb?did=1041533291&Fmt=7&clientId=5241&RQT=309&VName=PQD. Accessed Sept. 13, 2010.
- Forgione DA, Smith PC. Medical tourism and its impact on the US health care system. J Health Care Finance. 2007;34(1):27-35.
- Lancaster J. Surgeries, side trips for “medical tourists.” The Washington Post website. Available at: www.washingtonpost.com/wp-dyn/articles/A497432004Oct20.html. Accessed Sept. 13, 2010.
- Horowitz MD, Rosensweig JA, Jones CA. Medical tourism: Globaliz-ation of the healthcare marketplace. MedGenMed. 2007;9(4):33.
- Milstein A, Smith M. Will the surgical world become flat? Health Aff (Millwood). 2007;26(1):137-141.
- New AMA guidelines on medical tourism. AMA website. Available at: www.ama-assn.org/ama1/pub/upload/mm/31/medicaltourism.pdf. Accessed March 26, 2010.
- Anand G. The Henry Ford of heart surgery. Wall Street Journal website. Available at: online.wsj.com/article/SB12587589288795811.html.
- Einhorn B. Outsourcing the patients. Business Week website. Available at: www.businessweek.com/magazine/content/08_12/b40760367 77780.htm. Accessed Sept. 13, 2010.
- . Hartman M, Martin A, Nuccio O, Catlin A, et al. Health spending growth at a historic low in 2008. Health Aff (Millwood). 2010;29(1): 147-155.
- Milstein A, Smith M. America’s new refugees—seeking affordable surgery offshore. N Engl J Med. 2006;355(16):1637-1640.
Generation Next
If imitation is the sincerest form of flattery, then hospitalists have a lot to crow about. For the same reasons that sparked the original hospital medicine movement, HM’s specialist colleagues are flocking to the HM model.
“I switched because your impact with consultation is limited,” says geriatrician-hospitalist Jeffrey Farber, MD, assistant professor of geriatrics and palliative medicine and director of the Mobile Acute Care for the Elderly Service (MACE) at Mount Sinai Hospital in New York City. As the former director of the Department of Geriatrics’ consult service, Dr. Farber adds, “I like being able to call the shots and direct the care.”
He’s not the only one. Neurologists, surgeons, and even dermatologists and otolaryngologists have been establishing inpatient services based on the HM model. While many of these programs first begin in the academic setting, where resident work-hour limits necessitate faculty coverage, community hospitals increasingly are turning to specialist hospitalists to address patient-safety and treatment-innovation issues.
According to a leading surgical hospitalist, more than 250 such programs exist throughout the country.
Shaun Frost, MD, FACP, SFHM, chair of SHM’s Membership Committee and SHM’s Emergency Medicine Task Force, an SHM board member, and regional medical director for Brentwood, Tenn.-based Cogent Healthcare, views the growth of specialty hospitalist programs as a positive development. “In many ways, [this trend] is confirmatory regarding the key reasons for creation of the hospital movement,” he says.
For example, mirroring the performance of adult inpatient hospitalist programs, pediatric hospitalist programs have now documented improved throughput, increased efficiency, and increased patient satisfaction, especially when such programs combine pediatric emergency department and pediatric inpatient coverage.1
“We’ve all been inspired by the success of the medical hospitalist model, and we want to acknowledge and credit them for being the trailblazers and pioneers who are leading the way,” adds John Maa, MD, FACS, assistant professor in the Department of Surgery, assistant chair of the Surgery Quality Improvement Program, and director of the Surgical Hospitalist Program at the University of California at San Francisco (UCSF). Dr. Maa and colleagues introduced the surgical hospitalist program at UCSF in July 2005.

—David Likosky, MD, FHM, neurohospitalist, stroke program director, Evergreen Hospital Medical Center, Seattle
What’s Driving the Trend?
The impetus for adopting and adapting the HM model varies across medical specialties. For some, it was necessity; for others, it was a way to extend coverage or streamline the hospital stay; and for still others, it was a matter of personal choice.
“We couldn’t continue in the old paradigm and deliver safe care, because it was traditionally resident-dependent,” says Dr. Maa, explaining that the 80-hour resident workweek restriction mandated by the Accreditation Council for Graduate Medical Education (ACGME) “annihilated” the old-school model.
The goal in organizing the Society of Dermatology Hospitalists (SDH), according to SDH cofounder Lindy P. Fox, MD, assistant professor of clinical dermatology and director of the hospital consultation service at UCSF, was to ensure 24/7 coverage by a dedicated group of dermatologists whose skill set is focused on inpatient care, and who, because of their involvement with the university hospital, are probably more comfortable with the nuances of inpatient dermatologic care than their outpatient-based colleagues. The SDH currently has 20 members representing about 15 academic programs.
Innovations in stroke treatment caused a “sea change” for the field of neurology, says David Likosky, MD, SFHM, hospitalist and stroke program director at Evergreen Hospital Medical Center in Seattle. Dr. Likosky, who is board-certified in neurology and internal medicine, says the HM model allows neurohospitalists to enjoy a work-life balance.
“It used to be that neurologists didn’t have to get out of bed at night for most strokes. But with innovations in stroke treatments, that’s all changed,” Dr. Likosky says. “It really helped to give birth to the neurohospitalist movement.”
A recent survey on the current scope of neurohospitalists’ practice presented by Dr. Likosky and colleagues at the American Academy of Neurology found that 8% of those surveyed were full-time neurohospitalists. The number might seem small, but it might be a matter of perception. The same study showed 73% of neurologists surveyed listed inpatient neurology care as their primary practice focus.2
Another driver for the neurohospitalist movement was that it became unfeasible to staff inpatient neurology services with physicians who maintained offices “across town,” observes S. Andrew Josephson, MD, director of the neurohospitalist program and inpatient neurology at UCSF. “Stroke is just one example of a disease that has so many emergent therapies that hospitals decided they needed a neurologist on site to make those types of treatment decisions.”
At a quaternary-care center such as UCSF, the requirements for otolaryngology expertise have increased exponentially, says Andrew H. Murr, MD, FACS, vice-chair of the Department of Otolaryngology/Head and Neck Surgery at UCSF. “For instance, our hospital has a huge transplant volume. Often, patients are on immuno-compromising medications that create the specter of fungal sinusitis,” he says. “We also get called to the operating room or ICU when patients have breathing problems and require surgical airways or other complicated intubation schemes. All of these problems require a lot of time, effort, and special expertise.”
Since September of last year, Dr. Murr’s department has been using office space adjacent to the hospital as headquarters for a full-time otolaryngologist whose sole responsibility is to cover inpatient work. Increased complexity of otolaryngologic-related problems, increased ED commitment, and a simple matter of logistics prompted the move. The Department of Otolaryngology moved 10 minutes away from the hospital, so literally running across the street for an otolaryngology consult was no longer an option.
Today, the hospital duty is linked to the department’s call schedule. Dr. Murr anticipates the department soon will establish a full-time faculty position to create a hospitalist niche within the department.
Usefulness Affirmed

Good results already have been demonstrated for the hospitalist model in other specialties. In the first two years of the surgical hospitalist program at UCSF, response times for surgical consultations averaged less than 20 minutes; the average wait for patients with acute appendicitis to undergo surgery was cut in half; and the number of billable consults rose by almost 200%.3
Heidi Wald, MD, MSPH, FHM, a 2009 Health and Aging Policy Fellow, and two hospitalist colleagues studied the impact of hospitalist programs on acute-care geriatrics and found a paucity of geriatric-care approaches.4 “The employment of geriatrics-trained clinicians by hospitalist programs is one approach to supporting generalist-hospitalists and inclining group culture toward clinical geriatric concerns,” the authors wrote. “Programs that purposefully hired geriatricians and gerontology nurse-practitioners used them to staff geriatrics services.”
Dr. Wald, assistant professor of medicine in the division of Health Care Policy Research and a hospitalist at the University of Colorado Denver, says trends in patient demographics and patient-safety initiatives will drive the proliferation of more geriatrician-hospitalists and geriatrics-focused services in the future. “The median age of the hospital population is increasing,” she notes, “and there are not enough geriatricians to deal with every elderly patient.”
Mount Sinai’s Dr. Farber is in the process of submitting for publication two years’ worth of data about the MACE service at Mount Sinai, which will evaluate the effect of MACE on costs, length of stay, and rehospitalization rates.
Variations on a Theme
The dermatology HM model at UCSF more closely resembles a consultative practice model. UCSF’s dermatology hospitalists do not admit patients. Still, says SDH’s Dr. Fox, because of their conversance with inpatient care and round-the-clock availability, dermatology hospitalists are invaluable. They help colleagues “puzzle out” the causes of cutaneous manifestations of system disease, quickly initiate state of the art treatment for hospital-acquired skin conditions, and improve outcomes for hospitalized patients with skin diseases.
“We see our charge as being multifold,” Dr. Fox explains. “We provide continuity of care for patients who are frequently hospitalized; we keep up with the medical literature; we are comfortable with and know the nuances of hospital operations; and we provide education to residents, house staff, and colleagues.”
In Denver, the Acute Care for the Elderly (ACE) service operated by the internal-medicine hospitalist group has only informal ties to the Department of Medicine’s Geriatrics Division, Dr. Wald says. Although not a closed geriatric-care unit, the service concentrates elderly patients on one inpatient service and introduces the tenets of geriatric care—multidisciplinary approach, functional assessment, early discharge planning, mitigating the hazards of hospitalization, and patient and family-centered care—into a hospitalist milieu.
Surgical hospitalist models also vary by setting, and continue to evolve as surgeons examine processes to determine what works and what doesn’t. At UCSF, the original model relied on surgeons taking call for seven days running. “You probably couldn’t do that continuously for your career,” says Dr. Maa, who worked the seven-day call schedule for 3 1/2 years.
The program has been modified so that the surgical hospitalists now work three- or four-day stretches.
Another successful variation involves one surgeon taking all the daytime shifts, while others rotate in for the PM shifts and weekends.
A Win-Win for Hospitalists?
Does the proliferation of specialty hospitalists create competition for patients? That could be a possibility, says Dr. Frost, should other specialty hospitalists become interested in providing care for the “bread and butter” pathologies.
“For instance, if neurohospitalists were interested in evaluating and managing patients with TIAs (transient ischemic attacks), or cardiohospitalists were interested in managing patients with low-risk chest pain, then there could be some competition,” Dr. Frost says. Although possible, he senses it isn’t a likely scenario.
What’s more likely, according to neurohospitalist Dr. Likosky, is cross-fertilization between specialties, where hospitalists who interface with their specialty colleagues gain the benefit of on-site, in-service education. “Many hospitalists feel that they were not adequately trained in neurologic illnesses, and yet, by default, they have become the first-line providers of inpatient neurologic care nationally,” Dr. Likosky says. “The neurohospitalist model is a way of getting at that issue. I don’t think that we are in competition. I think we are welcome partners.”
Dr. Likosky and fellow neurohospitalists Dr. Josephson and W. David Freeman, MD, assistant professor in the department of neurology and critical care at the Mayo Clinic College of Medicine in Jacksonville, Fla., offered the first neurology precourse in April at HM10 in Washington, D.C., and more and more hospitalist meetings are including neurohospitalist courses on their schedules.
Increased education also is a benefit of Mount Sinai’s adaptation of the MACE concept, Dr. Farber says. Because the hospitalist-run MACE patients are located throughout the hospital, the team conducts nursing grand rounds to educate other hospital staff about geriatrics-centered HM principles.

—John Maa, MD, FACS, assistant professor, Department of Surgery; assistant chair, Surgery Quality Improvement Program; director, Surgical Hospitalist Program, University of California at San Francisco
Economies of Scale
Dr. Fox, the dermatology hospitalist, is the first to admit that UCSF’s practice model probably works best in a large, tertiary-care, academic medical center. However, the potential exists for extension into rural settings with telemedicine models and trained physician assistants or nurse practitioners, she notes.
Dr. Farber agrees the HM model is adaptable to a variety of medical specialties; he foresees geriatric hospitalists working in community settings. “Even in smaller hospitals with fewer discharges, there will be a sizable subset of admissions of patients at risk for high utilization of resources,” he says. “Many of Medicare’s hospital-acquired conditions are geriatrics-related, such as catheter-associated urinary tract infections, central-line infections, and falls. The investment [in geriatrician-hospitalist teams] could be justified if you track the outcomes of these high-risk patients over time and see whether you’re reducing length of stay, direct costs, and readmissions.”
Dr. Likosky says the benefits of the neurohospitalist model closely mirror those of the HM model, and although volumes are lower, the benefits “remain significant even in relatively small hospitals.” His American Academy of Neurology (AAN) survey backs up this observation: Neurohospitalists were about evenly split between academic and private settings (49% and 51%, respectively). “Unlike dermatology, neurologic diagnoses are very common as either a primary or secondary reason for admission to the hospital,” Dr. Likosky says.
In the community setting, surgical hospitalist programs provide a new answer for ED call coverage, Dr. Maa says. Surgical practices often approach the medical center leadership to negotiate a stipend, then contribute salary support so that a new surgeon can be recruited to join the practice. This physician—usually a younger surgeon—then is hired in the role of a surgicalist so that timely patient care and surgeon availability can be ensured.
In rural settings, however, even this model might not be feasible, Dr. Maa says, because surgical practices could be comprised of only one or two surgeons. “We will have to think differently about telemedicine, telesurgery, and having ERs equipped with video monitors so that the ED physician can examine the patient while a surgeon, at a remote centralized area, can provide input,” he says.
Adoption of the hospitalist model by other specialties shows no sign of slowing down. That’s good news for HM and patient care, Dr. Maa says.
“This represents a transformation of the way an academic medical center is structured,” he adds. “We’ve traditionally prioritized research ahead of patient care, but this model is inverting that. It is patient-centered, making them the priority, and answers the question, ‘How can we reconfigure what we have to take better care of patients?’ And that’s why I think we’ll succeed.” TH
Gretchen Henkel is a freelance writer based in California.
References
- Krugman SD, Suggs A, Photowala HY, et al. Redefining the community pediatric hospitalist: the combined pediatric ED/inpatient unit. Ped Emerg Car. 2007;23(1):33-37.
- Likosky D. Is it time for neurohospitalists? Neurology. 2009;72(9):859-860.
- Maa J, Carter JT, Gosnell JE, et al. The surgical hospitalist: a new model for emergency surgical care. J Am Coll Surg. 2007;205(5):704-711.
- Wald H, Huddleston J, Kramer A. Is there a geriatrician in the house? Geriatric care approaches in hospitalist programs. J Hosp Med. 2006;1(1):29-35.
Unique Factors Propel Proliferation of “ists” at Washington Hospital
By Gretchen Henkel

“Ists” are multiplying at Providence Regional Medical Center in Everett, Wash. (PRMCE), about 25 miles north of Seattle. The medical hospitalist team manages 90% of the hospital’s medical patients and comprises 34 FTEs, with nocturnists and a palliative-care service; other in-house services include general surgery hospitalists, critical-care hospitalists, orthopedic hospitalists, neurology hospitalists, pediatric hospitalists, and obstetrics hospitalists.
So many “ists” under one roof is unusual for a community-based medical center. One reason for the trend is a highly successful hospitalist program that’s caused other specialists to take notice of the increase in quality metrics and job satisfaction.
“For some reason, we were blessed with an early decision by the hospitalists to acculturate themselves with the hospital’s mission,” says Joanne C. Roberts, MD, FACP, chief of the division of medicine, hospice, and palliative medicine at PRMCE.
The medical hospitalists quickly instituted standardization, quality, and utilization measures, and tied their performance to incentives, says HM medical director Jefferey S. Winningham, MD. For example, every hospitalist is required to leave voicemails for referring physicians upon admittance and discharge of their patients. A 95% compliance rate—validated by surveys of referring physicians—yields bonuses for the HM team.
Quality scores have increased dramatically since 2003, when the hospitalist program took off. PRMCE chief medical officer Larry Schechter, MD, says that the hospitalists’ success has increased the willingness of other specialists to adopt the HM model for delivering inpatient care.
Another factor in the swift adoption of specialist hospitalists: Except for the intensivist service—recipient of the American Association of Critical-Care Nurses’ 2008-2009 Beacon Award for Care Excellence—most of PRMCE’s programs are staffed with physician members of Everett Clinic, a large multispecialty group. “The secret of this community is the large medical groups,” Dr. Roberts says. “Everybody plays well together, especially at the senior leadership level.”
Fewer administrators means nimble decision-making, Dr. Schechter notes. Hospitalists’ internal teamwork is continuously reinforced through bimonthly team meetings; with hospital administrators in steering committee meetings, the hospitalist program has “set a high bar and brought the community together,” Dr. Winningham says.
As PRMCE grows—a new, 12-story tower is set to open in 2011—the hospital is poised to attain its mission of becoming a regional referral center. “To deliver quality at the lowest cost is a really serious enterprise,” Dr. Roberts says, “so getting the hospitalists engaged in that value proposition has been challenging but delightfully fun.”
If imitation is the sincerest form of flattery, then hospitalists have a lot to crow about. For the same reasons that sparked the original hospital medicine movement, HM’s specialist colleagues are flocking to the HM model.
“I switched because your impact with consultation is limited,” says geriatrician-hospitalist Jeffrey Farber, MD, assistant professor of geriatrics and palliative medicine and director of the Mobile Acute Care for the Elderly Service (MACE) at Mount Sinai Hospital in New York City. As the former director of the Department of Geriatrics’ consult service, Dr. Farber adds, “I like being able to call the shots and direct the care.”
He’s not the only one. Neurologists, surgeons, and even dermatologists and otolaryngologists have been establishing inpatient services based on the HM model. While many of these programs first begin in the academic setting, where resident work-hour limits necessitate faculty coverage, community hospitals increasingly are turning to specialist hospitalists to address patient-safety and treatment-innovation issues.
According to a leading surgical hospitalist, more than 250 such programs exist throughout the country.
Shaun Frost, MD, FACP, SFHM, chair of SHM’s Membership Committee and SHM’s Emergency Medicine Task Force, an SHM board member, and regional medical director for Brentwood, Tenn.-based Cogent Healthcare, views the growth of specialty hospitalist programs as a positive development. “In many ways, [this trend] is confirmatory regarding the key reasons for creation of the hospital movement,” he says.
For example, mirroring the performance of adult inpatient hospitalist programs, pediatric hospitalist programs have now documented improved throughput, increased efficiency, and increased patient satisfaction, especially when such programs combine pediatric emergency department and pediatric inpatient coverage.1
“We’ve all been inspired by the success of the medical hospitalist model, and we want to acknowledge and credit them for being the trailblazers and pioneers who are leading the way,” adds John Maa, MD, FACS, assistant professor in the Department of Surgery, assistant chair of the Surgery Quality Improvement Program, and director of the Surgical Hospitalist Program at the University of California at San Francisco (UCSF). Dr. Maa and colleagues introduced the surgical hospitalist program at UCSF in July 2005.
—David Likosky, MD, FHM, neurohospitalist, stroke program director, Evergreen Hospital Medical Center, Seattle
What’s Driving the Trend?
The impetus for adopting and adapting the HM model varies across medical specialties. For some, it was necessity; for others, it was a way to extend coverage or streamline the hospital stay; and for still others, it was a matter of personal choice.
“We couldn’t continue in the old paradigm and deliver safe care, because it was traditionally resident-dependent,” says Dr. Maa, explaining that the 80-hour resident workweek restriction mandated by the Accreditation Council for Graduate Medical Education (ACGME) “annihilated” the old-school model.
The goal in organizing the Society of Dermatology Hospitalists (SDH), according to SDH cofounder Lindy P. Fox, MD, assistant professor of clinical dermatology and director of the hospital consultation service at UCSF, was to ensure 24/7 coverage by a dedicated group of dermatologists whose skill set is focused on inpatient care, and who, because of their involvement with the university hospital, are probably more comfortable with the nuances of inpatient dermatologic care than their outpatient-based colleagues. The SDH currently has 20 members representing about 15 academic programs.
Innovations in stroke treatment caused a “sea change” for the field of neurology, says David Likosky, MD, SFHM, hospitalist and stroke program director at Evergreen Hospital Medical Center in Seattle. Dr. Likosky, who is board-certified in neurology and internal medicine, says the HM model allows neurohospitalists to enjoy a work-life balance.
“It used to be that neurologists didn’t have to get out of bed at night for most strokes. But with innovations in stroke treatments, that’s all changed,” Dr. Likosky says. “It really helped to give birth to the neurohospitalist movement.”
A recent survey on the current scope of neurohospitalists’ practice presented by Dr. Likosky and colleagues at the American Academy of Neurology found that 8% of those surveyed were full-time neurohospitalists. The number might seem small, but it might be a matter of perception. The same study showed 73% of neurologists surveyed listed inpatient neurology care as their primary practice focus.2
Another driver for the neurohospitalist movement was that it became unfeasible to staff inpatient neurology services with physicians who maintained offices “across town,” observes S. Andrew Josephson, MD, director of the neurohospitalist program and inpatient neurology at UCSF. “Stroke is just one example of a disease that has so many emergent therapies that hospitals decided they needed a neurologist on site to make those types of treatment decisions.”
At a quaternary-care center such as UCSF, the requirements for otolaryngology expertise have increased exponentially, says Andrew H. Murr, MD, FACS, vice-chair of the Department of Otolaryngology/Head and Neck Surgery at UCSF. “For instance, our hospital has a huge transplant volume. Often, patients are on immuno-compromising medications that create the specter of fungal sinusitis,” he says. “We also get called to the operating room or ICU when patients have breathing problems and require surgical airways or other complicated intubation schemes. All of these problems require a lot of time, effort, and special expertise.”
Since September of last year, Dr. Murr’s department has been using office space adjacent to the hospital as headquarters for a full-time otolaryngologist whose sole responsibility is to cover inpatient work. Increased complexity of otolaryngologic-related problems, increased ED commitment, and a simple matter of logistics prompted the move. The Department of Otolaryngology moved 10 minutes away from the hospital, so literally running across the street for an otolaryngology consult was no longer an option.
Today, the hospital duty is linked to the department’s call schedule. Dr. Murr anticipates the department soon will establish a full-time faculty position to create a hospitalist niche within the department.
Usefulness Affirmed
Good results already have been demonstrated for the hospitalist model in other specialties. In the first two years of the surgical hospitalist program at UCSF, response times for surgical consultations averaged less than 20 minutes; the average wait for patients with acute appendicitis to undergo surgery was cut in half; and the number of billable consults rose by almost 200%.3
Heidi Wald, MD, MSPH, FHM, a 2009 Health and Aging Policy Fellow, and two hospitalist colleagues studied the impact of hospitalist programs on acute-care geriatrics and found a paucity of geriatric-care approaches.4 “The employment of geriatrics-trained clinicians by hospitalist programs is one approach to supporting generalist-hospitalists and inclining group culture toward clinical geriatric concerns,” the authors wrote. “Programs that purposefully hired geriatricians and gerontology nurse-practitioners used them to staff geriatrics services.”
Dr. Wald, assistant professor of medicine in the division of Health Care Policy Research and a hospitalist at the University of Colorado Denver, says trends in patient demographics and patient-safety initiatives will drive the proliferation of more geriatrician-hospitalists and geriatrics-focused services in the future. “The median age of the hospital population is increasing,” she notes, “and there are not enough geriatricians to deal with every elderly patient.”
Mount Sinai’s Dr. Farber is in the process of submitting for publication two years’ worth of data about the MACE service at Mount Sinai, which will evaluate the effect of MACE on costs, length of stay, and rehospitalization rates.
Variations on a Theme
The dermatology HM model at UCSF more closely resembles a consultative practice model. UCSF’s dermatology hospitalists do not admit patients. Still, says SDH’s Dr. Fox, because of their conversance with inpatient care and round-the-clock availability, dermatology hospitalists are invaluable. They help colleagues “puzzle out” the causes of cutaneous manifestations of system disease, quickly initiate state of the art treatment for hospital-acquired skin conditions, and improve outcomes for hospitalized patients with skin diseases.
“We see our charge as being multifold,” Dr. Fox explains. “We provide continuity of care for patients who are frequently hospitalized; we keep up with the medical literature; we are comfortable with and know the nuances of hospital operations; and we provide education to residents, house staff, and colleagues.”
In Denver, the Acute Care for the Elderly (ACE) service operated by the internal-medicine hospitalist group has only informal ties to the Department of Medicine’s Geriatrics Division, Dr. Wald says. Although not a closed geriatric-care unit, the service concentrates elderly patients on one inpatient service and introduces the tenets of geriatric care—multidisciplinary approach, functional assessment, early discharge planning, mitigating the hazards of hospitalization, and patient and family-centered care—into a hospitalist milieu.
Surgical hospitalist models also vary by setting, and continue to evolve as surgeons examine processes to determine what works and what doesn’t. At UCSF, the original model relied on surgeons taking call for seven days running. “You probably couldn’t do that continuously for your career,” says Dr. Maa, who worked the seven-day call schedule for 3 1/2 years.
The program has been modified so that the surgical hospitalists now work three- or four-day stretches.
Another successful variation involves one surgeon taking all the daytime shifts, while others rotate in for the PM shifts and weekends.
A Win-Win for Hospitalists?
Does the proliferation of specialty hospitalists create competition for patients? That could be a possibility, says Dr. Frost, should other specialty hospitalists become interested in providing care for the “bread and butter” pathologies.
“For instance, if neurohospitalists were interested in evaluating and managing patients with TIAs (transient ischemic attacks), or cardiohospitalists were interested in managing patients with low-risk chest pain, then there could be some competition,” Dr. Frost says. Although possible, he senses it isn’t a likely scenario.
What’s more likely, according to neurohospitalist Dr. Likosky, is cross-fertilization between specialties, where hospitalists who interface with their specialty colleagues gain the benefit of on-site, in-service education. “Many hospitalists feel that they were not adequately trained in neurologic illnesses, and yet, by default, they have become the first-line providers of inpatient neurologic care nationally,” Dr. Likosky says. “The neurohospitalist model is a way of getting at that issue. I don’t think that we are in competition. I think we are welcome partners.”
Dr. Likosky and fellow neurohospitalists Dr. Josephson and W. David Freeman, MD, assistant professor in the department of neurology and critical care at the Mayo Clinic College of Medicine in Jacksonville, Fla., offered the first neurology precourse in April at HM10 in Washington, D.C., and more and more hospitalist meetings are including neurohospitalist courses on their schedules.
Increased education also is a benefit of Mount Sinai’s adaptation of the MACE concept, Dr. Farber says. Because the hospitalist-run MACE patients are located throughout the hospital, the team conducts nursing grand rounds to educate other hospital staff about geriatrics-centered HM principles.
—John Maa, MD, FACS, assistant professor, Department of Surgery; assistant chair, Surgery Quality Improvement Program; director, Surgical Hospitalist Program, University of California at San Francisco
Economies of Scale
Dr. Fox, the dermatology hospitalist, is the first to admit that UCSF’s practice model probably works best in a large, tertiary-care, academic medical center. However, the potential exists for extension into rural settings with telemedicine models and trained physician assistants or nurse practitioners, she notes.
Dr. Farber agrees the HM model is adaptable to a variety of medical specialties; he foresees geriatric hospitalists working in community settings. “Even in smaller hospitals with fewer discharges, there will be a sizable subset of admissions of patients at risk for high utilization of resources,” he says. “Many of Medicare’s hospital-acquired conditions are geriatrics-related, such as catheter-associated urinary tract infections, central-line infections, and falls. The investment [in geriatrician-hospitalist teams] could be justified if you track the outcomes of these high-risk patients over time and see whether you’re reducing length of stay, direct costs, and readmissions.”
Dr. Likosky says the benefits of the neurohospitalist model closely mirror those of the HM model, and although volumes are lower, the benefits “remain significant even in relatively small hospitals.” His American Academy of Neurology (AAN) survey backs up this observation: Neurohospitalists were about evenly split between academic and private settings (49% and 51%, respectively). “Unlike dermatology, neurologic diagnoses are very common as either a primary or secondary reason for admission to the hospital,” Dr. Likosky says.
In the community setting, surgical hospitalist programs provide a new answer for ED call coverage, Dr. Maa says. Surgical practices often approach the medical center leadership to negotiate a stipend, then contribute salary support so that a new surgeon can be recruited to join the practice. This physician—usually a younger surgeon—then is hired in the role of a surgicalist so that timely patient care and surgeon availability can be ensured.
In rural settings, however, even this model might not be feasible, Dr. Maa says, because surgical practices could be comprised of only one or two surgeons. “We will have to think differently about telemedicine, telesurgery, and having ERs equipped with video monitors so that the ED physician can examine the patient while a surgeon, at a remote centralized area, can provide input,” he says.
Adoption of the hospitalist model by other specialties shows no sign of slowing down. That’s good news for HM and patient care, Dr. Maa says.
“This represents a transformation of the way an academic medical center is structured,” he adds. “We’ve traditionally prioritized research ahead of patient care, but this model is inverting that. It is patient-centered, making them the priority, and answers the question, ‘How can we reconfigure what we have to take better care of patients?’ And that’s why I think we’ll succeed.” TH
Gretchen Henkel is a freelance writer based in California.
References
- Krugman SD, Suggs A, Photowala HY, et al. Redefining the community pediatric hospitalist: the combined pediatric ED/inpatient unit. Ped Emerg Car. 2007;23(1):33-37.
- Likosky D. Is it time for neurohospitalists? Neurology. 2009;72(9):859-860.
- Maa J, Carter JT, Gosnell JE, et al. The surgical hospitalist: a new model for emergency surgical care. J Am Coll Surg. 2007;205(5):704-711.
- Wald H, Huddleston J, Kramer A. Is there a geriatrician in the house? Geriatric care approaches in hospitalist programs. J Hosp Med. 2006;1(1):29-35.
Unique Factors Propel Proliferation of “ists” at Washington Hospital
By Gretchen Henkel
“Ists” are multiplying at Providence Regional Medical Center in Everett, Wash. (PRMCE), about 25 miles north of Seattle. The medical hospitalist team manages 90% of the hospital’s medical patients and comprises 34 FTEs, with nocturnists and a palliative-care service; other in-house services include general surgery hospitalists, critical-care hospitalists, orthopedic hospitalists, neurology hospitalists, pediatric hospitalists, and obstetrics hospitalists.
So many “ists” under one roof is unusual for a community-based medical center. One reason for the trend is a highly successful hospitalist program that’s caused other specialists to take notice of the increase in quality metrics and job satisfaction.
“For some reason, we were blessed with an early decision by the hospitalists to acculturate themselves with the hospital’s mission,” says Joanne C. Roberts, MD, FACP, chief of the division of medicine, hospice, and palliative medicine at PRMCE.
The medical hospitalists quickly instituted standardization, quality, and utilization measures, and tied their performance to incentives, says HM medical director Jefferey S. Winningham, MD. For example, every hospitalist is required to leave voicemails for referring physicians upon admittance and discharge of their patients. A 95% compliance rate—validated by surveys of referring physicians—yields bonuses for the HM team.
Quality scores have increased dramatically since 2003, when the hospitalist program took off. PRMCE chief medical officer Larry Schechter, MD, says that the hospitalists’ success has increased the willingness of other specialists to adopt the HM model for delivering inpatient care.
Another factor in the swift adoption of specialist hospitalists: Except for the intensivist service—recipient of the American Association of Critical-Care Nurses’ 2008-2009 Beacon Award for Care Excellence—most of PRMCE’s programs are staffed with physician members of Everett Clinic, a large multispecialty group. “The secret of this community is the large medical groups,” Dr. Roberts says. “Everybody plays well together, especially at the senior leadership level.”
Fewer administrators means nimble decision-making, Dr. Schechter notes. Hospitalists’ internal teamwork is continuously reinforced through bimonthly team meetings; with hospital administrators in steering committee meetings, the hospitalist program has “set a high bar and brought the community together,” Dr. Winningham says.
As PRMCE grows—a new, 12-story tower is set to open in 2011—the hospital is poised to attain its mission of becoming a regional referral center. “To deliver quality at the lowest cost is a really serious enterprise,” Dr. Roberts says, “so getting the hospitalists engaged in that value proposition has been challenging but delightfully fun.”
If imitation is the sincerest form of flattery, then hospitalists have a lot to crow about. For the same reasons that sparked the original hospital medicine movement, HM’s specialist colleagues are flocking to the HM model.
“I switched because your impact with consultation is limited,” says geriatrician-hospitalist Jeffrey Farber, MD, assistant professor of geriatrics and palliative medicine and director of the Mobile Acute Care for the Elderly Service (MACE) at Mount Sinai Hospital in New York City. As the former director of the Department of Geriatrics’ consult service, Dr. Farber adds, “I like being able to call the shots and direct the care.”
He’s not the only one. Neurologists, surgeons, and even dermatologists and otolaryngologists have been establishing inpatient services based on the HM model. While many of these programs first begin in the academic setting, where resident work-hour limits necessitate faculty coverage, community hospitals increasingly are turning to specialist hospitalists to address patient-safety and treatment-innovation issues.
According to a leading surgical hospitalist, more than 250 such programs exist throughout the country.
Shaun Frost, MD, FACP, SFHM, chair of SHM’s Membership Committee and SHM’s Emergency Medicine Task Force, an SHM board member, and regional medical director for Brentwood, Tenn.-based Cogent Healthcare, views the growth of specialty hospitalist programs as a positive development. “In many ways, [this trend] is confirmatory regarding the key reasons for creation of the hospital movement,” he says.
For example, mirroring the performance of adult inpatient hospitalist programs, pediatric hospitalist programs have now documented improved throughput, increased efficiency, and increased patient satisfaction, especially when such programs combine pediatric emergency department and pediatric inpatient coverage.1
“We’ve all been inspired by the success of the medical hospitalist model, and we want to acknowledge and credit them for being the trailblazers and pioneers who are leading the way,” adds John Maa, MD, FACS, assistant professor in the Department of Surgery, assistant chair of the Surgery Quality Improvement Program, and director of the Surgical Hospitalist Program at the University of California at San Francisco (UCSF). Dr. Maa and colleagues introduced the surgical hospitalist program at UCSF in July 2005.
—David Likosky, MD, FHM, neurohospitalist, stroke program director, Evergreen Hospital Medical Center, Seattle
What’s Driving the Trend?
The impetus for adopting and adapting the HM model varies across medical specialties. For some, it was necessity; for others, it was a way to extend coverage or streamline the hospital stay; and for still others, it was a matter of personal choice.
“We couldn’t continue in the old paradigm and deliver safe care, because it was traditionally resident-dependent,” says Dr. Maa, explaining that the 80-hour resident workweek restriction mandated by the Accreditation Council for Graduate Medical Education (ACGME) “annihilated” the old-school model.
The goal in organizing the Society of Dermatology Hospitalists (SDH), according to SDH cofounder Lindy P. Fox, MD, assistant professor of clinical dermatology and director of the hospital consultation service at UCSF, was to ensure 24/7 coverage by a dedicated group of dermatologists whose skill set is focused on inpatient care, and who, because of their involvement with the university hospital, are probably more comfortable with the nuances of inpatient dermatologic care than their outpatient-based colleagues. The SDH currently has 20 members representing about 15 academic programs.
Innovations in stroke treatment caused a “sea change” for the field of neurology, says David Likosky, MD, SFHM, hospitalist and stroke program director at Evergreen Hospital Medical Center in Seattle. Dr. Likosky, who is board-certified in neurology and internal medicine, says the HM model allows neurohospitalists to enjoy a work-life balance.
“It used to be that neurologists didn’t have to get out of bed at night for most strokes. But with innovations in stroke treatments, that’s all changed,” Dr. Likosky says. “It really helped to give birth to the neurohospitalist movement.”
A recent survey on the current scope of neurohospitalists’ practice presented by Dr. Likosky and colleagues at the American Academy of Neurology found that 8% of those surveyed were full-time neurohospitalists. The number might seem small, but it might be a matter of perception. The same study showed 73% of neurologists surveyed listed inpatient neurology care as their primary practice focus.2
Another driver for the neurohospitalist movement was that it became unfeasible to staff inpatient neurology services with physicians who maintained offices “across town,” observes S. Andrew Josephson, MD, director of the neurohospitalist program and inpatient neurology at UCSF. “Stroke is just one example of a disease that has so many emergent therapies that hospitals decided they needed a neurologist on site to make those types of treatment decisions.”
At a quaternary-care center such as UCSF, the requirements for otolaryngology expertise have increased exponentially, says Andrew H. Murr, MD, FACS, vice-chair of the Department of Otolaryngology/Head and Neck Surgery at UCSF. “For instance, our hospital has a huge transplant volume. Often, patients are on immuno-compromising medications that create the specter of fungal sinusitis,” he says. “We also get called to the operating room or ICU when patients have breathing problems and require surgical airways or other complicated intubation schemes. All of these problems require a lot of time, effort, and special expertise.”
Since September of last year, Dr. Murr’s department has been using office space adjacent to the hospital as headquarters for a full-time otolaryngologist whose sole responsibility is to cover inpatient work. Increased complexity of otolaryngologic-related problems, increased ED commitment, and a simple matter of logistics prompted the move. The Department of Otolaryngology moved 10 minutes away from the hospital, so literally running across the street for an otolaryngology consult was no longer an option.
Today, the hospital duty is linked to the department’s call schedule. Dr. Murr anticipates the department soon will establish a full-time faculty position to create a hospitalist niche within the department.
Usefulness Affirmed
Good results already have been demonstrated for the hospitalist model in other specialties. In the first two years of the surgical hospitalist program at UCSF, response times for surgical consultations averaged less than 20 minutes; the average wait for patients with acute appendicitis to undergo surgery was cut in half; and the number of billable consults rose by almost 200%.3
Heidi Wald, MD, MSPH, FHM, a 2009 Health and Aging Policy Fellow, and two hospitalist colleagues studied the impact of hospitalist programs on acute-care geriatrics and found a paucity of geriatric-care approaches.4 “The employment of geriatrics-trained clinicians by hospitalist programs is one approach to supporting generalist-hospitalists and inclining group culture toward clinical geriatric concerns,” the authors wrote. “Programs that purposefully hired geriatricians and gerontology nurse-practitioners used them to staff geriatrics services.”
Dr. Wald, assistant professor of medicine in the division of Health Care Policy Research and a hospitalist at the University of Colorado Denver, says trends in patient demographics and patient-safety initiatives will drive the proliferation of more geriatrician-hospitalists and geriatrics-focused services in the future. “The median age of the hospital population is increasing,” she notes, “and there are not enough geriatricians to deal with every elderly patient.”
Mount Sinai’s Dr. Farber is in the process of submitting for publication two years’ worth of data about the MACE service at Mount Sinai, which will evaluate the effect of MACE on costs, length of stay, and rehospitalization rates.
Variations on a Theme
The dermatology HM model at UCSF more closely resembles a consultative practice model. UCSF’s dermatology hospitalists do not admit patients. Still, says SDH’s Dr. Fox, because of their conversance with inpatient care and round-the-clock availability, dermatology hospitalists are invaluable. They help colleagues “puzzle out” the causes of cutaneous manifestations of system disease, quickly initiate state of the art treatment for hospital-acquired skin conditions, and improve outcomes for hospitalized patients with skin diseases.
“We see our charge as being multifold,” Dr. Fox explains. “We provide continuity of care for patients who are frequently hospitalized; we keep up with the medical literature; we are comfortable with and know the nuances of hospital operations; and we provide education to residents, house staff, and colleagues.”
In Denver, the Acute Care for the Elderly (ACE) service operated by the internal-medicine hospitalist group has only informal ties to the Department of Medicine’s Geriatrics Division, Dr. Wald says. Although not a closed geriatric-care unit, the service concentrates elderly patients on one inpatient service and introduces the tenets of geriatric care—multidisciplinary approach, functional assessment, early discharge planning, mitigating the hazards of hospitalization, and patient and family-centered care—into a hospitalist milieu.
Surgical hospitalist models also vary by setting, and continue to evolve as surgeons examine processes to determine what works and what doesn’t. At UCSF, the original model relied on surgeons taking call for seven days running. “You probably couldn’t do that continuously for your career,” says Dr. Maa, who worked the seven-day call schedule for 3 1/2 years.
The program has been modified so that the surgical hospitalists now work three- or four-day stretches.
Another successful variation involves one surgeon taking all the daytime shifts, while others rotate in for the PM shifts and weekends.
A Win-Win for Hospitalists?
Does the proliferation of specialty hospitalists create competition for patients? That could be a possibility, says Dr. Frost, should other specialty hospitalists become interested in providing care for the “bread and butter” pathologies.
“For instance, if neurohospitalists were interested in evaluating and managing patients with TIAs (transient ischemic attacks), or cardiohospitalists were interested in managing patients with low-risk chest pain, then there could be some competition,” Dr. Frost says. Although possible, he senses it isn’t a likely scenario.
What’s more likely, according to neurohospitalist Dr. Likosky, is cross-fertilization between specialties, where hospitalists who interface with their specialty colleagues gain the benefit of on-site, in-service education. “Many hospitalists feel that they were not adequately trained in neurologic illnesses, and yet, by default, they have become the first-line providers of inpatient neurologic care nationally,” Dr. Likosky says. “The neurohospitalist model is a way of getting at that issue. I don’t think that we are in competition. I think we are welcome partners.”
Dr. Likosky and fellow neurohospitalists Dr. Josephson and W. David Freeman, MD, assistant professor in the department of neurology and critical care at the Mayo Clinic College of Medicine in Jacksonville, Fla., offered the first neurology precourse in April at HM10 in Washington, D.C., and more and more hospitalist meetings are including neurohospitalist courses on their schedules.
Increased education also is a benefit of Mount Sinai’s adaptation of the MACE concept, Dr. Farber says. Because the hospitalist-run MACE patients are located throughout the hospital, the team conducts nursing grand rounds to educate other hospital staff about geriatrics-centered HM principles.
—John Maa, MD, FACS, assistant professor, Department of Surgery; assistant chair, Surgery Quality Improvement Program; director, Surgical Hospitalist Program, University of California at San Francisco
Economies of Scale
Dr. Fox, the dermatology hospitalist, is the first to admit that UCSF’s practice model probably works best in a large, tertiary-care, academic medical center. However, the potential exists for extension into rural settings with telemedicine models and trained physician assistants or nurse practitioners, she notes.
Dr. Farber agrees the HM model is adaptable to a variety of medical specialties; he foresees geriatric hospitalists working in community settings. “Even in smaller hospitals with fewer discharges, there will be a sizable subset of admissions of patients at risk for high utilization of resources,” he says. “Many of Medicare’s hospital-acquired conditions are geriatrics-related, such as catheter-associated urinary tract infections, central-line infections, and falls. The investment [in geriatrician-hospitalist teams] could be justified if you track the outcomes of these high-risk patients over time and see whether you’re reducing length of stay, direct costs, and readmissions.”
Dr. Likosky says the benefits of the neurohospitalist model closely mirror those of the HM model, and although volumes are lower, the benefits “remain significant even in relatively small hospitals.” His American Academy of Neurology (AAN) survey backs up this observation: Neurohospitalists were about evenly split between academic and private settings (49% and 51%, respectively). “Unlike dermatology, neurologic diagnoses are very common as either a primary or secondary reason for admission to the hospital,” Dr. Likosky says.
In the community setting, surgical hospitalist programs provide a new answer for ED call coverage, Dr. Maa says. Surgical practices often approach the medical center leadership to negotiate a stipend, then contribute salary support so that a new surgeon can be recruited to join the practice. This physician—usually a younger surgeon—then is hired in the role of a surgicalist so that timely patient care and surgeon availability can be ensured.
In rural settings, however, even this model might not be feasible, Dr. Maa says, because surgical practices could be comprised of only one or two surgeons. “We will have to think differently about telemedicine, telesurgery, and having ERs equipped with video monitors so that the ED physician can examine the patient while a surgeon, at a remote centralized area, can provide input,” he says.
Adoption of the hospitalist model by other specialties shows no sign of slowing down. That’s good news for HM and patient care, Dr. Maa says.
“This represents a transformation of the way an academic medical center is structured,” he adds. “We’ve traditionally prioritized research ahead of patient care, but this model is inverting that. It is patient-centered, making them the priority, and answers the question, ‘How can we reconfigure what we have to take better care of patients?’ And that’s why I think we’ll succeed.” TH
Gretchen Henkel is a freelance writer based in California.
References
- Krugman SD, Suggs A, Photowala HY, et al. Redefining the community pediatric hospitalist: the combined pediatric ED/inpatient unit. Ped Emerg Car. 2007;23(1):33-37.
- Likosky D. Is it time for neurohospitalists? Neurology. 2009;72(9):859-860.
- Maa J, Carter JT, Gosnell JE, et al. The surgical hospitalist: a new model for emergency surgical care. J Am Coll Surg. 2007;205(5):704-711.
- Wald H, Huddleston J, Kramer A. Is there a geriatrician in the house? Geriatric care approaches in hospitalist programs. J Hosp Med. 2006;1(1):29-35.
Unique Factors Propel Proliferation of “ists” at Washington Hospital
By Gretchen Henkel
“Ists” are multiplying at Providence Regional Medical Center in Everett, Wash. (PRMCE), about 25 miles north of Seattle. The medical hospitalist team manages 90% of the hospital’s medical patients and comprises 34 FTEs, with nocturnists and a palliative-care service; other in-house services include general surgery hospitalists, critical-care hospitalists, orthopedic hospitalists, neurology hospitalists, pediatric hospitalists, and obstetrics hospitalists.
So many “ists” under one roof is unusual for a community-based medical center. One reason for the trend is a highly successful hospitalist program that’s caused other specialists to take notice of the increase in quality metrics and job satisfaction.
“For some reason, we were blessed with an early decision by the hospitalists to acculturate themselves with the hospital’s mission,” says Joanne C. Roberts, MD, FACP, chief of the division of medicine, hospice, and palliative medicine at PRMCE.
The medical hospitalists quickly instituted standardization, quality, and utilization measures, and tied their performance to incentives, says HM medical director Jefferey S. Winningham, MD. For example, every hospitalist is required to leave voicemails for referring physicians upon admittance and discharge of their patients. A 95% compliance rate—validated by surveys of referring physicians—yields bonuses for the HM team.
Quality scores have increased dramatically since 2003, when the hospitalist program took off. PRMCE chief medical officer Larry Schechter, MD, says that the hospitalists’ success has increased the willingness of other specialists to adopt the HM model for delivering inpatient care.
Another factor in the swift adoption of specialist hospitalists: Except for the intensivist service—recipient of the American Association of Critical-Care Nurses’ 2008-2009 Beacon Award for Care Excellence—most of PRMCE’s programs are staffed with physician members of Everett Clinic, a large multispecialty group. “The secret of this community is the large medical groups,” Dr. Roberts says. “Everybody plays well together, especially at the senior leadership level.”
Fewer administrators means nimble decision-making, Dr. Schechter notes. Hospitalists’ internal teamwork is continuously reinforced through bimonthly team meetings; with hospital administrators in steering committee meetings, the hospitalist program has “set a high bar and brought the community together,” Dr. Winningham says.
As PRMCE grows—a new, 12-story tower is set to open in 2011—the hospital is poised to attain its mission of becoming a regional referral center. “To deliver quality at the lowest cost is a really serious enterprise,” Dr. Roberts says, “so getting the hospitalists engaged in that value proposition has been challenging but delightfully fun.”
ONLINE EXCLUSIVE: HM pioneer Bob Wachter, MD, MHM, discusses the growing trend of specialist-hospitalists
Bob Wachter, MD, MHM, has watched the hospitalist movement grow from its infancy in the mid-1990s to more than 30,000 hospitalists practicing nationwide today. As professor and chief of the Division of Hospital Medicine and associate chairman of the Department of Medicine at the University of California at San Francisco, and chief of the medical service at UCSF Medical Center, Dr. Wachter also has watched the HM model spread to other medical specialties, including a handful of departments in his own hospital. The Hospitalist caught up with Dr. Wachter and found out what he thinks about the spread of the HM model.
Question: Do specialist-hospitalist programs threaten to siphon off your medical hospitalist workforce, or are they a boon?
Answer: Having specialized physicians focus on hospital care is a powerful model. Not only are they available all the time, but they are keeping up with innovations in their field. More importantly, they get involved in system improvement in a way that the part-time hospital person will not.

—Bob Wachter, MD, MHM
Q: Are there direct benefits to the hospitalist on the floor?
A: I think it creates a vehicle for collegiality, interchange, and learning across the specialties, which is harder to come by when we’re in the hospital all the time, but the consults we’re interacting with may not be.
Q: Aren’t hospitalists already comanaging patients with neurosurgery, hematology/oncology, and orthopedics at your institution? How are specialist hospitalists different?
A: Neurohospitalists focus their professional practice on the hospitalized care of patients with neurological diseases—they perform the same function for those patients as we do for medical patients. That is, they admit patients, supervise their overall care, and discharge them. On our neurosurgery service, which has a census of 50 patients, the surgeons are in the operating room much of the day. Their post-surgical patients often have multiple medical comorbidities (heart failure, high blood pressures, diabetes, etc.), which is where the medical hospitalist comes in to comanage and coordinate their medical care.
We probably need new lingo to distinguish between medical hospitalists comanaging specialty patients and specialty hospitalists, because it can be confusing to people.
Q: Is this model sustainable in the community and rural settings, where specialists are in short supply?
A: There is a size below which you probably cannot support a specialty hospitalist. But larger places can, and their value is not only what they do at that individual hospital, but the fact that they can teach and do research and (quality improvement) that may help influence care beyond their organization’s walls.
—GH
Bob Wachter, MD, MHM, has watched the hospitalist movement grow from its infancy in the mid-1990s to more than 30,000 hospitalists practicing nationwide today. As professor and chief of the Division of Hospital Medicine and associate chairman of the Department of Medicine at the University of California at San Francisco, and chief of the medical service at UCSF Medical Center, Dr. Wachter also has watched the HM model spread to other medical specialties, including a handful of departments in his own hospital. The Hospitalist caught up with Dr. Wachter and found out what he thinks about the spread of the HM model.
Question: Do specialist-hospitalist programs threaten to siphon off your medical hospitalist workforce, or are they a boon?
Answer: Having specialized physicians focus on hospital care is a powerful model. Not only are they available all the time, but they are keeping up with innovations in their field. More importantly, they get involved in system improvement in a way that the part-time hospital person will not.
—Bob Wachter, MD, MHM
Q: Are there direct benefits to the hospitalist on the floor?
A: I think it creates a vehicle for collegiality, interchange, and learning across the specialties, which is harder to come by when we’re in the hospital all the time, but the consults we’re interacting with may not be.
Q: Aren’t hospitalists already comanaging patients with neurosurgery, hematology/oncology, and orthopedics at your institution? How are specialist hospitalists different?
A: Neurohospitalists focus their professional practice on the hospitalized care of patients with neurological diseases—they perform the same function for those patients as we do for medical patients. That is, they admit patients, supervise their overall care, and discharge them. On our neurosurgery service, which has a census of 50 patients, the surgeons are in the operating room much of the day. Their post-surgical patients often have multiple medical comorbidities (heart failure, high blood pressures, diabetes, etc.), which is where the medical hospitalist comes in to comanage and coordinate their medical care.
We probably need new lingo to distinguish between medical hospitalists comanaging specialty patients and specialty hospitalists, because it can be confusing to people.
Q: Is this model sustainable in the community and rural settings, where specialists are in short supply?
A: There is a size below which you probably cannot support a specialty hospitalist. But larger places can, and their value is not only what they do at that individual hospital, but the fact that they can teach and do research and (quality improvement) that may help influence care beyond their organization’s walls.
—GH
Bob Wachter, MD, MHM, has watched the hospitalist movement grow from its infancy in the mid-1990s to more than 30,000 hospitalists practicing nationwide today. As professor and chief of the Division of Hospital Medicine and associate chairman of the Department of Medicine at the University of California at San Francisco, and chief of the medical service at UCSF Medical Center, Dr. Wachter also has watched the HM model spread to other medical specialties, including a handful of departments in his own hospital. The Hospitalist caught up with Dr. Wachter and found out what he thinks about the spread of the HM model.
Question: Do specialist-hospitalist programs threaten to siphon off your medical hospitalist workforce, or are they a boon?
Answer: Having specialized physicians focus on hospital care is a powerful model. Not only are they available all the time, but they are keeping up with innovations in their field. More importantly, they get involved in system improvement in a way that the part-time hospital person will not.
—Bob Wachter, MD, MHM
Q: Are there direct benefits to the hospitalist on the floor?
A: I think it creates a vehicle for collegiality, interchange, and learning across the specialties, which is harder to come by when we’re in the hospital all the time, but the consults we’re interacting with may not be.
Q: Aren’t hospitalists already comanaging patients with neurosurgery, hematology/oncology, and orthopedics at your institution? How are specialist hospitalists different?
A: Neurohospitalists focus their professional practice on the hospitalized care of patients with neurological diseases—they perform the same function for those patients as we do for medical patients. That is, they admit patients, supervise their overall care, and discharge them. On our neurosurgery service, which has a census of 50 patients, the surgeons are in the operating room much of the day. Their post-surgical patients often have multiple medical comorbidities (heart failure, high blood pressures, diabetes, etc.), which is where the medical hospitalist comes in to comanage and coordinate their medical care.
We probably need new lingo to distinguish between medical hospitalists comanaging specialty patients and specialty hospitalists, because it can be confusing to people.
Q: Is this model sustainable in the community and rural settings, where specialists are in short supply?
A: There is a size below which you probably cannot support a specialty hospitalist. But larger places can, and their value is not only what they do at that individual hospital, but the fact that they can teach and do research and (quality improvement) that may help influence care beyond their organization’s walls.
—GH
Innovative Use of Scribes in the Inpatient Setting
Over the past couple of decades, the ever-increasing medical-legal, financial, and patient-safety demands have led to a mushrooming of the amount of documentation needed during patient care, especially in the inpatient setting. With the advent of HM, that burden simply shifted to hospitalists, along with rapidly expanding patient loads as PCPs started delegating inpatient care. The problem was further compounded in teaching hospitals by a gradual decline in resident support as patient caps and work-hour limits were instituted.
Not surprisingly, the quality and accuracy of physicians’ progress notes started to suffer. It became frequently difficult to remember the details of encounters from earlier in the day, and fatigue sometimes led to details essential to continuity of care being left out completely.
A potential—and very intriguing—solution presented itself, however, as we were designing family-centered team rounds. Apparently, the ED group at the adjacent Abbott-Northwestern Hospital in Minneapolis had been using scribes for several years. The scribes captured the providers’ notes during each encounter, and the group had developed a polished system of scribe recruitment and training (mostly pre-med students awaiting acceptance to medical schools).
But would this model work in the inpatient setting where workflow was completely different? This was a total unknown, given that there has been no precedent in the literature about inpatient scribe utilization. Although relatively meager in number, the published articles about outpatient use of scribes were generally favorable, with the authors noting improved productivity and increased patient and staff satisfaction.1,2,3,4
Operationally, the main difference between inpatient and outpatient scribe use lied in the rounding mechanism itself; it was not just a provider-patient interaction, as in the ED, but rather a sometimes cacophonous collection of multiple inputs from families, providers, students, residents, nurses, and ancillary staff. The challenge here was to train the scribes (natural ability played a significant role) to produce a coherent document out of this interaction; the document had to accurately reflect current status and plans of care. The first step was to create a template for the daily progress notes with all the necessary headings, as well as age-appropriate normal exams, with the ability to directly import from the EMR such dynamic data as vital signs, medication lists, and lab results.
Each morning prior to rounds, the scribe was provided a list of patients to be rounded on, and the scribe spent about 30 minutes creating partial notes on each patient, as well as a brief patient identification statement. This proved to be a significant time-saver during rounds and allowed the scribes to keep up with the care team. Each note was pre-pended with the following statements, as recommended by the hospital’s risk-management team:
- I, (scribe name), am serving as a scribe to document services personally performed by (hospitalist name), MD, based on my observation and the provider’s statements to me.
- I, (hospitalist name), MD, attest that (scribe name) is acting in a scribe capacity, has observed my performance of the services, and has documented them in accordance with my direction.
A computer-on-wheels (COW) station was assigned to the scribes and accompanied the rounding team into the patient rooms, making it possible for them to follow the interactions in real time. The scribes were encouraged to hold their hands up and interrupt the conversation at any time if they needed clarification, something that happened rather infrequently. On the other hand, the care team was directed to speak clearly and the residents were instructed to present their cases using the same format as the progress-note template, thus minimizing guesswork on the part of the scribes. The only part of the interaction the scribes could not transcribe directly was the physical examination, and typically the attending physician dictated abnormal findings as well as systems not assessed, if any, at the end. All the scribe-generated notes were forwarded to the rounding provider’s EMR inbox and reviewed by the latter, amended when necessary, and signed electronically. The review of the scribe-generated notes proved to be initially a time-consuming process, typically two hours. However, as the scribes gained experience, the time commitment on the part of the providers decreased rapidly; after about three months, the time spent was about 30 minutes on busy days, even less otherwise, with a concomitant increase in satisfaction with the scribing process.
Not too unexpectedly, our transcription service initially pushed back on this idea because of their fear of job loss. However, this issue was resolved by eliminating the need for outsourcing overflow dictations. In addition, the relative terseness of the scribed notes did not sit well initially with some of our colleagues used to excessive verbosity, and this issue again gradually faded away as physicians realized that all the necessary information for care was preserved.
Does a scribe program make sense in all situations? Not likely. This kind of setup will work best in busy tertiary-care centers with residency programs and family-centered team rounds. Furthermore, a nearby college or university is a must if cost-efficient hiring of pre-med students is to be possible.
Walid Maalouli, MD, FAAP,
medical director, hospitalist department,
Children’s Hospitals & Clinics of Minnesota, Minneapolis
References
- Arya R, Salovich DM, Ohman-Strickland P, Merlin MA. Impact of scribes on performance indicators in the emergency department. Acad Emerg Med. 2010;17(5):490- 494.
- Koshy S, Feustel PJ, Hong M, Kogan BA. Scribes in an ambulatory urology practice: patient and physician satisfaction. J Urol. 2010;184(1):258-262.
- Conn J. Getting it in writing. Docs using scribes to ease the transition to EHRs. Mod Healthc. 2010;40(6):30,32.
- Expanded scribe role boosts staff morale. ED Manag. 2009;21(7):75-77.
Over the past couple of decades, the ever-increasing medical-legal, financial, and patient-safety demands have led to a mushrooming of the amount of documentation needed during patient care, especially in the inpatient setting. With the advent of HM, that burden simply shifted to hospitalists, along with rapidly expanding patient loads as PCPs started delegating inpatient care. The problem was further compounded in teaching hospitals by a gradual decline in resident support as patient caps and work-hour limits were instituted.
Not surprisingly, the quality and accuracy of physicians’ progress notes started to suffer. It became frequently difficult to remember the details of encounters from earlier in the day, and fatigue sometimes led to details essential to continuity of care being left out completely.
A potential—and very intriguing—solution presented itself, however, as we were designing family-centered team rounds. Apparently, the ED group at the adjacent Abbott-Northwestern Hospital in Minneapolis had been using scribes for several years. The scribes captured the providers’ notes during each encounter, and the group had developed a polished system of scribe recruitment and training (mostly pre-med students awaiting acceptance to medical schools).
But would this model work in the inpatient setting where workflow was completely different? This was a total unknown, given that there has been no precedent in the literature about inpatient scribe utilization. Although relatively meager in number, the published articles about outpatient use of scribes were generally favorable, with the authors noting improved productivity and increased patient and staff satisfaction.1,2,3,4
Operationally, the main difference between inpatient and outpatient scribe use lied in the rounding mechanism itself; it was not just a provider-patient interaction, as in the ED, but rather a sometimes cacophonous collection of multiple inputs from families, providers, students, residents, nurses, and ancillary staff. The challenge here was to train the scribes (natural ability played a significant role) to produce a coherent document out of this interaction; the document had to accurately reflect current status and plans of care. The first step was to create a template for the daily progress notes with all the necessary headings, as well as age-appropriate normal exams, with the ability to directly import from the EMR such dynamic data as vital signs, medication lists, and lab results.
Each morning prior to rounds, the scribe was provided a list of patients to be rounded on, and the scribe spent about 30 minutes creating partial notes on each patient, as well as a brief patient identification statement. This proved to be a significant time-saver during rounds and allowed the scribes to keep up with the care team. Each note was pre-pended with the following statements, as recommended by the hospital’s risk-management team:
- I, (scribe name), am serving as a scribe to document services personally performed by (hospitalist name), MD, based on my observation and the provider’s statements to me.
- I, (hospitalist name), MD, attest that (scribe name) is acting in a scribe capacity, has observed my performance of the services, and has documented them in accordance with my direction.
A computer-on-wheels (COW) station was assigned to the scribes and accompanied the rounding team into the patient rooms, making it possible for them to follow the interactions in real time. The scribes were encouraged to hold their hands up and interrupt the conversation at any time if they needed clarification, something that happened rather infrequently. On the other hand, the care team was directed to speak clearly and the residents were instructed to present their cases using the same format as the progress-note template, thus minimizing guesswork on the part of the scribes. The only part of the interaction the scribes could not transcribe directly was the physical examination, and typically the attending physician dictated abnormal findings as well as systems not assessed, if any, at the end. All the scribe-generated notes were forwarded to the rounding provider’s EMR inbox and reviewed by the latter, amended when necessary, and signed electronically. The review of the scribe-generated notes proved to be initially a time-consuming process, typically two hours. However, as the scribes gained experience, the time commitment on the part of the providers decreased rapidly; after about three months, the time spent was about 30 minutes on busy days, even less otherwise, with a concomitant increase in satisfaction with the scribing process.
Not too unexpectedly, our transcription service initially pushed back on this idea because of their fear of job loss. However, this issue was resolved by eliminating the need for outsourcing overflow dictations. In addition, the relative terseness of the scribed notes did not sit well initially with some of our colleagues used to excessive verbosity, and this issue again gradually faded away as physicians realized that all the necessary information for care was preserved.
Does a scribe program make sense in all situations? Not likely. This kind of setup will work best in busy tertiary-care centers with residency programs and family-centered team rounds. Furthermore, a nearby college or university is a must if cost-efficient hiring of pre-med students is to be possible.
Walid Maalouli, MD, FAAP,
medical director, hospitalist department,
Children’s Hospitals & Clinics of Minnesota, Minneapolis
References
- Arya R, Salovich DM, Ohman-Strickland P, Merlin MA. Impact of scribes on performance indicators in the emergency department. Acad Emerg Med. 2010;17(5):490- 494.
- Koshy S, Feustel PJ, Hong M, Kogan BA. Scribes in an ambulatory urology practice: patient and physician satisfaction. J Urol. 2010;184(1):258-262.
- Conn J. Getting it in writing. Docs using scribes to ease the transition to EHRs. Mod Healthc. 2010;40(6):30,32.
- Expanded scribe role boosts staff morale. ED Manag. 2009;21(7):75-77.
Over the past couple of decades, the ever-increasing medical-legal, financial, and patient-safety demands have led to a mushrooming of the amount of documentation needed during patient care, especially in the inpatient setting. With the advent of HM, that burden simply shifted to hospitalists, along with rapidly expanding patient loads as PCPs started delegating inpatient care. The problem was further compounded in teaching hospitals by a gradual decline in resident support as patient caps and work-hour limits were instituted.
Not surprisingly, the quality and accuracy of physicians’ progress notes started to suffer. It became frequently difficult to remember the details of encounters from earlier in the day, and fatigue sometimes led to details essential to continuity of care being left out completely.
A potential—and very intriguing—solution presented itself, however, as we were designing family-centered team rounds. Apparently, the ED group at the adjacent Abbott-Northwestern Hospital in Minneapolis had been using scribes for several years. The scribes captured the providers’ notes during each encounter, and the group had developed a polished system of scribe recruitment and training (mostly pre-med students awaiting acceptance to medical schools).
But would this model work in the inpatient setting where workflow was completely different? This was a total unknown, given that there has been no precedent in the literature about inpatient scribe utilization. Although relatively meager in number, the published articles about outpatient use of scribes were generally favorable, with the authors noting improved productivity and increased patient and staff satisfaction.1,2,3,4
Operationally, the main difference between inpatient and outpatient scribe use lied in the rounding mechanism itself; it was not just a provider-patient interaction, as in the ED, but rather a sometimes cacophonous collection of multiple inputs from families, providers, students, residents, nurses, and ancillary staff. The challenge here was to train the scribes (natural ability played a significant role) to produce a coherent document out of this interaction; the document had to accurately reflect current status and plans of care. The first step was to create a template for the daily progress notes with all the necessary headings, as well as age-appropriate normal exams, with the ability to directly import from the EMR such dynamic data as vital signs, medication lists, and lab results.
Each morning prior to rounds, the scribe was provided a list of patients to be rounded on, and the scribe spent about 30 minutes creating partial notes on each patient, as well as a brief patient identification statement. This proved to be a significant time-saver during rounds and allowed the scribes to keep up with the care team. Each note was pre-pended with the following statements, as recommended by the hospital’s risk-management team:
- I, (scribe name), am serving as a scribe to document services personally performed by (hospitalist name), MD, based on my observation and the provider’s statements to me.
- I, (hospitalist name), MD, attest that (scribe name) is acting in a scribe capacity, has observed my performance of the services, and has documented them in accordance with my direction.
A computer-on-wheels (COW) station was assigned to the scribes and accompanied the rounding team into the patient rooms, making it possible for them to follow the interactions in real time. The scribes were encouraged to hold their hands up and interrupt the conversation at any time if they needed clarification, something that happened rather infrequently. On the other hand, the care team was directed to speak clearly and the residents were instructed to present their cases using the same format as the progress-note template, thus minimizing guesswork on the part of the scribes. The only part of the interaction the scribes could not transcribe directly was the physical examination, and typically the attending physician dictated abnormal findings as well as systems not assessed, if any, at the end. All the scribe-generated notes were forwarded to the rounding provider’s EMR inbox and reviewed by the latter, amended when necessary, and signed electronically. The review of the scribe-generated notes proved to be initially a time-consuming process, typically two hours. However, as the scribes gained experience, the time commitment on the part of the providers decreased rapidly; after about three months, the time spent was about 30 minutes on busy days, even less otherwise, with a concomitant increase in satisfaction with the scribing process.
Not too unexpectedly, our transcription service initially pushed back on this idea because of their fear of job loss. However, this issue was resolved by eliminating the need for outsourcing overflow dictations. In addition, the relative terseness of the scribed notes did not sit well initially with some of our colleagues used to excessive verbosity, and this issue again gradually faded away as physicians realized that all the necessary information for care was preserved.
Does a scribe program make sense in all situations? Not likely. This kind of setup will work best in busy tertiary-care centers with residency programs and family-centered team rounds. Furthermore, a nearby college or university is a must if cost-efficient hiring of pre-med students is to be possible.
Walid Maalouli, MD, FAAP,
medical director, hospitalist department,
Children’s Hospitals & Clinics of Minnesota, Minneapolis
References
- Arya R, Salovich DM, Ohman-Strickland P, Merlin MA. Impact of scribes on performance indicators in the emergency department. Acad Emerg Med. 2010;17(5):490- 494.
- Koshy S, Feustel PJ, Hong M, Kogan BA. Scribes in an ambulatory urology practice: patient and physician satisfaction. J Urol. 2010;184(1):258-262.
- Conn J. Getting it in writing. Docs using scribes to ease the transition to EHRs. Mod Healthc. 2010;40(6):30,32.
- Expanded scribe role boosts staff morale. ED Manag. 2009;21(7):75-77.
Can You Hear Me Now?
In the past three years, SHM has brought in-depth quality-improvement (QI) programs to nearly every state in the country.
Between its three major mentored implementation projects—Project BOOST (Better Outcomes for Older Adults through Safe Transitions), Glycemic Control Mentored Implemen-tation, and the Venous Thromboembolism (VTE) Collaborative—SHM has worked with more than 100 hospitals across the country and in Canada. SHM is expanding these three programs to additional hospitals and actively developing other QI initiatives.
“SHM’s quality-improvement programs focus on real change, and they have made a substantial impact,” says Joe Miller, SHM’s senior vice president and chief solutions officer. “Hospitalists using SHM’s quality-improvement methods have impacted the care of tens of thousands of hospitalized patients.”
SHM’s programs all use a mix of in-depth mentoring led by national experts and specially designed resource toolkits that enable hospitalists to lead major initiatives within their hospitals. The programs also facilitate “peer learning,” allowing hospitalists to learn from one another.
Project BOOST, which is designed to reduce unplanned readmissions to the hospital, has received national attention. In early 2010, SHM teamed with Blue Cross/Blue Shield of Michigan and the University of Michigan to bring the program to more than a dozen hospitals in that state. SHM also announced a new collaboration with the California HealthCare Foundation to implement Project BOOST in more than 20 hospitals in California.
“Healthcare reform is creating a new focus on quality improvement,” Miller says. “SHM is bringing a multidisciplinary approach to transforming inpatient care to hospitals across the country.” TH
Chapter Updates
Milwaukee/SE Wisconsin
The Milwaukee/SE Wisconsin chapter held a meeting June 10 at Bacchus Restaurant in Milwaukee, at which congratulations were doled out to chapter member Eric Siegal, MD, SFHM, on his election to SHM’s board of directors. As chair of SHM’s Public Policy Committee, Dr. Siegal advocates for such issues as the Physician Quality Reporting Initiative (PQRI).
The chapter also acknowledged Dr. Len Scarpinato of St. Luke’s Hospital, who achieved Senior Fellow in Hospital Medicine (SFHM) designation and was honored at HM10 in April in Washington, D.C. As the regional director of Cogent Healthcare in southeast Wisconsin, Dr. Scarpinato has been instrumental in bringing hospitalists together to network and exchange innovative ideas.
Chapter member Jeanette Kalupa, DNP, ACNP-BC, APNP, of St. Luke’s was mentioned in the opening presentation at HM10 for her work as co-chair of the Nonphysician Providers Committee. Despite a busy HM10 schedule, Drs. Don Lee, Wes Lafferty, Scarpinato, Betty Tucker, and Peter Quandt took time out for a White House tour.
Greater Baltimore Area
The Greater Baltimore Area chapter of SHM met June 16 at Linwood’s Restaurant in Owings Mills, Md. Dr. Suzanne Mitchell spoke on “Relating to the Patient.” The meeting, sponsored by Merck, attracted 50 hospitalists and guests from 10 HM groups.
Los Angeles
The latest Los Angeles chapter meeting was held July 29. The featured speaker was Darrell Harrington, MD, associate medical director for Graduate Medical Education and chief of the division of general internal medicine at Harbor-UCLA Medical Center. Dr. Harrington delivered a presentation about maximizing DVT and PE quality measures. The chapter’s next meeting will be held in the fall.
Fellow in Hospital Medicine Spotlight
James C. Pile, MD, FACP, SFHM

Dr. Pile is an associate professor of medicine, interim director of hospital medicine, and associate program director of the internal residency program at the MetroHealth Campus of Case Western Reserve University in Cleveland. As a 10-year SHM member, he has been heavily involved in the growth of the Journal of Hospital Medicine, for which he is now deputy editor. He is an active member of the Annual Meeting and Education committees, and is former physician editor of The Hospitalist.
Undergraduate: Kings College in Briarcliff Manor, N.Y.
Medical school: Ohio State University College of Medicine, Columbus.
Internship and residency: University Hospitals of Cleveland.
Fellowship: Infectious Disease, National Naval Medicine Center, Bethesda, Md.
Notable: Prior to working as a hospitalist, Dr. Pile served as a battalion surgeon with Marine infantry on the front lines of the first Gulf War. He also worked as a general practitioner and infectious-disease specialist. His current interests lie in medical education, anti-microbial stewardship, and perioperative medicine.
Quotable: “I continue to see hospital medicine being front and center in patient safety in this country. … That is our whole reason for being, essentially. I anticipate us continuing to grow and develop into the real national leaders in quality improvement in the inpatient setting.”
FYI: Dr. Pile is an avid cyclist. He recently completed a one-day, 200-mile ride, and during his time in medical school, he biked from Seattle to New York City. He loves traveling and spending time with his wife and two daughters.
— Sarah Gelotte
SHAPE the Landscape of Academic Hospital Medicine: Participate in the Academic Hospitalist Survey
The recently released State of Hospital Medicine: 2010 Report Based on 2009 Data provides an unprecedented look at the factors shaping the specialty. However, for academic hospitalists, the picture can be very different. That is why SHM and the Medical Group Management Association (MGMA) are embarking on their first joint survey of academic hospitalists.

Academic HM groups—including groups at community-based teaching hospitals—can participate in the survey now through Nov. 5 by logging on to www6.mgma.com, or by contacting MGMA’s Survey Operations Department at 877-275-6462, Ext. 1895.
“Academic hospitalists and executive leaders at academic institutions need to know how they stack up against their peers in the field,” says Leslie Flores, SHM’s senior advisor for practice management. “Participating in this survey is the first step in providing an in-depth resource that identifies the major trends in academic hospital medicine.”
Like the new State of Hospital Medicine report, the academic report will provide data on hospitalist compensation and productivity, staffing information, and financial support. It also will examine the organizational structure of academic hospitalist practices and how academic hospitalists allocate their time between clinical, research, and teaching responsibilities. The new report also will feature information about medical-school and research funding.
MGMA will publish its standard academic survey results early next spring. Hospitalist-specific data will also be published in the 2011 State of Hospital Medicine report, to be released next summer.
In the past three years, SHM has brought in-depth quality-improvement (QI) programs to nearly every state in the country.
Between its three major mentored implementation projects—Project BOOST (Better Outcomes for Older Adults through Safe Transitions), Glycemic Control Mentored Implemen-tation, and the Venous Thromboembolism (VTE) Collaborative—SHM has worked with more than 100 hospitals across the country and in Canada. SHM is expanding these three programs to additional hospitals and actively developing other QI initiatives.
“SHM’s quality-improvement programs focus on real change, and they have made a substantial impact,” says Joe Miller, SHM’s senior vice president and chief solutions officer. “Hospitalists using SHM’s quality-improvement methods have impacted the care of tens of thousands of hospitalized patients.”
SHM’s programs all use a mix of in-depth mentoring led by national experts and specially designed resource toolkits that enable hospitalists to lead major initiatives within their hospitals. The programs also facilitate “peer learning,” allowing hospitalists to learn from one another.
Project BOOST, which is designed to reduce unplanned readmissions to the hospital, has received national attention. In early 2010, SHM teamed with Blue Cross/Blue Shield of Michigan and the University of Michigan to bring the program to more than a dozen hospitals in that state. SHM also announced a new collaboration with the California HealthCare Foundation to implement Project BOOST in more than 20 hospitals in California.
“Healthcare reform is creating a new focus on quality improvement,” Miller says. “SHM is bringing a multidisciplinary approach to transforming inpatient care to hospitals across the country.” TH
Chapter Updates
Milwaukee/SE Wisconsin
The Milwaukee/SE Wisconsin chapter held a meeting June 10 at Bacchus Restaurant in Milwaukee, at which congratulations were doled out to chapter member Eric Siegal, MD, SFHM, on his election to SHM’s board of directors. As chair of SHM’s Public Policy Committee, Dr. Siegal advocates for such issues as the Physician Quality Reporting Initiative (PQRI).
The chapter also acknowledged Dr. Len Scarpinato of St. Luke’s Hospital, who achieved Senior Fellow in Hospital Medicine (SFHM) designation and was honored at HM10 in April in Washington, D.C. As the regional director of Cogent Healthcare in southeast Wisconsin, Dr. Scarpinato has been instrumental in bringing hospitalists together to network and exchange innovative ideas.
Chapter member Jeanette Kalupa, DNP, ACNP-BC, APNP, of St. Luke’s was mentioned in the opening presentation at HM10 for her work as co-chair of the Nonphysician Providers Committee. Despite a busy HM10 schedule, Drs. Don Lee, Wes Lafferty, Scarpinato, Betty Tucker, and Peter Quandt took time out for a White House tour.
Greater Baltimore Area
The Greater Baltimore Area chapter of SHM met June 16 at Linwood’s Restaurant in Owings Mills, Md. Dr. Suzanne Mitchell spoke on “Relating to the Patient.” The meeting, sponsored by Merck, attracted 50 hospitalists and guests from 10 HM groups.
Los Angeles
The latest Los Angeles chapter meeting was held July 29. The featured speaker was Darrell Harrington, MD, associate medical director for Graduate Medical Education and chief of the division of general internal medicine at Harbor-UCLA Medical Center. Dr. Harrington delivered a presentation about maximizing DVT and PE quality measures. The chapter’s next meeting will be held in the fall.
Fellow in Hospital Medicine Spotlight
James C. Pile, MD, FACP, SFHM
Dr. Pile is an associate professor of medicine, interim director of hospital medicine, and associate program director of the internal residency program at the MetroHealth Campus of Case Western Reserve University in Cleveland. As a 10-year SHM member, he has been heavily involved in the growth of the Journal of Hospital Medicine, for which he is now deputy editor. He is an active member of the Annual Meeting and Education committees, and is former physician editor of The Hospitalist.
Undergraduate: Kings College in Briarcliff Manor, N.Y.
Medical school: Ohio State University College of Medicine, Columbus.
Internship and residency: University Hospitals of Cleveland.
Fellowship: Infectious Disease, National Naval Medicine Center, Bethesda, Md.
Notable: Prior to working as a hospitalist, Dr. Pile served as a battalion surgeon with Marine infantry on the front lines of the first Gulf War. He also worked as a general practitioner and infectious-disease specialist. His current interests lie in medical education, anti-microbial stewardship, and perioperative medicine.
Quotable: “I continue to see hospital medicine being front and center in patient safety in this country. … That is our whole reason for being, essentially. I anticipate us continuing to grow and develop into the real national leaders in quality improvement in the inpatient setting.”
FYI: Dr. Pile is an avid cyclist. He recently completed a one-day, 200-mile ride, and during his time in medical school, he biked from Seattle to New York City. He loves traveling and spending time with his wife and two daughters.
— Sarah Gelotte
SHAPE the Landscape of Academic Hospital Medicine: Participate in the Academic Hospitalist Survey
The recently released State of Hospital Medicine: 2010 Report Based on 2009 Data provides an unprecedented look at the factors shaping the specialty. However, for academic hospitalists, the picture can be very different. That is why SHM and the Medical Group Management Association (MGMA) are embarking on their first joint survey of academic hospitalists.
Academic HM groups—including groups at community-based teaching hospitals—can participate in the survey now through Nov. 5 by logging on to www6.mgma.com, or by contacting MGMA’s Survey Operations Department at 877-275-6462, Ext. 1895.
“Academic hospitalists and executive leaders at academic institutions need to know how they stack up against their peers in the field,” says Leslie Flores, SHM’s senior advisor for practice management. “Participating in this survey is the first step in providing an in-depth resource that identifies the major trends in academic hospital medicine.”
Like the new State of Hospital Medicine report, the academic report will provide data on hospitalist compensation and productivity, staffing information, and financial support. It also will examine the organizational structure of academic hospitalist practices and how academic hospitalists allocate their time between clinical, research, and teaching responsibilities. The new report also will feature information about medical-school and research funding.
MGMA will publish its standard academic survey results early next spring. Hospitalist-specific data will also be published in the 2011 State of Hospital Medicine report, to be released next summer.
In the past three years, SHM has brought in-depth quality-improvement (QI) programs to nearly every state in the country.
Between its three major mentored implementation projects—Project BOOST (Better Outcomes for Older Adults through Safe Transitions), Glycemic Control Mentored Implemen-tation, and the Venous Thromboembolism (VTE) Collaborative—SHM has worked with more than 100 hospitals across the country and in Canada. SHM is expanding these three programs to additional hospitals and actively developing other QI initiatives.
“SHM’s quality-improvement programs focus on real change, and they have made a substantial impact,” says Joe Miller, SHM’s senior vice president and chief solutions officer. “Hospitalists using SHM’s quality-improvement methods have impacted the care of tens of thousands of hospitalized patients.”
SHM’s programs all use a mix of in-depth mentoring led by national experts and specially designed resource toolkits that enable hospitalists to lead major initiatives within their hospitals. The programs also facilitate “peer learning,” allowing hospitalists to learn from one another.
Project BOOST, which is designed to reduce unplanned readmissions to the hospital, has received national attention. In early 2010, SHM teamed with Blue Cross/Blue Shield of Michigan and the University of Michigan to bring the program to more than a dozen hospitals in that state. SHM also announced a new collaboration with the California HealthCare Foundation to implement Project BOOST in more than 20 hospitals in California.
“Healthcare reform is creating a new focus on quality improvement,” Miller says. “SHM is bringing a multidisciplinary approach to transforming inpatient care to hospitals across the country.” TH
Chapter Updates
Milwaukee/SE Wisconsin
The Milwaukee/SE Wisconsin chapter held a meeting June 10 at Bacchus Restaurant in Milwaukee, at which congratulations were doled out to chapter member Eric Siegal, MD, SFHM, on his election to SHM’s board of directors. As chair of SHM’s Public Policy Committee, Dr. Siegal advocates for such issues as the Physician Quality Reporting Initiative (PQRI).
The chapter also acknowledged Dr. Len Scarpinato of St. Luke’s Hospital, who achieved Senior Fellow in Hospital Medicine (SFHM) designation and was honored at HM10 in April in Washington, D.C. As the regional director of Cogent Healthcare in southeast Wisconsin, Dr. Scarpinato has been instrumental in bringing hospitalists together to network and exchange innovative ideas.
Chapter member Jeanette Kalupa, DNP, ACNP-BC, APNP, of St. Luke’s was mentioned in the opening presentation at HM10 for her work as co-chair of the Nonphysician Providers Committee. Despite a busy HM10 schedule, Drs. Don Lee, Wes Lafferty, Scarpinato, Betty Tucker, and Peter Quandt took time out for a White House tour.
Greater Baltimore Area
The Greater Baltimore Area chapter of SHM met June 16 at Linwood’s Restaurant in Owings Mills, Md. Dr. Suzanne Mitchell spoke on “Relating to the Patient.” The meeting, sponsored by Merck, attracted 50 hospitalists and guests from 10 HM groups.
Los Angeles
The latest Los Angeles chapter meeting was held July 29. The featured speaker was Darrell Harrington, MD, associate medical director for Graduate Medical Education and chief of the division of general internal medicine at Harbor-UCLA Medical Center. Dr. Harrington delivered a presentation about maximizing DVT and PE quality measures. The chapter’s next meeting will be held in the fall.
Fellow in Hospital Medicine Spotlight
James C. Pile, MD, FACP, SFHM
Dr. Pile is an associate professor of medicine, interim director of hospital medicine, and associate program director of the internal residency program at the MetroHealth Campus of Case Western Reserve University in Cleveland. As a 10-year SHM member, he has been heavily involved in the growth of the Journal of Hospital Medicine, for which he is now deputy editor. He is an active member of the Annual Meeting and Education committees, and is former physician editor of The Hospitalist.
Undergraduate: Kings College in Briarcliff Manor, N.Y.
Medical school: Ohio State University College of Medicine, Columbus.
Internship and residency: University Hospitals of Cleveland.
Fellowship: Infectious Disease, National Naval Medicine Center, Bethesda, Md.
Notable: Prior to working as a hospitalist, Dr. Pile served as a battalion surgeon with Marine infantry on the front lines of the first Gulf War. He also worked as a general practitioner and infectious-disease specialist. His current interests lie in medical education, anti-microbial stewardship, and perioperative medicine.
Quotable: “I continue to see hospital medicine being front and center in patient safety in this country. … That is our whole reason for being, essentially. I anticipate us continuing to grow and develop into the real national leaders in quality improvement in the inpatient setting.”
FYI: Dr. Pile is an avid cyclist. He recently completed a one-day, 200-mile ride, and during his time in medical school, he biked from Seattle to New York City. He loves traveling and spending time with his wife and two daughters.
— Sarah Gelotte
SHAPE the Landscape of Academic Hospital Medicine: Participate in the Academic Hospitalist Survey
The recently released State of Hospital Medicine: 2010 Report Based on 2009 Data provides an unprecedented look at the factors shaping the specialty. However, for academic hospitalists, the picture can be very different. That is why SHM and the Medical Group Management Association (MGMA) are embarking on their first joint survey of academic hospitalists.
Academic HM groups—including groups at community-based teaching hospitals—can participate in the survey now through Nov. 5 by logging on to www6.mgma.com, or by contacting MGMA’s Survey Operations Department at 877-275-6462, Ext. 1895.
“Academic hospitalists and executive leaders at academic institutions need to know how they stack up against their peers in the field,” says Leslie Flores, SHM’s senior advisor for practice management. “Participating in this survey is the first step in providing an in-depth resource that identifies the major trends in academic hospital medicine.”
Like the new State of Hospital Medicine report, the academic report will provide data on hospitalist compensation and productivity, staffing information, and financial support. It also will examine the organizational structure of academic hospitalist practices and how academic hospitalists allocate their time between clinical, research, and teaching responsibilities. The new report also will feature information about medical-school and research funding.
MGMA will publish its standard academic survey results early next spring. Hospitalist-specific data will also be published in the 2011 State of Hospital Medicine report, to be released next summer.
Market Watch
New Generics
- Anastrazole tablets (generic Arimidex)1
- Azelastine hydrochloride ophthalmic solution 0.05% (generic Optivar)2
- Aztreonam for injection in single-dose vials of 1 g/20 mL and 2 g/30 mL (generic Azactam)3
- Bupropion hydrochloride extended-release 150-mg tablets (generic Zyban)4
- Meropenem injection, USP, IV, 500-mg and 1-g vials (generic Merrem IV)5
- Levetiracetam injection in 100 mg/1 mL and 500 mg/5 mL single-use vials (generic Keppra injection)6
- Tacrolimus 5-mg capsules (generic Prograf)7
- Trandolapril/verapamil tablets (generic Tarka)8
- Valacyclovir hydrochloride tablets, USP (generic Valtrex)9
- Venlafaxine extended-release capsules (generic Effexor XR)10
New Drugs, Indications, Approval Recommendations
- The Alair Bronchial Thermoplasty System is the first device to be FDA-approved for treating severe and persistent asthma.11 It is to be used by adults who are still symptomatic despite treatment with high-dose inhaled corticosteroids (ICS) and long-acting beta-agonists (LABAs). Radiofrequency signals are converted into heat that warms the lining of targeted airways via bronchoscope. There are a number of contraindications and warnings for this device. Treatment is delivered using a standard bronchoscope under moderate sedation.
- Buprenorphine Transdermal System (Butrans) is FDA-approved to treat moderate to severe chronic pain in patients requiring continuous, around-the-clock opioid analgesia for an extended period of time.12 It is a Schedule III controlled substance and will be available in early 2011 in 5 mcg/hour, 10 mcg/hour, and 20 mcg/hour dosage strengths. Patches continuously release the drug over seven days.
- Denosumab injection (Prolia) has been approved by the FDA for treating postmenopausal women with osteoporosis at high risk for fractures.13
- Fingolimod (FTY720), an oral sphingosine 1-phosphate receptor (S1PR) modulator and disease-modifying treatment for relapsing-remitting multiple sclerosis (RRMS), has received a positive review by an FDA Advisory Committee.14 The committee voted 25-0, stating that in clinical trials to date that FTY720 has demonstrated substantial evidence of effectiveness in patients with RRMS, reducing the frequency of clinical exacerbations. This agent works by retaining lymphocytes in the lymph nodes, preventing them from entering the central nervous system to cause damage. This lymphocyte retention is reversible, allowing circulating lymphocytes to regain normal levels if treatment is stopped.
- Ketorolac tromethamine intranasal (Sprix) is FDA-approved for treating acute moderate to moderately severe pain requiring opioid-level analgesia for up to five days.15 Even though it is administered intranasally, gastrointestinal hemorrhage, bleeding, and cardiovascular risks are included in the labeling as adverse events.
- HCV Rapid Antibody Test (OraQuick) has been approved by the FDA for use in patients 15 and older to identify hepatitis C virus (HCV) antibodies.16 Available as a test strip, it identifies HCV antibodies within 20 minutes, which allows patients to more quickly present for evaluation and treatment.
- Lopinavir/ritonavir (Kaletra) has been approved by the FDA for once-daily dosing for treatment-experienced HIV patients.17 The agent had been approved for once-daily treatment for therapy-naive patients.
Pipeline
- HPV vaccine (Gardasil) is being evaluated by the FDA in order to potentially expand its indication to include women 27 to 45 years old.18 A decision is expected by the end of the year.
- Roflumilast is a phosphodiesterase 4 (PDE4) enzyme inhibitor that targets underlying inflammation in COPD patients.19 The FDA has issued a complete response letter for Roflumilast, which was filed as a potential treatment to reduce COPD exacerbations associated with chronic bronchitis in patients at risk for exacerbations. No new clinical trials have been requested.
Product Discontinuation
- Estradiol vaginal tablets 10 mcg (Vagifem) will replace estradiol vaginal tablets 25 mcg to treat the symptoms of atrophic vaginitis due to menopause.20 Sales of the 25-mcg formulation were discontinued July 31.
Medication Safety
GlaxoSmithKline has received reports of dispensing errors related to rosiglitazone (Avandia), glimepiride (Amaryl), rosiglitazone/metformin (Avandamet), candesartan (Atacand), and warfarin (Coumadin). In some instances, the patient received the wrong medication (one severe case led to impaired mental status). Errors likely occurred due to illegible written prescriptions and/or incorrectly interpreted, labeled, and filled prescriptions. Some of these products have similar dosage strengths and also look alike, leading to the errors.21
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Teva gets FDA approval for generic cancer drug. Forbes.com website. Available at: http://www.forbes.com/feeds/ap/2010/06/28/business-health-care-us-teva-pharmaceutical-industries-fda_7726375.html. Accessed June 29, 2010.
- Sun Pharma bags FDA approval for generic Optivar. Pharmaceutical Business Review website. Available at: http://regulatoryaffairs.pharmaceutical-business-review.com/news/sun_pharma_bags_fda_approval_for_generic_optivar_100622/. Accessed June 25, 2010.
- APP Pharmaceuticals Inc receives FDA approval for generic Aztreonam for injection, USP. TradingMarkets.com website. Available at: http://www.tradingmarkets.com/news/stock-alert/appx_apcvz_app-pharmaceuticals-inc-receives-fda-approval-for-generic-aztreonam-for-injection-usp-995249.html. Accessed June 24, 2010.
- Mylan gets FDA approval for generic Zyban. Forbes.com website. Available at: http://www.forbes.com/feeds/prnewswire/2010/05/04/prnewswire201005040700PR_NEWS_USPR_____NE98210.html. Accessed June 25, 2010.
- Hospira receives FDA approval for Meropenem for injection, USP (I.V.) Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192733.php. Accessed June 24, 2010.
- Sun Pharma announces USFDA approval for generic Keppra injection. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192275.php. Accessed June 24, 2010.
- Watson’s generic Prograf 5 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1443895. Accessed July 7, 2010.
- Glenmark arm gets US FDA nod for Tarka generic; stk up. Money Control website. Available at: http://www.moneycontrol.com/news/buzzing-stocks/glenmark-gets-us-fda-nod-for-tarka-generic-stk-up_460856.html. Accessed June 25, 2010.
- Watson’s generic Valtrex 500 mg and 1000 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1430538&highlight=. Accessed June 25, 2010.
- Walsh S. FDA approves first generic Effexor extended release capsules to treat major depressive disorder. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217624.htm Accessed June 29, 2010.
- Waknine Y. FDA approves first non-drug treatment for severe, persistent asthma. Medscape website. Available at: www.medscape.com/viewarticle/720922. Accessed June 30, 2010.
- Butrans transdermal system approved for chronic pain. Monthly Prescribing Reference website. Available at: www.empr.com/butrans-transdermal-system-approved-for-chronic-pain/article/173803/. Accessed July 7, 2010.
- Amgen’s Prolia garners FDA approval. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=BDE45B4D9F3F4C4A9326074859FF661F&logRowId=366890. Accessed June 30, 2010.
- FDA advisory committee unanimously recommends approval of Novartis investigational treatment FTY720 to treat relapsing remitting MS. Novartis Pharmaceuticals Corporation website. Available at: www.pharma.us.novartis.com/newsroom/press-release.jsp?PRID=2284. Accessed June 29, 2010.
- Roxro announces FDA approval of Sprix. Sprix website. Available at: www.sprix.com/docs/SPRIX-approval-press-release.pdf. Accessed June 29, 2010.
- FDA approves rapid test for antibodies to hepatitis C virus. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217318. Accessed July 7, 2010.
- Abbott receives FDA approval for once-daily dosing of Kaletra (lopinavir/ritonavir) for treatment-experienced patients. Abbott website. Available at: www.abbott.com/global/url/pressRelease/en_US/60.5:5/Press_Release_0849.htm. Accessed June 30, 2010.
- Dane L. FDA extends review of Merck & Co.’s Gardasil for use in older women. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=2843FE3BFE2B44C5B463DBA787F213ED&logRowId=369474. Accessed July 7, 2010.
- Forest Laboratories and Nycomed receive complete response letter for Roflumilast. Forest Laboratories website. Available at: www.frx.com/news/PressRelease.aspx?ID=1428047. Accessed July 25, 2010.
- Vagifem 10 mcg to replace Vagifem 25 mcg formulation for atrophic vaginitis due to menopause. Novo Nordisk website. Available at: http://press.novonordisk-us.com/index.php?s=43&item=252. Accessed June 29, 2010.
- Dear Pharmacist Letter, June 2010. Important Drug Warnings: Medication Dispensing Errors; GlaxoSmithKline.
- New Jersey State Board of Pharmacy News, April 2010;24:2-3.
New Generics
- Anastrazole tablets (generic Arimidex)1
- Azelastine hydrochloride ophthalmic solution 0.05% (generic Optivar)2
- Aztreonam for injection in single-dose vials of 1 g/20 mL and 2 g/30 mL (generic Azactam)3
- Bupropion hydrochloride extended-release 150-mg tablets (generic Zyban)4
- Meropenem injection, USP, IV, 500-mg and 1-g vials (generic Merrem IV)5
- Levetiracetam injection in 100 mg/1 mL and 500 mg/5 mL single-use vials (generic Keppra injection)6
- Tacrolimus 5-mg capsules (generic Prograf)7
- Trandolapril/verapamil tablets (generic Tarka)8
- Valacyclovir hydrochloride tablets, USP (generic Valtrex)9
- Venlafaxine extended-release capsules (generic Effexor XR)10
New Drugs, Indications, Approval Recommendations
- The Alair Bronchial Thermoplasty System is the first device to be FDA-approved for treating severe and persistent asthma.11 It is to be used by adults who are still symptomatic despite treatment with high-dose inhaled corticosteroids (ICS) and long-acting beta-agonists (LABAs). Radiofrequency signals are converted into heat that warms the lining of targeted airways via bronchoscope. There are a number of contraindications and warnings for this device. Treatment is delivered using a standard bronchoscope under moderate sedation.
- Buprenorphine Transdermal System (Butrans) is FDA-approved to treat moderate to severe chronic pain in patients requiring continuous, around-the-clock opioid analgesia for an extended period of time.12 It is a Schedule III controlled substance and will be available in early 2011 in 5 mcg/hour, 10 mcg/hour, and 20 mcg/hour dosage strengths. Patches continuously release the drug over seven days.
- Denosumab injection (Prolia) has been approved by the FDA for treating postmenopausal women with osteoporosis at high risk for fractures.13
- Fingolimod (FTY720), an oral sphingosine 1-phosphate receptor (S1PR) modulator and disease-modifying treatment for relapsing-remitting multiple sclerosis (RRMS), has received a positive review by an FDA Advisory Committee.14 The committee voted 25-0, stating that in clinical trials to date that FTY720 has demonstrated substantial evidence of effectiveness in patients with RRMS, reducing the frequency of clinical exacerbations. This agent works by retaining lymphocytes in the lymph nodes, preventing them from entering the central nervous system to cause damage. This lymphocyte retention is reversible, allowing circulating lymphocytes to regain normal levels if treatment is stopped.
- Ketorolac tromethamine intranasal (Sprix) is FDA-approved for treating acute moderate to moderately severe pain requiring opioid-level analgesia for up to five days.15 Even though it is administered intranasally, gastrointestinal hemorrhage, bleeding, and cardiovascular risks are included in the labeling as adverse events.
- HCV Rapid Antibody Test (OraQuick) has been approved by the FDA for use in patients 15 and older to identify hepatitis C virus (HCV) antibodies.16 Available as a test strip, it identifies HCV antibodies within 20 minutes, which allows patients to more quickly present for evaluation and treatment.
- Lopinavir/ritonavir (Kaletra) has been approved by the FDA for once-daily dosing for treatment-experienced HIV patients.17 The agent had been approved for once-daily treatment for therapy-naive patients.
Pipeline
- HPV vaccine (Gardasil) is being evaluated by the FDA in order to potentially expand its indication to include women 27 to 45 years old.18 A decision is expected by the end of the year.
- Roflumilast is a phosphodiesterase 4 (PDE4) enzyme inhibitor that targets underlying inflammation in COPD patients.19 The FDA has issued a complete response letter for Roflumilast, which was filed as a potential treatment to reduce COPD exacerbations associated with chronic bronchitis in patients at risk for exacerbations. No new clinical trials have been requested.
Product Discontinuation
- Estradiol vaginal tablets 10 mcg (Vagifem) will replace estradiol vaginal tablets 25 mcg to treat the symptoms of atrophic vaginitis due to menopause.20 Sales of the 25-mcg formulation were discontinued July 31.
Medication Safety
GlaxoSmithKline has received reports of dispensing errors related to rosiglitazone (Avandia), glimepiride (Amaryl), rosiglitazone/metformin (Avandamet), candesartan (Atacand), and warfarin (Coumadin). In some instances, the patient received the wrong medication (one severe case led to impaired mental status). Errors likely occurred due to illegible written prescriptions and/or incorrectly interpreted, labeled, and filled prescriptions. Some of these products have similar dosage strengths and also look alike, leading to the errors.21
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Teva gets FDA approval for generic cancer drug. Forbes.com website. Available at: http://www.forbes.com/feeds/ap/2010/06/28/business-health-care-us-teva-pharmaceutical-industries-fda_7726375.html. Accessed June 29, 2010.
- Sun Pharma bags FDA approval for generic Optivar. Pharmaceutical Business Review website. Available at: http://regulatoryaffairs.pharmaceutical-business-review.com/news/sun_pharma_bags_fda_approval_for_generic_optivar_100622/. Accessed June 25, 2010.
- APP Pharmaceuticals Inc receives FDA approval for generic Aztreonam for injection, USP. TradingMarkets.com website. Available at: http://www.tradingmarkets.com/news/stock-alert/appx_apcvz_app-pharmaceuticals-inc-receives-fda-approval-for-generic-aztreonam-for-injection-usp-995249.html. Accessed June 24, 2010.
- Mylan gets FDA approval for generic Zyban. Forbes.com website. Available at: http://www.forbes.com/feeds/prnewswire/2010/05/04/prnewswire201005040700PR_NEWS_USPR_____NE98210.html. Accessed June 25, 2010.
- Hospira receives FDA approval for Meropenem for injection, USP (I.V.) Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192733.php. Accessed June 24, 2010.
- Sun Pharma announces USFDA approval for generic Keppra injection. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192275.php. Accessed June 24, 2010.
- Watson’s generic Prograf 5 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1443895. Accessed July 7, 2010.
- Glenmark arm gets US FDA nod for Tarka generic; stk up. Money Control website. Available at: http://www.moneycontrol.com/news/buzzing-stocks/glenmark-gets-us-fda-nod-for-tarka-generic-stk-up_460856.html. Accessed June 25, 2010.
- Watson’s generic Valtrex 500 mg and 1000 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1430538&highlight=. Accessed June 25, 2010.
- Walsh S. FDA approves first generic Effexor extended release capsules to treat major depressive disorder. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217624.htm Accessed June 29, 2010.
- Waknine Y. FDA approves first non-drug treatment for severe, persistent asthma. Medscape website. Available at: www.medscape.com/viewarticle/720922. Accessed June 30, 2010.
- Butrans transdermal system approved for chronic pain. Monthly Prescribing Reference website. Available at: www.empr.com/butrans-transdermal-system-approved-for-chronic-pain/article/173803/. Accessed July 7, 2010.
- Amgen’s Prolia garners FDA approval. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=BDE45B4D9F3F4C4A9326074859FF661F&logRowId=366890. Accessed June 30, 2010.
- FDA advisory committee unanimously recommends approval of Novartis investigational treatment FTY720 to treat relapsing remitting MS. Novartis Pharmaceuticals Corporation website. Available at: www.pharma.us.novartis.com/newsroom/press-release.jsp?PRID=2284. Accessed June 29, 2010.
- Roxro announces FDA approval of Sprix. Sprix website. Available at: www.sprix.com/docs/SPRIX-approval-press-release.pdf. Accessed June 29, 2010.
- FDA approves rapid test for antibodies to hepatitis C virus. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217318. Accessed July 7, 2010.
- Abbott receives FDA approval for once-daily dosing of Kaletra (lopinavir/ritonavir) for treatment-experienced patients. Abbott website. Available at: www.abbott.com/global/url/pressRelease/en_US/60.5:5/Press_Release_0849.htm. Accessed June 30, 2010.
- Dane L. FDA extends review of Merck & Co.’s Gardasil for use in older women. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=2843FE3BFE2B44C5B463DBA787F213ED&logRowId=369474. Accessed July 7, 2010.
- Forest Laboratories and Nycomed receive complete response letter for Roflumilast. Forest Laboratories website. Available at: www.frx.com/news/PressRelease.aspx?ID=1428047. Accessed July 25, 2010.
- Vagifem 10 mcg to replace Vagifem 25 mcg formulation for atrophic vaginitis due to menopause. Novo Nordisk website. Available at: http://press.novonordisk-us.com/index.php?s=43&item=252. Accessed June 29, 2010.
- Dear Pharmacist Letter, June 2010. Important Drug Warnings: Medication Dispensing Errors; GlaxoSmithKline.
- New Jersey State Board of Pharmacy News, April 2010;24:2-3.
New Generics
- Anastrazole tablets (generic Arimidex)1
- Azelastine hydrochloride ophthalmic solution 0.05% (generic Optivar)2
- Aztreonam for injection in single-dose vials of 1 g/20 mL and 2 g/30 mL (generic Azactam)3
- Bupropion hydrochloride extended-release 150-mg tablets (generic Zyban)4
- Meropenem injection, USP, IV, 500-mg and 1-g vials (generic Merrem IV)5
- Levetiracetam injection in 100 mg/1 mL and 500 mg/5 mL single-use vials (generic Keppra injection)6
- Tacrolimus 5-mg capsules (generic Prograf)7
- Trandolapril/verapamil tablets (generic Tarka)8
- Valacyclovir hydrochloride tablets, USP (generic Valtrex)9
- Venlafaxine extended-release capsules (generic Effexor XR)10
New Drugs, Indications, Approval Recommendations
- The Alair Bronchial Thermoplasty System is the first device to be FDA-approved for treating severe and persistent asthma.11 It is to be used by adults who are still symptomatic despite treatment with high-dose inhaled corticosteroids (ICS) and long-acting beta-agonists (LABAs). Radiofrequency signals are converted into heat that warms the lining of targeted airways via bronchoscope. There are a number of contraindications and warnings for this device. Treatment is delivered using a standard bronchoscope under moderate sedation.
- Buprenorphine Transdermal System (Butrans) is FDA-approved to treat moderate to severe chronic pain in patients requiring continuous, around-the-clock opioid analgesia for an extended period of time.12 It is a Schedule III controlled substance and will be available in early 2011 in 5 mcg/hour, 10 mcg/hour, and 20 mcg/hour dosage strengths. Patches continuously release the drug over seven days.
- Denosumab injection (Prolia) has been approved by the FDA for treating postmenopausal women with osteoporosis at high risk for fractures.13
- Fingolimod (FTY720), an oral sphingosine 1-phosphate receptor (S1PR) modulator and disease-modifying treatment for relapsing-remitting multiple sclerosis (RRMS), has received a positive review by an FDA Advisory Committee.14 The committee voted 25-0, stating that in clinical trials to date that FTY720 has demonstrated substantial evidence of effectiveness in patients with RRMS, reducing the frequency of clinical exacerbations. This agent works by retaining lymphocytes in the lymph nodes, preventing them from entering the central nervous system to cause damage. This lymphocyte retention is reversible, allowing circulating lymphocytes to regain normal levels if treatment is stopped.
- Ketorolac tromethamine intranasal (Sprix) is FDA-approved for treating acute moderate to moderately severe pain requiring opioid-level analgesia for up to five days.15 Even though it is administered intranasally, gastrointestinal hemorrhage, bleeding, and cardiovascular risks are included in the labeling as adverse events.
- HCV Rapid Antibody Test (OraQuick) has been approved by the FDA for use in patients 15 and older to identify hepatitis C virus (HCV) antibodies.16 Available as a test strip, it identifies HCV antibodies within 20 minutes, which allows patients to more quickly present for evaluation and treatment.
- Lopinavir/ritonavir (Kaletra) has been approved by the FDA for once-daily dosing for treatment-experienced HIV patients.17 The agent had been approved for once-daily treatment for therapy-naive patients.
Pipeline
- HPV vaccine (Gardasil) is being evaluated by the FDA in order to potentially expand its indication to include women 27 to 45 years old.18 A decision is expected by the end of the year.
- Roflumilast is a phosphodiesterase 4 (PDE4) enzyme inhibitor that targets underlying inflammation in COPD patients.19 The FDA has issued a complete response letter for Roflumilast, which was filed as a potential treatment to reduce COPD exacerbations associated with chronic bronchitis in patients at risk for exacerbations. No new clinical trials have been requested.
Product Discontinuation
- Estradiol vaginal tablets 10 mcg (Vagifem) will replace estradiol vaginal tablets 25 mcg to treat the symptoms of atrophic vaginitis due to menopause.20 Sales of the 25-mcg formulation were discontinued July 31.
Medication Safety
GlaxoSmithKline has received reports of dispensing errors related to rosiglitazone (Avandia), glimepiride (Amaryl), rosiglitazone/metformin (Avandamet), candesartan (Atacand), and warfarin (Coumadin). In some instances, the patient received the wrong medication (one severe case led to impaired mental status). Errors likely occurred due to illegible written prescriptions and/or incorrectly interpreted, labeled, and filled prescriptions. Some of these products have similar dosage strengths and also look alike, leading to the errors.21
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Teva gets FDA approval for generic cancer drug. Forbes.com website. Available at: http://www.forbes.com/feeds/ap/2010/06/28/business-health-care-us-teva-pharmaceutical-industries-fda_7726375.html. Accessed June 29, 2010.
- Sun Pharma bags FDA approval for generic Optivar. Pharmaceutical Business Review website. Available at: http://regulatoryaffairs.pharmaceutical-business-review.com/news/sun_pharma_bags_fda_approval_for_generic_optivar_100622/. Accessed June 25, 2010.
- APP Pharmaceuticals Inc receives FDA approval for generic Aztreonam for injection, USP. TradingMarkets.com website. Available at: http://www.tradingmarkets.com/news/stock-alert/appx_apcvz_app-pharmaceuticals-inc-receives-fda-approval-for-generic-aztreonam-for-injection-usp-995249.html. Accessed June 24, 2010.
- Mylan gets FDA approval for generic Zyban. Forbes.com website. Available at: http://www.forbes.com/feeds/prnewswire/2010/05/04/prnewswire201005040700PR_NEWS_USPR_____NE98210.html. Accessed June 25, 2010.
- Hospira receives FDA approval for Meropenem for injection, USP (I.V.) Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192733.php. Accessed June 24, 2010.
- Sun Pharma announces USFDA approval for generic Keppra injection. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192275.php. Accessed June 24, 2010.
- Watson’s generic Prograf 5 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1443895. Accessed July 7, 2010.
- Glenmark arm gets US FDA nod for Tarka generic; stk up. Money Control website. Available at: http://www.moneycontrol.com/news/buzzing-stocks/glenmark-gets-us-fda-nod-for-tarka-generic-stk-up_460856.html. Accessed June 25, 2010.
- Watson’s generic Valtrex 500 mg and 1000 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1430538&highlight=. Accessed June 25, 2010.
- Walsh S. FDA approves first generic Effexor extended release capsules to treat major depressive disorder. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217624.htm Accessed June 29, 2010.
- Waknine Y. FDA approves first non-drug treatment for severe, persistent asthma. Medscape website. Available at: www.medscape.com/viewarticle/720922. Accessed June 30, 2010.
- Butrans transdermal system approved for chronic pain. Monthly Prescribing Reference website. Available at: www.empr.com/butrans-transdermal-system-approved-for-chronic-pain/article/173803/. Accessed July 7, 2010.
- Amgen’s Prolia garners FDA approval. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=BDE45B4D9F3F4C4A9326074859FF661F&logRowId=366890. Accessed June 30, 2010.
- FDA advisory committee unanimously recommends approval of Novartis investigational treatment FTY720 to treat relapsing remitting MS. Novartis Pharmaceuticals Corporation website. Available at: www.pharma.us.novartis.com/newsroom/press-release.jsp?PRID=2284. Accessed June 29, 2010.
- Roxro announces FDA approval of Sprix. Sprix website. Available at: www.sprix.com/docs/SPRIX-approval-press-release.pdf. Accessed June 29, 2010.
- FDA approves rapid test for antibodies to hepatitis C virus. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217318. Accessed July 7, 2010.
- Abbott receives FDA approval for once-daily dosing of Kaletra (lopinavir/ritonavir) for treatment-experienced patients. Abbott website. Available at: www.abbott.com/global/url/pressRelease/en_US/60.5:5/Press_Release_0849.htm. Accessed June 30, 2010.
- Dane L. FDA extends review of Merck & Co.’s Gardasil for use in older women. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=2843FE3BFE2B44C5B463DBA787F213ED&logRowId=369474. Accessed July 7, 2010.
- Forest Laboratories and Nycomed receive complete response letter for Roflumilast. Forest Laboratories website. Available at: www.frx.com/news/PressRelease.aspx?ID=1428047. Accessed July 25, 2010.
- Vagifem 10 mcg to replace Vagifem 25 mcg formulation for atrophic vaginitis due to menopause. Novo Nordisk website. Available at: http://press.novonordisk-us.com/index.php?s=43&item=252. Accessed June 29, 2010.
- Dear Pharmacist Letter, June 2010. Important Drug Warnings: Medication Dispensing Errors; GlaxoSmithKline.
- New Jersey State Board of Pharmacy News, April 2010;24:2-3.
In the Literature: HM-Related Research You Need to Know
In This Edition
Literature at a Glance
A guide to this month’s studies
- Effect of early follow-up on readmission rates
- Heart rate control and outcomes in atrial fibrillation
- Pneumococcal vaccine to prevent stroke and MI
- Long-term outcomes of endovascular repair of AAA
- Insurance and outcomes in myocardial infarction
- Risk of gastrointestinal bleeding and cardiovascular outcomes with concurrent PPI and clopidogrel use
- CT in patients with suspected coronary artery disease
Reduced 30-Day Readmission Rate for Patients Discharged from Hospitals with Higher Rates of Early Follow-Up
Clinical question: Is early follow-up after discharge for heart failure associated with a reduction in readmission rates?
Background: Readmission for heart failure is very frequent and often unplanned. Early follow-up visits after discharge have been hypothesized to reduce readmissions but have been undefined.
Study design: Retrospective cohort study.
Setting: Patients with Medicare inpatient claims data linked to the OPTIMIZE-HF and GWTG-HF registries.
Synopsis: The study included 30,136 patients >65 years old with the principal discharge diagnosis of heart failure from 2003 to 2006. Hospitals were stratified into quartiles based upon the median arrival rate to “early” (within one week after discharge) follow-up appointments. Ranges of arrival rates to these appointments ranged from Quartile 1 (Q1) (<32.4% of patients) to Q4 (>44.5%). Readmission rates were highest in the lowest quartile of “early” follow-up (Q1: 23.3%; Q2: 20.5%; Q3: 20.5%; Q4: 20.5%, P<0.001). No mortality difference was seen.
The study also examined whether the physician following the patient after discharge impacted the readmission rate for these same quartiles, comparing cardiologists to generalists and comparing the same physician at discharge and follow-up (defined as “continuity”) versus different physicians. Follow-up with continuity or a cardiologist did not reduce readmissions.
Interestingly, nearly all markers of quality were best in Q1 and Q2 hospitals, which had the lowest arrival rates to appointments, which might reflect patient-centered rather than hospital-centered issues.
Bottom line: Hospitals with low “early” follow-up appointment rates after discharge have a higher readmission rate, although causality is not established.
Citation: Hernandez AF, Greiner MA, Fonarow GC, et al. Relationship between early physician follow-up and 30-day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA. 2010;303 (17):1716-1722.
Strict Heart Rate Control Is Not Necessary in Management of Chronic Atrial Fibrillation
Clinical question: Is lenient heart rate control inferior to strict heart rate control in preventing cardiovascular events in patients with chronic atrial fibrillation?
Background: Guidelines generally call for the use of medications to achieve strict heart rate control in the management of chronic atrial fibrillation, but the optimal level of heart rate control necessary to avoid cardiovascular events remains uncertain.
Study design: Prospectively randomized, noninferiority trial.
Setting: Thirty-three medical centers in the Netherlands.
Synopsis: The study looked at 614 patients with permanent atrial fibrillation; 311 patients were randomized to lenient control and 303 to strict control. Calcium channel blockers, beta-blockers, or digoxin were dose-adjusted to control heart rate below 110 beats per minute (bpm) in the lenient control group versus 80 bpm in the strict control group.
Thirty-eight patients (12.9%) in the lenient control group and 43 (14.9%) in the strict control group reached the primary composite outcome of significant cardiovascular events (death, heart failure, stroke, embolism, major bleeding, major arrhythmia, need for pacemaker, or severe drug adverse event). Although no statistical difference in the frequency of these events between groups was detected, the study was dramatically underpowered due to unanticipated low event rates.
Bottom line: Although the lenient control group had far fewer outpatient visits and a trend toward improved outcomes, no definite conclusion regarding the management of permanent atrial fibrillation can be drawn from this underpowered noninferiority trial.
Citation: Van Gelder IC, Groenveld HF, Crijns HJ, et al. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med. 2010;362(15):1363-1373.
Pneumococcal Vaccine Does Not Reduce the Risk of Stroke or Myocardial Infarction
Clinical question: Does pneumococcal vaccination reduce the risk of acute myocardial infarction (MI) and stroke?
Background: Studies have demonstrated that influenza vaccination reduces the risk of cardiac and cerebrovascular events. A single study has shown similar outcomes for the pneumococcal vaccination, although the study was limited by confounders and selection bias.
Study design: Retrospective cohort.
Setting: Large HMO in California.
Synopsis: More than 84,000 men participating in the California Men’s Health Study (CMHS) and enrolled in the Kaiser Permanente health plan were categorized as unvaccinated or vaccinated with the pneumococcal vaccine. Vaccinated patients had 10.73 first MIs and 5.30 strokes per 1,000 person-years, compared with unvaccinated patients who incurred 6.07 MIs and 1.90 strokes per 1,000 unvaccinated person-years based on ICD-9 codes.
Even with propensity scoring to minimize selection bias, no clear evidence of benefit was observed. One significant limitation is that 80% of the unvaccinated patients were younger than 60 years old, whereas 74% of the vaccinated patients were 60 or older; this might represent selection bias that cannot be overcome with propensity scoring.
Bottom line: In a population of men older than age 45, pneumococcal vaccination does not appear to reduce the risk of acute MI or stroke.
Citation: Tseng HF, Slezak JM, Quinn VP, et al. Pneumococcal vaccination and risk of acute myocardial infarction and stroke in men. JAMA. 2010;303(17):1699-1706.
No Durable Mortality Benefit from Endovascular Repair of Enlarged Abdominal Aortic Aneurysm
Clinical question: What is the cost and mortality benefit of endovascular versus open repair of abdominal aneurysms?
Background: Previous studies demonstrated a 30-day mortality benefit using endovascular repair over open surgical repair of large abdominal aortic aneurysms. Limited longer-term data are available assessing the durability of these findings.
Study design: Randomized controlled trial.
Setting: Thirty-seven hospitals in the United Kingdom.
Synopsis: Researchers looked at 1,252 patients who were at least 60 years old with a large abdominal aortic aneurysm (>5.5 cm) on CT scan. The patients were randomized to open versus endovascular repair and followed for a median of six years postoperatively. An early, postoperative, all-cause mortality benefit was observed for endovascular repair (1.8%) compared with open repair (4.3%), but no benefit was seen after six months of follow-up, driven by secondary aneurysm ruptures with endovascular grafts. Graft-related complications in all time periods were higher in the endovascular repair group, highest from 0 to 6 months (nearly 50% of patients), and were associated with an increased cost.
Bottom line: Immediate postoperative mortality benefit of endovascular repair is not sustained for abdominal aortic aneurysm beyond six months postoperatively.
Citation: The United Kingdom EVAR trial investigators. Endovascular versus open repair of abdominal aortic aneurysm. N Engl J Med. 2010:362(20):1863-1870.
Financial Constraints Delay Presentation in Patients Suffering from Acute Myocardial Infarction
Clinical question: Does being underinsured or uninsured delay individuals from seeking treatment for emergency medical care?
Background: The number of underinsured or uninsured Americans is growing. Studies have shown that patients with financial concerns avoid routine preventive and chronic medical care; however, similar avoidance has not been defined clearly for patients seeking emergent care.
Study design: Prospective cohort study.
Setting: Twenty-four urban hospitals in the U.S. included in a multisite, acute myocardial infarction (AMI) registry.
Synopsis: Of the 3,721 patients enrolled in the AMI registry, 61.7% of the cohort was insured and without financial concerns that prevented them from seeking care. These patients were less likely to have delays in care related to AMI compared with patients who were insured with financial concerns (18.5% of the cohort; OR 1.22; 95% confidence interval [CI], 1.06-1.40) or uninsured (19.8%; OR 1.30; 95% CI, 1.12-1.51) in all time frames after symptom onset. Patients were less likely to undergo PCI or thrombolysis if the delay to presentation was more than six hours.
After adjustment for confounding factors, the authors concluded that uninsured and underinsured patients were likely to delay presentation to the hospital. Despite these findings, alternative etiologies for delays in care are likely to be more significant, as insurance considerations only account for an 8% difference between the well-insured group (39.3% delayed seeking care >6 hours) and the uninsured group (48.6%). These etiologies are ill-defined.
Bottom line: Underinsured or uninsured patients have a small but significant delay in seeking treatment for AMI due to financial concerns.
Citation: Smolderen KG, Spertus JA, Nallamothu BK, et al. Health care insurance, financial concerns in accessing care, and delays to hospital presentation in acute myocardial infarction. JAMA. 2010;303 (14):1392-1400.
Concurrent Use of PPIs and Clopidogrel Decrease Hospitalizations for Gastroduodenal Bleeding without Significant Increase in Adverse Cardiovascular Events
Clinical question: Does concomitant use of proton-pump inhibitors (PPIs) and clopidogrel affect the risks of hospitalizations for gastroduodenal bleeding and serious cardiovascular events?
Background: PPIs commonly are prescribed with clopidogrel to reduce the risk of serious gastroduodenal bleeding. Recent observational studies suggest that concurrent PPI and clopidogrel administration might increase the risk of cardiovascular events compared with clopidogrel alone.
Study design: Retrospective cohort.
Setting: Tennessee Medicaid program.
Synopsis: Researchers identified 20,596 patients hospitalized for acute MI, revascularization, or unstable angina, and prescribed clopidogrel. Of this cohort, 7,593 were initial concurrent PPI users—62% used pantoprazole and 9% used omeprazole. Hospitalizations for gastroduodenal bleeding were reduced by 50% (HR 0.50 [95% CI, 0.39-0.65]) in concurrent users of PPIs and clopidogrel, compared with nonusers of PPIs.
Concurrent use was not associated with a statistically significant increase in serious cardiovascular diseases (HR, 0.99 [95% CI, 0.82-1.19]), defined as acute MI, sudden cardiac death, nonfatal or fatal stroke, or other cardiovascular deaths.
Subgroup analyses of individual PPIs and patients undergoing percutaneous coronary interventions also showed no increased risk of serious cardiovascular events. This study could differ from previous observational studies because far fewer patients were on omeprazole, the most potent inhibitor of clopidogrel.
Bottom line: In patients treated with clopidogrel, PPI users had 50% fewer hospitalizations for gastroduodenal bleeding compared with nonusers. Concurrent use of clopidogrel and PPIs, most of which was pantoprazole, was not associated with a significant increase in serious cardiovascular events.
Citation: Ray WA, Murray KT, Griffin MR, et al. Outcomes with concurrent use of clopidogrel and proton-pump inhibitors. Ann Intern Med. 2010;152(6):337-345.
CTCA a Promising, Noninvasive Option in Evaluating Patients with Suspected Coronary Artery Disease
Clinical question: How does computed tomography coronary angiography (CTCA) compare to noninvasive stress testing for diagnosing coronary artery disease (CAD)?
Background: CTCA is a newer, noninvasive test that has a high diagnostic accuracy for CAD, but its clinical role in the evaluation of patients with chest symptoms is unclear.
Study design: Observational study.
Setting: Single academic center in the Netherlands.
Synopsis: Five hundred seventeen eligible patients were evaluated with stress testing and CTCA. The patients were classified as having a low (<20%), intermediate (20%-80%), or high (>80%) pretest probability of CAD based on the Duke clinical score. Using coronary angiography as the gold standard, stress-testing was found to be less accurate than CTCA in all of the patient groups. In patients with low and intermediate pretest probabilities, a negative CTCA had a post-test probability of 0% and 1%, respectively. On the other hand, patients with an intermediate pretest probability and a positive CTCA had a post-test probability of 94% (CI, 89%-97%). In patients with an initial high pretest probability, stress-testing and CTCA confirmed disease in most cases.
The results of this study suggest that CTCA is particularly useful in evaluating patients with an intermediate pretest probability.
Patients were ineligible in this study if they had acute coronary syndromes, previous coronary stent placement, coronary artery bypass surgery, or myocardial infarction. It is important to note that because anatomic lesions seen on imaging (CTCA and coronary angiography) are not always functionally significant, CTCA might have seemed more accurate and clinically useful than it actually is. The investigators also acknowledge that further studies are necessary before CTCA can be accepted as a first-line diagnostic test.
Bottom line: In patients with an intermediate pretest probability of CAD, a negative CTCA is valuable in excluding coronary artery disease, thereby reducing the need for invasive coronary angiography in this group.
Citation: Weustink AC, Mollet NR, Neefjes LA, et al. Diagnostic accuracy and clinical utility of noninvasive testing for coronary artery disease. Ann Intern Med. 2010;152(10):630-639. TH
PEDIATRIC HM LITerature
Neonatal Nonhemolytic Hyperbilirubinemia Not Associated with Long-Term Cognitive or Neuropsychiatric Disability

Clinical question: Is exposure to neonatal nonhemolytic hyperbilirubinemia associated with negative long-term cognitive effects?
Background: Guidelines for the treatment of neonatal hyperbilirubinemia focus on the prevention of rare but potentially devastating consequences: bilirubin encephalopathy and subsequent kernicterus. Small studies have raised concerns regarding the potential for long-term cognitive disability in infants exposed to severe hyperbilirubinemia without kernicterus. This association primarily has been noted in patients with severe hemolytic hyperbilirubinemia; the relationship in nonhemolytic cases is less clear.
Study design: Retrospective, population-based cohort study.
Setting: Fifth Military Conscription District of Denmark.
Synopsis: All 18-year-old male conscripts born from 1977 to 1983 had data extracted from a national discharge registry with respect to maximum total serum bilirubin (TSB-max) and other clinical details. Infants born <35 weeks or of multiple gestation, age >14 days at TSB-max, or with hemolytic disease were excluded. TSB-max was analyzed as a categorical and dichotomous variable. Data were then compared to a validated Danish intelligence test administered at military draft conscription and the presence of neuropsychiatric diagnoses.
Of those examined, 463 men exceeded the cutoff for TSB-max, compared with 12,718 controls. There were no significant differences between groups with respect to the presence of neuropsychiatric diagnoses or cognitive performance.
This study benefits from its population-based design and use of an inclusive national database. However, cognitive performance is notoriously difficult to study, owing to the numerous potential confounders, many of which could not be ascertained retrospectively from the registry. Additional limitations were that the Danish thresholds for phototherapy and exchange transfusion were 240 μmol/L and 340 μmol/L (or approximately 14 mg/dL and 20 mg/dL), respectively, and only 25 newborns were exposed to levels greater than 340 μmol/L.
Although no dose response association was noted between 240 μmol/L and 340 μmol/L, no conclusions may be drawn regarding significantly higher levels.
Bottom line: Neonatal nonhemolytic hyperbilirubinemia requiring phototherapy is unlikely to be associated with long-term cognitive or neuropsychiatric disability.
Citation: Ebbesen F, Ehrenstein V, Traeger M, Nielsen GL. Neonatal non-hemolytic hyperbilirubinemia: a prevalence study of adult neuropsychiatric disability and cognitive function in 463 male Danish conscripts. Arch Dis Child. 2010;95(8):583-587.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Effect of early follow-up on readmission rates
- Heart rate control and outcomes in atrial fibrillation
- Pneumococcal vaccine to prevent stroke and MI
- Long-term outcomes of endovascular repair of AAA
- Insurance and outcomes in myocardial infarction
- Risk of gastrointestinal bleeding and cardiovascular outcomes with concurrent PPI and clopidogrel use
- CT in patients with suspected coronary artery disease
Reduced 30-Day Readmission Rate for Patients Discharged from Hospitals with Higher Rates of Early Follow-Up
Clinical question: Is early follow-up after discharge for heart failure associated with a reduction in readmission rates?
Background: Readmission for heart failure is very frequent and often unplanned. Early follow-up visits after discharge have been hypothesized to reduce readmissions but have been undefined.
Study design: Retrospective cohort study.
Setting: Patients with Medicare inpatient claims data linked to the OPTIMIZE-HF and GWTG-HF registries.
Synopsis: The study included 30,136 patients >65 years old with the principal discharge diagnosis of heart failure from 2003 to 2006. Hospitals were stratified into quartiles based upon the median arrival rate to “early” (within one week after discharge) follow-up appointments. Ranges of arrival rates to these appointments ranged from Quartile 1 (Q1) (<32.4% of patients) to Q4 (>44.5%). Readmission rates were highest in the lowest quartile of “early” follow-up (Q1: 23.3%; Q2: 20.5%; Q3: 20.5%; Q4: 20.5%, P<0.001). No mortality difference was seen.
The study also examined whether the physician following the patient after discharge impacted the readmission rate for these same quartiles, comparing cardiologists to generalists and comparing the same physician at discharge and follow-up (defined as “continuity”) versus different physicians. Follow-up with continuity or a cardiologist did not reduce readmissions.
Interestingly, nearly all markers of quality were best in Q1 and Q2 hospitals, which had the lowest arrival rates to appointments, which might reflect patient-centered rather than hospital-centered issues.
Bottom line: Hospitals with low “early” follow-up appointment rates after discharge have a higher readmission rate, although causality is not established.
Citation: Hernandez AF, Greiner MA, Fonarow GC, et al. Relationship between early physician follow-up and 30-day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA. 2010;303 (17):1716-1722.
Strict Heart Rate Control Is Not Necessary in Management of Chronic Atrial Fibrillation
Clinical question: Is lenient heart rate control inferior to strict heart rate control in preventing cardiovascular events in patients with chronic atrial fibrillation?
Background: Guidelines generally call for the use of medications to achieve strict heart rate control in the management of chronic atrial fibrillation, but the optimal level of heart rate control necessary to avoid cardiovascular events remains uncertain.
Study design: Prospectively randomized, noninferiority trial.
Setting: Thirty-three medical centers in the Netherlands.
Synopsis: The study looked at 614 patients with permanent atrial fibrillation; 311 patients were randomized to lenient control and 303 to strict control. Calcium channel blockers, beta-blockers, or digoxin were dose-adjusted to control heart rate below 110 beats per minute (bpm) in the lenient control group versus 80 bpm in the strict control group.
Thirty-eight patients (12.9%) in the lenient control group and 43 (14.9%) in the strict control group reached the primary composite outcome of significant cardiovascular events (death, heart failure, stroke, embolism, major bleeding, major arrhythmia, need for pacemaker, or severe drug adverse event). Although no statistical difference in the frequency of these events between groups was detected, the study was dramatically underpowered due to unanticipated low event rates.
Bottom line: Although the lenient control group had far fewer outpatient visits and a trend toward improved outcomes, no definite conclusion regarding the management of permanent atrial fibrillation can be drawn from this underpowered noninferiority trial.
Citation: Van Gelder IC, Groenveld HF, Crijns HJ, et al. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med. 2010;362(15):1363-1373.
Pneumococcal Vaccine Does Not Reduce the Risk of Stroke or Myocardial Infarction
Clinical question: Does pneumococcal vaccination reduce the risk of acute myocardial infarction (MI) and stroke?
Background: Studies have demonstrated that influenza vaccination reduces the risk of cardiac and cerebrovascular events. A single study has shown similar outcomes for the pneumococcal vaccination, although the study was limited by confounders and selection bias.
Study design: Retrospective cohort.
Setting: Large HMO in California.
Synopsis: More than 84,000 men participating in the California Men’s Health Study (CMHS) and enrolled in the Kaiser Permanente health plan were categorized as unvaccinated or vaccinated with the pneumococcal vaccine. Vaccinated patients had 10.73 first MIs and 5.30 strokes per 1,000 person-years, compared with unvaccinated patients who incurred 6.07 MIs and 1.90 strokes per 1,000 unvaccinated person-years based on ICD-9 codes.
Even with propensity scoring to minimize selection bias, no clear evidence of benefit was observed. One significant limitation is that 80% of the unvaccinated patients were younger than 60 years old, whereas 74% of the vaccinated patients were 60 or older; this might represent selection bias that cannot be overcome with propensity scoring.
Bottom line: In a population of men older than age 45, pneumococcal vaccination does not appear to reduce the risk of acute MI or stroke.
Citation: Tseng HF, Slezak JM, Quinn VP, et al. Pneumococcal vaccination and risk of acute myocardial infarction and stroke in men. JAMA. 2010;303(17):1699-1706.
No Durable Mortality Benefit from Endovascular Repair of Enlarged Abdominal Aortic Aneurysm
Clinical question: What is the cost and mortality benefit of endovascular versus open repair of abdominal aneurysms?
Background: Previous studies demonstrated a 30-day mortality benefit using endovascular repair over open surgical repair of large abdominal aortic aneurysms. Limited longer-term data are available assessing the durability of these findings.
Study design: Randomized controlled trial.
Setting: Thirty-seven hospitals in the United Kingdom.
Synopsis: Researchers looked at 1,252 patients who were at least 60 years old with a large abdominal aortic aneurysm (>5.5 cm) on CT scan. The patients were randomized to open versus endovascular repair and followed for a median of six years postoperatively. An early, postoperative, all-cause mortality benefit was observed for endovascular repair (1.8%) compared with open repair (4.3%), but no benefit was seen after six months of follow-up, driven by secondary aneurysm ruptures with endovascular grafts. Graft-related complications in all time periods were higher in the endovascular repair group, highest from 0 to 6 months (nearly 50% of patients), and were associated with an increased cost.
Bottom line: Immediate postoperative mortality benefit of endovascular repair is not sustained for abdominal aortic aneurysm beyond six months postoperatively.
Citation: The United Kingdom EVAR trial investigators. Endovascular versus open repair of abdominal aortic aneurysm. N Engl J Med. 2010:362(20):1863-1870.
Financial Constraints Delay Presentation in Patients Suffering from Acute Myocardial Infarction
Clinical question: Does being underinsured or uninsured delay individuals from seeking treatment for emergency medical care?
Background: The number of underinsured or uninsured Americans is growing. Studies have shown that patients with financial concerns avoid routine preventive and chronic medical care; however, similar avoidance has not been defined clearly for patients seeking emergent care.
Study design: Prospective cohort study.
Setting: Twenty-four urban hospitals in the U.S. included in a multisite, acute myocardial infarction (AMI) registry.
Synopsis: Of the 3,721 patients enrolled in the AMI registry, 61.7% of the cohort was insured and without financial concerns that prevented them from seeking care. These patients were less likely to have delays in care related to AMI compared with patients who were insured with financial concerns (18.5% of the cohort; OR 1.22; 95% confidence interval [CI], 1.06-1.40) or uninsured (19.8%; OR 1.30; 95% CI, 1.12-1.51) in all time frames after symptom onset. Patients were less likely to undergo PCI or thrombolysis if the delay to presentation was more than six hours.
After adjustment for confounding factors, the authors concluded that uninsured and underinsured patients were likely to delay presentation to the hospital. Despite these findings, alternative etiologies for delays in care are likely to be more significant, as insurance considerations only account for an 8% difference between the well-insured group (39.3% delayed seeking care >6 hours) and the uninsured group (48.6%). These etiologies are ill-defined.
Bottom line: Underinsured or uninsured patients have a small but significant delay in seeking treatment for AMI due to financial concerns.
Citation: Smolderen KG, Spertus JA, Nallamothu BK, et al. Health care insurance, financial concerns in accessing care, and delays to hospital presentation in acute myocardial infarction. JAMA. 2010;303 (14):1392-1400.
Concurrent Use of PPIs and Clopidogrel Decrease Hospitalizations for Gastroduodenal Bleeding without Significant Increase in Adverse Cardiovascular Events
Clinical question: Does concomitant use of proton-pump inhibitors (PPIs) and clopidogrel affect the risks of hospitalizations for gastroduodenal bleeding and serious cardiovascular events?
Background: PPIs commonly are prescribed with clopidogrel to reduce the risk of serious gastroduodenal bleeding. Recent observational studies suggest that concurrent PPI and clopidogrel administration might increase the risk of cardiovascular events compared with clopidogrel alone.
Study design: Retrospective cohort.
Setting: Tennessee Medicaid program.
Synopsis: Researchers identified 20,596 patients hospitalized for acute MI, revascularization, or unstable angina, and prescribed clopidogrel. Of this cohort, 7,593 were initial concurrent PPI users—62% used pantoprazole and 9% used omeprazole. Hospitalizations for gastroduodenal bleeding were reduced by 50% (HR 0.50 [95% CI, 0.39-0.65]) in concurrent users of PPIs and clopidogrel, compared with nonusers of PPIs.
Concurrent use was not associated with a statistically significant increase in serious cardiovascular diseases (HR, 0.99 [95% CI, 0.82-1.19]), defined as acute MI, sudden cardiac death, nonfatal or fatal stroke, or other cardiovascular deaths.
Subgroup analyses of individual PPIs and patients undergoing percutaneous coronary interventions also showed no increased risk of serious cardiovascular events. This study could differ from previous observational studies because far fewer patients were on omeprazole, the most potent inhibitor of clopidogrel.
Bottom line: In patients treated with clopidogrel, PPI users had 50% fewer hospitalizations for gastroduodenal bleeding compared with nonusers. Concurrent use of clopidogrel and PPIs, most of which was pantoprazole, was not associated with a significant increase in serious cardiovascular events.
Citation: Ray WA, Murray KT, Griffin MR, et al. Outcomes with concurrent use of clopidogrel and proton-pump inhibitors. Ann Intern Med. 2010;152(6):337-345.
CTCA a Promising, Noninvasive Option in Evaluating Patients with Suspected Coronary Artery Disease
Clinical question: How does computed tomography coronary angiography (CTCA) compare to noninvasive stress testing for diagnosing coronary artery disease (CAD)?
Background: CTCA is a newer, noninvasive test that has a high diagnostic accuracy for CAD, but its clinical role in the evaluation of patients with chest symptoms is unclear.
Study design: Observational study.
Setting: Single academic center in the Netherlands.
Synopsis: Five hundred seventeen eligible patients were evaluated with stress testing and CTCA. The patients were classified as having a low (<20%), intermediate (20%-80%), or high (>80%) pretest probability of CAD based on the Duke clinical score. Using coronary angiography as the gold standard, stress-testing was found to be less accurate than CTCA in all of the patient groups. In patients with low and intermediate pretest probabilities, a negative CTCA had a post-test probability of 0% and 1%, respectively. On the other hand, patients with an intermediate pretest probability and a positive CTCA had a post-test probability of 94% (CI, 89%-97%). In patients with an initial high pretest probability, stress-testing and CTCA confirmed disease in most cases.
The results of this study suggest that CTCA is particularly useful in evaluating patients with an intermediate pretest probability.
Patients were ineligible in this study if they had acute coronary syndromes, previous coronary stent placement, coronary artery bypass surgery, or myocardial infarction. It is important to note that because anatomic lesions seen on imaging (CTCA and coronary angiography) are not always functionally significant, CTCA might have seemed more accurate and clinically useful than it actually is. The investigators also acknowledge that further studies are necessary before CTCA can be accepted as a first-line diagnostic test.
Bottom line: In patients with an intermediate pretest probability of CAD, a negative CTCA is valuable in excluding coronary artery disease, thereby reducing the need for invasive coronary angiography in this group.
Citation: Weustink AC, Mollet NR, Neefjes LA, et al. Diagnostic accuracy and clinical utility of noninvasive testing for coronary artery disease. Ann Intern Med. 2010;152(10):630-639. TH
PEDIATRIC HM LITerature
Neonatal Nonhemolytic Hyperbilirubinemia Not Associated with Long-Term Cognitive or Neuropsychiatric Disability
Clinical question: Is exposure to neonatal nonhemolytic hyperbilirubinemia associated with negative long-term cognitive effects?
Background: Guidelines for the treatment of neonatal hyperbilirubinemia focus on the prevention of rare but potentially devastating consequences: bilirubin encephalopathy and subsequent kernicterus. Small studies have raised concerns regarding the potential for long-term cognitive disability in infants exposed to severe hyperbilirubinemia without kernicterus. This association primarily has been noted in patients with severe hemolytic hyperbilirubinemia; the relationship in nonhemolytic cases is less clear.
Study design: Retrospective, population-based cohort study.
Setting: Fifth Military Conscription District of Denmark.
Synopsis: All 18-year-old male conscripts born from 1977 to 1983 had data extracted from a national discharge registry with respect to maximum total serum bilirubin (TSB-max) and other clinical details. Infants born <35 weeks or of multiple gestation, age >14 days at TSB-max, or with hemolytic disease were excluded. TSB-max was analyzed as a categorical and dichotomous variable. Data were then compared to a validated Danish intelligence test administered at military draft conscription and the presence of neuropsychiatric diagnoses.
Of those examined, 463 men exceeded the cutoff for TSB-max, compared with 12,718 controls. There were no significant differences between groups with respect to the presence of neuropsychiatric diagnoses or cognitive performance.
This study benefits from its population-based design and use of an inclusive national database. However, cognitive performance is notoriously difficult to study, owing to the numerous potential confounders, many of which could not be ascertained retrospectively from the registry. Additional limitations were that the Danish thresholds for phototherapy and exchange transfusion were 240 μmol/L and 340 μmol/L (or approximately 14 mg/dL and 20 mg/dL), respectively, and only 25 newborns were exposed to levels greater than 340 μmol/L.
Although no dose response association was noted between 240 μmol/L and 340 μmol/L, no conclusions may be drawn regarding significantly higher levels.
Bottom line: Neonatal nonhemolytic hyperbilirubinemia requiring phototherapy is unlikely to be associated with long-term cognitive or neuropsychiatric disability.
Citation: Ebbesen F, Ehrenstein V, Traeger M, Nielsen GL. Neonatal non-hemolytic hyperbilirubinemia: a prevalence study of adult neuropsychiatric disability and cognitive function in 463 male Danish conscripts. Arch Dis Child. 2010;95(8):583-587.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Effect of early follow-up on readmission rates
- Heart rate control and outcomes in atrial fibrillation
- Pneumococcal vaccine to prevent stroke and MI
- Long-term outcomes of endovascular repair of AAA
- Insurance and outcomes in myocardial infarction
- Risk of gastrointestinal bleeding and cardiovascular outcomes with concurrent PPI and clopidogrel use
- CT in patients with suspected coronary artery disease
Reduced 30-Day Readmission Rate for Patients Discharged from Hospitals with Higher Rates of Early Follow-Up
Clinical question: Is early follow-up after discharge for heart failure associated with a reduction in readmission rates?
Background: Readmission for heart failure is very frequent and often unplanned. Early follow-up visits after discharge have been hypothesized to reduce readmissions but have been undefined.
Study design: Retrospective cohort study.
Setting: Patients with Medicare inpatient claims data linked to the OPTIMIZE-HF and GWTG-HF registries.
Synopsis: The study included 30,136 patients >65 years old with the principal discharge diagnosis of heart failure from 2003 to 2006. Hospitals were stratified into quartiles based upon the median arrival rate to “early” (within one week after discharge) follow-up appointments. Ranges of arrival rates to these appointments ranged from Quartile 1 (Q1) (<32.4% of patients) to Q4 (>44.5%). Readmission rates were highest in the lowest quartile of “early” follow-up (Q1: 23.3%; Q2: 20.5%; Q3: 20.5%; Q4: 20.5%, P<0.001). No mortality difference was seen.
The study also examined whether the physician following the patient after discharge impacted the readmission rate for these same quartiles, comparing cardiologists to generalists and comparing the same physician at discharge and follow-up (defined as “continuity”) versus different physicians. Follow-up with continuity or a cardiologist did not reduce readmissions.
Interestingly, nearly all markers of quality were best in Q1 and Q2 hospitals, which had the lowest arrival rates to appointments, which might reflect patient-centered rather than hospital-centered issues.
Bottom line: Hospitals with low “early” follow-up appointment rates after discharge have a higher readmission rate, although causality is not established.
Citation: Hernandez AF, Greiner MA, Fonarow GC, et al. Relationship between early physician follow-up and 30-day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA. 2010;303 (17):1716-1722.
Strict Heart Rate Control Is Not Necessary in Management of Chronic Atrial Fibrillation
Clinical question: Is lenient heart rate control inferior to strict heart rate control in preventing cardiovascular events in patients with chronic atrial fibrillation?
Background: Guidelines generally call for the use of medications to achieve strict heart rate control in the management of chronic atrial fibrillation, but the optimal level of heart rate control necessary to avoid cardiovascular events remains uncertain.
Study design: Prospectively randomized, noninferiority trial.
Setting: Thirty-three medical centers in the Netherlands.
Synopsis: The study looked at 614 patients with permanent atrial fibrillation; 311 patients were randomized to lenient control and 303 to strict control. Calcium channel blockers, beta-blockers, or digoxin were dose-adjusted to control heart rate below 110 beats per minute (bpm) in the lenient control group versus 80 bpm in the strict control group.
Thirty-eight patients (12.9%) in the lenient control group and 43 (14.9%) in the strict control group reached the primary composite outcome of significant cardiovascular events (death, heart failure, stroke, embolism, major bleeding, major arrhythmia, need for pacemaker, or severe drug adverse event). Although no statistical difference in the frequency of these events between groups was detected, the study was dramatically underpowered due to unanticipated low event rates.
Bottom line: Although the lenient control group had far fewer outpatient visits and a trend toward improved outcomes, no definite conclusion regarding the management of permanent atrial fibrillation can be drawn from this underpowered noninferiority trial.
Citation: Van Gelder IC, Groenveld HF, Crijns HJ, et al. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med. 2010;362(15):1363-1373.
Pneumococcal Vaccine Does Not Reduce the Risk of Stroke or Myocardial Infarction
Clinical question: Does pneumococcal vaccination reduce the risk of acute myocardial infarction (MI) and stroke?
Background: Studies have demonstrated that influenza vaccination reduces the risk of cardiac and cerebrovascular events. A single study has shown similar outcomes for the pneumococcal vaccination, although the study was limited by confounders and selection bias.
Study design: Retrospective cohort.
Setting: Large HMO in California.
Synopsis: More than 84,000 men participating in the California Men’s Health Study (CMHS) and enrolled in the Kaiser Permanente health plan were categorized as unvaccinated or vaccinated with the pneumococcal vaccine. Vaccinated patients had 10.73 first MIs and 5.30 strokes per 1,000 person-years, compared with unvaccinated patients who incurred 6.07 MIs and 1.90 strokes per 1,000 unvaccinated person-years based on ICD-9 codes.
Even with propensity scoring to minimize selection bias, no clear evidence of benefit was observed. One significant limitation is that 80% of the unvaccinated patients were younger than 60 years old, whereas 74% of the vaccinated patients were 60 or older; this might represent selection bias that cannot be overcome with propensity scoring.
Bottom line: In a population of men older than age 45, pneumococcal vaccination does not appear to reduce the risk of acute MI or stroke.
Citation: Tseng HF, Slezak JM, Quinn VP, et al. Pneumococcal vaccination and risk of acute myocardial infarction and stroke in men. JAMA. 2010;303(17):1699-1706.
No Durable Mortality Benefit from Endovascular Repair of Enlarged Abdominal Aortic Aneurysm
Clinical question: What is the cost and mortality benefit of endovascular versus open repair of abdominal aneurysms?
Background: Previous studies demonstrated a 30-day mortality benefit using endovascular repair over open surgical repair of large abdominal aortic aneurysms. Limited longer-term data are available assessing the durability of these findings.
Study design: Randomized controlled trial.
Setting: Thirty-seven hospitals in the United Kingdom.
Synopsis: Researchers looked at 1,252 patients who were at least 60 years old with a large abdominal aortic aneurysm (>5.5 cm) on CT scan. The patients were randomized to open versus endovascular repair and followed for a median of six years postoperatively. An early, postoperative, all-cause mortality benefit was observed for endovascular repair (1.8%) compared with open repair (4.3%), but no benefit was seen after six months of follow-up, driven by secondary aneurysm ruptures with endovascular grafts. Graft-related complications in all time periods were higher in the endovascular repair group, highest from 0 to 6 months (nearly 50% of patients), and were associated with an increased cost.
Bottom line: Immediate postoperative mortality benefit of endovascular repair is not sustained for abdominal aortic aneurysm beyond six months postoperatively.
Citation: The United Kingdom EVAR trial investigators. Endovascular versus open repair of abdominal aortic aneurysm. N Engl J Med. 2010:362(20):1863-1870.
Financial Constraints Delay Presentation in Patients Suffering from Acute Myocardial Infarction
Clinical question: Does being underinsured or uninsured delay individuals from seeking treatment for emergency medical care?
Background: The number of underinsured or uninsured Americans is growing. Studies have shown that patients with financial concerns avoid routine preventive and chronic medical care; however, similar avoidance has not been defined clearly for patients seeking emergent care.
Study design: Prospective cohort study.
Setting: Twenty-four urban hospitals in the U.S. included in a multisite, acute myocardial infarction (AMI) registry.
Synopsis: Of the 3,721 patients enrolled in the AMI registry, 61.7% of the cohort was insured and without financial concerns that prevented them from seeking care. These patients were less likely to have delays in care related to AMI compared with patients who were insured with financial concerns (18.5% of the cohort; OR 1.22; 95% confidence interval [CI], 1.06-1.40) or uninsured (19.8%; OR 1.30; 95% CI, 1.12-1.51) in all time frames after symptom onset. Patients were less likely to undergo PCI or thrombolysis if the delay to presentation was more than six hours.
After adjustment for confounding factors, the authors concluded that uninsured and underinsured patients were likely to delay presentation to the hospital. Despite these findings, alternative etiologies for delays in care are likely to be more significant, as insurance considerations only account for an 8% difference between the well-insured group (39.3% delayed seeking care >6 hours) and the uninsured group (48.6%). These etiologies are ill-defined.
Bottom line: Underinsured or uninsured patients have a small but significant delay in seeking treatment for AMI due to financial concerns.
Citation: Smolderen KG, Spertus JA, Nallamothu BK, et al. Health care insurance, financial concerns in accessing care, and delays to hospital presentation in acute myocardial infarction. JAMA. 2010;303 (14):1392-1400.
Concurrent Use of PPIs and Clopidogrel Decrease Hospitalizations for Gastroduodenal Bleeding without Significant Increase in Adverse Cardiovascular Events
Clinical question: Does concomitant use of proton-pump inhibitors (PPIs) and clopidogrel affect the risks of hospitalizations for gastroduodenal bleeding and serious cardiovascular events?
Background: PPIs commonly are prescribed with clopidogrel to reduce the risk of serious gastroduodenal bleeding. Recent observational studies suggest that concurrent PPI and clopidogrel administration might increase the risk of cardiovascular events compared with clopidogrel alone.
Study design: Retrospective cohort.
Setting: Tennessee Medicaid program.
Synopsis: Researchers identified 20,596 patients hospitalized for acute MI, revascularization, or unstable angina, and prescribed clopidogrel. Of this cohort, 7,593 were initial concurrent PPI users—62% used pantoprazole and 9% used omeprazole. Hospitalizations for gastroduodenal bleeding were reduced by 50% (HR 0.50 [95% CI, 0.39-0.65]) in concurrent users of PPIs and clopidogrel, compared with nonusers of PPIs.
Concurrent use was not associated with a statistically significant increase in serious cardiovascular diseases (HR, 0.99 [95% CI, 0.82-1.19]), defined as acute MI, sudden cardiac death, nonfatal or fatal stroke, or other cardiovascular deaths.
Subgroup analyses of individual PPIs and patients undergoing percutaneous coronary interventions also showed no increased risk of serious cardiovascular events. This study could differ from previous observational studies because far fewer patients were on omeprazole, the most potent inhibitor of clopidogrel.
Bottom line: In patients treated with clopidogrel, PPI users had 50% fewer hospitalizations for gastroduodenal bleeding compared with nonusers. Concurrent use of clopidogrel and PPIs, most of which was pantoprazole, was not associated with a significant increase in serious cardiovascular events.
Citation: Ray WA, Murray KT, Griffin MR, et al. Outcomes with concurrent use of clopidogrel and proton-pump inhibitors. Ann Intern Med. 2010;152(6):337-345.
CTCA a Promising, Noninvasive Option in Evaluating Patients with Suspected Coronary Artery Disease
Clinical question: How does computed tomography coronary angiography (CTCA) compare to noninvasive stress testing for diagnosing coronary artery disease (CAD)?
Background: CTCA is a newer, noninvasive test that has a high diagnostic accuracy for CAD, but its clinical role in the evaluation of patients with chest symptoms is unclear.
Study design: Observational study.
Setting: Single academic center in the Netherlands.
Synopsis: Five hundred seventeen eligible patients were evaluated with stress testing and CTCA. The patients were classified as having a low (<20%), intermediate (20%-80%), or high (>80%) pretest probability of CAD based on the Duke clinical score. Using coronary angiography as the gold standard, stress-testing was found to be less accurate than CTCA in all of the patient groups. In patients with low and intermediate pretest probabilities, a negative CTCA had a post-test probability of 0% and 1%, respectively. On the other hand, patients with an intermediate pretest probability and a positive CTCA had a post-test probability of 94% (CI, 89%-97%). In patients with an initial high pretest probability, stress-testing and CTCA confirmed disease in most cases.
The results of this study suggest that CTCA is particularly useful in evaluating patients with an intermediate pretest probability.
Patients were ineligible in this study if they had acute coronary syndromes, previous coronary stent placement, coronary artery bypass surgery, or myocardial infarction. It is important to note that because anatomic lesions seen on imaging (CTCA and coronary angiography) are not always functionally significant, CTCA might have seemed more accurate and clinically useful than it actually is. The investigators also acknowledge that further studies are necessary before CTCA can be accepted as a first-line diagnostic test.
Bottom line: In patients with an intermediate pretest probability of CAD, a negative CTCA is valuable in excluding coronary artery disease, thereby reducing the need for invasive coronary angiography in this group.
Citation: Weustink AC, Mollet NR, Neefjes LA, et al. Diagnostic accuracy and clinical utility of noninvasive testing for coronary artery disease. Ann Intern Med. 2010;152(10):630-639. TH
PEDIATRIC HM LITerature
Neonatal Nonhemolytic Hyperbilirubinemia Not Associated with Long-Term Cognitive or Neuropsychiatric Disability
Clinical question: Is exposure to neonatal nonhemolytic hyperbilirubinemia associated with negative long-term cognitive effects?
Background: Guidelines for the treatment of neonatal hyperbilirubinemia focus on the prevention of rare but potentially devastating consequences: bilirubin encephalopathy and subsequent kernicterus. Small studies have raised concerns regarding the potential for long-term cognitive disability in infants exposed to severe hyperbilirubinemia without kernicterus. This association primarily has been noted in patients with severe hemolytic hyperbilirubinemia; the relationship in nonhemolytic cases is less clear.
Study design: Retrospective, population-based cohort study.
Setting: Fifth Military Conscription District of Denmark.
Synopsis: All 18-year-old male conscripts born from 1977 to 1983 had data extracted from a national discharge registry with respect to maximum total serum bilirubin (TSB-max) and other clinical details. Infants born <35 weeks or of multiple gestation, age >14 days at TSB-max, or with hemolytic disease were excluded. TSB-max was analyzed as a categorical and dichotomous variable. Data were then compared to a validated Danish intelligence test administered at military draft conscription and the presence of neuropsychiatric diagnoses.
Of those examined, 463 men exceeded the cutoff for TSB-max, compared with 12,718 controls. There were no significant differences between groups with respect to the presence of neuropsychiatric diagnoses or cognitive performance.
This study benefits from its population-based design and use of an inclusive national database. However, cognitive performance is notoriously difficult to study, owing to the numerous potential confounders, many of which could not be ascertained retrospectively from the registry. Additional limitations were that the Danish thresholds for phototherapy and exchange transfusion were 240 μmol/L and 340 μmol/L (or approximately 14 mg/dL and 20 mg/dL), respectively, and only 25 newborns were exposed to levels greater than 340 μmol/L.
Although no dose response association was noted between 240 μmol/L and 340 μmol/L, no conclusions may be drawn regarding significantly higher levels.
Bottom line: Neonatal nonhemolytic hyperbilirubinemia requiring phototherapy is unlikely to be associated with long-term cognitive or neuropsychiatric disability.
Citation: Ebbesen F, Ehrenstein V, Traeger M, Nielsen GL. Neonatal non-hemolytic hyperbilirubinemia: a prevalence study of adult neuropsychiatric disability and cognitive function in 463 male Danish conscripts. Arch Dis Child. 2010;95(8):583-587.