User login
"Peel the Onion" to Avoid Common Mistakes With a Hospital's Offer of an Electronic Medical Records System
What's Eating You? Ixodes Ticks
Update on Pediatric Psoriasis, Part 2: Therapeutic Management
UPDATE: PELVIC FLOOR DYSFUNCTION
When a woman has advanced prolapse of the anterior vaginal wall, it is highly likely that she has apical prolapse as well. Consider a study by Rooney and associates that determined that clinically significant vault prolapse is present in most women who have anterior vaginal prolapse of stage II or higher.1 For that reason, suspension of the vaginal apex should be considered whenever surgical treatment of anterior wall defects is planned.
Sacrocolpopexy involves suspension of the vaginal vault from the anterior longitudinal ligament of the sacrum, using Y-shaped mesh to augment native tissue (FIGURE).2 It is an effective, durable treatment for vaginal apical prolapse. With a success rate approaching 93%, this procedure has become the gold standard for repair of vault prolapse. Among its advantages are maximization of vaginal depth and preservation of a normal vaginal axis.
Sacrocolpopexy preserves the vaginal axis
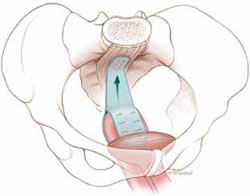
With the vaginal vault suspended from the anterior longitudinal
ligament of the sacrum, the normal vaginal axis is preserved
and vaginal depth is maximized.
Sacrocolpopexy can be performed via the abdominal, laparoscopic, or robotic-assisted approach (TABLE 1). Minimally invasive techniques are attractive because they involve faster recovery than abdominal sacrocolpopexy does. Minimally invasive techniques have also advanced to the point that they are both effective and durable. However, these advantages must be weighed against the effort required to learn the techniques, as well as their higher cost.
TABLE 1
How the 3 approaches to sacrocolpopexy compare
| Approach | Advantages and disadvantages |
|---|---|
| Abdominal | Shortest operative time No significant Trendelenburg position required Highest estimated blood loss Longest length of stay Low rate of complications Longest postoperative recovery Well-established long-term durability |
| Laparoscopic | Longer operative time Moderate Trendelenburg position required Lower estimated blood loss Shorter length of stay Surgical technique least similar to abdominal procedure Low rate of complications Shorter postoperative recovery Long-term durability less firmly established |
| Robotic-assisted | Longest operative time Steep Trendelenburg position required Lower estimated blood loss Shorter length of stay Surgical technique resembles that of abdominal approach Low rate of complications Shorter postoperative recovery Long-term durability appears to be good |
In this article, we highlight:
- a comparison of the laparoscopic and abdominal approaches to sacrocolpopexy
- an investigation of the learning curve associated with robotic-assisted sacrocolpopexy
- a study exploring the durability of robotic-assisted repair
- an estimate of the costs associated with each route of operation.
Laparoscopic vs abdominal sacrocolpopexy—how do they compare?
Paraiso MF, Walters MD, Rackley RR, Melek S, Hugney C. Laparoscopic and abdominal sacral colpopexies: a comparative cohort study. Am J Obstet Gynecol. 2005;192(5):1752–1758.
When surgeons at the Cleveland Clinic performed a retrospective cohort study to compare laparoscopic and abdominal sacrocolpopexy, they found significantly longer operative time with the laparoscopic route, with an average difference of 51 minutes (P < .0001). However, the laparoscopic approach was associated with lower blood loss (although there was no difference between groups in hematocrit on postoperative day 1); shorter hospital stay (average of 1.8 days versus 4 days [P < .001]); and comparable rates of intraoperative and postoperative complications.
Details of the trial
Paraiso and colleagues reviewed the medical charts of 56 consecutive patients who had undergone laparoscopic sacrocolpopexy, comparing them with the charts of 61 consecutive patients who had undergone the procedure using the abdominal approach. The operations had been performed between 1998 and 2003 for treatment of posthysterectomy vaginal prolapse.
The groups underwent similar rates of concurrent procedures. The laparotomy group had a significantly higher number of Burch procedures (P = .007), and the laparoscopic group had a significantly higher rate of adhesiolysis (P = .002).
Among the complications noted— which occurred at comparable rates between groups—were cystotomy, enterotomy, need for transfusion, deep-vein thrombosis, ileus, small bowel obstruction, wound infection, ventral hernia, mesh erosion, and recurrent prolapse. One laparoscopic case was converted to laparotomy because of excessive bleeding during the rectopexy portion of the operation.
Laparoscopy may have taken longer than this trial suggests
This study is one of very few well-designed trials comparing laparoscopic sacrocolpopexy to the historical gold standard of abdominal sacrocolpopexy for vault prolapse.
Twenty-eight percent of laparoscopic procedures in this study used tacking devices in lieu of suturing. Had suturing been performed universally, an even greater difference in surgical time may have been observed.
There may also be differences between groups in the durability of the two types of repair, an outcome not included in this particular study.
The laparoscopic approach offers a shorter hospital stay with no increase in intraoperative or postoperative complications, compared with abdominal sacrocolpopexy. However, it entails a significantly longer operative time than the abdominal approach does.
How steep is the learning curve for robotic-assisted sacrocolpopexy?
Akl MN, Long JB, Giles DL, et al. Robotic-assisted sacrocolpopexy: technique and learning curve. Surg Endosc. 2009;23(10):2390–2394.
Akl and coworkers reviewed the medical records of all patients who had undergone robotic-assisted sacrocolpopexy at the Mayo Clinics in Arizona and Florida between 2004 and 2007. All operations were performed by the same four urogynecologists, with an average operative time of 197.9 minutes (standard deviation, ± 66.8 minutes). However, after the first 10 cases, the operative time decreased by 64.3 minutes—a decline of 25.4% (P < .01; 95% confidence interval [CI], 16.1–112.4 minutes).
Details of the trial
Researchers collected baseline information on participants’ age, stage of prolapse, and concomitant procedures. They also gathered data on average operative time, estimated blood loss, intraoperative and postoperative complications, conversion to laparotomy, and length of hospitalization.
Of 80 women who had advanced pelvic organ prolapse (stage III/IV) who underwent robotic-assisted sacrocolpopexy, 88% underwent concomitant robotic and vaginal procedures, including robotic supracervical hysterectomy, Burch procedure, paravaginal repair, lysis of adhesions, bilateral salpingooophorectomy, vaginal cystocele or rectocele repair, and placement of a midurethral sling.
Estimated blood loss for the robotic-assisted approach ranged from 25 mL to 300 mL, with a mean loss of 96.8 mL. Average length of hospitalization was 2.6 days. Four cases (5%) were converted to laparotomy because of limited exposure and one intraoperative bladder injury. Other intraoperative complications included small-bowel injury during trocar placement and one ureteral injury. Postoperative complications included one case of ileus and five (6%) vaginal mesh erosions. Three patients developed recurrent prolapse and underwent subsequent correction.
Learning curve could have been measured more precisely
The authors did not specifically measure the learning curve for robotic-assisted sacrocolpopexy, as they took into account the concomitant procedures. For this reason, the decrease in operative time observed after 10 cases may not accurately reflect an improvement in the performance of sacrocolpopexy.
Akl and colleagues consider this detail to be a strength of the study because most women who undergo prolapse surgery have concomitant procedures. However, recording the length of time it took to perform the sacrocolpopexy portion of the procedure would have been more accurate.
The average length of stay approached that of the abdominal route. Length of stay may decline as a surgeon gains experience with the robotic-assisted approach.
Robotic-assisted sacrocolpopexy has a steep learning curve with respect to technique and surgical time.
Does robotic-assisted sacrocolpopexy provide durable support?
Elliott DS, Krambeck AE, Chow GK. Long-term results of robotic assisted laparoscopic sacrocolpopexy for the treatment of high grade vaginal vault prolapse. J Urol. 2006;176(2):655–659.
Among the few recent series reporting long-term outcomes after robotic-assisted sacrocolpopexy is this observational study from the Mayo Clinic. It involved 30 women who underwent the operation for the treatment of Baden Walker grade 4/4 posthysterectomy vaginal vault prolapse. The authors concluded that advanced prolapse can be treated with robotic-assisted sacrocolpopexy with long-term success and minimal complications.
Details of the trial
Of 30 women in this trial, 52% underwent an anti-incontinence procedure at the time of sacrocolpopexy. Women who had multiple vaginal defects or a history of abdominal surgery were excluded from the study.
Average operative time was 3.1 hours (range, 2.15–4.75 hours) in the early phase of development of operative technique (described in the manuscript) but diminished over time to an average of 2.5 hours.
Twenty-nine patients were discharged from the hospital after an overnight stay. Very few immediate postoperative complications were observed. Two patients experienced mild port-site infections that required outpatient treatment, and one patient had persistent vaginal bleeding from the incision made during the anti-incontinence procedure.
Most patients were followed for at least 1 year
The mean follow-up in this study was 24 months (range, 16–39 months). During this period, 21 women were followed for a full year. Long-term observation revealed that the repair of vault prolapse remained successful in 19 of these women.
One patient experienced recurrent prolapse 7 months after surgery. Another developed a rectocele 9 months after sacrocolpopexy. Vaginal mesh erosions occurred in two patients within 6 months after the procedure; both patients were treated with outpatient resection of the exposed mesh, with no recurrence of the prolapse.
Although a larger sample size and longer follow-up would be ideal, this study demonstrates a low rate of recurrent prolapse 1 year after the procedure.
Robotic sacrocolpopexy appears to provide long-term durability for the treatment of advanced vaginal vault prolapse.
Depending on where you practice, you may have as many as three options: abdominal, laparoscopic, or robotic-assisted. Here are basic questions you should address when choosing one:
- How familiar are you with the technique? if the answer is “not much,” you can anticipate that the cost and time required to perform it will be significantly higher.
- Are the appropriate instruments and surgical team available?
- Does the patient have comorbidities? Consider, for example, the fact that she may not be able to tolerate a steep Trendelenberg position—required for the robotic-assisted approach—if she has severe cardiac or pulmonary disease. However, if she has a risk of poor wound healing, a large abdominal incision may not be advisable and postoperative immobility can be risky. if she is obese, laparoscopic or robotic port placement is challenging, but visualization and retraction will be easier. The need for anticoagulation is another consideration, as it will affect estimated blood loss and the choice of an incision, among other things.
- Let’s not forget the patient. Given the pros and cons, what approach does she prefer?
How much do laparoscopic, abdominal, and robotic-assisted sacrocolpopexy cost?
Judd JP, Siddiqui NY, Barnett JC, et al. Cost-minimization analysis of robotic-assisted, laparoscopic, and abdominal sacrocolpopexy. J Minim Invasive Gynecol. 2010;17: 493–499.
This cost-minimization analysis concluded that robotic-assisted sacrocolpopexy incurs the highest hospital charges but is reimbursed by Medicare at a rate similar to reimbursement for the abdominal and laparoscopic routes (TABLE 2).
TABLE 2
Cost of sacrocolpopexy is significant—especially using the robotic approach
| Approach | Cost of a procedure | Operative time, min (range) |
|---|---|---|
| Robotic-assisted | $8,508 | 328 (130–383) |
| Laparoscopic | $7,353 | 269 (97–334) |
| Abdominal | $5,792 | 170 (110–286) |
| Source: Judd JP, Siddiqui NY, Barnett JC, Visco AG, Havrilesky LJ, Wu JM. Cost-minimization analysis of robotic-assisted, laparoscopic, and abdominal sacrocolpopexy. J Minim invasive Gynecol. 2010;17(4):493–499. | ||
The analysis accounted for realistic practices, such as the inclusion of concurrent hysterectomy and other procedures.
Details of the trial
Surgeons from Duke University developed a decision-analysis model in which a hypothetical group of women with advanced vaginal prolapse could choose between one of the three routes of sacrocolpopexy: abdominal, laparoscopic, or robotic-assisted. Researchers postulated two different scenarios:
- the hospital had ownership of a robotic system
- the hospital invested in the initial purchase and maintenance of such a system.
Researchers reviewed the literature to formulate their estimates of operative time, rate of conversion to laparotomy, rate of transfusion, and length of hospital stay. In addition, the costs of initial anesthesia setup, professional fees, per-minute intraoperative fees, and postanesthesia care were applied to each approach. Operating room costs per minute and the cost of disposable items such as drapes, gowns, gloves, and single-use instruments were added. For the robotic approach, the costs of reusable instruments were distributed across 10 operations. Reusable instruments for laparoscopic and abdominal surgery were assumed to incur no additional investment. Last, postoperative care—including laboratory tests, pharmacy usage, and the need for a hospital room—were individualized for each route of surgery and applied to the cost.
Costs were estimated in 2008 US dollars, based on procedure costs incurred at Duke University Medical Center.
Physician reimbursement data were obtained from Medicare reimbursement rates for anesthesia and from surgeon Current Procedural Terminology (CPT) codes specific to each procedure.
Quality-of-life assessments were not measured. Nor was the cost to society of the postoperative loss of productivity and wages for each surgical route. Had these losses been recognized, the authors observed, the cost of robotic surgery may have been lower.
The cost of robotic surgery was equivalent to the cost of laparoscopy in only two instances:
- when the operative time of robotic surgery was reduced to 149 minutes
- when the cost of robotic disposable items was less than $2,132 (reduced from a baseline cost of $3,293).
Robotic sacrocolpopexy is costly. this is an important consideration when implementing new technology. cost-saving scenarios are useful to maximize patient benefit and minimize financial burden.
We want to hear from you! Tell us what you think.
When a woman has advanced prolapse of the anterior vaginal wall, it is highly likely that she has apical prolapse as well. Consider a study by Rooney and associates that determined that clinically significant vault prolapse is present in most women who have anterior vaginal prolapse of stage II or higher.1 For that reason, suspension of the vaginal apex should be considered whenever surgical treatment of anterior wall defects is planned.
Sacrocolpopexy involves suspension of the vaginal vault from the anterior longitudinal ligament of the sacrum, using Y-shaped mesh to augment native tissue (FIGURE).2 It is an effective, durable treatment for vaginal apical prolapse. With a success rate approaching 93%, this procedure has become the gold standard for repair of vault prolapse. Among its advantages are maximization of vaginal depth and preservation of a normal vaginal axis.
Sacrocolpopexy preserves the vaginal axis
With the vaginal vault suspended from the anterior longitudinal
ligament of the sacrum, the normal vaginal axis is preserved
and vaginal depth is maximized.
Sacrocolpopexy can be performed via the abdominal, laparoscopic, or robotic-assisted approach (TABLE 1). Minimally invasive techniques are attractive because they involve faster recovery than abdominal sacrocolpopexy does. Minimally invasive techniques have also advanced to the point that they are both effective and durable. However, these advantages must be weighed against the effort required to learn the techniques, as well as their higher cost.
TABLE 1
How the 3 approaches to sacrocolpopexy compare
| Approach | Advantages and disadvantages |
|---|---|
| Abdominal | Shortest operative time No significant Trendelenburg position required Highest estimated blood loss Longest length of stay Low rate of complications Longest postoperative recovery Well-established long-term durability |
| Laparoscopic | Longer operative time Moderate Trendelenburg position required Lower estimated blood loss Shorter length of stay Surgical technique least similar to abdominal procedure Low rate of complications Shorter postoperative recovery Long-term durability less firmly established |
| Robotic-assisted | Longest operative time Steep Trendelenburg position required Lower estimated blood loss Shorter length of stay Surgical technique resembles that of abdominal approach Low rate of complications Shorter postoperative recovery Long-term durability appears to be good |
In this article, we highlight:
- a comparison of the laparoscopic and abdominal approaches to sacrocolpopexy
- an investigation of the learning curve associated with robotic-assisted sacrocolpopexy
- a study exploring the durability of robotic-assisted repair
- an estimate of the costs associated with each route of operation.
Laparoscopic vs abdominal sacrocolpopexy—how do they compare?
Paraiso MF, Walters MD, Rackley RR, Melek S, Hugney C. Laparoscopic and abdominal sacral colpopexies: a comparative cohort study. Am J Obstet Gynecol. 2005;192(5):1752–1758.
When surgeons at the Cleveland Clinic performed a retrospective cohort study to compare laparoscopic and abdominal sacrocolpopexy, they found significantly longer operative time with the laparoscopic route, with an average difference of 51 minutes (P < .0001). However, the laparoscopic approach was associated with lower blood loss (although there was no difference between groups in hematocrit on postoperative day 1); shorter hospital stay (average of 1.8 days versus 4 days [P < .001]); and comparable rates of intraoperative and postoperative complications.
Details of the trial
Paraiso and colleagues reviewed the medical charts of 56 consecutive patients who had undergone laparoscopic sacrocolpopexy, comparing them with the charts of 61 consecutive patients who had undergone the procedure using the abdominal approach. The operations had been performed between 1998 and 2003 for treatment of posthysterectomy vaginal prolapse.
The groups underwent similar rates of concurrent procedures. The laparotomy group had a significantly higher number of Burch procedures (P = .007), and the laparoscopic group had a significantly higher rate of adhesiolysis (P = .002).
Among the complications noted— which occurred at comparable rates between groups—were cystotomy, enterotomy, need for transfusion, deep-vein thrombosis, ileus, small bowel obstruction, wound infection, ventral hernia, mesh erosion, and recurrent prolapse. One laparoscopic case was converted to laparotomy because of excessive bleeding during the rectopexy portion of the operation.
Laparoscopy may have taken longer than this trial suggests
This study is one of very few well-designed trials comparing laparoscopic sacrocolpopexy to the historical gold standard of abdominal sacrocolpopexy for vault prolapse.
Twenty-eight percent of laparoscopic procedures in this study used tacking devices in lieu of suturing. Had suturing been performed universally, an even greater difference in surgical time may have been observed.
There may also be differences between groups in the durability of the two types of repair, an outcome not included in this particular study.
The laparoscopic approach offers a shorter hospital stay with no increase in intraoperative or postoperative complications, compared with abdominal sacrocolpopexy. However, it entails a significantly longer operative time than the abdominal approach does.
How steep is the learning curve for robotic-assisted sacrocolpopexy?
Akl MN, Long JB, Giles DL, et al. Robotic-assisted sacrocolpopexy: technique and learning curve. Surg Endosc. 2009;23(10):2390–2394.
Akl and coworkers reviewed the medical records of all patients who had undergone robotic-assisted sacrocolpopexy at the Mayo Clinics in Arizona and Florida between 2004 and 2007. All operations were performed by the same four urogynecologists, with an average operative time of 197.9 minutes (standard deviation, ± 66.8 minutes). However, after the first 10 cases, the operative time decreased by 64.3 minutes—a decline of 25.4% (P < .01; 95% confidence interval [CI], 16.1–112.4 minutes).
Details of the trial
Researchers collected baseline information on participants’ age, stage of prolapse, and concomitant procedures. They also gathered data on average operative time, estimated blood loss, intraoperative and postoperative complications, conversion to laparotomy, and length of hospitalization.
Of 80 women who had advanced pelvic organ prolapse (stage III/IV) who underwent robotic-assisted sacrocolpopexy, 88% underwent concomitant robotic and vaginal procedures, including robotic supracervical hysterectomy, Burch procedure, paravaginal repair, lysis of adhesions, bilateral salpingooophorectomy, vaginal cystocele or rectocele repair, and placement of a midurethral sling.
Estimated blood loss for the robotic-assisted approach ranged from 25 mL to 300 mL, with a mean loss of 96.8 mL. Average length of hospitalization was 2.6 days. Four cases (5%) were converted to laparotomy because of limited exposure and one intraoperative bladder injury. Other intraoperative complications included small-bowel injury during trocar placement and one ureteral injury. Postoperative complications included one case of ileus and five (6%) vaginal mesh erosions. Three patients developed recurrent prolapse and underwent subsequent correction.
Learning curve could have been measured more precisely
The authors did not specifically measure the learning curve for robotic-assisted sacrocolpopexy, as they took into account the concomitant procedures. For this reason, the decrease in operative time observed after 10 cases may not accurately reflect an improvement in the performance of sacrocolpopexy.
Akl and colleagues consider this detail to be a strength of the study because most women who undergo prolapse surgery have concomitant procedures. However, recording the length of time it took to perform the sacrocolpopexy portion of the procedure would have been more accurate.
The average length of stay approached that of the abdominal route. Length of stay may decline as a surgeon gains experience with the robotic-assisted approach.
Robotic-assisted sacrocolpopexy has a steep learning curve with respect to technique and surgical time.
Does robotic-assisted sacrocolpopexy provide durable support?
Elliott DS, Krambeck AE, Chow GK. Long-term results of robotic assisted laparoscopic sacrocolpopexy for the treatment of high grade vaginal vault prolapse. J Urol. 2006;176(2):655–659.
Among the few recent series reporting long-term outcomes after robotic-assisted sacrocolpopexy is this observational study from the Mayo Clinic. It involved 30 women who underwent the operation for the treatment of Baden Walker grade 4/4 posthysterectomy vaginal vault prolapse. The authors concluded that advanced prolapse can be treated with robotic-assisted sacrocolpopexy with long-term success and minimal complications.
Details of the trial
Of 30 women in this trial, 52% underwent an anti-incontinence procedure at the time of sacrocolpopexy. Women who had multiple vaginal defects or a history of abdominal surgery were excluded from the study.
Average operative time was 3.1 hours (range, 2.15–4.75 hours) in the early phase of development of operative technique (described in the manuscript) but diminished over time to an average of 2.5 hours.
Twenty-nine patients were discharged from the hospital after an overnight stay. Very few immediate postoperative complications were observed. Two patients experienced mild port-site infections that required outpatient treatment, and one patient had persistent vaginal bleeding from the incision made during the anti-incontinence procedure.
Most patients were followed for at least 1 year
The mean follow-up in this study was 24 months (range, 16–39 months). During this period, 21 women were followed for a full year. Long-term observation revealed that the repair of vault prolapse remained successful in 19 of these women.
One patient experienced recurrent prolapse 7 months after surgery. Another developed a rectocele 9 months after sacrocolpopexy. Vaginal mesh erosions occurred in two patients within 6 months after the procedure; both patients were treated with outpatient resection of the exposed mesh, with no recurrence of the prolapse.
Although a larger sample size and longer follow-up would be ideal, this study demonstrates a low rate of recurrent prolapse 1 year after the procedure.
Robotic sacrocolpopexy appears to provide long-term durability for the treatment of advanced vaginal vault prolapse.
Depending on where you practice, you may have as many as three options: abdominal, laparoscopic, or robotic-assisted. Here are basic questions you should address when choosing one:
- How familiar are you with the technique? if the answer is “not much,” you can anticipate that the cost and time required to perform it will be significantly higher.
- Are the appropriate instruments and surgical team available?
- Does the patient have comorbidities? Consider, for example, the fact that she may not be able to tolerate a steep Trendelenberg position—required for the robotic-assisted approach—if she has severe cardiac or pulmonary disease. However, if she has a risk of poor wound healing, a large abdominal incision may not be advisable and postoperative immobility can be risky. if she is obese, laparoscopic or robotic port placement is challenging, but visualization and retraction will be easier. The need for anticoagulation is another consideration, as it will affect estimated blood loss and the choice of an incision, among other things.
- Let’s not forget the patient. Given the pros and cons, what approach does she prefer?
How much do laparoscopic, abdominal, and robotic-assisted sacrocolpopexy cost?
Judd JP, Siddiqui NY, Barnett JC, et al. Cost-minimization analysis of robotic-assisted, laparoscopic, and abdominal sacrocolpopexy. J Minim Invasive Gynecol. 2010;17: 493–499.
This cost-minimization analysis concluded that robotic-assisted sacrocolpopexy incurs the highest hospital charges but is reimbursed by Medicare at a rate similar to reimbursement for the abdominal and laparoscopic routes (TABLE 2).
TABLE 2
Cost of sacrocolpopexy is significant—especially using the robotic approach
| Approach | Cost of a procedure | Operative time, min (range) |
|---|---|---|
| Robotic-assisted | $8,508 | 328 (130–383) |
| Laparoscopic | $7,353 | 269 (97–334) |
| Abdominal | $5,792 | 170 (110–286) |
| Source: Judd JP, Siddiqui NY, Barnett JC, Visco AG, Havrilesky LJ, Wu JM. Cost-minimization analysis of robotic-assisted, laparoscopic, and abdominal sacrocolpopexy. J Minim invasive Gynecol. 2010;17(4):493–499. | ||
The analysis accounted for realistic practices, such as the inclusion of concurrent hysterectomy and other procedures.
Details of the trial
Surgeons from Duke University developed a decision-analysis model in which a hypothetical group of women with advanced vaginal prolapse could choose between one of the three routes of sacrocolpopexy: abdominal, laparoscopic, or robotic-assisted. Researchers postulated two different scenarios:
- the hospital had ownership of a robotic system
- the hospital invested in the initial purchase and maintenance of such a system.
Researchers reviewed the literature to formulate their estimates of operative time, rate of conversion to laparotomy, rate of transfusion, and length of hospital stay. In addition, the costs of initial anesthesia setup, professional fees, per-minute intraoperative fees, and postanesthesia care were applied to each approach. Operating room costs per minute and the cost of disposable items such as drapes, gowns, gloves, and single-use instruments were added. For the robotic approach, the costs of reusable instruments were distributed across 10 operations. Reusable instruments for laparoscopic and abdominal surgery were assumed to incur no additional investment. Last, postoperative care—including laboratory tests, pharmacy usage, and the need for a hospital room—were individualized for each route of surgery and applied to the cost.
Costs were estimated in 2008 US dollars, based on procedure costs incurred at Duke University Medical Center.
Physician reimbursement data were obtained from Medicare reimbursement rates for anesthesia and from surgeon Current Procedural Terminology (CPT) codes specific to each procedure.
Quality-of-life assessments were not measured. Nor was the cost to society of the postoperative loss of productivity and wages for each surgical route. Had these losses been recognized, the authors observed, the cost of robotic surgery may have been lower.
The cost of robotic surgery was equivalent to the cost of laparoscopy in only two instances:
- when the operative time of robotic surgery was reduced to 149 minutes
- when the cost of robotic disposable items was less than $2,132 (reduced from a baseline cost of $3,293).
Robotic sacrocolpopexy is costly. this is an important consideration when implementing new technology. cost-saving scenarios are useful to maximize patient benefit and minimize financial burden.
We want to hear from you! Tell us what you think.
When a woman has advanced prolapse of the anterior vaginal wall, it is highly likely that she has apical prolapse as well. Consider a study by Rooney and associates that determined that clinically significant vault prolapse is present in most women who have anterior vaginal prolapse of stage II or higher.1 For that reason, suspension of the vaginal apex should be considered whenever surgical treatment of anterior wall defects is planned.
Sacrocolpopexy involves suspension of the vaginal vault from the anterior longitudinal ligament of the sacrum, using Y-shaped mesh to augment native tissue (FIGURE).2 It is an effective, durable treatment for vaginal apical prolapse. With a success rate approaching 93%, this procedure has become the gold standard for repair of vault prolapse. Among its advantages are maximization of vaginal depth and preservation of a normal vaginal axis.
Sacrocolpopexy preserves the vaginal axis
With the vaginal vault suspended from the anterior longitudinal
ligament of the sacrum, the normal vaginal axis is preserved
and vaginal depth is maximized.
Sacrocolpopexy can be performed via the abdominal, laparoscopic, or robotic-assisted approach (TABLE 1). Minimally invasive techniques are attractive because they involve faster recovery than abdominal sacrocolpopexy does. Minimally invasive techniques have also advanced to the point that they are both effective and durable. However, these advantages must be weighed against the effort required to learn the techniques, as well as their higher cost.
TABLE 1
How the 3 approaches to sacrocolpopexy compare
| Approach | Advantages and disadvantages |
|---|---|
| Abdominal | Shortest operative time No significant Trendelenburg position required Highest estimated blood loss Longest length of stay Low rate of complications Longest postoperative recovery Well-established long-term durability |
| Laparoscopic | Longer operative time Moderate Trendelenburg position required Lower estimated blood loss Shorter length of stay Surgical technique least similar to abdominal procedure Low rate of complications Shorter postoperative recovery Long-term durability less firmly established |
| Robotic-assisted | Longest operative time Steep Trendelenburg position required Lower estimated blood loss Shorter length of stay Surgical technique resembles that of abdominal approach Low rate of complications Shorter postoperative recovery Long-term durability appears to be good |
In this article, we highlight:
- a comparison of the laparoscopic and abdominal approaches to sacrocolpopexy
- an investigation of the learning curve associated with robotic-assisted sacrocolpopexy
- a study exploring the durability of robotic-assisted repair
- an estimate of the costs associated with each route of operation.
Laparoscopic vs abdominal sacrocolpopexy—how do they compare?
Paraiso MF, Walters MD, Rackley RR, Melek S, Hugney C. Laparoscopic and abdominal sacral colpopexies: a comparative cohort study. Am J Obstet Gynecol. 2005;192(5):1752–1758.
When surgeons at the Cleveland Clinic performed a retrospective cohort study to compare laparoscopic and abdominal sacrocolpopexy, they found significantly longer operative time with the laparoscopic route, with an average difference of 51 minutes (P < .0001). However, the laparoscopic approach was associated with lower blood loss (although there was no difference between groups in hematocrit on postoperative day 1); shorter hospital stay (average of 1.8 days versus 4 days [P < .001]); and comparable rates of intraoperative and postoperative complications.
Details of the trial
Paraiso and colleagues reviewed the medical charts of 56 consecutive patients who had undergone laparoscopic sacrocolpopexy, comparing them with the charts of 61 consecutive patients who had undergone the procedure using the abdominal approach. The operations had been performed between 1998 and 2003 for treatment of posthysterectomy vaginal prolapse.
The groups underwent similar rates of concurrent procedures. The laparotomy group had a significantly higher number of Burch procedures (P = .007), and the laparoscopic group had a significantly higher rate of adhesiolysis (P = .002).
Among the complications noted— which occurred at comparable rates between groups—were cystotomy, enterotomy, need for transfusion, deep-vein thrombosis, ileus, small bowel obstruction, wound infection, ventral hernia, mesh erosion, and recurrent prolapse. One laparoscopic case was converted to laparotomy because of excessive bleeding during the rectopexy portion of the operation.
Laparoscopy may have taken longer than this trial suggests
This study is one of very few well-designed trials comparing laparoscopic sacrocolpopexy to the historical gold standard of abdominal sacrocolpopexy for vault prolapse.
Twenty-eight percent of laparoscopic procedures in this study used tacking devices in lieu of suturing. Had suturing been performed universally, an even greater difference in surgical time may have been observed.
There may also be differences between groups in the durability of the two types of repair, an outcome not included in this particular study.
The laparoscopic approach offers a shorter hospital stay with no increase in intraoperative or postoperative complications, compared with abdominal sacrocolpopexy. However, it entails a significantly longer operative time than the abdominal approach does.
How steep is the learning curve for robotic-assisted sacrocolpopexy?
Akl MN, Long JB, Giles DL, et al. Robotic-assisted sacrocolpopexy: technique and learning curve. Surg Endosc. 2009;23(10):2390–2394.
Akl and coworkers reviewed the medical records of all patients who had undergone robotic-assisted sacrocolpopexy at the Mayo Clinics in Arizona and Florida between 2004 and 2007. All operations were performed by the same four urogynecologists, with an average operative time of 197.9 minutes (standard deviation, ± 66.8 minutes). However, after the first 10 cases, the operative time decreased by 64.3 minutes—a decline of 25.4% (P < .01; 95% confidence interval [CI], 16.1–112.4 minutes).
Details of the trial
Researchers collected baseline information on participants’ age, stage of prolapse, and concomitant procedures. They also gathered data on average operative time, estimated blood loss, intraoperative and postoperative complications, conversion to laparotomy, and length of hospitalization.
Of 80 women who had advanced pelvic organ prolapse (stage III/IV) who underwent robotic-assisted sacrocolpopexy, 88% underwent concomitant robotic and vaginal procedures, including robotic supracervical hysterectomy, Burch procedure, paravaginal repair, lysis of adhesions, bilateral salpingooophorectomy, vaginal cystocele or rectocele repair, and placement of a midurethral sling.
Estimated blood loss for the robotic-assisted approach ranged from 25 mL to 300 mL, with a mean loss of 96.8 mL. Average length of hospitalization was 2.6 days. Four cases (5%) were converted to laparotomy because of limited exposure and one intraoperative bladder injury. Other intraoperative complications included small-bowel injury during trocar placement and one ureteral injury. Postoperative complications included one case of ileus and five (6%) vaginal mesh erosions. Three patients developed recurrent prolapse and underwent subsequent correction.
Learning curve could have been measured more precisely
The authors did not specifically measure the learning curve for robotic-assisted sacrocolpopexy, as they took into account the concomitant procedures. For this reason, the decrease in operative time observed after 10 cases may not accurately reflect an improvement in the performance of sacrocolpopexy.
Akl and colleagues consider this detail to be a strength of the study because most women who undergo prolapse surgery have concomitant procedures. However, recording the length of time it took to perform the sacrocolpopexy portion of the procedure would have been more accurate.
The average length of stay approached that of the abdominal route. Length of stay may decline as a surgeon gains experience with the robotic-assisted approach.
Robotic-assisted sacrocolpopexy has a steep learning curve with respect to technique and surgical time.
Does robotic-assisted sacrocolpopexy provide durable support?
Elliott DS, Krambeck AE, Chow GK. Long-term results of robotic assisted laparoscopic sacrocolpopexy for the treatment of high grade vaginal vault prolapse. J Urol. 2006;176(2):655–659.
Among the few recent series reporting long-term outcomes after robotic-assisted sacrocolpopexy is this observational study from the Mayo Clinic. It involved 30 women who underwent the operation for the treatment of Baden Walker grade 4/4 posthysterectomy vaginal vault prolapse. The authors concluded that advanced prolapse can be treated with robotic-assisted sacrocolpopexy with long-term success and minimal complications.
Details of the trial
Of 30 women in this trial, 52% underwent an anti-incontinence procedure at the time of sacrocolpopexy. Women who had multiple vaginal defects or a history of abdominal surgery were excluded from the study.
Average operative time was 3.1 hours (range, 2.15–4.75 hours) in the early phase of development of operative technique (described in the manuscript) but diminished over time to an average of 2.5 hours.
Twenty-nine patients were discharged from the hospital after an overnight stay. Very few immediate postoperative complications were observed. Two patients experienced mild port-site infections that required outpatient treatment, and one patient had persistent vaginal bleeding from the incision made during the anti-incontinence procedure.
Most patients were followed for at least 1 year
The mean follow-up in this study was 24 months (range, 16–39 months). During this period, 21 women were followed for a full year. Long-term observation revealed that the repair of vault prolapse remained successful in 19 of these women.
One patient experienced recurrent prolapse 7 months after surgery. Another developed a rectocele 9 months after sacrocolpopexy. Vaginal mesh erosions occurred in two patients within 6 months after the procedure; both patients were treated with outpatient resection of the exposed mesh, with no recurrence of the prolapse.
Although a larger sample size and longer follow-up would be ideal, this study demonstrates a low rate of recurrent prolapse 1 year after the procedure.
Robotic sacrocolpopexy appears to provide long-term durability for the treatment of advanced vaginal vault prolapse.
Depending on where you practice, you may have as many as three options: abdominal, laparoscopic, or robotic-assisted. Here are basic questions you should address when choosing one:
- How familiar are you with the technique? if the answer is “not much,” you can anticipate that the cost and time required to perform it will be significantly higher.
- Are the appropriate instruments and surgical team available?
- Does the patient have comorbidities? Consider, for example, the fact that she may not be able to tolerate a steep Trendelenberg position—required for the robotic-assisted approach—if she has severe cardiac or pulmonary disease. However, if she has a risk of poor wound healing, a large abdominal incision may not be advisable and postoperative immobility can be risky. if she is obese, laparoscopic or robotic port placement is challenging, but visualization and retraction will be easier. The need for anticoagulation is another consideration, as it will affect estimated blood loss and the choice of an incision, among other things.
- Let’s not forget the patient. Given the pros and cons, what approach does she prefer?
How much do laparoscopic, abdominal, and robotic-assisted sacrocolpopexy cost?
Judd JP, Siddiqui NY, Barnett JC, et al. Cost-minimization analysis of robotic-assisted, laparoscopic, and abdominal sacrocolpopexy. J Minim Invasive Gynecol. 2010;17: 493–499.
This cost-minimization analysis concluded that robotic-assisted sacrocolpopexy incurs the highest hospital charges but is reimbursed by Medicare at a rate similar to reimbursement for the abdominal and laparoscopic routes (TABLE 2).
TABLE 2
Cost of sacrocolpopexy is significant—especially using the robotic approach
| Approach | Cost of a procedure | Operative time, min (range) |
|---|---|---|
| Robotic-assisted | $8,508 | 328 (130–383) |
| Laparoscopic | $7,353 | 269 (97–334) |
| Abdominal | $5,792 | 170 (110–286) |
| Source: Judd JP, Siddiqui NY, Barnett JC, Visco AG, Havrilesky LJ, Wu JM. Cost-minimization analysis of robotic-assisted, laparoscopic, and abdominal sacrocolpopexy. J Minim invasive Gynecol. 2010;17(4):493–499. | ||
The analysis accounted for realistic practices, such as the inclusion of concurrent hysterectomy and other procedures.
Details of the trial
Surgeons from Duke University developed a decision-analysis model in which a hypothetical group of women with advanced vaginal prolapse could choose between one of the three routes of sacrocolpopexy: abdominal, laparoscopic, or robotic-assisted. Researchers postulated two different scenarios:
- the hospital had ownership of a robotic system
- the hospital invested in the initial purchase and maintenance of such a system.
Researchers reviewed the literature to formulate their estimates of operative time, rate of conversion to laparotomy, rate of transfusion, and length of hospital stay. In addition, the costs of initial anesthesia setup, professional fees, per-minute intraoperative fees, and postanesthesia care were applied to each approach. Operating room costs per minute and the cost of disposable items such as drapes, gowns, gloves, and single-use instruments were added. For the robotic approach, the costs of reusable instruments were distributed across 10 operations. Reusable instruments for laparoscopic and abdominal surgery were assumed to incur no additional investment. Last, postoperative care—including laboratory tests, pharmacy usage, and the need for a hospital room—were individualized for each route of surgery and applied to the cost.
Costs were estimated in 2008 US dollars, based on procedure costs incurred at Duke University Medical Center.
Physician reimbursement data were obtained from Medicare reimbursement rates for anesthesia and from surgeon Current Procedural Terminology (CPT) codes specific to each procedure.
Quality-of-life assessments were not measured. Nor was the cost to society of the postoperative loss of productivity and wages for each surgical route. Had these losses been recognized, the authors observed, the cost of robotic surgery may have been lower.
The cost of robotic surgery was equivalent to the cost of laparoscopy in only two instances:
- when the operative time of robotic surgery was reduced to 149 minutes
- when the cost of robotic disposable items was less than $2,132 (reduced from a baseline cost of $3,293).
Robotic sacrocolpopexy is costly. this is an important consideration when implementing new technology. cost-saving scenarios are useful to maximize patient benefit and minimize financial burden.
We want to hear from you! Tell us what you think.
Doxepin for insomnia
Low-dose doxepin—3 mg and 6 mg—has demonstrated efficacy for insomnia characterized by frequent or early-morning awakenings and an inability to return to sleep (Table 1).1 FDA-approved in March 2010, doxepin (3 mg and 6 mg) is only the second insomnia medication not designated as a controlled substance and thus may be of special value in patients with a history of substance abuse.
Table 1
Doxepin: Fast facts
| Brand name: Silenor |
| Indication: Insomnia characterized by difficulty with sleep maintenance |
| Approval date: March 2010 |
| Availability date: September 7, 2010 |
| Manufacturer: Somaxon Pharmaceuticals |
| Dosage forms: 3 mg and 6 mg tablets |
| Recommended dosage: 3 mg or 6 mg once daily within 30 minutes of bedtime |
Clinical implications
Ramelteon, the other hypnotic that is not a controlled substance, is indicated for sleep initiation insomnia (ie, inability to fall asleep). In contrast, low-dose doxepin is for patients with sleep maintenance insomnia, which is waking up frequently or early in the morning and not falling back asleep.1,2 A tricyclic antidepressant first approved in 1969, doxepin has long been available in larger doses (10-, 25-, 50-, 75-, 100-, and 150-mg capsules) to treat depression and anxiety and as a topical preparation (5% cream) for pruritus, but not in dosages <10 mg. An inexpensive generic doxepin oral solution (10 mg/ml) is available and can be titrated to smaller dosages by a dropper. Liquid doxepin costs 10 to 20 cents per dose. A pharmacist can provide a dropper, and patients should mix the medication in 4 ounces of water, milk, or juice; 0.3 ml of liquid doxepin contains 3 mg of active ingredient and 0.6 ml of solution contains 6 mg of doxepin. These other dosage forms of doxepin, however, are not FDA-approved for insomnia. (The retail price of low-dose doxepin was not available when this article went to press.)
How it works
Doxepin’s mechanism of action for treating depression and insomnia remains unknown. The antidepressant effect of doxepin is thought to result from inhibition of serotonin and norepinephrine reuptake at the synaptic cleft. Animal studies have shown anticholinergic and antihistaminergic activity with doxepin.2 Doxepin is a potent histamine antagonist—predominantly at the H1 receptor—and its binding potency to the H1 receptor is approximately 100-times higher than its binding potency for monoamine transporters (serotonin and norepinephrine).2,3 Brain histamine is believed to be 1 of the key elements in maintaining wakefulness, and the activation of the H1 receptor is thought to play an important role in mediating arousal. Blockade of the H1 receptor by doxepin likely plays a role in reducing wakefulness. Typically, therapeutic doses of antidepressants with anti-histaminergic properties, such as doxepin at antidepressant doses, amitriptyline, or desipramine, do not selectively block H1 receptors, but act at cholinergic, serotonergic, adrenergic, histaminergic, and muscarinic receptors, which can cause adverse effects.3 However, low doses of doxepin (1, 3, and 6 mg) can achieve selective H1 blockade.4,5 Patients taking >25 mg/d of doxepin may report clinically significant anticholinergic effects.
Pharmacokinetics
When doxepin, 6 mg, was administered to healthy, fasting patients, time to maximum concentration (Tmax) was 3.5 hours. Peak plasma concentration (Cmax) increased in a dose-related fashion when doxepin was increased from 3 mg to 6 mg. Doxepin, 6 mg, taken with a high-fat meal resulted in area under the curve increase of 41%, Cmax increase of 15%, and almost 3-hour delay in Tmax. Therefore, to prevent a delay in onset of action and to minimize the likelihood of daytime sedation, doxepin should not be taken within 3 hours of a meal.1-3
Doxepin is metabolized primarily by the liver’s cytochrome P450 (CYP) 2C19 and CYP2D6 enzymes; CYP1A2 and CYP2D6 are involved to a lesser extent. If doxepin is coadministered with drugs that inhibit these isoenzymes, such as fluoxetine and paroxetine, doxepin blood levels may increase. Doxepin does not seem to induce CYP isoenzymes. This medication is metabolized by demethylation and oxidation; the primary metabolite is nordoxepin (N-desmethyldoxepin), which later undergoes glucuronide conjugation. The half-life is 15 hours for doxepin and 31 hours for nordoxepin. Doxepin is excreted in urine primarily as glucuronide conjugate.1-3
Coadministration with cimetidine, an inhibitor of CYP isoenzymes, could double the doxepin plasma concentration; therefore, patients taking cimetidine should not exceed 3 mg/d of doxepin.
Efficacy
Doxepin reduced insomnia symptoms in 3 pilot studies at doses of 10, 25, and 50 mg, and in 2 phase III randomized, double-blind, placebo-controlled clinical trials using 1, 3, and 6 mg (Table 2).4,5 Clinical studies lasted up to 3 months.1-3,6-8
In the first phase III trial, 67 patients, age 18 to 64 with chronic primary insomnia, were randomly assigned to placebo or 1 mg, 3 mg, or 6 mg of doxepin for 2 nights. All patients received all treatments, and each treatment was followed by 8 hours of polysomnography (PSG) evaluation in a sleep laboratory.4 In this study, patients taking doxepin at all doses achieved improvement in objective (PSG-defined) and subjective (patient-reported) measures of sleep duration and sleep maintenance. Wake after sleep onset (WASO), total sleep time (TST), and sleep efficiency (SE) improved with all doxepin doses, and wake time during sleep (WTDS)—which was the primary study endpoint—decreased with 3 mg and 6 mg doses, but not with 1 mg or placebo. In addition, PSG indicators of early-morning awakenings (terminal insomnia) were reduced, as shown by an increase in SE during the final third of the night and the 7th and 8th hours of sleep (1, 3, and 6 mg doses) and a reduction in wake time after sleep (WTAS) during the final third of the night (6 mg only). The effects on sleep duration and maintenance were more robust with 3 mg and 6 mg doses. Improved sleep onset was seen only with the 6 mg dose. Next-day alertness was assessed using the Visual Analogue Scale (VAS) for sleepiness, and the Digit-Symbol Substitution Test (DSST) and the Symbol-Copying Task (SCT) for psychomotor function. No statistically significant differences were found among placebo and any of the doxepin doses on the VAS, DSST, or SCT.
Doxepin was well tolerated. Reported adverse events were mild or moderate. Headaches and somnolence were reported by >2% of patients. The incidence of adverse events, including next-day sedation, was similar to that of placebo. Additionally, there were no spontaneous reports of anticholinergic side effects, which are associated with higher doxepin doses.4
The second phase III trial examined safety and efficacy of 1, 3, and 6 mg doxepin in patients age ≥65.5 Seventy-six adults with primary insomnia were randomly assigned to receive placebo or doxepin for 2 nights; all patients received all treatments, and each treatment was followed by an 8-hour PSG. Patients taking any doxepin dose achieved objective and subjective improvement in sleep duration and sleep maintenance, which lasted into the final hours of the night. WTDS (primary study endpoint), WASO, TST, and overall SE improved at all doxepin doses compared with placebo, and WTAS and SE at hours 7 and 8 improved at doxepin doses of 3 mg and 6 mg compared with placebo. These findings suggest that doxepin, 3 mg and 6 mg, can help older insomnia patients with early morning awakenings.
In this study, no statistically significant differences were found among placebo and any doxepin doses on VAS, DSST, or SCT or next-day residual sedation. The incidence of side effects was low and similar to that of placebo. Adverse events were mild or moderate; 1 incident of chest pain was reported, but it was determined not to be of cardiac origin and not related to study drug. There were no spontaneous reports of anticholinergic side effects associated with higher doses of doxepin. There were no reports of memory impairment.5
Table 2
Evidence of effectiveness of doxepin for insomnia
| Study | Subjects | Dosages | Results |
|---|---|---|---|
| Roth et al, 20074; phase III, randomized, multi-center, double-blind, placebo-controlled, 4-period crossover, dose-response study | 67 patients age 18 to 64 with chronic primary insomnia | 1, 3, or 6 mg given once daily at bedtime for 2 nights | Improvement vs placebo in PSG-defined WASO, TST, SE, and SE during the final third of the night. 6-mg dose significantly reduced subjective latency to sleep onset. Safety profile of all 3 doses was comparable to placebo. No difference in residual sedation |
| Scharf et al, 20085; phase III, randomized, multi-center, double-blind, placebo-controlled, 4-period crossover, dose-response study | 76 patients age ≥65 with primary insomnia | 1, 3, or 6 mg at bedtime for 2 nights | Reduction vs placebo in WTDS and WASO at all 3 doses. Increase in TST and SE at all 3 doses. No difference in number of awakenings after sleep onset and latency to persistent sleep at all 3 doses. WTAS was reduced only at 3 and 6 mg doses. Patient-reported WTAS was decreased at all doses. Patient-reported latency to sleep onset decreased only with 6 mg. Safety profile of all 3 doses was comparable to placebo and there were no differences among placebo and all 3 doses doxepin in next-day sleepiness or psychomotor function |
| PSG: polysomnography; SE: sleep efficiency; TST: total sleep time; WASO: wake after sleep onset; WTAS: wake time after sleep; WTDS: wake time during sleep Source: References 4,5 | |||
Tolerability
Clinical studies that evaluated the safety of doxepin lasted up to 3 months. Somnolence/sedation, nausea, and upper respiratory tract infection were reported by >2% of patients taking doxepin and were more common than in patients treated with placebo.1 All reported adverse events were mild to moderate.
Doxepin appears to be better tolerated at hypnotic doses (3 mg and 6 mg) than at antidepressant doses (50 to 300 mg/d), although direct comparative studies are not available.2,4,5 Additionally, psycho-motor function assessed using DSST and SCT and next-day sedation assessed using VAS in patients receiving hypnotic doses of doxepin (1 and 3 mg) were the same as placebo. Two studies noted small-to-modest decreases in DSST, SCT, and VAS when doxepin, 6 mg, was administered.1 Patients taking doxepin at antidepressant doses report significant anticholinergic side effects, including sedation, confusion, urinary retention, constipation, blurred vision, and dry mouth. Hypotension also has been reported at antidepressant doses, and there seems to be a dose-dependant cardiotoxicity, with higher incidence of adverse effects occurring at higher doses of the drug.
Severe toxicity or death from overdose is presumably less likely with hypnotic doses of doxepin than with higher doses, although this has not been systematically explored. If an insomniac overdosed on a 30-day supply of an hypnotic dose (3 or 6 mg), he or she would take only 90 to 180 mg of doxepin, which would be unlikely to cause severe toxicity or death.2-4
Symptoms of withdrawal and rebound insomnia—an increase in WASO compared with baseline after discontinuing the medication—were assessed in a 35-day double-blind study of adults with chronic insomnia.1 There was no evidence of withdrawal syndrome as measured by Tyler’s Symptom Checklist after doxepin 3 mg and 6 mg was discontinued. Discontinuation period-emergent nausea and vomiting was noted in 5% of patients taking 6 mg of doxepin, but not in those taking placebo or 3 mg of doxepin. There was no evidence of rebound insomnia after doxepin 3 mg and 6 mg was discontinued.1
Contraindications
Doxepin is contraindicated in patients with hypersensitivity to doxepin hydrochloride, with severe urinary retention, with narrow angle glaucoma, and who have used monoamine oxidase inhibitors (MAOIs) within the previous 2 weeks. Serious adverse effects, including hypertensive crisis and death, have been reported with coadministration of MAOIs and certain drugs, such as serotonergic antidepressants and some opioids derivatives. There are no reports of concomitant use of doxepin with MAOIs.1
Dosing
In adults, the recommended hypnotic dose for doxepin is 6 mg taken 30 minutes before bedtime. For patients age ≥65, the recommended starting hypnotic dose is 3 mg 30 minutes before bedtime, which can be increased to 6 mg if indicated.1
Related Resources
- Doghramji K, Grewal R, Markov D. Evaluation and management of insomnia in the psychiatric setting. Focus. 2009;8(4):441-454.
- Psychiatric Clinics of North America. December 2006. All articles in this issue address sleep disorders encountered in psychiatric practice.
- National Sleep Foundation. www.sleepfoundation.org.
Drug Brand Names
- Amitriptyline • Elavil
- Cimetidine • Tagamet
- Desipramine • Norpramin
- Doxepin (3 mg and 6 mg) • Silenor
- Doxepin (10 to 150 mg, oral) • Sinequan
- Doxepin cream • Prudoxin
- Fluoxetine • Prozac
- Paroxetine • Paxil
- Ramelteon • Rozerem
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Silenor [package insert]. San Diego, CA: Somaxon; 2010.
2. Goforth HW. Low-dose doxepin for the treatment of insomnia: emerging data. Expert Opin Pharmacother. 2009;10(10):1649-1655.
3. Stahl SM. Selective histamine H1 antagonism: novel hypnotic and pharmacologic actions challenge classical notions of antihistamines. CNS Spectr. 2008;13(12):1027-1038.
4. Roth T, Rogowski R, Hull S, et al. Efficacy and safety of doxepin 1 mg, 3 mg, and 6 mg in adults with primary insomnia. Sleep. 2007;30(11):1555-1561.
5. Scharf M, Rogowski R, Hull S, et al. Efficacy and safety of doxepin 1 mg, 3 mg, and 6 mg in elderly patients with primary insomnia: a randomized, double-blind, placebo-controlled crossover study. J Clin Psychiatry. 2008;69:1557-1564.
6. Hajak G, Rodenbeck A, Adler L, et al. Nocturnal melatonin secretion and sleep after doxepin administration in chronic primary insomnia. Pharmacopsychiatry. 1996;29:187-192.
7. Hajak G, Rodenbeck A, Voderholzer U, et al. Doxepin in the treatment of primary insomnia: a placebo-controlled, double-blind, polysomnographic study. J Clin Psychiatry. 2001;62:453-463.
8. Rodenbeck A, Cohrs S, Jordan W, et al. The sleep-improving effects of doxepin are paralleled by a normalized plasma cortisol secretion in primary insomnia. A placebo-controlled, double-blind, randomized, cross-over study followed by an open treatment for 3 weeks. Psychopharmacology. 2003;170:423-428.
Low-dose doxepin—3 mg and 6 mg—has demonstrated efficacy for insomnia characterized by frequent or early-morning awakenings and an inability to return to sleep (Table 1).1 FDA-approved in March 2010, doxepin (3 mg and 6 mg) is only the second insomnia medication not designated as a controlled substance and thus may be of special value in patients with a history of substance abuse.
Table 1
Doxepin: Fast facts
| Brand name: Silenor |
| Indication: Insomnia characterized by difficulty with sleep maintenance |
| Approval date: March 2010 |
| Availability date: September 7, 2010 |
| Manufacturer: Somaxon Pharmaceuticals |
| Dosage forms: 3 mg and 6 mg tablets |
| Recommended dosage: 3 mg or 6 mg once daily within 30 minutes of bedtime |
Clinical implications
Ramelteon, the other hypnotic that is not a controlled substance, is indicated for sleep initiation insomnia (ie, inability to fall asleep). In contrast, low-dose doxepin is for patients with sleep maintenance insomnia, which is waking up frequently or early in the morning and not falling back asleep.1,2 A tricyclic antidepressant first approved in 1969, doxepin has long been available in larger doses (10-, 25-, 50-, 75-, 100-, and 150-mg capsules) to treat depression and anxiety and as a topical preparation (5% cream) for pruritus, but not in dosages <10 mg. An inexpensive generic doxepin oral solution (10 mg/ml) is available and can be titrated to smaller dosages by a dropper. Liquid doxepin costs 10 to 20 cents per dose. A pharmacist can provide a dropper, and patients should mix the medication in 4 ounces of water, milk, or juice; 0.3 ml of liquid doxepin contains 3 mg of active ingredient and 0.6 ml of solution contains 6 mg of doxepin. These other dosage forms of doxepin, however, are not FDA-approved for insomnia. (The retail price of low-dose doxepin was not available when this article went to press.)
How it works
Doxepin’s mechanism of action for treating depression and insomnia remains unknown. The antidepressant effect of doxepin is thought to result from inhibition of serotonin and norepinephrine reuptake at the synaptic cleft. Animal studies have shown anticholinergic and antihistaminergic activity with doxepin.2 Doxepin is a potent histamine antagonist—predominantly at the H1 receptor—and its binding potency to the H1 receptor is approximately 100-times higher than its binding potency for monoamine transporters (serotonin and norepinephrine).2,3 Brain histamine is believed to be 1 of the key elements in maintaining wakefulness, and the activation of the H1 receptor is thought to play an important role in mediating arousal. Blockade of the H1 receptor by doxepin likely plays a role in reducing wakefulness. Typically, therapeutic doses of antidepressants with anti-histaminergic properties, such as doxepin at antidepressant doses, amitriptyline, or desipramine, do not selectively block H1 receptors, but act at cholinergic, serotonergic, adrenergic, histaminergic, and muscarinic receptors, which can cause adverse effects.3 However, low doses of doxepin (1, 3, and 6 mg) can achieve selective H1 blockade.4,5 Patients taking >25 mg/d of doxepin may report clinically significant anticholinergic effects.
Pharmacokinetics
When doxepin, 6 mg, was administered to healthy, fasting patients, time to maximum concentration (Tmax) was 3.5 hours. Peak plasma concentration (Cmax) increased in a dose-related fashion when doxepin was increased from 3 mg to 6 mg. Doxepin, 6 mg, taken with a high-fat meal resulted in area under the curve increase of 41%, Cmax increase of 15%, and almost 3-hour delay in Tmax. Therefore, to prevent a delay in onset of action and to minimize the likelihood of daytime sedation, doxepin should not be taken within 3 hours of a meal.1-3
Doxepin is metabolized primarily by the liver’s cytochrome P450 (CYP) 2C19 and CYP2D6 enzymes; CYP1A2 and CYP2D6 are involved to a lesser extent. If doxepin is coadministered with drugs that inhibit these isoenzymes, such as fluoxetine and paroxetine, doxepin blood levels may increase. Doxepin does not seem to induce CYP isoenzymes. This medication is metabolized by demethylation and oxidation; the primary metabolite is nordoxepin (N-desmethyldoxepin), which later undergoes glucuronide conjugation. The half-life is 15 hours for doxepin and 31 hours for nordoxepin. Doxepin is excreted in urine primarily as glucuronide conjugate.1-3
Coadministration with cimetidine, an inhibitor of CYP isoenzymes, could double the doxepin plasma concentration; therefore, patients taking cimetidine should not exceed 3 mg/d of doxepin.
Efficacy
Doxepin reduced insomnia symptoms in 3 pilot studies at doses of 10, 25, and 50 mg, and in 2 phase III randomized, double-blind, placebo-controlled clinical trials using 1, 3, and 6 mg (Table 2).4,5 Clinical studies lasted up to 3 months.1-3,6-8
In the first phase III trial, 67 patients, age 18 to 64 with chronic primary insomnia, were randomly assigned to placebo or 1 mg, 3 mg, or 6 mg of doxepin for 2 nights. All patients received all treatments, and each treatment was followed by 8 hours of polysomnography (PSG) evaluation in a sleep laboratory.4 In this study, patients taking doxepin at all doses achieved improvement in objective (PSG-defined) and subjective (patient-reported) measures of sleep duration and sleep maintenance. Wake after sleep onset (WASO), total sleep time (TST), and sleep efficiency (SE) improved with all doxepin doses, and wake time during sleep (WTDS)—which was the primary study endpoint—decreased with 3 mg and 6 mg doses, but not with 1 mg or placebo. In addition, PSG indicators of early-morning awakenings (terminal insomnia) were reduced, as shown by an increase in SE during the final third of the night and the 7th and 8th hours of sleep (1, 3, and 6 mg doses) and a reduction in wake time after sleep (WTAS) during the final third of the night (6 mg only). The effects on sleep duration and maintenance were more robust with 3 mg and 6 mg doses. Improved sleep onset was seen only with the 6 mg dose. Next-day alertness was assessed using the Visual Analogue Scale (VAS) for sleepiness, and the Digit-Symbol Substitution Test (DSST) and the Symbol-Copying Task (SCT) for psychomotor function. No statistically significant differences were found among placebo and any of the doxepin doses on the VAS, DSST, or SCT.
Doxepin was well tolerated. Reported adverse events were mild or moderate. Headaches and somnolence were reported by >2% of patients. The incidence of adverse events, including next-day sedation, was similar to that of placebo. Additionally, there were no spontaneous reports of anticholinergic side effects, which are associated with higher doxepin doses.4
The second phase III trial examined safety and efficacy of 1, 3, and 6 mg doxepin in patients age ≥65.5 Seventy-six adults with primary insomnia were randomly assigned to receive placebo or doxepin for 2 nights; all patients received all treatments, and each treatment was followed by an 8-hour PSG. Patients taking any doxepin dose achieved objective and subjective improvement in sleep duration and sleep maintenance, which lasted into the final hours of the night. WTDS (primary study endpoint), WASO, TST, and overall SE improved at all doxepin doses compared with placebo, and WTAS and SE at hours 7 and 8 improved at doxepin doses of 3 mg and 6 mg compared with placebo. These findings suggest that doxepin, 3 mg and 6 mg, can help older insomnia patients with early morning awakenings.
In this study, no statistically significant differences were found among placebo and any doxepin doses on VAS, DSST, or SCT or next-day residual sedation. The incidence of side effects was low and similar to that of placebo. Adverse events were mild or moderate; 1 incident of chest pain was reported, but it was determined not to be of cardiac origin and not related to study drug. There were no spontaneous reports of anticholinergic side effects associated with higher doses of doxepin. There were no reports of memory impairment.5
Table 2
Evidence of effectiveness of doxepin for insomnia
| Study | Subjects | Dosages | Results |
|---|---|---|---|
| Roth et al, 20074; phase III, randomized, multi-center, double-blind, placebo-controlled, 4-period crossover, dose-response study | 67 patients age 18 to 64 with chronic primary insomnia | 1, 3, or 6 mg given once daily at bedtime for 2 nights | Improvement vs placebo in PSG-defined WASO, TST, SE, and SE during the final third of the night. 6-mg dose significantly reduced subjective latency to sleep onset. Safety profile of all 3 doses was comparable to placebo. No difference in residual sedation |
| Scharf et al, 20085; phase III, randomized, multi-center, double-blind, placebo-controlled, 4-period crossover, dose-response study | 76 patients age ≥65 with primary insomnia | 1, 3, or 6 mg at bedtime for 2 nights | Reduction vs placebo in WTDS and WASO at all 3 doses. Increase in TST and SE at all 3 doses. No difference in number of awakenings after sleep onset and latency to persistent sleep at all 3 doses. WTAS was reduced only at 3 and 6 mg doses. Patient-reported WTAS was decreased at all doses. Patient-reported latency to sleep onset decreased only with 6 mg. Safety profile of all 3 doses was comparable to placebo and there were no differences among placebo and all 3 doses doxepin in next-day sleepiness or psychomotor function |
| PSG: polysomnography; SE: sleep efficiency; TST: total sleep time; WASO: wake after sleep onset; WTAS: wake time after sleep; WTDS: wake time during sleep Source: References 4,5 | |||
Tolerability
Clinical studies that evaluated the safety of doxepin lasted up to 3 months. Somnolence/sedation, nausea, and upper respiratory tract infection were reported by >2% of patients taking doxepin and were more common than in patients treated with placebo.1 All reported adverse events were mild to moderate.
Doxepin appears to be better tolerated at hypnotic doses (3 mg and 6 mg) than at antidepressant doses (50 to 300 mg/d), although direct comparative studies are not available.2,4,5 Additionally, psycho-motor function assessed using DSST and SCT and next-day sedation assessed using VAS in patients receiving hypnotic doses of doxepin (1 and 3 mg) were the same as placebo. Two studies noted small-to-modest decreases in DSST, SCT, and VAS when doxepin, 6 mg, was administered.1 Patients taking doxepin at antidepressant doses report significant anticholinergic side effects, including sedation, confusion, urinary retention, constipation, blurred vision, and dry mouth. Hypotension also has been reported at antidepressant doses, and there seems to be a dose-dependant cardiotoxicity, with higher incidence of adverse effects occurring at higher doses of the drug.
Severe toxicity or death from overdose is presumably less likely with hypnotic doses of doxepin than with higher doses, although this has not been systematically explored. If an insomniac overdosed on a 30-day supply of an hypnotic dose (3 or 6 mg), he or she would take only 90 to 180 mg of doxepin, which would be unlikely to cause severe toxicity or death.2-4
Symptoms of withdrawal and rebound insomnia—an increase in WASO compared with baseline after discontinuing the medication—were assessed in a 35-day double-blind study of adults with chronic insomnia.1 There was no evidence of withdrawal syndrome as measured by Tyler’s Symptom Checklist after doxepin 3 mg and 6 mg was discontinued. Discontinuation period-emergent nausea and vomiting was noted in 5% of patients taking 6 mg of doxepin, but not in those taking placebo or 3 mg of doxepin. There was no evidence of rebound insomnia after doxepin 3 mg and 6 mg was discontinued.1
Contraindications
Doxepin is contraindicated in patients with hypersensitivity to doxepin hydrochloride, with severe urinary retention, with narrow angle glaucoma, and who have used monoamine oxidase inhibitors (MAOIs) within the previous 2 weeks. Serious adverse effects, including hypertensive crisis and death, have been reported with coadministration of MAOIs and certain drugs, such as serotonergic antidepressants and some opioids derivatives. There are no reports of concomitant use of doxepin with MAOIs.1
Dosing
In adults, the recommended hypnotic dose for doxepin is 6 mg taken 30 minutes before bedtime. For patients age ≥65, the recommended starting hypnotic dose is 3 mg 30 minutes before bedtime, which can be increased to 6 mg if indicated.1
Related Resources
- Doghramji K, Grewal R, Markov D. Evaluation and management of insomnia in the psychiatric setting. Focus. 2009;8(4):441-454.
- Psychiatric Clinics of North America. December 2006. All articles in this issue address sleep disorders encountered in psychiatric practice.
- National Sleep Foundation. www.sleepfoundation.org.
Drug Brand Names
- Amitriptyline • Elavil
- Cimetidine • Tagamet
- Desipramine • Norpramin
- Doxepin (3 mg and 6 mg) • Silenor
- Doxepin (10 to 150 mg, oral) • Sinequan
- Doxepin cream • Prudoxin
- Fluoxetine • Prozac
- Paroxetine • Paxil
- Ramelteon • Rozerem
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Low-dose doxepin—3 mg and 6 mg—has demonstrated efficacy for insomnia characterized by frequent or early-morning awakenings and an inability to return to sleep (Table 1).1 FDA-approved in March 2010, doxepin (3 mg and 6 mg) is only the second insomnia medication not designated as a controlled substance and thus may be of special value in patients with a history of substance abuse.
Table 1
Doxepin: Fast facts
| Brand name: Silenor |
| Indication: Insomnia characterized by difficulty with sleep maintenance |
| Approval date: March 2010 |
| Availability date: September 7, 2010 |
| Manufacturer: Somaxon Pharmaceuticals |
| Dosage forms: 3 mg and 6 mg tablets |
| Recommended dosage: 3 mg or 6 mg once daily within 30 minutes of bedtime |
Clinical implications
Ramelteon, the other hypnotic that is not a controlled substance, is indicated for sleep initiation insomnia (ie, inability to fall asleep). In contrast, low-dose doxepin is for patients with sleep maintenance insomnia, which is waking up frequently or early in the morning and not falling back asleep.1,2 A tricyclic antidepressant first approved in 1969, doxepin has long been available in larger doses (10-, 25-, 50-, 75-, 100-, and 150-mg capsules) to treat depression and anxiety and as a topical preparation (5% cream) for pruritus, but not in dosages <10 mg. An inexpensive generic doxepin oral solution (10 mg/ml) is available and can be titrated to smaller dosages by a dropper. Liquid doxepin costs 10 to 20 cents per dose. A pharmacist can provide a dropper, and patients should mix the medication in 4 ounces of water, milk, or juice; 0.3 ml of liquid doxepin contains 3 mg of active ingredient and 0.6 ml of solution contains 6 mg of doxepin. These other dosage forms of doxepin, however, are not FDA-approved for insomnia. (The retail price of low-dose doxepin was not available when this article went to press.)
How it works
Doxepin’s mechanism of action for treating depression and insomnia remains unknown. The antidepressant effect of doxepin is thought to result from inhibition of serotonin and norepinephrine reuptake at the synaptic cleft. Animal studies have shown anticholinergic and antihistaminergic activity with doxepin.2 Doxepin is a potent histamine antagonist—predominantly at the H1 receptor—and its binding potency to the H1 receptor is approximately 100-times higher than its binding potency for monoamine transporters (serotonin and norepinephrine).2,3 Brain histamine is believed to be 1 of the key elements in maintaining wakefulness, and the activation of the H1 receptor is thought to play an important role in mediating arousal. Blockade of the H1 receptor by doxepin likely plays a role in reducing wakefulness. Typically, therapeutic doses of antidepressants with anti-histaminergic properties, such as doxepin at antidepressant doses, amitriptyline, or desipramine, do not selectively block H1 receptors, but act at cholinergic, serotonergic, adrenergic, histaminergic, and muscarinic receptors, which can cause adverse effects.3 However, low doses of doxepin (1, 3, and 6 mg) can achieve selective H1 blockade.4,5 Patients taking >25 mg/d of doxepin may report clinically significant anticholinergic effects.
Pharmacokinetics
When doxepin, 6 mg, was administered to healthy, fasting patients, time to maximum concentration (Tmax) was 3.5 hours. Peak plasma concentration (Cmax) increased in a dose-related fashion when doxepin was increased from 3 mg to 6 mg. Doxepin, 6 mg, taken with a high-fat meal resulted in area under the curve increase of 41%, Cmax increase of 15%, and almost 3-hour delay in Tmax. Therefore, to prevent a delay in onset of action and to minimize the likelihood of daytime sedation, doxepin should not be taken within 3 hours of a meal.1-3
Doxepin is metabolized primarily by the liver’s cytochrome P450 (CYP) 2C19 and CYP2D6 enzymes; CYP1A2 and CYP2D6 are involved to a lesser extent. If doxepin is coadministered with drugs that inhibit these isoenzymes, such as fluoxetine and paroxetine, doxepin blood levels may increase. Doxepin does not seem to induce CYP isoenzymes. This medication is metabolized by demethylation and oxidation; the primary metabolite is nordoxepin (N-desmethyldoxepin), which later undergoes glucuronide conjugation. The half-life is 15 hours for doxepin and 31 hours for nordoxepin. Doxepin is excreted in urine primarily as glucuronide conjugate.1-3
Coadministration with cimetidine, an inhibitor of CYP isoenzymes, could double the doxepin plasma concentration; therefore, patients taking cimetidine should not exceed 3 mg/d of doxepin.
Efficacy
Doxepin reduced insomnia symptoms in 3 pilot studies at doses of 10, 25, and 50 mg, and in 2 phase III randomized, double-blind, placebo-controlled clinical trials using 1, 3, and 6 mg (Table 2).4,5 Clinical studies lasted up to 3 months.1-3,6-8
In the first phase III trial, 67 patients, age 18 to 64 with chronic primary insomnia, were randomly assigned to placebo or 1 mg, 3 mg, or 6 mg of doxepin for 2 nights. All patients received all treatments, and each treatment was followed by 8 hours of polysomnography (PSG) evaluation in a sleep laboratory.4 In this study, patients taking doxepin at all doses achieved improvement in objective (PSG-defined) and subjective (patient-reported) measures of sleep duration and sleep maintenance. Wake after sleep onset (WASO), total sleep time (TST), and sleep efficiency (SE) improved with all doxepin doses, and wake time during sleep (WTDS)—which was the primary study endpoint—decreased with 3 mg and 6 mg doses, but not with 1 mg or placebo. In addition, PSG indicators of early-morning awakenings (terminal insomnia) were reduced, as shown by an increase in SE during the final third of the night and the 7th and 8th hours of sleep (1, 3, and 6 mg doses) and a reduction in wake time after sleep (WTAS) during the final third of the night (6 mg only). The effects on sleep duration and maintenance were more robust with 3 mg and 6 mg doses. Improved sleep onset was seen only with the 6 mg dose. Next-day alertness was assessed using the Visual Analogue Scale (VAS) for sleepiness, and the Digit-Symbol Substitution Test (DSST) and the Symbol-Copying Task (SCT) for psychomotor function. No statistically significant differences were found among placebo and any of the doxepin doses on the VAS, DSST, or SCT.
Doxepin was well tolerated. Reported adverse events were mild or moderate. Headaches and somnolence were reported by >2% of patients. The incidence of adverse events, including next-day sedation, was similar to that of placebo. Additionally, there were no spontaneous reports of anticholinergic side effects, which are associated with higher doxepin doses.4
The second phase III trial examined safety and efficacy of 1, 3, and 6 mg doxepin in patients age ≥65.5 Seventy-six adults with primary insomnia were randomly assigned to receive placebo or doxepin for 2 nights; all patients received all treatments, and each treatment was followed by an 8-hour PSG. Patients taking any doxepin dose achieved objective and subjective improvement in sleep duration and sleep maintenance, which lasted into the final hours of the night. WTDS (primary study endpoint), WASO, TST, and overall SE improved at all doxepin doses compared with placebo, and WTAS and SE at hours 7 and 8 improved at doxepin doses of 3 mg and 6 mg compared with placebo. These findings suggest that doxepin, 3 mg and 6 mg, can help older insomnia patients with early morning awakenings.
In this study, no statistically significant differences were found among placebo and any doxepin doses on VAS, DSST, or SCT or next-day residual sedation. The incidence of side effects was low and similar to that of placebo. Adverse events were mild or moderate; 1 incident of chest pain was reported, but it was determined not to be of cardiac origin and not related to study drug. There were no spontaneous reports of anticholinergic side effects associated with higher doses of doxepin. There were no reports of memory impairment.5
Table 2
Evidence of effectiveness of doxepin for insomnia
| Study | Subjects | Dosages | Results |
|---|---|---|---|
| Roth et al, 20074; phase III, randomized, multi-center, double-blind, placebo-controlled, 4-period crossover, dose-response study | 67 patients age 18 to 64 with chronic primary insomnia | 1, 3, or 6 mg given once daily at bedtime for 2 nights | Improvement vs placebo in PSG-defined WASO, TST, SE, and SE during the final third of the night. 6-mg dose significantly reduced subjective latency to sleep onset. Safety profile of all 3 doses was comparable to placebo. No difference in residual sedation |
| Scharf et al, 20085; phase III, randomized, multi-center, double-blind, placebo-controlled, 4-period crossover, dose-response study | 76 patients age ≥65 with primary insomnia | 1, 3, or 6 mg at bedtime for 2 nights | Reduction vs placebo in WTDS and WASO at all 3 doses. Increase in TST and SE at all 3 doses. No difference in number of awakenings after sleep onset and latency to persistent sleep at all 3 doses. WTAS was reduced only at 3 and 6 mg doses. Patient-reported WTAS was decreased at all doses. Patient-reported latency to sleep onset decreased only with 6 mg. Safety profile of all 3 doses was comparable to placebo and there were no differences among placebo and all 3 doses doxepin in next-day sleepiness or psychomotor function |
| PSG: polysomnography; SE: sleep efficiency; TST: total sleep time; WASO: wake after sleep onset; WTAS: wake time after sleep; WTDS: wake time during sleep Source: References 4,5 | |||
Tolerability
Clinical studies that evaluated the safety of doxepin lasted up to 3 months. Somnolence/sedation, nausea, and upper respiratory tract infection were reported by >2% of patients taking doxepin and were more common than in patients treated with placebo.1 All reported adverse events were mild to moderate.
Doxepin appears to be better tolerated at hypnotic doses (3 mg and 6 mg) than at antidepressant doses (50 to 300 mg/d), although direct comparative studies are not available.2,4,5 Additionally, psycho-motor function assessed using DSST and SCT and next-day sedation assessed using VAS in patients receiving hypnotic doses of doxepin (1 and 3 mg) were the same as placebo. Two studies noted small-to-modest decreases in DSST, SCT, and VAS when doxepin, 6 mg, was administered.1 Patients taking doxepin at antidepressant doses report significant anticholinergic side effects, including sedation, confusion, urinary retention, constipation, blurred vision, and dry mouth. Hypotension also has been reported at antidepressant doses, and there seems to be a dose-dependant cardiotoxicity, with higher incidence of adverse effects occurring at higher doses of the drug.
Severe toxicity or death from overdose is presumably less likely with hypnotic doses of doxepin than with higher doses, although this has not been systematically explored. If an insomniac overdosed on a 30-day supply of an hypnotic dose (3 or 6 mg), he or she would take only 90 to 180 mg of doxepin, which would be unlikely to cause severe toxicity or death.2-4
Symptoms of withdrawal and rebound insomnia—an increase in WASO compared with baseline after discontinuing the medication—were assessed in a 35-day double-blind study of adults with chronic insomnia.1 There was no evidence of withdrawal syndrome as measured by Tyler’s Symptom Checklist after doxepin 3 mg and 6 mg was discontinued. Discontinuation period-emergent nausea and vomiting was noted in 5% of patients taking 6 mg of doxepin, but not in those taking placebo or 3 mg of doxepin. There was no evidence of rebound insomnia after doxepin 3 mg and 6 mg was discontinued.1
Contraindications
Doxepin is contraindicated in patients with hypersensitivity to doxepin hydrochloride, with severe urinary retention, with narrow angle glaucoma, and who have used monoamine oxidase inhibitors (MAOIs) within the previous 2 weeks. Serious adverse effects, including hypertensive crisis and death, have been reported with coadministration of MAOIs and certain drugs, such as serotonergic antidepressants and some opioids derivatives. There are no reports of concomitant use of doxepin with MAOIs.1
Dosing
In adults, the recommended hypnotic dose for doxepin is 6 mg taken 30 minutes before bedtime. For patients age ≥65, the recommended starting hypnotic dose is 3 mg 30 minutes before bedtime, which can be increased to 6 mg if indicated.1
Related Resources
- Doghramji K, Grewal R, Markov D. Evaluation and management of insomnia in the psychiatric setting. Focus. 2009;8(4):441-454.
- Psychiatric Clinics of North America. December 2006. All articles in this issue address sleep disorders encountered in psychiatric practice.
- National Sleep Foundation. www.sleepfoundation.org.
Drug Brand Names
- Amitriptyline • Elavil
- Cimetidine • Tagamet
- Desipramine • Norpramin
- Doxepin (3 mg and 6 mg) • Silenor
- Doxepin (10 to 150 mg, oral) • Sinequan
- Doxepin cream • Prudoxin
- Fluoxetine • Prozac
- Paroxetine • Paxil
- Ramelteon • Rozerem
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Silenor [package insert]. San Diego, CA: Somaxon; 2010.
2. Goforth HW. Low-dose doxepin for the treatment of insomnia: emerging data. Expert Opin Pharmacother. 2009;10(10):1649-1655.
3. Stahl SM. Selective histamine H1 antagonism: novel hypnotic and pharmacologic actions challenge classical notions of antihistamines. CNS Spectr. 2008;13(12):1027-1038.
4. Roth T, Rogowski R, Hull S, et al. Efficacy and safety of doxepin 1 mg, 3 mg, and 6 mg in adults with primary insomnia. Sleep. 2007;30(11):1555-1561.
5. Scharf M, Rogowski R, Hull S, et al. Efficacy and safety of doxepin 1 mg, 3 mg, and 6 mg in elderly patients with primary insomnia: a randomized, double-blind, placebo-controlled crossover study. J Clin Psychiatry. 2008;69:1557-1564.
6. Hajak G, Rodenbeck A, Adler L, et al. Nocturnal melatonin secretion and sleep after doxepin administration in chronic primary insomnia. Pharmacopsychiatry. 1996;29:187-192.
7. Hajak G, Rodenbeck A, Voderholzer U, et al. Doxepin in the treatment of primary insomnia: a placebo-controlled, double-blind, polysomnographic study. J Clin Psychiatry. 2001;62:453-463.
8. Rodenbeck A, Cohrs S, Jordan W, et al. The sleep-improving effects of doxepin are paralleled by a normalized plasma cortisol secretion in primary insomnia. A placebo-controlled, double-blind, randomized, cross-over study followed by an open treatment for 3 weeks. Psychopharmacology. 2003;170:423-428.
1. Silenor [package insert]. San Diego, CA: Somaxon; 2010.
2. Goforth HW. Low-dose doxepin for the treatment of insomnia: emerging data. Expert Opin Pharmacother. 2009;10(10):1649-1655.
3. Stahl SM. Selective histamine H1 antagonism: novel hypnotic and pharmacologic actions challenge classical notions of antihistamines. CNS Spectr. 2008;13(12):1027-1038.
4. Roth T, Rogowski R, Hull S, et al. Efficacy and safety of doxepin 1 mg, 3 mg, and 6 mg in adults with primary insomnia. Sleep. 2007;30(11):1555-1561.
5. Scharf M, Rogowski R, Hull S, et al. Efficacy and safety of doxepin 1 mg, 3 mg, and 6 mg in elderly patients with primary insomnia: a randomized, double-blind, placebo-controlled crossover study. J Clin Psychiatry. 2008;69:1557-1564.
6. Hajak G, Rodenbeck A, Adler L, et al. Nocturnal melatonin secretion and sleep after doxepin administration in chronic primary insomnia. Pharmacopsychiatry. 1996;29:187-192.
7. Hajak G, Rodenbeck A, Voderholzer U, et al. Doxepin in the treatment of primary insomnia: a placebo-controlled, double-blind, polysomnographic study. J Clin Psychiatry. 2001;62:453-463.
8. Rodenbeck A, Cohrs S, Jordan W, et al. The sleep-improving effects of doxepin are paralleled by a normalized plasma cortisol secretion in primary insomnia. A placebo-controlled, double-blind, randomized, cross-over study followed by an open treatment for 3 weeks. Psychopharmacology. 2003;170:423-428.
Question BPD outcomes
In Drs. Ali M. Hashmi and Dennis Vowell’s article “The manipulative self-harmer” (Cases That Test Your Skills, Current Psychiatry, June 2010, p. 44-48), the authors regard the patient’s outcome (“Recently she was placed in a more restrictive setting because her hostile and self-destructive behavior escalated”) as characteristic of borderline personality disorder (BPD) (“Ms. L is no different from most axis II Cluster B disordered patients.”). In my view, this is the greatest risk of calling a patient borderline—it tends to justify poor outcomes by thinking that it is just characteristic of the illness. Instead, shouldn’t we worry that our treatment may be suboptimal? Maybe we are missing something?
For example, Ms. L may have some degree of bipolarity (see the Harvard Bipolarity Index as a characterization of that concept, incorporating but going beyond the DSM-IV-TR) that could account for their observation, “Her mood and behavior continue to oscillate; she is relatively calm and satisfied 1 week, angry and assaultive the next.” Instead of concluding, “this stormy course is expected…” the authors should be wondering whether they might be contributing to it by restarting venlafaxine despite simultaneous carbamazepine initiation. Granted, the possibilities of bipolarity and antidepressant-induced rapid cycling are complex considerations, because we lack solid footing for differentiating BPD and bipolar disorder and for determining causality when a patient experiences rapid mood changes while taking an antidepressant. These are controversial issues, but why present the case as though it’s illustrative of accepted principles? I find it perfectly illustrative of how badly we’re floundering as a field.
Jim Phelps, MD
PsychEducation.org
Corvallis, OR
The authors respond
Dr. Phelps’ contention is that our observation that Ms. L’s “hostile and self-destructive behavior” makes her “no different from most axis II Cluster B disordered patients” somehow understates the extent of her illness, perhaps leading to poorer outcomes. Negative countertransference toward such patients is the norm and handling it empathically is an integral part of the treatment relationship. This is true even though the severity of Ms. L’s personality pathology, as evidenced by her placement in the “911 program,” may not be representative of all patients with BPD.
We agree that “the possibilities of…antidepressant-induced rapid cycling are complex considerations.” Even experts disagree on this. In fact, as we pointed out, Ms. L resisted medication tapers, at one point insisting that high doses of fluoxetine and venafaxine be used together for depression, a request we denied specifically for fear of worsening her mood lability. Fluoxetine was discontinued and venlafaxine restarted at a lower dose to treat her persistent depression as well as to help with her chronic back pain. Because by this time she was taking carbamazepine as well, we felt the risk was acceptable. Her positive long-term outcome has validated our approach.
We disagree that psychiatry is “floundering” as a field. In fact, exchanges like this are a core component of placing our specialty on a more solid, scientific basis to position it for future challenges.
Ali M. Hashmi, MD
Medical director
Mid-South Health Systems
Jonesboro, AR
Clinical instructor
Department of psychiatry
University of Arkansas for Medical Science
College of Medicine
Little Rock, AR
Dennis Vowell, PsyD
Clinical psychologist
Mid-South Health Systems
Paragould, AR
In Drs. Ali M. Hashmi and Dennis Vowell’s article “The manipulative self-harmer” (Cases That Test Your Skills, Current Psychiatry, June 2010, p. 44-48), the authors regard the patient’s outcome (“Recently she was placed in a more restrictive setting because her hostile and self-destructive behavior escalated”) as characteristic of borderline personality disorder (BPD) (“Ms. L is no different from most axis II Cluster B disordered patients.”). In my view, this is the greatest risk of calling a patient borderline—it tends to justify poor outcomes by thinking that it is just characteristic of the illness. Instead, shouldn’t we worry that our treatment may be suboptimal? Maybe we are missing something?
For example, Ms. L may have some degree of bipolarity (see the Harvard Bipolarity Index as a characterization of that concept, incorporating but going beyond the DSM-IV-TR) that could account for their observation, “Her mood and behavior continue to oscillate; she is relatively calm and satisfied 1 week, angry and assaultive the next.” Instead of concluding, “this stormy course is expected…” the authors should be wondering whether they might be contributing to it by restarting venlafaxine despite simultaneous carbamazepine initiation. Granted, the possibilities of bipolarity and antidepressant-induced rapid cycling are complex considerations, because we lack solid footing for differentiating BPD and bipolar disorder and for determining causality when a patient experiences rapid mood changes while taking an antidepressant. These are controversial issues, but why present the case as though it’s illustrative of accepted principles? I find it perfectly illustrative of how badly we’re floundering as a field.
Jim Phelps, MD
PsychEducation.org
Corvallis, OR
The authors respond
Dr. Phelps’ contention is that our observation that Ms. L’s “hostile and self-destructive behavior” makes her “no different from most axis II Cluster B disordered patients” somehow understates the extent of her illness, perhaps leading to poorer outcomes. Negative countertransference toward such patients is the norm and handling it empathically is an integral part of the treatment relationship. This is true even though the severity of Ms. L’s personality pathology, as evidenced by her placement in the “911 program,” may not be representative of all patients with BPD.
We agree that “the possibilities of…antidepressant-induced rapid cycling are complex considerations.” Even experts disagree on this. In fact, as we pointed out, Ms. L resisted medication tapers, at one point insisting that high doses of fluoxetine and venafaxine be used together for depression, a request we denied specifically for fear of worsening her mood lability. Fluoxetine was discontinued and venlafaxine restarted at a lower dose to treat her persistent depression as well as to help with her chronic back pain. Because by this time she was taking carbamazepine as well, we felt the risk was acceptable. Her positive long-term outcome has validated our approach.
We disagree that psychiatry is “floundering” as a field. In fact, exchanges like this are a core component of placing our specialty on a more solid, scientific basis to position it for future challenges.
Ali M. Hashmi, MD
Medical director
Mid-South Health Systems
Jonesboro, AR
Clinical instructor
Department of psychiatry
University of Arkansas for Medical Science
College of Medicine
Little Rock, AR
Dennis Vowell, PsyD
Clinical psychologist
Mid-South Health Systems
Paragould, AR
In Drs. Ali M. Hashmi and Dennis Vowell’s article “The manipulative self-harmer” (Cases That Test Your Skills, Current Psychiatry, June 2010, p. 44-48), the authors regard the patient’s outcome (“Recently she was placed in a more restrictive setting because her hostile and self-destructive behavior escalated”) as characteristic of borderline personality disorder (BPD) (“Ms. L is no different from most axis II Cluster B disordered patients.”). In my view, this is the greatest risk of calling a patient borderline—it tends to justify poor outcomes by thinking that it is just characteristic of the illness. Instead, shouldn’t we worry that our treatment may be suboptimal? Maybe we are missing something?
For example, Ms. L may have some degree of bipolarity (see the Harvard Bipolarity Index as a characterization of that concept, incorporating but going beyond the DSM-IV-TR) that could account for their observation, “Her mood and behavior continue to oscillate; she is relatively calm and satisfied 1 week, angry and assaultive the next.” Instead of concluding, “this stormy course is expected…” the authors should be wondering whether they might be contributing to it by restarting venlafaxine despite simultaneous carbamazepine initiation. Granted, the possibilities of bipolarity and antidepressant-induced rapid cycling are complex considerations, because we lack solid footing for differentiating BPD and bipolar disorder and for determining causality when a patient experiences rapid mood changes while taking an antidepressant. These are controversial issues, but why present the case as though it’s illustrative of accepted principles? I find it perfectly illustrative of how badly we’re floundering as a field.
Jim Phelps, MD
PsychEducation.org
Corvallis, OR
The authors respond
Dr. Phelps’ contention is that our observation that Ms. L’s “hostile and self-destructive behavior” makes her “no different from most axis II Cluster B disordered patients” somehow understates the extent of her illness, perhaps leading to poorer outcomes. Negative countertransference toward such patients is the norm and handling it empathically is an integral part of the treatment relationship. This is true even though the severity of Ms. L’s personality pathology, as evidenced by her placement in the “911 program,” may not be representative of all patients with BPD.
We agree that “the possibilities of…antidepressant-induced rapid cycling are complex considerations.” Even experts disagree on this. In fact, as we pointed out, Ms. L resisted medication tapers, at one point insisting that high doses of fluoxetine and venafaxine be used together for depression, a request we denied specifically for fear of worsening her mood lability. Fluoxetine was discontinued and venlafaxine restarted at a lower dose to treat her persistent depression as well as to help with her chronic back pain. Because by this time she was taking carbamazepine as well, we felt the risk was acceptable. Her positive long-term outcome has validated our approach.
We disagree that psychiatry is “floundering” as a field. In fact, exchanges like this are a core component of placing our specialty on a more solid, scientific basis to position it for future challenges.
Ali M. Hashmi, MD
Medical director
Mid-South Health Systems
Jonesboro, AR
Clinical instructor
Department of psychiatry
University of Arkansas for Medical Science
College of Medicine
Little Rock, AR
Dennis Vowell, PsyD
Clinical psychologist
Mid-South Health Systems
Paragould, AR
CAM for your anxious patient: What the evidence says

The number of people with psychiatric disorders who use complementary and alternative medicine (CAM) is on the rise. In surveys of patients seeking psychiatric care, estimates of CAM use range from 8% to 57%; the most frequent uses are for depression and anxiety disorders. A population-based study in the United States found that 9% of respondents had anxiety attacks and 57% of these individuals had used CAM.1 Similarly, in a Finnish population-based study (N=5,987) 35% of subjects reported some form of CAM use in the previous year; those with comorbid anxiety and depressive disorders used CAM most frequently.2
Unfortunately, a MEDLINE search shows that the number of studies examining psychotropic medications dwarfs the number of studies on even the most common CAM treatments used for psychiatric disorders. Far more patients with diagnosed mental disorders are studied in trials of standard treatments than CAM treatments. Because very few studies evaluate the cost-effectiveness of CAM treatments for psychiatric disorders, the risk-to-benefit ratio is difficult to calculate. Although several CAM treatments for depressive disorders have enough support to be considered options,3 CAM options for anxiety disorders are fewer and have less evidence of efficacy.
For these reasons, it is hard to recommend any CAM treatment as first line. Despite the relative lack of high quality research on CAM treatment outcomes, high rates of CAM use make it critical for clinicians to understand what treatments are available—or at least which treatments should be favored if patients are intent on trying them. We review the current research for yoga, exercise, bibliotherapy, and the dietary supplements kava and inositol for treating anxiety disorders and suggest those that warrant consideration for patients who do not respond, respond partially, or suffer from side effects from selective serotonin reuptake inhibitors (SSRIs) or benzodiazepines.
Limitations of CAM research
There are several limitations to the research literature on CAM approaches for anxiety disorders.4 First, there is a wide diversity of practices considered alternative or complementary and various ways in which these methods are applied across cultures. Some authors consider complementary medicines to be only herbal remedies, whereas others include individual therapies such as acupuncture, aromatherapy, herbal therapy, homeopathy, iridology, naturopathy, and reflexology.5 This article defines “alternative” treatments as those other than a form of psychotherapy or an FDA-approved medication that substitute for standard psychiatric treatment, and “complementary” approaches as those used to augment standard psychiatric treatments.
Anxiety and stress are ubiquitous, perhaps motivating interest in CAM options and prompting research on heterogeneous groups of individuals with poorly defined clinical syndromes or with isolated symptoms of anxiety or subjective distress. Few studies examine well-defined patient groups with diagnosed anxiety disorders. There are also multiple research design problems, including poorly specified treatments, poorly chosen placebos, and interpreting nonsignificant differences from established treatments as equivalence in underpowered studies.
The CAM treatments reviewed in this article have ≥2 randomized controlled trials (RCTs) that support their use for patients with diagnosed anxiety disorders, and ≥1 study that shows that the treatment can induce remission.
Yoga
In 2005 Kirkwood et al carried out the first systematic review of research evidence for the effectiveness of yoga in anxiety treatment.6 Of 19 studies identified, 4 RCTs and 1 nonrandomized trial met their inclusion criteria, which were an anxiety disorder diagnosis, use of yoga or yoga-based exercises alone, and anxiety rating scales used as outcome measures. Most found significant improvement in anxiety symptoms with yoga compared with placebo. Details of the 5 trials evaluated in Kirkwood’s review are summarized in Table 1.7-11
Since the 2005 review, 3 additional studies of yoga and anxiety have been published, but none would meet Kirkwood’s inclusion criteria. One that evaluated a heterogeneous group of patients using an intervention with multiple components—only 1 of which was yoga—found the intervention significantly reduced anxiety scores.12 A second study comparing yoga with relaxation in 131 patients with mild-to-moderate stress but no anxiety disorder diagnosis showed yoga was as effective as relaxation in improving anxiety symptoms as measured by the anxiety subscale of the State Trait Personality Inventory.13 In a study of 183 nonrandomized survivors of the 2004 southeast Asia tsunami with posttraumatic stress disorder (PTSD) symptoms, yoga-based breathing either alone or paired with trauma reduction exposure techniques significantly reduced PTSD symptoms compared with wait-list controls.14
Conclusion. Few controlled studies evaluated yoga for anxiety disorders, and all have significant methodologic limitations and/or poor methodology reporting. The diagnostic conditions treated and both yoga interventions and control conditions varied. However, these limited results are encouraging, particularly for treatment of obsessive-compulsive disorder (OCD). There is little information regarding safety or contraindications of yoga. Reported attrition rates were high in most studies, which may raise concerns about patient motivation and compliance.
Table 1
Evidence on the effectiveness of yoga for anxiety disorders
| Study | Design | Results |
|---|---|---|
| Vahia et al, 19737 | 36 patients with psychoneurosis randomly assigned to yoga (N=15) or a control intervention of relaxation, postures, breathing, and writing (N=12) | Significant difference between groups in TAS scores after but not before treatment. Reduction in mean TAS score for yoga group but not control group |
| Vahia et al,19738 | 39 patients received 6 weeks of yoga (N=21) or medication (amitriptyline and chlordiazepoxide on a variable dosage schedule) (N=18) | Yoga showed significantly greater reductions in TAS in this non-randomized sample |
| Sahasi et al, 19899 | 91 patients randomly assigned to yoga practiced daily for 40 minutes (N=38) or diazepam at unspecified frequency or doses (N=53) for 3 months | Mean reduction in IPAT with yoga (3.39, P < .05) vs control group (0.36, P > .05). Attrition rate was 21.1% in yoga group and 66% in controls |
| Sharma et al, 199110 | 71 patients with anxiety neurosis randomly assigned to 1-week yoga training, then daily practice (N=41) or control (N=30, placebo capsule) | HAM-A measured at 3 weekly intervals for 12 weeks. Significant between group mean difference at 3 weeks (greater improvement in yoga group compared with controls). Significant improvement in yoga group between 3 and 6 weeks but not for controls |
| Shannahoff-Khalsa et al, 199911 | 21 OCD patients randomly assigned to kundalini yoga (N=11) or relaxation and mindfulness meditation (N=10). Multiple outcome measures; Y-BOCS was primary | Seven in each group completed 3 months; patients who practiced yoga demonstrated greater improvements on Y-BOCS. Intent-to-treat analysis (Y-BOCS) for the baseline and 3-month tests showed that only the yoga group improved. Groups were merged for an additional year of yoga; at 15 months, the final group (N=11) improved 71% on the Y-BOCS |
| HAM-A: Hamilton Anxiety Rating scale; IPAT: Institute for Personality and Ability Testing, Anxiety Scale; OCD: obsessive-compulsive disorder; TAS: Taylor’s Anxiety Scale; Y-BOCS: Yale-Brown Obsessive Compulsive Scale | ||
Exercise
The literature examining the relationship between exercise and depression is extensive, but much less has been published about exercise in patients with anxiety disorders (Table 2).15-17 In a 10-week trial, Broocks and colleagues compared clomipramine, exercise (running), and placebo in 46 outpatients with panic disorder.15 Both exercise and clomipramine, 112.5 mg/d, significantly reduced panic symptoms compared with placebo, but clomipramine was more effective and faster-acting.
A more recent RCT compared group cognitive-behavioral therapy (GCBT) plus a home-based walking program vs GCBT and in 21 patients with panic disorder, generalized anxiety disorder (GAD), or social phobia.16 Compared with GCBT plus educational sessions, GCBT plus walking had a significant effect on self-reported depression, anxiety, and stress. Results differed by diagnosis; the most marked effects occurred in individuals with social phobia, whereas benefits for those with panic disorder or GAD were questionable.
Fifteen patients with OCD were recruited to participate in a 12-week, moderate-intensity aerobic exercise program added to their standard behavioral and/or pharmacologic treatment.17 Subjects demonstrated improvement in negative mood, anxiety, obsessions, and compulsions after each exercise session. Changes after each session persisted over the 12-week intervention, although the magnitude attenuated over the duration of the intervention.
Conclusion. Although initial results from small trials suggest exercise may help improve anxiety symptoms, further studies are needed to determine how to best use exercise training to treat anxious patients, specifically regarding dose-response relationship, differences in effectiveness between aerobic and resistance training, and the mechanisms by which exercise improves psychiatric symptoms.
Table 2
Exercise for anxiety: More research is needed
| Study | Design | Results |
|---|---|---|
| Broocks et al, 199915 | 46 patients with panic disorder randomly assigned to 10 weeks of running, clomipramine, or wplacebo pills | Both exercise and clomipramine resulted in significant decreases in symptoms but clomipramine improved symptoms earlier and more effectively |
| Merom et al, 200816 | 21 patients with panic disorder, GAD, or social phobia randomly assigned to GCBT and either a home-based walking program or educational sessions | GCBT plus walking had a significant effect on depression, anxiety, and stress compared with GCBT plus educational sessions |
| Abrantes et al, 200917 | 15 patients with OCD assigned to a 12-week exercise intervention that was added to their standard behavioral and/or pharmacologic treatment | Subjects reported improved mood, anxiety, obsessions, and compulsions after each exercise session |
| GAD: generalized anxiety disorder; GCBT: group cognitive-behavioral therapy | ||
Bibliotherapy
Investigation of bibliotherapy for treatment of anxiety disorders has been limited (Table 3).18-20 A 2009 RCT demonstrated that for 21 patients with mild-to-moderate social phobia, bibliotherapy—in the form of an 8-week self-directed CBT program with minimal therapist involvement—was superior to a wait-list control and induced clinically significant change in approximately one-third of patients.20
Rapee et al randomly assigned 267 children age 6 to 12 with anxiety disorders to bibliotherapy that consisted of parents treating their children in the home with written materials, 9 sessions of GCBT, or a wait-list control condition.19 Bibliotherapy provided by parents demonstrated benefit compared with wait-listing but was not as efficacious as GCBT at post-treatment and 3-month follow-up.
Lidren and colleagues randomly assigned 36 adult patients with panic disorder to bibliotherapy, group therapy combined with bibliotherapy, or a waitlist.18 Both treatments were more effective than wait-listing in reducing the frequency of panic attacks, severity of physical panic symptoms, catastrophic cognitions, agoraphobic avoidance, and depression. Both interventions maintained their effects at 3-and 6-month follow-up and produced clinically significant change in most patients.
Conclusion. Some preliminary evidence supports the effectiveness of bibliotherapy for social anxiety disorder, childhood anxiety disorders, and panic disorder.
Table 3
Preliminary evidence supports bibliotherapy for select anxiety disorders
| Study | Design | Results |
|---|---|---|
| Lidren et al, 199418 | 36 adults with panic disorder randomly assigned to bibliotherapy, bibliotherapy plus group therapy, or wait-list control | Both bibliotherapy and bibliotherapy plus group therapy were more effective than wait-listing in reducing the frequency of panic attacks and severity of physical panic symptoms |
| Rapee et al, 200619 | 267 children with anxiety disorders randomly assigned to bibliotherapy (parents treating their children in the home with written materials with no therapist contact), 9 sessions of group CBT, or wait-list control | Parent-delivered bibliotherapy was beneficial compared with wait-listing but was not as efficacious as group CBT |
| Abramowitz et al, 200920 | 21 patients with mild-to-moderate social phobia underwent an 8-week self-directed CBT program with minimal therapist involvement | Bibliotherapy was superior to wait-listing. One-third of patients experienced clinically significant change |
| CBT: cognitive-behavioral therapy | ||
Dietary supplements
Many dietary and herbal supplements are purported to have therapeutic efficacy for anxiety symptoms. Because of inadequate FDA regulation of manufacturing and marketing of these agents, most of these supplements have not been tested on patients with anxiety disorders.21 Limited evidence supports the use of kava for GAD and inositol for panic disorder (Table 4).22-28
Kava. Multiple double-blind RCTs found kava (Piper methysticum)—a plant indigenous to South Pacific islands—has effects greater than placebo and comparable to standard treatments for mild to moderately severe GAD. A Cochrane meta-analysis22 of 11 trials with 645 participants concluded that kava is effective for reducing GAD symptoms, with risks comparable to standard treatments for up to 6 months of use.
Case reports of kava-associated liver toxicity led to a marketing ban in Canada in 2000, followed shortly by Germany, Australia, and the United Kingdom. In 2002 the FDA issued a Consumer Advisory29 discouraging kava use. Since then a flurry of research has looked for sources of possible toxicity, including individual sensitivities,29 excessive dosing, use of toxic parts of the kava plant instead of the roots,30,31 interactions with other hepatoactive substances, and non-water based extraction methods. RCTs demonstrating kava’s efficacy and safety were characterized by careful dosing supervision, use of standardized kava extracts, and avoidance of interactions with other hepatoactive medications or CAM treatments. Doses ≤300 mg/d are recommended.22
RCTs that used the standardized acetone extract WS149023 found that women and younger adults show more positive effects from kava, and showed no liver toxicity when used for 1 to 24 weeks. A recent RCT that used kava extracts obtained via water-based methods showed kava had significant anxiolytic effects.24 However, a study of liver toxicity reports found that water-based extractions, acetonic extractions, and ethanol extractions all have been associated with toxic hepatic reactions.32 Aqueous extraction does not guarantee safety, and the extraction solvent does not cause toxicity. A recent report of a severe liver reaction to the native drink by a tourist in Samoa33 suggests that aqueous extractions from the root stock— the type of kava used by South Pacific islanders—also can be unsafe.
Conclusion. Multiple RCTs have found kava relatively safe and effective for treating anxiety symptoms. Caution is necessary, however, because of reports of liver toxicity associated with its use. Physician oversight and monitoring of kava use are appropriate.
Inositol. Evidence from RCTs suggests inositol, a natural isomer of glucose and a precursor in the phosphatidylinositol cycle, can significantly improve panic disorder symptoms.25-28 In 1 trial, efficacy and side effects were comparable to fluvoxamine.28 Effective doses ranged from 12 g/d to 18 g/d. Researchers tested inositol as monotherapy or augmentation to SSRIs for patients with mild-to-moderate OCD. In small double-blind crossover RCTs, inositol monotherapy significantly reduced Yale-Brown Obsessive Compulsive Scale scores compared with placebo26 but inositol augmentation added nothing to the effects of SSRIs.27
Conclusion. Inositol appears to be effective in improving symptoms of panic disorder. Its use for other anxiety disorders is unproven.
Table 4
Dietary supplements for anxiety disorders
| Study | Design | Results |
|---|---|---|
| Kava | ||
| Pittler et al, 200322 | Meta-analysis of 11 RCTs with a total of 645 GAD patients | Compared with placebo, kava significantly reduced anxiety as measured by total HAM-A score |
| Witte et al, 200523 | Meta-analysis of 6 RCTs using kava extract WS1490 in patients with nonpsychotic anxiety disorders | Kava reduced HAM-A score more than placebo and seemed to be more effective in women and younger adults |
| Sarris et al, 200924 | 60 adults with ≥1 month of elevated generalized anxiety randomly assigned to an aqueous extract of kava | Aqueous-extract kava was significantly more effective than placebo in reducing HAM-A score |
| Inositol | ||
| Benjamin et al, 199525 | 21 patients with panic disorder with or without agoraphobia randomly assigned to inositol, 12 g/d, or placebo | Inositol significantly reduced frequency and severity of panic attacks and severity of agoraphobia compared with placebo |
| Fux et al, 199626 | 13 OCD patients randomly assigned to inositol,18 g/d, or placebo for 6 weeks | Patients taking inositol had significantly lower Y-BOCS scores compared with those receiving placebo |
| Fux et al, 199927 | 10 OCD patients receiving an SSRI randomly assigned to augmentation with inositol, 18 g/d, or placebo for 6 weeks | No significant differences between treatments |
| Palatnik et al, 200128 | In a crossover trial, 20 panic disorder patients completed 1 month of inositol, up to 18 g/d, and 1 month of fluvoxamine, up to 150 mg/d | Improvements in HAM-A, CGI, and agoraphobia scores were similar for both treatments |
| CGI: Clinical Global Impression scale; GAD: generalized anxiety disorder; HAM-A: Hamilton Anxiety Rating scale; OCD: obsessive-compulsive disorder; RCTs: randomized controlled trials; SSRI: selective serotonin reuptake inhibitor; Y-BOCS: Yale-Brown Obsessive Compulsive Scale | ||
Supervision is recommended
The evidence base for most CAM interventions commonly used for anxiety is relatively poor and recent systematic reviews found few methodologically rigorous studies. This has not, however, diminished CAM treatments’ popularity. Despite a paucity of high-quality studies regarding CAM for anxiety disorders, there is enough data supporting yoga, exercise, bibliotherapy, kava, and inositol to allow psychiatrists to collaborate with patients who wish to try these treatments. Advise patients that they may need physician supervision similar to that used with standard psychiatric treatments.
Related Resources
- National Center for Complementary and Alternative Medicine. http://nccam.nih.gov.
- The Journal of Alternative and Complementary Medicine. www.liebertonline.com/loi/acm.
- MedlinePlus: Complementary and Alternative Medicine. www.nlm.nih.gov/medlineplus/complementaryandalternativemedicine.html.
Drug Brand Names
- Amitriptyline • Elavil
- Chlordiazepoxide • Librium
- Clomipramine • Anafranil
- Diazepam • Valium
- Fluvoxamine • Luvox
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Kessler RC, Soukup J, Davis RB, et al. The use of complementary and alternative therapies to treat anxiety and depression in the United States. Am J Psychiatry. 2001;158(2):289-294.
2. Wahlström M, Sihvo S, Haukkala A, et al. Use of mental health services and complementary and alternative medicine in persons with common mental disorders. Acta Psychiatr Scand. 2008;118(1):73-80.
3. Saeed SA, Bloch RM, Antonacci DJ, et al. CAM for your depressed patient: 6 recommended options. Current Psychiatry. 2009;8(10):39-47.
4. Pilkington K. Searching for CAM evidence: an evaluation of therapy-specific search strategies. J Altern Complement Med. 2007;13(4):451-459.
5. van der Watt G, Laugharne J, Janca A. Complementary and alternative medicine in the treatment of anxiety and depression. Curr Opin Psychiatry. 2008;21(1):37-42.
6. Kirkwood G, Rampes H, Tuffrey V, et al. Yoga for anxiety: a systematic review of the research evidence. Br J Sports Med. 2005;39(12):884-891.
7. Vahia NS, Doongaji DR, Jeste DV, et al. Psychophysiologic therapy based on the concepts of Patanjali. A new approach to the treatment of neurotic and psychosomatic disorders. Am J Psychother. 1973;27(4):557-565.
8. Vahia NS, Doongaji DR, Jeste DV, et al. Further experience with the therapy based upon concepts of Patanjali in the treatment of psychiatric disorders. Indian J Psychiatry. 1973;15(1):32-37.
9. Sahasi G, Mohan D, Kacker C. Effectiveness of yogic techniques in the management of anxiety. J Pers Clin Stud. 1989;5(1):51-55.
10. Sharma I, Azmi SA, Settiwar RM. Evaluation of the effect of pranayama in anxiety state. Alternative Medicine. 1991;3:227-235.
11. Shannahoff-Khalsa DS, Ray LE, Levine S, et al. Randomized controlled trial of yogic meditation techniques for patients with obsessive-compulsive disorder. CNS Spectr. 1999;4(12):34-47.
12. Gupta N, Khera S, Vempati RP, et al. Effect of yoga based lifestyle intervention on state and trait anxiety. Indian J Physiol Pharmacol. 2006;50(1):41-47.
13. Smith C, Hancock H, Blake-Mortimer J, et al. A randomised comparative trial of yoga and relaxation to reduce stress and anxiety. Complement Ther Med. 2007;15(2):77-83.
14. Descilo T, Vedamurtachar A, Gerbarg PL, et al. Effects of a yoga breath intervention alone and in combination with an exposure therapy for post-traumatic stress disorder and depression in survivors of the 2004 South-East Asia tsunami. Acta Psychiatr Scand. 2010;121(4):289-300.
15. Broocks A, Bandelow B, Pekrun G, et al. Comparison of aerobic exercise, clomipramine, and placebo in the treatment of panic disorder. Am J Psychiatry. 1998;155(5):603-609.
16. Merom D, Phongsavan P, Wagner R, et al. Promoting walking as an adjunct intervention to group cognitive behavioral therapy for anxiety disorders—a pilot group randomized trial. J Anxiety Disord. 2008;22(6):959-968.
17. Abrantes AM, Strong DR, Cohn A, et al. Acute changes in obsessions and compulsions following moderate-intensity aerobic exercise among patients with obsessive-compulsive disorder. J Anxiety Disord. 2009;23(7):923-927.
18. Lidren DM, Watkins PL, Gould RA, et al. A comparison of bibliotherapy and group therapy in the treatment of panic disorder. J Consult Clin Psychol. 1994;62(4):865-869.
19. Rapee RM, Abbott MJ, Lyneham HJ. Bibliotherapy for children with anxiety disorders using written materials for parents: a randomized controlled trial. J Consult Clin Psychol. 2006;74(3):436-444.
20. Abramowitz JS, Moore EL, Braddock AE, et al. Self-help cognitive-behavioral therapy with minimal therapist contact for social phobia: a controlled trial. J Behav Ther Exp Psychiatry. 2009;40(1):98-105.
21. Saeed SA, Bloch RM, Antonacci DJ. Herbal and dietary supplements for treatment of anxiety disorders. Am Fam Physician. 2007;76(4):549-556.
22. Pittler MH, Ernst E. Kava extract for treating anxiety. Cochrane Database Syst Rev. 2003;(1):CD003383.-
23. Witte S, Loew D, Gaus W. Meta-analysis of the efficacy of the acetonic kava-kava extract WS1490 in patients with non-psychotic anxiety disorders. Phytother Res. 2005;19(3):183-188.
24. Sarris J, Kavanagh DJ, Byrne G, et al. The Kava Anxiety Depression Spectrum Study (KADSS): a randomized, placebo-controlled crossover trial using an aqueous extract of piper methysticum. Psychopharmacology (Berl). 2009;205:399-407.
25. Benjamin J, Levine J, Fux M, et al. Double-blind, placebo-controlled, crossover trial of inositol treatment for panic disorder. Am J Psychiatry. 1995;152(7):1084-1086.
26. Fux M, Levine J, Aviv A, et al. Inositol treatment of obsessive-compulsive disorder. Am J Psychiatry. 1996;153(9):1219-1221.
27. Fux M, Benjamin J, Belmaker RH. Inositol versus placebo augmentation of serotonin reuptake inhibitors in the treatment of obsessive-compulsive disorder: a double-blind cross-over study. Int J Neuropsychopharmcol. 1999;2(3):193-195.
28. Palatnik A, Frolov K, Fux M, et al. Double-blind, controlled, crossover trial of inositol versus fluvoxamine for the treatment of panic disorder. J Clin Psychopharmacol. 2001;21(3):335-339.
29. US Food and Drug Administration. Consumer advisory: kava-containing dietary supplements may be associated with severe injury. Available at: http://www.fda.gov/Food/ResourcesForYou/Consumers/ucm085482.htm. Accessed August 25, 2010.
30. Dragull K, Yoshida WY, Tang CS. Piperidine alkaloids from piper methysticum. Phytochemistry. 2003;63(2):193-198.
31. Simkins A, Thurston D, Colyar M, et al. Nature’s wrath? A closer look at complications with five popular herbs. Adv Nurse Pract. 2005;13(6):55-56.
32. Teschke R, Genthner A, Wolff A. Kava hepatotoxicity: comparison of aqueous, ethanolic, acetonic kava extracts and kava-herbs mixtures. J Ethnopharmacol. 2009;123(3):378-384.
33. Christl SU, Seifert A, Seeler D. Toxic hepatitis after consumption of traditional kava preparation. J Travel Med. 2009;16(1):55-56.
The number of people with psychiatric disorders who use complementary and alternative medicine (CAM) is on the rise. In surveys of patients seeking psychiatric care, estimates of CAM use range from 8% to 57%; the most frequent uses are for depression and anxiety disorders. A population-based study in the United States found that 9% of respondents had anxiety attacks and 57% of these individuals had used CAM.1 Similarly, in a Finnish population-based study (N=5,987) 35% of subjects reported some form of CAM use in the previous year; those with comorbid anxiety and depressive disorders used CAM most frequently.2
Unfortunately, a MEDLINE search shows that the number of studies examining psychotropic medications dwarfs the number of studies on even the most common CAM treatments used for psychiatric disorders. Far more patients with diagnosed mental disorders are studied in trials of standard treatments than CAM treatments. Because very few studies evaluate the cost-effectiveness of CAM treatments for psychiatric disorders, the risk-to-benefit ratio is difficult to calculate. Although several CAM treatments for depressive disorders have enough support to be considered options,3 CAM options for anxiety disorders are fewer and have less evidence of efficacy.
For these reasons, it is hard to recommend any CAM treatment as first line. Despite the relative lack of high quality research on CAM treatment outcomes, high rates of CAM use make it critical for clinicians to understand what treatments are available—or at least which treatments should be favored if patients are intent on trying them. We review the current research for yoga, exercise, bibliotherapy, and the dietary supplements kava and inositol for treating anxiety disorders and suggest those that warrant consideration for patients who do not respond, respond partially, or suffer from side effects from selective serotonin reuptake inhibitors (SSRIs) or benzodiazepines.
Limitations of CAM research
There are several limitations to the research literature on CAM approaches for anxiety disorders.4 First, there is a wide diversity of practices considered alternative or complementary and various ways in which these methods are applied across cultures. Some authors consider complementary medicines to be only herbal remedies, whereas others include individual therapies such as acupuncture, aromatherapy, herbal therapy, homeopathy, iridology, naturopathy, and reflexology.5 This article defines “alternative” treatments as those other than a form of psychotherapy or an FDA-approved medication that substitute for standard psychiatric treatment, and “complementary” approaches as those used to augment standard psychiatric treatments.
Anxiety and stress are ubiquitous, perhaps motivating interest in CAM options and prompting research on heterogeneous groups of individuals with poorly defined clinical syndromes or with isolated symptoms of anxiety or subjective distress. Few studies examine well-defined patient groups with diagnosed anxiety disorders. There are also multiple research design problems, including poorly specified treatments, poorly chosen placebos, and interpreting nonsignificant differences from established treatments as equivalence in underpowered studies.
The CAM treatments reviewed in this article have ≥2 randomized controlled trials (RCTs) that support their use for patients with diagnosed anxiety disorders, and ≥1 study that shows that the treatment can induce remission.
Yoga
In 2005 Kirkwood et al carried out the first systematic review of research evidence for the effectiveness of yoga in anxiety treatment.6 Of 19 studies identified, 4 RCTs and 1 nonrandomized trial met their inclusion criteria, which were an anxiety disorder diagnosis, use of yoga or yoga-based exercises alone, and anxiety rating scales used as outcome measures. Most found significant improvement in anxiety symptoms with yoga compared with placebo. Details of the 5 trials evaluated in Kirkwood’s review are summarized in Table 1.7-11
Since the 2005 review, 3 additional studies of yoga and anxiety have been published, but none would meet Kirkwood’s inclusion criteria. One that evaluated a heterogeneous group of patients using an intervention with multiple components—only 1 of which was yoga—found the intervention significantly reduced anxiety scores.12 A second study comparing yoga with relaxation in 131 patients with mild-to-moderate stress but no anxiety disorder diagnosis showed yoga was as effective as relaxation in improving anxiety symptoms as measured by the anxiety subscale of the State Trait Personality Inventory.13 In a study of 183 nonrandomized survivors of the 2004 southeast Asia tsunami with posttraumatic stress disorder (PTSD) symptoms, yoga-based breathing either alone or paired with trauma reduction exposure techniques significantly reduced PTSD symptoms compared with wait-list controls.14
Conclusion. Few controlled studies evaluated yoga for anxiety disorders, and all have significant methodologic limitations and/or poor methodology reporting. The diagnostic conditions treated and both yoga interventions and control conditions varied. However, these limited results are encouraging, particularly for treatment of obsessive-compulsive disorder (OCD). There is little information regarding safety or contraindications of yoga. Reported attrition rates were high in most studies, which may raise concerns about patient motivation and compliance.
Table 1
Evidence on the effectiveness of yoga for anxiety disorders
| Study | Design | Results |
|---|---|---|
| Vahia et al, 19737 | 36 patients with psychoneurosis randomly assigned to yoga (N=15) or a control intervention of relaxation, postures, breathing, and writing (N=12) | Significant difference between groups in TAS scores after but not before treatment. Reduction in mean TAS score for yoga group but not control group |
| Vahia et al,19738 | 39 patients received 6 weeks of yoga (N=21) or medication (amitriptyline and chlordiazepoxide on a variable dosage schedule) (N=18) | Yoga showed significantly greater reductions in TAS in this non-randomized sample |
| Sahasi et al, 19899 | 91 patients randomly assigned to yoga practiced daily for 40 minutes (N=38) or diazepam at unspecified frequency or doses (N=53) for 3 months | Mean reduction in IPAT with yoga (3.39, P < .05) vs control group (0.36, P > .05). Attrition rate was 21.1% in yoga group and 66% in controls |
| Sharma et al, 199110 | 71 patients with anxiety neurosis randomly assigned to 1-week yoga training, then daily practice (N=41) or control (N=30, placebo capsule) | HAM-A measured at 3 weekly intervals for 12 weeks. Significant between group mean difference at 3 weeks (greater improvement in yoga group compared with controls). Significant improvement in yoga group between 3 and 6 weeks but not for controls |
| Shannahoff-Khalsa et al, 199911 | 21 OCD patients randomly assigned to kundalini yoga (N=11) or relaxation and mindfulness meditation (N=10). Multiple outcome measures; Y-BOCS was primary | Seven in each group completed 3 months; patients who practiced yoga demonstrated greater improvements on Y-BOCS. Intent-to-treat analysis (Y-BOCS) for the baseline and 3-month tests showed that only the yoga group improved. Groups were merged for an additional year of yoga; at 15 months, the final group (N=11) improved 71% on the Y-BOCS |
| HAM-A: Hamilton Anxiety Rating scale; IPAT: Institute for Personality and Ability Testing, Anxiety Scale; OCD: obsessive-compulsive disorder; TAS: Taylor’s Anxiety Scale; Y-BOCS: Yale-Brown Obsessive Compulsive Scale | ||
Exercise
The literature examining the relationship between exercise and depression is extensive, but much less has been published about exercise in patients with anxiety disorders (Table 2).15-17 In a 10-week trial, Broocks and colleagues compared clomipramine, exercise (running), and placebo in 46 outpatients with panic disorder.15 Both exercise and clomipramine, 112.5 mg/d, significantly reduced panic symptoms compared with placebo, but clomipramine was more effective and faster-acting.
A more recent RCT compared group cognitive-behavioral therapy (GCBT) plus a home-based walking program vs GCBT and in 21 patients with panic disorder, generalized anxiety disorder (GAD), or social phobia.16 Compared with GCBT plus educational sessions, GCBT plus walking had a significant effect on self-reported depression, anxiety, and stress. Results differed by diagnosis; the most marked effects occurred in individuals with social phobia, whereas benefits for those with panic disorder or GAD were questionable.
Fifteen patients with OCD were recruited to participate in a 12-week, moderate-intensity aerobic exercise program added to their standard behavioral and/or pharmacologic treatment.17 Subjects demonstrated improvement in negative mood, anxiety, obsessions, and compulsions after each exercise session. Changes after each session persisted over the 12-week intervention, although the magnitude attenuated over the duration of the intervention.
Conclusion. Although initial results from small trials suggest exercise may help improve anxiety symptoms, further studies are needed to determine how to best use exercise training to treat anxious patients, specifically regarding dose-response relationship, differences in effectiveness between aerobic and resistance training, and the mechanisms by which exercise improves psychiatric symptoms.
Table 2
Exercise for anxiety: More research is needed
| Study | Design | Results |
|---|---|---|
| Broocks et al, 199915 | 46 patients with panic disorder randomly assigned to 10 weeks of running, clomipramine, or wplacebo pills | Both exercise and clomipramine resulted in significant decreases in symptoms but clomipramine improved symptoms earlier and more effectively |
| Merom et al, 200816 | 21 patients with panic disorder, GAD, or social phobia randomly assigned to GCBT and either a home-based walking program or educational sessions | GCBT plus walking had a significant effect on depression, anxiety, and stress compared with GCBT plus educational sessions |
| Abrantes et al, 200917 | 15 patients with OCD assigned to a 12-week exercise intervention that was added to their standard behavioral and/or pharmacologic treatment | Subjects reported improved mood, anxiety, obsessions, and compulsions after each exercise session |
| GAD: generalized anxiety disorder; GCBT: group cognitive-behavioral therapy | ||
Bibliotherapy
Investigation of bibliotherapy for treatment of anxiety disorders has been limited (Table 3).18-20 A 2009 RCT demonstrated that for 21 patients with mild-to-moderate social phobia, bibliotherapy—in the form of an 8-week self-directed CBT program with minimal therapist involvement—was superior to a wait-list control and induced clinically significant change in approximately one-third of patients.20
Rapee et al randomly assigned 267 children age 6 to 12 with anxiety disorders to bibliotherapy that consisted of parents treating their children in the home with written materials, 9 sessions of GCBT, or a wait-list control condition.19 Bibliotherapy provided by parents demonstrated benefit compared with wait-listing but was not as efficacious as GCBT at post-treatment and 3-month follow-up.
Lidren and colleagues randomly assigned 36 adult patients with panic disorder to bibliotherapy, group therapy combined with bibliotherapy, or a waitlist.18 Both treatments were more effective than wait-listing in reducing the frequency of panic attacks, severity of physical panic symptoms, catastrophic cognitions, agoraphobic avoidance, and depression. Both interventions maintained their effects at 3-and 6-month follow-up and produced clinically significant change in most patients.
Conclusion. Some preliminary evidence supports the effectiveness of bibliotherapy for social anxiety disorder, childhood anxiety disorders, and panic disorder.
Table 3
Preliminary evidence supports bibliotherapy for select anxiety disorders
| Study | Design | Results |
|---|---|---|
| Lidren et al, 199418 | 36 adults with panic disorder randomly assigned to bibliotherapy, bibliotherapy plus group therapy, or wait-list control | Both bibliotherapy and bibliotherapy plus group therapy were more effective than wait-listing in reducing the frequency of panic attacks and severity of physical panic symptoms |
| Rapee et al, 200619 | 267 children with anxiety disorders randomly assigned to bibliotherapy (parents treating their children in the home with written materials with no therapist contact), 9 sessions of group CBT, or wait-list control | Parent-delivered bibliotherapy was beneficial compared with wait-listing but was not as efficacious as group CBT |
| Abramowitz et al, 200920 | 21 patients with mild-to-moderate social phobia underwent an 8-week self-directed CBT program with minimal therapist involvement | Bibliotherapy was superior to wait-listing. One-third of patients experienced clinically significant change |
| CBT: cognitive-behavioral therapy | ||
Dietary supplements
Many dietary and herbal supplements are purported to have therapeutic efficacy for anxiety symptoms. Because of inadequate FDA regulation of manufacturing and marketing of these agents, most of these supplements have not been tested on patients with anxiety disorders.21 Limited evidence supports the use of kava for GAD and inositol for panic disorder (Table 4).22-28
Kava. Multiple double-blind RCTs found kava (Piper methysticum)—a plant indigenous to South Pacific islands—has effects greater than placebo and comparable to standard treatments for mild to moderately severe GAD. A Cochrane meta-analysis22 of 11 trials with 645 participants concluded that kava is effective for reducing GAD symptoms, with risks comparable to standard treatments for up to 6 months of use.
Case reports of kava-associated liver toxicity led to a marketing ban in Canada in 2000, followed shortly by Germany, Australia, and the United Kingdom. In 2002 the FDA issued a Consumer Advisory29 discouraging kava use. Since then a flurry of research has looked for sources of possible toxicity, including individual sensitivities,29 excessive dosing, use of toxic parts of the kava plant instead of the roots,30,31 interactions with other hepatoactive substances, and non-water based extraction methods. RCTs demonstrating kava’s efficacy and safety were characterized by careful dosing supervision, use of standardized kava extracts, and avoidance of interactions with other hepatoactive medications or CAM treatments. Doses ≤300 mg/d are recommended.22
RCTs that used the standardized acetone extract WS149023 found that women and younger adults show more positive effects from kava, and showed no liver toxicity when used for 1 to 24 weeks. A recent RCT that used kava extracts obtained via water-based methods showed kava had significant anxiolytic effects.24 However, a study of liver toxicity reports found that water-based extractions, acetonic extractions, and ethanol extractions all have been associated with toxic hepatic reactions.32 Aqueous extraction does not guarantee safety, and the extraction solvent does not cause toxicity. A recent report of a severe liver reaction to the native drink by a tourist in Samoa33 suggests that aqueous extractions from the root stock— the type of kava used by South Pacific islanders—also can be unsafe.
Conclusion. Multiple RCTs have found kava relatively safe and effective for treating anxiety symptoms. Caution is necessary, however, because of reports of liver toxicity associated with its use. Physician oversight and monitoring of kava use are appropriate.
Inositol. Evidence from RCTs suggests inositol, a natural isomer of glucose and a precursor in the phosphatidylinositol cycle, can significantly improve panic disorder symptoms.25-28 In 1 trial, efficacy and side effects were comparable to fluvoxamine.28 Effective doses ranged from 12 g/d to 18 g/d. Researchers tested inositol as monotherapy or augmentation to SSRIs for patients with mild-to-moderate OCD. In small double-blind crossover RCTs, inositol monotherapy significantly reduced Yale-Brown Obsessive Compulsive Scale scores compared with placebo26 but inositol augmentation added nothing to the effects of SSRIs.27
Conclusion. Inositol appears to be effective in improving symptoms of panic disorder. Its use for other anxiety disorders is unproven.
Table 4
Dietary supplements for anxiety disorders
| Study | Design | Results |
|---|---|---|
| Kava | ||
| Pittler et al, 200322 | Meta-analysis of 11 RCTs with a total of 645 GAD patients | Compared with placebo, kava significantly reduced anxiety as measured by total HAM-A score |
| Witte et al, 200523 | Meta-analysis of 6 RCTs using kava extract WS1490 in patients with nonpsychotic anxiety disorders | Kava reduced HAM-A score more than placebo and seemed to be more effective in women and younger adults |
| Sarris et al, 200924 | 60 adults with ≥1 month of elevated generalized anxiety randomly assigned to an aqueous extract of kava | Aqueous-extract kava was significantly more effective than placebo in reducing HAM-A score |
| Inositol | ||
| Benjamin et al, 199525 | 21 patients with panic disorder with or without agoraphobia randomly assigned to inositol, 12 g/d, or placebo | Inositol significantly reduced frequency and severity of panic attacks and severity of agoraphobia compared with placebo |
| Fux et al, 199626 | 13 OCD patients randomly assigned to inositol,18 g/d, or placebo for 6 weeks | Patients taking inositol had significantly lower Y-BOCS scores compared with those receiving placebo |
| Fux et al, 199927 | 10 OCD patients receiving an SSRI randomly assigned to augmentation with inositol, 18 g/d, or placebo for 6 weeks | No significant differences between treatments |
| Palatnik et al, 200128 | In a crossover trial, 20 panic disorder patients completed 1 month of inositol, up to 18 g/d, and 1 month of fluvoxamine, up to 150 mg/d | Improvements in HAM-A, CGI, and agoraphobia scores were similar for both treatments |
| CGI: Clinical Global Impression scale; GAD: generalized anxiety disorder; HAM-A: Hamilton Anxiety Rating scale; OCD: obsessive-compulsive disorder; RCTs: randomized controlled trials; SSRI: selective serotonin reuptake inhibitor; Y-BOCS: Yale-Brown Obsessive Compulsive Scale | ||
Supervision is recommended
The evidence base for most CAM interventions commonly used for anxiety is relatively poor and recent systematic reviews found few methodologically rigorous studies. This has not, however, diminished CAM treatments’ popularity. Despite a paucity of high-quality studies regarding CAM for anxiety disorders, there is enough data supporting yoga, exercise, bibliotherapy, kava, and inositol to allow psychiatrists to collaborate with patients who wish to try these treatments. Advise patients that they may need physician supervision similar to that used with standard psychiatric treatments.
Related Resources
- National Center for Complementary and Alternative Medicine. http://nccam.nih.gov.
- The Journal of Alternative and Complementary Medicine. www.liebertonline.com/loi/acm.
- MedlinePlus: Complementary and Alternative Medicine. www.nlm.nih.gov/medlineplus/complementaryandalternativemedicine.html.
Drug Brand Names
- Amitriptyline • Elavil
- Chlordiazepoxide • Librium
- Clomipramine • Anafranil
- Diazepam • Valium
- Fluvoxamine • Luvox
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
The number of people with psychiatric disorders who use complementary and alternative medicine (CAM) is on the rise. In surveys of patients seeking psychiatric care, estimates of CAM use range from 8% to 57%; the most frequent uses are for depression and anxiety disorders. A population-based study in the United States found that 9% of respondents had anxiety attacks and 57% of these individuals had used CAM.1 Similarly, in a Finnish population-based study (N=5,987) 35% of subjects reported some form of CAM use in the previous year; those with comorbid anxiety and depressive disorders used CAM most frequently.2
Unfortunately, a MEDLINE search shows that the number of studies examining psychotropic medications dwarfs the number of studies on even the most common CAM treatments used for psychiatric disorders. Far more patients with diagnosed mental disorders are studied in trials of standard treatments than CAM treatments. Because very few studies evaluate the cost-effectiveness of CAM treatments for psychiatric disorders, the risk-to-benefit ratio is difficult to calculate. Although several CAM treatments for depressive disorders have enough support to be considered options,3 CAM options for anxiety disorders are fewer and have less evidence of efficacy.
For these reasons, it is hard to recommend any CAM treatment as first line. Despite the relative lack of high quality research on CAM treatment outcomes, high rates of CAM use make it critical for clinicians to understand what treatments are available—or at least which treatments should be favored if patients are intent on trying them. We review the current research for yoga, exercise, bibliotherapy, and the dietary supplements kava and inositol for treating anxiety disorders and suggest those that warrant consideration for patients who do not respond, respond partially, or suffer from side effects from selective serotonin reuptake inhibitors (SSRIs) or benzodiazepines.
Limitations of CAM research
There are several limitations to the research literature on CAM approaches for anxiety disorders.4 First, there is a wide diversity of practices considered alternative or complementary and various ways in which these methods are applied across cultures. Some authors consider complementary medicines to be only herbal remedies, whereas others include individual therapies such as acupuncture, aromatherapy, herbal therapy, homeopathy, iridology, naturopathy, and reflexology.5 This article defines “alternative” treatments as those other than a form of psychotherapy or an FDA-approved medication that substitute for standard psychiatric treatment, and “complementary” approaches as those used to augment standard psychiatric treatments.
Anxiety and stress are ubiquitous, perhaps motivating interest in CAM options and prompting research on heterogeneous groups of individuals with poorly defined clinical syndromes or with isolated symptoms of anxiety or subjective distress. Few studies examine well-defined patient groups with diagnosed anxiety disorders. There are also multiple research design problems, including poorly specified treatments, poorly chosen placebos, and interpreting nonsignificant differences from established treatments as equivalence in underpowered studies.
The CAM treatments reviewed in this article have ≥2 randomized controlled trials (RCTs) that support their use for patients with diagnosed anxiety disorders, and ≥1 study that shows that the treatment can induce remission.
Yoga
In 2005 Kirkwood et al carried out the first systematic review of research evidence for the effectiveness of yoga in anxiety treatment.6 Of 19 studies identified, 4 RCTs and 1 nonrandomized trial met their inclusion criteria, which were an anxiety disorder diagnosis, use of yoga or yoga-based exercises alone, and anxiety rating scales used as outcome measures. Most found significant improvement in anxiety symptoms with yoga compared with placebo. Details of the 5 trials evaluated in Kirkwood’s review are summarized in Table 1.7-11
Since the 2005 review, 3 additional studies of yoga and anxiety have been published, but none would meet Kirkwood’s inclusion criteria. One that evaluated a heterogeneous group of patients using an intervention with multiple components—only 1 of which was yoga—found the intervention significantly reduced anxiety scores.12 A second study comparing yoga with relaxation in 131 patients with mild-to-moderate stress but no anxiety disorder diagnosis showed yoga was as effective as relaxation in improving anxiety symptoms as measured by the anxiety subscale of the State Trait Personality Inventory.13 In a study of 183 nonrandomized survivors of the 2004 southeast Asia tsunami with posttraumatic stress disorder (PTSD) symptoms, yoga-based breathing either alone or paired with trauma reduction exposure techniques significantly reduced PTSD symptoms compared with wait-list controls.14
Conclusion. Few controlled studies evaluated yoga for anxiety disorders, and all have significant methodologic limitations and/or poor methodology reporting. The diagnostic conditions treated and both yoga interventions and control conditions varied. However, these limited results are encouraging, particularly for treatment of obsessive-compulsive disorder (OCD). There is little information regarding safety or contraindications of yoga. Reported attrition rates were high in most studies, which may raise concerns about patient motivation and compliance.
Table 1
Evidence on the effectiveness of yoga for anxiety disorders
| Study | Design | Results |
|---|---|---|
| Vahia et al, 19737 | 36 patients with psychoneurosis randomly assigned to yoga (N=15) or a control intervention of relaxation, postures, breathing, and writing (N=12) | Significant difference between groups in TAS scores after but not before treatment. Reduction in mean TAS score for yoga group but not control group |
| Vahia et al,19738 | 39 patients received 6 weeks of yoga (N=21) or medication (amitriptyline and chlordiazepoxide on a variable dosage schedule) (N=18) | Yoga showed significantly greater reductions in TAS in this non-randomized sample |
| Sahasi et al, 19899 | 91 patients randomly assigned to yoga practiced daily for 40 minutes (N=38) or diazepam at unspecified frequency or doses (N=53) for 3 months | Mean reduction in IPAT with yoga (3.39, P < .05) vs control group (0.36, P > .05). Attrition rate was 21.1% in yoga group and 66% in controls |
| Sharma et al, 199110 | 71 patients with anxiety neurosis randomly assigned to 1-week yoga training, then daily practice (N=41) or control (N=30, placebo capsule) | HAM-A measured at 3 weekly intervals for 12 weeks. Significant between group mean difference at 3 weeks (greater improvement in yoga group compared with controls). Significant improvement in yoga group between 3 and 6 weeks but not for controls |
| Shannahoff-Khalsa et al, 199911 | 21 OCD patients randomly assigned to kundalini yoga (N=11) or relaxation and mindfulness meditation (N=10). Multiple outcome measures; Y-BOCS was primary | Seven in each group completed 3 months; patients who practiced yoga demonstrated greater improvements on Y-BOCS. Intent-to-treat analysis (Y-BOCS) for the baseline and 3-month tests showed that only the yoga group improved. Groups were merged for an additional year of yoga; at 15 months, the final group (N=11) improved 71% on the Y-BOCS |
| HAM-A: Hamilton Anxiety Rating scale; IPAT: Institute for Personality and Ability Testing, Anxiety Scale; OCD: obsessive-compulsive disorder; TAS: Taylor’s Anxiety Scale; Y-BOCS: Yale-Brown Obsessive Compulsive Scale | ||
Exercise
The literature examining the relationship between exercise and depression is extensive, but much less has been published about exercise in patients with anxiety disorders (Table 2).15-17 In a 10-week trial, Broocks and colleagues compared clomipramine, exercise (running), and placebo in 46 outpatients with panic disorder.15 Both exercise and clomipramine, 112.5 mg/d, significantly reduced panic symptoms compared with placebo, but clomipramine was more effective and faster-acting.
A more recent RCT compared group cognitive-behavioral therapy (GCBT) plus a home-based walking program vs GCBT and in 21 patients with panic disorder, generalized anxiety disorder (GAD), or social phobia.16 Compared with GCBT plus educational sessions, GCBT plus walking had a significant effect on self-reported depression, anxiety, and stress. Results differed by diagnosis; the most marked effects occurred in individuals with social phobia, whereas benefits for those with panic disorder or GAD were questionable.
Fifteen patients with OCD were recruited to participate in a 12-week, moderate-intensity aerobic exercise program added to their standard behavioral and/or pharmacologic treatment.17 Subjects demonstrated improvement in negative mood, anxiety, obsessions, and compulsions after each exercise session. Changes after each session persisted over the 12-week intervention, although the magnitude attenuated over the duration of the intervention.
Conclusion. Although initial results from small trials suggest exercise may help improve anxiety symptoms, further studies are needed to determine how to best use exercise training to treat anxious patients, specifically regarding dose-response relationship, differences in effectiveness between aerobic and resistance training, and the mechanisms by which exercise improves psychiatric symptoms.
Table 2
Exercise for anxiety: More research is needed
| Study | Design | Results |
|---|---|---|
| Broocks et al, 199915 | 46 patients with panic disorder randomly assigned to 10 weeks of running, clomipramine, or wplacebo pills | Both exercise and clomipramine resulted in significant decreases in symptoms but clomipramine improved symptoms earlier and more effectively |
| Merom et al, 200816 | 21 patients with panic disorder, GAD, or social phobia randomly assigned to GCBT and either a home-based walking program or educational sessions | GCBT plus walking had a significant effect on depression, anxiety, and stress compared with GCBT plus educational sessions |
| Abrantes et al, 200917 | 15 patients with OCD assigned to a 12-week exercise intervention that was added to their standard behavioral and/or pharmacologic treatment | Subjects reported improved mood, anxiety, obsessions, and compulsions after each exercise session |
| GAD: generalized anxiety disorder; GCBT: group cognitive-behavioral therapy | ||
Bibliotherapy
Investigation of bibliotherapy for treatment of anxiety disorders has been limited (Table 3).18-20 A 2009 RCT demonstrated that for 21 patients with mild-to-moderate social phobia, bibliotherapy—in the form of an 8-week self-directed CBT program with minimal therapist involvement—was superior to a wait-list control and induced clinically significant change in approximately one-third of patients.20
Rapee et al randomly assigned 267 children age 6 to 12 with anxiety disorders to bibliotherapy that consisted of parents treating their children in the home with written materials, 9 sessions of GCBT, or a wait-list control condition.19 Bibliotherapy provided by parents demonstrated benefit compared with wait-listing but was not as efficacious as GCBT at post-treatment and 3-month follow-up.
Lidren and colleagues randomly assigned 36 adult patients with panic disorder to bibliotherapy, group therapy combined with bibliotherapy, or a waitlist.18 Both treatments were more effective than wait-listing in reducing the frequency of panic attacks, severity of physical panic symptoms, catastrophic cognitions, agoraphobic avoidance, and depression. Both interventions maintained their effects at 3-and 6-month follow-up and produced clinically significant change in most patients.
Conclusion. Some preliminary evidence supports the effectiveness of bibliotherapy for social anxiety disorder, childhood anxiety disorders, and panic disorder.
Table 3
Preliminary evidence supports bibliotherapy for select anxiety disorders
| Study | Design | Results |
|---|---|---|
| Lidren et al, 199418 | 36 adults with panic disorder randomly assigned to bibliotherapy, bibliotherapy plus group therapy, or wait-list control | Both bibliotherapy and bibliotherapy plus group therapy were more effective than wait-listing in reducing the frequency of panic attacks and severity of physical panic symptoms |
| Rapee et al, 200619 | 267 children with anxiety disorders randomly assigned to bibliotherapy (parents treating their children in the home with written materials with no therapist contact), 9 sessions of group CBT, or wait-list control | Parent-delivered bibliotherapy was beneficial compared with wait-listing but was not as efficacious as group CBT |
| Abramowitz et al, 200920 | 21 patients with mild-to-moderate social phobia underwent an 8-week self-directed CBT program with minimal therapist involvement | Bibliotherapy was superior to wait-listing. One-third of patients experienced clinically significant change |
| CBT: cognitive-behavioral therapy | ||
Dietary supplements
Many dietary and herbal supplements are purported to have therapeutic efficacy for anxiety symptoms. Because of inadequate FDA regulation of manufacturing and marketing of these agents, most of these supplements have not been tested on patients with anxiety disorders.21 Limited evidence supports the use of kava for GAD and inositol for panic disorder (Table 4).22-28
Kava. Multiple double-blind RCTs found kava (Piper methysticum)—a plant indigenous to South Pacific islands—has effects greater than placebo and comparable to standard treatments for mild to moderately severe GAD. A Cochrane meta-analysis22 of 11 trials with 645 participants concluded that kava is effective for reducing GAD symptoms, with risks comparable to standard treatments for up to 6 months of use.
Case reports of kava-associated liver toxicity led to a marketing ban in Canada in 2000, followed shortly by Germany, Australia, and the United Kingdom. In 2002 the FDA issued a Consumer Advisory29 discouraging kava use. Since then a flurry of research has looked for sources of possible toxicity, including individual sensitivities,29 excessive dosing, use of toxic parts of the kava plant instead of the roots,30,31 interactions with other hepatoactive substances, and non-water based extraction methods. RCTs demonstrating kava’s efficacy and safety were characterized by careful dosing supervision, use of standardized kava extracts, and avoidance of interactions with other hepatoactive medications or CAM treatments. Doses ≤300 mg/d are recommended.22
RCTs that used the standardized acetone extract WS149023 found that women and younger adults show more positive effects from kava, and showed no liver toxicity when used for 1 to 24 weeks. A recent RCT that used kava extracts obtained via water-based methods showed kava had significant anxiolytic effects.24 However, a study of liver toxicity reports found that water-based extractions, acetonic extractions, and ethanol extractions all have been associated with toxic hepatic reactions.32 Aqueous extraction does not guarantee safety, and the extraction solvent does not cause toxicity. A recent report of a severe liver reaction to the native drink by a tourist in Samoa33 suggests that aqueous extractions from the root stock— the type of kava used by South Pacific islanders—also can be unsafe.
Conclusion. Multiple RCTs have found kava relatively safe and effective for treating anxiety symptoms. Caution is necessary, however, because of reports of liver toxicity associated with its use. Physician oversight and monitoring of kava use are appropriate.
Inositol. Evidence from RCTs suggests inositol, a natural isomer of glucose and a precursor in the phosphatidylinositol cycle, can significantly improve panic disorder symptoms.25-28 In 1 trial, efficacy and side effects were comparable to fluvoxamine.28 Effective doses ranged from 12 g/d to 18 g/d. Researchers tested inositol as monotherapy or augmentation to SSRIs for patients with mild-to-moderate OCD. In small double-blind crossover RCTs, inositol monotherapy significantly reduced Yale-Brown Obsessive Compulsive Scale scores compared with placebo26 but inositol augmentation added nothing to the effects of SSRIs.27
Conclusion. Inositol appears to be effective in improving symptoms of panic disorder. Its use for other anxiety disorders is unproven.
Table 4
Dietary supplements for anxiety disorders
| Study | Design | Results |
|---|---|---|
| Kava | ||
| Pittler et al, 200322 | Meta-analysis of 11 RCTs with a total of 645 GAD patients | Compared with placebo, kava significantly reduced anxiety as measured by total HAM-A score |
| Witte et al, 200523 | Meta-analysis of 6 RCTs using kava extract WS1490 in patients with nonpsychotic anxiety disorders | Kava reduced HAM-A score more than placebo and seemed to be more effective in women and younger adults |
| Sarris et al, 200924 | 60 adults with ≥1 month of elevated generalized anxiety randomly assigned to an aqueous extract of kava | Aqueous-extract kava was significantly more effective than placebo in reducing HAM-A score |
| Inositol | ||
| Benjamin et al, 199525 | 21 patients with panic disorder with or without agoraphobia randomly assigned to inositol, 12 g/d, or placebo | Inositol significantly reduced frequency and severity of panic attacks and severity of agoraphobia compared with placebo |
| Fux et al, 199626 | 13 OCD patients randomly assigned to inositol,18 g/d, or placebo for 6 weeks | Patients taking inositol had significantly lower Y-BOCS scores compared with those receiving placebo |
| Fux et al, 199927 | 10 OCD patients receiving an SSRI randomly assigned to augmentation with inositol, 18 g/d, or placebo for 6 weeks | No significant differences between treatments |
| Palatnik et al, 200128 | In a crossover trial, 20 panic disorder patients completed 1 month of inositol, up to 18 g/d, and 1 month of fluvoxamine, up to 150 mg/d | Improvements in HAM-A, CGI, and agoraphobia scores were similar for both treatments |
| CGI: Clinical Global Impression scale; GAD: generalized anxiety disorder; HAM-A: Hamilton Anxiety Rating scale; OCD: obsessive-compulsive disorder; RCTs: randomized controlled trials; SSRI: selective serotonin reuptake inhibitor; Y-BOCS: Yale-Brown Obsessive Compulsive Scale | ||
Supervision is recommended
The evidence base for most CAM interventions commonly used for anxiety is relatively poor and recent systematic reviews found few methodologically rigorous studies. This has not, however, diminished CAM treatments’ popularity. Despite a paucity of high-quality studies regarding CAM for anxiety disorders, there is enough data supporting yoga, exercise, bibliotherapy, kava, and inositol to allow psychiatrists to collaborate with patients who wish to try these treatments. Advise patients that they may need physician supervision similar to that used with standard psychiatric treatments.
Related Resources
- National Center for Complementary and Alternative Medicine. http://nccam.nih.gov.
- The Journal of Alternative and Complementary Medicine. www.liebertonline.com/loi/acm.
- MedlinePlus: Complementary and Alternative Medicine. www.nlm.nih.gov/medlineplus/complementaryandalternativemedicine.html.
Drug Brand Names
- Amitriptyline • Elavil
- Chlordiazepoxide • Librium
- Clomipramine • Anafranil
- Diazepam • Valium
- Fluvoxamine • Luvox
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Kessler RC, Soukup J, Davis RB, et al. The use of complementary and alternative therapies to treat anxiety and depression in the United States. Am J Psychiatry. 2001;158(2):289-294.
2. Wahlström M, Sihvo S, Haukkala A, et al. Use of mental health services and complementary and alternative medicine in persons with common mental disorders. Acta Psychiatr Scand. 2008;118(1):73-80.
3. Saeed SA, Bloch RM, Antonacci DJ, et al. CAM for your depressed patient: 6 recommended options. Current Psychiatry. 2009;8(10):39-47.
4. Pilkington K. Searching for CAM evidence: an evaluation of therapy-specific search strategies. J Altern Complement Med. 2007;13(4):451-459.
5. van der Watt G, Laugharne J, Janca A. Complementary and alternative medicine in the treatment of anxiety and depression. Curr Opin Psychiatry. 2008;21(1):37-42.
6. Kirkwood G, Rampes H, Tuffrey V, et al. Yoga for anxiety: a systematic review of the research evidence. Br J Sports Med. 2005;39(12):884-891.
7. Vahia NS, Doongaji DR, Jeste DV, et al. Psychophysiologic therapy based on the concepts of Patanjali. A new approach to the treatment of neurotic and psychosomatic disorders. Am J Psychother. 1973;27(4):557-565.
8. Vahia NS, Doongaji DR, Jeste DV, et al. Further experience with the therapy based upon concepts of Patanjali in the treatment of psychiatric disorders. Indian J Psychiatry. 1973;15(1):32-37.
9. Sahasi G, Mohan D, Kacker C. Effectiveness of yogic techniques in the management of anxiety. J Pers Clin Stud. 1989;5(1):51-55.
10. Sharma I, Azmi SA, Settiwar RM. Evaluation of the effect of pranayama in anxiety state. Alternative Medicine. 1991;3:227-235.
11. Shannahoff-Khalsa DS, Ray LE, Levine S, et al. Randomized controlled trial of yogic meditation techniques for patients with obsessive-compulsive disorder. CNS Spectr. 1999;4(12):34-47.
12. Gupta N, Khera S, Vempati RP, et al. Effect of yoga based lifestyle intervention on state and trait anxiety. Indian J Physiol Pharmacol. 2006;50(1):41-47.
13. Smith C, Hancock H, Blake-Mortimer J, et al. A randomised comparative trial of yoga and relaxation to reduce stress and anxiety. Complement Ther Med. 2007;15(2):77-83.
14. Descilo T, Vedamurtachar A, Gerbarg PL, et al. Effects of a yoga breath intervention alone and in combination with an exposure therapy for post-traumatic stress disorder and depression in survivors of the 2004 South-East Asia tsunami. Acta Psychiatr Scand. 2010;121(4):289-300.
15. Broocks A, Bandelow B, Pekrun G, et al. Comparison of aerobic exercise, clomipramine, and placebo in the treatment of panic disorder. Am J Psychiatry. 1998;155(5):603-609.
16. Merom D, Phongsavan P, Wagner R, et al. Promoting walking as an adjunct intervention to group cognitive behavioral therapy for anxiety disorders—a pilot group randomized trial. J Anxiety Disord. 2008;22(6):959-968.
17. Abrantes AM, Strong DR, Cohn A, et al. Acute changes in obsessions and compulsions following moderate-intensity aerobic exercise among patients with obsessive-compulsive disorder. J Anxiety Disord. 2009;23(7):923-927.
18. Lidren DM, Watkins PL, Gould RA, et al. A comparison of bibliotherapy and group therapy in the treatment of panic disorder. J Consult Clin Psychol. 1994;62(4):865-869.
19. Rapee RM, Abbott MJ, Lyneham HJ. Bibliotherapy for children with anxiety disorders using written materials for parents: a randomized controlled trial. J Consult Clin Psychol. 2006;74(3):436-444.
20. Abramowitz JS, Moore EL, Braddock AE, et al. Self-help cognitive-behavioral therapy with minimal therapist contact for social phobia: a controlled trial. J Behav Ther Exp Psychiatry. 2009;40(1):98-105.
21. Saeed SA, Bloch RM, Antonacci DJ. Herbal and dietary supplements for treatment of anxiety disorders. Am Fam Physician. 2007;76(4):549-556.
22. Pittler MH, Ernst E. Kava extract for treating anxiety. Cochrane Database Syst Rev. 2003;(1):CD003383.-
23. Witte S, Loew D, Gaus W. Meta-analysis of the efficacy of the acetonic kava-kava extract WS1490 in patients with non-psychotic anxiety disorders. Phytother Res. 2005;19(3):183-188.
24. Sarris J, Kavanagh DJ, Byrne G, et al. The Kava Anxiety Depression Spectrum Study (KADSS): a randomized, placebo-controlled crossover trial using an aqueous extract of piper methysticum. Psychopharmacology (Berl). 2009;205:399-407.
25. Benjamin J, Levine J, Fux M, et al. Double-blind, placebo-controlled, crossover trial of inositol treatment for panic disorder. Am J Psychiatry. 1995;152(7):1084-1086.
26. Fux M, Levine J, Aviv A, et al. Inositol treatment of obsessive-compulsive disorder. Am J Psychiatry. 1996;153(9):1219-1221.
27. Fux M, Benjamin J, Belmaker RH. Inositol versus placebo augmentation of serotonin reuptake inhibitors in the treatment of obsessive-compulsive disorder: a double-blind cross-over study. Int J Neuropsychopharmcol. 1999;2(3):193-195.
28. Palatnik A, Frolov K, Fux M, et al. Double-blind, controlled, crossover trial of inositol versus fluvoxamine for the treatment of panic disorder. J Clin Psychopharmacol. 2001;21(3):335-339.
29. US Food and Drug Administration. Consumer advisory: kava-containing dietary supplements may be associated with severe injury. Available at: http://www.fda.gov/Food/ResourcesForYou/Consumers/ucm085482.htm. Accessed August 25, 2010.
30. Dragull K, Yoshida WY, Tang CS. Piperidine alkaloids from piper methysticum. Phytochemistry. 2003;63(2):193-198.
31. Simkins A, Thurston D, Colyar M, et al. Nature’s wrath? A closer look at complications with five popular herbs. Adv Nurse Pract. 2005;13(6):55-56.
32. Teschke R, Genthner A, Wolff A. Kava hepatotoxicity: comparison of aqueous, ethanolic, acetonic kava extracts and kava-herbs mixtures. J Ethnopharmacol. 2009;123(3):378-384.
33. Christl SU, Seifert A, Seeler D. Toxic hepatitis after consumption of traditional kava preparation. J Travel Med. 2009;16(1):55-56.
1. Kessler RC, Soukup J, Davis RB, et al. The use of complementary and alternative therapies to treat anxiety and depression in the United States. Am J Psychiatry. 2001;158(2):289-294.
2. Wahlström M, Sihvo S, Haukkala A, et al. Use of mental health services and complementary and alternative medicine in persons with common mental disorders. Acta Psychiatr Scand. 2008;118(1):73-80.
3. Saeed SA, Bloch RM, Antonacci DJ, et al. CAM for your depressed patient: 6 recommended options. Current Psychiatry. 2009;8(10):39-47.
4. Pilkington K. Searching for CAM evidence: an evaluation of therapy-specific search strategies. J Altern Complement Med. 2007;13(4):451-459.
5. van der Watt G, Laugharne J, Janca A. Complementary and alternative medicine in the treatment of anxiety and depression. Curr Opin Psychiatry. 2008;21(1):37-42.
6. Kirkwood G, Rampes H, Tuffrey V, et al. Yoga for anxiety: a systematic review of the research evidence. Br J Sports Med. 2005;39(12):884-891.
7. Vahia NS, Doongaji DR, Jeste DV, et al. Psychophysiologic therapy based on the concepts of Patanjali. A new approach to the treatment of neurotic and psychosomatic disorders. Am J Psychother. 1973;27(4):557-565.
8. Vahia NS, Doongaji DR, Jeste DV, et al. Further experience with the therapy based upon concepts of Patanjali in the treatment of psychiatric disorders. Indian J Psychiatry. 1973;15(1):32-37.
9. Sahasi G, Mohan D, Kacker C. Effectiveness of yogic techniques in the management of anxiety. J Pers Clin Stud. 1989;5(1):51-55.
10. Sharma I, Azmi SA, Settiwar RM. Evaluation of the effect of pranayama in anxiety state. Alternative Medicine. 1991;3:227-235.
11. Shannahoff-Khalsa DS, Ray LE, Levine S, et al. Randomized controlled trial of yogic meditation techniques for patients with obsessive-compulsive disorder. CNS Spectr. 1999;4(12):34-47.
12. Gupta N, Khera S, Vempati RP, et al. Effect of yoga based lifestyle intervention on state and trait anxiety. Indian J Physiol Pharmacol. 2006;50(1):41-47.
13. Smith C, Hancock H, Blake-Mortimer J, et al. A randomised comparative trial of yoga and relaxation to reduce stress and anxiety. Complement Ther Med. 2007;15(2):77-83.
14. Descilo T, Vedamurtachar A, Gerbarg PL, et al. Effects of a yoga breath intervention alone and in combination with an exposure therapy for post-traumatic stress disorder and depression in survivors of the 2004 South-East Asia tsunami. Acta Psychiatr Scand. 2010;121(4):289-300.
15. Broocks A, Bandelow B, Pekrun G, et al. Comparison of aerobic exercise, clomipramine, and placebo in the treatment of panic disorder. Am J Psychiatry. 1998;155(5):603-609.
16. Merom D, Phongsavan P, Wagner R, et al. Promoting walking as an adjunct intervention to group cognitive behavioral therapy for anxiety disorders—a pilot group randomized trial. J Anxiety Disord. 2008;22(6):959-968.
17. Abrantes AM, Strong DR, Cohn A, et al. Acute changes in obsessions and compulsions following moderate-intensity aerobic exercise among patients with obsessive-compulsive disorder. J Anxiety Disord. 2009;23(7):923-927.
18. Lidren DM, Watkins PL, Gould RA, et al. A comparison of bibliotherapy and group therapy in the treatment of panic disorder. J Consult Clin Psychol. 1994;62(4):865-869.
19. Rapee RM, Abbott MJ, Lyneham HJ. Bibliotherapy for children with anxiety disorders using written materials for parents: a randomized controlled trial. J Consult Clin Psychol. 2006;74(3):436-444.
20. Abramowitz JS, Moore EL, Braddock AE, et al. Self-help cognitive-behavioral therapy with minimal therapist contact for social phobia: a controlled trial. J Behav Ther Exp Psychiatry. 2009;40(1):98-105.
21. Saeed SA, Bloch RM, Antonacci DJ. Herbal and dietary supplements for treatment of anxiety disorders. Am Fam Physician. 2007;76(4):549-556.
22. Pittler MH, Ernst E. Kava extract for treating anxiety. Cochrane Database Syst Rev. 2003;(1):CD003383.-
23. Witte S, Loew D, Gaus W. Meta-analysis of the efficacy of the acetonic kava-kava extract WS1490 in patients with non-psychotic anxiety disorders. Phytother Res. 2005;19(3):183-188.
24. Sarris J, Kavanagh DJ, Byrne G, et al. The Kava Anxiety Depression Spectrum Study (KADSS): a randomized, placebo-controlled crossover trial using an aqueous extract of piper methysticum. Psychopharmacology (Berl). 2009;205:399-407.
25. Benjamin J, Levine J, Fux M, et al. Double-blind, placebo-controlled, crossover trial of inositol treatment for panic disorder. Am J Psychiatry. 1995;152(7):1084-1086.
26. Fux M, Levine J, Aviv A, et al. Inositol treatment of obsessive-compulsive disorder. Am J Psychiatry. 1996;153(9):1219-1221.
27. Fux M, Benjamin J, Belmaker RH. Inositol versus placebo augmentation of serotonin reuptake inhibitors in the treatment of obsessive-compulsive disorder: a double-blind cross-over study. Int J Neuropsychopharmcol. 1999;2(3):193-195.
28. Palatnik A, Frolov K, Fux M, et al. Double-blind, controlled, crossover trial of inositol versus fluvoxamine for the treatment of panic disorder. J Clin Psychopharmacol. 2001;21(3):335-339.
29. US Food and Drug Administration. Consumer advisory: kava-containing dietary supplements may be associated with severe injury. Available at: http://www.fda.gov/Food/ResourcesForYou/Consumers/ucm085482.htm. Accessed August 25, 2010.
30. Dragull K, Yoshida WY, Tang CS. Piperidine alkaloids from piper methysticum. Phytochemistry. 2003;63(2):193-198.
31. Simkins A, Thurston D, Colyar M, et al. Nature’s wrath? A closer look at complications with five popular herbs. Adv Nurse Pract. 2005;13(6):55-56.
32. Teschke R, Genthner A, Wolff A. Kava hepatotoxicity: comparison of aqueous, ethanolic, acetonic kava extracts and kava-herbs mixtures. J Ethnopharmacol. 2009;123(3):378-384.
33. Christl SU, Seifert A, Seeler D. Toxic hepatitis after consumption of traditional kava preparation. J Travel Med. 2009;16(1):55-56.
Management of Dental Emergencies
As general pediatricians, you should feel confident in your ability to diagnose and manage dental trauma and emergencies. Bumped teeth that are not loose, bruised gums, and aphthous ulcers are dental emergencies that you can evaluate and treat in your office, for example.
In contrast, referral is warranted after trauma loosens a tooth, breaks it, or causes the tooth to come out (avulsion). In addition, a child who presents with extreme pain, an abscessed tooth, or a tooth pushed out of position should be referred to a specialist. Dental cellulitis and severe soft tissue injuries of the mouth are other reasons I typically see these children.
An avulsed permanent tooth should be replaced quickly, within seconds or minutes. The longer the tooth is out of the mouth, the poorer the prognosis. Do not handle the root surface, but do rinse lightly and quickly to remove foreign material. If it is impossible to reimplant the tooth immediately, instruct parents to store the tooth in milk or saline for transport to the dentist.
Once the child reaches a specialist, treatment may include reimplantation with a splint to stabilize the tooth, prescriptions for systemic antibiotics and oral antimicrobials, and pulp therapy. Inform parents that most displaced permanent teeth undergo pulpal necrosis and require initiation of root canal therapy 1 week after stabilization.
In contrast, primary teeth usually are not reimplanted. If a patient comes in with a “baby tooth” that has been knocked out, then just pass it on to the tooth fairy.
The good news is most tooth injuries are self-evident. Signs of trauma include discoloration and patient reports of pain associated with tooth movement, chewing, palpation, and/or sensitivity to hot or cold food or drinks.
If you see facial swelling, however, expand your differential diagnosis to include etiologies beyond the teeth or gingival tissue. Infections and allergic reactions, for example, also can cause substantial gingival swelling. Rule out ear infections, swollen lymph nodes, and strep throat and viral infections, because these can mimic dental concerns.
If a child presents after trauma with a fractured tooth, make sure to remove any tooth fragments before suturing nearby tissue, including lacerated lips. Hemorrhage control, cleansing, and suturing, as indicated, are important management tips for such soft tissue wounds. Antibiotics are recommended for all “through and through” lacerations.
Establish a working relationship with pediatric dentists and oral surgeons in your community. When a child requires immediate care, these specialists can provide telephone advice on how to handle the emergency and/or be a source of immediate referral for the patient.
A dentist never wants to see a child for the first time during a traumatic situation. Instead, each patient should see a dentist by age 1 to establish a dental home. A child who visits the dentist on a regular basis will become familiar with the provider and more comfortable in the event of a dental emergency. Education of parents on optimal oral health, prevention of problems, and appropriate dental development are other benefits of early, routine dental care.
I recommend the American Academy of Pediatrics Section on Pediatric Dentistry and Oral Health's new curriculum called Protecting All Children's Teeth (PACT): A Pediatric Oral Health Training Program (www.aap.org/oralhealth/pact.cfm
Some dental emergencies can be evaluated and treated in your office, according to Tonya Fuqua, D.D.S.
Source Courtesy Cook Children's Hospital
As general pediatricians, you should feel confident in your ability to diagnose and manage dental trauma and emergencies. Bumped teeth that are not loose, bruised gums, and aphthous ulcers are dental emergencies that you can evaluate and treat in your office, for example.
In contrast, referral is warranted after trauma loosens a tooth, breaks it, or causes the tooth to come out (avulsion). In addition, a child who presents with extreme pain, an abscessed tooth, or a tooth pushed out of position should be referred to a specialist. Dental cellulitis and severe soft tissue injuries of the mouth are other reasons I typically see these children.
An avulsed permanent tooth should be replaced quickly, within seconds or minutes. The longer the tooth is out of the mouth, the poorer the prognosis. Do not handle the root surface, but do rinse lightly and quickly to remove foreign material. If it is impossible to reimplant the tooth immediately, instruct parents to store the tooth in milk or saline for transport to the dentist.
Once the child reaches a specialist, treatment may include reimplantation with a splint to stabilize the tooth, prescriptions for systemic antibiotics and oral antimicrobials, and pulp therapy. Inform parents that most displaced permanent teeth undergo pulpal necrosis and require initiation of root canal therapy 1 week after stabilization.
In contrast, primary teeth usually are not reimplanted. If a patient comes in with a “baby tooth” that has been knocked out, then just pass it on to the tooth fairy.
The good news is most tooth injuries are self-evident. Signs of trauma include discoloration and patient reports of pain associated with tooth movement, chewing, palpation, and/or sensitivity to hot or cold food or drinks.
If you see facial swelling, however, expand your differential diagnosis to include etiologies beyond the teeth or gingival tissue. Infections and allergic reactions, for example, also can cause substantial gingival swelling. Rule out ear infections, swollen lymph nodes, and strep throat and viral infections, because these can mimic dental concerns.
If a child presents after trauma with a fractured tooth, make sure to remove any tooth fragments before suturing nearby tissue, including lacerated lips. Hemorrhage control, cleansing, and suturing, as indicated, are important management tips for such soft tissue wounds. Antibiotics are recommended for all “through and through” lacerations.
Establish a working relationship with pediatric dentists and oral surgeons in your community. When a child requires immediate care, these specialists can provide telephone advice on how to handle the emergency and/or be a source of immediate referral for the patient.
A dentist never wants to see a child for the first time during a traumatic situation. Instead, each patient should see a dentist by age 1 to establish a dental home. A child who visits the dentist on a regular basis will become familiar with the provider and more comfortable in the event of a dental emergency. Education of parents on optimal oral health, prevention of problems, and appropriate dental development are other benefits of early, routine dental care.
I recommend the American Academy of Pediatrics Section on Pediatric Dentistry and Oral Health's new curriculum called Protecting All Children's Teeth (PACT): A Pediatric Oral Health Training Program (www.aap.org/oralhealth/pact.cfm
Some dental emergencies can be evaluated and treated in your office, according to Tonya Fuqua, D.D.S.
Source Courtesy Cook Children's Hospital
As general pediatricians, you should feel confident in your ability to diagnose and manage dental trauma and emergencies. Bumped teeth that are not loose, bruised gums, and aphthous ulcers are dental emergencies that you can evaluate and treat in your office, for example.
In contrast, referral is warranted after trauma loosens a tooth, breaks it, or causes the tooth to come out (avulsion). In addition, a child who presents with extreme pain, an abscessed tooth, or a tooth pushed out of position should be referred to a specialist. Dental cellulitis and severe soft tissue injuries of the mouth are other reasons I typically see these children.
An avulsed permanent tooth should be replaced quickly, within seconds or minutes. The longer the tooth is out of the mouth, the poorer the prognosis. Do not handle the root surface, but do rinse lightly and quickly to remove foreign material. If it is impossible to reimplant the tooth immediately, instruct parents to store the tooth in milk or saline for transport to the dentist.
Once the child reaches a specialist, treatment may include reimplantation with a splint to stabilize the tooth, prescriptions for systemic antibiotics and oral antimicrobials, and pulp therapy. Inform parents that most displaced permanent teeth undergo pulpal necrosis and require initiation of root canal therapy 1 week after stabilization.
In contrast, primary teeth usually are not reimplanted. If a patient comes in with a “baby tooth” that has been knocked out, then just pass it on to the tooth fairy.
The good news is most tooth injuries are self-evident. Signs of trauma include discoloration and patient reports of pain associated with tooth movement, chewing, palpation, and/or sensitivity to hot or cold food or drinks.
If you see facial swelling, however, expand your differential diagnosis to include etiologies beyond the teeth or gingival tissue. Infections and allergic reactions, for example, also can cause substantial gingival swelling. Rule out ear infections, swollen lymph nodes, and strep throat and viral infections, because these can mimic dental concerns.
If a child presents after trauma with a fractured tooth, make sure to remove any tooth fragments before suturing nearby tissue, including lacerated lips. Hemorrhage control, cleansing, and suturing, as indicated, are important management tips for such soft tissue wounds. Antibiotics are recommended for all “through and through” lacerations.
Establish a working relationship with pediatric dentists and oral surgeons in your community. When a child requires immediate care, these specialists can provide telephone advice on how to handle the emergency and/or be a source of immediate referral for the patient.
A dentist never wants to see a child for the first time during a traumatic situation. Instead, each patient should see a dentist by age 1 to establish a dental home. A child who visits the dentist on a regular basis will become familiar with the provider and more comfortable in the event of a dental emergency. Education of parents on optimal oral health, prevention of problems, and appropriate dental development are other benefits of early, routine dental care.
I recommend the American Academy of Pediatrics Section on Pediatric Dentistry and Oral Health's new curriculum called Protecting All Children's Teeth (PACT): A Pediatric Oral Health Training Program (www.aap.org/oralhealth/pact.cfm
Some dental emergencies can be evaluated and treated in your office, according to Tonya Fuqua, D.D.S.
Source Courtesy Cook Children's Hospital
Kids and Divorce: A Long-Term Commitment
Divorce is so common in the United States – ending about half of all marriages – that it will affect many patients and families in your practice. If your practice has about 2,000 children and adolescents from about 1,500 families, for example, hundreds of families will be dealing with predivorce marital tension, the divorce itself, or postdivorce concerns.
Start by screening for family functioning at every annual visit. Specifically, try to identify strife and stress early on, at a time when your inventions have the greatest preventive impact. Ask open-ended questions such as, “How are things going in the family?” or “Is there any tension or discord in the family or in the marriage?”
I recommend using the broader term “discord” because it will pick up a pending divorce and also identify other family stressors for the child. For example, research indicates that the years of arguing and fighting that often precede divorce may be more damaging to the child in the long term than the divorce itself.
Once you identify marital or family stress, strive for the following three long-term goals to optimize a healthy outcome for the child.
▸ First, make sure the child continues to function well in school, with peers, in activities, and in areas of self-esteem. The firr certain key signs that a child is not functioning well. Persistently lower school performance is one sign. Most children are't concentrate or perform as well at school in the year of the divorce, but it is a warning sign if the problems persist. Determine whether the child is still having difficulty adjusting to the divorce, and assess if there is ongoing discord or fighting about visitation, custody, child rearing, or finances after the divorce. Another warning sign is the child who drops an after-school activity during a divorce crisis, and fails to retume itin the next school year.
How a child relates to friends after the divorce can be important. In particular, ascertain how young or midadolescents treat members of the opposite sex. Look for patterns in their relationships that repeat some of the dysfunctional behaviors of their parents' marriage. Keep in mind that children are often unaware that they are repeating these family patterns.
For example, are girls who are adversely affected by divorce especially vulnerable to getting involved with older teenagers who might take advantage of them? Do you see any evidence of longing in the girls, or signs that they are seeking to replace something missing in their paternal relationship? This type of behavior is much less likely if the girl has had a good relationship with her father before, during, and after the divorce.
With teenage boys, consider how they treat their girlfriends. Is the boy supportive in his relationships, or does he have girlfriend after girlfriend because of a callous or insensitive attitude?
Referral for a mental health evaluation might be appropriate if you see a pattern of continuing dysfunction in a major area of the child's life or of unsatisfactory relationships as these younger teenagers enter high school, particularly if they are alienated from a parent.
▸ Second, ensure that parents are open and willing to answer the child's questions as the child tries to make sense of the divorce at each developmental stage. Help postdivorce families encourage the child to ask questions on an ongoing basis. If divorce happened when the child was a toddler, for example, they are going to have questions 5, 10, and 15 years later that they could not conceptualize until they reached the appropriate developmental point.
Parents may need your advice on how best to talk to their 5- or 8-year-old, a time when information should be concrete and straightforward. In contrast, a 14-year-old may be able to understand more conceptual and nuanced answers to their questions. For example, a younger child is unlikely to think about the divorce in terms of an extramarital affair or the impact on their college finances, but that may not be the case when the child is 14 or 15 years old. Keep in mind that many adolescents do not ask parents such difficult questions unless they are given permission in advance, and it's at a time when they feel safe and at ease.
▸ Third, counsel the family to facilitate a good relationship between the child and each parent over the long term. When families come to me and there is a lot of tension about visitation, custody, and money, I often focus them on the long-term goals. I ask, “What kind of relationship do you want with your child 10 and 15 years from now?”; “What is likely to result in a good long-term relationship with them?”; “Do you want to be able to be at their wedding?”; “Do you want to be close to your grandchildren?” Going all out for an extra few hours of visitation or not paying a bill is not likely to help achieve these long-term goals.
Again, early screening and intervention make your job easier. If a patient or family comes to you after years of negativity and a court fight over a bitter divorce, your ability to intervene effectively is already very limited.
Divorce is often an angry and divisive time. You can advise parents not to act out of anger by offering examples of divorcing parents who invested a lot of time and energy into winning short-term victories, only to see their efforts backfire later. Some parents believe that the child will be closer to them if they can make the child angry at the spouse. But children who feel they have to betray one parent to please the other often become resentful of this role over time.
In contrast, children who observe their parents working together with a sense of harmony and cooperation to make the custody, visitation, financial, and other arrangements successful are much less likely to blame themselves for the divorce. They also are much less likely to feel guilty when they connect more to one parent or the other at different points in their development.
It is important to monitor your patients for long-term effects of divorce up to and including the time you transition them to an adult care provider. Ask the older adolescent questions such as, “How do you feel about the divorce now, looking back on it [5, 10, or 15] years later?”; “How do you think it's affected you?”; and “Are there any things you'd like to change?”
If you do a review of how they integrated the divorce when they are in 10th or 11th grade, you will still have time to address any unresolved issues. If the child is distant with one parent, you can at least wonder if this is a point in time to reconnect and repair that relationship before the teenager goes to work or college and moves to being fully independent.
Pediatricians often have limited time to intervene. Some find this work very gratifying and feel comfortable with divorce-related issues. Others may choose to refer the patient to a social worker, psychologist, or child and adolescent psychiatrist, according to the severity of the situation. Some pediatric practices are fortunate to have a full- or part-time social worker.
If you want to counsel but your time is limited, consider offering a divorced-parent discussion and education group in your practice. You and/or a social worker could facilitate this forum. This resource can help parents share their experiences and strategies to ensure that children emerge as happy and healthy as possible after a divorce. In addition, this intervention can be cost-neutral if you charge parents a nominal fee.
Divorce is so common in the United States – ending about half of all marriages – that it will affect many patients and families in your practice. If your practice has about 2,000 children and adolescents from about 1,500 families, for example, hundreds of families will be dealing with predivorce marital tension, the divorce itself, or postdivorce concerns.
Start by screening for family functioning at every annual visit. Specifically, try to identify strife and stress early on, at a time when your inventions have the greatest preventive impact. Ask open-ended questions such as, “How are things going in the family?” or “Is there any tension or discord in the family or in the marriage?”
I recommend using the broader term “discord” because it will pick up a pending divorce and also identify other family stressors for the child. For example, research indicates that the years of arguing and fighting that often precede divorce may be more damaging to the child in the long term than the divorce itself.
Once you identify marital or family stress, strive for the following three long-term goals to optimize a healthy outcome for the child.
▸ First, make sure the child continues to function well in school, with peers, in activities, and in areas of self-esteem. The firr certain key signs that a child is not functioning well. Persistently lower school performance is one sign. Most children are't concentrate or perform as well at school in the year of the divorce, but it is a warning sign if the problems persist. Determine whether the child is still having difficulty adjusting to the divorce, and assess if there is ongoing discord or fighting about visitation, custody, child rearing, or finances after the divorce. Another warning sign is the child who drops an after-school activity during a divorce crisis, and fails to retume itin the next school year.
How a child relates to friends after the divorce can be important. In particular, ascertain how young or midadolescents treat members of the opposite sex. Look for patterns in their relationships that repeat some of the dysfunctional behaviors of their parents' marriage. Keep in mind that children are often unaware that they are repeating these family patterns.
For example, are girls who are adversely affected by divorce especially vulnerable to getting involved with older teenagers who might take advantage of them? Do you see any evidence of longing in the girls, or signs that they are seeking to replace something missing in their paternal relationship? This type of behavior is much less likely if the girl has had a good relationship with her father before, during, and after the divorce.
With teenage boys, consider how they treat their girlfriends. Is the boy supportive in his relationships, or does he have girlfriend after girlfriend because of a callous or insensitive attitude?
Referral for a mental health evaluation might be appropriate if you see a pattern of continuing dysfunction in a major area of the child's life or of unsatisfactory relationships as these younger teenagers enter high school, particularly if they are alienated from a parent.
▸ Second, ensure that parents are open and willing to answer the child's questions as the child tries to make sense of the divorce at each developmental stage. Help postdivorce families encourage the child to ask questions on an ongoing basis. If divorce happened when the child was a toddler, for example, they are going to have questions 5, 10, and 15 years later that they could not conceptualize until they reached the appropriate developmental point.
Parents may need your advice on how best to talk to their 5- or 8-year-old, a time when information should be concrete and straightforward. In contrast, a 14-year-old may be able to understand more conceptual and nuanced answers to their questions. For example, a younger child is unlikely to think about the divorce in terms of an extramarital affair or the impact on their college finances, but that may not be the case when the child is 14 or 15 years old. Keep in mind that many adolescents do not ask parents such difficult questions unless they are given permission in advance, and it's at a time when they feel safe and at ease.
▸ Third, counsel the family to facilitate a good relationship between the child and each parent over the long term. When families come to me and there is a lot of tension about visitation, custody, and money, I often focus them on the long-term goals. I ask, “What kind of relationship do you want with your child 10 and 15 years from now?”; “What is likely to result in a good long-term relationship with them?”; “Do you want to be able to be at their wedding?”; “Do you want to be close to your grandchildren?” Going all out for an extra few hours of visitation or not paying a bill is not likely to help achieve these long-term goals.
Again, early screening and intervention make your job easier. If a patient or family comes to you after years of negativity and a court fight over a bitter divorce, your ability to intervene effectively is already very limited.
Divorce is often an angry and divisive time. You can advise parents not to act out of anger by offering examples of divorcing parents who invested a lot of time and energy into winning short-term victories, only to see their efforts backfire later. Some parents believe that the child will be closer to them if they can make the child angry at the spouse. But children who feel they have to betray one parent to please the other often become resentful of this role over time.
In contrast, children who observe their parents working together with a sense of harmony and cooperation to make the custody, visitation, financial, and other arrangements successful are much less likely to blame themselves for the divorce. They also are much less likely to feel guilty when they connect more to one parent or the other at different points in their development.
It is important to monitor your patients for long-term effects of divorce up to and including the time you transition them to an adult care provider. Ask the older adolescent questions such as, “How do you feel about the divorce now, looking back on it [5, 10, or 15] years later?”; “How do you think it's affected you?”; and “Are there any things you'd like to change?”
If you do a review of how they integrated the divorce when they are in 10th or 11th grade, you will still have time to address any unresolved issues. If the child is distant with one parent, you can at least wonder if this is a point in time to reconnect and repair that relationship before the teenager goes to work or college and moves to being fully independent.
Pediatricians often have limited time to intervene. Some find this work very gratifying and feel comfortable with divorce-related issues. Others may choose to refer the patient to a social worker, psychologist, or child and adolescent psychiatrist, according to the severity of the situation. Some pediatric practices are fortunate to have a full- or part-time social worker.
If you want to counsel but your time is limited, consider offering a divorced-parent discussion and education group in your practice. You and/or a social worker could facilitate this forum. This resource can help parents share their experiences and strategies to ensure that children emerge as happy and healthy as possible after a divorce. In addition, this intervention can be cost-neutral if you charge parents a nominal fee.
Divorce is so common in the United States – ending about half of all marriages – that it will affect many patients and families in your practice. If your practice has about 2,000 children and adolescents from about 1,500 families, for example, hundreds of families will be dealing with predivorce marital tension, the divorce itself, or postdivorce concerns.
Start by screening for family functioning at every annual visit. Specifically, try to identify strife and stress early on, at a time when your inventions have the greatest preventive impact. Ask open-ended questions such as, “How are things going in the family?” or “Is there any tension or discord in the family or in the marriage?”
I recommend using the broader term “discord” because it will pick up a pending divorce and also identify other family stressors for the child. For example, research indicates that the years of arguing and fighting that often precede divorce may be more damaging to the child in the long term than the divorce itself.
Once you identify marital or family stress, strive for the following three long-term goals to optimize a healthy outcome for the child.
▸ First, make sure the child continues to function well in school, with peers, in activities, and in areas of self-esteem. The firr certain key signs that a child is not functioning well. Persistently lower school performance is one sign. Most children are't concentrate or perform as well at school in the year of the divorce, but it is a warning sign if the problems persist. Determine whether the child is still having difficulty adjusting to the divorce, and assess if there is ongoing discord or fighting about visitation, custody, child rearing, or finances after the divorce. Another warning sign is the child who drops an after-school activity during a divorce crisis, and fails to retume itin the next school year.
How a child relates to friends after the divorce can be important. In particular, ascertain how young or midadolescents treat members of the opposite sex. Look for patterns in their relationships that repeat some of the dysfunctional behaviors of their parents' marriage. Keep in mind that children are often unaware that they are repeating these family patterns.
For example, are girls who are adversely affected by divorce especially vulnerable to getting involved with older teenagers who might take advantage of them? Do you see any evidence of longing in the girls, or signs that they are seeking to replace something missing in their paternal relationship? This type of behavior is much less likely if the girl has had a good relationship with her father before, during, and after the divorce.
With teenage boys, consider how they treat their girlfriends. Is the boy supportive in his relationships, or does he have girlfriend after girlfriend because of a callous or insensitive attitude?
Referral for a mental health evaluation might be appropriate if you see a pattern of continuing dysfunction in a major area of the child's life or of unsatisfactory relationships as these younger teenagers enter high school, particularly if they are alienated from a parent.
▸ Second, ensure that parents are open and willing to answer the child's questions as the child tries to make sense of the divorce at each developmental stage. Help postdivorce families encourage the child to ask questions on an ongoing basis. If divorce happened when the child was a toddler, for example, they are going to have questions 5, 10, and 15 years later that they could not conceptualize until they reached the appropriate developmental point.
Parents may need your advice on how best to talk to their 5- or 8-year-old, a time when information should be concrete and straightforward. In contrast, a 14-year-old may be able to understand more conceptual and nuanced answers to their questions. For example, a younger child is unlikely to think about the divorce in terms of an extramarital affair or the impact on their college finances, but that may not be the case when the child is 14 or 15 years old. Keep in mind that many adolescents do not ask parents such difficult questions unless they are given permission in advance, and it's at a time when they feel safe and at ease.
▸ Third, counsel the family to facilitate a good relationship between the child and each parent over the long term. When families come to me and there is a lot of tension about visitation, custody, and money, I often focus them on the long-term goals. I ask, “What kind of relationship do you want with your child 10 and 15 years from now?”; “What is likely to result in a good long-term relationship with them?”; “Do you want to be able to be at their wedding?”; “Do you want to be close to your grandchildren?” Going all out for an extra few hours of visitation or not paying a bill is not likely to help achieve these long-term goals.
Again, early screening and intervention make your job easier. If a patient or family comes to you after years of negativity and a court fight over a bitter divorce, your ability to intervene effectively is already very limited.
Divorce is often an angry and divisive time. You can advise parents not to act out of anger by offering examples of divorcing parents who invested a lot of time and energy into winning short-term victories, only to see their efforts backfire later. Some parents believe that the child will be closer to them if they can make the child angry at the spouse. But children who feel they have to betray one parent to please the other often become resentful of this role over time.
In contrast, children who observe their parents working together with a sense of harmony and cooperation to make the custody, visitation, financial, and other arrangements successful are much less likely to blame themselves for the divorce. They also are much less likely to feel guilty when they connect more to one parent or the other at different points in their development.
It is important to monitor your patients for long-term effects of divorce up to and including the time you transition them to an adult care provider. Ask the older adolescent questions such as, “How do you feel about the divorce now, looking back on it [5, 10, or 15] years later?”; “How do you think it's affected you?”; and “Are there any things you'd like to change?”
If you do a review of how they integrated the divorce when they are in 10th or 11th grade, you will still have time to address any unresolved issues. If the child is distant with one parent, you can at least wonder if this is a point in time to reconnect and repair that relationship before the teenager goes to work or college and moves to being fully independent.
Pediatricians often have limited time to intervene. Some find this work very gratifying and feel comfortable with divorce-related issues. Others may choose to refer the patient to a social worker, psychologist, or child and adolescent psychiatrist, according to the severity of the situation. Some pediatric practices are fortunate to have a full- or part-time social worker.
If you want to counsel but your time is limited, consider offering a divorced-parent discussion and education group in your practice. You and/or a social worker could facilitate this forum. This resource can help parents share their experiences and strategies to ensure that children emerge as happy and healthy as possible after a divorce. In addition, this intervention can be cost-neutral if you charge parents a nominal fee.
Spotlight on Physicians' Safety in Hospitals
Hospitalists should take care to remember the potentially violent offenders and situations that surround them daily at work, says a member of SHM's Practice Management Committee.
Michael Radzienda, MD, SFHM, vice president of hospital medicine and clinical effectiveness at Vanguard Health System in Southborough, Mass., says the recent shooting of a doctor at Johns Hopkins Hospital in Baltimore serves as a stark reminder that violence in the hospital is a concern for providers more than ever. To Dr. Radzienda's mind, that includes patients attacking doctors or patients attacking other patients.
"It's a newer issue for hospitalists, but one that they need to pay attention to," Dr. Radzienda says. "The volume of high-risk interactions that a hospitalist might have is significant compared to what that volume might have looked like 10 years ago before the hospitalist (model) took off."
And while one might think the incident at Johns Hopkins is enough to shine a lasting spotlight on the issue, a report from The Joint Commission this summer on hospital violence faded relatively quickly after its issuance. The commission's Sentinel Event Database, in fact, includes a category of assault, rape, and homicide (combined) with 256 reports since 1995, a number the organization suggests is under-reported. The commission's latest report, published in June, found that since 2004, hospitals have reported "significant increases in reports of assault, rape, and homicide, with the greater number of reports in the last three years."
The report recommends physicians learn techniques to identify potentially violent patients, implement violence de-escalation approaches, and even conduct violence audits to help determine an institution’s safety protocols.
Dr. Radzienda understands that training time and resources are stretched thin, but he says more focus on violence would be helpful to institutions and individual physicians. "The problem is someone needs to recognize this type of thing," he says. "But how do you prioritize that?"
Hospitalists should take care to remember the potentially violent offenders and situations that surround them daily at work, says a member of SHM's Practice Management Committee.
Michael Radzienda, MD, SFHM, vice president of hospital medicine and clinical effectiveness at Vanguard Health System in Southborough, Mass., says the recent shooting of a doctor at Johns Hopkins Hospital in Baltimore serves as a stark reminder that violence in the hospital is a concern for providers more than ever. To Dr. Radzienda's mind, that includes patients attacking doctors or patients attacking other patients.
"It's a newer issue for hospitalists, but one that they need to pay attention to," Dr. Radzienda says. "The volume of high-risk interactions that a hospitalist might have is significant compared to what that volume might have looked like 10 years ago before the hospitalist (model) took off."
And while one might think the incident at Johns Hopkins is enough to shine a lasting spotlight on the issue, a report from The Joint Commission this summer on hospital violence faded relatively quickly after its issuance. The commission's Sentinel Event Database, in fact, includes a category of assault, rape, and homicide (combined) with 256 reports since 1995, a number the organization suggests is under-reported. The commission's latest report, published in June, found that since 2004, hospitals have reported "significant increases in reports of assault, rape, and homicide, with the greater number of reports in the last three years."
The report recommends physicians learn techniques to identify potentially violent patients, implement violence de-escalation approaches, and even conduct violence audits to help determine an institution’s safety protocols.
Dr. Radzienda understands that training time and resources are stretched thin, but he says more focus on violence would be helpful to institutions and individual physicians. "The problem is someone needs to recognize this type of thing," he says. "But how do you prioritize that?"
Hospitalists should take care to remember the potentially violent offenders and situations that surround them daily at work, says a member of SHM's Practice Management Committee.
Michael Radzienda, MD, SFHM, vice president of hospital medicine and clinical effectiveness at Vanguard Health System in Southborough, Mass., says the recent shooting of a doctor at Johns Hopkins Hospital in Baltimore serves as a stark reminder that violence in the hospital is a concern for providers more than ever. To Dr. Radzienda's mind, that includes patients attacking doctors or patients attacking other patients.
"It's a newer issue for hospitalists, but one that they need to pay attention to," Dr. Radzienda says. "The volume of high-risk interactions that a hospitalist might have is significant compared to what that volume might have looked like 10 years ago before the hospitalist (model) took off."
And while one might think the incident at Johns Hopkins is enough to shine a lasting spotlight on the issue, a report from The Joint Commission this summer on hospital violence faded relatively quickly after its issuance. The commission's Sentinel Event Database, in fact, includes a category of assault, rape, and homicide (combined) with 256 reports since 1995, a number the organization suggests is under-reported. The commission's latest report, published in June, found that since 2004, hospitals have reported "significant increases in reports of assault, rape, and homicide, with the greater number of reports in the last three years."
The report recommends physicians learn techniques to identify potentially violent patients, implement violence de-escalation approaches, and even conduct violence audits to help determine an institution’s safety protocols.
Dr. Radzienda understands that training time and resources are stretched thin, but he says more focus on violence would be helpful to institutions and individual physicians. "The problem is someone needs to recognize this type of thing," he says. "But how do you prioritize that?"