User login
How accurate is stress radionuclide imaging for diagnosis of CAD?
Stress radionuclide testing is a moderately accurate test compared with coronary angiography for the diagnosis of coronary artery disease (CAD) in intermediate-risk individuals.
Variations in technique of imaging (planar or single-photon emission computed tomography [SPECT]) and stress (exercise or pharmacologic) do not significantly alter the accuracy of this test, although there is some evidence for decreased accuracy in women (strength of recommendation [SOR]: A, based on multiple meta-analyses). Abnormal stress radionuclide screening in vascular surgical candidates also predicts an increased rate of perioperative cardiac events (SOR: A, based on meta-analysis).
Evidence summary
Stress radionuclide imaging—specifically its diagnostic accuracy—has been the subject of numerous studies. Detrano et al1 reported the first pooled data (56 studies); they concluded that estimates of sensitivity (85%) and specificity (85%) are biased by studies that were not blinded, included subjects with prior myocardial infarction (MI), or had a work-up (verification) bias (ie, use of the gold standard test is affected by the result on the test under question).
Another systematic review reported estimates of sensitivity ranging from 68% to 96% and specificity from 65% to 100%.2 The review was accompanied by a position paper from the American College of Physicians stating that the test may be appropriate for a patient with intermediate risk of coronary artery disease.3
Four meta-analyses report diagnostic accuracy of radionuclide cardiac imaging (Table). Kwok et al6 analyzed data on women only and found decreased diagnostic accuracy in this population. Kim et al7 analyzed pharmacologic stressors used with SPECT and confirmed that accuracy is near that of exercise SPECT. Patient-centered outcomes were reported in a meta-analysis of dipyridamole-thallium imaging in the preoperative evaluation of vascular surgery patients. The summary odds ratio for any perioperative cardiac event (in patients with abnormal tests) was 3.5 (95% confidence interval [CI], 2.5–4.8); the odds ratio for MI or cardiac death was 3.9 (95% CI, 2.5–5.6), leading the authors to conclude that there is sound evidence to use radionuclide testing in intermedi.ate-risk patients during preoperative screening.8
TABLE
Diagnostic accuracy reported in meta-analyses of cardiac radionuclide SPECT imaging
| Authors, year | Studies | Sn % (95% CI) | Sp % (95% CI) | LR+ | LR– |
|---|---|---|---|---|---|
| Garber and Solomon 19944 | 8 | 88 (73–98) | 77 (53–96) | 3.8 | 0.16 |
| Fleischmann et al, et al 19985 | 27 | 87 (86–88) | 64 (60–68) | 2.4 | 0.20 |
| Kwok et al, 19966 | 3 | 78 (69–87) | 58 (51–66) | 1.9 | 0.38 |
| Kim et al, 20017 | 44 | 90 (89–92)* | 75 (70–79)* | 3.6 | 0.13 |
| 89 (84–93)† | 65 (54–74)† | 2.5 | 0.17 | ||
| 82(77–87)‡ | 73 (70–79)‡ | 3.0 | 0.25 | ||
| *Adenosine SPECT | |||||
| †Dipyridamole SPECT | |||||
| ‡Dobutamine SPECT | |||||
| SPECT, single-photon emission computed tomography; SN, sensitivity; Sp, specifity; LR+, positive likelihood ratio; LR–, negative likelihood ratio; Cl, confidence interval | |||||
Recommendations from others
The American Heart Association/American College Cardiology (AHA/ACC) Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures and the American Society of Nuclear Cardiology updated guidelines for cardiac radionuclide imaging in 2003. In this consensus statement (a nonsystematic review of literature and expert opinion), they reported test characteristics to detect a 50% angiographic lesion as follows—exercise SPECT: sensitivity 87%, specificity 73%; vasodilator (adenosine or dipyridamole) SPECT: sensitivity 89%, specificity 75%. They noted that quantitative analysis performs as well as qualitative analysis of radionuclide images. Gated SPECT is slightly more specific and just as sensitive as nongated SPECT.
The Taskforce recommended that radionuclide perfusion scans be performed in patients with baseline electrocardiogram (ECG) abnormalities (such as left bundle branch block, hypertrophy, digitalis effect, etc), patients who cannot perform an exercise stress test, and to assess the functional effect of indeterminate lesions found on angiography. They also note that the repeat use of radionuclide testing 3 to 5 years after an event in asymptomatic high-risk patients and the initial use of radionuclide testing in patients at very high risk are both somewhat controversial, but the weight of limited evidence suggests some benefit to their use.9
ECG stress still the choice; image those with abnormal ECG or unable to exercise
David Kilgore, MD
Tacoma Family Medicine, Tacoma, Wash
Primary care providers frequently face the question of how best to evaluate patients with suspected CAD. Recent studies and expert opinion appear to give conflicting advice regarding the merits of plain exercise ECG vs stress imaging. Information on accuracy doesn’t always indicate which test is best for a patient.
Though quoted sensitivities and specificities for exercise ECG typically appear lower than those for stress imaging, costs for stress imaging are significantly higher, and numerous recent studies are demonstrating mortality outcome differences obtainable from physiologic information found in exercise testing (exercise capacity, blood pressure and pulse changes, time to angina).
Currently, the best choice for evaluation appears to be summarized by the 2003 AHA/ACC practice guidelines, which endorse exercise ECG for patients (women included) with intermediate pretest risk, and normal resting ECG for those who are unable to exercise. Stress imaging is cost effective for those patients with abnormal baseline ECG (left bundle branch block, ST abnormalities), or who are unable to exercise.
1. Detrano R, Janosi A, Lyons KP, Marcondes G, Abbassi N, Froelicher VF. Factors affecting sensitivity and specificity of a diagnostic test: the exercise thallium scintigram. Am J Med 1988;84:699-710.
2. Kotler TS, Diamond GA. Exercise thallium-201 scintigraphy in the diagnosis and prognosis of coronary artery disease. Ann Intern Med 1990;113:684-702.
3. Efficacy of exercise thallium-201 scintigraphy in diagnosis and prognosis of coronary artery disease. American College of Physicians. Ann Intern Med 1990;113:703-704.
4. Garber AM, Solomon NA. Cost-effectiveness of alternative test strategies for the diagnosis of coronary artery disease. Ann Intern Med 1999;130:719-728.
5. Fleischmann KE, Hunink MG, Kuntz KM, Douglas PS. Exercise echocardiography or exercise SPECT imaging? A meta-analysis of diagnostic test performance. JAMA 1998;280:913-920.
6. Kwok Y, Kim C, Grady D, Segal M, Redberg R. Meta-analysis of exercise testing to detect coronary artery disease in women. Am J Cardiol 1999;83:660-666.
7. Kim C, Kwok YS, Heagerty P, Redberg R. Pharmacologic stress testing for coronary artery disease diagnosis: A meta-analysis. Am Heart J 2001;142:934-944.
8. Shaw LJ, Eagle KA, Gersh BJ, Miller DD. Meta-analysis of intravenous dipyridamole-thallium-201 imaging (1985–1994) and dobutamine echocardiography (1991–1994) for risk stratification before vascular surgery. J Am Coll Cardiol 1996;27:787-798.
9. Klocke FJ, Baird MG, Bateman TM, et al. ACC/AHA/ASNC guidelines for the clinical use of cardiac radionuclide imaging: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. ACC/AHA/ASNC Committee to Revise the 1995 Guidelines for the Clinical Use of Radionuclide Imaging. Available at: www.acc.org/clinical/guidelines/radio/rni_fulltext.pdf. Accessed on December 14, 2003.
Stress radionuclide testing is a moderately accurate test compared with coronary angiography for the diagnosis of coronary artery disease (CAD) in intermediate-risk individuals.
Variations in technique of imaging (planar or single-photon emission computed tomography [SPECT]) and stress (exercise or pharmacologic) do not significantly alter the accuracy of this test, although there is some evidence for decreased accuracy in women (strength of recommendation [SOR]: A, based on multiple meta-analyses). Abnormal stress radionuclide screening in vascular surgical candidates also predicts an increased rate of perioperative cardiac events (SOR: A, based on meta-analysis).
Evidence summary
Stress radionuclide imaging—specifically its diagnostic accuracy—has been the subject of numerous studies. Detrano et al1 reported the first pooled data (56 studies); they concluded that estimates of sensitivity (85%) and specificity (85%) are biased by studies that were not blinded, included subjects with prior myocardial infarction (MI), or had a work-up (verification) bias (ie, use of the gold standard test is affected by the result on the test under question).
Another systematic review reported estimates of sensitivity ranging from 68% to 96% and specificity from 65% to 100%.2 The review was accompanied by a position paper from the American College of Physicians stating that the test may be appropriate for a patient with intermediate risk of coronary artery disease.3
Four meta-analyses report diagnostic accuracy of radionuclide cardiac imaging (Table). Kwok et al6 analyzed data on women only and found decreased diagnostic accuracy in this population. Kim et al7 analyzed pharmacologic stressors used with SPECT and confirmed that accuracy is near that of exercise SPECT. Patient-centered outcomes were reported in a meta-analysis of dipyridamole-thallium imaging in the preoperative evaluation of vascular surgery patients. The summary odds ratio for any perioperative cardiac event (in patients with abnormal tests) was 3.5 (95% confidence interval [CI], 2.5–4.8); the odds ratio for MI or cardiac death was 3.9 (95% CI, 2.5–5.6), leading the authors to conclude that there is sound evidence to use radionuclide testing in intermedi.ate-risk patients during preoperative screening.8
TABLE
Diagnostic accuracy reported in meta-analyses of cardiac radionuclide SPECT imaging
| Authors, year | Studies | Sn % (95% CI) | Sp % (95% CI) | LR+ | LR– |
|---|---|---|---|---|---|
| Garber and Solomon 19944 | 8 | 88 (73–98) | 77 (53–96) | 3.8 | 0.16 |
| Fleischmann et al, et al 19985 | 27 | 87 (86–88) | 64 (60–68) | 2.4 | 0.20 |
| Kwok et al, 19966 | 3 | 78 (69–87) | 58 (51–66) | 1.9 | 0.38 |
| Kim et al, 20017 | 44 | 90 (89–92)* | 75 (70–79)* | 3.6 | 0.13 |
| 89 (84–93)† | 65 (54–74)† | 2.5 | 0.17 | ||
| 82(77–87)‡ | 73 (70–79)‡ | 3.0 | 0.25 | ||
| *Adenosine SPECT | |||||
| †Dipyridamole SPECT | |||||
| ‡Dobutamine SPECT | |||||
| SPECT, single-photon emission computed tomography; SN, sensitivity; Sp, specifity; LR+, positive likelihood ratio; LR–, negative likelihood ratio; Cl, confidence interval | |||||
Recommendations from others
The American Heart Association/American College Cardiology (AHA/ACC) Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures and the American Society of Nuclear Cardiology updated guidelines for cardiac radionuclide imaging in 2003. In this consensus statement (a nonsystematic review of literature and expert opinion), they reported test characteristics to detect a 50% angiographic lesion as follows—exercise SPECT: sensitivity 87%, specificity 73%; vasodilator (adenosine or dipyridamole) SPECT: sensitivity 89%, specificity 75%. They noted that quantitative analysis performs as well as qualitative analysis of radionuclide images. Gated SPECT is slightly more specific and just as sensitive as nongated SPECT.
The Taskforce recommended that radionuclide perfusion scans be performed in patients with baseline electrocardiogram (ECG) abnormalities (such as left bundle branch block, hypertrophy, digitalis effect, etc), patients who cannot perform an exercise stress test, and to assess the functional effect of indeterminate lesions found on angiography. They also note that the repeat use of radionuclide testing 3 to 5 years after an event in asymptomatic high-risk patients and the initial use of radionuclide testing in patients at very high risk are both somewhat controversial, but the weight of limited evidence suggests some benefit to their use.9
ECG stress still the choice; image those with abnormal ECG or unable to exercise
David Kilgore, MD
Tacoma Family Medicine, Tacoma, Wash
Primary care providers frequently face the question of how best to evaluate patients with suspected CAD. Recent studies and expert opinion appear to give conflicting advice regarding the merits of plain exercise ECG vs stress imaging. Information on accuracy doesn’t always indicate which test is best for a patient.
Though quoted sensitivities and specificities for exercise ECG typically appear lower than those for stress imaging, costs for stress imaging are significantly higher, and numerous recent studies are demonstrating mortality outcome differences obtainable from physiologic information found in exercise testing (exercise capacity, blood pressure and pulse changes, time to angina).
Currently, the best choice for evaluation appears to be summarized by the 2003 AHA/ACC practice guidelines, which endorse exercise ECG for patients (women included) with intermediate pretest risk, and normal resting ECG for those who are unable to exercise. Stress imaging is cost effective for those patients with abnormal baseline ECG (left bundle branch block, ST abnormalities), or who are unable to exercise.
Stress radionuclide testing is a moderately accurate test compared with coronary angiography for the diagnosis of coronary artery disease (CAD) in intermediate-risk individuals.
Variations in technique of imaging (planar or single-photon emission computed tomography [SPECT]) and stress (exercise or pharmacologic) do not significantly alter the accuracy of this test, although there is some evidence for decreased accuracy in women (strength of recommendation [SOR]: A, based on multiple meta-analyses). Abnormal stress radionuclide screening in vascular surgical candidates also predicts an increased rate of perioperative cardiac events (SOR: A, based on meta-analysis).
Evidence summary
Stress radionuclide imaging—specifically its diagnostic accuracy—has been the subject of numerous studies. Detrano et al1 reported the first pooled data (56 studies); they concluded that estimates of sensitivity (85%) and specificity (85%) are biased by studies that were not blinded, included subjects with prior myocardial infarction (MI), or had a work-up (verification) bias (ie, use of the gold standard test is affected by the result on the test under question).
Another systematic review reported estimates of sensitivity ranging from 68% to 96% and specificity from 65% to 100%.2 The review was accompanied by a position paper from the American College of Physicians stating that the test may be appropriate for a patient with intermediate risk of coronary artery disease.3
Four meta-analyses report diagnostic accuracy of radionuclide cardiac imaging (Table). Kwok et al6 analyzed data on women only and found decreased diagnostic accuracy in this population. Kim et al7 analyzed pharmacologic stressors used with SPECT and confirmed that accuracy is near that of exercise SPECT. Patient-centered outcomes were reported in a meta-analysis of dipyridamole-thallium imaging in the preoperative evaluation of vascular surgery patients. The summary odds ratio for any perioperative cardiac event (in patients with abnormal tests) was 3.5 (95% confidence interval [CI], 2.5–4.8); the odds ratio for MI or cardiac death was 3.9 (95% CI, 2.5–5.6), leading the authors to conclude that there is sound evidence to use radionuclide testing in intermedi.ate-risk patients during preoperative screening.8
TABLE
Diagnostic accuracy reported in meta-analyses of cardiac radionuclide SPECT imaging
| Authors, year | Studies | Sn % (95% CI) | Sp % (95% CI) | LR+ | LR– |
|---|---|---|---|---|---|
| Garber and Solomon 19944 | 8 | 88 (73–98) | 77 (53–96) | 3.8 | 0.16 |
| Fleischmann et al, et al 19985 | 27 | 87 (86–88) | 64 (60–68) | 2.4 | 0.20 |
| Kwok et al, 19966 | 3 | 78 (69–87) | 58 (51–66) | 1.9 | 0.38 |
| Kim et al, 20017 | 44 | 90 (89–92)* | 75 (70–79)* | 3.6 | 0.13 |
| 89 (84–93)† | 65 (54–74)† | 2.5 | 0.17 | ||
| 82(77–87)‡ | 73 (70–79)‡ | 3.0 | 0.25 | ||
| *Adenosine SPECT | |||||
| †Dipyridamole SPECT | |||||
| ‡Dobutamine SPECT | |||||
| SPECT, single-photon emission computed tomography; SN, sensitivity; Sp, specifity; LR+, positive likelihood ratio; LR–, negative likelihood ratio; Cl, confidence interval | |||||
Recommendations from others
The American Heart Association/American College Cardiology (AHA/ACC) Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures and the American Society of Nuclear Cardiology updated guidelines for cardiac radionuclide imaging in 2003. In this consensus statement (a nonsystematic review of literature and expert opinion), they reported test characteristics to detect a 50% angiographic lesion as follows—exercise SPECT: sensitivity 87%, specificity 73%; vasodilator (adenosine or dipyridamole) SPECT: sensitivity 89%, specificity 75%. They noted that quantitative analysis performs as well as qualitative analysis of radionuclide images. Gated SPECT is slightly more specific and just as sensitive as nongated SPECT.
The Taskforce recommended that radionuclide perfusion scans be performed in patients with baseline electrocardiogram (ECG) abnormalities (such as left bundle branch block, hypertrophy, digitalis effect, etc), patients who cannot perform an exercise stress test, and to assess the functional effect of indeterminate lesions found on angiography. They also note that the repeat use of radionuclide testing 3 to 5 years after an event in asymptomatic high-risk patients and the initial use of radionuclide testing in patients at very high risk are both somewhat controversial, but the weight of limited evidence suggests some benefit to their use.9
ECG stress still the choice; image those with abnormal ECG or unable to exercise
David Kilgore, MD
Tacoma Family Medicine, Tacoma, Wash
Primary care providers frequently face the question of how best to evaluate patients with suspected CAD. Recent studies and expert opinion appear to give conflicting advice regarding the merits of plain exercise ECG vs stress imaging. Information on accuracy doesn’t always indicate which test is best for a patient.
Though quoted sensitivities and specificities for exercise ECG typically appear lower than those for stress imaging, costs for stress imaging are significantly higher, and numerous recent studies are demonstrating mortality outcome differences obtainable from physiologic information found in exercise testing (exercise capacity, blood pressure and pulse changes, time to angina).
Currently, the best choice for evaluation appears to be summarized by the 2003 AHA/ACC practice guidelines, which endorse exercise ECG for patients (women included) with intermediate pretest risk, and normal resting ECG for those who are unable to exercise. Stress imaging is cost effective for those patients with abnormal baseline ECG (left bundle branch block, ST abnormalities), or who are unable to exercise.
1. Detrano R, Janosi A, Lyons KP, Marcondes G, Abbassi N, Froelicher VF. Factors affecting sensitivity and specificity of a diagnostic test: the exercise thallium scintigram. Am J Med 1988;84:699-710.
2. Kotler TS, Diamond GA. Exercise thallium-201 scintigraphy in the diagnosis and prognosis of coronary artery disease. Ann Intern Med 1990;113:684-702.
3. Efficacy of exercise thallium-201 scintigraphy in diagnosis and prognosis of coronary artery disease. American College of Physicians. Ann Intern Med 1990;113:703-704.
4. Garber AM, Solomon NA. Cost-effectiveness of alternative test strategies for the diagnosis of coronary artery disease. Ann Intern Med 1999;130:719-728.
5. Fleischmann KE, Hunink MG, Kuntz KM, Douglas PS. Exercise echocardiography or exercise SPECT imaging? A meta-analysis of diagnostic test performance. JAMA 1998;280:913-920.
6. Kwok Y, Kim C, Grady D, Segal M, Redberg R. Meta-analysis of exercise testing to detect coronary artery disease in women. Am J Cardiol 1999;83:660-666.
7. Kim C, Kwok YS, Heagerty P, Redberg R. Pharmacologic stress testing for coronary artery disease diagnosis: A meta-analysis. Am Heart J 2001;142:934-944.
8. Shaw LJ, Eagle KA, Gersh BJ, Miller DD. Meta-analysis of intravenous dipyridamole-thallium-201 imaging (1985–1994) and dobutamine echocardiography (1991–1994) for risk stratification before vascular surgery. J Am Coll Cardiol 1996;27:787-798.
9. Klocke FJ, Baird MG, Bateman TM, et al. ACC/AHA/ASNC guidelines for the clinical use of cardiac radionuclide imaging: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. ACC/AHA/ASNC Committee to Revise the 1995 Guidelines for the Clinical Use of Radionuclide Imaging. Available at: www.acc.org/clinical/guidelines/radio/rni_fulltext.pdf. Accessed on December 14, 2003.
1. Detrano R, Janosi A, Lyons KP, Marcondes G, Abbassi N, Froelicher VF. Factors affecting sensitivity and specificity of a diagnostic test: the exercise thallium scintigram. Am J Med 1988;84:699-710.
2. Kotler TS, Diamond GA. Exercise thallium-201 scintigraphy in the diagnosis and prognosis of coronary artery disease. Ann Intern Med 1990;113:684-702.
3. Efficacy of exercise thallium-201 scintigraphy in diagnosis and prognosis of coronary artery disease. American College of Physicians. Ann Intern Med 1990;113:703-704.
4. Garber AM, Solomon NA. Cost-effectiveness of alternative test strategies for the diagnosis of coronary artery disease. Ann Intern Med 1999;130:719-728.
5. Fleischmann KE, Hunink MG, Kuntz KM, Douglas PS. Exercise echocardiography or exercise SPECT imaging? A meta-analysis of diagnostic test performance. JAMA 1998;280:913-920.
6. Kwok Y, Kim C, Grady D, Segal M, Redberg R. Meta-analysis of exercise testing to detect coronary artery disease in women. Am J Cardiol 1999;83:660-666.
7. Kim C, Kwok YS, Heagerty P, Redberg R. Pharmacologic stress testing for coronary artery disease diagnosis: A meta-analysis. Am Heart J 2001;142:934-944.
8. Shaw LJ, Eagle KA, Gersh BJ, Miller DD. Meta-analysis of intravenous dipyridamole-thallium-201 imaging (1985–1994) and dobutamine echocardiography (1991–1994) for risk stratification before vascular surgery. J Am Coll Cardiol 1996;27:787-798.
9. Klocke FJ, Baird MG, Bateman TM, et al. ACC/AHA/ASNC guidelines for the clinical use of cardiac radionuclide imaging: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. ACC/AHA/ASNC Committee to Revise the 1995 Guidelines for the Clinical Use of Radionuclide Imaging. Available at: www.acc.org/clinical/guidelines/radio/rni_fulltext.pdf. Accessed on December 14, 2003.
Evidence-based answers from the Family Physicians Inquiries Network
Do ACE inhibitors prevent nephropathy in type 2 diabetes without proteinuria?
Angiotensin-converting enzyme (ACE) inhibitors make a significant difference for patients with diabetes as a whole. If patients both with and without microalbuminuria are included together, ACE inhibitors significantly reduce the progression of the albumin excretion rate (strength of recommendation [SOR]: A, based on multiple randomized controlled trials) and the development of overt nephropathy (SOR: A, based on 1 randomized controlled trial).
However, studying diabetes without microalbuminuria separately, the effect of ACE inhibitors on progression to nephropathy does not reach statistical significance. This applies to both type 1 and 2 diabetes (SOR: A, based on randomized controlled trials with heterogenous results). Results are contradictory regarding whether ACE inhibition delays new onset of diabetic microalbuminuria.
Evidence summary
There are 3 prospective randomized controlled trials studying the effect of ACE inhibitors on albumin excretion for patients with diabetes who do not have microalbuminuria. A 2-year randomized controlled trial compared lisinopril (Prinivil; Zestril) 10 mg/d with placebo in 530 normotensive adults (aged 20–59 years) with insulin-dependent diabetes, defined as those diagnosed with diabetes before age 36 and using continuous insulin therapy within 1 year of diagnosis. At the beginning of the study, 90 patients had microalbuminuria—defined as an albumin excretion rate (AER) >29 mg/24 hr—and 440 patients did not. When the results for all patients who had and did not have microalbuminuria were combined, there was a significantly smaller rise in the AER for the lisinopril group vs the placebo group (3.2 mg/24 hr lower; P=.03). However, for the patients without initial microalbuminuria, the reduction in the rise of AER with lisinopril was not significant (1.4 mg/24 hr lower; P=.10). The decreased rate of developing new microalbuminuria was also not significant (relative risk reduction [RRR]=12.7%; P=.10).1
A subsequent trial compared enalapril (Vasotec) 10 mg/d with placebo in 194 normotensive patients (aged 40–60) with type 2 diabetes and without microalbuminuria, defined as AER >30 mg/24 hr. Over the 6-year course of the study, the AER in the placebo group rose from 10.8 mg/24 hr to 26.5 mg/24 hr. The AER of the treatment group dropped from 11.6 mg/24 hr initially to 9.7 mg/24 hr at 2 years, then rose to 15.8 mg/24 hr at 6 years. Enalapril significantly slowed the rise in AER (RRR=0.4; P=.001). Nineteen percent of the placebo group developed microalbuminuria, compared with 6.5% of those taking enalapril (absolute risk reduction[ARR]=12.5%; number needed to treat=8; P=.042). While this study described a modest and statistically significant renal protective effect of enalapril, it did not use an intention-to-treat analysis.2
MICRO-HOPE, a subset of the HOPE trial, studied ramipril (Altace) 10 mg/d vs placebo in 2437 patients with diabetes who did not have clinical proteinuria. Patients were aged 55 years or older and had either a previous cardiovascular event or at least 1 other cardiovascular risk factor. There were 1140 patients with microalbuminuria, defined as an albumin/creatinine ratio 2 mg/mmol, and 2437 patients without. After 4.5 years, 10% of patients had developed overt nephropathy, defined as albumin/creatinine >36 mg/mmol.
When all patients in the study were examined together, ramipril provided significant renal protection over placebo (RRR=24%; ARR=1%; P=.027). It also lowered the risk of MI by 22%, stroke by 33%, and cardiovascular death by 37%. But in a separate analysis of the patients without microalbuminuria, ramipril did not significantly reduce overt nephropathy (P=.50). Ramipril also did not significantly reduce the risk of developing new microalbuminuria in this group (RRR=9%; P=.17). Further, for patients without microalbuminuria, ramipril did not reduce the combined outcomes of myocardial infarction, stroke, or cardiovascular death (odds ratio=0.85; 95% CI, 0.70–1.02).3
Recommendations from others
We could find no guidelines recommending for or against the use of ACE inhibitors for patients with diabetes without microalbuminuria.
ACE inhibitors should still be used in most patients with type 2 diabetes
Joseph Saseen, PharmD, FCCP, BCPS
University of Colorado Health Sciences Center, Denver
ACE inhibitors do not prevent the development of type 2 diabetic nephropathy. In contrast to type 1 diabetes, cardiovascular disease is the primary cause of death in type 2. The HOPE study demonstrated that ACE inhibitor therapy significantly reduces cardiovascular events in type 2 diabetes independent of hypertension status.4 These benefits are so compelling that the American Diabetes Association strongly recommends ACE inhibitor therapy for type 2 diabetics aged ≥55 years with 1 additional risk factor.5 Despite not preventing the development of nephropathy, ACE inhibitors should be used for most patients with type 2 diabetes for cardiovascular risk reduction.
1. Randomised placebo-controlled trial of lisinopril in normotensive patients with insulin-dependent diabetes and normoalbuminuria or microalbuminuria. The EUCLID Study Group. Lancet 1997;349:1787-1792.
2. Ravid M, Brosh D, Levi Z, Bar-Dayan Y, Ravid D, Rachmani R. Use of enalapril to attenuate decline in renal function in normotensive, normoalbuminuric patients with type 2 diabetes mellitus. A randomized, controlled trial. Ann Intern Med 1998;128:982-988.
3. Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE study and MICRO-HOPE substudy. Heart Outcomes Prevention Evaluation Study Investigators. Lancet 2000;355:253-259.
4. Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. The Heart Outcomes Prevention Evaluation Study Investigators. N Engl J Med 2000;342:145-153.
5. Arauz-Pacheco C, Parrott MA, Raskin P. American Diabetes Association. Treatment of hypertension in adults with diabetes. Diabetes Care 2003;26 Suppl 1:S80-S82.
Angiotensin-converting enzyme (ACE) inhibitors make a significant difference for patients with diabetes as a whole. If patients both with and without microalbuminuria are included together, ACE inhibitors significantly reduce the progression of the albumin excretion rate (strength of recommendation [SOR]: A, based on multiple randomized controlled trials) and the development of overt nephropathy (SOR: A, based on 1 randomized controlled trial).
However, studying diabetes without microalbuminuria separately, the effect of ACE inhibitors on progression to nephropathy does not reach statistical significance. This applies to both type 1 and 2 diabetes (SOR: A, based on randomized controlled trials with heterogenous results). Results are contradictory regarding whether ACE inhibition delays new onset of diabetic microalbuminuria.
Evidence summary
There are 3 prospective randomized controlled trials studying the effect of ACE inhibitors on albumin excretion for patients with diabetes who do not have microalbuminuria. A 2-year randomized controlled trial compared lisinopril (Prinivil; Zestril) 10 mg/d with placebo in 530 normotensive adults (aged 20–59 years) with insulin-dependent diabetes, defined as those diagnosed with diabetes before age 36 and using continuous insulin therapy within 1 year of diagnosis. At the beginning of the study, 90 patients had microalbuminuria—defined as an albumin excretion rate (AER) >29 mg/24 hr—and 440 patients did not. When the results for all patients who had and did not have microalbuminuria were combined, there was a significantly smaller rise in the AER for the lisinopril group vs the placebo group (3.2 mg/24 hr lower; P=.03). However, for the patients without initial microalbuminuria, the reduction in the rise of AER with lisinopril was not significant (1.4 mg/24 hr lower; P=.10). The decreased rate of developing new microalbuminuria was also not significant (relative risk reduction [RRR]=12.7%; P=.10).1
A subsequent trial compared enalapril (Vasotec) 10 mg/d with placebo in 194 normotensive patients (aged 40–60) with type 2 diabetes and without microalbuminuria, defined as AER >30 mg/24 hr. Over the 6-year course of the study, the AER in the placebo group rose from 10.8 mg/24 hr to 26.5 mg/24 hr. The AER of the treatment group dropped from 11.6 mg/24 hr initially to 9.7 mg/24 hr at 2 years, then rose to 15.8 mg/24 hr at 6 years. Enalapril significantly slowed the rise in AER (RRR=0.4; P=.001). Nineteen percent of the placebo group developed microalbuminuria, compared with 6.5% of those taking enalapril (absolute risk reduction[ARR]=12.5%; number needed to treat=8; P=.042). While this study described a modest and statistically significant renal protective effect of enalapril, it did not use an intention-to-treat analysis.2
MICRO-HOPE, a subset of the HOPE trial, studied ramipril (Altace) 10 mg/d vs placebo in 2437 patients with diabetes who did not have clinical proteinuria. Patients were aged 55 years or older and had either a previous cardiovascular event or at least 1 other cardiovascular risk factor. There were 1140 patients with microalbuminuria, defined as an albumin/creatinine ratio 2 mg/mmol, and 2437 patients without. After 4.5 years, 10% of patients had developed overt nephropathy, defined as albumin/creatinine >36 mg/mmol.
When all patients in the study were examined together, ramipril provided significant renal protection over placebo (RRR=24%; ARR=1%; P=.027). It also lowered the risk of MI by 22%, stroke by 33%, and cardiovascular death by 37%. But in a separate analysis of the patients without microalbuminuria, ramipril did not significantly reduce overt nephropathy (P=.50). Ramipril also did not significantly reduce the risk of developing new microalbuminuria in this group (RRR=9%; P=.17). Further, for patients without microalbuminuria, ramipril did not reduce the combined outcomes of myocardial infarction, stroke, or cardiovascular death (odds ratio=0.85; 95% CI, 0.70–1.02).3
Recommendations from others
We could find no guidelines recommending for or against the use of ACE inhibitors for patients with diabetes without microalbuminuria.
ACE inhibitors should still be used in most patients with type 2 diabetes
Joseph Saseen, PharmD, FCCP, BCPS
University of Colorado Health Sciences Center, Denver
ACE inhibitors do not prevent the development of type 2 diabetic nephropathy. In contrast to type 1 diabetes, cardiovascular disease is the primary cause of death in type 2. The HOPE study demonstrated that ACE inhibitor therapy significantly reduces cardiovascular events in type 2 diabetes independent of hypertension status.4 These benefits are so compelling that the American Diabetes Association strongly recommends ACE inhibitor therapy for type 2 diabetics aged ≥55 years with 1 additional risk factor.5 Despite not preventing the development of nephropathy, ACE inhibitors should be used for most patients with type 2 diabetes for cardiovascular risk reduction.
Angiotensin-converting enzyme (ACE) inhibitors make a significant difference for patients with diabetes as a whole. If patients both with and without microalbuminuria are included together, ACE inhibitors significantly reduce the progression of the albumin excretion rate (strength of recommendation [SOR]: A, based on multiple randomized controlled trials) and the development of overt nephropathy (SOR: A, based on 1 randomized controlled trial).
However, studying diabetes without microalbuminuria separately, the effect of ACE inhibitors on progression to nephropathy does not reach statistical significance. This applies to both type 1 and 2 diabetes (SOR: A, based on randomized controlled trials with heterogenous results). Results are contradictory regarding whether ACE inhibition delays new onset of diabetic microalbuminuria.
Evidence summary
There are 3 prospective randomized controlled trials studying the effect of ACE inhibitors on albumin excretion for patients with diabetes who do not have microalbuminuria. A 2-year randomized controlled trial compared lisinopril (Prinivil; Zestril) 10 mg/d with placebo in 530 normotensive adults (aged 20–59 years) with insulin-dependent diabetes, defined as those diagnosed with diabetes before age 36 and using continuous insulin therapy within 1 year of diagnosis. At the beginning of the study, 90 patients had microalbuminuria—defined as an albumin excretion rate (AER) >29 mg/24 hr—and 440 patients did not. When the results for all patients who had and did not have microalbuminuria were combined, there was a significantly smaller rise in the AER for the lisinopril group vs the placebo group (3.2 mg/24 hr lower; P=.03). However, for the patients without initial microalbuminuria, the reduction in the rise of AER with lisinopril was not significant (1.4 mg/24 hr lower; P=.10). The decreased rate of developing new microalbuminuria was also not significant (relative risk reduction [RRR]=12.7%; P=.10).1
A subsequent trial compared enalapril (Vasotec) 10 mg/d with placebo in 194 normotensive patients (aged 40–60) with type 2 diabetes and without microalbuminuria, defined as AER >30 mg/24 hr. Over the 6-year course of the study, the AER in the placebo group rose from 10.8 mg/24 hr to 26.5 mg/24 hr. The AER of the treatment group dropped from 11.6 mg/24 hr initially to 9.7 mg/24 hr at 2 years, then rose to 15.8 mg/24 hr at 6 years. Enalapril significantly slowed the rise in AER (RRR=0.4; P=.001). Nineteen percent of the placebo group developed microalbuminuria, compared with 6.5% of those taking enalapril (absolute risk reduction[ARR]=12.5%; number needed to treat=8; P=.042). While this study described a modest and statistically significant renal protective effect of enalapril, it did not use an intention-to-treat analysis.2
MICRO-HOPE, a subset of the HOPE trial, studied ramipril (Altace) 10 mg/d vs placebo in 2437 patients with diabetes who did not have clinical proteinuria. Patients were aged 55 years or older and had either a previous cardiovascular event or at least 1 other cardiovascular risk factor. There were 1140 patients with microalbuminuria, defined as an albumin/creatinine ratio 2 mg/mmol, and 2437 patients without. After 4.5 years, 10% of patients had developed overt nephropathy, defined as albumin/creatinine >36 mg/mmol.
When all patients in the study were examined together, ramipril provided significant renal protection over placebo (RRR=24%; ARR=1%; P=.027). It also lowered the risk of MI by 22%, stroke by 33%, and cardiovascular death by 37%. But in a separate analysis of the patients without microalbuminuria, ramipril did not significantly reduce overt nephropathy (P=.50). Ramipril also did not significantly reduce the risk of developing new microalbuminuria in this group (RRR=9%; P=.17). Further, for patients without microalbuminuria, ramipril did not reduce the combined outcomes of myocardial infarction, stroke, or cardiovascular death (odds ratio=0.85; 95% CI, 0.70–1.02).3
Recommendations from others
We could find no guidelines recommending for or against the use of ACE inhibitors for patients with diabetes without microalbuminuria.
ACE inhibitors should still be used in most patients with type 2 diabetes
Joseph Saseen, PharmD, FCCP, BCPS
University of Colorado Health Sciences Center, Denver
ACE inhibitors do not prevent the development of type 2 diabetic nephropathy. In contrast to type 1 diabetes, cardiovascular disease is the primary cause of death in type 2. The HOPE study demonstrated that ACE inhibitor therapy significantly reduces cardiovascular events in type 2 diabetes independent of hypertension status.4 These benefits are so compelling that the American Diabetes Association strongly recommends ACE inhibitor therapy for type 2 diabetics aged ≥55 years with 1 additional risk factor.5 Despite not preventing the development of nephropathy, ACE inhibitors should be used for most patients with type 2 diabetes for cardiovascular risk reduction.
1. Randomised placebo-controlled trial of lisinopril in normotensive patients with insulin-dependent diabetes and normoalbuminuria or microalbuminuria. The EUCLID Study Group. Lancet 1997;349:1787-1792.
2. Ravid M, Brosh D, Levi Z, Bar-Dayan Y, Ravid D, Rachmani R. Use of enalapril to attenuate decline in renal function in normotensive, normoalbuminuric patients with type 2 diabetes mellitus. A randomized, controlled trial. Ann Intern Med 1998;128:982-988.
3. Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE study and MICRO-HOPE substudy. Heart Outcomes Prevention Evaluation Study Investigators. Lancet 2000;355:253-259.
4. Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. The Heart Outcomes Prevention Evaluation Study Investigators. N Engl J Med 2000;342:145-153.
5. Arauz-Pacheco C, Parrott MA, Raskin P. American Diabetes Association. Treatment of hypertension in adults with diabetes. Diabetes Care 2003;26 Suppl 1:S80-S82.
1. Randomised placebo-controlled trial of lisinopril in normotensive patients with insulin-dependent diabetes and normoalbuminuria or microalbuminuria. The EUCLID Study Group. Lancet 1997;349:1787-1792.
2. Ravid M, Brosh D, Levi Z, Bar-Dayan Y, Ravid D, Rachmani R. Use of enalapril to attenuate decline in renal function in normotensive, normoalbuminuric patients with type 2 diabetes mellitus. A randomized, controlled trial. Ann Intern Med 1998;128:982-988.
3. Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE study and MICRO-HOPE substudy. Heart Outcomes Prevention Evaluation Study Investigators. Lancet 2000;355:253-259.
4. Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. The Heart Outcomes Prevention Evaluation Study Investigators. N Engl J Med 2000;342:145-153.
5. Arauz-Pacheco C, Parrott MA, Raskin P. American Diabetes Association. Treatment of hypertension in adults with diabetes. Diabetes Care 2003;26 Suppl 1:S80-S82.
Evidence-based answers from the Family Physicians Inquiries Network
Are liver function tests required for patients taking isoniazid for latent TB?
Routine liver function test monitoring is not required for all patients on isoniazid therapy for latent tuberculosis (TB) infection (strength of recommendation: B, based on case series). No clinical trials have studied the potential risks and benefits of routinely monitoring liver function tests for all patients taking isoniazid for latent TB infection. Data from 2 case series suggest that routine liver function test monitoring leads to withdrawal of isoniazid prophylaxis from about 6% of patients because of abnormal lab results.1,2 This is 10 to 60 times the hepatitis rate found in case series using a symptom-based monitoring strategy.3,6 Data are insufficient, however, to conclude that routine liver function test monitoring leads to a lower rate of fatal isoniazid hepatitis compared with a strategy of symptom-based screening. Given that complete recovery from nonfatal hepatitis is the rule, and that patients withdrawn from isoniazid prophylaxis remain at risk for developing active tuberculosis, current evidence does not support routine liver function test monitoring for all patients.
Evidence summary
Several large population-based case series have tried to define the incidence of isoniazid-induced hepatitis and fatal hepatitis. Because these series differed in patient selection, diagnostic criteria for hepatitis, and toxicity monitoring strategies, and because their data span decades, they provide limited insight. Data from 6 large case series1,3-7 and 1 pooled compilation of published and unpublished reports8 are summarized in the Table.
Two studies1,2 that defined hepatitis as asymptomatic liver function test elevation (>5 times normal) on monthly screening found a 6% to 6.4% incidence of hepatitis, a rate 10 to 60 times higher than 4 case series3-6 that relied on symptom-based monitoring. A pooled analysis of more than 200,000 patients receiving isoniazid prophylaxis and monitored according to 1983 American Thoracic Society guidelines reported an intermediate hepatitis rate (1.2%) and only 2 deaths.8 Mortality from isoniazid hepatitis is rare, whichever monitoring strategy is selected. Some deaths attributed to isoniazid prophylaxis may also have had other contributing causes, such as unrecognized hepatitis C; most cases and deaths reported in these large series occurred before testing for hepatitis C became available in 1991.
Symptom-based monitoring strategies require stopping isoniazid promptly if symptoms of hepatotoxicity develop. In a series of 62 fatal cases of probable or possible isoniazid hepatitis, 42% had been monitored at least monthly for symptoms, and 38% stopped isoniazid within 1 week of symptom onset.9 Seven of the 8 patients receiving a liver transplant following the development of fulminant, isoniazid-related hepatitis continued to take the drug for a least 10 days after onset of symptoms of hepatotoxicity.10
Several series report increasing hepatitis risk with advancing age.1,3,5,6 In 1 series,3 rates were 3/1000 in those aged 20 to 34 years, 12/1000 in those aged 35 to 49 years, 23/1000 in those aged 50 to 64 years, and 8/1000 after age 65.
TABLE
INH hepatitis incidence and mortality rates: summary of the largest case series
| Study | Time period | Monitoring strategy | Hepatitis definition | No. of patients | No. of hepatitis cases | No. of fatal cases mortality rate |
|---|---|---|---|---|---|---|
| Byrd1 | ~early/mid 1970s | Monthly symptom and LFT screening | AST >5x normal, with or without symptoms | 1000 | 64 (6.4%) | 0 |
| Salpeter8 | 1983-early 1990s | Presumed to follow 1983 ATS guidelinesa | Not defined | 202,497 | 2,459 (1.2%) | 2 (0.001%) |
| Kopanoff3 | July 1971 to Nov. 1972 | Monthly symptom-based screening | AST ≥250 Karmen units or ALT>AST, and no other cause | 13,838 | 92 (0.66%) | 8 (0.06%) |
| IUATCP4 | mid-1970s | Every-4-week symptom-based screening | Not defined | 20,840 | 95 (0.5%) | 3 (0.014%) |
| Dash4 | Jan. 1973 to June 1977 | Monthly symptom based screening | Jaundice, scleral icterus, or “hepatitis” notation | 5300 | 15 (0.37%)b | 1 (.019%) |
| Nolan6 | Jan. 1989 to 1 December 1995 | Monthly symptom-based screening | AST >5x normal with symptoms, and no other cause | 11,141 | 11 (0.1%) | 0 |
| LoBue7 | July 1999 to Nov. 2002 | Monthly clinical monitoring, routine LFTs for patients >34 before 2000 | LFTs >3x normal with symptoms, or LFTs >5x normal without symptoms | 3,788 | 10 (0.3%) | 0 |
| a Withhold treatment in presence of active liver disease, limit prophylaxis of patients aged >35 to those at highest risk of developing active disease, baseline and periodic LFTs for those over 35, discontinue isoniazid if transaminases exceed 3 to 5 times normal. | ||||||
| b Calculation based on life-table analysis, because of high dropout rate during treatment LFT, liver function test; AST, aspartate transaminase; ALT, alanine transaminase; IUSTCP, International Union Against Tuberculosis Committee on Prophylaxis | ||||||
Recommendations From Others
The Centers for Disease Control and Prevention (CDC) and the American Thoracic Society joint guidelines for the treatment of latent TB infection state that baseline laboratory testing is not routinely indicated, even for persons aged >35 years, but may be considered for patients who are taking other hepatotoxic medications or have chronic medical conditions.11
Baseline measurements of bilirubin and aspartate transaminase (AST) or alanine transaminase (ALT) along with monthly liver function test monitoring are recommended for patients with pre-existing liver disease, patients at risk for chronic liver disease, patients with HIV infection, pregnant or postpartum women, and regular users of alcohol. All patients should be evaluated at least monthly for symptoms of hepatitis, and liver function tests should also be obtained for patients with symptoms compatible with hepatotoxicity. The guideline suggests that isoniazid be stopped if liver function tests exceed 5 times the upper limits of normal, or 3 times the upper limits of normal if the patient is symptomatic. The Canadian Tuberculosis Standards (5th ed, 2000) recommend baseline AST before isoniazid preventive therapy is started, and regular monitoring in those with pre-existing liver disease, a history of ethanol abuse, or age ≥35 years.12
Patients need to understand risks and benefits of TB treatment
Lauren DeAlleaume, MD
University of Colorado Health Sciences Center, Denver
As the number of immigrants increases, FPs will see more patients at high risk for TB. Patients whose risk of developing active TB exceeds the risk of isoniazid toxicity should be tested (targeted testing). It is challenging to ensure an asymptomatic patient completes a 9-month course of therapy while undergoing monthly monitoring for symptoms of isoniazid toxicity. Overall, only 60% of patients complete a full course of isoniazid. Clinical and public health systems that make it easier for patients to follow-up can enhance compliance.
Patients need to understand the benefits of treatment and the symptoms of isoniazid toxicity. The CDC recommends clinical monitoring without routine blood testing for patients of any age without additional risk factors for isoniazid hepatitis. Excessive monitoring can lead to premature discontinuation of therapy because 10%–20% of patients develop some liver function test elevation. The CDC has an excellent course on the basics of latent TB testing and treatment ( at www.phppo.cdc.gov/phtn/tbmodules/Default.htm). Patient education materials and risk assessment and monitoring forms can be obtained from state health departments.
1. Byrd RB, Horn BR, Solomon DA, Griggs GA. Toxic effects of isoniazid in tuberculosis chemoprophylaxis. Role of biochemical monitoring in 1,000 patients. JAMA 1979;241:1239-1241.
2. Stuart RL, Wilson J, Grayson ML. Isoniazid toxicity in health care workers. Clin Infect Dis 1999;28:895-897.
3. Kopanoff DE, Snider DE, Jr, Caras GJ. Isoniazid-related hepatitis: a U.S. Public Health Service cooperative surveillance study. Am Rev Respir Dis 1978;117:991-1001.
4. Efficacy of various durations of isoniazid preventive therapy for tuberculosis: five years of follow-up in the IUAT trial. International Union Against Tuberculosis Committee on Prophylaxis. Bull World Health Organ 1982;60:555-564.
5. Dash LA, Comstock GW, Flynn JP. Isoniazid preventive therapy: retrospect and prospect. Am Rev Respir Dis 1980;121:1039-1044.
6. Dash CM, Goldberg SV, Buskin SE. Hepatotoxicity associated with isoniazid preventive therapy; a 7-year survey from a public health tuberculosis clinic. JAMA 1999;281:1014-1018.
7. LoBue PA, Moser KS. Use of isoniazid for latent tuberculosis infection in a public health clinic. Am J Respir Crit Care Med 2003;168:443-447.
8. Salpeter SR. Fatal isoniazid-induced hepatitis. Its risk during chemoprophylaxis. West J Med 1993;159:560-564.
9. Millard PS, Wilcosky TC, Reade-Christopher SJ, Weber DJ. Isoniazid-related fatal hepatitis. West J Med 1996;164:486-491.
10. Centers for Disease Control and Prevention. Severe isoniazid-associated hepatitis—New York, 1991–1993. MMWR Morb Mortal Wkly Rep 42:545-547.
11. Targeted tuberculin testing and treatment of latent tuberculosis infection. American Thoracic Society. MMWR Recomm Rep 2000;49(RR-6):1-51.
12. Canadian Tuberculosis Standards 2000. 5th ed. Available at: www.lung.ca/tb/TBStandards_Eng.pdf. Accessed on November 28, 2003.
Routine liver function test monitoring is not required for all patients on isoniazid therapy for latent tuberculosis (TB) infection (strength of recommendation: B, based on case series). No clinical trials have studied the potential risks and benefits of routinely monitoring liver function tests for all patients taking isoniazid for latent TB infection. Data from 2 case series suggest that routine liver function test monitoring leads to withdrawal of isoniazid prophylaxis from about 6% of patients because of abnormal lab results.1,2 This is 10 to 60 times the hepatitis rate found in case series using a symptom-based monitoring strategy.3,6 Data are insufficient, however, to conclude that routine liver function test monitoring leads to a lower rate of fatal isoniazid hepatitis compared with a strategy of symptom-based screening. Given that complete recovery from nonfatal hepatitis is the rule, and that patients withdrawn from isoniazid prophylaxis remain at risk for developing active tuberculosis, current evidence does not support routine liver function test monitoring for all patients.
Evidence summary
Several large population-based case series have tried to define the incidence of isoniazid-induced hepatitis and fatal hepatitis. Because these series differed in patient selection, diagnostic criteria for hepatitis, and toxicity monitoring strategies, and because their data span decades, they provide limited insight. Data from 6 large case series1,3-7 and 1 pooled compilation of published and unpublished reports8 are summarized in the Table.
Two studies1,2 that defined hepatitis as asymptomatic liver function test elevation (>5 times normal) on monthly screening found a 6% to 6.4% incidence of hepatitis, a rate 10 to 60 times higher than 4 case series3-6 that relied on symptom-based monitoring. A pooled analysis of more than 200,000 patients receiving isoniazid prophylaxis and monitored according to 1983 American Thoracic Society guidelines reported an intermediate hepatitis rate (1.2%) and only 2 deaths.8 Mortality from isoniazid hepatitis is rare, whichever monitoring strategy is selected. Some deaths attributed to isoniazid prophylaxis may also have had other contributing causes, such as unrecognized hepatitis C; most cases and deaths reported in these large series occurred before testing for hepatitis C became available in 1991.
Symptom-based monitoring strategies require stopping isoniazid promptly if symptoms of hepatotoxicity develop. In a series of 62 fatal cases of probable or possible isoniazid hepatitis, 42% had been monitored at least monthly for symptoms, and 38% stopped isoniazid within 1 week of symptom onset.9 Seven of the 8 patients receiving a liver transplant following the development of fulminant, isoniazid-related hepatitis continued to take the drug for a least 10 days after onset of symptoms of hepatotoxicity.10
Several series report increasing hepatitis risk with advancing age.1,3,5,6 In 1 series,3 rates were 3/1000 in those aged 20 to 34 years, 12/1000 in those aged 35 to 49 years, 23/1000 in those aged 50 to 64 years, and 8/1000 after age 65.
TABLE
INH hepatitis incidence and mortality rates: summary of the largest case series
| Study | Time period | Monitoring strategy | Hepatitis definition | No. of patients | No. of hepatitis cases | No. of fatal cases mortality rate |
|---|---|---|---|---|---|---|
| Byrd1 | ~early/mid 1970s | Monthly symptom and LFT screening | AST >5x normal, with or without symptoms | 1000 | 64 (6.4%) | 0 |
| Salpeter8 | 1983-early 1990s | Presumed to follow 1983 ATS guidelinesa | Not defined | 202,497 | 2,459 (1.2%) | 2 (0.001%) |
| Kopanoff3 | July 1971 to Nov. 1972 | Monthly symptom-based screening | AST ≥250 Karmen units or ALT>AST, and no other cause | 13,838 | 92 (0.66%) | 8 (0.06%) |
| IUATCP4 | mid-1970s | Every-4-week symptom-based screening | Not defined | 20,840 | 95 (0.5%) | 3 (0.014%) |
| Dash4 | Jan. 1973 to June 1977 | Monthly symptom based screening | Jaundice, scleral icterus, or “hepatitis” notation | 5300 | 15 (0.37%)b | 1 (.019%) |
| Nolan6 | Jan. 1989 to 1 December 1995 | Monthly symptom-based screening | AST >5x normal with symptoms, and no other cause | 11,141 | 11 (0.1%) | 0 |
| LoBue7 | July 1999 to Nov. 2002 | Monthly clinical monitoring, routine LFTs for patients >34 before 2000 | LFTs >3x normal with symptoms, or LFTs >5x normal without symptoms | 3,788 | 10 (0.3%) | 0 |
| a Withhold treatment in presence of active liver disease, limit prophylaxis of patients aged >35 to those at highest risk of developing active disease, baseline and periodic LFTs for those over 35, discontinue isoniazid if transaminases exceed 3 to 5 times normal. | ||||||
| b Calculation based on life-table analysis, because of high dropout rate during treatment LFT, liver function test; AST, aspartate transaminase; ALT, alanine transaminase; IUSTCP, International Union Against Tuberculosis Committee on Prophylaxis | ||||||
Recommendations From Others
The Centers for Disease Control and Prevention (CDC) and the American Thoracic Society joint guidelines for the treatment of latent TB infection state that baseline laboratory testing is not routinely indicated, even for persons aged >35 years, but may be considered for patients who are taking other hepatotoxic medications or have chronic medical conditions.11
Baseline measurements of bilirubin and aspartate transaminase (AST) or alanine transaminase (ALT) along with monthly liver function test monitoring are recommended for patients with pre-existing liver disease, patients at risk for chronic liver disease, patients with HIV infection, pregnant or postpartum women, and regular users of alcohol. All patients should be evaluated at least monthly for symptoms of hepatitis, and liver function tests should also be obtained for patients with symptoms compatible with hepatotoxicity. The guideline suggests that isoniazid be stopped if liver function tests exceed 5 times the upper limits of normal, or 3 times the upper limits of normal if the patient is symptomatic. The Canadian Tuberculosis Standards (5th ed, 2000) recommend baseline AST before isoniazid preventive therapy is started, and regular monitoring in those with pre-existing liver disease, a history of ethanol abuse, or age ≥35 years.12
Patients need to understand risks and benefits of TB treatment
Lauren DeAlleaume, MD
University of Colorado Health Sciences Center, Denver
As the number of immigrants increases, FPs will see more patients at high risk for TB. Patients whose risk of developing active TB exceeds the risk of isoniazid toxicity should be tested (targeted testing). It is challenging to ensure an asymptomatic patient completes a 9-month course of therapy while undergoing monthly monitoring for symptoms of isoniazid toxicity. Overall, only 60% of patients complete a full course of isoniazid. Clinical and public health systems that make it easier for patients to follow-up can enhance compliance.
Patients need to understand the benefits of treatment and the symptoms of isoniazid toxicity. The CDC recommends clinical monitoring without routine blood testing for patients of any age without additional risk factors for isoniazid hepatitis. Excessive monitoring can lead to premature discontinuation of therapy because 10%–20% of patients develop some liver function test elevation. The CDC has an excellent course on the basics of latent TB testing and treatment ( at www.phppo.cdc.gov/phtn/tbmodules/Default.htm). Patient education materials and risk assessment and monitoring forms can be obtained from state health departments.
Routine liver function test monitoring is not required for all patients on isoniazid therapy for latent tuberculosis (TB) infection (strength of recommendation: B, based on case series). No clinical trials have studied the potential risks and benefits of routinely monitoring liver function tests for all patients taking isoniazid for latent TB infection. Data from 2 case series suggest that routine liver function test monitoring leads to withdrawal of isoniazid prophylaxis from about 6% of patients because of abnormal lab results.1,2 This is 10 to 60 times the hepatitis rate found in case series using a symptom-based monitoring strategy.3,6 Data are insufficient, however, to conclude that routine liver function test monitoring leads to a lower rate of fatal isoniazid hepatitis compared with a strategy of symptom-based screening. Given that complete recovery from nonfatal hepatitis is the rule, and that patients withdrawn from isoniazid prophylaxis remain at risk for developing active tuberculosis, current evidence does not support routine liver function test monitoring for all patients.
Evidence summary
Several large population-based case series have tried to define the incidence of isoniazid-induced hepatitis and fatal hepatitis. Because these series differed in patient selection, diagnostic criteria for hepatitis, and toxicity monitoring strategies, and because their data span decades, they provide limited insight. Data from 6 large case series1,3-7 and 1 pooled compilation of published and unpublished reports8 are summarized in the Table.
Two studies1,2 that defined hepatitis as asymptomatic liver function test elevation (>5 times normal) on monthly screening found a 6% to 6.4% incidence of hepatitis, a rate 10 to 60 times higher than 4 case series3-6 that relied on symptom-based monitoring. A pooled analysis of more than 200,000 patients receiving isoniazid prophylaxis and monitored according to 1983 American Thoracic Society guidelines reported an intermediate hepatitis rate (1.2%) and only 2 deaths.8 Mortality from isoniazid hepatitis is rare, whichever monitoring strategy is selected. Some deaths attributed to isoniazid prophylaxis may also have had other contributing causes, such as unrecognized hepatitis C; most cases and deaths reported in these large series occurred before testing for hepatitis C became available in 1991.
Symptom-based monitoring strategies require stopping isoniazid promptly if symptoms of hepatotoxicity develop. In a series of 62 fatal cases of probable or possible isoniazid hepatitis, 42% had been monitored at least monthly for symptoms, and 38% stopped isoniazid within 1 week of symptom onset.9 Seven of the 8 patients receiving a liver transplant following the development of fulminant, isoniazid-related hepatitis continued to take the drug for a least 10 days after onset of symptoms of hepatotoxicity.10
Several series report increasing hepatitis risk with advancing age.1,3,5,6 In 1 series,3 rates were 3/1000 in those aged 20 to 34 years, 12/1000 in those aged 35 to 49 years, 23/1000 in those aged 50 to 64 years, and 8/1000 after age 65.
TABLE
INH hepatitis incidence and mortality rates: summary of the largest case series
| Study | Time period | Monitoring strategy | Hepatitis definition | No. of patients | No. of hepatitis cases | No. of fatal cases mortality rate |
|---|---|---|---|---|---|---|
| Byrd1 | ~early/mid 1970s | Monthly symptom and LFT screening | AST >5x normal, with or without symptoms | 1000 | 64 (6.4%) | 0 |
| Salpeter8 | 1983-early 1990s | Presumed to follow 1983 ATS guidelinesa | Not defined | 202,497 | 2,459 (1.2%) | 2 (0.001%) |
| Kopanoff3 | July 1971 to Nov. 1972 | Monthly symptom-based screening | AST ≥250 Karmen units or ALT>AST, and no other cause | 13,838 | 92 (0.66%) | 8 (0.06%) |
| IUATCP4 | mid-1970s | Every-4-week symptom-based screening | Not defined | 20,840 | 95 (0.5%) | 3 (0.014%) |
| Dash4 | Jan. 1973 to June 1977 | Monthly symptom based screening | Jaundice, scleral icterus, or “hepatitis” notation | 5300 | 15 (0.37%)b | 1 (.019%) |
| Nolan6 | Jan. 1989 to 1 December 1995 | Monthly symptom-based screening | AST >5x normal with symptoms, and no other cause | 11,141 | 11 (0.1%) | 0 |
| LoBue7 | July 1999 to Nov. 2002 | Monthly clinical monitoring, routine LFTs for patients >34 before 2000 | LFTs >3x normal with symptoms, or LFTs >5x normal without symptoms | 3,788 | 10 (0.3%) | 0 |
| a Withhold treatment in presence of active liver disease, limit prophylaxis of patients aged >35 to those at highest risk of developing active disease, baseline and periodic LFTs for those over 35, discontinue isoniazid if transaminases exceed 3 to 5 times normal. | ||||||
| b Calculation based on life-table analysis, because of high dropout rate during treatment LFT, liver function test; AST, aspartate transaminase; ALT, alanine transaminase; IUSTCP, International Union Against Tuberculosis Committee on Prophylaxis | ||||||
Recommendations From Others
The Centers for Disease Control and Prevention (CDC) and the American Thoracic Society joint guidelines for the treatment of latent TB infection state that baseline laboratory testing is not routinely indicated, even for persons aged >35 years, but may be considered for patients who are taking other hepatotoxic medications or have chronic medical conditions.11
Baseline measurements of bilirubin and aspartate transaminase (AST) or alanine transaminase (ALT) along with monthly liver function test monitoring are recommended for patients with pre-existing liver disease, patients at risk for chronic liver disease, patients with HIV infection, pregnant or postpartum women, and regular users of alcohol. All patients should be evaluated at least monthly for symptoms of hepatitis, and liver function tests should also be obtained for patients with symptoms compatible with hepatotoxicity. The guideline suggests that isoniazid be stopped if liver function tests exceed 5 times the upper limits of normal, or 3 times the upper limits of normal if the patient is symptomatic. The Canadian Tuberculosis Standards (5th ed, 2000) recommend baseline AST before isoniazid preventive therapy is started, and regular monitoring in those with pre-existing liver disease, a history of ethanol abuse, or age ≥35 years.12
Patients need to understand risks and benefits of TB treatment
Lauren DeAlleaume, MD
University of Colorado Health Sciences Center, Denver
As the number of immigrants increases, FPs will see more patients at high risk for TB. Patients whose risk of developing active TB exceeds the risk of isoniazid toxicity should be tested (targeted testing). It is challenging to ensure an asymptomatic patient completes a 9-month course of therapy while undergoing monthly monitoring for symptoms of isoniazid toxicity. Overall, only 60% of patients complete a full course of isoniazid. Clinical and public health systems that make it easier for patients to follow-up can enhance compliance.
Patients need to understand the benefits of treatment and the symptoms of isoniazid toxicity. The CDC recommends clinical monitoring without routine blood testing for patients of any age without additional risk factors for isoniazid hepatitis. Excessive monitoring can lead to premature discontinuation of therapy because 10%–20% of patients develop some liver function test elevation. The CDC has an excellent course on the basics of latent TB testing and treatment ( at www.phppo.cdc.gov/phtn/tbmodules/Default.htm). Patient education materials and risk assessment and monitoring forms can be obtained from state health departments.
1. Byrd RB, Horn BR, Solomon DA, Griggs GA. Toxic effects of isoniazid in tuberculosis chemoprophylaxis. Role of biochemical monitoring in 1,000 patients. JAMA 1979;241:1239-1241.
2. Stuart RL, Wilson J, Grayson ML. Isoniazid toxicity in health care workers. Clin Infect Dis 1999;28:895-897.
3. Kopanoff DE, Snider DE, Jr, Caras GJ. Isoniazid-related hepatitis: a U.S. Public Health Service cooperative surveillance study. Am Rev Respir Dis 1978;117:991-1001.
4. Efficacy of various durations of isoniazid preventive therapy for tuberculosis: five years of follow-up in the IUAT trial. International Union Against Tuberculosis Committee on Prophylaxis. Bull World Health Organ 1982;60:555-564.
5. Dash LA, Comstock GW, Flynn JP. Isoniazid preventive therapy: retrospect and prospect. Am Rev Respir Dis 1980;121:1039-1044.
6. Dash CM, Goldberg SV, Buskin SE. Hepatotoxicity associated with isoniazid preventive therapy; a 7-year survey from a public health tuberculosis clinic. JAMA 1999;281:1014-1018.
7. LoBue PA, Moser KS. Use of isoniazid for latent tuberculosis infection in a public health clinic. Am J Respir Crit Care Med 2003;168:443-447.
8. Salpeter SR. Fatal isoniazid-induced hepatitis. Its risk during chemoprophylaxis. West J Med 1993;159:560-564.
9. Millard PS, Wilcosky TC, Reade-Christopher SJ, Weber DJ. Isoniazid-related fatal hepatitis. West J Med 1996;164:486-491.
10. Centers for Disease Control and Prevention. Severe isoniazid-associated hepatitis—New York, 1991–1993. MMWR Morb Mortal Wkly Rep 42:545-547.
11. Targeted tuberculin testing and treatment of latent tuberculosis infection. American Thoracic Society. MMWR Recomm Rep 2000;49(RR-6):1-51.
12. Canadian Tuberculosis Standards 2000. 5th ed. Available at: www.lung.ca/tb/TBStandards_Eng.pdf. Accessed on November 28, 2003.
1. Byrd RB, Horn BR, Solomon DA, Griggs GA. Toxic effects of isoniazid in tuberculosis chemoprophylaxis. Role of biochemical monitoring in 1,000 patients. JAMA 1979;241:1239-1241.
2. Stuart RL, Wilson J, Grayson ML. Isoniazid toxicity in health care workers. Clin Infect Dis 1999;28:895-897.
3. Kopanoff DE, Snider DE, Jr, Caras GJ. Isoniazid-related hepatitis: a U.S. Public Health Service cooperative surveillance study. Am Rev Respir Dis 1978;117:991-1001.
4. Efficacy of various durations of isoniazid preventive therapy for tuberculosis: five years of follow-up in the IUAT trial. International Union Against Tuberculosis Committee on Prophylaxis. Bull World Health Organ 1982;60:555-564.
5. Dash LA, Comstock GW, Flynn JP. Isoniazid preventive therapy: retrospect and prospect. Am Rev Respir Dis 1980;121:1039-1044.
6. Dash CM, Goldberg SV, Buskin SE. Hepatotoxicity associated with isoniazid preventive therapy; a 7-year survey from a public health tuberculosis clinic. JAMA 1999;281:1014-1018.
7. LoBue PA, Moser KS. Use of isoniazid for latent tuberculosis infection in a public health clinic. Am J Respir Crit Care Med 2003;168:443-447.
8. Salpeter SR. Fatal isoniazid-induced hepatitis. Its risk during chemoprophylaxis. West J Med 1993;159:560-564.
9. Millard PS, Wilcosky TC, Reade-Christopher SJ, Weber DJ. Isoniazid-related fatal hepatitis. West J Med 1996;164:486-491.
10. Centers for Disease Control and Prevention. Severe isoniazid-associated hepatitis—New York, 1991–1993. MMWR Morb Mortal Wkly Rep 42:545-547.
11. Targeted tuberculin testing and treatment of latent tuberculosis infection. American Thoracic Society. MMWR Recomm Rep 2000;49(RR-6):1-51.
12. Canadian Tuberculosis Standards 2000. 5th ed. Available at: www.lung.ca/tb/TBStandards_Eng.pdf. Accessed on November 28, 2003.
Evidence-based answers from the Family Physicians Inquiries Network
Is folate supplementation indicated for patients with CAD?
There is insufficient evidence to advocate the routine use of folate supplementation for the treatment of coronary artery disease (CAD). High levels of serum homocysteine have been associated in several studies with an increased risk for CAD (strength of recommendation [SOR]: B, associated in case-control studies). Folate supplementation decreases the level of serum homocysteine (SOR: A, meta-analysis of randomized controlled trials). This indirect evidence suggests that folate supplementation may be of benefit in slowing the progress of arteriosclerosis.
Two randomized controlled trials measuring the clinical benefits of folate supplementation for patients with CAD have been completed, with differing results. One study showed no benefit of 0.5 mg/d of folate for patients with stable CAD already on statin therapy. The other study found that patients given 1 mg/d of folate with vitamins B6 and B12 had a decreased restenosis rate after percutaneous coronary intervention (PCI) (SOR: B, conflicting randomized controlled trials).
It is possible that larger doses of folate are needed to be of clinical benefit, or that the addition of vitamins B6 and B12 are needed for synergy. Several randomized control trials are underway to further assess folate’s affect on CAD.
Evidence summary
Hyperhomocysteinemia is defined as a fasting plasma homocysteine level 15 μmol/L, although levels >10 μmol/L appear to have detrimental effects on risk profiles for CAD and arteriosclerosis.1 In 22 of 27 retrospective case-control studies, patients with CAD had significantly higher plasma homocysteine levels than control subjects (odds ratio [OR]=1.2–10.9, after adjustment for other CAD risk factors).2,3 However, only 4 of 7 prospective nested case-control trials showed a correlation between elevated homocysteine and myocardial infarction (MI) and coronary death.2
A meta-analysis of 12 randomized controlled trials found that folate supplementation, with vitamin B6 and B12, reduces plasma homocysteine levels.4 However, the long-term clinical cons quences of these interventions are unknown. At doses of 1 gm/d folate has no known side-effects.5
Two randomized, placebo-controlled trials of folate reporting clinical endpoints have been completed. One study analyzed folate supplementation in a patient population with known, stable CAD and found no difference in clinical endpoints at 24 months.6 In this study, 593 patients were randomized to receive either 0.5 mg/d of folic acid or placebo. The primary study endpoint was a composite of events including: overall mortality, sudden death, MI, stroke, and major vascular surgery. The study was powered to detect a 50% reduction in clinical events based on existing observational data in populations with CAD. An event rate of 15% for the 2-year interval was assumed.6 All patients in this study were on statin therapy prior to initiation of folate supplementation.
The second study analyzed folate supplementation in 553 post-PCI patients. Patients were treated with 1 mg of folate plus 10 mg of vitamin B6 and 400 μg of vitamin B12 for 6 months after the PCI. After a mean follow-up of 11 months, the rate of restenosis requiring revascularization was lower in the vitamin-treated study arm (9.9% vs 16% restenosis rate; relative risk [RR]=0.62; 95% confidence interval [CI], 0.40–0.97; number needed to treat=16).7 There was also a nonsignificant trend toward fewer deaths and MIs in the treated arm at both 6 and 12 months after intervention (death: 1.5% vs 2.8%; RR=0.54; 95% CI, 0.016–1.7; MI: 2.6% vs 4.3%; RR=0.60; 95% CI, 0.24–1.51). Statin use was similar in both control (71%) and treatment groups (69%).
Recommendations from others
The American Heart Association and American College of Cardiology do not recommend the routine use of high-dose folic acid or B-vitamin supplements for the primary or secondary prevention of cardiovascular events. The AHA recommendation is to meet recommended daily allowances of folate (400 μg), B12 (2.4 μg), and B6 (1.7 mg) primarily through a balanced diet, with use of supplements if diet alone does not meet the above requirements.8 Since 1998, wheat flour has been supplemented with folate, adding an estimated 100 μg/day to the average American diet.8
The Canadian Task Force on Preventive Health Care (CTFPHC) finds insufficient evidence to advocate screening for hyperhomocysteinemia and rely on expert opinion to advocate treatment in select, high-risk populations.2 Currently, the CTFPHC advocates meeting the recommended daily allowance of folate, B12, and B6.2
Folate for CAD an unanswered question
James M. Gill, MD, MPH
Christianacare Health System, Wilmington, Del
Folate seems like a simple, inexpensive, and relatively benign way to improve care. It is no wonder that many physicians have been recommending folate to their patients with CAD for years. However, as responsible physicians, we need more comprehensive evidence on the benefit of folate before making such universal recommendations.
Several points are important: first, most of the evidence on folate is from observational studies. Only 1 interventional study has shown benefit for patients with CAD, and this study used folate in combination with vitamins B6 and B12. Therefore, if physicians are going to recommend folate supplementation to their patients with CAD, they should recommend this combination rather than folate alone. Also, since this study only included patients who are post-PTCA, it may not apply to all patients with CAD. In short, there is still a fair amount of uncertainty in the answer to this clinical question. We should discuss this uncertainty with our patients, and come to a mutual decision based on preferences.
1. Ford ES, Smith SJ, Stroup DF, Steinberg KK, Mueller PW, Thacker SB. Homocyst(e)ine and cardiovascular disease: a systematic review of the evidence with special emphasis on case-control studies and nested case-control studies. Int J Epidemiol 2002;31:59-70.
2. Booth GL, Wang EE. Preventive health care, 2000 update: screening and management of hyperhomocysteinemia for the prevention of coronary artery disease events. The Canadian Task Force on Preventive Health Care. CMAJ 2000;163:21-29.
3. Bandolier Library. Homocysteine and heart disease: an update. Available at: http://www.jr2.ox.ac.uk/bandolier/booth/cardiac/homheart.html. Accessed on May 29, 2003.
4. Lowering blood homocysteine with folic acid based supplements: meta-analysis of randomised trials. Homocysteine Lowering Trialists’ Collaboration. BMJ 1998;316:894-898.
5. Fairfield KM, Fletcher RH. Vitamins for chronic disease prevention in adults: scientific review. JAMA 2002;287:3116-3126.
6. Liem A, Reynierse-Buitenwerf GH, Zwinderman AH, Jukema JW, van Veldhuisen DJ. Secondary prevention with folic acid: Effects on clinical outcomes. J Am Coll Cardiol 2003;41:2105-2113.
7. Schnyder G, Roffi M, Flammer Y, Pin R, Hess OM. Effect of homocysteine-lowering therapy with folic acid, vitamin B12, and vitamin B6 on clinical outcome after percutaneous coronary intervention: the Swiss Heart study: a randomized controlled trial. JAMA 2002;288:973-979.
8. American Heart Association. AHA Science Advisory: Homocyst(e)ine, Diet, and Cardiovascular Diseases. Available at: http://www.americanheart.org. Accessed on May 29, 2003.
There is insufficient evidence to advocate the routine use of folate supplementation for the treatment of coronary artery disease (CAD). High levels of serum homocysteine have been associated in several studies with an increased risk for CAD (strength of recommendation [SOR]: B, associated in case-control studies). Folate supplementation decreases the level of serum homocysteine (SOR: A, meta-analysis of randomized controlled trials). This indirect evidence suggests that folate supplementation may be of benefit in slowing the progress of arteriosclerosis.
Two randomized controlled trials measuring the clinical benefits of folate supplementation for patients with CAD have been completed, with differing results. One study showed no benefit of 0.5 mg/d of folate for patients with stable CAD already on statin therapy. The other study found that patients given 1 mg/d of folate with vitamins B6 and B12 had a decreased restenosis rate after percutaneous coronary intervention (PCI) (SOR: B, conflicting randomized controlled trials).
It is possible that larger doses of folate are needed to be of clinical benefit, or that the addition of vitamins B6 and B12 are needed for synergy. Several randomized control trials are underway to further assess folate’s affect on CAD.
Evidence summary
Hyperhomocysteinemia is defined as a fasting plasma homocysteine level 15 μmol/L, although levels >10 μmol/L appear to have detrimental effects on risk profiles for CAD and arteriosclerosis.1 In 22 of 27 retrospective case-control studies, patients with CAD had significantly higher plasma homocysteine levels than control subjects (odds ratio [OR]=1.2–10.9, after adjustment for other CAD risk factors).2,3 However, only 4 of 7 prospective nested case-control trials showed a correlation between elevated homocysteine and myocardial infarction (MI) and coronary death.2
A meta-analysis of 12 randomized controlled trials found that folate supplementation, with vitamin B6 and B12, reduces plasma homocysteine levels.4 However, the long-term clinical cons quences of these interventions are unknown. At doses of 1 gm/d folate has no known side-effects.5
Two randomized, placebo-controlled trials of folate reporting clinical endpoints have been completed. One study analyzed folate supplementation in a patient population with known, stable CAD and found no difference in clinical endpoints at 24 months.6 In this study, 593 patients were randomized to receive either 0.5 mg/d of folic acid or placebo. The primary study endpoint was a composite of events including: overall mortality, sudden death, MI, stroke, and major vascular surgery. The study was powered to detect a 50% reduction in clinical events based on existing observational data in populations with CAD. An event rate of 15% for the 2-year interval was assumed.6 All patients in this study were on statin therapy prior to initiation of folate supplementation.
The second study analyzed folate supplementation in 553 post-PCI patients. Patients were treated with 1 mg of folate plus 10 mg of vitamin B6 and 400 μg of vitamin B12 for 6 months after the PCI. After a mean follow-up of 11 months, the rate of restenosis requiring revascularization was lower in the vitamin-treated study arm (9.9% vs 16% restenosis rate; relative risk [RR]=0.62; 95% confidence interval [CI], 0.40–0.97; number needed to treat=16).7 There was also a nonsignificant trend toward fewer deaths and MIs in the treated arm at both 6 and 12 months after intervention (death: 1.5% vs 2.8%; RR=0.54; 95% CI, 0.016–1.7; MI: 2.6% vs 4.3%; RR=0.60; 95% CI, 0.24–1.51). Statin use was similar in both control (71%) and treatment groups (69%).
Recommendations from others
The American Heart Association and American College of Cardiology do not recommend the routine use of high-dose folic acid or B-vitamin supplements for the primary or secondary prevention of cardiovascular events. The AHA recommendation is to meet recommended daily allowances of folate (400 μg), B12 (2.4 μg), and B6 (1.7 mg) primarily through a balanced diet, with use of supplements if diet alone does not meet the above requirements.8 Since 1998, wheat flour has been supplemented with folate, adding an estimated 100 μg/day to the average American diet.8
The Canadian Task Force on Preventive Health Care (CTFPHC) finds insufficient evidence to advocate screening for hyperhomocysteinemia and rely on expert opinion to advocate treatment in select, high-risk populations.2 Currently, the CTFPHC advocates meeting the recommended daily allowance of folate, B12, and B6.2
Folate for CAD an unanswered question
James M. Gill, MD, MPH
Christianacare Health System, Wilmington, Del
Folate seems like a simple, inexpensive, and relatively benign way to improve care. It is no wonder that many physicians have been recommending folate to their patients with CAD for years. However, as responsible physicians, we need more comprehensive evidence on the benefit of folate before making such universal recommendations.
Several points are important: first, most of the evidence on folate is from observational studies. Only 1 interventional study has shown benefit for patients with CAD, and this study used folate in combination with vitamins B6 and B12. Therefore, if physicians are going to recommend folate supplementation to their patients with CAD, they should recommend this combination rather than folate alone. Also, since this study only included patients who are post-PTCA, it may not apply to all patients with CAD. In short, there is still a fair amount of uncertainty in the answer to this clinical question. We should discuss this uncertainty with our patients, and come to a mutual decision based on preferences.
There is insufficient evidence to advocate the routine use of folate supplementation for the treatment of coronary artery disease (CAD). High levels of serum homocysteine have been associated in several studies with an increased risk for CAD (strength of recommendation [SOR]: B, associated in case-control studies). Folate supplementation decreases the level of serum homocysteine (SOR: A, meta-analysis of randomized controlled trials). This indirect evidence suggests that folate supplementation may be of benefit in slowing the progress of arteriosclerosis.
Two randomized controlled trials measuring the clinical benefits of folate supplementation for patients with CAD have been completed, with differing results. One study showed no benefit of 0.5 mg/d of folate for patients with stable CAD already on statin therapy. The other study found that patients given 1 mg/d of folate with vitamins B6 and B12 had a decreased restenosis rate after percutaneous coronary intervention (PCI) (SOR: B, conflicting randomized controlled trials).
It is possible that larger doses of folate are needed to be of clinical benefit, or that the addition of vitamins B6 and B12 are needed for synergy. Several randomized control trials are underway to further assess folate’s affect on CAD.
Evidence summary
Hyperhomocysteinemia is defined as a fasting plasma homocysteine level 15 μmol/L, although levels >10 μmol/L appear to have detrimental effects on risk profiles for CAD and arteriosclerosis.1 In 22 of 27 retrospective case-control studies, patients with CAD had significantly higher plasma homocysteine levels than control subjects (odds ratio [OR]=1.2–10.9, after adjustment for other CAD risk factors).2,3 However, only 4 of 7 prospective nested case-control trials showed a correlation between elevated homocysteine and myocardial infarction (MI) and coronary death.2
A meta-analysis of 12 randomized controlled trials found that folate supplementation, with vitamin B6 and B12, reduces plasma homocysteine levels.4 However, the long-term clinical cons quences of these interventions are unknown. At doses of 1 gm/d folate has no known side-effects.5
Two randomized, placebo-controlled trials of folate reporting clinical endpoints have been completed. One study analyzed folate supplementation in a patient population with known, stable CAD and found no difference in clinical endpoints at 24 months.6 In this study, 593 patients were randomized to receive either 0.5 mg/d of folic acid or placebo. The primary study endpoint was a composite of events including: overall mortality, sudden death, MI, stroke, and major vascular surgery. The study was powered to detect a 50% reduction in clinical events based on existing observational data in populations with CAD. An event rate of 15% for the 2-year interval was assumed.6 All patients in this study were on statin therapy prior to initiation of folate supplementation.
The second study analyzed folate supplementation in 553 post-PCI patients. Patients were treated with 1 mg of folate plus 10 mg of vitamin B6 and 400 μg of vitamin B12 for 6 months after the PCI. After a mean follow-up of 11 months, the rate of restenosis requiring revascularization was lower in the vitamin-treated study arm (9.9% vs 16% restenosis rate; relative risk [RR]=0.62; 95% confidence interval [CI], 0.40–0.97; number needed to treat=16).7 There was also a nonsignificant trend toward fewer deaths and MIs in the treated arm at both 6 and 12 months after intervention (death: 1.5% vs 2.8%; RR=0.54; 95% CI, 0.016–1.7; MI: 2.6% vs 4.3%; RR=0.60; 95% CI, 0.24–1.51). Statin use was similar in both control (71%) and treatment groups (69%).
Recommendations from others
The American Heart Association and American College of Cardiology do not recommend the routine use of high-dose folic acid or B-vitamin supplements for the primary or secondary prevention of cardiovascular events. The AHA recommendation is to meet recommended daily allowances of folate (400 μg), B12 (2.4 μg), and B6 (1.7 mg) primarily through a balanced diet, with use of supplements if diet alone does not meet the above requirements.8 Since 1998, wheat flour has been supplemented with folate, adding an estimated 100 μg/day to the average American diet.8
The Canadian Task Force on Preventive Health Care (CTFPHC) finds insufficient evidence to advocate screening for hyperhomocysteinemia and rely on expert opinion to advocate treatment in select, high-risk populations.2 Currently, the CTFPHC advocates meeting the recommended daily allowance of folate, B12, and B6.2
Folate for CAD an unanswered question
James M. Gill, MD, MPH
Christianacare Health System, Wilmington, Del
Folate seems like a simple, inexpensive, and relatively benign way to improve care. It is no wonder that many physicians have been recommending folate to their patients with CAD for years. However, as responsible physicians, we need more comprehensive evidence on the benefit of folate before making such universal recommendations.
Several points are important: first, most of the evidence on folate is from observational studies. Only 1 interventional study has shown benefit for patients with CAD, and this study used folate in combination with vitamins B6 and B12. Therefore, if physicians are going to recommend folate supplementation to their patients with CAD, they should recommend this combination rather than folate alone. Also, since this study only included patients who are post-PTCA, it may not apply to all patients with CAD. In short, there is still a fair amount of uncertainty in the answer to this clinical question. We should discuss this uncertainty with our patients, and come to a mutual decision based on preferences.
1. Ford ES, Smith SJ, Stroup DF, Steinberg KK, Mueller PW, Thacker SB. Homocyst(e)ine and cardiovascular disease: a systematic review of the evidence with special emphasis on case-control studies and nested case-control studies. Int J Epidemiol 2002;31:59-70.
2. Booth GL, Wang EE. Preventive health care, 2000 update: screening and management of hyperhomocysteinemia for the prevention of coronary artery disease events. The Canadian Task Force on Preventive Health Care. CMAJ 2000;163:21-29.
3. Bandolier Library. Homocysteine and heart disease: an update. Available at: http://www.jr2.ox.ac.uk/bandolier/booth/cardiac/homheart.html. Accessed on May 29, 2003.
4. Lowering blood homocysteine with folic acid based supplements: meta-analysis of randomised trials. Homocysteine Lowering Trialists’ Collaboration. BMJ 1998;316:894-898.
5. Fairfield KM, Fletcher RH. Vitamins for chronic disease prevention in adults: scientific review. JAMA 2002;287:3116-3126.
6. Liem A, Reynierse-Buitenwerf GH, Zwinderman AH, Jukema JW, van Veldhuisen DJ. Secondary prevention with folic acid: Effects on clinical outcomes. J Am Coll Cardiol 2003;41:2105-2113.
7. Schnyder G, Roffi M, Flammer Y, Pin R, Hess OM. Effect of homocysteine-lowering therapy with folic acid, vitamin B12, and vitamin B6 on clinical outcome after percutaneous coronary intervention: the Swiss Heart study: a randomized controlled trial. JAMA 2002;288:973-979.
8. American Heart Association. AHA Science Advisory: Homocyst(e)ine, Diet, and Cardiovascular Diseases. Available at: http://www.americanheart.org. Accessed on May 29, 2003.
1. Ford ES, Smith SJ, Stroup DF, Steinberg KK, Mueller PW, Thacker SB. Homocyst(e)ine and cardiovascular disease: a systematic review of the evidence with special emphasis on case-control studies and nested case-control studies. Int J Epidemiol 2002;31:59-70.
2. Booth GL, Wang EE. Preventive health care, 2000 update: screening and management of hyperhomocysteinemia for the prevention of coronary artery disease events. The Canadian Task Force on Preventive Health Care. CMAJ 2000;163:21-29.
3. Bandolier Library. Homocysteine and heart disease: an update. Available at: http://www.jr2.ox.ac.uk/bandolier/booth/cardiac/homheart.html. Accessed on May 29, 2003.
4. Lowering blood homocysteine with folic acid based supplements: meta-analysis of randomised trials. Homocysteine Lowering Trialists’ Collaboration. BMJ 1998;316:894-898.
5. Fairfield KM, Fletcher RH. Vitamins for chronic disease prevention in adults: scientific review. JAMA 2002;287:3116-3126.
6. Liem A, Reynierse-Buitenwerf GH, Zwinderman AH, Jukema JW, van Veldhuisen DJ. Secondary prevention with folic acid: Effects on clinical outcomes. J Am Coll Cardiol 2003;41:2105-2113.
7. Schnyder G, Roffi M, Flammer Y, Pin R, Hess OM. Effect of homocysteine-lowering therapy with folic acid, vitamin B12, and vitamin B6 on clinical outcome after percutaneous coronary intervention: the Swiss Heart study: a randomized controlled trial. JAMA 2002;288:973-979.
8. American Heart Association. AHA Science Advisory: Homocyst(e)ine, Diet, and Cardiovascular Diseases. Available at: http://www.americanheart.org. Accessed on May 29, 2003.
Evidence-based answers from the Family Physicians Inquiries Network
Do antipyretics prolong febrile illness?
Antipyretics appear to have minor and variable effects on the course of febrile illness. Aspirin and acetaminophen do not prolong the course of rhinovirus illness, although they may prolong the period of viral shedding and worsen nasal congestion (strength of recommendation [SOR]: A–, based on small randomized controlled trials).
Acetaminophen did not affect symptoms, overall condition, or time to complete healing in children with varicella, although it increased the time to total scabbing of lesions (SOR: A, based on a small randomized controlled trial). Aspirin and acetaminophen may prolong influenza A illness (SOR: C, based on a poor-quality, retrospective observational study).
Acetaminophen may prolong the course of Shigella sonnei infection (SOR: B–, based on a small retrospective cohort study). It does not affect malaria cure rate, and there are insufficient data to assess clearance of Plasmodium falciparum (SOR: C, based on small randomized controlled trials with heterogeneous results).
Evidence summary
Acetaminophen has a different mechanism of action from other antipyretics. It halts the production of prostaglandin in the brain but not in the periphery, solely lowering fever. Aspirin and other nonsteroidal anti-inflammatory agents inhibit both central and peripheral cyclooxygenase and may cause multiple effects in addition to temperature reduction. Clinical outcome studies of their antipyretic effects are inconclusive.1
A randomized controlled trial involving 60 volunteers given intranasal rhinovirus type 2 monitored the effect of aspirin, acetaminophen, ibuprofen, or placebo on virus shedding, immune response, and clinical status. There was no difference in duration of illness. There was a trend toward longer duration of virus shedding in the aspirin and acetaminophen groups, but serum neutralizing antibody response was suppressed (P<.05 vs placebo). Aspirin and acetaminophen worsened symptoms of turbinate edema and nasal obstruction (P<.05 vs placebo).2
In 2 double-blind trials, 45 adults infected with rhinovirus were given aspirin or placebo for 5 days, beginning on the day after viral exposure (as opposed to the typical use in response to symptoms). Aspirin treatment improved symptoms of conjunctivitis significantly, but did not change the duration of illness. Other symptoms (headache, sneezing, chills, malaise, nasal discharge) were not significantly different. Aspirin increased the amount of viral shedding by 36% in 1 trial and 17% in the other (P<.01), potentially increasing risk of spread.3
In a randomized controlled trial evaluating antipyretic effects on the duration or severity of childhood varicella, 31 children received placebo and 37 received acetaminophen for 4 days. There was no difference in itching, appetite, activity, or overall condition between the 2 groups. Children treated with acetaminophen took 1.1 days longer to total scabbing (P<.05), although the number of days until the appearance of the last new vesicle and the time to total healing were unchanged. The duration of viral shedding was not measured, but it is possible that the delay in healing of lesions would prolong viral shedding as well.4
A retrospective observational study of 54 volunteers demonstrated prolonged illness in subjects infected with influenza A that received antipyretic therapy. Patients who got antipyretics were sick 3.5 days longer than those who did not (8.8 ± 2.3 days vs 5.3 ± 3.0 days; P<.001). Only patients with temperatures >38.9°C on 2 readings 6 hours apart received antipyretics, indicating that the longer course correlated with greater severity of illness as well as with antipyretic use.
In the same study, antipyretics were associated with a trend towards prolonged duration of illness in a group of 21 patients infected with S sonnei (4.6 ± 2.1 days with antipyretics vs 1.9 ± 1.6 days without; P=not significant).5
A Cochrane review examined 3 trials of acetaminophen vs placebo for fever in 128 adults and children with P falciparum malaria. Although fever clearance varied between the trials, the malaria cure rate was similar in all, and the review concluded that data were insufficient to evaluate an effect on parasitemia.6
Recommendations from others
We found no recommendations regarding the use of antipyretics and their effect on the duration of febrile illness.
The risk-benefit ratio of antipyretics may not be as favorable as you think
Jon O. Neher, MD
Valley Medical Center Family Medicine Residency
The doctor’s recommendation, “Take two aspirin and call me in the morning,” is an enduring stereotype, not an evidence-based therapy for a fever. This review reevaluates the simplistic notion that antipyretics are uniformly beneficial and safe in febrile illnesses.
Surprisingly, there appear to be some negative impacts from using antipyretics for common disease states without much clear benefit. It can be argued that the studies are small and purported negative consequences modest. Still, enough evidence exists to warrant more research and to cause clinicians to consider that the risk-to-benefit ratio of these medications may not be as favorable as once thought.
1. Mackowiak PA, Plaisance KI. Benefits and risks of antipyretic therapy. Ann N Y Acad Sci 1998;856:214-223.
2. Graham NM, Burrell CJ, Douglas RM, Debelle P, Davies L. Adverse effects of aspirin, acetaminophen, and ibuprofen on immune function, viral shedding, and clinical status in rhinovirus-infected volunteers. J Infect Dis 1990;162:1277-1282.
3. Stanley ED, Jackson GG, Panusarn C, Rubenis M, Dirda V. Increased virus shedding with aspirin treatment of rhinovirus infection. JAMA 1975;231:1248-1251.
4. Doran TF, De Angelis C, Baumgardner RA, Mellits ED. Acetaminophen: more harm than good for chickenpox? J Pediatr 1989;114:1045-1048.
5. Plaisance KI, Kudaravalli S, Wasserman SS, Levine MM, Mackowiak PA. Effect of antipyretic therapy on the duration of illness in experimental influenza A, Shigella sonnei, and Rickettsia rickettsii infections. Pharmacotherapy 2000;20:1417-1422.
6. Meremikwu M, Logan K, Garner P. Antipyretic measures for treating fever in malaria (Cochrane Review). The Cochrane Library, Issue 2, 2002. Oxford: Update Software; 2002.
Antipyretics appear to have minor and variable effects on the course of febrile illness. Aspirin and acetaminophen do not prolong the course of rhinovirus illness, although they may prolong the period of viral shedding and worsen nasal congestion (strength of recommendation [SOR]: A–, based on small randomized controlled trials).
Acetaminophen did not affect symptoms, overall condition, or time to complete healing in children with varicella, although it increased the time to total scabbing of lesions (SOR: A, based on a small randomized controlled trial). Aspirin and acetaminophen may prolong influenza A illness (SOR: C, based on a poor-quality, retrospective observational study).
Acetaminophen may prolong the course of Shigella sonnei infection (SOR: B–, based on a small retrospective cohort study). It does not affect malaria cure rate, and there are insufficient data to assess clearance of Plasmodium falciparum (SOR: C, based on small randomized controlled trials with heterogeneous results).
Evidence summary
Acetaminophen has a different mechanism of action from other antipyretics. It halts the production of prostaglandin in the brain but not in the periphery, solely lowering fever. Aspirin and other nonsteroidal anti-inflammatory agents inhibit both central and peripheral cyclooxygenase and may cause multiple effects in addition to temperature reduction. Clinical outcome studies of their antipyretic effects are inconclusive.1
A randomized controlled trial involving 60 volunteers given intranasal rhinovirus type 2 monitored the effect of aspirin, acetaminophen, ibuprofen, or placebo on virus shedding, immune response, and clinical status. There was no difference in duration of illness. There was a trend toward longer duration of virus shedding in the aspirin and acetaminophen groups, but serum neutralizing antibody response was suppressed (P<.05 vs placebo). Aspirin and acetaminophen worsened symptoms of turbinate edema and nasal obstruction (P<.05 vs placebo).2
In 2 double-blind trials, 45 adults infected with rhinovirus were given aspirin or placebo for 5 days, beginning on the day after viral exposure (as opposed to the typical use in response to symptoms). Aspirin treatment improved symptoms of conjunctivitis significantly, but did not change the duration of illness. Other symptoms (headache, sneezing, chills, malaise, nasal discharge) were not significantly different. Aspirin increased the amount of viral shedding by 36% in 1 trial and 17% in the other (P<.01), potentially increasing risk of spread.3
In a randomized controlled trial evaluating antipyretic effects on the duration or severity of childhood varicella, 31 children received placebo and 37 received acetaminophen for 4 days. There was no difference in itching, appetite, activity, or overall condition between the 2 groups. Children treated with acetaminophen took 1.1 days longer to total scabbing (P<.05), although the number of days until the appearance of the last new vesicle and the time to total healing were unchanged. The duration of viral shedding was not measured, but it is possible that the delay in healing of lesions would prolong viral shedding as well.4
A retrospective observational study of 54 volunteers demonstrated prolonged illness in subjects infected with influenza A that received antipyretic therapy. Patients who got antipyretics were sick 3.5 days longer than those who did not (8.8 ± 2.3 days vs 5.3 ± 3.0 days; P<.001). Only patients with temperatures >38.9°C on 2 readings 6 hours apart received antipyretics, indicating that the longer course correlated with greater severity of illness as well as with antipyretic use.
In the same study, antipyretics were associated with a trend towards prolonged duration of illness in a group of 21 patients infected with S sonnei (4.6 ± 2.1 days with antipyretics vs 1.9 ± 1.6 days without; P=not significant).5
A Cochrane review examined 3 trials of acetaminophen vs placebo for fever in 128 adults and children with P falciparum malaria. Although fever clearance varied between the trials, the malaria cure rate was similar in all, and the review concluded that data were insufficient to evaluate an effect on parasitemia.6
Recommendations from others
We found no recommendations regarding the use of antipyretics and their effect on the duration of febrile illness.
The risk-benefit ratio of antipyretics may not be as favorable as you think
Jon O. Neher, MD
Valley Medical Center Family Medicine Residency
The doctor’s recommendation, “Take two aspirin and call me in the morning,” is an enduring stereotype, not an evidence-based therapy for a fever. This review reevaluates the simplistic notion that antipyretics are uniformly beneficial and safe in febrile illnesses.
Surprisingly, there appear to be some negative impacts from using antipyretics for common disease states without much clear benefit. It can be argued that the studies are small and purported negative consequences modest. Still, enough evidence exists to warrant more research and to cause clinicians to consider that the risk-to-benefit ratio of these medications may not be as favorable as once thought.
Antipyretics appear to have minor and variable effects on the course of febrile illness. Aspirin and acetaminophen do not prolong the course of rhinovirus illness, although they may prolong the period of viral shedding and worsen nasal congestion (strength of recommendation [SOR]: A–, based on small randomized controlled trials).
Acetaminophen did not affect symptoms, overall condition, or time to complete healing in children with varicella, although it increased the time to total scabbing of lesions (SOR: A, based on a small randomized controlled trial). Aspirin and acetaminophen may prolong influenza A illness (SOR: C, based on a poor-quality, retrospective observational study).
Acetaminophen may prolong the course of Shigella sonnei infection (SOR: B–, based on a small retrospective cohort study). It does not affect malaria cure rate, and there are insufficient data to assess clearance of Plasmodium falciparum (SOR: C, based on small randomized controlled trials with heterogeneous results).
Evidence summary
Acetaminophen has a different mechanism of action from other antipyretics. It halts the production of prostaglandin in the brain but not in the periphery, solely lowering fever. Aspirin and other nonsteroidal anti-inflammatory agents inhibit both central and peripheral cyclooxygenase and may cause multiple effects in addition to temperature reduction. Clinical outcome studies of their antipyretic effects are inconclusive.1
A randomized controlled trial involving 60 volunteers given intranasal rhinovirus type 2 monitored the effect of aspirin, acetaminophen, ibuprofen, or placebo on virus shedding, immune response, and clinical status. There was no difference in duration of illness. There was a trend toward longer duration of virus shedding in the aspirin and acetaminophen groups, but serum neutralizing antibody response was suppressed (P<.05 vs placebo). Aspirin and acetaminophen worsened symptoms of turbinate edema and nasal obstruction (P<.05 vs placebo).2
In 2 double-blind trials, 45 adults infected with rhinovirus were given aspirin or placebo for 5 days, beginning on the day after viral exposure (as opposed to the typical use in response to symptoms). Aspirin treatment improved symptoms of conjunctivitis significantly, but did not change the duration of illness. Other symptoms (headache, sneezing, chills, malaise, nasal discharge) were not significantly different. Aspirin increased the amount of viral shedding by 36% in 1 trial and 17% in the other (P<.01), potentially increasing risk of spread.3
In a randomized controlled trial evaluating antipyretic effects on the duration or severity of childhood varicella, 31 children received placebo and 37 received acetaminophen for 4 days. There was no difference in itching, appetite, activity, or overall condition between the 2 groups. Children treated with acetaminophen took 1.1 days longer to total scabbing (P<.05), although the number of days until the appearance of the last new vesicle and the time to total healing were unchanged. The duration of viral shedding was not measured, but it is possible that the delay in healing of lesions would prolong viral shedding as well.4
A retrospective observational study of 54 volunteers demonstrated prolonged illness in subjects infected with influenza A that received antipyretic therapy. Patients who got antipyretics were sick 3.5 days longer than those who did not (8.8 ± 2.3 days vs 5.3 ± 3.0 days; P<.001). Only patients with temperatures >38.9°C on 2 readings 6 hours apart received antipyretics, indicating that the longer course correlated with greater severity of illness as well as with antipyretic use.
In the same study, antipyretics were associated with a trend towards prolonged duration of illness in a group of 21 patients infected with S sonnei (4.6 ± 2.1 days with antipyretics vs 1.9 ± 1.6 days without; P=not significant).5
A Cochrane review examined 3 trials of acetaminophen vs placebo for fever in 128 adults and children with P falciparum malaria. Although fever clearance varied between the trials, the malaria cure rate was similar in all, and the review concluded that data were insufficient to evaluate an effect on parasitemia.6
Recommendations from others
We found no recommendations regarding the use of antipyretics and their effect on the duration of febrile illness.
The risk-benefit ratio of antipyretics may not be as favorable as you think
Jon O. Neher, MD
Valley Medical Center Family Medicine Residency
The doctor’s recommendation, “Take two aspirin and call me in the morning,” is an enduring stereotype, not an evidence-based therapy for a fever. This review reevaluates the simplistic notion that antipyretics are uniformly beneficial and safe in febrile illnesses.
Surprisingly, there appear to be some negative impacts from using antipyretics for common disease states without much clear benefit. It can be argued that the studies are small and purported negative consequences modest. Still, enough evidence exists to warrant more research and to cause clinicians to consider that the risk-to-benefit ratio of these medications may not be as favorable as once thought.
1. Mackowiak PA, Plaisance KI. Benefits and risks of antipyretic therapy. Ann N Y Acad Sci 1998;856:214-223.
2. Graham NM, Burrell CJ, Douglas RM, Debelle P, Davies L. Adverse effects of aspirin, acetaminophen, and ibuprofen on immune function, viral shedding, and clinical status in rhinovirus-infected volunteers. J Infect Dis 1990;162:1277-1282.
3. Stanley ED, Jackson GG, Panusarn C, Rubenis M, Dirda V. Increased virus shedding with aspirin treatment of rhinovirus infection. JAMA 1975;231:1248-1251.
4. Doran TF, De Angelis C, Baumgardner RA, Mellits ED. Acetaminophen: more harm than good for chickenpox? J Pediatr 1989;114:1045-1048.
5. Plaisance KI, Kudaravalli S, Wasserman SS, Levine MM, Mackowiak PA. Effect of antipyretic therapy on the duration of illness in experimental influenza A, Shigella sonnei, and Rickettsia rickettsii infections. Pharmacotherapy 2000;20:1417-1422.
6. Meremikwu M, Logan K, Garner P. Antipyretic measures for treating fever in malaria (Cochrane Review). The Cochrane Library, Issue 2, 2002. Oxford: Update Software; 2002.
1. Mackowiak PA, Plaisance KI. Benefits and risks of antipyretic therapy. Ann N Y Acad Sci 1998;856:214-223.
2. Graham NM, Burrell CJ, Douglas RM, Debelle P, Davies L. Adverse effects of aspirin, acetaminophen, and ibuprofen on immune function, viral shedding, and clinical status in rhinovirus-infected volunteers. J Infect Dis 1990;162:1277-1282.
3. Stanley ED, Jackson GG, Panusarn C, Rubenis M, Dirda V. Increased virus shedding with aspirin treatment of rhinovirus infection. JAMA 1975;231:1248-1251.
4. Doran TF, De Angelis C, Baumgardner RA, Mellits ED. Acetaminophen: more harm than good for chickenpox? J Pediatr 1989;114:1045-1048.
5. Plaisance KI, Kudaravalli S, Wasserman SS, Levine MM, Mackowiak PA. Effect of antipyretic therapy on the duration of illness in experimental influenza A, Shigella sonnei, and Rickettsia rickettsii infections. Pharmacotherapy 2000;20:1417-1422.
6. Meremikwu M, Logan K, Garner P. Antipyretic measures for treating fever in malaria (Cochrane Review). The Cochrane Library, Issue 2, 2002. Oxford: Update Software; 2002.
Evidence-based answers from the Family Physicians Inquiries Network
Are inhalers with spacers better than nebulizers for children with asthma?
Metered-dose inhalers with a spacer (MDI/S) are as good as, or better than, nebulizers for children with asthma. This is based on numerous randomized controlled trials that compared outcomes such as hospital admission rates, asthma severity scores, and pulmonary function scores (strength of recommendation: A, based on consistent randomized controlled trials and meta-analysis).
Evidence summary
A Cochrane review of 10 randomized controlled trials comparing nebulizers with MDI/S, both in adults and in children aged >2 years, showed a substantial trend towards improvement in hospital admission rates with MDI/S use. Sample size for each study was small, ranging from 18 to 152 patients, with a total sample size of 880 children and 444 adults.
The relative risk of admission for MDI/S vs nebulizer for children was 0.65 (95% confidence interval, 0.4–1.06). Secondary outcomes were equivalent or slightly improved, including duration in the emergency department, changes in respiratory rate, blood gases, pulse, tremor, symptoms score, lung function, and use of steroids. Patients with life-threatening asthma (for example, those considered for ventilation) or other chronic illnesses were excluded.1
All but 1 of these studies were set in the emergency department and all involved the use of one of a variety of spacers with the MDI, such as the Aerochamber or Inspirease. Whether these efficacy studies can be translated into daily outpatient clinical practice remains unclear. Emergency departments typically have higher staffing levels, and study subjects and their parents may have received more MDI/S training than is practical in many office settings.
While most of the data were for children aged 2 years and older, 1 study published after the Cochrane review did show a lower admission rate in 85 patients who were 2 to 24 months in the MDI/S group.2 Controlling for the initial Pulmonary Index score, children using an MDI and Aerochamber spacer were admitted less often (5% vs 20%, number needed to treat=7; P=.05) than children using nebulizers. Since the results of this single small trial are the only data available for this younger age group, using MDI/S instead of nebulizers should be done with caution for children aged <2 years.
Another randomized controlled trial of 152 patients found no difference in primary outcomes of asthma severity score, oxygen saturation, and percent predicted peak expiratory flow rate (PEFR). Several secondary outcomes slightly favored MDI/S: number of treatments given, whether steroids were used, change in heart rate, side effects, rate of hospital admission, and treatment time in the emergency department.3
A smaller double-blinded randomized controlled trial of 33 children aged 6 to 14 years showed no difference in MDI/S vs nebulizer, as measured by clinical score, respiratory rate, oxygen saturation, and forced expiratory volume at 1 second (FEV1).4 The researchers calculated the study had 90% power to detect a clinically meaningful difference in FEV1 of 12% of the predicted value between the groups.
Other review articles reach the same conclusion. One article reviewed the literature from 1980 to 1996 and examined 17 prospective clinical trials. Outcomes measured included pulmonary function measures and clinical scores. The researchers recommended that MDI/S be used due to clinical benefit, safety, lower cost, personnel time, and speed and ease of administration.5
A review article from the British literature examined 3 randomized controlled trials involving 51 patients and found no superiority of nebulizer vs MDI/S.6 A similar review article examined 14 randomized controlled trials for beta-agonist delivery for patients aged 5 to 15 with stable asthma. They found no obvious benefit of 1 type of device over another, including nebulizer, MDI/S, and dry powder inhalers.7 These last 2 articles claimed to be systematic reviews, although they do not clearly state their search methodology.
Researchers used a wide variety of spacers in all aforementioned studies; accordingly, one cannot be recommended as superior to others. The degree of teaching given to parents and children about MDI/S use was not described in any of the trials.
FIGURE
MDI with spacer is beneficial when used properly
Recommendations from others
Guidelines from the Global Health Initiative for Asthma, a collaboration of the National Heart, Lung and Blood Institute and the World Health Organization, recommend MDI/S for children with asthma due to increased efficacy and decreased cost (revised in 2002). Specifically, they recommend a spacer with a face mask for infants and preschool children, a mouthpiece and spacer for children aged 4 to 6 years, and a dry powder inhaler or breath-activated device from age 6 onwards.8 Cincinnati Children’s Hospital’s evidence-based guidelines from 1998 also recommend MDI/S for children aged >1 year with acute asthma exacerbations.9 This guideline suggests using 4 to 8 puffs from a 90 μg albuterol MDI at 1- to 2-minute intervals every 20 minutes for 1 hour, then every 1 to 4 hours subsequently.
Use MDIs with spacers in all but the youngest patients
Grant Hoekzema, MD
Mercy Family Medicine Residency, St. Louis, Mo
Until recently, using a nebulizer for the wheezing child or infant seemed intuitively to be the most effective way to deliver bronchodilators. However, with recent data showing that MDIs with spacers are just as effective, I have been using MDIs with spacers for all but my youngest patients. Parents as well as physicians may need to be convinced that using less technology in this case is better for their child. In some cases, parental acceptance of therapy necessitates using a nebulizer.
1. Cates CJ, Rowe BH, Bara A. Holding chambers versus nebulisers for beta-agonist treatment of acute asthma (Cochrane Review). The Cochrane Library, Issue 2, 2002. Oxford: Update Software, last updated February 21, 2002.
2. Delgado A, Chou KJ, Silver EJ, Crain EF. Nebulizers vs metered dose-inhalers with spacers for bronchodilator therapy to treat wheezing in children aged 2 to 24 months in a pediatric emergency department. Arch Pediatr Adolesc Med 2003;157:76-80.
3. Chou KJ, Cunningham SJ, Crain EF. Metered-dose inhalers with spacers vs nebulizers for pediatric asthma. Arch Pediatr Adolesc Med 1995;149:201-205.
4. Kerem E, Levison H, Schuh S, et al. Efficacy of albuterol administered by nebulizer versus spacer device in children with acute asthma. J Pediatr 1993;123:313-317.
5. Amirav I, Newhouse MT. Metered-dose inhaler accessory devices in acute asthma: efficacy and comparison with nebulizers: a literature review. Arch Pediatr Adolesc Med 1997;151:876-882.
6. Brocklebank D, Ram F, Wright J, et al. Comparison of the effectiveness of inhaler devices in asthma and chronic obstructive airways disease: a systematic review of the literature. Health Technol Assess 2001;5:1-149.
7. Peters J, Stevenson M, Beverley C, Lim JN, Smith S. The clinical effectiveness and cost-effectiveness of inhaler devices used in the routine management of chronic asthma in older children: a systematic review and economic evaluation. Health Technol Assess 2002;6:1-167.
8. National Heart, Lung and Blood Institute (NHLBI), World Health Organization (WHO). Global Initiative for Asthma: Global Strategy for Asthma Management and Prevention. 2002. Available at: http://www.ginasthma.com/workshop.pdf. Accessed on December 3, 2003. Updated from: NHLBI/WHO Workshop Report: Global Strategy for Asthma Management and Prevention, issued January 1995. NIH Publication No. 02-3659.
9. Evidence-Based Clinical Practice Guideline for Managing an Acute Exacerbation of Asthma. Cincinnati, Ohio: Cincinnati Childrens’ Hospital Medical Center; 1998 (revised 2002). Available at: http://www.cincinnatichildrens.org/svc/dept-div/health-policy/ev-based/asthma.htm. Accessed on December 3, 2003.
Metered-dose inhalers with a spacer (MDI/S) are as good as, or better than, nebulizers for children with asthma. This is based on numerous randomized controlled trials that compared outcomes such as hospital admission rates, asthma severity scores, and pulmonary function scores (strength of recommendation: A, based on consistent randomized controlled trials and meta-analysis).
Evidence summary
A Cochrane review of 10 randomized controlled trials comparing nebulizers with MDI/S, both in adults and in children aged >2 years, showed a substantial trend towards improvement in hospital admission rates with MDI/S use. Sample size for each study was small, ranging from 18 to 152 patients, with a total sample size of 880 children and 444 adults.
The relative risk of admission for MDI/S vs nebulizer for children was 0.65 (95% confidence interval, 0.4–1.06). Secondary outcomes were equivalent or slightly improved, including duration in the emergency department, changes in respiratory rate, blood gases, pulse, tremor, symptoms score, lung function, and use of steroids. Patients with life-threatening asthma (for example, those considered for ventilation) or other chronic illnesses were excluded.1
All but 1 of these studies were set in the emergency department and all involved the use of one of a variety of spacers with the MDI, such as the Aerochamber or Inspirease. Whether these efficacy studies can be translated into daily outpatient clinical practice remains unclear. Emergency departments typically have higher staffing levels, and study subjects and their parents may have received more MDI/S training than is practical in many office settings.
While most of the data were for children aged 2 years and older, 1 study published after the Cochrane review did show a lower admission rate in 85 patients who were 2 to 24 months in the MDI/S group.2 Controlling for the initial Pulmonary Index score, children using an MDI and Aerochamber spacer were admitted less often (5% vs 20%, number needed to treat=7; P=.05) than children using nebulizers. Since the results of this single small trial are the only data available for this younger age group, using MDI/S instead of nebulizers should be done with caution for children aged <2 years.
Another randomized controlled trial of 152 patients found no difference in primary outcomes of asthma severity score, oxygen saturation, and percent predicted peak expiratory flow rate (PEFR). Several secondary outcomes slightly favored MDI/S: number of treatments given, whether steroids were used, change in heart rate, side effects, rate of hospital admission, and treatment time in the emergency department.3
A smaller double-blinded randomized controlled trial of 33 children aged 6 to 14 years showed no difference in MDI/S vs nebulizer, as measured by clinical score, respiratory rate, oxygen saturation, and forced expiratory volume at 1 second (FEV1).4 The researchers calculated the study had 90% power to detect a clinically meaningful difference in FEV1 of 12% of the predicted value between the groups.
Other review articles reach the same conclusion. One article reviewed the literature from 1980 to 1996 and examined 17 prospective clinical trials. Outcomes measured included pulmonary function measures and clinical scores. The researchers recommended that MDI/S be used due to clinical benefit, safety, lower cost, personnel time, and speed and ease of administration.5
A review article from the British literature examined 3 randomized controlled trials involving 51 patients and found no superiority of nebulizer vs MDI/S.6 A similar review article examined 14 randomized controlled trials for beta-agonist delivery for patients aged 5 to 15 with stable asthma. They found no obvious benefit of 1 type of device over another, including nebulizer, MDI/S, and dry powder inhalers.7 These last 2 articles claimed to be systematic reviews, although they do not clearly state their search methodology.
Researchers used a wide variety of spacers in all aforementioned studies; accordingly, one cannot be recommended as superior to others. The degree of teaching given to parents and children about MDI/S use was not described in any of the trials.
FIGURE
MDI with spacer is beneficial when used properly
Recommendations from others
Guidelines from the Global Health Initiative for Asthma, a collaboration of the National Heart, Lung and Blood Institute and the World Health Organization, recommend MDI/S for children with asthma due to increased efficacy and decreased cost (revised in 2002). Specifically, they recommend a spacer with a face mask for infants and preschool children, a mouthpiece and spacer for children aged 4 to 6 years, and a dry powder inhaler or breath-activated device from age 6 onwards.8 Cincinnati Children’s Hospital’s evidence-based guidelines from 1998 also recommend MDI/S for children aged >1 year with acute asthma exacerbations.9 This guideline suggests using 4 to 8 puffs from a 90 μg albuterol MDI at 1- to 2-minute intervals every 20 minutes for 1 hour, then every 1 to 4 hours subsequently.
Use MDIs with spacers in all but the youngest patients
Grant Hoekzema, MD
Mercy Family Medicine Residency, St. Louis, Mo
Until recently, using a nebulizer for the wheezing child or infant seemed intuitively to be the most effective way to deliver bronchodilators. However, with recent data showing that MDIs with spacers are just as effective, I have been using MDIs with spacers for all but my youngest patients. Parents as well as physicians may need to be convinced that using less technology in this case is better for their child. In some cases, parental acceptance of therapy necessitates using a nebulizer.
Metered-dose inhalers with a spacer (MDI/S) are as good as, or better than, nebulizers for children with asthma. This is based on numerous randomized controlled trials that compared outcomes such as hospital admission rates, asthma severity scores, and pulmonary function scores (strength of recommendation: A, based on consistent randomized controlled trials and meta-analysis).
Evidence summary
A Cochrane review of 10 randomized controlled trials comparing nebulizers with MDI/S, both in adults and in children aged >2 years, showed a substantial trend towards improvement in hospital admission rates with MDI/S use. Sample size for each study was small, ranging from 18 to 152 patients, with a total sample size of 880 children and 444 adults.
The relative risk of admission for MDI/S vs nebulizer for children was 0.65 (95% confidence interval, 0.4–1.06). Secondary outcomes were equivalent or slightly improved, including duration in the emergency department, changes in respiratory rate, blood gases, pulse, tremor, symptoms score, lung function, and use of steroids. Patients with life-threatening asthma (for example, those considered for ventilation) or other chronic illnesses were excluded.1
All but 1 of these studies were set in the emergency department and all involved the use of one of a variety of spacers with the MDI, such as the Aerochamber or Inspirease. Whether these efficacy studies can be translated into daily outpatient clinical practice remains unclear. Emergency departments typically have higher staffing levels, and study subjects and their parents may have received more MDI/S training than is practical in many office settings.
While most of the data were for children aged 2 years and older, 1 study published after the Cochrane review did show a lower admission rate in 85 patients who were 2 to 24 months in the MDI/S group.2 Controlling for the initial Pulmonary Index score, children using an MDI and Aerochamber spacer were admitted less often (5% vs 20%, number needed to treat=7; P=.05) than children using nebulizers. Since the results of this single small trial are the only data available for this younger age group, using MDI/S instead of nebulizers should be done with caution for children aged <2 years.
Another randomized controlled trial of 152 patients found no difference in primary outcomes of asthma severity score, oxygen saturation, and percent predicted peak expiratory flow rate (PEFR). Several secondary outcomes slightly favored MDI/S: number of treatments given, whether steroids were used, change in heart rate, side effects, rate of hospital admission, and treatment time in the emergency department.3
A smaller double-blinded randomized controlled trial of 33 children aged 6 to 14 years showed no difference in MDI/S vs nebulizer, as measured by clinical score, respiratory rate, oxygen saturation, and forced expiratory volume at 1 second (FEV1).4 The researchers calculated the study had 90% power to detect a clinically meaningful difference in FEV1 of 12% of the predicted value between the groups.
Other review articles reach the same conclusion. One article reviewed the literature from 1980 to 1996 and examined 17 prospective clinical trials. Outcomes measured included pulmonary function measures and clinical scores. The researchers recommended that MDI/S be used due to clinical benefit, safety, lower cost, personnel time, and speed and ease of administration.5
A review article from the British literature examined 3 randomized controlled trials involving 51 patients and found no superiority of nebulizer vs MDI/S.6 A similar review article examined 14 randomized controlled trials for beta-agonist delivery for patients aged 5 to 15 with stable asthma. They found no obvious benefit of 1 type of device over another, including nebulizer, MDI/S, and dry powder inhalers.7 These last 2 articles claimed to be systematic reviews, although they do not clearly state their search methodology.
Researchers used a wide variety of spacers in all aforementioned studies; accordingly, one cannot be recommended as superior to others. The degree of teaching given to parents and children about MDI/S use was not described in any of the trials.
FIGURE
MDI with spacer is beneficial when used properly
Recommendations from others
Guidelines from the Global Health Initiative for Asthma, a collaboration of the National Heart, Lung and Blood Institute and the World Health Organization, recommend MDI/S for children with asthma due to increased efficacy and decreased cost (revised in 2002). Specifically, they recommend a spacer with a face mask for infants and preschool children, a mouthpiece and spacer for children aged 4 to 6 years, and a dry powder inhaler or breath-activated device from age 6 onwards.8 Cincinnati Children’s Hospital’s evidence-based guidelines from 1998 also recommend MDI/S for children aged >1 year with acute asthma exacerbations.9 This guideline suggests using 4 to 8 puffs from a 90 μg albuterol MDI at 1- to 2-minute intervals every 20 minutes for 1 hour, then every 1 to 4 hours subsequently.
Use MDIs with spacers in all but the youngest patients
Grant Hoekzema, MD
Mercy Family Medicine Residency, St. Louis, Mo
Until recently, using a nebulizer for the wheezing child or infant seemed intuitively to be the most effective way to deliver bronchodilators. However, with recent data showing that MDIs with spacers are just as effective, I have been using MDIs with spacers for all but my youngest patients. Parents as well as physicians may need to be convinced that using less technology in this case is better for their child. In some cases, parental acceptance of therapy necessitates using a nebulizer.
1. Cates CJ, Rowe BH, Bara A. Holding chambers versus nebulisers for beta-agonist treatment of acute asthma (Cochrane Review). The Cochrane Library, Issue 2, 2002. Oxford: Update Software, last updated February 21, 2002.
2. Delgado A, Chou KJ, Silver EJ, Crain EF. Nebulizers vs metered dose-inhalers with spacers for bronchodilator therapy to treat wheezing in children aged 2 to 24 months in a pediatric emergency department. Arch Pediatr Adolesc Med 2003;157:76-80.
3. Chou KJ, Cunningham SJ, Crain EF. Metered-dose inhalers with spacers vs nebulizers for pediatric asthma. Arch Pediatr Adolesc Med 1995;149:201-205.
4. Kerem E, Levison H, Schuh S, et al. Efficacy of albuterol administered by nebulizer versus spacer device in children with acute asthma. J Pediatr 1993;123:313-317.
5. Amirav I, Newhouse MT. Metered-dose inhaler accessory devices in acute asthma: efficacy and comparison with nebulizers: a literature review. Arch Pediatr Adolesc Med 1997;151:876-882.
6. Brocklebank D, Ram F, Wright J, et al. Comparison of the effectiveness of inhaler devices in asthma and chronic obstructive airways disease: a systematic review of the literature. Health Technol Assess 2001;5:1-149.
7. Peters J, Stevenson M, Beverley C, Lim JN, Smith S. The clinical effectiveness and cost-effectiveness of inhaler devices used in the routine management of chronic asthma in older children: a systematic review and economic evaluation. Health Technol Assess 2002;6:1-167.
8. National Heart, Lung and Blood Institute (NHLBI), World Health Organization (WHO). Global Initiative for Asthma: Global Strategy for Asthma Management and Prevention. 2002. Available at: http://www.ginasthma.com/workshop.pdf. Accessed on December 3, 2003. Updated from: NHLBI/WHO Workshop Report: Global Strategy for Asthma Management and Prevention, issued January 1995. NIH Publication No. 02-3659.
9. Evidence-Based Clinical Practice Guideline for Managing an Acute Exacerbation of Asthma. Cincinnati, Ohio: Cincinnati Childrens’ Hospital Medical Center; 1998 (revised 2002). Available at: http://www.cincinnatichildrens.org/svc/dept-div/health-policy/ev-based/asthma.htm. Accessed on December 3, 2003.
1. Cates CJ, Rowe BH, Bara A. Holding chambers versus nebulisers for beta-agonist treatment of acute asthma (Cochrane Review). The Cochrane Library, Issue 2, 2002. Oxford: Update Software, last updated February 21, 2002.
2. Delgado A, Chou KJ, Silver EJ, Crain EF. Nebulizers vs metered dose-inhalers with spacers for bronchodilator therapy to treat wheezing in children aged 2 to 24 months in a pediatric emergency department. Arch Pediatr Adolesc Med 2003;157:76-80.
3. Chou KJ, Cunningham SJ, Crain EF. Metered-dose inhalers with spacers vs nebulizers for pediatric asthma. Arch Pediatr Adolesc Med 1995;149:201-205.
4. Kerem E, Levison H, Schuh S, et al. Efficacy of albuterol administered by nebulizer versus spacer device in children with acute asthma. J Pediatr 1993;123:313-317.
5. Amirav I, Newhouse MT. Metered-dose inhaler accessory devices in acute asthma: efficacy and comparison with nebulizers: a literature review. Arch Pediatr Adolesc Med 1997;151:876-882.
6. Brocklebank D, Ram F, Wright J, et al. Comparison of the effectiveness of inhaler devices in asthma and chronic obstructive airways disease: a systematic review of the literature. Health Technol Assess 2001;5:1-149.
7. Peters J, Stevenson M, Beverley C, Lim JN, Smith S. The clinical effectiveness and cost-effectiveness of inhaler devices used in the routine management of chronic asthma in older children: a systematic review and economic evaluation. Health Technol Assess 2002;6:1-167.
8. National Heart, Lung and Blood Institute (NHLBI), World Health Organization (WHO). Global Initiative for Asthma: Global Strategy for Asthma Management and Prevention. 2002. Available at: http://www.ginasthma.com/workshop.pdf. Accessed on December 3, 2003. Updated from: NHLBI/WHO Workshop Report: Global Strategy for Asthma Management and Prevention, issued January 1995. NIH Publication No. 02-3659.
9. Evidence-Based Clinical Practice Guideline for Managing an Acute Exacerbation of Asthma. Cincinnati, Ohio: Cincinnati Childrens’ Hospital Medical Center; 1998 (revised 2002). Available at: http://www.cincinnatichildrens.org/svc/dept-div/health-policy/ev-based/asthma.htm. Accessed on December 3, 2003.
Evidence-based answers from the Family Physicians Inquiries Network
Do systemic corticosteroids lessen symptoms in acute exacerbations of COPD?
Systemic corticosteroids improve measures of dyspnea in patients with acute exacerbations of chronic obstructive pulmonary disease (COPD) (strength of recommendation [SOR]: A, meta-analysis of 2 small randomized controlled trials). The optimal dose of systemic corticosteroids to achieve these benefits is uncertain. An international consensus panel recommended 30 to 40 mg of oral prednisone daily for 10 to 14 days as a reasonable compromise of efficacy and safety (SOR: C, consensus expert opinion).
Evidence summary
Three systematic reviews addressing the efficacy of systemic corticosteroids in managing acute exacerbations of COPD found consistent, good-quality evidence supporting short courses of systemic steroids. The improvement in outcomes included decreases in airflow obstruction, treatment failure, and length of hospital stay.1-3
The optimal initial doses of systemic corticosteroids to achieve these benefits are uncertain. Variable study designs limit combining study results into a dose-response curve, and there are no comparative trials of high- vs low-dose regimens. A panel consensus judgment from a collaboration of the National Heart, Lung, and Blood Institute and the World Health Organization recommended 30–40 mg of oral prednisone daily for 10 to 14 days.4
A Cochrane systematic review analyzed 7 randomized, placebo-controlled trials of systemic steroids for acute exacerbations of COPD.1 While most of the studies reporting symptom outcomes used disparate methods of measurement, 2 small studies5,6 reported changes in quality of life using validated visual analogue scales. This allowed their results to be combined into a summary estimate of the effect of corticosteroids compared with placebo. Combining the visual analogue scales using a standardized mean difference showed a significant improvement of this summary quality of life measure in the steroid-treated group.
Other small randomized controlled trials of systemic steroids1 demonstrated trends towards improvement in symptom outcomes. A Taiwanese study randomized 138 patients presenting to an emergency department to treatment with 100 mg intravenous hydrocortisone or placebo within 15 minutes of arrival.1 Using a 6-point scale, patients gave self-assessments of the severity of their attack on arrival and at 6 hours. Compared with placebo, the steroid group showed a 6-hour improvement of uncertain significance.
Similarly, a British trial of 30 mg prednisone vs placebo in 56 inpatients with acute exacerbations of COPD measured a daily composite symptom score based on 7 pulmonary and functional symptoms.8 There was a nonsignificant trend towards greater improvement in the steroid-treated group.
Finally, a multicenter, 3-armed, placebo-controlled, double-blinded, parallel design study enrolled 199 COPD inpatients, who were randomized to oral prednisone, inhaled budesonide, or placebo treatment groups.9 Dyspnea was assessed using a validated, modified Borg scale every 12 hours for 72 hours. The reduction in the modified Borg scale rating was of comparable magnitude in the 3 groups, but again there was a nonsignificant greater reduction in the systemic steroid group compared with both the placebo and inhaled budesonide groups. Power calculations were not provided, so it is unclear whether sample size in this study was sufficient to detect important differences in outcomes.
Three randomized controlled trials prospectively measured adverse events rates of systemic steroids in acute exacerbations of COPD.9-11 Hyperglycemia or glycosuria was more common in the steroid-treated groups. The SCCOPE study, the largest of the 3 trials, found hyperglycemia requiring treatment occurred in a greater proportion of the steroid-treated group than placebo (15% vs 4%; P=.002; number needed to harm=9).
Recommendations from others
A recent review provides a concise summary of practice guidelines for the management of acute exacerbations of COPD from widely recognized professional societies.12 Systemic steroids are endorsed in the evidence-based systematic review guidelines from the American College of Chest Physicians–American Society of Internal Medicine, along with the National Heart, Lung, and Blood Institute with the World Health Organization cosponsored Global Initiative for Chronic Obstructive Lung Disease (GOLD), and the consensus guidelines of the American Thoracic Society.13
Lack of long-term benefits emphasize need for prevention
Donald Briscoe, MD
CHRISTUS St. Joseph Family Practice Residency, Houston, TX
It is reassuring to see that there is good evidence to support what most practicing physicians already do—use steroids for acute exacerbations of COPD. Along with inhaled anticholinergics, beta-agonists and (sometimes) antibiotics, short-term measures of patient oriented outcomes seem to be improved. Questions still remain regarding the optimal dosing, route of administration, and length of therapy needed. The lack of evidence of long-term outcome benefits emphasizes, to me, the need for improved efforts at primary and secondary prevention, such as smoking prevention and cessation interventions, annual influenza vaccination, and routine pneumococcal vaccination in our COPD patients.
1. Wood-Baker R, Walters EH, Gibson P. Oral corticos-teroids for acute exacerbations of chronic obstructive pulmonary disease (Cochrane Review). The Cochrane Library, issue 4, 2003. Updated January 12, 2001.
2. McCrory DC, Brown C, Gelfand SE, Bach PB. Management of acute exacerbations of COPD: a summary and appraisal of published evidence. Chest 2001;119:1190-1209.
3. Singh JM, Palda VA, Stanbrook MB, Chapman KR. Corticosteroid therapy for patients with acute exacerbations of chronic obstructive pulmonary disease. Arch Intern Med 2002;162:2527-2536.
4. Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS. GOLD Scientific Committee. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop Summary. Am J Respir Crit Care Med 2001;163:1256-1276.
5. Thompson WH, Nielson CP, Carvalho P, Charan NB, Crowley JJ. Controlled trial of oral prednisone in outpatients with acute COPD exacerbation. Am J Respir Crit Care Med 1996;154:407-412.
6. Wood-Baker R, Wilinson J, Pearce M, Ryan G. A double-blind, placebo-controlled trial of corticosteroids for acute exacerbations of chronic obstructive pulmonary disease. Aust N Z J Med 1998;28:262.-
7. Bullard MJ, Liaw SJ, Tsai YH, Min HP. Early corticosteroid use in acute exacerbations of chronic airflow obstruction. Am J Emerg Med 1996;14:139-143.
8. Davies L, Angus RM, Calverley PM. Oral corticosteroids in patients admitted to hospital with exacerbations of chronic obstructive pulmonary disease: a prospective randomised controlled trial. Lancet 1999;354:456-460.
9. Maltais F, Ostinelli J, Bourbeau J, et al. Comparison of nebulized budesonide and oral prednisolone with placebo in the treatment of acute exacerbations of chronic obstructive pulmonary disease: a randomized controlled trial. Am J Respir Crit Care Med 2002;165:698-703.
10. Albert RK, Martin TR, Lewis SW. Controlled clinical trial of methylprednisolone in patients with chronic bronchitis and acute respiratory insufficiency. Ann Intern Med 1980;92:753-758.
11. Niewoehner DE, Erbland ML, Deupree RH, et al. Effect of systemic glucocorticoids on exacerbations of chronic obstructive pulmonary disease. Department of Veterans Affairs Cooperative Study Group. N Engl J Med 1999;340:1941-1947.
12. Stoller JK. Clinical practice. Acute exacerbations of chronic obstructive pulmonary disease. N Engl J Med 2002;346:988-994.
13. Niewoehner DE, Erbland M, Collins D. Glucocorticoids for chronic obstructive pulmonary disease [letter]. N Engl J Med 1999;341:1772-1773.
Systemic corticosteroids improve measures of dyspnea in patients with acute exacerbations of chronic obstructive pulmonary disease (COPD) (strength of recommendation [SOR]: A, meta-analysis of 2 small randomized controlled trials). The optimal dose of systemic corticosteroids to achieve these benefits is uncertain. An international consensus panel recommended 30 to 40 mg of oral prednisone daily for 10 to 14 days as a reasonable compromise of efficacy and safety (SOR: C, consensus expert opinion).
Evidence summary
Three systematic reviews addressing the efficacy of systemic corticosteroids in managing acute exacerbations of COPD found consistent, good-quality evidence supporting short courses of systemic steroids. The improvement in outcomes included decreases in airflow obstruction, treatment failure, and length of hospital stay.1-3
The optimal initial doses of systemic corticosteroids to achieve these benefits are uncertain. Variable study designs limit combining study results into a dose-response curve, and there are no comparative trials of high- vs low-dose regimens. A panel consensus judgment from a collaboration of the National Heart, Lung, and Blood Institute and the World Health Organization recommended 30–40 mg of oral prednisone daily for 10 to 14 days.4
A Cochrane systematic review analyzed 7 randomized, placebo-controlled trials of systemic steroids for acute exacerbations of COPD.1 While most of the studies reporting symptom outcomes used disparate methods of measurement, 2 small studies5,6 reported changes in quality of life using validated visual analogue scales. This allowed their results to be combined into a summary estimate of the effect of corticosteroids compared with placebo. Combining the visual analogue scales using a standardized mean difference showed a significant improvement of this summary quality of life measure in the steroid-treated group.
Other small randomized controlled trials of systemic steroids1 demonstrated trends towards improvement in symptom outcomes. A Taiwanese study randomized 138 patients presenting to an emergency department to treatment with 100 mg intravenous hydrocortisone or placebo within 15 minutes of arrival.1 Using a 6-point scale, patients gave self-assessments of the severity of their attack on arrival and at 6 hours. Compared with placebo, the steroid group showed a 6-hour improvement of uncertain significance.
Similarly, a British trial of 30 mg prednisone vs placebo in 56 inpatients with acute exacerbations of COPD measured a daily composite symptom score based on 7 pulmonary and functional symptoms.8 There was a nonsignificant trend towards greater improvement in the steroid-treated group.
Finally, a multicenter, 3-armed, placebo-controlled, double-blinded, parallel design study enrolled 199 COPD inpatients, who were randomized to oral prednisone, inhaled budesonide, or placebo treatment groups.9 Dyspnea was assessed using a validated, modified Borg scale every 12 hours for 72 hours. The reduction in the modified Borg scale rating was of comparable magnitude in the 3 groups, but again there was a nonsignificant greater reduction in the systemic steroid group compared with both the placebo and inhaled budesonide groups. Power calculations were not provided, so it is unclear whether sample size in this study was sufficient to detect important differences in outcomes.
Three randomized controlled trials prospectively measured adverse events rates of systemic steroids in acute exacerbations of COPD.9-11 Hyperglycemia or glycosuria was more common in the steroid-treated groups. The SCCOPE study, the largest of the 3 trials, found hyperglycemia requiring treatment occurred in a greater proportion of the steroid-treated group than placebo (15% vs 4%; P=.002; number needed to harm=9).
Recommendations from others
A recent review provides a concise summary of practice guidelines for the management of acute exacerbations of COPD from widely recognized professional societies.12 Systemic steroids are endorsed in the evidence-based systematic review guidelines from the American College of Chest Physicians–American Society of Internal Medicine, along with the National Heart, Lung, and Blood Institute with the World Health Organization cosponsored Global Initiative for Chronic Obstructive Lung Disease (GOLD), and the consensus guidelines of the American Thoracic Society.13
Lack of long-term benefits emphasize need for prevention
Donald Briscoe, MD
CHRISTUS St. Joseph Family Practice Residency, Houston, TX
It is reassuring to see that there is good evidence to support what most practicing physicians already do—use steroids for acute exacerbations of COPD. Along with inhaled anticholinergics, beta-agonists and (sometimes) antibiotics, short-term measures of patient oriented outcomes seem to be improved. Questions still remain regarding the optimal dosing, route of administration, and length of therapy needed. The lack of evidence of long-term outcome benefits emphasizes, to me, the need for improved efforts at primary and secondary prevention, such as smoking prevention and cessation interventions, annual influenza vaccination, and routine pneumococcal vaccination in our COPD patients.
Systemic corticosteroids improve measures of dyspnea in patients with acute exacerbations of chronic obstructive pulmonary disease (COPD) (strength of recommendation [SOR]: A, meta-analysis of 2 small randomized controlled trials). The optimal dose of systemic corticosteroids to achieve these benefits is uncertain. An international consensus panel recommended 30 to 40 mg of oral prednisone daily for 10 to 14 days as a reasonable compromise of efficacy and safety (SOR: C, consensus expert opinion).
Evidence summary
Three systematic reviews addressing the efficacy of systemic corticosteroids in managing acute exacerbations of COPD found consistent, good-quality evidence supporting short courses of systemic steroids. The improvement in outcomes included decreases in airflow obstruction, treatment failure, and length of hospital stay.1-3
The optimal initial doses of systemic corticosteroids to achieve these benefits are uncertain. Variable study designs limit combining study results into a dose-response curve, and there are no comparative trials of high- vs low-dose regimens. A panel consensus judgment from a collaboration of the National Heart, Lung, and Blood Institute and the World Health Organization recommended 30–40 mg of oral prednisone daily for 10 to 14 days.4
A Cochrane systematic review analyzed 7 randomized, placebo-controlled trials of systemic steroids for acute exacerbations of COPD.1 While most of the studies reporting symptom outcomes used disparate methods of measurement, 2 small studies5,6 reported changes in quality of life using validated visual analogue scales. This allowed their results to be combined into a summary estimate of the effect of corticosteroids compared with placebo. Combining the visual analogue scales using a standardized mean difference showed a significant improvement of this summary quality of life measure in the steroid-treated group.
Other small randomized controlled trials of systemic steroids1 demonstrated trends towards improvement in symptom outcomes. A Taiwanese study randomized 138 patients presenting to an emergency department to treatment with 100 mg intravenous hydrocortisone or placebo within 15 minutes of arrival.1 Using a 6-point scale, patients gave self-assessments of the severity of their attack on arrival and at 6 hours. Compared with placebo, the steroid group showed a 6-hour improvement of uncertain significance.
Similarly, a British trial of 30 mg prednisone vs placebo in 56 inpatients with acute exacerbations of COPD measured a daily composite symptom score based on 7 pulmonary and functional symptoms.8 There was a nonsignificant trend towards greater improvement in the steroid-treated group.
Finally, a multicenter, 3-armed, placebo-controlled, double-blinded, parallel design study enrolled 199 COPD inpatients, who were randomized to oral prednisone, inhaled budesonide, or placebo treatment groups.9 Dyspnea was assessed using a validated, modified Borg scale every 12 hours for 72 hours. The reduction in the modified Borg scale rating was of comparable magnitude in the 3 groups, but again there was a nonsignificant greater reduction in the systemic steroid group compared with both the placebo and inhaled budesonide groups. Power calculations were not provided, so it is unclear whether sample size in this study was sufficient to detect important differences in outcomes.
Three randomized controlled trials prospectively measured adverse events rates of systemic steroids in acute exacerbations of COPD.9-11 Hyperglycemia or glycosuria was more common in the steroid-treated groups. The SCCOPE study, the largest of the 3 trials, found hyperglycemia requiring treatment occurred in a greater proportion of the steroid-treated group than placebo (15% vs 4%; P=.002; number needed to harm=9).
Recommendations from others
A recent review provides a concise summary of practice guidelines for the management of acute exacerbations of COPD from widely recognized professional societies.12 Systemic steroids are endorsed in the evidence-based systematic review guidelines from the American College of Chest Physicians–American Society of Internal Medicine, along with the National Heart, Lung, and Blood Institute with the World Health Organization cosponsored Global Initiative for Chronic Obstructive Lung Disease (GOLD), and the consensus guidelines of the American Thoracic Society.13
Lack of long-term benefits emphasize need for prevention
Donald Briscoe, MD
CHRISTUS St. Joseph Family Practice Residency, Houston, TX
It is reassuring to see that there is good evidence to support what most practicing physicians already do—use steroids for acute exacerbations of COPD. Along with inhaled anticholinergics, beta-agonists and (sometimes) antibiotics, short-term measures of patient oriented outcomes seem to be improved. Questions still remain regarding the optimal dosing, route of administration, and length of therapy needed. The lack of evidence of long-term outcome benefits emphasizes, to me, the need for improved efforts at primary and secondary prevention, such as smoking prevention and cessation interventions, annual influenza vaccination, and routine pneumococcal vaccination in our COPD patients.
1. Wood-Baker R, Walters EH, Gibson P. Oral corticos-teroids for acute exacerbations of chronic obstructive pulmonary disease (Cochrane Review). The Cochrane Library, issue 4, 2003. Updated January 12, 2001.
2. McCrory DC, Brown C, Gelfand SE, Bach PB. Management of acute exacerbations of COPD: a summary and appraisal of published evidence. Chest 2001;119:1190-1209.
3. Singh JM, Palda VA, Stanbrook MB, Chapman KR. Corticosteroid therapy for patients with acute exacerbations of chronic obstructive pulmonary disease. Arch Intern Med 2002;162:2527-2536.
4. Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS. GOLD Scientific Committee. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop Summary. Am J Respir Crit Care Med 2001;163:1256-1276.
5. Thompson WH, Nielson CP, Carvalho P, Charan NB, Crowley JJ. Controlled trial of oral prednisone in outpatients with acute COPD exacerbation. Am J Respir Crit Care Med 1996;154:407-412.
6. Wood-Baker R, Wilinson J, Pearce M, Ryan G. A double-blind, placebo-controlled trial of corticosteroids for acute exacerbations of chronic obstructive pulmonary disease. Aust N Z J Med 1998;28:262.-
7. Bullard MJ, Liaw SJ, Tsai YH, Min HP. Early corticosteroid use in acute exacerbations of chronic airflow obstruction. Am J Emerg Med 1996;14:139-143.
8. Davies L, Angus RM, Calverley PM. Oral corticosteroids in patients admitted to hospital with exacerbations of chronic obstructive pulmonary disease: a prospective randomised controlled trial. Lancet 1999;354:456-460.
9. Maltais F, Ostinelli J, Bourbeau J, et al. Comparison of nebulized budesonide and oral prednisolone with placebo in the treatment of acute exacerbations of chronic obstructive pulmonary disease: a randomized controlled trial. Am J Respir Crit Care Med 2002;165:698-703.
10. Albert RK, Martin TR, Lewis SW. Controlled clinical trial of methylprednisolone in patients with chronic bronchitis and acute respiratory insufficiency. Ann Intern Med 1980;92:753-758.
11. Niewoehner DE, Erbland ML, Deupree RH, et al. Effect of systemic glucocorticoids on exacerbations of chronic obstructive pulmonary disease. Department of Veterans Affairs Cooperative Study Group. N Engl J Med 1999;340:1941-1947.
12. Stoller JK. Clinical practice. Acute exacerbations of chronic obstructive pulmonary disease. N Engl J Med 2002;346:988-994.
13. Niewoehner DE, Erbland M, Collins D. Glucocorticoids for chronic obstructive pulmonary disease [letter]. N Engl J Med 1999;341:1772-1773.
1. Wood-Baker R, Walters EH, Gibson P. Oral corticos-teroids for acute exacerbations of chronic obstructive pulmonary disease (Cochrane Review). The Cochrane Library, issue 4, 2003. Updated January 12, 2001.
2. McCrory DC, Brown C, Gelfand SE, Bach PB. Management of acute exacerbations of COPD: a summary and appraisal of published evidence. Chest 2001;119:1190-1209.
3. Singh JM, Palda VA, Stanbrook MB, Chapman KR. Corticosteroid therapy for patients with acute exacerbations of chronic obstructive pulmonary disease. Arch Intern Med 2002;162:2527-2536.
4. Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS. GOLD Scientific Committee. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop Summary. Am J Respir Crit Care Med 2001;163:1256-1276.
5. Thompson WH, Nielson CP, Carvalho P, Charan NB, Crowley JJ. Controlled trial of oral prednisone in outpatients with acute COPD exacerbation. Am J Respir Crit Care Med 1996;154:407-412.
6. Wood-Baker R, Wilinson J, Pearce M, Ryan G. A double-blind, placebo-controlled trial of corticosteroids for acute exacerbations of chronic obstructive pulmonary disease. Aust N Z J Med 1998;28:262.-
7. Bullard MJ, Liaw SJ, Tsai YH, Min HP. Early corticosteroid use in acute exacerbations of chronic airflow obstruction. Am J Emerg Med 1996;14:139-143.
8. Davies L, Angus RM, Calverley PM. Oral corticosteroids in patients admitted to hospital with exacerbations of chronic obstructive pulmonary disease: a prospective randomised controlled trial. Lancet 1999;354:456-460.
9. Maltais F, Ostinelli J, Bourbeau J, et al. Comparison of nebulized budesonide and oral prednisolone with placebo in the treatment of acute exacerbations of chronic obstructive pulmonary disease: a randomized controlled trial. Am J Respir Crit Care Med 2002;165:698-703.
10. Albert RK, Martin TR, Lewis SW. Controlled clinical trial of methylprednisolone in patients with chronic bronchitis and acute respiratory insufficiency. Ann Intern Med 1980;92:753-758.
11. Niewoehner DE, Erbland ML, Deupree RH, et al. Effect of systemic glucocorticoids on exacerbations of chronic obstructive pulmonary disease. Department of Veterans Affairs Cooperative Study Group. N Engl J Med 1999;340:1941-1947.
12. Stoller JK. Clinical practice. Acute exacerbations of chronic obstructive pulmonary disease. N Engl J Med 2002;346:988-994.
13. Niewoehner DE, Erbland M, Collins D. Glucocorticoids for chronic obstructive pulmonary disease [letter]. N Engl J Med 1999;341:1772-1773.
Evidence-based answers from the Family Physicians Inquiries Network
What is the best hypnotic for use in the elderly?
Short-acting hypnotics such as zolpidem (Ambien) or zaleplon (Sonata) are the preferred hypnotics in the elderly because of an improved side-effect profile compared with traditional hypnotics such as benzodiazepines (strength of recommendation: B, based on extrapolations of randomized controlled trials). Zolpidem and zaleplon have a quick onset and short duration of action, making them less likely to cause residual sedation, cognitive changes, and falls than benzodiazepines. More comparative clinical trials in the elderly are needed to determine if zolpidem and zaleplon are truly safer than benzodiazepines in this population. Hypnotics should be prescribed on a short-term, intermittent basis as part of a comprehensive treatment plan that addresses any underlying causes of poor sleep.
Evidence summary
Zolpidem and zaleplon
Zolpidem and zaleplon differ structurally from benzodiazepines but act at the benzodiazepine receptor.1 Due to their rapid absorption and short half-lives, they are particularly helpful for patients who have trouble falling asleep.2 They have been shown to decrease sleep latency, increase total sleep time, and increase sleep efficiency without disturbing sleep architecture or adversely affecting memory.1
Comparative studies in the elderly have demonstrated that zolpidem is as effective as triazolam,3 and that zaleplon is more effective than placebo at decreasing sleep latency and improving sleep quality.4 Tolerance, withdrawal symptoms, or rebound insomnia occur less frequently than with benzodi-azepines,1 but zolpidem increased risk of hip fracture in a case control study (adjusted odds ratio=1.95, 95% confidence interval, 1.09–3.51).5
Side effects of zolpidem and zaleplon are considered dose-related, and a lower dose of 5 mg is recommended for older patients.2 Efficacy of intermittent use of zolpidem has been demonstrated in clinical studies,1 a practice that could potentially decrease risk of side effects. Overall, if a hypnotic is desired for an older adult, zolpidem and zaleplon are preferred because of their improved side-effect profiles compared with older hypnotics such as benzodiazepines, chloral hydrate, over-the-counter sleep aids, and antidepressants (see Table ).
TABLE 1
Adverse effects of hypnotics in the elderly
| Hypnotic | Adverse effect |
|---|---|
| Benzodiazepines | Somnolence, anterograde amnesia, falls, hip fracture, rebound insomnia, tolerance, dependence, impaired sleep architecture2,3,5 |
| Antihistamines | Somnolence, dry mouth, constipation, urinary retention, blurred vision, cognitive changes3 |
| Valerian | Headache, excitability, uneasiness, cardiac disturbances, insomnia, drowsiness, withdrawal symptoms10 |
| Melatonin | Headache, depressive symptoms, daytime fatigue and drowsiness, dizziness, abdominal cramps, reduced alertness10 |
| Chloral hydrate | Nausea, vomiting, diarrhea, may increase effects of warfarin, overdose potential3,8 |
| Tricyclic antidepressants | Dry mouth, constipation, urinary retention, blurred vision, cognitive changes, orthostatic hypotension, somnolence, worsening of chronic heart failure, overdose potential, cardiac conduction abnormalities2,3 |
| Trazodone | Somnolence, orthostatic hypotension, dry mouth, priapism3 |
| Zolpidem | Drowsiness, headache, dizziness, somnolence, fatigue, agitation, nightmares, diarrhea, myalgia, arthralgia, anterograde amnesia1,10 |
| Zaleplon | Headache, dizziness, somnolence, short-term amnesic effects, next-day memory impairment, mild rebound insomnia1,10 |
Benzodiazepines
Benzodiazepines have been used since the 1960s for their hypnotic, anxiolytic, anticonvulsant, muscle-relaxing, and amnesic properties. A recent meta-analysis showed that benzodiazepines improve sleep latency by only 4.2 minutes compared with placebo.6 Although benzodiazepines increase sleep time and efficiency, patients quickly develop tolerance to the hypnotic effects.7 Additional problems associated with benzodiazepines include dependence, rebound insomnia, residual sedation, falls, hip fractures, and detrimental effects on sleep architecture.7
Chloral hydrate
Chloral hydrate has a narrow therapeutic index and is not recommended for the treatment of insomnia.8 Tolerance to its effects develops after only 2 weeks of use, and drug interactions with warfarin can occur.2
Over-the-counter sleep aids
Most over-the-counter sleep aids contain diphen-hydramine, a long-acting antihistamine that is considered less effective than benzodiazepines. The anticholinergic properties of antihistamines can result in cognitive changes and urinary retention in the elderly.8 Melatonin and valerian are “natural” hypnotics that are available without a prescription,9 but their safety and efficacy are not regulated by the FDA.8
Antidepressants
Antidepressants with sedative effects, such as tricyclic antidepressants and trazodone, have been used for insomnia, but minimal data support the efficacy or safety of this approach.8 Tricyclic antidepressants may exacerbate restless legs syndrome and periodic limb movement disorder,8 cause anticholinergic side effects, worsen chronic heart failure, and cause ortho-static hypotension and falls.2 Although tra-zodone is not a tricyclic antidepressant, it can cause dry mouth, orthostatic hypotension, and (rarely) priapism.2
Recommendations from others
A Canadian consensus statement published in 2003 supports the use of non-benzodiazepines such as zolpidem and zaleplon due to improved tolerability, and less withdrawal and abuse potential compared with benzodiazepines.7 The National Heart, Lung and Blood Institute Working Group on Insomnia recommends the use of short-acting hypnotics for short-term management of insomnia, but does not differentiate between short-acting benzodiazepines and the newer hypnotics such as zolpidem and zale-plon.8 Geriatric experts recommend that long-acting benzodiazepines, barbiturates, and amitriptyline be avoided in the elderly due to the risk of adverse drug events.10
Question the patient about sleep habits
David Cravens, MD, MSPH
Department of Family & Community Medicine, University of Missouri–Columbia
Sleep complaints are common in the elderly. However, before prescribing a hypnotic, determine the elderly patient’s sleep habits: often daytime naps plus nighttime sleep add up to adequate sleep. Encourage measures to avoid daytime naps if nighttime sleep is more important. Second, discuss sleep hygiene, such as avoiding evening caffeine or excessive alcohol, and avoiding using bed for activities other than sleeping, such as watching TV, reading, and the like. Determine whether sleep problems are part of a larger problem requiring evaluation, such as medication effects, depression, or obstructive sleep apnea. Finally, consider costs: although not a true hypnotic, trazodone at doses of 25–50 mg is a very effective and well-tolerated soporific at about one-tenth the cost of 5 mg of zolpidem or zaleplon.
1. Terzano MG, Rossi M, Palomba V, Smerien A, Parrino L. New drugs for insomnia: comparative tolerability of zopiclone, zolpi-dem and zaleplon. Drug Saf 2003;26:261-282.
2. McEvoy GK, Miller J, Litvak K, et al. AHFS Drug Information. Bethesda, MD: American Society of Health-System Pharmacists; 2003;2400-2405.
3. Roger M, Attali P, Coquelin JP. Multicenter, double-blind, controlled comparison of zolpidem and triazolam in elderly patients with insomnia. Clin Ther 1993;15:127-136.
4. Hedner J, Yaeche R, Emilien G, Farr I, Salinas E. Zaleplon shortens subjective sleep latency and improves subjective sleep quality in elderly patients with insomnia. The Zaleplon Clinical Investigator Study Group. Int J Geriatr Psychiatry 2000;15:704-712.
5. Wang PS, Bohn RL, Glynn RJ, Mogun H, Avom J. Zolpidem use and hip fractures in older people. J Am Geriatr Soc 2001;49:1685-1690.
6. Holbrook AM, Crowther R, Lotter A, Cheng C, King D. Meta-analysis of benzodiazepine use in the treatment of insomnia. CMAJ 2000;162:225-233.
7. Montplaisir J, Hawa R, Moller H, et al. Zopiclone and zaleplon vs benzodiazepines in the treatment of insomnia: Canadian consensus statement. Hum Psychopharmacol 2003;18:29-38.
8. Insomnia: assessment and management in primary care. National Heart, Lung, and Blood Institute Working Group on Insomnia. Am Fam Physician 1999;59:3029-3038.
9. Jellin JM, Gregory P, Batz F, et al. Pharmacist’s Letter/Prescriber’s Letter Natural Medicines Comprehensive Database. 3rd ed. Stockton, Calif: Therapeutic Research Faculty; 2000;723-7251052-1053.
10. Beers MH. Explicit criteria for determining potentially inappropriate medication use by the elderly. An update. Arch Intern Med 1997;157:1531-1536.
Short-acting hypnotics such as zolpidem (Ambien) or zaleplon (Sonata) are the preferred hypnotics in the elderly because of an improved side-effect profile compared with traditional hypnotics such as benzodiazepines (strength of recommendation: B, based on extrapolations of randomized controlled trials). Zolpidem and zaleplon have a quick onset and short duration of action, making them less likely to cause residual sedation, cognitive changes, and falls than benzodiazepines. More comparative clinical trials in the elderly are needed to determine if zolpidem and zaleplon are truly safer than benzodiazepines in this population. Hypnotics should be prescribed on a short-term, intermittent basis as part of a comprehensive treatment plan that addresses any underlying causes of poor sleep.
Evidence summary
Zolpidem and zaleplon
Zolpidem and zaleplon differ structurally from benzodiazepines but act at the benzodiazepine receptor.1 Due to their rapid absorption and short half-lives, they are particularly helpful for patients who have trouble falling asleep.2 They have been shown to decrease sleep latency, increase total sleep time, and increase sleep efficiency without disturbing sleep architecture or adversely affecting memory.1
Comparative studies in the elderly have demonstrated that zolpidem is as effective as triazolam,3 and that zaleplon is more effective than placebo at decreasing sleep latency and improving sleep quality.4 Tolerance, withdrawal symptoms, or rebound insomnia occur less frequently than with benzodi-azepines,1 but zolpidem increased risk of hip fracture in a case control study (adjusted odds ratio=1.95, 95% confidence interval, 1.09–3.51).5
Side effects of zolpidem and zaleplon are considered dose-related, and a lower dose of 5 mg is recommended for older patients.2 Efficacy of intermittent use of zolpidem has been demonstrated in clinical studies,1 a practice that could potentially decrease risk of side effects. Overall, if a hypnotic is desired for an older adult, zolpidem and zaleplon are preferred because of their improved side-effect profiles compared with older hypnotics such as benzodiazepines, chloral hydrate, over-the-counter sleep aids, and antidepressants (see Table ).
TABLE 1
Adverse effects of hypnotics in the elderly
| Hypnotic | Adverse effect |
|---|---|
| Benzodiazepines | Somnolence, anterograde amnesia, falls, hip fracture, rebound insomnia, tolerance, dependence, impaired sleep architecture2,3,5 |
| Antihistamines | Somnolence, dry mouth, constipation, urinary retention, blurred vision, cognitive changes3 |
| Valerian | Headache, excitability, uneasiness, cardiac disturbances, insomnia, drowsiness, withdrawal symptoms10 |
| Melatonin | Headache, depressive symptoms, daytime fatigue and drowsiness, dizziness, abdominal cramps, reduced alertness10 |
| Chloral hydrate | Nausea, vomiting, diarrhea, may increase effects of warfarin, overdose potential3,8 |
| Tricyclic antidepressants | Dry mouth, constipation, urinary retention, blurred vision, cognitive changes, orthostatic hypotension, somnolence, worsening of chronic heart failure, overdose potential, cardiac conduction abnormalities2,3 |
| Trazodone | Somnolence, orthostatic hypotension, dry mouth, priapism3 |
| Zolpidem | Drowsiness, headache, dizziness, somnolence, fatigue, agitation, nightmares, diarrhea, myalgia, arthralgia, anterograde amnesia1,10 |
| Zaleplon | Headache, dizziness, somnolence, short-term amnesic effects, next-day memory impairment, mild rebound insomnia1,10 |
Benzodiazepines
Benzodiazepines have been used since the 1960s for their hypnotic, anxiolytic, anticonvulsant, muscle-relaxing, and amnesic properties. A recent meta-analysis showed that benzodiazepines improve sleep latency by only 4.2 minutes compared with placebo.6 Although benzodiazepines increase sleep time and efficiency, patients quickly develop tolerance to the hypnotic effects.7 Additional problems associated with benzodiazepines include dependence, rebound insomnia, residual sedation, falls, hip fractures, and detrimental effects on sleep architecture.7
Chloral hydrate
Chloral hydrate has a narrow therapeutic index and is not recommended for the treatment of insomnia.8 Tolerance to its effects develops after only 2 weeks of use, and drug interactions with warfarin can occur.2
Over-the-counter sleep aids
Most over-the-counter sleep aids contain diphen-hydramine, a long-acting antihistamine that is considered less effective than benzodiazepines. The anticholinergic properties of antihistamines can result in cognitive changes and urinary retention in the elderly.8 Melatonin and valerian are “natural” hypnotics that are available without a prescription,9 but their safety and efficacy are not regulated by the FDA.8
Antidepressants
Antidepressants with sedative effects, such as tricyclic antidepressants and trazodone, have been used for insomnia, but minimal data support the efficacy or safety of this approach.8 Tricyclic antidepressants may exacerbate restless legs syndrome and periodic limb movement disorder,8 cause anticholinergic side effects, worsen chronic heart failure, and cause ortho-static hypotension and falls.2 Although tra-zodone is not a tricyclic antidepressant, it can cause dry mouth, orthostatic hypotension, and (rarely) priapism.2
Recommendations from others
A Canadian consensus statement published in 2003 supports the use of non-benzodiazepines such as zolpidem and zaleplon due to improved tolerability, and less withdrawal and abuse potential compared with benzodiazepines.7 The National Heart, Lung and Blood Institute Working Group on Insomnia recommends the use of short-acting hypnotics for short-term management of insomnia, but does not differentiate between short-acting benzodiazepines and the newer hypnotics such as zolpidem and zale-plon.8 Geriatric experts recommend that long-acting benzodiazepines, barbiturates, and amitriptyline be avoided in the elderly due to the risk of adverse drug events.10
Question the patient about sleep habits
David Cravens, MD, MSPH
Department of Family & Community Medicine, University of Missouri–Columbia
Sleep complaints are common in the elderly. However, before prescribing a hypnotic, determine the elderly patient’s sleep habits: often daytime naps plus nighttime sleep add up to adequate sleep. Encourage measures to avoid daytime naps if nighttime sleep is more important. Second, discuss sleep hygiene, such as avoiding evening caffeine or excessive alcohol, and avoiding using bed for activities other than sleeping, such as watching TV, reading, and the like. Determine whether sleep problems are part of a larger problem requiring evaluation, such as medication effects, depression, or obstructive sleep apnea. Finally, consider costs: although not a true hypnotic, trazodone at doses of 25–50 mg is a very effective and well-tolerated soporific at about one-tenth the cost of 5 mg of zolpidem or zaleplon.
Short-acting hypnotics such as zolpidem (Ambien) or zaleplon (Sonata) are the preferred hypnotics in the elderly because of an improved side-effect profile compared with traditional hypnotics such as benzodiazepines (strength of recommendation: B, based on extrapolations of randomized controlled trials). Zolpidem and zaleplon have a quick onset and short duration of action, making them less likely to cause residual sedation, cognitive changes, and falls than benzodiazepines. More comparative clinical trials in the elderly are needed to determine if zolpidem and zaleplon are truly safer than benzodiazepines in this population. Hypnotics should be prescribed on a short-term, intermittent basis as part of a comprehensive treatment plan that addresses any underlying causes of poor sleep.
Evidence summary
Zolpidem and zaleplon
Zolpidem and zaleplon differ structurally from benzodiazepines but act at the benzodiazepine receptor.1 Due to their rapid absorption and short half-lives, they are particularly helpful for patients who have trouble falling asleep.2 They have been shown to decrease sleep latency, increase total sleep time, and increase sleep efficiency without disturbing sleep architecture or adversely affecting memory.1
Comparative studies in the elderly have demonstrated that zolpidem is as effective as triazolam,3 and that zaleplon is more effective than placebo at decreasing sleep latency and improving sleep quality.4 Tolerance, withdrawal symptoms, or rebound insomnia occur less frequently than with benzodi-azepines,1 but zolpidem increased risk of hip fracture in a case control study (adjusted odds ratio=1.95, 95% confidence interval, 1.09–3.51).5
Side effects of zolpidem and zaleplon are considered dose-related, and a lower dose of 5 mg is recommended for older patients.2 Efficacy of intermittent use of zolpidem has been demonstrated in clinical studies,1 a practice that could potentially decrease risk of side effects. Overall, if a hypnotic is desired for an older adult, zolpidem and zaleplon are preferred because of their improved side-effect profiles compared with older hypnotics such as benzodiazepines, chloral hydrate, over-the-counter sleep aids, and antidepressants (see Table ).
TABLE 1
Adverse effects of hypnotics in the elderly
| Hypnotic | Adverse effect |
|---|---|
| Benzodiazepines | Somnolence, anterograde amnesia, falls, hip fracture, rebound insomnia, tolerance, dependence, impaired sleep architecture2,3,5 |
| Antihistamines | Somnolence, dry mouth, constipation, urinary retention, blurred vision, cognitive changes3 |
| Valerian | Headache, excitability, uneasiness, cardiac disturbances, insomnia, drowsiness, withdrawal symptoms10 |
| Melatonin | Headache, depressive symptoms, daytime fatigue and drowsiness, dizziness, abdominal cramps, reduced alertness10 |
| Chloral hydrate | Nausea, vomiting, diarrhea, may increase effects of warfarin, overdose potential3,8 |
| Tricyclic antidepressants | Dry mouth, constipation, urinary retention, blurred vision, cognitive changes, orthostatic hypotension, somnolence, worsening of chronic heart failure, overdose potential, cardiac conduction abnormalities2,3 |
| Trazodone | Somnolence, orthostatic hypotension, dry mouth, priapism3 |
| Zolpidem | Drowsiness, headache, dizziness, somnolence, fatigue, agitation, nightmares, diarrhea, myalgia, arthralgia, anterograde amnesia1,10 |
| Zaleplon | Headache, dizziness, somnolence, short-term amnesic effects, next-day memory impairment, mild rebound insomnia1,10 |
Benzodiazepines
Benzodiazepines have been used since the 1960s for their hypnotic, anxiolytic, anticonvulsant, muscle-relaxing, and amnesic properties. A recent meta-analysis showed that benzodiazepines improve sleep latency by only 4.2 minutes compared with placebo.6 Although benzodiazepines increase sleep time and efficiency, patients quickly develop tolerance to the hypnotic effects.7 Additional problems associated with benzodiazepines include dependence, rebound insomnia, residual sedation, falls, hip fractures, and detrimental effects on sleep architecture.7
Chloral hydrate
Chloral hydrate has a narrow therapeutic index and is not recommended for the treatment of insomnia.8 Tolerance to its effects develops after only 2 weeks of use, and drug interactions with warfarin can occur.2
Over-the-counter sleep aids
Most over-the-counter sleep aids contain diphen-hydramine, a long-acting antihistamine that is considered less effective than benzodiazepines. The anticholinergic properties of antihistamines can result in cognitive changes and urinary retention in the elderly.8 Melatonin and valerian are “natural” hypnotics that are available without a prescription,9 but their safety and efficacy are not regulated by the FDA.8
Antidepressants
Antidepressants with sedative effects, such as tricyclic antidepressants and trazodone, have been used for insomnia, but minimal data support the efficacy or safety of this approach.8 Tricyclic antidepressants may exacerbate restless legs syndrome and periodic limb movement disorder,8 cause anticholinergic side effects, worsen chronic heart failure, and cause ortho-static hypotension and falls.2 Although tra-zodone is not a tricyclic antidepressant, it can cause dry mouth, orthostatic hypotension, and (rarely) priapism.2
Recommendations from others
A Canadian consensus statement published in 2003 supports the use of non-benzodiazepines such as zolpidem and zaleplon due to improved tolerability, and less withdrawal and abuse potential compared with benzodiazepines.7 The National Heart, Lung and Blood Institute Working Group on Insomnia recommends the use of short-acting hypnotics for short-term management of insomnia, but does not differentiate between short-acting benzodiazepines and the newer hypnotics such as zolpidem and zale-plon.8 Geriatric experts recommend that long-acting benzodiazepines, barbiturates, and amitriptyline be avoided in the elderly due to the risk of adverse drug events.10
Question the patient about sleep habits
David Cravens, MD, MSPH
Department of Family & Community Medicine, University of Missouri–Columbia
Sleep complaints are common in the elderly. However, before prescribing a hypnotic, determine the elderly patient’s sleep habits: often daytime naps plus nighttime sleep add up to adequate sleep. Encourage measures to avoid daytime naps if nighttime sleep is more important. Second, discuss sleep hygiene, such as avoiding evening caffeine or excessive alcohol, and avoiding using bed for activities other than sleeping, such as watching TV, reading, and the like. Determine whether sleep problems are part of a larger problem requiring evaluation, such as medication effects, depression, or obstructive sleep apnea. Finally, consider costs: although not a true hypnotic, trazodone at doses of 25–50 mg is a very effective and well-tolerated soporific at about one-tenth the cost of 5 mg of zolpidem or zaleplon.
1. Terzano MG, Rossi M, Palomba V, Smerien A, Parrino L. New drugs for insomnia: comparative tolerability of zopiclone, zolpi-dem and zaleplon. Drug Saf 2003;26:261-282.
2. McEvoy GK, Miller J, Litvak K, et al. AHFS Drug Information. Bethesda, MD: American Society of Health-System Pharmacists; 2003;2400-2405.
3. Roger M, Attali P, Coquelin JP. Multicenter, double-blind, controlled comparison of zolpidem and triazolam in elderly patients with insomnia. Clin Ther 1993;15:127-136.
4. Hedner J, Yaeche R, Emilien G, Farr I, Salinas E. Zaleplon shortens subjective sleep latency and improves subjective sleep quality in elderly patients with insomnia. The Zaleplon Clinical Investigator Study Group. Int J Geriatr Psychiatry 2000;15:704-712.
5. Wang PS, Bohn RL, Glynn RJ, Mogun H, Avom J. Zolpidem use and hip fractures in older people. J Am Geriatr Soc 2001;49:1685-1690.
6. Holbrook AM, Crowther R, Lotter A, Cheng C, King D. Meta-analysis of benzodiazepine use in the treatment of insomnia. CMAJ 2000;162:225-233.
7. Montplaisir J, Hawa R, Moller H, et al. Zopiclone and zaleplon vs benzodiazepines in the treatment of insomnia: Canadian consensus statement. Hum Psychopharmacol 2003;18:29-38.
8. Insomnia: assessment and management in primary care. National Heart, Lung, and Blood Institute Working Group on Insomnia. Am Fam Physician 1999;59:3029-3038.
9. Jellin JM, Gregory P, Batz F, et al. Pharmacist’s Letter/Prescriber’s Letter Natural Medicines Comprehensive Database. 3rd ed. Stockton, Calif: Therapeutic Research Faculty; 2000;723-7251052-1053.
10. Beers MH. Explicit criteria for determining potentially inappropriate medication use by the elderly. An update. Arch Intern Med 1997;157:1531-1536.
1. Terzano MG, Rossi M, Palomba V, Smerien A, Parrino L. New drugs for insomnia: comparative tolerability of zopiclone, zolpi-dem and zaleplon. Drug Saf 2003;26:261-282.
2. McEvoy GK, Miller J, Litvak K, et al. AHFS Drug Information. Bethesda, MD: American Society of Health-System Pharmacists; 2003;2400-2405.
3. Roger M, Attali P, Coquelin JP. Multicenter, double-blind, controlled comparison of zolpidem and triazolam in elderly patients with insomnia. Clin Ther 1993;15:127-136.
4. Hedner J, Yaeche R, Emilien G, Farr I, Salinas E. Zaleplon shortens subjective sleep latency and improves subjective sleep quality in elderly patients with insomnia. The Zaleplon Clinical Investigator Study Group. Int J Geriatr Psychiatry 2000;15:704-712.
5. Wang PS, Bohn RL, Glynn RJ, Mogun H, Avom J. Zolpidem use and hip fractures in older people. J Am Geriatr Soc 2001;49:1685-1690.
6. Holbrook AM, Crowther R, Lotter A, Cheng C, King D. Meta-analysis of benzodiazepine use in the treatment of insomnia. CMAJ 2000;162:225-233.
7. Montplaisir J, Hawa R, Moller H, et al. Zopiclone and zaleplon vs benzodiazepines in the treatment of insomnia: Canadian consensus statement. Hum Psychopharmacol 2003;18:29-38.
8. Insomnia: assessment and management in primary care. National Heart, Lung, and Blood Institute Working Group on Insomnia. Am Fam Physician 1999;59:3029-3038.
9. Jellin JM, Gregory P, Batz F, et al. Pharmacist’s Letter/Prescriber’s Letter Natural Medicines Comprehensive Database. 3rd ed. Stockton, Calif: Therapeutic Research Faculty; 2000;723-7251052-1053.
10. Beers MH. Explicit criteria for determining potentially inappropriate medication use by the elderly. An update. Arch Intern Med 1997;157:1531-1536.
Evidence-based answers from the Family Physicians Inquiries Network
Do statins cause myopathy?
If statins (HMG-CoA reductase inhibitors) cause myopathy, the risk is very low (strength of recommendation [SOR]: A). There is no direct evidence to answer this question. A pooled analysis of randomized controlled trials found similar myopathy rates in patients taking statins and placebo. However, a large cohort study revealed a very small but statistically significant increased risk of myopathy in patients taking statins (number needed to harm=10,000/year).
Case reports suggest a myopathy risk for all statins, including fatal rhabdomyolysis. Risk of myopathy may increase with higher statin doses, certain comorbid states (eg, hypothyroidism, renal insufficiency [especially with diabetes], recent trauma, perioperative periods, advanced age, small body frame) and concurrent medications, including fibrates, cyclosporine, azole antifungals, and macrolide antibiotics (SOR: B). No studies have directly compared myopathy rates among statins, and there is no good evidence to suggest any differences. No controlled study has directly examined statin rechallenge in patients with previous myopathy; however, case reports and expert opinion support this practice (SOR: B).
Evidence summary
There is little evidence that statins cause myopathy. Synthesis is difficult because definitions of myopathy types differ among investigators. Proposed clinical syndrome definitions are myalgia (muscle weakness or ache with normal creatine kinase), myositis (symptoms with increased creatine kinase), and rhabdomyolysis (symptoms, markedly elevated creatine kinase, and renal insufficiency) as subsets of the more general term myopathy.1 The Table summarizes myopathy data from 30 statin trials analyzed in a recent systematic review, showing similar myopathy rates in statin and placebo patients.2 There may be a lower myopathy rate in these trials than in routine clinical practice because of stricter exclusion criteria and more intense monitoring.
A large well-done British epidemiologic cohort study (n=96,193) found an increased rate of myopathy (broadly defined, not requiring creatine kinase elevation) among patients taking statins, with an absolute rate difference of 1 per 10,000 person-years.3 A small study of 21 patients on statins with muscle symptoms but normal creatine kinases described 4 patients who were able to distinguish statins from placebo, with objective reversible weakness and abnormal muscle biopsies.4 Postmarket voluntary clinician reports point to statin myopathy in this and other countries;5-7 these include 3339 rhabdomyolysis FDA reports (1990 to March 2002).2
Though some assert differential myopathy rates among statins based on cell research, case reports, or differences in metabolic clearance, no studies directly compare clinical myopathy rates among statins. There is no good evidence of a differential myopathy risk among statins currently available in the US.1-2 Cerivastatin, however, was withdrawn from the US market because of a fatal rhabdomyolysis rate 16 to 80 times higher than other statins based on FDA reports using a denominator of prescription volume (3.16 fatal cases/million prescriptions vs 0.15 for the statin class as a whole).6
It is unknown whether previous myopathy, however defined, increases the risk of future myopathy with statin rechallenge. A tabular analysis of 74 published case reports of statin-associated rhabdomyolysis from a MEDLINE search covering 1985 to 2000 reported that in most cases the statin was safely restarted after stopping presumed interactive drugs (exact numbers not reported).8 In the AFCAPS/TexCAPS trial, 20 of 21 statin patients (out of a study population of 3304) who had elevated creatine kinase (>10 times the upper limits of normal) recovered with continued lovastatin treatment, while the other patient resumed treatment after a brief interruption without further elevations.9 The EXCEL trial (n=8245) of various lovastatin dosages included routine creatine kinase tests every 6 weeks for 48 weeks. Five lovastatin patients had muscle symptoms with creatine kinases >10 times the upper limits of normal, and in the 2 who continued treatment, symptoms and creatine kinase became normal.10 Of note, creatine kinase elevation of any kind at least once during 48 weeks occurred in 28.9% of placebo patients, arguing against routine creatine kinase screening in statin patients.
Case studies suggest an increased myopathy risk when statins are given with various medications, including fibrates, cyclosporine, azole antifungals, warfarin, nefazodone, and macrolide antibiotics.4,6,8 Pravastatin and fluvastatin, which are not metabolized by the P450 CYP3A4 pathway, may be safer to use because of fewer drug interactions.2,8 Likewise, certain comorbid states such as hypothyroidism, renal insufficiency (especially in patients with diabetes), recent trauma, and perioperative periods, as well as advanced age, small body frame, and multiple medications may increase statin myopathy risk.1,2,7,8
TABLE
Pooled myopathy data from 30 randomized controlled statin trials
| Trials | Total patients | Statin patients | Placebo patients | |
|---|---|---|---|---|
| Myalgia | 5 | 33,929 | 0.3–32.9% | 0–33.3% |
| Creatine kinase elevation | 9 | 33,921 | 0–0.64% | 0–0.58% |
| Myositis* | 18 | 58,237 | 0.17% | 0.15% |
| Rhabdomyolysis | 20 | 70,126 | 0.020% | 0.014% |
| *Creatine kinase >10 times upper limit of normal | ||||
| Adapted and calculated from Thompson PD, et al. JAMA 2003; 289:1681–1690.2 | ||||
Recommendations from others
A 2002 Clinical Advisory, jointly issued by the American College of Cardiology, the American Heart Association, and the National Heart, Lung and Blood Institute, asserted that statins carry a small but definite myopathy risk.1 It recommended against routine creatine kinase tests, reserving them for patients who develop muscle symptoms. It also recommended stopping statins when muscle symptoms with creatine kinase elevations >10 times the upper limits of normal occur, with consideration of restarting statins later at a lower dose if symptoms and elevated creatine kinase resolve. Careful monitoring of patients at higher risk of statin myopathy is also recommended.
Benefits of statins outweigh the risks
Joseph Saseen, PharmD, BCPS
University of Colorado Health Sciences Center, Denver
Contrary to popular belief, statin-associated myopathy is a rare adverse event. Drug-drug interactions and comorbid diseases (especially chronic kidney disease) increase myopathy risk. Given the overwhelming evidence demonstrating reduced morbidity and mortality with statins, benefits outweigh risks in patients with elevated low-density lipoprotein cholesterol. Data supporting myopathy management strategies are limited, but support stopping statin therapy in patients with myopathy (muscle aches/pain with elevated creatine kinase), and restarting, possibly with a different statin, after symptoms resolve. Myopathy should not be confused with myalgia (muscle aches/pain with normal creatine kinase). Myalgia requires interrupting treatment only for patients with persistent muscle aches/pain while on statin therapy.
1. Pasternak RC, Smith SC, Jr, Biarey-Merz CN, Grundy SM, Cleeman JI, Lenfant C. ACC/AHA/NHLBI clinical advisory on the use and safety of statins. J Am Coll Cardiol 2002;40:567-572.
2. Thompson PD, Clarkson P, Karas RH. Statin-associated myopathy. JAMA 2003;289:1681-1690.
3. Gaist D, Rodriquez LA, Huerta C, Hallas J, Sindrup SH. Lipid-lowering drugs and risk of myopathy: a population-based follow-up study. Epidemiology 2001;12:565-569.
4. Phillips PS, Haas RH, Bannykh S, et al. Statin-associated myopathy with normal creatine kinase levels. Ann Intern Med 2002;137:581-585.
5. Omar MA, Wilson JP. FDA adverse event reports on statin-associated rhabdomyolysis. Ann Pharmacother 2002;36:288-295.
6. Staffa JA, Chang J, Green L. Cerivastatin and reports of fatal rhabdomyolysis. N Engl J Med 2002;346:539-540.
7. Ucar M, Mjorndal T, Dahlqvist R. HMG-CoA reductase inhibitors and myotoxicity. Drug Saf 2000;6:441-447.
8. Omar MA, Wilson JP, Cox TS. Rhabdomyolysis and HMG-CoA reductase inhibitors. Ann Pharmacother 2001;35:1096-1107.
9. Downs JR, Clearfield M, Tyroler HA, et al. Air Force/Texas Coronary Atherosclerosis Prevention Study (AFCAPS/TexCAPS): Additional perspectives on tolerability of long-term treatment with lovastatin. Am J Cardiol 2001;87:1074-1079.
10. Bradford RH, Shear CL, Chremos AN, et al. Expanded Clinical Evaluation of Lovastatin (EXCEL) study results. I. Efficacy in modifying plasma lipoproteins and adverse event profile in 8245 patients with moderate hypercholes-terolemia. Arch Intern Med 1991;151:43-49.
If statins (HMG-CoA reductase inhibitors) cause myopathy, the risk is very low (strength of recommendation [SOR]: A). There is no direct evidence to answer this question. A pooled analysis of randomized controlled trials found similar myopathy rates in patients taking statins and placebo. However, a large cohort study revealed a very small but statistically significant increased risk of myopathy in patients taking statins (number needed to harm=10,000/year).
Case reports suggest a myopathy risk for all statins, including fatal rhabdomyolysis. Risk of myopathy may increase with higher statin doses, certain comorbid states (eg, hypothyroidism, renal insufficiency [especially with diabetes], recent trauma, perioperative periods, advanced age, small body frame) and concurrent medications, including fibrates, cyclosporine, azole antifungals, and macrolide antibiotics (SOR: B). No studies have directly compared myopathy rates among statins, and there is no good evidence to suggest any differences. No controlled study has directly examined statin rechallenge in patients with previous myopathy; however, case reports and expert opinion support this practice (SOR: B).
Evidence summary
There is little evidence that statins cause myopathy. Synthesis is difficult because definitions of myopathy types differ among investigators. Proposed clinical syndrome definitions are myalgia (muscle weakness or ache with normal creatine kinase), myositis (symptoms with increased creatine kinase), and rhabdomyolysis (symptoms, markedly elevated creatine kinase, and renal insufficiency) as subsets of the more general term myopathy.1 The Table summarizes myopathy data from 30 statin trials analyzed in a recent systematic review, showing similar myopathy rates in statin and placebo patients.2 There may be a lower myopathy rate in these trials than in routine clinical practice because of stricter exclusion criteria and more intense monitoring.
A large well-done British epidemiologic cohort study (n=96,193) found an increased rate of myopathy (broadly defined, not requiring creatine kinase elevation) among patients taking statins, with an absolute rate difference of 1 per 10,000 person-years.3 A small study of 21 patients on statins with muscle symptoms but normal creatine kinases described 4 patients who were able to distinguish statins from placebo, with objective reversible weakness and abnormal muscle biopsies.4 Postmarket voluntary clinician reports point to statin myopathy in this and other countries;5-7 these include 3339 rhabdomyolysis FDA reports (1990 to March 2002).2
Though some assert differential myopathy rates among statins based on cell research, case reports, or differences in metabolic clearance, no studies directly compare clinical myopathy rates among statins. There is no good evidence of a differential myopathy risk among statins currently available in the US.1-2 Cerivastatin, however, was withdrawn from the US market because of a fatal rhabdomyolysis rate 16 to 80 times higher than other statins based on FDA reports using a denominator of prescription volume (3.16 fatal cases/million prescriptions vs 0.15 for the statin class as a whole).6
It is unknown whether previous myopathy, however defined, increases the risk of future myopathy with statin rechallenge. A tabular analysis of 74 published case reports of statin-associated rhabdomyolysis from a MEDLINE search covering 1985 to 2000 reported that in most cases the statin was safely restarted after stopping presumed interactive drugs (exact numbers not reported).8 In the AFCAPS/TexCAPS trial, 20 of 21 statin patients (out of a study population of 3304) who had elevated creatine kinase (>10 times the upper limits of normal) recovered with continued lovastatin treatment, while the other patient resumed treatment after a brief interruption without further elevations.9 The EXCEL trial (n=8245) of various lovastatin dosages included routine creatine kinase tests every 6 weeks for 48 weeks. Five lovastatin patients had muscle symptoms with creatine kinases >10 times the upper limits of normal, and in the 2 who continued treatment, symptoms and creatine kinase became normal.10 Of note, creatine kinase elevation of any kind at least once during 48 weeks occurred in 28.9% of placebo patients, arguing against routine creatine kinase screening in statin patients.
Case studies suggest an increased myopathy risk when statins are given with various medications, including fibrates, cyclosporine, azole antifungals, warfarin, nefazodone, and macrolide antibiotics.4,6,8 Pravastatin and fluvastatin, which are not metabolized by the P450 CYP3A4 pathway, may be safer to use because of fewer drug interactions.2,8 Likewise, certain comorbid states such as hypothyroidism, renal insufficiency (especially in patients with diabetes), recent trauma, and perioperative periods, as well as advanced age, small body frame, and multiple medications may increase statin myopathy risk.1,2,7,8
TABLE
Pooled myopathy data from 30 randomized controlled statin trials
| Trials | Total patients | Statin patients | Placebo patients | |
|---|---|---|---|---|
| Myalgia | 5 | 33,929 | 0.3–32.9% | 0–33.3% |
| Creatine kinase elevation | 9 | 33,921 | 0–0.64% | 0–0.58% |
| Myositis* | 18 | 58,237 | 0.17% | 0.15% |
| Rhabdomyolysis | 20 | 70,126 | 0.020% | 0.014% |
| *Creatine kinase >10 times upper limit of normal | ||||
| Adapted and calculated from Thompson PD, et al. JAMA 2003; 289:1681–1690.2 | ||||
Recommendations from others
A 2002 Clinical Advisory, jointly issued by the American College of Cardiology, the American Heart Association, and the National Heart, Lung and Blood Institute, asserted that statins carry a small but definite myopathy risk.1 It recommended against routine creatine kinase tests, reserving them for patients who develop muscle symptoms. It also recommended stopping statins when muscle symptoms with creatine kinase elevations >10 times the upper limits of normal occur, with consideration of restarting statins later at a lower dose if symptoms and elevated creatine kinase resolve. Careful monitoring of patients at higher risk of statin myopathy is also recommended.
Benefits of statins outweigh the risks
Joseph Saseen, PharmD, BCPS
University of Colorado Health Sciences Center, Denver
Contrary to popular belief, statin-associated myopathy is a rare adverse event. Drug-drug interactions and comorbid diseases (especially chronic kidney disease) increase myopathy risk. Given the overwhelming evidence demonstrating reduced morbidity and mortality with statins, benefits outweigh risks in patients with elevated low-density lipoprotein cholesterol. Data supporting myopathy management strategies are limited, but support stopping statin therapy in patients with myopathy (muscle aches/pain with elevated creatine kinase), and restarting, possibly with a different statin, after symptoms resolve. Myopathy should not be confused with myalgia (muscle aches/pain with normal creatine kinase). Myalgia requires interrupting treatment only for patients with persistent muscle aches/pain while on statin therapy.
If statins (HMG-CoA reductase inhibitors) cause myopathy, the risk is very low (strength of recommendation [SOR]: A). There is no direct evidence to answer this question. A pooled analysis of randomized controlled trials found similar myopathy rates in patients taking statins and placebo. However, a large cohort study revealed a very small but statistically significant increased risk of myopathy in patients taking statins (number needed to harm=10,000/year).
Case reports suggest a myopathy risk for all statins, including fatal rhabdomyolysis. Risk of myopathy may increase with higher statin doses, certain comorbid states (eg, hypothyroidism, renal insufficiency [especially with diabetes], recent trauma, perioperative periods, advanced age, small body frame) and concurrent medications, including fibrates, cyclosporine, azole antifungals, and macrolide antibiotics (SOR: B). No studies have directly compared myopathy rates among statins, and there is no good evidence to suggest any differences. No controlled study has directly examined statin rechallenge in patients with previous myopathy; however, case reports and expert opinion support this practice (SOR: B).
Evidence summary
There is little evidence that statins cause myopathy. Synthesis is difficult because definitions of myopathy types differ among investigators. Proposed clinical syndrome definitions are myalgia (muscle weakness or ache with normal creatine kinase), myositis (symptoms with increased creatine kinase), and rhabdomyolysis (symptoms, markedly elevated creatine kinase, and renal insufficiency) as subsets of the more general term myopathy.1 The Table summarizes myopathy data from 30 statin trials analyzed in a recent systematic review, showing similar myopathy rates in statin and placebo patients.2 There may be a lower myopathy rate in these trials than in routine clinical practice because of stricter exclusion criteria and more intense monitoring.
A large well-done British epidemiologic cohort study (n=96,193) found an increased rate of myopathy (broadly defined, not requiring creatine kinase elevation) among patients taking statins, with an absolute rate difference of 1 per 10,000 person-years.3 A small study of 21 patients on statins with muscle symptoms but normal creatine kinases described 4 patients who were able to distinguish statins from placebo, with objective reversible weakness and abnormal muscle biopsies.4 Postmarket voluntary clinician reports point to statin myopathy in this and other countries;5-7 these include 3339 rhabdomyolysis FDA reports (1990 to March 2002).2
Though some assert differential myopathy rates among statins based on cell research, case reports, or differences in metabolic clearance, no studies directly compare clinical myopathy rates among statins. There is no good evidence of a differential myopathy risk among statins currently available in the US.1-2 Cerivastatin, however, was withdrawn from the US market because of a fatal rhabdomyolysis rate 16 to 80 times higher than other statins based on FDA reports using a denominator of prescription volume (3.16 fatal cases/million prescriptions vs 0.15 for the statin class as a whole).6
It is unknown whether previous myopathy, however defined, increases the risk of future myopathy with statin rechallenge. A tabular analysis of 74 published case reports of statin-associated rhabdomyolysis from a MEDLINE search covering 1985 to 2000 reported that in most cases the statin was safely restarted after stopping presumed interactive drugs (exact numbers not reported).8 In the AFCAPS/TexCAPS trial, 20 of 21 statin patients (out of a study population of 3304) who had elevated creatine kinase (>10 times the upper limits of normal) recovered with continued lovastatin treatment, while the other patient resumed treatment after a brief interruption without further elevations.9 The EXCEL trial (n=8245) of various lovastatin dosages included routine creatine kinase tests every 6 weeks for 48 weeks. Five lovastatin patients had muscle symptoms with creatine kinases >10 times the upper limits of normal, and in the 2 who continued treatment, symptoms and creatine kinase became normal.10 Of note, creatine kinase elevation of any kind at least once during 48 weeks occurred in 28.9% of placebo patients, arguing against routine creatine kinase screening in statin patients.
Case studies suggest an increased myopathy risk when statins are given with various medications, including fibrates, cyclosporine, azole antifungals, warfarin, nefazodone, and macrolide antibiotics.4,6,8 Pravastatin and fluvastatin, which are not metabolized by the P450 CYP3A4 pathway, may be safer to use because of fewer drug interactions.2,8 Likewise, certain comorbid states such as hypothyroidism, renal insufficiency (especially in patients with diabetes), recent trauma, and perioperative periods, as well as advanced age, small body frame, and multiple medications may increase statin myopathy risk.1,2,7,8
TABLE
Pooled myopathy data from 30 randomized controlled statin trials
| Trials | Total patients | Statin patients | Placebo patients | |
|---|---|---|---|---|
| Myalgia | 5 | 33,929 | 0.3–32.9% | 0–33.3% |
| Creatine kinase elevation | 9 | 33,921 | 0–0.64% | 0–0.58% |
| Myositis* | 18 | 58,237 | 0.17% | 0.15% |
| Rhabdomyolysis | 20 | 70,126 | 0.020% | 0.014% |
| *Creatine kinase >10 times upper limit of normal | ||||
| Adapted and calculated from Thompson PD, et al. JAMA 2003; 289:1681–1690.2 | ||||
Recommendations from others
A 2002 Clinical Advisory, jointly issued by the American College of Cardiology, the American Heart Association, and the National Heart, Lung and Blood Institute, asserted that statins carry a small but definite myopathy risk.1 It recommended against routine creatine kinase tests, reserving them for patients who develop muscle symptoms. It also recommended stopping statins when muscle symptoms with creatine kinase elevations >10 times the upper limits of normal occur, with consideration of restarting statins later at a lower dose if symptoms and elevated creatine kinase resolve. Careful monitoring of patients at higher risk of statin myopathy is also recommended.
Benefits of statins outweigh the risks
Joseph Saseen, PharmD, BCPS
University of Colorado Health Sciences Center, Denver
Contrary to popular belief, statin-associated myopathy is a rare adverse event. Drug-drug interactions and comorbid diseases (especially chronic kidney disease) increase myopathy risk. Given the overwhelming evidence demonstrating reduced morbidity and mortality with statins, benefits outweigh risks in patients with elevated low-density lipoprotein cholesterol. Data supporting myopathy management strategies are limited, but support stopping statin therapy in patients with myopathy (muscle aches/pain with elevated creatine kinase), and restarting, possibly with a different statin, after symptoms resolve. Myopathy should not be confused with myalgia (muscle aches/pain with normal creatine kinase). Myalgia requires interrupting treatment only for patients with persistent muscle aches/pain while on statin therapy.
1. Pasternak RC, Smith SC, Jr, Biarey-Merz CN, Grundy SM, Cleeman JI, Lenfant C. ACC/AHA/NHLBI clinical advisory on the use and safety of statins. J Am Coll Cardiol 2002;40:567-572.
2. Thompson PD, Clarkson P, Karas RH. Statin-associated myopathy. JAMA 2003;289:1681-1690.
3. Gaist D, Rodriquez LA, Huerta C, Hallas J, Sindrup SH. Lipid-lowering drugs and risk of myopathy: a population-based follow-up study. Epidemiology 2001;12:565-569.
4. Phillips PS, Haas RH, Bannykh S, et al. Statin-associated myopathy with normal creatine kinase levels. Ann Intern Med 2002;137:581-585.
5. Omar MA, Wilson JP. FDA adverse event reports on statin-associated rhabdomyolysis. Ann Pharmacother 2002;36:288-295.
6. Staffa JA, Chang J, Green L. Cerivastatin and reports of fatal rhabdomyolysis. N Engl J Med 2002;346:539-540.
7. Ucar M, Mjorndal T, Dahlqvist R. HMG-CoA reductase inhibitors and myotoxicity. Drug Saf 2000;6:441-447.
8. Omar MA, Wilson JP, Cox TS. Rhabdomyolysis and HMG-CoA reductase inhibitors. Ann Pharmacother 2001;35:1096-1107.
9. Downs JR, Clearfield M, Tyroler HA, et al. Air Force/Texas Coronary Atherosclerosis Prevention Study (AFCAPS/TexCAPS): Additional perspectives on tolerability of long-term treatment with lovastatin. Am J Cardiol 2001;87:1074-1079.
10. Bradford RH, Shear CL, Chremos AN, et al. Expanded Clinical Evaluation of Lovastatin (EXCEL) study results. I. Efficacy in modifying plasma lipoproteins and adverse event profile in 8245 patients with moderate hypercholes-terolemia. Arch Intern Med 1991;151:43-49.
1. Pasternak RC, Smith SC, Jr, Biarey-Merz CN, Grundy SM, Cleeman JI, Lenfant C. ACC/AHA/NHLBI clinical advisory on the use and safety of statins. J Am Coll Cardiol 2002;40:567-572.
2. Thompson PD, Clarkson P, Karas RH. Statin-associated myopathy. JAMA 2003;289:1681-1690.
3. Gaist D, Rodriquez LA, Huerta C, Hallas J, Sindrup SH. Lipid-lowering drugs and risk of myopathy: a population-based follow-up study. Epidemiology 2001;12:565-569.
4. Phillips PS, Haas RH, Bannykh S, et al. Statin-associated myopathy with normal creatine kinase levels. Ann Intern Med 2002;137:581-585.
5. Omar MA, Wilson JP. FDA adverse event reports on statin-associated rhabdomyolysis. Ann Pharmacother 2002;36:288-295.
6. Staffa JA, Chang J, Green L. Cerivastatin and reports of fatal rhabdomyolysis. N Engl J Med 2002;346:539-540.
7. Ucar M, Mjorndal T, Dahlqvist R. HMG-CoA reductase inhibitors and myotoxicity. Drug Saf 2000;6:441-447.
8. Omar MA, Wilson JP, Cox TS. Rhabdomyolysis and HMG-CoA reductase inhibitors. Ann Pharmacother 2001;35:1096-1107.
9. Downs JR, Clearfield M, Tyroler HA, et al. Air Force/Texas Coronary Atherosclerosis Prevention Study (AFCAPS/TexCAPS): Additional perspectives on tolerability of long-term treatment with lovastatin. Am J Cardiol 2001;87:1074-1079.
10. Bradford RH, Shear CL, Chremos AN, et al. Expanded Clinical Evaluation of Lovastatin (EXCEL) study results. I. Efficacy in modifying plasma lipoproteins and adverse event profile in 8245 patients with moderate hypercholes-terolemia. Arch Intern Med 1991;151:43-49.
Evidence-based answers from the Family Physicians Inquiries Network
What is the best way to manage benign paroxysmal positional vertigo?
A simple repositioning maneuver, such as the Epley maneuver (Figures 1 and 2 ), performed by an experienced clinician, can provide symptom relief from benign paroxysmal positional vertigo (BPPV) lasting at least 1 month (strength of recommendation [SOR]: A, systematic review of randomized controlled trials). Medical therapy with benzodiazepines for vestibular suppression provides no proven benefit for BPPV (SOR: B, 1 small randomized controlled trial). For undifferentiated dizziness, vestibular rehabilitation may provide symptomatic relief (SOR: B, 1 randomized controlled trial).
FIGURE 1
Cause of BPPVE
FIGURE 2
Pley maneuver for BPPV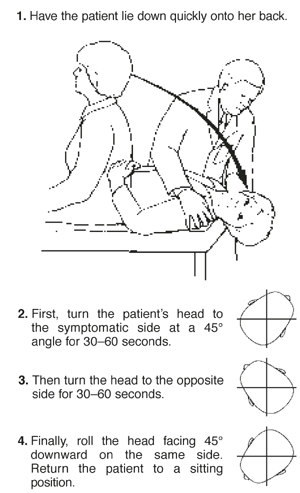
BPPV is characterized by brief, self-limited episodes of vertigo, provoked by typical position changes. This condition may result from free-floating debris in the endolymph of the posterior semicircular canal. This debris moves with position change, causing an abnormal perception of movement and classic symptoms of vertigo. Dix-Hallpike testing aids in the diagnosis, but treatment is often prescribed empirically.1
The most widely studied treatments for BPPV are the single-treatment repositioning techniques, such as the Epley maneuver.2A Cochrane review of treatments for BPPV yielded 11 trials, of which 9 were excluded due to a high risk of bias.3 The 2 remaining trials compared the Epley maneuver with a sham procedure among 86 patients referred to specialty care.4,5 Outcomes included conversion of the Dix-Hallpike test from positive to negative, as well as resolution of symptoms by patient report. Assessment occurred 1–4 weeks following the intervention in the 2 trials.4,5 Pooled data yielded odds ratios in favor of treatment for both objective testing (OR=5.67; 95% confidence interval [CI], 2.21–14.56) and symptom resolution (OR=4.92; 95% CI, 1.84–13.16), with no adverse outcomes reported.3We found no trials comparing the Epley maneuver with either vestibular habituation therapy or surgical management of BPPV.
There is no direct evidence for vestibular rehabilitation in BPPV. In a trial of vestibular rehabilitation for prolonged, undifferentiated dizziness, patients were randomized to usual care (n=76) or treatment with two 30-minute home education sessions at baseline and 6 weeks (n=67). A nurse, who had received 2 weeks of training, led the sessions, which included basic education on the vestibular system, causes of dizziness, and the rationale for exercise therapy. The nurse then taught the patients 8 sets of standard head and body movements to be performed twice daily. At 6 months, 69% of the treatment group vs 37% of the control group reported subjective improvement (OR=3.8 at 6 months; 95% CI, 1.6–8.7).6
Lorazepam and diazepam had no effect in 1 small randomized controlled trial.7 In this study, 25 BPPV patients from specialty clinics were randomized to placebo, diazepam 5 mg, or lorazepam 1 mg 3 times daily for 4 weeks. Patients reported dizziness on a 10-point scale at baseline and after 4 weeks of therapy. Nystagmus severity was also assessed using a 10-point scale at baseline and within 2 days following completion of treatment. The authors found no significant difference between the treatment and placebo arms; however, the study may have been underpowered to detect a clinically significant difference.
Recommendations from others
The Vestibular Disorders Association recommends the Epley maneuver as first-line treatment for BPPV, as does the Mayo Clinic.8,9 The National Institute on Deafness and Other Communication Disorders suggests that vestibular rehabilitation may be useful as a treatment for dizziness depending on the cause.10
Use otolith repositioning maneuvers
Grant Hoekzema, MD
Mercy Family Medicine Residency, St. Louis, MO
Although BPPV has a benign long-term outcome, it can be quite bothersome to patients and I have always felt compelled to offer some trial of therapy. Given the overall success and the relative safety of otolith repositioning maneuvers, such as the Epley maneuver, it has become my practice to refer patients to a physical therapist or other provider trained in these techniques. This makes sense from a pathophysiologic standpoint as well. I reserve antihistamines, such as meclizine, for those patients who have frequent, daily symptoms and who have not benefited from otolith repositioning.
1. Dix MR, Hallpike CS. Pathology, symptomatology and diagnosis of certain common disorders of the vestibular system. Proc Roy Soc Med 1952;45:341-354.
2. Epley JM. The canalith repositioning procedure: for treatment of benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg 1992;107:399-404.
3. Hilton M, Pinder D. The Epley (canalith repositioning) manoeuvre for benign paroxysmal positional vertigo (Cochrane Review). In: The Cochrane Library, Issue 3, 2003. Oxford: Update Software, last updated October 25, 2001.
4. Lynn S, Pool A, Rose D, Brey R, Suman V. Randomized trial of the canalith repositioning procedure. Otolaryngol Head Neck Surg 1995;113:712-720.
5. Froehling DA, Bowen JM, Mohr DN, et al. The canalith repositioning procedure for the treatment of benign paroxysmal positional vertigo: a randomized controlled trial. Mayo Clin Proc 2000;75:695-700.
6. Yardley L, Beech S, Zander L, Evans T, Weinman J. A randomized controlled trial of exercise therapy for dizziness and vertigo in primary care. Br J Gen Pract 1998;48:1136-1140.
7. McClure JA, Willett JM. Lorazepam and diazepam in the treatment of benign paroxysmal vertigo. J Otolaryngol 1980;9:472-477.
8. Mayo Clinic website. Vestibular rehabilitation. Available at www.mayoclinic.org/balance-rst/vestrehab.html. Accessed on October 8, 2003.
9. Vestibular Disorders Association (VEDA) website. Benign Paroxysmal Positional Vertigo (BPPV). March 1995 (modified April 17, 2003). Available at www.vestibular.org/bppv.html. Accessed on October 8, 2003.
10. National Institute on Deafness and Other Communication Disorders. Balance disorders. Available at www.nidcd.nih.gov/health/balance/balance_disorders.asp. Accessed on October 8, 2003.
A simple repositioning maneuver, such as the Epley maneuver (Figures 1 and 2 ), performed by an experienced clinician, can provide symptom relief from benign paroxysmal positional vertigo (BPPV) lasting at least 1 month (strength of recommendation [SOR]: A, systematic review of randomized controlled trials). Medical therapy with benzodiazepines for vestibular suppression provides no proven benefit for BPPV (SOR: B, 1 small randomized controlled trial). For undifferentiated dizziness, vestibular rehabilitation may provide symptomatic relief (SOR: B, 1 randomized controlled trial).
FIGURE 1
Cause of BPPVE
FIGURE 2
Pley maneuver for BPPV
BPPV is characterized by brief, self-limited episodes of vertigo, provoked by typical position changes. This condition may result from free-floating debris in the endolymph of the posterior semicircular canal. This debris moves with position change, causing an abnormal perception of movement and classic symptoms of vertigo. Dix-Hallpike testing aids in the diagnosis, but treatment is often prescribed empirically.1
The most widely studied treatments for BPPV are the single-treatment repositioning techniques, such as the Epley maneuver.2A Cochrane review of treatments for BPPV yielded 11 trials, of which 9 were excluded due to a high risk of bias.3 The 2 remaining trials compared the Epley maneuver with a sham procedure among 86 patients referred to specialty care.4,5 Outcomes included conversion of the Dix-Hallpike test from positive to negative, as well as resolution of symptoms by patient report. Assessment occurred 1–4 weeks following the intervention in the 2 trials.4,5 Pooled data yielded odds ratios in favor of treatment for both objective testing (OR=5.67; 95% confidence interval [CI], 2.21–14.56) and symptom resolution (OR=4.92; 95% CI, 1.84–13.16), with no adverse outcomes reported.3We found no trials comparing the Epley maneuver with either vestibular habituation therapy or surgical management of BPPV.
There is no direct evidence for vestibular rehabilitation in BPPV. In a trial of vestibular rehabilitation for prolonged, undifferentiated dizziness, patients were randomized to usual care (n=76) or treatment with two 30-minute home education sessions at baseline and 6 weeks (n=67). A nurse, who had received 2 weeks of training, led the sessions, which included basic education on the vestibular system, causes of dizziness, and the rationale for exercise therapy. The nurse then taught the patients 8 sets of standard head and body movements to be performed twice daily. At 6 months, 69% of the treatment group vs 37% of the control group reported subjective improvement (OR=3.8 at 6 months; 95% CI, 1.6–8.7).6
Lorazepam and diazepam had no effect in 1 small randomized controlled trial.7 In this study, 25 BPPV patients from specialty clinics were randomized to placebo, diazepam 5 mg, or lorazepam 1 mg 3 times daily for 4 weeks. Patients reported dizziness on a 10-point scale at baseline and after 4 weeks of therapy. Nystagmus severity was also assessed using a 10-point scale at baseline and within 2 days following completion of treatment. The authors found no significant difference between the treatment and placebo arms; however, the study may have been underpowered to detect a clinically significant difference.
Recommendations from others
The Vestibular Disorders Association recommends the Epley maneuver as first-line treatment for BPPV, as does the Mayo Clinic.8,9 The National Institute on Deafness and Other Communication Disorders suggests that vestibular rehabilitation may be useful as a treatment for dizziness depending on the cause.10
Use otolith repositioning maneuvers
Grant Hoekzema, MD
Mercy Family Medicine Residency, St. Louis, MO
Although BPPV has a benign long-term outcome, it can be quite bothersome to patients and I have always felt compelled to offer some trial of therapy. Given the overall success and the relative safety of otolith repositioning maneuvers, such as the Epley maneuver, it has become my practice to refer patients to a physical therapist or other provider trained in these techniques. This makes sense from a pathophysiologic standpoint as well. I reserve antihistamines, such as meclizine, for those patients who have frequent, daily symptoms and who have not benefited from otolith repositioning.
A simple repositioning maneuver, such as the Epley maneuver (Figures 1 and 2 ), performed by an experienced clinician, can provide symptom relief from benign paroxysmal positional vertigo (BPPV) lasting at least 1 month (strength of recommendation [SOR]: A, systematic review of randomized controlled trials). Medical therapy with benzodiazepines for vestibular suppression provides no proven benefit for BPPV (SOR: B, 1 small randomized controlled trial). For undifferentiated dizziness, vestibular rehabilitation may provide symptomatic relief (SOR: B, 1 randomized controlled trial).
FIGURE 1
Cause of BPPVE
FIGURE 2
Pley maneuver for BPPV
BPPV is characterized by brief, self-limited episodes of vertigo, provoked by typical position changes. This condition may result from free-floating debris in the endolymph of the posterior semicircular canal. This debris moves with position change, causing an abnormal perception of movement and classic symptoms of vertigo. Dix-Hallpike testing aids in the diagnosis, but treatment is often prescribed empirically.1
The most widely studied treatments for BPPV are the single-treatment repositioning techniques, such as the Epley maneuver.2A Cochrane review of treatments for BPPV yielded 11 trials, of which 9 were excluded due to a high risk of bias.3 The 2 remaining trials compared the Epley maneuver with a sham procedure among 86 patients referred to specialty care.4,5 Outcomes included conversion of the Dix-Hallpike test from positive to negative, as well as resolution of symptoms by patient report. Assessment occurred 1–4 weeks following the intervention in the 2 trials.4,5 Pooled data yielded odds ratios in favor of treatment for both objective testing (OR=5.67; 95% confidence interval [CI], 2.21–14.56) and symptom resolution (OR=4.92; 95% CI, 1.84–13.16), with no adverse outcomes reported.3We found no trials comparing the Epley maneuver with either vestibular habituation therapy or surgical management of BPPV.
There is no direct evidence for vestibular rehabilitation in BPPV. In a trial of vestibular rehabilitation for prolonged, undifferentiated dizziness, patients were randomized to usual care (n=76) or treatment with two 30-minute home education sessions at baseline and 6 weeks (n=67). A nurse, who had received 2 weeks of training, led the sessions, which included basic education on the vestibular system, causes of dizziness, and the rationale for exercise therapy. The nurse then taught the patients 8 sets of standard head and body movements to be performed twice daily. At 6 months, 69% of the treatment group vs 37% of the control group reported subjective improvement (OR=3.8 at 6 months; 95% CI, 1.6–8.7).6
Lorazepam and diazepam had no effect in 1 small randomized controlled trial.7 In this study, 25 BPPV patients from specialty clinics were randomized to placebo, diazepam 5 mg, or lorazepam 1 mg 3 times daily for 4 weeks. Patients reported dizziness on a 10-point scale at baseline and after 4 weeks of therapy. Nystagmus severity was also assessed using a 10-point scale at baseline and within 2 days following completion of treatment. The authors found no significant difference between the treatment and placebo arms; however, the study may have been underpowered to detect a clinically significant difference.
Recommendations from others
The Vestibular Disorders Association recommends the Epley maneuver as first-line treatment for BPPV, as does the Mayo Clinic.8,9 The National Institute on Deafness and Other Communication Disorders suggests that vestibular rehabilitation may be useful as a treatment for dizziness depending on the cause.10
Use otolith repositioning maneuvers
Grant Hoekzema, MD
Mercy Family Medicine Residency, St. Louis, MO
Although BPPV has a benign long-term outcome, it can be quite bothersome to patients and I have always felt compelled to offer some trial of therapy. Given the overall success and the relative safety of otolith repositioning maneuvers, such as the Epley maneuver, it has become my practice to refer patients to a physical therapist or other provider trained in these techniques. This makes sense from a pathophysiologic standpoint as well. I reserve antihistamines, such as meclizine, for those patients who have frequent, daily symptoms and who have not benefited from otolith repositioning.
1. Dix MR, Hallpike CS. Pathology, symptomatology and diagnosis of certain common disorders of the vestibular system. Proc Roy Soc Med 1952;45:341-354.
2. Epley JM. The canalith repositioning procedure: for treatment of benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg 1992;107:399-404.
3. Hilton M, Pinder D. The Epley (canalith repositioning) manoeuvre for benign paroxysmal positional vertigo (Cochrane Review). In: The Cochrane Library, Issue 3, 2003. Oxford: Update Software, last updated October 25, 2001.
4. Lynn S, Pool A, Rose D, Brey R, Suman V. Randomized trial of the canalith repositioning procedure. Otolaryngol Head Neck Surg 1995;113:712-720.
5. Froehling DA, Bowen JM, Mohr DN, et al. The canalith repositioning procedure for the treatment of benign paroxysmal positional vertigo: a randomized controlled trial. Mayo Clin Proc 2000;75:695-700.
6. Yardley L, Beech S, Zander L, Evans T, Weinman J. A randomized controlled trial of exercise therapy for dizziness and vertigo in primary care. Br J Gen Pract 1998;48:1136-1140.
7. McClure JA, Willett JM. Lorazepam and diazepam in the treatment of benign paroxysmal vertigo. J Otolaryngol 1980;9:472-477.
8. Mayo Clinic website. Vestibular rehabilitation. Available at www.mayoclinic.org/balance-rst/vestrehab.html. Accessed on October 8, 2003.
9. Vestibular Disorders Association (VEDA) website. Benign Paroxysmal Positional Vertigo (BPPV). March 1995 (modified April 17, 2003). Available at www.vestibular.org/bppv.html. Accessed on October 8, 2003.
10. National Institute on Deafness and Other Communication Disorders. Balance disorders. Available at www.nidcd.nih.gov/health/balance/balance_disorders.asp. Accessed on October 8, 2003.
1. Dix MR, Hallpike CS. Pathology, symptomatology and diagnosis of certain common disorders of the vestibular system. Proc Roy Soc Med 1952;45:341-354.
2. Epley JM. The canalith repositioning procedure: for treatment of benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg 1992;107:399-404.
3. Hilton M, Pinder D. The Epley (canalith repositioning) manoeuvre for benign paroxysmal positional vertigo (Cochrane Review). In: The Cochrane Library, Issue 3, 2003. Oxford: Update Software, last updated October 25, 2001.
4. Lynn S, Pool A, Rose D, Brey R, Suman V. Randomized trial of the canalith repositioning procedure. Otolaryngol Head Neck Surg 1995;113:712-720.
5. Froehling DA, Bowen JM, Mohr DN, et al. The canalith repositioning procedure for the treatment of benign paroxysmal positional vertigo: a randomized controlled trial. Mayo Clin Proc 2000;75:695-700.
6. Yardley L, Beech S, Zander L, Evans T, Weinman J. A randomized controlled trial of exercise therapy for dizziness and vertigo in primary care. Br J Gen Pract 1998;48:1136-1140.
7. McClure JA, Willett JM. Lorazepam and diazepam in the treatment of benign paroxysmal vertigo. J Otolaryngol 1980;9:472-477.
8. Mayo Clinic website. Vestibular rehabilitation. Available at www.mayoclinic.org/balance-rst/vestrehab.html. Accessed on October 8, 2003.
9. Vestibular Disorders Association (VEDA) website. Benign Paroxysmal Positional Vertigo (BPPV). March 1995 (modified April 17, 2003). Available at www.vestibular.org/bppv.html. Accessed on October 8, 2003.
10. National Institute on Deafness and Other Communication Disorders. Balance disorders. Available at www.nidcd.nih.gov/health/balance/balance_disorders.asp. Accessed on October 8, 2003.
Evidence-based answers from the Family Physicians Inquiries Network