User login
Avoiding “shotgun” treatment: New thoughts on endometriosis-associated pelvic pain
CASE: Resurgent, worsening dysmenorrhea
A 32-year-old woman (G2P2) with a history of 2 spontaneous vaginal deliveries presents to your office after 10 months of severe, worsening dysmenorrhea. Shortly after she developed severe dysmenorrhea, she began to experience daily pain in her lower abdomen and pelvis. This pain occurred in the midline, bilateral lower quadrants, and rectum. She also developed deep dyspareunia.
She has a history of dysmenorrhea from adolescence but has otherwise been healthy and pain-free until the past 10 months. She has tried oral contraceptives and nonsteroidal anti-inflammatory drugs, without success. She is happily married, and her medical history is unremarkable except for a bout of Lyme disease 6 months before the onset of pain, at which time she also developed symptoms of fatigue.
A physical examination is remarkable for unilateral thickening and shortening of the left uterosacral ligament, dense scarring, and tenderness at the posterior fornix, with poor uterine mobility. Magnetic resonance imaging reveals findings consistent with the physical examination.
What is causing her pain after such a long phase without it? And what treatments should you offer her?
Endometriosis represents the ectopic presence of endometrial glands and stroma. The most common sites of endometriotic implants are the uterosacral ligaments, cul-de-sac peritoneum, and ovarian fossae. Most clinicians are aware that the location of an endometriosis implant does not predict the location of pain experienced by the patient. An understanding of both abdominal and pelvic neuroanatomy may help clarify this phenomenon, as may knowledge of the concept of viscerosomatic convergence.1–3
Not only does the location of the endometriosis implant fail to predict the location of pain, but the level or stage of disease (in other words, the amount of endometriosis present) does not accurately predict the level of pain.4,5 In fact, some women with histopathologically confirmed endometriosis have no pain whatsoever.
When managing chronic pelvic pain (CPP), we need to consider mechanisms of pain when endometriosis is the primary pain driver, as well as when endometriosis is present but irrelevant to the patient’s pain (TABLE 1).
In this article, I focus on the role of endometriosis in CPP, including the role of the central nervous system (CNS) and other entities that may influence the pain threshold. This discussion is intended to help shift the current paradigm of thought about endometriosis and its association with CPP.
Numerous mechanisms drive pain in endometriosis
There are 2 main anatomic levels at which to consider pain associated with endometriosis—the local level (the endometriosis itself) and the level of the spinal cord and brain. Although emerging evidence points to a significant interaction between local anatomic disease and higher-order neurologically mediated pain,6–8 each level should be considered separately during selection of treatment.
At the most basic level, endometriosis is a disease of inflammation. Although the presence of inflammatory mediators is associated with the presence of endometriosis, the amount of endometriosis does not correlate with the amount of inflammatory mediators. Inflammatory mediators such as interleukin (IL) 1, IL-6, IL-8, human monocyte chemoattractant protein 1, RANTES (Regulated on Activation Normal T cell Expressed and Secreted), and tumor necrosis factor alpha are found in significantly higher concentrations in the peritoneal fluid of women with endometriosis, compared with women without endometriosis. The inflammatory mediators are produced by both endometriotic lesions and the surrounding peritoneum (Figure). This set of inflammatory mediators not only leads to angiogenesis and endometriosis tissue maintenance but also to neurogenesis.9 It is from this inflammatory environment that other pathogenic mechanisms can operate.

For example, when dorsal root ganglia are exposed to the peritoneal fluid of women with endometriosis, as opposed to the peritoneal fluid of women without endometriosis, there is a significant differential in the growth of sensory versus sympathetic neurites.10 This phenomenon translates into increased visceral pain sensitivity. In fact, it is this neurogenesis and increased neuronal responsiveness that are responsible for the upregulation of pain mediated by the spinal cord and brain.
A familiar but imperfectly understood theory is that of central sensitization. When there are prolonged and repeated pain impulses from peripheral sources, the CNS responds anatomically and biochemically by changing the processing of those pain signals. Even after the stimulus (in this case endometriosis) is removed for such high-intensity nociceptive signals, increasing excitability can continue. The result is chronic pain that is unresponsive or poorly responsive to treatment; in some cases, the chronic pain may even mimic the original anatomic site of the pain.
Central sensitization generally involves 2 phases: hyperalgesia, in which the excitatory threshold of the nerve is reset, leading to a lowered stimulatory requirement, and allodynia, in which normally harmless stimuli are interpreted as pain. During the allodynia phase, fibers (eg, C-fibers) that typically carry nonpainful information are recruited to become pain transmitters.
The pain threshold—and why it is important
The concept of the pain threshold is both complex and elusive. It can be defined as the point at which a stimulus begins to be perceived as painful. The pain threshold may be dependent on multiple variables, including gender, genetic issues (a concentration of mu receptors), a history of abuse, socioeconomic status, current and past levels of depression, earlier pain experiences, and psychosocial stressors.
The pain threshold is important because it changes over time. For example, a patient with endometriosis may experience isolated dysmenorrhea as a teen but, over time, may develop a pattern of chronic daily pain and depression. Or a woman with CPP may respond well to initial therapies but worsen after a stressful life event such as death of a loved one or new stressors at work. An understanding of the many variables that can alter the pain threshold can lead to more effective counseling and treatment and help us avoid unnecessary therapies.
Multiple types of pain can coexist in 1 patient
Clinicians who care for women with endometriosis and CPP should have an understanding of the mechanism of their pain, including the differences between nociceptive somatic, nociceptive visceral, and neuropathic pain (TABLE 2). All 3 types of pain can exist in a single patient with CPP.

Nociceptive somatic pain generally originates in somatic structures such as muscle, ligament, bone, and tendons. Women with endometriosis often have somatic pain, for 2 main reasons.11 First, skeletal muscles respond adversely to long-term inflammatory stimuli,12 and endometriosis is primarily a disease of inflammation. Long-term inflammatory stimuli may lead to atrophy and spasm. Second, the presence of inflammation in the muscle likely leads to worsening hyperalgesia with increasing muscle activity.13 This can lead to and explain pain in the pelvic floor, abdominal wall muscles, hips, thighs, buttocks, and lower back. Once this is understood, treatments can be targeted to the underlying mechanisms and specific muscle groups.
Nociceptive visceral pain generally indicates pain originating in visceral structures. In the pelvis, visceral structures of main concern are the uterus, ovaries, fallopian tubes, vagina (upper two-thirds), bladder, ureters, sigmoid colon, rectum, and, most importantly related to endometriosis, the visceral peritoneum.
In the case of visceral pain, the likely associated mechanisms are inflammation as well as local nerve growth.14,15 Local inflammation in turn leads to scarring and visceral hyperalgesia.16 Over a long period of time, local visceral hyperalgesia can lead to spinal wind-up and central sensitization. Spinal wind-up is the spinal cord’s expansion of signals from peripheral nociceptors associated with C-fibers. It likely stems from a prolonged, intense, and persistent generation of afferent nociceptive impulses. When this occurs, CNS pathways are well established and sensations of pain can remain even after careful surgery to remove sources of inflammation and anatomic deformity (visceral scarring). For this reason, early radical resection of endometriosis in women with endometriosis-associated pelvic pain may be more likely than later surgery to reduce or eliminate pain. Otherwise, reoperation rates may be high and later surgeries may fail to yield histopathology for endometrial glands and stroma.17
Neuropathic pain generally reflects damage to or dysfunction of either the peripheral nervous system or the CNS. Endometriosis-associated pain is also neuropathic in nature and occurs through multiple mechanisms.
There is good evidence to support the development of abnormal nerve growth in and around areas of endometriosis. When such nerve fibers exist, they serve only a pathologic function. This abnormal nerve growth is induced by multiple molecules, including nerve growth factor and vascular endothelial growth factor.7 It is likely that once high-density areas of sensitized nerves develop, peripheral nerves also become sensitized by endometriosis-associated inflammatory cytokines.16 When there are abnormal nerve growth and elevated levels of peripheral nerve sensitization, the nerves most often recruited are C-fibers, unmyeli-nated fibers largely associated with both peripheral and central neuropathic pain. When C-fibers are recruited, the ratio of C-fibers to autonomic afferent pain fibers increases.
In endometriosis, persistent inflammatory signals lead to an increase in the excitability of peripheral nerves, thereby significantly increasing transmitted pain signals and likely reducing the body’s ability to suppress pain.
Some of the peripheral nerve changes I have described may be observed via magnetic resonance tractography (MRT), which highlights neuronal tracts over long distances. Fractional anisotropy values measured by MRT yield information about the quality of neuronal structures. In women with endometriosis, fractional anisotropy values in the peripheral nerve roots of S1, S2, and S3 appear to be lower than those in women without endometriosis,18 indicating disruption of the normally myelinated nerve structure.
It’s time to abandon nontargeted treatments
Endometriosis-associated CPP remains a challenging heterogeneous and multifactorial disease state. In the past, treatments such as gonadotropin-releasing hormone agonists have been prescribed without an appropriate consideration of the disease and its mechanism of associated pain. In our CPP specialty practice, we have abandoned such nontargeted approaches. By developing an understanding of central sensitization, local neurologic responses to inflammation, and the pain threshold, clinicians are more likely to select a treatment targeted to specific mechanisms. Such an approach is superior to the traditional “shotgun” approach to treatment, which can produce harmful side effects and have high long-term failure rates. As Stratton and colleagues observed, “traditional methods of classifying endometriosis-associated pain based on disease, duration, and anatomy are inadequate and should be replaced by a mechanism-based evaluation.”19 Future clinical care and research will necessarily focus on specific disease etiologies and pain mechanisms if we are to continue to improve the care of women with CPP.
Case: Resolved
Because the history, physical examination, and imaging are strongly suggestive of endometriosis, the patient is counseled about the treatments most likely to be effective, which include medical therapies such as centrally acting agents (gabapentin, pregabalin, tricyclic antidepressants) and local treatments such as placement of a levonorgestrel-releasing intrauterine system or surgical resection. She elects to undergo total laparoscopic hysterectomy with bilateral salpingectomy and radical resection of endometriosis. Histopathology confirms adenomyosis and deep infiltrating endometriosis, including implants on the rectovaginal septum. The patient remains pain-free at her 2-year follow-up.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. Brumovsky PR, Gebhart GF. Visceral organ cross-sensitization—an integrated perspective. Auton Neurosci. 2010;153(1–2):106–115.
2. Schwartz ES, Gebhart GF. Visceral pain. Curr Top Behav Neurosci. 2014;20:171–197.
3. Gebhart GF. Visceral pain—peripheral sensitization. Gut. 2000;47(suppl 4):54–58.
4. Fukaya T, Hoshiai H, Yajima A. Is pelvic endometriosis always associated with chronic pain? A retrospective study of 618 cases diagnosed by laparoscopy. Am J Obstet Gynecol. 1993;169(3):719–722.
5. Vercellini P, Trespidi L, De GO, Cortesi I, Parazzini F, Crosignani PG. Endometriosis and pelvic pain: relation to disease stage and localization. Fertil Steril. 1996;65(2):299–304.
6. Brawn J, Morotti M, Zondervan KT, Becker CM, Vincent K. Central changes associated with chronic pelvic pain and endometriosis. Hum Reprod Update. 2014;20(5):737–747.
7. Morotti M, Vincent K, Brawn J, Zondervan KT, Becker CM. Peripheral changes in endometriosis-associated pain. Hum Reprod Update. 2014;20(5):717–736.
8. Neziri AY, Bersinger NA, Andersen OK, Arendt-Nielsen L, Mueller MD, Curatolo M. Correlation between altered central pain processing and concentration of peritoneal fluid inflammatory cytokines in endometriosis patients with chronic pelvic pain. Reg Anesth Pain Med. 2014;39(3):181–184.
9. Asante A, Taylor RN. Endometriosis: the role of neuroangiogenesis. Annu Rev Physiol. 2011;73:163–182.
10. Arnold J, Barcena de Arellano ML, Ruster C, et al. Imbalance between sympathetic and sensory innervation in peritoneal endometriosis. Brain Behav Immun. 2012;26(1):132–141.
11. Warren JW, Morozov V, Howard FM. Could chronic pelvic pain be a functional somatic syndrome? Am J Obstet Gynecol. 2011;205(3):199–205.
12. Korotkova M, Lundberg IE. The skeletal muscle arachidonic acid cascade in health and inflammatory disease. Nat Rev Rheumatol. 2014;10(5):295–303.
13. Sluka KA, Rasmussen LA. Fatiguing exercise enhances hyperalgesia to muscle inflammation. Pain. 2010;148(2):188–197.
14. McKinnon B, Bersinger NA, Wotzkow C, Mueller MD. Endometriosis-associated nerve fibers, peritoneal fluid cytokine concentrations, and pain in endometriotic lesions from different locations. Fertil Steril. 2012;97(2):373–380.
15. Anaf V, El Nakadi I, De Moor V, Chapron C, Pistofidis G, Noel JC. Increased nerve density in deep infiltrating endometriotic nodules. Gynecol Obstet Invest. 2011;71(2):112–117.
16. McKinnon BD, Bertschi D, Bersinger NA, Mueller MD. Inflammation and nerve fiber interaction in endometriotic pain. Trends Endocrinol Metab. 2015;26(1):1–10.
17. Redwine DB. Conservative laparoscopic excision of endometriosis by sharp dissection: life table analysis of reoperation and persistent or recurrent disease. Fertil Steril. 1991;56(4):628–634.
18. Manganaro L, Porpora MG, Vinci V, et al. Diffusion tensor imaging and tractography to evaluate sacral nerve root abnormalities in endometriosis-related pain: a pilot study. Eur Radiol. 2014;24(1):95–101.
19. Stratton P, Khachikyan I, Sinaii N, Ortiz R, Shah J. Association of chronic pelvic pain and endometriosis with signs of sensitization and myofascial pain. Obstet Gynecol. 2015;125(3):719–728.

Kenneth A. Levey, MD, MPH
Dr. Levey is Assistant Clinical Professor of Obstetrics and Gynecology at Weill-Cornell Medical College in New York, New York.
The author reports that he is a speaker for Surgiquest and Intuitive Surgical.
Kenneth A. Levey, MD, MPH
Dr. Levey is Assistant Clinical Professor of Obstetrics and Gynecology at Weill-Cornell Medical College in New York, New York.
The author reports that he is a speaker for Surgiquest and Intuitive Surgical.
Kenneth A. Levey, MD, MPH
Dr. Levey is Assistant Clinical Professor of Obstetrics and Gynecology at Weill-Cornell Medical College in New York, New York.
The author reports that he is a speaker for Surgiquest and Intuitive Surgical.
CASE: Resurgent, worsening dysmenorrhea
A 32-year-old woman (G2P2) with a history of 2 spontaneous vaginal deliveries presents to your office after 10 months of severe, worsening dysmenorrhea. Shortly after she developed severe dysmenorrhea, she began to experience daily pain in her lower abdomen and pelvis. This pain occurred in the midline, bilateral lower quadrants, and rectum. She also developed deep dyspareunia.
She has a history of dysmenorrhea from adolescence but has otherwise been healthy and pain-free until the past 10 months. She has tried oral contraceptives and nonsteroidal anti-inflammatory drugs, without success. She is happily married, and her medical history is unremarkable except for a bout of Lyme disease 6 months before the onset of pain, at which time she also developed symptoms of fatigue.
A physical examination is remarkable for unilateral thickening and shortening of the left uterosacral ligament, dense scarring, and tenderness at the posterior fornix, with poor uterine mobility. Magnetic resonance imaging reveals findings consistent with the physical examination.
What is causing her pain after such a long phase without it? And what treatments should you offer her?
Endometriosis represents the ectopic presence of endometrial glands and stroma. The most common sites of endometriotic implants are the uterosacral ligaments, cul-de-sac peritoneum, and ovarian fossae. Most clinicians are aware that the location of an endometriosis implant does not predict the location of pain experienced by the patient. An understanding of both abdominal and pelvic neuroanatomy may help clarify this phenomenon, as may knowledge of the concept of viscerosomatic convergence.1–3
Not only does the location of the endometriosis implant fail to predict the location of pain, but the level or stage of disease (in other words, the amount of endometriosis present) does not accurately predict the level of pain.4,5 In fact, some women with histopathologically confirmed endometriosis have no pain whatsoever.
When managing chronic pelvic pain (CPP), we need to consider mechanisms of pain when endometriosis is the primary pain driver, as well as when endometriosis is present but irrelevant to the patient’s pain (TABLE 1).
In this article, I focus on the role of endometriosis in CPP, including the role of the central nervous system (CNS) and other entities that may influence the pain threshold. This discussion is intended to help shift the current paradigm of thought about endometriosis and its association with CPP.
Numerous mechanisms drive pain in endometriosis
There are 2 main anatomic levels at which to consider pain associated with endometriosis—the local level (the endometriosis itself) and the level of the spinal cord and brain. Although emerging evidence points to a significant interaction between local anatomic disease and higher-order neurologically mediated pain,6–8 each level should be considered separately during selection of treatment.
At the most basic level, endometriosis is a disease of inflammation. Although the presence of inflammatory mediators is associated with the presence of endometriosis, the amount of endometriosis does not correlate with the amount of inflammatory mediators. Inflammatory mediators such as interleukin (IL) 1, IL-6, IL-8, human monocyte chemoattractant protein 1, RANTES (Regulated on Activation Normal T cell Expressed and Secreted), and tumor necrosis factor alpha are found in significantly higher concentrations in the peritoneal fluid of women with endometriosis, compared with women without endometriosis. The inflammatory mediators are produced by both endometriotic lesions and the surrounding peritoneum (Figure). This set of inflammatory mediators not only leads to angiogenesis and endometriosis tissue maintenance but also to neurogenesis.9 It is from this inflammatory environment that other pathogenic mechanisms can operate.
For example, when dorsal root ganglia are exposed to the peritoneal fluid of women with endometriosis, as opposed to the peritoneal fluid of women without endometriosis, there is a significant differential in the growth of sensory versus sympathetic neurites.10 This phenomenon translates into increased visceral pain sensitivity. In fact, it is this neurogenesis and increased neuronal responsiveness that are responsible for the upregulation of pain mediated by the spinal cord and brain.
A familiar but imperfectly understood theory is that of central sensitization. When there are prolonged and repeated pain impulses from peripheral sources, the CNS responds anatomically and biochemically by changing the processing of those pain signals. Even after the stimulus (in this case endometriosis) is removed for such high-intensity nociceptive signals, increasing excitability can continue. The result is chronic pain that is unresponsive or poorly responsive to treatment; in some cases, the chronic pain may even mimic the original anatomic site of the pain.
Central sensitization generally involves 2 phases: hyperalgesia, in which the excitatory threshold of the nerve is reset, leading to a lowered stimulatory requirement, and allodynia, in which normally harmless stimuli are interpreted as pain. During the allodynia phase, fibers (eg, C-fibers) that typically carry nonpainful information are recruited to become pain transmitters.
The pain threshold—and why it is important
The concept of the pain threshold is both complex and elusive. It can be defined as the point at which a stimulus begins to be perceived as painful. The pain threshold may be dependent on multiple variables, including gender, genetic issues (a concentration of mu receptors), a history of abuse, socioeconomic status, current and past levels of depression, earlier pain experiences, and psychosocial stressors.
The pain threshold is important because it changes over time. For example, a patient with endometriosis may experience isolated dysmenorrhea as a teen but, over time, may develop a pattern of chronic daily pain and depression. Or a woman with CPP may respond well to initial therapies but worsen after a stressful life event such as death of a loved one or new stressors at work. An understanding of the many variables that can alter the pain threshold can lead to more effective counseling and treatment and help us avoid unnecessary therapies.
Multiple types of pain can coexist in 1 patient
Clinicians who care for women with endometriosis and CPP should have an understanding of the mechanism of their pain, including the differences between nociceptive somatic, nociceptive visceral, and neuropathic pain (TABLE 2). All 3 types of pain can exist in a single patient with CPP.
Nociceptive somatic pain generally originates in somatic structures such as muscle, ligament, bone, and tendons. Women with endometriosis often have somatic pain, for 2 main reasons.11 First, skeletal muscles respond adversely to long-term inflammatory stimuli,12 and endometriosis is primarily a disease of inflammation. Long-term inflammatory stimuli may lead to atrophy and spasm. Second, the presence of inflammation in the muscle likely leads to worsening hyperalgesia with increasing muscle activity.13 This can lead to and explain pain in the pelvic floor, abdominal wall muscles, hips, thighs, buttocks, and lower back. Once this is understood, treatments can be targeted to the underlying mechanisms and specific muscle groups.
Nociceptive visceral pain generally indicates pain originating in visceral structures. In the pelvis, visceral structures of main concern are the uterus, ovaries, fallopian tubes, vagina (upper two-thirds), bladder, ureters, sigmoid colon, rectum, and, most importantly related to endometriosis, the visceral peritoneum.
In the case of visceral pain, the likely associated mechanisms are inflammation as well as local nerve growth.14,15 Local inflammation in turn leads to scarring and visceral hyperalgesia.16 Over a long period of time, local visceral hyperalgesia can lead to spinal wind-up and central sensitization. Spinal wind-up is the spinal cord’s expansion of signals from peripheral nociceptors associated with C-fibers. It likely stems from a prolonged, intense, and persistent generation of afferent nociceptive impulses. When this occurs, CNS pathways are well established and sensations of pain can remain even after careful surgery to remove sources of inflammation and anatomic deformity (visceral scarring). For this reason, early radical resection of endometriosis in women with endometriosis-associated pelvic pain may be more likely than later surgery to reduce or eliminate pain. Otherwise, reoperation rates may be high and later surgeries may fail to yield histopathology for endometrial glands and stroma.17
Neuropathic pain generally reflects damage to or dysfunction of either the peripheral nervous system or the CNS. Endometriosis-associated pain is also neuropathic in nature and occurs through multiple mechanisms.
There is good evidence to support the development of abnormal nerve growth in and around areas of endometriosis. When such nerve fibers exist, they serve only a pathologic function. This abnormal nerve growth is induced by multiple molecules, including nerve growth factor and vascular endothelial growth factor.7 It is likely that once high-density areas of sensitized nerves develop, peripheral nerves also become sensitized by endometriosis-associated inflammatory cytokines.16 When there are abnormal nerve growth and elevated levels of peripheral nerve sensitization, the nerves most often recruited are C-fibers, unmyeli-nated fibers largely associated with both peripheral and central neuropathic pain. When C-fibers are recruited, the ratio of C-fibers to autonomic afferent pain fibers increases.
In endometriosis, persistent inflammatory signals lead to an increase in the excitability of peripheral nerves, thereby significantly increasing transmitted pain signals and likely reducing the body’s ability to suppress pain.
Some of the peripheral nerve changes I have described may be observed via magnetic resonance tractography (MRT), which highlights neuronal tracts over long distances. Fractional anisotropy values measured by MRT yield information about the quality of neuronal structures. In women with endometriosis, fractional anisotropy values in the peripheral nerve roots of S1, S2, and S3 appear to be lower than those in women without endometriosis,18 indicating disruption of the normally myelinated nerve structure.
It’s time to abandon nontargeted treatments
Endometriosis-associated CPP remains a challenging heterogeneous and multifactorial disease state. In the past, treatments such as gonadotropin-releasing hormone agonists have been prescribed without an appropriate consideration of the disease and its mechanism of associated pain. In our CPP specialty practice, we have abandoned such nontargeted approaches. By developing an understanding of central sensitization, local neurologic responses to inflammation, and the pain threshold, clinicians are more likely to select a treatment targeted to specific mechanisms. Such an approach is superior to the traditional “shotgun” approach to treatment, which can produce harmful side effects and have high long-term failure rates. As Stratton and colleagues observed, “traditional methods of classifying endometriosis-associated pain based on disease, duration, and anatomy are inadequate and should be replaced by a mechanism-based evaluation.”19 Future clinical care and research will necessarily focus on specific disease etiologies and pain mechanisms if we are to continue to improve the care of women with CPP.
Case: Resolved
Because the history, physical examination, and imaging are strongly suggestive of endometriosis, the patient is counseled about the treatments most likely to be effective, which include medical therapies such as centrally acting agents (gabapentin, pregabalin, tricyclic antidepressants) and local treatments such as placement of a levonorgestrel-releasing intrauterine system or surgical resection. She elects to undergo total laparoscopic hysterectomy with bilateral salpingectomy and radical resection of endometriosis. Histopathology confirms adenomyosis and deep infiltrating endometriosis, including implants on the rectovaginal septum. The patient remains pain-free at her 2-year follow-up.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
CASE: Resurgent, worsening dysmenorrhea
A 32-year-old woman (G2P2) with a history of 2 spontaneous vaginal deliveries presents to your office after 10 months of severe, worsening dysmenorrhea. Shortly after she developed severe dysmenorrhea, she began to experience daily pain in her lower abdomen and pelvis. This pain occurred in the midline, bilateral lower quadrants, and rectum. She also developed deep dyspareunia.
She has a history of dysmenorrhea from adolescence but has otherwise been healthy and pain-free until the past 10 months. She has tried oral contraceptives and nonsteroidal anti-inflammatory drugs, without success. She is happily married, and her medical history is unremarkable except for a bout of Lyme disease 6 months before the onset of pain, at which time she also developed symptoms of fatigue.
A physical examination is remarkable for unilateral thickening and shortening of the left uterosacral ligament, dense scarring, and tenderness at the posterior fornix, with poor uterine mobility. Magnetic resonance imaging reveals findings consistent with the physical examination.
What is causing her pain after such a long phase without it? And what treatments should you offer her?
Endometriosis represents the ectopic presence of endometrial glands and stroma. The most common sites of endometriotic implants are the uterosacral ligaments, cul-de-sac peritoneum, and ovarian fossae. Most clinicians are aware that the location of an endometriosis implant does not predict the location of pain experienced by the patient. An understanding of both abdominal and pelvic neuroanatomy may help clarify this phenomenon, as may knowledge of the concept of viscerosomatic convergence.1–3
Not only does the location of the endometriosis implant fail to predict the location of pain, but the level or stage of disease (in other words, the amount of endometriosis present) does not accurately predict the level of pain.4,5 In fact, some women with histopathologically confirmed endometriosis have no pain whatsoever.
When managing chronic pelvic pain (CPP), we need to consider mechanisms of pain when endometriosis is the primary pain driver, as well as when endometriosis is present but irrelevant to the patient’s pain (TABLE 1).
In this article, I focus on the role of endometriosis in CPP, including the role of the central nervous system (CNS) and other entities that may influence the pain threshold. This discussion is intended to help shift the current paradigm of thought about endometriosis and its association with CPP.
Numerous mechanisms drive pain in endometriosis
There are 2 main anatomic levels at which to consider pain associated with endometriosis—the local level (the endometriosis itself) and the level of the spinal cord and brain. Although emerging evidence points to a significant interaction between local anatomic disease and higher-order neurologically mediated pain,6–8 each level should be considered separately during selection of treatment.
At the most basic level, endometriosis is a disease of inflammation. Although the presence of inflammatory mediators is associated with the presence of endometriosis, the amount of endometriosis does not correlate with the amount of inflammatory mediators. Inflammatory mediators such as interleukin (IL) 1, IL-6, IL-8, human monocyte chemoattractant protein 1, RANTES (Regulated on Activation Normal T cell Expressed and Secreted), and tumor necrosis factor alpha are found in significantly higher concentrations in the peritoneal fluid of women with endometriosis, compared with women without endometriosis. The inflammatory mediators are produced by both endometriotic lesions and the surrounding peritoneum (Figure). This set of inflammatory mediators not only leads to angiogenesis and endometriosis tissue maintenance but also to neurogenesis.9 It is from this inflammatory environment that other pathogenic mechanisms can operate.
For example, when dorsal root ganglia are exposed to the peritoneal fluid of women with endometriosis, as opposed to the peritoneal fluid of women without endometriosis, there is a significant differential in the growth of sensory versus sympathetic neurites.10 This phenomenon translates into increased visceral pain sensitivity. In fact, it is this neurogenesis and increased neuronal responsiveness that are responsible for the upregulation of pain mediated by the spinal cord and brain.
A familiar but imperfectly understood theory is that of central sensitization. When there are prolonged and repeated pain impulses from peripheral sources, the CNS responds anatomically and biochemically by changing the processing of those pain signals. Even after the stimulus (in this case endometriosis) is removed for such high-intensity nociceptive signals, increasing excitability can continue. The result is chronic pain that is unresponsive or poorly responsive to treatment; in some cases, the chronic pain may even mimic the original anatomic site of the pain.
Central sensitization generally involves 2 phases: hyperalgesia, in which the excitatory threshold of the nerve is reset, leading to a lowered stimulatory requirement, and allodynia, in which normally harmless stimuli are interpreted as pain. During the allodynia phase, fibers (eg, C-fibers) that typically carry nonpainful information are recruited to become pain transmitters.
The pain threshold—and why it is important
The concept of the pain threshold is both complex and elusive. It can be defined as the point at which a stimulus begins to be perceived as painful. The pain threshold may be dependent on multiple variables, including gender, genetic issues (a concentration of mu receptors), a history of abuse, socioeconomic status, current and past levels of depression, earlier pain experiences, and psychosocial stressors.
The pain threshold is important because it changes over time. For example, a patient with endometriosis may experience isolated dysmenorrhea as a teen but, over time, may develop a pattern of chronic daily pain and depression. Or a woman with CPP may respond well to initial therapies but worsen after a stressful life event such as death of a loved one or new stressors at work. An understanding of the many variables that can alter the pain threshold can lead to more effective counseling and treatment and help us avoid unnecessary therapies.
Multiple types of pain can coexist in 1 patient
Clinicians who care for women with endometriosis and CPP should have an understanding of the mechanism of their pain, including the differences between nociceptive somatic, nociceptive visceral, and neuropathic pain (TABLE 2). All 3 types of pain can exist in a single patient with CPP.
Nociceptive somatic pain generally originates in somatic structures such as muscle, ligament, bone, and tendons. Women with endometriosis often have somatic pain, for 2 main reasons.11 First, skeletal muscles respond adversely to long-term inflammatory stimuli,12 and endometriosis is primarily a disease of inflammation. Long-term inflammatory stimuli may lead to atrophy and spasm. Second, the presence of inflammation in the muscle likely leads to worsening hyperalgesia with increasing muscle activity.13 This can lead to and explain pain in the pelvic floor, abdominal wall muscles, hips, thighs, buttocks, and lower back. Once this is understood, treatments can be targeted to the underlying mechanisms and specific muscle groups.
Nociceptive visceral pain generally indicates pain originating in visceral structures. In the pelvis, visceral structures of main concern are the uterus, ovaries, fallopian tubes, vagina (upper two-thirds), bladder, ureters, sigmoid colon, rectum, and, most importantly related to endometriosis, the visceral peritoneum.
In the case of visceral pain, the likely associated mechanisms are inflammation as well as local nerve growth.14,15 Local inflammation in turn leads to scarring and visceral hyperalgesia.16 Over a long period of time, local visceral hyperalgesia can lead to spinal wind-up and central sensitization. Spinal wind-up is the spinal cord’s expansion of signals from peripheral nociceptors associated with C-fibers. It likely stems from a prolonged, intense, and persistent generation of afferent nociceptive impulses. When this occurs, CNS pathways are well established and sensations of pain can remain even after careful surgery to remove sources of inflammation and anatomic deformity (visceral scarring). For this reason, early radical resection of endometriosis in women with endometriosis-associated pelvic pain may be more likely than later surgery to reduce or eliminate pain. Otherwise, reoperation rates may be high and later surgeries may fail to yield histopathology for endometrial glands and stroma.17
Neuropathic pain generally reflects damage to or dysfunction of either the peripheral nervous system or the CNS. Endometriosis-associated pain is also neuropathic in nature and occurs through multiple mechanisms.
There is good evidence to support the development of abnormal nerve growth in and around areas of endometriosis. When such nerve fibers exist, they serve only a pathologic function. This abnormal nerve growth is induced by multiple molecules, including nerve growth factor and vascular endothelial growth factor.7 It is likely that once high-density areas of sensitized nerves develop, peripheral nerves also become sensitized by endometriosis-associated inflammatory cytokines.16 When there are abnormal nerve growth and elevated levels of peripheral nerve sensitization, the nerves most often recruited are C-fibers, unmyeli-nated fibers largely associated with both peripheral and central neuropathic pain. When C-fibers are recruited, the ratio of C-fibers to autonomic afferent pain fibers increases.
In endometriosis, persistent inflammatory signals lead to an increase in the excitability of peripheral nerves, thereby significantly increasing transmitted pain signals and likely reducing the body’s ability to suppress pain.
Some of the peripheral nerve changes I have described may be observed via magnetic resonance tractography (MRT), which highlights neuronal tracts over long distances. Fractional anisotropy values measured by MRT yield information about the quality of neuronal structures. In women with endometriosis, fractional anisotropy values in the peripheral nerve roots of S1, S2, and S3 appear to be lower than those in women without endometriosis,18 indicating disruption of the normally myelinated nerve structure.
It’s time to abandon nontargeted treatments
Endometriosis-associated CPP remains a challenging heterogeneous and multifactorial disease state. In the past, treatments such as gonadotropin-releasing hormone agonists have been prescribed without an appropriate consideration of the disease and its mechanism of associated pain. In our CPP specialty practice, we have abandoned such nontargeted approaches. By developing an understanding of central sensitization, local neurologic responses to inflammation, and the pain threshold, clinicians are more likely to select a treatment targeted to specific mechanisms. Such an approach is superior to the traditional “shotgun” approach to treatment, which can produce harmful side effects and have high long-term failure rates. As Stratton and colleagues observed, “traditional methods of classifying endometriosis-associated pain based on disease, duration, and anatomy are inadequate and should be replaced by a mechanism-based evaluation.”19 Future clinical care and research will necessarily focus on specific disease etiologies and pain mechanisms if we are to continue to improve the care of women with CPP.
Case: Resolved
Because the history, physical examination, and imaging are strongly suggestive of endometriosis, the patient is counseled about the treatments most likely to be effective, which include medical therapies such as centrally acting agents (gabapentin, pregabalin, tricyclic antidepressants) and local treatments such as placement of a levonorgestrel-releasing intrauterine system or surgical resection. She elects to undergo total laparoscopic hysterectomy with bilateral salpingectomy and radical resection of endometriosis. Histopathology confirms adenomyosis and deep infiltrating endometriosis, including implants on the rectovaginal septum. The patient remains pain-free at her 2-year follow-up.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. Brumovsky PR, Gebhart GF. Visceral organ cross-sensitization—an integrated perspective. Auton Neurosci. 2010;153(1–2):106–115.
2. Schwartz ES, Gebhart GF. Visceral pain. Curr Top Behav Neurosci. 2014;20:171–197.
3. Gebhart GF. Visceral pain—peripheral sensitization. Gut. 2000;47(suppl 4):54–58.
4. Fukaya T, Hoshiai H, Yajima A. Is pelvic endometriosis always associated with chronic pain? A retrospective study of 618 cases diagnosed by laparoscopy. Am J Obstet Gynecol. 1993;169(3):719–722.
5. Vercellini P, Trespidi L, De GO, Cortesi I, Parazzini F, Crosignani PG. Endometriosis and pelvic pain: relation to disease stage and localization. Fertil Steril. 1996;65(2):299–304.
6. Brawn J, Morotti M, Zondervan KT, Becker CM, Vincent K. Central changes associated with chronic pelvic pain and endometriosis. Hum Reprod Update. 2014;20(5):737–747.
7. Morotti M, Vincent K, Brawn J, Zondervan KT, Becker CM. Peripheral changes in endometriosis-associated pain. Hum Reprod Update. 2014;20(5):717–736.
8. Neziri AY, Bersinger NA, Andersen OK, Arendt-Nielsen L, Mueller MD, Curatolo M. Correlation between altered central pain processing and concentration of peritoneal fluid inflammatory cytokines in endometriosis patients with chronic pelvic pain. Reg Anesth Pain Med. 2014;39(3):181–184.
9. Asante A, Taylor RN. Endometriosis: the role of neuroangiogenesis. Annu Rev Physiol. 2011;73:163–182.
10. Arnold J, Barcena de Arellano ML, Ruster C, et al. Imbalance between sympathetic and sensory innervation in peritoneal endometriosis. Brain Behav Immun. 2012;26(1):132–141.
11. Warren JW, Morozov V, Howard FM. Could chronic pelvic pain be a functional somatic syndrome? Am J Obstet Gynecol. 2011;205(3):199–205.
12. Korotkova M, Lundberg IE. The skeletal muscle arachidonic acid cascade in health and inflammatory disease. Nat Rev Rheumatol. 2014;10(5):295–303.
13. Sluka KA, Rasmussen LA. Fatiguing exercise enhances hyperalgesia to muscle inflammation. Pain. 2010;148(2):188–197.
14. McKinnon B, Bersinger NA, Wotzkow C, Mueller MD. Endometriosis-associated nerve fibers, peritoneal fluid cytokine concentrations, and pain in endometriotic lesions from different locations. Fertil Steril. 2012;97(2):373–380.
15. Anaf V, El Nakadi I, De Moor V, Chapron C, Pistofidis G, Noel JC. Increased nerve density in deep infiltrating endometriotic nodules. Gynecol Obstet Invest. 2011;71(2):112–117.
16. McKinnon BD, Bertschi D, Bersinger NA, Mueller MD. Inflammation and nerve fiber interaction in endometriotic pain. Trends Endocrinol Metab. 2015;26(1):1–10.
17. Redwine DB. Conservative laparoscopic excision of endometriosis by sharp dissection: life table analysis of reoperation and persistent or recurrent disease. Fertil Steril. 1991;56(4):628–634.
18. Manganaro L, Porpora MG, Vinci V, et al. Diffusion tensor imaging and tractography to evaluate sacral nerve root abnormalities in endometriosis-related pain: a pilot study. Eur Radiol. 2014;24(1):95–101.
19. Stratton P, Khachikyan I, Sinaii N, Ortiz R, Shah J. Association of chronic pelvic pain and endometriosis with signs of sensitization and myofascial pain. Obstet Gynecol. 2015;125(3):719–728.
1. Brumovsky PR, Gebhart GF. Visceral organ cross-sensitization—an integrated perspective. Auton Neurosci. 2010;153(1–2):106–115.
2. Schwartz ES, Gebhart GF. Visceral pain. Curr Top Behav Neurosci. 2014;20:171–197.
3. Gebhart GF. Visceral pain—peripheral sensitization. Gut. 2000;47(suppl 4):54–58.
4. Fukaya T, Hoshiai H, Yajima A. Is pelvic endometriosis always associated with chronic pain? A retrospective study of 618 cases diagnosed by laparoscopy. Am J Obstet Gynecol. 1993;169(3):719–722.
5. Vercellini P, Trespidi L, De GO, Cortesi I, Parazzini F, Crosignani PG. Endometriosis and pelvic pain: relation to disease stage and localization. Fertil Steril. 1996;65(2):299–304.
6. Brawn J, Morotti M, Zondervan KT, Becker CM, Vincent K. Central changes associated with chronic pelvic pain and endometriosis. Hum Reprod Update. 2014;20(5):737–747.
7. Morotti M, Vincent K, Brawn J, Zondervan KT, Becker CM. Peripheral changes in endometriosis-associated pain. Hum Reprod Update. 2014;20(5):717–736.
8. Neziri AY, Bersinger NA, Andersen OK, Arendt-Nielsen L, Mueller MD, Curatolo M. Correlation between altered central pain processing and concentration of peritoneal fluid inflammatory cytokines in endometriosis patients with chronic pelvic pain. Reg Anesth Pain Med. 2014;39(3):181–184.
9. Asante A, Taylor RN. Endometriosis: the role of neuroangiogenesis. Annu Rev Physiol. 2011;73:163–182.
10. Arnold J, Barcena de Arellano ML, Ruster C, et al. Imbalance between sympathetic and sensory innervation in peritoneal endometriosis. Brain Behav Immun. 2012;26(1):132–141.
11. Warren JW, Morozov V, Howard FM. Could chronic pelvic pain be a functional somatic syndrome? Am J Obstet Gynecol. 2011;205(3):199–205.
12. Korotkova M, Lundberg IE. The skeletal muscle arachidonic acid cascade in health and inflammatory disease. Nat Rev Rheumatol. 2014;10(5):295–303.
13. Sluka KA, Rasmussen LA. Fatiguing exercise enhances hyperalgesia to muscle inflammation. Pain. 2010;148(2):188–197.
14. McKinnon B, Bersinger NA, Wotzkow C, Mueller MD. Endometriosis-associated nerve fibers, peritoneal fluid cytokine concentrations, and pain in endometriotic lesions from different locations. Fertil Steril. 2012;97(2):373–380.
15. Anaf V, El Nakadi I, De Moor V, Chapron C, Pistofidis G, Noel JC. Increased nerve density in deep infiltrating endometriotic nodules. Gynecol Obstet Invest. 2011;71(2):112–117.
16. McKinnon BD, Bertschi D, Bersinger NA, Mueller MD. Inflammation and nerve fiber interaction in endometriotic pain. Trends Endocrinol Metab. 2015;26(1):1–10.
17. Redwine DB. Conservative laparoscopic excision of endometriosis by sharp dissection: life table analysis of reoperation and persistent or recurrent disease. Fertil Steril. 1991;56(4):628–634.
18. Manganaro L, Porpora MG, Vinci V, et al. Diffusion tensor imaging and tractography to evaluate sacral nerve root abnormalities in endometriosis-related pain: a pilot study. Eur Radiol. 2014;24(1):95–101.
19. Stratton P, Khachikyan I, Sinaii N, Ortiz R, Shah J. Association of chronic pelvic pain and endometriosis with signs of sensitization and myofascial pain. Obstet Gynecol. 2015;125(3):719–728.
In This Article
- The pain threshold and why it is important
- Types of pain and their implications
- It’s time to abandon nontargeted treatments
On the Scent of Cancer
Cancers exude odors that dogs can sniff with high accuracy, but dogs may get distracted in a clinical setting. Thus, researchers at Kyushu University in Fukuoka, Japan, turned to nematodes. In the Nematode Scent Detection Test (NSDT), the researchers tested the cancer-sensing ability of Caenorhabditis elegans (C. elegans) on 242 urine samples: 218 controls and 24 samples from patients with cancer.
Related: Nephrotic Syndrome Is a Marker for Occult Cancer
C. elegans performed remarkably well, with 95.8% sensitivity and 95% specificity. The positive predictive value was 67.6%; efficiency was 95%. Strikingly, the nematode was able to diagnose various cancer types tested at stage 0 or 1.
Related: Do Age and Gender Matter in Colorectal Cancer?
The researchers tout the NSDT’s “outstanding” characteristics: high accuracy, low cost, painlessness, convenience, and speed. However, despite its nose for cancer, C. elegans can’t identify the organs harboring the cancer cells, the researchers say. Therefore, they suggest the test might best be combined with existing and new methods of diagnosis, such as metabolomic analyses.
Source
Hirotsu T, Sonoda H, Uozumi T, et al. PLoS ONE. 10(3):e0118699.
doi: 10.1371/journal.pone.0118699.
Cancers exude odors that dogs can sniff with high accuracy, but dogs may get distracted in a clinical setting. Thus, researchers at Kyushu University in Fukuoka, Japan, turned to nematodes. In the Nematode Scent Detection Test (NSDT), the researchers tested the cancer-sensing ability of Caenorhabditis elegans (C. elegans) on 242 urine samples: 218 controls and 24 samples from patients with cancer.
Related: Nephrotic Syndrome Is a Marker for Occult Cancer
C. elegans performed remarkably well, with 95.8% sensitivity and 95% specificity. The positive predictive value was 67.6%; efficiency was 95%. Strikingly, the nematode was able to diagnose various cancer types tested at stage 0 or 1.
Related: Do Age and Gender Matter in Colorectal Cancer?
The researchers tout the NSDT’s “outstanding” characteristics: high accuracy, low cost, painlessness, convenience, and speed. However, despite its nose for cancer, C. elegans can’t identify the organs harboring the cancer cells, the researchers say. Therefore, they suggest the test might best be combined with existing and new methods of diagnosis, such as metabolomic analyses.
Source
Hirotsu T, Sonoda H, Uozumi T, et al. PLoS ONE. 10(3):e0118699.
doi: 10.1371/journal.pone.0118699.
Cancers exude odors that dogs can sniff with high accuracy, but dogs may get distracted in a clinical setting. Thus, researchers at Kyushu University in Fukuoka, Japan, turned to nematodes. In the Nematode Scent Detection Test (NSDT), the researchers tested the cancer-sensing ability of Caenorhabditis elegans (C. elegans) on 242 urine samples: 218 controls and 24 samples from patients with cancer.
Related: Nephrotic Syndrome Is a Marker for Occult Cancer
C. elegans performed remarkably well, with 95.8% sensitivity and 95% specificity. The positive predictive value was 67.6%; efficiency was 95%. Strikingly, the nematode was able to diagnose various cancer types tested at stage 0 or 1.
Related: Do Age and Gender Matter in Colorectal Cancer?
The researchers tout the NSDT’s “outstanding” characteristics: high accuracy, low cost, painlessness, convenience, and speed. However, despite its nose for cancer, C. elegans can’t identify the organs harboring the cancer cells, the researchers say. Therefore, they suggest the test might best be combined with existing and new methods of diagnosis, such as metabolomic analyses.
Source
Hirotsu T, Sonoda H, Uozumi T, et al. PLoS ONE. 10(3):e0118699.
doi: 10.1371/journal.pone.0118699.
Depression and Substance Abuse Intensify Suicide Risk
Posttraumatic stress disorder (PTSD), traumatic brain injury (TBI), and chronic pain have affected so many veterans that this combination has become known as the polytrauma clinical triad (PCT). Individually and together, they have also been linked to an increased risk of suicide-related behavior (SRB), but no studies have examined the “unique or combined contributions” of the PCT among Operation Iraqi Freedom/Operation Enduring Freedom veterans, say researchers from South Texas Veterans Health Care System and the University of Texas, both in San Antonio; Edith Nourse Rogers Memorial VA Hospital in Bedford, Massachusetts; the Center for Applied Health Research in Temple, Texas; and the University of Utah in Salt Lake City.
Related: Active-Duty Suicide Rates Remain High
Thus, the researchers designed a study to help determine whether PTSD, TBI, and pain are more strongly associated with suicide in certain combinations as well as how they compare as risk indicators with other disorders, such as depression and substance abuse.
Related: Jonathan Woodson on Military Health Readiness
In this retrospective study of 211,652 veterans, 5,653 (2.6%) had demonstrated SRB—either ideation, attempt (suicide and self-inflicted injury), or both. But although veterans in the PCT had a greater risk of SRB, the co-occurrence of all 3 conditions did not increase risk above that associated with PTSD, depression, or substance abuse alone. Instead, adding depression or substance abuse to PTSD increased the risk of suicidal ideation by more than 4-fold.
Related: Clay Hunt Suicide Prevention Bill Signed by President Obama
Their findings reassert the importance of depression and substance abuse as additional risk factors for suicide among veterans, particularly those with comorbid PTSD, the researchers say. It is more essential than ever, they urge, to ensure that all veterans receive appropriate screening and treatment for symptoms of depression and substance abuse. They suggest an assessment template that targets subgroups at highest risk for depression and substance abuse, especially in conjunction with PTSD, as red flags warranting additional screening, care integration, and follow-up.
Source
Finley EP, Bollinger M, Noël PH, et al. Am J Public Health. 2015;105(2):380-387.
doi: 10.2105/AJPH.2014.301957.
Posttraumatic stress disorder (PTSD), traumatic brain injury (TBI), and chronic pain have affected so many veterans that this combination has become known as the polytrauma clinical triad (PCT). Individually and together, they have also been linked to an increased risk of suicide-related behavior (SRB), but no studies have examined the “unique or combined contributions” of the PCT among Operation Iraqi Freedom/Operation Enduring Freedom veterans, say researchers from South Texas Veterans Health Care System and the University of Texas, both in San Antonio; Edith Nourse Rogers Memorial VA Hospital in Bedford, Massachusetts; the Center for Applied Health Research in Temple, Texas; and the University of Utah in Salt Lake City.
Related: Active-Duty Suicide Rates Remain High
Thus, the researchers designed a study to help determine whether PTSD, TBI, and pain are more strongly associated with suicide in certain combinations as well as how they compare as risk indicators with other disorders, such as depression and substance abuse.
Related: Jonathan Woodson on Military Health Readiness
In this retrospective study of 211,652 veterans, 5,653 (2.6%) had demonstrated SRB—either ideation, attempt (suicide and self-inflicted injury), or both. But although veterans in the PCT had a greater risk of SRB, the co-occurrence of all 3 conditions did not increase risk above that associated with PTSD, depression, or substance abuse alone. Instead, adding depression or substance abuse to PTSD increased the risk of suicidal ideation by more than 4-fold.
Related: Clay Hunt Suicide Prevention Bill Signed by President Obama
Their findings reassert the importance of depression and substance abuse as additional risk factors for suicide among veterans, particularly those with comorbid PTSD, the researchers say. It is more essential than ever, they urge, to ensure that all veterans receive appropriate screening and treatment for symptoms of depression and substance abuse. They suggest an assessment template that targets subgroups at highest risk for depression and substance abuse, especially in conjunction with PTSD, as red flags warranting additional screening, care integration, and follow-up.
Source
Finley EP, Bollinger M, Noël PH, et al. Am J Public Health. 2015;105(2):380-387.
doi: 10.2105/AJPH.2014.301957.
Posttraumatic stress disorder (PTSD), traumatic brain injury (TBI), and chronic pain have affected so many veterans that this combination has become known as the polytrauma clinical triad (PCT). Individually and together, they have also been linked to an increased risk of suicide-related behavior (SRB), but no studies have examined the “unique or combined contributions” of the PCT among Operation Iraqi Freedom/Operation Enduring Freedom veterans, say researchers from South Texas Veterans Health Care System and the University of Texas, both in San Antonio; Edith Nourse Rogers Memorial VA Hospital in Bedford, Massachusetts; the Center for Applied Health Research in Temple, Texas; and the University of Utah in Salt Lake City.
Related: Active-Duty Suicide Rates Remain High
Thus, the researchers designed a study to help determine whether PTSD, TBI, and pain are more strongly associated with suicide in certain combinations as well as how they compare as risk indicators with other disorders, such as depression and substance abuse.
Related: Jonathan Woodson on Military Health Readiness
In this retrospective study of 211,652 veterans, 5,653 (2.6%) had demonstrated SRB—either ideation, attempt (suicide and self-inflicted injury), or both. But although veterans in the PCT had a greater risk of SRB, the co-occurrence of all 3 conditions did not increase risk above that associated with PTSD, depression, or substance abuse alone. Instead, adding depression or substance abuse to PTSD increased the risk of suicidal ideation by more than 4-fold.
Related: Clay Hunt Suicide Prevention Bill Signed by President Obama
Their findings reassert the importance of depression and substance abuse as additional risk factors for suicide among veterans, particularly those with comorbid PTSD, the researchers say. It is more essential than ever, they urge, to ensure that all veterans receive appropriate screening and treatment for symptoms of depression and substance abuse. They suggest an assessment template that targets subgroups at highest risk for depression and substance abuse, especially in conjunction with PTSD, as red flags warranting additional screening, care integration, and follow-up.
Source
Finley EP, Bollinger M, Noël PH, et al. Am J Public Health. 2015;105(2):380-387.
doi: 10.2105/AJPH.2014.301957.
The Cost of Unused Medications
Studies analyzing the causes of and patterns associated with polypharmacy have increased over the past decade.1-3 Disadvantages to polypharmacy include but are not limited to higher risk of drug-drug interactions, greater potential for adverse effects (AEs), higher risk of nonadherence, and higher costs for the patient and health care systems.1 Compounding the disadvantages associated with polypharmacy, medication storage and disposal are areas of environmental concern. A recent study by Wieczorkiewicz and colleagues examined how patients use, store, and dispose of medications and found that “almost all respondents had excess and leftover medications in their homes.”4 The authors concluded that both overprescribing and poor medication adherence contribute to excess medications at home.
As health care systems become more fiscally responsible, it is beneficial to review prescribing and dispensing patterns, which contribute to polypharmacy and excess medications in patient homes. One of the specific areas that came to the attention of the authors was the number of medication returns received at Evans Army Community Hospital (EACH). As Wiesczorkiewicz and colleagues discovered, it is common that medicine cabinets are filled with expired drugs or medications no longer in use. Although some of these medications can be disposed of in the trash or toilets, some facilities take back unused drugs.5
In an attempt to keep patients and the environment safe, EACH takes back unused medications daily for destruction. These patient returns must be destroyed for both legal and ethical reasons, because there is the potential that medications that have left the system may have been adulterated. The purpose of this quality improvement (QI) project was to evaluate the cost of patient medication returns and explore any additional sources of waste in the prescribing and dispensing processes.
Methods
As a QI project assessing current prescribing and dispensing processes and improving patient-centered performance, Institutional Review Board approval was not required. The QI project and manuscript submission did receive approval from the EACH Command Team. Patient prescription returns were collected at the main and outlying hospital pharmacies between December 16, 2012, and April 5, 2013. Patients were encouraged to bring all medications to clinic visits, and if it was determined that the patient was no longer taking the medication or that the medication was discontinued, the clinician would bring the medication(s) to the patient return collection bin for destruction.
Related: New Guidance on Compounded Drugs
Patients also presented medications no longer used to the pharmacy for the patient return collection bin. A pharmacy technician recorded the medication name, strength, original amount prescribed, and the number of tablets/capsules remaining in the vial. Quantities dispensed greater than the quantities prescribed were later segregated for additional analysis. The brand name of the product was recorded only when the brand name was dispensed. The cost per unit was obtained from the pharmaceutical distributor and recorded to quantify the total cost of each prescription and the total cost of the medications returned. Medications that were classified as hazardous waste were assessed, as were all other medications, and then were segregated to the hospital’s satellite accumulation point for disposal by the Directorate of Public Works Environmental Division. Partial creams and ointments were excluded from the analysis, because the total amount returned was not easily quantifiable.
Results
The total value of the medications collected from December 16, 2012, through April 5, 2013, was $63,183 (1,174 prescriptions). Furthermore, there was the cost of the vials; printer ink; labels; labor to pay pharmacists to process, check, and dispense the medications; and the time of technician staff to fill the prescriptions and later sort the medications to look for hazardous waste and controlled substances. These additional expenses were not quantified and therefore were not included in the aforementioned value.
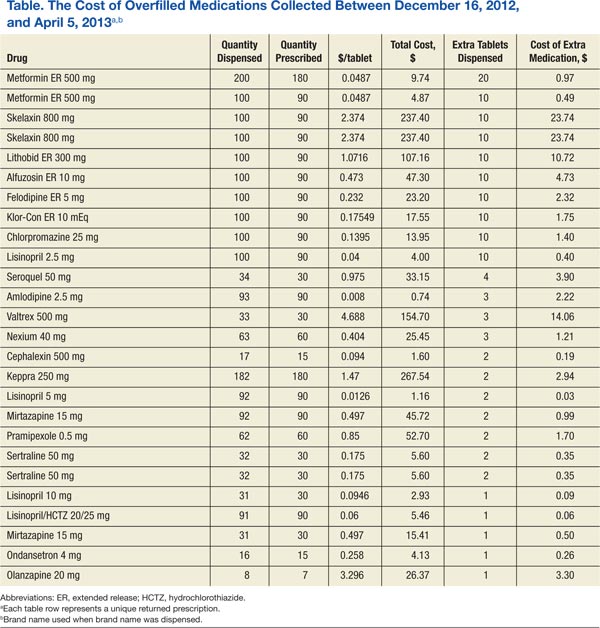
A subanalysis was conducted after it was observed that several prescriptions had greater quantities dispensed than the quantity prescribed (Table). An excess of $102.41 was dispensed and later collected during the study period. Of the 26 prescriptions that were overfilled, 10 were not due to human error but were intentionally overfilled as evidenced by sealed manufacturer bottles; the cost of the medications overfilled for these 10 prescriptions was $70.26.
The top returned drugs in descending order were lisinopril (42), bupropion (32), prazosin (28), gabapentin (27), and ondansetron (26). The top classifications of medications returned in descending order were antidepressants (198), antihypertensives (185), anticonvulsants (61), antilipemics (60), antibiotics (57), and antipsychotics (57). Also noteworthy is that a total of 91 prescriptions (7.8%) for over-the-counter (OTC) products were returned.
Discussion
As suggested by Wieczorkiewicz and colleagues, prescribing and dispensing patterns may be contributing to the accumulation of unwanted and unused medications.4 Patient feedback would also give insight to this problem. Furthermore, the data highlighted improvement opportunities related to back order/shortage and high-dollar medications. Additional exploration into prescribing, dispensing, and consumer patterns as well as potential cost-saving strategies addressing the aforementioned processes is warranted.
Prescribing Patterns
An editorial by Ruef addressed overprescribing patterns and hypothesized that prescribers may be more cautious and prescribe antibiotics (without laboratory confirmation), because if medications are not prescribed, patients with a potentially serious, quickly developing infection may experience an adverse outcome.6 Additionally, there is the anticipation and pressure from patients to receive a medication. Although only 60 of the 1,174 prescriptions were antibiotics or antifungals, one could easily insert other indications into this rationale.
Related: Pharmacists in the Emergency Department: Feasibility and Cost
During the collection period, the problem of polypharmacy stemming from the emergency department (ED), independent of this QI project, was brought to the authors’ attention. Consequently, data were collected from patients who presented for what was perceived (by both the patient and the pharmacy) as a high number of prescriptions from the ED. The data were reviewed and analyzed to determine whether there were any correlations between perceived excessive prescribing and the patient medication return data.
This study found that of 54 patient visits, there were a total of 324 prescriptions with a median of 6 prescriptions per person. The majority (56%) of these prescriptions were for OTC medications. The top 5 medications prescribed were ibuprofen, acetaminophen, ondansetron, oxymetazoline, and pseudoephedrine; 4 of which are OTC medications. The top 5 classifications of medications were decongestants, nonsteroidal anti-inflammatory drugs, analgesics, antibiotics, and antiemetics.
In contrast to the patient return data with 5 of the 6 top medications prescribed for chronic conditions, it is no surprise that the top 5 ED medications were prescribed for acute conditions. Ondansetron, which costs up to $0.37 per tablet, was one of the top prescribed medications from the ED and one of the most frequently returned medications. One might question whether this was a misuse of ED resources, considering patients were seen in this costly setting and received OTC medications. Further study of misappropriation of resources in the ED and trends from other clinic areas are needed.
Dispensing Patterns
In addition, it was observed that the pharmacy was overfilling prescriptions. Inaccurate quantities dispensed may have been due to human error and also due to staff belief that it would cost more (in staff time) to count the exact quantity prescribed for medications supplied in a manufacturer bottle near the amount needed for the prescription. It has been noted by pharmacy staff that deviation from exact counts is only done with medications that do not have a significant cost per tablet or capsule. The cost of medications intentionally overfilled was $70.26—not an insignificant source of waste.
Related: Pharmacist-Managed Collaborative Practice for Chronic Stable Angina
Medications returned to stock (because patients never picked up the prescription) were not used for future prescriptions but rather placed in the patient return collection for destruction. After this practice was noted, these returned-to-stock products were segregated to evaluate the value of the medications that could have been used for future prescriptions. Seventy-six prescriptions could have been dispensed, and the value of these unused medications was $3,049. Whereas civilian retail settings would not allow the practice of destroying medications that can otherwise be dispensed, this practice was permitted at EACH.
Consumer Patterns
It was hypothesized in this study that patients were returning medications because the prescriber switched the medication, the patient ultimately did not need the medication because symptoms resolved on their own, the patient may have had an AE or tolerance issues, the patient died, the dose was adjusted, or the patient had duplicate prescriptions. Further exploration regarding patients’ perspectives should be considered.
Back Orders and Shortages
Similar to many other institutions across the country, EACH has been affected by drug product shortages. There are a number of contributing factors to these shortages, including raw and bulk material unavailability, manufacturer difficulties and regulatory issues, voluntary recalls, change in product formulation or manufacturer, unexpected increases in demand, and shifts in clinical practice.7
An example of a recently recalled medication is atorvastatin. Historical data indicate that EACH paid $0.08 per tablet ($6.77 for a 90-day supply). After the generic manufacturer recalled atorvastatin, the brand-name product needed to be ordered, which cost $1.93 per tablet (or $173.70 for a 90-day supply). During the study, 370 atorvastatin tablets were returned, 90 of which were the brand-name tablets. It was unfortunate that this quantity was dispensed, considering these tablets were destroyed. If it is possible to limit quantities dispensed on manufacturer recall/ back order products until the price is more reasonable, without a significant disruption in patient care, pharmacies may consider policy changes.
High-Dollar Medications
Although the cost of a number of generic medications may be negligible, a number of medications continue to have a significant associated cost. Of the prescriptions returned, 170 cost > $100. Of these, 16 prescriptions cost > $500, and the total was > $13,000.
The U.S. Air Force had a high dollar program, in which patients were limited to a 30-day supply if the 30-day supply cost > $500 for treatment of a chronic condition. The staff burden and difficulty of maintaining such a program is unknown; however, the program is thought-provoking. Specifically, instead of dispensing 90-day supplies, the facility might consider limiting expensive prescriptions to ≤ 30 days for medications with additional refills if needed. Quantity limitations are already implemented for medications such as sildenafil, migraine medications, and opioids.
There is clearly a financial burden that needs to be addressed, and as this study evaluated the waste involved in patient returns, additional sources of waste were illuminated. Lean Six Sigma highlights several forms of waste: transportation, inventory, motion, waiting, overprocessing, overproduction, and defects/errors.8,9 This study found that there were several forms of waste in the prescribing and dispensing processes. Specifically, the authors found inventory mismanagement, overprocessing (overprescribing), overproduction (dispensing more than prescribed), possible misuse of costly resources, and defects/errors.
Limitations
The results of this QI project were limited to unused medications that patients returned to the facility. Returning unused medications is neither requested nor mandatory. Therefore, it is estimated that the true amount of unused medications that could be returned for destruction is vastly greater than the brief collection obtained in this data set. Furthermore, this collection is only a snapshot at one military treatment facility. With multiple facilities within the DoD, the total amount and value of unused medications is likely to be immensely greater than the $63,000 collected in this study.
Additionally, the cost to discard hazardous waste medications was not quantified. Evans Army Community Hospital pays $1.95 per lb for disposal of hazardous waste medications (eg, fluticasone/salmeterol, albuterol, warfarin, insulins), but this financial burden was not addressed in this QI project.
Recommendations
There are a number of behaviors that could be addressed to reduce the waste observed in this study:
- Prescribers should reevaluate prescribing habits to assess whether they are overprescribing medications. They may consider asking the patient whether they plan to take the medication prior to writing the prescription. If the patient is not agreeable to the treatment plan, then the treatment plan may need to be reevaluated.
- Facilities may consider a policy that allows no more than a 30-day supply for new medication prescriptions. Patients should have a follow-up to determine whether the treatment is effective or whether there are AEs, and a new maintenance prescription may be written at that time.
- Pharmacies should ensure that pharmacists fill the quantity prescribed. Prescriptions that have overfills in quantities are considered misbranded.
- Pharmacies should enforce policies for returning to stock the prescriptions that were prepared but never dispensed to patients.
- For medications that are on back order or in short supply, prescribers should consider changing the quantity dispensed to a 30-day supply (or less as appropriate) with refills.
- Pharmacies should consider limiting quantities of high-dollar medications and adding refills for any additional therapy needed.
- Hospitals should evaluate patient use of emergency resources. Other local health treatment facilities outline clearly for patients what constitutes an emergency and what does not. A similar policy change should be considered at EACH.
Summary
Polypharmacy is an increasing problem in today’s medical field. Consequently, unwanted and unused medications accumulate in patients’ homes. In an attempt to keep patients and the environment safe, EACH takes back unused medications every day for destruction. During the collection period of patient returns from December 16, 2012, through April 5, 2013, > $63,000 of unused medications were returned for destruction, which did not include the cost of labor or additional supplies. These data illuminated possible prescribing and dispensing patterns contributing to this waste and inspired further exploration of additional sources of waste, such as overprocessing, overproduction, inventory mismanagement, misuse of resources, and defects/ errors. This study highlighted a number of strategies that, if implemented, may significantly reduce the deficit burden and reduce costs associated with polypharmacy.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Kaur G. Polypharmacy: The past, present and the future. J Adv Pharm Technol Res. 2013;4(4):224-225.
2. Calderón-Larrañaga A, Gimeno-Feliu LA, González-Rubio F, et al. Polypharmacy patterns: Unravelling systematic associations between prescribed medications. PLoS One. 2013;8(12):e84967.
3. Murray MD, Kroenke K. Polypharmacy and medication adherence: Small steps on a long road. J Gen Intern Med. 2001;16(2):137-139.
4. Wieczorkiewicz SM, Kassamali Z, Danziger LH. Behind closed doors: Medication storage and disposal in the home. Ann Pharmacother. 2013;47(4):482-489.
5. U.S. Food and Drug Administration. How to dispose of unused medicines. U.S. Department of Health and Human Services Website. http://www.fda.gov/forconsumers/consumerupdates/ucm101653.htm. Updated February 18, 2015. Accessed March 11, 2015.
6. Ruef C. Why do physicians prescribe antibiotics? Infect. 2011;39(4):287.
7. ASHP Expert Panel on Drug Product Shortages; Fox ER, Birt A, James KB, Kokko H, Salverson S, Soflin DL. ASHP Guidelines on Managing Drug Product Shortages in Hospitals and Health Systems. Am J Health Syst Pharm. 2009;66(15):1399-1406.
8. George M, Rowlands D, Kastle B. What is Lean Six Sigma? New York, NY: McGraw-Hill; 2004.
9. Womack JP, Jones DT. Lean Thinking: Banish Waste and Create Wealth in Your Corporation. New York, NY: Free Press; 2003.
Studies analyzing the causes of and patterns associated with polypharmacy have increased over the past decade.1-3 Disadvantages to polypharmacy include but are not limited to higher risk of drug-drug interactions, greater potential for adverse effects (AEs), higher risk of nonadherence, and higher costs for the patient and health care systems.1 Compounding the disadvantages associated with polypharmacy, medication storage and disposal are areas of environmental concern. A recent study by Wieczorkiewicz and colleagues examined how patients use, store, and dispose of medications and found that “almost all respondents had excess and leftover medications in their homes.”4 The authors concluded that both overprescribing and poor medication adherence contribute to excess medications at home.
As health care systems become more fiscally responsible, it is beneficial to review prescribing and dispensing patterns, which contribute to polypharmacy and excess medications in patient homes. One of the specific areas that came to the attention of the authors was the number of medication returns received at Evans Army Community Hospital (EACH). As Wiesczorkiewicz and colleagues discovered, it is common that medicine cabinets are filled with expired drugs or medications no longer in use. Although some of these medications can be disposed of in the trash or toilets, some facilities take back unused drugs.5
In an attempt to keep patients and the environment safe, EACH takes back unused medications daily for destruction. These patient returns must be destroyed for both legal and ethical reasons, because there is the potential that medications that have left the system may have been adulterated. The purpose of this quality improvement (QI) project was to evaluate the cost of patient medication returns and explore any additional sources of waste in the prescribing and dispensing processes.
Methods
As a QI project assessing current prescribing and dispensing processes and improving patient-centered performance, Institutional Review Board approval was not required. The QI project and manuscript submission did receive approval from the EACH Command Team. Patient prescription returns were collected at the main and outlying hospital pharmacies between December 16, 2012, and April 5, 2013. Patients were encouraged to bring all medications to clinic visits, and if it was determined that the patient was no longer taking the medication or that the medication was discontinued, the clinician would bring the medication(s) to the patient return collection bin for destruction.
Related: New Guidance on Compounded Drugs
Patients also presented medications no longer used to the pharmacy for the patient return collection bin. A pharmacy technician recorded the medication name, strength, original amount prescribed, and the number of tablets/capsules remaining in the vial. Quantities dispensed greater than the quantities prescribed were later segregated for additional analysis. The brand name of the product was recorded only when the brand name was dispensed. The cost per unit was obtained from the pharmaceutical distributor and recorded to quantify the total cost of each prescription and the total cost of the medications returned. Medications that were classified as hazardous waste were assessed, as were all other medications, and then were segregated to the hospital’s satellite accumulation point for disposal by the Directorate of Public Works Environmental Division. Partial creams and ointments were excluded from the analysis, because the total amount returned was not easily quantifiable.
Results
The total value of the medications collected from December 16, 2012, through April 5, 2013, was $63,183 (1,174 prescriptions). Furthermore, there was the cost of the vials; printer ink; labels; labor to pay pharmacists to process, check, and dispense the medications; and the time of technician staff to fill the prescriptions and later sort the medications to look for hazardous waste and controlled substances. These additional expenses were not quantified and therefore were not included in the aforementioned value.
A subanalysis was conducted after it was observed that several prescriptions had greater quantities dispensed than the quantity prescribed (Table). An excess of $102.41 was dispensed and later collected during the study period. Of the 26 prescriptions that were overfilled, 10 were not due to human error but were intentionally overfilled as evidenced by sealed manufacturer bottles; the cost of the medications overfilled for these 10 prescriptions was $70.26.
The top returned drugs in descending order were lisinopril (42), bupropion (32), prazosin (28), gabapentin (27), and ondansetron (26). The top classifications of medications returned in descending order were antidepressants (198), antihypertensives (185), anticonvulsants (61), antilipemics (60), antibiotics (57), and antipsychotics (57). Also noteworthy is that a total of 91 prescriptions (7.8%) for over-the-counter (OTC) products were returned.
Discussion
As suggested by Wieczorkiewicz and colleagues, prescribing and dispensing patterns may be contributing to the accumulation of unwanted and unused medications.4 Patient feedback would also give insight to this problem. Furthermore, the data highlighted improvement opportunities related to back order/shortage and high-dollar medications. Additional exploration into prescribing, dispensing, and consumer patterns as well as potential cost-saving strategies addressing the aforementioned processes is warranted.
Prescribing Patterns
An editorial by Ruef addressed overprescribing patterns and hypothesized that prescribers may be more cautious and prescribe antibiotics (without laboratory confirmation), because if medications are not prescribed, patients with a potentially serious, quickly developing infection may experience an adverse outcome.6 Additionally, there is the anticipation and pressure from patients to receive a medication. Although only 60 of the 1,174 prescriptions were antibiotics or antifungals, one could easily insert other indications into this rationale.
Related: Pharmacists in the Emergency Department: Feasibility and Cost
During the collection period, the problem of polypharmacy stemming from the emergency department (ED), independent of this QI project, was brought to the authors’ attention. Consequently, data were collected from patients who presented for what was perceived (by both the patient and the pharmacy) as a high number of prescriptions from the ED. The data were reviewed and analyzed to determine whether there were any correlations between perceived excessive prescribing and the patient medication return data.
This study found that of 54 patient visits, there were a total of 324 prescriptions with a median of 6 prescriptions per person. The majority (56%) of these prescriptions were for OTC medications. The top 5 medications prescribed were ibuprofen, acetaminophen, ondansetron, oxymetazoline, and pseudoephedrine; 4 of which are OTC medications. The top 5 classifications of medications were decongestants, nonsteroidal anti-inflammatory drugs, analgesics, antibiotics, and antiemetics.
In contrast to the patient return data with 5 of the 6 top medications prescribed for chronic conditions, it is no surprise that the top 5 ED medications were prescribed for acute conditions. Ondansetron, which costs up to $0.37 per tablet, was one of the top prescribed medications from the ED and one of the most frequently returned medications. One might question whether this was a misuse of ED resources, considering patients were seen in this costly setting and received OTC medications. Further study of misappropriation of resources in the ED and trends from other clinic areas are needed.
Dispensing Patterns
In addition, it was observed that the pharmacy was overfilling prescriptions. Inaccurate quantities dispensed may have been due to human error and also due to staff belief that it would cost more (in staff time) to count the exact quantity prescribed for medications supplied in a manufacturer bottle near the amount needed for the prescription. It has been noted by pharmacy staff that deviation from exact counts is only done with medications that do not have a significant cost per tablet or capsule. The cost of medications intentionally overfilled was $70.26—not an insignificant source of waste.
Related: Pharmacist-Managed Collaborative Practice for Chronic Stable Angina
Medications returned to stock (because patients never picked up the prescription) were not used for future prescriptions but rather placed in the patient return collection for destruction. After this practice was noted, these returned-to-stock products were segregated to evaluate the value of the medications that could have been used for future prescriptions. Seventy-six prescriptions could have been dispensed, and the value of these unused medications was $3,049. Whereas civilian retail settings would not allow the practice of destroying medications that can otherwise be dispensed, this practice was permitted at EACH.
Consumer Patterns
It was hypothesized in this study that patients were returning medications because the prescriber switched the medication, the patient ultimately did not need the medication because symptoms resolved on their own, the patient may have had an AE or tolerance issues, the patient died, the dose was adjusted, or the patient had duplicate prescriptions. Further exploration regarding patients’ perspectives should be considered.
Back Orders and Shortages
Similar to many other institutions across the country, EACH has been affected by drug product shortages. There are a number of contributing factors to these shortages, including raw and bulk material unavailability, manufacturer difficulties and regulatory issues, voluntary recalls, change in product formulation or manufacturer, unexpected increases in demand, and shifts in clinical practice.7
An example of a recently recalled medication is atorvastatin. Historical data indicate that EACH paid $0.08 per tablet ($6.77 for a 90-day supply). After the generic manufacturer recalled atorvastatin, the brand-name product needed to be ordered, which cost $1.93 per tablet (or $173.70 for a 90-day supply). During the study, 370 atorvastatin tablets were returned, 90 of which were the brand-name tablets. It was unfortunate that this quantity was dispensed, considering these tablets were destroyed. If it is possible to limit quantities dispensed on manufacturer recall/ back order products until the price is more reasonable, without a significant disruption in patient care, pharmacies may consider policy changes.
High-Dollar Medications
Although the cost of a number of generic medications may be negligible, a number of medications continue to have a significant associated cost. Of the prescriptions returned, 170 cost > $100. Of these, 16 prescriptions cost > $500, and the total was > $13,000.
The U.S. Air Force had a high dollar program, in which patients were limited to a 30-day supply if the 30-day supply cost > $500 for treatment of a chronic condition. The staff burden and difficulty of maintaining such a program is unknown; however, the program is thought-provoking. Specifically, instead of dispensing 90-day supplies, the facility might consider limiting expensive prescriptions to ≤ 30 days for medications with additional refills if needed. Quantity limitations are already implemented for medications such as sildenafil, migraine medications, and opioids.
There is clearly a financial burden that needs to be addressed, and as this study evaluated the waste involved in patient returns, additional sources of waste were illuminated. Lean Six Sigma highlights several forms of waste: transportation, inventory, motion, waiting, overprocessing, overproduction, and defects/errors.8,9 This study found that there were several forms of waste in the prescribing and dispensing processes. Specifically, the authors found inventory mismanagement, overprocessing (overprescribing), overproduction (dispensing more than prescribed), possible misuse of costly resources, and defects/errors.
Limitations
The results of this QI project were limited to unused medications that patients returned to the facility. Returning unused medications is neither requested nor mandatory. Therefore, it is estimated that the true amount of unused medications that could be returned for destruction is vastly greater than the brief collection obtained in this data set. Furthermore, this collection is only a snapshot at one military treatment facility. With multiple facilities within the DoD, the total amount and value of unused medications is likely to be immensely greater than the $63,000 collected in this study.
Additionally, the cost to discard hazardous waste medications was not quantified. Evans Army Community Hospital pays $1.95 per lb for disposal of hazardous waste medications (eg, fluticasone/salmeterol, albuterol, warfarin, insulins), but this financial burden was not addressed in this QI project.
Recommendations
There are a number of behaviors that could be addressed to reduce the waste observed in this study:
- Prescribers should reevaluate prescribing habits to assess whether they are overprescribing medications. They may consider asking the patient whether they plan to take the medication prior to writing the prescription. If the patient is not agreeable to the treatment plan, then the treatment plan may need to be reevaluated.
- Facilities may consider a policy that allows no more than a 30-day supply for new medication prescriptions. Patients should have a follow-up to determine whether the treatment is effective or whether there are AEs, and a new maintenance prescription may be written at that time.
- Pharmacies should ensure that pharmacists fill the quantity prescribed. Prescriptions that have overfills in quantities are considered misbranded.
- Pharmacies should enforce policies for returning to stock the prescriptions that were prepared but never dispensed to patients.
- For medications that are on back order or in short supply, prescribers should consider changing the quantity dispensed to a 30-day supply (or less as appropriate) with refills.
- Pharmacies should consider limiting quantities of high-dollar medications and adding refills for any additional therapy needed.
- Hospitals should evaluate patient use of emergency resources. Other local health treatment facilities outline clearly for patients what constitutes an emergency and what does not. A similar policy change should be considered at EACH.
Summary
Polypharmacy is an increasing problem in today’s medical field. Consequently, unwanted and unused medications accumulate in patients’ homes. In an attempt to keep patients and the environment safe, EACH takes back unused medications every day for destruction. During the collection period of patient returns from December 16, 2012, through April 5, 2013, > $63,000 of unused medications were returned for destruction, which did not include the cost of labor or additional supplies. These data illuminated possible prescribing and dispensing patterns contributing to this waste and inspired further exploration of additional sources of waste, such as overprocessing, overproduction, inventory mismanagement, misuse of resources, and defects/ errors. This study highlighted a number of strategies that, if implemented, may significantly reduce the deficit burden and reduce costs associated with polypharmacy.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Studies analyzing the causes of and patterns associated with polypharmacy have increased over the past decade.1-3 Disadvantages to polypharmacy include but are not limited to higher risk of drug-drug interactions, greater potential for adverse effects (AEs), higher risk of nonadherence, and higher costs for the patient and health care systems.1 Compounding the disadvantages associated with polypharmacy, medication storage and disposal are areas of environmental concern. A recent study by Wieczorkiewicz and colleagues examined how patients use, store, and dispose of medications and found that “almost all respondents had excess and leftover medications in their homes.”4 The authors concluded that both overprescribing and poor medication adherence contribute to excess medications at home.
As health care systems become more fiscally responsible, it is beneficial to review prescribing and dispensing patterns, which contribute to polypharmacy and excess medications in patient homes. One of the specific areas that came to the attention of the authors was the number of medication returns received at Evans Army Community Hospital (EACH). As Wiesczorkiewicz and colleagues discovered, it is common that medicine cabinets are filled with expired drugs or medications no longer in use. Although some of these medications can be disposed of in the trash or toilets, some facilities take back unused drugs.5
In an attempt to keep patients and the environment safe, EACH takes back unused medications daily for destruction. These patient returns must be destroyed for both legal and ethical reasons, because there is the potential that medications that have left the system may have been adulterated. The purpose of this quality improvement (QI) project was to evaluate the cost of patient medication returns and explore any additional sources of waste in the prescribing and dispensing processes.
Methods
As a QI project assessing current prescribing and dispensing processes and improving patient-centered performance, Institutional Review Board approval was not required. The QI project and manuscript submission did receive approval from the EACH Command Team. Patient prescription returns were collected at the main and outlying hospital pharmacies between December 16, 2012, and April 5, 2013. Patients were encouraged to bring all medications to clinic visits, and if it was determined that the patient was no longer taking the medication or that the medication was discontinued, the clinician would bring the medication(s) to the patient return collection bin for destruction.
Related: New Guidance on Compounded Drugs
Patients also presented medications no longer used to the pharmacy for the patient return collection bin. A pharmacy technician recorded the medication name, strength, original amount prescribed, and the number of tablets/capsules remaining in the vial. Quantities dispensed greater than the quantities prescribed were later segregated for additional analysis. The brand name of the product was recorded only when the brand name was dispensed. The cost per unit was obtained from the pharmaceutical distributor and recorded to quantify the total cost of each prescription and the total cost of the medications returned. Medications that were classified as hazardous waste were assessed, as were all other medications, and then were segregated to the hospital’s satellite accumulation point for disposal by the Directorate of Public Works Environmental Division. Partial creams and ointments were excluded from the analysis, because the total amount returned was not easily quantifiable.
Results
The total value of the medications collected from December 16, 2012, through April 5, 2013, was $63,183 (1,174 prescriptions). Furthermore, there was the cost of the vials; printer ink; labels; labor to pay pharmacists to process, check, and dispense the medications; and the time of technician staff to fill the prescriptions and later sort the medications to look for hazardous waste and controlled substances. These additional expenses were not quantified and therefore were not included in the aforementioned value.
A subanalysis was conducted after it was observed that several prescriptions had greater quantities dispensed than the quantity prescribed (Table). An excess of $102.41 was dispensed and later collected during the study period. Of the 26 prescriptions that were overfilled, 10 were not due to human error but were intentionally overfilled as evidenced by sealed manufacturer bottles; the cost of the medications overfilled for these 10 prescriptions was $70.26.
The top returned drugs in descending order were lisinopril (42), bupropion (32), prazosin (28), gabapentin (27), and ondansetron (26). The top classifications of medications returned in descending order were antidepressants (198), antihypertensives (185), anticonvulsants (61), antilipemics (60), antibiotics (57), and antipsychotics (57). Also noteworthy is that a total of 91 prescriptions (7.8%) for over-the-counter (OTC) products were returned.
Discussion
As suggested by Wieczorkiewicz and colleagues, prescribing and dispensing patterns may be contributing to the accumulation of unwanted and unused medications.4 Patient feedback would also give insight to this problem. Furthermore, the data highlighted improvement opportunities related to back order/shortage and high-dollar medications. Additional exploration into prescribing, dispensing, and consumer patterns as well as potential cost-saving strategies addressing the aforementioned processes is warranted.
Prescribing Patterns
An editorial by Ruef addressed overprescribing patterns and hypothesized that prescribers may be more cautious and prescribe antibiotics (without laboratory confirmation), because if medications are not prescribed, patients with a potentially serious, quickly developing infection may experience an adverse outcome.6 Additionally, there is the anticipation and pressure from patients to receive a medication. Although only 60 of the 1,174 prescriptions were antibiotics or antifungals, one could easily insert other indications into this rationale.
Related: Pharmacists in the Emergency Department: Feasibility and Cost
During the collection period, the problem of polypharmacy stemming from the emergency department (ED), independent of this QI project, was brought to the authors’ attention. Consequently, data were collected from patients who presented for what was perceived (by both the patient and the pharmacy) as a high number of prescriptions from the ED. The data were reviewed and analyzed to determine whether there were any correlations between perceived excessive prescribing and the patient medication return data.
This study found that of 54 patient visits, there were a total of 324 prescriptions with a median of 6 prescriptions per person. The majority (56%) of these prescriptions were for OTC medications. The top 5 medications prescribed were ibuprofen, acetaminophen, ondansetron, oxymetazoline, and pseudoephedrine; 4 of which are OTC medications. The top 5 classifications of medications were decongestants, nonsteroidal anti-inflammatory drugs, analgesics, antibiotics, and antiemetics.
In contrast to the patient return data with 5 of the 6 top medications prescribed for chronic conditions, it is no surprise that the top 5 ED medications were prescribed for acute conditions. Ondansetron, which costs up to $0.37 per tablet, was one of the top prescribed medications from the ED and one of the most frequently returned medications. One might question whether this was a misuse of ED resources, considering patients were seen in this costly setting and received OTC medications. Further study of misappropriation of resources in the ED and trends from other clinic areas are needed.
Dispensing Patterns
In addition, it was observed that the pharmacy was overfilling prescriptions. Inaccurate quantities dispensed may have been due to human error and also due to staff belief that it would cost more (in staff time) to count the exact quantity prescribed for medications supplied in a manufacturer bottle near the amount needed for the prescription. It has been noted by pharmacy staff that deviation from exact counts is only done with medications that do not have a significant cost per tablet or capsule. The cost of medications intentionally overfilled was $70.26—not an insignificant source of waste.
Related: Pharmacist-Managed Collaborative Practice for Chronic Stable Angina
Medications returned to stock (because patients never picked up the prescription) were not used for future prescriptions but rather placed in the patient return collection for destruction. After this practice was noted, these returned-to-stock products were segregated to evaluate the value of the medications that could have been used for future prescriptions. Seventy-six prescriptions could have been dispensed, and the value of these unused medications was $3,049. Whereas civilian retail settings would not allow the practice of destroying medications that can otherwise be dispensed, this practice was permitted at EACH.
Consumer Patterns
It was hypothesized in this study that patients were returning medications because the prescriber switched the medication, the patient ultimately did not need the medication because symptoms resolved on their own, the patient may have had an AE or tolerance issues, the patient died, the dose was adjusted, or the patient had duplicate prescriptions. Further exploration regarding patients’ perspectives should be considered.
Back Orders and Shortages
Similar to many other institutions across the country, EACH has been affected by drug product shortages. There are a number of contributing factors to these shortages, including raw and bulk material unavailability, manufacturer difficulties and regulatory issues, voluntary recalls, change in product formulation or manufacturer, unexpected increases in demand, and shifts in clinical practice.7
An example of a recently recalled medication is atorvastatin. Historical data indicate that EACH paid $0.08 per tablet ($6.77 for a 90-day supply). After the generic manufacturer recalled atorvastatin, the brand-name product needed to be ordered, which cost $1.93 per tablet (or $173.70 for a 90-day supply). During the study, 370 atorvastatin tablets were returned, 90 of which were the brand-name tablets. It was unfortunate that this quantity was dispensed, considering these tablets were destroyed. If it is possible to limit quantities dispensed on manufacturer recall/ back order products until the price is more reasonable, without a significant disruption in patient care, pharmacies may consider policy changes.
High-Dollar Medications
Although the cost of a number of generic medications may be negligible, a number of medications continue to have a significant associated cost. Of the prescriptions returned, 170 cost > $100. Of these, 16 prescriptions cost > $500, and the total was > $13,000.
The U.S. Air Force had a high dollar program, in which patients were limited to a 30-day supply if the 30-day supply cost > $500 for treatment of a chronic condition. The staff burden and difficulty of maintaining such a program is unknown; however, the program is thought-provoking. Specifically, instead of dispensing 90-day supplies, the facility might consider limiting expensive prescriptions to ≤ 30 days for medications with additional refills if needed. Quantity limitations are already implemented for medications such as sildenafil, migraine medications, and opioids.
There is clearly a financial burden that needs to be addressed, and as this study evaluated the waste involved in patient returns, additional sources of waste were illuminated. Lean Six Sigma highlights several forms of waste: transportation, inventory, motion, waiting, overprocessing, overproduction, and defects/errors.8,9 This study found that there were several forms of waste in the prescribing and dispensing processes. Specifically, the authors found inventory mismanagement, overprocessing (overprescribing), overproduction (dispensing more than prescribed), possible misuse of costly resources, and defects/errors.
Limitations
The results of this QI project were limited to unused medications that patients returned to the facility. Returning unused medications is neither requested nor mandatory. Therefore, it is estimated that the true amount of unused medications that could be returned for destruction is vastly greater than the brief collection obtained in this data set. Furthermore, this collection is only a snapshot at one military treatment facility. With multiple facilities within the DoD, the total amount and value of unused medications is likely to be immensely greater than the $63,000 collected in this study.
Additionally, the cost to discard hazardous waste medications was not quantified. Evans Army Community Hospital pays $1.95 per lb for disposal of hazardous waste medications (eg, fluticasone/salmeterol, albuterol, warfarin, insulins), but this financial burden was not addressed in this QI project.
Recommendations
There are a number of behaviors that could be addressed to reduce the waste observed in this study:
- Prescribers should reevaluate prescribing habits to assess whether they are overprescribing medications. They may consider asking the patient whether they plan to take the medication prior to writing the prescription. If the patient is not agreeable to the treatment plan, then the treatment plan may need to be reevaluated.
- Facilities may consider a policy that allows no more than a 30-day supply for new medication prescriptions. Patients should have a follow-up to determine whether the treatment is effective or whether there are AEs, and a new maintenance prescription may be written at that time.
- Pharmacies should ensure that pharmacists fill the quantity prescribed. Prescriptions that have overfills in quantities are considered misbranded.
- Pharmacies should enforce policies for returning to stock the prescriptions that were prepared but never dispensed to patients.
- For medications that are on back order or in short supply, prescribers should consider changing the quantity dispensed to a 30-day supply (or less as appropriate) with refills.
- Pharmacies should consider limiting quantities of high-dollar medications and adding refills for any additional therapy needed.
- Hospitals should evaluate patient use of emergency resources. Other local health treatment facilities outline clearly for patients what constitutes an emergency and what does not. A similar policy change should be considered at EACH.
Summary
Polypharmacy is an increasing problem in today’s medical field. Consequently, unwanted and unused medications accumulate in patients’ homes. In an attempt to keep patients and the environment safe, EACH takes back unused medications every day for destruction. During the collection period of patient returns from December 16, 2012, through April 5, 2013, > $63,000 of unused medications were returned for destruction, which did not include the cost of labor or additional supplies. These data illuminated possible prescribing and dispensing patterns contributing to this waste and inspired further exploration of additional sources of waste, such as overprocessing, overproduction, inventory mismanagement, misuse of resources, and defects/ errors. This study highlighted a number of strategies that, if implemented, may significantly reduce the deficit burden and reduce costs associated with polypharmacy.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Kaur G. Polypharmacy: The past, present and the future. J Adv Pharm Technol Res. 2013;4(4):224-225.
2. Calderón-Larrañaga A, Gimeno-Feliu LA, González-Rubio F, et al. Polypharmacy patterns: Unravelling systematic associations between prescribed medications. PLoS One. 2013;8(12):e84967.
3. Murray MD, Kroenke K. Polypharmacy and medication adherence: Small steps on a long road. J Gen Intern Med. 2001;16(2):137-139.
4. Wieczorkiewicz SM, Kassamali Z, Danziger LH. Behind closed doors: Medication storage and disposal in the home. Ann Pharmacother. 2013;47(4):482-489.
5. U.S. Food and Drug Administration. How to dispose of unused medicines. U.S. Department of Health and Human Services Website. http://www.fda.gov/forconsumers/consumerupdates/ucm101653.htm. Updated February 18, 2015. Accessed March 11, 2015.
6. Ruef C. Why do physicians prescribe antibiotics? Infect. 2011;39(4):287.
7. ASHP Expert Panel on Drug Product Shortages; Fox ER, Birt A, James KB, Kokko H, Salverson S, Soflin DL. ASHP Guidelines on Managing Drug Product Shortages in Hospitals and Health Systems. Am J Health Syst Pharm. 2009;66(15):1399-1406.
8. George M, Rowlands D, Kastle B. What is Lean Six Sigma? New York, NY: McGraw-Hill; 2004.
9. Womack JP, Jones DT. Lean Thinking: Banish Waste and Create Wealth in Your Corporation. New York, NY: Free Press; 2003.
1. Kaur G. Polypharmacy: The past, present and the future. J Adv Pharm Technol Res. 2013;4(4):224-225.
2. Calderón-Larrañaga A, Gimeno-Feliu LA, González-Rubio F, et al. Polypharmacy patterns: Unravelling systematic associations between prescribed medications. PLoS One. 2013;8(12):e84967.
3. Murray MD, Kroenke K. Polypharmacy and medication adherence: Small steps on a long road. J Gen Intern Med. 2001;16(2):137-139.
4. Wieczorkiewicz SM, Kassamali Z, Danziger LH. Behind closed doors: Medication storage and disposal in the home. Ann Pharmacother. 2013;47(4):482-489.
5. U.S. Food and Drug Administration. How to dispose of unused medicines. U.S. Department of Health and Human Services Website. http://www.fda.gov/forconsumers/consumerupdates/ucm101653.htm. Updated February 18, 2015. Accessed March 11, 2015.
6. Ruef C. Why do physicians prescribe antibiotics? Infect. 2011;39(4):287.
7. ASHP Expert Panel on Drug Product Shortages; Fox ER, Birt A, James KB, Kokko H, Salverson S, Soflin DL. ASHP Guidelines on Managing Drug Product Shortages in Hospitals and Health Systems. Am J Health Syst Pharm. 2009;66(15):1399-1406.
8. George M, Rowlands D, Kastle B. What is Lean Six Sigma? New York, NY: McGraw-Hill; 2004.
9. Womack JP, Jones DT. Lean Thinking: Banish Waste and Create Wealth in Your Corporation. New York, NY: Free Press; 2003.

Weight Loss Promotes Nonbariatric Surgery Medical Clearance
The prevalence of overweight and obesity has continued to increase over the past several decades.1,2 Data specific to the veteran population indicates prevalence rates are considerably higher than that of the general population, with overweight or obese veteran women and men at 68.4% and 73%, respectively.3-6
Traditional weight-loss programs (> 1,200 calories per day) fail to produce the degree of weight loss required to reduce surgical risk to a safe level for individuals with a body mass index (BMI) > 35. In contrast, intensive weight-loss programs using very low calorie diets (< 800 calories per day) combined with lifestyle modifications have been effective in generating considerable weight loss. These intensive weight-loss programs have also improved comorbid conditions such as insulin resistance, diabetes, hypertension, hyperlipidemia, and hypertriglyceridemia.7-10 Additionally, these programs have reduced surgical risks by decreasing operative time and reducing hospital length of stay.11,12 Weight loss not only improves surgical risk, but also impacts health care resource allocation.
Related: A Call to Action: Intensive Lifestyle Intervention Against Diabesity
Very low calorie diets have proven to be safe for preoperative weight loss. One prospective study evaluated the safety of a weight-reduction program with 30 patients with morbid obesity and whose elective surgery had been postponed due to patient’s weight status.13 Study participants lost ≥ 15% of their body weight. Subsequently, only 15 patients underwent surgery. Surgery was no longer indicated for 4 participants, 9 did not have surgery for reasons that were unreported, and 2 discontinued the diet. The authors suggested a very low calorie diet program is suitable for preoperative weight reduction in morbid obesity without significant complications.
Most investigations of preoperative very low calorie diets included only those patients awaiting bariatric surgery. These studies confirmed bariatric preoperative weight loss correlates with reduced postoperative complications.11,14,15 Additionally, the National Surgery Quality Improvement Program analysis of bariatric outcomes identified superobesity (defined as > 350 pounds) as a preoperative risk factor associated with postoperative complications.16
Related: Minimally Invasive Surgical Treatments for Obstructive Sleep Apnea
Obesity-related intra- and postoperative complications during elective surgeries are concerning because of the increasing number of obese surgical patients. With a growing aging population and rising rates of obesity, the number of total knee arthroplasties (TKAs) are increasing and now surpass total hip arthoplasties.17 The risk of intra-operative surgical complications is higher in patients with an elevated BMI than in those without, including higher blood transfusion requirements as a result of operative blood loss, difficulty in identifying anatomy leading to iatrogenic damage, or malalignment of the prosthesis.18-20
The risk of postoperative complications in obese patients is reported with rates as high as 32% and is primarily caused by superficial and deep surgical site infections and postoperative venous thromboembolic complications.18,19,21,22 One retrospective study evaluated prevalence, pattern, and severity of 7,721 postoperative complications in obese and nonobese surgical patients occurring within 30 days of surgery.23 Obese patients had significantly higher rates of postoperative myocardial infarction, wound infection, nerve injury, and urinary tract infections. The evidence suggests a higher risk of intra- and postoperative complications of TKA in obese patients, but there remains continued controversy in this area. Furthermore, there is a paucity of data regarding actual postponement or cancellation rate in elective procedures related to obesity. There is a lack of literature evaluating the impact of significant preoperative weight loss by nonsurgical interventions on outcomes of subsequent elective surgery.
The primary aim of this study was to determine whether a medically supervised, very low calorie weight loss program (Optifast, Nestlé Health Science) could safely and effectively produce the weight loss necessary to achieve surgical clearance at the Phoenix VA Health Care System (PVAHCS). The secondary aim was to determine whether a decrease in medication utilization during the diet intervention would offset the cost of the nutrition intervention.
Methods
This was a prospective, theory-based pilot study exploring weight status in response to a very low calorie diet, utilizing a quasi-experimental design. The PVAHCS Institutional Review Board approved the study.
Subjects participated in a medically supervised weight-loss program, including a liquid-meal replacement and weekly education administered by a registered dietitian. Twenty male and female veterans with obesity who had been denied medically indicated nonbariatric elective surgery due to obesity/morbid obesity and who met the study’s inclusion criteria were recruited.
Inclusion criteria included veterans aged 18 to 70 years, BMI > 30, and a nutritional consult for weight loss prior to elective (nonbariatric) surgery. The exclusion criteria included active medical conditions for which weight loss would be contraindicated, active alcohol or substance abuse, and psychological issues that could prevent compliance.
Screening Measures
A complete metabolic panel and prealbumin levels were assessed at baseline and used as indicators of overall electrolyte, hydration, and nutritional status. A complete blood count and thyroid stimulating test were used to rule out anemia, infections, and thyroid disorders. Because rapid weight loss may precipitate serious ventricular arrhythmias, an electrocardiogram was performed at baseline and after each 50 pounds of weight loss.
Intervention
Subjects consumed 5 Optifast packets per day (each mixed with 6-10 ounces of water), providing 800 calories per day (34% protein, 49% carbohydrate, and 17% fat; with 100% of the Dietary Reference Intake for vitamins and minerals). Participants were enrolled in the program for a minimum of 6 weeks and a maximum of 16 weeks.
The research dietitian provided participants with weekly modules focused on lifestyle and education plans developed by Nestlé (eTable 1). Concentrating initially on behavior modification techniques and later introducing concepts dealing with food minimized distracting stimuli for participants. Subjects were required to consume an additional 2 quarts of noncaloric liquid to maintain hydration and were educated not to consume any liquids or solids containing calories. Subjects were required to maintain a diary on timing of Optifast and fluid consumption. Caffeine intake was limited (< 200 mg per day) because of its effects on fluid loss, cardiac stimulation, and irritation to the gastric mucosa. Participants served as their own controls.
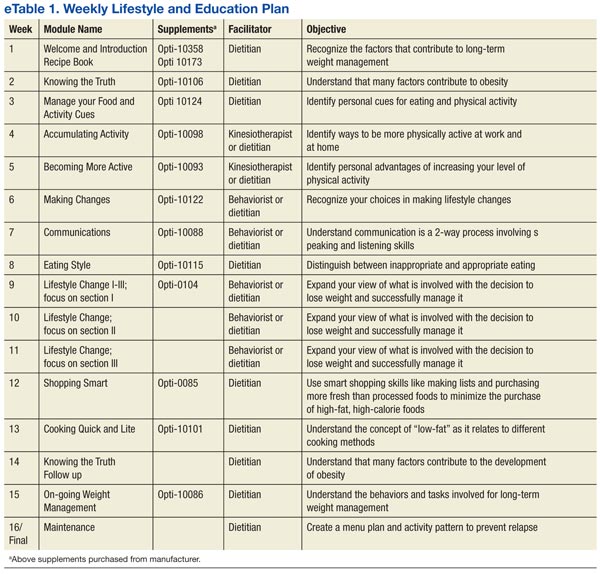
Three weeks prior to completing the liquid diet, patients were instructed on a 3-week dietary transition plan, incorporating solid foods into their meal plan. Transition guidelines used the plate method, based on recommendations from the Dietary Guidelines for Americans to assist individuals in making healthy food choices, as patients were transitioned from the liquid to solid food.24 During transition week 1, subjects consumed 4 shakes per day and 1 meal (885 kcal per day); the second transition week consisted of 3 shakes and 2 meals (1,030 kcal per day); and the final transition week included 1 shake and 3 meals (1,080 kcal per day).
Outcome Measurements
Subjects were weighed weekly. To assess dietary compliance, participants were given a log to record daily intake of the liquid diet, additional liquids consumed, and physical activity. Bioelectrical impedance analysis was used pre- and postintervention to determine body composition, including body fat percentile.
Biochemical outcome measures affected by very low calorie diets (lipids, hemoglobin A1c, fasting glucose) were measured at baseline and every 4 weeks, and clinical outcomes were measured weekly. A BodyGem hand-held indirect calorimeter measured resting energy expenditure (REE) to monitor caloric needs during weight loss and to guide the transition to solid food. Medication use related to obesity was recorded weekly, and the total medication costs were calculated pre- and postintervention.
Medication Management
Blood pressure was monitored weekly. If a patient was prescribed warfarin, the primary care provider and pharmacist were alerted, because it was anticipated that dosages would change with weight loss. Patients on insulin had a 50% reduction on week 1, and subsequent adjustments were made at the discretion of the provider based on glucose monitoring. Oral hypoglycemic agent adjustments were also made based on glucose monitoring.
All patients were prescribed ursodeoxycholic acid 300 mg twice a day to reduce the risk of gallstone formation.25 Psyllium was provided to prevent constipation, a commonly reported adverse event (AE) of Optifast. Over-the-counter lactase additives were recommended for patients with known lactose intolerance. As recommended by the Optifast program, patients were instructed to avoid nonsteroidal anti-inflammatory drugs, aspirin and laxatives, amphetamines/stimulants, pseudoephedrine, and sugar-containing medications. Medications were adjusted according to clinical practices.
Statistical Analysis
Distributions of continuous measurements at the beginning (baseline) and end (follow-up) of the study and changes in these measurements (follow-up minus baseline) were tested for normality using the Shapiro-Wilk test. Where both baseline and follow-up values of a given measurement were distributed normally, both baseline and follow-up values are shown as mean ± SD (Table 1). If ≥ 1 baseline and follow-up measurements were not normally distributed, both baseline and follow-up measurements are shown as median with interquartile range. Changes in measurements are either shown as mean ± SD or median and interquartile range as appropriate. Significance of the former changes was evaluated with a paired t test; whereas the latter changes were evaluated with a Wilcoxon signed rank test.
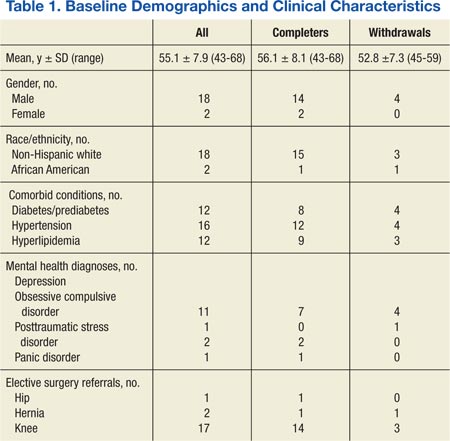
Results
A total of 65 veterans were referred to the program. Eighteen male and 2 female veterans ranging from ages 43 to 68 years, with a mean age of 55 years (SD ± 7.9) consented to participate; 16 (80%) completed the study. Four subjects dropped out; 1 due to lactose intolerance uncontrolled by lactase, 1 due to exacerbation of obsessive compulsive disorder, 1 moved out of state, and 1 opted out before beginning the dietary intervention. Comorbidities included psychiatric diagnoses (80%), hypertension (80%), diabetes (60%), and hyperlipidemia (60%). Baseline characteristics were not different between those who withdrew and those who completed the study (Table 1). Study outcomes based on intent-to-treat analysis are presented in Table 2.
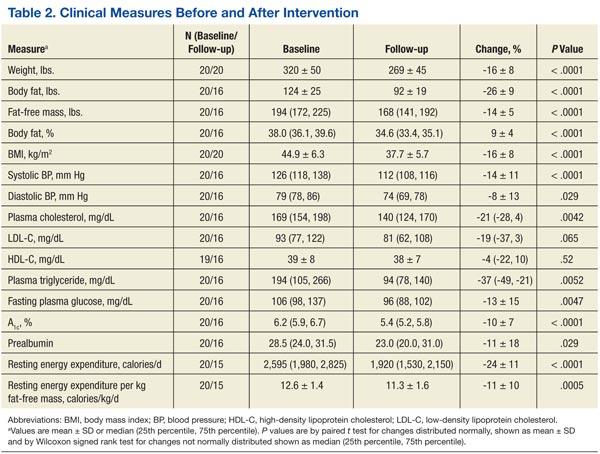
BMI decreased linearly during the intervention (Figure 1). In 10 subjects, the change in BMI postintervention was both statistically (-16 ± 8%, P < .0001) and clinically significant and sufficient for surgical clearance. Eight (40%) had surgery and 2 (10%) no longer needed surgery due to self-reported improved quality of life and decreased pain. Despite the clinically and statistically significant weight loss, 14.5% of the weight lost was fat-free mass; decrease in body fat was 9% ± 4% (P < .0001).
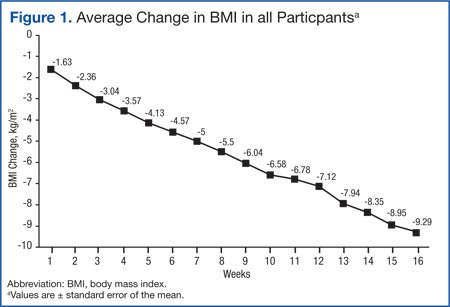
All study subjects consumed 5 Optifast packets per day for at least 10 weeks and no longer than 16 weeks. Of the participants who completed the intervention, the majority elected to continue the intervention time to 16 weeks; however 1 participant went to week 10 and 2 participants completed through week 13. Nonadherence in this protocol was defined as > 2 weeks of weight gain. Two participants gained weight for 6 and 7 weeks, respectively.
Mean systolic blood pressure, plasma triglyceride and fasting glucose levels, A1c, and REE levels decreased significantly postintervention. Additionally, patients experienced either dose reduction or discontinuation of diabetes or hypertension medication use postintervention (Figure 2). Discontinued diabetes medications included rosiglitazone (n = 1), glyburide (n = 1), and metformin (n = 2). Discontinued or reduced antihypertensives included furosemide (n = 1), thiazides (n = 3), beta blockers (n = 1), angiotensin-converting enzyme inhibitors (n = 4), calcium channel blockers (n = 2), and angiotensin II receptor antagonists (n = 2).
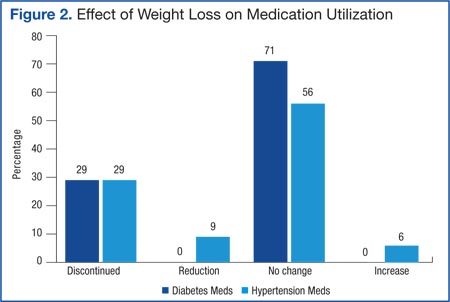
Discussion
To the authors’ knowledge, this was the first study using a low calorie liquid diet to achieve weight loss to qualify for nonbariatric elective surgery. This diet provides an alternative intervention for individuals who would otherwise be denied elective surgery due to extreme obesity. Eighty percent of participants completed 10 to 16 weeks of the 800 calorie liquid diet plan with significant weight loss of 16 BMI ± 8%. The intervention was well tolerated without significant AEs.
It is difficult to compare these results to prior studies, as the target populations differ. Previous studies utilizing calorie levels < 800 calories per day included mostly women and consequently, their preintervention weights were lower than in the current study population.10 This study population was predominately older males with a high prevalence of comorbid medical and psychiatric conditions. Despite these demographic and clinical differences, improvements in biochemistries were similar to those demonstrated previously.8-10 The observations for beneficial changes in cardiovascular and glycemic risk factors and reduced medication use related to weight loss and calorie control are consistent with previous results.8-10
Related: Moral Questions Surrounding Bariatric Surgery
To the authors’ knowledge, REE has not been reported in earlier investigations of very low calorie diet interventions. This study found significant decreases in REE, which was measured pre- and postintervention. Participants were given postintervention REE value and individualized meal plans were developed from this number. An interesting and unexpected finding was that this number seemed to provide useful reinforcement for patients as they transitioned to solid food. This may have helped improve adherence to meal plans. Despite concerns regarding possible weight gain, the weight loss continued at a similar rate during the transition, demonstrating that continued weight loss can occur with a combination of food and liquid diet.
The need for elective surgery may have increased motivation to adhere to this weight-loss program. The dropout rate was 20%; lower than previous studies using very low calorie diets and substantially better than traditional weight-loss programs.8,9
An unexpected finding was that 10% of participants who qualified for knee replacement surgery chose to postpone surgery due to decreased pain and improved quality of life. Over the past 20 years, the estimated cost of 1 TKA was $15,000 with an estimated $9 billion spent annually for this procedure in the U.S.26 Importantly, obesity increases the risk of TKA revision surgeries, which are both expensive (average cost of Medicare-covered TKA revision surgeries is $73,696) and projected to increase 66% over the next 25 years.27 Weight loss prior to surgery not only may decrease risk for revisions of TKA, but in some cases also may delay or eliminate the need for surgery.
Although there are significant costs associated with certain weight loss programs, the savings associated with reducing the need for surgery would be substantially greater than that associated with the dietary intervention. The estimated private sector cost of an 18-week weight-loss program (12-week liquid with 6-week transition) is $3,500 per participant. This study program was estimated to cost $2,400 per participant for the 16-week (13-week liquid diet and 3-week transition) program. Patients with obesity awaiting orthopedic, gastrointestinal, or neurosurgery were often referred for bariatric surgery to obtain weight loss. Bariatric surgery averages $17,000 to $26,000, which is more expensive than this diet program.28
The majority of AEs observed in this intervention were expected and similar to other studies.10 Among the 20 participants, 18 experienced a total of 60 AEs, of which 38 (63%) were considered to be study-related. Although constipation was a known AE, 25% of participants subjectively complained of decrease in frequency of bowel movements. The 2 most frequent and unanticipated AEs were increased blood urea nitrogen/ creatinine (n = 9) and reduced sodium (n = 7).
Nonadherence was often related but not limited to the following: inappropriate social cues for eating, lack of social support, sabotage by family or peers, filling an emotional void with food, and/or psychological eating related to depression and posttraumatic stress disorder. Prior to starting a similar intervention, a complete mental health assessment for individuals with known or suspected mental health diagnoses seems warranted.
Conclusion
The study limitations are its small and predominantly male sample size and lack of a randomized control. Nonetheless, this study demonstrated the feasibility of the medically supervised weight loss program to obtain the necessary weight loss in 50% of the veterans (with higher comorbidities and more advanced age). Because of the results of this investigation, the authors have initiated a randomized controlled trial utilizing this intervention. The Optifast program had a high success rate, was cost-effective, and may obviate the need for surgery.
Acknowledgements
This work was supported by pilot funding from the Department Veterans Affairs awarded on a competitive basis to Julie Kurtz. Additional support was provided by the Department of Veterans Affairs. The authors would like to acknowledge the contribution of Julie Stoneroad-Vedda, PA-C, MPAS, Northern Arizona VA Health Care System in Prescott.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence and trends in obesity among US adults, 1999-2000. JAMA. 2002;288(14):1723-1727.
2. Ogden CL, Flegal KM, Carroll MD, Johnson CL. Prevalence and trends in overweight among US children and adolescents, 1999-2000. JAMA. 2002;288(14):1728-1732.
3. Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999-2008. JAMA. 2010;303(3):235-241.
4. Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM. Prevalence of high body mass index in US children and adolescents, 2007-2008. JAMA. 2010;303(3):242-249.
5. Flegal KM, Carroll MD, Kit BK, Ogden CL. Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999-2010. JAMA. 2012;307(5):491-497.
6. Das SR, Kinsinger LS, Yancy WS Jr, et al. Obesity prevalence among veterans at Veterans Affairs medical facilities. Am J Prev Med. 2005;28(3):291-294.
7. Drawert S, Bedford K, Largent D. Change in glucose, blood pressure, and cholesterol with weight loss in medically obese patients. Obes Res. 1996;4(suppl 1):67S.
8. Kirschner MA, Schneider G, Ertel NH, Gorman J. An eight-year experience with very-low-calorie formula diet for control of major obesity. Int J Obes. 1988;12(1):69-80.
9. Wadden TA, Foster GD, Letizia KA, Stunkard AJ. A multicenter evaluation of a proprietary weight reduction program for the treatment of marked obesity. Arch Intern Med. 1992;152(5):961-966.
10. Anderson JW, Brinkman-Kaplan VL, Lee H, Wood CL. Relationship of weight loss to cardiovascular risk factors in morbidly obese individuals. J Am Coll Nutr. 1994;13(3):256-261.
11. Huerta S, Dredar S, Hayden E, et al. Preoperative weight loss decreases the operative time of gastric bypass at a Veterans Administration hospital. Obes Surg. 2008;18(5):508-512.
12. Still CD, Benotti P, Wood GC, et al. Outcomes of preoperative weight loss in high-risk patients undergoing gastric bypass surgery. Arch Surg. 2007;142(10):994-998; discussion 999.
13. Pekkarinen, T, Mustajoki P. Use of a very low- calorie diet in preoperative weight loss: Efficacy and safety. Obes Res. 1997;5(6):595-602.
14. Van Nieuwenhove Y, Dambrauskas Z, Campillo-Soto A, et al. Preoperative very low-calorie diet and operative outcome after laparoscopic gastric bypass: A randomized multicenter study. Arch Surg. 2011;146(11):1300-1305.
15. Hauser DL, Titchner RL, Wilson MA, Eid GM. Long-term outcomes of laparoscopic Roux-en-Y gastric bypass in US veterans. Obes Surg. 2010;20(3):283-289.
16. Livingston EH, Arterburn D, Schifftner TL, Henderson WG, DePalma RG. National Surgical Quality Improvement Program analysis of bariatric operations: Modifiable risk factors contribute to bariatric surgical adverse outcomes. J Am Coll Surg. 2006;203(5):625-633.
17. National Joint Registry. 11th Annual Report 2014: National Joint Registry for England and Wales and Northern Ireland. Hemel Hempsted, England: National Joint Registry; 2014.
18. Pritchett JW, Bortel DT. Knee replacement in morbidly obese women. Surg Gynecol Obstet. 1991;173(2):119-122.
19. Winiarsky R, Barth P, Lotke P. Total knee arthroplasty in morbidly obese patients. J Bone Joint Surg Am. 1998;80(12):1770-1774.
20. Krushell RJ, Fingeroth RJ. Primary total knee arthroplasty in morbidly obese patients: A 5- to 14-year follow-up study. J Arthroplasty. 2007;22 (6 suppl 2):77-80.
21. Sridhar MS, Jarrett CD, Xerogeanes JW, Labib SA. Obesity and symptomatic osteoarthritis of the knee. J Bone Joint Surg Br. 2012;94(4):433-440.
22. Amin AK, Clayton RA, Patton JT, Gaston M, Cook RE, Brenkel IJ. Total knee replacement in morbidly obese patients: Results of a prospective, matched study. J Bone Joint Surg Br. 2006;88(10):1321-1326.
23. Bamgbade OA, Rutter TW, Nafiu OO, Dorje P. Postoperative complications in obese and nonobese patients. World J Surg. 2007;31(3):556-560; discussion 561.
24. U.S. Department of Agriculture, U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2010. 7th ed. Washington, DC: U.S. Government Printing Office; 2010.
25. Kamrath RO, Plummer LJ, Sadur CN, et al. Cholelithiasis in patients treated with a very-low-calorie diet. Am J Clin Nutr. 1992;56(suppl 1):255S-257S.
26. Cram P, Lu X, Kates SL, Singh JA, Li Y, Wolf BR. Total knee arthroplasty volume, utilization, and outcomes among Medicare beneficiaries, 1991-2010. JAMA. 2012;308(12):1227-1236.
27. Lavernia C, Lee DJ, Hernandez VH. The increasing financial burden of knee revision surgery in the United States. Clin Orthop Relat Res. 2006;446: 221-226.
28. Cremieux PY, Buchwald H, Shikora SA, Ghosh A, Yang HE, Buessing M. A study on the economic impact of bariatric surgery. Am J Manag Care. 2008;14(9):589-596.
The prevalence of overweight and obesity has continued to increase over the past several decades.1,2 Data specific to the veteran population indicates prevalence rates are considerably higher than that of the general population, with overweight or obese veteran women and men at 68.4% and 73%, respectively.3-6
Traditional weight-loss programs (> 1,200 calories per day) fail to produce the degree of weight loss required to reduce surgical risk to a safe level for individuals with a body mass index (BMI) > 35. In contrast, intensive weight-loss programs using very low calorie diets (< 800 calories per day) combined with lifestyle modifications have been effective in generating considerable weight loss. These intensive weight-loss programs have also improved comorbid conditions such as insulin resistance, diabetes, hypertension, hyperlipidemia, and hypertriglyceridemia.7-10 Additionally, these programs have reduced surgical risks by decreasing operative time and reducing hospital length of stay.11,12 Weight loss not only improves surgical risk, but also impacts health care resource allocation.
Related: A Call to Action: Intensive Lifestyle Intervention Against Diabesity
Very low calorie diets have proven to be safe for preoperative weight loss. One prospective study evaluated the safety of a weight-reduction program with 30 patients with morbid obesity and whose elective surgery had been postponed due to patient’s weight status.13 Study participants lost ≥ 15% of their body weight. Subsequently, only 15 patients underwent surgery. Surgery was no longer indicated for 4 participants, 9 did not have surgery for reasons that were unreported, and 2 discontinued the diet. The authors suggested a very low calorie diet program is suitable for preoperative weight reduction in morbid obesity without significant complications.
Most investigations of preoperative very low calorie diets included only those patients awaiting bariatric surgery. These studies confirmed bariatric preoperative weight loss correlates with reduced postoperative complications.11,14,15 Additionally, the National Surgery Quality Improvement Program analysis of bariatric outcomes identified superobesity (defined as > 350 pounds) as a preoperative risk factor associated with postoperative complications.16
Related: Minimally Invasive Surgical Treatments for Obstructive Sleep Apnea
Obesity-related intra- and postoperative complications during elective surgeries are concerning because of the increasing number of obese surgical patients. With a growing aging population and rising rates of obesity, the number of total knee arthroplasties (TKAs) are increasing and now surpass total hip arthoplasties.17 The risk of intra-operative surgical complications is higher in patients with an elevated BMI than in those without, including higher blood transfusion requirements as a result of operative blood loss, difficulty in identifying anatomy leading to iatrogenic damage, or malalignment of the prosthesis.18-20
The risk of postoperative complications in obese patients is reported with rates as high as 32% and is primarily caused by superficial and deep surgical site infections and postoperative venous thromboembolic complications.18,19,21,22 One retrospective study evaluated prevalence, pattern, and severity of 7,721 postoperative complications in obese and nonobese surgical patients occurring within 30 days of surgery.23 Obese patients had significantly higher rates of postoperative myocardial infarction, wound infection, nerve injury, and urinary tract infections. The evidence suggests a higher risk of intra- and postoperative complications of TKA in obese patients, but there remains continued controversy in this area. Furthermore, there is a paucity of data regarding actual postponement or cancellation rate in elective procedures related to obesity. There is a lack of literature evaluating the impact of significant preoperative weight loss by nonsurgical interventions on outcomes of subsequent elective surgery.
The primary aim of this study was to determine whether a medically supervised, very low calorie weight loss program (Optifast, Nestlé Health Science) could safely and effectively produce the weight loss necessary to achieve surgical clearance at the Phoenix VA Health Care System (PVAHCS). The secondary aim was to determine whether a decrease in medication utilization during the diet intervention would offset the cost of the nutrition intervention.
Methods
This was a prospective, theory-based pilot study exploring weight status in response to a very low calorie diet, utilizing a quasi-experimental design. The PVAHCS Institutional Review Board approved the study.
Subjects participated in a medically supervised weight-loss program, including a liquid-meal replacement and weekly education administered by a registered dietitian. Twenty male and female veterans with obesity who had been denied medically indicated nonbariatric elective surgery due to obesity/morbid obesity and who met the study’s inclusion criteria were recruited.
Inclusion criteria included veterans aged 18 to 70 years, BMI > 30, and a nutritional consult for weight loss prior to elective (nonbariatric) surgery. The exclusion criteria included active medical conditions for which weight loss would be contraindicated, active alcohol or substance abuse, and psychological issues that could prevent compliance.
Screening Measures
A complete metabolic panel and prealbumin levels were assessed at baseline and used as indicators of overall electrolyte, hydration, and nutritional status. A complete blood count and thyroid stimulating test were used to rule out anemia, infections, and thyroid disorders. Because rapid weight loss may precipitate serious ventricular arrhythmias, an electrocardiogram was performed at baseline and after each 50 pounds of weight loss.
Intervention
Subjects consumed 5 Optifast packets per day (each mixed with 6-10 ounces of water), providing 800 calories per day (34% protein, 49% carbohydrate, and 17% fat; with 100% of the Dietary Reference Intake for vitamins and minerals). Participants were enrolled in the program for a minimum of 6 weeks and a maximum of 16 weeks.
The research dietitian provided participants with weekly modules focused on lifestyle and education plans developed by Nestlé (eTable 1). Concentrating initially on behavior modification techniques and later introducing concepts dealing with food minimized distracting stimuli for participants. Subjects were required to consume an additional 2 quarts of noncaloric liquid to maintain hydration and were educated not to consume any liquids or solids containing calories. Subjects were required to maintain a diary on timing of Optifast and fluid consumption. Caffeine intake was limited (< 200 mg per day) because of its effects on fluid loss, cardiac stimulation, and irritation to the gastric mucosa. Participants served as their own controls.
Three weeks prior to completing the liquid diet, patients were instructed on a 3-week dietary transition plan, incorporating solid foods into their meal plan. Transition guidelines used the plate method, based on recommendations from the Dietary Guidelines for Americans to assist individuals in making healthy food choices, as patients were transitioned from the liquid to solid food.24 During transition week 1, subjects consumed 4 shakes per day and 1 meal (885 kcal per day); the second transition week consisted of 3 shakes and 2 meals (1,030 kcal per day); and the final transition week included 1 shake and 3 meals (1,080 kcal per day).
Outcome Measurements
Subjects were weighed weekly. To assess dietary compliance, participants were given a log to record daily intake of the liquid diet, additional liquids consumed, and physical activity. Bioelectrical impedance analysis was used pre- and postintervention to determine body composition, including body fat percentile.
Biochemical outcome measures affected by very low calorie diets (lipids, hemoglobin A1c, fasting glucose) were measured at baseline and every 4 weeks, and clinical outcomes were measured weekly. A BodyGem hand-held indirect calorimeter measured resting energy expenditure (REE) to monitor caloric needs during weight loss and to guide the transition to solid food. Medication use related to obesity was recorded weekly, and the total medication costs were calculated pre- and postintervention.
Medication Management
Blood pressure was monitored weekly. If a patient was prescribed warfarin, the primary care provider and pharmacist were alerted, because it was anticipated that dosages would change with weight loss. Patients on insulin had a 50% reduction on week 1, and subsequent adjustments were made at the discretion of the provider based on glucose monitoring. Oral hypoglycemic agent adjustments were also made based on glucose monitoring.
All patients were prescribed ursodeoxycholic acid 300 mg twice a day to reduce the risk of gallstone formation.25 Psyllium was provided to prevent constipation, a commonly reported adverse event (AE) of Optifast. Over-the-counter lactase additives were recommended for patients with known lactose intolerance. As recommended by the Optifast program, patients were instructed to avoid nonsteroidal anti-inflammatory drugs, aspirin and laxatives, amphetamines/stimulants, pseudoephedrine, and sugar-containing medications. Medications were adjusted according to clinical practices.
Statistical Analysis
Distributions of continuous measurements at the beginning (baseline) and end (follow-up) of the study and changes in these measurements (follow-up minus baseline) were tested for normality using the Shapiro-Wilk test. Where both baseline and follow-up values of a given measurement were distributed normally, both baseline and follow-up values are shown as mean ± SD (Table 1). If ≥ 1 baseline and follow-up measurements were not normally distributed, both baseline and follow-up measurements are shown as median with interquartile range. Changes in measurements are either shown as mean ± SD or median and interquartile range as appropriate. Significance of the former changes was evaluated with a paired t test; whereas the latter changes were evaluated with a Wilcoxon signed rank test.
Results
A total of 65 veterans were referred to the program. Eighteen male and 2 female veterans ranging from ages 43 to 68 years, with a mean age of 55 years (SD ± 7.9) consented to participate; 16 (80%) completed the study. Four subjects dropped out; 1 due to lactose intolerance uncontrolled by lactase, 1 due to exacerbation of obsessive compulsive disorder, 1 moved out of state, and 1 opted out before beginning the dietary intervention. Comorbidities included psychiatric diagnoses (80%), hypertension (80%), diabetes (60%), and hyperlipidemia (60%). Baseline characteristics were not different between those who withdrew and those who completed the study (Table 1). Study outcomes based on intent-to-treat analysis are presented in Table 2.
BMI decreased linearly during the intervention (Figure 1). In 10 subjects, the change in BMI postintervention was both statistically (-16 ± 8%, P < .0001) and clinically significant and sufficient for surgical clearance. Eight (40%) had surgery and 2 (10%) no longer needed surgery due to self-reported improved quality of life and decreased pain. Despite the clinically and statistically significant weight loss, 14.5% of the weight lost was fat-free mass; decrease in body fat was 9% ± 4% (P < .0001).
All study subjects consumed 5 Optifast packets per day for at least 10 weeks and no longer than 16 weeks. Of the participants who completed the intervention, the majority elected to continue the intervention time to 16 weeks; however 1 participant went to week 10 and 2 participants completed through week 13. Nonadherence in this protocol was defined as > 2 weeks of weight gain. Two participants gained weight for 6 and 7 weeks, respectively.
Mean systolic blood pressure, plasma triglyceride and fasting glucose levels, A1c, and REE levels decreased significantly postintervention. Additionally, patients experienced either dose reduction or discontinuation of diabetes or hypertension medication use postintervention (Figure 2). Discontinued diabetes medications included rosiglitazone (n = 1), glyburide (n = 1), and metformin (n = 2). Discontinued or reduced antihypertensives included furosemide (n = 1), thiazides (n = 3), beta blockers (n = 1), angiotensin-converting enzyme inhibitors (n = 4), calcium channel blockers (n = 2), and angiotensin II receptor antagonists (n = 2).
Discussion
To the authors’ knowledge, this was the first study using a low calorie liquid diet to achieve weight loss to qualify for nonbariatric elective surgery. This diet provides an alternative intervention for individuals who would otherwise be denied elective surgery due to extreme obesity. Eighty percent of participants completed 10 to 16 weeks of the 800 calorie liquid diet plan with significant weight loss of 16 BMI ± 8%. The intervention was well tolerated without significant AEs.
It is difficult to compare these results to prior studies, as the target populations differ. Previous studies utilizing calorie levels < 800 calories per day included mostly women and consequently, their preintervention weights were lower than in the current study population.10 This study population was predominately older males with a high prevalence of comorbid medical and psychiatric conditions. Despite these demographic and clinical differences, improvements in biochemistries were similar to those demonstrated previously.8-10 The observations for beneficial changes in cardiovascular and glycemic risk factors and reduced medication use related to weight loss and calorie control are consistent with previous results.8-10
Related: Moral Questions Surrounding Bariatric Surgery
To the authors’ knowledge, REE has not been reported in earlier investigations of very low calorie diet interventions. This study found significant decreases in REE, which was measured pre- and postintervention. Participants were given postintervention REE value and individualized meal plans were developed from this number. An interesting and unexpected finding was that this number seemed to provide useful reinforcement for patients as they transitioned to solid food. This may have helped improve adherence to meal plans. Despite concerns regarding possible weight gain, the weight loss continued at a similar rate during the transition, demonstrating that continued weight loss can occur with a combination of food and liquid diet.
The need for elective surgery may have increased motivation to adhere to this weight-loss program. The dropout rate was 20%; lower than previous studies using very low calorie diets and substantially better than traditional weight-loss programs.8,9
An unexpected finding was that 10% of participants who qualified for knee replacement surgery chose to postpone surgery due to decreased pain and improved quality of life. Over the past 20 years, the estimated cost of 1 TKA was $15,000 with an estimated $9 billion spent annually for this procedure in the U.S.26 Importantly, obesity increases the risk of TKA revision surgeries, which are both expensive (average cost of Medicare-covered TKA revision surgeries is $73,696) and projected to increase 66% over the next 25 years.27 Weight loss prior to surgery not only may decrease risk for revisions of TKA, but in some cases also may delay or eliminate the need for surgery.
Although there are significant costs associated with certain weight loss programs, the savings associated with reducing the need for surgery would be substantially greater than that associated with the dietary intervention. The estimated private sector cost of an 18-week weight-loss program (12-week liquid with 6-week transition) is $3,500 per participant. This study program was estimated to cost $2,400 per participant for the 16-week (13-week liquid diet and 3-week transition) program. Patients with obesity awaiting orthopedic, gastrointestinal, or neurosurgery were often referred for bariatric surgery to obtain weight loss. Bariatric surgery averages $17,000 to $26,000, which is more expensive than this diet program.28
The majority of AEs observed in this intervention were expected and similar to other studies.10 Among the 20 participants, 18 experienced a total of 60 AEs, of which 38 (63%) were considered to be study-related. Although constipation was a known AE, 25% of participants subjectively complained of decrease in frequency of bowel movements. The 2 most frequent and unanticipated AEs were increased blood urea nitrogen/ creatinine (n = 9) and reduced sodium (n = 7).
Nonadherence was often related but not limited to the following: inappropriate social cues for eating, lack of social support, sabotage by family or peers, filling an emotional void with food, and/or psychological eating related to depression and posttraumatic stress disorder. Prior to starting a similar intervention, a complete mental health assessment for individuals with known or suspected mental health diagnoses seems warranted.
Conclusion
The study limitations are its small and predominantly male sample size and lack of a randomized control. Nonetheless, this study demonstrated the feasibility of the medically supervised weight loss program to obtain the necessary weight loss in 50% of the veterans (with higher comorbidities and more advanced age). Because of the results of this investigation, the authors have initiated a randomized controlled trial utilizing this intervention. The Optifast program had a high success rate, was cost-effective, and may obviate the need for surgery.
Acknowledgements
This work was supported by pilot funding from the Department Veterans Affairs awarded on a competitive basis to Julie Kurtz. Additional support was provided by the Department of Veterans Affairs. The authors would like to acknowledge the contribution of Julie Stoneroad-Vedda, PA-C, MPAS, Northern Arizona VA Health Care System in Prescott.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
The prevalence of overweight and obesity has continued to increase over the past several decades.1,2 Data specific to the veteran population indicates prevalence rates are considerably higher than that of the general population, with overweight or obese veteran women and men at 68.4% and 73%, respectively.3-6
Traditional weight-loss programs (> 1,200 calories per day) fail to produce the degree of weight loss required to reduce surgical risk to a safe level for individuals with a body mass index (BMI) > 35. In contrast, intensive weight-loss programs using very low calorie diets (< 800 calories per day) combined with lifestyle modifications have been effective in generating considerable weight loss. These intensive weight-loss programs have also improved comorbid conditions such as insulin resistance, diabetes, hypertension, hyperlipidemia, and hypertriglyceridemia.7-10 Additionally, these programs have reduced surgical risks by decreasing operative time and reducing hospital length of stay.11,12 Weight loss not only improves surgical risk, but also impacts health care resource allocation.
Related: A Call to Action: Intensive Lifestyle Intervention Against Diabesity
Very low calorie diets have proven to be safe for preoperative weight loss. One prospective study evaluated the safety of a weight-reduction program with 30 patients with morbid obesity and whose elective surgery had been postponed due to patient’s weight status.13 Study participants lost ≥ 15% of their body weight. Subsequently, only 15 patients underwent surgery. Surgery was no longer indicated for 4 participants, 9 did not have surgery for reasons that were unreported, and 2 discontinued the diet. The authors suggested a very low calorie diet program is suitable for preoperative weight reduction in morbid obesity without significant complications.
Most investigations of preoperative very low calorie diets included only those patients awaiting bariatric surgery. These studies confirmed bariatric preoperative weight loss correlates with reduced postoperative complications.11,14,15 Additionally, the National Surgery Quality Improvement Program analysis of bariatric outcomes identified superobesity (defined as > 350 pounds) as a preoperative risk factor associated with postoperative complications.16
Related: Minimally Invasive Surgical Treatments for Obstructive Sleep Apnea
Obesity-related intra- and postoperative complications during elective surgeries are concerning because of the increasing number of obese surgical patients. With a growing aging population and rising rates of obesity, the number of total knee arthroplasties (TKAs) are increasing and now surpass total hip arthoplasties.17 The risk of intra-operative surgical complications is higher in patients with an elevated BMI than in those without, including higher blood transfusion requirements as a result of operative blood loss, difficulty in identifying anatomy leading to iatrogenic damage, or malalignment of the prosthesis.18-20
The risk of postoperative complications in obese patients is reported with rates as high as 32% and is primarily caused by superficial and deep surgical site infections and postoperative venous thromboembolic complications.18,19,21,22 One retrospective study evaluated prevalence, pattern, and severity of 7,721 postoperative complications in obese and nonobese surgical patients occurring within 30 days of surgery.23 Obese patients had significantly higher rates of postoperative myocardial infarction, wound infection, nerve injury, and urinary tract infections. The evidence suggests a higher risk of intra- and postoperative complications of TKA in obese patients, but there remains continued controversy in this area. Furthermore, there is a paucity of data regarding actual postponement or cancellation rate in elective procedures related to obesity. There is a lack of literature evaluating the impact of significant preoperative weight loss by nonsurgical interventions on outcomes of subsequent elective surgery.
The primary aim of this study was to determine whether a medically supervised, very low calorie weight loss program (Optifast, Nestlé Health Science) could safely and effectively produce the weight loss necessary to achieve surgical clearance at the Phoenix VA Health Care System (PVAHCS). The secondary aim was to determine whether a decrease in medication utilization during the diet intervention would offset the cost of the nutrition intervention.
Methods
This was a prospective, theory-based pilot study exploring weight status in response to a very low calorie diet, utilizing a quasi-experimental design. The PVAHCS Institutional Review Board approved the study.
Subjects participated in a medically supervised weight-loss program, including a liquid-meal replacement and weekly education administered by a registered dietitian. Twenty male and female veterans with obesity who had been denied medically indicated nonbariatric elective surgery due to obesity/morbid obesity and who met the study’s inclusion criteria were recruited.
Inclusion criteria included veterans aged 18 to 70 years, BMI > 30, and a nutritional consult for weight loss prior to elective (nonbariatric) surgery. The exclusion criteria included active medical conditions for which weight loss would be contraindicated, active alcohol or substance abuse, and psychological issues that could prevent compliance.
Screening Measures
A complete metabolic panel and prealbumin levels were assessed at baseline and used as indicators of overall electrolyte, hydration, and nutritional status. A complete blood count and thyroid stimulating test were used to rule out anemia, infections, and thyroid disorders. Because rapid weight loss may precipitate serious ventricular arrhythmias, an electrocardiogram was performed at baseline and after each 50 pounds of weight loss.
Intervention
Subjects consumed 5 Optifast packets per day (each mixed with 6-10 ounces of water), providing 800 calories per day (34% protein, 49% carbohydrate, and 17% fat; with 100% of the Dietary Reference Intake for vitamins and minerals). Participants were enrolled in the program for a minimum of 6 weeks and a maximum of 16 weeks.
The research dietitian provided participants with weekly modules focused on lifestyle and education plans developed by Nestlé (eTable 1). Concentrating initially on behavior modification techniques and later introducing concepts dealing with food minimized distracting stimuli for participants. Subjects were required to consume an additional 2 quarts of noncaloric liquid to maintain hydration and were educated not to consume any liquids or solids containing calories. Subjects were required to maintain a diary on timing of Optifast and fluid consumption. Caffeine intake was limited (< 200 mg per day) because of its effects on fluid loss, cardiac stimulation, and irritation to the gastric mucosa. Participants served as their own controls.
Three weeks prior to completing the liquid diet, patients were instructed on a 3-week dietary transition plan, incorporating solid foods into their meal plan. Transition guidelines used the plate method, based on recommendations from the Dietary Guidelines for Americans to assist individuals in making healthy food choices, as patients were transitioned from the liquid to solid food.24 During transition week 1, subjects consumed 4 shakes per day and 1 meal (885 kcal per day); the second transition week consisted of 3 shakes and 2 meals (1,030 kcal per day); and the final transition week included 1 shake and 3 meals (1,080 kcal per day).
Outcome Measurements
Subjects were weighed weekly. To assess dietary compliance, participants were given a log to record daily intake of the liquid diet, additional liquids consumed, and physical activity. Bioelectrical impedance analysis was used pre- and postintervention to determine body composition, including body fat percentile.
Biochemical outcome measures affected by very low calorie diets (lipids, hemoglobin A1c, fasting glucose) were measured at baseline and every 4 weeks, and clinical outcomes were measured weekly. A BodyGem hand-held indirect calorimeter measured resting energy expenditure (REE) to monitor caloric needs during weight loss and to guide the transition to solid food. Medication use related to obesity was recorded weekly, and the total medication costs were calculated pre- and postintervention.
Medication Management
Blood pressure was monitored weekly. If a patient was prescribed warfarin, the primary care provider and pharmacist were alerted, because it was anticipated that dosages would change with weight loss. Patients on insulin had a 50% reduction on week 1, and subsequent adjustments were made at the discretion of the provider based on glucose monitoring. Oral hypoglycemic agent adjustments were also made based on glucose monitoring.
All patients were prescribed ursodeoxycholic acid 300 mg twice a day to reduce the risk of gallstone formation.25 Psyllium was provided to prevent constipation, a commonly reported adverse event (AE) of Optifast. Over-the-counter lactase additives were recommended for patients with known lactose intolerance. As recommended by the Optifast program, patients were instructed to avoid nonsteroidal anti-inflammatory drugs, aspirin and laxatives, amphetamines/stimulants, pseudoephedrine, and sugar-containing medications. Medications were adjusted according to clinical practices.
Statistical Analysis
Distributions of continuous measurements at the beginning (baseline) and end (follow-up) of the study and changes in these measurements (follow-up minus baseline) were tested for normality using the Shapiro-Wilk test. Where both baseline and follow-up values of a given measurement were distributed normally, both baseline and follow-up values are shown as mean ± SD (Table 1). If ≥ 1 baseline and follow-up measurements were not normally distributed, both baseline and follow-up measurements are shown as median with interquartile range. Changes in measurements are either shown as mean ± SD or median and interquartile range as appropriate. Significance of the former changes was evaluated with a paired t test; whereas the latter changes were evaluated with a Wilcoxon signed rank test.
Results
A total of 65 veterans were referred to the program. Eighteen male and 2 female veterans ranging from ages 43 to 68 years, with a mean age of 55 years (SD ± 7.9) consented to participate; 16 (80%) completed the study. Four subjects dropped out; 1 due to lactose intolerance uncontrolled by lactase, 1 due to exacerbation of obsessive compulsive disorder, 1 moved out of state, and 1 opted out before beginning the dietary intervention. Comorbidities included psychiatric diagnoses (80%), hypertension (80%), diabetes (60%), and hyperlipidemia (60%). Baseline characteristics were not different between those who withdrew and those who completed the study (Table 1). Study outcomes based on intent-to-treat analysis are presented in Table 2.
BMI decreased linearly during the intervention (Figure 1). In 10 subjects, the change in BMI postintervention was both statistically (-16 ± 8%, P < .0001) and clinically significant and sufficient for surgical clearance. Eight (40%) had surgery and 2 (10%) no longer needed surgery due to self-reported improved quality of life and decreased pain. Despite the clinically and statistically significant weight loss, 14.5% of the weight lost was fat-free mass; decrease in body fat was 9% ± 4% (P < .0001).
All study subjects consumed 5 Optifast packets per day for at least 10 weeks and no longer than 16 weeks. Of the participants who completed the intervention, the majority elected to continue the intervention time to 16 weeks; however 1 participant went to week 10 and 2 participants completed through week 13. Nonadherence in this protocol was defined as > 2 weeks of weight gain. Two participants gained weight for 6 and 7 weeks, respectively.
Mean systolic blood pressure, plasma triglyceride and fasting glucose levels, A1c, and REE levels decreased significantly postintervention. Additionally, patients experienced either dose reduction or discontinuation of diabetes or hypertension medication use postintervention (Figure 2). Discontinued diabetes medications included rosiglitazone (n = 1), glyburide (n = 1), and metformin (n = 2). Discontinued or reduced antihypertensives included furosemide (n = 1), thiazides (n = 3), beta blockers (n = 1), angiotensin-converting enzyme inhibitors (n = 4), calcium channel blockers (n = 2), and angiotensin II receptor antagonists (n = 2).
Discussion
To the authors’ knowledge, this was the first study using a low calorie liquid diet to achieve weight loss to qualify for nonbariatric elective surgery. This diet provides an alternative intervention for individuals who would otherwise be denied elective surgery due to extreme obesity. Eighty percent of participants completed 10 to 16 weeks of the 800 calorie liquid diet plan with significant weight loss of 16 BMI ± 8%. The intervention was well tolerated without significant AEs.
It is difficult to compare these results to prior studies, as the target populations differ. Previous studies utilizing calorie levels < 800 calories per day included mostly women and consequently, their preintervention weights were lower than in the current study population.10 This study population was predominately older males with a high prevalence of comorbid medical and psychiatric conditions. Despite these demographic and clinical differences, improvements in biochemistries were similar to those demonstrated previously.8-10 The observations for beneficial changes in cardiovascular and glycemic risk factors and reduced medication use related to weight loss and calorie control are consistent with previous results.8-10
Related: Moral Questions Surrounding Bariatric Surgery
To the authors’ knowledge, REE has not been reported in earlier investigations of very low calorie diet interventions. This study found significant decreases in REE, which was measured pre- and postintervention. Participants were given postintervention REE value and individualized meal plans were developed from this number. An interesting and unexpected finding was that this number seemed to provide useful reinforcement for patients as they transitioned to solid food. This may have helped improve adherence to meal plans. Despite concerns regarding possible weight gain, the weight loss continued at a similar rate during the transition, demonstrating that continued weight loss can occur with a combination of food and liquid diet.
The need for elective surgery may have increased motivation to adhere to this weight-loss program. The dropout rate was 20%; lower than previous studies using very low calorie diets and substantially better than traditional weight-loss programs.8,9
An unexpected finding was that 10% of participants who qualified for knee replacement surgery chose to postpone surgery due to decreased pain and improved quality of life. Over the past 20 years, the estimated cost of 1 TKA was $15,000 with an estimated $9 billion spent annually for this procedure in the U.S.26 Importantly, obesity increases the risk of TKA revision surgeries, which are both expensive (average cost of Medicare-covered TKA revision surgeries is $73,696) and projected to increase 66% over the next 25 years.27 Weight loss prior to surgery not only may decrease risk for revisions of TKA, but in some cases also may delay or eliminate the need for surgery.
Although there are significant costs associated with certain weight loss programs, the savings associated with reducing the need for surgery would be substantially greater than that associated with the dietary intervention. The estimated private sector cost of an 18-week weight-loss program (12-week liquid with 6-week transition) is $3,500 per participant. This study program was estimated to cost $2,400 per participant for the 16-week (13-week liquid diet and 3-week transition) program. Patients with obesity awaiting orthopedic, gastrointestinal, or neurosurgery were often referred for bariatric surgery to obtain weight loss. Bariatric surgery averages $17,000 to $26,000, which is more expensive than this diet program.28
The majority of AEs observed in this intervention were expected and similar to other studies.10 Among the 20 participants, 18 experienced a total of 60 AEs, of which 38 (63%) were considered to be study-related. Although constipation was a known AE, 25% of participants subjectively complained of decrease in frequency of bowel movements. The 2 most frequent and unanticipated AEs were increased blood urea nitrogen/ creatinine (n = 9) and reduced sodium (n = 7).
Nonadherence was often related but not limited to the following: inappropriate social cues for eating, lack of social support, sabotage by family or peers, filling an emotional void with food, and/or psychological eating related to depression and posttraumatic stress disorder. Prior to starting a similar intervention, a complete mental health assessment for individuals with known or suspected mental health diagnoses seems warranted.
Conclusion
The study limitations are its small and predominantly male sample size and lack of a randomized control. Nonetheless, this study demonstrated the feasibility of the medically supervised weight loss program to obtain the necessary weight loss in 50% of the veterans (with higher comorbidities and more advanced age). Because of the results of this investigation, the authors have initiated a randomized controlled trial utilizing this intervention. The Optifast program had a high success rate, was cost-effective, and may obviate the need for surgery.
Acknowledgements
This work was supported by pilot funding from the Department Veterans Affairs awarded on a competitive basis to Julie Kurtz. Additional support was provided by the Department of Veterans Affairs. The authors would like to acknowledge the contribution of Julie Stoneroad-Vedda, PA-C, MPAS, Northern Arizona VA Health Care System in Prescott.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence and trends in obesity among US adults, 1999-2000. JAMA. 2002;288(14):1723-1727.
2. Ogden CL, Flegal KM, Carroll MD, Johnson CL. Prevalence and trends in overweight among US children and adolescents, 1999-2000. JAMA. 2002;288(14):1728-1732.
3. Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999-2008. JAMA. 2010;303(3):235-241.
4. Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM. Prevalence of high body mass index in US children and adolescents, 2007-2008. JAMA. 2010;303(3):242-249.
5. Flegal KM, Carroll MD, Kit BK, Ogden CL. Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999-2010. JAMA. 2012;307(5):491-497.
6. Das SR, Kinsinger LS, Yancy WS Jr, et al. Obesity prevalence among veterans at Veterans Affairs medical facilities. Am J Prev Med. 2005;28(3):291-294.
7. Drawert S, Bedford K, Largent D. Change in glucose, blood pressure, and cholesterol with weight loss in medically obese patients. Obes Res. 1996;4(suppl 1):67S.
8. Kirschner MA, Schneider G, Ertel NH, Gorman J. An eight-year experience with very-low-calorie formula diet for control of major obesity. Int J Obes. 1988;12(1):69-80.
9. Wadden TA, Foster GD, Letizia KA, Stunkard AJ. A multicenter evaluation of a proprietary weight reduction program for the treatment of marked obesity. Arch Intern Med. 1992;152(5):961-966.
10. Anderson JW, Brinkman-Kaplan VL, Lee H, Wood CL. Relationship of weight loss to cardiovascular risk factors in morbidly obese individuals. J Am Coll Nutr. 1994;13(3):256-261.
11. Huerta S, Dredar S, Hayden E, et al. Preoperative weight loss decreases the operative time of gastric bypass at a Veterans Administration hospital. Obes Surg. 2008;18(5):508-512.
12. Still CD, Benotti P, Wood GC, et al. Outcomes of preoperative weight loss in high-risk patients undergoing gastric bypass surgery. Arch Surg. 2007;142(10):994-998; discussion 999.
13. Pekkarinen, T, Mustajoki P. Use of a very low- calorie diet in preoperative weight loss: Efficacy and safety. Obes Res. 1997;5(6):595-602.
14. Van Nieuwenhove Y, Dambrauskas Z, Campillo-Soto A, et al. Preoperative very low-calorie diet and operative outcome after laparoscopic gastric bypass: A randomized multicenter study. Arch Surg. 2011;146(11):1300-1305.
15. Hauser DL, Titchner RL, Wilson MA, Eid GM. Long-term outcomes of laparoscopic Roux-en-Y gastric bypass in US veterans. Obes Surg. 2010;20(3):283-289.
16. Livingston EH, Arterburn D, Schifftner TL, Henderson WG, DePalma RG. National Surgical Quality Improvement Program analysis of bariatric operations: Modifiable risk factors contribute to bariatric surgical adverse outcomes. J Am Coll Surg. 2006;203(5):625-633.
17. National Joint Registry. 11th Annual Report 2014: National Joint Registry for England and Wales and Northern Ireland. Hemel Hempsted, England: National Joint Registry; 2014.
18. Pritchett JW, Bortel DT. Knee replacement in morbidly obese women. Surg Gynecol Obstet. 1991;173(2):119-122.
19. Winiarsky R, Barth P, Lotke P. Total knee arthroplasty in morbidly obese patients. J Bone Joint Surg Am. 1998;80(12):1770-1774.
20. Krushell RJ, Fingeroth RJ. Primary total knee arthroplasty in morbidly obese patients: A 5- to 14-year follow-up study. J Arthroplasty. 2007;22 (6 suppl 2):77-80.
21. Sridhar MS, Jarrett CD, Xerogeanes JW, Labib SA. Obesity and symptomatic osteoarthritis of the knee. J Bone Joint Surg Br. 2012;94(4):433-440.
22. Amin AK, Clayton RA, Patton JT, Gaston M, Cook RE, Brenkel IJ. Total knee replacement in morbidly obese patients: Results of a prospective, matched study. J Bone Joint Surg Br. 2006;88(10):1321-1326.
23. Bamgbade OA, Rutter TW, Nafiu OO, Dorje P. Postoperative complications in obese and nonobese patients. World J Surg. 2007;31(3):556-560; discussion 561.
24. U.S. Department of Agriculture, U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2010. 7th ed. Washington, DC: U.S. Government Printing Office; 2010.
25. Kamrath RO, Plummer LJ, Sadur CN, et al. Cholelithiasis in patients treated with a very-low-calorie diet. Am J Clin Nutr. 1992;56(suppl 1):255S-257S.
26. Cram P, Lu X, Kates SL, Singh JA, Li Y, Wolf BR. Total knee arthroplasty volume, utilization, and outcomes among Medicare beneficiaries, 1991-2010. JAMA. 2012;308(12):1227-1236.
27. Lavernia C, Lee DJ, Hernandez VH. The increasing financial burden of knee revision surgery in the United States. Clin Orthop Relat Res. 2006;446: 221-226.
28. Cremieux PY, Buchwald H, Shikora SA, Ghosh A, Yang HE, Buessing M. A study on the economic impact of bariatric surgery. Am J Manag Care. 2008;14(9):589-596.
1. Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence and trends in obesity among US adults, 1999-2000. JAMA. 2002;288(14):1723-1727.
2. Ogden CL, Flegal KM, Carroll MD, Johnson CL. Prevalence and trends in overweight among US children and adolescents, 1999-2000. JAMA. 2002;288(14):1728-1732.
3. Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999-2008. JAMA. 2010;303(3):235-241.
4. Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM. Prevalence of high body mass index in US children and adolescents, 2007-2008. JAMA. 2010;303(3):242-249.
5. Flegal KM, Carroll MD, Kit BK, Ogden CL. Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999-2010. JAMA. 2012;307(5):491-497.
6. Das SR, Kinsinger LS, Yancy WS Jr, et al. Obesity prevalence among veterans at Veterans Affairs medical facilities. Am J Prev Med. 2005;28(3):291-294.
7. Drawert S, Bedford K, Largent D. Change in glucose, blood pressure, and cholesterol with weight loss in medically obese patients. Obes Res. 1996;4(suppl 1):67S.
8. Kirschner MA, Schneider G, Ertel NH, Gorman J. An eight-year experience with very-low-calorie formula diet for control of major obesity. Int J Obes. 1988;12(1):69-80.
9. Wadden TA, Foster GD, Letizia KA, Stunkard AJ. A multicenter evaluation of a proprietary weight reduction program for the treatment of marked obesity. Arch Intern Med. 1992;152(5):961-966.
10. Anderson JW, Brinkman-Kaplan VL, Lee H, Wood CL. Relationship of weight loss to cardiovascular risk factors in morbidly obese individuals. J Am Coll Nutr. 1994;13(3):256-261.
11. Huerta S, Dredar S, Hayden E, et al. Preoperative weight loss decreases the operative time of gastric bypass at a Veterans Administration hospital. Obes Surg. 2008;18(5):508-512.
12. Still CD, Benotti P, Wood GC, et al. Outcomes of preoperative weight loss in high-risk patients undergoing gastric bypass surgery. Arch Surg. 2007;142(10):994-998; discussion 999.
13. Pekkarinen, T, Mustajoki P. Use of a very low- calorie diet in preoperative weight loss: Efficacy and safety. Obes Res. 1997;5(6):595-602.
14. Van Nieuwenhove Y, Dambrauskas Z, Campillo-Soto A, et al. Preoperative very low-calorie diet and operative outcome after laparoscopic gastric bypass: A randomized multicenter study. Arch Surg. 2011;146(11):1300-1305.
15. Hauser DL, Titchner RL, Wilson MA, Eid GM. Long-term outcomes of laparoscopic Roux-en-Y gastric bypass in US veterans. Obes Surg. 2010;20(3):283-289.
16. Livingston EH, Arterburn D, Schifftner TL, Henderson WG, DePalma RG. National Surgical Quality Improvement Program analysis of bariatric operations: Modifiable risk factors contribute to bariatric surgical adverse outcomes. J Am Coll Surg. 2006;203(5):625-633.
17. National Joint Registry. 11th Annual Report 2014: National Joint Registry for England and Wales and Northern Ireland. Hemel Hempsted, England: National Joint Registry; 2014.
18. Pritchett JW, Bortel DT. Knee replacement in morbidly obese women. Surg Gynecol Obstet. 1991;173(2):119-122.
19. Winiarsky R, Barth P, Lotke P. Total knee arthroplasty in morbidly obese patients. J Bone Joint Surg Am. 1998;80(12):1770-1774.
20. Krushell RJ, Fingeroth RJ. Primary total knee arthroplasty in morbidly obese patients: A 5- to 14-year follow-up study. J Arthroplasty. 2007;22 (6 suppl 2):77-80.
21. Sridhar MS, Jarrett CD, Xerogeanes JW, Labib SA. Obesity and symptomatic osteoarthritis of the knee. J Bone Joint Surg Br. 2012;94(4):433-440.
22. Amin AK, Clayton RA, Patton JT, Gaston M, Cook RE, Brenkel IJ. Total knee replacement in morbidly obese patients: Results of a prospective, matched study. J Bone Joint Surg Br. 2006;88(10):1321-1326.
23. Bamgbade OA, Rutter TW, Nafiu OO, Dorje P. Postoperative complications in obese and nonobese patients. World J Surg. 2007;31(3):556-560; discussion 561.
24. U.S. Department of Agriculture, U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2010. 7th ed. Washington, DC: U.S. Government Printing Office; 2010.
25. Kamrath RO, Plummer LJ, Sadur CN, et al. Cholelithiasis in patients treated with a very-low-calorie diet. Am J Clin Nutr. 1992;56(suppl 1):255S-257S.
26. Cram P, Lu X, Kates SL, Singh JA, Li Y, Wolf BR. Total knee arthroplasty volume, utilization, and outcomes among Medicare beneficiaries, 1991-2010. JAMA. 2012;308(12):1227-1236.
27. Lavernia C, Lee DJ, Hernandez VH. The increasing financial burden of knee revision surgery in the United States. Clin Orthop Relat Res. 2006;446: 221-226.
28. Cremieux PY, Buchwald H, Shikora SA, Ghosh A, Yang HE, Buessing M. A study on the economic impact of bariatric surgery. Am J Manag Care. 2008;14(9):589-596.
Venous Thromboembolism Prophylaxis in Acutely Ill Veterans With Respiratory Disease
Venous thromboembolism (VTE), including deep venous thrombosis (DVT) and pulmonary embolism, is an important public health concern. Deep venous thrombosis is estimated to affect 10% to 20% of medical (nonsurgical) patients, 15% to 40% of stroke patients, and 10% to 80% of critical care patients who are not prophylaxed.1 Venous thromboembolism is associated with significant resource utilization, long-term sequelae, recurrent events, and sudden death.2
The current guidelines of the American College of Chest Physicians recommend use of pharmacologic thromboprophylaxis as the preferred strategy for nonsurgical (or medical) patients (IB, formerly IA, recommendation) and for critically ill patients (2C recommendation) at low risk for bleeding.1,3 Mechanical (or nonpharmacologic) thromboprophylaxis (eg, intermittent pneumatic compression) is an alternative for those at increased risk for bleeding (2C recommendation).3 Pharmacologic thromboprophylaxis in high-risk patients, similar to those studied in randomized controlled clinical trials, reduces the occurrence of symptomatic DVT by 34 events per 1,000 patients treated.3 However, data are conflicting regarding mortality benefit.4,5
Related: Trends in Venous Thromboembolism
The Joint Commission adopted any thromboprophylaxis (measure includes pharmacologic or nonpharmacologic strategies) as a core discretionary measure in the ORYX (National Quality Hospital Measures) program. The ORYX measurements are intended to support Joint Commission-accredited organizations in institutional quality improvement efforts. The thromboprophylaxis core measure became effective May 2009 and remains as an option for hospitals to meet the 4 core measure set accreditation requirement. A top-performing hospital should provide this measure to applicable patients ≥ 95% of the time, according to the Joint Commission.6 The Joint Commission does not encourage use of any risk assessment model (RAM), such as the Padua Prediction Score to preferentially select high-risk medical patients.3
A disparity exists between thromboprophylaxis recommendations and practices in the nonsurgical patient, even when electronic prompts or alerts are available (eTables 1 and 2). In the U.S., pharmacologic thromboprophylaxis is administered to 23.6% to 81.1% of medical patients and 37.9% to 79.4% of critical care patients.7-21 In most cases, these rates are liberal estimates, because they include patients who are already on therapeutic anticoagulation or may have received only 1 prophylactic dose during hospitalization.8-11,13-20 When studies exclude patients receiving therapeutic (or treatment doses) anti-coagulation, pharmacologic thromboprophylaxis rates are substantially lower, typically 31% to 33% for medical patients and 37.9% for critical care patients.7,12,21 Furthermore, when studies examine appropriateness of thromboprophylaxis (eg, within the first 2 days of hospitalization or at the correct dose, correct time, or predefined duration), calculations are often less robust.10,11,13,14,22,23
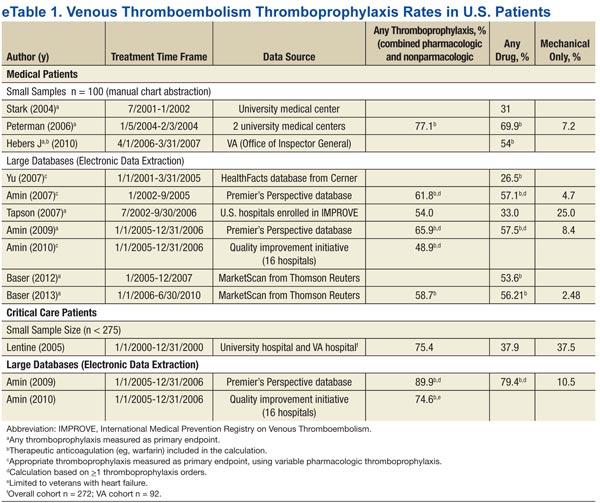
The VHA uses thromboprophylaxis of surgical patients as an external peer review (EPR) performance measure (PM). With the great attention to this national measure, Altom and colleagues reported 89.9% of surgeries adhered.24 Before 2015, VTE thromboprophylaxis EPR PM did not exist. However, the VHA has initiated efforts to assure that providers are adherent to the new indications, which include VTE prophylaxis and treatment.
There is little published literature evaluating VHA performance.Quraishi and colleagues reported a pharmacologic prophylaxis rate of 63% in nonsurgical patients at a single VAMC, facilitated by the use of an admission VTE order set. Unfortunately, their estimate allowed inclusion of 5% of patients receiving treatment doses of anticoagulation and failed to provide any estimates on regimen appropriateness (eg, correct dose, correct time, or correct duration).18 Lentine and colleagues documented a pharmacologic thromboprophylaxis rate of 48% for a subset of veteran critical care patients who were not already receiving indicated therapeutic anticoagulants.21
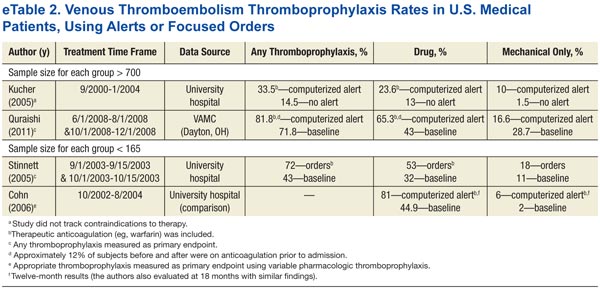
Veterans have poorer health status, more medical conditions, and higher medical resource use than do nonveterans; therefore, it is postulated that veterans can derive clinical benefit from improved attention to thromboprophylaxis benchmarking, performance improvement, and potentially, implementation of electronic alerts or reminder tools.25 Nationally, VHA has no formal inpatient reminder tools to trigger use of thromboprophylaxis for high-risk medical patients, although individual health care systems may have created alerts or tools. Some studies demonstrated that order sets and electronic tools are helpful, whereas others demonstrated potential for harm.17-20,26,27
For any hospitalization at the VA Tennessee Valley Healthcare System (TVHS), the only electronic prompt to order VTE thromboprophylaxis occurs when the admission order set is completed. But the prompt can be readily bypassed if the quick admission orders are selected. Although no further electronic prompts in the Computerized Patient Record System (CPRS) are invoked following admission, the authors hypothesized that the rate of VTE thromboprophylaxis, specifically pharmacologic, in a subset of veterans with respiratory disease will be higher than the usual published rates.
Purpose and Relevance
This study’s primary aim was to assess the rate of pharmacologic VTE prophylaxis in veterans with pulmonary disease who were admitted for a nonsurgical stay. The 2 secondary aims were to determine whether thromboprophylaxis was appropriate and to characterize whether differences exist for pharmacologic prophylaxis according to level of care (medical critical care unit [CCU] vs acute care medical ward).
Related: Prevention of Venous Thromboembolism After Total Joint Replacement: Rivaroxaban Update
This analysis emphasizes pharmacologic thromboprophylaxis instead of the combined endpoint of pharmacologic plus nonpharmacologic thromboprophylaxis traditionally used and will supplement the limited literature in 2 understudied cohorts: (1) nonsurgical veteran patients, specifically where advanced computerized thromboprophylaxis alerts are not in use; and (2) patients with the VTE risk factor of respiratory disease.1,7-9,12,13,15,16,18,21
Study Design
This observational study used retrospectively collected data. The data were extracted electronically from the VISN 9 data warehouse by a Decision Support Services analyst and manually validated by an investigator using the CPRS. Prior to initiation of research activities, the VHA Institutional Review Board and the Research and Development Committee at the facility level approved the study.
Sampling
Patients assigned to the treating specialties of medicine and medical critical care during fiscal years 2006 to 2008, admitted for ≥ 24 hours, and discharged with a diagnosis of chronic obstructive pulmonary disease (COPD), asthma, or acute, severe respiratory disease (eg, patients requiring mechanical ventilation) were eligible for inclusion. The authors also elected to include patients with asthma, because this diagnosis commonly overlaps with COPD and reflects real-world clinical practice and diagnostic challenges.28 Pneumonia and other infectious pulmonary conditions were not a qualifying diagnosis for study inclusion.
Patients were excluded if aged > 79 years, because it is difficult to maintain de-identification in a small sample of inpatients in this age category. Unfortunately, octogenarians have the highest rate of VTE per 100,000 population and would gain substantial benefit from prophylaxis.29 Similar to other VHA and non-VHA investigators, this study excluded patients who were prescribed therapeutic anticoagulation.7,12,21,30 The authors believe continuation of therapeutic (or treatment) anticoagulation does not measure a clinical decision to use pharmacologic thromboprophylaxis, and any interruption of therapeutic anticoagulation suggests that prophylactic anticoagulation is not warranted.
Related: Pulmonary Vein Thrombosis Associated With Metastatic Carcinoma
Additionally, patients were excluded if length of stay (LOS) exceeded 14 days, if known or potential contraindications to thromboprophylaxis existed, or if laboratory data that were needed to assess for contraindications were missing from the electronic data set. Known or potential contraindications included active hemorrhage, hemorrhage within the past 3 months, recent administration of packed red blood cells, bacterial endocarditis, known coagulopathy, recent or current heparin-induced thrombocytopenia, or a potential coagulopathy (International Normalized Ratio > 1.5, platelets < 50,000, or an activated partial thromboplastin time > 41 sec).
Contraindications were conservative in construct and were similar to the exclusion-based VTE checklist for the nonsurgical patient.31 The authors did not examine the electronic data set for the contraindication of epidural or spinal anesthesia, because neither is commonly used in the medical ward or medical CCU. The authors also did not exclude patients with a creatinine clearance (CrCl) < 10 mL/min (a relative contraindication to VTE thromboprophylaxis), although these patients may be at an increased risk for bleeding complications.32
Endpoints and Measures
The primary endpoint of this study was the rate of any pharmacologic thromboprophylaxis (eg, ≥ 1 doses), similar to the endpoint selected by other investigators.7-9,12,13,15,16 Secondary endpoints included VTE protected time period on thromboprophylaxis, therapeutic appropriateness ratio for heparin and enoxaparin doses combined, and pharmacologic thromboprophylaxis rates according to level and location of care.
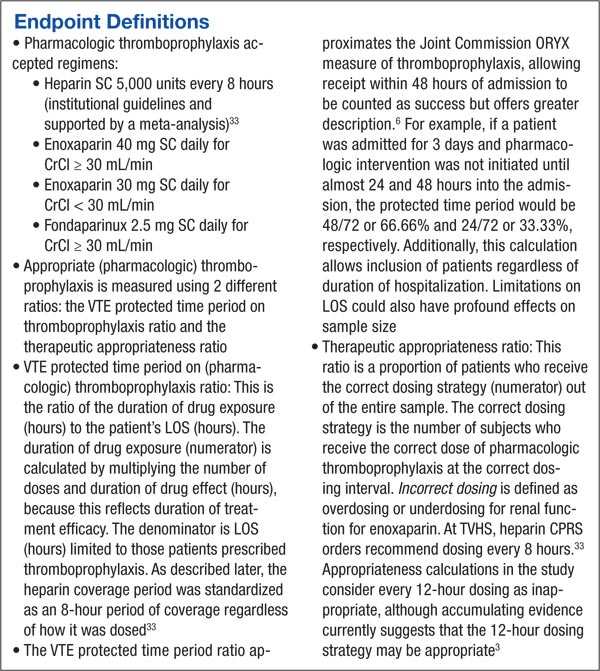
Sample Size
Although data have been forthcoming, at the time of study inception no studies documented the rate of pharmacologic thromboprophylaxis alone (defined as use of ≥ 1 dose of a pharmacologic agent) in patients with the VTE risk factor of respiratory disease.15,23 However, an average combined pharmacologic and nonpharmacologic thromboprophylaxis rate of 48.8% was determined from available studies.11,14 Although this percentage is an overestimate of pharmacologic thromboprophylaxis rates alone, this value was used to determine a sample size for the cohort.
About 122 subjects would be needed to provide 80% power and a significance level of < 0.05 to assess the hypothesis that pharmacologic prophylaxis rates at TVHS would exceed 60%. Additionally calculated was the sample size necessary to find a 20% expected difference in thromboprophylaxis rates according to location of care (eg, medical ward vs medical CCU), the secondary endpoint. This sample size was calculated to be 180 subjects, or 90 patients in each arm, to provide 80% power and a significance level (2-tailed alpha) of < 0.05. Subsequently, up to 130 patients from each location of care were randomly selected for study inclusion.
Data Analysis
A chi square test was used to compare groups on categorical variables. SPSS version 16.0 (SPSS Chicago, IL) was used for data analysis.
Results
A sample of 3,762 hospitalizations for veterans with COPD, asthma, or acute, severe respiratory disease who received inpatient care in the medical ward or medical CCU were extracted from the data warehouse.
Electronic Data Set
An investigator reviewed the electronic data set, and exclusion criteria that could be ascertained electronically were applied. The primary reasons for exclusion were age (18.4%), potential coagulopathy (14.5%), recent transfusion (14.6%), use of therapeutic anticoagulation (11%), or an extended LOS (7%). Less common reasons for exclusion were coagulation disorders (1.4%), heparin-induced thrombocytopenia (1.2%), recent hemorrhage (1.1%), or missing baseline laboratory values (3.2%). Subsequently, the potential sample of subjects declined to 1,018 (27%) hospitalizations. Of the remaining hospitalizations, 46 and 972 were medical CCU and nonsurgical (medical) inpatients, respectively.
In line with the sampling plan, 130 (13.4%) medical ward hospitalizations were selected using a random number generator. As the ICU sample was smaller than anticipated, the convenience sample of all 46 hospitalizations was used.
Manual Chart Abstraction
Manual chart abstraction (n = 176) clarified physician/provider decision making (eg, some patients were not appropriate for thromboprophylaxis due to upcoming invasive procedures), medical history that could not be extracted by ICD-9 coding (eg, recent non-VHA admissions for medical conditions that were contraindications to prophylaxis), and anticoagulation dosing. These exclusions led to an additional 52 (29.5%) excluded hospitalizations. Reasons for manual exclusion included recent bleeding or at high risk for bleeding (18, 34.6%), incorrect classification as nonsurgical or elective admission (5, 9.6%), no diagnosis of lung disease (21, 40.4%), invasive procedures planned (4, 7.7%), treatment anticoagulant doses selected (4, 7.7%), or patient transferred to a non-VA medical facility due to acuity level (1, 1.9%). One patient was excluded for multiple reasons.
Baseline Demographics
The sample was an elderly, male (98%), white (79.8%) cohort (Table 1). No patients were aged < 40 years. Racial information was missing for 5.6% of the patients. The chief pulmonary diagnosis was COPD, and few patients had new onset, acute, severe respiratory disease (3.2%) prompting admission, because pneumonia was not included as a qualifying diagnosis. Median body mass index (BMI) was 26.31. The median LOS was 3.8 days for the overall cohort and 4.1 days for those receiving pharmacologic thromboprophylaxis, although for the latter group a larger proportion of patients were hospitalized for < 3 days. Renal function, according to endpoint definitions, was for using enoxaparin as the appropriate strategy for thromboprophylaxis for the majority (97.5%) of hospitalizations.
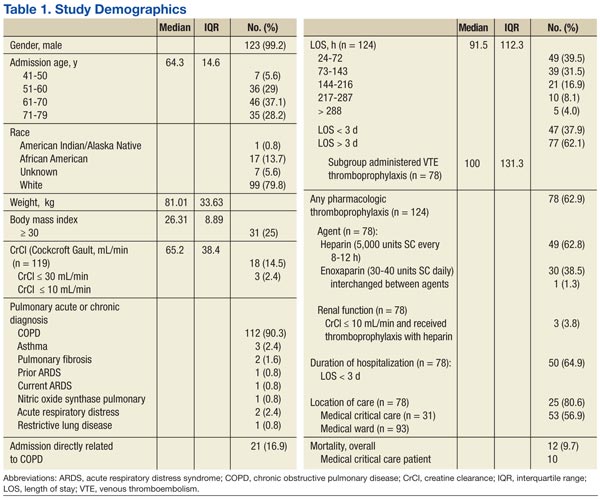
Primary and Secondary Endpoints
Of those receiving pharmacologic thromboprophylaxis, heparin was prescribed most often (62.8%). One patient received both heparin and enoxaparin during a single hospitalization.
Pharmacologic thromboprophylaxis was more common in the medical CCU subgroup (80.6%) compared with the nonsurgical patient (56.9%). Pharmacologic thromboprophylaxis was used in 62.9% of patients (n = 124). However, the therapeutic appropriateness ratio was reduced to 58% of the entire sample (n = 124), because 6 patients of the cohort receiving thromboprophylaxis (n = 78) were prescribed suboptimal doses: Specifically, 1 patient was underdosed and 1 overdosed when prescribed enoxaparin (2, 2.6%). Four patients (5.1%) received underdoses of heparin, based on institutional guidance. For those prescribed pharmacologic thromboprophylaxis, the VTE protected time period ratio was 82.8% (Table 2). Overall inpatient mortality rate was low (12, 9.7%). Most deceased patients were managed in the medical CCU (10, 83.3%) and did receive pharmacologic thromboprophylaxis (10, 83.3%).
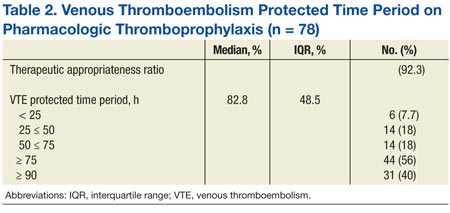
Discussion
This study demonstrated moderate rates of VTE pharmacologic thromboprophylaxis, because 62.9% of nonsurgical patients with respiratory disease who were hospitalized for various reasons were prophylaxed with either SC heparin or enoxaparin. This rate represents active clinical decision making, because there was no indication to prescribe anticoagulation at therapeutic doses. As expected, pharmacologic thromboprophylaxis was more common in the critical care subgroup (80.6%) compared with the nonsurgical patients (56.9%). Although the study did not meet the intended sample size for this subgroup analysis, results were statistically significant for location of care (P = .014) and may be beneficial for future study design by other investigators.
As early studies of nonsurgical and critical care patients document ≤ 40% of patients receive pharmacologic thromboprophylaxis, this study’s performance seems better.7,12,21 Recently, VHA investigators Quraishi and colleagues seemed to document similar findings. Although 63% of medical patients at the Dayton VAMC in Ohio received appropriate pharmacologic thromboprophylaxis, this value must be tempered by the proportion of subjects receiving therapeutic anticoagulation (5.4%).18
Similar to this study’s results, recent studies of nonveterans document pharmacologic thromboprophylaxis rates of 41% to 51.8%, 41% to 65.9%, and 74.6% to 89.9% in patients with respiratory disease, nonsurgical patients, and critical care patients, respectively. Although findings seem similar to this study’s results, adjustments in estimates again must be made, because these estimates included patients on therapeutic anticoagulation.12,14-16 This study’s results found that 58% of the patient cohort met the therapeutic appropriateness ratio, because they were administered pharmacologic thromboprophylaxis and received correct doses at indicated dosing intervals.
Because stringent exclusion criteria that minimized use of pharmacologic thromboprophylaxis in patients at risk for bleeding were applied, a higher rate of use was expected. This difference between expected and actual rates likely occurred because patient care is individualized and not all factors can be readily assessed in an observational study using retrospective data.
Additionally, for patients who remain ambulatory or have an invasive procedure, thromboprophylaxis may be appropriately delayed past the first 24-hour window of therapy or even temporarily interrupted. Subsequently, the measure of thromboprophylaxis initiation within the first 24 to 48 hours of admission was not elected. Instead, an alternative endpoint of VTE protected time period on thromboprophylaxis was selected. When thromboprophylaxis was used, the median period of protection was 83% of the time period hospitalized for this subgroup. Standardizing to a 7-day period, a VTE protected time period of 83% is coverage for 5.81 days. This would support the Joint Commission ORYX measure that allows for the receipt of thromboprophylaxis within 48 hours of admission to be counted as a success.6
Unfortunately, the authors did not assess whether mechanical thromboprophylaxis was provided to the remaining one-third of patients not receiving pharmacologic thromboprophylaxis. As a result, the complete data set is lacking, which would document whether the Joint Commission measure of ≥ 95% of the time was achieved. Therefore, the claim that TVHS is a top performing hospital for this ORYX measure cannot be made.
Although this study demonstrated a low mortality rate, this rate was not selected as a measure of interest, since one meta-analysis has demonstrated no mortality benefit from VTE thromboprophylaxis.4 Although in-hospital mortality may be an appropriate measure for critical care patients, most of the study patients did not meet this criterion.21 Last, mortality should be assessed no earlier than 30 days from admission.17 Subsequently, statistical assessment and conclusions from this measure are not relevant.
Limitations
A number of limitations hindered the generalizability of the results. This was an observational study using retrospectively collected data. The sample was narrowed to those with chronic respiratory disease, which has been less studied and typically examined in concert with acute processes, such as pneumonia. The demographic was primarily white males. The BMI of subjects enrolled in this study (26 kg/m2) was lower than the BMI of nonveteran subjects with COPD (28.6 kg/m2), nonveteran subjects with COPD and VTE (29 kg/m2), or veteran nonsurgical patients receiving thromboprophylaxis (29 kg/m2).18,34,35
The exclusion criteria resulted in a 73% reduction in the cohort and severely limited the number of medical critical care patients included. However, the problem of a small cohort was anticipated.
Other researchers conducting a prospective VHA thromboprophylaxis study found only 7.6% of veterans screened were eligible for enrollment, although 25% of subjects were anticipated by chart review. Two of the 3 primary reasons for trial exclusion were indication for therapeutic anticoagulation and contraindications to heparin (other than thrombocytopenia), and these were also primary reasons for exclusion in this study.30 Subsequently, the cohort appropriate for thromboprophylaxis in VHA seems relatively small.
Additionally, mobility is difficult to judge in a chart review. Day-to-day clinical assessments of mobility lead to individualization of care, including delayed initiation and timely termination of thromboprophylaxis. It is also possible that a significant portion of the patients had mechanical thromboprophylaxis, because they may have had an unrecognized risk factor for bleeding or patient preferences were considered. Last, some veterans may have classified as palliative care, and VTE prophylaxis may have been omitted for comfort care purposes.32
This study was not designed to evaluate the Padua Prediction Score, which categorizes risk and ration-alizes use of thromboprophylaxis for nonsurgical patients.3 This tool eliminates many of the established risk factors for VTE, including COPD, which was a qualifying diagnosis for inclusion in this study.1 It is not clear how the Padua Prediction Score would categorize the inpatient veteran population. Veterans clearly have poorer health status, more medical conditions, and higher medical resource use compared with the general patient population.25
Veterans with COPD have a higher comorbid illness burden than that of veterans without COPD.36 Chronic obstructive pulmonary disease is associated with VTE development, and when VTE develops in patients with COPD, mortality is greater than that of patients without COPD.37,38 VTE mortality may be related to an increased likelihood of fatal pulmonary embolism.39 Therefore, the authors recommend that VHA conduct studies to examine the Padua Prediction Score and potentially other RAMs that include COPD subjects, to determine what tool should be used in VHA.32
The authors also recommend that VHA evaluate how to improve thromboprophylaxis care with time-based studies. Since manual extraction to determine study inclusion was a time-consuming process, this time frame likely was a barrier to physician implementation of pharmacologic thromboprophylaxis. Therefore an electronic tool that serves as a daily reminder for subjects calculated as high risk for VTE but low risk for bleeding may improve clinical outcomes.
Conclusions
Overall, about one-third of patients did not receive potentially indicated pharmacologic thromboprophylaxis on the medical wards. Use of pharmacologic thromboprophylaxis in medical CCU patients was robust (80%). Doses and dosing intervals were appropriate for > 90% of patients, and therapy clearly was started early and continued for much of the at-risk period, as the VTE protected time period exceeded 80%. Although computerized tools were limited, the authors feel their modest pharmacologic thromboprophylaxis rate is related to the facility’s teaching hospital affiliation or the provider mix, because TVHS is one of the largest VA cardiology centers in the U.S.7,8,13
As it was challenging and time consuming to locate eligible subjects, it may also prove difficult for the admitting physician to have the same luxury of time to look for specific at-risk diagnoses in the medical record and evaluate for exclusions to therapy. If electronic alerts and reminder tools were included in clinical pharmacy inpatient templates, the authors believe the frequency of pharmacologic thromboprophylaxis would further improve in the facility. Also, the authors encourage VHA researchers to further evaluate VTE prophylaxis RAM, the role of daily electronic reminders, and tools to calculate VTE and bleeding risk.
Acknowledgements
The authors are grateful to James Minnis, PharmD, BCPS, and April Ungar, PharmD, BCPS, for their contributions to the study design. This material is the result of work supported with resources and the use of facilities at the VA Tennessee Valley Healthcare System.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Geerts WH, Bergquist D, Pineo G, et al; American College of Chest Physicians. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(suppl 6):381S-453S.
2. Go AS, Mozaffarian D, Roger VL, et al; on behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics–2013 update: A report from the American Heart Association. Circulation. 2013;127(1):e6-e245.
3. Kahn SR, Lim W, Dunn AS, et al; American College of Chest Physicians. Prevention of VTE in nonsurgical patients: Antithrombotic Therapy and Prevention of Thrombosis 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2)(suppl):e195S-e226S.
4. Wein L, Wein S, Haas SJ, Shaw J, Krum H. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients: A meta-analysis of randomized controlled trials. Arch Intern Med. 2007;167(14):1476-1486.
5. Ruiz EM, Utrilla GB, Alvarez JL, Perrin RS. Effectiveness and safety of thromboprophylaxis with enoxaparin in medical inpatients. Thromb Res. 2011;128(5):440-445.
6. The Joint Commission. Specifications Manual for National Hospital Inpatient Quality Measures. http://www.jointcommission.org/specifications_manual_for_national_hospital_inpatient_quality _measures.aspx. The Joint Commission Website. Accessed March 5, 2015.
7. Stark JE, Kilzer WJ. Venous thromboembolic prophylaxis in hospitalized medical patients. Ann Pharmacother. 2004;38(1):36-40.
8. Peterman CM, Kolansky DM, Spinler SA. Prophylaxis against venous thromboembolism in acutely ill medical patients: An observational study. Pharmacotherapy. 2006;26(8):1086-1090.
9. Herbers J, Zarter S. Prevention of venous thromboembolism in Department of Veterans Affairs hospitals. J Hosp Med. 2010;5(1):E21-E25.
10. Yu HT, Dylan ML, Lin J, Dubois RW. Hospitals’ compliance with prophylaxis guidelines for venous thromboembolism. Am J Health-Syst Pharm. 2007;64(1):69-76.
11. Amin A, Stemkowski S, Lin J, Yang G. Thromboprophylaxis rates in US medical centers: Success or failure? J Thromb Haemost. 2007;5(8):1610-1616.
12. Tapson VF, Decousus H, Pini M, et al; IMPROVE Investigators. Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: Findings from the International Medical Prevention Registry on Venous Thromboembolism. Chest. 2007;132(3):936-945.
13. Amin AN, Stemkowski S, Lin J, Yang G. Inpatient thromboprophylaxis use in U.S. hospitals: Adherence to the Seventh American College of Chest Physician’s recommendations for at-risk medical and surgical patients. J Hosp Med. 2009;4(8):E15-E21.
14. Amin A, Spyropoulos AC, Dobesh P, et al. Are hospitals delivering appropriate VTE prevention? The venous thromboembolism study to assess the rate of thromboprophylaxis (VTE Start). J Thromb Thrombolysis. 2010;29(3):326-339.
15. Baser O, Liu X, Phatak H, Wang L, et al. Venous thromboembolism prophylaxis and clinical consequences in medically ill patients. Am J Ther. 2013:20(2):132-142.
16. Baser O, Sengupta N, Dysinger A, Wang L. Thromboembolism prophylaxis in medical inpatients: Effect on outcomes and costs. Am J Manag Care. 2012;18(6):294-302.
17. Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005;352(10):969-977.
18. Quraishi MB, Mathew R, Lowes A, et al. Venous thromboembolism prophylaxis and the impact of standardized guidelines: Is a computer-based approach enough? J Clin Outcomes Manage. 2011;18(11):505-512.
19. Stinnett JM, Pendleton R, Skordos L, Wheeler M, Rodgers GM. Venous thromboembolism prophylaxis in medically ill patients and the development of strategies to improve prophylaxis rates. Am J Hematol. 2005;78(3):167-172.
20. Cohn SL, Adekile A, Mahabir V. Improved use of thromboprophylaxis for deep vein thrombosis following an educational intervention. J Hosp Med. 2006;1(6):331-338.
21. Lentine KL, Flavin KE, Gould MK. Variability in the use of thromboprophylaxis and outcomes in critically ill medical patients. Am J Med. 2005;118(12):1373-1380.
22. Pendergraft T, Liu X, Edelsberg J, Phatak H, et al. Prophylaxis against venous thromboembolism in hospitalized medically ill patients. Circ Cardiovasc Qual Outcomes. 2013;6(1):75-82.
23. Rothberg MB, Lahti M, Pekow PS, Lindenauer PK. Venous thromboembolism prophylaxis among medical patients at US hospitals. J Gen Intern Med. 2010;25(6):489-494.
24. Altom LK, Deierhoi RJ, Grams J, et al. Association between Surgical Care Improvement Program venous thromboembolism measures and postoperative events. Am J Surg. 2012;204(5):591-597.
25. Agha Z, Lofgren RP, VanRuiswyk JV, Layde PM. Are patients at Veterans Affairs medical centers sicker? A comparative analysis of health status and medical resource use. Arch Intern Med. 2000;160(21): 3252-3257.
26. Pham DQ, Pham AQ, Ullah E, McFarlane SI, Payne R. Short communication: Evaluating the appropriateness of thromboprophylaxis in an acute care setting using a computerised reminder, through order-entry system. Int J Clin Pract. 2008;62(1):134-137.
27. Khanna R, Vittinghoff E, Maselli J, Auerbach A. Unintended consequences of a standard admission order set on venous thromboembolism prophylaxis and patient outcomes. J Gen Intern Med. 2011;27(3):318-324.
28. Barr RG, Celli VR, Mannino DM, et al. Comorbidities, patient knowledge, and disease management in a national sample of patients with COPD. Am J Med. 2009;122(4):348-355.
29. Centers for Disease Control and Prevention. Venous thromboembolism in adult hospitalizations – United States, 2007-2009. (MMWR) Morbidity & Mortality Weekly Report. 2012;61(22):401-404.
30. Lederle FA, Sacks JN, Fiore L, et al. The prophylaxis of medical patients for thromboembolism pilot study. Am J Med. 2006;119(1):54-59.
31. Dobromirski M, Cohen AT. How I manage venous thromboembolism risk in hospitalized medical patients. Blood. 2012;120(8):1562-1569.
32. Polich AL, Etherton GM, Knezevich JT, Rousek JB, Masek CM, Hallbeck MS. Can eliminating risk stratification improve medical residents’ adherence to venous thromboembolism prophylaxis? Acad Med. 2011;86(12):1518-1524.
33. King CS, Holley AB, Jackson JL, Shorr AF, Moores LK. Twice vs three times daily heparin dosing for thromboembolism prophylaxis in the general medical population: A metaanalysis. Chest. 2007;131(2):507-516.
34. Piazza G, Goldhaber SZ, Kroll A, Goldberg RJ, Emery C, Spencer FA. Venous thromboembolism in patients with chronic obstructive pulmonary disease. Am J Med. 2012;125(10):1010-1018.
35. Niewoehner DE, Lokhnygina Y, Rice K, et al. Risk indexes for exacerbations and hospitalizations due to COPD. Chest. 2007;131(1):20-28.
36. Sharafkhaneh A. Peterson NJ, Yu HJ, Dalal AA, Johnson ML, Hanania NA. Burden of COPD in a government health care system: A retrospective observational study using data from the US Veterans Affairs population. Int J Chron Obstruct Pulmon Dis. 2010;5:125-132.
37. Shetty R, Seddighzadeh A, Piazza G, Goldhaber SZ. Chronic obstructive pulmonary disease and deep venous thrombosis: a prevalent combination. J Thromb Thrombolysis. 2008;26(1):35-40.
38. Carson JL, Terrin ML, Duff A, Kelley MA. Pulmonary embolism and mortality in patients with COPD. Chest. 1996;110(5):1212-1219.
39. Huerta C, Johansson S, Wallander MA, García Rodríguez LA. Risk factors and short-term mortality of venous thromboembolism diagnosed in the primary care setting in the United Kingdom. Arch Intern Med. 2007;167(9):935-943.
Venous thromboembolism (VTE), including deep venous thrombosis (DVT) and pulmonary embolism, is an important public health concern. Deep venous thrombosis is estimated to affect 10% to 20% of medical (nonsurgical) patients, 15% to 40% of stroke patients, and 10% to 80% of critical care patients who are not prophylaxed.1 Venous thromboembolism is associated with significant resource utilization, long-term sequelae, recurrent events, and sudden death.2
The current guidelines of the American College of Chest Physicians recommend use of pharmacologic thromboprophylaxis as the preferred strategy for nonsurgical (or medical) patients (IB, formerly IA, recommendation) and for critically ill patients (2C recommendation) at low risk for bleeding.1,3 Mechanical (or nonpharmacologic) thromboprophylaxis (eg, intermittent pneumatic compression) is an alternative for those at increased risk for bleeding (2C recommendation).3 Pharmacologic thromboprophylaxis in high-risk patients, similar to those studied in randomized controlled clinical trials, reduces the occurrence of symptomatic DVT by 34 events per 1,000 patients treated.3 However, data are conflicting regarding mortality benefit.4,5
Related: Trends in Venous Thromboembolism
The Joint Commission adopted any thromboprophylaxis (measure includes pharmacologic or nonpharmacologic strategies) as a core discretionary measure in the ORYX (National Quality Hospital Measures) program. The ORYX measurements are intended to support Joint Commission-accredited organizations in institutional quality improvement efforts. The thromboprophylaxis core measure became effective May 2009 and remains as an option for hospitals to meet the 4 core measure set accreditation requirement. A top-performing hospital should provide this measure to applicable patients ≥ 95% of the time, according to the Joint Commission.6 The Joint Commission does not encourage use of any risk assessment model (RAM), such as the Padua Prediction Score to preferentially select high-risk medical patients.3
A disparity exists between thromboprophylaxis recommendations and practices in the nonsurgical patient, even when electronic prompts or alerts are available (eTables 1 and 2). In the U.S., pharmacologic thromboprophylaxis is administered to 23.6% to 81.1% of medical patients and 37.9% to 79.4% of critical care patients.7-21 In most cases, these rates are liberal estimates, because they include patients who are already on therapeutic anticoagulation or may have received only 1 prophylactic dose during hospitalization.8-11,13-20 When studies exclude patients receiving therapeutic (or treatment doses) anti-coagulation, pharmacologic thromboprophylaxis rates are substantially lower, typically 31% to 33% for medical patients and 37.9% for critical care patients.7,12,21 Furthermore, when studies examine appropriateness of thromboprophylaxis (eg, within the first 2 days of hospitalization or at the correct dose, correct time, or predefined duration), calculations are often less robust.10,11,13,14,22,23
The VHA uses thromboprophylaxis of surgical patients as an external peer review (EPR) performance measure (PM). With the great attention to this national measure, Altom and colleagues reported 89.9% of surgeries adhered.24 Before 2015, VTE thromboprophylaxis EPR PM did not exist. However, the VHA has initiated efforts to assure that providers are adherent to the new indications, which include VTE prophylaxis and treatment.
There is little published literature evaluating VHA performance.Quraishi and colleagues reported a pharmacologic prophylaxis rate of 63% in nonsurgical patients at a single VAMC, facilitated by the use of an admission VTE order set. Unfortunately, their estimate allowed inclusion of 5% of patients receiving treatment doses of anticoagulation and failed to provide any estimates on regimen appropriateness (eg, correct dose, correct time, or correct duration).18 Lentine and colleagues documented a pharmacologic thromboprophylaxis rate of 48% for a subset of veteran critical care patients who were not already receiving indicated therapeutic anticoagulants.21
Veterans have poorer health status, more medical conditions, and higher medical resource use than do nonveterans; therefore, it is postulated that veterans can derive clinical benefit from improved attention to thromboprophylaxis benchmarking, performance improvement, and potentially, implementation of electronic alerts or reminder tools.25 Nationally, VHA has no formal inpatient reminder tools to trigger use of thromboprophylaxis for high-risk medical patients, although individual health care systems may have created alerts or tools. Some studies demonstrated that order sets and electronic tools are helpful, whereas others demonstrated potential for harm.17-20,26,27
For any hospitalization at the VA Tennessee Valley Healthcare System (TVHS), the only electronic prompt to order VTE thromboprophylaxis occurs when the admission order set is completed. But the prompt can be readily bypassed if the quick admission orders are selected. Although no further electronic prompts in the Computerized Patient Record System (CPRS) are invoked following admission, the authors hypothesized that the rate of VTE thromboprophylaxis, specifically pharmacologic, in a subset of veterans with respiratory disease will be higher than the usual published rates.
Purpose and Relevance
This study’s primary aim was to assess the rate of pharmacologic VTE prophylaxis in veterans with pulmonary disease who were admitted for a nonsurgical stay. The 2 secondary aims were to determine whether thromboprophylaxis was appropriate and to characterize whether differences exist for pharmacologic prophylaxis according to level of care (medical critical care unit [CCU] vs acute care medical ward).
Related: Prevention of Venous Thromboembolism After Total Joint Replacement: Rivaroxaban Update
This analysis emphasizes pharmacologic thromboprophylaxis instead of the combined endpoint of pharmacologic plus nonpharmacologic thromboprophylaxis traditionally used and will supplement the limited literature in 2 understudied cohorts: (1) nonsurgical veteran patients, specifically where advanced computerized thromboprophylaxis alerts are not in use; and (2) patients with the VTE risk factor of respiratory disease.1,7-9,12,13,15,16,18,21
Study Design
This observational study used retrospectively collected data. The data were extracted electronically from the VISN 9 data warehouse by a Decision Support Services analyst and manually validated by an investigator using the CPRS. Prior to initiation of research activities, the VHA Institutional Review Board and the Research and Development Committee at the facility level approved the study.
Sampling
Patients assigned to the treating specialties of medicine and medical critical care during fiscal years 2006 to 2008, admitted for ≥ 24 hours, and discharged with a diagnosis of chronic obstructive pulmonary disease (COPD), asthma, or acute, severe respiratory disease (eg, patients requiring mechanical ventilation) were eligible for inclusion. The authors also elected to include patients with asthma, because this diagnosis commonly overlaps with COPD and reflects real-world clinical practice and diagnostic challenges.28 Pneumonia and other infectious pulmonary conditions were not a qualifying diagnosis for study inclusion.
Patients were excluded if aged > 79 years, because it is difficult to maintain de-identification in a small sample of inpatients in this age category. Unfortunately, octogenarians have the highest rate of VTE per 100,000 population and would gain substantial benefit from prophylaxis.29 Similar to other VHA and non-VHA investigators, this study excluded patients who were prescribed therapeutic anticoagulation.7,12,21,30 The authors believe continuation of therapeutic (or treatment) anticoagulation does not measure a clinical decision to use pharmacologic thromboprophylaxis, and any interruption of therapeutic anticoagulation suggests that prophylactic anticoagulation is not warranted.
Related: Pulmonary Vein Thrombosis Associated With Metastatic Carcinoma
Additionally, patients were excluded if length of stay (LOS) exceeded 14 days, if known or potential contraindications to thromboprophylaxis existed, or if laboratory data that were needed to assess for contraindications were missing from the electronic data set. Known or potential contraindications included active hemorrhage, hemorrhage within the past 3 months, recent administration of packed red blood cells, bacterial endocarditis, known coagulopathy, recent or current heparin-induced thrombocytopenia, or a potential coagulopathy (International Normalized Ratio > 1.5, platelets < 50,000, or an activated partial thromboplastin time > 41 sec).
Contraindications were conservative in construct and were similar to the exclusion-based VTE checklist for the nonsurgical patient.31 The authors did not examine the electronic data set for the contraindication of epidural or spinal anesthesia, because neither is commonly used in the medical ward or medical CCU. The authors also did not exclude patients with a creatinine clearance (CrCl) < 10 mL/min (a relative contraindication to VTE thromboprophylaxis), although these patients may be at an increased risk for bleeding complications.32
Endpoints and Measures
The primary endpoint of this study was the rate of any pharmacologic thromboprophylaxis (eg, ≥ 1 doses), similar to the endpoint selected by other investigators.7-9,12,13,15,16 Secondary endpoints included VTE protected time period on thromboprophylaxis, therapeutic appropriateness ratio for heparin and enoxaparin doses combined, and pharmacologic thromboprophylaxis rates according to level and location of care.
Sample Size
Although data have been forthcoming, at the time of study inception no studies documented the rate of pharmacologic thromboprophylaxis alone (defined as use of ≥ 1 dose of a pharmacologic agent) in patients with the VTE risk factor of respiratory disease.15,23 However, an average combined pharmacologic and nonpharmacologic thromboprophylaxis rate of 48.8% was determined from available studies.11,14 Although this percentage is an overestimate of pharmacologic thromboprophylaxis rates alone, this value was used to determine a sample size for the cohort.
About 122 subjects would be needed to provide 80% power and a significance level of < 0.05 to assess the hypothesis that pharmacologic prophylaxis rates at TVHS would exceed 60%. Additionally calculated was the sample size necessary to find a 20% expected difference in thromboprophylaxis rates according to location of care (eg, medical ward vs medical CCU), the secondary endpoint. This sample size was calculated to be 180 subjects, or 90 patients in each arm, to provide 80% power and a significance level (2-tailed alpha) of < 0.05. Subsequently, up to 130 patients from each location of care were randomly selected for study inclusion.
Data Analysis
A chi square test was used to compare groups on categorical variables. SPSS version 16.0 (SPSS Chicago, IL) was used for data analysis.
Results
A sample of 3,762 hospitalizations for veterans with COPD, asthma, or acute, severe respiratory disease who received inpatient care in the medical ward or medical CCU were extracted from the data warehouse.
Electronic Data Set
An investigator reviewed the electronic data set, and exclusion criteria that could be ascertained electronically were applied. The primary reasons for exclusion were age (18.4%), potential coagulopathy (14.5%), recent transfusion (14.6%), use of therapeutic anticoagulation (11%), or an extended LOS (7%). Less common reasons for exclusion were coagulation disorders (1.4%), heparin-induced thrombocytopenia (1.2%), recent hemorrhage (1.1%), or missing baseline laboratory values (3.2%). Subsequently, the potential sample of subjects declined to 1,018 (27%) hospitalizations. Of the remaining hospitalizations, 46 and 972 were medical CCU and nonsurgical (medical) inpatients, respectively.
In line with the sampling plan, 130 (13.4%) medical ward hospitalizations were selected using a random number generator. As the ICU sample was smaller than anticipated, the convenience sample of all 46 hospitalizations was used.
Manual Chart Abstraction
Manual chart abstraction (n = 176) clarified physician/provider decision making (eg, some patients were not appropriate for thromboprophylaxis due to upcoming invasive procedures), medical history that could not be extracted by ICD-9 coding (eg, recent non-VHA admissions for medical conditions that were contraindications to prophylaxis), and anticoagulation dosing. These exclusions led to an additional 52 (29.5%) excluded hospitalizations. Reasons for manual exclusion included recent bleeding or at high risk for bleeding (18, 34.6%), incorrect classification as nonsurgical or elective admission (5, 9.6%), no diagnosis of lung disease (21, 40.4%), invasive procedures planned (4, 7.7%), treatment anticoagulant doses selected (4, 7.7%), or patient transferred to a non-VA medical facility due to acuity level (1, 1.9%). One patient was excluded for multiple reasons.
Baseline Demographics
The sample was an elderly, male (98%), white (79.8%) cohort (Table 1). No patients were aged < 40 years. Racial information was missing for 5.6% of the patients. The chief pulmonary diagnosis was COPD, and few patients had new onset, acute, severe respiratory disease (3.2%) prompting admission, because pneumonia was not included as a qualifying diagnosis. Median body mass index (BMI) was 26.31. The median LOS was 3.8 days for the overall cohort and 4.1 days for those receiving pharmacologic thromboprophylaxis, although for the latter group a larger proportion of patients were hospitalized for < 3 days. Renal function, according to endpoint definitions, was for using enoxaparin as the appropriate strategy for thromboprophylaxis for the majority (97.5%) of hospitalizations.
Primary and Secondary Endpoints
Of those receiving pharmacologic thromboprophylaxis, heparin was prescribed most often (62.8%). One patient received both heparin and enoxaparin during a single hospitalization.
Pharmacologic thromboprophylaxis was more common in the medical CCU subgroup (80.6%) compared with the nonsurgical patient (56.9%). Pharmacologic thromboprophylaxis was used in 62.9% of patients (n = 124). However, the therapeutic appropriateness ratio was reduced to 58% of the entire sample (n = 124), because 6 patients of the cohort receiving thromboprophylaxis (n = 78) were prescribed suboptimal doses: Specifically, 1 patient was underdosed and 1 overdosed when prescribed enoxaparin (2, 2.6%). Four patients (5.1%) received underdoses of heparin, based on institutional guidance. For those prescribed pharmacologic thromboprophylaxis, the VTE protected time period ratio was 82.8% (Table 2). Overall inpatient mortality rate was low (12, 9.7%). Most deceased patients were managed in the medical CCU (10, 83.3%) and did receive pharmacologic thromboprophylaxis (10, 83.3%).
Discussion
This study demonstrated moderate rates of VTE pharmacologic thromboprophylaxis, because 62.9% of nonsurgical patients with respiratory disease who were hospitalized for various reasons were prophylaxed with either SC heparin or enoxaparin. This rate represents active clinical decision making, because there was no indication to prescribe anticoagulation at therapeutic doses. As expected, pharmacologic thromboprophylaxis was more common in the critical care subgroup (80.6%) compared with the nonsurgical patients (56.9%). Although the study did not meet the intended sample size for this subgroup analysis, results were statistically significant for location of care (P = .014) and may be beneficial for future study design by other investigators.
As early studies of nonsurgical and critical care patients document ≤ 40% of patients receive pharmacologic thromboprophylaxis, this study’s performance seems better.7,12,21 Recently, VHA investigators Quraishi and colleagues seemed to document similar findings. Although 63% of medical patients at the Dayton VAMC in Ohio received appropriate pharmacologic thromboprophylaxis, this value must be tempered by the proportion of subjects receiving therapeutic anticoagulation (5.4%).18
Similar to this study’s results, recent studies of nonveterans document pharmacologic thromboprophylaxis rates of 41% to 51.8%, 41% to 65.9%, and 74.6% to 89.9% in patients with respiratory disease, nonsurgical patients, and critical care patients, respectively. Although findings seem similar to this study’s results, adjustments in estimates again must be made, because these estimates included patients on therapeutic anticoagulation.12,14-16 This study’s results found that 58% of the patient cohort met the therapeutic appropriateness ratio, because they were administered pharmacologic thromboprophylaxis and received correct doses at indicated dosing intervals.
Because stringent exclusion criteria that minimized use of pharmacologic thromboprophylaxis in patients at risk for bleeding were applied, a higher rate of use was expected. This difference between expected and actual rates likely occurred because patient care is individualized and not all factors can be readily assessed in an observational study using retrospective data.
Additionally, for patients who remain ambulatory or have an invasive procedure, thromboprophylaxis may be appropriately delayed past the first 24-hour window of therapy or even temporarily interrupted. Subsequently, the measure of thromboprophylaxis initiation within the first 24 to 48 hours of admission was not elected. Instead, an alternative endpoint of VTE protected time period on thromboprophylaxis was selected. When thromboprophylaxis was used, the median period of protection was 83% of the time period hospitalized for this subgroup. Standardizing to a 7-day period, a VTE protected time period of 83% is coverage for 5.81 days. This would support the Joint Commission ORYX measure that allows for the receipt of thromboprophylaxis within 48 hours of admission to be counted as a success.6
Unfortunately, the authors did not assess whether mechanical thromboprophylaxis was provided to the remaining one-third of patients not receiving pharmacologic thromboprophylaxis. As a result, the complete data set is lacking, which would document whether the Joint Commission measure of ≥ 95% of the time was achieved. Therefore, the claim that TVHS is a top performing hospital for this ORYX measure cannot be made.
Although this study demonstrated a low mortality rate, this rate was not selected as a measure of interest, since one meta-analysis has demonstrated no mortality benefit from VTE thromboprophylaxis.4 Although in-hospital mortality may be an appropriate measure for critical care patients, most of the study patients did not meet this criterion.21 Last, mortality should be assessed no earlier than 30 days from admission.17 Subsequently, statistical assessment and conclusions from this measure are not relevant.
Limitations
A number of limitations hindered the generalizability of the results. This was an observational study using retrospectively collected data. The sample was narrowed to those with chronic respiratory disease, which has been less studied and typically examined in concert with acute processes, such as pneumonia. The demographic was primarily white males. The BMI of subjects enrolled in this study (26 kg/m2) was lower than the BMI of nonveteran subjects with COPD (28.6 kg/m2), nonveteran subjects with COPD and VTE (29 kg/m2), or veteran nonsurgical patients receiving thromboprophylaxis (29 kg/m2).18,34,35
The exclusion criteria resulted in a 73% reduction in the cohort and severely limited the number of medical critical care patients included. However, the problem of a small cohort was anticipated.
Other researchers conducting a prospective VHA thromboprophylaxis study found only 7.6% of veterans screened were eligible for enrollment, although 25% of subjects were anticipated by chart review. Two of the 3 primary reasons for trial exclusion were indication for therapeutic anticoagulation and contraindications to heparin (other than thrombocytopenia), and these were also primary reasons for exclusion in this study.30 Subsequently, the cohort appropriate for thromboprophylaxis in VHA seems relatively small.
Additionally, mobility is difficult to judge in a chart review. Day-to-day clinical assessments of mobility lead to individualization of care, including delayed initiation and timely termination of thromboprophylaxis. It is also possible that a significant portion of the patients had mechanical thromboprophylaxis, because they may have had an unrecognized risk factor for bleeding or patient preferences were considered. Last, some veterans may have classified as palliative care, and VTE prophylaxis may have been omitted for comfort care purposes.32
This study was not designed to evaluate the Padua Prediction Score, which categorizes risk and ration-alizes use of thromboprophylaxis for nonsurgical patients.3 This tool eliminates many of the established risk factors for VTE, including COPD, which was a qualifying diagnosis for inclusion in this study.1 It is not clear how the Padua Prediction Score would categorize the inpatient veteran population. Veterans clearly have poorer health status, more medical conditions, and higher medical resource use compared with the general patient population.25
Veterans with COPD have a higher comorbid illness burden than that of veterans without COPD.36 Chronic obstructive pulmonary disease is associated with VTE development, and when VTE develops in patients with COPD, mortality is greater than that of patients without COPD.37,38 VTE mortality may be related to an increased likelihood of fatal pulmonary embolism.39 Therefore, the authors recommend that VHA conduct studies to examine the Padua Prediction Score and potentially other RAMs that include COPD subjects, to determine what tool should be used in VHA.32
The authors also recommend that VHA evaluate how to improve thromboprophylaxis care with time-based studies. Since manual extraction to determine study inclusion was a time-consuming process, this time frame likely was a barrier to physician implementation of pharmacologic thromboprophylaxis. Therefore an electronic tool that serves as a daily reminder for subjects calculated as high risk for VTE but low risk for bleeding may improve clinical outcomes.
Conclusions
Overall, about one-third of patients did not receive potentially indicated pharmacologic thromboprophylaxis on the medical wards. Use of pharmacologic thromboprophylaxis in medical CCU patients was robust (80%). Doses and dosing intervals were appropriate for > 90% of patients, and therapy clearly was started early and continued for much of the at-risk period, as the VTE protected time period exceeded 80%. Although computerized tools were limited, the authors feel their modest pharmacologic thromboprophylaxis rate is related to the facility’s teaching hospital affiliation or the provider mix, because TVHS is one of the largest VA cardiology centers in the U.S.7,8,13
As it was challenging and time consuming to locate eligible subjects, it may also prove difficult for the admitting physician to have the same luxury of time to look for specific at-risk diagnoses in the medical record and evaluate for exclusions to therapy. If electronic alerts and reminder tools were included in clinical pharmacy inpatient templates, the authors believe the frequency of pharmacologic thromboprophylaxis would further improve in the facility. Also, the authors encourage VHA researchers to further evaluate VTE prophylaxis RAM, the role of daily electronic reminders, and tools to calculate VTE and bleeding risk.
Acknowledgements
The authors are grateful to James Minnis, PharmD, BCPS, and April Ungar, PharmD, BCPS, for their contributions to the study design. This material is the result of work supported with resources and the use of facilities at the VA Tennessee Valley Healthcare System.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Venous thromboembolism (VTE), including deep venous thrombosis (DVT) and pulmonary embolism, is an important public health concern. Deep venous thrombosis is estimated to affect 10% to 20% of medical (nonsurgical) patients, 15% to 40% of stroke patients, and 10% to 80% of critical care patients who are not prophylaxed.1 Venous thromboembolism is associated with significant resource utilization, long-term sequelae, recurrent events, and sudden death.2
The current guidelines of the American College of Chest Physicians recommend use of pharmacologic thromboprophylaxis as the preferred strategy for nonsurgical (or medical) patients (IB, formerly IA, recommendation) and for critically ill patients (2C recommendation) at low risk for bleeding.1,3 Mechanical (or nonpharmacologic) thromboprophylaxis (eg, intermittent pneumatic compression) is an alternative for those at increased risk for bleeding (2C recommendation).3 Pharmacologic thromboprophylaxis in high-risk patients, similar to those studied in randomized controlled clinical trials, reduces the occurrence of symptomatic DVT by 34 events per 1,000 patients treated.3 However, data are conflicting regarding mortality benefit.4,5
Related: Trends in Venous Thromboembolism
The Joint Commission adopted any thromboprophylaxis (measure includes pharmacologic or nonpharmacologic strategies) as a core discretionary measure in the ORYX (National Quality Hospital Measures) program. The ORYX measurements are intended to support Joint Commission-accredited organizations in institutional quality improvement efforts. The thromboprophylaxis core measure became effective May 2009 and remains as an option for hospitals to meet the 4 core measure set accreditation requirement. A top-performing hospital should provide this measure to applicable patients ≥ 95% of the time, according to the Joint Commission.6 The Joint Commission does not encourage use of any risk assessment model (RAM), such as the Padua Prediction Score to preferentially select high-risk medical patients.3
A disparity exists between thromboprophylaxis recommendations and practices in the nonsurgical patient, even when electronic prompts or alerts are available (eTables 1 and 2). In the U.S., pharmacologic thromboprophylaxis is administered to 23.6% to 81.1% of medical patients and 37.9% to 79.4% of critical care patients.7-21 In most cases, these rates are liberal estimates, because they include patients who are already on therapeutic anticoagulation or may have received only 1 prophylactic dose during hospitalization.8-11,13-20 When studies exclude patients receiving therapeutic (or treatment doses) anti-coagulation, pharmacologic thromboprophylaxis rates are substantially lower, typically 31% to 33% for medical patients and 37.9% for critical care patients.7,12,21 Furthermore, when studies examine appropriateness of thromboprophylaxis (eg, within the first 2 days of hospitalization or at the correct dose, correct time, or predefined duration), calculations are often less robust.10,11,13,14,22,23
The VHA uses thromboprophylaxis of surgical patients as an external peer review (EPR) performance measure (PM). With the great attention to this national measure, Altom and colleagues reported 89.9% of surgeries adhered.24 Before 2015, VTE thromboprophylaxis EPR PM did not exist. However, the VHA has initiated efforts to assure that providers are adherent to the new indications, which include VTE prophylaxis and treatment.
There is little published literature evaluating VHA performance.Quraishi and colleagues reported a pharmacologic prophylaxis rate of 63% in nonsurgical patients at a single VAMC, facilitated by the use of an admission VTE order set. Unfortunately, their estimate allowed inclusion of 5% of patients receiving treatment doses of anticoagulation and failed to provide any estimates on regimen appropriateness (eg, correct dose, correct time, or correct duration).18 Lentine and colleagues documented a pharmacologic thromboprophylaxis rate of 48% for a subset of veteran critical care patients who were not already receiving indicated therapeutic anticoagulants.21
Veterans have poorer health status, more medical conditions, and higher medical resource use than do nonveterans; therefore, it is postulated that veterans can derive clinical benefit from improved attention to thromboprophylaxis benchmarking, performance improvement, and potentially, implementation of electronic alerts or reminder tools.25 Nationally, VHA has no formal inpatient reminder tools to trigger use of thromboprophylaxis for high-risk medical patients, although individual health care systems may have created alerts or tools. Some studies demonstrated that order sets and electronic tools are helpful, whereas others demonstrated potential for harm.17-20,26,27
For any hospitalization at the VA Tennessee Valley Healthcare System (TVHS), the only electronic prompt to order VTE thromboprophylaxis occurs when the admission order set is completed. But the prompt can be readily bypassed if the quick admission orders are selected. Although no further electronic prompts in the Computerized Patient Record System (CPRS) are invoked following admission, the authors hypothesized that the rate of VTE thromboprophylaxis, specifically pharmacologic, in a subset of veterans with respiratory disease will be higher than the usual published rates.
Purpose and Relevance
This study’s primary aim was to assess the rate of pharmacologic VTE prophylaxis in veterans with pulmonary disease who were admitted for a nonsurgical stay. The 2 secondary aims were to determine whether thromboprophylaxis was appropriate and to characterize whether differences exist for pharmacologic prophylaxis according to level of care (medical critical care unit [CCU] vs acute care medical ward).
Related: Prevention of Venous Thromboembolism After Total Joint Replacement: Rivaroxaban Update
This analysis emphasizes pharmacologic thromboprophylaxis instead of the combined endpoint of pharmacologic plus nonpharmacologic thromboprophylaxis traditionally used and will supplement the limited literature in 2 understudied cohorts: (1) nonsurgical veteran patients, specifically where advanced computerized thromboprophylaxis alerts are not in use; and (2) patients with the VTE risk factor of respiratory disease.1,7-9,12,13,15,16,18,21
Study Design
This observational study used retrospectively collected data. The data were extracted electronically from the VISN 9 data warehouse by a Decision Support Services analyst and manually validated by an investigator using the CPRS. Prior to initiation of research activities, the VHA Institutional Review Board and the Research and Development Committee at the facility level approved the study.
Sampling
Patients assigned to the treating specialties of medicine and medical critical care during fiscal years 2006 to 2008, admitted for ≥ 24 hours, and discharged with a diagnosis of chronic obstructive pulmonary disease (COPD), asthma, or acute, severe respiratory disease (eg, patients requiring mechanical ventilation) were eligible for inclusion. The authors also elected to include patients with asthma, because this diagnosis commonly overlaps with COPD and reflects real-world clinical practice and diagnostic challenges.28 Pneumonia and other infectious pulmonary conditions were not a qualifying diagnosis for study inclusion.
Patients were excluded if aged > 79 years, because it is difficult to maintain de-identification in a small sample of inpatients in this age category. Unfortunately, octogenarians have the highest rate of VTE per 100,000 population and would gain substantial benefit from prophylaxis.29 Similar to other VHA and non-VHA investigators, this study excluded patients who were prescribed therapeutic anticoagulation.7,12,21,30 The authors believe continuation of therapeutic (or treatment) anticoagulation does not measure a clinical decision to use pharmacologic thromboprophylaxis, and any interruption of therapeutic anticoagulation suggests that prophylactic anticoagulation is not warranted.
Related: Pulmonary Vein Thrombosis Associated With Metastatic Carcinoma
Additionally, patients were excluded if length of stay (LOS) exceeded 14 days, if known or potential contraindications to thromboprophylaxis existed, or if laboratory data that were needed to assess for contraindications were missing from the electronic data set. Known or potential contraindications included active hemorrhage, hemorrhage within the past 3 months, recent administration of packed red blood cells, bacterial endocarditis, known coagulopathy, recent or current heparin-induced thrombocytopenia, or a potential coagulopathy (International Normalized Ratio > 1.5, platelets < 50,000, or an activated partial thromboplastin time > 41 sec).
Contraindications were conservative in construct and were similar to the exclusion-based VTE checklist for the nonsurgical patient.31 The authors did not examine the electronic data set for the contraindication of epidural or spinal anesthesia, because neither is commonly used in the medical ward or medical CCU. The authors also did not exclude patients with a creatinine clearance (CrCl) < 10 mL/min (a relative contraindication to VTE thromboprophylaxis), although these patients may be at an increased risk for bleeding complications.32
Endpoints and Measures
The primary endpoint of this study was the rate of any pharmacologic thromboprophylaxis (eg, ≥ 1 doses), similar to the endpoint selected by other investigators.7-9,12,13,15,16 Secondary endpoints included VTE protected time period on thromboprophylaxis, therapeutic appropriateness ratio for heparin and enoxaparin doses combined, and pharmacologic thromboprophylaxis rates according to level and location of care.
Sample Size
Although data have been forthcoming, at the time of study inception no studies documented the rate of pharmacologic thromboprophylaxis alone (defined as use of ≥ 1 dose of a pharmacologic agent) in patients with the VTE risk factor of respiratory disease.15,23 However, an average combined pharmacologic and nonpharmacologic thromboprophylaxis rate of 48.8% was determined from available studies.11,14 Although this percentage is an overestimate of pharmacologic thromboprophylaxis rates alone, this value was used to determine a sample size for the cohort.
About 122 subjects would be needed to provide 80% power and a significance level of < 0.05 to assess the hypothesis that pharmacologic prophylaxis rates at TVHS would exceed 60%. Additionally calculated was the sample size necessary to find a 20% expected difference in thromboprophylaxis rates according to location of care (eg, medical ward vs medical CCU), the secondary endpoint. This sample size was calculated to be 180 subjects, or 90 patients in each arm, to provide 80% power and a significance level (2-tailed alpha) of < 0.05. Subsequently, up to 130 patients from each location of care were randomly selected for study inclusion.
Data Analysis
A chi square test was used to compare groups on categorical variables. SPSS version 16.0 (SPSS Chicago, IL) was used for data analysis.
Results
A sample of 3,762 hospitalizations for veterans with COPD, asthma, or acute, severe respiratory disease who received inpatient care in the medical ward or medical CCU were extracted from the data warehouse.
Electronic Data Set
An investigator reviewed the electronic data set, and exclusion criteria that could be ascertained electronically were applied. The primary reasons for exclusion were age (18.4%), potential coagulopathy (14.5%), recent transfusion (14.6%), use of therapeutic anticoagulation (11%), or an extended LOS (7%). Less common reasons for exclusion were coagulation disorders (1.4%), heparin-induced thrombocytopenia (1.2%), recent hemorrhage (1.1%), or missing baseline laboratory values (3.2%). Subsequently, the potential sample of subjects declined to 1,018 (27%) hospitalizations. Of the remaining hospitalizations, 46 and 972 were medical CCU and nonsurgical (medical) inpatients, respectively.
In line with the sampling plan, 130 (13.4%) medical ward hospitalizations were selected using a random number generator. As the ICU sample was smaller than anticipated, the convenience sample of all 46 hospitalizations was used.
Manual Chart Abstraction
Manual chart abstraction (n = 176) clarified physician/provider decision making (eg, some patients were not appropriate for thromboprophylaxis due to upcoming invasive procedures), medical history that could not be extracted by ICD-9 coding (eg, recent non-VHA admissions for medical conditions that were contraindications to prophylaxis), and anticoagulation dosing. These exclusions led to an additional 52 (29.5%) excluded hospitalizations. Reasons for manual exclusion included recent bleeding or at high risk for bleeding (18, 34.6%), incorrect classification as nonsurgical or elective admission (5, 9.6%), no diagnosis of lung disease (21, 40.4%), invasive procedures planned (4, 7.7%), treatment anticoagulant doses selected (4, 7.7%), or patient transferred to a non-VA medical facility due to acuity level (1, 1.9%). One patient was excluded for multiple reasons.
Baseline Demographics
The sample was an elderly, male (98%), white (79.8%) cohort (Table 1). No patients were aged < 40 years. Racial information was missing for 5.6% of the patients. The chief pulmonary diagnosis was COPD, and few patients had new onset, acute, severe respiratory disease (3.2%) prompting admission, because pneumonia was not included as a qualifying diagnosis. Median body mass index (BMI) was 26.31. The median LOS was 3.8 days for the overall cohort and 4.1 days for those receiving pharmacologic thromboprophylaxis, although for the latter group a larger proportion of patients were hospitalized for < 3 days. Renal function, according to endpoint definitions, was for using enoxaparin as the appropriate strategy for thromboprophylaxis for the majority (97.5%) of hospitalizations.
Primary and Secondary Endpoints
Of those receiving pharmacologic thromboprophylaxis, heparin was prescribed most often (62.8%). One patient received both heparin and enoxaparin during a single hospitalization.
Pharmacologic thromboprophylaxis was more common in the medical CCU subgroup (80.6%) compared with the nonsurgical patient (56.9%). Pharmacologic thromboprophylaxis was used in 62.9% of patients (n = 124). However, the therapeutic appropriateness ratio was reduced to 58% of the entire sample (n = 124), because 6 patients of the cohort receiving thromboprophylaxis (n = 78) were prescribed suboptimal doses: Specifically, 1 patient was underdosed and 1 overdosed when prescribed enoxaparin (2, 2.6%). Four patients (5.1%) received underdoses of heparin, based on institutional guidance. For those prescribed pharmacologic thromboprophylaxis, the VTE protected time period ratio was 82.8% (Table 2). Overall inpatient mortality rate was low (12, 9.7%). Most deceased patients were managed in the medical CCU (10, 83.3%) and did receive pharmacologic thromboprophylaxis (10, 83.3%).
Discussion
This study demonstrated moderate rates of VTE pharmacologic thromboprophylaxis, because 62.9% of nonsurgical patients with respiratory disease who were hospitalized for various reasons were prophylaxed with either SC heparin or enoxaparin. This rate represents active clinical decision making, because there was no indication to prescribe anticoagulation at therapeutic doses. As expected, pharmacologic thromboprophylaxis was more common in the critical care subgroup (80.6%) compared with the nonsurgical patients (56.9%). Although the study did not meet the intended sample size for this subgroup analysis, results were statistically significant for location of care (P = .014) and may be beneficial for future study design by other investigators.
As early studies of nonsurgical and critical care patients document ≤ 40% of patients receive pharmacologic thromboprophylaxis, this study’s performance seems better.7,12,21 Recently, VHA investigators Quraishi and colleagues seemed to document similar findings. Although 63% of medical patients at the Dayton VAMC in Ohio received appropriate pharmacologic thromboprophylaxis, this value must be tempered by the proportion of subjects receiving therapeutic anticoagulation (5.4%).18
Similar to this study’s results, recent studies of nonveterans document pharmacologic thromboprophylaxis rates of 41% to 51.8%, 41% to 65.9%, and 74.6% to 89.9% in patients with respiratory disease, nonsurgical patients, and critical care patients, respectively. Although findings seem similar to this study’s results, adjustments in estimates again must be made, because these estimates included patients on therapeutic anticoagulation.12,14-16 This study’s results found that 58% of the patient cohort met the therapeutic appropriateness ratio, because they were administered pharmacologic thromboprophylaxis and received correct doses at indicated dosing intervals.
Because stringent exclusion criteria that minimized use of pharmacologic thromboprophylaxis in patients at risk for bleeding were applied, a higher rate of use was expected. This difference between expected and actual rates likely occurred because patient care is individualized and not all factors can be readily assessed in an observational study using retrospective data.
Additionally, for patients who remain ambulatory or have an invasive procedure, thromboprophylaxis may be appropriately delayed past the first 24-hour window of therapy or even temporarily interrupted. Subsequently, the measure of thromboprophylaxis initiation within the first 24 to 48 hours of admission was not elected. Instead, an alternative endpoint of VTE protected time period on thromboprophylaxis was selected. When thromboprophylaxis was used, the median period of protection was 83% of the time period hospitalized for this subgroup. Standardizing to a 7-day period, a VTE protected time period of 83% is coverage for 5.81 days. This would support the Joint Commission ORYX measure that allows for the receipt of thromboprophylaxis within 48 hours of admission to be counted as a success.6
Unfortunately, the authors did not assess whether mechanical thromboprophylaxis was provided to the remaining one-third of patients not receiving pharmacologic thromboprophylaxis. As a result, the complete data set is lacking, which would document whether the Joint Commission measure of ≥ 95% of the time was achieved. Therefore, the claim that TVHS is a top performing hospital for this ORYX measure cannot be made.
Although this study demonstrated a low mortality rate, this rate was not selected as a measure of interest, since one meta-analysis has demonstrated no mortality benefit from VTE thromboprophylaxis.4 Although in-hospital mortality may be an appropriate measure for critical care patients, most of the study patients did not meet this criterion.21 Last, mortality should be assessed no earlier than 30 days from admission.17 Subsequently, statistical assessment and conclusions from this measure are not relevant.
Limitations
A number of limitations hindered the generalizability of the results. This was an observational study using retrospectively collected data. The sample was narrowed to those with chronic respiratory disease, which has been less studied and typically examined in concert with acute processes, such as pneumonia. The demographic was primarily white males. The BMI of subjects enrolled in this study (26 kg/m2) was lower than the BMI of nonveteran subjects with COPD (28.6 kg/m2), nonveteran subjects with COPD and VTE (29 kg/m2), or veteran nonsurgical patients receiving thromboprophylaxis (29 kg/m2).18,34,35
The exclusion criteria resulted in a 73% reduction in the cohort and severely limited the number of medical critical care patients included. However, the problem of a small cohort was anticipated.
Other researchers conducting a prospective VHA thromboprophylaxis study found only 7.6% of veterans screened were eligible for enrollment, although 25% of subjects were anticipated by chart review. Two of the 3 primary reasons for trial exclusion were indication for therapeutic anticoagulation and contraindications to heparin (other than thrombocytopenia), and these were also primary reasons for exclusion in this study.30 Subsequently, the cohort appropriate for thromboprophylaxis in VHA seems relatively small.
Additionally, mobility is difficult to judge in a chart review. Day-to-day clinical assessments of mobility lead to individualization of care, including delayed initiation and timely termination of thromboprophylaxis. It is also possible that a significant portion of the patients had mechanical thromboprophylaxis, because they may have had an unrecognized risk factor for bleeding or patient preferences were considered. Last, some veterans may have classified as palliative care, and VTE prophylaxis may have been omitted for comfort care purposes.32
This study was not designed to evaluate the Padua Prediction Score, which categorizes risk and ration-alizes use of thromboprophylaxis for nonsurgical patients.3 This tool eliminates many of the established risk factors for VTE, including COPD, which was a qualifying diagnosis for inclusion in this study.1 It is not clear how the Padua Prediction Score would categorize the inpatient veteran population. Veterans clearly have poorer health status, more medical conditions, and higher medical resource use compared with the general patient population.25
Veterans with COPD have a higher comorbid illness burden than that of veterans without COPD.36 Chronic obstructive pulmonary disease is associated with VTE development, and when VTE develops in patients with COPD, mortality is greater than that of patients without COPD.37,38 VTE mortality may be related to an increased likelihood of fatal pulmonary embolism.39 Therefore, the authors recommend that VHA conduct studies to examine the Padua Prediction Score and potentially other RAMs that include COPD subjects, to determine what tool should be used in VHA.32
The authors also recommend that VHA evaluate how to improve thromboprophylaxis care with time-based studies. Since manual extraction to determine study inclusion was a time-consuming process, this time frame likely was a barrier to physician implementation of pharmacologic thromboprophylaxis. Therefore an electronic tool that serves as a daily reminder for subjects calculated as high risk for VTE but low risk for bleeding may improve clinical outcomes.
Conclusions
Overall, about one-third of patients did not receive potentially indicated pharmacologic thromboprophylaxis on the medical wards. Use of pharmacologic thromboprophylaxis in medical CCU patients was robust (80%). Doses and dosing intervals were appropriate for > 90% of patients, and therapy clearly was started early and continued for much of the at-risk period, as the VTE protected time period exceeded 80%. Although computerized tools were limited, the authors feel their modest pharmacologic thromboprophylaxis rate is related to the facility’s teaching hospital affiliation or the provider mix, because TVHS is one of the largest VA cardiology centers in the U.S.7,8,13
As it was challenging and time consuming to locate eligible subjects, it may also prove difficult for the admitting physician to have the same luxury of time to look for specific at-risk diagnoses in the medical record and evaluate for exclusions to therapy. If electronic alerts and reminder tools were included in clinical pharmacy inpatient templates, the authors believe the frequency of pharmacologic thromboprophylaxis would further improve in the facility. Also, the authors encourage VHA researchers to further evaluate VTE prophylaxis RAM, the role of daily electronic reminders, and tools to calculate VTE and bleeding risk.
Acknowledgements
The authors are grateful to James Minnis, PharmD, BCPS, and April Ungar, PharmD, BCPS, for their contributions to the study design. This material is the result of work supported with resources and the use of facilities at the VA Tennessee Valley Healthcare System.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Geerts WH, Bergquist D, Pineo G, et al; American College of Chest Physicians. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(suppl 6):381S-453S.
2. Go AS, Mozaffarian D, Roger VL, et al; on behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics–2013 update: A report from the American Heart Association. Circulation. 2013;127(1):e6-e245.
3. Kahn SR, Lim W, Dunn AS, et al; American College of Chest Physicians. Prevention of VTE in nonsurgical patients: Antithrombotic Therapy and Prevention of Thrombosis 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2)(suppl):e195S-e226S.
4. Wein L, Wein S, Haas SJ, Shaw J, Krum H. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients: A meta-analysis of randomized controlled trials. Arch Intern Med. 2007;167(14):1476-1486.
5. Ruiz EM, Utrilla GB, Alvarez JL, Perrin RS. Effectiveness and safety of thromboprophylaxis with enoxaparin in medical inpatients. Thromb Res. 2011;128(5):440-445.
6. The Joint Commission. Specifications Manual for National Hospital Inpatient Quality Measures. http://www.jointcommission.org/specifications_manual_for_national_hospital_inpatient_quality _measures.aspx. The Joint Commission Website. Accessed March 5, 2015.
7. Stark JE, Kilzer WJ. Venous thromboembolic prophylaxis in hospitalized medical patients. Ann Pharmacother. 2004;38(1):36-40.
8. Peterman CM, Kolansky DM, Spinler SA. Prophylaxis against venous thromboembolism in acutely ill medical patients: An observational study. Pharmacotherapy. 2006;26(8):1086-1090.
9. Herbers J, Zarter S. Prevention of venous thromboembolism in Department of Veterans Affairs hospitals. J Hosp Med. 2010;5(1):E21-E25.
10. Yu HT, Dylan ML, Lin J, Dubois RW. Hospitals’ compliance with prophylaxis guidelines for venous thromboembolism. Am J Health-Syst Pharm. 2007;64(1):69-76.
11. Amin A, Stemkowski S, Lin J, Yang G. Thromboprophylaxis rates in US medical centers: Success or failure? J Thromb Haemost. 2007;5(8):1610-1616.
12. Tapson VF, Decousus H, Pini M, et al; IMPROVE Investigators. Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: Findings from the International Medical Prevention Registry on Venous Thromboembolism. Chest. 2007;132(3):936-945.
13. Amin AN, Stemkowski S, Lin J, Yang G. Inpatient thromboprophylaxis use in U.S. hospitals: Adherence to the Seventh American College of Chest Physician’s recommendations for at-risk medical and surgical patients. J Hosp Med. 2009;4(8):E15-E21.
14. Amin A, Spyropoulos AC, Dobesh P, et al. Are hospitals delivering appropriate VTE prevention? The venous thromboembolism study to assess the rate of thromboprophylaxis (VTE Start). J Thromb Thrombolysis. 2010;29(3):326-339.
15. Baser O, Liu X, Phatak H, Wang L, et al. Venous thromboembolism prophylaxis and clinical consequences in medically ill patients. Am J Ther. 2013:20(2):132-142.
16. Baser O, Sengupta N, Dysinger A, Wang L. Thromboembolism prophylaxis in medical inpatients: Effect on outcomes and costs. Am J Manag Care. 2012;18(6):294-302.
17. Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005;352(10):969-977.
18. Quraishi MB, Mathew R, Lowes A, et al. Venous thromboembolism prophylaxis and the impact of standardized guidelines: Is a computer-based approach enough? J Clin Outcomes Manage. 2011;18(11):505-512.
19. Stinnett JM, Pendleton R, Skordos L, Wheeler M, Rodgers GM. Venous thromboembolism prophylaxis in medically ill patients and the development of strategies to improve prophylaxis rates. Am J Hematol. 2005;78(3):167-172.
20. Cohn SL, Adekile A, Mahabir V. Improved use of thromboprophylaxis for deep vein thrombosis following an educational intervention. J Hosp Med. 2006;1(6):331-338.
21. Lentine KL, Flavin KE, Gould MK. Variability in the use of thromboprophylaxis and outcomes in critically ill medical patients. Am J Med. 2005;118(12):1373-1380.
22. Pendergraft T, Liu X, Edelsberg J, Phatak H, et al. Prophylaxis against venous thromboembolism in hospitalized medically ill patients. Circ Cardiovasc Qual Outcomes. 2013;6(1):75-82.
23. Rothberg MB, Lahti M, Pekow PS, Lindenauer PK. Venous thromboembolism prophylaxis among medical patients at US hospitals. J Gen Intern Med. 2010;25(6):489-494.
24. Altom LK, Deierhoi RJ, Grams J, et al. Association between Surgical Care Improvement Program venous thromboembolism measures and postoperative events. Am J Surg. 2012;204(5):591-597.
25. Agha Z, Lofgren RP, VanRuiswyk JV, Layde PM. Are patients at Veterans Affairs medical centers sicker? A comparative analysis of health status and medical resource use. Arch Intern Med. 2000;160(21): 3252-3257.
26. Pham DQ, Pham AQ, Ullah E, McFarlane SI, Payne R. Short communication: Evaluating the appropriateness of thromboprophylaxis in an acute care setting using a computerised reminder, through order-entry system. Int J Clin Pract. 2008;62(1):134-137.
27. Khanna R, Vittinghoff E, Maselli J, Auerbach A. Unintended consequences of a standard admission order set on venous thromboembolism prophylaxis and patient outcomes. J Gen Intern Med. 2011;27(3):318-324.
28. Barr RG, Celli VR, Mannino DM, et al. Comorbidities, patient knowledge, and disease management in a national sample of patients with COPD. Am J Med. 2009;122(4):348-355.
29. Centers for Disease Control and Prevention. Venous thromboembolism in adult hospitalizations – United States, 2007-2009. (MMWR) Morbidity & Mortality Weekly Report. 2012;61(22):401-404.
30. Lederle FA, Sacks JN, Fiore L, et al. The prophylaxis of medical patients for thromboembolism pilot study. Am J Med. 2006;119(1):54-59.
31. Dobromirski M, Cohen AT. How I manage venous thromboembolism risk in hospitalized medical patients. Blood. 2012;120(8):1562-1569.
32. Polich AL, Etherton GM, Knezevich JT, Rousek JB, Masek CM, Hallbeck MS. Can eliminating risk stratification improve medical residents’ adherence to venous thromboembolism prophylaxis? Acad Med. 2011;86(12):1518-1524.
33. King CS, Holley AB, Jackson JL, Shorr AF, Moores LK. Twice vs three times daily heparin dosing for thromboembolism prophylaxis in the general medical population: A metaanalysis. Chest. 2007;131(2):507-516.
34. Piazza G, Goldhaber SZ, Kroll A, Goldberg RJ, Emery C, Spencer FA. Venous thromboembolism in patients with chronic obstructive pulmonary disease. Am J Med. 2012;125(10):1010-1018.
35. Niewoehner DE, Lokhnygina Y, Rice K, et al. Risk indexes for exacerbations and hospitalizations due to COPD. Chest. 2007;131(1):20-28.
36. Sharafkhaneh A. Peterson NJ, Yu HJ, Dalal AA, Johnson ML, Hanania NA. Burden of COPD in a government health care system: A retrospective observational study using data from the US Veterans Affairs population. Int J Chron Obstruct Pulmon Dis. 2010;5:125-132.
37. Shetty R, Seddighzadeh A, Piazza G, Goldhaber SZ. Chronic obstructive pulmonary disease and deep venous thrombosis: a prevalent combination. J Thromb Thrombolysis. 2008;26(1):35-40.
38. Carson JL, Terrin ML, Duff A, Kelley MA. Pulmonary embolism and mortality in patients with COPD. Chest. 1996;110(5):1212-1219.
39. Huerta C, Johansson S, Wallander MA, García Rodríguez LA. Risk factors and short-term mortality of venous thromboembolism diagnosed in the primary care setting in the United Kingdom. Arch Intern Med. 2007;167(9):935-943.
1. Geerts WH, Bergquist D, Pineo G, et al; American College of Chest Physicians. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(suppl 6):381S-453S.
2. Go AS, Mozaffarian D, Roger VL, et al; on behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics–2013 update: A report from the American Heart Association. Circulation. 2013;127(1):e6-e245.
3. Kahn SR, Lim W, Dunn AS, et al; American College of Chest Physicians. Prevention of VTE in nonsurgical patients: Antithrombotic Therapy and Prevention of Thrombosis 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2)(suppl):e195S-e226S.
4. Wein L, Wein S, Haas SJ, Shaw J, Krum H. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients: A meta-analysis of randomized controlled trials. Arch Intern Med. 2007;167(14):1476-1486.
5. Ruiz EM, Utrilla GB, Alvarez JL, Perrin RS. Effectiveness and safety of thromboprophylaxis with enoxaparin in medical inpatients. Thromb Res. 2011;128(5):440-445.
6. The Joint Commission. Specifications Manual for National Hospital Inpatient Quality Measures. http://www.jointcommission.org/specifications_manual_for_national_hospital_inpatient_quality _measures.aspx. The Joint Commission Website. Accessed March 5, 2015.
7. Stark JE, Kilzer WJ. Venous thromboembolic prophylaxis in hospitalized medical patients. Ann Pharmacother. 2004;38(1):36-40.
8. Peterman CM, Kolansky DM, Spinler SA. Prophylaxis against venous thromboembolism in acutely ill medical patients: An observational study. Pharmacotherapy. 2006;26(8):1086-1090.
9. Herbers J, Zarter S. Prevention of venous thromboembolism in Department of Veterans Affairs hospitals. J Hosp Med. 2010;5(1):E21-E25.
10. Yu HT, Dylan ML, Lin J, Dubois RW. Hospitals’ compliance with prophylaxis guidelines for venous thromboembolism. Am J Health-Syst Pharm. 2007;64(1):69-76.
11. Amin A, Stemkowski S, Lin J, Yang G. Thromboprophylaxis rates in US medical centers: Success or failure? J Thromb Haemost. 2007;5(8):1610-1616.
12. Tapson VF, Decousus H, Pini M, et al; IMPROVE Investigators. Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: Findings from the International Medical Prevention Registry on Venous Thromboembolism. Chest. 2007;132(3):936-945.
13. Amin AN, Stemkowski S, Lin J, Yang G. Inpatient thromboprophylaxis use in U.S. hospitals: Adherence to the Seventh American College of Chest Physician’s recommendations for at-risk medical and surgical patients. J Hosp Med. 2009;4(8):E15-E21.
14. Amin A, Spyropoulos AC, Dobesh P, et al. Are hospitals delivering appropriate VTE prevention? The venous thromboembolism study to assess the rate of thromboprophylaxis (VTE Start). J Thromb Thrombolysis. 2010;29(3):326-339.
15. Baser O, Liu X, Phatak H, Wang L, et al. Venous thromboembolism prophylaxis and clinical consequences in medically ill patients. Am J Ther. 2013:20(2):132-142.
16. Baser O, Sengupta N, Dysinger A, Wang L. Thromboembolism prophylaxis in medical inpatients: Effect on outcomes and costs. Am J Manag Care. 2012;18(6):294-302.
17. Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005;352(10):969-977.
18. Quraishi MB, Mathew R, Lowes A, et al. Venous thromboembolism prophylaxis and the impact of standardized guidelines: Is a computer-based approach enough? J Clin Outcomes Manage. 2011;18(11):505-512.
19. Stinnett JM, Pendleton R, Skordos L, Wheeler M, Rodgers GM. Venous thromboembolism prophylaxis in medically ill patients and the development of strategies to improve prophylaxis rates. Am J Hematol. 2005;78(3):167-172.
20. Cohn SL, Adekile A, Mahabir V. Improved use of thromboprophylaxis for deep vein thrombosis following an educational intervention. J Hosp Med. 2006;1(6):331-338.
21. Lentine KL, Flavin KE, Gould MK. Variability in the use of thromboprophylaxis and outcomes in critically ill medical patients. Am J Med. 2005;118(12):1373-1380.
22. Pendergraft T, Liu X, Edelsberg J, Phatak H, et al. Prophylaxis against venous thromboembolism in hospitalized medically ill patients. Circ Cardiovasc Qual Outcomes. 2013;6(1):75-82.
23. Rothberg MB, Lahti M, Pekow PS, Lindenauer PK. Venous thromboembolism prophylaxis among medical patients at US hospitals. J Gen Intern Med. 2010;25(6):489-494.
24. Altom LK, Deierhoi RJ, Grams J, et al. Association between Surgical Care Improvement Program venous thromboembolism measures and postoperative events. Am J Surg. 2012;204(5):591-597.
25. Agha Z, Lofgren RP, VanRuiswyk JV, Layde PM. Are patients at Veterans Affairs medical centers sicker? A comparative analysis of health status and medical resource use. Arch Intern Med. 2000;160(21): 3252-3257.
26. Pham DQ, Pham AQ, Ullah E, McFarlane SI, Payne R. Short communication: Evaluating the appropriateness of thromboprophylaxis in an acute care setting using a computerised reminder, through order-entry system. Int J Clin Pract. 2008;62(1):134-137.
27. Khanna R, Vittinghoff E, Maselli J, Auerbach A. Unintended consequences of a standard admission order set on venous thromboembolism prophylaxis and patient outcomes. J Gen Intern Med. 2011;27(3):318-324.
28. Barr RG, Celli VR, Mannino DM, et al. Comorbidities, patient knowledge, and disease management in a national sample of patients with COPD. Am J Med. 2009;122(4):348-355.
29. Centers for Disease Control and Prevention. Venous thromboembolism in adult hospitalizations – United States, 2007-2009. (MMWR) Morbidity & Mortality Weekly Report. 2012;61(22):401-404.
30. Lederle FA, Sacks JN, Fiore L, et al. The prophylaxis of medical patients for thromboembolism pilot study. Am J Med. 2006;119(1):54-59.
31. Dobromirski M, Cohen AT. How I manage venous thromboembolism risk in hospitalized medical patients. Blood. 2012;120(8):1562-1569.
32. Polich AL, Etherton GM, Knezevich JT, Rousek JB, Masek CM, Hallbeck MS. Can eliminating risk stratification improve medical residents’ adherence to venous thromboembolism prophylaxis? Acad Med. 2011;86(12):1518-1524.
33. King CS, Holley AB, Jackson JL, Shorr AF, Moores LK. Twice vs three times daily heparin dosing for thromboembolism prophylaxis in the general medical population: A metaanalysis. Chest. 2007;131(2):507-516.
34. Piazza G, Goldhaber SZ, Kroll A, Goldberg RJ, Emery C, Spencer FA. Venous thromboembolism in patients with chronic obstructive pulmonary disease. Am J Med. 2012;125(10):1010-1018.
35. Niewoehner DE, Lokhnygina Y, Rice K, et al. Risk indexes for exacerbations and hospitalizations due to COPD. Chest. 2007;131(1):20-28.
36. Sharafkhaneh A. Peterson NJ, Yu HJ, Dalal AA, Johnson ML, Hanania NA. Burden of COPD in a government health care system: A retrospective observational study using data from the US Veterans Affairs population. Int J Chron Obstruct Pulmon Dis. 2010;5:125-132.
37. Shetty R, Seddighzadeh A, Piazza G, Goldhaber SZ. Chronic obstructive pulmonary disease and deep venous thrombosis: a prevalent combination. J Thromb Thrombolysis. 2008;26(1):35-40.
38. Carson JL, Terrin ML, Duff A, Kelley MA. Pulmonary embolism and mortality in patients with COPD. Chest. 1996;110(5):1212-1219.
39. Huerta C, Johansson S, Wallander MA, García Rodríguez LA. Risk factors and short-term mortality of venous thromboembolism diagnosed in the primary care setting in the United Kingdom. Arch Intern Med. 2007;167(9):935-943.
High-Yield Biopsy Technique for Subepidermal Blisters
The traditional approach for confirming the diagnosis of subepidermal blistering diseases such as bullous pemphigoid (BP), epidermolysis bullosa acquisita (EBA), dermatitis herpetifor-mis (DH), and linear IgA bullous dermatosis (LABD) requires 2 punch biopsies: one from perilesional skin for direct immunofluorescence (DIF) and one from lesional skin for light microscopy using hematoxylin and eosin (H&E) stain.1-4 These conditions are distinguished by a combination of features appreciated on H&E-stained sections, DIF, and indirect immunofluorescence for a subset of disorders. Additional information may be provided by DIF or indirect immunofluorescence utilizing the salt-split skin technique to differentiate BP (in which linear IgG deposition is identified by immunofluorescence on the roof of salt-split skin) from EBA and antiepiligrin cicatricial pemphigoid (in which linear IgG deposition is identified by immunofluorescence along the floor of the salt-split skin), which is more rare.4 One bisected punch biopsy of a subepidermal blister yields salt-split skin–like information through standard DIF and supersedes the need for the more cumbersome salt-split skin technique.
Serologic tests for the presence of circulating antibodies to BP180 and BP230 represent an emerging technology that can confirm the diagnosis of BP, but it has been difficult to identify clinically useful autoantibodies to confirm diagnoses of EBA and LABD.5-7 Serologic tests for tissue transglutaminase IgA antibodies may be useful in the diagnosis of DH.8 We present a cost-effective approach to biopsy in the diagnosis of subepidermal blistering diseases that provides the necessary diagnostic information to distinguish relevant disease processes.
Subepidermal Blistering Diseases
Bullous pemphigoid commonly presents with widespread tense bullae of varying sizes on an erythematous base or on otherwise normal skin.9 Some cases of BP present not with bullae but with pruritic, urticarial, plaquelike, or papular lesions. Bullous pemphigoid commonly involves flexural surfaces and the trunk but can appear anywhere on the skin. The induction of blisters by shearing with mechanical pressure on perilesional skin (Nikolsky sign) is not characteristically present in BP as it is in pemphigus vulgaris.10 Epidermolysis bullosa acquisita can mimic BP in the development of widespread tense bullae, but blisters typically appear on areas of the skin that are prone to trauma (eg, toes, knees, elbows, hands). Crusted erosions, scarring, and milia also are clinical manifestations of EBA.11 Dermatitis herpetiformis presents with grouped vesicles, papulovesicles, plaques, and excoriations that are symmetrically distributed on extensor surfaces of the skin but also can occur on the buttocks, scalp, and other areas of the skin.12,13 Although it may mimic both BP and DH, LABD frequently is less pruritic than these other conditions.14,15 Linear IgA bullous dermatosis also demonstrates the characteristic finding of multiple bullae that form concentrically around a crusted area of skin. This physical finding is known as a string of pearls. Linear IgA bullous dermatosis typically occurs in childhood and may resolve without treatment in months to years.16
Traditional Biopsy Approach
A review of several articles from the literature and multiple dermatology and dermatopathology textbooks revealed uniform recommendations for biopsy of subepidermal blistering conditions that manifest as tense blisters.1-4,9-23 A biopsy of early lesional skin or of a blister for light microscopy with H&E stain and biopsy of perilesional skin for DIF is recommended.1-4,9-23 Three review articles specifically suggested biopsy of “perilesional skin” for DIF.1-3 The majority of textbooks we reviewed also suggested that perilesional skin, or skin adjacent to a zone of erythema in the case of DH, should be sampled for DIF to assist in the diagnosis of BP, EBA, DH, and LABD.4,9-21 Biopsy of adjacent or nonlesional skin or skin around the lesion for DIF also was recommended by other textbooks for diagnosis of subepidermal blistering diseases.22,23 Perilesional skin is chosen because it is critical that the epidermis be included for adequate immunofluorescence studies.5,20 Biopsy of healed and crusted lesions should be avoided.24
Recommended Alternative Approach
A single punch biopsy produces the best possible specimen for light microscopy with H&E stain and DIF if it is obtained via one of 2 methods.
The first method involves choosing a small, 1- to 2-mm tense blister.25 Use an 8-mm punch centered on the blister that includes at least 3 mm of circumferential perilesional skin (Figures 1 and 2).20 Holding the specimen with forceps, use a no. 15 scalpel blade to bisect the blister with a sawing motion. Place half of the specimen in formalin for H&E staining and the other half in Zeus (or Michel) medium for DIF (Figure 3).
|
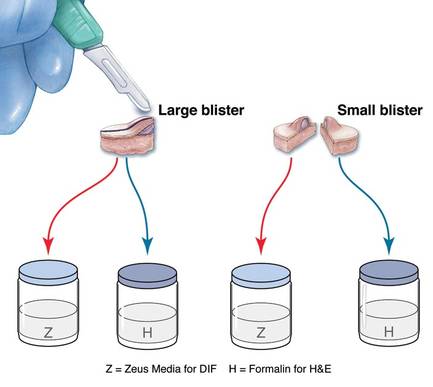
|
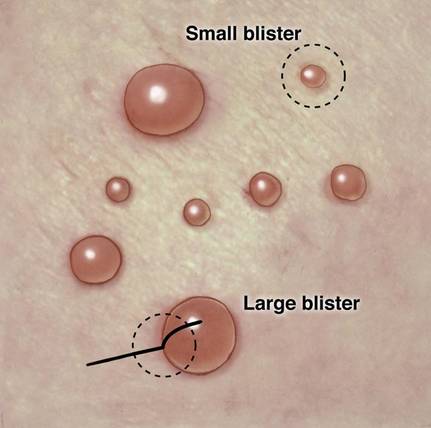
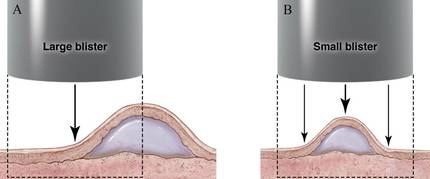
The second method is to choose any large blister and, utilizing a surgical marker, draw a line from the roof of the blister onto the adjacent perilesional skin (Figure 1).20,24 After blotting with an alcohol pad so as not to remove the mark, anesthetize the site with lidocaine 1% with epinephrine,24 then take an 8-mm punch biopsy encompassing 75% perilesional skin and 25% of the blister centered on the line (Figure 2). After separating the punch specimen from the subcutaneous tissue with surgical scissors, hold the tissue with forceps and bisect the specimen with a no. 15 scalpel blade. Use a sawing motion along the line drawn in the prior steps. Submit half of the biopsy for H&E staining in formalin and the other half for DIF in Zeus (or Michel) medium (Figure 3).
Advantages
This approach offers several advantages. First, when biopsying either a small or large tense blister with this technique, only 1 invasive procedure, not 2 separate biopsies, is required. Therefore, our proposed procedures can be done quickly and efficiently with the least morbidity and scarring. Secondly, because the patient is billed for 1 biopsy instead of 2, the single punch biopsy technique is more cost effective.
The bisected specimen resulting from complete excision of a small blister or from biopsy of a larger blister that includes 75% perilesional skin and 25% from the blister cavity also provides the best tissue specimen for interpretation of the subepidermal blistering processes via H&E staining.4,20,24 When traditional unmarked punch specimens of a blister margin are sent to the laboratory in formalin for H&E staining, the technician that grosses the specimen may or may not bisect the specimen demonstrating the edge of the blister at the point where the epidermis is separated from the papillary dermis.
Finally, when the DIF specimen is prepared using either of these 2 approaches, the immunoprecipitants can be seen at the dermoepidermal junction or in the papillary dermis in the perilesional portion of the specimen.2,4 Additionally, the immunoprecipitant may be identified on the roof or floor of the blister. Although this approach has not been studied in a systematic fashion, we believe this technique provides “bonus” information (eg, the same information gained from salt-split skin indirect immunofluorescence to demonstrate if immunoprecipitants are deposited in the roof or floor of the blister).
Limitations
It is critical for the pathologist or technician grossing these specimens to understand this technique and ensure that the cut edge of each half punch specimen is properly embedded for both H&E and DIF specimens. Additionally, with either recommended technique, if the portion of perilesional skin is not sufficient and the epidermis completely separates from the dermis, interpretation of both the H&E staining and DIF sections is substantially compromised.20 Therefore, an 8-mm disposable punch is recommended to avoid mangling the specimens when they are bisected and to ensure that the epithelium is not lost. This technique is less suitable for blistering processes with a positive Nikolsky sign, such as pemphigus and toxic epidermal necrolysis, because the small area of perilesional skin adjacent to the blister may detach completely, requiring the epidermis and dermis to be evaluated separately or, in the worst-case scenario, the epidermis may be lost in processing.
Conclusion
Bisecting a single punch biopsy on subepidermal blisters provides the best specimen for H&E staining and DIF. The single punch biopsy technique also differentiates BP and EBA without utilizing salt-split skin immunofluorescence studies. This technique is more efficient and cost effective than the traditional approach of multiple biopsies on subepidermal blisters.
1. Kasperkiewicz M, Zillikens D, Schmidt E. Pemphigoid diseases: pathogenesis, diagnosis, and treatment. Autoimmunity. 2012;45:55-70.
2. Mihai S, Sitaru C. Immunopathology and molecular diagnosis of autoimmune bullous diseases. J Cell Mol Med. 2007;11:462-481.
3. Yeh SW, Ahmed B, Sami N, et al. Blistering disorders: diagnosis and treatment. Dermatol Ther. 2003;16:214-223.
4. Vesicular and bullous diseases. In: Habif TP. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. Edinburgh, Scotland: Mosby Elsevier; 2010:635-670.
5. Schmidt E, della Torre R, Borradori L. Clinical features and practical diagnosis of bullous pemphigoid. Dermatol Clin. 2011;29:427-438.
6. Caux F. Diagnosis and clinical features of epidermolysis bullosa acquisita. Dermatol Clin. 2011;29:485-491.
7. Terra JB, Jonkman MF, Diercks GF, et al. Low sensitivity of type VII collagen enzyme-linked immunosorbent assay in epidermolysis bullosa acquisita: serration pattern analysis on skin biopsy is required for diagnosis. Br J Dermatol. 2013;169:164-167.
8. Plotnikova N, Miller JL. Dermatitis herpetiformis. Skin Therapy Lett. 2013;18:1-3.
9. Culton DA, Liu Z, Diaz LA. Bullous pemphigoid. In: Goldsmith LA, Katz SI, Gilchrest BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill; 2012. http://accessmedicine.mhmedi cal.com.proxy.kcumb.edu/content.aspx?bookid=392& Sectionid=41138755. Accessed June 24, 2013.
10. Bernard P, Borradori L. Pemphigoid group. In: Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Edinburgh, Scotland: Saunders Elsevier; 2012:475-490.
11. Woodley DT, Chen M. Epidermolysis bullosa acquisita. In: Goldsmith LA, Katz SI, Gilchrest, BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill; 2012. http://access medicine.mhmedical.com.proxy.kcumb.edu/content.aspx?bookid=392&Sectionid=41138759. Accessed June 24, 2013.
12. Chronic blistering dermatoses. In: James WD, Berger TG, Elston DM. Andrew’s Diseases of the Skin. 11th ed. London, England: Saunders Elsevier; 2011:448-467.
13. Ronaghy A, Katz SI, Hall RP. Dermatitis herpetiformis. In: Goldsmith LA, Katz SI, Gilchrest, BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill; 2012. http://accessmedicine.mhmedical.com.proxy.kcumb.edu/content.aspx?bookid=392&Sectionid=41138760. Accessed June 24, 2013.
14. Hull CM, Zone JJ. Dermatitis herpetiformis and linear IgA bullous dermatosis. In: Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Edinburgh, Scotland: Saunders Elsevier; 2012:491-500.
15. Rao CL, Hall RP III. Linear immunoglobulin a dermatosis and chronic bullous disease of childhood. In: Goldsmith LA, Katz SI, Gilchrest BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill; 2012. http://accessmedicine.mhmedical.com.proxy.kcumb.edu/content.aspx?bookid=392&Sectionid=41138757. Accessed June 24, 2013.
16. Bullous disorders of childhood. In: Paller AS, Mancini AJ. Hurwitz Clinical Pediatric Dermatology: A Textbook of Skin Disorders of Childhood and Adolescence. 4th ed. Philadelphia, PA: Saunders Elsevier; 2011:303-320.
17. Inherited and autoimmune subepidermal blistering diseases. In: Caljone E, Brenn T, Lazar A, et al. McKee’s Pathology of the Skin: With Clinical Correlations. 4th ed. Edinburgh, Scotland: Elsevier Saunders; 2012:99-150.
18. Elenitsas R, Ming ME. Biopsy techniques. In: Elder DE, Elenitsas R, Johnson BL Jr, et al, eds. Lever’s Histopathology of the Skin. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008:5-6.
19. Wu H, Brandling-Bennett HA, Harrist TJ. Noninfectious vesiculobullous and vesiculopustular diseases. In: Elder DE, Elenitsas R, Johnson BL Jr, et al, eds. Lever’s Histopathology of the Skin. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008:235-278.
20. Smoller BR, Kohler S. Subepidermal vesicular dermatitis. In: Barnhill RL, Crowson AN, eds. Textbook of Dermatopathology. New York, NY: McGraw-Hill; 2004:167-194.
21. Junkins-Hopkins JM, Busam KJ. Blistering skin diseases. In: Busam KJ, ed. Dermatopathology. 2nd ed. Philadelphia, PA: Saunders Elsevier; 2010:207-248.
22. High, WA. Blistering diseases. In: Elston DM, Ferringer T, Ko C, et al, eds. Dermatopathology. Edinburgh, Scotland: Saunders Elsevier; 2009:161-172.
23. The vesicobullous reaction pattern. In: Weedon D. Weedon’s Skin Pathology. 3rd ed. Edinburgh, Scotland; Churchill Livingstone/Elsevier; 2009:93-148.
24. Alguire PC, Mathes BM. Skin biopsy techniques for the internist. J Gen Intern Med. 1998;13:46-54.
25. Sina B, Kao GF, Deng AC, et al. Skin biopsy for inflammatory and common neoplastic skin diseases: optimum time, best location and preferred techniques. a critical review. J Cutan Pathol. 2009;36:505-510.
The traditional approach for confirming the diagnosis of subepidermal blistering diseases such as bullous pemphigoid (BP), epidermolysis bullosa acquisita (EBA), dermatitis herpetifor-mis (DH), and linear IgA bullous dermatosis (LABD) requires 2 punch biopsies: one from perilesional skin for direct immunofluorescence (DIF) and one from lesional skin for light microscopy using hematoxylin and eosin (H&E) stain.1-4 These conditions are distinguished by a combination of features appreciated on H&E-stained sections, DIF, and indirect immunofluorescence for a subset of disorders. Additional information may be provided by DIF or indirect immunofluorescence utilizing the salt-split skin technique to differentiate BP (in which linear IgG deposition is identified by immunofluorescence on the roof of salt-split skin) from EBA and antiepiligrin cicatricial pemphigoid (in which linear IgG deposition is identified by immunofluorescence along the floor of the salt-split skin), which is more rare.4 One bisected punch biopsy of a subepidermal blister yields salt-split skin–like information through standard DIF and supersedes the need for the more cumbersome salt-split skin technique.
Serologic tests for the presence of circulating antibodies to BP180 and BP230 represent an emerging technology that can confirm the diagnosis of BP, but it has been difficult to identify clinically useful autoantibodies to confirm diagnoses of EBA and LABD.5-7 Serologic tests for tissue transglutaminase IgA antibodies may be useful in the diagnosis of DH.8 We present a cost-effective approach to biopsy in the diagnosis of subepidermal blistering diseases that provides the necessary diagnostic information to distinguish relevant disease processes.
Subepidermal Blistering Diseases
Bullous pemphigoid commonly presents with widespread tense bullae of varying sizes on an erythematous base or on otherwise normal skin.9 Some cases of BP present not with bullae but with pruritic, urticarial, plaquelike, or papular lesions. Bullous pemphigoid commonly involves flexural surfaces and the trunk but can appear anywhere on the skin. The induction of blisters by shearing with mechanical pressure on perilesional skin (Nikolsky sign) is not characteristically present in BP as it is in pemphigus vulgaris.10 Epidermolysis bullosa acquisita can mimic BP in the development of widespread tense bullae, but blisters typically appear on areas of the skin that are prone to trauma (eg, toes, knees, elbows, hands). Crusted erosions, scarring, and milia also are clinical manifestations of EBA.11 Dermatitis herpetiformis presents with grouped vesicles, papulovesicles, plaques, and excoriations that are symmetrically distributed on extensor surfaces of the skin but also can occur on the buttocks, scalp, and other areas of the skin.12,13 Although it may mimic both BP and DH, LABD frequently is less pruritic than these other conditions.14,15 Linear IgA bullous dermatosis also demonstrates the characteristic finding of multiple bullae that form concentrically around a crusted area of skin. This physical finding is known as a string of pearls. Linear IgA bullous dermatosis typically occurs in childhood and may resolve without treatment in months to years.16
Traditional Biopsy Approach
A review of several articles from the literature and multiple dermatology and dermatopathology textbooks revealed uniform recommendations for biopsy of subepidermal blistering conditions that manifest as tense blisters.1-4,9-23 A biopsy of early lesional skin or of a blister for light microscopy with H&E stain and biopsy of perilesional skin for DIF is recommended.1-4,9-23 Three review articles specifically suggested biopsy of “perilesional skin” for DIF.1-3 The majority of textbooks we reviewed also suggested that perilesional skin, or skin adjacent to a zone of erythema in the case of DH, should be sampled for DIF to assist in the diagnosis of BP, EBA, DH, and LABD.4,9-21 Biopsy of adjacent or nonlesional skin or skin around the lesion for DIF also was recommended by other textbooks for diagnosis of subepidermal blistering diseases.22,23 Perilesional skin is chosen because it is critical that the epidermis be included for adequate immunofluorescence studies.5,20 Biopsy of healed and crusted lesions should be avoided.24
Recommended Alternative Approach
A single punch biopsy produces the best possible specimen for light microscopy with H&E stain and DIF if it is obtained via one of 2 methods.
The first method involves choosing a small, 1- to 2-mm tense blister.25 Use an 8-mm punch centered on the blister that includes at least 3 mm of circumferential perilesional skin (Figures 1 and 2).20 Holding the specimen with forceps, use a no. 15 scalpel blade to bisect the blister with a sawing motion. Place half of the specimen in formalin for H&E staining and the other half in Zeus (or Michel) medium for DIF (Figure 3).
|
|
|
The second method is to choose any large blister and, utilizing a surgical marker, draw a line from the roof of the blister onto the adjacent perilesional skin (Figure 1).20,24 After blotting with an alcohol pad so as not to remove the mark, anesthetize the site with lidocaine 1% with epinephrine,24 then take an 8-mm punch biopsy encompassing 75% perilesional skin and 25% of the blister centered on the line (Figure 2). After separating the punch specimen from the subcutaneous tissue with surgical scissors, hold the tissue with forceps and bisect the specimen with a no. 15 scalpel blade. Use a sawing motion along the line drawn in the prior steps. Submit half of the biopsy for H&E staining in formalin and the other half for DIF in Zeus (or Michel) medium (Figure 3).
Advantages
This approach offers several advantages. First, when biopsying either a small or large tense blister with this technique, only 1 invasive procedure, not 2 separate biopsies, is required. Therefore, our proposed procedures can be done quickly and efficiently with the least morbidity and scarring. Secondly, because the patient is billed for 1 biopsy instead of 2, the single punch biopsy technique is more cost effective.
The bisected specimen resulting from complete excision of a small blister or from biopsy of a larger blister that includes 75% perilesional skin and 25% from the blister cavity also provides the best tissue specimen for interpretation of the subepidermal blistering processes via H&E staining.4,20,24 When traditional unmarked punch specimens of a blister margin are sent to the laboratory in formalin for H&E staining, the technician that grosses the specimen may or may not bisect the specimen demonstrating the edge of the blister at the point where the epidermis is separated from the papillary dermis.
Finally, when the DIF specimen is prepared using either of these 2 approaches, the immunoprecipitants can be seen at the dermoepidermal junction or in the papillary dermis in the perilesional portion of the specimen.2,4 Additionally, the immunoprecipitant may be identified on the roof or floor of the blister. Although this approach has not been studied in a systematic fashion, we believe this technique provides “bonus” information (eg, the same information gained from salt-split skin indirect immunofluorescence to demonstrate if immunoprecipitants are deposited in the roof or floor of the blister).
Limitations
It is critical for the pathologist or technician grossing these specimens to understand this technique and ensure that the cut edge of each half punch specimen is properly embedded for both H&E and DIF specimens. Additionally, with either recommended technique, if the portion of perilesional skin is not sufficient and the epidermis completely separates from the dermis, interpretation of both the H&E staining and DIF sections is substantially compromised.20 Therefore, an 8-mm disposable punch is recommended to avoid mangling the specimens when they are bisected and to ensure that the epithelium is not lost. This technique is less suitable for blistering processes with a positive Nikolsky sign, such as pemphigus and toxic epidermal necrolysis, because the small area of perilesional skin adjacent to the blister may detach completely, requiring the epidermis and dermis to be evaluated separately or, in the worst-case scenario, the epidermis may be lost in processing.
Conclusion
Bisecting a single punch biopsy on subepidermal blisters provides the best specimen for H&E staining and DIF. The single punch biopsy technique also differentiates BP and EBA without utilizing salt-split skin immunofluorescence studies. This technique is more efficient and cost effective than the traditional approach of multiple biopsies on subepidermal blisters.
The traditional approach for confirming the diagnosis of subepidermal blistering diseases such as bullous pemphigoid (BP), epidermolysis bullosa acquisita (EBA), dermatitis herpetifor-mis (DH), and linear IgA bullous dermatosis (LABD) requires 2 punch biopsies: one from perilesional skin for direct immunofluorescence (DIF) and one from lesional skin for light microscopy using hematoxylin and eosin (H&E) stain.1-4 These conditions are distinguished by a combination of features appreciated on H&E-stained sections, DIF, and indirect immunofluorescence for a subset of disorders. Additional information may be provided by DIF or indirect immunofluorescence utilizing the salt-split skin technique to differentiate BP (in which linear IgG deposition is identified by immunofluorescence on the roof of salt-split skin) from EBA and antiepiligrin cicatricial pemphigoid (in which linear IgG deposition is identified by immunofluorescence along the floor of the salt-split skin), which is more rare.4 One bisected punch biopsy of a subepidermal blister yields salt-split skin–like information through standard DIF and supersedes the need for the more cumbersome salt-split skin technique.
Serologic tests for the presence of circulating antibodies to BP180 and BP230 represent an emerging technology that can confirm the diagnosis of BP, but it has been difficult to identify clinically useful autoantibodies to confirm diagnoses of EBA and LABD.5-7 Serologic tests for tissue transglutaminase IgA antibodies may be useful in the diagnosis of DH.8 We present a cost-effective approach to biopsy in the diagnosis of subepidermal blistering diseases that provides the necessary diagnostic information to distinguish relevant disease processes.
Subepidermal Blistering Diseases
Bullous pemphigoid commonly presents with widespread tense bullae of varying sizes on an erythematous base or on otherwise normal skin.9 Some cases of BP present not with bullae but with pruritic, urticarial, plaquelike, or papular lesions. Bullous pemphigoid commonly involves flexural surfaces and the trunk but can appear anywhere on the skin. The induction of blisters by shearing with mechanical pressure on perilesional skin (Nikolsky sign) is not characteristically present in BP as it is in pemphigus vulgaris.10 Epidermolysis bullosa acquisita can mimic BP in the development of widespread tense bullae, but blisters typically appear on areas of the skin that are prone to trauma (eg, toes, knees, elbows, hands). Crusted erosions, scarring, and milia also are clinical manifestations of EBA.11 Dermatitis herpetiformis presents with grouped vesicles, papulovesicles, plaques, and excoriations that are symmetrically distributed on extensor surfaces of the skin but also can occur on the buttocks, scalp, and other areas of the skin.12,13 Although it may mimic both BP and DH, LABD frequently is less pruritic than these other conditions.14,15 Linear IgA bullous dermatosis also demonstrates the characteristic finding of multiple bullae that form concentrically around a crusted area of skin. This physical finding is known as a string of pearls. Linear IgA bullous dermatosis typically occurs in childhood and may resolve without treatment in months to years.16
Traditional Biopsy Approach
A review of several articles from the literature and multiple dermatology and dermatopathology textbooks revealed uniform recommendations for biopsy of subepidermal blistering conditions that manifest as tense blisters.1-4,9-23 A biopsy of early lesional skin or of a blister for light microscopy with H&E stain and biopsy of perilesional skin for DIF is recommended.1-4,9-23 Three review articles specifically suggested biopsy of “perilesional skin” for DIF.1-3 The majority of textbooks we reviewed also suggested that perilesional skin, or skin adjacent to a zone of erythema in the case of DH, should be sampled for DIF to assist in the diagnosis of BP, EBA, DH, and LABD.4,9-21 Biopsy of adjacent or nonlesional skin or skin around the lesion for DIF also was recommended by other textbooks for diagnosis of subepidermal blistering diseases.22,23 Perilesional skin is chosen because it is critical that the epidermis be included for adequate immunofluorescence studies.5,20 Biopsy of healed and crusted lesions should be avoided.24
Recommended Alternative Approach
A single punch biopsy produces the best possible specimen for light microscopy with H&E stain and DIF if it is obtained via one of 2 methods.
The first method involves choosing a small, 1- to 2-mm tense blister.25 Use an 8-mm punch centered on the blister that includes at least 3 mm of circumferential perilesional skin (Figures 1 and 2).20 Holding the specimen with forceps, use a no. 15 scalpel blade to bisect the blister with a sawing motion. Place half of the specimen in formalin for H&E staining and the other half in Zeus (or Michel) medium for DIF (Figure 3).
|
|
|
The second method is to choose any large blister and, utilizing a surgical marker, draw a line from the roof of the blister onto the adjacent perilesional skin (Figure 1).20,24 After blotting with an alcohol pad so as not to remove the mark, anesthetize the site with lidocaine 1% with epinephrine,24 then take an 8-mm punch biopsy encompassing 75% perilesional skin and 25% of the blister centered on the line (Figure 2). After separating the punch specimen from the subcutaneous tissue with surgical scissors, hold the tissue with forceps and bisect the specimen with a no. 15 scalpel blade. Use a sawing motion along the line drawn in the prior steps. Submit half of the biopsy for H&E staining in formalin and the other half for DIF in Zeus (or Michel) medium (Figure 3).
Advantages
This approach offers several advantages. First, when biopsying either a small or large tense blister with this technique, only 1 invasive procedure, not 2 separate biopsies, is required. Therefore, our proposed procedures can be done quickly and efficiently with the least morbidity and scarring. Secondly, because the patient is billed for 1 biopsy instead of 2, the single punch biopsy technique is more cost effective.
The bisected specimen resulting from complete excision of a small blister or from biopsy of a larger blister that includes 75% perilesional skin and 25% from the blister cavity also provides the best tissue specimen for interpretation of the subepidermal blistering processes via H&E staining.4,20,24 When traditional unmarked punch specimens of a blister margin are sent to the laboratory in formalin for H&E staining, the technician that grosses the specimen may or may not bisect the specimen demonstrating the edge of the blister at the point where the epidermis is separated from the papillary dermis.
Finally, when the DIF specimen is prepared using either of these 2 approaches, the immunoprecipitants can be seen at the dermoepidermal junction or in the papillary dermis in the perilesional portion of the specimen.2,4 Additionally, the immunoprecipitant may be identified on the roof or floor of the blister. Although this approach has not been studied in a systematic fashion, we believe this technique provides “bonus” information (eg, the same information gained from salt-split skin indirect immunofluorescence to demonstrate if immunoprecipitants are deposited in the roof or floor of the blister).
Limitations
It is critical for the pathologist or technician grossing these specimens to understand this technique and ensure that the cut edge of each half punch specimen is properly embedded for both H&E and DIF specimens. Additionally, with either recommended technique, if the portion of perilesional skin is not sufficient and the epidermis completely separates from the dermis, interpretation of both the H&E staining and DIF sections is substantially compromised.20 Therefore, an 8-mm disposable punch is recommended to avoid mangling the specimens when they are bisected and to ensure that the epithelium is not lost. This technique is less suitable for blistering processes with a positive Nikolsky sign, such as pemphigus and toxic epidermal necrolysis, because the small area of perilesional skin adjacent to the blister may detach completely, requiring the epidermis and dermis to be evaluated separately or, in the worst-case scenario, the epidermis may be lost in processing.
Conclusion
Bisecting a single punch biopsy on subepidermal blisters provides the best specimen for H&E staining and DIF. The single punch biopsy technique also differentiates BP and EBA without utilizing salt-split skin immunofluorescence studies. This technique is more efficient and cost effective than the traditional approach of multiple biopsies on subepidermal blisters.
1. Kasperkiewicz M, Zillikens D, Schmidt E. Pemphigoid diseases: pathogenesis, diagnosis, and treatment. Autoimmunity. 2012;45:55-70.
2. Mihai S, Sitaru C. Immunopathology and molecular diagnosis of autoimmune bullous diseases. J Cell Mol Med. 2007;11:462-481.
3. Yeh SW, Ahmed B, Sami N, et al. Blistering disorders: diagnosis and treatment. Dermatol Ther. 2003;16:214-223.
4. Vesicular and bullous diseases. In: Habif TP. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. Edinburgh, Scotland: Mosby Elsevier; 2010:635-670.
5. Schmidt E, della Torre R, Borradori L. Clinical features and practical diagnosis of bullous pemphigoid. Dermatol Clin. 2011;29:427-438.
6. Caux F. Diagnosis and clinical features of epidermolysis bullosa acquisita. Dermatol Clin. 2011;29:485-491.
7. Terra JB, Jonkman MF, Diercks GF, et al. Low sensitivity of type VII collagen enzyme-linked immunosorbent assay in epidermolysis bullosa acquisita: serration pattern analysis on skin biopsy is required for diagnosis. Br J Dermatol. 2013;169:164-167.
8. Plotnikova N, Miller JL. Dermatitis herpetiformis. Skin Therapy Lett. 2013;18:1-3.
9. Culton DA, Liu Z, Diaz LA. Bullous pemphigoid. In: Goldsmith LA, Katz SI, Gilchrest BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill; 2012. http://accessmedicine.mhmedi cal.com.proxy.kcumb.edu/content.aspx?bookid=392& Sectionid=41138755. Accessed June 24, 2013.
10. Bernard P, Borradori L. Pemphigoid group. In: Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Edinburgh, Scotland: Saunders Elsevier; 2012:475-490.
11. Woodley DT, Chen M. Epidermolysis bullosa acquisita. In: Goldsmith LA, Katz SI, Gilchrest, BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill; 2012. http://access medicine.mhmedical.com.proxy.kcumb.edu/content.aspx?bookid=392&Sectionid=41138759. Accessed June 24, 2013.
12. Chronic blistering dermatoses. In: James WD, Berger TG, Elston DM. Andrew’s Diseases of the Skin. 11th ed. London, England: Saunders Elsevier; 2011:448-467.
13. Ronaghy A, Katz SI, Hall RP. Dermatitis herpetiformis. In: Goldsmith LA, Katz SI, Gilchrest, BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill; 2012. http://accessmedicine.mhmedical.com.proxy.kcumb.edu/content.aspx?bookid=392&Sectionid=41138760. Accessed June 24, 2013.
14. Hull CM, Zone JJ. Dermatitis herpetiformis and linear IgA bullous dermatosis. In: Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Edinburgh, Scotland: Saunders Elsevier; 2012:491-500.
15. Rao CL, Hall RP III. Linear immunoglobulin a dermatosis and chronic bullous disease of childhood. In: Goldsmith LA, Katz SI, Gilchrest BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill; 2012. http://accessmedicine.mhmedical.com.proxy.kcumb.edu/content.aspx?bookid=392&Sectionid=41138757. Accessed June 24, 2013.
16. Bullous disorders of childhood. In: Paller AS, Mancini AJ. Hurwitz Clinical Pediatric Dermatology: A Textbook of Skin Disorders of Childhood and Adolescence. 4th ed. Philadelphia, PA: Saunders Elsevier; 2011:303-320.
17. Inherited and autoimmune subepidermal blistering diseases. In: Caljone E, Brenn T, Lazar A, et al. McKee’s Pathology of the Skin: With Clinical Correlations. 4th ed. Edinburgh, Scotland: Elsevier Saunders; 2012:99-150.
18. Elenitsas R, Ming ME. Biopsy techniques. In: Elder DE, Elenitsas R, Johnson BL Jr, et al, eds. Lever’s Histopathology of the Skin. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008:5-6.
19. Wu H, Brandling-Bennett HA, Harrist TJ. Noninfectious vesiculobullous and vesiculopustular diseases. In: Elder DE, Elenitsas R, Johnson BL Jr, et al, eds. Lever’s Histopathology of the Skin. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008:235-278.
20. Smoller BR, Kohler S. Subepidermal vesicular dermatitis. In: Barnhill RL, Crowson AN, eds. Textbook of Dermatopathology. New York, NY: McGraw-Hill; 2004:167-194.
21. Junkins-Hopkins JM, Busam KJ. Blistering skin diseases. In: Busam KJ, ed. Dermatopathology. 2nd ed. Philadelphia, PA: Saunders Elsevier; 2010:207-248.
22. High, WA. Blistering diseases. In: Elston DM, Ferringer T, Ko C, et al, eds. Dermatopathology. Edinburgh, Scotland: Saunders Elsevier; 2009:161-172.
23. The vesicobullous reaction pattern. In: Weedon D. Weedon’s Skin Pathology. 3rd ed. Edinburgh, Scotland; Churchill Livingstone/Elsevier; 2009:93-148.
24. Alguire PC, Mathes BM. Skin biopsy techniques for the internist. J Gen Intern Med. 1998;13:46-54.
25. Sina B, Kao GF, Deng AC, et al. Skin biopsy for inflammatory and common neoplastic skin diseases: optimum time, best location and preferred techniques. a critical review. J Cutan Pathol. 2009;36:505-510.
1. Kasperkiewicz M, Zillikens D, Schmidt E. Pemphigoid diseases: pathogenesis, diagnosis, and treatment. Autoimmunity. 2012;45:55-70.
2. Mihai S, Sitaru C. Immunopathology and molecular diagnosis of autoimmune bullous diseases. J Cell Mol Med. 2007;11:462-481.
3. Yeh SW, Ahmed B, Sami N, et al. Blistering disorders: diagnosis and treatment. Dermatol Ther. 2003;16:214-223.
4. Vesicular and bullous diseases. In: Habif TP. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. Edinburgh, Scotland: Mosby Elsevier; 2010:635-670.
5. Schmidt E, della Torre R, Borradori L. Clinical features and practical diagnosis of bullous pemphigoid. Dermatol Clin. 2011;29:427-438.
6. Caux F. Diagnosis and clinical features of epidermolysis bullosa acquisita. Dermatol Clin. 2011;29:485-491.
7. Terra JB, Jonkman MF, Diercks GF, et al. Low sensitivity of type VII collagen enzyme-linked immunosorbent assay in epidermolysis bullosa acquisita: serration pattern analysis on skin biopsy is required for diagnosis. Br J Dermatol. 2013;169:164-167.
8. Plotnikova N, Miller JL. Dermatitis herpetiformis. Skin Therapy Lett. 2013;18:1-3.
9. Culton DA, Liu Z, Diaz LA. Bullous pemphigoid. In: Goldsmith LA, Katz SI, Gilchrest BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill; 2012. http://accessmedicine.mhmedi cal.com.proxy.kcumb.edu/content.aspx?bookid=392& Sectionid=41138755. Accessed June 24, 2013.
10. Bernard P, Borradori L. Pemphigoid group. In: Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Edinburgh, Scotland: Saunders Elsevier; 2012:475-490.
11. Woodley DT, Chen M. Epidermolysis bullosa acquisita. In: Goldsmith LA, Katz SI, Gilchrest, BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill; 2012. http://access medicine.mhmedical.com.proxy.kcumb.edu/content.aspx?bookid=392&Sectionid=41138759. Accessed June 24, 2013.
12. Chronic blistering dermatoses. In: James WD, Berger TG, Elston DM. Andrew’s Diseases of the Skin. 11th ed. London, England: Saunders Elsevier; 2011:448-467.
13. Ronaghy A, Katz SI, Hall RP. Dermatitis herpetiformis. In: Goldsmith LA, Katz SI, Gilchrest, BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill; 2012. http://accessmedicine.mhmedical.com.proxy.kcumb.edu/content.aspx?bookid=392&Sectionid=41138760. Accessed June 24, 2013.
14. Hull CM, Zone JJ. Dermatitis herpetiformis and linear IgA bullous dermatosis. In: Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Edinburgh, Scotland: Saunders Elsevier; 2012:491-500.
15. Rao CL, Hall RP III. Linear immunoglobulin a dermatosis and chronic bullous disease of childhood. In: Goldsmith LA, Katz SI, Gilchrest BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill; 2012. http://accessmedicine.mhmedical.com.proxy.kcumb.edu/content.aspx?bookid=392&Sectionid=41138757. Accessed June 24, 2013.
16. Bullous disorders of childhood. In: Paller AS, Mancini AJ. Hurwitz Clinical Pediatric Dermatology: A Textbook of Skin Disorders of Childhood and Adolescence. 4th ed. Philadelphia, PA: Saunders Elsevier; 2011:303-320.
17. Inherited and autoimmune subepidermal blistering diseases. In: Caljone E, Brenn T, Lazar A, et al. McKee’s Pathology of the Skin: With Clinical Correlations. 4th ed. Edinburgh, Scotland: Elsevier Saunders; 2012:99-150.
18. Elenitsas R, Ming ME. Biopsy techniques. In: Elder DE, Elenitsas R, Johnson BL Jr, et al, eds. Lever’s Histopathology of the Skin. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008:5-6.
19. Wu H, Brandling-Bennett HA, Harrist TJ. Noninfectious vesiculobullous and vesiculopustular diseases. In: Elder DE, Elenitsas R, Johnson BL Jr, et al, eds. Lever’s Histopathology of the Skin. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008:235-278.
20. Smoller BR, Kohler S. Subepidermal vesicular dermatitis. In: Barnhill RL, Crowson AN, eds. Textbook of Dermatopathology. New York, NY: McGraw-Hill; 2004:167-194.
21. Junkins-Hopkins JM, Busam KJ. Blistering skin diseases. In: Busam KJ, ed. Dermatopathology. 2nd ed. Philadelphia, PA: Saunders Elsevier; 2010:207-248.
22. High, WA. Blistering diseases. In: Elston DM, Ferringer T, Ko C, et al, eds. Dermatopathology. Edinburgh, Scotland: Saunders Elsevier; 2009:161-172.
23. The vesicobullous reaction pattern. In: Weedon D. Weedon’s Skin Pathology. 3rd ed. Edinburgh, Scotland; Churchill Livingstone/Elsevier; 2009:93-148.
24. Alguire PC, Mathes BM. Skin biopsy techniques for the internist. J Gen Intern Med. 1998;13:46-54.
25. Sina B, Kao GF, Deng AC, et al. Skin biopsy for inflammatory and common neoplastic skin diseases: optimum time, best location and preferred techniques. a critical review. J Cutan Pathol. 2009;36:505-510.
Practice Points
- Allergic contact dermatitis, pemphigoid, dermatitis herpetiformis, acquired epidermolysis bullosa, and porphyria cutanea tarda produce tense blisters.
- Biopsy of the edge point of a tense blister localizes immunoglobulin to the floor versus the roof on
direct immunofluorescence. - A punch biopsy should include 75% perilesional skin at the edge of a blister.
- Marking the blister with a skin marker will assure that the tissue is properly oriented when bisected at the bedside.
How Much Is Too Much Cancer Screening?
Overdetection—when a cancerous lesion is found that would otherwise not have caused any symptoms or early death—is considered the most important adverse effect (AE) of cancer screening, leading to unnecessary tests and treatment. But when do nonclinicians believe detection crosses that threshold?
Researchers from the University of Oxford in the United Kingdom (UK) surveyed 1,000 adults about 3 types of cancer screening: breast, prostate, and bowel. For each type, they presented the absolute number of cases per year in the UK and described the treatment, including AEs. They also presented 2 hypothetical screening scenarios, both of which represented a population of 1,000 adults with a 5% incidence of cancer and 1% cancer-specific mortality. The first scenario represented a 10% reduction of cancer-specific mortality as a result of screening; the second a 50% reduction. All information was presented in written format with absolute numbers and in graphics, to aid understanding. Throughout, the researchers used the term overdetection, rather than overdiagnosis, to avoid confusion with misdiagnosis (something documented in earlier studies).
Related: Timely Assessment of Cancer Symptoms
Of the survey respondents, 48 had a previous cancer diagnosis and 54% had been screened for cancer at least once.
The researchers found significantly higher screening acceptance rates for the 50% reduction compared with the 10% reduction (P < .001), although, they add, “acceptability of overdetection did not increase 5-fold when benefit increased 5-fold.” Women accepted more overdetection in breast cancer than in bowel cancer; men accepted more overdetection in prostate cancer than in bowel cancer.
Related: Early Cancer Detection Helps Underserved Women
Across all scenarios, 3.5% to 7.4% of people said they would not accept any level of overdetection. By contrast, 7.1% to 13.9% would accept the entire population of 1,000 people being overdetected to avoid 1 or 5 people dying of cancer.
Patient education leaflets rarely discuss overdetection, the researchers noted. Clearly, there is room for more education, and not only for potential patients, but also for health care providers. Evidence suggests, they say, that clinicians have an equally poor understanding of diagnostic accuracy.
Source
Van den Bruel A, Jones C, Yang Y, Oke J, Hewitson P. BMJ. 2015;350:h980.
doi: 10.1136/bmj.h980.
Overdetection—when a cancerous lesion is found that would otherwise not have caused any symptoms or early death—is considered the most important adverse effect (AE) of cancer screening, leading to unnecessary tests and treatment. But when do nonclinicians believe detection crosses that threshold?
Researchers from the University of Oxford in the United Kingdom (UK) surveyed 1,000 adults about 3 types of cancer screening: breast, prostate, and bowel. For each type, they presented the absolute number of cases per year in the UK and described the treatment, including AEs. They also presented 2 hypothetical screening scenarios, both of which represented a population of 1,000 adults with a 5% incidence of cancer and 1% cancer-specific mortality. The first scenario represented a 10% reduction of cancer-specific mortality as a result of screening; the second a 50% reduction. All information was presented in written format with absolute numbers and in graphics, to aid understanding. Throughout, the researchers used the term overdetection, rather than overdiagnosis, to avoid confusion with misdiagnosis (something documented in earlier studies).
Related: Timely Assessment of Cancer Symptoms
Of the survey respondents, 48 had a previous cancer diagnosis and 54% had been screened for cancer at least once.
The researchers found significantly higher screening acceptance rates for the 50% reduction compared with the 10% reduction (P < .001), although, they add, “acceptability of overdetection did not increase 5-fold when benefit increased 5-fold.” Women accepted more overdetection in breast cancer than in bowel cancer; men accepted more overdetection in prostate cancer than in bowel cancer.
Related: Early Cancer Detection Helps Underserved Women
Across all scenarios, 3.5% to 7.4% of people said they would not accept any level of overdetection. By contrast, 7.1% to 13.9% would accept the entire population of 1,000 people being overdetected to avoid 1 or 5 people dying of cancer.
Patient education leaflets rarely discuss overdetection, the researchers noted. Clearly, there is room for more education, and not only for potential patients, but also for health care providers. Evidence suggests, they say, that clinicians have an equally poor understanding of diagnostic accuracy.
Source
Van den Bruel A, Jones C, Yang Y, Oke J, Hewitson P. BMJ. 2015;350:h980.
doi: 10.1136/bmj.h980.
Overdetection—when a cancerous lesion is found that would otherwise not have caused any symptoms or early death—is considered the most important adverse effect (AE) of cancer screening, leading to unnecessary tests and treatment. But when do nonclinicians believe detection crosses that threshold?
Researchers from the University of Oxford in the United Kingdom (UK) surveyed 1,000 adults about 3 types of cancer screening: breast, prostate, and bowel. For each type, they presented the absolute number of cases per year in the UK and described the treatment, including AEs. They also presented 2 hypothetical screening scenarios, both of which represented a population of 1,000 adults with a 5% incidence of cancer and 1% cancer-specific mortality. The first scenario represented a 10% reduction of cancer-specific mortality as a result of screening; the second a 50% reduction. All information was presented in written format with absolute numbers and in graphics, to aid understanding. Throughout, the researchers used the term overdetection, rather than overdiagnosis, to avoid confusion with misdiagnosis (something documented in earlier studies).
Related: Timely Assessment of Cancer Symptoms
Of the survey respondents, 48 had a previous cancer diagnosis and 54% had been screened for cancer at least once.
The researchers found significantly higher screening acceptance rates for the 50% reduction compared with the 10% reduction (P < .001), although, they add, “acceptability of overdetection did not increase 5-fold when benefit increased 5-fold.” Women accepted more overdetection in breast cancer than in bowel cancer; men accepted more overdetection in prostate cancer than in bowel cancer.
Related: Early Cancer Detection Helps Underserved Women
Across all scenarios, 3.5% to 7.4% of people said they would not accept any level of overdetection. By contrast, 7.1% to 13.9% would accept the entire population of 1,000 people being overdetected to avoid 1 or 5 people dying of cancer.
Patient education leaflets rarely discuss overdetection, the researchers noted. Clearly, there is room for more education, and not only for potential patients, but also for health care providers. Evidence suggests, they say, that clinicians have an equally poor understanding of diagnostic accuracy.
Source
Van den Bruel A, Jones C, Yang Y, Oke J, Hewitson P. BMJ. 2015;350:h980.
doi: 10.1136/bmj.h980.
A Systematic Review of Tibialis Anterior Tendon Rupture Treatments and Outcomes
Subcutaneous rupture of the tibialis anterior (TA) tendon has been reported predominantly in case reports and small case series because of the relative rarity of the injury. Unlike traumatic lacerations or open injuries to the tendon, subcutaneous injuries often go unnoticed by patients because of compensation by surrounding dorsiflexors of the foot and toes—namely, the extensor hallucis longus (EHL) and the extensor digitorum longus (EDL).1 This can delay presentation to an orthopedic surgeon and lead to difficulties in treatment, such as allograft or autograft being required if primary repair is no longer possible. Case reports and series have described treatment methods as well as anecdotal evidence of outcomes after operative repair or conservative treatment, but there have been no comprehensive systematic reviews of outcomes after various types of treatment. Authors have come to conclusions about expected outcomes based on patient age, time to treatment, treatment used, and other variables, but no reviews have examined these variables across multiple studies. Given the low level of the evidence presented in most of these reports, it is difficult to perform a meta-analysis of the data.
Instead, we systematically reviewed 87 cases from all pertinent studies and examined commonly reported data, such as patient age, time to treatment, treatment used, and outcome. Using the PICO (population, intervention, comparison, outcome) model for systematic reviews, we looked at patients who had closed, spontaneous, complete rupture of the TA tendon and underwent operative repair or conservative treatment of the injury. Outcomes surveyed included successful operative repair or conservative treatment, as measured by objective systems, such as MMSS (Manual Muscle Strength Scale) score, AOFAS (American Orthopaedic Foot and Ankle Society) hindfoot score, and FAOS (Foot and Ankle Outcome Score) testing, or by subjective description of posttreatment outcome.
We intend this review to serve as a guide for surgeons who find themselves treating a ruptured TA tendon, a relatively rare injury. They will be able to select the operative technique or conservative treatment that best matches the patient’s needs, based on comparison with previous case studies.
Materials and Methods
The cases reviewed for this study were found through a comprehensive PubMed search and an independent review of references cited in similar articles. Articles included were published between 1975 and 2012, inclusive. The latest search was performed on March 22, 2013. The search criteria were tibialis anterior [Title/Abstract] OR anterior tibial [Title/Abstract] AND rupture [Title/Abstract]) AND surgery. Only English-language articles, or articles already translated into English, were included. Eligible studies described cases of closed tendon rupture. No traumatic lacerations or open ruptures were included. If a study described both open and subcutaneous ruptures, only the subcutaneous cases were included. Further, partial ruptures were not included. In addition, ruptures caused directly by a known comorbid condition—for example, a rupture caused by a gouty tophaceous deposit at the site of rupture2—were not included. Data were extracted from publications independently and analyzed in a Microsoft Excel workbook (Microsoft, Redmond, Washington). Variables examined included patient age and sex, side involved, time to treatment, mechanism of injury, defect size, predisposing comorbidities, surgery or conservative treatment, type of operative repair (if applicable), graft used (if applicable), pretreatment function (by independent scoring system, if applicable), and posttreatment function. These variables were not necessarily reported in all the studies.
A potential bias exists in our PubMed search. As the query was specific for studies that included operative repair of a ruptured TA tendon, case studies that involved only conservative treatment were excluded. However, the primary goal of this review was to compare operative possibilities and the patient characteristics and outcomes associated with these surgeries.
Results
Figure 1 shows the criteria used to select eligible papers for review. Twenty-three papers matched the criteria.3-25 Data were independently extracted from these papers, as described in the Methods section. Again, not all variables were reported by all authors. Sammarco and colleagues21 reported time to treatment as a mean for 2 groups: 8 cases defined as “early” treatment (mean time to treatment, 0.625 months) and 11 defined as “late” treatment (mean time to treatment, 10.7 months). These mean times were therefore used independently for each case in calculating mean time to treatment for this systematic review.
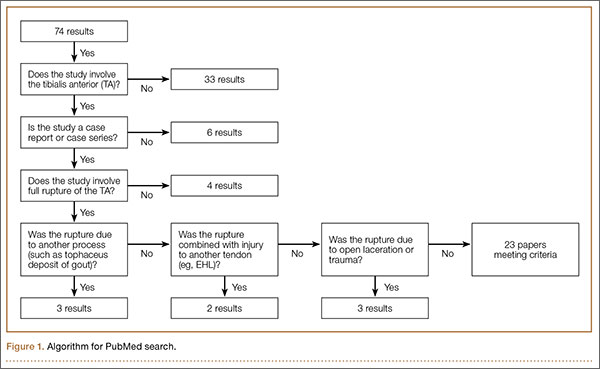
Table 1 lists the demographics. There were 40 male and 25 female patients, and 22 cases in which sex was not specified. Mean age was 63.9 years (surgery group), 72.4 years (conservative treatment group), and 65.8 years (overall). Of the 87 patients, 72 underwent surgery, and 15 were treated with conservative measures.
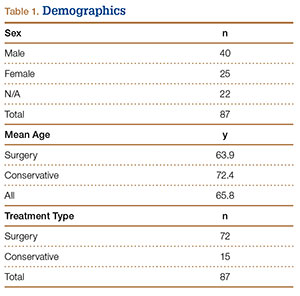
Table 2 lists the operative techniques identified. Of the 72 surgeries, 23 were primary repairs, 12 were primary repairs of the anatomical insertion, and 18 involved use of autograft.
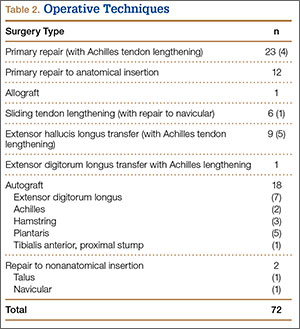
Time to treatment was available for 54 of the 87 cases (Table 3). Primary repair was most often performed in cases in which the injury was less than 3 months old, and autograft was most often used in cases in which the injury occurred more than 3 months before presentation.
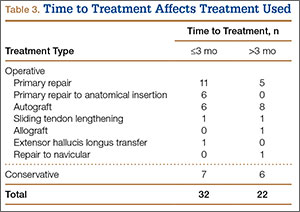
Posttreatment outcome scores were available for 59 cases. Only 3 authors reported preoperative scores.5,21,24 None of the authors who used conservative treatment measures reported pretreatment scores. Scores used included the MMSS score (26 cases), the AOFAS hindfoot score (16 cases),26 the FAOS (17 cases),27 and the Tinetti gait and balance score (3 cases; the author also used the MMSS score).28Table 4 lists the mean posttreatment scores for patients who underwent surgery and patients treated conservatively. AOFAS, MMSS, and Tinetti scores and FAOS were used by authors presenting operative treatment outcomes. Only posttreatment FAOS was available for both surgery (84.4/100) and conservative treatment (69.4/100).
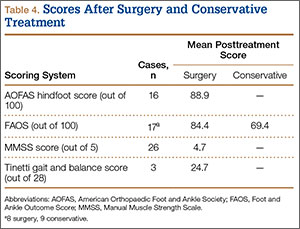
Discussion
Closed rupture of the TA tendon is a relatively rare entity occurring mostly in older patients without any history of acute, traumatic injury. Some patients, however, recall a particular moment of rupture, often accompanied immediately by pain and swelling, which eventually resolve. Later sequelae include footdrop with associated steppage gait and a palpable mass on the dorsal aspect of the ankle.3,21 Chronic TA tendon rupture can also lead to clawing of the toes as the other foot extensors (EHL, EDL) overcompensate. Cohen and Gordon1 described the case of a patient who ruptured a TA tendon 25 years earlier and then, in the absence of operative repair, developed hypertrophy of the EHL and the EDL. This extensor substitution led to hammer toes and plantar prominence of the metatarsal heads, ultimately leading to moderate pain and a neuroma. Although this particular outcome is likely rare, the more common sequelae of footdrop, flatfoot, Achilles tendon contracture, and compromised gait are reason enough to consider operative repair for any ruptured TA tendon.
Most previous studies of TA tendon rupture were case reports and case studies. In the largest series, Sammarco and colleagues21 described 19 cases of closed rupture. These included 3 traumatic cases, 1 by blunt trauma to the tendon and 2 of open laceration, all treated surgically with various methods. Unfortunately, these 3 traumatic cases were not separated in the authors’ analysis and therefore had to be included in this systematic review. Including them here did not compromise our goals in this review, which included examining typical patient demographics and the most common methods of operative repair.
Conservative measures remain a treatment possibility for some patients. We found that patients treated with conservative measures historically have been older (mean age, 72.4 years) than patients treated surgically (mean age, 63.9 years). However, advanced age itself is not a contraindication for operative repair of a TA tendon rupture, and authors have described positive outcomes for active, elderly (>70 years) patients who wanted to maintain their activity level and therefore opted for operative repair.7,8,10,13,16,24 Ouzounian and Anderson18 described functional limitations (eg, persistent footdrop, slapfoot gait, limitations in walking) after conservative treatment with an ankle-foot orthosis. Operative repair offers the chance for better functional outcome for patients who are surgical candidates and lead even a mildly active lifestyle.
Of operative repair methods, primary repair is used most often. This technique, however, must be allowed by the gap between the 2 ruptured ends after débridement of any necrotic tissue. If the distal stump is not viable, primary repair of the proximal stump to the native anatomical insertion is feasible. Figure 2, reprinted from a case report by Rajagopalan and colleagues,19 shows a ligament–osseous reattachment of the proximal stump using suture anchors to the medial cuneiform. Both primary repair and repair to the anatomical insertion can be augmented with Achilles tendon lengthening if needed to achieve balance between flexor and extensor functions of the ankle.
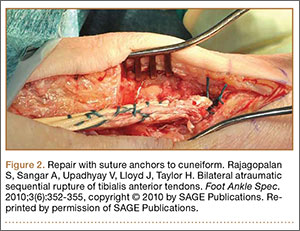
If the gap between the 2 stumps cannot be covered by the native tendon, then autograft, another surgical technique with positive outcomes, can be used. The most popular autograft sites historically have been the EDL, Achilles, and plantaris tendons. In addition, Goehring and Liakos9 described 3 cases of good results with semitendinosus autograft. Sapkas and colleagues22 used a free-sliding TA graft harvested from the healthy tissue of the proximal tendon stump. Their technique is depicted in Figure 3. Sliding tendon lengthening, well described by Trout and colleagues24 in a case study, is feasible for use of the native tendon when there is a gap to bridge between the 2 stumps of ruptured tendon. EHL or EDL transfer with or without Achilles lengthening is another option, albeit historically less often used.6,7 This technique is depicted in Figure 4, reprinted from a case series by Ellington and colleagues,7 who used EHL transfer with and without Achilles tendon lengthening in 9 cases.
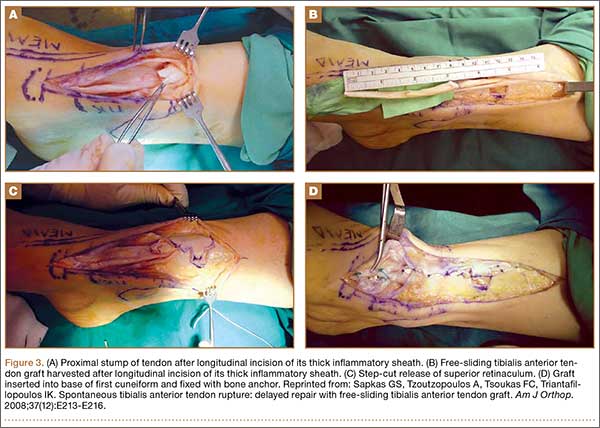
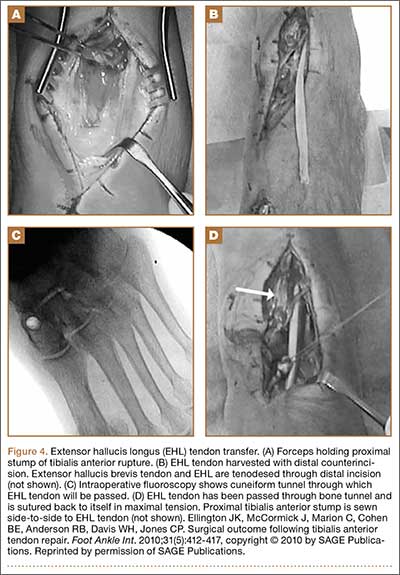
Last, less popular techniques have included repair to sites other than the medial cuneiform, including the neck of the talus and the navicular bone.10,13 An Achilles tendon allograft was used in a case described by Aderinto and Gross3 to repair a ruptured tendon found incidentally on preoperative examination for a scheduled knee arthroplasty. The patient had a postoperative MMSS score of 4/5.
Overall, primary repair is clearly preferred, but successful outcomes can be achieved by other means. As Table 3 shows, primary repair is more often used for ruptures less than 3 months old, and autograft for older ruptures. Although which operative technique to use can be decided after necrotic tissue is débrided, surgeons should try to ascertain age of injury ahead of time so that, going into surgery, they will have a better idea of the feasibility of primary repair.
Posttreatment ankle scores were not widely available. As Table 4 indicates, only FAOS was used for the conservative treatment cases. However, raw mean FAOS and raw mean AOFAS hindfoot, MMSS, and Tinetti scores showed that good outcomes and high scores can be achieved with surgery. Further, the mean FAOS reported by Gwynne-Jones and colleagues10 and Markarian and colleagues13 showed a clinically significant difference between surgery and conservative treatment. DiDomenico and colleagues,5 Sammarco and colleagues,21 and Trout and colleagues24 were the only authors who reported pretreatment and posttreatment scores.
We intend this systematic review of the literature on closed TA rupture to serve as a guide for surgeons who find themselves treating this relatively rare injury, which often presents with only a chief complaint of the foot catching while walking. Overall, the literature shows that operative repair provides very good outcomes for many patients. Patients who are surgical candidates and amenable to surgery can be counseled that operative repair leads to fewer sequelae, such as persistent footdrop and flatfooted gait, with a strong likelihood of return to baseline activity status. Patients who are not surgical candidates or are strongly against surgery can be offered conservative treatment with an ankle-foot orthosis or physical therapy, but they should also be counseled that persistent gait abnormalities and weakness in dorsiflexion are likely outcomes. Surgeons must also consider age of injury (time from probable rupture to presentation), estimating a particular moment of rupture if unknown by the patient. They can then gauge the feasibility of primary repair and, during surgery, decide which technique (primary repair, tendon transfer, autograft, or other technique) will produce the best results. They can also use scores such as the FAOS and the AOFAS hindfoot, MMSS, and Tinetti scores to compare preoperative and postoperative function, though subjective reports of return to previous activity can also serve as markers of successful repair.
This review highlights the need for further study regarding the treatment of TA ruptures. Larger, randomized studies with validated scoring systems for preoperative and postoperative function would offer more insight onto the best treatment options for these complex injuries.
1. Cohen DA, Gordon DH. The long-term effects of an untreated tibialis anterior tendon rupture. J Am Podiatr Med Assoc. 1999;89(3):149-152.
2. Jerome JTJ, Varghese M, Sankaran B, Thomas S, Thirumagal SK. Tibialis anterior tendon rupture in gout—case report and literature review. Foot Ankle Surg. 2008;14(3):166-169.
3. Aderinto J, Gross A. Delayed repair of tibialis anterior tendon rupture with Achilles tendon allograft. J Foot Ankle Surg. 2011;50(3):340-342.
4. Constantinou M, Wilson A. Traumatic tear of tibialis anterior during a Gaelic football game: a case report. Br J Sports Med. 2004;38(6):e30.
5. DiDomenico LA, Williams K, Petrolla AF. Spontaneous rupture of the anterior tibial tendon in a diabetic patient: results of operative treatment. J Foot Ankle Surg. 2008;47(5):463-467.
6. Dooley BJ, Kudelka P, Menelaus MB. Subcutaneous rupture of the tendon of tibialis anterior. J Bone Joint Surg Br. 1980;62(4):471-472.
7. Ellington JK, McCormick J, Marion C, et al. Surgical outcome following tibialis anterior tendon repair. Foot Ankle Int. 2010;31(5):412-417.
8. ElMaraghy A, Devereaux MW. Bone tunnel fixation for repair of tibialis anterior tendon rupture. Foot Ankle Surg. 2010;16(2):e47-e50.
9. Goehring M, Liakos P. Long-term outcomes following anterior tibialis tendon reconstruction with hamstring autograft in a series of 3 cases. J Foot Ankle Surg. 2009;48(2):196-202.
10. Gwynne-Jones D, Garneti N, Wyatt M. Closed tibialis anterior tendon rupture: a case series. Foot Ankle Int. 2009;30(8):758-762.
11. Kashyap S, Prince R. Spontaneous rupture of the tibialis anterior tendon. A case report. Clin Orthop. 1987;(216):159-161.
12. Kausch T, Rütt J. Subcutaneous rupture of the tibialis anterior tendon: review of the literature and a case report. Arch Orthop Trauma Surg. 1998;117(4-5):290-293.
13. Markarian GG, Kelikian AS, Brage M, Trainor T, Dias L. Anterior tibialis tendon ruptures: an outcome analysis of operative versus nonoperative treatment. Foot Ankle Int. 1998;19(12):792-802.
14. Meyn MA Jr. Closed rupture of the anterior tibial tendon. A case report and review of the literature. Clin Orthop. 1975;(113):154-157.
15. Miller RR, Mahan KT. Closed rupture of the anterior tibial tendon. A case report. J Am Podiatr Med Assoc. 1998;88(8):394-399.
16. Neumayer F, Djembi YR, Gerin A, Masquelet AC. Closed rupture of the tibialis anterior tendon: a report of 2 cases. J Foot Ankle Surg. 2009;48(4):457-461.
17. Otte S, Klinger HM, Lorenz F, Haerer T. Operative treatment in case of a closed rupture of the anterior tibial tendon. Arch Orthop Trauma Surg. 2002;122(3):188-190.
18. Ouzounian TJ, Anderson R. Anterior tibial tendon rupture. Foot Ankle Int. 1995;16(7):406-410.
19. Rajagopalan S, Sangar A, Upadhyay V, Lloyd J, Taylor H. Bilateral atraumatic sequential rupture of tibialis anterior tendons. Foot Ankle Spec. 2010;3(6):352-355.
20. Rimoldi RL, Oberlander MA, Waldrop JI, Hunter SC. Acute rupture of the tibialis anterior tendon: a case report. Foot Ankle. 1991;12(3):176-177.
21. Sammarco VJ, Sammarco GJ, Henning C, Chaim S. Surgical repair of acute and chronic tibialis anterior tendon ruptures. J Bone Joint Surg Am. 2009;91(2):325-332.
22. Sapkas GS, Tzoutzopoulos A, Tsoukas FC, Triantafillopoulos IK. Spontaneous tibialis anterior tendon rupture: delayed repair with free-sliding tibialis anterior tendon graft. Am J Orthop. 2008;37(12):E213-E216.
23. Stuart MJ. Traumatic disruption of the anterior tibial tendon while cross-country skiing. A case report. Clin Orthop. 1992;(281):193-194.
24. Trout BM, Hosey G, Wertheimer SJ. Rupture of the tibialis anterior tendon. J Foot Ankle Surg. 2000;39(1):54-58.
25. Van Acker G, Pingen F, Luitse J, Goslings C. Rupture of the tibialis anterior tendon. Acta Orthop Belg. 2006;72(1):105-107.
26. Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. 1994;15(7):349-353.
27. Roos EM, Brandsson S, Karlsson J. Validation of the foot and ankle outcome score for ankle ligament reconstruction. Foot Ankle Int. 2001;22(10):788-794.
28. Tinetti ME, Williams TF, Mayewski R. Fall risk index for elderly patients based on number of chronic disabilities. Am J Med. 1986;80(3):429-434.
Subcutaneous rupture of the tibialis anterior (TA) tendon has been reported predominantly in case reports and small case series because of the relative rarity of the injury. Unlike traumatic lacerations or open injuries to the tendon, subcutaneous injuries often go unnoticed by patients because of compensation by surrounding dorsiflexors of the foot and toes—namely, the extensor hallucis longus (EHL) and the extensor digitorum longus (EDL).1 This can delay presentation to an orthopedic surgeon and lead to difficulties in treatment, such as allograft or autograft being required if primary repair is no longer possible. Case reports and series have described treatment methods as well as anecdotal evidence of outcomes after operative repair or conservative treatment, but there have been no comprehensive systematic reviews of outcomes after various types of treatment. Authors have come to conclusions about expected outcomes based on patient age, time to treatment, treatment used, and other variables, but no reviews have examined these variables across multiple studies. Given the low level of the evidence presented in most of these reports, it is difficult to perform a meta-analysis of the data.
Instead, we systematically reviewed 87 cases from all pertinent studies and examined commonly reported data, such as patient age, time to treatment, treatment used, and outcome. Using the PICO (population, intervention, comparison, outcome) model for systematic reviews, we looked at patients who had closed, spontaneous, complete rupture of the TA tendon and underwent operative repair or conservative treatment of the injury. Outcomes surveyed included successful operative repair or conservative treatment, as measured by objective systems, such as MMSS (Manual Muscle Strength Scale) score, AOFAS (American Orthopaedic Foot and Ankle Society) hindfoot score, and FAOS (Foot and Ankle Outcome Score) testing, or by subjective description of posttreatment outcome.
We intend this review to serve as a guide for surgeons who find themselves treating a ruptured TA tendon, a relatively rare injury. They will be able to select the operative technique or conservative treatment that best matches the patient’s needs, based on comparison with previous case studies.
Materials and Methods
The cases reviewed for this study were found through a comprehensive PubMed search and an independent review of references cited in similar articles. Articles included were published between 1975 and 2012, inclusive. The latest search was performed on March 22, 2013. The search criteria were tibialis anterior [Title/Abstract] OR anterior tibial [Title/Abstract] AND rupture [Title/Abstract]) AND surgery. Only English-language articles, or articles already translated into English, were included. Eligible studies described cases of closed tendon rupture. No traumatic lacerations or open ruptures were included. If a study described both open and subcutaneous ruptures, only the subcutaneous cases were included. Further, partial ruptures were not included. In addition, ruptures caused directly by a known comorbid condition—for example, a rupture caused by a gouty tophaceous deposit at the site of rupture2—were not included. Data were extracted from publications independently and analyzed in a Microsoft Excel workbook (Microsoft, Redmond, Washington). Variables examined included patient age and sex, side involved, time to treatment, mechanism of injury, defect size, predisposing comorbidities, surgery or conservative treatment, type of operative repair (if applicable), graft used (if applicable), pretreatment function (by independent scoring system, if applicable), and posttreatment function. These variables were not necessarily reported in all the studies.
A potential bias exists in our PubMed search. As the query was specific for studies that included operative repair of a ruptured TA tendon, case studies that involved only conservative treatment were excluded. However, the primary goal of this review was to compare operative possibilities and the patient characteristics and outcomes associated with these surgeries.
Results
Figure 1 shows the criteria used to select eligible papers for review. Twenty-three papers matched the criteria.3-25 Data were independently extracted from these papers, as described in the Methods section. Again, not all variables were reported by all authors. Sammarco and colleagues21 reported time to treatment as a mean for 2 groups: 8 cases defined as “early” treatment (mean time to treatment, 0.625 months) and 11 defined as “late” treatment (mean time to treatment, 10.7 months). These mean times were therefore used independently for each case in calculating mean time to treatment for this systematic review.
Table 1 lists the demographics. There were 40 male and 25 female patients, and 22 cases in which sex was not specified. Mean age was 63.9 years (surgery group), 72.4 years (conservative treatment group), and 65.8 years (overall). Of the 87 patients, 72 underwent surgery, and 15 were treated with conservative measures.
Table 2 lists the operative techniques identified. Of the 72 surgeries, 23 were primary repairs, 12 were primary repairs of the anatomical insertion, and 18 involved use of autograft.
Time to treatment was available for 54 of the 87 cases (Table 3). Primary repair was most often performed in cases in which the injury was less than 3 months old, and autograft was most often used in cases in which the injury occurred more than 3 months before presentation.
Posttreatment outcome scores were available for 59 cases. Only 3 authors reported preoperative scores.5,21,24 None of the authors who used conservative treatment measures reported pretreatment scores. Scores used included the MMSS score (26 cases), the AOFAS hindfoot score (16 cases),26 the FAOS (17 cases),27 and the Tinetti gait and balance score (3 cases; the author also used the MMSS score).28Table 4 lists the mean posttreatment scores for patients who underwent surgery and patients treated conservatively. AOFAS, MMSS, and Tinetti scores and FAOS were used by authors presenting operative treatment outcomes. Only posttreatment FAOS was available for both surgery (84.4/100) and conservative treatment (69.4/100).
Discussion
Closed rupture of the TA tendon is a relatively rare entity occurring mostly in older patients without any history of acute, traumatic injury. Some patients, however, recall a particular moment of rupture, often accompanied immediately by pain and swelling, which eventually resolve. Later sequelae include footdrop with associated steppage gait and a palpable mass on the dorsal aspect of the ankle.3,21 Chronic TA tendon rupture can also lead to clawing of the toes as the other foot extensors (EHL, EDL) overcompensate. Cohen and Gordon1 described the case of a patient who ruptured a TA tendon 25 years earlier and then, in the absence of operative repair, developed hypertrophy of the EHL and the EDL. This extensor substitution led to hammer toes and plantar prominence of the metatarsal heads, ultimately leading to moderate pain and a neuroma. Although this particular outcome is likely rare, the more common sequelae of footdrop, flatfoot, Achilles tendon contracture, and compromised gait are reason enough to consider operative repair for any ruptured TA tendon.
Most previous studies of TA tendon rupture were case reports and case studies. In the largest series, Sammarco and colleagues21 described 19 cases of closed rupture. These included 3 traumatic cases, 1 by blunt trauma to the tendon and 2 of open laceration, all treated surgically with various methods. Unfortunately, these 3 traumatic cases were not separated in the authors’ analysis and therefore had to be included in this systematic review. Including them here did not compromise our goals in this review, which included examining typical patient demographics and the most common methods of operative repair.
Conservative measures remain a treatment possibility for some patients. We found that patients treated with conservative measures historically have been older (mean age, 72.4 years) than patients treated surgically (mean age, 63.9 years). However, advanced age itself is not a contraindication for operative repair of a TA tendon rupture, and authors have described positive outcomes for active, elderly (>70 years) patients who wanted to maintain their activity level and therefore opted for operative repair.7,8,10,13,16,24 Ouzounian and Anderson18 described functional limitations (eg, persistent footdrop, slapfoot gait, limitations in walking) after conservative treatment with an ankle-foot orthosis. Operative repair offers the chance for better functional outcome for patients who are surgical candidates and lead even a mildly active lifestyle.
Of operative repair methods, primary repair is used most often. This technique, however, must be allowed by the gap between the 2 ruptured ends after débridement of any necrotic tissue. If the distal stump is not viable, primary repair of the proximal stump to the native anatomical insertion is feasible. Figure 2, reprinted from a case report by Rajagopalan and colleagues,19 shows a ligament–osseous reattachment of the proximal stump using suture anchors to the medial cuneiform. Both primary repair and repair to the anatomical insertion can be augmented with Achilles tendon lengthening if needed to achieve balance between flexor and extensor functions of the ankle.
If the gap between the 2 stumps cannot be covered by the native tendon, then autograft, another surgical technique with positive outcomes, can be used. The most popular autograft sites historically have been the EDL, Achilles, and plantaris tendons. In addition, Goehring and Liakos9 described 3 cases of good results with semitendinosus autograft. Sapkas and colleagues22 used a free-sliding TA graft harvested from the healthy tissue of the proximal tendon stump. Their technique is depicted in Figure 3. Sliding tendon lengthening, well described by Trout and colleagues24 in a case study, is feasible for use of the native tendon when there is a gap to bridge between the 2 stumps of ruptured tendon. EHL or EDL transfer with or without Achilles lengthening is another option, albeit historically less often used.6,7 This technique is depicted in Figure 4, reprinted from a case series by Ellington and colleagues,7 who used EHL transfer with and without Achilles tendon lengthening in 9 cases.
Last, less popular techniques have included repair to sites other than the medial cuneiform, including the neck of the talus and the navicular bone.10,13 An Achilles tendon allograft was used in a case described by Aderinto and Gross3 to repair a ruptured tendon found incidentally on preoperative examination for a scheduled knee arthroplasty. The patient had a postoperative MMSS score of 4/5.
Overall, primary repair is clearly preferred, but successful outcomes can be achieved by other means. As Table 3 shows, primary repair is more often used for ruptures less than 3 months old, and autograft for older ruptures. Although which operative technique to use can be decided after necrotic tissue is débrided, surgeons should try to ascertain age of injury ahead of time so that, going into surgery, they will have a better idea of the feasibility of primary repair.
Posttreatment ankle scores were not widely available. As Table 4 indicates, only FAOS was used for the conservative treatment cases. However, raw mean FAOS and raw mean AOFAS hindfoot, MMSS, and Tinetti scores showed that good outcomes and high scores can be achieved with surgery. Further, the mean FAOS reported by Gwynne-Jones and colleagues10 and Markarian and colleagues13 showed a clinically significant difference between surgery and conservative treatment. DiDomenico and colleagues,5 Sammarco and colleagues,21 and Trout and colleagues24 were the only authors who reported pretreatment and posttreatment scores.
We intend this systematic review of the literature on closed TA rupture to serve as a guide for surgeons who find themselves treating this relatively rare injury, which often presents with only a chief complaint of the foot catching while walking. Overall, the literature shows that operative repair provides very good outcomes for many patients. Patients who are surgical candidates and amenable to surgery can be counseled that operative repair leads to fewer sequelae, such as persistent footdrop and flatfooted gait, with a strong likelihood of return to baseline activity status. Patients who are not surgical candidates or are strongly against surgery can be offered conservative treatment with an ankle-foot orthosis or physical therapy, but they should also be counseled that persistent gait abnormalities and weakness in dorsiflexion are likely outcomes. Surgeons must also consider age of injury (time from probable rupture to presentation), estimating a particular moment of rupture if unknown by the patient. They can then gauge the feasibility of primary repair and, during surgery, decide which technique (primary repair, tendon transfer, autograft, or other technique) will produce the best results. They can also use scores such as the FAOS and the AOFAS hindfoot, MMSS, and Tinetti scores to compare preoperative and postoperative function, though subjective reports of return to previous activity can also serve as markers of successful repair.
This review highlights the need for further study regarding the treatment of TA ruptures. Larger, randomized studies with validated scoring systems for preoperative and postoperative function would offer more insight onto the best treatment options for these complex injuries.
Subcutaneous rupture of the tibialis anterior (TA) tendon has been reported predominantly in case reports and small case series because of the relative rarity of the injury. Unlike traumatic lacerations or open injuries to the tendon, subcutaneous injuries often go unnoticed by patients because of compensation by surrounding dorsiflexors of the foot and toes—namely, the extensor hallucis longus (EHL) and the extensor digitorum longus (EDL).1 This can delay presentation to an orthopedic surgeon and lead to difficulties in treatment, such as allograft or autograft being required if primary repair is no longer possible. Case reports and series have described treatment methods as well as anecdotal evidence of outcomes after operative repair or conservative treatment, but there have been no comprehensive systematic reviews of outcomes after various types of treatment. Authors have come to conclusions about expected outcomes based on patient age, time to treatment, treatment used, and other variables, but no reviews have examined these variables across multiple studies. Given the low level of the evidence presented in most of these reports, it is difficult to perform a meta-analysis of the data.
Instead, we systematically reviewed 87 cases from all pertinent studies and examined commonly reported data, such as patient age, time to treatment, treatment used, and outcome. Using the PICO (population, intervention, comparison, outcome) model for systematic reviews, we looked at patients who had closed, spontaneous, complete rupture of the TA tendon and underwent operative repair or conservative treatment of the injury. Outcomes surveyed included successful operative repair or conservative treatment, as measured by objective systems, such as MMSS (Manual Muscle Strength Scale) score, AOFAS (American Orthopaedic Foot and Ankle Society) hindfoot score, and FAOS (Foot and Ankle Outcome Score) testing, or by subjective description of posttreatment outcome.
We intend this review to serve as a guide for surgeons who find themselves treating a ruptured TA tendon, a relatively rare injury. They will be able to select the operative technique or conservative treatment that best matches the patient’s needs, based on comparison with previous case studies.
Materials and Methods
The cases reviewed for this study were found through a comprehensive PubMed search and an independent review of references cited in similar articles. Articles included were published between 1975 and 2012, inclusive. The latest search was performed on March 22, 2013. The search criteria were tibialis anterior [Title/Abstract] OR anterior tibial [Title/Abstract] AND rupture [Title/Abstract]) AND surgery. Only English-language articles, or articles already translated into English, were included. Eligible studies described cases of closed tendon rupture. No traumatic lacerations or open ruptures were included. If a study described both open and subcutaneous ruptures, only the subcutaneous cases were included. Further, partial ruptures were not included. In addition, ruptures caused directly by a known comorbid condition—for example, a rupture caused by a gouty tophaceous deposit at the site of rupture2—were not included. Data were extracted from publications independently and analyzed in a Microsoft Excel workbook (Microsoft, Redmond, Washington). Variables examined included patient age and sex, side involved, time to treatment, mechanism of injury, defect size, predisposing comorbidities, surgery or conservative treatment, type of operative repair (if applicable), graft used (if applicable), pretreatment function (by independent scoring system, if applicable), and posttreatment function. These variables were not necessarily reported in all the studies.
A potential bias exists in our PubMed search. As the query was specific for studies that included operative repair of a ruptured TA tendon, case studies that involved only conservative treatment were excluded. However, the primary goal of this review was to compare operative possibilities and the patient characteristics and outcomes associated with these surgeries.
Results
Figure 1 shows the criteria used to select eligible papers for review. Twenty-three papers matched the criteria.3-25 Data were independently extracted from these papers, as described in the Methods section. Again, not all variables were reported by all authors. Sammarco and colleagues21 reported time to treatment as a mean for 2 groups: 8 cases defined as “early” treatment (mean time to treatment, 0.625 months) and 11 defined as “late” treatment (mean time to treatment, 10.7 months). These mean times were therefore used independently for each case in calculating mean time to treatment for this systematic review.
Table 1 lists the demographics. There were 40 male and 25 female patients, and 22 cases in which sex was not specified. Mean age was 63.9 years (surgery group), 72.4 years (conservative treatment group), and 65.8 years (overall). Of the 87 patients, 72 underwent surgery, and 15 were treated with conservative measures.
Table 2 lists the operative techniques identified. Of the 72 surgeries, 23 were primary repairs, 12 were primary repairs of the anatomical insertion, and 18 involved use of autograft.
Time to treatment was available for 54 of the 87 cases (Table 3). Primary repair was most often performed in cases in which the injury was less than 3 months old, and autograft was most often used in cases in which the injury occurred more than 3 months before presentation.
Posttreatment outcome scores were available for 59 cases. Only 3 authors reported preoperative scores.5,21,24 None of the authors who used conservative treatment measures reported pretreatment scores. Scores used included the MMSS score (26 cases), the AOFAS hindfoot score (16 cases),26 the FAOS (17 cases),27 and the Tinetti gait and balance score (3 cases; the author also used the MMSS score).28Table 4 lists the mean posttreatment scores for patients who underwent surgery and patients treated conservatively. AOFAS, MMSS, and Tinetti scores and FAOS were used by authors presenting operative treatment outcomes. Only posttreatment FAOS was available for both surgery (84.4/100) and conservative treatment (69.4/100).
Discussion
Closed rupture of the TA tendon is a relatively rare entity occurring mostly in older patients without any history of acute, traumatic injury. Some patients, however, recall a particular moment of rupture, often accompanied immediately by pain and swelling, which eventually resolve. Later sequelae include footdrop with associated steppage gait and a palpable mass on the dorsal aspect of the ankle.3,21 Chronic TA tendon rupture can also lead to clawing of the toes as the other foot extensors (EHL, EDL) overcompensate. Cohen and Gordon1 described the case of a patient who ruptured a TA tendon 25 years earlier and then, in the absence of operative repair, developed hypertrophy of the EHL and the EDL. This extensor substitution led to hammer toes and plantar prominence of the metatarsal heads, ultimately leading to moderate pain and a neuroma. Although this particular outcome is likely rare, the more common sequelae of footdrop, flatfoot, Achilles tendon contracture, and compromised gait are reason enough to consider operative repair for any ruptured TA tendon.
Most previous studies of TA tendon rupture were case reports and case studies. In the largest series, Sammarco and colleagues21 described 19 cases of closed rupture. These included 3 traumatic cases, 1 by blunt trauma to the tendon and 2 of open laceration, all treated surgically with various methods. Unfortunately, these 3 traumatic cases were not separated in the authors’ analysis and therefore had to be included in this systematic review. Including them here did not compromise our goals in this review, which included examining typical patient demographics and the most common methods of operative repair.
Conservative measures remain a treatment possibility for some patients. We found that patients treated with conservative measures historically have been older (mean age, 72.4 years) than patients treated surgically (mean age, 63.9 years). However, advanced age itself is not a contraindication for operative repair of a TA tendon rupture, and authors have described positive outcomes for active, elderly (>70 years) patients who wanted to maintain their activity level and therefore opted for operative repair.7,8,10,13,16,24 Ouzounian and Anderson18 described functional limitations (eg, persistent footdrop, slapfoot gait, limitations in walking) after conservative treatment with an ankle-foot orthosis. Operative repair offers the chance for better functional outcome for patients who are surgical candidates and lead even a mildly active lifestyle.
Of operative repair methods, primary repair is used most often. This technique, however, must be allowed by the gap between the 2 ruptured ends after débridement of any necrotic tissue. If the distal stump is not viable, primary repair of the proximal stump to the native anatomical insertion is feasible. Figure 2, reprinted from a case report by Rajagopalan and colleagues,19 shows a ligament–osseous reattachment of the proximal stump using suture anchors to the medial cuneiform. Both primary repair and repair to the anatomical insertion can be augmented with Achilles tendon lengthening if needed to achieve balance between flexor and extensor functions of the ankle.
If the gap between the 2 stumps cannot be covered by the native tendon, then autograft, another surgical technique with positive outcomes, can be used. The most popular autograft sites historically have been the EDL, Achilles, and plantaris tendons. In addition, Goehring and Liakos9 described 3 cases of good results with semitendinosus autograft. Sapkas and colleagues22 used a free-sliding TA graft harvested from the healthy tissue of the proximal tendon stump. Their technique is depicted in Figure 3. Sliding tendon lengthening, well described by Trout and colleagues24 in a case study, is feasible for use of the native tendon when there is a gap to bridge between the 2 stumps of ruptured tendon. EHL or EDL transfer with or without Achilles lengthening is another option, albeit historically less often used.6,7 This technique is depicted in Figure 4, reprinted from a case series by Ellington and colleagues,7 who used EHL transfer with and without Achilles tendon lengthening in 9 cases.
Last, less popular techniques have included repair to sites other than the medial cuneiform, including the neck of the talus and the navicular bone.10,13 An Achilles tendon allograft was used in a case described by Aderinto and Gross3 to repair a ruptured tendon found incidentally on preoperative examination for a scheduled knee arthroplasty. The patient had a postoperative MMSS score of 4/5.
Overall, primary repair is clearly preferred, but successful outcomes can be achieved by other means. As Table 3 shows, primary repair is more often used for ruptures less than 3 months old, and autograft for older ruptures. Although which operative technique to use can be decided after necrotic tissue is débrided, surgeons should try to ascertain age of injury ahead of time so that, going into surgery, they will have a better idea of the feasibility of primary repair.
Posttreatment ankle scores were not widely available. As Table 4 indicates, only FAOS was used for the conservative treatment cases. However, raw mean FAOS and raw mean AOFAS hindfoot, MMSS, and Tinetti scores showed that good outcomes and high scores can be achieved with surgery. Further, the mean FAOS reported by Gwynne-Jones and colleagues10 and Markarian and colleagues13 showed a clinically significant difference between surgery and conservative treatment. DiDomenico and colleagues,5 Sammarco and colleagues,21 and Trout and colleagues24 were the only authors who reported pretreatment and posttreatment scores.
We intend this systematic review of the literature on closed TA rupture to serve as a guide for surgeons who find themselves treating this relatively rare injury, which often presents with only a chief complaint of the foot catching while walking. Overall, the literature shows that operative repair provides very good outcomes for many patients. Patients who are surgical candidates and amenable to surgery can be counseled that operative repair leads to fewer sequelae, such as persistent footdrop and flatfooted gait, with a strong likelihood of return to baseline activity status. Patients who are not surgical candidates or are strongly against surgery can be offered conservative treatment with an ankle-foot orthosis or physical therapy, but they should also be counseled that persistent gait abnormalities and weakness in dorsiflexion are likely outcomes. Surgeons must also consider age of injury (time from probable rupture to presentation), estimating a particular moment of rupture if unknown by the patient. They can then gauge the feasibility of primary repair and, during surgery, decide which technique (primary repair, tendon transfer, autograft, or other technique) will produce the best results. They can also use scores such as the FAOS and the AOFAS hindfoot, MMSS, and Tinetti scores to compare preoperative and postoperative function, though subjective reports of return to previous activity can also serve as markers of successful repair.
This review highlights the need for further study regarding the treatment of TA ruptures. Larger, randomized studies with validated scoring systems for preoperative and postoperative function would offer more insight onto the best treatment options for these complex injuries.
1. Cohen DA, Gordon DH. The long-term effects of an untreated tibialis anterior tendon rupture. J Am Podiatr Med Assoc. 1999;89(3):149-152.
2. Jerome JTJ, Varghese M, Sankaran B, Thomas S, Thirumagal SK. Tibialis anterior tendon rupture in gout—case report and literature review. Foot Ankle Surg. 2008;14(3):166-169.
3. Aderinto J, Gross A. Delayed repair of tibialis anterior tendon rupture with Achilles tendon allograft. J Foot Ankle Surg. 2011;50(3):340-342.
4. Constantinou M, Wilson A. Traumatic tear of tibialis anterior during a Gaelic football game: a case report. Br J Sports Med. 2004;38(6):e30.
5. DiDomenico LA, Williams K, Petrolla AF. Spontaneous rupture of the anterior tibial tendon in a diabetic patient: results of operative treatment. J Foot Ankle Surg. 2008;47(5):463-467.
6. Dooley BJ, Kudelka P, Menelaus MB. Subcutaneous rupture of the tendon of tibialis anterior. J Bone Joint Surg Br. 1980;62(4):471-472.
7. Ellington JK, McCormick J, Marion C, et al. Surgical outcome following tibialis anterior tendon repair. Foot Ankle Int. 2010;31(5):412-417.
8. ElMaraghy A, Devereaux MW. Bone tunnel fixation for repair of tibialis anterior tendon rupture. Foot Ankle Surg. 2010;16(2):e47-e50.
9. Goehring M, Liakos P. Long-term outcomes following anterior tibialis tendon reconstruction with hamstring autograft in a series of 3 cases. J Foot Ankle Surg. 2009;48(2):196-202.
10. Gwynne-Jones D, Garneti N, Wyatt M. Closed tibialis anterior tendon rupture: a case series. Foot Ankle Int. 2009;30(8):758-762.
11. Kashyap S, Prince R. Spontaneous rupture of the tibialis anterior tendon. A case report. Clin Orthop. 1987;(216):159-161.
12. Kausch T, Rütt J. Subcutaneous rupture of the tibialis anterior tendon: review of the literature and a case report. Arch Orthop Trauma Surg. 1998;117(4-5):290-293.
13. Markarian GG, Kelikian AS, Brage M, Trainor T, Dias L. Anterior tibialis tendon ruptures: an outcome analysis of operative versus nonoperative treatment. Foot Ankle Int. 1998;19(12):792-802.
14. Meyn MA Jr. Closed rupture of the anterior tibial tendon. A case report and review of the literature. Clin Orthop. 1975;(113):154-157.
15. Miller RR, Mahan KT. Closed rupture of the anterior tibial tendon. A case report. J Am Podiatr Med Assoc. 1998;88(8):394-399.
16. Neumayer F, Djembi YR, Gerin A, Masquelet AC. Closed rupture of the tibialis anterior tendon: a report of 2 cases. J Foot Ankle Surg. 2009;48(4):457-461.
17. Otte S, Klinger HM, Lorenz F, Haerer T. Operative treatment in case of a closed rupture of the anterior tibial tendon. Arch Orthop Trauma Surg. 2002;122(3):188-190.
18. Ouzounian TJ, Anderson R. Anterior tibial tendon rupture. Foot Ankle Int. 1995;16(7):406-410.
19. Rajagopalan S, Sangar A, Upadhyay V, Lloyd J, Taylor H. Bilateral atraumatic sequential rupture of tibialis anterior tendons. Foot Ankle Spec. 2010;3(6):352-355.
20. Rimoldi RL, Oberlander MA, Waldrop JI, Hunter SC. Acute rupture of the tibialis anterior tendon: a case report. Foot Ankle. 1991;12(3):176-177.
21. Sammarco VJ, Sammarco GJ, Henning C, Chaim S. Surgical repair of acute and chronic tibialis anterior tendon ruptures. J Bone Joint Surg Am. 2009;91(2):325-332.
22. Sapkas GS, Tzoutzopoulos A, Tsoukas FC, Triantafillopoulos IK. Spontaneous tibialis anterior tendon rupture: delayed repair with free-sliding tibialis anterior tendon graft. Am J Orthop. 2008;37(12):E213-E216.
23. Stuart MJ. Traumatic disruption of the anterior tibial tendon while cross-country skiing. A case report. Clin Orthop. 1992;(281):193-194.
24. Trout BM, Hosey G, Wertheimer SJ. Rupture of the tibialis anterior tendon. J Foot Ankle Surg. 2000;39(1):54-58.
25. Van Acker G, Pingen F, Luitse J, Goslings C. Rupture of the tibialis anterior tendon. Acta Orthop Belg. 2006;72(1):105-107.
26. Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. 1994;15(7):349-353.
27. Roos EM, Brandsson S, Karlsson J. Validation of the foot and ankle outcome score for ankle ligament reconstruction. Foot Ankle Int. 2001;22(10):788-794.
28. Tinetti ME, Williams TF, Mayewski R. Fall risk index for elderly patients based on number of chronic disabilities. Am J Med. 1986;80(3):429-434.
1. Cohen DA, Gordon DH. The long-term effects of an untreated tibialis anterior tendon rupture. J Am Podiatr Med Assoc. 1999;89(3):149-152.
2. Jerome JTJ, Varghese M, Sankaran B, Thomas S, Thirumagal SK. Tibialis anterior tendon rupture in gout—case report and literature review. Foot Ankle Surg. 2008;14(3):166-169.
3. Aderinto J, Gross A. Delayed repair of tibialis anterior tendon rupture with Achilles tendon allograft. J Foot Ankle Surg. 2011;50(3):340-342.
4. Constantinou M, Wilson A. Traumatic tear of tibialis anterior during a Gaelic football game: a case report. Br J Sports Med. 2004;38(6):e30.
5. DiDomenico LA, Williams K, Petrolla AF. Spontaneous rupture of the anterior tibial tendon in a diabetic patient: results of operative treatment. J Foot Ankle Surg. 2008;47(5):463-467.
6. Dooley BJ, Kudelka P, Menelaus MB. Subcutaneous rupture of the tendon of tibialis anterior. J Bone Joint Surg Br. 1980;62(4):471-472.
7. Ellington JK, McCormick J, Marion C, et al. Surgical outcome following tibialis anterior tendon repair. Foot Ankle Int. 2010;31(5):412-417.
8. ElMaraghy A, Devereaux MW. Bone tunnel fixation for repair of tibialis anterior tendon rupture. Foot Ankle Surg. 2010;16(2):e47-e50.
9. Goehring M, Liakos P. Long-term outcomes following anterior tibialis tendon reconstruction with hamstring autograft in a series of 3 cases. J Foot Ankle Surg. 2009;48(2):196-202.
10. Gwynne-Jones D, Garneti N, Wyatt M. Closed tibialis anterior tendon rupture: a case series. Foot Ankle Int. 2009;30(8):758-762.
11. Kashyap S, Prince R. Spontaneous rupture of the tibialis anterior tendon. A case report. Clin Orthop. 1987;(216):159-161.
12. Kausch T, Rütt J. Subcutaneous rupture of the tibialis anterior tendon: review of the literature and a case report. Arch Orthop Trauma Surg. 1998;117(4-5):290-293.
13. Markarian GG, Kelikian AS, Brage M, Trainor T, Dias L. Anterior tibialis tendon ruptures: an outcome analysis of operative versus nonoperative treatment. Foot Ankle Int. 1998;19(12):792-802.
14. Meyn MA Jr. Closed rupture of the anterior tibial tendon. A case report and review of the literature. Clin Orthop. 1975;(113):154-157.
15. Miller RR, Mahan KT. Closed rupture of the anterior tibial tendon. A case report. J Am Podiatr Med Assoc. 1998;88(8):394-399.
16. Neumayer F, Djembi YR, Gerin A, Masquelet AC. Closed rupture of the tibialis anterior tendon: a report of 2 cases. J Foot Ankle Surg. 2009;48(4):457-461.
17. Otte S, Klinger HM, Lorenz F, Haerer T. Operative treatment in case of a closed rupture of the anterior tibial tendon. Arch Orthop Trauma Surg. 2002;122(3):188-190.
18. Ouzounian TJ, Anderson R. Anterior tibial tendon rupture. Foot Ankle Int. 1995;16(7):406-410.
19. Rajagopalan S, Sangar A, Upadhyay V, Lloyd J, Taylor H. Bilateral atraumatic sequential rupture of tibialis anterior tendons. Foot Ankle Spec. 2010;3(6):352-355.
20. Rimoldi RL, Oberlander MA, Waldrop JI, Hunter SC. Acute rupture of the tibialis anterior tendon: a case report. Foot Ankle. 1991;12(3):176-177.
21. Sammarco VJ, Sammarco GJ, Henning C, Chaim S. Surgical repair of acute and chronic tibialis anterior tendon ruptures. J Bone Joint Surg Am. 2009;91(2):325-332.
22. Sapkas GS, Tzoutzopoulos A, Tsoukas FC, Triantafillopoulos IK. Spontaneous tibialis anterior tendon rupture: delayed repair with free-sliding tibialis anterior tendon graft. Am J Orthop. 2008;37(12):E213-E216.
23. Stuart MJ. Traumatic disruption of the anterior tibial tendon while cross-country skiing. A case report. Clin Orthop. 1992;(281):193-194.
24. Trout BM, Hosey G, Wertheimer SJ. Rupture of the tibialis anterior tendon. J Foot Ankle Surg. 2000;39(1):54-58.
25. Van Acker G, Pingen F, Luitse J, Goslings C. Rupture of the tibialis anterior tendon. Acta Orthop Belg. 2006;72(1):105-107.
26. Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. 1994;15(7):349-353.
27. Roos EM, Brandsson S, Karlsson J. Validation of the foot and ankle outcome score for ankle ligament reconstruction. Foot Ankle Int. 2001;22(10):788-794.
28. Tinetti ME, Williams TF, Mayewski R. Fall risk index for elderly patients based on number of chronic disabilities. Am J Med. 1986;80(3):429-434.

Endometriosis: Expert answers to 7 crucial questions on diagnosis
CASE Is her chronic pelvic pain caused by endometriosis?
M.L. is a 32-year-old nulliparous woman who is referred to your office by her primary care provider for chronic pelvic pain. She reports severe dysmenorrhea as her main symptom, but she also mentions dyspareunia. She says these symptoms have been present for several years but have increased in intensity gradually. She asks what you consider to be the most likely diagnosis.
What potential diagnoses do you mention to her? And how do you identify the cause of her pain?
Although endometriosis—the presence of endometrial tissue outside the uterus—affects at least 5 million women of reproductive age in the United States alone, it can be a challenging diagnosis for several reasons.
“Endometriosis is a great masquerader,” says Linda Giudice, MD, PhD. “It presents with a variety of pain patterns, intensities, and triggers. It can also involve symptoms that overlap those of other disorders, including disorders of the gastrointestinal and urinary tracts.”
Although endometriosis falls within the differential diagnosis of chronic pelvic pain, “it is usually not high on the list in the primary care setting (adult and adolescent),” Dr. Giudice adds. She is the Robert B. Jaffe, MD, Endowed Professor in the reproductive sciences and chair of obstetrics, gynecology, and reproductive sciences at the University of California, San Francisco.
John R. Lue, MD, MPH, an author of the most recent practice bulletin on endometriosis from the American College of Obstetricians and Gynecologists,1 sees the situation similarly.
“The main challenge in the diagnosis of endometriosis is that its presentation mimics other causes of chronic pelvic pain,” he says. “Pelvic pain due to endometriosis is usually chronic (lasting ≥6 months). It is associated with dysmenorrhea in 50% to 90% of cases, as well as with dyspareunia, deep pelvic pain, and lower abdominal pain with or without back and loin pain. The pain can occur unpredictably and intermittently throughout the menstrual cycle or it can be continuous. In addition, it can be dull, throbbing, or sharp and may be exacerbated by physical activity.2,3 Up to 20% of women with endometriosis have concurrent pain conditions.”4 Dr. Lue is associate professor, chief of the section of general obstetrics and gynecology, and medical director of women’s ambulatory services at the Medical College of Georgia and Georgia Regents University in Augusta, Georgia.
Among other diseases of the female pelvis that have relatively similar presentation, Dr. Lue adds, are pathologies of the:
- uterus (adenomyosis, fibroids)
- fallopian tube (hydrosalpinx)
- ovaries (ovarian cysts)
- bladder (interstitial cystitis)
- bowel (irritable bowel syndrome)
- musculoskeletal system (piriformis syndrome).
Before pelvic pain is attributed to endometriosis, he says, the provider should rule out bowel, bladder, musculoskeletal, and psychiatric causes.
This article focuses on 7 questions, the answers of which are critical to narrowing in on the diagnosis of endometriosis, including essential factors to consider in the patient history, imaging and other diagnostic tools, and considerations in surgical exploration. In the second and third installments of this in-depth series on endometriosis, pain and infertility will be the respective subjects of investigation.
Several theories explain the “why” of endometriosis
A dominant theory is that peritoneal endometrial implants arise from retrograde menstruation, during which endometrial tissue passes through the fallopian tubes into the pelvis, says John R. Lue, MD, MPH. Dr. Lue is associate professor and chief of the section of general obstetrics and gynecology and medical director of women’s ambulatory services at the Medical College of Georgia and Georgia Regents University in Augusta, Georgia.
“Additional theories include immune dysfunction that interferes with clearing of endometrial lesions in the pelvis, as well as genetic alterations that lead to growth dysregulation,” he says.1 “These theories all have merit, and it is likely that the pathogenesis of endometriosis is multifactorial.”
Another strong theory involves the homeobox (HOX) genes, “which mediate embryonic development,” says Dr. Lue.2,3 “These genes are translated into transcription factors that regulate downstream genes necessary for growth and differentiation. It has been demonstrated that HOX genes play an analogous role in endometrial development during the adult menstrual cycle.4 HOX gene expression regulates the growth and development of the human endometrium.5 The expression of HOX genes A10 and A11 varies in response to sex steroids during the menstrual cycle, with dramatic upregulation in the mid-secretory phase,” says Dr. Lue. Recent studies suggest that these genes “play a major role” in endometriosis.6
“Since ovarian endometriomas are clonal and lesions usually have genetic mutations, such somatic mutations with subsequent growth dysregulation may also be etiologic factors,” says Dr. Lue.1,7,8 “Disease at distant sites may be caused by lymphatic or hematogenous spread or metaplastic transformation.”
References
1. Giudice LC, Swierz LM, Burney RO. Edometriosis. In: Jameson JL, DeGroot LJ, eds. Endocrinology. 6th ed. New York, NY: Elsevier; 2010:2356–2370.
2. Krumlauf R. Hox genes in vertebrate development. Cell. 1992;78(2):191–201.
3. McGinnis W, Krumlauf R. Homeobox genes and axial patterning. Cell. 1992;68(2):283–302.
4. Taylor H, Igarashi P, Olive D, Arici A. Sex steroids mediate HOXA11 expression in the human peri-implantation endometrium. J Clin Endocrinol Metab. 1999;84(3):1129–1135.
5. Taylor H, Vanden Heuvel GB, Igarashi P. A conserved HOX axis in the mouse and human female reproductive system: late establishment and persistent adult expression of the HOXA cluster genes. Biol Reprod. 1997;57(6):1338–1345.
6. Taylor HS, Bagot C, Kardana A. HOX gene expression is altered in the endometrium of women with endometriosis. Hum Reprod. 1999;14(5):1328–1331.
7. Practice Committee of the American Society for Reproductive Medicine. Treatment of pelvic pain associated with endometriosis. Fertil Steril. 2008;90(5 suppl):S260–S269.
8. Bulun SE. Endometriosis. N Engl J Med. 2009;360(3):268–279.
1. Why such a long delay in diagnosis?
Investigators exploring the length of time between a patient’s presentation with symptoms and diagnosis have found it to be particularly long for endometriosis, ranging from 6 to 11 years.
Because endometriosis is usually not high on the list of differential diagnoses for chronic pelvic pain in the primary care setting, a patient may not be referred to a gynecologist unless those symptoms include severe dysmenorrhea, dyspareunia, or similar findings. Once the referral is made, the gynecologist “will usually try contraceptive steroids, nonsteroidal anti-inflammatory drugs, or second-line progestins before a diagnosis is made,” says Dr. Giudice.5
The delay in diagnosis “is astounding,” she adds, “and has its roots in empiric medical therapies and a combination of patients fearing a diagnosis of cancer and reluctance of gynecologists to perform laparoscopy on adolescents.”6
Another possible cause of diagnostic delay: Some adolescent girls may not realize when their pain is severe. Because they may have always experienced a high degree of pain since menarche, they may assume it to be a normal aspect of womanhood and delay seeking help, says Pamela Stratton, MD, chief of the gynecology consult service at the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
2. Have any biomarkers proved to be useful diagnostic tools?
Any biomarker proven to reliably identify endometriosis would be a boon to medicine, as it would provide a noninvasive or minimally invasive alternative to diagnostic laparoscopy, the current gold standard. Regrettably, the search for such a biomarker has produced “disappointing results,” says Dr. Giudice.
“Recent systematic reviews of all proposed endometriosis-related biomarkers over the last 25 years in serum, plasma, urine, and endometrium could not identify an unequivocally clinically useful biomarker or panel of biomarkers,” she notes.7,8 “This is due mainly to low numbers of subjects, small populations for validations, cycle/hormonal- and disease stage-dependence, poorly defined controls, and low sensitivity and specificity.”
One hopeful development: “Whole genome transcriptomics of archived endometrial tissue and machine learning found several classifiers to diagnose and stage endometriosis with high accuracy that were validated on an independent sample set,” says Dr. Giudice.9 “However, these data now warrant a prospective, multisite study for further validation.”
Environmental factors, estrogen, and endometriosis
“There is increasing evidence that in utero and also adult exposures to endocrine-disrupting chemicals (EDCs) play a role in the pathogenesis and progression of disease,” says Linda Giudice, MD, PhD, the Robert B. Jaffe, MD, Endowed Professor in the reproductive sciences and chair of obstetrics, gynecology, and reproductive sciences at the University of California, San Francisco.
“For example, the Nurses’ Health Study II, a prospective cohort study of more than 80,000 women, revealed that daughters exposed to diethylstilbestrol (DES) had an 80% increased risk (odds ratio [OR], 1.8; 95% confidence interval [CI], 1.2–2.8) of developing endometriosis,” she says.1
“Also, dioxin (TCDD) exposure in rats in utero on gestational day 8 increased the size of endometriosis lesions when combined with an adult exposure,” Dr. Giudice says.2 Although we do not know the precise mechanisms underlying in utero events that result in disease onset as a teen or adult, abnormal programming of the female reproductive tract by EDCs and similar agents is believed to play a role, she says.3
Because estrogen is essential for endometriosis lesions and associated symptoms to progress, “EDCs that have either estrogenic activity or interfere with estrogen metabolism or action, or both, have been proposed as contributors to progression of disease. Abundant animal data using nonhuman primate and rodent models and exposures to organochlorines and other EDCs support this hypothesis,” Dr. Giudice says.4
“The weight of human evidence of associations of EDCs and the risk of endometriosis in adult women depends on the class of endocrine disrupter,” Dr. Giudice continues. “Strongest correlations are with polychlorobiphenyls (PCBs), where 10 of 12 studies found significant odds of disease and circulating or omental fat concentrations of these compounds. PCBs inhibit peripheral natural killer cell activity and interleukin 1b and 12 production, relevant to the immune component of endometriosis progression.”
“Significant risk has also been associated with organochlorines (in three of three studies) and perfluorochemicals. In contrast, data linking endometriosis with exposures to dioxins, phthalates, and bisphenol A are equivocal, with some studies finding significant odds ratios and others failing to find significant correlations. Interestingly, dioxins have a significant association with deep infiltrating endometriotic lesions.”5
References
1. Missmer SA, Hankinson SE, Spiegelman D, Barbieri RL, Michels KB, Hunter DJ. In utero exposures and the incidence of endometriosis. Fertil Steril. 2004;82(6):1501–1508.
2. Cummings AM, Hedge JM, Birnbaum LS. Effects on prenatal exposure to TCDD on the promotion of endometriotic lesion growth by TCDD in adult female rats and mice. Toxicol Sci. 1999;52(1):45–49.
3. Bulun SE. Endometriosis. N Engl J Med. 2009;360(3):268–279.
4. Crain DA, Janssen SJ, Edwards TM, et al. Female reproductive disorders: the roles of endocrine disrupting compounds and developmental timing. Fertil Steril. 2008;90(4):911–940.
5. Heilier JF, Donnez J, Nackers F, et al. Environmental and host-associated risk factors in endometriosis and deep endometriotic nodules: a matched case-control study. Environ Res. 2007;103(1):121–129.
3. What aspects of the patient history are key?
Dr. Stratton recommends that clinicians begin their evaluation of the patient with pain by asking her to describe that pain—how long she has had it, when it occurs, and which areas are affected.
“Most women with endometriosis-associated pain have chronic pelvic pain,” Dr. Stratton continues.5 “Up to 90% of those have dysmenorrhea or cyclic pain with menses.”10 In addition, women with endometriosis “commonly report having pain with any bleeding or spotting. About 30% of women diagnosed with endometriosis initially present to their gynecologist with dyspareunia.”11
“Episodic pain with menses may become more constant, lasting for many days of the month,” says Dr. Stratton. “Women with dyschezia or dysuria may have endometriosis lesions associated with the bowel or bladder, respectively.12 When women with these symptoms do not have lesions on bowel or bladder, these pain symptoms may occur because of higher peritoneal hormone and inflammatory factor levels or because adjacent organs share the neural networks.”
Dr. Giudice views the history similarly.
“I believe listening to the patient is essential in evaluating the possibility of her having endometriosis. This involves asking her to describe where her pain is, grading it on a scale of 1 to 10, identifying when in her cycle it occurs, and learning what makes it better or worse,” she says.
“It also is important to assess the quality of the pain,” Dr. Giudice says. “Does it radiate, does it limit her daily activities, does it interfere with her relationships, intercourse, work, school? Is it associated with bowel movements, urination, other pain syndromes?”
“Having a pain questionnaire is a great help so that patients have a chance to reflect on these and other questions that help to frame the pain associated with endometriosis when they come for consultation,” she adds.
By determining if pain is associated with menstruation or spotting, the clinician is better informed about the value of menstrual suppression, says Dr. Stratton. “Determining what makes the pain better or worse can help define triggers which, if treated, can decrease the likelihood of episodes of pain.”
“A detailed history of any medical or surgical treatments and their outcome is helpful in guiding future treatment,” she adds. “While hormonal therapy has been a mainstay of treatment, in some women, some hormonal treatments may worsen pain or have unacceptable side effects like worsening depression or anxiety. In addition, some pain—especially that associated with deep lesions—may be relieved by surgical treatment13,14; pain that worsened after surgery may suggest neural damage.”
“As there is an engagement of the central nervous system, endometriosis is considered a central sensitivity syndrome in which women may also have other sites of pain,” Dr. Stratton says. “Thus, obtaining a history about current symptoms or prior diagnosis of irritable bowel syndrome, interstitial cystitis/painful bladder, migraines, fibromyalgia, or chronic fatigue syndrome is beneficial.10,15–17 Facilitating treatment for these comorbidities is a key principle in helping women with endometriosis-associated pain, as any condition that triggers or perpetuates pain warrants treatment.”
4. What should the physical exam entail?
“An abdominal exam and a pelvic exam are essential in evaluating pain in a woman when endometriosis is suspected,” says Dr. Giudice. “Sometimes the latter is challenging in young teens and can be deferred.” Overall, however, “the pelvic exam can give insight into pain triggers, adnexal masses (possible endometriomas) and mobility of pelvic organs. A rectovaginal exam is important in evaluating deep infiltrating disease and to gauge the pelvic pain landscape overall. In addition, palpating the pelvic floor musculature is important to distinguish pelvic floor muscle spasm from endometriosis pain.”
“The challenge for clinicians is to think beyond the endometrial implants, taking into account multiple factors that influence pain perception,” says Dr. Stratton. During the examination, the clinician should begin by mapping the regions of pain in the abdomen and back, “distinguishing musculoskeletal pain from deep pain. Determining whether pains are focused or diffuse is also important.”
Dr. Stratton recommends that the routine pelvic exam be modified because a standard bimanual exam “confuses pain signals from the pelvic floor, abdominal wall, bladder, and other viscera. For this reason, a pain-oriented assessment is mandatory.”
Begin with a single digital examination to map tender areas, Dr. Stratton advises. Then consider the size, shape, and mobility of reproductive and pelvic organs. “A bimanual exam will help identify adnexal masses like endometriomas,” she says.
Endometriomas usually are not associated with pain, she adds, but “they are associated with deep infiltrating lesions. Nodularity along the uterosacral ligaments, limited reproductive organ mobility, and thickening of the rectovaginal septum also suggest deep infiltrating lesions. Importantly, deep infiltrating lesions are the lesion type most associated with pain.”18,19
5. Is imaging useful in the diagnosis of endometriosis?
Laparoscopy remains the gold standard for diagnosis of endometriosis, observes Steven R. Goldstein, MD. Visualization of endometriotic implants at the time of surgery—with histologic assessment—offers definitive confirmation of the diagnosis. The physical examination, too, can offer a strong suggestion of endometriosis, he says. Dr. Goldstein is professor of obstetrics and gynecology at New York University School of Medicine and director of gynecologic ultrasound and co-director of bone densitometry at New York University Medical Center in New York City. He serves on the OBG Management Board of Editors.
“In the past, the pelvic examination and history often were the sine qua non for patients with pain,” Dr. Goldstein says. “Extreme dysmenorrhea and pain between periods, especially with intercourse, defecation, and exercise, all increased the suspicion of endometriosis. People used to talk about feeling nodularity in the uterosacral ligaments and finding decreased mobility of pelvic structures—but I don’t have any question that the skill of today’s gynecologists in doing a bimanual pelvic exam is a fraction of what it was in years gone by because they haven’t had the necessity of experience. The first thing they do if there’s any question is they send the patient for an ultrasound.”
Of course, ultrasound can be especially helpful in identifying endometriomas—sometimes called “chocolate cysts”—in the ovary. Endometriomas can have a solid appearance on ultrasound, says Dr. Goldstein, because the fluid they contain (dried blood) is sonolucent or pure black on ultrasound, similar to amniotic fluid or the fluid seen in the bladder. “This ‘chocolate’ fluid contained in endometriomas is homogeneous, particulate, and very monotonous in its appearance, in contrast to the internal echoes observed in hemorrhagic corpus lutea, which are very cobweblike and can sometimes mimic papillary projections,” he adds.
“What’s absolutely essential when imaging a suspected endometrioma by ultrasound is that there be no evidence of any blood flow contained within that structure. Because it’s dried blood, it shouldn’t have any vascularity. If you see blood flow inside what you would call an endometrioma, you need to rethink your diagnosis,” he says.
In some cases, a supposed endometriomalacks a black, sonolucent appearance, but “the clinician often can tell that it’s a cystic structure by the very bright posterior wall—what we call posterior wall acoustic enhancement—even though the interior of the structure may appear sort of grayish or whitish rather than the pure black of a simple cyst. It’s still fluid-filled,” Dr. Goldstein says.
In some instances, even endometriotic nodules can be imaged by ultrasound, he adds. “There’s an increasing body of literature that suggests that, if you look carefully in people with deep infiltrating endometriosis, you can often see solid-appearing nodules in the rectovaginal septum or between the uterus and bladder. With the kind of resolution that we now have with the vaginal probe, some of these nodules can be seen. That’s somewhat new, and it’s a function of 2 things—people looking for endometriosis and the better resolution of more modern equipment.”
Dr. Goldstein believes that magnetic resonance imaging (MRI) is “almost never” indicated in the diagnosis of endometriosis. A more helpful approach would be a consultative ultrasound with someone with more experience. However, when that is not available, or “in areas where you have excellent backup in terms of pelvic MRI, that may be the way to go. I don’t think so,” he demurs, “and some of my colleagues would be very upset at the thought of needing to use MRI to diagnose endometriosis. But in the occasional confusing or difficult case, depending on the quality of the referral pattern you have, it might make sense,” he says.
6. When is diagnostic laparoscopy clearly indicated?
Dr. Giudice believes that laparoscopy—with the intention to treat endometriosis, if present—“is essential when first-line medical therapy fails or when pain is acute and severe.”5
Dr. Stratton concurs. “Any woman with chronic pain wants to know what is causing the pain,” she says. Therefore, “women report a benefit from knowing that their pain is associated with endometriosis.6 However, diagnostic laparoscopy alone, with the sole purpose of determining the presence of endometriosis but not treating the lesions, is no longer performed, as it poses little benefit to the patient other than peace of mind.”
“The general trend in the United States has been to first use hormonal treatments when the diagnosis of endometriosis is suspected, prior to performing surgery,” Dr. Stratton says.1 In many cases, by using cyclic combined hormonal contraceptives to reduce menstrual flow or “suppressing menstruation with continuous combined hormonal contraceptives,” gonadotropin-releasing hormone analogues (combined with progestin to prevent bone loss), “or continuous progestin alone may be effective in decreasing pain. Not surprisingly, these hormonal approaches are effective for any chronic pelvic pain, even for women who do not have the surgical diagnosis of endometriosis.”20
“When the first-line approach to chronic pelvic pain is hormonal treatment, laparoscopy is considered when these medical treatments have failed to control the pain or are poorly tolerated, or when the diagnosis of endometriosis is in question,” Dr. Stratton says.
“Laparoscopy to treat endometriomas is indicated if an endometrioma is enlarging, measures more than 4 cm in diameter, or if the diagnosis of an ovarian mass is in question,” she explains. “While surgeons have previously been aggressive in removing endometriomas, this practice may have negative consequences on ovarian function. Because endometriomas are pseudocysts, removing them completely leads to the removal of viable ovarian tissue and may diminish ovarian reserve.”21,22
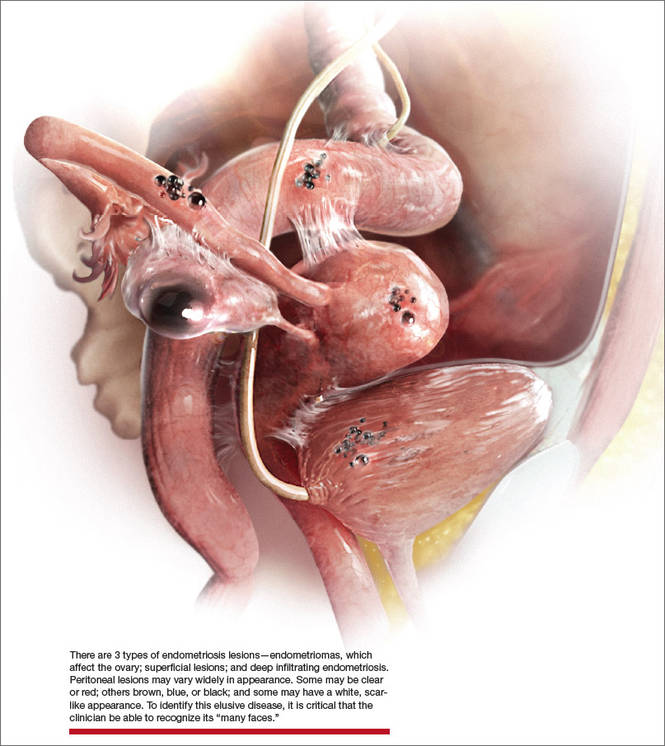
7. What is the surgical appearance of endometriosis?
Dr. Giudice returns to the enigmatic nature of endometriosis in addressing this question, mentioning its “many faces” at the time of surgery. “It is imperative that the surgeon recognize the disease in its many forms,” she says. “Also, it is especially helpful at the time of surgery if suspected lesions are biopsied and sent to pathology to have the diagnosis made unequivocally.”5
As for the surgical appearance of endometriosis, Dr. Stratton notes that there are 3 types of lesions—“superficial lesions, deep infiltrating lesions, and endometriomas. Endometriomas occur almost exclusively in the ovary and are pseudocysts without an identifiable cystic lining. They vary in dimension from a few millimeters to several centimeters.”
“Superficial peritoneal endometriosis lesions have a variable appearance, with some lesions being clear or red, some brown, blue or black, and some having a white appearance, like a scar,” says Dr. Stratton. “Endometriosis can be diagnosed on histologic examination of any of these lesion types.
“Overall, single-color lesions have similar frequencies of biopsy-confirmed endometriosis (59% to 62%),” she says.23 “These lesion appearances likely represent different stages of development of endometriosis, with red or clear lesions occurring first, soon after endometrial tissue implantation; black, blue, or brown lesions occurring later, in response to the hormones varying in the menstrual cycle; and white lesions occurring as the lesions age. Deep infiltrating lesions generally have blue/black or white features.”
“Wide, deep, multiple-color lesions in the cul-de-sac, ovarian fossa or uterosacral ligaments are most likely endometriosis,” Dr. Stratton adds.23 Only lesions with multiple colors have a significantly higher percentage of positive biopsies (76%). Importantly, over half of women with only subtle lesions (small red or white lesions) have endometriosis.
CASE Resolved
You tell the patient that endometriosis is one of the possible diagnoses for her chronic pelvic pain, and you take a focused history. During a pelvic examination, you observe that her right ovary lacks mobility, and you map a number of trigger points for her pain. Transvaginal ultrasound results suggest the presence of nodules in the rectovaginal septum. You begin empiric treatment with continuous combined hormonal contraceptives to suppress menstruation. On her next visit, the patient reports reduced but still bothersome pain. Laparoscopy reveals a 2-cm endometrioma in the right ovary and deep infiltrating lesions in the cul-de-sac. The endometrioma is resected. Histology confirms the diagnosis of endometriosis.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. American College of Obstetricians and Gynecologists. Practice Bulletin #114: Management of endometriosis. Obstet Gynecol. 2010;116(1):223–236.
2. Sanfilippo JS, Wakim NG, Schikler KN, Yussman MA. Endometriosis in association with uterine anomaly. Am J Obstet Gynecol. 1986;154(1):39–43.
3. Taylor HS, Bagot C, Kardana A. HOX gene expression is altered in the endometrium of women with endometriosis. Hum Reprod. 1999;14(5):1328–1331.
4. Berkley KJ, Stratton P. Mechanisms: lessons from translational studies of endometriosis. In: Giamberardino MA, ed. Visceral Pain: Clinical, Pathophysiological and Therapeutic Aspects. Oxford, UK: Oxford University Press; 2009:39–50.
5. Giudice LC. Clinical practice: endometriosis. N Engl J Med. 2010;362(25):2389–2398.
6. Ballard K, Lowton K, Wright J. What’s the delay: a qualitative study of women’s experiences of reaching a diagnosis of endometriosis. Fertil Steril. 2006;86(5):1296–1301.
7. May KE, Conduit-Hulbert SA, Villar J, Kirtley S, Kennedy SH, Becker CM. Peripheral biomarkers of endometriosis: a systematic review. Hum Reprod Update. 2010;16(6):651–674.
8. May KE, Villar J, Kirtley S, Kennedy SH, Becker CM. Endometrial alterations in endometriosis: a systematic review of putative biomarkers. Hum Reprod Update. 2011;17(5):637–653.
9. Tamaresis JS, Irwin JC, Goldfien GA, et al. Molecular classification of endometriosis and disease stage using high-dimensional genomic data. Endocrinology. 2014;155(12):4986–4999.
10. Sinaii N, Cleary SD, Ballweg ML, Nieman LK, Stratton P. High rates of autoimmune and endocrine disorders, fibromyalgia, chronic fatigue syndrome and atopic diseases among women with endometriosis: a survey analysis. Hum Reprod. 2002;17(10):2715–2724.
11. De Graaff AA, D’Hooghe TM, Dunselman GA, et al. The significant effect of endometriosis on physical, mental and social wellbeing: results from an international cross-sectional survey. Hum Reprod. 2013;28(10):2677–2685.
12. Lafay Pillet MC, Huchon C, Santulli P, Borghese B, Chapron C, Fauconnier A. A clinical score can predict associated deep infiltrating endometriosis before surgery for an endometrioma. Hum Reprod. 2014;29(8):1666–1676.
13. Healey M, Cheng C, Kaur H. To excise or ablate endometriosis? A prospective randomized double-blinded trial after 5-year follow-up. J Minim Invasive Gynecol. 2014;21(6):999–1004.
14. Anaf V, El Nakadi I, De Moor V, Chapron C, Pistofidis G, Noel JC. Increased nerve density in deep infiltrating endometriotic nodules. Gynecol Obstet Invest. 2011;71(2):112–117.
15. Stratton P, Berkley KJ. Chronic pelvic pain and endometriosis: translational evidence of the relationship and implications. Hum Reprod Update. 2011;17(3):327–346.
16. Karp BI, Sinaii N, Nieman LK, Silberstein SD, Stratton P. Migraine in women with chronic pelvic pain with and without endometriosis. Fertil Steril. 2011;95(3):895–899.
17. Berkley KJ. A life of pelvic pain. Physiol Behav. 2005;86(3):272–280.
18. Fauconnier A, Chapron C. Endometriosis and pelvic pain: epidemiological evidence of the relationship and implications. Hum Reprod Update. 2005;11(6):595–606.
19. Vercellini P, Fedele L, Aimi G, Pietropaolo G, Consonni D, Crosignani PG. Association between endometriosis stage, lesion type, patient characteristics and severity of pelvic pain symptoms: a multivariate analysis of over 1000 patients. Hum Reprod. 2007;22(1):266–271.
20. Ling FW. Randomized controlled trial of depot leuprolide in patients with chronic pelvic pain and clinically suspected endometriosis. Pelvic Pain Study Group. Obstet Gynecol. 1999;93(1):51–58.
21. Muzii L, Di Tucci C, Di Feliciantonio M, Marchetti C, Perniola G, Panici PB. The effect of surgery for endometrioma on ovarian reserve evaluated by antral follicle count: a systematic review and meta-analysis. Hum Reprod. 2014;29(10):2190–2198.
22. Muzii L, Luciano AA, Zupi E, Panici PB. Effect of surgery for endometrioma on ovarian function: a different point of view. J Minim Invasive Gynecol. 2014;21(4):531–533.
23. Stegmann BJ, Sinaii N, Liu S, et al. Using location, color, size, and depth to characterize and identify endometriosis lesions in a cohort of 133 women. Fertil Steril. 2008;89(6):1632–1636.
Janelle Yates, Senior Editor
Experts featured in this article
| Linda C. Giudice, MD, PhD, is the Robert B. Jaffe, MD, Endowed Professor in the Reproductive Sciences and Chair of Obstetrics, Gynecology, and Reproductive Sciences at the University of California, San Francisco. |
| Steven R. Goldstein, MD, is Professor of Obstetrics and Gynecology at New York University School of Medicine; and Director of Gynecologic Ultrasound and Co-Director of Bone Densitometry at New York University Medical Center in New York City. He serves on the OBG Management Board of Editors. |
| John R. Lue, MD, MPH, is Associate Professor and Chief of the Section of General Obstetrics and Gynecology and Medical Director of Women’s Ambulatory Services at the Medical College of Georgia and Georgia Regents University in Augusta, Georgia. |
| Pamela Stratton, MD, is Chief of the Gynecology Consult Service, Program in Reproductive and Adult Endocrinology, at the Eunice Kennedy Shriver National Institute of Child Health and Human Development in Bethesda, Maryland. |



Dr. Guidice reports that she receives support from NIH/NICHD for research on endometriosis pathophysiology and diagnostic classified development. Dr. Goldstein reports that he has an equipment loan with Philips Ultrasound. Dr. Lue and Dr. Stratton report no financial relationships relevant to this article.
Janelle Yates, Senior Editor
Experts featured in this article
| Linda C. Giudice, MD, PhD, is the Robert B. Jaffe, MD, Endowed Professor in the Reproductive Sciences and Chair of Obstetrics, Gynecology, and Reproductive Sciences at the University of California, San Francisco. |
| Steven R. Goldstein, MD, is Professor of Obstetrics and Gynecology at New York University School of Medicine; and Director of Gynecologic Ultrasound and Co-Director of Bone Densitometry at New York University Medical Center in New York City. He serves on the OBG Management Board of Editors. |
| John R. Lue, MD, MPH, is Associate Professor and Chief of the Section of General Obstetrics and Gynecology and Medical Director of Women’s Ambulatory Services at the Medical College of Georgia and Georgia Regents University in Augusta, Georgia. |
| Pamela Stratton, MD, is Chief of the Gynecology Consult Service, Program in Reproductive and Adult Endocrinology, at the Eunice Kennedy Shriver National Institute of Child Health and Human Development in Bethesda, Maryland. |
Dr. Guidice reports that she receives support from NIH/NICHD for research on endometriosis pathophysiology and diagnostic classified development. Dr. Goldstein reports that he has an equipment loan with Philips Ultrasound. Dr. Lue and Dr. Stratton report no financial relationships relevant to this article.
Janelle Yates, Senior Editor
Experts featured in this article
| Linda C. Giudice, MD, PhD, is the Robert B. Jaffe, MD, Endowed Professor in the Reproductive Sciences and Chair of Obstetrics, Gynecology, and Reproductive Sciences at the University of California, San Francisco. |
| Steven R. Goldstein, MD, is Professor of Obstetrics and Gynecology at New York University School of Medicine; and Director of Gynecologic Ultrasound and Co-Director of Bone Densitometry at New York University Medical Center in New York City. He serves on the OBG Management Board of Editors. |
| John R. Lue, MD, MPH, is Associate Professor and Chief of the Section of General Obstetrics and Gynecology and Medical Director of Women’s Ambulatory Services at the Medical College of Georgia and Georgia Regents University in Augusta, Georgia. |
| Pamela Stratton, MD, is Chief of the Gynecology Consult Service, Program in Reproductive and Adult Endocrinology, at the Eunice Kennedy Shriver National Institute of Child Health and Human Development in Bethesda, Maryland. |
Dr. Guidice reports that she receives support from NIH/NICHD for research on endometriosis pathophysiology and diagnostic classified development. Dr. Goldstein reports that he has an equipment loan with Philips Ultrasound. Dr. Lue and Dr. Stratton report no financial relationships relevant to this article.
CASE Is her chronic pelvic pain caused by endometriosis?
M.L. is a 32-year-old nulliparous woman who is referred to your office by her primary care provider for chronic pelvic pain. She reports severe dysmenorrhea as her main symptom, but she also mentions dyspareunia. She says these symptoms have been present for several years but have increased in intensity gradually. She asks what you consider to be the most likely diagnosis.
What potential diagnoses do you mention to her? And how do you identify the cause of her pain?
Although endometriosis—the presence of endometrial tissue outside the uterus—affects at least 5 million women of reproductive age in the United States alone, it can be a challenging diagnosis for several reasons.
“Endometriosis is a great masquerader,” says Linda Giudice, MD, PhD. “It presents with a variety of pain patterns, intensities, and triggers. It can also involve symptoms that overlap those of other disorders, including disorders of the gastrointestinal and urinary tracts.”
Although endometriosis falls within the differential diagnosis of chronic pelvic pain, “it is usually not high on the list in the primary care setting (adult and adolescent),” Dr. Giudice adds. She is the Robert B. Jaffe, MD, Endowed Professor in the reproductive sciences and chair of obstetrics, gynecology, and reproductive sciences at the University of California, San Francisco.
John R. Lue, MD, MPH, an author of the most recent practice bulletin on endometriosis from the American College of Obstetricians and Gynecologists,1 sees the situation similarly.
“The main challenge in the diagnosis of endometriosis is that its presentation mimics other causes of chronic pelvic pain,” he says. “Pelvic pain due to endometriosis is usually chronic (lasting ≥6 months). It is associated with dysmenorrhea in 50% to 90% of cases, as well as with dyspareunia, deep pelvic pain, and lower abdominal pain with or without back and loin pain. The pain can occur unpredictably and intermittently throughout the menstrual cycle or it can be continuous. In addition, it can be dull, throbbing, or sharp and may be exacerbated by physical activity.2,3 Up to 20% of women with endometriosis have concurrent pain conditions.”4 Dr. Lue is associate professor, chief of the section of general obstetrics and gynecology, and medical director of women’s ambulatory services at the Medical College of Georgia and Georgia Regents University in Augusta, Georgia.
Among other diseases of the female pelvis that have relatively similar presentation, Dr. Lue adds, are pathologies of the:
- uterus (adenomyosis, fibroids)
- fallopian tube (hydrosalpinx)
- ovaries (ovarian cysts)
- bladder (interstitial cystitis)
- bowel (irritable bowel syndrome)
- musculoskeletal system (piriformis syndrome).
Before pelvic pain is attributed to endometriosis, he says, the provider should rule out bowel, bladder, musculoskeletal, and psychiatric causes.
This article focuses on 7 questions, the answers of which are critical to narrowing in on the diagnosis of endometriosis, including essential factors to consider in the patient history, imaging and other diagnostic tools, and considerations in surgical exploration. In the second and third installments of this in-depth series on endometriosis, pain and infertility will be the respective subjects of investigation.
Several theories explain the “why” of endometriosis
A dominant theory is that peritoneal endometrial implants arise from retrograde menstruation, during which endometrial tissue passes through the fallopian tubes into the pelvis, says John R. Lue, MD, MPH. Dr. Lue is associate professor and chief of the section of general obstetrics and gynecology and medical director of women’s ambulatory services at the Medical College of Georgia and Georgia Regents University in Augusta, Georgia.
“Additional theories include immune dysfunction that interferes with clearing of endometrial lesions in the pelvis, as well as genetic alterations that lead to growth dysregulation,” he says.1 “These theories all have merit, and it is likely that the pathogenesis of endometriosis is multifactorial.”
Another strong theory involves the homeobox (HOX) genes, “which mediate embryonic development,” says Dr. Lue.2,3 “These genes are translated into transcription factors that regulate downstream genes necessary for growth and differentiation. It has been demonstrated that HOX genes play an analogous role in endometrial development during the adult menstrual cycle.4 HOX gene expression regulates the growth and development of the human endometrium.5 The expression of HOX genes A10 and A11 varies in response to sex steroids during the menstrual cycle, with dramatic upregulation in the mid-secretory phase,” says Dr. Lue. Recent studies suggest that these genes “play a major role” in endometriosis.6
“Since ovarian endometriomas are clonal and lesions usually have genetic mutations, such somatic mutations with subsequent growth dysregulation may also be etiologic factors,” says Dr. Lue.1,7,8 “Disease at distant sites may be caused by lymphatic or hematogenous spread or metaplastic transformation.”
References
1. Giudice LC, Swierz LM, Burney RO. Edometriosis. In: Jameson JL, DeGroot LJ, eds. Endocrinology. 6th ed. New York, NY: Elsevier; 2010:2356–2370.
2. Krumlauf R. Hox genes in vertebrate development. Cell. 1992;78(2):191–201.
3. McGinnis W, Krumlauf R. Homeobox genes and axial patterning. Cell. 1992;68(2):283–302.
4. Taylor H, Igarashi P, Olive D, Arici A. Sex steroids mediate HOXA11 expression in the human peri-implantation endometrium. J Clin Endocrinol Metab. 1999;84(3):1129–1135.
5. Taylor H, Vanden Heuvel GB, Igarashi P. A conserved HOX axis in the mouse and human female reproductive system: late establishment and persistent adult expression of the HOXA cluster genes. Biol Reprod. 1997;57(6):1338–1345.
6. Taylor HS, Bagot C, Kardana A. HOX gene expression is altered in the endometrium of women with endometriosis. Hum Reprod. 1999;14(5):1328–1331.
7. Practice Committee of the American Society for Reproductive Medicine. Treatment of pelvic pain associated with endometriosis. Fertil Steril. 2008;90(5 suppl):S260–S269.
8. Bulun SE. Endometriosis. N Engl J Med. 2009;360(3):268–279.
1. Why such a long delay in diagnosis?
Investigators exploring the length of time between a patient’s presentation with symptoms and diagnosis have found it to be particularly long for endometriosis, ranging from 6 to 11 years.
Because endometriosis is usually not high on the list of differential diagnoses for chronic pelvic pain in the primary care setting, a patient may not be referred to a gynecologist unless those symptoms include severe dysmenorrhea, dyspareunia, or similar findings. Once the referral is made, the gynecologist “will usually try contraceptive steroids, nonsteroidal anti-inflammatory drugs, or second-line progestins before a diagnosis is made,” says Dr. Giudice.5
The delay in diagnosis “is astounding,” she adds, “and has its roots in empiric medical therapies and a combination of patients fearing a diagnosis of cancer and reluctance of gynecologists to perform laparoscopy on adolescents.”6
Another possible cause of diagnostic delay: Some adolescent girls may not realize when their pain is severe. Because they may have always experienced a high degree of pain since menarche, they may assume it to be a normal aspect of womanhood and delay seeking help, says Pamela Stratton, MD, chief of the gynecology consult service at the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
2. Have any biomarkers proved to be useful diagnostic tools?
Any biomarker proven to reliably identify endometriosis would be a boon to medicine, as it would provide a noninvasive or minimally invasive alternative to diagnostic laparoscopy, the current gold standard. Regrettably, the search for such a biomarker has produced “disappointing results,” says Dr. Giudice.
“Recent systematic reviews of all proposed endometriosis-related biomarkers over the last 25 years in serum, plasma, urine, and endometrium could not identify an unequivocally clinically useful biomarker or panel of biomarkers,” she notes.7,8 “This is due mainly to low numbers of subjects, small populations for validations, cycle/hormonal- and disease stage-dependence, poorly defined controls, and low sensitivity and specificity.”
One hopeful development: “Whole genome transcriptomics of archived endometrial tissue and machine learning found several classifiers to diagnose and stage endometriosis with high accuracy that were validated on an independent sample set,” says Dr. Giudice.9 “However, these data now warrant a prospective, multisite study for further validation.”
Environmental factors, estrogen, and endometriosis
“There is increasing evidence that in utero and also adult exposures to endocrine-disrupting chemicals (EDCs) play a role in the pathogenesis and progression of disease,” says Linda Giudice, MD, PhD, the Robert B. Jaffe, MD, Endowed Professor in the reproductive sciences and chair of obstetrics, gynecology, and reproductive sciences at the University of California, San Francisco.
“For example, the Nurses’ Health Study II, a prospective cohort study of more than 80,000 women, revealed that daughters exposed to diethylstilbestrol (DES) had an 80% increased risk (odds ratio [OR], 1.8; 95% confidence interval [CI], 1.2–2.8) of developing endometriosis,” she says.1
“Also, dioxin (TCDD) exposure in rats in utero on gestational day 8 increased the size of endometriosis lesions when combined with an adult exposure,” Dr. Giudice says.2 Although we do not know the precise mechanisms underlying in utero events that result in disease onset as a teen or adult, abnormal programming of the female reproductive tract by EDCs and similar agents is believed to play a role, she says.3
Because estrogen is essential for endometriosis lesions and associated symptoms to progress, “EDCs that have either estrogenic activity or interfere with estrogen metabolism or action, or both, have been proposed as contributors to progression of disease. Abundant animal data using nonhuman primate and rodent models and exposures to organochlorines and other EDCs support this hypothesis,” Dr. Giudice says.4
“The weight of human evidence of associations of EDCs and the risk of endometriosis in adult women depends on the class of endocrine disrupter,” Dr. Giudice continues. “Strongest correlations are with polychlorobiphenyls (PCBs), where 10 of 12 studies found significant odds of disease and circulating or omental fat concentrations of these compounds. PCBs inhibit peripheral natural killer cell activity and interleukin 1b and 12 production, relevant to the immune component of endometriosis progression.”
“Significant risk has also been associated with organochlorines (in three of three studies) and perfluorochemicals. In contrast, data linking endometriosis with exposures to dioxins, phthalates, and bisphenol A are equivocal, with some studies finding significant odds ratios and others failing to find significant correlations. Interestingly, dioxins have a significant association with deep infiltrating endometriotic lesions.”5
References
1. Missmer SA, Hankinson SE, Spiegelman D, Barbieri RL, Michels KB, Hunter DJ. In utero exposures and the incidence of endometriosis. Fertil Steril. 2004;82(6):1501–1508.
2. Cummings AM, Hedge JM, Birnbaum LS. Effects on prenatal exposure to TCDD on the promotion of endometriotic lesion growth by TCDD in adult female rats and mice. Toxicol Sci. 1999;52(1):45–49.
3. Bulun SE. Endometriosis. N Engl J Med. 2009;360(3):268–279.
4. Crain DA, Janssen SJ, Edwards TM, et al. Female reproductive disorders: the roles of endocrine disrupting compounds and developmental timing. Fertil Steril. 2008;90(4):911–940.
5. Heilier JF, Donnez J, Nackers F, et al. Environmental and host-associated risk factors in endometriosis and deep endometriotic nodules: a matched case-control study. Environ Res. 2007;103(1):121–129.
3. What aspects of the patient history are key?
Dr. Stratton recommends that clinicians begin their evaluation of the patient with pain by asking her to describe that pain—how long she has had it, when it occurs, and which areas are affected.
“Most women with endometriosis-associated pain have chronic pelvic pain,” Dr. Stratton continues.5 “Up to 90% of those have dysmenorrhea or cyclic pain with menses.”10 In addition, women with endometriosis “commonly report having pain with any bleeding or spotting. About 30% of women diagnosed with endometriosis initially present to their gynecologist with dyspareunia.”11
“Episodic pain with menses may become more constant, lasting for many days of the month,” says Dr. Stratton. “Women with dyschezia or dysuria may have endometriosis lesions associated with the bowel or bladder, respectively.12 When women with these symptoms do not have lesions on bowel or bladder, these pain symptoms may occur because of higher peritoneal hormone and inflammatory factor levels or because adjacent organs share the neural networks.”
Dr. Giudice views the history similarly.
“I believe listening to the patient is essential in evaluating the possibility of her having endometriosis. This involves asking her to describe where her pain is, grading it on a scale of 1 to 10, identifying when in her cycle it occurs, and learning what makes it better or worse,” she says.
“It also is important to assess the quality of the pain,” Dr. Giudice says. “Does it radiate, does it limit her daily activities, does it interfere with her relationships, intercourse, work, school? Is it associated with bowel movements, urination, other pain syndromes?”
“Having a pain questionnaire is a great help so that patients have a chance to reflect on these and other questions that help to frame the pain associated with endometriosis when they come for consultation,” she adds.
By determining if pain is associated with menstruation or spotting, the clinician is better informed about the value of menstrual suppression, says Dr. Stratton. “Determining what makes the pain better or worse can help define triggers which, if treated, can decrease the likelihood of episodes of pain.”
“A detailed history of any medical or surgical treatments and their outcome is helpful in guiding future treatment,” she adds. “While hormonal therapy has been a mainstay of treatment, in some women, some hormonal treatments may worsen pain or have unacceptable side effects like worsening depression or anxiety. In addition, some pain—especially that associated with deep lesions—may be relieved by surgical treatment13,14; pain that worsened after surgery may suggest neural damage.”
“As there is an engagement of the central nervous system, endometriosis is considered a central sensitivity syndrome in which women may also have other sites of pain,” Dr. Stratton says. “Thus, obtaining a history about current symptoms or prior diagnosis of irritable bowel syndrome, interstitial cystitis/painful bladder, migraines, fibromyalgia, or chronic fatigue syndrome is beneficial.10,15–17 Facilitating treatment for these comorbidities is a key principle in helping women with endometriosis-associated pain, as any condition that triggers or perpetuates pain warrants treatment.”
4. What should the physical exam entail?
“An abdominal exam and a pelvic exam are essential in evaluating pain in a woman when endometriosis is suspected,” says Dr. Giudice. “Sometimes the latter is challenging in young teens and can be deferred.” Overall, however, “the pelvic exam can give insight into pain triggers, adnexal masses (possible endometriomas) and mobility of pelvic organs. A rectovaginal exam is important in evaluating deep infiltrating disease and to gauge the pelvic pain landscape overall. In addition, palpating the pelvic floor musculature is important to distinguish pelvic floor muscle spasm from endometriosis pain.”
“The challenge for clinicians is to think beyond the endometrial implants, taking into account multiple factors that influence pain perception,” says Dr. Stratton. During the examination, the clinician should begin by mapping the regions of pain in the abdomen and back, “distinguishing musculoskeletal pain from deep pain. Determining whether pains are focused or diffuse is also important.”
Dr. Stratton recommends that the routine pelvic exam be modified because a standard bimanual exam “confuses pain signals from the pelvic floor, abdominal wall, bladder, and other viscera. For this reason, a pain-oriented assessment is mandatory.”
Begin with a single digital examination to map tender areas, Dr. Stratton advises. Then consider the size, shape, and mobility of reproductive and pelvic organs. “A bimanual exam will help identify adnexal masses like endometriomas,” she says.
Endometriomas usually are not associated with pain, she adds, but “they are associated with deep infiltrating lesions. Nodularity along the uterosacral ligaments, limited reproductive organ mobility, and thickening of the rectovaginal septum also suggest deep infiltrating lesions. Importantly, deep infiltrating lesions are the lesion type most associated with pain.”18,19
5. Is imaging useful in the diagnosis of endometriosis?
Laparoscopy remains the gold standard for diagnosis of endometriosis, observes Steven R. Goldstein, MD. Visualization of endometriotic implants at the time of surgery—with histologic assessment—offers definitive confirmation of the diagnosis. The physical examination, too, can offer a strong suggestion of endometriosis, he says. Dr. Goldstein is professor of obstetrics and gynecology at New York University School of Medicine and director of gynecologic ultrasound and co-director of bone densitometry at New York University Medical Center in New York City. He serves on the OBG Management Board of Editors.
“In the past, the pelvic examination and history often were the sine qua non for patients with pain,” Dr. Goldstein says. “Extreme dysmenorrhea and pain between periods, especially with intercourse, defecation, and exercise, all increased the suspicion of endometriosis. People used to talk about feeling nodularity in the uterosacral ligaments and finding decreased mobility of pelvic structures—but I don’t have any question that the skill of today’s gynecologists in doing a bimanual pelvic exam is a fraction of what it was in years gone by because they haven’t had the necessity of experience. The first thing they do if there’s any question is they send the patient for an ultrasound.”
Of course, ultrasound can be especially helpful in identifying endometriomas—sometimes called “chocolate cysts”—in the ovary. Endometriomas can have a solid appearance on ultrasound, says Dr. Goldstein, because the fluid they contain (dried blood) is sonolucent or pure black on ultrasound, similar to amniotic fluid or the fluid seen in the bladder. “This ‘chocolate’ fluid contained in endometriomas is homogeneous, particulate, and very monotonous in its appearance, in contrast to the internal echoes observed in hemorrhagic corpus lutea, which are very cobweblike and can sometimes mimic papillary projections,” he adds.
“What’s absolutely essential when imaging a suspected endometrioma by ultrasound is that there be no evidence of any blood flow contained within that structure. Because it’s dried blood, it shouldn’t have any vascularity. If you see blood flow inside what you would call an endometrioma, you need to rethink your diagnosis,” he says.
In some cases, a supposed endometriomalacks a black, sonolucent appearance, but “the clinician often can tell that it’s a cystic structure by the very bright posterior wall—what we call posterior wall acoustic enhancement—even though the interior of the structure may appear sort of grayish or whitish rather than the pure black of a simple cyst. It’s still fluid-filled,” Dr. Goldstein says.
In some instances, even endometriotic nodules can be imaged by ultrasound, he adds. “There’s an increasing body of literature that suggests that, if you look carefully in people with deep infiltrating endometriosis, you can often see solid-appearing nodules in the rectovaginal septum or between the uterus and bladder. With the kind of resolution that we now have with the vaginal probe, some of these nodules can be seen. That’s somewhat new, and it’s a function of 2 things—people looking for endometriosis and the better resolution of more modern equipment.”
Dr. Goldstein believes that magnetic resonance imaging (MRI) is “almost never” indicated in the diagnosis of endometriosis. A more helpful approach would be a consultative ultrasound with someone with more experience. However, when that is not available, or “in areas where you have excellent backup in terms of pelvic MRI, that may be the way to go. I don’t think so,” he demurs, “and some of my colleagues would be very upset at the thought of needing to use MRI to diagnose endometriosis. But in the occasional confusing or difficult case, depending on the quality of the referral pattern you have, it might make sense,” he says.
6. When is diagnostic laparoscopy clearly indicated?
Dr. Giudice believes that laparoscopy—with the intention to treat endometriosis, if present—“is essential when first-line medical therapy fails or when pain is acute and severe.”5
Dr. Stratton concurs. “Any woman with chronic pain wants to know what is causing the pain,” she says. Therefore, “women report a benefit from knowing that their pain is associated with endometriosis.6 However, diagnostic laparoscopy alone, with the sole purpose of determining the presence of endometriosis but not treating the lesions, is no longer performed, as it poses little benefit to the patient other than peace of mind.”
“The general trend in the United States has been to first use hormonal treatments when the diagnosis of endometriosis is suspected, prior to performing surgery,” Dr. Stratton says.1 In many cases, by using cyclic combined hormonal contraceptives to reduce menstrual flow or “suppressing menstruation with continuous combined hormonal contraceptives,” gonadotropin-releasing hormone analogues (combined with progestin to prevent bone loss), “or continuous progestin alone may be effective in decreasing pain. Not surprisingly, these hormonal approaches are effective for any chronic pelvic pain, even for women who do not have the surgical diagnosis of endometriosis.”20
“When the first-line approach to chronic pelvic pain is hormonal treatment, laparoscopy is considered when these medical treatments have failed to control the pain or are poorly tolerated, or when the diagnosis of endometriosis is in question,” Dr. Stratton says.
“Laparoscopy to treat endometriomas is indicated if an endometrioma is enlarging, measures more than 4 cm in diameter, or if the diagnosis of an ovarian mass is in question,” she explains. “While surgeons have previously been aggressive in removing endometriomas, this practice may have negative consequences on ovarian function. Because endometriomas are pseudocysts, removing them completely leads to the removal of viable ovarian tissue and may diminish ovarian reserve.”21,22
7. What is the surgical appearance of endometriosis?
Dr. Giudice returns to the enigmatic nature of endometriosis in addressing this question, mentioning its “many faces” at the time of surgery. “It is imperative that the surgeon recognize the disease in its many forms,” she says. “Also, it is especially helpful at the time of surgery if suspected lesions are biopsied and sent to pathology to have the diagnosis made unequivocally.”5
As for the surgical appearance of endometriosis, Dr. Stratton notes that there are 3 types of lesions—“superficial lesions, deep infiltrating lesions, and endometriomas. Endometriomas occur almost exclusively in the ovary and are pseudocysts without an identifiable cystic lining. They vary in dimension from a few millimeters to several centimeters.”
“Superficial peritoneal endometriosis lesions have a variable appearance, with some lesions being clear or red, some brown, blue or black, and some having a white appearance, like a scar,” says Dr. Stratton. “Endometriosis can be diagnosed on histologic examination of any of these lesion types.
“Overall, single-color lesions have similar frequencies of biopsy-confirmed endometriosis (59% to 62%),” she says.23 “These lesion appearances likely represent different stages of development of endometriosis, with red or clear lesions occurring first, soon after endometrial tissue implantation; black, blue, or brown lesions occurring later, in response to the hormones varying in the menstrual cycle; and white lesions occurring as the lesions age. Deep infiltrating lesions generally have blue/black or white features.”
“Wide, deep, multiple-color lesions in the cul-de-sac, ovarian fossa or uterosacral ligaments are most likely endometriosis,” Dr. Stratton adds.23 Only lesions with multiple colors have a significantly higher percentage of positive biopsies (76%). Importantly, over half of women with only subtle lesions (small red or white lesions) have endometriosis.
CASE Resolved
You tell the patient that endometriosis is one of the possible diagnoses for her chronic pelvic pain, and you take a focused history. During a pelvic examination, you observe that her right ovary lacks mobility, and you map a number of trigger points for her pain. Transvaginal ultrasound results suggest the presence of nodules in the rectovaginal septum. You begin empiric treatment with continuous combined hormonal contraceptives to suppress menstruation. On her next visit, the patient reports reduced but still bothersome pain. Laparoscopy reveals a 2-cm endometrioma in the right ovary and deep infiltrating lesions in the cul-de-sac. The endometrioma is resected. Histology confirms the diagnosis of endometriosis.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
CASE Is her chronic pelvic pain caused by endometriosis?
M.L. is a 32-year-old nulliparous woman who is referred to your office by her primary care provider for chronic pelvic pain. She reports severe dysmenorrhea as her main symptom, but she also mentions dyspareunia. She says these symptoms have been present for several years but have increased in intensity gradually. She asks what you consider to be the most likely diagnosis.
What potential diagnoses do you mention to her? And how do you identify the cause of her pain?
Although endometriosis—the presence of endometrial tissue outside the uterus—affects at least 5 million women of reproductive age in the United States alone, it can be a challenging diagnosis for several reasons.
“Endometriosis is a great masquerader,” says Linda Giudice, MD, PhD. “It presents with a variety of pain patterns, intensities, and triggers. It can also involve symptoms that overlap those of other disorders, including disorders of the gastrointestinal and urinary tracts.”
Although endometriosis falls within the differential diagnosis of chronic pelvic pain, “it is usually not high on the list in the primary care setting (adult and adolescent),” Dr. Giudice adds. She is the Robert B. Jaffe, MD, Endowed Professor in the reproductive sciences and chair of obstetrics, gynecology, and reproductive sciences at the University of California, San Francisco.
John R. Lue, MD, MPH, an author of the most recent practice bulletin on endometriosis from the American College of Obstetricians and Gynecologists,1 sees the situation similarly.
“The main challenge in the diagnosis of endometriosis is that its presentation mimics other causes of chronic pelvic pain,” he says. “Pelvic pain due to endometriosis is usually chronic (lasting ≥6 months). It is associated with dysmenorrhea in 50% to 90% of cases, as well as with dyspareunia, deep pelvic pain, and lower abdominal pain with or without back and loin pain. The pain can occur unpredictably and intermittently throughout the menstrual cycle or it can be continuous. In addition, it can be dull, throbbing, or sharp and may be exacerbated by physical activity.2,3 Up to 20% of women with endometriosis have concurrent pain conditions.”4 Dr. Lue is associate professor, chief of the section of general obstetrics and gynecology, and medical director of women’s ambulatory services at the Medical College of Georgia and Georgia Regents University in Augusta, Georgia.
Among other diseases of the female pelvis that have relatively similar presentation, Dr. Lue adds, are pathologies of the:
- uterus (adenomyosis, fibroids)
- fallopian tube (hydrosalpinx)
- ovaries (ovarian cysts)
- bladder (interstitial cystitis)
- bowel (irritable bowel syndrome)
- musculoskeletal system (piriformis syndrome).
Before pelvic pain is attributed to endometriosis, he says, the provider should rule out bowel, bladder, musculoskeletal, and psychiatric causes.
This article focuses on 7 questions, the answers of which are critical to narrowing in on the diagnosis of endometriosis, including essential factors to consider in the patient history, imaging and other diagnostic tools, and considerations in surgical exploration. In the second and third installments of this in-depth series on endometriosis, pain and infertility will be the respective subjects of investigation.
Several theories explain the “why” of endometriosis
A dominant theory is that peritoneal endometrial implants arise from retrograde menstruation, during which endometrial tissue passes through the fallopian tubes into the pelvis, says John R. Lue, MD, MPH. Dr. Lue is associate professor and chief of the section of general obstetrics and gynecology and medical director of women’s ambulatory services at the Medical College of Georgia and Georgia Regents University in Augusta, Georgia.
“Additional theories include immune dysfunction that interferes with clearing of endometrial lesions in the pelvis, as well as genetic alterations that lead to growth dysregulation,” he says.1 “These theories all have merit, and it is likely that the pathogenesis of endometriosis is multifactorial.”
Another strong theory involves the homeobox (HOX) genes, “which mediate embryonic development,” says Dr. Lue.2,3 “These genes are translated into transcription factors that regulate downstream genes necessary for growth and differentiation. It has been demonstrated that HOX genes play an analogous role in endometrial development during the adult menstrual cycle.4 HOX gene expression regulates the growth and development of the human endometrium.5 The expression of HOX genes A10 and A11 varies in response to sex steroids during the menstrual cycle, with dramatic upregulation in the mid-secretory phase,” says Dr. Lue. Recent studies suggest that these genes “play a major role” in endometriosis.6
“Since ovarian endometriomas are clonal and lesions usually have genetic mutations, such somatic mutations with subsequent growth dysregulation may also be etiologic factors,” says Dr. Lue.1,7,8 “Disease at distant sites may be caused by lymphatic or hematogenous spread or metaplastic transformation.”
References
1. Giudice LC, Swierz LM, Burney RO. Edometriosis. In: Jameson JL, DeGroot LJ, eds. Endocrinology. 6th ed. New York, NY: Elsevier; 2010:2356–2370.
2. Krumlauf R. Hox genes in vertebrate development. Cell. 1992;78(2):191–201.
3. McGinnis W, Krumlauf R. Homeobox genes and axial patterning. Cell. 1992;68(2):283–302.
4. Taylor H, Igarashi P, Olive D, Arici A. Sex steroids mediate HOXA11 expression in the human peri-implantation endometrium. J Clin Endocrinol Metab. 1999;84(3):1129–1135.
5. Taylor H, Vanden Heuvel GB, Igarashi P. A conserved HOX axis in the mouse and human female reproductive system: late establishment and persistent adult expression of the HOXA cluster genes. Biol Reprod. 1997;57(6):1338–1345.
6. Taylor HS, Bagot C, Kardana A. HOX gene expression is altered in the endometrium of women with endometriosis. Hum Reprod. 1999;14(5):1328–1331.
7. Practice Committee of the American Society for Reproductive Medicine. Treatment of pelvic pain associated with endometriosis. Fertil Steril. 2008;90(5 suppl):S260–S269.
8. Bulun SE. Endometriosis. N Engl J Med. 2009;360(3):268–279.
1. Why such a long delay in diagnosis?
Investigators exploring the length of time between a patient’s presentation with symptoms and diagnosis have found it to be particularly long for endometriosis, ranging from 6 to 11 years.
Because endometriosis is usually not high on the list of differential diagnoses for chronic pelvic pain in the primary care setting, a patient may not be referred to a gynecologist unless those symptoms include severe dysmenorrhea, dyspareunia, or similar findings. Once the referral is made, the gynecologist “will usually try contraceptive steroids, nonsteroidal anti-inflammatory drugs, or second-line progestins before a diagnosis is made,” says Dr. Giudice.5
The delay in diagnosis “is astounding,” she adds, “and has its roots in empiric medical therapies and a combination of patients fearing a diagnosis of cancer and reluctance of gynecologists to perform laparoscopy on adolescents.”6
Another possible cause of diagnostic delay: Some adolescent girls may not realize when their pain is severe. Because they may have always experienced a high degree of pain since menarche, they may assume it to be a normal aspect of womanhood and delay seeking help, says Pamela Stratton, MD, chief of the gynecology consult service at the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
2. Have any biomarkers proved to be useful diagnostic tools?
Any biomarker proven to reliably identify endometriosis would be a boon to medicine, as it would provide a noninvasive or minimally invasive alternative to diagnostic laparoscopy, the current gold standard. Regrettably, the search for such a biomarker has produced “disappointing results,” says Dr. Giudice.
“Recent systematic reviews of all proposed endometriosis-related biomarkers over the last 25 years in serum, plasma, urine, and endometrium could not identify an unequivocally clinically useful biomarker or panel of biomarkers,” she notes.7,8 “This is due mainly to low numbers of subjects, small populations for validations, cycle/hormonal- and disease stage-dependence, poorly defined controls, and low sensitivity and specificity.”
One hopeful development: “Whole genome transcriptomics of archived endometrial tissue and machine learning found several classifiers to diagnose and stage endometriosis with high accuracy that were validated on an independent sample set,” says Dr. Giudice.9 “However, these data now warrant a prospective, multisite study for further validation.”
Environmental factors, estrogen, and endometriosis
“There is increasing evidence that in utero and also adult exposures to endocrine-disrupting chemicals (EDCs) play a role in the pathogenesis and progression of disease,” says Linda Giudice, MD, PhD, the Robert B. Jaffe, MD, Endowed Professor in the reproductive sciences and chair of obstetrics, gynecology, and reproductive sciences at the University of California, San Francisco.
“For example, the Nurses’ Health Study II, a prospective cohort study of more than 80,000 women, revealed that daughters exposed to diethylstilbestrol (DES) had an 80% increased risk (odds ratio [OR], 1.8; 95% confidence interval [CI], 1.2–2.8) of developing endometriosis,” she says.1
“Also, dioxin (TCDD) exposure in rats in utero on gestational day 8 increased the size of endometriosis lesions when combined with an adult exposure,” Dr. Giudice says.2 Although we do not know the precise mechanisms underlying in utero events that result in disease onset as a teen or adult, abnormal programming of the female reproductive tract by EDCs and similar agents is believed to play a role, she says.3
Because estrogen is essential for endometriosis lesions and associated symptoms to progress, “EDCs that have either estrogenic activity or interfere with estrogen metabolism or action, or both, have been proposed as contributors to progression of disease. Abundant animal data using nonhuman primate and rodent models and exposures to organochlorines and other EDCs support this hypothesis,” Dr. Giudice says.4
“The weight of human evidence of associations of EDCs and the risk of endometriosis in adult women depends on the class of endocrine disrupter,” Dr. Giudice continues. “Strongest correlations are with polychlorobiphenyls (PCBs), where 10 of 12 studies found significant odds of disease and circulating or omental fat concentrations of these compounds. PCBs inhibit peripheral natural killer cell activity and interleukin 1b and 12 production, relevant to the immune component of endometriosis progression.”
“Significant risk has also been associated with organochlorines (in three of three studies) and perfluorochemicals. In contrast, data linking endometriosis with exposures to dioxins, phthalates, and bisphenol A are equivocal, with some studies finding significant odds ratios and others failing to find significant correlations. Interestingly, dioxins have a significant association with deep infiltrating endometriotic lesions.”5
References
1. Missmer SA, Hankinson SE, Spiegelman D, Barbieri RL, Michels KB, Hunter DJ. In utero exposures and the incidence of endometriosis. Fertil Steril. 2004;82(6):1501–1508.
2. Cummings AM, Hedge JM, Birnbaum LS. Effects on prenatal exposure to TCDD on the promotion of endometriotic lesion growth by TCDD in adult female rats and mice. Toxicol Sci. 1999;52(1):45–49.
3. Bulun SE. Endometriosis. N Engl J Med. 2009;360(3):268–279.
4. Crain DA, Janssen SJ, Edwards TM, et al. Female reproductive disorders: the roles of endocrine disrupting compounds and developmental timing. Fertil Steril. 2008;90(4):911–940.
5. Heilier JF, Donnez J, Nackers F, et al. Environmental and host-associated risk factors in endometriosis and deep endometriotic nodules: a matched case-control study. Environ Res. 2007;103(1):121–129.
3. What aspects of the patient history are key?
Dr. Stratton recommends that clinicians begin their evaluation of the patient with pain by asking her to describe that pain—how long she has had it, when it occurs, and which areas are affected.
“Most women with endometriosis-associated pain have chronic pelvic pain,” Dr. Stratton continues.5 “Up to 90% of those have dysmenorrhea or cyclic pain with menses.”10 In addition, women with endometriosis “commonly report having pain with any bleeding or spotting. About 30% of women diagnosed with endometriosis initially present to their gynecologist with dyspareunia.”11
“Episodic pain with menses may become more constant, lasting for many days of the month,” says Dr. Stratton. “Women with dyschezia or dysuria may have endometriosis lesions associated with the bowel or bladder, respectively.12 When women with these symptoms do not have lesions on bowel or bladder, these pain symptoms may occur because of higher peritoneal hormone and inflammatory factor levels or because adjacent organs share the neural networks.”
Dr. Giudice views the history similarly.
“I believe listening to the patient is essential in evaluating the possibility of her having endometriosis. This involves asking her to describe where her pain is, grading it on a scale of 1 to 10, identifying when in her cycle it occurs, and learning what makes it better or worse,” she says.
“It also is important to assess the quality of the pain,” Dr. Giudice says. “Does it radiate, does it limit her daily activities, does it interfere with her relationships, intercourse, work, school? Is it associated with bowel movements, urination, other pain syndromes?”
“Having a pain questionnaire is a great help so that patients have a chance to reflect on these and other questions that help to frame the pain associated with endometriosis when they come for consultation,” she adds.
By determining if pain is associated with menstruation or spotting, the clinician is better informed about the value of menstrual suppression, says Dr. Stratton. “Determining what makes the pain better or worse can help define triggers which, if treated, can decrease the likelihood of episodes of pain.”
“A detailed history of any medical or surgical treatments and their outcome is helpful in guiding future treatment,” she adds. “While hormonal therapy has been a mainstay of treatment, in some women, some hormonal treatments may worsen pain or have unacceptable side effects like worsening depression or anxiety. In addition, some pain—especially that associated with deep lesions—may be relieved by surgical treatment13,14; pain that worsened after surgery may suggest neural damage.”
“As there is an engagement of the central nervous system, endometriosis is considered a central sensitivity syndrome in which women may also have other sites of pain,” Dr. Stratton says. “Thus, obtaining a history about current symptoms or prior diagnosis of irritable bowel syndrome, interstitial cystitis/painful bladder, migraines, fibromyalgia, or chronic fatigue syndrome is beneficial.10,15–17 Facilitating treatment for these comorbidities is a key principle in helping women with endometriosis-associated pain, as any condition that triggers or perpetuates pain warrants treatment.”
4. What should the physical exam entail?
“An abdominal exam and a pelvic exam are essential in evaluating pain in a woman when endometriosis is suspected,” says Dr. Giudice. “Sometimes the latter is challenging in young teens and can be deferred.” Overall, however, “the pelvic exam can give insight into pain triggers, adnexal masses (possible endometriomas) and mobility of pelvic organs. A rectovaginal exam is important in evaluating deep infiltrating disease and to gauge the pelvic pain landscape overall. In addition, palpating the pelvic floor musculature is important to distinguish pelvic floor muscle spasm from endometriosis pain.”
“The challenge for clinicians is to think beyond the endometrial implants, taking into account multiple factors that influence pain perception,” says Dr. Stratton. During the examination, the clinician should begin by mapping the regions of pain in the abdomen and back, “distinguishing musculoskeletal pain from deep pain. Determining whether pains are focused or diffuse is also important.”
Dr. Stratton recommends that the routine pelvic exam be modified because a standard bimanual exam “confuses pain signals from the pelvic floor, abdominal wall, bladder, and other viscera. For this reason, a pain-oriented assessment is mandatory.”
Begin with a single digital examination to map tender areas, Dr. Stratton advises. Then consider the size, shape, and mobility of reproductive and pelvic organs. “A bimanual exam will help identify adnexal masses like endometriomas,” she says.
Endometriomas usually are not associated with pain, she adds, but “they are associated with deep infiltrating lesions. Nodularity along the uterosacral ligaments, limited reproductive organ mobility, and thickening of the rectovaginal septum also suggest deep infiltrating lesions. Importantly, deep infiltrating lesions are the lesion type most associated with pain.”18,19
5. Is imaging useful in the diagnosis of endometriosis?
Laparoscopy remains the gold standard for diagnosis of endometriosis, observes Steven R. Goldstein, MD. Visualization of endometriotic implants at the time of surgery—with histologic assessment—offers definitive confirmation of the diagnosis. The physical examination, too, can offer a strong suggestion of endometriosis, he says. Dr. Goldstein is professor of obstetrics and gynecology at New York University School of Medicine and director of gynecologic ultrasound and co-director of bone densitometry at New York University Medical Center in New York City. He serves on the OBG Management Board of Editors.
“In the past, the pelvic examination and history often were the sine qua non for patients with pain,” Dr. Goldstein says. “Extreme dysmenorrhea and pain between periods, especially with intercourse, defecation, and exercise, all increased the suspicion of endometriosis. People used to talk about feeling nodularity in the uterosacral ligaments and finding decreased mobility of pelvic structures—but I don’t have any question that the skill of today’s gynecologists in doing a bimanual pelvic exam is a fraction of what it was in years gone by because they haven’t had the necessity of experience. The first thing they do if there’s any question is they send the patient for an ultrasound.”
Of course, ultrasound can be especially helpful in identifying endometriomas—sometimes called “chocolate cysts”—in the ovary. Endometriomas can have a solid appearance on ultrasound, says Dr. Goldstein, because the fluid they contain (dried blood) is sonolucent or pure black on ultrasound, similar to amniotic fluid or the fluid seen in the bladder. “This ‘chocolate’ fluid contained in endometriomas is homogeneous, particulate, and very monotonous in its appearance, in contrast to the internal echoes observed in hemorrhagic corpus lutea, which are very cobweblike and can sometimes mimic papillary projections,” he adds.
“What’s absolutely essential when imaging a suspected endometrioma by ultrasound is that there be no evidence of any blood flow contained within that structure. Because it’s dried blood, it shouldn’t have any vascularity. If you see blood flow inside what you would call an endometrioma, you need to rethink your diagnosis,” he says.
In some cases, a supposed endometriomalacks a black, sonolucent appearance, but “the clinician often can tell that it’s a cystic structure by the very bright posterior wall—what we call posterior wall acoustic enhancement—even though the interior of the structure may appear sort of grayish or whitish rather than the pure black of a simple cyst. It’s still fluid-filled,” Dr. Goldstein says.
In some instances, even endometriotic nodules can be imaged by ultrasound, he adds. “There’s an increasing body of literature that suggests that, if you look carefully in people with deep infiltrating endometriosis, you can often see solid-appearing nodules in the rectovaginal septum or between the uterus and bladder. With the kind of resolution that we now have with the vaginal probe, some of these nodules can be seen. That’s somewhat new, and it’s a function of 2 things—people looking for endometriosis and the better resolution of more modern equipment.”
Dr. Goldstein believes that magnetic resonance imaging (MRI) is “almost never” indicated in the diagnosis of endometriosis. A more helpful approach would be a consultative ultrasound with someone with more experience. However, when that is not available, or “in areas where you have excellent backup in terms of pelvic MRI, that may be the way to go. I don’t think so,” he demurs, “and some of my colleagues would be very upset at the thought of needing to use MRI to diagnose endometriosis. But in the occasional confusing or difficult case, depending on the quality of the referral pattern you have, it might make sense,” he says.
6. When is diagnostic laparoscopy clearly indicated?
Dr. Giudice believes that laparoscopy—with the intention to treat endometriosis, if present—“is essential when first-line medical therapy fails or when pain is acute and severe.”5
Dr. Stratton concurs. “Any woman with chronic pain wants to know what is causing the pain,” she says. Therefore, “women report a benefit from knowing that their pain is associated with endometriosis.6 However, diagnostic laparoscopy alone, with the sole purpose of determining the presence of endometriosis but not treating the lesions, is no longer performed, as it poses little benefit to the patient other than peace of mind.”
“The general trend in the United States has been to first use hormonal treatments when the diagnosis of endometriosis is suspected, prior to performing surgery,” Dr. Stratton says.1 In many cases, by using cyclic combined hormonal contraceptives to reduce menstrual flow or “suppressing menstruation with continuous combined hormonal contraceptives,” gonadotropin-releasing hormone analogues (combined with progestin to prevent bone loss), “or continuous progestin alone may be effective in decreasing pain. Not surprisingly, these hormonal approaches are effective for any chronic pelvic pain, even for women who do not have the surgical diagnosis of endometriosis.”20
“When the first-line approach to chronic pelvic pain is hormonal treatment, laparoscopy is considered when these medical treatments have failed to control the pain or are poorly tolerated, or when the diagnosis of endometriosis is in question,” Dr. Stratton says.
“Laparoscopy to treat endometriomas is indicated if an endometrioma is enlarging, measures more than 4 cm in diameter, or if the diagnosis of an ovarian mass is in question,” she explains. “While surgeons have previously been aggressive in removing endometriomas, this practice may have negative consequences on ovarian function. Because endometriomas are pseudocysts, removing them completely leads to the removal of viable ovarian tissue and may diminish ovarian reserve.”21,22
7. What is the surgical appearance of endometriosis?
Dr. Giudice returns to the enigmatic nature of endometriosis in addressing this question, mentioning its “many faces” at the time of surgery. “It is imperative that the surgeon recognize the disease in its many forms,” she says. “Also, it is especially helpful at the time of surgery if suspected lesions are biopsied and sent to pathology to have the diagnosis made unequivocally.”5
As for the surgical appearance of endometriosis, Dr. Stratton notes that there are 3 types of lesions—“superficial lesions, deep infiltrating lesions, and endometriomas. Endometriomas occur almost exclusively in the ovary and are pseudocysts without an identifiable cystic lining. They vary in dimension from a few millimeters to several centimeters.”
“Superficial peritoneal endometriosis lesions have a variable appearance, with some lesions being clear or red, some brown, blue or black, and some having a white appearance, like a scar,” says Dr. Stratton. “Endometriosis can be diagnosed on histologic examination of any of these lesion types.
“Overall, single-color lesions have similar frequencies of biopsy-confirmed endometriosis (59% to 62%),” she says.23 “These lesion appearances likely represent different stages of development of endometriosis, with red or clear lesions occurring first, soon after endometrial tissue implantation; black, blue, or brown lesions occurring later, in response to the hormones varying in the menstrual cycle; and white lesions occurring as the lesions age. Deep infiltrating lesions generally have blue/black or white features.”
“Wide, deep, multiple-color lesions in the cul-de-sac, ovarian fossa or uterosacral ligaments are most likely endometriosis,” Dr. Stratton adds.23 Only lesions with multiple colors have a significantly higher percentage of positive biopsies (76%). Importantly, over half of women with only subtle lesions (small red or white lesions) have endometriosis.
CASE Resolved
You tell the patient that endometriosis is one of the possible diagnoses for her chronic pelvic pain, and you take a focused history. During a pelvic examination, you observe that her right ovary lacks mobility, and you map a number of trigger points for her pain. Transvaginal ultrasound results suggest the presence of nodules in the rectovaginal septum. You begin empiric treatment with continuous combined hormonal contraceptives to suppress menstruation. On her next visit, the patient reports reduced but still bothersome pain. Laparoscopy reveals a 2-cm endometrioma in the right ovary and deep infiltrating lesions in the cul-de-sac. The endometrioma is resected. Histology confirms the diagnosis of endometriosis.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. American College of Obstetricians and Gynecologists. Practice Bulletin #114: Management of endometriosis. Obstet Gynecol. 2010;116(1):223–236.
2. Sanfilippo JS, Wakim NG, Schikler KN, Yussman MA. Endometriosis in association with uterine anomaly. Am J Obstet Gynecol. 1986;154(1):39–43.
3. Taylor HS, Bagot C, Kardana A. HOX gene expression is altered in the endometrium of women with endometriosis. Hum Reprod. 1999;14(5):1328–1331.
4. Berkley KJ, Stratton P. Mechanisms: lessons from translational studies of endometriosis. In: Giamberardino MA, ed. Visceral Pain: Clinical, Pathophysiological and Therapeutic Aspects. Oxford, UK: Oxford University Press; 2009:39–50.
5. Giudice LC. Clinical practice: endometriosis. N Engl J Med. 2010;362(25):2389–2398.
6. Ballard K, Lowton K, Wright J. What’s the delay: a qualitative study of women’s experiences of reaching a diagnosis of endometriosis. Fertil Steril. 2006;86(5):1296–1301.
7. May KE, Conduit-Hulbert SA, Villar J, Kirtley S, Kennedy SH, Becker CM. Peripheral biomarkers of endometriosis: a systematic review. Hum Reprod Update. 2010;16(6):651–674.
8. May KE, Villar J, Kirtley S, Kennedy SH, Becker CM. Endometrial alterations in endometriosis: a systematic review of putative biomarkers. Hum Reprod Update. 2011;17(5):637–653.
9. Tamaresis JS, Irwin JC, Goldfien GA, et al. Molecular classification of endometriosis and disease stage using high-dimensional genomic data. Endocrinology. 2014;155(12):4986–4999.
10. Sinaii N, Cleary SD, Ballweg ML, Nieman LK, Stratton P. High rates of autoimmune and endocrine disorders, fibromyalgia, chronic fatigue syndrome and atopic diseases among women with endometriosis: a survey analysis. Hum Reprod. 2002;17(10):2715–2724.
11. De Graaff AA, D’Hooghe TM, Dunselman GA, et al. The significant effect of endometriosis on physical, mental and social wellbeing: results from an international cross-sectional survey. Hum Reprod. 2013;28(10):2677–2685.
12. Lafay Pillet MC, Huchon C, Santulli P, Borghese B, Chapron C, Fauconnier A. A clinical score can predict associated deep infiltrating endometriosis before surgery for an endometrioma. Hum Reprod. 2014;29(8):1666–1676.
13. Healey M, Cheng C, Kaur H. To excise or ablate endometriosis? A prospective randomized double-blinded trial after 5-year follow-up. J Minim Invasive Gynecol. 2014;21(6):999–1004.
14. Anaf V, El Nakadi I, De Moor V, Chapron C, Pistofidis G, Noel JC. Increased nerve density in deep infiltrating endometriotic nodules. Gynecol Obstet Invest. 2011;71(2):112–117.
15. Stratton P, Berkley KJ. Chronic pelvic pain and endometriosis: translational evidence of the relationship and implications. Hum Reprod Update. 2011;17(3):327–346.
16. Karp BI, Sinaii N, Nieman LK, Silberstein SD, Stratton P. Migraine in women with chronic pelvic pain with and without endometriosis. Fertil Steril. 2011;95(3):895–899.
17. Berkley KJ. A life of pelvic pain. Physiol Behav. 2005;86(3):272–280.
18. Fauconnier A, Chapron C. Endometriosis and pelvic pain: epidemiological evidence of the relationship and implications. Hum Reprod Update. 2005;11(6):595–606.
19. Vercellini P, Fedele L, Aimi G, Pietropaolo G, Consonni D, Crosignani PG. Association between endometriosis stage, lesion type, patient characteristics and severity of pelvic pain symptoms: a multivariate analysis of over 1000 patients. Hum Reprod. 2007;22(1):266–271.
20. Ling FW. Randomized controlled trial of depot leuprolide in patients with chronic pelvic pain and clinically suspected endometriosis. Pelvic Pain Study Group. Obstet Gynecol. 1999;93(1):51–58.
21. Muzii L, Di Tucci C, Di Feliciantonio M, Marchetti C, Perniola G, Panici PB. The effect of surgery for endometrioma on ovarian reserve evaluated by antral follicle count: a systematic review and meta-analysis. Hum Reprod. 2014;29(10):2190–2198.
22. Muzii L, Luciano AA, Zupi E, Panici PB. Effect of surgery for endometrioma on ovarian function: a different point of view. J Minim Invasive Gynecol. 2014;21(4):531–533.
23. Stegmann BJ, Sinaii N, Liu S, et al. Using location, color, size, and depth to characterize and identify endometriosis lesions in a cohort of 133 women. Fertil Steril. 2008;89(6):1632–1636.
1. American College of Obstetricians and Gynecologists. Practice Bulletin #114: Management of endometriosis. Obstet Gynecol. 2010;116(1):223–236.
2. Sanfilippo JS, Wakim NG, Schikler KN, Yussman MA. Endometriosis in association with uterine anomaly. Am J Obstet Gynecol. 1986;154(1):39–43.
3. Taylor HS, Bagot C, Kardana A. HOX gene expression is altered in the endometrium of women with endometriosis. Hum Reprod. 1999;14(5):1328–1331.
4. Berkley KJ, Stratton P. Mechanisms: lessons from translational studies of endometriosis. In: Giamberardino MA, ed. Visceral Pain: Clinical, Pathophysiological and Therapeutic Aspects. Oxford, UK: Oxford University Press; 2009:39–50.
5. Giudice LC. Clinical practice: endometriosis. N Engl J Med. 2010;362(25):2389–2398.
6. Ballard K, Lowton K, Wright J. What’s the delay: a qualitative study of women’s experiences of reaching a diagnosis of endometriosis. Fertil Steril. 2006;86(5):1296–1301.
7. May KE, Conduit-Hulbert SA, Villar J, Kirtley S, Kennedy SH, Becker CM. Peripheral biomarkers of endometriosis: a systematic review. Hum Reprod Update. 2010;16(6):651–674.
8. May KE, Villar J, Kirtley S, Kennedy SH, Becker CM. Endometrial alterations in endometriosis: a systematic review of putative biomarkers. Hum Reprod Update. 2011;17(5):637–653.
9. Tamaresis JS, Irwin JC, Goldfien GA, et al. Molecular classification of endometriosis and disease stage using high-dimensional genomic data. Endocrinology. 2014;155(12):4986–4999.
10. Sinaii N, Cleary SD, Ballweg ML, Nieman LK, Stratton P. High rates of autoimmune and endocrine disorders, fibromyalgia, chronic fatigue syndrome and atopic diseases among women with endometriosis: a survey analysis. Hum Reprod. 2002;17(10):2715–2724.
11. De Graaff AA, D’Hooghe TM, Dunselman GA, et al. The significant effect of endometriosis on physical, mental and social wellbeing: results from an international cross-sectional survey. Hum Reprod. 2013;28(10):2677–2685.
12. Lafay Pillet MC, Huchon C, Santulli P, Borghese B, Chapron C, Fauconnier A. A clinical score can predict associated deep infiltrating endometriosis before surgery for an endometrioma. Hum Reprod. 2014;29(8):1666–1676.
13. Healey M, Cheng C, Kaur H. To excise or ablate endometriosis? A prospective randomized double-blinded trial after 5-year follow-up. J Minim Invasive Gynecol. 2014;21(6):999–1004.
14. Anaf V, El Nakadi I, De Moor V, Chapron C, Pistofidis G, Noel JC. Increased nerve density in deep infiltrating endometriotic nodules. Gynecol Obstet Invest. 2011;71(2):112–117.
15. Stratton P, Berkley KJ. Chronic pelvic pain and endometriosis: translational evidence of the relationship and implications. Hum Reprod Update. 2011;17(3):327–346.
16. Karp BI, Sinaii N, Nieman LK, Silberstein SD, Stratton P. Migraine in women with chronic pelvic pain with and without endometriosis. Fertil Steril. 2011;95(3):895–899.
17. Berkley KJ. A life of pelvic pain. Physiol Behav. 2005;86(3):272–280.
18. Fauconnier A, Chapron C. Endometriosis and pelvic pain: epidemiological evidence of the relationship and implications. Hum Reprod Update. 2005;11(6):595–606.
19. Vercellini P, Fedele L, Aimi G, Pietropaolo G, Consonni D, Crosignani PG. Association between endometriosis stage, lesion type, patient characteristics and severity of pelvic pain symptoms: a multivariate analysis of over 1000 patients. Hum Reprod. 2007;22(1):266–271.
20. Ling FW. Randomized controlled trial of depot leuprolide in patients with chronic pelvic pain and clinically suspected endometriosis. Pelvic Pain Study Group. Obstet Gynecol. 1999;93(1):51–58.
21. Muzii L, Di Tucci C, Di Feliciantonio M, Marchetti C, Perniola G, Panici PB. The effect of surgery for endometrioma on ovarian reserve evaluated by antral follicle count: a systematic review and meta-analysis. Hum Reprod. 2014;29(10):2190–2198.
22. Muzii L, Luciano AA, Zupi E, Panici PB. Effect of surgery for endometrioma on ovarian function: a different point of view. J Minim Invasive Gynecol. 2014;21(4):531–533.
23. Stegmann BJ, Sinaii N, Liu S, et al. Using location, color, size, and depth to characterize and identify endometriosis lesions in a cohort of 133 women. Fertil Steril. 2008;89(6):1632–1636.
IN THIS ARTICLE
- The “why” of endometriosis
- Is imaging useful?
- When is diagnostic laparoscopy clearly indicated?
- Environmental factors, estrogen, and endometriosis