User login
Medical Management of Ectopic Pregnancy: Early Diagnosis is Key
Ectopic pregnancy is a significant health risk to women during their childbearing years; approximately 6% of all pregnancy-related deaths are due to ectopic pregnancy.1-3 Some 1% to 2% of all pregnancies in the United States each year—approximately 100,000 cases—are ectopic, with an estimated annual cost of care approaching $1.1 billion.4 The incidence of ectopic pregnancy has increased in the past 20 years; in one analysis, ectopic pregnancy was diagnosed in 18% of women who presented to an emergency department (ED) with first trimester vaginal bleeding, abdominal pain, or both.5 This growing prevalence is attributed to a number of factors, including the sensitivity of current diagnostic methods in detecting early ectopic pregnancy, the greater incidence of salpingitis, and the growing use of assisted reproductive technologies.2,6
While the number of ectopic pregnancies is on the rise, the proportion of patients requiring hospitalization for surgical treatment of ectopic pregnancy has decreased significantly. Today, for appropriate patients, many clinicians manage ectopic pregnancy on an outpatient basis using the drug methotrexate.6
In this article, we will present an overview of the current status of medical management of ectopic pregnancy, along with a case study. The case study describes a patient diagnosed with an unruptured ectopic pregnancy who was managed medically with methotrexate. It illustrates how, with early diagnosis, clinicians can intervene to make medical management an effective treatment option in selected situations.
The patient reported a history of oral contraceptive use until approximately three months prior to this pregnancy. She was taking no medications and had no known drug allergies. Her previous pregnancies included two uncomplicated vaginal births at term and one miscarriage at six to seven weeks’ gestation two years ago. She also reported a dilation and curettage after the miscarriage. Her medical, surgical, and gynecologic histories were otherwise noncontributory. A review of systems was otherwise negative.
Sexual history revealed that the patient was married and monogamous with her husband of five years. She disclosed four previous sexual partners and inconsistent use of condoms with those partners; no current condom use was reported. Seven years ago, she tested positive for gonorrhea and chlamydia and was treated concurrently with her partner. Subsequent diagnostics were negative. She reported vaginal intercourse but no oral sex and denied any other sexual contact. All partners had been male.
On the next page: Diagnosis and case continuation >>
DIAGNOSIS
There is some variation in the presentation of women experiencing ectopic pregnancy; this may be due to differences in the pathologic mechanisms of ectopic pregnancy. Patients may be asymptomatic, hemodynamically compromised, or somewhere in between.3 Typical clinical signs include abdominal pain, amenorrhea, and vaginal bleeding. Approximately 40% to 50% of patients present with vaginal bleeding, 50% may have a palpable adnexal mass, and 75% may have abdominal tenderness.3 Only about 50% of women with ectopic pregnancies present with these typical symptoms.3
The patient may also experience common symptoms of early pregnancy, such as nausea, fatigue, and breast fullness. Worrisome signs and symptoms, including abdominal guarding, hypotension, tachycardia, shock, shoulder pain from peritoneal irritation, dizziness, fever, and vomiting, may also be present.3,7 Approximately 20% of patients with ectopic pregnancies are hemodynamically compromised at presentation, which is highly suggestive of rupture.3
Risk factors
Risk factors for ectopic pregnancy include previous ectopic pregnancy; previous tubal procedures; history of sexually transmitted disease or genital infections; infertility; use of assisted reproductive technology; previous abdominal or pelvic surgery; smoking; pelvic inflammatory disease; exposure in utero to diethylstilbestrol; and previous intrauterine device use.2,5,7,8 Knowledge of these risk factors can help identify a patient with an ectopic pregnancy.
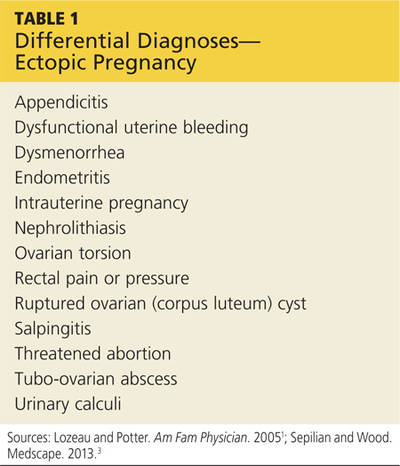
The diagnosis of ectopic pregnancy is most certainly a clinical challenge. The differential diagnosis is based upon history and physical findings; the list can be lengthy if both vaginal bleeding and abdominal pain (nonspecific symptoms common in women who miscarry) are present.7 Prompt completion of diagnostic testing is critical in making a definitive diagnosis. Possible diagnoses are listed in Table 1.
CASE Upon examination, the patient appeared comfortable and relaxed, and there were no signs of distress. Blood pressure was 100/65 mm Hg, pulse rate was 72 beats/min, and temperature was 99.0°F. There was no tenderness upon abdominal examination. Pelvic examination revealed a small amount of brown vaginal discharge but no active bleeding or pooled blood, clots, or tissue. The cervical os was closed, and positive Chadwick sign was present. Bimanual examination revealed no cervical motion tenderness. The uterus was soft, mobile, and nontender, and consistent in size with a gestation at eight weeks. There were no palpable adnexa, ovaries, or masses. There was no pain with bimanual examination and no evidence of tenderness at the posterior fornix. The remainder of the physical examination was unremarkable.
It is important to note that examination results in the case patient are not unusual in a woman with a small, unruptured ectopic pregnancy. All findings were normal except for the scant brown vaginal discharge. Abdominal and adnexal tenderness are common, as is a palpable adnexal mass; but absence of a detectable mass does not exclude ectopic pregnancy.1 Pathologic findings may include severe abdominal tenderness and pain, significant vaginal bleeding, passage of clots, tachycardia, and orthostatic hypotension.
Diagnostic workup
Laboratory tests are critical to making an accurate diagnosis for women whose history and physical examination results are consistent with ectopic pregnancy. Assessment for ectopic pregnancy should include a urine pregnancy test, transvaginal ultrasound, measurement of serum ß-human chorionic gonadotropin (ß-hCG) level, and occasionally, diagnostic curettage.1 Once the diagnosis is confirmed, a complete blood count (CBC) is necessary to assess anemia and platelet functioning. Coagulation tests may be required for worrisome bleeding. Blood type, Rh status, and antibody screen are also necessary to determine whether a patient who is Rh D-negative will require Rh immune globulin. See Table 2 for the patient’s laboratory test results.
In a patient with a ß-hCG level greater than the discriminatory cutoff value of 1,500 to 1,800 mIU/mL, the level above which an intrauterine gestational sac is visible on transvaginal ultrasound in a normal pregnancy, an empty uterus is considered an ectopic pregnancy until proven otherwise.3 In a definite intrauterine pregnancy of about six weeks’ gestation, transvaginal ultrasound reveals a gestational sac that contains a yolk sac and a fetal pole.3
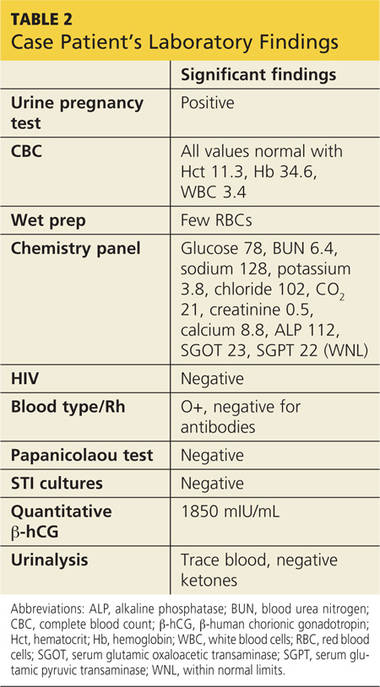
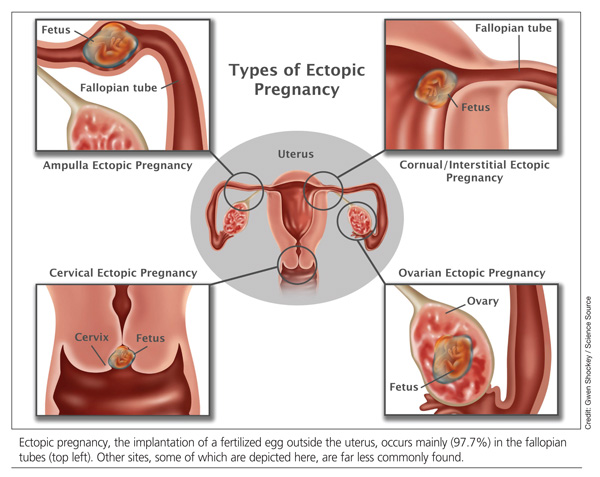
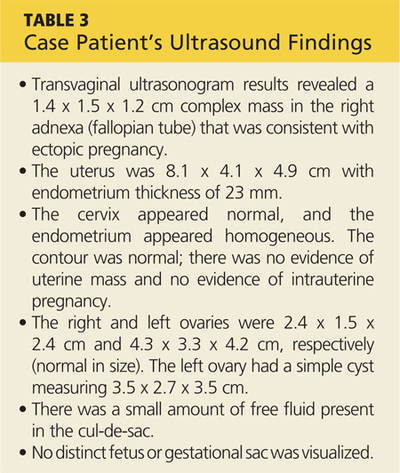
CASE The patient’s presenting symptoms, combined with a positive pregnancy test, ß-hCG level of 1,850 mIU/mL, and a complex adnexal mass in the right fallopian tube, were highly suggestive of an unruptured ectopic pregnancy (see Table 3 for the patient’s transvaginal ultrasound findings). There was also a secondary finding of a corpus luteum cyst. Other diagnoses were ruled out, and the patient was diagnosed with an unruptured ectopic pregnancy.
On the next page: Treatment >>
TREATMENT
A patient with an ectopic pregnancy who presents with pain and hemodynamic instability should be referred immediately for appropriate surgical care.7 Otherwise, once the diagnosis of ectopic pregnancy is confirmed, the patient should be referred to an obstetric specialist. Treatments for ectopic pregnancy include expectant management and surgery—which will be discussed briefly—and medical management, which is the focus of this review.5
Expectant management
Most ectopic pregnancies are diagnosed early as a result of accurate, minimally invasive and noninvasive diagnostic tools and greater awareness of risk factors. Since the natural course of early ectopic pregnancy is often self-limited, eventually resulting in tubal abortion or reabsorption, expectant management is a viable option.9
This treatment option may be considered if the patient is asymptomatic; ß-hCG is < 200 mIU/mL; the ectopic mass is < 3 cm; and no fetal heartbeat is present.1,2 With this approach, patients must be willing to accept the risk for tubal rupture and agree to close monitoring of ß-hCG levels. The ß-hCG level must be measured every 24 to 48 hours in order to determine if it is declining adequately, plateauing, or increasing.2,5
Surgery
For the hemodynamically unstable patient, the treatment decision is relatively straightforward. Optimal treatment for a ruptured ectopic pregnancy is immediate surgery, which may include salpingostomy or salpingectomy.10 Surgery may also be considered for hemodynamically stable patients with nonruptured ectopic pregnancies; in addition to her clinical presentation, overall management may be driven by a patient’s preferences.5 Salpingostomy and salpingectomy can be performed either laparoscopically or via laparotomy, depending on the specific situation.
Medical management
The use of methotrexate for the management of unruptured ectopic pregnancy was introduced in the early 1980s.11 Initially, protocols called for multiple doses administered during the course of an inpatient stay. Further research led to revised treatment recommendations and today, medical management most often consists of a single dose of methotrexate with outpatient follow-up.3
Methotrexate is a folic acid antagonist often used as an antimetabolite chemotherapeutic agent. In ectopic pregnancy, it inhibits growth of the rapidly dividing trophoblastic cells and ultimately ends the pregnancy.2 Outcomes of medical management are comparable to those of surgical treatment, including the potential for future normal pregnancies.2,5
An analysis of US trends in ectopic pregnancy management from 2002-2007 revealed that the use of methotrexate increased from 11.1% to 35.1% during that time, while the use of surgical approaches declined from 90% to 65%.10 Medical management of ectopic pregnancy eliminates the costs of surgery, anesthesia, and hospitalization and avoids potential complications of surgery and anesthesia.
Appropriate candidates
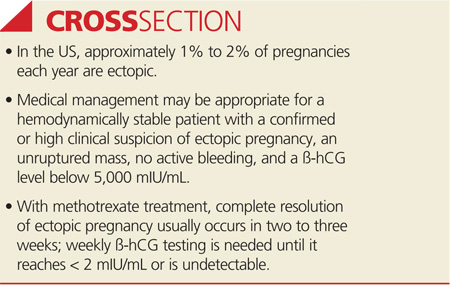
A hemodynamically stable patient with a confirmed or high clinical suspicion of ectopic pregnancy, an unruptured mass, no active bleeding, and low ß-hCG levels (< 5,000 mIU/mL) can be considered for methotrexate therapy.2,3,9 It is critical that medically managed patients be willing and able to adhere to all follow-up appointments.9 Before initiating treatment, normal serum creatinine and transaminase levels should be confirmed, and there should be no evidence of significant anemia, leukopenia, or thrombocytopenia.2 To detect any adverse effects of methotrexate on renal, hepatic, and hematologic functioning, these tests are repeated one week after administration.2
Contraindications
Contraindications to methotrexate treatment include breastfeeding, immunodeficiency, alcoholism, alcoholic liver disease or other chronic liver disease, preexisting blood dyscrasias (eg, bone marrow hypoplasia, leukopenia, thrombocytopenia, or significant anemia), known sensitivity to methotrexate, active pulmonary disease, peptic ulcer, and hepatic, renal, or hematologic dysfunction. Relative contraindications are a gestational sac larger than 3.5 cm and embryonic cardiac motion.2
On the next page: Patient education >>
PATIENT EDUCATION AND INFORMED CONSENT
A diagnosis of unruptured ectopic pregnancy requires patient education about the condition and its treatment options. The clinician should explain what an ectopic pregnancy is and distinguish between unruptured and ruptured. A discussion of the benefits and risks of each treatment option for which the patient is an appropriate candidate, as well as what to anticipate during treatment, is needed. Emotional support for impending pregnancy loss should also be provided.
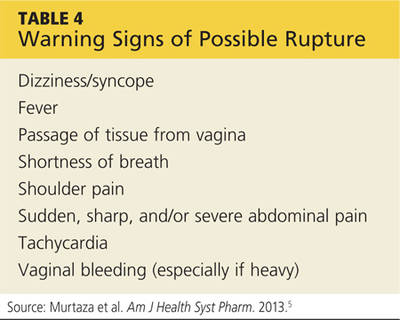
For patients who choose medical management, education includes methotrexate-specific information and written instructions to follow after methotrexate administration. Patients must be instructed about the use of safety precautions after treatment (eg, the toilet should be double-flushed with the lid closed during the first 72 hours after treatment to prevent exposing others to methotrexate in urine and stool), the need for adherence to follow-up visits, and warning signs of a possible rupture.5 These warning signs are listed in Table 4.
The most common adverse effects of methotrexate are gastrointestinal (nausea, vomiting, stomatitis). Patients should be advised to avoid alcohol, NSAIDs, folic acid supplements, excessive sun exposure (due to photosensitivity), strenuous exercise, and sexual intercourse until ß-hCG has returned to nonpregnant levels. Other adverse effects may include a temporary elevation in liver enzymes and rarely, alopecia. Abdominal pain may occur a few days after methotrexate administration, likely from the cytotoxic effects of the drug on the trophoblastic tissue.
Informed consent is required prior to methotrexate administration. The patient must be advised of the potential risks of medical management with methotrexate, including rupture of the ectopic pregnancy during treatment, inadvertent administration of methotrexate in the presence of an early intrauterine embryo, allergic reaction to methotrexate, and methotrexate-induced pneumonitis.5
CASE After lengthy discussion of the treatment options, the patient chose medical management with methotrexate. She verbalized her understanding of the teaching provided and signed an informed consent document.
METHOTREXATE REGIMENS
Protocols for single-dose, two-dose, and fixed multidose methotrexate regimens are described in the medical literature, according to a 2008 American Congress of Obstetricians and Gynecologists practice bulletin.2 A 2013 practice committee opinion of the American Society for Reproductive Medicine (ASRM) indicates that single-dose and multiple-dose regimens are used most often.12
With methotrexate treatment, complete resolution of ectopic pregnancy usually occurs in two to three weeks but may require up to six to eight weeks, depending on how high the ß-hCG level is when treatment begins.12
Single-dose
In the single-dose regimen, an intramuscular (IM) injection of methotrexate 50 mg/m2 is administered on day 1. The ß-hCG levels are measured on days 4 and 7 after administration; a decrease of at least 15% in the ß-hCG level should be observed. The ß-hCG level is then measured weekly until it reaches < 2 mIU/mL or is undetectable.2 If the level does not decline, a repeat dose of methotrexate can be given, with measurement of ß-hCG on days 4 and 7 after the repeat dose. If the ß-hCG level fails to decrease, additional methotrexate or surgical intervention should be considered.
The single-dose regimen is more frequently used and is most successful when ß-hCG levels are low (< 5,000 mIU/mL), the ectopic mass is small
(< 3.5 cm), and embryonic cardiac activity is not observed on ultrasound.2,3 Patients with ß-hCG levels > 5,000 mIU/mL may be appropriate candidates for additional doses of methotrexate.2 In fact, the single-dose protocol provides for repeat doses of methotrexate if the ß-hCG level is not decreasing adequately.12
Multiple-dose
With the multiple-dose regimen, methotrexate 1 mg/kg IM is administered on days 1, 3, 5, and 7; on days 2, 4, 6, and 8, the patient receives leucovorin (folinic acid) 0.1 mg/kg IM. The ß-hCG level is measured on days methotrexate is administered; once the minimum 15% decline is observed, ß-hCG is measured weekly until a nonpregnant level is reached.12
The patient received a single dose of methotrexate 50 mg/m2 IM on day 1 and returned to the clinic for follow-up on days 4 and 7 posttreatment. On day 4, her ß-hCG level was 1,060 mIU/mL; on day 7, it was 470 mIU/mL. Also on day 7, blood was drawn for a CBC and comprehensive metabolic panel; results were within normal limits. The patient continued weekly follow-up until her ß-hCG level decreased to < 2 mIU/mL.
On the next page: Follow-up and conclusion >>
FOLLOW-UP AND REFERRALS
Close monitoring of ß-hCG levels, as described previously, is essential after methotrexate treatment in order to confirm that the pregnancy has been terminated and reduce the risk for tubal rupture. Clinicians should also be sensitive to the sequelae of loss of a pregnancy and refer patients as needed to appropriate health care professionals for grief support.
CASE The patient was referred to an obstetrics clinic and reported for all scheduled follow-up appointments. She was discharged from care after a full reduction in her ß-hCG to nonpregnant levels. While at the clinic, the patient was referred to social services for psychosocial counseling.
CONCLUSION
Ectopic implantation is a serious complication that may occur during the first trimester of pregnancy. Worldwide, it is the leading cause of maternal death in the first trimester. For women who meet specific criteria, outpatient treatment of early ectopic pregnancy with methotrexate avoids surgery and decreases the overall cost of care. Medical management and conservative surgical management offer the patient comparable outcomes for tubal patency preservation and risk for ectopic pregnancy recurrence.11
REFERENCES
1. Lozeau AM, Potter B. Diagnosis and management of ectopic pregnancy. Am Fam Physician. 2005;72(9):1707-1714.
2. American Congress of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 94: medical management of ectopic pregnancy. Obstet Gynecol. 2008;111(6):1479-1485.
3. Sepilian VP, Wood E. Ectopic pregnancy. http://emedicine.medscape.com/article/2041923-overview. Medscape. Accessed June 19, 2014.
4. Stein JC, Wang R, Adler N, et al. Emergency physician ultrasonography for evaluating patients at risk for ectopic pregnancy: a meta-analysis. Ann Emerg Med. 2010;56(6):674-683.
5. Murtaza UI, Ortmann MJ, Mando-Vandrick J, Lee ASD. Management of first-trimester complications in the emergency department. Am J Health Syst Pharm. 2013;70(2):99-111.
6. Sewell CA, Cundiff GW. Trends for inpatient treatment of tubal pregnancy in Maryland. Am J Obstet Gynecol. 2002;186(3):404-408.
7. Nama V, Manyonda I. Tubal ectopic pregnancy: diagnosis and management. Arch Gynecol Obstet. 2009;279(4):443-453.
8. Barnhart KT, Sammel MD, Gracia CR, et al. Risk factors for ectopic pregnancy in women with symptomatic first-trimester pregnancies. Fertil Steril. 2006;86(1):36-43.
9. Hajenius PJ, Mol F, Mol BW, et al. Interventions for tubal ectopic pregnancy. Cochrane Database Syst Rev. 2007;(1):CD000324.
10. Hoover KW, Tao G, Kent CK. Trends in the diagnosis and treatment of ectopic pregnancy in the United States. Obstet Gynecol. 2010;115(3): 495-502.
11. Autry A. Medical treatment of ectopic pregnancy: is there something new? Obstet Gynecol. 2013;122(4):733.
12. The Practice Committee of the American Society for Reproductive Medicine. Medical treatment of ectopic pregnancy: a committee opinion. Fertil Steril. 2013;100(3):638-644.
Ectopic pregnancy is a significant health risk to women during their childbearing years; approximately 6% of all pregnancy-related deaths are due to ectopic pregnancy.1-3 Some 1% to 2% of all pregnancies in the United States each year—approximately 100,000 cases—are ectopic, with an estimated annual cost of care approaching $1.1 billion.4 The incidence of ectopic pregnancy has increased in the past 20 years; in one analysis, ectopic pregnancy was diagnosed in 18% of women who presented to an emergency department (ED) with first trimester vaginal bleeding, abdominal pain, or both.5 This growing prevalence is attributed to a number of factors, including the sensitivity of current diagnostic methods in detecting early ectopic pregnancy, the greater incidence of salpingitis, and the growing use of assisted reproductive technologies.2,6
While the number of ectopic pregnancies is on the rise, the proportion of patients requiring hospitalization for surgical treatment of ectopic pregnancy has decreased significantly. Today, for appropriate patients, many clinicians manage ectopic pregnancy on an outpatient basis using the drug methotrexate.6
In this article, we will present an overview of the current status of medical management of ectopic pregnancy, along with a case study. The case study describes a patient diagnosed with an unruptured ectopic pregnancy who was managed medically with methotrexate. It illustrates how, with early diagnosis, clinicians can intervene to make medical management an effective treatment option in selected situations.
The patient reported a history of oral contraceptive use until approximately three months prior to this pregnancy. She was taking no medications and had no known drug allergies. Her previous pregnancies included two uncomplicated vaginal births at term and one miscarriage at six to seven weeks’ gestation two years ago. She also reported a dilation and curettage after the miscarriage. Her medical, surgical, and gynecologic histories were otherwise noncontributory. A review of systems was otherwise negative.
Sexual history revealed that the patient was married and monogamous with her husband of five years. She disclosed four previous sexual partners and inconsistent use of condoms with those partners; no current condom use was reported. Seven years ago, she tested positive for gonorrhea and chlamydia and was treated concurrently with her partner. Subsequent diagnostics were negative. She reported vaginal intercourse but no oral sex and denied any other sexual contact. All partners had been male.
On the next page: Diagnosis and case continuation >>
DIAGNOSIS
There is some variation in the presentation of women experiencing ectopic pregnancy; this may be due to differences in the pathologic mechanisms of ectopic pregnancy. Patients may be asymptomatic, hemodynamically compromised, or somewhere in between.3 Typical clinical signs include abdominal pain, amenorrhea, and vaginal bleeding. Approximately 40% to 50% of patients present with vaginal bleeding, 50% may have a palpable adnexal mass, and 75% may have abdominal tenderness.3 Only about 50% of women with ectopic pregnancies present with these typical symptoms.3
The patient may also experience common symptoms of early pregnancy, such as nausea, fatigue, and breast fullness. Worrisome signs and symptoms, including abdominal guarding, hypotension, tachycardia, shock, shoulder pain from peritoneal irritation, dizziness, fever, and vomiting, may also be present.3,7 Approximately 20% of patients with ectopic pregnancies are hemodynamically compromised at presentation, which is highly suggestive of rupture.3
Risk factors
Risk factors for ectopic pregnancy include previous ectopic pregnancy; previous tubal procedures; history of sexually transmitted disease or genital infections; infertility; use of assisted reproductive technology; previous abdominal or pelvic surgery; smoking; pelvic inflammatory disease; exposure in utero to diethylstilbestrol; and previous intrauterine device use.2,5,7,8 Knowledge of these risk factors can help identify a patient with an ectopic pregnancy.
The diagnosis of ectopic pregnancy is most certainly a clinical challenge. The differential diagnosis is based upon history and physical findings; the list can be lengthy if both vaginal bleeding and abdominal pain (nonspecific symptoms common in women who miscarry) are present.7 Prompt completion of diagnostic testing is critical in making a definitive diagnosis. Possible diagnoses are listed in Table 1.
CASE Upon examination, the patient appeared comfortable and relaxed, and there were no signs of distress. Blood pressure was 100/65 mm Hg, pulse rate was 72 beats/min, and temperature was 99.0°F. There was no tenderness upon abdominal examination. Pelvic examination revealed a small amount of brown vaginal discharge but no active bleeding or pooled blood, clots, or tissue. The cervical os was closed, and positive Chadwick sign was present. Bimanual examination revealed no cervical motion tenderness. The uterus was soft, mobile, and nontender, and consistent in size with a gestation at eight weeks. There were no palpable adnexa, ovaries, or masses. There was no pain with bimanual examination and no evidence of tenderness at the posterior fornix. The remainder of the physical examination was unremarkable.
It is important to note that examination results in the case patient are not unusual in a woman with a small, unruptured ectopic pregnancy. All findings were normal except for the scant brown vaginal discharge. Abdominal and adnexal tenderness are common, as is a palpable adnexal mass; but absence of a detectable mass does not exclude ectopic pregnancy.1 Pathologic findings may include severe abdominal tenderness and pain, significant vaginal bleeding, passage of clots, tachycardia, and orthostatic hypotension.
Diagnostic workup
Laboratory tests are critical to making an accurate diagnosis for women whose history and physical examination results are consistent with ectopic pregnancy. Assessment for ectopic pregnancy should include a urine pregnancy test, transvaginal ultrasound, measurement of serum ß-human chorionic gonadotropin (ß-hCG) level, and occasionally, diagnostic curettage.1 Once the diagnosis is confirmed, a complete blood count (CBC) is necessary to assess anemia and platelet functioning. Coagulation tests may be required for worrisome bleeding. Blood type, Rh status, and antibody screen are also necessary to determine whether a patient who is Rh D-negative will require Rh immune globulin. See Table 2 for the patient’s laboratory test results.
In a patient with a ß-hCG level greater than the discriminatory cutoff value of 1,500 to 1,800 mIU/mL, the level above which an intrauterine gestational sac is visible on transvaginal ultrasound in a normal pregnancy, an empty uterus is considered an ectopic pregnancy until proven otherwise.3 In a definite intrauterine pregnancy of about six weeks’ gestation, transvaginal ultrasound reveals a gestational sac that contains a yolk sac and a fetal pole.3
CASE The patient’s presenting symptoms, combined with a positive pregnancy test, ß-hCG level of 1,850 mIU/mL, and a complex adnexal mass in the right fallopian tube, were highly suggestive of an unruptured ectopic pregnancy (see Table 3 for the patient’s transvaginal ultrasound findings). There was also a secondary finding of a corpus luteum cyst. Other diagnoses were ruled out, and the patient was diagnosed with an unruptured ectopic pregnancy.
On the next page: Treatment >>
TREATMENT
A patient with an ectopic pregnancy who presents with pain and hemodynamic instability should be referred immediately for appropriate surgical care.7 Otherwise, once the diagnosis of ectopic pregnancy is confirmed, the patient should be referred to an obstetric specialist. Treatments for ectopic pregnancy include expectant management and surgery—which will be discussed briefly—and medical management, which is the focus of this review.5
Expectant management
Most ectopic pregnancies are diagnosed early as a result of accurate, minimally invasive and noninvasive diagnostic tools and greater awareness of risk factors. Since the natural course of early ectopic pregnancy is often self-limited, eventually resulting in tubal abortion or reabsorption, expectant management is a viable option.9
This treatment option may be considered if the patient is asymptomatic; ß-hCG is < 200 mIU/mL; the ectopic mass is < 3 cm; and no fetal heartbeat is present.1,2 With this approach, patients must be willing to accept the risk for tubal rupture and agree to close monitoring of ß-hCG levels. The ß-hCG level must be measured every 24 to 48 hours in order to determine if it is declining adequately, plateauing, or increasing.2,5
Surgery
For the hemodynamically unstable patient, the treatment decision is relatively straightforward. Optimal treatment for a ruptured ectopic pregnancy is immediate surgery, which may include salpingostomy or salpingectomy.10 Surgery may also be considered for hemodynamically stable patients with nonruptured ectopic pregnancies; in addition to her clinical presentation, overall management may be driven by a patient’s preferences.5 Salpingostomy and salpingectomy can be performed either laparoscopically or via laparotomy, depending on the specific situation.
Medical management
The use of methotrexate for the management of unruptured ectopic pregnancy was introduced in the early 1980s.11 Initially, protocols called for multiple doses administered during the course of an inpatient stay. Further research led to revised treatment recommendations and today, medical management most often consists of a single dose of methotrexate with outpatient follow-up.3
Methotrexate is a folic acid antagonist often used as an antimetabolite chemotherapeutic agent. In ectopic pregnancy, it inhibits growth of the rapidly dividing trophoblastic cells and ultimately ends the pregnancy.2 Outcomes of medical management are comparable to those of surgical treatment, including the potential for future normal pregnancies.2,5
An analysis of US trends in ectopic pregnancy management from 2002-2007 revealed that the use of methotrexate increased from 11.1% to 35.1% during that time, while the use of surgical approaches declined from 90% to 65%.10 Medical management of ectopic pregnancy eliminates the costs of surgery, anesthesia, and hospitalization and avoids potential complications of surgery and anesthesia.
Appropriate candidates
A hemodynamically stable patient with a confirmed or high clinical suspicion of ectopic pregnancy, an unruptured mass, no active bleeding, and low ß-hCG levels (< 5,000 mIU/mL) can be considered for methotrexate therapy.2,3,9 It is critical that medically managed patients be willing and able to adhere to all follow-up appointments.9 Before initiating treatment, normal serum creatinine and transaminase levels should be confirmed, and there should be no evidence of significant anemia, leukopenia, or thrombocytopenia.2 To detect any adverse effects of methotrexate on renal, hepatic, and hematologic functioning, these tests are repeated one week after administration.2
Contraindications
Contraindications to methotrexate treatment include breastfeeding, immunodeficiency, alcoholism, alcoholic liver disease or other chronic liver disease, preexisting blood dyscrasias (eg, bone marrow hypoplasia, leukopenia, thrombocytopenia, or significant anemia), known sensitivity to methotrexate, active pulmonary disease, peptic ulcer, and hepatic, renal, or hematologic dysfunction. Relative contraindications are a gestational sac larger than 3.5 cm and embryonic cardiac motion.2
On the next page: Patient education >>
PATIENT EDUCATION AND INFORMED CONSENT
A diagnosis of unruptured ectopic pregnancy requires patient education about the condition and its treatment options. The clinician should explain what an ectopic pregnancy is and distinguish between unruptured and ruptured. A discussion of the benefits and risks of each treatment option for which the patient is an appropriate candidate, as well as what to anticipate during treatment, is needed. Emotional support for impending pregnancy loss should also be provided.
For patients who choose medical management, education includes methotrexate-specific information and written instructions to follow after methotrexate administration. Patients must be instructed about the use of safety precautions after treatment (eg, the toilet should be double-flushed with the lid closed during the first 72 hours after treatment to prevent exposing others to methotrexate in urine and stool), the need for adherence to follow-up visits, and warning signs of a possible rupture.5 These warning signs are listed in Table 4.
The most common adverse effects of methotrexate are gastrointestinal (nausea, vomiting, stomatitis). Patients should be advised to avoid alcohol, NSAIDs, folic acid supplements, excessive sun exposure (due to photosensitivity), strenuous exercise, and sexual intercourse until ß-hCG has returned to nonpregnant levels. Other adverse effects may include a temporary elevation in liver enzymes and rarely, alopecia. Abdominal pain may occur a few days after methotrexate administration, likely from the cytotoxic effects of the drug on the trophoblastic tissue.
Informed consent is required prior to methotrexate administration. The patient must be advised of the potential risks of medical management with methotrexate, including rupture of the ectopic pregnancy during treatment, inadvertent administration of methotrexate in the presence of an early intrauterine embryo, allergic reaction to methotrexate, and methotrexate-induced pneumonitis.5
CASE After lengthy discussion of the treatment options, the patient chose medical management with methotrexate. She verbalized her understanding of the teaching provided and signed an informed consent document.
METHOTREXATE REGIMENS
Protocols for single-dose, two-dose, and fixed multidose methotrexate regimens are described in the medical literature, according to a 2008 American Congress of Obstetricians and Gynecologists practice bulletin.2 A 2013 practice committee opinion of the American Society for Reproductive Medicine (ASRM) indicates that single-dose and multiple-dose regimens are used most often.12
With methotrexate treatment, complete resolution of ectopic pregnancy usually occurs in two to three weeks but may require up to six to eight weeks, depending on how high the ß-hCG level is when treatment begins.12
Single-dose
In the single-dose regimen, an intramuscular (IM) injection of methotrexate 50 mg/m2 is administered on day 1. The ß-hCG levels are measured on days 4 and 7 after administration; a decrease of at least 15% in the ß-hCG level should be observed. The ß-hCG level is then measured weekly until it reaches < 2 mIU/mL or is undetectable.2 If the level does not decline, a repeat dose of methotrexate can be given, with measurement of ß-hCG on days 4 and 7 after the repeat dose. If the ß-hCG level fails to decrease, additional methotrexate or surgical intervention should be considered.
The single-dose regimen is more frequently used and is most successful when ß-hCG levels are low (< 5,000 mIU/mL), the ectopic mass is small
(< 3.5 cm), and embryonic cardiac activity is not observed on ultrasound.2,3 Patients with ß-hCG levels > 5,000 mIU/mL may be appropriate candidates for additional doses of methotrexate.2 In fact, the single-dose protocol provides for repeat doses of methotrexate if the ß-hCG level is not decreasing adequately.12
Multiple-dose
With the multiple-dose regimen, methotrexate 1 mg/kg IM is administered on days 1, 3, 5, and 7; on days 2, 4, 6, and 8, the patient receives leucovorin (folinic acid) 0.1 mg/kg IM. The ß-hCG level is measured on days methotrexate is administered; once the minimum 15% decline is observed, ß-hCG is measured weekly until a nonpregnant level is reached.12
The patient received a single dose of methotrexate 50 mg/m2 IM on day 1 and returned to the clinic for follow-up on days 4 and 7 posttreatment. On day 4, her ß-hCG level was 1,060 mIU/mL; on day 7, it was 470 mIU/mL. Also on day 7, blood was drawn for a CBC and comprehensive metabolic panel; results were within normal limits. The patient continued weekly follow-up until her ß-hCG level decreased to < 2 mIU/mL.
On the next page: Follow-up and conclusion >>
FOLLOW-UP AND REFERRALS
Close monitoring of ß-hCG levels, as described previously, is essential after methotrexate treatment in order to confirm that the pregnancy has been terminated and reduce the risk for tubal rupture. Clinicians should also be sensitive to the sequelae of loss of a pregnancy and refer patients as needed to appropriate health care professionals for grief support.
CASE The patient was referred to an obstetrics clinic and reported for all scheduled follow-up appointments. She was discharged from care after a full reduction in her ß-hCG to nonpregnant levels. While at the clinic, the patient was referred to social services for psychosocial counseling.
CONCLUSION
Ectopic implantation is a serious complication that may occur during the first trimester of pregnancy. Worldwide, it is the leading cause of maternal death in the first trimester. For women who meet specific criteria, outpatient treatment of early ectopic pregnancy with methotrexate avoids surgery and decreases the overall cost of care. Medical management and conservative surgical management offer the patient comparable outcomes for tubal patency preservation and risk for ectopic pregnancy recurrence.11
REFERENCES
1. Lozeau AM, Potter B. Diagnosis and management of ectopic pregnancy. Am Fam Physician. 2005;72(9):1707-1714.
2. American Congress of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 94: medical management of ectopic pregnancy. Obstet Gynecol. 2008;111(6):1479-1485.
3. Sepilian VP, Wood E. Ectopic pregnancy. http://emedicine.medscape.com/article/2041923-overview. Medscape. Accessed June 19, 2014.
4. Stein JC, Wang R, Adler N, et al. Emergency physician ultrasonography for evaluating patients at risk for ectopic pregnancy: a meta-analysis. Ann Emerg Med. 2010;56(6):674-683.
5. Murtaza UI, Ortmann MJ, Mando-Vandrick J, Lee ASD. Management of first-trimester complications in the emergency department. Am J Health Syst Pharm. 2013;70(2):99-111.
6. Sewell CA, Cundiff GW. Trends for inpatient treatment of tubal pregnancy in Maryland. Am J Obstet Gynecol. 2002;186(3):404-408.
7. Nama V, Manyonda I. Tubal ectopic pregnancy: diagnosis and management. Arch Gynecol Obstet. 2009;279(4):443-453.
8. Barnhart KT, Sammel MD, Gracia CR, et al. Risk factors for ectopic pregnancy in women with symptomatic first-trimester pregnancies. Fertil Steril. 2006;86(1):36-43.
9. Hajenius PJ, Mol F, Mol BW, et al. Interventions for tubal ectopic pregnancy. Cochrane Database Syst Rev. 2007;(1):CD000324.
10. Hoover KW, Tao G, Kent CK. Trends in the diagnosis and treatment of ectopic pregnancy in the United States. Obstet Gynecol. 2010;115(3): 495-502.
11. Autry A. Medical treatment of ectopic pregnancy: is there something new? Obstet Gynecol. 2013;122(4):733.
12. The Practice Committee of the American Society for Reproductive Medicine. Medical treatment of ectopic pregnancy: a committee opinion. Fertil Steril. 2013;100(3):638-644.
Ectopic pregnancy is a significant health risk to women during their childbearing years; approximately 6% of all pregnancy-related deaths are due to ectopic pregnancy.1-3 Some 1% to 2% of all pregnancies in the United States each year—approximately 100,000 cases—are ectopic, with an estimated annual cost of care approaching $1.1 billion.4 The incidence of ectopic pregnancy has increased in the past 20 years; in one analysis, ectopic pregnancy was diagnosed in 18% of women who presented to an emergency department (ED) with first trimester vaginal bleeding, abdominal pain, or both.5 This growing prevalence is attributed to a number of factors, including the sensitivity of current diagnostic methods in detecting early ectopic pregnancy, the greater incidence of salpingitis, and the growing use of assisted reproductive technologies.2,6
While the number of ectopic pregnancies is on the rise, the proportion of patients requiring hospitalization for surgical treatment of ectopic pregnancy has decreased significantly. Today, for appropriate patients, many clinicians manage ectopic pregnancy on an outpatient basis using the drug methotrexate.6
In this article, we will present an overview of the current status of medical management of ectopic pregnancy, along with a case study. The case study describes a patient diagnosed with an unruptured ectopic pregnancy who was managed medically with methotrexate. It illustrates how, with early diagnosis, clinicians can intervene to make medical management an effective treatment option in selected situations.
The patient reported a history of oral contraceptive use until approximately three months prior to this pregnancy. She was taking no medications and had no known drug allergies. Her previous pregnancies included two uncomplicated vaginal births at term and one miscarriage at six to seven weeks’ gestation two years ago. She also reported a dilation and curettage after the miscarriage. Her medical, surgical, and gynecologic histories were otherwise noncontributory. A review of systems was otherwise negative.
Sexual history revealed that the patient was married and monogamous with her husband of five years. She disclosed four previous sexual partners and inconsistent use of condoms with those partners; no current condom use was reported. Seven years ago, she tested positive for gonorrhea and chlamydia and was treated concurrently with her partner. Subsequent diagnostics were negative. She reported vaginal intercourse but no oral sex and denied any other sexual contact. All partners had been male.
On the next page: Diagnosis and case continuation >>
DIAGNOSIS
There is some variation in the presentation of women experiencing ectopic pregnancy; this may be due to differences in the pathologic mechanisms of ectopic pregnancy. Patients may be asymptomatic, hemodynamically compromised, or somewhere in between.3 Typical clinical signs include abdominal pain, amenorrhea, and vaginal bleeding. Approximately 40% to 50% of patients present with vaginal bleeding, 50% may have a palpable adnexal mass, and 75% may have abdominal tenderness.3 Only about 50% of women with ectopic pregnancies present with these typical symptoms.3
The patient may also experience common symptoms of early pregnancy, such as nausea, fatigue, and breast fullness. Worrisome signs and symptoms, including abdominal guarding, hypotension, tachycardia, shock, shoulder pain from peritoneal irritation, dizziness, fever, and vomiting, may also be present.3,7 Approximately 20% of patients with ectopic pregnancies are hemodynamically compromised at presentation, which is highly suggestive of rupture.3
Risk factors
Risk factors for ectopic pregnancy include previous ectopic pregnancy; previous tubal procedures; history of sexually transmitted disease or genital infections; infertility; use of assisted reproductive technology; previous abdominal or pelvic surgery; smoking; pelvic inflammatory disease; exposure in utero to diethylstilbestrol; and previous intrauterine device use.2,5,7,8 Knowledge of these risk factors can help identify a patient with an ectopic pregnancy.
The diagnosis of ectopic pregnancy is most certainly a clinical challenge. The differential diagnosis is based upon history and physical findings; the list can be lengthy if both vaginal bleeding and abdominal pain (nonspecific symptoms common in women who miscarry) are present.7 Prompt completion of diagnostic testing is critical in making a definitive diagnosis. Possible diagnoses are listed in Table 1.
CASE Upon examination, the patient appeared comfortable and relaxed, and there were no signs of distress. Blood pressure was 100/65 mm Hg, pulse rate was 72 beats/min, and temperature was 99.0°F. There was no tenderness upon abdominal examination. Pelvic examination revealed a small amount of brown vaginal discharge but no active bleeding or pooled blood, clots, or tissue. The cervical os was closed, and positive Chadwick sign was present. Bimanual examination revealed no cervical motion tenderness. The uterus was soft, mobile, and nontender, and consistent in size with a gestation at eight weeks. There were no palpable adnexa, ovaries, or masses. There was no pain with bimanual examination and no evidence of tenderness at the posterior fornix. The remainder of the physical examination was unremarkable.
It is important to note that examination results in the case patient are not unusual in a woman with a small, unruptured ectopic pregnancy. All findings were normal except for the scant brown vaginal discharge. Abdominal and adnexal tenderness are common, as is a palpable adnexal mass; but absence of a detectable mass does not exclude ectopic pregnancy.1 Pathologic findings may include severe abdominal tenderness and pain, significant vaginal bleeding, passage of clots, tachycardia, and orthostatic hypotension.
Diagnostic workup
Laboratory tests are critical to making an accurate diagnosis for women whose history and physical examination results are consistent with ectopic pregnancy. Assessment for ectopic pregnancy should include a urine pregnancy test, transvaginal ultrasound, measurement of serum ß-human chorionic gonadotropin (ß-hCG) level, and occasionally, diagnostic curettage.1 Once the diagnosis is confirmed, a complete blood count (CBC) is necessary to assess anemia and platelet functioning. Coagulation tests may be required for worrisome bleeding. Blood type, Rh status, and antibody screen are also necessary to determine whether a patient who is Rh D-negative will require Rh immune globulin. See Table 2 for the patient’s laboratory test results.
In a patient with a ß-hCG level greater than the discriminatory cutoff value of 1,500 to 1,800 mIU/mL, the level above which an intrauterine gestational sac is visible on transvaginal ultrasound in a normal pregnancy, an empty uterus is considered an ectopic pregnancy until proven otherwise.3 In a definite intrauterine pregnancy of about six weeks’ gestation, transvaginal ultrasound reveals a gestational sac that contains a yolk sac and a fetal pole.3
CASE The patient’s presenting symptoms, combined with a positive pregnancy test, ß-hCG level of 1,850 mIU/mL, and a complex adnexal mass in the right fallopian tube, were highly suggestive of an unruptured ectopic pregnancy (see Table 3 for the patient’s transvaginal ultrasound findings). There was also a secondary finding of a corpus luteum cyst. Other diagnoses were ruled out, and the patient was diagnosed with an unruptured ectopic pregnancy.
On the next page: Treatment >>
TREATMENT
A patient with an ectopic pregnancy who presents with pain and hemodynamic instability should be referred immediately for appropriate surgical care.7 Otherwise, once the diagnosis of ectopic pregnancy is confirmed, the patient should be referred to an obstetric specialist. Treatments for ectopic pregnancy include expectant management and surgery—which will be discussed briefly—and medical management, which is the focus of this review.5
Expectant management
Most ectopic pregnancies are diagnosed early as a result of accurate, minimally invasive and noninvasive diagnostic tools and greater awareness of risk factors. Since the natural course of early ectopic pregnancy is often self-limited, eventually resulting in tubal abortion or reabsorption, expectant management is a viable option.9
This treatment option may be considered if the patient is asymptomatic; ß-hCG is < 200 mIU/mL; the ectopic mass is < 3 cm; and no fetal heartbeat is present.1,2 With this approach, patients must be willing to accept the risk for tubal rupture and agree to close monitoring of ß-hCG levels. The ß-hCG level must be measured every 24 to 48 hours in order to determine if it is declining adequately, plateauing, or increasing.2,5
Surgery
For the hemodynamically unstable patient, the treatment decision is relatively straightforward. Optimal treatment for a ruptured ectopic pregnancy is immediate surgery, which may include salpingostomy or salpingectomy.10 Surgery may also be considered for hemodynamically stable patients with nonruptured ectopic pregnancies; in addition to her clinical presentation, overall management may be driven by a patient’s preferences.5 Salpingostomy and salpingectomy can be performed either laparoscopically or via laparotomy, depending on the specific situation.
Medical management
The use of methotrexate for the management of unruptured ectopic pregnancy was introduced in the early 1980s.11 Initially, protocols called for multiple doses administered during the course of an inpatient stay. Further research led to revised treatment recommendations and today, medical management most often consists of a single dose of methotrexate with outpatient follow-up.3
Methotrexate is a folic acid antagonist often used as an antimetabolite chemotherapeutic agent. In ectopic pregnancy, it inhibits growth of the rapidly dividing trophoblastic cells and ultimately ends the pregnancy.2 Outcomes of medical management are comparable to those of surgical treatment, including the potential for future normal pregnancies.2,5
An analysis of US trends in ectopic pregnancy management from 2002-2007 revealed that the use of methotrexate increased from 11.1% to 35.1% during that time, while the use of surgical approaches declined from 90% to 65%.10 Medical management of ectopic pregnancy eliminates the costs of surgery, anesthesia, and hospitalization and avoids potential complications of surgery and anesthesia.
Appropriate candidates
A hemodynamically stable patient with a confirmed or high clinical suspicion of ectopic pregnancy, an unruptured mass, no active bleeding, and low ß-hCG levels (< 5,000 mIU/mL) can be considered for methotrexate therapy.2,3,9 It is critical that medically managed patients be willing and able to adhere to all follow-up appointments.9 Before initiating treatment, normal serum creatinine and transaminase levels should be confirmed, and there should be no evidence of significant anemia, leukopenia, or thrombocytopenia.2 To detect any adverse effects of methotrexate on renal, hepatic, and hematologic functioning, these tests are repeated one week after administration.2
Contraindications
Contraindications to methotrexate treatment include breastfeeding, immunodeficiency, alcoholism, alcoholic liver disease or other chronic liver disease, preexisting blood dyscrasias (eg, bone marrow hypoplasia, leukopenia, thrombocytopenia, or significant anemia), known sensitivity to methotrexate, active pulmonary disease, peptic ulcer, and hepatic, renal, or hematologic dysfunction. Relative contraindications are a gestational sac larger than 3.5 cm and embryonic cardiac motion.2
On the next page: Patient education >>
PATIENT EDUCATION AND INFORMED CONSENT
A diagnosis of unruptured ectopic pregnancy requires patient education about the condition and its treatment options. The clinician should explain what an ectopic pregnancy is and distinguish between unruptured and ruptured. A discussion of the benefits and risks of each treatment option for which the patient is an appropriate candidate, as well as what to anticipate during treatment, is needed. Emotional support for impending pregnancy loss should also be provided.
For patients who choose medical management, education includes methotrexate-specific information and written instructions to follow after methotrexate administration. Patients must be instructed about the use of safety precautions after treatment (eg, the toilet should be double-flushed with the lid closed during the first 72 hours after treatment to prevent exposing others to methotrexate in urine and stool), the need for adherence to follow-up visits, and warning signs of a possible rupture.5 These warning signs are listed in Table 4.
The most common adverse effects of methotrexate are gastrointestinal (nausea, vomiting, stomatitis). Patients should be advised to avoid alcohol, NSAIDs, folic acid supplements, excessive sun exposure (due to photosensitivity), strenuous exercise, and sexual intercourse until ß-hCG has returned to nonpregnant levels. Other adverse effects may include a temporary elevation in liver enzymes and rarely, alopecia. Abdominal pain may occur a few days after methotrexate administration, likely from the cytotoxic effects of the drug on the trophoblastic tissue.
Informed consent is required prior to methotrexate administration. The patient must be advised of the potential risks of medical management with methotrexate, including rupture of the ectopic pregnancy during treatment, inadvertent administration of methotrexate in the presence of an early intrauterine embryo, allergic reaction to methotrexate, and methotrexate-induced pneumonitis.5
CASE After lengthy discussion of the treatment options, the patient chose medical management with methotrexate. She verbalized her understanding of the teaching provided and signed an informed consent document.
METHOTREXATE REGIMENS
Protocols for single-dose, two-dose, and fixed multidose methotrexate regimens are described in the medical literature, according to a 2008 American Congress of Obstetricians and Gynecologists practice bulletin.2 A 2013 practice committee opinion of the American Society for Reproductive Medicine (ASRM) indicates that single-dose and multiple-dose regimens are used most often.12
With methotrexate treatment, complete resolution of ectopic pregnancy usually occurs in two to three weeks but may require up to six to eight weeks, depending on how high the ß-hCG level is when treatment begins.12
Single-dose
In the single-dose regimen, an intramuscular (IM) injection of methotrexate 50 mg/m2 is administered on day 1. The ß-hCG levels are measured on days 4 and 7 after administration; a decrease of at least 15% in the ß-hCG level should be observed. The ß-hCG level is then measured weekly until it reaches < 2 mIU/mL or is undetectable.2 If the level does not decline, a repeat dose of methotrexate can be given, with measurement of ß-hCG on days 4 and 7 after the repeat dose. If the ß-hCG level fails to decrease, additional methotrexate or surgical intervention should be considered.
The single-dose regimen is more frequently used and is most successful when ß-hCG levels are low (< 5,000 mIU/mL), the ectopic mass is small
(< 3.5 cm), and embryonic cardiac activity is not observed on ultrasound.2,3 Patients with ß-hCG levels > 5,000 mIU/mL may be appropriate candidates for additional doses of methotrexate.2 In fact, the single-dose protocol provides for repeat doses of methotrexate if the ß-hCG level is not decreasing adequately.12
Multiple-dose
With the multiple-dose regimen, methotrexate 1 mg/kg IM is administered on days 1, 3, 5, and 7; on days 2, 4, 6, and 8, the patient receives leucovorin (folinic acid) 0.1 mg/kg IM. The ß-hCG level is measured on days methotrexate is administered; once the minimum 15% decline is observed, ß-hCG is measured weekly until a nonpregnant level is reached.12
The patient received a single dose of methotrexate 50 mg/m2 IM on day 1 and returned to the clinic for follow-up on days 4 and 7 posttreatment. On day 4, her ß-hCG level was 1,060 mIU/mL; on day 7, it was 470 mIU/mL. Also on day 7, blood was drawn for a CBC and comprehensive metabolic panel; results were within normal limits. The patient continued weekly follow-up until her ß-hCG level decreased to < 2 mIU/mL.
On the next page: Follow-up and conclusion >>
FOLLOW-UP AND REFERRALS
Close monitoring of ß-hCG levels, as described previously, is essential after methotrexate treatment in order to confirm that the pregnancy has been terminated and reduce the risk for tubal rupture. Clinicians should also be sensitive to the sequelae of loss of a pregnancy and refer patients as needed to appropriate health care professionals for grief support.
CASE The patient was referred to an obstetrics clinic and reported for all scheduled follow-up appointments. She was discharged from care after a full reduction in her ß-hCG to nonpregnant levels. While at the clinic, the patient was referred to social services for psychosocial counseling.
CONCLUSION
Ectopic implantation is a serious complication that may occur during the first trimester of pregnancy. Worldwide, it is the leading cause of maternal death in the first trimester. For women who meet specific criteria, outpatient treatment of early ectopic pregnancy with methotrexate avoids surgery and decreases the overall cost of care. Medical management and conservative surgical management offer the patient comparable outcomes for tubal patency preservation and risk for ectopic pregnancy recurrence.11
REFERENCES
1. Lozeau AM, Potter B. Diagnosis and management of ectopic pregnancy. Am Fam Physician. 2005;72(9):1707-1714.
2. American Congress of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 94: medical management of ectopic pregnancy. Obstet Gynecol. 2008;111(6):1479-1485.
3. Sepilian VP, Wood E. Ectopic pregnancy. http://emedicine.medscape.com/article/2041923-overview. Medscape. Accessed June 19, 2014.
4. Stein JC, Wang R, Adler N, et al. Emergency physician ultrasonography for evaluating patients at risk for ectopic pregnancy: a meta-analysis. Ann Emerg Med. 2010;56(6):674-683.
5. Murtaza UI, Ortmann MJ, Mando-Vandrick J, Lee ASD. Management of first-trimester complications in the emergency department. Am J Health Syst Pharm. 2013;70(2):99-111.
6. Sewell CA, Cundiff GW. Trends for inpatient treatment of tubal pregnancy in Maryland. Am J Obstet Gynecol. 2002;186(3):404-408.
7. Nama V, Manyonda I. Tubal ectopic pregnancy: diagnosis and management. Arch Gynecol Obstet. 2009;279(4):443-453.
8. Barnhart KT, Sammel MD, Gracia CR, et al. Risk factors for ectopic pregnancy in women with symptomatic first-trimester pregnancies. Fertil Steril. 2006;86(1):36-43.
9. Hajenius PJ, Mol F, Mol BW, et al. Interventions for tubal ectopic pregnancy. Cochrane Database Syst Rev. 2007;(1):CD000324.
10. Hoover KW, Tao G, Kent CK. Trends in the diagnosis and treatment of ectopic pregnancy in the United States. Obstet Gynecol. 2010;115(3): 495-502.
11. Autry A. Medical treatment of ectopic pregnancy: is there something new? Obstet Gynecol. 2013;122(4):733.
12. The Practice Committee of the American Society for Reproductive Medicine. Medical treatment of ectopic pregnancy: a committee opinion. Fertil Steril. 2013;100(3):638-644.

Aspiration of a Dental Tool During a Crown Placement Procedure
There are many reports in the medical and dental literature of complications arising from a routine delivery of dental care. One complication can include physical injury from swallowing or aspirating foreign objects.1 However, a review of such literature presents a scarcity of documented instances and no long-term evaluation of the aforementioned events.2,3
This report presents the case of a patient who aspirated a hex driver tool during a procedure to place a crown on a dental implant. The aspirated object was subsequently removed through flexible fiberoptic bronchoscopy without complications.
Case Report
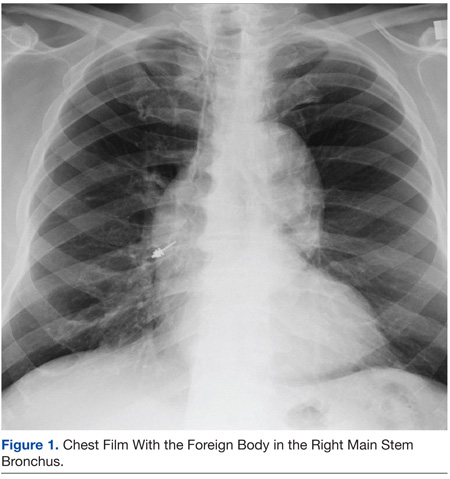
An 83-year-old man was referred to the Pulmonary and Critical Care Department of the VA Caribbean Healthcare System in San Juan, Puerto Rico, after a hex driver tool was lost during a procedure to place a crown on a dental implant, performed under topical anesthesia. It was first thought that the patient swallowed the hex driver, since he never experienced or complained of coughing or shortness of breath. A chest radiograph revealed a metal object lying within the right main stem bronchus, for which the patient was referred to the Pulmonary and Critical Care Department (Figure 1).
The patient’s past medical history was remarkable for hypertension and hypercholesterolemia. Outpatient medications included hydrochlorothiazide, simvastatin, aspirin, felodipine, and lorazepam. He had no previous history of dysphagia or neurologic disease. A physical examination revealed expiratory and inspiratory wheezing localized to the right lower lobe without associated rhonchi or crackles. No distress, shortness of breath, or coughing was noted.
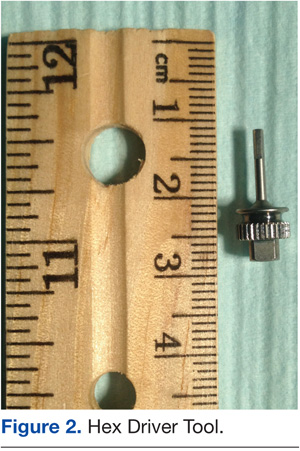
A flexible fiberoptic bronchoscopy was performed under conscious sedation with 3 mg of IV midazolam and topical anesthesia with nebulized 4% lidocaine. No mucosal edema, hyperemia, or structural damage was noted during direct visualization of both the right and left bronchopulmonary segments. A metallic object was visualized at the entrance of the right lower lobe. The foreign object had irregular borders, providing multiple edges that made it suitable to be embraced (Figure 2).
Using a radial jaw single-use biopsy forceps 1.8 mm, the physician clinched and retrieved the object through the bronchoscope. The object was retrieved on the same day of the dental procedure almost 5 hours after it was aspirated. The patient tolerated the procedure well; no coughing, oxygen desaturation, or bleeding occurred during the procedure.
After a few hours of observation, a postprocedural radiograph confirmed the removal of the foreign body without evidence of pneumothorax. The patient was discharged, and 24 hours after the incident remained asymptomatic without chest pain, cough, hemoptysis, sputum production, or fever.
Discussion
Foreign-body aspiration and inadvertent swallowing remains underrecognized by clinicians. In the U.S., more than 2,700 people, including more than 300 children, die of foreign-body aspiration each year.4,5 Aspiration or ingestion of a foreign body during a dental procedure is serious and potentially fatal.6 Some of the consequences of an aspirated object are complete or partial airway obstruction, respiratory distress and failure, pneumothorax, and hemorrhage.7 In addition, inadvertent aspiration of foreign objects in asymptomatic patients may not be evident for months, resulting in late complications as postobstructive pneumonia, bronchiectasis, or lung abscess.8 Early recognition and diagnosis of these events are crucial to prevent complications.
Accidental aspiration of foreign objects during dental procedures is not as common as is swallowing. In the normal population, the foreign object enters the gastrointestinal tract in about 92.5% of the time, and the tracheobronchial tree in 7.5% of these instances.
A 10-year review done at the School of Dentistry of the University of North Carolina reported 36 incidents of lost instruments during dental procedures. In only 1 case, an object was aspirated, 25 of the 36 cases were secondary to ingestion, and in the remaining 10 incidents, swallowing or aspiration was ruled out by radiography or after the object’s removal from the patient’s mouth.2 Previous reviews about foreign-body aspiration in adults have reported dental appliances as the second most commonly aspirated foreign objects.4 Of all aspirated objects, the most common site of impaction is the right lower lobe; however, aspiration has been reported in all pulmonary lobes.6
Available literature recognizes that impaction of aspirated objects occurred in 56% of instances within the right lower lobe and 33% in the left lower lobe.7,9 Identification of risk factors for aspiration is important for any patient who will undergo dental procedures, such as advanced age (ie, elderly patients may have a decreased gag reflex); neurologic conditions, such as stroke; dementia and other degenerative diseases; the use of topical anesthesia; and altered states of consciousness associated with the use of IV sedation.1,2
The key sign that most dentists recognize when patients aspirate an object during a dental procedure is coughing. It has been reported that coughing resulting from aspiration of foreign objects may range from mild to severe. In this case, the patient was completely asymptomatic during the procedure. The only clue of possible object aspiration was the reported tool loss by the dentist. It is important to always examine, account for, and review all equipment used during dental procedures. Assessment for any lost objects or missing parts of instruments should be done promptly with a high degree of suspicion for possible swallowing or aspiration if an object is missing.
It has been recommended to use a gauze throat screen and rubber dam and to avoid a supine position during a procedure, among other techniques, to minimize risk of ingestion or aspiration.2 Imaging studies should be used for further evaluation of the patient; however, some instruments, such as dental pieces and impression material, may not be identified by plain films. In those cases, further evaluation with more sophisticated imaging techniques, such as computed tomography (CT), should be considered.1-10
In a previous case report of a patient who aspirated a third molar during a dental procedure, a chest film failed to identify it. A chest CT was performed, and the object showed in the right main stem bronchus. In another instance, aspiration of impression material in a 45-year-old man was not observed by chest radiography. In this case, the history of coughing and respiratory symptoms days after the procedure pointed toward aspiration of an object as the culprit, with subsequent identification and removal by flexible fiberoptic bronchoscopy.1-11
Bronchoscopy is the treatment of choice for extraction of aspirated foreign bodies; however, there is still a debate about whether to use flexible or rigid bronchoscopy. The decision is usually made based on the object size, localization, medical facility, and personnel expertise. The rigid bronchoscope has the advantages of offering better control and visualization of the airway and easier use of removal instruments. Its primary disadvantage is that the procedure needs to be done in the operating room under general anesthesia. Flexible fiberoptic bronchoscopy done under conscious sedation and topical anesthesia may be as effective as rigid bronchoscopy and even superior in the case of smaller and more distal impacted objects.10-14
In this case, flexible fiberoptic bronchoscopy was used successfully for the removal of the foreign object. Biopsy forceps were used to grasp the object and retrieve it from the airway without complication.
Conclusion
Aspiration of foreign objects during a dental procedure is a potential life-threatening complication. A high-level of suspicion is needed for early diagnosis and referral of the patient for extraction of the object and further avoidance of complications. Flexible fiberoptic bronchoscopy is a feasible procedure for removal of objects within the airway.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc. , the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Cameron SM, Whitlock WL, Tabor MS. Foreign body aspiration in dentistry: A review. J Am Dent Assoc. 1996;127(8):1224-1229.
2. Tiwana KK, Morton T, Tiwana PS. Aspiration and ingestion in dental practice: A 10-year institutional review. J Am Dent Assoc. 2004;135(9):1287-1291.
3. Susini G, Pommel L, Camps J. Accidental ingestion and aspiration of root canal instruments and other dental foreign bodies in a French population. Int Endod J. 2007;40(8):585-589.
4. Fields RT Jr, Schow SR. Aspiration and ingestion of foreign bodies in oral and maxillofacial surgery: A review of the literature and report of five cases. J Oral Maxillofac Surg. 1998;56(9):1091-1098.
5. Black RE, Johnson DG, Matlak ME. Bronchoscopic removal of aspirated foreign bodies in children. J Pediatr Surg. 1994;29(5):682-684.
6. Limper AH, Prakash UBS. Tracheobronchial foreign bodies in adults. Ann Intern Med. 1990;112(8):604-609.
7. Bas¸oglu OK, Buduneli N, Cagirici U, Turhan K, Aysan T. Pulmonary aspiration of a two-unit bridge during a deep sleep. J Oral Rehabil. 2005;32(6):461-463.
8. Mahmoud M, Imam S, Patel H, King M. Foreign body aspiration of a dental bridge in the left main stem bronchus. Case Rep Med. 2012;2012:1-4.
9. Jackson C, Jackson CL. Diseases of the Air and Food Passages of Foreign-Body Origin. Philadelphia, PA: Saunders; 1936.
10. Zitzmann NU, Elsasser S, Fried R, Marinello CP. Foreign body ingestion and aspiration. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88(6):657-660.
11. Elgazzar RF, Abdelhady AI, Sadakah AA. Aspiration of an impacted lower third molar during its surgical removal under local anaesthesia. Int J Oral Maxillofac Surg. 2007;36(4):362-364.
12. Tu CY, Chen HJ, Chen W, Liu YH, Chen CH. A feasible approach for extraction of dental prostheses from the airway by flexible bronchoscopy in concert with wire loops snares. Laryngoscope. 2007;117(7):1280-1282.
13. Ospina JC, Ludemann JP. Aspiration of an extracted molar: Case report. J Can Dent Assoc. 2005;71(8):581-583.
14. Cohen S, Pine H, Drake A. Use of rigid and flexible bronchoscopy among pediatric otolaryngologists. Arch Otoralyngol Head Neck Surg. 2001;127(5):505-509.
There are many reports in the medical and dental literature of complications arising from a routine delivery of dental care. One complication can include physical injury from swallowing or aspirating foreign objects.1 However, a review of such literature presents a scarcity of documented instances and no long-term evaluation of the aforementioned events.2,3
This report presents the case of a patient who aspirated a hex driver tool during a procedure to place a crown on a dental implant. The aspirated object was subsequently removed through flexible fiberoptic bronchoscopy without complications.
Case Report
An 83-year-old man was referred to the Pulmonary and Critical Care Department of the VA Caribbean Healthcare System in San Juan, Puerto Rico, after a hex driver tool was lost during a procedure to place a crown on a dental implant, performed under topical anesthesia. It was first thought that the patient swallowed the hex driver, since he never experienced or complained of coughing or shortness of breath. A chest radiograph revealed a metal object lying within the right main stem bronchus, for which the patient was referred to the Pulmonary and Critical Care Department (Figure 1).
The patient’s past medical history was remarkable for hypertension and hypercholesterolemia. Outpatient medications included hydrochlorothiazide, simvastatin, aspirin, felodipine, and lorazepam. He had no previous history of dysphagia or neurologic disease. A physical examination revealed expiratory and inspiratory wheezing localized to the right lower lobe without associated rhonchi or crackles. No distress, shortness of breath, or coughing was noted.
A flexible fiberoptic bronchoscopy was performed under conscious sedation with 3 mg of IV midazolam and topical anesthesia with nebulized 4% lidocaine. No mucosal edema, hyperemia, or structural damage was noted during direct visualization of both the right and left bronchopulmonary segments. A metallic object was visualized at the entrance of the right lower lobe. The foreign object had irregular borders, providing multiple edges that made it suitable to be embraced (Figure 2).
Using a radial jaw single-use biopsy forceps 1.8 mm, the physician clinched and retrieved the object through the bronchoscope. The object was retrieved on the same day of the dental procedure almost 5 hours after it was aspirated. The patient tolerated the procedure well; no coughing, oxygen desaturation, or bleeding occurred during the procedure.
After a few hours of observation, a postprocedural radiograph confirmed the removal of the foreign body without evidence of pneumothorax. The patient was discharged, and 24 hours after the incident remained asymptomatic without chest pain, cough, hemoptysis, sputum production, or fever.
Discussion
Foreign-body aspiration and inadvertent swallowing remains underrecognized by clinicians. In the U.S., more than 2,700 people, including more than 300 children, die of foreign-body aspiration each year.4,5 Aspiration or ingestion of a foreign body during a dental procedure is serious and potentially fatal.6 Some of the consequences of an aspirated object are complete or partial airway obstruction, respiratory distress and failure, pneumothorax, and hemorrhage.7 In addition, inadvertent aspiration of foreign objects in asymptomatic patients may not be evident for months, resulting in late complications as postobstructive pneumonia, bronchiectasis, or lung abscess.8 Early recognition and diagnosis of these events are crucial to prevent complications.
Accidental aspiration of foreign objects during dental procedures is not as common as is swallowing. In the normal population, the foreign object enters the gastrointestinal tract in about 92.5% of the time, and the tracheobronchial tree in 7.5% of these instances.
A 10-year review done at the School of Dentistry of the University of North Carolina reported 36 incidents of lost instruments during dental procedures. In only 1 case, an object was aspirated, 25 of the 36 cases were secondary to ingestion, and in the remaining 10 incidents, swallowing or aspiration was ruled out by radiography or after the object’s removal from the patient’s mouth.2 Previous reviews about foreign-body aspiration in adults have reported dental appliances as the second most commonly aspirated foreign objects.4 Of all aspirated objects, the most common site of impaction is the right lower lobe; however, aspiration has been reported in all pulmonary lobes.6
Available literature recognizes that impaction of aspirated objects occurred in 56% of instances within the right lower lobe and 33% in the left lower lobe.7,9 Identification of risk factors for aspiration is important for any patient who will undergo dental procedures, such as advanced age (ie, elderly patients may have a decreased gag reflex); neurologic conditions, such as stroke; dementia and other degenerative diseases; the use of topical anesthesia; and altered states of consciousness associated with the use of IV sedation.1,2
The key sign that most dentists recognize when patients aspirate an object during a dental procedure is coughing. It has been reported that coughing resulting from aspiration of foreign objects may range from mild to severe. In this case, the patient was completely asymptomatic during the procedure. The only clue of possible object aspiration was the reported tool loss by the dentist. It is important to always examine, account for, and review all equipment used during dental procedures. Assessment for any lost objects or missing parts of instruments should be done promptly with a high degree of suspicion for possible swallowing or aspiration if an object is missing.
It has been recommended to use a gauze throat screen and rubber dam and to avoid a supine position during a procedure, among other techniques, to minimize risk of ingestion or aspiration.2 Imaging studies should be used for further evaluation of the patient; however, some instruments, such as dental pieces and impression material, may not be identified by plain films. In those cases, further evaluation with more sophisticated imaging techniques, such as computed tomography (CT), should be considered.1-10
In a previous case report of a patient who aspirated a third molar during a dental procedure, a chest film failed to identify it. A chest CT was performed, and the object showed in the right main stem bronchus. In another instance, aspiration of impression material in a 45-year-old man was not observed by chest radiography. In this case, the history of coughing and respiratory symptoms days after the procedure pointed toward aspiration of an object as the culprit, with subsequent identification and removal by flexible fiberoptic bronchoscopy.1-11
Bronchoscopy is the treatment of choice for extraction of aspirated foreign bodies; however, there is still a debate about whether to use flexible or rigid bronchoscopy. The decision is usually made based on the object size, localization, medical facility, and personnel expertise. The rigid bronchoscope has the advantages of offering better control and visualization of the airway and easier use of removal instruments. Its primary disadvantage is that the procedure needs to be done in the operating room under general anesthesia. Flexible fiberoptic bronchoscopy done under conscious sedation and topical anesthesia may be as effective as rigid bronchoscopy and even superior in the case of smaller and more distal impacted objects.10-14
In this case, flexible fiberoptic bronchoscopy was used successfully for the removal of the foreign object. Biopsy forceps were used to grasp the object and retrieve it from the airway without complication.
Conclusion
Aspiration of foreign objects during a dental procedure is a potential life-threatening complication. A high-level of suspicion is needed for early diagnosis and referral of the patient for extraction of the object and further avoidance of complications. Flexible fiberoptic bronchoscopy is a feasible procedure for removal of objects within the airway.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc. , the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
There are many reports in the medical and dental literature of complications arising from a routine delivery of dental care. One complication can include physical injury from swallowing or aspirating foreign objects.1 However, a review of such literature presents a scarcity of documented instances and no long-term evaluation of the aforementioned events.2,3
This report presents the case of a patient who aspirated a hex driver tool during a procedure to place a crown on a dental implant. The aspirated object was subsequently removed through flexible fiberoptic bronchoscopy without complications.
Case Report
An 83-year-old man was referred to the Pulmonary and Critical Care Department of the VA Caribbean Healthcare System in San Juan, Puerto Rico, after a hex driver tool was lost during a procedure to place a crown on a dental implant, performed under topical anesthesia. It was first thought that the patient swallowed the hex driver, since he never experienced or complained of coughing or shortness of breath. A chest radiograph revealed a metal object lying within the right main stem bronchus, for which the patient was referred to the Pulmonary and Critical Care Department (Figure 1).
The patient’s past medical history was remarkable for hypertension and hypercholesterolemia. Outpatient medications included hydrochlorothiazide, simvastatin, aspirin, felodipine, and lorazepam. He had no previous history of dysphagia or neurologic disease. A physical examination revealed expiratory and inspiratory wheezing localized to the right lower lobe without associated rhonchi or crackles. No distress, shortness of breath, or coughing was noted.
A flexible fiberoptic bronchoscopy was performed under conscious sedation with 3 mg of IV midazolam and topical anesthesia with nebulized 4% lidocaine. No mucosal edema, hyperemia, or structural damage was noted during direct visualization of both the right and left bronchopulmonary segments. A metallic object was visualized at the entrance of the right lower lobe. The foreign object had irregular borders, providing multiple edges that made it suitable to be embraced (Figure 2).
Using a radial jaw single-use biopsy forceps 1.8 mm, the physician clinched and retrieved the object through the bronchoscope. The object was retrieved on the same day of the dental procedure almost 5 hours after it was aspirated. The patient tolerated the procedure well; no coughing, oxygen desaturation, or bleeding occurred during the procedure.
After a few hours of observation, a postprocedural radiograph confirmed the removal of the foreign body without evidence of pneumothorax. The patient was discharged, and 24 hours after the incident remained asymptomatic without chest pain, cough, hemoptysis, sputum production, or fever.
Discussion
Foreign-body aspiration and inadvertent swallowing remains underrecognized by clinicians. In the U.S., more than 2,700 people, including more than 300 children, die of foreign-body aspiration each year.4,5 Aspiration or ingestion of a foreign body during a dental procedure is serious and potentially fatal.6 Some of the consequences of an aspirated object are complete or partial airway obstruction, respiratory distress and failure, pneumothorax, and hemorrhage.7 In addition, inadvertent aspiration of foreign objects in asymptomatic patients may not be evident for months, resulting in late complications as postobstructive pneumonia, bronchiectasis, or lung abscess.8 Early recognition and diagnosis of these events are crucial to prevent complications.
Accidental aspiration of foreign objects during dental procedures is not as common as is swallowing. In the normal population, the foreign object enters the gastrointestinal tract in about 92.5% of the time, and the tracheobronchial tree in 7.5% of these instances.
A 10-year review done at the School of Dentistry of the University of North Carolina reported 36 incidents of lost instruments during dental procedures. In only 1 case, an object was aspirated, 25 of the 36 cases were secondary to ingestion, and in the remaining 10 incidents, swallowing or aspiration was ruled out by radiography or after the object’s removal from the patient’s mouth.2 Previous reviews about foreign-body aspiration in adults have reported dental appliances as the second most commonly aspirated foreign objects.4 Of all aspirated objects, the most common site of impaction is the right lower lobe; however, aspiration has been reported in all pulmonary lobes.6
Available literature recognizes that impaction of aspirated objects occurred in 56% of instances within the right lower lobe and 33% in the left lower lobe.7,9 Identification of risk factors for aspiration is important for any patient who will undergo dental procedures, such as advanced age (ie, elderly patients may have a decreased gag reflex); neurologic conditions, such as stroke; dementia and other degenerative diseases; the use of topical anesthesia; and altered states of consciousness associated with the use of IV sedation.1,2
The key sign that most dentists recognize when patients aspirate an object during a dental procedure is coughing. It has been reported that coughing resulting from aspiration of foreign objects may range from mild to severe. In this case, the patient was completely asymptomatic during the procedure. The only clue of possible object aspiration was the reported tool loss by the dentist. It is important to always examine, account for, and review all equipment used during dental procedures. Assessment for any lost objects or missing parts of instruments should be done promptly with a high degree of suspicion for possible swallowing or aspiration if an object is missing.
It has been recommended to use a gauze throat screen and rubber dam and to avoid a supine position during a procedure, among other techniques, to minimize risk of ingestion or aspiration.2 Imaging studies should be used for further evaluation of the patient; however, some instruments, such as dental pieces and impression material, may not be identified by plain films. In those cases, further evaluation with more sophisticated imaging techniques, such as computed tomography (CT), should be considered.1-10
In a previous case report of a patient who aspirated a third molar during a dental procedure, a chest film failed to identify it. A chest CT was performed, and the object showed in the right main stem bronchus. In another instance, aspiration of impression material in a 45-year-old man was not observed by chest radiography. In this case, the history of coughing and respiratory symptoms days after the procedure pointed toward aspiration of an object as the culprit, with subsequent identification and removal by flexible fiberoptic bronchoscopy.1-11
Bronchoscopy is the treatment of choice for extraction of aspirated foreign bodies; however, there is still a debate about whether to use flexible or rigid bronchoscopy. The decision is usually made based on the object size, localization, medical facility, and personnel expertise. The rigid bronchoscope has the advantages of offering better control and visualization of the airway and easier use of removal instruments. Its primary disadvantage is that the procedure needs to be done in the operating room under general anesthesia. Flexible fiberoptic bronchoscopy done under conscious sedation and topical anesthesia may be as effective as rigid bronchoscopy and even superior in the case of smaller and more distal impacted objects.10-14
In this case, flexible fiberoptic bronchoscopy was used successfully for the removal of the foreign object. Biopsy forceps were used to grasp the object and retrieve it from the airway without complication.
Conclusion
Aspiration of foreign objects during a dental procedure is a potential life-threatening complication. A high-level of suspicion is needed for early diagnosis and referral of the patient for extraction of the object and further avoidance of complications. Flexible fiberoptic bronchoscopy is a feasible procedure for removal of objects within the airway.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc. , the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Cameron SM, Whitlock WL, Tabor MS. Foreign body aspiration in dentistry: A review. J Am Dent Assoc. 1996;127(8):1224-1229.
2. Tiwana KK, Morton T, Tiwana PS. Aspiration and ingestion in dental practice: A 10-year institutional review. J Am Dent Assoc. 2004;135(9):1287-1291.
3. Susini G, Pommel L, Camps J. Accidental ingestion and aspiration of root canal instruments and other dental foreign bodies in a French population. Int Endod J. 2007;40(8):585-589.
4. Fields RT Jr, Schow SR. Aspiration and ingestion of foreign bodies in oral and maxillofacial surgery: A review of the literature and report of five cases. J Oral Maxillofac Surg. 1998;56(9):1091-1098.
5. Black RE, Johnson DG, Matlak ME. Bronchoscopic removal of aspirated foreign bodies in children. J Pediatr Surg. 1994;29(5):682-684.
6. Limper AH, Prakash UBS. Tracheobronchial foreign bodies in adults. Ann Intern Med. 1990;112(8):604-609.
7. Bas¸oglu OK, Buduneli N, Cagirici U, Turhan K, Aysan T. Pulmonary aspiration of a two-unit bridge during a deep sleep. J Oral Rehabil. 2005;32(6):461-463.
8. Mahmoud M, Imam S, Patel H, King M. Foreign body aspiration of a dental bridge in the left main stem bronchus. Case Rep Med. 2012;2012:1-4.
9. Jackson C, Jackson CL. Diseases of the Air and Food Passages of Foreign-Body Origin. Philadelphia, PA: Saunders; 1936.
10. Zitzmann NU, Elsasser S, Fried R, Marinello CP. Foreign body ingestion and aspiration. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88(6):657-660.
11. Elgazzar RF, Abdelhady AI, Sadakah AA. Aspiration of an impacted lower third molar during its surgical removal under local anaesthesia. Int J Oral Maxillofac Surg. 2007;36(4):362-364.
12. Tu CY, Chen HJ, Chen W, Liu YH, Chen CH. A feasible approach for extraction of dental prostheses from the airway by flexible bronchoscopy in concert with wire loops snares. Laryngoscope. 2007;117(7):1280-1282.
13. Ospina JC, Ludemann JP. Aspiration of an extracted molar: Case report. J Can Dent Assoc. 2005;71(8):581-583.
14. Cohen S, Pine H, Drake A. Use of rigid and flexible bronchoscopy among pediatric otolaryngologists. Arch Otoralyngol Head Neck Surg. 2001;127(5):505-509.
1. Cameron SM, Whitlock WL, Tabor MS. Foreign body aspiration in dentistry: A review. J Am Dent Assoc. 1996;127(8):1224-1229.
2. Tiwana KK, Morton T, Tiwana PS. Aspiration and ingestion in dental practice: A 10-year institutional review. J Am Dent Assoc. 2004;135(9):1287-1291.
3. Susini G, Pommel L, Camps J. Accidental ingestion and aspiration of root canal instruments and other dental foreign bodies in a French population. Int Endod J. 2007;40(8):585-589.
4. Fields RT Jr, Schow SR. Aspiration and ingestion of foreign bodies in oral and maxillofacial surgery: A review of the literature and report of five cases. J Oral Maxillofac Surg. 1998;56(9):1091-1098.
5. Black RE, Johnson DG, Matlak ME. Bronchoscopic removal of aspirated foreign bodies in children. J Pediatr Surg. 1994;29(5):682-684.
6. Limper AH, Prakash UBS. Tracheobronchial foreign bodies in adults. Ann Intern Med. 1990;112(8):604-609.
7. Bas¸oglu OK, Buduneli N, Cagirici U, Turhan K, Aysan T. Pulmonary aspiration of a two-unit bridge during a deep sleep. J Oral Rehabil. 2005;32(6):461-463.
8. Mahmoud M, Imam S, Patel H, King M. Foreign body aspiration of a dental bridge in the left main stem bronchus. Case Rep Med. 2012;2012:1-4.
9. Jackson C, Jackson CL. Diseases of the Air and Food Passages of Foreign-Body Origin. Philadelphia, PA: Saunders; 1936.
10. Zitzmann NU, Elsasser S, Fried R, Marinello CP. Foreign body ingestion and aspiration. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88(6):657-660.
11. Elgazzar RF, Abdelhady AI, Sadakah AA. Aspiration of an impacted lower third molar during its surgical removal under local anaesthesia. Int J Oral Maxillofac Surg. 2007;36(4):362-364.
12. Tu CY, Chen HJ, Chen W, Liu YH, Chen CH. A feasible approach for extraction of dental prostheses from the airway by flexible bronchoscopy in concert with wire loops snares. Laryngoscope. 2007;117(7):1280-1282.
13. Ospina JC, Ludemann JP. Aspiration of an extracted molar: Case report. J Can Dent Assoc. 2005;71(8):581-583.
14. Cohen S, Pine H, Drake A. Use of rigid and flexible bronchoscopy among pediatric otolaryngologists. Arch Otoralyngol Head Neck Surg. 2001;127(5):505-509.
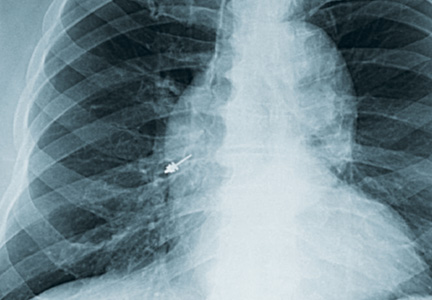
Minimally Invasive Surgical Treatments for Obstructive Sleep Apnea
Obstructive sleep apnea (OSA) is recognized primarily as a problem of the upper airway. Although narrowing or actual obstruction of the airway during the night can be found in only 1 or 2 areas of the upper airway, most often sleep apnea involves the entire pharyngeal upper airway passages. Three regions are considered to be of major concern: the nasal cavity region, the retropalatal region, and the retrolingual region. As the level of these 3 regions descends, the volume of tissue from the nose to the base of the tongue increases significantly. This leads to increased difficulty treating OSA with each descending region as well as to a lower success rate overall. Sometimes, the problem causing OSA is limited to only 1 region but may involve 2 or even all 3 regions.1
Continuous positive airway pressure (CPAP) therapy and other positive airway pressure (PAP) therapies have been considered a safe and effective treatment for OSA. Unfortunately, compliance rates, even among patients who use it to successfully eliminate their symptoms, can vary from 50% to 70%. Complaints about using CPAP and other PAP therapies range from skin irritation, discomfort to the nose or nasal passages, and eye problems to claustrophobia from wearing a mask. Patients who are unable or unwilling to use CPAP therapy can be candidates for surgical treatment of OSA.2
This article discusses surgical options for adult patients who have OSA who choose not to use CPAP therapy, the reasons to perform surgery for adults who have OSA, and the desired outcomes of surgery for OSA with a focus on minimally invasive procedures. Interventions for pediatric patients are not addressed.
Treatment Options
Treatments other than CPAP can help lessen the severity of OSA. Noninvasive treatments include weight loss, positional treatment (avoiding sleeping on one’s back), and oral appliances. Practice parameters from the American Academy of Sleep Medicine (AASM) for the treatment of OSA include dietary weight loss in addition to the primary therapy. An improvement in the apnea-hypopnea index (AHI) may occur with dietary weight loss.3
Major weight loss through the use of bariatric surgery has been shown to be effective in treating OSA and obesity hypoventilation syndrome (OHS), which is defined as daytime hypercapnia and hypoxemia (PaCO2 > 45 mm Hg and PaO2 < 70 mm Hg at sea level) in an obese patient (body mass index [BMI] > 30 kg/m2) with sleep-disordered breathing in the absence of any other cause of hypoventilation.4 Some individuals may have both conditions. However, CPAP therapy should not be discontinued even when major weight loss occurs until repeat polysomnography has been performed. Major weight loss may cure OHS and help improve the severity of OSA but will not totally resolve the condition.4 According to Woodson, sleep apnea in patients who are morbidly obese may be different from traditional OSA as rapid eye movement (REM), REM-related apneas, and hypoventilation occur more often in this population. Although weight loss is strongly recommended for patients with OSA, bariatric surgery is not recommended as the sole treatment for traditional OSA.5
Positional therapy, wherein the patient avoids the supine position, can be effective as a secondary or supplemental therapy in addition to treatment with CPAP. Guidelines recommend this primarily for individuals who have a lower AHI when in the nonsupine position than when lying on their backs. Patients who benefit from positional therapy tend to be younger, less obese, and with a less severe condition. The AASM practice parameter was based on 3 level II studies—randomized trials with high alpha and beta levels.6 One of the level II studies compared supine with an upright position, stating: “Because not all patients normalize AHI when non-supine, the committee’s opinion is that correction of OSA by position should be documented with an appropriate test.” Special pillows have been described in 2 papers reviewed by AASM, which seemed to improve OSA.6
The AASM guidelines state that oral appliances are indicated for some patients, although they are not as efficacious in treating OSA as CPAP therapy. Oral appliances are recommended for patients with mild to moderate OSA who have not responded to CPAP therapy, cannot tolerate CPAP therapy, are not appropriate for treatment with CPAP for some reason, or fail treatment with CPAP along with other behavioral measures, such as weight loss or positional therapy.6
In addition, the AASM guidelines recommend that patients with severe OSA, “should have an initial trial of nasal CPAP because greater effectiveness has been shown with this intervention than with the use of oral appliances. Upper airway surgery (including tonsillectomy and adenoidectomy, craniofacial operations, and tracheostomy) may also supersede use of oral appliances in patients for whom these operations are predicted to be highly effective in treating sleep apnea.”6
Nasal expiratory positive end pressure (EPAP) devices may be helpful in treating OSA in some patients. These devices contain a mechanical valve with very low inspiratory resistance but high expiratory resistance. The device has an adhesive and is applied by the patient to create a seal. Exhalation causes a high expiratory resistance that splints the upper airway open. This increases the resistance of the airway to close on inspiration.7 An EPAP device is recommended for potential use in mild to moderate OSA for patients who either have an intolerance to CPAP therapy or have failed to respond to it.8
Finally, there are major surgeries performed by oral surgeons that can benefit some patients with OSA. One of these is maxillomandibular advancement (MMA). According to the AASM practice parameter: MMA “involves simultaneous advancement of the maxilla and mandible through sagittal split osteotomies. It provides enlargement of the retrolingual airway and some advancement of the retropalatal airway.”9 It is indicated as a surgical treatment for patients with severe OSA who are either unwilling or do not tolerate CPAP treatment. These individuals would not benefit from an oral appliance (recommended for mild to moderate OSA) or would find it undesirable.9
There is also stepwise or multilevel surgery (MLS) that can be performed. These include a number of combined procedures, which address multiple sites with narrowing in the upper airway. Frequently, MLS will consist of
2 phases: the first involves use of the uvulopalatopharyngoplasty (UPPP) procedure “and or genioglossus advancement and hyoid myotomy (GAHM). The second phase surgeries consist of utilizing maxillary and mandibular advancement osteotomy (MMO), offered to those failing Phase I surgeries.”9
OSA Surgical Procedures
Tracheostomies are first estimated to have been performed in 2000 BC.10 Performing a tracheostomy to bypass the upper airway was used in the 1960s and 1970s for the treatment of OSA and for many years was the only treatment available for people with Pickwickian syndrome (OHS) and nocturnal upper airway obstruction. The procedure was generally not tolerated or accepted by patients, even though it improved their quality of life and added to their life expectancy. Once CPAP treatment proved successful for OSA, tracheostomy has rarely been necessary.11
Uvulopalatopharyngoplasty surgery was introduced in 1981. The aim of this surgery is to decrease snoring and treat OSA by removing obstructive tissues, enlarging the cross-sectional portion of the upper airway, and bypassing the upper airway. Tissue that is removed includes the tonsils, uvula, and the distal portion of the soft palate.12
Woodson considers surgery for OSA to be the third-line of treatment. The first-line treatment would be CPAP therapy, and second-line therapy would include oral appliances to enlarge the airway or retain the tongue (if the individual has no dentition). The intent of surgery falls into 3 categories: curative, salvage, and ancillary.
In a chronic disease such as OSA, “many may question whether a cure exists.” Instead of eliminating OSA, the curative intent is definitively to reduce symptoms and disease morbidity for long periods. The criteria for defining a responder or cure to surgery for OSA are found in Table 1.5
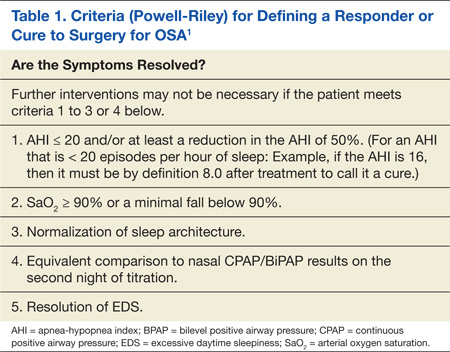
Surgery for salvage aims at treating patients who have failed CPAP therapy. Successful treatment with the intent of salvage can occur with a lessening of disease severity, including morbidity and mortality, but not necessarily totally eliminating the symptoms. Finally, ancillary surgery for OSA aims to combine a surgical procedure with the first-line therapy (positive pressure) to add an additional therapeutic benefit. The combination of CPAP and ancillary procedures may be of the most benefit to patients with OSA.5
As mentioned previously, the AASM has developed practice parameters for the treatment of OSA, including surgery. Desired outcomes of treatment for OSA include the resolution of symptoms and clinical signs, normalization of the quality of sleep, AHI, and levels of oxyhemoglobin saturation. It is recognized that normalization of the AHI may not reverse all the components of OSA, and up to 22% of patients continue to have residual hypersomnia with CPAP therapy.9
Despite this, most studies that show significant benefits in lowering cardiovascular risk, mortality rates, symptoms, and neurocognitive effects have also shown significant reductions in the AHI.9 Therefore, the AASM puts a high value on treating OSA with the goal of normalization of the AHI. There exists a lack of quality studies and good evidence regarding the effectiveness of surgical procedures of the upper airway as treatment for OSA. Despite this, the AASM recommendation is that “all reasonable treatment alternatives for OSA be discussed in a manner that allows the patient to make an informed decision.”9
Types of OSA Surgeries
Surgery for OSA can be divided into 2 categories, invasive surgery and minimally invasive surgery (Table 2). Invasive surgeries for OSA have a higher risk of complications and postoperative pain.9
Invasive Surgery
The UPPP surgery is perhaps the best-known invasive procedure for treating OSA. A meta-analysis of 15 studies on UPPP outcomes found overall improvement in AHI of 33% but with postoperative AHI remaining elevated at an average of 29.8 events per hour.13
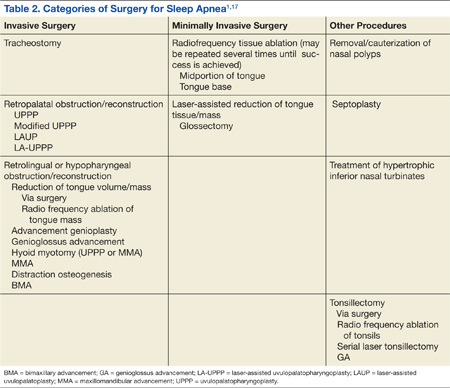
Adverse effects for the procedure include changes in taste, dysphagia, nasal regurgitation, and voice alterations. Seven of the 15 studies reported at least 1 death following the UPPP procedure. The effects of UPPP surgery on systemic and cardiovascular sequelae of OSA are not fully known and need to be further researched. 13
Another invasive procedure that is similar to the UPPP is the laser-assisted uvulopalatoplasty (LAUP) procedure. First reported in 1990, LAUP was developed as a procedure to eliminate snoring and was found to be effective. Other studies have been conducted since then, but there are inconsistencies in the specific types of procedures performed and a lack of detailed data analysis.
Adverse effects of the LAUP procedure include minor bleeding, globus sensation, local infection, minor dysphagia and dysphonia, and transient velopharyngeal insufficiency.14 However, studies have also shown that about one-quarter of the participants developed persistent dysphagia or mild to moderate scar fibrosis. Postoperative swelling can reduce an already narrow airway, and the use of sedatives or narcotics can make this problem worse. Some studies have noted structural changes following this procedure that lower airway resistance, resulting in the collapse of the upper airway and the narrowing of the airway during inhalation with worsening OSA.13,14
Practice parameters for the LAUP procedure were developed by the AASM in 1994. The AASM recommended against using LAUP to treat OSA (and other sleep-related breathing disorders) and against substituting LAUP for UPPP surgery. The AASM also suggested criteria for choosing candidates for LAUP and urged that patients be given full information about the procedure and a preoperative evaluation from their provider.5,14
Minimally Invasive Surgery
Radiofrequency surgery and soft palate implants are considered minimally invasive procedures, according to the criteria established in a study by Maurer.11 Various nasal surgeries (eg, septoplasty, adenoidectomy, and polyp removal) could also be considered minimally invasive and are often performed in patients with OSA to improve tolerance of CPAP by improving the ability to breathe nasally. However, nasal surgery with improvement of nasal breathing has not been found to have a significant impact on adults who have OSA. An advantage of nasal surgery is that some studies have shown longer use of CPAP therapy, up to 2 hours longer per night.5
With radiofrequency of the tongue base, high-frequency radio waves, either monopolar or bipolar, are used to coagulate the interstitial tissue at the base of the tongue. This, in turn, leads to necrosis and scarring, which then leads to stiffening of the tissue and in some cases, volume reduction. The surgeon controls the temperature to avoid overdosing and tissue carbonization. A number of lesions are produced during a session and the number of sessions necessary for full treatment varies per surgeon and the technical system used in procedures.
Although radiofrequency ablation (RFA) has been used on the tonsils and soft palate, RFA is currently available only to patients with OSA on the tongue base. A reduction in AHI of 33% on average was achieved in a review of 6 studies, and the reduction was stable over a 2-year period.11 The average presurgery AHI was 39.5, and the average postsurgery AHI was 28.7. In this same review, the average Epworth Sleepiness Scale (ESS) (a commonly used subjective tool to measure levels of daytime sleepiness) score was 10.4 presurgery and 4.5 postsurgery.11
A Chinese study looked at complications from RFA of the tongue base. According to the abstract (the article was written in Chinese), 1 patient (n = 193) developed a fatal arrhythmia. The authors’ recommendation was for close monitoring after surgery until the swelling subsided.15
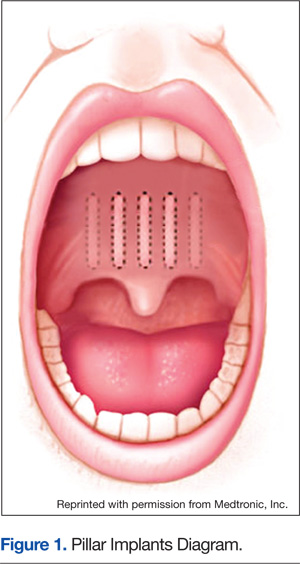
With soft palate implants, small cylinders of woven polyester (“polyethylene terephthalate, commonly marketed as Dacron polyester”) yarn, 18 mm long by 2 mm diameter, are inserted at the junction of the hard palate and soft palate. Placed into the proximal soft palate tissue, these implants are designed to stiffen the soft palate “through fibrotic tissue encapsulation and tissue ingrowth over time.” Many patients with only snoring or mild to moderate OSA have found improvement with this procedure. Improved reduction of snoring was found in 1 study (n = 79), which looked at the use of Pillar implants to reduce snoring (Figure 1). This reduction of snoring occurred in patients with lower AHI levels before the procedure.16 Mauer reviewed 3 studies of the palatal implants and found a pooled reduction of 26% in AHI after placement.11
Criteria for Surgery
The mechanism that causes collapse of a patient’s airway will vary from one person to the next. Variables include age, body weight, anatomy, and body position. Thus, different findings will require different surgical techniques, and there is no one-size-fits-all surgery for OSA.11
A thorough physical examination of the upper airway is important. Maurer recommends considering the use of videoendoscopy under sedation, which allows a view of the mechanism and site of obstruction, with pressure catheters inserted to collect data. This procedure was developed in the 1990s to improve the analysis of obstruction within the upper airway. Unfortunately, the data are unclear about whether this aids in the surgical outcome.11 Powell stated that sleep endoscopy is currently considered investigational because medication-induced sleep may differ from natural sleep without medication.1
Nasopharyngoscopy, using fiberoptics, and lateral cephalometric analysis have been used for several years as primary diagnostic tools for patients being considered for a surgical procedure for OSA. Some new imaging procedures (eg, 3-D imaging coupled with advanced software programs) have been developed that may be helpful to assess regions that are constricted as well as provide a more exact measurement of the airway from the nose to the larynx.1
Risks and Complications of Surgery
The higher risk of anesthesia-related complications during or after surgery related to OSA is one reason that surgery is usually considered to be the third-line of treatment. Patients with OSA commonly have hypertension and other cardiovascular disease, which adds to the risk of anesthesia-related complications. Patients who have anatomical abnormalities of the jaw or portions of the upper airway will also be at a higher risk. Initial intubation and providing anesthesia during procedures may be more difficult for patients with these jaw or airway abnormalities. Postsurgical pain management with opioids contributes to the higher rate of apnea. After extubation, the incidence of apnea has been found to be higher in the population with OSA as well.17
A study published in 2001 used a case-control matched population methodology to examine patients who were undergoing elective surgeries for either hip or knee joint replacements. Significant differences in overall complication rates were found among the patients with OSA (n = 101) compared with those of the control group (n = 101). These differences were not related to the type of anesthesia, narcotic use after surgery, or the type of operation performed. The OSA group had a significantly higher number of patients who required higher flow rates of oxygen postoperatively and for a longer period. Serious complications, including the reintubation of 2 patients and unplanned intensive care unit (ICU) transfers, were noted in the patients with OSA (24%) compared with the control group (P = .004). The mean length of hospital stay was significantly longer for patients with OSA (6.8 + 2.8 days) compared with those in the control group (5.1 + 4.1 days, P = .007).18
The OSA group in the aforementioned study was divided into 2 types during this investigation: one group (n = 36) included patients undiagnosed with OSA until after their surgery (mean 1.8 years); the other group (n = 65) had a confirmed diagnosis at the time of surgery. All 36 in the first group and 32 from the second group with diagnosed OSA did not use CPAP therapy at home; a total of 68 patients (67.3%) who had not received therapy before the surgery. The 33 patients with diagnosed OSA (32.7%) who did use CPAP therapy before surgery had lower complication rates, including shorter hospital stays (6.0 + 2.1 days) compared with their counterparts with untreated OSA (7.2 + 3.1 days). The authors surmised that there might be a carryover protective effect at least for the first postoperative day.18
A retrospective study examined patients with OSA who had outpatient surgical procedures performed under either major regional anesthesia (central neuraxial) or general anesthesia. The study looked at the first outpatient surgical procedure for the patient with OSA following the diagnosis except for otorhinolaryngologic surgeries, which were excluded from the study. The 234 patients with OSA were then matched to the same number of control patients who had also had outpatient surgical procedures (excluding the otorhinolaryngologic procedures). The researchers noted a higher incidence of endotracheal intubation in the OSA group (79.9% vs 73.9% in the control group, P = .017).
The OSA group was less likely to have a laryngeal mask airway used during surgery for their airway management (5.1% vs 10.7% in the control group, P = .017). The only significantly different complication between the 2 groups was unplanned admissions to an ICU in the postoperative period (although numbers/percentages were not listed in the article). However, there was no difference in the overall unplanned hospital admission rate between the 2 groups. One limitation to this study was that the control group had not been tested for OSA, and therefore, it was possible that some in the control group might have had undiagnosed OSA.19
It is recommended that the surgeon and anesthesiologist ask about a diagnosis of OSA or sleep apnea symptoms during the preanesthesia assessment for any surgery. The provider performing the preoperative physical examination should pay attention to the circumference of the neck, chin-throat length, Mallampati classification, mandible position, and BMI. Any findings that suggest undiagnosed OSA should prompt further evaluation before any elective surgery.
Those who are at risk of OSA anesthesia-related complications should be offered regional anesthesia if possible. It is undesirable to premedicate with sedatives or opioids for this population. The sniffing position during surgery has been found to reduce the collapsibility of the airway and improve its dimensions. All patients who use CPAP therapy at home should have this therapy available for use in the recovery room with the lateral position preferred.17
Outpatient surgery using sedation and local anesthetics can also be a higher risk for patients with OSA. The unprotected, potentially problematic airway is still a serious concern. Patients requiring short procedures may do well with titrated sedation if well positioned and appropriately selected for this before the procedure. Clinicians must be prepared to handle any complications that occur. One complication that occurs commonly in obese patients related to a smaller functional residual capacity is rapid oxygen desaturation.17
A Chinese study evaluated complications in patients who had received tongue base reduction through RFA. Complications, both intraoperative and postoperative, included hematoma of the tongue base, bleeding, altered taste, an abscess at the base of the tongue, speech dysfunction, numbness, and deviation of the tongue extension movement. One cardiac death occurred 37 hours following surgery related to swelling of the tongue base and pain, which aggravated sleep apnea and nocturnal hypoxemia and induced a fatal arrhythmia.15
The Future of OSA Treatments
Research is underway to evaluate the effectiveness of an implanted system to stimulate the hypoglossal nerve with the intent of activating the upper airway musculature. A small study of 8 patients found improvement in the degree of upper airway collapsibility and the severity of OSA. Continued research on the device is focusing on the parameters for the nerve stimulation. The criteria for patient selection are also being established.20
Another study of hypoglossal nerve stimulation (HNS) evaluated 21 patients who were unable to tolerate CPAP therapy. The researchers found significant improvement in AHI (43.1 + 17.5 to 19.5 + 16.7); Functional Outcomes of Sleep Questionnaire (14.4 + 2.0 to 16.7 + 2.2); ESS (12.1 + 4.7 to 8.1 + 4.4); Beck Depression Inventory (15.8 + 9.0 to 9.7 + 7.6); and the Calgary Sleep Apnea Quality of Life Index (3.2 + 1.0 to 4.9 to 4.9 + 1.3). The researchers concluded HNS decreased OSA-related symptoms and the severity of OSA.21 At least one of these devices, the Inspire device, has been approved for use in Europe (Figure 2).22 In addition, the FDA has approve the Inspire Upper Airway Stimulation therapy for use in a subset of patients with moderate to severe OSA who are unable to use CPAP.23
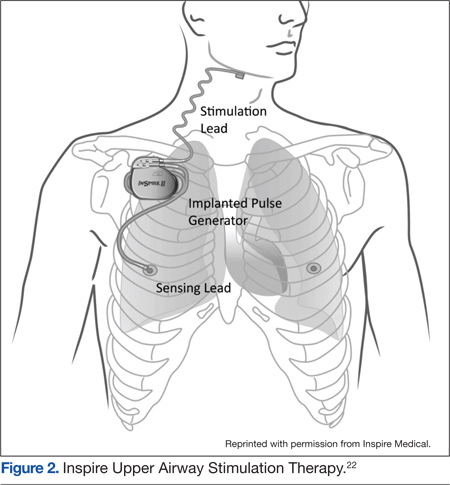
A recent study investigated the effect of HNS on the severity of OSA among patients who had moderate to severe OSA and had not had a response to CPAP therapy. The HNS was associated with significant improvement in reducing the frequency of respiratory events. The median AHI at 12 months decreased from 29.3 events per hour to 9.0 events per hour (P < .001), and the number of times per hour of sleep that the blood oxygen level dropped by ≥ 4% from the baseline (oxygen desaturation index score) decreased from 25.4 to 7.4 events per hour (P < .001).24
Another area being studied is the development of a device to advance the tongue. Forty-two patients had mandibular bone anchors inserted with a flexible tether connected to a surgically inserted anchor in the posterior tongue. Unfortunately, 31% of the participants developed tissue anchor barb fractures that were asymptomatic and detected through radiography. At this time, the failure rate does not warrant clinical use. However, some patients showed significant improvement in multiple measures for sleep apnea, and more research is ongoing with the device.25
Similarly, a surgically inserted tongue pin that connects to an oral device during sleep has been studied. This pin prevents the tongue from moving back and obstructing the upper airway. Polysomnographies were performed both before and after and showed an increased rate of apnea in the 10 subjects. Visualization with magnetic resonance imaging showed that the upper airway was not kept open by this fixation device. Additional research with a modified design for the device is recommended.26
Reshaping of the epiglottis using a CO2 laser has been studied with cadaver specimens. The researchers believe scar formation following the reshaping would aid in retraction of the epiglottis anteriorly. Studies with animals are being conducted with different laser types. Future studies involving selected patients with OSA who have epiglottis malformations would be the next step.27
More studies about both minimally invasive and invasive surgeries for OSA are needed. There are many unanswered questions, including the timing of follow-up assessments, how long to observe a patient after surgery, whether the use of multilevel surgery affects the rate of relapse, and what are the best follow-up tools to use. Research needs to be performed in diverse populations, including gender, race/ethnicity, and age groups. Complications of surgical procedures need to be studied and clarified over both short- and long-term periods.9
Conclusions
Although there have been some successes in using surgical procedures to treat OSA, CPAP therapy remains the first-line treatment. Invasive surgeries have higher rates of complications and risks than do those of minimally invasive procedures. There are also additional risks related to the use of anesthesia both during and after surgery. Referrals for surgery should include information about a diagnosis of OSA, and patients should be instructed to discuss this with the anesthesiologist or certified nurse anesthetist.
With careful selection by the surgeon and sleep providers, patients who do not tolerate CPAP therapy or respond to other noninvasive interventions can benefit from a surgical procedure. Minimally invasive surgeries are less risky for the patient and should be considered.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
WEB EXCLUSIVE CASE STUDY
A Physical Examination of the Upper Airway by an Ear, Nose, and Throat Physician
1. Powell NB. Contemporary surgery for obstructive sleep apnea syndrome. Clin Exp Otorhinolaryngol. 2009;2(3):107-114.
2. Shine NP, Lewis RH. Transpalatal advancement paryngoplasty for obstructive sleep apnea syndrome: Results and analysis of failures. Arch Otolaryngol Head Neck Surg. 2009;135(5): 434-438.
3. Morgenthaler TI, Kapen S, Lee-Chiong T; American Academy of Sleep Medicine. Practice parameters for the medical therapy of obstructive sleep apnea. Sleep. 2006;29(8):1031-1035.
4. Aigner MJ, Sikka P, Whitfield P. Obesity hypoventilation syndrome: What is it? How is it treated? Is there a cure? Bariatric Nursing and Surgical Patient Care. 2009;4(2):109-113.
5. Woodson BT. Non-pressure therapies for obstructive sleep apnea: Surgery and oral appliances. Respir Care. 2010;55(10):1314-1321.
6. Kushida CA, Morgenthaler TI, Littner MR, et al; American Academy of Sleep Medicine. Practice parameters for the treatment of snoring and Obstructive Sleep Apnea with oral appliances: An update for 2005. Sleep. 2006;29(2):240-243.
7. Berry RB, Kryger MH, Massie CA. A novel nasal expiratory positive airway pressure (EPAP) device for the treatment of obstructive sleep apnea: A randomized controlled trial. Sleep. 2011;34(4):479-485.
8. Kryger MH, Berry RB, Massie CA. Long-term use of a nasal expiratory positive airway pressure (EPAP) device as a treatment of obstructive sleep apnea (OSA). J Clin Sleep Med. 2011;7(5):449-453.
9. Aurora RN, Casey KR, Kristo D, et al; American Academy of Sleep Medicine. Practice parameters for the surgical modifications of the upper airway for obstructive sleep apnea in adults. Sleep. 2010;33(10):1408-1413.
10. Szmuk P, Ezri T, Evron S, Roth Y, Katz J. A brief history of tracheostomy and tracheal intubation, from the Bronze Age to the space age. Intensive Care Med. 2008;34(2):222-228.
11. Maurer JT. Update on surgical treatment for sleep apnoea. Swiss Med Wkly. 2009;139(43-44):624-629.
12. Franklin KA, Anttila H, Axelsson S, et al. Effects and side-effects of surgery for snoring and obsructive sleep apnea—a systematic review. Sleep. 2009;32(1):27-36.
13. Caples SM, Rowley JA, Prinsell JR, et al. Surgical modifications of the upper airway for obstructive sleep apnea in adults: A systematic review and meta-analysis. Sleep. 2010; 33(10):1396-1407.
14. Littner M, Kushida CA, Hartse K, et al. Practice parameters for the use of laser-assisted uvulopalatoplasty: An update for 2000. Sleep. 2001;24(5):603-619.
15. Chen JH, Luo ZH, Yang XL, Zhu MW, Tao ZZ. Complications of tongue base reduction with radiofrequency tissue ablation on obstructive sleep apnea hypopnea syndrome. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2010;45(7):574-577. (Abstract, full text in Chinese.)
16. Gillespie MB, Smith JE, Clarke J, Nguyen SA. Effectiveness of Pillar palatal implants for snoring management. Otolaryngol Head Neck Surg. 2009;140(3):363-368.
17. Ephros HD, Madani M, Yalamanchili SC. Surgical treatment of snoring and obstructive sleep apnoea. Indian J Med Res. 2010;131:267-276.
18. Gupta RM, Parvizi J, Hanssen AD, Gay PC. Postoperative complications in patients with obstructive sleep apnea syndrome undergoing hip or knee replacement: A case-control study. Mayo Clin Proc. 2001;76(9):897-905.
19. Sabers C, Plevak DJ, Schroeder DR, Warner DO. The diagnosis of obstructive sleep apnea as a risk factor for unanticipated admissions in outpatient surgery. Anesth Analg. 2003;96(5):1328-1335.
20. Kerzirian EJ, Boudewyns A, Eisele DW, et al. Electrical stimulation of the hypoglossal nerve in the treatment of obstructive sleep apnea. Sleep Med Rev. 2010;14(5):299-305.
21. Eastwood PR, Barnes M, Walsh JH, et al. Treating obstructive sleep apnea with hypoglossal nerve stimulation. Sleep. 2011;34(11):1479-1486.
22. Inspire Medical. STAR Trial. Inspire Medical Website. http://www.inspiresleep.com/star-trial.php. Accessed May 7, 2014.
23. FDA approves Inspire Upper Airway Stimulation (UAS) therapy for obstructive sleep apnea [press release]. Inspire Medical Website. http://www.inspiresleep.com/pdf/FDA-Approval-Press-Release-final-20140501.pdf.
Accessed May 29, 2014.
24. Strollo PJ Jr, Soose RJ, Maurer JT, et al. Upper-airway stimulation for obstructive sleep apnea. N Engl J Med. 2014;370(2):139-149.
25. Woodson BT, Steward DL, Mickelson S, Huntley T, Goldberg A. Multicenter study of a novel adjustable tongue-advancement device for obstructive sleep apnea. Otolaryngol Head Neck Surg. 2010;143(4):585-590.
26. Punke C, Schöentag C, Hortian B, et al. Tongue fixation system for therapy of sleeping disorders. A feasibility study. HNO. 2010;58(12):1184-1189. (Abstract, full text in German).
27. Bourolinas C, Hajiioannou J, Sobol E, Velegrakis G, Helidonis E. Epiglottis reshaping using CO2: A minimally invasive technique and its potential applications. Head Face Med. 2008;4:15.
Obstructive sleep apnea (OSA) is recognized primarily as a problem of the upper airway. Although narrowing or actual obstruction of the airway during the night can be found in only 1 or 2 areas of the upper airway, most often sleep apnea involves the entire pharyngeal upper airway passages. Three regions are considered to be of major concern: the nasal cavity region, the retropalatal region, and the retrolingual region. As the level of these 3 regions descends, the volume of tissue from the nose to the base of the tongue increases significantly. This leads to increased difficulty treating OSA with each descending region as well as to a lower success rate overall. Sometimes, the problem causing OSA is limited to only 1 region but may involve 2 or even all 3 regions.1
Continuous positive airway pressure (CPAP) therapy and other positive airway pressure (PAP) therapies have been considered a safe and effective treatment for OSA. Unfortunately, compliance rates, even among patients who use it to successfully eliminate their symptoms, can vary from 50% to 70%. Complaints about using CPAP and other PAP therapies range from skin irritation, discomfort to the nose or nasal passages, and eye problems to claustrophobia from wearing a mask. Patients who are unable or unwilling to use CPAP therapy can be candidates for surgical treatment of OSA.2
This article discusses surgical options for adult patients who have OSA who choose not to use CPAP therapy, the reasons to perform surgery for adults who have OSA, and the desired outcomes of surgery for OSA with a focus on minimally invasive procedures. Interventions for pediatric patients are not addressed.
Treatment Options
Treatments other than CPAP can help lessen the severity of OSA. Noninvasive treatments include weight loss, positional treatment (avoiding sleeping on one’s back), and oral appliances. Practice parameters from the American Academy of Sleep Medicine (AASM) for the treatment of OSA include dietary weight loss in addition to the primary therapy. An improvement in the apnea-hypopnea index (AHI) may occur with dietary weight loss.3
Major weight loss through the use of bariatric surgery has been shown to be effective in treating OSA and obesity hypoventilation syndrome (OHS), which is defined as daytime hypercapnia and hypoxemia (PaCO2 > 45 mm Hg and PaO2 < 70 mm Hg at sea level) in an obese patient (body mass index [BMI] > 30 kg/m2) with sleep-disordered breathing in the absence of any other cause of hypoventilation.4 Some individuals may have both conditions. However, CPAP therapy should not be discontinued even when major weight loss occurs until repeat polysomnography has been performed. Major weight loss may cure OHS and help improve the severity of OSA but will not totally resolve the condition.4 According to Woodson, sleep apnea in patients who are morbidly obese may be different from traditional OSA as rapid eye movement (REM), REM-related apneas, and hypoventilation occur more often in this population. Although weight loss is strongly recommended for patients with OSA, bariatric surgery is not recommended as the sole treatment for traditional OSA.5
Positional therapy, wherein the patient avoids the supine position, can be effective as a secondary or supplemental therapy in addition to treatment with CPAP. Guidelines recommend this primarily for individuals who have a lower AHI when in the nonsupine position than when lying on their backs. Patients who benefit from positional therapy tend to be younger, less obese, and with a less severe condition. The AASM practice parameter was based on 3 level II studies—randomized trials with high alpha and beta levels.6 One of the level II studies compared supine with an upright position, stating: “Because not all patients normalize AHI when non-supine, the committee’s opinion is that correction of OSA by position should be documented with an appropriate test.” Special pillows have been described in 2 papers reviewed by AASM, which seemed to improve OSA.6
The AASM guidelines state that oral appliances are indicated for some patients, although they are not as efficacious in treating OSA as CPAP therapy. Oral appliances are recommended for patients with mild to moderate OSA who have not responded to CPAP therapy, cannot tolerate CPAP therapy, are not appropriate for treatment with CPAP for some reason, or fail treatment with CPAP along with other behavioral measures, such as weight loss or positional therapy.6
In addition, the AASM guidelines recommend that patients with severe OSA, “should have an initial trial of nasal CPAP because greater effectiveness has been shown with this intervention than with the use of oral appliances. Upper airway surgery (including tonsillectomy and adenoidectomy, craniofacial operations, and tracheostomy) may also supersede use of oral appliances in patients for whom these operations are predicted to be highly effective in treating sleep apnea.”6
Nasal expiratory positive end pressure (EPAP) devices may be helpful in treating OSA in some patients. These devices contain a mechanical valve with very low inspiratory resistance but high expiratory resistance. The device has an adhesive and is applied by the patient to create a seal. Exhalation causes a high expiratory resistance that splints the upper airway open. This increases the resistance of the airway to close on inspiration.7 An EPAP device is recommended for potential use in mild to moderate OSA for patients who either have an intolerance to CPAP therapy or have failed to respond to it.8
Finally, there are major surgeries performed by oral surgeons that can benefit some patients with OSA. One of these is maxillomandibular advancement (MMA). According to the AASM practice parameter: MMA “involves simultaneous advancement of the maxilla and mandible through sagittal split osteotomies. It provides enlargement of the retrolingual airway and some advancement of the retropalatal airway.”9 It is indicated as a surgical treatment for patients with severe OSA who are either unwilling or do not tolerate CPAP treatment. These individuals would not benefit from an oral appliance (recommended for mild to moderate OSA) or would find it undesirable.9
There is also stepwise or multilevel surgery (MLS) that can be performed. These include a number of combined procedures, which address multiple sites with narrowing in the upper airway. Frequently, MLS will consist of
2 phases: the first involves use of the uvulopalatopharyngoplasty (UPPP) procedure “and or genioglossus advancement and hyoid myotomy (GAHM). The second phase surgeries consist of utilizing maxillary and mandibular advancement osteotomy (MMO), offered to those failing Phase I surgeries.”9
OSA Surgical Procedures
Tracheostomies are first estimated to have been performed in 2000 BC.10 Performing a tracheostomy to bypass the upper airway was used in the 1960s and 1970s for the treatment of OSA and for many years was the only treatment available for people with Pickwickian syndrome (OHS) and nocturnal upper airway obstruction. The procedure was generally not tolerated or accepted by patients, even though it improved their quality of life and added to their life expectancy. Once CPAP treatment proved successful for OSA, tracheostomy has rarely been necessary.11
Uvulopalatopharyngoplasty surgery was introduced in 1981. The aim of this surgery is to decrease snoring and treat OSA by removing obstructive tissues, enlarging the cross-sectional portion of the upper airway, and bypassing the upper airway. Tissue that is removed includes the tonsils, uvula, and the distal portion of the soft palate.12
Woodson considers surgery for OSA to be the third-line of treatment. The first-line treatment would be CPAP therapy, and second-line therapy would include oral appliances to enlarge the airway or retain the tongue (if the individual has no dentition). The intent of surgery falls into 3 categories: curative, salvage, and ancillary.
In a chronic disease such as OSA, “many may question whether a cure exists.” Instead of eliminating OSA, the curative intent is definitively to reduce symptoms and disease morbidity for long periods. The criteria for defining a responder or cure to surgery for OSA are found in Table 1.5
Surgery for salvage aims at treating patients who have failed CPAP therapy. Successful treatment with the intent of salvage can occur with a lessening of disease severity, including morbidity and mortality, but not necessarily totally eliminating the symptoms. Finally, ancillary surgery for OSA aims to combine a surgical procedure with the first-line therapy (positive pressure) to add an additional therapeutic benefit. The combination of CPAP and ancillary procedures may be of the most benefit to patients with OSA.5
As mentioned previously, the AASM has developed practice parameters for the treatment of OSA, including surgery. Desired outcomes of treatment for OSA include the resolution of symptoms and clinical signs, normalization of the quality of sleep, AHI, and levels of oxyhemoglobin saturation. It is recognized that normalization of the AHI may not reverse all the components of OSA, and up to 22% of patients continue to have residual hypersomnia with CPAP therapy.9
Despite this, most studies that show significant benefits in lowering cardiovascular risk, mortality rates, symptoms, and neurocognitive effects have also shown significant reductions in the AHI.9 Therefore, the AASM puts a high value on treating OSA with the goal of normalization of the AHI. There exists a lack of quality studies and good evidence regarding the effectiveness of surgical procedures of the upper airway as treatment for OSA. Despite this, the AASM recommendation is that “all reasonable treatment alternatives for OSA be discussed in a manner that allows the patient to make an informed decision.”9
Types of OSA Surgeries
Surgery for OSA can be divided into 2 categories, invasive surgery and minimally invasive surgery (Table 2). Invasive surgeries for OSA have a higher risk of complications and postoperative pain.9
Invasive Surgery
The UPPP surgery is perhaps the best-known invasive procedure for treating OSA. A meta-analysis of 15 studies on UPPP outcomes found overall improvement in AHI of 33% but with postoperative AHI remaining elevated at an average of 29.8 events per hour.13
Adverse effects for the procedure include changes in taste, dysphagia, nasal regurgitation, and voice alterations. Seven of the 15 studies reported at least 1 death following the UPPP procedure. The effects of UPPP surgery on systemic and cardiovascular sequelae of OSA are not fully known and need to be further researched. 13
Another invasive procedure that is similar to the UPPP is the laser-assisted uvulopalatoplasty (LAUP) procedure. First reported in 1990, LAUP was developed as a procedure to eliminate snoring and was found to be effective. Other studies have been conducted since then, but there are inconsistencies in the specific types of procedures performed and a lack of detailed data analysis.
Adverse effects of the LAUP procedure include minor bleeding, globus sensation, local infection, minor dysphagia and dysphonia, and transient velopharyngeal insufficiency.14 However, studies have also shown that about one-quarter of the participants developed persistent dysphagia or mild to moderate scar fibrosis. Postoperative swelling can reduce an already narrow airway, and the use of sedatives or narcotics can make this problem worse. Some studies have noted structural changes following this procedure that lower airway resistance, resulting in the collapse of the upper airway and the narrowing of the airway during inhalation with worsening OSA.13,14
Practice parameters for the LAUP procedure were developed by the AASM in 1994. The AASM recommended against using LAUP to treat OSA (and other sleep-related breathing disorders) and against substituting LAUP for UPPP surgery. The AASM also suggested criteria for choosing candidates for LAUP and urged that patients be given full information about the procedure and a preoperative evaluation from their provider.5,14
Minimally Invasive Surgery
Radiofrequency surgery and soft palate implants are considered minimally invasive procedures, according to the criteria established in a study by Maurer.11 Various nasal surgeries (eg, septoplasty, adenoidectomy, and polyp removal) could also be considered minimally invasive and are often performed in patients with OSA to improve tolerance of CPAP by improving the ability to breathe nasally. However, nasal surgery with improvement of nasal breathing has not been found to have a significant impact on adults who have OSA. An advantage of nasal surgery is that some studies have shown longer use of CPAP therapy, up to 2 hours longer per night.5
With radiofrequency of the tongue base, high-frequency radio waves, either monopolar or bipolar, are used to coagulate the interstitial tissue at the base of the tongue. This, in turn, leads to necrosis and scarring, which then leads to stiffening of the tissue and in some cases, volume reduction. The surgeon controls the temperature to avoid overdosing and tissue carbonization. A number of lesions are produced during a session and the number of sessions necessary for full treatment varies per surgeon and the technical system used in procedures.
Although radiofrequency ablation (RFA) has been used on the tonsils and soft palate, RFA is currently available only to patients with OSA on the tongue base. A reduction in AHI of 33% on average was achieved in a review of 6 studies, and the reduction was stable over a 2-year period.11 The average presurgery AHI was 39.5, and the average postsurgery AHI was 28.7. In this same review, the average Epworth Sleepiness Scale (ESS) (a commonly used subjective tool to measure levels of daytime sleepiness) score was 10.4 presurgery and 4.5 postsurgery.11
A Chinese study looked at complications from RFA of the tongue base. According to the abstract (the article was written in Chinese), 1 patient (n = 193) developed a fatal arrhythmia. The authors’ recommendation was for close monitoring after surgery until the swelling subsided.15
With soft palate implants, small cylinders of woven polyester (“polyethylene terephthalate, commonly marketed as Dacron polyester”) yarn, 18 mm long by 2 mm diameter, are inserted at the junction of the hard palate and soft palate. Placed into the proximal soft palate tissue, these implants are designed to stiffen the soft palate “through fibrotic tissue encapsulation and tissue ingrowth over time.” Many patients with only snoring or mild to moderate OSA have found improvement with this procedure. Improved reduction of snoring was found in 1 study (n = 79), which looked at the use of Pillar implants to reduce snoring (Figure 1). This reduction of snoring occurred in patients with lower AHI levels before the procedure.16 Mauer reviewed 3 studies of the palatal implants and found a pooled reduction of 26% in AHI after placement.11
Criteria for Surgery
The mechanism that causes collapse of a patient’s airway will vary from one person to the next. Variables include age, body weight, anatomy, and body position. Thus, different findings will require different surgical techniques, and there is no one-size-fits-all surgery for OSA.11
A thorough physical examination of the upper airway is important. Maurer recommends considering the use of videoendoscopy under sedation, which allows a view of the mechanism and site of obstruction, with pressure catheters inserted to collect data. This procedure was developed in the 1990s to improve the analysis of obstruction within the upper airway. Unfortunately, the data are unclear about whether this aids in the surgical outcome.11 Powell stated that sleep endoscopy is currently considered investigational because medication-induced sleep may differ from natural sleep without medication.1
Nasopharyngoscopy, using fiberoptics, and lateral cephalometric analysis have been used for several years as primary diagnostic tools for patients being considered for a surgical procedure for OSA. Some new imaging procedures (eg, 3-D imaging coupled with advanced software programs) have been developed that may be helpful to assess regions that are constricted as well as provide a more exact measurement of the airway from the nose to the larynx.1
Risks and Complications of Surgery
The higher risk of anesthesia-related complications during or after surgery related to OSA is one reason that surgery is usually considered to be the third-line of treatment. Patients with OSA commonly have hypertension and other cardiovascular disease, which adds to the risk of anesthesia-related complications. Patients who have anatomical abnormalities of the jaw or portions of the upper airway will also be at a higher risk. Initial intubation and providing anesthesia during procedures may be more difficult for patients with these jaw or airway abnormalities. Postsurgical pain management with opioids contributes to the higher rate of apnea. After extubation, the incidence of apnea has been found to be higher in the population with OSA as well.17
A study published in 2001 used a case-control matched population methodology to examine patients who were undergoing elective surgeries for either hip or knee joint replacements. Significant differences in overall complication rates were found among the patients with OSA (n = 101) compared with those of the control group (n = 101). These differences were not related to the type of anesthesia, narcotic use after surgery, or the type of operation performed. The OSA group had a significantly higher number of patients who required higher flow rates of oxygen postoperatively and for a longer period. Serious complications, including the reintubation of 2 patients and unplanned intensive care unit (ICU) transfers, were noted in the patients with OSA (24%) compared with the control group (P = .004). The mean length of hospital stay was significantly longer for patients with OSA (6.8 + 2.8 days) compared with those in the control group (5.1 + 4.1 days, P = .007).18
The OSA group in the aforementioned study was divided into 2 types during this investigation: one group (n = 36) included patients undiagnosed with OSA until after their surgery (mean 1.8 years); the other group (n = 65) had a confirmed diagnosis at the time of surgery. All 36 in the first group and 32 from the second group with diagnosed OSA did not use CPAP therapy at home; a total of 68 patients (67.3%) who had not received therapy before the surgery. The 33 patients with diagnosed OSA (32.7%) who did use CPAP therapy before surgery had lower complication rates, including shorter hospital stays (6.0 + 2.1 days) compared with their counterparts with untreated OSA (7.2 + 3.1 days). The authors surmised that there might be a carryover protective effect at least for the first postoperative day.18
A retrospective study examined patients with OSA who had outpatient surgical procedures performed under either major regional anesthesia (central neuraxial) or general anesthesia. The study looked at the first outpatient surgical procedure for the patient with OSA following the diagnosis except for otorhinolaryngologic surgeries, which were excluded from the study. The 234 patients with OSA were then matched to the same number of control patients who had also had outpatient surgical procedures (excluding the otorhinolaryngologic procedures). The researchers noted a higher incidence of endotracheal intubation in the OSA group (79.9% vs 73.9% in the control group, P = .017).
The OSA group was less likely to have a laryngeal mask airway used during surgery for their airway management (5.1% vs 10.7% in the control group, P = .017). The only significantly different complication between the 2 groups was unplanned admissions to an ICU in the postoperative period (although numbers/percentages were not listed in the article). However, there was no difference in the overall unplanned hospital admission rate between the 2 groups. One limitation to this study was that the control group had not been tested for OSA, and therefore, it was possible that some in the control group might have had undiagnosed OSA.19
It is recommended that the surgeon and anesthesiologist ask about a diagnosis of OSA or sleep apnea symptoms during the preanesthesia assessment for any surgery. The provider performing the preoperative physical examination should pay attention to the circumference of the neck, chin-throat length, Mallampati classification, mandible position, and BMI. Any findings that suggest undiagnosed OSA should prompt further evaluation before any elective surgery.
Those who are at risk of OSA anesthesia-related complications should be offered regional anesthesia if possible. It is undesirable to premedicate with sedatives or opioids for this population. The sniffing position during surgery has been found to reduce the collapsibility of the airway and improve its dimensions. All patients who use CPAP therapy at home should have this therapy available for use in the recovery room with the lateral position preferred.17
Outpatient surgery using sedation and local anesthetics can also be a higher risk for patients with OSA. The unprotected, potentially problematic airway is still a serious concern. Patients requiring short procedures may do well with titrated sedation if well positioned and appropriately selected for this before the procedure. Clinicians must be prepared to handle any complications that occur. One complication that occurs commonly in obese patients related to a smaller functional residual capacity is rapid oxygen desaturation.17
A Chinese study evaluated complications in patients who had received tongue base reduction through RFA. Complications, both intraoperative and postoperative, included hematoma of the tongue base, bleeding, altered taste, an abscess at the base of the tongue, speech dysfunction, numbness, and deviation of the tongue extension movement. One cardiac death occurred 37 hours following surgery related to swelling of the tongue base and pain, which aggravated sleep apnea and nocturnal hypoxemia and induced a fatal arrhythmia.15
The Future of OSA Treatments
Research is underway to evaluate the effectiveness of an implanted system to stimulate the hypoglossal nerve with the intent of activating the upper airway musculature. A small study of 8 patients found improvement in the degree of upper airway collapsibility and the severity of OSA. Continued research on the device is focusing on the parameters for the nerve stimulation. The criteria for patient selection are also being established.20
Another study of hypoglossal nerve stimulation (HNS) evaluated 21 patients who were unable to tolerate CPAP therapy. The researchers found significant improvement in AHI (43.1 + 17.5 to 19.5 + 16.7); Functional Outcomes of Sleep Questionnaire (14.4 + 2.0 to 16.7 + 2.2); ESS (12.1 + 4.7 to 8.1 + 4.4); Beck Depression Inventory (15.8 + 9.0 to 9.7 + 7.6); and the Calgary Sleep Apnea Quality of Life Index (3.2 + 1.0 to 4.9 to 4.9 + 1.3). The researchers concluded HNS decreased OSA-related symptoms and the severity of OSA.21 At least one of these devices, the Inspire device, has been approved for use in Europe (Figure 2).22 In addition, the FDA has approve the Inspire Upper Airway Stimulation therapy for use in a subset of patients with moderate to severe OSA who are unable to use CPAP.23
A recent study investigated the effect of HNS on the severity of OSA among patients who had moderate to severe OSA and had not had a response to CPAP therapy. The HNS was associated with significant improvement in reducing the frequency of respiratory events. The median AHI at 12 months decreased from 29.3 events per hour to 9.0 events per hour (P < .001), and the number of times per hour of sleep that the blood oxygen level dropped by ≥ 4% from the baseline (oxygen desaturation index score) decreased from 25.4 to 7.4 events per hour (P < .001).24
Another area being studied is the development of a device to advance the tongue. Forty-two patients had mandibular bone anchors inserted with a flexible tether connected to a surgically inserted anchor in the posterior tongue. Unfortunately, 31% of the participants developed tissue anchor barb fractures that were asymptomatic and detected through radiography. At this time, the failure rate does not warrant clinical use. However, some patients showed significant improvement in multiple measures for sleep apnea, and more research is ongoing with the device.25
Similarly, a surgically inserted tongue pin that connects to an oral device during sleep has been studied. This pin prevents the tongue from moving back and obstructing the upper airway. Polysomnographies were performed both before and after and showed an increased rate of apnea in the 10 subjects. Visualization with magnetic resonance imaging showed that the upper airway was not kept open by this fixation device. Additional research with a modified design for the device is recommended.26
Reshaping of the epiglottis using a CO2 laser has been studied with cadaver specimens. The researchers believe scar formation following the reshaping would aid in retraction of the epiglottis anteriorly. Studies with animals are being conducted with different laser types. Future studies involving selected patients with OSA who have epiglottis malformations would be the next step.27
More studies about both minimally invasive and invasive surgeries for OSA are needed. There are many unanswered questions, including the timing of follow-up assessments, how long to observe a patient after surgery, whether the use of multilevel surgery affects the rate of relapse, and what are the best follow-up tools to use. Research needs to be performed in diverse populations, including gender, race/ethnicity, and age groups. Complications of surgical procedures need to be studied and clarified over both short- and long-term periods.9
Conclusions
Although there have been some successes in using surgical procedures to treat OSA, CPAP therapy remains the first-line treatment. Invasive surgeries have higher rates of complications and risks than do those of minimally invasive procedures. There are also additional risks related to the use of anesthesia both during and after surgery. Referrals for surgery should include information about a diagnosis of OSA, and patients should be instructed to discuss this with the anesthesiologist or certified nurse anesthetist.
With careful selection by the surgeon and sleep providers, patients who do not tolerate CPAP therapy or respond to other noninvasive interventions can benefit from a surgical procedure. Minimally invasive surgeries are less risky for the patient and should be considered.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
WEB EXCLUSIVE CASE STUDY
A Physical Examination of the Upper Airway by an Ear, Nose, and Throat Physician
Obstructive sleep apnea (OSA) is recognized primarily as a problem of the upper airway. Although narrowing or actual obstruction of the airway during the night can be found in only 1 or 2 areas of the upper airway, most often sleep apnea involves the entire pharyngeal upper airway passages. Three regions are considered to be of major concern: the nasal cavity region, the retropalatal region, and the retrolingual region. As the level of these 3 regions descends, the volume of tissue from the nose to the base of the tongue increases significantly. This leads to increased difficulty treating OSA with each descending region as well as to a lower success rate overall. Sometimes, the problem causing OSA is limited to only 1 region but may involve 2 or even all 3 regions.1
Continuous positive airway pressure (CPAP) therapy and other positive airway pressure (PAP) therapies have been considered a safe and effective treatment for OSA. Unfortunately, compliance rates, even among patients who use it to successfully eliminate their symptoms, can vary from 50% to 70%. Complaints about using CPAP and other PAP therapies range from skin irritation, discomfort to the nose or nasal passages, and eye problems to claustrophobia from wearing a mask. Patients who are unable or unwilling to use CPAP therapy can be candidates for surgical treatment of OSA.2
This article discusses surgical options for adult patients who have OSA who choose not to use CPAP therapy, the reasons to perform surgery for adults who have OSA, and the desired outcomes of surgery for OSA with a focus on minimally invasive procedures. Interventions for pediatric patients are not addressed.
Treatment Options
Treatments other than CPAP can help lessen the severity of OSA. Noninvasive treatments include weight loss, positional treatment (avoiding sleeping on one’s back), and oral appliances. Practice parameters from the American Academy of Sleep Medicine (AASM) for the treatment of OSA include dietary weight loss in addition to the primary therapy. An improvement in the apnea-hypopnea index (AHI) may occur with dietary weight loss.3
Major weight loss through the use of bariatric surgery has been shown to be effective in treating OSA and obesity hypoventilation syndrome (OHS), which is defined as daytime hypercapnia and hypoxemia (PaCO2 > 45 mm Hg and PaO2 < 70 mm Hg at sea level) in an obese patient (body mass index [BMI] > 30 kg/m2) with sleep-disordered breathing in the absence of any other cause of hypoventilation.4 Some individuals may have both conditions. However, CPAP therapy should not be discontinued even when major weight loss occurs until repeat polysomnography has been performed. Major weight loss may cure OHS and help improve the severity of OSA but will not totally resolve the condition.4 According to Woodson, sleep apnea in patients who are morbidly obese may be different from traditional OSA as rapid eye movement (REM), REM-related apneas, and hypoventilation occur more often in this population. Although weight loss is strongly recommended for patients with OSA, bariatric surgery is not recommended as the sole treatment for traditional OSA.5
Positional therapy, wherein the patient avoids the supine position, can be effective as a secondary or supplemental therapy in addition to treatment with CPAP. Guidelines recommend this primarily for individuals who have a lower AHI when in the nonsupine position than when lying on their backs. Patients who benefit from positional therapy tend to be younger, less obese, and with a less severe condition. The AASM practice parameter was based on 3 level II studies—randomized trials with high alpha and beta levels.6 One of the level II studies compared supine with an upright position, stating: “Because not all patients normalize AHI when non-supine, the committee’s opinion is that correction of OSA by position should be documented with an appropriate test.” Special pillows have been described in 2 papers reviewed by AASM, which seemed to improve OSA.6
The AASM guidelines state that oral appliances are indicated for some patients, although they are not as efficacious in treating OSA as CPAP therapy. Oral appliances are recommended for patients with mild to moderate OSA who have not responded to CPAP therapy, cannot tolerate CPAP therapy, are not appropriate for treatment with CPAP for some reason, or fail treatment with CPAP along with other behavioral measures, such as weight loss or positional therapy.6
In addition, the AASM guidelines recommend that patients with severe OSA, “should have an initial trial of nasal CPAP because greater effectiveness has been shown with this intervention than with the use of oral appliances. Upper airway surgery (including tonsillectomy and adenoidectomy, craniofacial operations, and tracheostomy) may also supersede use of oral appliances in patients for whom these operations are predicted to be highly effective in treating sleep apnea.”6
Nasal expiratory positive end pressure (EPAP) devices may be helpful in treating OSA in some patients. These devices contain a mechanical valve with very low inspiratory resistance but high expiratory resistance. The device has an adhesive and is applied by the patient to create a seal. Exhalation causes a high expiratory resistance that splints the upper airway open. This increases the resistance of the airway to close on inspiration.7 An EPAP device is recommended for potential use in mild to moderate OSA for patients who either have an intolerance to CPAP therapy or have failed to respond to it.8
Finally, there are major surgeries performed by oral surgeons that can benefit some patients with OSA. One of these is maxillomandibular advancement (MMA). According to the AASM practice parameter: MMA “involves simultaneous advancement of the maxilla and mandible through sagittal split osteotomies. It provides enlargement of the retrolingual airway and some advancement of the retropalatal airway.”9 It is indicated as a surgical treatment for patients with severe OSA who are either unwilling or do not tolerate CPAP treatment. These individuals would not benefit from an oral appliance (recommended for mild to moderate OSA) or would find it undesirable.9
There is also stepwise or multilevel surgery (MLS) that can be performed. These include a number of combined procedures, which address multiple sites with narrowing in the upper airway. Frequently, MLS will consist of
2 phases: the first involves use of the uvulopalatopharyngoplasty (UPPP) procedure “and or genioglossus advancement and hyoid myotomy (GAHM). The second phase surgeries consist of utilizing maxillary and mandibular advancement osteotomy (MMO), offered to those failing Phase I surgeries.”9
OSA Surgical Procedures
Tracheostomies are first estimated to have been performed in 2000 BC.10 Performing a tracheostomy to bypass the upper airway was used in the 1960s and 1970s for the treatment of OSA and for many years was the only treatment available for people with Pickwickian syndrome (OHS) and nocturnal upper airway obstruction. The procedure was generally not tolerated or accepted by patients, even though it improved their quality of life and added to their life expectancy. Once CPAP treatment proved successful for OSA, tracheostomy has rarely been necessary.11
Uvulopalatopharyngoplasty surgery was introduced in 1981. The aim of this surgery is to decrease snoring and treat OSA by removing obstructive tissues, enlarging the cross-sectional portion of the upper airway, and bypassing the upper airway. Tissue that is removed includes the tonsils, uvula, and the distal portion of the soft palate.12
Woodson considers surgery for OSA to be the third-line of treatment. The first-line treatment would be CPAP therapy, and second-line therapy would include oral appliances to enlarge the airway or retain the tongue (if the individual has no dentition). The intent of surgery falls into 3 categories: curative, salvage, and ancillary.
In a chronic disease such as OSA, “many may question whether a cure exists.” Instead of eliminating OSA, the curative intent is definitively to reduce symptoms and disease morbidity for long periods. The criteria for defining a responder or cure to surgery for OSA are found in Table 1.5
Surgery for salvage aims at treating patients who have failed CPAP therapy. Successful treatment with the intent of salvage can occur with a lessening of disease severity, including morbidity and mortality, but not necessarily totally eliminating the symptoms. Finally, ancillary surgery for OSA aims to combine a surgical procedure with the first-line therapy (positive pressure) to add an additional therapeutic benefit. The combination of CPAP and ancillary procedures may be of the most benefit to patients with OSA.5
As mentioned previously, the AASM has developed practice parameters for the treatment of OSA, including surgery. Desired outcomes of treatment for OSA include the resolution of symptoms and clinical signs, normalization of the quality of sleep, AHI, and levels of oxyhemoglobin saturation. It is recognized that normalization of the AHI may not reverse all the components of OSA, and up to 22% of patients continue to have residual hypersomnia with CPAP therapy.9
Despite this, most studies that show significant benefits in lowering cardiovascular risk, mortality rates, symptoms, and neurocognitive effects have also shown significant reductions in the AHI.9 Therefore, the AASM puts a high value on treating OSA with the goal of normalization of the AHI. There exists a lack of quality studies and good evidence regarding the effectiveness of surgical procedures of the upper airway as treatment for OSA. Despite this, the AASM recommendation is that “all reasonable treatment alternatives for OSA be discussed in a manner that allows the patient to make an informed decision.”9
Types of OSA Surgeries
Surgery for OSA can be divided into 2 categories, invasive surgery and minimally invasive surgery (Table 2). Invasive surgeries for OSA have a higher risk of complications and postoperative pain.9
Invasive Surgery
The UPPP surgery is perhaps the best-known invasive procedure for treating OSA. A meta-analysis of 15 studies on UPPP outcomes found overall improvement in AHI of 33% but with postoperative AHI remaining elevated at an average of 29.8 events per hour.13
Adverse effects for the procedure include changes in taste, dysphagia, nasal regurgitation, and voice alterations. Seven of the 15 studies reported at least 1 death following the UPPP procedure. The effects of UPPP surgery on systemic and cardiovascular sequelae of OSA are not fully known and need to be further researched. 13
Another invasive procedure that is similar to the UPPP is the laser-assisted uvulopalatoplasty (LAUP) procedure. First reported in 1990, LAUP was developed as a procedure to eliminate snoring and was found to be effective. Other studies have been conducted since then, but there are inconsistencies in the specific types of procedures performed and a lack of detailed data analysis.
Adverse effects of the LAUP procedure include minor bleeding, globus sensation, local infection, minor dysphagia and dysphonia, and transient velopharyngeal insufficiency.14 However, studies have also shown that about one-quarter of the participants developed persistent dysphagia or mild to moderate scar fibrosis. Postoperative swelling can reduce an already narrow airway, and the use of sedatives or narcotics can make this problem worse. Some studies have noted structural changes following this procedure that lower airway resistance, resulting in the collapse of the upper airway and the narrowing of the airway during inhalation with worsening OSA.13,14
Practice parameters for the LAUP procedure were developed by the AASM in 1994. The AASM recommended against using LAUP to treat OSA (and other sleep-related breathing disorders) and against substituting LAUP for UPPP surgery. The AASM also suggested criteria for choosing candidates for LAUP and urged that patients be given full information about the procedure and a preoperative evaluation from their provider.5,14
Minimally Invasive Surgery
Radiofrequency surgery and soft palate implants are considered minimally invasive procedures, according to the criteria established in a study by Maurer.11 Various nasal surgeries (eg, septoplasty, adenoidectomy, and polyp removal) could also be considered minimally invasive and are often performed in patients with OSA to improve tolerance of CPAP by improving the ability to breathe nasally. However, nasal surgery with improvement of nasal breathing has not been found to have a significant impact on adults who have OSA. An advantage of nasal surgery is that some studies have shown longer use of CPAP therapy, up to 2 hours longer per night.5
With radiofrequency of the tongue base, high-frequency radio waves, either monopolar or bipolar, are used to coagulate the interstitial tissue at the base of the tongue. This, in turn, leads to necrosis and scarring, which then leads to stiffening of the tissue and in some cases, volume reduction. The surgeon controls the temperature to avoid overdosing and tissue carbonization. A number of lesions are produced during a session and the number of sessions necessary for full treatment varies per surgeon and the technical system used in procedures.
Although radiofrequency ablation (RFA) has been used on the tonsils and soft palate, RFA is currently available only to patients with OSA on the tongue base. A reduction in AHI of 33% on average was achieved in a review of 6 studies, and the reduction was stable over a 2-year period.11 The average presurgery AHI was 39.5, and the average postsurgery AHI was 28.7. In this same review, the average Epworth Sleepiness Scale (ESS) (a commonly used subjective tool to measure levels of daytime sleepiness) score was 10.4 presurgery and 4.5 postsurgery.11
A Chinese study looked at complications from RFA of the tongue base. According to the abstract (the article was written in Chinese), 1 patient (n = 193) developed a fatal arrhythmia. The authors’ recommendation was for close monitoring after surgery until the swelling subsided.15
With soft palate implants, small cylinders of woven polyester (“polyethylene terephthalate, commonly marketed as Dacron polyester”) yarn, 18 mm long by 2 mm diameter, are inserted at the junction of the hard palate and soft palate. Placed into the proximal soft palate tissue, these implants are designed to stiffen the soft palate “through fibrotic tissue encapsulation and tissue ingrowth over time.” Many patients with only snoring or mild to moderate OSA have found improvement with this procedure. Improved reduction of snoring was found in 1 study (n = 79), which looked at the use of Pillar implants to reduce snoring (Figure 1). This reduction of snoring occurred in patients with lower AHI levels before the procedure.16 Mauer reviewed 3 studies of the palatal implants and found a pooled reduction of 26% in AHI after placement.11
Criteria for Surgery
The mechanism that causes collapse of a patient’s airway will vary from one person to the next. Variables include age, body weight, anatomy, and body position. Thus, different findings will require different surgical techniques, and there is no one-size-fits-all surgery for OSA.11
A thorough physical examination of the upper airway is important. Maurer recommends considering the use of videoendoscopy under sedation, which allows a view of the mechanism and site of obstruction, with pressure catheters inserted to collect data. This procedure was developed in the 1990s to improve the analysis of obstruction within the upper airway. Unfortunately, the data are unclear about whether this aids in the surgical outcome.11 Powell stated that sleep endoscopy is currently considered investigational because medication-induced sleep may differ from natural sleep without medication.1
Nasopharyngoscopy, using fiberoptics, and lateral cephalometric analysis have been used for several years as primary diagnostic tools for patients being considered for a surgical procedure for OSA. Some new imaging procedures (eg, 3-D imaging coupled with advanced software programs) have been developed that may be helpful to assess regions that are constricted as well as provide a more exact measurement of the airway from the nose to the larynx.1
Risks and Complications of Surgery
The higher risk of anesthesia-related complications during or after surgery related to OSA is one reason that surgery is usually considered to be the third-line of treatment. Patients with OSA commonly have hypertension and other cardiovascular disease, which adds to the risk of anesthesia-related complications. Patients who have anatomical abnormalities of the jaw or portions of the upper airway will also be at a higher risk. Initial intubation and providing anesthesia during procedures may be more difficult for patients with these jaw or airway abnormalities. Postsurgical pain management with opioids contributes to the higher rate of apnea. After extubation, the incidence of apnea has been found to be higher in the population with OSA as well.17
A study published in 2001 used a case-control matched population methodology to examine patients who were undergoing elective surgeries for either hip or knee joint replacements. Significant differences in overall complication rates were found among the patients with OSA (n = 101) compared with those of the control group (n = 101). These differences were not related to the type of anesthesia, narcotic use after surgery, or the type of operation performed. The OSA group had a significantly higher number of patients who required higher flow rates of oxygen postoperatively and for a longer period. Serious complications, including the reintubation of 2 patients and unplanned intensive care unit (ICU) transfers, were noted in the patients with OSA (24%) compared with the control group (P = .004). The mean length of hospital stay was significantly longer for patients with OSA (6.8 + 2.8 days) compared with those in the control group (5.1 + 4.1 days, P = .007).18
The OSA group in the aforementioned study was divided into 2 types during this investigation: one group (n = 36) included patients undiagnosed with OSA until after their surgery (mean 1.8 years); the other group (n = 65) had a confirmed diagnosis at the time of surgery. All 36 in the first group and 32 from the second group with diagnosed OSA did not use CPAP therapy at home; a total of 68 patients (67.3%) who had not received therapy before the surgery. The 33 patients with diagnosed OSA (32.7%) who did use CPAP therapy before surgery had lower complication rates, including shorter hospital stays (6.0 + 2.1 days) compared with their counterparts with untreated OSA (7.2 + 3.1 days). The authors surmised that there might be a carryover protective effect at least for the first postoperative day.18
A retrospective study examined patients with OSA who had outpatient surgical procedures performed under either major regional anesthesia (central neuraxial) or general anesthesia. The study looked at the first outpatient surgical procedure for the patient with OSA following the diagnosis except for otorhinolaryngologic surgeries, which were excluded from the study. The 234 patients with OSA were then matched to the same number of control patients who had also had outpatient surgical procedures (excluding the otorhinolaryngologic procedures). The researchers noted a higher incidence of endotracheal intubation in the OSA group (79.9% vs 73.9% in the control group, P = .017).
The OSA group was less likely to have a laryngeal mask airway used during surgery for their airway management (5.1% vs 10.7% in the control group, P = .017). The only significantly different complication between the 2 groups was unplanned admissions to an ICU in the postoperative period (although numbers/percentages were not listed in the article). However, there was no difference in the overall unplanned hospital admission rate between the 2 groups. One limitation to this study was that the control group had not been tested for OSA, and therefore, it was possible that some in the control group might have had undiagnosed OSA.19
It is recommended that the surgeon and anesthesiologist ask about a diagnosis of OSA or sleep apnea symptoms during the preanesthesia assessment for any surgery. The provider performing the preoperative physical examination should pay attention to the circumference of the neck, chin-throat length, Mallampati classification, mandible position, and BMI. Any findings that suggest undiagnosed OSA should prompt further evaluation before any elective surgery.
Those who are at risk of OSA anesthesia-related complications should be offered regional anesthesia if possible. It is undesirable to premedicate with sedatives or opioids for this population. The sniffing position during surgery has been found to reduce the collapsibility of the airway and improve its dimensions. All patients who use CPAP therapy at home should have this therapy available for use in the recovery room with the lateral position preferred.17
Outpatient surgery using sedation and local anesthetics can also be a higher risk for patients with OSA. The unprotected, potentially problematic airway is still a serious concern. Patients requiring short procedures may do well with titrated sedation if well positioned and appropriately selected for this before the procedure. Clinicians must be prepared to handle any complications that occur. One complication that occurs commonly in obese patients related to a smaller functional residual capacity is rapid oxygen desaturation.17
A Chinese study evaluated complications in patients who had received tongue base reduction through RFA. Complications, both intraoperative and postoperative, included hematoma of the tongue base, bleeding, altered taste, an abscess at the base of the tongue, speech dysfunction, numbness, and deviation of the tongue extension movement. One cardiac death occurred 37 hours following surgery related to swelling of the tongue base and pain, which aggravated sleep apnea and nocturnal hypoxemia and induced a fatal arrhythmia.15
The Future of OSA Treatments
Research is underway to evaluate the effectiveness of an implanted system to stimulate the hypoglossal nerve with the intent of activating the upper airway musculature. A small study of 8 patients found improvement in the degree of upper airway collapsibility and the severity of OSA. Continued research on the device is focusing on the parameters for the nerve stimulation. The criteria for patient selection are also being established.20
Another study of hypoglossal nerve stimulation (HNS) evaluated 21 patients who were unable to tolerate CPAP therapy. The researchers found significant improvement in AHI (43.1 + 17.5 to 19.5 + 16.7); Functional Outcomes of Sleep Questionnaire (14.4 + 2.0 to 16.7 + 2.2); ESS (12.1 + 4.7 to 8.1 + 4.4); Beck Depression Inventory (15.8 + 9.0 to 9.7 + 7.6); and the Calgary Sleep Apnea Quality of Life Index (3.2 + 1.0 to 4.9 to 4.9 + 1.3). The researchers concluded HNS decreased OSA-related symptoms and the severity of OSA.21 At least one of these devices, the Inspire device, has been approved for use in Europe (Figure 2).22 In addition, the FDA has approve the Inspire Upper Airway Stimulation therapy for use in a subset of patients with moderate to severe OSA who are unable to use CPAP.23
A recent study investigated the effect of HNS on the severity of OSA among patients who had moderate to severe OSA and had not had a response to CPAP therapy. The HNS was associated with significant improvement in reducing the frequency of respiratory events. The median AHI at 12 months decreased from 29.3 events per hour to 9.0 events per hour (P < .001), and the number of times per hour of sleep that the blood oxygen level dropped by ≥ 4% from the baseline (oxygen desaturation index score) decreased from 25.4 to 7.4 events per hour (P < .001).24
Another area being studied is the development of a device to advance the tongue. Forty-two patients had mandibular bone anchors inserted with a flexible tether connected to a surgically inserted anchor in the posterior tongue. Unfortunately, 31% of the participants developed tissue anchor barb fractures that were asymptomatic and detected through radiography. At this time, the failure rate does not warrant clinical use. However, some patients showed significant improvement in multiple measures for sleep apnea, and more research is ongoing with the device.25
Similarly, a surgically inserted tongue pin that connects to an oral device during sleep has been studied. This pin prevents the tongue from moving back and obstructing the upper airway. Polysomnographies were performed both before and after and showed an increased rate of apnea in the 10 subjects. Visualization with magnetic resonance imaging showed that the upper airway was not kept open by this fixation device. Additional research with a modified design for the device is recommended.26
Reshaping of the epiglottis using a CO2 laser has been studied with cadaver specimens. The researchers believe scar formation following the reshaping would aid in retraction of the epiglottis anteriorly. Studies with animals are being conducted with different laser types. Future studies involving selected patients with OSA who have epiglottis malformations would be the next step.27
More studies about both minimally invasive and invasive surgeries for OSA are needed. There are many unanswered questions, including the timing of follow-up assessments, how long to observe a patient after surgery, whether the use of multilevel surgery affects the rate of relapse, and what are the best follow-up tools to use. Research needs to be performed in diverse populations, including gender, race/ethnicity, and age groups. Complications of surgical procedures need to be studied and clarified over both short- and long-term periods.9
Conclusions
Although there have been some successes in using surgical procedures to treat OSA, CPAP therapy remains the first-line treatment. Invasive surgeries have higher rates of complications and risks than do those of minimally invasive procedures. There are also additional risks related to the use of anesthesia both during and after surgery. Referrals for surgery should include information about a diagnosis of OSA, and patients should be instructed to discuss this with the anesthesiologist or certified nurse anesthetist.
With careful selection by the surgeon and sleep providers, patients who do not tolerate CPAP therapy or respond to other noninvasive interventions can benefit from a surgical procedure. Minimally invasive surgeries are less risky for the patient and should be considered.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
WEB EXCLUSIVE CASE STUDY
A Physical Examination of the Upper Airway by an Ear, Nose, and Throat Physician
1. Powell NB. Contemporary surgery for obstructive sleep apnea syndrome. Clin Exp Otorhinolaryngol. 2009;2(3):107-114.
2. Shine NP, Lewis RH. Transpalatal advancement paryngoplasty for obstructive sleep apnea syndrome: Results and analysis of failures. Arch Otolaryngol Head Neck Surg. 2009;135(5): 434-438.
3. Morgenthaler TI, Kapen S, Lee-Chiong T; American Academy of Sleep Medicine. Practice parameters for the medical therapy of obstructive sleep apnea. Sleep. 2006;29(8):1031-1035.
4. Aigner MJ, Sikka P, Whitfield P. Obesity hypoventilation syndrome: What is it? How is it treated? Is there a cure? Bariatric Nursing and Surgical Patient Care. 2009;4(2):109-113.
5. Woodson BT. Non-pressure therapies for obstructive sleep apnea: Surgery and oral appliances. Respir Care. 2010;55(10):1314-1321.
6. Kushida CA, Morgenthaler TI, Littner MR, et al; American Academy of Sleep Medicine. Practice parameters for the treatment of snoring and Obstructive Sleep Apnea with oral appliances: An update for 2005. Sleep. 2006;29(2):240-243.
7. Berry RB, Kryger MH, Massie CA. A novel nasal expiratory positive airway pressure (EPAP) device for the treatment of obstructive sleep apnea: A randomized controlled trial. Sleep. 2011;34(4):479-485.
8. Kryger MH, Berry RB, Massie CA. Long-term use of a nasal expiratory positive airway pressure (EPAP) device as a treatment of obstructive sleep apnea (OSA). J Clin Sleep Med. 2011;7(5):449-453.
9. Aurora RN, Casey KR, Kristo D, et al; American Academy of Sleep Medicine. Practice parameters for the surgical modifications of the upper airway for obstructive sleep apnea in adults. Sleep. 2010;33(10):1408-1413.
10. Szmuk P, Ezri T, Evron S, Roth Y, Katz J. A brief history of tracheostomy and tracheal intubation, from the Bronze Age to the space age. Intensive Care Med. 2008;34(2):222-228.
11. Maurer JT. Update on surgical treatment for sleep apnoea. Swiss Med Wkly. 2009;139(43-44):624-629.
12. Franklin KA, Anttila H, Axelsson S, et al. Effects and side-effects of surgery for snoring and obsructive sleep apnea—a systematic review. Sleep. 2009;32(1):27-36.
13. Caples SM, Rowley JA, Prinsell JR, et al. Surgical modifications of the upper airway for obstructive sleep apnea in adults: A systematic review and meta-analysis. Sleep. 2010; 33(10):1396-1407.
14. Littner M, Kushida CA, Hartse K, et al. Practice parameters for the use of laser-assisted uvulopalatoplasty: An update for 2000. Sleep. 2001;24(5):603-619.
15. Chen JH, Luo ZH, Yang XL, Zhu MW, Tao ZZ. Complications of tongue base reduction with radiofrequency tissue ablation on obstructive sleep apnea hypopnea syndrome. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2010;45(7):574-577. (Abstract, full text in Chinese.)
16. Gillespie MB, Smith JE, Clarke J, Nguyen SA. Effectiveness of Pillar palatal implants for snoring management. Otolaryngol Head Neck Surg. 2009;140(3):363-368.
17. Ephros HD, Madani M, Yalamanchili SC. Surgical treatment of snoring and obstructive sleep apnoea. Indian J Med Res. 2010;131:267-276.
18. Gupta RM, Parvizi J, Hanssen AD, Gay PC. Postoperative complications in patients with obstructive sleep apnea syndrome undergoing hip or knee replacement: A case-control study. Mayo Clin Proc. 2001;76(9):897-905.
19. Sabers C, Plevak DJ, Schroeder DR, Warner DO. The diagnosis of obstructive sleep apnea as a risk factor for unanticipated admissions in outpatient surgery. Anesth Analg. 2003;96(5):1328-1335.
20. Kerzirian EJ, Boudewyns A, Eisele DW, et al. Electrical stimulation of the hypoglossal nerve in the treatment of obstructive sleep apnea. Sleep Med Rev. 2010;14(5):299-305.
21. Eastwood PR, Barnes M, Walsh JH, et al. Treating obstructive sleep apnea with hypoglossal nerve stimulation. Sleep. 2011;34(11):1479-1486.
22. Inspire Medical. STAR Trial. Inspire Medical Website. http://www.inspiresleep.com/star-trial.php. Accessed May 7, 2014.
23. FDA approves Inspire Upper Airway Stimulation (UAS) therapy for obstructive sleep apnea [press release]. Inspire Medical Website. http://www.inspiresleep.com/pdf/FDA-Approval-Press-Release-final-20140501.pdf.
Accessed May 29, 2014.
24. Strollo PJ Jr, Soose RJ, Maurer JT, et al. Upper-airway stimulation for obstructive sleep apnea. N Engl J Med. 2014;370(2):139-149.
25. Woodson BT, Steward DL, Mickelson S, Huntley T, Goldberg A. Multicenter study of a novel adjustable tongue-advancement device for obstructive sleep apnea. Otolaryngol Head Neck Surg. 2010;143(4):585-590.
26. Punke C, Schöentag C, Hortian B, et al. Tongue fixation system for therapy of sleeping disorders. A feasibility study. HNO. 2010;58(12):1184-1189. (Abstract, full text in German).
27. Bourolinas C, Hajiioannou J, Sobol E, Velegrakis G, Helidonis E. Epiglottis reshaping using CO2: A minimally invasive technique and its potential applications. Head Face Med. 2008;4:15.
1. Powell NB. Contemporary surgery for obstructive sleep apnea syndrome. Clin Exp Otorhinolaryngol. 2009;2(3):107-114.
2. Shine NP, Lewis RH. Transpalatal advancement paryngoplasty for obstructive sleep apnea syndrome: Results and analysis of failures. Arch Otolaryngol Head Neck Surg. 2009;135(5): 434-438.
3. Morgenthaler TI, Kapen S, Lee-Chiong T; American Academy of Sleep Medicine. Practice parameters for the medical therapy of obstructive sleep apnea. Sleep. 2006;29(8):1031-1035.
4. Aigner MJ, Sikka P, Whitfield P. Obesity hypoventilation syndrome: What is it? How is it treated? Is there a cure? Bariatric Nursing and Surgical Patient Care. 2009;4(2):109-113.
5. Woodson BT. Non-pressure therapies for obstructive sleep apnea: Surgery and oral appliances. Respir Care. 2010;55(10):1314-1321.
6. Kushida CA, Morgenthaler TI, Littner MR, et al; American Academy of Sleep Medicine. Practice parameters for the treatment of snoring and Obstructive Sleep Apnea with oral appliances: An update for 2005. Sleep. 2006;29(2):240-243.
7. Berry RB, Kryger MH, Massie CA. A novel nasal expiratory positive airway pressure (EPAP) device for the treatment of obstructive sleep apnea: A randomized controlled trial. Sleep. 2011;34(4):479-485.
8. Kryger MH, Berry RB, Massie CA. Long-term use of a nasal expiratory positive airway pressure (EPAP) device as a treatment of obstructive sleep apnea (OSA). J Clin Sleep Med. 2011;7(5):449-453.
9. Aurora RN, Casey KR, Kristo D, et al; American Academy of Sleep Medicine. Practice parameters for the surgical modifications of the upper airway for obstructive sleep apnea in adults. Sleep. 2010;33(10):1408-1413.
10. Szmuk P, Ezri T, Evron S, Roth Y, Katz J. A brief history of tracheostomy and tracheal intubation, from the Bronze Age to the space age. Intensive Care Med. 2008;34(2):222-228.
11. Maurer JT. Update on surgical treatment for sleep apnoea. Swiss Med Wkly. 2009;139(43-44):624-629.
12. Franklin KA, Anttila H, Axelsson S, et al. Effects and side-effects of surgery for snoring and obsructive sleep apnea—a systematic review. Sleep. 2009;32(1):27-36.
13. Caples SM, Rowley JA, Prinsell JR, et al. Surgical modifications of the upper airway for obstructive sleep apnea in adults: A systematic review and meta-analysis. Sleep. 2010; 33(10):1396-1407.
14. Littner M, Kushida CA, Hartse K, et al. Practice parameters for the use of laser-assisted uvulopalatoplasty: An update for 2000. Sleep. 2001;24(5):603-619.
15. Chen JH, Luo ZH, Yang XL, Zhu MW, Tao ZZ. Complications of tongue base reduction with radiofrequency tissue ablation on obstructive sleep apnea hypopnea syndrome. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2010;45(7):574-577. (Abstract, full text in Chinese.)
16. Gillespie MB, Smith JE, Clarke J, Nguyen SA. Effectiveness of Pillar palatal implants for snoring management. Otolaryngol Head Neck Surg. 2009;140(3):363-368.
17. Ephros HD, Madani M, Yalamanchili SC. Surgical treatment of snoring and obstructive sleep apnoea. Indian J Med Res. 2010;131:267-276.
18. Gupta RM, Parvizi J, Hanssen AD, Gay PC. Postoperative complications in patients with obstructive sleep apnea syndrome undergoing hip or knee replacement: A case-control study. Mayo Clin Proc. 2001;76(9):897-905.
19. Sabers C, Plevak DJ, Schroeder DR, Warner DO. The diagnosis of obstructive sleep apnea as a risk factor for unanticipated admissions in outpatient surgery. Anesth Analg. 2003;96(5):1328-1335.
20. Kerzirian EJ, Boudewyns A, Eisele DW, et al. Electrical stimulation of the hypoglossal nerve in the treatment of obstructive sleep apnea. Sleep Med Rev. 2010;14(5):299-305.
21. Eastwood PR, Barnes M, Walsh JH, et al. Treating obstructive sleep apnea with hypoglossal nerve stimulation. Sleep. 2011;34(11):1479-1486.
22. Inspire Medical. STAR Trial. Inspire Medical Website. http://www.inspiresleep.com/star-trial.php. Accessed May 7, 2014.
23. FDA approves Inspire Upper Airway Stimulation (UAS) therapy for obstructive sleep apnea [press release]. Inspire Medical Website. http://www.inspiresleep.com/pdf/FDA-Approval-Press-Release-final-20140501.pdf.
Accessed May 29, 2014.
24. Strollo PJ Jr, Soose RJ, Maurer JT, et al. Upper-airway stimulation for obstructive sleep apnea. N Engl J Med. 2014;370(2):139-149.
25. Woodson BT, Steward DL, Mickelson S, Huntley T, Goldberg A. Multicenter study of a novel adjustable tongue-advancement device for obstructive sleep apnea. Otolaryngol Head Neck Surg. 2010;143(4):585-590.
26. Punke C, Schöentag C, Hortian B, et al. Tongue fixation system for therapy of sleeping disorders. A feasibility study. HNO. 2010;58(12):1184-1189. (Abstract, full text in German).
27. Bourolinas C, Hajiioannou J, Sobol E, Velegrakis G, Helidonis E. Epiglottis reshaping using CO2: A minimally invasive technique and its potential applications. Head Face Med. 2008;4:15.
Antimicrobial Stewardship in an Outpatient Parenteral Antibiotic Therapy Program
Antimicrobial stewardship activities have been in place at the Edward Hines, Jr. VA Hospital in Hines, Illinois, since 1988. Initial activities, including antimicrobial restriction and the start of an outpatient-infusion program justified and led to dedicated funding for hiring the first infectious diseases (ID) clinical pharmacist. This position was initiated in 1992 and has been maintained since then. The committed multidisciplinary team, including ID physicians, ID clinical pharmacists, venous access nurses (VAN), microbiologists, infection control practitioners, and an outpatient-infusion coordinator have led stewardship activities at this VA.
One of the first efforts of the team was the development of the outpatient parenteral antibiotic therapy (OPAT) program.1 The program began in 1989 and has served more than 1,200 veterans. Outpatient parenteral antibiotic therapy is only one component of the stewardship program, which provides safe, effective, and cost-minimizing care for veterans, and is the focus of this article.
Background
Complex medical care and escalating costs have pushed all but the most seriously ill patients out of the hospital setting for care delivery. The reality is that patients who might have received care for non–life-threatening problems in a hospital bed are now relegated to an outpatient status. Beginning in the 1970s, OPAT has been used to facilitate the cost-effective, safe administration of antibiotics as an alternative to an extensive, expensive hospital stay.2 Initially developed for use in a nonhospital health care setting, the administration of antibiotics under the guidance of a health care provider (HCP) has now been extended to a self-administered infusion program.3,4 Under the latter, patients and caregivers are educated to safely administer IV antibiotics for extended periods at home.
This program uses elements of both health care–associated OPAT and self-administered OPAT (S-OPAT) to accomplish its goals: (1) safe, effective administration of antibiotic therapy to a variety of patients; (2) reduction in bed days of care (BDOC); (3) reduction of the economic burden to the hospitals’ global budgets; and (4) reduction in the incidence of common nosocomially-acquired infections, including those caused by Clostridium difficile (C difficile), methicillin-resistant Staphylococcus aureus, and vancomycin-resistant enterococcus.3
The advantages of S-OPAT have been fully realized in a variety of countries, enabling patients to receive necessary therapy in the comfort of their homes and providing them with the ability to lead normal lives without the confinement of a protracted hospital stay.5-7
Description of OPAT
The outpatient-infusion team provides specialized care for patients in accordance with the OPAT national guidelines from patient screening to program discharge.8 The dedicated staff include the OPAT nurse coordinator, VAN, pharmacists, and ID consultants. The VAN places the venous access device (VAD), educates the patient and caregiver in the care and safety of the catheter, aseptic technique, and infusion of the selected antimicrobial agent, and monitors the laboratory work. The VA may contract an outside nursing agency to provide support and reinforcement of IV administration for the patient and caregiver.
The pharmacists oversee the pharmacokinetics and pharmacodynamics of the antimicrobials as well as monitor for any toxicities that could potentially arise during and after therapy. The ID consultants identify the infection, collaborate with the pharmacists to select the most appropriate antimicrobial regimen, and determine the duration of required therapy. The team then regularly monitors the patient in the ID clinic until there is evidence of infection resolution.
Primary care providers who want to enroll patients in the OPAT program place a formal electronic consult to the ID team for antibiotic recommendation, to the outpatient infusion team for assessment of potential outpatient therapy, and to the venous access team for insertion of the VAD. The consults are completed after receiving consent from the patient, developing a patient-centered treatment plan, and determining the patient’s ability to comprehend and adhere to the program requirements. The patient or caregiver must be able to competently demonstrate aseptic technique for IV administration prior to discharge. The pharmacist educates the patient or caregiver about the stability, storage requirements, and potential adverse drug reactions of the antimicrobial.
Eligible patients must have resolved their acute medical problems and require > 1 week of therapy to treat their infection. Patients chosen for OPAT or S-OPAT must have a suitable living environment with access to a refrigerator, a telephone, and transportation to return to the hospital for follow-up. Most patients and caregivers are eager to learn and recognize the advantages of home-based care.
The VANs are a central component of the program. They maintain open communication with the patient during the entire treatment course and help triage issues to the appropriate HCP. In addition, they are responsible for submitting catheter-related bloodstream infection (CRBSI) information to the hospital administration, which then gets reported to the National Healthcare Safety Network (NHSN).
Not all patients qualify for S-OPAT. Other options include returning to the hospital daily for infusions, being discharged to a skilled care facility, or arranging for a VA-contracted agency to provide nursing care while the VA provides all required medications and supplies.
On completion of OPAT, patients are asked to evaluate the program. The anonymous survey includes open-ended questions for patients to better express their experience with the program and staff. Patients are given the opportunity to suggest improvements and provide overall feedback. The team for quality assurance and patient satisfaction reviews every survey, which is used as a tool to improve team functions.
Data are also collected in the OPAT program to measure efficacy and monitor for safety. Data obtained from the start of the program in February 1989 through fiscal year (FY) 2011 include the number of patients who were candidates for outpatient-infusion therapy, type of infection, antibiotic selection, CRBSIs, hospital readmission rates, cost savings, and patient satisfaction.
Results
The Edward Hines, Jr. VA Hospital has a proven, successful OPAT program. Most of the patients in the program during the study period were men, which reflects a typical VA population. Patients with spinal cord injury comprised a large portion of those treated. Table 1 provides the number of patients treated and lists the frequency of infections. The data are divided into 3 periods. From 1989 to September 30, 1995, OPAT used other VADs before using peripherally inserted central catheters. During the second period (October 1, 1995-September 30, 2003), patients remained with a VAD for an average of 48.6 days; whereas in Period 3 (October 1, 2003-September 30, 2011), the patients had a VAD average of 34.7 days. Consequently, with fewer VAD days, there was a decreased incidence of complications (Table 2).
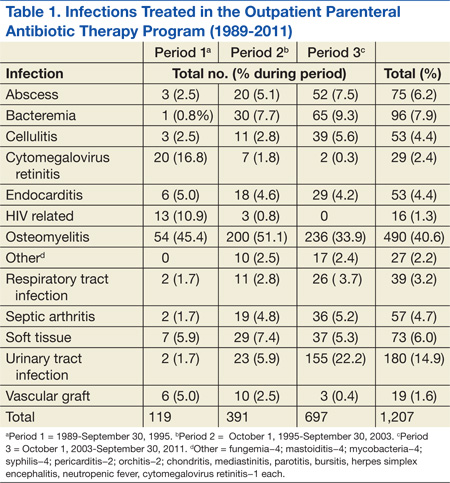
Osteomyelitis accounted for the majority of the infections (40.6%), which required ≥ 6 weeks of therapy. Complicated urinary tract infection (UTI), including pyelonephritis, perinephric abscess, and complicated cystitis, was the next most common (14.9%). Bacteremia was the third most common infection (7.9%), whereas abscesses of a diverse variety affected 6.2%, including brain, liver, intra-abdominal, soft tissue, and epidural abscesses. Endocarditis and septic arthritis accounted for 4.4% and 4.7%, respectively, of infected patients.
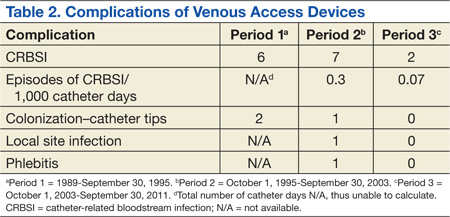
Three periods of the OPAT program were selected at random (1996, 2003, and 2011) to examine trends in antimicrobial selection. Overall, ceftriaxone was the most commonly used antibiotic (35%). Vancomycin was the next most commonly prescribed (27%). Since its 2001 FDA approval, ertapenem has become the third most commonly prescribed antibiotic for the OPAT program (11%). As expected, antimicrobial agents that have to be dosed more frequently than twice a day were rarely used for OPAT. In addition, there was low usage of aminoglycosides due to the need for the close monitoring of levels and potential toxicity.
Outcomes
Catheter Complications
The majority of catheter complications occurring in the first period were multifactorial, relating to nursing education, product selection, program development, insertion techniques, and a less comprehensive infection control program.
Hospital Readmissions
A snapshot of FY 2011 data was used to evaluate hospital readmissions. One hundred one patients were reviewed. Of these patients, 9 (9%) were readmitted to the hospital at some point after being discharged from OPAT. Readmission due to complications of OPAT was found in 2 of the 9 patients. One was due to an adverse drug reaction from the antibiotic; the other was due to a possible relapse of a hip osteomyelitis.
Cost Analysis
The OPAT program has resulted in a total savings to the global hospital budget from the deferred BDOC of more than $65 million (Table 3) since 1989. The OPAT program eliminated > 47,000 days of inpatient care. In FY 2009 the program cost the hospital $691.35 for each of the 106 patients enrolled (total cost: $73,283.10). This included all IV supplies, antimicrobials, visiting nurse costs when applicable, as well as nursing and pharmacy time dedicated to training the patient and making therapeutic decisions. Expenses for 3,109 BDOC would have cost about $6,218,000. The outpatient-infusion program saved the hospital nearly $6 million in 2009 alone.
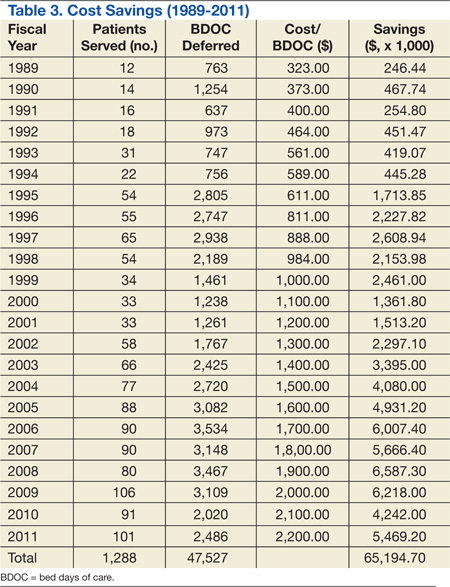
Patient Satisfaction
About 60% of the patients discharged from the OPAT program responded to an evaluation survey. The feedback was overwhelmingly positive with about 99% of respondents reporting satisfaction relating to an improved quality of life. Most of the positive comments were directed toward the outpatient-infusion coordinator for resolving issues, being easily accessible, and acting as a patient advocate.
Discussion
The number and types of reasons for OPAT have grown with the knowledge that it is a safe, cost-effective method for the delivery of parenteral antimicrobials. In the early years of the program, before effective antiretroviral therapy was available, cytomegalovirus retinitis was the second most commonly treated infection of the OPAT program. In recent years, the rise of multidrug-resistant organisms has led to limited oral treatment options for UTIs, which are now the second most commonly treated infection of OPAT. Osteomyelitis clearly remains the top indication for OPAT because it requires long-term therapy. Ceftriaxone remains the drug of choice due to once-daily dosing, spectrum of activity, overall safety, and cost-effectiveness.
Catheter complication rates in the OPAT program were lower than those reported in the literature. According to the 2009 NHSN report, the catheter complication rate in the inpatient long-term care units was 1.0 CRBSI/1,000 catheter days.9 Moreover, this program has been instrumental in providing care that otherwise would be administered through the use of home health agencies.
In the private sector, OPAT is frequently contracted to agencies that provide the same type of service to outpatients who have insurance. These agencies charge for the antimicrobials, IV supplies, nursing visits, and laboratory costs for patient-safety monitoring. Use of an agency could raise expenses by a factor of 8-fold or more above the cost of a hospital-based OPAT program, an estimate based on a comparison with a local federally contracted home-infusion agency that provides specialized home-infusion services at a cost.
Although costs related to hospital readmissions were not factored in to the cost savings calculations, the rate of readmission was low in the snapshot analysis that was conducted at the Edward Hines, Jr. VA Hospital. It is believed that this is the result of the close follow-up and continuity of care that the patients in this OPAT program received.
In addition to cost containment, the data reflect the safe, effective care that resulted from treatment outside the hospital setting. One of the key attributes that has made the Edward Hines, Jr. VA Hospital OPAT program unique is that it is recognized in the community as the only VA facility in the area to provide OPAT as an option for the veteran patient. Other VA facilities in the area contract with home-infusion agencies, which are responsible for supplying the antibiotics and nursing care. The Edward Hines, Jr. VA Hospital is the only VA hospital in VISN 12 that has a facility-supported program that provides all supplies and antimicrobials from the VA—a major contributing factor to the cost savings. Continuity of care is provided to the patient who transitions from inpatient to outpatient status with the same team of providers contributing to the significant patient satisfaction that the program has engendered.
Conclusions
One of the main benefits realized with this transition of antibiotic therapy to the home setting is the avoidance of newly acquired nosocomial infections, including C difficile infection, fungal, and multidrug-resistant bacterial infections. Other benefits include early IV to oral switch in therapy when the patient is deemed a candidate, the ability to go back to work sooner, and the ability to receive treatment in the comfort of the patient’s home. Plans for data collection may include a more in-depth review of repeat admissions due to unresolved infections and the number of patients who are unable to complete OPAT at home.
The Edward Hines, Jr. VA Hospital OPAT program has shown that in a large, federally-funded hospital, OPAT is safe, cost-effective, convenient and leads to increased patient satisfaction in a diverse group of veterans.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Lentino JR, Pachucki CT, Byrne R, Lau MT, Bayer D. Parenteral antibiotic therapy: A home-based program. Fed Pract. 2000;17(4):10-15.
2. Paladino JA, Poretz D. Outpatient parenteral antimicrobial therapy today. Clin Infect Dis. 2010;51(suppl 2):S198-S208.
3. Matthews PC, Conlon CP, Berendt AR, et al. Outpatient parenteral antimicrobial therapy (OPAT): Is it safe for selected patients to self-administer at home? A retrospective analysis of a large cohort over 13 years. J Antimicrob Chemother. 2007;60(2):356-362.
4. Ingram PR, Sulaiman Z, Chua A, Fisher DA. Comment on: Outpatient parenteral antibiotic therapy (OPAT): Is it safe for selected patients to self-administer at home? A retrospective analysis of a large cohort over 13 years. J Antimicrob Chemother. 2008;61(1):226-227.
5. Bernard L, El-Hajj, Pron B, et al. Outpatient parenteral antimicrobial therapy (OPAT) for the treatment of osteomyelitis: Evaluation of efficacy, tolerance and cost. J Clin Pharm Ther. 2001;26(6):445-451.
6. Yong C, Fisher DA, Sklar GE, Li SC. A cost analysis of outpatient parenteral antibiotic therapy (OPAT): An Asian perspective. Int J Antimicrob Agents. 2009;33(1):46-51.
7. Tice AD, Hoaglund PA, Nolet B, McKinnon PS, Mozaffari E. Cost perspectives for outpatient intravenous antimicrobial therapy. Pharmacotherapy. 2002;22(2 Pt 2):63S-70S.
8. Tice AD, Rehm SJ, Dalovisio JR, et al. Practice guidelines for outpatient parenteral antimicrobial therapy. Clin Infect Dis. 2004;38(12):1651-1672.
9. Edwards JR, Peterson KD, Mu Y, et al. National Healthcare Safety Network (NHSN) report: Data summary for 2006 through 2008, issued December 2009. Am J Infect Control. 2009;37(10):783-805.
Antimicrobial stewardship activities have been in place at the Edward Hines, Jr. VA Hospital in Hines, Illinois, since 1988. Initial activities, including antimicrobial restriction and the start of an outpatient-infusion program justified and led to dedicated funding for hiring the first infectious diseases (ID) clinical pharmacist. This position was initiated in 1992 and has been maintained since then. The committed multidisciplinary team, including ID physicians, ID clinical pharmacists, venous access nurses (VAN), microbiologists, infection control practitioners, and an outpatient-infusion coordinator have led stewardship activities at this VA.
One of the first efforts of the team was the development of the outpatient parenteral antibiotic therapy (OPAT) program.1 The program began in 1989 and has served more than 1,200 veterans. Outpatient parenteral antibiotic therapy is only one component of the stewardship program, which provides safe, effective, and cost-minimizing care for veterans, and is the focus of this article.
Background
Complex medical care and escalating costs have pushed all but the most seriously ill patients out of the hospital setting for care delivery. The reality is that patients who might have received care for non–life-threatening problems in a hospital bed are now relegated to an outpatient status. Beginning in the 1970s, OPAT has been used to facilitate the cost-effective, safe administration of antibiotics as an alternative to an extensive, expensive hospital stay.2 Initially developed for use in a nonhospital health care setting, the administration of antibiotics under the guidance of a health care provider (HCP) has now been extended to a self-administered infusion program.3,4 Under the latter, patients and caregivers are educated to safely administer IV antibiotics for extended periods at home.
This program uses elements of both health care–associated OPAT and self-administered OPAT (S-OPAT) to accomplish its goals: (1) safe, effective administration of antibiotic therapy to a variety of patients; (2) reduction in bed days of care (BDOC); (3) reduction of the economic burden to the hospitals’ global budgets; and (4) reduction in the incidence of common nosocomially-acquired infections, including those caused by Clostridium difficile (C difficile), methicillin-resistant Staphylococcus aureus, and vancomycin-resistant enterococcus.3
The advantages of S-OPAT have been fully realized in a variety of countries, enabling patients to receive necessary therapy in the comfort of their homes and providing them with the ability to lead normal lives without the confinement of a protracted hospital stay.5-7
Description of OPAT
The outpatient-infusion team provides specialized care for patients in accordance with the OPAT national guidelines from patient screening to program discharge.8 The dedicated staff include the OPAT nurse coordinator, VAN, pharmacists, and ID consultants. The VAN places the venous access device (VAD), educates the patient and caregiver in the care and safety of the catheter, aseptic technique, and infusion of the selected antimicrobial agent, and monitors the laboratory work. The VA may contract an outside nursing agency to provide support and reinforcement of IV administration for the patient and caregiver.
The pharmacists oversee the pharmacokinetics and pharmacodynamics of the antimicrobials as well as monitor for any toxicities that could potentially arise during and after therapy. The ID consultants identify the infection, collaborate with the pharmacists to select the most appropriate antimicrobial regimen, and determine the duration of required therapy. The team then regularly monitors the patient in the ID clinic until there is evidence of infection resolution.
Primary care providers who want to enroll patients in the OPAT program place a formal electronic consult to the ID team for antibiotic recommendation, to the outpatient infusion team for assessment of potential outpatient therapy, and to the venous access team for insertion of the VAD. The consults are completed after receiving consent from the patient, developing a patient-centered treatment plan, and determining the patient’s ability to comprehend and adhere to the program requirements. The patient or caregiver must be able to competently demonstrate aseptic technique for IV administration prior to discharge. The pharmacist educates the patient or caregiver about the stability, storage requirements, and potential adverse drug reactions of the antimicrobial.
Eligible patients must have resolved their acute medical problems and require > 1 week of therapy to treat their infection. Patients chosen for OPAT or S-OPAT must have a suitable living environment with access to a refrigerator, a telephone, and transportation to return to the hospital for follow-up. Most patients and caregivers are eager to learn and recognize the advantages of home-based care.
The VANs are a central component of the program. They maintain open communication with the patient during the entire treatment course and help triage issues to the appropriate HCP. In addition, they are responsible for submitting catheter-related bloodstream infection (CRBSI) information to the hospital administration, which then gets reported to the National Healthcare Safety Network (NHSN).
Not all patients qualify for S-OPAT. Other options include returning to the hospital daily for infusions, being discharged to a skilled care facility, or arranging for a VA-contracted agency to provide nursing care while the VA provides all required medications and supplies.
On completion of OPAT, patients are asked to evaluate the program. The anonymous survey includes open-ended questions for patients to better express their experience with the program and staff. Patients are given the opportunity to suggest improvements and provide overall feedback. The team for quality assurance and patient satisfaction reviews every survey, which is used as a tool to improve team functions.
Data are also collected in the OPAT program to measure efficacy and monitor for safety. Data obtained from the start of the program in February 1989 through fiscal year (FY) 2011 include the number of patients who were candidates for outpatient-infusion therapy, type of infection, antibiotic selection, CRBSIs, hospital readmission rates, cost savings, and patient satisfaction.
Results
The Edward Hines, Jr. VA Hospital has a proven, successful OPAT program. Most of the patients in the program during the study period were men, which reflects a typical VA population. Patients with spinal cord injury comprised a large portion of those treated. Table 1 provides the number of patients treated and lists the frequency of infections. The data are divided into 3 periods. From 1989 to September 30, 1995, OPAT used other VADs before using peripherally inserted central catheters. During the second period (October 1, 1995-September 30, 2003), patients remained with a VAD for an average of 48.6 days; whereas in Period 3 (October 1, 2003-September 30, 2011), the patients had a VAD average of 34.7 days. Consequently, with fewer VAD days, there was a decreased incidence of complications (Table 2).
Osteomyelitis accounted for the majority of the infections (40.6%), which required ≥ 6 weeks of therapy. Complicated urinary tract infection (UTI), including pyelonephritis, perinephric abscess, and complicated cystitis, was the next most common (14.9%). Bacteremia was the third most common infection (7.9%), whereas abscesses of a diverse variety affected 6.2%, including brain, liver, intra-abdominal, soft tissue, and epidural abscesses. Endocarditis and septic arthritis accounted for 4.4% and 4.7%, respectively, of infected patients.
Three periods of the OPAT program were selected at random (1996, 2003, and 2011) to examine trends in antimicrobial selection. Overall, ceftriaxone was the most commonly used antibiotic (35%). Vancomycin was the next most commonly prescribed (27%). Since its 2001 FDA approval, ertapenem has become the third most commonly prescribed antibiotic for the OPAT program (11%). As expected, antimicrobial agents that have to be dosed more frequently than twice a day were rarely used for OPAT. In addition, there was low usage of aminoglycosides due to the need for the close monitoring of levels and potential toxicity.
Outcomes
Catheter Complications
The majority of catheter complications occurring in the first period were multifactorial, relating to nursing education, product selection, program development, insertion techniques, and a less comprehensive infection control program.
Hospital Readmissions
A snapshot of FY 2011 data was used to evaluate hospital readmissions. One hundred one patients were reviewed. Of these patients, 9 (9%) were readmitted to the hospital at some point after being discharged from OPAT. Readmission due to complications of OPAT was found in 2 of the 9 patients. One was due to an adverse drug reaction from the antibiotic; the other was due to a possible relapse of a hip osteomyelitis.
Cost Analysis
The OPAT program has resulted in a total savings to the global hospital budget from the deferred BDOC of more than $65 million (Table 3) since 1989. The OPAT program eliminated > 47,000 days of inpatient care. In FY 2009 the program cost the hospital $691.35 for each of the 106 patients enrolled (total cost: $73,283.10). This included all IV supplies, antimicrobials, visiting nurse costs when applicable, as well as nursing and pharmacy time dedicated to training the patient and making therapeutic decisions. Expenses for 3,109 BDOC would have cost about $6,218,000. The outpatient-infusion program saved the hospital nearly $6 million in 2009 alone.
Patient Satisfaction
About 60% of the patients discharged from the OPAT program responded to an evaluation survey. The feedback was overwhelmingly positive with about 99% of respondents reporting satisfaction relating to an improved quality of life. Most of the positive comments were directed toward the outpatient-infusion coordinator for resolving issues, being easily accessible, and acting as a patient advocate.
Discussion
The number and types of reasons for OPAT have grown with the knowledge that it is a safe, cost-effective method for the delivery of parenteral antimicrobials. In the early years of the program, before effective antiretroviral therapy was available, cytomegalovirus retinitis was the second most commonly treated infection of the OPAT program. In recent years, the rise of multidrug-resistant organisms has led to limited oral treatment options for UTIs, which are now the second most commonly treated infection of OPAT. Osteomyelitis clearly remains the top indication for OPAT because it requires long-term therapy. Ceftriaxone remains the drug of choice due to once-daily dosing, spectrum of activity, overall safety, and cost-effectiveness.
Catheter complication rates in the OPAT program were lower than those reported in the literature. According to the 2009 NHSN report, the catheter complication rate in the inpatient long-term care units was 1.0 CRBSI/1,000 catheter days.9 Moreover, this program has been instrumental in providing care that otherwise would be administered through the use of home health agencies.
In the private sector, OPAT is frequently contracted to agencies that provide the same type of service to outpatients who have insurance. These agencies charge for the antimicrobials, IV supplies, nursing visits, and laboratory costs for patient-safety monitoring. Use of an agency could raise expenses by a factor of 8-fold or more above the cost of a hospital-based OPAT program, an estimate based on a comparison with a local federally contracted home-infusion agency that provides specialized home-infusion services at a cost.
Although costs related to hospital readmissions were not factored in to the cost savings calculations, the rate of readmission was low in the snapshot analysis that was conducted at the Edward Hines, Jr. VA Hospital. It is believed that this is the result of the close follow-up and continuity of care that the patients in this OPAT program received.
In addition to cost containment, the data reflect the safe, effective care that resulted from treatment outside the hospital setting. One of the key attributes that has made the Edward Hines, Jr. VA Hospital OPAT program unique is that it is recognized in the community as the only VA facility in the area to provide OPAT as an option for the veteran patient. Other VA facilities in the area contract with home-infusion agencies, which are responsible for supplying the antibiotics and nursing care. The Edward Hines, Jr. VA Hospital is the only VA hospital in VISN 12 that has a facility-supported program that provides all supplies and antimicrobials from the VA—a major contributing factor to the cost savings. Continuity of care is provided to the patient who transitions from inpatient to outpatient status with the same team of providers contributing to the significant patient satisfaction that the program has engendered.
Conclusions
One of the main benefits realized with this transition of antibiotic therapy to the home setting is the avoidance of newly acquired nosocomial infections, including C difficile infection, fungal, and multidrug-resistant bacterial infections. Other benefits include early IV to oral switch in therapy when the patient is deemed a candidate, the ability to go back to work sooner, and the ability to receive treatment in the comfort of the patient’s home. Plans for data collection may include a more in-depth review of repeat admissions due to unresolved infections and the number of patients who are unable to complete OPAT at home.
The Edward Hines, Jr. VA Hospital OPAT program has shown that in a large, federally-funded hospital, OPAT is safe, cost-effective, convenient and leads to increased patient satisfaction in a diverse group of veterans.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Antimicrobial stewardship activities have been in place at the Edward Hines, Jr. VA Hospital in Hines, Illinois, since 1988. Initial activities, including antimicrobial restriction and the start of an outpatient-infusion program justified and led to dedicated funding for hiring the first infectious diseases (ID) clinical pharmacist. This position was initiated in 1992 and has been maintained since then. The committed multidisciplinary team, including ID physicians, ID clinical pharmacists, venous access nurses (VAN), microbiologists, infection control practitioners, and an outpatient-infusion coordinator have led stewardship activities at this VA.
One of the first efforts of the team was the development of the outpatient parenteral antibiotic therapy (OPAT) program.1 The program began in 1989 and has served more than 1,200 veterans. Outpatient parenteral antibiotic therapy is only one component of the stewardship program, which provides safe, effective, and cost-minimizing care for veterans, and is the focus of this article.
Background
Complex medical care and escalating costs have pushed all but the most seriously ill patients out of the hospital setting for care delivery. The reality is that patients who might have received care for non–life-threatening problems in a hospital bed are now relegated to an outpatient status. Beginning in the 1970s, OPAT has been used to facilitate the cost-effective, safe administration of antibiotics as an alternative to an extensive, expensive hospital stay.2 Initially developed for use in a nonhospital health care setting, the administration of antibiotics under the guidance of a health care provider (HCP) has now been extended to a self-administered infusion program.3,4 Under the latter, patients and caregivers are educated to safely administer IV antibiotics for extended periods at home.
This program uses elements of both health care–associated OPAT and self-administered OPAT (S-OPAT) to accomplish its goals: (1) safe, effective administration of antibiotic therapy to a variety of patients; (2) reduction in bed days of care (BDOC); (3) reduction of the economic burden to the hospitals’ global budgets; and (4) reduction in the incidence of common nosocomially-acquired infections, including those caused by Clostridium difficile (C difficile), methicillin-resistant Staphylococcus aureus, and vancomycin-resistant enterococcus.3
The advantages of S-OPAT have been fully realized in a variety of countries, enabling patients to receive necessary therapy in the comfort of their homes and providing them with the ability to lead normal lives without the confinement of a protracted hospital stay.5-7
Description of OPAT
The outpatient-infusion team provides specialized care for patients in accordance with the OPAT national guidelines from patient screening to program discharge.8 The dedicated staff include the OPAT nurse coordinator, VAN, pharmacists, and ID consultants. The VAN places the venous access device (VAD), educates the patient and caregiver in the care and safety of the catheter, aseptic technique, and infusion of the selected antimicrobial agent, and monitors the laboratory work. The VA may contract an outside nursing agency to provide support and reinforcement of IV administration for the patient and caregiver.
The pharmacists oversee the pharmacokinetics and pharmacodynamics of the antimicrobials as well as monitor for any toxicities that could potentially arise during and after therapy. The ID consultants identify the infection, collaborate with the pharmacists to select the most appropriate antimicrobial regimen, and determine the duration of required therapy. The team then regularly monitors the patient in the ID clinic until there is evidence of infection resolution.
Primary care providers who want to enroll patients in the OPAT program place a formal electronic consult to the ID team for antibiotic recommendation, to the outpatient infusion team for assessment of potential outpatient therapy, and to the venous access team for insertion of the VAD. The consults are completed after receiving consent from the patient, developing a patient-centered treatment plan, and determining the patient’s ability to comprehend and adhere to the program requirements. The patient or caregiver must be able to competently demonstrate aseptic technique for IV administration prior to discharge. The pharmacist educates the patient or caregiver about the stability, storage requirements, and potential adverse drug reactions of the antimicrobial.
Eligible patients must have resolved their acute medical problems and require > 1 week of therapy to treat their infection. Patients chosen for OPAT or S-OPAT must have a suitable living environment with access to a refrigerator, a telephone, and transportation to return to the hospital for follow-up. Most patients and caregivers are eager to learn and recognize the advantages of home-based care.
The VANs are a central component of the program. They maintain open communication with the patient during the entire treatment course and help triage issues to the appropriate HCP. In addition, they are responsible for submitting catheter-related bloodstream infection (CRBSI) information to the hospital administration, which then gets reported to the National Healthcare Safety Network (NHSN).
Not all patients qualify for S-OPAT. Other options include returning to the hospital daily for infusions, being discharged to a skilled care facility, or arranging for a VA-contracted agency to provide nursing care while the VA provides all required medications and supplies.
On completion of OPAT, patients are asked to evaluate the program. The anonymous survey includes open-ended questions for patients to better express their experience with the program and staff. Patients are given the opportunity to suggest improvements and provide overall feedback. The team for quality assurance and patient satisfaction reviews every survey, which is used as a tool to improve team functions.
Data are also collected in the OPAT program to measure efficacy and monitor for safety. Data obtained from the start of the program in February 1989 through fiscal year (FY) 2011 include the number of patients who were candidates for outpatient-infusion therapy, type of infection, antibiotic selection, CRBSIs, hospital readmission rates, cost savings, and patient satisfaction.
Results
The Edward Hines, Jr. VA Hospital has a proven, successful OPAT program. Most of the patients in the program during the study period were men, which reflects a typical VA population. Patients with spinal cord injury comprised a large portion of those treated. Table 1 provides the number of patients treated and lists the frequency of infections. The data are divided into 3 periods. From 1989 to September 30, 1995, OPAT used other VADs before using peripherally inserted central catheters. During the second period (October 1, 1995-September 30, 2003), patients remained with a VAD for an average of 48.6 days; whereas in Period 3 (October 1, 2003-September 30, 2011), the patients had a VAD average of 34.7 days. Consequently, with fewer VAD days, there was a decreased incidence of complications (Table 2).
Osteomyelitis accounted for the majority of the infections (40.6%), which required ≥ 6 weeks of therapy. Complicated urinary tract infection (UTI), including pyelonephritis, perinephric abscess, and complicated cystitis, was the next most common (14.9%). Bacteremia was the third most common infection (7.9%), whereas abscesses of a diverse variety affected 6.2%, including brain, liver, intra-abdominal, soft tissue, and epidural abscesses. Endocarditis and septic arthritis accounted for 4.4% and 4.7%, respectively, of infected patients.
Three periods of the OPAT program were selected at random (1996, 2003, and 2011) to examine trends in antimicrobial selection. Overall, ceftriaxone was the most commonly used antibiotic (35%). Vancomycin was the next most commonly prescribed (27%). Since its 2001 FDA approval, ertapenem has become the third most commonly prescribed antibiotic for the OPAT program (11%). As expected, antimicrobial agents that have to be dosed more frequently than twice a day were rarely used for OPAT. In addition, there was low usage of aminoglycosides due to the need for the close monitoring of levels and potential toxicity.
Outcomes
Catheter Complications
The majority of catheter complications occurring in the first period were multifactorial, relating to nursing education, product selection, program development, insertion techniques, and a less comprehensive infection control program.
Hospital Readmissions
A snapshot of FY 2011 data was used to evaluate hospital readmissions. One hundred one patients were reviewed. Of these patients, 9 (9%) were readmitted to the hospital at some point after being discharged from OPAT. Readmission due to complications of OPAT was found in 2 of the 9 patients. One was due to an adverse drug reaction from the antibiotic; the other was due to a possible relapse of a hip osteomyelitis.
Cost Analysis
The OPAT program has resulted in a total savings to the global hospital budget from the deferred BDOC of more than $65 million (Table 3) since 1989. The OPAT program eliminated > 47,000 days of inpatient care. In FY 2009 the program cost the hospital $691.35 for each of the 106 patients enrolled (total cost: $73,283.10). This included all IV supplies, antimicrobials, visiting nurse costs when applicable, as well as nursing and pharmacy time dedicated to training the patient and making therapeutic decisions. Expenses for 3,109 BDOC would have cost about $6,218,000. The outpatient-infusion program saved the hospital nearly $6 million in 2009 alone.
Patient Satisfaction
About 60% of the patients discharged from the OPAT program responded to an evaluation survey. The feedback was overwhelmingly positive with about 99% of respondents reporting satisfaction relating to an improved quality of life. Most of the positive comments were directed toward the outpatient-infusion coordinator for resolving issues, being easily accessible, and acting as a patient advocate.
Discussion
The number and types of reasons for OPAT have grown with the knowledge that it is a safe, cost-effective method for the delivery of parenteral antimicrobials. In the early years of the program, before effective antiretroviral therapy was available, cytomegalovirus retinitis was the second most commonly treated infection of the OPAT program. In recent years, the rise of multidrug-resistant organisms has led to limited oral treatment options for UTIs, which are now the second most commonly treated infection of OPAT. Osteomyelitis clearly remains the top indication for OPAT because it requires long-term therapy. Ceftriaxone remains the drug of choice due to once-daily dosing, spectrum of activity, overall safety, and cost-effectiveness.
Catheter complication rates in the OPAT program were lower than those reported in the literature. According to the 2009 NHSN report, the catheter complication rate in the inpatient long-term care units was 1.0 CRBSI/1,000 catheter days.9 Moreover, this program has been instrumental in providing care that otherwise would be administered through the use of home health agencies.
In the private sector, OPAT is frequently contracted to agencies that provide the same type of service to outpatients who have insurance. These agencies charge for the antimicrobials, IV supplies, nursing visits, and laboratory costs for patient-safety monitoring. Use of an agency could raise expenses by a factor of 8-fold or more above the cost of a hospital-based OPAT program, an estimate based on a comparison with a local federally contracted home-infusion agency that provides specialized home-infusion services at a cost.
Although costs related to hospital readmissions were not factored in to the cost savings calculations, the rate of readmission was low in the snapshot analysis that was conducted at the Edward Hines, Jr. VA Hospital. It is believed that this is the result of the close follow-up and continuity of care that the patients in this OPAT program received.
In addition to cost containment, the data reflect the safe, effective care that resulted from treatment outside the hospital setting. One of the key attributes that has made the Edward Hines, Jr. VA Hospital OPAT program unique is that it is recognized in the community as the only VA facility in the area to provide OPAT as an option for the veteran patient. Other VA facilities in the area contract with home-infusion agencies, which are responsible for supplying the antibiotics and nursing care. The Edward Hines, Jr. VA Hospital is the only VA hospital in VISN 12 that has a facility-supported program that provides all supplies and antimicrobials from the VA—a major contributing factor to the cost savings. Continuity of care is provided to the patient who transitions from inpatient to outpatient status with the same team of providers contributing to the significant patient satisfaction that the program has engendered.
Conclusions
One of the main benefits realized with this transition of antibiotic therapy to the home setting is the avoidance of newly acquired nosocomial infections, including C difficile infection, fungal, and multidrug-resistant bacterial infections. Other benefits include early IV to oral switch in therapy when the patient is deemed a candidate, the ability to go back to work sooner, and the ability to receive treatment in the comfort of the patient’s home. Plans for data collection may include a more in-depth review of repeat admissions due to unresolved infections and the number of patients who are unable to complete OPAT at home.
The Edward Hines, Jr. VA Hospital OPAT program has shown that in a large, federally-funded hospital, OPAT is safe, cost-effective, convenient and leads to increased patient satisfaction in a diverse group of veterans.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Lentino JR, Pachucki CT, Byrne R, Lau MT, Bayer D. Parenteral antibiotic therapy: A home-based program. Fed Pract. 2000;17(4):10-15.
2. Paladino JA, Poretz D. Outpatient parenteral antimicrobial therapy today. Clin Infect Dis. 2010;51(suppl 2):S198-S208.
3. Matthews PC, Conlon CP, Berendt AR, et al. Outpatient parenteral antimicrobial therapy (OPAT): Is it safe for selected patients to self-administer at home? A retrospective analysis of a large cohort over 13 years. J Antimicrob Chemother. 2007;60(2):356-362.
4. Ingram PR, Sulaiman Z, Chua A, Fisher DA. Comment on: Outpatient parenteral antibiotic therapy (OPAT): Is it safe for selected patients to self-administer at home? A retrospective analysis of a large cohort over 13 years. J Antimicrob Chemother. 2008;61(1):226-227.
5. Bernard L, El-Hajj, Pron B, et al. Outpatient parenteral antimicrobial therapy (OPAT) for the treatment of osteomyelitis: Evaluation of efficacy, tolerance and cost. J Clin Pharm Ther. 2001;26(6):445-451.
6. Yong C, Fisher DA, Sklar GE, Li SC. A cost analysis of outpatient parenteral antibiotic therapy (OPAT): An Asian perspective. Int J Antimicrob Agents. 2009;33(1):46-51.
7. Tice AD, Hoaglund PA, Nolet B, McKinnon PS, Mozaffari E. Cost perspectives for outpatient intravenous antimicrobial therapy. Pharmacotherapy. 2002;22(2 Pt 2):63S-70S.
8. Tice AD, Rehm SJ, Dalovisio JR, et al. Practice guidelines for outpatient parenteral antimicrobial therapy. Clin Infect Dis. 2004;38(12):1651-1672.
9. Edwards JR, Peterson KD, Mu Y, et al. National Healthcare Safety Network (NHSN) report: Data summary for 2006 through 2008, issued December 2009. Am J Infect Control. 2009;37(10):783-805.
1. Lentino JR, Pachucki CT, Byrne R, Lau MT, Bayer D. Parenteral antibiotic therapy: A home-based program. Fed Pract. 2000;17(4):10-15.
2. Paladino JA, Poretz D. Outpatient parenteral antimicrobial therapy today. Clin Infect Dis. 2010;51(suppl 2):S198-S208.
3. Matthews PC, Conlon CP, Berendt AR, et al. Outpatient parenteral antimicrobial therapy (OPAT): Is it safe for selected patients to self-administer at home? A retrospective analysis of a large cohort over 13 years. J Antimicrob Chemother. 2007;60(2):356-362.
4. Ingram PR, Sulaiman Z, Chua A, Fisher DA. Comment on: Outpatient parenteral antibiotic therapy (OPAT): Is it safe for selected patients to self-administer at home? A retrospective analysis of a large cohort over 13 years. J Antimicrob Chemother. 2008;61(1):226-227.
5. Bernard L, El-Hajj, Pron B, et al. Outpatient parenteral antimicrobial therapy (OPAT) for the treatment of osteomyelitis: Evaluation of efficacy, tolerance and cost. J Clin Pharm Ther. 2001;26(6):445-451.
6. Yong C, Fisher DA, Sklar GE, Li SC. A cost analysis of outpatient parenteral antibiotic therapy (OPAT): An Asian perspective. Int J Antimicrob Agents. 2009;33(1):46-51.
7. Tice AD, Hoaglund PA, Nolet B, McKinnon PS, Mozaffari E. Cost perspectives for outpatient intravenous antimicrobial therapy. Pharmacotherapy. 2002;22(2 Pt 2):63S-70S.
8. Tice AD, Rehm SJ, Dalovisio JR, et al. Practice guidelines for outpatient parenteral antimicrobial therapy. Clin Infect Dis. 2004;38(12):1651-1672.
9. Edwards JR, Peterson KD, Mu Y, et al. National Healthcare Safety Network (NHSN) report: Data summary for 2006 through 2008, issued December 2009. Am J Infect Control. 2009;37(10):783-805.
Psychogenic Nonepileptic Seizures
From the Department of Neurology, University of Maryland School of Medicine, Baltimore, MD.
Abstracts
- Objective: To provide a review of psychogenic nonepileptic seizures, including a discussion of the diagnosis, treatment, and clinical significance of the disorder.
- Methods: Review of the relevant literature.
- Results: Psychogenic nonepileptic seizures are a common and potentially disabling neurologic disorder. They are most prevalent in young adults, and more commonly seen in women versus men. Certain psychosocial variables may impact the development of the condition. The diagnosis is made through a detailed history and observation of clinical events in conjunction with video EEG monitoring. Neuropsychological testing is an important component in the evaluation. Treatment includes establishment of an accurate diagnosis, management of any underlying psychiatric diagnoses, and regular follow-up with a neurologist or trained care provider.
- Conclusion: Psychogenic nonepileptic seizures represent a complex interaction between neurologic and psychological factors. Obtaining an accurate diagnosis through the use of video EEG monitoring and clinical observation is an important initial step in treatment and improved quality of life in this patient population.
Psychogenic nonepileptic seizures (PNES) are commonly encountered in outpatient specialty epilepsy clinics as well as inpatient epilepsy monitoring units. They comprise approximately 20% of all refractory seizure disorders referred to specialty epilepsy centers [1–4]. PNES are thought to be psychological in origin as opposed to arising from abnormal electrical discharges as in epileptic seizures. PNES may be more frequent and disabling than epileptic seizures, and patients with PNES may report worse outcomes [5,6]. Increased utilization of long-term video EEG monitoring along with greater recognition of psychogenic neurologic disorders has allowed for improved diagnosis of PNES. However, many diagnostic and therapeutic challenges remain. There are often delays in obtaining an accurate diagnosis, and optimal management remains challenging, often leading to inappropriate, ineffective, and costly treatment, sometimes for many years [6–8].
Epidemiology
PNES are seen across the spectrum of age-groups, from children [9,10] to elderly persons, but they most often occur in young adults between the ages of 15 to 35 years [1,8]. Caution should be used when considering this diagnosis in infants or young children, in whom it is more common to see physiologic events that may mimic epileptic seizures, including gastroesophageal reflux, shuddering, night terrors, or breath holding spells [1,9,10].
PNES are prevalent within epilepsy practices. Patients with PNES comprise approximately 5% to 20% patients thought to have intractable epilepsy seen in outpatient centers, and within epilepsy monitoring units they account for 10% to 40% of patients [1,2,6,8]. A population-based study approximates the incidence of PNES at 1.4 per 100,000 people and 3.4 per 100,000 people between the ages of 15 to 24 years [4].
There is a female preponderance in PNES, which is similar to other conversion and somatoform disorders. Overall, women comprise approximately 70% to 80% of patients with the PNES diagnosis [1,2,6]. There are psychosocial variables that are seen in some patients with this disorder. An important factor that has been described is past history of sexual or physical abuse. In one series, there was a history of sexual abuse in almost 25% of patients with PNES, and history of either sexual abuse, physical abuse, or both in 32% of patients [11]. A history of sexual and/or physical abuse is not exclusive to these patients, and can certainly be seen in patients with epilepsy as well. For example, in a control population of epilepsy patients, there was a reported rate of past sexual or physical abuse approaching 9% [12].
A prior history of head trauma, often of a relatively mild degree, has been described as a potential inciting factor for some cases of PNES [6,13]. In the literature, studies report that as many as 20% of PNES patients attributed their seizures to head trauma, often rather mild head trauma [6,14].
Historcial Context
Historically, what today are called PNES originate with the concept of hysteria, a medical diagnosis in women that can be traced to antiquity [15,16]. By the late 1800s, one of the founders of neurology, Jean Charcot, established hysterical seizures as an important clinical entity with his detailed, elegant descriptions of patients. Charcot formulated clinical methods for distinguishing hysteria and particularly hysterical seizures from epilepsy. He presumed that hysteria and epilepsy were closely related, and he termed seizures due to hysteria as “hysteroepilepsy” or “epileptiform” hysteria. Charcot proposed that hysterical seizures were organic disorders of the brain, like other forms of seizures and epilepsy, and emphasized their relation to disturbance of the female reproductive system [17,18]. Charcot utilized techniques such as manipulation of “hysterogenic zones” and ovarian compression as well as suggestion to both treat and provoke hysteria and hysterical seizures, which he described and documented [17,18]. One of Charcot’s most celebrated students, Sigmund Freud, observed Charcot’s demonstrations but drew different conclusions. He theorized that hysteria and hysterical seizures were not organic disorders of the brain as Charcot proposed, but were rather emotional disorders of the unconscious mind due to repressed energies or drives. Based largely the theories of Freud and Charcot, individuals with hysteria were distinguished from those with epilepsy, with hysterical seizures related to psychological dysfunction while epileptic seizures were associated with physical or organic brain disorders [15,16].
With the introduction of EEG recording in the 1930s, it became possible to characterize epilepsy as an electrical disorder of the brain with associated EEG changes and more effectively distinguish it from hysterical seizures, which did not have such abnormalities. In addition, in the first half of the 20th century, the nature of hysteria as seen and diagnosed by physicians seemed to change. The dramatic, theatrical convulsions described by Charcot and his contemporaries appeared less commonly, while disorders such as chronic pain seemed to increase [1,19].
However, by the 1960s, several reports confirmed that hysterical seizures were actually still prevalent. Newer terms like “pseudoseizures” were used to describe these disorders because the term “hysteria” was thought to be somewhat derogatory, anti-feminist, and antiquated [20,21]. In the 1970s and thereafter, with the increasing availability of video EEG monitoring and growth of inpatient epilepsy monitoring units, it was discovered that these hysterical, pseudo-, or what were also by then termed psychogenic seizures, were actually still common [1,22].
More recently, it has been recognized that the pendulum in some cases may have swung too far in regard to the diagnosis of this disorder. Some rare patients with seizures initially diagnosed as PNES may actually have forms of epileptic seizures such as frontal lobe epilepsy or related physiological disorders rather than psychogenic causes for their episodes [1,23]. These types of epileptic seizures can be very difficult to diagnose properly unless one appreciates how they present and manifest and remains vigilant for them during evaluation [1,23].
Terminology
There is an ongoing debate regarding the appropriate terminology for psychogenic events, and there is no uniform standardized definition or classification at this time. The term that is currently preferred within the epilepsy community for seizures of psychological origin that are thought to be associated with conversion, somatization, or dissociative disorders is “psychogenic nonepileptic seizures” (PNES). This terminology is felt to be non-disparaging and more neutral as compared with other terms such as pseudoseizures, which were previously favored. Nonepileptic seizures or nonepileptic events are broader terms meant to incorporate both physiologic and psychological causes for disorders that are mistaken for epilepsy. PNES are widely defined as paroxysmal events that appear similar to epileptic seizures but are not due to abnormal electrical discharges in the brain and as noted, are typically thought to be related or caused by conversion, somatization, or dissociative disorders.
Physiologic nonepileptic events are another category of physical disorders that may be mistaken for epilepsy. The underlying causes differ between age-groups, and can include conditions such as cardiac arrhythmias, migraine variants, syncope, or metabolic abnormalities. Physiologic nonepileptic seizures account for only a small proportion of all patients with nonepileptic seizures or events [1]. In general, any patient with a psychological disorder that causes symptoms that are mistaken for epilepsy can be said to have PNES.
Clinical Characteristics And Presentation
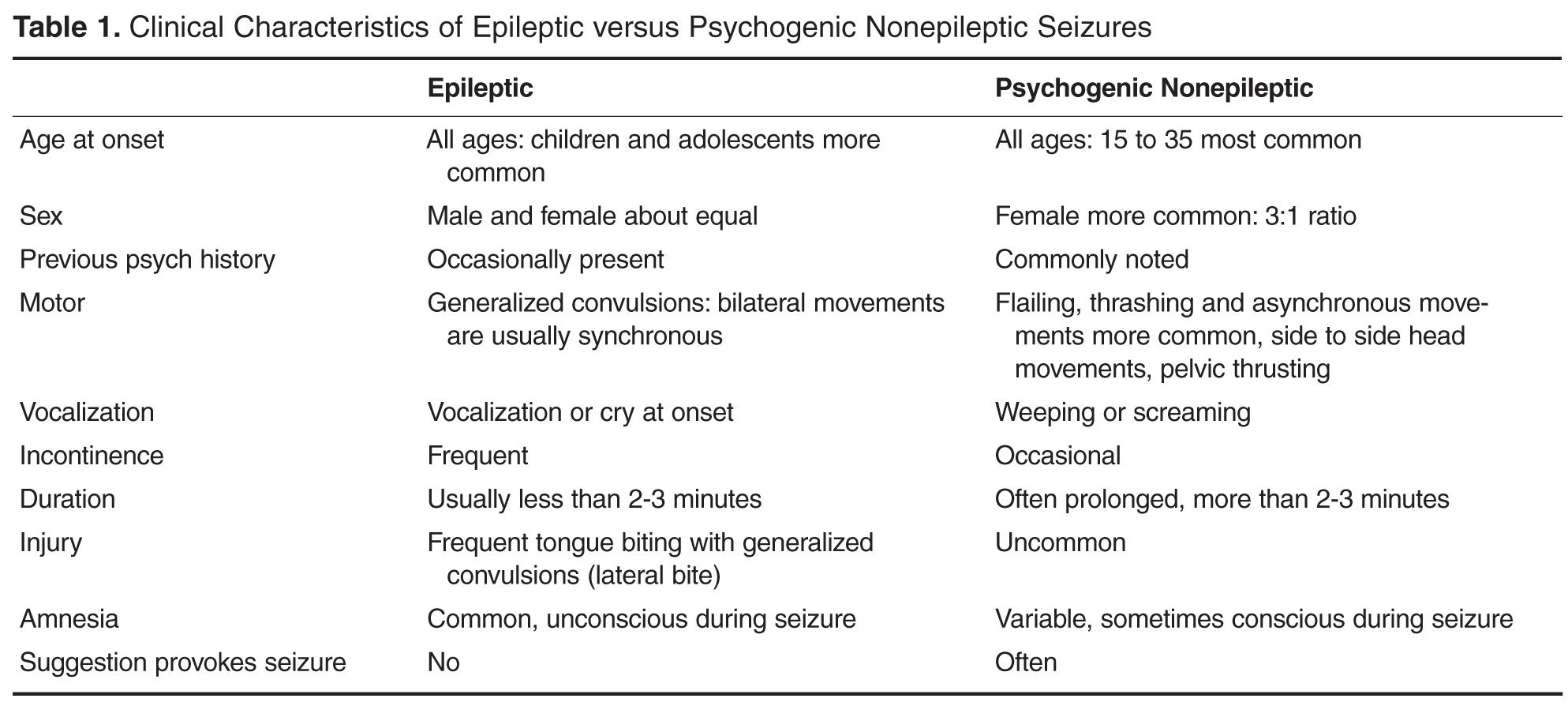
The duration of PNES is often significantly longer than that seen in epileptic seizures, which usually last less than 3 minutes, excluding the postictal period. PNES may also exhibit waxing and waning convulsive activity, although this finding can certainly be seen in epileptic seizures as well. PNES may be shown to have distractibility with external stimuli. Additionally, the movements in PNES may appear asymmetric, asynchronous, or purposeful, although this is not diagnostic for this disorder. This may contrast with the well-defined, synchronous tonic-clonic activity typically seen in epileptic seizures [1,24,25]. Back arching and pelvic thrusting movements can also be seen in PNES. Despite these differences, it may still be challenging to distinguish the semi-purposeful behaviors of PNES from the automatisms of certain focal epileptic seizures. The often bizarre-appearing, hypermotor activity that can be seen in frontal lobe seizures is often especially difficult to differentiate from PNES [1,23].
Another important consideration is that consciousness is preserved in PNES, while consciousness and responsiveness are frequently impaired in epileptic seizures. Patients with PNES are often apparently unresponsive during events, although there is no true impairment of awareness. Other characteristics that are more commonly seen in PNES are crying and eye closure [26]. Self-injury and incontinence may be reported, but they are less often clearly witnessed or documented [27,28]. Additionally, although patients may at times appear to be asleep at seizure onset, EEG recordings document the patient to actually be asleep in less than 1% of cases [29]. While epileptic seizures often respond well to antiepileptic medications, PNES characteristically do not [1,3,6,8].
In certain situations, provocation maneuvers may be utilized in order to reproduce PNES in patients undergoing EEG monitoring. In comparison to epileptic seizures, suggestion and emotional stimuli are more likely to trigger psychogenic events [1]. Methods utilized to provoke PNES may include saline injections, placement of a tuning fork on the head or body, or even hypnosis, when a suggestion is concurrently provided that such maneuvers can trigger the patient’s seizures [1,30,31]. When evaluating seizures that are provoked in such a manner, it is important to consider whether or not the event captured is in fact a typical event for the patient, or whether the provocation has uncovered a different, atypical event. Given that PNES and epileptic seizures can co-exist within the same patient, care should be taken to avoid making a diagnosis based on capturing an atypical event, or capturing only a subset of a patient’s seizure types. This could result in failure to make an accurate and thorough diagnosis [23]. There is debate regarding the ethics of provoking seizures by way of suggestion. Some members of the epilepsy community feel that provoking seizures through suggestion is inherently deceitful, and therefore can damage the physician-patient relationship. Others assert that such provocative testing can be undertaken in an honest manner, and can ultimately help achieve an accurate diagnosis for the patient [32].
As previously mentioned, there is a proportion of patients who have co-existing epileptic seizures and PNES, and obtaining an accurate diagnosis can be especially challenging in this group. Studies have reported that around 10% to 40% of patients with PNES also have epilepsy [1,22,23,33]. Care must be taken to distinguish between differences in seizure types and if necessary, video EEG monitoring may be needed to capture both seizure types for an accurate diagnosis. This testing can then be useful in education with families and caregivers who may be shown the videos with consent from the patient in order to guide future care.
Evaluation And Diagnosis
As in much of neurology, a thorough history, along with detailed clinical observation remains essential in the diagnosis of patients with PNES and for distinguishing these events from epilepsy. Video EEG monitoring of seizures is a key adjunct to the history and clinical observation in diagnosing this condition [1,2]. Long-term video EEG monitoring is considered the “gold standard” in the characterization and differential diagnosis of seizures. Additional potentially helpful diagnostic techniques include video EEG-monitored seizure provocation, serum prolactin levels, single photon emission computed tomography, and neuropsychological testing.
Video EEG Monitoring
![]()
EEG monitoring for characterization of clinical events can be conducted on an ambulatory or outpatient basis or in dedicated inpatient epilepsy monitoring units. Ambulatory monitoring can be useful in the case of patients who report seizures that are more frequent in their home environment or in patients with frequent events. If events are infrequent, then inpatient monitoring may be more efficacious [1]. With longer-term inpatient monitoring, antiepileptic medications can be withdrawn in a supervised setting, in order to lower the seizure threshold as well as to safely discontinue medications that may not be necessary. Such medication titrations are typically not safe in an unsupervised outpatient setting. Some ambulatory EEG monitoring systems do allow for simultaneous video and EEG recording. However, an advantage to inpatient monitoring, which is not afforded in the outpatient setting, is the ability for nursing staff or physicians to perform clinical testing during events to assess for patient responsiveness and other features. Additionally, with inpatient monitoring, EEG technicians can routinely assess for any technical problems with the electrodes or recording system.
Another benefit of video EEG monitoring is that the state (waking, drowsy, or asleep) of the patient at the onset of an event can be established. While epileptic seizures can arise from any state, PNES most often occur from wakefulness. Patients with PNES may appear to be asleep at the onset of events, and they may report seizures from sleep. Video EEG monitoring can help to establish the waking or sleep state of the patient that may aid in diagnosis [29].
Prolactin Levels
Serum prolactin levels may be helpful in the diagnosis of PNES [35,36]. Following generalized tonic-clonic or complex partial epileptic seizures, the serum prolactin can rise from two to threefold to five to tenfold [37]. The maximal rise in serum prolactin occurs in the initial 20 to 60 minutes after the seizure [35–37]. A similar rise in serum prolactin would not be expected in PNES. Although prolactin levels may have some utility in diagnosis, they are not currently routinely ordered as part of a standard admission to most inpatient epilepsy monitoring units. This may be due in part to the fact that false-positive and false-negative results can occur with these levels [37–39]. For example, there may not be a rise in the prolactin level after a simple partial seizure or more subtle complex partial seizure.
Neuropsychological Testing
Neuropsychological testing is also a key component in the evaluation and diagnosis of PNES. Ideally, a mental health provider with a background in psychological assessment and neuropsychological intervention for patients with psychogenic disorders would perform the evaluation [40,41].
The goal of the evaluation should not solely focused on whether the patient suffers from nonepileptic or epileptic seizures. An epileptologist upon review of clinical, electrographic, and neuropsychological data better makes this determination. Moreover, neuropsychological testing cannot in itself either diagnose or exclude the possibility that a seizure disorder is nonepileptic because of the considerable overlap between epileptic and nonepileptic test results [40,41]. Neuropsychological evaluations aid this assessment by (1) determining the potential or likelihood of significant contributing psychopathology or cognitive difficulties, (2) defining the nature of the associated psychological or psychosocial issues, and (3) assessing how a patient might benefit from various psychologically based interventions [1]. The testing may identify psychological problems that can guide treatment after diagnosis.
Delays in Diagnosis
Correct and prompt diagnosis is essential for patients with PNES as is appropriate referral to a knowledgeable trained mental health professional. On average, patients with PNES are diagnosed 7.2 years after manifestation (SD 9.3 years), with mean delay of 5 to 7 years. Younger age, interictal epileptiform potentials in the EEG, and anticonvulsant treatment are associated with longer delays [42,43]. Delays are also thought to occur because of problems with “ownership” of these patients. Although typically neurologists are involved in the diagnosis of PNES, often using video EEG monitoring done in an inpatient setting, the next step is often a referral to a psychiatrist or mental health care provider. There are sometimes delays in the initial referral to the neurologist, delays in referral to specialists for video EEG testing, and also to the physicians, psychologists or social workers who may provide treatment. Another disconnect can occur if patients are “lost to follow-up” if they receive a referral for mental health care and either do not follow up on this on their own, or if the reason for this care is not fully explained. In addition, many mental health professionals are not trained in the evaluation and treatment of psychogenic symptoms and may even feel uncomfortable in dealing with these patients [13,44].
Many studies have been suggestive that delays in diagnosis may result in poorer outcomes [45,46], while other studies have suggested that patients who have an acute diagnosis of PNES upon presentation may do particularly well [8,47–49]. Some of the most recent large outcome studies suggest that there may be no worsening of outcome associated with delays in diagnosis and that outcome was predicted by other factors [50–52].
Management
Management of patients with PNES is similar to that for patients with other types of so-called abnormal illness behavior, although there remains a relative paucity of evidence for specific treatment strategies for PNES [1]. The first consideration should be the manner in which the diagnosis of PNES is presented to the patient and family. It is important to be honest with the patient and demonstrate a positive approach to the diagnosis [53]. The physician should emphasize as favorable or good news the fact that the patient does not have epilepsy, and should also stress that the disorder, although serious and "real," does not require treatment with antiepileptic medications and that once stress or emotional issues are resolved, the patient has the potential to gain better control of these events [1,54,55]. Nevertheless, not all patients readily accept the diagnosis or this type of approach. Some patients may seek other opinions, and this should not be discouraged. An adversarial relationship with the patient should be avoided. The patient should be encouraged to return if desired, and records should be made available to other health care providers to avoid duplication of services.
After the diagnosis of PNES is presented, supportive measures should be initiated. PNES patients may benefit from education and support that can be provided by the neurologist or primary care physician [1]. If the neuropsychological assessment suggests a clinical profile that requires a professional mental health intervention, then an appropriate referral should be made. Regular follow-up visits for the patient with the neurologist are useful even if a mental health professional is involved [49,56]. This allows the patient to get medical attention without demonstrating illness behavior. Patient education and support are stressed at these visits. Because family issues are often important contributing factors, physicians should consider involving family members in visits with consent of the patient [1].
A variety of treatment strategies are employed for the management of PNES including cognitive behavioral therapy (CBT), group and family therapy, antidepressant medication, and other forms of rehabilitation [5,57,58]. A 2007 Cochrane review that identified 608 references for non-medication PNES treatments found that only 3 studies met criteria for a randomized controlled trial. One of the more recently favored treatment options for PNES that has been applied to the treatment of various somatoform disorders and other psychiatric disorders in the past is CBT [57,59,60]. This form of psychotherapy can be administered by trained personnel in a time-limited fashion using defined protocols. The basis of this treatment is that the patient learns to increase awareness of their dysfunctional thoughts and learns new ways to respond to them [57,58]. To date, several groups have reported results of nonrandomized trials as well as case reports and case series which have established the utility of this treatment. There have been reports of significant reductions in seizure frequency and this treatment strategy appears very promising [61–65]. Preliminary randomized controlled trials have also been piloted and are also suggestive that this may be a validated treatment approach [66].
Prognosis
The outcomes of patients with PNES vary. Long-term follow-up studies show that about half of all patients with PNES function reasonably well following their diagnosis. However, only approximately one-third of patients will completely stop having seizures or related problems, and approximately 50% percent have poor functional outcomes [1,2,50]. When the diagnosis of PNES is based on reliable criteria such a video EEG monitoring, misdiagnosis is unlikely. Instead, the usual cause for a poor outcome is related to a patient’s chronic psychological and social problems[1,8,22,50].
It is noteworthy that children with PNES appear to have a much better prognosis than adults [9,10]. In fact, the etiology in children may be related more to transient stress and coping disorders, while adults are more likely to have PNES within the context of more chronic psychological maladjustment, such as personality disorders [10]. Another factor that accounts for the better outcomes in children is that they are usually properly diagnosed earlier in the course of their disorder [9,10].
Patients with milder psychopathology respond better to supportive educational or behavioral therapeutic approaches. In contrast, patients with more severe psychopathology and factitious disorders more often have associated chronic personality problems and correspondingly, a poorer prognosis [1,50]. Also it appears that patients who continue to be followed by the diagnosing neurologist or center do better than patients who are not seen after diagnosis [49,67]. As knowledge about the nature of PNES and their associated psychopathology is gained, better treatment strategies can be developed that will improve the care and prognosis of these difficult and challenging patients.
A large study of 164 patients who were followed for 10 years were considered to have “poor outcome” in general but favorable factors included higher education, younger age of onset and diagnosis, and less “dramatic” attacks, defined as lack of “positive motor features, no ictal incontinence or tongue biting.” These findings were consistent with prior studies [52,68].
In addition, the patients who tended to have less seizures and do better long term, had less somatoform and dissociative symptoms on psychometric testing [51]. These findings are often explained by the theory that patients who do not do well have poor coping strategies to deal with stress and anxiety and that in a sense, these patients have emotional dysregulation.
Special Issues
Coexisting Epileptic and Psychogenic Nonepileptic Seizures
A complicating factor in diagnosis is that both PNES and epileptic seizures may occur in a single patient. Indeed, approximately 10% to 40% of patients identified to have PNES also have been reported to have epileptic seizures [1,23,33,56]. There are several possible explanations for this. Some patients with epilepsy may learn that seizures result in attention and fill certain psychological needs. Alternatively, they may have concomitant neurologic problems, personality disorders, cognitive deficits, or impaired coping mechanisms that predispose them to psychogenic symptoms [69–71]. Fortunately, in such patients with combined seizure disorders, the epileptic seizures are usually well controlled or of only historical relevance at the time a patient develops PNES [1,22,23,33,72–74].
In other patients, both epileptic and PNES may start simultaneously, making management even more complex. In such patients, we have found it particularly helpful to focus on the semiology of seizure manifestations as recorded by video EEG monitoring to distinguish PNES from the epileptic seizures. We then direct our treatment of the patient according to the semiology manifesting at that time. We also have found it useful to show the videos of seizures to family members or caregivers with patient consent to help them understand how to respond best to a patient’s symptoms when epileptic and PNES co-exist.
Misdiagnosis of Psychogenic Nonepileptic Seizures
Sometimes events that are initially diagnosed as nonepileptic actually prove to be epileptic. Such events can be called “pseudo-pseudo” or “epileptic-nonepileptic” seizures [1]. Frontal lobe seizures in particular may not be associated with significant EEG changes ictally and therefore misdiagnosed as PNES [23,75,76]. Clinical presentation and proper diagnosis of these types of events warrant emphasis.
Notable manifestations of frontal lobe seizures that may easily be confused with hysterical behavior include shouting, laughing, cursing, clapping, snapping, genital manipulation, pelvic thrusting, pedaling, running, kicking, and thrashing [23,75–77]. Not all of these behaviors are specific for frontal lobe seizures. For example, bicycling leg movements have also been reported in seizures originating from the temporal lobe [78].
Summary
PNES represent a common yet challenging problem within neurology. This is due to the difficulty in diagnosis as well as lack of effective and widely available treatment options. Overall outcomes of patients with PNES vary, and may relate to an individual patient’s chronic psychological and social problems. However, an accurate and timely diagnosis remains critical and can help provide direction for implementing appropriate treatment.
Corresponding author: Jennifer Hopp, MD, Department of Neurology, University of Maryland Medical Center, Room S12C09, 22 South Greene Street, Baltimore, MD 21201, [email protected].
Financial disclosures: None.
1. Krumholz A. Nonepileptic seizures: diagnosis and management. Neurology 1999;S76–83.
2. Meierkord H, Will B, Fish D, Shorvon S. The clinical features and prognosis of pseudoseizures diagnosed using video-EEG telemetry. Neurology 1991;41:1643–6.
3. Lesser RP. Psychogenic seizures. Neurology 1996;46:1499–1507.
4. Sigurdardottir KR, Olafsson E. Incidence of psychogenic seizures in adults: a population-based study in Iceland. Epilepsia 1998;39:857–62.
5. Szaflarski JP, Szaflarski M, Hughes C, et al. Psychopathology and quality of life: psychogenic non-epileptic seizures versus epilepsy. Med Sci Monit 2003 9:CR113–8.
6. Barry E, Krumholz A, Bergey C, et al. Nonepileptic posttraumatic seizures. Epilepsia 1998;39:427–31.
7. Pakalnis A, Drake ME, Phillips B. Neuropsychiatric aspects of psychogenic status epilepticus. Neurology 1991;41;1104–6.
8. Walzack TS, Papacostas S, Williams DT, et al. Outcome after the diagnosis of psychogenic nonepileptic seizures. Epilepsia 1995;36:1131–7.
9. Metrick ME, Ritter FJ, Gates JR, et al. Nonepileptic events in childhood. Epilepsia 1991;32:322–8.
10. Wyllie E, Friedman D, Luders H, et al. Outcome of psychogenic seizures in children and adolescents compared to adults. Neurology 1991;41:742–4.
11. Duncan R, Oto M. Predictors of antecedent factors in psychogenic nonepileptic attacks: multivariate analysis. Neurology 2008;71:1000–5.
12. Alper K, Devinsky O, Perrine K, et al. Nonepileptic seizures and childhood sexual and physical abuse. Neurology 1993; 43:1950–3.
13. LaFrance WC Jr, Devinsky O. The treatment of nonepileptic seizures: historical perspectives and future directions. Epilepsia 2004;45 Suppl 2:15–21.
14. Westbrook LE, Devinsky O, Geocadin R. Nonepileptic seizures after head injury. Epilepsia 1998;39:978–82.
15. Slavney PR. Perspectives on hysteria. Baltimore: Johns Hopkins University Press; 1990.
16. Veith I. Hysteria: the history of a disease. Chicago: University of Chicago Press; 1965.
17. Goetz CG. Charcot the clinician. The Tuesday lessons. New York: Raven Press; 1987.
18. Massey EW, McHenry LC. Hysteroepilepsy in the nineteenth century: Charcot and Gowers. Neurology 1986;36:65–7.
19. Zeigler FJ, Imboden JB, Meyer E. Contemporary conversion reactions: a clinical study. Am J Psychiatry 1960;116:901–10.
20. Liske E, Forster FM. Pseudoseizures: a problem in the diagnosis and management of epileptic patients. Neurology 1964;14:41–9.
21. Diagnostic and statistical manual of mental disorders. DSM-IV 4th ed. American Psychiatric Association. Washington, DC; 1995.
22. Krumholz A, Niedermeyer, E. Psychogenic seizures: a clinical study with follow-up data. Neurology 1983; 33:498-502.
23. Krumholz A, Ting T. Co-existing epileptic and nonepileptic seizures. in imitators of epilepsy. 2nd ed. In: Kaplan PW, Fisher RS, editors. New York: Demos Medical Publishing; 2005:261–76.
24. Gates JR, Ramani V, Whalen S, Loewenson R. Ictal characteristics of pseudoseizures. Arch Neurol 1985;42:1183–87.
25. Leis AA, Ross MA, Summers AK. Psychogenic seizures: Ictal characteristics and diagnostic pitfalls. Neurology 1992;42:95–9.
26. Walczak TS, Bogolioubov. Weeping during psychogenic nonepileptic seizures. Epilepsia 1996;37:207–10.
27. Bergen D, Ristanovic R. Weeping is a common element during psychogenic nonepileptic seizures. Arch Neurol 1993;50:1059–60.
28. Peguero E, Abou-Khalil B, Fakhoury, Mathews G. Self-injury and incontinence in psychogenic seizures. Epilepsia 1995;36:586–91.
29. Orbach D, Ritaccio A, Devinsky O. Psychogenic, nonepileptic seizures associated with video-EEG-verified sleep. Epilepsia 2003;44:64–8.
30. Walczak TS, Williams DT, Berton W. Utility and reliability of placebo infusion in the evaluation of patients with seizures. Neurology 1994;44:394–99.
31. Bazil CW, Kothari M, Luciano D, et al. Provocation of nonepileptic seizures by suggestion in a general seizure population. Epilepsia 1994;35:768–70.
32. Devinsky O, Fisher RS. Ethical use of placebos and provocative testing in diagnosing nonepileptic seizures. Neurology 1996;47:866–70.
33. Lesser RP, Lueders H, Dinner DS. Evidence for epilepsy is rare in patients with psychogenic seizures. Neurology 1983; 33:502–4.
34. Barre MA, Burnstine TH, Fisher RS, Lesser RP. Electroencephalographic changes during simple partial seizures. Epilepsia 1994;35:715–20.
35. Trimble MR. Serum prolactin levels in epilepsy and hysteria. BMJ 1978;2:1682.
36. Laxer KD, Mullooly JP, Howell B. Prolactin changes after seizures classified by EEG monitoring. Neurology 1985; 35:31–5.
37. Pritchard PB, Wannamaker BB, Sagel J, et al. Endocrine function following complex partial seizures. Ann Neurol 1983;14:27–32.
38. Malkowicz DE, Legido A, Jackel RA, et al. Prolactin secretion following repetitive seizures. Neurology 1995;45:448–52.
39. Oribe E, Rohullah A, Nissenbaum E, Boal B. Serum prolactin concentrations are elevated after syncope. Neurology 1996;47:60–2.
40. Henrichs TF, Tucker DM, Farha J, Novelly RA. MMPI indices in the identification of patients evidencing pseudoseizures. Epilepsia 1988;29:184–8.
41. Wilkus RJ, Dodrill CB. Factors affecting the outcome of MMPI and neuropsychological assessments of psychogenic and epileptic seizure patients. Epilepsia 1989;30:339–47.
42. DeTimary P, Fouchet P, Sylin M, et al. Non–epileptic seizures: delayed diagnosis in patients presenting with electroencephalographic (EEG) or clinical signs of epileptic seizures. Seizure 2002;11:193–7.
43. Reuber M, Fernandez G, et al. Diagnostic delay in psychogenic nonepileptic seizures. Neurology 2002;58:493–5.
44. Rosenbaum DH, et al. Outpatient multidisciplinary management of non-epileptic seizures. In: Rowan AJ, Gates Jr, editors. Non-epileptic seizures. 1st ed. Stoneham, MA: Butterworth-Heinemann; 1993:275–83.
45. Lempert T, Schmidt D. Natural history and outcome of psychogenic seizures: a clinical study in 50 patients. J Neurol 1990;237:35–8.
46. Selwa LM, Geyer J, Nikakhtar N, et al. Nonepileptic seizure outcome varies by type of spell and duration of illness. Epilepsia 2000;41:1330–4.
47. Buchanan N, Snars J. Pseudoseizures (non epileptic attack disorder): clinical management and outcome in 50 patients. Seizure 1993;2:141–6.
48. Kanner AM. More controversies on the treatment of psychogenic pseudoseizures: an addendum. Epilepsy Behav 2003;4:360–4.
49. Aboukasm A, Mahr G, Gahry BR, et al. Retrospective analysis of the effects of psychotherapeutic interventions on outcomes of psychogenic nonepileptic seizures. Epilepsia 1998;39:470–3.
50. Reuber M, Pukrop T, Bauer J, et al. Outcome in psychogenic nonepileptic seizures: 1 to 10-year follow-up in 164 patients. Ann Neurol 2003;53:305–11.
51. McKenzie P, Oto M, Russell A, Pelosi A, Duncan R. Early outcomes and predictors in 260 patients with psychogenic nonepileptic seizures (PNES). Neurology 2010;74:64–9.
52. Kanner AM, Parra J, Frey M, et al. Psychiatric and neurologic predictors of psychogenic pseudoseizure outcome. Neurology 1999;53:933–8.
53. Shen W, Bowman ES, Markand ON. Presenting the diagnosis of pseudoseizure. Neurology 1990; 40:756–9.
54. Friedman JH, LaFrance Jr WC. Psychogenic disorders: the need to speak plainly. Arch Neurol 2010;67:753–5.
55. LaFrance Jr WC. Psychogenic nonepileptic “seizures” or “attacks”? It’s not just semantics: “Seizures.” Neurology 2010;75: 87–8.
56. Ramsay RE, Cohen A, Brown MC. Coexisting epilepsy and non-epileptic seizures. In: Non-epileptic seizures. Butterworth-Heinemann; 1998:47–54.
57. Stone J, Carson A, Sharpe M. Functional symptoms in neurology: management. J Neurol Neurosurg Psychiatry. 2005;6(Suppl 1):i13–i21.
58. LaFrance WC Jr, Bjornaes H. Designing treatment plans based on etiology of psychogenic nonepileptic seizures. In: Schachter SC, LaFrance WC Jr, editors. Gates and Rowan’s nonepileptic seizures. 3rd ed. New York: Cambridge University Press; 2010:266–80.
59. Kroenke K, Swindle R. Cognitive-behavioral therapy for somatization and symptom syndromes: a critical review of controlled clinical trials. Psychother Psychosom 200;69:205–15.
60. Kroenke K. Efficacy of treatment of somatoform disorders: a review of randomized controlled trials. Psychosom Med 2007:69:881–8.
61. LaFrance WC Jr, Miller IW, Ryan CE, et al. Cognitive behavioral therapy for psychogenic nonepileptic seizures. Epilepsy Behav 2009;14:591–6.
62. Chalder T. Non-epileptic attacks: a cognitive behavioral approach in a single case with a four-year follow-up. Clin Psychol Psychother 1996;3:291–7.
63. Betts T, Duffy N. Non-epileptic attack disorder (pseudoseizures) and sexual abuse: a review. In: Gram L, Johannessen SI, Osterman PE, et al, editors. Pseudo-epileptic seizures. Petersfield, UK: Wrightson Biomedical Publishing; 1993:55–66.
64. Lesser RP. Treatment and outcome of psychogenic nonepileptic seizures. Epilepsy Currents 2003;3:198–200.
65. Ramani V. Review of psychiatric treatment strategies in non-epileptic seizures. In: Rowan AJ, Gates JR, eds. Non-epileptic Seizures. 1st ed. Stoneham, MA: Butterworth Heinemann; 1993:259–67.
66. Goldstein LH, Chalder T, Chigwedere C, et al. Cognitive-behavioral therapy for psychogenic nonepileptic seizures: a pilot RCT. Neurology 2010;74:1986–94.
67. Bennet C, So NM, Smith WB, Thompson K. Structured treatment improves the outcome of nonepileptic events. Epilepsia 1997;38(Suppl 8):214.
68. McDade G, Brown SW. Non-epileptic seizures: management and predictive factors of outcome. Seizure 1992;1:7–10.
69. Bowman ES. Etiology and clinical course of pseudoseizures: relationship to trauma, depression, and dissociation. Psychosomatics 1993;34:333–42.
70. Bowman ES, Markand ON. Psychodynamics and psychiatric diagnoses of pseudoseizure subjects. Am J Psychiatry 1996;153:57–63.
71. Vanderzant CW, Giordani B, Berent S, et al. Personality of patients with pseudoseizures. Neurology 1986;36:664–8.
72. Benbadis SR, Agrawal V, Tatum WO. How many patients with psychogenic nonepileptic seizures also have epilepsy? Neurology 2001; 57:915–7.
73. Glosser G, Roberts D, et al. Nonepileptic seizures after resective epilepsy surgery. Epilepsia 1999; 40:1750–4.
74. Reuber M, Kral T. New-onset psychogenic seizures after intracranial neurosurgery. Acta Neurochir (Wien) 2002; 144:901–7.
75. Williamson P, Spencer D, Spencer S, et al. Complex partial seizures of frontal lobe origin. Ann Neurol 1985;18:497–504.
76. Saygi S, Katz A, Marks D, et al. Frontal lobe partial seizures and psychogenic seizures: comparison of clinical and ictal characteristics. Neurology 1992;42:1274–7.
77. Waterman K, Purves S, Kosaka B, et al. An epileptic syndrome caused by mesial frontal lobe seizure foci. Neurology 1987; 37:577–82.
78. Sussman N, Jackel R, Kaplan L, et al. Bicycling movements as a manifestation of complex partial seizures of temporal lobe origin. Epilepsia 1989;30:527–31.
From the Department of Neurology, University of Maryland School of Medicine, Baltimore, MD.
Abstracts
- Objective: To provide a review of psychogenic nonepileptic seizures, including a discussion of the diagnosis, treatment, and clinical significance of the disorder.
- Methods: Review of the relevant literature.
- Results: Psychogenic nonepileptic seizures are a common and potentially disabling neurologic disorder. They are most prevalent in young adults, and more commonly seen in women versus men. Certain psychosocial variables may impact the development of the condition. The diagnosis is made through a detailed history and observation of clinical events in conjunction with video EEG monitoring. Neuropsychological testing is an important component in the evaluation. Treatment includes establishment of an accurate diagnosis, management of any underlying psychiatric diagnoses, and regular follow-up with a neurologist or trained care provider.
- Conclusion: Psychogenic nonepileptic seizures represent a complex interaction between neurologic and psychological factors. Obtaining an accurate diagnosis through the use of video EEG monitoring and clinical observation is an important initial step in treatment and improved quality of life in this patient population.
Psychogenic nonepileptic seizures (PNES) are commonly encountered in outpatient specialty epilepsy clinics as well as inpatient epilepsy monitoring units. They comprise approximately 20% of all refractory seizure disorders referred to specialty epilepsy centers [1–4]. PNES are thought to be psychological in origin as opposed to arising from abnormal electrical discharges as in epileptic seizures. PNES may be more frequent and disabling than epileptic seizures, and patients with PNES may report worse outcomes [5,6]. Increased utilization of long-term video EEG monitoring along with greater recognition of psychogenic neurologic disorders has allowed for improved diagnosis of PNES. However, many diagnostic and therapeutic challenges remain. There are often delays in obtaining an accurate diagnosis, and optimal management remains challenging, often leading to inappropriate, ineffective, and costly treatment, sometimes for many years [6–8].
Epidemiology
PNES are seen across the spectrum of age-groups, from children [9,10] to elderly persons, but they most often occur in young adults between the ages of 15 to 35 years [1,8]. Caution should be used when considering this diagnosis in infants or young children, in whom it is more common to see physiologic events that may mimic epileptic seizures, including gastroesophageal reflux, shuddering, night terrors, or breath holding spells [1,9,10].
PNES are prevalent within epilepsy practices. Patients with PNES comprise approximately 5% to 20% patients thought to have intractable epilepsy seen in outpatient centers, and within epilepsy monitoring units they account for 10% to 40% of patients [1,2,6,8]. A population-based study approximates the incidence of PNES at 1.4 per 100,000 people and 3.4 per 100,000 people between the ages of 15 to 24 years [4].
There is a female preponderance in PNES, which is similar to other conversion and somatoform disorders. Overall, women comprise approximately 70% to 80% of patients with the PNES diagnosis [1,2,6]. There are psychosocial variables that are seen in some patients with this disorder. An important factor that has been described is past history of sexual or physical abuse. In one series, there was a history of sexual abuse in almost 25% of patients with PNES, and history of either sexual abuse, physical abuse, or both in 32% of patients [11]. A history of sexual and/or physical abuse is not exclusive to these patients, and can certainly be seen in patients with epilepsy as well. For example, in a control population of epilepsy patients, there was a reported rate of past sexual or physical abuse approaching 9% [12].
A prior history of head trauma, often of a relatively mild degree, has been described as a potential inciting factor for some cases of PNES [6,13]. In the literature, studies report that as many as 20% of PNES patients attributed their seizures to head trauma, often rather mild head trauma [6,14].
Historcial Context
Historically, what today are called PNES originate with the concept of hysteria, a medical diagnosis in women that can be traced to antiquity [15,16]. By the late 1800s, one of the founders of neurology, Jean Charcot, established hysterical seizures as an important clinical entity with his detailed, elegant descriptions of patients. Charcot formulated clinical methods for distinguishing hysteria and particularly hysterical seizures from epilepsy. He presumed that hysteria and epilepsy were closely related, and he termed seizures due to hysteria as “hysteroepilepsy” or “epileptiform” hysteria. Charcot proposed that hysterical seizures were organic disorders of the brain, like other forms of seizures and epilepsy, and emphasized their relation to disturbance of the female reproductive system [17,18]. Charcot utilized techniques such as manipulation of “hysterogenic zones” and ovarian compression as well as suggestion to both treat and provoke hysteria and hysterical seizures, which he described and documented [17,18]. One of Charcot’s most celebrated students, Sigmund Freud, observed Charcot’s demonstrations but drew different conclusions. He theorized that hysteria and hysterical seizures were not organic disorders of the brain as Charcot proposed, but were rather emotional disorders of the unconscious mind due to repressed energies or drives. Based largely the theories of Freud and Charcot, individuals with hysteria were distinguished from those with epilepsy, with hysterical seizures related to psychological dysfunction while epileptic seizures were associated with physical or organic brain disorders [15,16].
With the introduction of EEG recording in the 1930s, it became possible to characterize epilepsy as an electrical disorder of the brain with associated EEG changes and more effectively distinguish it from hysterical seizures, which did not have such abnormalities. In addition, in the first half of the 20th century, the nature of hysteria as seen and diagnosed by physicians seemed to change. The dramatic, theatrical convulsions described by Charcot and his contemporaries appeared less commonly, while disorders such as chronic pain seemed to increase [1,19].
However, by the 1960s, several reports confirmed that hysterical seizures were actually still prevalent. Newer terms like “pseudoseizures” were used to describe these disorders because the term “hysteria” was thought to be somewhat derogatory, anti-feminist, and antiquated [20,21]. In the 1970s and thereafter, with the increasing availability of video EEG monitoring and growth of inpatient epilepsy monitoring units, it was discovered that these hysterical, pseudo-, or what were also by then termed psychogenic seizures, were actually still common [1,22].
More recently, it has been recognized that the pendulum in some cases may have swung too far in regard to the diagnosis of this disorder. Some rare patients with seizures initially diagnosed as PNES may actually have forms of epileptic seizures such as frontal lobe epilepsy or related physiological disorders rather than psychogenic causes for their episodes [1,23]. These types of epileptic seizures can be very difficult to diagnose properly unless one appreciates how they present and manifest and remains vigilant for them during evaluation [1,23].
Terminology
There is an ongoing debate regarding the appropriate terminology for psychogenic events, and there is no uniform standardized definition or classification at this time. The term that is currently preferred within the epilepsy community for seizures of psychological origin that are thought to be associated with conversion, somatization, or dissociative disorders is “psychogenic nonepileptic seizures” (PNES). This terminology is felt to be non-disparaging and more neutral as compared with other terms such as pseudoseizures, which were previously favored. Nonepileptic seizures or nonepileptic events are broader terms meant to incorporate both physiologic and psychological causes for disorders that are mistaken for epilepsy. PNES are widely defined as paroxysmal events that appear similar to epileptic seizures but are not due to abnormal electrical discharges in the brain and as noted, are typically thought to be related or caused by conversion, somatization, or dissociative disorders.
Physiologic nonepileptic events are another category of physical disorders that may be mistaken for epilepsy. The underlying causes differ between age-groups, and can include conditions such as cardiac arrhythmias, migraine variants, syncope, or metabolic abnormalities. Physiologic nonepileptic seizures account for only a small proportion of all patients with nonepileptic seizures or events [1]. In general, any patient with a psychological disorder that causes symptoms that are mistaken for epilepsy can be said to have PNES.
Clinical Characteristics And Presentation
The duration of PNES is often significantly longer than that seen in epileptic seizures, which usually last less than 3 minutes, excluding the postictal period. PNES may also exhibit waxing and waning convulsive activity, although this finding can certainly be seen in epileptic seizures as well. PNES may be shown to have distractibility with external stimuli. Additionally, the movements in PNES may appear asymmetric, asynchronous, or purposeful, although this is not diagnostic for this disorder. This may contrast with the well-defined, synchronous tonic-clonic activity typically seen in epileptic seizures [1,24,25]. Back arching and pelvic thrusting movements can also be seen in PNES. Despite these differences, it may still be challenging to distinguish the semi-purposeful behaviors of PNES from the automatisms of certain focal epileptic seizures. The often bizarre-appearing, hypermotor activity that can be seen in frontal lobe seizures is often especially difficult to differentiate from PNES [1,23].
Another important consideration is that consciousness is preserved in PNES, while consciousness and responsiveness are frequently impaired in epileptic seizures. Patients with PNES are often apparently unresponsive during events, although there is no true impairment of awareness. Other characteristics that are more commonly seen in PNES are crying and eye closure [26]. Self-injury and incontinence may be reported, but they are less often clearly witnessed or documented [27,28]. Additionally, although patients may at times appear to be asleep at seizure onset, EEG recordings document the patient to actually be asleep in less than 1% of cases [29]. While epileptic seizures often respond well to antiepileptic medications, PNES characteristically do not [1,3,6,8].
In certain situations, provocation maneuvers may be utilized in order to reproduce PNES in patients undergoing EEG monitoring. In comparison to epileptic seizures, suggestion and emotional stimuli are more likely to trigger psychogenic events [1]. Methods utilized to provoke PNES may include saline injections, placement of a tuning fork on the head or body, or even hypnosis, when a suggestion is concurrently provided that such maneuvers can trigger the patient’s seizures [1,30,31]. When evaluating seizures that are provoked in such a manner, it is important to consider whether or not the event captured is in fact a typical event for the patient, or whether the provocation has uncovered a different, atypical event. Given that PNES and epileptic seizures can co-exist within the same patient, care should be taken to avoid making a diagnosis based on capturing an atypical event, or capturing only a subset of a patient’s seizure types. This could result in failure to make an accurate and thorough diagnosis [23]. There is debate regarding the ethics of provoking seizures by way of suggestion. Some members of the epilepsy community feel that provoking seizures through suggestion is inherently deceitful, and therefore can damage the physician-patient relationship. Others assert that such provocative testing can be undertaken in an honest manner, and can ultimately help achieve an accurate diagnosis for the patient [32].
As previously mentioned, there is a proportion of patients who have co-existing epileptic seizures and PNES, and obtaining an accurate diagnosis can be especially challenging in this group. Studies have reported that around 10% to 40% of patients with PNES also have epilepsy [1,22,23,33]. Care must be taken to distinguish between differences in seizure types and if necessary, video EEG monitoring may be needed to capture both seizure types for an accurate diagnosis. This testing can then be useful in education with families and caregivers who may be shown the videos with consent from the patient in order to guide future care.
Evaluation And Diagnosis
As in much of neurology, a thorough history, along with detailed clinical observation remains essential in the diagnosis of patients with PNES and for distinguishing these events from epilepsy. Video EEG monitoring of seizures is a key adjunct to the history and clinical observation in diagnosing this condition [1,2]. Long-term video EEG monitoring is considered the “gold standard” in the characterization and differential diagnosis of seizures. Additional potentially helpful diagnostic techniques include video EEG-monitored seizure provocation, serum prolactin levels, single photon emission computed tomography, and neuropsychological testing.
Video EEG Monitoring
![]()
EEG monitoring for characterization of clinical events can be conducted on an ambulatory or outpatient basis or in dedicated inpatient epilepsy monitoring units. Ambulatory monitoring can be useful in the case of patients who report seizures that are more frequent in their home environment or in patients with frequent events. If events are infrequent, then inpatient monitoring may be more efficacious [1]. With longer-term inpatient monitoring, antiepileptic medications can be withdrawn in a supervised setting, in order to lower the seizure threshold as well as to safely discontinue medications that may not be necessary. Such medication titrations are typically not safe in an unsupervised outpatient setting. Some ambulatory EEG monitoring systems do allow for simultaneous video and EEG recording. However, an advantage to inpatient monitoring, which is not afforded in the outpatient setting, is the ability for nursing staff or physicians to perform clinical testing during events to assess for patient responsiveness and other features. Additionally, with inpatient monitoring, EEG technicians can routinely assess for any technical problems with the electrodes or recording system.
Another benefit of video EEG monitoring is that the state (waking, drowsy, or asleep) of the patient at the onset of an event can be established. While epileptic seizures can arise from any state, PNES most often occur from wakefulness. Patients with PNES may appear to be asleep at the onset of events, and they may report seizures from sleep. Video EEG monitoring can help to establish the waking or sleep state of the patient that may aid in diagnosis [29].
Prolactin Levels
Serum prolactin levels may be helpful in the diagnosis of PNES [35,36]. Following generalized tonic-clonic or complex partial epileptic seizures, the serum prolactin can rise from two to threefold to five to tenfold [37]. The maximal rise in serum prolactin occurs in the initial 20 to 60 minutes after the seizure [35–37]. A similar rise in serum prolactin would not be expected in PNES. Although prolactin levels may have some utility in diagnosis, they are not currently routinely ordered as part of a standard admission to most inpatient epilepsy monitoring units. This may be due in part to the fact that false-positive and false-negative results can occur with these levels [37–39]. For example, there may not be a rise in the prolactin level after a simple partial seizure or more subtle complex partial seizure.
Neuropsychological Testing
Neuropsychological testing is also a key component in the evaluation and diagnosis of PNES. Ideally, a mental health provider with a background in psychological assessment and neuropsychological intervention for patients with psychogenic disorders would perform the evaluation [40,41].
The goal of the evaluation should not solely focused on whether the patient suffers from nonepileptic or epileptic seizures. An epileptologist upon review of clinical, electrographic, and neuropsychological data better makes this determination. Moreover, neuropsychological testing cannot in itself either diagnose or exclude the possibility that a seizure disorder is nonepileptic because of the considerable overlap between epileptic and nonepileptic test results [40,41]. Neuropsychological evaluations aid this assessment by (1) determining the potential or likelihood of significant contributing psychopathology or cognitive difficulties, (2) defining the nature of the associated psychological or psychosocial issues, and (3) assessing how a patient might benefit from various psychologically based interventions [1]. The testing may identify psychological problems that can guide treatment after diagnosis.
Delays in Diagnosis
Correct and prompt diagnosis is essential for patients with PNES as is appropriate referral to a knowledgeable trained mental health professional. On average, patients with PNES are diagnosed 7.2 years after manifestation (SD 9.3 years), with mean delay of 5 to 7 years. Younger age, interictal epileptiform potentials in the EEG, and anticonvulsant treatment are associated with longer delays [42,43]. Delays are also thought to occur because of problems with “ownership” of these patients. Although typically neurologists are involved in the diagnosis of PNES, often using video EEG monitoring done in an inpatient setting, the next step is often a referral to a psychiatrist or mental health care provider. There are sometimes delays in the initial referral to the neurologist, delays in referral to specialists for video EEG testing, and also to the physicians, psychologists or social workers who may provide treatment. Another disconnect can occur if patients are “lost to follow-up” if they receive a referral for mental health care and either do not follow up on this on their own, or if the reason for this care is not fully explained. In addition, many mental health professionals are not trained in the evaluation and treatment of psychogenic symptoms and may even feel uncomfortable in dealing with these patients [13,44].
Many studies have been suggestive that delays in diagnosis may result in poorer outcomes [45,46], while other studies have suggested that patients who have an acute diagnosis of PNES upon presentation may do particularly well [8,47–49]. Some of the most recent large outcome studies suggest that there may be no worsening of outcome associated with delays in diagnosis and that outcome was predicted by other factors [50–52].
Management
Management of patients with PNES is similar to that for patients with other types of so-called abnormal illness behavior, although there remains a relative paucity of evidence for specific treatment strategies for PNES [1]. The first consideration should be the manner in which the diagnosis of PNES is presented to the patient and family. It is important to be honest with the patient and demonstrate a positive approach to the diagnosis [53]. The physician should emphasize as favorable or good news the fact that the patient does not have epilepsy, and should also stress that the disorder, although serious and "real," does not require treatment with antiepileptic medications and that once stress or emotional issues are resolved, the patient has the potential to gain better control of these events [1,54,55]. Nevertheless, not all patients readily accept the diagnosis or this type of approach. Some patients may seek other opinions, and this should not be discouraged. An adversarial relationship with the patient should be avoided. The patient should be encouraged to return if desired, and records should be made available to other health care providers to avoid duplication of services.
After the diagnosis of PNES is presented, supportive measures should be initiated. PNES patients may benefit from education and support that can be provided by the neurologist or primary care physician [1]. If the neuropsychological assessment suggests a clinical profile that requires a professional mental health intervention, then an appropriate referral should be made. Regular follow-up visits for the patient with the neurologist are useful even if a mental health professional is involved [49,56]. This allows the patient to get medical attention without demonstrating illness behavior. Patient education and support are stressed at these visits. Because family issues are often important contributing factors, physicians should consider involving family members in visits with consent of the patient [1].
A variety of treatment strategies are employed for the management of PNES including cognitive behavioral therapy (CBT), group and family therapy, antidepressant medication, and other forms of rehabilitation [5,57,58]. A 2007 Cochrane review that identified 608 references for non-medication PNES treatments found that only 3 studies met criteria for a randomized controlled trial. One of the more recently favored treatment options for PNES that has been applied to the treatment of various somatoform disorders and other psychiatric disorders in the past is CBT [57,59,60]. This form of psychotherapy can be administered by trained personnel in a time-limited fashion using defined protocols. The basis of this treatment is that the patient learns to increase awareness of their dysfunctional thoughts and learns new ways to respond to them [57,58]. To date, several groups have reported results of nonrandomized trials as well as case reports and case series which have established the utility of this treatment. There have been reports of significant reductions in seizure frequency and this treatment strategy appears very promising [61–65]. Preliminary randomized controlled trials have also been piloted and are also suggestive that this may be a validated treatment approach [66].
Prognosis
The outcomes of patients with PNES vary. Long-term follow-up studies show that about half of all patients with PNES function reasonably well following their diagnosis. However, only approximately one-third of patients will completely stop having seizures or related problems, and approximately 50% percent have poor functional outcomes [1,2,50]. When the diagnosis of PNES is based on reliable criteria such a video EEG monitoring, misdiagnosis is unlikely. Instead, the usual cause for a poor outcome is related to a patient’s chronic psychological and social problems[1,8,22,50].
It is noteworthy that children with PNES appear to have a much better prognosis than adults [9,10]. In fact, the etiology in children may be related more to transient stress and coping disorders, while adults are more likely to have PNES within the context of more chronic psychological maladjustment, such as personality disorders [10]. Another factor that accounts for the better outcomes in children is that they are usually properly diagnosed earlier in the course of their disorder [9,10].
Patients with milder psychopathology respond better to supportive educational or behavioral therapeutic approaches. In contrast, patients with more severe psychopathology and factitious disorders more often have associated chronic personality problems and correspondingly, a poorer prognosis [1,50]. Also it appears that patients who continue to be followed by the diagnosing neurologist or center do better than patients who are not seen after diagnosis [49,67]. As knowledge about the nature of PNES and their associated psychopathology is gained, better treatment strategies can be developed that will improve the care and prognosis of these difficult and challenging patients.
A large study of 164 patients who were followed for 10 years were considered to have “poor outcome” in general but favorable factors included higher education, younger age of onset and diagnosis, and less “dramatic” attacks, defined as lack of “positive motor features, no ictal incontinence or tongue biting.” These findings were consistent with prior studies [52,68].
In addition, the patients who tended to have less seizures and do better long term, had less somatoform and dissociative symptoms on psychometric testing [51]. These findings are often explained by the theory that patients who do not do well have poor coping strategies to deal with stress and anxiety and that in a sense, these patients have emotional dysregulation.
Special Issues
Coexisting Epileptic and Psychogenic Nonepileptic Seizures
A complicating factor in diagnosis is that both PNES and epileptic seizures may occur in a single patient. Indeed, approximately 10% to 40% of patients identified to have PNES also have been reported to have epileptic seizures [1,23,33,56]. There are several possible explanations for this. Some patients with epilepsy may learn that seizures result in attention and fill certain psychological needs. Alternatively, they may have concomitant neurologic problems, personality disorders, cognitive deficits, or impaired coping mechanisms that predispose them to psychogenic symptoms [69–71]. Fortunately, in such patients with combined seizure disorders, the epileptic seizures are usually well controlled or of only historical relevance at the time a patient develops PNES [1,22,23,33,72–74].
In other patients, both epileptic and PNES may start simultaneously, making management even more complex. In such patients, we have found it particularly helpful to focus on the semiology of seizure manifestations as recorded by video EEG monitoring to distinguish PNES from the epileptic seizures. We then direct our treatment of the patient according to the semiology manifesting at that time. We also have found it useful to show the videos of seizures to family members or caregivers with patient consent to help them understand how to respond best to a patient’s symptoms when epileptic and PNES co-exist.
Misdiagnosis of Psychogenic Nonepileptic Seizures
Sometimes events that are initially diagnosed as nonepileptic actually prove to be epileptic. Such events can be called “pseudo-pseudo” or “epileptic-nonepileptic” seizures [1]. Frontal lobe seizures in particular may not be associated with significant EEG changes ictally and therefore misdiagnosed as PNES [23,75,76]. Clinical presentation and proper diagnosis of these types of events warrant emphasis.
Notable manifestations of frontal lobe seizures that may easily be confused with hysterical behavior include shouting, laughing, cursing, clapping, snapping, genital manipulation, pelvic thrusting, pedaling, running, kicking, and thrashing [23,75–77]. Not all of these behaviors are specific for frontal lobe seizures. For example, bicycling leg movements have also been reported in seizures originating from the temporal lobe [78].
Summary
PNES represent a common yet challenging problem within neurology. This is due to the difficulty in diagnosis as well as lack of effective and widely available treatment options. Overall outcomes of patients with PNES vary, and may relate to an individual patient’s chronic psychological and social problems. However, an accurate and timely diagnosis remains critical and can help provide direction for implementing appropriate treatment.
Corresponding author: Jennifer Hopp, MD, Department of Neurology, University of Maryland Medical Center, Room S12C09, 22 South Greene Street, Baltimore, MD 21201, [email protected].
Financial disclosures: None.
From the Department of Neurology, University of Maryland School of Medicine, Baltimore, MD.
Abstracts
- Objective: To provide a review of psychogenic nonepileptic seizures, including a discussion of the diagnosis, treatment, and clinical significance of the disorder.
- Methods: Review of the relevant literature.
- Results: Psychogenic nonepileptic seizures are a common and potentially disabling neurologic disorder. They are most prevalent in young adults, and more commonly seen in women versus men. Certain psychosocial variables may impact the development of the condition. The diagnosis is made through a detailed history and observation of clinical events in conjunction with video EEG monitoring. Neuropsychological testing is an important component in the evaluation. Treatment includes establishment of an accurate diagnosis, management of any underlying psychiatric diagnoses, and regular follow-up with a neurologist or trained care provider.
- Conclusion: Psychogenic nonepileptic seizures represent a complex interaction between neurologic and psychological factors. Obtaining an accurate diagnosis through the use of video EEG monitoring and clinical observation is an important initial step in treatment and improved quality of life in this patient population.
Psychogenic nonepileptic seizures (PNES) are commonly encountered in outpatient specialty epilepsy clinics as well as inpatient epilepsy monitoring units. They comprise approximately 20% of all refractory seizure disorders referred to specialty epilepsy centers [1–4]. PNES are thought to be psychological in origin as opposed to arising from abnormal electrical discharges as in epileptic seizures. PNES may be more frequent and disabling than epileptic seizures, and patients with PNES may report worse outcomes [5,6]. Increased utilization of long-term video EEG monitoring along with greater recognition of psychogenic neurologic disorders has allowed for improved diagnosis of PNES. However, many diagnostic and therapeutic challenges remain. There are often delays in obtaining an accurate diagnosis, and optimal management remains challenging, often leading to inappropriate, ineffective, and costly treatment, sometimes for many years [6–8].
Epidemiology
PNES are seen across the spectrum of age-groups, from children [9,10] to elderly persons, but they most often occur in young adults between the ages of 15 to 35 years [1,8]. Caution should be used when considering this diagnosis in infants or young children, in whom it is more common to see physiologic events that may mimic epileptic seizures, including gastroesophageal reflux, shuddering, night terrors, or breath holding spells [1,9,10].
PNES are prevalent within epilepsy practices. Patients with PNES comprise approximately 5% to 20% patients thought to have intractable epilepsy seen in outpatient centers, and within epilepsy monitoring units they account for 10% to 40% of patients [1,2,6,8]. A population-based study approximates the incidence of PNES at 1.4 per 100,000 people and 3.4 per 100,000 people between the ages of 15 to 24 years [4].
There is a female preponderance in PNES, which is similar to other conversion and somatoform disorders. Overall, women comprise approximately 70% to 80% of patients with the PNES diagnosis [1,2,6]. There are psychosocial variables that are seen in some patients with this disorder. An important factor that has been described is past history of sexual or physical abuse. In one series, there was a history of sexual abuse in almost 25% of patients with PNES, and history of either sexual abuse, physical abuse, or both in 32% of patients [11]. A history of sexual and/or physical abuse is not exclusive to these patients, and can certainly be seen in patients with epilepsy as well. For example, in a control population of epilepsy patients, there was a reported rate of past sexual or physical abuse approaching 9% [12].
A prior history of head trauma, often of a relatively mild degree, has been described as a potential inciting factor for some cases of PNES [6,13]. In the literature, studies report that as many as 20% of PNES patients attributed their seizures to head trauma, often rather mild head trauma [6,14].
Historcial Context
Historically, what today are called PNES originate with the concept of hysteria, a medical diagnosis in women that can be traced to antiquity [15,16]. By the late 1800s, one of the founders of neurology, Jean Charcot, established hysterical seizures as an important clinical entity with his detailed, elegant descriptions of patients. Charcot formulated clinical methods for distinguishing hysteria and particularly hysterical seizures from epilepsy. He presumed that hysteria and epilepsy were closely related, and he termed seizures due to hysteria as “hysteroepilepsy” or “epileptiform” hysteria. Charcot proposed that hysterical seizures were organic disorders of the brain, like other forms of seizures and epilepsy, and emphasized their relation to disturbance of the female reproductive system [17,18]. Charcot utilized techniques such as manipulation of “hysterogenic zones” and ovarian compression as well as suggestion to both treat and provoke hysteria and hysterical seizures, which he described and documented [17,18]. One of Charcot’s most celebrated students, Sigmund Freud, observed Charcot’s demonstrations but drew different conclusions. He theorized that hysteria and hysterical seizures were not organic disorders of the brain as Charcot proposed, but were rather emotional disorders of the unconscious mind due to repressed energies or drives. Based largely the theories of Freud and Charcot, individuals with hysteria were distinguished from those with epilepsy, with hysterical seizures related to psychological dysfunction while epileptic seizures were associated with physical or organic brain disorders [15,16].
With the introduction of EEG recording in the 1930s, it became possible to characterize epilepsy as an electrical disorder of the brain with associated EEG changes and more effectively distinguish it from hysterical seizures, which did not have such abnormalities. In addition, in the first half of the 20th century, the nature of hysteria as seen and diagnosed by physicians seemed to change. The dramatic, theatrical convulsions described by Charcot and his contemporaries appeared less commonly, while disorders such as chronic pain seemed to increase [1,19].
However, by the 1960s, several reports confirmed that hysterical seizures were actually still prevalent. Newer terms like “pseudoseizures” were used to describe these disorders because the term “hysteria” was thought to be somewhat derogatory, anti-feminist, and antiquated [20,21]. In the 1970s and thereafter, with the increasing availability of video EEG monitoring and growth of inpatient epilepsy monitoring units, it was discovered that these hysterical, pseudo-, or what were also by then termed psychogenic seizures, were actually still common [1,22].
More recently, it has been recognized that the pendulum in some cases may have swung too far in regard to the diagnosis of this disorder. Some rare patients with seizures initially diagnosed as PNES may actually have forms of epileptic seizures such as frontal lobe epilepsy or related physiological disorders rather than psychogenic causes for their episodes [1,23]. These types of epileptic seizures can be very difficult to diagnose properly unless one appreciates how they present and manifest and remains vigilant for them during evaluation [1,23].
Terminology
There is an ongoing debate regarding the appropriate terminology for psychogenic events, and there is no uniform standardized definition or classification at this time. The term that is currently preferred within the epilepsy community for seizures of psychological origin that are thought to be associated with conversion, somatization, or dissociative disorders is “psychogenic nonepileptic seizures” (PNES). This terminology is felt to be non-disparaging and more neutral as compared with other terms such as pseudoseizures, which were previously favored. Nonepileptic seizures or nonepileptic events are broader terms meant to incorporate both physiologic and psychological causes for disorders that are mistaken for epilepsy. PNES are widely defined as paroxysmal events that appear similar to epileptic seizures but are not due to abnormal electrical discharges in the brain and as noted, are typically thought to be related or caused by conversion, somatization, or dissociative disorders.
Physiologic nonepileptic events are another category of physical disorders that may be mistaken for epilepsy. The underlying causes differ between age-groups, and can include conditions such as cardiac arrhythmias, migraine variants, syncope, or metabolic abnormalities. Physiologic nonepileptic seizures account for only a small proportion of all patients with nonepileptic seizures or events [1]. In general, any patient with a psychological disorder that causes symptoms that are mistaken for epilepsy can be said to have PNES.
Clinical Characteristics And Presentation
The duration of PNES is often significantly longer than that seen in epileptic seizures, which usually last less than 3 minutes, excluding the postictal period. PNES may also exhibit waxing and waning convulsive activity, although this finding can certainly be seen in epileptic seizures as well. PNES may be shown to have distractibility with external stimuli. Additionally, the movements in PNES may appear asymmetric, asynchronous, or purposeful, although this is not diagnostic for this disorder. This may contrast with the well-defined, synchronous tonic-clonic activity typically seen in epileptic seizures [1,24,25]. Back arching and pelvic thrusting movements can also be seen in PNES. Despite these differences, it may still be challenging to distinguish the semi-purposeful behaviors of PNES from the automatisms of certain focal epileptic seizures. The often bizarre-appearing, hypermotor activity that can be seen in frontal lobe seizures is often especially difficult to differentiate from PNES [1,23].
Another important consideration is that consciousness is preserved in PNES, while consciousness and responsiveness are frequently impaired in epileptic seizures. Patients with PNES are often apparently unresponsive during events, although there is no true impairment of awareness. Other characteristics that are more commonly seen in PNES are crying and eye closure [26]. Self-injury and incontinence may be reported, but they are less often clearly witnessed or documented [27,28]. Additionally, although patients may at times appear to be asleep at seizure onset, EEG recordings document the patient to actually be asleep in less than 1% of cases [29]. While epileptic seizures often respond well to antiepileptic medications, PNES characteristically do not [1,3,6,8].
In certain situations, provocation maneuvers may be utilized in order to reproduce PNES in patients undergoing EEG monitoring. In comparison to epileptic seizures, suggestion and emotional stimuli are more likely to trigger psychogenic events [1]. Methods utilized to provoke PNES may include saline injections, placement of a tuning fork on the head or body, or even hypnosis, when a suggestion is concurrently provided that such maneuvers can trigger the patient’s seizures [1,30,31]. When evaluating seizures that are provoked in such a manner, it is important to consider whether or not the event captured is in fact a typical event for the patient, or whether the provocation has uncovered a different, atypical event. Given that PNES and epileptic seizures can co-exist within the same patient, care should be taken to avoid making a diagnosis based on capturing an atypical event, or capturing only a subset of a patient’s seizure types. This could result in failure to make an accurate and thorough diagnosis [23]. There is debate regarding the ethics of provoking seizures by way of suggestion. Some members of the epilepsy community feel that provoking seizures through suggestion is inherently deceitful, and therefore can damage the physician-patient relationship. Others assert that such provocative testing can be undertaken in an honest manner, and can ultimately help achieve an accurate diagnosis for the patient [32].
As previously mentioned, there is a proportion of patients who have co-existing epileptic seizures and PNES, and obtaining an accurate diagnosis can be especially challenging in this group. Studies have reported that around 10% to 40% of patients with PNES also have epilepsy [1,22,23,33]. Care must be taken to distinguish between differences in seizure types and if necessary, video EEG monitoring may be needed to capture both seizure types for an accurate diagnosis. This testing can then be useful in education with families and caregivers who may be shown the videos with consent from the patient in order to guide future care.
Evaluation And Diagnosis
As in much of neurology, a thorough history, along with detailed clinical observation remains essential in the diagnosis of patients with PNES and for distinguishing these events from epilepsy. Video EEG monitoring of seizures is a key adjunct to the history and clinical observation in diagnosing this condition [1,2]. Long-term video EEG monitoring is considered the “gold standard” in the characterization and differential diagnosis of seizures. Additional potentially helpful diagnostic techniques include video EEG-monitored seizure provocation, serum prolactin levels, single photon emission computed tomography, and neuropsychological testing.
Video EEG Monitoring
![]()
EEG monitoring for characterization of clinical events can be conducted on an ambulatory or outpatient basis or in dedicated inpatient epilepsy monitoring units. Ambulatory monitoring can be useful in the case of patients who report seizures that are more frequent in their home environment or in patients with frequent events. If events are infrequent, then inpatient monitoring may be more efficacious [1]. With longer-term inpatient monitoring, antiepileptic medications can be withdrawn in a supervised setting, in order to lower the seizure threshold as well as to safely discontinue medications that may not be necessary. Such medication titrations are typically not safe in an unsupervised outpatient setting. Some ambulatory EEG monitoring systems do allow for simultaneous video and EEG recording. However, an advantage to inpatient monitoring, which is not afforded in the outpatient setting, is the ability for nursing staff or physicians to perform clinical testing during events to assess for patient responsiveness and other features. Additionally, with inpatient monitoring, EEG technicians can routinely assess for any technical problems with the electrodes or recording system.
Another benefit of video EEG monitoring is that the state (waking, drowsy, or asleep) of the patient at the onset of an event can be established. While epileptic seizures can arise from any state, PNES most often occur from wakefulness. Patients with PNES may appear to be asleep at the onset of events, and they may report seizures from sleep. Video EEG monitoring can help to establish the waking or sleep state of the patient that may aid in diagnosis [29].
Prolactin Levels
Serum prolactin levels may be helpful in the diagnosis of PNES [35,36]. Following generalized tonic-clonic or complex partial epileptic seizures, the serum prolactin can rise from two to threefold to five to tenfold [37]. The maximal rise in serum prolactin occurs in the initial 20 to 60 minutes after the seizure [35–37]. A similar rise in serum prolactin would not be expected in PNES. Although prolactin levels may have some utility in diagnosis, they are not currently routinely ordered as part of a standard admission to most inpatient epilepsy monitoring units. This may be due in part to the fact that false-positive and false-negative results can occur with these levels [37–39]. For example, there may not be a rise in the prolactin level after a simple partial seizure or more subtle complex partial seizure.
Neuropsychological Testing
Neuropsychological testing is also a key component in the evaluation and diagnosis of PNES. Ideally, a mental health provider with a background in psychological assessment and neuropsychological intervention for patients with psychogenic disorders would perform the evaluation [40,41].
The goal of the evaluation should not solely focused on whether the patient suffers from nonepileptic or epileptic seizures. An epileptologist upon review of clinical, electrographic, and neuropsychological data better makes this determination. Moreover, neuropsychological testing cannot in itself either diagnose or exclude the possibility that a seizure disorder is nonepileptic because of the considerable overlap between epileptic and nonepileptic test results [40,41]. Neuropsychological evaluations aid this assessment by (1) determining the potential or likelihood of significant contributing psychopathology or cognitive difficulties, (2) defining the nature of the associated psychological or psychosocial issues, and (3) assessing how a patient might benefit from various psychologically based interventions [1]. The testing may identify psychological problems that can guide treatment after diagnosis.
Delays in Diagnosis
Correct and prompt diagnosis is essential for patients with PNES as is appropriate referral to a knowledgeable trained mental health professional. On average, patients with PNES are diagnosed 7.2 years after manifestation (SD 9.3 years), with mean delay of 5 to 7 years. Younger age, interictal epileptiform potentials in the EEG, and anticonvulsant treatment are associated with longer delays [42,43]. Delays are also thought to occur because of problems with “ownership” of these patients. Although typically neurologists are involved in the diagnosis of PNES, often using video EEG monitoring done in an inpatient setting, the next step is often a referral to a psychiatrist or mental health care provider. There are sometimes delays in the initial referral to the neurologist, delays in referral to specialists for video EEG testing, and also to the physicians, psychologists or social workers who may provide treatment. Another disconnect can occur if patients are “lost to follow-up” if they receive a referral for mental health care and either do not follow up on this on their own, or if the reason for this care is not fully explained. In addition, many mental health professionals are not trained in the evaluation and treatment of psychogenic symptoms and may even feel uncomfortable in dealing with these patients [13,44].
Many studies have been suggestive that delays in diagnosis may result in poorer outcomes [45,46], while other studies have suggested that patients who have an acute diagnosis of PNES upon presentation may do particularly well [8,47–49]. Some of the most recent large outcome studies suggest that there may be no worsening of outcome associated with delays in diagnosis and that outcome was predicted by other factors [50–52].
Management
Management of patients with PNES is similar to that for patients with other types of so-called abnormal illness behavior, although there remains a relative paucity of evidence for specific treatment strategies for PNES [1]. The first consideration should be the manner in which the diagnosis of PNES is presented to the patient and family. It is important to be honest with the patient and demonstrate a positive approach to the diagnosis [53]. The physician should emphasize as favorable or good news the fact that the patient does not have epilepsy, and should also stress that the disorder, although serious and "real," does not require treatment with antiepileptic medications and that once stress or emotional issues are resolved, the patient has the potential to gain better control of these events [1,54,55]. Nevertheless, not all patients readily accept the diagnosis or this type of approach. Some patients may seek other opinions, and this should not be discouraged. An adversarial relationship with the patient should be avoided. The patient should be encouraged to return if desired, and records should be made available to other health care providers to avoid duplication of services.
After the diagnosis of PNES is presented, supportive measures should be initiated. PNES patients may benefit from education and support that can be provided by the neurologist or primary care physician [1]. If the neuropsychological assessment suggests a clinical profile that requires a professional mental health intervention, then an appropriate referral should be made. Regular follow-up visits for the patient with the neurologist are useful even if a mental health professional is involved [49,56]. This allows the patient to get medical attention without demonstrating illness behavior. Patient education and support are stressed at these visits. Because family issues are often important contributing factors, physicians should consider involving family members in visits with consent of the patient [1].
A variety of treatment strategies are employed for the management of PNES including cognitive behavioral therapy (CBT), group and family therapy, antidepressant medication, and other forms of rehabilitation [5,57,58]. A 2007 Cochrane review that identified 608 references for non-medication PNES treatments found that only 3 studies met criteria for a randomized controlled trial. One of the more recently favored treatment options for PNES that has been applied to the treatment of various somatoform disorders and other psychiatric disorders in the past is CBT [57,59,60]. This form of psychotherapy can be administered by trained personnel in a time-limited fashion using defined protocols. The basis of this treatment is that the patient learns to increase awareness of their dysfunctional thoughts and learns new ways to respond to them [57,58]. To date, several groups have reported results of nonrandomized trials as well as case reports and case series which have established the utility of this treatment. There have been reports of significant reductions in seizure frequency and this treatment strategy appears very promising [61–65]. Preliminary randomized controlled trials have also been piloted and are also suggestive that this may be a validated treatment approach [66].
Prognosis
The outcomes of patients with PNES vary. Long-term follow-up studies show that about half of all patients with PNES function reasonably well following their diagnosis. However, only approximately one-third of patients will completely stop having seizures or related problems, and approximately 50% percent have poor functional outcomes [1,2,50]. When the diagnosis of PNES is based on reliable criteria such a video EEG monitoring, misdiagnosis is unlikely. Instead, the usual cause for a poor outcome is related to a patient’s chronic psychological and social problems[1,8,22,50].
It is noteworthy that children with PNES appear to have a much better prognosis than adults [9,10]. In fact, the etiology in children may be related more to transient stress and coping disorders, while adults are more likely to have PNES within the context of more chronic psychological maladjustment, such as personality disorders [10]. Another factor that accounts for the better outcomes in children is that they are usually properly diagnosed earlier in the course of their disorder [9,10].
Patients with milder psychopathology respond better to supportive educational or behavioral therapeutic approaches. In contrast, patients with more severe psychopathology and factitious disorders more often have associated chronic personality problems and correspondingly, a poorer prognosis [1,50]. Also it appears that patients who continue to be followed by the diagnosing neurologist or center do better than patients who are not seen after diagnosis [49,67]. As knowledge about the nature of PNES and their associated psychopathology is gained, better treatment strategies can be developed that will improve the care and prognosis of these difficult and challenging patients.
A large study of 164 patients who were followed for 10 years were considered to have “poor outcome” in general but favorable factors included higher education, younger age of onset and diagnosis, and less “dramatic” attacks, defined as lack of “positive motor features, no ictal incontinence or tongue biting.” These findings were consistent with prior studies [52,68].
In addition, the patients who tended to have less seizures and do better long term, had less somatoform and dissociative symptoms on psychometric testing [51]. These findings are often explained by the theory that patients who do not do well have poor coping strategies to deal with stress and anxiety and that in a sense, these patients have emotional dysregulation.
Special Issues
Coexisting Epileptic and Psychogenic Nonepileptic Seizures
A complicating factor in diagnosis is that both PNES and epileptic seizures may occur in a single patient. Indeed, approximately 10% to 40% of patients identified to have PNES also have been reported to have epileptic seizures [1,23,33,56]. There are several possible explanations for this. Some patients with epilepsy may learn that seizures result in attention and fill certain psychological needs. Alternatively, they may have concomitant neurologic problems, personality disorders, cognitive deficits, or impaired coping mechanisms that predispose them to psychogenic symptoms [69–71]. Fortunately, in such patients with combined seizure disorders, the epileptic seizures are usually well controlled or of only historical relevance at the time a patient develops PNES [1,22,23,33,72–74].
In other patients, both epileptic and PNES may start simultaneously, making management even more complex. In such patients, we have found it particularly helpful to focus on the semiology of seizure manifestations as recorded by video EEG monitoring to distinguish PNES from the epileptic seizures. We then direct our treatment of the patient according to the semiology manifesting at that time. We also have found it useful to show the videos of seizures to family members or caregivers with patient consent to help them understand how to respond best to a patient’s symptoms when epileptic and PNES co-exist.
Misdiagnosis of Psychogenic Nonepileptic Seizures
Sometimes events that are initially diagnosed as nonepileptic actually prove to be epileptic. Such events can be called “pseudo-pseudo” or “epileptic-nonepileptic” seizures [1]. Frontal lobe seizures in particular may not be associated with significant EEG changes ictally and therefore misdiagnosed as PNES [23,75,76]. Clinical presentation and proper diagnosis of these types of events warrant emphasis.
Notable manifestations of frontal lobe seizures that may easily be confused with hysterical behavior include shouting, laughing, cursing, clapping, snapping, genital manipulation, pelvic thrusting, pedaling, running, kicking, and thrashing [23,75–77]. Not all of these behaviors are specific for frontal lobe seizures. For example, bicycling leg movements have also been reported in seizures originating from the temporal lobe [78].
Summary
PNES represent a common yet challenging problem within neurology. This is due to the difficulty in diagnosis as well as lack of effective and widely available treatment options. Overall outcomes of patients with PNES vary, and may relate to an individual patient’s chronic psychological and social problems. However, an accurate and timely diagnosis remains critical and can help provide direction for implementing appropriate treatment.
Corresponding author: Jennifer Hopp, MD, Department of Neurology, University of Maryland Medical Center, Room S12C09, 22 South Greene Street, Baltimore, MD 21201, [email protected].
Financial disclosures: None.
1. Krumholz A. Nonepileptic seizures: diagnosis and management. Neurology 1999;S76–83.
2. Meierkord H, Will B, Fish D, Shorvon S. The clinical features and prognosis of pseudoseizures diagnosed using video-EEG telemetry. Neurology 1991;41:1643–6.
3. Lesser RP. Psychogenic seizures. Neurology 1996;46:1499–1507.
4. Sigurdardottir KR, Olafsson E. Incidence of psychogenic seizures in adults: a population-based study in Iceland. Epilepsia 1998;39:857–62.
5. Szaflarski JP, Szaflarski M, Hughes C, et al. Psychopathology and quality of life: psychogenic non-epileptic seizures versus epilepsy. Med Sci Monit 2003 9:CR113–8.
6. Barry E, Krumholz A, Bergey C, et al. Nonepileptic posttraumatic seizures. Epilepsia 1998;39:427–31.
7. Pakalnis A, Drake ME, Phillips B. Neuropsychiatric aspects of psychogenic status epilepticus. Neurology 1991;41;1104–6.
8. Walzack TS, Papacostas S, Williams DT, et al. Outcome after the diagnosis of psychogenic nonepileptic seizures. Epilepsia 1995;36:1131–7.
9. Metrick ME, Ritter FJ, Gates JR, et al. Nonepileptic events in childhood. Epilepsia 1991;32:322–8.
10. Wyllie E, Friedman D, Luders H, et al. Outcome of psychogenic seizures in children and adolescents compared to adults. Neurology 1991;41:742–4.
11. Duncan R, Oto M. Predictors of antecedent factors in psychogenic nonepileptic attacks: multivariate analysis. Neurology 2008;71:1000–5.
12. Alper K, Devinsky O, Perrine K, et al. Nonepileptic seizures and childhood sexual and physical abuse. Neurology 1993; 43:1950–3.
13. LaFrance WC Jr, Devinsky O. The treatment of nonepileptic seizures: historical perspectives and future directions. Epilepsia 2004;45 Suppl 2:15–21.
14. Westbrook LE, Devinsky O, Geocadin R. Nonepileptic seizures after head injury. Epilepsia 1998;39:978–82.
15. Slavney PR. Perspectives on hysteria. Baltimore: Johns Hopkins University Press; 1990.
16. Veith I. Hysteria: the history of a disease. Chicago: University of Chicago Press; 1965.
17. Goetz CG. Charcot the clinician. The Tuesday lessons. New York: Raven Press; 1987.
18. Massey EW, McHenry LC. Hysteroepilepsy in the nineteenth century: Charcot and Gowers. Neurology 1986;36:65–7.
19. Zeigler FJ, Imboden JB, Meyer E. Contemporary conversion reactions: a clinical study. Am J Psychiatry 1960;116:901–10.
20. Liske E, Forster FM. Pseudoseizures: a problem in the diagnosis and management of epileptic patients. Neurology 1964;14:41–9.
21. Diagnostic and statistical manual of mental disorders. DSM-IV 4th ed. American Psychiatric Association. Washington, DC; 1995.
22. Krumholz A, Niedermeyer, E. Psychogenic seizures: a clinical study with follow-up data. Neurology 1983; 33:498-502.
23. Krumholz A, Ting T. Co-existing epileptic and nonepileptic seizures. in imitators of epilepsy. 2nd ed. In: Kaplan PW, Fisher RS, editors. New York: Demos Medical Publishing; 2005:261–76.
24. Gates JR, Ramani V, Whalen S, Loewenson R. Ictal characteristics of pseudoseizures. Arch Neurol 1985;42:1183–87.
25. Leis AA, Ross MA, Summers AK. Psychogenic seizures: Ictal characteristics and diagnostic pitfalls. Neurology 1992;42:95–9.
26. Walczak TS, Bogolioubov. Weeping during psychogenic nonepileptic seizures. Epilepsia 1996;37:207–10.
27. Bergen D, Ristanovic R. Weeping is a common element during psychogenic nonepileptic seizures. Arch Neurol 1993;50:1059–60.
28. Peguero E, Abou-Khalil B, Fakhoury, Mathews G. Self-injury and incontinence in psychogenic seizures. Epilepsia 1995;36:586–91.
29. Orbach D, Ritaccio A, Devinsky O. Psychogenic, nonepileptic seizures associated with video-EEG-verified sleep. Epilepsia 2003;44:64–8.
30. Walczak TS, Williams DT, Berton W. Utility and reliability of placebo infusion in the evaluation of patients with seizures. Neurology 1994;44:394–99.
31. Bazil CW, Kothari M, Luciano D, et al. Provocation of nonepileptic seizures by suggestion in a general seizure population. Epilepsia 1994;35:768–70.
32. Devinsky O, Fisher RS. Ethical use of placebos and provocative testing in diagnosing nonepileptic seizures. Neurology 1996;47:866–70.
33. Lesser RP, Lueders H, Dinner DS. Evidence for epilepsy is rare in patients with psychogenic seizures. Neurology 1983; 33:502–4.
34. Barre MA, Burnstine TH, Fisher RS, Lesser RP. Electroencephalographic changes during simple partial seizures. Epilepsia 1994;35:715–20.
35. Trimble MR. Serum prolactin levels in epilepsy and hysteria. BMJ 1978;2:1682.
36. Laxer KD, Mullooly JP, Howell B. Prolactin changes after seizures classified by EEG monitoring. Neurology 1985; 35:31–5.
37. Pritchard PB, Wannamaker BB, Sagel J, et al. Endocrine function following complex partial seizures. Ann Neurol 1983;14:27–32.
38. Malkowicz DE, Legido A, Jackel RA, et al. Prolactin secretion following repetitive seizures. Neurology 1995;45:448–52.
39. Oribe E, Rohullah A, Nissenbaum E, Boal B. Serum prolactin concentrations are elevated after syncope. Neurology 1996;47:60–2.
40. Henrichs TF, Tucker DM, Farha J, Novelly RA. MMPI indices in the identification of patients evidencing pseudoseizures. Epilepsia 1988;29:184–8.
41. Wilkus RJ, Dodrill CB. Factors affecting the outcome of MMPI and neuropsychological assessments of psychogenic and epileptic seizure patients. Epilepsia 1989;30:339–47.
42. DeTimary P, Fouchet P, Sylin M, et al. Non–epileptic seizures: delayed diagnosis in patients presenting with electroencephalographic (EEG) or clinical signs of epileptic seizures. Seizure 2002;11:193–7.
43. Reuber M, Fernandez G, et al. Diagnostic delay in psychogenic nonepileptic seizures. Neurology 2002;58:493–5.
44. Rosenbaum DH, et al. Outpatient multidisciplinary management of non-epileptic seizures. In: Rowan AJ, Gates Jr, editors. Non-epileptic seizures. 1st ed. Stoneham, MA: Butterworth-Heinemann; 1993:275–83.
45. Lempert T, Schmidt D. Natural history and outcome of psychogenic seizures: a clinical study in 50 patients. J Neurol 1990;237:35–8.
46. Selwa LM, Geyer J, Nikakhtar N, et al. Nonepileptic seizure outcome varies by type of spell and duration of illness. Epilepsia 2000;41:1330–4.
47. Buchanan N, Snars J. Pseudoseizures (non epileptic attack disorder): clinical management and outcome in 50 patients. Seizure 1993;2:141–6.
48. Kanner AM. More controversies on the treatment of psychogenic pseudoseizures: an addendum. Epilepsy Behav 2003;4:360–4.
49. Aboukasm A, Mahr G, Gahry BR, et al. Retrospective analysis of the effects of psychotherapeutic interventions on outcomes of psychogenic nonepileptic seizures. Epilepsia 1998;39:470–3.
50. Reuber M, Pukrop T, Bauer J, et al. Outcome in psychogenic nonepileptic seizures: 1 to 10-year follow-up in 164 patients. Ann Neurol 2003;53:305–11.
51. McKenzie P, Oto M, Russell A, Pelosi A, Duncan R. Early outcomes and predictors in 260 patients with psychogenic nonepileptic seizures (PNES). Neurology 2010;74:64–9.
52. Kanner AM, Parra J, Frey M, et al. Psychiatric and neurologic predictors of psychogenic pseudoseizure outcome. Neurology 1999;53:933–8.
53. Shen W, Bowman ES, Markand ON. Presenting the diagnosis of pseudoseizure. Neurology 1990; 40:756–9.
54. Friedman JH, LaFrance Jr WC. Psychogenic disorders: the need to speak plainly. Arch Neurol 2010;67:753–5.
55. LaFrance Jr WC. Psychogenic nonepileptic “seizures” or “attacks”? It’s not just semantics: “Seizures.” Neurology 2010;75: 87–8.
56. Ramsay RE, Cohen A, Brown MC. Coexisting epilepsy and non-epileptic seizures. In: Non-epileptic seizures. Butterworth-Heinemann; 1998:47–54.
57. Stone J, Carson A, Sharpe M. Functional symptoms in neurology: management. J Neurol Neurosurg Psychiatry. 2005;6(Suppl 1):i13–i21.
58. LaFrance WC Jr, Bjornaes H. Designing treatment plans based on etiology of psychogenic nonepileptic seizures. In: Schachter SC, LaFrance WC Jr, editors. Gates and Rowan’s nonepileptic seizures. 3rd ed. New York: Cambridge University Press; 2010:266–80.
59. Kroenke K, Swindle R. Cognitive-behavioral therapy for somatization and symptom syndromes: a critical review of controlled clinical trials. Psychother Psychosom 200;69:205–15.
60. Kroenke K. Efficacy of treatment of somatoform disorders: a review of randomized controlled trials. Psychosom Med 2007:69:881–8.
61. LaFrance WC Jr, Miller IW, Ryan CE, et al. Cognitive behavioral therapy for psychogenic nonepileptic seizures. Epilepsy Behav 2009;14:591–6.
62. Chalder T. Non-epileptic attacks: a cognitive behavioral approach in a single case with a four-year follow-up. Clin Psychol Psychother 1996;3:291–7.
63. Betts T, Duffy N. Non-epileptic attack disorder (pseudoseizures) and sexual abuse: a review. In: Gram L, Johannessen SI, Osterman PE, et al, editors. Pseudo-epileptic seizures. Petersfield, UK: Wrightson Biomedical Publishing; 1993:55–66.
64. Lesser RP. Treatment and outcome of psychogenic nonepileptic seizures. Epilepsy Currents 2003;3:198–200.
65. Ramani V. Review of psychiatric treatment strategies in non-epileptic seizures. In: Rowan AJ, Gates JR, eds. Non-epileptic Seizures. 1st ed. Stoneham, MA: Butterworth Heinemann; 1993:259–67.
66. Goldstein LH, Chalder T, Chigwedere C, et al. Cognitive-behavioral therapy for psychogenic nonepileptic seizures: a pilot RCT. Neurology 2010;74:1986–94.
67. Bennet C, So NM, Smith WB, Thompson K. Structured treatment improves the outcome of nonepileptic events. Epilepsia 1997;38(Suppl 8):214.
68. McDade G, Brown SW. Non-epileptic seizures: management and predictive factors of outcome. Seizure 1992;1:7–10.
69. Bowman ES. Etiology and clinical course of pseudoseizures: relationship to trauma, depression, and dissociation. Psychosomatics 1993;34:333–42.
70. Bowman ES, Markand ON. Psychodynamics and psychiatric diagnoses of pseudoseizure subjects. Am J Psychiatry 1996;153:57–63.
71. Vanderzant CW, Giordani B, Berent S, et al. Personality of patients with pseudoseizures. Neurology 1986;36:664–8.
72. Benbadis SR, Agrawal V, Tatum WO. How many patients with psychogenic nonepileptic seizures also have epilepsy? Neurology 2001; 57:915–7.
73. Glosser G, Roberts D, et al. Nonepileptic seizures after resective epilepsy surgery. Epilepsia 1999; 40:1750–4.
74. Reuber M, Kral T. New-onset psychogenic seizures after intracranial neurosurgery. Acta Neurochir (Wien) 2002; 144:901–7.
75. Williamson P, Spencer D, Spencer S, et al. Complex partial seizures of frontal lobe origin. Ann Neurol 1985;18:497–504.
76. Saygi S, Katz A, Marks D, et al. Frontal lobe partial seizures and psychogenic seizures: comparison of clinical and ictal characteristics. Neurology 1992;42:1274–7.
77. Waterman K, Purves S, Kosaka B, et al. An epileptic syndrome caused by mesial frontal lobe seizure foci. Neurology 1987; 37:577–82.
78. Sussman N, Jackel R, Kaplan L, et al. Bicycling movements as a manifestation of complex partial seizures of temporal lobe origin. Epilepsia 1989;30:527–31.
1. Krumholz A. Nonepileptic seizures: diagnosis and management. Neurology 1999;S76–83.
2. Meierkord H, Will B, Fish D, Shorvon S. The clinical features and prognosis of pseudoseizures diagnosed using video-EEG telemetry. Neurology 1991;41:1643–6.
3. Lesser RP. Psychogenic seizures. Neurology 1996;46:1499–1507.
4. Sigurdardottir KR, Olafsson E. Incidence of psychogenic seizures in adults: a population-based study in Iceland. Epilepsia 1998;39:857–62.
5. Szaflarski JP, Szaflarski M, Hughes C, et al. Psychopathology and quality of life: psychogenic non-epileptic seizures versus epilepsy. Med Sci Monit 2003 9:CR113–8.
6. Barry E, Krumholz A, Bergey C, et al. Nonepileptic posttraumatic seizures. Epilepsia 1998;39:427–31.
7. Pakalnis A, Drake ME, Phillips B. Neuropsychiatric aspects of psychogenic status epilepticus. Neurology 1991;41;1104–6.
8. Walzack TS, Papacostas S, Williams DT, et al. Outcome after the diagnosis of psychogenic nonepileptic seizures. Epilepsia 1995;36:1131–7.
9. Metrick ME, Ritter FJ, Gates JR, et al. Nonepileptic events in childhood. Epilepsia 1991;32:322–8.
10. Wyllie E, Friedman D, Luders H, et al. Outcome of psychogenic seizures in children and adolescents compared to adults. Neurology 1991;41:742–4.
11. Duncan R, Oto M. Predictors of antecedent factors in psychogenic nonepileptic attacks: multivariate analysis. Neurology 2008;71:1000–5.
12. Alper K, Devinsky O, Perrine K, et al. Nonepileptic seizures and childhood sexual and physical abuse. Neurology 1993; 43:1950–3.
13. LaFrance WC Jr, Devinsky O. The treatment of nonepileptic seizures: historical perspectives and future directions. Epilepsia 2004;45 Suppl 2:15–21.
14. Westbrook LE, Devinsky O, Geocadin R. Nonepileptic seizures after head injury. Epilepsia 1998;39:978–82.
15. Slavney PR. Perspectives on hysteria. Baltimore: Johns Hopkins University Press; 1990.
16. Veith I. Hysteria: the history of a disease. Chicago: University of Chicago Press; 1965.
17. Goetz CG. Charcot the clinician. The Tuesday lessons. New York: Raven Press; 1987.
18. Massey EW, McHenry LC. Hysteroepilepsy in the nineteenth century: Charcot and Gowers. Neurology 1986;36:65–7.
19. Zeigler FJ, Imboden JB, Meyer E. Contemporary conversion reactions: a clinical study. Am J Psychiatry 1960;116:901–10.
20. Liske E, Forster FM. Pseudoseizures: a problem in the diagnosis and management of epileptic patients. Neurology 1964;14:41–9.
21. Diagnostic and statistical manual of mental disorders. DSM-IV 4th ed. American Psychiatric Association. Washington, DC; 1995.
22. Krumholz A, Niedermeyer, E. Psychogenic seizures: a clinical study with follow-up data. Neurology 1983; 33:498-502.
23. Krumholz A, Ting T. Co-existing epileptic and nonepileptic seizures. in imitators of epilepsy. 2nd ed. In: Kaplan PW, Fisher RS, editors. New York: Demos Medical Publishing; 2005:261–76.
24. Gates JR, Ramani V, Whalen S, Loewenson R. Ictal characteristics of pseudoseizures. Arch Neurol 1985;42:1183–87.
25. Leis AA, Ross MA, Summers AK. Psychogenic seizures: Ictal characteristics and diagnostic pitfalls. Neurology 1992;42:95–9.
26. Walczak TS, Bogolioubov. Weeping during psychogenic nonepileptic seizures. Epilepsia 1996;37:207–10.
27. Bergen D, Ristanovic R. Weeping is a common element during psychogenic nonepileptic seizures. Arch Neurol 1993;50:1059–60.
28. Peguero E, Abou-Khalil B, Fakhoury, Mathews G. Self-injury and incontinence in psychogenic seizures. Epilepsia 1995;36:586–91.
29. Orbach D, Ritaccio A, Devinsky O. Psychogenic, nonepileptic seizures associated with video-EEG-verified sleep. Epilepsia 2003;44:64–8.
30. Walczak TS, Williams DT, Berton W. Utility and reliability of placebo infusion in the evaluation of patients with seizures. Neurology 1994;44:394–99.
31. Bazil CW, Kothari M, Luciano D, et al. Provocation of nonepileptic seizures by suggestion in a general seizure population. Epilepsia 1994;35:768–70.
32. Devinsky O, Fisher RS. Ethical use of placebos and provocative testing in diagnosing nonepileptic seizures. Neurology 1996;47:866–70.
33. Lesser RP, Lueders H, Dinner DS. Evidence for epilepsy is rare in patients with psychogenic seizures. Neurology 1983; 33:502–4.
34. Barre MA, Burnstine TH, Fisher RS, Lesser RP. Electroencephalographic changes during simple partial seizures. Epilepsia 1994;35:715–20.
35. Trimble MR. Serum prolactin levels in epilepsy and hysteria. BMJ 1978;2:1682.
36. Laxer KD, Mullooly JP, Howell B. Prolactin changes after seizures classified by EEG monitoring. Neurology 1985; 35:31–5.
37. Pritchard PB, Wannamaker BB, Sagel J, et al. Endocrine function following complex partial seizures. Ann Neurol 1983;14:27–32.
38. Malkowicz DE, Legido A, Jackel RA, et al. Prolactin secretion following repetitive seizures. Neurology 1995;45:448–52.
39. Oribe E, Rohullah A, Nissenbaum E, Boal B. Serum prolactin concentrations are elevated after syncope. Neurology 1996;47:60–2.
40. Henrichs TF, Tucker DM, Farha J, Novelly RA. MMPI indices in the identification of patients evidencing pseudoseizures. Epilepsia 1988;29:184–8.
41. Wilkus RJ, Dodrill CB. Factors affecting the outcome of MMPI and neuropsychological assessments of psychogenic and epileptic seizure patients. Epilepsia 1989;30:339–47.
42. DeTimary P, Fouchet P, Sylin M, et al. Non–epileptic seizures: delayed diagnosis in patients presenting with electroencephalographic (EEG) or clinical signs of epileptic seizures. Seizure 2002;11:193–7.
43. Reuber M, Fernandez G, et al. Diagnostic delay in psychogenic nonepileptic seizures. Neurology 2002;58:493–5.
44. Rosenbaum DH, et al. Outpatient multidisciplinary management of non-epileptic seizures. In: Rowan AJ, Gates Jr, editors. Non-epileptic seizures. 1st ed. Stoneham, MA: Butterworth-Heinemann; 1993:275–83.
45. Lempert T, Schmidt D. Natural history and outcome of psychogenic seizures: a clinical study in 50 patients. J Neurol 1990;237:35–8.
46. Selwa LM, Geyer J, Nikakhtar N, et al. Nonepileptic seizure outcome varies by type of spell and duration of illness. Epilepsia 2000;41:1330–4.
47. Buchanan N, Snars J. Pseudoseizures (non epileptic attack disorder): clinical management and outcome in 50 patients. Seizure 1993;2:141–6.
48. Kanner AM. More controversies on the treatment of psychogenic pseudoseizures: an addendum. Epilepsy Behav 2003;4:360–4.
49. Aboukasm A, Mahr G, Gahry BR, et al. Retrospective analysis of the effects of psychotherapeutic interventions on outcomes of psychogenic nonepileptic seizures. Epilepsia 1998;39:470–3.
50. Reuber M, Pukrop T, Bauer J, et al. Outcome in psychogenic nonepileptic seizures: 1 to 10-year follow-up in 164 patients. Ann Neurol 2003;53:305–11.
51. McKenzie P, Oto M, Russell A, Pelosi A, Duncan R. Early outcomes and predictors in 260 patients with psychogenic nonepileptic seizures (PNES). Neurology 2010;74:64–9.
52. Kanner AM, Parra J, Frey M, et al. Psychiatric and neurologic predictors of psychogenic pseudoseizure outcome. Neurology 1999;53:933–8.
53. Shen W, Bowman ES, Markand ON. Presenting the diagnosis of pseudoseizure. Neurology 1990; 40:756–9.
54. Friedman JH, LaFrance Jr WC. Psychogenic disorders: the need to speak plainly. Arch Neurol 2010;67:753–5.
55. LaFrance Jr WC. Psychogenic nonepileptic “seizures” or “attacks”? It’s not just semantics: “Seizures.” Neurology 2010;75: 87–8.
56. Ramsay RE, Cohen A, Brown MC. Coexisting epilepsy and non-epileptic seizures. In: Non-epileptic seizures. Butterworth-Heinemann; 1998:47–54.
57. Stone J, Carson A, Sharpe M. Functional symptoms in neurology: management. J Neurol Neurosurg Psychiatry. 2005;6(Suppl 1):i13–i21.
58. LaFrance WC Jr, Bjornaes H. Designing treatment plans based on etiology of psychogenic nonepileptic seizures. In: Schachter SC, LaFrance WC Jr, editors. Gates and Rowan’s nonepileptic seizures. 3rd ed. New York: Cambridge University Press; 2010:266–80.
59. Kroenke K, Swindle R. Cognitive-behavioral therapy for somatization and symptom syndromes: a critical review of controlled clinical trials. Psychother Psychosom 200;69:205–15.
60. Kroenke K. Efficacy of treatment of somatoform disorders: a review of randomized controlled trials. Psychosom Med 2007:69:881–8.
61. LaFrance WC Jr, Miller IW, Ryan CE, et al. Cognitive behavioral therapy for psychogenic nonepileptic seizures. Epilepsy Behav 2009;14:591–6.
62. Chalder T. Non-epileptic attacks: a cognitive behavioral approach in a single case with a four-year follow-up. Clin Psychol Psychother 1996;3:291–7.
63. Betts T, Duffy N. Non-epileptic attack disorder (pseudoseizures) and sexual abuse: a review. In: Gram L, Johannessen SI, Osterman PE, et al, editors. Pseudo-epileptic seizures. Petersfield, UK: Wrightson Biomedical Publishing; 1993:55–66.
64. Lesser RP. Treatment and outcome of psychogenic nonepileptic seizures. Epilepsy Currents 2003;3:198–200.
65. Ramani V. Review of psychiatric treatment strategies in non-epileptic seizures. In: Rowan AJ, Gates JR, eds. Non-epileptic Seizures. 1st ed. Stoneham, MA: Butterworth Heinemann; 1993:259–67.
66. Goldstein LH, Chalder T, Chigwedere C, et al. Cognitive-behavioral therapy for psychogenic nonepileptic seizures: a pilot RCT. Neurology 2010;74:1986–94.
67. Bennet C, So NM, Smith WB, Thompson K. Structured treatment improves the outcome of nonepileptic events. Epilepsia 1997;38(Suppl 8):214.
68. McDade G, Brown SW. Non-epileptic seizures: management and predictive factors of outcome. Seizure 1992;1:7–10.
69. Bowman ES. Etiology and clinical course of pseudoseizures: relationship to trauma, depression, and dissociation. Psychosomatics 1993;34:333–42.
70. Bowman ES, Markand ON. Psychodynamics and psychiatric diagnoses of pseudoseizure subjects. Am J Psychiatry 1996;153:57–63.
71. Vanderzant CW, Giordani B, Berent S, et al. Personality of patients with pseudoseizures. Neurology 1986;36:664–8.
72. Benbadis SR, Agrawal V, Tatum WO. How many patients with psychogenic nonepileptic seizures also have epilepsy? Neurology 2001; 57:915–7.
73. Glosser G, Roberts D, et al. Nonepileptic seizures after resective epilepsy surgery. Epilepsia 1999; 40:1750–4.
74. Reuber M, Kral T. New-onset psychogenic seizures after intracranial neurosurgery. Acta Neurochir (Wien) 2002; 144:901–7.
75. Williamson P, Spencer D, Spencer S, et al. Complex partial seizures of frontal lobe origin. Ann Neurol 1985;18:497–504.
76. Saygi S, Katz A, Marks D, et al. Frontal lobe partial seizures and psychogenic seizures: comparison of clinical and ictal characteristics. Neurology 1992;42:1274–7.
77. Waterman K, Purves S, Kosaka B, et al. An epileptic syndrome caused by mesial frontal lobe seizure foci. Neurology 1987; 37:577–82.
78. Sussman N, Jackel R, Kaplan L, et al. Bicycling movements as a manifestation of complex partial seizures of temporal lobe origin. Epilepsia 1989;30:527–31.
Finding the Optimum in the Use of Elective Percutaneous Coronary Intervention
From the VA Eastern Colorado Health Care System, University of Colorado School of Medicine, and the Colorado Cardiovascular Outcomes Research Group, Denver and Aurora, CO.
Abstract
- Objective: To review the use of elective percutaneous coronary intervention (PCI), evaluate what is currently known about elective PCI in the context of appropriate use criteria, and offer insight into next steps to optimize the use of elective PCI to achieve high-quality care.
- Methods: Review of the scientific literature, appropriate use criteria, and professional society guidelines relevant to elective PCI.
- Results: Recent studies have demonstrated as many as 1 in 6 elective PCIs are inappropriate as determined by appropriate use criteria. These inappropriate PCIs are not anticipated to benefit patients and result in unnecessary patient risk and cost. While these studies are consistent with regard to overuse of elective PCI, less is known about potential underuse of PCI for elective indications. We lack health status data on populations of ischemic heart disease patients to inform PCI underuse that may contribute to patient symptom burden, functional status, and quality of life. Optimal use of PCI will be attained with longitudinal capture of patient-reported health status, study of factors contributing to overuse and underuse, refinement of the appropriate use criteria with particular focus on patient-centered measures, and incorporation of patient preference and shared decision making into appropriateness evaluation tools.
- Conclusion: The use of elective PCI is less than optimal in current clinical practice. Continued effort is needed to ensure elective PCI is targeted to patients with anticipated benefit and use of the procedure is aligned with patient preferences.
Providing the right care to the right patient at the right time is essential to the practice of high-quality care. Reducing overuse of health care services is part of this equation, and initiatives to reduce inappropriate use and to encourage physicians and patients to “choose wisely” have been introduced [1]. One procedure that is being examined with a focus on appropriateness is percutaneous coronary intervention (PCI). This procedure is common (nearly 1 million inpatient PCI procedures performed in 2010), presents risks to the patient, and is expensive (attributable cost approximately $10 billion in 2010) [2,3]. While the clinical benefit of PCI in acute settings such as ST-segment elevation myocardial infarction is well established [4], the benefit of PCI in nonacute (elective) settings is less robust [5–7]. Prior studies have demonstrated PCI for stable ischemic heart disease does not result in mortality benefit [6]. Furthermore, PCI as an initial strategy for symptom relief of stable angina may offer little benefit relative to medications alone [5]. Given that PCI is common, costly, and associated with both short- and long-term risks [8,9], ensuring this therapy is provided to the right patient at the right time is important.
In 2009, appropriate use criteria (AUC) were developed by 6 professional organizations to support the rational and judicious use of PCI [10]; a focused update was published in 2012 [11]. In this review, we discuss the recommendations for appropriate use and their application and offer thoughts on next steps to optimize the use of elective PCI as part of high-quality care.
Variation in the Use of PCI
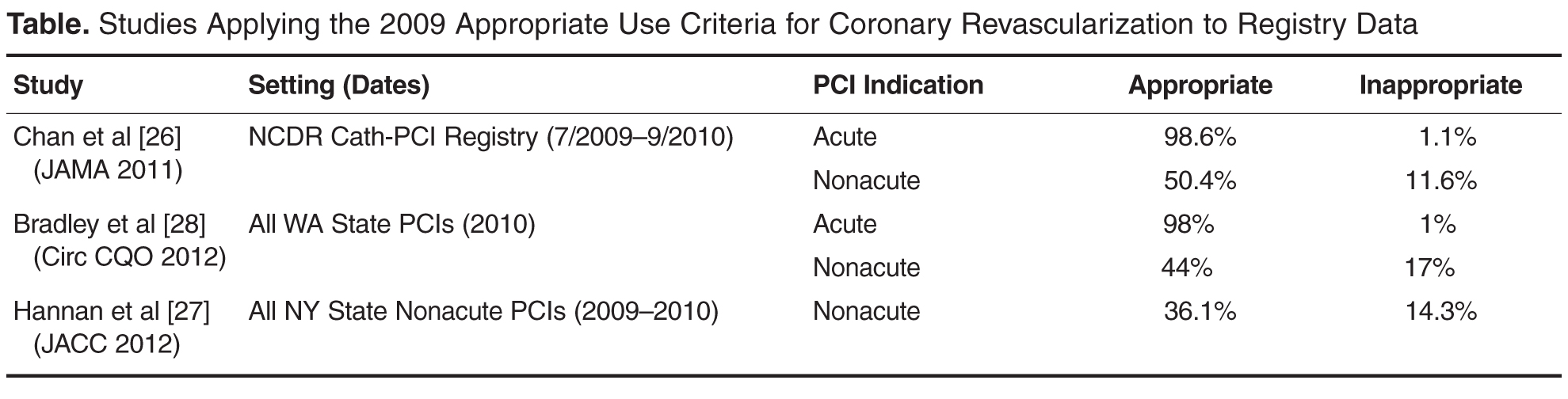
Additionally, significant public attention has been focused on the issue of overuse after lay press investigations into community practice patterns. In particular, a case study presented in the New York Times highlighted the community of Elyria, Ohio, which was found to have a PCI rate that was 4 times the national average [16]. This investigation sparked public debate and further focused attention on the issue of overuse of elective PCI. Conversely, others have pointed to data that suggest underuse of coronary procedural care, particularly among women and racial and ethnic minorities [17–22].
Appropriate Use Criteria
Development Methodology
AUC for PCI, which were developed through the collaborative efforts of 6 major cardiovascular professional organizations, are intended to support the effective, efficient, and equitable use of PCI [10,11]. They were developed in response to a growing need to support rational use of cardiovascular procedures as part of high-quality care. The methods of development for the AUC have been described in detail in the criteria publications [10,11]. We briefly review these methods here.
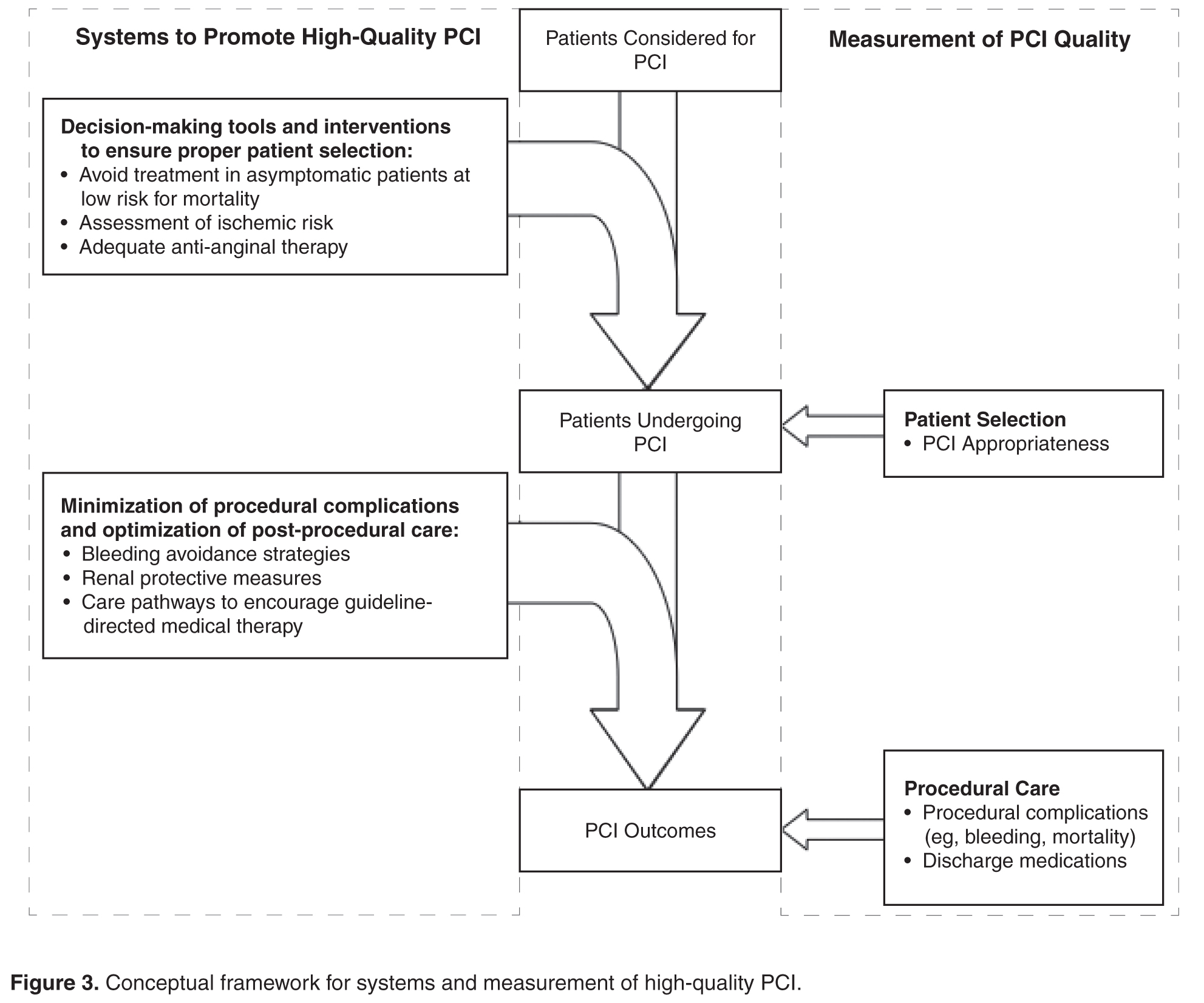
Panel members first individually assigned ratings to each clinical scenario that ranged from 1 (least appropriate) to 9 (most appropriate). This was followed by an in-person meeting in which technical panel members discussed scenarios for which there was wide variation in appropriateness assessment. After this meeting, technical panel members again assigned ratings for each scenario from 1 to 9. After this second round, the median values for the pooled ratings were used as the appropriateness classification for each scenario. Scenarios with median values of 1–3 were classified as “inappropriate,” 4–6 as “uncertain,” and 7–9 as “appropriate.” A rating of “appropriate” represented clinical scenarios in which the indication is considered generally acceptable and likely to improve health outcomes or survival. A rating of “uncertain” represented clinical scenarios where the indication may be reasonable but more research is necessary to further understand the relative benefits and risks of PCI in this setting. Finally, a rating of “inappropriate” represented clinical scenarios in which the indication is not generally acceptable as it is unlikely to improve health outcomes or survival.
The approach used for AUC development appears to be valid, as Class III indications for PCI in the ACC/AHA clinical guideline [24] (Class III = PCI should NOT be performed since it is not helpful and may be harmful) and AUC scenarios rated as inappropriate are in 100% agreement (personal communication, Ralph Brindis, past president of the American College of Cardiology).
Application
It is important to remember that the AUC are intended to aid in patient selection and are not absolute. Unique clinical factors and patient preference cannot feasibly be captured by the AUC scenarios. It should also be noted that the intent of the AUC is not to be punitive but rather to identify and assess variation in practice patterns. To reflect this intent, the terminology applied to appropriateness ratings has recently changed. Clinical scenarios previously classified as “inappropriate” are now termed “rarely appropriate” and clinical scenarios classified as “uncertain” are now termed “may be appropriate.”
Although the AUC were developed to help evaluate practice patterns of care delivery and serve as guides for clinical decision making, they were not intended to serve as mandates for or against treatment in individual patients or to be tied to reimbursement for individual patients. Despite this, health care organizations and payors have used other AUC documents for incentive pay and prior authorization programs, specifically for cardiovascular imaging [25]. Use of the AUC in this manner may still be reasonable if application and measurement is at the level of the practice, rather than the individual patient, but much remains to be understood about the implications of applying AUC in reimbursement
decisions.
Refinement
The AUC for PCI are designed to be dynamic and continually updated. As additional evidence becomes available regarding the efficacy of PCI in specific clinical scenarios, there will be ongoing efforts to update the AUC to reflect this new evidence. This is highlighted by the first update to the AUC occurring less than 3 years after the original publication date [11].
In addition to perpetual review of the data used to inform scenario ratings, there are opportunities to improve measurement of the clinical variables that are considered in rating PCI appropriateness (eg, clinical presentation, symptom severity, ischemia severity, extent of medical therapy, extent of anatomic disease). For example, in the current AUC, symptom severity is dependent on clinician assessment using the Canadian Cardiovascular Society Classification [25]. Moving toward a patient-centered assessment of symptom severity would ensure that the AUC more closely reflect the patient-perceived symptom burden. Further, the use of a patient-centered instrument would reduce the possibility of physician manipulation of symptom severity to influence the apparent appropriateness of PCI. There are similar opportunities to improve reporting of noninvasive stress test data, such as through standardized reporting of ischemic risk. Finally, the use of physiologic assessments of stenosis severity (eg, fractional flow reserve) and quantitative coronary angiography to standardize interpretations of diagnostic angiography may further optimize the assessment of PCI appropriateness.
Application of the Appropriate Use Criteria in Clinical Practice—Study Results
 Application of the AUC to clinical practice has highlighted potential overuse of PCI (Table). The first report came from applying the AUC to the National Cardiovascular Data Registry (NCDR) CathPCI Registry [26]. In this study of more than 500,000 PCIs from over 1000 facilities across the country, the authors found that PCIs performed in the acute setting (STEMI, NSTEMI, and high-risk unstable angina) were almost uniformly classified as appropriate. However, for nonacute (elective) PCI, application of the AUC resulted in the classification of 50% as appropriate, 38% as uncertain, and 12% as inappropriate. The majority of patients who received inappropriate PCI had a low-risk stress test (72%) or were asymptomatic (54%). Additionally, 96% of patients who received PCI classified as inappropriate had not been given a trial of adequate anti-anginal therapy. This analysis was supported by subsequent analyses of 2 other state-specific registries (New York and Washington), which found similar rates of PCI for nonacute indications rated as inappropriate [27,28]. Additionally, all 3 studies showed wide facility-level variation in the percentage of appropriate and inappropriate PCI for elective indications.
Application of the AUC to clinical practice has highlighted potential overuse of PCI (Table). The first report came from applying the AUC to the National Cardiovascular Data Registry (NCDR) CathPCI Registry [26]. In this study of more than 500,000 PCIs from over 1000 facilities across the country, the authors found that PCIs performed in the acute setting (STEMI, NSTEMI, and high-risk unstable angina) were almost uniformly classified as appropriate. However, for nonacute (elective) PCI, application of the AUC resulted in the classification of 50% as appropriate, 38% as uncertain, and 12% as inappropriate. The majority of patients who received inappropriate PCI had a low-risk stress test (72%) or were asymptomatic (54%). Additionally, 96% of patients who received PCI classified as inappropriate had not been given a trial of adequate anti-anginal therapy. This analysis was supported by subsequent analyses of 2 other state-specific registries (New York and Washington), which found similar rates of PCI for nonacute indications rated as inappropriate [27,28]. Additionally, all 3 studies showed wide facility-level variation in the percentage of appropriate and inappropriate PCI for elective indications.
These studies also highlight a gap in preprocedural care. The anticipated benefit of elective PCI is related to patient symptom burden, adequacy of anti-anginal therapy, and ischemic risk as determined by noninvasive stress testing. However, 30% to 50% of patients undergo elective PCI without evidence of preprocedural stress testing. Attempts are being made to address this gap with the recent release of PCI performance measures [29]. These performance measures, intended for cardiac catheterization labs, include comprehensive documentation of the indication for PCI, which is central to determination of appropriateness. This integration of procedural indication into a performance measure marks the first such occurrence in cardiology.
As documentation of procedural indication and appropriateness have become part and parcel of assessing quality of care, concerns about “gaming” have become more pertinent. Providers who perform PCI could potentially enhance the appearance of appropriateness by overstating the clinical symptom burden or stress test findings. The incorporation of validated, patient-centered health status questionnaires along with data audit programs have been proposed as measures to prevent this type of abuse. Addressing quality gaps in preprocedural assessment and documentation is critical to optimizing use of elective PCI [28].
The apparent overuse of PCI for elective indications may be a reflection of our fragmented, fee-for-service health care delivery system. However, recent studies challenge these assumptions. In a Canadian study, Ko et al found that 18% of elective PCIs were classified as inappropriate, a proportion similar to what had been found previously in the United States [30]. In a US study of Medicare beneficiaries, Matlock and colleagues observed a fourfold regional variation in use of elective coronary angiography and PCI in both Medicare fee-for-service and capitated Medicare Advantage beneficiaries [31]. Collectively, these studies suggest barriers to optimal patient selection for invasive coronary procedures in both capitated and fee-for-service health care systems. Without addressing factors that contribute to variation in the absence of fee-for-service incentives, efforts to improve integration and reduce fee-for-service reimbursement may be inadequate to optimize PCI use.
Evaluating Underuse
While potential underuse of PCI has been described for acute indications [17–22], study of underuse of PCI for elective indications is more challenging. Population data on the effect of underuse of elective PCI on patient symptom burden, functional status, and quality of life is lacking.
A population-based study from Australia highlights the potential importance of underuse in the care of patients with stable coronary disease. This study assessed symptom burden among patients with chronic stable angina using the Seattle Angina Questionnaire and included patients cared for by 207 primary care practitioners [32]. The authors noted that there was considerable variation in patient symptom burden between practices, with 14% of practices having no patients with more than 1 episode of angina per week and 18% of clinics having more than half of enrolled patients with at least 1 episode of angina per week. The authors postulate that this variability may be due to differences among providers in the identification and management of angina, including using PCI to minimize symptom burden.
In the Ko study mentioned earlier, the AUC was used to examine potential underuse of coronary revascularization procedures. In this study, they analyzed the association between AUC ratings and outcomes in patients undergoing diagnostic coronary angiography [30]. Of patients considered “appropriate” for revascularization following completion of diagnostic angiography, only 69% underwent revascularization. However, the clinical aspects that influence the decision to proceed with revascularization may not be fully captured in this study. Thus, the true degree of underuse of PCI remains elusive.
In summary, the relative lack of data that would allow for the assessment of underuse of elective PCI is an important quality concern. Health systems should work to systematically capture patient-reported health status, including symptom burden data, to identify inadequate symptom control and potential underuse of procedural care for CAD.
Facilitating Optimal Use
 In current practice, the AUC hold promise to minimize the overuse of elective PCI. This likely involves addressing processes occurring upstream of the cardiac catheterization lab, including employing systems to ensure that procedures are avoided in patients who are unlikely to benefit (eg, asymptomatic, low ischemic burden) (Figure 3) [33]. Studying hospitals that already have low rates of inappropriate PCI may inform the design and dissemination of strategies that will help improve patient selection at hospitals with higher rates. Although professional organizations have developed tools intended to facilitate appropriateness evaluation at the point-of-care [34], the use of these tools are likely to be sporadic without greater integration into the health care delivery system. Further, these applications are currently limited to determination of appropriateness of PCI after completion of the diagnostic coronary angiogram. Identifying processes prior to catheterization that contribute to PCI appropriateness may also streamline appropriate ad hoc PCI, as the need to reassess appropriateness after the diagnostic angiogram may be mitigated.
In current practice, the AUC hold promise to minimize the overuse of elective PCI. This likely involves addressing processes occurring upstream of the cardiac catheterization lab, including employing systems to ensure that procedures are avoided in patients who are unlikely to benefit (eg, asymptomatic, low ischemic burden) (Figure 3) [33]. Studying hospitals that already have low rates of inappropriate PCI may inform the design and dissemination of strategies that will help improve patient selection at hospitals with higher rates. Although professional organizations have developed tools intended to facilitate appropriateness evaluation at the point-of-care [34], the use of these tools are likely to be sporadic without greater integration into the health care delivery system. Further, these applications are currently limited to determination of appropriateness of PCI after completion of the diagnostic coronary angiogram. Identifying processes prior to catheterization that contribute to PCI appropriateness may also streamline appropriate ad hoc PCI, as the need to reassess appropriateness after the diagnostic angiogram may be mitigated.
Significant barriers exist to the application of the AUC for determination of procedural underuse. As described above, we lack adequate data to ascertain gaps in symptom management that could be mitigated by proper use of PCI. Further study of symptom burden in populations of patients with coronary artery disease is needed. This may help in the identification of patient populations whose symptom burden may warrant consideration of invasive coronary procedures, including coronary angiography and PCI.
Finally, it is important to note that the AUC are based on technical considerations, ie, practice guidelines and trial evidence. They do not take into consideration patient preferences. For example, PCI can be technically appropriate for the scenario but inappropriate for the individual if the procedure is not desired by the patient. Similarly, a procedure may be of uncertain benefit but appropriate if the patient desires more aggressive procedural care and has a full understanding of the risks and benefits. Currently, we fail to convey this information to patients, as evidenced by patients’ overestimation of the benefits of PCI [34]. As we continue to work toward optimal use of PCI, we must not only address the technical appropriateness of care, but move toward incorporating patient preferences through a robust process of shared decision-making.
Corresponding author: Preston M. Schneider, MD, VA Eastern Colorado Health Care System, Cardiology Section (111B), 1055 Clermont St., Denver, CO 80220, [email protected].
Funding/support: Dr. Schneider is supported by a T32 training grant from the National Institutes of Health (5T32HL00
7822-15). Dr. Bradley is supported by a Career Development Award (HSR&D-CDA2 10-199) from VA Health Services Research & Development.
Financial disclosures: None.
1. Cassel CK, Guest JA. Choosing wisely: helping physicians and patients make smart decisions about their care. JAMA 2012;307:1801–2.
2. Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics—2013 update: a report from the American Heart Association. Circulation 2013;127:e6–e245.
3. HCUPnet: A tool for identifying, tracking, and analyzing national hospital statistics. Accessed 22 Oct 2013 at http://hcupnet.ahrq.gov/HCUPnet.jsp?Parms=
H4sIAAAAAAAAABXBMQ6AIBAEwC9JAg.gsLAhRvjAnnuXgGihFb9XZwYe3EhLdpN2h2aIcsnQLCp9jQVbLDN3ksq
DnSeqVXzNfIAP9mtmLy0rZhdIAAAA83D0C2BCAE02DD1508408B2C5C094F1ADF6E788C&JS=Y.
4. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet 2003;361:13–20.
5. Boden WE, O’Rourke RA, Teo KK, et al. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med 2007;356:1503–16.
6. Boden WE, O’Rourke RA, Teo KK, et al. Impact of optimal medical therapy with or without percutaneous coronary intervention on long-term cardiovascular end points in patients with stable coronary artery disease (from the COURAGE Trial). Am J Cardiol 2009;104:1–4.
7. Stergiopoulos K, Brown DL. Initial coronary stent implantation with medical therapy vs medical therapy alone for stable coronary artery disease: Meta-analysis of randomized controlled trials. Arch Intern Med 2012;172:312–9.
8. McCullough PA, Adam A, Becker CR, et al. Epidemiology and prognostic implications of contrast-induced nephropathy. Contrast-Induc Nephrop Clin Insights Pract Guid Rep CIN Consens Work Panel 2006;98:5–13.
9. Roe MT, Messenger JC, Weintraub WS, et al. Treatments, trends, and outcomes of acute myocardial infarction and percutaneous coronary intervention. J Am Coll Cardiol 2010;56:254–63.
10. Patel MR, Dehmer GJ, Hirshfeld JW, et al. ACCF/SCAI/STS/AATS/AHA/ASNC 2009 Appropriateness Criteria for Coronary Revascularization: A Report by the American College of Cardiology Foundation Appropriateness Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, and the American Society of Nuclear Cardiology Endorsed by the American Society of Echocardiography, the Heart Failure Society of America, and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol 2009;53:530–53.
11. Patel MR, Dehmer GJ, Hirshfeld JW, et al. ACCF/SCAI/STS/AATS/AHA/ASNC/HFSA/SCCT 2012 Appropriate Use Criteria for Coronary Revascularization Focused Update: A Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, American Society of Nuclear Cardiology, and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol 2012;59:857–81.
12. Dartmouth Atlas of Health Care. Accessed 8 Jan 2014 at www.dartmouthatlas.org.
13. Dartmouth Atlas of Health Care: Studies of surgical variation. Cardiac surgery report. 2005. Accessed 8 Jan 2014 at www.dartmouthatlas.org/publications/reports.aspx.
14. Fisher ES, Wennberg DE, Stukel TA, et al. The implications of regional variations in medicare spending. part 1: the content, quality, and accessibility of care. Ann Intern Med 2003;138:273–87.
15. Fisher ES, Wennberg DE, Stukel TA, et al. The implications of regional variations in medicare spending. part 2: health outcomes and satisfaction with care. Ann Intern Med 2003;138:288–98.
16. Abelson R. Heart procedure is off the charts in an Ohio city. New York Times 2006. Accessed 23 Apr 2013 at www.nytimes.com/2006/08/18/business/18stent.html.
17. Akhter N, Milford-Beland S, Roe MT, et al. Gender differences among patients with acute coronary syndromes undergoing percutaneous coronary intervention in the American College of Cardiology-National Cardiovascular Data Registry (ACC-NCDR). Am Heart J 2009;157:141–8.
18. Blomkalns AL, Chen AY, Hochman JS, et al. Gender disparities in the diagnosis and treatment of non–ST-segment elevation acute coronary syndromesLarge-scale observations from the CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the American College of Cardiology/American Heart Association Guidelines) National Quality Improvement Initiative. J Am Coll Cardiol 2005;45:832–7.
19. Daly C, Clemens F, Lopez Sendon JL, et al. Gender differences in the management and clinical outcome of stable angina. Circulation 2006;113:490–8.
20. Groeneveld PW, Heidenreich PA, Garber AM. Racial disparity in cardiac procedures and mortality among long-term survivors of cardiac arrest. Circulation 2003;108:286–91.
21. Hannan EL, Zhong Y, Walford G, et al. Underutilization of percutaneous coronary intervention for ST-elevation myocardial infarction in Medicaid patients relative to private insurance patients. J Intervent Cardiol 2013;26:470–81.
22. Sonel AF, Good CB, Mulgund J, et al. Racial variations in treatment and outcomes of black and white patients with high-risk non–ST-elevation acute coronary syndromes: insights From CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the ACC/AHA Guidelines?). Circulation 2005;111:1225–32.
23. Patel MR, Spertus JA, Brindis RG, et al. ACCF proposed method for evaluating the appropriateness of cardiovascular imaging. J Am Coll Cardiol 2005;46:1606–13.
24. Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI Guideline for percutaneous coronary intervention: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation 2011;124:2574–609.
25. Campeau L. Letter: Grading of angina pectoris. Circulation 1976;54:522–3.
26. Chan PS, Patel MR, Klein LW, et al. Appropriateness of percutaneous coronary intervention. JAMA 2011;306:53–61.
27. Hannan EL, Cozzens K, Samadashvili Z, et al. Appropriateness of coronary revascularization for patients without acute coronary syndromes. J Am Coll Cardiol 2012;59:1870–6.
28. Bradley SM, Maynard C, Bryson CL. Appropriateness of percutaneous coronary interventions in Washington State. Circ Cardiovasc Qual Outcomes 2012;5:445–53.
29. Nallamothu BK, Tommaso CL, Anderson HV, et al. ACC/AHA/SCAI/AMA–Convened PCPI/NCQA 2013 Performance measures for adults undergoing percutaneous coronary intervention. A report of the American College of Cardiology/American Heart Association Task Force on Performance Measures, the Society for Cardiovascular Angiography and Interventions, the American Medical Association–Convened Physician Consortium for Performance Improvement, and the National Committee for Quality Assurance. J Am Coll Cardiol 2014;63:722–45.
30. Ko DT, Guo H, Wijeysundera HC, et al. Assessing the association of appropriateness of coronary revascularization and clinical outcomes for patients with stable coronary artery disease. J Am Coll Cardiol 2012;60:1876–84.
31. Matlock DD, Groeneveld PW, Sidney S, et al. Geographic variation in cardiovascular procedure use among medicare fee-for-service vs medicare advantage beneficiaries. JAMA 2013;310:155–62.
32. Beltrame JF, Weekes AJ, Morgan C, et al. The prevalence of weekly angina among patients with chronic stable angina in primary care practices: The coronary artery disease in general practice (cadence) study. Arch Intern Med 2009;169:1491–9.
33. Bradley SM, Spertus JA, Nallamothu BK, et al. The association between patient selection for diagnostic coronary angiography and hospital-level PCI appropriateness: Insights from the NCDR. Circ Cardiovasc Qual Outcomes 2013;6:A1. Accessed 20 Nov 2013 at http://circoutcomes.ahajournals.org/cgi/content/short/6/3_MeetingAbstracts/A1?rss=1.
34. Lee J, Chuu K, Spertus J, et al. Patients overestimate the potential benefits of elective percutaneous coronary intervention. Mo Med 2012;109:79.
From the VA Eastern Colorado Health Care System, University of Colorado School of Medicine, and the Colorado Cardiovascular Outcomes Research Group, Denver and Aurora, CO.
Abstract
- Objective: To review the use of elective percutaneous coronary intervention (PCI), evaluate what is currently known about elective PCI in the context of appropriate use criteria, and offer insight into next steps to optimize the use of elective PCI to achieve high-quality care.
- Methods: Review of the scientific literature, appropriate use criteria, and professional society guidelines relevant to elective PCI.
- Results: Recent studies have demonstrated as many as 1 in 6 elective PCIs are inappropriate as determined by appropriate use criteria. These inappropriate PCIs are not anticipated to benefit patients and result in unnecessary patient risk and cost. While these studies are consistent with regard to overuse of elective PCI, less is known about potential underuse of PCI for elective indications. We lack health status data on populations of ischemic heart disease patients to inform PCI underuse that may contribute to patient symptom burden, functional status, and quality of life. Optimal use of PCI will be attained with longitudinal capture of patient-reported health status, study of factors contributing to overuse and underuse, refinement of the appropriate use criteria with particular focus on patient-centered measures, and incorporation of patient preference and shared decision making into appropriateness evaluation tools.
- Conclusion: The use of elective PCI is less than optimal in current clinical practice. Continued effort is needed to ensure elective PCI is targeted to patients with anticipated benefit and use of the procedure is aligned with patient preferences.
Providing the right care to the right patient at the right time is essential to the practice of high-quality care. Reducing overuse of health care services is part of this equation, and initiatives to reduce inappropriate use and to encourage physicians and patients to “choose wisely” have been introduced [1]. One procedure that is being examined with a focus on appropriateness is percutaneous coronary intervention (PCI). This procedure is common (nearly 1 million inpatient PCI procedures performed in 2010), presents risks to the patient, and is expensive (attributable cost approximately $10 billion in 2010) [2,3]. While the clinical benefit of PCI in acute settings such as ST-segment elevation myocardial infarction is well established [4], the benefit of PCI in nonacute (elective) settings is less robust [5–7]. Prior studies have demonstrated PCI for stable ischemic heart disease does not result in mortality benefit [6]. Furthermore, PCI as an initial strategy for symptom relief of stable angina may offer little benefit relative to medications alone [5]. Given that PCI is common, costly, and associated with both short- and long-term risks [8,9], ensuring this therapy is provided to the right patient at the right time is important.
In 2009, appropriate use criteria (AUC) were developed by 6 professional organizations to support the rational and judicious use of PCI [10]; a focused update was published in 2012 [11]. In this review, we discuss the recommendations for appropriate use and their application and offer thoughts on next steps to optimize the use of elective PCI as part of high-quality care.
Variation in the Use of PCI
Additionally, significant public attention has been focused on the issue of overuse after lay press investigations into community practice patterns. In particular, a case study presented in the New York Times highlighted the community of Elyria, Ohio, which was found to have a PCI rate that was 4 times the national average [16]. This investigation sparked public debate and further focused attention on the issue of overuse of elective PCI. Conversely, others have pointed to data that suggest underuse of coronary procedural care, particularly among women and racial and ethnic minorities [17–22].
Appropriate Use Criteria
Development Methodology
AUC for PCI, which were developed through the collaborative efforts of 6 major cardiovascular professional organizations, are intended to support the effective, efficient, and equitable use of PCI [10,11]. They were developed in response to a growing need to support rational use of cardiovascular procedures as part of high-quality care. The methods of development for the AUC have been described in detail in the criteria publications [10,11]. We briefly review these methods here.
Panel members first individually assigned ratings to each clinical scenario that ranged from 1 (least appropriate) to 9 (most appropriate). This was followed by an in-person meeting in which technical panel members discussed scenarios for which there was wide variation in appropriateness assessment. After this meeting, technical panel members again assigned ratings for each scenario from 1 to 9. After this second round, the median values for the pooled ratings were used as the appropriateness classification for each scenario. Scenarios with median values of 1–3 were classified as “inappropriate,” 4–6 as “uncertain,” and 7–9 as “appropriate.” A rating of “appropriate” represented clinical scenarios in which the indication is considered generally acceptable and likely to improve health outcomes or survival. A rating of “uncertain” represented clinical scenarios where the indication may be reasonable but more research is necessary to further understand the relative benefits and risks of PCI in this setting. Finally, a rating of “inappropriate” represented clinical scenarios in which the indication is not generally acceptable as it is unlikely to improve health outcomes or survival.
The approach used for AUC development appears to be valid, as Class III indications for PCI in the ACC/AHA clinical guideline [24] (Class III = PCI should NOT be performed since it is not helpful and may be harmful) and AUC scenarios rated as inappropriate are in 100% agreement (personal communication, Ralph Brindis, past president of the American College of Cardiology).
Application
It is important to remember that the AUC are intended to aid in patient selection and are not absolute. Unique clinical factors and patient preference cannot feasibly be captured by the AUC scenarios. It should also be noted that the intent of the AUC is not to be punitive but rather to identify and assess variation in practice patterns. To reflect this intent, the terminology applied to appropriateness ratings has recently changed. Clinical scenarios previously classified as “inappropriate” are now termed “rarely appropriate” and clinical scenarios classified as “uncertain” are now termed “may be appropriate.”
Although the AUC were developed to help evaluate practice patterns of care delivery and serve as guides for clinical decision making, they were not intended to serve as mandates for or against treatment in individual patients or to be tied to reimbursement for individual patients. Despite this, health care organizations and payors have used other AUC documents for incentive pay and prior authorization programs, specifically for cardiovascular imaging [25]. Use of the AUC in this manner may still be reasonable if application and measurement is at the level of the practice, rather than the individual patient, but much remains to be understood about the implications of applying AUC in reimbursement
decisions.
Refinement
The AUC for PCI are designed to be dynamic and continually updated. As additional evidence becomes available regarding the efficacy of PCI in specific clinical scenarios, there will be ongoing efforts to update the AUC to reflect this new evidence. This is highlighted by the first update to the AUC occurring less than 3 years after the original publication date [11].
In addition to perpetual review of the data used to inform scenario ratings, there are opportunities to improve measurement of the clinical variables that are considered in rating PCI appropriateness (eg, clinical presentation, symptom severity, ischemia severity, extent of medical therapy, extent of anatomic disease). For example, in the current AUC, symptom severity is dependent on clinician assessment using the Canadian Cardiovascular Society Classification [25]. Moving toward a patient-centered assessment of symptom severity would ensure that the AUC more closely reflect the patient-perceived symptom burden. Further, the use of a patient-centered instrument would reduce the possibility of physician manipulation of symptom severity to influence the apparent appropriateness of PCI. There are similar opportunities to improve reporting of noninvasive stress test data, such as through standardized reporting of ischemic risk. Finally, the use of physiologic assessments of stenosis severity (eg, fractional flow reserve) and quantitative coronary angiography to standardize interpretations of diagnostic angiography may further optimize the assessment of PCI appropriateness.
Application of the Appropriate Use Criteria in Clinical Practice—Study Results
Application of the AUC to clinical practice has highlighted potential overuse of PCI (Table). The first report came from applying the AUC to the National Cardiovascular Data Registry (NCDR) CathPCI Registry [26]. In this study of more than 500,000 PCIs from over 1000 facilities across the country, the authors found that PCIs performed in the acute setting (STEMI, NSTEMI, and high-risk unstable angina) were almost uniformly classified as appropriate. However, for nonacute (elective) PCI, application of the AUC resulted in the classification of 50% as appropriate, 38% as uncertain, and 12% as inappropriate. The majority of patients who received inappropriate PCI had a low-risk stress test (72%) or were asymptomatic (54%). Additionally, 96% of patients who received PCI classified as inappropriate had not been given a trial of adequate anti-anginal therapy. This analysis was supported by subsequent analyses of 2 other state-specific registries (New York and Washington), which found similar rates of PCI for nonacute indications rated as inappropriate [27,28]. Additionally, all 3 studies showed wide facility-level variation in the percentage of appropriate and inappropriate PCI for elective indications.
These studies also highlight a gap in preprocedural care. The anticipated benefit of elective PCI is related to patient symptom burden, adequacy of anti-anginal therapy, and ischemic risk as determined by noninvasive stress testing. However, 30% to 50% of patients undergo elective PCI without evidence of preprocedural stress testing. Attempts are being made to address this gap with the recent release of PCI performance measures [29]. These performance measures, intended for cardiac catheterization labs, include comprehensive documentation of the indication for PCI, which is central to determination of appropriateness. This integration of procedural indication into a performance measure marks the first such occurrence in cardiology.
As documentation of procedural indication and appropriateness have become part and parcel of assessing quality of care, concerns about “gaming” have become more pertinent. Providers who perform PCI could potentially enhance the appearance of appropriateness by overstating the clinical symptom burden or stress test findings. The incorporation of validated, patient-centered health status questionnaires along with data audit programs have been proposed as measures to prevent this type of abuse. Addressing quality gaps in preprocedural assessment and documentation is critical to optimizing use of elective PCI [28].
The apparent overuse of PCI for elective indications may be a reflection of our fragmented, fee-for-service health care delivery system. However, recent studies challenge these assumptions. In a Canadian study, Ko et al found that 18% of elective PCIs were classified as inappropriate, a proportion similar to what had been found previously in the United States [30]. In a US study of Medicare beneficiaries, Matlock and colleagues observed a fourfold regional variation in use of elective coronary angiography and PCI in both Medicare fee-for-service and capitated Medicare Advantage beneficiaries [31]. Collectively, these studies suggest barriers to optimal patient selection for invasive coronary procedures in both capitated and fee-for-service health care systems. Without addressing factors that contribute to variation in the absence of fee-for-service incentives, efforts to improve integration and reduce fee-for-service reimbursement may be inadequate to optimize PCI use.
Evaluating Underuse
While potential underuse of PCI has been described for acute indications [17–22], study of underuse of PCI for elective indications is more challenging. Population data on the effect of underuse of elective PCI on patient symptom burden, functional status, and quality of life is lacking.
A population-based study from Australia highlights the potential importance of underuse in the care of patients with stable coronary disease. This study assessed symptom burden among patients with chronic stable angina using the Seattle Angina Questionnaire and included patients cared for by 207 primary care practitioners [32]. The authors noted that there was considerable variation in patient symptom burden between practices, with 14% of practices having no patients with more than 1 episode of angina per week and 18% of clinics having more than half of enrolled patients with at least 1 episode of angina per week. The authors postulate that this variability may be due to differences among providers in the identification and management of angina, including using PCI to minimize symptom burden.
In the Ko study mentioned earlier, the AUC was used to examine potential underuse of coronary revascularization procedures. In this study, they analyzed the association between AUC ratings and outcomes in patients undergoing diagnostic coronary angiography [30]. Of patients considered “appropriate” for revascularization following completion of diagnostic angiography, only 69% underwent revascularization. However, the clinical aspects that influence the decision to proceed with revascularization may not be fully captured in this study. Thus, the true degree of underuse of PCI remains elusive.
In summary, the relative lack of data that would allow for the assessment of underuse of elective PCI is an important quality concern. Health systems should work to systematically capture patient-reported health status, including symptom burden data, to identify inadequate symptom control and potential underuse of procedural care for CAD.
Facilitating Optimal Use
In current practice, the AUC hold promise to minimize the overuse of elective PCI. This likely involves addressing processes occurring upstream of the cardiac catheterization lab, including employing systems to ensure that procedures are avoided in patients who are unlikely to benefit (eg, asymptomatic, low ischemic burden) (Figure 3) [33]. Studying hospitals that already have low rates of inappropriate PCI may inform the design and dissemination of strategies that will help improve patient selection at hospitals with higher rates. Although professional organizations have developed tools intended to facilitate appropriateness evaluation at the point-of-care [34], the use of these tools are likely to be sporadic without greater integration into the health care delivery system. Further, these applications are currently limited to determination of appropriateness of PCI after completion of the diagnostic coronary angiogram. Identifying processes prior to catheterization that contribute to PCI appropriateness may also streamline appropriate ad hoc PCI, as the need to reassess appropriateness after the diagnostic angiogram may be mitigated.
Significant barriers exist to the application of the AUC for determination of procedural underuse. As described above, we lack adequate data to ascertain gaps in symptom management that could be mitigated by proper use of PCI. Further study of symptom burden in populations of patients with coronary artery disease is needed. This may help in the identification of patient populations whose symptom burden may warrant consideration of invasive coronary procedures, including coronary angiography and PCI.
Finally, it is important to note that the AUC are based on technical considerations, ie, practice guidelines and trial evidence. They do not take into consideration patient preferences. For example, PCI can be technically appropriate for the scenario but inappropriate for the individual if the procedure is not desired by the patient. Similarly, a procedure may be of uncertain benefit but appropriate if the patient desires more aggressive procedural care and has a full understanding of the risks and benefits. Currently, we fail to convey this information to patients, as evidenced by patients’ overestimation of the benefits of PCI [34]. As we continue to work toward optimal use of PCI, we must not only address the technical appropriateness of care, but move toward incorporating patient preferences through a robust process of shared decision-making.
Corresponding author: Preston M. Schneider, MD, VA Eastern Colorado Health Care System, Cardiology Section (111B), 1055 Clermont St., Denver, CO 80220, [email protected].
Funding/support: Dr. Schneider is supported by a T32 training grant from the National Institutes of Health (5T32HL00
7822-15). Dr. Bradley is supported by a Career Development Award (HSR&D-CDA2 10-199) from VA Health Services Research & Development.
Financial disclosures: None.
From the VA Eastern Colorado Health Care System, University of Colorado School of Medicine, and the Colorado Cardiovascular Outcomes Research Group, Denver and Aurora, CO.
Abstract
- Objective: To review the use of elective percutaneous coronary intervention (PCI), evaluate what is currently known about elective PCI in the context of appropriate use criteria, and offer insight into next steps to optimize the use of elective PCI to achieve high-quality care.
- Methods: Review of the scientific literature, appropriate use criteria, and professional society guidelines relevant to elective PCI.
- Results: Recent studies have demonstrated as many as 1 in 6 elective PCIs are inappropriate as determined by appropriate use criteria. These inappropriate PCIs are not anticipated to benefit patients and result in unnecessary patient risk and cost. While these studies are consistent with regard to overuse of elective PCI, less is known about potential underuse of PCI for elective indications. We lack health status data on populations of ischemic heart disease patients to inform PCI underuse that may contribute to patient symptom burden, functional status, and quality of life. Optimal use of PCI will be attained with longitudinal capture of patient-reported health status, study of factors contributing to overuse and underuse, refinement of the appropriate use criteria with particular focus on patient-centered measures, and incorporation of patient preference and shared decision making into appropriateness evaluation tools.
- Conclusion: The use of elective PCI is less than optimal in current clinical practice. Continued effort is needed to ensure elective PCI is targeted to patients with anticipated benefit and use of the procedure is aligned with patient preferences.
Providing the right care to the right patient at the right time is essential to the practice of high-quality care. Reducing overuse of health care services is part of this equation, and initiatives to reduce inappropriate use and to encourage physicians and patients to “choose wisely” have been introduced [1]. One procedure that is being examined with a focus on appropriateness is percutaneous coronary intervention (PCI). This procedure is common (nearly 1 million inpatient PCI procedures performed in 2010), presents risks to the patient, and is expensive (attributable cost approximately $10 billion in 2010) [2,3]. While the clinical benefit of PCI in acute settings such as ST-segment elevation myocardial infarction is well established [4], the benefit of PCI in nonacute (elective) settings is less robust [5–7]. Prior studies have demonstrated PCI for stable ischemic heart disease does not result in mortality benefit [6]. Furthermore, PCI as an initial strategy for symptom relief of stable angina may offer little benefit relative to medications alone [5]. Given that PCI is common, costly, and associated with both short- and long-term risks [8,9], ensuring this therapy is provided to the right patient at the right time is important.
In 2009, appropriate use criteria (AUC) were developed by 6 professional organizations to support the rational and judicious use of PCI [10]; a focused update was published in 2012 [11]. In this review, we discuss the recommendations for appropriate use and their application and offer thoughts on next steps to optimize the use of elective PCI as part of high-quality care.
Variation in the Use of PCI
Additionally, significant public attention has been focused on the issue of overuse after lay press investigations into community practice patterns. In particular, a case study presented in the New York Times highlighted the community of Elyria, Ohio, which was found to have a PCI rate that was 4 times the national average [16]. This investigation sparked public debate and further focused attention on the issue of overuse of elective PCI. Conversely, others have pointed to data that suggest underuse of coronary procedural care, particularly among women and racial and ethnic minorities [17–22].
Appropriate Use Criteria
Development Methodology
AUC for PCI, which were developed through the collaborative efforts of 6 major cardiovascular professional organizations, are intended to support the effective, efficient, and equitable use of PCI [10,11]. They were developed in response to a growing need to support rational use of cardiovascular procedures as part of high-quality care. The methods of development for the AUC have been described in detail in the criteria publications [10,11]. We briefly review these methods here.
Panel members first individually assigned ratings to each clinical scenario that ranged from 1 (least appropriate) to 9 (most appropriate). This was followed by an in-person meeting in which technical panel members discussed scenarios for which there was wide variation in appropriateness assessment. After this meeting, technical panel members again assigned ratings for each scenario from 1 to 9. After this second round, the median values for the pooled ratings were used as the appropriateness classification for each scenario. Scenarios with median values of 1–3 were classified as “inappropriate,” 4–6 as “uncertain,” and 7–9 as “appropriate.” A rating of “appropriate” represented clinical scenarios in which the indication is considered generally acceptable and likely to improve health outcomes or survival. A rating of “uncertain” represented clinical scenarios where the indication may be reasonable but more research is necessary to further understand the relative benefits and risks of PCI in this setting. Finally, a rating of “inappropriate” represented clinical scenarios in which the indication is not generally acceptable as it is unlikely to improve health outcomes or survival.
The approach used for AUC development appears to be valid, as Class III indications for PCI in the ACC/AHA clinical guideline [24] (Class III = PCI should NOT be performed since it is not helpful and may be harmful) and AUC scenarios rated as inappropriate are in 100% agreement (personal communication, Ralph Brindis, past president of the American College of Cardiology).
Application
It is important to remember that the AUC are intended to aid in patient selection and are not absolute. Unique clinical factors and patient preference cannot feasibly be captured by the AUC scenarios. It should also be noted that the intent of the AUC is not to be punitive but rather to identify and assess variation in practice patterns. To reflect this intent, the terminology applied to appropriateness ratings has recently changed. Clinical scenarios previously classified as “inappropriate” are now termed “rarely appropriate” and clinical scenarios classified as “uncertain” are now termed “may be appropriate.”
Although the AUC were developed to help evaluate practice patterns of care delivery and serve as guides for clinical decision making, they were not intended to serve as mandates for or against treatment in individual patients or to be tied to reimbursement for individual patients. Despite this, health care organizations and payors have used other AUC documents for incentive pay and prior authorization programs, specifically for cardiovascular imaging [25]. Use of the AUC in this manner may still be reasonable if application and measurement is at the level of the practice, rather than the individual patient, but much remains to be understood about the implications of applying AUC in reimbursement
decisions.
Refinement
The AUC for PCI are designed to be dynamic and continually updated. As additional evidence becomes available regarding the efficacy of PCI in specific clinical scenarios, there will be ongoing efforts to update the AUC to reflect this new evidence. This is highlighted by the first update to the AUC occurring less than 3 years after the original publication date [11].
In addition to perpetual review of the data used to inform scenario ratings, there are opportunities to improve measurement of the clinical variables that are considered in rating PCI appropriateness (eg, clinical presentation, symptom severity, ischemia severity, extent of medical therapy, extent of anatomic disease). For example, in the current AUC, symptom severity is dependent on clinician assessment using the Canadian Cardiovascular Society Classification [25]. Moving toward a patient-centered assessment of symptom severity would ensure that the AUC more closely reflect the patient-perceived symptom burden. Further, the use of a patient-centered instrument would reduce the possibility of physician manipulation of symptom severity to influence the apparent appropriateness of PCI. There are similar opportunities to improve reporting of noninvasive stress test data, such as through standardized reporting of ischemic risk. Finally, the use of physiologic assessments of stenosis severity (eg, fractional flow reserve) and quantitative coronary angiography to standardize interpretations of diagnostic angiography may further optimize the assessment of PCI appropriateness.
Application of the Appropriate Use Criteria in Clinical Practice—Study Results
Application of the AUC to clinical practice has highlighted potential overuse of PCI (Table). The first report came from applying the AUC to the National Cardiovascular Data Registry (NCDR) CathPCI Registry [26]. In this study of more than 500,000 PCIs from over 1000 facilities across the country, the authors found that PCIs performed in the acute setting (STEMI, NSTEMI, and high-risk unstable angina) were almost uniformly classified as appropriate. However, for nonacute (elective) PCI, application of the AUC resulted in the classification of 50% as appropriate, 38% as uncertain, and 12% as inappropriate. The majority of patients who received inappropriate PCI had a low-risk stress test (72%) or were asymptomatic (54%). Additionally, 96% of patients who received PCI classified as inappropriate had not been given a trial of adequate anti-anginal therapy. This analysis was supported by subsequent analyses of 2 other state-specific registries (New York and Washington), which found similar rates of PCI for nonacute indications rated as inappropriate [27,28]. Additionally, all 3 studies showed wide facility-level variation in the percentage of appropriate and inappropriate PCI for elective indications.
These studies also highlight a gap in preprocedural care. The anticipated benefit of elective PCI is related to patient symptom burden, adequacy of anti-anginal therapy, and ischemic risk as determined by noninvasive stress testing. However, 30% to 50% of patients undergo elective PCI without evidence of preprocedural stress testing. Attempts are being made to address this gap with the recent release of PCI performance measures [29]. These performance measures, intended for cardiac catheterization labs, include comprehensive documentation of the indication for PCI, which is central to determination of appropriateness. This integration of procedural indication into a performance measure marks the first such occurrence in cardiology.
As documentation of procedural indication and appropriateness have become part and parcel of assessing quality of care, concerns about “gaming” have become more pertinent. Providers who perform PCI could potentially enhance the appearance of appropriateness by overstating the clinical symptom burden or stress test findings. The incorporation of validated, patient-centered health status questionnaires along with data audit programs have been proposed as measures to prevent this type of abuse. Addressing quality gaps in preprocedural assessment and documentation is critical to optimizing use of elective PCI [28].
The apparent overuse of PCI for elective indications may be a reflection of our fragmented, fee-for-service health care delivery system. However, recent studies challenge these assumptions. In a Canadian study, Ko et al found that 18% of elective PCIs were classified as inappropriate, a proportion similar to what had been found previously in the United States [30]. In a US study of Medicare beneficiaries, Matlock and colleagues observed a fourfold regional variation in use of elective coronary angiography and PCI in both Medicare fee-for-service and capitated Medicare Advantage beneficiaries [31]. Collectively, these studies suggest barriers to optimal patient selection for invasive coronary procedures in both capitated and fee-for-service health care systems. Without addressing factors that contribute to variation in the absence of fee-for-service incentives, efforts to improve integration and reduce fee-for-service reimbursement may be inadequate to optimize PCI use.
Evaluating Underuse
While potential underuse of PCI has been described for acute indications [17–22], study of underuse of PCI for elective indications is more challenging. Population data on the effect of underuse of elective PCI on patient symptom burden, functional status, and quality of life is lacking.
A population-based study from Australia highlights the potential importance of underuse in the care of patients with stable coronary disease. This study assessed symptom burden among patients with chronic stable angina using the Seattle Angina Questionnaire and included patients cared for by 207 primary care practitioners [32]. The authors noted that there was considerable variation in patient symptom burden between practices, with 14% of practices having no patients with more than 1 episode of angina per week and 18% of clinics having more than half of enrolled patients with at least 1 episode of angina per week. The authors postulate that this variability may be due to differences among providers in the identification and management of angina, including using PCI to minimize symptom burden.
In the Ko study mentioned earlier, the AUC was used to examine potential underuse of coronary revascularization procedures. In this study, they analyzed the association between AUC ratings and outcomes in patients undergoing diagnostic coronary angiography [30]. Of patients considered “appropriate” for revascularization following completion of diagnostic angiography, only 69% underwent revascularization. However, the clinical aspects that influence the decision to proceed with revascularization may not be fully captured in this study. Thus, the true degree of underuse of PCI remains elusive.
In summary, the relative lack of data that would allow for the assessment of underuse of elective PCI is an important quality concern. Health systems should work to systematically capture patient-reported health status, including symptom burden data, to identify inadequate symptom control and potential underuse of procedural care for CAD.
Facilitating Optimal Use
In current practice, the AUC hold promise to minimize the overuse of elective PCI. This likely involves addressing processes occurring upstream of the cardiac catheterization lab, including employing systems to ensure that procedures are avoided in patients who are unlikely to benefit (eg, asymptomatic, low ischemic burden) (Figure 3) [33]. Studying hospitals that already have low rates of inappropriate PCI may inform the design and dissemination of strategies that will help improve patient selection at hospitals with higher rates. Although professional organizations have developed tools intended to facilitate appropriateness evaluation at the point-of-care [34], the use of these tools are likely to be sporadic without greater integration into the health care delivery system. Further, these applications are currently limited to determination of appropriateness of PCI after completion of the diagnostic coronary angiogram. Identifying processes prior to catheterization that contribute to PCI appropriateness may also streamline appropriate ad hoc PCI, as the need to reassess appropriateness after the diagnostic angiogram may be mitigated.
Significant barriers exist to the application of the AUC for determination of procedural underuse. As described above, we lack adequate data to ascertain gaps in symptom management that could be mitigated by proper use of PCI. Further study of symptom burden in populations of patients with coronary artery disease is needed. This may help in the identification of patient populations whose symptom burden may warrant consideration of invasive coronary procedures, including coronary angiography and PCI.
Finally, it is important to note that the AUC are based on technical considerations, ie, practice guidelines and trial evidence. They do not take into consideration patient preferences. For example, PCI can be technically appropriate for the scenario but inappropriate for the individual if the procedure is not desired by the patient. Similarly, a procedure may be of uncertain benefit but appropriate if the patient desires more aggressive procedural care and has a full understanding of the risks and benefits. Currently, we fail to convey this information to patients, as evidenced by patients’ overestimation of the benefits of PCI [34]. As we continue to work toward optimal use of PCI, we must not only address the technical appropriateness of care, but move toward incorporating patient preferences through a robust process of shared decision-making.
Corresponding author: Preston M. Schneider, MD, VA Eastern Colorado Health Care System, Cardiology Section (111B), 1055 Clermont St., Denver, CO 80220, [email protected].
Funding/support: Dr. Schneider is supported by a T32 training grant from the National Institutes of Health (5T32HL00
7822-15). Dr. Bradley is supported by a Career Development Award (HSR&D-CDA2 10-199) from VA Health Services Research & Development.
Financial disclosures: None.
1. Cassel CK, Guest JA. Choosing wisely: helping physicians and patients make smart decisions about their care. JAMA 2012;307:1801–2.
2. Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics—2013 update: a report from the American Heart Association. Circulation 2013;127:e6–e245.
3. HCUPnet: A tool for identifying, tracking, and analyzing national hospital statistics. Accessed 22 Oct 2013 at http://hcupnet.ahrq.gov/HCUPnet.jsp?Parms=
H4sIAAAAAAAAABXBMQ6AIBAEwC9JAg.gsLAhRvjAnnuXgGihFb9XZwYe3EhLdpN2h2aIcsnQLCp9jQVbLDN3ksq
DnSeqVXzNfIAP9mtmLy0rZhdIAAAA83D0C2BCAE02DD1508408B2C5C094F1ADF6E788C&JS=Y.
4. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet 2003;361:13–20.
5. Boden WE, O’Rourke RA, Teo KK, et al. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med 2007;356:1503–16.
6. Boden WE, O’Rourke RA, Teo KK, et al. Impact of optimal medical therapy with or without percutaneous coronary intervention on long-term cardiovascular end points in patients with stable coronary artery disease (from the COURAGE Trial). Am J Cardiol 2009;104:1–4.
7. Stergiopoulos K, Brown DL. Initial coronary stent implantation with medical therapy vs medical therapy alone for stable coronary artery disease: Meta-analysis of randomized controlled trials. Arch Intern Med 2012;172:312–9.
8. McCullough PA, Adam A, Becker CR, et al. Epidemiology and prognostic implications of contrast-induced nephropathy. Contrast-Induc Nephrop Clin Insights Pract Guid Rep CIN Consens Work Panel 2006;98:5–13.
9. Roe MT, Messenger JC, Weintraub WS, et al. Treatments, trends, and outcomes of acute myocardial infarction and percutaneous coronary intervention. J Am Coll Cardiol 2010;56:254–63.
10. Patel MR, Dehmer GJ, Hirshfeld JW, et al. ACCF/SCAI/STS/AATS/AHA/ASNC 2009 Appropriateness Criteria for Coronary Revascularization: A Report by the American College of Cardiology Foundation Appropriateness Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, and the American Society of Nuclear Cardiology Endorsed by the American Society of Echocardiography, the Heart Failure Society of America, and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol 2009;53:530–53.
11. Patel MR, Dehmer GJ, Hirshfeld JW, et al. ACCF/SCAI/STS/AATS/AHA/ASNC/HFSA/SCCT 2012 Appropriate Use Criteria for Coronary Revascularization Focused Update: A Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, American Society of Nuclear Cardiology, and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol 2012;59:857–81.
12. Dartmouth Atlas of Health Care. Accessed 8 Jan 2014 at www.dartmouthatlas.org.
13. Dartmouth Atlas of Health Care: Studies of surgical variation. Cardiac surgery report. 2005. Accessed 8 Jan 2014 at www.dartmouthatlas.org/publications/reports.aspx.
14. Fisher ES, Wennberg DE, Stukel TA, et al. The implications of regional variations in medicare spending. part 1: the content, quality, and accessibility of care. Ann Intern Med 2003;138:273–87.
15. Fisher ES, Wennberg DE, Stukel TA, et al. The implications of regional variations in medicare spending. part 2: health outcomes and satisfaction with care. Ann Intern Med 2003;138:288–98.
16. Abelson R. Heart procedure is off the charts in an Ohio city. New York Times 2006. Accessed 23 Apr 2013 at www.nytimes.com/2006/08/18/business/18stent.html.
17. Akhter N, Milford-Beland S, Roe MT, et al. Gender differences among patients with acute coronary syndromes undergoing percutaneous coronary intervention in the American College of Cardiology-National Cardiovascular Data Registry (ACC-NCDR). Am Heart J 2009;157:141–8.
18. Blomkalns AL, Chen AY, Hochman JS, et al. Gender disparities in the diagnosis and treatment of non–ST-segment elevation acute coronary syndromesLarge-scale observations from the CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the American College of Cardiology/American Heart Association Guidelines) National Quality Improvement Initiative. J Am Coll Cardiol 2005;45:832–7.
19. Daly C, Clemens F, Lopez Sendon JL, et al. Gender differences in the management and clinical outcome of stable angina. Circulation 2006;113:490–8.
20. Groeneveld PW, Heidenreich PA, Garber AM. Racial disparity in cardiac procedures and mortality among long-term survivors of cardiac arrest. Circulation 2003;108:286–91.
21. Hannan EL, Zhong Y, Walford G, et al. Underutilization of percutaneous coronary intervention for ST-elevation myocardial infarction in Medicaid patients relative to private insurance patients. J Intervent Cardiol 2013;26:470–81.
22. Sonel AF, Good CB, Mulgund J, et al. Racial variations in treatment and outcomes of black and white patients with high-risk non–ST-elevation acute coronary syndromes: insights From CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the ACC/AHA Guidelines?). Circulation 2005;111:1225–32.
23. Patel MR, Spertus JA, Brindis RG, et al. ACCF proposed method for evaluating the appropriateness of cardiovascular imaging. J Am Coll Cardiol 2005;46:1606–13.
24. Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI Guideline for percutaneous coronary intervention: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation 2011;124:2574–609.
25. Campeau L. Letter: Grading of angina pectoris. Circulation 1976;54:522–3.
26. Chan PS, Patel MR, Klein LW, et al. Appropriateness of percutaneous coronary intervention. JAMA 2011;306:53–61.
27. Hannan EL, Cozzens K, Samadashvili Z, et al. Appropriateness of coronary revascularization for patients without acute coronary syndromes. J Am Coll Cardiol 2012;59:1870–6.
28. Bradley SM, Maynard C, Bryson CL. Appropriateness of percutaneous coronary interventions in Washington State. Circ Cardiovasc Qual Outcomes 2012;5:445–53.
29. Nallamothu BK, Tommaso CL, Anderson HV, et al. ACC/AHA/SCAI/AMA–Convened PCPI/NCQA 2013 Performance measures for adults undergoing percutaneous coronary intervention. A report of the American College of Cardiology/American Heart Association Task Force on Performance Measures, the Society for Cardiovascular Angiography and Interventions, the American Medical Association–Convened Physician Consortium for Performance Improvement, and the National Committee for Quality Assurance. J Am Coll Cardiol 2014;63:722–45.
30. Ko DT, Guo H, Wijeysundera HC, et al. Assessing the association of appropriateness of coronary revascularization and clinical outcomes for patients with stable coronary artery disease. J Am Coll Cardiol 2012;60:1876–84.
31. Matlock DD, Groeneveld PW, Sidney S, et al. Geographic variation in cardiovascular procedure use among medicare fee-for-service vs medicare advantage beneficiaries. JAMA 2013;310:155–62.
32. Beltrame JF, Weekes AJ, Morgan C, et al. The prevalence of weekly angina among patients with chronic stable angina in primary care practices: The coronary artery disease in general practice (cadence) study. Arch Intern Med 2009;169:1491–9.
33. Bradley SM, Spertus JA, Nallamothu BK, et al. The association between patient selection for diagnostic coronary angiography and hospital-level PCI appropriateness: Insights from the NCDR. Circ Cardiovasc Qual Outcomes 2013;6:A1. Accessed 20 Nov 2013 at http://circoutcomes.ahajournals.org/cgi/content/short/6/3_MeetingAbstracts/A1?rss=1.
34. Lee J, Chuu K, Spertus J, et al. Patients overestimate the potential benefits of elective percutaneous coronary intervention. Mo Med 2012;109:79.
1. Cassel CK, Guest JA. Choosing wisely: helping physicians and patients make smart decisions about their care. JAMA 2012;307:1801–2.
2. Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics—2013 update: a report from the American Heart Association. Circulation 2013;127:e6–e245.
3. HCUPnet: A tool for identifying, tracking, and analyzing national hospital statistics. Accessed 22 Oct 2013 at http://hcupnet.ahrq.gov/HCUPnet.jsp?Parms=
H4sIAAAAAAAAABXBMQ6AIBAEwC9JAg.gsLAhRvjAnnuXgGihFb9XZwYe3EhLdpN2h2aIcsnQLCp9jQVbLDN3ksq
DnSeqVXzNfIAP9mtmLy0rZhdIAAAA83D0C2BCAE02DD1508408B2C5C094F1ADF6E788C&JS=Y.
4. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet 2003;361:13–20.
5. Boden WE, O’Rourke RA, Teo KK, et al. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med 2007;356:1503–16.
6. Boden WE, O’Rourke RA, Teo KK, et al. Impact of optimal medical therapy with or without percutaneous coronary intervention on long-term cardiovascular end points in patients with stable coronary artery disease (from the COURAGE Trial). Am J Cardiol 2009;104:1–4.
7. Stergiopoulos K, Brown DL. Initial coronary stent implantation with medical therapy vs medical therapy alone for stable coronary artery disease: Meta-analysis of randomized controlled trials. Arch Intern Med 2012;172:312–9.
8. McCullough PA, Adam A, Becker CR, et al. Epidemiology and prognostic implications of contrast-induced nephropathy. Contrast-Induc Nephrop Clin Insights Pract Guid Rep CIN Consens Work Panel 2006;98:5–13.
9. Roe MT, Messenger JC, Weintraub WS, et al. Treatments, trends, and outcomes of acute myocardial infarction and percutaneous coronary intervention. J Am Coll Cardiol 2010;56:254–63.
10. Patel MR, Dehmer GJ, Hirshfeld JW, et al. ACCF/SCAI/STS/AATS/AHA/ASNC 2009 Appropriateness Criteria for Coronary Revascularization: A Report by the American College of Cardiology Foundation Appropriateness Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, and the American Society of Nuclear Cardiology Endorsed by the American Society of Echocardiography, the Heart Failure Society of America, and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol 2009;53:530–53.
11. Patel MR, Dehmer GJ, Hirshfeld JW, et al. ACCF/SCAI/STS/AATS/AHA/ASNC/HFSA/SCCT 2012 Appropriate Use Criteria for Coronary Revascularization Focused Update: A Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, American Society of Nuclear Cardiology, and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol 2012;59:857–81.
12. Dartmouth Atlas of Health Care. Accessed 8 Jan 2014 at www.dartmouthatlas.org.
13. Dartmouth Atlas of Health Care: Studies of surgical variation. Cardiac surgery report. 2005. Accessed 8 Jan 2014 at www.dartmouthatlas.org/publications/reports.aspx.
14. Fisher ES, Wennberg DE, Stukel TA, et al. The implications of regional variations in medicare spending. part 1: the content, quality, and accessibility of care. Ann Intern Med 2003;138:273–87.
15. Fisher ES, Wennberg DE, Stukel TA, et al. The implications of regional variations in medicare spending. part 2: health outcomes and satisfaction with care. Ann Intern Med 2003;138:288–98.
16. Abelson R. Heart procedure is off the charts in an Ohio city. New York Times 2006. Accessed 23 Apr 2013 at www.nytimes.com/2006/08/18/business/18stent.html.
17. Akhter N, Milford-Beland S, Roe MT, et al. Gender differences among patients with acute coronary syndromes undergoing percutaneous coronary intervention in the American College of Cardiology-National Cardiovascular Data Registry (ACC-NCDR). Am Heart J 2009;157:141–8.
18. Blomkalns AL, Chen AY, Hochman JS, et al. Gender disparities in the diagnosis and treatment of non–ST-segment elevation acute coronary syndromesLarge-scale observations from the CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the American College of Cardiology/American Heart Association Guidelines) National Quality Improvement Initiative. J Am Coll Cardiol 2005;45:832–7.
19. Daly C, Clemens F, Lopez Sendon JL, et al. Gender differences in the management and clinical outcome of stable angina. Circulation 2006;113:490–8.
20. Groeneveld PW, Heidenreich PA, Garber AM. Racial disparity in cardiac procedures and mortality among long-term survivors of cardiac arrest. Circulation 2003;108:286–91.
21. Hannan EL, Zhong Y, Walford G, et al. Underutilization of percutaneous coronary intervention for ST-elevation myocardial infarction in Medicaid patients relative to private insurance patients. J Intervent Cardiol 2013;26:470–81.
22. Sonel AF, Good CB, Mulgund J, et al. Racial variations in treatment and outcomes of black and white patients with high-risk non–ST-elevation acute coronary syndromes: insights From CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the ACC/AHA Guidelines?). Circulation 2005;111:1225–32.
23. Patel MR, Spertus JA, Brindis RG, et al. ACCF proposed method for evaluating the appropriateness of cardiovascular imaging. J Am Coll Cardiol 2005;46:1606–13.
24. Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI Guideline for percutaneous coronary intervention: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation 2011;124:2574–609.
25. Campeau L. Letter: Grading of angina pectoris. Circulation 1976;54:522–3.
26. Chan PS, Patel MR, Klein LW, et al. Appropriateness of percutaneous coronary intervention. JAMA 2011;306:53–61.
27. Hannan EL, Cozzens K, Samadashvili Z, et al. Appropriateness of coronary revascularization for patients without acute coronary syndromes. J Am Coll Cardiol 2012;59:1870–6.
28. Bradley SM, Maynard C, Bryson CL. Appropriateness of percutaneous coronary interventions in Washington State. Circ Cardiovasc Qual Outcomes 2012;5:445–53.
29. Nallamothu BK, Tommaso CL, Anderson HV, et al. ACC/AHA/SCAI/AMA–Convened PCPI/NCQA 2013 Performance measures for adults undergoing percutaneous coronary intervention. A report of the American College of Cardiology/American Heart Association Task Force on Performance Measures, the Society for Cardiovascular Angiography and Interventions, the American Medical Association–Convened Physician Consortium for Performance Improvement, and the National Committee for Quality Assurance. J Am Coll Cardiol 2014;63:722–45.
30. Ko DT, Guo H, Wijeysundera HC, et al. Assessing the association of appropriateness of coronary revascularization and clinical outcomes for patients with stable coronary artery disease. J Am Coll Cardiol 2012;60:1876–84.
31. Matlock DD, Groeneveld PW, Sidney S, et al. Geographic variation in cardiovascular procedure use among medicare fee-for-service vs medicare advantage beneficiaries. JAMA 2013;310:155–62.
32. Beltrame JF, Weekes AJ, Morgan C, et al. The prevalence of weekly angina among patients with chronic stable angina in primary care practices: The coronary artery disease in general practice (cadence) study. Arch Intern Med 2009;169:1491–9.
33. Bradley SM, Spertus JA, Nallamothu BK, et al. The association between patient selection for diagnostic coronary angiography and hospital-level PCI appropriateness: Insights from the NCDR. Circ Cardiovasc Qual Outcomes 2013;6:A1. Accessed 20 Nov 2013 at http://circoutcomes.ahajournals.org/cgi/content/short/6/3_MeetingAbstracts/A1?rss=1.
34. Lee J, Chuu K, Spertus J, et al. Patients overestimate the potential benefits of elective percutaneous coronary intervention. Mo Med 2012;109:79.
General Anesthesia May Raise Risk of Dementia
A history of surgery with anesthesia may raise the risk of dementia for some patients, particularly those who have been repeatedly exposed to general anesthesia (GA), say researchers from China Medical University in Taichung, Taiwan.
Their study of 26,725 patients, including 5,345 newly diagnosed with dementia and a 21,380 person control group of patients without dementia, evaluated the effects of 3 types of GA: endotracheal tube intubation (ETGA); intravenous injection (IVGA) or intramuscular injection (IMGA); and heavy sedation. The patients were also divided into subgroups: a group of high-risk patients who underwent cardiac, orthopedic, or emergency surgery; moderate-risk patients who underwent general surgery, neurosurgery, gynecologic surgery, cosmetic, rectal, thoracic, or digestive surgery; and patients who underwent other surgeries, such as dental. Patients who did not receive anesthesia were grouped as with or without surgery.
Of the patients with dementia, 32% were exposed to ETGA and 9.3% were exposed to IVGA or IMGA. Exposure to both types of anesthesia was higher in the patients with dementia. Nearly 0.5% of the total sample was exposed to heavy sedation.
The patients who were exposed to ETGA, IVGA, or IMGA had a higher risk of dementia after the researchers adjusted for age, sex, depression, diabetes, hypertension, stroke, and atherosclerosis, all of which were also independent, significant risk factors for dementia. Patients who had been exposed 2 or more times to GA had the highest risk of developing dementia. Heavy sedation was not associated with increased risk.
The relationship between surgery with GA and dementia is complex, the researchers say, because patients who receive anesthesia all undergo surgery. Hospitalization has been associated with the development of dementia, with multiple potential mechanisms. Surgery and GA may play individual or synergistic roles in the development of dementia, with the risk heightened by a patient’s comorbidities.
Further, the researchers say, the inhalation of general anesthetics may have neurotoxic effects that correlate with dementia. The major pathologic hallmark of Alzheimer dementia (AD) is excessive accumulation of amyloid beta (Aβ) protein in the brain. Exposure to inhalational general anesthetics may promote AD processes by inducing apoptosis and Aβ generation.
If surgery with general anesthesia is unavoidable, the researchers advise using less-toxic anesthetics, particularly in elderly patients with systemic vascular comorbidities.
Source
Chen C-W, Lin C-C, Chen K-B, Kuo Y-C, Li C-Y, Chung C-J. Alzheimers Dement. 2014;10(2):196-204.
doi: 10.1016/j.jalz.2013.05.1766.
A history of surgery with anesthesia may raise the risk of dementia for some patients, particularly those who have been repeatedly exposed to general anesthesia (GA), say researchers from China Medical University in Taichung, Taiwan.
Their study of 26,725 patients, including 5,345 newly diagnosed with dementia and a 21,380 person control group of patients without dementia, evaluated the effects of 3 types of GA: endotracheal tube intubation (ETGA); intravenous injection (IVGA) or intramuscular injection (IMGA); and heavy sedation. The patients were also divided into subgroups: a group of high-risk patients who underwent cardiac, orthopedic, or emergency surgery; moderate-risk patients who underwent general surgery, neurosurgery, gynecologic surgery, cosmetic, rectal, thoracic, or digestive surgery; and patients who underwent other surgeries, such as dental. Patients who did not receive anesthesia were grouped as with or without surgery.
Of the patients with dementia, 32% were exposed to ETGA and 9.3% were exposed to IVGA or IMGA. Exposure to both types of anesthesia was higher in the patients with dementia. Nearly 0.5% of the total sample was exposed to heavy sedation.
The patients who were exposed to ETGA, IVGA, or IMGA had a higher risk of dementia after the researchers adjusted for age, sex, depression, diabetes, hypertension, stroke, and atherosclerosis, all of which were also independent, significant risk factors for dementia. Patients who had been exposed 2 or more times to GA had the highest risk of developing dementia. Heavy sedation was not associated with increased risk.
The relationship between surgery with GA and dementia is complex, the researchers say, because patients who receive anesthesia all undergo surgery. Hospitalization has been associated with the development of dementia, with multiple potential mechanisms. Surgery and GA may play individual or synergistic roles in the development of dementia, with the risk heightened by a patient’s comorbidities.
Further, the researchers say, the inhalation of general anesthetics may have neurotoxic effects that correlate with dementia. The major pathologic hallmark of Alzheimer dementia (AD) is excessive accumulation of amyloid beta (Aβ) protein in the brain. Exposure to inhalational general anesthetics may promote AD processes by inducing apoptosis and Aβ generation.
If surgery with general anesthesia is unavoidable, the researchers advise using less-toxic anesthetics, particularly in elderly patients with systemic vascular comorbidities.
Source
Chen C-W, Lin C-C, Chen K-B, Kuo Y-C, Li C-Y, Chung C-J. Alzheimers Dement. 2014;10(2):196-204.
doi: 10.1016/j.jalz.2013.05.1766.
A history of surgery with anesthesia may raise the risk of dementia for some patients, particularly those who have been repeatedly exposed to general anesthesia (GA), say researchers from China Medical University in Taichung, Taiwan.
Their study of 26,725 patients, including 5,345 newly diagnosed with dementia and a 21,380 person control group of patients without dementia, evaluated the effects of 3 types of GA: endotracheal tube intubation (ETGA); intravenous injection (IVGA) or intramuscular injection (IMGA); and heavy sedation. The patients were also divided into subgroups: a group of high-risk patients who underwent cardiac, orthopedic, or emergency surgery; moderate-risk patients who underwent general surgery, neurosurgery, gynecologic surgery, cosmetic, rectal, thoracic, or digestive surgery; and patients who underwent other surgeries, such as dental. Patients who did not receive anesthesia were grouped as with or without surgery.
Of the patients with dementia, 32% were exposed to ETGA and 9.3% were exposed to IVGA or IMGA. Exposure to both types of anesthesia was higher in the patients with dementia. Nearly 0.5% of the total sample was exposed to heavy sedation.
The patients who were exposed to ETGA, IVGA, or IMGA had a higher risk of dementia after the researchers adjusted for age, sex, depression, diabetes, hypertension, stroke, and atherosclerosis, all of which were also independent, significant risk factors for dementia. Patients who had been exposed 2 or more times to GA had the highest risk of developing dementia. Heavy sedation was not associated with increased risk.
The relationship between surgery with GA and dementia is complex, the researchers say, because patients who receive anesthesia all undergo surgery. Hospitalization has been associated with the development of dementia, with multiple potential mechanisms. Surgery and GA may play individual or synergistic roles in the development of dementia, with the risk heightened by a patient’s comorbidities.
Further, the researchers say, the inhalation of general anesthetics may have neurotoxic effects that correlate with dementia. The major pathologic hallmark of Alzheimer dementia (AD) is excessive accumulation of amyloid beta (Aβ) protein in the brain. Exposure to inhalational general anesthetics may promote AD processes by inducing apoptosis and Aβ generation.
If surgery with general anesthesia is unavoidable, the researchers advise using less-toxic anesthetics, particularly in elderly patients with systemic vascular comorbidities.
Source
Chen C-W, Lin C-C, Chen K-B, Kuo Y-C, Li C-Y, Chung C-J. Alzheimers Dement. 2014;10(2):196-204.
doi: 10.1016/j.jalz.2013.05.1766.
Autism: Why the rise in rates?

For many years, articles about autism cited prevalence rates of approximately 7 in 10,000.1 Over the past few years, however, there appears to have been an explosion in the rate at which autism is diagnosed: More recent estimates range from about 30 in 10,0002 to one in 68.3 References to an autism epidemic appear to have originated in a 2002 California legislative report suggesting a 273% increase in autism from 1987 to 1998.4
Concerns about rising rates of autism, however, are not new. In 1943, Leo Kanner, MD, a psychiatrist and pioneer in the study of autism, published a paper titled, “Autistic disturbances of affective contact.”5 The result? “Almost overnight, the country seemed to be populated by a multitude of autistic children,” he later observed.6
To what should we attribute the current rise in reported autism rates? Even a casual review of the autism literature suggests a number of potential causes that may account for at least a portion of the recent increase.
We know more about the disorder
In his paper, Kanner described the “peculiarities” of 11 children whom he had cared for.5 While several had been diagnosed with mental retardation, childhood schizophrenia, or both, what stood out to Kanner was an “autistic aloneness” evident from the beginning of life. This was in contrast to childhood schizophrenia, in which a child experienced a departure from previously normal interrelations. His insight contributed to our understanding of what is now recognized as autism spectrum disorder (ASD).
Also in 1943, Hans Asperger, MD, was studying families with children exhibiting behaviors similar to those described by Kanner. The following year, Asperger published an article (in German) describing these children. Unfortunately, this paper—titled “Autistic psychopathy in childhood”7—was not translated into English until the early 1990s.8
Since Kanner and Asperger first called attention to the disorder, there have been numerous changes in societal and medical understanding of autism. Bruno Bettelheim, PhD, an Austrian-born child psychologist with a particular interest in emotionally disturbed children, theorized that poor maternal bonding and lack of maternal affection were responsible for autistic characteristics.9 Bernard Rimland, PhD, a psychologist and the father of an autistic child, argued for a biological basis of the disorder.10 Rimland’s theory of autism as a neurodevelopmental disorder with an unidentified organic etiology is most consistent with current medical opinion.
Definitions and diagnostic criteria have evolved
The first edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM) was published in 1952.11 Although it was nearly a decade after Dr. Kanner clearly described autism as an entity separate from childhood schizophrenia, the word autism was used in this edition only once—to describe psychotic reactions associated with schizophrenia. Similarly, autism was referred to only in relation to childhood schizophrenia in the DSMII,12 published in 1968.
DSM-III adds diagnostic criteria. In DSM-III (1980),13 specific diagnostic criteria for infantile autism and pervasive developmental disorder (PDD) appeared for the first time. Both diagnoses were clearly contrasted with a diagnosis of schizophrenia, and were used to identify children who exhibited a pervasive lack of responsiveness to others.
The DSM-III-Revised (R) (1987)14 added a classification scheme more consistent with the current standard. It included: 1) qualitative impairment in reciprocal social interaction; 2) qualitative impairment in communication and imaginative activity; and 3) restricted activity/interests.
PDD Not Otherwise Specified was also included, and served to identify those who had qualitative impairments in social interaction and communication skills but did not meet the full criteria for autism disorder or PDD.
The publication of DSM-IV (1994)15 brought another change: Specific criteria were outlined for the diagnoses of Asperger syndrome, Rett syndrome, and childhood disintegrative disorders; in the DSM-IV-Text Revision (TR) (2000),16 this structure remained relatively stable.
DSM-5 (2013) took another step, consolidating these various disorders into a single, unifying diagnosis of ASD.17 Significant controversy surrounded this change, with some viewing it as an oversimplification that does not accurately reflect important distinctions among divergent disorders18 and others arguing that it will result in unrecognized cases and exclusion of affected individuals.19 Notably, a recent study using concurrent DSM-IV and DSM-5 criteria to diagnose autism and PDD in more than 4000 children documented a high level of agreement between them.20
Diagnostic tools have improved
As the number of children diagnosed with autism has increased, so have efforts to more accurately diagnose autism as a distinct disorder.
In the 1960s, guidelines for diagnosing autism focused primarily on Kanner’s original descriptive criteria. Even in the 1980s, after DSM-III criteria identified autism as a distinct disorder, children were being evaluated with generalized developmental screening tools focused on behaviors characteristic of a severe mental handicap, without differentiating between autistic and nonautistic children.
Early autism-specific observational and structured interview tools (eg, Childhood Autism Rating Scale,21 Autism Diagnostic Interview [ADI],22 and Autistic Diagnostic Observation Schedule)23 emerged from a need for standardized diagnostic instruments that were comparable and reproducible.24 But because these tools were highly specific and initially studied in research settings with high-risk populations, they lacked the sensitivity to identify children at risk in the general population, particularly those with milder symptoms.
As the diagnosis of autism became more standardized following publication of the DSM III-R in 1987, developmental specialists were able to construct increasingly sensitive evaluation tools. The ADI was revised25 to facilitate earlier and more efficient diagnosis, allowing for assessment of children as young as 19 months of age. The Checklist for Autism in Toddlers (CHAT)26 and subsequent modification (M-CHAT)27 were among the earliest and most effective screening tools, appropriate for use in children as young as 16 months old.
Tools that followed the original CHAT (eg, the Autism Spectrum Screening Questionnaire [ASSQ]28) were adapted to better identify high-functioning children with Asperger syndrome, as well as those with autism.
Another revision of the M-CHAT—the M-CHAT-R/F (Revised with Follow-up) was validated earlier this year. In a study involving 16,000 children, 95% of those who had positive tests were found to have some form of developmental delay and almost half (47%) received an ASD diagnosis.29
Other diagnostic aids are being explored as a means of promoting earlier identification of ASD. For example, a blood test to identify differences in gene expression between children with and without ASD30 has shown initial promise, particularly in males. This test is licensed by SynapDx (Lexington, Mass) and a clinical trial to evaluate it has begun.
Results of another study demonstrating normalization of brain activity in autistic children after they’ve undergone intensive treatment31 raise the possibility of using cortical activation as measured by electroencephalography as an early biomarker for autism.
Treatment options, advocacy affect rate of diagnosis
Improvements in diagnosis and targeted identification of potentially treatable symptoms32 led to the development of new treatment options. And greater use of day care and preschool programs prompted networking among parents, who touted the benefits of early evaluation, diagnosis, and treatment. Earlier screening, not surprisingly, led to an increase in the target population.
|
Local as well as national advocacy groups, led primarily by parents, have become powerful voices for improvements in services offered to children with autism. And research studies with varying degrees of sophistication continue to be published, further fueling the demand for school systems to provide supportive learning environments as required by the Individuals with Disabilities Education Act, initially enacted in 1975 and amended in 2004.33
Federal and state funds in the form of Medicaid waivers are available to provide long-term care services in home and community settings, while private insurers typically pay for associated treatment modalities for those with an autism diagnosis, including physical, occupational, and speech therapy, among other services.
Finally, politicians and celebrities with personal connections to autism have joined the effort to increase awareness and improve the quality and availability of services—further assuring that autism is recognized as a legitimate, definable, and treatable disorder.
As an autism diagnosis has become more socially acceptable, it has at times replaced diagnoses of learning disability and mental retardation, a trend known as “diagnostic substitution.”34 Indeed, having a child with an ASD diagnosis often makes it possible for parents to secure services that might otherwise be unavailable to them.
Is the incidence of autism linked to the environment?
Numerous environmental, nutritional, and pharmaceutical changes have been cited as reasons for what is perceived as an increasing incidence of autism in recent years. For example, some contend that greater use of food preservatives and greater exposure of young children to environmental toxins are contributing factors.35
Thimerosal. Perhaps most notable is the assertion—since disproven—that thimerosal, a substance previously used in the manufacture of several childhood vaccines, was a leading cause of autism.36,37 In fact, one study documented an increase in autism after thimerosal had been discontinued.38 (For more on the thimerosal controversy, see “Autism: 5 misconceptions that can complicate care”.)
Autism comorbidity. As autism is frequently comorbid with other developmental disabilities, advances in medical technology that have led to a decline in neonatal death and overall mortality among the disabled may mean more survivors are subsequently diagnosed with an autism comorbidity.
Biological factors. Recent studies suggest that advanced paternal age can increase the risk of autism.39 Twin studies suggest moderate genetic heritability, along with a substantial environmental contribution to the development of autism.40 And new research suggests that maternal stressors during pregnancy—eg, trauma, illness, or substance abuse—may increase a child’s risk of developing autism, among other psychiatric disorders.41
The important role you play in the diagnosis of autism
It is clear that autism is more common than previously thought3 and that various factors are at work. Ensuring that children are promptly and properly evaluated begins when primary care physicians take parents’ concerns seriously and keep an eye out for common symptoms and characteristic developmental delays that may be evident even in the first year of life.
If symptoms are not severe enough to be detected in the child’s first several years, the next likely presentation will be when a parent gets a call from school suggesting that their child be tested for autism. While this delayed presentation suggests a higher level of functioning, a full evaluation, including the use of questionnaires such as the Social Responsiveness Scale42 and ASSQ,28 and appropriate referrals are still vital.
Puberty is another time when characteristics suggestive of autism that escaped earlier detection may be noted, and vague behavioral issues or concerns about intellectual impairment may become sufficiently troublesome to prompt a thorough evaluation. While behavioral therapy can be very helpful in such cases, medical therapy directed at co-occurring conditions (ie, a mood or anxiety disorder, including obsessive-compulsive disorder) may also provide significant benefit.
Whatever the age of the child, his or her parents should be counseled as to the general nature of autism, reassured of the availability of treatment options and given the appropriate referrals, and encouraged to learn more by availing themselves of resources (TABLE) and support groups. A consumer update from the US Food and Drug Administration titled “Beware of false or misleading claims for treating autism” (http://www.fda.gov/ForConsumers/ConsumerUpdates/ucm394757.htm) will be helpful for many parents, as well.
CORRESPONDENCE
Robert G. Zylstra, EdD, LCSW, Department of Family Medicine, The University of Tennessee College of Medicine, 110 East Third Street, Chattanooga, TN 37403; [email protected]
1. Prater C, Zylstra R. Autism: a medical primer. Am Fam Physician. 2002;66:1667-1674.
2. Nassar N, Dixon G, Bourke J, et al. Autism spectrum disorders in young children: effect of changes in diagnostic practices. Int J Epidemiol. 2009;38:1245-1254.
3. Developmental Disabilities Monitoring Network Surveillance Year 2010 Principal Investigators; Centers for Disease Control and Prevention (CDC). Prevalence of autism spectrum disorder among children aged 8 years - Autism and Developmental Disabilities Monitoring Network, 11 sites, United States, 2010. MMWR Surveill Summ. 2014;63:1-21.
4. Report to the legislature on the principle findings from the epidemiology of autism in California: a comprehensive pilot study. State of California Department of Developmental Services Web site. Available at: http://www.dds.ca.gov/Autism/docs/study_final.pdf. Accessed May 1, 2014.
5. Kanner L. Autistic disturbances of affective contact. Nervous Child. 1943;2:217-250.
6. Kanner L. Infantile autism and the schizophrenias. Behav Sci. 1965;10:412-420.
7. Asperger H. Die ‘autistischen psychopathen’ im kindesalter. Archiv für Psychiatrie und Nervenkrankheiten. 1944;117:76-136.
8. Frith U. Autism and Asperger Syndrome. Cambridge, UK: Cambridge University Press; 1991.
9. Bettelheim B. The empty fortress: Infantile autism and the birth of the self. New York: Free Press; 1972.
10. Rimland B. Infantile autism: The syndrome and its implications for a neural theory of behavior. New York: Appleton-Century- Crofts; 1964.
11. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: American Psychiatric Association; 1952.
12. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 2nd ed. Washington, DC: American Psychiatric Association;1968.
13. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 3rd ed. Washington, DC: American Psychiatric Association; 1980.
14. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 3rd ed, revised. Washington, DC: American Psychiatric Association; 1987.
15. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association; 1994.
16. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed, text revision. Washington: DC: American Psychiatric Association; 2000.
17. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Publishing; 2013.
18. Ghaziuddin M. Brief report: Should the DMS-V drop Asperger Syndrome? J Autism Dev Disord. 2010;40:1146-1148.
19. Wing L, Gould J, Gillberg C. Autism spectrum disorders in the DSM-V: better or worse than the DSM-IV? Res Dev Disabil. 2011;32:768-773.
20. Huerta M, Bishop S, Duncan A, et al. Application of DSM-5 criteria for Autism Spectrum Disorder to three samples of children with DSM-IV diagnoses of pervasive developmental disorders. Am J Psychiatry. 2012;169:1056-1064.
21. Schopler E, Reichler RJ, DeVellis RF. Toward objective classification of childhood autism: Childhood Autism Rating Scale (CARS). J Autism Dev Disord. 1980;10:91-103.
22. Le Couteur A, Rutter M, Lord C, et al. Autism diagnostic interview: a standardized investigator-based instrument. J Autism Dev Disord. 1989;19:363-387.
23. Lord C, Rutter M, Goode S, et al. Autism diagnostic observation schedule: a standardized observation of communicative and social behavior. J Autism Dev Disord. 1989;19:185-212.
24. Zwaigenbaum L. Advances in the early detection of autism. Curr Opin Neurol. 2010;23:97-102.
25. Lord C, Rutter M, Le Couteur A. Autism Diagnostic Interview-Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J Autism Dev Disord. 1994;24:659-685.
26. Baron-Cohen S, Allen J, Gillberg C. Can autism be detected at 18 months? The needle, the haystack, and the CHAT. Br J Psychiatry. 1992;161:839-843.
27. Robins DL, Fein D, Barton ML, et al. The Modified Checklist for Autism in Toddlers: an initial study investigating the early detection of autism and pervasive developmental disorders. J Autism Dev Disord. 2001;31:131-144.
28. Ehlers S, Gilberg C, Wing L. A screening questionnaire for Asperger syndrome and other high-functioning autism spectrum disorders in school age children. J Autism Dev Disord. 1999;29:129-141.
29. Robins DL, Casagrande K, Barton M, et al. Validation of the modified checklist for Autism in toddlers, revised with followup (M-CHAT-R/F). Pediatrics. 2014;133:37-45.
30. Kong SW, Collins CD, Shimizu-Motohashi Y, et al. Characteristics and predictive value of blood transcriptome signature in males with autism spectrum disorders. PLoS One. 2012;7:e49475.
31. Dawson G, Jones EJ, Merkle K, et al. Early behavioral intervention is associated with normalized brain activity in young children with autism. J Am Acad Child Adolesc Psychiatry. 2012;51:1150-1159.
32. Autism ALARM. National Center for Medical Home Implementation Web site. Available at: http://www.medicalhomeinfo.org/downloads/pdfs/AutismAlarm.pdf. Accessed March 4, 2013.
33. IDEA. Autism Community Web site. Available at: http://www.autism-community.com/education/idea/. Accessed April 25, 2014.
34. Shattuck P. The contribution of diagnostic substitution to the growing administrative prevalence of autism in US special education. Pediatrics. 2006;117:1028-1037.
35. Landrigan P. What causes autism? Exploring the environmental contribution. Curr Opin Pediatr. 2010;22:219-225.
36. The great thimerosal cover-up: Mercury, vaccines, autism and your child’s health. Natural Health News & Scientific Discoveries Web site. Available at: http://www.naturalnews.com/011764_thimerosal_mercury.html. Accessed March 4, 2013.
37. Price CS, Thompson WW, Goodson B, et al. Prenatal and infant exposure to thimerosal from vaccines and immunoglobulins and risk of autism. Pediatrics. 2010;126:656-664.
38. Fombonne E, Zakarian R, Bennett A, et al. Pervasive developmental disorders in Montreal, Quebec, Canada: prevalence and links with immunizations. Pediatrics. 2006;118:e139-e150.
39. Flatscher-Bader T, Foldi CJ, Chong S, et al. Increased de novo copy number variants in the offspring of older males. Transl Psychiatry. 2011;1:e34.
40. Hallmayer J, Cleveland S, Torres A, et al. Genetic heritability and shared environmental factors among twin pairs with autism. Arch Gen Psychiatry. 2011;68:1095-1102.
41. Fine R, Zhang J, Stevens HE. Prenatal stress and inhibitory neuron systems: implications for neuropsychiatric disorders Mol Psychiatry. 2014 April 22. [Epub ahead of print].
42. Joshi G, Petty DR, Fried R, et al. Discriminant and concurrent validity of a simplified DSM-based structured diagnostic instrument for the assessment of autism spectrum disorders in youth and young adults. BMC Psychiatry. 2011;11:204.
For many years, articles about autism cited prevalence rates of approximately 7 in 10,000.1 Over the past few years, however, there appears to have been an explosion in the rate at which autism is diagnosed: More recent estimates range from about 30 in 10,0002 to one in 68.3 References to an autism epidemic appear to have originated in a 2002 California legislative report suggesting a 273% increase in autism from 1987 to 1998.4
Concerns about rising rates of autism, however, are not new. In 1943, Leo Kanner, MD, a psychiatrist and pioneer in the study of autism, published a paper titled, “Autistic disturbances of affective contact.”5 The result? “Almost overnight, the country seemed to be populated by a multitude of autistic children,” he later observed.6
To what should we attribute the current rise in reported autism rates? Even a casual review of the autism literature suggests a number of potential causes that may account for at least a portion of the recent increase.
We know more about the disorder
In his paper, Kanner described the “peculiarities” of 11 children whom he had cared for.5 While several had been diagnosed with mental retardation, childhood schizophrenia, or both, what stood out to Kanner was an “autistic aloneness” evident from the beginning of life. This was in contrast to childhood schizophrenia, in which a child experienced a departure from previously normal interrelations. His insight contributed to our understanding of what is now recognized as autism spectrum disorder (ASD).
Also in 1943, Hans Asperger, MD, was studying families with children exhibiting behaviors similar to those described by Kanner. The following year, Asperger published an article (in German) describing these children. Unfortunately, this paper—titled “Autistic psychopathy in childhood”7—was not translated into English until the early 1990s.8
Since Kanner and Asperger first called attention to the disorder, there have been numerous changes in societal and medical understanding of autism. Bruno Bettelheim, PhD, an Austrian-born child psychologist with a particular interest in emotionally disturbed children, theorized that poor maternal bonding and lack of maternal affection were responsible for autistic characteristics.9 Bernard Rimland, PhD, a psychologist and the father of an autistic child, argued for a biological basis of the disorder.10 Rimland’s theory of autism as a neurodevelopmental disorder with an unidentified organic etiology is most consistent with current medical opinion.
Definitions and diagnostic criteria have evolved
The first edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM) was published in 1952.11 Although it was nearly a decade after Dr. Kanner clearly described autism as an entity separate from childhood schizophrenia, the word autism was used in this edition only once—to describe psychotic reactions associated with schizophrenia. Similarly, autism was referred to only in relation to childhood schizophrenia in the DSMII,12 published in 1968.
DSM-III adds diagnostic criteria. In DSM-III (1980),13 specific diagnostic criteria for infantile autism and pervasive developmental disorder (PDD) appeared for the first time. Both diagnoses were clearly contrasted with a diagnosis of schizophrenia, and were used to identify children who exhibited a pervasive lack of responsiveness to others.
The DSM-III-Revised (R) (1987)14 added a classification scheme more consistent with the current standard. It included: 1) qualitative impairment in reciprocal social interaction; 2) qualitative impairment in communication and imaginative activity; and 3) restricted activity/interests.
PDD Not Otherwise Specified was also included, and served to identify those who had qualitative impairments in social interaction and communication skills but did not meet the full criteria for autism disorder or PDD.
The publication of DSM-IV (1994)15 brought another change: Specific criteria were outlined for the diagnoses of Asperger syndrome, Rett syndrome, and childhood disintegrative disorders; in the DSM-IV-Text Revision (TR) (2000),16 this structure remained relatively stable.
DSM-5 (2013) took another step, consolidating these various disorders into a single, unifying diagnosis of ASD.17 Significant controversy surrounded this change, with some viewing it as an oversimplification that does not accurately reflect important distinctions among divergent disorders18 and others arguing that it will result in unrecognized cases and exclusion of affected individuals.19 Notably, a recent study using concurrent DSM-IV and DSM-5 criteria to diagnose autism and PDD in more than 4000 children documented a high level of agreement between them.20
Diagnostic tools have improved
As the number of children diagnosed with autism has increased, so have efforts to more accurately diagnose autism as a distinct disorder.
In the 1960s, guidelines for diagnosing autism focused primarily on Kanner’s original descriptive criteria. Even in the 1980s, after DSM-III criteria identified autism as a distinct disorder, children were being evaluated with generalized developmental screening tools focused on behaviors characteristic of a severe mental handicap, without differentiating between autistic and nonautistic children.
Early autism-specific observational and structured interview tools (eg, Childhood Autism Rating Scale,21 Autism Diagnostic Interview [ADI],22 and Autistic Diagnostic Observation Schedule)23 emerged from a need for standardized diagnostic instruments that were comparable and reproducible.24 But because these tools were highly specific and initially studied in research settings with high-risk populations, they lacked the sensitivity to identify children at risk in the general population, particularly those with milder symptoms.
As the diagnosis of autism became more standardized following publication of the DSM III-R in 1987, developmental specialists were able to construct increasingly sensitive evaluation tools. The ADI was revised25 to facilitate earlier and more efficient diagnosis, allowing for assessment of children as young as 19 months of age. The Checklist for Autism in Toddlers (CHAT)26 and subsequent modification (M-CHAT)27 were among the earliest and most effective screening tools, appropriate for use in children as young as 16 months old.
Tools that followed the original CHAT (eg, the Autism Spectrum Screening Questionnaire [ASSQ]28) were adapted to better identify high-functioning children with Asperger syndrome, as well as those with autism.
Another revision of the M-CHAT—the M-CHAT-R/F (Revised with Follow-up) was validated earlier this year. In a study involving 16,000 children, 95% of those who had positive tests were found to have some form of developmental delay and almost half (47%) received an ASD diagnosis.29
Other diagnostic aids are being explored as a means of promoting earlier identification of ASD. For example, a blood test to identify differences in gene expression between children with and without ASD30 has shown initial promise, particularly in males. This test is licensed by SynapDx (Lexington, Mass) and a clinical trial to evaluate it has begun.
Results of another study demonstrating normalization of brain activity in autistic children after they’ve undergone intensive treatment31 raise the possibility of using cortical activation as measured by electroencephalography as an early biomarker for autism.
Treatment options, advocacy affect rate of diagnosis
Improvements in diagnosis and targeted identification of potentially treatable symptoms32 led to the development of new treatment options. And greater use of day care and preschool programs prompted networking among parents, who touted the benefits of early evaluation, diagnosis, and treatment. Earlier screening, not surprisingly, led to an increase in the target population.
|
Local as well as national advocacy groups, led primarily by parents, have become powerful voices for improvements in services offered to children with autism. And research studies with varying degrees of sophistication continue to be published, further fueling the demand for school systems to provide supportive learning environments as required by the Individuals with Disabilities Education Act, initially enacted in 1975 and amended in 2004.33
Federal and state funds in the form of Medicaid waivers are available to provide long-term care services in home and community settings, while private insurers typically pay for associated treatment modalities for those with an autism diagnosis, including physical, occupational, and speech therapy, among other services.
Finally, politicians and celebrities with personal connections to autism have joined the effort to increase awareness and improve the quality and availability of services—further assuring that autism is recognized as a legitimate, definable, and treatable disorder.
As an autism diagnosis has become more socially acceptable, it has at times replaced diagnoses of learning disability and mental retardation, a trend known as “diagnostic substitution.”34 Indeed, having a child with an ASD diagnosis often makes it possible for parents to secure services that might otherwise be unavailable to them.
Is the incidence of autism linked to the environment?
Numerous environmental, nutritional, and pharmaceutical changes have been cited as reasons for what is perceived as an increasing incidence of autism in recent years. For example, some contend that greater use of food preservatives and greater exposure of young children to environmental toxins are contributing factors.35
Thimerosal. Perhaps most notable is the assertion—since disproven—that thimerosal, a substance previously used in the manufacture of several childhood vaccines, was a leading cause of autism.36,37 In fact, one study documented an increase in autism after thimerosal had been discontinued.38 (For more on the thimerosal controversy, see “Autism: 5 misconceptions that can complicate care”.)
Autism comorbidity. As autism is frequently comorbid with other developmental disabilities, advances in medical technology that have led to a decline in neonatal death and overall mortality among the disabled may mean more survivors are subsequently diagnosed with an autism comorbidity.
Biological factors. Recent studies suggest that advanced paternal age can increase the risk of autism.39 Twin studies suggest moderate genetic heritability, along with a substantial environmental contribution to the development of autism.40 And new research suggests that maternal stressors during pregnancy—eg, trauma, illness, or substance abuse—may increase a child’s risk of developing autism, among other psychiatric disorders.41
The important role you play in the diagnosis of autism
It is clear that autism is more common than previously thought3 and that various factors are at work. Ensuring that children are promptly and properly evaluated begins when primary care physicians take parents’ concerns seriously and keep an eye out for common symptoms and characteristic developmental delays that may be evident even in the first year of life.
If symptoms are not severe enough to be detected in the child’s first several years, the next likely presentation will be when a parent gets a call from school suggesting that their child be tested for autism. While this delayed presentation suggests a higher level of functioning, a full evaluation, including the use of questionnaires such as the Social Responsiveness Scale42 and ASSQ,28 and appropriate referrals are still vital.
Puberty is another time when characteristics suggestive of autism that escaped earlier detection may be noted, and vague behavioral issues or concerns about intellectual impairment may become sufficiently troublesome to prompt a thorough evaluation. While behavioral therapy can be very helpful in such cases, medical therapy directed at co-occurring conditions (ie, a mood or anxiety disorder, including obsessive-compulsive disorder) may also provide significant benefit.
Whatever the age of the child, his or her parents should be counseled as to the general nature of autism, reassured of the availability of treatment options and given the appropriate referrals, and encouraged to learn more by availing themselves of resources (TABLE) and support groups. A consumer update from the US Food and Drug Administration titled “Beware of false or misleading claims for treating autism” (http://www.fda.gov/ForConsumers/ConsumerUpdates/ucm394757.htm) will be helpful for many parents, as well.
CORRESPONDENCE
Robert G. Zylstra, EdD, LCSW, Department of Family Medicine, The University of Tennessee College of Medicine, 110 East Third Street, Chattanooga, TN 37403; [email protected]
For many years, articles about autism cited prevalence rates of approximately 7 in 10,000.1 Over the past few years, however, there appears to have been an explosion in the rate at which autism is diagnosed: More recent estimates range from about 30 in 10,0002 to one in 68.3 References to an autism epidemic appear to have originated in a 2002 California legislative report suggesting a 273% increase in autism from 1987 to 1998.4
Concerns about rising rates of autism, however, are not new. In 1943, Leo Kanner, MD, a psychiatrist and pioneer in the study of autism, published a paper titled, “Autistic disturbances of affective contact.”5 The result? “Almost overnight, the country seemed to be populated by a multitude of autistic children,” he later observed.6
To what should we attribute the current rise in reported autism rates? Even a casual review of the autism literature suggests a number of potential causes that may account for at least a portion of the recent increase.
We know more about the disorder
In his paper, Kanner described the “peculiarities” of 11 children whom he had cared for.5 While several had been diagnosed with mental retardation, childhood schizophrenia, or both, what stood out to Kanner was an “autistic aloneness” evident from the beginning of life. This was in contrast to childhood schizophrenia, in which a child experienced a departure from previously normal interrelations. His insight contributed to our understanding of what is now recognized as autism spectrum disorder (ASD).
Also in 1943, Hans Asperger, MD, was studying families with children exhibiting behaviors similar to those described by Kanner. The following year, Asperger published an article (in German) describing these children. Unfortunately, this paper—titled “Autistic psychopathy in childhood”7—was not translated into English until the early 1990s.8
Since Kanner and Asperger first called attention to the disorder, there have been numerous changes in societal and medical understanding of autism. Bruno Bettelheim, PhD, an Austrian-born child psychologist with a particular interest in emotionally disturbed children, theorized that poor maternal bonding and lack of maternal affection were responsible for autistic characteristics.9 Bernard Rimland, PhD, a psychologist and the father of an autistic child, argued for a biological basis of the disorder.10 Rimland’s theory of autism as a neurodevelopmental disorder with an unidentified organic etiology is most consistent with current medical opinion.
Definitions and diagnostic criteria have evolved
The first edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM) was published in 1952.11 Although it was nearly a decade after Dr. Kanner clearly described autism as an entity separate from childhood schizophrenia, the word autism was used in this edition only once—to describe psychotic reactions associated with schizophrenia. Similarly, autism was referred to only in relation to childhood schizophrenia in the DSMII,12 published in 1968.
DSM-III adds diagnostic criteria. In DSM-III (1980),13 specific diagnostic criteria for infantile autism and pervasive developmental disorder (PDD) appeared for the first time. Both diagnoses were clearly contrasted with a diagnosis of schizophrenia, and were used to identify children who exhibited a pervasive lack of responsiveness to others.
The DSM-III-Revised (R) (1987)14 added a classification scheme more consistent with the current standard. It included: 1) qualitative impairment in reciprocal social interaction; 2) qualitative impairment in communication and imaginative activity; and 3) restricted activity/interests.
PDD Not Otherwise Specified was also included, and served to identify those who had qualitative impairments in social interaction and communication skills but did not meet the full criteria for autism disorder or PDD.
The publication of DSM-IV (1994)15 brought another change: Specific criteria were outlined for the diagnoses of Asperger syndrome, Rett syndrome, and childhood disintegrative disorders; in the DSM-IV-Text Revision (TR) (2000),16 this structure remained relatively stable.
DSM-5 (2013) took another step, consolidating these various disorders into a single, unifying diagnosis of ASD.17 Significant controversy surrounded this change, with some viewing it as an oversimplification that does not accurately reflect important distinctions among divergent disorders18 and others arguing that it will result in unrecognized cases and exclusion of affected individuals.19 Notably, a recent study using concurrent DSM-IV and DSM-5 criteria to diagnose autism and PDD in more than 4000 children documented a high level of agreement between them.20
Diagnostic tools have improved
As the number of children diagnosed with autism has increased, so have efforts to more accurately diagnose autism as a distinct disorder.
In the 1960s, guidelines for diagnosing autism focused primarily on Kanner’s original descriptive criteria. Even in the 1980s, after DSM-III criteria identified autism as a distinct disorder, children were being evaluated with generalized developmental screening tools focused on behaviors characteristic of a severe mental handicap, without differentiating between autistic and nonautistic children.
Early autism-specific observational and structured interview tools (eg, Childhood Autism Rating Scale,21 Autism Diagnostic Interview [ADI],22 and Autistic Diagnostic Observation Schedule)23 emerged from a need for standardized diagnostic instruments that were comparable and reproducible.24 But because these tools were highly specific and initially studied in research settings with high-risk populations, they lacked the sensitivity to identify children at risk in the general population, particularly those with milder symptoms.
As the diagnosis of autism became more standardized following publication of the DSM III-R in 1987, developmental specialists were able to construct increasingly sensitive evaluation tools. The ADI was revised25 to facilitate earlier and more efficient diagnosis, allowing for assessment of children as young as 19 months of age. The Checklist for Autism in Toddlers (CHAT)26 and subsequent modification (M-CHAT)27 were among the earliest and most effective screening tools, appropriate for use in children as young as 16 months old.
Tools that followed the original CHAT (eg, the Autism Spectrum Screening Questionnaire [ASSQ]28) were adapted to better identify high-functioning children with Asperger syndrome, as well as those with autism.
Another revision of the M-CHAT—the M-CHAT-R/F (Revised with Follow-up) was validated earlier this year. In a study involving 16,000 children, 95% of those who had positive tests were found to have some form of developmental delay and almost half (47%) received an ASD diagnosis.29
Other diagnostic aids are being explored as a means of promoting earlier identification of ASD. For example, a blood test to identify differences in gene expression between children with and without ASD30 has shown initial promise, particularly in males. This test is licensed by SynapDx (Lexington, Mass) and a clinical trial to evaluate it has begun.
Results of another study demonstrating normalization of brain activity in autistic children after they’ve undergone intensive treatment31 raise the possibility of using cortical activation as measured by electroencephalography as an early biomarker for autism.
Treatment options, advocacy affect rate of diagnosis
Improvements in diagnosis and targeted identification of potentially treatable symptoms32 led to the development of new treatment options. And greater use of day care and preschool programs prompted networking among parents, who touted the benefits of early evaluation, diagnosis, and treatment. Earlier screening, not surprisingly, led to an increase in the target population.
|
Local as well as national advocacy groups, led primarily by parents, have become powerful voices for improvements in services offered to children with autism. And research studies with varying degrees of sophistication continue to be published, further fueling the demand for school systems to provide supportive learning environments as required by the Individuals with Disabilities Education Act, initially enacted in 1975 and amended in 2004.33
Federal and state funds in the form of Medicaid waivers are available to provide long-term care services in home and community settings, while private insurers typically pay for associated treatment modalities for those with an autism diagnosis, including physical, occupational, and speech therapy, among other services.
Finally, politicians and celebrities with personal connections to autism have joined the effort to increase awareness and improve the quality and availability of services—further assuring that autism is recognized as a legitimate, definable, and treatable disorder.
As an autism diagnosis has become more socially acceptable, it has at times replaced diagnoses of learning disability and mental retardation, a trend known as “diagnostic substitution.”34 Indeed, having a child with an ASD diagnosis often makes it possible for parents to secure services that might otherwise be unavailable to them.
Is the incidence of autism linked to the environment?
Numerous environmental, nutritional, and pharmaceutical changes have been cited as reasons for what is perceived as an increasing incidence of autism in recent years. For example, some contend that greater use of food preservatives and greater exposure of young children to environmental toxins are contributing factors.35
Thimerosal. Perhaps most notable is the assertion—since disproven—that thimerosal, a substance previously used in the manufacture of several childhood vaccines, was a leading cause of autism.36,37 In fact, one study documented an increase in autism after thimerosal had been discontinued.38 (For more on the thimerosal controversy, see “Autism: 5 misconceptions that can complicate care”.)
Autism comorbidity. As autism is frequently comorbid with other developmental disabilities, advances in medical technology that have led to a decline in neonatal death and overall mortality among the disabled may mean more survivors are subsequently diagnosed with an autism comorbidity.
Biological factors. Recent studies suggest that advanced paternal age can increase the risk of autism.39 Twin studies suggest moderate genetic heritability, along with a substantial environmental contribution to the development of autism.40 And new research suggests that maternal stressors during pregnancy—eg, trauma, illness, or substance abuse—may increase a child’s risk of developing autism, among other psychiatric disorders.41
The important role you play in the diagnosis of autism
It is clear that autism is more common than previously thought3 and that various factors are at work. Ensuring that children are promptly and properly evaluated begins when primary care physicians take parents’ concerns seriously and keep an eye out for common symptoms and characteristic developmental delays that may be evident even in the first year of life.
If symptoms are not severe enough to be detected in the child’s first several years, the next likely presentation will be when a parent gets a call from school suggesting that their child be tested for autism. While this delayed presentation suggests a higher level of functioning, a full evaluation, including the use of questionnaires such as the Social Responsiveness Scale42 and ASSQ,28 and appropriate referrals are still vital.
Puberty is another time when characteristics suggestive of autism that escaped earlier detection may be noted, and vague behavioral issues or concerns about intellectual impairment may become sufficiently troublesome to prompt a thorough evaluation. While behavioral therapy can be very helpful in such cases, medical therapy directed at co-occurring conditions (ie, a mood or anxiety disorder, including obsessive-compulsive disorder) may also provide significant benefit.
Whatever the age of the child, his or her parents should be counseled as to the general nature of autism, reassured of the availability of treatment options and given the appropriate referrals, and encouraged to learn more by availing themselves of resources (TABLE) and support groups. A consumer update from the US Food and Drug Administration titled “Beware of false or misleading claims for treating autism” (http://www.fda.gov/ForConsumers/ConsumerUpdates/ucm394757.htm) will be helpful for many parents, as well.
CORRESPONDENCE
Robert G. Zylstra, EdD, LCSW, Department of Family Medicine, The University of Tennessee College of Medicine, 110 East Third Street, Chattanooga, TN 37403; [email protected]
1. Prater C, Zylstra R. Autism: a medical primer. Am Fam Physician. 2002;66:1667-1674.
2. Nassar N, Dixon G, Bourke J, et al. Autism spectrum disorders in young children: effect of changes in diagnostic practices. Int J Epidemiol. 2009;38:1245-1254.
3. Developmental Disabilities Monitoring Network Surveillance Year 2010 Principal Investigators; Centers for Disease Control and Prevention (CDC). Prevalence of autism spectrum disorder among children aged 8 years - Autism and Developmental Disabilities Monitoring Network, 11 sites, United States, 2010. MMWR Surveill Summ. 2014;63:1-21.
4. Report to the legislature on the principle findings from the epidemiology of autism in California: a comprehensive pilot study. State of California Department of Developmental Services Web site. Available at: http://www.dds.ca.gov/Autism/docs/study_final.pdf. Accessed May 1, 2014.
5. Kanner L. Autistic disturbances of affective contact. Nervous Child. 1943;2:217-250.
6. Kanner L. Infantile autism and the schizophrenias. Behav Sci. 1965;10:412-420.
7. Asperger H. Die ‘autistischen psychopathen’ im kindesalter. Archiv für Psychiatrie und Nervenkrankheiten. 1944;117:76-136.
8. Frith U. Autism and Asperger Syndrome. Cambridge, UK: Cambridge University Press; 1991.
9. Bettelheim B. The empty fortress: Infantile autism and the birth of the self. New York: Free Press; 1972.
10. Rimland B. Infantile autism: The syndrome and its implications for a neural theory of behavior. New York: Appleton-Century- Crofts; 1964.
11. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: American Psychiatric Association; 1952.
12. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 2nd ed. Washington, DC: American Psychiatric Association;1968.
13. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 3rd ed. Washington, DC: American Psychiatric Association; 1980.
14. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 3rd ed, revised. Washington, DC: American Psychiatric Association; 1987.
15. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association; 1994.
16. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed, text revision. Washington: DC: American Psychiatric Association; 2000.
17. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Publishing; 2013.
18. Ghaziuddin M. Brief report: Should the DMS-V drop Asperger Syndrome? J Autism Dev Disord. 2010;40:1146-1148.
19. Wing L, Gould J, Gillberg C. Autism spectrum disorders in the DSM-V: better or worse than the DSM-IV? Res Dev Disabil. 2011;32:768-773.
20. Huerta M, Bishop S, Duncan A, et al. Application of DSM-5 criteria for Autism Spectrum Disorder to three samples of children with DSM-IV diagnoses of pervasive developmental disorders. Am J Psychiatry. 2012;169:1056-1064.
21. Schopler E, Reichler RJ, DeVellis RF. Toward objective classification of childhood autism: Childhood Autism Rating Scale (CARS). J Autism Dev Disord. 1980;10:91-103.
22. Le Couteur A, Rutter M, Lord C, et al. Autism diagnostic interview: a standardized investigator-based instrument. J Autism Dev Disord. 1989;19:363-387.
23. Lord C, Rutter M, Goode S, et al. Autism diagnostic observation schedule: a standardized observation of communicative and social behavior. J Autism Dev Disord. 1989;19:185-212.
24. Zwaigenbaum L. Advances in the early detection of autism. Curr Opin Neurol. 2010;23:97-102.
25. Lord C, Rutter M, Le Couteur A. Autism Diagnostic Interview-Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J Autism Dev Disord. 1994;24:659-685.
26. Baron-Cohen S, Allen J, Gillberg C. Can autism be detected at 18 months? The needle, the haystack, and the CHAT. Br J Psychiatry. 1992;161:839-843.
27. Robins DL, Fein D, Barton ML, et al. The Modified Checklist for Autism in Toddlers: an initial study investigating the early detection of autism and pervasive developmental disorders. J Autism Dev Disord. 2001;31:131-144.
28. Ehlers S, Gilberg C, Wing L. A screening questionnaire for Asperger syndrome and other high-functioning autism spectrum disorders in school age children. J Autism Dev Disord. 1999;29:129-141.
29. Robins DL, Casagrande K, Barton M, et al. Validation of the modified checklist for Autism in toddlers, revised with followup (M-CHAT-R/F). Pediatrics. 2014;133:37-45.
30. Kong SW, Collins CD, Shimizu-Motohashi Y, et al. Characteristics and predictive value of blood transcriptome signature in males with autism spectrum disorders. PLoS One. 2012;7:e49475.
31. Dawson G, Jones EJ, Merkle K, et al. Early behavioral intervention is associated with normalized brain activity in young children with autism. J Am Acad Child Adolesc Psychiatry. 2012;51:1150-1159.
32. Autism ALARM. National Center for Medical Home Implementation Web site. Available at: http://www.medicalhomeinfo.org/downloads/pdfs/AutismAlarm.pdf. Accessed March 4, 2013.
33. IDEA. Autism Community Web site. Available at: http://www.autism-community.com/education/idea/. Accessed April 25, 2014.
34. Shattuck P. The contribution of diagnostic substitution to the growing administrative prevalence of autism in US special education. Pediatrics. 2006;117:1028-1037.
35. Landrigan P. What causes autism? Exploring the environmental contribution. Curr Opin Pediatr. 2010;22:219-225.
36. The great thimerosal cover-up: Mercury, vaccines, autism and your child’s health. Natural Health News & Scientific Discoveries Web site. Available at: http://www.naturalnews.com/011764_thimerosal_mercury.html. Accessed March 4, 2013.
37. Price CS, Thompson WW, Goodson B, et al. Prenatal and infant exposure to thimerosal from vaccines and immunoglobulins and risk of autism. Pediatrics. 2010;126:656-664.
38. Fombonne E, Zakarian R, Bennett A, et al. Pervasive developmental disorders in Montreal, Quebec, Canada: prevalence and links with immunizations. Pediatrics. 2006;118:e139-e150.
39. Flatscher-Bader T, Foldi CJ, Chong S, et al. Increased de novo copy number variants in the offspring of older males. Transl Psychiatry. 2011;1:e34.
40. Hallmayer J, Cleveland S, Torres A, et al. Genetic heritability and shared environmental factors among twin pairs with autism. Arch Gen Psychiatry. 2011;68:1095-1102.
41. Fine R, Zhang J, Stevens HE. Prenatal stress and inhibitory neuron systems: implications for neuropsychiatric disorders Mol Psychiatry. 2014 April 22. [Epub ahead of print].
42. Joshi G, Petty DR, Fried R, et al. Discriminant and concurrent validity of a simplified DSM-based structured diagnostic instrument for the assessment of autism spectrum disorders in youth and young adults. BMC Psychiatry. 2011;11:204.
1. Prater C, Zylstra R. Autism: a medical primer. Am Fam Physician. 2002;66:1667-1674.
2. Nassar N, Dixon G, Bourke J, et al. Autism spectrum disorders in young children: effect of changes in diagnostic practices. Int J Epidemiol. 2009;38:1245-1254.
3. Developmental Disabilities Monitoring Network Surveillance Year 2010 Principal Investigators; Centers for Disease Control and Prevention (CDC). Prevalence of autism spectrum disorder among children aged 8 years - Autism and Developmental Disabilities Monitoring Network, 11 sites, United States, 2010. MMWR Surveill Summ. 2014;63:1-21.
4. Report to the legislature on the principle findings from the epidemiology of autism in California: a comprehensive pilot study. State of California Department of Developmental Services Web site. Available at: http://www.dds.ca.gov/Autism/docs/study_final.pdf. Accessed May 1, 2014.
5. Kanner L. Autistic disturbances of affective contact. Nervous Child. 1943;2:217-250.
6. Kanner L. Infantile autism and the schizophrenias. Behav Sci. 1965;10:412-420.
7. Asperger H. Die ‘autistischen psychopathen’ im kindesalter. Archiv für Psychiatrie und Nervenkrankheiten. 1944;117:76-136.
8. Frith U. Autism and Asperger Syndrome. Cambridge, UK: Cambridge University Press; 1991.
9. Bettelheim B. The empty fortress: Infantile autism and the birth of the self. New York: Free Press; 1972.
10. Rimland B. Infantile autism: The syndrome and its implications for a neural theory of behavior. New York: Appleton-Century- Crofts; 1964.
11. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: American Psychiatric Association; 1952.
12. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 2nd ed. Washington, DC: American Psychiatric Association;1968.
13. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 3rd ed. Washington, DC: American Psychiatric Association; 1980.
14. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 3rd ed, revised. Washington, DC: American Psychiatric Association; 1987.
15. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association; 1994.
16. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed, text revision. Washington: DC: American Psychiatric Association; 2000.
17. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Publishing; 2013.
18. Ghaziuddin M. Brief report: Should the DMS-V drop Asperger Syndrome? J Autism Dev Disord. 2010;40:1146-1148.
19. Wing L, Gould J, Gillberg C. Autism spectrum disorders in the DSM-V: better or worse than the DSM-IV? Res Dev Disabil. 2011;32:768-773.
20. Huerta M, Bishop S, Duncan A, et al. Application of DSM-5 criteria for Autism Spectrum Disorder to three samples of children with DSM-IV diagnoses of pervasive developmental disorders. Am J Psychiatry. 2012;169:1056-1064.
21. Schopler E, Reichler RJ, DeVellis RF. Toward objective classification of childhood autism: Childhood Autism Rating Scale (CARS). J Autism Dev Disord. 1980;10:91-103.
22. Le Couteur A, Rutter M, Lord C, et al. Autism diagnostic interview: a standardized investigator-based instrument. J Autism Dev Disord. 1989;19:363-387.
23. Lord C, Rutter M, Goode S, et al. Autism diagnostic observation schedule: a standardized observation of communicative and social behavior. J Autism Dev Disord. 1989;19:185-212.
24. Zwaigenbaum L. Advances in the early detection of autism. Curr Opin Neurol. 2010;23:97-102.
25. Lord C, Rutter M, Le Couteur A. Autism Diagnostic Interview-Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J Autism Dev Disord. 1994;24:659-685.
26. Baron-Cohen S, Allen J, Gillberg C. Can autism be detected at 18 months? The needle, the haystack, and the CHAT. Br J Psychiatry. 1992;161:839-843.
27. Robins DL, Fein D, Barton ML, et al. The Modified Checklist for Autism in Toddlers: an initial study investigating the early detection of autism and pervasive developmental disorders. J Autism Dev Disord. 2001;31:131-144.
28. Ehlers S, Gilberg C, Wing L. A screening questionnaire for Asperger syndrome and other high-functioning autism spectrum disorders in school age children. J Autism Dev Disord. 1999;29:129-141.
29. Robins DL, Casagrande K, Barton M, et al. Validation of the modified checklist for Autism in toddlers, revised with followup (M-CHAT-R/F). Pediatrics. 2014;133:37-45.
30. Kong SW, Collins CD, Shimizu-Motohashi Y, et al. Characteristics and predictive value of blood transcriptome signature in males with autism spectrum disorders. PLoS One. 2012;7:e49475.
31. Dawson G, Jones EJ, Merkle K, et al. Early behavioral intervention is associated with normalized brain activity in young children with autism. J Am Acad Child Adolesc Psychiatry. 2012;51:1150-1159.
32. Autism ALARM. National Center for Medical Home Implementation Web site. Available at: http://www.medicalhomeinfo.org/downloads/pdfs/AutismAlarm.pdf. Accessed March 4, 2013.
33. IDEA. Autism Community Web site. Available at: http://www.autism-community.com/education/idea/. Accessed April 25, 2014.
34. Shattuck P. The contribution of diagnostic substitution to the growing administrative prevalence of autism in US special education. Pediatrics. 2006;117:1028-1037.
35. Landrigan P. What causes autism? Exploring the environmental contribution. Curr Opin Pediatr. 2010;22:219-225.
36. The great thimerosal cover-up: Mercury, vaccines, autism and your child’s health. Natural Health News & Scientific Discoveries Web site. Available at: http://www.naturalnews.com/011764_thimerosal_mercury.html. Accessed March 4, 2013.
37. Price CS, Thompson WW, Goodson B, et al. Prenatal and infant exposure to thimerosal from vaccines and immunoglobulins and risk of autism. Pediatrics. 2010;126:656-664.
38. Fombonne E, Zakarian R, Bennett A, et al. Pervasive developmental disorders in Montreal, Quebec, Canada: prevalence and links with immunizations. Pediatrics. 2006;118:e139-e150.
39. Flatscher-Bader T, Foldi CJ, Chong S, et al. Increased de novo copy number variants in the offspring of older males. Transl Psychiatry. 2011;1:e34.
40. Hallmayer J, Cleveland S, Torres A, et al. Genetic heritability and shared environmental factors among twin pairs with autism. Arch Gen Psychiatry. 2011;68:1095-1102.
41. Fine R, Zhang J, Stevens HE. Prenatal stress and inhibitory neuron systems: implications for neuropsychiatric disorders Mol Psychiatry. 2014 April 22. [Epub ahead of print].
42. Joshi G, Petty DR, Fried R, et al. Discriminant and concurrent validity of a simplified DSM-based structured diagnostic instrument for the assessment of autism spectrum disorders in youth and young adults. BMC Psychiatry. 2011;11:204.

Appropriate Analgesic Use in the Emergency Department
Pain, one of the most common reasons patients present to the ED, may be a primary complaint or a warning sign encouraging further evaluation. The decision to treat pain is one of the most frequent therapeutic decisions made by emergency physicians (EPs) and involves a variety of options and considerations. Moreover, the decision of how to treat pain similarly encompasses a wide selection of variables, including etiology and severity of the pain; intravenous (IV) access; medication allergies; renal function; alcohol use; rapidity of onset; patients’ vital signs; patient preference; and mode of transport upon discharge. Given all of these considerations, there is no perfect analgesic to suit every circumstance. Rather, EPs must tailor their analgesic selection to the individual clinical situation and patient.
The literature over the past 20 years is replete with studies demonstrating the undertreatment or inadequate treatment of pain in the ED.1-5 Often referred to as oligoanalgesia,6 contributing factors include physician concerns regarding adverse side effects, secondary gain, and drug addiction. In addition, the increasing pressure placed on EPs to diagnose and dispose patients quickly likely relegates pain control to a secondary concern.
Further complicating the issue, physicians’ own prejudices and perceptions appear to influence their analgesic prescription practice. For example, several studies have demonstrated that black patients do not receive prescriptions for analgesics similar to those written for white patients in general, and particularly not for opioid analgesics. In a meta-analysis of pain treatment disparity studies, blacks were 22% less likely than whites to receive any analgesics, and 29% less likely than whites to receive opioid treatment for the same type of painful conditions.7 Likewise, Hispanic/Latino patients were also 22% less likely than their white counterparts to receive opioid treatment for similar pain.7 Physicians must keep these common biases in mind when treating patients for pain.
The administration of analgesics and the prescription habits of physicians has never been under greater scrutiny. The Centers for Medicare and Medicaid Services has benchmarked “median time to pain management for long bone fractures” as a core measure, possibly affecting hospital reimbursement rates. Similarly, every patient satisfaction survey specifically inquires about the timeliness and adequacy of pain control. At the same time, though, the increasing problem of prescription opioid abuse has become the nation’s fastest growing drug problem. In 2013, prescription drug abuse was second only to marijuana as the most abused drug category.8 Contributing to this problem are the frequency and ease with which many physicians prescribe opioids. From 1997 to 2007, the milligram-per-person use of prescription opioids in the United States increased from 74 mg per year to 369 mg per year—an increase of 402%.9 As a result, some legislators are now calling for mandatory educational sessions for any physician prescribing medications containing opioids.
Though there are many classes of medications used to treat pain, and numerous individual drugs within each class, this article focuses on several of the more commonly prescribed medications in the ED, including their mechanisms of action, advantages, and disadvantages. The management of pediatric pain and procedural sedation and analgesia are not discussed in this review, as each of these topics deserves a separate detailed discussion.
Recognizing and Quantifying Pain
The first step in treating pain appropriately is recognition. Physicians must specifically inquire about pain and not rely solely on a patient’s unprompted complaint. Several pain scales exist, including the Faces Pain Scale (ie, pictorial representation of a smiling face on one end indicating “no pain” to a frowning face on the opposite end); the verbal quantitative scale or numerical rating scale (ie, “how would you rate your pain on a scale of 0 to 10, with 10 the worst pain ever?”); and the visual analog scale (ie, a 10-cm linear scale marked at one end with “no pain” and “worst pain imaginable” at the opposite end).10,11 Probably the most commonly used scale in the ED is some variation of the numerical rating scale (NRS).1
Each of these scales has its own advantages and disadvantages, but the important point is that patients are given the opportunity to express the type and degree of pain to the healthcare provider. In addition, a pain scale provides a starting point against which the practitioner (or later practitioners) can determine the success (or failure) of a pain treatment strategy.
Three-Step Ladder
In 1996, the World Health Organization developed a three-step analgesic ladder to guide the management of cancer pain.12 Its use has been expanded over time to include treating pain of noncancer etiology. Mild pain (NRS of 1 to 3) is considered Step 1; moderate pain (NRS 4 to 6) is considered Step 2; and severe pain (NRS 7 to 10) is Step 3. For Step 1 (mild pain), acetaminophen or a nonsteroidal anti-inflammatory drug (NSAID) is recommended. For Step 2 (moderate pain), a weak opioid (ie, codeine or hydrocodone) with or without acetaminophen or an NSAID is recommended. Finally, for Step 3 (severe pain), a strong opioid such as morphine or hydromorphone is recommended.
Again, the purpose of the ladder is not to provide a strict protocol for adherence, but rather to provide a reasonable starting point as a guide to the clinician. The key to its successful use is reassessment of the patient to determine if adequate pain relief is achieved.
Routes of Administration
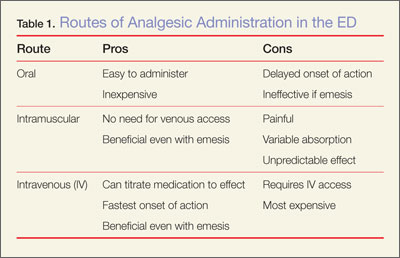
Acetaminophen
Acetaminophen, the active ingredient in Tylenol, was first marketed in the United States in 1955 as an antipyretic and pain reliever.13 It is a synthetic centrally acting analgesic that is metabolized in the liver. Acetaminophen has been used alone or in combination in hundreds of formulations to treat a wide variety of pain and fever-related conditions. In the ED setting, acetaminophen is frequently used as an antipyretic and—either alone or in combination with opioids—for oral pain control.
Acetaminophen is very well tolerated by most patients, with minimal gastrointestinal (GI) distress. It is inexpensive, and the wide variety of formulations (eg, liquid, tablet, suppository) make it useful in a number of clinical scenarios. Acetaminophen is generally considered to be the only nonopioid analgesic that is safe in pregnancy,14 and it has no sedative or addictive effects.
There are, however, some disadvantages to using acetaminophen. Concerns about its safety and accidental overdose have recently led to the introduction of a 4,000-mg maximum daily dose recommendation15 and heightened concern over using multiple medications containing acetaminophen. In January 2014, the US Food and Drug Administration recommended that no combination medication contain more than 325 mg of acetaminophen because of the risk of toxicity when multiple drugs containing acetaminophen are consumed.
In addition to concerns of inadvertent overdose, another disadvantage of acetaminophen is that while it may be an effective antipyretic and analgesic, it has little or no anti-inflammatory properties. Therefore, in cases requiring an anti-inflammatory agent, an NSAID, when appropriate, would be the more effective option.
NSAIDs
Nonsteroidal anti-inflammatory drugs function by inhibiting prostaglandin production in the cyclooxygenase 1 and 2 (COX-1 and COX-2) pathways. Ibuprofen, indomethacin, ketorolac, naproxen, and other NSAIDs are chiefly utilized to control pain, inflammation, and fever via the oral route. As production of various prostaglandins via the COX-2 pathway is thought to contribute to fever, inflammation, and pain, inhibition of this pathway by NSAIDs can help alleviate these symptoms. The COX-1 pathway contributes many factors important to the protection and health of the GI tract, and inhibition of this pathway can lead to GI distress and damage. Unfortunately, the most commonly used and available NSAIDs inhibit both COX pathways simultaneously, and in doing so, prompt the GI symptoms which are the most common adverse side effects of therapy. In addition to GI effects of the COX-1 and COX-2 inhibitors, there are also concerns over the associated antiplatelet effects in patients undergoing surgery or potentially suffering from occult or intracranial bleeding.13
Ibuprofen
This is the most commonly used NSAID in the United States and is available without a prescription. Ibuprofen is typically used to treat mild-to-moderate pain from a musculoskeletal or inflammatory source. As an oral nonprescription medication, it can be used advantageously to treat acute pain in the ED and continued in the outpatient setting. Ibuprofen is neither sedating nor addicting, with a rapid onset of action and a plasma half-life of approximately 2 hours.13 However, there is a dose-dependent feature which allows large doses (eg, 800 mg) to be spaced-out every 8 hours while maintaining effective analgesia. Typical doses range from 200 mg to 800 mg orally every 6 to 8 hours, with a maximum dose of 3.2 g/d. Patients should be instructed to take each dose with a meal or snack to help alleviate GI side effects.
The greatest advantage of ibuprofen and other NSAIDs is their effect on inflammation and the ability to treat the inflammatory cause of pain—not just the symptom. Nonsteroidal anti-inflammatory drugs are well tolerated by most patients and can be obtained without prescription at low cost. Additionally, doses of ibuprofen and acetaminophen can be alternated.
Ketorolac
Often marketed as Toradol, ketorolac is a powerful NSAID available in IV, IM, and oral formulations. Typical doses are 30 mg IV, 60 mg IM, or 10 mg orally every 4 to 6 hours (maximum of 40 mg/d). The basic pharmacology and mechanism of action of ketorolac are similar to ibuprofen. Though ketorolac is useful to treat more severe pain, it should only be used for short-term management of pain (ie, 5 days or less). Ketorolac is often used for postoperative pain, but also is helpful for pain control in patients using opioids. It has been shown to be effective for acute renal colic and can also provide relief for migraine headaches.16,17 In a direct comparison between ketorolac and meperidine (Demerol) for patients suffering from renal stones, ketorolac was found to be more effective and provide longer lasting pain relief.18
The major concern regarding ketorolac relates to potential renal toxicity, and thus caution should be undertaken in prescribing it to patients with known or suspected renal disease. Although this risk is associated with even a single dose, multiple doses increase the danger and therefore should be avoided.
Ketorolac should also be used with caution in patients with asthma. As a subset of asthma patients will experience severe bronchospasm after NSAID administration, clinicians should always determine whether a patient can tolerate NSAIDs.
Renal Toxicity and GI Effects
Concerns over renal toxicity and potential GI distress are the chief disadvantages of NSAID use. While renal toxicity has been reported in patients without pre-existing kidney dysfunction, it is of much greater concern in patients with pre-existing renal disease or decreased glomerular filtration rate. For this reason, care must be exercised when prescribing NSAIDS to elderly patients, patients with diabetes mellitus, or patients with hypertension (or even worse, a combination of these). Prolonged use of NSAIDs can also cause upper GI bleeding. Nonsteroidal anti-inflammatory drugs are contraindicated in pregnant patients.
Opioid analgesics
Morphine
Morphine is the prototypical compound in the opioid class, and has been utilized for more than two centuries since its isolation in 1804.19 Other opioid compounds include codeine, hydrocodone, oxycodone, morphine, and hydromorphone, which represent different functional groups substituted onto the base morphine molecule. All share similar pharmacology, differing primarily only in potency. The onset of action for codeine, hydrocodone, and oxycodone is 30 to 60 minutes when taken orally, with a peak time of 60 to 90 minutes. Codeine and hydrocodone are at the weak-end of the spectrum (Step 2 medications), while morphine and hydromorphone are more potent (Step 3 medications). The majority of opioids and their metabolites are primarily excreted renally (90%-95%).20 Therefore, care must be exercised regarding dosing and frequency when used in patients with renal insufficiency or disease.
Morphine has several features that make it an attractive analgesic for use in the ED. The ability to administer morphine via IV, IM, subcutaneous, or oral route; its quick onset of action; and safety profile are all advantageous. The onset of action is 5 to 10 minutes when given IV. For oral administration, it is 30 to 60 minutes (similar to the other opioids discussed) and can be given as a tablet or syrup.
Morphine decreases the severity of pain, with an apparent increase in tolerance for any remaining discomfort. The potency and central action of morphine make it ideal for managing moderate and severe pain.
As with other analgesics, morphine and its related compounds have associated drawbacks, of which respiratory depression is the most feared, though this is uncommon at therapeutic doses. The respiratory depressant effect is more pronounced in patients with underlying lung disease, depressed mental status, or concurrent use of sedating medication (eg, benzodiazepines).
Another disadvantage to morphine is that it can cause hypotension, limiting its use in certain clinical situations. Repeated or prolonged use may cause slowing or complete arrest of peristaltic waves in the GI tract, which can lead to significant constipation. Pruritus and nausea are two other frequently reported side effects and may necessitate, respectively, coadministration of diphenhydramine (eg, Benadryl) or an antiemetic (eg, Phenergan or Zofran). As an opioid, morphine is potentially addictive, though it is generally thought to require significant intake over several weeks before such problems arise.
The sedation caused by morphine is also of concern, as patients who are under its influence immediately following discharge cannot safely drive, and may actually not be safe to walk or even utilize public transportation. This concern can be lessened by verifying the patient’s mode of transport prior to administration of the medication, ensuring that patients are not overly sedated at the time of discharge and, as much as possible, accompanied home by an adult relative or friend. In comparison to other frequently used opioids, several features can be considered. The duration of action for codeine, hydromorphone, and morphine is similar at 3 to 5 hours.
Hydromorphone
Hydromorphone (Dilaudid) is approximately seven times more potent than morphine, but otherwise very similar. It is frequently the IV opioid of choice for severe pain and also appears to cause pruritus less frequently than morphine. Hydromorphone has a rapid onset of action (1-5 minutes IV; 15-30 minutes orally) and can be titrated to effect when given via the IV route, making it an ideal agent for the pain associated with long bone or pelvic fractures, vasoocclusive crises in patients with sickle cell disease, and renal colic. The oral formulation of hydromorphone can be utilized for severe pain in the appropriate patient population, usually at a dose of 2 to 4 mg every 4 hours.
Codeine
Codeine is frequently prescribed in combination with acetaminophen in a product marketed as Tylenol #3 for mild-to-moderate pain. Because codeine is metabolized in the liver to morphine, it is contraindicated in patients with morphine allergy. Also, the clinician must be aware that codeine is ineffective in 7% to 10% of the population due to an enzyme deficiency.
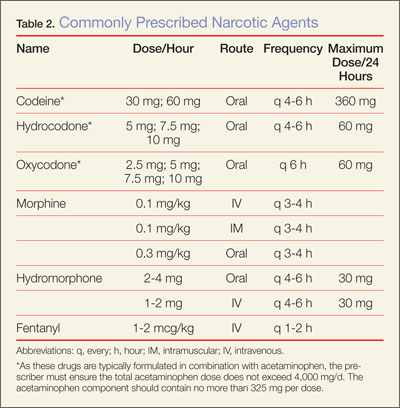
Hydrocodone and oxycodone, which are often combined with acetaminophen and marketed respectively as Vicodin and Percocet, are two additional commonly used compounds in the oral treatment of moderate-to-severe pain. There are numerous preparations containing various strengths of both the opioid and acetaminophen components. Utilizing these medications as initial pain control in the ED can be beneficial, as therapy can be continued as an outpatient. Table 2 provides dosing and frequency information, but the clinician must also be aware of the total amount of acetaminophen administered, especially when being used in conjunction with other medications containing acetaminophen.
Tramadol
Tramadol (Ultram), another oral analgesic with opioid properties, affects several neurotransmitters and is less reliant on the opioid receptors compared to the opioid compounds described above. It is used to treat moderate-to-severe pain and can be considered another option along with codeine, hydrocodone, and oxycodone for oral pain control. Although the complete mechanism of action for tramadol is poorly understood, it appears to be effective in patients who do not respond well to pure opioids, and in patients with neuropathic pain or persistent pain of unclear etiology (eg, fibromyalgia).19 Because of its limited interaction with opioid receptors, tramadol has less potential for abuse and addiction than the opioids. It is also available in several combinations with acetaminophen or ibuprofen.
Conclusion
The ideal medication for treating pain in the ED is one that is effective, easy to administer, and has minimal adverse or residual effects. Generally, the least potent medication that will control pain should be chosen initially. When treating minor traumatic or musculoskeletal pain, initiating pain control with oral medication in the ED may provide patients with relief during imaging or splinting, and help control pain until they can fill outpatient prescriptions. All of the medications discussed in this article can be given in the oral form. However, IV usage may be appropriate when there is need for rapid onset of action, to titrate the medication, or for ease of administration in patients who are vomiting or unable to take anything orally.
When prescribing analgesics for pain control after discharge, the clinician must consider potential relative and absolute contraindications. For acetaminophen, liver toxicity is the major concern, and care must be taken not to exceed recommended daily dosing limits with the multitude of available products containing acetaminophen. Physicians should avoid recommending or prescribing acetaminophen to patients with liver disease (ie, cirrhosis) or habitual alcohol abuse.
Nonsteroidal anti-inflammatory drugs such as ibuprofen and naproxen carry the risk of renal damage, as well as concerns about antiplatelet activity. Because of the tendency for renal function to decline with age, caution must be exercised in using these compounds in older patients and those with preexisting renal dysfunction.
Opioid-containing medications are known for their potency in pain control, but also for their side effects. The most common side effect involves the GI tract, with nausea, vomiting, and constipation. The most dangerous side effect of opioids is respiratory depression; fortunately, this is rarely seen with therapeutic doses. However, somnolence and decreased coordination are significant concerns when prescribing opioids to elderly patients or those already at risk for falls.
There is no ideal single medication to treat all types of pain or situations. However, the choice of medication begins with a decision by the EP to treat pain. Utilizing a stepwise approach, oral medication will usually be effective for mild pain, but IV narcotics will probably be required for severe pain. Frequent reassessment of the patient is critically important for successful pain management in the ED.
Dr Byers is an emergency physician at the Presbyterian Medical Group, department of emergency medicine, Presbyterian Healthcare Services, Albuquerque, New Mexico. Dr Counselman is a distinguished professor of emergency medicine and chairman, department of emergency medicine, Eastern Virginia Medical School and Emergency Physicians of Tidewater, Norfolk, Virginia. He is also associate editor-in-chief of the Emergency Medicine editorial board.
- Todd KH. Pain assessment instruments for use in the emergency department. Emerg Med Clin North Am. 2005;23(2):285-295.
- Cordell WH, Keene KK, Giles BK, Jones JB, Jones JH, Brizendine EJ. The high prevalence of pain in emergency medical care. Am J Emerg Med. 2002;20(3):165-169.
- Tcherny-Lessenot S, Karwowski-Soulié F, Lamarche-Vadel A, Ginsburg C, Brunet F, Vidal-Trecan G. Management and relief of pain in an emergency department from the adult patients’ perspective. J Pain Symptom Manage. 2003;25(6):539-546.
- Karwowski-Soulié F, Lessenot-Tcherny S, Lamarche-Vadel A, et al. Pain in an emergency department: an audit. Eur J Emerg Med. 2006;13(4):218-224.
- Fosnocht DE, Swanson ER, Barton ED. Changing attitudes about pain and pain control in emergency medicine. Emerg Med Clin North Am. 2005;23(2):297-306.
- Wilson JE, Pendelton JM. Oligoanalgesia in the emergency department. Am J Emerg Med. 1989;7(6):620-623.
- Meghani SH, Byun E, Gallagher RM. Time to take stock: a meta-analysis and systemic review of analgesic treatment disparities for pain in the United States. Pain Med. 2012;13(2):150-174.
- Johnston LD, O’Malley PM, Miech RA, Bachman JG, Schutenberg JE; The University of Michigan Institute for Social Research. Monitoring the future: 2013 overview key findings of on adolescent drug use. http://www.monitoringthefuture.org/pubs/monographs/mtf-overview2013.pdf. Accessed June 6, 2014.
- Manchikanti L, Fellow B, Ailinani H, Pampati V. Therapeutic use, abuse, and nonmedical use of opioids: a ten year perspective. Pain Physician. 2010;13(5):401-435.
- Silka PA, Roth MM, Moreno G, Merrill L, Geiderman JM. Pain scores improve analgesic administration patterns for trauma patients in the emergency department. Acad Emerg Med. 2004;11(3):264-270.
- Nelson BP, Cohen D, Lander O, Crawford N, Viccellio AW, Singer AJ. Mandated pain scales improve frequency of ED analgesic administration. Am J Emerg Med. 2004;22(7):582-585.
- World Health Organization. Cancer pain relief with a guide to opioid availability 2nd ed. 1996. http://whqlibdoc.who.int/publications/9241544821.pdf. Accessed June 6, 2014.
- Grosser T, Smyth EM, FitzGerald GA. Anti-inflammatory, antipyretic, and analgesic agents: pharmacotherapy of gout. In: Brunton LL, Chabner BA, Knollman BC, eds. Goodman and Gilman’s The Pharmacological Basis of Therapeutics. 12th ed. China: The McGraw Hill Companies; 2011:959-1004.
- Scialli AR, Ang R, Breitmeyer J, Royal MA. A review of the literature on the effects of acetaminophen on pregnancy outcome. Reprod Toxicol. 2010;30(4):495-507.
- Schilling A, Corey R, Leonard M, Eghtesad B. Acetaminophen: old drug, new warnings. Cleveland Clin J Med. 2010;77(1):19-27.
- Shrestha M, Singh R, Moreden J, Hayes JE. Ketorolac vs chlorpromazine in the treatment of acute migraine without aura. A prospective, randomized, double-blind trial. Arch Intern Med.1996;156(15):1725-1728.
- Turkewitz LJ, Casaly JS, Dawson GA, Wirth O, Hurst RJ, Gillette PL. Self-administration of parenteral ketorolac tromethamine for head pain. Headache. 1992;32(9):452-454.
- Larkin GL, Peacock WF 4th, Pearl SM, Blair GA, D’Amico F. Efficacy of ketorolac tromethamine versus meperidine in the ED treatment of acute renal colic. Am J Emerg Med. 1999;17(1):6-10.
- Yaksh TL, Wallace MS. Opiods, analgesia and pain management. In: Brunton LL, Chabner BA, Knollman BC, eds. Goodman and Gilman’s The Pharmacological Basis of Therapeutics. 12th ed. China: The McGraw Hill Companies; 2011:481-526.
- DeSandre PL, Quest TE. Management of cancer-related pain. Hematol Oncol Clin N Am. 2010;24(3):643-658.
Pain, one of the most common reasons patients present to the ED, may be a primary complaint or a warning sign encouraging further evaluation. The decision to treat pain is one of the most frequent therapeutic decisions made by emergency physicians (EPs) and involves a variety of options and considerations. Moreover, the decision of how to treat pain similarly encompasses a wide selection of variables, including etiology and severity of the pain; intravenous (IV) access; medication allergies; renal function; alcohol use; rapidity of onset; patients’ vital signs; patient preference; and mode of transport upon discharge. Given all of these considerations, there is no perfect analgesic to suit every circumstance. Rather, EPs must tailor their analgesic selection to the individual clinical situation and patient.
The literature over the past 20 years is replete with studies demonstrating the undertreatment or inadequate treatment of pain in the ED.1-5 Often referred to as oligoanalgesia,6 contributing factors include physician concerns regarding adverse side effects, secondary gain, and drug addiction. In addition, the increasing pressure placed on EPs to diagnose and dispose patients quickly likely relegates pain control to a secondary concern.
Further complicating the issue, physicians’ own prejudices and perceptions appear to influence their analgesic prescription practice. For example, several studies have demonstrated that black patients do not receive prescriptions for analgesics similar to those written for white patients in general, and particularly not for opioid analgesics. In a meta-analysis of pain treatment disparity studies, blacks were 22% less likely than whites to receive any analgesics, and 29% less likely than whites to receive opioid treatment for the same type of painful conditions.7 Likewise, Hispanic/Latino patients were also 22% less likely than their white counterparts to receive opioid treatment for similar pain.7 Physicians must keep these common biases in mind when treating patients for pain.
The administration of analgesics and the prescription habits of physicians has never been under greater scrutiny. The Centers for Medicare and Medicaid Services has benchmarked “median time to pain management for long bone fractures” as a core measure, possibly affecting hospital reimbursement rates. Similarly, every patient satisfaction survey specifically inquires about the timeliness and adequacy of pain control. At the same time, though, the increasing problem of prescription opioid abuse has become the nation’s fastest growing drug problem. In 2013, prescription drug abuse was second only to marijuana as the most abused drug category.8 Contributing to this problem are the frequency and ease with which many physicians prescribe opioids. From 1997 to 2007, the milligram-per-person use of prescription opioids in the United States increased from 74 mg per year to 369 mg per year—an increase of 402%.9 As a result, some legislators are now calling for mandatory educational sessions for any physician prescribing medications containing opioids.
Though there are many classes of medications used to treat pain, and numerous individual drugs within each class, this article focuses on several of the more commonly prescribed medications in the ED, including their mechanisms of action, advantages, and disadvantages. The management of pediatric pain and procedural sedation and analgesia are not discussed in this review, as each of these topics deserves a separate detailed discussion.
Recognizing and Quantifying Pain
The first step in treating pain appropriately is recognition. Physicians must specifically inquire about pain and not rely solely on a patient’s unprompted complaint. Several pain scales exist, including the Faces Pain Scale (ie, pictorial representation of a smiling face on one end indicating “no pain” to a frowning face on the opposite end); the verbal quantitative scale or numerical rating scale (ie, “how would you rate your pain on a scale of 0 to 10, with 10 the worst pain ever?”); and the visual analog scale (ie, a 10-cm linear scale marked at one end with “no pain” and “worst pain imaginable” at the opposite end).10,11 Probably the most commonly used scale in the ED is some variation of the numerical rating scale (NRS).1
Each of these scales has its own advantages and disadvantages, but the important point is that patients are given the opportunity to express the type and degree of pain to the healthcare provider. In addition, a pain scale provides a starting point against which the practitioner (or later practitioners) can determine the success (or failure) of a pain treatment strategy.
Three-Step Ladder
In 1996, the World Health Organization developed a three-step analgesic ladder to guide the management of cancer pain.12 Its use has been expanded over time to include treating pain of noncancer etiology. Mild pain (NRS of 1 to 3) is considered Step 1; moderate pain (NRS 4 to 6) is considered Step 2; and severe pain (NRS 7 to 10) is Step 3. For Step 1 (mild pain), acetaminophen or a nonsteroidal anti-inflammatory drug (NSAID) is recommended. For Step 2 (moderate pain), a weak opioid (ie, codeine or hydrocodone) with or without acetaminophen or an NSAID is recommended. Finally, for Step 3 (severe pain), a strong opioid such as morphine or hydromorphone is recommended.
Again, the purpose of the ladder is not to provide a strict protocol for adherence, but rather to provide a reasonable starting point as a guide to the clinician. The key to its successful use is reassessment of the patient to determine if adequate pain relief is achieved.
Routes of Administration
Acetaminophen
Acetaminophen, the active ingredient in Tylenol, was first marketed in the United States in 1955 as an antipyretic and pain reliever.13 It is a synthetic centrally acting analgesic that is metabolized in the liver. Acetaminophen has been used alone or in combination in hundreds of formulations to treat a wide variety of pain and fever-related conditions. In the ED setting, acetaminophen is frequently used as an antipyretic and—either alone or in combination with opioids—for oral pain control.
Acetaminophen is very well tolerated by most patients, with minimal gastrointestinal (GI) distress. It is inexpensive, and the wide variety of formulations (eg, liquid, tablet, suppository) make it useful in a number of clinical scenarios. Acetaminophen is generally considered to be the only nonopioid analgesic that is safe in pregnancy,14 and it has no sedative or addictive effects.
There are, however, some disadvantages to using acetaminophen. Concerns about its safety and accidental overdose have recently led to the introduction of a 4,000-mg maximum daily dose recommendation15 and heightened concern over using multiple medications containing acetaminophen. In January 2014, the US Food and Drug Administration recommended that no combination medication contain more than 325 mg of acetaminophen because of the risk of toxicity when multiple drugs containing acetaminophen are consumed.
In addition to concerns of inadvertent overdose, another disadvantage of acetaminophen is that while it may be an effective antipyretic and analgesic, it has little or no anti-inflammatory properties. Therefore, in cases requiring an anti-inflammatory agent, an NSAID, when appropriate, would be the more effective option.
NSAIDs
Nonsteroidal anti-inflammatory drugs function by inhibiting prostaglandin production in the cyclooxygenase 1 and 2 (COX-1 and COX-2) pathways. Ibuprofen, indomethacin, ketorolac, naproxen, and other NSAIDs are chiefly utilized to control pain, inflammation, and fever via the oral route. As production of various prostaglandins via the COX-2 pathway is thought to contribute to fever, inflammation, and pain, inhibition of this pathway by NSAIDs can help alleviate these symptoms. The COX-1 pathway contributes many factors important to the protection and health of the GI tract, and inhibition of this pathway can lead to GI distress and damage. Unfortunately, the most commonly used and available NSAIDs inhibit both COX pathways simultaneously, and in doing so, prompt the GI symptoms which are the most common adverse side effects of therapy. In addition to GI effects of the COX-1 and COX-2 inhibitors, there are also concerns over the associated antiplatelet effects in patients undergoing surgery or potentially suffering from occult or intracranial bleeding.13
Ibuprofen
This is the most commonly used NSAID in the United States and is available without a prescription. Ibuprofen is typically used to treat mild-to-moderate pain from a musculoskeletal or inflammatory source. As an oral nonprescription medication, it can be used advantageously to treat acute pain in the ED and continued in the outpatient setting. Ibuprofen is neither sedating nor addicting, with a rapid onset of action and a plasma half-life of approximately 2 hours.13 However, there is a dose-dependent feature which allows large doses (eg, 800 mg) to be spaced-out every 8 hours while maintaining effective analgesia. Typical doses range from 200 mg to 800 mg orally every 6 to 8 hours, with a maximum dose of 3.2 g/d. Patients should be instructed to take each dose with a meal or snack to help alleviate GI side effects.
The greatest advantage of ibuprofen and other NSAIDs is their effect on inflammation and the ability to treat the inflammatory cause of pain—not just the symptom. Nonsteroidal anti-inflammatory drugs are well tolerated by most patients and can be obtained without prescription at low cost. Additionally, doses of ibuprofen and acetaminophen can be alternated.
Ketorolac
Often marketed as Toradol, ketorolac is a powerful NSAID available in IV, IM, and oral formulations. Typical doses are 30 mg IV, 60 mg IM, or 10 mg orally every 4 to 6 hours (maximum of 40 mg/d). The basic pharmacology and mechanism of action of ketorolac are similar to ibuprofen. Though ketorolac is useful to treat more severe pain, it should only be used for short-term management of pain (ie, 5 days or less). Ketorolac is often used for postoperative pain, but also is helpful for pain control in patients using opioids. It has been shown to be effective for acute renal colic and can also provide relief for migraine headaches.16,17 In a direct comparison between ketorolac and meperidine (Demerol) for patients suffering from renal stones, ketorolac was found to be more effective and provide longer lasting pain relief.18
The major concern regarding ketorolac relates to potential renal toxicity, and thus caution should be undertaken in prescribing it to patients with known or suspected renal disease. Although this risk is associated with even a single dose, multiple doses increase the danger and therefore should be avoided.
Ketorolac should also be used with caution in patients with asthma. As a subset of asthma patients will experience severe bronchospasm after NSAID administration, clinicians should always determine whether a patient can tolerate NSAIDs.
Renal Toxicity and GI Effects
Concerns over renal toxicity and potential GI distress are the chief disadvantages of NSAID use. While renal toxicity has been reported in patients without pre-existing kidney dysfunction, it is of much greater concern in patients with pre-existing renal disease or decreased glomerular filtration rate. For this reason, care must be exercised when prescribing NSAIDS to elderly patients, patients with diabetes mellitus, or patients with hypertension (or even worse, a combination of these). Prolonged use of NSAIDs can also cause upper GI bleeding. Nonsteroidal anti-inflammatory drugs are contraindicated in pregnant patients.
Opioid analgesics
Morphine
Morphine is the prototypical compound in the opioid class, and has been utilized for more than two centuries since its isolation in 1804.19 Other opioid compounds include codeine, hydrocodone, oxycodone, morphine, and hydromorphone, which represent different functional groups substituted onto the base morphine molecule. All share similar pharmacology, differing primarily only in potency. The onset of action for codeine, hydrocodone, and oxycodone is 30 to 60 minutes when taken orally, with a peak time of 60 to 90 minutes. Codeine and hydrocodone are at the weak-end of the spectrum (Step 2 medications), while morphine and hydromorphone are more potent (Step 3 medications). The majority of opioids and their metabolites are primarily excreted renally (90%-95%).20 Therefore, care must be exercised regarding dosing and frequency when used in patients with renal insufficiency or disease.
Morphine has several features that make it an attractive analgesic for use in the ED. The ability to administer morphine via IV, IM, subcutaneous, or oral route; its quick onset of action; and safety profile are all advantageous. The onset of action is 5 to 10 minutes when given IV. For oral administration, it is 30 to 60 minutes (similar to the other opioids discussed) and can be given as a tablet or syrup.
Morphine decreases the severity of pain, with an apparent increase in tolerance for any remaining discomfort. The potency and central action of morphine make it ideal for managing moderate and severe pain.
As with other analgesics, morphine and its related compounds have associated drawbacks, of which respiratory depression is the most feared, though this is uncommon at therapeutic doses. The respiratory depressant effect is more pronounced in patients with underlying lung disease, depressed mental status, or concurrent use of sedating medication (eg, benzodiazepines).
Another disadvantage to morphine is that it can cause hypotension, limiting its use in certain clinical situations. Repeated or prolonged use may cause slowing or complete arrest of peristaltic waves in the GI tract, which can lead to significant constipation. Pruritus and nausea are two other frequently reported side effects and may necessitate, respectively, coadministration of diphenhydramine (eg, Benadryl) or an antiemetic (eg, Phenergan or Zofran). As an opioid, morphine is potentially addictive, though it is generally thought to require significant intake over several weeks before such problems arise.
The sedation caused by morphine is also of concern, as patients who are under its influence immediately following discharge cannot safely drive, and may actually not be safe to walk or even utilize public transportation. This concern can be lessened by verifying the patient’s mode of transport prior to administration of the medication, ensuring that patients are not overly sedated at the time of discharge and, as much as possible, accompanied home by an adult relative or friend. In comparison to other frequently used opioids, several features can be considered. The duration of action for codeine, hydromorphone, and morphine is similar at 3 to 5 hours.
Hydromorphone
Hydromorphone (Dilaudid) is approximately seven times more potent than morphine, but otherwise very similar. It is frequently the IV opioid of choice for severe pain and also appears to cause pruritus less frequently than morphine. Hydromorphone has a rapid onset of action (1-5 minutes IV; 15-30 minutes orally) and can be titrated to effect when given via the IV route, making it an ideal agent for the pain associated with long bone or pelvic fractures, vasoocclusive crises in patients with sickle cell disease, and renal colic. The oral formulation of hydromorphone can be utilized for severe pain in the appropriate patient population, usually at a dose of 2 to 4 mg every 4 hours.
Codeine
Codeine is frequently prescribed in combination with acetaminophen in a product marketed as Tylenol #3 for mild-to-moderate pain. Because codeine is metabolized in the liver to morphine, it is contraindicated in patients with morphine allergy. Also, the clinician must be aware that codeine is ineffective in 7% to 10% of the population due to an enzyme deficiency.
Hydrocodone and oxycodone, which are often combined with acetaminophen and marketed respectively as Vicodin and Percocet, are two additional commonly used compounds in the oral treatment of moderate-to-severe pain. There are numerous preparations containing various strengths of both the opioid and acetaminophen components. Utilizing these medications as initial pain control in the ED can be beneficial, as therapy can be continued as an outpatient. Table 2 provides dosing and frequency information, but the clinician must also be aware of the total amount of acetaminophen administered, especially when being used in conjunction with other medications containing acetaminophen.
Tramadol
Tramadol (Ultram), another oral analgesic with opioid properties, affects several neurotransmitters and is less reliant on the opioid receptors compared to the opioid compounds described above. It is used to treat moderate-to-severe pain and can be considered another option along with codeine, hydrocodone, and oxycodone for oral pain control. Although the complete mechanism of action for tramadol is poorly understood, it appears to be effective in patients who do not respond well to pure opioids, and in patients with neuropathic pain or persistent pain of unclear etiology (eg, fibromyalgia).19 Because of its limited interaction with opioid receptors, tramadol has less potential for abuse and addiction than the opioids. It is also available in several combinations with acetaminophen or ibuprofen.
Conclusion
The ideal medication for treating pain in the ED is one that is effective, easy to administer, and has minimal adverse or residual effects. Generally, the least potent medication that will control pain should be chosen initially. When treating minor traumatic or musculoskeletal pain, initiating pain control with oral medication in the ED may provide patients with relief during imaging or splinting, and help control pain until they can fill outpatient prescriptions. All of the medications discussed in this article can be given in the oral form. However, IV usage may be appropriate when there is need for rapid onset of action, to titrate the medication, or for ease of administration in patients who are vomiting or unable to take anything orally.
When prescribing analgesics for pain control after discharge, the clinician must consider potential relative and absolute contraindications. For acetaminophen, liver toxicity is the major concern, and care must be taken not to exceed recommended daily dosing limits with the multitude of available products containing acetaminophen. Physicians should avoid recommending or prescribing acetaminophen to patients with liver disease (ie, cirrhosis) or habitual alcohol abuse.
Nonsteroidal anti-inflammatory drugs such as ibuprofen and naproxen carry the risk of renal damage, as well as concerns about antiplatelet activity. Because of the tendency for renal function to decline with age, caution must be exercised in using these compounds in older patients and those with preexisting renal dysfunction.
Opioid-containing medications are known for their potency in pain control, but also for their side effects. The most common side effect involves the GI tract, with nausea, vomiting, and constipation. The most dangerous side effect of opioids is respiratory depression; fortunately, this is rarely seen with therapeutic doses. However, somnolence and decreased coordination are significant concerns when prescribing opioids to elderly patients or those already at risk for falls.
There is no ideal single medication to treat all types of pain or situations. However, the choice of medication begins with a decision by the EP to treat pain. Utilizing a stepwise approach, oral medication will usually be effective for mild pain, but IV narcotics will probably be required for severe pain. Frequent reassessment of the patient is critically important for successful pain management in the ED.
Dr Byers is an emergency physician at the Presbyterian Medical Group, department of emergency medicine, Presbyterian Healthcare Services, Albuquerque, New Mexico. Dr Counselman is a distinguished professor of emergency medicine and chairman, department of emergency medicine, Eastern Virginia Medical School and Emergency Physicians of Tidewater, Norfolk, Virginia. He is also associate editor-in-chief of the Emergency Medicine editorial board.
Pain, one of the most common reasons patients present to the ED, may be a primary complaint or a warning sign encouraging further evaluation. The decision to treat pain is one of the most frequent therapeutic decisions made by emergency physicians (EPs) and involves a variety of options and considerations. Moreover, the decision of how to treat pain similarly encompasses a wide selection of variables, including etiology and severity of the pain; intravenous (IV) access; medication allergies; renal function; alcohol use; rapidity of onset; patients’ vital signs; patient preference; and mode of transport upon discharge. Given all of these considerations, there is no perfect analgesic to suit every circumstance. Rather, EPs must tailor their analgesic selection to the individual clinical situation and patient.
The literature over the past 20 years is replete with studies demonstrating the undertreatment or inadequate treatment of pain in the ED.1-5 Often referred to as oligoanalgesia,6 contributing factors include physician concerns regarding adverse side effects, secondary gain, and drug addiction. In addition, the increasing pressure placed on EPs to diagnose and dispose patients quickly likely relegates pain control to a secondary concern.
Further complicating the issue, physicians’ own prejudices and perceptions appear to influence their analgesic prescription practice. For example, several studies have demonstrated that black patients do not receive prescriptions for analgesics similar to those written for white patients in general, and particularly not for opioid analgesics. In a meta-analysis of pain treatment disparity studies, blacks were 22% less likely than whites to receive any analgesics, and 29% less likely than whites to receive opioid treatment for the same type of painful conditions.7 Likewise, Hispanic/Latino patients were also 22% less likely than their white counterparts to receive opioid treatment for similar pain.7 Physicians must keep these common biases in mind when treating patients for pain.
The administration of analgesics and the prescription habits of physicians has never been under greater scrutiny. The Centers for Medicare and Medicaid Services has benchmarked “median time to pain management for long bone fractures” as a core measure, possibly affecting hospital reimbursement rates. Similarly, every patient satisfaction survey specifically inquires about the timeliness and adequacy of pain control. At the same time, though, the increasing problem of prescription opioid abuse has become the nation’s fastest growing drug problem. In 2013, prescription drug abuse was second only to marijuana as the most abused drug category.8 Contributing to this problem are the frequency and ease with which many physicians prescribe opioids. From 1997 to 2007, the milligram-per-person use of prescription opioids in the United States increased from 74 mg per year to 369 mg per year—an increase of 402%.9 As a result, some legislators are now calling for mandatory educational sessions for any physician prescribing medications containing opioids.
Though there are many classes of medications used to treat pain, and numerous individual drugs within each class, this article focuses on several of the more commonly prescribed medications in the ED, including their mechanisms of action, advantages, and disadvantages. The management of pediatric pain and procedural sedation and analgesia are not discussed in this review, as each of these topics deserves a separate detailed discussion.
Recognizing and Quantifying Pain
The first step in treating pain appropriately is recognition. Physicians must specifically inquire about pain and not rely solely on a patient’s unprompted complaint. Several pain scales exist, including the Faces Pain Scale (ie, pictorial representation of a smiling face on one end indicating “no pain” to a frowning face on the opposite end); the verbal quantitative scale or numerical rating scale (ie, “how would you rate your pain on a scale of 0 to 10, with 10 the worst pain ever?”); and the visual analog scale (ie, a 10-cm linear scale marked at one end with “no pain” and “worst pain imaginable” at the opposite end).10,11 Probably the most commonly used scale in the ED is some variation of the numerical rating scale (NRS).1
Each of these scales has its own advantages and disadvantages, but the important point is that patients are given the opportunity to express the type and degree of pain to the healthcare provider. In addition, a pain scale provides a starting point against which the practitioner (or later practitioners) can determine the success (or failure) of a pain treatment strategy.
Three-Step Ladder
In 1996, the World Health Organization developed a three-step analgesic ladder to guide the management of cancer pain.12 Its use has been expanded over time to include treating pain of noncancer etiology. Mild pain (NRS of 1 to 3) is considered Step 1; moderate pain (NRS 4 to 6) is considered Step 2; and severe pain (NRS 7 to 10) is Step 3. For Step 1 (mild pain), acetaminophen or a nonsteroidal anti-inflammatory drug (NSAID) is recommended. For Step 2 (moderate pain), a weak opioid (ie, codeine or hydrocodone) with or without acetaminophen or an NSAID is recommended. Finally, for Step 3 (severe pain), a strong opioid such as morphine or hydromorphone is recommended.
Again, the purpose of the ladder is not to provide a strict protocol for adherence, but rather to provide a reasonable starting point as a guide to the clinician. The key to its successful use is reassessment of the patient to determine if adequate pain relief is achieved.
Routes of Administration
Acetaminophen
Acetaminophen, the active ingredient in Tylenol, was first marketed in the United States in 1955 as an antipyretic and pain reliever.13 It is a synthetic centrally acting analgesic that is metabolized in the liver. Acetaminophen has been used alone or in combination in hundreds of formulations to treat a wide variety of pain and fever-related conditions. In the ED setting, acetaminophen is frequently used as an antipyretic and—either alone or in combination with opioids—for oral pain control.
Acetaminophen is very well tolerated by most patients, with minimal gastrointestinal (GI) distress. It is inexpensive, and the wide variety of formulations (eg, liquid, tablet, suppository) make it useful in a number of clinical scenarios. Acetaminophen is generally considered to be the only nonopioid analgesic that is safe in pregnancy,14 and it has no sedative or addictive effects.
There are, however, some disadvantages to using acetaminophen. Concerns about its safety and accidental overdose have recently led to the introduction of a 4,000-mg maximum daily dose recommendation15 and heightened concern over using multiple medications containing acetaminophen. In January 2014, the US Food and Drug Administration recommended that no combination medication contain more than 325 mg of acetaminophen because of the risk of toxicity when multiple drugs containing acetaminophen are consumed.
In addition to concerns of inadvertent overdose, another disadvantage of acetaminophen is that while it may be an effective antipyretic and analgesic, it has little or no anti-inflammatory properties. Therefore, in cases requiring an anti-inflammatory agent, an NSAID, when appropriate, would be the more effective option.
NSAIDs
Nonsteroidal anti-inflammatory drugs function by inhibiting prostaglandin production in the cyclooxygenase 1 and 2 (COX-1 and COX-2) pathways. Ibuprofen, indomethacin, ketorolac, naproxen, and other NSAIDs are chiefly utilized to control pain, inflammation, and fever via the oral route. As production of various prostaglandins via the COX-2 pathway is thought to contribute to fever, inflammation, and pain, inhibition of this pathway by NSAIDs can help alleviate these symptoms. The COX-1 pathway contributes many factors important to the protection and health of the GI tract, and inhibition of this pathway can lead to GI distress and damage. Unfortunately, the most commonly used and available NSAIDs inhibit both COX pathways simultaneously, and in doing so, prompt the GI symptoms which are the most common adverse side effects of therapy. In addition to GI effects of the COX-1 and COX-2 inhibitors, there are also concerns over the associated antiplatelet effects in patients undergoing surgery or potentially suffering from occult or intracranial bleeding.13
Ibuprofen
This is the most commonly used NSAID in the United States and is available without a prescription. Ibuprofen is typically used to treat mild-to-moderate pain from a musculoskeletal or inflammatory source. As an oral nonprescription medication, it can be used advantageously to treat acute pain in the ED and continued in the outpatient setting. Ibuprofen is neither sedating nor addicting, with a rapid onset of action and a plasma half-life of approximately 2 hours.13 However, there is a dose-dependent feature which allows large doses (eg, 800 mg) to be spaced-out every 8 hours while maintaining effective analgesia. Typical doses range from 200 mg to 800 mg orally every 6 to 8 hours, with a maximum dose of 3.2 g/d. Patients should be instructed to take each dose with a meal or snack to help alleviate GI side effects.
The greatest advantage of ibuprofen and other NSAIDs is their effect on inflammation and the ability to treat the inflammatory cause of pain—not just the symptom. Nonsteroidal anti-inflammatory drugs are well tolerated by most patients and can be obtained without prescription at low cost. Additionally, doses of ibuprofen and acetaminophen can be alternated.
Ketorolac
Often marketed as Toradol, ketorolac is a powerful NSAID available in IV, IM, and oral formulations. Typical doses are 30 mg IV, 60 mg IM, or 10 mg orally every 4 to 6 hours (maximum of 40 mg/d). The basic pharmacology and mechanism of action of ketorolac are similar to ibuprofen. Though ketorolac is useful to treat more severe pain, it should only be used for short-term management of pain (ie, 5 days or less). Ketorolac is often used for postoperative pain, but also is helpful for pain control in patients using opioids. It has been shown to be effective for acute renal colic and can also provide relief for migraine headaches.16,17 In a direct comparison between ketorolac and meperidine (Demerol) for patients suffering from renal stones, ketorolac was found to be more effective and provide longer lasting pain relief.18
The major concern regarding ketorolac relates to potential renal toxicity, and thus caution should be undertaken in prescribing it to patients with known or suspected renal disease. Although this risk is associated with even a single dose, multiple doses increase the danger and therefore should be avoided.
Ketorolac should also be used with caution in patients with asthma. As a subset of asthma patients will experience severe bronchospasm after NSAID administration, clinicians should always determine whether a patient can tolerate NSAIDs.
Renal Toxicity and GI Effects
Concerns over renal toxicity and potential GI distress are the chief disadvantages of NSAID use. While renal toxicity has been reported in patients without pre-existing kidney dysfunction, it is of much greater concern in patients with pre-existing renal disease or decreased glomerular filtration rate. For this reason, care must be exercised when prescribing NSAIDS to elderly patients, patients with diabetes mellitus, or patients with hypertension (or even worse, a combination of these). Prolonged use of NSAIDs can also cause upper GI bleeding. Nonsteroidal anti-inflammatory drugs are contraindicated in pregnant patients.
Opioid analgesics
Morphine
Morphine is the prototypical compound in the opioid class, and has been utilized for more than two centuries since its isolation in 1804.19 Other opioid compounds include codeine, hydrocodone, oxycodone, morphine, and hydromorphone, which represent different functional groups substituted onto the base morphine molecule. All share similar pharmacology, differing primarily only in potency. The onset of action for codeine, hydrocodone, and oxycodone is 30 to 60 minutes when taken orally, with a peak time of 60 to 90 minutes. Codeine and hydrocodone are at the weak-end of the spectrum (Step 2 medications), while morphine and hydromorphone are more potent (Step 3 medications). The majority of opioids and their metabolites are primarily excreted renally (90%-95%).20 Therefore, care must be exercised regarding dosing and frequency when used in patients with renal insufficiency or disease.
Morphine has several features that make it an attractive analgesic for use in the ED. The ability to administer morphine via IV, IM, subcutaneous, or oral route; its quick onset of action; and safety profile are all advantageous. The onset of action is 5 to 10 minutes when given IV. For oral administration, it is 30 to 60 minutes (similar to the other opioids discussed) and can be given as a tablet or syrup.
Morphine decreases the severity of pain, with an apparent increase in tolerance for any remaining discomfort. The potency and central action of morphine make it ideal for managing moderate and severe pain.
As with other analgesics, morphine and its related compounds have associated drawbacks, of which respiratory depression is the most feared, though this is uncommon at therapeutic doses. The respiratory depressant effect is more pronounced in patients with underlying lung disease, depressed mental status, or concurrent use of sedating medication (eg, benzodiazepines).
Another disadvantage to morphine is that it can cause hypotension, limiting its use in certain clinical situations. Repeated or prolonged use may cause slowing or complete arrest of peristaltic waves in the GI tract, which can lead to significant constipation. Pruritus and nausea are two other frequently reported side effects and may necessitate, respectively, coadministration of diphenhydramine (eg, Benadryl) or an antiemetic (eg, Phenergan or Zofran). As an opioid, morphine is potentially addictive, though it is generally thought to require significant intake over several weeks before such problems arise.
The sedation caused by morphine is also of concern, as patients who are under its influence immediately following discharge cannot safely drive, and may actually not be safe to walk or even utilize public transportation. This concern can be lessened by verifying the patient’s mode of transport prior to administration of the medication, ensuring that patients are not overly sedated at the time of discharge and, as much as possible, accompanied home by an adult relative or friend. In comparison to other frequently used opioids, several features can be considered. The duration of action for codeine, hydromorphone, and morphine is similar at 3 to 5 hours.
Hydromorphone
Hydromorphone (Dilaudid) is approximately seven times more potent than morphine, but otherwise very similar. It is frequently the IV opioid of choice for severe pain and also appears to cause pruritus less frequently than morphine. Hydromorphone has a rapid onset of action (1-5 minutes IV; 15-30 minutes orally) and can be titrated to effect when given via the IV route, making it an ideal agent for the pain associated with long bone or pelvic fractures, vasoocclusive crises in patients with sickle cell disease, and renal colic. The oral formulation of hydromorphone can be utilized for severe pain in the appropriate patient population, usually at a dose of 2 to 4 mg every 4 hours.
Codeine
Codeine is frequently prescribed in combination with acetaminophen in a product marketed as Tylenol #3 for mild-to-moderate pain. Because codeine is metabolized in the liver to morphine, it is contraindicated in patients with morphine allergy. Also, the clinician must be aware that codeine is ineffective in 7% to 10% of the population due to an enzyme deficiency.
Hydrocodone and oxycodone, which are often combined with acetaminophen and marketed respectively as Vicodin and Percocet, are two additional commonly used compounds in the oral treatment of moderate-to-severe pain. There are numerous preparations containing various strengths of both the opioid and acetaminophen components. Utilizing these medications as initial pain control in the ED can be beneficial, as therapy can be continued as an outpatient. Table 2 provides dosing and frequency information, but the clinician must also be aware of the total amount of acetaminophen administered, especially when being used in conjunction with other medications containing acetaminophen.
Tramadol
Tramadol (Ultram), another oral analgesic with opioid properties, affects several neurotransmitters and is less reliant on the opioid receptors compared to the opioid compounds described above. It is used to treat moderate-to-severe pain and can be considered another option along with codeine, hydrocodone, and oxycodone for oral pain control. Although the complete mechanism of action for tramadol is poorly understood, it appears to be effective in patients who do not respond well to pure opioids, and in patients with neuropathic pain or persistent pain of unclear etiology (eg, fibromyalgia).19 Because of its limited interaction with opioid receptors, tramadol has less potential for abuse and addiction than the opioids. It is also available in several combinations with acetaminophen or ibuprofen.
Conclusion
The ideal medication for treating pain in the ED is one that is effective, easy to administer, and has minimal adverse or residual effects. Generally, the least potent medication that will control pain should be chosen initially. When treating minor traumatic or musculoskeletal pain, initiating pain control with oral medication in the ED may provide patients with relief during imaging or splinting, and help control pain until they can fill outpatient prescriptions. All of the medications discussed in this article can be given in the oral form. However, IV usage may be appropriate when there is need for rapid onset of action, to titrate the medication, or for ease of administration in patients who are vomiting or unable to take anything orally.
When prescribing analgesics for pain control after discharge, the clinician must consider potential relative and absolute contraindications. For acetaminophen, liver toxicity is the major concern, and care must be taken not to exceed recommended daily dosing limits with the multitude of available products containing acetaminophen. Physicians should avoid recommending or prescribing acetaminophen to patients with liver disease (ie, cirrhosis) or habitual alcohol abuse.
Nonsteroidal anti-inflammatory drugs such as ibuprofen and naproxen carry the risk of renal damage, as well as concerns about antiplatelet activity. Because of the tendency for renal function to decline with age, caution must be exercised in using these compounds in older patients and those with preexisting renal dysfunction.
Opioid-containing medications are known for their potency in pain control, but also for their side effects. The most common side effect involves the GI tract, with nausea, vomiting, and constipation. The most dangerous side effect of opioids is respiratory depression; fortunately, this is rarely seen with therapeutic doses. However, somnolence and decreased coordination are significant concerns when prescribing opioids to elderly patients or those already at risk for falls.
There is no ideal single medication to treat all types of pain or situations. However, the choice of medication begins with a decision by the EP to treat pain. Utilizing a stepwise approach, oral medication will usually be effective for mild pain, but IV narcotics will probably be required for severe pain. Frequent reassessment of the patient is critically important for successful pain management in the ED.
Dr Byers is an emergency physician at the Presbyterian Medical Group, department of emergency medicine, Presbyterian Healthcare Services, Albuquerque, New Mexico. Dr Counselman is a distinguished professor of emergency medicine and chairman, department of emergency medicine, Eastern Virginia Medical School and Emergency Physicians of Tidewater, Norfolk, Virginia. He is also associate editor-in-chief of the Emergency Medicine editorial board.
- Todd KH. Pain assessment instruments for use in the emergency department. Emerg Med Clin North Am. 2005;23(2):285-295.
- Cordell WH, Keene KK, Giles BK, Jones JB, Jones JH, Brizendine EJ. The high prevalence of pain in emergency medical care. Am J Emerg Med. 2002;20(3):165-169.
- Tcherny-Lessenot S, Karwowski-Soulié F, Lamarche-Vadel A, Ginsburg C, Brunet F, Vidal-Trecan G. Management and relief of pain in an emergency department from the adult patients’ perspective. J Pain Symptom Manage. 2003;25(6):539-546.
- Karwowski-Soulié F, Lessenot-Tcherny S, Lamarche-Vadel A, et al. Pain in an emergency department: an audit. Eur J Emerg Med. 2006;13(4):218-224.
- Fosnocht DE, Swanson ER, Barton ED. Changing attitudes about pain and pain control in emergency medicine. Emerg Med Clin North Am. 2005;23(2):297-306.
- Wilson JE, Pendelton JM. Oligoanalgesia in the emergency department. Am J Emerg Med. 1989;7(6):620-623.
- Meghani SH, Byun E, Gallagher RM. Time to take stock: a meta-analysis and systemic review of analgesic treatment disparities for pain in the United States. Pain Med. 2012;13(2):150-174.
- Johnston LD, O’Malley PM, Miech RA, Bachman JG, Schutenberg JE; The University of Michigan Institute for Social Research. Monitoring the future: 2013 overview key findings of on adolescent drug use. http://www.monitoringthefuture.org/pubs/monographs/mtf-overview2013.pdf. Accessed June 6, 2014.
- Manchikanti L, Fellow B, Ailinani H, Pampati V. Therapeutic use, abuse, and nonmedical use of opioids: a ten year perspective. Pain Physician. 2010;13(5):401-435.
- Silka PA, Roth MM, Moreno G, Merrill L, Geiderman JM. Pain scores improve analgesic administration patterns for trauma patients in the emergency department. Acad Emerg Med. 2004;11(3):264-270.
- Nelson BP, Cohen D, Lander O, Crawford N, Viccellio AW, Singer AJ. Mandated pain scales improve frequency of ED analgesic administration. Am J Emerg Med. 2004;22(7):582-585.
- World Health Organization. Cancer pain relief with a guide to opioid availability 2nd ed. 1996. http://whqlibdoc.who.int/publications/9241544821.pdf. Accessed June 6, 2014.
- Grosser T, Smyth EM, FitzGerald GA. Anti-inflammatory, antipyretic, and analgesic agents: pharmacotherapy of gout. In: Brunton LL, Chabner BA, Knollman BC, eds. Goodman and Gilman’s The Pharmacological Basis of Therapeutics. 12th ed. China: The McGraw Hill Companies; 2011:959-1004.
- Scialli AR, Ang R, Breitmeyer J, Royal MA. A review of the literature on the effects of acetaminophen on pregnancy outcome. Reprod Toxicol. 2010;30(4):495-507.
- Schilling A, Corey R, Leonard M, Eghtesad B. Acetaminophen: old drug, new warnings. Cleveland Clin J Med. 2010;77(1):19-27.
- Shrestha M, Singh R, Moreden J, Hayes JE. Ketorolac vs chlorpromazine in the treatment of acute migraine without aura. A prospective, randomized, double-blind trial. Arch Intern Med.1996;156(15):1725-1728.
- Turkewitz LJ, Casaly JS, Dawson GA, Wirth O, Hurst RJ, Gillette PL. Self-administration of parenteral ketorolac tromethamine for head pain. Headache. 1992;32(9):452-454.
- Larkin GL, Peacock WF 4th, Pearl SM, Blair GA, D’Amico F. Efficacy of ketorolac tromethamine versus meperidine in the ED treatment of acute renal colic. Am J Emerg Med. 1999;17(1):6-10.
- Yaksh TL, Wallace MS. Opiods, analgesia and pain management. In: Brunton LL, Chabner BA, Knollman BC, eds. Goodman and Gilman’s The Pharmacological Basis of Therapeutics. 12th ed. China: The McGraw Hill Companies; 2011:481-526.
- DeSandre PL, Quest TE. Management of cancer-related pain. Hematol Oncol Clin N Am. 2010;24(3):643-658.
- Todd KH. Pain assessment instruments for use in the emergency department. Emerg Med Clin North Am. 2005;23(2):285-295.
- Cordell WH, Keene KK, Giles BK, Jones JB, Jones JH, Brizendine EJ. The high prevalence of pain in emergency medical care. Am J Emerg Med. 2002;20(3):165-169.
- Tcherny-Lessenot S, Karwowski-Soulié F, Lamarche-Vadel A, Ginsburg C, Brunet F, Vidal-Trecan G. Management and relief of pain in an emergency department from the adult patients’ perspective. J Pain Symptom Manage. 2003;25(6):539-546.
- Karwowski-Soulié F, Lessenot-Tcherny S, Lamarche-Vadel A, et al. Pain in an emergency department: an audit. Eur J Emerg Med. 2006;13(4):218-224.
- Fosnocht DE, Swanson ER, Barton ED. Changing attitudes about pain and pain control in emergency medicine. Emerg Med Clin North Am. 2005;23(2):297-306.
- Wilson JE, Pendelton JM. Oligoanalgesia in the emergency department. Am J Emerg Med. 1989;7(6):620-623.
- Meghani SH, Byun E, Gallagher RM. Time to take stock: a meta-analysis and systemic review of analgesic treatment disparities for pain in the United States. Pain Med. 2012;13(2):150-174.
- Johnston LD, O’Malley PM, Miech RA, Bachman JG, Schutenberg JE; The University of Michigan Institute for Social Research. Monitoring the future: 2013 overview key findings of on adolescent drug use. http://www.monitoringthefuture.org/pubs/monographs/mtf-overview2013.pdf. Accessed June 6, 2014.
- Manchikanti L, Fellow B, Ailinani H, Pampati V. Therapeutic use, abuse, and nonmedical use of opioids: a ten year perspective. Pain Physician. 2010;13(5):401-435.
- Silka PA, Roth MM, Moreno G, Merrill L, Geiderman JM. Pain scores improve analgesic administration patterns for trauma patients in the emergency department. Acad Emerg Med. 2004;11(3):264-270.
- Nelson BP, Cohen D, Lander O, Crawford N, Viccellio AW, Singer AJ. Mandated pain scales improve frequency of ED analgesic administration. Am J Emerg Med. 2004;22(7):582-585.
- World Health Organization. Cancer pain relief with a guide to opioid availability 2nd ed. 1996. http://whqlibdoc.who.int/publications/9241544821.pdf. Accessed June 6, 2014.
- Grosser T, Smyth EM, FitzGerald GA. Anti-inflammatory, antipyretic, and analgesic agents: pharmacotherapy of gout. In: Brunton LL, Chabner BA, Knollman BC, eds. Goodman and Gilman’s The Pharmacological Basis of Therapeutics. 12th ed. China: The McGraw Hill Companies; 2011:959-1004.
- Scialli AR, Ang R, Breitmeyer J, Royal MA. A review of the literature on the effects of acetaminophen on pregnancy outcome. Reprod Toxicol. 2010;30(4):495-507.
- Schilling A, Corey R, Leonard M, Eghtesad B. Acetaminophen: old drug, new warnings. Cleveland Clin J Med. 2010;77(1):19-27.
- Shrestha M, Singh R, Moreden J, Hayes JE. Ketorolac vs chlorpromazine in the treatment of acute migraine without aura. A prospective, randomized, double-blind trial. Arch Intern Med.1996;156(15):1725-1728.
- Turkewitz LJ, Casaly JS, Dawson GA, Wirth O, Hurst RJ, Gillette PL. Self-administration of parenteral ketorolac tromethamine for head pain. Headache. 1992;32(9):452-454.
- Larkin GL, Peacock WF 4th, Pearl SM, Blair GA, D’Amico F. Efficacy of ketorolac tromethamine versus meperidine in the ED treatment of acute renal colic. Am J Emerg Med. 1999;17(1):6-10.
- Yaksh TL, Wallace MS. Opiods, analgesia and pain management. In: Brunton LL, Chabner BA, Knollman BC, eds. Goodman and Gilman’s The Pharmacological Basis of Therapeutics. 12th ed. China: The McGraw Hill Companies; 2011:481-526.
- DeSandre PL, Quest TE. Management of cancer-related pain. Hematol Oncol Clin N Am. 2010;24(3):643-658.

The Geriatric ED and Clinical Protocols for the Emergency Care of Older Adults
Case 1
An 82-year-old man presented to the ED accompanied by his son, who stated that his father “had not been acting right” for the past 2 days. The patient was combative, yelling “Go away,” and was intermittently more confused than his baseline; he was also eating and drinking less than usual. He had a history of mild dementia, noninsulin-dependent diabetes, hypertension, and arthritis; there were no recent changes in his medication. The patient lived alone in an apartment across the hall from his son and had home healthcare aide 4 hours a day, 3 days a week. He was independent of activities of daily living (ADL), but needed help with shopping and cooking.
At presentation, the patient’s vital signs were: temperature, afebrile; heart rate (HR), 94 beats/minute; blood pressure (BP), 146/92 mm hg; respiratory rate (RR), 22 breaths/minute. Oxygen (O2) saturation was 96% on room air. A finger-stick glucose test was 103 mg/dL. He was hyperalert and agitated, and did not appear oriented to place or time. There were no focal neurological deficits; mucous membranes were mildly dry; and faint crackles were heard at the right base of the lungs. The patient was placed on a monitor in a curtained room in the ED, and was given 2 L O2 via nasal cannula, which improved O2 saturation to 99%. With his son present, an intravenous (IV) line was placed and blood was drawn. An electrocardiogram (ECG) showed a sinus rhythm without ischemic findings.
During evaluation, the patient continued to pull at the monitor lines and attempted to get off the stretcher. To calm his agitation, he was given haloperidol 2.5 mg and lorazepam 1 mg; 10 minutes after administration, he became sedated and difficult to arouse. His vital signs remained stable.
Laboratory analysis revealed a white blood cell count (WBC) of 12.5 K/uL, a negative troponin, a brain natriuretic peptide (BNP) of 80 pg/mL, and normal blood urea nitrogen (BUN) and creatinine levels. Urinalysis was negative for infection, but chest X-ray showed a right lower lobe infiltrate. Blood cultures were drawn, and the patient was continued on maintenance fluids and started on IV antibiotics to cover community-acquired pneumonia. He was admitted to the hospital for pneumonia and altered mental status.
As the patient’s sedative state was followed by periods of agitation, he was treated with additional haloperidol and lorazepam by the inpatient medical team, which resulted in further sedation. On hospital day 3, his urinary output decreased. He was given an IV bolus of 3 L normal saline over 6 hours, after which his mental status began to improve, and he was switched to oral antibiotics. His mental status returned to baseline and O2 saturation was 99% on room air. He was discharged home on hospital day 5 accompanied by his son.
Case 2
A 75-year-old man was brought to the ED with a 3-day history of worsening dyspnea on exertion, increased orthopnea, and increased bilateral lower extremity edema. He had a history of congestive heart failure (CHF), with an ejection fraction of 40%, and had been on 40 mg of furosemide daily at home; there were no recent changes to his medication. The patient was independent of ADL at baseline, living with his wife in a home with stairs.
His vital signs at presentation were: temperature, afebrile; HR, 86 beats/minute; BP, 160/90 mm hg; RR 30 breaths/minute; O2 saturation was 92% on room air. The patient had increased work of breathing and was speaking in four- to five-word sentences. Pulmonary examination revealed crackles half way up bilaterally. He also had 2+ pitting edema bilaterally in his lower extremities. He was otherwise alert and oriented.
On 4 L O2 via nasal cannula, the patient’s O2 saturation was 98%. Laboratory analysis revealed a BNP of 600 pg/mL, negative troponin, and normal creatinine level. Urinalysis was negative for evidence of infection. An ECG showed no changes, and chest X-ray revealed mild pulmonary congestion without an infiltrate. In the ED, an indwelling urinary catheter (IUC) was placed to monitor urinary output before the patient was given 40 mg of IV furosemide for diuresis. The patient was then admitted for management of exacerbation of CHF. As the medical team was preparing to discharge him on hospital day 2, his wife noticed that he was confused and not acting “like himself.” An investigation for causes of delirium included evaluation for infectious disease, which revealed an elevated WBC of 14.0 K/uL, stable creatinine; and urinalysis positive for bacteria, WBCs, leukocyte esterase, and nitrites. Since chest X-ray showed resolution of the vascular congestion, the patient no longer required supplemental O2.
The IUC was removed, and the patient was started on IV antibiotics for a urinary tract infection (UTI) secondary to IUC placement. The inpatient stay was prolonged for an additional 3 days until his delirium cleared and he could be continued on oral antibiotics as an outpatient.
Discussion
There is nothing extraordinary about these two cases. Every day elderly adults present to EDs throughout the country with confusion caused by pneumonia and dehydration that is sometimes initially attributed to worsening dementia and then complicated or prolonged by overuse of powerful sedating medications. Also, complications resulting from IUCs inserted in the ED all too often prolong hospitalizations. But by using protocols designed for better, more efficient emergency care of elderly patients, their ED care can be substantially improved and any subsequent inpatient care shortened.
The older adult population (ages 65 years and older) often presents to the ED with similar complaints to their younger counterparts—eg, chest pain, abdominal pain, dyspnea. However, the history, physical examination, and social assessment of elderly patients usually lead to a more comprehensive work-up, as older adults tend to present in an atypical fashion for both illness and trauma, thus necessitating a broader differential. In addition, they are more susceptible to adverse reactions from medications and procedures.
Regardless of the ultimate diagnosis, simply presenting to an ED as a patient (and sometimes spending many hours there) places older adults at elevated risk of morbidity and mortality. The challenge is to develop reliable tools to streamline the management of this population in order to increase diagnostic accuracy, decrease adverse events, and improve patient outcomes.
Clinical Protocols
Clinical protocols are one way in which we can educate and standardize the practice of multiple levels of provider, including nurses, midlevel providers, and physicians. Adopting protocols is natural for EPs—the key is to make sure the clinical protocol to be implemented is designed or modified for the ED setting in which it will be implemented.
In our ED, we have recently implemented the following two protocols for common scenarios in older adults: (1) assessment and management of delirium; and (2) decreased use of IUCs. These protocols employ the following stepwise project plan:
- Focus groups involving nurses, midlevels, residents, and attendings to assess ED provider knowledge, attitudes, and practice patterns regarding the clinical issue in older adult patients, and to guide development of the clinical protocol by understanding needs and constraints of the current ED environment;
- An extensive literature review of the clinical topic;
- Development of the clinical protocol by the workgroup;
- Implementation of protocol after multiple educational sessions using a scripted slide presentation to ensure all providers receive the same information; and
- Subsequent data analysis from the electronic medical record to assess the impact (ie, outcome) of the protocol.
Delirium
Delirium is a common syndrome in older adults, but is often unrecognized despite its clinical importance. Although 7% to 17% of older adults who present to the ED suffer from delirium,1-6 emergency physicians (EPs) miss 64% to 83% of cases, and 12% to 38% of patients with unrecognized delirium are actually discharged from the ED.1,6-8 Unfortunately, patients discharged from the ED with undetected delirium are three times more likely to die within 3 months than those whose delirium was recognized.
Life-threatening causes are more apt to be recognized early on in the ED. With this in mind, we developed a new, comprehensive, evidence-based protocol for recognition, diagnosis, management, and disposition of agitated delirium in older adults in the ED, with a focus on identifying and treating the commonly missed contributing causes: analgesia, bladder-urine retention, constipation, dehydration, environment, and medications.9
IUC Placement in the ED
The second protocol implemented at our institution is a new, evidence-based protocol for the placement, management, and reassessment of IUCs. As emphasized by the National American College of Emergency Physicians (ACEP) 2013 Choosing Wisely Campaign,10 inserting an IUC is a procedure that should be undertaken judiciously as it is associated with an elevated risk of infection, delirium, falls, and other adverse events. As of 2008, the Centers for Medicare and Medicaid Services no longer reimburses for hospital-acquired catheter-associated UTIs.11
After conducting focus groups of our ED providers, we learned that IUCs are placed more frequently than needed—often for reasons of convenience—and are rarely reassessed or removed if the patient is admitted to the hospital. Thus, our protocol highlights appropriate, possibly appropriate, and inappropriate indications for IUC placement, with an emphasis on trying alternative modes of urine collection, communicating among healthcare providers regarding the necessity of an IUC, and reassessment of the patient for IUC removal.
Our protocols have yielded early promising results, but further research is underway to determine their specific impact. The goal is to create a protocol that is feasible and effective for the specific institution and department to which it is applied. By ensuring all members of the healthcare team are involved in the development and design of a protocol, there is ownership of its implementation and use, with the overarching goal of improving patient care.
Geriatric ED Guidelines
In the beginning of 2014, new consensus-based Geriatric Emergency Department (GED) guidelines were published in order to “provide a standardized set of guidelines that can effectively improve the care of the geriatric population and are feasible to implement in the ED.”12 These guidelines are the result of a 2-year effort by representatives from ACEP, the American Geriatrics Society, the Society of Academic Emergency Medicine, and the Emergency Nurses Association, who were committed to optimizing the emergency-care delivery model for geriatrics. The participants encompassed both academic and community providers and included clinicians and researchers. These guidelines were formulated based on an 80% consensus among the representatives and, when possible, validated using existing literature at the time.
The genesis of the GED guidelines was multifactorial. In addition to the formation and rapid growth of geriatric interest groups and sections within EM academic organizations over the last 14 years, as well as the development of geriatric core competencies for EM residents in training, the 2010 Census Data results sharply outlined the details of the rapidly growing population of older adults in the United States. This acted as an alarm highlighting the need for a structured document containing best practice recommendations from geriatric emergency healthcare providers, researchers, and advocates. “The subsequent increased need for healthcare for this burgeoning geriatric population represents an unprecedented and overwhelming challenge to the American healthcare system as a whole and to emergency departments specifically,” the authors of the GED guidelines noted.
In response to a growing national interest in geriatric ED patients and an ever-increasing competition to attract patients from this demographic by EDs across the country, there has been a surge of self-designated GEDs during the last few years. Currently, more than 70 hospitals claim to have GEDs, raising the question of what sort of geriatric patient care is actually being delivered in these EDs. The question is of increased importance because very few of these “GEDs” are in academic centers or are associated with thought leaders in EM. In fact, when 30 self-designated GEDs that were snowball sampled in 2013 by researchers who asked what specific changes they had made toward the goal of improving care for the elderly, several rescinded this self-designation.
Because of heightened concerns for the needs of the increasing geriatric population overall, and the rise in the proportion of ED visits by this demographic, the authors of the GED guidelines state that “the contemporary emergency medicine management model may not be adequate for geriatric adults,” and offer the new GED guidelines as a basis on which EDs can consider ways to improve care for older adults while addressing the unique needs of this population. The GED guidelines propose specific methods and processes by which ED care of the elderly can be optimized. The authors note that “similar programs designed for other age groups (pediatrics) or directed towards specific diseases (STEMI, stroke, and trauma) have improved the care both in individual EDs and system-wide, resulting in better, more cost-effective care and ultimately better patient outcomes.”
The GED guidelines consist of 40 specific recommendations in six general categories: (1) staffing/administration; (2) equipment/supplies; (3) education; (4) policies/procedures/protocols; (5) follow-up/transitions of care; and (6) quality-improvement measures. This template outlines how to construct an effective GED program. The following highlights recommendations for each of these categories:
Staffing/Administration. Set qualifications and responsibilities for the medical director, nurse manager, staff physicians, nurses, and specialists, as well as accessibility to specialist ancillary services, with the goal of establishing hospital site-specific staff and coordination of local resources.
Equipment/Supplies. Develop potential physical and structural enhancements that address issues of mobility, comfort, safety, and behavioral needs (including memory cues and sensorial perception) while decreasing iatrogenic complications, such as the development of pressure ulcers (eg, the use of reclining chairs and pressure-redistributing foam mattresses).
Education. Provide nurse and clinical provider education and specialty-specific training focusing on contemporary, research-based geriatric-specific material, with regular assessment for interdisciplinary core competencies.
Policies/Procedures/Protocols. Implement a directed, comprehensive approach to facilitate screening and assessment of geriatric patients for added needs/post-ED adverse outcomes, as well as validated, ED-feasible screening tools/instruments for delirium and dementia, medication management, falls, use of urinary catheters, and the provision of palliative care.
Follow-up/Transitions of Care. Design discharge processes best suited for older patients (eg, large-font instructions), as well as collaborate with community resources to provide home-health services and home safety assessment in order to facilitate care following discharge.
Quality Improvement. Implement a system to collect and monitor pertinent and prevalent geriatric emergency care indicators (eg, incidence of injurious falls and documentation of fall risk assessment) designed to increase staff education and program success.
The authors clearly state that the GED guidelines represent recommendations. They are not a mandate for every ED, nor are they a list that requires 100% compliance. Instead, the document provides the potential steps to be taken, the rationale for these recommendations, and an outline of the resources available to aid in the transition from theory to implementation in any ED. The goal is to ensure better, safer, and age-appropriate treatment. In summary, these guidelines represent an effort to improve and even transform emergency care for older adults on the brink of one of the most significant challenges facing our healthcare system both in and beyond the ED.
Moving forward, the authors of the GED guidelines have defined a plan that “includes dissemination, implementation, adaptation, and refinement.” In addition to approval by each of the organization’s board of directors and the copyright of the material in 2013, the ED guidelines have now been widely disseminated through publication in numerous news articles (including international publications) and discussions on satellite radio. Tracking of new GEDs is planned. In addition, the prioritization of the guidelines is underway using a modified Delphi method, with the express purpose of assessing the relative potential benefits and harms associated with each recommendation by providing a weighted list from most important to least important.
A “Geriatric Emergency Department Boot Camp” is being developed to bring the recommendations to hospitals interested in “geriatricizing” their EDs. Geriatric EM leaders will act as consultants, providing training and a toolbox of resources. Specific reviews and revisions of the GED guidelines will take place in a 4- to 5-year cycle. Clearly, a next important step is the development of a GED certification system based on outcome studies of the individual components.
Criticisms of the GED guidelines have already been voiced among some EM providers. Specific concerns include a fear of partitioning the ED (as has occurred with pediatrics); an increase in cost and decreased efficiency; the need to maintain general expertise among EM physicians; the lack of evidence-based data upon which the recommendations were made; the fact that some guidelines were extrapolated from other clinical settings; and the belief that these changes will be too logistically difficult and take too much time.
The fact remains that the wave of geriatric patients (the “silver tsunami”) is already beginning to hit the shores of our hospitals. And GEDs are already here to help absorb the impact. The lack of iron-clad evidence for many of the recommendations should not be an absolute obstacle, but rather part of the natural evolution and improvement of similar endeavors. Nor should GEDs contain empty beds while younger adults sit in the waiting room, or conversely, force the elderly to wait for space in the GED when there are empty beds in the main ED. Ideally, the GED should be the location where the ED staff can implement these guidelines, which they can afterwards utilize in any part of the ED. These guidelines are designed to provide the best available expert opinion on how to deliver better geriatric care in the ED. The imperative for this goal is clear and necessitates this educated “leap-of-faith.” Change is never easy and often comes with an upfront cost of time, resources, and money. Moreover, there is nothing in a well-designed GED that may not also benefit, or at least will not adversely affect care of a younger adult as well. Therefore, flexibility and optimal utilization of space in a busy ED need not be sacrificed.
Conclusion
To improve diagnostic evaluation and care of the increasing number of geriatric patients presenting to the ED, reliable tools, protocols, and guidelines must be developed and implemented to ensure diagnostic accuracy, decrease adverse events, and improve patient outcomes. Fortunately, the new GED consensus guidelines are flexible and do not need to be wholly embraced—lending themselves to modifications and institution-specific adoptions. The “protocolization” and implementation of the guidelines may improve patient flow, operational efficiency, and, most importantly, the quality of care delivered. And likely, these guidelines will provide the foundation for future education and research into the improved emergency care of older adults.
The GED guidelines can be accessed at http://www.saem.org/docs/education/geri_ed_guidelines_final.pdf?sfvrsn=2.
Dr Stern is an assistant professor of medicine and codirector, geriatric emergency medicine fellowship, department of emergency medicine, New York-Presbyterian Hospital/Weill Cornell Medical Center, New York; and an assistant attending physician, department of emergency medicine, New York-Presbyterian Hospital.
Dr Mulcare is an instructor of medicine and an assistant attending physician, department of emergency medicine, New York-Presbyterian Hospital/Weill Cornell Medical Center, New York. She is a former fellow of geriatric emergency medicine.
- Lewis LM, Miller DK, Morley JE, Nork MJ, Lasater LC. Unrecognized delirium in ED geriatric patients. Am J Emerg Med. 1995;13(2):142-145.
- Naughton BJ, Moran M, Ghaly Y, Michalakes C. Computed tomography scanning and delirium in elder patients. Acad Emerg Med. 1997;4(12):1107-1110.
- Naughton BJ, Moran MB, Kadah H, Heman-Ackah Y, Longano J. Delirium and other cognitive impairment in older adults in an emergency department. Ann Emerg Med. 1995;25(6):751-755.
- Hustey FM, Meldon SW. The prevalence and documentation of impaired mental status in elderly emergency department patients. Ann Emerg Med. 2002;39(3):248-253.
- Hustey FM, Meldon SW, Smith MD, Lex CK. The effect of mental status screening on the care of elderly emergency department patients. Ann Emerg Med. 2003;41(5):678-684.
- Elie M, Rousseau F, Cole M, Primeau F, McCusker J, Bellavance F. Prevalence and detection of delirium in elderly emergency department patients. CMAJ. 2000;163(8):977-981.
- Han JH, Zimmerman EE, Cutler N, et al. Delirium in older emergency department patients: recognition, risk factors, and psychomotor subtypes. Acad Emerg Med. 2009;16(3):193-200.
- Sanders AB. Missed delirium in older emergency department patients: a quality-of-care problem. Ann Emerg Med. 2002;39(3):338-341.
- Rosen T, Connors S, Halpern A, et al. Improving emergency department identification and management of agitated delirium in older adults: implementation and impact assessment of a comprehensive clinical protocol emphasizing commonly missed contributing causes using an A-B-C-D-E-F mnemonic. Sys Qual Rev J. 2013;11(special issue):203,204. http://www.nypsystem.org/pdf/System-Quality-Review-2013.pdf. Accessed June 4, 2014.
- Choosing Wisely: ACEP Lists 5 Tests to Question. Medscape Web site. http://www.medscape.com/viewarticle/812600. Accessed June 4, 2014.
- Wald HL, Kramer AM. Nonpayment for harms resulting from medical care: catheter-associated urinary tract infections. JAMA. 2007;298(23):2782-2784.
- American College of Emergency Physicians; American Geriatrics Society; Emergency Nurses Association; Society for Academic Emergency Medicine. Geriatric Emergency Department Guidelines. http://www.saem.org/docs/education/geri_ed_guidelines_final.pdf?sfvrsn=2. Accessed June 4, 2014.
Case 1
An 82-year-old man presented to the ED accompanied by his son, who stated that his father “had not been acting right” for the past 2 days. The patient was combative, yelling “Go away,” and was intermittently more confused than his baseline; he was also eating and drinking less than usual. He had a history of mild dementia, noninsulin-dependent diabetes, hypertension, and arthritis; there were no recent changes in his medication. The patient lived alone in an apartment across the hall from his son and had home healthcare aide 4 hours a day, 3 days a week. He was independent of activities of daily living (ADL), but needed help with shopping and cooking.
At presentation, the patient’s vital signs were: temperature, afebrile; heart rate (HR), 94 beats/minute; blood pressure (BP), 146/92 mm hg; respiratory rate (RR), 22 breaths/minute. Oxygen (O2) saturation was 96% on room air. A finger-stick glucose test was 103 mg/dL. He was hyperalert and agitated, and did not appear oriented to place or time. There were no focal neurological deficits; mucous membranes were mildly dry; and faint crackles were heard at the right base of the lungs. The patient was placed on a monitor in a curtained room in the ED, and was given 2 L O2 via nasal cannula, which improved O2 saturation to 99%. With his son present, an intravenous (IV) line was placed and blood was drawn. An electrocardiogram (ECG) showed a sinus rhythm without ischemic findings.
During evaluation, the patient continued to pull at the monitor lines and attempted to get off the stretcher. To calm his agitation, he was given haloperidol 2.5 mg and lorazepam 1 mg; 10 minutes after administration, he became sedated and difficult to arouse. His vital signs remained stable.
Laboratory analysis revealed a white blood cell count (WBC) of 12.5 K/uL, a negative troponin, a brain natriuretic peptide (BNP) of 80 pg/mL, and normal blood urea nitrogen (BUN) and creatinine levels. Urinalysis was negative for infection, but chest X-ray showed a right lower lobe infiltrate. Blood cultures were drawn, and the patient was continued on maintenance fluids and started on IV antibiotics to cover community-acquired pneumonia. He was admitted to the hospital for pneumonia and altered mental status.
As the patient’s sedative state was followed by periods of agitation, he was treated with additional haloperidol and lorazepam by the inpatient medical team, which resulted in further sedation. On hospital day 3, his urinary output decreased. He was given an IV bolus of 3 L normal saline over 6 hours, after which his mental status began to improve, and he was switched to oral antibiotics. His mental status returned to baseline and O2 saturation was 99% on room air. He was discharged home on hospital day 5 accompanied by his son.
Case 2
A 75-year-old man was brought to the ED with a 3-day history of worsening dyspnea on exertion, increased orthopnea, and increased bilateral lower extremity edema. He had a history of congestive heart failure (CHF), with an ejection fraction of 40%, and had been on 40 mg of furosemide daily at home; there were no recent changes to his medication. The patient was independent of ADL at baseline, living with his wife in a home with stairs.
His vital signs at presentation were: temperature, afebrile; HR, 86 beats/minute; BP, 160/90 mm hg; RR 30 breaths/minute; O2 saturation was 92% on room air. The patient had increased work of breathing and was speaking in four- to five-word sentences. Pulmonary examination revealed crackles half way up bilaterally. He also had 2+ pitting edema bilaterally in his lower extremities. He was otherwise alert and oriented.
On 4 L O2 via nasal cannula, the patient’s O2 saturation was 98%. Laboratory analysis revealed a BNP of 600 pg/mL, negative troponin, and normal creatinine level. Urinalysis was negative for evidence of infection. An ECG showed no changes, and chest X-ray revealed mild pulmonary congestion without an infiltrate. In the ED, an indwelling urinary catheter (IUC) was placed to monitor urinary output before the patient was given 40 mg of IV furosemide for diuresis. The patient was then admitted for management of exacerbation of CHF. As the medical team was preparing to discharge him on hospital day 2, his wife noticed that he was confused and not acting “like himself.” An investigation for causes of delirium included evaluation for infectious disease, which revealed an elevated WBC of 14.0 K/uL, stable creatinine; and urinalysis positive for bacteria, WBCs, leukocyte esterase, and nitrites. Since chest X-ray showed resolution of the vascular congestion, the patient no longer required supplemental O2.
The IUC was removed, and the patient was started on IV antibiotics for a urinary tract infection (UTI) secondary to IUC placement. The inpatient stay was prolonged for an additional 3 days until his delirium cleared and he could be continued on oral antibiotics as an outpatient.
Discussion
There is nothing extraordinary about these two cases. Every day elderly adults present to EDs throughout the country with confusion caused by pneumonia and dehydration that is sometimes initially attributed to worsening dementia and then complicated or prolonged by overuse of powerful sedating medications. Also, complications resulting from IUCs inserted in the ED all too often prolong hospitalizations. But by using protocols designed for better, more efficient emergency care of elderly patients, their ED care can be substantially improved and any subsequent inpatient care shortened.
The older adult population (ages 65 years and older) often presents to the ED with similar complaints to their younger counterparts—eg, chest pain, abdominal pain, dyspnea. However, the history, physical examination, and social assessment of elderly patients usually lead to a more comprehensive work-up, as older adults tend to present in an atypical fashion for both illness and trauma, thus necessitating a broader differential. In addition, they are more susceptible to adverse reactions from medications and procedures.
Regardless of the ultimate diagnosis, simply presenting to an ED as a patient (and sometimes spending many hours there) places older adults at elevated risk of morbidity and mortality. The challenge is to develop reliable tools to streamline the management of this population in order to increase diagnostic accuracy, decrease adverse events, and improve patient outcomes.
Clinical Protocols
Clinical protocols are one way in which we can educate and standardize the practice of multiple levels of provider, including nurses, midlevel providers, and physicians. Adopting protocols is natural for EPs—the key is to make sure the clinical protocol to be implemented is designed or modified for the ED setting in which it will be implemented.
In our ED, we have recently implemented the following two protocols for common scenarios in older adults: (1) assessment and management of delirium; and (2) decreased use of IUCs. These protocols employ the following stepwise project plan:
- Focus groups involving nurses, midlevels, residents, and attendings to assess ED provider knowledge, attitudes, and practice patterns regarding the clinical issue in older adult patients, and to guide development of the clinical protocol by understanding needs and constraints of the current ED environment;
- An extensive literature review of the clinical topic;
- Development of the clinical protocol by the workgroup;
- Implementation of protocol after multiple educational sessions using a scripted slide presentation to ensure all providers receive the same information; and
- Subsequent data analysis from the electronic medical record to assess the impact (ie, outcome) of the protocol.
Delirium
Delirium is a common syndrome in older adults, but is often unrecognized despite its clinical importance. Although 7% to 17% of older adults who present to the ED suffer from delirium,1-6 emergency physicians (EPs) miss 64% to 83% of cases, and 12% to 38% of patients with unrecognized delirium are actually discharged from the ED.1,6-8 Unfortunately, patients discharged from the ED with undetected delirium are three times more likely to die within 3 months than those whose delirium was recognized.
Life-threatening causes are more apt to be recognized early on in the ED. With this in mind, we developed a new, comprehensive, evidence-based protocol for recognition, diagnosis, management, and disposition of agitated delirium in older adults in the ED, with a focus on identifying and treating the commonly missed contributing causes: analgesia, bladder-urine retention, constipation, dehydration, environment, and medications.9
IUC Placement in the ED
The second protocol implemented at our institution is a new, evidence-based protocol for the placement, management, and reassessment of IUCs. As emphasized by the National American College of Emergency Physicians (ACEP) 2013 Choosing Wisely Campaign,10 inserting an IUC is a procedure that should be undertaken judiciously as it is associated with an elevated risk of infection, delirium, falls, and other adverse events. As of 2008, the Centers for Medicare and Medicaid Services no longer reimburses for hospital-acquired catheter-associated UTIs.11
After conducting focus groups of our ED providers, we learned that IUCs are placed more frequently than needed—often for reasons of convenience—and are rarely reassessed or removed if the patient is admitted to the hospital. Thus, our protocol highlights appropriate, possibly appropriate, and inappropriate indications for IUC placement, with an emphasis on trying alternative modes of urine collection, communicating among healthcare providers regarding the necessity of an IUC, and reassessment of the patient for IUC removal.
Our protocols have yielded early promising results, but further research is underway to determine their specific impact. The goal is to create a protocol that is feasible and effective for the specific institution and department to which it is applied. By ensuring all members of the healthcare team are involved in the development and design of a protocol, there is ownership of its implementation and use, with the overarching goal of improving patient care.
Geriatric ED Guidelines
In the beginning of 2014, new consensus-based Geriatric Emergency Department (GED) guidelines were published in order to “provide a standardized set of guidelines that can effectively improve the care of the geriatric population and are feasible to implement in the ED.”12 These guidelines are the result of a 2-year effort by representatives from ACEP, the American Geriatrics Society, the Society of Academic Emergency Medicine, and the Emergency Nurses Association, who were committed to optimizing the emergency-care delivery model for geriatrics. The participants encompassed both academic and community providers and included clinicians and researchers. These guidelines were formulated based on an 80% consensus among the representatives and, when possible, validated using existing literature at the time.
The genesis of the GED guidelines was multifactorial. In addition to the formation and rapid growth of geriatric interest groups and sections within EM academic organizations over the last 14 years, as well as the development of geriatric core competencies for EM residents in training, the 2010 Census Data results sharply outlined the details of the rapidly growing population of older adults in the United States. This acted as an alarm highlighting the need for a structured document containing best practice recommendations from geriatric emergency healthcare providers, researchers, and advocates. “The subsequent increased need for healthcare for this burgeoning geriatric population represents an unprecedented and overwhelming challenge to the American healthcare system as a whole and to emergency departments specifically,” the authors of the GED guidelines noted.
In response to a growing national interest in geriatric ED patients and an ever-increasing competition to attract patients from this demographic by EDs across the country, there has been a surge of self-designated GEDs during the last few years. Currently, more than 70 hospitals claim to have GEDs, raising the question of what sort of geriatric patient care is actually being delivered in these EDs. The question is of increased importance because very few of these “GEDs” are in academic centers or are associated with thought leaders in EM. In fact, when 30 self-designated GEDs that were snowball sampled in 2013 by researchers who asked what specific changes they had made toward the goal of improving care for the elderly, several rescinded this self-designation.
Because of heightened concerns for the needs of the increasing geriatric population overall, and the rise in the proportion of ED visits by this demographic, the authors of the GED guidelines state that “the contemporary emergency medicine management model may not be adequate for geriatric adults,” and offer the new GED guidelines as a basis on which EDs can consider ways to improve care for older adults while addressing the unique needs of this population. The GED guidelines propose specific methods and processes by which ED care of the elderly can be optimized. The authors note that “similar programs designed for other age groups (pediatrics) or directed towards specific diseases (STEMI, stroke, and trauma) have improved the care both in individual EDs and system-wide, resulting in better, more cost-effective care and ultimately better patient outcomes.”
The GED guidelines consist of 40 specific recommendations in six general categories: (1) staffing/administration; (2) equipment/supplies; (3) education; (4) policies/procedures/protocols; (5) follow-up/transitions of care; and (6) quality-improvement measures. This template outlines how to construct an effective GED program. The following highlights recommendations for each of these categories:
Staffing/Administration. Set qualifications and responsibilities for the medical director, nurse manager, staff physicians, nurses, and specialists, as well as accessibility to specialist ancillary services, with the goal of establishing hospital site-specific staff and coordination of local resources.
Equipment/Supplies. Develop potential physical and structural enhancements that address issues of mobility, comfort, safety, and behavioral needs (including memory cues and sensorial perception) while decreasing iatrogenic complications, such as the development of pressure ulcers (eg, the use of reclining chairs and pressure-redistributing foam mattresses).
Education. Provide nurse and clinical provider education and specialty-specific training focusing on contemporary, research-based geriatric-specific material, with regular assessment for interdisciplinary core competencies.
Policies/Procedures/Protocols. Implement a directed, comprehensive approach to facilitate screening and assessment of geriatric patients for added needs/post-ED adverse outcomes, as well as validated, ED-feasible screening tools/instruments for delirium and dementia, medication management, falls, use of urinary catheters, and the provision of palliative care.
Follow-up/Transitions of Care. Design discharge processes best suited for older patients (eg, large-font instructions), as well as collaborate with community resources to provide home-health services and home safety assessment in order to facilitate care following discharge.
Quality Improvement. Implement a system to collect and monitor pertinent and prevalent geriatric emergency care indicators (eg, incidence of injurious falls and documentation of fall risk assessment) designed to increase staff education and program success.
The authors clearly state that the GED guidelines represent recommendations. They are not a mandate for every ED, nor are they a list that requires 100% compliance. Instead, the document provides the potential steps to be taken, the rationale for these recommendations, and an outline of the resources available to aid in the transition from theory to implementation in any ED. The goal is to ensure better, safer, and age-appropriate treatment. In summary, these guidelines represent an effort to improve and even transform emergency care for older adults on the brink of one of the most significant challenges facing our healthcare system both in and beyond the ED.
Moving forward, the authors of the GED guidelines have defined a plan that “includes dissemination, implementation, adaptation, and refinement.” In addition to approval by each of the organization’s board of directors and the copyright of the material in 2013, the ED guidelines have now been widely disseminated through publication in numerous news articles (including international publications) and discussions on satellite radio. Tracking of new GEDs is planned. In addition, the prioritization of the guidelines is underway using a modified Delphi method, with the express purpose of assessing the relative potential benefits and harms associated with each recommendation by providing a weighted list from most important to least important.
A “Geriatric Emergency Department Boot Camp” is being developed to bring the recommendations to hospitals interested in “geriatricizing” their EDs. Geriatric EM leaders will act as consultants, providing training and a toolbox of resources. Specific reviews and revisions of the GED guidelines will take place in a 4- to 5-year cycle. Clearly, a next important step is the development of a GED certification system based on outcome studies of the individual components.
Criticisms of the GED guidelines have already been voiced among some EM providers. Specific concerns include a fear of partitioning the ED (as has occurred with pediatrics); an increase in cost and decreased efficiency; the need to maintain general expertise among EM physicians; the lack of evidence-based data upon which the recommendations were made; the fact that some guidelines were extrapolated from other clinical settings; and the belief that these changes will be too logistically difficult and take too much time.
The fact remains that the wave of geriatric patients (the “silver tsunami”) is already beginning to hit the shores of our hospitals. And GEDs are already here to help absorb the impact. The lack of iron-clad evidence for many of the recommendations should not be an absolute obstacle, but rather part of the natural evolution and improvement of similar endeavors. Nor should GEDs contain empty beds while younger adults sit in the waiting room, or conversely, force the elderly to wait for space in the GED when there are empty beds in the main ED. Ideally, the GED should be the location where the ED staff can implement these guidelines, which they can afterwards utilize in any part of the ED. These guidelines are designed to provide the best available expert opinion on how to deliver better geriatric care in the ED. The imperative for this goal is clear and necessitates this educated “leap-of-faith.” Change is never easy and often comes with an upfront cost of time, resources, and money. Moreover, there is nothing in a well-designed GED that may not also benefit, or at least will not adversely affect care of a younger adult as well. Therefore, flexibility and optimal utilization of space in a busy ED need not be sacrificed.
Conclusion
To improve diagnostic evaluation and care of the increasing number of geriatric patients presenting to the ED, reliable tools, protocols, and guidelines must be developed and implemented to ensure diagnostic accuracy, decrease adverse events, and improve patient outcomes. Fortunately, the new GED consensus guidelines are flexible and do not need to be wholly embraced—lending themselves to modifications and institution-specific adoptions. The “protocolization” and implementation of the guidelines may improve patient flow, operational efficiency, and, most importantly, the quality of care delivered. And likely, these guidelines will provide the foundation for future education and research into the improved emergency care of older adults.
The GED guidelines can be accessed at http://www.saem.org/docs/education/geri_ed_guidelines_final.pdf?sfvrsn=2.
Dr Stern is an assistant professor of medicine and codirector, geriatric emergency medicine fellowship, department of emergency medicine, New York-Presbyterian Hospital/Weill Cornell Medical Center, New York; and an assistant attending physician, department of emergency medicine, New York-Presbyterian Hospital.
Dr Mulcare is an instructor of medicine and an assistant attending physician, department of emergency medicine, New York-Presbyterian Hospital/Weill Cornell Medical Center, New York. She is a former fellow of geriatric emergency medicine.
Case 1
An 82-year-old man presented to the ED accompanied by his son, who stated that his father “had not been acting right” for the past 2 days. The patient was combative, yelling “Go away,” and was intermittently more confused than his baseline; he was also eating and drinking less than usual. He had a history of mild dementia, noninsulin-dependent diabetes, hypertension, and arthritis; there were no recent changes in his medication. The patient lived alone in an apartment across the hall from his son and had home healthcare aide 4 hours a day, 3 days a week. He was independent of activities of daily living (ADL), but needed help with shopping and cooking.
At presentation, the patient’s vital signs were: temperature, afebrile; heart rate (HR), 94 beats/minute; blood pressure (BP), 146/92 mm hg; respiratory rate (RR), 22 breaths/minute. Oxygen (O2) saturation was 96% on room air. A finger-stick glucose test was 103 mg/dL. He was hyperalert and agitated, and did not appear oriented to place or time. There were no focal neurological deficits; mucous membranes were mildly dry; and faint crackles were heard at the right base of the lungs. The patient was placed on a monitor in a curtained room in the ED, and was given 2 L O2 via nasal cannula, which improved O2 saturation to 99%. With his son present, an intravenous (IV) line was placed and blood was drawn. An electrocardiogram (ECG) showed a sinus rhythm without ischemic findings.
During evaluation, the patient continued to pull at the monitor lines and attempted to get off the stretcher. To calm his agitation, he was given haloperidol 2.5 mg and lorazepam 1 mg; 10 minutes after administration, he became sedated and difficult to arouse. His vital signs remained stable.
Laboratory analysis revealed a white blood cell count (WBC) of 12.5 K/uL, a negative troponin, a brain natriuretic peptide (BNP) of 80 pg/mL, and normal blood urea nitrogen (BUN) and creatinine levels. Urinalysis was negative for infection, but chest X-ray showed a right lower lobe infiltrate. Blood cultures were drawn, and the patient was continued on maintenance fluids and started on IV antibiotics to cover community-acquired pneumonia. He was admitted to the hospital for pneumonia and altered mental status.
As the patient’s sedative state was followed by periods of agitation, he was treated with additional haloperidol and lorazepam by the inpatient medical team, which resulted in further sedation. On hospital day 3, his urinary output decreased. He was given an IV bolus of 3 L normal saline over 6 hours, after which his mental status began to improve, and he was switched to oral antibiotics. His mental status returned to baseline and O2 saturation was 99% on room air. He was discharged home on hospital day 5 accompanied by his son.
Case 2
A 75-year-old man was brought to the ED with a 3-day history of worsening dyspnea on exertion, increased orthopnea, and increased bilateral lower extremity edema. He had a history of congestive heart failure (CHF), with an ejection fraction of 40%, and had been on 40 mg of furosemide daily at home; there were no recent changes to his medication. The patient was independent of ADL at baseline, living with his wife in a home with stairs.
His vital signs at presentation were: temperature, afebrile; HR, 86 beats/minute; BP, 160/90 mm hg; RR 30 breaths/minute; O2 saturation was 92% on room air. The patient had increased work of breathing and was speaking in four- to five-word sentences. Pulmonary examination revealed crackles half way up bilaterally. He also had 2+ pitting edema bilaterally in his lower extremities. He was otherwise alert and oriented.
On 4 L O2 via nasal cannula, the patient’s O2 saturation was 98%. Laboratory analysis revealed a BNP of 600 pg/mL, negative troponin, and normal creatinine level. Urinalysis was negative for evidence of infection. An ECG showed no changes, and chest X-ray revealed mild pulmonary congestion without an infiltrate. In the ED, an indwelling urinary catheter (IUC) was placed to monitor urinary output before the patient was given 40 mg of IV furosemide for diuresis. The patient was then admitted for management of exacerbation of CHF. As the medical team was preparing to discharge him on hospital day 2, his wife noticed that he was confused and not acting “like himself.” An investigation for causes of delirium included evaluation for infectious disease, which revealed an elevated WBC of 14.0 K/uL, stable creatinine; and urinalysis positive for bacteria, WBCs, leukocyte esterase, and nitrites. Since chest X-ray showed resolution of the vascular congestion, the patient no longer required supplemental O2.
The IUC was removed, and the patient was started on IV antibiotics for a urinary tract infection (UTI) secondary to IUC placement. The inpatient stay was prolonged for an additional 3 days until his delirium cleared and he could be continued on oral antibiotics as an outpatient.
Discussion
There is nothing extraordinary about these two cases. Every day elderly adults present to EDs throughout the country with confusion caused by pneumonia and dehydration that is sometimes initially attributed to worsening dementia and then complicated or prolonged by overuse of powerful sedating medications. Also, complications resulting from IUCs inserted in the ED all too often prolong hospitalizations. But by using protocols designed for better, more efficient emergency care of elderly patients, their ED care can be substantially improved and any subsequent inpatient care shortened.
The older adult population (ages 65 years and older) often presents to the ED with similar complaints to their younger counterparts—eg, chest pain, abdominal pain, dyspnea. However, the history, physical examination, and social assessment of elderly patients usually lead to a more comprehensive work-up, as older adults tend to present in an atypical fashion for both illness and trauma, thus necessitating a broader differential. In addition, they are more susceptible to adverse reactions from medications and procedures.
Regardless of the ultimate diagnosis, simply presenting to an ED as a patient (and sometimes spending many hours there) places older adults at elevated risk of morbidity and mortality. The challenge is to develop reliable tools to streamline the management of this population in order to increase diagnostic accuracy, decrease adverse events, and improve patient outcomes.
Clinical Protocols
Clinical protocols are one way in which we can educate and standardize the practice of multiple levels of provider, including nurses, midlevel providers, and physicians. Adopting protocols is natural for EPs—the key is to make sure the clinical protocol to be implemented is designed or modified for the ED setting in which it will be implemented.
In our ED, we have recently implemented the following two protocols for common scenarios in older adults: (1) assessment and management of delirium; and (2) decreased use of IUCs. These protocols employ the following stepwise project plan:
- Focus groups involving nurses, midlevels, residents, and attendings to assess ED provider knowledge, attitudes, and practice patterns regarding the clinical issue in older adult patients, and to guide development of the clinical protocol by understanding needs and constraints of the current ED environment;
- An extensive literature review of the clinical topic;
- Development of the clinical protocol by the workgroup;
- Implementation of protocol after multiple educational sessions using a scripted slide presentation to ensure all providers receive the same information; and
- Subsequent data analysis from the electronic medical record to assess the impact (ie, outcome) of the protocol.
Delirium
Delirium is a common syndrome in older adults, but is often unrecognized despite its clinical importance. Although 7% to 17% of older adults who present to the ED suffer from delirium,1-6 emergency physicians (EPs) miss 64% to 83% of cases, and 12% to 38% of patients with unrecognized delirium are actually discharged from the ED.1,6-8 Unfortunately, patients discharged from the ED with undetected delirium are three times more likely to die within 3 months than those whose delirium was recognized.
Life-threatening causes are more apt to be recognized early on in the ED. With this in mind, we developed a new, comprehensive, evidence-based protocol for recognition, diagnosis, management, and disposition of agitated delirium in older adults in the ED, with a focus on identifying and treating the commonly missed contributing causes: analgesia, bladder-urine retention, constipation, dehydration, environment, and medications.9
IUC Placement in the ED
The second protocol implemented at our institution is a new, evidence-based protocol for the placement, management, and reassessment of IUCs. As emphasized by the National American College of Emergency Physicians (ACEP) 2013 Choosing Wisely Campaign,10 inserting an IUC is a procedure that should be undertaken judiciously as it is associated with an elevated risk of infection, delirium, falls, and other adverse events. As of 2008, the Centers for Medicare and Medicaid Services no longer reimburses for hospital-acquired catheter-associated UTIs.11
After conducting focus groups of our ED providers, we learned that IUCs are placed more frequently than needed—often for reasons of convenience—and are rarely reassessed or removed if the patient is admitted to the hospital. Thus, our protocol highlights appropriate, possibly appropriate, and inappropriate indications for IUC placement, with an emphasis on trying alternative modes of urine collection, communicating among healthcare providers regarding the necessity of an IUC, and reassessment of the patient for IUC removal.
Our protocols have yielded early promising results, but further research is underway to determine their specific impact. The goal is to create a protocol that is feasible and effective for the specific institution and department to which it is applied. By ensuring all members of the healthcare team are involved in the development and design of a protocol, there is ownership of its implementation and use, with the overarching goal of improving patient care.
Geriatric ED Guidelines
In the beginning of 2014, new consensus-based Geriatric Emergency Department (GED) guidelines were published in order to “provide a standardized set of guidelines that can effectively improve the care of the geriatric population and are feasible to implement in the ED.”12 These guidelines are the result of a 2-year effort by representatives from ACEP, the American Geriatrics Society, the Society of Academic Emergency Medicine, and the Emergency Nurses Association, who were committed to optimizing the emergency-care delivery model for geriatrics. The participants encompassed both academic and community providers and included clinicians and researchers. These guidelines were formulated based on an 80% consensus among the representatives and, when possible, validated using existing literature at the time.
The genesis of the GED guidelines was multifactorial. In addition to the formation and rapid growth of geriatric interest groups and sections within EM academic organizations over the last 14 years, as well as the development of geriatric core competencies for EM residents in training, the 2010 Census Data results sharply outlined the details of the rapidly growing population of older adults in the United States. This acted as an alarm highlighting the need for a structured document containing best practice recommendations from geriatric emergency healthcare providers, researchers, and advocates. “The subsequent increased need for healthcare for this burgeoning geriatric population represents an unprecedented and overwhelming challenge to the American healthcare system as a whole and to emergency departments specifically,” the authors of the GED guidelines noted.
In response to a growing national interest in geriatric ED patients and an ever-increasing competition to attract patients from this demographic by EDs across the country, there has been a surge of self-designated GEDs during the last few years. Currently, more than 70 hospitals claim to have GEDs, raising the question of what sort of geriatric patient care is actually being delivered in these EDs. The question is of increased importance because very few of these “GEDs” are in academic centers or are associated with thought leaders in EM. In fact, when 30 self-designated GEDs that were snowball sampled in 2013 by researchers who asked what specific changes they had made toward the goal of improving care for the elderly, several rescinded this self-designation.
Because of heightened concerns for the needs of the increasing geriatric population overall, and the rise in the proportion of ED visits by this demographic, the authors of the GED guidelines state that “the contemporary emergency medicine management model may not be adequate for geriatric adults,” and offer the new GED guidelines as a basis on which EDs can consider ways to improve care for older adults while addressing the unique needs of this population. The GED guidelines propose specific methods and processes by which ED care of the elderly can be optimized. The authors note that “similar programs designed for other age groups (pediatrics) or directed towards specific diseases (STEMI, stroke, and trauma) have improved the care both in individual EDs and system-wide, resulting in better, more cost-effective care and ultimately better patient outcomes.”
The GED guidelines consist of 40 specific recommendations in six general categories: (1) staffing/administration; (2) equipment/supplies; (3) education; (4) policies/procedures/protocols; (5) follow-up/transitions of care; and (6) quality-improvement measures. This template outlines how to construct an effective GED program. The following highlights recommendations for each of these categories:
Staffing/Administration. Set qualifications and responsibilities for the medical director, nurse manager, staff physicians, nurses, and specialists, as well as accessibility to specialist ancillary services, with the goal of establishing hospital site-specific staff and coordination of local resources.
Equipment/Supplies. Develop potential physical and structural enhancements that address issues of mobility, comfort, safety, and behavioral needs (including memory cues and sensorial perception) while decreasing iatrogenic complications, such as the development of pressure ulcers (eg, the use of reclining chairs and pressure-redistributing foam mattresses).
Education. Provide nurse and clinical provider education and specialty-specific training focusing on contemporary, research-based geriatric-specific material, with regular assessment for interdisciplinary core competencies.
Policies/Procedures/Protocols. Implement a directed, comprehensive approach to facilitate screening and assessment of geriatric patients for added needs/post-ED adverse outcomes, as well as validated, ED-feasible screening tools/instruments for delirium and dementia, medication management, falls, use of urinary catheters, and the provision of palliative care.
Follow-up/Transitions of Care. Design discharge processes best suited for older patients (eg, large-font instructions), as well as collaborate with community resources to provide home-health services and home safety assessment in order to facilitate care following discharge.
Quality Improvement. Implement a system to collect and monitor pertinent and prevalent geriatric emergency care indicators (eg, incidence of injurious falls and documentation of fall risk assessment) designed to increase staff education and program success.
The authors clearly state that the GED guidelines represent recommendations. They are not a mandate for every ED, nor are they a list that requires 100% compliance. Instead, the document provides the potential steps to be taken, the rationale for these recommendations, and an outline of the resources available to aid in the transition from theory to implementation in any ED. The goal is to ensure better, safer, and age-appropriate treatment. In summary, these guidelines represent an effort to improve and even transform emergency care for older adults on the brink of one of the most significant challenges facing our healthcare system both in and beyond the ED.
Moving forward, the authors of the GED guidelines have defined a plan that “includes dissemination, implementation, adaptation, and refinement.” In addition to approval by each of the organization’s board of directors and the copyright of the material in 2013, the ED guidelines have now been widely disseminated through publication in numerous news articles (including international publications) and discussions on satellite radio. Tracking of new GEDs is planned. In addition, the prioritization of the guidelines is underway using a modified Delphi method, with the express purpose of assessing the relative potential benefits and harms associated with each recommendation by providing a weighted list from most important to least important.
A “Geriatric Emergency Department Boot Camp” is being developed to bring the recommendations to hospitals interested in “geriatricizing” their EDs. Geriatric EM leaders will act as consultants, providing training and a toolbox of resources. Specific reviews and revisions of the GED guidelines will take place in a 4- to 5-year cycle. Clearly, a next important step is the development of a GED certification system based on outcome studies of the individual components.
Criticisms of the GED guidelines have already been voiced among some EM providers. Specific concerns include a fear of partitioning the ED (as has occurred with pediatrics); an increase in cost and decreased efficiency; the need to maintain general expertise among EM physicians; the lack of evidence-based data upon which the recommendations were made; the fact that some guidelines were extrapolated from other clinical settings; and the belief that these changes will be too logistically difficult and take too much time.
The fact remains that the wave of geriatric patients (the “silver tsunami”) is already beginning to hit the shores of our hospitals. And GEDs are already here to help absorb the impact. The lack of iron-clad evidence for many of the recommendations should not be an absolute obstacle, but rather part of the natural evolution and improvement of similar endeavors. Nor should GEDs contain empty beds while younger adults sit in the waiting room, or conversely, force the elderly to wait for space in the GED when there are empty beds in the main ED. Ideally, the GED should be the location where the ED staff can implement these guidelines, which they can afterwards utilize in any part of the ED. These guidelines are designed to provide the best available expert opinion on how to deliver better geriatric care in the ED. The imperative for this goal is clear and necessitates this educated “leap-of-faith.” Change is never easy and often comes with an upfront cost of time, resources, and money. Moreover, there is nothing in a well-designed GED that may not also benefit, or at least will not adversely affect care of a younger adult as well. Therefore, flexibility and optimal utilization of space in a busy ED need not be sacrificed.
Conclusion
To improve diagnostic evaluation and care of the increasing number of geriatric patients presenting to the ED, reliable tools, protocols, and guidelines must be developed and implemented to ensure diagnostic accuracy, decrease adverse events, and improve patient outcomes. Fortunately, the new GED consensus guidelines are flexible and do not need to be wholly embraced—lending themselves to modifications and institution-specific adoptions. The “protocolization” and implementation of the guidelines may improve patient flow, operational efficiency, and, most importantly, the quality of care delivered. And likely, these guidelines will provide the foundation for future education and research into the improved emergency care of older adults.
The GED guidelines can be accessed at http://www.saem.org/docs/education/geri_ed_guidelines_final.pdf?sfvrsn=2.
Dr Stern is an assistant professor of medicine and codirector, geriatric emergency medicine fellowship, department of emergency medicine, New York-Presbyterian Hospital/Weill Cornell Medical Center, New York; and an assistant attending physician, department of emergency medicine, New York-Presbyterian Hospital.
Dr Mulcare is an instructor of medicine and an assistant attending physician, department of emergency medicine, New York-Presbyterian Hospital/Weill Cornell Medical Center, New York. She is a former fellow of geriatric emergency medicine.
- Lewis LM, Miller DK, Morley JE, Nork MJ, Lasater LC. Unrecognized delirium in ED geriatric patients. Am J Emerg Med. 1995;13(2):142-145.
- Naughton BJ, Moran M, Ghaly Y, Michalakes C. Computed tomography scanning and delirium in elder patients. Acad Emerg Med. 1997;4(12):1107-1110.
- Naughton BJ, Moran MB, Kadah H, Heman-Ackah Y, Longano J. Delirium and other cognitive impairment in older adults in an emergency department. Ann Emerg Med. 1995;25(6):751-755.
- Hustey FM, Meldon SW. The prevalence and documentation of impaired mental status in elderly emergency department patients. Ann Emerg Med. 2002;39(3):248-253.
- Hustey FM, Meldon SW, Smith MD, Lex CK. The effect of mental status screening on the care of elderly emergency department patients. Ann Emerg Med. 2003;41(5):678-684.
- Elie M, Rousseau F, Cole M, Primeau F, McCusker J, Bellavance F. Prevalence and detection of delirium in elderly emergency department patients. CMAJ. 2000;163(8):977-981.
- Han JH, Zimmerman EE, Cutler N, et al. Delirium in older emergency department patients: recognition, risk factors, and psychomotor subtypes. Acad Emerg Med. 2009;16(3):193-200.
- Sanders AB. Missed delirium in older emergency department patients: a quality-of-care problem. Ann Emerg Med. 2002;39(3):338-341.
- Rosen T, Connors S, Halpern A, et al. Improving emergency department identification and management of agitated delirium in older adults: implementation and impact assessment of a comprehensive clinical protocol emphasizing commonly missed contributing causes using an A-B-C-D-E-F mnemonic. Sys Qual Rev J. 2013;11(special issue):203,204. http://www.nypsystem.org/pdf/System-Quality-Review-2013.pdf. Accessed June 4, 2014.
- Choosing Wisely: ACEP Lists 5 Tests to Question. Medscape Web site. http://www.medscape.com/viewarticle/812600. Accessed June 4, 2014.
- Wald HL, Kramer AM. Nonpayment for harms resulting from medical care: catheter-associated urinary tract infections. JAMA. 2007;298(23):2782-2784.
- American College of Emergency Physicians; American Geriatrics Society; Emergency Nurses Association; Society for Academic Emergency Medicine. Geriatric Emergency Department Guidelines. http://www.saem.org/docs/education/geri_ed_guidelines_final.pdf?sfvrsn=2. Accessed June 4, 2014.
- Lewis LM, Miller DK, Morley JE, Nork MJ, Lasater LC. Unrecognized delirium in ED geriatric patients. Am J Emerg Med. 1995;13(2):142-145.
- Naughton BJ, Moran M, Ghaly Y, Michalakes C. Computed tomography scanning and delirium in elder patients. Acad Emerg Med. 1997;4(12):1107-1110.
- Naughton BJ, Moran MB, Kadah H, Heman-Ackah Y, Longano J. Delirium and other cognitive impairment in older adults in an emergency department. Ann Emerg Med. 1995;25(6):751-755.
- Hustey FM, Meldon SW. The prevalence and documentation of impaired mental status in elderly emergency department patients. Ann Emerg Med. 2002;39(3):248-253.
- Hustey FM, Meldon SW, Smith MD, Lex CK. The effect of mental status screening on the care of elderly emergency department patients. Ann Emerg Med. 2003;41(5):678-684.
- Elie M, Rousseau F, Cole M, Primeau F, McCusker J, Bellavance F. Prevalence and detection of delirium in elderly emergency department patients. CMAJ. 2000;163(8):977-981.
- Han JH, Zimmerman EE, Cutler N, et al. Delirium in older emergency department patients: recognition, risk factors, and psychomotor subtypes. Acad Emerg Med. 2009;16(3):193-200.
- Sanders AB. Missed delirium in older emergency department patients: a quality-of-care problem. Ann Emerg Med. 2002;39(3):338-341.
- Rosen T, Connors S, Halpern A, et al. Improving emergency department identification and management of agitated delirium in older adults: implementation and impact assessment of a comprehensive clinical protocol emphasizing commonly missed contributing causes using an A-B-C-D-E-F mnemonic. Sys Qual Rev J. 2013;11(special issue):203,204. http://www.nypsystem.org/pdf/System-Quality-Review-2013.pdf. Accessed June 4, 2014.
- Choosing Wisely: ACEP Lists 5 Tests to Question. Medscape Web site. http://www.medscape.com/viewarticle/812600. Accessed June 4, 2014.
- Wald HL, Kramer AM. Nonpayment for harms resulting from medical care: catheter-associated urinary tract infections. JAMA. 2007;298(23):2782-2784.
- American College of Emergency Physicians; American Geriatrics Society; Emergency Nurses Association; Society for Academic Emergency Medicine. Geriatric Emergency Department Guidelines. http://www.saem.org/docs/education/geri_ed_guidelines_final.pdf?sfvrsn=2. Accessed June 4, 2014.
