User login
Low, high dose vancomycin equally effective in C. difficile
DENVER – Oral vancomycin at a dose of 125 mg four times daily is just as effective as is a dose of 250 mg or higher given at the same frequency in the treatment of diarrhea associated with Clostridium difficile infection, judging from the results from a retrospective study.
Use of the lower dosing regimen has the potential to decrease treatment costs without worsening outcomes, Philip Chung, Pharm.D., said in an interview before the annual Interscience Conference on Antimicrobial Agents and Chemotherapy, where the study was presented.
According to current recommendations, oral vancomycin 125 mg q.i.d. is the treatment of choice for severe uncomplicated C. difficile infection. To date, no studies have shown the use of oral vancomycin doses higher than 125 mg q.i.d. to be more efficacious than the recommended 125 mg q.i.d. in this setting, said Dr. Chung, clinical pharmacy manager of infectious diseases at Montefiore Medical Center, New York.

"Prior to 2008, prescribers at our institution frequently requested vancomycin doses higher than the recommended 125 mg q.i.d. for treatment of [C. difficile infection] despite the absence of data showing added benefits with the higher dosing regimens," he said. "This practice not only increases medication and/or preparation costs, but it may also increase the potential for untoward effects in patients being treated with the higher doses (e.g., increased risks for vancomycin-resistant enterococci colonization or higher likelihood to further alter the GI flora)."
Since the inception of the Antimicrobial Stewardship Program at Montefiore Medical Center in 2008, Dr. Chung and his associates observed a shift in oral vancomycin prescribing practices from a higher dosing regimen to a lower dosing regimen. "Because of this change in practice, we wished to evaluate the efficacy of the different oral vancomycin dosing regimen in order to ensure treatment outcomes remained unchanged at our institution," he said. To do so, the researchers retrospectively reviewed clinical outcomes of 300 adult patients treated with oral vancomycin at the medical center between 2006 and 2010. They looked at clinical parameters, concomitant antibiotics, in-hospital mortality, and 30-day readmission.
The primary endpoint was clinical improvement at 72 hours of oral vancomycin. Secondary endpoints included clinical improvement at end of therapy or discharge, length of stay, in-hospital mortality, and 30-day readmission rate.
Of the 300 patients, 197 were prescribed oral vancomycin 125 mg q.i.d. (low-dose group) and 103 patients were prescribed 250 mg or higher q.i.d. (high-dose group). Dr. Chung and his associates reported that clinical improvement assessed 72 hours after starting oral vancomycin therapy was observed in 85% and 86% of patients in the low- and high-dose groups, respectively (P less than 0.05). Rates of clinical improvement at end of therapy or time of hospital discharge between the two groups were also found to be similar (93% vs. 96%), as were total length of hospital stay (20 days vs. 19 days), in-hospital mortality (15% vs. 23%), and rates of 30-day readmission (34% vs. 24%).
"The finding that oral vancomycin 125 mg q.i.d. works as well as higher doses for severe uncomplicated C. difficile infection for the most part is not a surprise to us, as some evidence already exists in the literature," said Dr. Chung, also of Albert Einstein College of Medicine in New York. "Our finding only confirmed what is already known."
Limitations include the fact that this is a single-center study, and that it is subject to selection bias because of its retrospective design, Dr. Chung said. "However, we took steps to ensure that all patients treated with oral vancomycin who had laboratory-confirmed [C. difficile infection] and symptoms consistent with [C. difficile infection] were included in the study," he said.
Dr. Chung said that he had no relevant financial conflicts to disclose.
DENVER – Oral vancomycin at a dose of 125 mg four times daily is just as effective as is a dose of 250 mg or higher given at the same frequency in the treatment of diarrhea associated with Clostridium difficile infection, judging from the results from a retrospective study.
Use of the lower dosing regimen has the potential to decrease treatment costs without worsening outcomes, Philip Chung, Pharm.D., said in an interview before the annual Interscience Conference on Antimicrobial Agents and Chemotherapy, where the study was presented.
According to current recommendations, oral vancomycin 125 mg q.i.d. is the treatment of choice for severe uncomplicated C. difficile infection. To date, no studies have shown the use of oral vancomycin doses higher than 125 mg q.i.d. to be more efficacious than the recommended 125 mg q.i.d. in this setting, said Dr. Chung, clinical pharmacy manager of infectious diseases at Montefiore Medical Center, New York.
"Prior to 2008, prescribers at our institution frequently requested vancomycin doses higher than the recommended 125 mg q.i.d. for treatment of [C. difficile infection] despite the absence of data showing added benefits with the higher dosing regimens," he said. "This practice not only increases medication and/or preparation costs, but it may also increase the potential for untoward effects in patients being treated with the higher doses (e.g., increased risks for vancomycin-resistant enterococci colonization or higher likelihood to further alter the GI flora)."
Since the inception of the Antimicrobial Stewardship Program at Montefiore Medical Center in 2008, Dr. Chung and his associates observed a shift in oral vancomycin prescribing practices from a higher dosing regimen to a lower dosing regimen. "Because of this change in practice, we wished to evaluate the efficacy of the different oral vancomycin dosing regimen in order to ensure treatment outcomes remained unchanged at our institution," he said. To do so, the researchers retrospectively reviewed clinical outcomes of 300 adult patients treated with oral vancomycin at the medical center between 2006 and 2010. They looked at clinical parameters, concomitant antibiotics, in-hospital mortality, and 30-day readmission.
The primary endpoint was clinical improvement at 72 hours of oral vancomycin. Secondary endpoints included clinical improvement at end of therapy or discharge, length of stay, in-hospital mortality, and 30-day readmission rate.
Of the 300 patients, 197 were prescribed oral vancomycin 125 mg q.i.d. (low-dose group) and 103 patients were prescribed 250 mg or higher q.i.d. (high-dose group). Dr. Chung and his associates reported that clinical improvement assessed 72 hours after starting oral vancomycin therapy was observed in 85% and 86% of patients in the low- and high-dose groups, respectively (P less than 0.05). Rates of clinical improvement at end of therapy or time of hospital discharge between the two groups were also found to be similar (93% vs. 96%), as were total length of hospital stay (20 days vs. 19 days), in-hospital mortality (15% vs. 23%), and rates of 30-day readmission (34% vs. 24%).
"The finding that oral vancomycin 125 mg q.i.d. works as well as higher doses for severe uncomplicated C. difficile infection for the most part is not a surprise to us, as some evidence already exists in the literature," said Dr. Chung, also of Albert Einstein College of Medicine in New York. "Our finding only confirmed what is already known."
Limitations include the fact that this is a single-center study, and that it is subject to selection bias because of its retrospective design, Dr. Chung said. "However, we took steps to ensure that all patients treated with oral vancomycin who had laboratory-confirmed [C. difficile infection] and symptoms consistent with [C. difficile infection] were included in the study," he said.
Dr. Chung said that he had no relevant financial conflicts to disclose.
DENVER – Oral vancomycin at a dose of 125 mg four times daily is just as effective as is a dose of 250 mg or higher given at the same frequency in the treatment of diarrhea associated with Clostridium difficile infection, judging from the results from a retrospective study.
Use of the lower dosing regimen has the potential to decrease treatment costs without worsening outcomes, Philip Chung, Pharm.D., said in an interview before the annual Interscience Conference on Antimicrobial Agents and Chemotherapy, where the study was presented.
According to current recommendations, oral vancomycin 125 mg q.i.d. is the treatment of choice for severe uncomplicated C. difficile infection. To date, no studies have shown the use of oral vancomycin doses higher than 125 mg q.i.d. to be more efficacious than the recommended 125 mg q.i.d. in this setting, said Dr. Chung, clinical pharmacy manager of infectious diseases at Montefiore Medical Center, New York.
"Prior to 2008, prescribers at our institution frequently requested vancomycin doses higher than the recommended 125 mg q.i.d. for treatment of [C. difficile infection] despite the absence of data showing added benefits with the higher dosing regimens," he said. "This practice not only increases medication and/or preparation costs, but it may also increase the potential for untoward effects in patients being treated with the higher doses (e.g., increased risks for vancomycin-resistant enterococci colonization or higher likelihood to further alter the GI flora)."
Since the inception of the Antimicrobial Stewardship Program at Montefiore Medical Center in 2008, Dr. Chung and his associates observed a shift in oral vancomycin prescribing practices from a higher dosing regimen to a lower dosing regimen. "Because of this change in practice, we wished to evaluate the efficacy of the different oral vancomycin dosing regimen in order to ensure treatment outcomes remained unchanged at our institution," he said. To do so, the researchers retrospectively reviewed clinical outcomes of 300 adult patients treated with oral vancomycin at the medical center between 2006 and 2010. They looked at clinical parameters, concomitant antibiotics, in-hospital mortality, and 30-day readmission.
The primary endpoint was clinical improvement at 72 hours of oral vancomycin. Secondary endpoints included clinical improvement at end of therapy or discharge, length of stay, in-hospital mortality, and 30-day readmission rate.
Of the 300 patients, 197 were prescribed oral vancomycin 125 mg q.i.d. (low-dose group) and 103 patients were prescribed 250 mg or higher q.i.d. (high-dose group). Dr. Chung and his associates reported that clinical improvement assessed 72 hours after starting oral vancomycin therapy was observed in 85% and 86% of patients in the low- and high-dose groups, respectively (P less than 0.05). Rates of clinical improvement at end of therapy or time of hospital discharge between the two groups were also found to be similar (93% vs. 96%), as were total length of hospital stay (20 days vs. 19 days), in-hospital mortality (15% vs. 23%), and rates of 30-day readmission (34% vs. 24%).
"The finding that oral vancomycin 125 mg q.i.d. works as well as higher doses for severe uncomplicated C. difficile infection for the most part is not a surprise to us, as some evidence already exists in the literature," said Dr. Chung, also of Albert Einstein College of Medicine in New York. "Our finding only confirmed what is already known."
Limitations include the fact that this is a single-center study, and that it is subject to selection bias because of its retrospective design, Dr. Chung said. "However, we took steps to ensure that all patients treated with oral vancomycin who had laboratory-confirmed [C. difficile infection] and symptoms consistent with [C. difficile infection] were included in the study," he said.
Dr. Chung said that he had no relevant financial conflicts to disclose.
AT ICAAC 2013

AHA statement spotlights severe pediatric obesity
Earn 0.25 hours AMA PRA Category 1 credit: Read this article, and click the link at the end to take the post-test.
An estimated 4%-6% of children and adolescents in the United States are severely obese, and the prevalence appears to be on the uptick.
At the same time, existing treatments for the condition are limited in effectiveness and lack widespread availability, a nine-member writing group of experts led by Aaron S. Kelly, Ph.D., reported in a scientific statement from the American Heart Association.
"Severe obesity in young people has grave health consequences," said Dr. Kelly in a press statement. "It’s a much more serious childhood disease than obesity."
The condition "demands attention and clinical management, because if left unchecked, it will have a profound effect on those it afflicts and will place a significant economic and clinical services burden on the future health care system," the writing group cautionedonline Sept. 9 in Circulation. It emphasized that stakeholders at all levels "will need to work together to engage the growing problem of severe pediatric obesity."
The 17-page statement includes a recommendation to define children over age 2 as severely obese if they have either a body mass index that’s at least 20%higher than the 95th percentile for their sex and age, or a BMI score of 35 kg/mm2 or higher (Circulation 2013 Sept. 9 [doi:10.1161/CIR.0b013e3182a5cfb3]). According to estimates from the National Health and Nutrition Examination Survey dating back to 1999, 4%-6% of children and adolescents in the United States currently fall into this category. Those same data suggest that severe obesity is the fastest-growing subcategory of obesity in youth.
Dr. Kelly of the division of epidemiology and clinical research in the department of pediatrics at the University of Minnesota, Minneapolis, and his associates discussed numerous associated health risks from being severely obese as a child, in particular the mounting evidence from clinical and population-based studies regarding its link to the development of cardiovascular disease (CVD). "Importantly, obesity and CVD risk factors associated with obesity have been linked to early atherosclerosis in pathological studies of the coronary arteries and aorta in adolescents and young adults," the writing group stated.
Other associated health risks that threaten this subset of patients include hyperinsulinemia, insulin resistance, and prediabetes; obstructive sleep apnea syndrome; nonalcoholic fatty liver disease; musculoskeletal problems; depression and other psychosocial problems; and disordered eating.
Although data regarding the long-term risks of severe pediatric obesity are sparse, the authors noted, "it is well established that obese youth (probably because of the strong tracking of adiposity into adulthood) are more likely to have adverse levels of cardiovascular and metabolic risk factors later in life. Higher BMI is associated with tracking in the higher levels of both blood pressure and lipids in longitudinal pediatric cohort studies. Adolescents with a higher degree of obesity are also much more likely to demonstrate CVD risk factor clustering over time. Rate and degree of obesity development are also important."
The writing group characterized current treatment options for severe pediatric obesity as limited, as most standard approaches to weight loss are insufficient for this group. As for medications, orlistat is the only agent approved for weight loss in adolescents. The largest study of its use in adolescents reported a 2.4% reduction in BMI over the course of 12 months (JAMA 2005;293:2873-83). Other agents that have been studied for pediatric obesity include metformin and exenatide. To date, the "results have demonstrated that treatment elicits only modest reductions in BMI/weight and has relatively little impact on the cardiometabolic risk factor profile in obese youth," the experts wrote. Two weight loss medications recently approved by the Food and Drug Administration to treat obesity in adults, lorcaserin and the combination of phentermine and topiramate, have never been studied in children.
Dr. Kelly and his associates went on to note that bariatric surgery "has generally been effective in reducing body mass index and improving cardiovascular and metabolic risk factors; however, reports of long-term outcomes are few, many youth with severe obesity do not qualify for surgery, and access is limited by lack of insurance coverage."
The scientific statement, which is endorsed by the Obesity Society, includes "a call to action" for innovative ways to "fill the gap between lifestyle/medication and surgery." Proposals include conducting more research on bariatric surgery’s effects and safety; evaluating the effectiveness of lifestyle modification interventions, including adherence to dietary and physical activity plans; funding research to find other useful interventions, including better drugs and medical devices; and recognizing severe obesity as a chronic disease requiring ongoing care and management.
"The task ahead will be arduous and complicated, but the high prevalence and serious consequences of severe obesity require us to commit time, intellectual capital, and financial resources to address it," the writing group concluded.
Dr. Kelly disclosed that he has received research grants from Amylin Pharmaceuticals, the National Institutes of Health/National Institute of Neurological Disorders and Stroke, and the Thrasher Research Fund. He is also a consultant to Novo Nordisk. One other writing group member, Dr. Thomas H. Inge, disclosed that he has received a research grant from Ethicon Endosurgery.
To earn 0.25 hours AMA PRA Category 1 credit after reading this article, take the post-test here.
This is a wonderful and yet frightening manuscript that summarizes why we must be so concerned about childhood obesity and overweight. Additionally worrisome is the high prevalence of severe obesity in very young children. More research is definitely warranted and needed, particularly regarding effective interventions, but with so many children already affected and suffering, we can't wait to act. However, currently the majority of pediatricians across the United States are unable to see a child for "only" having childhood obesity or overweight because these visits are rejected for payment by the majority of Medicaid and private insurance carriers in most states. There are some states and insurance carriers that reimburse an obesity or weight management visit, but for most pediatricians and other health professionals, we have to wait until the child develops a complication of their weight before we can see them to address their excess weight. This is very frustrating.

|
| Dr. Stephen Pont |
In November 2011, Medicare approved intensive outpatient treatment for adults with obesity; however, the majority of insurance providers for children, both Medicaid and private payers, still do not recognize childhood obesity as a reimbursable reason for a child to visit their pediatrician - or other health care professional - to address their weight. If you are interested in working in this area of advocacy, the American Academy of Pediatrics section on obesity would love to work with you. Beyond the walls of our clinics, pediatricians and other health professionals must also work in our communities. We must advocate and lead healthy community change so that healthy choices are easier to make where our patients live. Then as we help empower our patients in our clinics, they can return to communities where the healthier choice is much easier to make.
Stephen Pont, M.D., M.P.H., is a pediatrician at Dell Children's Medical Center in Austin, Tex., and chair of the American Academy of Pediatrics section on obesity. (On Twitter @DrStephenPont). He said he had no relevant financial disclosures.
This is a wonderful and yet frightening manuscript that summarizes why we must be so concerned about childhood obesity and overweight. Additionally worrisome is the high prevalence of severe obesity in very young children. More research is definitely warranted and needed, particularly regarding effective interventions, but with so many children already affected and suffering, we can't wait to act. However, currently the majority of pediatricians across the United States are unable to see a child for "only" having childhood obesity or overweight because these visits are rejected for payment by the majority of Medicaid and private insurance carriers in most states. There are some states and insurance carriers that reimburse an obesity or weight management visit, but for most pediatricians and other health professionals, we have to wait until the child develops a complication of their weight before we can see them to address their excess weight. This is very frustrating.
|
|
| Dr. Stephen Pont |
In November 2011, Medicare approved intensive outpatient treatment for adults with obesity; however, the majority of insurance providers for children, both Medicaid and private payers, still do not recognize childhood obesity as a reimbursable reason for a child to visit their pediatrician - or other health care professional - to address their weight. If you are interested in working in this area of advocacy, the American Academy of Pediatrics section on obesity would love to work with you. Beyond the walls of our clinics, pediatricians and other health professionals must also work in our communities. We must advocate and lead healthy community change so that healthy choices are easier to make where our patients live. Then as we help empower our patients in our clinics, they can return to communities where the healthier choice is much easier to make.
Stephen Pont, M.D., M.P.H., is a pediatrician at Dell Children's Medical Center in Austin, Tex., and chair of the American Academy of Pediatrics section on obesity. (On Twitter @DrStephenPont). He said he had no relevant financial disclosures.
This is a wonderful and yet frightening manuscript that summarizes why we must be so concerned about childhood obesity and overweight. Additionally worrisome is the high prevalence of severe obesity in very young children. More research is definitely warranted and needed, particularly regarding effective interventions, but with so many children already affected and suffering, we can't wait to act. However, currently the majority of pediatricians across the United States are unable to see a child for "only" having childhood obesity or overweight because these visits are rejected for payment by the majority of Medicaid and private insurance carriers in most states. There are some states and insurance carriers that reimburse an obesity or weight management visit, but for most pediatricians and other health professionals, we have to wait until the child develops a complication of their weight before we can see them to address their excess weight. This is very frustrating.
|
|
| Dr. Stephen Pont |
In November 2011, Medicare approved intensive outpatient treatment for adults with obesity; however, the majority of insurance providers for children, both Medicaid and private payers, still do not recognize childhood obesity as a reimbursable reason for a child to visit their pediatrician - or other health care professional - to address their weight. If you are interested in working in this area of advocacy, the American Academy of Pediatrics section on obesity would love to work with you. Beyond the walls of our clinics, pediatricians and other health professionals must also work in our communities. We must advocate and lead healthy community change so that healthy choices are easier to make where our patients live. Then as we help empower our patients in our clinics, they can return to communities where the healthier choice is much easier to make.
Stephen Pont, M.D., M.P.H., is a pediatrician at Dell Children's Medical Center in Austin, Tex., and chair of the American Academy of Pediatrics section on obesity. (On Twitter @DrStephenPont). He said he had no relevant financial disclosures.
Earn 0.25 hours AMA PRA Category 1 credit: Read this article, and click the link at the end to take the post-test.
An estimated 4%-6% of children and adolescents in the United States are severely obese, and the prevalence appears to be on the uptick.
At the same time, existing treatments for the condition are limited in effectiveness and lack widespread availability, a nine-member writing group of experts led by Aaron S. Kelly, Ph.D., reported in a scientific statement from the American Heart Association.
"Severe obesity in young people has grave health consequences," said Dr. Kelly in a press statement. "It’s a much more serious childhood disease than obesity."
The condition "demands attention and clinical management, because if left unchecked, it will have a profound effect on those it afflicts and will place a significant economic and clinical services burden on the future health care system," the writing group cautionedonline Sept. 9 in Circulation. It emphasized that stakeholders at all levels "will need to work together to engage the growing problem of severe pediatric obesity."
The 17-page statement includes a recommendation to define children over age 2 as severely obese if they have either a body mass index that’s at least 20%higher than the 95th percentile for their sex and age, or a BMI score of 35 kg/mm2 or higher (Circulation 2013 Sept. 9 [doi:10.1161/CIR.0b013e3182a5cfb3]). According to estimates from the National Health and Nutrition Examination Survey dating back to 1999, 4%-6% of children and adolescents in the United States currently fall into this category. Those same data suggest that severe obesity is the fastest-growing subcategory of obesity in youth.
Dr. Kelly of the division of epidemiology and clinical research in the department of pediatrics at the University of Minnesota, Minneapolis, and his associates discussed numerous associated health risks from being severely obese as a child, in particular the mounting evidence from clinical and population-based studies regarding its link to the development of cardiovascular disease (CVD). "Importantly, obesity and CVD risk factors associated with obesity have been linked to early atherosclerosis in pathological studies of the coronary arteries and aorta in adolescents and young adults," the writing group stated.
Other associated health risks that threaten this subset of patients include hyperinsulinemia, insulin resistance, and prediabetes; obstructive sleep apnea syndrome; nonalcoholic fatty liver disease; musculoskeletal problems; depression and other psychosocial problems; and disordered eating.
Although data regarding the long-term risks of severe pediatric obesity are sparse, the authors noted, "it is well established that obese youth (probably because of the strong tracking of adiposity into adulthood) are more likely to have adverse levels of cardiovascular and metabolic risk factors later in life. Higher BMI is associated with tracking in the higher levels of both blood pressure and lipids in longitudinal pediatric cohort studies. Adolescents with a higher degree of obesity are also much more likely to demonstrate CVD risk factor clustering over time. Rate and degree of obesity development are also important."
The writing group characterized current treatment options for severe pediatric obesity as limited, as most standard approaches to weight loss are insufficient for this group. As for medications, orlistat is the only agent approved for weight loss in adolescents. The largest study of its use in adolescents reported a 2.4% reduction in BMI over the course of 12 months (JAMA 2005;293:2873-83). Other agents that have been studied for pediatric obesity include metformin and exenatide. To date, the "results have demonstrated that treatment elicits only modest reductions in BMI/weight and has relatively little impact on the cardiometabolic risk factor profile in obese youth," the experts wrote. Two weight loss medications recently approved by the Food and Drug Administration to treat obesity in adults, lorcaserin and the combination of phentermine and topiramate, have never been studied in children.
Dr. Kelly and his associates went on to note that bariatric surgery "has generally been effective in reducing body mass index and improving cardiovascular and metabolic risk factors; however, reports of long-term outcomes are few, many youth with severe obesity do not qualify for surgery, and access is limited by lack of insurance coverage."
The scientific statement, which is endorsed by the Obesity Society, includes "a call to action" for innovative ways to "fill the gap between lifestyle/medication and surgery." Proposals include conducting more research on bariatric surgery’s effects and safety; evaluating the effectiveness of lifestyle modification interventions, including adherence to dietary and physical activity plans; funding research to find other useful interventions, including better drugs and medical devices; and recognizing severe obesity as a chronic disease requiring ongoing care and management.
"The task ahead will be arduous and complicated, but the high prevalence and serious consequences of severe obesity require us to commit time, intellectual capital, and financial resources to address it," the writing group concluded.
Dr. Kelly disclosed that he has received research grants from Amylin Pharmaceuticals, the National Institutes of Health/National Institute of Neurological Disorders and Stroke, and the Thrasher Research Fund. He is also a consultant to Novo Nordisk. One other writing group member, Dr. Thomas H. Inge, disclosed that he has received a research grant from Ethicon Endosurgery.
To earn 0.25 hours AMA PRA Category 1 credit after reading this article, take the post-test here.
Earn 0.25 hours AMA PRA Category 1 credit: Read this article, and click the link at the end to take the post-test.
An estimated 4%-6% of children and adolescents in the United States are severely obese, and the prevalence appears to be on the uptick.
At the same time, existing treatments for the condition are limited in effectiveness and lack widespread availability, a nine-member writing group of experts led by Aaron S. Kelly, Ph.D., reported in a scientific statement from the American Heart Association.
"Severe obesity in young people has grave health consequences," said Dr. Kelly in a press statement. "It’s a much more serious childhood disease than obesity."
The condition "demands attention and clinical management, because if left unchecked, it will have a profound effect on those it afflicts and will place a significant economic and clinical services burden on the future health care system," the writing group cautionedonline Sept. 9 in Circulation. It emphasized that stakeholders at all levels "will need to work together to engage the growing problem of severe pediatric obesity."
The 17-page statement includes a recommendation to define children over age 2 as severely obese if they have either a body mass index that’s at least 20%higher than the 95th percentile for their sex and age, or a BMI score of 35 kg/mm2 or higher (Circulation 2013 Sept. 9 [doi:10.1161/CIR.0b013e3182a5cfb3]). According to estimates from the National Health and Nutrition Examination Survey dating back to 1999, 4%-6% of children and adolescents in the United States currently fall into this category. Those same data suggest that severe obesity is the fastest-growing subcategory of obesity in youth.
Dr. Kelly of the division of epidemiology and clinical research in the department of pediatrics at the University of Minnesota, Minneapolis, and his associates discussed numerous associated health risks from being severely obese as a child, in particular the mounting evidence from clinical and population-based studies regarding its link to the development of cardiovascular disease (CVD). "Importantly, obesity and CVD risk factors associated with obesity have been linked to early atherosclerosis in pathological studies of the coronary arteries and aorta in adolescents and young adults," the writing group stated.
Other associated health risks that threaten this subset of patients include hyperinsulinemia, insulin resistance, and prediabetes; obstructive sleep apnea syndrome; nonalcoholic fatty liver disease; musculoskeletal problems; depression and other psychosocial problems; and disordered eating.
Although data regarding the long-term risks of severe pediatric obesity are sparse, the authors noted, "it is well established that obese youth (probably because of the strong tracking of adiposity into adulthood) are more likely to have adverse levels of cardiovascular and metabolic risk factors later in life. Higher BMI is associated with tracking in the higher levels of both blood pressure and lipids in longitudinal pediatric cohort studies. Adolescents with a higher degree of obesity are also much more likely to demonstrate CVD risk factor clustering over time. Rate and degree of obesity development are also important."
The writing group characterized current treatment options for severe pediatric obesity as limited, as most standard approaches to weight loss are insufficient for this group. As for medications, orlistat is the only agent approved for weight loss in adolescents. The largest study of its use in adolescents reported a 2.4% reduction in BMI over the course of 12 months (JAMA 2005;293:2873-83). Other agents that have been studied for pediatric obesity include metformin and exenatide. To date, the "results have demonstrated that treatment elicits only modest reductions in BMI/weight and has relatively little impact on the cardiometabolic risk factor profile in obese youth," the experts wrote. Two weight loss medications recently approved by the Food and Drug Administration to treat obesity in adults, lorcaserin and the combination of phentermine and topiramate, have never been studied in children.
Dr. Kelly and his associates went on to note that bariatric surgery "has generally been effective in reducing body mass index and improving cardiovascular and metabolic risk factors; however, reports of long-term outcomes are few, many youth with severe obesity do not qualify for surgery, and access is limited by lack of insurance coverage."
The scientific statement, which is endorsed by the Obesity Society, includes "a call to action" for innovative ways to "fill the gap between lifestyle/medication and surgery." Proposals include conducting more research on bariatric surgery’s effects and safety; evaluating the effectiveness of lifestyle modification interventions, including adherence to dietary and physical activity plans; funding research to find other useful interventions, including better drugs and medical devices; and recognizing severe obesity as a chronic disease requiring ongoing care and management.
"The task ahead will be arduous and complicated, but the high prevalence and serious consequences of severe obesity require us to commit time, intellectual capital, and financial resources to address it," the writing group concluded.
Dr. Kelly disclosed that he has received research grants from Amylin Pharmaceuticals, the National Institutes of Health/National Institute of Neurological Disorders and Stroke, and the Thrasher Research Fund. He is also a consultant to Novo Nordisk. One other writing group member, Dr. Thomas H. Inge, disclosed that he has received a research grant from Ethicon Endosurgery.
To earn 0.25 hours AMA PRA Category 1 credit after reading this article, take the post-test here.
FROM CIRCULATION

New Anticoagulants for Thromboprophylaxis After Total Knee Arthroplasty
Fecal incontinence: New therapies, age-old problem
Fecal incontinence is a socially embarrassing condition that affects approximately 18 million adults in the United States.1 Its true incidence is likely much higher than reported, however, as many patients are reluctant to discuss it.
A recent study found that nearly 20% of women experience fecal incontinence at least once a year, and 9.5% experience it al least once a month.2 Only 28% of these women had ever discussed their symptoms with a physician, however.3 Women who did seek care were more likely to consult a family physician or internist (75%) than a gynecologist (7%).3
Until recently, few options were available for patients with fecal incontinence who had not benefited from conservative measures. Many patients simply had to live with their symptoms or undergo a diverting ostomy to control the chronic involuntary drainage.
Recent years have seen the development of new minimally invasive and highly successful techniques to treat fecal incontinence. Greater awareness of the prevalence of fecal incontinence and its devastating impact on quality of life is needed for this problem to be fully addressed, however. In this article, we review the recommended evaluation of a patient who reports fecal incontinence and describe the range of treatment options.
Fecal incontinence is a symptom, not a diagnosis
Although the most common historical factor contributing to fecal incontinence is obstetric trauma, there are several other causes of this condition. A detailed history and physical examination are vital to determine whether the patient is experiencing true fecal incontinence, or whether she is leaking for other reasons—so-called pseudo-incontinence.
Conditions that can mimic fecal incontinence include:
- prolapsing hemorrhoids
- anal fistula
- sexually transmitted infection
- benign or malignant anorectal neoplasms
- dermatologic conditions.
True fecal incontinence may be active (loss of stool despite the patient’s best effort to control it) or passive (loss of stool without the patient’s awareness). Among the causes of true fecal incontinence are:
- anal sphincter injury (obstetric tear, anorectal surgery such as fistulotomy, or trauma)
- denervation of the pelvic floor from pudendal nerve injury during childbirth
- chronic rectal prolapse
- neurologic conditions (spina bifida, myelomeningocele)
- noncompliant rectum from inflammatory bowel disease
- radiation proctitis.
The maintenance of continence requires a complex interaction between the sphincter muscle, the puborectalis muscle (which acts as a sling), rectal capacity and compliance, stool volume and frequency, and neurologic mechanisms.
Diagnosis and management require an experienced physician
We believe that patients reporting fecal incontinence are best worked up and managed by a physician who is well versed in the various diagnoses associated with fecal incontinence, as well as the most current treatments.
Diagnosis entails some detective work
When a patient reports fecal incontinence, she should be asked to elaborate on the circumstances surrounding the complaint and the frequency of its occurrence, duration of symptoms, and nature of the incontinence (gas, liquid, or solid).
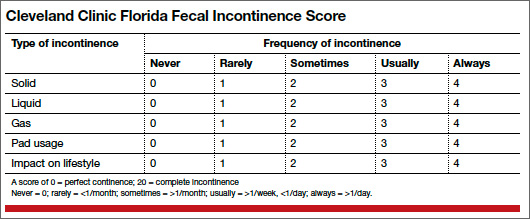
Validated quality-of-life instruments, such as the Cleveland Clinic Florida Fecal Incontinence Score (CCF-FIS) may be helpful in documenting the severity of the symptoms and improvement after treatment (TABLE).4
One factor that current scoring systems fail to capture is urgency. In many instances, urgency is the symptom most distressing to the patient. Be sure to ask about it.
A detailed obstetric history also is important. It is not uncommon for a patient to develop symptoms 20 years or longer after the injury. Also review the patient’s medical history for inflammatory bowel disease, neurologic disorders, and any history of pelvic radiation for help in determining the cause of symptoms.
In addition, ask the patient about any other pelvic floor symptoms, such as voiding dysfunction and problems with pelvic organ prolapse. And question her about stool consistency and frequency. In some cases, diarrhea can lead to fecal incontinence and is usually managed conservatively.
Physical exam: Focus on the perineum and anus
A detailed physical examination is warranted to determine the state of the patient’s sphincter musculature and rule out other causes of pseudo-incontinence, such as hemorrhoids or anal fistula. Inspect the perineum for thinning of the perineal body and scars from prior surgery.
A patulous anus may be a sign of rectal prolapse. To check for it, ask the patient to strain on the commode. If rectal prolapse is present, it will become apparent upon straining. If prolapse is detected, surgical treatment of the prolapse would be the first step in managing the incontinence.
A simple test of neurologic function is to try to elicit an anal “wink” in response to a pinprick.
A digital rectal exam allows the assessment of resting and squeeze tone, as well as the use of accessory muscles, such as the gluteus maximus, during squeezing.
Rigid or flexible proctoscopy may be indicated to rule out inflammatory bowel disease, radiation proctitis, and rectal neoplasm, depending on the patient’s history.
A few diagnostic adjuncts can help
Several adjuncts to physical examination can provide more detailed information about the patient’s condition and facilitate the development of an individualized treatment plan. For example, if rectal prolapse, rectocele with delayed emptying, or enterocele is suspected, consider defecography. If voiding dysfunction coexists with the fecal incontinence, urodynamic testing and cystoscopy may be indicated.
We routinely perform physiology testing and endoanal ultrasound if surgery is planned to address the fecal incontinence, although routine use of these adjuncts is controversial. Because many patients can be managed with conservative medical measures, we do not find it necessary to perform these tests at the time of the first visit.
Anal physiology testing includes manometry (a measure of both resting and squeeze tone) and pudendal nerve terminal motor latency testing.
Manometry can help quantify the severity of muscle weakness and determine the presence or absence of normal anal reflexes. Pudendal nerve testing assesses the innervation of the anal sphincter. There is some evidence that patients who have a pudendal neuropathy have a poor outcome with sphincteroplasty,5 although that evidence is controversial. The findings from physiology studies have not been correlated with outcomes of newer treatments, such as sacral neuromodulation (InterStim, Medtronic, Minneapolis, Minnesota). Each physiology lab uses different equipment, so “normal” values vary between institutions.
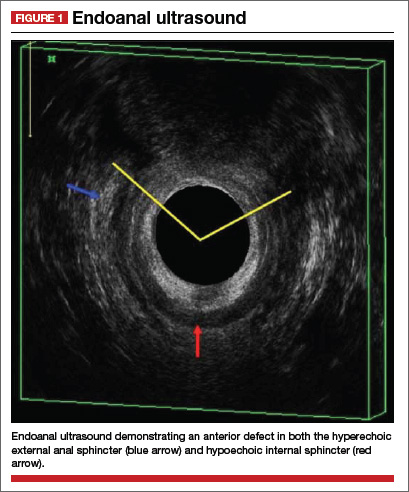
Endoanal ultrasound is easily performed in an office setting. It is well tolerated and provides anatomic detail of the sphincter musculature. We use a 13-MHz rotating probe to provide 3D imaging of the anal canal. The internal sphincter is represented by a hypoechoic circle surrounded by the hyperechoic external sphincter (FIGURE 1).
In the hands of an experienced examiner, the sensitivity and specificity of endoanal ultrasound in detecting sphincter defects approaches 100%.6,7 Ultrasound also enables measurement of the perineal body. A normal perineal body measures 10 to 15 mm.
For treatment, try conservative measures first
Bulking agents (fiber), constipating agents (loperamide, etc.), or a laxative regimen with scheduled disimpactions (in patients who have pelvic outlet constipation and overflow incontinence) often can control the symptoms of fecal incontinence, making further interventions unnecessary.
Biofeedback is another option. It uses visual, auditory, and sensory information to train patients to better control anal sphincter muscle function.
A recent randomized study found manometric biofeedback to be superior to simple Kegel exercises in improving fecal continence.8 In this study, 76% of patients in the biofeedback group experienced symptom improvement, compared with 41% of patients in the pelvic floor exercise group (P <.001). The long-term benefits of biofeedback are less clear, and patients often need to be reminded to perform their exercises at home and to attend occasional refresher-training sessions. Nevertheless, biofeedback is an important noninvasive option for patients in whom medical management has failed.
Minimally invasive options are now available
Over the past 2 years, minimally invasive treatments for fecal incontinence have emerged, including an implantable sacral neuromodulation device (InterStim) and an injectable dextranomer (Solesta; Salix Pharmaceuticals, Raleigh, North Carolina). Previously, the only surgical option for fecal incontinence was a sphincter repair if a defect was present. The new options may help patients improve their quality of life without having to undergo major surgery.
No one has directly compared the outcomes of these procedures when they are performed by a colorectal surgeon versus a physician of another specialty. It is our belief that the treating physician should have a strong interest in caring for these complex patients and a good working knowledge of the various treatment options.
Related Article Obstetric anal sphincter injury: 7 critical questions about care Ranee Thakar, MD, MRCOG (February 2008)
Sacral neuromodulation
This technique initially was developed for the treatment of overactive bladder and nonobstructive urinary retention and has been used in the United States for the past 15 years for these indications. Improvement in fecal continence was observed in these patients, prompting further studies of its efficacy. In 2011, it was approved by the US Food and Drug Administration (FDA) for the treatment of fecal incontinence. It has since revolutionized the treatment of this disorder, offering a minimally invasive and highly successful alternative to sphincteroplasty.
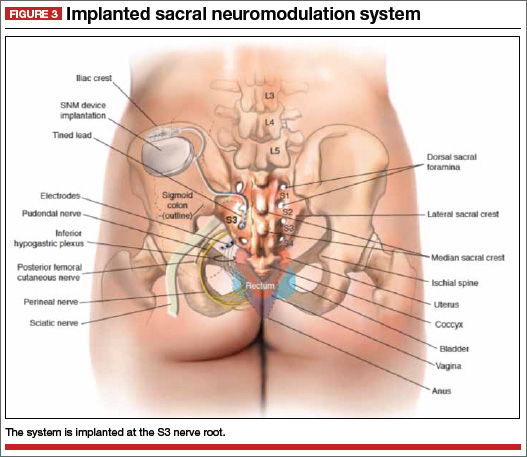
The InterStim procedure is the only therapeutic modality to include a test phase. The outpatient procedure involves sterile placement of an electrode through the S3 foramen to stimulate the S3 nerve root using fluoroscopic guidance (FIGURES 2 and 3). Patients who experience at least 50% improvement in symptoms are then offered placement of a permanent stimulator.
In most series, approximately 90% of patients have a positive test and progress to implantation. A recent US multicenter clinical trial indicated that 86% of patients achieved an improvement in continence of at least 50%, and 40% of patients were completely continent at 3 years.9 The number of episodes of incontinence decreased from a mean of 9.4/week to 1.7/week.9 Quality of life also improved greatly. Few complications have been reported, the most notable of which is infection (10.8% in the US multicenter trial9).
Another advantage of sacral neuromodulation: It can be used successfully in patients with external sphincter defects as large as 120º. A study by Tjandra and colleagues found that 65% of patients experienced improvement in symptoms of at least 50%, and 47% of patients (more than 50% of whom had external sphincter defects as large as 120º) became completely continent.10
The only variable shown to predict success with sacral neuromodulation is a positive response to the test implant procedure.
In our experience, this procedure is easy to perform and well tolerated, even in elderly patients with multiple comorbidities. The procedure has the additional advantage of potentially improving concomitant urinary symptoms as well.
The major disadvantage of sacral neuromodulation is its cost, although most major insurance carriers cover it. There is no well-conducted cost-effectiveness analysis comparing this modality to other treatments.
Related Article Interstim: An implantable device for implacable urinary symptoms Deborah L. Myers, MD (October 2006)
Injectable agents
Several biocompatible bulking agents have been tested in the treatment of fecal incontinence. These compounds traditionally have been used to treat mild fecal incontinence, or to treat patients with isolated internal sphincter defects.
More recently, an injectable dextranomer in stabilized hyaluronic acid was approved by the FDA and marketed as Solesta. Graf and colleagues randomly allocated 136 patients to injection and 70 patients to sham injection. Patients with external sphincter defects were excluded. At 6 months, 52% of patients in the active treatment group experienced an improvement in continence of at least 50%, compared with 31% of patients injected with placebo.11
The advantage of this procedure is its minimally invasive nature (submucosal injection performed in the office). The disadvantage: a lack of long-term efficacy data, although unpublished data suggest that patients who improve after an injection see a durable response at 3 years.
This easy, office-based treatment is ideal for patients with minor incontinence or persistent symptoms after another procedure.
Sphincter repair
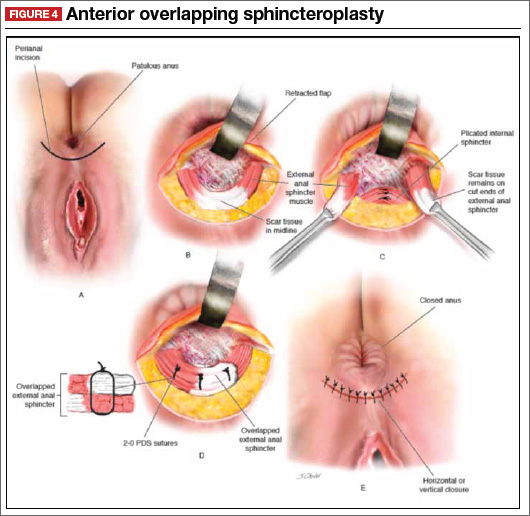
Anterior sphincteroplasty has been the mainstay of surgical treatment for patients with a sphincter defect. With the patient in a dorsal lithotomy or prone position on the operating-room table, a transverse perineal incision is made, and the ends of the severed sphincter muscle are located and mobilized. The repair then can be performed in an end-to-end manner or by overlapping the muscles in the anterior midline (FIGURE 4).
Some of the debatable technical issues of this procedure include:
- whether to overlap the muscles or scar tissue
- whether to repair internal and external defects together or separately
- how the age of the patient affects the outcome.
In regard to the first issue, there may be a superior outcome with overlapping repairs, but they carry a higher risk of dyspareunia and evacuation difficulties. Some surgeons will attempt a separate repair of the internal and external sphincter muscles if it appears feasible. Most often, both muscles are tethered together with scar tissue and separate repair is not possible. There are no conclusive data to demonstrate the superiority of either approach.
As for age, the traditional teaching was that older patients do not benefit from this procedure as much as younger patients do. However, a recent study found no differences in the CCF-FIS score in patients older than age 60, compared with younger patients.12 Investigators concluded that sphincteroplasty can be offered to both young and older patients.12
Although sphincteroplasty often leads to excellent short-term improvement, with 60% to 90% of patients experiencing a good or excellent outcome, nearly all series indicate a decline over the long term (>5 years). A recent systematic review found that as few as 12% of patients experience a good or excellent result, depending on the series.13
We offer sphincter repair to young women with a new sphincter defect after delivery. For older patients, we offer sacral neuromodulation as a first-line treatment.
Other surgical options
We believe that most patients with fecal incontinence can be managed using conservative measures, sacral neuromodulation, injectable dextranomer, or sphincter repair. However, several other options are available.
Artificial bowel sphincter
The artificial bowel sphincter was first described in 1987 and has been modified over the years. The system currently is marketed as the Acticon Neosphincter (American Medical Systems, Minnetonka, Minnesota). The procedure involves the creation of a subcutaneous tunnel around the anus so that an inflatable cuff can be positioned there. A pump then is tunneled through a Pfannenstiel incision to the labia or scrotum, and a reservoir is positioned in the space of Retzius. The device maintains continence by keeping the cuff inflated during the resting state and by pumping fluid from the cuff to the reservoir when the patient needs to evacuate.
The major barrier to utilization of the artificial bowel sphincter is infection. In a series of 112 patients who were implanted with the sphincter, 384 device-related adverse events occurred in 99 patients.14 A total of 73 revision operations were required in 51 patients (46%). Twenty-five percent of patients developed infection that required surgical revision, and 37% had the device explanted. Eighty-five percent of patients with a functional device had a successful outcome.14
Given the device-related challenges and infectious complications, patients should be considered for less invasive treatments before being offered an artificial bowel
sphincter.
Radiofrequency current
The Secca procedure (Curon Medical, Fremont, California) involves the application of radiofrequency current to the anal canal to generate thermal energy. This procedure causes contraction of collagen fibers, which are permanently shortened, and leads to tightening of the muscle. It is performed under intravenous sedation on an outpatient basis.
This approach is indicated for patients with mild to moderate fecal incontinence who have not responded to conservative management. An external sphincter defect is a contraindication.
Small, nonrandomized studies have found improvement in the CCF-FIS score in patients treated with this approach.15 The major limitation of this treatment is the lack of high-level clinical evidence demonstrating its efficacy and safety.
Antegrade continence enema
This approach, also known as the Malone procedure, is usually reserved for debilitating incontinence or constipation in the pediatric population. An appendicostomy is constructed at the navel, allowing daily introduction of a catheter and antegrade enema. The purpose is to perform rapid, controlled emptying of the colon at times chosen by the patient. It is also reserved as a last resort for patients considering an ostomy.
Adult patients with neurologic problems, such as spina bifida, may be candidates for this procedure, provided they are highly motivated.
Fecal diversion
Creation of a colostomy or ileostomy is usually the last resort for a patient with fecal incontinence. We are fortunate that there are an increasing number of options that may improve the patient’s condition before colostomy is required.
If fecal diversion is chosen by the patient, it is important to involve an enterostomal therapist for site marking and patient education. A well-constructed ostomy is essential, as this option often is permanent.
Up and coming options
A novel treatment approach for fecal incontinence is the magnetic anal sphincter. The device, marketed as the FENIX Continence Restoration System (Torax Medical, Shoreview, Minnesota) consists of a series of titanium beads with magnetic cores that are interlinked with titanium wires. The device is designed to encircle the external anal sphincter muscle, reinforce the sphincter, and expand to allow passage of stool at a socially appropriate time.
Preliminary data from 16 patients indicate a mean decrease in the number of episodes of incontinence from 7.2/week to 0.7/week, as well as a mean reduction in the CCF-FIS score from 17.2 to 8.7.16 Two devices were removed due to infection, and one device passed spontaneously after disconnection of the suture.16
This device is not approved by the FDA, but it may become a promising treatment if its safety and efficacy can be established in larger clinical trials.
The TOPAS sling (American Medical Systems) is currently being studied in a Phase 3, multicenter, nonrandomized, clinical trial (NCT01090739) for the treatment of fecal incontinence.17 The sling is implanted using a minimally invasive transobturator approach; two needle-passers deliver the sling assembly. Two small posterior incisions facilitate the postanal placement of the mesh.
This procedure replicates the anorectal angle created by the puborectalis muscle. Although it may become a minimally invasive treatment in the future, final results of the Phase 3 trial are not expected until 2016.
Tibial nerve stimulation is commonly used for urinary urge incontinence. Several small series have documented modest success with its application to fecal incontinence.18
The outpatient procedure involves the insertion of a needle electrode three fingerbreadths above the medial malleolus, followed by electrical stimulation. The current is slowly increased until a sensory or motor response (tingling under the sole of the foot or great toe plantar flexion) is elicited. Treatment necessitates several outpatient sessions.
In a recent series, the mean CCF-FIS decreased from 12.2/20 at baseline to 9.1/20 after treatment (P <.0001).18
The role of this procedure in the treatment algorithm for fecal incontinence remains to be determined.
What we offer patients
Fecal incontinence is a debilitating condition with an increasing number of potential therapeutic options. It clearly is under-recognized by patients and physicians alike.
After a thorough work-up, conservative treatment options should be offered first. When those fail, we generally recommend a trial of sacral neuromodulation for patients with no sphincter defect. When a sphincter defect is present, we counsel the patient about the merits of sphincter repair versus a trial of neuromodulation. These options have the most robust data supporting their clinical use, and have been used successfully in our own practices.
Given the continuous development of other therapeutic modalities, it is likely that future treatments will involve a stepwise progression of approaches. The need for colostomy should diminish in coming years as more minimally invasive techniques become available.
- Whitehead WE, Borrud L, Goode PS, et al. Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology. 2009;137(2):512–517.
- Brown HW, Wexner SD, Segall MM, et al. Accidental bowel leakage in the mature women’s health study: prevalence and predictors. Int Clin Pract. 2012;66(11):1101–1108.
- Brown HW, Wexner SD, Segall MM, et al. Quality of life in women with accidental bowel leakage. Int Clin Pract. 2012;66(11):1109–1116.
- Jorge JM, Wexner SD. Etiology and management of fecal incontinence. Dis Colon Rectum. 1993;36(1):77–97.
- Sangwan YP, Collar JA, Barrett RC, et al. Unilateral pudendal neuropathy. Impact on outcomes of anal sphincter repair. Dis Colon Rectum. 1996;39(6):686–689.
- Deen KI, Kumar D, Williams JG, et al. Anal sphincter defects. Correlation between endoanal ultrasound and surgery. Ann Surg. 1993;218(2):201–205.
- Oberwalder M, Thaler K, Baig MK, et al. Anal ultrasound and endosonographic measurement of perineal body thickness: a new evaluation for fecal incontinence in females. Surg Endosc. 2004;18(4):650–654.
- Heymen S, Scarlett Y, Jones K, et al. Randomized controlled trial shows biofeedback to be superior to pelvic floor exercises for fecal incontinence. Dis Colon Rectum. 2009;52(10):1730–1737.
- Mellgren AF, Wexner SD, Coller JA, et al. Long-term efficacy and safety of sacral nerve stimulation for fecal incontinence. Dis Colon Rectum. 2011:54(9):1065–1075.
- Tjandra JJ, Chan MK, Yeh CH, et al. Sacral nerve stimulation is more effective than optimal medical therapy for severe fecal incontinence: a randomized, controlled study. Dis Colon Rectum. 2008;51(5):494–502.
- Graf W, Mellgren A, Matzel K, et al. Efficacy of a dextranomer in stabilized hyaluronic acid for treatment of faecal incontinence: a randomized, sham-controlled trial. Lancet. 2011;377(9770):997–1003.
- El-Gazzaz G, Zutshi M, Hannaway C, Gurland B, Hull T. Overlapping sphincter repair: does age matter? Dis Colon Rectum. 2012;55(3):256–261.
- Glasgow SC, Lowry AC. Long-term outcomes of anal sphincter repair for fecal incontinence: a systematic review. Dis Colon Rectum. 2012;55(4):482–490.
- Wong WD, Congliosi SM, Spencer MP, et al. The safety and efficacy of the artificial bowel sphincter for fecal incontinence: results from a multicenter cohort study. Dis Colon Rectum. 2002;45(9):1139–1153.
- Takahashi T, Morales M, Garcia-Osogobio S, et al. Secca procedure for the treatment of fecal incontinence: results of five-year follow-up. Dis Colon Rectum. 2008;51(3):355–359.
- Lehur PA, McNevin S, Buntzen S, et al. Magnetic anal sphincter augmentation for the treatment of fecal incontinence: a preliminary report from a feasibility study. Dis Colon Rectum. 2010;53(12):1604–1610.
- TOPAS sling. http://clinicaltrials.gov/ct2/show/NCT01090739. Accessed August 26, 2013.
- Hotouras A, Thaha MA, Allison ME, et al. Percutaneous tibial nerve stimulation (PTNS) in females with faecal incontinence: the impact of sphincter morphology and rectal sensation on the clinical outcome. Int J Colorectal Dis. 2012;27(7):927–930.
Fecal incontinence is a socially embarrassing condition that affects approximately 18 million adults in the United States.1 Its true incidence is likely much higher than reported, however, as many patients are reluctant to discuss it.
A recent study found that nearly 20% of women experience fecal incontinence at least once a year, and 9.5% experience it al least once a month.2 Only 28% of these women had ever discussed their symptoms with a physician, however.3 Women who did seek care were more likely to consult a family physician or internist (75%) than a gynecologist (7%).3
Until recently, few options were available for patients with fecal incontinence who had not benefited from conservative measures. Many patients simply had to live with their symptoms or undergo a diverting ostomy to control the chronic involuntary drainage.
Recent years have seen the development of new minimally invasive and highly successful techniques to treat fecal incontinence. Greater awareness of the prevalence of fecal incontinence and its devastating impact on quality of life is needed for this problem to be fully addressed, however. In this article, we review the recommended evaluation of a patient who reports fecal incontinence and describe the range of treatment options.
Fecal incontinence is a symptom, not a diagnosis
Although the most common historical factor contributing to fecal incontinence is obstetric trauma, there are several other causes of this condition. A detailed history and physical examination are vital to determine whether the patient is experiencing true fecal incontinence, or whether she is leaking for other reasons—so-called pseudo-incontinence.
Conditions that can mimic fecal incontinence include:
- prolapsing hemorrhoids
- anal fistula
- sexually transmitted infection
- benign or malignant anorectal neoplasms
- dermatologic conditions.
True fecal incontinence may be active (loss of stool despite the patient’s best effort to control it) or passive (loss of stool without the patient’s awareness). Among the causes of true fecal incontinence are:
- anal sphincter injury (obstetric tear, anorectal surgery such as fistulotomy, or trauma)
- denervation of the pelvic floor from pudendal nerve injury during childbirth
- chronic rectal prolapse
- neurologic conditions (spina bifida, myelomeningocele)
- noncompliant rectum from inflammatory bowel disease
- radiation proctitis.
The maintenance of continence requires a complex interaction between the sphincter muscle, the puborectalis muscle (which acts as a sling), rectal capacity and compliance, stool volume and frequency, and neurologic mechanisms.
Diagnosis and management require an experienced physician
We believe that patients reporting fecal incontinence are best worked up and managed by a physician who is well versed in the various diagnoses associated with fecal incontinence, as well as the most current treatments.
Diagnosis entails some detective work
When a patient reports fecal incontinence, she should be asked to elaborate on the circumstances surrounding the complaint and the frequency of its occurrence, duration of symptoms, and nature of the incontinence (gas, liquid, or solid).
Validated quality-of-life instruments, such as the Cleveland Clinic Florida Fecal Incontinence Score (CCF-FIS) may be helpful in documenting the severity of the symptoms and improvement after treatment (TABLE).4
One factor that current scoring systems fail to capture is urgency. In many instances, urgency is the symptom most distressing to the patient. Be sure to ask about it.
A detailed obstetric history also is important. It is not uncommon for a patient to develop symptoms 20 years or longer after the injury. Also review the patient’s medical history for inflammatory bowel disease, neurologic disorders, and any history of pelvic radiation for help in determining the cause of symptoms.
In addition, ask the patient about any other pelvic floor symptoms, such as voiding dysfunction and problems with pelvic organ prolapse. And question her about stool consistency and frequency. In some cases, diarrhea can lead to fecal incontinence and is usually managed conservatively.
Physical exam: Focus on the perineum and anus
A detailed physical examination is warranted to determine the state of the patient’s sphincter musculature and rule out other causes of pseudo-incontinence, such as hemorrhoids or anal fistula. Inspect the perineum for thinning of the perineal body and scars from prior surgery.
A patulous anus may be a sign of rectal prolapse. To check for it, ask the patient to strain on the commode. If rectal prolapse is present, it will become apparent upon straining. If prolapse is detected, surgical treatment of the prolapse would be the first step in managing the incontinence.
A simple test of neurologic function is to try to elicit an anal “wink” in response to a pinprick.
A digital rectal exam allows the assessment of resting and squeeze tone, as well as the use of accessory muscles, such as the gluteus maximus, during squeezing.
Rigid or flexible proctoscopy may be indicated to rule out inflammatory bowel disease, radiation proctitis, and rectal neoplasm, depending on the patient’s history.
A few diagnostic adjuncts can help
Several adjuncts to physical examination can provide more detailed information about the patient’s condition and facilitate the development of an individualized treatment plan. For example, if rectal prolapse, rectocele with delayed emptying, or enterocele is suspected, consider defecography. If voiding dysfunction coexists with the fecal incontinence, urodynamic testing and cystoscopy may be indicated.
We routinely perform physiology testing and endoanal ultrasound if surgery is planned to address the fecal incontinence, although routine use of these adjuncts is controversial. Because many patients can be managed with conservative medical measures, we do not find it necessary to perform these tests at the time of the first visit.
Anal physiology testing includes manometry (a measure of both resting and squeeze tone) and pudendal nerve terminal motor latency testing.
Manometry can help quantify the severity of muscle weakness and determine the presence or absence of normal anal reflexes. Pudendal nerve testing assesses the innervation of the anal sphincter. There is some evidence that patients who have a pudendal neuropathy have a poor outcome with sphincteroplasty,5 although that evidence is controversial. The findings from physiology studies have not been correlated with outcomes of newer treatments, such as sacral neuromodulation (InterStim, Medtronic, Minneapolis, Minnesota). Each physiology lab uses different equipment, so “normal” values vary between institutions.
Endoanal ultrasound is easily performed in an office setting. It is well tolerated and provides anatomic detail of the sphincter musculature. We use a 13-MHz rotating probe to provide 3D imaging of the anal canal. The internal sphincter is represented by a hypoechoic circle surrounded by the hyperechoic external sphincter (FIGURE 1).
In the hands of an experienced examiner, the sensitivity and specificity of endoanal ultrasound in detecting sphincter defects approaches 100%.6,7 Ultrasound also enables measurement of the perineal body. A normal perineal body measures 10 to 15 mm.
For treatment, try conservative measures first
Bulking agents (fiber), constipating agents (loperamide, etc.), or a laxative regimen with scheduled disimpactions (in patients who have pelvic outlet constipation and overflow incontinence) often can control the symptoms of fecal incontinence, making further interventions unnecessary.
Biofeedback is another option. It uses visual, auditory, and sensory information to train patients to better control anal sphincter muscle function.
A recent randomized study found manometric biofeedback to be superior to simple Kegel exercises in improving fecal continence.8 In this study, 76% of patients in the biofeedback group experienced symptom improvement, compared with 41% of patients in the pelvic floor exercise group (P <.001). The long-term benefits of biofeedback are less clear, and patients often need to be reminded to perform their exercises at home and to attend occasional refresher-training sessions. Nevertheless, biofeedback is an important noninvasive option for patients in whom medical management has failed.
Minimally invasive options are now available
Over the past 2 years, minimally invasive treatments for fecal incontinence have emerged, including an implantable sacral neuromodulation device (InterStim) and an injectable dextranomer (Solesta; Salix Pharmaceuticals, Raleigh, North Carolina). Previously, the only surgical option for fecal incontinence was a sphincter repair if a defect was present. The new options may help patients improve their quality of life without having to undergo major surgery.
No one has directly compared the outcomes of these procedures when they are performed by a colorectal surgeon versus a physician of another specialty. It is our belief that the treating physician should have a strong interest in caring for these complex patients and a good working knowledge of the various treatment options.
Related Article Obstetric anal sphincter injury: 7 critical questions about care Ranee Thakar, MD, MRCOG (February 2008)
Sacral neuromodulation
This technique initially was developed for the treatment of overactive bladder and nonobstructive urinary retention and has been used in the United States for the past 15 years for these indications. Improvement in fecal continence was observed in these patients, prompting further studies of its efficacy. In 2011, it was approved by the US Food and Drug Administration (FDA) for the treatment of fecal incontinence. It has since revolutionized the treatment of this disorder, offering a minimally invasive and highly successful alternative to sphincteroplasty.
The InterStim procedure is the only therapeutic modality to include a test phase. The outpatient procedure involves sterile placement of an electrode through the S3 foramen to stimulate the S3 nerve root using fluoroscopic guidance (FIGURES 2 and 3). Patients who experience at least 50% improvement in symptoms are then offered placement of a permanent stimulator.
In most series, approximately 90% of patients have a positive test and progress to implantation. A recent US multicenter clinical trial indicated that 86% of patients achieved an improvement in continence of at least 50%, and 40% of patients were completely continent at 3 years.9 The number of episodes of incontinence decreased from a mean of 9.4/week to 1.7/week.9 Quality of life also improved greatly. Few complications have been reported, the most notable of which is infection (10.8% in the US multicenter trial9).
Another advantage of sacral neuromodulation: It can be used successfully in patients with external sphincter defects as large as 120º. A study by Tjandra and colleagues found that 65% of patients experienced improvement in symptoms of at least 50%, and 47% of patients (more than 50% of whom had external sphincter defects as large as 120º) became completely continent.10
The only variable shown to predict success with sacral neuromodulation is a positive response to the test implant procedure.
In our experience, this procedure is easy to perform and well tolerated, even in elderly patients with multiple comorbidities. The procedure has the additional advantage of potentially improving concomitant urinary symptoms as well.
The major disadvantage of sacral neuromodulation is its cost, although most major insurance carriers cover it. There is no well-conducted cost-effectiveness analysis comparing this modality to other treatments.
Related Article Interstim: An implantable device for implacable urinary symptoms Deborah L. Myers, MD (October 2006)
Injectable agents
Several biocompatible bulking agents have been tested in the treatment of fecal incontinence. These compounds traditionally have been used to treat mild fecal incontinence, or to treat patients with isolated internal sphincter defects.
More recently, an injectable dextranomer in stabilized hyaluronic acid was approved by the FDA and marketed as Solesta. Graf and colleagues randomly allocated 136 patients to injection and 70 patients to sham injection. Patients with external sphincter defects were excluded. At 6 months, 52% of patients in the active treatment group experienced an improvement in continence of at least 50%, compared with 31% of patients injected with placebo.11
The advantage of this procedure is its minimally invasive nature (submucosal injection performed in the office). The disadvantage: a lack of long-term efficacy data, although unpublished data suggest that patients who improve after an injection see a durable response at 3 years.
This easy, office-based treatment is ideal for patients with minor incontinence or persistent symptoms after another procedure.
Sphincter repair
Anterior sphincteroplasty has been the mainstay of surgical treatment for patients with a sphincter defect. With the patient in a dorsal lithotomy or prone position on the operating-room table, a transverse perineal incision is made, and the ends of the severed sphincter muscle are located and mobilized. The repair then can be performed in an end-to-end manner or by overlapping the muscles in the anterior midline (FIGURE 4).
Some of the debatable technical issues of this procedure include:
- whether to overlap the muscles or scar tissue
- whether to repair internal and external defects together or separately
- how the age of the patient affects the outcome.
In regard to the first issue, there may be a superior outcome with overlapping repairs, but they carry a higher risk of dyspareunia and evacuation difficulties. Some surgeons will attempt a separate repair of the internal and external sphincter muscles if it appears feasible. Most often, both muscles are tethered together with scar tissue and separate repair is not possible. There are no conclusive data to demonstrate the superiority of either approach.
As for age, the traditional teaching was that older patients do not benefit from this procedure as much as younger patients do. However, a recent study found no differences in the CCF-FIS score in patients older than age 60, compared with younger patients.12 Investigators concluded that sphincteroplasty can be offered to both young and older patients.12
Although sphincteroplasty often leads to excellent short-term improvement, with 60% to 90% of patients experiencing a good or excellent outcome, nearly all series indicate a decline over the long term (>5 years). A recent systematic review found that as few as 12% of patients experience a good or excellent result, depending on the series.13
We offer sphincter repair to young women with a new sphincter defect after delivery. For older patients, we offer sacral neuromodulation as a first-line treatment.
Other surgical options
We believe that most patients with fecal incontinence can be managed using conservative measures, sacral neuromodulation, injectable dextranomer, or sphincter repair. However, several other options are available.
Artificial bowel sphincter
The artificial bowel sphincter was first described in 1987 and has been modified over the years. The system currently is marketed as the Acticon Neosphincter (American Medical Systems, Minnetonka, Minnesota). The procedure involves the creation of a subcutaneous tunnel around the anus so that an inflatable cuff can be positioned there. A pump then is tunneled through a Pfannenstiel incision to the labia or scrotum, and a reservoir is positioned in the space of Retzius. The device maintains continence by keeping the cuff inflated during the resting state and by pumping fluid from the cuff to the reservoir when the patient needs to evacuate.
The major barrier to utilization of the artificial bowel sphincter is infection. In a series of 112 patients who were implanted with the sphincter, 384 device-related adverse events occurred in 99 patients.14 A total of 73 revision operations were required in 51 patients (46%). Twenty-five percent of patients developed infection that required surgical revision, and 37% had the device explanted. Eighty-five percent of patients with a functional device had a successful outcome.14
Given the device-related challenges and infectious complications, patients should be considered for less invasive treatments before being offered an artificial bowel
sphincter.
Radiofrequency current
The Secca procedure (Curon Medical, Fremont, California) involves the application of radiofrequency current to the anal canal to generate thermal energy. This procedure causes contraction of collagen fibers, which are permanently shortened, and leads to tightening of the muscle. It is performed under intravenous sedation on an outpatient basis.
This approach is indicated for patients with mild to moderate fecal incontinence who have not responded to conservative management. An external sphincter defect is a contraindication.
Small, nonrandomized studies have found improvement in the CCF-FIS score in patients treated with this approach.15 The major limitation of this treatment is the lack of high-level clinical evidence demonstrating its efficacy and safety.
Antegrade continence enema
This approach, also known as the Malone procedure, is usually reserved for debilitating incontinence or constipation in the pediatric population. An appendicostomy is constructed at the navel, allowing daily introduction of a catheter and antegrade enema. The purpose is to perform rapid, controlled emptying of the colon at times chosen by the patient. It is also reserved as a last resort for patients considering an ostomy.
Adult patients with neurologic problems, such as spina bifida, may be candidates for this procedure, provided they are highly motivated.
Fecal diversion
Creation of a colostomy or ileostomy is usually the last resort for a patient with fecal incontinence. We are fortunate that there are an increasing number of options that may improve the patient’s condition before colostomy is required.
If fecal diversion is chosen by the patient, it is important to involve an enterostomal therapist for site marking and patient education. A well-constructed ostomy is essential, as this option often is permanent.
Up and coming options
A novel treatment approach for fecal incontinence is the magnetic anal sphincter. The device, marketed as the FENIX Continence Restoration System (Torax Medical, Shoreview, Minnesota) consists of a series of titanium beads with magnetic cores that are interlinked with titanium wires. The device is designed to encircle the external anal sphincter muscle, reinforce the sphincter, and expand to allow passage of stool at a socially appropriate time.
Preliminary data from 16 patients indicate a mean decrease in the number of episodes of incontinence from 7.2/week to 0.7/week, as well as a mean reduction in the CCF-FIS score from 17.2 to 8.7.16 Two devices were removed due to infection, and one device passed spontaneously after disconnection of the suture.16
This device is not approved by the FDA, but it may become a promising treatment if its safety and efficacy can be established in larger clinical trials.
The TOPAS sling (American Medical Systems) is currently being studied in a Phase 3, multicenter, nonrandomized, clinical trial (NCT01090739) for the treatment of fecal incontinence.17 The sling is implanted using a minimally invasive transobturator approach; two needle-passers deliver the sling assembly. Two small posterior incisions facilitate the postanal placement of the mesh.
This procedure replicates the anorectal angle created by the puborectalis muscle. Although it may become a minimally invasive treatment in the future, final results of the Phase 3 trial are not expected until 2016.
Tibial nerve stimulation is commonly used for urinary urge incontinence. Several small series have documented modest success with its application to fecal incontinence.18
The outpatient procedure involves the insertion of a needle electrode three fingerbreadths above the medial malleolus, followed by electrical stimulation. The current is slowly increased until a sensory or motor response (tingling under the sole of the foot or great toe plantar flexion) is elicited. Treatment necessitates several outpatient sessions.
In a recent series, the mean CCF-FIS decreased from 12.2/20 at baseline to 9.1/20 after treatment (P <.0001).18
The role of this procedure in the treatment algorithm for fecal incontinence remains to be determined.
What we offer patients
Fecal incontinence is a debilitating condition with an increasing number of potential therapeutic options. It clearly is under-recognized by patients and physicians alike.
After a thorough work-up, conservative treatment options should be offered first. When those fail, we generally recommend a trial of sacral neuromodulation for patients with no sphincter defect. When a sphincter defect is present, we counsel the patient about the merits of sphincter repair versus a trial of neuromodulation. These options have the most robust data supporting their clinical use, and have been used successfully in our own practices.
Given the continuous development of other therapeutic modalities, it is likely that future treatments will involve a stepwise progression of approaches. The need for colostomy should diminish in coming years as more minimally invasive techniques become available.
Fecal incontinence is a socially embarrassing condition that affects approximately 18 million adults in the United States.1 Its true incidence is likely much higher than reported, however, as many patients are reluctant to discuss it.
A recent study found that nearly 20% of women experience fecal incontinence at least once a year, and 9.5% experience it al least once a month.2 Only 28% of these women had ever discussed their symptoms with a physician, however.3 Women who did seek care were more likely to consult a family physician or internist (75%) than a gynecologist (7%).3
Until recently, few options were available for patients with fecal incontinence who had not benefited from conservative measures. Many patients simply had to live with their symptoms or undergo a diverting ostomy to control the chronic involuntary drainage.
Recent years have seen the development of new minimally invasive and highly successful techniques to treat fecal incontinence. Greater awareness of the prevalence of fecal incontinence and its devastating impact on quality of life is needed for this problem to be fully addressed, however. In this article, we review the recommended evaluation of a patient who reports fecal incontinence and describe the range of treatment options.
Fecal incontinence is a symptom, not a diagnosis
Although the most common historical factor contributing to fecal incontinence is obstetric trauma, there are several other causes of this condition. A detailed history and physical examination are vital to determine whether the patient is experiencing true fecal incontinence, or whether she is leaking for other reasons—so-called pseudo-incontinence.
Conditions that can mimic fecal incontinence include:
- prolapsing hemorrhoids
- anal fistula
- sexually transmitted infection
- benign or malignant anorectal neoplasms
- dermatologic conditions.
True fecal incontinence may be active (loss of stool despite the patient’s best effort to control it) or passive (loss of stool without the patient’s awareness). Among the causes of true fecal incontinence are:
- anal sphincter injury (obstetric tear, anorectal surgery such as fistulotomy, or trauma)
- denervation of the pelvic floor from pudendal nerve injury during childbirth
- chronic rectal prolapse
- neurologic conditions (spina bifida, myelomeningocele)
- noncompliant rectum from inflammatory bowel disease
- radiation proctitis.
The maintenance of continence requires a complex interaction between the sphincter muscle, the puborectalis muscle (which acts as a sling), rectal capacity and compliance, stool volume and frequency, and neurologic mechanisms.
Diagnosis and management require an experienced physician
We believe that patients reporting fecal incontinence are best worked up and managed by a physician who is well versed in the various diagnoses associated with fecal incontinence, as well as the most current treatments.
Diagnosis entails some detective work
When a patient reports fecal incontinence, she should be asked to elaborate on the circumstances surrounding the complaint and the frequency of its occurrence, duration of symptoms, and nature of the incontinence (gas, liquid, or solid).
Validated quality-of-life instruments, such as the Cleveland Clinic Florida Fecal Incontinence Score (CCF-FIS) may be helpful in documenting the severity of the symptoms and improvement after treatment (TABLE).4
One factor that current scoring systems fail to capture is urgency. In many instances, urgency is the symptom most distressing to the patient. Be sure to ask about it.
A detailed obstetric history also is important. It is not uncommon for a patient to develop symptoms 20 years or longer after the injury. Also review the patient’s medical history for inflammatory bowel disease, neurologic disorders, and any history of pelvic radiation for help in determining the cause of symptoms.
In addition, ask the patient about any other pelvic floor symptoms, such as voiding dysfunction and problems with pelvic organ prolapse. And question her about stool consistency and frequency. In some cases, diarrhea can lead to fecal incontinence and is usually managed conservatively.
Physical exam: Focus on the perineum and anus
A detailed physical examination is warranted to determine the state of the patient’s sphincter musculature and rule out other causes of pseudo-incontinence, such as hemorrhoids or anal fistula. Inspect the perineum for thinning of the perineal body and scars from prior surgery.
A patulous anus may be a sign of rectal prolapse. To check for it, ask the patient to strain on the commode. If rectal prolapse is present, it will become apparent upon straining. If prolapse is detected, surgical treatment of the prolapse would be the first step in managing the incontinence.
A simple test of neurologic function is to try to elicit an anal “wink” in response to a pinprick.
A digital rectal exam allows the assessment of resting and squeeze tone, as well as the use of accessory muscles, such as the gluteus maximus, during squeezing.
Rigid or flexible proctoscopy may be indicated to rule out inflammatory bowel disease, radiation proctitis, and rectal neoplasm, depending on the patient’s history.
A few diagnostic adjuncts can help
Several adjuncts to physical examination can provide more detailed information about the patient’s condition and facilitate the development of an individualized treatment plan. For example, if rectal prolapse, rectocele with delayed emptying, or enterocele is suspected, consider defecography. If voiding dysfunction coexists with the fecal incontinence, urodynamic testing and cystoscopy may be indicated.
We routinely perform physiology testing and endoanal ultrasound if surgery is planned to address the fecal incontinence, although routine use of these adjuncts is controversial. Because many patients can be managed with conservative medical measures, we do not find it necessary to perform these tests at the time of the first visit.
Anal physiology testing includes manometry (a measure of both resting and squeeze tone) and pudendal nerve terminal motor latency testing.
Manometry can help quantify the severity of muscle weakness and determine the presence or absence of normal anal reflexes. Pudendal nerve testing assesses the innervation of the anal sphincter. There is some evidence that patients who have a pudendal neuropathy have a poor outcome with sphincteroplasty,5 although that evidence is controversial. The findings from physiology studies have not been correlated with outcomes of newer treatments, such as sacral neuromodulation (InterStim, Medtronic, Minneapolis, Minnesota). Each physiology lab uses different equipment, so “normal” values vary between institutions.
Endoanal ultrasound is easily performed in an office setting. It is well tolerated and provides anatomic detail of the sphincter musculature. We use a 13-MHz rotating probe to provide 3D imaging of the anal canal. The internal sphincter is represented by a hypoechoic circle surrounded by the hyperechoic external sphincter (FIGURE 1).
In the hands of an experienced examiner, the sensitivity and specificity of endoanal ultrasound in detecting sphincter defects approaches 100%.6,7 Ultrasound also enables measurement of the perineal body. A normal perineal body measures 10 to 15 mm.
For treatment, try conservative measures first
Bulking agents (fiber), constipating agents (loperamide, etc.), or a laxative regimen with scheduled disimpactions (in patients who have pelvic outlet constipation and overflow incontinence) often can control the symptoms of fecal incontinence, making further interventions unnecessary.
Biofeedback is another option. It uses visual, auditory, and sensory information to train patients to better control anal sphincter muscle function.
A recent randomized study found manometric biofeedback to be superior to simple Kegel exercises in improving fecal continence.8 In this study, 76% of patients in the biofeedback group experienced symptom improvement, compared with 41% of patients in the pelvic floor exercise group (P <.001). The long-term benefits of biofeedback are less clear, and patients often need to be reminded to perform their exercises at home and to attend occasional refresher-training sessions. Nevertheless, biofeedback is an important noninvasive option for patients in whom medical management has failed.
Minimally invasive options are now available
Over the past 2 years, minimally invasive treatments for fecal incontinence have emerged, including an implantable sacral neuromodulation device (InterStim) and an injectable dextranomer (Solesta; Salix Pharmaceuticals, Raleigh, North Carolina). Previously, the only surgical option for fecal incontinence was a sphincter repair if a defect was present. The new options may help patients improve their quality of life without having to undergo major surgery.
No one has directly compared the outcomes of these procedures when they are performed by a colorectal surgeon versus a physician of another specialty. It is our belief that the treating physician should have a strong interest in caring for these complex patients and a good working knowledge of the various treatment options.
Related Article Obstetric anal sphincter injury: 7 critical questions about care Ranee Thakar, MD, MRCOG (February 2008)
Sacral neuromodulation
This technique initially was developed for the treatment of overactive bladder and nonobstructive urinary retention and has been used in the United States for the past 15 years for these indications. Improvement in fecal continence was observed in these patients, prompting further studies of its efficacy. In 2011, it was approved by the US Food and Drug Administration (FDA) for the treatment of fecal incontinence. It has since revolutionized the treatment of this disorder, offering a minimally invasive and highly successful alternative to sphincteroplasty.
The InterStim procedure is the only therapeutic modality to include a test phase. The outpatient procedure involves sterile placement of an electrode through the S3 foramen to stimulate the S3 nerve root using fluoroscopic guidance (FIGURES 2 and 3). Patients who experience at least 50% improvement in symptoms are then offered placement of a permanent stimulator.
In most series, approximately 90% of patients have a positive test and progress to implantation. A recent US multicenter clinical trial indicated that 86% of patients achieved an improvement in continence of at least 50%, and 40% of patients were completely continent at 3 years.9 The number of episodes of incontinence decreased from a mean of 9.4/week to 1.7/week.9 Quality of life also improved greatly. Few complications have been reported, the most notable of which is infection (10.8% in the US multicenter trial9).
Another advantage of sacral neuromodulation: It can be used successfully in patients with external sphincter defects as large as 120º. A study by Tjandra and colleagues found that 65% of patients experienced improvement in symptoms of at least 50%, and 47% of patients (more than 50% of whom had external sphincter defects as large as 120º) became completely continent.10
The only variable shown to predict success with sacral neuromodulation is a positive response to the test implant procedure.
In our experience, this procedure is easy to perform and well tolerated, even in elderly patients with multiple comorbidities. The procedure has the additional advantage of potentially improving concomitant urinary symptoms as well.
The major disadvantage of sacral neuromodulation is its cost, although most major insurance carriers cover it. There is no well-conducted cost-effectiveness analysis comparing this modality to other treatments.
Related Article Interstim: An implantable device for implacable urinary symptoms Deborah L. Myers, MD (October 2006)
Injectable agents
Several biocompatible bulking agents have been tested in the treatment of fecal incontinence. These compounds traditionally have been used to treat mild fecal incontinence, or to treat patients with isolated internal sphincter defects.
More recently, an injectable dextranomer in stabilized hyaluronic acid was approved by the FDA and marketed as Solesta. Graf and colleagues randomly allocated 136 patients to injection and 70 patients to sham injection. Patients with external sphincter defects were excluded. At 6 months, 52% of patients in the active treatment group experienced an improvement in continence of at least 50%, compared with 31% of patients injected with placebo.11
The advantage of this procedure is its minimally invasive nature (submucosal injection performed in the office). The disadvantage: a lack of long-term efficacy data, although unpublished data suggest that patients who improve after an injection see a durable response at 3 years.
This easy, office-based treatment is ideal for patients with minor incontinence or persistent symptoms after another procedure.
Sphincter repair
Anterior sphincteroplasty has been the mainstay of surgical treatment for patients with a sphincter defect. With the patient in a dorsal lithotomy or prone position on the operating-room table, a transverse perineal incision is made, and the ends of the severed sphincter muscle are located and mobilized. The repair then can be performed in an end-to-end manner or by overlapping the muscles in the anterior midline (FIGURE 4).
Some of the debatable technical issues of this procedure include:
- whether to overlap the muscles or scar tissue
- whether to repair internal and external defects together or separately
- how the age of the patient affects the outcome.
In regard to the first issue, there may be a superior outcome with overlapping repairs, but they carry a higher risk of dyspareunia and evacuation difficulties. Some surgeons will attempt a separate repair of the internal and external sphincter muscles if it appears feasible. Most often, both muscles are tethered together with scar tissue and separate repair is not possible. There are no conclusive data to demonstrate the superiority of either approach.
As for age, the traditional teaching was that older patients do not benefit from this procedure as much as younger patients do. However, a recent study found no differences in the CCF-FIS score in patients older than age 60, compared with younger patients.12 Investigators concluded that sphincteroplasty can be offered to both young and older patients.12
Although sphincteroplasty often leads to excellent short-term improvement, with 60% to 90% of patients experiencing a good or excellent outcome, nearly all series indicate a decline over the long term (>5 years). A recent systematic review found that as few as 12% of patients experience a good or excellent result, depending on the series.13
We offer sphincter repair to young women with a new sphincter defect after delivery. For older patients, we offer sacral neuromodulation as a first-line treatment.
Other surgical options
We believe that most patients with fecal incontinence can be managed using conservative measures, sacral neuromodulation, injectable dextranomer, or sphincter repair. However, several other options are available.
Artificial bowel sphincter
The artificial bowel sphincter was first described in 1987 and has been modified over the years. The system currently is marketed as the Acticon Neosphincter (American Medical Systems, Minnetonka, Minnesota). The procedure involves the creation of a subcutaneous tunnel around the anus so that an inflatable cuff can be positioned there. A pump then is tunneled through a Pfannenstiel incision to the labia or scrotum, and a reservoir is positioned in the space of Retzius. The device maintains continence by keeping the cuff inflated during the resting state and by pumping fluid from the cuff to the reservoir when the patient needs to evacuate.
The major barrier to utilization of the artificial bowel sphincter is infection. In a series of 112 patients who were implanted with the sphincter, 384 device-related adverse events occurred in 99 patients.14 A total of 73 revision operations were required in 51 patients (46%). Twenty-five percent of patients developed infection that required surgical revision, and 37% had the device explanted. Eighty-five percent of patients with a functional device had a successful outcome.14
Given the device-related challenges and infectious complications, patients should be considered for less invasive treatments before being offered an artificial bowel
sphincter.
Radiofrequency current
The Secca procedure (Curon Medical, Fremont, California) involves the application of radiofrequency current to the anal canal to generate thermal energy. This procedure causes contraction of collagen fibers, which are permanently shortened, and leads to tightening of the muscle. It is performed under intravenous sedation on an outpatient basis.
This approach is indicated for patients with mild to moderate fecal incontinence who have not responded to conservative management. An external sphincter defect is a contraindication.
Small, nonrandomized studies have found improvement in the CCF-FIS score in patients treated with this approach.15 The major limitation of this treatment is the lack of high-level clinical evidence demonstrating its efficacy and safety.
Antegrade continence enema
This approach, also known as the Malone procedure, is usually reserved for debilitating incontinence or constipation in the pediatric population. An appendicostomy is constructed at the navel, allowing daily introduction of a catheter and antegrade enema. The purpose is to perform rapid, controlled emptying of the colon at times chosen by the patient. It is also reserved as a last resort for patients considering an ostomy.
Adult patients with neurologic problems, such as spina bifida, may be candidates for this procedure, provided they are highly motivated.
Fecal diversion
Creation of a colostomy or ileostomy is usually the last resort for a patient with fecal incontinence. We are fortunate that there are an increasing number of options that may improve the patient’s condition before colostomy is required.
If fecal diversion is chosen by the patient, it is important to involve an enterostomal therapist for site marking and patient education. A well-constructed ostomy is essential, as this option often is permanent.
Up and coming options
A novel treatment approach for fecal incontinence is the magnetic anal sphincter. The device, marketed as the FENIX Continence Restoration System (Torax Medical, Shoreview, Minnesota) consists of a series of titanium beads with magnetic cores that are interlinked with titanium wires. The device is designed to encircle the external anal sphincter muscle, reinforce the sphincter, and expand to allow passage of stool at a socially appropriate time.
Preliminary data from 16 patients indicate a mean decrease in the number of episodes of incontinence from 7.2/week to 0.7/week, as well as a mean reduction in the CCF-FIS score from 17.2 to 8.7.16 Two devices were removed due to infection, and one device passed spontaneously after disconnection of the suture.16
This device is not approved by the FDA, but it may become a promising treatment if its safety and efficacy can be established in larger clinical trials.
The TOPAS sling (American Medical Systems) is currently being studied in a Phase 3, multicenter, nonrandomized, clinical trial (NCT01090739) for the treatment of fecal incontinence.17 The sling is implanted using a minimally invasive transobturator approach; two needle-passers deliver the sling assembly. Two small posterior incisions facilitate the postanal placement of the mesh.
This procedure replicates the anorectal angle created by the puborectalis muscle. Although it may become a minimally invasive treatment in the future, final results of the Phase 3 trial are not expected until 2016.
Tibial nerve stimulation is commonly used for urinary urge incontinence. Several small series have documented modest success with its application to fecal incontinence.18
The outpatient procedure involves the insertion of a needle electrode three fingerbreadths above the medial malleolus, followed by electrical stimulation. The current is slowly increased until a sensory or motor response (tingling under the sole of the foot or great toe plantar flexion) is elicited. Treatment necessitates several outpatient sessions.
In a recent series, the mean CCF-FIS decreased from 12.2/20 at baseline to 9.1/20 after treatment (P <.0001).18
The role of this procedure in the treatment algorithm for fecal incontinence remains to be determined.
What we offer patients
Fecal incontinence is a debilitating condition with an increasing number of potential therapeutic options. It clearly is under-recognized by patients and physicians alike.
After a thorough work-up, conservative treatment options should be offered first. When those fail, we generally recommend a trial of sacral neuromodulation for patients with no sphincter defect. When a sphincter defect is present, we counsel the patient about the merits of sphincter repair versus a trial of neuromodulation. These options have the most robust data supporting their clinical use, and have been used successfully in our own practices.
Given the continuous development of other therapeutic modalities, it is likely that future treatments will involve a stepwise progression of approaches. The need for colostomy should diminish in coming years as more minimally invasive techniques become available.
- Whitehead WE, Borrud L, Goode PS, et al. Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology. 2009;137(2):512–517.
- Brown HW, Wexner SD, Segall MM, et al. Accidental bowel leakage in the mature women’s health study: prevalence and predictors. Int Clin Pract. 2012;66(11):1101–1108.
- Brown HW, Wexner SD, Segall MM, et al. Quality of life in women with accidental bowel leakage. Int Clin Pract. 2012;66(11):1109–1116.
- Jorge JM, Wexner SD. Etiology and management of fecal incontinence. Dis Colon Rectum. 1993;36(1):77–97.
- Sangwan YP, Collar JA, Barrett RC, et al. Unilateral pudendal neuropathy. Impact on outcomes of anal sphincter repair. Dis Colon Rectum. 1996;39(6):686–689.
- Deen KI, Kumar D, Williams JG, et al. Anal sphincter defects. Correlation between endoanal ultrasound and surgery. Ann Surg. 1993;218(2):201–205.
- Oberwalder M, Thaler K, Baig MK, et al. Anal ultrasound and endosonographic measurement of perineal body thickness: a new evaluation for fecal incontinence in females. Surg Endosc. 2004;18(4):650–654.
- Heymen S, Scarlett Y, Jones K, et al. Randomized controlled trial shows biofeedback to be superior to pelvic floor exercises for fecal incontinence. Dis Colon Rectum. 2009;52(10):1730–1737.
- Mellgren AF, Wexner SD, Coller JA, et al. Long-term efficacy and safety of sacral nerve stimulation for fecal incontinence. Dis Colon Rectum. 2011:54(9):1065–1075.
- Tjandra JJ, Chan MK, Yeh CH, et al. Sacral nerve stimulation is more effective than optimal medical therapy for severe fecal incontinence: a randomized, controlled study. Dis Colon Rectum. 2008;51(5):494–502.
- Graf W, Mellgren A, Matzel K, et al. Efficacy of a dextranomer in stabilized hyaluronic acid for treatment of faecal incontinence: a randomized, sham-controlled trial. Lancet. 2011;377(9770):997–1003.
- El-Gazzaz G, Zutshi M, Hannaway C, Gurland B, Hull T. Overlapping sphincter repair: does age matter? Dis Colon Rectum. 2012;55(3):256–261.
- Glasgow SC, Lowry AC. Long-term outcomes of anal sphincter repair for fecal incontinence: a systematic review. Dis Colon Rectum. 2012;55(4):482–490.
- Wong WD, Congliosi SM, Spencer MP, et al. The safety and efficacy of the artificial bowel sphincter for fecal incontinence: results from a multicenter cohort study. Dis Colon Rectum. 2002;45(9):1139–1153.
- Takahashi T, Morales M, Garcia-Osogobio S, et al. Secca procedure for the treatment of fecal incontinence: results of five-year follow-up. Dis Colon Rectum. 2008;51(3):355–359.
- Lehur PA, McNevin S, Buntzen S, et al. Magnetic anal sphincter augmentation for the treatment of fecal incontinence: a preliminary report from a feasibility study. Dis Colon Rectum. 2010;53(12):1604–1610.
- TOPAS sling. http://clinicaltrials.gov/ct2/show/NCT01090739. Accessed August 26, 2013.
- Hotouras A, Thaha MA, Allison ME, et al. Percutaneous tibial nerve stimulation (PTNS) in females with faecal incontinence: the impact of sphincter morphology and rectal sensation on the clinical outcome. Int J Colorectal Dis. 2012;27(7):927–930.
- Whitehead WE, Borrud L, Goode PS, et al. Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology. 2009;137(2):512–517.
- Brown HW, Wexner SD, Segall MM, et al. Accidental bowel leakage in the mature women’s health study: prevalence and predictors. Int Clin Pract. 2012;66(11):1101–1108.
- Brown HW, Wexner SD, Segall MM, et al. Quality of life in women with accidental bowel leakage. Int Clin Pract. 2012;66(11):1109–1116.
- Jorge JM, Wexner SD. Etiology and management of fecal incontinence. Dis Colon Rectum. 1993;36(1):77–97.
- Sangwan YP, Collar JA, Barrett RC, et al. Unilateral pudendal neuropathy. Impact on outcomes of anal sphincter repair. Dis Colon Rectum. 1996;39(6):686–689.
- Deen KI, Kumar D, Williams JG, et al. Anal sphincter defects. Correlation between endoanal ultrasound and surgery. Ann Surg. 1993;218(2):201–205.
- Oberwalder M, Thaler K, Baig MK, et al. Anal ultrasound and endosonographic measurement of perineal body thickness: a new evaluation for fecal incontinence in females. Surg Endosc. 2004;18(4):650–654.
- Heymen S, Scarlett Y, Jones K, et al. Randomized controlled trial shows biofeedback to be superior to pelvic floor exercises for fecal incontinence. Dis Colon Rectum. 2009;52(10):1730–1737.
- Mellgren AF, Wexner SD, Coller JA, et al. Long-term efficacy and safety of sacral nerve stimulation for fecal incontinence. Dis Colon Rectum. 2011:54(9):1065–1075.
- Tjandra JJ, Chan MK, Yeh CH, et al. Sacral nerve stimulation is more effective than optimal medical therapy for severe fecal incontinence: a randomized, controlled study. Dis Colon Rectum. 2008;51(5):494–502.
- Graf W, Mellgren A, Matzel K, et al. Efficacy of a dextranomer in stabilized hyaluronic acid for treatment of faecal incontinence: a randomized, sham-controlled trial. Lancet. 2011;377(9770):997–1003.
- El-Gazzaz G, Zutshi M, Hannaway C, Gurland B, Hull T. Overlapping sphincter repair: does age matter? Dis Colon Rectum. 2012;55(3):256–261.
- Glasgow SC, Lowry AC. Long-term outcomes of anal sphincter repair for fecal incontinence: a systematic review. Dis Colon Rectum. 2012;55(4):482–490.
- Wong WD, Congliosi SM, Spencer MP, et al. The safety and efficacy of the artificial bowel sphincter for fecal incontinence: results from a multicenter cohort study. Dis Colon Rectum. 2002;45(9):1139–1153.
- Takahashi T, Morales M, Garcia-Osogobio S, et al. Secca procedure for the treatment of fecal incontinence: results of five-year follow-up. Dis Colon Rectum. 2008;51(3):355–359.
- Lehur PA, McNevin S, Buntzen S, et al. Magnetic anal sphincter augmentation for the treatment of fecal incontinence: a preliminary report from a feasibility study. Dis Colon Rectum. 2010;53(12):1604–1610.
- TOPAS sling. http://clinicaltrials.gov/ct2/show/NCT01090739. Accessed August 26, 2013.
- Hotouras A, Thaha MA, Allison ME, et al. Percutaneous tibial nerve stimulation (PTNS) in females with faecal incontinence: the impact of sphincter morphology and rectal sensation on the clinical outcome. Int J Colorectal Dis. 2012;27(7):927–930.
Pulsed Dye Laser for the Treatment of Nail Psoriasis

5 IUD myths dispelled
Long-acting reversible contraceptives (LARCs), which include intrauterine devices (IUDs), implants, and injectables, are being offered to more and more women because of their demonstrated safety, efficacy, and convenience. In other countries, as many as 50% of all women use an IUD, but the United States has been slow to adopt this option.1 In 2002, approximately 2% of US women used an IUD.2 That percentage rose to 5.2% between 2006 and 2008, according to a recent survey.3 In that survey, women consistently expressed a high degree of satisfaction with this method of contraception.3
So why aren’t more US women using an IUD?
A general fear of the IUD persists. Women may not even know why they fear the device; they may have simply heard that it is “bad for you.” The negative press the IUD has received in this country probably is related to poor outcomes associated with use of the Dalkon Shield IUD in the 1970s. As a reminder, the Dalkon Shield was blamed for many cases of pelvic inflammatory disease (PID) and other negative sequelae as a result of poor patient selection. In addition, some authorities believe the design of the device was severely flawed, with a string that permitted bacteria to get from the vagina to the uterus and tubes.
Today, clinicians and many patients are better educated about the prevention of chlamydia, the primary causative organism of PID and other sexually transmitted infections (STIs); patients also are better informed about safe sex practices. We now know that women should be screened for behaviors that could increase their risk for PID and render them poor candidates for the IUD.
Clinicians also have expressed concerns about reimbursement issues related to the IUD, as well as confusion and difficulty with insertion procedures and the potential for litigation. In this article, I address some of these issues in an attempt to increase the use of this highly effective contraceptive.
What’s available today
Today there are three IUDs available to US women (FIGURE):
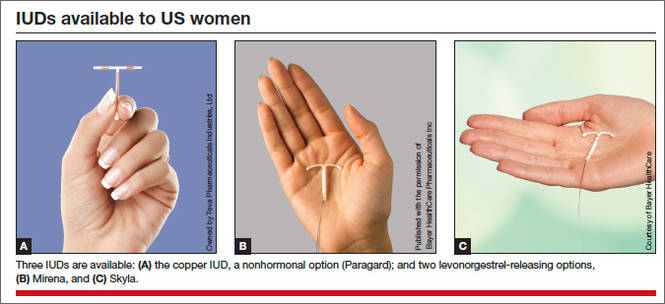
The Copper IUD (ParaGard)—This device can be used for at least 10 years, although, in many countries, it is considered “permanent reversible contraception.” It has the advantage of being nonhormonal, making it an important option for women who cannot or will not use a hormonal contraceptive. Pregnancy is prevented through a “foreign body” effect and the spermicidal action of copper ions. The combination of these two influences prevents fertilization.4
The levonorgestrel-releasing intrauterine system (LNG-IUS) (Mirena)—This IUD is recommended for 5 years of use but may remain effective for as long as 7 years. It contains 52 mg of levonorgestrel, which it releases at a rate of approximately 20 μg/day. In addition to the foreign body effect, this IUD prevents pregnancy through progestogenic mechanisms: It thickens cervical mucus, thins the endometrium, and reduces sperm capacitation.5
The "mini" LNG-IUS (Skyla)—This newly marketed IUD is recommended for 3 years of use. It contains 13.5 mg of levonorgestrel, which it releases at a rate of 14 μg/day. It has the same mechanism of action as Mirena but may be easier to insert owing to its slightly smaller size and preloaded inserter.
Myth #1: The IUD is not suitable for teens and nulliparous women
This myth arose out of concerns about the smaller uterine cavity and cervical diameter of teens and nulliparous women. Today we know that an IUD can be inserted safely in this population. Moreover, because adolescents are at high risk for unintended pregnancy, they stand to benefit uniquely from LARC options, including the IUD. As the American College of Obstetricians and Gynecologists (ACOG) recommends in a recent Committee Opinion on adolescents and LARCs, the IUD should be a “first-line” option for all women of reproductive age.6
Myth #2: An IUD should not be inserted immediately after childbirth
For many years, it was assumed that an IUD should be inserted in the postpartum period only after uterine involution was completed. However, in 2010, the Centers for Disease Control and Prevention (CDC) published medical eligibility criteria for contraceptive use, which included the following recommendations for breastfeeding or non–breast-feeding women:
• Mirena was given a Level 2 recommendation (advantages outweigh risks) for insertion within 10 minutes after delivery of the placenta
• The copper IUD was given a Level 1 recommendation (no restrictions) for insertion within the same time interval
• From 10 minutes to 4 weeks postpartum, both devices have a Level 2 recommendation for insertion
• Beyond 4 weeks, both devices have a Level 1 recommendation for insertion.7
Immediate post-delivery insertion of an IUD has several benefits, including:
• a reduction in the risk of unintended pregnancy in women who are not breastfeeding
• providing new mothers with a LARC method.
Myth #3: Antibiotics and NSAIDs should be administered
This myth arose from concerns about PID and insertion-related pain. However, a Cochrane Database review found no benefit for prophylactic use of antibiotics prior to insertion of the copper or LNG-IUS devices to prevent PID.8
In fact, data indicate that the incidence of PID is low among women who are appropriate candidates for an IUD. Similarly, Allen and colleagues found that nonsteroidal anti-inflammatory drugs (NSAIDs) did not ameliorate symptoms of cramping during or immediately after insertion of an IUD.9
Myth #4: IUD insertion is difficult
In reality, both the copper IUD and Mirena are easy to insert. In addition, the smaller LNG-IUS (Skyla) comes more completely preloaded in its inserter. In a published Phase 2 trial comparing Mirena with two smaller, lower-dose levonorgestrel-releasing devices, with the lowest-dose product corresponding to the marketed Skyla product, all 738 women given Mirena or the smaller devices experienced successful placement, with 98.5% of placements achieved on the first attempt.10
Various studies have been conducted to evaluate methods to ease insertion, including use of intracervical lidocaine, vaginal and/or oral administration of misoprostol (Cytotec), and vaginal estrogen creams. None was found to be effective in controlled trials. (See the sidebar, “Data-driven tactics for reducing pain on IUD insertion,” by Jennifer Gunter, MD, on page 28.) In the small percentage of women in whom it is difficult to pass a uterine sound through the external and internal os, cervical dilators may be beneficial. Gentle, progressive dilation can be accomplished easily with minimal discomfort to the patient, easing IUD insertion dramatically.
If a clinician does not insert IUDs on a frequent basis, it is prudent to look over the insertion procedure prior to the patient’s arrival. The procedure then can be reviewed with the patient as part of informed consent, which should be documented in the chart.
No steps in the recommended insertion procedure should be omitted, and charting should reflect each step:
1. Perform a bimanual exam
2. Document the appearance of the vagina and cervix
3. Use betadine or another cleansing solution on the cervical portio
4. Apply the tenaculum to the cervix (anterior lip if the uterus is anteverted, posterior lip if it is retroverted)
5. Sound the uterus to determine the optimal depth of IUD insertion. (The recommended uterine depth is 6 to 10 cm. A smaller uterus increases the likelihood of perforation, pain, and expulsion.)
6. Insert the IUD (and document the ease or difficulty of insertion)
7. Trim the string to an appropriate length
8. Assess the patient’s condition after insertion
9. Schedule a return visit in 4 weeks.
Related Article Let’s increase our use of IUDs and improve contraceptive effectiveness in this country Robert L. Barbieri, MD
Myth #5: Perforation is common
Uterine perforation occurs in approximately 1 in every 1,000 insertions.11 If perforation occurs with a copper IUD, remove the device to prevent the formation of intraperitoneal adhesions.12 The LNG-IUS devices do not produce this reaction, although most experts agree that they should be removed when a perforation occurs.13
Anecdotal evidence suggests that perforation may be more common among breastfeeding women, but this finding is far from definitive.
How to select an IUD for a patient: 3 case studies
CASE 1: Heavy bleeding and signs of endometriosis
Amelia, a 26-year-old nulliparous white woman, visits your office for routine examination and asks about her contraceptive options. She has no notable medical history. She has a body mass index (BMI) of 20.2 kg/m2 and exercises regularly. Menarche occurred at age 13. Her menstrual cycles are regular but are getting heavier; she now “soaks” a tampon every hour. She also complains that her cramps are more difficult to manage. She takes ibuprofen 600 mg every 6 hours during the days of heaviest bleeding and cramping, but that approach doesn’t seem to be effective lately. She is in a stable sexual relationship with her boyfriend of 2 years, now her fiancé. They have been using condoms consistently as contraception but don’t plan to start a family for a “few years.” Amelia reports that their sex life is good, although she has been experiencing pain with deep penetration for about 6 months.
Examination reveals a clear cervix and nontender uterus, although the uterus is retroverted. Palpation of the ovaries indicates that they are normal. Her main complaints: dysmenorrhea and heavy menstrual bleeding.
What contraceptive would you suggest?
Amelia would be a good candidate for the LNG-IUS because she is in a stable relationship and wants to postpone pregnancy for several years. Although she has some symptoms suggestive of endometriosis (dyspareunia), they could be relieved by this method.14 Because thinning of the endometrial lining is an inherent mechanism of action of the LNG-IUS, this method could reduce her heavy bleeding.
She should be advised of the risks and benefits of the LNG-IUS, which can be inserted when she begins her next menstrual cycle.
CASE 2: Mother of two with no immediate desire for pregnancy
Tamika is a 19-year-old black woman (G2P2) who has arrived at your clinic for her 6-week postpartum visit. She is not breastfeeding. Her BMI is 25.7 kg/m2. She reports that her baby and 2-year-old are doing “OK” and says she does not want to get pregnant again anytime soon. She is in a relationship with the father of her baby and says he is “working a good job and taking care of me.” Her menstrual cycles have always been normal, with no cramping or heavy bleeding.
Examination reveals that her cervix is clear, her uterus is anteverted and nontender, and her ovaries appear to be normal.
Would this patient be a good candidate for a LARC?
Tamika is an excellent candidate for the copper IUD or LNG-IUS and should be educated about both methods. If she chooses an IUD, it can be inserted at the start of her next menstrual period.
These first two cases illustrate the importance of making no assumptions on the basis of general patient characteristics. Although Tamika may appear to be at greater risk for STI than Amelia, such “typecasting” may lead to inappropriate counseling.
Related Article Malpositioned IUDs: When you should intervene (and when you should not)
At the time of IUD insertion, both patients should be instructed to check for the IUD string periodically, and this recommendation should be documented in their charts.
CASE 3: Anovulatory patient with heavy periods
Mary, 25, is a nulliparous Hispanic woman who has been referred by her primary care provider. She has a BMI of 35.4 kg/m2 and has had menstrual problems since menarche at the age of 14. She reports that her periods are irregular and very heavy, with intermittent pelvic pain that she manages, with some success, with ibuprofen. She has never had a sexual relationship, but she has a boyfriend now and asks about her contraceptive options.
On examination, you discover that Mary has pubic hair distribution over her inner thigh, with primary escutcheon and acanthosis nigricans on the inner thigh. Her vulva is marked by multiple sebaceous cysts, and a speculum exam shows a large amount of estrogenic mucus and a clear cervix. Her uterus is anteverted and nontender. Her ovaries are palpable but may be enlarged, and transvaginal ultrasound reveals that they are cystic. Her diagnosis: hirsutism with probable polycystic ovary syndrome.
Would an IUD be appropriate?
Mary is not a good candidate for an IUD. Neither the copper IUD nor the LNG-IUS would suppress ovarian function sufficiently to reduce the growth of multiple follicles that occurs with polycystic ovary syndrome. She would benefit from a hormonal method (specifically, a combination oral contraceptive) to suppress follicular activity.
Time for a renaissance?
The IUD may be making a comeback. With the unintended pregnancy rate remaining consistently at about 50%, it is important that we offer our patients contraceptive methods that maximize efficacy, safety, and convenience. Today’s IUDs meet all these criteria.
Data-driven tactics for reducing pain on IUD insertion
Many patients worry about the potential for pain with IUD insertion—and this concern can dissuade them from choosing the IUD as a contraceptive. This is regrettable because the IUD has the highest satisfaction rating among reversible contraceptives, as well as the greatest efficacy.
How much pain can your patient expect? In one recent prospective study involving 40 women who received either 1.2% lidocaine or saline infused 3 minutes before IUD insertion, 33% of women reported a pain score of 5 or higher (on a scale of 0–10) at tenaculum placement. This finding means that two-thirds of women had a pain score of 4 or lower. In fact, 46% of women had a pain score of 2 or below.15 (The mean pain scores for insertion were similar with lidocaine and placebo [3.0 vs 3.7, respectively; P=.4]).
Pain reducing options
The evidence validates (or fails to disprove) the value of the following interventions to make insertion more comfortable for patients:
• Naproxen (550 mg) administration 40 minutes prior to insertion. One small study found it to be better than placebo.9
• Nonopioid pain medication. One small, randomized, double-blinded clinical trial found that tramadol was even more effective than naproxen at relieving insertion-related pain.16
• Injection of lidocaine into the cervix. Although this intervention is common, data supporting it are scarce. One small, high-quality study found no benefit, compared with placebo. However, if you have had success with this approach in the past, I would not discourage you from continuing to offer it, as a single small study is insufficient to disprove it.15 More data are needed.
• Keeping the patient calm. Anxiety increases the perception of pain. Studies have demonstrated that women who expect pain at insertion are more likely to experience it. Encourage the patient to breathe diaphragmatically, and remind her that she is likely to be very happy with her choice of the IUD.
Many other interventions don’t seem to be effective, although they may be offered frequently. Unproven methods include administration of NSAIDs other than naproxen, use of misoprostol (which can increase cramping), application of topical lidocaine to the cervix, and insertion during menses (although the LNG-IUS is inserted during the menstrual period to render it effective during the first month of use).
The studies described here come from the general population of reproductive-age women. If a patient has cervical scarring or a history of difficult or painful insertion, she may be more likely to experience pain, and these data may not apply to her.
—Jennifer Gunter, MD
Dr. Gunter is an ObGyn in San Francisco. She is the author of The Preemie Primer: A Complete Guide for Parents of Premature Babies—from Birth through the Toddler Years and Beyond (Da Capo Press, 2010). Dr. Gunter blogs at www.drjengunter.com, and you can find her on Twitter at @DrJenGunter. She is an OBG Management Contributing Editor.
Dr. Gunter reports no financial relationships relevant to this article.
1. 2006 Pan EU study on female contraceptives [unpublished data]. Bayer Schering Pharma; 2007.
2. Moser WD, Martinex GM, Chandra A, Abma JC, Wilson SJ. Use of contraception and use of family planning services in the United States: 1982–2002. Advance data from vital and health statistics; No. 350. Hyattsville, Maryland: National Center for Health Statistics. 2004;350:1–36.
3. Finer LB, Jerman J, Kavanaugh ML. Changes in use of long-acting contraceptive methods in the United States, 2007–2009. Fertil Steril. 2012;98(4):893–897.
4. Ortiz ME, Croxatto HB, Bardin CW. Mechanisms of action of intrauterine devices. Obstet Gynecol Surv. 1996;51(12 Suppl):S42–S51.
5. Barbosa I, Olsson SE, Odlind V, Goncalves T, Coutinho E. Ovarian function after seven years’ use of a levonorgestrel IUD. Adv Contracept. 1995;11(2):85–95.
6. Committee on Adolescent Health Care Long-Acting Reversible Contraception Working Group; American College of Obstetricians and Gynecologists. Committee Opinion #539: Adolescents and long-acting reversible contraception: implants and intrauterine devices. Obstet Gynecol. 2012;120(4):983–988.
7. CDC. US medical eligibility criteria for contraceptive use, 2010. MMWR Early Release. http://www.cdc.gov/mmwr/pdf/rr/rr59e0528.pdf. Accessed August 18, 2013.
8. Grimes DA, Lopez LM, Schulz KF. Antibiotics for prevention with IUDs. Cochrane summaries. http://summaries.cochrane.org/CD001327/antibiotics-for-prevention-with-iuds. Published May 16, 2012. Accessed August 18, 2013.
9. Allen RH, Bartz D, Grimes DA, Hubacher D, O’Brien P. Interventions for pain with intrauterine device insertion. Cochrane Database Syst Rev. 2009; (3):CD007373.
10. Gemzell-Danielsson K, Schellschmidt I, Apter D. A randomized phase II study describing the efficacy, bleeding profile, and safety of two low-dose levonorgestrel-releasing intrauterine contraceptive systems and Mirena. Fertil Steril. 2012;97(3):616-622.e1-e3.
11. Grimes DA. Intrauterine devices (IUDs). In: Hatcher RA, ed. Contraceptive Technology. 19th ed. New York, New York: Ardent Media; 2007:117–143.
12. Hatcher RA. Contraceptive Technology. New York, New York: Ardent Media; 2011.
13. Adoni A, Ben C. The management of intrauterine devices following uterine perforation. Contraception. 1991;43(1):77.
14. Petta CA, Ferriani RA, Abrao MS, et al. Randomized clinical trial of a levonorgestrel-releasing intrauterine system and a depot GnRH analogue for the treatment of chronic pelvic pain in women with endometriosis. Hum Reprod. 2005;20(7):1993–1998.
15. Nelson AL, Fong JK. Intrauterine infusion of lidocaine does not reduce pain scores during IUD insertion. Contraception. 2013;88(1):37–40.
16. Karabayirli S, Ayrim AA, Muslu B. Comparison of the analgesic effects of oral tramadol and naproxen sodium on pain relief during IUD insertion. J Minim Invasive Gynecol. 2012;19(5):581–584.

Anne A. Moore, DNP, APN
Dr. Moore is Professor and Director of the Women’s Health Nurse Practitioner Program at the Vanderbilt University School of Nursing in Nashville, Tennessee. She serves on the OBG Management Board of Editors.
The author reports no financial relationships relevant to this article.
Anne A. Moore, DNP, APN
Dr. Moore is Professor and Director of the Women’s Health Nurse Practitioner Program at the Vanderbilt University School of Nursing in Nashville, Tennessee. She serves on the OBG Management Board of Editors.
The author reports no financial relationships relevant to this article.
Anne A. Moore, DNP, APN
Dr. Moore is Professor and Director of the Women’s Health Nurse Practitioner Program at the Vanderbilt University School of Nursing in Nashville, Tennessee. She serves on the OBG Management Board of Editors.
The author reports no financial relationships relevant to this article.
Long-acting reversible contraceptives (LARCs), which include intrauterine devices (IUDs), implants, and injectables, are being offered to more and more women because of their demonstrated safety, efficacy, and convenience. In other countries, as many as 50% of all women use an IUD, but the United States has been slow to adopt this option.1 In 2002, approximately 2% of US women used an IUD.2 That percentage rose to 5.2% between 2006 and 2008, according to a recent survey.3 In that survey, women consistently expressed a high degree of satisfaction with this method of contraception.3
So why aren’t more US women using an IUD?
A general fear of the IUD persists. Women may not even know why they fear the device; they may have simply heard that it is “bad for you.” The negative press the IUD has received in this country probably is related to poor outcomes associated with use of the Dalkon Shield IUD in the 1970s. As a reminder, the Dalkon Shield was blamed for many cases of pelvic inflammatory disease (PID) and other negative sequelae as a result of poor patient selection. In addition, some authorities believe the design of the device was severely flawed, with a string that permitted bacteria to get from the vagina to the uterus and tubes.
Today, clinicians and many patients are better educated about the prevention of chlamydia, the primary causative organism of PID and other sexually transmitted infections (STIs); patients also are better informed about safe sex practices. We now know that women should be screened for behaviors that could increase their risk for PID and render them poor candidates for the IUD.
Clinicians also have expressed concerns about reimbursement issues related to the IUD, as well as confusion and difficulty with insertion procedures and the potential for litigation. In this article, I address some of these issues in an attempt to increase the use of this highly effective contraceptive.
What’s available today
Today there are three IUDs available to US women (FIGURE):
The Copper IUD (ParaGard)—This device can be used for at least 10 years, although, in many countries, it is considered “permanent reversible contraception.” It has the advantage of being nonhormonal, making it an important option for women who cannot or will not use a hormonal contraceptive. Pregnancy is prevented through a “foreign body” effect and the spermicidal action of copper ions. The combination of these two influences prevents fertilization.4
The levonorgestrel-releasing intrauterine system (LNG-IUS) (Mirena)—This IUD is recommended for 5 years of use but may remain effective for as long as 7 years. It contains 52 mg of levonorgestrel, which it releases at a rate of approximately 20 μg/day. In addition to the foreign body effect, this IUD prevents pregnancy through progestogenic mechanisms: It thickens cervical mucus, thins the endometrium, and reduces sperm capacitation.5
The "mini" LNG-IUS (Skyla)—This newly marketed IUD is recommended for 3 years of use. It contains 13.5 mg of levonorgestrel, which it releases at a rate of 14 μg/day. It has the same mechanism of action as Mirena but may be easier to insert owing to its slightly smaller size and preloaded inserter.
Myth #1: The IUD is not suitable for teens and nulliparous women
This myth arose out of concerns about the smaller uterine cavity and cervical diameter of teens and nulliparous women. Today we know that an IUD can be inserted safely in this population. Moreover, because adolescents are at high risk for unintended pregnancy, they stand to benefit uniquely from LARC options, including the IUD. As the American College of Obstetricians and Gynecologists (ACOG) recommends in a recent Committee Opinion on adolescents and LARCs, the IUD should be a “first-line” option for all women of reproductive age.6
Myth #2: An IUD should not be inserted immediately after childbirth
For many years, it was assumed that an IUD should be inserted in the postpartum period only after uterine involution was completed. However, in 2010, the Centers for Disease Control and Prevention (CDC) published medical eligibility criteria for contraceptive use, which included the following recommendations for breastfeeding or non–breast-feeding women:
• Mirena was given a Level 2 recommendation (advantages outweigh risks) for insertion within 10 minutes after delivery of the placenta
• The copper IUD was given a Level 1 recommendation (no restrictions) for insertion within the same time interval
• From 10 minutes to 4 weeks postpartum, both devices have a Level 2 recommendation for insertion
• Beyond 4 weeks, both devices have a Level 1 recommendation for insertion.7
Immediate post-delivery insertion of an IUD has several benefits, including:
• a reduction in the risk of unintended pregnancy in women who are not breastfeeding
• providing new mothers with a LARC method.
Myth #3: Antibiotics and NSAIDs should be administered
This myth arose from concerns about PID and insertion-related pain. However, a Cochrane Database review found no benefit for prophylactic use of antibiotics prior to insertion of the copper or LNG-IUS devices to prevent PID.8
In fact, data indicate that the incidence of PID is low among women who are appropriate candidates for an IUD. Similarly, Allen and colleagues found that nonsteroidal anti-inflammatory drugs (NSAIDs) did not ameliorate symptoms of cramping during or immediately after insertion of an IUD.9
Myth #4: IUD insertion is difficult
In reality, both the copper IUD and Mirena are easy to insert. In addition, the smaller LNG-IUS (Skyla) comes more completely preloaded in its inserter. In a published Phase 2 trial comparing Mirena with two smaller, lower-dose levonorgestrel-releasing devices, with the lowest-dose product corresponding to the marketed Skyla product, all 738 women given Mirena or the smaller devices experienced successful placement, with 98.5% of placements achieved on the first attempt.10
Various studies have been conducted to evaluate methods to ease insertion, including use of intracervical lidocaine, vaginal and/or oral administration of misoprostol (Cytotec), and vaginal estrogen creams. None was found to be effective in controlled trials. (See the sidebar, “Data-driven tactics for reducing pain on IUD insertion,” by Jennifer Gunter, MD, on page 28.) In the small percentage of women in whom it is difficult to pass a uterine sound through the external and internal os, cervical dilators may be beneficial. Gentle, progressive dilation can be accomplished easily with minimal discomfort to the patient, easing IUD insertion dramatically.
If a clinician does not insert IUDs on a frequent basis, it is prudent to look over the insertion procedure prior to the patient’s arrival. The procedure then can be reviewed with the patient as part of informed consent, which should be documented in the chart.
No steps in the recommended insertion procedure should be omitted, and charting should reflect each step:
1. Perform a bimanual exam
2. Document the appearance of the vagina and cervix
3. Use betadine or another cleansing solution on the cervical portio
4. Apply the tenaculum to the cervix (anterior lip if the uterus is anteverted, posterior lip if it is retroverted)
5. Sound the uterus to determine the optimal depth of IUD insertion. (The recommended uterine depth is 6 to 10 cm. A smaller uterus increases the likelihood of perforation, pain, and expulsion.)
6. Insert the IUD (and document the ease or difficulty of insertion)
7. Trim the string to an appropriate length
8. Assess the patient’s condition after insertion
9. Schedule a return visit in 4 weeks.
Related Article Let’s increase our use of IUDs and improve contraceptive effectiveness in this country Robert L. Barbieri, MD
Myth #5: Perforation is common
Uterine perforation occurs in approximately 1 in every 1,000 insertions.11 If perforation occurs with a copper IUD, remove the device to prevent the formation of intraperitoneal adhesions.12 The LNG-IUS devices do not produce this reaction, although most experts agree that they should be removed when a perforation occurs.13
Anecdotal evidence suggests that perforation may be more common among breastfeeding women, but this finding is far from definitive.
How to select an IUD for a patient: 3 case studies
CASE 1: Heavy bleeding and signs of endometriosis
Amelia, a 26-year-old nulliparous white woman, visits your office for routine examination and asks about her contraceptive options. She has no notable medical history. She has a body mass index (BMI) of 20.2 kg/m2 and exercises regularly. Menarche occurred at age 13. Her menstrual cycles are regular but are getting heavier; she now “soaks” a tampon every hour. She also complains that her cramps are more difficult to manage. She takes ibuprofen 600 mg every 6 hours during the days of heaviest bleeding and cramping, but that approach doesn’t seem to be effective lately. She is in a stable sexual relationship with her boyfriend of 2 years, now her fiancé. They have been using condoms consistently as contraception but don’t plan to start a family for a “few years.” Amelia reports that their sex life is good, although she has been experiencing pain with deep penetration for about 6 months.
Examination reveals a clear cervix and nontender uterus, although the uterus is retroverted. Palpation of the ovaries indicates that they are normal. Her main complaints: dysmenorrhea and heavy menstrual bleeding.
What contraceptive would you suggest?
Amelia would be a good candidate for the LNG-IUS because she is in a stable relationship and wants to postpone pregnancy for several years. Although she has some symptoms suggestive of endometriosis (dyspareunia), they could be relieved by this method.14 Because thinning of the endometrial lining is an inherent mechanism of action of the LNG-IUS, this method could reduce her heavy bleeding.
She should be advised of the risks and benefits of the LNG-IUS, which can be inserted when she begins her next menstrual cycle.
CASE 2: Mother of two with no immediate desire for pregnancy
Tamika is a 19-year-old black woman (G2P2) who has arrived at your clinic for her 6-week postpartum visit. She is not breastfeeding. Her BMI is 25.7 kg/m2. She reports that her baby and 2-year-old are doing “OK” and says she does not want to get pregnant again anytime soon. She is in a relationship with the father of her baby and says he is “working a good job and taking care of me.” Her menstrual cycles have always been normal, with no cramping or heavy bleeding.
Examination reveals that her cervix is clear, her uterus is anteverted and nontender, and her ovaries appear to be normal.
Would this patient be a good candidate for a LARC?
Tamika is an excellent candidate for the copper IUD or LNG-IUS and should be educated about both methods. If she chooses an IUD, it can be inserted at the start of her next menstrual period.
These first two cases illustrate the importance of making no assumptions on the basis of general patient characteristics. Although Tamika may appear to be at greater risk for STI than Amelia, such “typecasting” may lead to inappropriate counseling.
Related Article Malpositioned IUDs: When you should intervene (and when you should not)
At the time of IUD insertion, both patients should be instructed to check for the IUD string periodically, and this recommendation should be documented in their charts.
CASE 3: Anovulatory patient with heavy periods
Mary, 25, is a nulliparous Hispanic woman who has been referred by her primary care provider. She has a BMI of 35.4 kg/m2 and has had menstrual problems since menarche at the age of 14. She reports that her periods are irregular and very heavy, with intermittent pelvic pain that she manages, with some success, with ibuprofen. She has never had a sexual relationship, but she has a boyfriend now and asks about her contraceptive options.
On examination, you discover that Mary has pubic hair distribution over her inner thigh, with primary escutcheon and acanthosis nigricans on the inner thigh. Her vulva is marked by multiple sebaceous cysts, and a speculum exam shows a large amount of estrogenic mucus and a clear cervix. Her uterus is anteverted and nontender. Her ovaries are palpable but may be enlarged, and transvaginal ultrasound reveals that they are cystic. Her diagnosis: hirsutism with probable polycystic ovary syndrome.
Would an IUD be appropriate?
Mary is not a good candidate for an IUD. Neither the copper IUD nor the LNG-IUS would suppress ovarian function sufficiently to reduce the growth of multiple follicles that occurs with polycystic ovary syndrome. She would benefit from a hormonal method (specifically, a combination oral contraceptive) to suppress follicular activity.
Time for a renaissance?
The IUD may be making a comeback. With the unintended pregnancy rate remaining consistently at about 50%, it is important that we offer our patients contraceptive methods that maximize efficacy, safety, and convenience. Today’s IUDs meet all these criteria.
Data-driven tactics for reducing pain on IUD insertion
Many patients worry about the potential for pain with IUD insertion—and this concern can dissuade them from choosing the IUD as a contraceptive. This is regrettable because the IUD has the highest satisfaction rating among reversible contraceptives, as well as the greatest efficacy.
How much pain can your patient expect? In one recent prospective study involving 40 women who received either 1.2% lidocaine or saline infused 3 minutes before IUD insertion, 33% of women reported a pain score of 5 or higher (on a scale of 0–10) at tenaculum placement. This finding means that two-thirds of women had a pain score of 4 or lower. In fact, 46% of women had a pain score of 2 or below.15 (The mean pain scores for insertion were similar with lidocaine and placebo [3.0 vs 3.7, respectively; P=.4]).
Pain reducing options
The evidence validates (or fails to disprove) the value of the following interventions to make insertion more comfortable for patients:
• Naproxen (550 mg) administration 40 minutes prior to insertion. One small study found it to be better than placebo.9
• Nonopioid pain medication. One small, randomized, double-blinded clinical trial found that tramadol was even more effective than naproxen at relieving insertion-related pain.16
• Injection of lidocaine into the cervix. Although this intervention is common, data supporting it are scarce. One small, high-quality study found no benefit, compared with placebo. However, if you have had success with this approach in the past, I would not discourage you from continuing to offer it, as a single small study is insufficient to disprove it.15 More data are needed.
• Keeping the patient calm. Anxiety increases the perception of pain. Studies have demonstrated that women who expect pain at insertion are more likely to experience it. Encourage the patient to breathe diaphragmatically, and remind her that she is likely to be very happy with her choice of the IUD.
Many other interventions don’t seem to be effective, although they may be offered frequently. Unproven methods include administration of NSAIDs other than naproxen, use of misoprostol (which can increase cramping), application of topical lidocaine to the cervix, and insertion during menses (although the LNG-IUS is inserted during the menstrual period to render it effective during the first month of use).
The studies described here come from the general population of reproductive-age women. If a patient has cervical scarring or a history of difficult or painful insertion, she may be more likely to experience pain, and these data may not apply to her.
—Jennifer Gunter, MD
Dr. Gunter is an ObGyn in San Francisco. She is the author of The Preemie Primer: A Complete Guide for Parents of Premature Babies—from Birth through the Toddler Years and Beyond (Da Capo Press, 2010). Dr. Gunter blogs at www.drjengunter.com, and you can find her on Twitter at @DrJenGunter. She is an OBG Management Contributing Editor.
Dr. Gunter reports no financial relationships relevant to this article.
Long-acting reversible contraceptives (LARCs), which include intrauterine devices (IUDs), implants, and injectables, are being offered to more and more women because of their demonstrated safety, efficacy, and convenience. In other countries, as many as 50% of all women use an IUD, but the United States has been slow to adopt this option.1 In 2002, approximately 2% of US women used an IUD.2 That percentage rose to 5.2% between 2006 and 2008, according to a recent survey.3 In that survey, women consistently expressed a high degree of satisfaction with this method of contraception.3
So why aren’t more US women using an IUD?
A general fear of the IUD persists. Women may not even know why they fear the device; they may have simply heard that it is “bad for you.” The negative press the IUD has received in this country probably is related to poor outcomes associated with use of the Dalkon Shield IUD in the 1970s. As a reminder, the Dalkon Shield was blamed for many cases of pelvic inflammatory disease (PID) and other negative sequelae as a result of poor patient selection. In addition, some authorities believe the design of the device was severely flawed, with a string that permitted bacteria to get from the vagina to the uterus and tubes.
Today, clinicians and many patients are better educated about the prevention of chlamydia, the primary causative organism of PID and other sexually transmitted infections (STIs); patients also are better informed about safe sex practices. We now know that women should be screened for behaviors that could increase their risk for PID and render them poor candidates for the IUD.
Clinicians also have expressed concerns about reimbursement issues related to the IUD, as well as confusion and difficulty with insertion procedures and the potential for litigation. In this article, I address some of these issues in an attempt to increase the use of this highly effective contraceptive.
What’s available today
Today there are three IUDs available to US women (FIGURE):
The Copper IUD (ParaGard)—This device can be used for at least 10 years, although, in many countries, it is considered “permanent reversible contraception.” It has the advantage of being nonhormonal, making it an important option for women who cannot or will not use a hormonal contraceptive. Pregnancy is prevented through a “foreign body” effect and the spermicidal action of copper ions. The combination of these two influences prevents fertilization.4
The levonorgestrel-releasing intrauterine system (LNG-IUS) (Mirena)—This IUD is recommended for 5 years of use but may remain effective for as long as 7 years. It contains 52 mg of levonorgestrel, which it releases at a rate of approximately 20 μg/day. In addition to the foreign body effect, this IUD prevents pregnancy through progestogenic mechanisms: It thickens cervical mucus, thins the endometrium, and reduces sperm capacitation.5
The "mini" LNG-IUS (Skyla)—This newly marketed IUD is recommended for 3 years of use. It contains 13.5 mg of levonorgestrel, which it releases at a rate of 14 μg/day. It has the same mechanism of action as Mirena but may be easier to insert owing to its slightly smaller size and preloaded inserter.
Myth #1: The IUD is not suitable for teens and nulliparous women
This myth arose out of concerns about the smaller uterine cavity and cervical diameter of teens and nulliparous women. Today we know that an IUD can be inserted safely in this population. Moreover, because adolescents are at high risk for unintended pregnancy, they stand to benefit uniquely from LARC options, including the IUD. As the American College of Obstetricians and Gynecologists (ACOG) recommends in a recent Committee Opinion on adolescents and LARCs, the IUD should be a “first-line” option for all women of reproductive age.6
Myth #2: An IUD should not be inserted immediately after childbirth
For many years, it was assumed that an IUD should be inserted in the postpartum period only after uterine involution was completed. However, in 2010, the Centers for Disease Control and Prevention (CDC) published medical eligibility criteria for contraceptive use, which included the following recommendations for breastfeeding or non–breast-feeding women:
• Mirena was given a Level 2 recommendation (advantages outweigh risks) for insertion within 10 minutes after delivery of the placenta
• The copper IUD was given a Level 1 recommendation (no restrictions) for insertion within the same time interval
• From 10 minutes to 4 weeks postpartum, both devices have a Level 2 recommendation for insertion
• Beyond 4 weeks, both devices have a Level 1 recommendation for insertion.7
Immediate post-delivery insertion of an IUD has several benefits, including:
• a reduction in the risk of unintended pregnancy in women who are not breastfeeding
• providing new mothers with a LARC method.
Myth #3: Antibiotics and NSAIDs should be administered
This myth arose from concerns about PID and insertion-related pain. However, a Cochrane Database review found no benefit for prophylactic use of antibiotics prior to insertion of the copper or LNG-IUS devices to prevent PID.8
In fact, data indicate that the incidence of PID is low among women who are appropriate candidates for an IUD. Similarly, Allen and colleagues found that nonsteroidal anti-inflammatory drugs (NSAIDs) did not ameliorate symptoms of cramping during or immediately after insertion of an IUD.9
Myth #4: IUD insertion is difficult
In reality, both the copper IUD and Mirena are easy to insert. In addition, the smaller LNG-IUS (Skyla) comes more completely preloaded in its inserter. In a published Phase 2 trial comparing Mirena with two smaller, lower-dose levonorgestrel-releasing devices, with the lowest-dose product corresponding to the marketed Skyla product, all 738 women given Mirena or the smaller devices experienced successful placement, with 98.5% of placements achieved on the first attempt.10
Various studies have been conducted to evaluate methods to ease insertion, including use of intracervical lidocaine, vaginal and/or oral administration of misoprostol (Cytotec), and vaginal estrogen creams. None was found to be effective in controlled trials. (See the sidebar, “Data-driven tactics for reducing pain on IUD insertion,” by Jennifer Gunter, MD, on page 28.) In the small percentage of women in whom it is difficult to pass a uterine sound through the external and internal os, cervical dilators may be beneficial. Gentle, progressive dilation can be accomplished easily with minimal discomfort to the patient, easing IUD insertion dramatically.
If a clinician does not insert IUDs on a frequent basis, it is prudent to look over the insertion procedure prior to the patient’s arrival. The procedure then can be reviewed with the patient as part of informed consent, which should be documented in the chart.
No steps in the recommended insertion procedure should be omitted, and charting should reflect each step:
1. Perform a bimanual exam
2. Document the appearance of the vagina and cervix
3. Use betadine or another cleansing solution on the cervical portio
4. Apply the tenaculum to the cervix (anterior lip if the uterus is anteverted, posterior lip if it is retroverted)
5. Sound the uterus to determine the optimal depth of IUD insertion. (The recommended uterine depth is 6 to 10 cm. A smaller uterus increases the likelihood of perforation, pain, and expulsion.)
6. Insert the IUD (and document the ease or difficulty of insertion)
7. Trim the string to an appropriate length
8. Assess the patient’s condition after insertion
9. Schedule a return visit in 4 weeks.
Related Article Let’s increase our use of IUDs and improve contraceptive effectiveness in this country Robert L. Barbieri, MD
Myth #5: Perforation is common
Uterine perforation occurs in approximately 1 in every 1,000 insertions.11 If perforation occurs with a copper IUD, remove the device to prevent the formation of intraperitoneal adhesions.12 The LNG-IUS devices do not produce this reaction, although most experts agree that they should be removed when a perforation occurs.13
Anecdotal evidence suggests that perforation may be more common among breastfeeding women, but this finding is far from definitive.
How to select an IUD for a patient: 3 case studies
CASE 1: Heavy bleeding and signs of endometriosis
Amelia, a 26-year-old nulliparous white woman, visits your office for routine examination and asks about her contraceptive options. She has no notable medical history. She has a body mass index (BMI) of 20.2 kg/m2 and exercises regularly. Menarche occurred at age 13. Her menstrual cycles are regular but are getting heavier; she now “soaks” a tampon every hour. She also complains that her cramps are more difficult to manage. She takes ibuprofen 600 mg every 6 hours during the days of heaviest bleeding and cramping, but that approach doesn’t seem to be effective lately. She is in a stable sexual relationship with her boyfriend of 2 years, now her fiancé. They have been using condoms consistently as contraception but don’t plan to start a family for a “few years.” Amelia reports that their sex life is good, although she has been experiencing pain with deep penetration for about 6 months.
Examination reveals a clear cervix and nontender uterus, although the uterus is retroverted. Palpation of the ovaries indicates that they are normal. Her main complaints: dysmenorrhea and heavy menstrual bleeding.
What contraceptive would you suggest?
Amelia would be a good candidate for the LNG-IUS because she is in a stable relationship and wants to postpone pregnancy for several years. Although she has some symptoms suggestive of endometriosis (dyspareunia), they could be relieved by this method.14 Because thinning of the endometrial lining is an inherent mechanism of action of the LNG-IUS, this method could reduce her heavy bleeding.
She should be advised of the risks and benefits of the LNG-IUS, which can be inserted when she begins her next menstrual cycle.
CASE 2: Mother of two with no immediate desire for pregnancy
Tamika is a 19-year-old black woman (G2P2) who has arrived at your clinic for her 6-week postpartum visit. She is not breastfeeding. Her BMI is 25.7 kg/m2. She reports that her baby and 2-year-old are doing “OK” and says she does not want to get pregnant again anytime soon. She is in a relationship with the father of her baby and says he is “working a good job and taking care of me.” Her menstrual cycles have always been normal, with no cramping or heavy bleeding.
Examination reveals that her cervix is clear, her uterus is anteverted and nontender, and her ovaries appear to be normal.
Would this patient be a good candidate for a LARC?
Tamika is an excellent candidate for the copper IUD or LNG-IUS and should be educated about both methods. If she chooses an IUD, it can be inserted at the start of her next menstrual period.
These first two cases illustrate the importance of making no assumptions on the basis of general patient characteristics. Although Tamika may appear to be at greater risk for STI than Amelia, such “typecasting” may lead to inappropriate counseling.
Related Article Malpositioned IUDs: When you should intervene (and when you should not)
At the time of IUD insertion, both patients should be instructed to check for the IUD string periodically, and this recommendation should be documented in their charts.
CASE 3: Anovulatory patient with heavy periods
Mary, 25, is a nulliparous Hispanic woman who has been referred by her primary care provider. She has a BMI of 35.4 kg/m2 and has had menstrual problems since menarche at the age of 14. She reports that her periods are irregular and very heavy, with intermittent pelvic pain that she manages, with some success, with ibuprofen. She has never had a sexual relationship, but she has a boyfriend now and asks about her contraceptive options.
On examination, you discover that Mary has pubic hair distribution over her inner thigh, with primary escutcheon and acanthosis nigricans on the inner thigh. Her vulva is marked by multiple sebaceous cysts, and a speculum exam shows a large amount of estrogenic mucus and a clear cervix. Her uterus is anteverted and nontender. Her ovaries are palpable but may be enlarged, and transvaginal ultrasound reveals that they are cystic. Her diagnosis: hirsutism with probable polycystic ovary syndrome.
Would an IUD be appropriate?
Mary is not a good candidate for an IUD. Neither the copper IUD nor the LNG-IUS would suppress ovarian function sufficiently to reduce the growth of multiple follicles that occurs with polycystic ovary syndrome. She would benefit from a hormonal method (specifically, a combination oral contraceptive) to suppress follicular activity.
Time for a renaissance?
The IUD may be making a comeback. With the unintended pregnancy rate remaining consistently at about 50%, it is important that we offer our patients contraceptive methods that maximize efficacy, safety, and convenience. Today’s IUDs meet all these criteria.
Data-driven tactics for reducing pain on IUD insertion
Many patients worry about the potential for pain with IUD insertion—and this concern can dissuade them from choosing the IUD as a contraceptive. This is regrettable because the IUD has the highest satisfaction rating among reversible contraceptives, as well as the greatest efficacy.
How much pain can your patient expect? In one recent prospective study involving 40 women who received either 1.2% lidocaine or saline infused 3 minutes before IUD insertion, 33% of women reported a pain score of 5 or higher (on a scale of 0–10) at tenaculum placement. This finding means that two-thirds of women had a pain score of 4 or lower. In fact, 46% of women had a pain score of 2 or below.15 (The mean pain scores for insertion were similar with lidocaine and placebo [3.0 vs 3.7, respectively; P=.4]).
Pain reducing options
The evidence validates (or fails to disprove) the value of the following interventions to make insertion more comfortable for patients:
• Naproxen (550 mg) administration 40 minutes prior to insertion. One small study found it to be better than placebo.9
• Nonopioid pain medication. One small, randomized, double-blinded clinical trial found that tramadol was even more effective than naproxen at relieving insertion-related pain.16
• Injection of lidocaine into the cervix. Although this intervention is common, data supporting it are scarce. One small, high-quality study found no benefit, compared with placebo. However, if you have had success with this approach in the past, I would not discourage you from continuing to offer it, as a single small study is insufficient to disprove it.15 More data are needed.
• Keeping the patient calm. Anxiety increases the perception of pain. Studies have demonstrated that women who expect pain at insertion are more likely to experience it. Encourage the patient to breathe diaphragmatically, and remind her that she is likely to be very happy with her choice of the IUD.
Many other interventions don’t seem to be effective, although they may be offered frequently. Unproven methods include administration of NSAIDs other than naproxen, use of misoprostol (which can increase cramping), application of topical lidocaine to the cervix, and insertion during menses (although the LNG-IUS is inserted during the menstrual period to render it effective during the first month of use).
The studies described here come from the general population of reproductive-age women. If a patient has cervical scarring or a history of difficult or painful insertion, she may be more likely to experience pain, and these data may not apply to her.
—Jennifer Gunter, MD
Dr. Gunter is an ObGyn in San Francisco. She is the author of The Preemie Primer: A Complete Guide for Parents of Premature Babies—from Birth through the Toddler Years and Beyond (Da Capo Press, 2010). Dr. Gunter blogs at www.drjengunter.com, and you can find her on Twitter at @DrJenGunter. She is an OBG Management Contributing Editor.
Dr. Gunter reports no financial relationships relevant to this article.
1. 2006 Pan EU study on female contraceptives [unpublished data]. Bayer Schering Pharma; 2007.
2. Moser WD, Martinex GM, Chandra A, Abma JC, Wilson SJ. Use of contraception and use of family planning services in the United States: 1982–2002. Advance data from vital and health statistics; No. 350. Hyattsville, Maryland: National Center for Health Statistics. 2004;350:1–36.
3. Finer LB, Jerman J, Kavanaugh ML. Changes in use of long-acting contraceptive methods in the United States, 2007–2009. Fertil Steril. 2012;98(4):893–897.
4. Ortiz ME, Croxatto HB, Bardin CW. Mechanisms of action of intrauterine devices. Obstet Gynecol Surv. 1996;51(12 Suppl):S42–S51.
5. Barbosa I, Olsson SE, Odlind V, Goncalves T, Coutinho E. Ovarian function after seven years’ use of a levonorgestrel IUD. Adv Contracept. 1995;11(2):85–95.
6. Committee on Adolescent Health Care Long-Acting Reversible Contraception Working Group; American College of Obstetricians and Gynecologists. Committee Opinion #539: Adolescents and long-acting reversible contraception: implants and intrauterine devices. Obstet Gynecol. 2012;120(4):983–988.
7. CDC. US medical eligibility criteria for contraceptive use, 2010. MMWR Early Release. http://www.cdc.gov/mmwr/pdf/rr/rr59e0528.pdf. Accessed August 18, 2013.
8. Grimes DA, Lopez LM, Schulz KF. Antibiotics for prevention with IUDs. Cochrane summaries. http://summaries.cochrane.org/CD001327/antibiotics-for-prevention-with-iuds. Published May 16, 2012. Accessed August 18, 2013.
9. Allen RH, Bartz D, Grimes DA, Hubacher D, O’Brien P. Interventions for pain with intrauterine device insertion. Cochrane Database Syst Rev. 2009; (3):CD007373.
10. Gemzell-Danielsson K, Schellschmidt I, Apter D. A randomized phase II study describing the efficacy, bleeding profile, and safety of two low-dose levonorgestrel-releasing intrauterine contraceptive systems and Mirena. Fertil Steril. 2012;97(3):616-622.e1-e3.
11. Grimes DA. Intrauterine devices (IUDs). In: Hatcher RA, ed. Contraceptive Technology. 19th ed. New York, New York: Ardent Media; 2007:117–143.
12. Hatcher RA. Contraceptive Technology. New York, New York: Ardent Media; 2011.
13. Adoni A, Ben C. The management of intrauterine devices following uterine perforation. Contraception. 1991;43(1):77.
14. Petta CA, Ferriani RA, Abrao MS, et al. Randomized clinical trial of a levonorgestrel-releasing intrauterine system and a depot GnRH analogue for the treatment of chronic pelvic pain in women with endometriosis. Hum Reprod. 2005;20(7):1993–1998.
15. Nelson AL, Fong JK. Intrauterine infusion of lidocaine does not reduce pain scores during IUD insertion. Contraception. 2013;88(1):37–40.
16. Karabayirli S, Ayrim AA, Muslu B. Comparison of the analgesic effects of oral tramadol and naproxen sodium on pain relief during IUD insertion. J Minim Invasive Gynecol. 2012;19(5):581–584.
1. 2006 Pan EU study on female contraceptives [unpublished data]. Bayer Schering Pharma; 2007.
2. Moser WD, Martinex GM, Chandra A, Abma JC, Wilson SJ. Use of contraception and use of family planning services in the United States: 1982–2002. Advance data from vital and health statistics; No. 350. Hyattsville, Maryland: National Center for Health Statistics. 2004;350:1–36.
3. Finer LB, Jerman J, Kavanaugh ML. Changes in use of long-acting contraceptive methods in the United States, 2007–2009. Fertil Steril. 2012;98(4):893–897.
4. Ortiz ME, Croxatto HB, Bardin CW. Mechanisms of action of intrauterine devices. Obstet Gynecol Surv. 1996;51(12 Suppl):S42–S51.
5. Barbosa I, Olsson SE, Odlind V, Goncalves T, Coutinho E. Ovarian function after seven years’ use of a levonorgestrel IUD. Adv Contracept. 1995;11(2):85–95.
6. Committee on Adolescent Health Care Long-Acting Reversible Contraception Working Group; American College of Obstetricians and Gynecologists. Committee Opinion #539: Adolescents and long-acting reversible contraception: implants and intrauterine devices. Obstet Gynecol. 2012;120(4):983–988.
7. CDC. US medical eligibility criteria for contraceptive use, 2010. MMWR Early Release. http://www.cdc.gov/mmwr/pdf/rr/rr59e0528.pdf. Accessed August 18, 2013.
8. Grimes DA, Lopez LM, Schulz KF. Antibiotics for prevention with IUDs. Cochrane summaries. http://summaries.cochrane.org/CD001327/antibiotics-for-prevention-with-iuds. Published May 16, 2012. Accessed August 18, 2013.
9. Allen RH, Bartz D, Grimes DA, Hubacher D, O’Brien P. Interventions for pain with intrauterine device insertion. Cochrane Database Syst Rev. 2009; (3):CD007373.
10. Gemzell-Danielsson K, Schellschmidt I, Apter D. A randomized phase II study describing the efficacy, bleeding profile, and safety of two low-dose levonorgestrel-releasing intrauterine contraceptive systems and Mirena. Fertil Steril. 2012;97(3):616-622.e1-e3.
11. Grimes DA. Intrauterine devices (IUDs). In: Hatcher RA, ed. Contraceptive Technology. 19th ed. New York, New York: Ardent Media; 2007:117–143.
12. Hatcher RA. Contraceptive Technology. New York, New York: Ardent Media; 2011.
13. Adoni A, Ben C. The management of intrauterine devices following uterine perforation. Contraception. 1991;43(1):77.
14. Petta CA, Ferriani RA, Abrao MS, et al. Randomized clinical trial of a levonorgestrel-releasing intrauterine system and a depot GnRH analogue for the treatment of chronic pelvic pain in women with endometriosis. Hum Reprod. 2005;20(7):1993–1998.
15. Nelson AL, Fong JK. Intrauterine infusion of lidocaine does not reduce pain scores during IUD insertion. Contraception. 2013;88(1):37–40.
16. Karabayirli S, Ayrim AA, Muslu B. Comparison of the analgesic effects of oral tramadol and naproxen sodium on pain relief during IUD insertion. J Minim Invasive Gynecol. 2012;19(5):581–584.
UPDATE ON TECHNOLOGY
The development of new medical technology continues at a brisk pace—and ObGyns and our patients often are the beneficiaries. Notable technological breakthroughs of the past include hormonal contraception, in vitro fertilization, the application of minimally invasive surgical devices and techniques to gynecologic procedures, and many other innovations.
The leaders in our specialty are innovators themselves, ever vigilant for developments that can help improve health and quality of life for our patients. Regrettably, however, many technologies spread widely before they are fully validated by published studies—or continue to be used long after a superior or less invasive intervention has come along. And many claims about new technology are based on marketing information rather than reliable data.
Another common occurrence in regard to published data: Findings in one well-defined sector of the population are extrapolated to all patients. Even clinicians who are careful about adopting new technology can overlook the fact that it was tested, and proven, in a subset of patients that may not be comparable to all their patients.
In this article, I offer two case studies that illustrate some of the challenges we face when it comes to applying scientific findings to our practice and assessing medical technologies. In both settings, the health of the patient should be our primary focus.
When it comes to technology, patient selection is key
CASE 1: Anovulatory patient requests endometrial ablation
A 34-year-old woman (G2P2) who is moderately obese (body mass index of 32 kg/m2) visits your office to request endometrial ablation to manage her irregular and heavy menses. She reached menarche at age 10, and her periods have been somewhat irregular ever since. She required ovarian stimulation with clomiphene citrate to achieve each of her pregnancies, and both children were delivered by cesarean section. She currently uses condoms for contraception but does not have a steady partner, and she desires no additional pregnancies.
The patient reports that her menses occur every 2 to 6 weeks, with flow lasting from 2 to 8 days. She is housebound for 2 days each cycle because of heavy flow and cramping. She takes no medications and has no other medical conditions.
On exam, she is centrally obese with a tender uterus that is 10- to 12-weeks’ size; no adnexal masses are palpable. All other findings are normal. A recent test for diabetes was negative, but her serum cholesterol and triglyceride levels are borderline elevated.
What intervention would you recommend to address the heavy bleeding?
With the advent of second-generation endometrial ablation devices in the late 1990s, women with refractory menorrhagia had a safe, reliable, minimally invasive alternative to hysterectomy that made it possible to treat the endometrial cavity without the technical challenges of resectoscopic surgery. More than 10 million women report menorrhagia each year in the United States—so it is no small problem.1,2 Global endometrial ablation devices make management possible in an office setting, and recovery is significantly shorter than with hysterectomy. The three most prominent nonhysteroscopic ablation devices are (FIGURE):

• NovaSure (Hologic) uses bipolar radiofrequency energy to ablate tissue. Its probe contains stretchable gold-plated fabric that conforms to the endometrial surface.
• Gynecare Thermachoice (Ethicon) consists of an intrauterine balloon that is filled with hot liquid (temperatures of roughly 87°C) to ablate the endometrium
• Her Option (CooperSurgical) is a cryoablation system that consists of an intrauterine probe that forms an ice ball (temperatures of roughly –90°C) that destroys the uterine lining. Several applications are required to treat the majority of the cavity.
Use of these devices is widespread, although a nonsurgical alternative—the levonorgestrel-releasing intrauterine system (LNG-IUS; Mirena)—was approved by the US Food and Drug Administration (FDA) in 2009 for the treatment of heavy menstrual bleeding.
Not only is the efficacy of the LNG-IUS for controlling menorrhagia equal to endometrial ablation, but it provides the additional benefits of reliable contraception and management of dysmenorrhea.
6 questions to ask before applying a technology
1. In which population was it studied?
One of the most important issues to consider when you are evaluating technology is the population in which it was studied. In other words, to whom do the findings apply?
Most endometrial ablation technologies were tested in women who had a uterus of normal size (mean, 8 cm) with no structural abnormalities (ie, no polyps or fibroids) and regular but very heavy periods. The findings from these studies now have been extrapolated in many cases to women who have hormonally induced abnormal bleeding, whose periods are irregular. That extrapolation may not be appropriate.
2. What is the diagnosis?
As the manufacturers of global endometrial ablation devices note, heavy menstrual bleeding may arise from an underlying condition, such as endometrial cancer, hormonal imbalance, fibroids, coagulopathy, and so on—and it is important to rule these conditions out before considering endometrial ablation.
For example, in Case 1, the patient is experiencing anovulatory cycles, as evidenced by her irregular menses and the need for ovulation induction to achieve her pregnancies. The success rate of endometrial ablation in the setting of chronic anovulation is unknown. Pivotal trials for all of the nonhysteroscopic endometrial ablation technologies required regular menses or failure of cyclic hormonal therapy prior to enrollment.
In addition, in Case 1, the patient has signs (an enlarged, tender uterus) that suggest the presence of adenomyosis. Endometrial ablation is not recommended as a treatment for women with this condition.
3. Will later surgery be required?
In one study from Kaiser Permanente of Northern California, 21% of women who underwent endometrial ablation for menorrhagia later underwent hysterectomy, and 3.9% underwent other uterine-sparing procedures to alleviate heavy bleeding.3
In that study, women younger than age 45 were 2.1 times more likely to require hysterectomy after endometrial ablation, compared with older women (95% confidence interval [CI], 1.8–2.4). The likelihood of hysterectomy increased with each decreasing stratum of age and exceeded 40% in women aged 40 years or younger.3
In a population-based retrospective cohort study from Scotland, 2,779 (19.7%) of 11,299 women who underwent endometrial ablation for heavy menstrual bleeding required hysterectomy later.4 Again, women who required hysterectomy after endometrial ablation tended to be younger than those who did not. Overall, 26.6% of women undergoing endometrial ablation for heavy menstrual bleeding required further surgery.4
And in a 5-year follow-up of patients participating in a randomized trial of uterine balloon therapy versus rollerball ablation, roughly 30% of women required subsequent surgery for heavy menstrual bleeding.5
The need for subsequent surgery following endometrial ablation is likely to be higher among women who do not match the profile of participants in pivotal trials of the devices. All patients considering endometrial ablation should be counseled about the possible need for further surgery.
Related Article The economics of surgical gynecology: How we can not only survive, but thrive, in the 21st Century Barbara S. Levy, MD
4. What is the patient's overall health?
Before selecting an intervention for heavy menstrual bleeding, it is important to consider the patient’s overall health. What comorbidities does she have? Is pain a component of her condition? If so, might she have endometriosis or adenomyosis, as our patient does? If pain is a significant component of her menorrhagia, is it cyclical—that is, does it correspond to the days of heaviest flow? Pain related to the passage of large clots during menses may respond well to endometrial ablation. Pelvic pain occurring before and after the flow probably won’t.
Also keep in mind that the patient in Case 1 has two risk factors for endometrial hyperplasia: anovulatory cycles and obesity. If she undergoes endometrial ablation and subsequently experiences abnormal uterine bleeding, the most prominent sign of endometrial hyperplasia, how will you assess her endometrium 5 years after ablation if she develops abnormal bleeding? Will you be able to adequately sample it?
5. Have less invasive options been tried?
Many of the women studied in pivotal trials of second-generation endometrial ablation devices failed medical therapy prior to undergoing ablation. Because medical therapy is less expensive and noninvasive, it makes sense to offer it before proceeding to surgery. Common pharmacologic approaches include nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives, and tranexamic acid.
In addition, as I mentioned earlier, Mirena is approved for treatment of heavy menstrual bleeding.
Medical therapy and Mirena should be offered prior to surgery because of their noninvasive, reversible nature. Most physicians now consider Mirena to be the first-line option for heavy menstrual bleeding in women who have normal anatomy.6
6. What is the cost of treatment?
With health-care expenses accelerating, we need to be mindful of the cost-effectiveness of the options we recommend.
Let’s assess the expense of managing the patient in Case 1. To address her desire for long-term contraception, we might offer tubal sterilization by laparoscopy followed by endometrial ablation (to address the heavy bleeding), which would require a general anesthetic and management in an ambulatory surgical facility.
If she opts for hysteroscopic sterilization prior to endometrial ablation, the sterilization procedure must be performed at least 3 months prior to ablation (according to FDA labeling) so that tubal occlusion can be demonstrated by hysterosalpingography (HSG) before the uterine cavity is scarred. This means that the patient would require two separate interventions. Although both procedures could be performed in an office setting, the patient would still require time away from work and family.
The cost for sterilization plus ablation in the office without anesthesia would be approximately $4,500 (including HSG) at Medicare rates. For a combined laparoscopic sterilization and endometrial ablation, costs would be higher because of the need for anesthesia and an ambulatory surgical facility. Another option that would address both the heavy bleeding and the need for contraception: oral contraceptives (OCs). The overall cost of this approach over 5 years would be $4,200 (60 months of OCs at $70/month), but it would be fully covered under the Affordable Care Act (ACA), so the patient would have no out-of-pocket expense. The cost of Mirena would be $1,000 ($850 for the device plus $150 for insertion), but it also would be fully covered under the ACA.
CASE 1: Resolved
You discuss the option of cyclic OCs with the patient. This approach would help control her irregular, heavy, and painful menses while providing good contraceptive coverage.
Although sterilization plus endometrial ablation is an option, you counsel the patient that the published “success” rates do not apply to her. Given her young age, obesity, and anovulatory status, endometrial ablation has a greater likelihood of failure. Further, when abnormal bleeding recurs, it may be difficult to assess this high-risk patient’s endometrium.
You also discuss Mirena, which would provide long-term contraception and also manage her menorrhagia and dysmenorrhea; indeed, it is FDA-approved for this indication. In fact, Mirena would address all of this patient’s concerns, offering superb contraception and reliable reductions in bleeding and pelvic pain in the setting of endometriosis and adenomyosis.
Overall, this woman is best served by a highly reliable approach that manages her contraceptive needs and her menorrhagia and dysmenorrhea while reducing her risk for endometrial hyperplasia and cancer. Given the long-term endometrial-sampling problems ablation would create, it is not an optimal solution for this woman.
What this evidence means for practice
When assessing technology, consider which patients it was tested in, your patient’s diagnosis and long-term health risks, the cost and success rate of the technology, and the availability of less invasive options.
How to assess new data on a technology or procedure
Gill SE, Mills BB. Physician opinions regarding elective bilateral salpingectomy with hysterectomy and for sterilization. JMIG. 2013;20(4):517–521.
CASE 2: A healthy patient seeks permanent contraception
At her annual well-woman visit, your 42-year-old patient (G3P3) asks to discuss permanent contraception now that she has completed her family. She has used OCs for more than 10 years without problems. She is a nonsmoker of normal weight (BMI of 22 kg/m2), with normal blood pressure and vital signs. Her family history is remarkable for the health of her parents and siblings: Her mother is 68 years old and well; her father, 70, also is healthy. There is no family history of breast or ovarian cancer, prostate cancer, or significant medical illness.
What options would you offer this patient? Given recent data suggesting that ovarian cancer may originate in the fallopian tubes, would you recommend prophylactic salpingectomy as her contraceptive method of choice?
This patient has many options. In describing them to her, it would be important to focus on the breadth of safe, reversible, long-acting contraceptives now available, including their respective risks, benefits, and long-term outcomes and costs. It also is important to consider the published data on these methods, weighing their relevance to her overall health and medical history. Although some data regarding the origin of ovarian cancer in the fallopian tubes may be especially compelling, it may not be wise to extrapolate it from a specific group of women to all patients, as we shall see.
Option 1: Cyclic OCs
This option should not be excluded, despite the need for daily dosing, because the patient has used it successfully for more than 10 years. OCs are highly effective and have the added benefits of reducing menstrual blood loss, alleviating cramps, and lowering the risks of endometrial and ovarian cancer.7
Option 2: LARC
Long-acting reversible contraceptive (LARC) methods include the LNG-IUS, the copper intrauterine device (IUD; ParaGard, Teva), and the etonogestrel implant (Nexplanon, Merck). Each of these contraceptives is similar to sterilization in terms of efficacy. None requires the interruption of sexual activity or weekly or monthly trips to the pharmacy.
The LNG-IUS and the etonogestrel implant have the added benefits of reducing menstrual blood loss and reducing or eliminating premenstrual symptoms and cramps in most women. In addition, they may reduce the risk of unopposed estrogen stimulation of the endometrium associated with perimenopausal anovulatory cycles.
Option 3: Transcervical tubal sterilization
This hysteroscopic method (Essure, Bayer) avoids the risks of general anesthesia, but successful bilateral placement may not be possible in a small percentage of women. It also requires a 3-month interval between placement and confirmation of tubal occlusion (via HSG). During this interval, alternative contraception must be used. Once occlusion is confirmed, this method is highly reliable.
Option 4: Laparoscopic sterilization
This approach was the method of choice prior to the introduction of Essure in 2002. There now is a resurgence of interest in laparoscopic sterilization due to recent publications describing the distal portion of the fallopian tube as the “true source” of high-grade serous ovarian cancers.
In pathologic analyses of fallopian tubes removed prophylactically from women with a BRCA 1 or 2 mutation, investigators found a significant rate of serous tubal intraepithelial carcinoma.8 Researchers began to study the genetics of these cancers and concluded that, in women with a BRCA mutation, high-grade serous carcinomas may arise from the distal fallopian tube.
Until recently, all of the literature on these tubal carcinomas related only to women with a specific tumor suppressor gene p53 mutation in the BRCA system. Other investigators then reviewed pathology specimens from women without a BRCA mutation who had high-grade serous carcinomas that were peritoneal, tubal, or ovarian in origin. They found serous tubal intraepithelial carcinomas in 33% to 59% of these women.9
“Research suggests that bilateral salpingectomy during hysterectomy for benign indications or as a sterilization procedure may have benefits, such as preventing tubal disease and cancer, without significant risks,” wrote Gill and Mills.10 In conducting a survey of US physicians to determine how widespread prophylactic salpingectomy is during benign hysterectomy or sterilization, they found that 54% of respondents performed bilateral salpingectomy during hysterectomy, usually to lower the risk of cancer (75%) and avoid the need for reoperation (49.1%). Of the 45.5% of respondents who did not perform bilateral salpingectomy during hysterectomy, most (69.4%) believed it has no benefit.10
Although 58% of respondents believed bilateral salpingectomy to be the most effective option for sterilization in women older than 35 years, they reported that they reserve it for women in whom one sterilization procedure has failed or for women who have tubal disease.10
As for the 45.5% of respondents who did not perform prophylactic salpingectomy, they offered as reasons their concern about increased operative time and the risk of complications, as well as a belief that it has no benefit.10
The lifetime risk of ovarian cancer in the general population is 1 in 70 women. Although it is possible that high-grade serous ovarian cancers originate in the distal fallopian tube, as the research to date suggests, it also is possible that we might find in-situ lesions in tissues other than the distal tube, suggesting a more global genetic defect underlying ovarian cancers in the peritoneal and müllerian tissues. Randomized trials are under way in an effort to determine whether excision of the fallopian tubes will prevent the majority of high-grade serous cancers. It will be many years, however, before the results of these trials are available.
CASE 2: Resolved
This patient has used combination OCs for more than 10 years, so her lifetime risk of ovarian cancer has been reduced by approximately 50%. Because her family history indicates that a BRCA mutation is highly unlikely, her lifetime risk of ovarian cancer now has declined from 1:70 to roughly 1:140.
Prophylactic salpingectomy might offer a very small reduction in this patient’s absolute risk of ovarian cancer—from 0.75% to 0.50% lifetime risk—but the current data are not robust enough to suggest that it should be recommended for her. The operation would carry the risks associated with general anesthesia and peritoneal access. Although these risks are small, there is a documented risk of death from laparoscopic sterilization procedures in the United States, from complications related to bowel injury, anesthesia, and hemorrhage.
For these reasons, I would counsel this patient that her best options for contraception are combination OCs, transcervical tubal sterilization, or a long-acting reversible contraceptive such as the IUD or implant.
Tell us what you think, at [email protected]. Please include your name and city and state.
1. Centers for Disease Control and Prevention. Blood disor-ders in women: heavy menstrual bleeding. http://www.cdc.gov/ncbddd/blooddisorders/women/menorrhagia.html. Updated December 12, 2011. Accessed August 15, 2013.
2. Centers for Disease Control and Prevention. Blood disorders in women: research. http://www.cdc.gov/ncbddd/blooddis orders/women/research.html. Updated December 12, 2011. Accessed August 15, 2013.
3. Longinotti K, Jacobson GF, Hung YY, Learman LA. Probability of hysterectomy after endometrial ablation. Obstet Gynecol. 2008;112(6):1214–1220.
4. Cooper K, Lee AJ, Chien P, Raja EA, Timmaraju V, Bhattacharya S. Outcomes following hysterectomy or endometrial ablation for heavy menstrual bleeding: retrospective analysis of hospital episode statistics in Scotland. BJOG. 2011;118(10):1171–1179.
5. Loffer FD, Grainger D. Five-year follow-up of patients participating in a randomized trial of uterine balloon therapy versus rollerball ablation for treatment of menorrhagia. J Am Assoc Gynecol Laparosc. 2002;9(4):429–435.
6. Sayre C. Beyond hysterectomy: Alternative options for heavy bleeding. NY Times. http://www.nytimes.com/ref/health/healthguide/esn-menorrhagia-ess.html. Published October 10, 2008. Accessed August 15, 2013.
7. Havrilesky LJ, Moorman PG, Lowery WJ, et al. Oral contraceptive pills as primary prevention for ovarian cancer. A systematic review and meta-analysis. Obstet Gynecol. 2013;122(1):139–147.
8. Kindelberger DW, Lee Y, Miron A, et al. Intraepithelial carcinoma of the fimbria and pelvic serous carcinoma: evidence for a causal relationship. Am J Surg Pathol. 2007; 31:161–169.
9. Crum CP, McKeon FD, Xian W. The oviduct and ovarian cancer: causality, clinical implications, and “targeted prevention.” Clin Obstet Gynecol. 2012;55(1):24–35.
10. Gill SE, Mills BB. Physician opinions regarding elective bilateral salpingectomy with hysterectomy and for sterilization. JMIG. 2013;20(4):517–521.

Barbara S. Levy, MD
Dr. Levy is Vice President for Health Policy at the American Congress of Obstetricians and Gynecologists in Washington, DC.
The author reports no financial relationships relevant to this article.
Barbara S. Levy, MD
Dr. Levy is Vice President for Health Policy at the American Congress of Obstetricians and Gynecologists in Washington, DC.
The author reports no financial relationships relevant to this article.
Barbara S. Levy, MD
Dr. Levy is Vice President for Health Policy at the American Congress of Obstetricians and Gynecologists in Washington, DC.
The author reports no financial relationships relevant to this article.
The development of new medical technology continues at a brisk pace—and ObGyns and our patients often are the beneficiaries. Notable technological breakthroughs of the past include hormonal contraception, in vitro fertilization, the application of minimally invasive surgical devices and techniques to gynecologic procedures, and many other innovations.
The leaders in our specialty are innovators themselves, ever vigilant for developments that can help improve health and quality of life for our patients. Regrettably, however, many technologies spread widely before they are fully validated by published studies—or continue to be used long after a superior or less invasive intervention has come along. And many claims about new technology are based on marketing information rather than reliable data.
Another common occurrence in regard to published data: Findings in one well-defined sector of the population are extrapolated to all patients. Even clinicians who are careful about adopting new technology can overlook the fact that it was tested, and proven, in a subset of patients that may not be comparable to all their patients.
In this article, I offer two case studies that illustrate some of the challenges we face when it comes to applying scientific findings to our practice and assessing medical technologies. In both settings, the health of the patient should be our primary focus.
When it comes to technology, patient selection is key
CASE 1: Anovulatory patient requests endometrial ablation
A 34-year-old woman (G2P2) who is moderately obese (body mass index of 32 kg/m2) visits your office to request endometrial ablation to manage her irregular and heavy menses. She reached menarche at age 10, and her periods have been somewhat irregular ever since. She required ovarian stimulation with clomiphene citrate to achieve each of her pregnancies, and both children were delivered by cesarean section. She currently uses condoms for contraception but does not have a steady partner, and she desires no additional pregnancies.
The patient reports that her menses occur every 2 to 6 weeks, with flow lasting from 2 to 8 days. She is housebound for 2 days each cycle because of heavy flow and cramping. She takes no medications and has no other medical conditions.
On exam, she is centrally obese with a tender uterus that is 10- to 12-weeks’ size; no adnexal masses are palpable. All other findings are normal. A recent test for diabetes was negative, but her serum cholesterol and triglyceride levels are borderline elevated.
What intervention would you recommend to address the heavy bleeding?
With the advent of second-generation endometrial ablation devices in the late 1990s, women with refractory menorrhagia had a safe, reliable, minimally invasive alternative to hysterectomy that made it possible to treat the endometrial cavity without the technical challenges of resectoscopic surgery. More than 10 million women report menorrhagia each year in the United States—so it is no small problem.1,2 Global endometrial ablation devices make management possible in an office setting, and recovery is significantly shorter than with hysterectomy. The three most prominent nonhysteroscopic ablation devices are (FIGURE):
• NovaSure (Hologic) uses bipolar radiofrequency energy to ablate tissue. Its probe contains stretchable gold-plated fabric that conforms to the endometrial surface.
• Gynecare Thermachoice (Ethicon) consists of an intrauterine balloon that is filled with hot liquid (temperatures of roughly 87°C) to ablate the endometrium
• Her Option (CooperSurgical) is a cryoablation system that consists of an intrauterine probe that forms an ice ball (temperatures of roughly –90°C) that destroys the uterine lining. Several applications are required to treat the majority of the cavity.
Use of these devices is widespread, although a nonsurgical alternative—the levonorgestrel-releasing intrauterine system (LNG-IUS; Mirena)—was approved by the US Food and Drug Administration (FDA) in 2009 for the treatment of heavy menstrual bleeding.
Not only is the efficacy of the LNG-IUS for controlling menorrhagia equal to endometrial ablation, but it provides the additional benefits of reliable contraception and management of dysmenorrhea.
6 questions to ask before applying a technology
1. In which population was it studied?
One of the most important issues to consider when you are evaluating technology is the population in which it was studied. In other words, to whom do the findings apply?
Most endometrial ablation technologies were tested in women who had a uterus of normal size (mean, 8 cm) with no structural abnormalities (ie, no polyps or fibroids) and regular but very heavy periods. The findings from these studies now have been extrapolated in many cases to women who have hormonally induced abnormal bleeding, whose periods are irregular. That extrapolation may not be appropriate.
2. What is the diagnosis?
As the manufacturers of global endometrial ablation devices note, heavy menstrual bleeding may arise from an underlying condition, such as endometrial cancer, hormonal imbalance, fibroids, coagulopathy, and so on—and it is important to rule these conditions out before considering endometrial ablation.
For example, in Case 1, the patient is experiencing anovulatory cycles, as evidenced by her irregular menses and the need for ovulation induction to achieve her pregnancies. The success rate of endometrial ablation in the setting of chronic anovulation is unknown. Pivotal trials for all of the nonhysteroscopic endometrial ablation technologies required regular menses or failure of cyclic hormonal therapy prior to enrollment.
In addition, in Case 1, the patient has signs (an enlarged, tender uterus) that suggest the presence of adenomyosis. Endometrial ablation is not recommended as a treatment for women with this condition.
3. Will later surgery be required?
In one study from Kaiser Permanente of Northern California, 21% of women who underwent endometrial ablation for menorrhagia later underwent hysterectomy, and 3.9% underwent other uterine-sparing procedures to alleviate heavy bleeding.3
In that study, women younger than age 45 were 2.1 times more likely to require hysterectomy after endometrial ablation, compared with older women (95% confidence interval [CI], 1.8–2.4). The likelihood of hysterectomy increased with each decreasing stratum of age and exceeded 40% in women aged 40 years or younger.3
In a population-based retrospective cohort study from Scotland, 2,779 (19.7%) of 11,299 women who underwent endometrial ablation for heavy menstrual bleeding required hysterectomy later.4 Again, women who required hysterectomy after endometrial ablation tended to be younger than those who did not. Overall, 26.6% of women undergoing endometrial ablation for heavy menstrual bleeding required further surgery.4
And in a 5-year follow-up of patients participating in a randomized trial of uterine balloon therapy versus rollerball ablation, roughly 30% of women required subsequent surgery for heavy menstrual bleeding.5
The need for subsequent surgery following endometrial ablation is likely to be higher among women who do not match the profile of participants in pivotal trials of the devices. All patients considering endometrial ablation should be counseled about the possible need for further surgery.
Related Article The economics of surgical gynecology: How we can not only survive, but thrive, in the 21st Century Barbara S. Levy, MD
4. What is the patient's overall health?
Before selecting an intervention for heavy menstrual bleeding, it is important to consider the patient’s overall health. What comorbidities does she have? Is pain a component of her condition? If so, might she have endometriosis or adenomyosis, as our patient does? If pain is a significant component of her menorrhagia, is it cyclical—that is, does it correspond to the days of heaviest flow? Pain related to the passage of large clots during menses may respond well to endometrial ablation. Pelvic pain occurring before and after the flow probably won’t.
Also keep in mind that the patient in Case 1 has two risk factors for endometrial hyperplasia: anovulatory cycles and obesity. If she undergoes endometrial ablation and subsequently experiences abnormal uterine bleeding, the most prominent sign of endometrial hyperplasia, how will you assess her endometrium 5 years after ablation if she develops abnormal bleeding? Will you be able to adequately sample it?
5. Have less invasive options been tried?
Many of the women studied in pivotal trials of second-generation endometrial ablation devices failed medical therapy prior to undergoing ablation. Because medical therapy is less expensive and noninvasive, it makes sense to offer it before proceeding to surgery. Common pharmacologic approaches include nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives, and tranexamic acid.
In addition, as I mentioned earlier, Mirena is approved for treatment of heavy menstrual bleeding.
Medical therapy and Mirena should be offered prior to surgery because of their noninvasive, reversible nature. Most physicians now consider Mirena to be the first-line option for heavy menstrual bleeding in women who have normal anatomy.6
6. What is the cost of treatment?
With health-care expenses accelerating, we need to be mindful of the cost-effectiveness of the options we recommend.
Let’s assess the expense of managing the patient in Case 1. To address her desire for long-term contraception, we might offer tubal sterilization by laparoscopy followed by endometrial ablation (to address the heavy bleeding), which would require a general anesthetic and management in an ambulatory surgical facility.
If she opts for hysteroscopic sterilization prior to endometrial ablation, the sterilization procedure must be performed at least 3 months prior to ablation (according to FDA labeling) so that tubal occlusion can be demonstrated by hysterosalpingography (HSG) before the uterine cavity is scarred. This means that the patient would require two separate interventions. Although both procedures could be performed in an office setting, the patient would still require time away from work and family.
The cost for sterilization plus ablation in the office without anesthesia would be approximately $4,500 (including HSG) at Medicare rates. For a combined laparoscopic sterilization and endometrial ablation, costs would be higher because of the need for anesthesia and an ambulatory surgical facility. Another option that would address both the heavy bleeding and the need for contraception: oral contraceptives (OCs). The overall cost of this approach over 5 years would be $4,200 (60 months of OCs at $70/month), but it would be fully covered under the Affordable Care Act (ACA), so the patient would have no out-of-pocket expense. The cost of Mirena would be $1,000 ($850 for the device plus $150 for insertion), but it also would be fully covered under the ACA.
CASE 1: Resolved
You discuss the option of cyclic OCs with the patient. This approach would help control her irregular, heavy, and painful menses while providing good contraceptive coverage.
Although sterilization plus endometrial ablation is an option, you counsel the patient that the published “success” rates do not apply to her. Given her young age, obesity, and anovulatory status, endometrial ablation has a greater likelihood of failure. Further, when abnormal bleeding recurs, it may be difficult to assess this high-risk patient’s endometrium.
You also discuss Mirena, which would provide long-term contraception and also manage her menorrhagia and dysmenorrhea; indeed, it is FDA-approved for this indication. In fact, Mirena would address all of this patient’s concerns, offering superb contraception and reliable reductions in bleeding and pelvic pain in the setting of endometriosis and adenomyosis.
Overall, this woman is best served by a highly reliable approach that manages her contraceptive needs and her menorrhagia and dysmenorrhea while reducing her risk for endometrial hyperplasia and cancer. Given the long-term endometrial-sampling problems ablation would create, it is not an optimal solution for this woman.
What this evidence means for practice
When assessing technology, consider which patients it was tested in, your patient’s diagnosis and long-term health risks, the cost and success rate of the technology, and the availability of less invasive options.
How to assess new data on a technology or procedure
Gill SE, Mills BB. Physician opinions regarding elective bilateral salpingectomy with hysterectomy and for sterilization. JMIG. 2013;20(4):517–521.
CASE 2: A healthy patient seeks permanent contraception
At her annual well-woman visit, your 42-year-old patient (G3P3) asks to discuss permanent contraception now that she has completed her family. She has used OCs for more than 10 years without problems. She is a nonsmoker of normal weight (BMI of 22 kg/m2), with normal blood pressure and vital signs. Her family history is remarkable for the health of her parents and siblings: Her mother is 68 years old and well; her father, 70, also is healthy. There is no family history of breast or ovarian cancer, prostate cancer, or significant medical illness.
What options would you offer this patient? Given recent data suggesting that ovarian cancer may originate in the fallopian tubes, would you recommend prophylactic salpingectomy as her contraceptive method of choice?
This patient has many options. In describing them to her, it would be important to focus on the breadth of safe, reversible, long-acting contraceptives now available, including their respective risks, benefits, and long-term outcomes and costs. It also is important to consider the published data on these methods, weighing their relevance to her overall health and medical history. Although some data regarding the origin of ovarian cancer in the fallopian tubes may be especially compelling, it may not be wise to extrapolate it from a specific group of women to all patients, as we shall see.
Option 1: Cyclic OCs
This option should not be excluded, despite the need for daily dosing, because the patient has used it successfully for more than 10 years. OCs are highly effective and have the added benefits of reducing menstrual blood loss, alleviating cramps, and lowering the risks of endometrial and ovarian cancer.7
Option 2: LARC
Long-acting reversible contraceptive (LARC) methods include the LNG-IUS, the copper intrauterine device (IUD; ParaGard, Teva), and the etonogestrel implant (Nexplanon, Merck). Each of these contraceptives is similar to sterilization in terms of efficacy. None requires the interruption of sexual activity or weekly or monthly trips to the pharmacy.
The LNG-IUS and the etonogestrel implant have the added benefits of reducing menstrual blood loss and reducing or eliminating premenstrual symptoms and cramps in most women. In addition, they may reduce the risk of unopposed estrogen stimulation of the endometrium associated with perimenopausal anovulatory cycles.
Option 3: Transcervical tubal sterilization
This hysteroscopic method (Essure, Bayer) avoids the risks of general anesthesia, but successful bilateral placement may not be possible in a small percentage of women. It also requires a 3-month interval between placement and confirmation of tubal occlusion (via HSG). During this interval, alternative contraception must be used. Once occlusion is confirmed, this method is highly reliable.
Option 4: Laparoscopic sterilization
This approach was the method of choice prior to the introduction of Essure in 2002. There now is a resurgence of interest in laparoscopic sterilization due to recent publications describing the distal portion of the fallopian tube as the “true source” of high-grade serous ovarian cancers.
In pathologic analyses of fallopian tubes removed prophylactically from women with a BRCA 1 or 2 mutation, investigators found a significant rate of serous tubal intraepithelial carcinoma.8 Researchers began to study the genetics of these cancers and concluded that, in women with a BRCA mutation, high-grade serous carcinomas may arise from the distal fallopian tube.
Until recently, all of the literature on these tubal carcinomas related only to women with a specific tumor suppressor gene p53 mutation in the BRCA system. Other investigators then reviewed pathology specimens from women without a BRCA mutation who had high-grade serous carcinomas that were peritoneal, tubal, or ovarian in origin. They found serous tubal intraepithelial carcinomas in 33% to 59% of these women.9
“Research suggests that bilateral salpingectomy during hysterectomy for benign indications or as a sterilization procedure may have benefits, such as preventing tubal disease and cancer, without significant risks,” wrote Gill and Mills.10 In conducting a survey of US physicians to determine how widespread prophylactic salpingectomy is during benign hysterectomy or sterilization, they found that 54% of respondents performed bilateral salpingectomy during hysterectomy, usually to lower the risk of cancer (75%) and avoid the need for reoperation (49.1%). Of the 45.5% of respondents who did not perform bilateral salpingectomy during hysterectomy, most (69.4%) believed it has no benefit.10
Although 58% of respondents believed bilateral salpingectomy to be the most effective option for sterilization in women older than 35 years, they reported that they reserve it for women in whom one sterilization procedure has failed or for women who have tubal disease.10
As for the 45.5% of respondents who did not perform prophylactic salpingectomy, they offered as reasons their concern about increased operative time and the risk of complications, as well as a belief that it has no benefit.10
The lifetime risk of ovarian cancer in the general population is 1 in 70 women. Although it is possible that high-grade serous ovarian cancers originate in the distal fallopian tube, as the research to date suggests, it also is possible that we might find in-situ lesions in tissues other than the distal tube, suggesting a more global genetic defect underlying ovarian cancers in the peritoneal and müllerian tissues. Randomized trials are under way in an effort to determine whether excision of the fallopian tubes will prevent the majority of high-grade serous cancers. It will be many years, however, before the results of these trials are available.
CASE 2: Resolved
This patient has used combination OCs for more than 10 years, so her lifetime risk of ovarian cancer has been reduced by approximately 50%. Because her family history indicates that a BRCA mutation is highly unlikely, her lifetime risk of ovarian cancer now has declined from 1:70 to roughly 1:140.
Prophylactic salpingectomy might offer a very small reduction in this patient’s absolute risk of ovarian cancer—from 0.75% to 0.50% lifetime risk—but the current data are not robust enough to suggest that it should be recommended for her. The operation would carry the risks associated with general anesthesia and peritoneal access. Although these risks are small, there is a documented risk of death from laparoscopic sterilization procedures in the United States, from complications related to bowel injury, anesthesia, and hemorrhage.
For these reasons, I would counsel this patient that her best options for contraception are combination OCs, transcervical tubal sterilization, or a long-acting reversible contraceptive such as the IUD or implant.
Tell us what you think, at [email protected]. Please include your name and city and state.
The development of new medical technology continues at a brisk pace—and ObGyns and our patients often are the beneficiaries. Notable technological breakthroughs of the past include hormonal contraception, in vitro fertilization, the application of minimally invasive surgical devices and techniques to gynecologic procedures, and many other innovations.
The leaders in our specialty are innovators themselves, ever vigilant for developments that can help improve health and quality of life for our patients. Regrettably, however, many technologies spread widely before they are fully validated by published studies—or continue to be used long after a superior or less invasive intervention has come along. And many claims about new technology are based on marketing information rather than reliable data.
Another common occurrence in regard to published data: Findings in one well-defined sector of the population are extrapolated to all patients. Even clinicians who are careful about adopting new technology can overlook the fact that it was tested, and proven, in a subset of patients that may not be comparable to all their patients.
In this article, I offer two case studies that illustrate some of the challenges we face when it comes to applying scientific findings to our practice and assessing medical technologies. In both settings, the health of the patient should be our primary focus.
When it comes to technology, patient selection is key
CASE 1: Anovulatory patient requests endometrial ablation
A 34-year-old woman (G2P2) who is moderately obese (body mass index of 32 kg/m2) visits your office to request endometrial ablation to manage her irregular and heavy menses. She reached menarche at age 10, and her periods have been somewhat irregular ever since. She required ovarian stimulation with clomiphene citrate to achieve each of her pregnancies, and both children were delivered by cesarean section. She currently uses condoms for contraception but does not have a steady partner, and she desires no additional pregnancies.
The patient reports that her menses occur every 2 to 6 weeks, with flow lasting from 2 to 8 days. She is housebound for 2 days each cycle because of heavy flow and cramping. She takes no medications and has no other medical conditions.
On exam, she is centrally obese with a tender uterus that is 10- to 12-weeks’ size; no adnexal masses are palpable. All other findings are normal. A recent test for diabetes was negative, but her serum cholesterol and triglyceride levels are borderline elevated.
What intervention would you recommend to address the heavy bleeding?
With the advent of second-generation endometrial ablation devices in the late 1990s, women with refractory menorrhagia had a safe, reliable, minimally invasive alternative to hysterectomy that made it possible to treat the endometrial cavity without the technical challenges of resectoscopic surgery. More than 10 million women report menorrhagia each year in the United States—so it is no small problem.1,2 Global endometrial ablation devices make management possible in an office setting, and recovery is significantly shorter than with hysterectomy. The three most prominent nonhysteroscopic ablation devices are (FIGURE):
• NovaSure (Hologic) uses bipolar radiofrequency energy to ablate tissue. Its probe contains stretchable gold-plated fabric that conforms to the endometrial surface.
• Gynecare Thermachoice (Ethicon) consists of an intrauterine balloon that is filled with hot liquid (temperatures of roughly 87°C) to ablate the endometrium
• Her Option (CooperSurgical) is a cryoablation system that consists of an intrauterine probe that forms an ice ball (temperatures of roughly –90°C) that destroys the uterine lining. Several applications are required to treat the majority of the cavity.
Use of these devices is widespread, although a nonsurgical alternative—the levonorgestrel-releasing intrauterine system (LNG-IUS; Mirena)—was approved by the US Food and Drug Administration (FDA) in 2009 for the treatment of heavy menstrual bleeding.
Not only is the efficacy of the LNG-IUS for controlling menorrhagia equal to endometrial ablation, but it provides the additional benefits of reliable contraception and management of dysmenorrhea.
6 questions to ask before applying a technology
1. In which population was it studied?
One of the most important issues to consider when you are evaluating technology is the population in which it was studied. In other words, to whom do the findings apply?
Most endometrial ablation technologies were tested in women who had a uterus of normal size (mean, 8 cm) with no structural abnormalities (ie, no polyps or fibroids) and regular but very heavy periods. The findings from these studies now have been extrapolated in many cases to women who have hormonally induced abnormal bleeding, whose periods are irregular. That extrapolation may not be appropriate.
2. What is the diagnosis?
As the manufacturers of global endometrial ablation devices note, heavy menstrual bleeding may arise from an underlying condition, such as endometrial cancer, hormonal imbalance, fibroids, coagulopathy, and so on—and it is important to rule these conditions out before considering endometrial ablation.
For example, in Case 1, the patient is experiencing anovulatory cycles, as evidenced by her irregular menses and the need for ovulation induction to achieve her pregnancies. The success rate of endometrial ablation in the setting of chronic anovulation is unknown. Pivotal trials for all of the nonhysteroscopic endometrial ablation technologies required regular menses or failure of cyclic hormonal therapy prior to enrollment.
In addition, in Case 1, the patient has signs (an enlarged, tender uterus) that suggest the presence of adenomyosis. Endometrial ablation is not recommended as a treatment for women with this condition.
3. Will later surgery be required?
In one study from Kaiser Permanente of Northern California, 21% of women who underwent endometrial ablation for menorrhagia later underwent hysterectomy, and 3.9% underwent other uterine-sparing procedures to alleviate heavy bleeding.3
In that study, women younger than age 45 were 2.1 times more likely to require hysterectomy after endometrial ablation, compared with older women (95% confidence interval [CI], 1.8–2.4). The likelihood of hysterectomy increased with each decreasing stratum of age and exceeded 40% in women aged 40 years or younger.3
In a population-based retrospective cohort study from Scotland, 2,779 (19.7%) of 11,299 women who underwent endometrial ablation for heavy menstrual bleeding required hysterectomy later.4 Again, women who required hysterectomy after endometrial ablation tended to be younger than those who did not. Overall, 26.6% of women undergoing endometrial ablation for heavy menstrual bleeding required further surgery.4
And in a 5-year follow-up of patients participating in a randomized trial of uterine balloon therapy versus rollerball ablation, roughly 30% of women required subsequent surgery for heavy menstrual bleeding.5
The need for subsequent surgery following endometrial ablation is likely to be higher among women who do not match the profile of participants in pivotal trials of the devices. All patients considering endometrial ablation should be counseled about the possible need for further surgery.
Related Article The economics of surgical gynecology: How we can not only survive, but thrive, in the 21st Century Barbara S. Levy, MD
4. What is the patient's overall health?
Before selecting an intervention for heavy menstrual bleeding, it is important to consider the patient’s overall health. What comorbidities does she have? Is pain a component of her condition? If so, might she have endometriosis or adenomyosis, as our patient does? If pain is a significant component of her menorrhagia, is it cyclical—that is, does it correspond to the days of heaviest flow? Pain related to the passage of large clots during menses may respond well to endometrial ablation. Pelvic pain occurring before and after the flow probably won’t.
Also keep in mind that the patient in Case 1 has two risk factors for endometrial hyperplasia: anovulatory cycles and obesity. If she undergoes endometrial ablation and subsequently experiences abnormal uterine bleeding, the most prominent sign of endometrial hyperplasia, how will you assess her endometrium 5 years after ablation if she develops abnormal bleeding? Will you be able to adequately sample it?
5. Have less invasive options been tried?
Many of the women studied in pivotal trials of second-generation endometrial ablation devices failed medical therapy prior to undergoing ablation. Because medical therapy is less expensive and noninvasive, it makes sense to offer it before proceeding to surgery. Common pharmacologic approaches include nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives, and tranexamic acid.
In addition, as I mentioned earlier, Mirena is approved for treatment of heavy menstrual bleeding.
Medical therapy and Mirena should be offered prior to surgery because of their noninvasive, reversible nature. Most physicians now consider Mirena to be the first-line option for heavy menstrual bleeding in women who have normal anatomy.6
6. What is the cost of treatment?
With health-care expenses accelerating, we need to be mindful of the cost-effectiveness of the options we recommend.
Let’s assess the expense of managing the patient in Case 1. To address her desire for long-term contraception, we might offer tubal sterilization by laparoscopy followed by endometrial ablation (to address the heavy bleeding), which would require a general anesthetic and management in an ambulatory surgical facility.
If she opts for hysteroscopic sterilization prior to endometrial ablation, the sterilization procedure must be performed at least 3 months prior to ablation (according to FDA labeling) so that tubal occlusion can be demonstrated by hysterosalpingography (HSG) before the uterine cavity is scarred. This means that the patient would require two separate interventions. Although both procedures could be performed in an office setting, the patient would still require time away from work and family.
The cost for sterilization plus ablation in the office without anesthesia would be approximately $4,500 (including HSG) at Medicare rates. For a combined laparoscopic sterilization and endometrial ablation, costs would be higher because of the need for anesthesia and an ambulatory surgical facility. Another option that would address both the heavy bleeding and the need for contraception: oral contraceptives (OCs). The overall cost of this approach over 5 years would be $4,200 (60 months of OCs at $70/month), but it would be fully covered under the Affordable Care Act (ACA), so the patient would have no out-of-pocket expense. The cost of Mirena would be $1,000 ($850 for the device plus $150 for insertion), but it also would be fully covered under the ACA.
CASE 1: Resolved
You discuss the option of cyclic OCs with the patient. This approach would help control her irregular, heavy, and painful menses while providing good contraceptive coverage.
Although sterilization plus endometrial ablation is an option, you counsel the patient that the published “success” rates do not apply to her. Given her young age, obesity, and anovulatory status, endometrial ablation has a greater likelihood of failure. Further, when abnormal bleeding recurs, it may be difficult to assess this high-risk patient’s endometrium.
You also discuss Mirena, which would provide long-term contraception and also manage her menorrhagia and dysmenorrhea; indeed, it is FDA-approved for this indication. In fact, Mirena would address all of this patient’s concerns, offering superb contraception and reliable reductions in bleeding and pelvic pain in the setting of endometriosis and adenomyosis.
Overall, this woman is best served by a highly reliable approach that manages her contraceptive needs and her menorrhagia and dysmenorrhea while reducing her risk for endometrial hyperplasia and cancer. Given the long-term endometrial-sampling problems ablation would create, it is not an optimal solution for this woman.
What this evidence means for practice
When assessing technology, consider which patients it was tested in, your patient’s diagnosis and long-term health risks, the cost and success rate of the technology, and the availability of less invasive options.
How to assess new data on a technology or procedure
Gill SE, Mills BB. Physician opinions regarding elective bilateral salpingectomy with hysterectomy and for sterilization. JMIG. 2013;20(4):517–521.
CASE 2: A healthy patient seeks permanent contraception
At her annual well-woman visit, your 42-year-old patient (G3P3) asks to discuss permanent contraception now that she has completed her family. She has used OCs for more than 10 years without problems. She is a nonsmoker of normal weight (BMI of 22 kg/m2), with normal blood pressure and vital signs. Her family history is remarkable for the health of her parents and siblings: Her mother is 68 years old and well; her father, 70, also is healthy. There is no family history of breast or ovarian cancer, prostate cancer, or significant medical illness.
What options would you offer this patient? Given recent data suggesting that ovarian cancer may originate in the fallopian tubes, would you recommend prophylactic salpingectomy as her contraceptive method of choice?
This patient has many options. In describing them to her, it would be important to focus on the breadth of safe, reversible, long-acting contraceptives now available, including their respective risks, benefits, and long-term outcomes and costs. It also is important to consider the published data on these methods, weighing their relevance to her overall health and medical history. Although some data regarding the origin of ovarian cancer in the fallopian tubes may be especially compelling, it may not be wise to extrapolate it from a specific group of women to all patients, as we shall see.
Option 1: Cyclic OCs
This option should not be excluded, despite the need for daily dosing, because the patient has used it successfully for more than 10 years. OCs are highly effective and have the added benefits of reducing menstrual blood loss, alleviating cramps, and lowering the risks of endometrial and ovarian cancer.7
Option 2: LARC
Long-acting reversible contraceptive (LARC) methods include the LNG-IUS, the copper intrauterine device (IUD; ParaGard, Teva), and the etonogestrel implant (Nexplanon, Merck). Each of these contraceptives is similar to sterilization in terms of efficacy. None requires the interruption of sexual activity or weekly or monthly trips to the pharmacy.
The LNG-IUS and the etonogestrel implant have the added benefits of reducing menstrual blood loss and reducing or eliminating premenstrual symptoms and cramps in most women. In addition, they may reduce the risk of unopposed estrogen stimulation of the endometrium associated with perimenopausal anovulatory cycles.
Option 3: Transcervical tubal sterilization
This hysteroscopic method (Essure, Bayer) avoids the risks of general anesthesia, but successful bilateral placement may not be possible in a small percentage of women. It also requires a 3-month interval between placement and confirmation of tubal occlusion (via HSG). During this interval, alternative contraception must be used. Once occlusion is confirmed, this method is highly reliable.
Option 4: Laparoscopic sterilization
This approach was the method of choice prior to the introduction of Essure in 2002. There now is a resurgence of interest in laparoscopic sterilization due to recent publications describing the distal portion of the fallopian tube as the “true source” of high-grade serous ovarian cancers.
In pathologic analyses of fallopian tubes removed prophylactically from women with a BRCA 1 or 2 mutation, investigators found a significant rate of serous tubal intraepithelial carcinoma.8 Researchers began to study the genetics of these cancers and concluded that, in women with a BRCA mutation, high-grade serous carcinomas may arise from the distal fallopian tube.
Until recently, all of the literature on these tubal carcinomas related only to women with a specific tumor suppressor gene p53 mutation in the BRCA system. Other investigators then reviewed pathology specimens from women without a BRCA mutation who had high-grade serous carcinomas that were peritoneal, tubal, or ovarian in origin. They found serous tubal intraepithelial carcinomas in 33% to 59% of these women.9
“Research suggests that bilateral salpingectomy during hysterectomy for benign indications or as a sterilization procedure may have benefits, such as preventing tubal disease and cancer, without significant risks,” wrote Gill and Mills.10 In conducting a survey of US physicians to determine how widespread prophylactic salpingectomy is during benign hysterectomy or sterilization, they found that 54% of respondents performed bilateral salpingectomy during hysterectomy, usually to lower the risk of cancer (75%) and avoid the need for reoperation (49.1%). Of the 45.5% of respondents who did not perform bilateral salpingectomy during hysterectomy, most (69.4%) believed it has no benefit.10
Although 58% of respondents believed bilateral salpingectomy to be the most effective option for sterilization in women older than 35 years, they reported that they reserve it for women in whom one sterilization procedure has failed or for women who have tubal disease.10
As for the 45.5% of respondents who did not perform prophylactic salpingectomy, they offered as reasons their concern about increased operative time and the risk of complications, as well as a belief that it has no benefit.10
The lifetime risk of ovarian cancer in the general population is 1 in 70 women. Although it is possible that high-grade serous ovarian cancers originate in the distal fallopian tube, as the research to date suggests, it also is possible that we might find in-situ lesions in tissues other than the distal tube, suggesting a more global genetic defect underlying ovarian cancers in the peritoneal and müllerian tissues. Randomized trials are under way in an effort to determine whether excision of the fallopian tubes will prevent the majority of high-grade serous cancers. It will be many years, however, before the results of these trials are available.
CASE 2: Resolved
This patient has used combination OCs for more than 10 years, so her lifetime risk of ovarian cancer has been reduced by approximately 50%. Because her family history indicates that a BRCA mutation is highly unlikely, her lifetime risk of ovarian cancer now has declined from 1:70 to roughly 1:140.
Prophylactic salpingectomy might offer a very small reduction in this patient’s absolute risk of ovarian cancer—from 0.75% to 0.50% lifetime risk—but the current data are not robust enough to suggest that it should be recommended for her. The operation would carry the risks associated with general anesthesia and peritoneal access. Although these risks are small, there is a documented risk of death from laparoscopic sterilization procedures in the United States, from complications related to bowel injury, anesthesia, and hemorrhage.
For these reasons, I would counsel this patient that her best options for contraception are combination OCs, transcervical tubal sterilization, or a long-acting reversible contraceptive such as the IUD or implant.
Tell us what you think, at [email protected]. Please include your name and city and state.
1. Centers for Disease Control and Prevention. Blood disor-ders in women: heavy menstrual bleeding. http://www.cdc.gov/ncbddd/blooddisorders/women/menorrhagia.html. Updated December 12, 2011. Accessed August 15, 2013.
2. Centers for Disease Control and Prevention. Blood disorders in women: research. http://www.cdc.gov/ncbddd/blooddis orders/women/research.html. Updated December 12, 2011. Accessed August 15, 2013.
3. Longinotti K, Jacobson GF, Hung YY, Learman LA. Probability of hysterectomy after endometrial ablation. Obstet Gynecol. 2008;112(6):1214–1220.
4. Cooper K, Lee AJ, Chien P, Raja EA, Timmaraju V, Bhattacharya S. Outcomes following hysterectomy or endometrial ablation for heavy menstrual bleeding: retrospective analysis of hospital episode statistics in Scotland. BJOG. 2011;118(10):1171–1179.
5. Loffer FD, Grainger D. Five-year follow-up of patients participating in a randomized trial of uterine balloon therapy versus rollerball ablation for treatment of menorrhagia. J Am Assoc Gynecol Laparosc. 2002;9(4):429–435.
6. Sayre C. Beyond hysterectomy: Alternative options for heavy bleeding. NY Times. http://www.nytimes.com/ref/health/healthguide/esn-menorrhagia-ess.html. Published October 10, 2008. Accessed August 15, 2013.
7. Havrilesky LJ, Moorman PG, Lowery WJ, et al. Oral contraceptive pills as primary prevention for ovarian cancer. A systematic review and meta-analysis. Obstet Gynecol. 2013;122(1):139–147.
8. Kindelberger DW, Lee Y, Miron A, et al. Intraepithelial carcinoma of the fimbria and pelvic serous carcinoma: evidence for a causal relationship. Am J Surg Pathol. 2007; 31:161–169.
9. Crum CP, McKeon FD, Xian W. The oviduct and ovarian cancer: causality, clinical implications, and “targeted prevention.” Clin Obstet Gynecol. 2012;55(1):24–35.
10. Gill SE, Mills BB. Physician opinions regarding elective bilateral salpingectomy with hysterectomy and for sterilization. JMIG. 2013;20(4):517–521.
1. Centers for Disease Control and Prevention. Blood disor-ders in women: heavy menstrual bleeding. http://www.cdc.gov/ncbddd/blooddisorders/women/menorrhagia.html. Updated December 12, 2011. Accessed August 15, 2013.
2. Centers for Disease Control and Prevention. Blood disorders in women: research. http://www.cdc.gov/ncbddd/blooddis orders/women/research.html. Updated December 12, 2011. Accessed August 15, 2013.
3. Longinotti K, Jacobson GF, Hung YY, Learman LA. Probability of hysterectomy after endometrial ablation. Obstet Gynecol. 2008;112(6):1214–1220.
4. Cooper K, Lee AJ, Chien P, Raja EA, Timmaraju V, Bhattacharya S. Outcomes following hysterectomy or endometrial ablation for heavy menstrual bleeding: retrospective analysis of hospital episode statistics in Scotland. BJOG. 2011;118(10):1171–1179.
5. Loffer FD, Grainger D. Five-year follow-up of patients participating in a randomized trial of uterine balloon therapy versus rollerball ablation for treatment of menorrhagia. J Am Assoc Gynecol Laparosc. 2002;9(4):429–435.
6. Sayre C. Beyond hysterectomy: Alternative options for heavy bleeding. NY Times. http://www.nytimes.com/ref/health/healthguide/esn-menorrhagia-ess.html. Published October 10, 2008. Accessed August 15, 2013.
7. Havrilesky LJ, Moorman PG, Lowery WJ, et al. Oral contraceptive pills as primary prevention for ovarian cancer. A systematic review and meta-analysis. Obstet Gynecol. 2013;122(1):139–147.
8. Kindelberger DW, Lee Y, Miron A, et al. Intraepithelial carcinoma of the fimbria and pelvic serous carcinoma: evidence for a causal relationship. Am J Surg Pathol. 2007; 31:161–169.
9. Crum CP, McKeon FD, Xian W. The oviduct and ovarian cancer: causality, clinical implications, and “targeted prevention.” Clin Obstet Gynecol. 2012;55(1):24–35.
10. Gill SE, Mills BB. Physician opinions regarding elective bilateral salpingectomy with hysterectomy and for sterilization. JMIG. 2013;20(4):517–521.
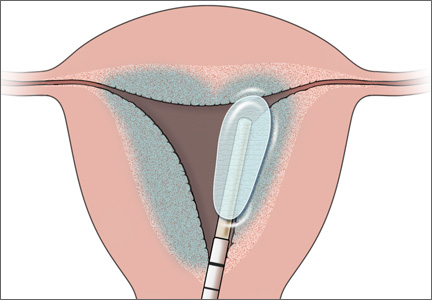
In Vino Veritas?

Pearls in clinical diagnosis of pertussis
VAIL, COLO. – One of the most useful signs that a young infant with an afebrile coughing illness has pertussis is the combination of an elevated white blood cell count of 20,000 cells/mcL or more plus a lymphocyte count of at least 10,000 cells/mcL.
"This is a pediatric pearl. It’s really a poor man’s way of diagnosing pertussis. It’s an effect of the pertussis toxin spreading throughout the neonate’s body, causing a very high white cell count with absolute lymphocytosis," Dr. Ann-Christine Nyquist said at a conference on pediatric infectious diseases sponsored by the Children’s Hospital Colorado.
This clinical pearl is part of a highly useful algorithm put forth by the Global Pertussis Initiative in an effort to update and standardize the case definitions of pertussis. Existing case definitions were developed more than 40 years ago and have numerous shortcomings.
The group developed a three-pronged, age-based algorithm, reflecting an understanding that the key manifestations of pertussis are different in infants aged 0-3 months, children aged 4 months to 9 years, and adolescents or adults.
According to the algorithm, the presence of an elevated WBC count with absolute lymphocytosis in an infant up to 3 months old with an afebrile illness and a cough of less than 3 weeks’ duration that’s increasing in frequency and severity is "virtually diagnostic" of pertussis (Clin. Infect. Dis. 2012;54:1756-64).
Another key feature of pertussis – and this one applies across the age spectrum, from infants to adults – is that the coryza remains watery and doesn’t become purulent, unlike in most viral respiratory infections.
"That green snotty nose doesn’t usually happen when kids have pertussis," explained Dr. Nyquist, professor of pediatrics at the University of Colorado, Denver.
Similarly, in patients of all ages the pertussis cough, even as it worsens, does not become truly productive.
To help nail down the diagnosis of pertussis in infants, the key question to ask parents is, "Is there an adult or adolescent in your family who’s had the most severe cough in their life?" Most infants with pertussis will have had close exposure to an older family member with a prolonged afebrile coughing illness, Dr. Nyquist noted.
In the 4-month to 9-year-old age group, the cough becomes more paroxysmal. The key indicators of pertussis in this age group, according to the Global Pertussis Initiative algorithm, are worsening paroxysmal nonproductive cough of at least 7 days’ duration in an afebrile child with nonpurulent coryza.
This same triad – worsening paroxysmal nonproductive cough, afebrile illness, and nonpurulent coryza – also has high sensitivity and good specificity for the clinical diagnosis of pertussis in adolescents and adults. In addition, the algorithm highlights another useful clue to the diagnosis in patients in this age range: the occurrence of sweating episodes between coughing paroxysms.
In terms of laboratory diagnostics, real-time PCR and culture of nasopharyngeal mucus are most useful in the first 3 weeks after illness onset. Serology is a challenge because the results are influenced by the effects of vaccination; it shouldn’t be used to diagnose pertussis within 1 year following inoculation with any pertussis vaccine because it’s impossible to tell if a positive result represents a response to the vaccine or to infection.
Also, serology can’t distinguish between Bordetella pertussis and B. parapertussis infection. Most PCR tests can. It’s an important distinction because B. parapertussis turns out to be the pathogen in roughly 15% of cases of coughing illnesses similar to pertussis. B. parapertussis infection isn’t vaccine preventable, and its treatment hasn’t been well studied.
The expert consensus is that direct fluorescent antibody testing should be discouraged as a tool to diagnose pertussis because of its unreliable sensitivity and specificity. IgG anti–pertussis toxin ELISA testing is superior to IgA anti–pertussis toxin ELISA, which has a high false-negative rate, Dr. Nyquist observed.
She reported having no financial relationships with any commercial interests.
VAIL, COLO. – One of the most useful signs that a young infant with an afebrile coughing illness has pertussis is the combination of an elevated white blood cell count of 20,000 cells/mcL or more plus a lymphocyte count of at least 10,000 cells/mcL.
"This is a pediatric pearl. It’s really a poor man’s way of diagnosing pertussis. It’s an effect of the pertussis toxin spreading throughout the neonate’s body, causing a very high white cell count with absolute lymphocytosis," Dr. Ann-Christine Nyquist said at a conference on pediatric infectious diseases sponsored by the Children’s Hospital Colorado.
This clinical pearl is part of a highly useful algorithm put forth by the Global Pertussis Initiative in an effort to update and standardize the case definitions of pertussis. Existing case definitions were developed more than 40 years ago and have numerous shortcomings.
The group developed a three-pronged, age-based algorithm, reflecting an understanding that the key manifestations of pertussis are different in infants aged 0-3 months, children aged 4 months to 9 years, and adolescents or adults.
According to the algorithm, the presence of an elevated WBC count with absolute lymphocytosis in an infant up to 3 months old with an afebrile illness and a cough of less than 3 weeks’ duration that’s increasing in frequency and severity is "virtually diagnostic" of pertussis (Clin. Infect. Dis. 2012;54:1756-64).
Another key feature of pertussis – and this one applies across the age spectrum, from infants to adults – is that the coryza remains watery and doesn’t become purulent, unlike in most viral respiratory infections.
"That green snotty nose doesn’t usually happen when kids have pertussis," explained Dr. Nyquist, professor of pediatrics at the University of Colorado, Denver.
Similarly, in patients of all ages the pertussis cough, even as it worsens, does not become truly productive.
To help nail down the diagnosis of pertussis in infants, the key question to ask parents is, "Is there an adult or adolescent in your family who’s had the most severe cough in their life?" Most infants with pertussis will have had close exposure to an older family member with a prolonged afebrile coughing illness, Dr. Nyquist noted.
In the 4-month to 9-year-old age group, the cough becomes more paroxysmal. The key indicators of pertussis in this age group, according to the Global Pertussis Initiative algorithm, are worsening paroxysmal nonproductive cough of at least 7 days’ duration in an afebrile child with nonpurulent coryza.
This same triad – worsening paroxysmal nonproductive cough, afebrile illness, and nonpurulent coryza – also has high sensitivity and good specificity for the clinical diagnosis of pertussis in adolescents and adults. In addition, the algorithm highlights another useful clue to the diagnosis in patients in this age range: the occurrence of sweating episodes between coughing paroxysms.
In terms of laboratory diagnostics, real-time PCR and culture of nasopharyngeal mucus are most useful in the first 3 weeks after illness onset. Serology is a challenge because the results are influenced by the effects of vaccination; it shouldn’t be used to diagnose pertussis within 1 year following inoculation with any pertussis vaccine because it’s impossible to tell if a positive result represents a response to the vaccine or to infection.
Also, serology can’t distinguish between Bordetella pertussis and B. parapertussis infection. Most PCR tests can. It’s an important distinction because B. parapertussis turns out to be the pathogen in roughly 15% of cases of coughing illnesses similar to pertussis. B. parapertussis infection isn’t vaccine preventable, and its treatment hasn’t been well studied.
The expert consensus is that direct fluorescent antibody testing should be discouraged as a tool to diagnose pertussis because of its unreliable sensitivity and specificity. IgG anti–pertussis toxin ELISA testing is superior to IgA anti–pertussis toxin ELISA, which has a high false-negative rate, Dr. Nyquist observed.
She reported having no financial relationships with any commercial interests.
VAIL, COLO. – One of the most useful signs that a young infant with an afebrile coughing illness has pertussis is the combination of an elevated white blood cell count of 20,000 cells/mcL or more plus a lymphocyte count of at least 10,000 cells/mcL.
"This is a pediatric pearl. It’s really a poor man’s way of diagnosing pertussis. It’s an effect of the pertussis toxin spreading throughout the neonate’s body, causing a very high white cell count with absolute lymphocytosis," Dr. Ann-Christine Nyquist said at a conference on pediatric infectious diseases sponsored by the Children’s Hospital Colorado.
This clinical pearl is part of a highly useful algorithm put forth by the Global Pertussis Initiative in an effort to update and standardize the case definitions of pertussis. Existing case definitions were developed more than 40 years ago and have numerous shortcomings.
The group developed a three-pronged, age-based algorithm, reflecting an understanding that the key manifestations of pertussis are different in infants aged 0-3 months, children aged 4 months to 9 years, and adolescents or adults.
According to the algorithm, the presence of an elevated WBC count with absolute lymphocytosis in an infant up to 3 months old with an afebrile illness and a cough of less than 3 weeks’ duration that’s increasing in frequency and severity is "virtually diagnostic" of pertussis (Clin. Infect. Dis. 2012;54:1756-64).
Another key feature of pertussis – and this one applies across the age spectrum, from infants to adults – is that the coryza remains watery and doesn’t become purulent, unlike in most viral respiratory infections.
"That green snotty nose doesn’t usually happen when kids have pertussis," explained Dr. Nyquist, professor of pediatrics at the University of Colorado, Denver.
Similarly, in patients of all ages the pertussis cough, even as it worsens, does not become truly productive.
To help nail down the diagnosis of pertussis in infants, the key question to ask parents is, "Is there an adult or adolescent in your family who’s had the most severe cough in their life?" Most infants with pertussis will have had close exposure to an older family member with a prolonged afebrile coughing illness, Dr. Nyquist noted.
In the 4-month to 9-year-old age group, the cough becomes more paroxysmal. The key indicators of pertussis in this age group, according to the Global Pertussis Initiative algorithm, are worsening paroxysmal nonproductive cough of at least 7 days’ duration in an afebrile child with nonpurulent coryza.
This same triad – worsening paroxysmal nonproductive cough, afebrile illness, and nonpurulent coryza – also has high sensitivity and good specificity for the clinical diagnosis of pertussis in adolescents and adults. In addition, the algorithm highlights another useful clue to the diagnosis in patients in this age range: the occurrence of sweating episodes between coughing paroxysms.
In terms of laboratory diagnostics, real-time PCR and culture of nasopharyngeal mucus are most useful in the first 3 weeks after illness onset. Serology is a challenge because the results are influenced by the effects of vaccination; it shouldn’t be used to diagnose pertussis within 1 year following inoculation with any pertussis vaccine because it’s impossible to tell if a positive result represents a response to the vaccine or to infection.
Also, serology can’t distinguish between Bordetella pertussis and B. parapertussis infection. Most PCR tests can. It’s an important distinction because B. parapertussis turns out to be the pathogen in roughly 15% of cases of coughing illnesses similar to pertussis. B. parapertussis infection isn’t vaccine preventable, and its treatment hasn’t been well studied.
The expert consensus is that direct fluorescent antibody testing should be discouraged as a tool to diagnose pertussis because of its unreliable sensitivity and specificity. IgG anti–pertussis toxin ELISA testing is superior to IgA anti–pertussis toxin ELISA, which has a high false-negative rate, Dr. Nyquist observed.
She reported having no financial relationships with any commercial interests.
Carbonation affects brain processing of sweet stimuli
Carbonation produces a decrease in the neural processing of sweetness-related signals, particularly those from sucrose, a small functional neuroimaging study shows.
The findings, which suggest that the combination of CO2 and sucrose might increase consumption of sucrose, could have implications for dietary interventions designed to regulate caloric intake, according to Dr. Francesco Di Salle of Salerno (Italy) University and his colleagues.
To assess the interference between CO2 and perception of sweetness, as well as the differential effects of CO2 on sucrose and aspartame-acesulfame, (As-Ac, an artificial sweetener combination commonly used in diet beverages), the investigators performed two functional magnetic resonance imaging (fMRI) experiments to evaluate changes in regional brain activity.
The first experiment, performed in nine volunteers, analyzed the effect of carbonation in four sweet Sprite-based solutions, including one carbonated and sweetened with sucrose, one noncarbonated and sweetened with sucrose, one carbonated and sweetened with As-Ac, and one noncarbonated and sweetened with As-Ac. The second experiment evaluated the spatial location of the strongest neural effects of sour taste and CO2 within the insular cortex of eight subjects.
On fMRI, the presence of carbonation in sweet solutions "independently of the sweetening agent, reduced neural activity in the anterior insula (AI), orbitofrontal cortex (OFC), and posterior pons ... the effect of carbonation on sucrose was much higher than on perception of As-Ac," they noted, explaining that "at the perceptual level ... carbonation reduced the perception of sweetness and the differences between the sensory profiles of sucrose and As-Ac."
This effect may increase sucrose intake, but is also favorable to diet beverage formulations being perceived as similar to regular beverage formulations, the investigators reported online May 28 ahead of print in Gastroenterology.
"It is also coherent with a process of prioritization among perceptual inputs (chemesthetic and gustatory information) deriving from the same body topography and converging to the same cortical regions (AI, OFC), they said (Gastroenterology 2013 [doi:10.1053/j.gastro.2013.05.041]).
To correlate neuroimaging with behavioral data, the ability of carbonation to modulate perception of sweetness was assessed in 14 subjects, who scored the level of perceived sweetness of the solutions on a visual analog scale ranging from 0 to 100 mm. The effect of 1,585 ppm of CO2 added to a 10% glucose solution on the perception of sweetness was also tested in seven subjects.
CO2 was able to significantly reduce sweet-induced taste perceptions as assessed by the volunteers’ visual analog scale recordings: The perception of Sprite-associated sweetness was significantly reduced by CO2 (48 vs. 63 and 48 vs. 55 for As-Ac and sucrose, respectively).
"Similarly, in the presence of carbonation, sweet-induced perception of a 10% glucose solution was significantly reduced (36 vs. 53), the investigators said.
Given the widespread use of CO2 in sweet beverages, the modulation of sweet perception by CO2 is of interest, they noted.
The findings, which suggest that CO2 modulates the perception of sweetness thereby reducing the global neural processing of sweetness, the processing of sucrose more than of As-Ac, and the processing difference between sweetening agents via modulation of the perception of sweetness, is "of utmost importance for designing carbonated beverages and is relevant to the regulation of caloric intake," they said.
"This effect is driven by the integration of information on gastric fullness and on nutrient depletion, conveyed to a brain network where the autonomic brainstem circuitry and tractus solitarius neurons play a critical role in homeostatic functions," they added.
It may be that taste and CO2-related information influence food choices and intake through integration in the tractus solitarius with input from the gastrointestinal tract, they suggested, explaining that "the reduced discrimination between sucrose and As-Ac induced by CO2 would promote the consumptions of low-calorie beverages and would converge with CO2-induced gastric distention in limiting caloric intake."
This study was supported in part by the Coca-Cola Company. One author, Dr. Rosario Cuomo, was sponsored by the Coca-Cola Company. The remaining authors reported having no disclosures.
Carbonation produces a decrease in the neural processing of sweetness-related signals, particularly those from sucrose, a small functional neuroimaging study shows.
The findings, which suggest that the combination of CO2 and sucrose might increase consumption of sucrose, could have implications for dietary interventions designed to regulate caloric intake, according to Dr. Francesco Di Salle of Salerno (Italy) University and his colleagues.
To assess the interference between CO2 and perception of sweetness, as well as the differential effects of CO2 on sucrose and aspartame-acesulfame, (As-Ac, an artificial sweetener combination commonly used in diet beverages), the investigators performed two functional magnetic resonance imaging (fMRI) experiments to evaluate changes in regional brain activity.
The first experiment, performed in nine volunteers, analyzed the effect of carbonation in four sweet Sprite-based solutions, including one carbonated and sweetened with sucrose, one noncarbonated and sweetened with sucrose, one carbonated and sweetened with As-Ac, and one noncarbonated and sweetened with As-Ac. The second experiment evaluated the spatial location of the strongest neural effects of sour taste and CO2 within the insular cortex of eight subjects.
On fMRI, the presence of carbonation in sweet solutions "independently of the sweetening agent, reduced neural activity in the anterior insula (AI), orbitofrontal cortex (OFC), and posterior pons ... the effect of carbonation on sucrose was much higher than on perception of As-Ac," they noted, explaining that "at the perceptual level ... carbonation reduced the perception of sweetness and the differences between the sensory profiles of sucrose and As-Ac."
This effect may increase sucrose intake, but is also favorable to diet beverage formulations being perceived as similar to regular beverage formulations, the investigators reported online May 28 ahead of print in Gastroenterology.
"It is also coherent with a process of prioritization among perceptual inputs (chemesthetic and gustatory information) deriving from the same body topography and converging to the same cortical regions (AI, OFC), they said (Gastroenterology 2013 [doi:10.1053/j.gastro.2013.05.041]).
To correlate neuroimaging with behavioral data, the ability of carbonation to modulate perception of sweetness was assessed in 14 subjects, who scored the level of perceived sweetness of the solutions on a visual analog scale ranging from 0 to 100 mm. The effect of 1,585 ppm of CO2 added to a 10% glucose solution on the perception of sweetness was also tested in seven subjects.
CO2 was able to significantly reduce sweet-induced taste perceptions as assessed by the volunteers’ visual analog scale recordings: The perception of Sprite-associated sweetness was significantly reduced by CO2 (48 vs. 63 and 48 vs. 55 for As-Ac and sucrose, respectively).
"Similarly, in the presence of carbonation, sweet-induced perception of a 10% glucose solution was significantly reduced (36 vs. 53), the investigators said.
Given the widespread use of CO2 in sweet beverages, the modulation of sweet perception by CO2 is of interest, they noted.
The findings, which suggest that CO2 modulates the perception of sweetness thereby reducing the global neural processing of sweetness, the processing of sucrose more than of As-Ac, and the processing difference between sweetening agents via modulation of the perception of sweetness, is "of utmost importance for designing carbonated beverages and is relevant to the regulation of caloric intake," they said.
"This effect is driven by the integration of information on gastric fullness and on nutrient depletion, conveyed to a brain network where the autonomic brainstem circuitry and tractus solitarius neurons play a critical role in homeostatic functions," they added.
It may be that taste and CO2-related information influence food choices and intake through integration in the tractus solitarius with input from the gastrointestinal tract, they suggested, explaining that "the reduced discrimination between sucrose and As-Ac induced by CO2 would promote the consumptions of low-calorie beverages and would converge with CO2-induced gastric distention in limiting caloric intake."
This study was supported in part by the Coca-Cola Company. One author, Dr. Rosario Cuomo, was sponsored by the Coca-Cola Company. The remaining authors reported having no disclosures.
Carbonation produces a decrease in the neural processing of sweetness-related signals, particularly those from sucrose, a small functional neuroimaging study shows.
The findings, which suggest that the combination of CO2 and sucrose might increase consumption of sucrose, could have implications for dietary interventions designed to regulate caloric intake, according to Dr. Francesco Di Salle of Salerno (Italy) University and his colleagues.
To assess the interference between CO2 and perception of sweetness, as well as the differential effects of CO2 on sucrose and aspartame-acesulfame, (As-Ac, an artificial sweetener combination commonly used in diet beverages), the investigators performed two functional magnetic resonance imaging (fMRI) experiments to evaluate changes in regional brain activity.
The first experiment, performed in nine volunteers, analyzed the effect of carbonation in four sweet Sprite-based solutions, including one carbonated and sweetened with sucrose, one noncarbonated and sweetened with sucrose, one carbonated and sweetened with As-Ac, and one noncarbonated and sweetened with As-Ac. The second experiment evaluated the spatial location of the strongest neural effects of sour taste and CO2 within the insular cortex of eight subjects.
On fMRI, the presence of carbonation in sweet solutions "independently of the sweetening agent, reduced neural activity in the anterior insula (AI), orbitofrontal cortex (OFC), and posterior pons ... the effect of carbonation on sucrose was much higher than on perception of As-Ac," they noted, explaining that "at the perceptual level ... carbonation reduced the perception of sweetness and the differences between the sensory profiles of sucrose and As-Ac."
This effect may increase sucrose intake, but is also favorable to diet beverage formulations being perceived as similar to regular beverage formulations, the investigators reported online May 28 ahead of print in Gastroenterology.
"It is also coherent with a process of prioritization among perceptual inputs (chemesthetic and gustatory information) deriving from the same body topography and converging to the same cortical regions (AI, OFC), they said (Gastroenterology 2013 [doi:10.1053/j.gastro.2013.05.041]).
To correlate neuroimaging with behavioral data, the ability of carbonation to modulate perception of sweetness was assessed in 14 subjects, who scored the level of perceived sweetness of the solutions on a visual analog scale ranging from 0 to 100 mm. The effect of 1,585 ppm of CO2 added to a 10% glucose solution on the perception of sweetness was also tested in seven subjects.
CO2 was able to significantly reduce sweet-induced taste perceptions as assessed by the volunteers’ visual analog scale recordings: The perception of Sprite-associated sweetness was significantly reduced by CO2 (48 vs. 63 and 48 vs. 55 for As-Ac and sucrose, respectively).
"Similarly, in the presence of carbonation, sweet-induced perception of a 10% glucose solution was significantly reduced (36 vs. 53), the investigators said.
Given the widespread use of CO2 in sweet beverages, the modulation of sweet perception by CO2 is of interest, they noted.
The findings, which suggest that CO2 modulates the perception of sweetness thereby reducing the global neural processing of sweetness, the processing of sucrose more than of As-Ac, and the processing difference between sweetening agents via modulation of the perception of sweetness, is "of utmost importance for designing carbonated beverages and is relevant to the regulation of caloric intake," they said.
"This effect is driven by the integration of information on gastric fullness and on nutrient depletion, conveyed to a brain network where the autonomic brainstem circuitry and tractus solitarius neurons play a critical role in homeostatic functions," they added.
It may be that taste and CO2-related information influence food choices and intake through integration in the tractus solitarius with input from the gastrointestinal tract, they suggested, explaining that "the reduced discrimination between sucrose and As-Ac induced by CO2 would promote the consumptions of low-calorie beverages and would converge with CO2-induced gastric distention in limiting caloric intake."
This study was supported in part by the Coca-Cola Company. One author, Dr. Rosario Cuomo, was sponsored by the Coca-Cola Company. The remaining authors reported having no disclosures.
FROM GASTROENTEROLOGY
