User login
Eczema of the eyelids? Think chemical allergy
LAS VEGAS – If a patient presents with eczema of the eyelids, or swollen eyelids that don’t respond to topical steroids, think about sending them for chemical testing, advised Dr. Janet M. Neigel.
"The eyelids are red and scaly, a little swollen, and it just never goes away," she said in an interview at the annual meeting of the American Academy of Cosmetic Surgery.
Dr. Neigel, a cosmetic surgeon in West Orange, N.J., said that over the past 5 years, she has seen increasing numbers of patients present with eczema localized to the eyelids or eyeball area that recurs like pesky crabgrass.
"I treat them with topical steroids," Dr. Neigel said. "It will get better, but it always comes back. Some of this is seasonal. It may only happen in the winter, when the air is drier and their skin tends to get drier. In others it can be all year long," she said. "It seems to be more common in women, but I see men with this condition, too. In men, it tends to present as a reddish eye and tearing," she noted.
In the majority of cases, the culprit turns out to be an allergy to chemicals including gold, nickel, tin, rubber, preservatives in shampoos and laundry detergent, and formaldehyde resin, which is used in nail polish. "There was one patient who was allergic to the preservative in eyedrops," Dr. Neigel recalled. "She was on several different eyedrops trying to treat the swollen eye area, and it was just making the condition worse."
Another patient’s eczema cleared only after she removed her wedding ring, Dr. Neigel said. "So she couldn’t wear any gold jewelry. In somebody else it was tin and nickel, so she couldn’t wear any cheap jewelry."
Ointments commonly used for cosmetic procedures also can cause trouble. "There is cross-reactivity between neomycin, tobramycin, and Neosporin," Dr. Neigel said. "One patient was applying Neosporin every time she bumped herself on different parts of her body, and her eyelids were the only things flaring up."
Dr. Neigel speculated that the reaction in such cases is localized to the eyelid because "it’s the thinnest skin in the body. It’s the most sensitive, and for some reason, the patients I’m seeing only have reactions there," she noted. So, for patients with allergic conjunctivitis or tearing for a contact dermatitis–type presentation around the eyeball or the eyelids, send them for chemical testing, she advised. "There’s a good chance you might clear things up and figure out what they’re truly reacting to – get to the source instead of just treating the problem symptomatically," she said.
Dr. Neigel said she had no relevant financial disclosures.
LAS VEGAS – If a patient presents with eczema of the eyelids, or swollen eyelids that don’t respond to topical steroids, think about sending them for chemical testing, advised Dr. Janet M. Neigel.
"The eyelids are red and scaly, a little swollen, and it just never goes away," she said in an interview at the annual meeting of the American Academy of Cosmetic Surgery.
Dr. Neigel, a cosmetic surgeon in West Orange, N.J., said that over the past 5 years, she has seen increasing numbers of patients present with eczema localized to the eyelids or eyeball area that recurs like pesky crabgrass.
"I treat them with topical steroids," Dr. Neigel said. "It will get better, but it always comes back. Some of this is seasonal. It may only happen in the winter, when the air is drier and their skin tends to get drier. In others it can be all year long," she said. "It seems to be more common in women, but I see men with this condition, too. In men, it tends to present as a reddish eye and tearing," she noted.
In the majority of cases, the culprit turns out to be an allergy to chemicals including gold, nickel, tin, rubber, preservatives in shampoos and laundry detergent, and formaldehyde resin, which is used in nail polish. "There was one patient who was allergic to the preservative in eyedrops," Dr. Neigel recalled. "She was on several different eyedrops trying to treat the swollen eye area, and it was just making the condition worse."
Another patient’s eczema cleared only after she removed her wedding ring, Dr. Neigel said. "So she couldn’t wear any gold jewelry. In somebody else it was tin and nickel, so she couldn’t wear any cheap jewelry."
Ointments commonly used for cosmetic procedures also can cause trouble. "There is cross-reactivity between neomycin, tobramycin, and Neosporin," Dr. Neigel said. "One patient was applying Neosporin every time she bumped herself on different parts of her body, and her eyelids were the only things flaring up."
Dr. Neigel speculated that the reaction in such cases is localized to the eyelid because "it’s the thinnest skin in the body. It’s the most sensitive, and for some reason, the patients I’m seeing only have reactions there," she noted. So, for patients with allergic conjunctivitis or tearing for a contact dermatitis–type presentation around the eyeball or the eyelids, send them for chemical testing, she advised. "There’s a good chance you might clear things up and figure out what they’re truly reacting to – get to the source instead of just treating the problem symptomatically," she said.
Dr. Neigel said she had no relevant financial disclosures.
LAS VEGAS – If a patient presents with eczema of the eyelids, or swollen eyelids that don’t respond to topical steroids, think about sending them for chemical testing, advised Dr. Janet M. Neigel.
"The eyelids are red and scaly, a little swollen, and it just never goes away," she said in an interview at the annual meeting of the American Academy of Cosmetic Surgery.
Dr. Neigel, a cosmetic surgeon in West Orange, N.J., said that over the past 5 years, she has seen increasing numbers of patients present with eczema localized to the eyelids or eyeball area that recurs like pesky crabgrass.
"I treat them with topical steroids," Dr. Neigel said. "It will get better, but it always comes back. Some of this is seasonal. It may only happen in the winter, when the air is drier and their skin tends to get drier. In others it can be all year long," she said. "It seems to be more common in women, but I see men with this condition, too. In men, it tends to present as a reddish eye and tearing," she noted.
In the majority of cases, the culprit turns out to be an allergy to chemicals including gold, nickel, tin, rubber, preservatives in shampoos and laundry detergent, and formaldehyde resin, which is used in nail polish. "There was one patient who was allergic to the preservative in eyedrops," Dr. Neigel recalled. "She was on several different eyedrops trying to treat the swollen eye area, and it was just making the condition worse."
Another patient’s eczema cleared only after she removed her wedding ring, Dr. Neigel said. "So she couldn’t wear any gold jewelry. In somebody else it was tin and nickel, so she couldn’t wear any cheap jewelry."
Ointments commonly used for cosmetic procedures also can cause trouble. "There is cross-reactivity between neomycin, tobramycin, and Neosporin," Dr. Neigel said. "One patient was applying Neosporin every time she bumped herself on different parts of her body, and her eyelids were the only things flaring up."
Dr. Neigel speculated that the reaction in such cases is localized to the eyelid because "it’s the thinnest skin in the body. It’s the most sensitive, and for some reason, the patients I’m seeing only have reactions there," she noted. So, for patients with allergic conjunctivitis or tearing for a contact dermatitis–type presentation around the eyeball or the eyelids, send them for chemical testing, she advised. "There’s a good chance you might clear things up and figure out what they’re truly reacting to – get to the source instead of just treating the problem symptomatically," she said.
Dr. Neigel said she had no relevant financial disclosures.
AT THE AACS ANNUAL MEETING
Scuba Diving Safety: A Case Report of Diving Injury in the Red Sea

Time Change and Acute Myocardial Infarction
Providing an Alternative Treatment Modality for Veterans: Establishing and Evaluating an Acupuncture Clinic in a VA Medical Center
Parsonage-Turner Syndrome: Diagnosis and Rehabilitation Strategies
Man, 57, With Dyspnea After Chiropractic Manipulation
A 57-year-old man presented to the emergency department (ED) with a two-day history of worsening shortness of breath, light-headedness, and back pain. The patient, who had a history of ankylosing spondylitis, had been receiving weekly therapy from a chiropractor for about 10 years. One week before presenting to the ED, he had begun to undergo daily manipulations under anesthesia (MUA)—an aggressive chiropractic procedure that is administered while the patient is under monitored, procedural sedation. After the second day of treatment, the patient began to experience worsening back pain and progressive light-headedness and shortness of breath.
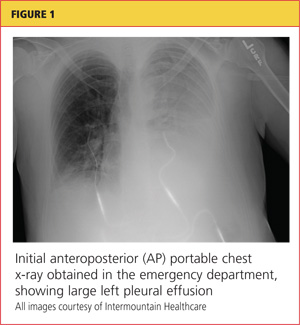
At a follow-up visit with his chiropractor, he was found to have decreased O2 saturation and was directed to go to the hospital for evaluation. On arrival at the ED, the patient was awake and alert. He had intact motor strength in all extremities, no sensory abnormalities, intact symmetric reflexes, and no bladder or bowel dysfunction, with a negative Babinski sign. His O2 saturation was 92% on 5 L of oxygen. An absence of breath sounds was noted on the left side.
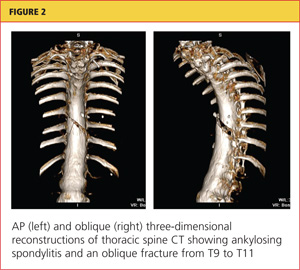
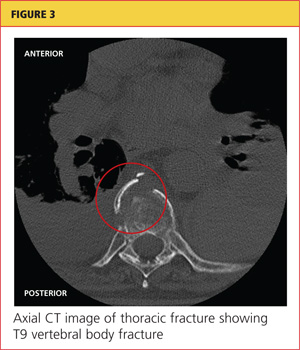
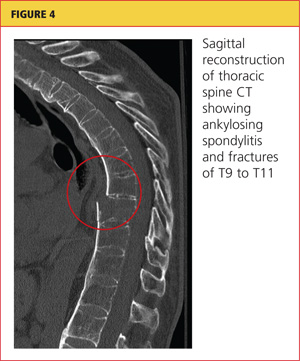
Chest x-ray (see Figure 1) was performed, which demonstrated complete opacification of the left hemithorax, consistent with a large pleural effusion or hemothorax. CT scan of the thoracic spine showed diffuse ankylosis. A complex oblique coronal and transversely oriented fracture with 7 mm of displacement was identified, beginning at the right anterior inferior lateral margin of the T8 vertebral body and extending centrally and inferiorly to the left and right into the T9 vertebral body. The fracture continued through the right T9-10 neural foramen and what was probably the right fused T9-10 facet joint. The fracture exited through the left superior and lateral margin of the T10 vertebral body and the left T10-11 neural foramen (see Figures 2, 3, and 4).
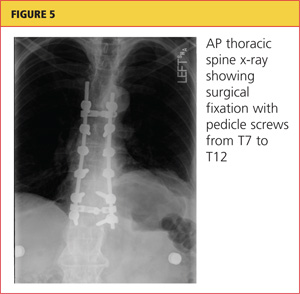
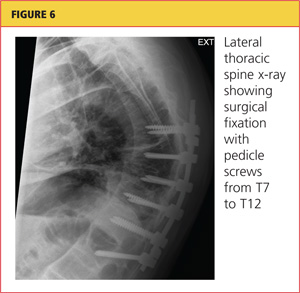
A chest tube was inserted in the ED, and 1,600 mL of old blood was immediately drained. The patient was admitted to the ICU on the trauma service. He was taken to surgery for open reduction and internal fixation of his unstable thoracic spine fracture on day 3 of hospitalization, after his pulmonary condition stabilized. Pedicle screws were placed from T7 through T12 during the spinal fusion. Good reduction of the fracture was observed following the spine surgery (see Figures 5 and 6). At the conclusion of surgery, an epidural catheter was placed in the thoracic spine to administer pain control.
After the spine portion of the procedure, the patient was repositioned and underwent video-assisted thoracoscopic surgery of the left hemithorax for evacuation of retained hemothorax. The patient tolerated the procedure well and was taken to the ICU for recovery.
On postoperative day 2, the patient complained of chest pain and experienced hypoxemia with activity. CT angiography of the chest demonstrated bilateral segmental and subsegmental pulmonary emboli. The epidural catheter was discontinued. Six hours later, a heparin drip was started, and the patient was transitioned to therapeutic enoxaparin and warfarin. When methicillin-sensitive Staphylococcus aureus (MSSA) was detected in his hemothorax fluid, he was treated with a course of nafcillin.
The patient was discharged to home on postoperative day 12. He has remained neurologically intact and has returned to his former work activities. He is not taking narcotic pain medications.
Discussion
Chiropractic care is a popular alternative health care modality in the United States. Researchers for the 2007 National Health Interview Study1 reported an annual use of chiropractic manipulation of 8.6%, while the Medical Expenditure Panel Survey2 data yielded an estimate of 12.6 million adults using chiropractic manipulation in 2006—translating to a prevalence of 5.6%. Despite the popularity of chiropractic medicine, few well-designed studies have been conducted to support its use.3,4 Because of its designation as an alternative therapy, however, chiropractic manipulation has not been subjected to rigorous efficacy and safety evaluations.5
Given the inconsistency of the evidence to support chiropractic manipulation, the practice's safety profile is a concern. The risks associated with spinal manipulation are generally described in case reports and small series. Most serious adverse events described in the literature are cerebrovascular in nature and tend to occur after cervical manipulation.6,7 Fractures after spine manipulation are exceedingly rare, and published literature on this topic consists of a few isolated case reports, with all fractures occurring in the cervical spine in patients with an underlying pathologic condition.8-10
In 2009, Gouveia et al5 reviewed the published literature regarding all adverse events resulting from chiropractic manipulation. The authors found one randomized controlled trial, two case-control studies, six prospective studies, 12 surveys, three retrospective studies, and 100 case reports. The spectrum of complications identified ranged from benign and transient, such as local discomfort, to far more serious: stroke, myelopathy, radiculopathy, subdural hematoma, spinal fluid leakage, cauda equina syndrome, herniated disc, diaphragmatic palsy, and vertebral fractures. The authors were unable to perform a true meta-analysis because of the heterogeneity of the data, but they concluded that complications associated with chiropractic procedures are "frequent."5
Manipulations Under Anesthesia
MUA is a procedure that combines chiropractic adjustments and manipulations with general anesthesia or procedural sedation.11 The theory behind this strategy is that the anesthesia or sedation reduces pain and muscle spasm that may hinder the manipulation, allowing the practitioner to more effectively break up joint adhesions and reduce segmental dysfunction than if the patient had not undergone anesthesia.11
MUA is generally indicated in patients who have not responded to a 4- to 8-week trial of traditional manipulation therapy.12 It is also considered in patients who have "painful and restricting muscular guarding [that] interferes with the performance of spinal adjustments, mobilizations, and soft tissue release techniques."13
In the chiropractic literature, between 3% and 10% of patients are estimated to be candidates for MUA.12,14 It is not completely clear, however, what diagnoses are most likely to be treated successfully with this technique. Contraindications to MUA are generally the same as those for manipulation in conscious patients. A published list of contraindications from the Committee for Manipulation under Anesthesia (2003)15 included malignancy with bony metastasis, tuberculosis of the bone, recent fracture, acute arthritis, acute gout, diabetic neuropathy, syphilitic articular lesions, excessive spinal osteoporosis, disk fragmentation, direct nerve root impingement, and evidence of cord or caudal compression by tumor, ankylosis, or other space-occupying lesions.
MUA generally begins with deep procedural sedation, managed by an anesthesiologist. Once an adequate level of sedation is achieved, the manipulations are performed. Both high- and low-velocity thrusts are used, but it is recommended that the force exerted should be much less, and the manipulations performed with more caution, than in patients who are not anesthetized.12
For the thoracic spine, the patient is manipulated in the supine position with the arms crossed over the chest. The practitioner places one hand in a fist under the spine with the other hand on the patient's crossed arms, then delivers an anterior-to-posterior thrust. This is repeated until all affected segments have been treated.11,12
Literature to support the use of MUA for various indications is largely anecdotal. The largest published series13 is of 177 patients with chronic spinal pain who each underwent three MUA sessions followed by four to six weeks of traditional manipulations. The authors found that pain, as measured by visual analog scale, was reduced by 62% in patients with cervical spine pain, and by 60% in patients with lumbar pain. No adverse events were reported in the study.
Kohlbeck and Haldeman12 reviewed the reported complications of MUA across all published literature. They found that in 17 published papers, the overall complication rate was 0.7%, mainly represented by transitory increased pain. No spinal fractures were reported.
This case demonstrates a rare but serious complication of chiropractic MUA. It is unclear exactly what mechanism of injury led to an unstable thoracic spine fracture with massive hemothorax, and the precise cause will probably never be known. The clinicians who treated the case patient find it curious that the reported rate of adverse events following this procedure is so low, but they suspect an element of reporting bias in the chiropractic literature.
Conclusion
Iatrogenic injury after chiropractic manipulation is uncommon, but it can be devastating. Few serious complications of chiropractic MUA have been reported, but the literature is lacking in well-designed research studies. Despite the dearth of clinical trials to support its safety and efficacy, use of MUA has continued in the chiropractic community. This case demonstrates that serious adverse outcomes can occur, and more rigorous studies are needed to delineate the true benefits and risks of this set of chiropractic procedures.
References
1. Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report. 2008;12:1-9.
2. Davis MA, Sirovich BE, Weeks WB. Utilization and expenditures on chiropractic care in the United States from 1997 to 2006. Health Serv Res. 2009;45:748-761.
3. Canadian Chiropractic Association; Canadian Federation of Chiropractic Regulatory Boards; Clinical Practice Guidelines Development Initiative; Guidelines Development Committee. Chiropractic clinical practice guideline: evidence-based treatment of adult neck pain not due to whiplash. J Can Chiropr Assoc. 2005;49:417-421.
4.
Hurwitz EL, Aker PD, Adams AH, et al. Manipulation and mobilization of the cervical spine: a systematic review of the literature. Spine (Phila Pa 1976). 1996;21:1746-1760.
5.Gouveia LO, Castanho P, Ferreira JJ. Safety of chiropractic interventions: a systematic review. Spine (Phila Pa 1976). 2009;34:E405-E413.
6. Di Fabio RP. Manipulation of the cervical spine: risks and benefits. Phys Ther. 1999;79:50-65.
7. Nadareishvili Z, Norris JW. Stroke from traumatic arterial dissection. Lancet. 1999;354:159-160.
8. Austin RT. Pathological vertebral fractures after spinal manipulation. Br Med J (Clin Res Ed). 1985;291:1114-1115.
9. Ea HK, Weber AJ, Yon F, Lioté F. Osteoporotic fracture of the dens revealed by cervical manipulation. Joint Bone Spine. 2004;71:246-250.
10. Schmitz A, Lutterbey G, von Engelhardt L, et al. Pathological cervical fracture after spinal manipulation in a pregnant patient. J Manipulative Physiol Ther. 2005;28:633-636.
11. Cremata E, Collins S, Clauson W, et al. Manipulation under anesthesia: a report of four cases. J Manipulative Physiol Ther. 2005;28:526-533.
12. Kohlbeck FJ, Haldeman S. Medication-assisted spinal manipulation. Spine J. 2002;2:288-302.
13. West DT, Mathews RS, Miller MR, Kent GM. Effective management of spinal pain in one hundred seventy-seven patients evaluated for manipulation under anesthesia. J Manipulative Physiol Ther. 1999;22:299-308.
14. Morey LW Jr. Osteopathic manipulation under general anesthesia. J Am Osteopath Assoc. 1973;73:116-127.
15. Tain L, Gunderson C, Cremata E, et al; Committee for Manipulation Under Anesthesia. Recommendations to the Industrial Medical Council Work Group of California for manipulation under anesthesia use for injured workers. Sacramento, CA: Industrial Medical Council; 2003.
A 57-year-old man presented to the emergency department (ED) with a two-day history of worsening shortness of breath, light-headedness, and back pain. The patient, who had a history of ankylosing spondylitis, had been receiving weekly therapy from a chiropractor for about 10 years. One week before presenting to the ED, he had begun to undergo daily manipulations under anesthesia (MUA)—an aggressive chiropractic procedure that is administered while the patient is under monitored, procedural sedation. After the second day of treatment, the patient began to experience worsening back pain and progressive light-headedness and shortness of breath.
At a follow-up visit with his chiropractor, he was found to have decreased O2 saturation and was directed to go to the hospital for evaluation. On arrival at the ED, the patient was awake and alert. He had intact motor strength in all extremities, no sensory abnormalities, intact symmetric reflexes, and no bladder or bowel dysfunction, with a negative Babinski sign. His O2 saturation was 92% on 5 L of oxygen. An absence of breath sounds was noted on the left side.
Chest x-ray (see Figure 1) was performed, which demonstrated complete opacification of the left hemithorax, consistent with a large pleural effusion or hemothorax. CT scan of the thoracic spine showed diffuse ankylosis. A complex oblique coronal and transversely oriented fracture with 7 mm of displacement was identified, beginning at the right anterior inferior lateral margin of the T8 vertebral body and extending centrally and inferiorly to the left and right into the T9 vertebral body. The fracture continued through the right T9-10 neural foramen and what was probably the right fused T9-10 facet joint. The fracture exited through the left superior and lateral margin of the T10 vertebral body and the left T10-11 neural foramen (see Figures 2, 3, and 4).
A chest tube was inserted in the ED, and 1,600 mL of old blood was immediately drained. The patient was admitted to the ICU on the trauma service. He was taken to surgery for open reduction and internal fixation of his unstable thoracic spine fracture on day 3 of hospitalization, after his pulmonary condition stabilized. Pedicle screws were placed from T7 through T12 during the spinal fusion. Good reduction of the fracture was observed following the spine surgery (see Figures 5 and 6). At the conclusion of surgery, an epidural catheter was placed in the thoracic spine to administer pain control.
After the spine portion of the procedure, the patient was repositioned and underwent video-assisted thoracoscopic surgery of the left hemithorax for evacuation of retained hemothorax. The patient tolerated the procedure well and was taken to the ICU for recovery.
On postoperative day 2, the patient complained of chest pain and experienced hypoxemia with activity. CT angiography of the chest demonstrated bilateral segmental and subsegmental pulmonary emboli. The epidural catheter was discontinued. Six hours later, a heparin drip was started, and the patient was transitioned to therapeutic enoxaparin and warfarin. When methicillin-sensitive Staphylococcus aureus (MSSA) was detected in his hemothorax fluid, he was treated with a course of nafcillin.
The patient was discharged to home on postoperative day 12. He has remained neurologically intact and has returned to his former work activities. He is not taking narcotic pain medications.
Discussion
Chiropractic care is a popular alternative health care modality in the United States. Researchers for the 2007 National Health Interview Study1 reported an annual use of chiropractic manipulation of 8.6%, while the Medical Expenditure Panel Survey2 data yielded an estimate of 12.6 million adults using chiropractic manipulation in 2006—translating to a prevalence of 5.6%. Despite the popularity of chiropractic medicine, few well-designed studies have been conducted to support its use.3,4 Because of its designation as an alternative therapy, however, chiropractic manipulation has not been subjected to rigorous efficacy and safety evaluations.5
Given the inconsistency of the evidence to support chiropractic manipulation, the practice's safety profile is a concern. The risks associated with spinal manipulation are generally described in case reports and small series. Most serious adverse events described in the literature are cerebrovascular in nature and tend to occur after cervical manipulation.6,7 Fractures after spine manipulation are exceedingly rare, and published literature on this topic consists of a few isolated case reports, with all fractures occurring in the cervical spine in patients with an underlying pathologic condition.8-10
In 2009, Gouveia et al5 reviewed the published literature regarding all adverse events resulting from chiropractic manipulation. The authors found one randomized controlled trial, two case-control studies, six prospective studies, 12 surveys, three retrospective studies, and 100 case reports. The spectrum of complications identified ranged from benign and transient, such as local discomfort, to far more serious: stroke, myelopathy, radiculopathy, subdural hematoma, spinal fluid leakage, cauda equina syndrome, herniated disc, diaphragmatic palsy, and vertebral fractures. The authors were unable to perform a true meta-analysis because of the heterogeneity of the data, but they concluded that complications associated with chiropractic procedures are "frequent."5
Manipulations Under Anesthesia
MUA is a procedure that combines chiropractic adjustments and manipulations with general anesthesia or procedural sedation.11 The theory behind this strategy is that the anesthesia or sedation reduces pain and muscle spasm that may hinder the manipulation, allowing the practitioner to more effectively break up joint adhesions and reduce segmental dysfunction than if the patient had not undergone anesthesia.11
MUA is generally indicated in patients who have not responded to a 4- to 8-week trial of traditional manipulation therapy.12 It is also considered in patients who have "painful and restricting muscular guarding [that] interferes with the performance of spinal adjustments, mobilizations, and soft tissue release techniques."13
In the chiropractic literature, between 3% and 10% of patients are estimated to be candidates for MUA.12,14 It is not completely clear, however, what diagnoses are most likely to be treated successfully with this technique. Contraindications to MUA are generally the same as those for manipulation in conscious patients. A published list of contraindications from the Committee for Manipulation under Anesthesia (2003)15 included malignancy with bony metastasis, tuberculosis of the bone, recent fracture, acute arthritis, acute gout, diabetic neuropathy, syphilitic articular lesions, excessive spinal osteoporosis, disk fragmentation, direct nerve root impingement, and evidence of cord or caudal compression by tumor, ankylosis, or other space-occupying lesions.
MUA generally begins with deep procedural sedation, managed by an anesthesiologist. Once an adequate level of sedation is achieved, the manipulations are performed. Both high- and low-velocity thrusts are used, but it is recommended that the force exerted should be much less, and the manipulations performed with more caution, than in patients who are not anesthetized.12
For the thoracic spine, the patient is manipulated in the supine position with the arms crossed over the chest. The practitioner places one hand in a fist under the spine with the other hand on the patient's crossed arms, then delivers an anterior-to-posterior thrust. This is repeated until all affected segments have been treated.11,12
Literature to support the use of MUA for various indications is largely anecdotal. The largest published series13 is of 177 patients with chronic spinal pain who each underwent three MUA sessions followed by four to six weeks of traditional manipulations. The authors found that pain, as measured by visual analog scale, was reduced by 62% in patients with cervical spine pain, and by 60% in patients with lumbar pain. No adverse events were reported in the study.
Kohlbeck and Haldeman12 reviewed the reported complications of MUA across all published literature. They found that in 17 published papers, the overall complication rate was 0.7%, mainly represented by transitory increased pain. No spinal fractures were reported.
This case demonstrates a rare but serious complication of chiropractic MUA. It is unclear exactly what mechanism of injury led to an unstable thoracic spine fracture with massive hemothorax, and the precise cause will probably never be known. The clinicians who treated the case patient find it curious that the reported rate of adverse events following this procedure is so low, but they suspect an element of reporting bias in the chiropractic literature.
Conclusion
Iatrogenic injury after chiropractic manipulation is uncommon, but it can be devastating. Few serious complications of chiropractic MUA have been reported, but the literature is lacking in well-designed research studies. Despite the dearth of clinical trials to support its safety and efficacy, use of MUA has continued in the chiropractic community. This case demonstrates that serious adverse outcomes can occur, and more rigorous studies are needed to delineate the true benefits and risks of this set of chiropractic procedures.
References
1. Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report. 2008;12:1-9.
2. Davis MA, Sirovich BE, Weeks WB. Utilization and expenditures on chiropractic care in the United States from 1997 to 2006. Health Serv Res. 2009;45:748-761.
3. Canadian Chiropractic Association; Canadian Federation of Chiropractic Regulatory Boards; Clinical Practice Guidelines Development Initiative; Guidelines Development Committee. Chiropractic clinical practice guideline: evidence-based treatment of adult neck pain not due to whiplash. J Can Chiropr Assoc. 2005;49:417-421.
4.
Hurwitz EL, Aker PD, Adams AH, et al. Manipulation and mobilization of the cervical spine: a systematic review of the literature. Spine (Phila Pa 1976). 1996;21:1746-1760.
5.Gouveia LO, Castanho P, Ferreira JJ. Safety of chiropractic interventions: a systematic review. Spine (Phila Pa 1976). 2009;34:E405-E413.
6. Di Fabio RP. Manipulation of the cervical spine: risks and benefits. Phys Ther. 1999;79:50-65.
7. Nadareishvili Z, Norris JW. Stroke from traumatic arterial dissection. Lancet. 1999;354:159-160.
8. Austin RT. Pathological vertebral fractures after spinal manipulation. Br Med J (Clin Res Ed). 1985;291:1114-1115.
9. Ea HK, Weber AJ, Yon F, Lioté F. Osteoporotic fracture of the dens revealed by cervical manipulation. Joint Bone Spine. 2004;71:246-250.
10. Schmitz A, Lutterbey G, von Engelhardt L, et al. Pathological cervical fracture after spinal manipulation in a pregnant patient. J Manipulative Physiol Ther. 2005;28:633-636.
11. Cremata E, Collins S, Clauson W, et al. Manipulation under anesthesia: a report of four cases. J Manipulative Physiol Ther. 2005;28:526-533.
12. Kohlbeck FJ, Haldeman S. Medication-assisted spinal manipulation. Spine J. 2002;2:288-302.
13. West DT, Mathews RS, Miller MR, Kent GM. Effective management of spinal pain in one hundred seventy-seven patients evaluated for manipulation under anesthesia. J Manipulative Physiol Ther. 1999;22:299-308.
14. Morey LW Jr. Osteopathic manipulation under general anesthesia. J Am Osteopath Assoc. 1973;73:116-127.
15. Tain L, Gunderson C, Cremata E, et al; Committee for Manipulation Under Anesthesia. Recommendations to the Industrial Medical Council Work Group of California for manipulation under anesthesia use for injured workers. Sacramento, CA: Industrial Medical Council; 2003.
A 57-year-old man presented to the emergency department (ED) with a two-day history of worsening shortness of breath, light-headedness, and back pain. The patient, who had a history of ankylosing spondylitis, had been receiving weekly therapy from a chiropractor for about 10 years. One week before presenting to the ED, he had begun to undergo daily manipulations under anesthesia (MUA)—an aggressive chiropractic procedure that is administered while the patient is under monitored, procedural sedation. After the second day of treatment, the patient began to experience worsening back pain and progressive light-headedness and shortness of breath.
At a follow-up visit with his chiropractor, he was found to have decreased O2 saturation and was directed to go to the hospital for evaluation. On arrival at the ED, the patient was awake and alert. He had intact motor strength in all extremities, no sensory abnormalities, intact symmetric reflexes, and no bladder or bowel dysfunction, with a negative Babinski sign. His O2 saturation was 92% on 5 L of oxygen. An absence of breath sounds was noted on the left side.
Chest x-ray (see Figure 1) was performed, which demonstrated complete opacification of the left hemithorax, consistent with a large pleural effusion or hemothorax. CT scan of the thoracic spine showed diffuse ankylosis. A complex oblique coronal and transversely oriented fracture with 7 mm of displacement was identified, beginning at the right anterior inferior lateral margin of the T8 vertebral body and extending centrally and inferiorly to the left and right into the T9 vertebral body. The fracture continued through the right T9-10 neural foramen and what was probably the right fused T9-10 facet joint. The fracture exited through the left superior and lateral margin of the T10 vertebral body and the left T10-11 neural foramen (see Figures 2, 3, and 4).
A chest tube was inserted in the ED, and 1,600 mL of old blood was immediately drained. The patient was admitted to the ICU on the trauma service. He was taken to surgery for open reduction and internal fixation of his unstable thoracic spine fracture on day 3 of hospitalization, after his pulmonary condition stabilized. Pedicle screws were placed from T7 through T12 during the spinal fusion. Good reduction of the fracture was observed following the spine surgery (see Figures 5 and 6). At the conclusion of surgery, an epidural catheter was placed in the thoracic spine to administer pain control.
After the spine portion of the procedure, the patient was repositioned and underwent video-assisted thoracoscopic surgery of the left hemithorax for evacuation of retained hemothorax. The patient tolerated the procedure well and was taken to the ICU for recovery.
On postoperative day 2, the patient complained of chest pain and experienced hypoxemia with activity. CT angiography of the chest demonstrated bilateral segmental and subsegmental pulmonary emboli. The epidural catheter was discontinued. Six hours later, a heparin drip was started, and the patient was transitioned to therapeutic enoxaparin and warfarin. When methicillin-sensitive Staphylococcus aureus (MSSA) was detected in his hemothorax fluid, he was treated with a course of nafcillin.
The patient was discharged to home on postoperative day 12. He has remained neurologically intact and has returned to his former work activities. He is not taking narcotic pain medications.
Discussion
Chiropractic care is a popular alternative health care modality in the United States. Researchers for the 2007 National Health Interview Study1 reported an annual use of chiropractic manipulation of 8.6%, while the Medical Expenditure Panel Survey2 data yielded an estimate of 12.6 million adults using chiropractic manipulation in 2006—translating to a prevalence of 5.6%. Despite the popularity of chiropractic medicine, few well-designed studies have been conducted to support its use.3,4 Because of its designation as an alternative therapy, however, chiropractic manipulation has not been subjected to rigorous efficacy and safety evaluations.5
Given the inconsistency of the evidence to support chiropractic manipulation, the practice's safety profile is a concern. The risks associated with spinal manipulation are generally described in case reports and small series. Most serious adverse events described in the literature are cerebrovascular in nature and tend to occur after cervical manipulation.6,7 Fractures after spine manipulation are exceedingly rare, and published literature on this topic consists of a few isolated case reports, with all fractures occurring in the cervical spine in patients with an underlying pathologic condition.8-10
In 2009, Gouveia et al5 reviewed the published literature regarding all adverse events resulting from chiropractic manipulation. The authors found one randomized controlled trial, two case-control studies, six prospective studies, 12 surveys, three retrospective studies, and 100 case reports. The spectrum of complications identified ranged from benign and transient, such as local discomfort, to far more serious: stroke, myelopathy, radiculopathy, subdural hematoma, spinal fluid leakage, cauda equina syndrome, herniated disc, diaphragmatic palsy, and vertebral fractures. The authors were unable to perform a true meta-analysis because of the heterogeneity of the data, but they concluded that complications associated with chiropractic procedures are "frequent."5
Manipulations Under Anesthesia
MUA is a procedure that combines chiropractic adjustments and manipulations with general anesthesia or procedural sedation.11 The theory behind this strategy is that the anesthesia or sedation reduces pain and muscle spasm that may hinder the manipulation, allowing the practitioner to more effectively break up joint adhesions and reduce segmental dysfunction than if the patient had not undergone anesthesia.11
MUA is generally indicated in patients who have not responded to a 4- to 8-week trial of traditional manipulation therapy.12 It is also considered in patients who have "painful and restricting muscular guarding [that] interferes with the performance of spinal adjustments, mobilizations, and soft tissue release techniques."13
In the chiropractic literature, between 3% and 10% of patients are estimated to be candidates for MUA.12,14 It is not completely clear, however, what diagnoses are most likely to be treated successfully with this technique. Contraindications to MUA are generally the same as those for manipulation in conscious patients. A published list of contraindications from the Committee for Manipulation under Anesthesia (2003)15 included malignancy with bony metastasis, tuberculosis of the bone, recent fracture, acute arthritis, acute gout, diabetic neuropathy, syphilitic articular lesions, excessive spinal osteoporosis, disk fragmentation, direct nerve root impingement, and evidence of cord or caudal compression by tumor, ankylosis, or other space-occupying lesions.
MUA generally begins with deep procedural sedation, managed by an anesthesiologist. Once an adequate level of sedation is achieved, the manipulations are performed. Both high- and low-velocity thrusts are used, but it is recommended that the force exerted should be much less, and the manipulations performed with more caution, than in patients who are not anesthetized.12
For the thoracic spine, the patient is manipulated in the supine position with the arms crossed over the chest. The practitioner places one hand in a fist under the spine with the other hand on the patient's crossed arms, then delivers an anterior-to-posterior thrust. This is repeated until all affected segments have been treated.11,12
Literature to support the use of MUA for various indications is largely anecdotal. The largest published series13 is of 177 patients with chronic spinal pain who each underwent three MUA sessions followed by four to six weeks of traditional manipulations. The authors found that pain, as measured by visual analog scale, was reduced by 62% in patients with cervical spine pain, and by 60% in patients with lumbar pain. No adverse events were reported in the study.
Kohlbeck and Haldeman12 reviewed the reported complications of MUA across all published literature. They found that in 17 published papers, the overall complication rate was 0.7%, mainly represented by transitory increased pain. No spinal fractures were reported.
This case demonstrates a rare but serious complication of chiropractic MUA. It is unclear exactly what mechanism of injury led to an unstable thoracic spine fracture with massive hemothorax, and the precise cause will probably never be known. The clinicians who treated the case patient find it curious that the reported rate of adverse events following this procedure is so low, but they suspect an element of reporting bias in the chiropractic literature.
Conclusion
Iatrogenic injury after chiropractic manipulation is uncommon, but it can be devastating. Few serious complications of chiropractic MUA have been reported, but the literature is lacking in well-designed research studies. Despite the dearth of clinical trials to support its safety and efficacy, use of MUA has continued in the chiropractic community. This case demonstrates that serious adverse outcomes can occur, and more rigorous studies are needed to delineate the true benefits and risks of this set of chiropractic procedures.
References
1. Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report. 2008;12:1-9.
2. Davis MA, Sirovich BE, Weeks WB. Utilization and expenditures on chiropractic care in the United States from 1997 to 2006. Health Serv Res. 2009;45:748-761.
3. Canadian Chiropractic Association; Canadian Federation of Chiropractic Regulatory Boards; Clinical Practice Guidelines Development Initiative; Guidelines Development Committee. Chiropractic clinical practice guideline: evidence-based treatment of adult neck pain not due to whiplash. J Can Chiropr Assoc. 2005;49:417-421.
4.
Hurwitz EL, Aker PD, Adams AH, et al. Manipulation and mobilization of the cervical spine: a systematic review of the literature. Spine (Phila Pa 1976). 1996;21:1746-1760.
5.Gouveia LO, Castanho P, Ferreira JJ. Safety of chiropractic interventions: a systematic review. Spine (Phila Pa 1976). 2009;34:E405-E413.
6. Di Fabio RP. Manipulation of the cervical spine: risks and benefits. Phys Ther. 1999;79:50-65.
7. Nadareishvili Z, Norris JW. Stroke from traumatic arterial dissection. Lancet. 1999;354:159-160.
8. Austin RT. Pathological vertebral fractures after spinal manipulation. Br Med J (Clin Res Ed). 1985;291:1114-1115.
9. Ea HK, Weber AJ, Yon F, Lioté F. Osteoporotic fracture of the dens revealed by cervical manipulation. Joint Bone Spine. 2004;71:246-250.
10. Schmitz A, Lutterbey G, von Engelhardt L, et al. Pathological cervical fracture after spinal manipulation in a pregnant patient. J Manipulative Physiol Ther. 2005;28:633-636.
11. Cremata E, Collins S, Clauson W, et al. Manipulation under anesthesia: a report of four cases. J Manipulative Physiol Ther. 2005;28:526-533.
12. Kohlbeck FJ, Haldeman S. Medication-assisted spinal manipulation. Spine J. 2002;2:288-302.
13. West DT, Mathews RS, Miller MR, Kent GM. Effective management of spinal pain in one hundred seventy-seven patients evaluated for manipulation under anesthesia. J Manipulative Physiol Ther. 1999;22:299-308.
14. Morey LW Jr. Osteopathic manipulation under general anesthesia. J Am Osteopath Assoc. 1973;73:116-127.
15. Tain L, Gunderson C, Cremata E, et al; Committee for Manipulation Under Anesthesia. Recommendations to the Industrial Medical Council Work Group of California for manipulation under anesthesia use for injured workers. Sacramento, CA: Industrial Medical Council; 2003.
Scuba Diving Safety: A Case Report of Diving Injury in the Red Sea
Cover

5 Points on Improving Rotator Cuff Healing
ajo, the american journal of orthopedics, rotator cuff healing, platelet-rich plasma, PRP, platelet-rich fibrin matrix, PRFM
ajo, the american journal of orthopedics, rotator cuff healing, platelet-rich plasma, PRP, platelet-rich fibrin matrix, PRFM
ajo, the american journal of orthopedics, rotator cuff healing, platelet-rich plasma, PRP, platelet-rich fibrin matrix, PRFM
UPDATE: MINIMALLY INVASIVE GYNECOLOGY
LARCs: Why they should be first-line contraceptive options
for your patients
Elizabeth O. Schmidt, MD; Tessa Madden, MD, MPH; Jeffrey F. Piepert, MD, PhD
(November 2012)
Let’s increase our use of IUDs and improve contraceptive effectiveness in this country
Robert L. Barbieri, MD (Editorial, August 2012)
Minimally invasive surgery
Amy Garcia, MD (Update, April 2012)
Your surgical toolbox should include topical hemostatic
agents—here is why
Lisa A. dos Santos, MD; Andrew W. Menzin, MD (Surgical Techniques, April 2012)
Minimally invasive surgery
Amy Garcia, MD (Update, April 2011)
The proliferation of terms to describe heavy menstrual bleeding sometimes seems never-ending. From “menometrorrhagia” to “uterine hemorrhage,” these terms pop up quickly and confuse discussion of one of the most widespread problems in gynecology.
Enter the International Federation of Gynecology and Obstetrics (FIGO), which decided to tackle the inconsistent terminology and lack of classification of causes of abnormal uterine bleeding (AUB) with an eye toward standardizing research, facilitating discussion, and informing management decisions.
In this article, I focus on three aspects of this effort:
- FIGO’s revamping of terminology and classification
- comparisons of outcomes of hysterectomy versus endometrial ablation and the levonorgestrel-releasing intrauterine system
- guidelines on management of AUB related to ovulatory disorders and endometrial hemostatic dysfunction.
FIGO revamps nomenclature for abnormal uterine bleeding
Munro MG, Critchley HO, Fraser IS. The FIGO systems for nomenclature and classification of causes of abnormal uterine bleeding in the reproductive years: who needs them? Am J Obstet Gynecol. 2012;207(4):259–265.
As early as 2004, FIGO began a process to standardize the nomenclature for defining both normal and abnormal uterine bleeding in reproductive-aged women who are not pregnant.1 This process was a response to a lack of consistency and continuity in the design and interpretation of basic science and clinical investigation related to the problem of AUB. Inconsistent definitions of AUB, such as “menorrhagia,” “metrorrhagia,” and “dysfunctional uterine bleeding,” along with the absence of standard categorization of the causes of AUB, have led to confusion and difficulties in comparing clinical trials and in finding significant, relevant, and even meaningful correlations among investigations of AUB. Applying information from asynchronous and often incomplete investigations to evidence-based clinical practice then becomes a challenge for the gynecologist.
Munro and colleagues summarize the process by which FIGO developed both a nomenclature system and a classification system of the causes of AUB, which were formally adopted by FIGO in 2010 and endorsed in 2012 by the American College of Obstetricians and Gynecologists (ACOG).1-6 The arduous process led to:
- a refined definition of chronic AUB
- a new category called acute AUB
- a method for describing the clinical dimensions of menstruation and the menstrual cycle according to the following parameters:
- regularity of onset
- frequency of onset
- duration of menstrual flow
- heaviness, or volume, of menstrual flow.
Wherever appropriate, the definitions of normal for these parameters were based on statistics from large population studies that used medians and 5th and 95th percentiles.
The term “heavy menstrual bleeding” (HMB) is used to describe a woman’s perception of increased menstrual volume, regardless of regularity, frequency, or duration. AUB is the overarching term to describe any departure from normal menstruation, as defined by the parameters listed above. A group of misleading terms commonly used to describe AUB were eliminated from the FIGO nomenclature system, including “dysfunctional uterine bleeding,” “menorrhagia,” “hypermenorrhea,” “menometrorrhagia,” “polymenorrhagia,” and “metrorrhagia.”
The causes of AUB are classified in nine categories that are arranged according to the acronym PALM-COEIN:
- Polyp
- Adenomyosis
- Leiomyoma
- Malignancy and hyperplasia
- Coagulopathy
- Ovulatory disorders
- Endometrial dysfunction
- Iatrogenic
- Not otherwise classified.
Leiomyoma are subclassified as submucous or other, with tertiary subcategorization for intramural, subserosal, and transmural lesions
In general, the components of the PALM group are discrete (structural) entities that are measurable visually via imaging or histopathology, or both, while the COEI (of the COEIN group) includes women for whom the AUB is unrelated to structural abnormalities.
The classification system provides the infrastructure for a thorough investigative process and a means to characterize AUB for an individual who may have one or more potential causes or contributors. Such a comprehensive assessment allows the basic scientist to identify pure populations for tissue and molecular studies, the clinical scientist to identify potential confounders when defining populations for clinical investigation, and the clinician, educator, and trainee to consider the multidimensional nature of AUB where asymptomatic “red herrings” may coexist with otherwise invisible disorders of menstrual function.
The FIGO Menstrual Disorders Working Group anticipates that widespread, international acceptance of the recommended terms, definitions, and classification for AUB will lead to improved and more meaningful communication in clinical trials and published research and will enhance communication between health-care providers and patients, leading to better management of AUB.
Use of the FIGO-recommended terms, definitions, and classification of AUB will lead to higher-quality clinical research and thorough clinical investigation into the causes of AUB, with improved management of patients.
How hysterectomy for AUB compares with less invasive treatment options
Matteson KA, Abed H, Wheeler TL II, et al; Society of Gynecologic Surgeons Systematic Review Group. A systematic review comparing hysterectomy with less invasive treatments for abnormal uterine bleeding. J Minim Invasive Gynecol. 2012;19(1):13–28.
To create reliable treatment recommendations for AUB, as defined by the FIGO classification system just described, in women with ovulatory disorders, endometrial hemostatic dysfunction, and concomitant leiomyoma, the Systematic Review Group (SRG) of the Society of Gynecologic Surgeons performed a systematic review of treatments. The analysis was intended to compare hysterectomy with less invasive treatment modalities. The SRG reviewed randomized, controlled trials of AUB treatment that compared hysterectomy with:
- endometrial ablation by resectoscopic loop, rollerball, or thermal balloon
- the LNG-IUS
- medical therapy.
This comprehensive review of literature published between 1950 and January 14, 2011 led the SRG to create seven categories of clinical outcomes:
- bleeding control
- quality of life
- pain
- sexual health
- patient satisfaction
- need for additional treatment
- adverse events.
Of the initial 5,503 titles identified, only 18 articles, representing nine clinical trials, contained data of adequate quality to meet criteria for review. Seven of the trials compared hysterectomy with ablation, one compared hysterectomy with the LNG-IUS, and one compared hysterectomy with medical therapy. As FIGO has pointed out, the lack of homogeneity of terminology used to describe AUB and classification of its causes prevented clinically applicable comparative analyses of treatment outcomes.
Here are some of the SRG’s findings:
- Control of bleeding. Only data regarding amenorrhea were sufficient for comparative analysis. The SRG was able to conclude only that there was moderate strength of evidence supporting the statement that bleeding is better controlled following hysterectomy than following ablation.
- Quality of life. Overall, studies that evaluated quality of life showed improvement after ablation and hysterectomy. The strength of evidence demonstrating no difference between hysterectomy and ablation in postoperative quality of life was moderate.
- Pain, general health, vitality, and social function. Three studies found statistically significant differences in validated dimensions of the SF-36 questionnaire favoring hysterectomy for pain, general health, vitality, and social function. Two of these three studies evaluated minimally invasive hysterectomy by the laparoscopic supracervical or vaginal approach. The strength of evidence on pain beyond the postoperative time period was low and favored hysterectomy over ablation.
- Sexual health. The strength of evidence related to sexual health was low and revealed no differences between hysterectomy and ablation.
- Patient satisfaction. Overall, the quality of evidence was very low, showing no difference between hysterectomy and ablation.
- Need for additional treatment. The quality of evidence was moderate and favored hysterectomy over ablation.
- Adverse events. Evidence of moderate quality favored ablation and the LNG-IUS over hysterectomy, and low-quality evidence favored medical therapy over hysterectomy (TABLES 1, 2).
TABLE 1
What the data reveal about hysterectomy versus ablation
| Parameter | Strength of evidence (comparison) | |
|---|---|---|
| Hysterectomy | Ablation | |
| Bleeding control | Moderate (F) | — |
| Quality of life | Moderate (S) | Moderate (S) |
| Lower pain | Low (F) | — |
| Sexual health | Low (S) | Low (S) |
| Patient satisfaction | Very low (S) | Very low (S) |
| Need for additional treatment | Moderate (F) | — |
| Adverse events | — | Moderate (F) |
| F=Evidence favors comparator; S=no difference between comparators | ||
TABLE 2
What the data reveal about hysterectomy versus the levonorgestrel-releasing intrauterine system (LNG-IUS)
| Parameter | Strength of evidence (comparison) | |
|---|---|---|
| Hysterectomy | LNG-IUS | |
| Bleeding control | Moderate (F) | — |
| Quality of life | Moderate (S) | Moderate (S) |
| Lower pain | Moderate (S) | Moderate (S) |
| Sexual health | Moderate (S) | Moderate (S) |
| Patient satisfaction | Moderate (S) | Moderate (S) |
| Need for additional treatment | Moderate (F) | — |
| Adverse events | — | Moderate (F) |
| F=Evidence favors comparator; S=no difference between comparators | ||
The SRG concluded that there are tradeoffs between treatment effectiveness and the risk of serious adverse events between hysterectomy, ablation, and the LNG-IUS. It recommended that clinicians be educated about the relative advantages and disadvantages of each option so that they can discuss them with patients.
The SRG developed clinical practice guidelines for the treatment of ovulatory disorders and endometrial hemostatic dysfunction associated with AUB (see below).
Gynecologists should educate each patient about the efficacy and risks of options available for the management of AUB in the context of specific symptoms to facilitate an informed choice.
Wheeler TL II, Murphy M, Rogers RG, et al; Society of Gynecologic Surgeons Systematic Review Group. Clinical practice guidelines for abnormal uterine bleeding: hysterectomy versus alternative therapy. J Minim Invasive Gynecol. 2012;19(1):81–87.
The SRG used the results of the systematic review just summarized to formulate clinical guidelines for the treatment of AUB related to ovulatory disorders and endometrial hemostatic dysfunction. Recommendations were assigned a grade for their strength on the basis of the quality of supporting evidence, the size of the net medical benefit, and other considerations, including values and preferences applied in judgments. The strength of the clinical recommendation is either “strong” or “weak” and indicates the degree to which one can be confident that adherence to the recommendation will do more good than harm. All of the clinical recommendations described below received a grade of “weak.”
One primary suggestion from the study group is patient counseling that must first determine the type of AUB and the degree of burden or distress for the patient, as well as the presence of any additional cycle-related symptoms. Consideration should be given to variables that may modify the inherent risks or benefits of each intervention for the particular patient, as well as her values and preferences regarding treatment harms, benefits, and potential outcomes. Counseling should assess the patient’s need for contraception, desire for future childbearing, and proximity to menopause, as well as any cultural preferences for management.
Based on the clinical evidence related to hysterectomy versus endometrial ablation, the SRG made the following recommendations:
- If the patient desires amenorrhea and less pain and wants to avoid additional therapy, hysterectomy is preferred
- If the patient wants to avoid adverse events and seeks a shorter hospital stay, endometrial ablation is preferred
- If the patient’s main desire is for improvement in overall quality of life or sexual health, either intervention is appropriate, depending on patient preferences.
There were no data available in the systematic review concerning newer technologies for nonhysteroscopic endometrial ablation versus hysterectomy.
Based on the clinical evidence related to hysterectomy versus the LNG-IUS, the SRG made the following recommendations:
- If the patient desires amenorrhea or seeks to avoid additional therapy, hysterectomy is preferred
- If the patient’s main preference is to avoid adverse events, the LNG-IUS is preferred
- If her preference is for improved quality of life or sexual health, either treatment can be offered.
Based on the clinical evidence related to hysterectomy versus systemic medication, the SRG made the following recommendations:
- If the patient wants to become amenorrheic or hopes to avoid further intervention, hysterectomy is recommended
- If she wants to avoid adverse events, medications are recommended
- If her main preference is overall improvement in quality of life, less pain, or improvement in sexual health, either hysterectomy or medication is appropriate.
Note that no standard therapy was given; medical agents included combined oral contraceptive pills, cyclic or continuous progestin, conjugated estrogen with or without progestin, and prostaglandin synthetase inhibitors, usually with hormonal therapy. There are no randomized, controlled trials of other medications such as nonsteroidal anti-inflammatory drugs or tranexamic acid versus hysterectomy.
The SRG cited three main difficulties in the development of clinical guidelines:
- a lack of well-developed randomized, controlled trials of alternative management versus hysterectomy, as well as inconsistent measurement and reporting among the few trials that exist
- a lack of uniformity in AUB diagnoses among the randomized, controlled trials evaluated
- inconsistent use of terminology related to AUB within the trials.
All of these challenges were addressed by the FIGO nomenclature and AUB classification recommendations. Adherence to the FIGO guidelines for future clinical research would eliminate the difficulties faced by this study group and lead to higher-quality clinical evidence that could form the basis of solid clinical recommendations for the treatment of AUB related to ovulatory disorders or endometrial hemostatic dysfunction.
“Decision-making about treatments of AUB requires discussion so a patient can choose a therapy that best fits her disease, her values, and her preferences and optimizes her chance for treatment success while minimizing risks,” the SRG concluded.
ACKNOWLEDGMENT. Thank you to Dr. Malcolm Munro and Dr. Anita Lee Sloan for their thoughtful reviews of this manuscript.
We want to hear from you! Tell us what you think.
TECHNIQUE ARTICLES?
CLICK HERE to access Surgical Technique articles published recently in OBG Management.
1. Munro MG, Critchley HO, Broder MS, Fraser IS. FIGO Working Group on Menstrual Disorders. FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int J Gynaecol Obstet. 2011;113(1):3-13.
2. Munro MG, Critchley HO, Broder MS, Fraser IS. FIGO Working Group on Menstrual Disorders. The FIGO classification of causes of abnormal bleeding in the reproductive years. Fertil Steril. 2011;95(7):2204-2208.
3. Critchley HO, Munro MG, Broder M, Fraser IS. A five-year international review process concerning terminologies and definitions for normal and abnormal uterine bleeding. Semin Reprod Med. 2011;29(5):377-382.
4. Fraser IS, Critchley HO, Broder M, Munro MG. The FIGO recommendations on terminologies and definitions for normal and abnormal uterine bleeding. Semin Reprod Med. 2011;29(5):383-390.
5. Munro MG, Critchley HO, Fraser IS. The flexible FIGO classification concept for underlying causes of abnormal uterine bleeding. Semin Reprod Med. 2011;29(5):391-399.
6. American College of Obstetricians and Gynecologists. Practice bulletin #128: Diagnosis of abnormal uterine bleeding in reproductive-aged women. Obstet Gynecol. 2012;120(1):207-211.

Amy Garcia, MD
Dr. Garcia is Director, Center for Women’s Surgery, Albuquerque, and Clinical Assistant Professor, Department of Obstetrics and Gynecology, University of New Mexico School of Medicine, Albuquerque, New Mexico.
The author reports no financial relationships relevant to this article.
Amy Garcia, MD
Dr. Garcia is Director, Center for Women’s Surgery, Albuquerque, and Clinical Assistant Professor, Department of Obstetrics and Gynecology, University of New Mexico School of Medicine, Albuquerque, New Mexico.
The author reports no financial relationships relevant to this article.
Amy Garcia, MD
Dr. Garcia is Director, Center for Women’s Surgery, Albuquerque, and Clinical Assistant Professor, Department of Obstetrics and Gynecology, University of New Mexico School of Medicine, Albuquerque, New Mexico.
The author reports no financial relationships relevant to this article.
LARCs: Why they should be first-line contraceptive options
for your patients
Elizabeth O. Schmidt, MD; Tessa Madden, MD, MPH; Jeffrey F. Piepert, MD, PhD
(November 2012)
Let’s increase our use of IUDs and improve contraceptive effectiveness in this country
Robert L. Barbieri, MD (Editorial, August 2012)
Minimally invasive surgery
Amy Garcia, MD (Update, April 2012)
Your surgical toolbox should include topical hemostatic
agents—here is why
Lisa A. dos Santos, MD; Andrew W. Menzin, MD (Surgical Techniques, April 2012)
Minimally invasive surgery
Amy Garcia, MD (Update, April 2011)
The proliferation of terms to describe heavy menstrual bleeding sometimes seems never-ending. From “menometrorrhagia” to “uterine hemorrhage,” these terms pop up quickly and confuse discussion of one of the most widespread problems in gynecology.
Enter the International Federation of Gynecology and Obstetrics (FIGO), which decided to tackle the inconsistent terminology and lack of classification of causes of abnormal uterine bleeding (AUB) with an eye toward standardizing research, facilitating discussion, and informing management decisions.
In this article, I focus on three aspects of this effort:
- FIGO’s revamping of terminology and classification
- comparisons of outcomes of hysterectomy versus endometrial ablation and the levonorgestrel-releasing intrauterine system
- guidelines on management of AUB related to ovulatory disorders and endometrial hemostatic dysfunction.
FIGO revamps nomenclature for abnormal uterine bleeding
Munro MG, Critchley HO, Fraser IS. The FIGO systems for nomenclature and classification of causes of abnormal uterine bleeding in the reproductive years: who needs them? Am J Obstet Gynecol. 2012;207(4):259–265.
As early as 2004, FIGO began a process to standardize the nomenclature for defining both normal and abnormal uterine bleeding in reproductive-aged women who are not pregnant.1 This process was a response to a lack of consistency and continuity in the design and interpretation of basic science and clinical investigation related to the problem of AUB. Inconsistent definitions of AUB, such as “menorrhagia,” “metrorrhagia,” and “dysfunctional uterine bleeding,” along with the absence of standard categorization of the causes of AUB, have led to confusion and difficulties in comparing clinical trials and in finding significant, relevant, and even meaningful correlations among investigations of AUB. Applying information from asynchronous and often incomplete investigations to evidence-based clinical practice then becomes a challenge for the gynecologist.
Munro and colleagues summarize the process by which FIGO developed both a nomenclature system and a classification system of the causes of AUB, which were formally adopted by FIGO in 2010 and endorsed in 2012 by the American College of Obstetricians and Gynecologists (ACOG).1-6 The arduous process led to:
- a refined definition of chronic AUB
- a new category called acute AUB
- a method for describing the clinical dimensions of menstruation and the menstrual cycle according to the following parameters:
- regularity of onset
- frequency of onset
- duration of menstrual flow
- heaviness, or volume, of menstrual flow.
Wherever appropriate, the definitions of normal for these parameters were based on statistics from large population studies that used medians and 5th and 95th percentiles.
The term “heavy menstrual bleeding” (HMB) is used to describe a woman’s perception of increased menstrual volume, regardless of regularity, frequency, or duration. AUB is the overarching term to describe any departure from normal menstruation, as defined by the parameters listed above. A group of misleading terms commonly used to describe AUB were eliminated from the FIGO nomenclature system, including “dysfunctional uterine bleeding,” “menorrhagia,” “hypermenorrhea,” “menometrorrhagia,” “polymenorrhagia,” and “metrorrhagia.”
The causes of AUB are classified in nine categories that are arranged according to the acronym PALM-COEIN:
- Polyp
- Adenomyosis
- Leiomyoma
- Malignancy and hyperplasia
- Coagulopathy
- Ovulatory disorders
- Endometrial dysfunction
- Iatrogenic
- Not otherwise classified.
Leiomyoma are subclassified as submucous or other, with tertiary subcategorization for intramural, subserosal, and transmural lesions
In general, the components of the PALM group are discrete (structural) entities that are measurable visually via imaging or histopathology, or both, while the COEI (of the COEIN group) includes women for whom the AUB is unrelated to structural abnormalities.
The classification system provides the infrastructure for a thorough investigative process and a means to characterize AUB for an individual who may have one or more potential causes or contributors. Such a comprehensive assessment allows the basic scientist to identify pure populations for tissue and molecular studies, the clinical scientist to identify potential confounders when defining populations for clinical investigation, and the clinician, educator, and trainee to consider the multidimensional nature of AUB where asymptomatic “red herrings” may coexist with otherwise invisible disorders of menstrual function.
The FIGO Menstrual Disorders Working Group anticipates that widespread, international acceptance of the recommended terms, definitions, and classification for AUB will lead to improved and more meaningful communication in clinical trials and published research and will enhance communication between health-care providers and patients, leading to better management of AUB.
Use of the FIGO-recommended terms, definitions, and classification of AUB will lead to higher-quality clinical research and thorough clinical investigation into the causes of AUB, with improved management of patients.
How hysterectomy for AUB compares with less invasive treatment options
Matteson KA, Abed H, Wheeler TL II, et al; Society of Gynecologic Surgeons Systematic Review Group. A systematic review comparing hysterectomy with less invasive treatments for abnormal uterine bleeding. J Minim Invasive Gynecol. 2012;19(1):13–28.
To create reliable treatment recommendations for AUB, as defined by the FIGO classification system just described, in women with ovulatory disorders, endometrial hemostatic dysfunction, and concomitant leiomyoma, the Systematic Review Group (SRG) of the Society of Gynecologic Surgeons performed a systematic review of treatments. The analysis was intended to compare hysterectomy with less invasive treatment modalities. The SRG reviewed randomized, controlled trials of AUB treatment that compared hysterectomy with:
- endometrial ablation by resectoscopic loop, rollerball, or thermal balloon
- the LNG-IUS
- medical therapy.
This comprehensive review of literature published between 1950 and January 14, 2011 led the SRG to create seven categories of clinical outcomes:
- bleeding control
- quality of life
- pain
- sexual health
- patient satisfaction
- need for additional treatment
- adverse events.
Of the initial 5,503 titles identified, only 18 articles, representing nine clinical trials, contained data of adequate quality to meet criteria for review. Seven of the trials compared hysterectomy with ablation, one compared hysterectomy with the LNG-IUS, and one compared hysterectomy with medical therapy. As FIGO has pointed out, the lack of homogeneity of terminology used to describe AUB and classification of its causes prevented clinically applicable comparative analyses of treatment outcomes.
Here are some of the SRG’s findings:
- Control of bleeding. Only data regarding amenorrhea were sufficient for comparative analysis. The SRG was able to conclude only that there was moderate strength of evidence supporting the statement that bleeding is better controlled following hysterectomy than following ablation.
- Quality of life. Overall, studies that evaluated quality of life showed improvement after ablation and hysterectomy. The strength of evidence demonstrating no difference between hysterectomy and ablation in postoperative quality of life was moderate.
- Pain, general health, vitality, and social function. Three studies found statistically significant differences in validated dimensions of the SF-36 questionnaire favoring hysterectomy for pain, general health, vitality, and social function. Two of these three studies evaluated minimally invasive hysterectomy by the laparoscopic supracervical or vaginal approach. The strength of evidence on pain beyond the postoperative time period was low and favored hysterectomy over ablation.
- Sexual health. The strength of evidence related to sexual health was low and revealed no differences between hysterectomy and ablation.
- Patient satisfaction. Overall, the quality of evidence was very low, showing no difference between hysterectomy and ablation.
- Need for additional treatment. The quality of evidence was moderate and favored hysterectomy over ablation.
- Adverse events. Evidence of moderate quality favored ablation and the LNG-IUS over hysterectomy, and low-quality evidence favored medical therapy over hysterectomy (TABLES 1, 2).
TABLE 1
What the data reveal about hysterectomy versus ablation
| Parameter | Strength of evidence (comparison) | |
|---|---|---|
| Hysterectomy | Ablation | |
| Bleeding control | Moderate (F) | — |
| Quality of life | Moderate (S) | Moderate (S) |
| Lower pain | Low (F) | — |
| Sexual health | Low (S) | Low (S) |
| Patient satisfaction | Very low (S) | Very low (S) |
| Need for additional treatment | Moderate (F) | — |
| Adverse events | — | Moderate (F) |
| F=Evidence favors comparator; S=no difference between comparators | ||
TABLE 2
What the data reveal about hysterectomy versus the levonorgestrel-releasing intrauterine system (LNG-IUS)
| Parameter | Strength of evidence (comparison) | |
|---|---|---|
| Hysterectomy | LNG-IUS | |
| Bleeding control | Moderate (F) | — |
| Quality of life | Moderate (S) | Moderate (S) |
| Lower pain | Moderate (S) | Moderate (S) |
| Sexual health | Moderate (S) | Moderate (S) |
| Patient satisfaction | Moderate (S) | Moderate (S) |
| Need for additional treatment | Moderate (F) | — |
| Adverse events | — | Moderate (F) |
| F=Evidence favors comparator; S=no difference between comparators | ||
The SRG concluded that there are tradeoffs between treatment effectiveness and the risk of serious adverse events between hysterectomy, ablation, and the LNG-IUS. It recommended that clinicians be educated about the relative advantages and disadvantages of each option so that they can discuss them with patients.
The SRG developed clinical practice guidelines for the treatment of ovulatory disorders and endometrial hemostatic dysfunction associated with AUB (see below).
Gynecologists should educate each patient about the efficacy and risks of options available for the management of AUB in the context of specific symptoms to facilitate an informed choice.
Wheeler TL II, Murphy M, Rogers RG, et al; Society of Gynecologic Surgeons Systematic Review Group. Clinical practice guidelines for abnormal uterine bleeding: hysterectomy versus alternative therapy. J Minim Invasive Gynecol. 2012;19(1):81–87.
The SRG used the results of the systematic review just summarized to formulate clinical guidelines for the treatment of AUB related to ovulatory disorders and endometrial hemostatic dysfunction. Recommendations were assigned a grade for their strength on the basis of the quality of supporting evidence, the size of the net medical benefit, and other considerations, including values and preferences applied in judgments. The strength of the clinical recommendation is either “strong” or “weak” and indicates the degree to which one can be confident that adherence to the recommendation will do more good than harm. All of the clinical recommendations described below received a grade of “weak.”
One primary suggestion from the study group is patient counseling that must first determine the type of AUB and the degree of burden or distress for the patient, as well as the presence of any additional cycle-related symptoms. Consideration should be given to variables that may modify the inherent risks or benefits of each intervention for the particular patient, as well as her values and preferences regarding treatment harms, benefits, and potential outcomes. Counseling should assess the patient’s need for contraception, desire for future childbearing, and proximity to menopause, as well as any cultural preferences for management.
Based on the clinical evidence related to hysterectomy versus endometrial ablation, the SRG made the following recommendations:
- If the patient desires amenorrhea and less pain and wants to avoid additional therapy, hysterectomy is preferred
- If the patient wants to avoid adverse events and seeks a shorter hospital stay, endometrial ablation is preferred
- If the patient’s main desire is for improvement in overall quality of life or sexual health, either intervention is appropriate, depending on patient preferences.
There were no data available in the systematic review concerning newer technologies for nonhysteroscopic endometrial ablation versus hysterectomy.
Based on the clinical evidence related to hysterectomy versus the LNG-IUS, the SRG made the following recommendations:
- If the patient desires amenorrhea or seeks to avoid additional therapy, hysterectomy is preferred
- If the patient’s main preference is to avoid adverse events, the LNG-IUS is preferred
- If her preference is for improved quality of life or sexual health, either treatment can be offered.
Based on the clinical evidence related to hysterectomy versus systemic medication, the SRG made the following recommendations:
- If the patient wants to become amenorrheic or hopes to avoid further intervention, hysterectomy is recommended
- If she wants to avoid adverse events, medications are recommended
- If her main preference is overall improvement in quality of life, less pain, or improvement in sexual health, either hysterectomy or medication is appropriate.
Note that no standard therapy was given; medical agents included combined oral contraceptive pills, cyclic or continuous progestin, conjugated estrogen with or without progestin, and prostaglandin synthetase inhibitors, usually with hormonal therapy. There are no randomized, controlled trials of other medications such as nonsteroidal anti-inflammatory drugs or tranexamic acid versus hysterectomy.
The SRG cited three main difficulties in the development of clinical guidelines:
- a lack of well-developed randomized, controlled trials of alternative management versus hysterectomy, as well as inconsistent measurement and reporting among the few trials that exist
- a lack of uniformity in AUB diagnoses among the randomized, controlled trials evaluated
- inconsistent use of terminology related to AUB within the trials.
All of these challenges were addressed by the FIGO nomenclature and AUB classification recommendations. Adherence to the FIGO guidelines for future clinical research would eliminate the difficulties faced by this study group and lead to higher-quality clinical evidence that could form the basis of solid clinical recommendations for the treatment of AUB related to ovulatory disorders or endometrial hemostatic dysfunction.
“Decision-making about treatments of AUB requires discussion so a patient can choose a therapy that best fits her disease, her values, and her preferences and optimizes her chance for treatment success while minimizing risks,” the SRG concluded.
ACKNOWLEDGMENT. Thank you to Dr. Malcolm Munro and Dr. Anita Lee Sloan for their thoughtful reviews of this manuscript.
We want to hear from you! Tell us what you think.
TECHNIQUE ARTICLES?
CLICK HERE to access Surgical Technique articles published recently in OBG Management.
LARCs: Why they should be first-line contraceptive options
for your patients
Elizabeth O. Schmidt, MD; Tessa Madden, MD, MPH; Jeffrey F. Piepert, MD, PhD
(November 2012)
Let’s increase our use of IUDs and improve contraceptive effectiveness in this country
Robert L. Barbieri, MD (Editorial, August 2012)
Minimally invasive surgery
Amy Garcia, MD (Update, April 2012)
Your surgical toolbox should include topical hemostatic
agents—here is why
Lisa A. dos Santos, MD; Andrew W. Menzin, MD (Surgical Techniques, April 2012)
Minimally invasive surgery
Amy Garcia, MD (Update, April 2011)
The proliferation of terms to describe heavy menstrual bleeding sometimes seems never-ending. From “menometrorrhagia” to “uterine hemorrhage,” these terms pop up quickly and confuse discussion of one of the most widespread problems in gynecology.
Enter the International Federation of Gynecology and Obstetrics (FIGO), which decided to tackle the inconsistent terminology and lack of classification of causes of abnormal uterine bleeding (AUB) with an eye toward standardizing research, facilitating discussion, and informing management decisions.
In this article, I focus on three aspects of this effort:
- FIGO’s revamping of terminology and classification
- comparisons of outcomes of hysterectomy versus endometrial ablation and the levonorgestrel-releasing intrauterine system
- guidelines on management of AUB related to ovulatory disorders and endometrial hemostatic dysfunction.
FIGO revamps nomenclature for abnormal uterine bleeding
Munro MG, Critchley HO, Fraser IS. The FIGO systems for nomenclature and classification of causes of abnormal uterine bleeding in the reproductive years: who needs them? Am J Obstet Gynecol. 2012;207(4):259–265.
As early as 2004, FIGO began a process to standardize the nomenclature for defining both normal and abnormal uterine bleeding in reproductive-aged women who are not pregnant.1 This process was a response to a lack of consistency and continuity in the design and interpretation of basic science and clinical investigation related to the problem of AUB. Inconsistent definitions of AUB, such as “menorrhagia,” “metrorrhagia,” and “dysfunctional uterine bleeding,” along with the absence of standard categorization of the causes of AUB, have led to confusion and difficulties in comparing clinical trials and in finding significant, relevant, and even meaningful correlations among investigations of AUB. Applying information from asynchronous and often incomplete investigations to evidence-based clinical practice then becomes a challenge for the gynecologist.
Munro and colleagues summarize the process by which FIGO developed both a nomenclature system and a classification system of the causes of AUB, which were formally adopted by FIGO in 2010 and endorsed in 2012 by the American College of Obstetricians and Gynecologists (ACOG).1-6 The arduous process led to:
- a refined definition of chronic AUB
- a new category called acute AUB
- a method for describing the clinical dimensions of menstruation and the menstrual cycle according to the following parameters:
- regularity of onset
- frequency of onset
- duration of menstrual flow
- heaviness, or volume, of menstrual flow.
Wherever appropriate, the definitions of normal for these parameters were based on statistics from large population studies that used medians and 5th and 95th percentiles.
The term “heavy menstrual bleeding” (HMB) is used to describe a woman’s perception of increased menstrual volume, regardless of regularity, frequency, or duration. AUB is the overarching term to describe any departure from normal menstruation, as defined by the parameters listed above. A group of misleading terms commonly used to describe AUB were eliminated from the FIGO nomenclature system, including “dysfunctional uterine bleeding,” “menorrhagia,” “hypermenorrhea,” “menometrorrhagia,” “polymenorrhagia,” and “metrorrhagia.”
The causes of AUB are classified in nine categories that are arranged according to the acronym PALM-COEIN:
- Polyp
- Adenomyosis
- Leiomyoma
- Malignancy and hyperplasia
- Coagulopathy
- Ovulatory disorders
- Endometrial dysfunction
- Iatrogenic
- Not otherwise classified.
Leiomyoma are subclassified as submucous or other, with tertiary subcategorization for intramural, subserosal, and transmural lesions
In general, the components of the PALM group are discrete (structural) entities that are measurable visually via imaging or histopathology, or both, while the COEI (of the COEIN group) includes women for whom the AUB is unrelated to structural abnormalities.
The classification system provides the infrastructure for a thorough investigative process and a means to characterize AUB for an individual who may have one or more potential causes or contributors. Such a comprehensive assessment allows the basic scientist to identify pure populations for tissue and molecular studies, the clinical scientist to identify potential confounders when defining populations for clinical investigation, and the clinician, educator, and trainee to consider the multidimensional nature of AUB where asymptomatic “red herrings” may coexist with otherwise invisible disorders of menstrual function.
The FIGO Menstrual Disorders Working Group anticipates that widespread, international acceptance of the recommended terms, definitions, and classification for AUB will lead to improved and more meaningful communication in clinical trials and published research and will enhance communication between health-care providers and patients, leading to better management of AUB.
Use of the FIGO-recommended terms, definitions, and classification of AUB will lead to higher-quality clinical research and thorough clinical investigation into the causes of AUB, with improved management of patients.
How hysterectomy for AUB compares with less invasive treatment options
Matteson KA, Abed H, Wheeler TL II, et al; Society of Gynecologic Surgeons Systematic Review Group. A systematic review comparing hysterectomy with less invasive treatments for abnormal uterine bleeding. J Minim Invasive Gynecol. 2012;19(1):13–28.
To create reliable treatment recommendations for AUB, as defined by the FIGO classification system just described, in women with ovulatory disorders, endometrial hemostatic dysfunction, and concomitant leiomyoma, the Systematic Review Group (SRG) of the Society of Gynecologic Surgeons performed a systematic review of treatments. The analysis was intended to compare hysterectomy with less invasive treatment modalities. The SRG reviewed randomized, controlled trials of AUB treatment that compared hysterectomy with:
- endometrial ablation by resectoscopic loop, rollerball, or thermal balloon
- the LNG-IUS
- medical therapy.
This comprehensive review of literature published between 1950 and January 14, 2011 led the SRG to create seven categories of clinical outcomes:
- bleeding control
- quality of life
- pain
- sexual health
- patient satisfaction
- need for additional treatment
- adverse events.
Of the initial 5,503 titles identified, only 18 articles, representing nine clinical trials, contained data of adequate quality to meet criteria for review. Seven of the trials compared hysterectomy with ablation, one compared hysterectomy with the LNG-IUS, and one compared hysterectomy with medical therapy. As FIGO has pointed out, the lack of homogeneity of terminology used to describe AUB and classification of its causes prevented clinically applicable comparative analyses of treatment outcomes.
Here are some of the SRG’s findings:
- Control of bleeding. Only data regarding amenorrhea were sufficient for comparative analysis. The SRG was able to conclude only that there was moderate strength of evidence supporting the statement that bleeding is better controlled following hysterectomy than following ablation.
- Quality of life. Overall, studies that evaluated quality of life showed improvement after ablation and hysterectomy. The strength of evidence demonstrating no difference between hysterectomy and ablation in postoperative quality of life was moderate.
- Pain, general health, vitality, and social function. Three studies found statistically significant differences in validated dimensions of the SF-36 questionnaire favoring hysterectomy for pain, general health, vitality, and social function. Two of these three studies evaluated minimally invasive hysterectomy by the laparoscopic supracervical or vaginal approach. The strength of evidence on pain beyond the postoperative time period was low and favored hysterectomy over ablation.
- Sexual health. The strength of evidence related to sexual health was low and revealed no differences between hysterectomy and ablation.
- Patient satisfaction. Overall, the quality of evidence was very low, showing no difference between hysterectomy and ablation.
- Need for additional treatment. The quality of evidence was moderate and favored hysterectomy over ablation.
- Adverse events. Evidence of moderate quality favored ablation and the LNG-IUS over hysterectomy, and low-quality evidence favored medical therapy over hysterectomy (TABLES 1, 2).
TABLE 1
What the data reveal about hysterectomy versus ablation
| Parameter | Strength of evidence (comparison) | |
|---|---|---|
| Hysterectomy | Ablation | |
| Bleeding control | Moderate (F) | — |
| Quality of life | Moderate (S) | Moderate (S) |
| Lower pain | Low (F) | — |
| Sexual health | Low (S) | Low (S) |
| Patient satisfaction | Very low (S) | Very low (S) |
| Need for additional treatment | Moderate (F) | — |
| Adverse events | — | Moderate (F) |
| F=Evidence favors comparator; S=no difference between comparators | ||
TABLE 2
What the data reveal about hysterectomy versus the levonorgestrel-releasing intrauterine system (LNG-IUS)
| Parameter | Strength of evidence (comparison) | |
|---|---|---|
| Hysterectomy | LNG-IUS | |
| Bleeding control | Moderate (F) | — |
| Quality of life | Moderate (S) | Moderate (S) |
| Lower pain | Moderate (S) | Moderate (S) |
| Sexual health | Moderate (S) | Moderate (S) |
| Patient satisfaction | Moderate (S) | Moderate (S) |
| Need for additional treatment | Moderate (F) | — |
| Adverse events | — | Moderate (F) |
| F=Evidence favors comparator; S=no difference between comparators | ||
The SRG concluded that there are tradeoffs between treatment effectiveness and the risk of serious adverse events between hysterectomy, ablation, and the LNG-IUS. It recommended that clinicians be educated about the relative advantages and disadvantages of each option so that they can discuss them with patients.
The SRG developed clinical practice guidelines for the treatment of ovulatory disorders and endometrial hemostatic dysfunction associated with AUB (see below).
Gynecologists should educate each patient about the efficacy and risks of options available for the management of AUB in the context of specific symptoms to facilitate an informed choice.
Wheeler TL II, Murphy M, Rogers RG, et al; Society of Gynecologic Surgeons Systematic Review Group. Clinical practice guidelines for abnormal uterine bleeding: hysterectomy versus alternative therapy. J Minim Invasive Gynecol. 2012;19(1):81–87.
The SRG used the results of the systematic review just summarized to formulate clinical guidelines for the treatment of AUB related to ovulatory disorders and endometrial hemostatic dysfunction. Recommendations were assigned a grade for their strength on the basis of the quality of supporting evidence, the size of the net medical benefit, and other considerations, including values and preferences applied in judgments. The strength of the clinical recommendation is either “strong” or “weak” and indicates the degree to which one can be confident that adherence to the recommendation will do more good than harm. All of the clinical recommendations described below received a grade of “weak.”
One primary suggestion from the study group is patient counseling that must first determine the type of AUB and the degree of burden or distress for the patient, as well as the presence of any additional cycle-related symptoms. Consideration should be given to variables that may modify the inherent risks or benefits of each intervention for the particular patient, as well as her values and preferences regarding treatment harms, benefits, and potential outcomes. Counseling should assess the patient’s need for contraception, desire for future childbearing, and proximity to menopause, as well as any cultural preferences for management.
Based on the clinical evidence related to hysterectomy versus endometrial ablation, the SRG made the following recommendations:
- If the patient desires amenorrhea and less pain and wants to avoid additional therapy, hysterectomy is preferred
- If the patient wants to avoid adverse events and seeks a shorter hospital stay, endometrial ablation is preferred
- If the patient’s main desire is for improvement in overall quality of life or sexual health, either intervention is appropriate, depending on patient preferences.
There were no data available in the systematic review concerning newer technologies for nonhysteroscopic endometrial ablation versus hysterectomy.
Based on the clinical evidence related to hysterectomy versus the LNG-IUS, the SRG made the following recommendations:
- If the patient desires amenorrhea or seeks to avoid additional therapy, hysterectomy is preferred
- If the patient’s main preference is to avoid adverse events, the LNG-IUS is preferred
- If her preference is for improved quality of life or sexual health, either treatment can be offered.
Based on the clinical evidence related to hysterectomy versus systemic medication, the SRG made the following recommendations:
- If the patient wants to become amenorrheic or hopes to avoid further intervention, hysterectomy is recommended
- If she wants to avoid adverse events, medications are recommended
- If her main preference is overall improvement in quality of life, less pain, or improvement in sexual health, either hysterectomy or medication is appropriate.
Note that no standard therapy was given; medical agents included combined oral contraceptive pills, cyclic or continuous progestin, conjugated estrogen with or without progestin, and prostaglandin synthetase inhibitors, usually with hormonal therapy. There are no randomized, controlled trials of other medications such as nonsteroidal anti-inflammatory drugs or tranexamic acid versus hysterectomy.
The SRG cited three main difficulties in the development of clinical guidelines:
- a lack of well-developed randomized, controlled trials of alternative management versus hysterectomy, as well as inconsistent measurement and reporting among the few trials that exist
- a lack of uniformity in AUB diagnoses among the randomized, controlled trials evaluated
- inconsistent use of terminology related to AUB within the trials.
All of these challenges were addressed by the FIGO nomenclature and AUB classification recommendations. Adherence to the FIGO guidelines for future clinical research would eliminate the difficulties faced by this study group and lead to higher-quality clinical evidence that could form the basis of solid clinical recommendations for the treatment of AUB related to ovulatory disorders or endometrial hemostatic dysfunction.
“Decision-making about treatments of AUB requires discussion so a patient can choose a therapy that best fits her disease, her values, and her preferences and optimizes her chance for treatment success while minimizing risks,” the SRG concluded.
ACKNOWLEDGMENT. Thank you to Dr. Malcolm Munro and Dr. Anita Lee Sloan for their thoughtful reviews of this manuscript.
We want to hear from you! Tell us what you think.
TECHNIQUE ARTICLES?
CLICK HERE to access Surgical Technique articles published recently in OBG Management.
1. Munro MG, Critchley HO, Broder MS, Fraser IS. FIGO Working Group on Menstrual Disorders. FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int J Gynaecol Obstet. 2011;113(1):3-13.
2. Munro MG, Critchley HO, Broder MS, Fraser IS. FIGO Working Group on Menstrual Disorders. The FIGO classification of causes of abnormal bleeding in the reproductive years. Fertil Steril. 2011;95(7):2204-2208.
3. Critchley HO, Munro MG, Broder M, Fraser IS. A five-year international review process concerning terminologies and definitions for normal and abnormal uterine bleeding. Semin Reprod Med. 2011;29(5):377-382.
4. Fraser IS, Critchley HO, Broder M, Munro MG. The FIGO recommendations on terminologies and definitions for normal and abnormal uterine bleeding. Semin Reprod Med. 2011;29(5):383-390.
5. Munro MG, Critchley HO, Fraser IS. The flexible FIGO classification concept for underlying causes of abnormal uterine bleeding. Semin Reprod Med. 2011;29(5):391-399.
6. American College of Obstetricians and Gynecologists. Practice bulletin #128: Diagnosis of abnormal uterine bleeding in reproductive-aged women. Obstet Gynecol. 2012;120(1):207-211.
1. Munro MG, Critchley HO, Broder MS, Fraser IS. FIGO Working Group on Menstrual Disorders. FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int J Gynaecol Obstet. 2011;113(1):3-13.
2. Munro MG, Critchley HO, Broder MS, Fraser IS. FIGO Working Group on Menstrual Disorders. The FIGO classification of causes of abnormal bleeding in the reproductive years. Fertil Steril. 2011;95(7):2204-2208.
3. Critchley HO, Munro MG, Broder M, Fraser IS. A five-year international review process concerning terminologies and definitions for normal and abnormal uterine bleeding. Semin Reprod Med. 2011;29(5):377-382.
4. Fraser IS, Critchley HO, Broder M, Munro MG. The FIGO recommendations on terminologies and definitions for normal and abnormal uterine bleeding. Semin Reprod Med. 2011;29(5):383-390.
5. Munro MG, Critchley HO, Fraser IS. The flexible FIGO classification concept for underlying causes of abnormal uterine bleeding. Semin Reprod Med. 2011;29(5):391-399.
6. American College of Obstetricians and Gynecologists. Practice bulletin #128: Diagnosis of abnormal uterine bleeding in reproductive-aged women. Obstet Gynecol. 2012;120(1):207-211.