User login
Letrozole versus clomiphene for ovulation induction
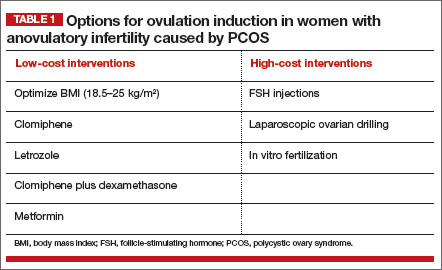
The three most common causes of infertility are anovulation, tubal occlusion, and abnormal semen parameters. The most common cause of anovulatory infertility is polycystic ovary syndrome (PCOS). Options for initial treatment of anovulatory infertility caused by PCOS include optimizing body mass index (BMI), clomiphene, clomiphene plus dexamethasone, and metformin (TABLE 1). If these low-cost interventions are not successful, high-cost interventions are often very effective treatments, and include follicle-stimulating hormone (FSH) injections, laparoscopic ovarian drilling, and in vitro fertilization.
For many couples, the high-cost interventions are prohibitively expensive. Recently, results of a high-quality randomized clinical trial published by Legro and colleagues in the New England Journal of Medicine indicate that letrozole is more effective than clomiphene for the treatment of anovulatory infertility in women with PCOS.1 Of great importance, letrozole was documented to be especially effective in women with a BMI greater than 30.3 kg/m2.
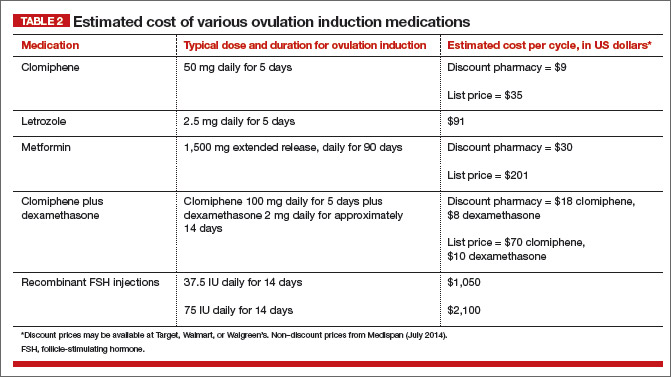
Letrozole is another low-cost option for couples with anovulatory infertility (TABLE 2), and you should consider it among your initial treatment choices. In this article, I outline when letrozole is your best first option for treatment.
Letrozole is more effective than clomiphene for ovulation induction in women with PCOS and BMI >30.3 kg/m2
Legro and colleagues1 randomly assigned 750 women with anovulatory infertility and PCOS to receive ovulation induction with either clomiphene or letrozole. The medications were prescribed using an escalating dose if ovulation did not occur. For clomiphene, the doses prescribed were 50 mg, 100 mg, and 150 mg. For letrozole, the doses were 2.5 mg, 5 mg, and 7.5 mg. The medications were given daily for 5 days on cycle days 3 to 7, following a spontaneous menses or a medroxyprogesterone acetate withdrawal bleed. Up to 5 cycles of ovulation induction were prescribed.
The ovulation rates for letrozole versus clomiphene were 61.7% and 48.3%, respectively (P<.001). The live birth rates for letrozole versus clomiphene were 27.5% and 19.1%, respectively (P = .007). Among women with a BMI of 30.3 kg/m2 or less, both letrozole and clomiphene treatment resulted in a similar live birth rate of approximately 30% to 35%. Among women with a BMI greater than 30.3 kg/m2, however, the live birth rates with letrozole versus clomiphene were approximately 20% and 10%, respectively.
Consequently, in my practice, I prioritize the use of letrozole for women with a BMI of 30 kg/m2 or greater.
Do not use anastrozole for ovulation induction
In a randomized trial of letrozole versus anastrozole for ovulation induction, 40 women with PCOS were randomly assigned to receive ovulation induction with letrozole (2.5 mg daily for 5 days) or anastrozole (1 mg daily for 5 days).2 The resulting ovulation rate was 84% for letrozole, compared with 60% for anastrozole (P<.05). The pregnancy rate also was significantly higher for letrozole (19% vs 10% for anastrozole, P<.05).
Investigators of two large randomized trials of anastrozole versus clomiphene reported that clomiphene was superior to anastrozole for induction of ovulation in the first cycle of treatment.3,4 Anastrozole, at doses of 1 mg, 5 mg, 10 mg, 20 mg, and 30 mg daily for 5 days, was less effective for ovulation induction in the first cycle of treatment than clomiphene at a dose of 50 mg.3,4
If an aromatase inhibitor is going to be prescribed for ovulation induction, I recommend the use of letrozole and recommend against the use of anastrozole.
Congenital malformations and ovulation induction
The administration of clomiphene or letrozole to pregnant rats has adverse fetal effects.5,6 For example, in pregnant rats a low dose of letrozole (0.003 mg/kg) has been reported to increase intrauterine mortality, fetal resorption, and postimplantation loss; decrease live births; and result in fetal anomalies, including dilation of the ureter and shortening of renal papillae.6
However, in the setting of ovulation induction, letrozole is not administered while the patient is pregnant and is discontinued many days before ovulation and conception. Consequently, the results observed in animal studies (with the medications administered to pregnant animals) may not be particularly relevant to the clinical situation where the fertility medication is discontinued before ovulation and conception.
It is important to exclude pregnancy prior to initiating treatment with letrozole or clomiphene.
Birth defects affect approximately 5% of newborns in the United States.7 The relative impact of maternal age, obesity, ovulation induction medicines, and a history of infertility on the rate of birth defects is not fully characterized and is a subject of intense research. To date, there is no strong and consistent evidence that ovulation induction agents, per se, significantly increase the rate of birth defects.
Tulandi and colleagues reported on 911 newborns conceived following ovulation induction with clomiphene or letrozole.8 Overall, the congenital malformation plus chromosomal abnormality rates associated with letrozole and clomiphene ovulation induction were 2.4% and 4.8%, respectively. The major congenital malformation rate for letrozole was 1.2%, and 3.0% for clomiphene.
Many women with anovulatory infertility and PCOS have a BMI of 30 kg/m2 or greater, and some are of advanced maternal age. It is known that women with such a BMI level have an increased risk of congenital malformations, including neural tube defects, spina bifida, septal anomalies, cleft palate, cleft lip, anorectal atresia, hydrocephaly, and limb reduction anomalies.9 The risk of gastroschisis is significantly reduced among obese pregnant women.9 Women aged 40 or older have an increased risk of having a fetus with cardiac defects, esophageal atresia, hypospadias, and craniosynostosis.10
Caution women of advanced maternal age with PCOS and a BMI of 30 kg/m2 or greater about the increased rate of congenital malformations associated with their age and elevated BMI.
Prioritize letrozole when BMI ≥30 kg/m2
I recommend that clomiphene should remain the first-line ovulation induction agent for women with PCOS and a BMI less than 30 kg/m2. This is because, among women with such a BMI level, both clomiphene and letrozole have similar efficacy, and clomiphene is approved by the US Food and Drug Administration for ovulation induction while letrozole is not.
However, for women with PCOS and a BMI of 30 kg/m2 or greater—a clinical situation where letrozole is about twice as effective as clomiphene—letrozole may be the preferred agent.
When prescribing letrozole, start with a dose of 2.5 mg daily for cycle days 3 to 7, following a spontaneous menses or progestin-induced bleed. If ovulation occurs, continue with the dose. If ovulation does not occur, increase the dose to 5 mg daily for cycle days 3 to 7. The maximal dose is 7.5 mg daily for cycle days 3 to 7. When prescribing letrozole, counsel your patient about the increased rate of congenital anomalies among women with an elevated BMI and the possible teratogenic effects of fertility medications.
The aromatase inhibitor letrozole is an important addition to our options for ovulation induction in women with PCOS. Will you start using letrozole for ovulation induction in your practice?
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. Legro RS, Brzyski RG, Diamond MP, et al; NICHD Reproductive Medicine Network. Letrozole versus clomiphene for infertility in the polycystic ovary syndrome. N Engl J Med. 2014;371(2):119–129.
2. Al-Omari WR, Sulaiman WR, Al-Hadithi N. Comparison of two aromatase inhibitors in women with clomiphene-resistant polycystic ovary syndrome. Int J Gynaecol Obstet. 2004;85(3):289–291.
3. Tredway D, Schertz JC, Bock D, Hemsey G, Diamond MP. Anastrozole vs. clomiphene citrate in infertile women with ovulatory dysfunction: a phase II, randomized, dose-finding study. Fertil Steril. 2011;95(5):1720–1724.
4. Tredway D, Schertz JC, Bock D, Hemsey G, Diamond MP. Anastrozole single-dose protocol in women with oligo- or anovulatory infertility: results of a randomized phase II dose-response study. Fertil Steril. 2011;95(5):1725–1729.
5. Clomid (clomiphene citrate tablets USP) [package insert]. Bridgewater, NJ: sanofi-aventis. http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/016131s026lbl.pdf. Revised October 2012. Accessed October 20, 2014.
6. Femara (letrozole tablets) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation. https://www.pharma.us.novartis.com/product/pi/pdf/Femara.pdf. Revised January 2014. Accessed October 20, 2014.
7. Christianson A, Howson CP, Modell B. March of Dimes Global Report on Birth Defects: Executive Summary. White Plains NY: March of Dimes Birth Defects Foundation; 2006:2–9. http://www.marchofdimes.com/materials/global-report-on-birth-defects-the-hidden-toll-of-dying-and-disabled-children-execu tive-summary.pdf. Accessed October 20, 2014.
8. Tulandi T, Martin J, Al-Fadhli R, et al. Congenital malformations among 911 newborns conceived after infertility with letrozole or clomiphene citrate. Fertil Steril. 2006;85(6):1761–1765.
9. Stothard KJ, Tennant PW, Bell R, Rankin J. Maternal overweight and obesity and the risk of congenital anomalies: a systemic review and meta-analysis. JAMA. 2009;301(6):636–650.
10. Gill SK, Broussard C, Devine O, Green RF, Rasmussen SA, Reefhuis J; National Birth Defects Prevention Study. Association between maternal age and birth defects of unknown etiology: United States, 1997–2007. Birth Defects Res A Clin Mol Teratol. 2012;94(12):1010–1018

Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
The three most common causes of infertility are anovulation, tubal occlusion, and abnormal semen parameters. The most common cause of anovulatory infertility is polycystic ovary syndrome (PCOS). Options for initial treatment of anovulatory infertility caused by PCOS include optimizing body mass index (BMI), clomiphene, clomiphene plus dexamethasone, and metformin (TABLE 1). If these low-cost interventions are not successful, high-cost interventions are often very effective treatments, and include follicle-stimulating hormone (FSH) injections, laparoscopic ovarian drilling, and in vitro fertilization.
For many couples, the high-cost interventions are prohibitively expensive. Recently, results of a high-quality randomized clinical trial published by Legro and colleagues in the New England Journal of Medicine indicate that letrozole is more effective than clomiphene for the treatment of anovulatory infertility in women with PCOS.1 Of great importance, letrozole was documented to be especially effective in women with a BMI greater than 30.3 kg/m2.
Letrozole is another low-cost option for couples with anovulatory infertility (TABLE 2), and you should consider it among your initial treatment choices. In this article, I outline when letrozole is your best first option for treatment.
Letrozole is more effective than clomiphene for ovulation induction in women with PCOS and BMI >30.3 kg/m2
Legro and colleagues1 randomly assigned 750 women with anovulatory infertility and PCOS to receive ovulation induction with either clomiphene or letrozole. The medications were prescribed using an escalating dose if ovulation did not occur. For clomiphene, the doses prescribed were 50 mg, 100 mg, and 150 mg. For letrozole, the doses were 2.5 mg, 5 mg, and 7.5 mg. The medications were given daily for 5 days on cycle days 3 to 7, following a spontaneous menses or a medroxyprogesterone acetate withdrawal bleed. Up to 5 cycles of ovulation induction were prescribed.
The ovulation rates for letrozole versus clomiphene were 61.7% and 48.3%, respectively (P<.001). The live birth rates for letrozole versus clomiphene were 27.5% and 19.1%, respectively (P = .007). Among women with a BMI of 30.3 kg/m2 or less, both letrozole and clomiphene treatment resulted in a similar live birth rate of approximately 30% to 35%. Among women with a BMI greater than 30.3 kg/m2, however, the live birth rates with letrozole versus clomiphene were approximately 20% and 10%, respectively.
Consequently, in my practice, I prioritize the use of letrozole for women with a BMI of 30 kg/m2 or greater.
Do not use anastrozole for ovulation induction
In a randomized trial of letrozole versus anastrozole for ovulation induction, 40 women with PCOS were randomly assigned to receive ovulation induction with letrozole (2.5 mg daily for 5 days) or anastrozole (1 mg daily for 5 days).2 The resulting ovulation rate was 84% for letrozole, compared with 60% for anastrozole (P<.05). The pregnancy rate also was significantly higher for letrozole (19% vs 10% for anastrozole, P<.05).
Investigators of two large randomized trials of anastrozole versus clomiphene reported that clomiphene was superior to anastrozole for induction of ovulation in the first cycle of treatment.3,4 Anastrozole, at doses of 1 mg, 5 mg, 10 mg, 20 mg, and 30 mg daily for 5 days, was less effective for ovulation induction in the first cycle of treatment than clomiphene at a dose of 50 mg.3,4
If an aromatase inhibitor is going to be prescribed for ovulation induction, I recommend the use of letrozole and recommend against the use of anastrozole.
Congenital malformations and ovulation induction
The administration of clomiphene or letrozole to pregnant rats has adverse fetal effects.5,6 For example, in pregnant rats a low dose of letrozole (0.003 mg/kg) has been reported to increase intrauterine mortality, fetal resorption, and postimplantation loss; decrease live births; and result in fetal anomalies, including dilation of the ureter and shortening of renal papillae.6
However, in the setting of ovulation induction, letrozole is not administered while the patient is pregnant and is discontinued many days before ovulation and conception. Consequently, the results observed in animal studies (with the medications administered to pregnant animals) may not be particularly relevant to the clinical situation where the fertility medication is discontinued before ovulation and conception.
It is important to exclude pregnancy prior to initiating treatment with letrozole or clomiphene.
Birth defects affect approximately 5% of newborns in the United States.7 The relative impact of maternal age, obesity, ovulation induction medicines, and a history of infertility on the rate of birth defects is not fully characterized and is a subject of intense research. To date, there is no strong and consistent evidence that ovulation induction agents, per se, significantly increase the rate of birth defects.
Tulandi and colleagues reported on 911 newborns conceived following ovulation induction with clomiphene or letrozole.8 Overall, the congenital malformation plus chromosomal abnormality rates associated with letrozole and clomiphene ovulation induction were 2.4% and 4.8%, respectively. The major congenital malformation rate for letrozole was 1.2%, and 3.0% for clomiphene.
Many women with anovulatory infertility and PCOS have a BMI of 30 kg/m2 or greater, and some are of advanced maternal age. It is known that women with such a BMI level have an increased risk of congenital malformations, including neural tube defects, spina bifida, septal anomalies, cleft palate, cleft lip, anorectal atresia, hydrocephaly, and limb reduction anomalies.9 The risk of gastroschisis is significantly reduced among obese pregnant women.9 Women aged 40 or older have an increased risk of having a fetus with cardiac defects, esophageal atresia, hypospadias, and craniosynostosis.10
Caution women of advanced maternal age with PCOS and a BMI of 30 kg/m2 or greater about the increased rate of congenital malformations associated with their age and elevated BMI.
Prioritize letrozole when BMI ≥30 kg/m2
I recommend that clomiphene should remain the first-line ovulation induction agent for women with PCOS and a BMI less than 30 kg/m2. This is because, among women with such a BMI level, both clomiphene and letrozole have similar efficacy, and clomiphene is approved by the US Food and Drug Administration for ovulation induction while letrozole is not.
However, for women with PCOS and a BMI of 30 kg/m2 or greater—a clinical situation where letrozole is about twice as effective as clomiphene—letrozole may be the preferred agent.
When prescribing letrozole, start with a dose of 2.5 mg daily for cycle days 3 to 7, following a spontaneous menses or progestin-induced bleed. If ovulation occurs, continue with the dose. If ovulation does not occur, increase the dose to 5 mg daily for cycle days 3 to 7. The maximal dose is 7.5 mg daily for cycle days 3 to 7. When prescribing letrozole, counsel your patient about the increased rate of congenital anomalies among women with an elevated BMI and the possible teratogenic effects of fertility medications.
The aromatase inhibitor letrozole is an important addition to our options for ovulation induction in women with PCOS. Will you start using letrozole for ovulation induction in your practice?
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
The three most common causes of infertility are anovulation, tubal occlusion, and abnormal semen parameters. The most common cause of anovulatory infertility is polycystic ovary syndrome (PCOS). Options for initial treatment of anovulatory infertility caused by PCOS include optimizing body mass index (BMI), clomiphene, clomiphene plus dexamethasone, and metformin (TABLE 1). If these low-cost interventions are not successful, high-cost interventions are often very effective treatments, and include follicle-stimulating hormone (FSH) injections, laparoscopic ovarian drilling, and in vitro fertilization.
For many couples, the high-cost interventions are prohibitively expensive. Recently, results of a high-quality randomized clinical trial published by Legro and colleagues in the New England Journal of Medicine indicate that letrozole is more effective than clomiphene for the treatment of anovulatory infertility in women with PCOS.1 Of great importance, letrozole was documented to be especially effective in women with a BMI greater than 30.3 kg/m2.
Letrozole is another low-cost option for couples with anovulatory infertility (TABLE 2), and you should consider it among your initial treatment choices. In this article, I outline when letrozole is your best first option for treatment.
Letrozole is more effective than clomiphene for ovulation induction in women with PCOS and BMI >30.3 kg/m2
Legro and colleagues1 randomly assigned 750 women with anovulatory infertility and PCOS to receive ovulation induction with either clomiphene or letrozole. The medications were prescribed using an escalating dose if ovulation did not occur. For clomiphene, the doses prescribed were 50 mg, 100 mg, and 150 mg. For letrozole, the doses were 2.5 mg, 5 mg, and 7.5 mg. The medications were given daily for 5 days on cycle days 3 to 7, following a spontaneous menses or a medroxyprogesterone acetate withdrawal bleed. Up to 5 cycles of ovulation induction were prescribed.
The ovulation rates for letrozole versus clomiphene were 61.7% and 48.3%, respectively (P<.001). The live birth rates for letrozole versus clomiphene were 27.5% and 19.1%, respectively (P = .007). Among women with a BMI of 30.3 kg/m2 or less, both letrozole and clomiphene treatment resulted in a similar live birth rate of approximately 30% to 35%. Among women with a BMI greater than 30.3 kg/m2, however, the live birth rates with letrozole versus clomiphene were approximately 20% and 10%, respectively.
Consequently, in my practice, I prioritize the use of letrozole for women with a BMI of 30 kg/m2 or greater.
Do not use anastrozole for ovulation induction
In a randomized trial of letrozole versus anastrozole for ovulation induction, 40 women with PCOS were randomly assigned to receive ovulation induction with letrozole (2.5 mg daily for 5 days) or anastrozole (1 mg daily for 5 days).2 The resulting ovulation rate was 84% for letrozole, compared with 60% for anastrozole (P<.05). The pregnancy rate also was significantly higher for letrozole (19% vs 10% for anastrozole, P<.05).
Investigators of two large randomized trials of anastrozole versus clomiphene reported that clomiphene was superior to anastrozole for induction of ovulation in the first cycle of treatment.3,4 Anastrozole, at doses of 1 mg, 5 mg, 10 mg, 20 mg, and 30 mg daily for 5 days, was less effective for ovulation induction in the first cycle of treatment than clomiphene at a dose of 50 mg.3,4
If an aromatase inhibitor is going to be prescribed for ovulation induction, I recommend the use of letrozole and recommend against the use of anastrozole.
Congenital malformations and ovulation induction
The administration of clomiphene or letrozole to pregnant rats has adverse fetal effects.5,6 For example, in pregnant rats a low dose of letrozole (0.003 mg/kg) has been reported to increase intrauterine mortality, fetal resorption, and postimplantation loss; decrease live births; and result in fetal anomalies, including dilation of the ureter and shortening of renal papillae.6
However, in the setting of ovulation induction, letrozole is not administered while the patient is pregnant and is discontinued many days before ovulation and conception. Consequently, the results observed in animal studies (with the medications administered to pregnant animals) may not be particularly relevant to the clinical situation where the fertility medication is discontinued before ovulation and conception.
It is important to exclude pregnancy prior to initiating treatment with letrozole or clomiphene.
Birth defects affect approximately 5% of newborns in the United States.7 The relative impact of maternal age, obesity, ovulation induction medicines, and a history of infertility on the rate of birth defects is not fully characterized and is a subject of intense research. To date, there is no strong and consistent evidence that ovulation induction agents, per se, significantly increase the rate of birth defects.
Tulandi and colleagues reported on 911 newborns conceived following ovulation induction with clomiphene or letrozole.8 Overall, the congenital malformation plus chromosomal abnormality rates associated with letrozole and clomiphene ovulation induction were 2.4% and 4.8%, respectively. The major congenital malformation rate for letrozole was 1.2%, and 3.0% for clomiphene.
Many women with anovulatory infertility and PCOS have a BMI of 30 kg/m2 or greater, and some are of advanced maternal age. It is known that women with such a BMI level have an increased risk of congenital malformations, including neural tube defects, spina bifida, septal anomalies, cleft palate, cleft lip, anorectal atresia, hydrocephaly, and limb reduction anomalies.9 The risk of gastroschisis is significantly reduced among obese pregnant women.9 Women aged 40 or older have an increased risk of having a fetus with cardiac defects, esophageal atresia, hypospadias, and craniosynostosis.10
Caution women of advanced maternal age with PCOS and a BMI of 30 kg/m2 or greater about the increased rate of congenital malformations associated with their age and elevated BMI.
Prioritize letrozole when BMI ≥30 kg/m2
I recommend that clomiphene should remain the first-line ovulation induction agent for women with PCOS and a BMI less than 30 kg/m2. This is because, among women with such a BMI level, both clomiphene and letrozole have similar efficacy, and clomiphene is approved by the US Food and Drug Administration for ovulation induction while letrozole is not.
However, for women with PCOS and a BMI of 30 kg/m2 or greater—a clinical situation where letrozole is about twice as effective as clomiphene—letrozole may be the preferred agent.
When prescribing letrozole, start with a dose of 2.5 mg daily for cycle days 3 to 7, following a spontaneous menses or progestin-induced bleed. If ovulation occurs, continue with the dose. If ovulation does not occur, increase the dose to 5 mg daily for cycle days 3 to 7. The maximal dose is 7.5 mg daily for cycle days 3 to 7. When prescribing letrozole, counsel your patient about the increased rate of congenital anomalies among women with an elevated BMI and the possible teratogenic effects of fertility medications.
The aromatase inhibitor letrozole is an important addition to our options for ovulation induction in women with PCOS. Will you start using letrozole for ovulation induction in your practice?
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. Legro RS, Brzyski RG, Diamond MP, et al; NICHD Reproductive Medicine Network. Letrozole versus clomiphene for infertility in the polycystic ovary syndrome. N Engl J Med. 2014;371(2):119–129.
2. Al-Omari WR, Sulaiman WR, Al-Hadithi N. Comparison of two aromatase inhibitors in women with clomiphene-resistant polycystic ovary syndrome. Int J Gynaecol Obstet. 2004;85(3):289–291.
3. Tredway D, Schertz JC, Bock D, Hemsey G, Diamond MP. Anastrozole vs. clomiphene citrate in infertile women with ovulatory dysfunction: a phase II, randomized, dose-finding study. Fertil Steril. 2011;95(5):1720–1724.
4. Tredway D, Schertz JC, Bock D, Hemsey G, Diamond MP. Anastrozole single-dose protocol in women with oligo- or anovulatory infertility: results of a randomized phase II dose-response study. Fertil Steril. 2011;95(5):1725–1729.
5. Clomid (clomiphene citrate tablets USP) [package insert]. Bridgewater, NJ: sanofi-aventis. http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/016131s026lbl.pdf. Revised October 2012. Accessed October 20, 2014.
6. Femara (letrozole tablets) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation. https://www.pharma.us.novartis.com/product/pi/pdf/Femara.pdf. Revised January 2014. Accessed October 20, 2014.
7. Christianson A, Howson CP, Modell B. March of Dimes Global Report on Birth Defects: Executive Summary. White Plains NY: March of Dimes Birth Defects Foundation; 2006:2–9. http://www.marchofdimes.com/materials/global-report-on-birth-defects-the-hidden-toll-of-dying-and-disabled-children-execu tive-summary.pdf. Accessed October 20, 2014.
8. Tulandi T, Martin J, Al-Fadhli R, et al. Congenital malformations among 911 newborns conceived after infertility with letrozole or clomiphene citrate. Fertil Steril. 2006;85(6):1761–1765.
9. Stothard KJ, Tennant PW, Bell R, Rankin J. Maternal overweight and obesity and the risk of congenital anomalies: a systemic review and meta-analysis. JAMA. 2009;301(6):636–650.
10. Gill SK, Broussard C, Devine O, Green RF, Rasmussen SA, Reefhuis J; National Birth Defects Prevention Study. Association between maternal age and birth defects of unknown etiology: United States, 1997–2007. Birth Defects Res A Clin Mol Teratol. 2012;94(12):1010–1018
1. Legro RS, Brzyski RG, Diamond MP, et al; NICHD Reproductive Medicine Network. Letrozole versus clomiphene for infertility in the polycystic ovary syndrome. N Engl J Med. 2014;371(2):119–129.
2. Al-Omari WR, Sulaiman WR, Al-Hadithi N. Comparison of two aromatase inhibitors in women with clomiphene-resistant polycystic ovary syndrome. Int J Gynaecol Obstet. 2004;85(3):289–291.
3. Tredway D, Schertz JC, Bock D, Hemsey G, Diamond MP. Anastrozole vs. clomiphene citrate in infertile women with ovulatory dysfunction: a phase II, randomized, dose-finding study. Fertil Steril. 2011;95(5):1720–1724.
4. Tredway D, Schertz JC, Bock D, Hemsey G, Diamond MP. Anastrozole single-dose protocol in women with oligo- or anovulatory infertility: results of a randomized phase II dose-response study. Fertil Steril. 2011;95(5):1725–1729.
5. Clomid (clomiphene citrate tablets USP) [package insert]. Bridgewater, NJ: sanofi-aventis. http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/016131s026lbl.pdf. Revised October 2012. Accessed October 20, 2014.
6. Femara (letrozole tablets) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation. https://www.pharma.us.novartis.com/product/pi/pdf/Femara.pdf. Revised January 2014. Accessed October 20, 2014.
7. Christianson A, Howson CP, Modell B. March of Dimes Global Report on Birth Defects: Executive Summary. White Plains NY: March of Dimes Birth Defects Foundation; 2006:2–9. http://www.marchofdimes.com/materials/global-report-on-birth-defects-the-hidden-toll-of-dying-and-disabled-children-execu tive-summary.pdf. Accessed October 20, 2014.
8. Tulandi T, Martin J, Al-Fadhli R, et al. Congenital malformations among 911 newborns conceived after infertility with letrozole or clomiphene citrate. Fertil Steril. 2006;85(6):1761–1765.
9. Stothard KJ, Tennant PW, Bell R, Rankin J. Maternal overweight and obesity and the risk of congenital anomalies: a systemic review and meta-analysis. JAMA. 2009;301(6):636–650.
10. Gill SK, Broussard C, Devine O, Green RF, Rasmussen SA, Reefhuis J; National Birth Defects Prevention Study. Association between maternal age and birth defects of unknown etiology: United States, 1997–2007. Birth Defects Res A Clin Mol Teratol. 2012;94(12):1010–1018
Road maps
One of the greatest challenges you may face as a pediatrician is in helping your patients and families navigate the mental health system. Nearly 20% of children will experience a psychiatric illness before they turn 18, and a quarter of those will go on to experience a persistent or severe psychiatric illness. Whether a patient is experiencing symptoms that are mild or severe, their parents are likely to come to you first for an assessment and for help in finding a referral to the appropriate specialist.
Unlike the smooth process to refer to a neurologist or orthopedist, accessing treatment for mental health problems is often confusing and frustrating. Because of reimbursement that is below the cost of providing care, many community hospitals have closed their divisions of child and adolescent psychiatry, and academic medical centers often have a long wait for a provider. If you go through a patient’s insurance, usually the list of providers is woefully out-of-date, with most of them not accepting new referrals or insurance or both. If mental health services are “carved out” to cut costs, the primary insurer has no direct control of mental health services, and the carve out company is looking for providers willing to accept lower reimbursement and limit longer-term treatments. Faced with reimbursement and administrative demands by the carve out company, child psychiatrists, psychologists, and social workers that once staffed these services have chosen fee-for-service private offices that do not accept any insurance, leaving many communities without access to adequate resources. In private practice, these providers are busy, face no administrative demands to justify their work, and earn two or three times what insurers reimburse.

So families often turn to their schools and their pediatricians when faced with a mood, anxiety, or behavioral problem. While there is no straightforward solution to this problem of access, we have put together a “road map” to what services might be available and to help you in your approach to these patients.
It is first important to consider that mental health and developmental questions are now a major part of pediatric primary care. The majority of your visits will be well child care and psychosocial. So a part, maybe a third or half of mental health concerns might now be considered a routine part of primary care. Many practices are now doing psychosocial screening and more states are mandating reimbursement of this screening. Typically screening includes a CHATfor autism (Checklist for Autism in Toddlers), a developmental screen if indicated, a Pediatric Symptom Checklist for school-age children and adolescents, a Hamilton Rating Scale for Depression in adolescents, and a CRAFFTfor adolescent substance abuse. Some practices include a Hamilton or other depression screen for mothers of newborns and toddlers as maternal depression has a serious impact on the child and is responsive to treatment. If screening is reimbursed, some of that money could go to fund an on-site social worker, who can also bill for patient contact services, and thus provide the practice with an on-site mental health presence at break-even cost. This social worker may be expert in referring to local resources, may be trained in psychotherapy, or may even lead groups for parents of recent divorce, new mothers, facing attention-deficit/hyperactivity disorder (ADHD), etc.
The best place to start for a family with psychosocial concerns is to do a brief review of your patient’s day to day functioning – school, friends, family, activities, and mood. What is your best assessment of the problem, how much of the child and family’s life is affected, and how severe is the problem? There are many mental health problems for which the first-line treatment is a trial of medication according to an algorithm that you can use following American Academy of Pediatrics guidelines. For example, if considering stimulant treatment for a 7-year-old with possible attention difficulties, you can use broad screening instruments like the Pediatric Symptom Checklist or Childhood Behavior Checklist as well as the Vanderbilt Assessment Scales or Conners questionnaire that are specific for ADHD. Many pediatricians also are comfortable treating adolescent depression with medication and with comanagement from a social worker with a master’s degree or a doctorate level psychologist. Of course, treating depression requires a more careful interview, consideration of suicide risk, and more frequent follow-up visits.

As first-line treatment for depression and anxiety usually starts with psychotherapy, it is important to consider how you will access this component of mental health care. For those that don’t have a licensed clinical social worker on-site providing cognitive-behavioral therapy, many busy pediatric practices will establish a relationship with a therapist or group that has agreed to accept their referrals and accepts insurance reimbursement. If you are not fortunate enough to already have such a relationship, it can be fruitful to speak with colleagues in a busier practice about whom they use. It also can be fruitful to reach out to the graduate programs in psychology (PhD or PsyD programs) or social work in your community, to find out if they have a referral service or would like to connect recent graduates trying to establish themselves with referring pediatricians. Having a resource located in your office (employed by you or renting space) is ideal.
When a patient is presenting with a more complex set of symptoms or fails to respond to your initial treatments, then you will want to locate an appropriate referral to a child psychiatrist. If your group is affiliated with an academic medical center, find out what the procedure is for referring to their child psychiatrists or to the child psychiatry trainees. Often there is easy availability early in the academic year (summer), when children are less likely to present with problems and a new crop of trainees has arrived. Academic medical centers also will often be a hub for a lot of research activity, and research programs are usually eager to enroll patients without regard to their insurance. Good studies will provide patients with a formalized assessment that will clarify the diagnostic picture, ensuring that a child is on the path to the right treatment. Cultivating a connection with the research coordinator can ensure that your group knows about opportunities for free care that is easier to access than most.
Many states require schools to provide testing to clarify whether psychiatric symptoms, developmental issues, or learning disabilities are affecting a student’s ability to perform in school. Your office can educate parents that they should go to the school with their concerns and request a formal assessment. If testing indicates a condition, the school system is often required to provide appropriate educational services, such as tutoring for learning disabilities, occupational therapy, and social skills support for children on the autism spectrum, and even counseling for children with anxiety, mood, and behavioral issues. Often, the school psychologist or social worker will be a valuable resource in providing direct care to children or helping you and the parents identify excellent treaters in the community. For children with severe and persistent psychiatric illness, many states require that schools provide or pay for the services that are necessary to educate each child. This can mean anything from paying for an after school social skills group to paying for a therapeutic boarding school. In these cases, it is often helpful to have established a relationship with an educational consultant. These are usually social workers with expertise in mental health issues and the state’s educational system and regulations, and they will partner with parents for a modest fee to educate and empower parents so that they might get appropriate services from their schools. Again, it can be fruitful to speak with trusted colleagues and find one who has identified a local consultant that they trust.
Some states and counties have tried to address the problem of accessing psychiatric care for children, but often these are programs that have not been adequately marketed to pediatricians or families, so they may be under utilized. In Massachusetts and Connecticut, there is the state Child Psychiatry Access Project, which provides all pediatricians with free access to a consulting child psychiatrist by phone. It requires that pediatricians are willing to treat children themselves with the support and guidance of a consulting child psychiatrist, but it will also provide a face-to-face diagnostic evaluation of that child by a child psychiatrist so that they can in turn provide the best guidance to the pediatrician. And it provides a care coordinator who will help to identify appropriate treaters, such as a cognitive-behavioral therapist or a psychopharmacologist who accept the family’s insurance, when the pediatrician is unable to provide the recommended treatment. An online investigation through your state’s or county’s Office of Mental Health or your local Medical Society can help your office identify what resources may exist in your community.
Finally, your most critical task after a parent has come to you with concerns about their child’s mood, thinking, or behavior, may be in educating and supporting those parents. Prepare the parents by explaining to them how the mental health system is more fragmented and frustrating than most other medical specialties. Remind them that psychiatric symptoms and illnesses are eminently treatable, and it will be worth patiently navigating this complex system to eventually access the right care for their child. It can be helpful to suggest to them that if they can possibly afford to pay out-of-pocket for the appropriate care, it will make excellent treatment much easier to access in a timely way. It can be meaningful for parents to hear from you that it is worthwhile for them to call or write their insurance company and complain if that company has restricted access to child psychiatric care. They are, after all, the customers of their insurance company, and it is the silence, shame, and stigma surrounding psychiatric illness that has enabled insurance companies to restrict access to effective care. Finally, it can be very powerful to connect parents with support or advocacy organizations that will help them in navigating this system and in speaking up to their insurance companies, state health, or education agencies or in the press in ways that will diminish the stigma that still surrounds these problems. The National Alliance on Mental Illness (www.nami.org), The Bazelon Center for Mental Health Law (www.bazelon.org), and the American Academy of Child and Adolescent Psychiatry (www.aacap.org) all have excellent online resources that also help identify local organizations and resources for parents. If insurance companies refused to pay for potentially life-saving chemotherapy for a pediatric cancer, you can imagine that there would be many parents protesting to those insurers, to the news, and even to their local or state governments. Mental health care should be no different, as the problems can be as disabling and life-threatening and effective treatments and even cures exist.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston. E-mail them at [email protected].
One of the greatest challenges you may face as a pediatrician is in helping your patients and families navigate the mental health system. Nearly 20% of children will experience a psychiatric illness before they turn 18, and a quarter of those will go on to experience a persistent or severe psychiatric illness. Whether a patient is experiencing symptoms that are mild or severe, their parents are likely to come to you first for an assessment and for help in finding a referral to the appropriate specialist.
Unlike the smooth process to refer to a neurologist or orthopedist, accessing treatment for mental health problems is often confusing and frustrating. Because of reimbursement that is below the cost of providing care, many community hospitals have closed their divisions of child and adolescent psychiatry, and academic medical centers often have a long wait for a provider. If you go through a patient’s insurance, usually the list of providers is woefully out-of-date, with most of them not accepting new referrals or insurance or both. If mental health services are “carved out” to cut costs, the primary insurer has no direct control of mental health services, and the carve out company is looking for providers willing to accept lower reimbursement and limit longer-term treatments. Faced with reimbursement and administrative demands by the carve out company, child psychiatrists, psychologists, and social workers that once staffed these services have chosen fee-for-service private offices that do not accept any insurance, leaving many communities without access to adequate resources. In private practice, these providers are busy, face no administrative demands to justify their work, and earn two or three times what insurers reimburse.
So families often turn to their schools and their pediatricians when faced with a mood, anxiety, or behavioral problem. While there is no straightforward solution to this problem of access, we have put together a “road map” to what services might be available and to help you in your approach to these patients.
It is first important to consider that mental health and developmental questions are now a major part of pediatric primary care. The majority of your visits will be well child care and psychosocial. So a part, maybe a third or half of mental health concerns might now be considered a routine part of primary care. Many practices are now doing psychosocial screening and more states are mandating reimbursement of this screening. Typically screening includes a CHATfor autism (Checklist for Autism in Toddlers), a developmental screen if indicated, a Pediatric Symptom Checklist for school-age children and adolescents, a Hamilton Rating Scale for Depression in adolescents, and a CRAFFTfor adolescent substance abuse. Some practices include a Hamilton or other depression screen for mothers of newborns and toddlers as maternal depression has a serious impact on the child and is responsive to treatment. If screening is reimbursed, some of that money could go to fund an on-site social worker, who can also bill for patient contact services, and thus provide the practice with an on-site mental health presence at break-even cost. This social worker may be expert in referring to local resources, may be trained in psychotherapy, or may even lead groups for parents of recent divorce, new mothers, facing attention-deficit/hyperactivity disorder (ADHD), etc.
The best place to start for a family with psychosocial concerns is to do a brief review of your patient’s day to day functioning – school, friends, family, activities, and mood. What is your best assessment of the problem, how much of the child and family’s life is affected, and how severe is the problem? There are many mental health problems for which the first-line treatment is a trial of medication according to an algorithm that you can use following American Academy of Pediatrics guidelines. For example, if considering stimulant treatment for a 7-year-old with possible attention difficulties, you can use broad screening instruments like the Pediatric Symptom Checklist or Childhood Behavior Checklist as well as the Vanderbilt Assessment Scales or Conners questionnaire that are specific for ADHD. Many pediatricians also are comfortable treating adolescent depression with medication and with comanagement from a social worker with a master’s degree or a doctorate level psychologist. Of course, treating depression requires a more careful interview, consideration of suicide risk, and more frequent follow-up visits.
As first-line treatment for depression and anxiety usually starts with psychotherapy, it is important to consider how you will access this component of mental health care. For those that don’t have a licensed clinical social worker on-site providing cognitive-behavioral therapy, many busy pediatric practices will establish a relationship with a therapist or group that has agreed to accept their referrals and accepts insurance reimbursement. If you are not fortunate enough to already have such a relationship, it can be fruitful to speak with colleagues in a busier practice about whom they use. It also can be fruitful to reach out to the graduate programs in psychology (PhD or PsyD programs) or social work in your community, to find out if they have a referral service or would like to connect recent graduates trying to establish themselves with referring pediatricians. Having a resource located in your office (employed by you or renting space) is ideal.
When a patient is presenting with a more complex set of symptoms or fails to respond to your initial treatments, then you will want to locate an appropriate referral to a child psychiatrist. If your group is affiliated with an academic medical center, find out what the procedure is for referring to their child psychiatrists or to the child psychiatry trainees. Often there is easy availability early in the academic year (summer), when children are less likely to present with problems and a new crop of trainees has arrived. Academic medical centers also will often be a hub for a lot of research activity, and research programs are usually eager to enroll patients without regard to their insurance. Good studies will provide patients with a formalized assessment that will clarify the diagnostic picture, ensuring that a child is on the path to the right treatment. Cultivating a connection with the research coordinator can ensure that your group knows about opportunities for free care that is easier to access than most.
Many states require schools to provide testing to clarify whether psychiatric symptoms, developmental issues, or learning disabilities are affecting a student’s ability to perform in school. Your office can educate parents that they should go to the school with their concerns and request a formal assessment. If testing indicates a condition, the school system is often required to provide appropriate educational services, such as tutoring for learning disabilities, occupational therapy, and social skills support for children on the autism spectrum, and even counseling for children with anxiety, mood, and behavioral issues. Often, the school psychologist or social worker will be a valuable resource in providing direct care to children or helping you and the parents identify excellent treaters in the community. For children with severe and persistent psychiatric illness, many states require that schools provide or pay for the services that are necessary to educate each child. This can mean anything from paying for an after school social skills group to paying for a therapeutic boarding school. In these cases, it is often helpful to have established a relationship with an educational consultant. These are usually social workers with expertise in mental health issues and the state’s educational system and regulations, and they will partner with parents for a modest fee to educate and empower parents so that they might get appropriate services from their schools. Again, it can be fruitful to speak with trusted colleagues and find one who has identified a local consultant that they trust.
Some states and counties have tried to address the problem of accessing psychiatric care for children, but often these are programs that have not been adequately marketed to pediatricians or families, so they may be under utilized. In Massachusetts and Connecticut, there is the state Child Psychiatry Access Project, which provides all pediatricians with free access to a consulting child psychiatrist by phone. It requires that pediatricians are willing to treat children themselves with the support and guidance of a consulting child psychiatrist, but it will also provide a face-to-face diagnostic evaluation of that child by a child psychiatrist so that they can in turn provide the best guidance to the pediatrician. And it provides a care coordinator who will help to identify appropriate treaters, such as a cognitive-behavioral therapist or a psychopharmacologist who accept the family’s insurance, when the pediatrician is unable to provide the recommended treatment. An online investigation through your state’s or county’s Office of Mental Health or your local Medical Society can help your office identify what resources may exist in your community.
Finally, your most critical task after a parent has come to you with concerns about their child’s mood, thinking, or behavior, may be in educating and supporting those parents. Prepare the parents by explaining to them how the mental health system is more fragmented and frustrating than most other medical specialties. Remind them that psychiatric symptoms and illnesses are eminently treatable, and it will be worth patiently navigating this complex system to eventually access the right care for their child. It can be helpful to suggest to them that if they can possibly afford to pay out-of-pocket for the appropriate care, it will make excellent treatment much easier to access in a timely way. It can be meaningful for parents to hear from you that it is worthwhile for them to call or write their insurance company and complain if that company has restricted access to child psychiatric care. They are, after all, the customers of their insurance company, and it is the silence, shame, and stigma surrounding psychiatric illness that has enabled insurance companies to restrict access to effective care. Finally, it can be very powerful to connect parents with support or advocacy organizations that will help them in navigating this system and in speaking up to their insurance companies, state health, or education agencies or in the press in ways that will diminish the stigma that still surrounds these problems. The National Alliance on Mental Illness (www.nami.org), The Bazelon Center for Mental Health Law (www.bazelon.org), and the American Academy of Child and Adolescent Psychiatry (www.aacap.org) all have excellent online resources that also help identify local organizations and resources for parents. If insurance companies refused to pay for potentially life-saving chemotherapy for a pediatric cancer, you can imagine that there would be many parents protesting to those insurers, to the news, and even to their local or state governments. Mental health care should be no different, as the problems can be as disabling and life-threatening and effective treatments and even cures exist.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston. E-mail them at [email protected].
One of the greatest challenges you may face as a pediatrician is in helping your patients and families navigate the mental health system. Nearly 20% of children will experience a psychiatric illness before they turn 18, and a quarter of those will go on to experience a persistent or severe psychiatric illness. Whether a patient is experiencing symptoms that are mild or severe, their parents are likely to come to you first for an assessment and for help in finding a referral to the appropriate specialist.
Unlike the smooth process to refer to a neurologist or orthopedist, accessing treatment for mental health problems is often confusing and frustrating. Because of reimbursement that is below the cost of providing care, many community hospitals have closed their divisions of child and adolescent psychiatry, and academic medical centers often have a long wait for a provider. If you go through a patient’s insurance, usually the list of providers is woefully out-of-date, with most of them not accepting new referrals or insurance or both. If mental health services are “carved out” to cut costs, the primary insurer has no direct control of mental health services, and the carve out company is looking for providers willing to accept lower reimbursement and limit longer-term treatments. Faced with reimbursement and administrative demands by the carve out company, child psychiatrists, psychologists, and social workers that once staffed these services have chosen fee-for-service private offices that do not accept any insurance, leaving many communities without access to adequate resources. In private practice, these providers are busy, face no administrative demands to justify their work, and earn two or three times what insurers reimburse.
So families often turn to their schools and their pediatricians when faced with a mood, anxiety, or behavioral problem. While there is no straightforward solution to this problem of access, we have put together a “road map” to what services might be available and to help you in your approach to these patients.
It is first important to consider that mental health and developmental questions are now a major part of pediatric primary care. The majority of your visits will be well child care and psychosocial. So a part, maybe a third or half of mental health concerns might now be considered a routine part of primary care. Many practices are now doing psychosocial screening and more states are mandating reimbursement of this screening. Typically screening includes a CHATfor autism (Checklist for Autism in Toddlers), a developmental screen if indicated, a Pediatric Symptom Checklist for school-age children and adolescents, a Hamilton Rating Scale for Depression in adolescents, and a CRAFFTfor adolescent substance abuse. Some practices include a Hamilton or other depression screen for mothers of newborns and toddlers as maternal depression has a serious impact on the child and is responsive to treatment. If screening is reimbursed, some of that money could go to fund an on-site social worker, who can also bill for patient contact services, and thus provide the practice with an on-site mental health presence at break-even cost. This social worker may be expert in referring to local resources, may be trained in psychotherapy, or may even lead groups for parents of recent divorce, new mothers, facing attention-deficit/hyperactivity disorder (ADHD), etc.
The best place to start for a family with psychosocial concerns is to do a brief review of your patient’s day to day functioning – school, friends, family, activities, and mood. What is your best assessment of the problem, how much of the child and family’s life is affected, and how severe is the problem? There are many mental health problems for which the first-line treatment is a trial of medication according to an algorithm that you can use following American Academy of Pediatrics guidelines. For example, if considering stimulant treatment for a 7-year-old with possible attention difficulties, you can use broad screening instruments like the Pediatric Symptom Checklist or Childhood Behavior Checklist as well as the Vanderbilt Assessment Scales or Conners questionnaire that are specific for ADHD. Many pediatricians also are comfortable treating adolescent depression with medication and with comanagement from a social worker with a master’s degree or a doctorate level psychologist. Of course, treating depression requires a more careful interview, consideration of suicide risk, and more frequent follow-up visits.
As first-line treatment for depression and anxiety usually starts with psychotherapy, it is important to consider how you will access this component of mental health care. For those that don’t have a licensed clinical social worker on-site providing cognitive-behavioral therapy, many busy pediatric practices will establish a relationship with a therapist or group that has agreed to accept their referrals and accepts insurance reimbursement. If you are not fortunate enough to already have such a relationship, it can be fruitful to speak with colleagues in a busier practice about whom they use. It also can be fruitful to reach out to the graduate programs in psychology (PhD or PsyD programs) or social work in your community, to find out if they have a referral service or would like to connect recent graduates trying to establish themselves with referring pediatricians. Having a resource located in your office (employed by you or renting space) is ideal.
When a patient is presenting with a more complex set of symptoms or fails to respond to your initial treatments, then you will want to locate an appropriate referral to a child psychiatrist. If your group is affiliated with an academic medical center, find out what the procedure is for referring to their child psychiatrists or to the child psychiatry trainees. Often there is easy availability early in the academic year (summer), when children are less likely to present with problems and a new crop of trainees has arrived. Academic medical centers also will often be a hub for a lot of research activity, and research programs are usually eager to enroll patients without regard to their insurance. Good studies will provide patients with a formalized assessment that will clarify the diagnostic picture, ensuring that a child is on the path to the right treatment. Cultivating a connection with the research coordinator can ensure that your group knows about opportunities for free care that is easier to access than most.
Many states require schools to provide testing to clarify whether psychiatric symptoms, developmental issues, or learning disabilities are affecting a student’s ability to perform in school. Your office can educate parents that they should go to the school with their concerns and request a formal assessment. If testing indicates a condition, the school system is often required to provide appropriate educational services, such as tutoring for learning disabilities, occupational therapy, and social skills support for children on the autism spectrum, and even counseling for children with anxiety, mood, and behavioral issues. Often, the school psychologist or social worker will be a valuable resource in providing direct care to children or helping you and the parents identify excellent treaters in the community. For children with severe and persistent psychiatric illness, many states require that schools provide or pay for the services that are necessary to educate each child. This can mean anything from paying for an after school social skills group to paying for a therapeutic boarding school. In these cases, it is often helpful to have established a relationship with an educational consultant. These are usually social workers with expertise in mental health issues and the state’s educational system and regulations, and they will partner with parents for a modest fee to educate and empower parents so that they might get appropriate services from their schools. Again, it can be fruitful to speak with trusted colleagues and find one who has identified a local consultant that they trust.
Some states and counties have tried to address the problem of accessing psychiatric care for children, but often these are programs that have not been adequately marketed to pediatricians or families, so they may be under utilized. In Massachusetts and Connecticut, there is the state Child Psychiatry Access Project, which provides all pediatricians with free access to a consulting child psychiatrist by phone. It requires that pediatricians are willing to treat children themselves with the support and guidance of a consulting child psychiatrist, but it will also provide a face-to-face diagnostic evaluation of that child by a child psychiatrist so that they can in turn provide the best guidance to the pediatrician. And it provides a care coordinator who will help to identify appropriate treaters, such as a cognitive-behavioral therapist or a psychopharmacologist who accept the family’s insurance, when the pediatrician is unable to provide the recommended treatment. An online investigation through your state’s or county’s Office of Mental Health or your local Medical Society can help your office identify what resources may exist in your community.
Finally, your most critical task after a parent has come to you with concerns about their child’s mood, thinking, or behavior, may be in educating and supporting those parents. Prepare the parents by explaining to them how the mental health system is more fragmented and frustrating than most other medical specialties. Remind them that psychiatric symptoms and illnesses are eminently treatable, and it will be worth patiently navigating this complex system to eventually access the right care for their child. It can be helpful to suggest to them that if they can possibly afford to pay out-of-pocket for the appropriate care, it will make excellent treatment much easier to access in a timely way. It can be meaningful for parents to hear from you that it is worthwhile for them to call or write their insurance company and complain if that company has restricted access to child psychiatric care. They are, after all, the customers of their insurance company, and it is the silence, shame, and stigma surrounding psychiatric illness that has enabled insurance companies to restrict access to effective care. Finally, it can be very powerful to connect parents with support or advocacy organizations that will help them in navigating this system and in speaking up to their insurance companies, state health, or education agencies or in the press in ways that will diminish the stigma that still surrounds these problems. The National Alliance on Mental Illness (www.nami.org), The Bazelon Center for Mental Health Law (www.bazelon.org), and the American Academy of Child and Adolescent Psychiatry (www.aacap.org) all have excellent online resources that also help identify local organizations and resources for parents. If insurance companies refused to pay for potentially life-saving chemotherapy for a pediatric cancer, you can imagine that there would be many parents protesting to those insurers, to the news, and even to their local or state governments. Mental health care should be no different, as the problems can be as disabling and life-threatening and effective treatments and even cures exist.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston. E-mail them at [email protected].

LAW & MEDICINE: ‘Defective and unreasonably dangerous’
Question: After statins had been in use for several years, data began to accumulate purporting to show that they increase the risk of diabetes. When Mrs. Smith learned that her recent diagnosis of diabetes might have something to do with the drug, she consulted a lawyer who began advertising for similar cases to consolidate them into a class action lawsuit. The legal theory (theories) seeking to prove product liability will be based on:
A. Contract law and breach of warranty.
B. Negligence in tort law.
C. Strict liability without requiring proof of fault.
D. A defective product that is unreasonably dangerous.
E. All of the above.
Answer:E. Should a prescription drug lead to harm, an injured party can sue the manufacturer who had placed it into the stream of commerce. The law of products liability governs this cause of action, wherein recovery is based on a number of legal theories, specifically negligence, breach of warranty, and strict liability. The latter is the most favored, as there is no need to prove fault or warranty. Products liability law also covers defective medical devices. The recent multimillion-dollar settlements and jury verdicts with Endo, Johnson & Johnson, Bard, and other manufacturers over their vaginal mesh devices are good examples.
In products liability, injured plaintiffs frequently claim a failure to warn of known risks, such as cardiovascular deaths caused by Vioxx, a nonsteroidal anti-inflammatory drug that was withdrawn in 2004. Merck, its manufacturer, has thus far won 11 and lost 3 of the cases that have gone to trial. Some of these judgments are under appeal; most notably, a Texas Court of Appeals recently reversed a $253 million award initially won by plaintiff Robert Ernst in the very first trial. However, the company has proposed $4.85 billion to settle tens of thousands of similar pending lawsuits. Other recent examples alleging failure to warn are heart attacks linked to the diabetes drug rosiglitazone and bladder cancer associated with the diabetes drug pioglitazone.
In 1963, the California Supreme Court bypassed the law of contracts and warranty in a seminal case of product-related injury, and introduced the notion of strict liability, which goes beyond simple negligence (Greenman v Yuba Power Products Inc., 377 P.2d 897 [Cal. 1963]). The strict liability approach centers on whether a product is defective and unreasonably dangerous, and it has now been adopted in virtually all jurisdictions.
The theory holds that a professional supplier who sells a product that is both defective and unreasonably dangerous is strictly liable to foreseeable plaintiffs. “Defective” is usually defined as product quality that is less than what a reasonable consumer expects. “Unreasonably dangerous” is a conclusion that the risks that result from its condition outweigh the product’s advantages.
Strict liability is not about negligence or fault, but about a social policy that shifts to the manufacturer the cost of compensating the injured consumer. To prevail, the plaintiff must show proximate cause, and assumption of risk is still a valid defense.
Statins, which are powerful HMG-CoA reductase inhibitors widely used to treat hypercholesterolemia, are currently at the center of pharmaceutical products litigation.
Pfizer, the manufacturer of Lipitor (atorvastatin) has become the target of numerous lawsuits alleging that the drug causes diabetes. Lipitor is the best-selling prescription drug ever, with sales reaching $130 billion since it was approved in 1996. In the United States alone, more than 29 million people have been prescribed this medication. The drug is highly effective in lowering serum cholesterol and is proven to reduce cardiovascular deaths.
A meta-analysis in 2010 revealed an increased risk of diabetes in patients taking statins (Lancet 2010;375:735-42). Statin therapy was associated with a 9% increased risk for incident diabetes; it was calculated that treatment of 255 patients with statins for 4 years resulted in 1 extra case of diabetes. An earlier smaller study had rejected this conclusion, but other studies were in support.
In 2012, the Food and Drug Administration (FDA) required the revision of the package insert of Lipitor and other statins to warn that their use had been linked to a small increased risk of diabetes.
In 2013, a large Canadian study confirmed the increased incidence of new-onset diabetes in patients taking atorvastatin (hazard ratio, 1.22) and simvastatin (hazard ratio, 1.10). This population-based cohort study involved nondiabetic patients age 66 years or older who started statins between 1997 and 2010 (BMJ 2013;346:f2610).
These and other results, coupled with the FDA-mandated revised labeling, have spawned the filing of nearly 1,000 lawsuits by patients who developed diabetes while taking statins, especially postmenopausal women. The rapid increase in the number of lawsuits may be related to the recent decision of a federal judicial panel on multidistrict litigation to consolidate all Lipitor diabetes lawsuits into a single federal courtroom in Charleston, S.C., as a class-action suit. The first case has yet to go to trial, but is expected to do so in 2015.
Previous products liability cases implicating statins have famously involved cerivastatin (Baycol), a one-time rival to Lipitor, for causing rhabdomyolysis. The drug was pulled from the market in 2001 after it reportedly caused 31 deaths. Bayer, its manufacturer, paid about $1 billion in 2005 to settle some 3,000 cases. An example of a medication causing diabetes is quetiapine (Seroquel), an antipsychotic drug manufactured by AstraZeneca, which in 2011 agreed to pay $647 million to settle more than 28,000 lawsuits.
However, the upcoming Lipitor litigation may be more difficult for the plaintiffs to win. Among some of the medico-legal questions to be addressed are:
1) Was there prior company knowledge of the risk and a failure to warn?
2) Were the patients harmed by the drug, given that diabetes is a very common disease and may be linked more to genetics and/or an underlying metabolic syndrome in those who are hyperlipidemic, hypertensive, or obese – the very same patients likely to be on a statin?
3) Is Lipitor a defective product, and is it unreasonably dangerous?
Despite the FDA-directed change in labeling, a number of scientists and the FDA itself have emphasized that the cardiac benefits of a statin drug are greater than any small increased risk of developing diabetes.
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].
Question: After statins had been in use for several years, data began to accumulate purporting to show that they increase the risk of diabetes. When Mrs. Smith learned that her recent diagnosis of diabetes might have something to do with the drug, she consulted a lawyer who began advertising for similar cases to consolidate them into a class action lawsuit. The legal theory (theories) seeking to prove product liability will be based on:
A. Contract law and breach of warranty.
B. Negligence in tort law.
C. Strict liability without requiring proof of fault.
D. A defective product that is unreasonably dangerous.
E. All of the above.
Answer:E. Should a prescription drug lead to harm, an injured party can sue the manufacturer who had placed it into the stream of commerce. The law of products liability governs this cause of action, wherein recovery is based on a number of legal theories, specifically negligence, breach of warranty, and strict liability. The latter is the most favored, as there is no need to prove fault or warranty. Products liability law also covers defective medical devices. The recent multimillion-dollar settlements and jury verdicts with Endo, Johnson & Johnson, Bard, and other manufacturers over their vaginal mesh devices are good examples.
In products liability, injured plaintiffs frequently claim a failure to warn of known risks, such as cardiovascular deaths caused by Vioxx, a nonsteroidal anti-inflammatory drug that was withdrawn in 2004. Merck, its manufacturer, has thus far won 11 and lost 3 of the cases that have gone to trial. Some of these judgments are under appeal; most notably, a Texas Court of Appeals recently reversed a $253 million award initially won by plaintiff Robert Ernst in the very first trial. However, the company has proposed $4.85 billion to settle tens of thousands of similar pending lawsuits. Other recent examples alleging failure to warn are heart attacks linked to the diabetes drug rosiglitazone and bladder cancer associated with the diabetes drug pioglitazone.
In 1963, the California Supreme Court bypassed the law of contracts and warranty in a seminal case of product-related injury, and introduced the notion of strict liability, which goes beyond simple negligence (Greenman v Yuba Power Products Inc., 377 P.2d 897 [Cal. 1963]). The strict liability approach centers on whether a product is defective and unreasonably dangerous, and it has now been adopted in virtually all jurisdictions.
The theory holds that a professional supplier who sells a product that is both defective and unreasonably dangerous is strictly liable to foreseeable plaintiffs. “Defective” is usually defined as product quality that is less than what a reasonable consumer expects. “Unreasonably dangerous” is a conclusion that the risks that result from its condition outweigh the product’s advantages.
Strict liability is not about negligence or fault, but about a social policy that shifts to the manufacturer the cost of compensating the injured consumer. To prevail, the plaintiff must show proximate cause, and assumption of risk is still a valid defense.
Statins, which are powerful HMG-CoA reductase inhibitors widely used to treat hypercholesterolemia, are currently at the center of pharmaceutical products litigation.
Pfizer, the manufacturer of Lipitor (atorvastatin) has become the target of numerous lawsuits alleging that the drug causes diabetes. Lipitor is the best-selling prescription drug ever, with sales reaching $130 billion since it was approved in 1996. In the United States alone, more than 29 million people have been prescribed this medication. The drug is highly effective in lowering serum cholesterol and is proven to reduce cardiovascular deaths.
A meta-analysis in 2010 revealed an increased risk of diabetes in patients taking statins (Lancet 2010;375:735-42). Statin therapy was associated with a 9% increased risk for incident diabetes; it was calculated that treatment of 255 patients with statins for 4 years resulted in 1 extra case of diabetes. An earlier smaller study had rejected this conclusion, but other studies were in support.
In 2012, the Food and Drug Administration (FDA) required the revision of the package insert of Lipitor and other statins to warn that their use had been linked to a small increased risk of diabetes.
In 2013, a large Canadian study confirmed the increased incidence of new-onset diabetes in patients taking atorvastatin (hazard ratio, 1.22) and simvastatin (hazard ratio, 1.10). This population-based cohort study involved nondiabetic patients age 66 years or older who started statins between 1997 and 2010 (BMJ 2013;346:f2610).
These and other results, coupled with the FDA-mandated revised labeling, have spawned the filing of nearly 1,000 lawsuits by patients who developed diabetes while taking statins, especially postmenopausal women. The rapid increase in the number of lawsuits may be related to the recent decision of a federal judicial panel on multidistrict litigation to consolidate all Lipitor diabetes lawsuits into a single federal courtroom in Charleston, S.C., as a class-action suit. The first case has yet to go to trial, but is expected to do so in 2015.
Previous products liability cases implicating statins have famously involved cerivastatin (Baycol), a one-time rival to Lipitor, for causing rhabdomyolysis. The drug was pulled from the market in 2001 after it reportedly caused 31 deaths. Bayer, its manufacturer, paid about $1 billion in 2005 to settle some 3,000 cases. An example of a medication causing diabetes is quetiapine (Seroquel), an antipsychotic drug manufactured by AstraZeneca, which in 2011 agreed to pay $647 million to settle more than 28,000 lawsuits.
However, the upcoming Lipitor litigation may be more difficult for the plaintiffs to win. Among some of the medico-legal questions to be addressed are:
1) Was there prior company knowledge of the risk and a failure to warn?
2) Were the patients harmed by the drug, given that diabetes is a very common disease and may be linked more to genetics and/or an underlying metabolic syndrome in those who are hyperlipidemic, hypertensive, or obese – the very same patients likely to be on a statin?
3) Is Lipitor a defective product, and is it unreasonably dangerous?
Despite the FDA-directed change in labeling, a number of scientists and the FDA itself have emphasized that the cardiac benefits of a statin drug are greater than any small increased risk of developing diabetes.
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].
Question: After statins had been in use for several years, data began to accumulate purporting to show that they increase the risk of diabetes. When Mrs. Smith learned that her recent diagnosis of diabetes might have something to do with the drug, she consulted a lawyer who began advertising for similar cases to consolidate them into a class action lawsuit. The legal theory (theories) seeking to prove product liability will be based on:
A. Contract law and breach of warranty.
B. Negligence in tort law.
C. Strict liability without requiring proof of fault.
D. A defective product that is unreasonably dangerous.
E. All of the above.
Answer:E. Should a prescription drug lead to harm, an injured party can sue the manufacturer who had placed it into the stream of commerce. The law of products liability governs this cause of action, wherein recovery is based on a number of legal theories, specifically negligence, breach of warranty, and strict liability. The latter is the most favored, as there is no need to prove fault or warranty. Products liability law also covers defective medical devices. The recent multimillion-dollar settlements and jury verdicts with Endo, Johnson & Johnson, Bard, and other manufacturers over their vaginal mesh devices are good examples.
In products liability, injured plaintiffs frequently claim a failure to warn of known risks, such as cardiovascular deaths caused by Vioxx, a nonsteroidal anti-inflammatory drug that was withdrawn in 2004. Merck, its manufacturer, has thus far won 11 and lost 3 of the cases that have gone to trial. Some of these judgments are under appeal; most notably, a Texas Court of Appeals recently reversed a $253 million award initially won by plaintiff Robert Ernst in the very first trial. However, the company has proposed $4.85 billion to settle tens of thousands of similar pending lawsuits. Other recent examples alleging failure to warn are heart attacks linked to the diabetes drug rosiglitazone and bladder cancer associated with the diabetes drug pioglitazone.
In 1963, the California Supreme Court bypassed the law of contracts and warranty in a seminal case of product-related injury, and introduced the notion of strict liability, which goes beyond simple negligence (Greenman v Yuba Power Products Inc., 377 P.2d 897 [Cal. 1963]). The strict liability approach centers on whether a product is defective and unreasonably dangerous, and it has now been adopted in virtually all jurisdictions.
The theory holds that a professional supplier who sells a product that is both defective and unreasonably dangerous is strictly liable to foreseeable plaintiffs. “Defective” is usually defined as product quality that is less than what a reasonable consumer expects. “Unreasonably dangerous” is a conclusion that the risks that result from its condition outweigh the product’s advantages.
Strict liability is not about negligence or fault, but about a social policy that shifts to the manufacturer the cost of compensating the injured consumer. To prevail, the plaintiff must show proximate cause, and assumption of risk is still a valid defense.
Statins, which are powerful HMG-CoA reductase inhibitors widely used to treat hypercholesterolemia, are currently at the center of pharmaceutical products litigation.
Pfizer, the manufacturer of Lipitor (atorvastatin) has become the target of numerous lawsuits alleging that the drug causes diabetes. Lipitor is the best-selling prescription drug ever, with sales reaching $130 billion since it was approved in 1996. In the United States alone, more than 29 million people have been prescribed this medication. The drug is highly effective in lowering serum cholesterol and is proven to reduce cardiovascular deaths.
A meta-analysis in 2010 revealed an increased risk of diabetes in patients taking statins (Lancet 2010;375:735-42). Statin therapy was associated with a 9% increased risk for incident diabetes; it was calculated that treatment of 255 patients with statins for 4 years resulted in 1 extra case of diabetes. An earlier smaller study had rejected this conclusion, but other studies were in support.
In 2012, the Food and Drug Administration (FDA) required the revision of the package insert of Lipitor and other statins to warn that their use had been linked to a small increased risk of diabetes.
In 2013, a large Canadian study confirmed the increased incidence of new-onset diabetes in patients taking atorvastatin (hazard ratio, 1.22) and simvastatin (hazard ratio, 1.10). This population-based cohort study involved nondiabetic patients age 66 years or older who started statins between 1997 and 2010 (BMJ 2013;346:f2610).
These and other results, coupled with the FDA-mandated revised labeling, have spawned the filing of nearly 1,000 lawsuits by patients who developed diabetes while taking statins, especially postmenopausal women. The rapid increase in the number of lawsuits may be related to the recent decision of a federal judicial panel on multidistrict litigation to consolidate all Lipitor diabetes lawsuits into a single federal courtroom in Charleston, S.C., as a class-action suit. The first case has yet to go to trial, but is expected to do so in 2015.
Previous products liability cases implicating statins have famously involved cerivastatin (Baycol), a one-time rival to Lipitor, for causing rhabdomyolysis. The drug was pulled from the market in 2001 after it reportedly caused 31 deaths. Bayer, its manufacturer, paid about $1 billion in 2005 to settle some 3,000 cases. An example of a medication causing diabetes is quetiapine (Seroquel), an antipsychotic drug manufactured by AstraZeneca, which in 2011 agreed to pay $647 million to settle more than 28,000 lawsuits.
However, the upcoming Lipitor litigation may be more difficult for the plaintiffs to win. Among some of the medico-legal questions to be addressed are:
1) Was there prior company knowledge of the risk and a failure to warn?
2) Were the patients harmed by the drug, given that diabetes is a very common disease and may be linked more to genetics and/or an underlying metabolic syndrome in those who are hyperlipidemic, hypertensive, or obese – the very same patients likely to be on a statin?
3) Is Lipitor a defective product, and is it unreasonably dangerous?
Despite the FDA-directed change in labeling, a number of scientists and the FDA itself have emphasized that the cardiac benefits of a statin drug are greater than any small increased risk of developing diabetes.
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].

PEARCE-INGS: The right questions
During an adolescent visit, we all can agree that getting answers to even the simplest of questions can be a day’s work. Despite the reason for the visit, it always is important to ask a few basic questions in hopes that it might unveil a less obvious condition, or one that potentially could cause harm later. Asking the right questions is as important as getting the right answer to make a correct diagnosis. Questions that are too general usually yield zero information for diagnostic purposes. Adolescents are concrete thinkers; therefore, if we don’t ask the question in several different ways, we are likely not to get the right answers, or any at all.
Two questions that I feel must be asked at every female-patient visit are, “When was your last period?” and “How often does your period come?” Answers to these two questions can assist in diagnosing several medical conditions that otherwise might have gone unnoticed.

Amenorrhea, or absence of menses, is established if a female has never had a period by age 15 years (primary) or has gone 6 months or greater without one (secondary). Primary amenorrhea is generally caused by genetic or anatomic abnormalities, and commonly is identified at an earlier age. But if the presentation of the genetic disorder is not classic, such as in Turner’s syndrome, it may go unnoticed and the first clue may be amenorrhea.
Pregnancy is an obvious consideration with amenorrhea. But the picture is a little less clear when light or irregular periods are present. Postmenarche menstrual cycles are commonly irregular and not without risk of pregnancy if the adolescent becomes sexually active. Also, a patient with an ectopic pregnancy tends to have oligomenorrhea before the amenorrhea. Therefore, regardless of age, if the periods are abnormal, a pregnancy test should be done.
Early polycystic ovarian syndrome (PCOS) also can present as irregular/ infrequent periods. Many of the common signs such as hirsutism or acne may be minor and not convincing. In an age where obesity is so common, a clear picture is less likely, so PCOS may not be considered. PCOS is the No. 1 cause of infertility in women, and if suspected should be worked up.
Anovulation or dysfunctional ovaries, as seen in PCOS, may not be obvious early on. As stated, oligomenorrhea is very common in the first few years following menarche, but persistent oligomenorrhea is not normal. General guidelines state that oligomenorrhea post menarche is likely to be a sign of anovulation if 1 year post menarche, less than four menstrual cycles; 2 years post menarche, less than six menstrual cycles; 3-5 years post menarche, less than eight menstrual cycles; and greater than 5 years post menarche, less than nine menstrual cycles. Heavy bleeding occurring less than every 21 days is also a sign.
Thyroid dysfunction is a common consideration when the menstrual cycle is abnormal, and we normally attribute heavy periods to hypothyroidism and amenorrhea or irregular periods to hyperthyroidism. The truth is thyroid dysfunction – regardless of whether the hormone is high or low – can present in either fashion. Other endocrine disorders – such as adrenal hyperplasia, prolactinomas, or metabolic syndromes – also disrupt the menstrual cycle, but initial presentations can be vague and only the prudent investigator will identify the disorder.
If the patient appears underweight, careful evaluation for anorexia should be done. Irregular periods present with caloric deprivation. Questions should be asked about body image to determine if this is a concern.
Once it is established that there is a menstrual dysfunction, a careful physical exam should follow. Screening labs and a pelvic ultrasound will help identify the dysfunction, but a referral to an endocrinologist still should follow if the results are equivocal or unclear.
As demonstrated, those two simple questions have the potential to unveil so many disorders that likely would go unnoticed for months to years. Every encounter is an opportunity to obtain information regardless of the chief complaint. Posing questions in several different ways lessens the likelihood that the question will be misunderstood and compensates for varied levels of intellect.
Remember, you have to ask the right question to get the right answer!
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at [email protected].
During an adolescent visit, we all can agree that getting answers to even the simplest of questions can be a day’s work. Despite the reason for the visit, it always is important to ask a few basic questions in hopes that it might unveil a less obvious condition, or one that potentially could cause harm later. Asking the right questions is as important as getting the right answer to make a correct diagnosis. Questions that are too general usually yield zero information for diagnostic purposes. Adolescents are concrete thinkers; therefore, if we don’t ask the question in several different ways, we are likely not to get the right answers, or any at all.
Two questions that I feel must be asked at every female-patient visit are, “When was your last period?” and “How often does your period come?” Answers to these two questions can assist in diagnosing several medical conditions that otherwise might have gone unnoticed.
Amenorrhea, or absence of menses, is established if a female has never had a period by age 15 years (primary) or has gone 6 months or greater without one (secondary). Primary amenorrhea is generally caused by genetic or anatomic abnormalities, and commonly is identified at an earlier age. But if the presentation of the genetic disorder is not classic, such as in Turner’s syndrome, it may go unnoticed and the first clue may be amenorrhea.
Pregnancy is an obvious consideration with amenorrhea. But the picture is a little less clear when light or irregular periods are present. Postmenarche menstrual cycles are commonly irregular and not without risk of pregnancy if the adolescent becomes sexually active. Also, a patient with an ectopic pregnancy tends to have oligomenorrhea before the amenorrhea. Therefore, regardless of age, if the periods are abnormal, a pregnancy test should be done.
Early polycystic ovarian syndrome (PCOS) also can present as irregular/ infrequent periods. Many of the common signs such as hirsutism or acne may be minor and not convincing. In an age where obesity is so common, a clear picture is less likely, so PCOS may not be considered. PCOS is the No. 1 cause of infertility in women, and if suspected should be worked up.
Anovulation or dysfunctional ovaries, as seen in PCOS, may not be obvious early on. As stated, oligomenorrhea is very common in the first few years following menarche, but persistent oligomenorrhea is not normal. General guidelines state that oligomenorrhea post menarche is likely to be a sign of anovulation if 1 year post menarche, less than four menstrual cycles; 2 years post menarche, less than six menstrual cycles; 3-5 years post menarche, less than eight menstrual cycles; and greater than 5 years post menarche, less than nine menstrual cycles. Heavy bleeding occurring less than every 21 days is also a sign.
Thyroid dysfunction is a common consideration when the menstrual cycle is abnormal, and we normally attribute heavy periods to hypothyroidism and amenorrhea or irregular periods to hyperthyroidism. The truth is thyroid dysfunction – regardless of whether the hormone is high or low – can present in either fashion. Other endocrine disorders – such as adrenal hyperplasia, prolactinomas, or metabolic syndromes – also disrupt the menstrual cycle, but initial presentations can be vague and only the prudent investigator will identify the disorder.
If the patient appears underweight, careful evaluation for anorexia should be done. Irregular periods present with caloric deprivation. Questions should be asked about body image to determine if this is a concern.
Once it is established that there is a menstrual dysfunction, a careful physical exam should follow. Screening labs and a pelvic ultrasound will help identify the dysfunction, but a referral to an endocrinologist still should follow if the results are equivocal or unclear.
As demonstrated, those two simple questions have the potential to unveil so many disorders that likely would go unnoticed for months to years. Every encounter is an opportunity to obtain information regardless of the chief complaint. Posing questions in several different ways lessens the likelihood that the question will be misunderstood and compensates for varied levels of intellect.
Remember, you have to ask the right question to get the right answer!
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at [email protected].
During an adolescent visit, we all can agree that getting answers to even the simplest of questions can be a day’s work. Despite the reason for the visit, it always is important to ask a few basic questions in hopes that it might unveil a less obvious condition, or one that potentially could cause harm later. Asking the right questions is as important as getting the right answer to make a correct diagnosis. Questions that are too general usually yield zero information for diagnostic purposes. Adolescents are concrete thinkers; therefore, if we don’t ask the question in several different ways, we are likely not to get the right answers, or any at all.
Two questions that I feel must be asked at every female-patient visit are, “When was your last period?” and “How often does your period come?” Answers to these two questions can assist in diagnosing several medical conditions that otherwise might have gone unnoticed.
Amenorrhea, or absence of menses, is established if a female has never had a period by age 15 years (primary) or has gone 6 months or greater without one (secondary). Primary amenorrhea is generally caused by genetic or anatomic abnormalities, and commonly is identified at an earlier age. But if the presentation of the genetic disorder is not classic, such as in Turner’s syndrome, it may go unnoticed and the first clue may be amenorrhea.
Pregnancy is an obvious consideration with amenorrhea. But the picture is a little less clear when light or irregular periods are present. Postmenarche menstrual cycles are commonly irregular and not without risk of pregnancy if the adolescent becomes sexually active. Also, a patient with an ectopic pregnancy tends to have oligomenorrhea before the amenorrhea. Therefore, regardless of age, if the periods are abnormal, a pregnancy test should be done.
Early polycystic ovarian syndrome (PCOS) also can present as irregular/ infrequent periods. Many of the common signs such as hirsutism or acne may be minor and not convincing. In an age where obesity is so common, a clear picture is less likely, so PCOS may not be considered. PCOS is the No. 1 cause of infertility in women, and if suspected should be worked up.
Anovulation or dysfunctional ovaries, as seen in PCOS, may not be obvious early on. As stated, oligomenorrhea is very common in the first few years following menarche, but persistent oligomenorrhea is not normal. General guidelines state that oligomenorrhea post menarche is likely to be a sign of anovulation if 1 year post menarche, less than four menstrual cycles; 2 years post menarche, less than six menstrual cycles; 3-5 years post menarche, less than eight menstrual cycles; and greater than 5 years post menarche, less than nine menstrual cycles. Heavy bleeding occurring less than every 21 days is also a sign.
Thyroid dysfunction is a common consideration when the menstrual cycle is abnormal, and we normally attribute heavy periods to hypothyroidism and amenorrhea or irregular periods to hyperthyroidism. The truth is thyroid dysfunction – regardless of whether the hormone is high or low – can present in either fashion. Other endocrine disorders – such as adrenal hyperplasia, prolactinomas, or metabolic syndromes – also disrupt the menstrual cycle, but initial presentations can be vague and only the prudent investigator will identify the disorder.
If the patient appears underweight, careful evaluation for anorexia should be done. Irregular periods present with caloric deprivation. Questions should be asked about body image to determine if this is a concern.
Once it is established that there is a menstrual dysfunction, a careful physical exam should follow. Screening labs and a pelvic ultrasound will help identify the dysfunction, but a referral to an endocrinologist still should follow if the results are equivocal or unclear.
As demonstrated, those two simple questions have the potential to unveil so many disorders that likely would go unnoticed for months to years. Every encounter is an opportunity to obtain information regardless of the chief complaint. Posing questions in several different ways lessens the likelihood that the question will be misunderstood and compensates for varied levels of intellect.
Remember, you have to ask the right question to get the right answer!
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at [email protected].

Gaining control over fecal incontinence
Fecal incontinence is a devastating and isolating condition. Sales of adult diapers are a $7 billion global market and the fastest-growing household products business. Which is where a lot of our patients with this condition remain – at home.
Fecal incontinence (FI) is a condition characterized by continuous or recurrent uncontrolled passage of fecal material. The prevalence may be as high as 15%. Risk factors include physical disabilities, dementia, diabetes, urinary incontinence, chronic diarrhea, and multiparity. One-third of patients will talk to us about it. Which for some of us may be suitable, given our inability to offer good treatments.
If patients do mention it, evaluation involves taking a good history. We need to differentiate incontinence from fecal urgency and frequency. Anorectal examination should look for a bilateral anal wink (absence suggests nerve damage). Some form of endoscopic examination should be performed in most patients. Further evaluation/referral will be based upon findings.
Treatment includes improving stool consistency (e.g., fiber for loose stool) and reducing frequency (e.g., loperamide for diarrhea), and this is generally where I start. Hyoscyamine may be helpful for post-meal leakage. Scheduled defecation and amitriptyline may be of benefit to some patients.
Dr. Henri Damon of Hospices Civils de Lyon, France, and his colleagues conducted a multicenter study of perineal retraining for FI (Dig. Liver Dis. 2014;46:237-42). The intervention included perineal retraining and biofeedback. The protocol was based upon 20 sessions of 30 minutes performed within a 4-month period. The intervention was standardized. Eighty patients were included in the control group, with 77 in the biofeedback group.
The success rate was significantly higher in the biofeedback group (57% vs. 37%; P < .021). Stool frequency, leakage, and urgency significantly decreased. Perineal retraining was significantly associated with a higher chance of self-rated improvement.
The take-home message is that perineal retraining is an effective component of FI treatment. Combining it with improved perianal skin hygiene, bowel habit ritualization, and the addition of fiber as a bulking agent and loperamide for diarrhea offers the greatest hope for patients suffering from this challenging condition.
Our job is to figure out where and how our patients can access the level of expertise needed to do the training.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. The opinions expressed in this article should not be used to diagnose or treat any medical condition, nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician.
Fecal incontinence is a devastating and isolating condition. Sales of adult diapers are a $7 billion global market and the fastest-growing household products business. Which is where a lot of our patients with this condition remain – at home.
Fecal incontinence (FI) is a condition characterized by continuous or recurrent uncontrolled passage of fecal material. The prevalence may be as high as 15%. Risk factors include physical disabilities, dementia, diabetes, urinary incontinence, chronic diarrhea, and multiparity. One-third of patients will talk to us about it. Which for some of us may be suitable, given our inability to offer good treatments.
If patients do mention it, evaluation involves taking a good history. We need to differentiate incontinence from fecal urgency and frequency. Anorectal examination should look for a bilateral anal wink (absence suggests nerve damage). Some form of endoscopic examination should be performed in most patients. Further evaluation/referral will be based upon findings.
Treatment includes improving stool consistency (e.g., fiber for loose stool) and reducing frequency (e.g., loperamide for diarrhea), and this is generally where I start. Hyoscyamine may be helpful for post-meal leakage. Scheduled defecation and amitriptyline may be of benefit to some patients.
Dr. Henri Damon of Hospices Civils de Lyon, France, and his colleagues conducted a multicenter study of perineal retraining for FI (Dig. Liver Dis. 2014;46:237-42). The intervention included perineal retraining and biofeedback. The protocol was based upon 20 sessions of 30 minutes performed within a 4-month period. The intervention was standardized. Eighty patients were included in the control group, with 77 in the biofeedback group.
The success rate was significantly higher in the biofeedback group (57% vs. 37%; P < .021). Stool frequency, leakage, and urgency significantly decreased. Perineal retraining was significantly associated with a higher chance of self-rated improvement.
The take-home message is that perineal retraining is an effective component of FI treatment. Combining it with improved perianal skin hygiene, bowel habit ritualization, and the addition of fiber as a bulking agent and loperamide for diarrhea offers the greatest hope for patients suffering from this challenging condition.
Our job is to figure out where and how our patients can access the level of expertise needed to do the training.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. The opinions expressed in this article should not be used to diagnose or treat any medical condition, nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician.
Fecal incontinence is a devastating and isolating condition. Sales of adult diapers are a $7 billion global market and the fastest-growing household products business. Which is where a lot of our patients with this condition remain – at home.
Fecal incontinence (FI) is a condition characterized by continuous or recurrent uncontrolled passage of fecal material. The prevalence may be as high as 15%. Risk factors include physical disabilities, dementia, diabetes, urinary incontinence, chronic diarrhea, and multiparity. One-third of patients will talk to us about it. Which for some of us may be suitable, given our inability to offer good treatments.
If patients do mention it, evaluation involves taking a good history. We need to differentiate incontinence from fecal urgency and frequency. Anorectal examination should look for a bilateral anal wink (absence suggests nerve damage). Some form of endoscopic examination should be performed in most patients. Further evaluation/referral will be based upon findings.
Treatment includes improving stool consistency (e.g., fiber for loose stool) and reducing frequency (e.g., loperamide for diarrhea), and this is generally where I start. Hyoscyamine may be helpful for post-meal leakage. Scheduled defecation and amitriptyline may be of benefit to some patients.
Dr. Henri Damon of Hospices Civils de Lyon, France, and his colleagues conducted a multicenter study of perineal retraining for FI (Dig. Liver Dis. 2014;46:237-42). The intervention included perineal retraining and biofeedback. The protocol was based upon 20 sessions of 30 minutes performed within a 4-month period. The intervention was standardized. Eighty patients were included in the control group, with 77 in the biofeedback group.
The success rate was significantly higher in the biofeedback group (57% vs. 37%; P < .021). Stool frequency, leakage, and urgency significantly decreased. Perineal retraining was significantly associated with a higher chance of self-rated improvement.
The take-home message is that perineal retraining is an effective component of FI treatment. Combining it with improved perianal skin hygiene, bowel habit ritualization, and the addition of fiber as a bulking agent and loperamide for diarrhea offers the greatest hope for patients suffering from this challenging condition.
Our job is to figure out where and how our patients can access the level of expertise needed to do the training.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. The opinions expressed in this article should not be used to diagnose or treat any medical condition, nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician.

In defense of the lowly case report
A few months ago, a nephrologist called me about a young, previously healthy health care worker who presented with an altered mental status, rapidly progressive renal failure, and rhabdomyolysis. It was an unusual combination of symptoms, and he had already ruled out the first things that came to my mind: drug toxicity, illicit drug use, thrombotic thrombocytopenic purpura-hemolytic-uremic syndrome. He wanted to know if I’d ever seen myositis present in this manner. I had not and could not think of ever having come across this as a possibility.
After powwowing with my bosses and coming up empty handed, I did what I do in these circumstances: I went to PubMed. Apart from illicit drug use, it seemed this constellation of symptoms was quite unusual. But there was one case report in an obscure emergency medicine journal from the 1980s, or perhaps it was the 1970s, of a patient that presented in just this manner and turned out to have Legionnaires’ disease.
I called the nephrologist back and told him about the case report. Although the patient had not reported a cough, he ran the test, and it came back positive.
Randomized, controlled trials are the philosopher’s stone of the scientific method, turning individual anecdotes into generalizable information, useful for large numbers of patients. But when doctors see unusual cases, we are often left with nothing but our own store of medical knowledge, informed by experience, imagination, and inquisitiveness. Intelligent speculation, to be sure, but hardly comforting to patient and physician alike.
It can be reassuring to know that other people have come across such unusual cases, just as it can be gratifying to know that our peers are interested in hearing our stories as well.
Counterfactuals are hard to come by in medicine, and we will never know what would have happened to the patient had I not seen that case report on PubMed. But the bias against case reports is such that it is probable that many illnesses remain undiagnosed simply because similar cases were deemed unworthy of publication.
There ought to be a repository of well-curated case reports. We are, all of us, made up of stories after all. And the stories that we tell are the art that temper this science we call Medicine.
Dr. Chan is a rheumatologist in Pawtucket, R.I.
A few months ago, a nephrologist called me about a young, previously healthy health care worker who presented with an altered mental status, rapidly progressive renal failure, and rhabdomyolysis. It was an unusual combination of symptoms, and he had already ruled out the first things that came to my mind: drug toxicity, illicit drug use, thrombotic thrombocytopenic purpura-hemolytic-uremic syndrome. He wanted to know if I’d ever seen myositis present in this manner. I had not and could not think of ever having come across this as a possibility.
After powwowing with my bosses and coming up empty handed, I did what I do in these circumstances: I went to PubMed. Apart from illicit drug use, it seemed this constellation of symptoms was quite unusual. But there was one case report in an obscure emergency medicine journal from the 1980s, or perhaps it was the 1970s, of a patient that presented in just this manner and turned out to have Legionnaires’ disease.
I called the nephrologist back and told him about the case report. Although the patient had not reported a cough, he ran the test, and it came back positive.
Randomized, controlled trials are the philosopher’s stone of the scientific method, turning individual anecdotes into generalizable information, useful for large numbers of patients. But when doctors see unusual cases, we are often left with nothing but our own store of medical knowledge, informed by experience, imagination, and inquisitiveness. Intelligent speculation, to be sure, but hardly comforting to patient and physician alike.
It can be reassuring to know that other people have come across such unusual cases, just as it can be gratifying to know that our peers are interested in hearing our stories as well.
Counterfactuals are hard to come by in medicine, and we will never know what would have happened to the patient had I not seen that case report on PubMed. But the bias against case reports is such that it is probable that many illnesses remain undiagnosed simply because similar cases were deemed unworthy of publication.
There ought to be a repository of well-curated case reports. We are, all of us, made up of stories after all. And the stories that we tell are the art that temper this science we call Medicine.
Dr. Chan is a rheumatologist in Pawtucket, R.I.
A few months ago, a nephrologist called me about a young, previously healthy health care worker who presented with an altered mental status, rapidly progressive renal failure, and rhabdomyolysis. It was an unusual combination of symptoms, and he had already ruled out the first things that came to my mind: drug toxicity, illicit drug use, thrombotic thrombocytopenic purpura-hemolytic-uremic syndrome. He wanted to know if I’d ever seen myositis present in this manner. I had not and could not think of ever having come across this as a possibility.
After powwowing with my bosses and coming up empty handed, I did what I do in these circumstances: I went to PubMed. Apart from illicit drug use, it seemed this constellation of symptoms was quite unusual. But there was one case report in an obscure emergency medicine journal from the 1980s, or perhaps it was the 1970s, of a patient that presented in just this manner and turned out to have Legionnaires’ disease.
I called the nephrologist back and told him about the case report. Although the patient had not reported a cough, he ran the test, and it came back positive.
Randomized, controlled trials are the philosopher’s stone of the scientific method, turning individual anecdotes into generalizable information, useful for large numbers of patients. But when doctors see unusual cases, we are often left with nothing but our own store of medical knowledge, informed by experience, imagination, and inquisitiveness. Intelligent speculation, to be sure, but hardly comforting to patient and physician alike.
It can be reassuring to know that other people have come across such unusual cases, just as it can be gratifying to know that our peers are interested in hearing our stories as well.
Counterfactuals are hard to come by in medicine, and we will never know what would have happened to the patient had I not seen that case report on PubMed. But the bias against case reports is such that it is probable that many illnesses remain undiagnosed simply because similar cases were deemed unworthy of publication.
There ought to be a repository of well-curated case reports. We are, all of us, made up of stories after all. And the stories that we tell are the art that temper this science we call Medicine.
Dr. Chan is a rheumatologist in Pawtucket, R.I.

For whom the Ebola tolls
Infectious diseases have been common topics in the news these past 2 months. Enterovirus EV-D68 and Ebola were the focus of sessions and plenary talks at this year’s American Academy of Pediatrics National Conference and Exposition. The new respiratory syncytial virus prophylaxis guidelines for this winter markedly narrowed the recommended recipient population (Pediatrics 2014;134:415-20). The revision of the 2006 bronchiolitis care guideline was released (Pediatrics 2014 [doi: 10.1542/peds.2014-2742]). And there has been an indictment in an alleged fraud involving HIV vaccine research.
As a moderator of a Listserv for pediatric hospitalists, I am interested in both the content of these discussions and the process by which they occur. Pediatric hospitalists could grouse a bit about the Centers for Disease Control and Prevention (CDC) being a few days slow in disseminating information about the EV-D68 epidemic, but we had no reason to doubt the veracity of that information. Our Listserv had posts from pediatric hospitalists in various cities. We discussed the utility of diagnostic tests; the treatment options and their effectiveness compared with other cases of bronchiolitis; and the impact on emergency department and inpatient census. When the virus 2 weeks later was tenuously associated with a rare paralytic syndrome, the Listserv activity peaked again.
Public reaction to Ebola seems to be at the other extreme. The contagion to two nurses and exposure of a lab supervisor at a Dallas hospital have expanded to impact hundreds of airline passengers and cruise ship passengers. Governors in New York and New Jersey took actions to increase monitoring at airports and establish quarantines. Now Maine is involved. Those actions did not always agree with the suggestions of the CDC. Between the Department of Veterans Affairs scandal, the CDC mishandling of small pox and anthrax in its labs, Wikileaks, and celebrities dissing vaccines, the general public’s trust in health information provided by the U.S. government must be near an all-time low just when credibility is needed most.
Does this sound familiar? George Santayana said, “Those who cannot remember the past are condemned to repeat it.” AIDS in 1981 was a new, lethal contagious disease without an effective treatment. Five cases of unusual pneumonia reported in 1981 have become a million people living with the infection. There were fear, stigmatization, recriminations, political posturing, and many deaths. In response, patient isolation practices changed dramatically. A massive research program ensued that has failed to find a vaccine or cure for HIV, but has developed an expensive ongoing treatment regimen that controls the disease in most people who can afford it. That has left out most people in Africa.
The United States now has an Ebola czar. Ron Klain has no experience with tropical infectious diseases. He was selected because he knows how things get done in Washington, D.C. I don’t see him becoming another C. Everett Koop, credible and comforting. For that status, the New York Times was impressed with the local version of that official.
“People need to feel like they are being given information, that things aren’t being kept from them, that they are being apprised of what’s known, and that we’re being honest. ...”
“Fear is a powerful thing,” she added, “and it’s often not rational. That’s when reliance on science and fact really has to be our North Star.” –Dr. Mary Travis Bassett, New York City Health Commissioner
On the spectrum between these two experiences with EV-D68 and Ebola lie the battles over respiratory syncytial virus prophylaxis and treatment. At the AAP National Conference and Exposition session discussing the 2014 palivizumab recommendations, there was great attention paid to having speakers from the audience identify any conflicts of interest they might have. The new guideline on caring for infants with bronchiolitis has emphasized the methodology of evidence-based medicine. Both these approaches (conflicts of interest and evidence-based medicine) are recent tools in the quest for truth and credibility.
Jack Nicholson said, “You can’t handle the truth!” Woodward and Bernstein, the investigative reporters of Watergate, recently eulogized their editor Ben Bradlee with “His one unbending principle was the quest for the truth and the necessity of that pursuit.”
I can’t add anything at this time to the search for truth in dealing with Ebola and what sort of quarantine policies should be in place. The credibility problem is in the hands of politicos. The balancing of communal safety and individual rights is in the hands of judges. But whatever choices are made, medical ethics requires that they be implemented with respect and with compassion, which includes WiFi access. That is in the hands of nurses and doctors. So I will close with a quote from a meditation written nearly 400 years ago by John Donne, an English poet and cleric, during his own 3-week battle with a near-fatal illness.
“No man is an island, entire of itself; ... any man’s death diminishes me, ... therefore never send to know for whom the bell tolls; it tolls for thee.”
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Dr. Powell said he had no relevant financial disclosures. E-mail him at [email protected].
Infectious diseases have been common topics in the news these past 2 months. Enterovirus EV-D68 and Ebola were the focus of sessions and plenary talks at this year’s American Academy of Pediatrics National Conference and Exposition. The new respiratory syncytial virus prophylaxis guidelines for this winter markedly narrowed the recommended recipient population (Pediatrics 2014;134:415-20). The revision of the 2006 bronchiolitis care guideline was released (Pediatrics 2014 [doi: 10.1542/peds.2014-2742]). And there has been an indictment in an alleged fraud involving HIV vaccine research.
As a moderator of a Listserv for pediatric hospitalists, I am interested in both the content of these discussions and the process by which they occur. Pediatric hospitalists could grouse a bit about the Centers for Disease Control and Prevention (CDC) being a few days slow in disseminating information about the EV-D68 epidemic, but we had no reason to doubt the veracity of that information. Our Listserv had posts from pediatric hospitalists in various cities. We discussed the utility of diagnostic tests; the treatment options and their effectiveness compared with other cases of bronchiolitis; and the impact on emergency department and inpatient census. When the virus 2 weeks later was tenuously associated with a rare paralytic syndrome, the Listserv activity peaked again.
Public reaction to Ebola seems to be at the other extreme. The contagion to two nurses and exposure of a lab supervisor at a Dallas hospital have expanded to impact hundreds of airline passengers and cruise ship passengers. Governors in New York and New Jersey took actions to increase monitoring at airports and establish quarantines. Now Maine is involved. Those actions did not always agree with the suggestions of the CDC. Between the Department of Veterans Affairs scandal, the CDC mishandling of small pox and anthrax in its labs, Wikileaks, and celebrities dissing vaccines, the general public’s trust in health information provided by the U.S. government must be near an all-time low just when credibility is needed most.
Does this sound familiar? George Santayana said, “Those who cannot remember the past are condemned to repeat it.” AIDS in 1981 was a new, lethal contagious disease without an effective treatment. Five cases of unusual pneumonia reported in 1981 have become a million people living with the infection. There were fear, stigmatization, recriminations, political posturing, and many deaths. In response, patient isolation practices changed dramatically. A massive research program ensued that has failed to find a vaccine or cure for HIV, but has developed an expensive ongoing treatment regimen that controls the disease in most people who can afford it. That has left out most people in Africa.
The United States now has an Ebola czar. Ron Klain has no experience with tropical infectious diseases. He was selected because he knows how things get done in Washington, D.C. I don’t see him becoming another C. Everett Koop, credible and comforting. For that status, the New York Times was impressed with the local version of that official.
“People need to feel like they are being given information, that things aren’t being kept from them, that they are being apprised of what’s known, and that we’re being honest. ...”
“Fear is a powerful thing,” she added, “and it’s often not rational. That’s when reliance on science and fact really has to be our North Star.” –Dr. Mary Travis Bassett, New York City Health Commissioner
On the spectrum between these two experiences with EV-D68 and Ebola lie the battles over respiratory syncytial virus prophylaxis and treatment. At the AAP National Conference and Exposition session discussing the 2014 palivizumab recommendations, there was great attention paid to having speakers from the audience identify any conflicts of interest they might have. The new guideline on caring for infants with bronchiolitis has emphasized the methodology of evidence-based medicine. Both these approaches (conflicts of interest and evidence-based medicine) are recent tools in the quest for truth and credibility.
Jack Nicholson said, “You can’t handle the truth!” Woodward and Bernstein, the investigative reporters of Watergate, recently eulogized their editor Ben Bradlee with “His one unbending principle was the quest for the truth and the necessity of that pursuit.”
I can’t add anything at this time to the search for truth in dealing with Ebola and what sort of quarantine policies should be in place. The credibility problem is in the hands of politicos. The balancing of communal safety and individual rights is in the hands of judges. But whatever choices are made, medical ethics requires that they be implemented with respect and with compassion, which includes WiFi access. That is in the hands of nurses and doctors. So I will close with a quote from a meditation written nearly 400 years ago by John Donne, an English poet and cleric, during his own 3-week battle with a near-fatal illness.
“No man is an island, entire of itself; ... any man’s death diminishes me, ... therefore never send to know for whom the bell tolls; it tolls for thee.”
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Dr. Powell said he had no relevant financial disclosures. E-mail him at [email protected].
Infectious diseases have been common topics in the news these past 2 months. Enterovirus EV-D68 and Ebola were the focus of sessions and plenary talks at this year’s American Academy of Pediatrics National Conference and Exposition. The new respiratory syncytial virus prophylaxis guidelines for this winter markedly narrowed the recommended recipient population (Pediatrics 2014;134:415-20). The revision of the 2006 bronchiolitis care guideline was released (Pediatrics 2014 [doi: 10.1542/peds.2014-2742]). And there has been an indictment in an alleged fraud involving HIV vaccine research.
As a moderator of a Listserv for pediatric hospitalists, I am interested in both the content of these discussions and the process by which they occur. Pediatric hospitalists could grouse a bit about the Centers for Disease Control and Prevention (CDC) being a few days slow in disseminating information about the EV-D68 epidemic, but we had no reason to doubt the veracity of that information. Our Listserv had posts from pediatric hospitalists in various cities. We discussed the utility of diagnostic tests; the treatment options and their effectiveness compared with other cases of bronchiolitis; and the impact on emergency department and inpatient census. When the virus 2 weeks later was tenuously associated with a rare paralytic syndrome, the Listserv activity peaked again.
Public reaction to Ebola seems to be at the other extreme. The contagion to two nurses and exposure of a lab supervisor at a Dallas hospital have expanded to impact hundreds of airline passengers and cruise ship passengers. Governors in New York and New Jersey took actions to increase monitoring at airports and establish quarantines. Now Maine is involved. Those actions did not always agree with the suggestions of the CDC. Between the Department of Veterans Affairs scandal, the CDC mishandling of small pox and anthrax in its labs, Wikileaks, and celebrities dissing vaccines, the general public’s trust in health information provided by the U.S. government must be near an all-time low just when credibility is needed most.
Does this sound familiar? George Santayana said, “Those who cannot remember the past are condemned to repeat it.” AIDS in 1981 was a new, lethal contagious disease without an effective treatment. Five cases of unusual pneumonia reported in 1981 have become a million people living with the infection. There were fear, stigmatization, recriminations, political posturing, and many deaths. In response, patient isolation practices changed dramatically. A massive research program ensued that has failed to find a vaccine or cure for HIV, but has developed an expensive ongoing treatment regimen that controls the disease in most people who can afford it. That has left out most people in Africa.
The United States now has an Ebola czar. Ron Klain has no experience with tropical infectious diseases. He was selected because he knows how things get done in Washington, D.C. I don’t see him becoming another C. Everett Koop, credible and comforting. For that status, the New York Times was impressed with the local version of that official.
“People need to feel like they are being given information, that things aren’t being kept from them, that they are being apprised of what’s known, and that we’re being honest. ...”
“Fear is a powerful thing,” she added, “and it’s often not rational. That’s when reliance on science and fact really has to be our North Star.” –Dr. Mary Travis Bassett, New York City Health Commissioner
On the spectrum between these two experiences with EV-D68 and Ebola lie the battles over respiratory syncytial virus prophylaxis and treatment. At the AAP National Conference and Exposition session discussing the 2014 palivizumab recommendations, there was great attention paid to having speakers from the audience identify any conflicts of interest they might have. The new guideline on caring for infants with bronchiolitis has emphasized the methodology of evidence-based medicine. Both these approaches (conflicts of interest and evidence-based medicine) are recent tools in the quest for truth and credibility.
Jack Nicholson said, “You can’t handle the truth!” Woodward and Bernstein, the investigative reporters of Watergate, recently eulogized their editor Ben Bradlee with “His one unbending principle was the quest for the truth and the necessity of that pursuit.”
I can’t add anything at this time to the search for truth in dealing with Ebola and what sort of quarantine policies should be in place. The credibility problem is in the hands of politicos. The balancing of communal safety and individual rights is in the hands of judges. But whatever choices are made, medical ethics requires that they be implemented with respect and with compassion, which includes WiFi access. That is in the hands of nurses and doctors. So I will close with a quote from a meditation written nearly 400 years ago by John Donne, an English poet and cleric, during his own 3-week battle with a near-fatal illness.
“No man is an island, entire of itself; ... any man’s death diminishes me, ... therefore never send to know for whom the bell tolls; it tolls for thee.”
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Dr. Powell said he had no relevant financial disclosures. E-mail him at [email protected].

For PE victim, would Wells’ have been enough?
Medicolegal review has the opportunity to become the morbidity and mortality conference of the modern era. The more we share in our collective failures, the less likely we are to repeat those same mistakes.
CR was a 69-year-old man who presented to the hospital for an elective total knee revision. He had a past medical history of obesity, hypertension, and chronic obstructive pulmonary disease (COPD).
Two weeks prior to the surgery, he received preoperative clearance from his primary care physician. CR had a morning surgery that went well and was without complication. He was transferred to the postanesthesia care unit in good condition with normal oxygen saturations on 2L of oxygen by nasal cannula. His postoperative orders included a routine hospitalist consultation for “medical management,” along with orders for daily low-molecular weight heparin for deep vein thrombosis (DVT) prophylaxis. CR arrived to the orthopedic floor later that afternoon. He did well overnight, and the next morning, he began working with physical therapy. After doing some exercises in the bed, CR had his oxygen removed so that he could ambulate. While up with the physical therapist, CR reported feeling “dizzy.” A chair was brought up behind him so that he could sit down. His oxygen saturation was 88%. CR was placed back on 2L of oxygen, but as he transferred from the chair to the bed his oxygen saturation fell further to 81%. CR had his oxygen increased to 3L and over the next half-hour, his oxygen saturation came up and stayed above 92%.

Dr. Hospitalist met CR about an hour after he worked with physical therapy. CR was without complaints at the time of the evaluation and had good oxygen saturations on 3L of oxygen. Dr. Hospitalist documented that CR denied chest pain, cough, or sputum production. On auscultation, CR had a scattered wheeze. Dr. Hospitalist dictated that his differential diagnosis included pulmonary embolism (PE). He ordered bronchodilator aerosols, a chest radiograph, a troponin and a brain natriuretic peptide (BNP) level. The chest radiograph was performed that afternoon and interpreted as “no acute process,” with no evidence for atelectasis.
Overnight, CR remained on oxygen via nasal cannula. The following morning his nurse noted that CR had bilateral edema in his legs. The labs ordered by Dr. Hospitalist the previous day were now in the chart – the troponin was 0.07 ng/mL (normal < 0.04 ng/ml) and the BNP was 205 pg/mL.
At 11 a.m., CR was again seen by physical therapy. While ambulating in his room, CR began to feel “dizzy” despite the use of oxygen, and he passed out falling to his knees. The therapist and several nurses got him back to a chair and increased his oxygen. He spontaneously regained consciousness, but within a few minutes CR passed out a second time and lost his pulse. Dr. Hospitalist and the surgeon responded to the code. He was unable to be resuscitated and was pronounced dead. An autopsy was performed and determined the cause of death to be massive saddle pulmonary embolism (PE).
Complaint:
A complaint was filed against the hospital, the surgeon, and Dr. Hospitalist for failure to prevent DVT, failure to diagnose PE, and failure to treat PE. The complaint alleged that had the standard of care been followed, CR would not have died postoperatively and would otherwise have had a normal life expectancy.
Scientific principles:

Orthopedic surgery patients are known to be at high risk for venous thromboembolism. In the absence of prophylaxis, postoperative PE is common and often a fatal disease. Nonetheless, even without prophylaxis, mortality from PE can be reduced by prompt diagnosis and therapy. Unfortunately, the clinical presentation of PE is variable and nonspecific; thus, diagnostic testing is necessary before confirming or excluding the diagnosis of PE. The diagnostic approach includes algorithms designed to efficiently diagnose PE while simultaneously avoiding unnecessary testing and minimizing the risk of missing clinically important cases. While there is consensus regarding the need for algorithms, there is no agreed-upon best approach.
Complaint rebuttal and discussion:
The defense responded that the first item in the complaint was baseless as the surgeon ordered both mechanical and low-molecular weight heparin prophylaxis for DVT. The plaintiff experts agreed and the surgeon was dismissed from the case prior to trial. The focus of the case was now on Dr. Hospitalist and his failure to diagnose and treat PE.
Dr. Hospitalist defended himself by arguing that CR suffered a sudden fatal PE on the day of his death despite appropriate prophylaxis and that the “dizziness” the prior day was unrelated. The defense explained that the day prior to his death, CR was simply orthostatic from his postanesthesia state, combined with opiate analgesics, and any hypoxia was from CR’s preexisting COPD.
Plaintiff experts replied that CR had virtually no symptoms for a COPD exacerbation (i.e., no cough, no sputum production), and there was no explanation for the elevated troponin other than PE. Plaintiff experts further alleged that Dr. Hospitalist failed to incorporate an algorithm, such as the modified Wells’ Criteria, into his diagnostic approach for PE. Had he done so, Dr. Hospitalist would have recognized that CR had a high enough clinical probability for PE to warrant empiric treatment and confirmatory testing. The defense responded that the use of the modified Wells’ Criteria was nothing but an arcane “academic” exercise that did not match real clinical practice.
Conclusion:
Acute pulmonary embolism is a well-known postoperative pulmonary complication. The diagnosis must be considered in any surgical patient that has postoperative shortness of breath or unexplained hypoxia. The importance of using an algorithm to determine the need for testing and treatment cannot be understated. In this case, the PE diagnosis was considered but no algorithm was used. The jury in this case deliberated for more than a day, but ultimately returned a full defense verdict.
Dr. Michota is director of academic affairs in the hospital medicine department at the Cleveland Clinic and medical editor of Hospitalist News. He has been involved in peer review both within and outside the legal system. Read past columns at eHospitalist news.com/Lessons.
Medicolegal review has the opportunity to become the morbidity and mortality conference of the modern era. The more we share in our collective failures, the less likely we are to repeat those same mistakes.
CR was a 69-year-old man who presented to the hospital for an elective total knee revision. He had a past medical history of obesity, hypertension, and chronic obstructive pulmonary disease (COPD).
Two weeks prior to the surgery, he received preoperative clearance from his primary care physician. CR had a morning surgery that went well and was without complication. He was transferred to the postanesthesia care unit in good condition with normal oxygen saturations on 2L of oxygen by nasal cannula. His postoperative orders included a routine hospitalist consultation for “medical management,” along with orders for daily low-molecular weight heparin for deep vein thrombosis (DVT) prophylaxis. CR arrived to the orthopedic floor later that afternoon. He did well overnight, and the next morning, he began working with physical therapy. After doing some exercises in the bed, CR had his oxygen removed so that he could ambulate. While up with the physical therapist, CR reported feeling “dizzy.” A chair was brought up behind him so that he could sit down. His oxygen saturation was 88%. CR was placed back on 2L of oxygen, but as he transferred from the chair to the bed his oxygen saturation fell further to 81%. CR had his oxygen increased to 3L and over the next half-hour, his oxygen saturation came up and stayed above 92%.
Dr. Hospitalist met CR about an hour after he worked with physical therapy. CR was without complaints at the time of the evaluation and had good oxygen saturations on 3L of oxygen. Dr. Hospitalist documented that CR denied chest pain, cough, or sputum production. On auscultation, CR had a scattered wheeze. Dr. Hospitalist dictated that his differential diagnosis included pulmonary embolism (PE). He ordered bronchodilator aerosols, a chest radiograph, a troponin and a brain natriuretic peptide (BNP) level. The chest radiograph was performed that afternoon and interpreted as “no acute process,” with no evidence for atelectasis.
Overnight, CR remained on oxygen via nasal cannula. The following morning his nurse noted that CR had bilateral edema in his legs. The labs ordered by Dr. Hospitalist the previous day were now in the chart – the troponin was 0.07 ng/mL (normal < 0.04 ng/ml) and the BNP was 205 pg/mL.
At 11 a.m., CR was again seen by physical therapy. While ambulating in his room, CR began to feel “dizzy” despite the use of oxygen, and he passed out falling to his knees. The therapist and several nurses got him back to a chair and increased his oxygen. He spontaneously regained consciousness, but within a few minutes CR passed out a second time and lost his pulse. Dr. Hospitalist and the surgeon responded to the code. He was unable to be resuscitated and was pronounced dead. An autopsy was performed and determined the cause of death to be massive saddle pulmonary embolism (PE).
Complaint:
A complaint was filed against the hospital, the surgeon, and Dr. Hospitalist for failure to prevent DVT, failure to diagnose PE, and failure to treat PE. The complaint alleged that had the standard of care been followed, CR would not have died postoperatively and would otherwise have had a normal life expectancy.
Scientific principles:
Orthopedic surgery patients are known to be at high risk for venous thromboembolism. In the absence of prophylaxis, postoperative PE is common and often a fatal disease. Nonetheless, even without prophylaxis, mortality from PE can be reduced by prompt diagnosis and therapy. Unfortunately, the clinical presentation of PE is variable and nonspecific; thus, diagnostic testing is necessary before confirming or excluding the diagnosis of PE. The diagnostic approach includes algorithms designed to efficiently diagnose PE while simultaneously avoiding unnecessary testing and minimizing the risk of missing clinically important cases. While there is consensus regarding the need for algorithms, there is no agreed-upon best approach.
Complaint rebuttal and discussion:
The defense responded that the first item in the complaint was baseless as the surgeon ordered both mechanical and low-molecular weight heparin prophylaxis for DVT. The plaintiff experts agreed and the surgeon was dismissed from the case prior to trial. The focus of the case was now on Dr. Hospitalist and his failure to diagnose and treat PE.
Dr. Hospitalist defended himself by arguing that CR suffered a sudden fatal PE on the day of his death despite appropriate prophylaxis and that the “dizziness” the prior day was unrelated. The defense explained that the day prior to his death, CR was simply orthostatic from his postanesthesia state, combined with opiate analgesics, and any hypoxia was from CR’s preexisting COPD.
Plaintiff experts replied that CR had virtually no symptoms for a COPD exacerbation (i.e., no cough, no sputum production), and there was no explanation for the elevated troponin other than PE. Plaintiff experts further alleged that Dr. Hospitalist failed to incorporate an algorithm, such as the modified Wells’ Criteria, into his diagnostic approach for PE. Had he done so, Dr. Hospitalist would have recognized that CR had a high enough clinical probability for PE to warrant empiric treatment and confirmatory testing. The defense responded that the use of the modified Wells’ Criteria was nothing but an arcane “academic” exercise that did not match real clinical practice.
Conclusion:
Acute pulmonary embolism is a well-known postoperative pulmonary complication. The diagnosis must be considered in any surgical patient that has postoperative shortness of breath or unexplained hypoxia. The importance of using an algorithm to determine the need for testing and treatment cannot be understated. In this case, the PE diagnosis was considered but no algorithm was used. The jury in this case deliberated for more than a day, but ultimately returned a full defense verdict.
Dr. Michota is director of academic affairs in the hospital medicine department at the Cleveland Clinic and medical editor of Hospitalist News. He has been involved in peer review both within and outside the legal system. Read past columns at eHospitalist news.com/Lessons.
Medicolegal review has the opportunity to become the morbidity and mortality conference of the modern era. The more we share in our collective failures, the less likely we are to repeat those same mistakes.
CR was a 69-year-old man who presented to the hospital for an elective total knee revision. He had a past medical history of obesity, hypertension, and chronic obstructive pulmonary disease (COPD).
Two weeks prior to the surgery, he received preoperative clearance from his primary care physician. CR had a morning surgery that went well and was without complication. He was transferred to the postanesthesia care unit in good condition with normal oxygen saturations on 2L of oxygen by nasal cannula. His postoperative orders included a routine hospitalist consultation for “medical management,” along with orders for daily low-molecular weight heparin for deep vein thrombosis (DVT) prophylaxis. CR arrived to the orthopedic floor later that afternoon. He did well overnight, and the next morning, he began working with physical therapy. After doing some exercises in the bed, CR had his oxygen removed so that he could ambulate. While up with the physical therapist, CR reported feeling “dizzy.” A chair was brought up behind him so that he could sit down. His oxygen saturation was 88%. CR was placed back on 2L of oxygen, but as he transferred from the chair to the bed his oxygen saturation fell further to 81%. CR had his oxygen increased to 3L and over the next half-hour, his oxygen saturation came up and stayed above 92%.
Dr. Hospitalist met CR about an hour after he worked with physical therapy. CR was without complaints at the time of the evaluation and had good oxygen saturations on 3L of oxygen. Dr. Hospitalist documented that CR denied chest pain, cough, or sputum production. On auscultation, CR had a scattered wheeze. Dr. Hospitalist dictated that his differential diagnosis included pulmonary embolism (PE). He ordered bronchodilator aerosols, a chest radiograph, a troponin and a brain natriuretic peptide (BNP) level. The chest radiograph was performed that afternoon and interpreted as “no acute process,” with no evidence for atelectasis.
Overnight, CR remained on oxygen via nasal cannula. The following morning his nurse noted that CR had bilateral edema in his legs. The labs ordered by Dr. Hospitalist the previous day were now in the chart – the troponin was 0.07 ng/mL (normal < 0.04 ng/ml) and the BNP was 205 pg/mL.
At 11 a.m., CR was again seen by physical therapy. While ambulating in his room, CR began to feel “dizzy” despite the use of oxygen, and he passed out falling to his knees. The therapist and several nurses got him back to a chair and increased his oxygen. He spontaneously regained consciousness, but within a few minutes CR passed out a second time and lost his pulse. Dr. Hospitalist and the surgeon responded to the code. He was unable to be resuscitated and was pronounced dead. An autopsy was performed and determined the cause of death to be massive saddle pulmonary embolism (PE).
Complaint:
A complaint was filed against the hospital, the surgeon, and Dr. Hospitalist for failure to prevent DVT, failure to diagnose PE, and failure to treat PE. The complaint alleged that had the standard of care been followed, CR would not have died postoperatively and would otherwise have had a normal life expectancy.
Scientific principles:
Orthopedic surgery patients are known to be at high risk for venous thromboembolism. In the absence of prophylaxis, postoperative PE is common and often a fatal disease. Nonetheless, even without prophylaxis, mortality from PE can be reduced by prompt diagnosis and therapy. Unfortunately, the clinical presentation of PE is variable and nonspecific; thus, diagnostic testing is necessary before confirming or excluding the diagnosis of PE. The diagnostic approach includes algorithms designed to efficiently diagnose PE while simultaneously avoiding unnecessary testing and minimizing the risk of missing clinically important cases. While there is consensus regarding the need for algorithms, there is no agreed-upon best approach.
Complaint rebuttal and discussion:
The defense responded that the first item in the complaint was baseless as the surgeon ordered both mechanical and low-molecular weight heparin prophylaxis for DVT. The plaintiff experts agreed and the surgeon was dismissed from the case prior to trial. The focus of the case was now on Dr. Hospitalist and his failure to diagnose and treat PE.
Dr. Hospitalist defended himself by arguing that CR suffered a sudden fatal PE on the day of his death despite appropriate prophylaxis and that the “dizziness” the prior day was unrelated. The defense explained that the day prior to his death, CR was simply orthostatic from his postanesthesia state, combined with opiate analgesics, and any hypoxia was from CR’s preexisting COPD.
Plaintiff experts replied that CR had virtually no symptoms for a COPD exacerbation (i.e., no cough, no sputum production), and there was no explanation for the elevated troponin other than PE. Plaintiff experts further alleged that Dr. Hospitalist failed to incorporate an algorithm, such as the modified Wells’ Criteria, into his diagnostic approach for PE. Had he done so, Dr. Hospitalist would have recognized that CR had a high enough clinical probability for PE to warrant empiric treatment and confirmatory testing. The defense responded that the use of the modified Wells’ Criteria was nothing but an arcane “academic” exercise that did not match real clinical practice.
Conclusion:
Acute pulmonary embolism is a well-known postoperative pulmonary complication. The diagnosis must be considered in any surgical patient that has postoperative shortness of breath or unexplained hypoxia. The importance of using an algorithm to determine the need for testing and treatment cannot be understated. In this case, the PE diagnosis was considered but no algorithm was used. The jury in this case deliberated for more than a day, but ultimately returned a full defense verdict.
Dr. Michota is director of academic affairs in the hospital medicine department at the Cleveland Clinic and medical editor of Hospitalist News. He has been involved in peer review both within and outside the legal system. Read past columns at eHospitalist news.com/Lessons.

Editorial: Ebola and Beyond

Why were actual events seemingly at odds with the initial risk assessments? In part, it was because the statements appear to have been based on several unrealistic premises. They presumed that everyone, from airport personnel to emergency department physicians and nurses, to hospital staff and administrators, would do everything right, every time, for every patient. More importantly, hospitals underestimated the staff and resources that would actually be needed to care for Ebola patients.
The CDC statements also seem to have included a leap of faith: if the spread of Ebola among healthcare workers could be minimized in one of the most medically underserved regions of the world, surely the most advanced healthcare system in the world could do even better. This belief, however, did not take into account that any deaths among patients, close contacts, or healthcare workers would never be considered acceptable in this country, and that intravenous transfusions, hemodialysis, and other advanced treatment measures unavailable in Africa, would expose a greater number of healthcare workers here to the risk of infection.
With absolutely no margin for error in the plans to prevent the spread of Ebola, ED triage professionals, nurses, and physicians have been placed under an enormous burden to get everything right, 100% of the time—a standard that is clearly beyond human capabilities. Should EPs and nurses be blamed for the failure to diagnose the first case and the inability to subsequently prevent two nurses from becoming infected?
I am virtually certain that every EP reading this has had at least one patient encounter that he or she wishes could be done over. Sometimes no harm results from a serious or potentially fatal omission or error; sometimes we are not so fortunate. Have you ever failed to notice an important piece of information in the EMR because it was not entered into the place where you are used to finding it—especially during and after EMR “downtime” periods? Have you ever experienced the pressures resulting from too many patients and too few beds, or the federal regulations calling for reduced lengths of stay and reduced short-term admissions, or of not having all of the resources you need to treat a patient just when you need them? If not, you are indeed fortunate. But to assume that none of these factors—and others—could possibly compromise efforts to diagnose, treat, and contain Ebola is almost “magical thinking.” Afterward, when not everything goes as well as the public had believed it would, our ability to continue basing sound medical practice on scientific facts instead of unsupported fears, is undermined.
As a result of the widespread reporting of early missteps in managing the first Ebola cases in the United States, we are in a much better position now to prevent, manage, and contain new cases, and to avoid the mind-numbing effects of the huge numbers of cases we witnessed with the spread of HIV and AIDS in the 1980s and 1990s. With everyone’s full attention, and more than a small degree of luck, we can successfully prevent or limit the number of future cases—efforts that hopefully will be furthered in the next few months by at least one effective vaccine and/or antiviral agent.
But, there will always be new and emerging infections that the world has never heard of to challenge us. So now would be a very good time to think of the training and resources necessary to deal with future contagious diseases and epidemics, and to plan on avoiding the use of words that may later come back to haunt us.
—Neal Flomenbaum, MD, New York
Why were actual events seemingly at odds with the initial risk assessments? In part, it was because the statements appear to have been based on several unrealistic premises. They presumed that everyone, from airport personnel to emergency department physicians and nurses, to hospital staff and administrators, would do everything right, every time, for every patient. More importantly, hospitals underestimated the staff and resources that would actually be needed to care for Ebola patients.
The CDC statements also seem to have included a leap of faith: if the spread of Ebola among healthcare workers could be minimized in one of the most medically underserved regions of the world, surely the most advanced healthcare system in the world could do even better. This belief, however, did not take into account that any deaths among patients, close contacts, or healthcare workers would never be considered acceptable in this country, and that intravenous transfusions, hemodialysis, and other advanced treatment measures unavailable in Africa, would expose a greater number of healthcare workers here to the risk of infection.
With absolutely no margin for error in the plans to prevent the spread of Ebola, ED triage professionals, nurses, and physicians have been placed under an enormous burden to get everything right, 100% of the time—a standard that is clearly beyond human capabilities. Should EPs and nurses be blamed for the failure to diagnose the first case and the inability to subsequently prevent two nurses from becoming infected?
I am virtually certain that every EP reading this has had at least one patient encounter that he or she wishes could be done over. Sometimes no harm results from a serious or potentially fatal omission or error; sometimes we are not so fortunate. Have you ever failed to notice an important piece of information in the EMR because it was not entered into the place where you are used to finding it—especially during and after EMR “downtime” periods? Have you ever experienced the pressures resulting from too many patients and too few beds, or the federal regulations calling for reduced lengths of stay and reduced short-term admissions, or of not having all of the resources you need to treat a patient just when you need them? If not, you are indeed fortunate. But to assume that none of these factors—and others—could possibly compromise efforts to diagnose, treat, and contain Ebola is almost “magical thinking.” Afterward, when not everything goes as well as the public had believed it would, our ability to continue basing sound medical practice on scientific facts instead of unsupported fears, is undermined.
As a result of the widespread reporting of early missteps in managing the first Ebola cases in the United States, we are in a much better position now to prevent, manage, and contain new cases, and to avoid the mind-numbing effects of the huge numbers of cases we witnessed with the spread of HIV and AIDS in the 1980s and 1990s. With everyone’s full attention, and more than a small degree of luck, we can successfully prevent or limit the number of future cases—efforts that hopefully will be furthered in the next few months by at least one effective vaccine and/or antiviral agent.
But, there will always be new and emerging infections that the world has never heard of to challenge us. So now would be a very good time to think of the training and resources necessary to deal with future contagious diseases and epidemics, and to plan on avoiding the use of words that may later come back to haunt us.
—Neal Flomenbaum, MD, New York
Why were actual events seemingly at odds with the initial risk assessments? In part, it was because the statements appear to have been based on several unrealistic premises. They presumed that everyone, from airport personnel to emergency department physicians and nurses, to hospital staff and administrators, would do everything right, every time, for every patient. More importantly, hospitals underestimated the staff and resources that would actually be needed to care for Ebola patients.
The CDC statements also seem to have included a leap of faith: if the spread of Ebola among healthcare workers could be minimized in one of the most medically underserved regions of the world, surely the most advanced healthcare system in the world could do even better. This belief, however, did not take into account that any deaths among patients, close contacts, or healthcare workers would never be considered acceptable in this country, and that intravenous transfusions, hemodialysis, and other advanced treatment measures unavailable in Africa, would expose a greater number of healthcare workers here to the risk of infection.
With absolutely no margin for error in the plans to prevent the spread of Ebola, ED triage professionals, nurses, and physicians have been placed under an enormous burden to get everything right, 100% of the time—a standard that is clearly beyond human capabilities. Should EPs and nurses be blamed for the failure to diagnose the first case and the inability to subsequently prevent two nurses from becoming infected?
I am virtually certain that every EP reading this has had at least one patient encounter that he or she wishes could be done over. Sometimes no harm results from a serious or potentially fatal omission or error; sometimes we are not so fortunate. Have you ever failed to notice an important piece of information in the EMR because it was not entered into the place where you are used to finding it—especially during and after EMR “downtime” periods? Have you ever experienced the pressures resulting from too many patients and too few beds, or the federal regulations calling for reduced lengths of stay and reduced short-term admissions, or of not having all of the resources you need to treat a patient just when you need them? If not, you are indeed fortunate. But to assume that none of these factors—and others—could possibly compromise efforts to diagnose, treat, and contain Ebola is almost “magical thinking.” Afterward, when not everything goes as well as the public had believed it would, our ability to continue basing sound medical practice on scientific facts instead of unsupported fears, is undermined.
As a result of the widespread reporting of early missteps in managing the first Ebola cases in the United States, we are in a much better position now to prevent, manage, and contain new cases, and to avoid the mind-numbing effects of the huge numbers of cases we witnessed with the spread of HIV and AIDS in the 1980s and 1990s. With everyone’s full attention, and more than a small degree of luck, we can successfully prevent or limit the number of future cases—efforts that hopefully will be furthered in the next few months by at least one effective vaccine and/or antiviral agent.
But, there will always be new and emerging infections that the world has never heard of to challenge us. So now would be a very good time to think of the training and resources necessary to deal with future contagious diseases and epidemics, and to plan on avoiding the use of words that may later come back to haunt us.
—Neal Flomenbaum, MD, New York
How to avoid diagnostic errors

As a generalist specialty, family medicine faces more diagnostic challenges than any other specialty because we see so many undifferentiated problems. However, only 2 family physicians attended this meeting: I was one, because of my research interests in proper use of lab testing, and John Ely, MD, from the University of Iowa, was the other. He has been researching diagnostic errors for most of his career. Dr. Ely has been testing an idea borrowed from aviation: using a diagnostic checklist. He developed a packet of note cards that lists the top 10 to 20 diagnoses for complaints commonly seen in family medicine, such as headache and abdominal pain. Before the patient leaves the exam room, he pulls out the appropriate checklist and goes through it out loud, just like a pilot before takeoff. He says for most patients, this process is pretty quick and it reassures both them and him that he has not missed an important diagnosis. (You can download Dr. Ely’s checklists from http://www.improvediagnosis.org/resource/resmgr/docs/diffdx.doc.)
How are the rest of us avoiding diagnostic errors? Some day IBM’s Watson or another diagnostic software program embedded in the electronic health record will guide us to the right diagnosis. In the meantime, I have developed a list of 7 low-tech ways to arrive at the correct diagnosis (and to rapidly correct a diagnostic error, should one occur):
2. Find out what dreaded diagnosis the patient believes he or she has so you can rule it in or out.
3. Don’t forget the pertinent past history. It makes a big difference if this is the patient’s first bad headache or the latest in a string of them.
4. Don’t skip the physical exam; even a negative exam, if documented properly, may keep you out of court.
5. Negotiate the diagnosis and treatment plan with the patient. This often brings out new information and new concerns.
6. Follow up, follow up, follow up, and do so in a timely manner.
7. Quickly reconsider your diagnosis and/or get a consultation if things are not going as expected.
As a generalist specialty, family medicine faces more diagnostic challenges than any other specialty because we see so many undifferentiated problems. However, only 2 family physicians attended this meeting: I was one, because of my research interests in proper use of lab testing, and John Ely, MD, from the University of Iowa, was the other. He has been researching diagnostic errors for most of his career. Dr. Ely has been testing an idea borrowed from aviation: using a diagnostic checklist. He developed a packet of note cards that lists the top 10 to 20 diagnoses for complaints commonly seen in family medicine, such as headache and abdominal pain. Before the patient leaves the exam room, he pulls out the appropriate checklist and goes through it out loud, just like a pilot before takeoff. He says for most patients, this process is pretty quick and it reassures both them and him that he has not missed an important diagnosis. (You can download Dr. Ely’s checklists from http://www.improvediagnosis.org/resource/resmgr/docs/diffdx.doc.)
How are the rest of us avoiding diagnostic errors? Some day IBM’s Watson or another diagnostic software program embedded in the electronic health record will guide us to the right diagnosis. In the meantime, I have developed a list of 7 low-tech ways to arrive at the correct diagnosis (and to rapidly correct a diagnostic error, should one occur):
2. Find out what dreaded diagnosis the patient believes he or she has so you can rule it in or out.
3. Don’t forget the pertinent past history. It makes a big difference if this is the patient’s first bad headache or the latest in a string of them.
4. Don’t skip the physical exam; even a negative exam, if documented properly, may keep you out of court.
5. Negotiate the diagnosis and treatment plan with the patient. This often brings out new information and new concerns.
6. Follow up, follow up, follow up, and do so in a timely manner.
7. Quickly reconsider your diagnosis and/or get a consultation if things are not going as expected.
As a generalist specialty, family medicine faces more diagnostic challenges than any other specialty because we see so many undifferentiated problems. However, only 2 family physicians attended this meeting: I was one, because of my research interests in proper use of lab testing, and John Ely, MD, from the University of Iowa, was the other. He has been researching diagnostic errors for most of his career. Dr. Ely has been testing an idea borrowed from aviation: using a diagnostic checklist. He developed a packet of note cards that lists the top 10 to 20 diagnoses for complaints commonly seen in family medicine, such as headache and abdominal pain. Before the patient leaves the exam room, he pulls out the appropriate checklist and goes through it out loud, just like a pilot before takeoff. He says for most patients, this process is pretty quick and it reassures both them and him that he has not missed an important diagnosis. (You can download Dr. Ely’s checklists from http://www.improvediagnosis.org/resource/resmgr/docs/diffdx.doc.)
How are the rest of us avoiding diagnostic errors? Some day IBM’s Watson or another diagnostic software program embedded in the electronic health record will guide us to the right diagnosis. In the meantime, I have developed a list of 7 low-tech ways to arrive at the correct diagnosis (and to rapidly correct a diagnostic error, should one occur):
2. Find out what dreaded diagnosis the patient believes he or she has so you can rule it in or out.
3. Don’t forget the pertinent past history. It makes a big difference if this is the patient’s first bad headache or the latest in a string of them.
4. Don’t skip the physical exam; even a negative exam, if documented properly, may keep you out of court.
5. Negotiate the diagnosis and treatment plan with the patient. This often brings out new information and new concerns.
6. Follow up, follow up, follow up, and do so in a timely manner.
7. Quickly reconsider your diagnosis and/or get a consultation if things are not going as expected.