User login
E-Focus on Pediatric Orthopedic Surgery
We are fortunate this month to have a variety of papers in pediatric orthopedic surgery, and they point out differences in treating children and adults.
In “Patient Survey of Weight Bearing and Physical Activity in In Situ Pinning for Slipped Capital Femoral Epiphysis,” Drs. Anand and Chorney’s findings clearly indicate that with a proper pinning for chronic SCFE, physical activity and weight bearing can be allowed as soon as the patient is comfortable after surgery, and the final result will be the same as if the patient had been restricted to long-term inactivity postoperatively. The issue of postoperative physical activity after pinning for acute SCFE was not addressed. Physical activity after pinning for acute SCFE is still not recommended until its effects on the complications of chondrolysis, aseptic necrosis, and nonunion are determined. But a similar study has not been done, probably because an acute slip is so uncommon and a multicenter study would be required.
Drs. Bradley, Tashjian, and Eberson, in “Irreducible Radial Head Dislocation in a Child,” have described an unusual case of a dislocated radial head in a 5-year-old that required open reduction. Their discussion of all the impediments to reduction is beautifully thought out. And their emphasis on this dislocation being unrecognized initially is important. To differentiate this irreducible dislocation from a congenital radial head dislocation is essential. The congenital radial head dislocation should not be reduced and trying to reduce it can only cause frustration in the surgeon and a bad elbow in the patient.
Drs. Weinberg, Friedman, Sood, and Crider, in “Tropical Myositis (Pyomyositis) in Children in Temperate Climates: A report of 3 cases on Long Island, New York, and a Review of the Literature” bring to our attention an uncommon (or frequently missed) infectious disease in children: muscle infection, or what is called pyomyositis in the United States and tropical myositis where it is most common, Uganda and New Guinea. The diagnosis is difficult to arrive at unless it is considered in cases of extremity pain and fever in the child. If a magnetic resonance image (MRI) looking at the soft tissues of the extremity is not obtained, the diagnosis will be missed. It makes you wonder how this diagnosis was positively made before the advent of the MRI—by a calculated guess perhaps. It would be best to isolate the organism before treatment, but this occurred in only 1 out of 3 of the authors’ cases. An attempt at needling the lesion, possibly under guided x-ray control, should be made. Although the organism most encountered is Staphylococcus aureus, in this country this may not be the case and the more resistant organisms should be considered.
Drs. Nanno, Sawaizumi, and Ito, in “Three Cases of Pediatric Monteggia Fracture-Dislocation Associated With Acute Plastic Bowing of the Ulna,” also discuss a frequently missed diagnosis—plastic deformation of the ulna with a dislocated radial head. This can only occur in a young child whose bone will bend before it breaks and then maintain its deformed shape. The bend in the ulna forces the radial head to sublux or dislocate and, because the deformed ulna does not go back to its original shape, the radial head is forced to maintain its dislocated position. The authors’ recommendation for correction of the deformed ulna before any attempt at reducing the dislocation is a must. The radial head will not remain reduced with an existing deformed ulna. The question to ask: Will the unbent ulna remain unbent after closed reduction, thereby allowing the radial head to remain in
place? It is my recommendation that the ulna be not just unbent but also manually or surgically fractured, so that the plastic deformation will not recur. A rigid intramedullary ulna nail after fracture will ensure that a recurrent deformation will not occur, which would allow a dislocation of the radial head to persist.
Drs. Fabregas, Jencikova-Celerin, Kreiger, and Dormans, in ”12-Year-Old Boy With Left Knee Pain,” involve us in a wonderful tour of the thinking required to make a diagnosis—especially given how complacent one can be with a teen-aged boy with knee pain, very common and usually not serious. If complete studies had not
been done and the seriousness of the complaint understood, the lesion would have been missed. The differential diagnosis on the plain films is a good, challenging exercise, especially given a lesion in this location. The discussion of the histology of the lesion and its treatment in a child is captivating.
We are fortunate this month to have a variety of papers in pediatric orthopedic surgery, and they point out differences in treating children and adults.
In “Patient Survey of Weight Bearing and Physical Activity in In Situ Pinning for Slipped Capital Femoral Epiphysis,” Drs. Anand and Chorney’s findings clearly indicate that with a proper pinning for chronic SCFE, physical activity and weight bearing can be allowed as soon as the patient is comfortable after surgery, and the final result will be the same as if the patient had been restricted to long-term inactivity postoperatively. The issue of postoperative physical activity after pinning for acute SCFE was not addressed. Physical activity after pinning for acute SCFE is still not recommended until its effects on the complications of chondrolysis, aseptic necrosis, and nonunion are determined. But a similar study has not been done, probably because an acute slip is so uncommon and a multicenter study would be required.
Drs. Bradley, Tashjian, and Eberson, in “Irreducible Radial Head Dislocation in a Child,” have described an unusual case of a dislocated radial head in a 5-year-old that required open reduction. Their discussion of all the impediments to reduction is beautifully thought out. And their emphasis on this dislocation being unrecognized initially is important. To differentiate this irreducible dislocation from a congenital radial head dislocation is essential. The congenital radial head dislocation should not be reduced and trying to reduce it can only cause frustration in the surgeon and a bad elbow in the patient.
Drs. Weinberg, Friedman, Sood, and Crider, in “Tropical Myositis (Pyomyositis) in Children in Temperate Climates: A report of 3 cases on Long Island, New York, and a Review of the Literature” bring to our attention an uncommon (or frequently missed) infectious disease in children: muscle infection, or what is called pyomyositis in the United States and tropical myositis where it is most common, Uganda and New Guinea. The diagnosis is difficult to arrive at unless it is considered in cases of extremity pain and fever in the child. If a magnetic resonance image (MRI) looking at the soft tissues of the extremity is not obtained, the diagnosis will be missed. It makes you wonder how this diagnosis was positively made before the advent of the MRI—by a calculated guess perhaps. It would be best to isolate the organism before treatment, but this occurred in only 1 out of 3 of the authors’ cases. An attempt at needling the lesion, possibly under guided x-ray control, should be made. Although the organism most encountered is Staphylococcus aureus, in this country this may not be the case and the more resistant organisms should be considered.
Drs. Nanno, Sawaizumi, and Ito, in “Three Cases of Pediatric Monteggia Fracture-Dislocation Associated With Acute Plastic Bowing of the Ulna,” also discuss a frequently missed diagnosis—plastic deformation of the ulna with a dislocated radial head. This can only occur in a young child whose bone will bend before it breaks and then maintain its deformed shape. The bend in the ulna forces the radial head to sublux or dislocate and, because the deformed ulna does not go back to its original shape, the radial head is forced to maintain its dislocated position. The authors’ recommendation for correction of the deformed ulna before any attempt at reducing the dislocation is a must. The radial head will not remain reduced with an existing deformed ulna. The question to ask: Will the unbent ulna remain unbent after closed reduction, thereby allowing the radial head to remain in
place? It is my recommendation that the ulna be not just unbent but also manually or surgically fractured, so that the plastic deformation will not recur. A rigid intramedullary ulna nail after fracture will ensure that a recurrent deformation will not occur, which would allow a dislocation of the radial head to persist.
Drs. Fabregas, Jencikova-Celerin, Kreiger, and Dormans, in ”12-Year-Old Boy With Left Knee Pain,” involve us in a wonderful tour of the thinking required to make a diagnosis—especially given how complacent one can be with a teen-aged boy with knee pain, very common and usually not serious. If complete studies had not
been done and the seriousness of the complaint understood, the lesion would have been missed. The differential diagnosis on the plain films is a good, challenging exercise, especially given a lesion in this location. The discussion of the histology of the lesion and its treatment in a child is captivating.
We are fortunate this month to have a variety of papers in pediatric orthopedic surgery, and they point out differences in treating children and adults.
In “Patient Survey of Weight Bearing and Physical Activity in In Situ Pinning for Slipped Capital Femoral Epiphysis,” Drs. Anand and Chorney’s findings clearly indicate that with a proper pinning for chronic SCFE, physical activity and weight bearing can be allowed as soon as the patient is comfortable after surgery, and the final result will be the same as if the patient had been restricted to long-term inactivity postoperatively. The issue of postoperative physical activity after pinning for acute SCFE was not addressed. Physical activity after pinning for acute SCFE is still not recommended until its effects on the complications of chondrolysis, aseptic necrosis, and nonunion are determined. But a similar study has not been done, probably because an acute slip is so uncommon and a multicenter study would be required.
Drs. Bradley, Tashjian, and Eberson, in “Irreducible Radial Head Dislocation in a Child,” have described an unusual case of a dislocated radial head in a 5-year-old that required open reduction. Their discussion of all the impediments to reduction is beautifully thought out. And their emphasis on this dislocation being unrecognized initially is important. To differentiate this irreducible dislocation from a congenital radial head dislocation is essential. The congenital radial head dislocation should not be reduced and trying to reduce it can only cause frustration in the surgeon and a bad elbow in the patient.
Drs. Weinberg, Friedman, Sood, and Crider, in “Tropical Myositis (Pyomyositis) in Children in Temperate Climates: A report of 3 cases on Long Island, New York, and a Review of the Literature” bring to our attention an uncommon (or frequently missed) infectious disease in children: muscle infection, or what is called pyomyositis in the United States and tropical myositis where it is most common, Uganda and New Guinea. The diagnosis is difficult to arrive at unless it is considered in cases of extremity pain and fever in the child. If a magnetic resonance image (MRI) looking at the soft tissues of the extremity is not obtained, the diagnosis will be missed. It makes you wonder how this diagnosis was positively made before the advent of the MRI—by a calculated guess perhaps. It would be best to isolate the organism before treatment, but this occurred in only 1 out of 3 of the authors’ cases. An attempt at needling the lesion, possibly under guided x-ray control, should be made. Although the organism most encountered is Staphylococcus aureus, in this country this may not be the case and the more resistant organisms should be considered.
Drs. Nanno, Sawaizumi, and Ito, in “Three Cases of Pediatric Monteggia Fracture-Dislocation Associated With Acute Plastic Bowing of the Ulna,” also discuss a frequently missed diagnosis—plastic deformation of the ulna with a dislocated radial head. This can only occur in a young child whose bone will bend before it breaks and then maintain its deformed shape. The bend in the ulna forces the radial head to sublux or dislocate and, because the deformed ulna does not go back to its original shape, the radial head is forced to maintain its dislocated position. The authors’ recommendation for correction of the deformed ulna before any attempt at reducing the dislocation is a must. The radial head will not remain reduced with an existing deformed ulna. The question to ask: Will the unbent ulna remain unbent after closed reduction, thereby allowing the radial head to remain in
place? It is my recommendation that the ulna be not just unbent but also manually or surgically fractured, so that the plastic deformation will not recur. A rigid intramedullary ulna nail after fracture will ensure that a recurrent deformation will not occur, which would allow a dislocation of the radial head to persist.
Drs. Fabregas, Jencikova-Celerin, Kreiger, and Dormans, in ”12-Year-Old Boy With Left Knee Pain,” involve us in a wonderful tour of the thinking required to make a diagnosis—especially given how complacent one can be with a teen-aged boy with knee pain, very common and usually not serious. If complete studies had not
been done and the seriousness of the complaint understood, the lesion would have been missed. The differential diagnosis on the plain films is a good, challenging exercise, especially given a lesion in this location. The discussion of the histology of the lesion and its treatment in a child is captivating.
Pediatric Orthopedic Imaging: More Isn’t Always Better
Three excellent instructional cases from Dr. Lawrence Wells and colleagues from
the Children’s Hospital of Philadelphia follow in this E-Focus on Imaging in Pediatric Orthopedics of the February issue of The American Journal of Orthopedics (AJO). These cases highlight the important role of imaging in the practice of pediatric orthopedics, particularly its usefulness in problem solving for conditions that are difficult to diagnose clinically. Given the wide array of imaging techniques currently available, there is a tendency for surgeons to over-investigate. But more isn’t always better.
For example, while magnetic resonance (MR) imaging has the well-known advantages of avoidance of the potential hazards of ionizing radiation, multiplanar imaging capability, and superior soft-tissue contrast and resolution, the relatively long time period for acquisition of MR images make it relatively user-unfriendly for imaging in children. Movement artifacts can be a big problem, leading to image degradation and interpretation difficulties. For young children, having to administer heavy sedation or general anesthesia often negates the benefits of this diagnostic technique. Multidetector computed tomography (CT) produces images of excellent quality and resolution, particularly of bone. However, the price to pay for the thinner contiguous slices that enable production of the beautiful reformatted 2-dimensional sagittal and coronal images, and the stunning 3-dimensional
(3D) images, is a markedly increased radiation dose to the young patient.
It appears that the solution lies in a return to basic principles of good clinical practice. As illustrated by these 3 pediatric orthopedic cases in this month’s AJO, formulating a provisional diagnosis and short list of differential diagnoses starts with a well-taken and detailed clinical history and a meticulous physical examination. Simple hematologic investigations should be interpreted in light of the clinical findings. Imaging should be reserved for problem solving and should not be considered as a screening tool. There must be an imaging plan that aims to
address the following questions: Is there a lesion? If so, what and where exactly is it? And how can I best treat this patient’s condition—in this respect, is imaging really necessary?
For orthopedic problems, the time-honored radiograph still remains the initial imaging investigation in today’s practice. Too often, more expensive and advanced imaging modalities are requested first, even when the diagnosis can be made on
the basis of the plain film. This is poor clinical practice, and it reflects a lack of training and common sense. Radiographs are readily available, technically easy to perform, and give an overview of bone and joint lesions. It is the imaging investigation of choice for the detection of fractures and dislocations and also for the diagnosis of bone tumors and many other bone conditions. CT should be considered a supplementary examination to radiographs and is helpful when radiographs are equivocal or findings are subtle. CT is particularly suited for complex skeletal anatomy, for example, the spine, scapula, pelvis, and hindfoot.
In pediatric patients, reconstructed 3D CT images are useful for sorting out congenital spinal deformities.
For children and adolescents, ultrasonography can be used in place of MR imaging for many indications, particularly for assessing superficial structures such as tendons, muscles, ligaments, blood vessels, and other soft tissues. However, performing musculoskeletal ultrasonography well entails a rather long and steep
learning curve before technical expertise can be achieved. More advanced techniques such as MR imaging, nuclear medicine imaging, and imaging-guided interventional procedures should be used sparingly.
In fact, less may be better. If in doubt, pause before asking for more imaging and do consult your friendly neighborhood musculoskeletal radiologist.
Three excellent instructional cases from Dr. Lawrence Wells and colleagues from
the Children’s Hospital of Philadelphia follow in this E-Focus on Imaging in Pediatric Orthopedics of the February issue of The American Journal of Orthopedics (AJO). These cases highlight the important role of imaging in the practice of pediatric orthopedics, particularly its usefulness in problem solving for conditions that are difficult to diagnose clinically. Given the wide array of imaging techniques currently available, there is a tendency for surgeons to over-investigate. But more isn’t always better.
For example, while magnetic resonance (MR) imaging has the well-known advantages of avoidance of the potential hazards of ionizing radiation, multiplanar imaging capability, and superior soft-tissue contrast and resolution, the relatively long time period for acquisition of MR images make it relatively user-unfriendly for imaging in children. Movement artifacts can be a big problem, leading to image degradation and interpretation difficulties. For young children, having to administer heavy sedation or general anesthesia often negates the benefits of this diagnostic technique. Multidetector computed tomography (CT) produces images of excellent quality and resolution, particularly of bone. However, the price to pay for the thinner contiguous slices that enable production of the beautiful reformatted 2-dimensional sagittal and coronal images, and the stunning 3-dimensional
(3D) images, is a markedly increased radiation dose to the young patient.
It appears that the solution lies in a return to basic principles of good clinical practice. As illustrated by these 3 pediatric orthopedic cases in this month’s AJO, formulating a provisional diagnosis and short list of differential diagnoses starts with a well-taken and detailed clinical history and a meticulous physical examination. Simple hematologic investigations should be interpreted in light of the clinical findings. Imaging should be reserved for problem solving and should not be considered as a screening tool. There must be an imaging plan that aims to
address the following questions: Is there a lesion? If so, what and where exactly is it? And how can I best treat this patient’s condition—in this respect, is imaging really necessary?
For orthopedic problems, the time-honored radiograph still remains the initial imaging investigation in today’s practice. Too often, more expensive and advanced imaging modalities are requested first, even when the diagnosis can be made on
the basis of the plain film. This is poor clinical practice, and it reflects a lack of training and common sense. Radiographs are readily available, technically easy to perform, and give an overview of bone and joint lesions. It is the imaging investigation of choice for the detection of fractures and dislocations and also for the diagnosis of bone tumors and many other bone conditions. CT should be considered a supplementary examination to radiographs and is helpful when radiographs are equivocal or findings are subtle. CT is particularly suited for complex skeletal anatomy, for example, the spine, scapula, pelvis, and hindfoot.
In pediatric patients, reconstructed 3D CT images are useful for sorting out congenital spinal deformities.
For children and adolescents, ultrasonography can be used in place of MR imaging for many indications, particularly for assessing superficial structures such as tendons, muscles, ligaments, blood vessels, and other soft tissues. However, performing musculoskeletal ultrasonography well entails a rather long and steep
learning curve before technical expertise can be achieved. More advanced techniques such as MR imaging, nuclear medicine imaging, and imaging-guided interventional procedures should be used sparingly.
In fact, less may be better. If in doubt, pause before asking for more imaging and do consult your friendly neighborhood musculoskeletal radiologist.
Three excellent instructional cases from Dr. Lawrence Wells and colleagues from
the Children’s Hospital of Philadelphia follow in this E-Focus on Imaging in Pediatric Orthopedics of the February issue of The American Journal of Orthopedics (AJO). These cases highlight the important role of imaging in the practice of pediatric orthopedics, particularly its usefulness in problem solving for conditions that are difficult to diagnose clinically. Given the wide array of imaging techniques currently available, there is a tendency for surgeons to over-investigate. But more isn’t always better.
For example, while magnetic resonance (MR) imaging has the well-known advantages of avoidance of the potential hazards of ionizing radiation, multiplanar imaging capability, and superior soft-tissue contrast and resolution, the relatively long time period for acquisition of MR images make it relatively user-unfriendly for imaging in children. Movement artifacts can be a big problem, leading to image degradation and interpretation difficulties. For young children, having to administer heavy sedation or general anesthesia often negates the benefits of this diagnostic technique. Multidetector computed tomography (CT) produces images of excellent quality and resolution, particularly of bone. However, the price to pay for the thinner contiguous slices that enable production of the beautiful reformatted 2-dimensional sagittal and coronal images, and the stunning 3-dimensional
(3D) images, is a markedly increased radiation dose to the young patient.
It appears that the solution lies in a return to basic principles of good clinical practice. As illustrated by these 3 pediatric orthopedic cases in this month’s AJO, formulating a provisional diagnosis and short list of differential diagnoses starts with a well-taken and detailed clinical history and a meticulous physical examination. Simple hematologic investigations should be interpreted in light of the clinical findings. Imaging should be reserved for problem solving and should not be considered as a screening tool. There must be an imaging plan that aims to
address the following questions: Is there a lesion? If so, what and where exactly is it? And how can I best treat this patient’s condition—in this respect, is imaging really necessary?
For orthopedic problems, the time-honored radiograph still remains the initial imaging investigation in today’s practice. Too often, more expensive and advanced imaging modalities are requested first, even when the diagnosis can be made on
the basis of the plain film. This is poor clinical practice, and it reflects a lack of training and common sense. Radiographs are readily available, technically easy to perform, and give an overview of bone and joint lesions. It is the imaging investigation of choice for the detection of fractures and dislocations and also for the diagnosis of bone tumors and many other bone conditions. CT should be considered a supplementary examination to radiographs and is helpful when radiographs are equivocal or findings are subtle. CT is particularly suited for complex skeletal anatomy, for example, the spine, scapula, pelvis, and hindfoot.
In pediatric patients, reconstructed 3D CT images are useful for sorting out congenital spinal deformities.
For children and adolescents, ultrasonography can be used in place of MR imaging for many indications, particularly for assessing superficial structures such as tendons, muscles, ligaments, blood vessels, and other soft tissues. However, performing musculoskeletal ultrasonography well entails a rather long and steep
learning curve before technical expertise can be achieved. More advanced techniques such as MR imaging, nuclear medicine imaging, and imaging-guided interventional procedures should be used sparingly.
In fact, less may be better. If in doubt, pause before asking for more imaging and do consult your friendly neighborhood musculoskeletal radiologist.
The Diagnosis and Treatment of Musculoskeletal Infections
Making a diagnosis is the expectation of every practicing physician. In most cases, our timely diagnosis leads to appropriate treatment and predictable outcomes. Currently, investigations must be justifiable and conclusions logical. With the high cost of health care, increased patient awareness, escalating medicolegal issues, and insurance pressures, we are held more accountable than ever before.
Our clinical reasoning starts with the acquisition of knowledge. Without knowledge, there is nothing to comprehend and without an ability to comprehend, we cannot apply knowledge in a reasonable way. For a first-year medical student, such an impeccable diagnosis seems hopelessly complex: 1) recognize and solicit meaningful signs and symptoms, 2) determine what systems are involved, 3) speculatively identify what pathologic processes are occurring, 4) differentiate one process from the other, 5) evaluate all pieces of information, and 6) anticipate the most likely course of the illness.
The association of certain musculoskeletal infections with specific microorganisms is an evidence-based, “knee-jerk” reflex linking diagnosis and treatment: for example, Salmonella enterica osteomyelitis and sickle cell anemia; staphylococcal periprosthetic total joint infections; gonoccocal pyarthrosis and pelvic inflammatory disease; Clostridium speticum gangrene in patients with carcinoma of the colon; community-acquired oxacillin-resistant Staphylococcus aureus wound infections in high school wrestlers.
These infection patterns link our clinical reasoning with specific knowledge. Such reasoning may not apply in any particular case if the practitioner does not “know” enough about the clinical problem. In North America, a Pseudomonas infection has become synonymous with a puncture wound to the foot in children wearing tennis shoes. But, what if the same injury occurs in a barefoot child in Tobago?
In the latter case, there is a recognized pattern that does not conform to reflex reasoning. We have no specific knowledge to make the connections or inferences about the environmental implications of the injury. To move forward, we start the deductive process of setting up hypotheses and gathering data to prove or disprove the cues.
Clinical Diagnosis Starts With the Acquisition of Knowledge
With expanded travel and economic opportunity, the boundaries of the world are shrinking. Political, economic, and social issues are driving unstoppable numbers of immigrants to seek new opportunities in foreign environments, bringing with them their own unique health issues, microflora, and disease tolerances. As evidenced in China’s 2004 “bird flu” crisis, globalization has now interlocked us with the rest of the world. We must now base our diagnoses on a consideration of the dynamic internal and external environments of any living being.
The 5 case reports in this section of The American Journal of Orthopedics are another reminder of our ongoing need to acquire reliable knowledge about the world in which we live. Our clinical and diagnostic thinking can no longer be based on a reflexive matching of a presenting problem to a similar and previously encountered situation.
In these articles, we read of an Echinococccus cyst in Cairo, a Staphylococcus lugdunensis osteomyelitis originating in Tobago, dematiaceous fungi in Minnesota, Salmonella enterica in Temple, Texas, and septic arthritis due to Gemella morbillorum in Winnipeg, Canada.
In each case in these reports, the clinical history elicited a suspicion of infection and the need for a biopsy/culture to confirm the cue. Adequate and multiple tissue samples serve to safeguard the investigation. If pathogens cannot be isolated with conventional methods, saved portions of the biopsy specimens can be smeared on special culture media and cut for histologic study.
To be in medical practice is to tolerate ambiguity. Not all diagnoses are straightforward. Increasingly, unfounded diagnoses are made when practitioners use 1 or 2 symptoms to jump start a premature conclusion, never taking time to consider the totality of a patient’s presentation. The painstaking process of collecting cues to generate a diagnosis transforms an unstructured problem into a structured problem. This is the acquisition of specific knowledge. What follows is a sequential, progressive, logical reasoning to comprehend and analyze before initiating treatment. ◾
Making a diagnosis is the expectation of every practicing physician. In most cases, our timely diagnosis leads to appropriate treatment and predictable outcomes. Currently, investigations must be justifiable and conclusions logical. With the high cost of health care, increased patient awareness, escalating medicolegal issues, and insurance pressures, we are held more accountable than ever before.
Our clinical reasoning starts with the acquisition of knowledge. Without knowledge, there is nothing to comprehend and without an ability to comprehend, we cannot apply knowledge in a reasonable way. For a first-year medical student, such an impeccable diagnosis seems hopelessly complex: 1) recognize and solicit meaningful signs and symptoms, 2) determine what systems are involved, 3) speculatively identify what pathologic processes are occurring, 4) differentiate one process from the other, 5) evaluate all pieces of information, and 6) anticipate the most likely course of the illness.
The association of certain musculoskeletal infections with specific microorganisms is an evidence-based, “knee-jerk” reflex linking diagnosis and treatment: for example, Salmonella enterica osteomyelitis and sickle cell anemia; staphylococcal periprosthetic total joint infections; gonoccocal pyarthrosis and pelvic inflammatory disease; Clostridium speticum gangrene in patients with carcinoma of the colon; community-acquired oxacillin-resistant Staphylococcus aureus wound infections in high school wrestlers.
These infection patterns link our clinical reasoning with specific knowledge. Such reasoning may not apply in any particular case if the practitioner does not “know” enough about the clinical problem. In North America, a Pseudomonas infection has become synonymous with a puncture wound to the foot in children wearing tennis shoes. But, what if the same injury occurs in a barefoot child in Tobago?
In the latter case, there is a recognized pattern that does not conform to reflex reasoning. We have no specific knowledge to make the connections or inferences about the environmental implications of the injury. To move forward, we start the deductive process of setting up hypotheses and gathering data to prove or disprove the cues.
Clinical Diagnosis Starts With the Acquisition of Knowledge
With expanded travel and economic opportunity, the boundaries of the world are shrinking. Political, economic, and social issues are driving unstoppable numbers of immigrants to seek new opportunities in foreign environments, bringing with them their own unique health issues, microflora, and disease tolerances. As evidenced in China’s 2004 “bird flu” crisis, globalization has now interlocked us with the rest of the world. We must now base our diagnoses on a consideration of the dynamic internal and external environments of any living being.
The 5 case reports in this section of The American Journal of Orthopedics are another reminder of our ongoing need to acquire reliable knowledge about the world in which we live. Our clinical and diagnostic thinking can no longer be based on a reflexive matching of a presenting problem to a similar and previously encountered situation.
In these articles, we read of an Echinococccus cyst in Cairo, a Staphylococcus lugdunensis osteomyelitis originating in Tobago, dematiaceous fungi in Minnesota, Salmonella enterica in Temple, Texas, and septic arthritis due to Gemella morbillorum in Winnipeg, Canada.
In each case in these reports, the clinical history elicited a suspicion of infection and the need for a biopsy/culture to confirm the cue. Adequate and multiple tissue samples serve to safeguard the investigation. If pathogens cannot be isolated with conventional methods, saved portions of the biopsy specimens can be smeared on special culture media and cut for histologic study.
To be in medical practice is to tolerate ambiguity. Not all diagnoses are straightforward. Increasingly, unfounded diagnoses are made when practitioners use 1 or 2 symptoms to jump start a premature conclusion, never taking time to consider the totality of a patient’s presentation. The painstaking process of collecting cues to generate a diagnosis transforms an unstructured problem into a structured problem. This is the acquisition of specific knowledge. What follows is a sequential, progressive, logical reasoning to comprehend and analyze before initiating treatment. ◾
Making a diagnosis is the expectation of every practicing physician. In most cases, our timely diagnosis leads to appropriate treatment and predictable outcomes. Currently, investigations must be justifiable and conclusions logical. With the high cost of health care, increased patient awareness, escalating medicolegal issues, and insurance pressures, we are held more accountable than ever before.
Our clinical reasoning starts with the acquisition of knowledge. Without knowledge, there is nothing to comprehend and without an ability to comprehend, we cannot apply knowledge in a reasonable way. For a first-year medical student, such an impeccable diagnosis seems hopelessly complex: 1) recognize and solicit meaningful signs and symptoms, 2) determine what systems are involved, 3) speculatively identify what pathologic processes are occurring, 4) differentiate one process from the other, 5) evaluate all pieces of information, and 6) anticipate the most likely course of the illness.
The association of certain musculoskeletal infections with specific microorganisms is an evidence-based, “knee-jerk” reflex linking diagnosis and treatment: for example, Salmonella enterica osteomyelitis and sickle cell anemia; staphylococcal periprosthetic total joint infections; gonoccocal pyarthrosis and pelvic inflammatory disease; Clostridium speticum gangrene in patients with carcinoma of the colon; community-acquired oxacillin-resistant Staphylococcus aureus wound infections in high school wrestlers.
These infection patterns link our clinical reasoning with specific knowledge. Such reasoning may not apply in any particular case if the practitioner does not “know” enough about the clinical problem. In North America, a Pseudomonas infection has become synonymous with a puncture wound to the foot in children wearing tennis shoes. But, what if the same injury occurs in a barefoot child in Tobago?
In the latter case, there is a recognized pattern that does not conform to reflex reasoning. We have no specific knowledge to make the connections or inferences about the environmental implications of the injury. To move forward, we start the deductive process of setting up hypotheses and gathering data to prove or disprove the cues.
Clinical Diagnosis Starts With the Acquisition of Knowledge
With expanded travel and economic opportunity, the boundaries of the world are shrinking. Political, economic, and social issues are driving unstoppable numbers of immigrants to seek new opportunities in foreign environments, bringing with them their own unique health issues, microflora, and disease tolerances. As evidenced in China’s 2004 “bird flu” crisis, globalization has now interlocked us with the rest of the world. We must now base our diagnoses on a consideration of the dynamic internal and external environments of any living being.
The 5 case reports in this section of The American Journal of Orthopedics are another reminder of our ongoing need to acquire reliable knowledge about the world in which we live. Our clinical and diagnostic thinking can no longer be based on a reflexive matching of a presenting problem to a similar and previously encountered situation.
In these articles, we read of an Echinococccus cyst in Cairo, a Staphylococcus lugdunensis osteomyelitis originating in Tobago, dematiaceous fungi in Minnesota, Salmonella enterica in Temple, Texas, and septic arthritis due to Gemella morbillorum in Winnipeg, Canada.
In each case in these reports, the clinical history elicited a suspicion of infection and the need for a biopsy/culture to confirm the cue. Adequate and multiple tissue samples serve to safeguard the investigation. If pathogens cannot be isolated with conventional methods, saved portions of the biopsy specimens can be smeared on special culture media and cut for histologic study.
To be in medical practice is to tolerate ambiguity. Not all diagnoses are straightforward. Increasingly, unfounded diagnoses are made when practitioners use 1 or 2 symptoms to jump start a premature conclusion, never taking time to consider the totality of a patient’s presentation. The painstaking process of collecting cues to generate a diagnosis transforms an unstructured problem into a structured problem. This is the acquisition of specific knowledge. What follows is a sequential, progressive, logical reasoning to comprehend and analyze before initiating treatment. ◾
Q: Following cesarean delivery, what is the optimal oxytocin infusion duration to prevent postpartum bleeding?
CASE: DISCONTINUED OXYTOCIN LEADS TO POSTPARTUM HEMORRHAGE
You have just completed a repeat cesarean delivery for a 41-year-old woman, now G2P2. You order an infusion of oxytocin, 20 U in 1 L lactated Ringer’s solution, to run at a rate of 125 mL/hr for 8 hours. Without informing you, the recovery room nurse discontinues the bag with the oxytocin solution and starts an infusion of lactated Ringer’s solution without oxytocin.
One hour later, you are called to the recovery room because your patient is having a postpartum hemorrhage (PPH). Physical examination shows that the uterus is boggy and above the level of the umbilicus. On bedside ultrasonography, the uterine cavity is demonstrated to contain minimal blood, and Doppler sonography does not demonstrate any vascular tissue within the uterine cavity. You diagnose uterine atony and initiate treatment. You massage the uterus, rapidly infuse 1 L crystalloid solution, place misoprostol 800 µg in the rectum, and reinitiate the oxytocin infusion. The uterine bleeding slows and then stops.
The following morning, the patient’s hematocrit has decreased from a preoperative value of 37% to 21%.
Could this case of PPH have been prevented?
Cesarean delivery is one of the most commonly performed major operations in developed countries. More than 1,250,000 cesarean deliveries are performed annually in the United States. In 2012, there were 3,952,937 births and a cesarean delivery rate of 32.8%.1 It is an important goal of obstetric care providers to continuously improve our approach to cesarean delivery in order to minimize the surgical risks of this procedure. Evidence-based, standardized protocols for cesarean delivery are critical to ensuring high- reliability surgical outcomes.
A key gap in cesarean delivery protocols is the lack of a nationwide, standardized approach to reducing the risk of postoperative bleeding by maintaining a continuous infusion of oxytocin in the hours immediately following cesarean delivery.
OXYTOCIN: A CRITICAL INTERVENTION TO PREVENT PPH
More than half of all maternal deaths occur in the 24 hours following delivery, with the most common cause being PPH.2 In addition to death, serious complications of PPH include coagulopathy, shock, emergency hysterectomy, transfusion complications, respiratory distress, and pituitary necrosis. Most cases of PPH that occur within 24 hours of delivery are caused by uterine atony.3 Other causes include retained products of conception, placenta accreta, infection, coagulation defects, and amniotic fluid embolism.
Administering a uterotonic such as oxytocin at the time of delivery reduces the risk of PPH by approximately 66% and the risk of maternal blood transfusion by about 65%.4 In order to prevent uterine atony and PPH, oxytocin should be routinely administered following birth of the baby or after delivery of the placenta. Appropriate doses following vaginal delivery are oxytocin 10 U administered intramuscularly or 10 U administered as a slow intravenous (IV) infusion.5 The onset of action of oxytocin is approximately 2 to 5 minutes after an intramuscular dose and 1 minute after an IV dose.6
Related article: Routine use of oxytocin at birth: just the right amount to prevent postpartum hemorrhage Robert L. Barbieri, MD (Editorial, July 2012)
OXYTOCIN AND CESAREAN DELIVERY
Many clinical trials have reported that during a cesarean delivery, the routine administration of a uterotonic agent following birth of the baby reduces the risk of uterine atony and excessive bleeding. Three uterotonics: oxytocin, misoprostol, and carbetocin (a long-acting oxytocin analogue, see SIDEBAR), have been reported to reduce the risk of excessive bleeding during cesarean delivery.7 Oxytocin is the uterotonic most commonly used during cesarean delivery in developed countries.

Related article: A new (to the US) first-line agent for heavy menstrual bleeding Robert L. Barbieri, MD (Editorial, October 2010)
In the United States, there is no standardized oxytocin regimen for prevention of uterine atony and hemorrhage at cesarean delivery. The most common regimen is to add 10–40 U of oxytocin in 1 L crystalloid solution and initiate the oxytocin infusion following delivery of the baby. Initially, the infusion is run at a rapid rate. Once the obstetrician reports that there is adequate uterine tone, the infusion rate is slowed to one that maintains uterine tone.
Some clinicians administer a single bolus of oxytocin following birth of the baby. However, a bolus of oxytocin commonly causes hypotension and, less commonly, ST segment changes on the electrocardiogram (EKG) suggestive of cardiac ischemia.8–10Many experts recommend against administering one large bolus of oxytocin over a short period of time and favor a continuous infusion.
At cesarean delivery, the minimum infusion rate of oxytocin that has been reported to avoid most cases of uterine atony, as reported by the obstetrician immediately following delivery, is approximately oxytocin 0.3 U/min.11 Oxytocin infusion rates of 0.2 U/min and 0.1 U/min were associated with uterine atony rates of 21% and 40%, respectively. An infusion rate of oxytocin 0.3 U/min can be achieved by the administration of 20 U of oxytocin in 1 L crystalloid solution at a rate of 15 mL/min until uterine tone is achieved. The oxytocin dose then can be titrated to maintain adequate uterine tone. Following completion of surgery, uterine tone can be maintained with a low-dose continuous infusion of oxytocin.
4- TO 8-HOUR OXYTOCIN RULE
A key gap in our cesarean delivery protocols is a standardized recommendation concerning the duration of the oxytocin infusion following cesarean delivery. To my knowledge, no national organization has made a firm recommendation concerning the duration of oxytocin infusion following cesarean delivery.
One recent clinical trial studied PPH following cesarean delivery utilizing two oxytocin regimens: a bolus of oxytocin following delivery of the baby versus a bolus of oxytocin followed by a 4-hour IV infusion of oxytocin.12 In this trial, 2,058 women undergoing a scheduled cesarean delivery with a singleton pregnancy were randomly assigned to an oxytocin bolus alone, oxytocin 5 U administered intravenously over 1 minute, or an oxytocin bolus plus a 4-hour oxytocin infusion at a rate of 10 U/hr. The 4-hour postoperative oxytocin infusion was formulated by adding 40 U of oxytocin to 500 mL saline and infusing the solution at 125 mL/hr, equivalent to 0.167 U of oxytocin per minute. In this trial, 65% of the women were undergoing a repeat cesarean delivery and 35% were undergoing a primary cesarean delivery.
The authors reported that women who received the oxytocin bolus alone were significantly more likely to be diagnosed with uterine atony requiring additional uterotonic treatment than women who received both the bolus and the 4-hour postoperative infusion (18.4% versus 12.2%, respectively; P <.001). There was no difference in the rate of PPH between the two groups.
The rate of PPH was 16% in women receiving an oxytocin bolus alone and 15.7% in women receiving both an oxytocin bolus and the continuous oxytocin infusion. However, among less experienced surgeons, the rate of PPH was significantly greater in the group that received the oxytocin bolus alone compared with the women receiving the bolus and continuous infusion (22.2% versus 17.3%, respectively). The authors concluded that obstetricians should consider using a 4-hour infusion of oxytocin following cesarean delivery to reduce the risk of uterine atony.
In a recent evidence-based review of optimal interventions in cesarean delivery, the authors recommended an IV infusion of 10 to 40 U of oxytocin administered over 4 to 8 hours after cesarean delivery.7 Following cesarean, an IV infusion of crystalloid solution is typically maintained for at least 4 to 8 hours. Consequently, adding oxytocin (which costs approximately $1 for 10 units) to the crystalloid infusion does not add substantially to the cost of the patient’s postoperative care and may reduce the risk of uterine atony and PPH.
Related article: Act fast when confronted by a coagulopathy postpartum Robert L. Barbieri, MD (Editorial, March 2012)
My bottom-line recommendation. In the United States, we should adopt a policy of maintaining a continuous infusion of oxytocin for 4 to 8 hours following a cesarean delivery. Following a 4- to 8-hour rule will decrease the rate of uterine atony and excessive bleeding, thereby improving the safety of our cesarean delivery surgery.
INSTANT POLL
How many hours following cesarean delivery do you think that an oxytocin infusion should be maintained to reduce the risk of uterine atony and postpartum hemorrhage?
If the patient is a Jehovah’s Witness and refuses the transfusion of all blood products, how many hours following cesarean delivery do you think that an oxytocin infusion should be maintained to reduce the risk of uterine atony and postpartum hemorrhage?
Tell us—at [email protected] Please include your name and city and state.
- Hamilton BE, Martin JA, Ventura SJ. National Vital Statistics Reports. Births: Preliminary Data for 2012. 2013;62(3). http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_03.pdf. Published September 6, 2013. Accessed March 18, 2014.
- AbouZahr C. Global burden of maternal death and disability. Br Med Bull. 2003;67:1–11.
- Combs CA, Murphy EL, Laros RK Jr. Factors associated with postpartum hemorrhage with vaginal birth. Obstet Gynecol. 1991;77(1):69–76.
- Begley CM, Gyte GM, Devane D, McGuire W, Weeks A. Active versus expectant management for women in the third stage of labour. Cochrane Database Syst Rev. 2011;(11):CD007412.
- Westhoff G, Cotter AM, Tolosa JE. Prophylactic oxytocin for the third stage of labour to prevent postpartum hemorrhage. Cochrane Database Syst Rev. 2013;(10):CD001808.
- Embrey MP. Simultaneous intramuscular injection of oxytocin and ergometrine: a tocographic study. BMJ. 1961;1(5241):1737–1738.
- Dahlke JD, Mendez-Figueroa H, Rouse DJ, Berghella V, Baxter JK, Chauhan SP. Evidence-based surgery for cesarean delivery: An updated systematic review. Am J Obstet Gynecol. 2013;209(4):294–306.
- Archer TL, Knape K, Liles D, Wheeler AS, Carter B. The hemodynamics of oxytocin and other vasoactive agents during neuraxial anesthesia for cesarean delivery: Findings in six cases. Int J Obstet Anesth. 2008;17(3):247–254.
- Jonsson M, Hanson U, Lidell C, Norden-Lindeberg S. ST depression at caesarean section and the relation to oxytocin dose. A randomized controlled trial. BJOG. 2010;117(1):76–83.
- Svanstrom MC, Biber B, Hanes M, Johansson G, Naslund U, Balfourds EM. Signs of myocardial ischaemia after injection of oxytocin: A randomized double-blind comparison of oxytocin and methylergometrine during caesarean section. Br J Anaesth. 2008;100(5):683–689.
- George RB, McKeen D, Chaplin AC, McLeod L. Up-down determination of the ED90 of oxytocin infusions for the prevention of postpartum uterine atony in parturients undergoing cesarean delivery. Can J Anesth. 2010;57(6):578–582.
- Sheehan SR, Montgomery AA, Carey M, et al; ECSSIT Study Group. Oxytocin bolus versus oxytocin bolus and infusion for control of blood loss at elective cesarean section: Double blind, placebo controlled, randomized trial. BMJ. 2011;343:d4661.

Robert L. Barbieri, MD
Editor in Chief, OBG Management
Chair, Obstetrics and Gynecology Brigham and Women’s Hospital, Boston, Massachusetts; Kate Macy Ladd Professor of Obstetrics, Gynecology and Reproductive Biology, Harvard Medical School, Boston
[email protected]
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief, OBG Management
Chair, Obstetrics and Gynecology Brigham and Women’s Hospital, Boston, Massachusetts; Kate Macy Ladd Professor of Obstetrics, Gynecology and Reproductive Biology, Harvard Medical School, Boston
[email protected]
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief, OBG Management
Chair, Obstetrics and Gynecology Brigham and Women’s Hospital, Boston, Massachusetts; Kate Macy Ladd Professor of Obstetrics, Gynecology and Reproductive Biology, Harvard Medical School, Boston
[email protected]
Dr. Barbieri reports no financial relationships relevant to this article.
CASE: DISCONTINUED OXYTOCIN LEADS TO POSTPARTUM HEMORRHAGE
You have just completed a repeat cesarean delivery for a 41-year-old woman, now G2P2. You order an infusion of oxytocin, 20 U in 1 L lactated Ringer’s solution, to run at a rate of 125 mL/hr for 8 hours. Without informing you, the recovery room nurse discontinues the bag with the oxytocin solution and starts an infusion of lactated Ringer’s solution without oxytocin.
One hour later, you are called to the recovery room because your patient is having a postpartum hemorrhage (PPH). Physical examination shows that the uterus is boggy and above the level of the umbilicus. On bedside ultrasonography, the uterine cavity is demonstrated to contain minimal blood, and Doppler sonography does not demonstrate any vascular tissue within the uterine cavity. You diagnose uterine atony and initiate treatment. You massage the uterus, rapidly infuse 1 L crystalloid solution, place misoprostol 800 µg in the rectum, and reinitiate the oxytocin infusion. The uterine bleeding slows and then stops.
The following morning, the patient’s hematocrit has decreased from a preoperative value of 37% to 21%.
Could this case of PPH have been prevented?
Cesarean delivery is one of the most commonly performed major operations in developed countries. More than 1,250,000 cesarean deliveries are performed annually in the United States. In 2012, there were 3,952,937 births and a cesarean delivery rate of 32.8%.1 It is an important goal of obstetric care providers to continuously improve our approach to cesarean delivery in order to minimize the surgical risks of this procedure. Evidence-based, standardized protocols for cesarean delivery are critical to ensuring high- reliability surgical outcomes.
A key gap in cesarean delivery protocols is the lack of a nationwide, standardized approach to reducing the risk of postoperative bleeding by maintaining a continuous infusion of oxytocin in the hours immediately following cesarean delivery.
OXYTOCIN: A CRITICAL INTERVENTION TO PREVENT PPH
More than half of all maternal deaths occur in the 24 hours following delivery, with the most common cause being PPH.2 In addition to death, serious complications of PPH include coagulopathy, shock, emergency hysterectomy, transfusion complications, respiratory distress, and pituitary necrosis. Most cases of PPH that occur within 24 hours of delivery are caused by uterine atony.3 Other causes include retained products of conception, placenta accreta, infection, coagulation defects, and amniotic fluid embolism.
Administering a uterotonic such as oxytocin at the time of delivery reduces the risk of PPH by approximately 66% and the risk of maternal blood transfusion by about 65%.4 In order to prevent uterine atony and PPH, oxytocin should be routinely administered following birth of the baby or after delivery of the placenta. Appropriate doses following vaginal delivery are oxytocin 10 U administered intramuscularly or 10 U administered as a slow intravenous (IV) infusion.5 The onset of action of oxytocin is approximately 2 to 5 minutes after an intramuscular dose and 1 minute after an IV dose.6
Related article: Routine use of oxytocin at birth: just the right amount to prevent postpartum hemorrhage Robert L. Barbieri, MD (Editorial, July 2012)
OXYTOCIN AND CESAREAN DELIVERY
Many clinical trials have reported that during a cesarean delivery, the routine administration of a uterotonic agent following birth of the baby reduces the risk of uterine atony and excessive bleeding. Three uterotonics: oxytocin, misoprostol, and carbetocin (a long-acting oxytocin analogue, see SIDEBAR), have been reported to reduce the risk of excessive bleeding during cesarean delivery.7 Oxytocin is the uterotonic most commonly used during cesarean delivery in developed countries.
Related article: A new (to the US) first-line agent for heavy menstrual bleeding Robert L. Barbieri, MD (Editorial, October 2010)
In the United States, there is no standardized oxytocin regimen for prevention of uterine atony and hemorrhage at cesarean delivery. The most common regimen is to add 10–40 U of oxytocin in 1 L crystalloid solution and initiate the oxytocin infusion following delivery of the baby. Initially, the infusion is run at a rapid rate. Once the obstetrician reports that there is adequate uterine tone, the infusion rate is slowed to one that maintains uterine tone.
Some clinicians administer a single bolus of oxytocin following birth of the baby. However, a bolus of oxytocin commonly causes hypotension and, less commonly, ST segment changes on the electrocardiogram (EKG) suggestive of cardiac ischemia.8–10Many experts recommend against administering one large bolus of oxytocin over a short period of time and favor a continuous infusion.
At cesarean delivery, the minimum infusion rate of oxytocin that has been reported to avoid most cases of uterine atony, as reported by the obstetrician immediately following delivery, is approximately oxytocin 0.3 U/min.11 Oxytocin infusion rates of 0.2 U/min and 0.1 U/min were associated with uterine atony rates of 21% and 40%, respectively. An infusion rate of oxytocin 0.3 U/min can be achieved by the administration of 20 U of oxytocin in 1 L crystalloid solution at a rate of 15 mL/min until uterine tone is achieved. The oxytocin dose then can be titrated to maintain adequate uterine tone. Following completion of surgery, uterine tone can be maintained with a low-dose continuous infusion of oxytocin.
4- TO 8-HOUR OXYTOCIN RULE
A key gap in our cesarean delivery protocols is a standardized recommendation concerning the duration of the oxytocin infusion following cesarean delivery. To my knowledge, no national organization has made a firm recommendation concerning the duration of oxytocin infusion following cesarean delivery.
One recent clinical trial studied PPH following cesarean delivery utilizing two oxytocin regimens: a bolus of oxytocin following delivery of the baby versus a bolus of oxytocin followed by a 4-hour IV infusion of oxytocin.12 In this trial, 2,058 women undergoing a scheduled cesarean delivery with a singleton pregnancy were randomly assigned to an oxytocin bolus alone, oxytocin 5 U administered intravenously over 1 minute, or an oxytocin bolus plus a 4-hour oxytocin infusion at a rate of 10 U/hr. The 4-hour postoperative oxytocin infusion was formulated by adding 40 U of oxytocin to 500 mL saline and infusing the solution at 125 mL/hr, equivalent to 0.167 U of oxytocin per minute. In this trial, 65% of the women were undergoing a repeat cesarean delivery and 35% were undergoing a primary cesarean delivery.
The authors reported that women who received the oxytocin bolus alone were significantly more likely to be diagnosed with uterine atony requiring additional uterotonic treatment than women who received both the bolus and the 4-hour postoperative infusion (18.4% versus 12.2%, respectively; P <.001). There was no difference in the rate of PPH between the two groups.
The rate of PPH was 16% in women receiving an oxytocin bolus alone and 15.7% in women receiving both an oxytocin bolus and the continuous oxytocin infusion. However, among less experienced surgeons, the rate of PPH was significantly greater in the group that received the oxytocin bolus alone compared with the women receiving the bolus and continuous infusion (22.2% versus 17.3%, respectively). The authors concluded that obstetricians should consider using a 4-hour infusion of oxytocin following cesarean delivery to reduce the risk of uterine atony.
In a recent evidence-based review of optimal interventions in cesarean delivery, the authors recommended an IV infusion of 10 to 40 U of oxytocin administered over 4 to 8 hours after cesarean delivery.7 Following cesarean, an IV infusion of crystalloid solution is typically maintained for at least 4 to 8 hours. Consequently, adding oxytocin (which costs approximately $1 for 10 units) to the crystalloid infusion does not add substantially to the cost of the patient’s postoperative care and may reduce the risk of uterine atony and PPH.
Related article: Act fast when confronted by a coagulopathy postpartum Robert L. Barbieri, MD (Editorial, March 2012)
My bottom-line recommendation. In the United States, we should adopt a policy of maintaining a continuous infusion of oxytocin for 4 to 8 hours following a cesarean delivery. Following a 4- to 8-hour rule will decrease the rate of uterine atony and excessive bleeding, thereby improving the safety of our cesarean delivery surgery.
INSTANT POLL
How many hours following cesarean delivery do you think that an oxytocin infusion should be maintained to reduce the risk of uterine atony and postpartum hemorrhage?
If the patient is a Jehovah’s Witness and refuses the transfusion of all blood products, how many hours following cesarean delivery do you think that an oxytocin infusion should be maintained to reduce the risk of uterine atony and postpartum hemorrhage?
Tell us—at [email protected] Please include your name and city and state.
CASE: DISCONTINUED OXYTOCIN LEADS TO POSTPARTUM HEMORRHAGE
You have just completed a repeat cesarean delivery for a 41-year-old woman, now G2P2. You order an infusion of oxytocin, 20 U in 1 L lactated Ringer’s solution, to run at a rate of 125 mL/hr for 8 hours. Without informing you, the recovery room nurse discontinues the bag with the oxytocin solution and starts an infusion of lactated Ringer’s solution without oxytocin.
One hour later, you are called to the recovery room because your patient is having a postpartum hemorrhage (PPH). Physical examination shows that the uterus is boggy and above the level of the umbilicus. On bedside ultrasonography, the uterine cavity is demonstrated to contain minimal blood, and Doppler sonography does not demonstrate any vascular tissue within the uterine cavity. You diagnose uterine atony and initiate treatment. You massage the uterus, rapidly infuse 1 L crystalloid solution, place misoprostol 800 µg in the rectum, and reinitiate the oxytocin infusion. The uterine bleeding slows and then stops.
The following morning, the patient’s hematocrit has decreased from a preoperative value of 37% to 21%.
Could this case of PPH have been prevented?
Cesarean delivery is one of the most commonly performed major operations in developed countries. More than 1,250,000 cesarean deliveries are performed annually in the United States. In 2012, there were 3,952,937 births and a cesarean delivery rate of 32.8%.1 It is an important goal of obstetric care providers to continuously improve our approach to cesarean delivery in order to minimize the surgical risks of this procedure. Evidence-based, standardized protocols for cesarean delivery are critical to ensuring high- reliability surgical outcomes.
A key gap in cesarean delivery protocols is the lack of a nationwide, standardized approach to reducing the risk of postoperative bleeding by maintaining a continuous infusion of oxytocin in the hours immediately following cesarean delivery.
OXYTOCIN: A CRITICAL INTERVENTION TO PREVENT PPH
More than half of all maternal deaths occur in the 24 hours following delivery, with the most common cause being PPH.2 In addition to death, serious complications of PPH include coagulopathy, shock, emergency hysterectomy, transfusion complications, respiratory distress, and pituitary necrosis. Most cases of PPH that occur within 24 hours of delivery are caused by uterine atony.3 Other causes include retained products of conception, placenta accreta, infection, coagulation defects, and amniotic fluid embolism.
Administering a uterotonic such as oxytocin at the time of delivery reduces the risk of PPH by approximately 66% and the risk of maternal blood transfusion by about 65%.4 In order to prevent uterine atony and PPH, oxytocin should be routinely administered following birth of the baby or after delivery of the placenta. Appropriate doses following vaginal delivery are oxytocin 10 U administered intramuscularly or 10 U administered as a slow intravenous (IV) infusion.5 The onset of action of oxytocin is approximately 2 to 5 minutes after an intramuscular dose and 1 minute after an IV dose.6
Related article: Routine use of oxytocin at birth: just the right amount to prevent postpartum hemorrhage Robert L. Barbieri, MD (Editorial, July 2012)
OXYTOCIN AND CESAREAN DELIVERY
Many clinical trials have reported that during a cesarean delivery, the routine administration of a uterotonic agent following birth of the baby reduces the risk of uterine atony and excessive bleeding. Three uterotonics: oxytocin, misoprostol, and carbetocin (a long-acting oxytocin analogue, see SIDEBAR), have been reported to reduce the risk of excessive bleeding during cesarean delivery.7 Oxytocin is the uterotonic most commonly used during cesarean delivery in developed countries.
Related article: A new (to the US) first-line agent for heavy menstrual bleeding Robert L. Barbieri, MD (Editorial, October 2010)
In the United States, there is no standardized oxytocin regimen for prevention of uterine atony and hemorrhage at cesarean delivery. The most common regimen is to add 10–40 U of oxytocin in 1 L crystalloid solution and initiate the oxytocin infusion following delivery of the baby. Initially, the infusion is run at a rapid rate. Once the obstetrician reports that there is adequate uterine tone, the infusion rate is slowed to one that maintains uterine tone.
Some clinicians administer a single bolus of oxytocin following birth of the baby. However, a bolus of oxytocin commonly causes hypotension and, less commonly, ST segment changes on the electrocardiogram (EKG) suggestive of cardiac ischemia.8–10Many experts recommend against administering one large bolus of oxytocin over a short period of time and favor a continuous infusion.
At cesarean delivery, the minimum infusion rate of oxytocin that has been reported to avoid most cases of uterine atony, as reported by the obstetrician immediately following delivery, is approximately oxytocin 0.3 U/min.11 Oxytocin infusion rates of 0.2 U/min and 0.1 U/min were associated with uterine atony rates of 21% and 40%, respectively. An infusion rate of oxytocin 0.3 U/min can be achieved by the administration of 20 U of oxytocin in 1 L crystalloid solution at a rate of 15 mL/min until uterine tone is achieved. The oxytocin dose then can be titrated to maintain adequate uterine tone. Following completion of surgery, uterine tone can be maintained with a low-dose continuous infusion of oxytocin.
4- TO 8-HOUR OXYTOCIN RULE
A key gap in our cesarean delivery protocols is a standardized recommendation concerning the duration of the oxytocin infusion following cesarean delivery. To my knowledge, no national organization has made a firm recommendation concerning the duration of oxytocin infusion following cesarean delivery.
One recent clinical trial studied PPH following cesarean delivery utilizing two oxytocin regimens: a bolus of oxytocin following delivery of the baby versus a bolus of oxytocin followed by a 4-hour IV infusion of oxytocin.12 In this trial, 2,058 women undergoing a scheduled cesarean delivery with a singleton pregnancy were randomly assigned to an oxytocin bolus alone, oxytocin 5 U administered intravenously over 1 minute, or an oxytocin bolus plus a 4-hour oxytocin infusion at a rate of 10 U/hr. The 4-hour postoperative oxytocin infusion was formulated by adding 40 U of oxytocin to 500 mL saline and infusing the solution at 125 mL/hr, equivalent to 0.167 U of oxytocin per minute. In this trial, 65% of the women were undergoing a repeat cesarean delivery and 35% were undergoing a primary cesarean delivery.
The authors reported that women who received the oxytocin bolus alone were significantly more likely to be diagnosed with uterine atony requiring additional uterotonic treatment than women who received both the bolus and the 4-hour postoperative infusion (18.4% versus 12.2%, respectively; P <.001). There was no difference in the rate of PPH between the two groups.
The rate of PPH was 16% in women receiving an oxytocin bolus alone and 15.7% in women receiving both an oxytocin bolus and the continuous oxytocin infusion. However, among less experienced surgeons, the rate of PPH was significantly greater in the group that received the oxytocin bolus alone compared with the women receiving the bolus and continuous infusion (22.2% versus 17.3%, respectively). The authors concluded that obstetricians should consider using a 4-hour infusion of oxytocin following cesarean delivery to reduce the risk of uterine atony.
In a recent evidence-based review of optimal interventions in cesarean delivery, the authors recommended an IV infusion of 10 to 40 U of oxytocin administered over 4 to 8 hours after cesarean delivery.7 Following cesarean, an IV infusion of crystalloid solution is typically maintained for at least 4 to 8 hours. Consequently, adding oxytocin (which costs approximately $1 for 10 units) to the crystalloid infusion does not add substantially to the cost of the patient’s postoperative care and may reduce the risk of uterine atony and PPH.
Related article: Act fast when confronted by a coagulopathy postpartum Robert L. Barbieri, MD (Editorial, March 2012)
My bottom-line recommendation. In the United States, we should adopt a policy of maintaining a continuous infusion of oxytocin for 4 to 8 hours following a cesarean delivery. Following a 4- to 8-hour rule will decrease the rate of uterine atony and excessive bleeding, thereby improving the safety of our cesarean delivery surgery.
INSTANT POLL
How many hours following cesarean delivery do you think that an oxytocin infusion should be maintained to reduce the risk of uterine atony and postpartum hemorrhage?
If the patient is a Jehovah’s Witness and refuses the transfusion of all blood products, how many hours following cesarean delivery do you think that an oxytocin infusion should be maintained to reduce the risk of uterine atony and postpartum hemorrhage?
Tell us—at [email protected] Please include your name and city and state.
- Hamilton BE, Martin JA, Ventura SJ. National Vital Statistics Reports. Births: Preliminary Data for 2012. 2013;62(3). http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_03.pdf. Published September 6, 2013. Accessed March 18, 2014.
- AbouZahr C. Global burden of maternal death and disability. Br Med Bull. 2003;67:1–11.
- Combs CA, Murphy EL, Laros RK Jr. Factors associated with postpartum hemorrhage with vaginal birth. Obstet Gynecol. 1991;77(1):69–76.
- Begley CM, Gyte GM, Devane D, McGuire W, Weeks A. Active versus expectant management for women in the third stage of labour. Cochrane Database Syst Rev. 2011;(11):CD007412.
- Westhoff G, Cotter AM, Tolosa JE. Prophylactic oxytocin for the third stage of labour to prevent postpartum hemorrhage. Cochrane Database Syst Rev. 2013;(10):CD001808.
- Embrey MP. Simultaneous intramuscular injection of oxytocin and ergometrine: a tocographic study. BMJ. 1961;1(5241):1737–1738.
- Dahlke JD, Mendez-Figueroa H, Rouse DJ, Berghella V, Baxter JK, Chauhan SP. Evidence-based surgery for cesarean delivery: An updated systematic review. Am J Obstet Gynecol. 2013;209(4):294–306.
- Archer TL, Knape K, Liles D, Wheeler AS, Carter B. The hemodynamics of oxytocin and other vasoactive agents during neuraxial anesthesia for cesarean delivery: Findings in six cases. Int J Obstet Anesth. 2008;17(3):247–254.
- Jonsson M, Hanson U, Lidell C, Norden-Lindeberg S. ST depression at caesarean section and the relation to oxytocin dose. A randomized controlled trial. BJOG. 2010;117(1):76–83.
- Svanstrom MC, Biber B, Hanes M, Johansson G, Naslund U, Balfourds EM. Signs of myocardial ischaemia after injection of oxytocin: A randomized double-blind comparison of oxytocin and methylergometrine during caesarean section. Br J Anaesth. 2008;100(5):683–689.
- George RB, McKeen D, Chaplin AC, McLeod L. Up-down determination of the ED90 of oxytocin infusions for the prevention of postpartum uterine atony in parturients undergoing cesarean delivery. Can J Anesth. 2010;57(6):578–582.
- Sheehan SR, Montgomery AA, Carey M, et al; ECSSIT Study Group. Oxytocin bolus versus oxytocin bolus and infusion for control of blood loss at elective cesarean section: Double blind, placebo controlled, randomized trial. BMJ. 2011;343:d4661.
- Hamilton BE, Martin JA, Ventura SJ. National Vital Statistics Reports. Births: Preliminary Data for 2012. 2013;62(3). http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_03.pdf. Published September 6, 2013. Accessed March 18, 2014.
- AbouZahr C. Global burden of maternal death and disability. Br Med Bull. 2003;67:1–11.
- Combs CA, Murphy EL, Laros RK Jr. Factors associated with postpartum hemorrhage with vaginal birth. Obstet Gynecol. 1991;77(1):69–76.
- Begley CM, Gyte GM, Devane D, McGuire W, Weeks A. Active versus expectant management for women in the third stage of labour. Cochrane Database Syst Rev. 2011;(11):CD007412.
- Westhoff G, Cotter AM, Tolosa JE. Prophylactic oxytocin for the third stage of labour to prevent postpartum hemorrhage. Cochrane Database Syst Rev. 2013;(10):CD001808.
- Embrey MP. Simultaneous intramuscular injection of oxytocin and ergometrine: a tocographic study. BMJ. 1961;1(5241):1737–1738.
- Dahlke JD, Mendez-Figueroa H, Rouse DJ, Berghella V, Baxter JK, Chauhan SP. Evidence-based surgery for cesarean delivery: An updated systematic review. Am J Obstet Gynecol. 2013;209(4):294–306.
- Archer TL, Knape K, Liles D, Wheeler AS, Carter B. The hemodynamics of oxytocin and other vasoactive agents during neuraxial anesthesia for cesarean delivery: Findings in six cases. Int J Obstet Anesth. 2008;17(3):247–254.
- Jonsson M, Hanson U, Lidell C, Norden-Lindeberg S. ST depression at caesarean section and the relation to oxytocin dose. A randomized controlled trial. BJOG. 2010;117(1):76–83.
- Svanstrom MC, Biber B, Hanes M, Johansson G, Naslund U, Balfourds EM. Signs of myocardial ischaemia after injection of oxytocin: A randomized double-blind comparison of oxytocin and methylergometrine during caesarean section. Br J Anaesth. 2008;100(5):683–689.
- George RB, McKeen D, Chaplin AC, McLeod L. Up-down determination of the ED90 of oxytocin infusions for the prevention of postpartum uterine atony in parturients undergoing cesarean delivery. Can J Anesth. 2010;57(6):578–582.
- Sheehan SR, Montgomery AA, Carey M, et al; ECSSIT Study Group. Oxytocin bolus versus oxytocin bolus and infusion for control of blood loss at elective cesarean section: Double blind, placebo controlled, randomized trial. BMJ. 2011;343:d4661.

Do You Love Your Job? Survey Says …
There is no doubt that nurse practitioners and physician assistants are in demand in the US workforce. A 2013 survey of more than 300 large multispecialty health care organizations indicated that about two-thirds of them had increased their NP/PA workforce and were projecting additional hiring in the next 12 months. Also of note: 31% of these organizations reported having an NP/PA in an administrative role (an increase from 20% in 2012).1
But along with being in demand, our jobs have become increasingly demanding. Health care is changing, not least because of a shortage of primary care physicians, baby boomers increasing their consumption of health care, an increase in chronic disease care, and the growing complexity of health care management. Historically, large studies by our national professional organizations have indicated that NPs and PAs are predominantly satisfied with their role and their future professional prospects. But is that still the case today?
With that question in mind, a quasi-scientific nationwide survey was conducted at the behest of NP Editor-in-Chief Marie-Eileen Onieal and myself. We wanted to determine whether PAs and NPs are satisfied with their work and the state of their profession. This survey, fielded over a two-week period in February, involved a self-selected sample derived from an invitation to almost 100,000 PAs and NPs via the Clinician Reviews mailing list, as well as a posting on the Web site. It should be noted here, for my statistician friends, that this sample may not be representative of the population—but it does create the opportunity for discussion. People who respond to these types of surveys tend to feel strongly, one way or another, about the issues; this questionnaire was no exception.
A total of 240 clinicians participated: 145 NPs (60%) and 95 PAs (40%). The majority (88% of NPs and 86% of PAs) reported being in clinical practice, and 29% of NP respondents and 45% of PA respondents indicated that they have been in their profession for more than 20 years.
Demographically, more women than men participated (NPs, 94%; PAs, 58%), 71% of respondents were between ages 50 and 69, and almost 90% were white. The last item begs the question of the professional satisfaction of nonwhite NPs and PAs. As in other medical fields, the NP and PA professions do not currently emulate the diversity of the US population—which is something we should strive for (perhaps a topic for a future editorial).
Most respondents had “very positive” feelings about their profession (NPs, 73%; PAs, 65%), and many reported feeling “somewhat positive” (NPs, 23%; PAs, 28%). Only 4% of NPs and 7% of PAs expressed negative feelings about the current state of their profession. Perhaps not surprisingly, the majority of both NPs (58%) and PAs (65%) also indicated feeling “very positive” about the future of their profession. Overall, 66% of NPs and 60% of PAs said they would choose the same profession if they had the opportunity again.
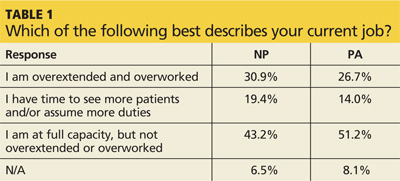
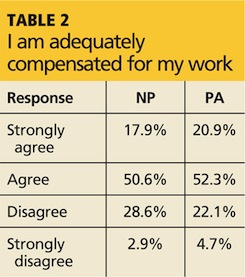
So what, if any, are the drawbacks to being a PA or NP? Well, with regard to workload, participants most commonly endorsed the response that they were working at full capacity but not overextended or overworked (NPs, 43%; PAs, 51%), and the majority felt they were adequately compensated for their work (NPs, 69%; PAs, 73%). However, a significant portion of the remaining respondents had less positive feelings on both subjects; Table 1 and Table 2 provide full data.
Continued on next page >>
The fact that almost one-third of NPs and one-fourth of PAs feel they are overextended and overworked is not lost here. This information is interesting in light of the projection that the workloads of NPs and PAs will increase with the introduction and expansion of team-based health care and with the implementation in primary care of the “medical home” practice model.
Participants were invited to append comments to their responses; these, while of course anecdotal, were rather illuminating of the mindset “in the trenches.” Many clinicians commented on the satisfaction they achieve from providing care and education to patients, their independence as practitioners, and the intellectual and instinctual challenges of diagnosis.
However, several voiced the opinion that NP and PA education programs are no longer as “competitive” as they used to be, noting that the expansion of such programs has led to a perceived attitude of “If you have the dough, you can go.” (As the dean of a PA program, I am of course concerned by this perspective.) This view of the educational system was also reflected in the response to a question about pursuit of a clinical doctorate, with 67% of NPs and 86% of PAs indicating they felt it would not enhance their ability to practice. (On the other hand, one wonders if this is because the majority of respondents are older and have been in the profession longer.)
A similar study by Jackson Healthcare (2012-2013) also noted high levels of job satisfaction among NPs and PAs, with only 5% reporting that they were “very dissatisfied.” In that survey, the five top drivers of NP/PA satisfaction included work environment (37%), patients (28%), compensation (27%), autonomy (21%), and growth opportunities (14%).2
In the same study, NPs and PAs were asked about negative aspects of their jobs. Respondents voiced concern over patient confusion with the NP/PA role, increased administrative duties, and problems with electronic medical records. A significant number mentioned a lack of understanding by physicians and others about the role PAs and NPs play in health care.2
The Jackson study corroborates our findings that overall, NPs and PAs are satisfied with our role and the future of our professions. Our professions continue to be critically important in responding to the converging trends in health care, so it is heartening to see that they continue to offer attractive, fulfilling opportunities to serve tomorrow’s health care needs. At the same time, it is evident that there are some areas with room for improvement. What are your thoughts (good and bad)?
Email me at [email protected].
REFERENCES
1. American Medical Group Association. Survey Reveals Advanced Practice Clinician Workforce Continues to Grow and Incentive Pay Is an Increasing Part of the Compensation Mix [press release]. February 12, 2014. www.amga.org/AboutAMGA/News/article_news.asp?k=727. Accessed February 28, 2014.
2. Jackson Healthcare. Advanced Practice Trends 2012-2013: An Attitude & Outlook on Nurse Practitioners and Physician Assistants. www.jacksonhealthcare.com/media/182734/advancedpracticetrendsreport_ebook0313_lr.pdf. Accessed March 21, 2014.
There is no doubt that nurse practitioners and physician assistants are in demand in the US workforce. A 2013 survey of more than 300 large multispecialty health care organizations indicated that about two-thirds of them had increased their NP/PA workforce and were projecting additional hiring in the next 12 months. Also of note: 31% of these organizations reported having an NP/PA in an administrative role (an increase from 20% in 2012).1
But along with being in demand, our jobs have become increasingly demanding. Health care is changing, not least because of a shortage of primary care physicians, baby boomers increasing their consumption of health care, an increase in chronic disease care, and the growing complexity of health care management. Historically, large studies by our national professional organizations have indicated that NPs and PAs are predominantly satisfied with their role and their future professional prospects. But is that still the case today?
With that question in mind, a quasi-scientific nationwide survey was conducted at the behest of NP Editor-in-Chief Marie-Eileen Onieal and myself. We wanted to determine whether PAs and NPs are satisfied with their work and the state of their profession. This survey, fielded over a two-week period in February, involved a self-selected sample derived from an invitation to almost 100,000 PAs and NPs via the Clinician Reviews mailing list, as well as a posting on the Web site. It should be noted here, for my statistician friends, that this sample may not be representative of the population—but it does create the opportunity for discussion. People who respond to these types of surveys tend to feel strongly, one way or another, about the issues; this questionnaire was no exception.
A total of 240 clinicians participated: 145 NPs (60%) and 95 PAs (40%). The majority (88% of NPs and 86% of PAs) reported being in clinical practice, and 29% of NP respondents and 45% of PA respondents indicated that they have been in their profession for more than 20 years.
Demographically, more women than men participated (NPs, 94%; PAs, 58%), 71% of respondents were between ages 50 and 69, and almost 90% were white. The last item begs the question of the professional satisfaction of nonwhite NPs and PAs. As in other medical fields, the NP and PA professions do not currently emulate the diversity of the US population—which is something we should strive for (perhaps a topic for a future editorial).
Most respondents had “very positive” feelings about their profession (NPs, 73%; PAs, 65%), and many reported feeling “somewhat positive” (NPs, 23%; PAs, 28%). Only 4% of NPs and 7% of PAs expressed negative feelings about the current state of their profession. Perhaps not surprisingly, the majority of both NPs (58%) and PAs (65%) also indicated feeling “very positive” about the future of their profession. Overall, 66% of NPs and 60% of PAs said they would choose the same profession if they had the opportunity again.
So what, if any, are the drawbacks to being a PA or NP? Well, with regard to workload, participants most commonly endorsed the response that they were working at full capacity but not overextended or overworked (NPs, 43%; PAs, 51%), and the majority felt they were adequately compensated for their work (NPs, 69%; PAs, 73%). However, a significant portion of the remaining respondents had less positive feelings on both subjects; Table 1 and Table 2 provide full data.
Continued on next page >>
The fact that almost one-third of NPs and one-fourth of PAs feel they are overextended and overworked is not lost here. This information is interesting in light of the projection that the workloads of NPs and PAs will increase with the introduction and expansion of team-based health care and with the implementation in primary care of the “medical home” practice model.
Participants were invited to append comments to their responses; these, while of course anecdotal, were rather illuminating of the mindset “in the trenches.” Many clinicians commented on the satisfaction they achieve from providing care and education to patients, their independence as practitioners, and the intellectual and instinctual challenges of diagnosis.
However, several voiced the opinion that NP and PA education programs are no longer as “competitive” as they used to be, noting that the expansion of such programs has led to a perceived attitude of “If you have the dough, you can go.” (As the dean of a PA program, I am of course concerned by this perspective.) This view of the educational system was also reflected in the response to a question about pursuit of a clinical doctorate, with 67% of NPs and 86% of PAs indicating they felt it would not enhance their ability to practice. (On the other hand, one wonders if this is because the majority of respondents are older and have been in the profession longer.)
A similar study by Jackson Healthcare (2012-2013) also noted high levels of job satisfaction among NPs and PAs, with only 5% reporting that they were “very dissatisfied.” In that survey, the five top drivers of NP/PA satisfaction included work environment (37%), patients (28%), compensation (27%), autonomy (21%), and growth opportunities (14%).2
In the same study, NPs and PAs were asked about negative aspects of their jobs. Respondents voiced concern over patient confusion with the NP/PA role, increased administrative duties, and problems with electronic medical records. A significant number mentioned a lack of understanding by physicians and others about the role PAs and NPs play in health care.2
The Jackson study corroborates our findings that overall, NPs and PAs are satisfied with our role and the future of our professions. Our professions continue to be critically important in responding to the converging trends in health care, so it is heartening to see that they continue to offer attractive, fulfilling opportunities to serve tomorrow’s health care needs. At the same time, it is evident that there are some areas with room for improvement. What are your thoughts (good and bad)?
Email me at [email protected].
REFERENCES
1. American Medical Group Association. Survey Reveals Advanced Practice Clinician Workforce Continues to Grow and Incentive Pay Is an Increasing Part of the Compensation Mix [press release]. February 12, 2014. www.amga.org/AboutAMGA/News/article_news.asp?k=727. Accessed February 28, 2014.
2. Jackson Healthcare. Advanced Practice Trends 2012-2013: An Attitude & Outlook on Nurse Practitioners and Physician Assistants. www.jacksonhealthcare.com/media/182734/advancedpracticetrendsreport_ebook0313_lr.pdf. Accessed March 21, 2014.
There is no doubt that nurse practitioners and physician assistants are in demand in the US workforce. A 2013 survey of more than 300 large multispecialty health care organizations indicated that about two-thirds of them had increased their NP/PA workforce and were projecting additional hiring in the next 12 months. Also of note: 31% of these organizations reported having an NP/PA in an administrative role (an increase from 20% in 2012).1
But along with being in demand, our jobs have become increasingly demanding. Health care is changing, not least because of a shortage of primary care physicians, baby boomers increasing their consumption of health care, an increase in chronic disease care, and the growing complexity of health care management. Historically, large studies by our national professional organizations have indicated that NPs and PAs are predominantly satisfied with their role and their future professional prospects. But is that still the case today?
With that question in mind, a quasi-scientific nationwide survey was conducted at the behest of NP Editor-in-Chief Marie-Eileen Onieal and myself. We wanted to determine whether PAs and NPs are satisfied with their work and the state of their profession. This survey, fielded over a two-week period in February, involved a self-selected sample derived from an invitation to almost 100,000 PAs and NPs via the Clinician Reviews mailing list, as well as a posting on the Web site. It should be noted here, for my statistician friends, that this sample may not be representative of the population—but it does create the opportunity for discussion. People who respond to these types of surveys tend to feel strongly, one way or another, about the issues; this questionnaire was no exception.
A total of 240 clinicians participated: 145 NPs (60%) and 95 PAs (40%). The majority (88% of NPs and 86% of PAs) reported being in clinical practice, and 29% of NP respondents and 45% of PA respondents indicated that they have been in their profession for more than 20 years.
Demographically, more women than men participated (NPs, 94%; PAs, 58%), 71% of respondents were between ages 50 and 69, and almost 90% were white. The last item begs the question of the professional satisfaction of nonwhite NPs and PAs. As in other medical fields, the NP and PA professions do not currently emulate the diversity of the US population—which is something we should strive for (perhaps a topic for a future editorial).
Most respondents had “very positive” feelings about their profession (NPs, 73%; PAs, 65%), and many reported feeling “somewhat positive” (NPs, 23%; PAs, 28%). Only 4% of NPs and 7% of PAs expressed negative feelings about the current state of their profession. Perhaps not surprisingly, the majority of both NPs (58%) and PAs (65%) also indicated feeling “very positive” about the future of their profession. Overall, 66% of NPs and 60% of PAs said they would choose the same profession if they had the opportunity again.
So what, if any, are the drawbacks to being a PA or NP? Well, with regard to workload, participants most commonly endorsed the response that they were working at full capacity but not overextended or overworked (NPs, 43%; PAs, 51%), and the majority felt they were adequately compensated for their work (NPs, 69%; PAs, 73%). However, a significant portion of the remaining respondents had less positive feelings on both subjects; Table 1 and Table 2 provide full data.
Continued on next page >>
The fact that almost one-third of NPs and one-fourth of PAs feel they are overextended and overworked is not lost here. This information is interesting in light of the projection that the workloads of NPs and PAs will increase with the introduction and expansion of team-based health care and with the implementation in primary care of the “medical home” practice model.
Participants were invited to append comments to their responses; these, while of course anecdotal, were rather illuminating of the mindset “in the trenches.” Many clinicians commented on the satisfaction they achieve from providing care and education to patients, their independence as practitioners, and the intellectual and instinctual challenges of diagnosis.
However, several voiced the opinion that NP and PA education programs are no longer as “competitive” as they used to be, noting that the expansion of such programs has led to a perceived attitude of “If you have the dough, you can go.” (As the dean of a PA program, I am of course concerned by this perspective.) This view of the educational system was also reflected in the response to a question about pursuit of a clinical doctorate, with 67% of NPs and 86% of PAs indicating they felt it would not enhance their ability to practice. (On the other hand, one wonders if this is because the majority of respondents are older and have been in the profession longer.)
A similar study by Jackson Healthcare (2012-2013) also noted high levels of job satisfaction among NPs and PAs, with only 5% reporting that they were “very dissatisfied.” In that survey, the five top drivers of NP/PA satisfaction included work environment (37%), patients (28%), compensation (27%), autonomy (21%), and growth opportunities (14%).2
In the same study, NPs and PAs were asked about negative aspects of their jobs. Respondents voiced concern over patient confusion with the NP/PA role, increased administrative duties, and problems with electronic medical records. A significant number mentioned a lack of understanding by physicians and others about the role PAs and NPs play in health care.2
The Jackson study corroborates our findings that overall, NPs and PAs are satisfied with our role and the future of our professions. Our professions continue to be critically important in responding to the converging trends in health care, so it is heartening to see that they continue to offer attractive, fulfilling opportunities to serve tomorrow’s health care needs. At the same time, it is evident that there are some areas with room for improvement. What are your thoughts (good and bad)?
Email me at [email protected].
REFERENCES
1. American Medical Group Association. Survey Reveals Advanced Practice Clinician Workforce Continues to Grow and Incentive Pay Is an Increasing Part of the Compensation Mix [press release]. February 12, 2014. www.amga.org/AboutAMGA/News/article_news.asp?k=727. Accessed February 28, 2014.
2. Jackson Healthcare. Advanced Practice Trends 2012-2013: An Attitude & Outlook on Nurse Practitioners and Physician Assistants. www.jacksonhealthcare.com/media/182734/advancedpracticetrendsreport_ebook0313_lr.pdf. Accessed March 21, 2014.
Delayed prescribing of antibiotics
While not a new phenomenon, antimicrobial resistance is an alarming and, arguably, still underappreciated public health problem. A mere 70 years after the introduction of antibiotics, we face the distinct possibility of a future without effective antibiotics for some infections. Such a reality will render select surgical operations, cancer chemotherapy, and organ transplants exceedingly dangerous.
The scarcity of new antimicrobial agents and the paucity of new agents in the drug development pipeline limit treatment options, particularly for patients with infections caused by multidrug-resistant organisms. Annually, multidrug resistant organisms cause an estimated 25,000 deaths in Europe and 12,000 deaths in the United States. In response to this threat, the Transatlantic Taskforce on Antimicrobial Resistance (TATFAR) was established and published their report with 17 recommendations.
Respiratory tract infections are one of the most common symptoms presenting to primary care. Overprescribing in this setting is rampant, driven largely by patient expectations and clinician need for expediency and desire to receive "high marks" for satisfaction. Available evidence has suggested that delayed antibiotic prescribing is effective. But what is the best method to delay antibiotic prescribing?
Researchers in the United Kingdom evaluated the comparative effectiveness of four different strategies of delayed antibiotic prescribing for patients not needing antibiotics right away:
• Recontact: Patients were asked to contact the office and leave a message for a clinician to prescribe an antibiotic.
• Postdated prescription: The prescription could be filled only after a certain date.
• Wait/Request: Patients were instructed to wait but could request an antibiotic from the front office.
• Delayed use: Patients received antibiotics but were asked to wait to use them.
A "no prescription" arm was added later in the trial. The primary outcome was symptom severity measured at the end of each day during days 2-4 of a two-week symptom diary. Secondary outcomes included antibiotic use and side effects.
No differences were observed between the four strategies with respect to symptom control. Antibiotic use did not differ significantly between strategies and the lowest use was reported in the no prescription arm. No significant differences were observed between groups in patient satisfaction. Complications were slightly higher in the no antibiotic group (2.5%), compared with the delayed groups (1.4%).
Delayed prescribing is associated with less than 40% of patients using an antibiotic. Given the current crisis with multidrug resistance, we should feel obligated to try one of the proposed strategies for delayed antibiotic prescription if patients do not need one right away.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. He reports no conflicts of interest.
While not a new phenomenon, antimicrobial resistance is an alarming and, arguably, still underappreciated public health problem. A mere 70 years after the introduction of antibiotics, we face the distinct possibility of a future without effective antibiotics for some infections. Such a reality will render select surgical operations, cancer chemotherapy, and organ transplants exceedingly dangerous.
The scarcity of new antimicrobial agents and the paucity of new agents in the drug development pipeline limit treatment options, particularly for patients with infections caused by multidrug-resistant organisms. Annually, multidrug resistant organisms cause an estimated 25,000 deaths in Europe and 12,000 deaths in the United States. In response to this threat, the Transatlantic Taskforce on Antimicrobial Resistance (TATFAR) was established and published their report with 17 recommendations.
Respiratory tract infections are one of the most common symptoms presenting to primary care. Overprescribing in this setting is rampant, driven largely by patient expectations and clinician need for expediency and desire to receive "high marks" for satisfaction. Available evidence has suggested that delayed antibiotic prescribing is effective. But what is the best method to delay antibiotic prescribing?
Researchers in the United Kingdom evaluated the comparative effectiveness of four different strategies of delayed antibiotic prescribing for patients not needing antibiotics right away:
• Recontact: Patients were asked to contact the office and leave a message for a clinician to prescribe an antibiotic.
• Postdated prescription: The prescription could be filled only after a certain date.
• Wait/Request: Patients were instructed to wait but could request an antibiotic from the front office.
• Delayed use: Patients received antibiotics but were asked to wait to use them.
A "no prescription" arm was added later in the trial. The primary outcome was symptom severity measured at the end of each day during days 2-4 of a two-week symptom diary. Secondary outcomes included antibiotic use and side effects.
No differences were observed between the four strategies with respect to symptom control. Antibiotic use did not differ significantly between strategies and the lowest use was reported in the no prescription arm. No significant differences were observed between groups in patient satisfaction. Complications were slightly higher in the no antibiotic group (2.5%), compared with the delayed groups (1.4%).
Delayed prescribing is associated with less than 40% of patients using an antibiotic. Given the current crisis with multidrug resistance, we should feel obligated to try one of the proposed strategies for delayed antibiotic prescription if patients do not need one right away.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. He reports no conflicts of interest.
While not a new phenomenon, antimicrobial resistance is an alarming and, arguably, still underappreciated public health problem. A mere 70 years after the introduction of antibiotics, we face the distinct possibility of a future without effective antibiotics for some infections. Such a reality will render select surgical operations, cancer chemotherapy, and organ transplants exceedingly dangerous.
The scarcity of new antimicrobial agents and the paucity of new agents in the drug development pipeline limit treatment options, particularly for patients with infections caused by multidrug-resistant organisms. Annually, multidrug resistant organisms cause an estimated 25,000 deaths in Europe and 12,000 deaths in the United States. In response to this threat, the Transatlantic Taskforce on Antimicrobial Resistance (TATFAR) was established and published their report with 17 recommendations.
Respiratory tract infections are one of the most common symptoms presenting to primary care. Overprescribing in this setting is rampant, driven largely by patient expectations and clinician need for expediency and desire to receive "high marks" for satisfaction. Available evidence has suggested that delayed antibiotic prescribing is effective. But what is the best method to delay antibiotic prescribing?
Researchers in the United Kingdom evaluated the comparative effectiveness of four different strategies of delayed antibiotic prescribing for patients not needing antibiotics right away:
• Recontact: Patients were asked to contact the office and leave a message for a clinician to prescribe an antibiotic.
• Postdated prescription: The prescription could be filled only after a certain date.
• Wait/Request: Patients were instructed to wait but could request an antibiotic from the front office.
• Delayed use: Patients received antibiotics but were asked to wait to use them.
A "no prescription" arm was added later in the trial. The primary outcome was symptom severity measured at the end of each day during days 2-4 of a two-week symptom diary. Secondary outcomes included antibiotic use and side effects.
No differences were observed between the four strategies with respect to symptom control. Antibiotic use did not differ significantly between strategies and the lowest use was reported in the no prescription arm. No significant differences were observed between groups in patient satisfaction. Complications were slightly higher in the no antibiotic group (2.5%), compared with the delayed groups (1.4%).
Delayed prescribing is associated with less than 40% of patients using an antibiotic. Given the current crisis with multidrug resistance, we should feel obligated to try one of the proposed strategies for delayed antibiotic prescription if patients do not need one right away.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. He reports no conflicts of interest.

Making Health Care More Accessible and Convenient
With great interest I read the article “Electronic Consult Experience: Making Health Care More Accessible and Convenient for Veterans.”1 The author, Barbara J. Siepierski, MD, described the successful implementation of the electronic consultation (e-consult). As a pulmonary staff physician at the James H. Quillen VAMC in Mountain Home, Tennessee, in VISN 9, I would like to add my experience as a subspecialist for the adaptation of the e-consult systemwide in the VA.
Several years ago, it became my responsibility to screen all the outpatient pulmonary consultations at the Mountain Home VAMC. The large number of outpatient consultations the pulmonary section received overwhelmed our physician and clinic resources and dictated that the individual veteran be prioritized. Also, it was hoped that screening the outpatient pulmonary consultations would ensure that laboratory and radiographic studies would be completed before the veterans’ clinic visits, thereby avoiding unnecessary visits and congestion of the pulmonary outpatient clinic.
When the e-consult was presented to the staff at the Mountain Home VAMC, many individual practitioners, including myself, were skeptical. I thought that nothing could or should replace the face-to-face visit and worried about medical-legal aspects of adopting this process. However, the benefits to our subspecialty pulmonary outpatient clinic have been enormous. There is now no wait time for new face-to-face consultations into the pulmonary outpatient clinic. There is no longer a need to prioritize the veterans into the pulmonary outpatient clinic.
It is my hope that the entire VA system will soon share the experience as expressed by Dr. Siepierski in VISN 11. This may be another example where the VA is leading the nation in health care.
Ryland P. Byrd Jr, MD
James H. Quillen VAMC
Mountain Home, Tennessee
Disclaimer
The opinions expressed in reader letters are those of the writers and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications, the U.S. Government, or any of its agencies.
Reference
1. Siepierski BJ. Electronic consult experience: Making health care more accessible and convenient for veterans. Fed Pract. 2013;30(12):38-40.
With great interest I read the article “Electronic Consult Experience: Making Health Care More Accessible and Convenient for Veterans.”1 The author, Barbara J. Siepierski, MD, described the successful implementation of the electronic consultation (e-consult). As a pulmonary staff physician at the James H. Quillen VAMC in Mountain Home, Tennessee, in VISN 9, I would like to add my experience as a subspecialist for the adaptation of the e-consult systemwide in the VA.
Several years ago, it became my responsibility to screen all the outpatient pulmonary consultations at the Mountain Home VAMC. The large number of outpatient consultations the pulmonary section received overwhelmed our physician and clinic resources and dictated that the individual veteran be prioritized. Also, it was hoped that screening the outpatient pulmonary consultations would ensure that laboratory and radiographic studies would be completed before the veterans’ clinic visits, thereby avoiding unnecessary visits and congestion of the pulmonary outpatient clinic.
When the e-consult was presented to the staff at the Mountain Home VAMC, many individual practitioners, including myself, were skeptical. I thought that nothing could or should replace the face-to-face visit and worried about medical-legal aspects of adopting this process. However, the benefits to our subspecialty pulmonary outpatient clinic have been enormous. There is now no wait time for new face-to-face consultations into the pulmonary outpatient clinic. There is no longer a need to prioritize the veterans into the pulmonary outpatient clinic.
It is my hope that the entire VA system will soon share the experience as expressed by Dr. Siepierski in VISN 11. This may be another example where the VA is leading the nation in health care.
Ryland P. Byrd Jr, MD
James H. Quillen VAMC
Mountain Home, Tennessee
Disclaimer
The opinions expressed in reader letters are those of the writers and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications, the U.S. Government, or any of its agencies.
Reference
1. Siepierski BJ. Electronic consult experience: Making health care more accessible and convenient for veterans. Fed Pract. 2013;30(12):38-40.
With great interest I read the article “Electronic Consult Experience: Making Health Care More Accessible and Convenient for Veterans.”1 The author, Barbara J. Siepierski, MD, described the successful implementation of the electronic consultation (e-consult). As a pulmonary staff physician at the James H. Quillen VAMC in Mountain Home, Tennessee, in VISN 9, I would like to add my experience as a subspecialist for the adaptation of the e-consult systemwide in the VA.
Several years ago, it became my responsibility to screen all the outpatient pulmonary consultations at the Mountain Home VAMC. The large number of outpatient consultations the pulmonary section received overwhelmed our physician and clinic resources and dictated that the individual veteran be prioritized. Also, it was hoped that screening the outpatient pulmonary consultations would ensure that laboratory and radiographic studies would be completed before the veterans’ clinic visits, thereby avoiding unnecessary visits and congestion of the pulmonary outpatient clinic.
When the e-consult was presented to the staff at the Mountain Home VAMC, many individual practitioners, including myself, were skeptical. I thought that nothing could or should replace the face-to-face visit and worried about medical-legal aspects of adopting this process. However, the benefits to our subspecialty pulmonary outpatient clinic have been enormous. There is now no wait time for new face-to-face consultations into the pulmonary outpatient clinic. There is no longer a need to prioritize the veterans into the pulmonary outpatient clinic.
It is my hope that the entire VA system will soon share the experience as expressed by Dr. Siepierski in VISN 11. This may be another example where the VA is leading the nation in health care.
Ryland P. Byrd Jr, MD
James H. Quillen VAMC
Mountain Home, Tennessee
Disclaimer
The opinions expressed in reader letters are those of the writers and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications, the U.S. Government, or any of its agencies.
Reference
1. Siepierski BJ. Electronic consult experience: Making health care more accessible and convenient for veterans. Fed Pract. 2013;30(12):38-40.
Breakfast of champions
I know that as a pediatrician I shouldn’t find it hard to keep up with parenting trends, but honestly, it’s exhausting! The new thing now is “grit,” right? I thought I had it down, but even here in the South, there are only so many ways to feed kids ground hominy before they complain, ironically demonstrating a complete lack of grit.
I like this grit concept, though. As parents, we get to do what we’ve always done: make our kids’ lives difficult for no reason. But now we can claim that we’re just preparing them for an economic landscape in which only the most determined workers will ever earn more than their parents. While those successful few feast on caviar and champagne, everyone else will have to eat...well, you know.
Hows and whys
Pediatricians are just so nice! It’s weird, right? I mean, we’re too nice. Apparently. the folks at the American Academy of Pediatrics and the ABIM Foundation agree, because they’ve teamed up to create the Choosing Wisely campaign, a coordinated multimedia strategy to help us learn how to say “no” to stuff. They knew, after all, that if they offered us this program we’d be too polite to turn it down.

Using evidence-based guidelines and surveys, the sponsors identified the Top 10 common pediatric interventions whose risks clearly outweighed their benefits, ranging from #10: Using home apnea monitors to prevent SIDS to #1: Treating viral upper respiratory infections with antibiotics. That one probably needs a #1a: Justifying doing #1 based on some lame excuse like green snot or a red throat. If you can convince yourself that green snot means a sinus infection, hopefully you can later convince yourself that a giant boil draining methicillin-resistant Staph aureus means a mosquito bite.
Not only does Choosing Wisely include a list of stuff not to do (antacids for “happy spittters,” anyone?), but it comes with video modules to teach pediatricians exactly how to tell parents that their kids do not need a CT scan for falling off the couch. Future modules will walk providers through explaining to their hospital administrators why their Press Ganey patient satisfaction scores have fallen.
Psych!
Do you find it scary how many patients you send for help with serious psychiatric conditions who never go? Is it possible that we would live in a perfectly sane world if only every child referred to a mental health provider actually went? Of course, in such a world we may never get another Miley Cyrus.
A group of researchers in Pittsburgh may have solved this problem: Every pediatrician’s office should have its own mental health provider. How good an answer is it? Among 321 kids sent for mental health referral, only 54% went when the provider was located somewhere else, compared with more than 99% when the provider was in the same office as the pediatrician.
Once they see these numbers, I expect psychiatrists to be lining up outside our doors begging to sublease our broom closets. Unless, of course, we already don’t have enough pediatric mental health providers to see the patients who do show up. Right. I may as well put those brooms back.
But why stop with co-located mental health services? My dream office would include a toy store, an ice cream shoppe, a day care, and a puppy adoption center. Of course with all that, we’d definitely need to add services for adult mental health.
Chemistry minor
This is the kind of quote I find scary: “It’s not a matter of if a child will be seriously poisoned or killed,” said Lee Cantrell, director of the San Diego division of the California Poison Control System and a professor of pharmacy at the University of California, San Francisco. “It’s a matter of when.”
What could this man, speaking to the New York Times for a March 23rd article, be talking about? Sarin gas? Methamphetamine? Whatever they put in Vienna sausages? What if I told you this potent neurotoxin was also brightly colored, attractively scented, and sold with no regulations whatsoever in non-child-safe bottles? No, it’s not 5-Hour Energy. Try nicotine refills for e-cigarettes. Now are you scared?
Depending on the concentration, e-cigarette liquid refills contain enough nicotine to send a child to the hospital just from spilling it on the skin. Drinking a bottle could be deadly. By now, you’ve already grasped the possible consequences: We have one more hazard to discuss at our well child visits. Hopefully before long, regulators will address these substances, with some grit.
David L. Hill, M.D., FAAP is the author of Dad to Dad: Parenting Like a Pro (AAP Publishing, 2012). He is also vice president of Cape Fear Pediatrics in Wilmington, N.C., and adjunct assistant professor of pediatrics at the University of North Carolina at Chapel Hill. He serves as Program Director for the AAP Council on Communications and Media and as an executive committee member of the North Carolina Pediatric Society. He has recorded commentaries for NPR's All Things Considered and provided content for various print, television, and Internet outlets.
I know that as a pediatrician I shouldn’t find it hard to keep up with parenting trends, but honestly, it’s exhausting! The new thing now is “grit,” right? I thought I had it down, but even here in the South, there are only so many ways to feed kids ground hominy before they complain, ironically demonstrating a complete lack of grit.
I like this grit concept, though. As parents, we get to do what we’ve always done: make our kids’ lives difficult for no reason. But now we can claim that we’re just preparing them for an economic landscape in which only the most determined workers will ever earn more than their parents. While those successful few feast on caviar and champagne, everyone else will have to eat...well, you know.
Hows and whys
Pediatricians are just so nice! It’s weird, right? I mean, we’re too nice. Apparently. the folks at the American Academy of Pediatrics and the ABIM Foundation agree, because they’ve teamed up to create the Choosing Wisely campaign, a coordinated multimedia strategy to help us learn how to say “no” to stuff. They knew, after all, that if they offered us this program we’d be too polite to turn it down.
Using evidence-based guidelines and surveys, the sponsors identified the Top 10 common pediatric interventions whose risks clearly outweighed their benefits, ranging from #10: Using home apnea monitors to prevent SIDS to #1: Treating viral upper respiratory infections with antibiotics. That one probably needs a #1a: Justifying doing #1 based on some lame excuse like green snot or a red throat. If you can convince yourself that green snot means a sinus infection, hopefully you can later convince yourself that a giant boil draining methicillin-resistant Staph aureus means a mosquito bite.
Not only does Choosing Wisely include a list of stuff not to do (antacids for “happy spittters,” anyone?), but it comes with video modules to teach pediatricians exactly how to tell parents that their kids do not need a CT scan for falling off the couch. Future modules will walk providers through explaining to their hospital administrators why their Press Ganey patient satisfaction scores have fallen.
Psych!
Do you find it scary how many patients you send for help with serious psychiatric conditions who never go? Is it possible that we would live in a perfectly sane world if only every child referred to a mental health provider actually went? Of course, in such a world we may never get another Miley Cyrus.
A group of researchers in Pittsburgh may have solved this problem: Every pediatrician’s office should have its own mental health provider. How good an answer is it? Among 321 kids sent for mental health referral, only 54% went when the provider was located somewhere else, compared with more than 99% when the provider was in the same office as the pediatrician.
Once they see these numbers, I expect psychiatrists to be lining up outside our doors begging to sublease our broom closets. Unless, of course, we already don’t have enough pediatric mental health providers to see the patients who do show up. Right. I may as well put those brooms back.
But why stop with co-located mental health services? My dream office would include a toy store, an ice cream shoppe, a day care, and a puppy adoption center. Of course with all that, we’d definitely need to add services for adult mental health.
Chemistry minor
This is the kind of quote I find scary: “It’s not a matter of if a child will be seriously poisoned or killed,” said Lee Cantrell, director of the San Diego division of the California Poison Control System and a professor of pharmacy at the University of California, San Francisco. “It’s a matter of when.”
What could this man, speaking to the New York Times for a March 23rd article, be talking about? Sarin gas? Methamphetamine? Whatever they put in Vienna sausages? What if I told you this potent neurotoxin was also brightly colored, attractively scented, and sold with no regulations whatsoever in non-child-safe bottles? No, it’s not 5-Hour Energy. Try nicotine refills for e-cigarettes. Now are you scared?
Depending on the concentration, e-cigarette liquid refills contain enough nicotine to send a child to the hospital just from spilling it on the skin. Drinking a bottle could be deadly. By now, you’ve already grasped the possible consequences: We have one more hazard to discuss at our well child visits. Hopefully before long, regulators will address these substances, with some grit.
David L. Hill, M.D., FAAP is the author of Dad to Dad: Parenting Like a Pro (AAP Publishing, 2012). He is also vice president of Cape Fear Pediatrics in Wilmington, N.C., and adjunct assistant professor of pediatrics at the University of North Carolina at Chapel Hill. He serves as Program Director for the AAP Council on Communications and Media and as an executive committee member of the North Carolina Pediatric Society. He has recorded commentaries for NPR's All Things Considered and provided content for various print, television, and Internet outlets.
I know that as a pediatrician I shouldn’t find it hard to keep up with parenting trends, but honestly, it’s exhausting! The new thing now is “grit,” right? I thought I had it down, but even here in the South, there are only so many ways to feed kids ground hominy before they complain, ironically demonstrating a complete lack of grit.
I like this grit concept, though. As parents, we get to do what we’ve always done: make our kids’ lives difficult for no reason. But now we can claim that we’re just preparing them for an economic landscape in which only the most determined workers will ever earn more than their parents. While those successful few feast on caviar and champagne, everyone else will have to eat...well, you know.
Hows and whys
Pediatricians are just so nice! It’s weird, right? I mean, we’re too nice. Apparently. the folks at the American Academy of Pediatrics and the ABIM Foundation agree, because they’ve teamed up to create the Choosing Wisely campaign, a coordinated multimedia strategy to help us learn how to say “no” to stuff. They knew, after all, that if they offered us this program we’d be too polite to turn it down.
Using evidence-based guidelines and surveys, the sponsors identified the Top 10 common pediatric interventions whose risks clearly outweighed their benefits, ranging from #10: Using home apnea monitors to prevent SIDS to #1: Treating viral upper respiratory infections with antibiotics. That one probably needs a #1a: Justifying doing #1 based on some lame excuse like green snot or a red throat. If you can convince yourself that green snot means a sinus infection, hopefully you can later convince yourself that a giant boil draining methicillin-resistant Staph aureus means a mosquito bite.
Not only does Choosing Wisely include a list of stuff not to do (antacids for “happy spittters,” anyone?), but it comes with video modules to teach pediatricians exactly how to tell parents that their kids do not need a CT scan for falling off the couch. Future modules will walk providers through explaining to their hospital administrators why their Press Ganey patient satisfaction scores have fallen.
Psych!
Do you find it scary how many patients you send for help with serious psychiatric conditions who never go? Is it possible that we would live in a perfectly sane world if only every child referred to a mental health provider actually went? Of course, in such a world we may never get another Miley Cyrus.
A group of researchers in Pittsburgh may have solved this problem: Every pediatrician’s office should have its own mental health provider. How good an answer is it? Among 321 kids sent for mental health referral, only 54% went when the provider was located somewhere else, compared with more than 99% when the provider was in the same office as the pediatrician.
Once they see these numbers, I expect psychiatrists to be lining up outside our doors begging to sublease our broom closets. Unless, of course, we already don’t have enough pediatric mental health providers to see the patients who do show up. Right. I may as well put those brooms back.
But why stop with co-located mental health services? My dream office would include a toy store, an ice cream shoppe, a day care, and a puppy adoption center. Of course with all that, we’d definitely need to add services for adult mental health.
Chemistry minor
This is the kind of quote I find scary: “It’s not a matter of if a child will be seriously poisoned or killed,” said Lee Cantrell, director of the San Diego division of the California Poison Control System and a professor of pharmacy at the University of California, San Francisco. “It’s a matter of when.”
What could this man, speaking to the New York Times for a March 23rd article, be talking about? Sarin gas? Methamphetamine? Whatever they put in Vienna sausages? What if I told you this potent neurotoxin was also brightly colored, attractively scented, and sold with no regulations whatsoever in non-child-safe bottles? No, it’s not 5-Hour Energy. Try nicotine refills for e-cigarettes. Now are you scared?
Depending on the concentration, e-cigarette liquid refills contain enough nicotine to send a child to the hospital just from spilling it on the skin. Drinking a bottle could be deadly. By now, you’ve already grasped the possible consequences: We have one more hazard to discuss at our well child visits. Hopefully before long, regulators will address these substances, with some grit.
David L. Hill, M.D., FAAP is the author of Dad to Dad: Parenting Like a Pro (AAP Publishing, 2012). He is also vice president of Cape Fear Pediatrics in Wilmington, N.C., and adjunct assistant professor of pediatrics at the University of North Carolina at Chapel Hill. He serves as Program Director for the AAP Council on Communications and Media and as an executive committee member of the North Carolina Pediatric Society. He has recorded commentaries for NPR's All Things Considered and provided content for various print, television, and Internet outlets.
Congressional Leadership Conference
Repealing the Sustainable Growth Rate, gestational diabetes, more residency positions for ob.gyns., and reducing liability were on the minds of ob.gyns. at the Congressional Leadership Conference this year.
Approximately 400 ob.gyns. attended the 32nd annual American College of Obstetricians and Gynecologists Congressional Leadership Conference (CLC) in Washington, D.C., during March 2-4. Forty-nine states plus Puerto Rico; Washington, D.C.; and Ontario were represented. The attendees learned about pending legislation and subsequently lobbied their legislators in Congress for their cosponsorship of four bills.
While Congress met the April 1 deadline to avoid the 24% Medicare pay cut called for by the Sustainable Growth Rate (SGR) formula, it did so via a 1-year patch and not by passing the comprehensive reform favored by many physicians. The SGR has created financial instability in health care. More than $150 billion has been spent to avoid physician payment cuts and the temporary patch will increase that cost. CLC attendees had asked their representatives and senators to cosponsor the Sustainable Growth Rate Repeal and Medicare Provider Modernization Act of 2014 (H.R. 4015). This bill would repeal the SGR and guarantee physicians 5 years of payment increases at 0.5% per year. The House passed H.R. 4015, but a modification was introduced and passed by a voice vote. That is the bill that ultimately went to the Senate and was passed, and that President Obama signed.

The Gestational Diabetes Act of 2013 (H.R. 1915/S. 907) provides funding for research and surveillance to improve screening for gestational diabetes and track women who have this diagnosis. This disease is estimated to affect 18% of all pregnancies and is increasing in frequency, according to the American Diabetes Association. Currently, there is minimal research being conducted on gestational diabetes.
The Training Tomorrow’s Doctors Today Act of 2013 (H.R. 1201) provides for 15,000 additional residency positions over the next 5 years. Currently, Medicare pays $3 billion for resident salaries (direct graduate medical education) and $6.4 billion for the higher cost of patient care in teaching hospitals (indirect GME). The number of federally funded residency slots has not increased since 1997. It is anticipated that there will be an 18% shortage of ob.gyns. by 2030 and 25% by 2050 if there is no increase in residency positions, according to ACOG. This bill requires hospitals receiving federal funding to allocate 25% of residency slots to primary care and general surgery. In this bill, ob.gyn. is considered primary care. The Senate does not have a companion bill.
The Saving Lives, Saving Cost Act of 2014 (H.R. 4106) was introduced in the House by a Republican lawyer and a Democratic physician. This bill provides for the option of a review by an independent medical review panel in a medical malpractice case where adherence to approved clinical guidelines can be used as a defense. This bill strives to cut medical costs by reducing the incidence of defensive medicine and frivolous lawsuits through the establishment of quality-promoting guidelines. At the time of the CLC, this bill had recently been introduced. There is no companion bill in the Senate.
The next CLC will be March 8-10, 2015.
Dr. Bohon is the American College of Obstetricians and Gynecologists’ D.C. Section Fellow Chair and a private practice ob.gyn. in Washington. She said she had no relevant financial disclosures. E-mail her at [email protected].
*This story was updated 4/3/2014
Repealing the Sustainable Growth Rate, gestational diabetes, more residency positions for ob.gyns., and reducing liability were on the minds of ob.gyns. at the Congressional Leadership Conference this year.
Approximately 400 ob.gyns. attended the 32nd annual American College of Obstetricians and Gynecologists Congressional Leadership Conference (CLC) in Washington, D.C., during March 2-4. Forty-nine states plus Puerto Rico; Washington, D.C.; and Ontario were represented. The attendees learned about pending legislation and subsequently lobbied their legislators in Congress for their cosponsorship of four bills.
While Congress met the April 1 deadline to avoid the 24% Medicare pay cut called for by the Sustainable Growth Rate (SGR) formula, it did so via a 1-year patch and not by passing the comprehensive reform favored by many physicians. The SGR has created financial instability in health care. More than $150 billion has been spent to avoid physician payment cuts and the temporary patch will increase that cost. CLC attendees had asked their representatives and senators to cosponsor the Sustainable Growth Rate Repeal and Medicare Provider Modernization Act of 2014 (H.R. 4015). This bill would repeal the SGR and guarantee physicians 5 years of payment increases at 0.5% per year. The House passed H.R. 4015, but a modification was introduced and passed by a voice vote. That is the bill that ultimately went to the Senate and was passed, and that President Obama signed.
The Gestational Diabetes Act of 2013 (H.R. 1915/S. 907) provides funding for research and surveillance to improve screening for gestational diabetes and track women who have this diagnosis. This disease is estimated to affect 18% of all pregnancies and is increasing in frequency, according to the American Diabetes Association. Currently, there is minimal research being conducted on gestational diabetes.
The Training Tomorrow’s Doctors Today Act of 2013 (H.R. 1201) provides for 15,000 additional residency positions over the next 5 years. Currently, Medicare pays $3 billion for resident salaries (direct graduate medical education) and $6.4 billion for the higher cost of patient care in teaching hospitals (indirect GME). The number of federally funded residency slots has not increased since 1997. It is anticipated that there will be an 18% shortage of ob.gyns. by 2030 and 25% by 2050 if there is no increase in residency positions, according to ACOG. This bill requires hospitals receiving federal funding to allocate 25% of residency slots to primary care and general surgery. In this bill, ob.gyn. is considered primary care. The Senate does not have a companion bill.
The Saving Lives, Saving Cost Act of 2014 (H.R. 4106) was introduced in the House by a Republican lawyer and a Democratic physician. This bill provides for the option of a review by an independent medical review panel in a medical malpractice case where adherence to approved clinical guidelines can be used as a defense. This bill strives to cut medical costs by reducing the incidence of defensive medicine and frivolous lawsuits through the establishment of quality-promoting guidelines. At the time of the CLC, this bill had recently been introduced. There is no companion bill in the Senate.
The next CLC will be March 8-10, 2015.
Dr. Bohon is the American College of Obstetricians and Gynecologists’ D.C. Section Fellow Chair and a private practice ob.gyn. in Washington. She said she had no relevant financial disclosures. E-mail her at [email protected].
*This story was updated 4/3/2014
Repealing the Sustainable Growth Rate, gestational diabetes, more residency positions for ob.gyns., and reducing liability were on the minds of ob.gyns. at the Congressional Leadership Conference this year.
Approximately 400 ob.gyns. attended the 32nd annual American College of Obstetricians and Gynecologists Congressional Leadership Conference (CLC) in Washington, D.C., during March 2-4. Forty-nine states plus Puerto Rico; Washington, D.C.; and Ontario were represented. The attendees learned about pending legislation and subsequently lobbied their legislators in Congress for their cosponsorship of four bills.
While Congress met the April 1 deadline to avoid the 24% Medicare pay cut called for by the Sustainable Growth Rate (SGR) formula, it did so via a 1-year patch and not by passing the comprehensive reform favored by many physicians. The SGR has created financial instability in health care. More than $150 billion has been spent to avoid physician payment cuts and the temporary patch will increase that cost. CLC attendees had asked their representatives and senators to cosponsor the Sustainable Growth Rate Repeal and Medicare Provider Modernization Act of 2014 (H.R. 4015). This bill would repeal the SGR and guarantee physicians 5 years of payment increases at 0.5% per year. The House passed H.R. 4015, but a modification was introduced and passed by a voice vote. That is the bill that ultimately went to the Senate and was passed, and that President Obama signed.
The Gestational Diabetes Act of 2013 (H.R. 1915/S. 907) provides funding for research and surveillance to improve screening for gestational diabetes and track women who have this diagnosis. This disease is estimated to affect 18% of all pregnancies and is increasing in frequency, according to the American Diabetes Association. Currently, there is minimal research being conducted on gestational diabetes.
The Training Tomorrow’s Doctors Today Act of 2013 (H.R. 1201) provides for 15,000 additional residency positions over the next 5 years. Currently, Medicare pays $3 billion for resident salaries (direct graduate medical education) and $6.4 billion for the higher cost of patient care in teaching hospitals (indirect GME). The number of federally funded residency slots has not increased since 1997. It is anticipated that there will be an 18% shortage of ob.gyns. by 2030 and 25% by 2050 if there is no increase in residency positions, according to ACOG. This bill requires hospitals receiving federal funding to allocate 25% of residency slots to primary care and general surgery. In this bill, ob.gyn. is considered primary care. The Senate does not have a companion bill.
The Saving Lives, Saving Cost Act of 2014 (H.R. 4106) was introduced in the House by a Republican lawyer and a Democratic physician. This bill provides for the option of a review by an independent medical review panel in a medical malpractice case where adherence to approved clinical guidelines can be used as a defense. This bill strives to cut medical costs by reducing the incidence of defensive medicine and frivolous lawsuits through the establishment of quality-promoting guidelines. At the time of the CLC, this bill had recently been introduced. There is no companion bill in the Senate.
The next CLC will be March 8-10, 2015.
Dr. Bohon is the American College of Obstetricians and Gynecologists’ D.C. Section Fellow Chair and a private practice ob.gyn. in Washington. She said she had no relevant financial disclosures. E-mail her at [email protected].
*This story was updated 4/3/2014

Editorial on ovarian teratoma linked to encephalitis came in handy!

Editorial on ovarian teratoma linked to encephalitis came in handy!
I enjoyed the recent editorial by Dr. Barbieri and Dr. Clark on the relationship between ovarian teratoma and encephalitis. Little did I know it would come in handy right away.
Recently, we were asked to see and operate on a 27-year-old patient with sudden onset of hallucinations, personality changes, and eventually a catatonic-like state (developed over 3 weeks but didn’t require intubation). All testing was negative for viral/bacterial encephalitis. A positive anti-N-methyl-D-aspartate (anti-NMDA)-receptor antibody screen and pelvic imaging revealed a probable teratoma in the right ovary.
We removed the right ovary. The teratoma was small but did have mature neural elements. The patient received the medical treatment outlined by Drs. Barbieri and Clark in their editorial. At the time of this writing, the patient is 3 weeks postsurgery and is talking, walking, eating, and will complete her rehab stay in the next week or so. Truly a remarkable improvement with notable progress every day.
Amazing such a case would arise shortly after I read this editorial—thank you!
John B. Gebhart, MD, MS
Mayo Clinic, Rochester, Minnesota
Dr. Barbieri responds
Dr. Clark and I thank Dr. Gebhart for alerting readers to his recent, very interesting, case of anti-NMDA-receptor antibody-induced encephalitis occurring in a woman with an ovarian teratoma. We hope that she recovers and can return to her full activities as quickly as possible.
Use supplementation, not replacement, for menopausal women
I thank Dr. Andrew M. Kaunitz for stating in his January 2014 commentary on estrogen therapy:
Human ovaries produce estradiol. Therefore, when production wanes, it makes sense to supplement (not replace!) with estradiol. That’s why I have been prescribing estradiol for many years rather than the more fashionable, trendy conjugated equine estrogens (Premarin, Pfizer).
This situation is similar to thyroid hormones. Again, we use supplementation in case of deficiency; replacement for surgical removal. Semantics is important.
Yasuo Ishida, MD
St. Louis, Missouri
Dr. Kaunitz responds
I appreciate Dr. Ishida’s thoughtful comments. It seems that in our practices, we are in agreement regarding our preferred oral estrogen.
How long should a patient push?
I don’t agree with Dr. Barbieri’s December editorial on the progress of labor. There is pushing, and then again there is pushing. All I seem to experience for my patients after 3 hours is marked perineal edema, not to mention the challenge of an impacted head when ultimately one does proceed with cesarean delivery. Persisting for more than 5 hours is not for me—or my patients.
Eugene Scioscia Jr., MD
Pittsburgh, Pennsylvania
Dr. Barbieri responds
I agree with Dr. Scioscia: Extending the hours of pushing is often accompanied by increasing edema and tissue friability in the birth canal and perineum.
The length of the second stage is not synonymous with “hours of pushing” and the data presented in the editorial focused on the length of the second stage.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about this or other current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected] Please include your name, city and state.
Editorial on ovarian teratoma linked to encephalitis came in handy!
I enjoyed the recent editorial by Dr. Barbieri and Dr. Clark on the relationship between ovarian teratoma and encephalitis. Little did I know it would come in handy right away.
Recently, we were asked to see and operate on a 27-year-old patient with sudden onset of hallucinations, personality changes, and eventually a catatonic-like state (developed over 3 weeks but didn’t require intubation). All testing was negative for viral/bacterial encephalitis. A positive anti-N-methyl-D-aspartate (anti-NMDA)-receptor antibody screen and pelvic imaging revealed a probable teratoma in the right ovary.
We removed the right ovary. The teratoma was small but did have mature neural elements. The patient received the medical treatment outlined by Drs. Barbieri and Clark in their editorial. At the time of this writing, the patient is 3 weeks postsurgery and is talking, walking, eating, and will complete her rehab stay in the next week or so. Truly a remarkable improvement with notable progress every day.
Amazing such a case would arise shortly after I read this editorial—thank you!
John B. Gebhart, MD, MS
Mayo Clinic, Rochester, Minnesota
Dr. Barbieri responds
Dr. Clark and I thank Dr. Gebhart for alerting readers to his recent, very interesting, case of anti-NMDA-receptor antibody-induced encephalitis occurring in a woman with an ovarian teratoma. We hope that she recovers and can return to her full activities as quickly as possible.
Use supplementation, not replacement, for menopausal women
I thank Dr. Andrew M. Kaunitz for stating in his January 2014 commentary on estrogen therapy:
Human ovaries produce estradiol. Therefore, when production wanes, it makes sense to supplement (not replace!) with estradiol. That’s why I have been prescribing estradiol for many years rather than the more fashionable, trendy conjugated equine estrogens (Premarin, Pfizer).
This situation is similar to thyroid hormones. Again, we use supplementation in case of deficiency; replacement for surgical removal. Semantics is important.
Yasuo Ishida, MD
St. Louis, Missouri
Dr. Kaunitz responds
I appreciate Dr. Ishida’s thoughtful comments. It seems that in our practices, we are in agreement regarding our preferred oral estrogen.
How long should a patient push?
I don’t agree with Dr. Barbieri’s December editorial on the progress of labor. There is pushing, and then again there is pushing. All I seem to experience for my patients after 3 hours is marked perineal edema, not to mention the challenge of an impacted head when ultimately one does proceed with cesarean delivery. Persisting for more than 5 hours is not for me—or my patients.
Eugene Scioscia Jr., MD
Pittsburgh, Pennsylvania
Dr. Barbieri responds
I agree with Dr. Scioscia: Extending the hours of pushing is often accompanied by increasing edema and tissue friability in the birth canal and perineum.
The length of the second stage is not synonymous with “hours of pushing” and the data presented in the editorial focused on the length of the second stage.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about this or other current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected] Please include your name, city and state.
Editorial on ovarian teratoma linked to encephalitis came in handy!
I enjoyed the recent editorial by Dr. Barbieri and Dr. Clark on the relationship between ovarian teratoma and encephalitis. Little did I know it would come in handy right away.
Recently, we were asked to see and operate on a 27-year-old patient with sudden onset of hallucinations, personality changes, and eventually a catatonic-like state (developed over 3 weeks but didn’t require intubation). All testing was negative for viral/bacterial encephalitis. A positive anti-N-methyl-D-aspartate (anti-NMDA)-receptor antibody screen and pelvic imaging revealed a probable teratoma in the right ovary.
We removed the right ovary. The teratoma was small but did have mature neural elements. The patient received the medical treatment outlined by Drs. Barbieri and Clark in their editorial. At the time of this writing, the patient is 3 weeks postsurgery and is talking, walking, eating, and will complete her rehab stay in the next week or so. Truly a remarkable improvement with notable progress every day.
Amazing such a case would arise shortly after I read this editorial—thank you!
John B. Gebhart, MD, MS
Mayo Clinic, Rochester, Minnesota
Dr. Barbieri responds
Dr. Clark and I thank Dr. Gebhart for alerting readers to his recent, very interesting, case of anti-NMDA-receptor antibody-induced encephalitis occurring in a woman with an ovarian teratoma. We hope that she recovers and can return to her full activities as quickly as possible.
Use supplementation, not replacement, for menopausal women
I thank Dr. Andrew M. Kaunitz for stating in his January 2014 commentary on estrogen therapy:
Human ovaries produce estradiol. Therefore, when production wanes, it makes sense to supplement (not replace!) with estradiol. That’s why I have been prescribing estradiol for many years rather than the more fashionable, trendy conjugated equine estrogens (Premarin, Pfizer).
This situation is similar to thyroid hormones. Again, we use supplementation in case of deficiency; replacement for surgical removal. Semantics is important.
Yasuo Ishida, MD
St. Louis, Missouri
Dr. Kaunitz responds
I appreciate Dr. Ishida’s thoughtful comments. It seems that in our practices, we are in agreement regarding our preferred oral estrogen.
How long should a patient push?
I don’t agree with Dr. Barbieri’s December editorial on the progress of labor. There is pushing, and then again there is pushing. All I seem to experience for my patients after 3 hours is marked perineal edema, not to mention the challenge of an impacted head when ultimately one does proceed with cesarean delivery. Persisting for more than 5 hours is not for me—or my patients.
Eugene Scioscia Jr., MD
Pittsburgh, Pennsylvania
Dr. Barbieri responds
I agree with Dr. Scioscia: Extending the hours of pushing is often accompanied by increasing edema and tissue friability in the birth canal and perineum.
The length of the second stage is not synonymous with “hours of pushing” and the data presented in the editorial focused on the length of the second stage.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about this or other current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected] Please include your name, city and state.