User login
Discontinuing Disease-Modifying Therapies in Nonactive Secondary Progressive MS:Review of the Evidence
Multiple sclerosis (MS) is an immune-mediated demyelinating disorder. There are 2 broad categories of MS: relapsing, also called active MS; and progressive MS. Unfortunately, there is no cure for MS, but disease-modifying therapies (DMTs) can help prevent relapses and new central nervous system lesions in people living with active MS. For patients with the most common type of MS, relapsing-remitting MS (RRMS), DMTs are typically continued for decades while the patient has active disease. RRMS will usually transition to secondary progressive MS (SPMS), which can present as active SPMS or nonactive SPMS. The latter is the type of MS most people with RRMS eventually experience.
A 2019 study estimated that nearly 1 million people in the United States were living with MS.1 This population estimate indicated the peak age-specific prevalence of MS was 55 to 64 years. Population data demonstrate improved mortality rates for people diagnosed with MS from 1997 to 2012 compared with prior years.2 Therefore, the management of nonactive SPMS is an increasingly significant area of need. There are currently no DMTs on the market approved for nonactive SPMS, and lifelong DMTs in these patients are neither indicated nor supported by evidence. Nevertheless, the discontinuation of DMTs in nonactive SPMS has been a long-debated topic with varied opinions on how and when to discontinue.
The 2018 American Academy of Neurology (AAN) guideline recommends that clinicians advise patients with SPMS to discontinue DMT use if they do not have ongoing relapses (or gadolinium-enhanced lesions on magnetic resonance imaging activity) or have not been ambulatory (Expanded Disability Status Scale [EDSS] ≥ 7) for ≥ 2 years.3 In recent years, there has been increased research on nonactive SPMS, specifically on discontinuation of DMTs. This clinical review assesses the recent evidence from a variety of standpoints, including the effect of discontinuing DMTs on the MS disease course and quality of life (QOL) and the perspectives of patients living with MS. Based on this evidence, a conversation guide will be presented as a framework to aid with the clinician-patient discussion on discontinuing MS DMTs.
Disease Modifying Therapies
Roos and colleagues used data from 2 large MS cohorts: MSBase and Observatoire Français de la Sclérose en Plaques (OFSEP) to compare high-efficacy vs low-efficacy DMT in both active and nonactive SPMS.4 In the active SPMS group, the strength of DMTs did not change disability progression, but high-efficacy DMTs reduced relapses better than the low-efficacy DMTs. On the other hand, the nonactive SPMS group saw no difference between DMTs in both relapse risk and disability progression. Another observational study of 221 patients with RRMS who discontinued DMTs noted that there were 2 independent predictors for the absence of relapse following DMT discontinuation: being aged > 45 years and the lack of relapse for ≥ 4 years prior to DMT discontinuation.5 Though these patients still may have been classified as RRMS, both these independent predictors for stability postdiscontinuation of DMTs are the typical characteristics of a nonactive SPMS patient.
Pathophysiology may help explain why DMT discontinuation seems to produce no adverse clinical outcomes in people with nonactive SPMS. Nonactive SPMS, which follows after RRMS, is largely correlated with age. In nonactive SPMS, there is less B and T lymphocyte migration across the blood-brain barrier. Furthermore, a lifetime of low-grade inflammation during the RRMS phase results in axonal damage and declined repair capacity, which produces the predominance of neurodegeneration in the nonactive SPMS disease process.6 This pathophysiologic difference between active and nonactive disease not only explains the different symptomatology of these MS subtypes, but also could explain why drugs that target the inflammatory processes more characteristic of active disease are not effective in nonactive SPMS.
Other recent studies explored the impact of age on DMT efficacy for patients with nonactive SPMS. A meta-analysis by Weidman and colleagues pooled trial data across multiple DMT classes in > 28,000 patients.7 The resulting regression model predicted zero efficacy of any DMT in patients who are aged > 53 years. High-efficacy DMTs only outperformed low-efficacy DMTs in people aged < 40.5 years. Another observational study by Hua and colleagues saw a similar result.8 This study included patients who discontinued DMT who were aged ≥ 60 years. The median follow-up time was 5.3 years. Of the 178 patients who discontinued DMTs, only 1 patient had a relapse. In this study, the age for participation provided a higher likelihood that patients included were in nonactive SPMS. Furthermore, the outcome reflects the typical presentation of nonactive SPMS where, despite the continuation or discontinuation of DMT, there was a lack of relapses. When comparing patients who discontinued DMTs with those who continued use, there was no significant difference in their 25-foot walk times, which is an objective marker for a more progressive symptom seen in nonactive MS.
The DISCOMS trial (NCT03073603) has been completed, but full results are not yet published. In this noninferiority trial, > 250 patients aged ≥ 55 years were assessed on a variety of outcomes, including relapses, EDSS score, and QOL. MS subtypes were considered at baseline, and subgroup analysis looking particularly at the SPMS population could provide further insight into its effect on MS course.
Quality of Life
Whether discontinuation of DMTs is worth considering in nonactive SPMS, it is also important to consider the risks and burdens associated with continuation. Medication administration burdens come with all MS DMTs whether there is the need to inject oneself, increased pill burden, or travel to an infusion clinic. The ever-rising costs of DMTs also can be a financial burden to the patient.9 All MS DMTs carry risks of adverse effects (AEs). These can range from a mild injection site reaction to severe infection, depending on the DMT used. Many of these severe AEs, such as opportunistic infections and cancer, have been associated with either an increased risk of occurrence and/or worsened outcomes in older adults who remain on DMTs, particularly moderate- to high-efficacy DMTs, such as sphingosine-1- phosphate receptor modulators, fumarates, natalizumab, alemtuzumab, cladribine, and anti-CD20 antibodies.10 In a 2019 survey of 377 patients with MS, 63.8% of respondents ranked safety as the most important reason they would consider discontinuing their DMTs.11 In addition, a real-world study comparing people with nonactive SPMS who continued DMTs vs those who discontinued found that discontinuers reported better QOL.8
Conversation Guide for Discontinuing Therapies
The 2019 survey that assessed reasons for discontinuation also asked people with nonactive SPMS whether they thought they were in a nonactive disease stage, and what was their likelihood they would stop DMTs.11 Interestingly, only 59.4% of respondents self-assessed their MS as nonactive, and just 11.9% of respondents were willing to discontinue DMTs.11 These results suggest that there may be a need for patient education about nonactive SPMS and the rationale to continue or discontinue DMTs. Thus, before broaching the topic of discontinuation, explaining the nonactive SPMS subtype is important.
Even with a good understanding of nonactive SPMS, patients may be hesitant to stop using DMTs that they previously relied on to keep their MS stable. The 2019 survey ranked physician recommendation as the third highest reason to discontinue DMTs.11 Taking the time to explain the clinical evidence for DMT discontinuation may help patients better understand a clinician’s recommendation and inspire more confidence.
Another important aspect of DMT discontinuation decision making is creating a plan for how the patient will be monitored to provide assurance if they experience a relapse. The 2019 survey asked patients what would be most important to them for their management plan after discontinuing DMT; magnetic resonance imaging and neurologic examination monitoring ranked the highest.11 The plan should include timing for follow-up appointments and imaging, providing the patient comfort in knowing their MS will be monitored and verified for the relapse stability that is expected from nonactive SPMS. In the rare case a relapse does occur, having a contingency plan and noting the possibility of restarting DMTs is an integral part of reassuring the patient that their decision to discontinue DMTs will be treated with the utmost caution and individualized to their needs.
Lastly, highlighting which aspects of MS treatment will continue to be a priority in nonactive SPMS, such as symptomatic medication management and nonpharmacologic therapy, is important for the patient to recognize that there are still opportunities to manage this phase of MS. There are many lifestyle modifications that can be considered complementary to medical management of MS at any stage of the disease. Vascular comorbidities, such as hypertension, hyperlipidemia, and diabetes, have been associated with more rapid disability progression in MS.12 Optimized management of these diseases may slow disability progression, in addition to the benefit of improved outcomes of the vascular comorbidity. Various formats of exercise have been studied in the MS population. A meta-analysis of aerobic, resistance, and combined exercise found benefits in these formats on health-related QOL.13
Many dietary strategies have been studied in MS. A recent network meta-analysis reviewed some of the more commonly studied diets, including low-fat, modified Mediterranean, ketogenic, anti-inflammatory, Paleolithic, intermittent fasting, and calorie restriction vs a usual diet.14 Although the overall quality of evidence was low, the Paleolithic and modified Mediterranean showed greater reductions in fatigue, as well as increased physical and
As with any health care decision, it is important to involve the patient in a joint decision regarding their care. This may mean giving the patient time to think about the information presented, do their own research, talk to family members or other clinicians, etc. The decision to discontinue DMT may not happen at the same appointment it is initially brought up at. It may even be reasonable to revisit the conversation later if discontinuation is not something the patient is amenable to at the time.
Conclusions
There is high-quality evidence that discontinuing DMTs in nonactive SPMS is not a major detriment to the MS disease course. Current literature also suggests that there may be benefits to discontinuation in this MS subtype in terms of QOL and meeting patient values. Additional research particularly in the nonactive SPMS population will continue to improve the knowledge and awareness of this aspect of MS DMT management. The growing evidence in this area may make discontinuation of DMT in nonactive SPMS a less-debatable topic, but it is still a major treatment decision that clinicians must thoroughly discuss with the patient to provide high-quality, patient-centered care.
1. Wallin MT, Culpepper WJ, Campbell JD, et al. The prevalence of MS in the United States: a population-based estimate using health claims data. Neurology. 2019;92(10):e1029-e1040. doi:10.1212/WNL.0000000000007035
2. Lunde HMB, Assmus J, Myhr KM, Bø L, Grytten N. Survival and cause of death in multiple sclerosis: a 60-year longitudinal population study. J Neurol Neurosurg Psychiatry. 2017;88(8):621-625. doi:10.1136/jnnp-2016-315238
3. Rae-Grant A, Day GS, Marrie RA, et al. Practice guideline recommendations summary: disease-modifying therapies for adults with multiple sclerosis: report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology. 2018;90(17):777-788. doi:10.1212/WNL.0000000000005347
4. Roos I, Leray E, Casey R, et al. Effects of high- and low-efficacy therapy in secondary progressive multiple sclerosis. Neurology. 2021;97(9):e869-e880. doi:10.1212/WNL.0000000000012354
5. Bsteh G, Feige J, Ehling R, et al. Discontinuation of disease-modifying therapies in multiple sclerosis - clinical outcome and prognostic factors. Mult Scler. 2017;23(9):1241-1248. doi:10.1177/1352458516675751
6. Musella A, Gentile A, Rizzo FR, et al. Interplay between age and neuroinflammation in multiple sclerosis: effects on motor and cognitive functions. Front Aging Neurosci. 2018;10:238. Published 2018 Aug 8. doi:10.3389/fnagi.2018.00238
7. Weideman AM, Tapia-Maltos MA, Johnson K, Greenwood M, Bielekova B. Meta-analysis of the age-dependent efficacy of multiple sclerosis treatments. Front Neurol. 2017;8:577. Published 2017 Nov 10. doi:10.3389/fneur.2017.00577
8. Hua LH, Harris H, Conway D, Thompson NR. Changes in patient-reported outcomes between continuers and discontinuers of disease modifying therapy in patients with multiple sclerosis over age 60. Mult Scler Relat Disord. 2019;30:252-256. doi:10.1016/j.msard.2019.02.028
9. San-Juan-Rodriguez A, Good CB, Heyman RA, Parekh N, Shrank WH, Hernandez I. Trends in prices, market share, and spending on self-administered disease-modifying therapies for multiple sclerosis in Medicare part D. JAMA Neurol. 2019;76(11):1386-1390. doi:10.1001/jamaneurol.2019.2711
10. Schweitzer F, Laurent S, Fink GR, et al. Age and the risks of high-efficacy disease modifying drugs in multiple sclerosis. Curr Opin Neurol. 2019;32(3):305-312. doi:10.1097/WCO.0000000000000701
11. McGinley MP, Cola PA, Fox RJ, Cohen JA, Corboy JJ, Miller D. Perspectives of individuals with multiple sclerosis on discontinuation of disease-modifying therapies. Mult Scler. 2020;26(12):1581-1589. doi:10.1177/1352458519867314
12. Marrie RA, Rudick R, Horwitz R, et al. Vascular comorbidity is associated with more rapid disability progression in multiple sclerosis. Neurology. 2010;74(13):1041-1047. doi:10.1212/WNL.0b013e3181d6b125
13. Flores VA, Šilic´ P, DuBose NG, Zheng P, Jeng B, Motl RW. Effects of aerobic, resistance, and combined exercise training on health-related quality of life in multiple sclerosis: Systematic review and meta-analysis. Mult Scler Relat Disord. 2023;75:104746. doi:10.1016/j.msard.2023.104746
14. Snetselaar LG, Cheek JJ, Fox SS, et al. Efficacy of diet on fatigue and quality of life in multiple sclerosis: a systematic review and network meta-analysis of randomized trials. Neurology. 2023;100(4):e357-e366. doi:10.1212/WNL.0000000000201371
Multiple sclerosis (MS) is an immune-mediated demyelinating disorder. There are 2 broad categories of MS: relapsing, also called active MS; and progressive MS. Unfortunately, there is no cure for MS, but disease-modifying therapies (DMTs) can help prevent relapses and new central nervous system lesions in people living with active MS. For patients with the most common type of MS, relapsing-remitting MS (RRMS), DMTs are typically continued for decades while the patient has active disease. RRMS will usually transition to secondary progressive MS (SPMS), which can present as active SPMS or nonactive SPMS. The latter is the type of MS most people with RRMS eventually experience.
A 2019 study estimated that nearly 1 million people in the United States were living with MS.1 This population estimate indicated the peak age-specific prevalence of MS was 55 to 64 years. Population data demonstrate improved mortality rates for people diagnosed with MS from 1997 to 2012 compared with prior years.2 Therefore, the management of nonactive SPMS is an increasingly significant area of need. There are currently no DMTs on the market approved for nonactive SPMS, and lifelong DMTs in these patients are neither indicated nor supported by evidence. Nevertheless, the discontinuation of DMTs in nonactive SPMS has been a long-debated topic with varied opinions on how and when to discontinue.
The 2018 American Academy of Neurology (AAN) guideline recommends that clinicians advise patients with SPMS to discontinue DMT use if they do not have ongoing relapses (or gadolinium-enhanced lesions on magnetic resonance imaging activity) or have not been ambulatory (Expanded Disability Status Scale [EDSS] ≥ 7) for ≥ 2 years.3 In recent years, there has been increased research on nonactive SPMS, specifically on discontinuation of DMTs. This clinical review assesses the recent evidence from a variety of standpoints, including the effect of discontinuing DMTs on the MS disease course and quality of life (QOL) and the perspectives of patients living with MS. Based on this evidence, a conversation guide will be presented as a framework to aid with the clinician-patient discussion on discontinuing MS DMTs.
Disease Modifying Therapies
Roos and colleagues used data from 2 large MS cohorts: MSBase and Observatoire Français de la Sclérose en Plaques (OFSEP) to compare high-efficacy vs low-efficacy DMT in both active and nonactive SPMS.4 In the active SPMS group, the strength of DMTs did not change disability progression, but high-efficacy DMTs reduced relapses better than the low-efficacy DMTs. On the other hand, the nonactive SPMS group saw no difference between DMTs in both relapse risk and disability progression. Another observational study of 221 patients with RRMS who discontinued DMTs noted that there were 2 independent predictors for the absence of relapse following DMT discontinuation: being aged > 45 years and the lack of relapse for ≥ 4 years prior to DMT discontinuation.5 Though these patients still may have been classified as RRMS, both these independent predictors for stability postdiscontinuation of DMTs are the typical characteristics of a nonactive SPMS patient.
Pathophysiology may help explain why DMT discontinuation seems to produce no adverse clinical outcomes in people with nonactive SPMS. Nonactive SPMS, which follows after RRMS, is largely correlated with age. In nonactive SPMS, there is less B and T lymphocyte migration across the blood-brain barrier. Furthermore, a lifetime of low-grade inflammation during the RRMS phase results in axonal damage and declined repair capacity, which produces the predominance of neurodegeneration in the nonactive SPMS disease process.6 This pathophysiologic difference between active and nonactive disease not only explains the different symptomatology of these MS subtypes, but also could explain why drugs that target the inflammatory processes more characteristic of active disease are not effective in nonactive SPMS.
Other recent studies explored the impact of age on DMT efficacy for patients with nonactive SPMS. A meta-analysis by Weidman and colleagues pooled trial data across multiple DMT classes in > 28,000 patients.7 The resulting regression model predicted zero efficacy of any DMT in patients who are aged > 53 years. High-efficacy DMTs only outperformed low-efficacy DMTs in people aged < 40.5 years. Another observational study by Hua and colleagues saw a similar result.8 This study included patients who discontinued DMT who were aged ≥ 60 years. The median follow-up time was 5.3 years. Of the 178 patients who discontinued DMTs, only 1 patient had a relapse. In this study, the age for participation provided a higher likelihood that patients included were in nonactive SPMS. Furthermore, the outcome reflects the typical presentation of nonactive SPMS where, despite the continuation or discontinuation of DMT, there was a lack of relapses. When comparing patients who discontinued DMTs with those who continued use, there was no significant difference in their 25-foot walk times, which is an objective marker for a more progressive symptom seen in nonactive MS.
The DISCOMS trial (NCT03073603) has been completed, but full results are not yet published. In this noninferiority trial, > 250 patients aged ≥ 55 years were assessed on a variety of outcomes, including relapses, EDSS score, and QOL. MS subtypes were considered at baseline, and subgroup analysis looking particularly at the SPMS population could provide further insight into its effect on MS course.
Quality of Life
Whether discontinuation of DMTs is worth considering in nonactive SPMS, it is also important to consider the risks and burdens associated with continuation. Medication administration burdens come with all MS DMTs whether there is the need to inject oneself, increased pill burden, or travel to an infusion clinic. The ever-rising costs of DMTs also can be a financial burden to the patient.9 All MS DMTs carry risks of adverse effects (AEs). These can range from a mild injection site reaction to severe infection, depending on the DMT used. Many of these severe AEs, such as opportunistic infections and cancer, have been associated with either an increased risk of occurrence and/or worsened outcomes in older adults who remain on DMTs, particularly moderate- to high-efficacy DMTs, such as sphingosine-1- phosphate receptor modulators, fumarates, natalizumab, alemtuzumab, cladribine, and anti-CD20 antibodies.10 In a 2019 survey of 377 patients with MS, 63.8% of respondents ranked safety as the most important reason they would consider discontinuing their DMTs.11 In addition, a real-world study comparing people with nonactive SPMS who continued DMTs vs those who discontinued found that discontinuers reported better QOL.8
Conversation Guide for Discontinuing Therapies
The 2019 survey that assessed reasons for discontinuation also asked people with nonactive SPMS whether they thought they were in a nonactive disease stage, and what was their likelihood they would stop DMTs.11 Interestingly, only 59.4% of respondents self-assessed their MS as nonactive, and just 11.9% of respondents were willing to discontinue DMTs.11 These results suggest that there may be a need for patient education about nonactive SPMS and the rationale to continue or discontinue DMTs. Thus, before broaching the topic of discontinuation, explaining the nonactive SPMS subtype is important.
Even with a good understanding of nonactive SPMS, patients may be hesitant to stop using DMTs that they previously relied on to keep their MS stable. The 2019 survey ranked physician recommendation as the third highest reason to discontinue DMTs.11 Taking the time to explain the clinical evidence for DMT discontinuation may help patients better understand a clinician’s recommendation and inspire more confidence.
Another important aspect of DMT discontinuation decision making is creating a plan for how the patient will be monitored to provide assurance if they experience a relapse. The 2019 survey asked patients what would be most important to them for their management plan after discontinuing DMT; magnetic resonance imaging and neurologic examination monitoring ranked the highest.11 The plan should include timing for follow-up appointments and imaging, providing the patient comfort in knowing their MS will be monitored and verified for the relapse stability that is expected from nonactive SPMS. In the rare case a relapse does occur, having a contingency plan and noting the possibility of restarting DMTs is an integral part of reassuring the patient that their decision to discontinue DMTs will be treated with the utmost caution and individualized to their needs.
Lastly, highlighting which aspects of MS treatment will continue to be a priority in nonactive SPMS, such as symptomatic medication management and nonpharmacologic therapy, is important for the patient to recognize that there are still opportunities to manage this phase of MS. There are many lifestyle modifications that can be considered complementary to medical management of MS at any stage of the disease. Vascular comorbidities, such as hypertension, hyperlipidemia, and diabetes, have been associated with more rapid disability progression in MS.12 Optimized management of these diseases may slow disability progression, in addition to the benefit of improved outcomes of the vascular comorbidity. Various formats of exercise have been studied in the MS population. A meta-analysis of aerobic, resistance, and combined exercise found benefits in these formats on health-related QOL.13
Many dietary strategies have been studied in MS. A recent network meta-analysis reviewed some of the more commonly studied diets, including low-fat, modified Mediterranean, ketogenic, anti-inflammatory, Paleolithic, intermittent fasting, and calorie restriction vs a usual diet.14 Although the overall quality of evidence was low, the Paleolithic and modified Mediterranean showed greater reductions in fatigue, as well as increased physical and
As with any health care decision, it is important to involve the patient in a joint decision regarding their care. This may mean giving the patient time to think about the information presented, do their own research, talk to family members or other clinicians, etc. The decision to discontinue DMT may not happen at the same appointment it is initially brought up at. It may even be reasonable to revisit the conversation later if discontinuation is not something the patient is amenable to at the time.
Conclusions
There is high-quality evidence that discontinuing DMTs in nonactive SPMS is not a major detriment to the MS disease course. Current literature also suggests that there may be benefits to discontinuation in this MS subtype in terms of QOL and meeting patient values. Additional research particularly in the nonactive SPMS population will continue to improve the knowledge and awareness of this aspect of MS DMT management. The growing evidence in this area may make discontinuation of DMT in nonactive SPMS a less-debatable topic, but it is still a major treatment decision that clinicians must thoroughly discuss with the patient to provide high-quality, patient-centered care.
Multiple sclerosis (MS) is an immune-mediated demyelinating disorder. There are 2 broad categories of MS: relapsing, also called active MS; and progressive MS. Unfortunately, there is no cure for MS, but disease-modifying therapies (DMTs) can help prevent relapses and new central nervous system lesions in people living with active MS. For patients with the most common type of MS, relapsing-remitting MS (RRMS), DMTs are typically continued for decades while the patient has active disease. RRMS will usually transition to secondary progressive MS (SPMS), which can present as active SPMS or nonactive SPMS. The latter is the type of MS most people with RRMS eventually experience.
A 2019 study estimated that nearly 1 million people in the United States were living with MS.1 This population estimate indicated the peak age-specific prevalence of MS was 55 to 64 years. Population data demonstrate improved mortality rates for people diagnosed with MS from 1997 to 2012 compared with prior years.2 Therefore, the management of nonactive SPMS is an increasingly significant area of need. There are currently no DMTs on the market approved for nonactive SPMS, and lifelong DMTs in these patients are neither indicated nor supported by evidence. Nevertheless, the discontinuation of DMTs in nonactive SPMS has been a long-debated topic with varied opinions on how and when to discontinue.
The 2018 American Academy of Neurology (AAN) guideline recommends that clinicians advise patients with SPMS to discontinue DMT use if they do not have ongoing relapses (or gadolinium-enhanced lesions on magnetic resonance imaging activity) or have not been ambulatory (Expanded Disability Status Scale [EDSS] ≥ 7) for ≥ 2 years.3 In recent years, there has been increased research on nonactive SPMS, specifically on discontinuation of DMTs. This clinical review assesses the recent evidence from a variety of standpoints, including the effect of discontinuing DMTs on the MS disease course and quality of life (QOL) and the perspectives of patients living with MS. Based on this evidence, a conversation guide will be presented as a framework to aid with the clinician-patient discussion on discontinuing MS DMTs.
Disease Modifying Therapies
Roos and colleagues used data from 2 large MS cohorts: MSBase and Observatoire Français de la Sclérose en Plaques (OFSEP) to compare high-efficacy vs low-efficacy DMT in both active and nonactive SPMS.4 In the active SPMS group, the strength of DMTs did not change disability progression, but high-efficacy DMTs reduced relapses better than the low-efficacy DMTs. On the other hand, the nonactive SPMS group saw no difference between DMTs in both relapse risk and disability progression. Another observational study of 221 patients with RRMS who discontinued DMTs noted that there were 2 independent predictors for the absence of relapse following DMT discontinuation: being aged > 45 years and the lack of relapse for ≥ 4 years prior to DMT discontinuation.5 Though these patients still may have been classified as RRMS, both these independent predictors for stability postdiscontinuation of DMTs are the typical characteristics of a nonactive SPMS patient.
Pathophysiology may help explain why DMT discontinuation seems to produce no adverse clinical outcomes in people with nonactive SPMS. Nonactive SPMS, which follows after RRMS, is largely correlated with age. In nonactive SPMS, there is less B and T lymphocyte migration across the blood-brain barrier. Furthermore, a lifetime of low-grade inflammation during the RRMS phase results in axonal damage and declined repair capacity, which produces the predominance of neurodegeneration in the nonactive SPMS disease process.6 This pathophysiologic difference between active and nonactive disease not only explains the different symptomatology of these MS subtypes, but also could explain why drugs that target the inflammatory processes more characteristic of active disease are not effective in nonactive SPMS.
Other recent studies explored the impact of age on DMT efficacy for patients with nonactive SPMS. A meta-analysis by Weidman and colleagues pooled trial data across multiple DMT classes in > 28,000 patients.7 The resulting regression model predicted zero efficacy of any DMT in patients who are aged > 53 years. High-efficacy DMTs only outperformed low-efficacy DMTs in people aged < 40.5 years. Another observational study by Hua and colleagues saw a similar result.8 This study included patients who discontinued DMT who were aged ≥ 60 years. The median follow-up time was 5.3 years. Of the 178 patients who discontinued DMTs, only 1 patient had a relapse. In this study, the age for participation provided a higher likelihood that patients included were in nonactive SPMS. Furthermore, the outcome reflects the typical presentation of nonactive SPMS where, despite the continuation or discontinuation of DMT, there was a lack of relapses. When comparing patients who discontinued DMTs with those who continued use, there was no significant difference in their 25-foot walk times, which is an objective marker for a more progressive symptom seen in nonactive MS.
The DISCOMS trial (NCT03073603) has been completed, but full results are not yet published. In this noninferiority trial, > 250 patients aged ≥ 55 years were assessed on a variety of outcomes, including relapses, EDSS score, and QOL. MS subtypes were considered at baseline, and subgroup analysis looking particularly at the SPMS population could provide further insight into its effect on MS course.
Quality of Life
Whether discontinuation of DMTs is worth considering in nonactive SPMS, it is also important to consider the risks and burdens associated with continuation. Medication administration burdens come with all MS DMTs whether there is the need to inject oneself, increased pill burden, or travel to an infusion clinic. The ever-rising costs of DMTs also can be a financial burden to the patient.9 All MS DMTs carry risks of adverse effects (AEs). These can range from a mild injection site reaction to severe infection, depending on the DMT used. Many of these severe AEs, such as opportunistic infections and cancer, have been associated with either an increased risk of occurrence and/or worsened outcomes in older adults who remain on DMTs, particularly moderate- to high-efficacy DMTs, such as sphingosine-1- phosphate receptor modulators, fumarates, natalizumab, alemtuzumab, cladribine, and anti-CD20 antibodies.10 In a 2019 survey of 377 patients with MS, 63.8% of respondents ranked safety as the most important reason they would consider discontinuing their DMTs.11 In addition, a real-world study comparing people with nonactive SPMS who continued DMTs vs those who discontinued found that discontinuers reported better QOL.8
Conversation Guide for Discontinuing Therapies
The 2019 survey that assessed reasons for discontinuation also asked people with nonactive SPMS whether they thought they were in a nonactive disease stage, and what was their likelihood they would stop DMTs.11 Interestingly, only 59.4% of respondents self-assessed their MS as nonactive, and just 11.9% of respondents were willing to discontinue DMTs.11 These results suggest that there may be a need for patient education about nonactive SPMS and the rationale to continue or discontinue DMTs. Thus, before broaching the topic of discontinuation, explaining the nonactive SPMS subtype is important.
Even with a good understanding of nonactive SPMS, patients may be hesitant to stop using DMTs that they previously relied on to keep their MS stable. The 2019 survey ranked physician recommendation as the third highest reason to discontinue DMTs.11 Taking the time to explain the clinical evidence for DMT discontinuation may help patients better understand a clinician’s recommendation and inspire more confidence.
Another important aspect of DMT discontinuation decision making is creating a plan for how the patient will be monitored to provide assurance if they experience a relapse. The 2019 survey asked patients what would be most important to them for their management plan after discontinuing DMT; magnetic resonance imaging and neurologic examination monitoring ranked the highest.11 The plan should include timing for follow-up appointments and imaging, providing the patient comfort in knowing their MS will be monitored and verified for the relapse stability that is expected from nonactive SPMS. In the rare case a relapse does occur, having a contingency plan and noting the possibility of restarting DMTs is an integral part of reassuring the patient that their decision to discontinue DMTs will be treated with the utmost caution and individualized to their needs.
Lastly, highlighting which aspects of MS treatment will continue to be a priority in nonactive SPMS, such as symptomatic medication management and nonpharmacologic therapy, is important for the patient to recognize that there are still opportunities to manage this phase of MS. There are many lifestyle modifications that can be considered complementary to medical management of MS at any stage of the disease. Vascular comorbidities, such as hypertension, hyperlipidemia, and diabetes, have been associated with more rapid disability progression in MS.12 Optimized management of these diseases may slow disability progression, in addition to the benefit of improved outcomes of the vascular comorbidity. Various formats of exercise have been studied in the MS population. A meta-analysis of aerobic, resistance, and combined exercise found benefits in these formats on health-related QOL.13
Many dietary strategies have been studied in MS. A recent network meta-analysis reviewed some of the more commonly studied diets, including low-fat, modified Mediterranean, ketogenic, anti-inflammatory, Paleolithic, intermittent fasting, and calorie restriction vs a usual diet.14 Although the overall quality of evidence was low, the Paleolithic and modified Mediterranean showed greater reductions in fatigue, as well as increased physical and
As with any health care decision, it is important to involve the patient in a joint decision regarding their care. This may mean giving the patient time to think about the information presented, do their own research, talk to family members or other clinicians, etc. The decision to discontinue DMT may not happen at the same appointment it is initially brought up at. It may even be reasonable to revisit the conversation later if discontinuation is not something the patient is amenable to at the time.
Conclusions
There is high-quality evidence that discontinuing DMTs in nonactive SPMS is not a major detriment to the MS disease course. Current literature also suggests that there may be benefits to discontinuation in this MS subtype in terms of QOL and meeting patient values. Additional research particularly in the nonactive SPMS population will continue to improve the knowledge and awareness of this aspect of MS DMT management. The growing evidence in this area may make discontinuation of DMT in nonactive SPMS a less-debatable topic, but it is still a major treatment decision that clinicians must thoroughly discuss with the patient to provide high-quality, patient-centered care.
1. Wallin MT, Culpepper WJ, Campbell JD, et al. The prevalence of MS in the United States: a population-based estimate using health claims data. Neurology. 2019;92(10):e1029-e1040. doi:10.1212/WNL.0000000000007035
2. Lunde HMB, Assmus J, Myhr KM, Bø L, Grytten N. Survival and cause of death in multiple sclerosis: a 60-year longitudinal population study. J Neurol Neurosurg Psychiatry. 2017;88(8):621-625. doi:10.1136/jnnp-2016-315238
3. Rae-Grant A, Day GS, Marrie RA, et al. Practice guideline recommendations summary: disease-modifying therapies for adults with multiple sclerosis: report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology. 2018;90(17):777-788. doi:10.1212/WNL.0000000000005347
4. Roos I, Leray E, Casey R, et al. Effects of high- and low-efficacy therapy in secondary progressive multiple sclerosis. Neurology. 2021;97(9):e869-e880. doi:10.1212/WNL.0000000000012354
5. Bsteh G, Feige J, Ehling R, et al. Discontinuation of disease-modifying therapies in multiple sclerosis - clinical outcome and prognostic factors. Mult Scler. 2017;23(9):1241-1248. doi:10.1177/1352458516675751
6. Musella A, Gentile A, Rizzo FR, et al. Interplay between age and neuroinflammation in multiple sclerosis: effects on motor and cognitive functions. Front Aging Neurosci. 2018;10:238. Published 2018 Aug 8. doi:10.3389/fnagi.2018.00238
7. Weideman AM, Tapia-Maltos MA, Johnson K, Greenwood M, Bielekova B. Meta-analysis of the age-dependent efficacy of multiple sclerosis treatments. Front Neurol. 2017;8:577. Published 2017 Nov 10. doi:10.3389/fneur.2017.00577
8. Hua LH, Harris H, Conway D, Thompson NR. Changes in patient-reported outcomes between continuers and discontinuers of disease modifying therapy in patients with multiple sclerosis over age 60. Mult Scler Relat Disord. 2019;30:252-256. doi:10.1016/j.msard.2019.02.028
9. San-Juan-Rodriguez A, Good CB, Heyman RA, Parekh N, Shrank WH, Hernandez I. Trends in prices, market share, and spending on self-administered disease-modifying therapies for multiple sclerosis in Medicare part D. JAMA Neurol. 2019;76(11):1386-1390. doi:10.1001/jamaneurol.2019.2711
10. Schweitzer F, Laurent S, Fink GR, et al. Age and the risks of high-efficacy disease modifying drugs in multiple sclerosis. Curr Opin Neurol. 2019;32(3):305-312. doi:10.1097/WCO.0000000000000701
11. McGinley MP, Cola PA, Fox RJ, Cohen JA, Corboy JJ, Miller D. Perspectives of individuals with multiple sclerosis on discontinuation of disease-modifying therapies. Mult Scler. 2020;26(12):1581-1589. doi:10.1177/1352458519867314
12. Marrie RA, Rudick R, Horwitz R, et al. Vascular comorbidity is associated with more rapid disability progression in multiple sclerosis. Neurology. 2010;74(13):1041-1047. doi:10.1212/WNL.0b013e3181d6b125
13. Flores VA, Šilic´ P, DuBose NG, Zheng P, Jeng B, Motl RW. Effects of aerobic, resistance, and combined exercise training on health-related quality of life in multiple sclerosis: Systematic review and meta-analysis. Mult Scler Relat Disord. 2023;75:104746. doi:10.1016/j.msard.2023.104746
14. Snetselaar LG, Cheek JJ, Fox SS, et al. Efficacy of diet on fatigue and quality of life in multiple sclerosis: a systematic review and network meta-analysis of randomized trials. Neurology. 2023;100(4):e357-e366. doi:10.1212/WNL.0000000000201371
1. Wallin MT, Culpepper WJ, Campbell JD, et al. The prevalence of MS in the United States: a population-based estimate using health claims data. Neurology. 2019;92(10):e1029-e1040. doi:10.1212/WNL.0000000000007035
2. Lunde HMB, Assmus J, Myhr KM, Bø L, Grytten N. Survival and cause of death in multiple sclerosis: a 60-year longitudinal population study. J Neurol Neurosurg Psychiatry. 2017;88(8):621-625. doi:10.1136/jnnp-2016-315238
3. Rae-Grant A, Day GS, Marrie RA, et al. Practice guideline recommendations summary: disease-modifying therapies for adults with multiple sclerosis: report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology. 2018;90(17):777-788. doi:10.1212/WNL.0000000000005347
4. Roos I, Leray E, Casey R, et al. Effects of high- and low-efficacy therapy in secondary progressive multiple sclerosis. Neurology. 2021;97(9):e869-e880. doi:10.1212/WNL.0000000000012354
5. Bsteh G, Feige J, Ehling R, et al. Discontinuation of disease-modifying therapies in multiple sclerosis - clinical outcome and prognostic factors. Mult Scler. 2017;23(9):1241-1248. doi:10.1177/1352458516675751
6. Musella A, Gentile A, Rizzo FR, et al. Interplay between age and neuroinflammation in multiple sclerosis: effects on motor and cognitive functions. Front Aging Neurosci. 2018;10:238. Published 2018 Aug 8. doi:10.3389/fnagi.2018.00238
7. Weideman AM, Tapia-Maltos MA, Johnson K, Greenwood M, Bielekova B. Meta-analysis of the age-dependent efficacy of multiple sclerosis treatments. Front Neurol. 2017;8:577. Published 2017 Nov 10. doi:10.3389/fneur.2017.00577
8. Hua LH, Harris H, Conway D, Thompson NR. Changes in patient-reported outcomes between continuers and discontinuers of disease modifying therapy in patients with multiple sclerosis over age 60. Mult Scler Relat Disord. 2019;30:252-256. doi:10.1016/j.msard.2019.02.028
9. San-Juan-Rodriguez A, Good CB, Heyman RA, Parekh N, Shrank WH, Hernandez I. Trends in prices, market share, and spending on self-administered disease-modifying therapies for multiple sclerosis in Medicare part D. JAMA Neurol. 2019;76(11):1386-1390. doi:10.1001/jamaneurol.2019.2711
10. Schweitzer F, Laurent S, Fink GR, et al. Age and the risks of high-efficacy disease modifying drugs in multiple sclerosis. Curr Opin Neurol. 2019;32(3):305-312. doi:10.1097/WCO.0000000000000701
11. McGinley MP, Cola PA, Fox RJ, Cohen JA, Corboy JJ, Miller D. Perspectives of individuals with multiple sclerosis on discontinuation of disease-modifying therapies. Mult Scler. 2020;26(12):1581-1589. doi:10.1177/1352458519867314
12. Marrie RA, Rudick R, Horwitz R, et al. Vascular comorbidity is associated with more rapid disability progression in multiple sclerosis. Neurology. 2010;74(13):1041-1047. doi:10.1212/WNL.0b013e3181d6b125
13. Flores VA, Šilic´ P, DuBose NG, Zheng P, Jeng B, Motl RW. Effects of aerobic, resistance, and combined exercise training on health-related quality of life in multiple sclerosis: Systematic review and meta-analysis. Mult Scler Relat Disord. 2023;75:104746. doi:10.1016/j.msard.2023.104746
14. Snetselaar LG, Cheek JJ, Fox SS, et al. Efficacy of diet on fatigue and quality of life in multiple sclerosis: a systematic review and network meta-analysis of randomized trials. Neurology. 2023;100(4):e357-e366. doi:10.1212/WNL.0000000000201371
Fireworks, Veterans, and PTSD: The Ironies of the Fourth of July
My first wish is to see this plague to Mankind, war, banished from the Earth; & the Sons and daughters of this World employed in more pleasing & innocent amusements than in preparing implements, & exercising them for the destruction of the human race.
General George Washington1
When I was a child, every Fourth of July holiday my father would take me to the military fireworks display at Fort Sam Houston in Texas. We would take our place in the long cascade of cars parked at the huge parade ground in front of Brooke Army Medical Center. It was the most spectacular display of the year not to be found anywhere else in the city. Army fire engines and medics were always on site in case anything went wrong, which rarely occurred thanks to the pyrotechnic experts who ran the display.
Later, when I began my psychiatric residency at the US Department of Veterans Affairs (VA) New Mexico Healthcare System, I quickly learned a darker truth about fireworks. What seemed to me and many other civilians in General Washington’s words, a “pleasing and innocent amusement,” instead was a distressing and terrifying revisiting of trauma for many service members and veterans, likely including my father, who was a World War II combat veteran.
Fireworks are so closely linked to the birth of our young nation that we often forget they were invented in China a millennia ago. Fireworks were first associated with the fledgling nation in the middle of the War of Independence. On July 4, 1776, representatives of the 13 colonies signed the Declaration of Independence. In one of several ironies of history, what was used at the initial commemorations was not fireworks but the very “implements of destruction,” to use Washington’s phrase—guns and cannons. The demonstrations of firepower were meant to be morale boosters. After the war, the dangers of the detonations were recognized, and firearms were replaced with the fireworks we still launch today.2
The country celebrates the holiday with cookouts, parades, brass band concerts, and of course fireworks. Added to the organized shows are the millions of citizens who demonstrate private patriotism by shooting off fireworks in their neighborhoods. In 2021, Americans spent $1.5 billion on fireworks, and 33% said they planned to attend a public display.3
However, people are increasingly recognizing the negative side of fireworks for wild and companion animals and the environment. Most of us who have dogs and I am sure cats, horses, and other animals dread the impending darkness of the Fourth as it signals the coming loud noise and the cringing, pacing animals who want to run yet have nowhere to go to be safe from the sound.4
Sitting in the clinic with veterans, I realized it was not only pets and wildlife that feared the ultimate American holiday but also the very individuals who fought to preserve the freedom those fireworks celebrate. The VA’s National Center for Posttraumatic Stress Disorder (PTSD) estimates that about 7% of veterans will meet the diagnostic criteria for PTSD in their lifetimes. The prevalence of PTSD differs, depending on the methodology used, era and type of services, and demographics. Some studies have found higher rates of PTSD in women, young veterans, and those who served in Vietnam. Among the veterans who receive health care at the VA, like those I saw in the clinic, 23 in 1000 may have PTSD.5
We, after all, are remarkably similar in physiology to other mammals, and not surprisingly, veterans with PTSD exhibit many of the same reactions to fireworks. The sights, sounds, and odor of fireworks, as well as the vocal responses of the crowd at large displays evoke memories that trigger fear and anxiety. Many veterans experience flashbacks in which they relive combat and training accidents and have nightmares of those events, interrupting sleep. The instinct of many veterans is to avoid the holiday altogether: Many patients I knew sought refuge in remote mountain campsites often to find that even there they were not safe from revelers.
Avoidance being a cardinal symptom and coping mechanism of PTSD, therapists advise other methods of managing the Fourth of July, such as distractions that are calming and people who are reassuring. Therapists often rehearse self-talk scripts and teach breathing exercises targeted to break the behavioral conditioning that links present innocuous sensory overstimulation with a past life-threatening danger. The heat of summer worsens the stress, cooling down literally and figuratively can help.6
Many VA medical centers send announcements to the media or have their experts do interviews to educate the public about the potentially traumatizing effects of fireworks. They also encourage veterans who are apprehensive about the holiday to seek additional mental health help, including the Veterans Crisis Line. With my patients, we started early and developed a preventive plan to manage the anticipatory apprehension and arrange a means of enduring the ordeal. I do not have data to prove it, but anecdotally I know from my years on-call that visits to VA emergency departments and admissions to our inpatient psychiatry unit always increased around Independence Day in part because some veterans used drugs and/or alcohol to dampen their stress response.
VA experts also have advice for the families and friends of veterans who want to reduce the impact of fireworks and other holiday activities on them. Many veterans will feel at once intensely present to the disturbing aspects like fireworks and crowds and at the same time, distant and separated from the more positive parts of celebrations like being with loved ones in the outdoors. We can simply ask the veterans in our lives and neighborhoods how the festivities affect them and how we can help them get through the long hot night.7 Yet it would not be America without some controversy, and opinions are divided even among veterans about whether yard signs that say, “Combat Veteran Lives Here Please Be Courteous With Fireworks” enhance or impede the effort to increase awareness of the connection between fireworks, veterans, and PTSD.8
This editorial began with my own story of enjoying fireworks to emphasize that my aim is not to ruin the fun but to ask us to think before we shoot and consider the veterans near us for whom our recreation may cause unnecessary distress. Fourth of July would not have been possible without the soldiers who fought and died in the American Revolution and all the conflicts since. We owe it to all who have worn the uniform for the United States of America to remember the extraordinary toll it has taken on their ability to live ordinary lives. Like General Washington, we should vow to end the wars that wounded them so future generations will be able to join in celebrating Independence Day.
1. From George Washington to David Humphreys, 25 July 1785. Accessed June 19, 2023. https://founders.archives.gov/documents/Washington/04-03-02-0142
2. Waxman OB. How fireworks became a Fourth of July tradition. TIME. Accessed June 19, 2023. https://time.com/4828701/first-fireworks-history-july-4th
3. Velasquez F. Here’s how much Americans are spending on food, alcohol, and fireworks this Fourth of July. Accessed June 19, 2023. https://www.cnbc.com/2021/07/04/how-much-americans-are-spending-on-fourth-of-july.html
4. Fireworks: growing evidence they distress animals builds case to restrict use. The Conversation. Accessed June 19, 2023. https://theconversation.com/fireworks-growing-evidence-they-distress-animals-builds-case-to-restrict-use-191472
5. US Department of Veterans Affairs. Epidemiology and impact of PTSD. Accessed June 17, 2023. https://www.ptsd.va.gov/professional/treat/essentials/epidemiology.asp#two,
6. US Department of Veterans Affairs. Independence Day celebrations can trigger PTSD in veterans. Press release. Accessed June 19, 2023. https://www.va.gov/new-jersey-health-care/news-releases/independence-day-celebrations-can-trigger-ptsd-in-veterans
7. Tips for veterans celebrating Independence Day. VA News. https://news.va.gov/62393/some-helpful-tips-to-remember-for-this-4th-of-july
8. Faith S. Veterans, July 4, and fireworks: don’t be courteous, just be American. Military.com. Accessed June 19, 2023. https://www.military.com/july-4th/veterans-july-4-and-fireworks-dont-be-courteous-just-be-american.html
My first wish is to see this plague to Mankind, war, banished from the Earth; & the Sons and daughters of this World employed in more pleasing & innocent amusements than in preparing implements, & exercising them for the destruction of the human race.
General George Washington1
When I was a child, every Fourth of July holiday my father would take me to the military fireworks display at Fort Sam Houston in Texas. We would take our place in the long cascade of cars parked at the huge parade ground in front of Brooke Army Medical Center. It was the most spectacular display of the year not to be found anywhere else in the city. Army fire engines and medics were always on site in case anything went wrong, which rarely occurred thanks to the pyrotechnic experts who ran the display.
Later, when I began my psychiatric residency at the US Department of Veterans Affairs (VA) New Mexico Healthcare System, I quickly learned a darker truth about fireworks. What seemed to me and many other civilians in General Washington’s words, a “pleasing and innocent amusement,” instead was a distressing and terrifying revisiting of trauma for many service members and veterans, likely including my father, who was a World War II combat veteran.
Fireworks are so closely linked to the birth of our young nation that we often forget they were invented in China a millennia ago. Fireworks were first associated with the fledgling nation in the middle of the War of Independence. On July 4, 1776, representatives of the 13 colonies signed the Declaration of Independence. In one of several ironies of history, what was used at the initial commemorations was not fireworks but the very “implements of destruction,” to use Washington’s phrase—guns and cannons. The demonstrations of firepower were meant to be morale boosters. After the war, the dangers of the detonations were recognized, and firearms were replaced with the fireworks we still launch today.2
The country celebrates the holiday with cookouts, parades, brass band concerts, and of course fireworks. Added to the organized shows are the millions of citizens who demonstrate private patriotism by shooting off fireworks in their neighborhoods. In 2021, Americans spent $1.5 billion on fireworks, and 33% said they planned to attend a public display.3
However, people are increasingly recognizing the negative side of fireworks for wild and companion animals and the environment. Most of us who have dogs and I am sure cats, horses, and other animals dread the impending darkness of the Fourth as it signals the coming loud noise and the cringing, pacing animals who want to run yet have nowhere to go to be safe from the sound.4
Sitting in the clinic with veterans, I realized it was not only pets and wildlife that feared the ultimate American holiday but also the very individuals who fought to preserve the freedom those fireworks celebrate. The VA’s National Center for Posttraumatic Stress Disorder (PTSD) estimates that about 7% of veterans will meet the diagnostic criteria for PTSD in their lifetimes. The prevalence of PTSD differs, depending on the methodology used, era and type of services, and demographics. Some studies have found higher rates of PTSD in women, young veterans, and those who served in Vietnam. Among the veterans who receive health care at the VA, like those I saw in the clinic, 23 in 1000 may have PTSD.5
We, after all, are remarkably similar in physiology to other mammals, and not surprisingly, veterans with PTSD exhibit many of the same reactions to fireworks. The sights, sounds, and odor of fireworks, as well as the vocal responses of the crowd at large displays evoke memories that trigger fear and anxiety. Many veterans experience flashbacks in which they relive combat and training accidents and have nightmares of those events, interrupting sleep. The instinct of many veterans is to avoid the holiday altogether: Many patients I knew sought refuge in remote mountain campsites often to find that even there they were not safe from revelers.
Avoidance being a cardinal symptom and coping mechanism of PTSD, therapists advise other methods of managing the Fourth of July, such as distractions that are calming and people who are reassuring. Therapists often rehearse self-talk scripts and teach breathing exercises targeted to break the behavioral conditioning that links present innocuous sensory overstimulation with a past life-threatening danger. The heat of summer worsens the stress, cooling down literally and figuratively can help.6
Many VA medical centers send announcements to the media or have their experts do interviews to educate the public about the potentially traumatizing effects of fireworks. They also encourage veterans who are apprehensive about the holiday to seek additional mental health help, including the Veterans Crisis Line. With my patients, we started early and developed a preventive plan to manage the anticipatory apprehension and arrange a means of enduring the ordeal. I do not have data to prove it, but anecdotally I know from my years on-call that visits to VA emergency departments and admissions to our inpatient psychiatry unit always increased around Independence Day in part because some veterans used drugs and/or alcohol to dampen their stress response.
VA experts also have advice for the families and friends of veterans who want to reduce the impact of fireworks and other holiday activities on them. Many veterans will feel at once intensely present to the disturbing aspects like fireworks and crowds and at the same time, distant and separated from the more positive parts of celebrations like being with loved ones in the outdoors. We can simply ask the veterans in our lives and neighborhoods how the festivities affect them and how we can help them get through the long hot night.7 Yet it would not be America without some controversy, and opinions are divided even among veterans about whether yard signs that say, “Combat Veteran Lives Here Please Be Courteous With Fireworks” enhance or impede the effort to increase awareness of the connection between fireworks, veterans, and PTSD.8
This editorial began with my own story of enjoying fireworks to emphasize that my aim is not to ruin the fun but to ask us to think before we shoot and consider the veterans near us for whom our recreation may cause unnecessary distress. Fourth of July would not have been possible without the soldiers who fought and died in the American Revolution and all the conflicts since. We owe it to all who have worn the uniform for the United States of America to remember the extraordinary toll it has taken on their ability to live ordinary lives. Like General Washington, we should vow to end the wars that wounded them so future generations will be able to join in celebrating Independence Day.
My first wish is to see this plague to Mankind, war, banished from the Earth; & the Sons and daughters of this World employed in more pleasing & innocent amusements than in preparing implements, & exercising them for the destruction of the human race.
General George Washington1
When I was a child, every Fourth of July holiday my father would take me to the military fireworks display at Fort Sam Houston in Texas. We would take our place in the long cascade of cars parked at the huge parade ground in front of Brooke Army Medical Center. It was the most spectacular display of the year not to be found anywhere else in the city. Army fire engines and medics were always on site in case anything went wrong, which rarely occurred thanks to the pyrotechnic experts who ran the display.
Later, when I began my psychiatric residency at the US Department of Veterans Affairs (VA) New Mexico Healthcare System, I quickly learned a darker truth about fireworks. What seemed to me and many other civilians in General Washington’s words, a “pleasing and innocent amusement,” instead was a distressing and terrifying revisiting of trauma for many service members and veterans, likely including my father, who was a World War II combat veteran.
Fireworks are so closely linked to the birth of our young nation that we often forget they were invented in China a millennia ago. Fireworks were first associated with the fledgling nation in the middle of the War of Independence. On July 4, 1776, representatives of the 13 colonies signed the Declaration of Independence. In one of several ironies of history, what was used at the initial commemorations was not fireworks but the very “implements of destruction,” to use Washington’s phrase—guns and cannons. The demonstrations of firepower were meant to be morale boosters. After the war, the dangers of the detonations were recognized, and firearms were replaced with the fireworks we still launch today.2
The country celebrates the holiday with cookouts, parades, brass band concerts, and of course fireworks. Added to the organized shows are the millions of citizens who demonstrate private patriotism by shooting off fireworks in their neighborhoods. In 2021, Americans spent $1.5 billion on fireworks, and 33% said they planned to attend a public display.3
However, people are increasingly recognizing the negative side of fireworks for wild and companion animals and the environment. Most of us who have dogs and I am sure cats, horses, and other animals dread the impending darkness of the Fourth as it signals the coming loud noise and the cringing, pacing animals who want to run yet have nowhere to go to be safe from the sound.4
Sitting in the clinic with veterans, I realized it was not only pets and wildlife that feared the ultimate American holiday but also the very individuals who fought to preserve the freedom those fireworks celebrate. The VA’s National Center for Posttraumatic Stress Disorder (PTSD) estimates that about 7% of veterans will meet the diagnostic criteria for PTSD in their lifetimes. The prevalence of PTSD differs, depending on the methodology used, era and type of services, and demographics. Some studies have found higher rates of PTSD in women, young veterans, and those who served in Vietnam. Among the veterans who receive health care at the VA, like those I saw in the clinic, 23 in 1000 may have PTSD.5
We, after all, are remarkably similar in physiology to other mammals, and not surprisingly, veterans with PTSD exhibit many of the same reactions to fireworks. The sights, sounds, and odor of fireworks, as well as the vocal responses of the crowd at large displays evoke memories that trigger fear and anxiety. Many veterans experience flashbacks in which they relive combat and training accidents and have nightmares of those events, interrupting sleep. The instinct of many veterans is to avoid the holiday altogether: Many patients I knew sought refuge in remote mountain campsites often to find that even there they were not safe from revelers.
Avoidance being a cardinal symptom and coping mechanism of PTSD, therapists advise other methods of managing the Fourth of July, such as distractions that are calming and people who are reassuring. Therapists often rehearse self-talk scripts and teach breathing exercises targeted to break the behavioral conditioning that links present innocuous sensory overstimulation with a past life-threatening danger. The heat of summer worsens the stress, cooling down literally and figuratively can help.6
Many VA medical centers send announcements to the media or have their experts do interviews to educate the public about the potentially traumatizing effects of fireworks. They also encourage veterans who are apprehensive about the holiday to seek additional mental health help, including the Veterans Crisis Line. With my patients, we started early and developed a preventive plan to manage the anticipatory apprehension and arrange a means of enduring the ordeal. I do not have data to prove it, but anecdotally I know from my years on-call that visits to VA emergency departments and admissions to our inpatient psychiatry unit always increased around Independence Day in part because some veterans used drugs and/or alcohol to dampen their stress response.
VA experts also have advice for the families and friends of veterans who want to reduce the impact of fireworks and other holiday activities on them. Many veterans will feel at once intensely present to the disturbing aspects like fireworks and crowds and at the same time, distant and separated from the more positive parts of celebrations like being with loved ones in the outdoors. We can simply ask the veterans in our lives and neighborhoods how the festivities affect them and how we can help them get through the long hot night.7 Yet it would not be America without some controversy, and opinions are divided even among veterans about whether yard signs that say, “Combat Veteran Lives Here Please Be Courteous With Fireworks” enhance or impede the effort to increase awareness of the connection between fireworks, veterans, and PTSD.8
This editorial began with my own story of enjoying fireworks to emphasize that my aim is not to ruin the fun but to ask us to think before we shoot and consider the veterans near us for whom our recreation may cause unnecessary distress. Fourth of July would not have been possible without the soldiers who fought and died in the American Revolution and all the conflicts since. We owe it to all who have worn the uniform for the United States of America to remember the extraordinary toll it has taken on their ability to live ordinary lives. Like General Washington, we should vow to end the wars that wounded them so future generations will be able to join in celebrating Independence Day.
1. From George Washington to David Humphreys, 25 July 1785. Accessed June 19, 2023. https://founders.archives.gov/documents/Washington/04-03-02-0142
2. Waxman OB. How fireworks became a Fourth of July tradition. TIME. Accessed June 19, 2023. https://time.com/4828701/first-fireworks-history-july-4th
3. Velasquez F. Here’s how much Americans are spending on food, alcohol, and fireworks this Fourth of July. Accessed June 19, 2023. https://www.cnbc.com/2021/07/04/how-much-americans-are-spending-on-fourth-of-july.html
4. Fireworks: growing evidence they distress animals builds case to restrict use. The Conversation. Accessed June 19, 2023. https://theconversation.com/fireworks-growing-evidence-they-distress-animals-builds-case-to-restrict-use-191472
5. US Department of Veterans Affairs. Epidemiology and impact of PTSD. Accessed June 17, 2023. https://www.ptsd.va.gov/professional/treat/essentials/epidemiology.asp#two,
6. US Department of Veterans Affairs. Independence Day celebrations can trigger PTSD in veterans. Press release. Accessed June 19, 2023. https://www.va.gov/new-jersey-health-care/news-releases/independence-day-celebrations-can-trigger-ptsd-in-veterans
7. Tips for veterans celebrating Independence Day. VA News. https://news.va.gov/62393/some-helpful-tips-to-remember-for-this-4th-of-july
8. Faith S. Veterans, July 4, and fireworks: don’t be courteous, just be American. Military.com. Accessed June 19, 2023. https://www.military.com/july-4th/veterans-july-4-and-fireworks-dont-be-courteous-just-be-american.html
1. From George Washington to David Humphreys, 25 July 1785. Accessed June 19, 2023. https://founders.archives.gov/documents/Washington/04-03-02-0142
2. Waxman OB. How fireworks became a Fourth of July tradition. TIME. Accessed June 19, 2023. https://time.com/4828701/first-fireworks-history-july-4th
3. Velasquez F. Here’s how much Americans are spending on food, alcohol, and fireworks this Fourth of July. Accessed June 19, 2023. https://www.cnbc.com/2021/07/04/how-much-americans-are-spending-on-fourth-of-july.html
4. Fireworks: growing evidence they distress animals builds case to restrict use. The Conversation. Accessed June 19, 2023. https://theconversation.com/fireworks-growing-evidence-they-distress-animals-builds-case-to-restrict-use-191472
5. US Department of Veterans Affairs. Epidemiology and impact of PTSD. Accessed June 17, 2023. https://www.ptsd.va.gov/professional/treat/essentials/epidemiology.asp#two,
6. US Department of Veterans Affairs. Independence Day celebrations can trigger PTSD in veterans. Press release. Accessed June 19, 2023. https://www.va.gov/new-jersey-health-care/news-releases/independence-day-celebrations-can-trigger-ptsd-in-veterans
7. Tips for veterans celebrating Independence Day. VA News. https://news.va.gov/62393/some-helpful-tips-to-remember-for-this-4th-of-july
8. Faith S. Veterans, July 4, and fireworks: don’t be courteous, just be American. Military.com. Accessed June 19, 2023. https://www.military.com/july-4th/veterans-july-4-and-fireworks-dont-be-courteous-just-be-american.html
Tirzepatide: Therapeutic titan or costly cure?
As a general practitioner with a specialist interest in diabetes, I am increasingly diagnosing younger people living with type 2 diabetes and obesity. Sadly, my youngest patient living with type 2 diabetes and obesity is only in her early 20s.
In fact, in England, there are now more people under the age of 40 years living with type 2 diabetes than type 1 diabetes. These younger individuals tend to present with very high hemoglobin A1c levels; I am routinely seeing double-digit A1c percentage levels in my practice. Indeed, the patient mentioned above presented with an A1c of more than 13%.
The lifetime cardiometabolic risk of individuals like her is considerable and very worrying: Younger adults with type 2 diabetes often have adverse cardiometabolic risk profiles at diagnosis, with higher body mass indices, marked dyslipidemia, hypertension, and abnormal liver profiles suggesting nonalcoholic fatty liver disease. The cumulative impact of this risk profile is a significant impact on quality and quantity of life. Evidence tells us that a younger age of diagnosis with type 2 diabetes is associated with an increased risk for premature death, especially from cardiovascular disease.
Early treatment intensification is warranted in younger individuals living with type 2 diabetes and obesity. My patient above is now on triple therapy with metformin, a sodium-glucose cotransporter 2 (SGLT2) inhibitor, and a glucagonlike peptide–1 (GLP-1) receptor agonist. I gave her an urgent referral to my local weight management service for weight, nutritional, and psychological support. I have also issued her a real-time continuous glucose monitoring (rt-CGM) device: Whilst she does not meet any current U.K. criteria for using rt-CGM, I feel that the role of CGM as an educational tool for her is invaluable and equally important to her pharmacologic therapies. We are in desperate need of effective pharmacologic and lifestyle interventions to tackle this epidemic of cardiometabolic disease in the young.
I attended the recent ADA 2023 congress in San Diego, including the presentation of the SURMOUNT-2 trial data. SURMOUNT-2 explored the efficacy and safety of the dual GLP-GIP agonist tirzepatide for weight management in patients with obesity and type 2 diabetes. Tirzepatide was associated with significant reductions in weight (average weight loss, 14-16 kg after 72 weeks) and glycemia (2.1% reduction in A1c after 72 weeks), as well as reductions in clinically meaningful cardiometabolic risk factors, including systolic blood pressure, liver enzymes, and fasting non–HDL cholesterol levels. The overall safety profile of tirzepatide was also reassuring and consistent with the GLP-1 class. Most adverse effects were gastrointestinal and of mild to moderate severity. These adverse effects decreased over time.
These results perfectly position tirzepatide for my younger patients like the young woman mentioned above. The significant improvements in weight, glycemia, and cardiometabolic risk factors will not only help mitigate her future cardiometabolic risk but also help the sustainability of the U.K.’s National Health System. The cost of diabetes to the NHS in the United Kingdom is more than 10% of the entire NHS budget for England and Wales. More than 80% of this cost, however, is related not to the medications and devices we prescribe for diabetes but to the downstream complications of diabetes, such as hospital admissions for cardiovascular events and amputations, as well as regular hospital attendance for dialysis for end-stage kidney disease.
There is no doubt, however, that modern obesity medications such as semaglutide and tirzepatide are expensive, and demand has been astronomical. This demand has been driven by private weight-management services and celebrity influencers, and has resulted in major U.K.-wide GLP-1 shortages.
This situation is tragically widening health inequalities, as many of my patients who have been on GLP-1 receptor agonists for many years are unable to obtain them. I am having to consider switching therapies, often to less efficacious options without the compelling cardiorenal benefits. Furthermore, the GLP-1 shortages have prevented GLP-1 initiation for my other high-risk younger patients, potentially increasing future cardiometabolic risk.
There remain unanswered questions for tirzepatide: What is the durability of effect of tirzepatide after 72 weeks (that is, the trial duration of SURMOUNT-2)? Crucially, what is the effect of withdrawal of tirzepatide on weight loss maintenance? Previous evidence has suggested weight regain after discontinuation of a GLP-1 receptor agonist for obesity. This, of course, has further financial and sustainability implications for health care systems such as the NHS.
Finally, we are increasingly seeing younger women of childbearing age with or at risk for cardiometabolic disease. Again, my patient above is one example. Many of the therapies we use for cardiometabolic disease management, including GLP-1 receptor agonists and tirzepatide, have not been studied, and hence have not been licensed in pregnant women. Therefore, frank discussions are required with patients about future family plans and the importance of contraception. Often, the significant weight loss seen with GLP-1 receptor agonists can improve hormonal profiles and fertility in women and result in unexpected pregnancies if robust contraception is not in place.
Tirzepatide has yet to be made commercially available in the United Kingdom, and its price has also yet to be set. But I already envision a clear role for tirzepatide in my treatment armamentarium. I will be positioning tirzepatide as my first injectable of choice after oral treatment escalation with metformin and an SGLT2 inhibitor in all my patients who require treatment intensification – not just my younger, higher-risk individuals. This may remain an aspirational goal until supply chains and cost are defined. There is no doubt, however, that the compelling weight and glycemic benefits of tirzepatide alongside individualized lifestyle interventions can help improve the quality and quantity of life of my patients living with type 2 diabetes and obesity.
Dr. Fernando is a general practitioner near Edinburgh. He reported receiving speaker fees from Eli Lilly and Novo Nordisk..
A version of this article first appeared on Medscape.com.
As a general practitioner with a specialist interest in diabetes, I am increasingly diagnosing younger people living with type 2 diabetes and obesity. Sadly, my youngest patient living with type 2 diabetes and obesity is only in her early 20s.
In fact, in England, there are now more people under the age of 40 years living with type 2 diabetes than type 1 diabetes. These younger individuals tend to present with very high hemoglobin A1c levels; I am routinely seeing double-digit A1c percentage levels in my practice. Indeed, the patient mentioned above presented with an A1c of more than 13%.
The lifetime cardiometabolic risk of individuals like her is considerable and very worrying: Younger adults with type 2 diabetes often have adverse cardiometabolic risk profiles at diagnosis, with higher body mass indices, marked dyslipidemia, hypertension, and abnormal liver profiles suggesting nonalcoholic fatty liver disease. The cumulative impact of this risk profile is a significant impact on quality and quantity of life. Evidence tells us that a younger age of diagnosis with type 2 diabetes is associated with an increased risk for premature death, especially from cardiovascular disease.
Early treatment intensification is warranted in younger individuals living with type 2 diabetes and obesity. My patient above is now on triple therapy with metformin, a sodium-glucose cotransporter 2 (SGLT2) inhibitor, and a glucagonlike peptide–1 (GLP-1) receptor agonist. I gave her an urgent referral to my local weight management service for weight, nutritional, and psychological support. I have also issued her a real-time continuous glucose monitoring (rt-CGM) device: Whilst she does not meet any current U.K. criteria for using rt-CGM, I feel that the role of CGM as an educational tool for her is invaluable and equally important to her pharmacologic therapies. We are in desperate need of effective pharmacologic and lifestyle interventions to tackle this epidemic of cardiometabolic disease in the young.
I attended the recent ADA 2023 congress in San Diego, including the presentation of the SURMOUNT-2 trial data. SURMOUNT-2 explored the efficacy and safety of the dual GLP-GIP agonist tirzepatide for weight management in patients with obesity and type 2 diabetes. Tirzepatide was associated with significant reductions in weight (average weight loss, 14-16 kg after 72 weeks) and glycemia (2.1% reduction in A1c after 72 weeks), as well as reductions in clinically meaningful cardiometabolic risk factors, including systolic blood pressure, liver enzymes, and fasting non–HDL cholesterol levels. The overall safety profile of tirzepatide was also reassuring and consistent with the GLP-1 class. Most adverse effects were gastrointestinal and of mild to moderate severity. These adverse effects decreased over time.
These results perfectly position tirzepatide for my younger patients like the young woman mentioned above. The significant improvements in weight, glycemia, and cardiometabolic risk factors will not only help mitigate her future cardiometabolic risk but also help the sustainability of the U.K.’s National Health System. The cost of diabetes to the NHS in the United Kingdom is more than 10% of the entire NHS budget for England and Wales. More than 80% of this cost, however, is related not to the medications and devices we prescribe for diabetes but to the downstream complications of diabetes, such as hospital admissions for cardiovascular events and amputations, as well as regular hospital attendance for dialysis for end-stage kidney disease.
There is no doubt, however, that modern obesity medications such as semaglutide and tirzepatide are expensive, and demand has been astronomical. This demand has been driven by private weight-management services and celebrity influencers, and has resulted in major U.K.-wide GLP-1 shortages.
This situation is tragically widening health inequalities, as many of my patients who have been on GLP-1 receptor agonists for many years are unable to obtain them. I am having to consider switching therapies, often to less efficacious options without the compelling cardiorenal benefits. Furthermore, the GLP-1 shortages have prevented GLP-1 initiation for my other high-risk younger patients, potentially increasing future cardiometabolic risk.
There remain unanswered questions for tirzepatide: What is the durability of effect of tirzepatide after 72 weeks (that is, the trial duration of SURMOUNT-2)? Crucially, what is the effect of withdrawal of tirzepatide on weight loss maintenance? Previous evidence has suggested weight regain after discontinuation of a GLP-1 receptor agonist for obesity. This, of course, has further financial and sustainability implications for health care systems such as the NHS.
Finally, we are increasingly seeing younger women of childbearing age with or at risk for cardiometabolic disease. Again, my patient above is one example. Many of the therapies we use for cardiometabolic disease management, including GLP-1 receptor agonists and tirzepatide, have not been studied, and hence have not been licensed in pregnant women. Therefore, frank discussions are required with patients about future family plans and the importance of contraception. Often, the significant weight loss seen with GLP-1 receptor agonists can improve hormonal profiles and fertility in women and result in unexpected pregnancies if robust contraception is not in place.
Tirzepatide has yet to be made commercially available in the United Kingdom, and its price has also yet to be set. But I already envision a clear role for tirzepatide in my treatment armamentarium. I will be positioning tirzepatide as my first injectable of choice after oral treatment escalation with metformin and an SGLT2 inhibitor in all my patients who require treatment intensification – not just my younger, higher-risk individuals. This may remain an aspirational goal until supply chains and cost are defined. There is no doubt, however, that the compelling weight and glycemic benefits of tirzepatide alongside individualized lifestyle interventions can help improve the quality and quantity of life of my patients living with type 2 diabetes and obesity.
Dr. Fernando is a general practitioner near Edinburgh. He reported receiving speaker fees from Eli Lilly and Novo Nordisk..
A version of this article first appeared on Medscape.com.
As a general practitioner with a specialist interest in diabetes, I am increasingly diagnosing younger people living with type 2 diabetes and obesity. Sadly, my youngest patient living with type 2 diabetes and obesity is only in her early 20s.
In fact, in England, there are now more people under the age of 40 years living with type 2 diabetes than type 1 diabetes. These younger individuals tend to present with very high hemoglobin A1c levels; I am routinely seeing double-digit A1c percentage levels in my practice. Indeed, the patient mentioned above presented with an A1c of more than 13%.
The lifetime cardiometabolic risk of individuals like her is considerable and very worrying: Younger adults with type 2 diabetes often have adverse cardiometabolic risk profiles at diagnosis, with higher body mass indices, marked dyslipidemia, hypertension, and abnormal liver profiles suggesting nonalcoholic fatty liver disease. The cumulative impact of this risk profile is a significant impact on quality and quantity of life. Evidence tells us that a younger age of diagnosis with type 2 diabetes is associated with an increased risk for premature death, especially from cardiovascular disease.
Early treatment intensification is warranted in younger individuals living with type 2 diabetes and obesity. My patient above is now on triple therapy with metformin, a sodium-glucose cotransporter 2 (SGLT2) inhibitor, and a glucagonlike peptide–1 (GLP-1) receptor agonist. I gave her an urgent referral to my local weight management service for weight, nutritional, and psychological support. I have also issued her a real-time continuous glucose monitoring (rt-CGM) device: Whilst she does not meet any current U.K. criteria for using rt-CGM, I feel that the role of CGM as an educational tool for her is invaluable and equally important to her pharmacologic therapies. We are in desperate need of effective pharmacologic and lifestyle interventions to tackle this epidemic of cardiometabolic disease in the young.
I attended the recent ADA 2023 congress in San Diego, including the presentation of the SURMOUNT-2 trial data. SURMOUNT-2 explored the efficacy and safety of the dual GLP-GIP agonist tirzepatide for weight management in patients with obesity and type 2 diabetes. Tirzepatide was associated with significant reductions in weight (average weight loss, 14-16 kg after 72 weeks) and glycemia (2.1% reduction in A1c after 72 weeks), as well as reductions in clinically meaningful cardiometabolic risk factors, including systolic blood pressure, liver enzymes, and fasting non–HDL cholesterol levels. The overall safety profile of tirzepatide was also reassuring and consistent with the GLP-1 class. Most adverse effects were gastrointestinal and of mild to moderate severity. These adverse effects decreased over time.
These results perfectly position tirzepatide for my younger patients like the young woman mentioned above. The significant improvements in weight, glycemia, and cardiometabolic risk factors will not only help mitigate her future cardiometabolic risk but also help the sustainability of the U.K.’s National Health System. The cost of diabetes to the NHS in the United Kingdom is more than 10% of the entire NHS budget for England and Wales. More than 80% of this cost, however, is related not to the medications and devices we prescribe for diabetes but to the downstream complications of diabetes, such as hospital admissions for cardiovascular events and amputations, as well as regular hospital attendance for dialysis for end-stage kidney disease.
There is no doubt, however, that modern obesity medications such as semaglutide and tirzepatide are expensive, and demand has been astronomical. This demand has been driven by private weight-management services and celebrity influencers, and has resulted in major U.K.-wide GLP-1 shortages.
This situation is tragically widening health inequalities, as many of my patients who have been on GLP-1 receptor agonists for many years are unable to obtain them. I am having to consider switching therapies, often to less efficacious options without the compelling cardiorenal benefits. Furthermore, the GLP-1 shortages have prevented GLP-1 initiation for my other high-risk younger patients, potentially increasing future cardiometabolic risk.
There remain unanswered questions for tirzepatide: What is the durability of effect of tirzepatide after 72 weeks (that is, the trial duration of SURMOUNT-2)? Crucially, what is the effect of withdrawal of tirzepatide on weight loss maintenance? Previous evidence has suggested weight regain after discontinuation of a GLP-1 receptor agonist for obesity. This, of course, has further financial and sustainability implications for health care systems such as the NHS.
Finally, we are increasingly seeing younger women of childbearing age with or at risk for cardiometabolic disease. Again, my patient above is one example. Many of the therapies we use for cardiometabolic disease management, including GLP-1 receptor agonists and tirzepatide, have not been studied, and hence have not been licensed in pregnant women. Therefore, frank discussions are required with patients about future family plans and the importance of contraception. Often, the significant weight loss seen with GLP-1 receptor agonists can improve hormonal profiles and fertility in women and result in unexpected pregnancies if robust contraception is not in place.
Tirzepatide has yet to be made commercially available in the United Kingdom, and its price has also yet to be set. But I already envision a clear role for tirzepatide in my treatment armamentarium. I will be positioning tirzepatide as my first injectable of choice after oral treatment escalation with metformin and an SGLT2 inhibitor in all my patients who require treatment intensification – not just my younger, higher-risk individuals. This may remain an aspirational goal until supply chains and cost are defined. There is no doubt, however, that the compelling weight and glycemic benefits of tirzepatide alongside individualized lifestyle interventions can help improve the quality and quantity of life of my patients living with type 2 diabetes and obesity.
Dr. Fernando is a general practitioner near Edinburgh. He reported receiving speaker fees from Eli Lilly and Novo Nordisk..
A version of this article first appeared on Medscape.com.
Beta cells from stem cells: Nearing a cure for type 1 diabetes?
This transcript has been edited for clarity.
Those of us in the field of diabetes have long wanted to cure type 1 diabetes, and there are little steps making me feel like this might be a possibility. One of those steps is that a company named Vertex – I’m actually on the steering committee for Vertex in terms of this project – has made beta cells from stem cells. Now, instead of waiting for a cadaveric donor, we can make little beta cells. They started giving them to people in human trials. The Food and Drug Administration has been cautious because it’s new, and I get that.
In the first part of these trials, we could only give half a dose of these beta cells. The doses were determined based on what we know from giving beta-cell transplants from cadaveric donors. We gave half a dose of these stem cell–derived beta cells to two people who were having episodes of severe hypoglycemia.
In patient 1, these beta cells worked incredibly well. He became insulin independent, and now after over a year, he’s basically free of his type 1 diabetes. Patient 2 received half a dose, and she did get some activity of the beta cells, but not enough to achieve insulin independence, so she got a second dose. Shortly after the second dose, she decided she didn’t want to participate in the trial anymore and she was lost to follow-up.
Patient 2 didn’t get the same response as patient 1, but then we moved on to four more patients who got a full dose to start with. Now, there’s a total of six patients. Of those additional four patients, one of them has now been followed for a year. Just like patient 1, he’s off insulin. It’s as though his body has normal beta cells and he’s doing great. For the next three patients, we don’t have enough follow-up data to tell you what’s going to happen to them at a year.
I can tell you that, in all six patients, the beta cells worked. They basically were producing insulin, they had positive C-peptide levels, and it showed that these beta cells work when given to human beings. Now the trial is going to start giving more patients these stem cell–derived beta cells.
One of the things that’s important to realize is that this is a very small sample size, at just six individuals. Even within those six individuals, there was variation in terms of the response to the treatment. Probably, just like with all things in medicine, there will be different doses, different ways in which people do respond, people who get off of insulin completely, and people who may require some ongoing insulin therapy. I have no idea what this is going to look like as we test this in more people.
Everybody did start making C-peptide, they were having an effect of these beta cells, and it was working. We’ll have to see how well it works, how well it works in whom, and how we’re going to be able to use these types of therapies in the future.
In terms of side effects, they were really related to immunosuppression. There were no real surprises, but again, this is a very small sample size.
In summary, I think this is really hopeful. I don’t like to give false hope, but each step of this development process has shown that these beta cells derived from stem cells do seem to work in human beings as native beta cells might. Hopefully, this portends a future of newer therapies in the treatment of people with type 1 diabetes. Thank you.
Dr. Peters is professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She has published more than 200 articles, reviews, and abstracts, and three books, on diabetes, and has been an investigator for more than 40 research studies. She has spoken internationally at over 400 programs and serves on many committees of several professional organizations She disclosed ties with Abbott Diabetes Care, AstraZeneca, Becton Dickinson, Boehringer Ingelheim Pharmaceuticals, Dexcom, Eli Lilly, Lexicon Pharmaceuticals, Livongo, MannKind Corporation, Medscape, Merck, Novo Nordisk, Omada Health, OptumHealth, Sanofi, and Zafgen.
A version of this article originally appeared on Medscape.com.
This transcript has been edited for clarity.
Those of us in the field of diabetes have long wanted to cure type 1 diabetes, and there are little steps making me feel like this might be a possibility. One of those steps is that a company named Vertex – I’m actually on the steering committee for Vertex in terms of this project – has made beta cells from stem cells. Now, instead of waiting for a cadaveric donor, we can make little beta cells. They started giving them to people in human trials. The Food and Drug Administration has been cautious because it’s new, and I get that.
In the first part of these trials, we could only give half a dose of these beta cells. The doses were determined based on what we know from giving beta-cell transplants from cadaveric donors. We gave half a dose of these stem cell–derived beta cells to two people who were having episodes of severe hypoglycemia.
In patient 1, these beta cells worked incredibly well. He became insulin independent, and now after over a year, he’s basically free of his type 1 diabetes. Patient 2 received half a dose, and she did get some activity of the beta cells, but not enough to achieve insulin independence, so she got a second dose. Shortly after the second dose, she decided she didn’t want to participate in the trial anymore and she was lost to follow-up.
Patient 2 didn’t get the same response as patient 1, but then we moved on to four more patients who got a full dose to start with. Now, there’s a total of six patients. Of those additional four patients, one of them has now been followed for a year. Just like patient 1, he’s off insulin. It’s as though his body has normal beta cells and he’s doing great. For the next three patients, we don’t have enough follow-up data to tell you what’s going to happen to them at a year.
I can tell you that, in all six patients, the beta cells worked. They basically were producing insulin, they had positive C-peptide levels, and it showed that these beta cells work when given to human beings. Now the trial is going to start giving more patients these stem cell–derived beta cells.
One of the things that’s important to realize is that this is a very small sample size, at just six individuals. Even within those six individuals, there was variation in terms of the response to the treatment. Probably, just like with all things in medicine, there will be different doses, different ways in which people do respond, people who get off of insulin completely, and people who may require some ongoing insulin therapy. I have no idea what this is going to look like as we test this in more people.
Everybody did start making C-peptide, they were having an effect of these beta cells, and it was working. We’ll have to see how well it works, how well it works in whom, and how we’re going to be able to use these types of therapies in the future.
In terms of side effects, they were really related to immunosuppression. There were no real surprises, but again, this is a very small sample size.
In summary, I think this is really hopeful. I don’t like to give false hope, but each step of this development process has shown that these beta cells derived from stem cells do seem to work in human beings as native beta cells might. Hopefully, this portends a future of newer therapies in the treatment of people with type 1 diabetes. Thank you.
Dr. Peters is professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She has published more than 200 articles, reviews, and abstracts, and three books, on diabetes, and has been an investigator for more than 40 research studies. She has spoken internationally at over 400 programs and serves on many committees of several professional organizations She disclosed ties with Abbott Diabetes Care, AstraZeneca, Becton Dickinson, Boehringer Ingelheim Pharmaceuticals, Dexcom, Eli Lilly, Lexicon Pharmaceuticals, Livongo, MannKind Corporation, Medscape, Merck, Novo Nordisk, Omada Health, OptumHealth, Sanofi, and Zafgen.
A version of this article originally appeared on Medscape.com.
This transcript has been edited for clarity.
Those of us in the field of diabetes have long wanted to cure type 1 diabetes, and there are little steps making me feel like this might be a possibility. One of those steps is that a company named Vertex – I’m actually on the steering committee for Vertex in terms of this project – has made beta cells from stem cells. Now, instead of waiting for a cadaveric donor, we can make little beta cells. They started giving them to people in human trials. The Food and Drug Administration has been cautious because it’s new, and I get that.
In the first part of these trials, we could only give half a dose of these beta cells. The doses were determined based on what we know from giving beta-cell transplants from cadaveric donors. We gave half a dose of these stem cell–derived beta cells to two people who were having episodes of severe hypoglycemia.
In patient 1, these beta cells worked incredibly well. He became insulin independent, and now after over a year, he’s basically free of his type 1 diabetes. Patient 2 received half a dose, and she did get some activity of the beta cells, but not enough to achieve insulin independence, so she got a second dose. Shortly after the second dose, she decided she didn’t want to participate in the trial anymore and she was lost to follow-up.
Patient 2 didn’t get the same response as patient 1, but then we moved on to four more patients who got a full dose to start with. Now, there’s a total of six patients. Of those additional four patients, one of them has now been followed for a year. Just like patient 1, he’s off insulin. It’s as though his body has normal beta cells and he’s doing great. For the next three patients, we don’t have enough follow-up data to tell you what’s going to happen to them at a year.
I can tell you that, in all six patients, the beta cells worked. They basically were producing insulin, they had positive C-peptide levels, and it showed that these beta cells work when given to human beings. Now the trial is going to start giving more patients these stem cell–derived beta cells.
One of the things that’s important to realize is that this is a very small sample size, at just six individuals. Even within those six individuals, there was variation in terms of the response to the treatment. Probably, just like with all things in medicine, there will be different doses, different ways in which people do respond, people who get off of insulin completely, and people who may require some ongoing insulin therapy. I have no idea what this is going to look like as we test this in more people.
Everybody did start making C-peptide, they were having an effect of these beta cells, and it was working. We’ll have to see how well it works, how well it works in whom, and how we’re going to be able to use these types of therapies in the future.
In terms of side effects, they were really related to immunosuppression. There were no real surprises, but again, this is a very small sample size.
In summary, I think this is really hopeful. I don’t like to give false hope, but each step of this development process has shown that these beta cells derived from stem cells do seem to work in human beings as native beta cells might. Hopefully, this portends a future of newer therapies in the treatment of people with type 1 diabetes. Thank you.
Dr. Peters is professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She has published more than 200 articles, reviews, and abstracts, and three books, on diabetes, and has been an investigator for more than 40 research studies. She has spoken internationally at over 400 programs and serves on many committees of several professional organizations She disclosed ties with Abbott Diabetes Care, AstraZeneca, Becton Dickinson, Boehringer Ingelheim Pharmaceuticals, Dexcom, Eli Lilly, Lexicon Pharmaceuticals, Livongo, MannKind Corporation, Medscape, Merck, Novo Nordisk, Omada Health, OptumHealth, Sanofi, and Zafgen.
A version of this article originally appeared on Medscape.com.
New DEA CME mandate affects 2 million prescribers
The Consolidated Appropriations Act of 2023 mandates that all Drug Enforcement Administration–registered physicians and health care providers complete a one-time, 8-hour CME training on managing and treating opioid and other substance abuse disorders. This requirement goes into effect on June 27, 2023. New DEA registrants must also comply. Veterinarians are exempt.
A DEA registration is required to prescribe any controlled substance. The DEA categorizes these as Schedule I-V, with V being the least likely to be abused (Table 1). For example, opioids like fentanyl, oxycodone, and morphine are Schedule II. Medications without abuse potential are not scheduled.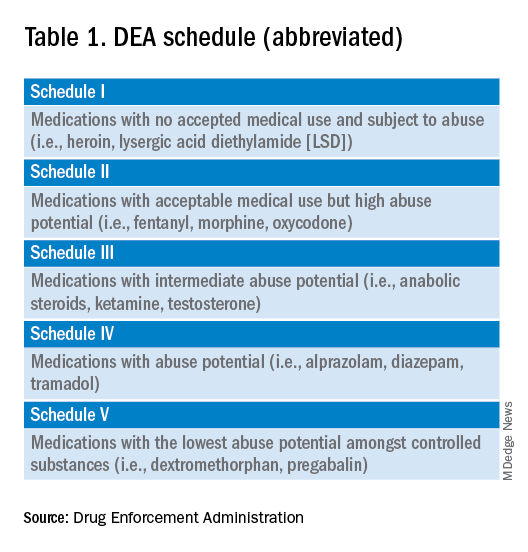
Will 16 million hours of opioid education save lives?
One should not underestimate the sweeping scope of this new federal requirement. DEA registrants include physicians and other health care providers such as nurse practitioners, physician assistants, and dentists. That is 8 hours per provider x 2 million providers: 16 million hours of CME!
Many states already require 1 or more hours of opioid training and pain management as part of their relicensure requirements (Table 2). To avoid redundancy, the DEA-mandated 8-hour training satisfies the various states’ requirements. 
An uncompensated mandate
Physicians are no strangers to lifelong learning and most eagerly pursue educational opportunities. Though some physicians may have CME time and stipends allocated by their employers, many others, such as the approximately 50,000 locum tenens doctors, do not. However, as enthusiastic as these physicians may be about this new CME course, they will likely lose a day of seeing patients (and income) to comply with this new obligation.
Not just pain doctors
The mandate’s broad brush includes many health care providers who hold DEA certificates but do not prescribe opioids. For example, as a general neurologist and epileptologist, I do not treat patients with chronic pain and cannot remember the last time I wrote an opioid prescription. However, I frequently prescribe lacosamide, a Schedule V drug. A surprisingly large number of antiseizure drugs are Schedule III, IV, or V drugs (Table 3).
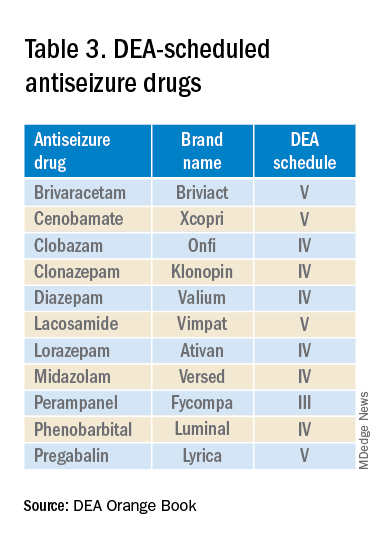
Real-world abuse?
How often scheduled antiseizure drugs are diverted or abused in an epilepsy population is unknown but appears to be infrequent. For example, perampanel abuse has not been reported despite its classification as a Schedule III drug. Anecdotally, in more than 40 years of clinical practice, I have never known a patient with epilepsy to abuse their antiseizure medications.
Take the course
Many organizations are happy to charge for the new 8-hour course. For example, the Tennessee Medical Association offers the training for $299 online or $400 in person. Materials from Elite Learning satisfy the 8-hour requirement for $80. However, NEJM Knowledge+ provides a complimentary 10-hour DEA-compliant course.
I recently completed the NEJM course. The information was thorough and took the whole 10 hours to finish. As excellent as it was, the content was only tangentially relevant to my clinical practice.
Conclusions
To obtain or renew a DEA certificate, neurologists, epilepsy specialists, and many other health care providers must comply with the new 8-hour CME opioid training mandate. Because the course requires 1 day to complete, health care providers would be prudent to obtain their CME well before their DEA certificate expires.
Though efforts to control the morbidity and mortality of the opioid epidemic are laudatory, perhaps the training should be more targeted to physicians who actually prescribe opioids rather than every DEA registrant. In the meantime, whether 16 million CME hours will save lives remains to be seen.
Dr. Wilner is professor of neurology at the University of Tennessee Health Science Center, Memphis. He reported a conflict of interest with Accordant Health Services.
A version of this article first appeared on Medscape.com.
The Consolidated Appropriations Act of 2023 mandates that all Drug Enforcement Administration–registered physicians and health care providers complete a one-time, 8-hour CME training on managing and treating opioid and other substance abuse disorders. This requirement goes into effect on June 27, 2023. New DEA registrants must also comply. Veterinarians are exempt.
A DEA registration is required to prescribe any controlled substance. The DEA categorizes these as Schedule I-V, with V being the least likely to be abused (Table 1). For example, opioids like fentanyl, oxycodone, and morphine are Schedule II. Medications without abuse potential are not scheduled.
Will 16 million hours of opioid education save lives?
One should not underestimate the sweeping scope of this new federal requirement. DEA registrants include physicians and other health care providers such as nurse practitioners, physician assistants, and dentists. That is 8 hours per provider x 2 million providers: 16 million hours of CME!
Many states already require 1 or more hours of opioid training and pain management as part of their relicensure requirements (Table 2). To avoid redundancy, the DEA-mandated 8-hour training satisfies the various states’ requirements.
An uncompensated mandate
Physicians are no strangers to lifelong learning and most eagerly pursue educational opportunities. Though some physicians may have CME time and stipends allocated by their employers, many others, such as the approximately 50,000 locum tenens doctors, do not. However, as enthusiastic as these physicians may be about this new CME course, they will likely lose a day of seeing patients (and income) to comply with this new obligation.
Not just pain doctors
The mandate’s broad brush includes many health care providers who hold DEA certificates but do not prescribe opioids. For example, as a general neurologist and epileptologist, I do not treat patients with chronic pain and cannot remember the last time I wrote an opioid prescription. However, I frequently prescribe lacosamide, a Schedule V drug. A surprisingly large number of antiseizure drugs are Schedule III, IV, or V drugs (Table 3).
Real-world abuse?
How often scheduled antiseizure drugs are diverted or abused in an epilepsy population is unknown but appears to be infrequent. For example, perampanel abuse has not been reported despite its classification as a Schedule III drug. Anecdotally, in more than 40 years of clinical practice, I have never known a patient with epilepsy to abuse their antiseizure medications.
Take the course
Many organizations are happy to charge for the new 8-hour course. For example, the Tennessee Medical Association offers the training for $299 online or $400 in person. Materials from Elite Learning satisfy the 8-hour requirement for $80. However, NEJM Knowledge+ provides a complimentary 10-hour DEA-compliant course.
I recently completed the NEJM course. The information was thorough and took the whole 10 hours to finish. As excellent as it was, the content was only tangentially relevant to my clinical practice.
Conclusions
To obtain or renew a DEA certificate, neurologists, epilepsy specialists, and many other health care providers must comply with the new 8-hour CME opioid training mandate. Because the course requires 1 day to complete, health care providers would be prudent to obtain their CME well before their DEA certificate expires.
Though efforts to control the morbidity and mortality of the opioid epidemic are laudatory, perhaps the training should be more targeted to physicians who actually prescribe opioids rather than every DEA registrant. In the meantime, whether 16 million CME hours will save lives remains to be seen.
Dr. Wilner is professor of neurology at the University of Tennessee Health Science Center, Memphis. He reported a conflict of interest with Accordant Health Services.
A version of this article first appeared on Medscape.com.
The Consolidated Appropriations Act of 2023 mandates that all Drug Enforcement Administration–registered physicians and health care providers complete a one-time, 8-hour CME training on managing and treating opioid and other substance abuse disorders. This requirement goes into effect on June 27, 2023. New DEA registrants must also comply. Veterinarians are exempt.
A DEA registration is required to prescribe any controlled substance. The DEA categorizes these as Schedule I-V, with V being the least likely to be abused (Table 1). For example, opioids like fentanyl, oxycodone, and morphine are Schedule II. Medications without abuse potential are not scheduled.
Will 16 million hours of opioid education save lives?
One should not underestimate the sweeping scope of this new federal requirement. DEA registrants include physicians and other health care providers such as nurse practitioners, physician assistants, and dentists. That is 8 hours per provider x 2 million providers: 16 million hours of CME!
Many states already require 1 or more hours of opioid training and pain management as part of their relicensure requirements (Table 2). To avoid redundancy, the DEA-mandated 8-hour training satisfies the various states’ requirements.
An uncompensated mandate
Physicians are no strangers to lifelong learning and most eagerly pursue educational opportunities. Though some physicians may have CME time and stipends allocated by their employers, many others, such as the approximately 50,000 locum tenens doctors, do not. However, as enthusiastic as these physicians may be about this new CME course, they will likely lose a day of seeing patients (and income) to comply with this new obligation.
Not just pain doctors
The mandate’s broad brush includes many health care providers who hold DEA certificates but do not prescribe opioids. For example, as a general neurologist and epileptologist, I do not treat patients with chronic pain and cannot remember the last time I wrote an opioid prescription. However, I frequently prescribe lacosamide, a Schedule V drug. A surprisingly large number of antiseizure drugs are Schedule III, IV, or V drugs (Table 3).
Real-world abuse?
How often scheduled antiseizure drugs are diverted or abused in an epilepsy population is unknown but appears to be infrequent. For example, perampanel abuse has not been reported despite its classification as a Schedule III drug. Anecdotally, in more than 40 years of clinical practice, I have never known a patient with epilepsy to abuse their antiseizure medications.
Take the course
Many organizations are happy to charge for the new 8-hour course. For example, the Tennessee Medical Association offers the training for $299 online or $400 in person. Materials from Elite Learning satisfy the 8-hour requirement for $80. However, NEJM Knowledge+ provides a complimentary 10-hour DEA-compliant course.
I recently completed the NEJM course. The information was thorough and took the whole 10 hours to finish. As excellent as it was, the content was only tangentially relevant to my clinical practice.
Conclusions
To obtain or renew a DEA certificate, neurologists, epilepsy specialists, and many other health care providers must comply with the new 8-hour CME opioid training mandate. Because the course requires 1 day to complete, health care providers would be prudent to obtain their CME well before their DEA certificate expires.
Though efforts to control the morbidity and mortality of the opioid epidemic are laudatory, perhaps the training should be more targeted to physicians who actually prescribe opioids rather than every DEA registrant. In the meantime, whether 16 million CME hours will save lives remains to be seen.
Dr. Wilner is professor of neurology at the University of Tennessee Health Science Center, Memphis. He reported a conflict of interest with Accordant Health Services.
A version of this article first appeared on Medscape.com.
The most important question in medicine
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
Today I am going to tell you the single best question you can ask any doctor, the one that has saved my butt countless times throughout my career, the one that every attending physician should be asking every intern and resident when they present a new case. That question: “What else could this be?”
I know, I know – “When you hear hoofbeats, think horses, not zebras.” I get it. But sometimes we get so good at our jobs, so good at recognizing horses, that we stop asking ourselves about zebras at all. You see this in a phenomenon known as “anchoring bias” where physicians, when presented with a diagnosis, tend to latch on to that diagnosis based on the first piece of information given, paying attention to data that support it and ignoring data that point in other directions.
That special question: “What else could this be?”, breaks through that barrier. It forces you, the medical team, everyone, to go through the exercise of real, old-fashioned differential diagnosis. And I promise that if you do this enough, at some point it will save someone’s life.
Though the concept of anchoring bias in medicine is broadly understood, it hasn’t been broadly studied until now, with this study appearing in JAMA Internal Medicine.
Here’s the setup.
The authors hypothesized that there would be substantial anchoring bias when patients with heart failure presented to the emergency department with shortness of breath if the triage “visit reason” section mentioned HF. We’re talking about the subtle difference between the following:
- Visit reason: Shortness of breath
- Visit reason: Shortness of breath/HF
People with HF can be short of breath for lots of reasons. HF exacerbation comes immediately to mind and it should. But there are obviously lots of answers to that “What else could this be?” question: pneumonia, pneumothorax, heart attack, COPD, and, of course, pulmonary embolism (PE).
The authors leveraged the nationwide VA database, allowing them to examine data from over 100,000 patients presenting to various VA EDs with shortness of breath. They then looked for particular tests – D-dimer, CT chest with contrast, V/Q scan, lower-extremity Doppler — that would suggest that the doctor was thinking about PE. The question, then, is whether mentioning HF in that little “visit reason” section would influence the likelihood of testing for PE.
I know what you’re thinking: Not everyone who is short of breath needs an evaluation for PE. And the authors did a nice job accounting for a variety of factors that might predict a PE workup: malignancy, recent surgery, elevated heart rate, low oxygen saturation, etc. Of course, some of those same factors might predict whether that triage nurse will write HF in the visit reason section. All of these things need to be accounted for statistically, and were, but – the unofficial Impact Factor motto reminds us that “there are always more confounders.”
But let’s dig into the results. I’m going to give you the raw numbers first. There were 4,392 people with HF whose visit reason section, in addition to noting shortness of breath, explicitly mentioned HF. Of those, 360 had PE testing and two had a PE diagnosed during that ED visit. So that’s around an 8% testing rate and a 0.5% hit rate for testing. But 43 people, presumably not tested in the ED, had a PE diagnosed within the next 30 days. Assuming that those PEs were present at the ED visit, that means the ED missed 95% of the PEs in the group with that HF label attached to them.
Let’s do the same thing for those whose visit reason just said “shortness of breath.”
Of the 103,627 people in that category, 13,886 were tested for PE and 231 of those tested positive. So that is an overall testing rate of around 13% and a hit rate of 1.7%. And 1,081 of these people had a PE diagnosed within 30 days. Assuming that those PEs were actually present at the ED visit, the docs missed 79% of them.
There’s one other thing to notice from the data: The overall PE rate (diagnosed by 30 days) was basically the same in both groups. That HF label does not really flag a group at lower risk for PE.
Yes, there are a lot of assumptions here, including that all PEs that were actually there in the ED got caught within 30 days, but the numbers do paint a picture. In this unadjusted analysis, it seems that the HF label leads to less testing and more missed PEs. Classic anchoring bias.
The adjusted analysis, accounting for all those PE risk factors, really didn’t change these results. You get nearly the same numbers and thus nearly the same conclusions.
Now, the main missing piece of this puzzle is in the mind of the clinician. We don’t know whether they didn’t consider PE or whether they considered PE but thought it unlikely. And in the end, it’s clear that the vast majority of people in this study did not have PE (though I suspect not all had a simple HF exacerbation). But this type of analysis is useful not only for the empiric evidence of the clinical impact of anchoring bias but because of the fact that it reminds us all to ask that all-important question: What else could this be?
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
Today I am going to tell you the single best question you can ask any doctor, the one that has saved my butt countless times throughout my career, the one that every attending physician should be asking every intern and resident when they present a new case. That question: “What else could this be?”
I know, I know – “When you hear hoofbeats, think horses, not zebras.” I get it. But sometimes we get so good at our jobs, so good at recognizing horses, that we stop asking ourselves about zebras at all. You see this in a phenomenon known as “anchoring bias” where physicians, when presented with a diagnosis, tend to latch on to that diagnosis based on the first piece of information given, paying attention to data that support it and ignoring data that point in other directions.
That special question: “What else could this be?”, breaks through that barrier. It forces you, the medical team, everyone, to go through the exercise of real, old-fashioned differential diagnosis. And I promise that if you do this enough, at some point it will save someone’s life.
Though the concept of anchoring bias in medicine is broadly understood, it hasn’t been broadly studied until now, with this study appearing in JAMA Internal Medicine.
Here’s the setup.
The authors hypothesized that there would be substantial anchoring bias when patients with heart failure presented to the emergency department with shortness of breath if the triage “visit reason” section mentioned HF. We’re talking about the subtle difference between the following:
- Visit reason: Shortness of breath
- Visit reason: Shortness of breath/HF
People with HF can be short of breath for lots of reasons. HF exacerbation comes immediately to mind and it should. But there are obviously lots of answers to that “What else could this be?” question: pneumonia, pneumothorax, heart attack, COPD, and, of course, pulmonary embolism (PE).
The authors leveraged the nationwide VA database, allowing them to examine data from over 100,000 patients presenting to various VA EDs with shortness of breath. They then looked for particular tests – D-dimer, CT chest with contrast, V/Q scan, lower-extremity Doppler — that would suggest that the doctor was thinking about PE. The question, then, is whether mentioning HF in that little “visit reason” section would influence the likelihood of testing for PE.
I know what you’re thinking: Not everyone who is short of breath needs an evaluation for PE. And the authors did a nice job accounting for a variety of factors that might predict a PE workup: malignancy, recent surgery, elevated heart rate, low oxygen saturation, etc. Of course, some of those same factors might predict whether that triage nurse will write HF in the visit reason section. All of these things need to be accounted for statistically, and were, but – the unofficial Impact Factor motto reminds us that “there are always more confounders.”
But let’s dig into the results. I’m going to give you the raw numbers first. There were 4,392 people with HF whose visit reason section, in addition to noting shortness of breath, explicitly mentioned HF. Of those, 360 had PE testing and two had a PE diagnosed during that ED visit. So that’s around an 8% testing rate and a 0.5% hit rate for testing. But 43 people, presumably not tested in the ED, had a PE diagnosed within the next 30 days. Assuming that those PEs were present at the ED visit, that means the ED missed 95% of the PEs in the group with that HF label attached to them.
Let’s do the same thing for those whose visit reason just said “shortness of breath.”
Of the 103,627 people in that category, 13,886 were tested for PE and 231 of those tested positive. So that is an overall testing rate of around 13% and a hit rate of 1.7%. And 1,081 of these people had a PE diagnosed within 30 days. Assuming that those PEs were actually present at the ED visit, the docs missed 79% of them.
There’s one other thing to notice from the data: The overall PE rate (diagnosed by 30 days) was basically the same in both groups. That HF label does not really flag a group at lower risk for PE.
Yes, there are a lot of assumptions here, including that all PEs that were actually there in the ED got caught within 30 days, but the numbers do paint a picture. In this unadjusted analysis, it seems that the HF label leads to less testing and more missed PEs. Classic anchoring bias.
The adjusted analysis, accounting for all those PE risk factors, really didn’t change these results. You get nearly the same numbers and thus nearly the same conclusions.
Now, the main missing piece of this puzzle is in the mind of the clinician. We don’t know whether they didn’t consider PE or whether they considered PE but thought it unlikely. And in the end, it’s clear that the vast majority of people in this study did not have PE (though I suspect not all had a simple HF exacerbation). But this type of analysis is useful not only for the empiric evidence of the clinical impact of anchoring bias but because of the fact that it reminds us all to ask that all-important question: What else could this be?
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
Today I am going to tell you the single best question you can ask any doctor, the one that has saved my butt countless times throughout my career, the one that every attending physician should be asking every intern and resident when they present a new case. That question: “What else could this be?”
I know, I know – “When you hear hoofbeats, think horses, not zebras.” I get it. But sometimes we get so good at our jobs, so good at recognizing horses, that we stop asking ourselves about zebras at all. You see this in a phenomenon known as “anchoring bias” where physicians, when presented with a diagnosis, tend to latch on to that diagnosis based on the first piece of information given, paying attention to data that support it and ignoring data that point in other directions.
That special question: “What else could this be?”, breaks through that barrier. It forces you, the medical team, everyone, to go through the exercise of real, old-fashioned differential diagnosis. And I promise that if you do this enough, at some point it will save someone’s life.
Though the concept of anchoring bias in medicine is broadly understood, it hasn’t been broadly studied until now, with this study appearing in JAMA Internal Medicine.
Here’s the setup.
The authors hypothesized that there would be substantial anchoring bias when patients with heart failure presented to the emergency department with shortness of breath if the triage “visit reason” section mentioned HF. We’re talking about the subtle difference between the following:
- Visit reason: Shortness of breath
- Visit reason: Shortness of breath/HF
People with HF can be short of breath for lots of reasons. HF exacerbation comes immediately to mind and it should. But there are obviously lots of answers to that “What else could this be?” question: pneumonia, pneumothorax, heart attack, COPD, and, of course, pulmonary embolism (PE).
The authors leveraged the nationwide VA database, allowing them to examine data from over 100,000 patients presenting to various VA EDs with shortness of breath. They then looked for particular tests – D-dimer, CT chest with contrast, V/Q scan, lower-extremity Doppler — that would suggest that the doctor was thinking about PE. The question, then, is whether mentioning HF in that little “visit reason” section would influence the likelihood of testing for PE.
I know what you’re thinking: Not everyone who is short of breath needs an evaluation for PE. And the authors did a nice job accounting for a variety of factors that might predict a PE workup: malignancy, recent surgery, elevated heart rate, low oxygen saturation, etc. Of course, some of those same factors might predict whether that triage nurse will write HF in the visit reason section. All of these things need to be accounted for statistically, and were, but – the unofficial Impact Factor motto reminds us that “there are always more confounders.”
But let’s dig into the results. I’m going to give you the raw numbers first. There were 4,392 people with HF whose visit reason section, in addition to noting shortness of breath, explicitly mentioned HF. Of those, 360 had PE testing and two had a PE diagnosed during that ED visit. So that’s around an 8% testing rate and a 0.5% hit rate for testing. But 43 people, presumably not tested in the ED, had a PE diagnosed within the next 30 days. Assuming that those PEs were present at the ED visit, that means the ED missed 95% of the PEs in the group with that HF label attached to them.
Let’s do the same thing for those whose visit reason just said “shortness of breath.”
Of the 103,627 people in that category, 13,886 were tested for PE and 231 of those tested positive. So that is an overall testing rate of around 13% and a hit rate of 1.7%. And 1,081 of these people had a PE diagnosed within 30 days. Assuming that those PEs were actually present at the ED visit, the docs missed 79% of them.
There’s one other thing to notice from the data: The overall PE rate (diagnosed by 30 days) was basically the same in both groups. That HF label does not really flag a group at lower risk for PE.
Yes, there are a lot of assumptions here, including that all PEs that were actually there in the ED got caught within 30 days, but the numbers do paint a picture. In this unadjusted analysis, it seems that the HF label leads to less testing and more missed PEs. Classic anchoring bias.
The adjusted analysis, accounting for all those PE risk factors, really didn’t change these results. You get nearly the same numbers and thus nearly the same conclusions.
Now, the main missing piece of this puzzle is in the mind of the clinician. We don’t know whether they didn’t consider PE or whether they considered PE but thought it unlikely. And in the end, it’s clear that the vast majority of people in this study did not have PE (though I suspect not all had a simple HF exacerbation). But this type of analysis is useful not only for the empiric evidence of the clinical impact of anchoring bias but because of the fact that it reminds us all to ask that all-important question: What else could this be?
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
In defense of artificial sweeteners
More than 140 million Americans use artificial sweeteners, a habit driven by the irrefutable fact that excess sugar is harmful. But I’m continually amazed by alarmist headlines on the topic.
In May, the World Health Organization (WHO) released a report to support its “conditional recommendation” against the use of non-sugar sweeteners (NSS) for weight control. Despite the WHO’s goal “to provide evidence-informed guidance,” the report includes the disclaimer that “The recommendation is based on evidence of low certainty.”
Low certainty is an accurate descriptor for the findings of many of the 280-plus studies in the report. That the guidance does not apply to patients with diabetes was easily lost in the repeated mentions of the perceived dangers of these sugar alternatives.
The review included various table-top and beverage sweeteners, including acesulfame K, aspartame, saccharin, sucralose, stevia, and stevia derivatives. Low-calorie sugars and sugar alcohols such as erythritol were excluded.
The WHO looked at long- and short-term trials, randomized controlled trials (RCTs), prospective studies, and case-control studies measuring a wide range of endpoints, from dental caries to cancer. The report highlighted that some findings cannot be attributed directly to NSS use but may simply be due to their substitution for sugar. Differences in outcomes due to sex, ethnicity, and body weight status could not be assessed either. And the WHO conceded the possibility of reverse causation in observational studies wherein higher-risk individuals may consume more NSS.
Nonnutritive sweeteners are given little credit for weight loss. “A significant difference in body weight and BMI was only observed in trials that reported a reduction in energy intake ... rather than primarily by an inherent property of NSS that can modulate body weight (independently of energy intake),” the report reads. But isn’t the desired effect of using an artificial sweetener instead of table sugar that you lower your calorie intake?
The WHO noted that weight loss was not sustained – a finding in nearly every weight loss trial in history and something more attributable to human nature than the sweetener one chooses.
The document outlines that meta-analyses of prospective cohort studies show that higher intakes of NSS were associated with an increased risk for type 2 diabetes and elevated fasting glucose, while meta-analyses of randomized trials suggest no significant effect on “biomarkers used in the assessment and diagnosis of diabetes and insulin resistance, including fasting glucose, fasting insulin and hemoglobin A1c.”
Similar disparities are noted with cardiovascular risk. Prospective trials suggest an increased risk for CVD, including stroke and its precursor, hypertension; but again, the RCT data found no evidence to suggest a significant effect “on biomarkers used in the assessment and diagnosis of CVDs, including blood pressure, low-density lipoprotein cholesterol and other blood lipids.”
Splenda and stevia under fire
Predictably, some in the nonnutritive sweetener industry are incensed.
Ted Gelov, CEO of Heartland Food Products Group, maker of Splenda, responded in a press release, “Every few years now it seems I have to come to you and clarify misleading headlines ... Suggesting that sweeteners like Splenda cannot have long-term benefits is a disservice to healthcare providers, their patients, and all consumers.”
Splenda has been on the U.S. market since 1999, and Mr. Gelov reportedly uses three to eight packets daily in his coffee and tea.
I reached out to Heartland and they sent me an eight-page document consisting of over 50 statements, summaries, and clinical trials supporting the safety of artificial sweeteners, including sucralose, an ingredient in Splenda. In 2016, Mr. Gelov rebutted claims that sucralose was linked to cancer in Swiss male mice. These “dramatized headlines are based on one flawed study by an isolated Italian research laboratory, the Ramazzini Institute,” Mr. Gelov wrote.
Another recent headline was about the DNA-damaging effects of sucralose-6-acetate (S6A) seen in an in vitro study published in the Journal of Toxicology and Environmental Health. According to the authors, commercial sucralose samples contain up to 0.67% S6A, a manufacturing impurity.
Despite many reports linking this study to Splenda, Heartland wrote that “Splenda and its ingredients were never studied or tested in this research. We, and our suppliers, rigorously and routinely test and monitor for any impurities in our products. We can confirm that S6A is not present in Splenda Brand sucralose down to the lowest detection limit possible, which is .001% sensitivity level.”
F. Perry Wilson, MD, director of Clinical and Translational Research Accelerator at Yale and a regular contributor to this news organization, took to Twitter to put this study in context: “The human exposure equivalent to sucralose would be 60 packets per day,” he pointed out. And the blood levels of S6A with normal consumption would not “come close to the DNA damage threshold noted in the article.”
Perhaps the most concerning scientific data suggesting a link between artificial sweetener use and ill health is a Cleveland Clinic study showing an association between higher blood levels of erythritol and adverse cardiovascular outcomes such as heart attack, stroke, or death. The researchers also found that erythritol, which is found in stevia and some keto food products, made platelet activation and clot formation easier.
When I asked about these findings, Heartland stated, “The study was primarily conducted on patients who were at an elevated risk of cardiovascular events due to their advanced age, elevated body mass and presence of pre-existing health conditions ... the stated findings were only an association and cannot imply causation.”
The main conclusion I’ve drawn on the topic of artificial sweeteners is that a lot of resources were wasted in performing underpowered, poorly designed trials on compounds that are already generally regarded as safe (GRAS) by the FDA. The WHO “conditional guideline” is, by its own description, based on a plethora of “low certainty” to “very low certainty” evidence.
The monies to produce the WHO report and many of these trials would have been better spent educating the public on the difference between simple and complex carbohydrates; the inflammatory and disease-producing effects of excess sugars; and how to prevent, diagnose, and treat diabetes.
If more trials on artificial sweeteners are planned, they should be performed on people doing human things – which does not include ingesting 60 packets of any sweetener in a single day.
In my personal N-of-1 trial, consuming sugar makes me crave more, feel sluggish, and gain weight. I don’t believe that NSS alone will control my weight. But I’ll continue to drink two cups of stevia-laced coffee every morning, take walks, avoid alcohol, eat my vegetables, and hope for the best.
Dr. Walton-Shirley is a clinical cardiologist in Nashville, Tenn. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
More than 140 million Americans use artificial sweeteners, a habit driven by the irrefutable fact that excess sugar is harmful. But I’m continually amazed by alarmist headlines on the topic.
In May, the World Health Organization (WHO) released a report to support its “conditional recommendation” against the use of non-sugar sweeteners (NSS) for weight control. Despite the WHO’s goal “to provide evidence-informed guidance,” the report includes the disclaimer that “The recommendation is based on evidence of low certainty.”
Low certainty is an accurate descriptor for the findings of many of the 280-plus studies in the report. That the guidance does not apply to patients with diabetes was easily lost in the repeated mentions of the perceived dangers of these sugar alternatives.
The review included various table-top and beverage sweeteners, including acesulfame K, aspartame, saccharin, sucralose, stevia, and stevia derivatives. Low-calorie sugars and sugar alcohols such as erythritol were excluded.
The WHO looked at long- and short-term trials, randomized controlled trials (RCTs), prospective studies, and case-control studies measuring a wide range of endpoints, from dental caries to cancer. The report highlighted that some findings cannot be attributed directly to NSS use but may simply be due to their substitution for sugar. Differences in outcomes due to sex, ethnicity, and body weight status could not be assessed either. And the WHO conceded the possibility of reverse causation in observational studies wherein higher-risk individuals may consume more NSS.
Nonnutritive sweeteners are given little credit for weight loss. “A significant difference in body weight and BMI was only observed in trials that reported a reduction in energy intake ... rather than primarily by an inherent property of NSS that can modulate body weight (independently of energy intake),” the report reads. But isn’t the desired effect of using an artificial sweetener instead of table sugar that you lower your calorie intake?
The WHO noted that weight loss was not sustained – a finding in nearly every weight loss trial in history and something more attributable to human nature than the sweetener one chooses.
The document outlines that meta-analyses of prospective cohort studies show that higher intakes of NSS were associated with an increased risk for type 2 diabetes and elevated fasting glucose, while meta-analyses of randomized trials suggest no significant effect on “biomarkers used in the assessment and diagnosis of diabetes and insulin resistance, including fasting glucose, fasting insulin and hemoglobin A1c.”
Similar disparities are noted with cardiovascular risk. Prospective trials suggest an increased risk for CVD, including stroke and its precursor, hypertension; but again, the RCT data found no evidence to suggest a significant effect “on biomarkers used in the assessment and diagnosis of CVDs, including blood pressure, low-density lipoprotein cholesterol and other blood lipids.”
Splenda and stevia under fire
Predictably, some in the nonnutritive sweetener industry are incensed.
Ted Gelov, CEO of Heartland Food Products Group, maker of Splenda, responded in a press release, “Every few years now it seems I have to come to you and clarify misleading headlines ... Suggesting that sweeteners like Splenda cannot have long-term benefits is a disservice to healthcare providers, their patients, and all consumers.”
Splenda has been on the U.S. market since 1999, and Mr. Gelov reportedly uses three to eight packets daily in his coffee and tea.
I reached out to Heartland and they sent me an eight-page document consisting of over 50 statements, summaries, and clinical trials supporting the safety of artificial sweeteners, including sucralose, an ingredient in Splenda. In 2016, Mr. Gelov rebutted claims that sucralose was linked to cancer in Swiss male mice. These “dramatized headlines are based on one flawed study by an isolated Italian research laboratory, the Ramazzini Institute,” Mr. Gelov wrote.
Another recent headline was about the DNA-damaging effects of sucralose-6-acetate (S6A) seen in an in vitro study published in the Journal of Toxicology and Environmental Health. According to the authors, commercial sucralose samples contain up to 0.67% S6A, a manufacturing impurity.
Despite many reports linking this study to Splenda, Heartland wrote that “Splenda and its ingredients were never studied or tested in this research. We, and our suppliers, rigorously and routinely test and monitor for any impurities in our products. We can confirm that S6A is not present in Splenda Brand sucralose down to the lowest detection limit possible, which is .001% sensitivity level.”
F. Perry Wilson, MD, director of Clinical and Translational Research Accelerator at Yale and a regular contributor to this news organization, took to Twitter to put this study in context: “The human exposure equivalent to sucralose would be 60 packets per day,” he pointed out. And the blood levels of S6A with normal consumption would not “come close to the DNA damage threshold noted in the article.”
Perhaps the most concerning scientific data suggesting a link between artificial sweetener use and ill health is a Cleveland Clinic study showing an association between higher blood levels of erythritol and adverse cardiovascular outcomes such as heart attack, stroke, or death. The researchers also found that erythritol, which is found in stevia and some keto food products, made platelet activation and clot formation easier.
When I asked about these findings, Heartland stated, “The study was primarily conducted on patients who were at an elevated risk of cardiovascular events due to their advanced age, elevated body mass and presence of pre-existing health conditions ... the stated findings were only an association and cannot imply causation.”
The main conclusion I’ve drawn on the topic of artificial sweeteners is that a lot of resources were wasted in performing underpowered, poorly designed trials on compounds that are already generally regarded as safe (GRAS) by the FDA. The WHO “conditional guideline” is, by its own description, based on a plethora of “low certainty” to “very low certainty” evidence.
The monies to produce the WHO report and many of these trials would have been better spent educating the public on the difference between simple and complex carbohydrates; the inflammatory and disease-producing effects of excess sugars; and how to prevent, diagnose, and treat diabetes.
If more trials on artificial sweeteners are planned, they should be performed on people doing human things – which does not include ingesting 60 packets of any sweetener in a single day.
In my personal N-of-1 trial, consuming sugar makes me crave more, feel sluggish, and gain weight. I don’t believe that NSS alone will control my weight. But I’ll continue to drink two cups of stevia-laced coffee every morning, take walks, avoid alcohol, eat my vegetables, and hope for the best.
Dr. Walton-Shirley is a clinical cardiologist in Nashville, Tenn. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
More than 140 million Americans use artificial sweeteners, a habit driven by the irrefutable fact that excess sugar is harmful. But I’m continually amazed by alarmist headlines on the topic.
In May, the World Health Organization (WHO) released a report to support its “conditional recommendation” against the use of non-sugar sweeteners (NSS) for weight control. Despite the WHO’s goal “to provide evidence-informed guidance,” the report includes the disclaimer that “The recommendation is based on evidence of low certainty.”
Low certainty is an accurate descriptor for the findings of many of the 280-plus studies in the report. That the guidance does not apply to patients with diabetes was easily lost in the repeated mentions of the perceived dangers of these sugar alternatives.
The review included various table-top and beverage sweeteners, including acesulfame K, aspartame, saccharin, sucralose, stevia, and stevia derivatives. Low-calorie sugars and sugar alcohols such as erythritol were excluded.
The WHO looked at long- and short-term trials, randomized controlled trials (RCTs), prospective studies, and case-control studies measuring a wide range of endpoints, from dental caries to cancer. The report highlighted that some findings cannot be attributed directly to NSS use but may simply be due to their substitution for sugar. Differences in outcomes due to sex, ethnicity, and body weight status could not be assessed either. And the WHO conceded the possibility of reverse causation in observational studies wherein higher-risk individuals may consume more NSS.
Nonnutritive sweeteners are given little credit for weight loss. “A significant difference in body weight and BMI was only observed in trials that reported a reduction in energy intake ... rather than primarily by an inherent property of NSS that can modulate body weight (independently of energy intake),” the report reads. But isn’t the desired effect of using an artificial sweetener instead of table sugar that you lower your calorie intake?
The WHO noted that weight loss was not sustained – a finding in nearly every weight loss trial in history and something more attributable to human nature than the sweetener one chooses.
The document outlines that meta-analyses of prospective cohort studies show that higher intakes of NSS were associated with an increased risk for type 2 diabetes and elevated fasting glucose, while meta-analyses of randomized trials suggest no significant effect on “biomarkers used in the assessment and diagnosis of diabetes and insulin resistance, including fasting glucose, fasting insulin and hemoglobin A1c.”
Similar disparities are noted with cardiovascular risk. Prospective trials suggest an increased risk for CVD, including stroke and its precursor, hypertension; but again, the RCT data found no evidence to suggest a significant effect “on biomarkers used in the assessment and diagnosis of CVDs, including blood pressure, low-density lipoprotein cholesterol and other blood lipids.”
Splenda and stevia under fire
Predictably, some in the nonnutritive sweetener industry are incensed.
Ted Gelov, CEO of Heartland Food Products Group, maker of Splenda, responded in a press release, “Every few years now it seems I have to come to you and clarify misleading headlines ... Suggesting that sweeteners like Splenda cannot have long-term benefits is a disservice to healthcare providers, their patients, and all consumers.”
Splenda has been on the U.S. market since 1999, and Mr. Gelov reportedly uses three to eight packets daily in his coffee and tea.
I reached out to Heartland and they sent me an eight-page document consisting of over 50 statements, summaries, and clinical trials supporting the safety of artificial sweeteners, including sucralose, an ingredient in Splenda. In 2016, Mr. Gelov rebutted claims that sucralose was linked to cancer in Swiss male mice. These “dramatized headlines are based on one flawed study by an isolated Italian research laboratory, the Ramazzini Institute,” Mr. Gelov wrote.
Another recent headline was about the DNA-damaging effects of sucralose-6-acetate (S6A) seen in an in vitro study published in the Journal of Toxicology and Environmental Health. According to the authors, commercial sucralose samples contain up to 0.67% S6A, a manufacturing impurity.
Despite many reports linking this study to Splenda, Heartland wrote that “Splenda and its ingredients were never studied or tested in this research. We, and our suppliers, rigorously and routinely test and monitor for any impurities in our products. We can confirm that S6A is not present in Splenda Brand sucralose down to the lowest detection limit possible, which is .001% sensitivity level.”
F. Perry Wilson, MD, director of Clinical and Translational Research Accelerator at Yale and a regular contributor to this news organization, took to Twitter to put this study in context: “The human exposure equivalent to sucralose would be 60 packets per day,” he pointed out. And the blood levels of S6A with normal consumption would not “come close to the DNA damage threshold noted in the article.”
Perhaps the most concerning scientific data suggesting a link between artificial sweetener use and ill health is a Cleveland Clinic study showing an association between higher blood levels of erythritol and adverse cardiovascular outcomes such as heart attack, stroke, or death. The researchers also found that erythritol, which is found in stevia and some keto food products, made platelet activation and clot formation easier.
When I asked about these findings, Heartland stated, “The study was primarily conducted on patients who were at an elevated risk of cardiovascular events due to their advanced age, elevated body mass and presence of pre-existing health conditions ... the stated findings were only an association and cannot imply causation.”
The main conclusion I’ve drawn on the topic of artificial sweeteners is that a lot of resources were wasted in performing underpowered, poorly designed trials on compounds that are already generally regarded as safe (GRAS) by the FDA. The WHO “conditional guideline” is, by its own description, based on a plethora of “low certainty” to “very low certainty” evidence.
The monies to produce the WHO report and many of these trials would have been better spent educating the public on the difference between simple and complex carbohydrates; the inflammatory and disease-producing effects of excess sugars; and how to prevent, diagnose, and treat diabetes.
If more trials on artificial sweeteners are planned, they should be performed on people doing human things – which does not include ingesting 60 packets of any sweetener in a single day.
In my personal N-of-1 trial, consuming sugar makes me crave more, feel sluggish, and gain weight. I don’t believe that NSS alone will control my weight. But I’ll continue to drink two cups of stevia-laced coffee every morning, take walks, avoid alcohol, eat my vegetables, and hope for the best.
Dr. Walton-Shirley is a clinical cardiologist in Nashville, Tenn. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Updates on pregnancy outcomes in transgender men
Despite increased societal gains, transgender individuals are still a medically and socially underserved group. The historic rise of antitransgender legislation and the overturning of Roe v. Wade, further compound existing health care disparities, particularly in the realm of contraception and pregnancy. Obstetrician-gynecologists and midwives are typically first-line providers when discussing family planning and fertility options for all patients assigned female at birth. Unfortunately,

Only individuals who are assigned female at birth and have a uterus are capable of pregnancy. This can include both cisgender women and nonbinary/transgender men. However, societal and medical institutions are struggling with this shift in perspective from a traditionally gendered role to a more inclusive one. Obstetrician-gynecologists and midwives can serve to bridge this gap between these patients and societal misconceptions surrounding transgender men who desire and experience pregnancy.
Providers need to remember that many transmasculine individuals will still retain their uterus and are therefore capable of getting pregnant. While testosterone causes amenorrhea, if patients are engaging in penile-vaginal intercourse, conception is still possible. If a patient does not desire pregnancy, all contraceptive options available for cisgender women, which also include combined oral contraceptives, should be offered.
For patients seeking to become pregnant, testosterone must be discontinued. Testosterone is teratogenic; it can cause abnormal urogenital development in the female fetus and should be avoided even prior to conception.1,2 The timing of testosterone discontinuation is debatable. There are no well-established guidelines dictating how early pregnancy can be attempted after cessation of testosterone, but typically if menses has resumed, the teratogenic effects of testosterone are less likely.
For amenorrheic patients on testosterone, menses will occur, on average, 3-6 months after testosterone is stopped. Of note, the longer that testosterone has been suspended, the greater the likelihood of achieving pregnancy.3 In a study by Light et al., 72% of patients conceived within 6 months of attempting pregnancy, 80% resumed menses within 6 months of stopping testosterone, and 20% of individuals conceived while they were amenorrheic from testosterone.4
Psychosocial support is an essential part of pregnancy care in transgender men. For some patients, pregnancy can worsen gender dysphoria, whereas others are empowered by the experience. Insurance companies may also deny obstetric care services to transgender males who have already changed their gender marker from female to male on insurance policies.
Whether transmasculine individuals are at higher risk for pregnancy complications is largely unknown, although emerging research in this field has yielded interesting results. While testosterone can cause vaginal atrophy, it does not seem to increase a patient’s risk of vaginal lacerations or their ability to have a successful vaginal delivery. For transgender men with significant discomfort around their genitalia, an elective cesarean section may be appropriate.5
More recently, Stroumsa et al. conducted an analysis of all deliveries at a Michigan institution from 2014 to 2018. Patients with male gender at the time of delivery or with the diagnostic code of gender dysphoria were identified as transgender.6 The primary outcome of this study was severe parental morbidity (such as amniotic fluid embolism, acute myocardial infarction, eclampsia, etc.), with secondary outcomes investigating rates of cesarean delivery and preterm birth.
During this time period, the researchers identified 256 transgender patients and 1.3 million cisgender patients in their Medicaid database and 1,651 transgender patients and 1.5 million cisgender patients in the commercial database who had experienced a delivery.6 Compared with cisgender patients, transgender patients in the Medicaid database were younger, less likely to be white, and more likely to have a chronic condition.6 Compared with cisgender patients in the commercial database, transgender patients experienced higher rates of anxiety and depression.6 Both transgender and cisgender patients had similar rates of severe parental morbidity. Ironically, rates of cesarean delivery were lower, compared with cisgender patients, in both the Medicaid and commercial databases, with no differences observed between rates of preterm birth.6
While more research is needed on pregnancy in transgender men, this analysis is not only one of the largest to date, but it also challenges many misconceptions providers have regarding pregnancy outcomes. Even though transmasculine patients may require additional medical interventions to achieve pregnancy, such as assisted reproductive technology, or increased psychosocial support during the process, these initial studies are reassuring. Based on current evidence, these patients are not at greater risk for perinatal complications than their cisgender counterparts.
Despite these encouraging findings, there are still several challenges faced by transgender men when it comes to getting pregnant. For instance, they may have difficulty accessing fertility services because of financial constraints or experience a lack of awareness or prejudice from providers; they might also be subject to discrimination or stigma within health care settings. As front-line providers for obstetrical care, we must lead the way towards improving the care for pregnant transmasculine individuals.
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa.
References
1. Light A et al. Family planning and contraception use in transgender men. Contraception. 2018 Oct. doi: 10.1016/j.contraception.2018.06.006.
2. Krempasky C et al. Contraception across the transmasculine spectrum. Am J Obstet Gynecol. 2020 Feb. doi: 10.1016/j.ajog.2019.07.043.
3. Obedin-Maliver J, De Haan G. “Gynecologic care for transgender patients” in Ferrando C, ed., Comprehensive Care of the Transgender Patient. Philadelphia: Elsevier, 2019. 131-51.
4. Light AD et al. Transgender men who experienced pregnancy after female-to-male gender transitioning. Obstet Gynecol. 2014 Dec. doi: 10.1097/AOG.0000000000000540.
5. Brandt JS et al. Transgender men, pregnancy, and the “new” advanced paternal age: A review of the literature. Maturitas. 2019 Oct. doi: 10.1016/j.maturitas.2019.07.004.
6. Stroumsa D et al. Pregnancy outcomes in a U.S. cohort of transgender people. JAMA. 2023 Jun 6. doi: 10.1001/jama.2023.7688.
Despite increased societal gains, transgender individuals are still a medically and socially underserved group. The historic rise of antitransgender legislation and the overturning of Roe v. Wade, further compound existing health care disparities, particularly in the realm of contraception and pregnancy. Obstetrician-gynecologists and midwives are typically first-line providers when discussing family planning and fertility options for all patients assigned female at birth. Unfortunately,
Only individuals who are assigned female at birth and have a uterus are capable of pregnancy. This can include both cisgender women and nonbinary/transgender men. However, societal and medical institutions are struggling with this shift in perspective from a traditionally gendered role to a more inclusive one. Obstetrician-gynecologists and midwives can serve to bridge this gap between these patients and societal misconceptions surrounding transgender men who desire and experience pregnancy.
Providers need to remember that many transmasculine individuals will still retain their uterus and are therefore capable of getting pregnant. While testosterone causes amenorrhea, if patients are engaging in penile-vaginal intercourse, conception is still possible. If a patient does not desire pregnancy, all contraceptive options available for cisgender women, which also include combined oral contraceptives, should be offered.
For patients seeking to become pregnant, testosterone must be discontinued. Testosterone is teratogenic; it can cause abnormal urogenital development in the female fetus and should be avoided even prior to conception.1,2 The timing of testosterone discontinuation is debatable. There are no well-established guidelines dictating how early pregnancy can be attempted after cessation of testosterone, but typically if menses has resumed, the teratogenic effects of testosterone are less likely.
For amenorrheic patients on testosterone, menses will occur, on average, 3-6 months after testosterone is stopped. Of note, the longer that testosterone has been suspended, the greater the likelihood of achieving pregnancy.3 In a study by Light et al., 72% of patients conceived within 6 months of attempting pregnancy, 80% resumed menses within 6 months of stopping testosterone, and 20% of individuals conceived while they were amenorrheic from testosterone.4
Psychosocial support is an essential part of pregnancy care in transgender men. For some patients, pregnancy can worsen gender dysphoria, whereas others are empowered by the experience. Insurance companies may also deny obstetric care services to transgender males who have already changed their gender marker from female to male on insurance policies.
Whether transmasculine individuals are at higher risk for pregnancy complications is largely unknown, although emerging research in this field has yielded interesting results. While testosterone can cause vaginal atrophy, it does not seem to increase a patient’s risk of vaginal lacerations or their ability to have a successful vaginal delivery. For transgender men with significant discomfort around their genitalia, an elective cesarean section may be appropriate.5
More recently, Stroumsa et al. conducted an analysis of all deliveries at a Michigan institution from 2014 to 2018. Patients with male gender at the time of delivery or with the diagnostic code of gender dysphoria were identified as transgender.6 The primary outcome of this study was severe parental morbidity (such as amniotic fluid embolism, acute myocardial infarction, eclampsia, etc.), with secondary outcomes investigating rates of cesarean delivery and preterm birth.
During this time period, the researchers identified 256 transgender patients and 1.3 million cisgender patients in their Medicaid database and 1,651 transgender patients and 1.5 million cisgender patients in the commercial database who had experienced a delivery.6 Compared with cisgender patients, transgender patients in the Medicaid database were younger, less likely to be white, and more likely to have a chronic condition.6 Compared with cisgender patients in the commercial database, transgender patients experienced higher rates of anxiety and depression.6 Both transgender and cisgender patients had similar rates of severe parental morbidity. Ironically, rates of cesarean delivery were lower, compared with cisgender patients, in both the Medicaid and commercial databases, with no differences observed between rates of preterm birth.6
While more research is needed on pregnancy in transgender men, this analysis is not only one of the largest to date, but it also challenges many misconceptions providers have regarding pregnancy outcomes. Even though transmasculine patients may require additional medical interventions to achieve pregnancy, such as assisted reproductive technology, or increased psychosocial support during the process, these initial studies are reassuring. Based on current evidence, these patients are not at greater risk for perinatal complications than their cisgender counterparts.
Despite these encouraging findings, there are still several challenges faced by transgender men when it comes to getting pregnant. For instance, they may have difficulty accessing fertility services because of financial constraints or experience a lack of awareness or prejudice from providers; they might also be subject to discrimination or stigma within health care settings. As front-line providers for obstetrical care, we must lead the way towards improving the care for pregnant transmasculine individuals.
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa.
References
1. Light A et al. Family planning and contraception use in transgender men. Contraception. 2018 Oct. doi: 10.1016/j.contraception.2018.06.006.
2. Krempasky C et al. Contraception across the transmasculine spectrum. Am J Obstet Gynecol. 2020 Feb. doi: 10.1016/j.ajog.2019.07.043.
3. Obedin-Maliver J, De Haan G. “Gynecologic care for transgender patients” in Ferrando C, ed., Comprehensive Care of the Transgender Patient. Philadelphia: Elsevier, 2019. 131-51.
4. Light AD et al. Transgender men who experienced pregnancy after female-to-male gender transitioning. Obstet Gynecol. 2014 Dec. doi: 10.1097/AOG.0000000000000540.
5. Brandt JS et al. Transgender men, pregnancy, and the “new” advanced paternal age: A review of the literature. Maturitas. 2019 Oct. doi: 10.1016/j.maturitas.2019.07.004.
6. Stroumsa D et al. Pregnancy outcomes in a U.S. cohort of transgender people. JAMA. 2023 Jun 6. doi: 10.1001/jama.2023.7688.
Despite increased societal gains, transgender individuals are still a medically and socially underserved group. The historic rise of antitransgender legislation and the overturning of Roe v. Wade, further compound existing health care disparities, particularly in the realm of contraception and pregnancy. Obstetrician-gynecologists and midwives are typically first-line providers when discussing family planning and fertility options for all patients assigned female at birth. Unfortunately,
Only individuals who are assigned female at birth and have a uterus are capable of pregnancy. This can include both cisgender women and nonbinary/transgender men. However, societal and medical institutions are struggling with this shift in perspective from a traditionally gendered role to a more inclusive one. Obstetrician-gynecologists and midwives can serve to bridge this gap between these patients and societal misconceptions surrounding transgender men who desire and experience pregnancy.
Providers need to remember that many transmasculine individuals will still retain their uterus and are therefore capable of getting pregnant. While testosterone causes amenorrhea, if patients are engaging in penile-vaginal intercourse, conception is still possible. If a patient does not desire pregnancy, all contraceptive options available for cisgender women, which also include combined oral contraceptives, should be offered.
For patients seeking to become pregnant, testosterone must be discontinued. Testosterone is teratogenic; it can cause abnormal urogenital development in the female fetus and should be avoided even prior to conception.1,2 The timing of testosterone discontinuation is debatable. There are no well-established guidelines dictating how early pregnancy can be attempted after cessation of testosterone, but typically if menses has resumed, the teratogenic effects of testosterone are less likely.
For amenorrheic patients on testosterone, menses will occur, on average, 3-6 months after testosterone is stopped. Of note, the longer that testosterone has been suspended, the greater the likelihood of achieving pregnancy.3 In a study by Light et al., 72% of patients conceived within 6 months of attempting pregnancy, 80% resumed menses within 6 months of stopping testosterone, and 20% of individuals conceived while they were amenorrheic from testosterone.4
Psychosocial support is an essential part of pregnancy care in transgender men. For some patients, pregnancy can worsen gender dysphoria, whereas others are empowered by the experience. Insurance companies may also deny obstetric care services to transgender males who have already changed their gender marker from female to male on insurance policies.
Whether transmasculine individuals are at higher risk for pregnancy complications is largely unknown, although emerging research in this field has yielded interesting results. While testosterone can cause vaginal atrophy, it does not seem to increase a patient’s risk of vaginal lacerations or their ability to have a successful vaginal delivery. For transgender men with significant discomfort around their genitalia, an elective cesarean section may be appropriate.5
More recently, Stroumsa et al. conducted an analysis of all deliveries at a Michigan institution from 2014 to 2018. Patients with male gender at the time of delivery or with the diagnostic code of gender dysphoria were identified as transgender.6 The primary outcome of this study was severe parental morbidity (such as amniotic fluid embolism, acute myocardial infarction, eclampsia, etc.), with secondary outcomes investigating rates of cesarean delivery and preterm birth.
During this time period, the researchers identified 256 transgender patients and 1.3 million cisgender patients in their Medicaid database and 1,651 transgender patients and 1.5 million cisgender patients in the commercial database who had experienced a delivery.6 Compared with cisgender patients, transgender patients in the Medicaid database were younger, less likely to be white, and more likely to have a chronic condition.6 Compared with cisgender patients in the commercial database, transgender patients experienced higher rates of anxiety and depression.6 Both transgender and cisgender patients had similar rates of severe parental morbidity. Ironically, rates of cesarean delivery were lower, compared with cisgender patients, in both the Medicaid and commercial databases, with no differences observed between rates of preterm birth.6
While more research is needed on pregnancy in transgender men, this analysis is not only one of the largest to date, but it also challenges many misconceptions providers have regarding pregnancy outcomes. Even though transmasculine patients may require additional medical interventions to achieve pregnancy, such as assisted reproductive technology, or increased psychosocial support during the process, these initial studies are reassuring. Based on current evidence, these patients are not at greater risk for perinatal complications than their cisgender counterparts.
Despite these encouraging findings, there are still several challenges faced by transgender men when it comes to getting pregnant. For instance, they may have difficulty accessing fertility services because of financial constraints or experience a lack of awareness or prejudice from providers; they might also be subject to discrimination or stigma within health care settings. As front-line providers for obstetrical care, we must lead the way towards improving the care for pregnant transmasculine individuals.
Dr. Brandt is an ob.gyn. and fellowship-trained gender-affirming surgeon in West Reading, Pa.
References
1. Light A et al. Family planning and contraception use in transgender men. Contraception. 2018 Oct. doi: 10.1016/j.contraception.2018.06.006.
2. Krempasky C et al. Contraception across the transmasculine spectrum. Am J Obstet Gynecol. 2020 Feb. doi: 10.1016/j.ajog.2019.07.043.
3. Obedin-Maliver J, De Haan G. “Gynecologic care for transgender patients” in Ferrando C, ed., Comprehensive Care of the Transgender Patient. Philadelphia: Elsevier, 2019. 131-51.
4. Light AD et al. Transgender men who experienced pregnancy after female-to-male gender transitioning. Obstet Gynecol. 2014 Dec. doi: 10.1097/AOG.0000000000000540.
5. Brandt JS et al. Transgender men, pregnancy, and the “new” advanced paternal age: A review of the literature. Maturitas. 2019 Oct. doi: 10.1016/j.maturitas.2019.07.004.
6. Stroumsa D et al. Pregnancy outcomes in a U.S. cohort of transgender people. JAMA. 2023 Jun 6. doi: 10.1001/jama.2023.7688.
Does ‘skeletal age’ describe fracture impact on mortality?
Thach Tran, MD, and colleagues introduced the concept of “skeletal age” in a recently published paper that aims to incorporate the impact of fragility, or low trauma, fractures – which can occur in patients with osteoporosis – on mortality risk.
They defined “skeletal age” as the age of the skeleton following a fragility fracture. This is calculated as the chronological age of the individual plus the number of years of “life lost” as a consequence of the specific fracture.
The risk for premature death following fragility fractures is concerning, with 22%-58% of patients with hip fracture dying within a year (Brauer et al.; Rapp et al.). Thus, it’s important to treat osteoporosis in a timely fashion to reduce the risk for such fractures and the excess mortality risk associated with them.
Implementation and uptake of such treatment, however, either before or after a fragility fracture, is far from optimal (Solomon et al). This may be because patients don’t fully understand the consequence of such a fracture, and outcomes measures currently in use (such as relative risk or hazard of mortality) are difficult to communicate to patients.
In the recent paper by Dr. Tran and colleagues, the authors examined the association between fractures and mortality based on sex, age, associated comorbidities, and fracture site. They pooled this information to create a “skeletal age” for each fracture site, using data from the Danish National Hospital Discharge Registry, which documents fractures and related mortality for all Danish people.
They examined mortality over a period of at least 2 years following a fragility fracture in individuals aged 50 or older, and reported that occurrence of any fragility fracture is associated with a 30%-45% increased risk for death, with the highest risk noted for hip and femur fractures (twofold increase). Fractures of the pelvis, vertebrae, humerus, ribs, clavicle, and lower leg were also associated with increased mortality risk, but no increase was seen with fractures of the forearm, knee, ankle, hand, or foot.
The number of years of life lost at any age depending on the fracture site is represented as a linear graph of skeletal age for any chronological age, for specific fracture sites, separated by sex.
For example, the skeletal age of a 50-year-old man who has a hip fracture is 57 years (7 years of life lost as a consequence of the fracture), while that for a 70-year-old man with the same fracture is 75 years (5 years of life lost because of the fracture). Similarly, the skeletal age of a 50-year-old man with a fracture of the pelvis, femur, vertebrae, and humerus is 55 years (5 years of life lost). Fractures of the lower leg, humerus, and clavicle lead to fewer lost years of life.
The authors are to be commended for creating a simple strategy to quantify mortality risk following low-impact or fragility fractures in older individuals; this could enable providers to communicate the importance of osteoporosis treatment more effectively to patients on the basis of their skeletal age, and for patients to better understand this information.
The study design appears reasonably robust as the authors considered many factors that might affect mortality risk, such as sex, age, and comorbidities, and the results are based on information from a very large number of people – 1.6 million.
However, there’s a major issue with the concept of “skeletal age” as proposed by Dr. Tran and colleagues. The term is already in use and defines the maturity of bones in children and adolescents, also called “bone age” (Greulich and Pyle 1959; Skeletal Age, Radiology Key). This is a real oversight and could cause confusion in interpreting “skeletal age.”
Skeletal age as currently defined in children and adolescents is influenced by chronological age, exposure to certain hormones, nutritional deficiencies, and systemic diseases, and is a predictor of adult height based on the skeletal age and current height. This concept is completely different from that being proposed by the authors in this paper. Dr. Tran and colleagues (and the reviewers of this paper) are probably not familiar with the use of the terminology in youth, which is a major oversight; they should consider changing the terminology given this overlap.
Further, fragility fractures can occur from osteoporosis at any age, and this study doesn’t provide information regarding years of life lost from occurrence of fragility fractures at younger ages, or the age at which mortality risk starts to increase (as the study was performed only in those aged 50 or older).
While the study takes into account general comorbidities in developing the model to define years of life lost, it doesn’t account for other factors that can influence fracture risk, such as lifestyle factors, activity level, and genetic risk (family history of osteoporosis, for example). Of note, the impact of additional fractures isn’t considered either and should be factored into future investigations.
Overall, the study is robust and important and provides valuable information regarding mortality risk from a fragility fracture in older people. However, there are some flaws that need to be considered and addressed, the most serious of which is that the term “skeletal age” has been in existence for decades, applied to a much younger age group, and its implications are completely different from those being proposed by the authors here.
A version of this article first appeared on Medscape.com.
Thach Tran, MD, and colleagues introduced the concept of “skeletal age” in a recently published paper that aims to incorporate the impact of fragility, or low trauma, fractures – which can occur in patients with osteoporosis – on mortality risk.
They defined “skeletal age” as the age of the skeleton following a fragility fracture. This is calculated as the chronological age of the individual plus the number of years of “life lost” as a consequence of the specific fracture.
The risk for premature death following fragility fractures is concerning, with 22%-58% of patients with hip fracture dying within a year (Brauer et al.; Rapp et al.). Thus, it’s important to treat osteoporosis in a timely fashion to reduce the risk for such fractures and the excess mortality risk associated with them.
Implementation and uptake of such treatment, however, either before or after a fragility fracture, is far from optimal (Solomon et al). This may be because patients don’t fully understand the consequence of such a fracture, and outcomes measures currently in use (such as relative risk or hazard of mortality) are difficult to communicate to patients.
In the recent paper by Dr. Tran and colleagues, the authors examined the association between fractures and mortality based on sex, age, associated comorbidities, and fracture site. They pooled this information to create a “skeletal age” for each fracture site, using data from the Danish National Hospital Discharge Registry, which documents fractures and related mortality for all Danish people.
They examined mortality over a period of at least 2 years following a fragility fracture in individuals aged 50 or older, and reported that occurrence of any fragility fracture is associated with a 30%-45% increased risk for death, with the highest risk noted for hip and femur fractures (twofold increase). Fractures of the pelvis, vertebrae, humerus, ribs, clavicle, and lower leg were also associated with increased mortality risk, but no increase was seen with fractures of the forearm, knee, ankle, hand, or foot.
The number of years of life lost at any age depending on the fracture site is represented as a linear graph of skeletal age for any chronological age, for specific fracture sites, separated by sex.
For example, the skeletal age of a 50-year-old man who has a hip fracture is 57 years (7 years of life lost as a consequence of the fracture), while that for a 70-year-old man with the same fracture is 75 years (5 years of life lost because of the fracture). Similarly, the skeletal age of a 50-year-old man with a fracture of the pelvis, femur, vertebrae, and humerus is 55 years (5 years of life lost). Fractures of the lower leg, humerus, and clavicle lead to fewer lost years of life.
The authors are to be commended for creating a simple strategy to quantify mortality risk following low-impact or fragility fractures in older individuals; this could enable providers to communicate the importance of osteoporosis treatment more effectively to patients on the basis of their skeletal age, and for patients to better understand this information.
The study design appears reasonably robust as the authors considered many factors that might affect mortality risk, such as sex, age, and comorbidities, and the results are based on information from a very large number of people – 1.6 million.
However, there’s a major issue with the concept of “skeletal age” as proposed by Dr. Tran and colleagues. The term is already in use and defines the maturity of bones in children and adolescents, also called “bone age” (Greulich and Pyle 1959; Skeletal Age, Radiology Key). This is a real oversight and could cause confusion in interpreting “skeletal age.”
Skeletal age as currently defined in children and adolescents is influenced by chronological age, exposure to certain hormones, nutritional deficiencies, and systemic diseases, and is a predictor of adult height based on the skeletal age and current height. This concept is completely different from that being proposed by the authors in this paper. Dr. Tran and colleagues (and the reviewers of this paper) are probably not familiar with the use of the terminology in youth, which is a major oversight; they should consider changing the terminology given this overlap.
Further, fragility fractures can occur from osteoporosis at any age, and this study doesn’t provide information regarding years of life lost from occurrence of fragility fractures at younger ages, or the age at which mortality risk starts to increase (as the study was performed only in those aged 50 or older).
While the study takes into account general comorbidities in developing the model to define years of life lost, it doesn’t account for other factors that can influence fracture risk, such as lifestyle factors, activity level, and genetic risk (family history of osteoporosis, for example). Of note, the impact of additional fractures isn’t considered either and should be factored into future investigations.
Overall, the study is robust and important and provides valuable information regarding mortality risk from a fragility fracture in older people. However, there are some flaws that need to be considered and addressed, the most serious of which is that the term “skeletal age” has been in existence for decades, applied to a much younger age group, and its implications are completely different from those being proposed by the authors here.
A version of this article first appeared on Medscape.com.
Thach Tran, MD, and colleagues introduced the concept of “skeletal age” in a recently published paper that aims to incorporate the impact of fragility, or low trauma, fractures – which can occur in patients with osteoporosis – on mortality risk.
They defined “skeletal age” as the age of the skeleton following a fragility fracture. This is calculated as the chronological age of the individual plus the number of years of “life lost” as a consequence of the specific fracture.
The risk for premature death following fragility fractures is concerning, with 22%-58% of patients with hip fracture dying within a year (Brauer et al.; Rapp et al.). Thus, it’s important to treat osteoporosis in a timely fashion to reduce the risk for such fractures and the excess mortality risk associated with them.
Implementation and uptake of such treatment, however, either before or after a fragility fracture, is far from optimal (Solomon et al). This may be because patients don’t fully understand the consequence of such a fracture, and outcomes measures currently in use (such as relative risk or hazard of mortality) are difficult to communicate to patients.
In the recent paper by Dr. Tran and colleagues, the authors examined the association between fractures and mortality based on sex, age, associated comorbidities, and fracture site. They pooled this information to create a “skeletal age” for each fracture site, using data from the Danish National Hospital Discharge Registry, which documents fractures and related mortality for all Danish people.
They examined mortality over a period of at least 2 years following a fragility fracture in individuals aged 50 or older, and reported that occurrence of any fragility fracture is associated with a 30%-45% increased risk for death, with the highest risk noted for hip and femur fractures (twofold increase). Fractures of the pelvis, vertebrae, humerus, ribs, clavicle, and lower leg were also associated with increased mortality risk, but no increase was seen with fractures of the forearm, knee, ankle, hand, or foot.
The number of years of life lost at any age depending on the fracture site is represented as a linear graph of skeletal age for any chronological age, for specific fracture sites, separated by sex.
For example, the skeletal age of a 50-year-old man who has a hip fracture is 57 years (7 years of life lost as a consequence of the fracture), while that for a 70-year-old man with the same fracture is 75 years (5 years of life lost because of the fracture). Similarly, the skeletal age of a 50-year-old man with a fracture of the pelvis, femur, vertebrae, and humerus is 55 years (5 years of life lost). Fractures of the lower leg, humerus, and clavicle lead to fewer lost years of life.
The authors are to be commended for creating a simple strategy to quantify mortality risk following low-impact or fragility fractures in older individuals; this could enable providers to communicate the importance of osteoporosis treatment more effectively to patients on the basis of their skeletal age, and for patients to better understand this information.
The study design appears reasonably robust as the authors considered many factors that might affect mortality risk, such as sex, age, and comorbidities, and the results are based on information from a very large number of people – 1.6 million.
However, there’s a major issue with the concept of “skeletal age” as proposed by Dr. Tran and colleagues. The term is already in use and defines the maturity of bones in children and adolescents, also called “bone age” (Greulich and Pyle 1959; Skeletal Age, Radiology Key). This is a real oversight and could cause confusion in interpreting “skeletal age.”
Skeletal age as currently defined in children and adolescents is influenced by chronological age, exposure to certain hormones, nutritional deficiencies, and systemic diseases, and is a predictor of adult height based on the skeletal age and current height. This concept is completely different from that being proposed by the authors in this paper. Dr. Tran and colleagues (and the reviewers of this paper) are probably not familiar with the use of the terminology in youth, which is a major oversight; they should consider changing the terminology given this overlap.
Further, fragility fractures can occur from osteoporosis at any age, and this study doesn’t provide information regarding years of life lost from occurrence of fragility fractures at younger ages, or the age at which mortality risk starts to increase (as the study was performed only in those aged 50 or older).
While the study takes into account general comorbidities in developing the model to define years of life lost, it doesn’t account for other factors that can influence fracture risk, such as lifestyle factors, activity level, and genetic risk (family history of osteoporosis, for example). Of note, the impact of additional fractures isn’t considered either and should be factored into future investigations.
Overall, the study is robust and important and provides valuable information regarding mortality risk from a fragility fracture in older people. However, there are some flaws that need to be considered and addressed, the most serious of which is that the term “skeletal age” has been in existence for decades, applied to a much younger age group, and its implications are completely different from those being proposed by the authors here.
A version of this article first appeared on Medscape.com.