User login
Self-talk overhaul may help patients achieve weight loss
It’s common knowledge that the recommended first-line treatment for obesity is behavioral or “lifestyle” intervention, with the goal of losing a modest amount of weight to gain significant health benefits. Unfortunately, when pursuing weight loss, patients often think they need to beat themselves up to stay motivated. I’ve heard patients call themselves “weak,” saying they need to “stop being lazy” and gain some self-control in order to be less of a “failure.” They label their bodies as “disgusting” and themselves as “worthless,” all because of their weight.
Some patients may worry that if they are kind to themselves or “too accepting” of their bodies, they’ll lose motivation to stick with their health behavior goals. That’s a question that my colleagues and I have explored in recent research that attempts to reduce weight stigma as part of standard weight-related care.
Misguided societal view drives blame game
This tendency for people to blame and disparage themselves for their weight is largely driven by the misguided societal view of body weight as an issue of personal responsibility. We’re constantly exposed to messages telling us that there’s a narrow range of acceptable body weights and sizes, and that if we have enough willpower and discipline to eat healthily and exercise, then we should be able to control our weight. These messages are prevalent in the news and in social media, but often they are communicated in health care settings too. Narratives of this kind usually ignore the complex environmental and biological factors that contribute to body size and shape, instead attributing high body weight to laziness and moral failings.
Such messages exemplify weight bias and stigma, or the negative attitudes toward and mistreatment of individuals with a high body weight. Given society’s harsh judgment of people with larger bodies, it’s no surprise that many individuals internalize these beliefs and stigmatize themselves for their weight. This internalized or self-directed stigma is known to be harmful to mental and physical health.
Contrary to beliefs that negative self-talk and self-blame can be motivators to improve health, we know that high levels of weight self-stigma are linked to unhealthy eating behaviors and less engagement in physical activity, among other poor health outcomes. Thus, ironically, internalizing weight stigma actually undermines efforts to lose weight and maintain weight loss, rather than motivating healthy behavior change.
Combating internalized weight stigma
How do we combat these negative weight messages in our culture and reduce, or ideally prevent, internalization of judgment and blame? Fundamental changes in policies, health care practices, and public attitudes are needed to eradicate weight stigma. While such initiatives are underway, there are many individuals who have already experienced and internalized weight stigma and need support now. Interventions such as peer support and psychological counseling may be helpful for challenging negative, internalized beliefs about weight; learning to cope with exposure to weight stigma without internalizing it; increasing self-acceptance and self-compassion; and feeling empowered to fight back against weight bias and stigma.
In our latest study, my colleagues and I tested the long-term effects of including a group intervention to address weight stigma in a standard behavioral weight management program. More than 100 adults with obesity who had experienced and internalized weight stigma were recruited for this clinical trial, which randomly assigned participants to receive either the Weight Bias Internalization and Stigma (Weight BIAS) program combined with standard behavioral weight loss treatment, or standard weight loss treatment alone.
The Weight BIAS program adapted evidence-based psychotherapy techniques to target weight self-stigma, while also providing peer support in a group treatment format. Specific topics included challenging myths and stereotypes about weight; identifying and changing negative thought patterns related to weight and how they affect emotions and behaviors; and responding to experiences of weight stigma.
For example, to challenge negative thoughts (for example, that they were a “failure” because of their weight), patients worked together to examine all of the evidence that proved these beliefs were not true, and came up with ideas for how to revise these thoughts to be less judgmental and more fair and accurate.
Other topics focused on building confidence, increasing body- and self-acceptance, and advocating for themselves and others who are mistreated because of their weight. Many patients shared examples of stigmatizing experiences in health care settings and discussed what they could say or do when facing judgment or discrimination from health care providers, as well as the importance of finding health care providers who treated them with respect. Group discussions also tied in information relevant to health behavior goals, such as overcoming self-consciousness about weight to enjoy physical activity.
Participants were offered weekly group meetings for 20 weeks, followed by a year of less frequent meetings. At the study’s end, participants in the group that received weight loss treatment with the Weight BIAS program on average lost about 7% of their starting weight, compared with an average weight loss of about 5% in the group that received weight loss treatment alone. Weight losses of these magnitudes are known to have meaningful health benefits. Results from our study showed comparable improvements in most outcomes across groups, with some added benefit of the Weight BIAS program for certain psychological and behavioral outcomes. These findings challenge the notion that reducing weight stigma and promoting body acceptance will undermine motivation to engage in healthy behaviors and lose weight. We found no such effect.
What did participants say?
When asked questions such as how much they liked the program, what they learned, and how they used the new skills and changed their self-perceptions, participants who received the Weight BIAS program gave higher ratings than those who received only the weight loss treatment. Positive feedback from free-response questions indicated that many participants identified social support as their favorite aspect of the program. Others highlighted how the program helped them to gain “the ability to think differently about myself and other people” and “an understanding that weight really is separate from the person.” They also described how they brought together the goals of weight loss and body and self-acceptance, saying, “I am more accepting of me and at the same time more dedicated to obtaining a healthier weight,” and “It’s okay to be happy the way I am and still want to change.”
Participants who didn’t receive the Weight BIAS program also shared positive feedback, writing that their favorite part of the program was “being part of such a supportive group of people who can relate to the things that I think and feel” and that they learned “how not to be so hard on myself.” This might suggest that even without an intervention specifically for weight stigma, providing respectful, compassionate care and peer support may help patients to feel less alone and to be kinder to themselves.
Our study results suggest that reducing negative self-talk and internalized beliefs about weight certainly won’t undermine treatment outcomes and may have some benefits beyond standard weight loss treatment. At the same time, we also all need to do our part to change how society views and treats people with larger bodies and prevent the harms of experiencing and internalizing weight stigma.
Research reported in this publication was supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under award number K23HL140176. The content is solely the responsibility of the author and does not necessarily reflect the official views of the National Institutes of Health.
Dr. Pearl is assistant professor, clinical and health psychology, University of Florida, Gainesville. She has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
It’s common knowledge that the recommended first-line treatment for obesity is behavioral or “lifestyle” intervention, with the goal of losing a modest amount of weight to gain significant health benefits. Unfortunately, when pursuing weight loss, patients often think they need to beat themselves up to stay motivated. I’ve heard patients call themselves “weak,” saying they need to “stop being lazy” and gain some self-control in order to be less of a “failure.” They label their bodies as “disgusting” and themselves as “worthless,” all because of their weight.
Some patients may worry that if they are kind to themselves or “too accepting” of their bodies, they’ll lose motivation to stick with their health behavior goals. That’s a question that my colleagues and I have explored in recent research that attempts to reduce weight stigma as part of standard weight-related care.
Misguided societal view drives blame game
This tendency for people to blame and disparage themselves for their weight is largely driven by the misguided societal view of body weight as an issue of personal responsibility. We’re constantly exposed to messages telling us that there’s a narrow range of acceptable body weights and sizes, and that if we have enough willpower and discipline to eat healthily and exercise, then we should be able to control our weight. These messages are prevalent in the news and in social media, but often they are communicated in health care settings too. Narratives of this kind usually ignore the complex environmental and biological factors that contribute to body size and shape, instead attributing high body weight to laziness and moral failings.
Such messages exemplify weight bias and stigma, or the negative attitudes toward and mistreatment of individuals with a high body weight. Given society’s harsh judgment of people with larger bodies, it’s no surprise that many individuals internalize these beliefs and stigmatize themselves for their weight. This internalized or self-directed stigma is known to be harmful to mental and physical health.
Contrary to beliefs that negative self-talk and self-blame can be motivators to improve health, we know that high levels of weight self-stigma are linked to unhealthy eating behaviors and less engagement in physical activity, among other poor health outcomes. Thus, ironically, internalizing weight stigma actually undermines efforts to lose weight and maintain weight loss, rather than motivating healthy behavior change.
Combating internalized weight stigma
How do we combat these negative weight messages in our culture and reduce, or ideally prevent, internalization of judgment and blame? Fundamental changes in policies, health care practices, and public attitudes are needed to eradicate weight stigma. While such initiatives are underway, there are many individuals who have already experienced and internalized weight stigma and need support now. Interventions such as peer support and psychological counseling may be helpful for challenging negative, internalized beliefs about weight; learning to cope with exposure to weight stigma without internalizing it; increasing self-acceptance and self-compassion; and feeling empowered to fight back against weight bias and stigma.
In our latest study, my colleagues and I tested the long-term effects of including a group intervention to address weight stigma in a standard behavioral weight management program. More than 100 adults with obesity who had experienced and internalized weight stigma were recruited for this clinical trial, which randomly assigned participants to receive either the Weight Bias Internalization and Stigma (Weight BIAS) program combined with standard behavioral weight loss treatment, or standard weight loss treatment alone.
The Weight BIAS program adapted evidence-based psychotherapy techniques to target weight self-stigma, while also providing peer support in a group treatment format. Specific topics included challenging myths and stereotypes about weight; identifying and changing negative thought patterns related to weight and how they affect emotions and behaviors; and responding to experiences of weight stigma.
For example, to challenge negative thoughts (for example, that they were a “failure” because of their weight), patients worked together to examine all of the evidence that proved these beliefs were not true, and came up with ideas for how to revise these thoughts to be less judgmental and more fair and accurate.
Other topics focused on building confidence, increasing body- and self-acceptance, and advocating for themselves and others who are mistreated because of their weight. Many patients shared examples of stigmatizing experiences in health care settings and discussed what they could say or do when facing judgment or discrimination from health care providers, as well as the importance of finding health care providers who treated them with respect. Group discussions also tied in information relevant to health behavior goals, such as overcoming self-consciousness about weight to enjoy physical activity.
Participants were offered weekly group meetings for 20 weeks, followed by a year of less frequent meetings. At the study’s end, participants in the group that received weight loss treatment with the Weight BIAS program on average lost about 7% of their starting weight, compared with an average weight loss of about 5% in the group that received weight loss treatment alone. Weight losses of these magnitudes are known to have meaningful health benefits. Results from our study showed comparable improvements in most outcomes across groups, with some added benefit of the Weight BIAS program for certain psychological and behavioral outcomes. These findings challenge the notion that reducing weight stigma and promoting body acceptance will undermine motivation to engage in healthy behaviors and lose weight. We found no such effect.
What did participants say?
When asked questions such as how much they liked the program, what they learned, and how they used the new skills and changed their self-perceptions, participants who received the Weight BIAS program gave higher ratings than those who received only the weight loss treatment. Positive feedback from free-response questions indicated that many participants identified social support as their favorite aspect of the program. Others highlighted how the program helped them to gain “the ability to think differently about myself and other people” and “an understanding that weight really is separate from the person.” They also described how they brought together the goals of weight loss and body and self-acceptance, saying, “I am more accepting of me and at the same time more dedicated to obtaining a healthier weight,” and “It’s okay to be happy the way I am and still want to change.”
Participants who didn’t receive the Weight BIAS program also shared positive feedback, writing that their favorite part of the program was “being part of such a supportive group of people who can relate to the things that I think and feel” and that they learned “how not to be so hard on myself.” This might suggest that even without an intervention specifically for weight stigma, providing respectful, compassionate care and peer support may help patients to feel less alone and to be kinder to themselves.
Our study results suggest that reducing negative self-talk and internalized beliefs about weight certainly won’t undermine treatment outcomes and may have some benefits beyond standard weight loss treatment. At the same time, we also all need to do our part to change how society views and treats people with larger bodies and prevent the harms of experiencing and internalizing weight stigma.
Research reported in this publication was supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under award number K23HL140176. The content is solely the responsibility of the author and does not necessarily reflect the official views of the National Institutes of Health.
Dr. Pearl is assistant professor, clinical and health psychology, University of Florida, Gainesville. She has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
It’s common knowledge that the recommended first-line treatment for obesity is behavioral or “lifestyle” intervention, with the goal of losing a modest amount of weight to gain significant health benefits. Unfortunately, when pursuing weight loss, patients often think they need to beat themselves up to stay motivated. I’ve heard patients call themselves “weak,” saying they need to “stop being lazy” and gain some self-control in order to be less of a “failure.” They label their bodies as “disgusting” and themselves as “worthless,” all because of their weight.
Some patients may worry that if they are kind to themselves or “too accepting” of their bodies, they’ll lose motivation to stick with their health behavior goals. That’s a question that my colleagues and I have explored in recent research that attempts to reduce weight stigma as part of standard weight-related care.
Misguided societal view drives blame game
This tendency for people to blame and disparage themselves for their weight is largely driven by the misguided societal view of body weight as an issue of personal responsibility. We’re constantly exposed to messages telling us that there’s a narrow range of acceptable body weights and sizes, and that if we have enough willpower and discipline to eat healthily and exercise, then we should be able to control our weight. These messages are prevalent in the news and in social media, but often they are communicated in health care settings too. Narratives of this kind usually ignore the complex environmental and biological factors that contribute to body size and shape, instead attributing high body weight to laziness and moral failings.
Such messages exemplify weight bias and stigma, or the negative attitudes toward and mistreatment of individuals with a high body weight. Given society’s harsh judgment of people with larger bodies, it’s no surprise that many individuals internalize these beliefs and stigmatize themselves for their weight. This internalized or self-directed stigma is known to be harmful to mental and physical health.
Contrary to beliefs that negative self-talk and self-blame can be motivators to improve health, we know that high levels of weight self-stigma are linked to unhealthy eating behaviors and less engagement in physical activity, among other poor health outcomes. Thus, ironically, internalizing weight stigma actually undermines efforts to lose weight and maintain weight loss, rather than motivating healthy behavior change.
Combating internalized weight stigma
How do we combat these negative weight messages in our culture and reduce, or ideally prevent, internalization of judgment and blame? Fundamental changes in policies, health care practices, and public attitudes are needed to eradicate weight stigma. While such initiatives are underway, there are many individuals who have already experienced and internalized weight stigma and need support now. Interventions such as peer support and psychological counseling may be helpful for challenging negative, internalized beliefs about weight; learning to cope with exposure to weight stigma without internalizing it; increasing self-acceptance and self-compassion; and feeling empowered to fight back against weight bias and stigma.
In our latest study, my colleagues and I tested the long-term effects of including a group intervention to address weight stigma in a standard behavioral weight management program. More than 100 adults with obesity who had experienced and internalized weight stigma were recruited for this clinical trial, which randomly assigned participants to receive either the Weight Bias Internalization and Stigma (Weight BIAS) program combined with standard behavioral weight loss treatment, or standard weight loss treatment alone.
The Weight BIAS program adapted evidence-based psychotherapy techniques to target weight self-stigma, while also providing peer support in a group treatment format. Specific topics included challenging myths and stereotypes about weight; identifying and changing negative thought patterns related to weight and how they affect emotions and behaviors; and responding to experiences of weight stigma.
For example, to challenge negative thoughts (for example, that they were a “failure” because of their weight), patients worked together to examine all of the evidence that proved these beliefs were not true, and came up with ideas for how to revise these thoughts to be less judgmental and more fair and accurate.
Other topics focused on building confidence, increasing body- and self-acceptance, and advocating for themselves and others who are mistreated because of their weight. Many patients shared examples of stigmatizing experiences in health care settings and discussed what they could say or do when facing judgment or discrimination from health care providers, as well as the importance of finding health care providers who treated them with respect. Group discussions also tied in information relevant to health behavior goals, such as overcoming self-consciousness about weight to enjoy physical activity.
Participants were offered weekly group meetings for 20 weeks, followed by a year of less frequent meetings. At the study’s end, participants in the group that received weight loss treatment with the Weight BIAS program on average lost about 7% of their starting weight, compared with an average weight loss of about 5% in the group that received weight loss treatment alone. Weight losses of these magnitudes are known to have meaningful health benefits. Results from our study showed comparable improvements in most outcomes across groups, with some added benefit of the Weight BIAS program for certain psychological and behavioral outcomes. These findings challenge the notion that reducing weight stigma and promoting body acceptance will undermine motivation to engage in healthy behaviors and lose weight. We found no such effect.
What did participants say?
When asked questions such as how much they liked the program, what they learned, and how they used the new skills and changed their self-perceptions, participants who received the Weight BIAS program gave higher ratings than those who received only the weight loss treatment. Positive feedback from free-response questions indicated that many participants identified social support as their favorite aspect of the program. Others highlighted how the program helped them to gain “the ability to think differently about myself and other people” and “an understanding that weight really is separate from the person.” They also described how they brought together the goals of weight loss and body and self-acceptance, saying, “I am more accepting of me and at the same time more dedicated to obtaining a healthier weight,” and “It’s okay to be happy the way I am and still want to change.”
Participants who didn’t receive the Weight BIAS program also shared positive feedback, writing that their favorite part of the program was “being part of such a supportive group of people who can relate to the things that I think and feel” and that they learned “how not to be so hard on myself.” This might suggest that even without an intervention specifically for weight stigma, providing respectful, compassionate care and peer support may help patients to feel less alone and to be kinder to themselves.
Our study results suggest that reducing negative self-talk and internalized beliefs about weight certainly won’t undermine treatment outcomes and may have some benefits beyond standard weight loss treatment. At the same time, we also all need to do our part to change how society views and treats people with larger bodies and prevent the harms of experiencing and internalizing weight stigma.
Research reported in this publication was supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under award number K23HL140176. The content is solely the responsibility of the author and does not necessarily reflect the official views of the National Institutes of Health.
Dr. Pearl is assistant professor, clinical and health psychology, University of Florida, Gainesville. She has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Protecting your practice data
While data protection is important in any industry, it is particularly critical in health care because in addition to the usual financial records, trade secrets, and other valuable data, confidential patient information is also at risk.
You may think that your computer vendor is responsible for safeguarding your data, but third parties can only do so much. And if your data is compromised, the ultimate responsibility is yours – not to mention the financial loss, and the damage to your practice’s reputation.

In addition to the security vulnerabilities inherent in any system, there are external vulnerabilities, such as weak passwords, viruses, and hacking (either externally or internally). And as hardware becomes more and more portable, there is the increasing risk of theft of platforms and storage media containing confidential data.
A close and ongoing relationship with your hardware and software vendors is essential to good data protection. Your office should have a permanent contact at each company, and you should talk to them regularly. Ask them what sort of firewalls, antivirus software, and other safeguards are in place to protect your system. Whenever they identify a bug or other vulnerability, you should know about it. They should tell you about each software update, what improvements it makes, and what defects it fixes. You should also know about any changes to your data encryption.
Encryption has become an essential component of data protection. It is especially important if you use portable devices such as laptops, pads, or smart phones to store and transport patient information. If you lose one of these devices, or a thumb drive or other storage media, HIPAA will probably not consider it a breach if the data it contains is encrypted.
Encryption isn’t perfect, of course. Log-in credentials can be stolen; and data that is stored in house is can be hacked with malware and phishing techniques, especially if the key to decryption is located on that server. And make sure that employees are not putting any medical data on their own private (unencrypted) devices.
Each employee should have his or her own password, and sharing should be strictly prohibited. Multifactor authentication is becoming increasingly popular for an extra level of security.
Your vendor should require you to change your passwords every few months. If it doesn’t, you need to establish a timetable to do it yourself. All passwords should be strong (no birthdays, pet names, etc.), and they shouldn’t be the same or similar to old passwords.
In some offices, I’ve been surprised to see that every employee has unrestricted access to all practice data. The vulnerabilities of such an arrangement are obvious. There is no reason why receptionists, for example, should have access to medical histories, and insurance people don’t need to know what medications a patient is on. Your vendor can help you design partitions that restrict each employee to only the information they need access to.
Ask if your vendor provides security training for employees. If not, look into hiring a security firm to do it. Regular security training can help employees to recognize data security attacks like phishing, and instills a heightened sense of security awareness and vigilance among staff. They will also gain a better understanding of the role they play in maintaining the overall security of your office.
It goes without saying that third parties, such as business vendors, payers, and managed care providers, should never have access to patient records or other personal health information.
Backing up data
I have written many times about the importance of regularly backing up your data. Industry statistics show that fully 10% of hard drives fail in any given year, and 43% of computer users lose one or more files every year in the form of clinical data, financial records, photos, email, documents, and other important information. Recovery of lost data, when it’s possible at all, can be very expensive.
Even if your EHR vendor backs up your data, you should consider making a separate backup of your own. Backup drives have been known to fail too; and if you decide to switch computer vendors, you don’t want to be at the mercy of the old company that might be reluctant to transfer your data without a hefty payment.
The first rule of backing up is to store your backup drives in a different location from your computers. Unfortunately, that’s a pain; and external drives can be lost or stolen, creating a HIPAA nightmare. So an increasingly popular alternative is automatic remote backup. Several companies offer that service, and the cost is very reasonable for individual computers. Backing up an entire office costs more, depending on how many computers and/or servers you have, but it’s still very reasonable and includes other services, such as operating system and network share support.
The procedure is simple: You create an account and tell the service which files you want copied. Your first backup can take a long time, often days, depending on how much data you are sending and how fast your Internet connection runs. After that the program runs in the background, copying only those files that have changed since the previous backup. Files are encrypted before leaving your computer, and they remain encrypted at the service’s data center, making them HIPAA compliant and, theoretically, only accessible by you.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
While data protection is important in any industry, it is particularly critical in health care because in addition to the usual financial records, trade secrets, and other valuable data, confidential patient information is also at risk.
You may think that your computer vendor is responsible for safeguarding your data, but third parties can only do so much. And if your data is compromised, the ultimate responsibility is yours – not to mention the financial loss, and the damage to your practice’s reputation.
In addition to the security vulnerabilities inherent in any system, there are external vulnerabilities, such as weak passwords, viruses, and hacking (either externally or internally). And as hardware becomes more and more portable, there is the increasing risk of theft of platforms and storage media containing confidential data.
A close and ongoing relationship with your hardware and software vendors is essential to good data protection. Your office should have a permanent contact at each company, and you should talk to them regularly. Ask them what sort of firewalls, antivirus software, and other safeguards are in place to protect your system. Whenever they identify a bug or other vulnerability, you should know about it. They should tell you about each software update, what improvements it makes, and what defects it fixes. You should also know about any changes to your data encryption.
Encryption has become an essential component of data protection. It is especially important if you use portable devices such as laptops, pads, or smart phones to store and transport patient information. If you lose one of these devices, or a thumb drive or other storage media, HIPAA will probably not consider it a breach if the data it contains is encrypted.
Encryption isn’t perfect, of course. Log-in credentials can be stolen; and data that is stored in house is can be hacked with malware and phishing techniques, especially if the key to decryption is located on that server. And make sure that employees are not putting any medical data on their own private (unencrypted) devices.
Each employee should have his or her own password, and sharing should be strictly prohibited. Multifactor authentication is becoming increasingly popular for an extra level of security.
Your vendor should require you to change your passwords every few months. If it doesn’t, you need to establish a timetable to do it yourself. All passwords should be strong (no birthdays, pet names, etc.), and they shouldn’t be the same or similar to old passwords.
In some offices, I’ve been surprised to see that every employee has unrestricted access to all practice data. The vulnerabilities of such an arrangement are obvious. There is no reason why receptionists, for example, should have access to medical histories, and insurance people don’t need to know what medications a patient is on. Your vendor can help you design partitions that restrict each employee to only the information they need access to.
Ask if your vendor provides security training for employees. If not, look into hiring a security firm to do it. Regular security training can help employees to recognize data security attacks like phishing, and instills a heightened sense of security awareness and vigilance among staff. They will also gain a better understanding of the role they play in maintaining the overall security of your office.
It goes without saying that third parties, such as business vendors, payers, and managed care providers, should never have access to patient records or other personal health information.
Backing up data
I have written many times about the importance of regularly backing up your data. Industry statistics show that fully 10% of hard drives fail in any given year, and 43% of computer users lose one or more files every year in the form of clinical data, financial records, photos, email, documents, and other important information. Recovery of lost data, when it’s possible at all, can be very expensive.
Even if your EHR vendor backs up your data, you should consider making a separate backup of your own. Backup drives have been known to fail too; and if you decide to switch computer vendors, you don’t want to be at the mercy of the old company that might be reluctant to transfer your data without a hefty payment.
The first rule of backing up is to store your backup drives in a different location from your computers. Unfortunately, that’s a pain; and external drives can be lost or stolen, creating a HIPAA nightmare. So an increasingly popular alternative is automatic remote backup. Several companies offer that service, and the cost is very reasonable for individual computers. Backing up an entire office costs more, depending on how many computers and/or servers you have, but it’s still very reasonable and includes other services, such as operating system and network share support.
The procedure is simple: You create an account and tell the service which files you want copied. Your first backup can take a long time, often days, depending on how much data you are sending and how fast your Internet connection runs. After that the program runs in the background, copying only those files that have changed since the previous backup. Files are encrypted before leaving your computer, and they remain encrypted at the service’s data center, making them HIPAA compliant and, theoretically, only accessible by you.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
While data protection is important in any industry, it is particularly critical in health care because in addition to the usual financial records, trade secrets, and other valuable data, confidential patient information is also at risk.
You may think that your computer vendor is responsible for safeguarding your data, but third parties can only do so much. And if your data is compromised, the ultimate responsibility is yours – not to mention the financial loss, and the damage to your practice’s reputation.
In addition to the security vulnerabilities inherent in any system, there are external vulnerabilities, such as weak passwords, viruses, and hacking (either externally or internally). And as hardware becomes more and more portable, there is the increasing risk of theft of platforms and storage media containing confidential data.
A close and ongoing relationship with your hardware and software vendors is essential to good data protection. Your office should have a permanent contact at each company, and you should talk to them regularly. Ask them what sort of firewalls, antivirus software, and other safeguards are in place to protect your system. Whenever they identify a bug or other vulnerability, you should know about it. They should tell you about each software update, what improvements it makes, and what defects it fixes. You should also know about any changes to your data encryption.
Encryption has become an essential component of data protection. It is especially important if you use portable devices such as laptops, pads, or smart phones to store and transport patient information. If you lose one of these devices, or a thumb drive or other storage media, HIPAA will probably not consider it a breach if the data it contains is encrypted.
Encryption isn’t perfect, of course. Log-in credentials can be stolen; and data that is stored in house is can be hacked with malware and phishing techniques, especially if the key to decryption is located on that server. And make sure that employees are not putting any medical data on their own private (unencrypted) devices.
Each employee should have his or her own password, and sharing should be strictly prohibited. Multifactor authentication is becoming increasingly popular for an extra level of security.
Your vendor should require you to change your passwords every few months. If it doesn’t, you need to establish a timetable to do it yourself. All passwords should be strong (no birthdays, pet names, etc.), and they shouldn’t be the same or similar to old passwords.
In some offices, I’ve been surprised to see that every employee has unrestricted access to all practice data. The vulnerabilities of such an arrangement are obvious. There is no reason why receptionists, for example, should have access to medical histories, and insurance people don’t need to know what medications a patient is on. Your vendor can help you design partitions that restrict each employee to only the information they need access to.
Ask if your vendor provides security training for employees. If not, look into hiring a security firm to do it. Regular security training can help employees to recognize data security attacks like phishing, and instills a heightened sense of security awareness and vigilance among staff. They will also gain a better understanding of the role they play in maintaining the overall security of your office.
It goes without saying that third parties, such as business vendors, payers, and managed care providers, should never have access to patient records or other personal health information.
Backing up data
I have written many times about the importance of regularly backing up your data. Industry statistics show that fully 10% of hard drives fail in any given year, and 43% of computer users lose one or more files every year in the form of clinical data, financial records, photos, email, documents, and other important information. Recovery of lost data, when it’s possible at all, can be very expensive.
Even if your EHR vendor backs up your data, you should consider making a separate backup of your own. Backup drives have been known to fail too; and if you decide to switch computer vendors, you don’t want to be at the mercy of the old company that might be reluctant to transfer your data without a hefty payment.
The first rule of backing up is to store your backup drives in a different location from your computers. Unfortunately, that’s a pain; and external drives can be lost or stolen, creating a HIPAA nightmare. So an increasingly popular alternative is automatic remote backup. Several companies offer that service, and the cost is very reasonable for individual computers. Backing up an entire office costs more, depending on how many computers and/or servers you have, but it’s still very reasonable and includes other services, such as operating system and network share support.
The procedure is simple: You create an account and tell the service which files you want copied. Your first backup can take a long time, often days, depending on how much data you are sending and how fast your Internet connection runs. After that the program runs in the background, copying only those files that have changed since the previous backup. Files are encrypted before leaving your computer, and they remain encrypted at the service’s data center, making them HIPAA compliant and, theoretically, only accessible by you.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].

The cardiopulmonary effects of mask wearing
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
There was a time when I would have had to explain to you what an N95 mask is, how it is designed to filter out 95% of fine particles, defined as stuff in the air less than 2.5 microns in size.
But of course, you know that now. The N95 had its moment – a moment that seemed to be passing as the concentration of airborne coronavirus particles decreased.
But, as the poet said, all that is less than 2.5 microns in size is not coronavirus. Wildfire smoke is also chock full of fine particulate matter. And so, N95s are having something of a comeback.
That’s why an article that took a deep look at what happens to our cardiovascular system when we wear N95 masks caught my eye.
Mask wearing has been the subject of intense debate around the country. While the vast majority of evidence, as well as the personal experience of thousands of doctors, suggests that wearing a mask has no significant physiologic effects, it’s not hard to find those who suggest that mask wearing depletes oxygen levels, or leads to infection, or has other bizarre effects.
In a world of conflicting opinions, a controlled study is a wonderful thing, and that’s what appeared in JAMA Network Open.
This isn’t a huge study, but it’s big enough to make some important conclusions. Thirty individuals, all young and healthy, half female, were enrolled. Each participant spent 3 days in a metabolic chamber; this is essentially a giant, airtight room where all the inputs (oxygen levels and so on) and outputs (carbon dioxide levels and so on) can be precisely measured.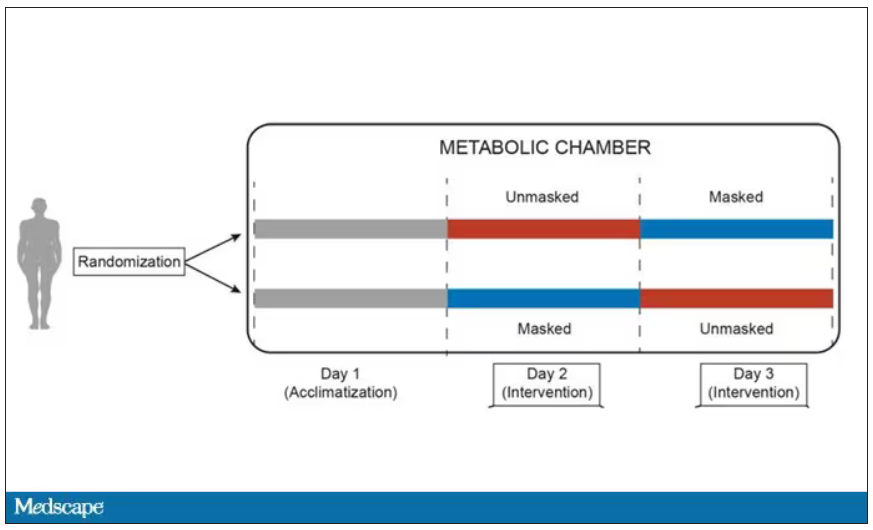
After a day of getting used to the environment, the participants spent a day either wearing an N95 mask or not for 16 waking hours. On the next day, they switched. Every other variable was controlled, from the calories in their diet to the temperature of the room itself.
They engaged in light exercise twice during the day – riding a stationary bike – and a host of physiologic parameters were measured. The question being, would the wearing of the mask for 16 hours straight change anything?
And the answer is yes, some things changed, but not by much.
Here’s a graph of the heart rate over time. You can see some separation, with higher heart rates during the mask-wearing day, particularly around 11 a.m. – when light exercise was scheduled.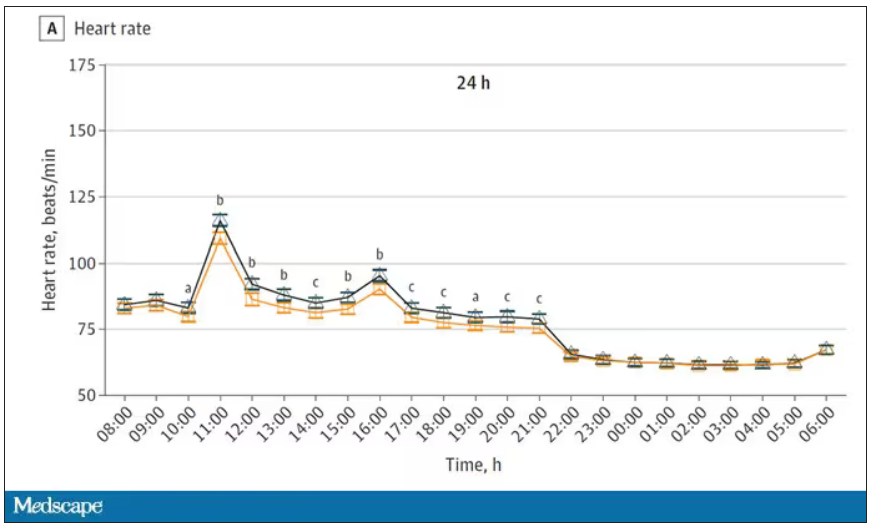
Zooming in on the exercise period makes the difference more clear. The heart rate was about eight beats/min higher while masked and engaging in exercise. Systolic blood pressure was about 6 mm Hg higher. Oxygen saturation was lower by 0.7%.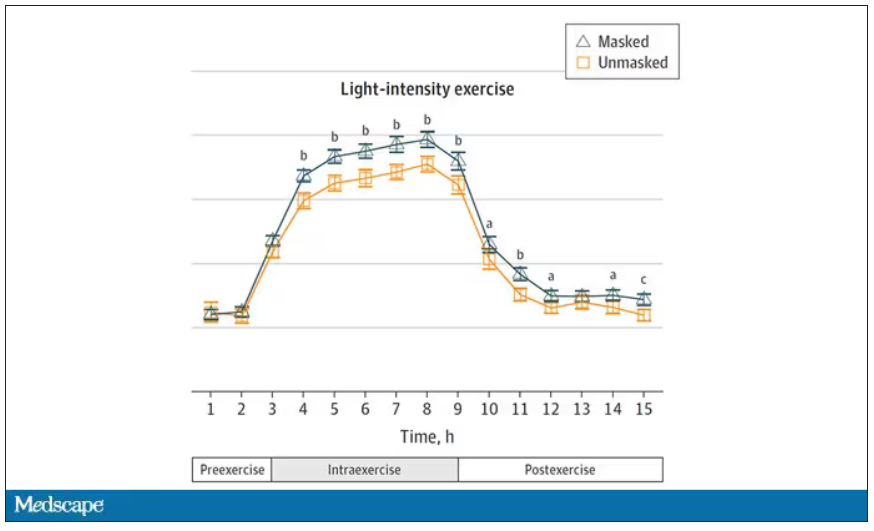
So yes, exercising while wearing an N95 mask might be different from exercising without an N95 mask. But nothing here looks dangerous to me. The 0.7% decrease in oxygen saturation is smaller than the typical measurement error of a pulse oximeter. The authors write that venous pH decreased during the masked day, which is of more interest to me as a nephrologist, but they don’t show that data even in the supplement. I suspect it didn’t decrease much.
They also showed that respiratory rate during exercise decreased in the masked condition. That doesn’t really make sense when you think about it in the context of the other findings, which are all suggestive of increased metabolic rate and sympathetic drive. Does that call the whole procedure into question? No, but it’s worth noting.
These were young, healthy people. You could certainly argue that those with more vulnerable cardiopulmonary status might have had different effects from mask wearing, but without a specific study in those people, it’s just conjecture. Clearly, this study lets us conclude that mask wearing at rest has less of an effect than mask wearing during exercise.
But remember that, in reality, we are wearing masks for a reason. One could imagine a study where this metabolic chamber was filled with wildfire smoke at a concentration similar to what we saw in New York. In that situation, we might find that wearing an N95 is quite helpful. The thing is, studying masks in isolation is useful because you can control so many variables. But masks aren’t used in isolation. In fact, that’s sort of their defining characteristic.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
There was a time when I would have had to explain to you what an N95 mask is, how it is designed to filter out 95% of fine particles, defined as stuff in the air less than 2.5 microns in size.
But of course, you know that now. The N95 had its moment – a moment that seemed to be passing as the concentration of airborne coronavirus particles decreased.
But, as the poet said, all that is less than 2.5 microns in size is not coronavirus. Wildfire smoke is also chock full of fine particulate matter. And so, N95s are having something of a comeback.
That’s why an article that took a deep look at what happens to our cardiovascular system when we wear N95 masks caught my eye.
Mask wearing has been the subject of intense debate around the country. While the vast majority of evidence, as well as the personal experience of thousands of doctors, suggests that wearing a mask has no significant physiologic effects, it’s not hard to find those who suggest that mask wearing depletes oxygen levels, or leads to infection, or has other bizarre effects.
In a world of conflicting opinions, a controlled study is a wonderful thing, and that’s what appeared in JAMA Network Open.
This isn’t a huge study, but it’s big enough to make some important conclusions. Thirty individuals, all young and healthy, half female, were enrolled. Each participant spent 3 days in a metabolic chamber; this is essentially a giant, airtight room where all the inputs (oxygen levels and so on) and outputs (carbon dioxide levels and so on) can be precisely measured.
After a day of getting used to the environment, the participants spent a day either wearing an N95 mask or not for 16 waking hours. On the next day, they switched. Every other variable was controlled, from the calories in their diet to the temperature of the room itself.
They engaged in light exercise twice during the day – riding a stationary bike – and a host of physiologic parameters were measured. The question being, would the wearing of the mask for 16 hours straight change anything?
And the answer is yes, some things changed, but not by much.
Here’s a graph of the heart rate over time. You can see some separation, with higher heart rates during the mask-wearing day, particularly around 11 a.m. – when light exercise was scheduled.
Zooming in on the exercise period makes the difference more clear. The heart rate was about eight beats/min higher while masked and engaging in exercise. Systolic blood pressure was about 6 mm Hg higher. Oxygen saturation was lower by 0.7%.
So yes, exercising while wearing an N95 mask might be different from exercising without an N95 mask. But nothing here looks dangerous to me. The 0.7% decrease in oxygen saturation is smaller than the typical measurement error of a pulse oximeter. The authors write that venous pH decreased during the masked day, which is of more interest to me as a nephrologist, but they don’t show that data even in the supplement. I suspect it didn’t decrease much.
They also showed that respiratory rate during exercise decreased in the masked condition. That doesn’t really make sense when you think about it in the context of the other findings, which are all suggestive of increased metabolic rate and sympathetic drive. Does that call the whole procedure into question? No, but it’s worth noting.
These were young, healthy people. You could certainly argue that those with more vulnerable cardiopulmonary status might have had different effects from mask wearing, but without a specific study in those people, it’s just conjecture. Clearly, this study lets us conclude that mask wearing at rest has less of an effect than mask wearing during exercise.
But remember that, in reality, we are wearing masks for a reason. One could imagine a study where this metabolic chamber was filled with wildfire smoke at a concentration similar to what we saw in New York. In that situation, we might find that wearing an N95 is quite helpful. The thing is, studying masks in isolation is useful because you can control so many variables. But masks aren’t used in isolation. In fact, that’s sort of their defining characteristic.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
There was a time when I would have had to explain to you what an N95 mask is, how it is designed to filter out 95% of fine particles, defined as stuff in the air less than 2.5 microns in size.
But of course, you know that now. The N95 had its moment – a moment that seemed to be passing as the concentration of airborne coronavirus particles decreased.
But, as the poet said, all that is less than 2.5 microns in size is not coronavirus. Wildfire smoke is also chock full of fine particulate matter. And so, N95s are having something of a comeback.
That’s why an article that took a deep look at what happens to our cardiovascular system when we wear N95 masks caught my eye.
Mask wearing has been the subject of intense debate around the country. While the vast majority of evidence, as well as the personal experience of thousands of doctors, suggests that wearing a mask has no significant physiologic effects, it’s not hard to find those who suggest that mask wearing depletes oxygen levels, or leads to infection, or has other bizarre effects.
In a world of conflicting opinions, a controlled study is a wonderful thing, and that’s what appeared in JAMA Network Open.
This isn’t a huge study, but it’s big enough to make some important conclusions. Thirty individuals, all young and healthy, half female, were enrolled. Each participant spent 3 days in a metabolic chamber; this is essentially a giant, airtight room where all the inputs (oxygen levels and so on) and outputs (carbon dioxide levels and so on) can be precisely measured.
After a day of getting used to the environment, the participants spent a day either wearing an N95 mask or not for 16 waking hours. On the next day, they switched. Every other variable was controlled, from the calories in their diet to the temperature of the room itself.
They engaged in light exercise twice during the day – riding a stationary bike – and a host of physiologic parameters were measured. The question being, would the wearing of the mask for 16 hours straight change anything?
And the answer is yes, some things changed, but not by much.
Here’s a graph of the heart rate over time. You can see some separation, with higher heart rates during the mask-wearing day, particularly around 11 a.m. – when light exercise was scheduled.
Zooming in on the exercise period makes the difference more clear. The heart rate was about eight beats/min higher while masked and engaging in exercise. Systolic blood pressure was about 6 mm Hg higher. Oxygen saturation was lower by 0.7%.
So yes, exercising while wearing an N95 mask might be different from exercising without an N95 mask. But nothing here looks dangerous to me. The 0.7% decrease in oxygen saturation is smaller than the typical measurement error of a pulse oximeter. The authors write that venous pH decreased during the masked day, which is of more interest to me as a nephrologist, but they don’t show that data even in the supplement. I suspect it didn’t decrease much.
They also showed that respiratory rate during exercise decreased in the masked condition. That doesn’t really make sense when you think about it in the context of the other findings, which are all suggestive of increased metabolic rate and sympathetic drive. Does that call the whole procedure into question? No, but it’s worth noting.
These were young, healthy people. You could certainly argue that those with more vulnerable cardiopulmonary status might have had different effects from mask wearing, but without a specific study in those people, it’s just conjecture. Clearly, this study lets us conclude that mask wearing at rest has less of an effect than mask wearing during exercise.
But remember that, in reality, we are wearing masks for a reason. One could imagine a study where this metabolic chamber was filled with wildfire smoke at a concentration similar to what we saw in New York. In that situation, we might find that wearing an N95 is quite helpful. The thing is, studying masks in isolation is useful because you can control so many variables. But masks aren’t used in isolation. In fact, that’s sort of their defining characteristic.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
PTSD: Children, adolescents, and all of us may be at risk
Not everyone will suffer an episode of posttraumatic stress disorder, even though everyday American life is characterized by a lot of uncertainty these days, particularly considering the proliferation of gun violence.

Also, everyone who does experience a traumatic event will not suffer an episode of PTSD – just as not everyone develops a heart attack or cancer, nor will everyone get every illness.
The data suggest that of those exposed to trauma, up to 25% of people will develop PTSD, according to Massachusetts General/McLean Hospital, Belmont, psychiatrist Kerry J. Ressler, MD, PhD, chief of the division of depression and anxiety disorders.
As I wrote in December 2022, our “kids” are not all right and psychiatry can help. I would say that many adolescents, and adults as well, may not be all right as we are terrorized not only by mass school shootings, but shootings happening almost anywhere and everywhere in our country: in supermarkets, hospitals, and shopping malls, at graduation parties, and on the streets.
According to a report published in Clinical Psychiatry News, a poll conducted by the American Psychiatric Association showed that most American adults [70%] reported that they were anxious or extremely anxious about keeping themselves or their families safe. APA President Rebecca W. Brendel, MD, JD, pointed out that there is “a lot of worry out there about economic uncertainty, about violence and how we are going to come out of this time period.”
Meanwhile, PTSD is still defined in the DSM-5 as exposure to actual or threatened death, serious injury, or sexual violence experienced directly, witnessing the traumatic event as it occurs to others, learning that a traumatic event occurred to a close family member or friend, or experiencing of traumatic events plus extreme exposure to aversive details of the event.
Examples of traumatic events can be numerous. They include natural disasters, man-made disasters, various types of assaults, war trauma, and severe illness with ICU experiences. I would add encounters with racism and bigotry – including homophobia when one fears for their very life or physical injury. This list includes only a few triggers that may invoke this disorder.
Interestingly, the DSM-5 excludes aversive exposure through electronic media, television, movies, or pictures. Including these aspects of trauma exposure would indeed increase PTSD diagnoses, and I believe this type of exposure needs to be included, especially considering how different people process information. Some viewers of media remain “outside” the events depicted on television, movies, or electronic media while others fit directly “into” the film or TV show. Even, for example, a news program, as evidenced by those people suffering from PTSD after viewing the Sept. 11, 2001, disaster on TV.
I have interviewed numerous people who witnessed Sept. 11 tragedies on TV, some during and some after the event, and they genuinely had experienced key factors of PTSD, including nightmares and intrusive recollections of the event. It’s important to include the ways in which people process information and events in order to make a correct diagnosis, in that “one [diagnostic] size does not fit all.”
PTSD at school
In my December column, I noted the fear of death that my generation and beyond experienced with the endless threat of nuclear war, which by its very nature meant death, and if not, the saying went “the living would envy the dead” – that is, in post–nuclear war.
As I pointed out in the column, that war never came and hopefully never will, yet the intensity of those many decades of threatened terror with regular school exercises of “hide under the desk” and “don’t look at the flash” left some with intrusive fearful thoughts, nightmares, and even visualization of atomic destruction, as well as the many scenes of destruction portrayed in news casts and films of nuclear explosions.
Clearly, most U.S. school children who participate in school lockdown drills will not suffer from PTSD episodes, but some will. If that “some” approaches 20% or even 10% or less, that will amount to a lot of kids.
I decided to interview two of my grandchildren, each living in different communities and attending different school systems, but both experiencing “lockdown drills.”
Jack, who is 13 and going into eighth grade, was quite clear regarding the drills and reported that in his age group, both he and the kids in his class felt scared while in lockdown. He told me some kids looked nervous. He mentioned that they were taught in school that if the “real thing” happened, the message was “hide, run, and fight.” I was curious and asked why not run first. He was quick to answer and said if you run, you might run into danger, so it’s better to hide and wait for help to arrive. I said to myself, if not PTSD, then being scared or nervous may also lead to anxiety or even to an anxiety disorder.
Next, I interviewed almost 11-year-old Charley, who is going into sixth grade. She was very clear about not at all being fearful or nervous during these drills and was confident that her classmates felt the same way. Then she explained that the school did a great job with a security officer and had locked doors all around that only opened from the inside. She was proud of the school and not fearful or worried at all.
The diverse views of these two young people surprised me but confirm that PTSD is not at all a given based on what is occurring in society. However, it should always be considered by clinicians if a child or adolescent begins to show signs consistent with PTSD.
These two interviews were quite short, but after I finished talking with Charley, she reported spontaneously that while she and her classmates were neither worried nor scared, some of their teachers did look nervous and seemed scared.
I was quite impressed with her sharpness and nuanced observation, and as noted, adults as well may be adversely affected by the entire concept of school lockdowns, as the awareness of their purpose rests in the forefront of their minds.
The way forward
So how do we prepare kids and adolescents for potential emotional problems like PTSD arising from lockdowns, even though most children or adults will not suffer any of these PTSD issues?
First, I believe that Second, it is important that school children be aware that if they feel bad in any way emotionally, they should speak to their parents, guardians, teachers, or school nurses.
Clearly, communicating simple problems without embarrassment or shame can lead to solutions, often quickly. Larger, more complicated issues may need professional intervention. Equally important, many mental health interventions need not be long in duration but client-centered, focused, and short term.
But what needs to be emphasized is that speaking and addressing what’s going on, if your thoughts and emotions are troubling, are in themselves therapeutic. Talk therapy works – especially if you get a new perspective on the old set of problems.
Dr. London is a practicing psychiatrist and has been a newspaper columnist for 35 years, specializing in and writing about short-term therapy, including cognitive-behavioral therapy and guided imagery. He is author of “Find Freedom Fast” (New York: Kettlehole Publishing, 2019). He has no conflicts of interest.
Not everyone will suffer an episode of posttraumatic stress disorder, even though everyday American life is characterized by a lot of uncertainty these days, particularly considering the proliferation of gun violence.
Also, everyone who does experience a traumatic event will not suffer an episode of PTSD – just as not everyone develops a heart attack or cancer, nor will everyone get every illness.
The data suggest that of those exposed to trauma, up to 25% of people will develop PTSD, according to Massachusetts General/McLean Hospital, Belmont, psychiatrist Kerry J. Ressler, MD, PhD, chief of the division of depression and anxiety disorders.
As I wrote in December 2022, our “kids” are not all right and psychiatry can help. I would say that many adolescents, and adults as well, may not be all right as we are terrorized not only by mass school shootings, but shootings happening almost anywhere and everywhere in our country: in supermarkets, hospitals, and shopping malls, at graduation parties, and on the streets.
According to a report published in Clinical Psychiatry News, a poll conducted by the American Psychiatric Association showed that most American adults [70%] reported that they were anxious or extremely anxious about keeping themselves or their families safe. APA President Rebecca W. Brendel, MD, JD, pointed out that there is “a lot of worry out there about economic uncertainty, about violence and how we are going to come out of this time period.”
Meanwhile, PTSD is still defined in the DSM-5 as exposure to actual or threatened death, serious injury, or sexual violence experienced directly, witnessing the traumatic event as it occurs to others, learning that a traumatic event occurred to a close family member or friend, or experiencing of traumatic events plus extreme exposure to aversive details of the event.
Examples of traumatic events can be numerous. They include natural disasters, man-made disasters, various types of assaults, war trauma, and severe illness with ICU experiences. I would add encounters with racism and bigotry – including homophobia when one fears for their very life or physical injury. This list includes only a few triggers that may invoke this disorder.
Interestingly, the DSM-5 excludes aversive exposure through electronic media, television, movies, or pictures. Including these aspects of trauma exposure would indeed increase PTSD diagnoses, and I believe this type of exposure needs to be included, especially considering how different people process information. Some viewers of media remain “outside” the events depicted on television, movies, or electronic media while others fit directly “into” the film or TV show. Even, for example, a news program, as evidenced by those people suffering from PTSD after viewing the Sept. 11, 2001, disaster on TV.
I have interviewed numerous people who witnessed Sept. 11 tragedies on TV, some during and some after the event, and they genuinely had experienced key factors of PTSD, including nightmares and intrusive recollections of the event. It’s important to include the ways in which people process information and events in order to make a correct diagnosis, in that “one [diagnostic] size does not fit all.”
PTSD at school
In my December column, I noted the fear of death that my generation and beyond experienced with the endless threat of nuclear war, which by its very nature meant death, and if not, the saying went “the living would envy the dead” – that is, in post–nuclear war.
As I pointed out in the column, that war never came and hopefully never will, yet the intensity of those many decades of threatened terror with regular school exercises of “hide under the desk” and “don’t look at the flash” left some with intrusive fearful thoughts, nightmares, and even visualization of atomic destruction, as well as the many scenes of destruction portrayed in news casts and films of nuclear explosions.
Clearly, most U.S. school children who participate in school lockdown drills will not suffer from PTSD episodes, but some will. If that “some” approaches 20% or even 10% or less, that will amount to a lot of kids.
I decided to interview two of my grandchildren, each living in different communities and attending different school systems, but both experiencing “lockdown drills.”
Jack, who is 13 and going into eighth grade, was quite clear regarding the drills and reported that in his age group, both he and the kids in his class felt scared while in lockdown. He told me some kids looked nervous. He mentioned that they were taught in school that if the “real thing” happened, the message was “hide, run, and fight.” I was curious and asked why not run first. He was quick to answer and said if you run, you might run into danger, so it’s better to hide and wait for help to arrive. I said to myself, if not PTSD, then being scared or nervous may also lead to anxiety or even to an anxiety disorder.
Next, I interviewed almost 11-year-old Charley, who is going into sixth grade. She was very clear about not at all being fearful or nervous during these drills and was confident that her classmates felt the same way. Then she explained that the school did a great job with a security officer and had locked doors all around that only opened from the inside. She was proud of the school and not fearful or worried at all.
The diverse views of these two young people surprised me but confirm that PTSD is not at all a given based on what is occurring in society. However, it should always be considered by clinicians if a child or adolescent begins to show signs consistent with PTSD.
These two interviews were quite short, but after I finished talking with Charley, she reported spontaneously that while she and her classmates were neither worried nor scared, some of their teachers did look nervous and seemed scared.
I was quite impressed with her sharpness and nuanced observation, and as noted, adults as well may be adversely affected by the entire concept of school lockdowns, as the awareness of their purpose rests in the forefront of their minds.
The way forward
So how do we prepare kids and adolescents for potential emotional problems like PTSD arising from lockdowns, even though most children or adults will not suffer any of these PTSD issues?
First, I believe that Second, it is important that school children be aware that if they feel bad in any way emotionally, they should speak to their parents, guardians, teachers, or school nurses.
Clearly, communicating simple problems without embarrassment or shame can lead to solutions, often quickly. Larger, more complicated issues may need professional intervention. Equally important, many mental health interventions need not be long in duration but client-centered, focused, and short term.
But what needs to be emphasized is that speaking and addressing what’s going on, if your thoughts and emotions are troubling, are in themselves therapeutic. Talk therapy works – especially if you get a new perspective on the old set of problems.
Dr. London is a practicing psychiatrist and has been a newspaper columnist for 35 years, specializing in and writing about short-term therapy, including cognitive-behavioral therapy and guided imagery. He is author of “Find Freedom Fast” (New York: Kettlehole Publishing, 2019). He has no conflicts of interest.
Not everyone will suffer an episode of posttraumatic stress disorder, even though everyday American life is characterized by a lot of uncertainty these days, particularly considering the proliferation of gun violence.
Also, everyone who does experience a traumatic event will not suffer an episode of PTSD – just as not everyone develops a heart attack or cancer, nor will everyone get every illness.
The data suggest that of those exposed to trauma, up to 25% of people will develop PTSD, according to Massachusetts General/McLean Hospital, Belmont, psychiatrist Kerry J. Ressler, MD, PhD, chief of the division of depression and anxiety disorders.
As I wrote in December 2022, our “kids” are not all right and psychiatry can help. I would say that many adolescents, and adults as well, may not be all right as we are terrorized not only by mass school shootings, but shootings happening almost anywhere and everywhere in our country: in supermarkets, hospitals, and shopping malls, at graduation parties, and on the streets.
According to a report published in Clinical Psychiatry News, a poll conducted by the American Psychiatric Association showed that most American adults [70%] reported that they were anxious or extremely anxious about keeping themselves or their families safe. APA President Rebecca W. Brendel, MD, JD, pointed out that there is “a lot of worry out there about economic uncertainty, about violence and how we are going to come out of this time period.”
Meanwhile, PTSD is still defined in the DSM-5 as exposure to actual or threatened death, serious injury, or sexual violence experienced directly, witnessing the traumatic event as it occurs to others, learning that a traumatic event occurred to a close family member or friend, or experiencing of traumatic events plus extreme exposure to aversive details of the event.
Examples of traumatic events can be numerous. They include natural disasters, man-made disasters, various types of assaults, war trauma, and severe illness with ICU experiences. I would add encounters with racism and bigotry – including homophobia when one fears for their very life or physical injury. This list includes only a few triggers that may invoke this disorder.
Interestingly, the DSM-5 excludes aversive exposure through electronic media, television, movies, or pictures. Including these aspects of trauma exposure would indeed increase PTSD diagnoses, and I believe this type of exposure needs to be included, especially considering how different people process information. Some viewers of media remain “outside” the events depicted on television, movies, or electronic media while others fit directly “into” the film or TV show. Even, for example, a news program, as evidenced by those people suffering from PTSD after viewing the Sept. 11, 2001, disaster on TV.
I have interviewed numerous people who witnessed Sept. 11 tragedies on TV, some during and some after the event, and they genuinely had experienced key factors of PTSD, including nightmares and intrusive recollections of the event. It’s important to include the ways in which people process information and events in order to make a correct diagnosis, in that “one [diagnostic] size does not fit all.”
PTSD at school
In my December column, I noted the fear of death that my generation and beyond experienced with the endless threat of nuclear war, which by its very nature meant death, and if not, the saying went “the living would envy the dead” – that is, in post–nuclear war.
As I pointed out in the column, that war never came and hopefully never will, yet the intensity of those many decades of threatened terror with regular school exercises of “hide under the desk” and “don’t look at the flash” left some with intrusive fearful thoughts, nightmares, and even visualization of atomic destruction, as well as the many scenes of destruction portrayed in news casts and films of nuclear explosions.
Clearly, most U.S. school children who participate in school lockdown drills will not suffer from PTSD episodes, but some will. If that “some” approaches 20% or even 10% or less, that will amount to a lot of kids.
I decided to interview two of my grandchildren, each living in different communities and attending different school systems, but both experiencing “lockdown drills.”
Jack, who is 13 and going into eighth grade, was quite clear regarding the drills and reported that in his age group, both he and the kids in his class felt scared while in lockdown. He told me some kids looked nervous. He mentioned that they were taught in school that if the “real thing” happened, the message was “hide, run, and fight.” I was curious and asked why not run first. He was quick to answer and said if you run, you might run into danger, so it’s better to hide and wait for help to arrive. I said to myself, if not PTSD, then being scared or nervous may also lead to anxiety or even to an anxiety disorder.
Next, I interviewed almost 11-year-old Charley, who is going into sixth grade. She was very clear about not at all being fearful or nervous during these drills and was confident that her classmates felt the same way. Then she explained that the school did a great job with a security officer and had locked doors all around that only opened from the inside. She was proud of the school and not fearful or worried at all.
The diverse views of these two young people surprised me but confirm that PTSD is not at all a given based on what is occurring in society. However, it should always be considered by clinicians if a child or adolescent begins to show signs consistent with PTSD.
These two interviews were quite short, but after I finished talking with Charley, she reported spontaneously that while she and her classmates were neither worried nor scared, some of their teachers did look nervous and seemed scared.
I was quite impressed with her sharpness and nuanced observation, and as noted, adults as well may be adversely affected by the entire concept of school lockdowns, as the awareness of their purpose rests in the forefront of their minds.
The way forward
So how do we prepare kids and adolescents for potential emotional problems like PTSD arising from lockdowns, even though most children or adults will not suffer any of these PTSD issues?
First, I believe that Second, it is important that school children be aware that if they feel bad in any way emotionally, they should speak to their parents, guardians, teachers, or school nurses.
Clearly, communicating simple problems without embarrassment or shame can lead to solutions, often quickly. Larger, more complicated issues may need professional intervention. Equally important, many mental health interventions need not be long in duration but client-centered, focused, and short term.
But what needs to be emphasized is that speaking and addressing what’s going on, if your thoughts and emotions are troubling, are in themselves therapeutic. Talk therapy works – especially if you get a new perspective on the old set of problems.
Dr. London is a practicing psychiatrist and has been a newspaper columnist for 35 years, specializing in and writing about short-term therapy, including cognitive-behavioral therapy and guided imagery. He is author of “Find Freedom Fast” (New York: Kettlehole Publishing, 2019). He has no conflicts of interest.
Applications of ChatGPT and Large Language Models in Medicine and Health Care: Benefits and Pitfalls
The development of [artificial intelligence] is as fundamental as the creation of the microprocessor, the personal computer, the Internet, and the mobile phone. It will change the way people work, learn, travel, get health care, and communicate with each other.
Bill Gates 1
As the world emerges from the pandemic and the health care system faces new challenges, technology has become an increasingly important tool for health care professionals (HCPs). One such technology is the large language model (LLM), which has the potential to revolutionize the health care industry. ChatGPT, a popular LLM developed by OpenAI, has gained particular attention in the medical community for its ability to pass the United States Medical Licensing Exam.2 This article will explore the benefits and potential pitfalls of using LLMs like ChatGPT in medicine and health care.
Benefits
HCP burnout is a serious issue that can lead to lower productivity, increased medical errors, and decreased patient satisfaction.3 LLMs can alleviate some administrative burdens on HCPs, allowing them to focus on patient care. By assisting with billing, coding, insurance claims, and organizing schedules, LLMs like ChatGPT can free up time for HCPs to focus on what they do best: providing quality patient care.4 ChatGPT also can assist with diagnoses by providing accurate and reliable information based on a vast amount of clinical data. By learning the relationships between different medical conditions, symptoms, and treatment options, ChatGPT can provide an appropriate differential diagnosis (Figure 1). 
Imaging medical specialists like radiologists, pathologists, dermatologists, and others can benefit from combining computer vision diagnostics with ChatGPT report creation abilities to streamline the diagnostic workflow and improve diagnostic accuracy (Figure 2). 
Although using ChatGPT and other LLMs in mental health care has potential benefits, it is essential to note that they are not a substitute for human interaction and personalized care. While ChatGPT can remember information from previous conversations, it cannot provide the same level of personalized, high-quality care that a professional therapist or HCP can. However, by augmenting the work of HCPs, ChatGPT and other LLMs have the potential to make mental health care more accessible and efficient. In addition to providing effective screening in underserved areas, ChatGPT technology may improve the competence of physician assistants and nurse practitioners in delivering mental health care. With the increased incidence of mental health problems in veterans, the pertinence of a ChatGPT-like feature will only increase with time.9
ChatGPT can also be integrated into health care organizations’ websites and mobile apps, providing patients instant access to medical information, self-care advice, symptom checkers, scheduling appointments, and arranging transportation. These features can reduce the burden on health care staff and help patients stay informed and motivated to take an active role in their health. Additionally, health care organizations can use ChatGPT to engage patients by providing reminders for medication renewals and assistance with self-care.4,6,10,11
The potential of artificial intelligence (AI) in the field of medical education and research is immense. According to a study by Gilson and colleagues, ChatGPT has shown promising results as a medical education tool.12 ChatGPT can simulate clinical scenarios, provide real-time feedback, and improve diagnostic skills. It also offers new interactive and personalized learning opportunities for medical students and HCPs.13 ChatGPT can help researchers by streamlining the process of data analysis. It can also administer surveys or questionnaires, facilitate data collection on preferences and experiences, and help in writing scientific publications.14 Nevertheless, to fully unlock the potential of these AI models, additional models that perform checks for factual accuracy, plagiarism, and copyright infringement must be developed.15,16
AI Bill of Rights
In order to protect the American public, the White House Office of Science and Technology Policy (OSTP) has released a blueprint for an AI Bill of Rights that emphasizes 5 principles to protect the public from the harmful effects of AI models, including safe and effective systems; algorithmic discrimination protection; data privacy; notice and explanation; and human alternatives, considerations, and fallback (Figure 3).17 
One of the biggest challenges with LLMs like ChatGPT is the prevalence of inaccurate information or so-called hallucinations.16 These inaccuracies stem from the inability of LLMs to distinguish between real and fake information. To prevent hallucinations, researchers have proposed several methods, including training models on more diverse data, using adversarial training methods, and human-in-the-loop approaches.21 In addition, medicine-specific models like GatorTron, medPaLM, and Almanac were developed, increasing the accuracy of factual results.22-24 Unfortunately, only the GatorTron model is available to the public through the NVIDIA developers’ program.25
Despite these shortcomings, the future of LLMs in health care is promising. Although these models will not replace HCPs, they can help reduce the unnecessary burden on them, prevent burnout, and enable HCPs and patients spend more time together. Establishing an official hospital AI oversight governing body that would promote best practices could ensure the trustworthy implementation of these new technologies.26
Conclusions
The use of ChatGPT and other LLMs in health care has the potential to revolutionize the industry. By assisting HCPs with administrative tasks, improving the accuracy and reliability of diagnoses, and engaging patients, ChatGPT can help health care organizations provide better care to their patients. While LLMs are not a substitute for human interaction and personalized care, they can augment the work of HCPs, making health care more accessible and efficient. As the health care industry continues to evolve, it will be exciting to see how ChatGPT and other LLMs are used to improve patient outcomes and quality of care. In addition, AI technologies like ChatGPT offer enormous potential in medical education and research. To ensure that the benefits outweigh the risks, developing trustworthy AI health care products and establishing oversight governing bodies to ensure their implementation is essential. By doing so, we can help HCPs focus on what matters most, providing high-quality care to patients.
Acknowledgments
This material is the result of work supported by resources and the use of facilities at the James A. Haley Veterans’ Hospital.
1. Bill Gates. The age of AI has begun. March 21, 2023. Accessed May 10, 2023. https://www.gatesnotes.com/the-age-of-ai-has-begun
2. Kung TH, Cheatham M, Medenilla A, et al. Performance of ChatGPT on USMLE: Potential for AI-assisted medical education using large language models. PLOS Digit Health. 2023;2(2):e0000198. Published 2023 Feb 9. doi:10.1371/journal.pdig.0000198
3. Shanafelt TD, West CP, Sinsky C, et al. Changes in burnout and satisfaction with work-life integration in physicians and the general US working population between 2011 and 2020. Mayo Clin Proc. 2022;97(3):491-506. doi:10.1016/j.mayocp.2021.11.021
4. Goodman RS, Patrinely JR Jr, Osterman T, Wheless L, Johnson DB. On the cusp: considering the impact of artificial intelligence language models in healthcare. Med. 2023;4(3):139-140. doi:10.1016/j.medj.2023.02.008
5. Will ChatGPT transform healthcare? Nat Med. 2023;29(3):505-506. doi:10.1038/s41591-023-02289-5
6. Hopkins AM, Logan JM, Kichenadasse G, Sorich MJ. Artificial intelligence chatbots will revolutionize how cancer patients access information: ChatGPT represents a paradigm-shift. JNCI Cancer Spectr. 2023;7(2):pkad010. doi:10.1093/jncics/pkad010
7. Babar Z, van Laarhoven T, Zanzotto FM, Marchiori E. Evaluating diagnostic content of AI-generated radiology reports of chest X-rays. Artif Intell Med. 2021;116:102075. doi:10.1016/j.artmed.2021.102075
8. Lecler A, Duron L, Soyer P. Revolutionizing radiology with GPT-based models: current applications, future possibilities and limitations of ChatGPT. Diagn Interv Imaging. 2023;S2211-5684(23)00027-X. doi:10.1016/j.diii.2023.02.003
9. Germain JM. Is ChatGPT smart enough to practice mental health therapy? March 23, 2023. Accessed May 11, 2023. https://www.technewsworld.com/story/is-chatgpt-smart-enough-to-practice-mental-health-therapy-178064.html
10. Cascella M, Montomoli J, Bellini V, Bignami E. Evaluating the feasibility of ChatGPT in healthcare: an analysis of multiple clinical and research scenarios. J Med Syst. 2023;47(1):33. Published 2023 Mar 4. doi:10.1007/s10916-023-01925-4
11. Jungwirth D, Haluza D. Artificial intelligence and public health: an exploratory study. Int J Environ Res Public Health. 2023;20(5):4541. Published 2023 Mar 3. doi:10.3390/ijerph20054541
12. Gilson A, Safranek CW, Huang T, et al. How does ChatGPT perform on the United States Medical Licensing Examination? The implications of large language models for medical education and knowledge assessment. JMIR Med Educ. 2023;9:e45312. Published 2023 Feb 8. doi:10.2196/45312
13. Eysenbach G. The role of ChatGPT, generative language models, and artificial intelligence in medical education: a conversation with ChatGPT and a call for papers. JMIR Med Educ. 2023;9:e46885. Published 2023 Mar 6. doi:10.2196/46885
14. Macdonald C, Adeloye D, Sheikh A, Rudan I. Can ChatGPT draft a research article? An example of population-level vaccine effectiveness analysis. J Glob Health. 2023;13:01003. Published 2023 Feb 17. doi:10.7189/jogh.13.01003
15. Masters K. Ethical use of artificial intelligence in health professions education: AMEE Guide No.158. Med Teach. 2023;1-11. doi:10.1080/0142159X.2023.2186203
16. Smith CS. Hallucinations could blunt ChatGPT’s success. IEEE Spectrum. March 13, 2023. Accessed May 11, 2023. https://spectrum.ieee.org/ai-hallucination
17. Executive Office of the President, Office of Science and Technology Policy. Blueprint for an AI Bill of Rights. Accessed May 11, 2023. https://www.whitehouse.gov/ostp/ai-bill-of-rights
18. Executive office of the President. Executive Order 13960: promoting the use of trustworthy artificial intelligence in the federal government. Fed Regist. 2020;89(236):78939-78943.
19. US Department of Commerce, National institute of Standards and Technology. Artificial Intelligence Risk Management Framework (AI RMF 1.0). Published January 2023. doi:10.6028/NIST.AI.100-1
20. Microsoft. Azure Cognitive Search—Cloud Search Service. Accessed May 11, 2023. https://azure.microsoft.com/en-us/products/search
21. Aiyappa R, An J, Kwak H, Ahn YY. Can we trust the evaluation on ChatGPT? March 22, 2023. Accessed May 11, 2023. https://arxiv.org/abs/2303.12767v1
22. Yang X, Chen A, Pournejatian N, et al. GatorTron: a large clinical language model to unlock patient information from unstructured electronic health records. Updated December 16, 2022. Accessed May 11, 2023. https://arxiv.org/abs/2203.03540v3
23. Singhal K, Azizi S, Tu T, et al. Large language models encode clinical knowledge. December 26, 2022. Accessed May 11, 2023. https://arxiv.org/abs/2212.13138v1
24. Zakka C, Chaurasia A, Shad R, Hiesinger W. Almanac: knowledge-grounded language models for clinical medicine. March 1, 2023. Accessed May 11, 2023. https://arxiv.org/abs/2303.01229v1
25. NVIDIA. GatorTron-OG. Accessed May 11, 2023. https://catalog.ngc.nvidia.com/orgs/nvidia/teams/clara/models/gatortron_og
26. Borkowski AA, Jakey CE, Thomas LB, Viswanadhan N, Mastorides SM. Establishing a hospital artificial intelligence committee to improve patient care. Fed Pract. 2022;39(8):334-336. doi:10.12788/fp.0299
The development of [artificial intelligence] is as fundamental as the creation of the microprocessor, the personal computer, the Internet, and the mobile phone. It will change the way people work, learn, travel, get health care, and communicate with each other.
Bill Gates 1
As the world emerges from the pandemic and the health care system faces new challenges, technology has become an increasingly important tool for health care professionals (HCPs). One such technology is the large language model (LLM), which has the potential to revolutionize the health care industry. ChatGPT, a popular LLM developed by OpenAI, has gained particular attention in the medical community for its ability to pass the United States Medical Licensing Exam.2 This article will explore the benefits and potential pitfalls of using LLMs like ChatGPT in medicine and health care.
Benefits
HCP burnout is a serious issue that can lead to lower productivity, increased medical errors, and decreased patient satisfaction.3 LLMs can alleviate some administrative burdens on HCPs, allowing them to focus on patient care. By assisting with billing, coding, insurance claims, and organizing schedules, LLMs like ChatGPT can free up time for HCPs to focus on what they do best: providing quality patient care.4 ChatGPT also can assist with diagnoses by providing accurate and reliable information based on a vast amount of clinical data. By learning the relationships between different medical conditions, symptoms, and treatment options, ChatGPT can provide an appropriate differential diagnosis (Figure 1).
Imaging medical specialists like radiologists, pathologists, dermatologists, and others can benefit from combining computer vision diagnostics with ChatGPT report creation abilities to streamline the diagnostic workflow and improve diagnostic accuracy (Figure 2).
Although using ChatGPT and other LLMs in mental health care has potential benefits, it is essential to note that they are not a substitute for human interaction and personalized care. While ChatGPT can remember information from previous conversations, it cannot provide the same level of personalized, high-quality care that a professional therapist or HCP can. However, by augmenting the work of HCPs, ChatGPT and other LLMs have the potential to make mental health care more accessible and efficient. In addition to providing effective screening in underserved areas, ChatGPT technology may improve the competence of physician assistants and nurse practitioners in delivering mental health care. With the increased incidence of mental health problems in veterans, the pertinence of a ChatGPT-like feature will only increase with time.9
ChatGPT can also be integrated into health care organizations’ websites and mobile apps, providing patients instant access to medical information, self-care advice, symptom checkers, scheduling appointments, and arranging transportation. These features can reduce the burden on health care staff and help patients stay informed and motivated to take an active role in their health. Additionally, health care organizations can use ChatGPT to engage patients by providing reminders for medication renewals and assistance with self-care.4,6,10,11
The potential of artificial intelligence (AI) in the field of medical education and research is immense. According to a study by Gilson and colleagues, ChatGPT has shown promising results as a medical education tool.12 ChatGPT can simulate clinical scenarios, provide real-time feedback, and improve diagnostic skills. It also offers new interactive and personalized learning opportunities for medical students and HCPs.13 ChatGPT can help researchers by streamlining the process of data analysis. It can also administer surveys or questionnaires, facilitate data collection on preferences and experiences, and help in writing scientific publications.14 Nevertheless, to fully unlock the potential of these AI models, additional models that perform checks for factual accuracy, plagiarism, and copyright infringement must be developed.15,16
AI Bill of Rights
In order to protect the American public, the White House Office of Science and Technology Policy (OSTP) has released a blueprint for an AI Bill of Rights that emphasizes 5 principles to protect the public from the harmful effects of AI models, including safe and effective systems; algorithmic discrimination protection; data privacy; notice and explanation; and human alternatives, considerations, and fallback (Figure 3).17
One of the biggest challenges with LLMs like ChatGPT is the prevalence of inaccurate information or so-called hallucinations.16 These inaccuracies stem from the inability of LLMs to distinguish between real and fake information. To prevent hallucinations, researchers have proposed several methods, including training models on more diverse data, using adversarial training methods, and human-in-the-loop approaches.21 In addition, medicine-specific models like GatorTron, medPaLM, and Almanac were developed, increasing the accuracy of factual results.22-24 Unfortunately, only the GatorTron model is available to the public through the NVIDIA developers’ program.25
Despite these shortcomings, the future of LLMs in health care is promising. Although these models will not replace HCPs, they can help reduce the unnecessary burden on them, prevent burnout, and enable HCPs and patients spend more time together. Establishing an official hospital AI oversight governing body that would promote best practices could ensure the trustworthy implementation of these new technologies.26
Conclusions
The use of ChatGPT and other LLMs in health care has the potential to revolutionize the industry. By assisting HCPs with administrative tasks, improving the accuracy and reliability of diagnoses, and engaging patients, ChatGPT can help health care organizations provide better care to their patients. While LLMs are not a substitute for human interaction and personalized care, they can augment the work of HCPs, making health care more accessible and efficient. As the health care industry continues to evolve, it will be exciting to see how ChatGPT and other LLMs are used to improve patient outcomes and quality of care. In addition, AI technologies like ChatGPT offer enormous potential in medical education and research. To ensure that the benefits outweigh the risks, developing trustworthy AI health care products and establishing oversight governing bodies to ensure their implementation is essential. By doing so, we can help HCPs focus on what matters most, providing high-quality care to patients.
Acknowledgments
This material is the result of work supported by resources and the use of facilities at the James A. Haley Veterans’ Hospital.
The development of [artificial intelligence] is as fundamental as the creation of the microprocessor, the personal computer, the Internet, and the mobile phone. It will change the way people work, learn, travel, get health care, and communicate with each other.
Bill Gates 1
As the world emerges from the pandemic and the health care system faces new challenges, technology has become an increasingly important tool for health care professionals (HCPs). One such technology is the large language model (LLM), which has the potential to revolutionize the health care industry. ChatGPT, a popular LLM developed by OpenAI, has gained particular attention in the medical community for its ability to pass the United States Medical Licensing Exam.2 This article will explore the benefits and potential pitfalls of using LLMs like ChatGPT in medicine and health care.
Benefits
HCP burnout is a serious issue that can lead to lower productivity, increased medical errors, and decreased patient satisfaction.3 LLMs can alleviate some administrative burdens on HCPs, allowing them to focus on patient care. By assisting with billing, coding, insurance claims, and organizing schedules, LLMs like ChatGPT can free up time for HCPs to focus on what they do best: providing quality patient care.4 ChatGPT also can assist with diagnoses by providing accurate and reliable information based on a vast amount of clinical data. By learning the relationships between different medical conditions, symptoms, and treatment options, ChatGPT can provide an appropriate differential diagnosis (Figure 1).
Imaging medical specialists like radiologists, pathologists, dermatologists, and others can benefit from combining computer vision diagnostics with ChatGPT report creation abilities to streamline the diagnostic workflow and improve diagnostic accuracy (Figure 2).
Although using ChatGPT and other LLMs in mental health care has potential benefits, it is essential to note that they are not a substitute for human interaction and personalized care. While ChatGPT can remember information from previous conversations, it cannot provide the same level of personalized, high-quality care that a professional therapist or HCP can. However, by augmenting the work of HCPs, ChatGPT and other LLMs have the potential to make mental health care more accessible and efficient. In addition to providing effective screening in underserved areas, ChatGPT technology may improve the competence of physician assistants and nurse practitioners in delivering mental health care. With the increased incidence of mental health problems in veterans, the pertinence of a ChatGPT-like feature will only increase with time.9
ChatGPT can also be integrated into health care organizations’ websites and mobile apps, providing patients instant access to medical information, self-care advice, symptom checkers, scheduling appointments, and arranging transportation. These features can reduce the burden on health care staff and help patients stay informed and motivated to take an active role in their health. Additionally, health care organizations can use ChatGPT to engage patients by providing reminders for medication renewals and assistance with self-care.4,6,10,11
The potential of artificial intelligence (AI) in the field of medical education and research is immense. According to a study by Gilson and colleagues, ChatGPT has shown promising results as a medical education tool.12 ChatGPT can simulate clinical scenarios, provide real-time feedback, and improve diagnostic skills. It also offers new interactive and personalized learning opportunities for medical students and HCPs.13 ChatGPT can help researchers by streamlining the process of data analysis. It can also administer surveys or questionnaires, facilitate data collection on preferences and experiences, and help in writing scientific publications.14 Nevertheless, to fully unlock the potential of these AI models, additional models that perform checks for factual accuracy, plagiarism, and copyright infringement must be developed.15,16
AI Bill of Rights
In order to protect the American public, the White House Office of Science and Technology Policy (OSTP) has released a blueprint for an AI Bill of Rights that emphasizes 5 principles to protect the public from the harmful effects of AI models, including safe and effective systems; algorithmic discrimination protection; data privacy; notice and explanation; and human alternatives, considerations, and fallback (Figure 3).17
One of the biggest challenges with LLMs like ChatGPT is the prevalence of inaccurate information or so-called hallucinations.16 These inaccuracies stem from the inability of LLMs to distinguish between real and fake information. To prevent hallucinations, researchers have proposed several methods, including training models on more diverse data, using adversarial training methods, and human-in-the-loop approaches.21 In addition, medicine-specific models like GatorTron, medPaLM, and Almanac were developed, increasing the accuracy of factual results.22-24 Unfortunately, only the GatorTron model is available to the public through the NVIDIA developers’ program.25
Despite these shortcomings, the future of LLMs in health care is promising. Although these models will not replace HCPs, they can help reduce the unnecessary burden on them, prevent burnout, and enable HCPs and patients spend more time together. Establishing an official hospital AI oversight governing body that would promote best practices could ensure the trustworthy implementation of these new technologies.26
Conclusions
The use of ChatGPT and other LLMs in health care has the potential to revolutionize the industry. By assisting HCPs with administrative tasks, improving the accuracy and reliability of diagnoses, and engaging patients, ChatGPT can help health care organizations provide better care to their patients. While LLMs are not a substitute for human interaction and personalized care, they can augment the work of HCPs, making health care more accessible and efficient. As the health care industry continues to evolve, it will be exciting to see how ChatGPT and other LLMs are used to improve patient outcomes and quality of care. In addition, AI technologies like ChatGPT offer enormous potential in medical education and research. To ensure that the benefits outweigh the risks, developing trustworthy AI health care products and establishing oversight governing bodies to ensure their implementation is essential. By doing so, we can help HCPs focus on what matters most, providing high-quality care to patients.
Acknowledgments
This material is the result of work supported by resources and the use of facilities at the James A. Haley Veterans’ Hospital.
1. Bill Gates. The age of AI has begun. March 21, 2023. Accessed May 10, 2023. https://www.gatesnotes.com/the-age-of-ai-has-begun
2. Kung TH, Cheatham M, Medenilla A, et al. Performance of ChatGPT on USMLE: Potential for AI-assisted medical education using large language models. PLOS Digit Health. 2023;2(2):e0000198. Published 2023 Feb 9. doi:10.1371/journal.pdig.0000198
3. Shanafelt TD, West CP, Sinsky C, et al. Changes in burnout and satisfaction with work-life integration in physicians and the general US working population between 2011 and 2020. Mayo Clin Proc. 2022;97(3):491-506. doi:10.1016/j.mayocp.2021.11.021
4. Goodman RS, Patrinely JR Jr, Osterman T, Wheless L, Johnson DB. On the cusp: considering the impact of artificial intelligence language models in healthcare. Med. 2023;4(3):139-140. doi:10.1016/j.medj.2023.02.008
5. Will ChatGPT transform healthcare? Nat Med. 2023;29(3):505-506. doi:10.1038/s41591-023-02289-5
6. Hopkins AM, Logan JM, Kichenadasse G, Sorich MJ. Artificial intelligence chatbots will revolutionize how cancer patients access information: ChatGPT represents a paradigm-shift. JNCI Cancer Spectr. 2023;7(2):pkad010. doi:10.1093/jncics/pkad010
7. Babar Z, van Laarhoven T, Zanzotto FM, Marchiori E. Evaluating diagnostic content of AI-generated radiology reports of chest X-rays. Artif Intell Med. 2021;116:102075. doi:10.1016/j.artmed.2021.102075
8. Lecler A, Duron L, Soyer P. Revolutionizing radiology with GPT-based models: current applications, future possibilities and limitations of ChatGPT. Diagn Interv Imaging. 2023;S2211-5684(23)00027-X. doi:10.1016/j.diii.2023.02.003
9. Germain JM. Is ChatGPT smart enough to practice mental health therapy? March 23, 2023. Accessed May 11, 2023. https://www.technewsworld.com/story/is-chatgpt-smart-enough-to-practice-mental-health-therapy-178064.html
10. Cascella M, Montomoli J, Bellini V, Bignami E. Evaluating the feasibility of ChatGPT in healthcare: an analysis of multiple clinical and research scenarios. J Med Syst. 2023;47(1):33. Published 2023 Mar 4. doi:10.1007/s10916-023-01925-4
11. Jungwirth D, Haluza D. Artificial intelligence and public health: an exploratory study. Int J Environ Res Public Health. 2023;20(5):4541. Published 2023 Mar 3. doi:10.3390/ijerph20054541
12. Gilson A, Safranek CW, Huang T, et al. How does ChatGPT perform on the United States Medical Licensing Examination? The implications of large language models for medical education and knowledge assessment. JMIR Med Educ. 2023;9:e45312. Published 2023 Feb 8. doi:10.2196/45312
13. Eysenbach G. The role of ChatGPT, generative language models, and artificial intelligence in medical education: a conversation with ChatGPT and a call for papers. JMIR Med Educ. 2023;9:e46885. Published 2023 Mar 6. doi:10.2196/46885
14. Macdonald C, Adeloye D, Sheikh A, Rudan I. Can ChatGPT draft a research article? An example of population-level vaccine effectiveness analysis. J Glob Health. 2023;13:01003. Published 2023 Feb 17. doi:10.7189/jogh.13.01003
15. Masters K. Ethical use of artificial intelligence in health professions education: AMEE Guide No.158. Med Teach. 2023;1-11. doi:10.1080/0142159X.2023.2186203
16. Smith CS. Hallucinations could blunt ChatGPT’s success. IEEE Spectrum. March 13, 2023. Accessed May 11, 2023. https://spectrum.ieee.org/ai-hallucination
17. Executive Office of the President, Office of Science and Technology Policy. Blueprint for an AI Bill of Rights. Accessed May 11, 2023. https://www.whitehouse.gov/ostp/ai-bill-of-rights
18. Executive office of the President. Executive Order 13960: promoting the use of trustworthy artificial intelligence in the federal government. Fed Regist. 2020;89(236):78939-78943.
19. US Department of Commerce, National institute of Standards and Technology. Artificial Intelligence Risk Management Framework (AI RMF 1.0). Published January 2023. doi:10.6028/NIST.AI.100-1
20. Microsoft. Azure Cognitive Search—Cloud Search Service. Accessed May 11, 2023. https://azure.microsoft.com/en-us/products/search
21. Aiyappa R, An J, Kwak H, Ahn YY. Can we trust the evaluation on ChatGPT? March 22, 2023. Accessed May 11, 2023. https://arxiv.org/abs/2303.12767v1
22. Yang X, Chen A, Pournejatian N, et al. GatorTron: a large clinical language model to unlock patient information from unstructured electronic health records. Updated December 16, 2022. Accessed May 11, 2023. https://arxiv.org/abs/2203.03540v3
23. Singhal K, Azizi S, Tu T, et al. Large language models encode clinical knowledge. December 26, 2022. Accessed May 11, 2023. https://arxiv.org/abs/2212.13138v1
24. Zakka C, Chaurasia A, Shad R, Hiesinger W. Almanac: knowledge-grounded language models for clinical medicine. March 1, 2023. Accessed May 11, 2023. https://arxiv.org/abs/2303.01229v1
25. NVIDIA. GatorTron-OG. Accessed May 11, 2023. https://catalog.ngc.nvidia.com/orgs/nvidia/teams/clara/models/gatortron_og
26. Borkowski AA, Jakey CE, Thomas LB, Viswanadhan N, Mastorides SM. Establishing a hospital artificial intelligence committee to improve patient care. Fed Pract. 2022;39(8):334-336. doi:10.12788/fp.0299
1. Bill Gates. The age of AI has begun. March 21, 2023. Accessed May 10, 2023. https://www.gatesnotes.com/the-age-of-ai-has-begun
2. Kung TH, Cheatham M, Medenilla A, et al. Performance of ChatGPT on USMLE: Potential for AI-assisted medical education using large language models. PLOS Digit Health. 2023;2(2):e0000198. Published 2023 Feb 9. doi:10.1371/journal.pdig.0000198
3. Shanafelt TD, West CP, Sinsky C, et al. Changes in burnout and satisfaction with work-life integration in physicians and the general US working population between 2011 and 2020. Mayo Clin Proc. 2022;97(3):491-506. doi:10.1016/j.mayocp.2021.11.021
4. Goodman RS, Patrinely JR Jr, Osterman T, Wheless L, Johnson DB. On the cusp: considering the impact of artificial intelligence language models in healthcare. Med. 2023;4(3):139-140. doi:10.1016/j.medj.2023.02.008
5. Will ChatGPT transform healthcare? Nat Med. 2023;29(3):505-506. doi:10.1038/s41591-023-02289-5
6. Hopkins AM, Logan JM, Kichenadasse G, Sorich MJ. Artificial intelligence chatbots will revolutionize how cancer patients access information: ChatGPT represents a paradigm-shift. JNCI Cancer Spectr. 2023;7(2):pkad010. doi:10.1093/jncics/pkad010
7. Babar Z, van Laarhoven T, Zanzotto FM, Marchiori E. Evaluating diagnostic content of AI-generated radiology reports of chest X-rays. Artif Intell Med. 2021;116:102075. doi:10.1016/j.artmed.2021.102075
8. Lecler A, Duron L, Soyer P. Revolutionizing radiology with GPT-based models: current applications, future possibilities and limitations of ChatGPT. Diagn Interv Imaging. 2023;S2211-5684(23)00027-X. doi:10.1016/j.diii.2023.02.003
9. Germain JM. Is ChatGPT smart enough to practice mental health therapy? March 23, 2023. Accessed May 11, 2023. https://www.technewsworld.com/story/is-chatgpt-smart-enough-to-practice-mental-health-therapy-178064.html
10. Cascella M, Montomoli J, Bellini V, Bignami E. Evaluating the feasibility of ChatGPT in healthcare: an analysis of multiple clinical and research scenarios. J Med Syst. 2023;47(1):33. Published 2023 Mar 4. doi:10.1007/s10916-023-01925-4
11. Jungwirth D, Haluza D. Artificial intelligence and public health: an exploratory study. Int J Environ Res Public Health. 2023;20(5):4541. Published 2023 Mar 3. doi:10.3390/ijerph20054541
12. Gilson A, Safranek CW, Huang T, et al. How does ChatGPT perform on the United States Medical Licensing Examination? The implications of large language models for medical education and knowledge assessment. JMIR Med Educ. 2023;9:e45312. Published 2023 Feb 8. doi:10.2196/45312
13. Eysenbach G. The role of ChatGPT, generative language models, and artificial intelligence in medical education: a conversation with ChatGPT and a call for papers. JMIR Med Educ. 2023;9:e46885. Published 2023 Mar 6. doi:10.2196/46885
14. Macdonald C, Adeloye D, Sheikh A, Rudan I. Can ChatGPT draft a research article? An example of population-level vaccine effectiveness analysis. J Glob Health. 2023;13:01003. Published 2023 Feb 17. doi:10.7189/jogh.13.01003
15. Masters K. Ethical use of artificial intelligence in health professions education: AMEE Guide No.158. Med Teach. 2023;1-11. doi:10.1080/0142159X.2023.2186203
16. Smith CS. Hallucinations could blunt ChatGPT’s success. IEEE Spectrum. March 13, 2023. Accessed May 11, 2023. https://spectrum.ieee.org/ai-hallucination
17. Executive Office of the President, Office of Science and Technology Policy. Blueprint for an AI Bill of Rights. Accessed May 11, 2023. https://www.whitehouse.gov/ostp/ai-bill-of-rights
18. Executive office of the President. Executive Order 13960: promoting the use of trustworthy artificial intelligence in the federal government. Fed Regist. 2020;89(236):78939-78943.
19. US Department of Commerce, National institute of Standards and Technology. Artificial Intelligence Risk Management Framework (AI RMF 1.0). Published January 2023. doi:10.6028/NIST.AI.100-1
20. Microsoft. Azure Cognitive Search—Cloud Search Service. Accessed May 11, 2023. https://azure.microsoft.com/en-us/products/search
21. Aiyappa R, An J, Kwak H, Ahn YY. Can we trust the evaluation on ChatGPT? March 22, 2023. Accessed May 11, 2023. https://arxiv.org/abs/2303.12767v1
22. Yang X, Chen A, Pournejatian N, et al. GatorTron: a large clinical language model to unlock patient information from unstructured electronic health records. Updated December 16, 2022. Accessed May 11, 2023. https://arxiv.org/abs/2203.03540v3
23. Singhal K, Azizi S, Tu T, et al. Large language models encode clinical knowledge. December 26, 2022. Accessed May 11, 2023. https://arxiv.org/abs/2212.13138v1
24. Zakka C, Chaurasia A, Shad R, Hiesinger W. Almanac: knowledge-grounded language models for clinical medicine. March 1, 2023. Accessed May 11, 2023. https://arxiv.org/abs/2303.01229v1
25. NVIDIA. GatorTron-OG. Accessed May 11, 2023. https://catalog.ngc.nvidia.com/orgs/nvidia/teams/clara/models/gatortron_og
26. Borkowski AA, Jakey CE, Thomas LB, Viswanadhan N, Mastorides SM. Establishing a hospital artificial intelligence committee to improve patient care. Fed Pract. 2022;39(8):334-336. doi:10.12788/fp.0299
WOW! You spend that much time on the EHR?
Unlike many of you, maybe even most of you, I can recall when my office records were handwritten, some would say scribbled, on pieces of paper. They were decipherable by a select few. Some veteran assistants never mastered the skill. Pages were sometimes lavishly illustrated with drawings of body parts, often because I couldn’t remember or spell the correct anatomic term. When I needed to send a referring letter to another provider I typed it myself because dictating never quite suited my personality.
When I joined a small primary care group, the computer-savvy lead physician and a programmer developed our own homegrown EHR. It relied on scanning documents, as so many of us still generated handwritten notes. Even the most vociferous Luddites among us loved the system from day 2.

However, for a variety of reasons, some defensible some just plain bad, our beloved system needed to be replaced after 7 years. We then invested in an off-the-shelf EHR system that promised more capabilities. We were told there would be a learning curve but the plateau would come quickly and we would enjoy our new electronic assistant.
You’ve lived the rest of the story. The learning curve was steep and long and the plateau was a time gobbler. I was probably the most efficient provider in the group, and after 6 months I was leaving the office an hour later than I had been and was seeing the same number of patients. Most of my coworkers were staying and/or working on the computer at home for an extra 2 hours. This change could be easily documented by speaking with our spouses and children. I understand from my colleagues who have stayed in the business that over the ensuing decade and a half since my first experience with the EHR, its insatiable appetite for a clinician’s time has not abated.
The authors of a recent article in Annals of Family Medicine offer up some advice on how this tragic situation might be brought under control. First, the investigators point out that the phenomenon of after-hours EHR work, sometimes referred to as WOW (work outside of work), has not gone unnoticed by health system administrators and vendors who develop and sell the EHRs. However, analyzing the voluminous data necessary is not any easy task and for the most part has resulted in metrics that cannot be easily applied over a variety of practice scenarios. Many health care organizations, even large ones, have simply given up and rely on the WOW data and recommendations provided by the vendors, obviously lending the situation a faint odor of conflict of interest.
The bottom line is that . It would seem to me just asking the spouses and significant others of the clinicians would be sufficient. But, authors of the paper have more specific recommendations. First, they suggest that time working on the computer outside of scheduled time with patients should be separated from any other calculation of EHR usage. They encourage vendors and time-management researchers to develop standardized and validated methods for measuring active EHR use. And, finally they recommend that all EHR work done outside of time scheduled with patients be attributed to WOW. They feel that clearly labeling it work outside of work offers health care organizations a better chance of developing policies that will address the scourge of burnout.
This, unfortunately, is another tragic example of how clinicians have lost control of our work environments. The fact that 20 years have passed and there is still no standardized method for determining how much time we spend on the computer is more evidence we need to raise our voices.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Unlike many of you, maybe even most of you, I can recall when my office records were handwritten, some would say scribbled, on pieces of paper. They were decipherable by a select few. Some veteran assistants never mastered the skill. Pages were sometimes lavishly illustrated with drawings of body parts, often because I couldn’t remember or spell the correct anatomic term. When I needed to send a referring letter to another provider I typed it myself because dictating never quite suited my personality.
When I joined a small primary care group, the computer-savvy lead physician and a programmer developed our own homegrown EHR. It relied on scanning documents, as so many of us still generated handwritten notes. Even the most vociferous Luddites among us loved the system from day 2.
However, for a variety of reasons, some defensible some just plain bad, our beloved system needed to be replaced after 7 years. We then invested in an off-the-shelf EHR system that promised more capabilities. We were told there would be a learning curve but the plateau would come quickly and we would enjoy our new electronic assistant.
You’ve lived the rest of the story. The learning curve was steep and long and the plateau was a time gobbler. I was probably the most efficient provider in the group, and after 6 months I was leaving the office an hour later than I had been and was seeing the same number of patients. Most of my coworkers were staying and/or working on the computer at home for an extra 2 hours. This change could be easily documented by speaking with our spouses and children. I understand from my colleagues who have stayed in the business that over the ensuing decade and a half since my first experience with the EHR, its insatiable appetite for a clinician’s time has not abated.
The authors of a recent article in Annals of Family Medicine offer up some advice on how this tragic situation might be brought under control. First, the investigators point out that the phenomenon of after-hours EHR work, sometimes referred to as WOW (work outside of work), has not gone unnoticed by health system administrators and vendors who develop and sell the EHRs. However, analyzing the voluminous data necessary is not any easy task and for the most part has resulted in metrics that cannot be easily applied over a variety of practice scenarios. Many health care organizations, even large ones, have simply given up and rely on the WOW data and recommendations provided by the vendors, obviously lending the situation a faint odor of conflict of interest.
The bottom line is that . It would seem to me just asking the spouses and significant others of the clinicians would be sufficient. But, authors of the paper have more specific recommendations. First, they suggest that time working on the computer outside of scheduled time with patients should be separated from any other calculation of EHR usage. They encourage vendors and time-management researchers to develop standardized and validated methods for measuring active EHR use. And, finally they recommend that all EHR work done outside of time scheduled with patients be attributed to WOW. They feel that clearly labeling it work outside of work offers health care organizations a better chance of developing policies that will address the scourge of burnout.
This, unfortunately, is another tragic example of how clinicians have lost control of our work environments. The fact that 20 years have passed and there is still no standardized method for determining how much time we spend on the computer is more evidence we need to raise our voices.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Unlike many of you, maybe even most of you, I can recall when my office records were handwritten, some would say scribbled, on pieces of paper. They were decipherable by a select few. Some veteran assistants never mastered the skill. Pages were sometimes lavishly illustrated with drawings of body parts, often because I couldn’t remember or spell the correct anatomic term. When I needed to send a referring letter to another provider I typed it myself because dictating never quite suited my personality.
When I joined a small primary care group, the computer-savvy lead physician and a programmer developed our own homegrown EHR. It relied on scanning documents, as so many of us still generated handwritten notes. Even the most vociferous Luddites among us loved the system from day 2.
However, for a variety of reasons, some defensible some just plain bad, our beloved system needed to be replaced after 7 years. We then invested in an off-the-shelf EHR system that promised more capabilities. We were told there would be a learning curve but the plateau would come quickly and we would enjoy our new electronic assistant.
You’ve lived the rest of the story. The learning curve was steep and long and the plateau was a time gobbler. I was probably the most efficient provider in the group, and after 6 months I was leaving the office an hour later than I had been and was seeing the same number of patients. Most of my coworkers were staying and/or working on the computer at home for an extra 2 hours. This change could be easily documented by speaking with our spouses and children. I understand from my colleagues who have stayed in the business that over the ensuing decade and a half since my first experience with the EHR, its insatiable appetite for a clinician’s time has not abated.
The authors of a recent article in Annals of Family Medicine offer up some advice on how this tragic situation might be brought under control. First, the investigators point out that the phenomenon of after-hours EHR work, sometimes referred to as WOW (work outside of work), has not gone unnoticed by health system administrators and vendors who develop and sell the EHRs. However, analyzing the voluminous data necessary is not any easy task and for the most part has resulted in metrics that cannot be easily applied over a variety of practice scenarios. Many health care organizations, even large ones, have simply given up and rely on the WOW data and recommendations provided by the vendors, obviously lending the situation a faint odor of conflict of interest.
The bottom line is that . It would seem to me just asking the spouses and significant others of the clinicians would be sufficient. But, authors of the paper have more specific recommendations. First, they suggest that time working on the computer outside of scheduled time with patients should be separated from any other calculation of EHR usage. They encourage vendors and time-management researchers to develop standardized and validated methods for measuring active EHR use. And, finally they recommend that all EHR work done outside of time scheduled with patients be attributed to WOW. They feel that clearly labeling it work outside of work offers health care organizations a better chance of developing policies that will address the scourge of burnout.
This, unfortunately, is another tragic example of how clinicians have lost control of our work environments. The fact that 20 years have passed and there is still no standardized method for determining how much time we spend on the computer is more evidence we need to raise our voices.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Daily multivitamins boost memory in older adults: A randomized trial
This transcript has been edited for clarity.
This is Dr. JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital. , known as COSMOS (Cocoa Supplement and Multivitamins Outcome Study). This is the second COSMOS trial to show a benefit of multivitamins on memory and cognition. This trial involved a collaboration between Brigham and Columbia University and was published in the American Journal of Clinical Nutrition. I’d like to acknowledge that I am a coauthor of this study, together with Dr. Howard Sesso, who co-leads the main COSMOS trial with me.
Preserving memory and cognitive function is of critical importance to older adults. Nutritional interventions play an important role because we know the brain requires several nutrients for optimal health, and deficiencies in one or more of these nutrients may accelerate cognitive decline. Some of the micronutrients that are known to be important for brain health include vitamin B12, thiamin, other B vitamins, lutein, magnesium, and zinc, among others.
The current trial included 3,500 participants aged 60 or older, looking at performance on a web-based memory test. The multivitamin group did significantly better than the placebo group on memory tests and word recall, a finding that was estimated as the equivalent of slowing age-related memory loss by about 3 years. The benefit was first seen at 1 year and was sustained across the 3 years of the trial.
Intriguingly, in both COSMOS and COSMOS-Web, and the earlier COSMOS-Mind study, which was done in collaboration with Wake Forest, the participants with a history of cardiovascular disease showed the greatest benefits from multivitamins, perhaps due to lower nutrient status. But the basis for this finding needs to be explored further.
A few important caveats need to be emphasized. First, multivitamins and other dietary supplements will never be a substitute for a healthy diet and healthy lifestyle and should not distract from those goals. But multivitamins may have a role as a complementary strategy. Another caveat is that the randomized trials tested recommended dietary allowances and not megadoses of these micronutrients. In fact, randomized trials of high doses of isolated micronutrients have not clearly shown cognitive benefits, and this suggests that more is not necessarily better and may be worse. High doses also may be associated with toxicity, or they may interfere with absorption or bioavailability of other nutrients.
In COSMOS, over the average 3.6 years of follow-up and in the earlier Physicians’ Health Study II, over 1 year of supplementation, multivitamins were found to be safe without any clear risks or safety concerns. A further caveat is that although Centrum Silver was tested in this trial, we would not expect that this is a brand-specific benefit, and other high-quality multivitamin brands would be expected to confer similar benefits. Of course, it’s important to check bottles for quality-control documentation such as the seals of the U.S. Pharmacopeia, National Science Foundation, ConsumerLab.com, and other auditors.
Overall, the finding that a daily multivitamin improved memory and slowed cognitive decline in two separate COSMOS randomized trials is exciting, suggesting that multivitamin supplementation holds promise as a safe, accessible, and affordable approach to protecting cognitive health in older adults. Further research will be needed to understand who is most likely to benefit and the biological mechanisms involved. Expert committees will have to look at the research and decide whether any changes in guidelines are indicated in the future.
Dr. Manson is Professor of Medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School and director of the Division of Preventive Medicine, Brigham and Women’s Hospital, both in Boston. She reported receiving funding/donations from Mars Symbioscience.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
This is Dr. JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital. , known as COSMOS (Cocoa Supplement and Multivitamins Outcome Study). This is the second COSMOS trial to show a benefit of multivitamins on memory and cognition. This trial involved a collaboration between Brigham and Columbia University and was published in the American Journal of Clinical Nutrition. I’d like to acknowledge that I am a coauthor of this study, together with Dr. Howard Sesso, who co-leads the main COSMOS trial with me.
Preserving memory and cognitive function is of critical importance to older adults. Nutritional interventions play an important role because we know the brain requires several nutrients for optimal health, and deficiencies in one or more of these nutrients may accelerate cognitive decline. Some of the micronutrients that are known to be important for brain health include vitamin B12, thiamin, other B vitamins, lutein, magnesium, and zinc, among others.
The current trial included 3,500 participants aged 60 or older, looking at performance on a web-based memory test. The multivitamin group did significantly better than the placebo group on memory tests and word recall, a finding that was estimated as the equivalent of slowing age-related memory loss by about 3 years. The benefit was first seen at 1 year and was sustained across the 3 years of the trial.
Intriguingly, in both COSMOS and COSMOS-Web, and the earlier COSMOS-Mind study, which was done in collaboration with Wake Forest, the participants with a history of cardiovascular disease showed the greatest benefits from multivitamins, perhaps due to lower nutrient status. But the basis for this finding needs to be explored further.
A few important caveats need to be emphasized. First, multivitamins and other dietary supplements will never be a substitute for a healthy diet and healthy lifestyle and should not distract from those goals. But multivitamins may have a role as a complementary strategy. Another caveat is that the randomized trials tested recommended dietary allowances and not megadoses of these micronutrients. In fact, randomized trials of high doses of isolated micronutrients have not clearly shown cognitive benefits, and this suggests that more is not necessarily better and may be worse. High doses also may be associated with toxicity, or they may interfere with absorption or bioavailability of other nutrients.
In COSMOS, over the average 3.6 years of follow-up and in the earlier Physicians’ Health Study II, over 1 year of supplementation, multivitamins were found to be safe without any clear risks or safety concerns. A further caveat is that although Centrum Silver was tested in this trial, we would not expect that this is a brand-specific benefit, and other high-quality multivitamin brands would be expected to confer similar benefits. Of course, it’s important to check bottles for quality-control documentation such as the seals of the U.S. Pharmacopeia, National Science Foundation, ConsumerLab.com, and other auditors.
Overall, the finding that a daily multivitamin improved memory and slowed cognitive decline in two separate COSMOS randomized trials is exciting, suggesting that multivitamin supplementation holds promise as a safe, accessible, and affordable approach to protecting cognitive health in older adults. Further research will be needed to understand who is most likely to benefit and the biological mechanisms involved. Expert committees will have to look at the research and decide whether any changes in guidelines are indicated in the future.
Dr. Manson is Professor of Medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School and director of the Division of Preventive Medicine, Brigham and Women’s Hospital, both in Boston. She reported receiving funding/donations from Mars Symbioscience.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
This is Dr. JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital. , known as COSMOS (Cocoa Supplement and Multivitamins Outcome Study). This is the second COSMOS trial to show a benefit of multivitamins on memory and cognition. This trial involved a collaboration between Brigham and Columbia University and was published in the American Journal of Clinical Nutrition. I’d like to acknowledge that I am a coauthor of this study, together with Dr. Howard Sesso, who co-leads the main COSMOS trial with me.
Preserving memory and cognitive function is of critical importance to older adults. Nutritional interventions play an important role because we know the brain requires several nutrients for optimal health, and deficiencies in one or more of these nutrients may accelerate cognitive decline. Some of the micronutrients that are known to be important for brain health include vitamin B12, thiamin, other B vitamins, lutein, magnesium, and zinc, among others.
The current trial included 3,500 participants aged 60 or older, looking at performance on a web-based memory test. The multivitamin group did significantly better than the placebo group on memory tests and word recall, a finding that was estimated as the equivalent of slowing age-related memory loss by about 3 years. The benefit was first seen at 1 year and was sustained across the 3 years of the trial.
Intriguingly, in both COSMOS and COSMOS-Web, and the earlier COSMOS-Mind study, which was done in collaboration with Wake Forest, the participants with a history of cardiovascular disease showed the greatest benefits from multivitamins, perhaps due to lower nutrient status. But the basis for this finding needs to be explored further.
A few important caveats need to be emphasized. First, multivitamins and other dietary supplements will never be a substitute for a healthy diet and healthy lifestyle and should not distract from those goals. But multivitamins may have a role as a complementary strategy. Another caveat is that the randomized trials tested recommended dietary allowances and not megadoses of these micronutrients. In fact, randomized trials of high doses of isolated micronutrients have not clearly shown cognitive benefits, and this suggests that more is not necessarily better and may be worse. High doses also may be associated with toxicity, or they may interfere with absorption or bioavailability of other nutrients.
In COSMOS, over the average 3.6 years of follow-up and in the earlier Physicians’ Health Study II, over 1 year of supplementation, multivitamins were found to be safe without any clear risks or safety concerns. A further caveat is that although Centrum Silver was tested in this trial, we would not expect that this is a brand-specific benefit, and other high-quality multivitamin brands would be expected to confer similar benefits. Of course, it’s important to check bottles for quality-control documentation such as the seals of the U.S. Pharmacopeia, National Science Foundation, ConsumerLab.com, and other auditors.
Overall, the finding that a daily multivitamin improved memory and slowed cognitive decline in two separate COSMOS randomized trials is exciting, suggesting that multivitamin supplementation holds promise as a safe, accessible, and affordable approach to protecting cognitive health in older adults. Further research will be needed to understand who is most likely to benefit and the biological mechanisms involved. Expert committees will have to look at the research and decide whether any changes in guidelines are indicated in the future.
Dr. Manson is Professor of Medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School and director of the Division of Preventive Medicine, Brigham and Women’s Hospital, both in Boston. She reported receiving funding/donations from Mars Symbioscience.
A version of this article first appeared on Medscape.com.
Feeling disconnected? Focus on what you can do
This is the exciting time of year when we graduate new classes of medical students and residents. Med school graduation brings mixed emotions; the new doctors and I both know residency will bring growth and challenges. Residency graduation is a wistful passage as well. It is so rewarding to welcome the newly board-certified family physicians to family medicine, but we miss them even as we orient a new class.
Every year, a few months (or even a few years) after graduation, I hear from a former resident, sometimes several. They ask to talk and, although it can be hard for them to explain exactly the ennui and disillusionment they’re feeling, their concerns boil down to: Is this all there is?
They are not burnt out, exactly, but they were hoping for more from their careers in family medicine.1 They find their hopes and expectations are not fulfilled by seeing patients in the office 8 hours per day, 4.5 days per week. Even those who report rewarding relationships with patients express less overall enthusiasm for jobs they were excited to start just months or years earlier.
Some of the difficulties I hear the graduates report are expected growing pains. It is a transition to go from supervised practice with attending backup to a setting where you are on your own, typically with a 4-fold increase in volume compared with residency. But the monotony is real for family physicians in full-time outpatient practice.
Research suggests an expanded scope of practice—including hospital medicine, obstetrics, and procedures—is associated with physician well-being.2,3 A broad scope of practice can bring stress, but it also brings meaning, and that meaning is protective to our well-being. However, a robust scope of practice is not always supported by medical groups or hospital systems, who prefer a more compartmentalized, widgetized physician.4 It would be easier for their algorithms if family physicians picked a lane and stayed in it. Alas, the broader our scope of practice, the healthier our population, the more equitable our care,5,6 and the happier our physicians.
The disconnect and hopelessness experienced by family physicians is more concerning. Many of my graduates report feeling disconnected from their patients, because they begin to feel disillusioned by the demands and requests that practice and patients place on them. The paperwork, “permission slips,” and requests for tests and studies not only feel overwhelming and exhausting but also create distance between physicians and patients.7 We want to help our patients, so we do the forms and order the tests. As the quantity of forms, slips, and requests adds up, we begin to feel resentful at what the forms take away: time with our patients, perhaps, or time with our families. We get angry at the forms and the “asks,” and then begin to get angry at the patients simply for having needs. Administrative burden is a hassle, but it is also insidiously destructive.8
Family physicians confront hopelessness when, day after day, we diagnose problems that no physician is likely to fix in a single office visit: chronic stress, family dysfunction, violence, unemployment, poverty, racism, loneliness, and the hopelessness of the patients themselves. This is not to say that we ignore these concerns or their impact on health. It is because we see and feel them, and deeply understand their consequences for our patients, that we grow frustrated with the lack of solutions.9,10
Thankfully, we have strong teams working at the policy level to improve the primary care and public health infrastructure so that we can maintain some hope that it will be better in the future. Sometimes when I counsel a former resident, they decide to join those teams so that they can work on the solutions. Others decide to expand their scope of practice. Others seek out virtual scribes to streamline charting and regain time. Some build better boundaries with their EHR inboxes.
The key is figuring out what we can do and making peace with our limits. When disillusionment hits, what we can do includes seeking connection and social contact and remembering that we are not trapped in our situation, even if we are practicing in a less-than-functional health care system. There are many ways to “be” a family physician—if what you’re doing isn’t working for you, look for opportunities (big or small) that make it better. We can all reach out to coaches, therapists, colleagues, and friends for support to remain steadfast in our purpose as family physicians. This support and the power of change means that from residency to the latter parts of our careers, we will continue to bring the tremendous good of family medicine to the communities we serve.
1. Coutinho AJ, Cochrane A, Stelter K, et al. Comparison of intended scope of practice for family medicine residents with reported scope of practice among practicing family physicians. JAMA. 2015;314:2364-2372. doi: 10.1001/jama.2015.13734
2. Weidner AKH, Phillips RL, Fang B, et al. Burnout and scope of practice in new family physicians. Ann Fam Med. 2018;16:200-205. doi: 10.1370/afm.2221
3. Zomahoun HT, Samson I, Sawadogo J, et al. Effects of the scope of practice on family physicians: a systematic review. BMC Family Practice. 2021;22. doi: 10.1186/s12875-020-01328-1
4. Killeen D, Jetty A, Peterson LE, et al. The association of practice type and the scope of care of family physicians. J Am Board Fam Med. 2023;36:79-87. doi: 10.3122/jabfm.2022.220172R1
5. Starfield B, Shi L, Macinko J. Contribution of primary care to health systems and health. Milbank Q. 2005;83:457-502. doi: 10.1111/j.1468-0009.2005.00409.x
6. Ferrer RL. Pursuing equity: contact with primary care and specialist clinicians by demographics, insurance, and health status. Ann Fam Med. 2007;5:492-502. doi: 10.1370/afm.746
7. Rao SK, Kimball AB, Lehrhoff SR, et al. The impact of administrative burden on academic physicians: results of a hospital-wide physician survey. Acad Med. 2017;92:237-243. doi: 10.1097/ACM.0000000000001461
8. McMahon LF, Rize K, Irby-Johnson N, et al. Designed to fail? The future of primary care. J Gen Intern Med. 2021;36:515-517. doi: 10.1007/s11606-020-06077-6
9. Welles CC, Tong A, Brereton E, et al. Sources of clinician burnout in providing care for underserved patients in a safety-net healthcare system. J Gen Intern Med. 2023;38:1468-1475. doi: 10.1007/s11606-022-07896-5
10. Kung A, Cheung T, Knox M, et al. Capacity to address social needs affects primary care clinician burnout. Ann Fam Med. 2019;17:487-494. doi: 10.1370/afm.2470
This is the exciting time of year when we graduate new classes of medical students and residents. Med school graduation brings mixed emotions; the new doctors and I both know residency will bring growth and challenges. Residency graduation is a wistful passage as well. It is so rewarding to welcome the newly board-certified family physicians to family medicine, but we miss them even as we orient a new class.
Every year, a few months (or even a few years) after graduation, I hear from a former resident, sometimes several. They ask to talk and, although it can be hard for them to explain exactly the ennui and disillusionment they’re feeling, their concerns boil down to: Is this all there is?
They are not burnt out, exactly, but they were hoping for more from their careers in family medicine.1 They find their hopes and expectations are not fulfilled by seeing patients in the office 8 hours per day, 4.5 days per week. Even those who report rewarding relationships with patients express less overall enthusiasm for jobs they were excited to start just months or years earlier.
Some of the difficulties I hear the graduates report are expected growing pains. It is a transition to go from supervised practice with attending backup to a setting where you are on your own, typically with a 4-fold increase in volume compared with residency. But the monotony is real for family physicians in full-time outpatient practice.
Research suggests an expanded scope of practice—including hospital medicine, obstetrics, and procedures—is associated with physician well-being.2,3 A broad scope of practice can bring stress, but it also brings meaning, and that meaning is protective to our well-being. However, a robust scope of practice is not always supported by medical groups or hospital systems, who prefer a more compartmentalized, widgetized physician.4 It would be easier for their algorithms if family physicians picked a lane and stayed in it. Alas, the broader our scope of practice, the healthier our population, the more equitable our care,5,6 and the happier our physicians.
The disconnect and hopelessness experienced by family physicians is more concerning. Many of my graduates report feeling disconnected from their patients, because they begin to feel disillusioned by the demands and requests that practice and patients place on them. The paperwork, “permission slips,” and requests for tests and studies not only feel overwhelming and exhausting but also create distance between physicians and patients.7 We want to help our patients, so we do the forms and order the tests. As the quantity of forms, slips, and requests adds up, we begin to feel resentful at what the forms take away: time with our patients, perhaps, or time with our families. We get angry at the forms and the “asks,” and then begin to get angry at the patients simply for having needs. Administrative burden is a hassle, but it is also insidiously destructive.8
Family physicians confront hopelessness when, day after day, we diagnose problems that no physician is likely to fix in a single office visit: chronic stress, family dysfunction, violence, unemployment, poverty, racism, loneliness, and the hopelessness of the patients themselves. This is not to say that we ignore these concerns or their impact on health. It is because we see and feel them, and deeply understand their consequences for our patients, that we grow frustrated with the lack of solutions.9,10
Thankfully, we have strong teams working at the policy level to improve the primary care and public health infrastructure so that we can maintain some hope that it will be better in the future. Sometimes when I counsel a former resident, they decide to join those teams so that they can work on the solutions. Others decide to expand their scope of practice. Others seek out virtual scribes to streamline charting and regain time. Some build better boundaries with their EHR inboxes.
The key is figuring out what we can do and making peace with our limits. When disillusionment hits, what we can do includes seeking connection and social contact and remembering that we are not trapped in our situation, even if we are practicing in a less-than-functional health care system. There are many ways to “be” a family physician—if what you’re doing isn’t working for you, look for opportunities (big or small) that make it better. We can all reach out to coaches, therapists, colleagues, and friends for support to remain steadfast in our purpose as family physicians. This support and the power of change means that from residency to the latter parts of our careers, we will continue to bring the tremendous good of family medicine to the communities we serve.
This is the exciting time of year when we graduate new classes of medical students and residents. Med school graduation brings mixed emotions; the new doctors and I both know residency will bring growth and challenges. Residency graduation is a wistful passage as well. It is so rewarding to welcome the newly board-certified family physicians to family medicine, but we miss them even as we orient a new class.
Every year, a few months (or even a few years) after graduation, I hear from a former resident, sometimes several. They ask to talk and, although it can be hard for them to explain exactly the ennui and disillusionment they’re feeling, their concerns boil down to: Is this all there is?
They are not burnt out, exactly, but they were hoping for more from their careers in family medicine.1 They find their hopes and expectations are not fulfilled by seeing patients in the office 8 hours per day, 4.5 days per week. Even those who report rewarding relationships with patients express less overall enthusiasm for jobs they were excited to start just months or years earlier.
Some of the difficulties I hear the graduates report are expected growing pains. It is a transition to go from supervised practice with attending backup to a setting where you are on your own, typically with a 4-fold increase in volume compared with residency. But the monotony is real for family physicians in full-time outpatient practice.
Research suggests an expanded scope of practice—including hospital medicine, obstetrics, and procedures—is associated with physician well-being.2,3 A broad scope of practice can bring stress, but it also brings meaning, and that meaning is protective to our well-being. However, a robust scope of practice is not always supported by medical groups or hospital systems, who prefer a more compartmentalized, widgetized physician.4 It would be easier for their algorithms if family physicians picked a lane and stayed in it. Alas, the broader our scope of practice, the healthier our population, the more equitable our care,5,6 and the happier our physicians.
The disconnect and hopelessness experienced by family physicians is more concerning. Many of my graduates report feeling disconnected from their patients, because they begin to feel disillusioned by the demands and requests that practice and patients place on them. The paperwork, “permission slips,” and requests for tests and studies not only feel overwhelming and exhausting but also create distance between physicians and patients.7 We want to help our patients, so we do the forms and order the tests. As the quantity of forms, slips, and requests adds up, we begin to feel resentful at what the forms take away: time with our patients, perhaps, or time with our families. We get angry at the forms and the “asks,” and then begin to get angry at the patients simply for having needs. Administrative burden is a hassle, but it is also insidiously destructive.8
Family physicians confront hopelessness when, day after day, we diagnose problems that no physician is likely to fix in a single office visit: chronic stress, family dysfunction, violence, unemployment, poverty, racism, loneliness, and the hopelessness of the patients themselves. This is not to say that we ignore these concerns or their impact on health. It is because we see and feel them, and deeply understand their consequences for our patients, that we grow frustrated with the lack of solutions.9,10
Thankfully, we have strong teams working at the policy level to improve the primary care and public health infrastructure so that we can maintain some hope that it will be better in the future. Sometimes when I counsel a former resident, they decide to join those teams so that they can work on the solutions. Others decide to expand their scope of practice. Others seek out virtual scribes to streamline charting and regain time. Some build better boundaries with their EHR inboxes.
The key is figuring out what we can do and making peace with our limits. When disillusionment hits, what we can do includes seeking connection and social contact and remembering that we are not trapped in our situation, even if we are practicing in a less-than-functional health care system. There are many ways to “be” a family physician—if what you’re doing isn’t working for you, look for opportunities (big or small) that make it better. We can all reach out to coaches, therapists, colleagues, and friends for support to remain steadfast in our purpose as family physicians. This support and the power of change means that from residency to the latter parts of our careers, we will continue to bring the tremendous good of family medicine to the communities we serve.
1. Coutinho AJ, Cochrane A, Stelter K, et al. Comparison of intended scope of practice for family medicine residents with reported scope of practice among practicing family physicians. JAMA. 2015;314:2364-2372. doi: 10.1001/jama.2015.13734
2. Weidner AKH, Phillips RL, Fang B, et al. Burnout and scope of practice in new family physicians. Ann Fam Med. 2018;16:200-205. doi: 10.1370/afm.2221
3. Zomahoun HT, Samson I, Sawadogo J, et al. Effects of the scope of practice on family physicians: a systematic review. BMC Family Practice. 2021;22. doi: 10.1186/s12875-020-01328-1
4. Killeen D, Jetty A, Peterson LE, et al. The association of practice type and the scope of care of family physicians. J Am Board Fam Med. 2023;36:79-87. doi: 10.3122/jabfm.2022.220172R1
5. Starfield B, Shi L, Macinko J. Contribution of primary care to health systems and health. Milbank Q. 2005;83:457-502. doi: 10.1111/j.1468-0009.2005.00409.x
6. Ferrer RL. Pursuing equity: contact with primary care and specialist clinicians by demographics, insurance, and health status. Ann Fam Med. 2007;5:492-502. doi: 10.1370/afm.746
7. Rao SK, Kimball AB, Lehrhoff SR, et al. The impact of administrative burden on academic physicians: results of a hospital-wide physician survey. Acad Med. 2017;92:237-243. doi: 10.1097/ACM.0000000000001461
8. McMahon LF, Rize K, Irby-Johnson N, et al. Designed to fail? The future of primary care. J Gen Intern Med. 2021;36:515-517. doi: 10.1007/s11606-020-06077-6
9. Welles CC, Tong A, Brereton E, et al. Sources of clinician burnout in providing care for underserved patients in a safety-net healthcare system. J Gen Intern Med. 2023;38:1468-1475. doi: 10.1007/s11606-022-07896-5
10. Kung A, Cheung T, Knox M, et al. Capacity to address social needs affects primary care clinician burnout. Ann Fam Med. 2019;17:487-494. doi: 10.1370/afm.2470
1. Coutinho AJ, Cochrane A, Stelter K, et al. Comparison of intended scope of practice for family medicine residents with reported scope of practice among practicing family physicians. JAMA. 2015;314:2364-2372. doi: 10.1001/jama.2015.13734
2. Weidner AKH, Phillips RL, Fang B, et al. Burnout and scope of practice in new family physicians. Ann Fam Med. 2018;16:200-205. doi: 10.1370/afm.2221
3. Zomahoun HT, Samson I, Sawadogo J, et al. Effects of the scope of practice on family physicians: a systematic review. BMC Family Practice. 2021;22. doi: 10.1186/s12875-020-01328-1
4. Killeen D, Jetty A, Peterson LE, et al. The association of practice type and the scope of care of family physicians. J Am Board Fam Med. 2023;36:79-87. doi: 10.3122/jabfm.2022.220172R1
5. Starfield B, Shi L, Macinko J. Contribution of primary care to health systems and health. Milbank Q. 2005;83:457-502. doi: 10.1111/j.1468-0009.2005.00409.x
6. Ferrer RL. Pursuing equity: contact with primary care and specialist clinicians by demographics, insurance, and health status. Ann Fam Med. 2007;5:492-502. doi: 10.1370/afm.746
7. Rao SK, Kimball AB, Lehrhoff SR, et al. The impact of administrative burden on academic physicians: results of a hospital-wide physician survey. Acad Med. 2017;92:237-243. doi: 10.1097/ACM.0000000000001461
8. McMahon LF, Rize K, Irby-Johnson N, et al. Designed to fail? The future of primary care. J Gen Intern Med. 2021;36:515-517. doi: 10.1007/s11606-020-06077-6
9. Welles CC, Tong A, Brereton E, et al. Sources of clinician burnout in providing care for underserved patients in a safety-net healthcare system. J Gen Intern Med. 2023;38:1468-1475. doi: 10.1007/s11606-022-07896-5
10. Kung A, Cheung T, Knox M, et al. Capacity to address social needs affects primary care clinician burnout. Ann Fam Med. 2019;17:487-494. doi: 10.1370/afm.2470
Did an unfair system help ADAURA win on overall survival?
Barry Bonds and Roger Clemens are two world-class baseball players who played well enough to earn enduring respect and admiration. However, their reputations have been permanently tainted by their use of performance-enhancing drugs. Although they are both undeniably gifted, we’ll never know where their natural talent ended and their unfair advantage began.
The medical oncology version of this scenario played out in front of our eyes at the ASCO 2023 Plenary Session featuring the ADAURA trial. In this case, the unfair advantage was clear: Nearly two-thirds of patients in the control arm did not cross over to a standard-of-care treatment at relapse.
The ADAURA trial tested the value of the third-generation oral EGFR inhibitor osimertinib vs. placebo for up to 3 years in patients with a resected stage IB-IIIA non–small cell lung cancer (NSCLC) harboring an activating EGFR mutation. Initially presented in the ASCO 2020 Plenary Session, the preliminary analysis for ADAURA demonstrated a remarkably favorable improvement in disease-free survival (DFS) in the osimertinib arm, which led to its prompt Food and Drug Administration approval in this setting.
At the time, I was among the more vocal critics of the fanfare around this trial. The DFS improvement was impressive but, in this context, represented a low threshold for FDA approval. We already knew that prior trials of other, less effective adjuvant EGFR inhibitors routinely improved DFS but ultimately failed to improve overall survival.
Although in some cases, a DFS benefit can be sufficient to warrant changing practice, I would argue that overall survival is the most critical endpoint in a curative setting by a wide margin. I would also argue that cost should be a consideration for a drug priced at $440,000 over 3 years in the United States. At the very least, we – patients, oncologists, payers – should want to clarify what we get for $440,000 per patient, especially if that money could be better spent on other things.
Of note, we need to know whether the same overall survival may be achieved in this setting by treating only patients whose disease relapses, avoiding both the cost and toxicity of continuous treatment.
The relevance of this question became even more acute when an updated version of the ADAURA trial showed that the DFS benefit from osimertinib began to erode immediately after patients completed active treatment. Although the DFS benefit remained excellent,
The overall survival data – the critical test in my mind – were presented at the ASCO Plenary Session. The results were highly positive, with a hazard ratio for overall survival of 0.49 and a similar benefit observed across all eligible disease stages.
As with the presentation of the DFS data in 2020, these results were accompanied by adulation during the session and fawning in the media. However, a subset of people in the audience, and on Twitter, voiced a major concern: In the control arm, only 38.5% of the patients whose disease had relapsed (79 of 205) ever received osimertinib.
Post-protocol treatment included reassurances that patients in the control arm were offered crossover to osimertinib, but this only occurred starting in April 2020 and only when the treating investigator requested it.
The fact that only a minority of patients in the control arm ever received osimertinib means that ADAURA is not a trial that tests adjuvant osimertinib to osimertinib at relapse, the prevailing standard of care in the United States and the preferred treatment in this setting, based on NCCN guidelines for patients with relapsed/metastatic EGFR mutation–positive NSCLC since the FDA approval in April 2018.
The change in standard of care in the United States and some other countries did not lead to an amendment in the trial, based on the argument that the trial was designed with DFS as the primary endpoint and that patients in the control arm are effectively off trial at relapse. That means patients would receive their country’s standard of care, which may be below, or different from, the standard in the United States or other parts of the world.
While defensible, others considered the low rate of osimertinib delivery in the control arm a serious flaw in the trial design and arguably an ethical problem.
Given this trial design, it’s important to question whether the trial magnified the difference in overall survival between the two arms compared with the standard of care in countries where adjuvant osimertinib will ultimately be marketed. Although I strongly suspect that the overall survival difference would have been significant without the disparity in access to osimertinib in the control arm, we will never know the magnitude of that difference.
With the current design, the trial demonstrates that osimertinib is associated with improved survival in 100% of patients with EGFR mutation–positive NSCLC who receive the agent vs. 38.5% of patients receiving it at some point after relapse.
At the end of the day, ADAURA followed conventional trial rules, which led to a windfall of accolades at the cost of suboptimal care for many of the patients randomly assigned to the control arm.
We need to decide as an oncology community whether we want to accept a system that confers rewards for stakeholders at the expense of patients enrolled in the trial.
We have developed a system that not only permits but depends on global trials enrolling many patients from countries with staging and off-protocol oncology care below standards of care in other parts of the world – effectively condoning and perpetuating disparities in optimal care globally. I am also saddened that some of the most respected leaders in our field have become upset when I question the ethics of accepting this system, one that I believe we have agency to change.
The question here is not whether osimertinib is a good drug; it is remarkably effective for patients with EGFR mutation–positive NSCLC. The question is how to design trials in a fair and balanced way that doesn’t compromise patient care or ethical standards.
If people think my assessment is too harsh, I openly welcome debate.
Bottom line: The ADAURA trial lays bare deeper problems with clinical trial design, and I would challenge readers to reflect on our clinical trial culture in oncology, which offers a system of rules that rewards denying the best identified care for patients on our clinical trials.
At the very least, should we celebrate these wins without fully acknowledging these problems?
Dr. West is clinical associate professor, department of medical oncology, City of Hope Comprehensive Cancer Care, Duarte, Calif. He reported conflicts of interest with Bristol-Myers Squibb, Boehringer Ingelheim, Spectrum, AstraZeneca, Celgene, Genentech/Roche, Pfizer, Merck, and Eli Lilly.
A version of this article first appeared on Medscape.com.
Barry Bonds and Roger Clemens are two world-class baseball players who played well enough to earn enduring respect and admiration. However, their reputations have been permanently tainted by their use of performance-enhancing drugs. Although they are both undeniably gifted, we’ll never know where their natural talent ended and their unfair advantage began.
The medical oncology version of this scenario played out in front of our eyes at the ASCO 2023 Plenary Session featuring the ADAURA trial. In this case, the unfair advantage was clear: Nearly two-thirds of patients in the control arm did not cross over to a standard-of-care treatment at relapse.
The ADAURA trial tested the value of the third-generation oral EGFR inhibitor osimertinib vs. placebo for up to 3 years in patients with a resected stage IB-IIIA non–small cell lung cancer (NSCLC) harboring an activating EGFR mutation. Initially presented in the ASCO 2020 Plenary Session, the preliminary analysis for ADAURA demonstrated a remarkably favorable improvement in disease-free survival (DFS) in the osimertinib arm, which led to its prompt Food and Drug Administration approval in this setting.
At the time, I was among the more vocal critics of the fanfare around this trial. The DFS improvement was impressive but, in this context, represented a low threshold for FDA approval. We already knew that prior trials of other, less effective adjuvant EGFR inhibitors routinely improved DFS but ultimately failed to improve overall survival.
Although in some cases, a DFS benefit can be sufficient to warrant changing practice, I would argue that overall survival is the most critical endpoint in a curative setting by a wide margin. I would also argue that cost should be a consideration for a drug priced at $440,000 over 3 years in the United States. At the very least, we – patients, oncologists, payers – should want to clarify what we get for $440,000 per patient, especially if that money could be better spent on other things.
Of note, we need to know whether the same overall survival may be achieved in this setting by treating only patients whose disease relapses, avoiding both the cost and toxicity of continuous treatment.
The relevance of this question became even more acute when an updated version of the ADAURA trial showed that the DFS benefit from osimertinib began to erode immediately after patients completed active treatment. Although the DFS benefit remained excellent,
The overall survival data – the critical test in my mind – were presented at the ASCO Plenary Session. The results were highly positive, with a hazard ratio for overall survival of 0.49 and a similar benefit observed across all eligible disease stages.
As with the presentation of the DFS data in 2020, these results were accompanied by adulation during the session and fawning in the media. However, a subset of people in the audience, and on Twitter, voiced a major concern: In the control arm, only 38.5% of the patients whose disease had relapsed (79 of 205) ever received osimertinib.
Post-protocol treatment included reassurances that patients in the control arm were offered crossover to osimertinib, but this only occurred starting in April 2020 and only when the treating investigator requested it.
The fact that only a minority of patients in the control arm ever received osimertinib means that ADAURA is not a trial that tests adjuvant osimertinib to osimertinib at relapse, the prevailing standard of care in the United States and the preferred treatment in this setting, based on NCCN guidelines for patients with relapsed/metastatic EGFR mutation–positive NSCLC since the FDA approval in April 2018.
The change in standard of care in the United States and some other countries did not lead to an amendment in the trial, based on the argument that the trial was designed with DFS as the primary endpoint and that patients in the control arm are effectively off trial at relapse. That means patients would receive their country’s standard of care, which may be below, or different from, the standard in the United States or other parts of the world.
While defensible, others considered the low rate of osimertinib delivery in the control arm a serious flaw in the trial design and arguably an ethical problem.
Given this trial design, it’s important to question whether the trial magnified the difference in overall survival between the two arms compared with the standard of care in countries where adjuvant osimertinib will ultimately be marketed. Although I strongly suspect that the overall survival difference would have been significant without the disparity in access to osimertinib in the control arm, we will never know the magnitude of that difference.
With the current design, the trial demonstrates that osimertinib is associated with improved survival in 100% of patients with EGFR mutation–positive NSCLC who receive the agent vs. 38.5% of patients receiving it at some point after relapse.
At the end of the day, ADAURA followed conventional trial rules, which led to a windfall of accolades at the cost of suboptimal care for many of the patients randomly assigned to the control arm.
We need to decide as an oncology community whether we want to accept a system that confers rewards for stakeholders at the expense of patients enrolled in the trial.
We have developed a system that not only permits but depends on global trials enrolling many patients from countries with staging and off-protocol oncology care below standards of care in other parts of the world – effectively condoning and perpetuating disparities in optimal care globally. I am also saddened that some of the most respected leaders in our field have become upset when I question the ethics of accepting this system, one that I believe we have agency to change.
The question here is not whether osimertinib is a good drug; it is remarkably effective for patients with EGFR mutation–positive NSCLC. The question is how to design trials in a fair and balanced way that doesn’t compromise patient care or ethical standards.
If people think my assessment is too harsh, I openly welcome debate.
Bottom line: The ADAURA trial lays bare deeper problems with clinical trial design, and I would challenge readers to reflect on our clinical trial culture in oncology, which offers a system of rules that rewards denying the best identified care for patients on our clinical trials.
At the very least, should we celebrate these wins without fully acknowledging these problems?
Dr. West is clinical associate professor, department of medical oncology, City of Hope Comprehensive Cancer Care, Duarte, Calif. He reported conflicts of interest with Bristol-Myers Squibb, Boehringer Ingelheim, Spectrum, AstraZeneca, Celgene, Genentech/Roche, Pfizer, Merck, and Eli Lilly.
A version of this article first appeared on Medscape.com.
Barry Bonds and Roger Clemens are two world-class baseball players who played well enough to earn enduring respect and admiration. However, their reputations have been permanently tainted by their use of performance-enhancing drugs. Although they are both undeniably gifted, we’ll never know where their natural talent ended and their unfair advantage began.
The medical oncology version of this scenario played out in front of our eyes at the ASCO 2023 Plenary Session featuring the ADAURA trial. In this case, the unfair advantage was clear: Nearly two-thirds of patients in the control arm did not cross over to a standard-of-care treatment at relapse.
The ADAURA trial tested the value of the third-generation oral EGFR inhibitor osimertinib vs. placebo for up to 3 years in patients with a resected stage IB-IIIA non–small cell lung cancer (NSCLC) harboring an activating EGFR mutation. Initially presented in the ASCO 2020 Plenary Session, the preliminary analysis for ADAURA demonstrated a remarkably favorable improvement in disease-free survival (DFS) in the osimertinib arm, which led to its prompt Food and Drug Administration approval in this setting.
At the time, I was among the more vocal critics of the fanfare around this trial. The DFS improvement was impressive but, in this context, represented a low threshold for FDA approval. We already knew that prior trials of other, less effective adjuvant EGFR inhibitors routinely improved DFS but ultimately failed to improve overall survival.
Although in some cases, a DFS benefit can be sufficient to warrant changing practice, I would argue that overall survival is the most critical endpoint in a curative setting by a wide margin. I would also argue that cost should be a consideration for a drug priced at $440,000 over 3 years in the United States. At the very least, we – patients, oncologists, payers – should want to clarify what we get for $440,000 per patient, especially if that money could be better spent on other things.
Of note, we need to know whether the same overall survival may be achieved in this setting by treating only patients whose disease relapses, avoiding both the cost and toxicity of continuous treatment.
The relevance of this question became even more acute when an updated version of the ADAURA trial showed that the DFS benefit from osimertinib began to erode immediately after patients completed active treatment. Although the DFS benefit remained excellent,
The overall survival data – the critical test in my mind – were presented at the ASCO Plenary Session. The results were highly positive, with a hazard ratio for overall survival of 0.49 and a similar benefit observed across all eligible disease stages.
As with the presentation of the DFS data in 2020, these results were accompanied by adulation during the session and fawning in the media. However, a subset of people in the audience, and on Twitter, voiced a major concern: In the control arm, only 38.5% of the patients whose disease had relapsed (79 of 205) ever received osimertinib.
Post-protocol treatment included reassurances that patients in the control arm were offered crossover to osimertinib, but this only occurred starting in April 2020 and only when the treating investigator requested it.
The fact that only a minority of patients in the control arm ever received osimertinib means that ADAURA is not a trial that tests adjuvant osimertinib to osimertinib at relapse, the prevailing standard of care in the United States and the preferred treatment in this setting, based on NCCN guidelines for patients with relapsed/metastatic EGFR mutation–positive NSCLC since the FDA approval in April 2018.
The change in standard of care in the United States and some other countries did not lead to an amendment in the trial, based on the argument that the trial was designed with DFS as the primary endpoint and that patients in the control arm are effectively off trial at relapse. That means patients would receive their country’s standard of care, which may be below, or different from, the standard in the United States or other parts of the world.
While defensible, others considered the low rate of osimertinib delivery in the control arm a serious flaw in the trial design and arguably an ethical problem.
Given this trial design, it’s important to question whether the trial magnified the difference in overall survival between the two arms compared with the standard of care in countries where adjuvant osimertinib will ultimately be marketed. Although I strongly suspect that the overall survival difference would have been significant without the disparity in access to osimertinib in the control arm, we will never know the magnitude of that difference.
With the current design, the trial demonstrates that osimertinib is associated with improved survival in 100% of patients with EGFR mutation–positive NSCLC who receive the agent vs. 38.5% of patients receiving it at some point after relapse.
At the end of the day, ADAURA followed conventional trial rules, which led to a windfall of accolades at the cost of suboptimal care for many of the patients randomly assigned to the control arm.
We need to decide as an oncology community whether we want to accept a system that confers rewards for stakeholders at the expense of patients enrolled in the trial.
We have developed a system that not only permits but depends on global trials enrolling many patients from countries with staging and off-protocol oncology care below standards of care in other parts of the world – effectively condoning and perpetuating disparities in optimal care globally. I am also saddened that some of the most respected leaders in our field have become upset when I question the ethics of accepting this system, one that I believe we have agency to change.
The question here is not whether osimertinib is a good drug; it is remarkably effective for patients with EGFR mutation–positive NSCLC. The question is how to design trials in a fair and balanced way that doesn’t compromise patient care or ethical standards.
If people think my assessment is too harsh, I openly welcome debate.
Bottom line: The ADAURA trial lays bare deeper problems with clinical trial design, and I would challenge readers to reflect on our clinical trial culture in oncology, which offers a system of rules that rewards denying the best identified care for patients on our clinical trials.
At the very least, should we celebrate these wins without fully acknowledging these problems?
Dr. West is clinical associate professor, department of medical oncology, City of Hope Comprehensive Cancer Care, Duarte, Calif. He reported conflicts of interest with Bristol-Myers Squibb, Boehringer Ingelheim, Spectrum, AstraZeneca, Celgene, Genentech/Roche, Pfizer, Merck, and Eli Lilly.
A version of this article first appeared on Medscape.com.