User login
Night owls may have greater risks of T2D and CVD
In the study involving 51 people, night owls metabolized fat less efficiently, showed less insulin sensitivity, and demonstrated lower physical fitness than early birds, lead author Steven K. Malin, PhD, of Rutgers University, New Brunswick, N.J., and colleagues reported.

Prior publications have suggested that night owls, formally known as “late chronotypes,” have an increased risk of obesity, type 2 diabetes, and cardiovascular disease, Dr. Malin said in an interview. But no previous research involved the gold-standard measurement tools used in this study, including euglycemic clamp and indirect calorimetry to quantify fat metabolism.
Dr. Malin also noted that this is the first study of its kind to characterize metabolism during both rest and exercise.
The study, published in Experimental Physiology, involved 24 early birds and 27 night owls classified by the Morning-Eveningness Questionnaire. All participants were sedentary, reporting less than one hour of structured exercise per week, and had metabolic syndrome according to Adult Treatment Panel III report criteria. Groups were otherwise demographically similar, with average ages in each group of approximately 54-55 years.
Compared with night owls, early birds were more physically active during the morning into midday. During exercise, they metabolized more fat and demonstrated greater physical fitness based on VO2max readings. At rest, early birds also came out ahead – they had higher fat oxidation and non–oxidative glucose disposal, suggesting more sensitivity to insulin.
“Collectively, this work highlights and supports chronotype as a potential risk factor related to type 2 diabetes and cardiovascular disease risk,” the investigators concluded.
Night owls have less metabolic control
Jed Friedman, PhD, director of OU Health Harold Hamm Diabetes Center at the University of Oklahoma Health Sciences Center, Oklahoma City, praised the study for the size of the groups the researchers compared with each other and how well matched those groups were, as well as the “state-of-the-art” measurement tools employed.

The findings show that night owls have “less metabolic control,” Dr. Friedman said in an interview.
“That’s a term that’s frequently invoked in [regard to] prediabetes,” he said. “Blood sugar goes up, because when you’re eating a high carbohydrate diet, your cells aren’t metabolizing sugar properly. That tends to raise your risk for a lot of diseases.”
Dr. Friedman added that the findings align with those of previous studies that have linked less sleep with changes in brain biology, and therefore behavior, especially in dietary choices.
“When you’re tired, the mechanisms for appetite control go haywire,” Dr. Friedman explained. “The evidence suggests that sugar is the primary driver for what people eat when they’re tired. That obviously has implications for diabetes and metabolic syndrome. So sleeping more really can help you control cravings.”
Dr. Friedman also noted that people who are tired tend to engage in less physical activity, further increasing their risk of metabolic issues. To control this risk, he advised people to return to their circadian rhythms, which could mean forgetting the midnight snack.
“Having a daily pattern that’s in sync with chronicity, or these daily rhythms, is associated with greater health,” Dr. Friedman said. “We’re not really made to eat at night. I think this [study] kind of reinforces that.”
Can a night owl become an early bird?
When asked if a person’s natural circadian rhythm can be later, Dr. Malin responded that chronotypes may be dictated by genetics and age, as well as external drivers like work schedule. For these reasons, it’s “tricky” to answer whether night owls can turn into early birds and reap the potential health benefits of making that shift.
“Given that so many life factors can influence what our routine entails, it’s hard to know if we [can] truly change our chronotype or if rather we [can] learn to manage,” Dr. Malin said. “In either case, there is some work that suggests people can adopt earlier bedtimes and waketimes through practical recommendations.”
Specifically, he suggested increasing physical activity during the day, and adjusting bedtimes gradually by 15-minute increments.
“Go to bed 15 minutes earlier then wake up 15 minutes earlier,” Dr. Malin said. “In time, and depending on how things are going, this can expand to another 15-minute window. Then, during the earlier time waking up, a person can engage in light physical activity to help with promoting general fitness. If they can get outside with sunlight, that would be great too, as the natural sunlight would provide cues to the circadian system to adjust.”
The study was supported by the National Institutes of Health. The investigators and Dr. Friedman disclosed no conflicts of interest.
In the study involving 51 people, night owls metabolized fat less efficiently, showed less insulin sensitivity, and demonstrated lower physical fitness than early birds, lead author Steven K. Malin, PhD, of Rutgers University, New Brunswick, N.J., and colleagues reported.
Prior publications have suggested that night owls, formally known as “late chronotypes,” have an increased risk of obesity, type 2 diabetes, and cardiovascular disease, Dr. Malin said in an interview. But no previous research involved the gold-standard measurement tools used in this study, including euglycemic clamp and indirect calorimetry to quantify fat metabolism.
Dr. Malin also noted that this is the first study of its kind to characterize metabolism during both rest and exercise.
The study, published in Experimental Physiology, involved 24 early birds and 27 night owls classified by the Morning-Eveningness Questionnaire. All participants were sedentary, reporting less than one hour of structured exercise per week, and had metabolic syndrome according to Adult Treatment Panel III report criteria. Groups were otherwise demographically similar, with average ages in each group of approximately 54-55 years.
Compared with night owls, early birds were more physically active during the morning into midday. During exercise, they metabolized more fat and demonstrated greater physical fitness based on VO2max readings. At rest, early birds also came out ahead – they had higher fat oxidation and non–oxidative glucose disposal, suggesting more sensitivity to insulin.
“Collectively, this work highlights and supports chronotype as a potential risk factor related to type 2 diabetes and cardiovascular disease risk,” the investigators concluded.
Night owls have less metabolic control
Jed Friedman, PhD, director of OU Health Harold Hamm Diabetes Center at the University of Oklahoma Health Sciences Center, Oklahoma City, praised the study for the size of the groups the researchers compared with each other and how well matched those groups were, as well as the “state-of-the-art” measurement tools employed.
The findings show that night owls have “less metabolic control,” Dr. Friedman said in an interview.
“That’s a term that’s frequently invoked in [regard to] prediabetes,” he said. “Blood sugar goes up, because when you’re eating a high carbohydrate diet, your cells aren’t metabolizing sugar properly. That tends to raise your risk for a lot of diseases.”
Dr. Friedman added that the findings align with those of previous studies that have linked less sleep with changes in brain biology, and therefore behavior, especially in dietary choices.
“When you’re tired, the mechanisms for appetite control go haywire,” Dr. Friedman explained. “The evidence suggests that sugar is the primary driver for what people eat when they’re tired. That obviously has implications for diabetes and metabolic syndrome. So sleeping more really can help you control cravings.”
Dr. Friedman also noted that people who are tired tend to engage in less physical activity, further increasing their risk of metabolic issues. To control this risk, he advised people to return to their circadian rhythms, which could mean forgetting the midnight snack.
“Having a daily pattern that’s in sync with chronicity, or these daily rhythms, is associated with greater health,” Dr. Friedman said. “We’re not really made to eat at night. I think this [study] kind of reinforces that.”
Can a night owl become an early bird?
When asked if a person’s natural circadian rhythm can be later, Dr. Malin responded that chronotypes may be dictated by genetics and age, as well as external drivers like work schedule. For these reasons, it’s “tricky” to answer whether night owls can turn into early birds and reap the potential health benefits of making that shift.
“Given that so many life factors can influence what our routine entails, it’s hard to know if we [can] truly change our chronotype or if rather we [can] learn to manage,” Dr. Malin said. “In either case, there is some work that suggests people can adopt earlier bedtimes and waketimes through practical recommendations.”
Specifically, he suggested increasing physical activity during the day, and adjusting bedtimes gradually by 15-minute increments.
“Go to bed 15 minutes earlier then wake up 15 minutes earlier,” Dr. Malin said. “In time, and depending on how things are going, this can expand to another 15-minute window. Then, during the earlier time waking up, a person can engage in light physical activity to help with promoting general fitness. If they can get outside with sunlight, that would be great too, as the natural sunlight would provide cues to the circadian system to adjust.”
The study was supported by the National Institutes of Health. The investigators and Dr. Friedman disclosed no conflicts of interest.
In the study involving 51 people, night owls metabolized fat less efficiently, showed less insulin sensitivity, and demonstrated lower physical fitness than early birds, lead author Steven K. Malin, PhD, of Rutgers University, New Brunswick, N.J., and colleagues reported.
Prior publications have suggested that night owls, formally known as “late chronotypes,” have an increased risk of obesity, type 2 diabetes, and cardiovascular disease, Dr. Malin said in an interview. But no previous research involved the gold-standard measurement tools used in this study, including euglycemic clamp and indirect calorimetry to quantify fat metabolism.
Dr. Malin also noted that this is the first study of its kind to characterize metabolism during both rest and exercise.
The study, published in Experimental Physiology, involved 24 early birds and 27 night owls classified by the Morning-Eveningness Questionnaire. All participants were sedentary, reporting less than one hour of structured exercise per week, and had metabolic syndrome according to Adult Treatment Panel III report criteria. Groups were otherwise demographically similar, with average ages in each group of approximately 54-55 years.
Compared with night owls, early birds were more physically active during the morning into midday. During exercise, they metabolized more fat and demonstrated greater physical fitness based on VO2max readings. At rest, early birds also came out ahead – they had higher fat oxidation and non–oxidative glucose disposal, suggesting more sensitivity to insulin.
“Collectively, this work highlights and supports chronotype as a potential risk factor related to type 2 diabetes and cardiovascular disease risk,” the investigators concluded.
Night owls have less metabolic control
Jed Friedman, PhD, director of OU Health Harold Hamm Diabetes Center at the University of Oklahoma Health Sciences Center, Oklahoma City, praised the study for the size of the groups the researchers compared with each other and how well matched those groups were, as well as the “state-of-the-art” measurement tools employed.
The findings show that night owls have “less metabolic control,” Dr. Friedman said in an interview.
“That’s a term that’s frequently invoked in [regard to] prediabetes,” he said. “Blood sugar goes up, because when you’re eating a high carbohydrate diet, your cells aren’t metabolizing sugar properly. That tends to raise your risk for a lot of diseases.”
Dr. Friedman added that the findings align with those of previous studies that have linked less sleep with changes in brain biology, and therefore behavior, especially in dietary choices.
“When you’re tired, the mechanisms for appetite control go haywire,” Dr. Friedman explained. “The evidence suggests that sugar is the primary driver for what people eat when they’re tired. That obviously has implications for diabetes and metabolic syndrome. So sleeping more really can help you control cravings.”
Dr. Friedman also noted that people who are tired tend to engage in less physical activity, further increasing their risk of metabolic issues. To control this risk, he advised people to return to their circadian rhythms, which could mean forgetting the midnight snack.
“Having a daily pattern that’s in sync with chronicity, or these daily rhythms, is associated with greater health,” Dr. Friedman said. “We’re not really made to eat at night. I think this [study] kind of reinforces that.”
Can a night owl become an early bird?
When asked if a person’s natural circadian rhythm can be later, Dr. Malin responded that chronotypes may be dictated by genetics and age, as well as external drivers like work schedule. For these reasons, it’s “tricky” to answer whether night owls can turn into early birds and reap the potential health benefits of making that shift.
“Given that so many life factors can influence what our routine entails, it’s hard to know if we [can] truly change our chronotype or if rather we [can] learn to manage,” Dr. Malin said. “In either case, there is some work that suggests people can adopt earlier bedtimes and waketimes through practical recommendations.”
Specifically, he suggested increasing physical activity during the day, and adjusting bedtimes gradually by 15-minute increments.
“Go to bed 15 minutes earlier then wake up 15 minutes earlier,” Dr. Malin said. “In time, and depending on how things are going, this can expand to another 15-minute window. Then, during the earlier time waking up, a person can engage in light physical activity to help with promoting general fitness. If they can get outside with sunlight, that would be great too, as the natural sunlight would provide cues to the circadian system to adjust.”
The study was supported by the National Institutes of Health. The investigators and Dr. Friedman disclosed no conflicts of interest.
FROM EXPERIMENTAL PHYSIOLOGY
Early bird gets the worm, night owl gets the diabetes
Metabolism a player in circadian rhythm section
Are you an early bird, or do you wake up and stare at your phone, wondering why you were up watching “The Crown” until 3 a.m.? Recent research suggests that people who wake up earlier tend to be more active during the day and burn more fat than those who sleep in. Fat builds up in the night owls, putting them at higher risk of type 2 diabetes and heart disease.
The study gives physicians something to think about when assessing a patient’s risk factors. “This could help medical professionals consider another behavioral factor contributing to disease risk,” Steven Malin, PhD, lead author of the study and expert in metabolism at Rutgers University in New Brunswick, N.J., said in The Guardian.
For the research, 51 participants were divided into night owls and early birds, depending on their answers to a questionnaire. They were examined, monitored for a week, and assessed while doing various activities. Those who woke up early tended to be more sensitive to insulin and burned off fat faster than those who woke up late, the researchers explained.
“Night owls are reported to have a higher risk of obesity, type 2 diabetes, and cardiovascular disease when compared with early birds,” Dr. Malin said. “A potential explanation is they become misaligned with their circadian rhythm for various reasons, but most notably among adults would be work.”
We all know that we may not be at our best when we throw off our internal clocks by going to sleep late and waking up early. Think about that next time you start another episode on Netflix at 2:57 a.m.
Mosquitoes, chemical cocktails, and glass sock beads
We all know that mosquitoes are annoying little disease vectors with a taste for human blood. One of the less-known things about mosquitoes is what attracts them to humans in the first place. It’s so less known that, until now, it was unknown. Oh sure, we knew that odor was involved, and that lactic acid was part of the odor equation, but what are the specific chemicals? Well, there’s carbon dioxide … and ammonia. Those were already known.
Ring Cardé, PhD, an entomologist at the University of California, Riverside, wasn’t convinced. “I suspected there was something undiscovered about the chemistry of odors luring the yellow fever mosquito. I wanted to nail down the exact blend,” he said in a statement from the university.
Dr. Cardé and his associates eventually figured out that the exact chemical cocktail attracting female Aedes aegypti mosquitoes was a combination of carbon dioxide plus two chemicals, 2-ketoglutaric acid and lactic acid. The odor from these chemicals enables mosquitoes to locate and land on their victim and “also encourages probing, the use of piercing mouthparts to find blood,” the university said.
This amazing destination of science is important, but we have to acknowledge the journey as well. To do that we turn to one of Dr. Cardé’s associates, Jan Bello, PhD, formerly of Cal-Riverside and now with insect pest control company Provivi. Turns out that 2-ketoglutaric acid is tricky stuff because the methods typically used to identify chemicals don’t work on it.
Dr. Bello employed a somewhat unorthodox chemical extraction method: He filled his socks with glass beads and walked around with the beads in his socks. 
“Wearing the beads felt almost like a massage, like squeezing stress balls full of sand, but with your feet,” Dr. Bello said. “The most frustrating part of doing it for a long time is that they would get stuck in between your toes, so it would be uncomfortable after a while.”
We hate when science gets stuck between our toes, but we love it when scientists write their own punchlines.
The MS drugs are better down where it’s wetter, take it from me
The myth of the mermaid is one with hundreds, if not thousands, of years of history. The ancient Greeks had the mythological siren, while the Babylonians depicted kulullû (which were mermen – never let the Babylonians be known as noninclusive) in artwork as far back as 1600 BC. Cultures as far flung as Japan, southern Africa, and New Zealand have folkloric figures similar to the mermaid. It is most decidedly not a creation of western Europe, Hans Christian Andersen, or Disney.
With that mild rant out of the way, let’s move to Germany and a group of researchers from the University of Bonn, who have not created a mermaid. They did, however, add human genes to a zebrafish for research purposes, which feels uncomfortably close. Nothing better than unholy animal-human hybrids, right?
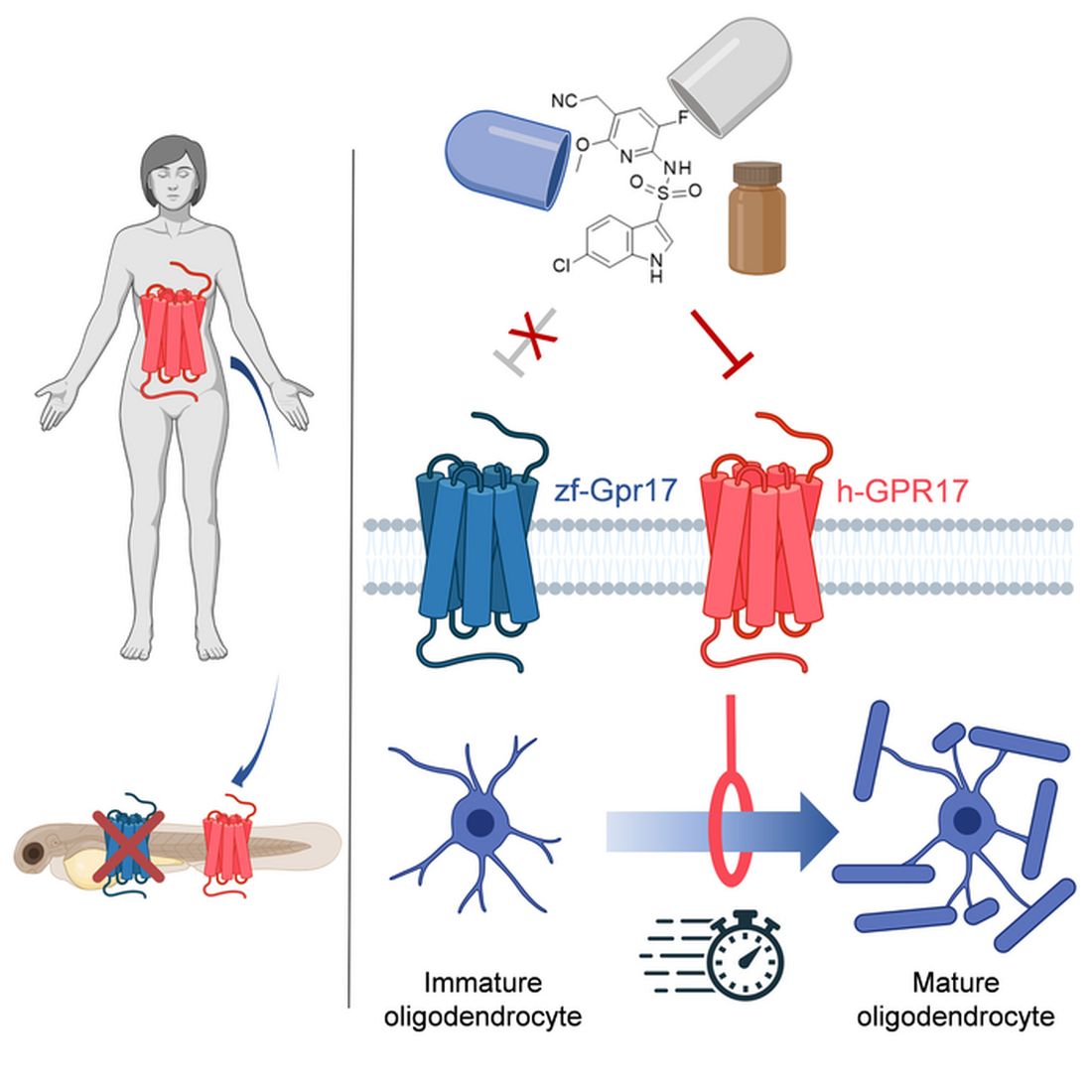
Stick with us here, because the researchers did have a good reason for their gene splicing. Zebrafish and humans both have the GPR17 receptor, which is highly active in nerve tissue. When GPR17 is overactivated, diseases such as multiple sclerosis can develop. Because the zebrafish has this receptor, which performs the same function in its body as in ours, it’s a prime candidate for replacement. Also, zebrafish larvae are transparent, which makes it very easy to observe a drug working.
That said, fish and humans are very far apart, genetically speaking. Big shock right there. But by replacing their GPR17 receptor with ours, the scientists have created a fish that we could test drug candidates on and be assured that they would also work on humans. Actually testing drugs for MS on these humanized zebrafish was beyond the scope of the study, but the researchers said that the new genes function normally in the fish larvae, making them a promising new avenue for MS drug development.
Can we all promise not to tell Disney that human DNA can be spliced into a fish without consequence? Otherwise, we’re just going to have to sit through another “Little Mermaid” adaptation in 30 years, this one in super live-action featuring actual, real-life mermaids. And we’re not ready for that level of man-made horror just yet.
Beware of the fly vomit
Picture this: You’re outside at a picnic or barbecue, loading a plate with food. In a brief moment of conversation a fly lands right on top of your sandwich. You shoo it away and think nothing more of it, eating the sandwich anyway. We’ve all been there.
A recent study is making us think again.
John Stoffolano, an entomology professor at the University of Massachusetts, Amherst, claims that too much attention has been focused on pathogen transmission by the biting, blood-feeding flies when really we should be taking note of the nonbiting, or synanthropic, flies we live with, which may have a greater impact on the transmission of pathogens right in our own homes.

Sure, blood-feeding flies can spread pathogens directly, but house flies vomit every time they land on something. Think about that.
The fly that sneakily swooped into your house from a tear in your window screen has just been outside in the neighbor’s garbage or sitting on dog poop and now has who knows what filling its crop, the tank in their body that serves as “a place to store food before it makes its way into the digestive tract where it will get turned into energy for the fly,” Dr. Stoffolano explained in a written statement.
Did that fly land right on the baked potato you were prepping for dinner before you shooed it away? Guess what? Before flying off it emitted excess water that has pathogens from whatever was in its crop. We don’t want to say your potato might have dog poop on it, but you get the idea. The crop doesn’t have a ton of digestive enzymes that would help neutralize pathogens, so whatever that fly regurgitated before buzzing off is still around for you to ingest and there’s not much you can do about it.
More research needs to be done about flies, but at the very least this study should make you think twice before eating that baked potato after a fly has been there.
Metabolism a player in circadian rhythm section
Are you an early bird, or do you wake up and stare at your phone, wondering why you were up watching “The Crown” until 3 a.m.? Recent research suggests that people who wake up earlier tend to be more active during the day and burn more fat than those who sleep in. Fat builds up in the night owls, putting them at higher risk of type 2 diabetes and heart disease.
The study gives physicians something to think about when assessing a patient’s risk factors. “This could help medical professionals consider another behavioral factor contributing to disease risk,” Steven Malin, PhD, lead author of the study and expert in metabolism at Rutgers University in New Brunswick, N.J., said in The Guardian.
For the research, 51 participants were divided into night owls and early birds, depending on their answers to a questionnaire. They were examined, monitored for a week, and assessed while doing various activities. Those who woke up early tended to be more sensitive to insulin and burned off fat faster than those who woke up late, the researchers explained.
“Night owls are reported to have a higher risk of obesity, type 2 diabetes, and cardiovascular disease when compared with early birds,” Dr. Malin said. “A potential explanation is they become misaligned with their circadian rhythm for various reasons, but most notably among adults would be work.”
We all know that we may not be at our best when we throw off our internal clocks by going to sleep late and waking up early. Think about that next time you start another episode on Netflix at 2:57 a.m.
Mosquitoes, chemical cocktails, and glass sock beads
We all know that mosquitoes are annoying little disease vectors with a taste for human blood. One of the less-known things about mosquitoes is what attracts them to humans in the first place. It’s so less known that, until now, it was unknown. Oh sure, we knew that odor was involved, and that lactic acid was part of the odor equation, but what are the specific chemicals? Well, there’s carbon dioxide … and ammonia. Those were already known.
Ring Cardé, PhD, an entomologist at the University of California, Riverside, wasn’t convinced. “I suspected there was something undiscovered about the chemistry of odors luring the yellow fever mosquito. I wanted to nail down the exact blend,” he said in a statement from the university.
Dr. Cardé and his associates eventually figured out that the exact chemical cocktail attracting female Aedes aegypti mosquitoes was a combination of carbon dioxide plus two chemicals, 2-ketoglutaric acid and lactic acid. The odor from these chemicals enables mosquitoes to locate and land on their victim and “also encourages probing, the use of piercing mouthparts to find blood,” the university said.
This amazing destination of science is important, but we have to acknowledge the journey as well. To do that we turn to one of Dr. Cardé’s associates, Jan Bello, PhD, formerly of Cal-Riverside and now with insect pest control company Provivi. Turns out that 2-ketoglutaric acid is tricky stuff because the methods typically used to identify chemicals don’t work on it.
Dr. Bello employed a somewhat unorthodox chemical extraction method: He filled his socks with glass beads and walked around with the beads in his socks.
“Wearing the beads felt almost like a massage, like squeezing stress balls full of sand, but with your feet,” Dr. Bello said. “The most frustrating part of doing it for a long time is that they would get stuck in between your toes, so it would be uncomfortable after a while.”
We hate when science gets stuck between our toes, but we love it when scientists write their own punchlines.
The MS drugs are better down where it’s wetter, take it from me
The myth of the mermaid is one with hundreds, if not thousands, of years of history. The ancient Greeks had the mythological siren, while the Babylonians depicted kulullû (which were mermen – never let the Babylonians be known as noninclusive) in artwork as far back as 1600 BC. Cultures as far flung as Japan, southern Africa, and New Zealand have folkloric figures similar to the mermaid. It is most decidedly not a creation of western Europe, Hans Christian Andersen, or Disney.
With that mild rant out of the way, let’s move to Germany and a group of researchers from the University of Bonn, who have not created a mermaid. They did, however, add human genes to a zebrafish for research purposes, which feels uncomfortably close. Nothing better than unholy animal-human hybrids, right?
Stick with us here, because the researchers did have a good reason for their gene splicing. Zebrafish and humans both have the GPR17 receptor, which is highly active in nerve tissue. When GPR17 is overactivated, diseases such as multiple sclerosis can develop. Because the zebrafish has this receptor, which performs the same function in its body as in ours, it’s a prime candidate for replacement. Also, zebrafish larvae are transparent, which makes it very easy to observe a drug working.
That said, fish and humans are very far apart, genetically speaking. Big shock right there. But by replacing their GPR17 receptor with ours, the scientists have created a fish that we could test drug candidates on and be assured that they would also work on humans. Actually testing drugs for MS on these humanized zebrafish was beyond the scope of the study, but the researchers said that the new genes function normally in the fish larvae, making them a promising new avenue for MS drug development.
Can we all promise not to tell Disney that human DNA can be spliced into a fish without consequence? Otherwise, we’re just going to have to sit through another “Little Mermaid” adaptation in 30 years, this one in super live-action featuring actual, real-life mermaids. And we’re not ready for that level of man-made horror just yet.
Beware of the fly vomit
Picture this: You’re outside at a picnic or barbecue, loading a plate with food. In a brief moment of conversation a fly lands right on top of your sandwich. You shoo it away and think nothing more of it, eating the sandwich anyway. We’ve all been there.
A recent study is making us think again.
John Stoffolano, an entomology professor at the University of Massachusetts, Amherst, claims that too much attention has been focused on pathogen transmission by the biting, blood-feeding flies when really we should be taking note of the nonbiting, or synanthropic, flies we live with, which may have a greater impact on the transmission of pathogens right in our own homes.
Sure, blood-feeding flies can spread pathogens directly, but house flies vomit every time they land on something. Think about that.
The fly that sneakily swooped into your house from a tear in your window screen has just been outside in the neighbor’s garbage or sitting on dog poop and now has who knows what filling its crop, the tank in their body that serves as “a place to store food before it makes its way into the digestive tract where it will get turned into energy for the fly,” Dr. Stoffolano explained in a written statement.
Did that fly land right on the baked potato you were prepping for dinner before you shooed it away? Guess what? Before flying off it emitted excess water that has pathogens from whatever was in its crop. We don’t want to say your potato might have dog poop on it, but you get the idea. The crop doesn’t have a ton of digestive enzymes that would help neutralize pathogens, so whatever that fly regurgitated before buzzing off is still around for you to ingest and there’s not much you can do about it.
More research needs to be done about flies, but at the very least this study should make you think twice before eating that baked potato after a fly has been there.
Metabolism a player in circadian rhythm section
Are you an early bird, or do you wake up and stare at your phone, wondering why you were up watching “The Crown” until 3 a.m.? Recent research suggests that people who wake up earlier tend to be more active during the day and burn more fat than those who sleep in. Fat builds up in the night owls, putting them at higher risk of type 2 diabetes and heart disease.
The study gives physicians something to think about when assessing a patient’s risk factors. “This could help medical professionals consider another behavioral factor contributing to disease risk,” Steven Malin, PhD, lead author of the study and expert in metabolism at Rutgers University in New Brunswick, N.J., said in The Guardian.
For the research, 51 participants were divided into night owls and early birds, depending on their answers to a questionnaire. They were examined, monitored for a week, and assessed while doing various activities. Those who woke up early tended to be more sensitive to insulin and burned off fat faster than those who woke up late, the researchers explained.
“Night owls are reported to have a higher risk of obesity, type 2 diabetes, and cardiovascular disease when compared with early birds,” Dr. Malin said. “A potential explanation is they become misaligned with their circadian rhythm for various reasons, but most notably among adults would be work.”
We all know that we may not be at our best when we throw off our internal clocks by going to sleep late and waking up early. Think about that next time you start another episode on Netflix at 2:57 a.m.
Mosquitoes, chemical cocktails, and glass sock beads
We all know that mosquitoes are annoying little disease vectors with a taste for human blood. One of the less-known things about mosquitoes is what attracts them to humans in the first place. It’s so less known that, until now, it was unknown. Oh sure, we knew that odor was involved, and that lactic acid was part of the odor equation, but what are the specific chemicals? Well, there’s carbon dioxide … and ammonia. Those were already known.
Ring Cardé, PhD, an entomologist at the University of California, Riverside, wasn’t convinced. “I suspected there was something undiscovered about the chemistry of odors luring the yellow fever mosquito. I wanted to nail down the exact blend,” he said in a statement from the university.
Dr. Cardé and his associates eventually figured out that the exact chemical cocktail attracting female Aedes aegypti mosquitoes was a combination of carbon dioxide plus two chemicals, 2-ketoglutaric acid and lactic acid. The odor from these chemicals enables mosquitoes to locate and land on their victim and “also encourages probing, the use of piercing mouthparts to find blood,” the university said.
This amazing destination of science is important, but we have to acknowledge the journey as well. To do that we turn to one of Dr. Cardé’s associates, Jan Bello, PhD, formerly of Cal-Riverside and now with insect pest control company Provivi. Turns out that 2-ketoglutaric acid is tricky stuff because the methods typically used to identify chemicals don’t work on it.
Dr. Bello employed a somewhat unorthodox chemical extraction method: He filled his socks with glass beads and walked around with the beads in his socks.
“Wearing the beads felt almost like a massage, like squeezing stress balls full of sand, but with your feet,” Dr. Bello said. “The most frustrating part of doing it for a long time is that they would get stuck in between your toes, so it would be uncomfortable after a while.”
We hate when science gets stuck between our toes, but we love it when scientists write their own punchlines.
The MS drugs are better down where it’s wetter, take it from me
The myth of the mermaid is one with hundreds, if not thousands, of years of history. The ancient Greeks had the mythological siren, while the Babylonians depicted kulullû (which were mermen – never let the Babylonians be known as noninclusive) in artwork as far back as 1600 BC. Cultures as far flung as Japan, southern Africa, and New Zealand have folkloric figures similar to the mermaid. It is most decidedly not a creation of western Europe, Hans Christian Andersen, or Disney.
With that mild rant out of the way, let’s move to Germany and a group of researchers from the University of Bonn, who have not created a mermaid. They did, however, add human genes to a zebrafish for research purposes, which feels uncomfortably close. Nothing better than unholy animal-human hybrids, right?
Stick with us here, because the researchers did have a good reason for their gene splicing. Zebrafish and humans both have the GPR17 receptor, which is highly active in nerve tissue. When GPR17 is overactivated, diseases such as multiple sclerosis can develop. Because the zebrafish has this receptor, which performs the same function in its body as in ours, it’s a prime candidate for replacement. Also, zebrafish larvae are transparent, which makes it very easy to observe a drug working.
That said, fish and humans are very far apart, genetically speaking. Big shock right there. But by replacing their GPR17 receptor with ours, the scientists have created a fish that we could test drug candidates on and be assured that they would also work on humans. Actually testing drugs for MS on these humanized zebrafish was beyond the scope of the study, but the researchers said that the new genes function normally in the fish larvae, making them a promising new avenue for MS drug development.
Can we all promise not to tell Disney that human DNA can be spliced into a fish without consequence? Otherwise, we’re just going to have to sit through another “Little Mermaid” adaptation in 30 years, this one in super live-action featuring actual, real-life mermaids. And we’re not ready for that level of man-made horror just yet.
Beware of the fly vomit
Picture this: You’re outside at a picnic or barbecue, loading a plate with food. In a brief moment of conversation a fly lands right on top of your sandwich. You shoo it away and think nothing more of it, eating the sandwich anyway. We’ve all been there.
A recent study is making us think again.
John Stoffolano, an entomology professor at the University of Massachusetts, Amherst, claims that too much attention has been focused on pathogen transmission by the biting, blood-feeding flies when really we should be taking note of the nonbiting, or synanthropic, flies we live with, which may have a greater impact on the transmission of pathogens right in our own homes.
Sure, blood-feeding flies can spread pathogens directly, but house flies vomit every time they land on something. Think about that.
The fly that sneakily swooped into your house from a tear in your window screen has just been outside in the neighbor’s garbage or sitting on dog poop and now has who knows what filling its crop, the tank in their body that serves as “a place to store food before it makes its way into the digestive tract where it will get turned into energy for the fly,” Dr. Stoffolano explained in a written statement.
Did that fly land right on the baked potato you were prepping for dinner before you shooed it away? Guess what? Before flying off it emitted excess water that has pathogens from whatever was in its crop. We don’t want to say your potato might have dog poop on it, but you get the idea. The crop doesn’t have a ton of digestive enzymes that would help neutralize pathogens, so whatever that fly regurgitated before buzzing off is still around for you to ingest and there’s not much you can do about it.
More research needs to be done about flies, but at the very least this study should make you think twice before eating that baked potato after a fly has been there.
Community-level actions could mitigate maternal mortality
Maternal mortality in the United States has been rising for several decades, but actions taken at the community level, as well as larger public health initiatives, have the potential to slow this trend, according to experts at a webinar sponsored by the National Institute for Health Care Management.
Maternal mortality in the United States increased by 14% from 2018 to 2020, according to data from the Centers for Disease Control and Prevention’s National Center for Health Statistics.
However, more than 80% of pregnancy-related deaths are preventable, according to 2017-2019 data from the Maternal Mortality Review Committees published online by the CDC. MMRCs include representatives of diverse clinical and nonclinical backgrounds who review the circumstances of pregnancy-related deaths.
In a webinar presented on Sept. 20, the NIHCM enlisted a panel of experts to discuss maternal mortality, the effect of changes to reproductive rights, and potential strategies to improve maternal health outcomes.
Maternal mortality is defined as “death while pregnant or within 42 days of the end of pregnancy, irrespective of the duration and site of pregnancy, from any cause related to pregnancy or its management,” according to the CDC.
Importantly, mortality rates in the United States are approximately three times higher in Black women compared with White women, said Ndidiamaka Amutah-Onukagha, PhD, MPH, of the Tufts University Center for Black Maternal Health & Reproductive Justice. Dr. Amutah-Onukagha addressed some of the potential issues that appear to drive the disparity in care.
The lack of diversity in the health care workforce has a significant effect on patient outcomes, Dr. Amutah-Onukagha said. Overall, Black newborns are more than twice as likely as White newborns to die during their first year of life, but this number is cut in half when Black infants are cared for by Black physicians, she emphasized.
Other factors that may affect disparities in maternal health care include limited access to prenatal care, discriminatory hospital protocols, and mistreatment by health care professionals, said Dr. Amutah-Onukagha. She cited data showing that maternal mortality rates were higher in rural compared with urban areas. “According to the American Hospital Association, half of rural hospitals have no obstetric care, leaving mothers in maternity care deserts; this exacerbates existing disparities,” she said.
In the webinar, Sindhu Srinivas, MD, a maternal-fetal medicine specialist at the University of Pennsylvania, explained how patient, community, and system factors play a role in the disparities in maternal care.
Overall, Black women have to travel further to receive care, which has implications for high-risk pregnancies, and patients on Medicaid have to wait longer for care, and are less likely to be referred, she added. Black women also have higher rates of preexisting conditions compared with other populations that put them in the high-risk category, such as high blood pressure, diabetes, obesity, or being HIV positive, she said.
Other factors contributing to persistent disparities in maternal care include sociodemographics, patient beliefs and knowledge, and psychological issues including stress, said Dr. Srinivas. Community factors, such as social networks, safety, and poverty, also play a role, as do clinician factors of implicit bias and communication skills, she said.
Strategies to reduce disparity
Dr. Srinivas presented several strategies to reduce disparities at various levels. At the policy level, interventions such as establishing a Maternal Mortality Review Committee, establishing a perinatal quality collaborative, and extending Medicaid for a full year postpartum could help improve outcomes, she said. Dr. Srinivas also encouraged clinicians to report maternal mortality data stratified by race and ethnicity, and to participate in the Alliance for Innovation on Maternal Health program (AIM), an initiative in partnership with the American College of Obstetrics and Gynecology.
Dr. Srinivas also proposed maternal health policies to develop payment models “to sustain and scale innovative solutions, and “preserve access to contraception and abortion care.”
For clinicians looking to have an immediate impact, the panelists agreed that working with community health centers can make a significant difference by improving access to maternal care. Consider opportunities for partnership between hospitals and health care delivery centers in the community, said Dr. Srinivas.
Also, don’t underestimate the value of doulas in the birthing process, Dr. Amutah-Onukagha said. She urged clinicians to advocate for doula reimbursement and to take advantage of opportunities for doulas to work with pregnant individuals at the community levels. Data suggest that doulas are associated with increased maternal care visits and with breastfeeding, she noted.
Adam Myers, MD, of the Blue Cross Blue Shield Association, also contributed to the webinar discussion with a key point: Having financial means and commercial coverage is not a buffer against adverse maternal outcomes for racial minorities.
Dr. Myers cited the latest Health of America Report, which included data up to April 2021 with surveys of Medicaid members and their experiences. According to the report, rates of severe maternal mortality (SMM) increased by 9% for commercially and Medicaid-insured women between 2018 and 2020.
Among commercially insured women, SMM was 53% higher among Black women than White women; among Medicaid-insured women, Black women had a 73% higher rate of SMM, compared with White women.
In addition, the report showed that significantly more mothers of color were not able to complete the recommended series of prenatal visits, mainly for reasons of scheduling and transportation, which were greater barriers than COVID-19, Dr. Myers said.
Based on the data, one specific risk profile rose to the top: “We believe women of color aged 35 or higher with comorbid conditions should be treated as very high risk for SMM,” Dr. Myers emphasized. He stressed the need to focus on transportation and scheduling barriers and expressed support for partnerships and health care delivery centers in the community to mitigate these issues.
Finally, Dr. Srinivas encouraged clinicians to have confidence in their expertise and make themselves heard to help their patients and improve maternal health for all. “Use your voice,” said Dr. Srinivas, “As physicians we don’t think of that as an important aspect of our work, or that we can’t articulate, but remember that we are experts, and sharing stories of patients who are impacted is incredibly powerful,” she said.
The presenters had no relevant financial conflicts to disclose.
Maternal mortality in the United States has been rising for several decades, but actions taken at the community level, as well as larger public health initiatives, have the potential to slow this trend, according to experts at a webinar sponsored by the National Institute for Health Care Management.
Maternal mortality in the United States increased by 14% from 2018 to 2020, according to data from the Centers for Disease Control and Prevention’s National Center for Health Statistics.
However, more than 80% of pregnancy-related deaths are preventable, according to 2017-2019 data from the Maternal Mortality Review Committees published online by the CDC. MMRCs include representatives of diverse clinical and nonclinical backgrounds who review the circumstances of pregnancy-related deaths.
In a webinar presented on Sept. 20, the NIHCM enlisted a panel of experts to discuss maternal mortality, the effect of changes to reproductive rights, and potential strategies to improve maternal health outcomes.
Maternal mortality is defined as “death while pregnant or within 42 days of the end of pregnancy, irrespective of the duration and site of pregnancy, from any cause related to pregnancy or its management,” according to the CDC.
Importantly, mortality rates in the United States are approximately three times higher in Black women compared with White women, said Ndidiamaka Amutah-Onukagha, PhD, MPH, of the Tufts University Center for Black Maternal Health & Reproductive Justice. Dr. Amutah-Onukagha addressed some of the potential issues that appear to drive the disparity in care.
The lack of diversity in the health care workforce has a significant effect on patient outcomes, Dr. Amutah-Onukagha said. Overall, Black newborns are more than twice as likely as White newborns to die during their first year of life, but this number is cut in half when Black infants are cared for by Black physicians, she emphasized.
Other factors that may affect disparities in maternal health care include limited access to prenatal care, discriminatory hospital protocols, and mistreatment by health care professionals, said Dr. Amutah-Onukagha. She cited data showing that maternal mortality rates were higher in rural compared with urban areas. “According to the American Hospital Association, half of rural hospitals have no obstetric care, leaving mothers in maternity care deserts; this exacerbates existing disparities,” she said.
In the webinar, Sindhu Srinivas, MD, a maternal-fetal medicine specialist at the University of Pennsylvania, explained how patient, community, and system factors play a role in the disparities in maternal care.
Overall, Black women have to travel further to receive care, which has implications for high-risk pregnancies, and patients on Medicaid have to wait longer for care, and are less likely to be referred, she added. Black women also have higher rates of preexisting conditions compared with other populations that put them in the high-risk category, such as high blood pressure, diabetes, obesity, or being HIV positive, she said.
Other factors contributing to persistent disparities in maternal care include sociodemographics, patient beliefs and knowledge, and psychological issues including stress, said Dr. Srinivas. Community factors, such as social networks, safety, and poverty, also play a role, as do clinician factors of implicit bias and communication skills, she said.
Strategies to reduce disparity
Dr. Srinivas presented several strategies to reduce disparities at various levels. At the policy level, interventions such as establishing a Maternal Mortality Review Committee, establishing a perinatal quality collaborative, and extending Medicaid for a full year postpartum could help improve outcomes, she said. Dr. Srinivas also encouraged clinicians to report maternal mortality data stratified by race and ethnicity, and to participate in the Alliance for Innovation on Maternal Health program (AIM), an initiative in partnership with the American College of Obstetrics and Gynecology.
Dr. Srinivas also proposed maternal health policies to develop payment models “to sustain and scale innovative solutions, and “preserve access to contraception and abortion care.”
For clinicians looking to have an immediate impact, the panelists agreed that working with community health centers can make a significant difference by improving access to maternal care. Consider opportunities for partnership between hospitals and health care delivery centers in the community, said Dr. Srinivas.
Also, don’t underestimate the value of doulas in the birthing process, Dr. Amutah-Onukagha said. She urged clinicians to advocate for doula reimbursement and to take advantage of opportunities for doulas to work with pregnant individuals at the community levels. Data suggest that doulas are associated with increased maternal care visits and with breastfeeding, she noted.
Adam Myers, MD, of the Blue Cross Blue Shield Association, also contributed to the webinar discussion with a key point: Having financial means and commercial coverage is not a buffer against adverse maternal outcomes for racial minorities.
Dr. Myers cited the latest Health of America Report, which included data up to April 2021 with surveys of Medicaid members and their experiences. According to the report, rates of severe maternal mortality (SMM) increased by 9% for commercially and Medicaid-insured women between 2018 and 2020.
Among commercially insured women, SMM was 53% higher among Black women than White women; among Medicaid-insured women, Black women had a 73% higher rate of SMM, compared with White women.
In addition, the report showed that significantly more mothers of color were not able to complete the recommended series of prenatal visits, mainly for reasons of scheduling and transportation, which were greater barriers than COVID-19, Dr. Myers said.
Based on the data, one specific risk profile rose to the top: “We believe women of color aged 35 or higher with comorbid conditions should be treated as very high risk for SMM,” Dr. Myers emphasized. He stressed the need to focus on transportation and scheduling barriers and expressed support for partnerships and health care delivery centers in the community to mitigate these issues.
Finally, Dr. Srinivas encouraged clinicians to have confidence in their expertise and make themselves heard to help their patients and improve maternal health for all. “Use your voice,” said Dr. Srinivas, “As physicians we don’t think of that as an important aspect of our work, or that we can’t articulate, but remember that we are experts, and sharing stories of patients who are impacted is incredibly powerful,” she said.
The presenters had no relevant financial conflicts to disclose.
Maternal mortality in the United States has been rising for several decades, but actions taken at the community level, as well as larger public health initiatives, have the potential to slow this trend, according to experts at a webinar sponsored by the National Institute for Health Care Management.
Maternal mortality in the United States increased by 14% from 2018 to 2020, according to data from the Centers for Disease Control and Prevention’s National Center for Health Statistics.
However, more than 80% of pregnancy-related deaths are preventable, according to 2017-2019 data from the Maternal Mortality Review Committees published online by the CDC. MMRCs include representatives of diverse clinical and nonclinical backgrounds who review the circumstances of pregnancy-related deaths.
In a webinar presented on Sept. 20, the NIHCM enlisted a panel of experts to discuss maternal mortality, the effect of changes to reproductive rights, and potential strategies to improve maternal health outcomes.
Maternal mortality is defined as “death while pregnant or within 42 days of the end of pregnancy, irrespective of the duration and site of pregnancy, from any cause related to pregnancy or its management,” according to the CDC.
Importantly, mortality rates in the United States are approximately three times higher in Black women compared with White women, said Ndidiamaka Amutah-Onukagha, PhD, MPH, of the Tufts University Center for Black Maternal Health & Reproductive Justice. Dr. Amutah-Onukagha addressed some of the potential issues that appear to drive the disparity in care.
The lack of diversity in the health care workforce has a significant effect on patient outcomes, Dr. Amutah-Onukagha said. Overall, Black newborns are more than twice as likely as White newborns to die during their first year of life, but this number is cut in half when Black infants are cared for by Black physicians, she emphasized.
Other factors that may affect disparities in maternal health care include limited access to prenatal care, discriminatory hospital protocols, and mistreatment by health care professionals, said Dr. Amutah-Onukagha. She cited data showing that maternal mortality rates were higher in rural compared with urban areas. “According to the American Hospital Association, half of rural hospitals have no obstetric care, leaving mothers in maternity care deserts; this exacerbates existing disparities,” she said.
In the webinar, Sindhu Srinivas, MD, a maternal-fetal medicine specialist at the University of Pennsylvania, explained how patient, community, and system factors play a role in the disparities in maternal care.
Overall, Black women have to travel further to receive care, which has implications for high-risk pregnancies, and patients on Medicaid have to wait longer for care, and are less likely to be referred, she added. Black women also have higher rates of preexisting conditions compared with other populations that put them in the high-risk category, such as high blood pressure, diabetes, obesity, or being HIV positive, she said.
Other factors contributing to persistent disparities in maternal care include sociodemographics, patient beliefs and knowledge, and psychological issues including stress, said Dr. Srinivas. Community factors, such as social networks, safety, and poverty, also play a role, as do clinician factors of implicit bias and communication skills, she said.
Strategies to reduce disparity
Dr. Srinivas presented several strategies to reduce disparities at various levels. At the policy level, interventions such as establishing a Maternal Mortality Review Committee, establishing a perinatal quality collaborative, and extending Medicaid for a full year postpartum could help improve outcomes, she said. Dr. Srinivas also encouraged clinicians to report maternal mortality data stratified by race and ethnicity, and to participate in the Alliance for Innovation on Maternal Health program (AIM), an initiative in partnership with the American College of Obstetrics and Gynecology.
Dr. Srinivas also proposed maternal health policies to develop payment models “to sustain and scale innovative solutions, and “preserve access to contraception and abortion care.”
For clinicians looking to have an immediate impact, the panelists agreed that working with community health centers can make a significant difference by improving access to maternal care. Consider opportunities for partnership between hospitals and health care delivery centers in the community, said Dr. Srinivas.
Also, don’t underestimate the value of doulas in the birthing process, Dr. Amutah-Onukagha said. She urged clinicians to advocate for doula reimbursement and to take advantage of opportunities for doulas to work with pregnant individuals at the community levels. Data suggest that doulas are associated with increased maternal care visits and with breastfeeding, she noted.
Adam Myers, MD, of the Blue Cross Blue Shield Association, also contributed to the webinar discussion with a key point: Having financial means and commercial coverage is not a buffer against adverse maternal outcomes for racial minorities.
Dr. Myers cited the latest Health of America Report, which included data up to April 2021 with surveys of Medicaid members and their experiences. According to the report, rates of severe maternal mortality (SMM) increased by 9% for commercially and Medicaid-insured women between 2018 and 2020.
Among commercially insured women, SMM was 53% higher among Black women than White women; among Medicaid-insured women, Black women had a 73% higher rate of SMM, compared with White women.
In addition, the report showed that significantly more mothers of color were not able to complete the recommended series of prenatal visits, mainly for reasons of scheduling and transportation, which were greater barriers than COVID-19, Dr. Myers said.
Based on the data, one specific risk profile rose to the top: “We believe women of color aged 35 or higher with comorbid conditions should be treated as very high risk for SMM,” Dr. Myers emphasized. He stressed the need to focus on transportation and scheduling barriers and expressed support for partnerships and health care delivery centers in the community to mitigate these issues.
Finally, Dr. Srinivas encouraged clinicians to have confidence in their expertise and make themselves heard to help their patients and improve maternal health for all. “Use your voice,” said Dr. Srinivas, “As physicians we don’t think of that as an important aspect of our work, or that we can’t articulate, but remember that we are experts, and sharing stories of patients who are impacted is incredibly powerful,” she said.
The presenters had no relevant financial conflicts to disclose.
Formula may be right for infants, but experts warn that toddlers don’t need it
Formulas for toddlers are a burgeoning business in the United States: Sales of the drinks more than doubled in recent years as companies convinced parents that their little ones needed the liquid boost. But many experts warn that these products, designed for children ages 1-3, fill no nutritional needs beyond what is available in a typical toddler diet, are subject to less regulation than infant formula, and are expensive.
In addition, some parents feed the toddler versions to infants even though they do not meet federal standards for infant formula and may not provide babies with adequate nutrients to sustain their growth.
Pediatricians and federal health officials say that when most children turn 1, they can begin drinking cow milk or an unsweetened plant-based milk substitute. In a 2019 “consensus” statement, the American Academy of Pediatrics and other health and nutrition organizations recommended against using toddler formulas, saying “they offer no unique nutritional value beyond what could be obtained with healthy foods; furthermore, they may contribute added sugars to the diet.” The toddler formulas often contain sweeteners and fats that add calories.
Some of the same companies that produce infant formula – including Enfamil, Gerber, and Similac – also make toddler formulas, as do some smaller, boutique brands that advertise that they have organic or other special qualities. Toddler formulas are available nearly everywhere infant formulas are sold and are marketed as providing extra nutrients to help children’s brain, immune system, and eye development, among other benefits. They are different from medical formulas prescribed for children with specific needs.
A 2020 study found that sales of toddler formula in the United States rose to $92 million in 2015 from $39 million in 2006.
Parents are often confused by the marketing for the formulas, according to a study led by Jennifer Harris, PhD, a marketing and public health researcher at the University of Connecticut, Hartford. She found that 60% of caregivers falsely believed toddler formulas have nutrients that toddlers can’t get from other foods.
Anthony Porto, MD, MPH, a pediatric gastroenterologist and pediatrics professor at Yale University, New Haven, Conn., said he is concerned these products could be giving toddlers more nutrients and calories than they need. Unlike what’s designed for infants, toddler formula has no nutritional regulations: Experts say standardizing a supplement to toddlers’ diets is impossible because no two children are alike.
In focus groups, Dr. Harris said, parents report feeding their children toddler formula to fill nutritional gaps when a child isn’t eating enough, a common concern among parents.
“Infants are often voracious eaters,” said Stephen Daniels, MD, chair of pediatrics at Children’s Hospital Colorado, Aurora. But at around a year of age, children’s growth plateaus, he said, and “they’re suddenly not hungry in the way they used to be anymore.” That can worry parents, he added, but “it’s a completely normal phenomenon.”
If parents have concerns about their children’s diet, Dr. Daniels said, they should consult a pediatrician or family doctor.
Blanche Lincoln, president of the Infant Nutrition Council of America, which represents the makers of Enfamil, Gerber, Similac, and store brands, said in an email that the toddler formulas can be helpful because they can fill “nutritional gaps during this period of transition to table foods.” Ms. Lincoln, a former U.S. senator from Arkansas, said the drinks “help contribute to the specific nutritional needs of toddlers by providing energy and important nutrients, as well as essential vitamins and minerals during this important period of growth and development.”
But toddler formula isn’t being ingested by toddlers alone – it’s also being fed to infants. In a recent study, Dr. Porto and colleagues found that 5% of infants’ parents reported giving their babies drinks marketed for the older age group. And Dr. Harris’ research indicated that 22% of parents of infants older than 6 months had fed their babies toddler formula in the previous month. Both studies were conducted before the recent infant formula shortage, which may have exacerbated the problem.
“Infant formulas and toddler formulas tend to be next to each other in the supermarket,” Dr. Harris said. “They look similar, but the toddler formulas are cheaper than the infant formulas. So people confuse them, and they grab the wrong one. Or they think: ‘Oh, this one is less expensive. I’ll get this one instead.’ ”
According to an email from Food and Drug Administration spokesperson Lindsay Haake, toddler drinks do not meet the definition of infant formula, so they are not subject to the same requirements. That means they do not have to undergo the clinical trials and pathogen safety testing that the infant versions do. “Unlike infant formulas, toddler formulas are not necessary to meet the nutritional needs of their intended consumers,” Ms. Haake said.
In a statement to KHN, the Infant Nutrition Council of America said: “Toddler drinks have a distinctive use and nutritional makeup from infant formula; the two are not interchangeable. The labeling of toddler nutritional drinks explicitly identifies the product as a toddler drink intended for children 12 months and older on the front of the package label.”
However, several expensive toddler formula brands made by smaller companies – often advertised as being made from goat milk, A2 whole milk (which lacks one common milk protein), or vegan ingredients that aren’t soy – do meet nutritional requirements for infants, and some advertise that.
Dr. Harris argued that this confuses parents, too, and shouldn’t be allowed. Just because a toddler formula has the nutritional ingredients required by the FDA for infant formula doesn’t mean it has met the other tests required of infant formula.
Federal regulators have not forced any of the companies to withdraw those products. In an email, FDA spokesperson Marianna Naum said: “The FDA does not comment on potential compliance actions.”
One company, Nature’s One, whose toddler formulas are named “Baby’s Only,” received warning letters a decade ago from the FDA about marketing them for infants. That case was closed in 2016. The company’s website says that Baby’s Only formula “meets nutrient requirements for infant” and that “Baby’s Only Organic® can be served up to 3 years of age.” Critics say that language implies the formula is fine for babies younger than 1. The company’s website and its Instagram account feature customer testimonials from parents who report feeding the formula to their infants, as well as pictures of infants drinking it.
Jay Highman, CEO and president of Nature’s One, said that Baby’s Only is clearly labeled as a toddler formula and that the back of the can states that “Baby’s Only is intended for a toddler 1 year of age or older OR when directed by a health care professional.” He also said that since the company launched in 1999, its formulas have met all the nutritional, manufacturing, and safety standards required of infant formula even though they don’t have to. “We behaved like we are an infant formula, but we were selling it as a toddler formula.”
He said that the clinical trials required by the FDA are a huge barrier to bringing a new infant formula to market and that many other countries don’t require a clinical trial. Baby’s Only recently completed a clinical trial, and the company expects to be able to sell it as an infant formula soon.
Yet pediatricians and nutritional experts continue to caution parents about using the toddler drinks. “There’s no question that infant formula is very important in the first year of life,” Dr. Daniels said. But he doesn’t recommend the toddler version “because it’s not that useful, because it’s confusing, because it’s expensive.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Formulas for toddlers are a burgeoning business in the United States: Sales of the drinks more than doubled in recent years as companies convinced parents that their little ones needed the liquid boost. But many experts warn that these products, designed for children ages 1-3, fill no nutritional needs beyond what is available in a typical toddler diet, are subject to less regulation than infant formula, and are expensive.
In addition, some parents feed the toddler versions to infants even though they do not meet federal standards for infant formula and may not provide babies with adequate nutrients to sustain their growth.
Pediatricians and federal health officials say that when most children turn 1, they can begin drinking cow milk or an unsweetened plant-based milk substitute. In a 2019 “consensus” statement, the American Academy of Pediatrics and other health and nutrition organizations recommended against using toddler formulas, saying “they offer no unique nutritional value beyond what could be obtained with healthy foods; furthermore, they may contribute added sugars to the diet.” The toddler formulas often contain sweeteners and fats that add calories.
Some of the same companies that produce infant formula – including Enfamil, Gerber, and Similac – also make toddler formulas, as do some smaller, boutique brands that advertise that they have organic or other special qualities. Toddler formulas are available nearly everywhere infant formulas are sold and are marketed as providing extra nutrients to help children’s brain, immune system, and eye development, among other benefits. They are different from medical formulas prescribed for children with specific needs.
A 2020 study found that sales of toddler formula in the United States rose to $92 million in 2015 from $39 million in 2006.
Parents are often confused by the marketing for the formulas, according to a study led by Jennifer Harris, PhD, a marketing and public health researcher at the University of Connecticut, Hartford. She found that 60% of caregivers falsely believed toddler formulas have nutrients that toddlers can’t get from other foods.
Anthony Porto, MD, MPH, a pediatric gastroenterologist and pediatrics professor at Yale University, New Haven, Conn., said he is concerned these products could be giving toddlers more nutrients and calories than they need. Unlike what’s designed for infants, toddler formula has no nutritional regulations: Experts say standardizing a supplement to toddlers’ diets is impossible because no two children are alike.
In focus groups, Dr. Harris said, parents report feeding their children toddler formula to fill nutritional gaps when a child isn’t eating enough, a common concern among parents.
“Infants are often voracious eaters,” said Stephen Daniels, MD, chair of pediatrics at Children’s Hospital Colorado, Aurora. But at around a year of age, children’s growth plateaus, he said, and “they’re suddenly not hungry in the way they used to be anymore.” That can worry parents, he added, but “it’s a completely normal phenomenon.”
If parents have concerns about their children’s diet, Dr. Daniels said, they should consult a pediatrician or family doctor.
Blanche Lincoln, president of the Infant Nutrition Council of America, which represents the makers of Enfamil, Gerber, Similac, and store brands, said in an email that the toddler formulas can be helpful because they can fill “nutritional gaps during this period of transition to table foods.” Ms. Lincoln, a former U.S. senator from Arkansas, said the drinks “help contribute to the specific nutritional needs of toddlers by providing energy and important nutrients, as well as essential vitamins and minerals during this important period of growth and development.”
But toddler formula isn’t being ingested by toddlers alone – it’s also being fed to infants. In a recent study, Dr. Porto and colleagues found that 5% of infants’ parents reported giving their babies drinks marketed for the older age group. And Dr. Harris’ research indicated that 22% of parents of infants older than 6 months had fed their babies toddler formula in the previous month. Both studies were conducted before the recent infant formula shortage, which may have exacerbated the problem.
“Infant formulas and toddler formulas tend to be next to each other in the supermarket,” Dr. Harris said. “They look similar, but the toddler formulas are cheaper than the infant formulas. So people confuse them, and they grab the wrong one. Or they think: ‘Oh, this one is less expensive. I’ll get this one instead.’ ”
According to an email from Food and Drug Administration spokesperson Lindsay Haake, toddler drinks do not meet the definition of infant formula, so they are not subject to the same requirements. That means they do not have to undergo the clinical trials and pathogen safety testing that the infant versions do. “Unlike infant formulas, toddler formulas are not necessary to meet the nutritional needs of their intended consumers,” Ms. Haake said.
In a statement to KHN, the Infant Nutrition Council of America said: “Toddler drinks have a distinctive use and nutritional makeup from infant formula; the two are not interchangeable. The labeling of toddler nutritional drinks explicitly identifies the product as a toddler drink intended for children 12 months and older on the front of the package label.”
However, several expensive toddler formula brands made by smaller companies – often advertised as being made from goat milk, A2 whole milk (which lacks one common milk protein), or vegan ingredients that aren’t soy – do meet nutritional requirements for infants, and some advertise that.
Dr. Harris argued that this confuses parents, too, and shouldn’t be allowed. Just because a toddler formula has the nutritional ingredients required by the FDA for infant formula doesn’t mean it has met the other tests required of infant formula.
Federal regulators have not forced any of the companies to withdraw those products. In an email, FDA spokesperson Marianna Naum said: “The FDA does not comment on potential compliance actions.”
One company, Nature’s One, whose toddler formulas are named “Baby’s Only,” received warning letters a decade ago from the FDA about marketing them for infants. That case was closed in 2016. The company’s website says that Baby’s Only formula “meets nutrient requirements for infant” and that “Baby’s Only Organic® can be served up to 3 years of age.” Critics say that language implies the formula is fine for babies younger than 1. The company’s website and its Instagram account feature customer testimonials from parents who report feeding the formula to their infants, as well as pictures of infants drinking it.
Jay Highman, CEO and president of Nature’s One, said that Baby’s Only is clearly labeled as a toddler formula and that the back of the can states that “Baby’s Only is intended for a toddler 1 year of age or older OR when directed by a health care professional.” He also said that since the company launched in 1999, its formulas have met all the nutritional, manufacturing, and safety standards required of infant formula even though they don’t have to. “We behaved like we are an infant formula, but we were selling it as a toddler formula.”
He said that the clinical trials required by the FDA are a huge barrier to bringing a new infant formula to market and that many other countries don’t require a clinical trial. Baby’s Only recently completed a clinical trial, and the company expects to be able to sell it as an infant formula soon.
Yet pediatricians and nutritional experts continue to caution parents about using the toddler drinks. “There’s no question that infant formula is very important in the first year of life,” Dr. Daniels said. But he doesn’t recommend the toddler version “because it’s not that useful, because it’s confusing, because it’s expensive.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Formulas for toddlers are a burgeoning business in the United States: Sales of the drinks more than doubled in recent years as companies convinced parents that their little ones needed the liquid boost. But many experts warn that these products, designed for children ages 1-3, fill no nutritional needs beyond what is available in a typical toddler diet, are subject to less regulation than infant formula, and are expensive.
In addition, some parents feed the toddler versions to infants even though they do not meet federal standards for infant formula and may not provide babies with adequate nutrients to sustain their growth.
Pediatricians and federal health officials say that when most children turn 1, they can begin drinking cow milk or an unsweetened plant-based milk substitute. In a 2019 “consensus” statement, the American Academy of Pediatrics and other health and nutrition organizations recommended against using toddler formulas, saying “they offer no unique nutritional value beyond what could be obtained with healthy foods; furthermore, they may contribute added sugars to the diet.” The toddler formulas often contain sweeteners and fats that add calories.
Some of the same companies that produce infant formula – including Enfamil, Gerber, and Similac – also make toddler formulas, as do some smaller, boutique brands that advertise that they have organic or other special qualities. Toddler formulas are available nearly everywhere infant formulas are sold and are marketed as providing extra nutrients to help children’s brain, immune system, and eye development, among other benefits. They are different from medical formulas prescribed for children with specific needs.
A 2020 study found that sales of toddler formula in the United States rose to $92 million in 2015 from $39 million in 2006.
Parents are often confused by the marketing for the formulas, according to a study led by Jennifer Harris, PhD, a marketing and public health researcher at the University of Connecticut, Hartford. She found that 60% of caregivers falsely believed toddler formulas have nutrients that toddlers can’t get from other foods.
Anthony Porto, MD, MPH, a pediatric gastroenterologist and pediatrics professor at Yale University, New Haven, Conn., said he is concerned these products could be giving toddlers more nutrients and calories than they need. Unlike what’s designed for infants, toddler formula has no nutritional regulations: Experts say standardizing a supplement to toddlers’ diets is impossible because no two children are alike.
In focus groups, Dr. Harris said, parents report feeding their children toddler formula to fill nutritional gaps when a child isn’t eating enough, a common concern among parents.
“Infants are often voracious eaters,” said Stephen Daniels, MD, chair of pediatrics at Children’s Hospital Colorado, Aurora. But at around a year of age, children’s growth plateaus, he said, and “they’re suddenly not hungry in the way they used to be anymore.” That can worry parents, he added, but “it’s a completely normal phenomenon.”
If parents have concerns about their children’s diet, Dr. Daniels said, they should consult a pediatrician or family doctor.
Blanche Lincoln, president of the Infant Nutrition Council of America, which represents the makers of Enfamil, Gerber, Similac, and store brands, said in an email that the toddler formulas can be helpful because they can fill “nutritional gaps during this period of transition to table foods.” Ms. Lincoln, a former U.S. senator from Arkansas, said the drinks “help contribute to the specific nutritional needs of toddlers by providing energy and important nutrients, as well as essential vitamins and minerals during this important period of growth and development.”
But toddler formula isn’t being ingested by toddlers alone – it’s also being fed to infants. In a recent study, Dr. Porto and colleagues found that 5% of infants’ parents reported giving their babies drinks marketed for the older age group. And Dr. Harris’ research indicated that 22% of parents of infants older than 6 months had fed their babies toddler formula in the previous month. Both studies were conducted before the recent infant formula shortage, which may have exacerbated the problem.
“Infant formulas and toddler formulas tend to be next to each other in the supermarket,” Dr. Harris said. “They look similar, but the toddler formulas are cheaper than the infant formulas. So people confuse them, and they grab the wrong one. Or they think: ‘Oh, this one is less expensive. I’ll get this one instead.’ ”
According to an email from Food and Drug Administration spokesperson Lindsay Haake, toddler drinks do not meet the definition of infant formula, so they are not subject to the same requirements. That means they do not have to undergo the clinical trials and pathogen safety testing that the infant versions do. “Unlike infant formulas, toddler formulas are not necessary to meet the nutritional needs of their intended consumers,” Ms. Haake said.
In a statement to KHN, the Infant Nutrition Council of America said: “Toddler drinks have a distinctive use and nutritional makeup from infant formula; the two are not interchangeable. The labeling of toddler nutritional drinks explicitly identifies the product as a toddler drink intended for children 12 months and older on the front of the package label.”
However, several expensive toddler formula brands made by smaller companies – often advertised as being made from goat milk, A2 whole milk (which lacks one common milk protein), or vegan ingredients that aren’t soy – do meet nutritional requirements for infants, and some advertise that.
Dr. Harris argued that this confuses parents, too, and shouldn’t be allowed. Just because a toddler formula has the nutritional ingredients required by the FDA for infant formula doesn’t mean it has met the other tests required of infant formula.
Federal regulators have not forced any of the companies to withdraw those products. In an email, FDA spokesperson Marianna Naum said: “The FDA does not comment on potential compliance actions.”
One company, Nature’s One, whose toddler formulas are named “Baby’s Only,” received warning letters a decade ago from the FDA about marketing them for infants. That case was closed in 2016. The company’s website says that Baby’s Only formula “meets nutrient requirements for infant” and that “Baby’s Only Organic® can be served up to 3 years of age.” Critics say that language implies the formula is fine for babies younger than 1. The company’s website and its Instagram account feature customer testimonials from parents who report feeding the formula to their infants, as well as pictures of infants drinking it.
Jay Highman, CEO and president of Nature’s One, said that Baby’s Only is clearly labeled as a toddler formula and that the back of the can states that “Baby’s Only is intended for a toddler 1 year of age or older OR when directed by a health care professional.” He also said that since the company launched in 1999, its formulas have met all the nutritional, manufacturing, and safety standards required of infant formula even though they don’t have to. “We behaved like we are an infant formula, but we were selling it as a toddler formula.”
He said that the clinical trials required by the FDA are a huge barrier to bringing a new infant formula to market and that many other countries don’t require a clinical trial. Baby’s Only recently completed a clinical trial, and the company expects to be able to sell it as an infant formula soon.
Yet pediatricians and nutritional experts continue to caution parents about using the toddler drinks. “There’s no question that infant formula is very important in the first year of life,” Dr. Daniels said. But he doesn’t recommend the toddler version “because it’s not that useful, because it’s confusing, because it’s expensive.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Online yoga program improves physical function in OA
Although pain did not significantly improve in the yoga group, participants only completed about two-thirds of the recommended sessions, suggesting that more benefit may be possible with greater adherence, wrote lead author Kim L. Bennell, PhD, of the University of Melbourne, and colleagues in the Annals of Internal Medicine.

“To date, an online yoga program specifically for people with knee osteoarthritis has not been investigated,” the investigators said. “The need for such evidence-based packaged online exercise programs is highlighted in the 2020 U.S. National Public Health Agenda for Osteoarthritis.”
Methods and results
The trial involved 212 adults aged 45 years or older with symptomatic knee osteoarthritis. All patients had access to online educational materials about managing osteoarthritis.
Half of the participants were randomized into the 12-week online yoga program. This self-directed, unsupervised course consisted of 12 prerecorded 30-minute instructional yoga sessions, each with a unique sequence of poses to be completed three times in one week before moving on to the next class the following week. After 12 weeks, these participants could choose to continue doing yoga via the online program for 12 additional weeks, if desired.
The primary outcomes were knee pain and physical function, gauged by a 10-point numerical rating scale and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), respectively. Adherence was defined as completion of at least 2 yoga sessions within the preceding week.
At the 12-week mark, the yoga group did not show any significant improvement in knee pain (–0.6; 95% confidence interval, –1.2 to 0.1), but they did achieve a mean 4-point reduction in WOMAC, suggesting significant improvement in knee function (–4.0; 95% CI, –6.8 to –1.3). Of note, however, this improvement was not enough to meet the threshold for minimal clinically important difference. At 24 weeks, the yoga group no longer showed significant improvement in knee function versus baseline.
“I don’t think a longer program would necessarily reduce knee pain, as benefits from a whole range of different types of exercise for knee osteoarthritis generally can show benefits within 8 weeks,” Dr. Bennell said in an interview.
Still, she noted that the average outcome in the trial may not represent what is possible if a patient commits to a regular yoga routine.
“I think it relates more to adherence [than duration], and I think benefits for knee pain would have been seen if a greater number of people had fully adhered to the program three times a week,” she said.
At 12 weeks, 68.8% of those in the yoga group were adherent, while just 28.4% were still adherent at week 24 after the optional extension period.
“As this was a self-directed program, adherence might be expected to be less than that of a supervised program,” Dr. Bennell noted.
Referring to unpublished data, Dr. Bennell said a sensitivity analysis showed that participants in the yoga group who completed yoga at least twice a week did show greater improvements in function and pain than those who did yoga less than twice per week.
“So it does suggest that adherence is important, as we might expect,” she said.
Another tool in the OA toolbox
Nick Trasolini, MD, of Wake Forest University School of Medicine, Winston-Salem, N.C., described the benefits in the trial as “modest” and noted that the improvement in function did not meet the threshold for minimal clinically important difference.
“Nevertheless,” he said in a written comment, “the [yoga] program was safe and associated with high participant satisfaction [mean satisfaction, 8 out of 10]. While this may not be the ‘silver bullet,’ it is another tool that we can offer to sufficiently motivated patients seeking non-operative solutions for knee osteoarthritis.”
Unfortunately, these tools remain “fraught with challenges,” Dr. Trasolini added.
“While multiple injection options are available (including corticosteroid, hyaluronic acid viscosupplementation, and biologic injections), the benefits of these injections can be short-lived,” he said. “This is frustrating to patients and physicians alike. Physical therapy is beneficial for knee osteoarthritis when deconditioning has led to decreased knee, hip, and core stability. However, physical therapy can be time consuming, painful, and cost prohibitive.”
In the present study, participants in the yoga group were somewhat willing (mean willingness, 5 out of 10) to pay for their 12-week yoga program. They reported that they would pay approximately $80 U.S. dollars for chance to do it all again.
The study was supported by grants from the National Health and Medical Research Council Program and the Centres of Research Excellence. The investigators disclosed additional relationships with Pfizer, Lilly, TLCBio, and others. Dr. Trasolini disclosed no relevant conflicts of interest.
Although pain did not significantly improve in the yoga group, participants only completed about two-thirds of the recommended sessions, suggesting that more benefit may be possible with greater adherence, wrote lead author Kim L. Bennell, PhD, of the University of Melbourne, and colleagues in the Annals of Internal Medicine.
“To date, an online yoga program specifically for people with knee osteoarthritis has not been investigated,” the investigators said. “The need for such evidence-based packaged online exercise programs is highlighted in the 2020 U.S. National Public Health Agenda for Osteoarthritis.”
Methods and results
The trial involved 212 adults aged 45 years or older with symptomatic knee osteoarthritis. All patients had access to online educational materials about managing osteoarthritis.
Half of the participants were randomized into the 12-week online yoga program. This self-directed, unsupervised course consisted of 12 prerecorded 30-minute instructional yoga sessions, each with a unique sequence of poses to be completed three times in one week before moving on to the next class the following week. After 12 weeks, these participants could choose to continue doing yoga via the online program for 12 additional weeks, if desired.
The primary outcomes were knee pain and physical function, gauged by a 10-point numerical rating scale and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), respectively. Adherence was defined as completion of at least 2 yoga sessions within the preceding week.
At the 12-week mark, the yoga group did not show any significant improvement in knee pain (–0.6; 95% confidence interval, –1.2 to 0.1), but they did achieve a mean 4-point reduction in WOMAC, suggesting significant improvement in knee function (–4.0; 95% CI, –6.8 to –1.3). Of note, however, this improvement was not enough to meet the threshold for minimal clinically important difference. At 24 weeks, the yoga group no longer showed significant improvement in knee function versus baseline.
“I don’t think a longer program would necessarily reduce knee pain, as benefits from a whole range of different types of exercise for knee osteoarthritis generally can show benefits within 8 weeks,” Dr. Bennell said in an interview.
Still, she noted that the average outcome in the trial may not represent what is possible if a patient commits to a regular yoga routine.
“I think it relates more to adherence [than duration], and I think benefits for knee pain would have been seen if a greater number of people had fully adhered to the program three times a week,” she said.
At 12 weeks, 68.8% of those in the yoga group were adherent, while just 28.4% were still adherent at week 24 after the optional extension period.
“As this was a self-directed program, adherence might be expected to be less than that of a supervised program,” Dr. Bennell noted.
Referring to unpublished data, Dr. Bennell said a sensitivity analysis showed that participants in the yoga group who completed yoga at least twice a week did show greater improvements in function and pain than those who did yoga less than twice per week.
“So it does suggest that adherence is important, as we might expect,” she said.
Another tool in the OA toolbox
Nick Trasolini, MD, of Wake Forest University School of Medicine, Winston-Salem, N.C., described the benefits in the trial as “modest” and noted that the improvement in function did not meet the threshold for minimal clinically important difference.
“Nevertheless,” he said in a written comment, “the [yoga] program was safe and associated with high participant satisfaction [mean satisfaction, 8 out of 10]. While this may not be the ‘silver bullet,’ it is another tool that we can offer to sufficiently motivated patients seeking non-operative solutions for knee osteoarthritis.”
Unfortunately, these tools remain “fraught with challenges,” Dr. Trasolini added.
“While multiple injection options are available (including corticosteroid, hyaluronic acid viscosupplementation, and biologic injections), the benefits of these injections can be short-lived,” he said. “This is frustrating to patients and physicians alike. Physical therapy is beneficial for knee osteoarthritis when deconditioning has led to decreased knee, hip, and core stability. However, physical therapy can be time consuming, painful, and cost prohibitive.”
In the present study, participants in the yoga group were somewhat willing (mean willingness, 5 out of 10) to pay for their 12-week yoga program. They reported that they would pay approximately $80 U.S. dollars for chance to do it all again.
The study was supported by grants from the National Health and Medical Research Council Program and the Centres of Research Excellence. The investigators disclosed additional relationships with Pfizer, Lilly, TLCBio, and others. Dr. Trasolini disclosed no relevant conflicts of interest.
Although pain did not significantly improve in the yoga group, participants only completed about two-thirds of the recommended sessions, suggesting that more benefit may be possible with greater adherence, wrote lead author Kim L. Bennell, PhD, of the University of Melbourne, and colleagues in the Annals of Internal Medicine.
“To date, an online yoga program specifically for people with knee osteoarthritis has not been investigated,” the investigators said. “The need for such evidence-based packaged online exercise programs is highlighted in the 2020 U.S. National Public Health Agenda for Osteoarthritis.”
Methods and results
The trial involved 212 adults aged 45 years or older with symptomatic knee osteoarthritis. All patients had access to online educational materials about managing osteoarthritis.
Half of the participants were randomized into the 12-week online yoga program. This self-directed, unsupervised course consisted of 12 prerecorded 30-minute instructional yoga sessions, each with a unique sequence of poses to be completed three times in one week before moving on to the next class the following week. After 12 weeks, these participants could choose to continue doing yoga via the online program for 12 additional weeks, if desired.
The primary outcomes were knee pain and physical function, gauged by a 10-point numerical rating scale and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), respectively. Adherence was defined as completion of at least 2 yoga sessions within the preceding week.
At the 12-week mark, the yoga group did not show any significant improvement in knee pain (–0.6; 95% confidence interval, –1.2 to 0.1), but they did achieve a mean 4-point reduction in WOMAC, suggesting significant improvement in knee function (–4.0; 95% CI, –6.8 to –1.3). Of note, however, this improvement was not enough to meet the threshold for minimal clinically important difference. At 24 weeks, the yoga group no longer showed significant improvement in knee function versus baseline.
“I don’t think a longer program would necessarily reduce knee pain, as benefits from a whole range of different types of exercise for knee osteoarthritis generally can show benefits within 8 weeks,” Dr. Bennell said in an interview.
Still, she noted that the average outcome in the trial may not represent what is possible if a patient commits to a regular yoga routine.
“I think it relates more to adherence [than duration], and I think benefits for knee pain would have been seen if a greater number of people had fully adhered to the program three times a week,” she said.
At 12 weeks, 68.8% of those in the yoga group were adherent, while just 28.4% were still adherent at week 24 after the optional extension period.
“As this was a self-directed program, adherence might be expected to be less than that of a supervised program,” Dr. Bennell noted.
Referring to unpublished data, Dr. Bennell said a sensitivity analysis showed that participants in the yoga group who completed yoga at least twice a week did show greater improvements in function and pain than those who did yoga less than twice per week.
“So it does suggest that adherence is important, as we might expect,” she said.
Another tool in the OA toolbox
Nick Trasolini, MD, of Wake Forest University School of Medicine, Winston-Salem, N.C., described the benefits in the trial as “modest” and noted that the improvement in function did not meet the threshold for minimal clinically important difference.
“Nevertheless,” he said in a written comment, “the [yoga] program was safe and associated with high participant satisfaction [mean satisfaction, 8 out of 10]. While this may not be the ‘silver bullet,’ it is another tool that we can offer to sufficiently motivated patients seeking non-operative solutions for knee osteoarthritis.”
Unfortunately, these tools remain “fraught with challenges,” Dr. Trasolini added.
“While multiple injection options are available (including corticosteroid, hyaluronic acid viscosupplementation, and biologic injections), the benefits of these injections can be short-lived,” he said. “This is frustrating to patients and physicians alike. Physical therapy is beneficial for knee osteoarthritis when deconditioning has led to decreased knee, hip, and core stability. However, physical therapy can be time consuming, painful, and cost prohibitive.”
In the present study, participants in the yoga group were somewhat willing (mean willingness, 5 out of 10) to pay for their 12-week yoga program. They reported that they would pay approximately $80 U.S. dollars for chance to do it all again.
The study was supported by grants from the National Health and Medical Research Council Program and the Centres of Research Excellence. The investigators disclosed additional relationships with Pfizer, Lilly, TLCBio, and others. Dr. Trasolini disclosed no relevant conflicts of interest.
FROM ANNALS OF INTERNAL MEDICINE
Family affair: OncBrothers host oncology hangout online
It’s hard out there for a small-town cancer doctor. Just ask Wederson M. Claudino, MD, who serves the town of Paducah in far western Kentucky. The nearest cities with significant numbers of hematologist/oncologists are hours away in cities like St. Louis and Nashville, Tenn., too far to go to talk shop over coffee, drinks, or lunch.
“It’s very challenging in a rural or small community,” he said. “I miss the opportunity to elaborate on a case.”
Now Dr. Claudino and hundreds of colleagues have discovered that useful cancer conversations are just a click away.

Urban and rural oncologists gather there to discuss new research, compare notes about challenging cases, and get to know each other.
“Following their Twitter feed and the comments and discussions make me feel like part of a bigger community,” Dr. Claudino said. And @OncBrothers is indeed a bustling Internet destination: The account’s 4,300 followers include hundreds who participate in discussions and offer perspective.
For instance, the brothers recently posted a poll asking followers how they’d treat a 55-year-old patient with non–small cell lung cancer. Nearly 250 people responded with their preferred approaches, and the survey thread included comments from oncologists from the City of Hope National Medical Center, the University of Florida, UC San Diego, and elsewhere.
In an interview, the Gosain brothers said the Twitter account is an outgrowth of their phone conversations in recent years, as they trained and settled into their early careers as general medical oncologists in smaller communities.
“After our clinic days, we’ll jump on the phone for 30-45 minutes. We’d talk about patients, how he would treat a case, and what I would do,” Rahul said. “We realized that we were living in a bubble, but we also thought that there are a lot more people in the same boat. They might jump at being able to do the same thing.”
Rahul recently became medical director at the new Wilmot Webster Cancer Center in Rochester, N.Y., after working in Corning, a tiny New York town just north of the Pennsylvania border. His brother Rohit is chair of hematology and oncology at the University of Pittsburgh’s Hillman Cancer Center in Jamestown, a small town at the western edge of New York.
“When we initially kicked off the Twitter account in August 2021, we didn’t realize the traction it would get,” Rohit said. “Now we realize that there really is a need for this.”
On an ordinary day, the @OncBrothers account may highlight research presented at a oncology conference, retweet posts by other oncologists about new guidelines or FDA drug approvals, and ask followers to consider how they’d handle a difficult case.
The brothers are especially thrilled when posts spawn discussions that draw voices from leading medical institutions who normally don’t interact much with community oncologists. “You’ll have someone from Sloan Kettering or Dana-Farber saying ‘This is what would do,’ ” Rahul said. “You have the brightest minds pitching in, and we get to learn from them.”
The Gosain brothers were both born in India and immigrated as children to Toronto. They each went to medical school in the Caribbean – for Rohit, it was after a stint as a computer engineer – and they each embraced oncology. “For me, it was about having the right mentors while I was doing my clinical rotations as a medical student and as a resident,” Rahul said. In addition, he said, “this field was moving and is still moving so fast. It really intrigued and excited me and made me want to be at the forefront of it.”
The fast-moving nature of oncology, in fact, was one of the drivers behind the daily conversations between the brothers and the subsequent creation of the @OncBrothers account. “Just last year, in 2021, there were 40 new drugs that were indicated for hematology-oncology,” Rahul said. “To stay on top of that is very, very hard.”
It’s especially difficult to figure out treatment plans when multiple options exist. A 2022 thread on @OncBrothers revealed a wide divergence of opinions about triple therapy in prostate cancer: The 322 respondents to a Twitter poll were sharply divided about the best three-drug combination from these options – docetaxel, daratumumab, abiraterone, androgen deprivation therapy, and alpha-reductase inhibitors.
To make things more challenging, community oncologists often are generalists who treat patients with a wide variety of cancers from prostate and lung to breast and colon. As a result, these oncologists must keep up on developments across the entire cancer field. Rohit highlighted a 2022 thread that polled users about the approach they’d take to another patient with non–small cell lung cancer; 474 people responded. The accompanying discussion emphasized the need for the next-generation sequencing (NGS).
“A significant portion of community oncologists are not even doing NGS testing, which is FDA-approved,” Rohit said. “There’s a huge gap that still exists, and we weren’t even aware of it. We continue to learn from these conversations.”
The brothers contend that there’s a crucial need for education among community oncologists in light of evidence suggesting that some cancer outcomes are worse than those in urban areas.
In fact, Rohit led a 2019 study published in the journal Cancer that found that overall survival in rural patients with neuroendocrine tumors trended toward worse outcomes than in urban patients.
“There are many factors such as financial burden, lack of education, and rural patients not willing to travel to the city,” Rohit said. “We need to be more creative and ask, ‘How can we equip our medical oncologist in rural settings to continue to do better?’ ”
What’s next for the OncBrothers? The Gosains have created a website (www.oncbrothers.com) that highlights their social media work, and they’re exploring options such as podcasts and short videos. “Our goal is to focus on how to continue to keep general medical oncologists up to date, informed, and educated so patients can get the best care close to home,” Rahul said. “We need to do better.”
It’s hard out there for a small-town cancer doctor. Just ask Wederson M. Claudino, MD, who serves the town of Paducah in far western Kentucky. The nearest cities with significant numbers of hematologist/oncologists are hours away in cities like St. Louis and Nashville, Tenn., too far to go to talk shop over coffee, drinks, or lunch.
“It’s very challenging in a rural or small community,” he said. “I miss the opportunity to elaborate on a case.”
Now Dr. Claudino and hundreds of colleagues have discovered that useful cancer conversations are just a click away.
Urban and rural oncologists gather there to discuss new research, compare notes about challenging cases, and get to know each other.
“Following their Twitter feed and the comments and discussions make me feel like part of a bigger community,” Dr. Claudino said. And @OncBrothers is indeed a bustling Internet destination: The account’s 4,300 followers include hundreds who participate in discussions and offer perspective.
For instance, the brothers recently posted a poll asking followers how they’d treat a 55-year-old patient with non–small cell lung cancer. Nearly 250 people responded with their preferred approaches, and the survey thread included comments from oncologists from the City of Hope National Medical Center, the University of Florida, UC San Diego, and elsewhere.
In an interview, the Gosain brothers said the Twitter account is an outgrowth of their phone conversations in recent years, as they trained and settled into their early careers as general medical oncologists in smaller communities.
“After our clinic days, we’ll jump on the phone for 30-45 minutes. We’d talk about patients, how he would treat a case, and what I would do,” Rahul said. “We realized that we were living in a bubble, but we also thought that there are a lot more people in the same boat. They might jump at being able to do the same thing.”
Rahul recently became medical director at the new Wilmot Webster Cancer Center in Rochester, N.Y., after working in Corning, a tiny New York town just north of the Pennsylvania border. His brother Rohit is chair of hematology and oncology at the University of Pittsburgh’s Hillman Cancer Center in Jamestown, a small town at the western edge of New York.
“When we initially kicked off the Twitter account in August 2021, we didn’t realize the traction it would get,” Rohit said. “Now we realize that there really is a need for this.”
On an ordinary day, the @OncBrothers account may highlight research presented at a oncology conference, retweet posts by other oncologists about new guidelines or FDA drug approvals, and ask followers to consider how they’d handle a difficult case.
The brothers are especially thrilled when posts spawn discussions that draw voices from leading medical institutions who normally don’t interact much with community oncologists. “You’ll have someone from Sloan Kettering or Dana-Farber saying ‘This is what would do,’ ” Rahul said. “You have the brightest minds pitching in, and we get to learn from them.”
The Gosain brothers were both born in India and immigrated as children to Toronto. They each went to medical school in the Caribbean – for Rohit, it was after a stint as a computer engineer – and they each embraced oncology. “For me, it was about having the right mentors while I was doing my clinical rotations as a medical student and as a resident,” Rahul said. In addition, he said, “this field was moving and is still moving so fast. It really intrigued and excited me and made me want to be at the forefront of it.”
The fast-moving nature of oncology, in fact, was one of the drivers behind the daily conversations between the brothers and the subsequent creation of the @OncBrothers account. “Just last year, in 2021, there were 40 new drugs that were indicated for hematology-oncology,” Rahul said. “To stay on top of that is very, very hard.”
It’s especially difficult to figure out treatment plans when multiple options exist. A 2022 thread on @OncBrothers revealed a wide divergence of opinions about triple therapy in prostate cancer: The 322 respondents to a Twitter poll were sharply divided about the best three-drug combination from these options – docetaxel, daratumumab, abiraterone, androgen deprivation therapy, and alpha-reductase inhibitors.
To make things more challenging, community oncologists often are generalists who treat patients with a wide variety of cancers from prostate and lung to breast and colon. As a result, these oncologists must keep up on developments across the entire cancer field. Rohit highlighted a 2022 thread that polled users about the approach they’d take to another patient with non–small cell lung cancer; 474 people responded. The accompanying discussion emphasized the need for the next-generation sequencing (NGS).
“A significant portion of community oncologists are not even doing NGS testing, which is FDA-approved,” Rohit said. “There’s a huge gap that still exists, and we weren’t even aware of it. We continue to learn from these conversations.”
The brothers contend that there’s a crucial need for education among community oncologists in light of evidence suggesting that some cancer outcomes are worse than those in urban areas.
In fact, Rohit led a 2019 study published in the journal Cancer that found that overall survival in rural patients with neuroendocrine tumors trended toward worse outcomes than in urban patients.
“There are many factors such as financial burden, lack of education, and rural patients not willing to travel to the city,” Rohit said. “We need to be more creative and ask, ‘How can we equip our medical oncologist in rural settings to continue to do better?’ ”
What’s next for the OncBrothers? The Gosains have created a website (www.oncbrothers.com) that highlights their social media work, and they’re exploring options such as podcasts and short videos. “Our goal is to focus on how to continue to keep general medical oncologists up to date, informed, and educated so patients can get the best care close to home,” Rahul said. “We need to do better.”
It’s hard out there for a small-town cancer doctor. Just ask Wederson M. Claudino, MD, who serves the town of Paducah in far western Kentucky. The nearest cities with significant numbers of hematologist/oncologists are hours away in cities like St. Louis and Nashville, Tenn., too far to go to talk shop over coffee, drinks, or lunch.
“It’s very challenging in a rural or small community,” he said. “I miss the opportunity to elaborate on a case.”
Now Dr. Claudino and hundreds of colleagues have discovered that useful cancer conversations are just a click away.
Urban and rural oncologists gather there to discuss new research, compare notes about challenging cases, and get to know each other.
“Following their Twitter feed and the comments and discussions make me feel like part of a bigger community,” Dr. Claudino said. And @OncBrothers is indeed a bustling Internet destination: The account’s 4,300 followers include hundreds who participate in discussions and offer perspective.
For instance, the brothers recently posted a poll asking followers how they’d treat a 55-year-old patient with non–small cell lung cancer. Nearly 250 people responded with their preferred approaches, and the survey thread included comments from oncologists from the City of Hope National Medical Center, the University of Florida, UC San Diego, and elsewhere.
In an interview, the Gosain brothers said the Twitter account is an outgrowth of their phone conversations in recent years, as they trained and settled into their early careers as general medical oncologists in smaller communities.
“After our clinic days, we’ll jump on the phone for 30-45 minutes. We’d talk about patients, how he would treat a case, and what I would do,” Rahul said. “We realized that we were living in a bubble, but we also thought that there are a lot more people in the same boat. They might jump at being able to do the same thing.”
Rahul recently became medical director at the new Wilmot Webster Cancer Center in Rochester, N.Y., after working in Corning, a tiny New York town just north of the Pennsylvania border. His brother Rohit is chair of hematology and oncology at the University of Pittsburgh’s Hillman Cancer Center in Jamestown, a small town at the western edge of New York.
“When we initially kicked off the Twitter account in August 2021, we didn’t realize the traction it would get,” Rohit said. “Now we realize that there really is a need for this.”
On an ordinary day, the @OncBrothers account may highlight research presented at a oncology conference, retweet posts by other oncologists about new guidelines or FDA drug approvals, and ask followers to consider how they’d handle a difficult case.
The brothers are especially thrilled when posts spawn discussions that draw voices from leading medical institutions who normally don’t interact much with community oncologists. “You’ll have someone from Sloan Kettering or Dana-Farber saying ‘This is what would do,’ ” Rahul said. “You have the brightest minds pitching in, and we get to learn from them.”
The Gosain brothers were both born in India and immigrated as children to Toronto. They each went to medical school in the Caribbean – for Rohit, it was after a stint as a computer engineer – and they each embraced oncology. “For me, it was about having the right mentors while I was doing my clinical rotations as a medical student and as a resident,” Rahul said. In addition, he said, “this field was moving and is still moving so fast. It really intrigued and excited me and made me want to be at the forefront of it.”
The fast-moving nature of oncology, in fact, was one of the drivers behind the daily conversations between the brothers and the subsequent creation of the @OncBrothers account. “Just last year, in 2021, there were 40 new drugs that were indicated for hematology-oncology,” Rahul said. “To stay on top of that is very, very hard.”
It’s especially difficult to figure out treatment plans when multiple options exist. A 2022 thread on @OncBrothers revealed a wide divergence of opinions about triple therapy in prostate cancer: The 322 respondents to a Twitter poll were sharply divided about the best three-drug combination from these options – docetaxel, daratumumab, abiraterone, androgen deprivation therapy, and alpha-reductase inhibitors.
To make things more challenging, community oncologists often are generalists who treat patients with a wide variety of cancers from prostate and lung to breast and colon. As a result, these oncologists must keep up on developments across the entire cancer field. Rohit highlighted a 2022 thread that polled users about the approach they’d take to another patient with non–small cell lung cancer; 474 people responded. The accompanying discussion emphasized the need for the next-generation sequencing (NGS).
“A significant portion of community oncologists are not even doing NGS testing, which is FDA-approved,” Rohit said. “There’s a huge gap that still exists, and we weren’t even aware of it. We continue to learn from these conversations.”
The brothers contend that there’s a crucial need for education among community oncologists in light of evidence suggesting that some cancer outcomes are worse than those in urban areas.
In fact, Rohit led a 2019 study published in the journal Cancer that found that overall survival in rural patients with neuroendocrine tumors trended toward worse outcomes than in urban patients.
“There are many factors such as financial burden, lack of education, and rural patients not willing to travel to the city,” Rohit said. “We need to be more creative and ask, ‘How can we equip our medical oncologist in rural settings to continue to do better?’ ”
What’s next for the OncBrothers? The Gosains have created a website (www.oncbrothers.com) that highlights their social media work, and they’re exploring options such as podcasts and short videos. “Our goal is to focus on how to continue to keep general medical oncologists up to date, informed, and educated so patients can get the best care close to home,” Rahul said. “We need to do better.”
House passes prior authorization bill, Senate path unclear
The path through the U.S. Senate is not yet certain for a bill intended to speed the prior authorization process of insurer-run Medicare Advantage plans, despite the measure having breezed through the House.
House leaders opted to move the Improving Seniors’ Timely Access to Care Act of 2021 (HR 3173) without requiring a roll-call vote. The measure was passed on Sept. 14 by a voice vote, an approach used in general with only uncontroversial measures that have broad support. The bill has 191 Democratic and 135 Republican sponsors, representing about three-quarters of the members of the House.
“There is no reason that patients should be waiting for medically appropriate care, especially when we know that this can lead to worse outcomes,” Rep. Earl Blumenauer (D-Ore.) said in a Sept. 14 speech on the House floor. “The fundamental promise of Medicare Advantage is undermined when people are delaying care, getting sicker, and ultimately costing Medicare more money.”
Rep. Greg Murphy, MD (R-N.C.), spoke on the House floor that day as well, bringing up cases he has seen in his own urology practice in which prior authorization delays disrupted medical care. One patient wound up in the hospital with abscess after an insurer denied an antibiotic prescription, Rep. Murphy said.
But the Senate appears unlikely at this time to move the prior authorization bill as a standalone measure. Instead, the bill may become part of a larger legislative package focused on health care that the Senate Finance Committee intends to prepare later this year.
The House-passed bill would require insurer-run Medicare plans to respond to expedited requests for prior authorization of services within 24 hours and to other requests within 7 days. This bill also would establish an electronic program for prior authorizations and mandate increased transparency as to how insurers use this tool.
CBO: Cost of change would be billions
In seeking to mandate changes in prior authorization, lawmakers likely will need to contend with the issue of a $16 billion cumulative cost estimate for the bill from the Congressional Budget Office. Members of Congress often seek to offset new spending by pairing bills that add to expected costs for the federal government with ones expected to produce savings.
Unlike Rep. Blumenauer, Rep. Murphy, and other backers of the prior authorization streamlining bill, CBO staff estimates that making the mandated changes would raise federal spending, inasmuch as there would be “a greater use of services.”
On Sept. 14, CBO issued a one-page report on the costs of the bill. The CBO report concerns only the bill in question, as is common practice with the office’s estimates.
Prior authorization changes would begin in fiscal 2025 and would add $899 million in spending, or outlays, that year, CBO said. The annual costs from the streamlined prior authorization practices through fiscal 2026 to 2032 range from $1.6 billion to $2.7 billion.
Looking at the CBO estimate against a backdrop of total Medicare Advantage costs, though, may provide important context.
The increases in spending estimated by CBO may suggest that there would be little change in federal spending as a result of streamlining prior authorization practices. These estimates of increased annual spending of $1.6 billion–$2.7 billion are only a small fraction of the current annual cost of insurer-run Medicare, and they represent an even smaller share of the projected expense.
The federal government last year spent about $350 billion on insurer-run plans, excluding Part D drug plan payments, according to the Medicare Advisory Payment Commission (MedPAC).
As of 2021, about 27 million people were enrolled in these plans, accounting for about 46% of the total Medicare population. Enrollment has doubled since 2010, MedPAC said, and it is expected to continue to grow. By 2027, insurer-run Medicare could cover 50% of the program’s population, a figure that may reach 53% by 2031.
Federal payments to these plans will accelerate in the years ahead as insurers attract more people eligible for Medicare as customers. Payments to these private health plans could rise from an expected $418 billion this year to $940.6 billion by 2031, according to the most recent Medicare trustees report.
Good intentions, poor implementation?
Insurer-run Medicare has long enjoyed deep bipartisan support in Congress. That’s due in part to its potential for reducing spending on what are considered low-value treatments, or ones considered unlikely to provide a significant medical benefit, but Rep. Blumenauer is among the members of Congress who see insurer-run Medicare as a path for preserving the giant federal health program. Traditional Medicare has far fewer restrictions on services, which sometimes opens a path for tests and treatments that offer less value for patients.
“I believe that the way traditional fee-for-service Medicare operates is not sustainable and that Medicare Advantage is one of the tools we can use to demonstrate how we can incentivize value,” Rep. Blumenauer said on the House floor. “But this is only possible when the program operates as intended. I have been deeply concerned about the reports of delays in care” caused by the clunky prior authorization processes.
He highlighted a recent report from the internal watchdog group for the Department of Health & Human Services that raises concerns about denials of appropriate care. About 18% of a set of payment denials examined by the Office of Inspector General of HHS in April actually met Medicare coverage rules and plan billing rules.
“For patients and their families, being told that you need to wait longer for care that your doctor tells you that you need is incredibly frustrating and frightening,” Rep. Blumenauer said. “There’s no comfort to be found in the fact that your insurance company needs time to decide if your doctor is right.”
Trends in prior authorization
The CBO report does not provide detail on what kind of medical spending would increase under a streamlined prior authorization process in insurer-run Medicare plans.
From trends reported in prior authorization, though, two factors could be at play in what appear to be relatively small estimated increases in Medicare spending from streamlined prior authorization.
One is the work already underway to create less burdensome electronic systems for these requests, such as the Fast Prior Authorization Technology Highway initiative run by the trade association America’s Health Insurance Plans.
The other factor could be the number of cases in which prior authorization merely causes delays in treatments and tests and thus simply postpones spending while adding to clinicians’ administrative work.
An analysis of prior authorization requests for dermatologic practices affiliated with the University of Utah may represent an extreme example. In a report published in JAMA Dermatology in 2020, researchers described what happened with requests made during 1 month, September 2016.
The approval rate for procedures was 99.6% – 100% (95 of 95) for Mohs surgery, and 96% (130 of 131, with 4 additional cases pending) for excisions. These findings supported calls for simplifying prior authorization procedures, “perhaps first by eliminating unnecessary PAs [prior authorizations] and appeals,” Aaron M. Secrest, MD, PhD, of the University of Utah, Salt Lake City, and coauthors wrote in the article.
Still, there is some evidence that insurer-run Medicare policies reduce the use of low-value care.
In a study published in JAMA Health Forum, Emily Boudreau, PhD, of insurer Humana Inc, and coauthors from Tufts University, Boston, and the University of Pennsylvania, Philadelphia investigated whether insurer-run Medicare could do a better job in reducing the amount of low-value care delivered than the traditional program. They analyzed a set of claims data from 2017 to 2019 for people enrolled in insurer-run and traditional Medicare.
They reported a rate of 23.07 low-value services provided per 100 people in insurer-run Medicare, compared with 25.39 for those in traditional Medicare. Some of the biggest differences reported in the article were in cancer screenings for older people.
As an example, the U.S. Preventive Services Task Force recommends that women older than 65 years not be screened for cervical cancer if they have undergone adequate screening in the past and are not at high risk for cervical cancer. There was an annual count of 1.76 screenings for cervical cancer per 100 women older than 65 in the insurer-run Medicare group versus 3.18 for those in traditional Medicare.
The Better Medicare Alliance issued a statement in favor of the House passage of the Improving Seniors’ Timely Access to Care Act.
In it, the group said the measure would “modernize prior authorization while protecting its essential function in facilitating safe, high-value, evidence-based care.” The alliance promotes use of insurer-run Medicare. The board of the Better Medicare Alliance includes executives who serve with firms that run Advantage plans as well as medical organizations and universities.
“With studies showing that up to one-quarter of all health care expenditures are wasted on services with no benefit to the patient, we need a robust, next-generation prior authorization program to deter low-value, and even harmful, care while protecting access to needed treatment and effective therapies,” said A. Mark Fendrick, MD, director of the University of Michigan’s Center for Value-Based Insurance Design in Ann Arbor, in a statement issued by the Better Medicare Alliance. He is a member of the group’s council of scholars.
On the House floor on September 14, Rep. Ami Bera, MD (D-Calif.), said he has heard from former colleagues and his medical school classmates that they now spend as much as 40% of their time on administrative work. These distractions from patient care are helping drive physicians away from the practice of medicine.
Still, the internist defended the basic premise of prior authorization while strongly appealing for better systems of handling it.
“Yes, there is a role for prior authorization in limited cases. There is also a role to go back and retrospectively look at how care is being delivered,” Rep. Bera said. “But what is happening today is a travesty. It wasn’t the intention of prior authorization. It is a prior authorization process gone awry.”
A version of this article first appeared on Medscape.com.
The path through the U.S. Senate is not yet certain for a bill intended to speed the prior authorization process of insurer-run Medicare Advantage plans, despite the measure having breezed through the House.
House leaders opted to move the Improving Seniors’ Timely Access to Care Act of 2021 (HR 3173) without requiring a roll-call vote. The measure was passed on Sept. 14 by a voice vote, an approach used in general with only uncontroversial measures that have broad support. The bill has 191 Democratic and 135 Republican sponsors, representing about three-quarters of the members of the House.
“There is no reason that patients should be waiting for medically appropriate care, especially when we know that this can lead to worse outcomes,” Rep. Earl Blumenauer (D-Ore.) said in a Sept. 14 speech on the House floor. “The fundamental promise of Medicare Advantage is undermined when people are delaying care, getting sicker, and ultimately costing Medicare more money.”
Rep. Greg Murphy, MD (R-N.C.), spoke on the House floor that day as well, bringing up cases he has seen in his own urology practice in which prior authorization delays disrupted medical care. One patient wound up in the hospital with abscess after an insurer denied an antibiotic prescription, Rep. Murphy said.
But the Senate appears unlikely at this time to move the prior authorization bill as a standalone measure. Instead, the bill may become part of a larger legislative package focused on health care that the Senate Finance Committee intends to prepare later this year.
The House-passed bill would require insurer-run Medicare plans to respond to expedited requests for prior authorization of services within 24 hours and to other requests within 7 days. This bill also would establish an electronic program for prior authorizations and mandate increased transparency as to how insurers use this tool.
CBO: Cost of change would be billions
In seeking to mandate changes in prior authorization, lawmakers likely will need to contend with the issue of a $16 billion cumulative cost estimate for the bill from the Congressional Budget Office. Members of Congress often seek to offset new spending by pairing bills that add to expected costs for the federal government with ones expected to produce savings.
Unlike Rep. Blumenauer, Rep. Murphy, and other backers of the prior authorization streamlining bill, CBO staff estimates that making the mandated changes would raise federal spending, inasmuch as there would be “a greater use of services.”
On Sept. 14, CBO issued a one-page report on the costs of the bill. The CBO report concerns only the bill in question, as is common practice with the office’s estimates.
Prior authorization changes would begin in fiscal 2025 and would add $899 million in spending, or outlays, that year, CBO said. The annual costs from the streamlined prior authorization practices through fiscal 2026 to 2032 range from $1.6 billion to $2.7 billion.
Looking at the CBO estimate against a backdrop of total Medicare Advantage costs, though, may provide important context.
The increases in spending estimated by CBO may suggest that there would be little change in federal spending as a result of streamlining prior authorization practices. These estimates of increased annual spending of $1.6 billion–$2.7 billion are only a small fraction of the current annual cost of insurer-run Medicare, and they represent an even smaller share of the projected expense.
The federal government last year spent about $350 billion on insurer-run plans, excluding Part D drug plan payments, according to the Medicare Advisory Payment Commission (MedPAC).
As of 2021, about 27 million people were enrolled in these plans, accounting for about 46% of the total Medicare population. Enrollment has doubled since 2010, MedPAC said, and it is expected to continue to grow. By 2027, insurer-run Medicare could cover 50% of the program’s population, a figure that may reach 53% by 2031.
Federal payments to these plans will accelerate in the years ahead as insurers attract more people eligible for Medicare as customers. Payments to these private health plans could rise from an expected $418 billion this year to $940.6 billion by 2031, according to the most recent Medicare trustees report.
Good intentions, poor implementation?
Insurer-run Medicare has long enjoyed deep bipartisan support in Congress. That’s due in part to its potential for reducing spending on what are considered low-value treatments, or ones considered unlikely to provide a significant medical benefit, but Rep. Blumenauer is among the members of Congress who see insurer-run Medicare as a path for preserving the giant federal health program. Traditional Medicare has far fewer restrictions on services, which sometimes opens a path for tests and treatments that offer less value for patients.
“I believe that the way traditional fee-for-service Medicare operates is not sustainable and that Medicare Advantage is one of the tools we can use to demonstrate how we can incentivize value,” Rep. Blumenauer said on the House floor. “But this is only possible when the program operates as intended. I have been deeply concerned about the reports of delays in care” caused by the clunky prior authorization processes.
He highlighted a recent report from the internal watchdog group for the Department of Health & Human Services that raises concerns about denials of appropriate care. About 18% of a set of payment denials examined by the Office of Inspector General of HHS in April actually met Medicare coverage rules and plan billing rules.
“For patients and their families, being told that you need to wait longer for care that your doctor tells you that you need is incredibly frustrating and frightening,” Rep. Blumenauer said. “There’s no comfort to be found in the fact that your insurance company needs time to decide if your doctor is right.”
Trends in prior authorization
The CBO report does not provide detail on what kind of medical spending would increase under a streamlined prior authorization process in insurer-run Medicare plans.
From trends reported in prior authorization, though, two factors could be at play in what appear to be relatively small estimated increases in Medicare spending from streamlined prior authorization.
One is the work already underway to create less burdensome electronic systems for these requests, such as the Fast Prior Authorization Technology Highway initiative run by the trade association America’s Health Insurance Plans.
The other factor could be the number of cases in which prior authorization merely causes delays in treatments and tests and thus simply postpones spending while adding to clinicians’ administrative work.
An analysis of prior authorization requests for dermatologic practices affiliated with the University of Utah may represent an extreme example. In a report published in JAMA Dermatology in 2020, researchers described what happened with requests made during 1 month, September 2016.
The approval rate for procedures was 99.6% – 100% (95 of 95) for Mohs surgery, and 96% (130 of 131, with 4 additional cases pending) for excisions. These findings supported calls for simplifying prior authorization procedures, “perhaps first by eliminating unnecessary PAs [prior authorizations] and appeals,” Aaron M. Secrest, MD, PhD, of the University of Utah, Salt Lake City, and coauthors wrote in the article.
Still, there is some evidence that insurer-run Medicare policies reduce the use of low-value care.
In a study published in JAMA Health Forum, Emily Boudreau, PhD, of insurer Humana Inc, and coauthors from Tufts University, Boston, and the University of Pennsylvania, Philadelphia investigated whether insurer-run Medicare could do a better job in reducing the amount of low-value care delivered than the traditional program. They analyzed a set of claims data from 2017 to 2019 for people enrolled in insurer-run and traditional Medicare.
They reported a rate of 23.07 low-value services provided per 100 people in insurer-run Medicare, compared with 25.39 for those in traditional Medicare. Some of the biggest differences reported in the article were in cancer screenings for older people.
As an example, the U.S. Preventive Services Task Force recommends that women older than 65 years not be screened for cervical cancer if they have undergone adequate screening in the past and are not at high risk for cervical cancer. There was an annual count of 1.76 screenings for cervical cancer per 100 women older than 65 in the insurer-run Medicare group versus 3.18 for those in traditional Medicare.
The Better Medicare Alliance issued a statement in favor of the House passage of the Improving Seniors’ Timely Access to Care Act.
In it, the group said the measure would “modernize prior authorization while protecting its essential function in facilitating safe, high-value, evidence-based care.” The alliance promotes use of insurer-run Medicare. The board of the Better Medicare Alliance includes executives who serve with firms that run Advantage plans as well as medical organizations and universities.
“With studies showing that up to one-quarter of all health care expenditures are wasted on services with no benefit to the patient, we need a robust, next-generation prior authorization program to deter low-value, and even harmful, care while protecting access to needed treatment and effective therapies,” said A. Mark Fendrick, MD, director of the University of Michigan’s Center for Value-Based Insurance Design in Ann Arbor, in a statement issued by the Better Medicare Alliance. He is a member of the group’s council of scholars.
On the House floor on September 14, Rep. Ami Bera, MD (D-Calif.), said he has heard from former colleagues and his medical school classmates that they now spend as much as 40% of their time on administrative work. These distractions from patient care are helping drive physicians away from the practice of medicine.
Still, the internist defended the basic premise of prior authorization while strongly appealing for better systems of handling it.
“Yes, there is a role for prior authorization in limited cases. There is also a role to go back and retrospectively look at how care is being delivered,” Rep. Bera said. “But what is happening today is a travesty. It wasn’t the intention of prior authorization. It is a prior authorization process gone awry.”
A version of this article first appeared on Medscape.com.
The path through the U.S. Senate is not yet certain for a bill intended to speed the prior authorization process of insurer-run Medicare Advantage plans, despite the measure having breezed through the House.
House leaders opted to move the Improving Seniors’ Timely Access to Care Act of 2021 (HR 3173) without requiring a roll-call vote. The measure was passed on Sept. 14 by a voice vote, an approach used in general with only uncontroversial measures that have broad support. The bill has 191 Democratic and 135 Republican sponsors, representing about three-quarters of the members of the House.
“There is no reason that patients should be waiting for medically appropriate care, especially when we know that this can lead to worse outcomes,” Rep. Earl Blumenauer (D-Ore.) said in a Sept. 14 speech on the House floor. “The fundamental promise of Medicare Advantage is undermined when people are delaying care, getting sicker, and ultimately costing Medicare more money.”
Rep. Greg Murphy, MD (R-N.C.), spoke on the House floor that day as well, bringing up cases he has seen in his own urology practice in which prior authorization delays disrupted medical care. One patient wound up in the hospital with abscess after an insurer denied an antibiotic prescription, Rep. Murphy said.
But the Senate appears unlikely at this time to move the prior authorization bill as a standalone measure. Instead, the bill may become part of a larger legislative package focused on health care that the Senate Finance Committee intends to prepare later this year.
The House-passed bill would require insurer-run Medicare plans to respond to expedited requests for prior authorization of services within 24 hours and to other requests within 7 days. This bill also would establish an electronic program for prior authorizations and mandate increased transparency as to how insurers use this tool.
CBO: Cost of change would be billions
In seeking to mandate changes in prior authorization, lawmakers likely will need to contend with the issue of a $16 billion cumulative cost estimate for the bill from the Congressional Budget Office. Members of Congress often seek to offset new spending by pairing bills that add to expected costs for the federal government with ones expected to produce savings.
Unlike Rep. Blumenauer, Rep. Murphy, and other backers of the prior authorization streamlining bill, CBO staff estimates that making the mandated changes would raise federal spending, inasmuch as there would be “a greater use of services.”
On Sept. 14, CBO issued a one-page report on the costs of the bill. The CBO report concerns only the bill in question, as is common practice with the office’s estimates.
Prior authorization changes would begin in fiscal 2025 and would add $899 million in spending, or outlays, that year, CBO said. The annual costs from the streamlined prior authorization practices through fiscal 2026 to 2032 range from $1.6 billion to $2.7 billion.
Looking at the CBO estimate against a backdrop of total Medicare Advantage costs, though, may provide important context.
The increases in spending estimated by CBO may suggest that there would be little change in federal spending as a result of streamlining prior authorization practices. These estimates of increased annual spending of $1.6 billion–$2.7 billion are only a small fraction of the current annual cost of insurer-run Medicare, and they represent an even smaller share of the projected expense.
The federal government last year spent about $350 billion on insurer-run plans, excluding Part D drug plan payments, according to the Medicare Advisory Payment Commission (MedPAC).
As of 2021, about 27 million people were enrolled in these plans, accounting for about 46% of the total Medicare population. Enrollment has doubled since 2010, MedPAC said, and it is expected to continue to grow. By 2027, insurer-run Medicare could cover 50% of the program’s population, a figure that may reach 53% by 2031.
Federal payments to these plans will accelerate in the years ahead as insurers attract more people eligible for Medicare as customers. Payments to these private health plans could rise from an expected $418 billion this year to $940.6 billion by 2031, according to the most recent Medicare trustees report.
Good intentions, poor implementation?
Insurer-run Medicare has long enjoyed deep bipartisan support in Congress. That’s due in part to its potential for reducing spending on what are considered low-value treatments, or ones considered unlikely to provide a significant medical benefit, but Rep. Blumenauer is among the members of Congress who see insurer-run Medicare as a path for preserving the giant federal health program. Traditional Medicare has far fewer restrictions on services, which sometimes opens a path for tests and treatments that offer less value for patients.
“I believe that the way traditional fee-for-service Medicare operates is not sustainable and that Medicare Advantage is one of the tools we can use to demonstrate how we can incentivize value,” Rep. Blumenauer said on the House floor. “But this is only possible when the program operates as intended. I have been deeply concerned about the reports of delays in care” caused by the clunky prior authorization processes.
He highlighted a recent report from the internal watchdog group for the Department of Health & Human Services that raises concerns about denials of appropriate care. About 18% of a set of payment denials examined by the Office of Inspector General of HHS in April actually met Medicare coverage rules and plan billing rules.
“For patients and their families, being told that you need to wait longer for care that your doctor tells you that you need is incredibly frustrating and frightening,” Rep. Blumenauer said. “There’s no comfort to be found in the fact that your insurance company needs time to decide if your doctor is right.”
Trends in prior authorization
The CBO report does not provide detail on what kind of medical spending would increase under a streamlined prior authorization process in insurer-run Medicare plans.
From trends reported in prior authorization, though, two factors could be at play in what appear to be relatively small estimated increases in Medicare spending from streamlined prior authorization.
One is the work already underway to create less burdensome electronic systems for these requests, such as the Fast Prior Authorization Technology Highway initiative run by the trade association America’s Health Insurance Plans.
The other factor could be the number of cases in which prior authorization merely causes delays in treatments and tests and thus simply postpones spending while adding to clinicians’ administrative work.
An analysis of prior authorization requests for dermatologic practices affiliated with the University of Utah may represent an extreme example. In a report published in JAMA Dermatology in 2020, researchers described what happened with requests made during 1 month, September 2016.
The approval rate for procedures was 99.6% – 100% (95 of 95) for Mohs surgery, and 96% (130 of 131, with 4 additional cases pending) for excisions. These findings supported calls for simplifying prior authorization procedures, “perhaps first by eliminating unnecessary PAs [prior authorizations] and appeals,” Aaron M. Secrest, MD, PhD, of the University of Utah, Salt Lake City, and coauthors wrote in the article.
Still, there is some evidence that insurer-run Medicare policies reduce the use of low-value care.
In a study published in JAMA Health Forum, Emily Boudreau, PhD, of insurer Humana Inc, and coauthors from Tufts University, Boston, and the University of Pennsylvania, Philadelphia investigated whether insurer-run Medicare could do a better job in reducing the amount of low-value care delivered than the traditional program. They analyzed a set of claims data from 2017 to 2019 for people enrolled in insurer-run and traditional Medicare.
They reported a rate of 23.07 low-value services provided per 100 people in insurer-run Medicare, compared with 25.39 for those in traditional Medicare. Some of the biggest differences reported in the article were in cancer screenings for older people.
As an example, the U.S. Preventive Services Task Force recommends that women older than 65 years not be screened for cervical cancer if they have undergone adequate screening in the past and are not at high risk for cervical cancer. There was an annual count of 1.76 screenings for cervical cancer per 100 women older than 65 in the insurer-run Medicare group versus 3.18 for those in traditional Medicare.
The Better Medicare Alliance issued a statement in favor of the House passage of the Improving Seniors’ Timely Access to Care Act.
In it, the group said the measure would “modernize prior authorization while protecting its essential function in facilitating safe, high-value, evidence-based care.” The alliance promotes use of insurer-run Medicare. The board of the Better Medicare Alliance includes executives who serve with firms that run Advantage plans as well as medical organizations and universities.
“With studies showing that up to one-quarter of all health care expenditures are wasted on services with no benefit to the patient, we need a robust, next-generation prior authorization program to deter low-value, and even harmful, care while protecting access to needed treatment and effective therapies,” said A. Mark Fendrick, MD, director of the University of Michigan’s Center for Value-Based Insurance Design in Ann Arbor, in a statement issued by the Better Medicare Alliance. He is a member of the group’s council of scholars.
On the House floor on September 14, Rep. Ami Bera, MD (D-Calif.), said he has heard from former colleagues and his medical school classmates that they now spend as much as 40% of their time on administrative work. These distractions from patient care are helping drive physicians away from the practice of medicine.
Still, the internist defended the basic premise of prior authorization while strongly appealing for better systems of handling it.
“Yes, there is a role for prior authorization in limited cases. There is also a role to go back and retrospectively look at how care is being delivered,” Rep. Bera said. “But what is happening today is a travesty. It wasn’t the intention of prior authorization. It is a prior authorization process gone awry.”
A version of this article first appeared on Medscape.com.
Royal family affliction or not, porphyria is treatable
European royal families may be enormously rich, but being a blueblood doesn’t always mean your blood is pristine. Queen Victoria’s DNA is famously believed to have silently bequeathed hemophilia to many of her descendants, including a great-grandson whose severe illness played a tragic role in spurring the Russian Revolution.
And that’s not all.
There’s plenty of skepticism about this theory, which seeks to explain the “madness” of King George III. But one thing is clear. If porphyria does indeed haunt the imperial bloodline that stretches to a new generation – the late Queen Elizabeth II’s great-grandchildren – any royal who’s afflicted going forward is likely to benefit mightily from modern treatment. While this disease may require lifelong vigilance, experts said in interviews that porphyria can often be controlled.
“If patients know they have the diagnosis, and they do the right things and avoid alcohol and risky drugs, most people will have few acute attacks,” said gastroenterologist Herbert Lloyd Bonkovsky, MD, of Wake Forest University, Winston-Salem, N.C., a leading porphyria specialist.
Heme infusions can also be helpful, he added, and the revolutionary new drug givosiran is available for those who suffer recurrent attacks. And “if all else fails, a successful liver transplant is curative” – as long as the transplanted liver doesn’t have porphyria, as happened in at least one case.
But, Dr. Bonkovsky cautioned, the diagnosis is often missed, in some cases for 15 years or more.
Diagnosing porphyria: Awareness and tests are crucial
Porphyria is caused when porphyins – essential components of hemoglobin – build up in the body, disrupting systems such as the nerves, skin, and gut. The urine can turn purplish, hence the condition’s name. (Porphyrus is the Greek word for purple.)
According to hematologist Danielle Nance, MD, of Banner MD Anderson Cancer Center in Gilbert, Ariz., acute intermittent porphyria “should be suspected in persons who have recurrent severe attacks of abdominal pain requiring strong pain medication to control symptoms, and there is no obvious physical cause.”
In such cases, practitioners should send out blood and urine for porphobilinogen (PBG) and delta-aminolevulinic acid (dALA or Delta-ALA) testing, Dr. Nance said. “These are almost always elevated, even between attacks, in persons with diagnoses of acute intermittent porphyria. Other types of porphyria, such as erythropoietic porphyria, may require additional testing. Genetic testing should be offered when a patient is suspected of having porphyria, as this can speed the diagnosis.”
The typical patient is a woman from age 18 to 55, often a young woman with recurrent abdominal pain that may occur during the second half of the menstrual cycle, Wake Forest’s Dr. Bonkovsky said. Constipation is common.
“She keeps coming to the clinic or emergency department, and no one knows what’s going on. Eventually, she tends to undergo an appendectomy, often a cholecystectomy, or sometimes gynecologic procedures without cure of the disease. Only after this long and arduous road of misdiagnosis does someone think it’s porphyria and do the correct tests.”
Dr. Bonkovsky led a 2014 study of 108 subjects (81% female) with acute porphyrias and found that the average time to a correct diagnosis was a whopping 15 years. Pain in the abdomen was the most common symptom (74%), followed by nausea/vomiting (73%), weakness (63%), and constipation (60%).
While underdiagnosis is common, porphyrias can also be overdiagnosed. According to Dr. Bonkovsky, a mild increase in urinary porphyrins is often misdiagnosed as porphyria when it may be a sign of liver disease or alcohol use, instead.
Hematologist Kleber Y. Fertrin, MD, PhD, of the University of Washington, Seattle, emphasized the importance of ordering the correct tests. “Urinary porphyrins are often inappropriately ordered because of their name. They are not diagnostic for acute hepatic porphyrias and may be nonspecifically elevated. It is paramount to get the labs from a reliable lab test experienced at performing diagnostic testing for porphyrias and make sure the urine sample needed is correctly obtained and preserved.”
New drug can control attacks, but it’s costly
Treatment should begin right away if porphyria is suspected, without waiting for confirmation, Dr. Nance said. “There are porphyria experts in the U.S. and in many other countries who can help practitioners interpret symptoms and testing results if there is uncertainty or if treatment options are unclear.”
Patients are counseled to avoid attack triggers and eat healthy diets, she said. “Persons with porphyria are encouraged to have a plan for home management of an attack and when to come to the hospital for symptoms that don’t respond to home therapy,” she said.
Dr. Fertrin said “the typical treatment for an acute porphyric attack is the use of intravenous glucose, as well as intravenous hemin infusions, along with pain medications and fluids as needed. Some patients may need medication for high blood pressure. For patients with recurrent attacks, prophylactic doses of hemin can be used.”
Another option is givosiran (Givlaari), the biggest recent advance in porphyria treatment. It was approved by the Food and Drug Administration for acute hepatic porphyria in 2019. “It’s an inhibitory mRNA that shuts down heme synthesis by downregulating aminolevulinic acid synthase,” said hematologist Thomas DeLoughery, MD, of Oregon Health & Science University, Portland.
A 2020 study coauthored by Dr. Bonkovsky found that the drug reduced the mean annualized attack rate in acute intermittent porphyria by 74%, compared with placebo (P < .001). “Givosiran led to lower levels of urinary ALA and porphobilinogen, fewer days of hemin use, and better daily scores for pain than placebo,” the study authors write. “Key adverse events that were observed more frequently in the givosiran group were elevations in serum aminotransferase levels, changes in serum creatinine levels and the estimated glomerular filtration rate, and injection-site reactions.”
Dr. Bonkovsky said the drug is appropriate in patients whose disease is not controlled by lifestyle interventions regarding alcohol, smoking, and substance use. However, while givosiran is helpful, “it’s not a cure,” he said. “Probably about 40% of patients have found the side effects such as nausea, fatigue, headaches, and liver injury to be too adverse and have not decided to take it in the long term.”
In addition, the drug costs about $500,000 a year, and insurers may balk at the expense. Still, specialists say it can be a good option. “Before givosiran, the standard therapy was hematin, which decreased the activity of the ALA synthase,” Dr. DeLoughery said. “This is a nasty drug that can inflame the blood vessels and is not all that effective.”
The royal family may be able to breathe easy
There are other forms of porphyria besides the acute type. Cutaneous porphryias can cause blistering from sunlight exposure, and treatment is avoidance of such triggers, Dr. Fertin said. “For a rare form called erythropoietic protoporphyria, there is a subcutaneous implant with a medication called afamelanotide that increases tolerance to sunlight.”
There’s another type: variegate porphyria, which UpToDate says is “characterized by cutaneous blistering and/or acute neurovisceral attacks.” In 1966, a mother-and-son psychiatrist team theorized that Britain’s King George III suffered from this type of porphyria.
However, researchers have sharply criticized the porphyria theory with regard to that king, and a recent theory now suggests that he actually had bipolar disorder. Dr. Fertin is among the skeptics, noting the high prevalence of porphyria in affected families.
“Since King George III would now have a living number of relatives of about 900 people, we would expect around 180 cases of variegate porphyria to be connected to him, and those are nowhere to be found,” he said. “The idea that it could cause progressive psychosis and dementia is also a misconception. We do not find that porphyria is the underlying cause of psychiatric conditions on their own. Many atypical symptoms of the king were attributed to variegate porphyria, and the few more typical symptoms he reportedly had, of abdominal pain and urine discoloration, can be more easily explained by common diseases, such as kidney stones or gallstones. Finally, attempts at obtaining genetic or biochemical evidence of porphyria from relatives of King George III have been negative or inconclusive.”
That’s good news for the royals, who have many other concerns these days.
Dr. Nance discloses research study funding from Alnylam (maker of Givlaari) and payments to participate in educational activities for patients and practitioners. Dr. Bonkovsky discloses relationships with drugmakers who have developed products to treat porphyria including Alnylam, Mitsubishi Tanabe, Recordati, and Disc. Dr. Fertin is subinvestigator in a clinical trial for a novel treatment for erythropoietic protoporphyria sponsored by Mitsubishi Tanabe. Dr. DeLoughery reports no disclosures.
European royal families may be enormously rich, but being a blueblood doesn’t always mean your blood is pristine. Queen Victoria’s DNA is famously believed to have silently bequeathed hemophilia to many of her descendants, including a great-grandson whose severe illness played a tragic role in spurring the Russian Revolution.
And that’s not all.
There’s plenty of skepticism about this theory, which seeks to explain the “madness” of King George III. But one thing is clear. If porphyria does indeed haunt the imperial bloodline that stretches to a new generation – the late Queen Elizabeth II’s great-grandchildren – any royal who’s afflicted going forward is likely to benefit mightily from modern treatment. While this disease may require lifelong vigilance, experts said in interviews that porphyria can often be controlled.
“If patients know they have the diagnosis, and they do the right things and avoid alcohol and risky drugs, most people will have few acute attacks,” said gastroenterologist Herbert Lloyd Bonkovsky, MD, of Wake Forest University, Winston-Salem, N.C., a leading porphyria specialist.
Heme infusions can also be helpful, he added, and the revolutionary new drug givosiran is available for those who suffer recurrent attacks. And “if all else fails, a successful liver transplant is curative” – as long as the transplanted liver doesn’t have porphyria, as happened in at least one case.
But, Dr. Bonkovsky cautioned, the diagnosis is often missed, in some cases for 15 years or more.
Diagnosing porphyria: Awareness and tests are crucial
Porphyria is caused when porphyins – essential components of hemoglobin – build up in the body, disrupting systems such as the nerves, skin, and gut. The urine can turn purplish, hence the condition’s name. (Porphyrus is the Greek word for purple.)
According to hematologist Danielle Nance, MD, of Banner MD Anderson Cancer Center in Gilbert, Ariz., acute intermittent porphyria “should be suspected in persons who have recurrent severe attacks of abdominal pain requiring strong pain medication to control symptoms, and there is no obvious physical cause.”
In such cases, practitioners should send out blood and urine for porphobilinogen (PBG) and delta-aminolevulinic acid (dALA or Delta-ALA) testing, Dr. Nance said. “These are almost always elevated, even between attacks, in persons with diagnoses of acute intermittent porphyria. Other types of porphyria, such as erythropoietic porphyria, may require additional testing. Genetic testing should be offered when a patient is suspected of having porphyria, as this can speed the diagnosis.”
The typical patient is a woman from age 18 to 55, often a young woman with recurrent abdominal pain that may occur during the second half of the menstrual cycle, Wake Forest’s Dr. Bonkovsky said. Constipation is common.
“She keeps coming to the clinic or emergency department, and no one knows what’s going on. Eventually, she tends to undergo an appendectomy, often a cholecystectomy, or sometimes gynecologic procedures without cure of the disease. Only after this long and arduous road of misdiagnosis does someone think it’s porphyria and do the correct tests.”
Dr. Bonkovsky led a 2014 study of 108 subjects (81% female) with acute porphyrias and found that the average time to a correct diagnosis was a whopping 15 years. Pain in the abdomen was the most common symptom (74%), followed by nausea/vomiting (73%), weakness (63%), and constipation (60%).
While underdiagnosis is common, porphyrias can also be overdiagnosed. According to Dr. Bonkovsky, a mild increase in urinary porphyrins is often misdiagnosed as porphyria when it may be a sign of liver disease or alcohol use, instead.
Hematologist Kleber Y. Fertrin, MD, PhD, of the University of Washington, Seattle, emphasized the importance of ordering the correct tests. “Urinary porphyrins are often inappropriately ordered because of their name. They are not diagnostic for acute hepatic porphyrias and may be nonspecifically elevated. It is paramount to get the labs from a reliable lab test experienced at performing diagnostic testing for porphyrias and make sure the urine sample needed is correctly obtained and preserved.”
New drug can control attacks, but it’s costly
Treatment should begin right away if porphyria is suspected, without waiting for confirmation, Dr. Nance said. “There are porphyria experts in the U.S. and in many other countries who can help practitioners interpret symptoms and testing results if there is uncertainty or if treatment options are unclear.”
Patients are counseled to avoid attack triggers and eat healthy diets, she said. “Persons with porphyria are encouraged to have a plan for home management of an attack and when to come to the hospital for symptoms that don’t respond to home therapy,” she said.
Dr. Fertrin said “the typical treatment for an acute porphyric attack is the use of intravenous glucose, as well as intravenous hemin infusions, along with pain medications and fluids as needed. Some patients may need medication for high blood pressure. For patients with recurrent attacks, prophylactic doses of hemin can be used.”
Another option is givosiran (Givlaari), the biggest recent advance in porphyria treatment. It was approved by the Food and Drug Administration for acute hepatic porphyria in 2019. “It’s an inhibitory mRNA that shuts down heme synthesis by downregulating aminolevulinic acid synthase,” said hematologist Thomas DeLoughery, MD, of Oregon Health & Science University, Portland.
A 2020 study coauthored by Dr. Bonkovsky found that the drug reduced the mean annualized attack rate in acute intermittent porphyria by 74%, compared with placebo (P < .001). “Givosiran led to lower levels of urinary ALA and porphobilinogen, fewer days of hemin use, and better daily scores for pain than placebo,” the study authors write. “Key adverse events that were observed more frequently in the givosiran group were elevations in serum aminotransferase levels, changes in serum creatinine levels and the estimated glomerular filtration rate, and injection-site reactions.”
Dr. Bonkovsky said the drug is appropriate in patients whose disease is not controlled by lifestyle interventions regarding alcohol, smoking, and substance use. However, while givosiran is helpful, “it’s not a cure,” he said. “Probably about 40% of patients have found the side effects such as nausea, fatigue, headaches, and liver injury to be too adverse and have not decided to take it in the long term.”
In addition, the drug costs about $500,000 a year, and insurers may balk at the expense. Still, specialists say it can be a good option. “Before givosiran, the standard therapy was hematin, which decreased the activity of the ALA synthase,” Dr. DeLoughery said. “This is a nasty drug that can inflame the blood vessels and is not all that effective.”
The royal family may be able to breathe easy
There are other forms of porphyria besides the acute type. Cutaneous porphryias can cause blistering from sunlight exposure, and treatment is avoidance of such triggers, Dr. Fertin said. “For a rare form called erythropoietic protoporphyria, there is a subcutaneous implant with a medication called afamelanotide that increases tolerance to sunlight.”
There’s another type: variegate porphyria, which UpToDate says is “characterized by cutaneous blistering and/or acute neurovisceral attacks.” In 1966, a mother-and-son psychiatrist team theorized that Britain’s King George III suffered from this type of porphyria.
However, researchers have sharply criticized the porphyria theory with regard to that king, and a recent theory now suggests that he actually had bipolar disorder. Dr. Fertin is among the skeptics, noting the high prevalence of porphyria in affected families.
“Since King George III would now have a living number of relatives of about 900 people, we would expect around 180 cases of variegate porphyria to be connected to him, and those are nowhere to be found,” he said. “The idea that it could cause progressive psychosis and dementia is also a misconception. We do not find that porphyria is the underlying cause of psychiatric conditions on their own. Many atypical symptoms of the king were attributed to variegate porphyria, and the few more typical symptoms he reportedly had, of abdominal pain and urine discoloration, can be more easily explained by common diseases, such as kidney stones or gallstones. Finally, attempts at obtaining genetic or biochemical evidence of porphyria from relatives of King George III have been negative or inconclusive.”
That’s good news for the royals, who have many other concerns these days.
Dr. Nance discloses research study funding from Alnylam (maker of Givlaari) and payments to participate in educational activities for patients and practitioners. Dr. Bonkovsky discloses relationships with drugmakers who have developed products to treat porphyria including Alnylam, Mitsubishi Tanabe, Recordati, and Disc. Dr. Fertin is subinvestigator in a clinical trial for a novel treatment for erythropoietic protoporphyria sponsored by Mitsubishi Tanabe. Dr. DeLoughery reports no disclosures.
European royal families may be enormously rich, but being a blueblood doesn’t always mean your blood is pristine. Queen Victoria’s DNA is famously believed to have silently bequeathed hemophilia to many of her descendants, including a great-grandson whose severe illness played a tragic role in spurring the Russian Revolution.
And that’s not all.
There’s plenty of skepticism about this theory, which seeks to explain the “madness” of King George III. But one thing is clear. If porphyria does indeed haunt the imperial bloodline that stretches to a new generation – the late Queen Elizabeth II’s great-grandchildren – any royal who’s afflicted going forward is likely to benefit mightily from modern treatment. While this disease may require lifelong vigilance, experts said in interviews that porphyria can often be controlled.
“If patients know they have the diagnosis, and they do the right things and avoid alcohol and risky drugs, most people will have few acute attacks,” said gastroenterologist Herbert Lloyd Bonkovsky, MD, of Wake Forest University, Winston-Salem, N.C., a leading porphyria specialist.
Heme infusions can also be helpful, he added, and the revolutionary new drug givosiran is available for those who suffer recurrent attacks. And “if all else fails, a successful liver transplant is curative” – as long as the transplanted liver doesn’t have porphyria, as happened in at least one case.
But, Dr. Bonkovsky cautioned, the diagnosis is often missed, in some cases for 15 years or more.
Diagnosing porphyria: Awareness and tests are crucial
Porphyria is caused when porphyins – essential components of hemoglobin – build up in the body, disrupting systems such as the nerves, skin, and gut. The urine can turn purplish, hence the condition’s name. (Porphyrus is the Greek word for purple.)
According to hematologist Danielle Nance, MD, of Banner MD Anderson Cancer Center in Gilbert, Ariz., acute intermittent porphyria “should be suspected in persons who have recurrent severe attacks of abdominal pain requiring strong pain medication to control symptoms, and there is no obvious physical cause.”
In such cases, practitioners should send out blood and urine for porphobilinogen (PBG) and delta-aminolevulinic acid (dALA or Delta-ALA) testing, Dr. Nance said. “These are almost always elevated, even between attacks, in persons with diagnoses of acute intermittent porphyria. Other types of porphyria, such as erythropoietic porphyria, may require additional testing. Genetic testing should be offered when a patient is suspected of having porphyria, as this can speed the diagnosis.”
The typical patient is a woman from age 18 to 55, often a young woman with recurrent abdominal pain that may occur during the second half of the menstrual cycle, Wake Forest’s Dr. Bonkovsky said. Constipation is common.
“She keeps coming to the clinic or emergency department, and no one knows what’s going on. Eventually, she tends to undergo an appendectomy, often a cholecystectomy, or sometimes gynecologic procedures without cure of the disease. Only after this long and arduous road of misdiagnosis does someone think it’s porphyria and do the correct tests.”
Dr. Bonkovsky led a 2014 study of 108 subjects (81% female) with acute porphyrias and found that the average time to a correct diagnosis was a whopping 15 years. Pain in the abdomen was the most common symptom (74%), followed by nausea/vomiting (73%), weakness (63%), and constipation (60%).
While underdiagnosis is common, porphyrias can also be overdiagnosed. According to Dr. Bonkovsky, a mild increase in urinary porphyrins is often misdiagnosed as porphyria when it may be a sign of liver disease or alcohol use, instead.
Hematologist Kleber Y. Fertrin, MD, PhD, of the University of Washington, Seattle, emphasized the importance of ordering the correct tests. “Urinary porphyrins are often inappropriately ordered because of their name. They are not diagnostic for acute hepatic porphyrias and may be nonspecifically elevated. It is paramount to get the labs from a reliable lab test experienced at performing diagnostic testing for porphyrias and make sure the urine sample needed is correctly obtained and preserved.”
New drug can control attacks, but it’s costly
Treatment should begin right away if porphyria is suspected, without waiting for confirmation, Dr. Nance said. “There are porphyria experts in the U.S. and in many other countries who can help practitioners interpret symptoms and testing results if there is uncertainty or if treatment options are unclear.”
Patients are counseled to avoid attack triggers and eat healthy diets, she said. “Persons with porphyria are encouraged to have a plan for home management of an attack and when to come to the hospital for symptoms that don’t respond to home therapy,” she said.
Dr. Fertrin said “the typical treatment for an acute porphyric attack is the use of intravenous glucose, as well as intravenous hemin infusions, along with pain medications and fluids as needed. Some patients may need medication for high blood pressure. For patients with recurrent attacks, prophylactic doses of hemin can be used.”
Another option is givosiran (Givlaari), the biggest recent advance in porphyria treatment. It was approved by the Food and Drug Administration for acute hepatic porphyria in 2019. “It’s an inhibitory mRNA that shuts down heme synthesis by downregulating aminolevulinic acid synthase,” said hematologist Thomas DeLoughery, MD, of Oregon Health & Science University, Portland.
A 2020 study coauthored by Dr. Bonkovsky found that the drug reduced the mean annualized attack rate in acute intermittent porphyria by 74%, compared with placebo (P < .001). “Givosiran led to lower levels of urinary ALA and porphobilinogen, fewer days of hemin use, and better daily scores for pain than placebo,” the study authors write. “Key adverse events that were observed more frequently in the givosiran group were elevations in serum aminotransferase levels, changes in serum creatinine levels and the estimated glomerular filtration rate, and injection-site reactions.”
Dr. Bonkovsky said the drug is appropriate in patients whose disease is not controlled by lifestyle interventions regarding alcohol, smoking, and substance use. However, while givosiran is helpful, “it’s not a cure,” he said. “Probably about 40% of patients have found the side effects such as nausea, fatigue, headaches, and liver injury to be too adverse and have not decided to take it in the long term.”
In addition, the drug costs about $500,000 a year, and insurers may balk at the expense. Still, specialists say it can be a good option. “Before givosiran, the standard therapy was hematin, which decreased the activity of the ALA synthase,” Dr. DeLoughery said. “This is a nasty drug that can inflame the blood vessels and is not all that effective.”
The royal family may be able to breathe easy
There are other forms of porphyria besides the acute type. Cutaneous porphryias can cause blistering from sunlight exposure, and treatment is avoidance of such triggers, Dr. Fertin said. “For a rare form called erythropoietic protoporphyria, there is a subcutaneous implant with a medication called afamelanotide that increases tolerance to sunlight.”
There’s another type: variegate porphyria, which UpToDate says is “characterized by cutaneous blistering and/or acute neurovisceral attacks.” In 1966, a mother-and-son psychiatrist team theorized that Britain’s King George III suffered from this type of porphyria.
However, researchers have sharply criticized the porphyria theory with regard to that king, and a recent theory now suggests that he actually had bipolar disorder. Dr. Fertin is among the skeptics, noting the high prevalence of porphyria in affected families.
“Since King George III would now have a living number of relatives of about 900 people, we would expect around 180 cases of variegate porphyria to be connected to him, and those are nowhere to be found,” he said. “The idea that it could cause progressive psychosis and dementia is also a misconception. We do not find that porphyria is the underlying cause of psychiatric conditions on their own. Many atypical symptoms of the king were attributed to variegate porphyria, and the few more typical symptoms he reportedly had, of abdominal pain and urine discoloration, can be more easily explained by common diseases, such as kidney stones or gallstones. Finally, attempts at obtaining genetic or biochemical evidence of porphyria from relatives of King George III have been negative or inconclusive.”
That’s good news for the royals, who have many other concerns these days.
Dr. Nance discloses research study funding from Alnylam (maker of Givlaari) and payments to participate in educational activities for patients and practitioners. Dr. Bonkovsky discloses relationships with drugmakers who have developed products to treat porphyria including Alnylam, Mitsubishi Tanabe, Recordati, and Disc. Dr. Fertin is subinvestigator in a clinical trial for a novel treatment for erythropoietic protoporphyria sponsored by Mitsubishi Tanabe. Dr. DeLoughery reports no disclosures.
WPATH removes age limits from transgender treatment guidelines
Long-awaited global transgender care guidelines have dropped, with no recommendations regarding age limits for treatment and surgery in teenagers but acknowledging the complexity of dealing with such adolescents amid lack of longitudinal research on the impact of transitioning gender.
The World Professional Association of Transgender Health published its latest standards of care (SOC8) as it opens its annual meeting on Sept. 16 in Montreal.![]()
These are “the most comprehensive set of guidelines ever produced to assist health care professionals around the world in support of transgender and gender diverse adults, adolescents, and children who are taking steps to live their lives authentically,” wrote WPATH President Walter Bouman, MD, PhD, and WPATH President-Elect Marci Bowers, MD, in a news release.
The SOC8 is the first update to guidance on the treatment of transgender individuals in 10 years and appears online in the International Journal of Transgender Health.
For the first time, the association wrote a chapter dedicated to transgender and gender-diverse adolescents – distinct from the child chapter.
The complexity of treating adolescents
WPATH officials said that this was owed to exponential growth in adolescent referral rates, more research on adolescent gender diversity–related care, and the unique developmental and care issues of this age group.
Until recently, there was limited information regarding the prevalence of gender diversity among adolescents. Studies from high-school samples indicate much higher rates than was earlier thought, with reports of up to 1.2% of participants identifying as transgender and up to 2.7% or more (for example, 7%-9%) experiencing some level of self-reported gender diversity, WPATH said.
The new chapter “applies to adolescents from the start of puberty until the legal age of majority (in most cases 18 years),” it stated.
However, WPATH did not go as far as to recommend lowering the age at which youth can receive cross-sex hormone therapy or gender-affirming surgeries, as earlier decreed in a draft of the guidelines. That draft suggested that young people could receive hormone therapy at age 14 years and surgeries for double mastectomies at age 15 years and for genital reassignment at age 17 years.
The exception was phalloplasty – surgery to construct a penis in female-to-male individuals – which WPATH stressed should not be performed under the age of 18 years owing to its complexity.
Now, the final SOC8 emphasizes that each transgender adolescent is unique, and decisions must be made on an individual basis, with no recommendations on specific ages for any treatment. This could be interpreted in many ways.
The SOC8 also acknowledges the “very rare” regret of individuals who have transitioned to the opposite gender and then changed their minds.
“[Health care] providers may consider the possibility an adolescent may regret gender-affirming decisions made during adolescence, and a young person will want to stop treatment and return to living in the birth-assigned gender role in the future. Providers may discuss this topic in a collaborative and trusting manner with the adolescent and their parents/caregivers before gender-affirming medical treatments are started,” it states.
WPATH, in addition, stressed the importance of counseling and supporting regretting patients, many who “expressed difficulties finding help during their detransition process and reported their detransition was an isolating experience during which they did not receive either sufficient or appropriate support.”
Although it doesn’t put a firm figure on the rate of regret overall, in its chapter on surgery, WPATH estimates that 0.3%-3.8% of transgender individuals regret gender-affirming surgery.
SOC8 also acknowledges “A pattern of uneven ratios by assigned sex has been reported in gender clinics, with assigned female-at-birth patients initiating care 2.5-7.1 times more frequently” than patients who were assigned male at birth.
And WPATH states in SOC8 that another phenomenon is the growing number of adolescents seeking care who had not previously experienced or expressed gender diversity during their childhood years.
It goes on to cite the 2018 paper of Lisa Littman, MD, MPH, now president of the Institute for Comprehensive Gender Dysphoria Research. Dr. Littman coined the term, “rapid-onset gender dysphoria” to describe this phenomenon; SOC8 refrains from using this phrase, but does acknowledge: “For a select subgroup of young people, susceptibility to social influence impacting gender may be an important differential to consider.”
SOC8 recommends that before any medical or surgical treatment is considered, health care professionals “undertake a comprehensive biopsychosocial assessment of adolescents who present with gender identity-related concerns and seek medical/surgical transition-related care.”
And it specifically mentions that transgender adolescents “show high rates of autism spectrum disorder/characteristics,” and notes that “other neurodevelopmental presentations and/or mental health challenges may also be present, (e.g., ADHD, intellectual disability, and psychotic disorders).”
Who uses WPATH to guide care? This is ‘a big unknown’
WPATH is an umbrella organization with offshoots in most Western nations, such as USPATH in the United States, EPATH in Europe, and AUSPATH and NZPATH in Australia and New Zealand.
However, it is not the only organization to issue guidance on the care of transgender individuals; several specialties take care of this patient population, including, but not limited to: pediatricians, endocrinologists, psychiatrists, psychologists and plastic surgeons.
The extent to which any health care professional, or professional body, follows WPATH guidance is extremely varied.
“There is nothing binding clinicians to the SOC, and the SOC is so broad and vague that anyone can say they’re following it but according to their own biases and interpretation,” Aaron Kimberly, a trans man and mental health clinician from the Gender Dysphoria Alliance, said in an interview.
In North America, some clinics practice full “informed consent” with no assessment and prescriptions at the first visit, Mr. Kimberly said, whereas others do comprehensive assessments.
“I think SOC should be observed. It shouldn’t just be people going rogue,” Erica Anderson, a clinical psychologist in Berkeley, Calif., former president of USPATH, and former member of WPATH, who is herself transgender, said in an interview. “The reason there are standards of care is because hundreds of scientists have weighed in – is it perfect? No. We have a long way to go. But you can’t just ignore whatever it is that we know and let people make their own decisions.”
A version of this article first appeared on Medscape.com.
Long-awaited global transgender care guidelines have dropped, with no recommendations regarding age limits for treatment and surgery in teenagers but acknowledging the complexity of dealing with such adolescents amid lack of longitudinal research on the impact of transitioning gender.
The World Professional Association of Transgender Health published its latest standards of care (SOC8) as it opens its annual meeting on Sept. 16 in Montreal.![]()
These are “the most comprehensive set of guidelines ever produced to assist health care professionals around the world in support of transgender and gender diverse adults, adolescents, and children who are taking steps to live their lives authentically,” wrote WPATH President Walter Bouman, MD, PhD, and WPATH President-Elect Marci Bowers, MD, in a news release.
The SOC8 is the first update to guidance on the treatment of transgender individuals in 10 years and appears online in the International Journal of Transgender Health.
For the first time, the association wrote a chapter dedicated to transgender and gender-diverse adolescents – distinct from the child chapter.
The complexity of treating adolescents
WPATH officials said that this was owed to exponential growth in adolescent referral rates, more research on adolescent gender diversity–related care, and the unique developmental and care issues of this age group.
Until recently, there was limited information regarding the prevalence of gender diversity among adolescents. Studies from high-school samples indicate much higher rates than was earlier thought, with reports of up to 1.2% of participants identifying as transgender and up to 2.7% or more (for example, 7%-9%) experiencing some level of self-reported gender diversity, WPATH said.
The new chapter “applies to adolescents from the start of puberty until the legal age of majority (in most cases 18 years),” it stated.
However, WPATH did not go as far as to recommend lowering the age at which youth can receive cross-sex hormone therapy or gender-affirming surgeries, as earlier decreed in a draft of the guidelines. That draft suggested that young people could receive hormone therapy at age 14 years and surgeries for double mastectomies at age 15 years and for genital reassignment at age 17 years.
The exception was phalloplasty – surgery to construct a penis in female-to-male individuals – which WPATH stressed should not be performed under the age of 18 years owing to its complexity.
Now, the final SOC8 emphasizes that each transgender adolescent is unique, and decisions must be made on an individual basis, with no recommendations on specific ages for any treatment. This could be interpreted in many ways.
The SOC8 also acknowledges the “very rare” regret of individuals who have transitioned to the opposite gender and then changed their minds.
“[Health care] providers may consider the possibility an adolescent may regret gender-affirming decisions made during adolescence, and a young person will want to stop treatment and return to living in the birth-assigned gender role in the future. Providers may discuss this topic in a collaborative and trusting manner with the adolescent and their parents/caregivers before gender-affirming medical treatments are started,” it states.
WPATH, in addition, stressed the importance of counseling and supporting regretting patients, many who “expressed difficulties finding help during their detransition process and reported their detransition was an isolating experience during which they did not receive either sufficient or appropriate support.”
Although it doesn’t put a firm figure on the rate of regret overall, in its chapter on surgery, WPATH estimates that 0.3%-3.8% of transgender individuals regret gender-affirming surgery.
SOC8 also acknowledges “A pattern of uneven ratios by assigned sex has been reported in gender clinics, with assigned female-at-birth patients initiating care 2.5-7.1 times more frequently” than patients who were assigned male at birth.
And WPATH states in SOC8 that another phenomenon is the growing number of adolescents seeking care who had not previously experienced or expressed gender diversity during their childhood years.
It goes on to cite the 2018 paper of Lisa Littman, MD, MPH, now president of the Institute for Comprehensive Gender Dysphoria Research. Dr. Littman coined the term, “rapid-onset gender dysphoria” to describe this phenomenon; SOC8 refrains from using this phrase, but does acknowledge: “For a select subgroup of young people, susceptibility to social influence impacting gender may be an important differential to consider.”
SOC8 recommends that before any medical or surgical treatment is considered, health care professionals “undertake a comprehensive biopsychosocial assessment of adolescents who present with gender identity-related concerns and seek medical/surgical transition-related care.”
And it specifically mentions that transgender adolescents “show high rates of autism spectrum disorder/characteristics,” and notes that “other neurodevelopmental presentations and/or mental health challenges may also be present, (e.g., ADHD, intellectual disability, and psychotic disorders).”
Who uses WPATH to guide care? This is ‘a big unknown’
WPATH is an umbrella organization with offshoots in most Western nations, such as USPATH in the United States, EPATH in Europe, and AUSPATH and NZPATH in Australia and New Zealand.
However, it is not the only organization to issue guidance on the care of transgender individuals; several specialties take care of this patient population, including, but not limited to: pediatricians, endocrinologists, psychiatrists, psychologists and plastic surgeons.
The extent to which any health care professional, or professional body, follows WPATH guidance is extremely varied.
“There is nothing binding clinicians to the SOC, and the SOC is so broad and vague that anyone can say they’re following it but according to their own biases and interpretation,” Aaron Kimberly, a trans man and mental health clinician from the Gender Dysphoria Alliance, said in an interview.
In North America, some clinics practice full “informed consent” with no assessment and prescriptions at the first visit, Mr. Kimberly said, whereas others do comprehensive assessments.
“I think SOC should be observed. It shouldn’t just be people going rogue,” Erica Anderson, a clinical psychologist in Berkeley, Calif., former president of USPATH, and former member of WPATH, who is herself transgender, said in an interview. “The reason there are standards of care is because hundreds of scientists have weighed in – is it perfect? No. We have a long way to go. But you can’t just ignore whatever it is that we know and let people make their own decisions.”
A version of this article first appeared on Medscape.com.
Long-awaited global transgender care guidelines have dropped, with no recommendations regarding age limits for treatment and surgery in teenagers but acknowledging the complexity of dealing with such adolescents amid lack of longitudinal research on the impact of transitioning gender.
The World Professional Association of Transgender Health published its latest standards of care (SOC8) as it opens its annual meeting on Sept. 16 in Montreal.![]()
These are “the most comprehensive set of guidelines ever produced to assist health care professionals around the world in support of transgender and gender diverse adults, adolescents, and children who are taking steps to live their lives authentically,” wrote WPATH President Walter Bouman, MD, PhD, and WPATH President-Elect Marci Bowers, MD, in a news release.
The SOC8 is the first update to guidance on the treatment of transgender individuals in 10 years and appears online in the International Journal of Transgender Health.
For the first time, the association wrote a chapter dedicated to transgender and gender-diverse adolescents – distinct from the child chapter.
The complexity of treating adolescents
WPATH officials said that this was owed to exponential growth in adolescent referral rates, more research on adolescent gender diversity–related care, and the unique developmental and care issues of this age group.
Until recently, there was limited information regarding the prevalence of gender diversity among adolescents. Studies from high-school samples indicate much higher rates than was earlier thought, with reports of up to 1.2% of participants identifying as transgender and up to 2.7% or more (for example, 7%-9%) experiencing some level of self-reported gender diversity, WPATH said.
The new chapter “applies to adolescents from the start of puberty until the legal age of majority (in most cases 18 years),” it stated.
However, WPATH did not go as far as to recommend lowering the age at which youth can receive cross-sex hormone therapy or gender-affirming surgeries, as earlier decreed in a draft of the guidelines. That draft suggested that young people could receive hormone therapy at age 14 years and surgeries for double mastectomies at age 15 years and for genital reassignment at age 17 years.
The exception was phalloplasty – surgery to construct a penis in female-to-male individuals – which WPATH stressed should not be performed under the age of 18 years owing to its complexity.
Now, the final SOC8 emphasizes that each transgender adolescent is unique, and decisions must be made on an individual basis, with no recommendations on specific ages for any treatment. This could be interpreted in many ways.
The SOC8 also acknowledges the “very rare” regret of individuals who have transitioned to the opposite gender and then changed their minds.
“[Health care] providers may consider the possibility an adolescent may regret gender-affirming decisions made during adolescence, and a young person will want to stop treatment and return to living in the birth-assigned gender role in the future. Providers may discuss this topic in a collaborative and trusting manner with the adolescent and their parents/caregivers before gender-affirming medical treatments are started,” it states.
WPATH, in addition, stressed the importance of counseling and supporting regretting patients, many who “expressed difficulties finding help during their detransition process and reported their detransition was an isolating experience during which they did not receive either sufficient or appropriate support.”
Although it doesn’t put a firm figure on the rate of regret overall, in its chapter on surgery, WPATH estimates that 0.3%-3.8% of transgender individuals regret gender-affirming surgery.
SOC8 also acknowledges “A pattern of uneven ratios by assigned sex has been reported in gender clinics, with assigned female-at-birth patients initiating care 2.5-7.1 times more frequently” than patients who were assigned male at birth.
And WPATH states in SOC8 that another phenomenon is the growing number of adolescents seeking care who had not previously experienced or expressed gender diversity during their childhood years.
It goes on to cite the 2018 paper of Lisa Littman, MD, MPH, now president of the Institute for Comprehensive Gender Dysphoria Research. Dr. Littman coined the term, “rapid-onset gender dysphoria” to describe this phenomenon; SOC8 refrains from using this phrase, but does acknowledge: “For a select subgroup of young people, susceptibility to social influence impacting gender may be an important differential to consider.”
SOC8 recommends that before any medical or surgical treatment is considered, health care professionals “undertake a comprehensive biopsychosocial assessment of adolescents who present with gender identity-related concerns and seek medical/surgical transition-related care.”
And it specifically mentions that transgender adolescents “show high rates of autism spectrum disorder/characteristics,” and notes that “other neurodevelopmental presentations and/or mental health challenges may also be present, (e.g., ADHD, intellectual disability, and psychotic disorders).”
Who uses WPATH to guide care? This is ‘a big unknown’
WPATH is an umbrella organization with offshoots in most Western nations, such as USPATH in the United States, EPATH in Europe, and AUSPATH and NZPATH in Australia and New Zealand.
However, it is not the only organization to issue guidance on the care of transgender individuals; several specialties take care of this patient population, including, but not limited to: pediatricians, endocrinologists, psychiatrists, psychologists and plastic surgeons.
The extent to which any health care professional, or professional body, follows WPATH guidance is extremely varied.
“There is nothing binding clinicians to the SOC, and the SOC is so broad and vague that anyone can say they’re following it but according to their own biases and interpretation,” Aaron Kimberly, a trans man and mental health clinician from the Gender Dysphoria Alliance, said in an interview.
In North America, some clinics practice full “informed consent” with no assessment and prescriptions at the first visit, Mr. Kimberly said, whereas others do comprehensive assessments.
“I think SOC should be observed. It shouldn’t just be people going rogue,” Erica Anderson, a clinical psychologist in Berkeley, Calif., former president of USPATH, and former member of WPATH, who is herself transgender, said in an interview. “The reason there are standards of care is because hundreds of scientists have weighed in – is it perfect? No. We have a long way to go. But you can’t just ignore whatever it is that we know and let people make their own decisions.”
A version of this article first appeared on Medscape.com.
FROM THE INTERNATIONAL JOURNAL OF TRANSGENDER HEALTH
A farewell to arms? Drug approvals based on single-arm trials can be flawed
PARIS – with results that should only be used, under certain conditions, for accelerated approvals that should then be followed by confirmatory studies.
In fact, many drugs approved over the last decade based solely on data from single-arm trials have been subsequently withdrawn when put through the rigors of a head-to-head randomized controlled trial, according to Bishal Gyawali, MD, PhD, from the department of oncology at Queen’s University, Kingston, Ont.
“Single-arm trials are not meant to provide confirmatory evidence sufficient for approval; However, that ship has sailed, and we have several drugs that are approved on the basis of single-arm trials, but we need to make sure that those approvals are accelerated or conditional approvals, not regular approval,” he said in a presentation included in a special session on drug approvals at the European Society for Medical Oncology Congress.
“We should not allow premature regular approval based on single-arm trials, because once a drug gets conditional approval, access is not an issue. Patients will have access to the drug anyway, but we should ensure that robust evidence follows, and long-term follow-up data are needed to develop confidence in the efficacy outcomes that are seen in single-arm trials,” he said.
In many cases, single-arm trials are large enough or of long enough duration that investigators could have reasonably performed a randomized controlled trial (RCT) in the first place, Dr. Gyawali added.
Why do single-arm trials?
The term “single-arm registration trial” is something of an oxymoron, he said, noting that the purpose of such trials should be whether to take the drug to a phase 3, randomized trial. But as authors of a 2019 study in JAMA Network Open showed, of a sample of phase 3 RCTs, 42% did not have a prior phase 2 trial, and 28% had a negative phase 2 trial. Single-arm trials may be acceptable for conditional drug approvals if all of the following conditions are met:
- A RCT is not possible because the disease is rare or randomization would be unethical.
- The safety of the drug is established and its potential benefits outweigh its risks.
- The drug is associated with a high and durable overall or objective response rate.
- The mechanism of action is supported by a strong scientific rationale, and if the drug may meet an unmet medical need.
Survival endpoints won’t do
Efficacy endpoints typically used in RCTs, such as progression-free survival (PFS) and overall survival (OS) can be misleading because they may be a result of the natural history of the disease and not the drug being tested, whereas ORRs are almost certainly reflective of the action of the drug itself, because spontaneous tumor regression is a rare phenomenon, Dr. Gyawali said.
He cautioned, however, that the ORR of placebo is not zero percent. For example in a 2018 study of sorafenib (Nexavar) versus placebo for advanced or refractory desmoid tumors, the ORR with the active drug was 33%, and the ORR for placebo was 20%.
It’s also open to question, he said, what constitutes an acceptably high ORR and duration of response, pointing to Food and Drug Administration accelerated approval of an indication for nivolumab (Opdivo) for treatment of patients with hepatocellular carcinoma (HCC) that had progressed on sorafenib. In the single-arm trial used as the basis for approval, the ORRs as assessed by an independent central review committee blinded to the results was 14.3%.
“So, nivolumab in hepatocellular cancer was approved on the basis of a response rate lower than that of placebo, albeit in a different tumor. But the point I’m trying to show here is we don’t have a good definition of what is a good response rate,” he said.
In July 2021, Bristol-Myers Squibb voluntarily withdrew the HCC indication for nivolumab, following negative results of the CheckMate 459 trial and a 5-4 vote against continuing the accelerated approval.
On second thought ...
Citing data compiled by Nathan I. Cherny, MD, from Shaare Zedek Medical Center, Jerusalem, Dr. Gyawali noted that 58 of 161 FDA approvals from 2017 to 2021 of drugs for adult solid tumors were based on single-arm trials. Of the 58 drugs, 39 received accelerated approvals, and 19 received regular approvals; of the 39 that received accelerated approvals, 4 were subsequently withdrawn, 8 were converted to regular approvals, and the remainder continued as accelerated approvals.
Interestingly, the median response rate among all the drugs was 40%, and did not differ between the type of approval received, suggesting that response rates are not predictive of whether a drug will receive a conditional or full-fledged go-ahead.
What’s rare and safe?
The definition of a rare disease in the United States is one that affects fewer than 40,000 per year, and in Europe it’s an incidence rate of less than 6 per 100,000 population, Dr. Gyawali noted. But he argued that even non–small cell lung cancer, the most common form of cancer in the world, could be considered rare if it is broken down into subtypes that are treated according to specific mutations that may occur in a relatively small number of patients.
He also noted that a specific drug’s safety, one of the most important criteria for granting approval to a drug based on a single-arm trial, can be difficult to judge without adequate controls for comparison.
Cherry-picking patients
Winette van der Graaf, MD, president of the European Organization for the Research and Treatment of Cancer, who attended the session where Dr. Gyawali’s presentation was played, said in an interview that clinicians should cast a critical eye on how trials are designed and conducted, including patient selection and choice of endpoints.
“One of the most obvious things to be concerned about is that we’re still having patients with good performance status enrolled, mostly PS 0 or 1, so how representative are these clinical trials for the patients we see in front of us on a daily basis?” she said.
“The other question is radiological endpoints, which we focus on with OS and PFS are most important for patients, especially if you consider that if patients may have asymptomatic disease, and we are only treating them with potentially toxic medication, what are we doing for them? Median overall survival when you look at all of these trials is only 4 months, so we really need to take into account how we affect patients in clinical trials,” she added.
Dr. van der Graaf emphasized that clinical trial investigators need to more routinely incorporate quality of life measures and other patient-reported outcomes in clinical trial results to help regulators and clinicians in practice get a better sense of the true clinical benefit of a new drug.
Dr. Gyawali did not disclose a funding source for his presentation. He reported consulting fees from Vivio Health and research grants from the American Society of Clinical Oncology. Dr. van der Graaf reported no conflicts of interest.
PARIS – with results that should only be used, under certain conditions, for accelerated approvals that should then be followed by confirmatory studies.
In fact, many drugs approved over the last decade based solely on data from single-arm trials have been subsequently withdrawn when put through the rigors of a head-to-head randomized controlled trial, according to Bishal Gyawali, MD, PhD, from the department of oncology at Queen’s University, Kingston, Ont.
“Single-arm trials are not meant to provide confirmatory evidence sufficient for approval; However, that ship has sailed, and we have several drugs that are approved on the basis of single-arm trials, but we need to make sure that those approvals are accelerated or conditional approvals, not regular approval,” he said in a presentation included in a special session on drug approvals at the European Society for Medical Oncology Congress.
“We should not allow premature regular approval based on single-arm trials, because once a drug gets conditional approval, access is not an issue. Patients will have access to the drug anyway, but we should ensure that robust evidence follows, and long-term follow-up data are needed to develop confidence in the efficacy outcomes that are seen in single-arm trials,” he said.
In many cases, single-arm trials are large enough or of long enough duration that investigators could have reasonably performed a randomized controlled trial (RCT) in the first place, Dr. Gyawali added.
Why do single-arm trials?
The term “single-arm registration trial” is something of an oxymoron, he said, noting that the purpose of such trials should be whether to take the drug to a phase 3, randomized trial. But as authors of a 2019 study in JAMA Network Open showed, of a sample of phase 3 RCTs, 42% did not have a prior phase 2 trial, and 28% had a negative phase 2 trial. Single-arm trials may be acceptable for conditional drug approvals if all of the following conditions are met:
- A RCT is not possible because the disease is rare or randomization would be unethical.
- The safety of the drug is established and its potential benefits outweigh its risks.
- The drug is associated with a high and durable overall or objective response rate.
- The mechanism of action is supported by a strong scientific rationale, and if the drug may meet an unmet medical need.
Survival endpoints won’t do
Efficacy endpoints typically used in RCTs, such as progression-free survival (PFS) and overall survival (OS) can be misleading because they may be a result of the natural history of the disease and not the drug being tested, whereas ORRs are almost certainly reflective of the action of the drug itself, because spontaneous tumor regression is a rare phenomenon, Dr. Gyawali said.
He cautioned, however, that the ORR of placebo is not zero percent. For example in a 2018 study of sorafenib (Nexavar) versus placebo for advanced or refractory desmoid tumors, the ORR with the active drug was 33%, and the ORR for placebo was 20%.
It’s also open to question, he said, what constitutes an acceptably high ORR and duration of response, pointing to Food and Drug Administration accelerated approval of an indication for nivolumab (Opdivo) for treatment of patients with hepatocellular carcinoma (HCC) that had progressed on sorafenib. In the single-arm trial used as the basis for approval, the ORRs as assessed by an independent central review committee blinded to the results was 14.3%.
“So, nivolumab in hepatocellular cancer was approved on the basis of a response rate lower than that of placebo, albeit in a different tumor. But the point I’m trying to show here is we don’t have a good definition of what is a good response rate,” he said.
In July 2021, Bristol-Myers Squibb voluntarily withdrew the HCC indication for nivolumab, following negative results of the CheckMate 459 trial and a 5-4 vote against continuing the accelerated approval.
On second thought ...
Citing data compiled by Nathan I. Cherny, MD, from Shaare Zedek Medical Center, Jerusalem, Dr. Gyawali noted that 58 of 161 FDA approvals from 2017 to 2021 of drugs for adult solid tumors were based on single-arm trials. Of the 58 drugs, 39 received accelerated approvals, and 19 received regular approvals; of the 39 that received accelerated approvals, 4 were subsequently withdrawn, 8 were converted to regular approvals, and the remainder continued as accelerated approvals.
Interestingly, the median response rate among all the drugs was 40%, and did not differ between the type of approval received, suggesting that response rates are not predictive of whether a drug will receive a conditional or full-fledged go-ahead.
What’s rare and safe?
The definition of a rare disease in the United States is one that affects fewer than 40,000 per year, and in Europe it’s an incidence rate of less than 6 per 100,000 population, Dr. Gyawali noted. But he argued that even non–small cell lung cancer, the most common form of cancer in the world, could be considered rare if it is broken down into subtypes that are treated according to specific mutations that may occur in a relatively small number of patients.
He also noted that a specific drug’s safety, one of the most important criteria for granting approval to a drug based on a single-arm trial, can be difficult to judge without adequate controls for comparison.
Cherry-picking patients
Winette van der Graaf, MD, president of the European Organization for the Research and Treatment of Cancer, who attended the session where Dr. Gyawali’s presentation was played, said in an interview that clinicians should cast a critical eye on how trials are designed and conducted, including patient selection and choice of endpoints.
“One of the most obvious things to be concerned about is that we’re still having patients with good performance status enrolled, mostly PS 0 or 1, so how representative are these clinical trials for the patients we see in front of us on a daily basis?” she said.
“The other question is radiological endpoints, which we focus on with OS and PFS are most important for patients, especially if you consider that if patients may have asymptomatic disease, and we are only treating them with potentially toxic medication, what are we doing for them? Median overall survival when you look at all of these trials is only 4 months, so we really need to take into account how we affect patients in clinical trials,” she added.
Dr. van der Graaf emphasized that clinical trial investigators need to more routinely incorporate quality of life measures and other patient-reported outcomes in clinical trial results to help regulators and clinicians in practice get a better sense of the true clinical benefit of a new drug.
Dr. Gyawali did not disclose a funding source for his presentation. He reported consulting fees from Vivio Health and research grants from the American Society of Clinical Oncology. Dr. van der Graaf reported no conflicts of interest.
PARIS – with results that should only be used, under certain conditions, for accelerated approvals that should then be followed by confirmatory studies.
In fact, many drugs approved over the last decade based solely on data from single-arm trials have been subsequently withdrawn when put through the rigors of a head-to-head randomized controlled trial, according to Bishal Gyawali, MD, PhD, from the department of oncology at Queen’s University, Kingston, Ont.
“Single-arm trials are not meant to provide confirmatory evidence sufficient for approval; However, that ship has sailed, and we have several drugs that are approved on the basis of single-arm trials, but we need to make sure that those approvals are accelerated or conditional approvals, not regular approval,” he said in a presentation included in a special session on drug approvals at the European Society for Medical Oncology Congress.
“We should not allow premature regular approval based on single-arm trials, because once a drug gets conditional approval, access is not an issue. Patients will have access to the drug anyway, but we should ensure that robust evidence follows, and long-term follow-up data are needed to develop confidence in the efficacy outcomes that are seen in single-arm trials,” he said.
In many cases, single-arm trials are large enough or of long enough duration that investigators could have reasonably performed a randomized controlled trial (RCT) in the first place, Dr. Gyawali added.
Why do single-arm trials?
The term “single-arm registration trial” is something of an oxymoron, he said, noting that the purpose of such trials should be whether to take the drug to a phase 3, randomized trial. But as authors of a 2019 study in JAMA Network Open showed, of a sample of phase 3 RCTs, 42% did not have a prior phase 2 trial, and 28% had a negative phase 2 trial. Single-arm trials may be acceptable for conditional drug approvals if all of the following conditions are met:
- A RCT is not possible because the disease is rare or randomization would be unethical.
- The safety of the drug is established and its potential benefits outweigh its risks.
- The drug is associated with a high and durable overall or objective response rate.
- The mechanism of action is supported by a strong scientific rationale, and if the drug may meet an unmet medical need.
Survival endpoints won’t do
Efficacy endpoints typically used in RCTs, such as progression-free survival (PFS) and overall survival (OS) can be misleading because they may be a result of the natural history of the disease and not the drug being tested, whereas ORRs are almost certainly reflective of the action of the drug itself, because spontaneous tumor regression is a rare phenomenon, Dr. Gyawali said.
He cautioned, however, that the ORR of placebo is not zero percent. For example in a 2018 study of sorafenib (Nexavar) versus placebo for advanced or refractory desmoid tumors, the ORR with the active drug was 33%, and the ORR for placebo was 20%.
It’s also open to question, he said, what constitutes an acceptably high ORR and duration of response, pointing to Food and Drug Administration accelerated approval of an indication for nivolumab (Opdivo) for treatment of patients with hepatocellular carcinoma (HCC) that had progressed on sorafenib. In the single-arm trial used as the basis for approval, the ORRs as assessed by an independent central review committee blinded to the results was 14.3%.
“So, nivolumab in hepatocellular cancer was approved on the basis of a response rate lower than that of placebo, albeit in a different tumor. But the point I’m trying to show here is we don’t have a good definition of what is a good response rate,” he said.
In July 2021, Bristol-Myers Squibb voluntarily withdrew the HCC indication for nivolumab, following negative results of the CheckMate 459 trial and a 5-4 vote against continuing the accelerated approval.
On second thought ...
Citing data compiled by Nathan I. Cherny, MD, from Shaare Zedek Medical Center, Jerusalem, Dr. Gyawali noted that 58 of 161 FDA approvals from 2017 to 2021 of drugs for adult solid tumors were based on single-arm trials. Of the 58 drugs, 39 received accelerated approvals, and 19 received regular approvals; of the 39 that received accelerated approvals, 4 were subsequently withdrawn, 8 were converted to regular approvals, and the remainder continued as accelerated approvals.
Interestingly, the median response rate among all the drugs was 40%, and did not differ between the type of approval received, suggesting that response rates are not predictive of whether a drug will receive a conditional or full-fledged go-ahead.
What’s rare and safe?
The definition of a rare disease in the United States is one that affects fewer than 40,000 per year, and in Europe it’s an incidence rate of less than 6 per 100,000 population, Dr. Gyawali noted. But he argued that even non–small cell lung cancer, the most common form of cancer in the world, could be considered rare if it is broken down into subtypes that are treated according to specific mutations that may occur in a relatively small number of patients.
He also noted that a specific drug’s safety, one of the most important criteria for granting approval to a drug based on a single-arm trial, can be difficult to judge without adequate controls for comparison.
Cherry-picking patients
Winette van der Graaf, MD, president of the European Organization for the Research and Treatment of Cancer, who attended the session where Dr. Gyawali’s presentation was played, said in an interview that clinicians should cast a critical eye on how trials are designed and conducted, including patient selection and choice of endpoints.
“One of the most obvious things to be concerned about is that we’re still having patients with good performance status enrolled, mostly PS 0 or 1, so how representative are these clinical trials for the patients we see in front of us on a daily basis?” she said.
“The other question is radiological endpoints, which we focus on with OS and PFS are most important for patients, especially if you consider that if patients may have asymptomatic disease, and we are only treating them with potentially toxic medication, what are we doing for them? Median overall survival when you look at all of these trials is only 4 months, so we really need to take into account how we affect patients in clinical trials,” she added.
Dr. van der Graaf emphasized that clinical trial investigators need to more routinely incorporate quality of life measures and other patient-reported outcomes in clinical trial results to help regulators and clinicians in practice get a better sense of the true clinical benefit of a new drug.
Dr. Gyawali did not disclose a funding source for his presentation. He reported consulting fees from Vivio Health and research grants from the American Society of Clinical Oncology. Dr. van der Graaf reported no conflicts of interest.
AT ESMO CONGRESS 2022