The US Department of Veterans Affairs (VA) has been integral in resident training. Resident surgical training requires a balance of supervision and autonomy, along with procedure repetition and appropriate feedback.1-3 Non-VA research has found that resident participation across various otolaryngology procedures, including thyroidectomy, neck dissection, and laryngectomy, does not increase patient morbidity.4-7 However, resident involvement in private and academic settings that included nonhead and neck procedures was linked to increased operative time and reduced productivity, as determined by work relative value units (wRVUs).7-13 This has also been identified in other specialties, including general surgery, orthopedics, and ophthalmology.14-16
Unlike the private sector, surgeon compensation at the VA is not as closely linked to operative productivity, offering a unique setting for resident training. While VA integration in otolaryngology residency programs increases resident case numbers, particularly in head and neck cases, the impact on VA patient outcomes and productivity is unknown.17 The use of larynxpreserving treatment modalities for laryngeal cancer has led to a decline in the number of total laryngectomies performed, which could potentially impact resident operative training for laryngectomies.18-20
This study sought to determine the impact of resident participation on operative time, wRVUs, and patient outcomes in veterans who underwent a total laryngectomy. This study was reviewed and approved by the MedStar Georgetown University Hospital Institutional Review Board and Research and Development Committee (#1595672).
Methods
A retrospective cohort of veterans nationwide who underwent total laryngectomy between 2001 and 2021, with or without neck dissection, was identified from the Veterans Affairs Surgical Quality Improvement Program (VASQIP). Data were extracted via the VA Informatics and Computing Infrastructure and patients were included based on Current Procedural Terminology codes for total laryngectomy, with or without neck dissection (31320, 31360, 31365). Laryngopharyngectomies, partial laryngectomies, and minimally invasive laryngectomies were excluded. VASQIP nurse data managers reviewed patient data for operative data, postoperative outcomes (including 30- day morbidity and mortality), and preoperative risk factors (Appendix).21
The VASQIP data provide the highest resident or postgraduate year (PGY) per surgery. PGY 1, 2, and 3 were considered junior residents and PGY ≥4, surgical fellows, and individuals who took research years during residency were considered senior residents. Cases performed by attending physicians alone were compared with those involving junior or senior residents.
Patient demographic data included age, body mass index, smoking and alcohol use, weight loss, and functional status. Consumption of any tobacco products within 12 months of surgery was considered tobacco use. Drinking on average ≥2 alcoholic beverages daily was considered alcohol use. Weight loss was defined as a 10% reduction in body weight within the 6 months before surgery, excluding patients enrolled in a weight loss program. Functional status was categorized as independent, partially dependent, totally dependent, and unknown.
Primary outcomes included operative time, wRVUs generated, and wRVUs generated per hour of operative time. Postoperative complications were recorded both as a continuous variable and as a binary variable for presence or absence of a complication. Additional outcome variables included length of postoperative hospital stay, return to the operating room (OR), and death within 30 days of surgery.
Statistical Analysis
Data were summarized using frequency and percentage for categorical variables and median with IQR for continuous variables. Data were also summarized based on resident involvement in the surgery and the PGY level of the residents involved. The occurrence of total laryngectomy, rate of complications, and patient return to the OR were summarized by year.
Univariate associations between resident involvement and surgical outcomes were analyzed using the Kruskal-Wallis test for continuous variables and the ÷2 test for categorical variables. A Fisher exact test was used when the cell count in the contingency table was < 5. The univariate associations between surgical outcomes and demographic/preoperative variables were examined using 2-sided Wilcoxon ranksum tests or Kruskal-Wallis tests between continuous variables and categorical variables, X2 or Fisher exact test between 2 categorical variables, and 2-sided Spearman correlation test between 2 continuous variables. A false-discovery rate approach was used for simultaneous posthoc tests to determine the adjusted P values for wRVUs generated/operative time for attending physicians alone vs with junior residents and for attending physicians alone vs with senior residents. Models were used to evaluate the effects of resident involvement on surgical outcomes, adjusting for variables that showed significant univariate associations. Linear regression models were used for operative time, wRVUs generated, wRVUs generated/operative time, and length of postoperative stay. A logistic regression model was used for death within 30 days. Models were not built for postoperative complications or patient return to the OR, as these were only statistically significantly associated with the patient’s preoperative functional status. A finding was considered significant if P < .05. All analyses were performed using statistical software RStudio Version 2023.03.0.
Results
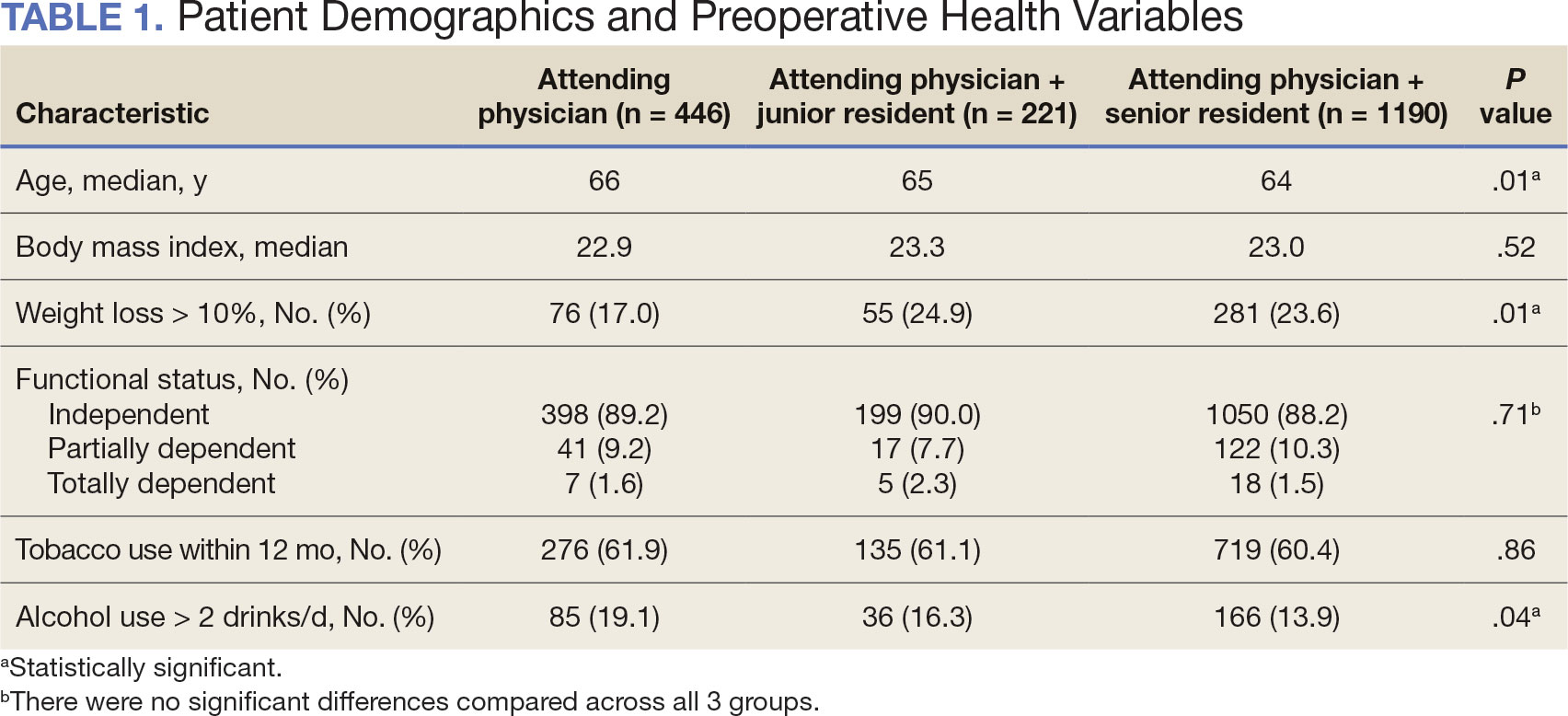
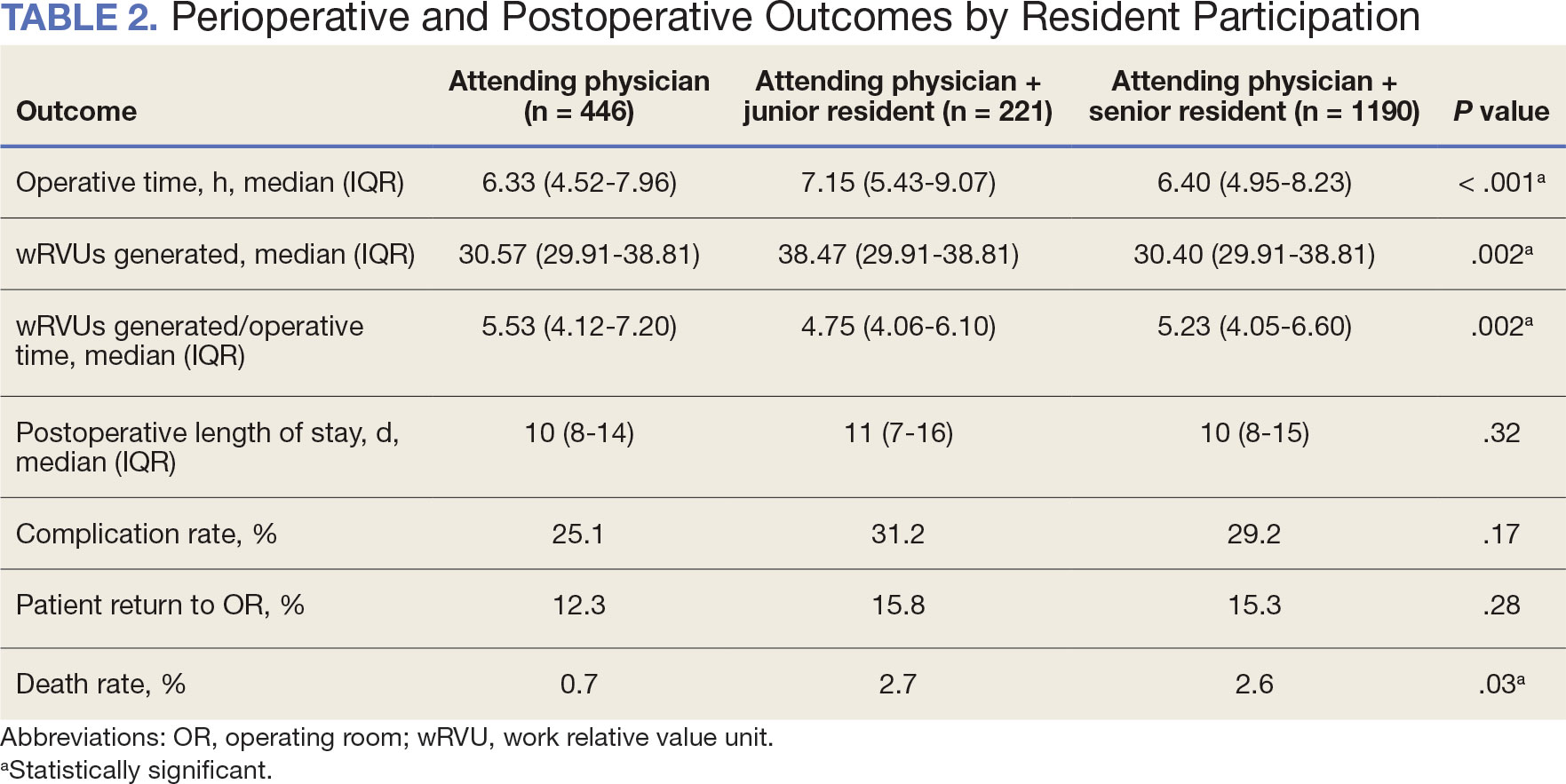
Between 2001 and 2021, 1857 patients who underwent total laryngectomy were identified from the VASQIP database nationwide. Most of the total laryngectomies were staffed by an attending physician with a senior resident (n = 1190, 64%), 446 (24%) were conducted by the attending physician alone, and 221 (12%) by an attending physician with a junior resident (Table 1). The mean operating time for an attending physician alone was 378 minutes, 384 minutes for an attending physician with a senior resident, and 432 minutes for an attending physician with a junior resident (Table 2). There was a statistically significant increase in operating time for laryngectomies with resident participation compared to attending physicians operating alone (P < .001).
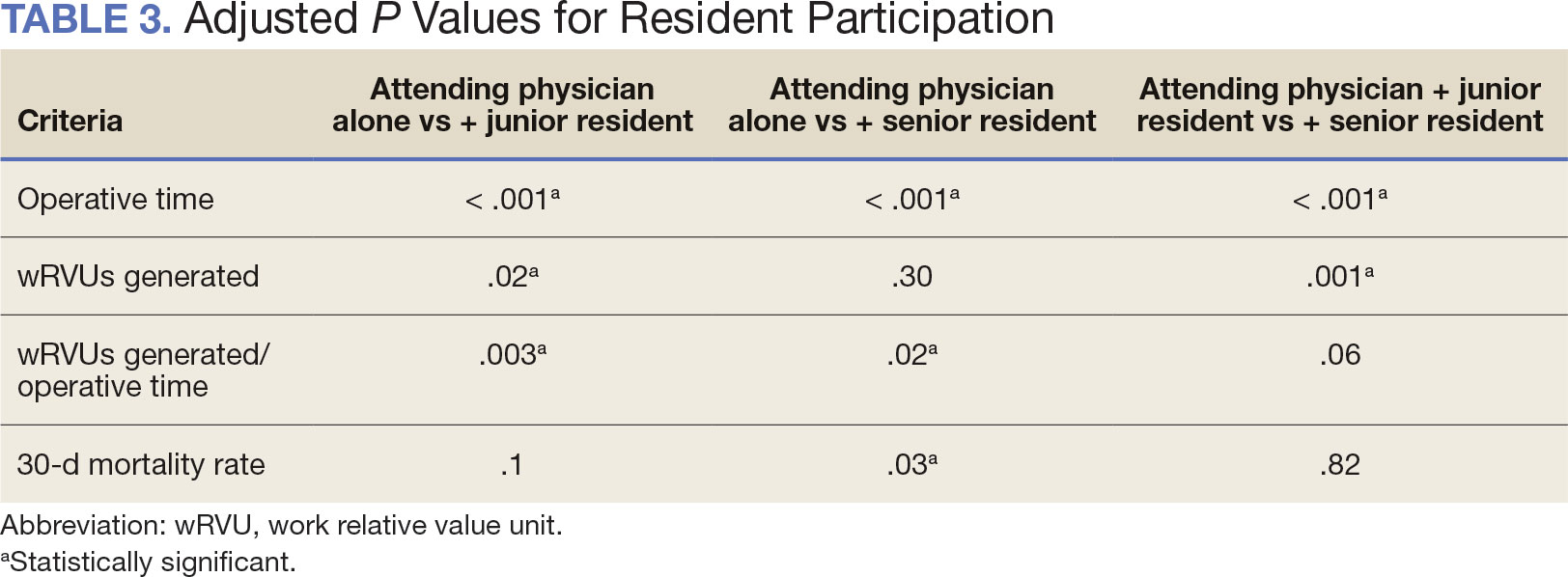
When the wRVUs generated/operative time was analyzed, there was a statistically significant difference between comparison groups. Total laryngectomies performed by attending physicians alone had the highest wRVUs generated/operative time (5.5), followed by laryngectomies performed by attending physicians with senior residents and laryngectomies performed by attending physicians with junior residents (5.2 and 4.8, respectively; P = .002). Table 3 describes adjusted P values for wRVUs generated/ operative time for total laryngectomies performed by attending physicians alone vs with junior residents (P = .003) and for attending physicians alone vs with senior residents (P = .02). Resident participation in total laryngectomies did not significantly impact the development or number of postoperative complications or the rate of return to the OR.
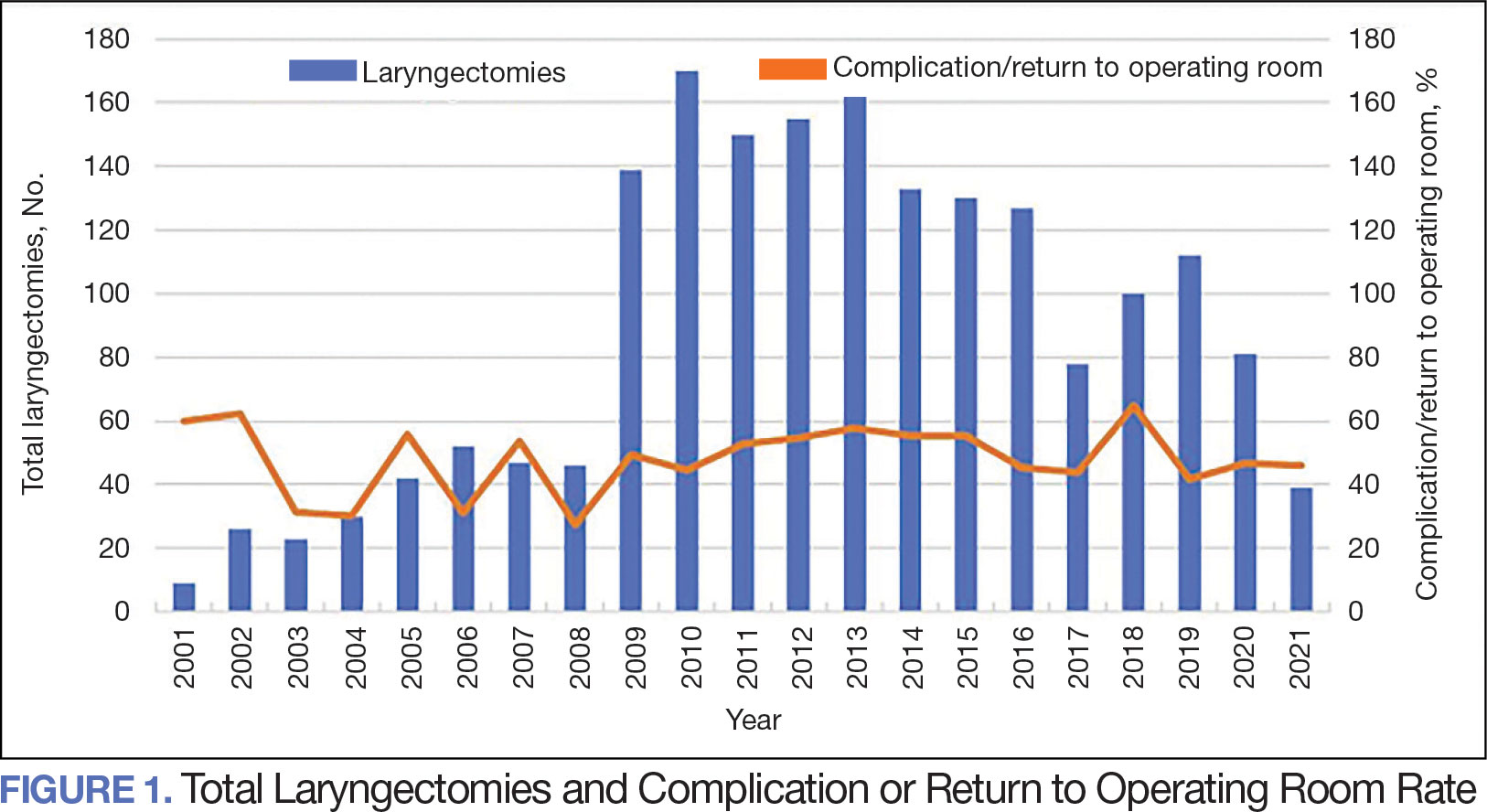
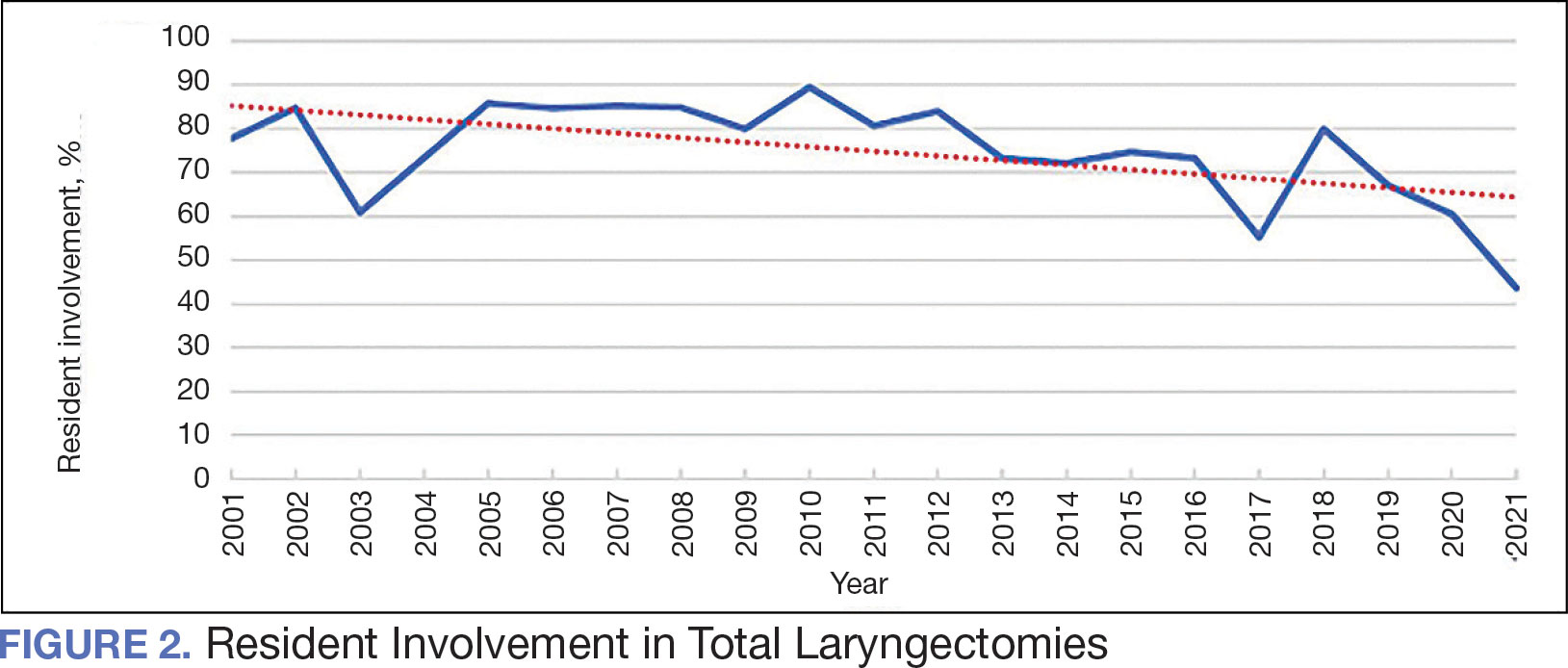
The number of laryngectomies performed in a single fiscal year peaked in 2010 at 170 cases (Figure 1). Between 2001 and 2021, the mean rates of postoperative complications (21.3%) and patient return to the OR (14.6%) did not significantly change. Resident participation in total laryngectomies also peaked in 2010 at 89.0% but has significantly declined, falling to a low of 43.6% in 2021 (Figure 2). From 2001 to 2011, the mean resident participation rate in total laryngectomies was 80.6%, compared with 68.3% from 2012 to 2021 (P < .001).
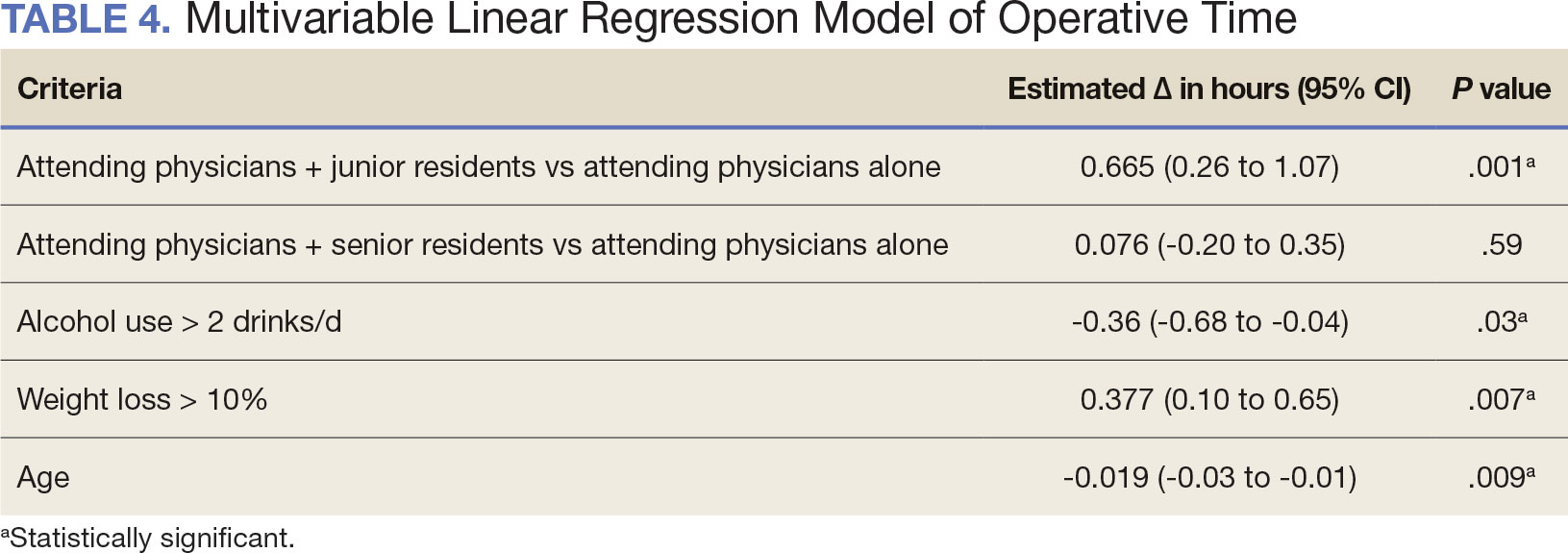
The effect of various demographic and preoperative characteristics on surgical outcomes was also analyzed. A linear regression model accounted for each variable significantly associated with operative time. On multivariable analysis, when all other variables were held constant, Table 4 shows the estimated change in operative time based on certain criteria. For instance, the operative time for attendings with junior residents surgeries was 40 minutes longer (95% CI, 16 to 64) than that of attending alone surgeries (P = .001). Furthermore, operative time decreased by 1.1 minutes (95% CI, 0.30 to 2.04) for each 1-year increase in patient age (P = .009).
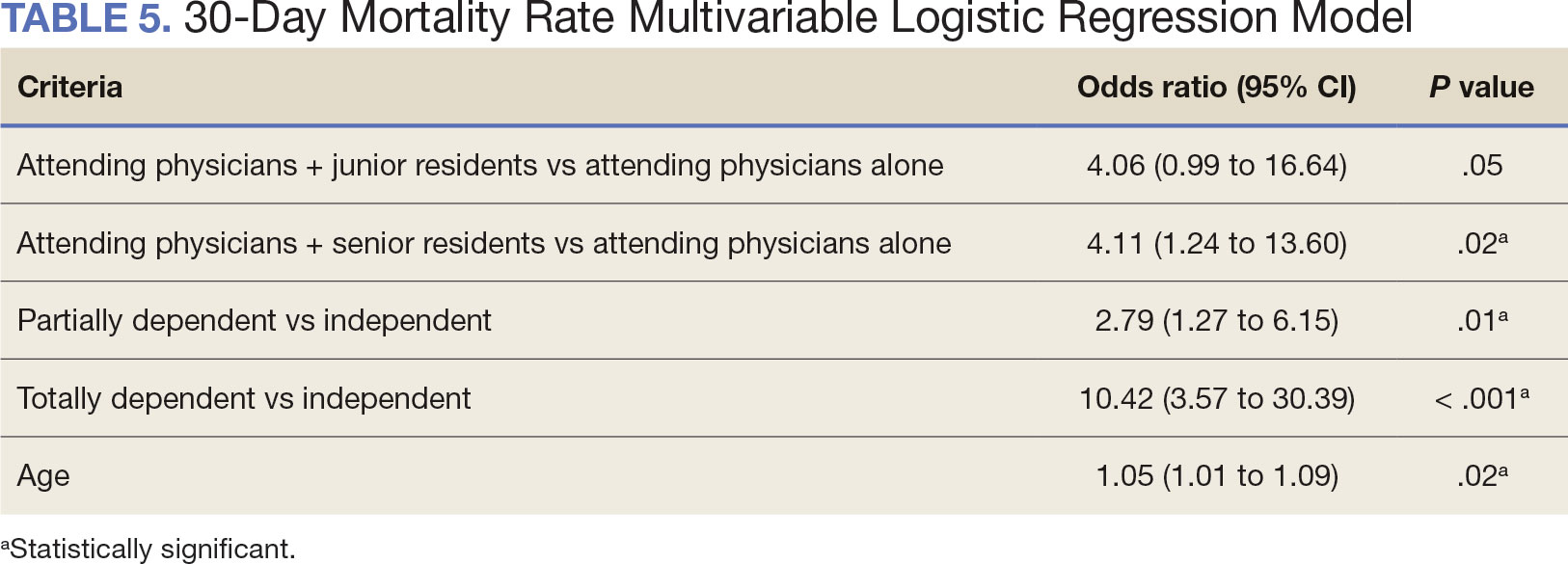
A multivariable logistic regression model evaluated the effect of resident involvement on 30-day mortality rates. Senior resident involvement (P = .02), partially dependent functional status (P = .01), totally dependent functional status (P < .001), and advanced age (P = .02) all were significantly associated with 30-day mortality (Table 5). When other variables remained constant, the odds of death for totally dependent patients were 10.4 times higher than that of patients with independent functional status. Thus, totally dependent functional status appeared to have a greater impact on this outcome than resident participation. The linear regression model for postoperative length of stay demonstrated that senior resident involvement (P = .04), functional status (partially dependent vs independent P < .001), and age (P = .03) were significantly associated with prolonged length of stay.
Discussion
Otolaryngology residency training is designed to educate future otolaryngologists through hands-on learning, adequate feedback, and supervision.1 Although this exposure is paramount for resident education, balancing appropriate supervision and autonomy while mitigating patient risk has been difficult. Numerous non-VA studies have reviewed the impact of resident participation on patient outcomes in various specialties, ranging from a single institution to the National Surgical Quality Improvement Program (NSQIP).4,5,7,22 This study is the first to describe the nationwide impact of resident participation on outcomes in veterans undergoing total laryngectomy.
This study found that resident participation increases operative time and decreases wRVUs generated/operative time without impacting complication rates or patient return to the OR. This reinforces the notion that under close supervision, resident participation does not negatively impact patient outcomes. Resident operative training requires time and dedication by the attending physician and surgical team, thereby increasing operative time. Because VA physician compensation is not linked with productivity as closely as it is in other private and academic settings, surgeons can dedicate more time to operative teaching. This study found that a total laryngectomy involving a junior resident took about 45 minutes longer than an attending physician working alone.
As expected, with longer operative times, the wRVUs generated/operative time ratio was lower in cases with resident participation. Even though resident participation leads to lower OR efficiency, their participation may not significantly impact ancillary costs.23 However, a recent study from NSQIP found an opportunity cost of $60.44 per hour for surgeons operating with a resident in head and neck cases.13
Postoperative complications and mortality are key measures of surgical outcomes in addition to operative time and efficiency. This study found that neither junior nor senior resident participation significantly increased complication rates or patient return to the OR. Despite declining resident involvement and the number of total laryngectomy surgeries in the VA, the complication rate has remained steady. The 30-day mortality rate was significantly higher in cases involving senior residents compared to cases with attending physicians alone. This could be a result of senior resident participation in more challenging cases, such as laryngectomies performed as salvage surgery following radiation. Residents are more often involved in cases with greater complexity at teaching institutions.24-26 Therefore, the higher mortality seen among laryngectomies with senior resident involvement is likely due to the higher complexity of those cases.
The proportion of resident involvement in laryngectomies at VA medical centers has been decreasing over time. Due to the single payer nature of the VA health care system and the number of complex and comorbid patients, the VA offers an invaluable space for resident education in the OR. The fact that less than half of laryngectomies in 2021 involved resident participation is noteworthy for residency training programs. As wRVU compensation models evolve, VA attending surgeons may face less pressure to move the case along, leading to a high potential for operative teaching. Therefore, complex cases, such as laryngectomies, are often ideal for resident participation in the VA.
The steady decline in total laryngectomies at the VA parallels the recent decrease seen in non-VA settings.20 This is due in part to the use of larynx-preserving treatment modalities for laryngeal cancer as well as decreases in the incidence of laryngeal cancer due to population level changes in smoking behaviors. 18,19 Although a laryngectomy is not a key indicator case as determined by the Accreditation Council for Graduate Medical Education, it is important for otolaryngology residents to be exposed to these cases and have a thorough understanding of the operative technique.27 Total laryngectomy was selected for this study because it is a complex and time-consuming surgery with somewhat standardized surgical steps. Unlike microvascular surgery that is very rarely performed by an attending physician alone, laryngectomies can be performed by attending physicians alone or with a resident.28
Limitations
Since this was a retrospective study, it was susceptible to errors in data entry and data extraction from the VASQIP database. Another limitation is the lack of preoperative treatment data on tumor stage and prior nonoperative treatment. For example, a salvage laryngectomy after treatment with radiation and/or chemoradiation is a higher risk procedure than an upfront laryngectomy. Senior resident involvement may be more common in patients undergoing salvage laryngectomy due to the high risk of postoperative fistula and other complications. This may have contributed to the association identified between senior resident participation and 30-day mortality.
Since we could not account for residents who took research years or were fellows, a senior resident may have been mislabeled as a junior resident or vice versa. However, because most research years occur following the third year of residency. We are confident that PGY-1, PGY-2, and PGY-3 is likely to capture junior residents. Other factors, such as coattending surgeon cases, medical student assistance, and fellow involvement may have also impacted the results of this study.
Conclusions
This study is the first to investigate the impact of resident participation on operative time, wRVUs generated, and complication rates in head and neck surgery at VA medical centers. It found that resident participation in total laryngectomies among veterans increased operative time and reduced wRVUs generated per hour but did not impact complication rate or patient return to the OR. The VA offers a unique and invaluable space for resident education and operative training, and the recent decline in resident participation among laryngectomies is important for residency programs to acknowledge and potentially address moving forward.
In contrast to oral cavity resections which can vary from partial glossectomies to composite resections, laryngectomy represents a homogenous procedure from which to draw meaningful conclusions about complication rates, operative time, and outcome. Future directions should include studying other types of head and neck surgery in the VA to determine whether the impact of resident participation mirrors the findings of this study.
References
Chung RS. How much time do surgical residents need to learn operative surgery? Am J Surg. 2005;190(3):351-353. doi:10.1016/j.amjsurg.2005.06.035
S, Darzi A. Defining quality in surgical training: perceptions of the profession. Am J Surg. 2014;207(4):628-636. doi:10.1016/j.amjsurg.2013.07.044
Bhatti NI, Ahmed A, Choi SS. Identifying quality indicators of surgical of surgical training: a national survey. Laryngoscope. 2015;125(12):2685-2689. doi:10.1002/lary.25262
Abt NB, Reh DD, Eisele DW, Francis HW, Gourin CG. Does resident participation influence otolaryngology-head and neck surgery morbidity and mortality? Laryngoscope. 2016;126(10):2263-2269. doi:10.1002/lary.25973
Jubbal KT, Chang D, Izaddoost SA, Pederson W, Zavlin D, Echo A. Resident involvement in microsurgery: an American College of Surgeons national surgical quality improvement program analysis. J Surg Educ. 2017;74(6):1124-1132. doi:10.1016/j.jsurg.2017.05.017
Kshirsagar RS, Chandy Z, Mahboubi H, Verma SP. Does resident involvement in thyroid surgery lead to increased postoperative complications? Laryngoscope. 2017;127(5):1242-1246. doi:10.1002/lary.26176
Vieira BL, Hernandez DJ, Qin C, Smith SS, Kim JY, Dutra JC. The impact of resident involvement on otolaryngology surgical outcomes. Laryngoscope. 2016;126(3):602-607. doi:10.1002/lary.25046
Advani V, Ahad S, Gonczy C, Markwell S, Hassan I. Does resident involvement effect surgical times and complication rates during laparoscopic appendectomy for uncomplicated appendicitis? An analysis of 16,849 cases from the ACS-NSQIP. Am J Surg. 2012;203(3):347-352. doi:10.1016/j.amjsurg.2011.08.015
Quinn NA, Alt JA, Ashby S, Orlandi RR. Time, resident involvement, and supply drive cost variability in septoplasty with turbinate reduction. Otolaryngol Head Neck Surg. 2018;159(2):310-314. doi:10.1177/0194599818765099
Leader BA, Wiebracht ND, Meinzen-Derr J, Ishman SL. The impact of resident involvement on tonsillectomy outcomes and surgical time. Laryngoscope. 2020;130(10):2481-2486. doi:10.1002/lary.28427
Muelleman T, Shew M, Muelleman RJ, et al. Impact of resident participation on operative time and outcomes in otologic surgery. Otolaryngol Head Neck Surg. 2018;158(1):151-154. doi:10.1177/0194599817737270
Puram SV, Kozin ED, Sethi R, et al. Impact of resident surgeons on procedure length based on common pediatric otolaryngology cases. Laryngoscope. 2015;125(4):991 -997. doi:10.1002/lary.24912
Chow MS, Gordon AJ, Talwar A, Lydiatt WM, Yueh B, Givi B. The RVU compensation model and head and neck surgical education. Laryngoscope. 2024;134(1):113-119. doi:10.1002/lary.30807
Papandria D, Rhee D, Ortega G, et al. Assessing trainee impact on operative time for common general surgical procedures in ACS-NSQIP. J Surg Educ. 2012;69(2):149-155. doi:10.1016/j.jsurg.2011.08.003
Pugely AJ, Gao Y, Martin CT, Callagh JJ, Weinstein SL, Marsh JL. The effect of resident participation on short-term outcomes after orthopaedic surgery. Clin Orthop Relat Res. 2014;472(7):2290-2300. doi:10.1007/s11999-014-3567-0
Hosler MR, Scott IU, Kunselman AR, Wolford KR, Oltra EZ, Murray WB. Impact of resident participation in cataract surgery on operative time and cost. Ophthalmology. 2012;119(1):95-98. doi:10.1016/j.ophtha.2011.06.026
Lanigan A, Spaw M, Donaghe C, Brennan J. The impact of the Veteran’s Affairs medical system on an otolaryngology residency training program. Mil Med. 2018;183(11-12):e671-e675. doi:10.1093/milmed/usy041
American Society of Clinical Oncology, Pfister DG, Laurie SA, et al. American Society of Clinical Oncology clinical practice guideline for the use of larynx-preservation strategies in the treatment of laryngeal cancer. J Clin Oncol. 2006;24(22):3693-3704. doi:10.1200/JCO.2006.07.4559
Forastiere AA, Ismaila N, Lewin JS, et al. Use of larynxpreservation strategies in the treatment of laryngeal cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2018;36(11):1143-1169. doi:10.1200/JCO.2017.75.7385
Verma SP, Mahboubi H. The changing landscape of total laryngectomy surgery. Otolaryngol Head Neck Surg. 2014;150(3):413-418. doi:10.1177/0194599813514515
Habermann EB, Harris AHS, Giori NJ. Large surgical databases with direct data abstraction: VASQIP and ACSNSQIP. J Bone Joint Surg Am. 2022;104(suppl 3):9-14. doi:10.2106/JBJS.22.00596
Benito DA, Mamidi I, Pasick LJ, et al. Evaluating resident involvement and the ‘July effect’ in parotidectomy. J Laryngol Otol. 2021;135(5):452-457. doi:10.1017/S0022215121000578
Hwang CS, Wichterman KA, Alfrey EJ. The cost of resident education. J Surg Res. 2010;163(1):18-23. doi:10.1016/j.jss.2010.03.013
Saliba AN, Taher AT, Tamim H, et al. Impact of resident involvement in surgery (IRIS-NSQIP): looking at the bigger picture based on the American College of Surgeons- NSQIP database. J Am Coll Surg. 2016; 222(1):30-40. doi:10.1016/j.jamcollsurg.2015.10.011
Khuri SF, Najjar SF, Daley J, et al. Comparison of surgical outcomes between teaching and nonteaching hospitals in the Department of Veterans Affairs. Ann Surg. 2001;234(3):370-383. doi:10.1097/00000658-200109000-00011
Relles DM, Burkhart RA, Pucci MJ et al. Does resident experience affect outcomes in complex abdominal surgery? Pancreaticoduodenectomy as an example. J Gastrointest Surg. 2014;18(2):279-285. doi:10.1007/s11605-013-2372-5
Brady JS, Crippen MM, Filimonov A, et al. The effect of training level on complications after free flap surgery of the head and neck. Am J Otolaryngol. 2017;38(5):560-564. doi:10.1016/j.amjoto.2017.06.001
John Andersona; Xue Geng, MSb; Jessica H. Maxwell, MD, MPHc,d
Author disclosures: The authors report no actual or potential conflicts of interest with regard to this article.
Author affiliationsL aGeorgetown University, Washington, District of Columbia bMedStar Georgetown University Hospital, Washington, District of Columbia cUniversity of Pittsburgh Medical Center, Pennsylvania dVeterans Affairs Pittsburgh Healthcare System, Pennsylvania
John Andersona; Xue Geng, MSb; Jessica H. Maxwell, MD, MPHc,d
Author disclosures: The authors report no actual or potential conflicts of interest with regard to this article.
Author affiliationsL aGeorgetown University, Washington, District of Columbia bMedStar Georgetown University Hospital, Washington, District of Columbia cUniversity of Pittsburgh Medical Center, Pennsylvania dVeterans Affairs Pittsburgh Healthcare System, Pennsylvania
Fed Pract. 2025;42(2). Published online February 15. doi:10.12788/fp.0550
Author and Disclosure Information
John Andersona; Xue Geng, MSb; Jessica H. Maxwell, MD, MPHc,d
Author disclosures: The authors report no actual or potential conflicts of interest with regard to this article.
Author affiliationsL aGeorgetown University, Washington, District of Columbia bMedStar Georgetown University Hospital, Washington, District of Columbia cUniversity of Pittsburgh Medical Center, Pennsylvania dVeterans Affairs Pittsburgh Healthcare System, Pennsylvania
The US Department of Veterans Affairs (VA) has been integral in resident training. Resident surgical training requires a balance of supervision and autonomy, along with procedure repetition and appropriate feedback.1-3 Non-VA research has found that resident participation across various otolaryngology procedures, including thyroidectomy, neck dissection, and laryngectomy, does not increase patient morbidity.4-7 However, resident involvement in private and academic settings that included nonhead and neck procedures was linked to increased operative time and reduced productivity, as determined by work relative value units (wRVUs).7-13 This has also been identified in other specialties, including general surgery, orthopedics, and ophthalmology.14-16
Unlike the private sector, surgeon compensation at the VA is not as closely linked to operative productivity, offering a unique setting for resident training. While VA integration in otolaryngology residency programs increases resident case numbers, particularly in head and neck cases, the impact on VA patient outcomes and productivity is unknown.17 The use of larynxpreserving treatment modalities for laryngeal cancer has led to a decline in the number of total laryngectomies performed, which could potentially impact resident operative training for laryngectomies.18-20
This study sought to determine the impact of resident participation on operative time, wRVUs, and patient outcomes in veterans who underwent a total laryngectomy. This study was reviewed and approved by the MedStar Georgetown University Hospital Institutional Review Board and Research and Development Committee (#1595672).
Methods
A retrospective cohort of veterans nationwide who underwent total laryngectomy between 2001 and 2021, with or without neck dissection, was identified from the Veterans Affairs Surgical Quality Improvement Program (VASQIP). Data were extracted via the VA Informatics and Computing Infrastructure and patients were included based on Current Procedural Terminology codes for total laryngectomy, with or without neck dissection (31320, 31360, 31365). Laryngopharyngectomies, partial laryngectomies, and minimally invasive laryngectomies were excluded. VASQIP nurse data managers reviewed patient data for operative data, postoperative outcomes (including 30- day morbidity and mortality), and preoperative risk factors (Appendix).21
The VASQIP data provide the highest resident or postgraduate year (PGY) per surgery. PGY 1, 2, and 3 were considered junior residents and PGY ≥4, surgical fellows, and individuals who took research years during residency were considered senior residents. Cases performed by attending physicians alone were compared with those involving junior or senior residents.
Patient demographic data included age, body mass index, smoking and alcohol use, weight loss, and functional status. Consumption of any tobacco products within 12 months of surgery was considered tobacco use. Drinking on average ≥2 alcoholic beverages daily was considered alcohol use. Weight loss was defined as a 10% reduction in body weight within the 6 months before surgery, excluding patients enrolled in a weight loss program. Functional status was categorized as independent, partially dependent, totally dependent, and unknown.
Primary outcomes included operative time, wRVUs generated, and wRVUs generated per hour of operative time. Postoperative complications were recorded both as a continuous variable and as a binary variable for presence or absence of a complication. Additional outcome variables included length of postoperative hospital stay, return to the operating room (OR), and death within 30 days of surgery.
Statistical Analysis
Data were summarized using frequency and percentage for categorical variables and median with IQR for continuous variables. Data were also summarized based on resident involvement in the surgery and the PGY level of the residents involved. The occurrence of total laryngectomy, rate of complications, and patient return to the OR were summarized by year.
Univariate associations between resident involvement and surgical outcomes were analyzed using the Kruskal-Wallis test for continuous variables and the ÷2 test for categorical variables. A Fisher exact test was used when the cell count in the contingency table was < 5. The univariate associations between surgical outcomes and demographic/preoperative variables were examined using 2-sided Wilcoxon ranksum tests or Kruskal-Wallis tests between continuous variables and categorical variables, X2 or Fisher exact test between 2 categorical variables, and 2-sided Spearman correlation test between 2 continuous variables. A false-discovery rate approach was used for simultaneous posthoc tests to determine the adjusted P values for wRVUs generated/operative time for attending physicians alone vs with junior residents and for attending physicians alone vs with senior residents. Models were used to evaluate the effects of resident involvement on surgical outcomes, adjusting for variables that showed significant univariate associations. Linear regression models were used for operative time, wRVUs generated, wRVUs generated/operative time, and length of postoperative stay. A logistic regression model was used for death within 30 days. Models were not built for postoperative complications or patient return to the OR, as these were only statistically significantly associated with the patient’s preoperative functional status. A finding was considered significant if P < .05. All analyses were performed using statistical software RStudio Version 2023.03.0.
Results
Between 2001 and 2021, 1857 patients who underwent total laryngectomy were identified from the VASQIP database nationwide. Most of the total laryngectomies were staffed by an attending physician with a senior resident (n = 1190, 64%), 446 (24%) were conducted by the attending physician alone, and 221 (12%) by an attending physician with a junior resident (Table 1). The mean operating time for an attending physician alone was 378 minutes, 384 minutes for an attending physician with a senior resident, and 432 minutes for an attending physician with a junior resident (Table 2). There was a statistically significant increase in operating time for laryngectomies with resident participation compared to attending physicians operating alone (P < .001).
When the wRVUs generated/operative time was analyzed, there was a statistically significant difference between comparison groups. Total laryngectomies performed by attending physicians alone had the highest wRVUs generated/operative time (5.5), followed by laryngectomies performed by attending physicians with senior residents and laryngectomies performed by attending physicians with junior residents (5.2 and 4.8, respectively; P = .002). Table 3 describes adjusted P values for wRVUs generated/ operative time for total laryngectomies performed by attending physicians alone vs with junior residents (P = .003) and for attending physicians alone vs with senior residents (P = .02). Resident participation in total laryngectomies did not significantly impact the development or number of postoperative complications or the rate of return to the OR.
The number of laryngectomies performed in a single fiscal year peaked in 2010 at 170 cases (Figure 1). Between 2001 and 2021, the mean rates of postoperative complications (21.3%) and patient return to the OR (14.6%) did not significantly change. Resident participation in total laryngectomies also peaked in 2010 at 89.0% but has significantly declined, falling to a low of 43.6% in 2021 (Figure 2). From 2001 to 2011, the mean resident participation rate in total laryngectomies was 80.6%, compared with 68.3% from 2012 to 2021 (P < .001).
The effect of various demographic and preoperative characteristics on surgical outcomes was also analyzed. A linear regression model accounted for each variable significantly associated with operative time. On multivariable analysis, when all other variables were held constant, Table 4 shows the estimated change in operative time based on certain criteria. For instance, the operative time for attendings with junior residents surgeries was 40 minutes longer (95% CI, 16 to 64) than that of attending alone surgeries (P = .001). Furthermore, operative time decreased by 1.1 minutes (95% CI, 0.30 to 2.04) for each 1-year increase in patient age (P = .009).
A multivariable logistic regression model evaluated the effect of resident involvement on 30-day mortality rates. Senior resident involvement (P = .02), partially dependent functional status (P = .01), totally dependent functional status (P < .001), and advanced age (P = .02) all were significantly associated with 30-day mortality (Table 5). When other variables remained constant, the odds of death for totally dependent patients were 10.4 times higher than that of patients with independent functional status. Thus, totally dependent functional status appeared to have a greater impact on this outcome than resident participation. The linear regression model for postoperative length of stay demonstrated that senior resident involvement (P = .04), functional status (partially dependent vs independent P < .001), and age (P = .03) were significantly associated with prolonged length of stay.
Discussion
Otolaryngology residency training is designed to educate future otolaryngologists through hands-on learning, adequate feedback, and supervision.1 Although this exposure is paramount for resident education, balancing appropriate supervision and autonomy while mitigating patient risk has been difficult. Numerous non-VA studies have reviewed the impact of resident participation on patient outcomes in various specialties, ranging from a single institution to the National Surgical Quality Improvement Program (NSQIP).4,5,7,22 This study is the first to describe the nationwide impact of resident participation on outcomes in veterans undergoing total laryngectomy.
This study found that resident participation increases operative time and decreases wRVUs generated/operative time without impacting complication rates or patient return to the OR. This reinforces the notion that under close supervision, resident participation does not negatively impact patient outcomes. Resident operative training requires time and dedication by the attending physician and surgical team, thereby increasing operative time. Because VA physician compensation is not linked with productivity as closely as it is in other private and academic settings, surgeons can dedicate more time to operative teaching. This study found that a total laryngectomy involving a junior resident took about 45 minutes longer than an attending physician working alone.
As expected, with longer operative times, the wRVUs generated/operative time ratio was lower in cases with resident participation. Even though resident participation leads to lower OR efficiency, their participation may not significantly impact ancillary costs.23 However, a recent study from NSQIP found an opportunity cost of $60.44 per hour for surgeons operating with a resident in head and neck cases.13
Postoperative complications and mortality are key measures of surgical outcomes in addition to operative time and efficiency. This study found that neither junior nor senior resident participation significantly increased complication rates or patient return to the OR. Despite declining resident involvement and the number of total laryngectomy surgeries in the VA, the complication rate has remained steady. The 30-day mortality rate was significantly higher in cases involving senior residents compared to cases with attending physicians alone. This could be a result of senior resident participation in more challenging cases, such as laryngectomies performed as salvage surgery following radiation. Residents are more often involved in cases with greater complexity at teaching institutions.24-26 Therefore, the higher mortality seen among laryngectomies with senior resident involvement is likely due to the higher complexity of those cases.
The proportion of resident involvement in laryngectomies at VA medical centers has been decreasing over time. Due to the single payer nature of the VA health care system and the number of complex and comorbid patients, the VA offers an invaluable space for resident education in the OR. The fact that less than half of laryngectomies in 2021 involved resident participation is noteworthy for residency training programs. As wRVU compensation models evolve, VA attending surgeons may face less pressure to move the case along, leading to a high potential for operative teaching. Therefore, complex cases, such as laryngectomies, are often ideal for resident participation in the VA.
The steady decline in total laryngectomies at the VA parallels the recent decrease seen in non-VA settings.20 This is due in part to the use of larynx-preserving treatment modalities for laryngeal cancer as well as decreases in the incidence of laryngeal cancer due to population level changes in smoking behaviors. 18,19 Although a laryngectomy is not a key indicator case as determined by the Accreditation Council for Graduate Medical Education, it is important for otolaryngology residents to be exposed to these cases and have a thorough understanding of the operative technique.27 Total laryngectomy was selected for this study because it is a complex and time-consuming surgery with somewhat standardized surgical steps. Unlike microvascular surgery that is very rarely performed by an attending physician alone, laryngectomies can be performed by attending physicians alone or with a resident.28
Limitations
Since this was a retrospective study, it was susceptible to errors in data entry and data extraction from the VASQIP database. Another limitation is the lack of preoperative treatment data on tumor stage and prior nonoperative treatment. For example, a salvage laryngectomy after treatment with radiation and/or chemoradiation is a higher risk procedure than an upfront laryngectomy. Senior resident involvement may be more common in patients undergoing salvage laryngectomy due to the high risk of postoperative fistula and other complications. This may have contributed to the association identified between senior resident participation and 30-day mortality.
Since we could not account for residents who took research years or were fellows, a senior resident may have been mislabeled as a junior resident or vice versa. However, because most research years occur following the third year of residency. We are confident that PGY-1, PGY-2, and PGY-3 is likely to capture junior residents. Other factors, such as coattending surgeon cases, medical student assistance, and fellow involvement may have also impacted the results of this study.
Conclusions
This study is the first to investigate the impact of resident participation on operative time, wRVUs generated, and complication rates in head and neck surgery at VA medical centers. It found that resident participation in total laryngectomies among veterans increased operative time and reduced wRVUs generated per hour but did not impact complication rate or patient return to the OR. The VA offers a unique and invaluable space for resident education and operative training, and the recent decline in resident participation among laryngectomies is important for residency programs to acknowledge and potentially address moving forward.
In contrast to oral cavity resections which can vary from partial glossectomies to composite resections, laryngectomy represents a homogenous procedure from which to draw meaningful conclusions about complication rates, operative time, and outcome. Future directions should include studying other types of head and neck surgery in the VA to determine whether the impact of resident participation mirrors the findings of this study.
The US Department of Veterans Affairs (VA) has been integral in resident training. Resident surgical training requires a balance of supervision and autonomy, along with procedure repetition and appropriate feedback.1-3 Non-VA research has found that resident participation across various otolaryngology procedures, including thyroidectomy, neck dissection, and laryngectomy, does not increase patient morbidity.4-7 However, resident involvement in private and academic settings that included nonhead and neck procedures was linked to increased operative time and reduced productivity, as determined by work relative value units (wRVUs).7-13 This has also been identified in other specialties, including general surgery, orthopedics, and ophthalmology.14-16
Unlike the private sector, surgeon compensation at the VA is not as closely linked to operative productivity, offering a unique setting for resident training. While VA integration in otolaryngology residency programs increases resident case numbers, particularly in head and neck cases, the impact on VA patient outcomes and productivity is unknown.17 The use of larynxpreserving treatment modalities for laryngeal cancer has led to a decline in the number of total laryngectomies performed, which could potentially impact resident operative training for laryngectomies.18-20
This study sought to determine the impact of resident participation on operative time, wRVUs, and patient outcomes in veterans who underwent a total laryngectomy. This study was reviewed and approved by the MedStar Georgetown University Hospital Institutional Review Board and Research and Development Committee (#1595672).
Methods
A retrospective cohort of veterans nationwide who underwent total laryngectomy between 2001 and 2021, with or without neck dissection, was identified from the Veterans Affairs Surgical Quality Improvement Program (VASQIP). Data were extracted via the VA Informatics and Computing Infrastructure and patients were included based on Current Procedural Terminology codes for total laryngectomy, with or without neck dissection (31320, 31360, 31365). Laryngopharyngectomies, partial laryngectomies, and minimally invasive laryngectomies were excluded. VASQIP nurse data managers reviewed patient data for operative data, postoperative outcomes (including 30- day morbidity and mortality), and preoperative risk factors (Appendix).21
The VASQIP data provide the highest resident or postgraduate year (PGY) per surgery. PGY 1, 2, and 3 were considered junior residents and PGY ≥4, surgical fellows, and individuals who took research years during residency were considered senior residents. Cases performed by attending physicians alone were compared with those involving junior or senior residents.
Patient demographic data included age, body mass index, smoking and alcohol use, weight loss, and functional status. Consumption of any tobacco products within 12 months of surgery was considered tobacco use. Drinking on average ≥2 alcoholic beverages daily was considered alcohol use. Weight loss was defined as a 10% reduction in body weight within the 6 months before surgery, excluding patients enrolled in a weight loss program. Functional status was categorized as independent, partially dependent, totally dependent, and unknown.
Primary outcomes included operative time, wRVUs generated, and wRVUs generated per hour of operative time. Postoperative complications were recorded both as a continuous variable and as a binary variable for presence or absence of a complication. Additional outcome variables included length of postoperative hospital stay, return to the operating room (OR), and death within 30 days of surgery.
Statistical Analysis
Data were summarized using frequency and percentage for categorical variables and median with IQR for continuous variables. Data were also summarized based on resident involvement in the surgery and the PGY level of the residents involved. The occurrence of total laryngectomy, rate of complications, and patient return to the OR were summarized by year.
Univariate associations between resident involvement and surgical outcomes were analyzed using the Kruskal-Wallis test for continuous variables and the ÷2 test for categorical variables. A Fisher exact test was used when the cell count in the contingency table was < 5. The univariate associations between surgical outcomes and demographic/preoperative variables were examined using 2-sided Wilcoxon ranksum tests or Kruskal-Wallis tests between continuous variables and categorical variables, X2 or Fisher exact test between 2 categorical variables, and 2-sided Spearman correlation test between 2 continuous variables. A false-discovery rate approach was used for simultaneous posthoc tests to determine the adjusted P values for wRVUs generated/operative time for attending physicians alone vs with junior residents and for attending physicians alone vs with senior residents. Models were used to evaluate the effects of resident involvement on surgical outcomes, adjusting for variables that showed significant univariate associations. Linear regression models were used for operative time, wRVUs generated, wRVUs generated/operative time, and length of postoperative stay. A logistic regression model was used for death within 30 days. Models were not built for postoperative complications or patient return to the OR, as these were only statistically significantly associated with the patient’s preoperative functional status. A finding was considered significant if P < .05. All analyses were performed using statistical software RStudio Version 2023.03.0.
Results
Between 2001 and 2021, 1857 patients who underwent total laryngectomy were identified from the VASQIP database nationwide. Most of the total laryngectomies were staffed by an attending physician with a senior resident (n = 1190, 64%), 446 (24%) were conducted by the attending physician alone, and 221 (12%) by an attending physician with a junior resident (Table 1). The mean operating time for an attending physician alone was 378 minutes, 384 minutes for an attending physician with a senior resident, and 432 minutes for an attending physician with a junior resident (Table 2). There was a statistically significant increase in operating time for laryngectomies with resident participation compared to attending physicians operating alone (P < .001).
When the wRVUs generated/operative time was analyzed, there was a statistically significant difference between comparison groups. Total laryngectomies performed by attending physicians alone had the highest wRVUs generated/operative time (5.5), followed by laryngectomies performed by attending physicians with senior residents and laryngectomies performed by attending physicians with junior residents (5.2 and 4.8, respectively; P = .002). Table 3 describes adjusted P values for wRVUs generated/ operative time for total laryngectomies performed by attending physicians alone vs with junior residents (P = .003) and for attending physicians alone vs with senior residents (P = .02). Resident participation in total laryngectomies did not significantly impact the development or number of postoperative complications or the rate of return to the OR.
The number of laryngectomies performed in a single fiscal year peaked in 2010 at 170 cases (Figure 1). Between 2001 and 2021, the mean rates of postoperative complications (21.3%) and patient return to the OR (14.6%) did not significantly change. Resident participation in total laryngectomies also peaked in 2010 at 89.0% but has significantly declined, falling to a low of 43.6% in 2021 (Figure 2). From 2001 to 2011, the mean resident participation rate in total laryngectomies was 80.6%, compared with 68.3% from 2012 to 2021 (P < .001).
The effect of various demographic and preoperative characteristics on surgical outcomes was also analyzed. A linear regression model accounted for each variable significantly associated with operative time. On multivariable analysis, when all other variables were held constant, Table 4 shows the estimated change in operative time based on certain criteria. For instance, the operative time for attendings with junior residents surgeries was 40 minutes longer (95% CI, 16 to 64) than that of attending alone surgeries (P = .001). Furthermore, operative time decreased by 1.1 minutes (95% CI, 0.30 to 2.04) for each 1-year increase in patient age (P = .009).
A multivariable logistic regression model evaluated the effect of resident involvement on 30-day mortality rates. Senior resident involvement (P = .02), partially dependent functional status (P = .01), totally dependent functional status (P < .001), and advanced age (P = .02) all were significantly associated with 30-day mortality (Table 5). When other variables remained constant, the odds of death for totally dependent patients were 10.4 times higher than that of patients with independent functional status. Thus, totally dependent functional status appeared to have a greater impact on this outcome than resident participation. The linear regression model for postoperative length of stay demonstrated that senior resident involvement (P = .04), functional status (partially dependent vs independent P < .001), and age (P = .03) were significantly associated with prolonged length of stay.
Discussion
Otolaryngology residency training is designed to educate future otolaryngologists through hands-on learning, adequate feedback, and supervision.1 Although this exposure is paramount for resident education, balancing appropriate supervision and autonomy while mitigating patient risk has been difficult. Numerous non-VA studies have reviewed the impact of resident participation on patient outcomes in various specialties, ranging from a single institution to the National Surgical Quality Improvement Program (NSQIP).4,5,7,22 This study is the first to describe the nationwide impact of resident participation on outcomes in veterans undergoing total laryngectomy.
This study found that resident participation increases operative time and decreases wRVUs generated/operative time without impacting complication rates or patient return to the OR. This reinforces the notion that under close supervision, resident participation does not negatively impact patient outcomes. Resident operative training requires time and dedication by the attending physician and surgical team, thereby increasing operative time. Because VA physician compensation is not linked with productivity as closely as it is in other private and academic settings, surgeons can dedicate more time to operative teaching. This study found that a total laryngectomy involving a junior resident took about 45 minutes longer than an attending physician working alone.
As expected, with longer operative times, the wRVUs generated/operative time ratio was lower in cases with resident participation. Even though resident participation leads to lower OR efficiency, their participation may not significantly impact ancillary costs.23 However, a recent study from NSQIP found an opportunity cost of $60.44 per hour for surgeons operating with a resident in head and neck cases.13
Postoperative complications and mortality are key measures of surgical outcomes in addition to operative time and efficiency. This study found that neither junior nor senior resident participation significantly increased complication rates or patient return to the OR. Despite declining resident involvement and the number of total laryngectomy surgeries in the VA, the complication rate has remained steady. The 30-day mortality rate was significantly higher in cases involving senior residents compared to cases with attending physicians alone. This could be a result of senior resident participation in more challenging cases, such as laryngectomies performed as salvage surgery following radiation. Residents are more often involved in cases with greater complexity at teaching institutions.24-26 Therefore, the higher mortality seen among laryngectomies with senior resident involvement is likely due to the higher complexity of those cases.
The proportion of resident involvement in laryngectomies at VA medical centers has been decreasing over time. Due to the single payer nature of the VA health care system and the number of complex and comorbid patients, the VA offers an invaluable space for resident education in the OR. The fact that less than half of laryngectomies in 2021 involved resident participation is noteworthy for residency training programs. As wRVU compensation models evolve, VA attending surgeons may face less pressure to move the case along, leading to a high potential for operative teaching. Therefore, complex cases, such as laryngectomies, are often ideal for resident participation in the VA.
The steady decline in total laryngectomies at the VA parallels the recent decrease seen in non-VA settings.20 This is due in part to the use of larynx-preserving treatment modalities for laryngeal cancer as well as decreases in the incidence of laryngeal cancer due to population level changes in smoking behaviors. 18,19 Although a laryngectomy is not a key indicator case as determined by the Accreditation Council for Graduate Medical Education, it is important for otolaryngology residents to be exposed to these cases and have a thorough understanding of the operative technique.27 Total laryngectomy was selected for this study because it is a complex and time-consuming surgery with somewhat standardized surgical steps. Unlike microvascular surgery that is very rarely performed by an attending physician alone, laryngectomies can be performed by attending physicians alone or with a resident.28
Limitations
Since this was a retrospective study, it was susceptible to errors in data entry and data extraction from the VASQIP database. Another limitation is the lack of preoperative treatment data on tumor stage and prior nonoperative treatment. For example, a salvage laryngectomy after treatment with radiation and/or chemoradiation is a higher risk procedure than an upfront laryngectomy. Senior resident involvement may be more common in patients undergoing salvage laryngectomy due to the high risk of postoperative fistula and other complications. This may have contributed to the association identified between senior resident participation and 30-day mortality.
Since we could not account for residents who took research years or were fellows, a senior resident may have been mislabeled as a junior resident or vice versa. However, because most research years occur following the third year of residency. We are confident that PGY-1, PGY-2, and PGY-3 is likely to capture junior residents. Other factors, such as coattending surgeon cases, medical student assistance, and fellow involvement may have also impacted the results of this study.
Conclusions
This study is the first to investigate the impact of resident participation on operative time, wRVUs generated, and complication rates in head and neck surgery at VA medical centers. It found that resident participation in total laryngectomies among veterans increased operative time and reduced wRVUs generated per hour but did not impact complication rate or patient return to the OR. The VA offers a unique and invaluable space for resident education and operative training, and the recent decline in resident participation among laryngectomies is important for residency programs to acknowledge and potentially address moving forward.
In contrast to oral cavity resections which can vary from partial glossectomies to composite resections, laryngectomy represents a homogenous procedure from which to draw meaningful conclusions about complication rates, operative time, and outcome. Future directions should include studying other types of head and neck surgery in the VA to determine whether the impact of resident participation mirrors the findings of this study.
References
Chung RS. How much time do surgical residents need to learn operative surgery? Am J Surg. 2005;190(3):351-353. doi:10.1016/j.amjsurg.2005.06.035
S, Darzi A. Defining quality in surgical training: perceptions of the profession. Am J Surg. 2014;207(4):628-636. doi:10.1016/j.amjsurg.2013.07.044
Bhatti NI, Ahmed A, Choi SS. Identifying quality indicators of surgical of surgical training: a national survey. Laryngoscope. 2015;125(12):2685-2689. doi:10.1002/lary.25262
Abt NB, Reh DD, Eisele DW, Francis HW, Gourin CG. Does resident participation influence otolaryngology-head and neck surgery morbidity and mortality? Laryngoscope. 2016;126(10):2263-2269. doi:10.1002/lary.25973
Jubbal KT, Chang D, Izaddoost SA, Pederson W, Zavlin D, Echo A. Resident involvement in microsurgery: an American College of Surgeons national surgical quality improvement program analysis. J Surg Educ. 2017;74(6):1124-1132. doi:10.1016/j.jsurg.2017.05.017
Kshirsagar RS, Chandy Z, Mahboubi H, Verma SP. Does resident involvement in thyroid surgery lead to increased postoperative complications? Laryngoscope. 2017;127(5):1242-1246. doi:10.1002/lary.26176
Vieira BL, Hernandez DJ, Qin C, Smith SS, Kim JY, Dutra JC. The impact of resident involvement on otolaryngology surgical outcomes. Laryngoscope. 2016;126(3):602-607. doi:10.1002/lary.25046
Advani V, Ahad S, Gonczy C, Markwell S, Hassan I. Does resident involvement effect surgical times and complication rates during laparoscopic appendectomy for uncomplicated appendicitis? An analysis of 16,849 cases from the ACS-NSQIP. Am J Surg. 2012;203(3):347-352. doi:10.1016/j.amjsurg.2011.08.015
Quinn NA, Alt JA, Ashby S, Orlandi RR. Time, resident involvement, and supply drive cost variability in septoplasty with turbinate reduction. Otolaryngol Head Neck Surg. 2018;159(2):310-314. doi:10.1177/0194599818765099
Leader BA, Wiebracht ND, Meinzen-Derr J, Ishman SL. The impact of resident involvement on tonsillectomy outcomes and surgical time. Laryngoscope. 2020;130(10):2481-2486. doi:10.1002/lary.28427
Muelleman T, Shew M, Muelleman RJ, et al. Impact of resident participation on operative time and outcomes in otologic surgery. Otolaryngol Head Neck Surg. 2018;158(1):151-154. doi:10.1177/0194599817737270
Puram SV, Kozin ED, Sethi R, et al. Impact of resident surgeons on procedure length based on common pediatric otolaryngology cases. Laryngoscope. 2015;125(4):991 -997. doi:10.1002/lary.24912
Chow MS, Gordon AJ, Talwar A, Lydiatt WM, Yueh B, Givi B. The RVU compensation model and head and neck surgical education. Laryngoscope. 2024;134(1):113-119. doi:10.1002/lary.30807
Papandria D, Rhee D, Ortega G, et al. Assessing trainee impact on operative time for common general surgical procedures in ACS-NSQIP. J Surg Educ. 2012;69(2):149-155. doi:10.1016/j.jsurg.2011.08.003
Pugely AJ, Gao Y, Martin CT, Callagh JJ, Weinstein SL, Marsh JL. The effect of resident participation on short-term outcomes after orthopaedic surgery. Clin Orthop Relat Res. 2014;472(7):2290-2300. doi:10.1007/s11999-014-3567-0
Hosler MR, Scott IU, Kunselman AR, Wolford KR, Oltra EZ, Murray WB. Impact of resident participation in cataract surgery on operative time and cost. Ophthalmology. 2012;119(1):95-98. doi:10.1016/j.ophtha.2011.06.026
Lanigan A, Spaw M, Donaghe C, Brennan J. The impact of the Veteran’s Affairs medical system on an otolaryngology residency training program. Mil Med. 2018;183(11-12):e671-e675. doi:10.1093/milmed/usy041
American Society of Clinical Oncology, Pfister DG, Laurie SA, et al. American Society of Clinical Oncology clinical practice guideline for the use of larynx-preservation strategies in the treatment of laryngeal cancer. J Clin Oncol. 2006;24(22):3693-3704. doi:10.1200/JCO.2006.07.4559
Forastiere AA, Ismaila N, Lewin JS, et al. Use of larynxpreservation strategies in the treatment of laryngeal cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2018;36(11):1143-1169. doi:10.1200/JCO.2017.75.7385
Verma SP, Mahboubi H. The changing landscape of total laryngectomy surgery. Otolaryngol Head Neck Surg. 2014;150(3):413-418. doi:10.1177/0194599813514515
Habermann EB, Harris AHS, Giori NJ. Large surgical databases with direct data abstraction: VASQIP and ACSNSQIP. J Bone Joint Surg Am. 2022;104(suppl 3):9-14. doi:10.2106/JBJS.22.00596
Benito DA, Mamidi I, Pasick LJ, et al. Evaluating resident involvement and the ‘July effect’ in parotidectomy. J Laryngol Otol. 2021;135(5):452-457. doi:10.1017/S0022215121000578
Hwang CS, Wichterman KA, Alfrey EJ. The cost of resident education. J Surg Res. 2010;163(1):18-23. doi:10.1016/j.jss.2010.03.013
Saliba AN, Taher AT, Tamim H, et al. Impact of resident involvement in surgery (IRIS-NSQIP): looking at the bigger picture based on the American College of Surgeons- NSQIP database. J Am Coll Surg. 2016; 222(1):30-40. doi:10.1016/j.jamcollsurg.2015.10.011
Khuri SF, Najjar SF, Daley J, et al. Comparison of surgical outcomes between teaching and nonteaching hospitals in the Department of Veterans Affairs. Ann Surg. 2001;234(3):370-383. doi:10.1097/00000658-200109000-00011
Relles DM, Burkhart RA, Pucci MJ et al. Does resident experience affect outcomes in complex abdominal surgery? Pancreaticoduodenectomy as an example. J Gastrointest Surg. 2014;18(2):279-285. doi:10.1007/s11605-013-2372-5
Brady JS, Crippen MM, Filimonov A, et al. The effect of training level on complications after free flap surgery of the head and neck. Am J Otolaryngol. 2017;38(5):560-564. doi:10.1016/j.amjoto.2017.06.001
References
Chung RS. How much time do surgical residents need to learn operative surgery? Am J Surg. 2005;190(3):351-353. doi:10.1016/j.amjsurg.2005.06.035
S, Darzi A. Defining quality in surgical training: perceptions of the profession. Am J Surg. 2014;207(4):628-636. doi:10.1016/j.amjsurg.2013.07.044
Bhatti NI, Ahmed A, Choi SS. Identifying quality indicators of surgical of surgical training: a national survey. Laryngoscope. 2015;125(12):2685-2689. doi:10.1002/lary.25262
Abt NB, Reh DD, Eisele DW, Francis HW, Gourin CG. Does resident participation influence otolaryngology-head and neck surgery morbidity and mortality? Laryngoscope. 2016;126(10):2263-2269. doi:10.1002/lary.25973
Jubbal KT, Chang D, Izaddoost SA, Pederson W, Zavlin D, Echo A. Resident involvement in microsurgery: an American College of Surgeons national surgical quality improvement program analysis. J Surg Educ. 2017;74(6):1124-1132. doi:10.1016/j.jsurg.2017.05.017
Kshirsagar RS, Chandy Z, Mahboubi H, Verma SP. Does resident involvement in thyroid surgery lead to increased postoperative complications? Laryngoscope. 2017;127(5):1242-1246. doi:10.1002/lary.26176
Vieira BL, Hernandez DJ, Qin C, Smith SS, Kim JY, Dutra JC. The impact of resident involvement on otolaryngology surgical outcomes. Laryngoscope. 2016;126(3):602-607. doi:10.1002/lary.25046
Advani V, Ahad S, Gonczy C, Markwell S, Hassan I. Does resident involvement effect surgical times and complication rates during laparoscopic appendectomy for uncomplicated appendicitis? An analysis of 16,849 cases from the ACS-NSQIP. Am J Surg. 2012;203(3):347-352. doi:10.1016/j.amjsurg.2011.08.015
Quinn NA, Alt JA, Ashby S, Orlandi RR. Time, resident involvement, and supply drive cost variability in septoplasty with turbinate reduction. Otolaryngol Head Neck Surg. 2018;159(2):310-314. doi:10.1177/0194599818765099
Leader BA, Wiebracht ND, Meinzen-Derr J, Ishman SL. The impact of resident involvement on tonsillectomy outcomes and surgical time. Laryngoscope. 2020;130(10):2481-2486. doi:10.1002/lary.28427
Muelleman T, Shew M, Muelleman RJ, et al. Impact of resident participation on operative time and outcomes in otologic surgery. Otolaryngol Head Neck Surg. 2018;158(1):151-154. doi:10.1177/0194599817737270
Puram SV, Kozin ED, Sethi R, et al. Impact of resident surgeons on procedure length based on common pediatric otolaryngology cases. Laryngoscope. 2015;125(4):991 -997. doi:10.1002/lary.24912
Chow MS, Gordon AJ, Talwar A, Lydiatt WM, Yueh B, Givi B. The RVU compensation model and head and neck surgical education. Laryngoscope. 2024;134(1):113-119. doi:10.1002/lary.30807
Papandria D, Rhee D, Ortega G, et al. Assessing trainee impact on operative time for common general surgical procedures in ACS-NSQIP. J Surg Educ. 2012;69(2):149-155. doi:10.1016/j.jsurg.2011.08.003
Pugely AJ, Gao Y, Martin CT, Callagh JJ, Weinstein SL, Marsh JL. The effect of resident participation on short-term outcomes after orthopaedic surgery. Clin Orthop Relat Res. 2014;472(7):2290-2300. doi:10.1007/s11999-014-3567-0
Hosler MR, Scott IU, Kunselman AR, Wolford KR, Oltra EZ, Murray WB. Impact of resident participation in cataract surgery on operative time and cost. Ophthalmology. 2012;119(1):95-98. doi:10.1016/j.ophtha.2011.06.026
Lanigan A, Spaw M, Donaghe C, Brennan J. The impact of the Veteran’s Affairs medical system on an otolaryngology residency training program. Mil Med. 2018;183(11-12):e671-e675. doi:10.1093/milmed/usy041
American Society of Clinical Oncology, Pfister DG, Laurie SA, et al. American Society of Clinical Oncology clinical practice guideline for the use of larynx-preservation strategies in the treatment of laryngeal cancer. J Clin Oncol. 2006;24(22):3693-3704. doi:10.1200/JCO.2006.07.4559
Forastiere AA, Ismaila N, Lewin JS, et al. Use of larynxpreservation strategies in the treatment of laryngeal cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2018;36(11):1143-1169. doi:10.1200/JCO.2017.75.7385
Verma SP, Mahboubi H. The changing landscape of total laryngectomy surgery. Otolaryngol Head Neck Surg. 2014;150(3):413-418. doi:10.1177/0194599813514515
Habermann EB, Harris AHS, Giori NJ. Large surgical databases with direct data abstraction: VASQIP and ACSNSQIP. J Bone Joint Surg Am. 2022;104(suppl 3):9-14. doi:10.2106/JBJS.22.00596
Benito DA, Mamidi I, Pasick LJ, et al. Evaluating resident involvement and the ‘July effect’ in parotidectomy. J Laryngol Otol. 2021;135(5):452-457. doi:10.1017/S0022215121000578
Hwang CS, Wichterman KA, Alfrey EJ. The cost of resident education. J Surg Res. 2010;163(1):18-23. doi:10.1016/j.jss.2010.03.013
Saliba AN, Taher AT, Tamim H, et al. Impact of resident involvement in surgery (IRIS-NSQIP): looking at the bigger picture based on the American College of Surgeons- NSQIP database. J Am Coll Surg. 2016; 222(1):30-40. doi:10.1016/j.jamcollsurg.2015.10.011
Khuri SF, Najjar SF, Daley J, et al. Comparison of surgical outcomes between teaching and nonteaching hospitals in the Department of Veterans Affairs. Ann Surg. 2001;234(3):370-383. doi:10.1097/00000658-200109000-00011
Relles DM, Burkhart RA, Pucci MJ et al. Does resident experience affect outcomes in complex abdominal surgery? Pancreaticoduodenectomy as an example. J Gastrointest Surg. 2014;18(2):279-285. doi:10.1007/s11605-013-2372-5
Brady JS, Crippen MM, Filimonov A, et al. The effect of training level on complications after free flap surgery of the head and neck. Am J Otolaryngol. 2017;38(5):560-564. doi:10.1016/j.amjoto.2017.06.001
Over half of pediatric rheumatology fellowship positions went unfilled in 2024, according to the National Resident Matching Program (NRMP). Comparatively, nearly all adult rheumatology positions were filled.
Across all 39 subspecialties in internal medicine and pediatrics, there was an 86% fill rate. In pediatric subspecialties, the fill rate was 78%. There were more than 10,200 applicants in this year’s medicine and pediatric specialties match — a 9% increase from 2023 — and 81% matched to a position.
The NRMP reported that adult rheumatology filled 129 (97.7%) of 132 programs, with 284 (99%) out of 287 positions filled. In 2024, there were five new programs and 11 more fellowship positions available compared with the previous year.
In pediatric rheumatology, 16 (44%) of 36 programs were filled, with 27 (49%) of 55 positions filled. This is a notable decrease from 2023, where pediatric rheumatology filled 21 of 38 programs (55%) and 32 (62%) of 52 positions.
This year, 27 of 30 applicants preferring pediatric rheumatology matched to a program, while in 2023 all 32 applicants that preferred pediatric rheumatology matched.
“It’s a little disappointing that our overall number of applicants have not gone up,” Jay Mehta, MD, the program director of the Children’s Hospital of Philadelphia’s pediatric rheumatology fellowship said in an interview with Medscape Medical News. “It’s an especially exciting time in pediatric rheumatology, with really fantastic breakthroughs in terms of treatments and diagnostics. Unfortunately, that excitement hasn’t necessarily translated into more interest in our field.”
Mehta noted that the number of applicants to pediatric rheumatology fellowships have remained relatively consistent. Since 2019, the number of applicants has ranged from 28 to 33.
“Given the low number of overall positions/programs it is hard to read too much into year-to-year differences,” added Kristen Hayward, MD, a pediatric rheumatologist at Seattle Children’s in Washington. “While this total number of applicants per year is steady, this number is insufficient to build an adequate workforce for our current needs, much less for the future.”
This year, matched applicants to pediatric rheumatology included 13 MD graduates, eight DO graduates, five foreign applicants, and one US citizen international medical graduate.
In adult rheumatology, matched applicants included 108 MD graduates, 97 foreign applicants, 41 DO graduates, and 38 US citizen international medical graduates. A total of 365 applicants preferred the specialty, and 76% matched to rheumatology. Seven applicants matched to another specialty, and the remaining 79 did not match to any program.
Rheumatology was one of several specialties offering at least 150 positions with a fill rate of over 98%. The other specialties included allergy and immunology, cardiovascular disease, clinical cardiac electrophysiology, endocrinology, gastroenterology, and hematology and oncology.
While some pediatric subspecialties like critical care medicine and cardiology had fill rates over 90%, many “cognitive subspecialties” beyond pediatric rheumatology also struggled to fill spots, Hayward noted. Only 37% of pediatric nephrology positions and 48% of pediatric infectious disease positions were filled this year, in addition to a decline in filled pediatric-residency positions overall, she added.
Mehta had no relevant disclosures. Hayward previously owned stock/stock options for AbbVie/Abbott, Cigna/Express Scripts, Merck, and Teva and has received an educational grant from Pfizer.
A version of this article first appeared on Medscape.com.
Over half of pediatric rheumatology fellowship positions went unfilled in 2024, according to the National Resident Matching Program (NRMP). Comparatively, nearly all adult rheumatology positions were filled.
Across all 39 subspecialties in internal medicine and pediatrics, there was an 86% fill rate. In pediatric subspecialties, the fill rate was 78%. There were more than 10,200 applicants in this year’s medicine and pediatric specialties match — a 9% increase from 2023 — and 81% matched to a position.
The NRMP reported that adult rheumatology filled 129 (97.7%) of 132 programs, with 284 (99%) out of 287 positions filled. In 2024, there were five new programs and 11 more fellowship positions available compared with the previous year.
In pediatric rheumatology, 16 (44%) of 36 programs were filled, with 27 (49%) of 55 positions filled. This is a notable decrease from 2023, where pediatric rheumatology filled 21 of 38 programs (55%) and 32 (62%) of 52 positions.
This year, 27 of 30 applicants preferring pediatric rheumatology matched to a program, while in 2023 all 32 applicants that preferred pediatric rheumatology matched.
“It’s a little disappointing that our overall number of applicants have not gone up,” Jay Mehta, MD, the program director of the Children’s Hospital of Philadelphia’s pediatric rheumatology fellowship said in an interview with Medscape Medical News. “It’s an especially exciting time in pediatric rheumatology, with really fantastic breakthroughs in terms of treatments and diagnostics. Unfortunately, that excitement hasn’t necessarily translated into more interest in our field.”
Mehta noted that the number of applicants to pediatric rheumatology fellowships have remained relatively consistent. Since 2019, the number of applicants has ranged from 28 to 33.
“Given the low number of overall positions/programs it is hard to read too much into year-to-year differences,” added Kristen Hayward, MD, a pediatric rheumatologist at Seattle Children’s in Washington. “While this total number of applicants per year is steady, this number is insufficient to build an adequate workforce for our current needs, much less for the future.”
This year, matched applicants to pediatric rheumatology included 13 MD graduates, eight DO graduates, five foreign applicants, and one US citizen international medical graduate.
In adult rheumatology, matched applicants included 108 MD graduates, 97 foreign applicants, 41 DO graduates, and 38 US citizen international medical graduates. A total of 365 applicants preferred the specialty, and 76% matched to rheumatology. Seven applicants matched to another specialty, and the remaining 79 did not match to any program.
Rheumatology was one of several specialties offering at least 150 positions with a fill rate of over 98%. The other specialties included allergy and immunology, cardiovascular disease, clinical cardiac electrophysiology, endocrinology, gastroenterology, and hematology and oncology.
While some pediatric subspecialties like critical care medicine and cardiology had fill rates over 90%, many “cognitive subspecialties” beyond pediatric rheumatology also struggled to fill spots, Hayward noted. Only 37% of pediatric nephrology positions and 48% of pediatric infectious disease positions were filled this year, in addition to a decline in filled pediatric-residency positions overall, she added.
Mehta had no relevant disclosures. Hayward previously owned stock/stock options for AbbVie/Abbott, Cigna/Express Scripts, Merck, and Teva and has received an educational grant from Pfizer.
A version of this article first appeared on Medscape.com.
Over half of pediatric rheumatology fellowship positions went unfilled in 2024, according to the National Resident Matching Program (NRMP). Comparatively, nearly all adult rheumatology positions were filled.
Across all 39 subspecialties in internal medicine and pediatrics, there was an 86% fill rate. In pediatric subspecialties, the fill rate was 78%. There were more than 10,200 applicants in this year’s medicine and pediatric specialties match — a 9% increase from 2023 — and 81% matched to a position.
The NRMP reported that adult rheumatology filled 129 (97.7%) of 132 programs, with 284 (99%) out of 287 positions filled. In 2024, there were five new programs and 11 more fellowship positions available compared with the previous year.
In pediatric rheumatology, 16 (44%) of 36 programs were filled, with 27 (49%) of 55 positions filled. This is a notable decrease from 2023, where pediatric rheumatology filled 21 of 38 programs (55%) and 32 (62%) of 52 positions.
This year, 27 of 30 applicants preferring pediatric rheumatology matched to a program, while in 2023 all 32 applicants that preferred pediatric rheumatology matched.
“It’s a little disappointing that our overall number of applicants have not gone up,” Jay Mehta, MD, the program director of the Children’s Hospital of Philadelphia’s pediatric rheumatology fellowship said in an interview with Medscape Medical News. “It’s an especially exciting time in pediatric rheumatology, with really fantastic breakthroughs in terms of treatments and diagnostics. Unfortunately, that excitement hasn’t necessarily translated into more interest in our field.”
Mehta noted that the number of applicants to pediatric rheumatology fellowships have remained relatively consistent. Since 2019, the number of applicants has ranged from 28 to 33.
“Given the low number of overall positions/programs it is hard to read too much into year-to-year differences,” added Kristen Hayward, MD, a pediatric rheumatologist at Seattle Children’s in Washington. “While this total number of applicants per year is steady, this number is insufficient to build an adequate workforce for our current needs, much less for the future.”
This year, matched applicants to pediatric rheumatology included 13 MD graduates, eight DO graduates, five foreign applicants, and one US citizen international medical graduate.
In adult rheumatology, matched applicants included 108 MD graduates, 97 foreign applicants, 41 DO graduates, and 38 US citizen international medical graduates. A total of 365 applicants preferred the specialty, and 76% matched to rheumatology. Seven applicants matched to another specialty, and the remaining 79 did not match to any program.
Rheumatology was one of several specialties offering at least 150 positions with a fill rate of over 98%. The other specialties included allergy and immunology, cardiovascular disease, clinical cardiac electrophysiology, endocrinology, gastroenterology, and hematology and oncology.
While some pediatric subspecialties like critical care medicine and cardiology had fill rates over 90%, many “cognitive subspecialties” beyond pediatric rheumatology also struggled to fill spots, Hayward noted. Only 37% of pediatric nephrology positions and 48% of pediatric infectious disease positions were filled this year, in addition to a decline in filled pediatric-residency positions overall, she added.
Mehta had no relevant disclosures. Hayward previously owned stock/stock options for AbbVie/Abbott, Cigna/Express Scripts, Merck, and Teva and has received an educational grant from Pfizer.
A version of this article first appeared on Medscape.com.
The sun often is rising in the rearview mirror as I travel with the University of New Mexico dermatology team from Albuquerque to our satellite clinic in Gallup, New Mexico. This twice-monthly trip—with a group usually comprising an attending physician, residents, and medical students—provides an invaluable opportunity for me to take part in delivering care to a majority Native American population and connects our institution and its trainees to the state’s rural and indigenous cultures and communities.
Community outreach is an important initiative for many dermatology residency training programs. Engaging with the community outside the clinic setting allows residents to hone their clinical skills, interact with and meet new people, and help to improve access to health care, especially for members of underserved populations.
Limited access to health care remains a pressing issue in the United States, especially for underserved and rural communities. There currently is no standardized way to measure access to care, but multiple contributing factors have been identified, including but not limited to patient wait times and throughput, provider turnover, ratio of dermatologists to patient population, insurance type, and patient outcomes.1 Fortunately, there are many ways for dermatology residents to get involved and improve access to dermatologic services in their communities, including skin cancer screenings, free clinics, and teledermatology.
Skin Cancer Screenings
More than 40% of community outreach initiatives offered by dermatology residency programs are related to skin cancer screening and prevention.2 The American Academy of Dermatology’s free skin cancer check program (https://www.aad.org/member/career/volunteer/spot) offers a way to participate in or even host a skin cancer screening in your community. Since 1985, this program has identified nearly 300,000 suspicious lesions and more than 30,000 suspected melanomas. Resources for setting up a skin cancer screening in your community are available on the program’s website. Residents may take this opportunity to teach medical students how to perform full-body skin examinations and/or practice making independent decisions as the supervisor for medical trainees. Skin cancer screening events not only expand access to care in underserved communities but also help residents feel more connected to the local community, especially if they have moved to a new location for their residency training.
Free Clinics
Engaging in educational opportunities offered through residency programs is another way to participate in community outreach. In particular, many programs are affiliated with a School of Medicine within their institution that allows residents to spearhead volunteer opportunities such as working at a free clinic. In fact, more than 30% of initiatives offered at dermatology residency programs are free general dermatology clinics.2 Residents are in the unique position of being both learners themselves as well as educators to trainees.3 As part of our role, we can provide crucial specialty care to the community by working in concert with medical students and while also familiarizing ourselves with treating populations that we may not reach in our daily clinical work. For example, by participating in free clinics, we can provide care to vulnerable populations who typically may have financial or time barriers that prevent them from seeking care at the institution-associated clinic, including individuals experiencing homelessness, patients who are uninsured, and individuals who cannot take time off work to pursue medical care. Our presence in the community helps to reduce barriers to specialty care, particularly in the field of dermatology where the access shortage in the context of rising skin cancer rates prompts public health concerns.4
Teledermatology
Teledermatology became a way to extend our reach in the community more than ever before during the COVID-19 pandemic. Advances in audio, visual, and data telecommunication have been particularly helpful in dermatology, a specialty that relies heavily on visual cues for diagnosis. Synchronous, asynchronous, and hybrid teledermatology services implemented during the pandemic have gained favor among patients and dermatologists and are still applied in current practice.5,6
For example, in the state of New Mexico (where there is a severe shortage of board-certified dermatologists to care for the state’s population), teledermatology has allowed rural providers of all specialties to consult University of New Mexico dermatologists by sending clinical photographs along with patient information and history via secure messaging. Instead of having the patient travel hundreds of miles to see the nearest dermatologist for their skin condition or endure long wait times to get in to see a specialist, primary providers now can initiate treatment or work-up for their patient’s skin issue in a timely manner with the use of teledermatology to consult specialists.
Teledermatology has demonstrated cost-effectiveness, accuracy, and efficiency in conveniently expanding access to care. It offers patients and dermatologists flexibility in receiving and delivering health care, respectively.7 As residents, learning how to navigate this technologic frontier in health care delivery is imperative, as it will remain a prevalent tool in the future care of our communities, particularly in underserved areas.
Final Thoughts
Through community outreach initiatives, dermatology residents have an opportunity not only to enrich our education but also to connect with and become closer to our patients. Skin cancer screenings, free clinics, and teledermatology have provided ways to reach more communities and remain important aspects of dermatology residency.
References
Patel B, Blalock TW. Defining “access to care” for dermatology at academic medical institutions. J Am Acad Dermatol. 2023;89:627-628. doi:10.1016/j.jaad.2023.03.014
Fritsche M, Maglakelidze N, Zaenglein A, et al. Community outreach initiatives in dermatology: cross-sectional study. Arch Dermatol Res. 2023;315:2693-2695. doi:10.1007/s00403-023-02629-y
Chiu LW. Teaching tips for dermatology residents. Cutis. 2024;113:E17-E19. doi:10.12788/cutis.1046
Duniphin DD. Limited access to dermatology specialty care: barriers and teledermatology. Dermatol Pract Concept. 2023;13:E2023031. doi:10.5826/dpc.1301a31
Ibrahim AE, Magdy M, Khalaf EM, et al. Teledermatology in the time of COVID-19. Int J Clin Pract. 2021;75:e15000. doi:10.1111/ijcp.15000
Farr MA, Duvic M, Joshi TP. Teledermatology during COVID-19: an updated review. Am J Clin Dermatol. 2021;22:467-475. doi:10.1007/s40257-021-00601-y
Lipner SR. Optimizing patient care with teledermatology: improving access, efficiency, and satisfaction. Cutis. 2024;114:63-64. doi:10.12788/cutis.1073
The sun often is rising in the rearview mirror as I travel with the University of New Mexico dermatology team from Albuquerque to our satellite clinic in Gallup, New Mexico. This twice-monthly trip—with a group usually comprising an attending physician, residents, and medical students—provides an invaluable opportunity for me to take part in delivering care to a majority Native American population and connects our institution and its trainees to the state’s rural and indigenous cultures and communities.
Community outreach is an important initiative for many dermatology residency training programs. Engaging with the community outside the clinic setting allows residents to hone their clinical skills, interact with and meet new people, and help to improve access to health care, especially for members of underserved populations.
Limited access to health care remains a pressing issue in the United States, especially for underserved and rural communities. There currently is no standardized way to measure access to care, but multiple contributing factors have been identified, including but not limited to patient wait times and throughput, provider turnover, ratio of dermatologists to patient population, insurance type, and patient outcomes.1 Fortunately, there are many ways for dermatology residents to get involved and improve access to dermatologic services in their communities, including skin cancer screenings, free clinics, and teledermatology.
Skin Cancer Screenings
More than 40% of community outreach initiatives offered by dermatology residency programs are related to skin cancer screening and prevention.2 The American Academy of Dermatology’s free skin cancer check program (https://www.aad.org/member/career/volunteer/spot) offers a way to participate in or even host a skin cancer screening in your community. Since 1985, this program has identified nearly 300,000 suspicious lesions and more than 30,000 suspected melanomas. Resources for setting up a skin cancer screening in your community are available on the program’s website. Residents may take this opportunity to teach medical students how to perform full-body skin examinations and/or practice making independent decisions as the supervisor for medical trainees. Skin cancer screening events not only expand access to care in underserved communities but also help residents feel more connected to the local community, especially if they have moved to a new location for their residency training.
Free Clinics
Engaging in educational opportunities offered through residency programs is another way to participate in community outreach. In particular, many programs are affiliated with a School of Medicine within their institution that allows residents to spearhead volunteer opportunities such as working at a free clinic. In fact, more than 30% of initiatives offered at dermatology residency programs are free general dermatology clinics.2 Residents are in the unique position of being both learners themselves as well as educators to trainees.3 As part of our role, we can provide crucial specialty care to the community by working in concert with medical students and while also familiarizing ourselves with treating populations that we may not reach in our daily clinical work. For example, by participating in free clinics, we can provide care to vulnerable populations who typically may have financial or time barriers that prevent them from seeking care at the institution-associated clinic, including individuals experiencing homelessness, patients who are uninsured, and individuals who cannot take time off work to pursue medical care. Our presence in the community helps to reduce barriers to specialty care, particularly in the field of dermatology where the access shortage in the context of rising skin cancer rates prompts public health concerns.4
Teledermatology
Teledermatology became a way to extend our reach in the community more than ever before during the COVID-19 pandemic. Advances in audio, visual, and data telecommunication have been particularly helpful in dermatology, a specialty that relies heavily on visual cues for diagnosis. Synchronous, asynchronous, and hybrid teledermatology services implemented during the pandemic have gained favor among patients and dermatologists and are still applied in current practice.5,6
For example, in the state of New Mexico (where there is a severe shortage of board-certified dermatologists to care for the state’s population), teledermatology has allowed rural providers of all specialties to consult University of New Mexico dermatologists by sending clinical photographs along with patient information and history via secure messaging. Instead of having the patient travel hundreds of miles to see the nearest dermatologist for their skin condition or endure long wait times to get in to see a specialist, primary providers now can initiate treatment or work-up for their patient’s skin issue in a timely manner with the use of teledermatology to consult specialists.
Teledermatology has demonstrated cost-effectiveness, accuracy, and efficiency in conveniently expanding access to care. It offers patients and dermatologists flexibility in receiving and delivering health care, respectively.7 As residents, learning how to navigate this technologic frontier in health care delivery is imperative, as it will remain a prevalent tool in the future care of our communities, particularly in underserved areas.
Final Thoughts
Through community outreach initiatives, dermatology residents have an opportunity not only to enrich our education but also to connect with and become closer to our patients. Skin cancer screenings, free clinics, and teledermatology have provided ways to reach more communities and remain important aspects of dermatology residency.
The sun often is rising in the rearview mirror as I travel with the University of New Mexico dermatology team from Albuquerque to our satellite clinic in Gallup, New Mexico. This twice-monthly trip—with a group usually comprising an attending physician, residents, and medical students—provides an invaluable opportunity for me to take part in delivering care to a majority Native American population and connects our institution and its trainees to the state’s rural and indigenous cultures and communities.
Community outreach is an important initiative for many dermatology residency training programs. Engaging with the community outside the clinic setting allows residents to hone their clinical skills, interact with and meet new people, and help to improve access to health care, especially for members of underserved populations.
Limited access to health care remains a pressing issue in the United States, especially for underserved and rural communities. There currently is no standardized way to measure access to care, but multiple contributing factors have been identified, including but not limited to patient wait times and throughput, provider turnover, ratio of dermatologists to patient population, insurance type, and patient outcomes.1 Fortunately, there are many ways for dermatology residents to get involved and improve access to dermatologic services in their communities, including skin cancer screenings, free clinics, and teledermatology.
Skin Cancer Screenings
More than 40% of community outreach initiatives offered by dermatology residency programs are related to skin cancer screening and prevention.2 The American Academy of Dermatology’s free skin cancer check program (https://www.aad.org/member/career/volunteer/spot) offers a way to participate in or even host a skin cancer screening in your community. Since 1985, this program has identified nearly 300,000 suspicious lesions and more than 30,000 suspected melanomas. Resources for setting up a skin cancer screening in your community are available on the program’s website. Residents may take this opportunity to teach medical students how to perform full-body skin examinations and/or practice making independent decisions as the supervisor for medical trainees. Skin cancer screening events not only expand access to care in underserved communities but also help residents feel more connected to the local community, especially if they have moved to a new location for their residency training.
Free Clinics
Engaging in educational opportunities offered through residency programs is another way to participate in community outreach. In particular, many programs are affiliated with a School of Medicine within their institution that allows residents to spearhead volunteer opportunities such as working at a free clinic. In fact, more than 30% of initiatives offered at dermatology residency programs are free general dermatology clinics.2 Residents are in the unique position of being both learners themselves as well as educators to trainees.3 As part of our role, we can provide crucial specialty care to the community by working in concert with medical students and while also familiarizing ourselves with treating populations that we may not reach in our daily clinical work. For example, by participating in free clinics, we can provide care to vulnerable populations who typically may have financial or time barriers that prevent them from seeking care at the institution-associated clinic, including individuals experiencing homelessness, patients who are uninsured, and individuals who cannot take time off work to pursue medical care. Our presence in the community helps to reduce barriers to specialty care, particularly in the field of dermatology where the access shortage in the context of rising skin cancer rates prompts public health concerns.4
Teledermatology
Teledermatology became a way to extend our reach in the community more than ever before during the COVID-19 pandemic. Advances in audio, visual, and data telecommunication have been particularly helpful in dermatology, a specialty that relies heavily on visual cues for diagnosis. Synchronous, asynchronous, and hybrid teledermatology services implemented during the pandemic have gained favor among patients and dermatologists and are still applied in current practice.5,6
For example, in the state of New Mexico (where there is a severe shortage of board-certified dermatologists to care for the state’s population), teledermatology has allowed rural providers of all specialties to consult University of New Mexico dermatologists by sending clinical photographs along with patient information and history via secure messaging. Instead of having the patient travel hundreds of miles to see the nearest dermatologist for their skin condition or endure long wait times to get in to see a specialist, primary providers now can initiate treatment or work-up for their patient’s skin issue in a timely manner with the use of teledermatology to consult specialists.
Teledermatology has demonstrated cost-effectiveness, accuracy, and efficiency in conveniently expanding access to care. It offers patients and dermatologists flexibility in receiving and delivering health care, respectively.7 As residents, learning how to navigate this technologic frontier in health care delivery is imperative, as it will remain a prevalent tool in the future care of our communities, particularly in underserved areas.
Final Thoughts
Through community outreach initiatives, dermatology residents have an opportunity not only to enrich our education but also to connect with and become closer to our patients. Skin cancer screenings, free clinics, and teledermatology have provided ways to reach more communities and remain important aspects of dermatology residency.
References
Patel B, Blalock TW. Defining “access to care” for dermatology at academic medical institutions. J Am Acad Dermatol. 2023;89:627-628. doi:10.1016/j.jaad.2023.03.014
Fritsche M, Maglakelidze N, Zaenglein A, et al. Community outreach initiatives in dermatology: cross-sectional study. Arch Dermatol Res. 2023;315:2693-2695. doi:10.1007/s00403-023-02629-y
Chiu LW. Teaching tips for dermatology residents. Cutis. 2024;113:E17-E19. doi:10.12788/cutis.1046
Duniphin DD. Limited access to dermatology specialty care: barriers and teledermatology. Dermatol Pract Concept. 2023;13:E2023031. doi:10.5826/dpc.1301a31
Ibrahim AE, Magdy M, Khalaf EM, et al. Teledermatology in the time of COVID-19. Int J Clin Pract. 2021;75:e15000. doi:10.1111/ijcp.15000
Farr MA, Duvic M, Joshi TP. Teledermatology during COVID-19: an updated review. Am J Clin Dermatol. 2021;22:467-475. doi:10.1007/s40257-021-00601-y
Lipner SR. Optimizing patient care with teledermatology: improving access, efficiency, and satisfaction. Cutis. 2024;114:63-64. doi:10.12788/cutis.1073
References
Patel B, Blalock TW. Defining “access to care” for dermatology at academic medical institutions. J Am Acad Dermatol. 2023;89:627-628. doi:10.1016/j.jaad.2023.03.014
Fritsche M, Maglakelidze N, Zaenglein A, et al. Community outreach initiatives in dermatology: cross-sectional study. Arch Dermatol Res. 2023;315:2693-2695. doi:10.1007/s00403-023-02629-y
Chiu LW. Teaching tips for dermatology residents. Cutis. 2024;113:E17-E19. doi:10.12788/cutis.1046
Duniphin DD. Limited access to dermatology specialty care: barriers and teledermatology. Dermatol Pract Concept. 2023;13:E2023031. doi:10.5826/dpc.1301a31
Ibrahim AE, Magdy M, Khalaf EM, et al. Teledermatology in the time of COVID-19. Int J Clin Pract. 2021;75:e15000. doi:10.1111/ijcp.15000
Farr MA, Duvic M, Joshi TP. Teledermatology during COVID-19: an updated review. Am J Clin Dermatol. 2021;22:467-475. doi:10.1007/s40257-021-00601-y
Lipner SR. Optimizing patient care with teledermatology: improving access, efficiency, and satisfaction. Cutis. 2024;114:63-64. doi:10.12788/cutis.1073
Case Presentation:A 65-year-old male veteran presented to the Veterans Affairs Boston Healthcare System (VABHS) emergency department with progressive fatigue, dyspnea on exertion, lightheadedness, and falls over the last month. New bilateral lower extremity numbness up to his knees developed in the week prior to admission and prompted him to seek care. Additional history included 2 episodes of transient loss of consciousness resulting in falls and a week of diarrhea, which had resolved. His medical history was notable for hypothyroidism secondary to Hashimoto thyroiditis, seizure disorder, vitiligo, treated hepatitis C virus (HCV) infection, alcohol use disorder in remission, diabetes mellitus, posttraumatic stress disorder, and traumatic brain injury. His medications included levothyroxine and carbamazepine. He previously worked as a barber but recently had stopped due to cognitive impairment. On initial evaluation, the patient's vital signs included a temperature of 36.3 °C, heart rate of 77 beats per minute, blood pressure of 139/83 mm Hg, respiratory rate of 18 breaths per minute, and 99% oxygen saturation while breathing ambient air. Physical examination was notable for a frail-appearing man in no acute distress. His conjunctivae were pale, and cardiac auscultation revealed a normal heart rate and irregularly irregular heart rhythm. A neurologic examination revealed decreased vibratory sensation in both feet, delayed and minimal speech, and a blunted affect. His skin was warm and dry with patchy hypopigmentation across the face and forehead. Laboratory results are shown in the Table. Testing 2 years previously found the patient's hemoglobin to be 11.4 g/dL and serum creatinine to be 1.7 mg/dL. A peripheral blood smear showed anisocytosis, hypochromia, decreased platelets, ovalocytes, elliptocytes, and rare teardrop cells, with no schistocytes present. Chest radiography and computed tomography of the head were unremarkable. An abdominal ultrasound revealed a complex hypoechoic mass with peripheral rim vascularity in the right hepatic lobe measuring 3.9 cm × 3.6 cm × 3.9 cm.
Lindsey Ulin, MD, Chief Medical Resident, VABHS and Brigham and Women’s Hospital (BWH):
To build the initial differential diagnosis, we are joined today by 3 internal medicine residents who were not involved in the care of this patient. Dr. Hickey, Dr. Ross and Dr. Manivannan, how did you approach this case?
Meghan Hickey, MD, Senior Internal Medicine Resident, VABHS and Boston Medical Center (BMC):
The constellation of fatigue, weakness, blunted affect, and delayed, minimal speech suggested central nervous system involvement, which I sought to unify with hemolytic anemia and his liver mass. The first diagnosis I considered was Wilson disease; however, this genetic disorder of copper metabolism often presents with liver failure or cirrhosis in young or middle-aged women, so this presentation would be atypical. Next, given the hypopigmentation was reported only on sun-exposed areas of the patient’s face, I considered possibilities other than vitiligo to avoid diagnostic anchoring. One such alternate diagnosis is porphyria cutanea tarda (PCT), which presents in middle-aged and older adults with a photosensitive dermatitis that can include acute sensory deficits. Manifestations of PCT can be triggered by alcohol consumption, though his alcohol use disorder was thought to be in remission, as well as HCV, for which he previously received treatment. However, anemia is uncommon in PCT, so the patient’s low hemoglobin would not be explained by this diagnosis. Lastly, I considered thrombotic thrombocytopenic purpura (TTP) given his anemia, thrombocytopenia, and neurologic symptoms; however, the patient did not have fever or a clear inciting cause, his renal dysfunction was relatively mild, and the peripheral blood smear revealed no schistocytes, which should be present in TTP.
TABLE Laboratory Results
Caroline Ross, MD, and Alan Manivannan, MD; Senior Internal Medicine Residents, VABHS and BMC:
We noted several salient features in the history and physical examination. First, we sought to explain the bilateral lower extremity numbness and decreased vibratory sensation in the feet leading to falls. We also considered his anemia and thrombocytopenia with signs of hemolysis including elevated lactate dehydrogenase (LDH), low haptoglobin, and elevated total bilirubin; however, with normal coagulation parameters. These results initially raised our concern for a thrombotic microangiopathy (TMA) such as TTP. However, the peripheral smear lacked schistocytes, making this less likely. The combination of his neurologic symptoms and TMA-like laboratory findings but without schistocytes raised our concern for vitamin B12 deficiency. Vitamin B12 deficiency can cause a pseudo-TMA picture with laboratory finding similar to TTP; however, schistocytes are typically absent. We also considered the possibility of hepatocellular carcinoma (HCC) with bone marrow infiltration leading to anemia given the finding of a liver mass on his abdominal ultrasound and low reticulocyte index. However, this would not explain his hemolysis. We also considered chronic disseminated intravascular coagulation in the setting of a malignancy as a contributor, but again, the smear lacked schistocytes and his coagulation parameters were normal. Finally, we considered a primary bone marrow process such as myelodysplastic syndrome due to the bicytopenia with poor bone marrow response and smear with tear drop cells and elliptocytes. However, we felt this was less likely as this would not explain his hemolytic anemia.
Dr. Ulin:
To refine the differential diagnosis, we are joined by an expert clinician who was also not involved in the care of this patient to describe his approach to this case. Dr. Orlander, can you walk us through your clinical reasoning?
Jay Orlander, MD, MPH: Professor of Medicine, Section of General Internal Medicine, Boston University Chobanian & Avedisian School of Medicine, Associate Chief, Medical Service, VABHS:
I will first comment on the hepatic mass. The hypoechoic liver mass with peripheral vascularity suggests a growing tumor. The patient has a history of substance use disorder with alcohol and treated HCV. He remains at increased risk for HCC even after prior successful HCV treatment and has 2 of 4 known risk factors for developing HCC— diabetes mellitus and alcohol use—the other 2 being underlying metabolic dysfunctionassociated steatotic liver disease (MASLD) and the presence of hepatic fibrosis, which we have not yet assessed. Worsening liver function can lead to cognitive issues and alcohol to peripheral neuropathy, but his story is not consistent with this. For his liver mass, I recommend a nonurgent magnetic resonance image for further evaluation.
Next, let’s consider his markedly elevated thyrotropin (TSH). Cognitive impairment along with lethargy, fatigue, and decreased exercise tolerance can be prominent features in severe hypothyroidism, but this diagnosis would not explain his hematologic findings.1
I view the principal finding of his laboratory testing as being that his bone marrow is failing to maintain adequate blood elements. He has a markedly low hematocrit along with low platelets and low-normal white blood cell counts. There is an absence of schistocytes on the blood smear, and after correcting his reticulocyte count for his degree of anemia (observed reticulocyte percentage [0.8%] x observed hematocrit [15.3%] / expected hematocrit [40%]), results in a reticulocyte index of 0.12, which is low. This suggests his bone marrow is failing to manufacture red blood cells at an appropriate rate. His haptoglobin is unmeasurable, so there is some free heme circulating. Hence, I infer that hemolysis and ineffective erythropoiesis are both occurring within the bone marrow, which also explains the slight elevation in bilirubin.
Intramedullary hemolysis with a markedly elevated LDH can be seen in severe vitamin B12 deficiency, which has many causes, but one cause in particular warrants consideration in this case: pernicious anemia. Pernicious anemia has an overall prevalence of about 0.1%, but is more common in older adults, and is estimated to be present in 2% to 3% of adults aged > 65 years.2 Prevalence is also increased in patients with other autoimmune diseases such as vitiligo and hypothyroidism, which our patient has.3 The pathophysiology of pernicious anemia relates to either autoimmune gastric parietal cell destruction and/or the development of antibodies against intrinsic factor, which is required for absorption of vitamin B12. Early disease may present with macrocytosis and a normal hemoglobin initially, but anemia develops over time if left untreated. When the primary cause of pernicious anemia is gastric parietal cell destruction, there is also an associated lack of stomach acid production (achlorhydria) with resulting poor micronutrient absorption; specifically, vitamin D, vitamin C, and iron. Hence, 30% of patients diagnosed with pernicious anemia have concurrent iron deficiency, which may counteract macrocytosis and result in a normal mean corpuscular volume. 4 Some medications are also poorly absorbed in achlorhydric states, such as levothyroxine, and treatment doses need to be increased, which could explain his markedly elevated TSH despite presumed medication adherence.
Vitamin B12 is essential for both the peripheral and central nervous systems. Longstanding severe B12 deficiency can explain all of his neurological and neurocognitive changes. The most common neurologic findings in B12 deficiency are symmetric paresthesias or numbness and gait problems. The sensory neuropathy affects the lower extremities more commonly than the upper. Untreated, patients can develop progressive weakness, ataxia, and orthostatic hypotension with syncope, as well as neuropsychiatric changes including depression or mood impairment, cognitive slowing, forgetfulness, and dementia.
Dr. Ulin:
Dr. Orlander, which pieces of objective data are most important in forming your differential diagnosis, and what tests would you obtain next?
Dr. Orlander:
The 3 most salient laboratory tests to me are a complete blood count, with all cell lines impacted but the hemoglobin and hematocrit most dramatically impacted, reticulocyte count of 0.8%, which is inappropriately low and hence suggests a hypoproliferative anemia, and the elevated LDH > 5000 IU/L.
Since my suspected diagnosis is pernicious anemia, I would obtain a blood smear looking for hypersegmented neutrophils, > 1 white blood cells with 5 lobes, or 1 with 6 lobes, which should clinch the diagnosis. Methylmalonic acid (MMA) levels are the most sensitive test for B12 deficiency, so I would also obtain that. Finally, I would check a B12 level, since in a patient with pernicious anemia, I would expect the level to be < 200 pg/mL.
Dr. Ulin:
Before we reveal the results of the patient’s additional workup, how do you approach interpreting B12 levels?
Dr. Orlander:
Measuring B12 can sometimes be problematic: the normal range is considered 200 to 900 pg/mL, but patients with measured low-normal levels in the range of 200 to 400 pg/mL can actually be physiologically deficient. There are also several common causes of falsely low and falsely high B12 levels in the absence of B12 deficiency. Hence, for patients with mild symptoms that could be due to B12 deficiency, many clinicians choose to just treat with B12 supplementation, deeming it safer to treat than miss an early diagnosis. B12 is involved in hydrogen transfer to convert MMA into succinyl-CoA and hence true vitamin B12 deficiency causes an increase in MMA.
Decreased production of vitamin B12 binding proteins, like haptocorrin, has been proposed as the mechanism for spurious low values.5 Certain conditions or medications can also cause spurious low serum vitamin B12 levels and thus might cause the appearance of vitamin B12 deficiency when the patient is not deficient. Examples include multiple myeloma, HIV infection, pregnancy, oral contraceptives, and phenytoin use. An example of spuriously low vitamin B12 level in pregnancy was demonstrated in a series of 50 pregnant individuals with low vitamin B12 levels (45-199 pg/mL), in whom metabolite testing for MMA and homocysteine showed no correlation with vitamin B12 level.6
Further complicating things, some conditions can cause spuriously increased vitamin B12 levels and thus might cause the appearance of normal vitamin B12 levels when the patient is actually deficient.7 Examples include occult malignancy, myeloproliferative neoplasms, alcoholic liver disease, kidney disease, and nitrous oxide exposure (the latter of which is unique in that it can also cause true vitamin B12 deficiency, as evidenced by clinical symptoms and high MMA levels).8,9
Lastly, autoantibodies to intrinsic factor in individuals with pernicious anemia may compete with intrinsic factor in the chemiluminescence assay and result in spuriously normal vitamin B12 levels in the presence of true deficiency.10-12 If the vitamin B12 level is very high (eg, 800 pg/mL), we do not worry about this effect in the absence of clinical features suggesting vitamin B12 deficiency; however, if the vitamin B12 level is borderline or low-normal and/or other clinical features suggest vitamin B12 deficiency, it is prudent to obtain other testing such as an MMA level.
Dr. Ulin:
We are also joined by Dr. Rahul Ganatra, who cared for the patient at the time the diagnosis was made. Dr. Ganatra, can you share the final diagnosis and provide an update on the patient?
Rahul Ganatra, MD, MPH, Director of Continuing Medical Education, VABHS:
The patient’s hemoglobin rose to 6.9 g/dL after transfusion of 2 units of packed red blood cells, and his dyspnea on exertion and fatigue improved. Iron studies, serum thiamine, serum folate, ADAMTS13 activity levels, and AM cortisol level were normal. Upon closer examination of the peripheral blood smear, rare hypersegmented neutrophils were noted. Serum B12 level returned below assay (< 146 pg/mL), and serum MMA was 50,800 nmol/L, confirming the diagnosis of severe vitamin B12 deficiency. Antibodies against intrinsic factor were detected, confirming the diagnosis of pernicious anemia. Treatment was initiated with intramuscular cyanocobalamin every other day and was transitioned to weekly dosing at the time of hospital discharge. After excluding adrenal insufficiency, his levothyroxine dose was increased. Finally, a liver mass biopsy confirmed a concomitant diagnosis of HCC. The patient was discharged home. Five weeks after discharge, his serum B12 level rose to > 1000 pg/mL, and 10 months after discharge, his TSH fell to 0.97 uIU/mL. Several months later, he underwent stereotactic body radiotherapy for the HCC. One year after his initial presentation, he has not resumed work as a barber.
References
Leigh H, Kramer SI. The psychiatric manifestations of endocrine disease. Adv Intern Med. 1984;29:413-445
Lenti MV, Rugge M, Lahner E, et al. Autoimmune gastritis. Nat Rev Dis Primers. 2020;6(1):56.doi:10.1038/s41572-020-0187-8
Toh BH, van Driel IR, Gleeson PA. Pernicious anemia. N Engl J Med. 1997;337(20):1441-1448. doi:10.1056/NEJM199711133372007
. Hershko C, Ronson A, Souroujon M, Maschler I, Heyd J, Patz J. Variable hematologic presentation of autoimmune gastritis: age-related progression from iron deficiency to cobalamin depletion. Blood. 2006;107(4):1673-1679. doi:10.1182/blood-2005-09-3534
Morkbak AL, Hvas AM, Milman N, Nexo E. Holotranscobalamin remains unchanged during pregnancy. Longitudinal changes of cobalamins and their binding proteins during pregnancy and postpartum. Haematologica. 2007;92(12):1711-1712. doi:10.3324/haematol.11636
Metz J, McGrath K, Bennett M, Hyland K, Bottiglieri T. Biochemical indices of vitamin B12 nutrition in pregnant patients with subnormal serum vitamin B12 levels. Am J Hematol. 1995;48(4):251-255. doi:10.1002/ajh.2830480409
Marsden P, Sharma AA, Rotella JA. Review article: clinical manifestations and outcomes of chronic nitrous oxide misuse: a systematic review. Emerg Med Australas. 2022;34(4):492- 503. doi:10.1111/1742-6723.13997
Hamilton MS, Blackmore S, Lee A. Possible cause of false normal B-12 assays. BMJ. 2006;333(7569):654-655. doi:10.1136/bmj.333.7569.654-c
Yang DT, Cook RJ. Spurious elevations of vitamin B12 with pernicious anemia. N Engl J Med. 2012;366(18):1742-1743. doi:10.1056/NEJMc1201655
Carmel R, Agrawal YP. Failures of cobalamin assays in pernicious anemia. N Engl J Med. 2012;367(4):385-386. doi:10.1056/NEJMc1204070
Green R. Vitamin B12 deficiency from the perspective of a practicing hematologist. Blood. May 11 2017;129(19):2603- 2611. doi:10.1182/blood-2016-10-569186
Miceli E, Lenti MV, Padula D, et al. Common features of patients with autoimmune atrophic gastritis. Clin Gastroenterol Hepatol. 2012;10(7):812-814.doi:10.1016/j.cgh.2012.02.018
Lindsey Ulin, MDa,b; Meghan Hickey, MDb,c; Caroline Ross, MDb,c; Alan Manivannan, MDb,c; Jay Orlander, MD, MPHb,d; Rahul B. Ganatra, MD, MPHb
Author affiliationsa Brigham and Women’s Hospital, Boston, Massachusetts bVeterans Affairs Boston Healthcare System, West Roxbury, Massachusetts c Boston Medical Center, Massachusetts dBoston University Chobanian & Avedisian School of Medicine, Massachusetts
Lindsey Ulin, MDa,b; Meghan Hickey, MDb,c; Caroline Ross, MDb,c; Alan Manivannan, MDb,c; Jay Orlander, MD, MPHb,d; Rahul B. Ganatra, MD, MPHb
Author affiliationsa Brigham and Women’s Hospital, Boston, Massachusetts bVeterans Affairs Boston Healthcare System, West Roxbury, Massachusetts c Boston Medical Center, Massachusetts dBoston University Chobanian & Avedisian School of Medicine, Massachusetts
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Fed Pract. 2024;41(10). Published online October 15. doi:10.12788/fp.0516
Author and Disclosure Information
Lindsey Ulin, MDa,b; Meghan Hickey, MDb,c; Caroline Ross, MDb,c; Alan Manivannan, MDb,c; Jay Orlander, MD, MPHb,d; Rahul B. Ganatra, MD, MPHb
Author affiliationsa Brigham and Women’s Hospital, Boston, Massachusetts bVeterans Affairs Boston Healthcare System, West Roxbury, Massachusetts c Boston Medical Center, Massachusetts dBoston University Chobanian & Avedisian School of Medicine, Massachusetts
Case Presentation:A 65-year-old male veteran presented to the Veterans Affairs Boston Healthcare System (VABHS) emergency department with progressive fatigue, dyspnea on exertion, lightheadedness, and falls over the last month. New bilateral lower extremity numbness up to his knees developed in the week prior to admission and prompted him to seek care. Additional history included 2 episodes of transient loss of consciousness resulting in falls and a week of diarrhea, which had resolved. His medical history was notable for hypothyroidism secondary to Hashimoto thyroiditis, seizure disorder, vitiligo, treated hepatitis C virus (HCV) infection, alcohol use disorder in remission, diabetes mellitus, posttraumatic stress disorder, and traumatic brain injury. His medications included levothyroxine and carbamazepine. He previously worked as a barber but recently had stopped due to cognitive impairment. On initial evaluation, the patient's vital signs included a temperature of 36.3 °C, heart rate of 77 beats per minute, blood pressure of 139/83 mm Hg, respiratory rate of 18 breaths per minute, and 99% oxygen saturation while breathing ambient air. Physical examination was notable for a frail-appearing man in no acute distress. His conjunctivae were pale, and cardiac auscultation revealed a normal heart rate and irregularly irregular heart rhythm. A neurologic examination revealed decreased vibratory sensation in both feet, delayed and minimal speech, and a blunted affect. His skin was warm and dry with patchy hypopigmentation across the face and forehead. Laboratory results are shown in the Table. Testing 2 years previously found the patient's hemoglobin to be 11.4 g/dL and serum creatinine to be 1.7 mg/dL. A peripheral blood smear showed anisocytosis, hypochromia, decreased platelets, ovalocytes, elliptocytes, and rare teardrop cells, with no schistocytes present. Chest radiography and computed tomography of the head were unremarkable. An abdominal ultrasound revealed a complex hypoechoic mass with peripheral rim vascularity in the right hepatic lobe measuring 3.9 cm × 3.6 cm × 3.9 cm.
Lindsey Ulin, MD, Chief Medical Resident, VABHS and Brigham and Women’s Hospital (BWH):
To build the initial differential diagnosis, we are joined today by 3 internal medicine residents who were not involved in the care of this patient. Dr. Hickey, Dr. Ross and Dr. Manivannan, how did you approach this case?
Meghan Hickey, MD, Senior Internal Medicine Resident, VABHS and Boston Medical Center (BMC):
The constellation of fatigue, weakness, blunted affect, and delayed, minimal speech suggested central nervous system involvement, which I sought to unify with hemolytic anemia and his liver mass. The first diagnosis I considered was Wilson disease; however, this genetic disorder of copper metabolism often presents with liver failure or cirrhosis in young or middle-aged women, so this presentation would be atypical. Next, given the hypopigmentation was reported only on sun-exposed areas of the patient’s face, I considered possibilities other than vitiligo to avoid diagnostic anchoring. One such alternate diagnosis is porphyria cutanea tarda (PCT), which presents in middle-aged and older adults with a photosensitive dermatitis that can include acute sensory deficits. Manifestations of PCT can be triggered by alcohol consumption, though his alcohol use disorder was thought to be in remission, as well as HCV, for which he previously received treatment. However, anemia is uncommon in PCT, so the patient’s low hemoglobin would not be explained by this diagnosis. Lastly, I considered thrombotic thrombocytopenic purpura (TTP) given his anemia, thrombocytopenia, and neurologic symptoms; however, the patient did not have fever or a clear inciting cause, his renal dysfunction was relatively mild, and the peripheral blood smear revealed no schistocytes, which should be present in TTP.
TABLE Laboratory Results
Caroline Ross, MD, and Alan Manivannan, MD; Senior Internal Medicine Residents, VABHS and BMC:
We noted several salient features in the history and physical examination. First, we sought to explain the bilateral lower extremity numbness and decreased vibratory sensation in the feet leading to falls. We also considered his anemia and thrombocytopenia with signs of hemolysis including elevated lactate dehydrogenase (LDH), low haptoglobin, and elevated total bilirubin; however, with normal coagulation parameters. These results initially raised our concern for a thrombotic microangiopathy (TMA) such as TTP. However, the peripheral smear lacked schistocytes, making this less likely. The combination of his neurologic symptoms and TMA-like laboratory findings but without schistocytes raised our concern for vitamin B12 deficiency. Vitamin B12 deficiency can cause a pseudo-TMA picture with laboratory finding similar to TTP; however, schistocytes are typically absent. We also considered the possibility of hepatocellular carcinoma (HCC) with bone marrow infiltration leading to anemia given the finding of a liver mass on his abdominal ultrasound and low reticulocyte index. However, this would not explain his hemolysis. We also considered chronic disseminated intravascular coagulation in the setting of a malignancy as a contributor, but again, the smear lacked schistocytes and his coagulation parameters were normal. Finally, we considered a primary bone marrow process such as myelodysplastic syndrome due to the bicytopenia with poor bone marrow response and smear with tear drop cells and elliptocytes. However, we felt this was less likely as this would not explain his hemolytic anemia.
Dr. Ulin:
To refine the differential diagnosis, we are joined by an expert clinician who was also not involved in the care of this patient to describe his approach to this case. Dr. Orlander, can you walk us through your clinical reasoning?
Jay Orlander, MD, MPH: Professor of Medicine, Section of General Internal Medicine, Boston University Chobanian & Avedisian School of Medicine, Associate Chief, Medical Service, VABHS:
I will first comment on the hepatic mass. The hypoechoic liver mass with peripheral vascularity suggests a growing tumor. The patient has a history of substance use disorder with alcohol and treated HCV. He remains at increased risk for HCC even after prior successful HCV treatment and has 2 of 4 known risk factors for developing HCC— diabetes mellitus and alcohol use—the other 2 being underlying metabolic dysfunctionassociated steatotic liver disease (MASLD) and the presence of hepatic fibrosis, which we have not yet assessed. Worsening liver function can lead to cognitive issues and alcohol to peripheral neuropathy, but his story is not consistent with this. For his liver mass, I recommend a nonurgent magnetic resonance image for further evaluation.
Next, let’s consider his markedly elevated thyrotropin (TSH). Cognitive impairment along with lethargy, fatigue, and decreased exercise tolerance can be prominent features in severe hypothyroidism, but this diagnosis would not explain his hematologic findings.1
I view the principal finding of his laboratory testing as being that his bone marrow is failing to maintain adequate blood elements. He has a markedly low hematocrit along with low platelets and low-normal white blood cell counts. There is an absence of schistocytes on the blood smear, and after correcting his reticulocyte count for his degree of anemia (observed reticulocyte percentage [0.8%] x observed hematocrit [15.3%] / expected hematocrit [40%]), results in a reticulocyte index of 0.12, which is low. This suggests his bone marrow is failing to manufacture red blood cells at an appropriate rate. His haptoglobin is unmeasurable, so there is some free heme circulating. Hence, I infer that hemolysis and ineffective erythropoiesis are both occurring within the bone marrow, which also explains the slight elevation in bilirubin.
Intramedullary hemolysis with a markedly elevated LDH can be seen in severe vitamin B12 deficiency, which has many causes, but one cause in particular warrants consideration in this case: pernicious anemia. Pernicious anemia has an overall prevalence of about 0.1%, but is more common in older adults, and is estimated to be present in 2% to 3% of adults aged > 65 years.2 Prevalence is also increased in patients with other autoimmune diseases such as vitiligo and hypothyroidism, which our patient has.3 The pathophysiology of pernicious anemia relates to either autoimmune gastric parietal cell destruction and/or the development of antibodies against intrinsic factor, which is required for absorption of vitamin B12. Early disease may present with macrocytosis and a normal hemoglobin initially, but anemia develops over time if left untreated. When the primary cause of pernicious anemia is gastric parietal cell destruction, there is also an associated lack of stomach acid production (achlorhydria) with resulting poor micronutrient absorption; specifically, vitamin D, vitamin C, and iron. Hence, 30% of patients diagnosed with pernicious anemia have concurrent iron deficiency, which may counteract macrocytosis and result in a normal mean corpuscular volume. 4 Some medications are also poorly absorbed in achlorhydric states, such as levothyroxine, and treatment doses need to be increased, which could explain his markedly elevated TSH despite presumed medication adherence.
Vitamin B12 is essential for both the peripheral and central nervous systems. Longstanding severe B12 deficiency can explain all of his neurological and neurocognitive changes. The most common neurologic findings in B12 deficiency are symmetric paresthesias or numbness and gait problems. The sensory neuropathy affects the lower extremities more commonly than the upper. Untreated, patients can develop progressive weakness, ataxia, and orthostatic hypotension with syncope, as well as neuropsychiatric changes including depression or mood impairment, cognitive slowing, forgetfulness, and dementia.
Dr. Ulin:
Dr. Orlander, which pieces of objective data are most important in forming your differential diagnosis, and what tests would you obtain next?
Dr. Orlander:
The 3 most salient laboratory tests to me are a complete blood count, with all cell lines impacted but the hemoglobin and hematocrit most dramatically impacted, reticulocyte count of 0.8%, which is inappropriately low and hence suggests a hypoproliferative anemia, and the elevated LDH > 5000 IU/L.
Since my suspected diagnosis is pernicious anemia, I would obtain a blood smear looking for hypersegmented neutrophils, > 1 white blood cells with 5 lobes, or 1 with 6 lobes, which should clinch the diagnosis. Methylmalonic acid (MMA) levels are the most sensitive test for B12 deficiency, so I would also obtain that. Finally, I would check a B12 level, since in a patient with pernicious anemia, I would expect the level to be < 200 pg/mL.
Dr. Ulin:
Before we reveal the results of the patient’s additional workup, how do you approach interpreting B12 levels?
Dr. Orlander:
Measuring B12 can sometimes be problematic: the normal range is considered 200 to 900 pg/mL, but patients with measured low-normal levels in the range of 200 to 400 pg/mL can actually be physiologically deficient. There are also several common causes of falsely low and falsely high B12 levels in the absence of B12 deficiency. Hence, for patients with mild symptoms that could be due to B12 deficiency, many clinicians choose to just treat with B12 supplementation, deeming it safer to treat than miss an early diagnosis. B12 is involved in hydrogen transfer to convert MMA into succinyl-CoA and hence true vitamin B12 deficiency causes an increase in MMA.
Decreased production of vitamin B12 binding proteins, like haptocorrin, has been proposed as the mechanism for spurious low values.5 Certain conditions or medications can also cause spurious low serum vitamin B12 levels and thus might cause the appearance of vitamin B12 deficiency when the patient is not deficient. Examples include multiple myeloma, HIV infection, pregnancy, oral contraceptives, and phenytoin use. An example of spuriously low vitamin B12 level in pregnancy was demonstrated in a series of 50 pregnant individuals with low vitamin B12 levels (45-199 pg/mL), in whom metabolite testing for MMA and homocysteine showed no correlation with vitamin B12 level.6
Further complicating things, some conditions can cause spuriously increased vitamin B12 levels and thus might cause the appearance of normal vitamin B12 levels when the patient is actually deficient.7 Examples include occult malignancy, myeloproliferative neoplasms, alcoholic liver disease, kidney disease, and nitrous oxide exposure (the latter of which is unique in that it can also cause true vitamin B12 deficiency, as evidenced by clinical symptoms and high MMA levels).8,9
Lastly, autoantibodies to intrinsic factor in individuals with pernicious anemia may compete with intrinsic factor in the chemiluminescence assay and result in spuriously normal vitamin B12 levels in the presence of true deficiency.10-12 If the vitamin B12 level is very high (eg, 800 pg/mL), we do not worry about this effect in the absence of clinical features suggesting vitamin B12 deficiency; however, if the vitamin B12 level is borderline or low-normal and/or other clinical features suggest vitamin B12 deficiency, it is prudent to obtain other testing such as an MMA level.
Dr. Ulin:
We are also joined by Dr. Rahul Ganatra, who cared for the patient at the time the diagnosis was made. Dr. Ganatra, can you share the final diagnosis and provide an update on the patient?
Rahul Ganatra, MD, MPH, Director of Continuing Medical Education, VABHS:
The patient’s hemoglobin rose to 6.9 g/dL after transfusion of 2 units of packed red blood cells, and his dyspnea on exertion and fatigue improved. Iron studies, serum thiamine, serum folate, ADAMTS13 activity levels, and AM cortisol level were normal. Upon closer examination of the peripheral blood smear, rare hypersegmented neutrophils were noted. Serum B12 level returned below assay (< 146 pg/mL), and serum MMA was 50,800 nmol/L, confirming the diagnosis of severe vitamin B12 deficiency. Antibodies against intrinsic factor were detected, confirming the diagnosis of pernicious anemia. Treatment was initiated with intramuscular cyanocobalamin every other day and was transitioned to weekly dosing at the time of hospital discharge. After excluding adrenal insufficiency, his levothyroxine dose was increased. Finally, a liver mass biopsy confirmed a concomitant diagnosis of HCC. The patient was discharged home. Five weeks after discharge, his serum B12 level rose to > 1000 pg/mL, and 10 months after discharge, his TSH fell to 0.97 uIU/mL. Several months later, he underwent stereotactic body radiotherapy for the HCC. One year after his initial presentation, he has not resumed work as a barber.
Case Presentation:A 65-year-old male veteran presented to the Veterans Affairs Boston Healthcare System (VABHS) emergency department with progressive fatigue, dyspnea on exertion, lightheadedness, and falls over the last month. New bilateral lower extremity numbness up to his knees developed in the week prior to admission and prompted him to seek care. Additional history included 2 episodes of transient loss of consciousness resulting in falls and a week of diarrhea, which had resolved. His medical history was notable for hypothyroidism secondary to Hashimoto thyroiditis, seizure disorder, vitiligo, treated hepatitis C virus (HCV) infection, alcohol use disorder in remission, diabetes mellitus, posttraumatic stress disorder, and traumatic brain injury. His medications included levothyroxine and carbamazepine. He previously worked as a barber but recently had stopped due to cognitive impairment. On initial evaluation, the patient's vital signs included a temperature of 36.3 °C, heart rate of 77 beats per minute, blood pressure of 139/83 mm Hg, respiratory rate of 18 breaths per minute, and 99% oxygen saturation while breathing ambient air. Physical examination was notable for a frail-appearing man in no acute distress. His conjunctivae were pale, and cardiac auscultation revealed a normal heart rate and irregularly irregular heart rhythm. A neurologic examination revealed decreased vibratory sensation in both feet, delayed and minimal speech, and a blunted affect. His skin was warm and dry with patchy hypopigmentation across the face and forehead. Laboratory results are shown in the Table. Testing 2 years previously found the patient's hemoglobin to be 11.4 g/dL and serum creatinine to be 1.7 mg/dL. A peripheral blood smear showed anisocytosis, hypochromia, decreased platelets, ovalocytes, elliptocytes, and rare teardrop cells, with no schistocytes present. Chest radiography and computed tomography of the head were unremarkable. An abdominal ultrasound revealed a complex hypoechoic mass with peripheral rim vascularity in the right hepatic lobe measuring 3.9 cm × 3.6 cm × 3.9 cm.
Lindsey Ulin, MD, Chief Medical Resident, VABHS and Brigham and Women’s Hospital (BWH):
To build the initial differential diagnosis, we are joined today by 3 internal medicine residents who were not involved in the care of this patient. Dr. Hickey, Dr. Ross and Dr. Manivannan, how did you approach this case?
Meghan Hickey, MD, Senior Internal Medicine Resident, VABHS and Boston Medical Center (BMC):
The constellation of fatigue, weakness, blunted affect, and delayed, minimal speech suggested central nervous system involvement, which I sought to unify with hemolytic anemia and his liver mass. The first diagnosis I considered was Wilson disease; however, this genetic disorder of copper metabolism often presents with liver failure or cirrhosis in young or middle-aged women, so this presentation would be atypical. Next, given the hypopigmentation was reported only on sun-exposed areas of the patient’s face, I considered possibilities other than vitiligo to avoid diagnostic anchoring. One such alternate diagnosis is porphyria cutanea tarda (PCT), which presents in middle-aged and older adults with a photosensitive dermatitis that can include acute sensory deficits. Manifestations of PCT can be triggered by alcohol consumption, though his alcohol use disorder was thought to be in remission, as well as HCV, for which he previously received treatment. However, anemia is uncommon in PCT, so the patient’s low hemoglobin would not be explained by this diagnosis. Lastly, I considered thrombotic thrombocytopenic purpura (TTP) given his anemia, thrombocytopenia, and neurologic symptoms; however, the patient did not have fever or a clear inciting cause, his renal dysfunction was relatively mild, and the peripheral blood smear revealed no schistocytes, which should be present in TTP.
TABLE Laboratory Results
Caroline Ross, MD, and Alan Manivannan, MD; Senior Internal Medicine Residents, VABHS and BMC:
We noted several salient features in the history and physical examination. First, we sought to explain the bilateral lower extremity numbness and decreased vibratory sensation in the feet leading to falls. We also considered his anemia and thrombocytopenia with signs of hemolysis including elevated lactate dehydrogenase (LDH), low haptoglobin, and elevated total bilirubin; however, with normal coagulation parameters. These results initially raised our concern for a thrombotic microangiopathy (TMA) such as TTP. However, the peripheral smear lacked schistocytes, making this less likely. The combination of his neurologic symptoms and TMA-like laboratory findings but without schistocytes raised our concern for vitamin B12 deficiency. Vitamin B12 deficiency can cause a pseudo-TMA picture with laboratory finding similar to TTP; however, schistocytes are typically absent. We also considered the possibility of hepatocellular carcinoma (HCC) with bone marrow infiltration leading to anemia given the finding of a liver mass on his abdominal ultrasound and low reticulocyte index. However, this would not explain his hemolysis. We also considered chronic disseminated intravascular coagulation in the setting of a malignancy as a contributor, but again, the smear lacked schistocytes and his coagulation parameters were normal. Finally, we considered a primary bone marrow process such as myelodysplastic syndrome due to the bicytopenia with poor bone marrow response and smear with tear drop cells and elliptocytes. However, we felt this was less likely as this would not explain his hemolytic anemia.
Dr. Ulin:
To refine the differential diagnosis, we are joined by an expert clinician who was also not involved in the care of this patient to describe his approach to this case. Dr. Orlander, can you walk us through your clinical reasoning?
Jay Orlander, MD, MPH: Professor of Medicine, Section of General Internal Medicine, Boston University Chobanian & Avedisian School of Medicine, Associate Chief, Medical Service, VABHS:
I will first comment on the hepatic mass. The hypoechoic liver mass with peripheral vascularity suggests a growing tumor. The patient has a history of substance use disorder with alcohol and treated HCV. He remains at increased risk for HCC even after prior successful HCV treatment and has 2 of 4 known risk factors for developing HCC— diabetes mellitus and alcohol use—the other 2 being underlying metabolic dysfunctionassociated steatotic liver disease (MASLD) and the presence of hepatic fibrosis, which we have not yet assessed. Worsening liver function can lead to cognitive issues and alcohol to peripheral neuropathy, but his story is not consistent with this. For his liver mass, I recommend a nonurgent magnetic resonance image for further evaluation.
Next, let’s consider his markedly elevated thyrotropin (TSH). Cognitive impairment along with lethargy, fatigue, and decreased exercise tolerance can be prominent features in severe hypothyroidism, but this diagnosis would not explain his hematologic findings.1
I view the principal finding of his laboratory testing as being that his bone marrow is failing to maintain adequate blood elements. He has a markedly low hematocrit along with low platelets and low-normal white blood cell counts. There is an absence of schistocytes on the blood smear, and after correcting his reticulocyte count for his degree of anemia (observed reticulocyte percentage [0.8%] x observed hematocrit [15.3%] / expected hematocrit [40%]), results in a reticulocyte index of 0.12, which is low. This suggests his bone marrow is failing to manufacture red blood cells at an appropriate rate. His haptoglobin is unmeasurable, so there is some free heme circulating. Hence, I infer that hemolysis and ineffective erythropoiesis are both occurring within the bone marrow, which also explains the slight elevation in bilirubin.
Intramedullary hemolysis with a markedly elevated LDH can be seen in severe vitamin B12 deficiency, which has many causes, but one cause in particular warrants consideration in this case: pernicious anemia. Pernicious anemia has an overall prevalence of about 0.1%, but is more common in older adults, and is estimated to be present in 2% to 3% of adults aged > 65 years.2 Prevalence is also increased in patients with other autoimmune diseases such as vitiligo and hypothyroidism, which our patient has.3 The pathophysiology of pernicious anemia relates to either autoimmune gastric parietal cell destruction and/or the development of antibodies against intrinsic factor, which is required for absorption of vitamin B12. Early disease may present with macrocytosis and a normal hemoglobin initially, but anemia develops over time if left untreated. When the primary cause of pernicious anemia is gastric parietal cell destruction, there is also an associated lack of stomach acid production (achlorhydria) with resulting poor micronutrient absorption; specifically, vitamin D, vitamin C, and iron. Hence, 30% of patients diagnosed with pernicious anemia have concurrent iron deficiency, which may counteract macrocytosis and result in a normal mean corpuscular volume. 4 Some medications are also poorly absorbed in achlorhydric states, such as levothyroxine, and treatment doses need to be increased, which could explain his markedly elevated TSH despite presumed medication adherence.
Vitamin B12 is essential for both the peripheral and central nervous systems. Longstanding severe B12 deficiency can explain all of his neurological and neurocognitive changes. The most common neurologic findings in B12 deficiency are symmetric paresthesias or numbness and gait problems. The sensory neuropathy affects the lower extremities more commonly than the upper. Untreated, patients can develop progressive weakness, ataxia, and orthostatic hypotension with syncope, as well as neuropsychiatric changes including depression or mood impairment, cognitive slowing, forgetfulness, and dementia.
Dr. Ulin:
Dr. Orlander, which pieces of objective data are most important in forming your differential diagnosis, and what tests would you obtain next?
Dr. Orlander:
The 3 most salient laboratory tests to me are a complete blood count, with all cell lines impacted but the hemoglobin and hematocrit most dramatically impacted, reticulocyte count of 0.8%, which is inappropriately low and hence suggests a hypoproliferative anemia, and the elevated LDH > 5000 IU/L.
Since my suspected diagnosis is pernicious anemia, I would obtain a blood smear looking for hypersegmented neutrophils, > 1 white blood cells with 5 lobes, or 1 with 6 lobes, which should clinch the diagnosis. Methylmalonic acid (MMA) levels are the most sensitive test for B12 deficiency, so I would also obtain that. Finally, I would check a B12 level, since in a patient with pernicious anemia, I would expect the level to be < 200 pg/mL.
Dr. Ulin:
Before we reveal the results of the patient’s additional workup, how do you approach interpreting B12 levels?
Dr. Orlander:
Measuring B12 can sometimes be problematic: the normal range is considered 200 to 900 pg/mL, but patients with measured low-normal levels in the range of 200 to 400 pg/mL can actually be physiologically deficient. There are also several common causes of falsely low and falsely high B12 levels in the absence of B12 deficiency. Hence, for patients with mild symptoms that could be due to B12 deficiency, many clinicians choose to just treat with B12 supplementation, deeming it safer to treat than miss an early diagnosis. B12 is involved in hydrogen transfer to convert MMA into succinyl-CoA and hence true vitamin B12 deficiency causes an increase in MMA.
Decreased production of vitamin B12 binding proteins, like haptocorrin, has been proposed as the mechanism for spurious low values.5 Certain conditions or medications can also cause spurious low serum vitamin B12 levels and thus might cause the appearance of vitamin B12 deficiency when the patient is not deficient. Examples include multiple myeloma, HIV infection, pregnancy, oral contraceptives, and phenytoin use. An example of spuriously low vitamin B12 level in pregnancy was demonstrated in a series of 50 pregnant individuals with low vitamin B12 levels (45-199 pg/mL), in whom metabolite testing for MMA and homocysteine showed no correlation with vitamin B12 level.6
Further complicating things, some conditions can cause spuriously increased vitamin B12 levels and thus might cause the appearance of normal vitamin B12 levels when the patient is actually deficient.7 Examples include occult malignancy, myeloproliferative neoplasms, alcoholic liver disease, kidney disease, and nitrous oxide exposure (the latter of which is unique in that it can also cause true vitamin B12 deficiency, as evidenced by clinical symptoms and high MMA levels).8,9
Lastly, autoantibodies to intrinsic factor in individuals with pernicious anemia may compete with intrinsic factor in the chemiluminescence assay and result in spuriously normal vitamin B12 levels in the presence of true deficiency.10-12 If the vitamin B12 level is very high (eg, 800 pg/mL), we do not worry about this effect in the absence of clinical features suggesting vitamin B12 deficiency; however, if the vitamin B12 level is borderline or low-normal and/or other clinical features suggest vitamin B12 deficiency, it is prudent to obtain other testing such as an MMA level.
Dr. Ulin:
We are also joined by Dr. Rahul Ganatra, who cared for the patient at the time the diagnosis was made. Dr. Ganatra, can you share the final diagnosis and provide an update on the patient?
Rahul Ganatra, MD, MPH, Director of Continuing Medical Education, VABHS:
The patient’s hemoglobin rose to 6.9 g/dL after transfusion of 2 units of packed red blood cells, and his dyspnea on exertion and fatigue improved. Iron studies, serum thiamine, serum folate, ADAMTS13 activity levels, and AM cortisol level were normal. Upon closer examination of the peripheral blood smear, rare hypersegmented neutrophils were noted. Serum B12 level returned below assay (< 146 pg/mL), and serum MMA was 50,800 nmol/L, confirming the diagnosis of severe vitamin B12 deficiency. Antibodies against intrinsic factor were detected, confirming the diagnosis of pernicious anemia. Treatment was initiated with intramuscular cyanocobalamin every other day and was transitioned to weekly dosing at the time of hospital discharge. After excluding adrenal insufficiency, his levothyroxine dose was increased. Finally, a liver mass biopsy confirmed a concomitant diagnosis of HCC. The patient was discharged home. Five weeks after discharge, his serum B12 level rose to > 1000 pg/mL, and 10 months after discharge, his TSH fell to 0.97 uIU/mL. Several months later, he underwent stereotactic body radiotherapy for the HCC. One year after his initial presentation, he has not resumed work as a barber.
References
Leigh H, Kramer SI. The psychiatric manifestations of endocrine disease. Adv Intern Med. 1984;29:413-445
Lenti MV, Rugge M, Lahner E, et al. Autoimmune gastritis. Nat Rev Dis Primers. 2020;6(1):56.doi:10.1038/s41572-020-0187-8
Toh BH, van Driel IR, Gleeson PA. Pernicious anemia. N Engl J Med. 1997;337(20):1441-1448. doi:10.1056/NEJM199711133372007
. Hershko C, Ronson A, Souroujon M, Maschler I, Heyd J, Patz J. Variable hematologic presentation of autoimmune gastritis: age-related progression from iron deficiency to cobalamin depletion. Blood. 2006;107(4):1673-1679. doi:10.1182/blood-2005-09-3534
Morkbak AL, Hvas AM, Milman N, Nexo E. Holotranscobalamin remains unchanged during pregnancy. Longitudinal changes of cobalamins and their binding proteins during pregnancy and postpartum. Haematologica. 2007;92(12):1711-1712. doi:10.3324/haematol.11636
Metz J, McGrath K, Bennett M, Hyland K, Bottiglieri T. Biochemical indices of vitamin B12 nutrition in pregnant patients with subnormal serum vitamin B12 levels. Am J Hematol. 1995;48(4):251-255. doi:10.1002/ajh.2830480409
Marsden P, Sharma AA, Rotella JA. Review article: clinical manifestations and outcomes of chronic nitrous oxide misuse: a systematic review. Emerg Med Australas. 2022;34(4):492- 503. doi:10.1111/1742-6723.13997
Hamilton MS, Blackmore S, Lee A. Possible cause of false normal B-12 assays. BMJ. 2006;333(7569):654-655. doi:10.1136/bmj.333.7569.654-c
Yang DT, Cook RJ. Spurious elevations of vitamin B12 with pernicious anemia. N Engl J Med. 2012;366(18):1742-1743. doi:10.1056/NEJMc1201655
Carmel R, Agrawal YP. Failures of cobalamin assays in pernicious anemia. N Engl J Med. 2012;367(4):385-386. doi:10.1056/NEJMc1204070
Green R. Vitamin B12 deficiency from the perspective of a practicing hematologist. Blood. May 11 2017;129(19):2603- 2611. doi:10.1182/blood-2016-10-569186
Miceli E, Lenti MV, Padula D, et al. Common features of patients with autoimmune atrophic gastritis. Clin Gastroenterol Hepatol. 2012;10(7):812-814.doi:10.1016/j.cgh.2012.02.018
References
Leigh H, Kramer SI. The psychiatric manifestations of endocrine disease. Adv Intern Med. 1984;29:413-445
Lenti MV, Rugge M, Lahner E, et al. Autoimmune gastritis. Nat Rev Dis Primers. 2020;6(1):56.doi:10.1038/s41572-020-0187-8
Toh BH, van Driel IR, Gleeson PA. Pernicious anemia. N Engl J Med. 1997;337(20):1441-1448. doi:10.1056/NEJM199711133372007
. Hershko C, Ronson A, Souroujon M, Maschler I, Heyd J, Patz J. Variable hematologic presentation of autoimmune gastritis: age-related progression from iron deficiency to cobalamin depletion. Blood. 2006;107(4):1673-1679. doi:10.1182/blood-2005-09-3534
Morkbak AL, Hvas AM, Milman N, Nexo E. Holotranscobalamin remains unchanged during pregnancy. Longitudinal changes of cobalamins and their binding proteins during pregnancy and postpartum. Haematologica. 2007;92(12):1711-1712. doi:10.3324/haematol.11636
Metz J, McGrath K, Bennett M, Hyland K, Bottiglieri T. Biochemical indices of vitamin B12 nutrition in pregnant patients with subnormal serum vitamin B12 levels. Am J Hematol. 1995;48(4):251-255. doi:10.1002/ajh.2830480409
Marsden P, Sharma AA, Rotella JA. Review article: clinical manifestations and outcomes of chronic nitrous oxide misuse: a systematic review. Emerg Med Australas. 2022;34(4):492- 503. doi:10.1111/1742-6723.13997
Hamilton MS, Blackmore S, Lee A. Possible cause of false normal B-12 assays. BMJ. 2006;333(7569):654-655. doi:10.1136/bmj.333.7569.654-c
Yang DT, Cook RJ. Spurious elevations of vitamin B12 with pernicious anemia. N Engl J Med. 2012;366(18):1742-1743. doi:10.1056/NEJMc1201655
Carmel R, Agrawal YP. Failures of cobalamin assays in pernicious anemia. N Engl J Med. 2012;367(4):385-386. doi:10.1056/NEJMc1204070
Green R. Vitamin B12 deficiency from the perspective of a practicing hematologist. Blood. May 11 2017;129(19):2603- 2611. doi:10.1182/blood-2016-10-569186
Miceli E, Lenti MV, Padula D, et al. Common features of patients with autoimmune atrophic gastritis. Clin Gastroenterol Hepatol. 2012;10(7):812-814.doi:10.1016/j.cgh.2012.02.018
Residency programs across the country may have a few more slots for incoming residents due to a recent bump in Medicare funding.
Case in point: The University of Alabama at Birmingham (UAB). The state has one of the top stroke rates in the country, and yet UAB has the only hospital in the state training future doctors to help stroke patients recover. “Our hospital cares for Alabama’s sickest patients, many who need rehabilitation services,” said Craig Hoesley, MD, senior associate dean for medical education, who oversees graduate medical education (GME) or residency programs.
After decades of stagnant support, a recent bump in Medicare funding will allow UAB to add two more physical medicine and rehabilitation residents to the four residencies already receiving such funding.
Medicare also awarded UAB more funding last year to add an addiction medicine fellowship, one of two such training programs in the state for the specialty that helps treat patients fighting addiction.
UAB is among healthcare systems and hospitals nationwide benefiting from a recent hike in Medicare funding for residency programs after some 25 years at the same level of federal support. Medicare is the largest funder of training positions. Otherwise, hospitals finance training through means such as state support.
The latest round of funding, which went into effect in July, adds 200 positions to the doctor pipeline, creating more openings for residents seeking positions after medical school.
In the next few months, the Centers for Medicare & Medicaid Services (CMS) will notify teaching hospitals whether they’ll receive the next round of Medicare funding for more residency positions. At that time, CMS will have awarded nearly half of the 1200 residency training slots Congress approved in the past few years. In 2020 — for the first time since 1996 — Congress approved adding 1000 residency slots at teaching hospitals nationwide. CMS awards the money for 200 slots each year for 5 years.
More than half of the initial round of funding focused on training primary care specialists, with other slots designated for mental health specialists. Last year, Congress also approved a separate allocation of 200 more Medicare-funded residency positions, with at least half designated for psychiatry and related subspecialty residencies to help meet the growing need for more mental health specialists. On August 1, CMS announced it would distribute the funds next year, effective in 2026.
The additional Medicare funding attempts to address the shortage of healthcare providers and ensure future access to care, including in rural and underserved communities. The Association of American Medical Colleges (AAMC) estimates the nation will face a shortage of up to 86,000 physicians by 2036, including primary care doctors and specialists.
In addition, more than 100 million Americans, nearly a third of the nation, don’t have access to primary care due to the physician shortages in their communities, according to the National Association of Community Health Centers.
Major medical organizations, medical schools, and hospital groups have been pushing for years for increased Medicare funding to train new doctors to keep up with the demand for healthcare services and offset the physician shortage. As a cost-saving measure, Medicare set its cap in 1996 for how much it will reimburse each hospital offering GME training. However, according to the medical groups that continue to advocate to Congress for more funding, the funding hasn’t kept pace with the growing healthcare needs or rising medical school enrollment.
Adding Residency Spots
In April, Dr. Hoesley of UAB spoke at a Congressional briefing among health systems and hospitals that benefited from the additional funding. He told Congressional leaders how the increased number of GME positions affects UAB Medicine and its ability to care for rural areas.
“We have entire counties in Alabama that don’t have physicians. One way to address the physician shortage is to grow the GME programs. The funding we received will help us grow these programs and care for residents in our state.”
Still, the Medicare funding is only a drop in the bucket, Dr. Hoesley said. “We rely on Medicare funding alongside other funding partners to train residents and expand our care across the state.” He said many UAB residency programs are over their Medicare funding cap and would like to grow, but they can’t without more funding.
Mount Sinai Health System in New York City also will be able to expand its residency program after receiving Medicare support in the latest round of funding. The health system will use the federal funds to train an additional vascular surgeon. Mount Sinai currently receives CMS funding to train three residents in the specialty.
Over a 5-year program, that means CMS funding will help train 20 residents in the specialty that treats blood vessel blockages and diseases of the veins and arteries generally associated with aging.
“The funding is amazing,” said Peter L. Faries, MD, a surgery professor and system chief of vascular surgery at the Icahn School of Medicine at Mount Sinai, New York City, who directs the residency program.
“We don’t have the capacity to provide an individual training program without the funding. It’s not economically feasible.”
The need for more vascular surgeons increases as the population continues to age, he said. Mount Sinai treats patients throughout New York, including underserved areas in Harlem, the Bronx, Washington Heights, Brooklyn, and Queens. “These individuals might not receive an appropriate level of vascular care if we don’t have clinicians to treat them.”
Of the recent funding, Dr. Faries said it’s taken the residency program 15 years of advocacy to increase by two slots. “It’s a long process to get funding.” Vascular training programs can remain very selective with Medicare funding, typically receiving two applicants for every position,” said Dr. Faries.
Pushing for More Funds
Nearly 98,000 students enrolled in medical school this year, according to the National Resident Matching Program. A total of 44,853 applicants vied for the 38,494 first-year residency positions and 3009 second-year slots, leaving 3350 medical school graduates without a match.
“There are not enough spots to meet the growing demand,” said Jesse M. Ehrenfeld, MD, MPH, immediate past president of the American Medical Association. “Graduate medical education funding has not kept up.”
Despite the increase in medical school graduates over the past two decades, Medicare-supported training opportunities remained frozen at the 1996 level. A limited number of training positions meant residency programs couldn’t expand the physician pipeline to offset an aging workforce, contributing to the shortage. “The way to solve this is to expand GME,” Dr. Ehrenfeld said. “We continue to advocate to remove the cap.”
Dr. Ehrenfeld also told this news organization that he doesn’t mind that Congress recently designated GME funding to certain specialties, such as psychiatry, because he believes the need is great for residency spots across the board. “The good news is people recognize it’s challenging to get much through Congress.” He’s optimistic, though, about recent legislative efforts to increase funding.
AAMC, representing about a third of the nation’s 1100 teaching hospitals and health systems, feels the same. Congress “acknowledges and continues to recognize that the shortage is not getting better, and one way to address it is to increase Medicare-supported GME positions,” said Leonard Marquez, senior director of government relations and legislative advocacy.
Still, he said that the Medicare funding bump is only making a small dent in the need. AAMC estimates the average cost to train residents is $23 billion annually, and Medicare only funds 20% of that, or $5 billion. “Our members are at the point where they say: We already can’t add new training positions,” Mr. Marquez said. He added that without increasing residency slots, patient care will suffer. “We have to do anything possible we can to increase access to care.”
Mr. Marquez also believes Medicare funding should increase residency positions across the specialty spectrum, not just for psychiatry and primary care. He said that the targeted funding may prevent some teaching hospitals from applying for residency positions if they need other types of specialists based on their community’s needs.
Among the current proposals before Congress, the Resident Physician Shortage Reduction Act of 2023 would add 14,000 Medicare-supported residency slots over 7 years. Mr. Marquez said it may be more realistic to expect fewer new slots. A decision on potential legislation is expected at the end of the year. He said that if the medical groups aren’t pleased with the decision, they’ll advocate again in 2025.
A version of this article first appeared on Medscape.com.
Residency programs across the country may have a few more slots for incoming residents due to a recent bump in Medicare funding.
Case in point: The University of Alabama at Birmingham (UAB). The state has one of the top stroke rates in the country, and yet UAB has the only hospital in the state training future doctors to help stroke patients recover. “Our hospital cares for Alabama’s sickest patients, many who need rehabilitation services,” said Craig Hoesley, MD, senior associate dean for medical education, who oversees graduate medical education (GME) or residency programs.
After decades of stagnant support, a recent bump in Medicare funding will allow UAB to add two more physical medicine and rehabilitation residents to the four residencies already receiving such funding.
Medicare also awarded UAB more funding last year to add an addiction medicine fellowship, one of two such training programs in the state for the specialty that helps treat patients fighting addiction.
UAB is among healthcare systems and hospitals nationwide benefiting from a recent hike in Medicare funding for residency programs after some 25 years at the same level of federal support. Medicare is the largest funder of training positions. Otherwise, hospitals finance training through means such as state support.
The latest round of funding, which went into effect in July, adds 200 positions to the doctor pipeline, creating more openings for residents seeking positions after medical school.
In the next few months, the Centers for Medicare & Medicaid Services (CMS) will notify teaching hospitals whether they’ll receive the next round of Medicare funding for more residency positions. At that time, CMS will have awarded nearly half of the 1200 residency training slots Congress approved in the past few years. In 2020 — for the first time since 1996 — Congress approved adding 1000 residency slots at teaching hospitals nationwide. CMS awards the money for 200 slots each year for 5 years.
More than half of the initial round of funding focused on training primary care specialists, with other slots designated for mental health specialists. Last year, Congress also approved a separate allocation of 200 more Medicare-funded residency positions, with at least half designated for psychiatry and related subspecialty residencies to help meet the growing need for more mental health specialists. On August 1, CMS announced it would distribute the funds next year, effective in 2026.
The additional Medicare funding attempts to address the shortage of healthcare providers and ensure future access to care, including in rural and underserved communities. The Association of American Medical Colleges (AAMC) estimates the nation will face a shortage of up to 86,000 physicians by 2036, including primary care doctors and specialists.
In addition, more than 100 million Americans, nearly a third of the nation, don’t have access to primary care due to the physician shortages in their communities, according to the National Association of Community Health Centers.
Major medical organizations, medical schools, and hospital groups have been pushing for years for increased Medicare funding to train new doctors to keep up with the demand for healthcare services and offset the physician shortage. As a cost-saving measure, Medicare set its cap in 1996 for how much it will reimburse each hospital offering GME training. However, according to the medical groups that continue to advocate to Congress for more funding, the funding hasn’t kept pace with the growing healthcare needs or rising medical school enrollment.
Adding Residency Spots
In April, Dr. Hoesley of UAB spoke at a Congressional briefing among health systems and hospitals that benefited from the additional funding. He told Congressional leaders how the increased number of GME positions affects UAB Medicine and its ability to care for rural areas.
“We have entire counties in Alabama that don’t have physicians. One way to address the physician shortage is to grow the GME programs. The funding we received will help us grow these programs and care for residents in our state.”
Still, the Medicare funding is only a drop in the bucket, Dr. Hoesley said. “We rely on Medicare funding alongside other funding partners to train residents and expand our care across the state.” He said many UAB residency programs are over their Medicare funding cap and would like to grow, but they can’t without more funding.
Mount Sinai Health System in New York City also will be able to expand its residency program after receiving Medicare support in the latest round of funding. The health system will use the federal funds to train an additional vascular surgeon. Mount Sinai currently receives CMS funding to train three residents in the specialty.
Over a 5-year program, that means CMS funding will help train 20 residents in the specialty that treats blood vessel blockages and diseases of the veins and arteries generally associated with aging.
“The funding is amazing,” said Peter L. Faries, MD, a surgery professor and system chief of vascular surgery at the Icahn School of Medicine at Mount Sinai, New York City, who directs the residency program.
“We don’t have the capacity to provide an individual training program without the funding. It’s not economically feasible.”
The need for more vascular surgeons increases as the population continues to age, he said. Mount Sinai treats patients throughout New York, including underserved areas in Harlem, the Bronx, Washington Heights, Brooklyn, and Queens. “These individuals might not receive an appropriate level of vascular care if we don’t have clinicians to treat them.”
Of the recent funding, Dr. Faries said it’s taken the residency program 15 years of advocacy to increase by two slots. “It’s a long process to get funding.” Vascular training programs can remain very selective with Medicare funding, typically receiving two applicants for every position,” said Dr. Faries.
Pushing for More Funds
Nearly 98,000 students enrolled in medical school this year, according to the National Resident Matching Program. A total of 44,853 applicants vied for the 38,494 first-year residency positions and 3009 second-year slots, leaving 3350 medical school graduates without a match.
“There are not enough spots to meet the growing demand,” said Jesse M. Ehrenfeld, MD, MPH, immediate past president of the American Medical Association. “Graduate medical education funding has not kept up.”
Despite the increase in medical school graduates over the past two decades, Medicare-supported training opportunities remained frozen at the 1996 level. A limited number of training positions meant residency programs couldn’t expand the physician pipeline to offset an aging workforce, contributing to the shortage. “The way to solve this is to expand GME,” Dr. Ehrenfeld said. “We continue to advocate to remove the cap.”
Dr. Ehrenfeld also told this news organization that he doesn’t mind that Congress recently designated GME funding to certain specialties, such as psychiatry, because he believes the need is great for residency spots across the board. “The good news is people recognize it’s challenging to get much through Congress.” He’s optimistic, though, about recent legislative efforts to increase funding.
AAMC, representing about a third of the nation’s 1100 teaching hospitals and health systems, feels the same. Congress “acknowledges and continues to recognize that the shortage is not getting better, and one way to address it is to increase Medicare-supported GME positions,” said Leonard Marquez, senior director of government relations and legislative advocacy.
Still, he said that the Medicare funding bump is only making a small dent in the need. AAMC estimates the average cost to train residents is $23 billion annually, and Medicare only funds 20% of that, or $5 billion. “Our members are at the point where they say: We already can’t add new training positions,” Mr. Marquez said. He added that without increasing residency slots, patient care will suffer. “We have to do anything possible we can to increase access to care.”
Mr. Marquez also believes Medicare funding should increase residency positions across the specialty spectrum, not just for psychiatry and primary care. He said that the targeted funding may prevent some teaching hospitals from applying for residency positions if they need other types of specialists based on their community’s needs.
Among the current proposals before Congress, the Resident Physician Shortage Reduction Act of 2023 would add 14,000 Medicare-supported residency slots over 7 years. Mr. Marquez said it may be more realistic to expect fewer new slots. A decision on potential legislation is expected at the end of the year. He said that if the medical groups aren’t pleased with the decision, they’ll advocate again in 2025.
A version of this article first appeared on Medscape.com.
Residency programs across the country may have a few more slots for incoming residents due to a recent bump in Medicare funding.
Case in point: The University of Alabama at Birmingham (UAB). The state has one of the top stroke rates in the country, and yet UAB has the only hospital in the state training future doctors to help stroke patients recover. “Our hospital cares for Alabama’s sickest patients, many who need rehabilitation services,” said Craig Hoesley, MD, senior associate dean for medical education, who oversees graduate medical education (GME) or residency programs.
After decades of stagnant support, a recent bump in Medicare funding will allow UAB to add two more physical medicine and rehabilitation residents to the four residencies already receiving such funding.
Medicare also awarded UAB more funding last year to add an addiction medicine fellowship, one of two such training programs in the state for the specialty that helps treat patients fighting addiction.
UAB is among healthcare systems and hospitals nationwide benefiting from a recent hike in Medicare funding for residency programs after some 25 years at the same level of federal support. Medicare is the largest funder of training positions. Otherwise, hospitals finance training through means such as state support.
The latest round of funding, which went into effect in July, adds 200 positions to the doctor pipeline, creating more openings for residents seeking positions after medical school.
In the next few months, the Centers for Medicare & Medicaid Services (CMS) will notify teaching hospitals whether they’ll receive the next round of Medicare funding for more residency positions. At that time, CMS will have awarded nearly half of the 1200 residency training slots Congress approved in the past few years. In 2020 — for the first time since 1996 — Congress approved adding 1000 residency slots at teaching hospitals nationwide. CMS awards the money for 200 slots each year for 5 years.
More than half of the initial round of funding focused on training primary care specialists, with other slots designated for mental health specialists. Last year, Congress also approved a separate allocation of 200 more Medicare-funded residency positions, with at least half designated for psychiatry and related subspecialty residencies to help meet the growing need for more mental health specialists. On August 1, CMS announced it would distribute the funds next year, effective in 2026.
The additional Medicare funding attempts to address the shortage of healthcare providers and ensure future access to care, including in rural and underserved communities. The Association of American Medical Colleges (AAMC) estimates the nation will face a shortage of up to 86,000 physicians by 2036, including primary care doctors and specialists.
In addition, more than 100 million Americans, nearly a third of the nation, don’t have access to primary care due to the physician shortages in their communities, according to the National Association of Community Health Centers.
Major medical organizations, medical schools, and hospital groups have been pushing for years for increased Medicare funding to train new doctors to keep up with the demand for healthcare services and offset the physician shortage. As a cost-saving measure, Medicare set its cap in 1996 for how much it will reimburse each hospital offering GME training. However, according to the medical groups that continue to advocate to Congress for more funding, the funding hasn’t kept pace with the growing healthcare needs or rising medical school enrollment.
Adding Residency Spots
In April, Dr. Hoesley of UAB spoke at a Congressional briefing among health systems and hospitals that benefited from the additional funding. He told Congressional leaders how the increased number of GME positions affects UAB Medicine and its ability to care for rural areas.
“We have entire counties in Alabama that don’t have physicians. One way to address the physician shortage is to grow the GME programs. The funding we received will help us grow these programs and care for residents in our state.”
Still, the Medicare funding is only a drop in the bucket, Dr. Hoesley said. “We rely on Medicare funding alongside other funding partners to train residents and expand our care across the state.” He said many UAB residency programs are over their Medicare funding cap and would like to grow, but they can’t without more funding.
Mount Sinai Health System in New York City also will be able to expand its residency program after receiving Medicare support in the latest round of funding. The health system will use the federal funds to train an additional vascular surgeon. Mount Sinai currently receives CMS funding to train three residents in the specialty.
Over a 5-year program, that means CMS funding will help train 20 residents in the specialty that treats blood vessel blockages and diseases of the veins and arteries generally associated with aging.
“The funding is amazing,” said Peter L. Faries, MD, a surgery professor and system chief of vascular surgery at the Icahn School of Medicine at Mount Sinai, New York City, who directs the residency program.
“We don’t have the capacity to provide an individual training program without the funding. It’s not economically feasible.”
The need for more vascular surgeons increases as the population continues to age, he said. Mount Sinai treats patients throughout New York, including underserved areas in Harlem, the Bronx, Washington Heights, Brooklyn, and Queens. “These individuals might not receive an appropriate level of vascular care if we don’t have clinicians to treat them.”
Of the recent funding, Dr. Faries said it’s taken the residency program 15 years of advocacy to increase by two slots. “It’s a long process to get funding.” Vascular training programs can remain very selective with Medicare funding, typically receiving two applicants for every position,” said Dr. Faries.
Pushing for More Funds
Nearly 98,000 students enrolled in medical school this year, according to the National Resident Matching Program. A total of 44,853 applicants vied for the 38,494 first-year residency positions and 3009 second-year slots, leaving 3350 medical school graduates without a match.
“There are not enough spots to meet the growing demand,” said Jesse M. Ehrenfeld, MD, MPH, immediate past president of the American Medical Association. “Graduate medical education funding has not kept up.”
Despite the increase in medical school graduates over the past two decades, Medicare-supported training opportunities remained frozen at the 1996 level. A limited number of training positions meant residency programs couldn’t expand the physician pipeline to offset an aging workforce, contributing to the shortage. “The way to solve this is to expand GME,” Dr. Ehrenfeld said. “We continue to advocate to remove the cap.”
Dr. Ehrenfeld also told this news organization that he doesn’t mind that Congress recently designated GME funding to certain specialties, such as psychiatry, because he believes the need is great for residency spots across the board. “The good news is people recognize it’s challenging to get much through Congress.” He’s optimistic, though, about recent legislative efforts to increase funding.
AAMC, representing about a third of the nation’s 1100 teaching hospitals and health systems, feels the same. Congress “acknowledges and continues to recognize that the shortage is not getting better, and one way to address it is to increase Medicare-supported GME positions,” said Leonard Marquez, senior director of government relations and legislative advocacy.
Still, he said that the Medicare funding bump is only making a small dent in the need. AAMC estimates the average cost to train residents is $23 billion annually, and Medicare only funds 20% of that, or $5 billion. “Our members are at the point where they say: We already can’t add new training positions,” Mr. Marquez said. He added that without increasing residency slots, patient care will suffer. “We have to do anything possible we can to increase access to care.”
Mr. Marquez also believes Medicare funding should increase residency positions across the specialty spectrum, not just for psychiatry and primary care. He said that the targeted funding may prevent some teaching hospitals from applying for residency positions if they need other types of specialists based on their community’s needs.
Among the current proposals before Congress, the Resident Physician Shortage Reduction Act of 2023 would add 14,000 Medicare-supported residency slots over 7 years. Mr. Marquez said it may be more realistic to expect fewer new slots. A decision on potential legislation is expected at the end of the year. He said that if the medical groups aren’t pleased with the decision, they’ll advocate again in 2025.
A version of this article first appeared on Medscape.com.
Diversity, equity, and inclusion (DEI) programs seek to improve dermatologic education and clinical care for an increasingly diverse patient population as well as to recruit and sustain a physician workforce that reflects the diversity of the patients they serve.1,2 In dermatology, only 4.2% and 3.0% of practicing dermatologists self-identify as being of Hispanic and African American ethnicity, respectively, compared with 18.5% and 13.4% of the general population, respectively.3 Creating an educational system that works to meet the goals of DEI is essential to improve health outcomes and address disparities. The lack of robust DEI-related curricula during residency training may limit the ability of practicing dermatologists to provide comprehensive and culturally sensitive care. It has been shown that racial concordance between patients and physicians has a positive impact on patient satisfaction by fostering a trusting patient-physician relationship.4
It is the responsibility of all dermatologists to create an environment where patients from any background can feel comfortable, which can be cultivated by establishing patient-centered communication and cultural humility.5 These skills can be strengthened via the implementation of DEI-related curricula during residency training. Augmenting exposure of these topics during training can optimize the delivery of dermatologic care by providing residents with the tools and confidence needed to care for patients of culturally diverse backgrounds. Enhancing DEI education is crucial to not only improve the recognition and treatment of dermatologic conditions in all skin and hair types but also to minimize misconceptions, stigma, health disparities, and discrimination faced by historically marginalized communities. Creating a culture of inclusion is of paramount importance to build successful relationships with patients and colleagues of culturally diverse backgrounds.6
There are multiple efforts underway to increase DEI education across the field of dermatology, including the development of DEI task forces in professional organizations and societies that serve to expand DEI-related research, mentorship, and education. The American Academy of Dermatology has been leading efforts to create a curriculum focused on skin of color, particularly addressing inadequate educational training on how dermatologic conditions manifest in this population.7 The Skin of Color Society has similar efforts underway and is developing a speakers bureau to give leading experts a platform to lecture dermatology trainees as well as patient and community audiences on various topics in skin of color.8 These are just 2 of many professional dermatology organizations that are advocating for expanded education on DEI; however, consistently integrating DEI-related topics into dermatology residency training curricula remains a gap in pedagogy. To identify the DEI-related topics of greatest relevance to the dermatology resident curricula, we implemented a modified electronic Delphi (e-Delphi) consensus process to provide standardized recommendations.
Methods
A 2-round modified e-Delphi method was utilized (Figure). An initial list of potential curricular topics was formulated by an expert panel consisting of 5 dermatologists from the Association of Professors of Dermatology DEI subcommittee and the American Academy of Dermatology Diversity Task Force (A.M.A., S.B., R.V., S.D.W., J.I.S.). Initial topics were selected via several meetings among the panel members to discuss existing DEI concerns and issues that were deemed relevant due to education gaps in residency training. The list of topics was further expanded with recommendations obtained via an email sent to dermatology program directors on the Association of Professors of Dermatology listserve, which solicited voluntary participation of academic dermatologists, including program directors and dermatology residents.
Methodology flowchart for electronic Delphi consensus study.
There were 2 voting rounds, with each round consisting of questions scored on a Likert scale ranging from 1 to 5 (1=not essential, 2=probably not essential, 3=neutral, 4=probably essential, 5=definitely essential). The inclusion criteria to classify a topic as necessary for integration into the dermatology residency curriculum included 95% (18/19) or more of respondents rating the topic as probably essential or definitely essential; if more than 90% (17/19) of respondents rated the topic as probably essential or definitely essential and less than 10% (2/19) rated it as not essential or probably not essential, the topic was still included as part of the suggested curriculum. Topics that received ratings of probably essential or definitely essential by less than 80% (15/19) of respondents were removed from consideration. The topics that did not meet inclusion or exclusion criteria during the first round of voting were refined by the e-Delphi steering committee (V.S.E-C. and F-A.R.) based on open-ended feedback from the voting group provided at the end of the survey and subsequently passed to the second round of voting.
Results
Participants—A total of 19 respondents participated in both voting rounds, the majority (80% [15/19]) of whom were program directors or dermatologists affiliated with academia or development of DEI education; the remaining 20% [4/19]) were dermatology residents.
Open-Ended Feedback—Voting group members were able to provide open-ended feedback for each of the sets of topics after the survey, which the steering committee utilized to modify the topics as needed for the final voting round. For example, “structural racism/discrimination” was originally mentioned as a topic, but several participants suggested including specific types of racism; therefore, the wording was changed to “racism: types, definitions” to encompass broader definitions and types of racism.
Survey Results—Two genres of topics were surveyed in each voting round: clinical and nonclinical. Participants voted on a total of 61 topics, with 23 ultimately selected in the final list of consensus curricular topics. Of those, 9 were clinical and 14 nonclinical. All topics deemed necessary for inclusion in residency curricula are presented in eTables 1 and 2.
During the first round of voting, the e-Delphi panel reached a consensus to include the following 17 topics as essential to dermatology residency training (along with the percentage of voters who classified them as probably essential or definitely essential): how to mitigate bias in clinical and workplace settings (100% [40/40]); social determinants of health-related disparities in dermatology (100% [40/40]); hairstyling practices across different hair textures (100% [40/40]); definitions and examples of microaggressions (97.50% [39/40]); definition, background, and types of bias (97.50% [39/40]); manifestations of bias in the clinical setting (97.44% [38/39]); racial and ethnic disparities in dermatology (97.44% [38/39]); keloids (97.37% [37/38]); differences in dermoscopic presentations in skin of color (97.30% [36/37]); skin cancer in patients with skin of color (97.30% [36/37]); disparities due to bias (95.00% [38/40]); how to apply cultural humility and safety to patients of different cultural backgrounds (94.87% [37/40]); best practices in providing care to patients with limited English proficiency (94.87% [37/40]); hair loss in patients with textured hair (94.74% [36/38]); pseudofolliculitis barbae and acne keloidalis nuchae (94.60% [35/37]); disparities regarding people experiencing homelessness (92.31% [36/39]); and definitions and types of racism and other forms of discrimination (92.31% [36/39]). eTable 1 provides a list of suggested resources to incorporate these topics into the educational components of residency curricula. The resources provided were not part of the voting process, and they were not considered in the consensus analysis; they are included here as suggested educational catalysts.
During the second round of voting, 25 topics were evaluated. Of those, the following 6 topics were proposed to be included as essential in residency training: differences in prevalence and presentation of common inflammatory disorders (100% [29/29]); manifestations of bias in the learning environment (96.55%); antiracist action and how to decrease the effects of structural racism in clinical and educational settings (96.55% [28/29]); diversity of images in dermatology education (96.55% [28/29]); pigmentary disorders and their psychological effects (96.55% [28/29]); and LGBTQ (lesbian, gay, bisexual, transgender, and queer) dermatologic health care (96.55% [28/29]). eTable 2 includes these topics as well as suggested resources to help incorporate them into training.
Comment
This study utilized a modified e-Delphi technique to identify relevant clinical and nonclinical DEI topics that should be incorporated into dermatology residency curricula. The panel members reached a consensus for 9 clinical DEI-related topics. The respondents agreed that the topics related to skin and hair conditions in patients with skin of color as well as textured hair were crucial to residency education. Skin cancer, hair loss, pseudofolliculitis barbae, acne keloidalis nuchae, keloids, pigmentary disorders, and their varying presentations in patients with skin of color were among the recommended topics. The panel also recommended educating residents on the variable visual presentations of inflammatory conditions in skin of color. Addressing the needs of diverse patients—for example, those belonging to the LGBTQ community—also was deemed important for inclusion.
The remaining 14 chosen topics were nonclinical items addressing concepts such as bias and health care disparities as well as cultural humility and safety.9 Cultural humility and safety focus on developing cultural awareness by creating a safe setting for patients rather than encouraging power relationships between them and their physicians. Various topics related to racism also were recommended to be included in residency curricula, including education on implementation of antiracist action in the workplace.
Many of the nonclinical topics are intertwined; for instance, learning about health care disparities in patients with limited English proficiency allows for improved best practices in delivering care to patients from this population. The first step in overcoming bias and subsequent disparities is acknowledging how the perpetuation of bias leads to disparities after being taught tools to recognize it.
Our group’s guidance on DEI topics should help dermatology residency program leaders as they design and refine program curricula. There are multiple avenues for incorporating education on these topics, including lectures, interactive workshops, role-playing sessions, book or journal clubs, and discussion circles. Many of these topics/programs may already be included in programs’ didactic curricula, which would minimize the burden of finding space to educate on these topics. Institutional cultural change is key to ensuring truly diverse, equitable, and inclusive workplaces. Educating tomorrow’s dermatologists on these topics is a first step toward achieving that cultural change.
Limitations—A limitation of this e-Delphi survey is that only a selection of experts in this field was included. Additionally, we were concerned that the Likert scale format and the bar we set for inclusion and exclusion may have failed to adequately capture participants’ nuanced opinions. As such, participants were able to provide open-ended feedback, and suggestions for alternate wording or other changes were considered by the steering committee. Finally, inclusion recommendations identified in this survey were developed specifically for US dermatology residents.
Conclusion
In this e-Delphi consensus assessment of DEI-related topics, we recommend the inclusion of 23 topics into dermatology residency program curricula to improve medical training and the patient-physician relationship as well as to create better health outcomes. We also provide specific sample resource recommendations in eTables 1 and 2 to facilitate inclusion of these topics into residency curricula across the country.
Lopez S, Lourido JO, Lim HW, et al. The call to action to increase racial and ethnic diversity in dermatology: a retrospective, cross-sectional study to monitor progress. J Am Acad Dermatol. 2020;86:E121-E123. doi:10.1016/j.jaad.2021.10.011
El-Kashlan N, Alexis A. Disparities in dermatology: a reflection. J Clin Aesthet Dermatol. 2022;15:27-29.
Laveist TA, Nuru-Jeter A. Is doctor-patient race concordance associated with greater satisfaction with care? J Health Soc Behav. 2002;43:296-306.
Street RL Jr, O’Malley KJ, Cooper LA, et al. Understanding concordance in patient-physician relationships: personal and ethnic dimensions of shared identity. Ann Fam Med. 2008;6:198-205. doi:10.1370/afm.821
Dadrass F, Bowers S, Shinkai K, et al. Diversity, equity, and inclusion in dermatology residency. Dermatol Clin. 2023;41:257-263. doi:10.1016/j.det.2022.10.006
Solchanyk D, Ekeh O, Saffran L, et al. Integrating cultural humility into the medical education curriculum: strategies for educators. Teach Learn Med. 2021;33:554-560. doi:10.1080/10401334.2021.1877711
Valerie S. Encarnación-Cortés is from the School of Medicine, University of Puerto Rico, Medical Sciences Campus, San Juan. Ivan Rodriguez and Drs. Elbuluk and Worswick are from the Department of Dermatology, University of Southern California, Los Angeles. Dr. Rinderknecht is from the School of Medicine, University of San Francisco, California. Dr. Admassu is from the Department of Dermatology, Medical College of Wisconsin, Milwaukee. Drs. Phillips and Pimentel are from the Department of Dermatology, Oregon Health and Science University, Portland. Dr. Castillo-Valladares is from the Department of Dermatology, University of California San Francisco. Dr. Tarbox is from the Department of Dermatology, Texas Tech University, Lubbock. Dr. Peebles is from the Department of Dermatology, Mid-Atlantic Permanente Medical Group, Rockville, Maryland. Dr. Stratman is from the Department of Dermatology, Marshfield Clinic Health System, Wisconsin. Dr. Altman is from the Department of Dermatology, University of New Mexico, Albuquerque. Dr. Parekh is from the Department of Dermatology, Baylor Scott and White Medical Center, Texas. Dr. Daveluy is from the Department of Dermatology, Wayne State University School of Medicine, Detroit. Dr. James is from the Department of Dermatology, Perelman School of Medicine, University of Pennsylvania, Philadelphia. Dr. Kim is from the Department of Dermatology, Baylor College of Medicine, Temple, Texas. Dr. Rosmarin is from the Department of Dermatology, School of Medicine, Indiana University, Indianapolis. Dr. Kakpovbia is from the Department of Dermatology, Grossman School of Medicine, New York University, New York. Dr. Silverberg is from the George Washington University School of Medicine and Health Sciences, Washington, DC. Dr. Bowers is from the Department of Dermatology, Stritch School of Medicine, Loyola University, Chicago. Dr. Vasquez is from the Department of Dermatology, University of Texas Southwestern Medical Center, Dallas. Dr. Ahmed is from the Division of Dermatology, Dell Medical School, University of Texas, Austin.
Several of the authors have relevant financial disclosures to report. Due to their length, the disclosures are listed in their entirety in the Appendix online at www.mdedge.com/dermatology.
The eTables are available in the Appendix online at www.mdedge.com/dermatology.
Correspondence: Valerie S. Encarnación-Cortés, BS ([email protected]).
Valerie S. Encarnación-Cortés is from the School of Medicine, University of Puerto Rico, Medical Sciences Campus, San Juan. Ivan Rodriguez and Drs. Elbuluk and Worswick are from the Department of Dermatology, University of Southern California, Los Angeles. Dr. Rinderknecht is from the School of Medicine, University of San Francisco, California. Dr. Admassu is from the Department of Dermatology, Medical College of Wisconsin, Milwaukee. Drs. Phillips and Pimentel are from the Department of Dermatology, Oregon Health and Science University, Portland. Dr. Castillo-Valladares is from the Department of Dermatology, University of California San Francisco. Dr. Tarbox is from the Department of Dermatology, Texas Tech University, Lubbock. Dr. Peebles is from the Department of Dermatology, Mid-Atlantic Permanente Medical Group, Rockville, Maryland. Dr. Stratman is from the Department of Dermatology, Marshfield Clinic Health System, Wisconsin. Dr. Altman is from the Department of Dermatology, University of New Mexico, Albuquerque. Dr. Parekh is from the Department of Dermatology, Baylor Scott and White Medical Center, Texas. Dr. Daveluy is from the Department of Dermatology, Wayne State University School of Medicine, Detroit. Dr. James is from the Department of Dermatology, Perelman School of Medicine, University of Pennsylvania, Philadelphia. Dr. Kim is from the Department of Dermatology, Baylor College of Medicine, Temple, Texas. Dr. Rosmarin is from the Department of Dermatology, School of Medicine, Indiana University, Indianapolis. Dr. Kakpovbia is from the Department of Dermatology, Grossman School of Medicine, New York University, New York. Dr. Silverberg is from the George Washington University School of Medicine and Health Sciences, Washington, DC. Dr. Bowers is from the Department of Dermatology, Stritch School of Medicine, Loyola University, Chicago. Dr. Vasquez is from the Department of Dermatology, University of Texas Southwestern Medical Center, Dallas. Dr. Ahmed is from the Division of Dermatology, Dell Medical School, University of Texas, Austin.
Several of the authors have relevant financial disclosures to report. Due to their length, the disclosures are listed in their entirety in the Appendix online at www.mdedge.com/dermatology.
The eTables are available in the Appendix online at www.mdedge.com/dermatology.
Correspondence: Valerie S. Encarnación-Cortés, BS ([email protected]).
Valerie S. Encarnación-Cortés is from the School of Medicine, University of Puerto Rico, Medical Sciences Campus, San Juan. Ivan Rodriguez and Drs. Elbuluk and Worswick are from the Department of Dermatology, University of Southern California, Los Angeles. Dr. Rinderknecht is from the School of Medicine, University of San Francisco, California. Dr. Admassu is from the Department of Dermatology, Medical College of Wisconsin, Milwaukee. Drs. Phillips and Pimentel are from the Department of Dermatology, Oregon Health and Science University, Portland. Dr. Castillo-Valladares is from the Department of Dermatology, University of California San Francisco. Dr. Tarbox is from the Department of Dermatology, Texas Tech University, Lubbock. Dr. Peebles is from the Department of Dermatology, Mid-Atlantic Permanente Medical Group, Rockville, Maryland. Dr. Stratman is from the Department of Dermatology, Marshfield Clinic Health System, Wisconsin. Dr. Altman is from the Department of Dermatology, University of New Mexico, Albuquerque. Dr. Parekh is from the Department of Dermatology, Baylor Scott and White Medical Center, Texas. Dr. Daveluy is from the Department of Dermatology, Wayne State University School of Medicine, Detroit. Dr. James is from the Department of Dermatology, Perelman School of Medicine, University of Pennsylvania, Philadelphia. Dr. Kim is from the Department of Dermatology, Baylor College of Medicine, Temple, Texas. Dr. Rosmarin is from the Department of Dermatology, School of Medicine, Indiana University, Indianapolis. Dr. Kakpovbia is from the Department of Dermatology, Grossman School of Medicine, New York University, New York. Dr. Silverberg is from the George Washington University School of Medicine and Health Sciences, Washington, DC. Dr. Bowers is from the Department of Dermatology, Stritch School of Medicine, Loyola University, Chicago. Dr. Vasquez is from the Department of Dermatology, University of Texas Southwestern Medical Center, Dallas. Dr. Ahmed is from the Division of Dermatology, Dell Medical School, University of Texas, Austin.
Several of the authors have relevant financial disclosures to report. Due to their length, the disclosures are listed in their entirety in the Appendix online at www.mdedge.com/dermatology.
The eTables are available in the Appendix online at www.mdedge.com/dermatology.
Correspondence: Valerie S. Encarnación-Cortés, BS ([email protected]).
Diversity, equity, and inclusion (DEI) programs seek to improve dermatologic education and clinical care for an increasingly diverse patient population as well as to recruit and sustain a physician workforce that reflects the diversity of the patients they serve.1,2 In dermatology, only 4.2% and 3.0% of practicing dermatologists self-identify as being of Hispanic and African American ethnicity, respectively, compared with 18.5% and 13.4% of the general population, respectively.3 Creating an educational system that works to meet the goals of DEI is essential to improve health outcomes and address disparities. The lack of robust DEI-related curricula during residency training may limit the ability of practicing dermatologists to provide comprehensive and culturally sensitive care. It has been shown that racial concordance between patients and physicians has a positive impact on patient satisfaction by fostering a trusting patient-physician relationship.4
It is the responsibility of all dermatologists to create an environment where patients from any background can feel comfortable, which can be cultivated by establishing patient-centered communication and cultural humility.5 These skills can be strengthened via the implementation of DEI-related curricula during residency training. Augmenting exposure of these topics during training can optimize the delivery of dermatologic care by providing residents with the tools and confidence needed to care for patients of culturally diverse backgrounds. Enhancing DEI education is crucial to not only improve the recognition and treatment of dermatologic conditions in all skin and hair types but also to minimize misconceptions, stigma, health disparities, and discrimination faced by historically marginalized communities. Creating a culture of inclusion is of paramount importance to build successful relationships with patients and colleagues of culturally diverse backgrounds.6
There are multiple efforts underway to increase DEI education across the field of dermatology, including the development of DEI task forces in professional organizations and societies that serve to expand DEI-related research, mentorship, and education. The American Academy of Dermatology has been leading efforts to create a curriculum focused on skin of color, particularly addressing inadequate educational training on how dermatologic conditions manifest in this population.7 The Skin of Color Society has similar efforts underway and is developing a speakers bureau to give leading experts a platform to lecture dermatology trainees as well as patient and community audiences on various topics in skin of color.8 These are just 2 of many professional dermatology organizations that are advocating for expanded education on DEI; however, consistently integrating DEI-related topics into dermatology residency training curricula remains a gap in pedagogy. To identify the DEI-related topics of greatest relevance to the dermatology resident curricula, we implemented a modified electronic Delphi (e-Delphi) consensus process to provide standardized recommendations.
Methods
A 2-round modified e-Delphi method was utilized (Figure). An initial list of potential curricular topics was formulated by an expert panel consisting of 5 dermatologists from the Association of Professors of Dermatology DEI subcommittee and the American Academy of Dermatology Diversity Task Force (A.M.A., S.B., R.V., S.D.W., J.I.S.). Initial topics were selected via several meetings among the panel members to discuss existing DEI concerns and issues that were deemed relevant due to education gaps in residency training. The list of topics was further expanded with recommendations obtained via an email sent to dermatology program directors on the Association of Professors of Dermatology listserve, which solicited voluntary participation of academic dermatologists, including program directors and dermatology residents.
Methodology flowchart for electronic Delphi consensus study.
There were 2 voting rounds, with each round consisting of questions scored on a Likert scale ranging from 1 to 5 (1=not essential, 2=probably not essential, 3=neutral, 4=probably essential, 5=definitely essential). The inclusion criteria to classify a topic as necessary for integration into the dermatology residency curriculum included 95% (18/19) or more of respondents rating the topic as probably essential or definitely essential; if more than 90% (17/19) of respondents rated the topic as probably essential or definitely essential and less than 10% (2/19) rated it as not essential or probably not essential, the topic was still included as part of the suggested curriculum. Topics that received ratings of probably essential or definitely essential by less than 80% (15/19) of respondents were removed from consideration. The topics that did not meet inclusion or exclusion criteria during the first round of voting were refined by the e-Delphi steering committee (V.S.E-C. and F-A.R.) based on open-ended feedback from the voting group provided at the end of the survey and subsequently passed to the second round of voting.
Results
Participants—A total of 19 respondents participated in both voting rounds, the majority (80% [15/19]) of whom were program directors or dermatologists affiliated with academia or development of DEI education; the remaining 20% [4/19]) were dermatology residents.
Open-Ended Feedback—Voting group members were able to provide open-ended feedback for each of the sets of topics after the survey, which the steering committee utilized to modify the topics as needed for the final voting round. For example, “structural racism/discrimination” was originally mentioned as a topic, but several participants suggested including specific types of racism; therefore, the wording was changed to “racism: types, definitions” to encompass broader definitions and types of racism.
Survey Results—Two genres of topics were surveyed in each voting round: clinical and nonclinical. Participants voted on a total of 61 topics, with 23 ultimately selected in the final list of consensus curricular topics. Of those, 9 were clinical and 14 nonclinical. All topics deemed necessary for inclusion in residency curricula are presented in eTables 1 and 2.
During the first round of voting, the e-Delphi panel reached a consensus to include the following 17 topics as essential to dermatology residency training (along with the percentage of voters who classified them as probably essential or definitely essential): how to mitigate bias in clinical and workplace settings (100% [40/40]); social determinants of health-related disparities in dermatology (100% [40/40]); hairstyling practices across different hair textures (100% [40/40]); definitions and examples of microaggressions (97.50% [39/40]); definition, background, and types of bias (97.50% [39/40]); manifestations of bias in the clinical setting (97.44% [38/39]); racial and ethnic disparities in dermatology (97.44% [38/39]); keloids (97.37% [37/38]); differences in dermoscopic presentations in skin of color (97.30% [36/37]); skin cancer in patients with skin of color (97.30% [36/37]); disparities due to bias (95.00% [38/40]); how to apply cultural humility and safety to patients of different cultural backgrounds (94.87% [37/40]); best practices in providing care to patients with limited English proficiency (94.87% [37/40]); hair loss in patients with textured hair (94.74% [36/38]); pseudofolliculitis barbae and acne keloidalis nuchae (94.60% [35/37]); disparities regarding people experiencing homelessness (92.31% [36/39]); and definitions and types of racism and other forms of discrimination (92.31% [36/39]). eTable 1 provides a list of suggested resources to incorporate these topics into the educational components of residency curricula. The resources provided were not part of the voting process, and they were not considered in the consensus analysis; they are included here as suggested educational catalysts.
During the second round of voting, 25 topics were evaluated. Of those, the following 6 topics were proposed to be included as essential in residency training: differences in prevalence and presentation of common inflammatory disorders (100% [29/29]); manifestations of bias in the learning environment (96.55%); antiracist action and how to decrease the effects of structural racism in clinical and educational settings (96.55% [28/29]); diversity of images in dermatology education (96.55% [28/29]); pigmentary disorders and their psychological effects (96.55% [28/29]); and LGBTQ (lesbian, gay, bisexual, transgender, and queer) dermatologic health care (96.55% [28/29]). eTable 2 includes these topics as well as suggested resources to help incorporate them into training.
Comment
This study utilized a modified e-Delphi technique to identify relevant clinical and nonclinical DEI topics that should be incorporated into dermatology residency curricula. The panel members reached a consensus for 9 clinical DEI-related topics. The respondents agreed that the topics related to skin and hair conditions in patients with skin of color as well as textured hair were crucial to residency education. Skin cancer, hair loss, pseudofolliculitis barbae, acne keloidalis nuchae, keloids, pigmentary disorders, and their varying presentations in patients with skin of color were among the recommended topics. The panel also recommended educating residents on the variable visual presentations of inflammatory conditions in skin of color. Addressing the needs of diverse patients—for example, those belonging to the LGBTQ community—also was deemed important for inclusion.
The remaining 14 chosen topics were nonclinical items addressing concepts such as bias and health care disparities as well as cultural humility and safety.9 Cultural humility and safety focus on developing cultural awareness by creating a safe setting for patients rather than encouraging power relationships between them and their physicians. Various topics related to racism also were recommended to be included in residency curricula, including education on implementation of antiracist action in the workplace.
Many of the nonclinical topics are intertwined; for instance, learning about health care disparities in patients with limited English proficiency allows for improved best practices in delivering care to patients from this population. The first step in overcoming bias and subsequent disparities is acknowledging how the perpetuation of bias leads to disparities after being taught tools to recognize it.
Our group’s guidance on DEI topics should help dermatology residency program leaders as they design and refine program curricula. There are multiple avenues for incorporating education on these topics, including lectures, interactive workshops, role-playing sessions, book or journal clubs, and discussion circles. Many of these topics/programs may already be included in programs’ didactic curricula, which would minimize the burden of finding space to educate on these topics. Institutional cultural change is key to ensuring truly diverse, equitable, and inclusive workplaces. Educating tomorrow’s dermatologists on these topics is a first step toward achieving that cultural change.
Limitations—A limitation of this e-Delphi survey is that only a selection of experts in this field was included. Additionally, we were concerned that the Likert scale format and the bar we set for inclusion and exclusion may have failed to adequately capture participants’ nuanced opinions. As such, participants were able to provide open-ended feedback, and suggestions for alternate wording or other changes were considered by the steering committee. Finally, inclusion recommendations identified in this survey were developed specifically for US dermatology residents.
Conclusion
In this e-Delphi consensus assessment of DEI-related topics, we recommend the inclusion of 23 topics into dermatology residency program curricula to improve medical training and the patient-physician relationship as well as to create better health outcomes. We also provide specific sample resource recommendations in eTables 1 and 2 to facilitate inclusion of these topics into residency curricula across the country.
Diversity, equity, and inclusion (DEI) programs seek to improve dermatologic education and clinical care for an increasingly diverse patient population as well as to recruit and sustain a physician workforce that reflects the diversity of the patients they serve.1,2 In dermatology, only 4.2% and 3.0% of practicing dermatologists self-identify as being of Hispanic and African American ethnicity, respectively, compared with 18.5% and 13.4% of the general population, respectively.3 Creating an educational system that works to meet the goals of DEI is essential to improve health outcomes and address disparities. The lack of robust DEI-related curricula during residency training may limit the ability of practicing dermatologists to provide comprehensive and culturally sensitive care. It has been shown that racial concordance between patients and physicians has a positive impact on patient satisfaction by fostering a trusting patient-physician relationship.4
It is the responsibility of all dermatologists to create an environment where patients from any background can feel comfortable, which can be cultivated by establishing patient-centered communication and cultural humility.5 These skills can be strengthened via the implementation of DEI-related curricula during residency training. Augmenting exposure of these topics during training can optimize the delivery of dermatologic care by providing residents with the tools and confidence needed to care for patients of culturally diverse backgrounds. Enhancing DEI education is crucial to not only improve the recognition and treatment of dermatologic conditions in all skin and hair types but also to minimize misconceptions, stigma, health disparities, and discrimination faced by historically marginalized communities. Creating a culture of inclusion is of paramount importance to build successful relationships with patients and colleagues of culturally diverse backgrounds.6
There are multiple efforts underway to increase DEI education across the field of dermatology, including the development of DEI task forces in professional organizations and societies that serve to expand DEI-related research, mentorship, and education. The American Academy of Dermatology has been leading efforts to create a curriculum focused on skin of color, particularly addressing inadequate educational training on how dermatologic conditions manifest in this population.7 The Skin of Color Society has similar efforts underway and is developing a speakers bureau to give leading experts a platform to lecture dermatology trainees as well as patient and community audiences on various topics in skin of color.8 These are just 2 of many professional dermatology organizations that are advocating for expanded education on DEI; however, consistently integrating DEI-related topics into dermatology residency training curricula remains a gap in pedagogy. To identify the DEI-related topics of greatest relevance to the dermatology resident curricula, we implemented a modified electronic Delphi (e-Delphi) consensus process to provide standardized recommendations.
Methods
A 2-round modified e-Delphi method was utilized (Figure). An initial list of potential curricular topics was formulated by an expert panel consisting of 5 dermatologists from the Association of Professors of Dermatology DEI subcommittee and the American Academy of Dermatology Diversity Task Force (A.M.A., S.B., R.V., S.D.W., J.I.S.). Initial topics were selected via several meetings among the panel members to discuss existing DEI concerns and issues that were deemed relevant due to education gaps in residency training. The list of topics was further expanded with recommendations obtained via an email sent to dermatology program directors on the Association of Professors of Dermatology listserve, which solicited voluntary participation of academic dermatologists, including program directors and dermatology residents.
Methodology flowchart for electronic Delphi consensus study.
There were 2 voting rounds, with each round consisting of questions scored on a Likert scale ranging from 1 to 5 (1=not essential, 2=probably not essential, 3=neutral, 4=probably essential, 5=definitely essential). The inclusion criteria to classify a topic as necessary for integration into the dermatology residency curriculum included 95% (18/19) or more of respondents rating the topic as probably essential or definitely essential; if more than 90% (17/19) of respondents rated the topic as probably essential or definitely essential and less than 10% (2/19) rated it as not essential or probably not essential, the topic was still included as part of the suggested curriculum. Topics that received ratings of probably essential or definitely essential by less than 80% (15/19) of respondents were removed from consideration. The topics that did not meet inclusion or exclusion criteria during the first round of voting were refined by the e-Delphi steering committee (V.S.E-C. and F-A.R.) based on open-ended feedback from the voting group provided at the end of the survey and subsequently passed to the second round of voting.
Results
Participants—A total of 19 respondents participated in both voting rounds, the majority (80% [15/19]) of whom were program directors or dermatologists affiliated with academia or development of DEI education; the remaining 20% [4/19]) were dermatology residents.
Open-Ended Feedback—Voting group members were able to provide open-ended feedback for each of the sets of topics after the survey, which the steering committee utilized to modify the topics as needed for the final voting round. For example, “structural racism/discrimination” was originally mentioned as a topic, but several participants suggested including specific types of racism; therefore, the wording was changed to “racism: types, definitions” to encompass broader definitions and types of racism.
Survey Results—Two genres of topics were surveyed in each voting round: clinical and nonclinical. Participants voted on a total of 61 topics, with 23 ultimately selected in the final list of consensus curricular topics. Of those, 9 were clinical and 14 nonclinical. All topics deemed necessary for inclusion in residency curricula are presented in eTables 1 and 2.
During the first round of voting, the e-Delphi panel reached a consensus to include the following 17 topics as essential to dermatology residency training (along with the percentage of voters who classified them as probably essential or definitely essential): how to mitigate bias in clinical and workplace settings (100% [40/40]); social determinants of health-related disparities in dermatology (100% [40/40]); hairstyling practices across different hair textures (100% [40/40]); definitions and examples of microaggressions (97.50% [39/40]); definition, background, and types of bias (97.50% [39/40]); manifestations of bias in the clinical setting (97.44% [38/39]); racial and ethnic disparities in dermatology (97.44% [38/39]); keloids (97.37% [37/38]); differences in dermoscopic presentations in skin of color (97.30% [36/37]); skin cancer in patients with skin of color (97.30% [36/37]); disparities due to bias (95.00% [38/40]); how to apply cultural humility and safety to patients of different cultural backgrounds (94.87% [37/40]); best practices in providing care to patients with limited English proficiency (94.87% [37/40]); hair loss in patients with textured hair (94.74% [36/38]); pseudofolliculitis barbae and acne keloidalis nuchae (94.60% [35/37]); disparities regarding people experiencing homelessness (92.31% [36/39]); and definitions and types of racism and other forms of discrimination (92.31% [36/39]). eTable 1 provides a list of suggested resources to incorporate these topics into the educational components of residency curricula. The resources provided were not part of the voting process, and they were not considered in the consensus analysis; they are included here as suggested educational catalysts.
During the second round of voting, 25 topics were evaluated. Of those, the following 6 topics were proposed to be included as essential in residency training: differences in prevalence and presentation of common inflammatory disorders (100% [29/29]); manifestations of bias in the learning environment (96.55%); antiracist action and how to decrease the effects of structural racism in clinical and educational settings (96.55% [28/29]); diversity of images in dermatology education (96.55% [28/29]); pigmentary disorders and their psychological effects (96.55% [28/29]); and LGBTQ (lesbian, gay, bisexual, transgender, and queer) dermatologic health care (96.55% [28/29]). eTable 2 includes these topics as well as suggested resources to help incorporate them into training.
Comment
This study utilized a modified e-Delphi technique to identify relevant clinical and nonclinical DEI topics that should be incorporated into dermatology residency curricula. The panel members reached a consensus for 9 clinical DEI-related topics. The respondents agreed that the topics related to skin and hair conditions in patients with skin of color as well as textured hair were crucial to residency education. Skin cancer, hair loss, pseudofolliculitis barbae, acne keloidalis nuchae, keloids, pigmentary disorders, and their varying presentations in patients with skin of color were among the recommended topics. The panel also recommended educating residents on the variable visual presentations of inflammatory conditions in skin of color. Addressing the needs of diverse patients—for example, those belonging to the LGBTQ community—also was deemed important for inclusion.
The remaining 14 chosen topics were nonclinical items addressing concepts such as bias and health care disparities as well as cultural humility and safety.9 Cultural humility and safety focus on developing cultural awareness by creating a safe setting for patients rather than encouraging power relationships between them and their physicians. Various topics related to racism also were recommended to be included in residency curricula, including education on implementation of antiracist action in the workplace.
Many of the nonclinical topics are intertwined; for instance, learning about health care disparities in patients with limited English proficiency allows for improved best practices in delivering care to patients from this population. The first step in overcoming bias and subsequent disparities is acknowledging how the perpetuation of bias leads to disparities after being taught tools to recognize it.
Our group’s guidance on DEI topics should help dermatology residency program leaders as they design and refine program curricula. There are multiple avenues for incorporating education on these topics, including lectures, interactive workshops, role-playing sessions, book or journal clubs, and discussion circles. Many of these topics/programs may already be included in programs’ didactic curricula, which would minimize the burden of finding space to educate on these topics. Institutional cultural change is key to ensuring truly diverse, equitable, and inclusive workplaces. Educating tomorrow’s dermatologists on these topics is a first step toward achieving that cultural change.
Limitations—A limitation of this e-Delphi survey is that only a selection of experts in this field was included. Additionally, we were concerned that the Likert scale format and the bar we set for inclusion and exclusion may have failed to adequately capture participants’ nuanced opinions. As such, participants were able to provide open-ended feedback, and suggestions for alternate wording or other changes were considered by the steering committee. Finally, inclusion recommendations identified in this survey were developed specifically for US dermatology residents.
Conclusion
In this e-Delphi consensus assessment of DEI-related topics, we recommend the inclusion of 23 topics into dermatology residency program curricula to improve medical training and the patient-physician relationship as well as to create better health outcomes. We also provide specific sample resource recommendations in eTables 1 and 2 to facilitate inclusion of these topics into residency curricula across the country.
Lopez S, Lourido JO, Lim HW, et al. The call to action to increase racial and ethnic diversity in dermatology: a retrospective, cross-sectional study to monitor progress. J Am Acad Dermatol. 2020;86:E121-E123. doi:10.1016/j.jaad.2021.10.011
El-Kashlan N, Alexis A. Disparities in dermatology: a reflection. J Clin Aesthet Dermatol. 2022;15:27-29.
Laveist TA, Nuru-Jeter A. Is doctor-patient race concordance associated with greater satisfaction with care? J Health Soc Behav. 2002;43:296-306.
Street RL Jr, O’Malley KJ, Cooper LA, et al. Understanding concordance in patient-physician relationships: personal and ethnic dimensions of shared identity. Ann Fam Med. 2008;6:198-205. doi:10.1370/afm.821
Dadrass F, Bowers S, Shinkai K, et al. Diversity, equity, and inclusion in dermatology residency. Dermatol Clin. 2023;41:257-263. doi:10.1016/j.det.2022.10.006
Solchanyk D, Ekeh O, Saffran L, et al. Integrating cultural humility into the medical education curriculum: strategies for educators. Teach Learn Med. 2021;33:554-560. doi:10.1080/10401334.2021.1877711
Lopez S, Lourido JO, Lim HW, et al. The call to action to increase racial and ethnic diversity in dermatology: a retrospective, cross-sectional study to monitor progress. J Am Acad Dermatol. 2020;86:E121-E123. doi:10.1016/j.jaad.2021.10.011
El-Kashlan N, Alexis A. Disparities in dermatology: a reflection. J Clin Aesthet Dermatol. 2022;15:27-29.
Laveist TA, Nuru-Jeter A. Is doctor-patient race concordance associated with greater satisfaction with care? J Health Soc Behav. 2002;43:296-306.
Street RL Jr, O’Malley KJ, Cooper LA, et al. Understanding concordance in patient-physician relationships: personal and ethnic dimensions of shared identity. Ann Fam Med. 2008;6:198-205. doi:10.1370/afm.821
Dadrass F, Bowers S, Shinkai K, et al. Diversity, equity, and inclusion in dermatology residency. Dermatol Clin. 2023;41:257-263. doi:10.1016/j.det.2022.10.006
Solchanyk D, Ekeh O, Saffran L, et al. Integrating cultural humility into the medical education curriculum: strategies for educators. Teach Learn Med. 2021;33:554-560. doi:10.1080/10401334.2021.1877711
Advancing curricula related to diversity, equity, and inclusion in dermatology training can improve health outcomes, address health care workforce disparities, and enhance clinical care for diverse patient populations.
Education on patient-centered communication, cultural humility, and the impact of social determinants of health results in dermatology residents who are better equipped with the necessary tools to effectively care for patients from diverse backgrounds.
Disallow All Ads
Content Gating
No Gating (article Unlocked/Free)
Alternative CME
Disqus Comments
Default
Gate On Date
Un-Gate On Date
Consolidated Pubs: Do Not Show Source Publication Logo
Dermatology remains one of the most competitive specialties in the residency match, with successful applicants demonstrating a well-rounded application reflecting not only their academic excellence but also their dedication to research, community service, and hands-on clinical experience.1 A growing emphasis on scholarly activities has made it crucial for applicants to stand out, with an increasing number opting to take gap years to engage in focused research endeavors.2 In highly competitive specialties such as dermatology, successful applicants now report more than 20 research items on average.3,4 This trend also is evident in primary care specialties, which have seen a 2- to 3-fold increase in reported research activities. The average unmatched applicant today lists more research items than the average matched applicant did a decade ago, underscoring the growing emphasis on scholarly activity.3
Ideally, graduate medical education should foster an environment of inquiry and scholarship, where residents develop new knowledge, evaluate research findings, and cultivate lifelong habits of inquiry. The Accreditation Council for Graduate Medical Education requires residents to engage in scholarship, such as case reports, research reviews, and original research.5 Research during residency has been linked to several benefits, including enhanced patient care through improved critical appraisal skills, clinical reasoning, and lifelong learning.6,7 Additionally, students and residents who publish research are more likely to achieve higher rank during residency and pursue careers in academic medicine, potentially helping to address the decline in clinician investigators.8,9 Publishing and presenting research also can enhance a residency program’s reputation, making it more attractive to competitive applicants, and may be beneficial for residents seeking jobs or fellowships.6
Dermatology residency programs vary in their structure and support for resident research. One survey revealed that many programs lack the necessary support, structure, and resources to effectively promote and maintain research training.1 Additionally, residents have less exposure to researchers who could serve as mentors due to the growing demands placed on attending physicians in teaching hospitals.10
The Research Arms Race
The growing emphasis on scholarly activity for residency and fellowship applicants coupled with the use of research productivity to differentiate candidates has led some to declare a “research arms race” in residency selection.3 As one author stated, “We need less research, better research, and research done for the right reasons.”11 Indeed, most articles authored by medical students are short reviews or case reports, with the majority (59% [207/350]) being cited zero times, according to one analysis.12 Given the variable research infrastructure between programs and the decreasing availability of research mentors despite the growing emphasis on scholarly activity, applicants face an unfortunate dilemma. Until the system changes, those who protest this research arms race by not engaging in substantial scholarly activity are less likely to match into competitive specialties. Thus, the race continues.
The Value of Mentorship
Resident research success is impacted by having an effective faculty research mentor.13 Although all medical research at the student or resident levels should be conducted with a faculty mentor to oversee it, finding a mentor can be challenging. If a resident’s program boasts a strong research infrastructure or prolific faculty, building relationships with potential mentors is a logical first step for residents wishing to engage in research; however, if suitable mentors are lacking, efforts should be made by residents to establish these connections elsewhere, such as attending society meetings to network with potential mentors and applying to formal mentorship programs (eg, the American Society for Dermatologic Surgery’s Preceptor Program, the Women’s Dermatologic Society’s Mentorship Award). Unsolicited email inquiries asking, “Hi Dr. X, my name is Y, and I was wondering if you have any research projects I could help with?” often go unanswered. Instead, consider emailing or approaching potential mentors with a more developed proposition, such as the following example:
Hello Dr. X, my name is Y. I have enjoyed reading your publications on A, which inspired me to think about B. I reviewed the literature and noticed a potential to enhance our current understanding on the topic. My team and I conducted a systematic review of the available literature and drafted a manuscript summarizing our findings. Given your expertise in this field, would you be willing to collaborate on this paper? We would be grateful for your critical eye, suggestions for improvement, and overall thoughts.
This approach demonstrates initiative, provides a clear plan, and shows respect for the mentor’s expertise, increasing the likelihood of a positive response and fruitful collaboration. Assuming the resident’s working draft meets the potential mentor’s basic expectations, such a display of initiative is likely to impress them, and they may then offer opportunities to engage in meaningful research projects in the future. Everyone benefits! These efforts to establish connections with mentors can pave the way to further collaboration and meaningful research opportunities for dermatology residents.
The Systematic Review: An Attractive Option For Residents
There are several potential avenues for students or residents interested in pursuing research. Case reports and case series are relatively easy to compile, can be completed quickly, and often require minimal guidance from a faculty mentor; however, case reports rank low in the research hierarchy. Conversely, prospective blinded clinical trials provide some of the highest-quality evidence available but are challenging to conduct without a practicing faculty member to provide a patient cohort, often require extensive funding, and may involve complex statistical analyses beyond the expertise of most students or residents. Additionally, they may take years to complete, often extending beyond residency or fellowship application deadlines.
Most medical applicants likely hold at least some hesitation in churning out vast amounts of low-quality research merely to boost their publication count for the match process. Ideally, those who pursue scholarly activity should be driven by a genuine desire to contribute meaningfully to the medical literature. One particularly valuable avenue for trainees wishing to engage in research is the systematic review, which aims to identify, evaluate, and summarize the findings of all relevant individual studies regarding a research topic and answer a focused question. If performed thoughtfully, a systematic review can meaningfully contribute to the medical literature without requiring access to a prospectively followed cohort of patients or the constant supervision of a faculty mentor. Sure, systematic reviews may not be as robust as prospective cohort clinical trials, but they often provide comprehensive insights and are considered valuable contributions to evidence-based medicine. With the help of co-residents or medical students, a medical reference librarian, and a statistician—along with a working understanding of universally accepted quality measures—a resident physician and their team can produce a systematic review that ultimately may merit publication in a top-tier medical journal.
The remainder of this column will outline a streamlined approach to the systematic review writing process, specifically tailored for medical residents who may not have affiliations to a prolific research department or established relationships with faculty mentors in their field of interest. The aim is to offer a basic framework to help residents navigate the complexities of conducting and writing a high-quality, impactful systematic review. It is important to emphasize that resident research should always be conducted under the guidance of a faculty mentor, and this approach is not intended to encourage independent research and publication by residents. Instead, it provides steps that can be undertaken with a foundational understanding of accepted principles, allowing residents to compile a working draft of a manuscript in collaboration with a trusted faculty mentor.
The Systematic Review: A Simple Approach
Step 1: Choose a Topic—Once a resident has decided to embark on conducting a systematic review, the first step is to choose a topic, which requires consideration of several factors to ensure relevance, feasibility, and impact. Begin by identifying areas of clinical uncertainty or controversy in which a comprehensive synthesis of the literature could provide valuable insights. Often, such a topic can be gleaned from the conclusion section of other primary studies; statements such as “further study is needed to determine the efficacy of X” or “systematic reviews would be beneficial to ascertaining the impact of Y” may be a great place to start.
Next, ensure that sufficient primary studies exist to support a robust review or meta-analysis by conducting a preliminary literature search, which will confirm that the chosen topic is both researchable and relevant. A narrow, focused, well-defined topic likely will prove more feasible to review than a broad, ill-defined one. Once a topic is selected, it is advisable to discuss it with a faculty mentor before starting the literature search to ensure the topic’s feasibility and clinical relevance, helping to guide your research in a meaningful direction.
When deciding between a systematic review and a meta-analysis, the nature of the research question is an influential factor. A systematic review is particularly suitable for addressing broad questions or topics when the aim is to summarize and synthesize all relevant research studies; for example, a systematic review may investigate the various treatment options for atopic dermatitis and their efficacy, which allows for a comprehensive overview of the available treatments—both the interventions and the outcomes. In contrast, a meta-analysis is ideal for collecting and statistically combining quantitative data from multiple primary studies, provided there are enough relevant studies available in the literature.
Step 2: Build a Team—Recruiting a skilled librarian to assist with Medical Subject Headings (MeSH) terms and retrieving relevant papers is crucial for conducting a high-quality systematic review or meta-analysis. Medical librarians specializing in health sciences enhance the efficiency, comprehensiveness, and reliability of your literature search, substantially boosting your work’s credibility. These librarians are well versed in medical databases such as PubMed and Embase. Begin by contacting your institution’s library services, as there often are valuable resources and personnel available to assist you. Personally, I was surprised to find a librarian at my institution specifically dedicated to helping medical residents with such projects! These professionals are eager to help, and if provided with the scope and goal of your project, they can deliver literature search results in a digestible format. Similarly, seeking the expertise of a medical statistician is crucial to the accuracy and legitimacy of your study. In your final paper, it is important to recognize the contributions of the librarian and statistician, either as co-authors or in the acknowledgments section.
In addition, recruiting colleagues or medical students can be an effective strategy to make the project more feasible and offer collaborative benefits for all parties involved. Given the growing emphasis on research for residency and fellowship admissions, there usually is no shortage of motivated volunteers.
Next, identify the software tool you will use for your systematic review. Options range from simple spreadsheets such as Microsoft Excel to reference managers such as EndNote or Mendeley or dedicated systematic review tools. Academic institutions may subscribe to paid services such as Covidence (https://www.covidence.org), or you can utilize free alternatives such as Rayyan (https://www.rayyan.ai). Investing time in learning to navigate dedicated systematic review software can greatly enhance efficiency and reduce frustrations compared to more basic methods. Ultimately, staying organized, thorough, and committed is key.
Step 3: Conduct the Literature Review—At this point, your research topic has been decided, a medical reference librarian has provided the results of a comprehensive literature search, and a software tool has been chosen. The next task is to read hundreds or thousands of papers—easy, right? With your dedicated team assembled, the workload can be divided and conquered. The first step involves screening out duplicate and irrelevant studies based on titles and abstracts. Next, review the remaining papers in more detail. Those that pass this preliminary screen should be read in their entirety, and only the papers relevant to the research topic should be included in the final synthesis. If there are uncertainties about a study’s relevance, consulting a faculty mentor is advisable. To ensure the systematic review is as thorough as possible, pay special attention to the references section of each paper, as cited references can reveal relevant studies that may have been missed in the literature search.
Once all relevant papers are compiled and read, the relevant data points should be extracted and imputed into a data sheet. Collaborating with a medical statistician is crucial at this stage, as they can provide guidance on the most effective ways to structure and input data. After all studies are included, the relevant statistical analyses on the resultant dataset can be run.
Step 4: Write the Paper—In 2020, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was developed to ensure transparent and complete reporting of systematic reviews. A full discussion of PRISMA guidelines is beyond the scope of this paper; Page et al14 provided a summary, checklist, and flow diagram that is available online (https://www.prisma-statement.org). Following the PRISMA checklist and guidelines ensures a high-quality, transparent, and reliable systematic review. These guidelines not only help streamline and simplify the writing process but also enhance its efficiency and effectiveness. Discovering the PRISMA checklist can be transformative, providing a valuable roadmap that guides the author through each step of the reporting process, helping to avoid common pitfalls. This structured approach ultimately leads to a more comprehensive and trustworthy review.
Step 5: Make Finishing Touches—At this stage in the systematic review process, the studies have been compiled and thoroughly analyzed and the statistical analysis has been conducted. The results have been organized within a structured framework following the PRISMA checklist. With these steps completed, the next task is to finalize the manuscript and seek a final review from the senior author or faculty mentor. To streamline this process, it is beneficial to adhere to the formatting guidelines of the specific medical journal you intend to submit to. Check the author guidelines on the journal’s website and review recent systematic reviews published there as a reference. Even if you have not chosen a journal yet, formatting your manuscript according to a prestigious journal’s general style provides a strong foundation that can be easily adapted to fit another journal’s requirements if necessary.
Final Thoughts
Designing and conducting a systematic review is no easy task, but it can be a valuable skill for dermatology residents aiming to contribute meaningfully to the medical literature. The process of compiling a systematic review offers an opportunity for developing critical research skills, from formulating a research question to synthesizing evidence and presenting findings in a clear methodical way. Engaging in systematic review writing not only enhances the resident’s understanding of a particular topic but also demonstrates a commitment to scholarly activity—a key factor in an increasingly competitive residency and fellowship application environment.
The basic steps outlined in this article are just one way in which residents can begin to navigate the complexities of medical research, specifically the systematic review process. By assembling a supportive team, utilizing available resources, and adhering to established guidelines such as PRISMA, one can produce a high-quality, impactful review. Ultimately, the systematic review process is not just about publication—it is about fostering a habit of inquiry, improving patient care, and contributing to the ever-evolving field of medicine. With dedication and collaboration, even the most challenging aspects of research can be tackled, paving the way for future opportunities and professional growth. In this way, perhaps one day the spirit of the “research race” can shift from a frantic sprint to a graceful marathon, where each mile is run with heart and every step is filled with purpose.
References
Anand P, Szeto MD, Flaten H, et al. Dermatology residency research policies: a 2021 national survey. Int J Womens Dermatol. 2021;7:787-792.
Costello CM, Harvey JA, Besch-Stokes JG, et al. The role research gap years play in a successful dermatology match. Int J Dermatol. 2022;61:226-230.
Elliott B, Carmody JB. Publish or perish: the research arms race in residency selection. J Grad Med Educ. 2023;15:524-527.
Bhuiya T, Makaryus AN. The importance of engaging in scientific research during medical training. Int J Angiol. 2023;32:153-157.
Seaburg LA, Wang AT, West CP, et al. Associations between resident physicians’ publications and clinical performance during residency training. BMC Med Educ. 2016;16:22.
West CP, Halvorsen AJ, McDonald FS. Scholarship during residency training: a controlled comparison study. Am J Med. 2011;124:983-987.e1.
Bhattacharya SD, Williams JB, De La Fuente SG, et al. Does protected research time during general surgery training contribute to graduates’ career choice? Am Surg. 2011;77:907-910.
Kralovec PD, Miller JA, Wellikson L, et al. The status of hospital medicine groups in the United States. J Hosp Med. 2006;1:75-80.
Altman DG. The scandal of poor medical research. BMJ. 1994;308:283-284.
Wickramasinghe DP, Perera CS, Senarathna S, et al. Patterns and trends of medical student research. BMC Med Educ. 2013;13:175.
Ercan-Fang NG, Mahmoud MA, Cottrell C, et al. Best practices in resident research—a national survey of high functioning internal medicine residency programs in resident research in USA. Am J Med Sci. 2021;361:23-29.
Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372.
Dermatology remains one of the most competitive specialties in the residency match, with successful applicants demonstrating a well-rounded application reflecting not only their academic excellence but also their dedication to research, community service, and hands-on clinical experience.1 A growing emphasis on scholarly activities has made it crucial for applicants to stand out, with an increasing number opting to take gap years to engage in focused research endeavors.2 In highly competitive specialties such as dermatology, successful applicants now report more than 20 research items on average.3,4 This trend also is evident in primary care specialties, which have seen a 2- to 3-fold increase in reported research activities. The average unmatched applicant today lists more research items than the average matched applicant did a decade ago, underscoring the growing emphasis on scholarly activity.3
Ideally, graduate medical education should foster an environment of inquiry and scholarship, where residents develop new knowledge, evaluate research findings, and cultivate lifelong habits of inquiry. The Accreditation Council for Graduate Medical Education requires residents to engage in scholarship, such as case reports, research reviews, and original research.5 Research during residency has been linked to several benefits, including enhanced patient care through improved critical appraisal skills, clinical reasoning, and lifelong learning.6,7 Additionally, students and residents who publish research are more likely to achieve higher rank during residency and pursue careers in academic medicine, potentially helping to address the decline in clinician investigators.8,9 Publishing and presenting research also can enhance a residency program’s reputation, making it more attractive to competitive applicants, and may be beneficial for residents seeking jobs or fellowships.6
Dermatology residency programs vary in their structure and support for resident research. One survey revealed that many programs lack the necessary support, structure, and resources to effectively promote and maintain research training.1 Additionally, residents have less exposure to researchers who could serve as mentors due to the growing demands placed on attending physicians in teaching hospitals.10
The Research Arms Race
The growing emphasis on scholarly activity for residency and fellowship applicants coupled with the use of research productivity to differentiate candidates has led some to declare a “research arms race” in residency selection.3 As one author stated, “We need less research, better research, and research done for the right reasons.”11 Indeed, most articles authored by medical students are short reviews or case reports, with the majority (59% [207/350]) being cited zero times, according to one analysis.12 Given the variable research infrastructure between programs and the decreasing availability of research mentors despite the growing emphasis on scholarly activity, applicants face an unfortunate dilemma. Until the system changes, those who protest this research arms race by not engaging in substantial scholarly activity are less likely to match into competitive specialties. Thus, the race continues.
The Value of Mentorship
Resident research success is impacted by having an effective faculty research mentor.13 Although all medical research at the student or resident levels should be conducted with a faculty mentor to oversee it, finding a mentor can be challenging. If a resident’s program boasts a strong research infrastructure or prolific faculty, building relationships with potential mentors is a logical first step for residents wishing to engage in research; however, if suitable mentors are lacking, efforts should be made by residents to establish these connections elsewhere, such as attending society meetings to network with potential mentors and applying to formal mentorship programs (eg, the American Society for Dermatologic Surgery’s Preceptor Program, the Women’s Dermatologic Society’s Mentorship Award). Unsolicited email inquiries asking, “Hi Dr. X, my name is Y, and I was wondering if you have any research projects I could help with?” often go unanswered. Instead, consider emailing or approaching potential mentors with a more developed proposition, such as the following example:
Hello Dr. X, my name is Y. I have enjoyed reading your publications on A, which inspired me to think about B. I reviewed the literature and noticed a potential to enhance our current understanding on the topic. My team and I conducted a systematic review of the available literature and drafted a manuscript summarizing our findings. Given your expertise in this field, would you be willing to collaborate on this paper? We would be grateful for your critical eye, suggestions for improvement, and overall thoughts.
This approach demonstrates initiative, provides a clear plan, and shows respect for the mentor’s expertise, increasing the likelihood of a positive response and fruitful collaboration. Assuming the resident’s working draft meets the potential mentor’s basic expectations, such a display of initiative is likely to impress them, and they may then offer opportunities to engage in meaningful research projects in the future. Everyone benefits! These efforts to establish connections with mentors can pave the way to further collaboration and meaningful research opportunities for dermatology residents.
The Systematic Review: An Attractive Option For Residents
There are several potential avenues for students or residents interested in pursuing research. Case reports and case series are relatively easy to compile, can be completed quickly, and often require minimal guidance from a faculty mentor; however, case reports rank low in the research hierarchy. Conversely, prospective blinded clinical trials provide some of the highest-quality evidence available but are challenging to conduct without a practicing faculty member to provide a patient cohort, often require extensive funding, and may involve complex statistical analyses beyond the expertise of most students or residents. Additionally, they may take years to complete, often extending beyond residency or fellowship application deadlines.
Most medical applicants likely hold at least some hesitation in churning out vast amounts of low-quality research merely to boost their publication count for the match process. Ideally, those who pursue scholarly activity should be driven by a genuine desire to contribute meaningfully to the medical literature. One particularly valuable avenue for trainees wishing to engage in research is the systematic review, which aims to identify, evaluate, and summarize the findings of all relevant individual studies regarding a research topic and answer a focused question. If performed thoughtfully, a systematic review can meaningfully contribute to the medical literature without requiring access to a prospectively followed cohort of patients or the constant supervision of a faculty mentor. Sure, systematic reviews may not be as robust as prospective cohort clinical trials, but they often provide comprehensive insights and are considered valuable contributions to evidence-based medicine. With the help of co-residents or medical students, a medical reference librarian, and a statistician—along with a working understanding of universally accepted quality measures—a resident physician and their team can produce a systematic review that ultimately may merit publication in a top-tier medical journal.
The remainder of this column will outline a streamlined approach to the systematic review writing process, specifically tailored for medical residents who may not have affiliations to a prolific research department or established relationships with faculty mentors in their field of interest. The aim is to offer a basic framework to help residents navigate the complexities of conducting and writing a high-quality, impactful systematic review. It is important to emphasize that resident research should always be conducted under the guidance of a faculty mentor, and this approach is not intended to encourage independent research and publication by residents. Instead, it provides steps that can be undertaken with a foundational understanding of accepted principles, allowing residents to compile a working draft of a manuscript in collaboration with a trusted faculty mentor.
The Systematic Review: A Simple Approach
Step 1: Choose a Topic—Once a resident has decided to embark on conducting a systematic review, the first step is to choose a topic, which requires consideration of several factors to ensure relevance, feasibility, and impact. Begin by identifying areas of clinical uncertainty or controversy in which a comprehensive synthesis of the literature could provide valuable insights. Often, such a topic can be gleaned from the conclusion section of other primary studies; statements such as “further study is needed to determine the efficacy of X” or “systematic reviews would be beneficial to ascertaining the impact of Y” may be a great place to start.
Next, ensure that sufficient primary studies exist to support a robust review or meta-analysis by conducting a preliminary literature search, which will confirm that the chosen topic is both researchable and relevant. A narrow, focused, well-defined topic likely will prove more feasible to review than a broad, ill-defined one. Once a topic is selected, it is advisable to discuss it with a faculty mentor before starting the literature search to ensure the topic’s feasibility and clinical relevance, helping to guide your research in a meaningful direction.
When deciding between a systematic review and a meta-analysis, the nature of the research question is an influential factor. A systematic review is particularly suitable for addressing broad questions or topics when the aim is to summarize and synthesize all relevant research studies; for example, a systematic review may investigate the various treatment options for atopic dermatitis and their efficacy, which allows for a comprehensive overview of the available treatments—both the interventions and the outcomes. In contrast, a meta-analysis is ideal for collecting and statistically combining quantitative data from multiple primary studies, provided there are enough relevant studies available in the literature.
Step 2: Build a Team—Recruiting a skilled librarian to assist with Medical Subject Headings (MeSH) terms and retrieving relevant papers is crucial for conducting a high-quality systematic review or meta-analysis. Medical librarians specializing in health sciences enhance the efficiency, comprehensiveness, and reliability of your literature search, substantially boosting your work’s credibility. These librarians are well versed in medical databases such as PubMed and Embase. Begin by contacting your institution’s library services, as there often are valuable resources and personnel available to assist you. Personally, I was surprised to find a librarian at my institution specifically dedicated to helping medical residents with such projects! These professionals are eager to help, and if provided with the scope and goal of your project, they can deliver literature search results in a digestible format. Similarly, seeking the expertise of a medical statistician is crucial to the accuracy and legitimacy of your study. In your final paper, it is important to recognize the contributions of the librarian and statistician, either as co-authors or in the acknowledgments section.
In addition, recruiting colleagues or medical students can be an effective strategy to make the project more feasible and offer collaborative benefits for all parties involved. Given the growing emphasis on research for residency and fellowship admissions, there usually is no shortage of motivated volunteers.
Next, identify the software tool you will use for your systematic review. Options range from simple spreadsheets such as Microsoft Excel to reference managers such as EndNote or Mendeley or dedicated systematic review tools. Academic institutions may subscribe to paid services such as Covidence (https://www.covidence.org), or you can utilize free alternatives such as Rayyan (https://www.rayyan.ai). Investing time in learning to navigate dedicated systematic review software can greatly enhance efficiency and reduce frustrations compared to more basic methods. Ultimately, staying organized, thorough, and committed is key.
Step 3: Conduct the Literature Review—At this point, your research topic has been decided, a medical reference librarian has provided the results of a comprehensive literature search, and a software tool has been chosen. The next task is to read hundreds or thousands of papers—easy, right? With your dedicated team assembled, the workload can be divided and conquered. The first step involves screening out duplicate and irrelevant studies based on titles and abstracts. Next, review the remaining papers in more detail. Those that pass this preliminary screen should be read in their entirety, and only the papers relevant to the research topic should be included in the final synthesis. If there are uncertainties about a study’s relevance, consulting a faculty mentor is advisable. To ensure the systematic review is as thorough as possible, pay special attention to the references section of each paper, as cited references can reveal relevant studies that may have been missed in the literature search.
Once all relevant papers are compiled and read, the relevant data points should be extracted and imputed into a data sheet. Collaborating with a medical statistician is crucial at this stage, as they can provide guidance on the most effective ways to structure and input data. After all studies are included, the relevant statistical analyses on the resultant dataset can be run.
Step 4: Write the Paper—In 2020, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was developed to ensure transparent and complete reporting of systematic reviews. A full discussion of PRISMA guidelines is beyond the scope of this paper; Page et al14 provided a summary, checklist, and flow diagram that is available online (https://www.prisma-statement.org). Following the PRISMA checklist and guidelines ensures a high-quality, transparent, and reliable systematic review. These guidelines not only help streamline and simplify the writing process but also enhance its efficiency and effectiveness. Discovering the PRISMA checklist can be transformative, providing a valuable roadmap that guides the author through each step of the reporting process, helping to avoid common pitfalls. This structured approach ultimately leads to a more comprehensive and trustworthy review.
Step 5: Make Finishing Touches—At this stage in the systematic review process, the studies have been compiled and thoroughly analyzed and the statistical analysis has been conducted. The results have been organized within a structured framework following the PRISMA checklist. With these steps completed, the next task is to finalize the manuscript and seek a final review from the senior author or faculty mentor. To streamline this process, it is beneficial to adhere to the formatting guidelines of the specific medical journal you intend to submit to. Check the author guidelines on the journal’s website and review recent systematic reviews published there as a reference. Even if you have not chosen a journal yet, formatting your manuscript according to a prestigious journal’s general style provides a strong foundation that can be easily adapted to fit another journal’s requirements if necessary.
Final Thoughts
Designing and conducting a systematic review is no easy task, but it can be a valuable skill for dermatology residents aiming to contribute meaningfully to the medical literature. The process of compiling a systematic review offers an opportunity for developing critical research skills, from formulating a research question to synthesizing evidence and presenting findings in a clear methodical way. Engaging in systematic review writing not only enhances the resident’s understanding of a particular topic but also demonstrates a commitment to scholarly activity—a key factor in an increasingly competitive residency and fellowship application environment.
The basic steps outlined in this article are just one way in which residents can begin to navigate the complexities of medical research, specifically the systematic review process. By assembling a supportive team, utilizing available resources, and adhering to established guidelines such as PRISMA, one can produce a high-quality, impactful review. Ultimately, the systematic review process is not just about publication—it is about fostering a habit of inquiry, improving patient care, and contributing to the ever-evolving field of medicine. With dedication and collaboration, even the most challenging aspects of research can be tackled, paving the way for future opportunities and professional growth. In this way, perhaps one day the spirit of the “research race” can shift from a frantic sprint to a graceful marathon, where each mile is run with heart and every step is filled with purpose.
Dermatology remains one of the most competitive specialties in the residency match, with successful applicants demonstrating a well-rounded application reflecting not only their academic excellence but also their dedication to research, community service, and hands-on clinical experience.1 A growing emphasis on scholarly activities has made it crucial for applicants to stand out, with an increasing number opting to take gap years to engage in focused research endeavors.2 In highly competitive specialties such as dermatology, successful applicants now report more than 20 research items on average.3,4 This trend also is evident in primary care specialties, which have seen a 2- to 3-fold increase in reported research activities. The average unmatched applicant today lists more research items than the average matched applicant did a decade ago, underscoring the growing emphasis on scholarly activity.3
Ideally, graduate medical education should foster an environment of inquiry and scholarship, where residents develop new knowledge, evaluate research findings, and cultivate lifelong habits of inquiry. The Accreditation Council for Graduate Medical Education requires residents to engage in scholarship, such as case reports, research reviews, and original research.5 Research during residency has been linked to several benefits, including enhanced patient care through improved critical appraisal skills, clinical reasoning, and lifelong learning.6,7 Additionally, students and residents who publish research are more likely to achieve higher rank during residency and pursue careers in academic medicine, potentially helping to address the decline in clinician investigators.8,9 Publishing and presenting research also can enhance a residency program’s reputation, making it more attractive to competitive applicants, and may be beneficial for residents seeking jobs or fellowships.6
Dermatology residency programs vary in their structure and support for resident research. One survey revealed that many programs lack the necessary support, structure, and resources to effectively promote and maintain research training.1 Additionally, residents have less exposure to researchers who could serve as mentors due to the growing demands placed on attending physicians in teaching hospitals.10
The Research Arms Race
The growing emphasis on scholarly activity for residency and fellowship applicants coupled with the use of research productivity to differentiate candidates has led some to declare a “research arms race” in residency selection.3 As one author stated, “We need less research, better research, and research done for the right reasons.”11 Indeed, most articles authored by medical students are short reviews or case reports, with the majority (59% [207/350]) being cited zero times, according to one analysis.12 Given the variable research infrastructure between programs and the decreasing availability of research mentors despite the growing emphasis on scholarly activity, applicants face an unfortunate dilemma. Until the system changes, those who protest this research arms race by not engaging in substantial scholarly activity are less likely to match into competitive specialties. Thus, the race continues.
The Value of Mentorship
Resident research success is impacted by having an effective faculty research mentor.13 Although all medical research at the student or resident levels should be conducted with a faculty mentor to oversee it, finding a mentor can be challenging. If a resident’s program boasts a strong research infrastructure or prolific faculty, building relationships with potential mentors is a logical first step for residents wishing to engage in research; however, if suitable mentors are lacking, efforts should be made by residents to establish these connections elsewhere, such as attending society meetings to network with potential mentors and applying to formal mentorship programs (eg, the American Society for Dermatologic Surgery’s Preceptor Program, the Women’s Dermatologic Society’s Mentorship Award). Unsolicited email inquiries asking, “Hi Dr. X, my name is Y, and I was wondering if you have any research projects I could help with?” often go unanswered. Instead, consider emailing or approaching potential mentors with a more developed proposition, such as the following example:
Hello Dr. X, my name is Y. I have enjoyed reading your publications on A, which inspired me to think about B. I reviewed the literature and noticed a potential to enhance our current understanding on the topic. My team and I conducted a systematic review of the available literature and drafted a manuscript summarizing our findings. Given your expertise in this field, would you be willing to collaborate on this paper? We would be grateful for your critical eye, suggestions for improvement, and overall thoughts.
This approach demonstrates initiative, provides a clear plan, and shows respect for the mentor’s expertise, increasing the likelihood of a positive response and fruitful collaboration. Assuming the resident’s working draft meets the potential mentor’s basic expectations, such a display of initiative is likely to impress them, and they may then offer opportunities to engage in meaningful research projects in the future. Everyone benefits! These efforts to establish connections with mentors can pave the way to further collaboration and meaningful research opportunities for dermatology residents.
The Systematic Review: An Attractive Option For Residents
There are several potential avenues for students or residents interested in pursuing research. Case reports and case series are relatively easy to compile, can be completed quickly, and often require minimal guidance from a faculty mentor; however, case reports rank low in the research hierarchy. Conversely, prospective blinded clinical trials provide some of the highest-quality evidence available but are challenging to conduct without a practicing faculty member to provide a patient cohort, often require extensive funding, and may involve complex statistical analyses beyond the expertise of most students or residents. Additionally, they may take years to complete, often extending beyond residency or fellowship application deadlines.
Most medical applicants likely hold at least some hesitation in churning out vast amounts of low-quality research merely to boost their publication count for the match process. Ideally, those who pursue scholarly activity should be driven by a genuine desire to contribute meaningfully to the medical literature. One particularly valuable avenue for trainees wishing to engage in research is the systematic review, which aims to identify, evaluate, and summarize the findings of all relevant individual studies regarding a research topic and answer a focused question. If performed thoughtfully, a systematic review can meaningfully contribute to the medical literature without requiring access to a prospectively followed cohort of patients or the constant supervision of a faculty mentor. Sure, systematic reviews may not be as robust as prospective cohort clinical trials, but they often provide comprehensive insights and are considered valuable contributions to evidence-based medicine. With the help of co-residents or medical students, a medical reference librarian, and a statistician—along with a working understanding of universally accepted quality measures—a resident physician and their team can produce a systematic review that ultimately may merit publication in a top-tier medical journal.
The remainder of this column will outline a streamlined approach to the systematic review writing process, specifically tailored for medical residents who may not have affiliations to a prolific research department or established relationships with faculty mentors in their field of interest. The aim is to offer a basic framework to help residents navigate the complexities of conducting and writing a high-quality, impactful systematic review. It is important to emphasize that resident research should always be conducted under the guidance of a faculty mentor, and this approach is not intended to encourage independent research and publication by residents. Instead, it provides steps that can be undertaken with a foundational understanding of accepted principles, allowing residents to compile a working draft of a manuscript in collaboration with a trusted faculty mentor.
The Systematic Review: A Simple Approach
Step 1: Choose a Topic—Once a resident has decided to embark on conducting a systematic review, the first step is to choose a topic, which requires consideration of several factors to ensure relevance, feasibility, and impact. Begin by identifying areas of clinical uncertainty or controversy in which a comprehensive synthesis of the literature could provide valuable insights. Often, such a topic can be gleaned from the conclusion section of other primary studies; statements such as “further study is needed to determine the efficacy of X” or “systematic reviews would be beneficial to ascertaining the impact of Y” may be a great place to start.
Next, ensure that sufficient primary studies exist to support a robust review or meta-analysis by conducting a preliminary literature search, which will confirm that the chosen topic is both researchable and relevant. A narrow, focused, well-defined topic likely will prove more feasible to review than a broad, ill-defined one. Once a topic is selected, it is advisable to discuss it with a faculty mentor before starting the literature search to ensure the topic’s feasibility and clinical relevance, helping to guide your research in a meaningful direction.
When deciding between a systematic review and a meta-analysis, the nature of the research question is an influential factor. A systematic review is particularly suitable for addressing broad questions or topics when the aim is to summarize and synthesize all relevant research studies; for example, a systematic review may investigate the various treatment options for atopic dermatitis and their efficacy, which allows for a comprehensive overview of the available treatments—both the interventions and the outcomes. In contrast, a meta-analysis is ideal for collecting and statistically combining quantitative data from multiple primary studies, provided there are enough relevant studies available in the literature.
Step 2: Build a Team—Recruiting a skilled librarian to assist with Medical Subject Headings (MeSH) terms and retrieving relevant papers is crucial for conducting a high-quality systematic review or meta-analysis. Medical librarians specializing in health sciences enhance the efficiency, comprehensiveness, and reliability of your literature search, substantially boosting your work’s credibility. These librarians are well versed in medical databases such as PubMed and Embase. Begin by contacting your institution’s library services, as there often are valuable resources and personnel available to assist you. Personally, I was surprised to find a librarian at my institution specifically dedicated to helping medical residents with such projects! These professionals are eager to help, and if provided with the scope and goal of your project, they can deliver literature search results in a digestible format. Similarly, seeking the expertise of a medical statistician is crucial to the accuracy and legitimacy of your study. In your final paper, it is important to recognize the contributions of the librarian and statistician, either as co-authors or in the acknowledgments section.
In addition, recruiting colleagues or medical students can be an effective strategy to make the project more feasible and offer collaborative benefits for all parties involved. Given the growing emphasis on research for residency and fellowship admissions, there usually is no shortage of motivated volunteers.
Next, identify the software tool you will use for your systematic review. Options range from simple spreadsheets such as Microsoft Excel to reference managers such as EndNote or Mendeley or dedicated systematic review tools. Academic institutions may subscribe to paid services such as Covidence (https://www.covidence.org), or you can utilize free alternatives such as Rayyan (https://www.rayyan.ai). Investing time in learning to navigate dedicated systematic review software can greatly enhance efficiency and reduce frustrations compared to more basic methods. Ultimately, staying organized, thorough, and committed is key.
Step 3: Conduct the Literature Review—At this point, your research topic has been decided, a medical reference librarian has provided the results of a comprehensive literature search, and a software tool has been chosen. The next task is to read hundreds or thousands of papers—easy, right? With your dedicated team assembled, the workload can be divided and conquered. The first step involves screening out duplicate and irrelevant studies based on titles and abstracts. Next, review the remaining papers in more detail. Those that pass this preliminary screen should be read in their entirety, and only the papers relevant to the research topic should be included in the final synthesis. If there are uncertainties about a study’s relevance, consulting a faculty mentor is advisable. To ensure the systematic review is as thorough as possible, pay special attention to the references section of each paper, as cited references can reveal relevant studies that may have been missed in the literature search.
Once all relevant papers are compiled and read, the relevant data points should be extracted and imputed into a data sheet. Collaborating with a medical statistician is crucial at this stage, as they can provide guidance on the most effective ways to structure and input data. After all studies are included, the relevant statistical analyses on the resultant dataset can be run.
Step 4: Write the Paper—In 2020, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was developed to ensure transparent and complete reporting of systematic reviews. A full discussion of PRISMA guidelines is beyond the scope of this paper; Page et al14 provided a summary, checklist, and flow diagram that is available online (https://www.prisma-statement.org). Following the PRISMA checklist and guidelines ensures a high-quality, transparent, and reliable systematic review. These guidelines not only help streamline and simplify the writing process but also enhance its efficiency and effectiveness. Discovering the PRISMA checklist can be transformative, providing a valuable roadmap that guides the author through each step of the reporting process, helping to avoid common pitfalls. This structured approach ultimately leads to a more comprehensive and trustworthy review.
Step 5: Make Finishing Touches—At this stage in the systematic review process, the studies have been compiled and thoroughly analyzed and the statistical analysis has been conducted. The results have been organized within a structured framework following the PRISMA checklist. With these steps completed, the next task is to finalize the manuscript and seek a final review from the senior author or faculty mentor. To streamline this process, it is beneficial to adhere to the formatting guidelines of the specific medical journal you intend to submit to. Check the author guidelines on the journal’s website and review recent systematic reviews published there as a reference. Even if you have not chosen a journal yet, formatting your manuscript according to a prestigious journal’s general style provides a strong foundation that can be easily adapted to fit another journal’s requirements if necessary.
Final Thoughts
Designing and conducting a systematic review is no easy task, but it can be a valuable skill for dermatology residents aiming to contribute meaningfully to the medical literature. The process of compiling a systematic review offers an opportunity for developing critical research skills, from formulating a research question to synthesizing evidence and presenting findings in a clear methodical way. Engaging in systematic review writing not only enhances the resident’s understanding of a particular topic but also demonstrates a commitment to scholarly activity—a key factor in an increasingly competitive residency and fellowship application environment.
The basic steps outlined in this article are just one way in which residents can begin to navigate the complexities of medical research, specifically the systematic review process. By assembling a supportive team, utilizing available resources, and adhering to established guidelines such as PRISMA, one can produce a high-quality, impactful review. Ultimately, the systematic review process is not just about publication—it is about fostering a habit of inquiry, improving patient care, and contributing to the ever-evolving field of medicine. With dedication and collaboration, even the most challenging aspects of research can be tackled, paving the way for future opportunities and professional growth. In this way, perhaps one day the spirit of the “research race” can shift from a frantic sprint to a graceful marathon, where each mile is run with heart and every step is filled with purpose.
References
Anand P, Szeto MD, Flaten H, et al. Dermatology residency research policies: a 2021 national survey. Int J Womens Dermatol. 2021;7:787-792.
Costello CM, Harvey JA, Besch-Stokes JG, et al. The role research gap years play in a successful dermatology match. Int J Dermatol. 2022;61:226-230.
Elliott B, Carmody JB. Publish or perish: the research arms race in residency selection. J Grad Med Educ. 2023;15:524-527.
Bhuiya T, Makaryus AN. The importance of engaging in scientific research during medical training. Int J Angiol. 2023;32:153-157.
Seaburg LA, Wang AT, West CP, et al. Associations between resident physicians’ publications and clinical performance during residency training. BMC Med Educ. 2016;16:22.
West CP, Halvorsen AJ, McDonald FS. Scholarship during residency training: a controlled comparison study. Am J Med. 2011;124:983-987.e1.
Bhattacharya SD, Williams JB, De La Fuente SG, et al. Does protected research time during general surgery training contribute to graduates’ career choice? Am Surg. 2011;77:907-910.
Kralovec PD, Miller JA, Wellikson L, et al. The status of hospital medicine groups in the United States. J Hosp Med. 2006;1:75-80.
Altman DG. The scandal of poor medical research. BMJ. 1994;308:283-284.
Wickramasinghe DP, Perera CS, Senarathna S, et al. Patterns and trends of medical student research. BMC Med Educ. 2013;13:175.
Ercan-Fang NG, Mahmoud MA, Cottrell C, et al. Best practices in resident research—a national survey of high functioning internal medicine residency programs in resident research in USA. Am J Med Sci. 2021;361:23-29.
Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372.
References
Anand P, Szeto MD, Flaten H, et al. Dermatology residency research policies: a 2021 national survey. Int J Womens Dermatol. 2021;7:787-792.
Costello CM, Harvey JA, Besch-Stokes JG, et al. The role research gap years play in a successful dermatology match. Int J Dermatol. 2022;61:226-230.
Elliott B, Carmody JB. Publish or perish: the research arms race in residency selection. J Grad Med Educ. 2023;15:524-527.
Bhuiya T, Makaryus AN. The importance of engaging in scientific research during medical training. Int J Angiol. 2023;32:153-157.
Seaburg LA, Wang AT, West CP, et al. Associations between resident physicians’ publications and clinical performance during residency training. BMC Med Educ. 2016;16:22.
West CP, Halvorsen AJ, McDonald FS. Scholarship during residency training: a controlled comparison study. Am J Med. 2011;124:983-987.e1.
Bhattacharya SD, Williams JB, De La Fuente SG, et al. Does protected research time during general surgery training contribute to graduates’ career choice? Am Surg. 2011;77:907-910.
Kralovec PD, Miller JA, Wellikson L, et al. The status of hospital medicine groups in the United States. J Hosp Med. 2006;1:75-80.
Altman DG. The scandal of poor medical research. BMJ. 1994;308:283-284.
Wickramasinghe DP, Perera CS, Senarathna S, et al. Patterns and trends of medical student research. BMC Med Educ. 2013;13:175.
Ercan-Fang NG, Mahmoud MA, Cottrell C, et al. Best practices in resident research—a national survey of high functioning internal medicine residency programs in resident research in USA. Am J Med Sci. 2021;361:23-29.
Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372.
Establishing a strong relationship with a research mentor is crucial for success in resident research. If your program lacks the necessary infrastructure, take the initiative to network at society meetings or apply for formal mentorship programs.
For residents facing limited access to patient cohorts and large datasets or those without access to a robust research infrastructure, conducting a systematic review is a valuable and feasible research option, allowing for meaningful contributions to the medical literature.
Disallow All Ads
Content Gating
No Gating (article Unlocked/Free)
Alternative CME
Disqus Comments
Default
Consolidated Pubs: Do Not Show Source Publication Logo
Applications for the CUTIS 2025 Resident Corner Column
The Cutis Editorial Board is now accepting applications for the 2025 Resident Corner column. The Editorial Board will select 2 to 3 residents to serve as the Resident Corner columnists for 1 year. Articles are posted online only at www.mdedge.com/dermatology but will be referenced in Index Medicus. All applicants must be current residents and will be in residency throughout 2025.
For consideration, send your curriculum vitae along with a brief (not to exceed 500 words) statement of why you enjoy Cutis and what you can offer your fellow residents in contributing a monthly column.
A signed letter of recommendation from the Director of the dermatology residency program also should be supplied.
All materials should be submitted via email to Alicia Sonners ([email protected]) by November 1. The residents who are selected to write the column for the upcoming year will be notified by November 15.
We look forward to continuing to educate dermatology residents on topics that are most important to them!
The Cutis Editorial Board is now accepting applications for the 2025 Resident Corner column. The Editorial Board will select 2 to 3 residents to serve as the Resident Corner columnists for 1 year. Articles are posted online only at www.mdedge.com/dermatology but will be referenced in Index Medicus. All applicants must be current residents and will be in residency throughout 2025.
For consideration, send your curriculum vitae along with a brief (not to exceed 500 words) statement of why you enjoy Cutis and what you can offer your fellow residents in contributing a monthly column.
A signed letter of recommendation from the Director of the dermatology residency program also should be supplied.
All materials should be submitted via email to Alicia Sonners ([email protected]) by November 1. The residents who are selected to write the column for the upcoming year will be notified by November 15.
We look forward to continuing to educate dermatology residents on topics that are most important to them!
The Cutis Editorial Board is now accepting applications for the 2025 Resident Corner column. The Editorial Board will select 2 to 3 residents to serve as the Resident Corner columnists for 1 year. Articles are posted online only at www.mdedge.com/dermatology but will be referenced in Index Medicus. All applicants must be current residents and will be in residency throughout 2025.
For consideration, send your curriculum vitae along with a brief (not to exceed 500 words) statement of why you enjoy Cutis and what you can offer your fellow residents in contributing a monthly column.
A signed letter of recommendation from the Director of the dermatology residency program also should be supplied.
All materials should be submitted via email to Alicia Sonners ([email protected]) by November 1. The residents who are selected to write the column for the upcoming year will be notified by November 15.
We look forward to continuing to educate dermatology residents on topics that are most important to them!
Hello. I’m Mark Lewis, director of gastrointestinal (GI) oncology at Intermountain Health in Utah. I’m speaking from the 2024 ASCO Annual Meeting in Chicago, where we’ve seen some interesting, new data in GI cancers.
If you allow me, I’d like to go in a craniocaudal fashion. It’s my anatomic mnemonic. I think that’s appropriate because our plenary session yesterday kicked off with some exciting data in esophageal cancer, specifically esophageal adenocarcinoma.
This was the long-awaited ESOPEC trial. It’s a phase 3 study looking at perioperative FLOT (5-FU/leucovorin/oxaliplatin/docetaxel), a chemo triplet, vs the CROSS protocol, which is neoadjuvant chemoradiation with carboplatin and paclitaxel. The primary endpoint was overall survival, and at first blush, FLOT looked to be the true winner. There were some really remarkable milestones in this study, and I have some reservations about the FLOT arm that I’ll raise in just a second.
The investigators are to be commended because in a truly deadly disease, they reported a 5-year overall survival in half of the patients who were receiving FLOT. That is truly commendable and really a milestone in our field. The reason I take a little bit of issue with the trial is that I still have some questions about methodology.
It wasn’t that long ago at ASCO GI that there was a really heated debate called “FLOT or Not” — not in this precise setting, but asking the question, do we think that patients with upper GI malignancy are even fit enough to handle a chemo triplet like FLOT?
The reason I bring that up now in 2024 is that, to my surprise, and I think to many others’, there was a lower-than-expected completion rate of the patients in this trial who were receiving the CROSS regimen. The number of people who were able to complete that in full was about two-thirds, which compared with a historical control from a trial scheme that first emerged over a decade ago that used to be over 90% completion. I found that quite strange.
I also think this trial suffers a little bit, and unavoidably, from the evolution of care that’s happened since it was first enrolling. Of course, I refer to adjuvant immunotherapy. Now, the real question is whether there is synergy between patients who receive radiation upfront and then adjuvant nivolumab, as per CheckMate 577.
In her plenary discussion, I thought Dr. Karyn Goodman did a masterful job — I would encourage you to watch it on ASCO’s website —discussing how we can take all these data and reconcile them for optimal patient outcome. She ultimately suggested that we might deploy all four modalities in the management of these people.
She proposed a paradigm with a PET-adapted, upfront induction chemotherapy, then moving to chemoradiation, then moving to surgery, and finally moving to immunotherapy. That is all four of the traditional arms of oncology. I find that really rather remarkable. Watch that space. This is a great trial with really remarkable survival data, but I’m not entirely convinced that the CROSS arm was given its due.
Next up, I want to talk about pancreas cancer, which is something near and dear to my heart. It affects about one in four of my patients and it remains, unfortunately, a highly lethal disease. I think the top-line news from this meeting is that the KRAS mutation is druggable. I’m probably showing my age, but when I did my fellowship in 2009 through 2012, I was taught that KRAS was sort of the undruggable mutation par excellence. At this meeting, we’ve seen maturing data in regard to targeting KRAS G12C with both sotorasib and adagrasib. The disease control rates are astounding, at 80% and more, which is really remarkable. I wouldn’t have believed that even a few years ago.
I’m even more excited about how we bring a rising tide that can lift all boats and apply this to other KRAS mutations, and not just KRAS G12C but all KRAS mutations. I think that’s coming, hopefully, with the pan-RAS inhibitors, because once that happens — if that happens; I’ll try not to be irrationally exuberant — that would take the traditional mutation found in almost all pancreas cancers and really make it its own Achilles heel. I think that could be such a huge leap forward.
Another matter, however, that remains unresolved at this meeting is in the neoadjuvant setting with pancreatic ductal adenocarcinoma. There’s still equipoise, actually, between neoadjuvant gemcitabine, paclitaxel, and FOLFIRINOX. I thought that that was very well spelled out by some of our Dutch colleagues, who continue to do great work in a variety of cancers, including colorectal.
Where I’d like to move next is colorectal cancer. Of course, immunotherapy remains a hot topic at all of these conferences. There were three different aspects of immunotherapy I’d like to highlight at this conference in regard to colon and rectal cancer.
First, Dr. Heinz-Josef Lenz presented updated data from CheckMate 8HW, which looked at nivolumab and ipilimumab (nivo/ipi) vs chemotherapy in the first line for MSI-high or mismatch repair–deficient colon cancer. Once again, the data we’ve had now for several years at the 2-year mark are incredibly impressive. The 2-year progression-free survival (PFS) rates for nivo/ipi are above 70% and down at around 14% for chemo.
What was impressive about this meeting is that Dr. Lenz presented PFS2, trying to determine the impact, if any, of subsequent therapy. What was going on here, which I think was ethically responsible by the investigators, was crossover. About two-thirds of the chemo arm crossed over to any form of immuno-oncology (IO), and just under a half crossed over to nivo and ipi. The PFS benefits continued with up-front IO. The way that Dr. Lenz phrased it is that you really never get the chance to win back the benefit that you would derive by giving immunotherapy first line to someone who has MSI-high or mismatch repair–deficient metastatic colon cancer.
One thing that’s still not settled in my mind, though, is, does this really dethrone single-agent immunotherapy, such as pembrolizumab in KEYNOTE-177? What I’m really driving at is the ipilimumab. Is the juice worth the squeeze? Is the addition of an anti-CTLA4 agent worth the toxicity that we know comes along with that mechanism of action? Watch this space.
I was also really interested in NEOPRISM-CRC, which looked at the role of immunotherapy in neoadjuvant down-staging of radiographically high-risk stage II or stage III colon cancer. Here, the investigators really make a strong case that, up front in these potentially respectable cases, not only should we know about mismatch repair deficiency but we should actually be interrogating further for tumor mutational burden (TMB).
They had TMB-high patients. In fact, the median TMB was 42 mutations per megabase, with really impressive down-staging using three cycles of every-3-week pembrolizumab before surgery. Again, I really think we’re at an exciting time where, even for colon cancer that looks operable up front, we might actually have the opportunity to improve pathologic and clinical complete responses before and after surgery.
Finally, I want to bring up what continues to amaze me. Two years ago, at ASCO 2022, we heard from Dr. Andrea Cercek and the Memorial Sloan Kettering group about the incredible experience they were having with neoadjuvant, or frankly, definitive dostarlimab in mismatch repair–deficient locally advanced rectal cancer.
I remember being at the conference and there was simultaneous publication of that abstract in The New York Times because it was so remarkable. There was a 100% clinical complete response. The patients didn’t require radiation, they didn’t require chemotherapy, and they didn’t require surgery for locally advanced rectal cancer, provided there was this vulnerability of mismatch-repair deficiency.
Now, 2 years later, Dr. Cercek and her group have updated those data with more than 40 patients, and again, a 100% clinical complete response, including mature, complete responses at over a year in about 20 patients. Again, we are really doing our rectal cancer patients a disservice if we’re not checking for mismatch-repair deficiency upfront, and especially if we’re not talking about them in multidisciplinary conferences.
One of the things that absolutely blows my mind about rectal cancer is just how complicated it’s becoming. I think it is the standard of care to discuss these cases upfront with radiation oncology, surgical oncology, medical oncology, and pathology.
Maybe the overarching message I would take from everything I’ve said today is that the oncologist without the pathologist is blind. It’s really a dyad, a partnership that guides optimal medical oncology care. As much as I love ASCO, I often wish we had more of our pathology colleagues here. I look forward to taking all the findings from this meeting back to the tumor board and really having a dynamic dialogue.
Dr. Lewis is director, Department of Gastrointestinal Oncology, Intermountain Health, Salt Lake City, Utah. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Hello. I’m Mark Lewis, director of gastrointestinal (GI) oncology at Intermountain Health in Utah. I’m speaking from the 2024 ASCO Annual Meeting in Chicago, where we’ve seen some interesting, new data in GI cancers.
If you allow me, I’d like to go in a craniocaudal fashion. It’s my anatomic mnemonic. I think that’s appropriate because our plenary session yesterday kicked off with some exciting data in esophageal cancer, specifically esophageal adenocarcinoma.
This was the long-awaited ESOPEC trial. It’s a phase 3 study looking at perioperative FLOT (5-FU/leucovorin/oxaliplatin/docetaxel), a chemo triplet, vs the CROSS protocol, which is neoadjuvant chemoradiation with carboplatin and paclitaxel. The primary endpoint was overall survival, and at first blush, FLOT looked to be the true winner. There were some really remarkable milestones in this study, and I have some reservations about the FLOT arm that I’ll raise in just a second.
The investigators are to be commended because in a truly deadly disease, they reported a 5-year overall survival in half of the patients who were receiving FLOT. That is truly commendable and really a milestone in our field. The reason I take a little bit of issue with the trial is that I still have some questions about methodology.
It wasn’t that long ago at ASCO GI that there was a really heated debate called “FLOT or Not” — not in this precise setting, but asking the question, do we think that patients with upper GI malignancy are even fit enough to handle a chemo triplet like FLOT?
The reason I bring that up now in 2024 is that, to my surprise, and I think to many others’, there was a lower-than-expected completion rate of the patients in this trial who were receiving the CROSS regimen. The number of people who were able to complete that in full was about two-thirds, which compared with a historical control from a trial scheme that first emerged over a decade ago that used to be over 90% completion. I found that quite strange.
I also think this trial suffers a little bit, and unavoidably, from the evolution of care that’s happened since it was first enrolling. Of course, I refer to adjuvant immunotherapy. Now, the real question is whether there is synergy between patients who receive radiation upfront and then adjuvant nivolumab, as per CheckMate 577.
In her plenary discussion, I thought Dr. Karyn Goodman did a masterful job — I would encourage you to watch it on ASCO’s website —discussing how we can take all these data and reconcile them for optimal patient outcome. She ultimately suggested that we might deploy all four modalities in the management of these people.
She proposed a paradigm with a PET-adapted, upfront induction chemotherapy, then moving to chemoradiation, then moving to surgery, and finally moving to immunotherapy. That is all four of the traditional arms of oncology. I find that really rather remarkable. Watch that space. This is a great trial with really remarkable survival data, but I’m not entirely convinced that the CROSS arm was given its due.
Next up, I want to talk about pancreas cancer, which is something near and dear to my heart. It affects about one in four of my patients and it remains, unfortunately, a highly lethal disease. I think the top-line news from this meeting is that the KRAS mutation is druggable. I’m probably showing my age, but when I did my fellowship in 2009 through 2012, I was taught that KRAS was sort of the undruggable mutation par excellence. At this meeting, we’ve seen maturing data in regard to targeting KRAS G12C with both sotorasib and adagrasib. The disease control rates are astounding, at 80% and more, which is really remarkable. I wouldn’t have believed that even a few years ago.
I’m even more excited about how we bring a rising tide that can lift all boats and apply this to other KRAS mutations, and not just KRAS G12C but all KRAS mutations. I think that’s coming, hopefully, with the pan-RAS inhibitors, because once that happens — if that happens; I’ll try not to be irrationally exuberant — that would take the traditional mutation found in almost all pancreas cancers and really make it its own Achilles heel. I think that could be such a huge leap forward.
Another matter, however, that remains unresolved at this meeting is in the neoadjuvant setting with pancreatic ductal adenocarcinoma. There’s still equipoise, actually, between neoadjuvant gemcitabine, paclitaxel, and FOLFIRINOX. I thought that that was very well spelled out by some of our Dutch colleagues, who continue to do great work in a variety of cancers, including colorectal.
Where I’d like to move next is colorectal cancer. Of course, immunotherapy remains a hot topic at all of these conferences. There were three different aspects of immunotherapy I’d like to highlight at this conference in regard to colon and rectal cancer.
First, Dr. Heinz-Josef Lenz presented updated data from CheckMate 8HW, which looked at nivolumab and ipilimumab (nivo/ipi) vs chemotherapy in the first line for MSI-high or mismatch repair–deficient colon cancer. Once again, the data we’ve had now for several years at the 2-year mark are incredibly impressive. The 2-year progression-free survival (PFS) rates for nivo/ipi are above 70% and down at around 14% for chemo.
What was impressive about this meeting is that Dr. Lenz presented PFS2, trying to determine the impact, if any, of subsequent therapy. What was going on here, which I think was ethically responsible by the investigators, was crossover. About two-thirds of the chemo arm crossed over to any form of immuno-oncology (IO), and just under a half crossed over to nivo and ipi. The PFS benefits continued with up-front IO. The way that Dr. Lenz phrased it is that you really never get the chance to win back the benefit that you would derive by giving immunotherapy first line to someone who has MSI-high or mismatch repair–deficient metastatic colon cancer.
One thing that’s still not settled in my mind, though, is, does this really dethrone single-agent immunotherapy, such as pembrolizumab in KEYNOTE-177? What I’m really driving at is the ipilimumab. Is the juice worth the squeeze? Is the addition of an anti-CTLA4 agent worth the toxicity that we know comes along with that mechanism of action? Watch this space.
I was also really interested in NEOPRISM-CRC, which looked at the role of immunotherapy in neoadjuvant down-staging of radiographically high-risk stage II or stage III colon cancer. Here, the investigators really make a strong case that, up front in these potentially respectable cases, not only should we know about mismatch repair deficiency but we should actually be interrogating further for tumor mutational burden (TMB).
They had TMB-high patients. In fact, the median TMB was 42 mutations per megabase, with really impressive down-staging using three cycles of every-3-week pembrolizumab before surgery. Again, I really think we’re at an exciting time where, even for colon cancer that looks operable up front, we might actually have the opportunity to improve pathologic and clinical complete responses before and after surgery.
Finally, I want to bring up what continues to amaze me. Two years ago, at ASCO 2022, we heard from Dr. Andrea Cercek and the Memorial Sloan Kettering group about the incredible experience they were having with neoadjuvant, or frankly, definitive dostarlimab in mismatch repair–deficient locally advanced rectal cancer.
I remember being at the conference and there was simultaneous publication of that abstract in The New York Times because it was so remarkable. There was a 100% clinical complete response. The patients didn’t require radiation, they didn’t require chemotherapy, and they didn’t require surgery for locally advanced rectal cancer, provided there was this vulnerability of mismatch-repair deficiency.
Now, 2 years later, Dr. Cercek and her group have updated those data with more than 40 patients, and again, a 100% clinical complete response, including mature, complete responses at over a year in about 20 patients. Again, we are really doing our rectal cancer patients a disservice if we’re not checking for mismatch-repair deficiency upfront, and especially if we’re not talking about them in multidisciplinary conferences.
One of the things that absolutely blows my mind about rectal cancer is just how complicated it’s becoming. I think it is the standard of care to discuss these cases upfront with radiation oncology, surgical oncology, medical oncology, and pathology.
Maybe the overarching message I would take from everything I’ve said today is that the oncologist without the pathologist is blind. It’s really a dyad, a partnership that guides optimal medical oncology care. As much as I love ASCO, I often wish we had more of our pathology colleagues here. I look forward to taking all the findings from this meeting back to the tumor board and really having a dynamic dialogue.
Dr. Lewis is director, Department of Gastrointestinal Oncology, Intermountain Health, Salt Lake City, Utah. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. I’m Mark Lewis, director of gastrointestinal (GI) oncology at Intermountain Health in Utah. I’m speaking from the 2024 ASCO Annual Meeting in Chicago, where we’ve seen some interesting, new data in GI cancers.
If you allow me, I’d like to go in a craniocaudal fashion. It’s my anatomic mnemonic. I think that’s appropriate because our plenary session yesterday kicked off with some exciting data in esophageal cancer, specifically esophageal adenocarcinoma.
This was the long-awaited ESOPEC trial. It’s a phase 3 study looking at perioperative FLOT (5-FU/leucovorin/oxaliplatin/docetaxel), a chemo triplet, vs the CROSS protocol, which is neoadjuvant chemoradiation with carboplatin and paclitaxel. The primary endpoint was overall survival, and at first blush, FLOT looked to be the true winner. There were some really remarkable milestones in this study, and I have some reservations about the FLOT arm that I’ll raise in just a second.
The investigators are to be commended because in a truly deadly disease, they reported a 5-year overall survival in half of the patients who were receiving FLOT. That is truly commendable and really a milestone in our field. The reason I take a little bit of issue with the trial is that I still have some questions about methodology.
It wasn’t that long ago at ASCO GI that there was a really heated debate called “FLOT or Not” — not in this precise setting, but asking the question, do we think that patients with upper GI malignancy are even fit enough to handle a chemo triplet like FLOT?
The reason I bring that up now in 2024 is that, to my surprise, and I think to many others’, there was a lower-than-expected completion rate of the patients in this trial who were receiving the CROSS regimen. The number of people who were able to complete that in full was about two-thirds, which compared with a historical control from a trial scheme that first emerged over a decade ago that used to be over 90% completion. I found that quite strange.
I also think this trial suffers a little bit, and unavoidably, from the evolution of care that’s happened since it was first enrolling. Of course, I refer to adjuvant immunotherapy. Now, the real question is whether there is synergy between patients who receive radiation upfront and then adjuvant nivolumab, as per CheckMate 577.
In her plenary discussion, I thought Dr. Karyn Goodman did a masterful job — I would encourage you to watch it on ASCO’s website —discussing how we can take all these data and reconcile them for optimal patient outcome. She ultimately suggested that we might deploy all four modalities in the management of these people.
She proposed a paradigm with a PET-adapted, upfront induction chemotherapy, then moving to chemoradiation, then moving to surgery, and finally moving to immunotherapy. That is all four of the traditional arms of oncology. I find that really rather remarkable. Watch that space. This is a great trial with really remarkable survival data, but I’m not entirely convinced that the CROSS arm was given its due.
Next up, I want to talk about pancreas cancer, which is something near and dear to my heart. It affects about one in four of my patients and it remains, unfortunately, a highly lethal disease. I think the top-line news from this meeting is that the KRAS mutation is druggable. I’m probably showing my age, but when I did my fellowship in 2009 through 2012, I was taught that KRAS was sort of the undruggable mutation par excellence. At this meeting, we’ve seen maturing data in regard to targeting KRAS G12C with both sotorasib and adagrasib. The disease control rates are astounding, at 80% and more, which is really remarkable. I wouldn’t have believed that even a few years ago.
I’m even more excited about how we bring a rising tide that can lift all boats and apply this to other KRAS mutations, and not just KRAS G12C but all KRAS mutations. I think that’s coming, hopefully, with the pan-RAS inhibitors, because once that happens — if that happens; I’ll try not to be irrationally exuberant — that would take the traditional mutation found in almost all pancreas cancers and really make it its own Achilles heel. I think that could be such a huge leap forward.
Another matter, however, that remains unresolved at this meeting is in the neoadjuvant setting with pancreatic ductal adenocarcinoma. There’s still equipoise, actually, between neoadjuvant gemcitabine, paclitaxel, and FOLFIRINOX. I thought that that was very well spelled out by some of our Dutch colleagues, who continue to do great work in a variety of cancers, including colorectal.
Where I’d like to move next is colorectal cancer. Of course, immunotherapy remains a hot topic at all of these conferences. There were three different aspects of immunotherapy I’d like to highlight at this conference in regard to colon and rectal cancer.
First, Dr. Heinz-Josef Lenz presented updated data from CheckMate 8HW, which looked at nivolumab and ipilimumab (nivo/ipi) vs chemotherapy in the first line for MSI-high or mismatch repair–deficient colon cancer. Once again, the data we’ve had now for several years at the 2-year mark are incredibly impressive. The 2-year progression-free survival (PFS) rates for nivo/ipi are above 70% and down at around 14% for chemo.
What was impressive about this meeting is that Dr. Lenz presented PFS2, trying to determine the impact, if any, of subsequent therapy. What was going on here, which I think was ethically responsible by the investigators, was crossover. About two-thirds of the chemo arm crossed over to any form of immuno-oncology (IO), and just under a half crossed over to nivo and ipi. The PFS benefits continued with up-front IO. The way that Dr. Lenz phrased it is that you really never get the chance to win back the benefit that you would derive by giving immunotherapy first line to someone who has MSI-high or mismatch repair–deficient metastatic colon cancer.
One thing that’s still not settled in my mind, though, is, does this really dethrone single-agent immunotherapy, such as pembrolizumab in KEYNOTE-177? What I’m really driving at is the ipilimumab. Is the juice worth the squeeze? Is the addition of an anti-CTLA4 agent worth the toxicity that we know comes along with that mechanism of action? Watch this space.
I was also really interested in NEOPRISM-CRC, which looked at the role of immunotherapy in neoadjuvant down-staging of radiographically high-risk stage II or stage III colon cancer. Here, the investigators really make a strong case that, up front in these potentially respectable cases, not only should we know about mismatch repair deficiency but we should actually be interrogating further for tumor mutational burden (TMB).
They had TMB-high patients. In fact, the median TMB was 42 mutations per megabase, with really impressive down-staging using three cycles of every-3-week pembrolizumab before surgery. Again, I really think we’re at an exciting time where, even for colon cancer that looks operable up front, we might actually have the opportunity to improve pathologic and clinical complete responses before and after surgery.
Finally, I want to bring up what continues to amaze me. Two years ago, at ASCO 2022, we heard from Dr. Andrea Cercek and the Memorial Sloan Kettering group about the incredible experience they were having with neoadjuvant, or frankly, definitive dostarlimab in mismatch repair–deficient locally advanced rectal cancer.
I remember being at the conference and there was simultaneous publication of that abstract in The New York Times because it was so remarkable. There was a 100% clinical complete response. The patients didn’t require radiation, they didn’t require chemotherapy, and they didn’t require surgery for locally advanced rectal cancer, provided there was this vulnerability of mismatch-repair deficiency.
Now, 2 years later, Dr. Cercek and her group have updated those data with more than 40 patients, and again, a 100% clinical complete response, including mature, complete responses at over a year in about 20 patients. Again, we are really doing our rectal cancer patients a disservice if we’re not checking for mismatch-repair deficiency upfront, and especially if we’re not talking about them in multidisciplinary conferences.
One of the things that absolutely blows my mind about rectal cancer is just how complicated it’s becoming. I think it is the standard of care to discuss these cases upfront with radiation oncology, surgical oncology, medical oncology, and pathology.
Maybe the overarching message I would take from everything I’ve said today is that the oncologist without the pathologist is blind. It’s really a dyad, a partnership that guides optimal medical oncology care. As much as I love ASCO, I often wish we had more of our pathology colleagues here. I look forward to taking all the findings from this meeting back to the tumor board and really having a dynamic dialogue.
Dr. Lewis is director, Department of Gastrointestinal Oncology, Intermountain Health, Salt Lake City, Utah. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Treatment for chronic hypertension in pregnancy with labetalol showed no significant differences in maternal or neonatal outcomes, compared with treatment with nifedipine, new research indicates.
The open-label, multicenter, randomized CHAP (Chronic Hypertension in Pregnancy) trial showed that treating mild chronic hypertension was better than delaying treatment until severe hypertension developed, but still unclear was whether, or to what extent, the choice of first-line treatment affected outcomes.
Researchers, led by Ayodeji A. Sanusi, MD, MPH, with the Division of Maternal and Fetal Medicine at the University of Alabama at Birmingham, conducted a secondary analysis of CHAP to compare the primary treatments. Mild chronic hypertension in the study was defined as blood pressure of 140-159/90-104 mmHg before 20 weeks of gestation.
Three Comparisons
Three comparisons were performed in 2292 participants based on medications prescribed at enrollment: 720 (31.4%) received labetalol; 417 (18.2%) initially received nifedipine; and 1155 (50.4%) had standard care. Labetalol was compared with standard care; nifedipine was compared with standard care; and labetalol was compared with nifedipine.
The primary outcome was occurrence of superimposed preeclampsia with severe features; preterm birth before 35 weeks of gestation; placental abruption; or fetal or neonatal death. The key secondary outcome was a small-for-gestational age neonate. Researchers also compared adverse effects between groups.
Among the results were the following:
The primary outcome occurred in 30.1% in the labetalol group; 31.2% in the nifedipine group; and 37% in the standard care group.
Risk of the primary outcome was lower among those receiving treatment. For labetalol vs standard care, the adjusted relative risk (RR) was 0.82; 95% confidence interval (CI), 0.72-0.94. For nifedipine vs standard care, the adjusted RR was 0.84; 95% CI, 0.71-0.99. There was no significant difference in risk when labetalol was compared with nifedipine (adjusted RR, 0.98; 95% CI, 0.82-1.18).
There were no significant differences in numbers of small-for-gestational age neonates or serious adverse events between those who received labetalol and those using nifedipine.
Any adverse events were significantly more common with nifedipine, compared with labetalol (35.7% vs 28.3%, P = .009), and with nifedipine, compared with standard care (35.7% vs 26.3%, P = .0003). Adverse event rates were not significantly higher with labetalol when compared with standard care (28.3% vs 26.3%, P = .34). The most frequently reported adverse events were headache, medication intolerance, dizziness, nausea, dyspepsia, neonatal jaundice, and vomiting.
“Thus, labetalol compared with nifedipine appeared to have fewer adverse events and to be better tolerated,” the authors write. They note that labetalol, a third-generation mixed alpha- and beta-adrenergic antagonist, is contraindicated for those who have obstructive pulmonary disease and nifedipine, a dihydropyridine calcium channel blocker, is contraindicated in people with tachycardia.
The authors write that their results align with other studies that have not found differences between labetalol and nifedipine. “[O]ur findings support the use of either labetalol or nifedipine as initial first-line agents for the management of mild chronic hypertension in pregnancy to reduce the risk of adverse maternal and other perinatal outcomes with no increased risk of fetal harm,” the authors write.
Dr. Sanusi reports no relevant financial relationships. Full coauthor disclosures are available with the full text of the paper.
Treatment for chronic hypertension in pregnancy with labetalol showed no significant differences in maternal or neonatal outcomes, compared with treatment with nifedipine, new research indicates.
The open-label, multicenter, randomized CHAP (Chronic Hypertension in Pregnancy) trial showed that treating mild chronic hypertension was better than delaying treatment until severe hypertension developed, but still unclear was whether, or to what extent, the choice of first-line treatment affected outcomes.
Researchers, led by Ayodeji A. Sanusi, MD, MPH, with the Division of Maternal and Fetal Medicine at the University of Alabama at Birmingham, conducted a secondary analysis of CHAP to compare the primary treatments. Mild chronic hypertension in the study was defined as blood pressure of 140-159/90-104 mmHg before 20 weeks of gestation.
Three Comparisons
Three comparisons were performed in 2292 participants based on medications prescribed at enrollment: 720 (31.4%) received labetalol; 417 (18.2%) initially received nifedipine; and 1155 (50.4%) had standard care. Labetalol was compared with standard care; nifedipine was compared with standard care; and labetalol was compared with nifedipine.
The primary outcome was occurrence of superimposed preeclampsia with severe features; preterm birth before 35 weeks of gestation; placental abruption; or fetal or neonatal death. The key secondary outcome was a small-for-gestational age neonate. Researchers also compared adverse effects between groups.
Among the results were the following:
The primary outcome occurred in 30.1% in the labetalol group; 31.2% in the nifedipine group; and 37% in the standard care group.
Risk of the primary outcome was lower among those receiving treatment. For labetalol vs standard care, the adjusted relative risk (RR) was 0.82; 95% confidence interval (CI), 0.72-0.94. For nifedipine vs standard care, the adjusted RR was 0.84; 95% CI, 0.71-0.99. There was no significant difference in risk when labetalol was compared with nifedipine (adjusted RR, 0.98; 95% CI, 0.82-1.18).
There were no significant differences in numbers of small-for-gestational age neonates or serious adverse events between those who received labetalol and those using nifedipine.
Any adverse events were significantly more common with nifedipine, compared with labetalol (35.7% vs 28.3%, P = .009), and with nifedipine, compared with standard care (35.7% vs 26.3%, P = .0003). Adverse event rates were not significantly higher with labetalol when compared with standard care (28.3% vs 26.3%, P = .34). The most frequently reported adverse events were headache, medication intolerance, dizziness, nausea, dyspepsia, neonatal jaundice, and vomiting.
“Thus, labetalol compared with nifedipine appeared to have fewer adverse events and to be better tolerated,” the authors write. They note that labetalol, a third-generation mixed alpha- and beta-adrenergic antagonist, is contraindicated for those who have obstructive pulmonary disease and nifedipine, a dihydropyridine calcium channel blocker, is contraindicated in people with tachycardia.
The authors write that their results align with other studies that have not found differences between labetalol and nifedipine. “[O]ur findings support the use of either labetalol or nifedipine as initial first-line agents for the management of mild chronic hypertension in pregnancy to reduce the risk of adverse maternal and other perinatal outcomes with no increased risk of fetal harm,” the authors write.
Dr. Sanusi reports no relevant financial relationships. Full coauthor disclosures are available with the full text of the paper.
Treatment for chronic hypertension in pregnancy with labetalol showed no significant differences in maternal or neonatal outcomes, compared with treatment with nifedipine, new research indicates.
The open-label, multicenter, randomized CHAP (Chronic Hypertension in Pregnancy) trial showed that treating mild chronic hypertension was better than delaying treatment until severe hypertension developed, but still unclear was whether, or to what extent, the choice of first-line treatment affected outcomes.
Researchers, led by Ayodeji A. Sanusi, MD, MPH, with the Division of Maternal and Fetal Medicine at the University of Alabama at Birmingham, conducted a secondary analysis of CHAP to compare the primary treatments. Mild chronic hypertension in the study was defined as blood pressure of 140-159/90-104 mmHg before 20 weeks of gestation.
Three Comparisons
Three comparisons were performed in 2292 participants based on medications prescribed at enrollment: 720 (31.4%) received labetalol; 417 (18.2%) initially received nifedipine; and 1155 (50.4%) had standard care. Labetalol was compared with standard care; nifedipine was compared with standard care; and labetalol was compared with nifedipine.
The primary outcome was occurrence of superimposed preeclampsia with severe features; preterm birth before 35 weeks of gestation; placental abruption; or fetal or neonatal death. The key secondary outcome was a small-for-gestational age neonate. Researchers also compared adverse effects between groups.
Among the results were the following:
The primary outcome occurred in 30.1% in the labetalol group; 31.2% in the nifedipine group; and 37% in the standard care group.
Risk of the primary outcome was lower among those receiving treatment. For labetalol vs standard care, the adjusted relative risk (RR) was 0.82; 95% confidence interval (CI), 0.72-0.94. For nifedipine vs standard care, the adjusted RR was 0.84; 95% CI, 0.71-0.99. There was no significant difference in risk when labetalol was compared with nifedipine (adjusted RR, 0.98; 95% CI, 0.82-1.18).
There were no significant differences in numbers of small-for-gestational age neonates or serious adverse events between those who received labetalol and those using nifedipine.
Any adverse events were significantly more common with nifedipine, compared with labetalol (35.7% vs 28.3%, P = .009), and with nifedipine, compared with standard care (35.7% vs 26.3%, P = .0003). Adverse event rates were not significantly higher with labetalol when compared with standard care (28.3% vs 26.3%, P = .34). The most frequently reported adverse events were headache, medication intolerance, dizziness, nausea, dyspepsia, neonatal jaundice, and vomiting.
“Thus, labetalol compared with nifedipine appeared to have fewer adverse events and to be better tolerated,” the authors write. They note that labetalol, a third-generation mixed alpha- and beta-adrenergic antagonist, is contraindicated for those who have obstructive pulmonary disease and nifedipine, a dihydropyridine calcium channel blocker, is contraindicated in people with tachycardia.
The authors write that their results align with other studies that have not found differences between labetalol and nifedipine. “[O]ur findings support the use of either labetalol or nifedipine as initial first-line agents for the management of mild chronic hypertension in pregnancy to reduce the risk of adverse maternal and other perinatal outcomes with no increased risk of fetal harm,” the authors write.
Dr. Sanusi reports no relevant financial relationships. Full coauthor disclosures are available with the full text of the paper.