User login
Expert Reviews Options for Revitalizing Dystrophic Nails
LAS VEGAS —
“With the fingernails, we don’t often see onychomycosis, but with toenails, we certainly do,” Tracey C. Vlahovic, DPM, a professor at the Samuel Merritt University College of Podiatric Medicine, Oakland, California, said at the Society of Dermatology Physician Associates (SDPA) 22nd Annual Fall Dermatology Conference. “But toenails are subject to a lot of forces beyond just fungal [infections]. We have the wear and tear of wearing shoes, gait, and other physical activity.”

For example, she continued, some runners develop second-toenail dystrophy “because there’s constant repetitive trauma to the toenail, and [poorly fitting] shoes can contribute to that. Biomechanical issues are a unique consideration when you’re dealing with toenail issues.”
Vlahovic highlighted several options that can help improve the appearance of dystrophic nails as they recover or grow back:
Urea nail preparations: To temporarily soften the nail.
Genadur (hydroxypropyl chitosan): This product “is used mainly for psoriatic nails, but I use it for all different kinds of nail dystrophy,” she said.
DermaNail (acetyl mandelic acid solution): This can be used for brittle nails and fingernails. Vlahovic said she recommends it be used on toenails “in addition to the onychomycosis and other nail dystrophy treatments that I’m doing because it really helps to hydrate the nail unit.”
Kerasal Fungal Nail Renewal (ingredients include propylene glycol, urea, glycerin, and lactic acid): This product is used “for smoothing out the appearance of the nail,” she said.
KeryFlex: Applied in an office setting, this resin-based product restores the appearance of an individual’s natural nails. “It comes in two colors [and] absorbs the shock of what is going on mechanically with the feet,” Vlahovic said. “So, if I’m treating a ballet dancer performing en pointe, or a soccer player, it’s something I can use to protect the nail, but also to make it cosmetically more acceptable.”
NECPro: A nail reconstruction method that involves the use of a composite used mainly by podiatrists, it “helps you not only create a barrier, but to create a natural-looking color that matches your own nail color,” she said.
In Vlahovic’s experience, KeryFlex and NECPro last 6-8 weeks. “You can use nail polish on top of them if you’d like, but they’re basically cosmetic barriers to protect the nail unit,” she said.
Vlahovic has disclosed being a consultant and investigator for Ortho Dermatologics and Sagis Diagnostics.
A version of this article appeared on Medscape.com.
LAS VEGAS —
“With the fingernails, we don’t often see onychomycosis, but with toenails, we certainly do,” Tracey C. Vlahovic, DPM, a professor at the Samuel Merritt University College of Podiatric Medicine, Oakland, California, said at the Society of Dermatology Physician Associates (SDPA) 22nd Annual Fall Dermatology Conference. “But toenails are subject to a lot of forces beyond just fungal [infections]. We have the wear and tear of wearing shoes, gait, and other physical activity.”
For example, she continued, some runners develop second-toenail dystrophy “because there’s constant repetitive trauma to the toenail, and [poorly fitting] shoes can contribute to that. Biomechanical issues are a unique consideration when you’re dealing with toenail issues.”
Vlahovic highlighted several options that can help improve the appearance of dystrophic nails as they recover or grow back:
Urea nail preparations: To temporarily soften the nail.
Genadur (hydroxypropyl chitosan): This product “is used mainly for psoriatic nails, but I use it for all different kinds of nail dystrophy,” she said.
DermaNail (acetyl mandelic acid solution): This can be used for brittle nails and fingernails. Vlahovic said she recommends it be used on toenails “in addition to the onychomycosis and other nail dystrophy treatments that I’m doing because it really helps to hydrate the nail unit.”
Kerasal Fungal Nail Renewal (ingredients include propylene glycol, urea, glycerin, and lactic acid): This product is used “for smoothing out the appearance of the nail,” she said.
KeryFlex: Applied in an office setting, this resin-based product restores the appearance of an individual’s natural nails. “It comes in two colors [and] absorbs the shock of what is going on mechanically with the feet,” Vlahovic said. “So, if I’m treating a ballet dancer performing en pointe, or a soccer player, it’s something I can use to protect the nail, but also to make it cosmetically more acceptable.”
NECPro: A nail reconstruction method that involves the use of a composite used mainly by podiatrists, it “helps you not only create a barrier, but to create a natural-looking color that matches your own nail color,” she said.
In Vlahovic’s experience, KeryFlex and NECPro last 6-8 weeks. “You can use nail polish on top of them if you’d like, but they’re basically cosmetic barriers to protect the nail unit,” she said.
Vlahovic has disclosed being a consultant and investigator for Ortho Dermatologics and Sagis Diagnostics.
A version of this article appeared on Medscape.com.
LAS VEGAS —
“With the fingernails, we don’t often see onychomycosis, but with toenails, we certainly do,” Tracey C. Vlahovic, DPM, a professor at the Samuel Merritt University College of Podiatric Medicine, Oakland, California, said at the Society of Dermatology Physician Associates (SDPA) 22nd Annual Fall Dermatology Conference. “But toenails are subject to a lot of forces beyond just fungal [infections]. We have the wear and tear of wearing shoes, gait, and other physical activity.”
For example, she continued, some runners develop second-toenail dystrophy “because there’s constant repetitive trauma to the toenail, and [poorly fitting] shoes can contribute to that. Biomechanical issues are a unique consideration when you’re dealing with toenail issues.”
Vlahovic highlighted several options that can help improve the appearance of dystrophic nails as they recover or grow back:
Urea nail preparations: To temporarily soften the nail.
Genadur (hydroxypropyl chitosan): This product “is used mainly for psoriatic nails, but I use it for all different kinds of nail dystrophy,” she said.
DermaNail (acetyl mandelic acid solution): This can be used for brittle nails and fingernails. Vlahovic said she recommends it be used on toenails “in addition to the onychomycosis and other nail dystrophy treatments that I’m doing because it really helps to hydrate the nail unit.”
Kerasal Fungal Nail Renewal (ingredients include propylene glycol, urea, glycerin, and lactic acid): This product is used “for smoothing out the appearance of the nail,” she said.
KeryFlex: Applied in an office setting, this resin-based product restores the appearance of an individual’s natural nails. “It comes in two colors [and] absorbs the shock of what is going on mechanically with the feet,” Vlahovic said. “So, if I’m treating a ballet dancer performing en pointe, or a soccer player, it’s something I can use to protect the nail, but also to make it cosmetically more acceptable.”
NECPro: A nail reconstruction method that involves the use of a composite used mainly by podiatrists, it “helps you not only create a barrier, but to create a natural-looking color that matches your own nail color,” she said.
In Vlahovic’s experience, KeryFlex and NECPro last 6-8 weeks. “You can use nail polish on top of them if you’d like, but they’re basically cosmetic barriers to protect the nail unit,” she said.
Vlahovic has disclosed being a consultant and investigator for Ortho Dermatologics and Sagis Diagnostics.
A version of this article appeared on Medscape.com.
FROM SDPA 24
Does Antibiotic Use During Influenza Infection Worsen Lung Immunity?
TOPLINE:
Antibiotic use during influenza infection increases lung eosinophils, impairing immunity against secondary bacterial pneumonia. This study highlights the detrimental effects of antibiotics on lung health during viral infections.
METHODOLOGY:
- Researchers conducted a murine model study to evaluate the impact of antibiotic use during influenza infection on lung immunity. Mice were treated with a broad-spectrum antibiotic cocktail (vancomycin, neomycin, ampicillin, and metronidazole) starting 7 days before influenza infection.
- The study included intranasal infection with influenza virus followed by a secondary challenge with methicillin-resistant Staphylococcus aureus (MRSA).
- Finally, in sub-study, a total of three cohorts of hospitalized patients were evaluated to correlate eosinophil levels with antibiotic use, systemic inflammation, and outcomes.
TAKEAWAY:
- Antibiotic use during influenza infection impairs lung immunity, leading to increased lung eosinophils and reduced macrophage function.
- The study found that antibiotic treatment during influenza infection caused fungal dysbiosis, driving lung eosinophilia and impairing MRSA clearance.
- The detrimental effects of antibiotics on lung immunity were specific to the two-hit model of influenza followed by MRSA infection in mice.
- In hospitalized patients, eosinophil levels positively correlated with antibiotic use, systemic inflammation, and worsened outcomes.
IN PRACTICE:
“Our study highlights the pernicious effects of antibiotic use during viral infections and defines a mechanism whereby antibiotics perturb the gut mycobiome and result in lung eosinophilia. In turn, lung eosinophils, via release of MBP-1, suppress alveolar macrophage clearance of bacteria,” the authors of the study wrote.
SOURCE:
This study was led by Marilia Sanches Santos Rizzo Zuttion, Cedars-Sinai Medical Center in Los Angeles. It was published online in The Journal of Clinical Investigation.
LIMITATIONS:
This study’s limitations included the use of a murine model, which may not fully replicate human immune responses. Additionally, the study focused on a specific antibiotic cocktail, and results may vary with different antibiotics. The findings were also specific to the two-hit model of influenza followed by MRSA infection, limiting generalizability to other infections.
DISCLOSURES:
This study was supported by grants from the National Institutes of Health. Marilia Sanches Santos Rizzo Zuttion received research funding from Pfizer Inc. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Antibiotic use during influenza infection increases lung eosinophils, impairing immunity against secondary bacterial pneumonia. This study highlights the detrimental effects of antibiotics on lung health during viral infections.
METHODOLOGY:
- Researchers conducted a murine model study to evaluate the impact of antibiotic use during influenza infection on lung immunity. Mice were treated with a broad-spectrum antibiotic cocktail (vancomycin, neomycin, ampicillin, and metronidazole) starting 7 days before influenza infection.
- The study included intranasal infection with influenza virus followed by a secondary challenge with methicillin-resistant Staphylococcus aureus (MRSA).
- Finally, in sub-study, a total of three cohorts of hospitalized patients were evaluated to correlate eosinophil levels with antibiotic use, systemic inflammation, and outcomes.
TAKEAWAY:
- Antibiotic use during influenza infection impairs lung immunity, leading to increased lung eosinophils and reduced macrophage function.
- The study found that antibiotic treatment during influenza infection caused fungal dysbiosis, driving lung eosinophilia and impairing MRSA clearance.
- The detrimental effects of antibiotics on lung immunity were specific to the two-hit model of influenza followed by MRSA infection in mice.
- In hospitalized patients, eosinophil levels positively correlated with antibiotic use, systemic inflammation, and worsened outcomes.
IN PRACTICE:
“Our study highlights the pernicious effects of antibiotic use during viral infections and defines a mechanism whereby antibiotics perturb the gut mycobiome and result in lung eosinophilia. In turn, lung eosinophils, via release of MBP-1, suppress alveolar macrophage clearance of bacteria,” the authors of the study wrote.
SOURCE:
This study was led by Marilia Sanches Santos Rizzo Zuttion, Cedars-Sinai Medical Center in Los Angeles. It was published online in The Journal of Clinical Investigation.
LIMITATIONS:
This study’s limitations included the use of a murine model, which may not fully replicate human immune responses. Additionally, the study focused on a specific antibiotic cocktail, and results may vary with different antibiotics. The findings were also specific to the two-hit model of influenza followed by MRSA infection, limiting generalizability to other infections.
DISCLOSURES:
This study was supported by grants from the National Institutes of Health. Marilia Sanches Santos Rizzo Zuttion received research funding from Pfizer Inc. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Antibiotic use during influenza infection increases lung eosinophils, impairing immunity against secondary bacterial pneumonia. This study highlights the detrimental effects of antibiotics on lung health during viral infections.
METHODOLOGY:
- Researchers conducted a murine model study to evaluate the impact of antibiotic use during influenza infection on lung immunity. Mice were treated with a broad-spectrum antibiotic cocktail (vancomycin, neomycin, ampicillin, and metronidazole) starting 7 days before influenza infection.
- The study included intranasal infection with influenza virus followed by a secondary challenge with methicillin-resistant Staphylococcus aureus (MRSA).
- Finally, in sub-study, a total of three cohorts of hospitalized patients were evaluated to correlate eosinophil levels with antibiotic use, systemic inflammation, and outcomes.
TAKEAWAY:
- Antibiotic use during influenza infection impairs lung immunity, leading to increased lung eosinophils and reduced macrophage function.
- The study found that antibiotic treatment during influenza infection caused fungal dysbiosis, driving lung eosinophilia and impairing MRSA clearance.
- The detrimental effects of antibiotics on lung immunity were specific to the two-hit model of influenza followed by MRSA infection in mice.
- In hospitalized patients, eosinophil levels positively correlated with antibiotic use, systemic inflammation, and worsened outcomes.
IN PRACTICE:
“Our study highlights the pernicious effects of antibiotic use during viral infections and defines a mechanism whereby antibiotics perturb the gut mycobiome and result in lung eosinophilia. In turn, lung eosinophils, via release of MBP-1, suppress alveolar macrophage clearance of bacteria,” the authors of the study wrote.
SOURCE:
This study was led by Marilia Sanches Santos Rizzo Zuttion, Cedars-Sinai Medical Center in Los Angeles. It was published online in The Journal of Clinical Investigation.
LIMITATIONS:
This study’s limitations included the use of a murine model, which may not fully replicate human immune responses. Additionally, the study focused on a specific antibiotic cocktail, and results may vary with different antibiotics. The findings were also specific to the two-hit model of influenza followed by MRSA infection, limiting generalizability to other infections.
DISCLOSURES:
This study was supported by grants from the National Institutes of Health. Marilia Sanches Santos Rizzo Zuttion received research funding from Pfizer Inc. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Periodontitis Management: GPs Should Play a Role
Periodontitis is a chronic inflammatory disease that triggers a local immuno-inflammatory response, potentially leading to periodontal tissue destruction and tooth loss. Affecting 1.1 billion people worldwide, periodontitis is recognized as a significant public health issue. It is also linked to a number of other conditions, such as diabetes, cardiovascular disease, and respiratory disorders. The European Federation of Periodontology recently published a consensus report recommending that the optimal management of periodontitis should involve a collaboration between general practitioners (GPs) and oral health professionals.
Diabetes and Periodontitis
A bidirectional association exists between diabetes and periodontitis. Hyperglycemia accelerates periodontitis progression by promoting inflammation and hindering the healing process, while periodontitis is associated with higher hemoglobin A1c levels in patients with diabetes and an increased risk for diabetes development in others. Intervention studies have demonstrated the positive effect of glycemic control on periodontitis and vice versa, with periodontal treatment improving A1c levels.
GPs can raise awareness of the links between these conditions as well as emphasize the benefits of addressing both metabolic and periodontal abnormalities. They should refer patients with diabetes to oral health specialists and look for signs of periodontitis, such as bleeding gums and loose teeth, in patients with diabetes and those with prediabetes.
Cardiovascular Diseases and Periodontitis
Cardiovascular diseases and periodontitis are linked by their epidemiological associations and common biologic mechanisms. This connection can be explained by some of their shared risk factors, such as smoking and systemic inflammatory pathways. Although no intervention studies have shown a direct reduction in cardiovascular risk from periodontal care, two studies have demonstrated improvements in surrogate markers such as blood pressure and arterial stiffness. GPs should inquire about symptoms of periodontitis in cardiovascular patients and, if necessary, refer them to oral health specialists. Periodontal treatments, whether surgical or nonsurgical, pose no risk for patients receiving well-managed secondary preventive treatments.
Respiratory Diseases and Periodontitis
The primary evidence linking periodontitis with chronic respiratory diseases concerns chronic obstructive pulmonary disease (COPD). Individuals with periodontitis have a 33% higher risk of developing COPD, and patients with COPD and periodontitis may experience a greater decline in lung function. An established association also exists between periodontitis and obstructive sleep apnea, although the data remain inconclusive regarding a link with asthma. GPs should encourage patients with COPD to quit smoking, as it benefits both respiratory and oral health.
Finally, based on meta-analyses of COVID-19, experts note significant associations between periodontitis and the need for assisted ventilation or the risk for death during a COVID-19 infection.
This story was translated from Univadis France using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Periodontitis is a chronic inflammatory disease that triggers a local immuno-inflammatory response, potentially leading to periodontal tissue destruction and tooth loss. Affecting 1.1 billion people worldwide, periodontitis is recognized as a significant public health issue. It is also linked to a number of other conditions, such as diabetes, cardiovascular disease, and respiratory disorders. The European Federation of Periodontology recently published a consensus report recommending that the optimal management of periodontitis should involve a collaboration between general practitioners (GPs) and oral health professionals.
Diabetes and Periodontitis
A bidirectional association exists between diabetes and periodontitis. Hyperglycemia accelerates periodontitis progression by promoting inflammation and hindering the healing process, while periodontitis is associated with higher hemoglobin A1c levels in patients with diabetes and an increased risk for diabetes development in others. Intervention studies have demonstrated the positive effect of glycemic control on periodontitis and vice versa, with periodontal treatment improving A1c levels.
GPs can raise awareness of the links between these conditions as well as emphasize the benefits of addressing both metabolic and periodontal abnormalities. They should refer patients with diabetes to oral health specialists and look for signs of periodontitis, such as bleeding gums and loose teeth, in patients with diabetes and those with prediabetes.
Cardiovascular Diseases and Periodontitis
Cardiovascular diseases and periodontitis are linked by their epidemiological associations and common biologic mechanisms. This connection can be explained by some of their shared risk factors, such as smoking and systemic inflammatory pathways. Although no intervention studies have shown a direct reduction in cardiovascular risk from periodontal care, two studies have demonstrated improvements in surrogate markers such as blood pressure and arterial stiffness. GPs should inquire about symptoms of periodontitis in cardiovascular patients and, if necessary, refer them to oral health specialists. Periodontal treatments, whether surgical or nonsurgical, pose no risk for patients receiving well-managed secondary preventive treatments.
Respiratory Diseases and Periodontitis
The primary evidence linking periodontitis with chronic respiratory diseases concerns chronic obstructive pulmonary disease (COPD). Individuals with periodontitis have a 33% higher risk of developing COPD, and patients with COPD and periodontitis may experience a greater decline in lung function. An established association also exists between periodontitis and obstructive sleep apnea, although the data remain inconclusive regarding a link with asthma. GPs should encourage patients with COPD to quit smoking, as it benefits both respiratory and oral health.
Finally, based on meta-analyses of COVID-19, experts note significant associations between periodontitis and the need for assisted ventilation or the risk for death during a COVID-19 infection.
This story was translated from Univadis France using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Periodontitis is a chronic inflammatory disease that triggers a local immuno-inflammatory response, potentially leading to periodontal tissue destruction and tooth loss. Affecting 1.1 billion people worldwide, periodontitis is recognized as a significant public health issue. It is also linked to a number of other conditions, such as diabetes, cardiovascular disease, and respiratory disorders. The European Federation of Periodontology recently published a consensus report recommending that the optimal management of periodontitis should involve a collaboration between general practitioners (GPs) and oral health professionals.
Diabetes and Periodontitis
A bidirectional association exists between diabetes and periodontitis. Hyperglycemia accelerates periodontitis progression by promoting inflammation and hindering the healing process, while periodontitis is associated with higher hemoglobin A1c levels in patients with diabetes and an increased risk for diabetes development in others. Intervention studies have demonstrated the positive effect of glycemic control on periodontitis and vice versa, with periodontal treatment improving A1c levels.
GPs can raise awareness of the links between these conditions as well as emphasize the benefits of addressing both metabolic and periodontal abnormalities. They should refer patients with diabetes to oral health specialists and look for signs of periodontitis, such as bleeding gums and loose teeth, in patients with diabetes and those with prediabetes.
Cardiovascular Diseases and Periodontitis
Cardiovascular diseases and periodontitis are linked by their epidemiological associations and common biologic mechanisms. This connection can be explained by some of their shared risk factors, such as smoking and systemic inflammatory pathways. Although no intervention studies have shown a direct reduction in cardiovascular risk from periodontal care, two studies have demonstrated improvements in surrogate markers such as blood pressure and arterial stiffness. GPs should inquire about symptoms of periodontitis in cardiovascular patients and, if necessary, refer them to oral health specialists. Periodontal treatments, whether surgical or nonsurgical, pose no risk for patients receiving well-managed secondary preventive treatments.
Respiratory Diseases and Periodontitis
The primary evidence linking periodontitis with chronic respiratory diseases concerns chronic obstructive pulmonary disease (COPD). Individuals with periodontitis have a 33% higher risk of developing COPD, and patients with COPD and periodontitis may experience a greater decline in lung function. An established association also exists between periodontitis and obstructive sleep apnea, although the data remain inconclusive regarding a link with asthma. GPs should encourage patients with COPD to quit smoking, as it benefits both respiratory and oral health.
Finally, based on meta-analyses of COVID-19, experts note significant associations between periodontitis and the need for assisted ventilation or the risk for death during a COVID-19 infection.
This story was translated from Univadis France using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
New Cause of Sexually Transmitted Fungal Infection Reported in MSM
A dermatophyte known as Trichophyton mentagrophytes genotype VII (TMVII) has been identified as the cause of an emerging sexually transmitted fungal infection in four adults in the United States, according to a paper published in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report.
TMVII is a sexually transmitted fungus that causes genital tinea; the fungus might be misidentified as eczema, psoriasis, or other dermatologic conditions, Jason E. Zucker, MD, an infectious disease specialist at Columbia University Irving Medical Center, New York City, and colleagues wrote.

“Dermatophyte infections, including TMVII, are spread through direct skin-to-skin contact,” corresponding author Avrom S. Caplan, MD, a dermatologist at New York University Grossman School of Medicine, New York City, said in an interview.
“In the United States, to our knowledge, the infection has only been in MSM [men who have sex with men], but there have been reports of TMVII in Europe in non-MSM patients, including among patients who traveled to Southeast Asia for sex tourism or partners of people who have been infected with TMVII,” he said.
The four patients were diagnosed with tinea between April 2024 and July 2024, and fungal cultures and DNA sequencing identified TMVII as the cause of the infection. All four patients were cisgender men aged 30-39 years from New York City who reported recent sexual contact with other men; one was a sex worker, two had sex with each other, and one reported recent travel to Europe.
All four patients presented with rashes on the face, buttocks, or genitals; all were successfully treated with antifungals, the authors wrote.
Individuals with genital lesions who are sexually active should be seen by a healthcare provider, and TMVII should be considered, especially in the event of scaly, itchy, or inflamed rashes elsewhere on the body, Caplan told this news organization.
Additionally, “If someone presents for a medical evaluation and has ringworm on the buttocks, face, or elsewhere, especially if they are sexually active, the question of TMVII should arise, and the patient should be asked about possible genital lesions as well,” he said. “Any patient diagnosed with an STI [sexually transmitted infection], including MSM patients, should be evaluated appropriately for other STIs including TMVII.”
Continued surveillance and monitoring are needed to track TMVII and to better understand emerging infections, Caplan told this news organization. Clinicians can find more information and a dermatophyte registry via the American Academy of Dermatology websites on emerging diseases in general and dermatophytes in particular.
“We also need better access to testing and more rapid confirmatory testing to detect emerging dermatophyte strains and monitor antifungal resistance patterns,” Caplan added. “At this time, we do not have evidence to suggest there is antifungal resistance in TMVII, which also distinguishes it from T indotineae.”
Encourage Reporting and Identify New Infections
“Emerging infections can mimic noninfectious disease processes, which can make the diagnosis challenging,” Shirin A. Mazumder, MD, associate professor and infectious disease specialist at the University of Tennessee Health Science Center, Memphis, said in an interview.
“Monitoring emerging infections can be difficult if the cases are not reported and if the disease is not widespread,” Mazumder noted. Educating clinicians with case reports and encouraging them to report unusual cases to public health helps to overcome this challenge.
In the clinical setting, skin lesions that fail to respond or worsen with the application of topical steroids could be a red flag for TMVII, Mazumder told this news organization. “Since the skin findings of TMVII can closely resemble noninfectious processes such as eczema or psoriasis, the use of topical corticosteroids may have already been tried before the diagnosis of TMVII is considered.”
Also, location matters in making the diagnosis. TMVII lesions occur on the face, genitals, extremities, trunk, and buttocks. Obtaining a thorough sexual history is important because the fungus spreads from close contact through sexual exposure, Mazumder added.
The most effective treatment for TMVII infections remains to be determined, Mazumder said. “Treatment considerations such as combination treatment with oral and topical antifungal medications vs oral antifungal medication alone is something that needs further research along with the best treatment duration.”
“Determining the rate of transmissibility between contacts, when someone is considered to be the most infectious, how long someone is considered infectious once infected, and rates of reinfection are questions that may benefit from further study,” she added.
Although the current cases are reported in MSM, determining how TMVII affects other patient populations will be interesting as more cases are reported, said Mazumder. “Further understanding of how different degrees of immunosuppression affect TMVII disease course is another important consideration.”
Finally, determining the rate of long-term sequelae from TMVII infection and the rate of bacterial co-infection will help better understand TMVII, she said.
The researchers had no financial conflicts to disclose. Mazumder had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
A dermatophyte known as Trichophyton mentagrophytes genotype VII (TMVII) has been identified as the cause of an emerging sexually transmitted fungal infection in four adults in the United States, according to a paper published in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report.
TMVII is a sexually transmitted fungus that causes genital tinea; the fungus might be misidentified as eczema, psoriasis, or other dermatologic conditions, Jason E. Zucker, MD, an infectious disease specialist at Columbia University Irving Medical Center, New York City, and colleagues wrote.
“Dermatophyte infections, including TMVII, are spread through direct skin-to-skin contact,” corresponding author Avrom S. Caplan, MD, a dermatologist at New York University Grossman School of Medicine, New York City, said in an interview.
“In the United States, to our knowledge, the infection has only been in MSM [men who have sex with men], but there have been reports of TMVII in Europe in non-MSM patients, including among patients who traveled to Southeast Asia for sex tourism or partners of people who have been infected with TMVII,” he said.
The four patients were diagnosed with tinea between April 2024 and July 2024, and fungal cultures and DNA sequencing identified TMVII as the cause of the infection. All four patients were cisgender men aged 30-39 years from New York City who reported recent sexual contact with other men; one was a sex worker, two had sex with each other, and one reported recent travel to Europe.
All four patients presented with rashes on the face, buttocks, or genitals; all were successfully treated with antifungals, the authors wrote.
Individuals with genital lesions who are sexually active should be seen by a healthcare provider, and TMVII should be considered, especially in the event of scaly, itchy, or inflamed rashes elsewhere on the body, Caplan told this news organization.
Additionally, “If someone presents for a medical evaluation and has ringworm on the buttocks, face, or elsewhere, especially if they are sexually active, the question of TMVII should arise, and the patient should be asked about possible genital lesions as well,” he said. “Any patient diagnosed with an STI [sexually transmitted infection], including MSM patients, should be evaluated appropriately for other STIs including TMVII.”
Continued surveillance and monitoring are needed to track TMVII and to better understand emerging infections, Caplan told this news organization. Clinicians can find more information and a dermatophyte registry via the American Academy of Dermatology websites on emerging diseases in general and dermatophytes in particular.
“We also need better access to testing and more rapid confirmatory testing to detect emerging dermatophyte strains and monitor antifungal resistance patterns,” Caplan added. “At this time, we do not have evidence to suggest there is antifungal resistance in TMVII, which also distinguishes it from T indotineae.”
Encourage Reporting and Identify New Infections
“Emerging infections can mimic noninfectious disease processes, which can make the diagnosis challenging,” Shirin A. Mazumder, MD, associate professor and infectious disease specialist at the University of Tennessee Health Science Center, Memphis, said in an interview.
“Monitoring emerging infections can be difficult if the cases are not reported and if the disease is not widespread,” Mazumder noted. Educating clinicians with case reports and encouraging them to report unusual cases to public health helps to overcome this challenge.
In the clinical setting, skin lesions that fail to respond or worsen with the application of topical steroids could be a red flag for TMVII, Mazumder told this news organization. “Since the skin findings of TMVII can closely resemble noninfectious processes such as eczema or psoriasis, the use of topical corticosteroids may have already been tried before the diagnosis of TMVII is considered.”
Also, location matters in making the diagnosis. TMVII lesions occur on the face, genitals, extremities, trunk, and buttocks. Obtaining a thorough sexual history is important because the fungus spreads from close contact through sexual exposure, Mazumder added.
The most effective treatment for TMVII infections remains to be determined, Mazumder said. “Treatment considerations such as combination treatment with oral and topical antifungal medications vs oral antifungal medication alone is something that needs further research along with the best treatment duration.”
“Determining the rate of transmissibility between contacts, when someone is considered to be the most infectious, how long someone is considered infectious once infected, and rates of reinfection are questions that may benefit from further study,” she added.
Although the current cases are reported in MSM, determining how TMVII affects other patient populations will be interesting as more cases are reported, said Mazumder. “Further understanding of how different degrees of immunosuppression affect TMVII disease course is another important consideration.”
Finally, determining the rate of long-term sequelae from TMVII infection and the rate of bacterial co-infection will help better understand TMVII, she said.
The researchers had no financial conflicts to disclose. Mazumder had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
A dermatophyte known as Trichophyton mentagrophytes genotype VII (TMVII) has been identified as the cause of an emerging sexually transmitted fungal infection in four adults in the United States, according to a paper published in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report.
TMVII is a sexually transmitted fungus that causes genital tinea; the fungus might be misidentified as eczema, psoriasis, or other dermatologic conditions, Jason E. Zucker, MD, an infectious disease specialist at Columbia University Irving Medical Center, New York City, and colleagues wrote.
“Dermatophyte infections, including TMVII, are spread through direct skin-to-skin contact,” corresponding author Avrom S. Caplan, MD, a dermatologist at New York University Grossman School of Medicine, New York City, said in an interview.
“In the United States, to our knowledge, the infection has only been in MSM [men who have sex with men], but there have been reports of TMVII in Europe in non-MSM patients, including among patients who traveled to Southeast Asia for sex tourism or partners of people who have been infected with TMVII,” he said.
The four patients were diagnosed with tinea between April 2024 and July 2024, and fungal cultures and DNA sequencing identified TMVII as the cause of the infection. All four patients were cisgender men aged 30-39 years from New York City who reported recent sexual contact with other men; one was a sex worker, two had sex with each other, and one reported recent travel to Europe.
All four patients presented with rashes on the face, buttocks, or genitals; all were successfully treated with antifungals, the authors wrote.
Individuals with genital lesions who are sexually active should be seen by a healthcare provider, and TMVII should be considered, especially in the event of scaly, itchy, or inflamed rashes elsewhere on the body, Caplan told this news organization.
Additionally, “If someone presents for a medical evaluation and has ringworm on the buttocks, face, or elsewhere, especially if they are sexually active, the question of TMVII should arise, and the patient should be asked about possible genital lesions as well,” he said. “Any patient diagnosed with an STI [sexually transmitted infection], including MSM patients, should be evaluated appropriately for other STIs including TMVII.”
Continued surveillance and monitoring are needed to track TMVII and to better understand emerging infections, Caplan told this news organization. Clinicians can find more information and a dermatophyte registry via the American Academy of Dermatology websites on emerging diseases in general and dermatophytes in particular.
“We also need better access to testing and more rapid confirmatory testing to detect emerging dermatophyte strains and monitor antifungal resistance patterns,” Caplan added. “At this time, we do not have evidence to suggest there is antifungal resistance in TMVII, which also distinguishes it from T indotineae.”
Encourage Reporting and Identify New Infections
“Emerging infections can mimic noninfectious disease processes, which can make the diagnosis challenging,” Shirin A. Mazumder, MD, associate professor and infectious disease specialist at the University of Tennessee Health Science Center, Memphis, said in an interview.
“Monitoring emerging infections can be difficult if the cases are not reported and if the disease is not widespread,” Mazumder noted. Educating clinicians with case reports and encouraging them to report unusual cases to public health helps to overcome this challenge.
In the clinical setting, skin lesions that fail to respond or worsen with the application of topical steroids could be a red flag for TMVII, Mazumder told this news organization. “Since the skin findings of TMVII can closely resemble noninfectious processes such as eczema or psoriasis, the use of topical corticosteroids may have already been tried before the diagnosis of TMVII is considered.”
Also, location matters in making the diagnosis. TMVII lesions occur on the face, genitals, extremities, trunk, and buttocks. Obtaining a thorough sexual history is important because the fungus spreads from close contact through sexual exposure, Mazumder added.
The most effective treatment for TMVII infections remains to be determined, Mazumder said. “Treatment considerations such as combination treatment with oral and topical antifungal medications vs oral antifungal medication alone is something that needs further research along with the best treatment duration.”
“Determining the rate of transmissibility between contacts, when someone is considered to be the most infectious, how long someone is considered infectious once infected, and rates of reinfection are questions that may benefit from further study,” she added.
Although the current cases are reported in MSM, determining how TMVII affects other patient populations will be interesting as more cases are reported, said Mazumder. “Further understanding of how different degrees of immunosuppression affect TMVII disease course is another important consideration.”
Finally, determining the rate of long-term sequelae from TMVII infection and the rate of bacterial co-infection will help better understand TMVII, she said.
The researchers had no financial conflicts to disclose. Mazumder had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
FROM THE MMWR
Does Bezlotoxumab Boost FMT Efficacy in IBD Patients With Recurrent CDI?
PHILADELPHIA – , according to a randomized controlled trial.
“Given the high efficacy of FMT, the addition of bezlotoxumab may not provide a further reduction in CDI recurrence,” said study author Jessica R. Allegretti, MD, MPH, AGAF, with Brigham and Women’s Hospital and Harvard Medical School, Boston, Massachusetts.
Allegretti presented the findings during a plenary session at the annual meeting of the American College of Gastroenterology (ACG).

Common and Deadly
CDI is the most common cause of healthcare-associated infection in the United States, leading to roughly 4.8 billion in excess healthcare costs. There are an estimated 500,000 cases each year in the United States, with roughly 30,000 of those cases leading to death.
Patients with IBD have a prevalence of CDI that is 2.5- to 8-fold higher than in peers without IBD, and they also have 4.5-fold higher risk of recurrence. Sequelae of CDI in IBD include exacerbations of IBD, increased hospitalizations, escalation of IBD therapy, and colectomy.
FMT has been shown to be safe and effective in patients with IBD and rCDI.
Bezlotoxumab — a fully human monoclonal antibody that binds to C difficile toxin B — was approved by the US Food and Drug Administration (FDA) in 2016 to reduce the recurrence of CDI in patients aged 18 years and older.
However, there is only limited data on the value of combining these two strategies.
Allegretti and colleagues conducted a multicenter randomized controlled trial to evaluate the impact of FMT in combination with bezlotoxumab in patients with IBD and rCDI.
They enrolled 61 patients (mean age, 38 years, 54% men) with two or more episodes of CDI who received a single colonoscopic FMT. Twenty patients had Crohn’s disease, and 41 had ulcerative colitis.
Thirty patients were randomly allocated to receive a single bezlotoxumab infusion and 31 to receive a placebo infusion prior to FMT.
A total of five participants (8%) experienced a CDI recurrence with confirmed EIA+ stool –4 in the treatment group and 1 in the placebo group (13% vs 3%, P = .15).
Participants in the treatment group had higher odds of CDI recurrence, though this was not statistically significant (odds ratio [OR], 4.6; 95% CI, 0.5-43.9), Allegretti reported.
With regards to C difficile colonization, more patients in the treatment group were decolonized compared with placebo at week 1 (82% vs 68%, P = .22) and at week 12 (83% vs 72%, P = .34).
Steroid use at the time of FMT was associated with a significant increased risk of ongoing colonization of C difficile at week 12 post-FMT (OR, 4.90; 95% CI, 1.18-20.37; P = .03).
While there were no significant differences in IBD outcomes between groups, there were numerically higher rates of IBD improvement in the treatment group compared to the placebo group 56% vs 46%.
Only one patient had IBD worsen, and this patient was in the placebo group. There were no de novo IBD flares.
FMT alone and with bezlotoxumab were both safe and well tolerated. Two serious adverse events were reported; neither were deemed to be treatment-related.
“This is the first clinical trial to assess the clinical effect of FMT in combination with bezlotoxumab in patients with IBD and rCDI. The data suggest no clear efficacy benefit to this combination compared to FMT alone,” Allegretti told attendees.
“This finding is not surprising given the high rate of efficacy of FMT,” said Ashwin N. Ananthakrishnan, MD, MPH, AGAF, with Massachusetts General Hospital and Harvard Medical School, Boston, who was not involved in the study.

“It would have been interesting to compare bezlotoxumab vs FMT as primary treatment for recurrent CDI in this population,” Ananthakrishnan added.
This was an investigator-initiated study funded by Merck. Allegretti disclosed various relationships with Abbvie, Artugen, Bristol Myers Squibb, Ferring, Finch Therapeutics, Janssen, Merck, Pfizer, and Seres. Ananthakrishnan had no relevant disclosures.
A version of this article first appeared on Medscape.com.
PHILADELPHIA – , according to a randomized controlled trial.
“Given the high efficacy of FMT, the addition of bezlotoxumab may not provide a further reduction in CDI recurrence,” said study author Jessica R. Allegretti, MD, MPH, AGAF, with Brigham and Women’s Hospital and Harvard Medical School, Boston, Massachusetts.
Allegretti presented the findings during a plenary session at the annual meeting of the American College of Gastroenterology (ACG).
Common and Deadly
CDI is the most common cause of healthcare-associated infection in the United States, leading to roughly 4.8 billion in excess healthcare costs. There are an estimated 500,000 cases each year in the United States, with roughly 30,000 of those cases leading to death.
Patients with IBD have a prevalence of CDI that is 2.5- to 8-fold higher than in peers without IBD, and they also have 4.5-fold higher risk of recurrence. Sequelae of CDI in IBD include exacerbations of IBD, increased hospitalizations, escalation of IBD therapy, and colectomy.
FMT has been shown to be safe and effective in patients with IBD and rCDI.
Bezlotoxumab — a fully human monoclonal antibody that binds to C difficile toxin B — was approved by the US Food and Drug Administration (FDA) in 2016 to reduce the recurrence of CDI in patients aged 18 years and older.
However, there is only limited data on the value of combining these two strategies.
Allegretti and colleagues conducted a multicenter randomized controlled trial to evaluate the impact of FMT in combination with bezlotoxumab in patients with IBD and rCDI.
They enrolled 61 patients (mean age, 38 years, 54% men) with two or more episodes of CDI who received a single colonoscopic FMT. Twenty patients had Crohn’s disease, and 41 had ulcerative colitis.
Thirty patients were randomly allocated to receive a single bezlotoxumab infusion and 31 to receive a placebo infusion prior to FMT.
A total of five participants (8%) experienced a CDI recurrence with confirmed EIA+ stool –4 in the treatment group and 1 in the placebo group (13% vs 3%, P = .15).
Participants in the treatment group had higher odds of CDI recurrence, though this was not statistically significant (odds ratio [OR], 4.6; 95% CI, 0.5-43.9), Allegretti reported.
With regards to C difficile colonization, more patients in the treatment group were decolonized compared with placebo at week 1 (82% vs 68%, P = .22) and at week 12 (83% vs 72%, P = .34).
Steroid use at the time of FMT was associated with a significant increased risk of ongoing colonization of C difficile at week 12 post-FMT (OR, 4.90; 95% CI, 1.18-20.37; P = .03).
While there were no significant differences in IBD outcomes between groups, there were numerically higher rates of IBD improvement in the treatment group compared to the placebo group 56% vs 46%.
Only one patient had IBD worsen, and this patient was in the placebo group. There were no de novo IBD flares.
FMT alone and with bezlotoxumab were both safe and well tolerated. Two serious adverse events were reported; neither were deemed to be treatment-related.
“This is the first clinical trial to assess the clinical effect of FMT in combination with bezlotoxumab in patients with IBD and rCDI. The data suggest no clear efficacy benefit to this combination compared to FMT alone,” Allegretti told attendees.
“This finding is not surprising given the high rate of efficacy of FMT,” said Ashwin N. Ananthakrishnan, MD, MPH, AGAF, with Massachusetts General Hospital and Harvard Medical School, Boston, who was not involved in the study.
“It would have been interesting to compare bezlotoxumab vs FMT as primary treatment for recurrent CDI in this population,” Ananthakrishnan added.
This was an investigator-initiated study funded by Merck. Allegretti disclosed various relationships with Abbvie, Artugen, Bristol Myers Squibb, Ferring, Finch Therapeutics, Janssen, Merck, Pfizer, and Seres. Ananthakrishnan had no relevant disclosures.
A version of this article first appeared on Medscape.com.
PHILADELPHIA – , according to a randomized controlled trial.
“Given the high efficacy of FMT, the addition of bezlotoxumab may not provide a further reduction in CDI recurrence,” said study author Jessica R. Allegretti, MD, MPH, AGAF, with Brigham and Women’s Hospital and Harvard Medical School, Boston, Massachusetts.
Allegretti presented the findings during a plenary session at the annual meeting of the American College of Gastroenterology (ACG).
Common and Deadly
CDI is the most common cause of healthcare-associated infection in the United States, leading to roughly 4.8 billion in excess healthcare costs. There are an estimated 500,000 cases each year in the United States, with roughly 30,000 of those cases leading to death.
Patients with IBD have a prevalence of CDI that is 2.5- to 8-fold higher than in peers without IBD, and they also have 4.5-fold higher risk of recurrence. Sequelae of CDI in IBD include exacerbations of IBD, increased hospitalizations, escalation of IBD therapy, and colectomy.
FMT has been shown to be safe and effective in patients with IBD and rCDI.
Bezlotoxumab — a fully human monoclonal antibody that binds to C difficile toxin B — was approved by the US Food and Drug Administration (FDA) in 2016 to reduce the recurrence of CDI in patients aged 18 years and older.
However, there is only limited data on the value of combining these two strategies.
Allegretti and colleagues conducted a multicenter randomized controlled trial to evaluate the impact of FMT in combination with bezlotoxumab in patients with IBD and rCDI.
They enrolled 61 patients (mean age, 38 years, 54% men) with two or more episodes of CDI who received a single colonoscopic FMT. Twenty patients had Crohn’s disease, and 41 had ulcerative colitis.
Thirty patients were randomly allocated to receive a single bezlotoxumab infusion and 31 to receive a placebo infusion prior to FMT.
A total of five participants (8%) experienced a CDI recurrence with confirmed EIA+ stool –4 in the treatment group and 1 in the placebo group (13% vs 3%, P = .15).
Participants in the treatment group had higher odds of CDI recurrence, though this was not statistically significant (odds ratio [OR], 4.6; 95% CI, 0.5-43.9), Allegretti reported.
With regards to C difficile colonization, more patients in the treatment group were decolonized compared with placebo at week 1 (82% vs 68%, P = .22) and at week 12 (83% vs 72%, P = .34).
Steroid use at the time of FMT was associated with a significant increased risk of ongoing colonization of C difficile at week 12 post-FMT (OR, 4.90; 95% CI, 1.18-20.37; P = .03).
While there were no significant differences in IBD outcomes between groups, there were numerically higher rates of IBD improvement in the treatment group compared to the placebo group 56% vs 46%.
Only one patient had IBD worsen, and this patient was in the placebo group. There were no de novo IBD flares.
FMT alone and with bezlotoxumab were both safe and well tolerated. Two serious adverse events were reported; neither were deemed to be treatment-related.
“This is the first clinical trial to assess the clinical effect of FMT in combination with bezlotoxumab in patients with IBD and rCDI. The data suggest no clear efficacy benefit to this combination compared to FMT alone,” Allegretti told attendees.
“This finding is not surprising given the high rate of efficacy of FMT,” said Ashwin N. Ananthakrishnan, MD, MPH, AGAF, with Massachusetts General Hospital and Harvard Medical School, Boston, who was not involved in the study.
“It would have been interesting to compare bezlotoxumab vs FMT as primary treatment for recurrent CDI in this population,” Ananthakrishnan added.
This was an investigator-initiated study funded by Merck. Allegretti disclosed various relationships with Abbvie, Artugen, Bristol Myers Squibb, Ferring, Finch Therapeutics, Janssen, Merck, Pfizer, and Seres. Ananthakrishnan had no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM ACG 2024
Pemphigus, Bullous Pemphigoid Risk Increased After COVID-19 Infection
TOPLINE:
according to a study that also found that vaccination against COVID-19 is associated with a reduced risk for these conditions.
METHODOLOGY:
- Researchers conducted a population-based retrospective cohort study using data from the TriNetX Analytics Network, encompassing over 112 million electronic health records in the United States.
- The study compared the risk for AIBD within 3 months among individuals who had COVID-19 infection and no COVID-19 vaccination 6 months prior to the infection (n = 4,787,106), individuals who had COVID-19 vaccination but did not have COVID-19 infection (n = 3,466,536), and individuals who did not have COVID-19 infection or vaccination (n = 5,609,197).
- The mean age of the three groups was 44.9, 52.3, and 49.3 years, respectively.
- Propensity score matching included 4,408,748 individuals each for the comparison between COVID-19 infection and controls, 3,465,420 for COVID-19 vaccination and controls, and 3,362,850 for COVID-19 infection and vaccination. The mean follow-up ranged from 72.2 to 76.3 days.
TAKEAWAY:
- Individuals with COVID-19 infection showed a 50.8% increased risk for AIBD within 3 months (P < .001) compared with those without infection or vaccination. The risk was more pronounced for pemphigus (hazard ratio [HR], 2.432; P < .001) than bullous pemphigoid (HR, 1.376; P = .036).
- On the contrary, individuals who had the COVID-19 vaccination showed almost half the risk for AIBD (HR, 0.514; P < .001). The risk reduction was significant for pemphigus (HR, 0.477; P = .030), but not for bullous pemphigoid (HR, 0.846).
- When the infection and vaccination groups were compared, COVID-19 infection increased AIBD risk by more than threefold (HR, 3.130; P < .001), with a particularly high risk for pemphigus (HR, 5.508; P < .001). A significant risk was also seen for bullous pemphigoid (HR, 1.587; P = .008).
IN PRACTICE:
“The findings underscore the importance of vaccination not only in preventing severe COVID-19 outcomes but also in potentially protecting against autoimmune complications,” the authors wrote, adding that “this potential dual benefit of vaccination should be a key message in public health campaigns and clinical practice to enhance vaccine uptake and ultimately improve health outcomes.”
SOURCE:
The study was led by Philip Curman, MD, PhD, of the Dermato-Venereology Clinic at Karolinska University Hospital, Stockholm, Sweden, and was published online on November 7 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The retrospective design has inherent biases, there is potential underreporting of COVID-19 cases and vaccinations, and there is misallocation of individuals. Unmeasured confounding factors may be present.
DISCLOSURES:
This study was funded by grant from the State of Schleswig-Holstein. Two authors were employees of TriNetX. Some authors received financial support and travel grants from various sources, including TriNetX. Additional disclosures are noted in the article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
according to a study that also found that vaccination against COVID-19 is associated with a reduced risk for these conditions.
METHODOLOGY:
- Researchers conducted a population-based retrospective cohort study using data from the TriNetX Analytics Network, encompassing over 112 million electronic health records in the United States.
- The study compared the risk for AIBD within 3 months among individuals who had COVID-19 infection and no COVID-19 vaccination 6 months prior to the infection (n = 4,787,106), individuals who had COVID-19 vaccination but did not have COVID-19 infection (n = 3,466,536), and individuals who did not have COVID-19 infection or vaccination (n = 5,609,197).
- The mean age of the three groups was 44.9, 52.3, and 49.3 years, respectively.
- Propensity score matching included 4,408,748 individuals each for the comparison between COVID-19 infection and controls, 3,465,420 for COVID-19 vaccination and controls, and 3,362,850 for COVID-19 infection and vaccination. The mean follow-up ranged from 72.2 to 76.3 days.
TAKEAWAY:
- Individuals with COVID-19 infection showed a 50.8% increased risk for AIBD within 3 months (P < .001) compared with those without infection or vaccination. The risk was more pronounced for pemphigus (hazard ratio [HR], 2.432; P < .001) than bullous pemphigoid (HR, 1.376; P = .036).
- On the contrary, individuals who had the COVID-19 vaccination showed almost half the risk for AIBD (HR, 0.514; P < .001). The risk reduction was significant for pemphigus (HR, 0.477; P = .030), but not for bullous pemphigoid (HR, 0.846).
- When the infection and vaccination groups were compared, COVID-19 infection increased AIBD risk by more than threefold (HR, 3.130; P < .001), with a particularly high risk for pemphigus (HR, 5.508; P < .001). A significant risk was also seen for bullous pemphigoid (HR, 1.587; P = .008).
IN PRACTICE:
“The findings underscore the importance of vaccination not only in preventing severe COVID-19 outcomes but also in potentially protecting against autoimmune complications,” the authors wrote, adding that “this potential dual benefit of vaccination should be a key message in public health campaigns and clinical practice to enhance vaccine uptake and ultimately improve health outcomes.”
SOURCE:
The study was led by Philip Curman, MD, PhD, of the Dermato-Venereology Clinic at Karolinska University Hospital, Stockholm, Sweden, and was published online on November 7 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The retrospective design has inherent biases, there is potential underreporting of COVID-19 cases and vaccinations, and there is misallocation of individuals. Unmeasured confounding factors may be present.
DISCLOSURES:
This study was funded by grant from the State of Schleswig-Holstein. Two authors were employees of TriNetX. Some authors received financial support and travel grants from various sources, including TriNetX. Additional disclosures are noted in the article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
according to a study that also found that vaccination against COVID-19 is associated with a reduced risk for these conditions.
METHODOLOGY:
- Researchers conducted a population-based retrospective cohort study using data from the TriNetX Analytics Network, encompassing over 112 million electronic health records in the United States.
- The study compared the risk for AIBD within 3 months among individuals who had COVID-19 infection and no COVID-19 vaccination 6 months prior to the infection (n = 4,787,106), individuals who had COVID-19 vaccination but did not have COVID-19 infection (n = 3,466,536), and individuals who did not have COVID-19 infection or vaccination (n = 5,609,197).
- The mean age of the three groups was 44.9, 52.3, and 49.3 years, respectively.
- Propensity score matching included 4,408,748 individuals each for the comparison between COVID-19 infection and controls, 3,465,420 for COVID-19 vaccination and controls, and 3,362,850 for COVID-19 infection and vaccination. The mean follow-up ranged from 72.2 to 76.3 days.
TAKEAWAY:
- Individuals with COVID-19 infection showed a 50.8% increased risk for AIBD within 3 months (P < .001) compared with those without infection or vaccination. The risk was more pronounced for pemphigus (hazard ratio [HR], 2.432; P < .001) than bullous pemphigoid (HR, 1.376; P = .036).
- On the contrary, individuals who had the COVID-19 vaccination showed almost half the risk for AIBD (HR, 0.514; P < .001). The risk reduction was significant for pemphigus (HR, 0.477; P = .030), but not for bullous pemphigoid (HR, 0.846).
- When the infection and vaccination groups were compared, COVID-19 infection increased AIBD risk by more than threefold (HR, 3.130; P < .001), with a particularly high risk for pemphigus (HR, 5.508; P < .001). A significant risk was also seen for bullous pemphigoid (HR, 1.587; P = .008).
IN PRACTICE:
“The findings underscore the importance of vaccination not only in preventing severe COVID-19 outcomes but also in potentially protecting against autoimmune complications,” the authors wrote, adding that “this potential dual benefit of vaccination should be a key message in public health campaigns and clinical practice to enhance vaccine uptake and ultimately improve health outcomes.”
SOURCE:
The study was led by Philip Curman, MD, PhD, of the Dermato-Venereology Clinic at Karolinska University Hospital, Stockholm, Sweden, and was published online on November 7 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The retrospective design has inherent biases, there is potential underreporting of COVID-19 cases and vaccinations, and there is misallocation of individuals. Unmeasured confounding factors may be present.
DISCLOSURES:
This study was funded by grant from the State of Schleswig-Holstein. Two authors were employees of TriNetX. Some authors received financial support and travel grants from various sources, including TriNetX. Additional disclosures are noted in the article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
How Extreme Rainfall Amplifies Health Risks
Climate change is intensifying the variability of precipitation caused by extreme daily and overall rainfall events. Awareness of the effects of these events is crucial for understanding the complex health consequences of climate change. Physicians have often advised their patients to move to a better climate, and when they did, the recommendation was rarely based on precise scientific knowledge. However, the benefits of changing environments were often so evident that they were indisputable.
Today, advanced models, satellite imagery, and biological approaches such as environmental epigenetics are enhancing our understanding of health risks related to climate change.
Extreme Rainfall and Health
The increase in precipitation variability is linked to climate warming, which leads to higher atmospheric humidity and extreme rainfall events. These manifestations can cause rapid weather changes, increasing interactions with harmful aerosols and raising the risk for various cardiovascular and respiratory conditions. However, a full understanding of the association between rain and health has been hindered by conflicting results and methodological issues (limited geographical locations and short observation durations) in studies.
The association between rainfall intensity and health effects is likely nonlinear. Moderate precipitation can mitigate summer heat and help reduce air pollution, an effect that may lower some environmental health risks. Conversely, intense, low-frequency, short-duration rainfall events can have particularly harmful effects on health, as such events can trigger rapid weather changes, increased proliferation of pathogens, and a rise in the risk of various pollutants, potentially exacerbating health conditions.
Rain and Mortality
Using an intensity-duration-frequency model of three rainfall indices (high intensity, low frequency, short duration), a study published in October 2024 combined these with mortality data from 34 countries or regions. Researchers estimated associations between mortality (all cause, cardiovascular, and respiratory) and rainfall events with different return periods (the average time expected before an extreme event of a certain magnitude occurs again) and crucial effect modifiers, including climatic, socioeconomic, and urban environmental conditions.
The analysis included 109,954,744 deaths from all causes; 31,164,161 cardiovascular deaths; and 11,817,278 respiratory deaths. During the study period, from 1980 to 2020, a total of 50,913 rainfall events with a 1-year return period, 8362 events with a 2-year return period, and 3301 events with a 5-year return period were identified.
The most significant finding was a global positive association between all-cause mortality and extreme rainfall events with a 5-year return period. One day of extreme rainfall with a 5-year return period was associated with a cumulative relative risk (RRc) of 1.08 (95% CI, 1.05-1.11) for daily mortality from all causes. Rainfall events with a 2-year return period were associated with increased daily respiratory mortality (RRc, 1.14), while no significant effect was observed for cardiovascular mortality during the same period. Rainfall events with a 5-year return period were associated with an increased risk for both cardiovascular mortality (RRc, 1.05) and respiratory mortality (RRc, 1.29), with the respiratory mortality being significantly higher.
Points of Concern
According to the authors, moderate to high rainfall can exert protective effects through two main mechanisms: Improving air quality (rainfall can reduce the concentration of particulate matter 2.5 cm in diameter or less in the atmosphere) and behavioral changes in people (more time spent in enclosed environments, reducing direct exposure to outdoor air pollution and nonoptimal temperatures). As rainfall intensity increases, the initial protective effects may be overshadowed by a cascade of negative impacts including:
- Critical resource disruptions: Intense rainfall can cause severe disruptions to access to healthcare, infrastructure damage including power outages, and compromised water and food quality.
- Physiological effects: Increased humidity levels facilitate the growth of airborne pathogens, potentially triggering allergic reactions and respiratory issues, particularly in vulnerable individuals. Rapid shifts in atmospheric pressure and temperature fluctuations can lead to cardiovascular and respiratory complications.
- Indirect effects: Extreme rainfall can have profound effects on mental health, inducing stress and anxiety that may exacerbate pre-existing mental health conditions and indirectly contribute to increased overall mortality from nonexternal causes.
The intensity-response curves for the health effects of heavy rainfall showed a nonlinear trend, transitioning from a protective effect at moderate levels of rainfall to a risk for severe harm when rainfall intensity became extreme. Additionally, the significant effects of extreme events were modified by various types of climate and were more pronounced in areas characterized by low variability in precipitation or sparse vegetation cover.
The study demonstrated that various local factors, such as climatic conditions, climate type, and vegetation cover, can potentially influence cardiovascular and respiratory mortality and all-cause mortality related to precipitation. The findings may help physicians convey to their patients the impact of climate change on their health.
This story was translated from Univadis Italy using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Climate change is intensifying the variability of precipitation caused by extreme daily and overall rainfall events. Awareness of the effects of these events is crucial for understanding the complex health consequences of climate change. Physicians have often advised their patients to move to a better climate, and when they did, the recommendation was rarely based on precise scientific knowledge. However, the benefits of changing environments were often so evident that they were indisputable.
Today, advanced models, satellite imagery, and biological approaches such as environmental epigenetics are enhancing our understanding of health risks related to climate change.
Extreme Rainfall and Health
The increase in precipitation variability is linked to climate warming, which leads to higher atmospheric humidity and extreme rainfall events. These manifestations can cause rapid weather changes, increasing interactions with harmful aerosols and raising the risk for various cardiovascular and respiratory conditions. However, a full understanding of the association between rain and health has been hindered by conflicting results and methodological issues (limited geographical locations and short observation durations) in studies.
The association between rainfall intensity and health effects is likely nonlinear. Moderate precipitation can mitigate summer heat and help reduce air pollution, an effect that may lower some environmental health risks. Conversely, intense, low-frequency, short-duration rainfall events can have particularly harmful effects on health, as such events can trigger rapid weather changes, increased proliferation of pathogens, and a rise in the risk of various pollutants, potentially exacerbating health conditions.
Rain and Mortality
Using an intensity-duration-frequency model of three rainfall indices (high intensity, low frequency, short duration), a study published in October 2024 combined these with mortality data from 34 countries or regions. Researchers estimated associations between mortality (all cause, cardiovascular, and respiratory) and rainfall events with different return periods (the average time expected before an extreme event of a certain magnitude occurs again) and crucial effect modifiers, including climatic, socioeconomic, and urban environmental conditions.
The analysis included 109,954,744 deaths from all causes; 31,164,161 cardiovascular deaths; and 11,817,278 respiratory deaths. During the study period, from 1980 to 2020, a total of 50,913 rainfall events with a 1-year return period, 8362 events with a 2-year return period, and 3301 events with a 5-year return period were identified.
The most significant finding was a global positive association between all-cause mortality and extreme rainfall events with a 5-year return period. One day of extreme rainfall with a 5-year return period was associated with a cumulative relative risk (RRc) of 1.08 (95% CI, 1.05-1.11) for daily mortality from all causes. Rainfall events with a 2-year return period were associated with increased daily respiratory mortality (RRc, 1.14), while no significant effect was observed for cardiovascular mortality during the same period. Rainfall events with a 5-year return period were associated with an increased risk for both cardiovascular mortality (RRc, 1.05) and respiratory mortality (RRc, 1.29), with the respiratory mortality being significantly higher.
Points of Concern
According to the authors, moderate to high rainfall can exert protective effects through two main mechanisms: Improving air quality (rainfall can reduce the concentration of particulate matter 2.5 cm in diameter or less in the atmosphere) and behavioral changes in people (more time spent in enclosed environments, reducing direct exposure to outdoor air pollution and nonoptimal temperatures). As rainfall intensity increases, the initial protective effects may be overshadowed by a cascade of negative impacts including:
- Critical resource disruptions: Intense rainfall can cause severe disruptions to access to healthcare, infrastructure damage including power outages, and compromised water and food quality.
- Physiological effects: Increased humidity levels facilitate the growth of airborne pathogens, potentially triggering allergic reactions and respiratory issues, particularly in vulnerable individuals. Rapid shifts in atmospheric pressure and temperature fluctuations can lead to cardiovascular and respiratory complications.
- Indirect effects: Extreme rainfall can have profound effects on mental health, inducing stress and anxiety that may exacerbate pre-existing mental health conditions and indirectly contribute to increased overall mortality from nonexternal causes.
The intensity-response curves for the health effects of heavy rainfall showed a nonlinear trend, transitioning from a protective effect at moderate levels of rainfall to a risk for severe harm when rainfall intensity became extreme. Additionally, the significant effects of extreme events were modified by various types of climate and were more pronounced in areas characterized by low variability in precipitation or sparse vegetation cover.
The study demonstrated that various local factors, such as climatic conditions, climate type, and vegetation cover, can potentially influence cardiovascular and respiratory mortality and all-cause mortality related to precipitation. The findings may help physicians convey to their patients the impact of climate change on their health.
This story was translated from Univadis Italy using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Climate change is intensifying the variability of precipitation caused by extreme daily and overall rainfall events. Awareness of the effects of these events is crucial for understanding the complex health consequences of climate change. Physicians have often advised their patients to move to a better climate, and when they did, the recommendation was rarely based on precise scientific knowledge. However, the benefits of changing environments were often so evident that they were indisputable.
Today, advanced models, satellite imagery, and biological approaches such as environmental epigenetics are enhancing our understanding of health risks related to climate change.
Extreme Rainfall and Health
The increase in precipitation variability is linked to climate warming, which leads to higher atmospheric humidity and extreme rainfall events. These manifestations can cause rapid weather changes, increasing interactions with harmful aerosols and raising the risk for various cardiovascular and respiratory conditions. However, a full understanding of the association between rain and health has been hindered by conflicting results and methodological issues (limited geographical locations and short observation durations) in studies.
The association between rainfall intensity and health effects is likely nonlinear. Moderate precipitation can mitigate summer heat and help reduce air pollution, an effect that may lower some environmental health risks. Conversely, intense, low-frequency, short-duration rainfall events can have particularly harmful effects on health, as such events can trigger rapid weather changes, increased proliferation of pathogens, and a rise in the risk of various pollutants, potentially exacerbating health conditions.
Rain and Mortality
Using an intensity-duration-frequency model of three rainfall indices (high intensity, low frequency, short duration), a study published in October 2024 combined these with mortality data from 34 countries or regions. Researchers estimated associations between mortality (all cause, cardiovascular, and respiratory) and rainfall events with different return periods (the average time expected before an extreme event of a certain magnitude occurs again) and crucial effect modifiers, including climatic, socioeconomic, and urban environmental conditions.
The analysis included 109,954,744 deaths from all causes; 31,164,161 cardiovascular deaths; and 11,817,278 respiratory deaths. During the study period, from 1980 to 2020, a total of 50,913 rainfall events with a 1-year return period, 8362 events with a 2-year return period, and 3301 events with a 5-year return period were identified.
The most significant finding was a global positive association between all-cause mortality and extreme rainfall events with a 5-year return period. One day of extreme rainfall with a 5-year return period was associated with a cumulative relative risk (RRc) of 1.08 (95% CI, 1.05-1.11) for daily mortality from all causes. Rainfall events with a 2-year return period were associated with increased daily respiratory mortality (RRc, 1.14), while no significant effect was observed for cardiovascular mortality during the same period. Rainfall events with a 5-year return period were associated with an increased risk for both cardiovascular mortality (RRc, 1.05) and respiratory mortality (RRc, 1.29), with the respiratory mortality being significantly higher.
Points of Concern
According to the authors, moderate to high rainfall can exert protective effects through two main mechanisms: Improving air quality (rainfall can reduce the concentration of particulate matter 2.5 cm in diameter or less in the atmosphere) and behavioral changes in people (more time spent in enclosed environments, reducing direct exposure to outdoor air pollution and nonoptimal temperatures). As rainfall intensity increases, the initial protective effects may be overshadowed by a cascade of negative impacts including:
- Critical resource disruptions: Intense rainfall can cause severe disruptions to access to healthcare, infrastructure damage including power outages, and compromised water and food quality.
- Physiological effects: Increased humidity levels facilitate the growth of airborne pathogens, potentially triggering allergic reactions and respiratory issues, particularly in vulnerable individuals. Rapid shifts in atmospheric pressure and temperature fluctuations can lead to cardiovascular and respiratory complications.
- Indirect effects: Extreme rainfall can have profound effects on mental health, inducing stress and anxiety that may exacerbate pre-existing mental health conditions and indirectly contribute to increased overall mortality from nonexternal causes.
The intensity-response curves for the health effects of heavy rainfall showed a nonlinear trend, transitioning from a protective effect at moderate levels of rainfall to a risk for severe harm when rainfall intensity became extreme. Additionally, the significant effects of extreme events were modified by various types of climate and were more pronounced in areas characterized by low variability in precipitation or sparse vegetation cover.
The study demonstrated that various local factors, such as climatic conditions, climate type, and vegetation cover, can potentially influence cardiovascular and respiratory mortality and all-cause mortality related to precipitation. The findings may help physicians convey to their patients the impact of climate change on their health.
This story was translated from Univadis Italy using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Skin Fungal Infections Increasing in the United States
TOPLINE:
. Tinea unguium, tinea pedis, and tinea corporis were among the most common infections.
METHODOLOGY:
- Researchers analyzed data from the National Ambulatory Medical Care Survey and National Hospital Ambulatory Medical Care Survey from 2005 to 2016, to evaluate trends in the prevalence of SCFIs during this period.
- The analysis included over 13 billion ambulatory visits to nonfederally funded community, office-based physician practices, and emergency or outpatient departments in the United States, with an estimated 1,104,258,333 annual average.
- The Jonckheere-Terpstra nonparametric test for trend was used to determine the pattern of SCFI prevalence over the 12-year period.
TAKEAWAY:
- SCFIs constituted approximately 0.54% of all annual ambulatory visits, with an estimated 6,001,852 visits for SCFIs per year and over 72 million total visits for the infections during the study period.
- Tinea unguium, tinea pedis, and tinea corporis were the most common infections, comprising 20.5%, 12.2%, and 12.0% of the total visits, respectively.
- Researchers noted an increasing trend in annual SCFIs (P = .03).
IN PRACTICE:
“We observed a high burden of SCFIs among outpatient visits in the United States and an increasing trend in their prevalence,” the authors wrote. These results, they added, “highlight the importance of healthcare providers being able to identify, treat, and, when necessary, refer patients with SCFIs, as a high burden of disease is associated with a significant negative impact on the individual and population levels.”
SOURCE:
The study was co-led by Sarah L. Spaulding, BS, and A. Mitchel Wride, BA, from the Yale School of Medicine, New Haven, Connecticut, and was published online October 30 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The authors did not list any study limitations.
DISCLOSURES:
The lead authors were supported by Yale School of Medicine Medical Student Research Fellowships. Two other authors declared receiving consulting fees, research funding, and licensing fees outside the submitted work and also served on a data and safety monitoring board for Advarra Inc.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
. Tinea unguium, tinea pedis, and tinea corporis were among the most common infections.
METHODOLOGY:
- Researchers analyzed data from the National Ambulatory Medical Care Survey and National Hospital Ambulatory Medical Care Survey from 2005 to 2016, to evaluate trends in the prevalence of SCFIs during this period.
- The analysis included over 13 billion ambulatory visits to nonfederally funded community, office-based physician practices, and emergency or outpatient departments in the United States, with an estimated 1,104,258,333 annual average.
- The Jonckheere-Terpstra nonparametric test for trend was used to determine the pattern of SCFI prevalence over the 12-year period.
TAKEAWAY:
- SCFIs constituted approximately 0.54% of all annual ambulatory visits, with an estimated 6,001,852 visits for SCFIs per year and over 72 million total visits for the infections during the study period.
- Tinea unguium, tinea pedis, and tinea corporis were the most common infections, comprising 20.5%, 12.2%, and 12.0% of the total visits, respectively.
- Researchers noted an increasing trend in annual SCFIs (P = .03).
IN PRACTICE:
“We observed a high burden of SCFIs among outpatient visits in the United States and an increasing trend in their prevalence,” the authors wrote. These results, they added, “highlight the importance of healthcare providers being able to identify, treat, and, when necessary, refer patients with SCFIs, as a high burden of disease is associated with a significant negative impact on the individual and population levels.”
SOURCE:
The study was co-led by Sarah L. Spaulding, BS, and A. Mitchel Wride, BA, from the Yale School of Medicine, New Haven, Connecticut, and was published online October 30 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The authors did not list any study limitations.
DISCLOSURES:
The lead authors were supported by Yale School of Medicine Medical Student Research Fellowships. Two other authors declared receiving consulting fees, research funding, and licensing fees outside the submitted work and also served on a data and safety monitoring board for Advarra Inc.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
. Tinea unguium, tinea pedis, and tinea corporis were among the most common infections.
METHODOLOGY:
- Researchers analyzed data from the National Ambulatory Medical Care Survey and National Hospital Ambulatory Medical Care Survey from 2005 to 2016, to evaluate trends in the prevalence of SCFIs during this period.
- The analysis included over 13 billion ambulatory visits to nonfederally funded community, office-based physician practices, and emergency or outpatient departments in the United States, with an estimated 1,104,258,333 annual average.
- The Jonckheere-Terpstra nonparametric test for trend was used to determine the pattern of SCFI prevalence over the 12-year period.
TAKEAWAY:
- SCFIs constituted approximately 0.54% of all annual ambulatory visits, with an estimated 6,001,852 visits for SCFIs per year and over 72 million total visits for the infections during the study period.
- Tinea unguium, tinea pedis, and tinea corporis were the most common infections, comprising 20.5%, 12.2%, and 12.0% of the total visits, respectively.
- Researchers noted an increasing trend in annual SCFIs (P = .03).
IN PRACTICE:
“We observed a high burden of SCFIs among outpatient visits in the United States and an increasing trend in their prevalence,” the authors wrote. These results, they added, “highlight the importance of healthcare providers being able to identify, treat, and, when necessary, refer patients with SCFIs, as a high burden of disease is associated with a significant negative impact on the individual and population levels.”
SOURCE:
The study was co-led by Sarah L. Spaulding, BS, and A. Mitchel Wride, BA, from the Yale School of Medicine, New Haven, Connecticut, and was published online October 30 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The authors did not list any study limitations.
DISCLOSURES:
The lead authors were supported by Yale School of Medicine Medical Student Research Fellowships. Two other authors declared receiving consulting fees, research funding, and licensing fees outside the submitted work and also served on a data and safety monitoring board for Advarra Inc.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Silent Epidemic: Loneliness a Serious Threat to Both Brain and Body
In a world that is more connected than ever, a silent epidemic is taking its toll. Overall, one in three US adults report chronic loneliness — a condition so detrimental that it rivals smoking and obesity with respect to its negative effect on health and well-being. From anxiety and depression to life-threatening conditions like cardiovascular disease, stroke, and Alzheimer’s and Parkinson’s diseases, loneliness is more than an emotion — it’s a serious threat to both the brain and body.
In 2023, a US Surgeon General advisory raised the alarm about the national problem of loneliness and isolation, describing it as an epidemic.
“Given the significant health consequences of loneliness and isolation, we must prioritize building social connection in the same way we have prioritized other critical public health issues such as tobacco, obesity, and substance use disorders. Together, we can build a country that’s healthier, more resilient, less lonely, and more connected,” the report concluded.
But how, exactly, does chronic loneliness affect the physiology and function of the brain? What does the latest research reveal about the link between loneliness and neurologic and psychiatric illness, and what can clinicians do to address the issue?
This news organization spoke to multiple experts in the field to explore these issues.
A Major Risk Factor
Anna Finley, PhD, assistant professor of psychology at North Dakota State University, Fargo, explained that loneliness and social isolation are different entities. Social isolation is an objective measure of the number of people someone interacts with on a regular basis, whereas loneliness is a subjective feeling that occurs when close connections are lacking.
“These two things are not actually as related as you think they would be. People can feel lonely in a crowd or feel well connected with only a few friendships. It’s more about the quality of the connection and the quality of your perception of it. So someone could be in some very supportive relationships but still feel that there’s something missing,” she said in an interview.
So what do we know about how loneliness affects health? Evidence supporting the hypothesis that loneliness is an emerging risk factor for many diseases is steadily building.
Recently, the American Heart Association published a statement summarizing the evidence for a direct association between social isolation and loneliness and coronary heart disease and stroke mortality.
In addition, many studies have shown that individuals experiencing social isolation or loneliness have an increased risk for anxiety and depression, dementia, infectious disease, hospitalization, and all-cause death, even after adjusting for age and many other traditional risk factors.
One study revealed that eliminating loneliness has the potential to prevent nearly 20% of cases of depression in adults aged 50 years or older.
Indu Subramanian, MD, professor of neurology at the University of California, Los Angeles, and colleagues conducted a study involving patients with Parkinson’s disease, which showed that the negative impact of loneliness on disease severity was as significant as the positive effects of 30 minutes of daily exercise.
“The importance of loneliness is under-recognized and undervalued, and it poses a major risk for health outcomes and quality of life,” said Subramanian.
Subramanian noted that loneliness is stigmatizing, causing people to feel unlikable and blame themselves, which prevents them from opening up to doctors or loved ones about their struggle. At the same time, healthcare providers may not think to ask about loneliness or know about potential interventions. She emphasized that much more work is needed to address this issue.
Early Mortality Risk
Julianne Holt-Lunstad, PhD, professor of psychology and neuroscience at Brigham Young University in Provo, Utah, is the author of two large meta-analyses that suggest loneliness, social isolation, or living alone are independent risk factors for early mortality, increasing this risk by about a third — the equivalent to the risk of smoking 15 cigarettes per day.
“We have quite robust evidence across a number of health outcomes implicating the harmful effects of loneliness and social isolation. While these are observational studies and show mainly associations, we do have evidence from longitudinal studies that show lacking social connection, whether that be loneliness or social isolation, predicts subsequent worse outcomes, and most of these studies have adjusted for alternative kinds of explanations, like age, initial health status, lifestyle factors,” Holt-Lunstad said.
There is some evidence to suggest that isolation is more predictive of physical health outcomes, whereas loneliness is more predictive of mental health outcomes. That said, both isolation and loneliness have significant effects on mental and physical health outcomes, she noted.
There is also the question of whether loneliness is causing poor health or whether people who are in poor health feel lonely because poor health can lead to social isolation.
Finley said there’s probably a bit of both going on, but longitudinal studies, where loneliness is measured at a fixed timepoint then health outcomes are reported a few years later, suggest that loneliness is contributing to these adverse outcomes.
She added that there is also some evidence in animal models to suggest that loneliness is a causal risk factor for adverse health outcomes. “But you can’t ask a mouse or rat how lonely they’re feeling. All you can do is house them individually — removing them from social connection. This isn’t necessarily the same thing as loneliness in humans.”
Finley is studying mechanisms in the brain that may be involved in mediating the adverse health consequences of loneliness.
“What I’ve been seeing in the data so far is that it tends to be the self-report of how lonely folks are feeling that has the associations with differences in the brain, as opposed to the number of social connections people have. It does seem to be the more subjective, emotional perception of loneliness that is important.”
In a review of potential mechanisms involved, she concluded that it is dysregulated emotions and altered perceptions of social interactions that has profound impacts on the brain, suggesting that people who are lonely may have a tendency to interpret social cues in a negative way, preventing them from forming productive positive relationships.
Lack of Trust
One researcher who has studied this phenomenon is Dirk Scheele, PhD, professor of social neuroscience at Ruhr University Bochum in Germany.
“We were interested to find out why people remained lonely,” he said in an interview. “Loneliness is an unpleasant experience, and there are so many opportunities for social contacts nowadays, it’s not really clear at first sight why people are chronically lonely.”
To examine this question, Scheele and his team conducted a study in which functional MRI was used to examine the brain in otherwise healthy individuals with high or low loneliness scores while they played a trust game.
They also simulated a positive social interaction between participants and researchers, in which they talked about plans for a fictitious lottery win, and about their hobbies and interests, during which mood was measured with questionnaires, and saliva samples were collected to measure hormone levels.
Results showed that the high-lonely individuals had reduced activation in the insula cortex during the trust decisions. “This area of the brain is involved in the processing of bodily signals, such as ‘gut feelings.’ So reduced activity here could be interpreted as fewer gut feelings on who can be trusted,” Scheele explained.
The high-lonely individuals also had reduced responsiveness to the positive social interaction with a lower release of oxytocin and a smaller elevation in mood compared with the control individuals.
Scheele pointed out that there is some evidence that oxytocin might increase trust, and there is reduced release of endogenous oxytocin in high loneliness.
“Our results are consistent with the idea that loneliness is associated with negative biases about other people. So if we expect negative things from other people — for instance, that they cannot be trusted — then that would hamper further social interactions and could lead to loneliness,” he added.
A Role for Oxytocin?
In another study, the same researchers tested short-term (five weekly sessions) group psychotherapy to reduce loneliness using established techniques to target these negative biases. They also investigated whether the effects of this group psychotherapy could be augmented by administering intranasal oxytocin (vs placebo) before the group psychotherapy sessions.
Results showed that the group psychotherapy intervention reduced trait loneliness (loneliness experienced over a prolonged period). The oxytocin did not show a significant effect on trait loneliness, but there was a suggestion that it may enhance the reduction in state loneliness (how someone is feeling at a specific time) brought about by the psychotherapy sessions.
“We found that bonding within the groups was experienced as more positive in the oxytocin treated groups. It is possible that a longer intervention would be helpful for longer-term results,” Scheele concluded. “It’s not going to be a quick fix for loneliness, but there may be a role for oxytocin as an adjunct to psychotherapy.”
A Basic Human Need
Another loneliness researcher, Livia Tomova, PhD, assistant professor of psychology at Cardiff University in Wales, has used social isolation to induce loneliness in young people and found that this intervention was linked to brain patterns similar to those associated with hunger.
“We know that the drive to eat food is a very basic human need. We know quite well how it is represented in the brain,” she explained.
The researchers tested how the brains of the participants responded to seeing pictures of social interactions after they underwent a prolonged period of social isolation. In a subsequent session, the same people were asked to undergo food fasting and then underwent brain scans when looking at pictures of food. Results showed that the neural patterns were similar in the two situations with increased activity in the substantia nigra area within the midbrain.
“This area of the brain processes rewards and motivation. It consists primarily of dopamine neurons and increased activity corresponds to a feeling of craving something. So this area of the brain that controls essential homeostatic needs is activated when people feel lonely, suggesting that our need for social contact with others is potentially a very basic need similar to eating,” Tomova said.
Lower Gray Matter Volumes in Key Brain Areas
And another group from Germany has found that higher loneliness scores are negatively associated with specific brain regions responsible for memory, emotion regulation, and social processing.
Sandra Düzel, PhD, and colleagues from the Max Planck Institute for Human Development and the Charité – Universitätsmedizin Berlin, both in Berlin, Germany, reported a study in which individuals who reported higher loneliness had smaller gray matter volumes in brain regions such as the left amygdala, anterior hippocampus, and cerebellum, regions which are crucial for both emotional regulation and higher-order cognitive processes, such as self-reflection and executive function.
Düzel believes that possible mechanisms behind the link between loneliness and brain volume differences could include stress-related damage, with prolonged loneliness associated with elevated levels of stress hormones, which can damage the hippocampus over time, and reduced cognitive and social stimulation, which may contribute to brain volume reductions in regions critical for memory and emotional processing.
“Loneliness is often characterized by reduced social and environmental diversity, leading to less engagement with novel experiences and potentially lower hippocampal-striatal connectivity.
Since novelty-seeking and environmental diversity are associated with positive emotional states, individuals experiencing loneliness might benefit from increased exposure to new environments which could stimulate the brain’s reward circuits, fostering positive affect and potentially mitigating the emotional burden of loneliness,” she said.
Is Social Prescribing the Answer?
So are there enough data now to act and attempt to develop interventions to reduce loneliness? Most of these researchers believe so.
“I think we have enough information to act on this now. There are a number of national academies consensus reports, which suggest that, while certainly there are still gaps in our evidence and more to be learned, there is sufficient evidence that a concerning portion of the population seems to lack connection, and that the consequences are serious enough that we need to do something about it,” said Holt-Lunstad.
Some countries have introduced social prescribing where doctors can prescribe a group activity or a regular visit or telephone conversation with a supportive person.
Subramanian pointed out that it’s easier to implement in countries with national health services and may be more difficult to embrace in the US healthcare system.
“We are not so encouraged from a financial perspective to think about preventive care in the US. We don’t have an easy way to recognize in any tangible way the downstream of such activities in terms of preventing future problems. That is something we need to work on,” she said.
Finley cautioned that to work well, social prescribing will require an understanding of each person’s individual situation.
“Some people may only receive benefit of interacting with others if they are also getting some sort of support to address the social and emotional concerns that are tagging along with loneliness. I’m not sure that just telling people to go join their local gardening club or whatever will be the correct answer for everyone.”
She pointed out that many people will have issues in their life that are making it hard for them to be social. These could be mobility or financial challenges, care responsibilities, or concerns about illnesses or life events. “We need to figure out what would have the most bang for the person’s buck, so to speak, as an intervention. That could mean connecting them to a group relevant to their individual situation.”
Opportunity to Connect Not Enough?
Tomova believes that training people in social skills may be a better option. “It appears that some people who are chronically lonely seem to struggle to make relationships with others. So just encouraging them to interact with others more will not necessarily help. We need to better understand the pathways involved and who are the people who become ill. We can then develop and target better interventions and teach people coping strategies for that situation.”
Scheele agreed. “While just giving people the opportunity to connect may work for some, others who are experiencing really chronic loneliness may not benefit very much from this unless their negative belief systems are addressed.” He suggested some sort of psychotherapy may be helpful in this situation.
But at least all seem to agree that healthcare providers need to be more aware of loneliness as a health risk factor, try to identify people at risk, and to think about how best to support them.
Holt-Lunstad noted that one of the recommendations in the US Surgeon General’s advisory was to increase the education, training, and resources on loneliness for healthcare providers.
“If we want this to be addressed, we need to give healthcare providers the time, resources, and training in order to do that, otherwise, we are adding one more thing to an already overburdened system. They need to understand how important it is, and how it might help them take care of the patient.”
“Our hope is that we can start to reverse some of the trends that we are seeing, both in terms of the prevalence rates of loneliness, but also that we could start seeing improvements in health and other kinds of outcomes,” she concluded.
Progress is being made in increasing awareness about the dangers of chronic loneliness. It’s now recognized as a serious health risk, but there are actionable steps that can help. Loneliness doesn’t have to be a permanent condition for anyone, said Scheele.
Holt-Lunstad served as an adviser for Foundation for Social Connection, Global Initiative on Loneliness and Connection, and Nextdoor Neighborhood Vitality Board and received research grants/income from Templeton Foundation, Eventbrite, Foundation for Social Connection, and Triple-S Foundation. Subramanian served as a speaker bureau for Acorda Pharma. The other researchers reported no disclosures.
A version of this article first appeared on Medscape.com.
In a world that is more connected than ever, a silent epidemic is taking its toll. Overall, one in three US adults report chronic loneliness — a condition so detrimental that it rivals smoking and obesity with respect to its negative effect on health and well-being. From anxiety and depression to life-threatening conditions like cardiovascular disease, stroke, and Alzheimer’s and Parkinson’s diseases, loneliness is more than an emotion — it’s a serious threat to both the brain and body.
In 2023, a US Surgeon General advisory raised the alarm about the national problem of loneliness and isolation, describing it as an epidemic.
“Given the significant health consequences of loneliness and isolation, we must prioritize building social connection in the same way we have prioritized other critical public health issues such as tobacco, obesity, and substance use disorders. Together, we can build a country that’s healthier, more resilient, less lonely, and more connected,” the report concluded.
But how, exactly, does chronic loneliness affect the physiology and function of the brain? What does the latest research reveal about the link between loneliness and neurologic and psychiatric illness, and what can clinicians do to address the issue?
This news organization spoke to multiple experts in the field to explore these issues.
A Major Risk Factor
Anna Finley, PhD, assistant professor of psychology at North Dakota State University, Fargo, explained that loneliness and social isolation are different entities. Social isolation is an objective measure of the number of people someone interacts with on a regular basis, whereas loneliness is a subjective feeling that occurs when close connections are lacking.
“These two things are not actually as related as you think they would be. People can feel lonely in a crowd or feel well connected with only a few friendships. It’s more about the quality of the connection and the quality of your perception of it. So someone could be in some very supportive relationships but still feel that there’s something missing,” she said in an interview.
So what do we know about how loneliness affects health? Evidence supporting the hypothesis that loneliness is an emerging risk factor for many diseases is steadily building.
Recently, the American Heart Association published a statement summarizing the evidence for a direct association between social isolation and loneliness and coronary heart disease and stroke mortality.
In addition, many studies have shown that individuals experiencing social isolation or loneliness have an increased risk for anxiety and depression, dementia, infectious disease, hospitalization, and all-cause death, even after adjusting for age and many other traditional risk factors.
One study revealed that eliminating loneliness has the potential to prevent nearly 20% of cases of depression in adults aged 50 years or older.
Indu Subramanian, MD, professor of neurology at the University of California, Los Angeles, and colleagues conducted a study involving patients with Parkinson’s disease, which showed that the negative impact of loneliness on disease severity was as significant as the positive effects of 30 minutes of daily exercise.
“The importance of loneliness is under-recognized and undervalued, and it poses a major risk for health outcomes and quality of life,” said Subramanian.
Subramanian noted that loneliness is stigmatizing, causing people to feel unlikable and blame themselves, which prevents them from opening up to doctors or loved ones about their struggle. At the same time, healthcare providers may not think to ask about loneliness or know about potential interventions. She emphasized that much more work is needed to address this issue.
Early Mortality Risk
Julianne Holt-Lunstad, PhD, professor of psychology and neuroscience at Brigham Young University in Provo, Utah, is the author of two large meta-analyses that suggest loneliness, social isolation, or living alone are independent risk factors for early mortality, increasing this risk by about a third — the equivalent to the risk of smoking 15 cigarettes per day.
“We have quite robust evidence across a number of health outcomes implicating the harmful effects of loneliness and social isolation. While these are observational studies and show mainly associations, we do have evidence from longitudinal studies that show lacking social connection, whether that be loneliness or social isolation, predicts subsequent worse outcomes, and most of these studies have adjusted for alternative kinds of explanations, like age, initial health status, lifestyle factors,” Holt-Lunstad said.
There is some evidence to suggest that isolation is more predictive of physical health outcomes, whereas loneliness is more predictive of mental health outcomes. That said, both isolation and loneliness have significant effects on mental and physical health outcomes, she noted.
There is also the question of whether loneliness is causing poor health or whether people who are in poor health feel lonely because poor health can lead to social isolation.
Finley said there’s probably a bit of both going on, but longitudinal studies, where loneliness is measured at a fixed timepoint then health outcomes are reported a few years later, suggest that loneliness is contributing to these adverse outcomes.
She added that there is also some evidence in animal models to suggest that loneliness is a causal risk factor for adverse health outcomes. “But you can’t ask a mouse or rat how lonely they’re feeling. All you can do is house them individually — removing them from social connection. This isn’t necessarily the same thing as loneliness in humans.”
Finley is studying mechanisms in the brain that may be involved in mediating the adverse health consequences of loneliness.
“What I’ve been seeing in the data so far is that it tends to be the self-report of how lonely folks are feeling that has the associations with differences in the brain, as opposed to the number of social connections people have. It does seem to be the more subjective, emotional perception of loneliness that is important.”
In a review of potential mechanisms involved, she concluded that it is dysregulated emotions and altered perceptions of social interactions that has profound impacts on the brain, suggesting that people who are lonely may have a tendency to interpret social cues in a negative way, preventing them from forming productive positive relationships.
Lack of Trust
One researcher who has studied this phenomenon is Dirk Scheele, PhD, professor of social neuroscience at Ruhr University Bochum in Germany.
“We were interested to find out why people remained lonely,” he said in an interview. “Loneliness is an unpleasant experience, and there are so many opportunities for social contacts nowadays, it’s not really clear at first sight why people are chronically lonely.”
To examine this question, Scheele and his team conducted a study in which functional MRI was used to examine the brain in otherwise healthy individuals with high or low loneliness scores while they played a trust game.
They also simulated a positive social interaction between participants and researchers, in which they talked about plans for a fictitious lottery win, and about their hobbies and interests, during which mood was measured with questionnaires, and saliva samples were collected to measure hormone levels.
Results showed that the high-lonely individuals had reduced activation in the insula cortex during the trust decisions. “This area of the brain is involved in the processing of bodily signals, such as ‘gut feelings.’ So reduced activity here could be interpreted as fewer gut feelings on who can be trusted,” Scheele explained.
The high-lonely individuals also had reduced responsiveness to the positive social interaction with a lower release of oxytocin and a smaller elevation in mood compared with the control individuals.
Scheele pointed out that there is some evidence that oxytocin might increase trust, and there is reduced release of endogenous oxytocin in high loneliness.
“Our results are consistent with the idea that loneliness is associated with negative biases about other people. So if we expect negative things from other people — for instance, that they cannot be trusted — then that would hamper further social interactions and could lead to loneliness,” he added.
A Role for Oxytocin?
In another study, the same researchers tested short-term (five weekly sessions) group psychotherapy to reduce loneliness using established techniques to target these negative biases. They also investigated whether the effects of this group psychotherapy could be augmented by administering intranasal oxytocin (vs placebo) before the group psychotherapy sessions.
Results showed that the group psychotherapy intervention reduced trait loneliness (loneliness experienced over a prolonged period). The oxytocin did not show a significant effect on trait loneliness, but there was a suggestion that it may enhance the reduction in state loneliness (how someone is feeling at a specific time) brought about by the psychotherapy sessions.
“We found that bonding within the groups was experienced as more positive in the oxytocin treated groups. It is possible that a longer intervention would be helpful for longer-term results,” Scheele concluded. “It’s not going to be a quick fix for loneliness, but there may be a role for oxytocin as an adjunct to psychotherapy.”
A Basic Human Need
Another loneliness researcher, Livia Tomova, PhD, assistant professor of psychology at Cardiff University in Wales, has used social isolation to induce loneliness in young people and found that this intervention was linked to brain patterns similar to those associated with hunger.
“We know that the drive to eat food is a very basic human need. We know quite well how it is represented in the brain,” she explained.
The researchers tested how the brains of the participants responded to seeing pictures of social interactions after they underwent a prolonged period of social isolation. In a subsequent session, the same people were asked to undergo food fasting and then underwent brain scans when looking at pictures of food. Results showed that the neural patterns were similar in the two situations with increased activity in the substantia nigra area within the midbrain.
“This area of the brain processes rewards and motivation. It consists primarily of dopamine neurons and increased activity corresponds to a feeling of craving something. So this area of the brain that controls essential homeostatic needs is activated when people feel lonely, suggesting that our need for social contact with others is potentially a very basic need similar to eating,” Tomova said.
Lower Gray Matter Volumes in Key Brain Areas
And another group from Germany has found that higher loneliness scores are negatively associated with specific brain regions responsible for memory, emotion regulation, and social processing.
Sandra Düzel, PhD, and colleagues from the Max Planck Institute for Human Development and the Charité – Universitätsmedizin Berlin, both in Berlin, Germany, reported a study in which individuals who reported higher loneliness had smaller gray matter volumes in brain regions such as the left amygdala, anterior hippocampus, and cerebellum, regions which are crucial for both emotional regulation and higher-order cognitive processes, such as self-reflection and executive function.
Düzel believes that possible mechanisms behind the link between loneliness and brain volume differences could include stress-related damage, with prolonged loneliness associated with elevated levels of stress hormones, which can damage the hippocampus over time, and reduced cognitive and social stimulation, which may contribute to brain volume reductions in regions critical for memory and emotional processing.
“Loneliness is often characterized by reduced social and environmental diversity, leading to less engagement with novel experiences and potentially lower hippocampal-striatal connectivity.
Since novelty-seeking and environmental diversity are associated with positive emotional states, individuals experiencing loneliness might benefit from increased exposure to new environments which could stimulate the brain’s reward circuits, fostering positive affect and potentially mitigating the emotional burden of loneliness,” she said.
Is Social Prescribing the Answer?
So are there enough data now to act and attempt to develop interventions to reduce loneliness? Most of these researchers believe so.
“I think we have enough information to act on this now. There are a number of national academies consensus reports, which suggest that, while certainly there are still gaps in our evidence and more to be learned, there is sufficient evidence that a concerning portion of the population seems to lack connection, and that the consequences are serious enough that we need to do something about it,” said Holt-Lunstad.
Some countries have introduced social prescribing where doctors can prescribe a group activity or a regular visit or telephone conversation with a supportive person.
Subramanian pointed out that it’s easier to implement in countries with national health services and may be more difficult to embrace in the US healthcare system.
“We are not so encouraged from a financial perspective to think about preventive care in the US. We don’t have an easy way to recognize in any tangible way the downstream of such activities in terms of preventing future problems. That is something we need to work on,” she said.
Finley cautioned that to work well, social prescribing will require an understanding of each person’s individual situation.
“Some people may only receive benefit of interacting with others if they are also getting some sort of support to address the social and emotional concerns that are tagging along with loneliness. I’m not sure that just telling people to go join their local gardening club or whatever will be the correct answer for everyone.”
She pointed out that many people will have issues in their life that are making it hard for them to be social. These could be mobility or financial challenges, care responsibilities, or concerns about illnesses or life events. “We need to figure out what would have the most bang for the person’s buck, so to speak, as an intervention. That could mean connecting them to a group relevant to their individual situation.”
Opportunity to Connect Not Enough?
Tomova believes that training people in social skills may be a better option. “It appears that some people who are chronically lonely seem to struggle to make relationships with others. So just encouraging them to interact with others more will not necessarily help. We need to better understand the pathways involved and who are the people who become ill. We can then develop and target better interventions and teach people coping strategies for that situation.”
Scheele agreed. “While just giving people the opportunity to connect may work for some, others who are experiencing really chronic loneliness may not benefit very much from this unless their negative belief systems are addressed.” He suggested some sort of psychotherapy may be helpful in this situation.
But at least all seem to agree that healthcare providers need to be more aware of loneliness as a health risk factor, try to identify people at risk, and to think about how best to support them.
Holt-Lunstad noted that one of the recommendations in the US Surgeon General’s advisory was to increase the education, training, and resources on loneliness for healthcare providers.
“If we want this to be addressed, we need to give healthcare providers the time, resources, and training in order to do that, otherwise, we are adding one more thing to an already overburdened system. They need to understand how important it is, and how it might help them take care of the patient.”
“Our hope is that we can start to reverse some of the trends that we are seeing, both in terms of the prevalence rates of loneliness, but also that we could start seeing improvements in health and other kinds of outcomes,” she concluded.
Progress is being made in increasing awareness about the dangers of chronic loneliness. It’s now recognized as a serious health risk, but there are actionable steps that can help. Loneliness doesn’t have to be a permanent condition for anyone, said Scheele.
Holt-Lunstad served as an adviser for Foundation for Social Connection, Global Initiative on Loneliness and Connection, and Nextdoor Neighborhood Vitality Board and received research grants/income from Templeton Foundation, Eventbrite, Foundation for Social Connection, and Triple-S Foundation. Subramanian served as a speaker bureau for Acorda Pharma. The other researchers reported no disclosures.
A version of this article first appeared on Medscape.com.
In a world that is more connected than ever, a silent epidemic is taking its toll. Overall, one in three US adults report chronic loneliness — a condition so detrimental that it rivals smoking and obesity with respect to its negative effect on health and well-being. From anxiety and depression to life-threatening conditions like cardiovascular disease, stroke, and Alzheimer’s and Parkinson’s diseases, loneliness is more than an emotion — it’s a serious threat to both the brain and body.
In 2023, a US Surgeon General advisory raised the alarm about the national problem of loneliness and isolation, describing it as an epidemic.
“Given the significant health consequences of loneliness and isolation, we must prioritize building social connection in the same way we have prioritized other critical public health issues such as tobacco, obesity, and substance use disorders. Together, we can build a country that’s healthier, more resilient, less lonely, and more connected,” the report concluded.
But how, exactly, does chronic loneliness affect the physiology and function of the brain? What does the latest research reveal about the link between loneliness and neurologic and psychiatric illness, and what can clinicians do to address the issue?
This news organization spoke to multiple experts in the field to explore these issues.
A Major Risk Factor
Anna Finley, PhD, assistant professor of psychology at North Dakota State University, Fargo, explained that loneliness and social isolation are different entities. Social isolation is an objective measure of the number of people someone interacts with on a regular basis, whereas loneliness is a subjective feeling that occurs when close connections are lacking.
“These two things are not actually as related as you think they would be. People can feel lonely in a crowd or feel well connected with only a few friendships. It’s more about the quality of the connection and the quality of your perception of it. So someone could be in some very supportive relationships but still feel that there’s something missing,” she said in an interview.
So what do we know about how loneliness affects health? Evidence supporting the hypothesis that loneliness is an emerging risk factor for many diseases is steadily building.
Recently, the American Heart Association published a statement summarizing the evidence for a direct association between social isolation and loneliness and coronary heart disease and stroke mortality.
In addition, many studies have shown that individuals experiencing social isolation or loneliness have an increased risk for anxiety and depression, dementia, infectious disease, hospitalization, and all-cause death, even after adjusting for age and many other traditional risk factors.
One study revealed that eliminating loneliness has the potential to prevent nearly 20% of cases of depression in adults aged 50 years or older.
Indu Subramanian, MD, professor of neurology at the University of California, Los Angeles, and colleagues conducted a study involving patients with Parkinson’s disease, which showed that the negative impact of loneliness on disease severity was as significant as the positive effects of 30 minutes of daily exercise.
“The importance of loneliness is under-recognized and undervalued, and it poses a major risk for health outcomes and quality of life,” said Subramanian.
Subramanian noted that loneliness is stigmatizing, causing people to feel unlikable and blame themselves, which prevents them from opening up to doctors or loved ones about their struggle. At the same time, healthcare providers may not think to ask about loneliness or know about potential interventions. She emphasized that much more work is needed to address this issue.
Early Mortality Risk
Julianne Holt-Lunstad, PhD, professor of psychology and neuroscience at Brigham Young University in Provo, Utah, is the author of two large meta-analyses that suggest loneliness, social isolation, or living alone are independent risk factors for early mortality, increasing this risk by about a third — the equivalent to the risk of smoking 15 cigarettes per day.
“We have quite robust evidence across a number of health outcomes implicating the harmful effects of loneliness and social isolation. While these are observational studies and show mainly associations, we do have evidence from longitudinal studies that show lacking social connection, whether that be loneliness or social isolation, predicts subsequent worse outcomes, and most of these studies have adjusted for alternative kinds of explanations, like age, initial health status, lifestyle factors,” Holt-Lunstad said.
There is some evidence to suggest that isolation is more predictive of physical health outcomes, whereas loneliness is more predictive of mental health outcomes. That said, both isolation and loneliness have significant effects on mental and physical health outcomes, she noted.
There is also the question of whether loneliness is causing poor health or whether people who are in poor health feel lonely because poor health can lead to social isolation.
Finley said there’s probably a bit of both going on, but longitudinal studies, where loneliness is measured at a fixed timepoint then health outcomes are reported a few years later, suggest that loneliness is contributing to these adverse outcomes.
She added that there is also some evidence in animal models to suggest that loneliness is a causal risk factor for adverse health outcomes. “But you can’t ask a mouse or rat how lonely they’re feeling. All you can do is house them individually — removing them from social connection. This isn’t necessarily the same thing as loneliness in humans.”
Finley is studying mechanisms in the brain that may be involved in mediating the adverse health consequences of loneliness.
“What I’ve been seeing in the data so far is that it tends to be the self-report of how lonely folks are feeling that has the associations with differences in the brain, as opposed to the number of social connections people have. It does seem to be the more subjective, emotional perception of loneliness that is important.”
In a review of potential mechanisms involved, she concluded that it is dysregulated emotions and altered perceptions of social interactions that has profound impacts on the brain, suggesting that people who are lonely may have a tendency to interpret social cues in a negative way, preventing them from forming productive positive relationships.
Lack of Trust
One researcher who has studied this phenomenon is Dirk Scheele, PhD, professor of social neuroscience at Ruhr University Bochum in Germany.
“We were interested to find out why people remained lonely,” he said in an interview. “Loneliness is an unpleasant experience, and there are so many opportunities for social contacts nowadays, it’s not really clear at first sight why people are chronically lonely.”
To examine this question, Scheele and his team conducted a study in which functional MRI was used to examine the brain in otherwise healthy individuals with high or low loneliness scores while they played a trust game.
They also simulated a positive social interaction between participants and researchers, in which they talked about plans for a fictitious lottery win, and about their hobbies and interests, during which mood was measured with questionnaires, and saliva samples were collected to measure hormone levels.
Results showed that the high-lonely individuals had reduced activation in the insula cortex during the trust decisions. “This area of the brain is involved in the processing of bodily signals, such as ‘gut feelings.’ So reduced activity here could be interpreted as fewer gut feelings on who can be trusted,” Scheele explained.
The high-lonely individuals also had reduced responsiveness to the positive social interaction with a lower release of oxytocin and a smaller elevation in mood compared with the control individuals.
Scheele pointed out that there is some evidence that oxytocin might increase trust, and there is reduced release of endogenous oxytocin in high loneliness.
“Our results are consistent with the idea that loneliness is associated with negative biases about other people. So if we expect negative things from other people — for instance, that they cannot be trusted — then that would hamper further social interactions and could lead to loneliness,” he added.
A Role for Oxytocin?
In another study, the same researchers tested short-term (five weekly sessions) group psychotherapy to reduce loneliness using established techniques to target these negative biases. They also investigated whether the effects of this group psychotherapy could be augmented by administering intranasal oxytocin (vs placebo) before the group psychotherapy sessions.
Results showed that the group psychotherapy intervention reduced trait loneliness (loneliness experienced over a prolonged period). The oxytocin did not show a significant effect on trait loneliness, but there was a suggestion that it may enhance the reduction in state loneliness (how someone is feeling at a specific time) brought about by the psychotherapy sessions.
“We found that bonding within the groups was experienced as more positive in the oxytocin treated groups. It is possible that a longer intervention would be helpful for longer-term results,” Scheele concluded. “It’s not going to be a quick fix for loneliness, but there may be a role for oxytocin as an adjunct to psychotherapy.”
A Basic Human Need
Another loneliness researcher, Livia Tomova, PhD, assistant professor of psychology at Cardiff University in Wales, has used social isolation to induce loneliness in young people and found that this intervention was linked to brain patterns similar to those associated with hunger.
“We know that the drive to eat food is a very basic human need. We know quite well how it is represented in the brain,” she explained.
The researchers tested how the brains of the participants responded to seeing pictures of social interactions after they underwent a prolonged period of social isolation. In a subsequent session, the same people were asked to undergo food fasting and then underwent brain scans when looking at pictures of food. Results showed that the neural patterns were similar in the two situations with increased activity in the substantia nigra area within the midbrain.
“This area of the brain processes rewards and motivation. It consists primarily of dopamine neurons and increased activity corresponds to a feeling of craving something. So this area of the brain that controls essential homeostatic needs is activated when people feel lonely, suggesting that our need for social contact with others is potentially a very basic need similar to eating,” Tomova said.
Lower Gray Matter Volumes in Key Brain Areas
And another group from Germany has found that higher loneliness scores are negatively associated with specific brain regions responsible for memory, emotion regulation, and social processing.
Sandra Düzel, PhD, and colleagues from the Max Planck Institute for Human Development and the Charité – Universitätsmedizin Berlin, both in Berlin, Germany, reported a study in which individuals who reported higher loneliness had smaller gray matter volumes in brain regions such as the left amygdala, anterior hippocampus, and cerebellum, regions which are crucial for both emotional regulation and higher-order cognitive processes, such as self-reflection and executive function.
Düzel believes that possible mechanisms behind the link between loneliness and brain volume differences could include stress-related damage, with prolonged loneliness associated with elevated levels of stress hormones, which can damage the hippocampus over time, and reduced cognitive and social stimulation, which may contribute to brain volume reductions in regions critical for memory and emotional processing.
“Loneliness is often characterized by reduced social and environmental diversity, leading to less engagement with novel experiences and potentially lower hippocampal-striatal connectivity.
Since novelty-seeking and environmental diversity are associated with positive emotional states, individuals experiencing loneliness might benefit from increased exposure to new environments which could stimulate the brain’s reward circuits, fostering positive affect and potentially mitigating the emotional burden of loneliness,” she said.
Is Social Prescribing the Answer?
So are there enough data now to act and attempt to develop interventions to reduce loneliness? Most of these researchers believe so.
“I think we have enough information to act on this now. There are a number of national academies consensus reports, which suggest that, while certainly there are still gaps in our evidence and more to be learned, there is sufficient evidence that a concerning portion of the population seems to lack connection, and that the consequences are serious enough that we need to do something about it,” said Holt-Lunstad.
Some countries have introduced social prescribing where doctors can prescribe a group activity or a regular visit or telephone conversation with a supportive person.
Subramanian pointed out that it’s easier to implement in countries with national health services and may be more difficult to embrace in the US healthcare system.
“We are not so encouraged from a financial perspective to think about preventive care in the US. We don’t have an easy way to recognize in any tangible way the downstream of such activities in terms of preventing future problems. That is something we need to work on,” she said.
Finley cautioned that to work well, social prescribing will require an understanding of each person’s individual situation.
“Some people may only receive benefit of interacting with others if they are also getting some sort of support to address the social and emotional concerns that are tagging along with loneliness. I’m not sure that just telling people to go join their local gardening club or whatever will be the correct answer for everyone.”
She pointed out that many people will have issues in their life that are making it hard for them to be social. These could be mobility or financial challenges, care responsibilities, or concerns about illnesses or life events. “We need to figure out what would have the most bang for the person’s buck, so to speak, as an intervention. That could mean connecting them to a group relevant to their individual situation.”
Opportunity to Connect Not Enough?
Tomova believes that training people in social skills may be a better option. “It appears that some people who are chronically lonely seem to struggle to make relationships with others. So just encouraging them to interact with others more will not necessarily help. We need to better understand the pathways involved and who are the people who become ill. We can then develop and target better interventions and teach people coping strategies for that situation.”
Scheele agreed. “While just giving people the opportunity to connect may work for some, others who are experiencing really chronic loneliness may not benefit very much from this unless their negative belief systems are addressed.” He suggested some sort of psychotherapy may be helpful in this situation.
But at least all seem to agree that healthcare providers need to be more aware of loneliness as a health risk factor, try to identify people at risk, and to think about how best to support them.
Holt-Lunstad noted that one of the recommendations in the US Surgeon General’s advisory was to increase the education, training, and resources on loneliness for healthcare providers.
“If we want this to be addressed, we need to give healthcare providers the time, resources, and training in order to do that, otherwise, we are adding one more thing to an already overburdened system. They need to understand how important it is, and how it might help them take care of the patient.”
“Our hope is that we can start to reverse some of the trends that we are seeing, both in terms of the prevalence rates of loneliness, but also that we could start seeing improvements in health and other kinds of outcomes,” she concluded.
Progress is being made in increasing awareness about the dangers of chronic loneliness. It’s now recognized as a serious health risk, but there are actionable steps that can help. Loneliness doesn’t have to be a permanent condition for anyone, said Scheele.
Holt-Lunstad served as an adviser for Foundation for Social Connection, Global Initiative on Loneliness and Connection, and Nextdoor Neighborhood Vitality Board and received research grants/income from Templeton Foundation, Eventbrite, Foundation for Social Connection, and Triple-S Foundation. Subramanian served as a speaker bureau for Acorda Pharma. The other researchers reported no disclosures.
A version of this article first appeared on Medscape.com.
Lichenoid Drug Eruption Secondary to Apalutamide Treatment
To the Editor:
Lichenoid drug eruptions are lichen planus–like hypersensitivity reactions induced by medications. These reactions are rare but cause irritation to the skin, as extreme pruritus is common. One review of 300 consecutive cases of drug eruptions submitted to dermatopathology revealed that 12% of cases were classified as lichenoid drug reactions.1 Lichenoid dermatitis is characterized by extremely pruritic, scaly, eczematous or psoriasiform papules, often along the extensor surfaces and trunk.2 The pruritic nature of the rash can negatively impact quality of life. Treatment typically involves discontinuation of the offending medication, although complete resolution can take months, even after the drug is stopped. Although there have been some data suggesting that topical and/or oral corticosteroids can help with resolution, the rash can persist even with steroid treatment.2
The histopathologic findings of lichenoid drug eruptions show lichen planus–like changes such as hyperkeratosis, irregular acanthosis, and lichenoid interface dermatitis. Accordingly, idiopathic lichen planus is an important differential diagnosis for lichenoid drug eruptions; however, compared to idiopathic lichen planus, lichenoid drug eruptions are more likely to be associated with eosinophils and parakeratosis.1,3 In some cases, the histopathologic distinction between the 2 conditions is impossible, and clinical history needs to be considered to make a diagnosis.1 Drugs known to cause lichenoid drug reactions more commonly include angiotensin-converting enzyme inhibitors, beta blockers, thiazides, gold, penicillamine, and antimalarials.2 Lichenoid drug eruptions also have been documented in patients taking the second-generation nonsteroidal androgen receptor antagonist enzalutamide, which is used for the treatment of prostate cancer.4 More recently, the newer second-generation nonsteroidal androgen receptor antagonist apalutamide has been implicated in several cases of lichenoid drug eruptions.5,6
We present a case of an apalutamide-induced lichenoid drug eruption that was resistant to dose reduction and required discontinuation of treatment due to the negative impact on the patient’s quality of life. Once the rash resolved, the patient transitioned to enzalutamide without any adverse events (AEs).
A 72-year-old man with a history of metastatic prostate cancer (stage IVB) presented to the dermatology clinic with a 4-month history of a dry itchy rash on the face, chest, back, and legs that had developed 2 to 3 months after oncology started him on apalutamide. The patient initially received apalutamide 240 mg/d, which was reduced by his oncologist 3 months later to 180 mg/d following the appearance of the rash. Then apalutamide was held as he awaited improvement of the rash.
One week after the apalutamide was held, the patient presented to dermatology. He reported that he had tried over-the-counter ammonium lactate 12% lotion twice daily when the rash first developed without improvement. When the apalutamide was held, oncology prescribed mupirocin ointment 2% 3 times daily which yielded minimal relief. On physical examination, widespread lichenified papules and plaques were noted on the face, chest, back, and legs (Figure 1). Dermatology initially prescribed triamcinolone ointment 0.1% twice daily. A 4-mm punch biopsy specimen of the upper back revealed a lichenoid interface dermatitis with numerous eosinophils compatible with a lichenoid hypersensitivity reaction (Figure 2). Considering the clinical and histologic findings, a diagnosis of lichenoid drug eruption secondary to apalutamide treatment was made.

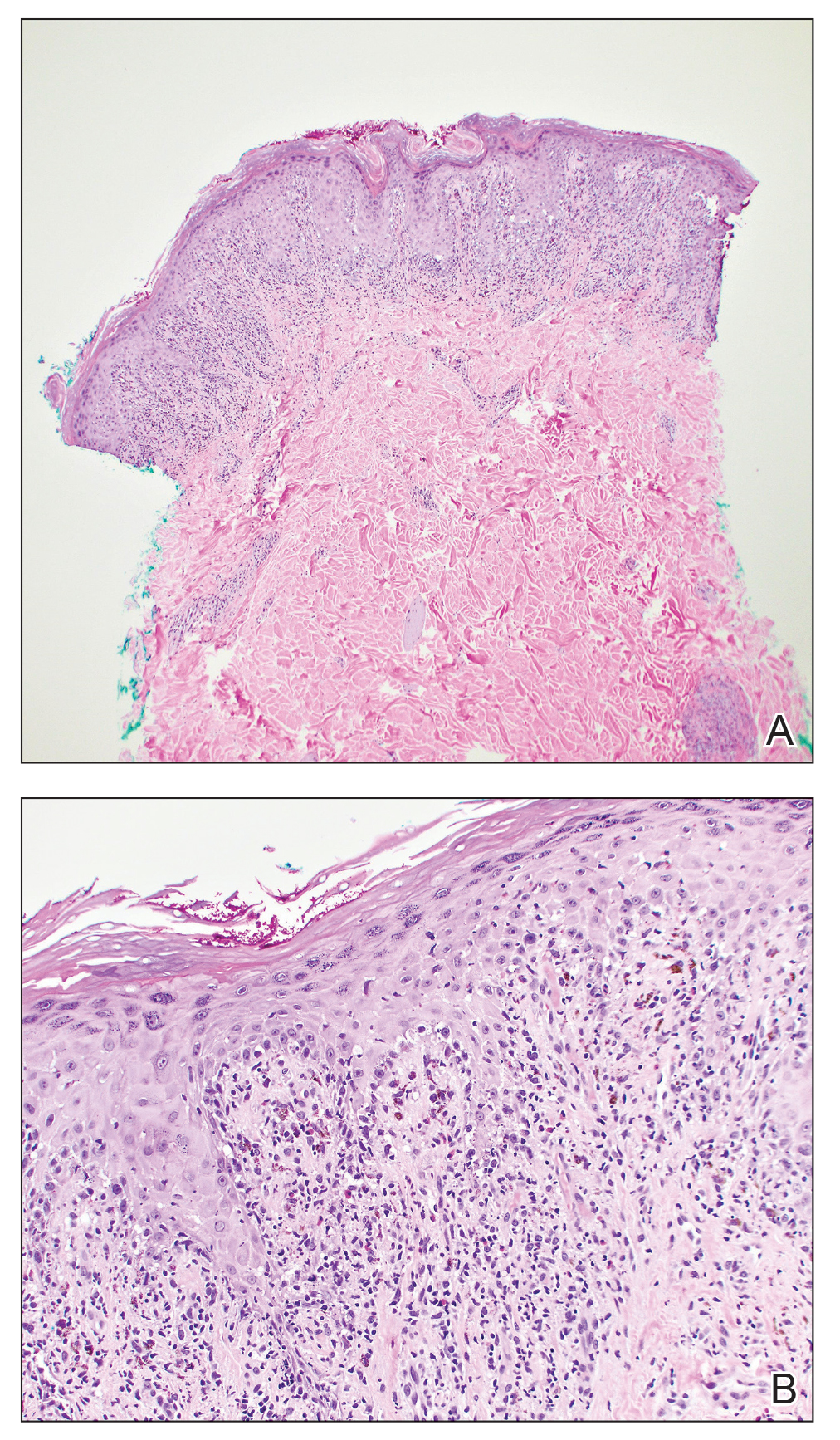
Two weeks after discontinuation of the medication, the rash improved, and the patient restarted apalutamide at a dosage of 120 mg/d; however, the rash re-emerged within 1 month and was resistant to the triamcinolone ointment 0.1%. Apalutamide was again discontinued, and oncology switched the patient to enzalutamide 160 mg/d in an effort to find a medication the patient could better tolerate. Two months after starting enzalutamide, the patient had resolution of the rash and no further dermatologic complications.
Apalutamide is a second-generation nonsteroidal androgen receptor antagonist used in the treatment of nonmetastatic castration-resistant prostate cancer (CRPC) and metastatic castration-sensitive prostate cancer (CSPC).7 It stops the spread and growth of prostate cancer cells by several different mechanisms, including competitively binding androgen receptors, preventing 5α-dihydrotestosterone from binding to androgen receptors, blocking androgen receptor nuclear translocation, impairing co-activator recruitment, and restraining androgen receptor DNA binding.7 The SPARTAN and TITAN phase 3 clinical trials demonstrated increased overall survival and time to progression with apalutamide in both nonmetastatic CRPC and metastatic CSPC. In both trials, the rash was shown to be an AE more commonly associated with apalutamide than placebo.8,9
Until recently, the characteristics of apalutamide-induced drug rashes have not been well described. One literature review reported 6 cases of cutaneous apalutamide-induced drug eruptions.5 Four (66.7%) of these eruptions were maculopapular rashes, only 2 of which were histologically classified as lichenoid in nature. The other 2 eruptions were classified as toxic epidermal necrosis.5 Another study of 303 patients with prostate cancer who were treated with apalutamide recorded the frequency and time to onset of dermatologic AEs.6 Seventy-one (23.4%) of the patients had dermatologic AEs, and of those, only 20 (28.2%) had AEs that resulted in interruptions in apalutamide therapy (with only 5 [25.0%] requiring medication discontinuation). Thirty-two (45.1%) patients were managed with topical or oral corticosteroids or dose modification. In this study, histopathology was examined in 8 cases (one of which had 2 biopsies for a total of 9 biopsies), 7 of which were consistent with lichenoid interface dermatitis.6
Lichenoid interface dermatitis is a rare manifestation of an apalutamide-induced drug eruption and also has been reported secondary to treatment with enzalutamide, another second-generation nonsteroidal androgen receptor antagonist.4 Enzalutamide was the first second-generation nonsteroidal androgen receptor antagonist approved for the treatment of prostate cancer. It originally was approved only for metastatic CRPC after docetaxel therapy in 2012, then later was expanded to metastatic and nonmetastatic CRPC in 2012 and 2018, respectively, as well as metastatic CSPC in 2019.7 Because enzalutamide is from the same medication class as apalutamide and has been on the market longer for the treatment of nonmetastatic CRPC and metastatic CSPC, it is not surprising that similar drug eruptions now are being reported secondary to apalutamide use as well.
It is important for providers to consider lichenoid drug eruptions in the differential diagnosis of pruritic rashes in patients taking second-generation nonsteroidal androgen receptor antagonists such as apalutamide or enzalutamide. Although dose reduction or treatment discontinuation have been the standard of care for patients with extremely pruritic lichenoid drug eruptions secondary to these medications, these are not ideal because they are important for cancer treatment. Interestingly, after our patient’s apalutamide-induced rash resolved and he was switched to enzalutamide, he did not develop any AEs. Based on our patient’s experience, physicians could consider switching their patients to another drug of the same class, as they may be able tolerate that medication. More research is needed to determine how commonly patients tolerate a different second-generation nonsteroidal androgen receptor antagonist after not tolerating another medication from the same class.
- Weyers W, Metze D. Histopathology of drug eruptions—general criteria, common patterns, and differential diagnosis. Dermatol Pract Concept. 2011;1:33-47. doi:10.5826/dpc.0101a09
- Cheraghlou S, Levy LL. Fixed drug eruption, bullous drug eruptions, and lichenoid drug eruptions. Clin Dermatol. 2020;38:679-692. doi:10.1016/j.clindermatol.2020.06.010
- Thompson DF, Skaehill PA. Drug-induced lichen planus. Pharmacotherapy. 1994;14:561-571.
- Khan S, Saizan AL, O’Brien K, et al. Diffuse hyperpigmented lichenoid drug eruption secondary to enzalutamide. Curr Probl Cancer Case Rep. 2022;5:100135. doi:10.1016/j.cpccr.2021.100135
- Katayama H, Saeki H, Osada S-I. Maculopapular drug eruption caused by apalutamide: case report and review of the literature. J Nippon Med Sch. 2022;89:550-554. doi:10.1272/jnms.JNMS.2022_89-503
- Pan A, Reingold RE, Zhao JL, et al. Dermatologic adverse events in prostate cancer patients treated with the androgen receptor inhibitor apalutamide. J Urol. 2022;207:1010-1019. doi:10.1097/JU.0000000000002425
- Rajaram P, Rivera A, Muthima K, et al. Second-generation androgen receptor antagonists as hormonal therapeutics for three forms of prostate cancer. Molecules. 2020;25:2448. doi:10.3390/molecules25102448
- Smith MR, Saad F, Chowdhury S, et al. Apalutamide treatment and metastasis-free survival in prostate cancer. N Engl J Med. 2018;378:1408-1418. doi:10.1056/NEJMoa1715546
- Chi KN, Agarwal N, Bjartell A, et al. Apalutamide for metastatic, castration-sensative prostate cancer. N Engl J Med. 2019;381:13-24. doi:10.1056/NEJMoa1903307
To the Editor:
Lichenoid drug eruptions are lichen planus–like hypersensitivity reactions induced by medications. These reactions are rare but cause irritation to the skin, as extreme pruritus is common. One review of 300 consecutive cases of drug eruptions submitted to dermatopathology revealed that 12% of cases were classified as lichenoid drug reactions.1 Lichenoid dermatitis is characterized by extremely pruritic, scaly, eczematous or psoriasiform papules, often along the extensor surfaces and trunk.2 The pruritic nature of the rash can negatively impact quality of life. Treatment typically involves discontinuation of the offending medication, although complete resolution can take months, even after the drug is stopped. Although there have been some data suggesting that topical and/or oral corticosteroids can help with resolution, the rash can persist even with steroid treatment.2
The histopathologic findings of lichenoid drug eruptions show lichen planus–like changes such as hyperkeratosis, irregular acanthosis, and lichenoid interface dermatitis. Accordingly, idiopathic lichen planus is an important differential diagnosis for lichenoid drug eruptions; however, compared to idiopathic lichen planus, lichenoid drug eruptions are more likely to be associated with eosinophils and parakeratosis.1,3 In some cases, the histopathologic distinction between the 2 conditions is impossible, and clinical history needs to be considered to make a diagnosis.1 Drugs known to cause lichenoid drug reactions more commonly include angiotensin-converting enzyme inhibitors, beta blockers, thiazides, gold, penicillamine, and antimalarials.2 Lichenoid drug eruptions also have been documented in patients taking the second-generation nonsteroidal androgen receptor antagonist enzalutamide, which is used for the treatment of prostate cancer.4 More recently, the newer second-generation nonsteroidal androgen receptor antagonist apalutamide has been implicated in several cases of lichenoid drug eruptions.5,6
We present a case of an apalutamide-induced lichenoid drug eruption that was resistant to dose reduction and required discontinuation of treatment due to the negative impact on the patient’s quality of life. Once the rash resolved, the patient transitioned to enzalutamide without any adverse events (AEs).
A 72-year-old man with a history of metastatic prostate cancer (stage IVB) presented to the dermatology clinic with a 4-month history of a dry itchy rash on the face, chest, back, and legs that had developed 2 to 3 months after oncology started him on apalutamide. The patient initially received apalutamide 240 mg/d, which was reduced by his oncologist 3 months later to 180 mg/d following the appearance of the rash. Then apalutamide was held as he awaited improvement of the rash.
One week after the apalutamide was held, the patient presented to dermatology. He reported that he had tried over-the-counter ammonium lactate 12% lotion twice daily when the rash first developed without improvement. When the apalutamide was held, oncology prescribed mupirocin ointment 2% 3 times daily which yielded minimal relief. On physical examination, widespread lichenified papules and plaques were noted on the face, chest, back, and legs (Figure 1). Dermatology initially prescribed triamcinolone ointment 0.1% twice daily. A 4-mm punch biopsy specimen of the upper back revealed a lichenoid interface dermatitis with numerous eosinophils compatible with a lichenoid hypersensitivity reaction (Figure 2). Considering the clinical and histologic findings, a diagnosis of lichenoid drug eruption secondary to apalutamide treatment was made.
Two weeks after discontinuation of the medication, the rash improved, and the patient restarted apalutamide at a dosage of 120 mg/d; however, the rash re-emerged within 1 month and was resistant to the triamcinolone ointment 0.1%. Apalutamide was again discontinued, and oncology switched the patient to enzalutamide 160 mg/d in an effort to find a medication the patient could better tolerate. Two months after starting enzalutamide, the patient had resolution of the rash and no further dermatologic complications.
Apalutamide is a second-generation nonsteroidal androgen receptor antagonist used in the treatment of nonmetastatic castration-resistant prostate cancer (CRPC) and metastatic castration-sensitive prostate cancer (CSPC).7 It stops the spread and growth of prostate cancer cells by several different mechanisms, including competitively binding androgen receptors, preventing 5α-dihydrotestosterone from binding to androgen receptors, blocking androgen receptor nuclear translocation, impairing co-activator recruitment, and restraining androgen receptor DNA binding.7 The SPARTAN and TITAN phase 3 clinical trials demonstrated increased overall survival and time to progression with apalutamide in both nonmetastatic CRPC and metastatic CSPC. In both trials, the rash was shown to be an AE more commonly associated with apalutamide than placebo.8,9
Until recently, the characteristics of apalutamide-induced drug rashes have not been well described. One literature review reported 6 cases of cutaneous apalutamide-induced drug eruptions.5 Four (66.7%) of these eruptions were maculopapular rashes, only 2 of which were histologically classified as lichenoid in nature. The other 2 eruptions were classified as toxic epidermal necrosis.5 Another study of 303 patients with prostate cancer who were treated with apalutamide recorded the frequency and time to onset of dermatologic AEs.6 Seventy-one (23.4%) of the patients had dermatologic AEs, and of those, only 20 (28.2%) had AEs that resulted in interruptions in apalutamide therapy (with only 5 [25.0%] requiring medication discontinuation). Thirty-two (45.1%) patients were managed with topical or oral corticosteroids or dose modification. In this study, histopathology was examined in 8 cases (one of which had 2 biopsies for a total of 9 biopsies), 7 of which were consistent with lichenoid interface dermatitis.6
Lichenoid interface dermatitis is a rare manifestation of an apalutamide-induced drug eruption and also has been reported secondary to treatment with enzalutamide, another second-generation nonsteroidal androgen receptor antagonist.4 Enzalutamide was the first second-generation nonsteroidal androgen receptor antagonist approved for the treatment of prostate cancer. It originally was approved only for metastatic CRPC after docetaxel therapy in 2012, then later was expanded to metastatic and nonmetastatic CRPC in 2012 and 2018, respectively, as well as metastatic CSPC in 2019.7 Because enzalutamide is from the same medication class as apalutamide and has been on the market longer for the treatment of nonmetastatic CRPC and metastatic CSPC, it is not surprising that similar drug eruptions now are being reported secondary to apalutamide use as well.
It is important for providers to consider lichenoid drug eruptions in the differential diagnosis of pruritic rashes in patients taking second-generation nonsteroidal androgen receptor antagonists such as apalutamide or enzalutamide. Although dose reduction or treatment discontinuation have been the standard of care for patients with extremely pruritic lichenoid drug eruptions secondary to these medications, these are not ideal because they are important for cancer treatment. Interestingly, after our patient’s apalutamide-induced rash resolved and he was switched to enzalutamide, he did not develop any AEs. Based on our patient’s experience, physicians could consider switching their patients to another drug of the same class, as they may be able tolerate that medication. More research is needed to determine how commonly patients tolerate a different second-generation nonsteroidal androgen receptor antagonist after not tolerating another medication from the same class.
To the Editor:
Lichenoid drug eruptions are lichen planus–like hypersensitivity reactions induced by medications. These reactions are rare but cause irritation to the skin, as extreme pruritus is common. One review of 300 consecutive cases of drug eruptions submitted to dermatopathology revealed that 12% of cases were classified as lichenoid drug reactions.1 Lichenoid dermatitis is characterized by extremely pruritic, scaly, eczematous or psoriasiform papules, often along the extensor surfaces and trunk.2 The pruritic nature of the rash can negatively impact quality of life. Treatment typically involves discontinuation of the offending medication, although complete resolution can take months, even after the drug is stopped. Although there have been some data suggesting that topical and/or oral corticosteroids can help with resolution, the rash can persist even with steroid treatment.2
The histopathologic findings of lichenoid drug eruptions show lichen planus–like changes such as hyperkeratosis, irregular acanthosis, and lichenoid interface dermatitis. Accordingly, idiopathic lichen planus is an important differential diagnosis for lichenoid drug eruptions; however, compared to idiopathic lichen planus, lichenoid drug eruptions are more likely to be associated with eosinophils and parakeratosis.1,3 In some cases, the histopathologic distinction between the 2 conditions is impossible, and clinical history needs to be considered to make a diagnosis.1 Drugs known to cause lichenoid drug reactions more commonly include angiotensin-converting enzyme inhibitors, beta blockers, thiazides, gold, penicillamine, and antimalarials.2 Lichenoid drug eruptions also have been documented in patients taking the second-generation nonsteroidal androgen receptor antagonist enzalutamide, which is used for the treatment of prostate cancer.4 More recently, the newer second-generation nonsteroidal androgen receptor antagonist apalutamide has been implicated in several cases of lichenoid drug eruptions.5,6
We present a case of an apalutamide-induced lichenoid drug eruption that was resistant to dose reduction and required discontinuation of treatment due to the negative impact on the patient’s quality of life. Once the rash resolved, the patient transitioned to enzalutamide without any adverse events (AEs).
A 72-year-old man with a history of metastatic prostate cancer (stage IVB) presented to the dermatology clinic with a 4-month history of a dry itchy rash on the face, chest, back, and legs that had developed 2 to 3 months after oncology started him on apalutamide. The patient initially received apalutamide 240 mg/d, which was reduced by his oncologist 3 months later to 180 mg/d following the appearance of the rash. Then apalutamide was held as he awaited improvement of the rash.
One week after the apalutamide was held, the patient presented to dermatology. He reported that he had tried over-the-counter ammonium lactate 12% lotion twice daily when the rash first developed without improvement. When the apalutamide was held, oncology prescribed mupirocin ointment 2% 3 times daily which yielded minimal relief. On physical examination, widespread lichenified papules and plaques were noted on the face, chest, back, and legs (Figure 1). Dermatology initially prescribed triamcinolone ointment 0.1% twice daily. A 4-mm punch biopsy specimen of the upper back revealed a lichenoid interface dermatitis with numerous eosinophils compatible with a lichenoid hypersensitivity reaction (Figure 2). Considering the clinical and histologic findings, a diagnosis of lichenoid drug eruption secondary to apalutamide treatment was made.
Two weeks after discontinuation of the medication, the rash improved, and the patient restarted apalutamide at a dosage of 120 mg/d; however, the rash re-emerged within 1 month and was resistant to the triamcinolone ointment 0.1%. Apalutamide was again discontinued, and oncology switched the patient to enzalutamide 160 mg/d in an effort to find a medication the patient could better tolerate. Two months after starting enzalutamide, the patient had resolution of the rash and no further dermatologic complications.
Apalutamide is a second-generation nonsteroidal androgen receptor antagonist used in the treatment of nonmetastatic castration-resistant prostate cancer (CRPC) and metastatic castration-sensitive prostate cancer (CSPC).7 It stops the spread and growth of prostate cancer cells by several different mechanisms, including competitively binding androgen receptors, preventing 5α-dihydrotestosterone from binding to androgen receptors, blocking androgen receptor nuclear translocation, impairing co-activator recruitment, and restraining androgen receptor DNA binding.7 The SPARTAN and TITAN phase 3 clinical trials demonstrated increased overall survival and time to progression with apalutamide in both nonmetastatic CRPC and metastatic CSPC. In both trials, the rash was shown to be an AE more commonly associated with apalutamide than placebo.8,9
Until recently, the characteristics of apalutamide-induced drug rashes have not been well described. One literature review reported 6 cases of cutaneous apalutamide-induced drug eruptions.5 Four (66.7%) of these eruptions were maculopapular rashes, only 2 of which were histologically classified as lichenoid in nature. The other 2 eruptions were classified as toxic epidermal necrosis.5 Another study of 303 patients with prostate cancer who were treated with apalutamide recorded the frequency and time to onset of dermatologic AEs.6 Seventy-one (23.4%) of the patients had dermatologic AEs, and of those, only 20 (28.2%) had AEs that resulted in interruptions in apalutamide therapy (with only 5 [25.0%] requiring medication discontinuation). Thirty-two (45.1%) patients were managed with topical or oral corticosteroids or dose modification. In this study, histopathology was examined in 8 cases (one of which had 2 biopsies for a total of 9 biopsies), 7 of which were consistent with lichenoid interface dermatitis.6
Lichenoid interface dermatitis is a rare manifestation of an apalutamide-induced drug eruption and also has been reported secondary to treatment with enzalutamide, another second-generation nonsteroidal androgen receptor antagonist.4 Enzalutamide was the first second-generation nonsteroidal androgen receptor antagonist approved for the treatment of prostate cancer. It originally was approved only for metastatic CRPC after docetaxel therapy in 2012, then later was expanded to metastatic and nonmetastatic CRPC in 2012 and 2018, respectively, as well as metastatic CSPC in 2019.7 Because enzalutamide is from the same medication class as apalutamide and has been on the market longer for the treatment of nonmetastatic CRPC and metastatic CSPC, it is not surprising that similar drug eruptions now are being reported secondary to apalutamide use as well.
It is important for providers to consider lichenoid drug eruptions in the differential diagnosis of pruritic rashes in patients taking second-generation nonsteroidal androgen receptor antagonists such as apalutamide or enzalutamide. Although dose reduction or treatment discontinuation have been the standard of care for patients with extremely pruritic lichenoid drug eruptions secondary to these medications, these are not ideal because they are important for cancer treatment. Interestingly, after our patient’s apalutamide-induced rash resolved and he was switched to enzalutamide, he did not develop any AEs. Based on our patient’s experience, physicians could consider switching their patients to another drug of the same class, as they may be able tolerate that medication. More research is needed to determine how commonly patients tolerate a different second-generation nonsteroidal androgen receptor antagonist after not tolerating another medication from the same class.
- Weyers W, Metze D. Histopathology of drug eruptions—general criteria, common patterns, and differential diagnosis. Dermatol Pract Concept. 2011;1:33-47. doi:10.5826/dpc.0101a09
- Cheraghlou S, Levy LL. Fixed drug eruption, bullous drug eruptions, and lichenoid drug eruptions. Clin Dermatol. 2020;38:679-692. doi:10.1016/j.clindermatol.2020.06.010
- Thompson DF, Skaehill PA. Drug-induced lichen planus. Pharmacotherapy. 1994;14:561-571.
- Khan S, Saizan AL, O’Brien K, et al. Diffuse hyperpigmented lichenoid drug eruption secondary to enzalutamide. Curr Probl Cancer Case Rep. 2022;5:100135. doi:10.1016/j.cpccr.2021.100135
- Katayama H, Saeki H, Osada S-I. Maculopapular drug eruption caused by apalutamide: case report and review of the literature. J Nippon Med Sch. 2022;89:550-554. doi:10.1272/jnms.JNMS.2022_89-503
- Pan A, Reingold RE, Zhao JL, et al. Dermatologic adverse events in prostate cancer patients treated with the androgen receptor inhibitor apalutamide. J Urol. 2022;207:1010-1019. doi:10.1097/JU.0000000000002425
- Rajaram P, Rivera A, Muthima K, et al. Second-generation androgen receptor antagonists as hormonal therapeutics for three forms of prostate cancer. Molecules. 2020;25:2448. doi:10.3390/molecules25102448
- Smith MR, Saad F, Chowdhury S, et al. Apalutamide treatment and metastasis-free survival in prostate cancer. N Engl J Med. 2018;378:1408-1418. doi:10.1056/NEJMoa1715546
- Chi KN, Agarwal N, Bjartell A, et al. Apalutamide for metastatic, castration-sensative prostate cancer. N Engl J Med. 2019;381:13-24. doi:10.1056/NEJMoa1903307
- Weyers W, Metze D. Histopathology of drug eruptions—general criteria, common patterns, and differential diagnosis. Dermatol Pract Concept. 2011;1:33-47. doi:10.5826/dpc.0101a09
- Cheraghlou S, Levy LL. Fixed drug eruption, bullous drug eruptions, and lichenoid drug eruptions. Clin Dermatol. 2020;38:679-692. doi:10.1016/j.clindermatol.2020.06.010
- Thompson DF, Skaehill PA. Drug-induced lichen planus. Pharmacotherapy. 1994;14:561-571.
- Khan S, Saizan AL, O’Brien K, et al. Diffuse hyperpigmented lichenoid drug eruption secondary to enzalutamide. Curr Probl Cancer Case Rep. 2022;5:100135. doi:10.1016/j.cpccr.2021.100135
- Katayama H, Saeki H, Osada S-I. Maculopapular drug eruption caused by apalutamide: case report and review of the literature. J Nippon Med Sch. 2022;89:550-554. doi:10.1272/jnms.JNMS.2022_89-503
- Pan A, Reingold RE, Zhao JL, et al. Dermatologic adverse events in prostate cancer patients treated with the androgen receptor inhibitor apalutamide. J Urol. 2022;207:1010-1019. doi:10.1097/JU.0000000000002425
- Rajaram P, Rivera A, Muthima K, et al. Second-generation androgen receptor antagonists as hormonal therapeutics for three forms of prostate cancer. Molecules. 2020;25:2448. doi:10.3390/molecules25102448
- Smith MR, Saad F, Chowdhury S, et al. Apalutamide treatment and metastasis-free survival in prostate cancer. N Engl J Med. 2018;378:1408-1418. doi:10.1056/NEJMoa1715546
- Chi KN, Agarwal N, Bjartell A, et al. Apalutamide for metastatic, castration-sensative prostate cancer. N Engl J Med. 2019;381:13-24. doi:10.1056/NEJMoa1903307
Practice Points
- Although it is rare, patients can develop lichenoid drug eruptions secondary to treatment with second-generation nonsteroidal androgen receptor antagonists such as apalutamide.
- If a patient develops a lichenoid drug eruption while taking a specific second-generation nonsteroidal androgen receptor antagonist, the entire class of medications should not be ruled out, as some patients can tolerate other drugs from that class.
