User login
OARSI: Bisphosphonate users less likely to undergo knee replacement
SEATTLE – Women with knee osteoarthritis who took bisphosphonates were 27% less likely to undergo joint replacement surgery than were women who didn’t take bisphosphonates in a U.K. cohort study of 3,928 propensity-matched users and nonusers, according to a report at the World Congress on Osteoarthritis.
“In older women with incident knee osteoarthritis, incident bisphosphonate use may be associated with lower risk of knee replacement than in nonusers,” said Dr. Tuhina Neogi of Boston University.

Dr. Neogi and her colleagues used data from The Health Improvement Network (THIN), a U.K. database of primary care patients, to identify women aged 50-89 years who received a diagnosis of knee osteoarthritis between 2003 and 2012. Patients were excluded if they were poor surgical candidates or were taking disease-modifying antirheumatic drugs, biologic agents, or other bone-active agents.
The researchers compared 1,964 women who subsequently started bisphosphonate therapy with 1,964 propensity score–matched women who did not. In 85% of the former, the bisphosphonate was alendronate, marketed as Fosamax in the United States.
During a mean follow-up of 3 years, the incidence rate of knee replacement was 21 cases per 1,000 patient-years among bisphosphonate users and 29 cases per 1,000 patient-years among nonusers, according to results reported at the meeting, which was sponsored by Osteoarthritis Research Society International.
In adjusted analyses, users had a significantly lower relative risk of undergoing this surgery (hazard ratio, 0.73), reported Dr. Neogi, who disclosed that she had no relevant conflicts of interest.
Sensitivity analyses showed an even stronger association in a separate cohort of patients matched by age, body mass index, and the duration of osteoarthritis (hazard ratio, 0.33) and a nonsignificant benefit when bisphosphonate users were instead compared against an active user group of women who initiated any other bone-modulating therapy.
“Now of course this is observational data from electronic medical records, so we cannot rule out the potential for residual bias,” she acknowledged. “Our sensitivity analyses were fairly consistent and provide some reassurance, but nonetheless, the magnitude of effect is still likely to be biased due to residual confounding.”
In an interview, Dr. Rik Lories, one of the session’s comoderators and a professor at the University of Leuven, Belgium, said that the study “is still far from practice changing. But the great thing about this research is that we are starting to split up what you would call the osteoarthritic diseases, taking osteoarthritis as the outcome [and showing] the underlying mechanisms of the different phenotypes being different.”

Dr. Neogi noted that subchrondral bone changes are prominent in knee osteoarthritis and that mechanical factors play a central role in the disease. At the same time, findings of trials of antiresorptive agents, including bisphosphonates, in knee osteoarthritis have been conflicting.
“There are a number of limitations to this study, including the fact that The Health Improvement Network does not have bone mineral density results. We tried to address this by accounting for a prior diagnosis of osteoporosis, fracture history, potential risk for fractures, body mass index, age, number of bone mineral density tests ordered, et cetera,” Dr. Neogi said. “Another limitation is that of the secular trends in use of bone-modulating agents over this time frame, and that precluded robust evaluation of the active user comparator analysis.
“Bone mineral density is still a major potential confounder here that can’t be adequately addressed,” she acknowledged.
SEATTLE – Women with knee osteoarthritis who took bisphosphonates were 27% less likely to undergo joint replacement surgery than were women who didn’t take bisphosphonates in a U.K. cohort study of 3,928 propensity-matched users and nonusers, according to a report at the World Congress on Osteoarthritis.
“In older women with incident knee osteoarthritis, incident bisphosphonate use may be associated with lower risk of knee replacement than in nonusers,” said Dr. Tuhina Neogi of Boston University.
Dr. Neogi and her colleagues used data from The Health Improvement Network (THIN), a U.K. database of primary care patients, to identify women aged 50-89 years who received a diagnosis of knee osteoarthritis between 2003 and 2012. Patients were excluded if they were poor surgical candidates or were taking disease-modifying antirheumatic drugs, biologic agents, or other bone-active agents.
The researchers compared 1,964 women who subsequently started bisphosphonate therapy with 1,964 propensity score–matched women who did not. In 85% of the former, the bisphosphonate was alendronate, marketed as Fosamax in the United States.
During a mean follow-up of 3 years, the incidence rate of knee replacement was 21 cases per 1,000 patient-years among bisphosphonate users and 29 cases per 1,000 patient-years among nonusers, according to results reported at the meeting, which was sponsored by Osteoarthritis Research Society International.
In adjusted analyses, users had a significantly lower relative risk of undergoing this surgery (hazard ratio, 0.73), reported Dr. Neogi, who disclosed that she had no relevant conflicts of interest.
Sensitivity analyses showed an even stronger association in a separate cohort of patients matched by age, body mass index, and the duration of osteoarthritis (hazard ratio, 0.33) and a nonsignificant benefit when bisphosphonate users were instead compared against an active user group of women who initiated any other bone-modulating therapy.
“Now of course this is observational data from electronic medical records, so we cannot rule out the potential for residual bias,” she acknowledged. “Our sensitivity analyses were fairly consistent and provide some reassurance, but nonetheless, the magnitude of effect is still likely to be biased due to residual confounding.”
In an interview, Dr. Rik Lories, one of the session’s comoderators and a professor at the University of Leuven, Belgium, said that the study “is still far from practice changing. But the great thing about this research is that we are starting to split up what you would call the osteoarthritic diseases, taking osteoarthritis as the outcome [and showing] the underlying mechanisms of the different phenotypes being different.”
Dr. Neogi noted that subchrondral bone changes are prominent in knee osteoarthritis and that mechanical factors play a central role in the disease. At the same time, findings of trials of antiresorptive agents, including bisphosphonates, in knee osteoarthritis have been conflicting.
“There are a number of limitations to this study, including the fact that The Health Improvement Network does not have bone mineral density results. We tried to address this by accounting for a prior diagnosis of osteoporosis, fracture history, potential risk for fractures, body mass index, age, number of bone mineral density tests ordered, et cetera,” Dr. Neogi said. “Another limitation is that of the secular trends in use of bone-modulating agents over this time frame, and that precluded robust evaluation of the active user comparator analysis.
“Bone mineral density is still a major potential confounder here that can’t be adequately addressed,” she acknowledged.
SEATTLE – Women with knee osteoarthritis who took bisphosphonates were 27% less likely to undergo joint replacement surgery than were women who didn’t take bisphosphonates in a U.K. cohort study of 3,928 propensity-matched users and nonusers, according to a report at the World Congress on Osteoarthritis.
“In older women with incident knee osteoarthritis, incident bisphosphonate use may be associated with lower risk of knee replacement than in nonusers,” said Dr. Tuhina Neogi of Boston University.
Dr. Neogi and her colleagues used data from The Health Improvement Network (THIN), a U.K. database of primary care patients, to identify women aged 50-89 years who received a diagnosis of knee osteoarthritis between 2003 and 2012. Patients were excluded if they were poor surgical candidates or were taking disease-modifying antirheumatic drugs, biologic agents, or other bone-active agents.
The researchers compared 1,964 women who subsequently started bisphosphonate therapy with 1,964 propensity score–matched women who did not. In 85% of the former, the bisphosphonate was alendronate, marketed as Fosamax in the United States.
During a mean follow-up of 3 years, the incidence rate of knee replacement was 21 cases per 1,000 patient-years among bisphosphonate users and 29 cases per 1,000 patient-years among nonusers, according to results reported at the meeting, which was sponsored by Osteoarthritis Research Society International.
In adjusted analyses, users had a significantly lower relative risk of undergoing this surgery (hazard ratio, 0.73), reported Dr. Neogi, who disclosed that she had no relevant conflicts of interest.
Sensitivity analyses showed an even stronger association in a separate cohort of patients matched by age, body mass index, and the duration of osteoarthritis (hazard ratio, 0.33) and a nonsignificant benefit when bisphosphonate users were instead compared against an active user group of women who initiated any other bone-modulating therapy.
“Now of course this is observational data from electronic medical records, so we cannot rule out the potential for residual bias,” she acknowledged. “Our sensitivity analyses were fairly consistent and provide some reassurance, but nonetheless, the magnitude of effect is still likely to be biased due to residual confounding.”
In an interview, Dr. Rik Lories, one of the session’s comoderators and a professor at the University of Leuven, Belgium, said that the study “is still far from practice changing. But the great thing about this research is that we are starting to split up what you would call the osteoarthritic diseases, taking osteoarthritis as the outcome [and showing] the underlying mechanisms of the different phenotypes being different.”
Dr. Neogi noted that subchrondral bone changes are prominent in knee osteoarthritis and that mechanical factors play a central role in the disease. At the same time, findings of trials of antiresorptive agents, including bisphosphonates, in knee osteoarthritis have been conflicting.
“There are a number of limitations to this study, including the fact that The Health Improvement Network does not have bone mineral density results. We tried to address this by accounting for a prior diagnosis of osteoporosis, fracture history, potential risk for fractures, body mass index, age, number of bone mineral density tests ordered, et cetera,” Dr. Neogi said. “Another limitation is that of the secular trends in use of bone-modulating agents over this time frame, and that precluded robust evaluation of the active user comparator analysis.
“Bone mineral density is still a major potential confounder here that can’t be adequately addressed,” she acknowledged.
AT OARSI 2015
Key clinical point: Bisphosphonate use by women with knee arthritis was associated with a reduced rate of knee surgery.
Major finding: Women who began using bisphosphonates had a 27% lower risk of total knee replacement surgery.
Data source: A cohort study of 3,928 women aged 50-89 who had knee osteoarthritis.
Disclosures: Dr. Neogi disclosed that she had no relevant conflicts of interest.
NASPAG: Hormonal add-back prevents GnRH-A–related bone loss in adolescents
ORLANDO – Hormonal add-back therapy using combination norethindrone acetate and conjugated equine estrogens was effective and better than norethindrone acetate plus placebo for preserving bone health and improving quality of life in adolescents receiving treatment with gonadotropin-releasing hormone agonists (GnRH-A) for endometriosis in a randomized, double-blind, placebo-controlled study.
Of 51 adolescents aged 15-22 years who were initiating GnRH-A therapy for endometriosis, 25 were randomized to receive add-back therapy with 5 mg daily oral norethindrone acetate (NA) plus 0.625 mg oral daily conjugated equine estrogens (CEE), and 26 were randomized to receive NA plus placebo; 18 and 16, respectively, completed the study.
Those in the combination-therapy group experienced significant increases over 12 months in both total body bone mineral content (BMC) and bone mineral density (BMD), compared with those who received NA plus placebo. BMC increased by nearly 40 g/unit scanned in the combination-therapy group, compared with about 12 g in the NA plus placebo group, and BMD increased more than 0.01 g/cm2, compared with no change in the NA plus placebo group, Dr. Amy D. DiVasta reported at the North American Society for Pediatric and Adolescent Gynecology annual meeting.
No losses of total hip or lumbar spine BMC or BMD occurred, said Dr. DiVasta of Boston Children’s Hospital.
Further, lean mass increased in the combination-therapy group at 12 months – by about 1.4 kg, compared with no change in the placebo group. No differences were seen between the groups in change in fat mass.
As for quality of life measures, overall physical health scores at baseline were significantly below the U.S. mean in both groups, and overall mental health scores were above the U.S. mean in both groups. Both groups improved over time on both measures; the increase in the Physical Component Summary scale scores on the SF-36 (Short Form 36 Health Survey) was significantly greater with combination-therapy group (increase from about 40 to 50 out of 100 ), compared with NA plus placebo (increase from about 40 to 45), but the increases on the Mental Component Summary scale scores were not statistically significant in either group, or between the groups.
The study subjects, who were treated for 12 months between 2008 and 2012, were at least 2 years post menarche at baseline and had a surgical diagnosis of endometriosis. The two treatment groups were similar with respect to baseline characteristics, including age, BMD Z score, and disease severity. No significant side effects were observed in either the combination or NA plus placebo group, Dr. DiVasta said, noting that laboratory tests included liver function tests and lipid levels.
Areal BMD, BMC, and body composition were measured by dual-energy X-ray absorptiometry (DXA) at baseline, 6 months, and 12 months. Anthropometrics, quality of life measures, and laboratory studies were conducted at 1, 3, 6, and 12 months.
GnRH-A are commonly utilized for endometriosis patients who fail primary therapy, such as NSAIDs or combined oral contraceptives, but long-term use is associated with deleterious effects on bone mineralization; adults have been shown to lose 5%-8% of BMD after 3-6 months of treatment, Dr. DiVasta noted.
Hormonal add-back therapy is a promising adjunct to counteract these effects and could be an important tool for protecting adolescents, who are at the greatest risk for the deleterious effects of GnRH-A therapy, she said.
In the current study, hormonal add-back did successfully protect bone health and improve quality of life for adolescents with endometriosis who were treated with 12 months of GnRH-A. Combination therapy with NA and CEE appears to be more effective for increasing total body BMC and BMD, lean mass, and physical health-related quality of life, as compared with NA monotherapy, she said.
The findings are limited by the inclusion of only skeletally mature young women, as the results may not be generalizable to growing girls. Also, DXA measures provide two-dimensional measures of bone mineral density, and do not yield information regarding skeletal strength or bone microarchitecture, she noted.
“Given the prevalence of endometriosis, our data suggest norethindrone plus estrogens to be a useful adjunctive therapy to prevent bone loss in these young women while they receive appropriate medical treatment for their underlying disease,” she concluded, noting that future work will explore the effects of add-back on the peripheral skeleton and bone strength.
This study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, the McCarthy Family Foundation, Thrasher Research Fund, and Boston Children’s Hospital department of medicine. Medications were provided by Abbott, Duramed Pharmaceuticals, and Wyeth Pharmaceuticals. Dr. DiVasta reported having no relevant financial disclosures.
ORLANDO – Hormonal add-back therapy using combination norethindrone acetate and conjugated equine estrogens was effective and better than norethindrone acetate plus placebo for preserving bone health and improving quality of life in adolescents receiving treatment with gonadotropin-releasing hormone agonists (GnRH-A) for endometriosis in a randomized, double-blind, placebo-controlled study.
Of 51 adolescents aged 15-22 years who were initiating GnRH-A therapy for endometriosis, 25 were randomized to receive add-back therapy with 5 mg daily oral norethindrone acetate (NA) plus 0.625 mg oral daily conjugated equine estrogens (CEE), and 26 were randomized to receive NA plus placebo; 18 and 16, respectively, completed the study.
Those in the combination-therapy group experienced significant increases over 12 months in both total body bone mineral content (BMC) and bone mineral density (BMD), compared with those who received NA plus placebo. BMC increased by nearly 40 g/unit scanned in the combination-therapy group, compared with about 12 g in the NA plus placebo group, and BMD increased more than 0.01 g/cm2, compared with no change in the NA plus placebo group, Dr. Amy D. DiVasta reported at the North American Society for Pediatric and Adolescent Gynecology annual meeting.
No losses of total hip or lumbar spine BMC or BMD occurred, said Dr. DiVasta of Boston Children’s Hospital.
Further, lean mass increased in the combination-therapy group at 12 months – by about 1.4 kg, compared with no change in the placebo group. No differences were seen between the groups in change in fat mass.
As for quality of life measures, overall physical health scores at baseline were significantly below the U.S. mean in both groups, and overall mental health scores were above the U.S. mean in both groups. Both groups improved over time on both measures; the increase in the Physical Component Summary scale scores on the SF-36 (Short Form 36 Health Survey) was significantly greater with combination-therapy group (increase from about 40 to 50 out of 100 ), compared with NA plus placebo (increase from about 40 to 45), but the increases on the Mental Component Summary scale scores were not statistically significant in either group, or between the groups.
The study subjects, who were treated for 12 months between 2008 and 2012, were at least 2 years post menarche at baseline and had a surgical diagnosis of endometriosis. The two treatment groups were similar with respect to baseline characteristics, including age, BMD Z score, and disease severity. No significant side effects were observed in either the combination or NA plus placebo group, Dr. DiVasta said, noting that laboratory tests included liver function tests and lipid levels.
Areal BMD, BMC, and body composition were measured by dual-energy X-ray absorptiometry (DXA) at baseline, 6 months, and 12 months. Anthropometrics, quality of life measures, and laboratory studies were conducted at 1, 3, 6, and 12 months.
GnRH-A are commonly utilized for endometriosis patients who fail primary therapy, such as NSAIDs or combined oral contraceptives, but long-term use is associated with deleterious effects on bone mineralization; adults have been shown to lose 5%-8% of BMD after 3-6 months of treatment, Dr. DiVasta noted.
Hormonal add-back therapy is a promising adjunct to counteract these effects and could be an important tool for protecting adolescents, who are at the greatest risk for the deleterious effects of GnRH-A therapy, she said.
In the current study, hormonal add-back did successfully protect bone health and improve quality of life for adolescents with endometriosis who were treated with 12 months of GnRH-A. Combination therapy with NA and CEE appears to be more effective for increasing total body BMC and BMD, lean mass, and physical health-related quality of life, as compared with NA monotherapy, she said.
The findings are limited by the inclusion of only skeletally mature young women, as the results may not be generalizable to growing girls. Also, DXA measures provide two-dimensional measures of bone mineral density, and do not yield information regarding skeletal strength or bone microarchitecture, she noted.
“Given the prevalence of endometriosis, our data suggest norethindrone plus estrogens to be a useful adjunctive therapy to prevent bone loss in these young women while they receive appropriate medical treatment for their underlying disease,” she concluded, noting that future work will explore the effects of add-back on the peripheral skeleton and bone strength.
This study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, the McCarthy Family Foundation, Thrasher Research Fund, and Boston Children’s Hospital department of medicine. Medications were provided by Abbott, Duramed Pharmaceuticals, and Wyeth Pharmaceuticals. Dr. DiVasta reported having no relevant financial disclosures.
ORLANDO – Hormonal add-back therapy using combination norethindrone acetate and conjugated equine estrogens was effective and better than norethindrone acetate plus placebo for preserving bone health and improving quality of life in adolescents receiving treatment with gonadotropin-releasing hormone agonists (GnRH-A) for endometriosis in a randomized, double-blind, placebo-controlled study.
Of 51 adolescents aged 15-22 years who were initiating GnRH-A therapy for endometriosis, 25 were randomized to receive add-back therapy with 5 mg daily oral norethindrone acetate (NA) plus 0.625 mg oral daily conjugated equine estrogens (CEE), and 26 were randomized to receive NA plus placebo; 18 and 16, respectively, completed the study.
Those in the combination-therapy group experienced significant increases over 12 months in both total body bone mineral content (BMC) and bone mineral density (BMD), compared with those who received NA plus placebo. BMC increased by nearly 40 g/unit scanned in the combination-therapy group, compared with about 12 g in the NA plus placebo group, and BMD increased more than 0.01 g/cm2, compared with no change in the NA plus placebo group, Dr. Amy D. DiVasta reported at the North American Society for Pediatric and Adolescent Gynecology annual meeting.
No losses of total hip or lumbar spine BMC or BMD occurred, said Dr. DiVasta of Boston Children’s Hospital.
Further, lean mass increased in the combination-therapy group at 12 months – by about 1.4 kg, compared with no change in the placebo group. No differences were seen between the groups in change in fat mass.
As for quality of life measures, overall physical health scores at baseline were significantly below the U.S. mean in both groups, and overall mental health scores were above the U.S. mean in both groups. Both groups improved over time on both measures; the increase in the Physical Component Summary scale scores on the SF-36 (Short Form 36 Health Survey) was significantly greater with combination-therapy group (increase from about 40 to 50 out of 100 ), compared with NA plus placebo (increase from about 40 to 45), but the increases on the Mental Component Summary scale scores were not statistically significant in either group, or between the groups.
The study subjects, who were treated for 12 months between 2008 and 2012, were at least 2 years post menarche at baseline and had a surgical diagnosis of endometriosis. The two treatment groups were similar with respect to baseline characteristics, including age, BMD Z score, and disease severity. No significant side effects were observed in either the combination or NA plus placebo group, Dr. DiVasta said, noting that laboratory tests included liver function tests and lipid levels.
Areal BMD, BMC, and body composition were measured by dual-energy X-ray absorptiometry (DXA) at baseline, 6 months, and 12 months. Anthropometrics, quality of life measures, and laboratory studies were conducted at 1, 3, 6, and 12 months.
GnRH-A are commonly utilized for endometriosis patients who fail primary therapy, such as NSAIDs or combined oral contraceptives, but long-term use is associated with deleterious effects on bone mineralization; adults have been shown to lose 5%-8% of BMD after 3-6 months of treatment, Dr. DiVasta noted.
Hormonal add-back therapy is a promising adjunct to counteract these effects and could be an important tool for protecting adolescents, who are at the greatest risk for the deleterious effects of GnRH-A therapy, she said.
In the current study, hormonal add-back did successfully protect bone health and improve quality of life for adolescents with endometriosis who were treated with 12 months of GnRH-A. Combination therapy with NA and CEE appears to be more effective for increasing total body BMC and BMD, lean mass, and physical health-related quality of life, as compared with NA monotherapy, she said.
The findings are limited by the inclusion of only skeletally mature young women, as the results may not be generalizable to growing girls. Also, DXA measures provide two-dimensional measures of bone mineral density, and do not yield information regarding skeletal strength or bone microarchitecture, she noted.
“Given the prevalence of endometriosis, our data suggest norethindrone plus estrogens to be a useful adjunctive therapy to prevent bone loss in these young women while they receive appropriate medical treatment for their underlying disease,” she concluded, noting that future work will explore the effects of add-back on the peripheral skeleton and bone strength.
This study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, the McCarthy Family Foundation, Thrasher Research Fund, and Boston Children’s Hospital department of medicine. Medications were provided by Abbott, Duramed Pharmaceuticals, and Wyeth Pharmaceuticals. Dr. DiVasta reported having no relevant financial disclosures.
AT THE NASPAG ANNUAL MEETING
Key clinical point: Add-back therapy could allow for safe long-term GnRH-A therapy in adolescents with endometriosis.
Major finding: Bone mineral content increased nearly 40 g/unit scanned in the combination therapy group vs. about 12 g in the norethindrone acetate plus placebo group.
Data source: A randomized, placebo-controlled study of 51 adolescents.
Disclosures: This study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, the McCarthy Family Foundation, Thrasher Research Fund, and Boston Children’s Hospital department of medicine. Medications were provided by Abbott, Duramed Pharmaceuticals, and Wyeth Pharmaceuticals. Dr. DiVasta reported having no relevant financial disclosures.
Hip replacements not just for the elderly anymore
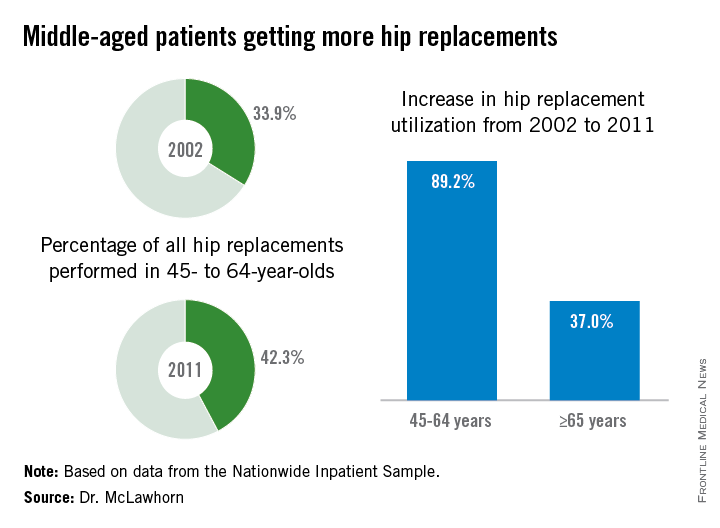
Hip replacement is becoming more common among middle-aged Americans at the same time as the number of surgeons who perform the procedure is declining, Dr. Alexander S. McLawhorn said at the annual meeting of the American Academy of Orthopaedic Surgeons in Las Vegas.
In 2011, patients aged 45-64 years underwent 42.3% of the hip replacements performed, compared with 33.9% in 2002. The number of replacements performed rose from approximately 68,000 in 2002 to 128,000 in 2011, an increase of 89.2%, compared with an increase of 37.0% among those aged 65 years and older, according to data from the Nationwide Inpatient Sample.
This “observed growth was best explained by an expansion of the middle-aged population in the United States. This particular age group is projected to continue expanding, and as such the demand for [hip replacement] in this active group of patients will likely continue to rise as well,” Dr. McLawhorn of the Hospital for Special Surgery, New York, said in a written statement.
According to membership data from the AAOS, however, the number of physicians performing hip replacements declined by almost 29% from 2002 to 2011, which will “increase the future revision burden” on those surgeons who are still doing the procedure, the investigators said.
Dr. McLawhorn had no conflicts to report, but one of his associates disclosed relationships with Ethicon, the Knee Society, Medtronic, Mekanika, and Zimmer.
Hip replacement is becoming more common among middle-aged Americans at the same time as the number of surgeons who perform the procedure is declining, Dr. Alexander S. McLawhorn said at the annual meeting of the American Academy of Orthopaedic Surgeons in Las Vegas.
In 2011, patients aged 45-64 years underwent 42.3% of the hip replacements performed, compared with 33.9% in 2002. The number of replacements performed rose from approximately 68,000 in 2002 to 128,000 in 2011, an increase of 89.2%, compared with an increase of 37.0% among those aged 65 years and older, according to data from the Nationwide Inpatient Sample.
This “observed growth was best explained by an expansion of the middle-aged population in the United States. This particular age group is projected to continue expanding, and as such the demand for [hip replacement] in this active group of patients will likely continue to rise as well,” Dr. McLawhorn of the Hospital for Special Surgery, New York, said in a written statement.
According to membership data from the AAOS, however, the number of physicians performing hip replacements declined by almost 29% from 2002 to 2011, which will “increase the future revision burden” on those surgeons who are still doing the procedure, the investigators said.
Dr. McLawhorn had no conflicts to report, but one of his associates disclosed relationships with Ethicon, the Knee Society, Medtronic, Mekanika, and Zimmer.
Hip replacement is becoming more common among middle-aged Americans at the same time as the number of surgeons who perform the procedure is declining, Dr. Alexander S. McLawhorn said at the annual meeting of the American Academy of Orthopaedic Surgeons in Las Vegas.
In 2011, patients aged 45-64 years underwent 42.3% of the hip replacements performed, compared with 33.9% in 2002. The number of replacements performed rose from approximately 68,000 in 2002 to 128,000 in 2011, an increase of 89.2%, compared with an increase of 37.0% among those aged 65 years and older, according to data from the Nationwide Inpatient Sample.
This “observed growth was best explained by an expansion of the middle-aged population in the United States. This particular age group is projected to continue expanding, and as such the demand for [hip replacement] in this active group of patients will likely continue to rise as well,” Dr. McLawhorn of the Hospital for Special Surgery, New York, said in a written statement.
According to membership data from the AAOS, however, the number of physicians performing hip replacements declined by almost 29% from 2002 to 2011, which will “increase the future revision burden” on those surgeons who are still doing the procedure, the investigators said.
Dr. McLawhorn had no conflicts to report, but one of his associates disclosed relationships with Ethicon, the Knee Society, Medtronic, Mekanika, and Zimmer.
FROM AAOS 2015

Universal bisphosphonates after wrist fracture prevent hip fractures but at a cost
Giving bone-strengthening medication routinely to all elderly women who sustain a wrist fracture would reduce subsequent hip fractures by about a quarter, but at a cost of over $200,000 per prevented fracture. Additionally, expanded bisphosphonate use could cause nearly 20,000 more atypical femur fractures in this population.
Dr. Suneel Bhat and his associates at Thomas Jefferson University, Philadelphia, used sophisticated modeling techniques to project costs and consequences of wider prescribing of bisphosphonates for bone fragility in women aged 65 years and older. Distal radius fracture is known to be associated with osteoporosis in women of this age, who are then at increased risk of subsequent fracture. Dr. Bhat presented his findings on March 24 at the annual meeting of the American Academy of Orthopaedic Surgeons in Las Vegas.
Study authors drew from the medical literature and publicly available Medicare data to obtain fracture incidence data and cost information for statistical modeling. Bhat and colleagues obtained age-specific incidence of distal radius fractures among women aged 65 and older, as well as rates of hip fracture following wrist fractures, both for those who did and did not receive the bisphosphonate risendronate. Atypical femur fracture is a known complication of bisphosphonate treatment for some patients; the risk of this complication and medication costs were drawn from the literature.
To assess the direct costs of hip fracture treatment, investigators used Medicare reimbursement data to price treatment components, including inpatient care as well as surgical and anesthesia services.
From these data, investigators used a modified Monte Carlo technique to obtain a cost and incidence model. This model predicted that 357,656 lifetime subsequent hip fractures would occur in elderly women with wrist fracture; this number would drop to 262,767 with universal bisphosphonate treatment. The cost for this savings, an aggregate $19.5 billion in drug costs, meant that each fracture prevented would cost $205,534. An additional 19,464 patients would sustain atypical femur fracture from risendronate treatment.
Average risendronate costs were estimated at $1,485/patient-year. This figure would have to fall to just $70/patient yearly to make risendronate treatment cost effective, Dr. Bhat calculated.
Giving bone-strengthening medication routinely to all elderly women who sustain a wrist fracture would reduce subsequent hip fractures by about a quarter, but at a cost of over $200,000 per prevented fracture. Additionally, expanded bisphosphonate use could cause nearly 20,000 more atypical femur fractures in this population.
Dr. Suneel Bhat and his associates at Thomas Jefferson University, Philadelphia, used sophisticated modeling techniques to project costs and consequences of wider prescribing of bisphosphonates for bone fragility in women aged 65 years and older. Distal radius fracture is known to be associated with osteoporosis in women of this age, who are then at increased risk of subsequent fracture. Dr. Bhat presented his findings on March 24 at the annual meeting of the American Academy of Orthopaedic Surgeons in Las Vegas.
Study authors drew from the medical literature and publicly available Medicare data to obtain fracture incidence data and cost information for statistical modeling. Bhat and colleagues obtained age-specific incidence of distal radius fractures among women aged 65 and older, as well as rates of hip fracture following wrist fractures, both for those who did and did not receive the bisphosphonate risendronate. Atypical femur fracture is a known complication of bisphosphonate treatment for some patients; the risk of this complication and medication costs were drawn from the literature.
To assess the direct costs of hip fracture treatment, investigators used Medicare reimbursement data to price treatment components, including inpatient care as well as surgical and anesthesia services.
From these data, investigators used a modified Monte Carlo technique to obtain a cost and incidence model. This model predicted that 357,656 lifetime subsequent hip fractures would occur in elderly women with wrist fracture; this number would drop to 262,767 with universal bisphosphonate treatment. The cost for this savings, an aggregate $19.5 billion in drug costs, meant that each fracture prevented would cost $205,534. An additional 19,464 patients would sustain atypical femur fracture from risendronate treatment.
Average risendronate costs were estimated at $1,485/patient-year. This figure would have to fall to just $70/patient yearly to make risendronate treatment cost effective, Dr. Bhat calculated.
Giving bone-strengthening medication routinely to all elderly women who sustain a wrist fracture would reduce subsequent hip fractures by about a quarter, but at a cost of over $200,000 per prevented fracture. Additionally, expanded bisphosphonate use could cause nearly 20,000 more atypical femur fractures in this population.
Dr. Suneel Bhat and his associates at Thomas Jefferson University, Philadelphia, used sophisticated modeling techniques to project costs and consequences of wider prescribing of bisphosphonates for bone fragility in women aged 65 years and older. Distal radius fracture is known to be associated with osteoporosis in women of this age, who are then at increased risk of subsequent fracture. Dr. Bhat presented his findings on March 24 at the annual meeting of the American Academy of Orthopaedic Surgeons in Las Vegas.
Study authors drew from the medical literature and publicly available Medicare data to obtain fracture incidence data and cost information for statistical modeling. Bhat and colleagues obtained age-specific incidence of distal radius fractures among women aged 65 and older, as well as rates of hip fracture following wrist fractures, both for those who did and did not receive the bisphosphonate risendronate. Atypical femur fracture is a known complication of bisphosphonate treatment for some patients; the risk of this complication and medication costs were drawn from the literature.
To assess the direct costs of hip fracture treatment, investigators used Medicare reimbursement data to price treatment components, including inpatient care as well as surgical and anesthesia services.
From these data, investigators used a modified Monte Carlo technique to obtain a cost and incidence model. This model predicted that 357,656 lifetime subsequent hip fractures would occur in elderly women with wrist fracture; this number would drop to 262,767 with universal bisphosphonate treatment. The cost for this savings, an aggregate $19.5 billion in drug costs, meant that each fracture prevented would cost $205,534. An additional 19,464 patients would sustain atypical femur fracture from risendronate treatment.
Average risendronate costs were estimated at $1,485/patient-year. This figure would have to fall to just $70/patient yearly to make risendronate treatment cost effective, Dr. Bhat calculated.
FROM AAOS 2015
Key clinical point: Savings from prevention of hip fractures with universal bisphosphonates after distal radius fractures in elderly women would be outweighed by drug costs.
Major findings: If all women 65 years of age and older who have had a distal radius fracture went on to receive bisphosphonate treatment, 94,888 lifetime hip fractures would be avoided, but at a cost of $205,534 per averted fracture, and with an additional 19,464 atypical femur fractures.
Data source: Modeling based on fracture incidence data and medication, surgical, and aftercare cost data drawn from literature review and publicly available Medicare databases.
Disclosures: Dr. Asif Ilyas reported publishing royalties and financial or material support from Jaypee Medical Publishers and is on the editorial or governing board of Orthopedic Clinics of North America. The other authors reported that they had no conflicts of interest.
Oral bisphosphonates linked with lower risk of endometrial cancer
A large prospective study found that among 89,918 women aged 50-79 years, bisphosphonate use was inversely associated with age-adjusted endometrial cancer risk, investigators reported. The study was published online Feb. 23 in the Journal of Clinical Oncology.
Crude incidence of endometrial cancer was 12 per 10,000 person-years for nonusers and 8 per 10,000 years for bisphosphonate users (bisphosphonate users: HR 0.76, 95% CI 0.61 to 0.94; P = .01). During the median 12.5-year follow up, 1,123 women (1,070 nonusers and 53 users) were diagnosed with endometrial cancer, reported Dr. Polly A. Newcomb and associates (J. Clin. Oncol. 2015 Feb. 23 [doi:10.1200/JCO.2014.58.6842]).
Bisphosphonate use was 2% at baseline and increased to 10% by year 6. It was treated as a time-varying never/ever variable that was updated at 1, 3, and 6 years. Compared with nonusers, bisphosphonate users were slightly older, leaner, more educated, and less likely to smoke.
This observational study is limited by the possibility of confounding factors. Women may have taken oral bisphosphonates because they had high fracture risk due to low endogenous estrogen from low weight, which is associated with low endometrial cancer risk. After the researchers controlled for weight and other confounding factors, such as fracture risk, the statistical analysis yielded similar measures of association (HR 0.80, 0.64 to 1.00; P = .05).
“In summary, our findings suggest that use of bisphosphonates is modestly associated with reduced endometrial cancer risk, a finding consistent with the inverse association between use of this medication and breast cancer risk,” wrote Dr. Newcomb of Fred Hutchinson Cancer and University of Washington Research Center, Seattle, and associates.
Dr. Newcomb and most coauthors had no disclosures. One coauthor reported consulting or advisory roles with Novartis, Pfizer, Genentech, Novo Nordisk, Genomic Health.
A large prospective study found that among 89,918 women aged 50-79 years, bisphosphonate use was inversely associated with age-adjusted endometrial cancer risk, investigators reported. The study was published online Feb. 23 in the Journal of Clinical Oncology.
Crude incidence of endometrial cancer was 12 per 10,000 person-years for nonusers and 8 per 10,000 years for bisphosphonate users (bisphosphonate users: HR 0.76, 95% CI 0.61 to 0.94; P = .01). During the median 12.5-year follow up, 1,123 women (1,070 nonusers and 53 users) were diagnosed with endometrial cancer, reported Dr. Polly A. Newcomb and associates (J. Clin. Oncol. 2015 Feb. 23 [doi:10.1200/JCO.2014.58.6842]).
Bisphosphonate use was 2% at baseline and increased to 10% by year 6. It was treated as a time-varying never/ever variable that was updated at 1, 3, and 6 years. Compared with nonusers, bisphosphonate users were slightly older, leaner, more educated, and less likely to smoke.
This observational study is limited by the possibility of confounding factors. Women may have taken oral bisphosphonates because they had high fracture risk due to low endogenous estrogen from low weight, which is associated with low endometrial cancer risk. After the researchers controlled for weight and other confounding factors, such as fracture risk, the statistical analysis yielded similar measures of association (HR 0.80, 0.64 to 1.00; P = .05).
“In summary, our findings suggest that use of bisphosphonates is modestly associated with reduced endometrial cancer risk, a finding consistent with the inverse association between use of this medication and breast cancer risk,” wrote Dr. Newcomb of Fred Hutchinson Cancer and University of Washington Research Center, Seattle, and associates.
Dr. Newcomb and most coauthors had no disclosures. One coauthor reported consulting or advisory roles with Novartis, Pfizer, Genentech, Novo Nordisk, Genomic Health.
A large prospective study found that among 89,918 women aged 50-79 years, bisphosphonate use was inversely associated with age-adjusted endometrial cancer risk, investigators reported. The study was published online Feb. 23 in the Journal of Clinical Oncology.
Crude incidence of endometrial cancer was 12 per 10,000 person-years for nonusers and 8 per 10,000 years for bisphosphonate users (bisphosphonate users: HR 0.76, 95% CI 0.61 to 0.94; P = .01). During the median 12.5-year follow up, 1,123 women (1,070 nonusers and 53 users) were diagnosed with endometrial cancer, reported Dr. Polly A. Newcomb and associates (J. Clin. Oncol. 2015 Feb. 23 [doi:10.1200/JCO.2014.58.6842]).
Bisphosphonate use was 2% at baseline and increased to 10% by year 6. It was treated as a time-varying never/ever variable that was updated at 1, 3, and 6 years. Compared with nonusers, bisphosphonate users were slightly older, leaner, more educated, and less likely to smoke.
This observational study is limited by the possibility of confounding factors. Women may have taken oral bisphosphonates because they had high fracture risk due to low endogenous estrogen from low weight, which is associated with low endometrial cancer risk. After the researchers controlled for weight and other confounding factors, such as fracture risk, the statistical analysis yielded similar measures of association (HR 0.80, 0.64 to 1.00; P = .05).
“In summary, our findings suggest that use of bisphosphonates is modestly associated with reduced endometrial cancer risk, a finding consistent with the inverse association between use of this medication and breast cancer risk,” wrote Dr. Newcomb of Fred Hutchinson Cancer and University of Washington Research Center, Seattle, and associates.
Dr. Newcomb and most coauthors had no disclosures. One coauthor reported consulting or advisory roles with Novartis, Pfizer, Genentech, Novo Nordisk, Genomic Health.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Oral bisphosphonate use was modestly associated with reduced risk of endometrial cancer.
Major finding: Risk of endometrial cancer was lower among bisphosphonate users: hazard ratio 0.76, 95% CI 0.61 to 0.94, P = .01.
Data source: The Women’s Health Initiative prospective cohort of 89,918 women with 1,123 cases of incident endometrial cancer.
Disclosures: Dr. Newcomb and most coauthors had no disclosures. One coauthor reported consulting or advisory roles with Novartis, Pfizer, Genentech, Novo Nordisk, Genomic Health.
Look for adverse events in patients with chronic urticaria
HOUSTON – The risk of adverse events may be cumulative over the lifetime of patients taking oral corticosteroids for urticaria.
Dr. Dennis Ledford, professor of medicine at the University of South Florida, Tampa, and his colleagues examined records of 12,647 patients culled from a commercial claims database between January 2008 and December 2012 who had taken oral corticosteroids for chronic idiopathic or spontaneous urticaria during a 12-month period. More than half (55%) used oral corticosteroids (mean dosage of 367.5 mg) for an average of 16.2 days. At follow-up, patients displayed adverse events at a rate of 27 per 100 patient-years.
Adverse events mostly included skeletal conditions such as osteoporosis and bone fractures, but investigators also noted diabetes, hypertension, lipid disorders, depression, mania, and cataracts, Dr. Ledford said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
More concerning, “there’s a cumulative risk,” Dr. Ledford said in an interview. “The more [prednisone equivalent] you take over your lifetime, the greater the chance is that you’re going to develop the side effects we’ve listed here.”
Using time-sensitive Cox regression models, Dr. Ledford and his colleagues determined that the risk for adverse events went up by 7% for each gram dose of prednisone equivalent to which patients were exposed after adjusting for age, sex, immunomodulator use, and Charlson Comorbidity Index. Only cataracts were not subject to the cumulative effects.
“The message of this fairly large analysis is that there are cumulative side effects to prednisone that may not be evident to the physician or clinician performing day-to-day care of patients,” Dr. Ledford said. “These effects are slow to develop and often present in areas of medicine that the physician treating urticaria would not take care of.”
Patients enrolled in this study had all been diagnosed with urticaria at either of two outpatient clinic visits at least 6 weeks apart in a single calendar year, or had received one diagnosis of urticaria and one of angioedema at two separate outpatient clinics at least 6 weeks apart. Patients were followed for at least 1 year after completion of the initial 12-month study period, until end of enrollment or end of study.
Dr. Ledford stressed the need to use noncorticosteroid therapies when treating chronic urticaria, such as calcineurin inhibitors – which also carry risks of hypertension and cancer – or omalizumab.
The study was funded by Genentech and Novartis Pharma AG which market omalizumab as Xolair. Dr. Ledford disclosed that he is affiliated with Genentech, Novartis Pharma AG, and a number of other pharmaceutical companies.
HOUSTON – The risk of adverse events may be cumulative over the lifetime of patients taking oral corticosteroids for urticaria.
Dr. Dennis Ledford, professor of medicine at the University of South Florida, Tampa, and his colleagues examined records of 12,647 patients culled from a commercial claims database between January 2008 and December 2012 who had taken oral corticosteroids for chronic idiopathic or spontaneous urticaria during a 12-month period. More than half (55%) used oral corticosteroids (mean dosage of 367.5 mg) for an average of 16.2 days. At follow-up, patients displayed adverse events at a rate of 27 per 100 patient-years.
Adverse events mostly included skeletal conditions such as osteoporosis and bone fractures, but investigators also noted diabetes, hypertension, lipid disorders, depression, mania, and cataracts, Dr. Ledford said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
More concerning, “there’s a cumulative risk,” Dr. Ledford said in an interview. “The more [prednisone equivalent] you take over your lifetime, the greater the chance is that you’re going to develop the side effects we’ve listed here.”
Using time-sensitive Cox regression models, Dr. Ledford and his colleagues determined that the risk for adverse events went up by 7% for each gram dose of prednisone equivalent to which patients were exposed after adjusting for age, sex, immunomodulator use, and Charlson Comorbidity Index. Only cataracts were not subject to the cumulative effects.
“The message of this fairly large analysis is that there are cumulative side effects to prednisone that may not be evident to the physician or clinician performing day-to-day care of patients,” Dr. Ledford said. “These effects are slow to develop and often present in areas of medicine that the physician treating urticaria would not take care of.”
Patients enrolled in this study had all been diagnosed with urticaria at either of two outpatient clinic visits at least 6 weeks apart in a single calendar year, or had received one diagnosis of urticaria and one of angioedema at two separate outpatient clinics at least 6 weeks apart. Patients were followed for at least 1 year after completion of the initial 12-month study period, until end of enrollment or end of study.
Dr. Ledford stressed the need to use noncorticosteroid therapies when treating chronic urticaria, such as calcineurin inhibitors – which also carry risks of hypertension and cancer – or omalizumab.
The study was funded by Genentech and Novartis Pharma AG which market omalizumab as Xolair. Dr. Ledford disclosed that he is affiliated with Genentech, Novartis Pharma AG, and a number of other pharmaceutical companies.
HOUSTON – The risk of adverse events may be cumulative over the lifetime of patients taking oral corticosteroids for urticaria.
Dr. Dennis Ledford, professor of medicine at the University of South Florida, Tampa, and his colleagues examined records of 12,647 patients culled from a commercial claims database between January 2008 and December 2012 who had taken oral corticosteroids for chronic idiopathic or spontaneous urticaria during a 12-month period. More than half (55%) used oral corticosteroids (mean dosage of 367.5 mg) for an average of 16.2 days. At follow-up, patients displayed adverse events at a rate of 27 per 100 patient-years.
Adverse events mostly included skeletal conditions such as osteoporosis and bone fractures, but investigators also noted diabetes, hypertension, lipid disorders, depression, mania, and cataracts, Dr. Ledford said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
More concerning, “there’s a cumulative risk,” Dr. Ledford said in an interview. “The more [prednisone equivalent] you take over your lifetime, the greater the chance is that you’re going to develop the side effects we’ve listed here.”
Using time-sensitive Cox regression models, Dr. Ledford and his colleagues determined that the risk for adverse events went up by 7% for each gram dose of prednisone equivalent to which patients were exposed after adjusting for age, sex, immunomodulator use, and Charlson Comorbidity Index. Only cataracts were not subject to the cumulative effects.
“The message of this fairly large analysis is that there are cumulative side effects to prednisone that may not be evident to the physician or clinician performing day-to-day care of patients,” Dr. Ledford said. “These effects are slow to develop and often present in areas of medicine that the physician treating urticaria would not take care of.”
Patients enrolled in this study had all been diagnosed with urticaria at either of two outpatient clinic visits at least 6 weeks apart in a single calendar year, or had received one diagnosis of urticaria and one of angioedema at two separate outpatient clinics at least 6 weeks apart. Patients were followed for at least 1 year after completion of the initial 12-month study period, until end of enrollment or end of study.
Dr. Ledford stressed the need to use noncorticosteroid therapies when treating chronic urticaria, such as calcineurin inhibitors – which also carry risks of hypertension and cancer – or omalizumab.
The study was funded by Genentech and Novartis Pharma AG which market omalizumab as Xolair. Dr. Ledford disclosed that he is affiliated with Genentech, Novartis Pharma AG, and a number of other pharmaceutical companies.
AT 2015 AAAAI ANNUAL MEETING
Key clinical point: The cumulative adverse events of oral corticosteroids may not present to the physician treating the patient for urticaria.
Major finding: The risk for adverse events went up by 7% for each gram dose of prednisone equivalent.
Data source: Retrospective cohort study of 12,647 patients selected from a commercial claims database from 2008 through 2012.
Disclosures: Study funded by Genentech and Novartis Pharma AG; Dr. Ledford is affiliated with Genentech, Novartis Pharma AG, and a number of other pharmaceutical companies.
Adults with eczema face increased risk of fracture and bone or joint injuries
Eczema in adulthood is directly associated with an increase in incidence of injuries that cause physical limitations, particularly fracture, bone, and joint injuries, according to the results of a prospective study published online in JAMA Dermatology.
“The risk of bone fracture and other injury causing limitation in adults with eczema has been largely unexplored,” noted Dr. Nitin Garg and Dr. Jonathan I. Silverberg of Northwestern University in Chicago.
“Patients with eczema may be at risk of fracture given their use of systemic corticosteroids, which may decrease bone mineral density [and] therefore, studies describing the prevalence of fracture among adults with eczema are needed,” they added (JAMA Dermatol. 2015;151:33-41 [doi:10.1001/jamadermatol.2014.2098]).

Dr. Garg and Dr. Silverberg used data from the 2012 National Health Interview Survey, which was conducted by the National Center for Health Statistics, to create their prospective, questionnaire-based study. The final analysis included 34,500 adults aged 18-85 years. They controlled for factors such as age, sex, race, Hispanic origin, household income, highest level of household education, family structure, and whether or not the subject was born in the United States.
The prevalence of self-reported eczema or skin allergy was 7.2%, the prevalence of any limitation-causing injury was 2.0%, and any limitation-causing injury in the past 12 months among adults was 7.2%. A fracture and bone or joint injury (FBJI) causing limitation was reported by 1.5% of the study population and other types of injury causing limitation were reported by 0.6%. The prevalence of FBJI causing limitation increased gradually with age, to peak in subjects aged 50-69 years, decreasing thereafter.
In a logistic regression analysis, adults with eczema had a 44% increased risk of any injury causing limitation (adjusted odds ratio, 1.44), and a 67% increased risk of FBJI (aOR, 1.67).
Adults with eczema who also reported experiencing fatigue (aOR, 1.59; 95% CI, 1.16-2.19), daytime sleepiness (aOR, 1.81), or insomnia (aOR, 1.74) had higher rates of FBJI than individuals with sleep symptoms but no eczema. Adults with both eczema and psychiatric or behavioral disorders also were more likely to experience FBJI than individuals suffering from eczema alone, or individuals suffering from psychiatric and behavioral disorders, but not eczema.
“Taken together, these data suggest that adult eczema is a previously unrecognized risk factor for fracture and other injury, emphasizing the importance of developing safer and more effective clinical interventions for itch and sleep problems in eczema, as well as preventive measures for injury risk reduction in eczema,” wrote Dr. Garg and Dr. Silverberg. The authors reported no relevant financial disclosures.
Eczema in adulthood is directly associated with an increase in incidence of injuries that cause physical limitations, particularly fracture, bone, and joint injuries, according to the results of a prospective study published online in JAMA Dermatology.
“The risk of bone fracture and other injury causing limitation in adults with eczema has been largely unexplored,” noted Dr. Nitin Garg and Dr. Jonathan I. Silverberg of Northwestern University in Chicago.
“Patients with eczema may be at risk of fracture given their use of systemic corticosteroids, which may decrease bone mineral density [and] therefore, studies describing the prevalence of fracture among adults with eczema are needed,” they added (JAMA Dermatol. 2015;151:33-41 [doi:10.1001/jamadermatol.2014.2098]).
Dr. Garg and Dr. Silverberg used data from the 2012 National Health Interview Survey, which was conducted by the National Center for Health Statistics, to create their prospective, questionnaire-based study. The final analysis included 34,500 adults aged 18-85 years. They controlled for factors such as age, sex, race, Hispanic origin, household income, highest level of household education, family structure, and whether or not the subject was born in the United States.
The prevalence of self-reported eczema or skin allergy was 7.2%, the prevalence of any limitation-causing injury was 2.0%, and any limitation-causing injury in the past 12 months among adults was 7.2%. A fracture and bone or joint injury (FBJI) causing limitation was reported by 1.5% of the study population and other types of injury causing limitation were reported by 0.6%. The prevalence of FBJI causing limitation increased gradually with age, to peak in subjects aged 50-69 years, decreasing thereafter.
In a logistic regression analysis, adults with eczema had a 44% increased risk of any injury causing limitation (adjusted odds ratio, 1.44), and a 67% increased risk of FBJI (aOR, 1.67).
Adults with eczema who also reported experiencing fatigue (aOR, 1.59; 95% CI, 1.16-2.19), daytime sleepiness (aOR, 1.81), or insomnia (aOR, 1.74) had higher rates of FBJI than individuals with sleep symptoms but no eczema. Adults with both eczema and psychiatric or behavioral disorders also were more likely to experience FBJI than individuals suffering from eczema alone, or individuals suffering from psychiatric and behavioral disorders, but not eczema.
“Taken together, these data suggest that adult eczema is a previously unrecognized risk factor for fracture and other injury, emphasizing the importance of developing safer and more effective clinical interventions for itch and sleep problems in eczema, as well as preventive measures for injury risk reduction in eczema,” wrote Dr. Garg and Dr. Silverberg. The authors reported no relevant financial disclosures.
Eczema in adulthood is directly associated with an increase in incidence of injuries that cause physical limitations, particularly fracture, bone, and joint injuries, according to the results of a prospective study published online in JAMA Dermatology.
“The risk of bone fracture and other injury causing limitation in adults with eczema has been largely unexplored,” noted Dr. Nitin Garg and Dr. Jonathan I. Silverberg of Northwestern University in Chicago.
“Patients with eczema may be at risk of fracture given their use of systemic corticosteroids, which may decrease bone mineral density [and] therefore, studies describing the prevalence of fracture among adults with eczema are needed,” they added (JAMA Dermatol. 2015;151:33-41 [doi:10.1001/jamadermatol.2014.2098]).
Dr. Garg and Dr. Silverberg used data from the 2012 National Health Interview Survey, which was conducted by the National Center for Health Statistics, to create their prospective, questionnaire-based study. The final analysis included 34,500 adults aged 18-85 years. They controlled for factors such as age, sex, race, Hispanic origin, household income, highest level of household education, family structure, and whether or not the subject was born in the United States.
The prevalence of self-reported eczema or skin allergy was 7.2%, the prevalence of any limitation-causing injury was 2.0%, and any limitation-causing injury in the past 12 months among adults was 7.2%. A fracture and bone or joint injury (FBJI) causing limitation was reported by 1.5% of the study population and other types of injury causing limitation were reported by 0.6%. The prevalence of FBJI causing limitation increased gradually with age, to peak in subjects aged 50-69 years, decreasing thereafter.
In a logistic regression analysis, adults with eczema had a 44% increased risk of any injury causing limitation (adjusted odds ratio, 1.44), and a 67% increased risk of FBJI (aOR, 1.67).
Adults with eczema who also reported experiencing fatigue (aOR, 1.59; 95% CI, 1.16-2.19), daytime sleepiness (aOR, 1.81), or insomnia (aOR, 1.74) had higher rates of FBJI than individuals with sleep symptoms but no eczema. Adults with both eczema and psychiatric or behavioral disorders also were more likely to experience FBJI than individuals suffering from eczema alone, or individuals suffering from psychiatric and behavioral disorders, but not eczema.
“Taken together, these data suggest that adult eczema is a previously unrecognized risk factor for fracture and other injury, emphasizing the importance of developing safer and more effective clinical interventions for itch and sleep problems in eczema, as well as preventive measures for injury risk reduction in eczema,” wrote Dr. Garg and Dr. Silverberg. The authors reported no relevant financial disclosures.
FROM JAMA DERMATOLOGY
Key clinical point: Eczema in adulthood is associated with an increased risk of limitation-causing injuries.
Major finding: Adults with eczema had a 67% increased risk of fracture and bone or joint injury (FBJI) causing limitation (aOR 1.67).
Data source: Prospective, questionnaire-based, cohort study of 34,500 adults aged 18-85 years from the 2012 National Health Interview Survey.
Disclosures: The authors reported no financial conflicts of interest.

Hot flashes linked to increased hip fracture risk
Hot flashes are associated with a significant increase in the risk of hip fracture, regardless of age, body mass index, and other confounders such as smoking, according to analysis of data from the Women’s Health Study.
The prospective, observational study among 4,867 women aged 50-79 years found a 78% increase in the risk of hip fracture among women with moderate to severe menopausal vasomotor symptoms at baseline, compared with women with no symptoms.

Vasomotor symptom severity was also inversely associated with bone mineral density (BMD) at both the femoral neck and the spine. Compared with women who had no vasomotor symptoms, those with moderate or severe symptoms had 0.015 g/cm2 lower femoral neck BMD and 0.016 g/cm2 lower lumbar spine BMD, according to an analysis published on Dec. 18 in the Journal of Clinical Endocrinology and Metabolism (2014 [doi:10.1210/jc.2014-3062]).
“Despite being younger and heavier than asymptomatic women, characteristics associated with higher BMD, women with moderate/severe [vasomotor symptoms] had a higher risk of hip fractures that was also independent of other established risk factors for fractures,” wrote Dr. Carolyn J. Crandall of the University of California, Los Angeles, and her colleagues.
The study was funded by the National Institutes of Health. Two of the study authors reported consulting and other financial relationships with drug and device companies.
Hot flashes are associated with a significant increase in the risk of hip fracture, regardless of age, body mass index, and other confounders such as smoking, according to analysis of data from the Women’s Health Study.
The prospective, observational study among 4,867 women aged 50-79 years found a 78% increase in the risk of hip fracture among women with moderate to severe menopausal vasomotor symptoms at baseline, compared with women with no symptoms.
Vasomotor symptom severity was also inversely associated with bone mineral density (BMD) at both the femoral neck and the spine. Compared with women who had no vasomotor symptoms, those with moderate or severe symptoms had 0.015 g/cm2 lower femoral neck BMD and 0.016 g/cm2 lower lumbar spine BMD, according to an analysis published on Dec. 18 in the Journal of Clinical Endocrinology and Metabolism (2014 [doi:10.1210/jc.2014-3062]).
“Despite being younger and heavier than asymptomatic women, characteristics associated with higher BMD, women with moderate/severe [vasomotor symptoms] had a higher risk of hip fractures that was also independent of other established risk factors for fractures,” wrote Dr. Carolyn J. Crandall of the University of California, Los Angeles, and her colleagues.
The study was funded by the National Institutes of Health. Two of the study authors reported consulting and other financial relationships with drug and device companies.
Hot flashes are associated with a significant increase in the risk of hip fracture, regardless of age, body mass index, and other confounders such as smoking, according to analysis of data from the Women’s Health Study.
The prospective, observational study among 4,867 women aged 50-79 years found a 78% increase in the risk of hip fracture among women with moderate to severe menopausal vasomotor symptoms at baseline, compared with women with no symptoms.
Vasomotor symptom severity was also inversely associated with bone mineral density (BMD) at both the femoral neck and the spine. Compared with women who had no vasomotor symptoms, those with moderate or severe symptoms had 0.015 g/cm2 lower femoral neck BMD and 0.016 g/cm2 lower lumbar spine BMD, according to an analysis published on Dec. 18 in the Journal of Clinical Endocrinology and Metabolism (2014 [doi:10.1210/jc.2014-3062]).
“Despite being younger and heavier than asymptomatic women, characteristics associated with higher BMD, women with moderate/severe [vasomotor symptoms] had a higher risk of hip fractures that was also independent of other established risk factors for fractures,” wrote Dr. Carolyn J. Crandall of the University of California, Los Angeles, and her colleagues.
The study was funded by the National Institutes of Health. Two of the study authors reported consulting and other financial relationships with drug and device companies.
FROM THE JOURNAL OF CLINICAL ENDOCRINOLOGY AND METABOLISM
Key clinical point: The severity of vasomotor menopause symptoms is associated with risk of hip fracture.
Major finding: Women with moderate to severe vasomotor symptoms have a 78% increase in their risk of hip fracture.
Data source: A prospective, observational study among 4,867 women aged 50-79 years.
Disclosures: The study was funded by the National Institutes of Health. Two of the study authors reported consulting and other financial relationships with drug and device companies.

Varying cutoffs of vitamin D add confusion to field
Efforts to reach agreement on how vitamin D deficiency is defined are complicated by the fact that the cutoff points used in reports from clinical laboratories vary widely.
“I think reporting is a great problem because primary care physicians are very hurried,” Dr. John F. Aloia said at a public conference on vitamin D sponsored by the National Institutes of Health. “When you look at the laboratory report, what you get is a column that’s normal and another column that’s low or high. The choice of the laboratories to choose their own cutpoints is really a problem. The other part of that reporting is using the low level of normal in a range at the RDA [recommended daily allowance].”
In its recently updated recommendations on vitamin D screening, the U.S. Preventive Services Task Force noted that variability between serum vitamin D assay methods “and between laboratories using the same methods may range from 10% to 20%, and classification of samples as ‘deficient’ or ‘nondeficient’ may vary by 4% to 32%, depending on which assay is used. Another factor that may complicate interpretation is that 25-(OH)D may act as a negative acute-phase reactant and its levels may decrease in response to inflammation. Lastly, whether common laboratory reference ranges are appropriate for all ethnic groups is unclear.”
Trying to exert influence on what ranges of serum vitamin D laboratories are using in reporting data “is an issue,” said Dr. Aloia, director of the Bone Mineral Research Center at Winthrop University Hospital, Mineola, N.Y., and professor of medicine at Stony Brook (N.Y.) University. “A laboratory can report anything it chooses to. For instance, the American College of Pathology and other [professional organizations] don’t have the responsibility for [the cut-offs in] those reports.”
Dr. Aloia favors translating the reporting of vitamin D levels based on something like Z scores, “so when you see lab reports, some of them will have a paragraph of explanation to guide the physician,” he explained. “We’re going to need that. We have to move away from just [a] cutpoint range and the lower level of the range being the RDA.”
Dr. Roger Bouillon, professor emeritus of internal medicine at the University of Leuven (Belgium), supports a threshold of 20 ng/mL serum vitamin D in adults. “I don’t like a range [of vitamin D]; they just need to have a level above 20 ng/mL. For me, a threshold is the best strategy on a population basis.”
During an open comment session, attendee Dr. Neil C. Binkley expressed concern over applying Z-score principles to the vitamin D field. “I love bone density measurement,” said Dr. Binkley, codirector of the Osteoporosis Clinical Center & Research Program at the University of Wisconsin, Madison, and past president of the International Society for Clinical Densitometry. “The T-score was in fact an advance in the field. But I can’t tell you how strongly I would urge you to not consider T-scores or Z-scores or something like that in the vitamin D field. Rather, I would urge that we do a better job at measuring 25-hydroxyvitamin D so our laboratories agree and have concise guidance for primary care. If you choose to go into the probability realm and the Z-scores, it is going to be a disaster.”
The presenters reported having no financial disclosures.
On Twitter @dougbrunk
Efforts to reach agreement on how vitamin D deficiency is defined are complicated by the fact that the cutoff points used in reports from clinical laboratories vary widely.
“I think reporting is a great problem because primary care physicians are very hurried,” Dr. John F. Aloia said at a public conference on vitamin D sponsored by the National Institutes of Health. “When you look at the laboratory report, what you get is a column that’s normal and another column that’s low or high. The choice of the laboratories to choose their own cutpoints is really a problem. The other part of that reporting is using the low level of normal in a range at the RDA [recommended daily allowance].”
In its recently updated recommendations on vitamin D screening, the U.S. Preventive Services Task Force noted that variability between serum vitamin D assay methods “and between laboratories using the same methods may range from 10% to 20%, and classification of samples as ‘deficient’ or ‘nondeficient’ may vary by 4% to 32%, depending on which assay is used. Another factor that may complicate interpretation is that 25-(OH)D may act as a negative acute-phase reactant and its levels may decrease in response to inflammation. Lastly, whether common laboratory reference ranges are appropriate for all ethnic groups is unclear.”
Trying to exert influence on what ranges of serum vitamin D laboratories are using in reporting data “is an issue,” said Dr. Aloia, director of the Bone Mineral Research Center at Winthrop University Hospital, Mineola, N.Y., and professor of medicine at Stony Brook (N.Y.) University. “A laboratory can report anything it chooses to. For instance, the American College of Pathology and other [professional organizations] don’t have the responsibility for [the cut-offs in] those reports.”
Dr. Aloia favors translating the reporting of vitamin D levels based on something like Z scores, “so when you see lab reports, some of them will have a paragraph of explanation to guide the physician,” he explained. “We’re going to need that. We have to move away from just [a] cutpoint range and the lower level of the range being the RDA.”
Dr. Roger Bouillon, professor emeritus of internal medicine at the University of Leuven (Belgium), supports a threshold of 20 ng/mL serum vitamin D in adults. “I don’t like a range [of vitamin D]; they just need to have a level above 20 ng/mL. For me, a threshold is the best strategy on a population basis.”
During an open comment session, attendee Dr. Neil C. Binkley expressed concern over applying Z-score principles to the vitamin D field. “I love bone density measurement,” said Dr. Binkley, codirector of the Osteoporosis Clinical Center & Research Program at the University of Wisconsin, Madison, and past president of the International Society for Clinical Densitometry. “The T-score was in fact an advance in the field. But I can’t tell you how strongly I would urge you to not consider T-scores or Z-scores or something like that in the vitamin D field. Rather, I would urge that we do a better job at measuring 25-hydroxyvitamin D so our laboratories agree and have concise guidance for primary care. If you choose to go into the probability realm and the Z-scores, it is going to be a disaster.”
The presenters reported having no financial disclosures.
On Twitter @dougbrunk
Efforts to reach agreement on how vitamin D deficiency is defined are complicated by the fact that the cutoff points used in reports from clinical laboratories vary widely.
“I think reporting is a great problem because primary care physicians are very hurried,” Dr. John F. Aloia said at a public conference on vitamin D sponsored by the National Institutes of Health. “When you look at the laboratory report, what you get is a column that’s normal and another column that’s low or high. The choice of the laboratories to choose their own cutpoints is really a problem. The other part of that reporting is using the low level of normal in a range at the RDA [recommended daily allowance].”
In its recently updated recommendations on vitamin D screening, the U.S. Preventive Services Task Force noted that variability between serum vitamin D assay methods “and between laboratories using the same methods may range from 10% to 20%, and classification of samples as ‘deficient’ or ‘nondeficient’ may vary by 4% to 32%, depending on which assay is used. Another factor that may complicate interpretation is that 25-(OH)D may act as a negative acute-phase reactant and its levels may decrease in response to inflammation. Lastly, whether common laboratory reference ranges are appropriate for all ethnic groups is unclear.”
Trying to exert influence on what ranges of serum vitamin D laboratories are using in reporting data “is an issue,” said Dr. Aloia, director of the Bone Mineral Research Center at Winthrop University Hospital, Mineola, N.Y., and professor of medicine at Stony Brook (N.Y.) University. “A laboratory can report anything it chooses to. For instance, the American College of Pathology and other [professional organizations] don’t have the responsibility for [the cut-offs in] those reports.”
Dr. Aloia favors translating the reporting of vitamin D levels based on something like Z scores, “so when you see lab reports, some of them will have a paragraph of explanation to guide the physician,” he explained. “We’re going to need that. We have to move away from just [a] cutpoint range and the lower level of the range being the RDA.”
Dr. Roger Bouillon, professor emeritus of internal medicine at the University of Leuven (Belgium), supports a threshold of 20 ng/mL serum vitamin D in adults. “I don’t like a range [of vitamin D]; they just need to have a level above 20 ng/mL. For me, a threshold is the best strategy on a population basis.”
During an open comment session, attendee Dr. Neil C. Binkley expressed concern over applying Z-score principles to the vitamin D field. “I love bone density measurement,” said Dr. Binkley, codirector of the Osteoporosis Clinical Center & Research Program at the University of Wisconsin, Madison, and past president of the International Society for Clinical Densitometry. “The T-score was in fact an advance in the field. But I can’t tell you how strongly I would urge you to not consider T-scores or Z-scores or something like that in the vitamin D field. Rather, I would urge that we do a better job at measuring 25-hydroxyvitamin D so our laboratories agree and have concise guidance for primary care. If you choose to go into the probability realm and the Z-scores, it is going to be a disaster.”
The presenters reported having no financial disclosures.
On Twitter @dougbrunk
FROM AN NIH PUBLIC CONFERENCE ON VITAMIN D
Bisphosphonates may protect against endometrial cancer
The use of nitrogenous bisphosphonates was associated with a nearly 50% reduction in the incidence of endometrial cancer among women in the PLCO, or Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial.
The endometrial cancer incidence rate among women in the study who reported ever using nitrogenous bisphosphonates was 8.7/10,000 person-years, compared with 17.7/10,000 person-years among those who reported never being exposed to nitrogenous bisphosphonates (rate ratio, 0.49), Sharon Hensley Alford, Ph.D., of the Henry Ford Health System, Detroit, and her colleagues reported online Dec. 22 in Cancer.

The effect was similar after adjustment for age, race, body mass index, smoking status, and use of hormone therapy (hazard ratio, 0.56). The effect was also similar for both type I and type II disease, although there were only nine cases of type II disease, so the finding did not reach statistical significance, the investigators reported (Cancer 2014 Dec. 22 [doi:10.1002/cncr.28952]).
PLCO study subjects included in the current analysis were 23,485 women aged 55-74 years at study entry between 1993 and 2001, who had no cancer diagnosed prior to year 5 of the study when they completed a supplemental questionnaire to assess bone medication use. The women were followed until last known contact, death, or endometrial cancer diagnosis.
The findings support those of preclinical studies demonstrating antitumor effects of bisphosphonates, and suggest that their use may protect against endometrial cancer, the investigators said.
“However, additional studies are needed that include other potential confounders and a larger sample so that type II endometrial cancer could be assessed more confidently,” they concluded, adding that a trial assessing for endometrial, breast, and colorectal cancer in postmenopausal women would be ideal.
The PLCO trial was funded by the National Institutes of Health. The authors reported having no relevant financial disclosures.
The use of nitrogenous bisphosphonates was associated with a nearly 50% reduction in the incidence of endometrial cancer among women in the PLCO, or Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial.
The endometrial cancer incidence rate among women in the study who reported ever using nitrogenous bisphosphonates was 8.7/10,000 person-years, compared with 17.7/10,000 person-years among those who reported never being exposed to nitrogenous bisphosphonates (rate ratio, 0.49), Sharon Hensley Alford, Ph.D., of the Henry Ford Health System, Detroit, and her colleagues reported online Dec. 22 in Cancer.
The effect was similar after adjustment for age, race, body mass index, smoking status, and use of hormone therapy (hazard ratio, 0.56). The effect was also similar for both type I and type II disease, although there were only nine cases of type II disease, so the finding did not reach statistical significance, the investigators reported (Cancer 2014 Dec. 22 [doi:10.1002/cncr.28952]).
PLCO study subjects included in the current analysis were 23,485 women aged 55-74 years at study entry between 1993 and 2001, who had no cancer diagnosed prior to year 5 of the study when they completed a supplemental questionnaire to assess bone medication use. The women were followed until last known contact, death, or endometrial cancer diagnosis.
The findings support those of preclinical studies demonstrating antitumor effects of bisphosphonates, and suggest that their use may protect against endometrial cancer, the investigators said.
“However, additional studies are needed that include other potential confounders and a larger sample so that type II endometrial cancer could be assessed more confidently,” they concluded, adding that a trial assessing for endometrial, breast, and colorectal cancer in postmenopausal women would be ideal.
The PLCO trial was funded by the National Institutes of Health. The authors reported having no relevant financial disclosures.
The use of nitrogenous bisphosphonates was associated with a nearly 50% reduction in the incidence of endometrial cancer among women in the PLCO, or Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial.
The endometrial cancer incidence rate among women in the study who reported ever using nitrogenous bisphosphonates was 8.7/10,000 person-years, compared with 17.7/10,000 person-years among those who reported never being exposed to nitrogenous bisphosphonates (rate ratio, 0.49), Sharon Hensley Alford, Ph.D., of the Henry Ford Health System, Detroit, and her colleagues reported online Dec. 22 in Cancer.
The effect was similar after adjustment for age, race, body mass index, smoking status, and use of hormone therapy (hazard ratio, 0.56). The effect was also similar for both type I and type II disease, although there were only nine cases of type II disease, so the finding did not reach statistical significance, the investigators reported (Cancer 2014 Dec. 22 [doi:10.1002/cncr.28952]).
PLCO study subjects included in the current analysis were 23,485 women aged 55-74 years at study entry between 1993 and 2001, who had no cancer diagnosed prior to year 5 of the study when they completed a supplemental questionnaire to assess bone medication use. The women were followed until last known contact, death, or endometrial cancer diagnosis.
The findings support those of preclinical studies demonstrating antitumor effects of bisphosphonates, and suggest that their use may protect against endometrial cancer, the investigators said.
“However, additional studies are needed that include other potential confounders and a larger sample so that type II endometrial cancer could be assessed more confidently,” they concluded, adding that a trial assessing for endometrial, breast, and colorectal cancer in postmenopausal women would be ideal.
The PLCO trial was funded by the National Institutes of Health. The authors reported having no relevant financial disclosures.
FROM CANCER
Key clinical point: Women with a history of bisphosphonate use had a reduced risk of developing endometrial cancer.
Major finding: The endometrial cancer incidence rate was 8.7 vs. 17.7/10,000 person-years for ever vs. never users of nitrogenous bisphosphonates (rate ratio, 0.49).
Data source: An analysis of data from 23,485 women from a randomized population-based trial.
Disclosures: The PLCO trial was funded by the National Institutes of Health. The authors reported having no financial disclosures.
