User login
‘Bigorexia’: Why teenage boys are obsessed with bulking up
Why are teenage boys obsessed with bulking up?
While the effects of Instagram on girls’ body image has long been documented – an article in The Wall Street Journal that was published this fall reported that Facebook knew Instagram was toxic for teen girls – teenage boys are under just as much pressure.
For adolescent boys, the goal is often to get superhero-size buff – and this is leading to anxiety, stress, excessive selfies, and, often, obsessive staring in the mirror to assess their “pec” progress.
So-called “bigorexia” – or extreme gym time, excessive focus on protein diets, and intense muscle-building goals – has hit new and concerning levels, according to a recent New York Times report.
Whether it’s the pandemic or TikTok that’s to blame, teen boys are pushing hard to achieve six-pack abs, with one-third of them in the U.S. trying to bulk up, according to a study published in the Journal of Adolescent Health. What’s more, 22% reported they’re engaging in muscle-enhancing behavior, including excess exercise, taking supplements or steroids, or eating more to bulk up, according to a study published in the International Journal of Eating Disorders.
“The pandemic and social media have been a perfect storm for eating disorders and body image issues for all teens, but this has been under-recognized in boys,” says Jason Nagata, MD, a pediatrician who specializes in adolescent medicine at the University of California, San Francisco. “Both are directly connected to an increase in muscle dysmorphia.”
While “bigorexia” is a newer term coined by mental health professionals, the concept of muscular dysmorphia isn’t, says Jennifer Bahrman, PhD, a licensed psychologist with McGovern Medical School at UTHealth Houston. This may be why about a third of boys ages 11-18 reported that they aren’t enamored with their bodies, according to a small survey published in 2019 in the Californian Journal of Health Promotion.
“When we think of dysmorphia, we think of girls having it, since we see it more in females,” says Dr. Bahrman, who works extensively with adolescents and athletes. “The interesting thing about muscular dysmorphia is that it’s the only body dysmorphic disorder that’s almost exclusively present in males.”
Social media’s role
Unlike other things in boys’ lives, like movies, TV, or even the uber-buff GI Joe doll, social media has created opportunities for young men to put their bodies on display – and become an influencer or get followers because of it.
“An everyday teen can become a celebrity,” Dr. Nagata says. “Then, thanks to social media algorithms, if a teenage boy likes or interacts with a post that features a muscular guy or is all about fitness, they’ll start getting all sorts of related content. They’ll get bombarded with tons of ads for protein shakes, for example, as well as bodybuilding equipment, and that will further distort reality.”
Before-and-after photos are also known to be quite misleading.
“Some of the most popular Instagram posts among teens feature people who have experienced a massive body transformation,” Dr. Nagata says. “It’s usually someone who lost a lot of weight or someone who was scrawny and then got muscular. The most drastic changes tend to get the most likes and are perpetuated the most and shared the most often with friends.”
But as many are aware, photos posted to social media are selected to tell the best story – with the best filters, lighting, and angles possible, however exaggerated.
“A guy will post his worst picture out of a thousand for his before shot and then post the best photo out of a thousand,” Dr. Nagata says. “This, in itself, can really confuse a teenager, because the story of this person’s changed body looks so realistic.”
Worse, these images tend to be damaging to your teenager’s self-esteem.
“When you see images of people you’re aspiring to look like, it can be very upsetting,” Dr. Bahrman says. “After all, it’s easy to think, ‘I’m doing all of these pushups, and I don’t look like this.’ From there, it’s easy to begin internalizing that something is wrong with you.”
Red flags to watch out for
If you’ve noticed that your son is obsessed with his appearance, weight, food, or exercise, take note. Also, notice if he’s asking you to buy protein powder or is spending more time at the gym than with his friends.
“Pay attention if he is withdrawing from friends and family because of his concerns about his appearance,” Dr. Nagata says. “For example, we often hear that a teenager will no longer eat family meals or at a restaurant because the protein content isn’t high enough or the food is too fatty.”
If you’re concerned, always make sure to discuss this with your son’s pediatrician.
“Ultimately, you want to make sure you share your concerns before your teen son becomes even more body-image obsessed,” Dr. Nagata says.
A version of this article first appeared on WebMD.com.
Why are teenage boys obsessed with bulking up?
While the effects of Instagram on girls’ body image has long been documented – an article in The Wall Street Journal that was published this fall reported that Facebook knew Instagram was toxic for teen girls – teenage boys are under just as much pressure.
For adolescent boys, the goal is often to get superhero-size buff – and this is leading to anxiety, stress, excessive selfies, and, often, obsessive staring in the mirror to assess their “pec” progress.
So-called “bigorexia” – or extreme gym time, excessive focus on protein diets, and intense muscle-building goals – has hit new and concerning levels, according to a recent New York Times report.
Whether it’s the pandemic or TikTok that’s to blame, teen boys are pushing hard to achieve six-pack abs, with one-third of them in the U.S. trying to bulk up, according to a study published in the Journal of Adolescent Health. What’s more, 22% reported they’re engaging in muscle-enhancing behavior, including excess exercise, taking supplements or steroids, or eating more to bulk up, according to a study published in the International Journal of Eating Disorders.
“The pandemic and social media have been a perfect storm for eating disorders and body image issues for all teens, but this has been under-recognized in boys,” says Jason Nagata, MD, a pediatrician who specializes in adolescent medicine at the University of California, San Francisco. “Both are directly connected to an increase in muscle dysmorphia.”
While “bigorexia” is a newer term coined by mental health professionals, the concept of muscular dysmorphia isn’t, says Jennifer Bahrman, PhD, a licensed psychologist with McGovern Medical School at UTHealth Houston. This may be why about a third of boys ages 11-18 reported that they aren’t enamored with their bodies, according to a small survey published in 2019 in the Californian Journal of Health Promotion.
“When we think of dysmorphia, we think of girls having it, since we see it more in females,” says Dr. Bahrman, who works extensively with adolescents and athletes. “The interesting thing about muscular dysmorphia is that it’s the only body dysmorphic disorder that’s almost exclusively present in males.”
Social media’s role
Unlike other things in boys’ lives, like movies, TV, or even the uber-buff GI Joe doll, social media has created opportunities for young men to put their bodies on display – and become an influencer or get followers because of it.
“An everyday teen can become a celebrity,” Dr. Nagata says. “Then, thanks to social media algorithms, if a teenage boy likes or interacts with a post that features a muscular guy or is all about fitness, they’ll start getting all sorts of related content. They’ll get bombarded with tons of ads for protein shakes, for example, as well as bodybuilding equipment, and that will further distort reality.”
Before-and-after photos are also known to be quite misleading.
“Some of the most popular Instagram posts among teens feature people who have experienced a massive body transformation,” Dr. Nagata says. “It’s usually someone who lost a lot of weight or someone who was scrawny and then got muscular. The most drastic changes tend to get the most likes and are perpetuated the most and shared the most often with friends.”
But as many are aware, photos posted to social media are selected to tell the best story – with the best filters, lighting, and angles possible, however exaggerated.
“A guy will post his worst picture out of a thousand for his before shot and then post the best photo out of a thousand,” Dr. Nagata says. “This, in itself, can really confuse a teenager, because the story of this person’s changed body looks so realistic.”
Worse, these images tend to be damaging to your teenager’s self-esteem.
“When you see images of people you’re aspiring to look like, it can be very upsetting,” Dr. Bahrman says. “After all, it’s easy to think, ‘I’m doing all of these pushups, and I don’t look like this.’ From there, it’s easy to begin internalizing that something is wrong with you.”
Red flags to watch out for
If you’ve noticed that your son is obsessed with his appearance, weight, food, or exercise, take note. Also, notice if he’s asking you to buy protein powder or is spending more time at the gym than with his friends.
“Pay attention if he is withdrawing from friends and family because of his concerns about his appearance,” Dr. Nagata says. “For example, we often hear that a teenager will no longer eat family meals or at a restaurant because the protein content isn’t high enough or the food is too fatty.”
If you’re concerned, always make sure to discuss this with your son’s pediatrician.
“Ultimately, you want to make sure you share your concerns before your teen son becomes even more body-image obsessed,” Dr. Nagata says.
A version of this article first appeared on WebMD.com.
Why are teenage boys obsessed with bulking up?
While the effects of Instagram on girls’ body image has long been documented – an article in The Wall Street Journal that was published this fall reported that Facebook knew Instagram was toxic for teen girls – teenage boys are under just as much pressure.
For adolescent boys, the goal is often to get superhero-size buff – and this is leading to anxiety, stress, excessive selfies, and, often, obsessive staring in the mirror to assess their “pec” progress.
So-called “bigorexia” – or extreme gym time, excessive focus on protein diets, and intense muscle-building goals – has hit new and concerning levels, according to a recent New York Times report.
Whether it’s the pandemic or TikTok that’s to blame, teen boys are pushing hard to achieve six-pack abs, with one-third of them in the U.S. trying to bulk up, according to a study published in the Journal of Adolescent Health. What’s more, 22% reported they’re engaging in muscle-enhancing behavior, including excess exercise, taking supplements or steroids, or eating more to bulk up, according to a study published in the International Journal of Eating Disorders.
“The pandemic and social media have been a perfect storm for eating disorders and body image issues for all teens, but this has been under-recognized in boys,” says Jason Nagata, MD, a pediatrician who specializes in adolescent medicine at the University of California, San Francisco. “Both are directly connected to an increase in muscle dysmorphia.”
While “bigorexia” is a newer term coined by mental health professionals, the concept of muscular dysmorphia isn’t, says Jennifer Bahrman, PhD, a licensed psychologist with McGovern Medical School at UTHealth Houston. This may be why about a third of boys ages 11-18 reported that they aren’t enamored with their bodies, according to a small survey published in 2019 in the Californian Journal of Health Promotion.
“When we think of dysmorphia, we think of girls having it, since we see it more in females,” says Dr. Bahrman, who works extensively with adolescents and athletes. “The interesting thing about muscular dysmorphia is that it’s the only body dysmorphic disorder that’s almost exclusively present in males.”
Social media’s role
Unlike other things in boys’ lives, like movies, TV, or even the uber-buff GI Joe doll, social media has created opportunities for young men to put their bodies on display – and become an influencer or get followers because of it.
“An everyday teen can become a celebrity,” Dr. Nagata says. “Then, thanks to social media algorithms, if a teenage boy likes or interacts with a post that features a muscular guy or is all about fitness, they’ll start getting all sorts of related content. They’ll get bombarded with tons of ads for protein shakes, for example, as well as bodybuilding equipment, and that will further distort reality.”
Before-and-after photos are also known to be quite misleading.
“Some of the most popular Instagram posts among teens feature people who have experienced a massive body transformation,” Dr. Nagata says. “It’s usually someone who lost a lot of weight or someone who was scrawny and then got muscular. The most drastic changes tend to get the most likes and are perpetuated the most and shared the most often with friends.”
But as many are aware, photos posted to social media are selected to tell the best story – with the best filters, lighting, and angles possible, however exaggerated.
“A guy will post his worst picture out of a thousand for his before shot and then post the best photo out of a thousand,” Dr. Nagata says. “This, in itself, can really confuse a teenager, because the story of this person’s changed body looks so realistic.”
Worse, these images tend to be damaging to your teenager’s self-esteem.
“When you see images of people you’re aspiring to look like, it can be very upsetting,” Dr. Bahrman says. “After all, it’s easy to think, ‘I’m doing all of these pushups, and I don’t look like this.’ From there, it’s easy to begin internalizing that something is wrong with you.”
Red flags to watch out for
If you’ve noticed that your son is obsessed with his appearance, weight, food, or exercise, take note. Also, notice if he’s asking you to buy protein powder or is spending more time at the gym than with his friends.
“Pay attention if he is withdrawing from friends and family because of his concerns about his appearance,” Dr. Nagata says. “For example, we often hear that a teenager will no longer eat family meals or at a restaurant because the protein content isn’t high enough or the food is too fatty.”
If you’re concerned, always make sure to discuss this with your son’s pediatrician.
“Ultimately, you want to make sure you share your concerns before your teen son becomes even more body-image obsessed,” Dr. Nagata says.
A version of this article first appeared on WebMD.com.
Food insecurity linked to metabolic syndrome in Hispanic/Latino youth
Severe food insecurity was associated with metabolic syndrome and unfavorable cardiometabolic markers in Hispanic/Latino youth, researchers report.
The findings, published March 16 in Pediatrics, highlight the need to investigate interventions that address food insecurity among Hispanic/Latino youth, a segment of the U.S. population at high risk of cardiometabolic complications.
“Among Hispanic/Latino youth, no study, to our knowledge has evaluated food insecurity’s role in metabolic syndrome and metabolic syndrome–relevant cardiometabolic markers in this population,” lead author Luis E. Maldonado, PhD, of the University of North Carolina at Chapel Hill, and colleagues explained.
The researchers conducted a cross-sectional study to evaluate the associations between lower household and child food security and metabolic syndrome, as well as clinically measured cardiometabolic markers, including fasting plasma glucose, waist circumference, triglycerides, systolic and diastolic blood pressure, and high-density lipoprotein cholesterol (HDL-C).
Household food security (high, marginal, low, very low) and child food security (high, marginal, low/very low) measures were evaluated separately, and were adjusted for participant age, sex, site, parental education, and poverty-income ratio.
Data were obtained from the Hispanic Community Children’s Health Study/Study of Latino Youth, a study of offspring of adults enrolled in the Hispanic Community Health Survey/Study of Latinos.
Results
The study cohort included 1,325 Hispanic/Latino youth aged 8-16 years. For both household food security and child food security, youth in the lowest food security category had significantly lower HDL-C compared with youth with high food security (household food security, –3.17; 95% confidence interval, –5.65 to –0.70; child food security, –1.81; 95% CI, –3.54 to –0.09).
In addition, low/very low compared with high child food security was associated with higher triglycerides (beta, 8.68; 95% CI, 1.75-15.61), higher fasting plasma glucose (beta, 1.37; 95% CI, 0.08-2.65), and metabolic syndrome composite variable expected log counts (beta, 2.12; 95% CI, 0.02-0.45).
Furthermore, the researchers found statistically significant interactions between each of the two food security measures and receipt of any food assistance in the previous year in models of triglycerides (P for interactions: household food security, .03 and child food security, .005) and HDL-C (P for interactions: household food security, .01 and child food security, .04).
After evaluating the effect of parental place of birth, they found a statistically significant association for triglycerides only (P for interactions: household food security, .05 and child food security, .008).
“Our study is among the first to document adverse associations between household and child food security measures with a metabolic syndrome score variable and several metabolic syndrome–relevant cardiometabolic markers among US Hispanic/Latino youth,” the researchers wrote.
The researchers acknowledged that the cross-sectional nature of the study was a key limitation; thus, causality could not be inferred.

“In the future, we plan to conduct more qualitative work to better understand how Hispanic/Latino families respond to food insecurity, which may identify the factors that shape their response,” study author Sandra S. Albrecht, PhD, of Columbia University, New York, NY, said in an interview.
Recommendations for pediatricians
Food insecurity researcher Yankun Wang, PhD candidate at Indiana University, Bloomington, commented: “I would recommend pediatricians pay more attention to children from low-income households since they are more likely to have mental and physical health issues due to food insecurity.
“It can be very helpful if pediatricians could help families obtain SNAP benefits, enroll youth in the school breakfast and lunch programs, and promote nutrition education in schools,” Mr. Wang added.
This study was supported by grant funding from the National Heart, Lung, and Blood Institute. The authors reported no relevant disclosures.
Severe food insecurity was associated with metabolic syndrome and unfavorable cardiometabolic markers in Hispanic/Latino youth, researchers report.
The findings, published March 16 in Pediatrics, highlight the need to investigate interventions that address food insecurity among Hispanic/Latino youth, a segment of the U.S. population at high risk of cardiometabolic complications.
“Among Hispanic/Latino youth, no study, to our knowledge has evaluated food insecurity’s role in metabolic syndrome and metabolic syndrome–relevant cardiometabolic markers in this population,” lead author Luis E. Maldonado, PhD, of the University of North Carolina at Chapel Hill, and colleagues explained.
The researchers conducted a cross-sectional study to evaluate the associations between lower household and child food security and metabolic syndrome, as well as clinically measured cardiometabolic markers, including fasting plasma glucose, waist circumference, triglycerides, systolic and diastolic blood pressure, and high-density lipoprotein cholesterol (HDL-C).
Household food security (high, marginal, low, very low) and child food security (high, marginal, low/very low) measures were evaluated separately, and were adjusted for participant age, sex, site, parental education, and poverty-income ratio.
Data were obtained from the Hispanic Community Children’s Health Study/Study of Latino Youth, a study of offspring of adults enrolled in the Hispanic Community Health Survey/Study of Latinos.
Results
The study cohort included 1,325 Hispanic/Latino youth aged 8-16 years. For both household food security and child food security, youth in the lowest food security category had significantly lower HDL-C compared with youth with high food security (household food security, –3.17; 95% confidence interval, –5.65 to –0.70; child food security, –1.81; 95% CI, –3.54 to –0.09).
In addition, low/very low compared with high child food security was associated with higher triglycerides (beta, 8.68; 95% CI, 1.75-15.61), higher fasting plasma glucose (beta, 1.37; 95% CI, 0.08-2.65), and metabolic syndrome composite variable expected log counts (beta, 2.12; 95% CI, 0.02-0.45).
Furthermore, the researchers found statistically significant interactions between each of the two food security measures and receipt of any food assistance in the previous year in models of triglycerides (P for interactions: household food security, .03 and child food security, .005) and HDL-C (P for interactions: household food security, .01 and child food security, .04).
After evaluating the effect of parental place of birth, they found a statistically significant association for triglycerides only (P for interactions: household food security, .05 and child food security, .008).
“Our study is among the first to document adverse associations between household and child food security measures with a metabolic syndrome score variable and several metabolic syndrome–relevant cardiometabolic markers among US Hispanic/Latino youth,” the researchers wrote.
The researchers acknowledged that the cross-sectional nature of the study was a key limitation; thus, causality could not be inferred.
“In the future, we plan to conduct more qualitative work to better understand how Hispanic/Latino families respond to food insecurity, which may identify the factors that shape their response,” study author Sandra S. Albrecht, PhD, of Columbia University, New York, NY, said in an interview.
Recommendations for pediatricians
Food insecurity researcher Yankun Wang, PhD candidate at Indiana University, Bloomington, commented: “I would recommend pediatricians pay more attention to children from low-income households since they are more likely to have mental and physical health issues due to food insecurity.
“It can be very helpful if pediatricians could help families obtain SNAP benefits, enroll youth in the school breakfast and lunch programs, and promote nutrition education in schools,” Mr. Wang added.
This study was supported by grant funding from the National Heart, Lung, and Blood Institute. The authors reported no relevant disclosures.
Severe food insecurity was associated with metabolic syndrome and unfavorable cardiometabolic markers in Hispanic/Latino youth, researchers report.
The findings, published March 16 in Pediatrics, highlight the need to investigate interventions that address food insecurity among Hispanic/Latino youth, a segment of the U.S. population at high risk of cardiometabolic complications.
“Among Hispanic/Latino youth, no study, to our knowledge has evaluated food insecurity’s role in metabolic syndrome and metabolic syndrome–relevant cardiometabolic markers in this population,” lead author Luis E. Maldonado, PhD, of the University of North Carolina at Chapel Hill, and colleagues explained.
The researchers conducted a cross-sectional study to evaluate the associations between lower household and child food security and metabolic syndrome, as well as clinically measured cardiometabolic markers, including fasting plasma glucose, waist circumference, triglycerides, systolic and diastolic blood pressure, and high-density lipoprotein cholesterol (HDL-C).
Household food security (high, marginal, low, very low) and child food security (high, marginal, low/very low) measures were evaluated separately, and were adjusted for participant age, sex, site, parental education, and poverty-income ratio.
Data were obtained from the Hispanic Community Children’s Health Study/Study of Latino Youth, a study of offspring of adults enrolled in the Hispanic Community Health Survey/Study of Latinos.
Results
The study cohort included 1,325 Hispanic/Latino youth aged 8-16 years. For both household food security and child food security, youth in the lowest food security category had significantly lower HDL-C compared with youth with high food security (household food security, –3.17; 95% confidence interval, –5.65 to –0.70; child food security, –1.81; 95% CI, –3.54 to –0.09).
In addition, low/very low compared with high child food security was associated with higher triglycerides (beta, 8.68; 95% CI, 1.75-15.61), higher fasting plasma glucose (beta, 1.37; 95% CI, 0.08-2.65), and metabolic syndrome composite variable expected log counts (beta, 2.12; 95% CI, 0.02-0.45).
Furthermore, the researchers found statistically significant interactions between each of the two food security measures and receipt of any food assistance in the previous year in models of triglycerides (P for interactions: household food security, .03 and child food security, .005) and HDL-C (P for interactions: household food security, .01 and child food security, .04).
After evaluating the effect of parental place of birth, they found a statistically significant association for triglycerides only (P for interactions: household food security, .05 and child food security, .008).
“Our study is among the first to document adverse associations between household and child food security measures with a metabolic syndrome score variable and several metabolic syndrome–relevant cardiometabolic markers among US Hispanic/Latino youth,” the researchers wrote.
The researchers acknowledged that the cross-sectional nature of the study was a key limitation; thus, causality could not be inferred.
“In the future, we plan to conduct more qualitative work to better understand how Hispanic/Latino families respond to food insecurity, which may identify the factors that shape their response,” study author Sandra S. Albrecht, PhD, of Columbia University, New York, NY, said in an interview.
Recommendations for pediatricians
Food insecurity researcher Yankun Wang, PhD candidate at Indiana University, Bloomington, commented: “I would recommend pediatricians pay more attention to children from low-income households since they are more likely to have mental and physical health issues due to food insecurity.
“It can be very helpful if pediatricians could help families obtain SNAP benefits, enroll youth in the school breakfast and lunch programs, and promote nutrition education in schools,” Mr. Wang added.
This study was supported by grant funding from the National Heart, Lung, and Blood Institute. The authors reported no relevant disclosures.
FROM PEDIATRICS
New guidance on palliative care for neurologic disorders
Palliative care includes much more than hospice services, lead author of the new position statement Lynne P. Taylor, MD, University of Washington, Seattle, and a fellow of the AAN, said in a press release.
“Neurologists provide palliative care to people living with life-altering neurologic illnesses not just at the end of life but throughout the course of a disease, improving their lives with symptom control,” Dr. Taylor added.
The position paper, developed by a joint committee of the AAN, American Neurological Association, and Child Neurology Society, was published online March 8 in Neurology.
Guidance across the lifespan
The new paper, an update of previous position statements, includes palliative care guidance for different neurologic disorders across the lifespan. For example, neuropalliative care for neonates deserves “extra consideration,” because one-third of pediatric deaths occur during the neonatal period, most often in the neonatal intensive care unit, and after withdrawal of life-sustaining interventions, the authors note.
For older children, neuropalliative care consultation benefits families trying to maximize the quality of the remainder of their child’s life. Decisionmaking must consider the child’s cognitive abilities, the diagnosis, the perceived level of suffering, parental values, and the family’s understanding of the prognosis, the authors note.
They note that discussions about prognosis are often difficult but critical. Previous research “supports that patients desire prognostic information even when prognosis is uncertain and appreciate when their physicians disclose the presence of that uncertainty,” the authors note.
Also important is engaging in shared decisionmaking with patients and families. “This approach requires the physician to elicit a patient’s goals, make recommendations based on whether medical treatments are likely to achieve those goals, and work with patients and families to finalize a treatment plan,” according to the new guidance.
Ethical considerations
When treatments are physiologically futile, clinicians need to explain why interventions that may cause harm and have no benefit are not offered.
The authors cite cardiopulmonary resuscitation in the setting of cardiac arrest from irreversible herniation as an example of futility in the context of neurologic disease.
When life-prolonging care is no longer an option, clinicians have an obligation to shift the focus of care to preserving quality of life and comfort as much as possible, they add.
Hospices, which provide comfort-focused medical care as well as psychosocial and spiritual support, are reserved for patients believed to be in the last 6 months of their life if their disease follows the expected course.
The investigators also broached ethical considerations for individual neurologic conditions. Concerns for disorders of consciousness include misdiagnosis or inaccurate prognostication, and serial examinations are needed to re-evaluate levels of cognition, psychological state, decisionmaking capacity, and disease trajectory.
In patients with locked-in syndrome, a state of irreversible paralysis, often with respiratory and vocal paralysis, consciousness may range from a chronic minimally conscious state to intact cognition.
Without careful examination, patients with preserved consciousness may be mistaken as having a disorder of consciousness and risk their decisional capacity being ignored, the researchers note.
These patients may need assistance from speech pathologists to identify techniques to enhance communication, such as careful “yes/no” questioning, communication boards, or advanced eye-gaze technology, they add.
Stroke, dementia, Parkinson’s guidance
For stroke, the guidance suggests neurologists encourage patients with retained decisionmaking capacity to complete advance care planning given the risk of recurrent stroke and loss of capacity in the future.
For dementia, a proper and timely diagnosis can help patients and their families prepare for the consequences of cognitive dysfunction and loss of autonomy while respecting their identified values, the authors write.
They note that for Parkinson’s disease, which is marked by slow functional and cognitive decline, neurologists must aim to anticipate and treat symptoms, address psychosocial and spiritual distress and caregiver burden, and engage patients and families in advance care planning before onset of cognitive impairment.
For patients with amyotrophic lateral sclerosis (ALS) and related disorders, clinicians should aim to document goals and treatment preferences prior to extreme weakness and aphonia.
It is also important to anticipate patient preferences for future disability-specific decisions, such as those related to feeding tubes and mechanical ventilation, and to identify the patient’s minimal acceptable outcome from these life-sustaining interventions.
On the topic of withdrawal of treatment, the paper notes that competent patients have the right to refuse life-prolonging therapies, including artificial nutrition, hydration, mechanical ventilation, and antibiotics. If physicians have a moral objection to removing life-support systems, they are obligated to transfer the care of the patient to another physician, the authors add.
Once a decision is made to forgo life-sustaining treatment, physicians should minimize subsequent suffering. The investigators note most symptoms at the end of life can be managed without sedation.
In broaching the “gap” in neurology training programs, the statement referred to a survey of 49 neurology residency programs. Results showed that 42% of respondents reported being dissatisfied with their palliative care education.
Well-timed update
Kate T. Brizzi, MD, a Boston neurologist with experience in hospice and palliative care, said the updated position statement is “well-timed” as neuropalliative care has evolved dramatically over the last decade.
“In the last several years, I’ve witnessed a significant increase in trainee interest in the field, and there is growing recognition of how a palliative care approach can improve patient care and hopefully outcomes,” said Dr. Brizzi.
She praised the authors for doing “an excellent job” in highlighting the ethical challenges facing the neurology provider, particularly as it relates to prognostication in an uncertain setting.
Dr. Brizzi noted communication tools that help facilitate discussions around shared decisionmaking “have enhanced our ability to meet the palliative care needs of our patients and can be incorporated by any provider.”
However, she added that the paper only briefly comments on the role of the neurologist in “lawful physician-hastened death.”
“I anticipate that this will be an area of further discussion in the neurology and palliative care community in the future, as requests for hastened death are frequently encountered from patients with serious neurologic illness,” she said.
Dr. Brizzi also noted the importance of understanding the reasons behind the request – and addressing patient worries related to end-of-life care, which can frequently help alleviate distress.
There was no targeted funding for this paper. Coauthor Salvador Cruz-Flores, MD, department of neurology, Texas Tech University Center, El Paso, reported participation on member adjudication committees for clinical trials for Novo Nordisk, Sunovion, and Galapagos. The remaining authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Palliative care includes much more than hospice services, lead author of the new position statement Lynne P. Taylor, MD, University of Washington, Seattle, and a fellow of the AAN, said in a press release.
“Neurologists provide palliative care to people living with life-altering neurologic illnesses not just at the end of life but throughout the course of a disease, improving their lives with symptom control,” Dr. Taylor added.
The position paper, developed by a joint committee of the AAN, American Neurological Association, and Child Neurology Society, was published online March 8 in Neurology.
Guidance across the lifespan
The new paper, an update of previous position statements, includes palliative care guidance for different neurologic disorders across the lifespan. For example, neuropalliative care for neonates deserves “extra consideration,” because one-third of pediatric deaths occur during the neonatal period, most often in the neonatal intensive care unit, and after withdrawal of life-sustaining interventions, the authors note.
For older children, neuropalliative care consultation benefits families trying to maximize the quality of the remainder of their child’s life. Decisionmaking must consider the child’s cognitive abilities, the diagnosis, the perceived level of suffering, parental values, and the family’s understanding of the prognosis, the authors note.
They note that discussions about prognosis are often difficult but critical. Previous research “supports that patients desire prognostic information even when prognosis is uncertain and appreciate when their physicians disclose the presence of that uncertainty,” the authors note.
Also important is engaging in shared decisionmaking with patients and families. “This approach requires the physician to elicit a patient’s goals, make recommendations based on whether medical treatments are likely to achieve those goals, and work with patients and families to finalize a treatment plan,” according to the new guidance.
Ethical considerations
When treatments are physiologically futile, clinicians need to explain why interventions that may cause harm and have no benefit are not offered.
The authors cite cardiopulmonary resuscitation in the setting of cardiac arrest from irreversible herniation as an example of futility in the context of neurologic disease.
When life-prolonging care is no longer an option, clinicians have an obligation to shift the focus of care to preserving quality of life and comfort as much as possible, they add.
Hospices, which provide comfort-focused medical care as well as psychosocial and spiritual support, are reserved for patients believed to be in the last 6 months of their life if their disease follows the expected course.
The investigators also broached ethical considerations for individual neurologic conditions. Concerns for disorders of consciousness include misdiagnosis or inaccurate prognostication, and serial examinations are needed to re-evaluate levels of cognition, psychological state, decisionmaking capacity, and disease trajectory.
In patients with locked-in syndrome, a state of irreversible paralysis, often with respiratory and vocal paralysis, consciousness may range from a chronic minimally conscious state to intact cognition.
Without careful examination, patients with preserved consciousness may be mistaken as having a disorder of consciousness and risk their decisional capacity being ignored, the researchers note.
These patients may need assistance from speech pathologists to identify techniques to enhance communication, such as careful “yes/no” questioning, communication boards, or advanced eye-gaze technology, they add.
Stroke, dementia, Parkinson’s guidance
For stroke, the guidance suggests neurologists encourage patients with retained decisionmaking capacity to complete advance care planning given the risk of recurrent stroke and loss of capacity in the future.
For dementia, a proper and timely diagnosis can help patients and their families prepare for the consequences of cognitive dysfunction and loss of autonomy while respecting their identified values, the authors write.
They note that for Parkinson’s disease, which is marked by slow functional and cognitive decline, neurologists must aim to anticipate and treat symptoms, address psychosocial and spiritual distress and caregiver burden, and engage patients and families in advance care planning before onset of cognitive impairment.
For patients with amyotrophic lateral sclerosis (ALS) and related disorders, clinicians should aim to document goals and treatment preferences prior to extreme weakness and aphonia.
It is also important to anticipate patient preferences for future disability-specific decisions, such as those related to feeding tubes and mechanical ventilation, and to identify the patient’s minimal acceptable outcome from these life-sustaining interventions.
On the topic of withdrawal of treatment, the paper notes that competent patients have the right to refuse life-prolonging therapies, including artificial nutrition, hydration, mechanical ventilation, and antibiotics. If physicians have a moral objection to removing life-support systems, they are obligated to transfer the care of the patient to another physician, the authors add.
Once a decision is made to forgo life-sustaining treatment, physicians should minimize subsequent suffering. The investigators note most symptoms at the end of life can be managed without sedation.
In broaching the “gap” in neurology training programs, the statement referred to a survey of 49 neurology residency programs. Results showed that 42% of respondents reported being dissatisfied with their palliative care education.
Well-timed update
Kate T. Brizzi, MD, a Boston neurologist with experience in hospice and palliative care, said the updated position statement is “well-timed” as neuropalliative care has evolved dramatically over the last decade.
“In the last several years, I’ve witnessed a significant increase in trainee interest in the field, and there is growing recognition of how a palliative care approach can improve patient care and hopefully outcomes,” said Dr. Brizzi.
She praised the authors for doing “an excellent job” in highlighting the ethical challenges facing the neurology provider, particularly as it relates to prognostication in an uncertain setting.
Dr. Brizzi noted communication tools that help facilitate discussions around shared decisionmaking “have enhanced our ability to meet the palliative care needs of our patients and can be incorporated by any provider.”
However, she added that the paper only briefly comments on the role of the neurologist in “lawful physician-hastened death.”
“I anticipate that this will be an area of further discussion in the neurology and palliative care community in the future, as requests for hastened death are frequently encountered from patients with serious neurologic illness,” she said.
Dr. Brizzi also noted the importance of understanding the reasons behind the request – and addressing patient worries related to end-of-life care, which can frequently help alleviate distress.
There was no targeted funding for this paper. Coauthor Salvador Cruz-Flores, MD, department of neurology, Texas Tech University Center, El Paso, reported participation on member adjudication committees for clinical trials for Novo Nordisk, Sunovion, and Galapagos. The remaining authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Palliative care includes much more than hospice services, lead author of the new position statement Lynne P. Taylor, MD, University of Washington, Seattle, and a fellow of the AAN, said in a press release.
“Neurologists provide palliative care to people living with life-altering neurologic illnesses not just at the end of life but throughout the course of a disease, improving their lives with symptom control,” Dr. Taylor added.
The position paper, developed by a joint committee of the AAN, American Neurological Association, and Child Neurology Society, was published online March 8 in Neurology.
Guidance across the lifespan
The new paper, an update of previous position statements, includes palliative care guidance for different neurologic disorders across the lifespan. For example, neuropalliative care for neonates deserves “extra consideration,” because one-third of pediatric deaths occur during the neonatal period, most often in the neonatal intensive care unit, and after withdrawal of life-sustaining interventions, the authors note.
For older children, neuropalliative care consultation benefits families trying to maximize the quality of the remainder of their child’s life. Decisionmaking must consider the child’s cognitive abilities, the diagnosis, the perceived level of suffering, parental values, and the family’s understanding of the prognosis, the authors note.
They note that discussions about prognosis are often difficult but critical. Previous research “supports that patients desire prognostic information even when prognosis is uncertain and appreciate when their physicians disclose the presence of that uncertainty,” the authors note.
Also important is engaging in shared decisionmaking with patients and families. “This approach requires the physician to elicit a patient’s goals, make recommendations based on whether medical treatments are likely to achieve those goals, and work with patients and families to finalize a treatment plan,” according to the new guidance.
Ethical considerations
When treatments are physiologically futile, clinicians need to explain why interventions that may cause harm and have no benefit are not offered.
The authors cite cardiopulmonary resuscitation in the setting of cardiac arrest from irreversible herniation as an example of futility in the context of neurologic disease.
When life-prolonging care is no longer an option, clinicians have an obligation to shift the focus of care to preserving quality of life and comfort as much as possible, they add.
Hospices, which provide comfort-focused medical care as well as psychosocial and spiritual support, are reserved for patients believed to be in the last 6 months of their life if their disease follows the expected course.
The investigators also broached ethical considerations for individual neurologic conditions. Concerns for disorders of consciousness include misdiagnosis or inaccurate prognostication, and serial examinations are needed to re-evaluate levels of cognition, psychological state, decisionmaking capacity, and disease trajectory.
In patients with locked-in syndrome, a state of irreversible paralysis, often with respiratory and vocal paralysis, consciousness may range from a chronic minimally conscious state to intact cognition.
Without careful examination, patients with preserved consciousness may be mistaken as having a disorder of consciousness and risk their decisional capacity being ignored, the researchers note.
These patients may need assistance from speech pathologists to identify techniques to enhance communication, such as careful “yes/no” questioning, communication boards, or advanced eye-gaze technology, they add.
Stroke, dementia, Parkinson’s guidance
For stroke, the guidance suggests neurologists encourage patients with retained decisionmaking capacity to complete advance care planning given the risk of recurrent stroke and loss of capacity in the future.
For dementia, a proper and timely diagnosis can help patients and their families prepare for the consequences of cognitive dysfunction and loss of autonomy while respecting their identified values, the authors write.
They note that for Parkinson’s disease, which is marked by slow functional and cognitive decline, neurologists must aim to anticipate and treat symptoms, address psychosocial and spiritual distress and caregiver burden, and engage patients and families in advance care planning before onset of cognitive impairment.
For patients with amyotrophic lateral sclerosis (ALS) and related disorders, clinicians should aim to document goals and treatment preferences prior to extreme weakness and aphonia.
It is also important to anticipate patient preferences for future disability-specific decisions, such as those related to feeding tubes and mechanical ventilation, and to identify the patient’s minimal acceptable outcome from these life-sustaining interventions.
On the topic of withdrawal of treatment, the paper notes that competent patients have the right to refuse life-prolonging therapies, including artificial nutrition, hydration, mechanical ventilation, and antibiotics. If physicians have a moral objection to removing life-support systems, they are obligated to transfer the care of the patient to another physician, the authors add.
Once a decision is made to forgo life-sustaining treatment, physicians should minimize subsequent suffering. The investigators note most symptoms at the end of life can be managed without sedation.
In broaching the “gap” in neurology training programs, the statement referred to a survey of 49 neurology residency programs. Results showed that 42% of respondents reported being dissatisfied with their palliative care education.
Well-timed update
Kate T. Brizzi, MD, a Boston neurologist with experience in hospice and palliative care, said the updated position statement is “well-timed” as neuropalliative care has evolved dramatically over the last decade.
“In the last several years, I’ve witnessed a significant increase in trainee interest in the field, and there is growing recognition of how a palliative care approach can improve patient care and hopefully outcomes,” said Dr. Brizzi.
She praised the authors for doing “an excellent job” in highlighting the ethical challenges facing the neurology provider, particularly as it relates to prognostication in an uncertain setting.
Dr. Brizzi noted communication tools that help facilitate discussions around shared decisionmaking “have enhanced our ability to meet the palliative care needs of our patients and can be incorporated by any provider.”
However, she added that the paper only briefly comments on the role of the neurologist in “lawful physician-hastened death.”
“I anticipate that this will be an area of further discussion in the neurology and palliative care community in the future, as requests for hastened death are frequently encountered from patients with serious neurologic illness,” she said.
Dr. Brizzi also noted the importance of understanding the reasons behind the request – and addressing patient worries related to end-of-life care, which can frequently help alleviate distress.
There was no targeted funding for this paper. Coauthor Salvador Cruz-Flores, MD, department of neurology, Texas Tech University Center, El Paso, reported participation on member adjudication committees for clinical trials for Novo Nordisk, Sunovion, and Galapagos. The remaining authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
From Neurology
Surveillance program highly predictive for early autism
A population-based developmental surveillance program showed high diagnostic accuracy in identifying autism in a community-based sample of infants, toddlers, and preschoolers, according to new data published online in JAMA Network Open.
Researchers, led by Josephine Barbaro, PhD, of Olga Tennison Autism Research Centre at La Trobe University, Bundoora, Australia, said their findings indicate the benefit of using early autism developmental surveillance from infancy to the preschool period rather than one-time screening.
For the study, maternal and child health nurses in Melbourne were trained to use the Social Attention and Communication Surveillance–Revised (SACS-R) and SACS-Preschool (SACS-PR) tools during well-child checkups at 11-30 months of age and at follow-up (42 months of age). Dr. Barbaro helped develop the SACS tools.
Children identified as being at high likelihood for autism (1-2 years of age: n = 327; 42 months of age: n = 168) and at low likelihood for autism plus concerns (42 months of age: n = 28) were referred by their nurse for diagnostic assessment by the researchers.
Diagnostic accuracy of the SACS-R and SACS-PR was determined by comparing likelihood for autism with children’s diagnostic outcome using clinical judgment based on standard autism assessments.
Researchers included 13,511 children ages 11 months to 42 months. Results indicated the SACS-R with SACS-PR (SACS-R+PR) had very high diagnostic accuracy for early autism detection.
According to the paper, SACS-R showed 83% positive predictive value (95% confidence interval, 0.77-0.87) and 99% estimated negative predictive value (95% CI, 0.01-0.02). Specificity (99.6%; 95% CI, 0.99-1.00) was high, with modest sensitivity (62%; 95% CI, 0.57-0.66). When the SACS-PR 42-month assessment was added, estimated sensitivity grew to 96% (95% CI, 0.94-0.98).
“Its greater accuracy, compared with psychometrics of commonly used autism screening tools when used in community-based samples, suggests that the SACS-R+PR can be used universally for the early identification of autism,” the authors wrote.
According to La Trobe University, the tool is used in 10 other countries around the world – among them China, Singapore, Poland, Japan, New Zealand, Nepal, and Bangladesh.
Early identification is crucial for children on the autism spectrum and their families because it facilitates early diagnosis and can help families get access to supports and services.
About 2% of the world’s population is on the autism spectrum. Some studies report prevalence of 4% or higher, the authors noted.
The authors called attention to a systematic review of universal autism screening in primary care, including the Infant-Toddler Checklist and the Modified Checklist for Autism in Toddlers and various versions. The authors of the review noted that few studies had enough participants to establish population sensitivity, specificity, and positive predictive value. Also, psychometric properties reported were modest and/or wide ranging, putting into question the diagnostic accuracy of the tools.
Dr. Barbaro and colleagues highlighted an advantage the current study offers. “A critical difference in this study was the use of a community-based sample rather than a clinical or high-likelihood sibling sample, which may not be representative of the general population of children on the autism spectrum because child outcomes, cognition, and autism prevalence vary by ascertainment strategy and multiplex or simplex status.”
The authors explained that, in the United States, The U.S. Preventive Services Task Force has said there is not enough evidence to recommend universal autism screening and instead recommends routine general developmental surveillance. The American Academy of Pediatrics recommends developmental surveillance between 9 and 30 months and autism-specific screening at 18 and 24 months because of the benefits of early supports and services.

Karen Pierce, PhD, codirector of the Autism Center of Excellence at University of California, San Diego, said in an interview that she was pleased to see that the researchers were able to identify a high percentage of children on the autism spectrum.
She said, however, that the system proposed in this paper involves a substantial amount of time for training the nurses.
The authors acknowledged that, saying, “there may be instances in which this could be impractical.”
Dr. Pierce said that, in the United States, parent questionnaires are combined with clinical judgment to decide which kids are at risk.
“It doesn’t take very much time to fill out these questionnaires,” she said. “That’s the sticking point. I’m not saying necessarily that it shouldn’t be adopted. It would be very hard, I think, to incorporate into current pediatric practice.”
She said a benefit of the SACS program is more hands-on observation of the child, beyond the parent report, which sometimes can reflect more emotionally how the parent is feeling about the child.
She pointed out it was impressive that the Australian team found virtually no false positives.
The researchers also identified an additional 168 children using the preschool version at 42 months who had actually passed at the earlier checkpoint, using the regular SACS-R.
“This underscores a supercritical point,” Dr. Pierce said. “Just because your child may have gotten screened at 12, 18, 24 months and they pass and everything’s looking great, it doesn’t necessarily mean at some point early in development around age 3 that there [wouldn’t] be some clearer signs of autism.”
She said in her own study, published in JAMA Pediatrics, 24% of their sample tested fine at first but were later identified as having autism.
“It underscores the need for repeat screening,” Dr. Pierce said. “That was a striking finding in this study.”
She also pointed out that the authors talk about the “false dichotomy” between screening and surveillance. “They are saying it doesn’t have to be that way. It can be a combined effort. We can have parents filling out screening tools and we can have more observational sessions with kids during checkups. It doesn’t have to be this rigid line between screening and surveillance. I would completely agree with that.”
Dr. Barbaro reported receiving grants from the Sir Robert Menzies Foundation and the Cooperative Research Centre for Living with Autism (Autism CRC) during the study. Funds are partially distributed to Dr. Barbaro for the background intellectual property. One coauthor reported grants from the Menzies Foundation and Autism CRC during the study. Another coauthor reported receiving salary from Autism CRC during the study. No other disclosures were reported. This work was supported by an Allied Health Sciences start-up grant from the Menzies Foundation and the Cooperative Research Centre for Living with Autism, established and supported under the Australian Government’s Cooperative Research Centres Program. Dr. Pierce reports no relevant financial relationships.
A population-based developmental surveillance program showed high diagnostic accuracy in identifying autism in a community-based sample of infants, toddlers, and preschoolers, according to new data published online in JAMA Network Open.
Researchers, led by Josephine Barbaro, PhD, of Olga Tennison Autism Research Centre at La Trobe University, Bundoora, Australia, said their findings indicate the benefit of using early autism developmental surveillance from infancy to the preschool period rather than one-time screening.
For the study, maternal and child health nurses in Melbourne were trained to use the Social Attention and Communication Surveillance–Revised (SACS-R) and SACS-Preschool (SACS-PR) tools during well-child checkups at 11-30 months of age and at follow-up (42 months of age). Dr. Barbaro helped develop the SACS tools.
Children identified as being at high likelihood for autism (1-2 years of age: n = 327; 42 months of age: n = 168) and at low likelihood for autism plus concerns (42 months of age: n = 28) were referred by their nurse for diagnostic assessment by the researchers.
Diagnostic accuracy of the SACS-R and SACS-PR was determined by comparing likelihood for autism with children’s diagnostic outcome using clinical judgment based on standard autism assessments.
Researchers included 13,511 children ages 11 months to 42 months. Results indicated the SACS-R with SACS-PR (SACS-R+PR) had very high diagnostic accuracy for early autism detection.
According to the paper, SACS-R showed 83% positive predictive value (95% confidence interval, 0.77-0.87) and 99% estimated negative predictive value (95% CI, 0.01-0.02). Specificity (99.6%; 95% CI, 0.99-1.00) was high, with modest sensitivity (62%; 95% CI, 0.57-0.66). When the SACS-PR 42-month assessment was added, estimated sensitivity grew to 96% (95% CI, 0.94-0.98).
“Its greater accuracy, compared with psychometrics of commonly used autism screening tools when used in community-based samples, suggests that the SACS-R+PR can be used universally for the early identification of autism,” the authors wrote.
According to La Trobe University, the tool is used in 10 other countries around the world – among them China, Singapore, Poland, Japan, New Zealand, Nepal, and Bangladesh.
Early identification is crucial for children on the autism spectrum and their families because it facilitates early diagnosis and can help families get access to supports and services.
About 2% of the world’s population is on the autism spectrum. Some studies report prevalence of 4% or higher, the authors noted.
The authors called attention to a systematic review of universal autism screening in primary care, including the Infant-Toddler Checklist and the Modified Checklist for Autism in Toddlers and various versions. The authors of the review noted that few studies had enough participants to establish population sensitivity, specificity, and positive predictive value. Also, psychometric properties reported were modest and/or wide ranging, putting into question the diagnostic accuracy of the tools.
Dr. Barbaro and colleagues highlighted an advantage the current study offers. “A critical difference in this study was the use of a community-based sample rather than a clinical or high-likelihood sibling sample, which may not be representative of the general population of children on the autism spectrum because child outcomes, cognition, and autism prevalence vary by ascertainment strategy and multiplex or simplex status.”
The authors explained that, in the United States, The U.S. Preventive Services Task Force has said there is not enough evidence to recommend universal autism screening and instead recommends routine general developmental surveillance. The American Academy of Pediatrics recommends developmental surveillance between 9 and 30 months and autism-specific screening at 18 and 24 months because of the benefits of early supports and services.
Karen Pierce, PhD, codirector of the Autism Center of Excellence at University of California, San Diego, said in an interview that she was pleased to see that the researchers were able to identify a high percentage of children on the autism spectrum.
She said, however, that the system proposed in this paper involves a substantial amount of time for training the nurses.
The authors acknowledged that, saying, “there may be instances in which this could be impractical.”
Dr. Pierce said that, in the United States, parent questionnaires are combined with clinical judgment to decide which kids are at risk.
“It doesn’t take very much time to fill out these questionnaires,” she said. “That’s the sticking point. I’m not saying necessarily that it shouldn’t be adopted. It would be very hard, I think, to incorporate into current pediatric practice.”
She said a benefit of the SACS program is more hands-on observation of the child, beyond the parent report, which sometimes can reflect more emotionally how the parent is feeling about the child.
She pointed out it was impressive that the Australian team found virtually no false positives.
The researchers also identified an additional 168 children using the preschool version at 42 months who had actually passed at the earlier checkpoint, using the regular SACS-R.
“This underscores a supercritical point,” Dr. Pierce said. “Just because your child may have gotten screened at 12, 18, 24 months and they pass and everything’s looking great, it doesn’t necessarily mean at some point early in development around age 3 that there [wouldn’t] be some clearer signs of autism.”
She said in her own study, published in JAMA Pediatrics, 24% of their sample tested fine at first but were later identified as having autism.
“It underscores the need for repeat screening,” Dr. Pierce said. “That was a striking finding in this study.”
She also pointed out that the authors talk about the “false dichotomy” between screening and surveillance. “They are saying it doesn’t have to be that way. It can be a combined effort. We can have parents filling out screening tools and we can have more observational sessions with kids during checkups. It doesn’t have to be this rigid line between screening and surveillance. I would completely agree with that.”
Dr. Barbaro reported receiving grants from the Sir Robert Menzies Foundation and the Cooperative Research Centre for Living with Autism (Autism CRC) during the study. Funds are partially distributed to Dr. Barbaro for the background intellectual property. One coauthor reported grants from the Menzies Foundation and Autism CRC during the study. Another coauthor reported receiving salary from Autism CRC during the study. No other disclosures were reported. This work was supported by an Allied Health Sciences start-up grant from the Menzies Foundation and the Cooperative Research Centre for Living with Autism, established and supported under the Australian Government’s Cooperative Research Centres Program. Dr. Pierce reports no relevant financial relationships.
A population-based developmental surveillance program showed high diagnostic accuracy in identifying autism in a community-based sample of infants, toddlers, and preschoolers, according to new data published online in JAMA Network Open.
Researchers, led by Josephine Barbaro, PhD, of Olga Tennison Autism Research Centre at La Trobe University, Bundoora, Australia, said their findings indicate the benefit of using early autism developmental surveillance from infancy to the preschool period rather than one-time screening.
For the study, maternal and child health nurses in Melbourne were trained to use the Social Attention and Communication Surveillance–Revised (SACS-R) and SACS-Preschool (SACS-PR) tools during well-child checkups at 11-30 months of age and at follow-up (42 months of age). Dr. Barbaro helped develop the SACS tools.
Children identified as being at high likelihood for autism (1-2 years of age: n = 327; 42 months of age: n = 168) and at low likelihood for autism plus concerns (42 months of age: n = 28) were referred by their nurse for diagnostic assessment by the researchers.
Diagnostic accuracy of the SACS-R and SACS-PR was determined by comparing likelihood for autism with children’s diagnostic outcome using clinical judgment based on standard autism assessments.
Researchers included 13,511 children ages 11 months to 42 months. Results indicated the SACS-R with SACS-PR (SACS-R+PR) had very high diagnostic accuracy for early autism detection.
According to the paper, SACS-R showed 83% positive predictive value (95% confidence interval, 0.77-0.87) and 99% estimated negative predictive value (95% CI, 0.01-0.02). Specificity (99.6%; 95% CI, 0.99-1.00) was high, with modest sensitivity (62%; 95% CI, 0.57-0.66). When the SACS-PR 42-month assessment was added, estimated sensitivity grew to 96% (95% CI, 0.94-0.98).
“Its greater accuracy, compared with psychometrics of commonly used autism screening tools when used in community-based samples, suggests that the SACS-R+PR can be used universally for the early identification of autism,” the authors wrote.
According to La Trobe University, the tool is used in 10 other countries around the world – among them China, Singapore, Poland, Japan, New Zealand, Nepal, and Bangladesh.
Early identification is crucial for children on the autism spectrum and their families because it facilitates early diagnosis and can help families get access to supports and services.
About 2% of the world’s population is on the autism spectrum. Some studies report prevalence of 4% or higher, the authors noted.
The authors called attention to a systematic review of universal autism screening in primary care, including the Infant-Toddler Checklist and the Modified Checklist for Autism in Toddlers and various versions. The authors of the review noted that few studies had enough participants to establish population sensitivity, specificity, and positive predictive value. Also, psychometric properties reported were modest and/or wide ranging, putting into question the diagnostic accuracy of the tools.
Dr. Barbaro and colleagues highlighted an advantage the current study offers. “A critical difference in this study was the use of a community-based sample rather than a clinical or high-likelihood sibling sample, which may not be representative of the general population of children on the autism spectrum because child outcomes, cognition, and autism prevalence vary by ascertainment strategy and multiplex or simplex status.”
The authors explained that, in the United States, The U.S. Preventive Services Task Force has said there is not enough evidence to recommend universal autism screening and instead recommends routine general developmental surveillance. The American Academy of Pediatrics recommends developmental surveillance between 9 and 30 months and autism-specific screening at 18 and 24 months because of the benefits of early supports and services.
Karen Pierce, PhD, codirector of the Autism Center of Excellence at University of California, San Diego, said in an interview that she was pleased to see that the researchers were able to identify a high percentage of children on the autism spectrum.
She said, however, that the system proposed in this paper involves a substantial amount of time for training the nurses.
The authors acknowledged that, saying, “there may be instances in which this could be impractical.”
Dr. Pierce said that, in the United States, parent questionnaires are combined with clinical judgment to decide which kids are at risk.
“It doesn’t take very much time to fill out these questionnaires,” she said. “That’s the sticking point. I’m not saying necessarily that it shouldn’t be adopted. It would be very hard, I think, to incorporate into current pediatric practice.”
She said a benefit of the SACS program is more hands-on observation of the child, beyond the parent report, which sometimes can reflect more emotionally how the parent is feeling about the child.
She pointed out it was impressive that the Australian team found virtually no false positives.
The researchers also identified an additional 168 children using the preschool version at 42 months who had actually passed at the earlier checkpoint, using the regular SACS-R.
“This underscores a supercritical point,” Dr. Pierce said. “Just because your child may have gotten screened at 12, 18, 24 months and they pass and everything’s looking great, it doesn’t necessarily mean at some point early in development around age 3 that there [wouldn’t] be some clearer signs of autism.”
She said in her own study, published in JAMA Pediatrics, 24% of their sample tested fine at first but were later identified as having autism.
“It underscores the need for repeat screening,” Dr. Pierce said. “That was a striking finding in this study.”
She also pointed out that the authors talk about the “false dichotomy” between screening and surveillance. “They are saying it doesn’t have to be that way. It can be a combined effort. We can have parents filling out screening tools and we can have more observational sessions with kids during checkups. It doesn’t have to be this rigid line between screening and surveillance. I would completely agree with that.”
Dr. Barbaro reported receiving grants from the Sir Robert Menzies Foundation and the Cooperative Research Centre for Living with Autism (Autism CRC) during the study. Funds are partially distributed to Dr. Barbaro for the background intellectual property. One coauthor reported grants from the Menzies Foundation and Autism CRC during the study. Another coauthor reported receiving salary from Autism CRC during the study. No other disclosures were reported. This work was supported by an Allied Health Sciences start-up grant from the Menzies Foundation and the Cooperative Research Centre for Living with Autism, established and supported under the Australian Government’s Cooperative Research Centres Program. Dr. Pierce reports no relevant financial relationships.
FROM JAMA NETWORK OPEN
Children and COVID: Decline in new cases reaches 7th week
New cases of COVID-19 in U.S. children have fallen to their lowest level since the beginning of the Delta surge in July of 2021, according to the American Academy of Pediatrics and the Children’s Hospital Association.
. Over those 7 weeks, new cases dropped over 96% from the 1.15 million reported for Jan. 14-20, based on data collected by the AAP and CHA from state and territorial health departments.
The last time that the weekly count was below 42,000 was July 16-22, 2021, when almost 39,000 cases were reported in the midst of the Delta upsurge. That was shortly after cases had reached their lowest point, 8,447, since the early stages of the pandemic in 2020, the AAP/CHA data show.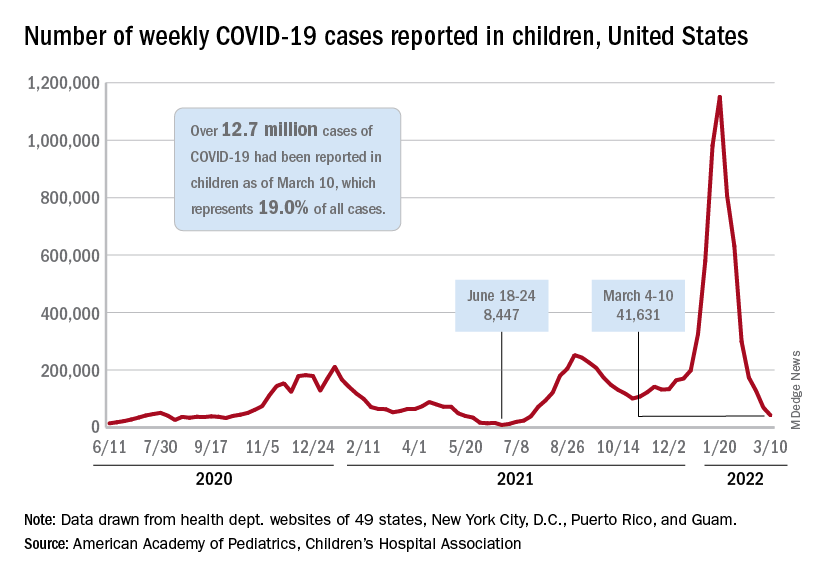
The cumulative number of pediatric cases is now up to 12.7 million, while the overall proportion of cases occurring in children held steady at 19.0% for the 4th week in a row, the AAP and CHA said in their weekly COVID-19 report. The Centers for Disease Control and Prevention, using an age range of 0-18 versus the states’ variety of ages, puts total cases at 11.7 million and deaths at 1,656 as of March 14.
Data from the CDC’s COVID-19–Associated Hospitalization Surveillance Network show that hospitalizations with laboratory-confirmed infection were down by 50% in children aged 0-4 years, by 63% among 5- to 11-year-olds, and by 58% in those aged 12-17 years for the week of Feb. 27 to March 5, compared with the week before.
The pace of vaccination continues to follow a similar trend, as the declines seen through February have continued into March. Cumulatively, 33.7% of children aged 5-11 have received at least one dose, and 26.8% are fully vaccinated, with corresponding numbers of 68.0% and 58.0% for children aged 12-17, the CDC reported on its COVID Data Tracker.
State-level data show that children aged 5-11 in Vermont, with a rate of 65%, are the most likely to have received at least one dose of COVID vaccine, while just 15% of 5- to 11-year-olds in Alabama, Louisiana, and Mississippi have gotten their first dose. Among children aged 12-17, that rate ranges from 40% in Wyoming to 94% in Hawaii, Massachusetts, and Rhode Island, the AAP said in a separate report based on CDC data.
In a recent report involving 1,364 children aged 5-15 years, two doses of the COVID-19 vaccine reduced the risk of infection from the Omicron variant by 31% in children aged 5-11 years and by 59% among children aged 12-15 years, said Ashley L. Fowlkes, ScD, of the CDC’s COVID-19 Emergency Response Team, and associates (MMWR 2022 Mar 11;71).
New cases of COVID-19 in U.S. children have fallen to their lowest level since the beginning of the Delta surge in July of 2021, according to the American Academy of Pediatrics and the Children’s Hospital Association.
. Over those 7 weeks, new cases dropped over 96% from the 1.15 million reported for Jan. 14-20, based on data collected by the AAP and CHA from state and territorial health departments.
The last time that the weekly count was below 42,000 was July 16-22, 2021, when almost 39,000 cases were reported in the midst of the Delta upsurge. That was shortly after cases had reached their lowest point, 8,447, since the early stages of the pandemic in 2020, the AAP/CHA data show.
The cumulative number of pediatric cases is now up to 12.7 million, while the overall proportion of cases occurring in children held steady at 19.0% for the 4th week in a row, the AAP and CHA said in their weekly COVID-19 report. The Centers for Disease Control and Prevention, using an age range of 0-18 versus the states’ variety of ages, puts total cases at 11.7 million and deaths at 1,656 as of March 14.
Data from the CDC’s COVID-19–Associated Hospitalization Surveillance Network show that hospitalizations with laboratory-confirmed infection were down by 50% in children aged 0-4 years, by 63% among 5- to 11-year-olds, and by 58% in those aged 12-17 years for the week of Feb. 27 to March 5, compared with the week before.
The pace of vaccination continues to follow a similar trend, as the declines seen through February have continued into March. Cumulatively, 33.7% of children aged 5-11 have received at least one dose, and 26.8% are fully vaccinated, with corresponding numbers of 68.0% and 58.0% for children aged 12-17, the CDC reported on its COVID Data Tracker.
State-level data show that children aged 5-11 in Vermont, with a rate of 65%, are the most likely to have received at least one dose of COVID vaccine, while just 15% of 5- to 11-year-olds in Alabama, Louisiana, and Mississippi have gotten their first dose. Among children aged 12-17, that rate ranges from 40% in Wyoming to 94% in Hawaii, Massachusetts, and Rhode Island, the AAP said in a separate report based on CDC data.
In a recent report involving 1,364 children aged 5-15 years, two doses of the COVID-19 vaccine reduced the risk of infection from the Omicron variant by 31% in children aged 5-11 years and by 59% among children aged 12-15 years, said Ashley L. Fowlkes, ScD, of the CDC’s COVID-19 Emergency Response Team, and associates (MMWR 2022 Mar 11;71).
New cases of COVID-19 in U.S. children have fallen to their lowest level since the beginning of the Delta surge in July of 2021, according to the American Academy of Pediatrics and the Children’s Hospital Association.
. Over those 7 weeks, new cases dropped over 96% from the 1.15 million reported for Jan. 14-20, based on data collected by the AAP and CHA from state and territorial health departments.
The last time that the weekly count was below 42,000 was July 16-22, 2021, when almost 39,000 cases were reported in the midst of the Delta upsurge. That was shortly after cases had reached their lowest point, 8,447, since the early stages of the pandemic in 2020, the AAP/CHA data show.
The cumulative number of pediatric cases is now up to 12.7 million, while the overall proportion of cases occurring in children held steady at 19.0% for the 4th week in a row, the AAP and CHA said in their weekly COVID-19 report. The Centers for Disease Control and Prevention, using an age range of 0-18 versus the states’ variety of ages, puts total cases at 11.7 million and deaths at 1,656 as of March 14.
Data from the CDC’s COVID-19–Associated Hospitalization Surveillance Network show that hospitalizations with laboratory-confirmed infection were down by 50% in children aged 0-4 years, by 63% among 5- to 11-year-olds, and by 58% in those aged 12-17 years for the week of Feb. 27 to March 5, compared with the week before.
The pace of vaccination continues to follow a similar trend, as the declines seen through February have continued into March. Cumulatively, 33.7% of children aged 5-11 have received at least one dose, and 26.8% are fully vaccinated, with corresponding numbers of 68.0% and 58.0% for children aged 12-17, the CDC reported on its COVID Data Tracker.
State-level data show that children aged 5-11 in Vermont, with a rate of 65%, are the most likely to have received at least one dose of COVID vaccine, while just 15% of 5- to 11-year-olds in Alabama, Louisiana, and Mississippi have gotten their first dose. Among children aged 12-17, that rate ranges from 40% in Wyoming to 94% in Hawaii, Massachusetts, and Rhode Island, the AAP said in a separate report based on CDC data.
In a recent report involving 1,364 children aged 5-15 years, two doses of the COVID-19 vaccine reduced the risk of infection from the Omicron variant by 31% in children aged 5-11 years and by 59% among children aged 12-15 years, said Ashley L. Fowlkes, ScD, of the CDC’s COVID-19 Emergency Response Team, and associates (MMWR 2022 Mar 11;71).
New JIA guidelines emphasize earlier DMARD use
Treatment of systemic juvenile idiopathic arthritis (sJIA) should emphasize early use of conventional synthetic and biologic disease-modifying antirheumatic drugs (DMARDs), compared with the previous reliance on NSAIDs and glucocorticoids, according to new guidelines from the American College of Rheumatology. The recently published 2021 guidelines focus on therapeutic approaches for oligoarthritis, temporomandibular joint (TMJ) arthritis, and sJIA.
“Systemic JIA should be treated early with biologics to rapidly bring disease under control and to avoid long-term use of glucocorticoids,” Karen Onel, MD, chief of the division of pediatric rheumatology at Weill Cornell Medicine, New York, and lead author of the guidelines, told this news organization. “Unfortunately, biologics can and are frequently denied for first-line use. For this reason, the guidelines are critically important as they demonstrate that first-line use of biologics are standard of care for the treatment of sJIA.”

The new publication is the second part of the ACR’s process to update JIA guidelines that began in 2017 and complements the release in 2019 of guidelines on the management of nonsystemic polyarthritis, sacroiliitis, and enthesitis, as well as a separate guidance on JIA-associated uveitis. The new guidelines include a second publication focused on nonpharmacologic therapies, medication monitoring, immunizations, and imaging. Both sets of guidelines grew out of a 15-member panel that included young adults with JIA and caregivers of children with JIA, and which required at least 70% agreement on recommendations.
“Though the scope of the two guidelines differed, one thing they had in common is the recognition of the importance of shared decision-making with the patient/caregiver,” Dr. Onel said. “Not every decision will be appropriate for every patient, which is why it was so instrumental to receive input from both patients and caregivers when creating these recommendations.”
Oligoarticular and TMJ arthritis
Oligoarticular and TMJ arthritis have similar recommendations, beginning with NSAIDs conditionally recommended and intra-articular glucocorticoids (IAGCs) strongly recommended as part of initial therapy. For oligoarticular arthritis, the guidelines specifically include a strong recommendation of triamcinolone hexacetonide as the preferred agent; no preferred agent is recommended for TMJ arthritis.

“The one thing that the panel was unanimous about was the use of triamcinolone hexacetonide for intra-articular steroid injections in oligoarticular kids,” Susan Shenoi, MBBS, MS, an associate professor and clinical director of pediatric rheumatology at Seattle Children’s Hospital and Research Center, said in an interview. “Triamcinolone hexacetonide has not been available recently, and through advocacy efforts, there is now a pathway to get that medication,” added Dr. Shenoi, a coauthor on the guidelines.
Dr. Onel said that “triamcinolone hexacetonide has been shown to be superior to alternative injectable glucocorticoids in achieving and maintaining remission in children with JIA,” but its unavailability meant physicians had to consider less effective, more potent, or more costly alternatives.” To address the shortage, “the FDA allowed the importation of one particular formulation of triamcinolone hexacetonide [Hexatrione 2%] specifically for joint injections in patients with JIA.”
The guidelines conditionally recommend against oral glucocorticoids for initial therapy for both oligoarticular and TMJ arthritis. In fact, throughout the guidelines it’s clear that the authors emphasize using steroids as little as possible, Dr. Shenoi said.
“Steroids are great anti-inflammatories, but in kids we worry about the long-term effects on growth and metabolism, and now we have many more DMARDs available,” Dr. Shenoi said.
The guidelines strongly recommend conventional synthetic DMARDs for patients with either of these diseases who cannot tolerate or do not respond to NSAIDs or IAGCs, with methotrexate conditionally recommended over leflunomide (Arava) for TMJ and over leflunomide, sulfasalazine (Azulfidine, Sulfazine), and hydroxychloroquine, respectively, for oligoarticular arthritis.
“NSAIDs remain widely used despite evidence supporting early use of DMARDs,” Dr. Onel said. “NSAIDs are readily available and familiar; however, they will not prevent disease progression. These guidelines should encourage short courses of NSAIDs only.”
If patients do not respond to or cannot tolerate NSAIDs, IAGCs, and at least one conventional DMARD, the guidelines strongly recommend a biologic DMARD for oligoarticular arthritis and conditionally recommend one for TMJ arthritis, without any preferences to the specific agent.
The guidelines also advise using validated disease activity measures to guide treatment decisions.
“The most important thing when you’re looking at these patients is to determine, do they have active disease or not?” Dr. Shenoi said. “If they have active disease, then you really want to step up therapy.” Using the relatively new concept of treat-to-target, Dr. Shenoi added that a crucial part of shared decision-making with the family is identifying the most appropriate target for that family “and then really trying hard to achieve that target.”
The guidelines also list risk factors for poor outcome that can be used to guide treatment decisions.
“Specific involvement of key joints, such as TMJ, wrist, sacroiliac, hip, and ankle, and other features were considered reasonable justification for early escalation of therapy,” Dr. Onel said. Other features included presence of erosive disease or enthesitis, delay in diagnosis, elevated levels of inflammation markers, and symmetric disease. “Moving quickly may be needed for a patient who is rapidly worsening, while moving slower may be appropriate for somebody who has improved substantially, but not fully.”
Systemic JIA with and without macrophage activation syndrome
For systemic JIA without macrophage activation syndrome (MAS), the guidelines similarly advise against oral glucocorticoids as initial monotherapy while conditionally recommending NSAIDs for initial monotherapy. Where the guidelines differ most from those for oligoarticular and TMJ arthritis is in progression of DMARD use, with a strong recommendation against conventional synthetic DMARDs as an initial monotherapy and interleukin-1 and IL-6 inhibitors conditionally recommended for initial monotherapy.
For patients who don’t adequately respond to NSAIDs or glucocorticoids, IL-1 and IL-6 inhibitors are strongly recommended over a single or combination of conventional DMARDs. Residual arthritis or an incomplete response to IL-1 or IL-6 inhibitors should lead next to biologic or conventional DMARDs instead of long-term glucocorticoids.
For patients with MAS, the guidelines conditionally recommend IL-1 and IL-6 inhibitors over calcineurin inhibitor monotherapy to reach inactive disease and MAS resolution, with glucocorticoids conditionally recommended in initial treatment. Again, however, for patients with incomplete responses to IL-1 or IL-6 inhibitors or with residual arthritis, the guidelines advise biologic or conventional DMARDs over long-term glucocorticoids.
In patients with sJIA with or without a history of MAS who have inactive disease, practitioners should taper and discontinue glucocorticoids (a strong recommendation). A conditional recommendation for tapering and discontinuing biologic DMARDs follows attainment of inactive disease.
Beyond pharmacology
Although many of the nonpharmacologic recommendations did not have strong evidence based on assessment with Grading of Recommendations Assessment, Development, and Evaluation methodology, consensus was more often the case than not, Dr. Onel said, such as with vaccination.
“There was strong support for the use of immunizations in children with JIA and specific guidance for children with JIA receiving immunosuppression, not on immunosuppression, and children who are underimmunized or unimmunized,” she said. “Although the supportive evidence was very low as per GRADE, panel members were strongly in favor [of immunizations], given risk of infection for immunosuppressed children as well as the preponderance of evidence in similar disease states, such as IBD [inflammatory bowel disease].”
An area with less consensus was whether to check antibody titers for vaccine-preventable childhood infections before beginning immunosuppressive medication, but more panelists opposed the practice than supported it, Dr. Onel said.
“Some panelists felt that the information might be useful for risk management in case of an outbreak or exposure,” she said. “Most believed that screening a fully immunized child was of low benefit and might delay treatment and incur unnecessary cost.”
The process of developing the documents also reveals where the biggest gaps are in research.
“One of the things that we should strive for in the future is really to do more systematic studies so we have better quality of evidence going forward,” Dr. Shenoi said. Overall, however, the guidelines also reveal the progress made in treatment of JIA.
“We now know some of the key cytokines that are involved in the disease pathogenesis, and we have effective therapies for some of these pathways,” Dr. Shenoi said. “We used to use a lot more toxic medication for systemic JIA, and in past decades, these patients used to be on steroids forever. Now we have targeted therapies, and we have some patients who don’t ever need steroids because people are moving toward targeted therapies and having good results. That’s a huge step forward in the field.”
The research was funded by the ACR. Dr. Shenoi has been a consultant for Pfizer. Dr. Onel disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Treatment of systemic juvenile idiopathic arthritis (sJIA) should emphasize early use of conventional synthetic and biologic disease-modifying antirheumatic drugs (DMARDs), compared with the previous reliance on NSAIDs and glucocorticoids, according to new guidelines from the American College of Rheumatology. The recently published 2021 guidelines focus on therapeutic approaches for oligoarthritis, temporomandibular joint (TMJ) arthritis, and sJIA.
“Systemic JIA should be treated early with biologics to rapidly bring disease under control and to avoid long-term use of glucocorticoids,” Karen Onel, MD, chief of the division of pediatric rheumatology at Weill Cornell Medicine, New York, and lead author of the guidelines, told this news organization. “Unfortunately, biologics can and are frequently denied for first-line use. For this reason, the guidelines are critically important as they demonstrate that first-line use of biologics are standard of care for the treatment of sJIA.”
The new publication is the second part of the ACR’s process to update JIA guidelines that began in 2017 and complements the release in 2019 of guidelines on the management of nonsystemic polyarthritis, sacroiliitis, and enthesitis, as well as a separate guidance on JIA-associated uveitis. The new guidelines include a second publication focused on nonpharmacologic therapies, medication monitoring, immunizations, and imaging. Both sets of guidelines grew out of a 15-member panel that included young adults with JIA and caregivers of children with JIA, and which required at least 70% agreement on recommendations.
“Though the scope of the two guidelines differed, one thing they had in common is the recognition of the importance of shared decision-making with the patient/caregiver,” Dr. Onel said. “Not every decision will be appropriate for every patient, which is why it was so instrumental to receive input from both patients and caregivers when creating these recommendations.”
Oligoarticular and TMJ arthritis
Oligoarticular and TMJ arthritis have similar recommendations, beginning with NSAIDs conditionally recommended and intra-articular glucocorticoids (IAGCs) strongly recommended as part of initial therapy. For oligoarticular arthritis, the guidelines specifically include a strong recommendation of triamcinolone hexacetonide as the preferred agent; no preferred agent is recommended for TMJ arthritis.
“The one thing that the panel was unanimous about was the use of triamcinolone hexacetonide for intra-articular steroid injections in oligoarticular kids,” Susan Shenoi, MBBS, MS, an associate professor and clinical director of pediatric rheumatology at Seattle Children’s Hospital and Research Center, said in an interview. “Triamcinolone hexacetonide has not been available recently, and through advocacy efforts, there is now a pathway to get that medication,” added Dr. Shenoi, a coauthor on the guidelines.
Dr. Onel said that “triamcinolone hexacetonide has been shown to be superior to alternative injectable glucocorticoids in achieving and maintaining remission in children with JIA,” but its unavailability meant physicians had to consider less effective, more potent, or more costly alternatives.” To address the shortage, “the FDA allowed the importation of one particular formulation of triamcinolone hexacetonide [Hexatrione 2%] specifically for joint injections in patients with JIA.”
The guidelines conditionally recommend against oral glucocorticoids for initial therapy for both oligoarticular and TMJ arthritis. In fact, throughout the guidelines it’s clear that the authors emphasize using steroids as little as possible, Dr. Shenoi said.
“Steroids are great anti-inflammatories, but in kids we worry about the long-term effects on growth and metabolism, and now we have many more DMARDs available,” Dr. Shenoi said.
The guidelines strongly recommend conventional synthetic DMARDs for patients with either of these diseases who cannot tolerate or do not respond to NSAIDs or IAGCs, with methotrexate conditionally recommended over leflunomide (Arava) for TMJ and over leflunomide, sulfasalazine (Azulfidine, Sulfazine), and hydroxychloroquine, respectively, for oligoarticular arthritis.
“NSAIDs remain widely used despite evidence supporting early use of DMARDs,” Dr. Onel said. “NSAIDs are readily available and familiar; however, they will not prevent disease progression. These guidelines should encourage short courses of NSAIDs only.”
If patients do not respond to or cannot tolerate NSAIDs, IAGCs, and at least one conventional DMARD, the guidelines strongly recommend a biologic DMARD for oligoarticular arthritis and conditionally recommend one for TMJ arthritis, without any preferences to the specific agent.
The guidelines also advise using validated disease activity measures to guide treatment decisions.
“The most important thing when you’re looking at these patients is to determine, do they have active disease or not?” Dr. Shenoi said. “If they have active disease, then you really want to step up therapy.” Using the relatively new concept of treat-to-target, Dr. Shenoi added that a crucial part of shared decision-making with the family is identifying the most appropriate target for that family “and then really trying hard to achieve that target.”
The guidelines also list risk factors for poor outcome that can be used to guide treatment decisions.
“Specific involvement of key joints, such as TMJ, wrist, sacroiliac, hip, and ankle, and other features were considered reasonable justification for early escalation of therapy,” Dr. Onel said. Other features included presence of erosive disease or enthesitis, delay in diagnosis, elevated levels of inflammation markers, and symmetric disease. “Moving quickly may be needed for a patient who is rapidly worsening, while moving slower may be appropriate for somebody who has improved substantially, but not fully.”
Systemic JIA with and without macrophage activation syndrome
For systemic JIA without macrophage activation syndrome (MAS), the guidelines similarly advise against oral glucocorticoids as initial monotherapy while conditionally recommending NSAIDs for initial monotherapy. Where the guidelines differ most from those for oligoarticular and TMJ arthritis is in progression of DMARD use, with a strong recommendation against conventional synthetic DMARDs as an initial monotherapy and interleukin-1 and IL-6 inhibitors conditionally recommended for initial monotherapy.
For patients who don’t adequately respond to NSAIDs or glucocorticoids, IL-1 and IL-6 inhibitors are strongly recommended over a single or combination of conventional DMARDs. Residual arthritis or an incomplete response to IL-1 or IL-6 inhibitors should lead next to biologic or conventional DMARDs instead of long-term glucocorticoids.
For patients with MAS, the guidelines conditionally recommend IL-1 and IL-6 inhibitors over calcineurin inhibitor monotherapy to reach inactive disease and MAS resolution, with glucocorticoids conditionally recommended in initial treatment. Again, however, for patients with incomplete responses to IL-1 or IL-6 inhibitors or with residual arthritis, the guidelines advise biologic or conventional DMARDs over long-term glucocorticoids.
In patients with sJIA with or without a history of MAS who have inactive disease, practitioners should taper and discontinue glucocorticoids (a strong recommendation). A conditional recommendation for tapering and discontinuing biologic DMARDs follows attainment of inactive disease.
Beyond pharmacology
Although many of the nonpharmacologic recommendations did not have strong evidence based on assessment with Grading of Recommendations Assessment, Development, and Evaluation methodology, consensus was more often the case than not, Dr. Onel said, such as with vaccination.
“There was strong support for the use of immunizations in children with JIA and specific guidance for children with JIA receiving immunosuppression, not on immunosuppression, and children who are underimmunized or unimmunized,” she said. “Although the supportive evidence was very low as per GRADE, panel members were strongly in favor [of immunizations], given risk of infection for immunosuppressed children as well as the preponderance of evidence in similar disease states, such as IBD [inflammatory bowel disease].”
An area with less consensus was whether to check antibody titers for vaccine-preventable childhood infections before beginning immunosuppressive medication, but more panelists opposed the practice than supported it, Dr. Onel said.
“Some panelists felt that the information might be useful for risk management in case of an outbreak or exposure,” she said. “Most believed that screening a fully immunized child was of low benefit and might delay treatment and incur unnecessary cost.”
The process of developing the documents also reveals where the biggest gaps are in research.
“One of the things that we should strive for in the future is really to do more systematic studies so we have better quality of evidence going forward,” Dr. Shenoi said. Overall, however, the guidelines also reveal the progress made in treatment of JIA.
“We now know some of the key cytokines that are involved in the disease pathogenesis, and we have effective therapies for some of these pathways,” Dr. Shenoi said. “We used to use a lot more toxic medication for systemic JIA, and in past decades, these patients used to be on steroids forever. Now we have targeted therapies, and we have some patients who don’t ever need steroids because people are moving toward targeted therapies and having good results. That’s a huge step forward in the field.”
The research was funded by the ACR. Dr. Shenoi has been a consultant for Pfizer. Dr. Onel disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Treatment of systemic juvenile idiopathic arthritis (sJIA) should emphasize early use of conventional synthetic and biologic disease-modifying antirheumatic drugs (DMARDs), compared with the previous reliance on NSAIDs and glucocorticoids, according to new guidelines from the American College of Rheumatology. The recently published 2021 guidelines focus on therapeutic approaches for oligoarthritis, temporomandibular joint (TMJ) arthritis, and sJIA.
“Systemic JIA should be treated early with biologics to rapidly bring disease under control and to avoid long-term use of glucocorticoids,” Karen Onel, MD, chief of the division of pediatric rheumatology at Weill Cornell Medicine, New York, and lead author of the guidelines, told this news organization. “Unfortunately, biologics can and are frequently denied for first-line use. For this reason, the guidelines are critically important as they demonstrate that first-line use of biologics are standard of care for the treatment of sJIA.”
The new publication is the second part of the ACR’s process to update JIA guidelines that began in 2017 and complements the release in 2019 of guidelines on the management of nonsystemic polyarthritis, sacroiliitis, and enthesitis, as well as a separate guidance on JIA-associated uveitis. The new guidelines include a second publication focused on nonpharmacologic therapies, medication monitoring, immunizations, and imaging. Both sets of guidelines grew out of a 15-member panel that included young adults with JIA and caregivers of children with JIA, and which required at least 70% agreement on recommendations.
“Though the scope of the two guidelines differed, one thing they had in common is the recognition of the importance of shared decision-making with the patient/caregiver,” Dr. Onel said. “Not every decision will be appropriate for every patient, which is why it was so instrumental to receive input from both patients and caregivers when creating these recommendations.”
Oligoarticular and TMJ arthritis
Oligoarticular and TMJ arthritis have similar recommendations, beginning with NSAIDs conditionally recommended and intra-articular glucocorticoids (IAGCs) strongly recommended as part of initial therapy. For oligoarticular arthritis, the guidelines specifically include a strong recommendation of triamcinolone hexacetonide as the preferred agent; no preferred agent is recommended for TMJ arthritis.
“The one thing that the panel was unanimous about was the use of triamcinolone hexacetonide for intra-articular steroid injections in oligoarticular kids,” Susan Shenoi, MBBS, MS, an associate professor and clinical director of pediatric rheumatology at Seattle Children’s Hospital and Research Center, said in an interview. “Triamcinolone hexacetonide has not been available recently, and through advocacy efforts, there is now a pathway to get that medication,” added Dr. Shenoi, a coauthor on the guidelines.
Dr. Onel said that “triamcinolone hexacetonide has been shown to be superior to alternative injectable glucocorticoids in achieving and maintaining remission in children with JIA,” but its unavailability meant physicians had to consider less effective, more potent, or more costly alternatives.” To address the shortage, “the FDA allowed the importation of one particular formulation of triamcinolone hexacetonide [Hexatrione 2%] specifically for joint injections in patients with JIA.”
The guidelines conditionally recommend against oral glucocorticoids for initial therapy for both oligoarticular and TMJ arthritis. In fact, throughout the guidelines it’s clear that the authors emphasize using steroids as little as possible, Dr. Shenoi said.
“Steroids are great anti-inflammatories, but in kids we worry about the long-term effects on growth and metabolism, and now we have many more DMARDs available,” Dr. Shenoi said.
The guidelines strongly recommend conventional synthetic DMARDs for patients with either of these diseases who cannot tolerate or do not respond to NSAIDs or IAGCs, with methotrexate conditionally recommended over leflunomide (Arava) for TMJ and over leflunomide, sulfasalazine (Azulfidine, Sulfazine), and hydroxychloroquine, respectively, for oligoarticular arthritis.
“NSAIDs remain widely used despite evidence supporting early use of DMARDs,” Dr. Onel said. “NSAIDs are readily available and familiar; however, they will not prevent disease progression. These guidelines should encourage short courses of NSAIDs only.”
If patients do not respond to or cannot tolerate NSAIDs, IAGCs, and at least one conventional DMARD, the guidelines strongly recommend a biologic DMARD for oligoarticular arthritis and conditionally recommend one for TMJ arthritis, without any preferences to the specific agent.
The guidelines also advise using validated disease activity measures to guide treatment decisions.
“The most important thing when you’re looking at these patients is to determine, do they have active disease or not?” Dr. Shenoi said. “If they have active disease, then you really want to step up therapy.” Using the relatively new concept of treat-to-target, Dr. Shenoi added that a crucial part of shared decision-making with the family is identifying the most appropriate target for that family “and then really trying hard to achieve that target.”
The guidelines also list risk factors for poor outcome that can be used to guide treatment decisions.
“Specific involvement of key joints, such as TMJ, wrist, sacroiliac, hip, and ankle, and other features were considered reasonable justification for early escalation of therapy,” Dr. Onel said. Other features included presence of erosive disease or enthesitis, delay in diagnosis, elevated levels of inflammation markers, and symmetric disease. “Moving quickly may be needed for a patient who is rapidly worsening, while moving slower may be appropriate for somebody who has improved substantially, but not fully.”
Systemic JIA with and without macrophage activation syndrome
For systemic JIA without macrophage activation syndrome (MAS), the guidelines similarly advise against oral glucocorticoids as initial monotherapy while conditionally recommending NSAIDs for initial monotherapy. Where the guidelines differ most from those for oligoarticular and TMJ arthritis is in progression of DMARD use, with a strong recommendation against conventional synthetic DMARDs as an initial monotherapy and interleukin-1 and IL-6 inhibitors conditionally recommended for initial monotherapy.
For patients who don’t adequately respond to NSAIDs or glucocorticoids, IL-1 and IL-6 inhibitors are strongly recommended over a single or combination of conventional DMARDs. Residual arthritis or an incomplete response to IL-1 or IL-6 inhibitors should lead next to biologic or conventional DMARDs instead of long-term glucocorticoids.
For patients with MAS, the guidelines conditionally recommend IL-1 and IL-6 inhibitors over calcineurin inhibitor monotherapy to reach inactive disease and MAS resolution, with glucocorticoids conditionally recommended in initial treatment. Again, however, for patients with incomplete responses to IL-1 or IL-6 inhibitors or with residual arthritis, the guidelines advise biologic or conventional DMARDs over long-term glucocorticoids.
In patients with sJIA with or without a history of MAS who have inactive disease, practitioners should taper and discontinue glucocorticoids (a strong recommendation). A conditional recommendation for tapering and discontinuing biologic DMARDs follows attainment of inactive disease.
Beyond pharmacology
Although many of the nonpharmacologic recommendations did not have strong evidence based on assessment with Grading of Recommendations Assessment, Development, and Evaluation methodology, consensus was more often the case than not, Dr. Onel said, such as with vaccination.
“There was strong support for the use of immunizations in children with JIA and specific guidance for children with JIA receiving immunosuppression, not on immunosuppression, and children who are underimmunized or unimmunized,” she said. “Although the supportive evidence was very low as per GRADE, panel members were strongly in favor [of immunizations], given risk of infection for immunosuppressed children as well as the preponderance of evidence in similar disease states, such as IBD [inflammatory bowel disease].”
An area with less consensus was whether to check antibody titers for vaccine-preventable childhood infections before beginning immunosuppressive medication, but more panelists opposed the practice than supported it, Dr. Onel said.
“Some panelists felt that the information might be useful for risk management in case of an outbreak or exposure,” she said. “Most believed that screening a fully immunized child was of low benefit and might delay treatment and incur unnecessary cost.”
The process of developing the documents also reveals where the biggest gaps are in research.
“One of the things that we should strive for in the future is really to do more systematic studies so we have better quality of evidence going forward,” Dr. Shenoi said. Overall, however, the guidelines also reveal the progress made in treatment of JIA.
“We now know some of the key cytokines that are involved in the disease pathogenesis, and we have effective therapies for some of these pathways,” Dr. Shenoi said. “We used to use a lot more toxic medication for systemic JIA, and in past decades, these patients used to be on steroids forever. Now we have targeted therapies, and we have some patients who don’t ever need steroids because people are moving toward targeted therapies and having good results. That’s a huge step forward in the field.”
The research was funded by the ACR. Dr. Shenoi has been a consultant for Pfizer. Dr. Onel disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ARTHRITIS & RHEUMATOLOGY
An 11-year-old female presented with skin discoloration on her back
Becker’s nevus
The history and physical exam are most consistent with Becker’s nevus, also known as Becker’s melanosis. This is a benign cutaneous hamartoma, usually found in males, characterized by a large, irregularly shaped brown patch, often with hypertrichosis.1 Becker’s nevus can be congenital but is more commonly noticed in late childhood or early adolescence, with thickening, increased pigmentation, and hair growth. Becker’s nevus is considered an overgrowth of epidermal pigment cells and hair follicles and is thought to be attributable to postzygotic mutations (with ACTB mutations most reported).1 It is often located unilaterally on the upper trunk but is occasionally present elsewhere on the body. Acne may occasionally develop within the nevus, which is believed to be triggered by puberty-associated androgens.1 The lesion tends to persist indefinitely but has no propensity for malignant transformation.

Becker’s nevus is generally an isolated skin lesion without other anomalies. However, in rare instances, it may be associated with ipsilateral breast hypoplasia or hypoplastic defects of the muscle, skin, or skeleton, which is known as Becker’s nevus syndrome.2 Treatment is not medically warranted for an isolated Becker’s nevus but may be pursued for cosmetic reasons. Although treatment is generally discouraged because of variable success, laser hair removal and laser therapy may be pursued to address the hypertrichosis and hyperpigmentation, respectively.
What is on the differential?
A café-au-lait macule (CALM) is a light- to dark-brown, oval lesion that commonly presents at birth or in early childhood. CALMs vary widely in size from less than 1.5 cm to more than 20 cm in diameter. They are asymptomatic and grow in proportion to the individual over time.3 Becker’s nevus can be distinguished from CALMs by the development of hypertrichosis, typical location and course, and other skin changes within the nevus.

Postinflammatory hyperpigmentation (PIH) is characterized by asymptomatic, darkened macules or patches that are brown to blue-gray in color. It is one of the most common causes of hyperpigmentation, particularly in skin of color, and can take months to years to resolve. PIH is caused by increased melanin production in response to a cutaneous inflammatory process, such as a drug reaction, allergy, mechanical or thermal injury, infection, phototoxicity, or an underlying skin condition.3 Our patient’s history with the lack of an inciting inflammatory process is more consistent with Becker’s nevus.
Erythema ab igne is a cutaneous reaction to heat that presents as a hyperpigmented patch with a reticular or mottled configuration and superficial venular telangiectasia. The lesion is initially erythematous and progresses to a pale pink to purplish dark-brown color.4 Causes include long-term use of a heating pad, laptop, electric blanket, or a hot water bottle. The absence of prolonged heat exposure in our patient’s history does not favor erythema ab igne.
Pigmentary mosaicism is characterized by a distinctive pattern of hyperpigmentation that follows the lines of ectodermal embryologic development, known as the lines of Blaschko.5 This condition is also known as linear and whorled nevoid hypermelanosis because of its streaky or swirl-like pattern. Pigmentary mosaicism can be present at birth or appear within the first few weeks of life. It is caused by genetic heterogeneity in neuroectodermal cells, which results in skin with areas of varying colors. Pigmentary mosaicism is unlikely in this case as our patient’s lesion does not follow the lines of Blaschko.
Ms. Laborada is a pediatric dermatology research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Dr. Eichenfield is the vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital. Ms. Laborada and Dr. Eichenfield have no relevant financial disclosures.
References
1. Atzmony L et al. J Cutan Pathol. 2020;47(8):681-5.
2. Danarti R et al. J Am Acad Dermatol. 2004;51(6):965-9.
3. Paller A and Mancini AJ. “Hurwitz Clinical Pediatric Dermatology: A textbook of skin disorders of childhood and adolescence” 4th ed. Philadelphia: Elsevier Saunders, 2011.
4. Patel DP. JAMA Dermatol. 2017;153(7):685.
5. Kromann AB et al. Orphanet J Rare Dis. 2018;13(1):39.
Becker’s nevus
The history and physical exam are most consistent with Becker’s nevus, also known as Becker’s melanosis. This is a benign cutaneous hamartoma, usually found in males, characterized by a large, irregularly shaped brown patch, often with hypertrichosis.1 Becker’s nevus can be congenital but is more commonly noticed in late childhood or early adolescence, with thickening, increased pigmentation, and hair growth. Becker’s nevus is considered an overgrowth of epidermal pigment cells and hair follicles and is thought to be attributable to postzygotic mutations (with ACTB mutations most reported).1 It is often located unilaterally on the upper trunk but is occasionally present elsewhere on the body. Acne may occasionally develop within the nevus, which is believed to be triggered by puberty-associated androgens.1 The lesion tends to persist indefinitely but has no propensity for malignant transformation.
Becker’s nevus is generally an isolated skin lesion without other anomalies. However, in rare instances, it may be associated with ipsilateral breast hypoplasia or hypoplastic defects of the muscle, skin, or skeleton, which is known as Becker’s nevus syndrome.2 Treatment is not medically warranted for an isolated Becker’s nevus but may be pursued for cosmetic reasons. Although treatment is generally discouraged because of variable success, laser hair removal and laser therapy may be pursued to address the hypertrichosis and hyperpigmentation, respectively.
What is on the differential?
A café-au-lait macule (CALM) is a light- to dark-brown, oval lesion that commonly presents at birth or in early childhood. CALMs vary widely in size from less than 1.5 cm to more than 20 cm in diameter. They are asymptomatic and grow in proportion to the individual over time.3 Becker’s nevus can be distinguished from CALMs by the development of hypertrichosis, typical location and course, and other skin changes within the nevus.
Postinflammatory hyperpigmentation (PIH) is characterized by asymptomatic, darkened macules or patches that are brown to blue-gray in color. It is one of the most common causes of hyperpigmentation, particularly in skin of color, and can take months to years to resolve. PIH is caused by increased melanin production in response to a cutaneous inflammatory process, such as a drug reaction, allergy, mechanical or thermal injury, infection, phototoxicity, or an underlying skin condition.3 Our patient’s history with the lack of an inciting inflammatory process is more consistent with Becker’s nevus.
Erythema ab igne is a cutaneous reaction to heat that presents as a hyperpigmented patch with a reticular or mottled configuration and superficial venular telangiectasia. The lesion is initially erythematous and progresses to a pale pink to purplish dark-brown color.4 Causes include long-term use of a heating pad, laptop, electric blanket, or a hot water bottle. The absence of prolonged heat exposure in our patient’s history does not favor erythema ab igne.
Pigmentary mosaicism is characterized by a distinctive pattern of hyperpigmentation that follows the lines of ectodermal embryologic development, known as the lines of Blaschko.5 This condition is also known as linear and whorled nevoid hypermelanosis because of its streaky or swirl-like pattern. Pigmentary mosaicism can be present at birth or appear within the first few weeks of life. It is caused by genetic heterogeneity in neuroectodermal cells, which results in skin with areas of varying colors. Pigmentary mosaicism is unlikely in this case as our patient’s lesion does not follow the lines of Blaschko.
Ms. Laborada is a pediatric dermatology research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Dr. Eichenfield is the vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital. Ms. Laborada and Dr. Eichenfield have no relevant financial disclosures.
References
1. Atzmony L et al. J Cutan Pathol. 2020;47(8):681-5.
2. Danarti R et al. J Am Acad Dermatol. 2004;51(6):965-9.
3. Paller A and Mancini AJ. “Hurwitz Clinical Pediatric Dermatology: A textbook of skin disorders of childhood and adolescence” 4th ed. Philadelphia: Elsevier Saunders, 2011.
4. Patel DP. JAMA Dermatol. 2017;153(7):685.
5. Kromann AB et al. Orphanet J Rare Dis. 2018;13(1):39.
Becker’s nevus
The history and physical exam are most consistent with Becker’s nevus, also known as Becker’s melanosis. This is a benign cutaneous hamartoma, usually found in males, characterized by a large, irregularly shaped brown patch, often with hypertrichosis.1 Becker’s nevus can be congenital but is more commonly noticed in late childhood or early adolescence, with thickening, increased pigmentation, and hair growth. Becker’s nevus is considered an overgrowth of epidermal pigment cells and hair follicles and is thought to be attributable to postzygotic mutations (with ACTB mutations most reported).1 It is often located unilaterally on the upper trunk but is occasionally present elsewhere on the body. Acne may occasionally develop within the nevus, which is believed to be triggered by puberty-associated androgens.1 The lesion tends to persist indefinitely but has no propensity for malignant transformation.
Becker’s nevus is generally an isolated skin lesion without other anomalies. However, in rare instances, it may be associated with ipsilateral breast hypoplasia or hypoplastic defects of the muscle, skin, or skeleton, which is known as Becker’s nevus syndrome.2 Treatment is not medically warranted for an isolated Becker’s nevus but may be pursued for cosmetic reasons. Although treatment is generally discouraged because of variable success, laser hair removal and laser therapy may be pursued to address the hypertrichosis and hyperpigmentation, respectively.
What is on the differential?
A café-au-lait macule (CALM) is a light- to dark-brown, oval lesion that commonly presents at birth or in early childhood. CALMs vary widely in size from less than 1.5 cm to more than 20 cm in diameter. They are asymptomatic and grow in proportion to the individual over time.3 Becker’s nevus can be distinguished from CALMs by the development of hypertrichosis, typical location and course, and other skin changes within the nevus.
Postinflammatory hyperpigmentation (PIH) is characterized by asymptomatic, darkened macules or patches that are brown to blue-gray in color. It is one of the most common causes of hyperpigmentation, particularly in skin of color, and can take months to years to resolve. PIH is caused by increased melanin production in response to a cutaneous inflammatory process, such as a drug reaction, allergy, mechanical or thermal injury, infection, phototoxicity, or an underlying skin condition.3 Our patient’s history with the lack of an inciting inflammatory process is more consistent with Becker’s nevus.
Erythema ab igne is a cutaneous reaction to heat that presents as a hyperpigmented patch with a reticular or mottled configuration and superficial venular telangiectasia. The lesion is initially erythematous and progresses to a pale pink to purplish dark-brown color.4 Causes include long-term use of a heating pad, laptop, electric blanket, or a hot water bottle. The absence of prolonged heat exposure in our patient’s history does not favor erythema ab igne.
Pigmentary mosaicism is characterized by a distinctive pattern of hyperpigmentation that follows the lines of ectodermal embryologic development, known as the lines of Blaschko.5 This condition is also known as linear and whorled nevoid hypermelanosis because of its streaky or swirl-like pattern. Pigmentary mosaicism can be present at birth or appear within the first few weeks of life. It is caused by genetic heterogeneity in neuroectodermal cells, which results in skin with areas of varying colors. Pigmentary mosaicism is unlikely in this case as our patient’s lesion does not follow the lines of Blaschko.
Ms. Laborada is a pediatric dermatology research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Dr. Eichenfield is the vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital. Ms. Laborada and Dr. Eichenfield have no relevant financial disclosures.
References
1. Atzmony L et al. J Cutan Pathol. 2020;47(8):681-5.
2. Danarti R et al. J Am Acad Dermatol. 2004;51(6):965-9.
3. Paller A and Mancini AJ. “Hurwitz Clinical Pediatric Dermatology: A textbook of skin disorders of childhood and adolescence” 4th ed. Philadelphia: Elsevier Saunders, 2011.
4. Patel DP. JAMA Dermatol. 2017;153(7):685.
5. Kromann AB et al. Orphanet J Rare Dis. 2018;13(1):39.

Cat ownership in childhood linked ‘conditionally’ to psychosis in adult males
Owning an outdoor cat as a child is associated with an increased risk of psychotic experiences in adulthood – but only in males, new research suggests.
Investigators found

The suspected culprit is not the cat itself but rather exposure to Toxoplasma gondii, a common parasite carried by rodents and sometimes found in cat feces. The study adds to a growing evidence showing exposure to T. gondii may be a risk factor for schizophrenia and other psychotic disorders.
“These are small pieces of evidence but it’s interesting to consider that there might be combinations of risk factors at play,” lead author Vincent Paquin, MD, psychiatry resident at McGill University, Montreal, said in an interview.
“And even if the magnitude of the risk is small at the individual level,” he added, “cats and Toxoplasma gondii are so present in our society that if we add up all these small potential effects then it becomes a potential public health question.”
The study was published online Jan. 30, 2022, in the Journal of Psychiatric Research.
Inconsistent evidence
T. gondii infects about 30% of the human population and is usually transmitted by cats. Most infections are asymptomatic, but T. gondii can cause toxoplasmosis in humans, which has been linked to increased risk of schizophrenia, suicide attempts, and more recently, mild cognitive impairment.
Although some studies show an association between cat ownership and increased risk of mental illness, the research findings have been inconsistent.
“The evidence has been mixed about the association between cat ownership and psychosis expression, so our approach was to consider whether specific factors or combinations of factors could explain this mixed evidence,” Dr. Paquin said.
For the study, 2206 individuals aged 18-40 years completed the Community Assessment of Psychic Experiences (CAPE-42) and a questionnaire to gather information about cat ownership at any time between birth and age 13 and if the cats lived exclusively indoors (nonhunting) or if they were allowed outside (rodent hunting).
Participants were also asked about the number of residential moves between birth and age 15, date and place of birth, lifetime history of head trauma, and tobacco smoking history.
Rodent-hunting cat ownership was associated with higher risk of psychosis in male participants, compared with owning no cat or a nonhunting cat. When the investigators added head trauma and residential moves to rodent-hunting cat ownership, psychosis risk was elevated in both men and women.
Independent of cat ownership, younger age, moving more than three times as a child, a history of head trauma, and being a smoker were all associated with higher psychosis risk.

The study wasn’t designed to explore potential biological mechanisms to explain the sex differences in psychosis risk seen among rodent-hunting cat owners, but “one possible explanation based on the animal model literature is that the neurobiological effects of parasitic exposure may be greater with male sex,” senior author Suzanne King, PhD, professor of psychiatry at McGill, said in an interview.
The new study is part of a larger, long-term project called EnviroGen, led by Dr. King, examining the environmental and genetic risk factors for schizophrenia.
Need for replication
Commenting on the findings, E. Fuller Torrey, MD, who was among the first researchers to identify a link between cat ownership, T. gondii infection, and schizophrenia, said the study is “an interesting addition to the studies of cat ownership in childhood as a risk factor for psychosis.”
Of the approximately 10 published studies on the topic, about half suggest a link between cat ownership and psychosis later in life, said Dr. Torrey, associate director for research at the Stanley Medical Research Institute in Rockville, Md.
“The Canadian study is interesting in that it is the first study that separates exposure to permanently indoor cats from cats that are allowed to go outdoors, and the results were positive only for outdoor cats,” Dr. Torrey said.
The study has limitations, Dr. Torrey added, including its retrospective design and the use of a self-report questionnaire to assess psychotic experiences in adulthood.
Also commenting on findings, James Kirkbride, PhD, professor of psychiatric and social epidemiology, University College London, noted the same limitations.
Dr. Kirkbride is the lead author of a 2017 study that showed no link between cat ownership and serious mental illness that included nearly 5,000 people born in 1991 or 1992 and followed until age 18. In this study, there was no link between psychosis and cat ownership during pregnancy or at ages 4 or 10 years.
“Researchers have long been fascinated with the idea that cat ownership may affect mental health. This paper may have them chasing their own tail,” Dr. Kirkbride said.
“Evidence of any association is limited to certain subgroups without a strong theoretical basis for why this may be the case,” he added. “The retrospective and cross-sectional nature of the survey also raise the possibility that the results are impacted by differential recall bias, as well as the broader issues of chance and unobserved confounding.”
Dr. King noted that recall bias is a limitation the researchers highlighted in their study, but “considering the exposures are relatively objective and factual, we do not believe the potential for recall bias is substantial.”
“Nonetheless, we strongly believe that replication of our results in prospective, population-representative cohorts will be crucial to making firmer conclusions,” he added.
The study was funded by grants from the Quebec Health Research Fund. The study authors and Dr. Kirkbride disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Owning an outdoor cat as a child is associated with an increased risk of psychotic experiences in adulthood – but only in males, new research suggests.
Investigators found
The suspected culprit is not the cat itself but rather exposure to Toxoplasma gondii, a common parasite carried by rodents and sometimes found in cat feces. The study adds to a growing evidence showing exposure to T. gondii may be a risk factor for schizophrenia and other psychotic disorders.
“These are small pieces of evidence but it’s interesting to consider that there might be combinations of risk factors at play,” lead author Vincent Paquin, MD, psychiatry resident at McGill University, Montreal, said in an interview.
“And even if the magnitude of the risk is small at the individual level,” he added, “cats and Toxoplasma gondii are so present in our society that if we add up all these small potential effects then it becomes a potential public health question.”
The study was published online Jan. 30, 2022, in the Journal of Psychiatric Research.
Inconsistent evidence
T. gondii infects about 30% of the human population and is usually transmitted by cats. Most infections are asymptomatic, but T. gondii can cause toxoplasmosis in humans, which has been linked to increased risk of schizophrenia, suicide attempts, and more recently, mild cognitive impairment.
Although some studies show an association between cat ownership and increased risk of mental illness, the research findings have been inconsistent.
“The evidence has been mixed about the association between cat ownership and psychosis expression, so our approach was to consider whether specific factors or combinations of factors could explain this mixed evidence,” Dr. Paquin said.
For the study, 2206 individuals aged 18-40 years completed the Community Assessment of Psychic Experiences (CAPE-42) and a questionnaire to gather information about cat ownership at any time between birth and age 13 and if the cats lived exclusively indoors (nonhunting) or if they were allowed outside (rodent hunting).
Participants were also asked about the number of residential moves between birth and age 15, date and place of birth, lifetime history of head trauma, and tobacco smoking history.
Rodent-hunting cat ownership was associated with higher risk of psychosis in male participants, compared with owning no cat or a nonhunting cat. When the investigators added head trauma and residential moves to rodent-hunting cat ownership, psychosis risk was elevated in both men and women.
Independent of cat ownership, younger age, moving more than three times as a child, a history of head trauma, and being a smoker were all associated with higher psychosis risk.
The study wasn’t designed to explore potential biological mechanisms to explain the sex differences in psychosis risk seen among rodent-hunting cat owners, but “one possible explanation based on the animal model literature is that the neurobiological effects of parasitic exposure may be greater with male sex,” senior author Suzanne King, PhD, professor of psychiatry at McGill, said in an interview.
The new study is part of a larger, long-term project called EnviroGen, led by Dr. King, examining the environmental and genetic risk factors for schizophrenia.
Need for replication
Commenting on the findings, E. Fuller Torrey, MD, who was among the first researchers to identify a link between cat ownership, T. gondii infection, and schizophrenia, said the study is “an interesting addition to the studies of cat ownership in childhood as a risk factor for psychosis.”
Of the approximately 10 published studies on the topic, about half suggest a link between cat ownership and psychosis later in life, said Dr. Torrey, associate director for research at the Stanley Medical Research Institute in Rockville, Md.
“The Canadian study is interesting in that it is the first study that separates exposure to permanently indoor cats from cats that are allowed to go outdoors, and the results were positive only for outdoor cats,” Dr. Torrey said.
The study has limitations, Dr. Torrey added, including its retrospective design and the use of a self-report questionnaire to assess psychotic experiences in adulthood.
Also commenting on findings, James Kirkbride, PhD, professor of psychiatric and social epidemiology, University College London, noted the same limitations.
Dr. Kirkbride is the lead author of a 2017 study that showed no link between cat ownership and serious mental illness that included nearly 5,000 people born in 1991 or 1992 and followed until age 18. In this study, there was no link between psychosis and cat ownership during pregnancy or at ages 4 or 10 years.
“Researchers have long been fascinated with the idea that cat ownership may affect mental health. This paper may have them chasing their own tail,” Dr. Kirkbride said.
“Evidence of any association is limited to certain subgroups without a strong theoretical basis for why this may be the case,” he added. “The retrospective and cross-sectional nature of the survey also raise the possibility that the results are impacted by differential recall bias, as well as the broader issues of chance and unobserved confounding.”
Dr. King noted that recall bias is a limitation the researchers highlighted in their study, but “considering the exposures are relatively objective and factual, we do not believe the potential for recall bias is substantial.”
“Nonetheless, we strongly believe that replication of our results in prospective, population-representative cohorts will be crucial to making firmer conclusions,” he added.
The study was funded by grants from the Quebec Health Research Fund. The study authors and Dr. Kirkbride disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Owning an outdoor cat as a child is associated with an increased risk of psychotic experiences in adulthood – but only in males, new research suggests.
Investigators found
The suspected culprit is not the cat itself but rather exposure to Toxoplasma gondii, a common parasite carried by rodents and sometimes found in cat feces. The study adds to a growing evidence showing exposure to T. gondii may be a risk factor for schizophrenia and other psychotic disorders.
“These are small pieces of evidence but it’s interesting to consider that there might be combinations of risk factors at play,” lead author Vincent Paquin, MD, psychiatry resident at McGill University, Montreal, said in an interview.
“And even if the magnitude of the risk is small at the individual level,” he added, “cats and Toxoplasma gondii are so present in our society that if we add up all these small potential effects then it becomes a potential public health question.”
The study was published online Jan. 30, 2022, in the Journal of Psychiatric Research.
Inconsistent evidence
T. gondii infects about 30% of the human population and is usually transmitted by cats. Most infections are asymptomatic, but T. gondii can cause toxoplasmosis in humans, which has been linked to increased risk of schizophrenia, suicide attempts, and more recently, mild cognitive impairment.
Although some studies show an association between cat ownership and increased risk of mental illness, the research findings have been inconsistent.
“The evidence has been mixed about the association between cat ownership and psychosis expression, so our approach was to consider whether specific factors or combinations of factors could explain this mixed evidence,” Dr. Paquin said.
For the study, 2206 individuals aged 18-40 years completed the Community Assessment of Psychic Experiences (CAPE-42) and a questionnaire to gather information about cat ownership at any time between birth and age 13 and if the cats lived exclusively indoors (nonhunting) or if they were allowed outside (rodent hunting).
Participants were also asked about the number of residential moves between birth and age 15, date and place of birth, lifetime history of head trauma, and tobacco smoking history.
Rodent-hunting cat ownership was associated with higher risk of psychosis in male participants, compared with owning no cat or a nonhunting cat. When the investigators added head trauma and residential moves to rodent-hunting cat ownership, psychosis risk was elevated in both men and women.
Independent of cat ownership, younger age, moving more than three times as a child, a history of head trauma, and being a smoker were all associated with higher psychosis risk.
The study wasn’t designed to explore potential biological mechanisms to explain the sex differences in psychosis risk seen among rodent-hunting cat owners, but “one possible explanation based on the animal model literature is that the neurobiological effects of parasitic exposure may be greater with male sex,” senior author Suzanne King, PhD, professor of psychiatry at McGill, said in an interview.
The new study is part of a larger, long-term project called EnviroGen, led by Dr. King, examining the environmental and genetic risk factors for schizophrenia.
Need for replication
Commenting on the findings, E. Fuller Torrey, MD, who was among the first researchers to identify a link between cat ownership, T. gondii infection, and schizophrenia, said the study is “an interesting addition to the studies of cat ownership in childhood as a risk factor for psychosis.”
Of the approximately 10 published studies on the topic, about half suggest a link between cat ownership and psychosis later in life, said Dr. Torrey, associate director for research at the Stanley Medical Research Institute in Rockville, Md.
“The Canadian study is interesting in that it is the first study that separates exposure to permanently indoor cats from cats that are allowed to go outdoors, and the results were positive only for outdoor cats,” Dr. Torrey said.
The study has limitations, Dr. Torrey added, including its retrospective design and the use of a self-report questionnaire to assess psychotic experiences in adulthood.
Also commenting on findings, James Kirkbride, PhD, professor of psychiatric and social epidemiology, University College London, noted the same limitations.
Dr. Kirkbride is the lead author of a 2017 study that showed no link between cat ownership and serious mental illness that included nearly 5,000 people born in 1991 or 1992 and followed until age 18. In this study, there was no link between psychosis and cat ownership during pregnancy or at ages 4 or 10 years.
“Researchers have long been fascinated with the idea that cat ownership may affect mental health. This paper may have them chasing their own tail,” Dr. Kirkbride said.
“Evidence of any association is limited to certain subgroups without a strong theoretical basis for why this may be the case,” he added. “The retrospective and cross-sectional nature of the survey also raise the possibility that the results are impacted by differential recall bias, as well as the broader issues of chance and unobserved confounding.”
Dr. King noted that recall bias is a limitation the researchers highlighted in their study, but “considering the exposures are relatively objective and factual, we do not believe the potential for recall bias is substantial.”
“Nonetheless, we strongly believe that replication of our results in prospective, population-representative cohorts will be crucial to making firmer conclusions,” he added.
The study was funded by grants from the Quebec Health Research Fund. The study authors and Dr. Kirkbride disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF PSYCHIATRIC RESEARCH
New guidelines on MRI use in patients with MS explained
MS affects approximately one million people in the United States. As family physicians, these guidelines are important to know, because we are often the ones who make the initial diagnosis of MS. Similarly, if we order the wrong imaging study, we can miss making an accurate diagnosis.

The new guidelines (MAGNIMS), which were sponsored by the Consortium of Multiple Sclerosis Centres, were published in August. The documents offers detailed guidance on the use of standardized MRI protocols as well as the use of IV gadolinium contrast agents, including in children and pregnant patients.
It is advised to use 3-D techniques (as opposed to two-dimensional) and it is noted that this is becoming more clinically available. Sagittal 3-D T2-weighted fluid-attenuated inversion recovery (FLAIR) is the core sequence considered for MS diagnosis and monitoring because of its high sensitivity. High-quality 2-D pulse sequences can be used alternatively when 3-D FLAIR is not available.
When 3 T scanners are not available, 1.5 T scanners are sufficient. However, 3 T scanners do have a higher detection rate for MS lesions. In evaluating the imaging, T2 lesion counts, gadolinium lesion counts, and interval changes should be reported.
The use of GBCAs (gadolinium-based contrast agents) is needed to diagnose MS and rule out other diseases. The time between injection of contrast should ideally be 10 minutes but no less than 5. Optic nerve MRI is recommended only in patients with atypical symptoms, such as new visual symptoms. Spinal cord MRI is also not routinely advised unless it is needed for prognosis.
When the initial MRI does not meet the full criteria of MS, brain MRI should be repeated every 6-12 months in suspected cases. The same modality should be used each time. After treatment is started, it is recommended to perform MRI without GBCAs for 3 months and annual follow ups. The use of GBCAs-free MRIs for routine follow up is a new recommendation compared to previous ones. However, if the use of GBCAs would change the management, then they should be utilized for monitoring.
The same imaging standards are recommended in pediatric patients. Spinal cord MRI should be utilized in kids with spinal cord symptoms or inconclusive brain MRI. Similar scan frequency is recommended as in adults. MRI is not contraindicated during pregnancy but should be decided on an individual basis. Standard protocols should be used as well as a magnetic field strength of 1.5 T. GBCAs should not be used during pregnancy. There are no limitations in the postpartum period.
The complete set of guidelines is quite extensive and adds to the previous guidelines published in 2017. They were first published in The Lancet Neurology.
While most of these patients will be referred to neurologists, as the primary care physician it is our responsibility to know all aspects of our patients’ diseases and treatments. While we may not be actively treating MS in these patients, we need to know their medications, how they interact with others, and how their disease is progressing
Additionally, we may be the ones asked to order MRIs for monitoring. It is imperative that we know the guidelines for how to do this.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at [email protected].
MS affects approximately one million people in the United States. As family physicians, these guidelines are important to know, because we are often the ones who make the initial diagnosis of MS. Similarly, if we order the wrong imaging study, we can miss making an accurate diagnosis.
The new guidelines (MAGNIMS), which were sponsored by the Consortium of Multiple Sclerosis Centres, were published in August. The documents offers detailed guidance on the use of standardized MRI protocols as well as the use of IV gadolinium contrast agents, including in children and pregnant patients.
It is advised to use 3-D techniques (as opposed to two-dimensional) and it is noted that this is becoming more clinically available. Sagittal 3-D T2-weighted fluid-attenuated inversion recovery (FLAIR) is the core sequence considered for MS diagnosis and monitoring because of its high sensitivity. High-quality 2-D pulse sequences can be used alternatively when 3-D FLAIR is not available.
When 3 T scanners are not available, 1.5 T scanners are sufficient. However, 3 T scanners do have a higher detection rate for MS lesions. In evaluating the imaging, T2 lesion counts, gadolinium lesion counts, and interval changes should be reported.
The use of GBCAs (gadolinium-based contrast agents) is needed to diagnose MS and rule out other diseases. The time between injection of contrast should ideally be 10 minutes but no less than 5. Optic nerve MRI is recommended only in patients with atypical symptoms, such as new visual symptoms. Spinal cord MRI is also not routinely advised unless it is needed for prognosis.
When the initial MRI does not meet the full criteria of MS, brain MRI should be repeated every 6-12 months in suspected cases. The same modality should be used each time. After treatment is started, it is recommended to perform MRI without GBCAs for 3 months and annual follow ups. The use of GBCAs-free MRIs for routine follow up is a new recommendation compared to previous ones. However, if the use of GBCAs would change the management, then they should be utilized for monitoring.
The same imaging standards are recommended in pediatric patients. Spinal cord MRI should be utilized in kids with spinal cord symptoms or inconclusive brain MRI. Similar scan frequency is recommended as in adults. MRI is not contraindicated during pregnancy but should be decided on an individual basis. Standard protocols should be used as well as a magnetic field strength of 1.5 T. GBCAs should not be used during pregnancy. There are no limitations in the postpartum period.
The complete set of guidelines is quite extensive and adds to the previous guidelines published in 2017. They were first published in The Lancet Neurology.
While most of these patients will be referred to neurologists, as the primary care physician it is our responsibility to know all aspects of our patients’ diseases and treatments. While we may not be actively treating MS in these patients, we need to know their medications, how they interact with others, and how their disease is progressing
Additionally, we may be the ones asked to order MRIs for monitoring. It is imperative that we know the guidelines for how to do this.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at [email protected].
MS affects approximately one million people in the United States. As family physicians, these guidelines are important to know, because we are often the ones who make the initial diagnosis of MS. Similarly, if we order the wrong imaging study, we can miss making an accurate diagnosis.
The new guidelines (MAGNIMS), which were sponsored by the Consortium of Multiple Sclerosis Centres, were published in August. The documents offers detailed guidance on the use of standardized MRI protocols as well as the use of IV gadolinium contrast agents, including in children and pregnant patients.
It is advised to use 3-D techniques (as opposed to two-dimensional) and it is noted that this is becoming more clinically available. Sagittal 3-D T2-weighted fluid-attenuated inversion recovery (FLAIR) is the core sequence considered for MS diagnosis and monitoring because of its high sensitivity. High-quality 2-D pulse sequences can be used alternatively when 3-D FLAIR is not available.
When 3 T scanners are not available, 1.5 T scanners are sufficient. However, 3 T scanners do have a higher detection rate for MS lesions. In evaluating the imaging, T2 lesion counts, gadolinium lesion counts, and interval changes should be reported.
The use of GBCAs (gadolinium-based contrast agents) is needed to diagnose MS and rule out other diseases. The time between injection of contrast should ideally be 10 minutes but no less than 5. Optic nerve MRI is recommended only in patients with atypical symptoms, such as new visual symptoms. Spinal cord MRI is also not routinely advised unless it is needed for prognosis.
When the initial MRI does not meet the full criteria of MS, brain MRI should be repeated every 6-12 months in suspected cases. The same modality should be used each time. After treatment is started, it is recommended to perform MRI without GBCAs for 3 months and annual follow ups. The use of GBCAs-free MRIs for routine follow up is a new recommendation compared to previous ones. However, if the use of GBCAs would change the management, then they should be utilized for monitoring.
The same imaging standards are recommended in pediatric patients. Spinal cord MRI should be utilized in kids with spinal cord symptoms or inconclusive brain MRI. Similar scan frequency is recommended as in adults. MRI is not contraindicated during pregnancy but should be decided on an individual basis. Standard protocols should be used as well as a magnetic field strength of 1.5 T. GBCAs should not be used during pregnancy. There are no limitations in the postpartum period.
The complete set of guidelines is quite extensive and adds to the previous guidelines published in 2017. They were first published in The Lancet Neurology.
While most of these patients will be referred to neurologists, as the primary care physician it is our responsibility to know all aspects of our patients’ diseases and treatments. While we may not be actively treating MS in these patients, we need to know their medications, how they interact with others, and how their disease is progressing
Additionally, we may be the ones asked to order MRIs for monitoring. It is imperative that we know the guidelines for how to do this.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at [email protected].
Is family reunification our goal?
This has been an unfortunate, but not an atypical year, for the children in Maine whose lives have intersected with the state’s Department of Health and Human Services. In 2021, 25 children died of abuse and neglect or in homes with prior involvement with the child protective system. Four cases not included in that number are currently listed as homicides. At a recent legislative hearing the grandmother of one of those victims told her story to the lawmaker.
Her grandson was removed from his mother’s custody at 3 months of age after a 2-year-old sibling overdosed on methadone. Father and grandmother became his caregivers but when the father was arrested the child was returned to the mother’s custody by a judge despite the pleas of the child’s court-appointed guardian. The child eventually returned to the care of his paternal aunt and father, but when the father was arrested again the then 3-year-old was returned to his mother. Within months he was dead with multiple fractures, including to his spine and with internal and intracranial bleeding (Overton P. Maine’s child welfare system failed a 3-year old who died, grandmother tells lawmakers. 2022 Feb 11. Portland Press Herald).

The grandmother questioned the legislators why a vulnerable child would be returned to the care of a woman with such an extensive history of involvement with the Department of Health and Human Services. While there may have been errors of judgment on the part of department staff, in large part the answer lies in the system’s emphasis on reunification. Like apple pie, motherhood, and more recently fatherhood, have been viewed as something deserving of our unquestioning efforts to preserve.
This is not a recent trend. Some of the most frustrating cases over my 40 years of practice involved the failure of the courts and in some cases social workers to place a child’s welfare in the proper perspective as court schedules and custody decisions were made. Too often the reunification of “the family” seemed to trump the needs of the child. Fortunately, I’m unaware of any of my patients who died as the result of these untimely and poorly made decisions. However, many of my patients lived in unsettled conditions never sure what the next week would bring while the system focused on giving an adult whose life was a mess one more chance to demonstrate his or her ability to parent.
Of course, there are occasions in which child protective workers have been too hasty in pulling a child from his or her parents. But, in my experience those cases pale next to the number of times in which children were exposed to home environments that threatened their psychological health and development. Yes, there are bad foster homes. Many foster homes might do a better job if they were working in a system that put a higher value on the emotional needs and safety of the children in making its custody decisions.
We have a governor here in Maine who has worked hard to do the right thing during the pandemic and has made child health a focus. However, her recent proposed appropriations bill appears to continue the focus on reunification by funneling money into programs such as family reunion training and coaching as well as a parent mentorship program. Certainly, one can’t argue that these kind of programs might be helpful to some families. On the other hand, we can’t let these programs create the impression that an intact family is our primary goal. Not every family is repairable, at least on a time schedule compatible with the emotional and health needs of the children.
I wouldn’t be surprised to learn that many of you have experienced a similar frustration when decisions based on an unrealistic goal of family reunification have put your patients at risk.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
This has been an unfortunate, but not an atypical year, for the children in Maine whose lives have intersected with the state’s Department of Health and Human Services. In 2021, 25 children died of abuse and neglect or in homes with prior involvement with the child protective system. Four cases not included in that number are currently listed as homicides. At a recent legislative hearing the grandmother of one of those victims told her story to the lawmaker.
Her grandson was removed from his mother’s custody at 3 months of age after a 2-year-old sibling overdosed on methadone. Father and grandmother became his caregivers but when the father was arrested the child was returned to the mother’s custody by a judge despite the pleas of the child’s court-appointed guardian. The child eventually returned to the care of his paternal aunt and father, but when the father was arrested again the then 3-year-old was returned to his mother. Within months he was dead with multiple fractures, including to his spine and with internal and intracranial bleeding (Overton P. Maine’s child welfare system failed a 3-year old who died, grandmother tells lawmakers. 2022 Feb 11. Portland Press Herald).
The grandmother questioned the legislators why a vulnerable child would be returned to the care of a woman with such an extensive history of involvement with the Department of Health and Human Services. While there may have been errors of judgment on the part of department staff, in large part the answer lies in the system’s emphasis on reunification. Like apple pie, motherhood, and more recently fatherhood, have been viewed as something deserving of our unquestioning efforts to preserve.
This is not a recent trend. Some of the most frustrating cases over my 40 years of practice involved the failure of the courts and in some cases social workers to place a child’s welfare in the proper perspective as court schedules and custody decisions were made. Too often the reunification of “the family” seemed to trump the needs of the child. Fortunately, I’m unaware of any of my patients who died as the result of these untimely and poorly made decisions. However, many of my patients lived in unsettled conditions never sure what the next week would bring while the system focused on giving an adult whose life was a mess one more chance to demonstrate his or her ability to parent.
Of course, there are occasions in which child protective workers have been too hasty in pulling a child from his or her parents. But, in my experience those cases pale next to the number of times in which children were exposed to home environments that threatened their psychological health and development. Yes, there are bad foster homes. Many foster homes might do a better job if they were working in a system that put a higher value on the emotional needs and safety of the children in making its custody decisions.
We have a governor here in Maine who has worked hard to do the right thing during the pandemic and has made child health a focus. However, her recent proposed appropriations bill appears to continue the focus on reunification by funneling money into programs such as family reunion training and coaching as well as a parent mentorship program. Certainly, one can’t argue that these kind of programs might be helpful to some families. On the other hand, we can’t let these programs create the impression that an intact family is our primary goal. Not every family is repairable, at least on a time schedule compatible with the emotional and health needs of the children.
I wouldn’t be surprised to learn that many of you have experienced a similar frustration when decisions based on an unrealistic goal of family reunification have put your patients at risk.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
This has been an unfortunate, but not an atypical year, for the children in Maine whose lives have intersected with the state’s Department of Health and Human Services. In 2021, 25 children died of abuse and neglect or in homes with prior involvement with the child protective system. Four cases not included in that number are currently listed as homicides. At a recent legislative hearing the grandmother of one of those victims told her story to the lawmaker.
Her grandson was removed from his mother’s custody at 3 months of age after a 2-year-old sibling overdosed on methadone. Father and grandmother became his caregivers but when the father was arrested the child was returned to the mother’s custody by a judge despite the pleas of the child’s court-appointed guardian. The child eventually returned to the care of his paternal aunt and father, but when the father was arrested again the then 3-year-old was returned to his mother. Within months he was dead with multiple fractures, including to his spine and with internal and intracranial bleeding (Overton P. Maine’s child welfare system failed a 3-year old who died, grandmother tells lawmakers. 2022 Feb 11. Portland Press Herald).
The grandmother questioned the legislators why a vulnerable child would be returned to the care of a woman with such an extensive history of involvement with the Department of Health and Human Services. While there may have been errors of judgment on the part of department staff, in large part the answer lies in the system’s emphasis on reunification. Like apple pie, motherhood, and more recently fatherhood, have been viewed as something deserving of our unquestioning efforts to preserve.
This is not a recent trend. Some of the most frustrating cases over my 40 years of practice involved the failure of the courts and in some cases social workers to place a child’s welfare in the proper perspective as court schedules and custody decisions were made. Too often the reunification of “the family” seemed to trump the needs of the child. Fortunately, I’m unaware of any of my patients who died as the result of these untimely and poorly made decisions. However, many of my patients lived in unsettled conditions never sure what the next week would bring while the system focused on giving an adult whose life was a mess one more chance to demonstrate his or her ability to parent.
Of course, there are occasions in which child protective workers have been too hasty in pulling a child from his or her parents. But, in my experience those cases pale next to the number of times in which children were exposed to home environments that threatened their psychological health and development. Yes, there are bad foster homes. Many foster homes might do a better job if they were working in a system that put a higher value on the emotional needs and safety of the children in making its custody decisions.
We have a governor here in Maine who has worked hard to do the right thing during the pandemic and has made child health a focus. However, her recent proposed appropriations bill appears to continue the focus on reunification by funneling money into programs such as family reunion training and coaching as well as a parent mentorship program. Certainly, one can’t argue that these kind of programs might be helpful to some families. On the other hand, we can’t let these programs create the impression that an intact family is our primary goal. Not every family is repairable, at least on a time schedule compatible with the emotional and health needs of the children.
I wouldn’t be surprised to learn that many of you have experienced a similar frustration when decisions based on an unrealistic goal of family reunification have put your patients at risk.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].