User login
Beware of the latest TikTok trend: Nasal spray tans
Although nasal spray tanning is being described as a new “viral” trend, it seems to have gotten its start as early as the spring of 2021. The tanning method appears to be especially popular in the United Kingdom, where self-tanning product brands have TikTok videos promoting nasal sprays.
The rising concerns of this and other viral TikTok trends has now prompted a bipartisan group of seven state attorneys general to launch an investigation.
“As children and teens already grapple with issues of anxiety, social pressure, and depression, we cannot allow social media to further harm their physical health and mental wellbeing,” Massachusetts Attorney General Maura Healey, a Democrat, said in a statement. “State attorneys general have an imperative to protect young people and seek more information about how companies like TikTok are influencing their daily lives.”
Ms. Healey, along with colleagues from California, Florida, Kentucky, Nebraska, New Jersey, Tennessee, and Vermont, will whether Chinese-based TikTok violates state consumer protection laws.
The trend of people shooting spray tan up their nose is just the latest in a long line of so-called TikTok challenges that have caused controversy, and often, injury.
In a February TikTok, put out by the British company So Tanned (@_sotanned), a young woman appears with text stating that she uses nasal spray “morning and night” and then adds self-tanning oral drops a half hour before getting into a tanning bed.
But, dermatologist Lily Talakoub, MD, of McLean, Va., posted a TikTok with the bold warning “DO NOT USE NASAL TANNING SPRAY!” In the video, the white coat–clad Dr. Talakoub is in the foreground of the TikTok made by @Sashawoodx.
“Don’t try this at home,” said Dr. Talakoub.
“Don’t try this even if you think it can make you tanner. It can cause nausea, vomiting, very bad side effects,” she said, adding “this can be very dangerous to your health.”
It’s also worth mentioning that self-tanning products are not approved by the Food and Drug Administration for inhalation.
Still, another U.K. company, 2btanned, posted a TikTok showing a user spraying the product up his nose and, in the comments, @2btanned suggested that the spray should be used at least a week or two before sun exposure “in order to get full effects.”
@Sashawoodx tells her viewers: “Don’t walk ... RUN for these products,” as she shows herself in several different outfits, squirting 2btanned spray up her nose. As of March 2, the TikTok video had been viewed over 212,000 times.
TikTokker @giannaarose, who has 125,000 followers, said in a video that she uses two to three sprays up the nose before stepping into the tanning bed. A commenter said, “this is scary but where do I buy it”.
The main ingredient in self-tanning products is dihydroxyacetone, or DHA. DHA, which is FDA-approved for use on skin, causes a chemical reaction when heat is applied, and a pigment is deposited on the skin.
Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, said, given that self-tanning products were never meant to be inhaled and that nasal sprays of any kind must be approved by the FDA, a company promoting the products is engaged in a dangerous game.
“People could go to jail over this,” said Dr. Friedman. What’s more, the products are unlikely to produce a tan.
“Because of the way self-tanners work, it would make no sense,” said Dr. Friedman.
“It’s purely a camouflage,” he said, adding that it does not produce melanin. Self-tanners were never intended to be inhaled, “so who knows what those ingredients would do to a different anatomical site like the inner passages of the nose.”
At a minimum, spraying into the nose could at cause irritation. But it could also potentially lead to acute or long-term damage, he said.
Some other spray ingredients, such as tyrosine and tyrosinase, are involved in producing melanin, but they only act within skin cells. If sprayed into the nose, the ingredients might produce melanin inside the nose, but not on the skin.
“This is not going to work,” said Dr. Friedman. “If anything, it could be dangerous.”
He added that there’s no such thing as a safe tan, and that self-tanning products offer no protection from dangerous ultraviolet rays. The nasal sprays are “quick fixes” that are not going to work.
“At the end of the day, just don’t inhale,” Dr. Friedman said.
A version of this article first appeared on WebMD.com.
Although nasal spray tanning is being described as a new “viral” trend, it seems to have gotten its start as early as the spring of 2021. The tanning method appears to be especially popular in the United Kingdom, where self-tanning product brands have TikTok videos promoting nasal sprays.
The rising concerns of this and other viral TikTok trends has now prompted a bipartisan group of seven state attorneys general to launch an investigation.
“As children and teens already grapple with issues of anxiety, social pressure, and depression, we cannot allow social media to further harm their physical health and mental wellbeing,” Massachusetts Attorney General Maura Healey, a Democrat, said in a statement. “State attorneys general have an imperative to protect young people and seek more information about how companies like TikTok are influencing their daily lives.”
Ms. Healey, along with colleagues from California, Florida, Kentucky, Nebraska, New Jersey, Tennessee, and Vermont, will whether Chinese-based TikTok violates state consumer protection laws.
The trend of people shooting spray tan up their nose is just the latest in a long line of so-called TikTok challenges that have caused controversy, and often, injury.
In a February TikTok, put out by the British company So Tanned (@_sotanned), a young woman appears with text stating that she uses nasal spray “morning and night” and then adds self-tanning oral drops a half hour before getting into a tanning bed.
But, dermatologist Lily Talakoub, MD, of McLean, Va., posted a TikTok with the bold warning “DO NOT USE NASAL TANNING SPRAY!” In the video, the white coat–clad Dr. Talakoub is in the foreground of the TikTok made by @Sashawoodx.
“Don’t try this at home,” said Dr. Talakoub.
“Don’t try this even if you think it can make you tanner. It can cause nausea, vomiting, very bad side effects,” she said, adding “this can be very dangerous to your health.”
It’s also worth mentioning that self-tanning products are not approved by the Food and Drug Administration for inhalation.
Still, another U.K. company, 2btanned, posted a TikTok showing a user spraying the product up his nose and, in the comments, @2btanned suggested that the spray should be used at least a week or two before sun exposure “in order to get full effects.”
@Sashawoodx tells her viewers: “Don’t walk ... RUN for these products,” as she shows herself in several different outfits, squirting 2btanned spray up her nose. As of March 2, the TikTok video had been viewed over 212,000 times.
TikTokker @giannaarose, who has 125,000 followers, said in a video that she uses two to three sprays up the nose before stepping into the tanning bed. A commenter said, “this is scary but where do I buy it”.
The main ingredient in self-tanning products is dihydroxyacetone, or DHA. DHA, which is FDA-approved for use on skin, causes a chemical reaction when heat is applied, and a pigment is deposited on the skin.
Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, said, given that self-tanning products were never meant to be inhaled and that nasal sprays of any kind must be approved by the FDA, a company promoting the products is engaged in a dangerous game.
“People could go to jail over this,” said Dr. Friedman. What’s more, the products are unlikely to produce a tan.
“Because of the way self-tanners work, it would make no sense,” said Dr. Friedman.
“It’s purely a camouflage,” he said, adding that it does not produce melanin. Self-tanners were never intended to be inhaled, “so who knows what those ingredients would do to a different anatomical site like the inner passages of the nose.”
At a minimum, spraying into the nose could at cause irritation. But it could also potentially lead to acute or long-term damage, he said.
Some other spray ingredients, such as tyrosine and tyrosinase, are involved in producing melanin, but they only act within skin cells. If sprayed into the nose, the ingredients might produce melanin inside the nose, but not on the skin.
“This is not going to work,” said Dr. Friedman. “If anything, it could be dangerous.”
He added that there’s no such thing as a safe tan, and that self-tanning products offer no protection from dangerous ultraviolet rays. The nasal sprays are “quick fixes” that are not going to work.
“At the end of the day, just don’t inhale,” Dr. Friedman said.
A version of this article first appeared on WebMD.com.
Although nasal spray tanning is being described as a new “viral” trend, it seems to have gotten its start as early as the spring of 2021. The tanning method appears to be especially popular in the United Kingdom, where self-tanning product brands have TikTok videos promoting nasal sprays.
The rising concerns of this and other viral TikTok trends has now prompted a bipartisan group of seven state attorneys general to launch an investigation.
“As children and teens already grapple with issues of anxiety, social pressure, and depression, we cannot allow social media to further harm their physical health and mental wellbeing,” Massachusetts Attorney General Maura Healey, a Democrat, said in a statement. “State attorneys general have an imperative to protect young people and seek more information about how companies like TikTok are influencing their daily lives.”
Ms. Healey, along with colleagues from California, Florida, Kentucky, Nebraska, New Jersey, Tennessee, and Vermont, will whether Chinese-based TikTok violates state consumer protection laws.
The trend of people shooting spray tan up their nose is just the latest in a long line of so-called TikTok challenges that have caused controversy, and often, injury.
In a February TikTok, put out by the British company So Tanned (@_sotanned), a young woman appears with text stating that she uses nasal spray “morning and night” and then adds self-tanning oral drops a half hour before getting into a tanning bed.
But, dermatologist Lily Talakoub, MD, of McLean, Va., posted a TikTok with the bold warning “DO NOT USE NASAL TANNING SPRAY!” In the video, the white coat–clad Dr. Talakoub is in the foreground of the TikTok made by @Sashawoodx.
“Don’t try this at home,” said Dr. Talakoub.
“Don’t try this even if you think it can make you tanner. It can cause nausea, vomiting, very bad side effects,” she said, adding “this can be very dangerous to your health.”
It’s also worth mentioning that self-tanning products are not approved by the Food and Drug Administration for inhalation.
Still, another U.K. company, 2btanned, posted a TikTok showing a user spraying the product up his nose and, in the comments, @2btanned suggested that the spray should be used at least a week or two before sun exposure “in order to get full effects.”
@Sashawoodx tells her viewers: “Don’t walk ... RUN for these products,” as she shows herself in several different outfits, squirting 2btanned spray up her nose. As of March 2, the TikTok video had been viewed over 212,000 times.
TikTokker @giannaarose, who has 125,000 followers, said in a video that she uses two to three sprays up the nose before stepping into the tanning bed. A commenter said, “this is scary but where do I buy it”.
The main ingredient in self-tanning products is dihydroxyacetone, or DHA. DHA, which is FDA-approved for use on skin, causes a chemical reaction when heat is applied, and a pigment is deposited on the skin.
Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, said, given that self-tanning products were never meant to be inhaled and that nasal sprays of any kind must be approved by the FDA, a company promoting the products is engaged in a dangerous game.
“People could go to jail over this,” said Dr. Friedman. What’s more, the products are unlikely to produce a tan.
“Because of the way self-tanners work, it would make no sense,” said Dr. Friedman.
“It’s purely a camouflage,” he said, adding that it does not produce melanin. Self-tanners were never intended to be inhaled, “so who knows what those ingredients would do to a different anatomical site like the inner passages of the nose.”
At a minimum, spraying into the nose could at cause irritation. But it could also potentially lead to acute or long-term damage, he said.
Some other spray ingredients, such as tyrosine and tyrosinase, are involved in producing melanin, but they only act within skin cells. If sprayed into the nose, the ingredients might produce melanin inside the nose, but not on the skin.
“This is not going to work,” said Dr. Friedman. “If anything, it could be dangerous.”
He added that there’s no such thing as a safe tan, and that self-tanning products offer no protection from dangerous ultraviolet rays. The nasal sprays are “quick fixes” that are not going to work.
“At the end of the day, just don’t inhale,” Dr. Friedman said.
A version of this article first appeared on WebMD.com.
Nirsevimab protects healthy infants from RSV
A single injection of the experimental agent nirsevimab ahead of respiratory syncytial virus (RSV) season protects healthy infants from lower respiratory tract infections associated with the pathogen, according to the results of a phase 3 study.
A previously published trial showed that a single dose of nirsevimab was effective in preterm infants. The ability to protect all babies from RSV, which causes bronchiolitis and pneumonia and is a leading cause of hospitalization for this age group, “would be a paradigm shift in the approach to this disease,” William Muller, MD, PhD, of the Lurie Children’s Hospital of Chicago and a coauthor of the study, said in a statement.
The primary endpoint of the study was medically attended lower respiratory tract infections linked to RSV. The single injection of nirsevimab was associated with a 74.5% reduction in such infections (P < .001), according to Dr. Muller’s group, who published their findings March 2 in the New England Journal of Medicine.
Nirsevimab, a monoclonal antibody to the RSV fusion protein being developed by AstraZeneca and Sanofi, has an extended half-life, which may allow one dose to confer protection throughout a season. The only approved option to prevent RSV, palivizumab (Synagis), is used for high-risk infants, and five injections are needed to cover a viral season.
Nearly 1,500 infants in more than 20 countries studied
To assess the effectiveness of nirsevimab in late-preterm and term infants, investigators at 160 sites randomly assigned 1,490 babies born at a gestational age of at least 35 weeks to receive an intramuscular injection of nirsevimab or placebo.
During the 150 days after injection, medically attended RSV-associated lower respiratory tract infections occurred in 12 of 994 infants who received nirsevimab, compared with 25 of 496 babies who received placebo (1.2% vs. 5%).
Six of 994 infants who received nirsevimab were hospitalized for RSV-associated lower respiratory tract infections, compared with 8 of 496 infants in the placebo group (0.6% vs. 1.6%; P = .07). The proportion of children hospitalized for any respiratory illness as a result of RSV was 0.9% among those who received nirsevimab, compared with 2.2% among those who received placebo.
Serious adverse events occurred in 6.8% of the nirsevimab group and 7.3% of the placebo group. None of these events, including three deaths in the nirsevimab group, was considered related to nirsevimab or placebo, according to the researchers. One infant who received nirsevimab had a generalized macular rash without systemic features that did not require treatment and resolved in 20 days, they said.
Antidrug antibodies were detected in 6.1% of the nirsevimab group and in 1.1% of the placebo group. These antidrug antibodies tended to develop later and did not affect nirsevimab pharmacokinetics during the RSV season, the researchers reported. How they might affect subsequent doses of nirsevimab is not known, they added.
In a separate report in the journal, researcher Joseph Domachowske, MD, SUNY Upstate Medical University, Syracuse, New York, and colleagues described safety results from an ongoing study of nirsevimab that includes infants with congenital heart disease, chronic lung disease, and prematurity.
In this trial, infants received nirsevimab or palivizumab, and the treatments appeared to have similar safety profiles, the authors reported.
Other approaches to RSV protection include passive antibodies acquired from maternal vaccination in pregnancy and active vaccination of infants.
The publication follows news last month that GlaxoSmithKline is pausing a maternal RSV vaccine trial, which “had the same goal of protecting babies against severe RSV infection,” said Louis Bont, MD, PhD, with University Medical Center Utrecht, the Netherlands.
RSV infection is one of the deadliest diseases during infancy, and the nirsevimab trial, conducted in more than 20 countries, is “gamechanging,” Dr. Bont told this news organization. Still, researchers will need to monitor for RSV resistance to this treatment, he said.
Whether nirsevimab prevents the development of reactive airway disease and asthma is another open question, he said.
“Finally, we need to keep in mind that RSV mortality is almost limited to the developing world, and it is unlikely that this novel drug will become available to these countries in the coming years,” Dr. Bont said. “Nevertheless, nirsevimab has the potential to seriously decrease the annual overwhelming number of RSV infected babies.”
Nirsevimab may have advantages in low- and middle-income countries, including its potential to be incorporated into established immunization programs and to be given seasonally, said Amy Sarah Ginsburg, MD, MPH, of the University of Washington, Seattle. “However, cost remains a significant factor, as does susceptibility to pathogen escape,” she said.
MedImmune/AstraZeneca and Sanofi funded the nirsevimab studies. UMC Utrecht has received research grants and fees for advisory work from AstraZeneca for RSV-related work by Bont.
A version of this article first appeared on Medscape.com.
A single injection of the experimental agent nirsevimab ahead of respiratory syncytial virus (RSV) season protects healthy infants from lower respiratory tract infections associated with the pathogen, according to the results of a phase 3 study.
A previously published trial showed that a single dose of nirsevimab was effective in preterm infants. The ability to protect all babies from RSV, which causes bronchiolitis and pneumonia and is a leading cause of hospitalization for this age group, “would be a paradigm shift in the approach to this disease,” William Muller, MD, PhD, of the Lurie Children’s Hospital of Chicago and a coauthor of the study, said in a statement.
The primary endpoint of the study was medically attended lower respiratory tract infections linked to RSV. The single injection of nirsevimab was associated with a 74.5% reduction in such infections (P < .001), according to Dr. Muller’s group, who published their findings March 2 in the New England Journal of Medicine.
Nirsevimab, a monoclonal antibody to the RSV fusion protein being developed by AstraZeneca and Sanofi, has an extended half-life, which may allow one dose to confer protection throughout a season. The only approved option to prevent RSV, palivizumab (Synagis), is used for high-risk infants, and five injections are needed to cover a viral season.
Nearly 1,500 infants in more than 20 countries studied
To assess the effectiveness of nirsevimab in late-preterm and term infants, investigators at 160 sites randomly assigned 1,490 babies born at a gestational age of at least 35 weeks to receive an intramuscular injection of nirsevimab or placebo.
During the 150 days after injection, medically attended RSV-associated lower respiratory tract infections occurred in 12 of 994 infants who received nirsevimab, compared with 25 of 496 babies who received placebo (1.2% vs. 5%).
Six of 994 infants who received nirsevimab were hospitalized for RSV-associated lower respiratory tract infections, compared with 8 of 496 infants in the placebo group (0.6% vs. 1.6%; P = .07). The proportion of children hospitalized for any respiratory illness as a result of RSV was 0.9% among those who received nirsevimab, compared with 2.2% among those who received placebo.
Serious adverse events occurred in 6.8% of the nirsevimab group and 7.3% of the placebo group. None of these events, including three deaths in the nirsevimab group, was considered related to nirsevimab or placebo, according to the researchers. One infant who received nirsevimab had a generalized macular rash without systemic features that did not require treatment and resolved in 20 days, they said.
Antidrug antibodies were detected in 6.1% of the nirsevimab group and in 1.1% of the placebo group. These antidrug antibodies tended to develop later and did not affect nirsevimab pharmacokinetics during the RSV season, the researchers reported. How they might affect subsequent doses of nirsevimab is not known, they added.
In a separate report in the journal, researcher Joseph Domachowske, MD, SUNY Upstate Medical University, Syracuse, New York, and colleagues described safety results from an ongoing study of nirsevimab that includes infants with congenital heart disease, chronic lung disease, and prematurity.
In this trial, infants received nirsevimab or palivizumab, and the treatments appeared to have similar safety profiles, the authors reported.
Other approaches to RSV protection include passive antibodies acquired from maternal vaccination in pregnancy and active vaccination of infants.
The publication follows news last month that GlaxoSmithKline is pausing a maternal RSV vaccine trial, which “had the same goal of protecting babies against severe RSV infection,” said Louis Bont, MD, PhD, with University Medical Center Utrecht, the Netherlands.
RSV infection is one of the deadliest diseases during infancy, and the nirsevimab trial, conducted in more than 20 countries, is “gamechanging,” Dr. Bont told this news organization. Still, researchers will need to monitor for RSV resistance to this treatment, he said.
Whether nirsevimab prevents the development of reactive airway disease and asthma is another open question, he said.
“Finally, we need to keep in mind that RSV mortality is almost limited to the developing world, and it is unlikely that this novel drug will become available to these countries in the coming years,” Dr. Bont said. “Nevertheless, nirsevimab has the potential to seriously decrease the annual overwhelming number of RSV infected babies.”
Nirsevimab may have advantages in low- and middle-income countries, including its potential to be incorporated into established immunization programs and to be given seasonally, said Amy Sarah Ginsburg, MD, MPH, of the University of Washington, Seattle. “However, cost remains a significant factor, as does susceptibility to pathogen escape,” she said.
MedImmune/AstraZeneca and Sanofi funded the nirsevimab studies. UMC Utrecht has received research grants and fees for advisory work from AstraZeneca for RSV-related work by Bont.
A version of this article first appeared on Medscape.com.
A single injection of the experimental agent nirsevimab ahead of respiratory syncytial virus (RSV) season protects healthy infants from lower respiratory tract infections associated with the pathogen, according to the results of a phase 3 study.
A previously published trial showed that a single dose of nirsevimab was effective in preterm infants. The ability to protect all babies from RSV, which causes bronchiolitis and pneumonia and is a leading cause of hospitalization for this age group, “would be a paradigm shift in the approach to this disease,” William Muller, MD, PhD, of the Lurie Children’s Hospital of Chicago and a coauthor of the study, said in a statement.
The primary endpoint of the study was medically attended lower respiratory tract infections linked to RSV. The single injection of nirsevimab was associated with a 74.5% reduction in such infections (P < .001), according to Dr. Muller’s group, who published their findings March 2 in the New England Journal of Medicine.
Nirsevimab, a monoclonal antibody to the RSV fusion protein being developed by AstraZeneca and Sanofi, has an extended half-life, which may allow one dose to confer protection throughout a season. The only approved option to prevent RSV, palivizumab (Synagis), is used for high-risk infants, and five injections are needed to cover a viral season.
Nearly 1,500 infants in more than 20 countries studied
To assess the effectiveness of nirsevimab in late-preterm and term infants, investigators at 160 sites randomly assigned 1,490 babies born at a gestational age of at least 35 weeks to receive an intramuscular injection of nirsevimab or placebo.
During the 150 days after injection, medically attended RSV-associated lower respiratory tract infections occurred in 12 of 994 infants who received nirsevimab, compared with 25 of 496 babies who received placebo (1.2% vs. 5%).
Six of 994 infants who received nirsevimab were hospitalized for RSV-associated lower respiratory tract infections, compared with 8 of 496 infants in the placebo group (0.6% vs. 1.6%; P = .07). The proportion of children hospitalized for any respiratory illness as a result of RSV was 0.9% among those who received nirsevimab, compared with 2.2% among those who received placebo.
Serious adverse events occurred in 6.8% of the nirsevimab group and 7.3% of the placebo group. None of these events, including three deaths in the nirsevimab group, was considered related to nirsevimab or placebo, according to the researchers. One infant who received nirsevimab had a generalized macular rash without systemic features that did not require treatment and resolved in 20 days, they said.
Antidrug antibodies were detected in 6.1% of the nirsevimab group and in 1.1% of the placebo group. These antidrug antibodies tended to develop later and did not affect nirsevimab pharmacokinetics during the RSV season, the researchers reported. How they might affect subsequent doses of nirsevimab is not known, they added.
In a separate report in the journal, researcher Joseph Domachowske, MD, SUNY Upstate Medical University, Syracuse, New York, and colleagues described safety results from an ongoing study of nirsevimab that includes infants with congenital heart disease, chronic lung disease, and prematurity.
In this trial, infants received nirsevimab or palivizumab, and the treatments appeared to have similar safety profiles, the authors reported.
Other approaches to RSV protection include passive antibodies acquired from maternal vaccination in pregnancy and active vaccination of infants.
The publication follows news last month that GlaxoSmithKline is pausing a maternal RSV vaccine trial, which “had the same goal of protecting babies against severe RSV infection,” said Louis Bont, MD, PhD, with University Medical Center Utrecht, the Netherlands.
RSV infection is one of the deadliest diseases during infancy, and the nirsevimab trial, conducted in more than 20 countries, is “gamechanging,” Dr. Bont told this news organization. Still, researchers will need to monitor for RSV resistance to this treatment, he said.
Whether nirsevimab prevents the development of reactive airway disease and asthma is another open question, he said.
“Finally, we need to keep in mind that RSV mortality is almost limited to the developing world, and it is unlikely that this novel drug will become available to these countries in the coming years,” Dr. Bont said. “Nevertheless, nirsevimab has the potential to seriously decrease the annual overwhelming number of RSV infected babies.”
Nirsevimab may have advantages in low- and middle-income countries, including its potential to be incorporated into established immunization programs and to be given seasonally, said Amy Sarah Ginsburg, MD, MPH, of the University of Washington, Seattle. “However, cost remains a significant factor, as does susceptibility to pathogen escape,” she said.
MedImmune/AstraZeneca and Sanofi funded the nirsevimab studies. UMC Utrecht has received research grants and fees for advisory work from AstraZeneca for RSV-related work by Bont.
A version of this article first appeared on Medscape.com.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Pediatric IBD increases cancer risk later in life
Children who are diagnosed with inflammatory bowel disease (IBD) are more than twice as likely to develop cancer, especially gastrointestinal cancer, later in life compared with the general pediatric population, a new meta-analysis suggests.
Although the overall incidence rate of cancer in this population is low, “we found a 2.4-fold increase in the relative rate of cancer among patients with pediatric-onset IBD compared with the general pediatric population, primarily associated with an increased rate of gastrointestinal cancers,” wrote senior author Tine Jess, MD, DMSci, Aalborg University, Copenhagen, and colleagues.
The study was published online March 1 in JAMA Network Open.
Previous research indicates that IBD is associated with an increased risk for colon, small bowel, and other types of cancer in adults, but the risk among children with IBD is not well understood.
In the current analysis, Dr. Jess and colleagues examined five population-based studies from North America and Europe, which included more than 19,800 participants with pediatric-onset IBD. Of these participants, 715 were later diagnosed with cancer.
Overall, the risk for cancer among individuals with pediatric-onset IBD was 2.4-fold higher than that of their peers without IBD, but those rates varied by IBD subtype. Those with Crohn’s disease, for instance, were about two times more likely to develop cancer, while those with ulcerative colitis were 2.6 times more likely to develop cancer later.
Two studies included in the meta-analysis broke down results by sex and found that the risk for cancer was higher among male versus female patients (pooled relative rates [pRR], 3.23 in men and 2.45 in women).
These two studies also calculated the risk for cancer by exposure to thiopurines. Patients receiving these immunosuppressive drugs had an increased relative rate of cancer (pRR, 2.09). Although numerically higher, this rate was not statistically higher compared with patients not exposed to the drugs (pRR, 1.82).
When looking at risk by cancer site, the authors consistently observed the highest relative rates for gastrointestinal cancers. Specifically, the investigators calculated a 55-fold increased risk for liver cancer (pRR, 55.4), followed by a 20-fold increased risk for colorectal cancer (pRR, 20.2), and a 16-fold increased risk for small bowel cancer (pRR, 16.2).
Despite such high estimates for gastrointestinal cancers, “this risk corresponds to a mean incidence rate of 0.3 cases of liver cancer, 0.6 cases of colorectal cancer, and 0.1 cases of small bowel cancer per 1,000 person-years in this population,” the authors noted.
In other words, “the overall incidence rate of cancer in this population is low,” at less than 3.3 cases per 1,000 person-years, the authors concluded.
Relative rates of extraintestinal cancers were even lower, with the highest risks for nonmelanoma skin cancer (pRR, 3.62), lymphoid cancer (pRR, 3.10), and melanoma (pRR, 2.05).
The authors suggest that identifying variables that might reduce cancer risk in pediatric patients who develop IBD could better shape management and prevention strategies.
CRC screening guidelines already recommend that children undergo a colonoscopy 6-8 years after being diagnosed with colitis extending beyond the rectum. Annual colonoscopy is also recommended for patients with primary sclerosing cholangitis from the time of diagnosis and annual screening for skin cancer is recommended for all patients with IBD.
The investigators further suggest that because ongoing inflammation is an important risk factor for cancer, early and adequate control of inflammation could be critical in the prevention of long-term complications.
The study was supported by a grant from the Danish National Research Foundation. Dr. Jess and coauthors Rahma Elmahdi, MD, Camilla Lemser, and Kristine Allin, MD, reported receiving grants from the Danish National Research Foundation National Center of Excellence during the conduct of the study. Coauthor Manasi Agrawal, MD, reported receiving grants from the National Institutes of Health/National Institute of Diabetes and Digestive and Kidney Diseases during the conduct of the study.
A version of this article first appeared on Medscape.com.
Children who are diagnosed with inflammatory bowel disease (IBD) are more than twice as likely to develop cancer, especially gastrointestinal cancer, later in life compared with the general pediatric population, a new meta-analysis suggests.
Although the overall incidence rate of cancer in this population is low, “we found a 2.4-fold increase in the relative rate of cancer among patients with pediatric-onset IBD compared with the general pediatric population, primarily associated with an increased rate of gastrointestinal cancers,” wrote senior author Tine Jess, MD, DMSci, Aalborg University, Copenhagen, and colleagues.
The study was published online March 1 in JAMA Network Open.
Previous research indicates that IBD is associated with an increased risk for colon, small bowel, and other types of cancer in adults, but the risk among children with IBD is not well understood.
In the current analysis, Dr. Jess and colleagues examined five population-based studies from North America and Europe, which included more than 19,800 participants with pediatric-onset IBD. Of these participants, 715 were later diagnosed with cancer.
Overall, the risk for cancer among individuals with pediatric-onset IBD was 2.4-fold higher than that of their peers without IBD, but those rates varied by IBD subtype. Those with Crohn’s disease, for instance, were about two times more likely to develop cancer, while those with ulcerative colitis were 2.6 times more likely to develop cancer later.
Two studies included in the meta-analysis broke down results by sex and found that the risk for cancer was higher among male versus female patients (pooled relative rates [pRR], 3.23 in men and 2.45 in women).
These two studies also calculated the risk for cancer by exposure to thiopurines. Patients receiving these immunosuppressive drugs had an increased relative rate of cancer (pRR, 2.09). Although numerically higher, this rate was not statistically higher compared with patients not exposed to the drugs (pRR, 1.82).
When looking at risk by cancer site, the authors consistently observed the highest relative rates for gastrointestinal cancers. Specifically, the investigators calculated a 55-fold increased risk for liver cancer (pRR, 55.4), followed by a 20-fold increased risk for colorectal cancer (pRR, 20.2), and a 16-fold increased risk for small bowel cancer (pRR, 16.2).
Despite such high estimates for gastrointestinal cancers, “this risk corresponds to a mean incidence rate of 0.3 cases of liver cancer, 0.6 cases of colorectal cancer, and 0.1 cases of small bowel cancer per 1,000 person-years in this population,” the authors noted.
In other words, “the overall incidence rate of cancer in this population is low,” at less than 3.3 cases per 1,000 person-years, the authors concluded.
Relative rates of extraintestinal cancers were even lower, with the highest risks for nonmelanoma skin cancer (pRR, 3.62), lymphoid cancer (pRR, 3.10), and melanoma (pRR, 2.05).
The authors suggest that identifying variables that might reduce cancer risk in pediatric patients who develop IBD could better shape management and prevention strategies.
CRC screening guidelines already recommend that children undergo a colonoscopy 6-8 years after being diagnosed with colitis extending beyond the rectum. Annual colonoscopy is also recommended for patients with primary sclerosing cholangitis from the time of diagnosis and annual screening for skin cancer is recommended for all patients with IBD.
The investigators further suggest that because ongoing inflammation is an important risk factor for cancer, early and adequate control of inflammation could be critical in the prevention of long-term complications.
The study was supported by a grant from the Danish National Research Foundation. Dr. Jess and coauthors Rahma Elmahdi, MD, Camilla Lemser, and Kristine Allin, MD, reported receiving grants from the Danish National Research Foundation National Center of Excellence during the conduct of the study. Coauthor Manasi Agrawal, MD, reported receiving grants from the National Institutes of Health/National Institute of Diabetes and Digestive and Kidney Diseases during the conduct of the study.
A version of this article first appeared on Medscape.com.
Children who are diagnosed with inflammatory bowel disease (IBD) are more than twice as likely to develop cancer, especially gastrointestinal cancer, later in life compared with the general pediatric population, a new meta-analysis suggests.
Although the overall incidence rate of cancer in this population is low, “we found a 2.4-fold increase in the relative rate of cancer among patients with pediatric-onset IBD compared with the general pediatric population, primarily associated with an increased rate of gastrointestinal cancers,” wrote senior author Tine Jess, MD, DMSci, Aalborg University, Copenhagen, and colleagues.
The study was published online March 1 in JAMA Network Open.
Previous research indicates that IBD is associated with an increased risk for colon, small bowel, and other types of cancer in adults, but the risk among children with IBD is not well understood.
In the current analysis, Dr. Jess and colleagues examined five population-based studies from North America and Europe, which included more than 19,800 participants with pediatric-onset IBD. Of these participants, 715 were later diagnosed with cancer.
Overall, the risk for cancer among individuals with pediatric-onset IBD was 2.4-fold higher than that of their peers without IBD, but those rates varied by IBD subtype. Those with Crohn’s disease, for instance, were about two times more likely to develop cancer, while those with ulcerative colitis were 2.6 times more likely to develop cancer later.
Two studies included in the meta-analysis broke down results by sex and found that the risk for cancer was higher among male versus female patients (pooled relative rates [pRR], 3.23 in men and 2.45 in women).
These two studies also calculated the risk for cancer by exposure to thiopurines. Patients receiving these immunosuppressive drugs had an increased relative rate of cancer (pRR, 2.09). Although numerically higher, this rate was not statistically higher compared with patients not exposed to the drugs (pRR, 1.82).
When looking at risk by cancer site, the authors consistently observed the highest relative rates for gastrointestinal cancers. Specifically, the investigators calculated a 55-fold increased risk for liver cancer (pRR, 55.4), followed by a 20-fold increased risk for colorectal cancer (pRR, 20.2), and a 16-fold increased risk for small bowel cancer (pRR, 16.2).
Despite such high estimates for gastrointestinal cancers, “this risk corresponds to a mean incidence rate of 0.3 cases of liver cancer, 0.6 cases of colorectal cancer, and 0.1 cases of small bowel cancer per 1,000 person-years in this population,” the authors noted.
In other words, “the overall incidence rate of cancer in this population is low,” at less than 3.3 cases per 1,000 person-years, the authors concluded.
Relative rates of extraintestinal cancers were even lower, with the highest risks for nonmelanoma skin cancer (pRR, 3.62), lymphoid cancer (pRR, 3.10), and melanoma (pRR, 2.05).
The authors suggest that identifying variables that might reduce cancer risk in pediatric patients who develop IBD could better shape management and prevention strategies.
CRC screening guidelines already recommend that children undergo a colonoscopy 6-8 years after being diagnosed with colitis extending beyond the rectum. Annual colonoscopy is also recommended for patients with primary sclerosing cholangitis from the time of diagnosis and annual screening for skin cancer is recommended for all patients with IBD.
The investigators further suggest that because ongoing inflammation is an important risk factor for cancer, early and adequate control of inflammation could be critical in the prevention of long-term complications.
The study was supported by a grant from the Danish National Research Foundation. Dr. Jess and coauthors Rahma Elmahdi, MD, Camilla Lemser, and Kristine Allin, MD, reported receiving grants from the Danish National Research Foundation National Center of Excellence during the conduct of the study. Coauthor Manasi Agrawal, MD, reported receiving grants from the National Institutes of Health/National Institute of Diabetes and Digestive and Kidney Diseases during the conduct of the study.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK
Debate heats up on how best to treat gender-questioning kids
The past week has seen heated debate about the complex issue of how to best treat children with gender dysphoria, with further developments in a number of U.S. states and in Sweden.
In the U.S., more states have moved to prevent the use of any medical treatment, such as puberty blockers or cross-sex hormones, in kids younger than the age of 18, most recently in a state Senate vote in Alabama last week, and in Texas, where Governor Greg Abbott is said to have ordered state agencies to investigate reports of gender-transition procedures on children as “child abuse.”
At least one parent has, because of this, established a crowdfunding page to try to raise money to move away from Texas, fearful of being accused of child abuse if their child with gender dysphoria receives hormone therapy. And a countersuit has been filed there by the ACLU of Texas and Lambda Legal, a civil rights organization, on behalf of one parent said to be under investigation.
But on the flip side, parents living in more liberal states – where children under the age of 18 can often get hormones to transition without parental consent – are considering moving out of them to protect their children. These parents are concerned that their kids do not know enough about the side effects of puberty blockers, or lifetime use of cross-sex hormones and its implications, to be able to make properly informed decisions at such a young age.
Meanwhile, Sweden has further tightened its restrictions on medical therapy to treat gender-questioning kids, with a recent announcement from its National Board of Health and Welfare (NBHW), on Feb. 22, urging restraint in hormone treatment of minors with gender dysphoria following a review by the agency there that assesses health technologies, the SBU.
Based on the review results, the NBHW’s overall conclusion is that the risks of puberty blocking and cross-sex hormone treatment for those under 18 currently outweigh the possible benefits for the group as a whole. The agency now says hormone treatment should only be offered in exceptional cases outside the framework of research, and principally, only in adolescents with childhood-onset gender dysphoria, as opposed to those who develop it during puberty, or in their teens, as is the case with most teenagers currently presenting.
At the same time, gender-affirming hormone treatment for adolescents who identify as transgender or nonbinary is associated with changes in depression and suicidality, according to a new U.S. survey published Feb. 25 in JAMA Network Health.
However, experts who spoke to this news organization were critical of the study, noting it was small, conducted in just 104 youth who were an average age of 15.8 years and of whom only 63% completed the survey at the final timepoint, just 1 year after starting therapy. In addition, there was no control group, among other limitations.
“The most worrying thing is that they haven’t described the pros and cons of the treatment that they are researching. We know that there are risks inherent in using gender-affirming medicine, as with all medications,” Anna Hutchinson, DClinPsych, of the Integrated Psychology Clinic, London, told this news organization.
“For example, when people with gender dysphoria use cross-sex hormones, there is a burden of treatment that can last a lifetime, both for those who benefit from the treatment and those who detransition or regret later on,” said Dr. Hutchinson, who has extensive experience of working with young people with issues related to sexuality or gender.
“This isn’t mentioned at all, which makes the paper appear quite biased towards using one approach for managing gender dysphoria and related distress, whilst not acknowledging any risks of doing so or considering alternatives,” she noted.
Why were some treated with hormones while others weren’t?
The newly published survey is by PhD student Diana M. Tordoff, MPH, of the Department of Epidemiology, University of Washington, Seattle, and colleagues. Published alongside was an invited commentary by Brett Dolotina, BS, of Massachusetts General Hospital, Boston, and Jack L. Turban, MD, MHS, of Stanford (Calif.) University.
The study was conducted at an urban multidisciplinary gender clinic in Seattle among transgender and nonbinary adolescents and young adults seeking gender-affirming care from August 2017 to June 2018. Data were analyzed from August 2020 to November 2021.
Participating in the study were 104 youths aged 13-20 years (mean age, 15.8 years), 63 transmasculine (born female) individuals (60.6%), 27 transfeminine (born male) individuals (26.0%), 10 nonbinary or gender-fluid individuals (9.6%), and four youths who responded, “I don’t know,” or did not respond to the gender-identity question (3.8%).
At baseline, 59 individuals (56.7%) had moderate-to-severe depression, 52 individuals (50.0%) had moderate-to-severe anxiety, and 45 individuals (43.3%) reported self-harm or suicidal thoughts.
By the end of the study, 69 youths (66.3%) had received puberty blockers, cross-sex hormones (testosterone for girls transitioning to male and estrogen for boys transitioning to female), or both interventions, while 35 youths had not received either intervention (33.7%).
After adjustment for temporal trends and potential confounders, there were a 60% lower odds of depression (adjusted odds ratio, 0.40; 95% confidence interval, 0.17-0.95) and 73% lower odds of suicidality (aOR, 0.27; 95% CI, 0.11-0.65) among youths who had initiated puberty blockers or cross-sex hormones.
There was no association between these treatments and anxiety, however (aOR, 1.01; 95% CI, 0.41-2.51).
Dr. Hutchinson points out that nonbinary and gender fluid “are not diagnostic or clinical terms,” adding, “there is no information about how the groups were chosen or if any of them met the criteria for gender dysphoria. It seems strange to not have measured gender dysphoria, both before and after interventions, in a group of children presenting with gender dysphoria.”
She adds: “I am questioning why ‘gender-affirming’ medicine appears to be being used here as a specific intervention for depression and suicidality? [That] wouldn’t usually be the first reason to commence these particular treatments. Why didn’t they provide therapy or antidepressant medication to this group of young people, as is routine for managing mood and/or suicidality in all other patient cohorts?”
In their commentary, Mr. Dolotina and Dr. Turban observe: “The rate of suicidality among the Tordoff et al. sample after receiving gender-affirming care was still much higher than national rates of suicidality among youth in the U.S., denoting that ... other mental health determinants must be addressed ... including gender minority stress.”
Small study, no control group, large loss to follow-up
Dr. Hutchinson also criticizes the small sample size of just 104 youth and “large loss to follow-up, whereby only 65 of those 104 [youth] completed the final survey in a short time [1 year].” This could indicate “that only the most satisfied kids stayed the course,” she suggests.
And importantly, the findings on depression and suicidality rely on the experience of only five people in the no-treatment group at 12 months, she points out.
Also, as the authors themselves acknowledge, they didn’t control for other psychiatric medicines that the participants might have been taking at baseline.
“It’s important to know more about all of this in order to draw accurate conclusions about what works, or does not, for whom,” noted Dr. Hutchinson.
Most patients, too, she notes, were females-to-males taking testosterone. Therefore, the finding that they experienced a reduction in depression might simply reflect the widely reported antidepressant effects of testosterone.
Also expressing concern about the small sample size and “lack of a control group” is Michelle Mackness, MC, a Canadian counselor in private practice who has experience working with gender-questioning individuals, detransitioners, and those experiencing complications related to their transition.
“Tordoff et al.’s assertion that there is a ‘robust evidence base’ supporting pediatric transition seems out-of-step with recent global developments in care policies and protocols for gender-questioning youth,” she points out.
“Neither the study authors or commentators acknowledge, let alone address, the fact that Finland, the U.K., and Sweden have recently determined that the evidence allegedly supporting medical interventions for pediatric transition is ‘inconclusive’,” she adds.
Asked to respond, Ms. Tordoff did not directly address this question. Rather, she reiterated to this news organization: “We found that receipt of puberty blockers and gender-affirming hormones was associated with a 60% lower odds of depression and a 73% lower odds of suicidal thoughts by the end of our study follow-up. We conducted extensive sensitivity analyses, which support the robustness of our study findings.”
She added: “These results are consistent with other recently published prospective cohort studies (please see citations provided within the manuscript).”
Parents may move states
It is this concern about the lifetime burden of treatment involved with transitioning that gives some parents of children with gender dysphoria pause for thought, especially those who live in more liberal U.S. states.
Indeed, two of America’s leading psychologists who work in this field, including one who is transgender herself, told this news organization in November they are now concerned about a lack of adequate psychological evaluations of youth with gender dysphoria before any medical treatment is considered.
So while one parent, Violet A., last week established a GoFundMe page for her child, entitled, “Help Us Move Isa to Safety,” stating she needed to move from Texas due to Governor Abbott’s pronouncements there “to a state that won’t consider me an abuser when I seek medical care for my trans child and potentially remove her from my custody,” some parents feel the need instead to move from more liberal states.
Some tell their stories anonymously, as they don’t want to risk causing their gender-questioning children further distress, as detailed on the Genspect website.
A version of this article first appeared on Medscape.com.
The past week has seen heated debate about the complex issue of how to best treat children with gender dysphoria, with further developments in a number of U.S. states and in Sweden.
In the U.S., more states have moved to prevent the use of any medical treatment, such as puberty blockers or cross-sex hormones, in kids younger than the age of 18, most recently in a state Senate vote in Alabama last week, and in Texas, where Governor Greg Abbott is said to have ordered state agencies to investigate reports of gender-transition procedures on children as “child abuse.”
At least one parent has, because of this, established a crowdfunding page to try to raise money to move away from Texas, fearful of being accused of child abuse if their child with gender dysphoria receives hormone therapy. And a countersuit has been filed there by the ACLU of Texas and Lambda Legal, a civil rights organization, on behalf of one parent said to be under investigation.
But on the flip side, parents living in more liberal states – where children under the age of 18 can often get hormones to transition without parental consent – are considering moving out of them to protect their children. These parents are concerned that their kids do not know enough about the side effects of puberty blockers, or lifetime use of cross-sex hormones and its implications, to be able to make properly informed decisions at such a young age.
Meanwhile, Sweden has further tightened its restrictions on medical therapy to treat gender-questioning kids, with a recent announcement from its National Board of Health and Welfare (NBHW), on Feb. 22, urging restraint in hormone treatment of minors with gender dysphoria following a review by the agency there that assesses health technologies, the SBU.
Based on the review results, the NBHW’s overall conclusion is that the risks of puberty blocking and cross-sex hormone treatment for those under 18 currently outweigh the possible benefits for the group as a whole. The agency now says hormone treatment should only be offered in exceptional cases outside the framework of research, and principally, only in adolescents with childhood-onset gender dysphoria, as opposed to those who develop it during puberty, or in their teens, as is the case with most teenagers currently presenting.
At the same time, gender-affirming hormone treatment for adolescents who identify as transgender or nonbinary is associated with changes in depression and suicidality, according to a new U.S. survey published Feb. 25 in JAMA Network Health.
However, experts who spoke to this news organization were critical of the study, noting it was small, conducted in just 104 youth who were an average age of 15.8 years and of whom only 63% completed the survey at the final timepoint, just 1 year after starting therapy. In addition, there was no control group, among other limitations.
“The most worrying thing is that they haven’t described the pros and cons of the treatment that they are researching. We know that there are risks inherent in using gender-affirming medicine, as with all medications,” Anna Hutchinson, DClinPsych, of the Integrated Psychology Clinic, London, told this news organization.
“For example, when people with gender dysphoria use cross-sex hormones, there is a burden of treatment that can last a lifetime, both for those who benefit from the treatment and those who detransition or regret later on,” said Dr. Hutchinson, who has extensive experience of working with young people with issues related to sexuality or gender.
“This isn’t mentioned at all, which makes the paper appear quite biased towards using one approach for managing gender dysphoria and related distress, whilst not acknowledging any risks of doing so or considering alternatives,” she noted.
Why were some treated with hormones while others weren’t?
The newly published survey is by PhD student Diana M. Tordoff, MPH, of the Department of Epidemiology, University of Washington, Seattle, and colleagues. Published alongside was an invited commentary by Brett Dolotina, BS, of Massachusetts General Hospital, Boston, and Jack L. Turban, MD, MHS, of Stanford (Calif.) University.
The study was conducted at an urban multidisciplinary gender clinic in Seattle among transgender and nonbinary adolescents and young adults seeking gender-affirming care from August 2017 to June 2018. Data were analyzed from August 2020 to November 2021.
Participating in the study were 104 youths aged 13-20 years (mean age, 15.8 years), 63 transmasculine (born female) individuals (60.6%), 27 transfeminine (born male) individuals (26.0%), 10 nonbinary or gender-fluid individuals (9.6%), and four youths who responded, “I don’t know,” or did not respond to the gender-identity question (3.8%).
At baseline, 59 individuals (56.7%) had moderate-to-severe depression, 52 individuals (50.0%) had moderate-to-severe anxiety, and 45 individuals (43.3%) reported self-harm or suicidal thoughts.
By the end of the study, 69 youths (66.3%) had received puberty blockers, cross-sex hormones (testosterone for girls transitioning to male and estrogen for boys transitioning to female), or both interventions, while 35 youths had not received either intervention (33.7%).
After adjustment for temporal trends and potential confounders, there were a 60% lower odds of depression (adjusted odds ratio, 0.40; 95% confidence interval, 0.17-0.95) and 73% lower odds of suicidality (aOR, 0.27; 95% CI, 0.11-0.65) among youths who had initiated puberty blockers or cross-sex hormones.
There was no association between these treatments and anxiety, however (aOR, 1.01; 95% CI, 0.41-2.51).
Dr. Hutchinson points out that nonbinary and gender fluid “are not diagnostic or clinical terms,” adding, “there is no information about how the groups were chosen or if any of them met the criteria for gender dysphoria. It seems strange to not have measured gender dysphoria, both before and after interventions, in a group of children presenting with gender dysphoria.”
She adds: “I am questioning why ‘gender-affirming’ medicine appears to be being used here as a specific intervention for depression and suicidality? [That] wouldn’t usually be the first reason to commence these particular treatments. Why didn’t they provide therapy or antidepressant medication to this group of young people, as is routine for managing mood and/or suicidality in all other patient cohorts?”
In their commentary, Mr. Dolotina and Dr. Turban observe: “The rate of suicidality among the Tordoff et al. sample after receiving gender-affirming care was still much higher than national rates of suicidality among youth in the U.S., denoting that ... other mental health determinants must be addressed ... including gender minority stress.”
Small study, no control group, large loss to follow-up
Dr. Hutchinson also criticizes the small sample size of just 104 youth and “large loss to follow-up, whereby only 65 of those 104 [youth] completed the final survey in a short time [1 year].” This could indicate “that only the most satisfied kids stayed the course,” she suggests.
And importantly, the findings on depression and suicidality rely on the experience of only five people in the no-treatment group at 12 months, she points out.
Also, as the authors themselves acknowledge, they didn’t control for other psychiatric medicines that the participants might have been taking at baseline.
“It’s important to know more about all of this in order to draw accurate conclusions about what works, or does not, for whom,” noted Dr. Hutchinson.
Most patients, too, she notes, were females-to-males taking testosterone. Therefore, the finding that they experienced a reduction in depression might simply reflect the widely reported antidepressant effects of testosterone.
Also expressing concern about the small sample size and “lack of a control group” is Michelle Mackness, MC, a Canadian counselor in private practice who has experience working with gender-questioning individuals, detransitioners, and those experiencing complications related to their transition.
“Tordoff et al.’s assertion that there is a ‘robust evidence base’ supporting pediatric transition seems out-of-step with recent global developments in care policies and protocols for gender-questioning youth,” she points out.
“Neither the study authors or commentators acknowledge, let alone address, the fact that Finland, the U.K., and Sweden have recently determined that the evidence allegedly supporting medical interventions for pediatric transition is ‘inconclusive’,” she adds.
Asked to respond, Ms. Tordoff did not directly address this question. Rather, she reiterated to this news organization: “We found that receipt of puberty blockers and gender-affirming hormones was associated with a 60% lower odds of depression and a 73% lower odds of suicidal thoughts by the end of our study follow-up. We conducted extensive sensitivity analyses, which support the robustness of our study findings.”
She added: “These results are consistent with other recently published prospective cohort studies (please see citations provided within the manuscript).”
Parents may move states
It is this concern about the lifetime burden of treatment involved with transitioning that gives some parents of children with gender dysphoria pause for thought, especially those who live in more liberal U.S. states.
Indeed, two of America’s leading psychologists who work in this field, including one who is transgender herself, told this news organization in November they are now concerned about a lack of adequate psychological evaluations of youth with gender dysphoria before any medical treatment is considered.
So while one parent, Violet A., last week established a GoFundMe page for her child, entitled, “Help Us Move Isa to Safety,” stating she needed to move from Texas due to Governor Abbott’s pronouncements there “to a state that won’t consider me an abuser when I seek medical care for my trans child and potentially remove her from my custody,” some parents feel the need instead to move from more liberal states.
Some tell their stories anonymously, as they don’t want to risk causing their gender-questioning children further distress, as detailed on the Genspect website.
A version of this article first appeared on Medscape.com.
The past week has seen heated debate about the complex issue of how to best treat children with gender dysphoria, with further developments in a number of U.S. states and in Sweden.
In the U.S., more states have moved to prevent the use of any medical treatment, such as puberty blockers or cross-sex hormones, in kids younger than the age of 18, most recently in a state Senate vote in Alabama last week, and in Texas, where Governor Greg Abbott is said to have ordered state agencies to investigate reports of gender-transition procedures on children as “child abuse.”
At least one parent has, because of this, established a crowdfunding page to try to raise money to move away from Texas, fearful of being accused of child abuse if their child with gender dysphoria receives hormone therapy. And a countersuit has been filed there by the ACLU of Texas and Lambda Legal, a civil rights organization, on behalf of one parent said to be under investigation.
But on the flip side, parents living in more liberal states – where children under the age of 18 can often get hormones to transition without parental consent – are considering moving out of them to protect their children. These parents are concerned that their kids do not know enough about the side effects of puberty blockers, or lifetime use of cross-sex hormones and its implications, to be able to make properly informed decisions at such a young age.
Meanwhile, Sweden has further tightened its restrictions on medical therapy to treat gender-questioning kids, with a recent announcement from its National Board of Health and Welfare (NBHW), on Feb. 22, urging restraint in hormone treatment of minors with gender dysphoria following a review by the agency there that assesses health technologies, the SBU.
Based on the review results, the NBHW’s overall conclusion is that the risks of puberty blocking and cross-sex hormone treatment for those under 18 currently outweigh the possible benefits for the group as a whole. The agency now says hormone treatment should only be offered in exceptional cases outside the framework of research, and principally, only in adolescents with childhood-onset gender dysphoria, as opposed to those who develop it during puberty, or in their teens, as is the case with most teenagers currently presenting.
At the same time, gender-affirming hormone treatment for adolescents who identify as transgender or nonbinary is associated with changes in depression and suicidality, according to a new U.S. survey published Feb. 25 in JAMA Network Health.
However, experts who spoke to this news organization were critical of the study, noting it was small, conducted in just 104 youth who were an average age of 15.8 years and of whom only 63% completed the survey at the final timepoint, just 1 year after starting therapy. In addition, there was no control group, among other limitations.
“The most worrying thing is that they haven’t described the pros and cons of the treatment that they are researching. We know that there are risks inherent in using gender-affirming medicine, as with all medications,” Anna Hutchinson, DClinPsych, of the Integrated Psychology Clinic, London, told this news organization.
“For example, when people with gender dysphoria use cross-sex hormones, there is a burden of treatment that can last a lifetime, both for those who benefit from the treatment and those who detransition or regret later on,” said Dr. Hutchinson, who has extensive experience of working with young people with issues related to sexuality or gender.
“This isn’t mentioned at all, which makes the paper appear quite biased towards using one approach for managing gender dysphoria and related distress, whilst not acknowledging any risks of doing so or considering alternatives,” she noted.
Why were some treated with hormones while others weren’t?
The newly published survey is by PhD student Diana M. Tordoff, MPH, of the Department of Epidemiology, University of Washington, Seattle, and colleagues. Published alongside was an invited commentary by Brett Dolotina, BS, of Massachusetts General Hospital, Boston, and Jack L. Turban, MD, MHS, of Stanford (Calif.) University.
The study was conducted at an urban multidisciplinary gender clinic in Seattle among transgender and nonbinary adolescents and young adults seeking gender-affirming care from August 2017 to June 2018. Data were analyzed from August 2020 to November 2021.
Participating in the study were 104 youths aged 13-20 years (mean age, 15.8 years), 63 transmasculine (born female) individuals (60.6%), 27 transfeminine (born male) individuals (26.0%), 10 nonbinary or gender-fluid individuals (9.6%), and four youths who responded, “I don’t know,” or did not respond to the gender-identity question (3.8%).
At baseline, 59 individuals (56.7%) had moderate-to-severe depression, 52 individuals (50.0%) had moderate-to-severe anxiety, and 45 individuals (43.3%) reported self-harm or suicidal thoughts.
By the end of the study, 69 youths (66.3%) had received puberty blockers, cross-sex hormones (testosterone for girls transitioning to male and estrogen for boys transitioning to female), or both interventions, while 35 youths had not received either intervention (33.7%).
After adjustment for temporal trends and potential confounders, there were a 60% lower odds of depression (adjusted odds ratio, 0.40; 95% confidence interval, 0.17-0.95) and 73% lower odds of suicidality (aOR, 0.27; 95% CI, 0.11-0.65) among youths who had initiated puberty blockers or cross-sex hormones.
There was no association between these treatments and anxiety, however (aOR, 1.01; 95% CI, 0.41-2.51).
Dr. Hutchinson points out that nonbinary and gender fluid “are not diagnostic or clinical terms,” adding, “there is no information about how the groups were chosen or if any of them met the criteria for gender dysphoria. It seems strange to not have measured gender dysphoria, both before and after interventions, in a group of children presenting with gender dysphoria.”
She adds: “I am questioning why ‘gender-affirming’ medicine appears to be being used here as a specific intervention for depression and suicidality? [That] wouldn’t usually be the first reason to commence these particular treatments. Why didn’t they provide therapy or antidepressant medication to this group of young people, as is routine for managing mood and/or suicidality in all other patient cohorts?”
In their commentary, Mr. Dolotina and Dr. Turban observe: “The rate of suicidality among the Tordoff et al. sample after receiving gender-affirming care was still much higher than national rates of suicidality among youth in the U.S., denoting that ... other mental health determinants must be addressed ... including gender minority stress.”
Small study, no control group, large loss to follow-up
Dr. Hutchinson also criticizes the small sample size of just 104 youth and “large loss to follow-up, whereby only 65 of those 104 [youth] completed the final survey in a short time [1 year].” This could indicate “that only the most satisfied kids stayed the course,” she suggests.
And importantly, the findings on depression and suicidality rely on the experience of only five people in the no-treatment group at 12 months, she points out.
Also, as the authors themselves acknowledge, they didn’t control for other psychiatric medicines that the participants might have been taking at baseline.
“It’s important to know more about all of this in order to draw accurate conclusions about what works, or does not, for whom,” noted Dr. Hutchinson.
Most patients, too, she notes, were females-to-males taking testosterone. Therefore, the finding that they experienced a reduction in depression might simply reflect the widely reported antidepressant effects of testosterone.
Also expressing concern about the small sample size and “lack of a control group” is Michelle Mackness, MC, a Canadian counselor in private practice who has experience working with gender-questioning individuals, detransitioners, and those experiencing complications related to their transition.
“Tordoff et al.’s assertion that there is a ‘robust evidence base’ supporting pediatric transition seems out-of-step with recent global developments in care policies and protocols for gender-questioning youth,” she points out.
“Neither the study authors or commentators acknowledge, let alone address, the fact that Finland, the U.K., and Sweden have recently determined that the evidence allegedly supporting medical interventions for pediatric transition is ‘inconclusive’,” she adds.
Asked to respond, Ms. Tordoff did not directly address this question. Rather, she reiterated to this news organization: “We found that receipt of puberty blockers and gender-affirming hormones was associated with a 60% lower odds of depression and a 73% lower odds of suicidal thoughts by the end of our study follow-up. We conducted extensive sensitivity analyses, which support the robustness of our study findings.”
She added: “These results are consistent with other recently published prospective cohort studies (please see citations provided within the manuscript).”
Parents may move states
It is this concern about the lifetime burden of treatment involved with transitioning that gives some parents of children with gender dysphoria pause for thought, especially those who live in more liberal U.S. states.
Indeed, two of America’s leading psychologists who work in this field, including one who is transgender herself, told this news organization in November they are now concerned about a lack of adequate psychological evaluations of youth with gender dysphoria before any medical treatment is considered.
So while one parent, Violet A., last week established a GoFundMe page for her child, entitled, “Help Us Move Isa to Safety,” stating she needed to move from Texas due to Governor Abbott’s pronouncements there “to a state that won’t consider me an abuser when I seek medical care for my trans child and potentially remove her from my custody,” some parents feel the need instead to move from more liberal states.
Some tell their stories anonymously, as they don’t want to risk causing their gender-questioning children further distress, as detailed on the Genspect website.
A version of this article first appeared on Medscape.com.
‘Robust’ increase in tics during the pandemic explained?
The findings should help answer questions surrounding a recent increase in tic disorders, lead author Jessica Frey, MD, a movement disorders fellow at the University of Florida, Gainesville, told this news organization.

“We’re trying to learn why there are new-onset explosive tic disorders [or] functional tic disorders, and to find ways to educate patients, parents, and the general public about what Tourette syndrome looks like – and how we can help patients have a better quality of life,” Dr. Frey said.
The findings will be presented at the American Academy of Neurology 2022 annual meeting in April.
‘Robust’ increase
A neurologic disorder that causes sudden repetitive involuntary muscle movements and sounds, Tourette syndrome typically develops in childhood, worsens in adolescence, and improves or completely disappears in adulthood, Dr. Frey noted.
The condition is often negatively portrayed in films, showing people using obscene gestures or vulgar language, she said. Although social media can be an “empowering tool” for tic sufferers, it is unregulated and can be a vehicle for “false information,” she added.
Dr. Frey noted that during the pandemic there has been a “robust” increase in use by teens of social media, particularly TikTok. At the same time, there have been reports of teen girls experiencing “explosive tic onset” that mimics videos from TikTok influencers.
The new analysis included 20 teens with a tic disorder, ranging in age from 11 to 21 years (average age, 16 years). About 45% of participants identified as male, 45% as female, and 10% as nonbinary.
The nature of the tic disorder varied widely among participants. Some had experienced tics for many years, while others only developed tics during the pandemic.
Participants completed a detailed survey, part of which inquired about where they received information about tics, such as from a doctor, media, parents, or teachers.
They were also asked to rank various social media platforms, including Tik Tok, Facebook, and YouTube on a five-point Likert scale as an information source about tics.
In addition, the survey inquired about tic severity and frequency, quality of life, and whether the pandemic or social media affected respondents’ tics.
Worsens quality of life
Results showed 65% of respondents used social media at least four to five times per day for an average of 5.6 hours per day. Approximately 90% reported increased use of social media during COVID.
Only 5% of participants reported using social media to provide information about tics.
About half of respondents indicated social media adversely affected their tics, and 85% said their tic frequency worsened during COVID.
Dr. Frey noted that because teens had to attend school virtually, that may have led to increased hours spent online.
There was no significant correlation between social media use and self-reported frequency of tics since the onset of COVID (Pearson correlation coefficient [R], –0.0055, P = .982).
However, there was a statistically significant correlation between social media use and tic severity (R, –0.496, P = .026) and quality of life (R, –0.447, P = .048).
These results suggest teenagers did not develop more tics, but rather the tics they already had worsened and affected their quality of life, Dr. Frey noted. She added that teens sometimes injure themselves while experiencing tics.
The full study has now enrolled 50 participants, and investigators anticipate that number to go up to 80. “We’re hoping to see more patterns emerge when we have a larger cohort of data available,” said Dr. Frey.
Asking parents to weigh in on the impact of social media on their child’s tic condition would be “a great idea for a follow-up study,” she added.
Symptoms exacerbated
Commenting on the findings, Tamara Pringsheim, MD, professor in the department of clinical neurosciences, psychiatry, pediatrics, and community health sciences at the University of Calgary (Alta.), said she also has noticed the impact of increased social media use on young patients with tics during the pandemic.

“Many young people report that seeing other people with tics, or ticlike behaviors, can exacerbate their own symptoms,” said Dr. Pringsheim, who is the university’s program lead on Tourette and pediatric movement disorders.
She noted a principle of the Comprehensive Behavioral Intervention for Tics, which is a nonpharmacologic technique demonstrated to reduce tic severity, is to identify antecedents or triggers for tics, and to learn to manage them. It might be a good idea to remind young patients of this principle, said Dr. Pringsheim, who was not associated with the current research.
“I suggest to young people who report specific social media content as a trigger for symptoms to recognize the effect of the exposure on their symptoms and make an informed choice about what they view and how much time they spend on social media,” she added.
The study did not receive any outside funding support. Dr. Frey has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The findings should help answer questions surrounding a recent increase in tic disorders, lead author Jessica Frey, MD, a movement disorders fellow at the University of Florida, Gainesville, told this news organization.
“We’re trying to learn why there are new-onset explosive tic disorders [or] functional tic disorders, and to find ways to educate patients, parents, and the general public about what Tourette syndrome looks like – and how we can help patients have a better quality of life,” Dr. Frey said.
The findings will be presented at the American Academy of Neurology 2022 annual meeting in April.
‘Robust’ increase
A neurologic disorder that causes sudden repetitive involuntary muscle movements and sounds, Tourette syndrome typically develops in childhood, worsens in adolescence, and improves or completely disappears in adulthood, Dr. Frey noted.
The condition is often negatively portrayed in films, showing people using obscene gestures or vulgar language, she said. Although social media can be an “empowering tool” for tic sufferers, it is unregulated and can be a vehicle for “false information,” she added.
Dr. Frey noted that during the pandemic there has been a “robust” increase in use by teens of social media, particularly TikTok. At the same time, there have been reports of teen girls experiencing “explosive tic onset” that mimics videos from TikTok influencers.
The new analysis included 20 teens with a tic disorder, ranging in age from 11 to 21 years (average age, 16 years). About 45% of participants identified as male, 45% as female, and 10% as nonbinary.
The nature of the tic disorder varied widely among participants. Some had experienced tics for many years, while others only developed tics during the pandemic.
Participants completed a detailed survey, part of which inquired about where they received information about tics, such as from a doctor, media, parents, or teachers.
They were also asked to rank various social media platforms, including Tik Tok, Facebook, and YouTube on a five-point Likert scale as an information source about tics.
In addition, the survey inquired about tic severity and frequency, quality of life, and whether the pandemic or social media affected respondents’ tics.
Worsens quality of life
Results showed 65% of respondents used social media at least four to five times per day for an average of 5.6 hours per day. Approximately 90% reported increased use of social media during COVID.
Only 5% of participants reported using social media to provide information about tics.
About half of respondents indicated social media adversely affected their tics, and 85% said their tic frequency worsened during COVID.
Dr. Frey noted that because teens had to attend school virtually, that may have led to increased hours spent online.
There was no significant correlation between social media use and self-reported frequency of tics since the onset of COVID (Pearson correlation coefficient [R], –0.0055, P = .982).
However, there was a statistically significant correlation between social media use and tic severity (R, –0.496, P = .026) and quality of life (R, –0.447, P = .048).
These results suggest teenagers did not develop more tics, but rather the tics they already had worsened and affected their quality of life, Dr. Frey noted. She added that teens sometimes injure themselves while experiencing tics.
The full study has now enrolled 50 participants, and investigators anticipate that number to go up to 80. “We’re hoping to see more patterns emerge when we have a larger cohort of data available,” said Dr. Frey.
Asking parents to weigh in on the impact of social media on their child’s tic condition would be “a great idea for a follow-up study,” she added.
Symptoms exacerbated
Commenting on the findings, Tamara Pringsheim, MD, professor in the department of clinical neurosciences, psychiatry, pediatrics, and community health sciences at the University of Calgary (Alta.), said she also has noticed the impact of increased social media use on young patients with tics during the pandemic.
“Many young people report that seeing other people with tics, or ticlike behaviors, can exacerbate their own symptoms,” said Dr. Pringsheim, who is the university’s program lead on Tourette and pediatric movement disorders.
She noted a principle of the Comprehensive Behavioral Intervention for Tics, which is a nonpharmacologic technique demonstrated to reduce tic severity, is to identify antecedents or triggers for tics, and to learn to manage them. It might be a good idea to remind young patients of this principle, said Dr. Pringsheim, who was not associated with the current research.
“I suggest to young people who report specific social media content as a trigger for symptoms to recognize the effect of the exposure on their symptoms and make an informed choice about what they view and how much time they spend on social media,” she added.
The study did not receive any outside funding support. Dr. Frey has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The findings should help answer questions surrounding a recent increase in tic disorders, lead author Jessica Frey, MD, a movement disorders fellow at the University of Florida, Gainesville, told this news organization.
“We’re trying to learn why there are new-onset explosive tic disorders [or] functional tic disorders, and to find ways to educate patients, parents, and the general public about what Tourette syndrome looks like – and how we can help patients have a better quality of life,” Dr. Frey said.
The findings will be presented at the American Academy of Neurology 2022 annual meeting in April.
‘Robust’ increase
A neurologic disorder that causes sudden repetitive involuntary muscle movements and sounds, Tourette syndrome typically develops in childhood, worsens in adolescence, and improves or completely disappears in adulthood, Dr. Frey noted.
The condition is often negatively portrayed in films, showing people using obscene gestures or vulgar language, she said. Although social media can be an “empowering tool” for tic sufferers, it is unregulated and can be a vehicle for “false information,” she added.
Dr. Frey noted that during the pandemic there has been a “robust” increase in use by teens of social media, particularly TikTok. At the same time, there have been reports of teen girls experiencing “explosive tic onset” that mimics videos from TikTok influencers.
The new analysis included 20 teens with a tic disorder, ranging in age from 11 to 21 years (average age, 16 years). About 45% of participants identified as male, 45% as female, and 10% as nonbinary.
The nature of the tic disorder varied widely among participants. Some had experienced tics for many years, while others only developed tics during the pandemic.
Participants completed a detailed survey, part of which inquired about where they received information about tics, such as from a doctor, media, parents, or teachers.
They were also asked to rank various social media platforms, including Tik Tok, Facebook, and YouTube on a five-point Likert scale as an information source about tics.
In addition, the survey inquired about tic severity and frequency, quality of life, and whether the pandemic or social media affected respondents’ tics.
Worsens quality of life
Results showed 65% of respondents used social media at least four to five times per day for an average of 5.6 hours per day. Approximately 90% reported increased use of social media during COVID.
Only 5% of participants reported using social media to provide information about tics.
About half of respondents indicated social media adversely affected their tics, and 85% said their tic frequency worsened during COVID.
Dr. Frey noted that because teens had to attend school virtually, that may have led to increased hours spent online.
There was no significant correlation between social media use and self-reported frequency of tics since the onset of COVID (Pearson correlation coefficient [R], –0.0055, P = .982).
However, there was a statistically significant correlation between social media use and tic severity (R, –0.496, P = .026) and quality of life (R, –0.447, P = .048).
These results suggest teenagers did not develop more tics, but rather the tics they already had worsened and affected their quality of life, Dr. Frey noted. She added that teens sometimes injure themselves while experiencing tics.
The full study has now enrolled 50 participants, and investigators anticipate that number to go up to 80. “We’re hoping to see more patterns emerge when we have a larger cohort of data available,” said Dr. Frey.
Asking parents to weigh in on the impact of social media on their child’s tic condition would be “a great idea for a follow-up study,” she added.
Symptoms exacerbated
Commenting on the findings, Tamara Pringsheim, MD, professor in the department of clinical neurosciences, psychiatry, pediatrics, and community health sciences at the University of Calgary (Alta.), said she also has noticed the impact of increased social media use on young patients with tics during the pandemic.
“Many young people report that seeing other people with tics, or ticlike behaviors, can exacerbate their own symptoms,” said Dr. Pringsheim, who is the university’s program lead on Tourette and pediatric movement disorders.
She noted a principle of the Comprehensive Behavioral Intervention for Tics, which is a nonpharmacologic technique demonstrated to reduce tic severity, is to identify antecedents or triggers for tics, and to learn to manage them. It might be a good idea to remind young patients of this principle, said Dr. Pringsheim, who was not associated with the current research.
“I suggest to young people who report specific social media content as a trigger for symptoms to recognize the effect of the exposure on their symptoms and make an informed choice about what they view and how much time they spend on social media,” she added.
The study did not receive any outside funding support. Dr. Frey has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
‘Striking’ differences in BP when wrong cuff size is used
Strong new evidence on the need to use an appropriately sized cuff in blood pressure measurement has come from the cross-sectional randomized trial Cuff(SZ).
The study found that in people in whom a small adult cuff was appropriate, systolic BP readings were on average 3.6 mm Hg lower when a regular adult size cuff was used.
However, systolic readings were on average 4.8 mm Hg higher when a regular cuff was used in people who required a large adult cuff and 19.5 mm Hg higher in those needing an extra-large cuff based on their mid-arm circumference.
The diastolic readings followed a similar pattern (-1.3 mm Hg, 1.8 mm Hg, and 7.4 mm Hg, respectively).
“We found that using the regular adult cuff in all individuals had striking differences in blood pressure,” lead author Tammy M. Brady, MD, PhD, Johns Hopkins University School of Medicine, Baltimore, told this news organization. “And that has a lot of clinical implications.”

She noted, for example, that people who required an extra-large cuff and were measured with a regular cuff had an average BP of 144/86.7 mm Hg, which is in the stage 2 hypertension range. But when the correct size cuff was used, the average BP was 124.5/79.3 mm Hg, or in the prehypertensive range.
Overall, the overestimation of BP due to using too small a cuff misclassified 39% of people as being hypertensive, while the underestimation of BP due to using a cuff that was too large missed 22% of people with hypertension.
“So, I think clinicians really need to have a renewed emphasis on cuff size, especially in populations where obesity is highly prevalent and many of their patients require extra-large cuffs, because those are the populations that are most impacted by mis-cuffing,” Dr. Brady said.
The findings were presented in an E-poster at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health (EPI/Lifestyle) 2022 conference sponsored by the American Heart Association.
Willie Lawrence, MD, chair of the AHA’s National Hypertension Control Initiative Advisory Committee, said in an interview that the magnitude of inaccuracy observed by the researchers “makes this a very, very important study.”
“Is it the first of its kind, no, but it’s incredibly important because it was so well done, and it comes at a time when people are once again dealing with issues around equity, and this study can have a significant impact on the state of hypertension in diverse communities,” said Dr. Lawrence, a cardiologist with Spectrum Health Lakeland, Benton Harbor, Michigan.
Previous studies examining the issue were older, had few participants, and used mercury sphygmomanometers instead of automated devices, which are typically recommended by professional societies for screening hypertension in adults, Dr. Brady explained.
For the Cuff Size Blood Pressure Measurement trial, 195 adults recruited from the community underwent 2 to 3 sets of 3 BP readings, 30 seconds apart, with an automated and validated device (Welch Allyn ProB 2000) using a BP cuff that was appropriated sized, one size lower, and one size higher. The order of cuff sizes was randomized. Before each set, patients walked for 2 minutes, followed by 5 minutes of rest to eliminate the potential effect of longer resting periods between tests on the results. The room was also kept quiet and participants were asked not to speak or use a smart phone.
Participants had a mean age of 54 years, 34% were male, 68% were Black, and 36% had a body mass index of at least 30 kg/m2, meeting the criteria for obesity.
Roughly one-half had a self-reported hypertension diagnosis, 31% had a systolic BP of 130 mm Hg or greater, and 26% had a diastolic BP of 80 mm Hg or greater.
Based on arm circumference (mean, 34 cm), the appropriate adult cuff size was small (20-25 cm) in 18%, regular (25.1-32 cm) in 28%, large (32.1-40 cm) in 34%, and extra-large (40.1-55 cm) in 21%.
Dr. Brady pointed out that the most recent hypertension guidelines detail sources of inaccuracy in BP measurement and say that if too small a cuff size is used, the blood pressure could be different by 2 to 11 mm Hg. “And what we show, is it can be anywhere from 5 to 20 mm Hg. So, I think that’s a significant difference from what studies have shown so far and is going to be very surprising to clinicians.”
A 2019 AHA scientific statement on the measurement of blood pressure stresses the importance of cuff size, and last year, the American Medical Association launched a new initiative to standardize training in BP measurement for future physicians and health care professionals.
Previous work also showed that children as young as 3 to 5 years of age often require an adult cuff size, and those in the 12- to 15-year age group may need an extra-large cuff, or what is often referred to as a thigh cuff, said Dr. Brady, who is also the medical director of the pediatric hypertension program at Johns Hopkins Children’s Center.
“Part of the problem is that many physicians aren’t often the one doing the measurement and that others may not be as in tune with some of these data and initiatives,” she said.
Other barriers are cost and availability. Offices and clinics don’t routinely stock multiple cuff sizes in exam rooms, and devices sold over the counter typically come with a regular adult cuff, Dr. Brady said. An extra cuff could add $25 to $50 on top of the $25 to $50 for the device for the growing number of patients measuring BP remotely.
“During the pandemic, I was trying to do telemedicine with my hypertensive patients, but the children who had significant obesity couldn’t afford or find blood pressure devices that had a cuff that was big enough for them,” she said. “It just wasn’t something that they could get. So I think people just don’t recognize how important this is.”
A version of this article first appeared on Medscape.com.
Strong new evidence on the need to use an appropriately sized cuff in blood pressure measurement has come from the cross-sectional randomized trial Cuff(SZ).
The study found that in people in whom a small adult cuff was appropriate, systolic BP readings were on average 3.6 mm Hg lower when a regular adult size cuff was used.
However, systolic readings were on average 4.8 mm Hg higher when a regular cuff was used in people who required a large adult cuff and 19.5 mm Hg higher in those needing an extra-large cuff based on their mid-arm circumference.
The diastolic readings followed a similar pattern (-1.3 mm Hg, 1.8 mm Hg, and 7.4 mm Hg, respectively).
“We found that using the regular adult cuff in all individuals had striking differences in blood pressure,” lead author Tammy M. Brady, MD, PhD, Johns Hopkins University School of Medicine, Baltimore, told this news organization. “And that has a lot of clinical implications.”
She noted, for example, that people who required an extra-large cuff and were measured with a regular cuff had an average BP of 144/86.7 mm Hg, which is in the stage 2 hypertension range. But when the correct size cuff was used, the average BP was 124.5/79.3 mm Hg, or in the prehypertensive range.
Overall, the overestimation of BP due to using too small a cuff misclassified 39% of people as being hypertensive, while the underestimation of BP due to using a cuff that was too large missed 22% of people with hypertension.
“So, I think clinicians really need to have a renewed emphasis on cuff size, especially in populations where obesity is highly prevalent and many of their patients require extra-large cuffs, because those are the populations that are most impacted by mis-cuffing,” Dr. Brady said.
The findings were presented in an E-poster at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health (EPI/Lifestyle) 2022 conference sponsored by the American Heart Association.
Willie Lawrence, MD, chair of the AHA’s National Hypertension Control Initiative Advisory Committee, said in an interview that the magnitude of inaccuracy observed by the researchers “makes this a very, very important study.”
“Is it the first of its kind, no, but it’s incredibly important because it was so well done, and it comes at a time when people are once again dealing with issues around equity, and this study can have a significant impact on the state of hypertension in diverse communities,” said Dr. Lawrence, a cardiologist with Spectrum Health Lakeland, Benton Harbor, Michigan.
Previous studies examining the issue were older, had few participants, and used mercury sphygmomanometers instead of automated devices, which are typically recommended by professional societies for screening hypertension in adults, Dr. Brady explained.
For the Cuff Size Blood Pressure Measurement trial, 195 adults recruited from the community underwent 2 to 3 sets of 3 BP readings, 30 seconds apart, with an automated and validated device (Welch Allyn ProB 2000) using a BP cuff that was appropriated sized, one size lower, and one size higher. The order of cuff sizes was randomized. Before each set, patients walked for 2 minutes, followed by 5 minutes of rest to eliminate the potential effect of longer resting periods between tests on the results. The room was also kept quiet and participants were asked not to speak or use a smart phone.
Participants had a mean age of 54 years, 34% were male, 68% were Black, and 36% had a body mass index of at least 30 kg/m2, meeting the criteria for obesity.
Roughly one-half had a self-reported hypertension diagnosis, 31% had a systolic BP of 130 mm Hg or greater, and 26% had a diastolic BP of 80 mm Hg or greater.
Based on arm circumference (mean, 34 cm), the appropriate adult cuff size was small (20-25 cm) in 18%, regular (25.1-32 cm) in 28%, large (32.1-40 cm) in 34%, and extra-large (40.1-55 cm) in 21%.
Dr. Brady pointed out that the most recent hypertension guidelines detail sources of inaccuracy in BP measurement and say that if too small a cuff size is used, the blood pressure could be different by 2 to 11 mm Hg. “And what we show, is it can be anywhere from 5 to 20 mm Hg. So, I think that’s a significant difference from what studies have shown so far and is going to be very surprising to clinicians.”
A 2019 AHA scientific statement on the measurement of blood pressure stresses the importance of cuff size, and last year, the American Medical Association launched a new initiative to standardize training in BP measurement for future physicians and health care professionals.
Previous work also showed that children as young as 3 to 5 years of age often require an adult cuff size, and those in the 12- to 15-year age group may need an extra-large cuff, or what is often referred to as a thigh cuff, said Dr. Brady, who is also the medical director of the pediatric hypertension program at Johns Hopkins Children’s Center.
“Part of the problem is that many physicians aren’t often the one doing the measurement and that others may not be as in tune with some of these data and initiatives,” she said.
Other barriers are cost and availability. Offices and clinics don’t routinely stock multiple cuff sizes in exam rooms, and devices sold over the counter typically come with a regular adult cuff, Dr. Brady said. An extra cuff could add $25 to $50 on top of the $25 to $50 for the device for the growing number of patients measuring BP remotely.
“During the pandemic, I was trying to do telemedicine with my hypertensive patients, but the children who had significant obesity couldn’t afford or find blood pressure devices that had a cuff that was big enough for them,” she said. “It just wasn’t something that they could get. So I think people just don’t recognize how important this is.”
A version of this article first appeared on Medscape.com.
Strong new evidence on the need to use an appropriately sized cuff in blood pressure measurement has come from the cross-sectional randomized trial Cuff(SZ).
The study found that in people in whom a small adult cuff was appropriate, systolic BP readings were on average 3.6 mm Hg lower when a regular adult size cuff was used.
However, systolic readings were on average 4.8 mm Hg higher when a regular cuff was used in people who required a large adult cuff and 19.5 mm Hg higher in those needing an extra-large cuff based on their mid-arm circumference.
The diastolic readings followed a similar pattern (-1.3 mm Hg, 1.8 mm Hg, and 7.4 mm Hg, respectively).
“We found that using the regular adult cuff in all individuals had striking differences in blood pressure,” lead author Tammy M. Brady, MD, PhD, Johns Hopkins University School of Medicine, Baltimore, told this news organization. “And that has a lot of clinical implications.”
She noted, for example, that people who required an extra-large cuff and were measured with a regular cuff had an average BP of 144/86.7 mm Hg, which is in the stage 2 hypertension range. But when the correct size cuff was used, the average BP was 124.5/79.3 mm Hg, or in the prehypertensive range.
Overall, the overestimation of BP due to using too small a cuff misclassified 39% of people as being hypertensive, while the underestimation of BP due to using a cuff that was too large missed 22% of people with hypertension.
“So, I think clinicians really need to have a renewed emphasis on cuff size, especially in populations where obesity is highly prevalent and many of their patients require extra-large cuffs, because those are the populations that are most impacted by mis-cuffing,” Dr. Brady said.
The findings were presented in an E-poster at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health (EPI/Lifestyle) 2022 conference sponsored by the American Heart Association.
Willie Lawrence, MD, chair of the AHA’s National Hypertension Control Initiative Advisory Committee, said in an interview that the magnitude of inaccuracy observed by the researchers “makes this a very, very important study.”
“Is it the first of its kind, no, but it’s incredibly important because it was so well done, and it comes at a time when people are once again dealing with issues around equity, and this study can have a significant impact on the state of hypertension in diverse communities,” said Dr. Lawrence, a cardiologist with Spectrum Health Lakeland, Benton Harbor, Michigan.
Previous studies examining the issue were older, had few participants, and used mercury sphygmomanometers instead of automated devices, which are typically recommended by professional societies for screening hypertension in adults, Dr. Brady explained.
For the Cuff Size Blood Pressure Measurement trial, 195 adults recruited from the community underwent 2 to 3 sets of 3 BP readings, 30 seconds apart, with an automated and validated device (Welch Allyn ProB 2000) using a BP cuff that was appropriated sized, one size lower, and one size higher. The order of cuff sizes was randomized. Before each set, patients walked for 2 minutes, followed by 5 minutes of rest to eliminate the potential effect of longer resting periods between tests on the results. The room was also kept quiet and participants were asked not to speak or use a smart phone.
Participants had a mean age of 54 years, 34% were male, 68% were Black, and 36% had a body mass index of at least 30 kg/m2, meeting the criteria for obesity.
Roughly one-half had a self-reported hypertension diagnosis, 31% had a systolic BP of 130 mm Hg or greater, and 26% had a diastolic BP of 80 mm Hg or greater.
Based on arm circumference (mean, 34 cm), the appropriate adult cuff size was small (20-25 cm) in 18%, regular (25.1-32 cm) in 28%, large (32.1-40 cm) in 34%, and extra-large (40.1-55 cm) in 21%.
Dr. Brady pointed out that the most recent hypertension guidelines detail sources of inaccuracy in BP measurement and say that if too small a cuff size is used, the blood pressure could be different by 2 to 11 mm Hg. “And what we show, is it can be anywhere from 5 to 20 mm Hg. So, I think that’s a significant difference from what studies have shown so far and is going to be very surprising to clinicians.”
A 2019 AHA scientific statement on the measurement of blood pressure stresses the importance of cuff size, and last year, the American Medical Association launched a new initiative to standardize training in BP measurement for future physicians and health care professionals.
Previous work also showed that children as young as 3 to 5 years of age often require an adult cuff size, and those in the 12- to 15-year age group may need an extra-large cuff, or what is often referred to as a thigh cuff, said Dr. Brady, who is also the medical director of the pediatric hypertension program at Johns Hopkins Children’s Center.
“Part of the problem is that many physicians aren’t often the one doing the measurement and that others may not be as in tune with some of these data and initiatives,” she said.
Other barriers are cost and availability. Offices and clinics don’t routinely stock multiple cuff sizes in exam rooms, and devices sold over the counter typically come with a regular adult cuff, Dr. Brady said. An extra cuff could add $25 to $50 on top of the $25 to $50 for the device for the growing number of patients measuring BP remotely.
“During the pandemic, I was trying to do telemedicine with my hypertensive patients, but the children who had significant obesity couldn’t afford or find blood pressure devices that had a cuff that was big enough for them,” she said. “It just wasn’t something that they could get. So I think people just don’t recognize how important this is.”
A version of this article first appeared on Medscape.com.
Azithromycin doesn’t prevent recurrent wheezing after acute infant RSV
Azithromycin administered for severe early-life respiratory syncytial virus (RSV) bronchiolitis did not prevent recurrent wheezing in affected children over the next 2-4 years, a randomized, single-center study found.
Antibiotics are frequently given to patients with RSV bronchiolitis, although this practice is not supported by American Academy of Pediatrics clinical guidelines. Many doctors will prescribe them anyway if they see redness in the ears or other signs of infection, lead author Avraham Beigelman, MD, a pediatric allergist and immunologist at Washington University in St. Louis, said in an interview.

The double-blind, placebo-controlled trial, presented at the 2022 meeting of the American Academy of Allergy, Asthma & Immunology in Phoenix, was simultaneously published online Feb. 27, 2022, in the New England Journal of Medicine–Evidence.
Since azithromycin has shown anti-inflammatory benefit in chronic lung diseases and is a mainstay of care in cystic fibrosis and had shown previous effects in RSV patients, this trial examined its potential for preventing future recurrent wheezing in infants hospitalized with RSV who are at risk for developing asthma later. About half of children admitted to the hospital for RSV will develop asthma by age 7, Dr. Beigelman said.
“We were very surprised that azithromycin didn’t help in this trial given our previous findings,” Dr. Beigelman said.
And while those given azithromycin versus those given a placebo showed no significant decrease in recurrent wheezing, there was a slight suggestion that treatment with antibiotics of any kind may increase the risk of later wheezing in infants hospitalized with the virus.
“The study was not designed to tease at the effects of different antibiotics or combinations of antibiotics, so we have to be very cautious about this trend,” Dr. Beigelman said. “There may be short-term effects and long-term effects. Certain antibiotics may affect the infant microbiome in other parts of the body, such as the gut, [in] a way that may predispose to asthma. But all these associations suggest that early-life antibiotics for viral infections are not good for you.”
He pointed to the longstanding question among clinicians whether it is the antibiotic that’s increasing the risk of the harm or the condition for which the antibiotic is prescribed. These exploratory data, however, suggest that antibiotics for RSV may be causing harm.
In pursuit of that hypothesis, his group has collected airway microbiome samples from these infants and plan to investigate whether bacteria colonizing the airway may interact with the antibiotics to increase wheezing. The researchers will analyze stool samples from the babies to see whether the gut microbiome may also play a role in wheezing and the subsequent risk of developing childhood asthma.
Study details
The trial prospectively enrolled 200 otherwise healthy babies aged 1-18 months who were hospitalized at St. Louis Children’s Hospital for acute RSV bronchiolitis. Although RSV is a very common pediatric virus, only bout 3% of babies will require hospitalization in order to receive oxygen, Dr. Beigelman said.
Babies were randomly assigned to receive placebo or oral azithromycin at 10 mg/kg daily for 7 days, followed by 5 mg/kg daily for 7 days. Randomization was stratified by recent open-label antibiotic use. The primary outcome was recurrent wheeze, defined as a third episode of post-RSV wheeze over the following 2-4 years.
The biologic activity of azithromycin was clear since nasal-wash interleukin at day 14 after randomization was lower in azithromycin-treated infants. But despite evidence of activity, the risk of post-RSV recurrent wheeze was similar in both arms: 47% in the azithromycin group versus 36% in the placebo group, for an adjusted hazard ratio of 1.45 (95% confidence interval, 0.92-2.29; P = .11).
Nor did azithromycin lower the risk of recurrent wheeze in babies already receiving other antibiotics at the time of enrollment (HR, 0.94; 95% CI, 0.43-2.07). As for antibiotic-naive participants receiving azithromycin, there was a slight signal of potential increased risk of developing recurrent wheezing (HR, 1.79; 95% CI, 1.03-3.1).
The bottom line? The findings support current clinical guidelines recommending against the use of antibiotics for RSV. “At the very least, azithromycin and antibiotics in general have no benefit in preventing recurrent wheeze, and there is a possibility they may be harmful,” Dr. Beigelman said.
This trial is funded by the National Heart, Lung, and Blood Institute. Dr. Beigelman reported relationships with AstraZeneca, Novartis, and Sanofi. Two study coauthors disclosed various ties to industry.
Azithromycin administered for severe early-life respiratory syncytial virus (RSV) bronchiolitis did not prevent recurrent wheezing in affected children over the next 2-4 years, a randomized, single-center study found.
Antibiotics are frequently given to patients with RSV bronchiolitis, although this practice is not supported by American Academy of Pediatrics clinical guidelines. Many doctors will prescribe them anyway if they see redness in the ears or other signs of infection, lead author Avraham Beigelman, MD, a pediatric allergist and immunologist at Washington University in St. Louis, said in an interview.
The double-blind, placebo-controlled trial, presented at the 2022 meeting of the American Academy of Allergy, Asthma & Immunology in Phoenix, was simultaneously published online Feb. 27, 2022, in the New England Journal of Medicine–Evidence.
Since azithromycin has shown anti-inflammatory benefit in chronic lung diseases and is a mainstay of care in cystic fibrosis and had shown previous effects in RSV patients, this trial examined its potential for preventing future recurrent wheezing in infants hospitalized with RSV who are at risk for developing asthma later. About half of children admitted to the hospital for RSV will develop asthma by age 7, Dr. Beigelman said.
“We were very surprised that azithromycin didn’t help in this trial given our previous findings,” Dr. Beigelman said.
And while those given azithromycin versus those given a placebo showed no significant decrease in recurrent wheezing, there was a slight suggestion that treatment with antibiotics of any kind may increase the risk of later wheezing in infants hospitalized with the virus.
“The study was not designed to tease at the effects of different antibiotics or combinations of antibiotics, so we have to be very cautious about this trend,” Dr. Beigelman said. “There may be short-term effects and long-term effects. Certain antibiotics may affect the infant microbiome in other parts of the body, such as the gut, [in] a way that may predispose to asthma. But all these associations suggest that early-life antibiotics for viral infections are not good for you.”
He pointed to the longstanding question among clinicians whether it is the antibiotic that’s increasing the risk of the harm or the condition for which the antibiotic is prescribed. These exploratory data, however, suggest that antibiotics for RSV may be causing harm.
In pursuit of that hypothesis, his group has collected airway microbiome samples from these infants and plan to investigate whether bacteria colonizing the airway may interact with the antibiotics to increase wheezing. The researchers will analyze stool samples from the babies to see whether the gut microbiome may also play a role in wheezing and the subsequent risk of developing childhood asthma.
Study details
The trial prospectively enrolled 200 otherwise healthy babies aged 1-18 months who were hospitalized at St. Louis Children’s Hospital for acute RSV bronchiolitis. Although RSV is a very common pediatric virus, only bout 3% of babies will require hospitalization in order to receive oxygen, Dr. Beigelman said.
Babies were randomly assigned to receive placebo or oral azithromycin at 10 mg/kg daily for 7 days, followed by 5 mg/kg daily for 7 days. Randomization was stratified by recent open-label antibiotic use. The primary outcome was recurrent wheeze, defined as a third episode of post-RSV wheeze over the following 2-4 years.
The biologic activity of azithromycin was clear since nasal-wash interleukin at day 14 after randomization was lower in azithromycin-treated infants. But despite evidence of activity, the risk of post-RSV recurrent wheeze was similar in both arms: 47% in the azithromycin group versus 36% in the placebo group, for an adjusted hazard ratio of 1.45 (95% confidence interval, 0.92-2.29; P = .11).
Nor did azithromycin lower the risk of recurrent wheeze in babies already receiving other antibiotics at the time of enrollment (HR, 0.94; 95% CI, 0.43-2.07). As for antibiotic-naive participants receiving azithromycin, there was a slight signal of potential increased risk of developing recurrent wheezing (HR, 1.79; 95% CI, 1.03-3.1).
The bottom line? The findings support current clinical guidelines recommending against the use of antibiotics for RSV. “At the very least, azithromycin and antibiotics in general have no benefit in preventing recurrent wheeze, and there is a possibility they may be harmful,” Dr. Beigelman said.
This trial is funded by the National Heart, Lung, and Blood Institute. Dr. Beigelman reported relationships with AstraZeneca, Novartis, and Sanofi. Two study coauthors disclosed various ties to industry.
Azithromycin administered for severe early-life respiratory syncytial virus (RSV) bronchiolitis did not prevent recurrent wheezing in affected children over the next 2-4 years, a randomized, single-center study found.
Antibiotics are frequently given to patients with RSV bronchiolitis, although this practice is not supported by American Academy of Pediatrics clinical guidelines. Many doctors will prescribe them anyway if they see redness in the ears or other signs of infection, lead author Avraham Beigelman, MD, a pediatric allergist and immunologist at Washington University in St. Louis, said in an interview.
The double-blind, placebo-controlled trial, presented at the 2022 meeting of the American Academy of Allergy, Asthma & Immunology in Phoenix, was simultaneously published online Feb. 27, 2022, in the New England Journal of Medicine–Evidence.
Since azithromycin has shown anti-inflammatory benefit in chronic lung diseases and is a mainstay of care in cystic fibrosis and had shown previous effects in RSV patients, this trial examined its potential for preventing future recurrent wheezing in infants hospitalized with RSV who are at risk for developing asthma later. About half of children admitted to the hospital for RSV will develop asthma by age 7, Dr. Beigelman said.
“We were very surprised that azithromycin didn’t help in this trial given our previous findings,” Dr. Beigelman said.
And while those given azithromycin versus those given a placebo showed no significant decrease in recurrent wheezing, there was a slight suggestion that treatment with antibiotics of any kind may increase the risk of later wheezing in infants hospitalized with the virus.
“The study was not designed to tease at the effects of different antibiotics or combinations of antibiotics, so we have to be very cautious about this trend,” Dr. Beigelman said. “There may be short-term effects and long-term effects. Certain antibiotics may affect the infant microbiome in other parts of the body, such as the gut, [in] a way that may predispose to asthma. But all these associations suggest that early-life antibiotics for viral infections are not good for you.”
He pointed to the longstanding question among clinicians whether it is the antibiotic that’s increasing the risk of the harm or the condition for which the antibiotic is prescribed. These exploratory data, however, suggest that antibiotics for RSV may be causing harm.
In pursuit of that hypothesis, his group has collected airway microbiome samples from these infants and plan to investigate whether bacteria colonizing the airway may interact with the antibiotics to increase wheezing. The researchers will analyze stool samples from the babies to see whether the gut microbiome may also play a role in wheezing and the subsequent risk of developing childhood asthma.
Study details
The trial prospectively enrolled 200 otherwise healthy babies aged 1-18 months who were hospitalized at St. Louis Children’s Hospital for acute RSV bronchiolitis. Although RSV is a very common pediatric virus, only bout 3% of babies will require hospitalization in order to receive oxygen, Dr. Beigelman said.
Babies were randomly assigned to receive placebo or oral azithromycin at 10 mg/kg daily for 7 days, followed by 5 mg/kg daily for 7 days. Randomization was stratified by recent open-label antibiotic use. The primary outcome was recurrent wheeze, defined as a third episode of post-RSV wheeze over the following 2-4 years.
The biologic activity of azithromycin was clear since nasal-wash interleukin at day 14 after randomization was lower in azithromycin-treated infants. But despite evidence of activity, the risk of post-RSV recurrent wheeze was similar in both arms: 47% in the azithromycin group versus 36% in the placebo group, for an adjusted hazard ratio of 1.45 (95% confidence interval, 0.92-2.29; P = .11).
Nor did azithromycin lower the risk of recurrent wheeze in babies already receiving other antibiotics at the time of enrollment (HR, 0.94; 95% CI, 0.43-2.07). As for antibiotic-naive participants receiving azithromycin, there was a slight signal of potential increased risk of developing recurrent wheezing (HR, 1.79; 95% CI, 1.03-3.1).
The bottom line? The findings support current clinical guidelines recommending against the use of antibiotics for RSV. “At the very least, azithromycin and antibiotics in general have no benefit in preventing recurrent wheeze, and there is a possibility they may be harmful,” Dr. Beigelman said.
This trial is funded by the National Heart, Lung, and Blood Institute. Dr. Beigelman reported relationships with AstraZeneca, Novartis, and Sanofi. Two study coauthors disclosed various ties to industry.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE–EVIDENCE
Needle-free epinephrine products could be available in 2023
Longstanding anxiety around use of epinephrine autoinjectors has prompted research into alternative delivery routes for this life-saving medication. Several companies presented posters on their needle-free epinephrine products at the American Academy of Allergy, Asthma & Immunology (AAAAI) Annual Meeting.
Intranasal formulations are under development at ARS Pharmaceuticals (San Diego) and Bryn Pharma (Raleigh, N.C.). And Aquestive Therapeutics (Warren, N.J.) is working on a sublingual film that delivers epinephrine prodrug when applied under the tongue.
Epinephrine is essential for stopping life-threatening allergic reactions, yet patients often don’t carry their autoinjectors and many hesitate to use them. “It’s needle phobia,” said ARS Pharmaceuticals CEO Richard Lowenthal in an interview with this news organization. “They’re afraid to use it. They don’t like to inject their children, so they hesitate.”
Both nasal sprays reached maximal plasma concentration in 20-30 minutes. ARS Pharmaceuticals compared its intranasal product (Neffy 1 mg) against manual intramuscular injection (0.3 mg) and two autoinjectors (EpiPen 0.3 mg and Symjepi 0.3 mg) by analyzing data from multiple randomized crossover Phase 1 studies examining pharmacokinetics and pharmacodynamics in 175 healthy adults. In this integrated analysis, EpiPen was fastest (20 minutes) at reaching maximal concentration (Tmax), followed by Symjepi and Neffy (both 30 minutes) and epinephrine 0.3 mg IM (45 minutes). In a human factors analysis, ARS Pharmaceuticals reported that untrained participants were able to administer the Neffy spray to themselves or another participant safely and effectively during a simulated emergency scenario.
Bryn Pharma compared pharmacokinetics of its nasal spray product (BRYN-NDS1C 6.6 mg) when self-administered or administered by trained professionals and found comparable profiles for each. Tmax values were also similar: 21.63 minutes (trained professional) and 19.82 minutes (self-administered).
Aquestive Therapeutics is developing a postage stamp-sized product (AQST-109) that delivers epinephrine and begins dissolving when placed under the tongue. No water or swallowing is required for administration, and its packaging is thinner and smaller than a credit card, according to CEO Keith Kendall.
Its analysis showed that the epinephrine reaches maximum plasma concentration in about 15 minutes, with a Tmax range narrower than that of the EpiPen. “The results showed dosing with AQST-109 resulted in PK concentration and Tmax values comparable to published data from autoinjectors,” said John Oppenheimer, MD, of Rutgers University School of Medicine, in a prerecorded poster summary.
Aquestive aims to move forward to the manufacture of registration batches and a pivotal pharmacokinetic study in the second half of 2022. Mr. Lowenthal said ARS Pharmaceuticals is hoping for approval and launch of its nasal spray by summer 2023.
“Having a non-needle delivery device would help many people overcome that fear and hopefully increase use in anaphylaxis,” said David Stukus, MD, an allergist-immunologist and professor of clinical pediatrics at Nationwide Children’s Hospital, Columbus, who was not involved with any of the studies on EpiPen alternatives. And “it’s not just food allergy – anaphylaxis can occur from venom stings, medications, or idiopathic causes.”
Mr. Lowenthal is the CEO of ARS Pharmaceuticals. Mr. Kendall is CEO of Aquestive Therapeutics. Dr. Oppenheimer is a consultant for Aquestive, GSK, Amgen, Sanofi, and Aimmune and sits on Aquestive’s advisory board. Dr. Stukus is a consultant for Novartis.
A version of this article first appeared on Medscape.com.
Longstanding anxiety around use of epinephrine autoinjectors has prompted research into alternative delivery routes for this life-saving medication. Several companies presented posters on their needle-free epinephrine products at the American Academy of Allergy, Asthma & Immunology (AAAAI) Annual Meeting.
Intranasal formulations are under development at ARS Pharmaceuticals (San Diego) and Bryn Pharma (Raleigh, N.C.). And Aquestive Therapeutics (Warren, N.J.) is working on a sublingual film that delivers epinephrine prodrug when applied under the tongue.
Epinephrine is essential for stopping life-threatening allergic reactions, yet patients often don’t carry their autoinjectors and many hesitate to use them. “It’s needle phobia,” said ARS Pharmaceuticals CEO Richard Lowenthal in an interview with this news organization. “They’re afraid to use it. They don’t like to inject their children, so they hesitate.”
Both nasal sprays reached maximal plasma concentration in 20-30 minutes. ARS Pharmaceuticals compared its intranasal product (Neffy 1 mg) against manual intramuscular injection (0.3 mg) and two autoinjectors (EpiPen 0.3 mg and Symjepi 0.3 mg) by analyzing data from multiple randomized crossover Phase 1 studies examining pharmacokinetics and pharmacodynamics in 175 healthy adults. In this integrated analysis, EpiPen was fastest (20 minutes) at reaching maximal concentration (Tmax), followed by Symjepi and Neffy (both 30 minutes) and epinephrine 0.3 mg IM (45 minutes). In a human factors analysis, ARS Pharmaceuticals reported that untrained participants were able to administer the Neffy spray to themselves or another participant safely and effectively during a simulated emergency scenario.
Bryn Pharma compared pharmacokinetics of its nasal spray product (BRYN-NDS1C 6.6 mg) when self-administered or administered by trained professionals and found comparable profiles for each. Tmax values were also similar: 21.63 minutes (trained professional) and 19.82 minutes (self-administered).
Aquestive Therapeutics is developing a postage stamp-sized product (AQST-109) that delivers epinephrine and begins dissolving when placed under the tongue. No water or swallowing is required for administration, and its packaging is thinner and smaller than a credit card, according to CEO Keith Kendall.
Its analysis showed that the epinephrine reaches maximum plasma concentration in about 15 minutes, with a Tmax range narrower than that of the EpiPen. “The results showed dosing with AQST-109 resulted in PK concentration and Tmax values comparable to published data from autoinjectors,” said John Oppenheimer, MD, of Rutgers University School of Medicine, in a prerecorded poster summary.
Aquestive aims to move forward to the manufacture of registration batches and a pivotal pharmacokinetic study in the second half of 2022. Mr. Lowenthal said ARS Pharmaceuticals is hoping for approval and launch of its nasal spray by summer 2023.
“Having a non-needle delivery device would help many people overcome that fear and hopefully increase use in anaphylaxis,” said David Stukus, MD, an allergist-immunologist and professor of clinical pediatrics at Nationwide Children’s Hospital, Columbus, who was not involved with any of the studies on EpiPen alternatives. And “it’s not just food allergy – anaphylaxis can occur from venom stings, medications, or idiopathic causes.”
Mr. Lowenthal is the CEO of ARS Pharmaceuticals. Mr. Kendall is CEO of Aquestive Therapeutics. Dr. Oppenheimer is a consultant for Aquestive, GSK, Amgen, Sanofi, and Aimmune and sits on Aquestive’s advisory board. Dr. Stukus is a consultant for Novartis.
A version of this article first appeared on Medscape.com.
Longstanding anxiety around use of epinephrine autoinjectors has prompted research into alternative delivery routes for this life-saving medication. Several companies presented posters on their needle-free epinephrine products at the American Academy of Allergy, Asthma & Immunology (AAAAI) Annual Meeting.
Intranasal formulations are under development at ARS Pharmaceuticals (San Diego) and Bryn Pharma (Raleigh, N.C.). And Aquestive Therapeutics (Warren, N.J.) is working on a sublingual film that delivers epinephrine prodrug when applied under the tongue.
Epinephrine is essential for stopping life-threatening allergic reactions, yet patients often don’t carry their autoinjectors and many hesitate to use them. “It’s needle phobia,” said ARS Pharmaceuticals CEO Richard Lowenthal in an interview with this news organization. “They’re afraid to use it. They don’t like to inject their children, so they hesitate.”
Both nasal sprays reached maximal plasma concentration in 20-30 minutes. ARS Pharmaceuticals compared its intranasal product (Neffy 1 mg) against manual intramuscular injection (0.3 mg) and two autoinjectors (EpiPen 0.3 mg and Symjepi 0.3 mg) by analyzing data from multiple randomized crossover Phase 1 studies examining pharmacokinetics and pharmacodynamics in 175 healthy adults. In this integrated analysis, EpiPen was fastest (20 minutes) at reaching maximal concentration (Tmax), followed by Symjepi and Neffy (both 30 minutes) and epinephrine 0.3 mg IM (45 minutes). In a human factors analysis, ARS Pharmaceuticals reported that untrained participants were able to administer the Neffy spray to themselves or another participant safely and effectively during a simulated emergency scenario.
Bryn Pharma compared pharmacokinetics of its nasal spray product (BRYN-NDS1C 6.6 mg) when self-administered or administered by trained professionals and found comparable profiles for each. Tmax values were also similar: 21.63 minutes (trained professional) and 19.82 minutes (self-administered).
Aquestive Therapeutics is developing a postage stamp-sized product (AQST-109) that delivers epinephrine and begins dissolving when placed under the tongue. No water or swallowing is required for administration, and its packaging is thinner and smaller than a credit card, according to CEO Keith Kendall.
Its analysis showed that the epinephrine reaches maximum plasma concentration in about 15 minutes, with a Tmax range narrower than that of the EpiPen. “The results showed dosing with AQST-109 resulted in PK concentration and Tmax values comparable to published data from autoinjectors,” said John Oppenheimer, MD, of Rutgers University School of Medicine, in a prerecorded poster summary.
Aquestive aims to move forward to the manufacture of registration batches and a pivotal pharmacokinetic study in the second half of 2022. Mr. Lowenthal said ARS Pharmaceuticals is hoping for approval and launch of its nasal spray by summer 2023.
“Having a non-needle delivery device would help many people overcome that fear and hopefully increase use in anaphylaxis,” said David Stukus, MD, an allergist-immunologist and professor of clinical pediatrics at Nationwide Children’s Hospital, Columbus, who was not involved with any of the studies on EpiPen alternatives. And “it’s not just food allergy – anaphylaxis can occur from venom stings, medications, or idiopathic causes.”
Mr. Lowenthal is the CEO of ARS Pharmaceuticals. Mr. Kendall is CEO of Aquestive Therapeutics. Dr. Oppenheimer is a consultant for Aquestive, GSK, Amgen, Sanofi, and Aimmune and sits on Aquestive’s advisory board. Dr. Stukus is a consultant for Novartis.
A version of this article first appeared on Medscape.com.
FROM AAAAI
GI involvement may signal risk for MIS-C after COVID
While evaluating an adolescent who had endured a several-day history of vomiting and diarrhea, I mentioned the likelihood of a viral causation, including SARS-CoV-2 infection. His well-informed mother responded, “He has no respiratory symptoms. Does COVID cause GI disease?”
Indeed, not only is the gastrointestinal tract a potential portal of entry of the virus but it may well be the site of mediation of both local and remote injury and thus a harbinger of more severe clinical phenotypes.
As we learn more about the clinical spectrum of COVID, it is becoming increasingly clear that certain features of GI tract involvement may allow us to establish a timeline of the clinical course and perhaps predict the outcome.
The GI tract’s involvement isn’t surprising
The ways in which the GI tract serves as a target organ of SARS-CoV-2 have been postulated in the literature. In part, this is related to the presence of abundant receptors for SARS-CoV-2 cell binding and internalization. The virus uses angiotensin-converting enzyme 2 receptors to enter various cells. These receptors are highly expressed on not only lung cells but also enterocytes. Binding of SARS-CoV-2 to ACE2 receptors allows GI involvement, leading to microscopic mucosal inflammation, increased permeability, and altered intestinal absorption.
The clinical GI manifestations of this include anorexia, nausea, vomiting, diarrhea, and abdominal pain, which may be the earliest, or sole, symptoms of COVID-19, often noted before the onset of fever or respiratory symptoms. In fact, John Ong, MBBS, and colleagues, in a discussion about patients with primary GI SARS-CoV-2 infection and symptoms, use the term “GI-COVID.”
Clinical course of GI manifestations
After SARS-CoV-2 exposure, adults most commonly present with respiratory symptoms, with GI symptoms reported in 10%-15% of cases. However, the overall incidence of GI involvement during SARS-CoV-2 infection varies according to age, with children more likely than adults to manifest intestinal symptoms.
There are also differences in incidence reported when comparing hospitalized with nonhospitalized individuals. In early reports from the onset of the COVID-19 pandemic, 11%-43% of hospitalized adult patients manifested GI symptoms. Of note, the presence of GI symptoms was associated with more severe disease and thus predictive of outcomes in those admitted to hospitals.
In a multicenter study that assessed pediatric inpatients with COVID-19, GI manifestations were present in 57% of patients and were the first manifestation in 14%. Adjusted by confounding factors, those with GI symptoms had a higher risk for pediatric intensive care unit admission. Patients admitted to the PICU also had higher serum C-reactive protein and aspartate aminotransferase values.
Emerging data on MIS-C
In previously healthy children and adolescents, the severe, life-threatening complication of multisystem inflammatory syndrome in children (MIS-C) may present 2-6 weeks after acute infection with SARS-CoV-2. MIS-C appears to be an immune activation syndrome and is presumed to be the delayed immunologic sequelae of mild/asymptomatic SARS-CoV-2 infection. This response manifests as hyperinflammation in conjunction with a peak in antibody production a few weeks later.
One report of 186 children with MIS-C in the United States noted that the involved organ system included the GI tract in 92%, followed by cardiovascular in 80%, hematologic in 76%, mucocutaneous in 74%, and respiratory in 70%. Affected children were hospitalized for a median of 7 days, with 80% requiring intensive care, 20% receiving mechanical ventilation, and 48% receiving vasoactive support; 2% died. In a similar study of patients hospitalized in New York, 88% had GI symptoms (abdominal pain, vomiting, and/or diarrhea). A retrospective chart review of patients with MIS-C found that the majority had GI symptoms with any portion of the GI tract potentially involved, but ileal and colonic inflammation predominated.
Elizabeth Whittaker, MD, and colleagues described the clinical characteristics of children in eight hospitals in England who met criteria for MIS-C that were temporally associated with SARS-CoV-2. At presentation, all of the patients manifested fever and nonspecific GI symptoms, including vomiting (45%), abdominal pain (53%), and diarrhea (52%). During hospitalization, 50% developed shock with evidence of myocardial dysfunction.
Ermias D. Belay, MD, and colleagues described the clinical characteristics of a large cohort of patients with MIS-C that were reported to the U.S. Centers for Disease Control and Prevention. Of 1,733 patients identified, GI symptoms were reported in 53%-67%. Over half developed hypotension or shock and were admitted for intensive care. Younger children more frequently presented with abdominal pain in contrast with adolescents, who more frequently manifest respiratory symptoms.
In a multicenter retrospective study of Italian children with COVID-19 that was conducted from the onset of the pandemic to early 2021, GI symptoms were noted in 38%. These manifestations were mild and self-limiting, comparable to other viral intestinal infections. However, a subset of children (9.5%) had severe GI manifestations of MIS-C, defined as a medical and/or radiologic diagnosis of acute abdomen, appendicitis, intussusception, pancreatitis, abdominal fluid collection, or diffuse adenomesenteritis requiring surgical consultation. Overall, 42% of this group underwent surgery. The authors noted that the clinical presentation of abdominal pain, lymphopenia, and increased C-reactive protein and ferritin levels were associated with a 9- to 30-fold increased probability of these severe sequelae. In addition, the severity of the GI manifestations was correlated with age (5-10 years: overall response, 8.33; >10 years: OR, 6.37). Again, the presence of GI symptoms was a harbinger of hospitalization and PICU admission.
Given that GI symptoms are a common presentation of MIS-C, its diagnosis may be delayed as clinicians first consider other GI/viral infections, inflammatory bowel disease, or Kawasaki disease. Prompt identification of GI involvement and awareness of the potential outcomes may guide the management and improve the outcome.
These studies provide a clear picture of the differential presenting features of COVID-19 and MIS-C. Although there may be other environmental/genetic factors that govern the incidence, impact, and manifestations, COVID’s status as an ongoing pandemic gives these observations worldwide relevance. This is evident in a recent report documenting pronounced GI symptoms in African children with COVID-19.
It should be noted, however, that the published data cited here reflect the impact of the initial variants of SARS-CoV-2. The GI binding, effects, and aftermath of infection with the Delta and Omicron variants is not yet known.
Cause and effect, or simply coincidental?
Some insight into MIS-C pathogenesis was provided by Lael M. Yonker, MD, and colleagues in their analysis of biospecimens from 100 children: 19 with MIS-C, 26 with acute COVID-19, and 55 controls. They demonstrated that in children with MIS-C the prolonged presence of SARS-CoV-2 in the GI tract led to the release of zonulin, a biomarker of intestinal permeability, with subsequent trafficking of SARS-CoV-2 antigens into the bloodstream, leading to hyperinflammation. They were then able to decrease plasma SARS-CoV-2 spike antigen levels and inflammatory markers, with resulting clinical improvement after administration of larazotide, a zonulin antagonist.
These observations regarding the potential mechanism and triggers of MIS-C may offer biomarkers for early detection and/or strategies for prevention and treatment of MIS-C.
Bottom line
The GI tract is the target of an immune-mediated inflammatory response that is triggered by SARS-CoV-2, with MIS-C being the major manifestation of the resultant high degree of inflammation. These observations will allow an increased awareness of nonrespiratory symptoms of SARS-CoV-2 infection by clinicians working in emergency departments and primary care settings.
Clues that may enhance the ability of pediatric clinicians to recognize the potential for severe GI involvement include the occurrence of abdominal pain, leukopenia, and elevated inflammatory markers. Their presence should raise suspicion of MIS-C and lead to early evaluation.
Of note, COVID-19 mRNA vaccination is associated with a lower incidence of MIS-C in adolescents. This underscores the importance of COVID vaccination for all eligible children. Yet, we clearly have our work cut out for us. Of 107 children with MIS-C who were hospitalized in France, 31% were adolescents eligible for vaccination; however, none had been fully vaccinated. At the end of 2021, CDC data noted that less than 1% of vaccine-eligible children (12-17 years) were fully vaccinated.
The Pfizer-BioNTech vaccine is now authorized for receipt by children aged 5-11 years, the age group that is at highest risk for MIS-C. However, despite the approval of vaccines for these younger children, there is limited access in some parts of the United States at a time of rising incidence.
We look forward to broad availability of pediatric vaccination strategies. In addition, with the intense focus on safe and effective therapeutics for SARS-CoV-2 infection, we hope to soon have strategies to prevent and/or treat the life-threatening manifestations and long-term consequences of MIS-C. For example, the recently reported central role of the gut microbiota in immunity against SARS-CoV-2 infection offer the possibility that “microbiota modulation” may both reduce GI injury and enhance vaccine efficacy.
Dr. Balistreri has disclosed no relevant financial relationships.
William F. Balistreri, MD, is the Dorothy M.M. Kersten Professor of Pediatrics; director emeritus, Pediatric Liver Care Center; medical director emeritus, liver transplantation; and professor, University of Cincinnati College of Medicine, department of pediatrics, Cincinnati Children’s Hospital Medical Center. He has served as director of the division of gastroenterology, hepatology, and nutrition at Cincinnati Children’s for 25 years and frequently covers gastroenterology, liver, and nutrition-related topics for this news organization. Dr Balistreri is currently editor-in-chief of the Journal of Pediatrics, having previously served as editor-in-chief of several journals and textbooks. He also became the first pediatrician to act as president of the American Association for the Study of Liver Diseases. In his spare time, he coaches youth lacrosse.
A version of this article first appeared on Medscape.com.
While evaluating an adolescent who had endured a several-day history of vomiting and diarrhea, I mentioned the likelihood of a viral causation, including SARS-CoV-2 infection. His well-informed mother responded, “He has no respiratory symptoms. Does COVID cause GI disease?”
Indeed, not only is the gastrointestinal tract a potential portal of entry of the virus but it may well be the site of mediation of both local and remote injury and thus a harbinger of more severe clinical phenotypes.
As we learn more about the clinical spectrum of COVID, it is becoming increasingly clear that certain features of GI tract involvement may allow us to establish a timeline of the clinical course and perhaps predict the outcome.
The GI tract’s involvement isn’t surprising
The ways in which the GI tract serves as a target organ of SARS-CoV-2 have been postulated in the literature. In part, this is related to the presence of abundant receptors for SARS-CoV-2 cell binding and internalization. The virus uses angiotensin-converting enzyme 2 receptors to enter various cells. These receptors are highly expressed on not only lung cells but also enterocytes. Binding of SARS-CoV-2 to ACE2 receptors allows GI involvement, leading to microscopic mucosal inflammation, increased permeability, and altered intestinal absorption.
The clinical GI manifestations of this include anorexia, nausea, vomiting, diarrhea, and abdominal pain, which may be the earliest, or sole, symptoms of COVID-19, often noted before the onset of fever or respiratory symptoms. In fact, John Ong, MBBS, and colleagues, in a discussion about patients with primary GI SARS-CoV-2 infection and symptoms, use the term “GI-COVID.”
Clinical course of GI manifestations
After SARS-CoV-2 exposure, adults most commonly present with respiratory symptoms, with GI symptoms reported in 10%-15% of cases. However, the overall incidence of GI involvement during SARS-CoV-2 infection varies according to age, with children more likely than adults to manifest intestinal symptoms.
There are also differences in incidence reported when comparing hospitalized with nonhospitalized individuals. In early reports from the onset of the COVID-19 pandemic, 11%-43% of hospitalized adult patients manifested GI symptoms. Of note, the presence of GI symptoms was associated with more severe disease and thus predictive of outcomes in those admitted to hospitals.
In a multicenter study that assessed pediatric inpatients with COVID-19, GI manifestations were present in 57% of patients and were the first manifestation in 14%. Adjusted by confounding factors, those with GI symptoms had a higher risk for pediatric intensive care unit admission. Patients admitted to the PICU also had higher serum C-reactive protein and aspartate aminotransferase values.
Emerging data on MIS-C
In previously healthy children and adolescents, the severe, life-threatening complication of multisystem inflammatory syndrome in children (MIS-C) may present 2-6 weeks after acute infection with SARS-CoV-2. MIS-C appears to be an immune activation syndrome and is presumed to be the delayed immunologic sequelae of mild/asymptomatic SARS-CoV-2 infection. This response manifests as hyperinflammation in conjunction with a peak in antibody production a few weeks later.
One report of 186 children with MIS-C in the United States noted that the involved organ system included the GI tract in 92%, followed by cardiovascular in 80%, hematologic in 76%, mucocutaneous in 74%, and respiratory in 70%. Affected children were hospitalized for a median of 7 days, with 80% requiring intensive care, 20% receiving mechanical ventilation, and 48% receiving vasoactive support; 2% died. In a similar study of patients hospitalized in New York, 88% had GI symptoms (abdominal pain, vomiting, and/or diarrhea). A retrospective chart review of patients with MIS-C found that the majority had GI symptoms with any portion of the GI tract potentially involved, but ileal and colonic inflammation predominated.
Elizabeth Whittaker, MD, and colleagues described the clinical characteristics of children in eight hospitals in England who met criteria for MIS-C that were temporally associated with SARS-CoV-2. At presentation, all of the patients manifested fever and nonspecific GI symptoms, including vomiting (45%), abdominal pain (53%), and diarrhea (52%). During hospitalization, 50% developed shock with evidence of myocardial dysfunction.
Ermias D. Belay, MD, and colleagues described the clinical characteristics of a large cohort of patients with MIS-C that were reported to the U.S. Centers for Disease Control and Prevention. Of 1,733 patients identified, GI symptoms were reported in 53%-67%. Over half developed hypotension or shock and were admitted for intensive care. Younger children more frequently presented with abdominal pain in contrast with adolescents, who more frequently manifest respiratory symptoms.
In a multicenter retrospective study of Italian children with COVID-19 that was conducted from the onset of the pandemic to early 2021, GI symptoms were noted in 38%. These manifestations were mild and self-limiting, comparable to other viral intestinal infections. However, a subset of children (9.5%) had severe GI manifestations of MIS-C, defined as a medical and/or radiologic diagnosis of acute abdomen, appendicitis, intussusception, pancreatitis, abdominal fluid collection, or diffuse adenomesenteritis requiring surgical consultation. Overall, 42% of this group underwent surgery. The authors noted that the clinical presentation of abdominal pain, lymphopenia, and increased C-reactive protein and ferritin levels were associated with a 9- to 30-fold increased probability of these severe sequelae. In addition, the severity of the GI manifestations was correlated with age (5-10 years: overall response, 8.33; >10 years: OR, 6.37). Again, the presence of GI symptoms was a harbinger of hospitalization and PICU admission.
Given that GI symptoms are a common presentation of MIS-C, its diagnosis may be delayed as clinicians first consider other GI/viral infections, inflammatory bowel disease, or Kawasaki disease. Prompt identification of GI involvement and awareness of the potential outcomes may guide the management and improve the outcome.
These studies provide a clear picture of the differential presenting features of COVID-19 and MIS-C. Although there may be other environmental/genetic factors that govern the incidence, impact, and manifestations, COVID’s status as an ongoing pandemic gives these observations worldwide relevance. This is evident in a recent report documenting pronounced GI symptoms in African children with COVID-19.
It should be noted, however, that the published data cited here reflect the impact of the initial variants of SARS-CoV-2. The GI binding, effects, and aftermath of infection with the Delta and Omicron variants is not yet known.
Cause and effect, or simply coincidental?
Some insight into MIS-C pathogenesis was provided by Lael M. Yonker, MD, and colleagues in their analysis of biospecimens from 100 children: 19 with MIS-C, 26 with acute COVID-19, and 55 controls. They demonstrated that in children with MIS-C the prolonged presence of SARS-CoV-2 in the GI tract led to the release of zonulin, a biomarker of intestinal permeability, with subsequent trafficking of SARS-CoV-2 antigens into the bloodstream, leading to hyperinflammation. They were then able to decrease plasma SARS-CoV-2 spike antigen levels and inflammatory markers, with resulting clinical improvement after administration of larazotide, a zonulin antagonist.
These observations regarding the potential mechanism and triggers of MIS-C may offer biomarkers for early detection and/or strategies for prevention and treatment of MIS-C.
Bottom line
The GI tract is the target of an immune-mediated inflammatory response that is triggered by SARS-CoV-2, with MIS-C being the major manifestation of the resultant high degree of inflammation. These observations will allow an increased awareness of nonrespiratory symptoms of SARS-CoV-2 infection by clinicians working in emergency departments and primary care settings.
Clues that may enhance the ability of pediatric clinicians to recognize the potential for severe GI involvement include the occurrence of abdominal pain, leukopenia, and elevated inflammatory markers. Their presence should raise suspicion of MIS-C and lead to early evaluation.
Of note, COVID-19 mRNA vaccination is associated with a lower incidence of MIS-C in adolescents. This underscores the importance of COVID vaccination for all eligible children. Yet, we clearly have our work cut out for us. Of 107 children with MIS-C who were hospitalized in France, 31% were adolescents eligible for vaccination; however, none had been fully vaccinated. At the end of 2021, CDC data noted that less than 1% of vaccine-eligible children (12-17 years) were fully vaccinated.
The Pfizer-BioNTech vaccine is now authorized for receipt by children aged 5-11 years, the age group that is at highest risk for MIS-C. However, despite the approval of vaccines for these younger children, there is limited access in some parts of the United States at a time of rising incidence.
We look forward to broad availability of pediatric vaccination strategies. In addition, with the intense focus on safe and effective therapeutics for SARS-CoV-2 infection, we hope to soon have strategies to prevent and/or treat the life-threatening manifestations and long-term consequences of MIS-C. For example, the recently reported central role of the gut microbiota in immunity against SARS-CoV-2 infection offer the possibility that “microbiota modulation” may both reduce GI injury and enhance vaccine efficacy.
Dr. Balistreri has disclosed no relevant financial relationships.
William F. Balistreri, MD, is the Dorothy M.M. Kersten Professor of Pediatrics; director emeritus, Pediatric Liver Care Center; medical director emeritus, liver transplantation; and professor, University of Cincinnati College of Medicine, department of pediatrics, Cincinnati Children’s Hospital Medical Center. He has served as director of the division of gastroenterology, hepatology, and nutrition at Cincinnati Children’s for 25 years and frequently covers gastroenterology, liver, and nutrition-related topics for this news organization. Dr Balistreri is currently editor-in-chief of the Journal of Pediatrics, having previously served as editor-in-chief of several journals and textbooks. He also became the first pediatrician to act as president of the American Association for the Study of Liver Diseases. In his spare time, he coaches youth lacrosse.
A version of this article first appeared on Medscape.com.
While evaluating an adolescent who had endured a several-day history of vomiting and diarrhea, I mentioned the likelihood of a viral causation, including SARS-CoV-2 infection. His well-informed mother responded, “He has no respiratory symptoms. Does COVID cause GI disease?”
Indeed, not only is the gastrointestinal tract a potential portal of entry of the virus but it may well be the site of mediation of both local and remote injury and thus a harbinger of more severe clinical phenotypes.
As we learn more about the clinical spectrum of COVID, it is becoming increasingly clear that certain features of GI tract involvement may allow us to establish a timeline of the clinical course and perhaps predict the outcome.
The GI tract’s involvement isn’t surprising
The ways in which the GI tract serves as a target organ of SARS-CoV-2 have been postulated in the literature. In part, this is related to the presence of abundant receptors for SARS-CoV-2 cell binding and internalization. The virus uses angiotensin-converting enzyme 2 receptors to enter various cells. These receptors are highly expressed on not only lung cells but also enterocytes. Binding of SARS-CoV-2 to ACE2 receptors allows GI involvement, leading to microscopic mucosal inflammation, increased permeability, and altered intestinal absorption.
The clinical GI manifestations of this include anorexia, nausea, vomiting, diarrhea, and abdominal pain, which may be the earliest, or sole, symptoms of COVID-19, often noted before the onset of fever or respiratory symptoms. In fact, John Ong, MBBS, and colleagues, in a discussion about patients with primary GI SARS-CoV-2 infection and symptoms, use the term “GI-COVID.”
Clinical course of GI manifestations
After SARS-CoV-2 exposure, adults most commonly present with respiratory symptoms, with GI symptoms reported in 10%-15% of cases. However, the overall incidence of GI involvement during SARS-CoV-2 infection varies according to age, with children more likely than adults to manifest intestinal symptoms.
There are also differences in incidence reported when comparing hospitalized with nonhospitalized individuals. In early reports from the onset of the COVID-19 pandemic, 11%-43% of hospitalized adult patients manifested GI symptoms. Of note, the presence of GI symptoms was associated with more severe disease and thus predictive of outcomes in those admitted to hospitals.
In a multicenter study that assessed pediatric inpatients with COVID-19, GI manifestations were present in 57% of patients and were the first manifestation in 14%. Adjusted by confounding factors, those with GI symptoms had a higher risk for pediatric intensive care unit admission. Patients admitted to the PICU also had higher serum C-reactive protein and aspartate aminotransferase values.
Emerging data on MIS-C
In previously healthy children and adolescents, the severe, life-threatening complication of multisystem inflammatory syndrome in children (MIS-C) may present 2-6 weeks after acute infection with SARS-CoV-2. MIS-C appears to be an immune activation syndrome and is presumed to be the delayed immunologic sequelae of mild/asymptomatic SARS-CoV-2 infection. This response manifests as hyperinflammation in conjunction with a peak in antibody production a few weeks later.
One report of 186 children with MIS-C in the United States noted that the involved organ system included the GI tract in 92%, followed by cardiovascular in 80%, hematologic in 76%, mucocutaneous in 74%, and respiratory in 70%. Affected children were hospitalized for a median of 7 days, with 80% requiring intensive care, 20% receiving mechanical ventilation, and 48% receiving vasoactive support; 2% died. In a similar study of patients hospitalized in New York, 88% had GI symptoms (abdominal pain, vomiting, and/or diarrhea). A retrospective chart review of patients with MIS-C found that the majority had GI symptoms with any portion of the GI tract potentially involved, but ileal and colonic inflammation predominated.
Elizabeth Whittaker, MD, and colleagues described the clinical characteristics of children in eight hospitals in England who met criteria for MIS-C that were temporally associated with SARS-CoV-2. At presentation, all of the patients manifested fever and nonspecific GI symptoms, including vomiting (45%), abdominal pain (53%), and diarrhea (52%). During hospitalization, 50% developed shock with evidence of myocardial dysfunction.
Ermias D. Belay, MD, and colleagues described the clinical characteristics of a large cohort of patients with MIS-C that were reported to the U.S. Centers for Disease Control and Prevention. Of 1,733 patients identified, GI symptoms were reported in 53%-67%. Over half developed hypotension or shock and were admitted for intensive care. Younger children more frequently presented with abdominal pain in contrast with adolescents, who more frequently manifest respiratory symptoms.
In a multicenter retrospective study of Italian children with COVID-19 that was conducted from the onset of the pandemic to early 2021, GI symptoms were noted in 38%. These manifestations were mild and self-limiting, comparable to other viral intestinal infections. However, a subset of children (9.5%) had severe GI manifestations of MIS-C, defined as a medical and/or radiologic diagnosis of acute abdomen, appendicitis, intussusception, pancreatitis, abdominal fluid collection, or diffuse adenomesenteritis requiring surgical consultation. Overall, 42% of this group underwent surgery. The authors noted that the clinical presentation of abdominal pain, lymphopenia, and increased C-reactive protein and ferritin levels were associated with a 9- to 30-fold increased probability of these severe sequelae. In addition, the severity of the GI manifestations was correlated with age (5-10 years: overall response, 8.33; >10 years: OR, 6.37). Again, the presence of GI symptoms was a harbinger of hospitalization and PICU admission.
Given that GI symptoms are a common presentation of MIS-C, its diagnosis may be delayed as clinicians first consider other GI/viral infections, inflammatory bowel disease, or Kawasaki disease. Prompt identification of GI involvement and awareness of the potential outcomes may guide the management and improve the outcome.
These studies provide a clear picture of the differential presenting features of COVID-19 and MIS-C. Although there may be other environmental/genetic factors that govern the incidence, impact, and manifestations, COVID’s status as an ongoing pandemic gives these observations worldwide relevance. This is evident in a recent report documenting pronounced GI symptoms in African children with COVID-19.
It should be noted, however, that the published data cited here reflect the impact of the initial variants of SARS-CoV-2. The GI binding, effects, and aftermath of infection with the Delta and Omicron variants is not yet known.
Cause and effect, or simply coincidental?
Some insight into MIS-C pathogenesis was provided by Lael M. Yonker, MD, and colleagues in their analysis of biospecimens from 100 children: 19 with MIS-C, 26 with acute COVID-19, and 55 controls. They demonstrated that in children with MIS-C the prolonged presence of SARS-CoV-2 in the GI tract led to the release of zonulin, a biomarker of intestinal permeability, with subsequent trafficking of SARS-CoV-2 antigens into the bloodstream, leading to hyperinflammation. They were then able to decrease plasma SARS-CoV-2 spike antigen levels and inflammatory markers, with resulting clinical improvement after administration of larazotide, a zonulin antagonist.
These observations regarding the potential mechanism and triggers of MIS-C may offer biomarkers for early detection and/or strategies for prevention and treatment of MIS-C.
Bottom line
The GI tract is the target of an immune-mediated inflammatory response that is triggered by SARS-CoV-2, with MIS-C being the major manifestation of the resultant high degree of inflammation. These observations will allow an increased awareness of nonrespiratory symptoms of SARS-CoV-2 infection by clinicians working in emergency departments and primary care settings.
Clues that may enhance the ability of pediatric clinicians to recognize the potential for severe GI involvement include the occurrence of abdominal pain, leukopenia, and elevated inflammatory markers. Their presence should raise suspicion of MIS-C and lead to early evaluation.
Of note, COVID-19 mRNA vaccination is associated with a lower incidence of MIS-C in adolescents. This underscores the importance of COVID vaccination for all eligible children. Yet, we clearly have our work cut out for us. Of 107 children with MIS-C who were hospitalized in France, 31% were adolescents eligible for vaccination; however, none had been fully vaccinated. At the end of 2021, CDC data noted that less than 1% of vaccine-eligible children (12-17 years) were fully vaccinated.
The Pfizer-BioNTech vaccine is now authorized for receipt by children aged 5-11 years, the age group that is at highest risk for MIS-C. However, despite the approval of vaccines for these younger children, there is limited access in some parts of the United States at a time of rising incidence.
We look forward to broad availability of pediatric vaccination strategies. In addition, with the intense focus on safe and effective therapeutics for SARS-CoV-2 infection, we hope to soon have strategies to prevent and/or treat the life-threatening manifestations and long-term consequences of MIS-C. For example, the recently reported central role of the gut microbiota in immunity against SARS-CoV-2 infection offer the possibility that “microbiota modulation” may both reduce GI injury and enhance vaccine efficacy.
Dr. Balistreri has disclosed no relevant financial relationships.
William F. Balistreri, MD, is the Dorothy M.M. Kersten Professor of Pediatrics; director emeritus, Pediatric Liver Care Center; medical director emeritus, liver transplantation; and professor, University of Cincinnati College of Medicine, department of pediatrics, Cincinnati Children’s Hospital Medical Center. He has served as director of the division of gastroenterology, hepatology, and nutrition at Cincinnati Children’s for 25 years and frequently covers gastroenterology, liver, and nutrition-related topics for this news organization. Dr Balistreri is currently editor-in-chief of the Journal of Pediatrics, having previously served as editor-in-chief of several journals and textbooks. He also became the first pediatrician to act as president of the American Association for the Study of Liver Diseases. In his spare time, he coaches youth lacrosse.
A version of this article first appeared on Medscape.com.
Children and COVID: New cases down to pre-Omicron level
New cases of COVID-19 in U.S. children dropped for the fifth consecutive week, but the rate of decline slowed considerably, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The national count of new cases has now fallen for five straight weeks since peaking Jan. 14-20, and this week’s figure is the lowest since the pre-Omicron days of mid-November, based on data collected by the AAP and CHA from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.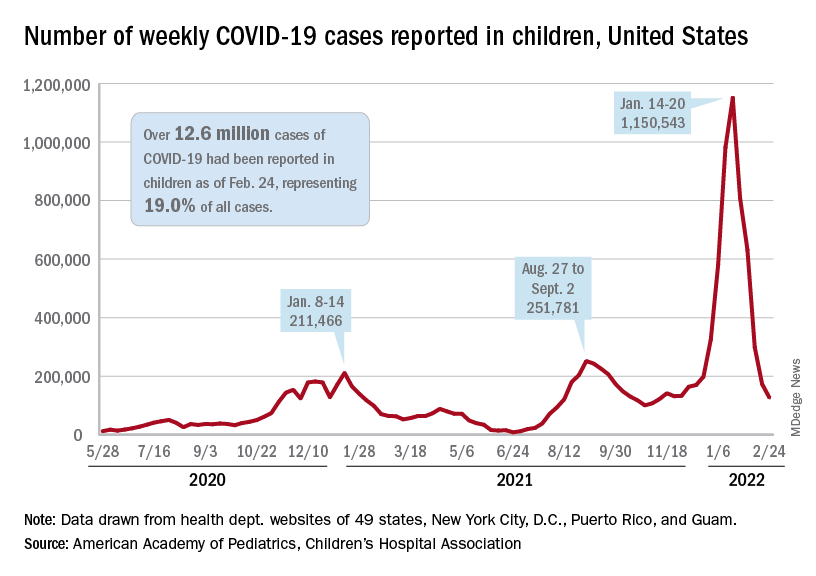
Over 12.6 million pediatric cases have been reported by those jurisdictions since the start of the pandemic, representing 19.0% of all cases in the United States, the AAP and CHA said in their weekly COVID report.
The highest cumulative rate among the states, 27.5%, can be found in Vermont, followed by New Hampshire (26.7%) and Alaska (26.6%). Alabama’s 12.1% is lower than any other jurisdiction, but the state stopped reporting during the summer of 2021, just as the Delta surge was beginning. The next two lowest states, Florida (12.8%) and Utah (13.9%), both define children as those aged 0-14 years, so the state with the lowest rate and no qualifiers is Idaho at 14.3%, the AAP/CHA data show.
The downward trend in new cases is reflected in other national measures. The daily rate of new hospital admissions for children aged 0-17 years was 0.32 per 100,000 population on Feb. 26, which is a drop of 75% since admissions peaked at 1.25 per 100,000 on Jan. 15, according to the Centers for Disease Control and Prevention.
The most recent 7-day average (Feb. 20-26) for child admissions with confirmed COVID-19 was 237 per day, compared with 914 per day during the peak week of Jan. 10-16. Emergency department visits with diagnosed COVID, measured as a percentage of all ED visits by age group, are down even more. The 7-day average was 1.2% on Feb. 25 for children aged 0-11 years, compared with a peak of 13.9% in mid-January, the CDC said on its COVID Data Tracker. The current rates for older children are even lower.
The decline of the Omicron surge over the last few weeks is allowing states to end mask mandates in schools around the country. The governors of California, Oregon, and Washington just announced that their states will be lifting their mask requirements on March 11, and New York State will end its mandate on March 2, while New York City is scheduled to go mask-free as of March 7, according to District Administration.
Those types of government moves, however, do not seem to be entirely supported by the public. In a survey conducted Feb. 9-21 by the Kaiser Family Foundation, 43% of the 1,502 respondents said that all students and staff should be required to wear masks in schools, while 40% said that there should be no mask requirements at all.
New cases of COVID-19 in U.S. children dropped for the fifth consecutive week, but the rate of decline slowed considerably, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The national count of new cases has now fallen for five straight weeks since peaking Jan. 14-20, and this week’s figure is the lowest since the pre-Omicron days of mid-November, based on data collected by the AAP and CHA from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.
Over 12.6 million pediatric cases have been reported by those jurisdictions since the start of the pandemic, representing 19.0% of all cases in the United States, the AAP and CHA said in their weekly COVID report.
The highest cumulative rate among the states, 27.5%, can be found in Vermont, followed by New Hampshire (26.7%) and Alaska (26.6%). Alabama’s 12.1% is lower than any other jurisdiction, but the state stopped reporting during the summer of 2021, just as the Delta surge was beginning. The next two lowest states, Florida (12.8%) and Utah (13.9%), both define children as those aged 0-14 years, so the state with the lowest rate and no qualifiers is Idaho at 14.3%, the AAP/CHA data show.
The downward trend in new cases is reflected in other national measures. The daily rate of new hospital admissions for children aged 0-17 years was 0.32 per 100,000 population on Feb. 26, which is a drop of 75% since admissions peaked at 1.25 per 100,000 on Jan. 15, according to the Centers for Disease Control and Prevention.
The most recent 7-day average (Feb. 20-26) for child admissions with confirmed COVID-19 was 237 per day, compared with 914 per day during the peak week of Jan. 10-16. Emergency department visits with diagnosed COVID, measured as a percentage of all ED visits by age group, are down even more. The 7-day average was 1.2% on Feb. 25 for children aged 0-11 years, compared with a peak of 13.9% in mid-January, the CDC said on its COVID Data Tracker. The current rates for older children are even lower.
The decline of the Omicron surge over the last few weeks is allowing states to end mask mandates in schools around the country. The governors of California, Oregon, and Washington just announced that their states will be lifting their mask requirements on March 11, and New York State will end its mandate on March 2, while New York City is scheduled to go mask-free as of March 7, according to District Administration.
Those types of government moves, however, do not seem to be entirely supported by the public. In a survey conducted Feb. 9-21 by the Kaiser Family Foundation, 43% of the 1,502 respondents said that all students and staff should be required to wear masks in schools, while 40% said that there should be no mask requirements at all.
New cases of COVID-19 in U.S. children dropped for the fifth consecutive week, but the rate of decline slowed considerably, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The national count of new cases has now fallen for five straight weeks since peaking Jan. 14-20, and this week’s figure is the lowest since the pre-Omicron days of mid-November, based on data collected by the AAP and CHA from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.
Over 12.6 million pediatric cases have been reported by those jurisdictions since the start of the pandemic, representing 19.0% of all cases in the United States, the AAP and CHA said in their weekly COVID report.
The highest cumulative rate among the states, 27.5%, can be found in Vermont, followed by New Hampshire (26.7%) and Alaska (26.6%). Alabama’s 12.1% is lower than any other jurisdiction, but the state stopped reporting during the summer of 2021, just as the Delta surge was beginning. The next two lowest states, Florida (12.8%) and Utah (13.9%), both define children as those aged 0-14 years, so the state with the lowest rate and no qualifiers is Idaho at 14.3%, the AAP/CHA data show.
The downward trend in new cases is reflected in other national measures. The daily rate of new hospital admissions for children aged 0-17 years was 0.32 per 100,000 population on Feb. 26, which is a drop of 75% since admissions peaked at 1.25 per 100,000 on Jan. 15, according to the Centers for Disease Control and Prevention.
The most recent 7-day average (Feb. 20-26) for child admissions with confirmed COVID-19 was 237 per day, compared with 914 per day during the peak week of Jan. 10-16. Emergency department visits with diagnosed COVID, measured as a percentage of all ED visits by age group, are down even more. The 7-day average was 1.2% on Feb. 25 for children aged 0-11 years, compared with a peak of 13.9% in mid-January, the CDC said on its COVID Data Tracker. The current rates for older children are even lower.
The decline of the Omicron surge over the last few weeks is allowing states to end mask mandates in schools around the country. The governors of California, Oregon, and Washington just announced that their states will be lifting their mask requirements on March 11, and New York State will end its mandate on March 2, while New York City is scheduled to go mask-free as of March 7, according to District Administration.
Those types of government moves, however, do not seem to be entirely supported by the public. In a survey conducted Feb. 9-21 by the Kaiser Family Foundation, 43% of the 1,502 respondents said that all students and staff should be required to wear masks in schools, while 40% said that there should be no mask requirements at all.