User login
When to Consider PCOS in Female Acne Patients
SAN DIEGO – Correctly diagnosed and adequately treated polycystic ovary syndrome can appreciably improve acne in a select group of female patients, according to Dr. Anne W. Lucky.
Dr. Lucky offered tips on evaluating and treating acne and PCOS at the annual meeting of the American Academy of Dermatology. She said that PCOS should be considered in female patients with early onset acne, acne that is refractory to conventional therapy, relapse that occurs after treatment with isotretinoin, persistence of acne beyond adolescence, or late onset of acne, she said.
Several laboratory tests are typically used to diagnose PCOS but agreement on which tests to use is limited. "This is somewhat controversial," said Dr. Lucky, a professor of dermatology at the University of Cincinnati. She recommended the following tests: free testosterone, DHEAS (dehydroepiandrosterone sulfate), and the ratio of LH (luteinizing hormone) to FSH (follicle-stimulating hormone). "If I have a good suspicion or find abnormalities – [I include] fasting glucose and insulin and a fasting lipid profile," she said.
Treatment options include combination oral contraceptives, glucocorticoids (for specific adrenal abnormalities), and anti-androgens among others.
"By and large, oral contraceptives are the No. 1 choice. I mentioned combination contraceptives because it’s the estrogen that’s helpful. Progesterone-only contraceptives can actually worsen acne," Dr. Lucky said. "We don’t treat girls before menarche because they don’t have a risk for pregnancy and we might influence bone growth if we treat too early. You can suspect PCOS very early but you may have to suspend your treatment until they get a little older."
Using contraceptives – especially in girls or adolescents -- usually involves discussions with a gynecologist, a parent, and the child. "Our biggest hurdle is that the teenage population has heard the word on the street that the pill is going to make them fat and they don’t want to take it. Actually [the gynecologists that I work with] tell me that the studies show that some children gain weight, some lose weight, but most stay the same weight with the combination pills," she said.
In the United States, spironolactone is the only antiandrogen treatment option. It works by being a competitive inhibitor of androgen receptors. The drug does not lower serum androgen levels, but it prevents the action of androgen – increasing estrogenicity. However, the use of spironolactone for PCOS is considered off label. The drug is indicated for the treatment of hypertension and the label carries a warning that it should only be used for this indication, Dr. Lucky noted.
Dr. Lucky reported that she has financial relationships with Amgen, Galderma, and Johnson & Johnson.
SAN DIEGO – Correctly diagnosed and adequately treated polycystic ovary syndrome can appreciably improve acne in a select group of female patients, according to Dr. Anne W. Lucky.
Dr. Lucky offered tips on evaluating and treating acne and PCOS at the annual meeting of the American Academy of Dermatology. She said that PCOS should be considered in female patients with early onset acne, acne that is refractory to conventional therapy, relapse that occurs after treatment with isotretinoin, persistence of acne beyond adolescence, or late onset of acne, she said.
Several laboratory tests are typically used to diagnose PCOS but agreement on which tests to use is limited. "This is somewhat controversial," said Dr. Lucky, a professor of dermatology at the University of Cincinnati. She recommended the following tests: free testosterone, DHEAS (dehydroepiandrosterone sulfate), and the ratio of LH (luteinizing hormone) to FSH (follicle-stimulating hormone). "If I have a good suspicion or find abnormalities – [I include] fasting glucose and insulin and a fasting lipid profile," she said.
Treatment options include combination oral contraceptives, glucocorticoids (for specific adrenal abnormalities), and anti-androgens among others.
"By and large, oral contraceptives are the No. 1 choice. I mentioned combination contraceptives because it’s the estrogen that’s helpful. Progesterone-only contraceptives can actually worsen acne," Dr. Lucky said. "We don’t treat girls before menarche because they don’t have a risk for pregnancy and we might influence bone growth if we treat too early. You can suspect PCOS very early but you may have to suspend your treatment until they get a little older."
Using contraceptives – especially in girls or adolescents -- usually involves discussions with a gynecologist, a parent, and the child. "Our biggest hurdle is that the teenage population has heard the word on the street that the pill is going to make them fat and they don’t want to take it. Actually [the gynecologists that I work with] tell me that the studies show that some children gain weight, some lose weight, but most stay the same weight with the combination pills," she said.
In the United States, spironolactone is the only antiandrogen treatment option. It works by being a competitive inhibitor of androgen receptors. The drug does not lower serum androgen levels, but it prevents the action of androgen – increasing estrogenicity. However, the use of spironolactone for PCOS is considered off label. The drug is indicated for the treatment of hypertension and the label carries a warning that it should only be used for this indication, Dr. Lucky noted.
Dr. Lucky reported that she has financial relationships with Amgen, Galderma, and Johnson & Johnson.
SAN DIEGO – Correctly diagnosed and adequately treated polycystic ovary syndrome can appreciably improve acne in a select group of female patients, according to Dr. Anne W. Lucky.
Dr. Lucky offered tips on evaluating and treating acne and PCOS at the annual meeting of the American Academy of Dermatology. She said that PCOS should be considered in female patients with early onset acne, acne that is refractory to conventional therapy, relapse that occurs after treatment with isotretinoin, persistence of acne beyond adolescence, or late onset of acne, she said.
Several laboratory tests are typically used to diagnose PCOS but agreement on which tests to use is limited. "This is somewhat controversial," said Dr. Lucky, a professor of dermatology at the University of Cincinnati. She recommended the following tests: free testosterone, DHEAS (dehydroepiandrosterone sulfate), and the ratio of LH (luteinizing hormone) to FSH (follicle-stimulating hormone). "If I have a good suspicion or find abnormalities – [I include] fasting glucose and insulin and a fasting lipid profile," she said.
Treatment options include combination oral contraceptives, glucocorticoids (for specific adrenal abnormalities), and anti-androgens among others.
"By and large, oral contraceptives are the No. 1 choice. I mentioned combination contraceptives because it’s the estrogen that’s helpful. Progesterone-only contraceptives can actually worsen acne," Dr. Lucky said. "We don’t treat girls before menarche because they don’t have a risk for pregnancy and we might influence bone growth if we treat too early. You can suspect PCOS very early but you may have to suspend your treatment until they get a little older."
Using contraceptives – especially in girls or adolescents -- usually involves discussions with a gynecologist, a parent, and the child. "Our biggest hurdle is that the teenage population has heard the word on the street that the pill is going to make them fat and they don’t want to take it. Actually [the gynecologists that I work with] tell me that the studies show that some children gain weight, some lose weight, but most stay the same weight with the combination pills," she said.
In the United States, spironolactone is the only antiandrogen treatment option. It works by being a competitive inhibitor of androgen receptors. The drug does not lower serum androgen levels, but it prevents the action of androgen – increasing estrogenicity. However, the use of spironolactone for PCOS is considered off label. The drug is indicated for the treatment of hypertension and the label carries a warning that it should only be used for this indication, Dr. Lucky noted.
Dr. Lucky reported that she has financial relationships with Amgen, Galderma, and Johnson & Johnson.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF DERMATOLOGY
FDA Panel: Approve Mirabegron for Overactive Bladder
SILVER SPRING, MD. – Physicians may soon have a first-in-class alternative to current treatments for overactive bladder, which may not always work and can have unpleasant side effects.
A Food and Drug Administration panel on April 5 voted 7-4 with 1 abstention that the overall benefit-risk assessment supports the approval of mirabegron for the treatment of overactive bladder.
Pharmacologic treatment options to date include muscarinic receptor antagonists, which can affect the salivary glands, intestines, and eyes, resulting in side effects such as dry mouth, constipation, and blurred vision, respectively.
Mirabegron is a first-in-class agonist of beta 3-adrenoceptors. Astellas Pharma developed the drug for the treatment of overactive bladder with symptoms of urge urinary incontinence, urgency, and urinary frequency. In the United States, the proposed dose is 50 mg once daily with or without food. However, a dose of 25 mg is reserved for patients with severe renal or moderate hepatic impairment. The formulation is an oral controlled-absorption system (extended-release) tablets. The drug is already approved in Japan.
"The committee has a sense that there is marginal efficacy, but overall the majority feels that the benefits outweigh the risks. This is seen as a new agent, which can potentially be used for individuals who have not had success with other available agents," summarized Dr. Julia V. Johnson, who is the chair of the advisory committee for reproductive health drugs. "With some caution and with some reservation the overall approval of the medication comes from this committee."
The committee also voted 8-4 that the data do provide substantial evidence of benefit for mirabegron in the treatment of overactive bladder. However, many members agreed that there was statistically-significant improvement in symptoms but questioned whether this would translate to a meaningful clinical difference.
The committee also voted 9-3 that adequate safety had been demonstrated for the drug. Committee members did express reservations about the paucity of data with regard to neoplasms, hepatotoxicity events, and hypersensitivity reactions.
The primary sources of data for the evaluation are three randomized placebo-controlled phase III trials. Supportive data included data from a single long-term (active-controlled) study, three phase II studies, and a phase II study in patients with symptomatic benign prostatic hyperplasia.
The three phase III trials lasted for 12 weeks with individuals randomized to receive mirabegron either 25 mg daily, or 50 mg daily, or placebo. Coprimary end points included change from baseline in the average number of micturitions in 24 hours and the change from baseline in the average number of incontinence episodes in 24 hours.
Mirabegron at a dose of 50 mg achieved the primary efficacy objectives in three phase III studies. Treatment with 50 mg mirabegron reduced the mean number of micturitions by 0.55/day, compared with placebo. Likewise, mirabegron reduced the mean number of incontinence episodes per day by 0.40, compared with placebo. Lastly, the mean volume per void increased by 11.9 mL with the drug, compared with placebo.
Committee members expressed some concern about increases in both blood pressure and pulse rate associated with the drug. There was also an increased incidence of urologic adverse events, particularly urinary tract infections of mild severity. The committee members were particularly concerned about an increased incidence of neoplasm serious adverse events – new malignant events – in the group on 100 mg mirabegron in the 1-year study, as well as hepatotoxicity events and hypersensitivity reactions. However, they noted that there was insufficient data to draw firm conclusions about these serious adverse events.
SILVER SPRING, MD. – Physicians may soon have a first-in-class alternative to current treatments for overactive bladder, which may not always work and can have unpleasant side effects.
A Food and Drug Administration panel on April 5 voted 7-4 with 1 abstention that the overall benefit-risk assessment supports the approval of mirabegron for the treatment of overactive bladder.
Pharmacologic treatment options to date include muscarinic receptor antagonists, which can affect the salivary glands, intestines, and eyes, resulting in side effects such as dry mouth, constipation, and blurred vision, respectively.
Mirabegron is a first-in-class agonist of beta 3-adrenoceptors. Astellas Pharma developed the drug for the treatment of overactive bladder with symptoms of urge urinary incontinence, urgency, and urinary frequency. In the United States, the proposed dose is 50 mg once daily with or without food. However, a dose of 25 mg is reserved for patients with severe renal or moderate hepatic impairment. The formulation is an oral controlled-absorption system (extended-release) tablets. The drug is already approved in Japan.
"The committee has a sense that there is marginal efficacy, but overall the majority feels that the benefits outweigh the risks. This is seen as a new agent, which can potentially be used for individuals who have not had success with other available agents," summarized Dr. Julia V. Johnson, who is the chair of the advisory committee for reproductive health drugs. "With some caution and with some reservation the overall approval of the medication comes from this committee."
The committee also voted 8-4 that the data do provide substantial evidence of benefit for mirabegron in the treatment of overactive bladder. However, many members agreed that there was statistically-significant improvement in symptoms but questioned whether this would translate to a meaningful clinical difference.
The committee also voted 9-3 that adequate safety had been demonstrated for the drug. Committee members did express reservations about the paucity of data with regard to neoplasms, hepatotoxicity events, and hypersensitivity reactions.
The primary sources of data for the evaluation are three randomized placebo-controlled phase III trials. Supportive data included data from a single long-term (active-controlled) study, three phase II studies, and a phase II study in patients with symptomatic benign prostatic hyperplasia.
The three phase III trials lasted for 12 weeks with individuals randomized to receive mirabegron either 25 mg daily, or 50 mg daily, or placebo. Coprimary end points included change from baseline in the average number of micturitions in 24 hours and the change from baseline in the average number of incontinence episodes in 24 hours.
Mirabegron at a dose of 50 mg achieved the primary efficacy objectives in three phase III studies. Treatment with 50 mg mirabegron reduced the mean number of micturitions by 0.55/day, compared with placebo. Likewise, mirabegron reduced the mean number of incontinence episodes per day by 0.40, compared with placebo. Lastly, the mean volume per void increased by 11.9 mL with the drug, compared with placebo.
Committee members expressed some concern about increases in both blood pressure and pulse rate associated with the drug. There was also an increased incidence of urologic adverse events, particularly urinary tract infections of mild severity. The committee members were particularly concerned about an increased incidence of neoplasm serious adverse events – new malignant events – in the group on 100 mg mirabegron in the 1-year study, as well as hepatotoxicity events and hypersensitivity reactions. However, they noted that there was insufficient data to draw firm conclusions about these serious adverse events.
SILVER SPRING, MD. – Physicians may soon have a first-in-class alternative to current treatments for overactive bladder, which may not always work and can have unpleasant side effects.
A Food and Drug Administration panel on April 5 voted 7-4 with 1 abstention that the overall benefit-risk assessment supports the approval of mirabegron for the treatment of overactive bladder.
Pharmacologic treatment options to date include muscarinic receptor antagonists, which can affect the salivary glands, intestines, and eyes, resulting in side effects such as dry mouth, constipation, and blurred vision, respectively.
Mirabegron is a first-in-class agonist of beta 3-adrenoceptors. Astellas Pharma developed the drug for the treatment of overactive bladder with symptoms of urge urinary incontinence, urgency, and urinary frequency. In the United States, the proposed dose is 50 mg once daily with or without food. However, a dose of 25 mg is reserved for patients with severe renal or moderate hepatic impairment. The formulation is an oral controlled-absorption system (extended-release) tablets. The drug is already approved in Japan.
"The committee has a sense that there is marginal efficacy, but overall the majority feels that the benefits outweigh the risks. This is seen as a new agent, which can potentially be used for individuals who have not had success with other available agents," summarized Dr. Julia V. Johnson, who is the chair of the advisory committee for reproductive health drugs. "With some caution and with some reservation the overall approval of the medication comes from this committee."
The committee also voted 8-4 that the data do provide substantial evidence of benefit for mirabegron in the treatment of overactive bladder. However, many members agreed that there was statistically-significant improvement in symptoms but questioned whether this would translate to a meaningful clinical difference.
The committee also voted 9-3 that adequate safety had been demonstrated for the drug. Committee members did express reservations about the paucity of data with regard to neoplasms, hepatotoxicity events, and hypersensitivity reactions.
The primary sources of data for the evaluation are three randomized placebo-controlled phase III trials. Supportive data included data from a single long-term (active-controlled) study, three phase II studies, and a phase II study in patients with symptomatic benign prostatic hyperplasia.
The three phase III trials lasted for 12 weeks with individuals randomized to receive mirabegron either 25 mg daily, or 50 mg daily, or placebo. Coprimary end points included change from baseline in the average number of micturitions in 24 hours and the change from baseline in the average number of incontinence episodes in 24 hours.
Mirabegron at a dose of 50 mg achieved the primary efficacy objectives in three phase III studies. Treatment with 50 mg mirabegron reduced the mean number of micturitions by 0.55/day, compared with placebo. Likewise, mirabegron reduced the mean number of incontinence episodes per day by 0.40, compared with placebo. Lastly, the mean volume per void increased by 11.9 mL with the drug, compared with placebo.
Committee members expressed some concern about increases in both blood pressure and pulse rate associated with the drug. There was also an increased incidence of urologic adverse events, particularly urinary tract infections of mild severity. The committee members were particularly concerned about an increased incidence of neoplasm serious adverse events – new malignant events – in the group on 100 mg mirabegron in the 1-year study, as well as hepatotoxicity events and hypersensitivity reactions. However, they noted that there was insufficient data to draw firm conclusions about these serious adverse events.
FROM A MEETING OF THE FDA'S REPRODUCTIVE HEALTH DRUGS ADVISORY COMMITTEE
IOM Report on Epilepsy Supports Comprehensive Approach
A new report released by the Institute of Medicine offers a unified public health plan for the epilepsies that focuses on public health surveillance and data collection, population and public health research, health policy and human services, and education.
Epilepsy represents "a complicated spectrum ... it impacts children but it also is growing very rapidly in senior citizens ... we have solutions and we need to come together as public and private communities to work with people with epilepsy, their families and their communities to make this report a reality," study chair Dr. Mary Jane England said at a press event.
The report, "Epilepsy Across the Spectrum: Promoting Health and Understanding," was released March 30.
"Our study sponsors are probably the most exciting part. The public and private sectors came together to ask the IOM [Institute of Medicine] to do this," Dr. England said. In all, 24 federal agencies and nonprofit organizations asked the IOM to examine the public health dimensions of the epilepsies. The study was sponsored by the U.S. Department of Health and Human Services and members of the Vision 20-20 collaborative, including the American Epilepsy Society (AES), Citizens United for Research in Epilepsy, the Epilepsy Foundation, and others.
"The focus that we’ve taken the most is that epilepsy is a spectrum of disorders; it’s not just one thing. There are many different types of seizures. There are many causes of seizures. So there are many syndromes and types of epilepsy," said Dr. England, who is also visiting professor of health policy and management at Boston University.
The study committee identified several cross-cutting themes during the development of this report: epilepsy is a common and complex neurologic disorder that often affects quality of life, a whole-patient perspective is needed, effective treatments are available but access falls far short, data are needed to improve epilepsy knowledge and care and to inform policy, and there is a need to strengthen health professionals’ education, as well as bolster education efforts for people with epilepsy and their families. Lastly, though equally important, the committee cited the need to eliminate the stigma associated with epilepsy.
In the resulting report, the committee highlighted gaps in the knowledge and management of epilepsy, and made 13 recommendations:
• Validation and implementation of standard definitions and criteria for epilepsy case ascertainment, health care and community services use and costs, and quality measurement.
• Continuation and expansion of collaborative surveillance efforts.
• Development and evaluation of prevention efforts for epilepsy and its consequences.
• Improvement in the early identification of epilepsy and its comorbid health conditions.
• Development and implementation of a national quality measurement and improvement strategy for epilepsy care.
• Establishment of epilepsy center accreditation and an Epilepsy Care Network.
• Improvement in health professionals’ education about the epilepsies.
• Improvement in the delivery and coordination of community services.
• Improvement in and expansion of educational opportunities for patients and families.
• Provision of information to media to improve awareness and eliminate stigma.
• Coordination of public awareness efforts.
• Continuation and expansion of Vision 20-20 working groups and collaborative partnerships.
• Engagement of people with epilepsy and their families in education, dissemination, and advocacy for improved epilepsy care and services.
The third recommendation focusing on developing and evaluating prevention efforts for epilepsy and its consequences – is of particular interest to both neurologic researchers and clinicians. The committee suggested that the Centers for Disease Control and Prevention partner with other stakeholders to develop and evaluate prevention efforts that focus on: preventing neurocysticercosis in high-risk populations; continuing prevention efforts for established risk factors of epilepsy (for example, traumatic brain injury, stroke, brain infections such as meningitis); preventing continued seizures in people with epilepsy and depression; reducing felt stigma; and preventing epilepsy-related causes of death, including accidents and injuries and suicide.
The fourth recommendation emphasizing the improvement of early identification of epilepsy and its comorbid health conditions also is relevant for clinicians. The committee recommends that the AES and American Academy of Neurology lead a collaborative effort with the wide range of relevant federal agencies and professional organizations to develop and validate screening tests for early identification of epilepsy in at-risk populations, establish and disseminate a standard screening protocol for comorbidities with currently approved screening tests, and establish and disseminate a screening tool for early identification of patients with persistent seizures to lead to earlier referrals to an epileptologist.
For more information, contact [email protected]. For free pdfs of the report, go to iom.edu/epilepsy.
The recent
release of the Institute
of Medicine’s report
“Epilepsy Across the Spectrum: Promoting Health and Understanding” provides a
broad view of gaps in epilepsy diagnosis, treatment, and professional and
public education about this spectrum of disorders.
Dr. Joseph F. Drazkowski |

The report provides a
glimpse of where the epilepsy community needs to be in the future. I’m not sure
that all of the recommendations are attainable in the immediate short term, but
I do think that the report has laudable goals as epilepsy is sure to become an
increasingly important health issue. It’s well known in the epilepsy world that
the elderly are disproportionately represented. As the population in the United States
ages and the number of baby boomers expands, they will require more care and
epilepsy services, not less. This tells me that the estimates in the report of
how many people have or will have epilepsy may be low. Certainly, if it’s not an
underestimate at this time, that number is certainly going to rise as the baby boomers
age.
Currently and
historically, there are certain images that are brought forth when you make the
diagnosis of epilepsy. There are all kinds of misconceptions about the
terminology. I think that standardizing the terminology used to discuss
epilepsy – as recommended in the report – will go a long way toward improving
understanding in providers, families, and persons with epilepsy.
While the committee
recommends looking at the prevention of epilepsy, I think that we have a long
way to go with regard to prevention. There are many modes of prevention.
Preventing injuries in high-impact sports such as football or motor sports is
one way of preventing epilepsy. However, prevention could take place in other
contexts after focused research. If two people present with seizure behavior,
we need to understand more fully why one person progresses to epilepsy and the
next person does not. If we can discern some of those factors, which I don’t
think are very well known at this time, we could prevent the development of
chronic seizures or epilepsy. We’re in our infancy in regard to that.
The report also
recommended epilepsy education for health professionals. Epilepsy is one of the
primary reasons for seeing a neurologist, but for the primary care provider or
other specialists, the number of people with epilepsy in their practice is
likely minimal. Most physicians can potentially manage a well-controlled
epilepsy patient, who is doing well taking a single medication and not having
any problems. However, in cases in which epilepsy is suspected but yet undiagnosed
or there’s intractability of seizures, a focused subspecialty evaluation should
be considered. This group may represent a significant portion of people with
epilepsy. No one would expect the family practitioner or the internist to care
for these complex individuals with medically refractory epilepsy who are taking
multiple medications, experiencing complex social challenges, or requiring a
surgical evaluation.
The committee also
emphasized and advocated for removing the considerable stigma associated with epilepsy
and raising public awareness of this spectrum of disorders. Right now, epilepsy
doesn’t seem have a champion for the disorder who has the cache to help raise
public awareness. The IOM report points out this often overlooked aspect of the
illness. Succeeding in the recommendation alone will go a long way to improving
the lives of people with epilepsy.
Dr. Joseph F. Drazkowski is with the department of
neurology at the Mayo Clinic, Scottsdale,
Ariz. He is the program director of
the Mayo’s fellowship in clinical neurophysiology, EEG, and epilepsy. He also
directs the EEG laboratory and codirects the epilepsy monitoring unit at the
Mayo Clinic Arizona.
His research interests have been focused primarily on social issues that
confront patients with epilepsy (especially driving and quality of life).
The recent
release of the Institute
of Medicine’s report
“Epilepsy Across the Spectrum: Promoting Health and Understanding” provides a
broad view of gaps in epilepsy diagnosis, treatment, and professional and
public education about this spectrum of disorders.
Dr. Joseph F. Drazkowski |
The report provides a
glimpse of where the epilepsy community needs to be in the future. I’m not sure
that all of the recommendations are attainable in the immediate short term, but
I do think that the report has laudable goals as epilepsy is sure to become an
increasingly important health issue. It’s well known in the epilepsy world that
the elderly are disproportionately represented. As the population in the United States
ages and the number of baby boomers expands, they will require more care and
epilepsy services, not less. This tells me that the estimates in the report of
how many people have or will have epilepsy may be low. Certainly, if it’s not an
underestimate at this time, that number is certainly going to rise as the baby boomers
age.
Currently and
historically, there are certain images that are brought forth when you make the
diagnosis of epilepsy. There are all kinds of misconceptions about the
terminology. I think that standardizing the terminology used to discuss
epilepsy – as recommended in the report – will go a long way toward improving
understanding in providers, families, and persons with epilepsy.
While the committee
recommends looking at the prevention of epilepsy, I think that we have a long
way to go with regard to prevention. There are many modes of prevention.
Preventing injuries in high-impact sports such as football or motor sports is
one way of preventing epilepsy. However, prevention could take place in other
contexts after focused research. If two people present with seizure behavior,
we need to understand more fully why one person progresses to epilepsy and the
next person does not. If we can discern some of those factors, which I don’t
think are very well known at this time, we could prevent the development of
chronic seizures or epilepsy. We’re in our infancy in regard to that.
The report also
recommended epilepsy education for health professionals. Epilepsy is one of the
primary reasons for seeing a neurologist, but for the primary care provider or
other specialists, the number of people with epilepsy in their practice is
likely minimal. Most physicians can potentially manage a well-controlled
epilepsy patient, who is doing well taking a single medication and not having
any problems. However, in cases in which epilepsy is suspected but yet undiagnosed
or there’s intractability of seizures, a focused subspecialty evaluation should
be considered. This group may represent a significant portion of people with
epilepsy. No one would expect the family practitioner or the internist to care
for these complex individuals with medically refractory epilepsy who are taking
multiple medications, experiencing complex social challenges, or requiring a
surgical evaluation.
The committee also
emphasized and advocated for removing the considerable stigma associated with epilepsy
and raising public awareness of this spectrum of disorders. Right now, epilepsy
doesn’t seem have a champion for the disorder who has the cache to help raise
public awareness. The IOM report points out this often overlooked aspect of the
illness. Succeeding in the recommendation alone will go a long way to improving
the lives of people with epilepsy.
Dr. Joseph F. Drazkowski is with the department of
neurology at the Mayo Clinic, Scottsdale,
Ariz. He is the program director of
the Mayo’s fellowship in clinical neurophysiology, EEG, and epilepsy. He also
directs the EEG laboratory and codirects the epilepsy monitoring unit at the
Mayo Clinic Arizona.
His research interests have been focused primarily on social issues that
confront patients with epilepsy (especially driving and quality of life).
The recent
release of the Institute
of Medicine’s report
“Epilepsy Across the Spectrum: Promoting Health and Understanding” provides a
broad view of gaps in epilepsy diagnosis, treatment, and professional and
public education about this spectrum of disorders.
Dr. Joseph F. Drazkowski |
The report provides a
glimpse of where the epilepsy community needs to be in the future. I’m not sure
that all of the recommendations are attainable in the immediate short term, but
I do think that the report has laudable goals as epilepsy is sure to become an
increasingly important health issue. It’s well known in the epilepsy world that
the elderly are disproportionately represented. As the population in the United States
ages and the number of baby boomers expands, they will require more care and
epilepsy services, not less. This tells me that the estimates in the report of
how many people have or will have epilepsy may be low. Certainly, if it’s not an
underestimate at this time, that number is certainly going to rise as the baby boomers
age.
Currently and
historically, there are certain images that are brought forth when you make the
diagnosis of epilepsy. There are all kinds of misconceptions about the
terminology. I think that standardizing the terminology used to discuss
epilepsy – as recommended in the report – will go a long way toward improving
understanding in providers, families, and persons with epilepsy.
While the committee
recommends looking at the prevention of epilepsy, I think that we have a long
way to go with regard to prevention. There are many modes of prevention.
Preventing injuries in high-impact sports such as football or motor sports is
one way of preventing epilepsy. However, prevention could take place in other
contexts after focused research. If two people present with seizure behavior,
we need to understand more fully why one person progresses to epilepsy and the
next person does not. If we can discern some of those factors, which I don’t
think are very well known at this time, we could prevent the development of
chronic seizures or epilepsy. We’re in our infancy in regard to that.
The report also
recommended epilepsy education for health professionals. Epilepsy is one of the
primary reasons for seeing a neurologist, but for the primary care provider or
other specialists, the number of people with epilepsy in their practice is
likely minimal. Most physicians can potentially manage a well-controlled
epilepsy patient, who is doing well taking a single medication and not having
any problems. However, in cases in which epilepsy is suspected but yet undiagnosed
or there’s intractability of seizures, a focused subspecialty evaluation should
be considered. This group may represent a significant portion of people with
epilepsy. No one would expect the family practitioner or the internist to care
for these complex individuals with medically refractory epilepsy who are taking
multiple medications, experiencing complex social challenges, or requiring a
surgical evaluation.
The committee also
emphasized and advocated for removing the considerable stigma associated with epilepsy
and raising public awareness of this spectrum of disorders. Right now, epilepsy
doesn’t seem have a champion for the disorder who has the cache to help raise
public awareness. The IOM report points out this often overlooked aspect of the
illness. Succeeding in the recommendation alone will go a long way to improving
the lives of people with epilepsy.
Dr. Joseph F. Drazkowski is with the department of
neurology at the Mayo Clinic, Scottsdale,
Ariz. He is the program director of
the Mayo’s fellowship in clinical neurophysiology, EEG, and epilepsy. He also
directs the EEG laboratory and codirects the epilepsy monitoring unit at the
Mayo Clinic Arizona.
His research interests have been focused primarily on social issues that
confront patients with epilepsy (especially driving and quality of life).
A new report released by the Institute of Medicine offers a unified public health plan for the epilepsies that focuses on public health surveillance and data collection, population and public health research, health policy and human services, and education.
Epilepsy represents "a complicated spectrum ... it impacts children but it also is growing very rapidly in senior citizens ... we have solutions and we need to come together as public and private communities to work with people with epilepsy, their families and their communities to make this report a reality," study chair Dr. Mary Jane England said at a press event.
The report, "Epilepsy Across the Spectrum: Promoting Health and Understanding," was released March 30.
"Our study sponsors are probably the most exciting part. The public and private sectors came together to ask the IOM [Institute of Medicine] to do this," Dr. England said. In all, 24 federal agencies and nonprofit organizations asked the IOM to examine the public health dimensions of the epilepsies. The study was sponsored by the U.S. Department of Health and Human Services and members of the Vision 20-20 collaborative, including the American Epilepsy Society (AES), Citizens United for Research in Epilepsy, the Epilepsy Foundation, and others.
"The focus that we’ve taken the most is that epilepsy is a spectrum of disorders; it’s not just one thing. There are many different types of seizures. There are many causes of seizures. So there are many syndromes and types of epilepsy," said Dr. England, who is also visiting professor of health policy and management at Boston University.
The study committee identified several cross-cutting themes during the development of this report: epilepsy is a common and complex neurologic disorder that often affects quality of life, a whole-patient perspective is needed, effective treatments are available but access falls far short, data are needed to improve epilepsy knowledge and care and to inform policy, and there is a need to strengthen health professionals’ education, as well as bolster education efforts for people with epilepsy and their families. Lastly, though equally important, the committee cited the need to eliminate the stigma associated with epilepsy.
In the resulting report, the committee highlighted gaps in the knowledge and management of epilepsy, and made 13 recommendations:
• Validation and implementation of standard definitions and criteria for epilepsy case ascertainment, health care and community services use and costs, and quality measurement.
• Continuation and expansion of collaborative surveillance efforts.
• Development and evaluation of prevention efforts for epilepsy and its consequences.
• Improvement in the early identification of epilepsy and its comorbid health conditions.
• Development and implementation of a national quality measurement and improvement strategy for epilepsy care.
• Establishment of epilepsy center accreditation and an Epilepsy Care Network.
• Improvement in health professionals’ education about the epilepsies.
• Improvement in the delivery and coordination of community services.
• Improvement in and expansion of educational opportunities for patients and families.
• Provision of information to media to improve awareness and eliminate stigma.
• Coordination of public awareness efforts.
• Continuation and expansion of Vision 20-20 working groups and collaborative partnerships.
• Engagement of people with epilepsy and their families in education, dissemination, and advocacy for improved epilepsy care and services.
The third recommendation focusing on developing and evaluating prevention efforts for epilepsy and its consequences – is of particular interest to both neurologic researchers and clinicians. The committee suggested that the Centers for Disease Control and Prevention partner with other stakeholders to develop and evaluate prevention efforts that focus on: preventing neurocysticercosis in high-risk populations; continuing prevention efforts for established risk factors of epilepsy (for example, traumatic brain injury, stroke, brain infections such as meningitis); preventing continued seizures in people with epilepsy and depression; reducing felt stigma; and preventing epilepsy-related causes of death, including accidents and injuries and suicide.
The fourth recommendation emphasizing the improvement of early identification of epilepsy and its comorbid health conditions also is relevant for clinicians. The committee recommends that the AES and American Academy of Neurology lead a collaborative effort with the wide range of relevant federal agencies and professional organizations to develop and validate screening tests for early identification of epilepsy in at-risk populations, establish and disseminate a standard screening protocol for comorbidities with currently approved screening tests, and establish and disseminate a screening tool for early identification of patients with persistent seizures to lead to earlier referrals to an epileptologist.
For more information, contact [email protected]. For free pdfs of the report, go to iom.edu/epilepsy.
A new report released by the Institute of Medicine offers a unified public health plan for the epilepsies that focuses on public health surveillance and data collection, population and public health research, health policy and human services, and education.
Epilepsy represents "a complicated spectrum ... it impacts children but it also is growing very rapidly in senior citizens ... we have solutions and we need to come together as public and private communities to work with people with epilepsy, their families and their communities to make this report a reality," study chair Dr. Mary Jane England said at a press event.
The report, "Epilepsy Across the Spectrum: Promoting Health and Understanding," was released March 30.
"Our study sponsors are probably the most exciting part. The public and private sectors came together to ask the IOM [Institute of Medicine] to do this," Dr. England said. In all, 24 federal agencies and nonprofit organizations asked the IOM to examine the public health dimensions of the epilepsies. The study was sponsored by the U.S. Department of Health and Human Services and members of the Vision 20-20 collaborative, including the American Epilepsy Society (AES), Citizens United for Research in Epilepsy, the Epilepsy Foundation, and others.
"The focus that we’ve taken the most is that epilepsy is a spectrum of disorders; it’s not just one thing. There are many different types of seizures. There are many causes of seizures. So there are many syndromes and types of epilepsy," said Dr. England, who is also visiting professor of health policy and management at Boston University.
The study committee identified several cross-cutting themes during the development of this report: epilepsy is a common and complex neurologic disorder that often affects quality of life, a whole-patient perspective is needed, effective treatments are available but access falls far short, data are needed to improve epilepsy knowledge and care and to inform policy, and there is a need to strengthen health professionals’ education, as well as bolster education efforts for people with epilepsy and their families. Lastly, though equally important, the committee cited the need to eliminate the stigma associated with epilepsy.
In the resulting report, the committee highlighted gaps in the knowledge and management of epilepsy, and made 13 recommendations:
• Validation and implementation of standard definitions and criteria for epilepsy case ascertainment, health care and community services use and costs, and quality measurement.
• Continuation and expansion of collaborative surveillance efforts.
• Development and evaluation of prevention efforts for epilepsy and its consequences.
• Improvement in the early identification of epilepsy and its comorbid health conditions.
• Development and implementation of a national quality measurement and improvement strategy for epilepsy care.
• Establishment of epilepsy center accreditation and an Epilepsy Care Network.
• Improvement in health professionals’ education about the epilepsies.
• Improvement in the delivery and coordination of community services.
• Improvement in and expansion of educational opportunities for patients and families.
• Provision of information to media to improve awareness and eliminate stigma.
• Coordination of public awareness efforts.
• Continuation and expansion of Vision 20-20 working groups and collaborative partnerships.
• Engagement of people with epilepsy and their families in education, dissemination, and advocacy for improved epilepsy care and services.
The third recommendation focusing on developing and evaluating prevention efforts for epilepsy and its consequences – is of particular interest to both neurologic researchers and clinicians. The committee suggested that the Centers for Disease Control and Prevention partner with other stakeholders to develop and evaluate prevention efforts that focus on: preventing neurocysticercosis in high-risk populations; continuing prevention efforts for established risk factors of epilepsy (for example, traumatic brain injury, stroke, brain infections such as meningitis); preventing continued seizures in people with epilepsy and depression; reducing felt stigma; and preventing epilepsy-related causes of death, including accidents and injuries and suicide.
The fourth recommendation emphasizing the improvement of early identification of epilepsy and its comorbid health conditions also is relevant for clinicians. The committee recommends that the AES and American Academy of Neurology lead a collaborative effort with the wide range of relevant federal agencies and professional organizations to develop and validate screening tests for early identification of epilepsy in at-risk populations, establish and disseminate a standard screening protocol for comorbidities with currently approved screening tests, and establish and disseminate a screening tool for early identification of patients with persistent seizures to lead to earlier referrals to an epileptologist.
For more information, contact [email protected]. For free pdfs of the report, go to iom.edu/epilepsy.
Investigational Psoriasis Drug Reduces Vessel Inflammation
SAN DIEGO – An investigational first-in-class drug not only improved plaque psoriasis but reduced atherosclerotic inflammation in major vessels, a study has shown.
At 12 weeks there was a dose-related response in inflammation in the most-diseased vessels. Those in the placebo group had a 4% decrease in the target-to-baseline ratio (a validated PET/CT measure of changes in vessel inflammation), while those on 20 mg and 80 mg of VB-201 had decreases of 7% and 13%.

"As we look at our patients with psoriasis, where cardiovascular risk factors are a huge public health problem, this type of approach may have multiple benefits for them," said Dr. Alexa B. Kimball, who presented the results at the annual meeting of the American Academy of Dermatology.
The results come from a phase II trial of 184 patients with moderate to severe plaque psoriasis and a PET/CT substudy of 47 patients with cardiovascular risk factors. The patients in the double-blind, randomized, placebo-controlled study received either 20 or 80 mg of VB-201 or placebo once daily for 12 weeks.
VB-201, a phospholipid analogue, is being developed by VBL Therapeutics as an oral disease-modifying agent for chronic immunoinflammatory disease and atherosclerosis inflammation, and is the first in the lecinoxoid molecular class.
The compound’s novel mechanism of action for the control and attenuation of chronic immunoinflammatory diseases is thought to be through the highly selective modulation of components of the innate immune system. The drug is proposed to work by inhibiting cell-surface toll-like receptor signal cascade. "It’s mimicking some of the native molecules, but this turns out to be specific to antigen-presenting cells, endothelial cells, and monocytes," said Dr. Kimball. Thus, chemokine-mediated migration of monocytes to inflamed tissue is limited.
In the subanalysis, patients had to have a target-to-baseline ratio on PET/CT scan that was greater than 1.6 in order to be eligible.
PET/CT was used to evaluate inflammation in the vessels over time. The primary endpoint in this substudy included the mean of the maximum values of the target-to-baseline ratio in the most-diseased segment of vessel. The secondary endpoint involved looking at all of the inflammation in the vessels to determine a mean value for the vessels in a given patient; these mean values were then used to calculate an overall mean value of inflammation.
"One of the challenges in cardiovascular studies looking at atherosclerotic disease is that the endpoint that you’re most interested in is actually myocardial infarction, typically," said Dr. Kimball. "This form of PET/CT has been shown to be a pretty sensitive measure for inflammation in these vessels and is being used in investigational settings to be a surrogate marker for risk."
In addition, the technique correlates well with histopathologic inflammation and with cardiovascular risk factors. "It also seems to be predictive of future clinical vascular events," she said. High-fluorine-18fluorodeoxyglucose uptake appears to correlate with future vascular events.
"We did enhance the substudy with patients with additional cardiovascular risk factors to make sure that we had a population at risk where we actually could see inflammation to begin with," she said.
In the substudy, 13 patients were on placebo, 18 were on 20 mg VB-201, and 16 were taking 80 mg VB-201. These patients were a little older and had such risk factors as vascular disease dyslipidemia, diabetes, and obesity. Many were on statins.
At 12 weeks, there was a dose-related response in inflammation in the most-diseased vessel. Those in the placebo group had a 4% decrease in target-to-baseline ratio, while those on 20 mg and 80 mg of VB-201 had decreases of 7% and 13%.
"To put that into context with high-dose statin therapy, we would typically see these types of responses in the 7%-10% reduction range usually over 6 months rather than just 3 months," said Dr. Kimball of the dermatology department at Massachusetts General Hospital in Boston.
In the main study, the researchers looked at the effects of the drug on plaque psoriasis, compared with placebo. The primary endpoint was a Psoriasis Area and Severity Index (PASI) score of 75.
The 184 patients were randomized to receive 20 mg VB-201 (66), 80 mg VB-201 (59), or placebo (59). The study cohort was primarily composed of overweight men (BMI approximately 30 kg/m2) with an average age of 45 years. Overall, the group had a baseline PASI score close to 20.
Statistically significant improvements were achieved on the Physician Global Assessment and Patient Global Assessment. In terms of PASI 75, "there was a dose response as well," said Dr. Kimball. "This is not a drug that is achieving high levels of PASI 90 or PASI 100 ... but there is some benefit."
"This drug is moving people from substantial severity to reduced severity ... It may not be a drug that clears psoriasis to zero, but you can move patients out of the severe category," she said.
"VBL-201 is thought to be – at least in these initial studies – quite well tolerated. ... The study met its primary endpoint in the PET-CT substudy, demonstrating a statistically significant reduction in vascular inflammation," Dr. Kimball noted. "Importantly, these reductions occurred also in patients who were on statin therapy."
There were no treatment-related serious adverse events; the overall rates of adverse events were similar for both doses of VB-201 drug and placebo.
The study was funded by VBL Pharmaceuticals. Dr. Kimball is a consultant for VBL and several other pharmaceutical companies.
SAN DIEGO – An investigational first-in-class drug not only improved plaque psoriasis but reduced atherosclerotic inflammation in major vessels, a study has shown.
At 12 weeks there was a dose-related response in inflammation in the most-diseased vessels. Those in the placebo group had a 4% decrease in the target-to-baseline ratio (a validated PET/CT measure of changes in vessel inflammation), while those on 20 mg and 80 mg of VB-201 had decreases of 7% and 13%.
"As we look at our patients with psoriasis, where cardiovascular risk factors are a huge public health problem, this type of approach may have multiple benefits for them," said Dr. Alexa B. Kimball, who presented the results at the annual meeting of the American Academy of Dermatology.
The results come from a phase II trial of 184 patients with moderate to severe plaque psoriasis and a PET/CT substudy of 47 patients with cardiovascular risk factors. The patients in the double-blind, randomized, placebo-controlled study received either 20 or 80 mg of VB-201 or placebo once daily for 12 weeks.
VB-201, a phospholipid analogue, is being developed by VBL Therapeutics as an oral disease-modifying agent for chronic immunoinflammatory disease and atherosclerosis inflammation, and is the first in the lecinoxoid molecular class.
The compound’s novel mechanism of action for the control and attenuation of chronic immunoinflammatory diseases is thought to be through the highly selective modulation of components of the innate immune system. The drug is proposed to work by inhibiting cell-surface toll-like receptor signal cascade. "It’s mimicking some of the native molecules, but this turns out to be specific to antigen-presenting cells, endothelial cells, and monocytes," said Dr. Kimball. Thus, chemokine-mediated migration of monocytes to inflamed tissue is limited.
In the subanalysis, patients had to have a target-to-baseline ratio on PET/CT scan that was greater than 1.6 in order to be eligible.
PET/CT was used to evaluate inflammation in the vessels over time. The primary endpoint in this substudy included the mean of the maximum values of the target-to-baseline ratio in the most-diseased segment of vessel. The secondary endpoint involved looking at all of the inflammation in the vessels to determine a mean value for the vessels in a given patient; these mean values were then used to calculate an overall mean value of inflammation.
"One of the challenges in cardiovascular studies looking at atherosclerotic disease is that the endpoint that you’re most interested in is actually myocardial infarction, typically," said Dr. Kimball. "This form of PET/CT has been shown to be a pretty sensitive measure for inflammation in these vessels and is being used in investigational settings to be a surrogate marker for risk."
In addition, the technique correlates well with histopathologic inflammation and with cardiovascular risk factors. "It also seems to be predictive of future clinical vascular events," she said. High-fluorine-18fluorodeoxyglucose uptake appears to correlate with future vascular events.
"We did enhance the substudy with patients with additional cardiovascular risk factors to make sure that we had a population at risk where we actually could see inflammation to begin with," she said.
In the substudy, 13 patients were on placebo, 18 were on 20 mg VB-201, and 16 were taking 80 mg VB-201. These patients were a little older and had such risk factors as vascular disease dyslipidemia, diabetes, and obesity. Many were on statins.
At 12 weeks, there was a dose-related response in inflammation in the most-diseased vessel. Those in the placebo group had a 4% decrease in target-to-baseline ratio, while those on 20 mg and 80 mg of VB-201 had decreases of 7% and 13%.
"To put that into context with high-dose statin therapy, we would typically see these types of responses in the 7%-10% reduction range usually over 6 months rather than just 3 months," said Dr. Kimball of the dermatology department at Massachusetts General Hospital in Boston.
In the main study, the researchers looked at the effects of the drug on plaque psoriasis, compared with placebo. The primary endpoint was a Psoriasis Area and Severity Index (PASI) score of 75.
The 184 patients were randomized to receive 20 mg VB-201 (66), 80 mg VB-201 (59), or placebo (59). The study cohort was primarily composed of overweight men (BMI approximately 30 kg/m2) with an average age of 45 years. Overall, the group had a baseline PASI score close to 20.
Statistically significant improvements were achieved on the Physician Global Assessment and Patient Global Assessment. In terms of PASI 75, "there was a dose response as well," said Dr. Kimball. "This is not a drug that is achieving high levels of PASI 90 or PASI 100 ... but there is some benefit."
"This drug is moving people from substantial severity to reduced severity ... It may not be a drug that clears psoriasis to zero, but you can move patients out of the severe category," she said.
"VBL-201 is thought to be – at least in these initial studies – quite well tolerated. ... The study met its primary endpoint in the PET-CT substudy, demonstrating a statistically significant reduction in vascular inflammation," Dr. Kimball noted. "Importantly, these reductions occurred also in patients who were on statin therapy."
There were no treatment-related serious adverse events; the overall rates of adverse events were similar for both doses of VB-201 drug and placebo.
The study was funded by VBL Pharmaceuticals. Dr. Kimball is a consultant for VBL and several other pharmaceutical companies.
SAN DIEGO – An investigational first-in-class drug not only improved plaque psoriasis but reduced atherosclerotic inflammation in major vessels, a study has shown.
At 12 weeks there was a dose-related response in inflammation in the most-diseased vessels. Those in the placebo group had a 4% decrease in the target-to-baseline ratio (a validated PET/CT measure of changes in vessel inflammation), while those on 20 mg and 80 mg of VB-201 had decreases of 7% and 13%.
"As we look at our patients with psoriasis, where cardiovascular risk factors are a huge public health problem, this type of approach may have multiple benefits for them," said Dr. Alexa B. Kimball, who presented the results at the annual meeting of the American Academy of Dermatology.
The results come from a phase II trial of 184 patients with moderate to severe plaque psoriasis and a PET/CT substudy of 47 patients with cardiovascular risk factors. The patients in the double-blind, randomized, placebo-controlled study received either 20 or 80 mg of VB-201 or placebo once daily for 12 weeks.
VB-201, a phospholipid analogue, is being developed by VBL Therapeutics as an oral disease-modifying agent for chronic immunoinflammatory disease and atherosclerosis inflammation, and is the first in the lecinoxoid molecular class.
The compound’s novel mechanism of action for the control and attenuation of chronic immunoinflammatory diseases is thought to be through the highly selective modulation of components of the innate immune system. The drug is proposed to work by inhibiting cell-surface toll-like receptor signal cascade. "It’s mimicking some of the native molecules, but this turns out to be specific to antigen-presenting cells, endothelial cells, and monocytes," said Dr. Kimball. Thus, chemokine-mediated migration of monocytes to inflamed tissue is limited.
In the subanalysis, patients had to have a target-to-baseline ratio on PET/CT scan that was greater than 1.6 in order to be eligible.
PET/CT was used to evaluate inflammation in the vessels over time. The primary endpoint in this substudy included the mean of the maximum values of the target-to-baseline ratio in the most-diseased segment of vessel. The secondary endpoint involved looking at all of the inflammation in the vessels to determine a mean value for the vessels in a given patient; these mean values were then used to calculate an overall mean value of inflammation.
"One of the challenges in cardiovascular studies looking at atherosclerotic disease is that the endpoint that you’re most interested in is actually myocardial infarction, typically," said Dr. Kimball. "This form of PET/CT has been shown to be a pretty sensitive measure for inflammation in these vessels and is being used in investigational settings to be a surrogate marker for risk."
In addition, the technique correlates well with histopathologic inflammation and with cardiovascular risk factors. "It also seems to be predictive of future clinical vascular events," she said. High-fluorine-18fluorodeoxyglucose uptake appears to correlate with future vascular events.
"We did enhance the substudy with patients with additional cardiovascular risk factors to make sure that we had a population at risk where we actually could see inflammation to begin with," she said.
In the substudy, 13 patients were on placebo, 18 were on 20 mg VB-201, and 16 were taking 80 mg VB-201. These patients were a little older and had such risk factors as vascular disease dyslipidemia, diabetes, and obesity. Many were on statins.
At 12 weeks, there was a dose-related response in inflammation in the most-diseased vessel. Those in the placebo group had a 4% decrease in target-to-baseline ratio, while those on 20 mg and 80 mg of VB-201 had decreases of 7% and 13%.
"To put that into context with high-dose statin therapy, we would typically see these types of responses in the 7%-10% reduction range usually over 6 months rather than just 3 months," said Dr. Kimball of the dermatology department at Massachusetts General Hospital in Boston.
In the main study, the researchers looked at the effects of the drug on plaque psoriasis, compared with placebo. The primary endpoint was a Psoriasis Area and Severity Index (PASI) score of 75.
The 184 patients were randomized to receive 20 mg VB-201 (66), 80 mg VB-201 (59), or placebo (59). The study cohort was primarily composed of overweight men (BMI approximately 30 kg/m2) with an average age of 45 years. Overall, the group had a baseline PASI score close to 20.
Statistically significant improvements were achieved on the Physician Global Assessment and Patient Global Assessment. In terms of PASI 75, "there was a dose response as well," said Dr. Kimball. "This is not a drug that is achieving high levels of PASI 90 or PASI 100 ... but there is some benefit."
"This drug is moving people from substantial severity to reduced severity ... It may not be a drug that clears psoriasis to zero, but you can move patients out of the severe category," she said.
"VBL-201 is thought to be – at least in these initial studies – quite well tolerated. ... The study met its primary endpoint in the PET-CT substudy, demonstrating a statistically significant reduction in vascular inflammation," Dr. Kimball noted. "Importantly, these reductions occurred also in patients who were on statin therapy."
There were no treatment-related serious adverse events; the overall rates of adverse events were similar for both doses of VB-201 drug and placebo.
The study was funded by VBL Pharmaceuticals. Dr. Kimball is a consultant for VBL and several other pharmaceutical companies.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF DERMATOLOGY
Major Finding: At 12 weeks there was a dose-related response in inflammation in the most-diseased vessels of patients with plaque psoriasis and cardiovascular risk factors: Those in the placebo group had a 4% decrease, while those on 20 mg and 80 mg of VB-201 had decreases of 7% and 13%.
Data Source: The phase II, double-blind, randomized placebo-controlled study enrolled 184 patients with moderate to severe psoriasis; a PET/CT substudy was done of 47 patients with cardiovascular risk factors.
Disclosures: The study was funded by VBL Pharmaceuticals. Dr. Kimball is a consultant for VBL and several other pharmaceutical companies.
Investigational Herpes Drug May Offer Alternative to Valacyclovir
Healing times for recurrences of herpes simplex virus 2 (HSV-2) for patients treated with ASP2151 were significantly better than placebo and were comparable to valacyclovir, based on the results of a phase-II randomized, double-blind study of 437 patients. The results were presented at the annual meeting of the American Academy of Dermatology.
The United States seroprevalence of HSV-2 is 16% among people aged 14-49 years. "Unlike other sexually-transmitted diseases that affect persons with a high level of sexual activity, HSV-2 affects even those with moderate-to-low sexual activity. It’s estimated that 18% of American women with a total of two to four lifetime sexual partners are seropositive for HSV-2," said Dr. Rachel Gordon of the Center for Clinical Studies at the University of Texas in Houston.
HSV is associated with significant morbidity and mortality. For example, those with genital herpes have a three-fold increased risk of acquiring HIV.
The current standard of care for these infections is the use of oral nucleoside analogues, such as valacyclovir (Valtrex). However, these drugs have some drawbacks. Their antiviral effect is dependent on the phosphorylation of viral thymidine kinase. "We know that viral replication can occur in the absence of viral thymidine kinase. In addition, there do exist HSV strains that have dysfunctional thymidine kinase that are immune to oral nucleoside analogues," said Dr. Gordon. "We know that sexual transmission does occur during suppressive therapy."
Helicase primase inhibitors target the virus helicase-primase complex, which is involved in DNA replication. In vitro studies have shown helicase-primase inhibitors to be more potent antivirals against both HSV-1 and HSV-2, compared with valacyclovir.
The researchers included 695 healthy adults with recurrent genital herpes. Of those, 437 (63%) experienced a recurrence and received treatment with ASP2151 (in doses of 100 mg, 200 mg, 400 mg, or 1,200 mg), valacyclovir 500 mg twice daily, or placebo.
Participants had to have at least 4 episodes of recurrent genital herpes in the last 12 months. If they received any sort of suppressive therapy within the last year, they had to have least one recurrence within stopping their suppressive therapy.
Patients, who received any dose of ASP2151, took the drug once a day for 3 days. Those who received valacyclovir took 500 mg twice a day for 3 days. Participants obtained swabs of their genital lesions within 6 hours of the first sign of recurrence. Then they initiated treatment and returned to the clinic within 24 hours of the first dose. The researchers did viral testing twice daily on days 2 and 6 and on days 8 and 10 if lesions were still present. Blood samples were drawn for pharmacokinetic analysis on days 1-4 and on day 17 (the end of the assessment period).
Patients were predominantly female (70%), with a mean age of 40 years. They typically had seven episodes per year. Half of the patients were only positive for HSV-2, while the other half were positive for HSV - 1 and HSV-2.
The primary endpoint for time to healing was significantly less for all active treatment groups, compared with placebo. Median healing times were 140 hours for placebo, 120 hours for ASP2151 100 mg, 106 hours for ASP2151 200 mg, 116 hours for ASP2151 400 mg, 102 hours for ASP2151 1,200 mg, and 114 hours for valacyclovir 500 mg.
The researchers calculated the hazard ratios for ASP2151 regimens and valacyclovir, compared with placebo: 1.40 for 100 mg of ASP2151, 1.40 for 200 mg of ASP2151, 1.25 for 400 mg of ASP2151, 1.72 for 1,200 mg of ASP2151, and 1.42 for valacyclovir. These results suggest similar efficacy for ASP2151 and valacyclovir, said Dr. Gordon.
In terms of duration of symptoms, all treatments were better than placebo, and ASP2151 regimens were comparable to valacyclovir. The most significant difference between placebo and all treatment regimens was duration of viral shedding. ASP2151 regimens were comparable to valacyclovir for viral shedding duration.
In ASP2151 treatment groups, the most common side effects were nausea, dizziness and headache. There were no severe adverse reactions.
The study was funded by Astellas Pharma. Dr. Gordon reported having no relevant disclosures.
Healing times for recurrences of herpes simplex virus 2 (HSV-2) for patients treated with ASP2151 were significantly better than placebo and were comparable to valacyclovir, based on the results of a phase-II randomized, double-blind study of 437 patients. The results were presented at the annual meeting of the American Academy of Dermatology.
The United States seroprevalence of HSV-2 is 16% among people aged 14-49 years. "Unlike other sexually-transmitted diseases that affect persons with a high level of sexual activity, HSV-2 affects even those with moderate-to-low sexual activity. It’s estimated that 18% of American women with a total of two to four lifetime sexual partners are seropositive for HSV-2," said Dr. Rachel Gordon of the Center for Clinical Studies at the University of Texas in Houston.
HSV is associated with significant morbidity and mortality. For example, those with genital herpes have a three-fold increased risk of acquiring HIV.
The current standard of care for these infections is the use of oral nucleoside analogues, such as valacyclovir (Valtrex). However, these drugs have some drawbacks. Their antiviral effect is dependent on the phosphorylation of viral thymidine kinase. "We know that viral replication can occur in the absence of viral thymidine kinase. In addition, there do exist HSV strains that have dysfunctional thymidine kinase that are immune to oral nucleoside analogues," said Dr. Gordon. "We know that sexual transmission does occur during suppressive therapy."
Helicase primase inhibitors target the virus helicase-primase complex, which is involved in DNA replication. In vitro studies have shown helicase-primase inhibitors to be more potent antivirals against both HSV-1 and HSV-2, compared with valacyclovir.
The researchers included 695 healthy adults with recurrent genital herpes. Of those, 437 (63%) experienced a recurrence and received treatment with ASP2151 (in doses of 100 mg, 200 mg, 400 mg, or 1,200 mg), valacyclovir 500 mg twice daily, or placebo.
Participants had to have at least 4 episodes of recurrent genital herpes in the last 12 months. If they received any sort of suppressive therapy within the last year, they had to have least one recurrence within stopping their suppressive therapy.
Patients, who received any dose of ASP2151, took the drug once a day for 3 days. Those who received valacyclovir took 500 mg twice a day for 3 days. Participants obtained swabs of their genital lesions within 6 hours of the first sign of recurrence. Then they initiated treatment and returned to the clinic within 24 hours of the first dose. The researchers did viral testing twice daily on days 2 and 6 and on days 8 and 10 if lesions were still present. Blood samples were drawn for pharmacokinetic analysis on days 1-4 and on day 17 (the end of the assessment period).
Patients were predominantly female (70%), with a mean age of 40 years. They typically had seven episodes per year. Half of the patients were only positive for HSV-2, while the other half were positive for HSV - 1 and HSV-2.
The primary endpoint for time to healing was significantly less for all active treatment groups, compared with placebo. Median healing times were 140 hours for placebo, 120 hours for ASP2151 100 mg, 106 hours for ASP2151 200 mg, 116 hours for ASP2151 400 mg, 102 hours for ASP2151 1,200 mg, and 114 hours for valacyclovir 500 mg.
The researchers calculated the hazard ratios for ASP2151 regimens and valacyclovir, compared with placebo: 1.40 for 100 mg of ASP2151, 1.40 for 200 mg of ASP2151, 1.25 for 400 mg of ASP2151, 1.72 for 1,200 mg of ASP2151, and 1.42 for valacyclovir. These results suggest similar efficacy for ASP2151 and valacyclovir, said Dr. Gordon.
In terms of duration of symptoms, all treatments were better than placebo, and ASP2151 regimens were comparable to valacyclovir. The most significant difference between placebo and all treatment regimens was duration of viral shedding. ASP2151 regimens were comparable to valacyclovir for viral shedding duration.
In ASP2151 treatment groups, the most common side effects were nausea, dizziness and headache. There were no severe adverse reactions.
The study was funded by Astellas Pharma. Dr. Gordon reported having no relevant disclosures.
Healing times for recurrences of herpes simplex virus 2 (HSV-2) for patients treated with ASP2151 were significantly better than placebo and were comparable to valacyclovir, based on the results of a phase-II randomized, double-blind study of 437 patients. The results were presented at the annual meeting of the American Academy of Dermatology.
The United States seroprevalence of HSV-2 is 16% among people aged 14-49 years. "Unlike other sexually-transmitted diseases that affect persons with a high level of sexual activity, HSV-2 affects even those with moderate-to-low sexual activity. It’s estimated that 18% of American women with a total of two to four lifetime sexual partners are seropositive for HSV-2," said Dr. Rachel Gordon of the Center for Clinical Studies at the University of Texas in Houston.
HSV is associated with significant morbidity and mortality. For example, those with genital herpes have a three-fold increased risk of acquiring HIV.
The current standard of care for these infections is the use of oral nucleoside analogues, such as valacyclovir (Valtrex). However, these drugs have some drawbacks. Their antiviral effect is dependent on the phosphorylation of viral thymidine kinase. "We know that viral replication can occur in the absence of viral thymidine kinase. In addition, there do exist HSV strains that have dysfunctional thymidine kinase that are immune to oral nucleoside analogues," said Dr. Gordon. "We know that sexual transmission does occur during suppressive therapy."
Helicase primase inhibitors target the virus helicase-primase complex, which is involved in DNA replication. In vitro studies have shown helicase-primase inhibitors to be more potent antivirals against both HSV-1 and HSV-2, compared with valacyclovir.
The researchers included 695 healthy adults with recurrent genital herpes. Of those, 437 (63%) experienced a recurrence and received treatment with ASP2151 (in doses of 100 mg, 200 mg, 400 mg, or 1,200 mg), valacyclovir 500 mg twice daily, or placebo.
Participants had to have at least 4 episodes of recurrent genital herpes in the last 12 months. If they received any sort of suppressive therapy within the last year, they had to have least one recurrence within stopping their suppressive therapy.
Patients, who received any dose of ASP2151, took the drug once a day for 3 days. Those who received valacyclovir took 500 mg twice a day for 3 days. Participants obtained swabs of their genital lesions within 6 hours of the first sign of recurrence. Then they initiated treatment and returned to the clinic within 24 hours of the first dose. The researchers did viral testing twice daily on days 2 and 6 and on days 8 and 10 if lesions were still present. Blood samples were drawn for pharmacokinetic analysis on days 1-4 and on day 17 (the end of the assessment period).
Patients were predominantly female (70%), with a mean age of 40 years. They typically had seven episodes per year. Half of the patients were only positive for HSV-2, while the other half were positive for HSV - 1 and HSV-2.
The primary endpoint for time to healing was significantly less for all active treatment groups, compared with placebo. Median healing times were 140 hours for placebo, 120 hours for ASP2151 100 mg, 106 hours for ASP2151 200 mg, 116 hours for ASP2151 400 mg, 102 hours for ASP2151 1,200 mg, and 114 hours for valacyclovir 500 mg.
The researchers calculated the hazard ratios for ASP2151 regimens and valacyclovir, compared with placebo: 1.40 for 100 mg of ASP2151, 1.40 for 200 mg of ASP2151, 1.25 for 400 mg of ASP2151, 1.72 for 1,200 mg of ASP2151, and 1.42 for valacyclovir. These results suggest similar efficacy for ASP2151 and valacyclovir, said Dr. Gordon.
In terms of duration of symptoms, all treatments were better than placebo, and ASP2151 regimens were comparable to valacyclovir. The most significant difference between placebo and all treatment regimens was duration of viral shedding. ASP2151 regimens were comparable to valacyclovir for viral shedding duration.
In ASP2151 treatment groups, the most common side effects were nausea, dizziness and headache. There were no severe adverse reactions.
The study was funded by Astellas Pharma. Dr. Gordon reported having no relevant disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF DERMATOLOGY
Major Finding: Median healing times were 140 hours for placebo, 120 hours for ASP2151 100 mg, 106 hours for ASP2151 200 mg, 116 hours for ASP2151 400 mg, 102 hours for ASP2151 1,200 mg, and 114 hours for valacyclovir 500 mg.
Data Source: The findings come from a phase-II randomized, double-blind study of 437 patients with genital herpes.
Disclosures: The study was funded by Astellas Pharma. Dr. Gordon reported having no relevant disclosures.
Acrylates Named Contact Allergen of the Year
SAN DIEGO – The ubiquitous acrylates take home the Contact Allergen of the Year title for 2012.
"We chose them because acrylates are everywhere in the environment," said Dr. Donald V. Belsito, who announced this year’s winner at the annual meeting of the American Contact Dermatitis Society.

Acrylates are plastic materials that are formed by the polymerization of monomers derived from acrylic or methacrylic acid. First used in Plexiglas, these compounds have a wide range of applications, including: paints, adhesives, dental composite resins, printing inks, and artificial nails. Acrylates also are used in a number of medical devices, including contact lenses, hearing aids, and bone cement for orthopedic endoprostheses.
While monomers are very strong irritants and allergens, fully polymerized acrylates are relatively inert. "Patch testing is tricky, and I think that’s something that we’re just finding out about the acrylates," said Dr. Belsito, a professor of clinical dermatology at Columbia University in New York. "They’re very volatile. The stability of the [patch test] allergens is a major issue, and they should be frozen or refrigerated."
In addition, the concentration necessary to reveal allergic sensitization is close to the irritancy threshold. These molecules also can induce active sensitization.
The North American Standard Series (Chemotechnique screening series) has been found to identify many cases of acrylate allergy caused by the inclusion of methyl methacrylate and ethyl acrylate in the series. However, clinicians should not rule out acrylate allergy even if the initial screening is negative. (Dermatitis 2011;22:98-101).
When patch tested, acrylate-allergic patients often display multiple positive tests. Previously, this was thought to be caused by cross-reaction. However, more recent analyses have shown that most acrylate-based industrial products contain many other acrylates as impurities – and thus are not included on the material safety data sheets.
"Many of the so-called cross reactions could in fact be concomitant reactions," noted Dr. Denis Sasseville in his article on acrylates, published in the January/February issue of Dermatitis (2012;23:6-16 [doi:10.1097/DER.obo13e31823d1b81]).
Methacrylates are tested at 2%, acrylates at 0.1%, and cyanoacrylates at 10%, according to Dr. Sasseville, who is a researcher in the division of dermatology at McGill University, Montreal. It is believed that patch testing with methyl methacrylate, 2-hydrorxymethyl methacrylate, ethyl acrylate, ethylene dimethacrylate, triethylene glycol diacrylate, and ethyl cyanoacrylate will identify most acrylate allergies.
The occupational exposure for dentists in particular is quite high; classic dental acrylics (including methyl acrylate) will cross through latex and vinyl gloves within minutes. Double gloving is suggested.
In one Finnish study of dental personnel, dentists and other dental personnel were most commonly exposed to 2-hydroxyethyl methacrylate, triethylene glycol dimethacrylate, and 3,3-bis[4-(2-hydroxy-3-methacryoxypropoxy) phenyl] propane (Contact Dermatitis 2007;57:324-30).
Both Dr. Belsito and Dr. Sasseville reported that they have no relevant disclosures.
SAN DIEGO – The ubiquitous acrylates take home the Contact Allergen of the Year title for 2012.
"We chose them because acrylates are everywhere in the environment," said Dr. Donald V. Belsito, who announced this year’s winner at the annual meeting of the American Contact Dermatitis Society.
Acrylates are plastic materials that are formed by the polymerization of monomers derived from acrylic or methacrylic acid. First used in Plexiglas, these compounds have a wide range of applications, including: paints, adhesives, dental composite resins, printing inks, and artificial nails. Acrylates also are used in a number of medical devices, including contact lenses, hearing aids, and bone cement for orthopedic endoprostheses.
While monomers are very strong irritants and allergens, fully polymerized acrylates are relatively inert. "Patch testing is tricky, and I think that’s something that we’re just finding out about the acrylates," said Dr. Belsito, a professor of clinical dermatology at Columbia University in New York. "They’re very volatile. The stability of the [patch test] allergens is a major issue, and they should be frozen or refrigerated."
In addition, the concentration necessary to reveal allergic sensitization is close to the irritancy threshold. These molecules also can induce active sensitization.
The North American Standard Series (Chemotechnique screening series) has been found to identify many cases of acrylate allergy caused by the inclusion of methyl methacrylate and ethyl acrylate in the series. However, clinicians should not rule out acrylate allergy even if the initial screening is negative. (Dermatitis 2011;22:98-101).
When patch tested, acrylate-allergic patients often display multiple positive tests. Previously, this was thought to be caused by cross-reaction. However, more recent analyses have shown that most acrylate-based industrial products contain many other acrylates as impurities – and thus are not included on the material safety data sheets.
"Many of the so-called cross reactions could in fact be concomitant reactions," noted Dr. Denis Sasseville in his article on acrylates, published in the January/February issue of Dermatitis (2012;23:6-16 [doi:10.1097/DER.obo13e31823d1b81]).
Methacrylates are tested at 2%, acrylates at 0.1%, and cyanoacrylates at 10%, according to Dr. Sasseville, who is a researcher in the division of dermatology at McGill University, Montreal. It is believed that patch testing with methyl methacrylate, 2-hydrorxymethyl methacrylate, ethyl acrylate, ethylene dimethacrylate, triethylene glycol diacrylate, and ethyl cyanoacrylate will identify most acrylate allergies.
The occupational exposure for dentists in particular is quite high; classic dental acrylics (including methyl acrylate) will cross through latex and vinyl gloves within minutes. Double gloving is suggested.
In one Finnish study of dental personnel, dentists and other dental personnel were most commonly exposed to 2-hydroxyethyl methacrylate, triethylene glycol dimethacrylate, and 3,3-bis[4-(2-hydroxy-3-methacryoxypropoxy) phenyl] propane (Contact Dermatitis 2007;57:324-30).
Both Dr. Belsito and Dr. Sasseville reported that they have no relevant disclosures.
SAN DIEGO – The ubiquitous acrylates take home the Contact Allergen of the Year title for 2012.
"We chose them because acrylates are everywhere in the environment," said Dr. Donald V. Belsito, who announced this year’s winner at the annual meeting of the American Contact Dermatitis Society.
Acrylates are plastic materials that are formed by the polymerization of monomers derived from acrylic or methacrylic acid. First used in Plexiglas, these compounds have a wide range of applications, including: paints, adhesives, dental composite resins, printing inks, and artificial nails. Acrylates also are used in a number of medical devices, including contact lenses, hearing aids, and bone cement for orthopedic endoprostheses.
While monomers are very strong irritants and allergens, fully polymerized acrylates are relatively inert. "Patch testing is tricky, and I think that’s something that we’re just finding out about the acrylates," said Dr. Belsito, a professor of clinical dermatology at Columbia University in New York. "They’re very volatile. The stability of the [patch test] allergens is a major issue, and they should be frozen or refrigerated."
In addition, the concentration necessary to reveal allergic sensitization is close to the irritancy threshold. These molecules also can induce active sensitization.
The North American Standard Series (Chemotechnique screening series) has been found to identify many cases of acrylate allergy caused by the inclusion of methyl methacrylate and ethyl acrylate in the series. However, clinicians should not rule out acrylate allergy even if the initial screening is negative. (Dermatitis 2011;22:98-101).
When patch tested, acrylate-allergic patients often display multiple positive tests. Previously, this was thought to be caused by cross-reaction. However, more recent analyses have shown that most acrylate-based industrial products contain many other acrylates as impurities – and thus are not included on the material safety data sheets.
"Many of the so-called cross reactions could in fact be concomitant reactions," noted Dr. Denis Sasseville in his article on acrylates, published in the January/February issue of Dermatitis (2012;23:6-16 [doi:10.1097/DER.obo13e31823d1b81]).
Methacrylates are tested at 2%, acrylates at 0.1%, and cyanoacrylates at 10%, according to Dr. Sasseville, who is a researcher in the division of dermatology at McGill University, Montreal. It is believed that patch testing with methyl methacrylate, 2-hydrorxymethyl methacrylate, ethyl acrylate, ethylene dimethacrylate, triethylene glycol diacrylate, and ethyl cyanoacrylate will identify most acrylate allergies.
The occupational exposure for dentists in particular is quite high; classic dental acrylics (including methyl acrylate) will cross through latex and vinyl gloves within minutes. Double gloving is suggested.
In one Finnish study of dental personnel, dentists and other dental personnel were most commonly exposed to 2-hydroxyethyl methacrylate, triethylene glycol dimethacrylate, and 3,3-bis[4-(2-hydroxy-3-methacryoxypropoxy) phenyl] propane (Contact Dermatitis 2007;57:324-30).
Both Dr. Belsito and Dr. Sasseville reported that they have no relevant disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN CONTACT DERMATITIS SOCIETY
IVC Filter Perforations Are Often Asymptomatic
ORLANDO – Roughly half of all inferior vena cava filter perforations voluntarily reported between 2000 and 2011 were asymptomatic and were noted as incidental findings on imaging studies, Dr. Emily A. Wood reported at the annual meeting of the American Venous Forum.
"An important thing to note about IVC perforation is that a large proportion of the patients are actually asymptomatic. Our study noted an average of 47% – almost half – of perforations were incidental findings on imaging," said Dr. Wood, a general surgery resident at Stony Brook (N.Y.) University.
IVC filter placement has more than doubled in the last decade – from 30,756 to 65,041 (J. Am. Coll. Radiol. 2011;8:483-9). While uncomplicated filter placement is a relatively straightforward ambulatory procedure, IVC filter registration and reporting of outcomes are not mandatory. Little is known about the number of adverse events related to these procedures. However, IVC perforation is an easily quantifiable event, said Dr. Wood.
The researchers used the Food and Drug Administration’s Manufacturer and User Facility Device Experience (MAUDE) database. They performed a retrospective review of 3,311 reported adverse events using filter/intravascular/cardiovascular product class search criteria from January 2000 to December 2011.
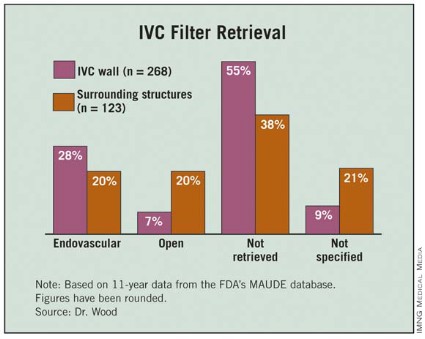
They excluded adverse event descriptions that did not specifically involve IVC perforation, including: device malfunction, failure to deploy device properly, migration/tilting, and cardiopulmonary system involvement. Outcomes of interest included clinical presentation, type of device utilized, and management (including retrievability rates).
The researchers found 391 (11%) instances of IVC perforation were reported over the 11-year period of interest. In particular, a fivefold increase in adverse events related to IVC perforation occurred from 2003 to 2004. The annual distribution of cases was 35 (12%); the annual accrual rate has not significantly increased. "Remember that this is not a universal registry and that it is voluntary. Thus, it is not entirely representative of the type of complications that actually occurred during those years," she said.
The most commonly involved structure was the aorta (43), followed by small bowel (36), vertebral body (14), and others. By far, the most commonly used filter type was the Bard G2 (168), followed by the Bard Recovery (59), the Cook Celect (46), and others.
"The majority of these filters are left in place, despite the adverse event. In other words, a perforation alone is not necessarily an indication for device removal," said Dr. Wood (see table).
IVC filter placement is not free from complications and therefore indications for filter placement should be carefully reviewed prior to any procedure. Retrievable filters are commonly involved in IVC perforation. "This gives more weight to the fact that these patients should be followed more closely and that a scheduled date for retrieval should be set, if indicated."
The authors reported that they have no relevant disclosures.
ORLANDO – Roughly half of all inferior vena cava filter perforations voluntarily reported between 2000 and 2011 were asymptomatic and were noted as incidental findings on imaging studies, Dr. Emily A. Wood reported at the annual meeting of the American Venous Forum.
"An important thing to note about IVC perforation is that a large proportion of the patients are actually asymptomatic. Our study noted an average of 47% – almost half – of perforations were incidental findings on imaging," said Dr. Wood, a general surgery resident at Stony Brook (N.Y.) University.
IVC filter placement has more than doubled in the last decade – from 30,756 to 65,041 (J. Am. Coll. Radiol. 2011;8:483-9). While uncomplicated filter placement is a relatively straightforward ambulatory procedure, IVC filter registration and reporting of outcomes are not mandatory. Little is known about the number of adverse events related to these procedures. However, IVC perforation is an easily quantifiable event, said Dr. Wood.
The researchers used the Food and Drug Administration’s Manufacturer and User Facility Device Experience (MAUDE) database. They performed a retrospective review of 3,311 reported adverse events using filter/intravascular/cardiovascular product class search criteria from January 2000 to December 2011.
They excluded adverse event descriptions that did not specifically involve IVC perforation, including: device malfunction, failure to deploy device properly, migration/tilting, and cardiopulmonary system involvement. Outcomes of interest included clinical presentation, type of device utilized, and management (including retrievability rates).
The researchers found 391 (11%) instances of IVC perforation were reported over the 11-year period of interest. In particular, a fivefold increase in adverse events related to IVC perforation occurred from 2003 to 2004. The annual distribution of cases was 35 (12%); the annual accrual rate has not significantly increased. "Remember that this is not a universal registry and that it is voluntary. Thus, it is not entirely representative of the type of complications that actually occurred during those years," she said.
The most commonly involved structure was the aorta (43), followed by small bowel (36), vertebral body (14), and others. By far, the most commonly used filter type was the Bard G2 (168), followed by the Bard Recovery (59), the Cook Celect (46), and others.
"The majority of these filters are left in place, despite the adverse event. In other words, a perforation alone is not necessarily an indication for device removal," said Dr. Wood (see table).
IVC filter placement is not free from complications and therefore indications for filter placement should be carefully reviewed prior to any procedure. Retrievable filters are commonly involved in IVC perforation. "This gives more weight to the fact that these patients should be followed more closely and that a scheduled date for retrieval should be set, if indicated."
The authors reported that they have no relevant disclosures.
ORLANDO – Roughly half of all inferior vena cava filter perforations voluntarily reported between 2000 and 2011 were asymptomatic and were noted as incidental findings on imaging studies, Dr. Emily A. Wood reported at the annual meeting of the American Venous Forum.
"An important thing to note about IVC perforation is that a large proportion of the patients are actually asymptomatic. Our study noted an average of 47% – almost half – of perforations were incidental findings on imaging," said Dr. Wood, a general surgery resident at Stony Brook (N.Y.) University.
IVC filter placement has more than doubled in the last decade – from 30,756 to 65,041 (J. Am. Coll. Radiol. 2011;8:483-9). While uncomplicated filter placement is a relatively straightforward ambulatory procedure, IVC filter registration and reporting of outcomes are not mandatory. Little is known about the number of adverse events related to these procedures. However, IVC perforation is an easily quantifiable event, said Dr. Wood.
The researchers used the Food and Drug Administration’s Manufacturer and User Facility Device Experience (MAUDE) database. They performed a retrospective review of 3,311 reported adverse events using filter/intravascular/cardiovascular product class search criteria from January 2000 to December 2011.
They excluded adverse event descriptions that did not specifically involve IVC perforation, including: device malfunction, failure to deploy device properly, migration/tilting, and cardiopulmonary system involvement. Outcomes of interest included clinical presentation, type of device utilized, and management (including retrievability rates).
The researchers found 391 (11%) instances of IVC perforation were reported over the 11-year period of interest. In particular, a fivefold increase in adverse events related to IVC perforation occurred from 2003 to 2004. The annual distribution of cases was 35 (12%); the annual accrual rate has not significantly increased. "Remember that this is not a universal registry and that it is voluntary. Thus, it is not entirely representative of the type of complications that actually occurred during those years," she said.
The most commonly involved structure was the aorta (43), followed by small bowel (36), vertebral body (14), and others. By far, the most commonly used filter type was the Bard G2 (168), followed by the Bard Recovery (59), the Cook Celect (46), and others.
"The majority of these filters are left in place, despite the adverse event. In other words, a perforation alone is not necessarily an indication for device removal," said Dr. Wood (see table).
IVC filter placement is not free from complications and therefore indications for filter placement should be carefully reviewed prior to any procedure. Retrievable filters are commonly involved in IVC perforation. "This gives more weight to the fact that these patients should be followed more closely and that a scheduled date for retrieval should be set, if indicated."
The authors reported that they have no relevant disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN VENOUS FORUM
Major Finding: Forty-seven percent of IVC filter perforations were incidental findings on imaging.
Data Source: The data are from a retrospective review of 3,311 cases reported in the Food and Drug Administration’s Manufacture and User Facility Device Experience (MAUDE) database between 2000 and 2011.
Disclosures: The authors reported that they have no relevant disclosures.
Cardiac Surgical Transfusions Linked to Infection Risk
FT. LAUDERDALE, FLA. – Transfusion of packed red blood cells during cardiac surgery is independently associated with increased risk of major infection, researchers reported, and – in a related study – pneumonia was found to be the most common infection associated with cardiac surgery.
Cardiac procedures with transfusions were associated with a significant risk of infection, such that "with every unit of blood, you had a significant increase in the risk of infection for the patient. It appears that there might be some sort of threshold in the 2- to 4-unit range, whereafter the risk really seems to increase. But statistically, even that first drop of blood carried an additional infectious risk," Dr. Keith A. Horvath said at the annual meeting of the Society of Thoracic Surgeons.
In a related study, researchers found pneumonia to be the most common infection associated with cardiac surgery. "Pneumonia, surprisingly, was the most common infection, at 2.4%. This was much more common than other infections that we certainly worry about and get a fair amount of press and literature on, specifically sternal wound infections," said Dr. Gorav Ailawadi of the University of Virginia in Charlottesville.
Data for 5,184 adult cardiac patients were used for both studies. The patients were prospectively enrolled in a 10-center infection registry between February and September, 2010. Captured data included infection occurrence, type, and organism. Adjudication was performed by an independent panel of infectious diseases experts.
Major infections evaluated in the study included deep incisional surgical (chest), deep incisional surgical (second incisions), empyema, endocarditis, mediastinitis, myocarditis, pneumonia, bloodstream infections, Clostridium difficile colitis, and cardiac device infections. Infections were defined by a combination of clinical, laboratory, and/or radiologic evidence (according to Centers for Disease Control and Prevention surveillance definitions) for a follow-up of 65 days.
The researchers included several types of surgical interventions: isolated coronary artery bypass graft (CABG), isolated valve surgery, CABG with valve surgery, surgery for heart failure, thoracic aortic surgery, and other procedures.
The mean patient age was 64 years, mean bypass time was 115 minutes, two-thirds (67%) were men, 71% had heart failure, a quarter (27%) had diabetes, 14% had chronic obstructive pulmonary disease (COPD), and 19% had prior cardiac surgery. Mean hemoglobin was 13.2 mg/dL.
There was a significant dose-dependent association between quantity of packed red blood cells (PRBCs) and risk of infection, with the crude risk increasing by an average of 29% with each PRBC unit.
Several factors increased the risk of infection, including severe COPD (relative risk, 1.85), preoperative creatinine levels greater than 1.5 mg/dL (RR, 1.72), heart failure (RR, 1.49), mild to moderate COPD (RR, 1.36), PRBCs per unit (RR, 1.24), and surgery time per 60 minutes (RR, 1.19).
Platelet transfusion occurred in 31% of patients. However, the use of platelets was associated with a decreased risk of infection (RR, 0.71). Cell Saver use was not related to infection.
Creatinine levels greater than 1.5 mg/dL (RR, 2.40) and PRBCs per unit (RR, 1.23) significantly increased the risk of death. Many factors significantly increased the length of stay, including creatinine levels greater than 1.5 mg/dL (RR, 1.26), severe COPD (RR, 1.41), mild to moderate COPD (RR, 1.14), heart failure (RR, 1.36), PRBCs (RR, 1.12), surgery time per 60 minutes (RR, 1.11), age of 65-79 years (RR, 1.21), and age older than 80 years (RR, 1.44). The use of platelets was associated with a decreased length of stay (RR, 0.71).
All risks of transfusion must be weighed against toleration anemia, which is also associated with adverse outcomes, according to Dr. Horvath, who is the director of the Cardiothoracic Surgery Research Program for the National Heart, Lung, and Blood Institute and a member of the Cardiothoracic Surgery Trials Network.
Efforts to reduce PRBC transfusions may significantly reduce major postoperative infections. Cell salvage and ultrafiltration could be viable alternatives, he noted.
In the second study, the researchers used the same dataset. Captured data included infection occurrence, type, timing, and organisms. Infections were adjudicated by an independent panel of infectious disease experts. The risk of pneumonia, mortality, and length of stay (time to discharge) were analyzed.
Major infections included bloodstream, pneumonia, C. difficile, deep sternal incisional, mediastinitis, deep groin/leg incisional, endocarditis, and empyema.
Pneumonia was diagnosed using the 2010 surveillance criteria from the CDC/National Healthcare Safety Network, including chest x-ray with new or progressive and persistent infiltrate; fever greater than 38° C; leukopenia (defined as fewer than 4,000 leukocytes per cc); leukocytosis (at least 12,000 leukocytes per cc); or altered mental status. At least two of the following must have been present as well: purulent sputum or change; cough, dyspnea, or tachypnea; rales or bronchial breath sounds; or worsening gas exchange. Duration of follow-up was 65 days.
In all, 31% had isolated CABG, 30% had isolated valve surgery, 11% had CABG and valve surgery, 6% had thoracic aortic surgery, 2% had left ventricular assist device (LVAD) implantation/heart transplant, and 20% were categorized as other.
Overall, 2.4% of patients in the registry had pneumonia, 1.1% had blood stream infection, 1% had C. difficile colitis, and 0.5% had deep sternal infections.
The overall mean time to infection was 19 days and the median was 14 days. The mean time to infection for pneumonia was 15 days. Overall, more than 40% of infections occurred after the index hospitalization. However, 68% and 66% of pneumonias and blood stream infections, respectively, occurred during hospitalization. The three most common organisms were Pseudomonas aeruginosa (12%), Enterobacter cloacae (8%), and Klebsiella pneumoniae (7%).
Increased risk of pneumonia was associated with surgery time (RR, 1.42), a creatinine level of at least 1.5 mg/dL (RR, 1.94), mild to moderate COPD (RR, 1.78), severe COPD (RR, 4.12), and heart failure (RR, 1.76). The reference category was those without COPD.
In terms of process-of-care factors, only nasal decontamination with mupirocin was associated with reduced risk of pneumonia (RR, 0.77). Nasal decontamination with other agents (RR, 1.44); antibiotics given within 24 hours after surgery (RR, 1.26) and within 48 hours postop (RR, 2.70); ventilator use of 24-48 hours (RR, 2.31) and more than 48 hours (RR, 4.58); nasogastric tube (RR, 2.07); and use of PRBCs (RR, 1.10) were all associated with increased risk of pneumonia.
In terms of mortality, "pneumonia, among all the factors analyzed, had the greatest association with mortality, with an odds ratio greater than seven ... which was far and away greater than anything else that was examined," said Dr. Ailawadi.
Pneumonia was significantly associated with an increased risk of mortality (RR, 7.07), as were heart failure (RR, 1.87), creatinine levels of at least 1.5 mg/dL (RR, 2.97), and surgery duration (1.27). However, black race appeared to be protective, with a significantly decreased risk of pneumonia (RR, 0.43).
Pneumonia significantly increased the length of stay by a median of 13 days (19 days with pneumonia and 6 days without). A number of factors – mild to moderate COPD, severe COPD, heart failure, creatinine levels of at least 1.5 mg/dL, surgery time, age of 65-79 years, age 80 years and older, and black or Hispanic race – were significantly associated with increased risk of longer length of stay. Male sex was significantly associated with decreased length of stay (RR, 0.79).
Both Dr. Horvath and Dr. Ailawadi reported that they have no relevant financial disclosures.
Cardiac procedures with transfusions, Dr. Keith A. Horvath, the Society of Thoracic Surgeons, Dr. Gorav Ailawadi, deep incisional surgical, deep incisional surgical, empyema, endocarditis, mediastinitis, myocarditis, pneumonia, bloodstream infections, Clostridium difficile colitis, and cardiac device infections,
FT. LAUDERDALE, FLA. – Transfusion of packed red blood cells during cardiac surgery is independently associated with increased risk of major infection, researchers reported, and – in a related study – pneumonia was found to be the most common infection associated with cardiac surgery.
Cardiac procedures with transfusions were associated with a significant risk of infection, such that "with every unit of blood, you had a significant increase in the risk of infection for the patient. It appears that there might be some sort of threshold in the 2- to 4-unit range, whereafter the risk really seems to increase. But statistically, even that first drop of blood carried an additional infectious risk," Dr. Keith A. Horvath said at the annual meeting of the Society of Thoracic Surgeons.
In a related study, researchers found pneumonia to be the most common infection associated with cardiac surgery. "Pneumonia, surprisingly, was the most common infection, at 2.4%. This was much more common than other infections that we certainly worry about and get a fair amount of press and literature on, specifically sternal wound infections," said Dr. Gorav Ailawadi of the University of Virginia in Charlottesville.
Data for 5,184 adult cardiac patients were used for both studies. The patients were prospectively enrolled in a 10-center infection registry between February and September, 2010. Captured data included infection occurrence, type, and organism. Adjudication was performed by an independent panel of infectious diseases experts.
Major infections evaluated in the study included deep incisional surgical (chest), deep incisional surgical (second incisions), empyema, endocarditis, mediastinitis, myocarditis, pneumonia, bloodstream infections, Clostridium difficile colitis, and cardiac device infections. Infections were defined by a combination of clinical, laboratory, and/or radiologic evidence (according to Centers for Disease Control and Prevention surveillance definitions) for a follow-up of 65 days.
The researchers included several types of surgical interventions: isolated coronary artery bypass graft (CABG), isolated valve surgery, CABG with valve surgery, surgery for heart failure, thoracic aortic surgery, and other procedures.
The mean patient age was 64 years, mean bypass time was 115 minutes, two-thirds (67%) were men, 71% had heart failure, a quarter (27%) had diabetes, 14% had chronic obstructive pulmonary disease (COPD), and 19% had prior cardiac surgery. Mean hemoglobin was 13.2 mg/dL.
There was a significant dose-dependent association between quantity of packed red blood cells (PRBCs) and risk of infection, with the crude risk increasing by an average of 29% with each PRBC unit.
Several factors increased the risk of infection, including severe COPD (relative risk, 1.85), preoperative creatinine levels greater than 1.5 mg/dL (RR, 1.72), heart failure (RR, 1.49), mild to moderate COPD (RR, 1.36), PRBCs per unit (RR, 1.24), and surgery time per 60 minutes (RR, 1.19).
Platelet transfusion occurred in 31% of patients. However, the use of platelets was associated with a decreased risk of infection (RR, 0.71). Cell Saver use was not related to infection.
Creatinine levels greater than 1.5 mg/dL (RR, 2.40) and PRBCs per unit (RR, 1.23) significantly increased the risk of death. Many factors significantly increased the length of stay, including creatinine levels greater than 1.5 mg/dL (RR, 1.26), severe COPD (RR, 1.41), mild to moderate COPD (RR, 1.14), heart failure (RR, 1.36), PRBCs (RR, 1.12), surgery time per 60 minutes (RR, 1.11), age of 65-79 years (RR, 1.21), and age older than 80 years (RR, 1.44). The use of platelets was associated with a decreased length of stay (RR, 0.71).
All risks of transfusion must be weighed against toleration anemia, which is also associated with adverse outcomes, according to Dr. Horvath, who is the director of the Cardiothoracic Surgery Research Program for the National Heart, Lung, and Blood Institute and a member of the Cardiothoracic Surgery Trials Network.
Efforts to reduce PRBC transfusions may significantly reduce major postoperative infections. Cell salvage and ultrafiltration could be viable alternatives, he noted.
In the second study, the researchers used the same dataset. Captured data included infection occurrence, type, timing, and organisms. Infections were adjudicated by an independent panel of infectious disease experts. The risk of pneumonia, mortality, and length of stay (time to discharge) were analyzed.
Major infections included bloodstream, pneumonia, C. difficile, deep sternal incisional, mediastinitis, deep groin/leg incisional, endocarditis, and empyema.
Pneumonia was diagnosed using the 2010 surveillance criteria from the CDC/National Healthcare Safety Network, including chest x-ray with new or progressive and persistent infiltrate; fever greater than 38° C; leukopenia (defined as fewer than 4,000 leukocytes per cc); leukocytosis (at least 12,000 leukocytes per cc); or altered mental status. At least two of the following must have been present as well: purulent sputum or change; cough, dyspnea, or tachypnea; rales or bronchial breath sounds; or worsening gas exchange. Duration of follow-up was 65 days.
In all, 31% had isolated CABG, 30% had isolated valve surgery, 11% had CABG and valve surgery, 6% had thoracic aortic surgery, 2% had left ventricular assist device (LVAD) implantation/heart transplant, and 20% were categorized as other.
Overall, 2.4% of patients in the registry had pneumonia, 1.1% had blood stream infection, 1% had C. difficile colitis, and 0.5% had deep sternal infections.
The overall mean time to infection was 19 days and the median was 14 days. The mean time to infection for pneumonia was 15 days. Overall, more than 40% of infections occurred after the index hospitalization. However, 68% and 66% of pneumonias and blood stream infections, respectively, occurred during hospitalization. The three most common organisms were Pseudomonas aeruginosa (12%), Enterobacter cloacae (8%), and Klebsiella pneumoniae (7%).
Increased risk of pneumonia was associated with surgery time (RR, 1.42), a creatinine level of at least 1.5 mg/dL (RR, 1.94), mild to moderate COPD (RR, 1.78), severe COPD (RR, 4.12), and heart failure (RR, 1.76). The reference category was those without COPD.
In terms of process-of-care factors, only nasal decontamination with mupirocin was associated with reduced risk of pneumonia (RR, 0.77). Nasal decontamination with other agents (RR, 1.44); antibiotics given within 24 hours after surgery (RR, 1.26) and within 48 hours postop (RR, 2.70); ventilator use of 24-48 hours (RR, 2.31) and more than 48 hours (RR, 4.58); nasogastric tube (RR, 2.07); and use of PRBCs (RR, 1.10) were all associated with increased risk of pneumonia.
In terms of mortality, "pneumonia, among all the factors analyzed, had the greatest association with mortality, with an odds ratio greater than seven ... which was far and away greater than anything else that was examined," said Dr. Ailawadi.
Pneumonia was significantly associated with an increased risk of mortality (RR, 7.07), as were heart failure (RR, 1.87), creatinine levels of at least 1.5 mg/dL (RR, 2.97), and surgery duration (1.27). However, black race appeared to be protective, with a significantly decreased risk of pneumonia (RR, 0.43).
Pneumonia significantly increased the length of stay by a median of 13 days (19 days with pneumonia and 6 days without). A number of factors – mild to moderate COPD, severe COPD, heart failure, creatinine levels of at least 1.5 mg/dL, surgery time, age of 65-79 years, age 80 years and older, and black or Hispanic race – were significantly associated with increased risk of longer length of stay. Male sex was significantly associated with decreased length of stay (RR, 0.79).
Both Dr. Horvath and Dr. Ailawadi reported that they have no relevant financial disclosures.
FT. LAUDERDALE, FLA. – Transfusion of packed red blood cells during cardiac surgery is independently associated with increased risk of major infection, researchers reported, and – in a related study – pneumonia was found to be the most common infection associated with cardiac surgery.
Cardiac procedures with transfusions were associated with a significant risk of infection, such that "with every unit of blood, you had a significant increase in the risk of infection for the patient. It appears that there might be some sort of threshold in the 2- to 4-unit range, whereafter the risk really seems to increase. But statistically, even that first drop of blood carried an additional infectious risk," Dr. Keith A. Horvath said at the annual meeting of the Society of Thoracic Surgeons.
In a related study, researchers found pneumonia to be the most common infection associated with cardiac surgery. "Pneumonia, surprisingly, was the most common infection, at 2.4%. This was much more common than other infections that we certainly worry about and get a fair amount of press and literature on, specifically sternal wound infections," said Dr. Gorav Ailawadi of the University of Virginia in Charlottesville.
Data for 5,184 adult cardiac patients were used for both studies. The patients were prospectively enrolled in a 10-center infection registry between February and September, 2010. Captured data included infection occurrence, type, and organism. Adjudication was performed by an independent panel of infectious diseases experts.
Major infections evaluated in the study included deep incisional surgical (chest), deep incisional surgical (second incisions), empyema, endocarditis, mediastinitis, myocarditis, pneumonia, bloodstream infections, Clostridium difficile colitis, and cardiac device infections. Infections were defined by a combination of clinical, laboratory, and/or radiologic evidence (according to Centers for Disease Control and Prevention surveillance definitions) for a follow-up of 65 days.
The researchers included several types of surgical interventions: isolated coronary artery bypass graft (CABG), isolated valve surgery, CABG with valve surgery, surgery for heart failure, thoracic aortic surgery, and other procedures.
The mean patient age was 64 years, mean bypass time was 115 minutes, two-thirds (67%) were men, 71% had heart failure, a quarter (27%) had diabetes, 14% had chronic obstructive pulmonary disease (COPD), and 19% had prior cardiac surgery. Mean hemoglobin was 13.2 mg/dL.
There was a significant dose-dependent association between quantity of packed red blood cells (PRBCs) and risk of infection, with the crude risk increasing by an average of 29% with each PRBC unit.
Several factors increased the risk of infection, including severe COPD (relative risk, 1.85), preoperative creatinine levels greater than 1.5 mg/dL (RR, 1.72), heart failure (RR, 1.49), mild to moderate COPD (RR, 1.36), PRBCs per unit (RR, 1.24), and surgery time per 60 minutes (RR, 1.19).
Platelet transfusion occurred in 31% of patients. However, the use of platelets was associated with a decreased risk of infection (RR, 0.71). Cell Saver use was not related to infection.
Creatinine levels greater than 1.5 mg/dL (RR, 2.40) and PRBCs per unit (RR, 1.23) significantly increased the risk of death. Many factors significantly increased the length of stay, including creatinine levels greater than 1.5 mg/dL (RR, 1.26), severe COPD (RR, 1.41), mild to moderate COPD (RR, 1.14), heart failure (RR, 1.36), PRBCs (RR, 1.12), surgery time per 60 minutes (RR, 1.11), age of 65-79 years (RR, 1.21), and age older than 80 years (RR, 1.44). The use of platelets was associated with a decreased length of stay (RR, 0.71).
All risks of transfusion must be weighed against toleration anemia, which is also associated with adverse outcomes, according to Dr. Horvath, who is the director of the Cardiothoracic Surgery Research Program for the National Heart, Lung, and Blood Institute and a member of the Cardiothoracic Surgery Trials Network.
Efforts to reduce PRBC transfusions may significantly reduce major postoperative infections. Cell salvage and ultrafiltration could be viable alternatives, he noted.
In the second study, the researchers used the same dataset. Captured data included infection occurrence, type, timing, and organisms. Infections were adjudicated by an independent panel of infectious disease experts. The risk of pneumonia, mortality, and length of stay (time to discharge) were analyzed.
Major infections included bloodstream, pneumonia, C. difficile, deep sternal incisional, mediastinitis, deep groin/leg incisional, endocarditis, and empyema.
Pneumonia was diagnosed using the 2010 surveillance criteria from the CDC/National Healthcare Safety Network, including chest x-ray with new or progressive and persistent infiltrate; fever greater than 38° C; leukopenia (defined as fewer than 4,000 leukocytes per cc); leukocytosis (at least 12,000 leukocytes per cc); or altered mental status. At least two of the following must have been present as well: purulent sputum or change; cough, dyspnea, or tachypnea; rales or bronchial breath sounds; or worsening gas exchange. Duration of follow-up was 65 days.
In all, 31% had isolated CABG, 30% had isolated valve surgery, 11% had CABG and valve surgery, 6% had thoracic aortic surgery, 2% had left ventricular assist device (LVAD) implantation/heart transplant, and 20% were categorized as other.
Overall, 2.4% of patients in the registry had pneumonia, 1.1% had blood stream infection, 1% had C. difficile colitis, and 0.5% had deep sternal infections.
The overall mean time to infection was 19 days and the median was 14 days. The mean time to infection for pneumonia was 15 days. Overall, more than 40% of infections occurred after the index hospitalization. However, 68% and 66% of pneumonias and blood stream infections, respectively, occurred during hospitalization. The three most common organisms were Pseudomonas aeruginosa (12%), Enterobacter cloacae (8%), and Klebsiella pneumoniae (7%).
Increased risk of pneumonia was associated with surgery time (RR, 1.42), a creatinine level of at least 1.5 mg/dL (RR, 1.94), mild to moderate COPD (RR, 1.78), severe COPD (RR, 4.12), and heart failure (RR, 1.76). The reference category was those without COPD.
In terms of process-of-care factors, only nasal decontamination with mupirocin was associated with reduced risk of pneumonia (RR, 0.77). Nasal decontamination with other agents (RR, 1.44); antibiotics given within 24 hours after surgery (RR, 1.26) and within 48 hours postop (RR, 2.70); ventilator use of 24-48 hours (RR, 2.31) and more than 48 hours (RR, 4.58); nasogastric tube (RR, 2.07); and use of PRBCs (RR, 1.10) were all associated with increased risk of pneumonia.
In terms of mortality, "pneumonia, among all the factors analyzed, had the greatest association with mortality, with an odds ratio greater than seven ... which was far and away greater than anything else that was examined," said Dr. Ailawadi.
Pneumonia was significantly associated with an increased risk of mortality (RR, 7.07), as were heart failure (RR, 1.87), creatinine levels of at least 1.5 mg/dL (RR, 2.97), and surgery duration (1.27). However, black race appeared to be protective, with a significantly decreased risk of pneumonia (RR, 0.43).
Pneumonia significantly increased the length of stay by a median of 13 days (19 days with pneumonia and 6 days without). A number of factors – mild to moderate COPD, severe COPD, heart failure, creatinine levels of at least 1.5 mg/dL, surgery time, age of 65-79 years, age 80 years and older, and black or Hispanic race – were significantly associated with increased risk of longer length of stay. Male sex was significantly associated with decreased length of stay (RR, 0.79).
Both Dr. Horvath and Dr. Ailawadi reported that they have no relevant financial disclosures.
Cardiac procedures with transfusions, Dr. Keith A. Horvath, the Society of Thoracic Surgeons, Dr. Gorav Ailawadi, deep incisional surgical, deep incisional surgical, empyema, endocarditis, mediastinitis, myocarditis, pneumonia, bloodstream infections, Clostridium difficile colitis, and cardiac device infections,
Cardiac procedures with transfusions, Dr. Keith A. Horvath, the Society of Thoracic Surgeons, Dr. Gorav Ailawadi, deep incisional surgical, deep incisional surgical, empyema, endocarditis, mediastinitis, myocarditis, pneumonia, bloodstream infections, Clostridium difficile colitis, and cardiac device infections,
FROM THE ANNUAL MEETING OF THE SOCIETY OF THORACIC SURGEONS
Major Finding: There was a significant dose-dependent association between quantity of packed red blood cells (PRBCs) and risk of infection, with the crude risk increasing by an average of 29% with each PRBC unit. Pneumonia was the most common infection at 2.4%.
Data Source: A total of 5,184 adult cardiac patients were prospectively enrolled in a 10-center infection registry between February and September 2010. Captured data included infection occurrence, type, and organism. Adjudication was performed by an independent panel of infectious diseases experts.
Disclosures: Both Dr. Horvath and Dr. Ailawadi reported that they have no relevant financial disclosures.
Sunburns Still Common Despite Protective Efforts
WASHINGTON – While the use of sun protection measures became more common between 2000 and 2010, there was not a corresponding decrease in sunburns, according to an analysis of national data.
Overall among women, staying in the shade, using sunscreen, and wearing clothing to the ankles increased significantly over time by 5%, 6%, and 5%, respectively, between 2000 and 2010. Similarly, among men, staying in the shade, sunscreen use, and wearing clothing to the ankles increased by 7%, 2%, and 5%, respectively. However, the overall prevalence of sunburn did not change significantly over those years. In 2010, 51% of women and 49% of men reported having at least one sunburn in the past year. The results come from a poster presented at the annual meeting of the American Society of Preventive Oncology.

The rates of melanoma and nonmelanoma skin cancers have increased in recent years. Monitoring and reporting sun-protective behaviors and sunburns over time are important ways to measure the impact of skin cancer prevention activity and to track progress toward Healthy People 2020 objectives, noted lead author Dawn M. Holman and her coinvestigators at the Centers for Disease Control and Prevention.
To estimate how commonly people engage in these behaviors that protect against sun exposure, the researchers used data from the National Health Interview Survey – Cancer Control Supplement, for years 2000, 2003, 2005, 2008, and 2010. The survey assessed the following behaviors as related to sun protection and sunburn: use of sunscreen, staying in the shade, wearing a wide-brimmed hat, wearing a long-sleeved shirt, and wearing long clothing to the ankles. Respondents reported their use as being: always, most of the time, sometimes, rarely, or never for each item. Respondents were also asked about the number of sunburns they’ve had in the last year.
Data were weighted to produce nationally representative estimates. Analyses were limited to those aged 18-29 years – age-adjusted to the 2000 U.S. population. The researchers estimated the percentage who reported engaging in each behavior always or most of the time and the percentage reporting one or more sunburns in the past year overall, by gender and by race/ethnicity.
Among women, using sunscreen (37%) and staying in the shade (35%) were the most common reported protective behaviors in 2010. Wearing a long-sleeved shirt (5%) and wearing a wide-brimmed hat (4%) were the least common. Black women were significantly less likely to report sunscreen use than were other racial/ethnic groups.
Among men, wearing long clothing to the ankles (33%) and staying in the shade (26%) were the most commonly reported behaviors in 2010. Fewer men reported using sunscreen (16%), wearing a long-sleeved shirt (8%), and wearing a wide-brimmed hat (7%). Of note, sunburn was significantly more common among non-Hispanic whites, compared with other racial/ethnic groups.
The results point to the "need for continued public health efforts to facilitate sun protection by: creating environments that support protective behaviors and by changing social norms regarding tanning and tanned skin. Facilitating sun protection may prevent sunburns and future increases in the burden of skin cancer," the researchers wrote.
The authors did not report whether they had any relevant financial interests.
WASHINGTON – While the use of sun protection measures became more common between 2000 and 2010, there was not a corresponding decrease in sunburns, according to an analysis of national data.
Overall among women, staying in the shade, using sunscreen, and wearing clothing to the ankles increased significantly over time by 5%, 6%, and 5%, respectively, between 2000 and 2010. Similarly, among men, staying in the shade, sunscreen use, and wearing clothing to the ankles increased by 7%, 2%, and 5%, respectively. However, the overall prevalence of sunburn did not change significantly over those years. In 2010, 51% of women and 49% of men reported having at least one sunburn in the past year. The results come from a poster presented at the annual meeting of the American Society of Preventive Oncology.
The rates of melanoma and nonmelanoma skin cancers have increased in recent years. Monitoring and reporting sun-protective behaviors and sunburns over time are important ways to measure the impact of skin cancer prevention activity and to track progress toward Healthy People 2020 objectives, noted lead author Dawn M. Holman and her coinvestigators at the Centers for Disease Control and Prevention.
To estimate how commonly people engage in these behaviors that protect against sun exposure, the researchers used data from the National Health Interview Survey – Cancer Control Supplement, for years 2000, 2003, 2005, 2008, and 2010. The survey assessed the following behaviors as related to sun protection and sunburn: use of sunscreen, staying in the shade, wearing a wide-brimmed hat, wearing a long-sleeved shirt, and wearing long clothing to the ankles. Respondents reported their use as being: always, most of the time, sometimes, rarely, or never for each item. Respondents were also asked about the number of sunburns they’ve had in the last year.
Data were weighted to produce nationally representative estimates. Analyses were limited to those aged 18-29 years – age-adjusted to the 2000 U.S. population. The researchers estimated the percentage who reported engaging in each behavior always or most of the time and the percentage reporting one or more sunburns in the past year overall, by gender and by race/ethnicity.
Among women, using sunscreen (37%) and staying in the shade (35%) were the most common reported protective behaviors in 2010. Wearing a long-sleeved shirt (5%) and wearing a wide-brimmed hat (4%) were the least common. Black women were significantly less likely to report sunscreen use than were other racial/ethnic groups.
Among men, wearing long clothing to the ankles (33%) and staying in the shade (26%) were the most commonly reported behaviors in 2010. Fewer men reported using sunscreen (16%), wearing a long-sleeved shirt (8%), and wearing a wide-brimmed hat (7%). Of note, sunburn was significantly more common among non-Hispanic whites, compared with other racial/ethnic groups.
The results point to the "need for continued public health efforts to facilitate sun protection by: creating environments that support protective behaviors and by changing social norms regarding tanning and tanned skin. Facilitating sun protection may prevent sunburns and future increases in the burden of skin cancer," the researchers wrote.
The authors did not report whether they had any relevant financial interests.
WASHINGTON – While the use of sun protection measures became more common between 2000 and 2010, there was not a corresponding decrease in sunburns, according to an analysis of national data.
Overall among women, staying in the shade, using sunscreen, and wearing clothing to the ankles increased significantly over time by 5%, 6%, and 5%, respectively, between 2000 and 2010. Similarly, among men, staying in the shade, sunscreen use, and wearing clothing to the ankles increased by 7%, 2%, and 5%, respectively. However, the overall prevalence of sunburn did not change significantly over those years. In 2010, 51% of women and 49% of men reported having at least one sunburn in the past year. The results come from a poster presented at the annual meeting of the American Society of Preventive Oncology.
The rates of melanoma and nonmelanoma skin cancers have increased in recent years. Monitoring and reporting sun-protective behaviors and sunburns over time are important ways to measure the impact of skin cancer prevention activity and to track progress toward Healthy People 2020 objectives, noted lead author Dawn M. Holman and her coinvestigators at the Centers for Disease Control and Prevention.
To estimate how commonly people engage in these behaviors that protect against sun exposure, the researchers used data from the National Health Interview Survey – Cancer Control Supplement, for years 2000, 2003, 2005, 2008, and 2010. The survey assessed the following behaviors as related to sun protection and sunburn: use of sunscreen, staying in the shade, wearing a wide-brimmed hat, wearing a long-sleeved shirt, and wearing long clothing to the ankles. Respondents reported their use as being: always, most of the time, sometimes, rarely, or never for each item. Respondents were also asked about the number of sunburns they’ve had in the last year.
Data were weighted to produce nationally representative estimates. Analyses were limited to those aged 18-29 years – age-adjusted to the 2000 U.S. population. The researchers estimated the percentage who reported engaging in each behavior always or most of the time and the percentage reporting one or more sunburns in the past year overall, by gender and by race/ethnicity.
Among women, using sunscreen (37%) and staying in the shade (35%) were the most common reported protective behaviors in 2010. Wearing a long-sleeved shirt (5%) and wearing a wide-brimmed hat (4%) were the least common. Black women were significantly less likely to report sunscreen use than were other racial/ethnic groups.
Among men, wearing long clothing to the ankles (33%) and staying in the shade (26%) were the most commonly reported behaviors in 2010. Fewer men reported using sunscreen (16%), wearing a long-sleeved shirt (8%), and wearing a wide-brimmed hat (7%). Of note, sunburn was significantly more common among non-Hispanic whites, compared with other racial/ethnic groups.
The results point to the "need for continued public health efforts to facilitate sun protection by: creating environments that support protective behaviors and by changing social norms regarding tanning and tanned skin. Facilitating sun protection may prevent sunburns and future increases in the burden of skin cancer," the researchers wrote.
The authors did not report whether they had any relevant financial interests.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF PREVENTIVE ONCOLOGY
Major Findings: In 2010, 51% of women and 49% of men reported having at least one sunburn in the past year. Sunburn was significantly more common among non-Hispanic whites, compared with other racial/ethnic groups.
Data Source: Researchers used data from the National Health Interview Survey – Cancer Control Supplement for years 2000, 2003, 2005, 2008, and 2010.
Disclosures: The authors did not report whether they had any relevant financial interests.
Infections, Pulmonary Complications Up Risk of Thrombotic Events
ORLANDO – Researchers have identified risk groups of common perioperative conditions that indicate an increased risk for venous thrombotic events during arterial reconstruction procedures in an analysis of a large administrative database.
The findings could lead to more aggressive venous thrombotic event (VTE) prophylaxis strategies for patients with those "risk families," Dr. Leila Mureebe said at the annual meeting of the American Venous Forum.

Infectious and pulmonary risk families were more commonly associated with VTE. Urinary and intestinal risk families were associated with a lower – although still important – risk of VTEs, said Dr. Mureebe, a vascular surgeon at Duke University in Durham, N.C.
Rates of deep vein thrombosis (DVT) and pulmonary embolism (PE) after common vascular procedures are poorly defined. However, determining the true incidence and/or prevalence would be impractical, she noted.
The researchers used administrative data from the National Inpatient Sample (NIS) to identify patients at increased risk of VTE by identifying associated pre- and postoperative factors. The NIS captures discharges by procedure, and is designed to approximate a 20% sample of U.S. community hospitals. All discharges from sampled hospitals are included in the NIS database, which contains clinical and resource-use information (typically included in a discharge abstract).
This study included all discharges during 2000-2008 with primary arterial operations (abdominal aortic aneurysm [open], aortobifemoral bypass, carotid endarterectomy, and infrainguinal bypass). Procedure codes were crossed by diagnosis code for DVT and PE diagnoses. Next the researchers subselected the population that was associated with VTE, including VTE discharges.
The incidence of VTE was 0.34% of 73,545 patients undergoing abdominal aortic aneurysm repair, 0.06% of 372,465 patients undergoing carotid endarterectomy, 0.27% of 50,415 patients undergoing aortobifemoral bypass, and 0.31% of 253,234 patients undergoing bypass graft.
"We then created risk families to capture the relatively common perioperative events," said Dr. Mureebe. The risk families included intestinal (ileus, small-bowel obstruction), pulmonary (aspiration, bronchitis, pneumonia, lobar pneumonia), urinary complications (urinary tract infection not otherwise specified, indwelling urinary catheter), infectious complications (postoperative infection, postoperative abscess, intra-abdominal infection, stitch abscess, subabscess, wound complications, septicemia, infection due to vascular device, and systemic inflammatory response syndrome), and cardiac (acute myocardial infarction, acute coronary occlusion without MI).
Potential confounders included age at admission, sex, a history of DVT/PE, and a history of a coagulopathy (clotting defect, thrombocytosis, heparin-induced thrombocytopenia, antithrombin deficiency, and mutations [factor V Leiden, prothrombin gene]). Logistic regression was used to assess the association between VTE and risk families. The model was adjusted for age and sex.
In all, 755,536 weighted procedures were identified. VTEs were found in 1,445 diagnoses, for an overall prevalence of 0.19%. "Interestingly, each family of complications was associated with a different risk of VTE," said Dr. Mureebe. The risk of intestinal family complications was 0.62%. Pulmonary, urinary, and infectious family risk rates were 1.2%, 0.66%, and 1.46%, respectively. "Cardiac fell out of all analyses and was not associated – at least in this dataset – with the development of VTEs."
Confounders were more strongly associated with VTEs, Dr. Mureebe noted. A history of VTE was associated with a 2.2% increased risk, and a history of coagulopathy was associated with a 1.68% increased risk.
"So, in addition to discrete risk families having increased risk, there’s also a different profile dependent upon the actual surgical procedure."
For example, in carotid endarterectomy – which is associated with an overall low risk of VTEs – "we really see a large contribution from these potential risk families," she said.
Dr. Mureebe did not report whether she had any relevant financial disclosures.
ORLANDO – Researchers have identified risk groups of common perioperative conditions that indicate an increased risk for venous thrombotic events during arterial reconstruction procedures in an analysis of a large administrative database.
The findings could lead to more aggressive venous thrombotic event (VTE) prophylaxis strategies for patients with those "risk families," Dr. Leila Mureebe said at the annual meeting of the American Venous Forum.
Infectious and pulmonary risk families were more commonly associated with VTE. Urinary and intestinal risk families were associated with a lower – although still important – risk of VTEs, said Dr. Mureebe, a vascular surgeon at Duke University in Durham, N.C.
Rates of deep vein thrombosis (DVT) and pulmonary embolism (PE) after common vascular procedures are poorly defined. However, determining the true incidence and/or prevalence would be impractical, she noted.
The researchers used administrative data from the National Inpatient Sample (NIS) to identify patients at increased risk of VTE by identifying associated pre- and postoperative factors. The NIS captures discharges by procedure, and is designed to approximate a 20% sample of U.S. community hospitals. All discharges from sampled hospitals are included in the NIS database, which contains clinical and resource-use information (typically included in a discharge abstract).
This study included all discharges during 2000-2008 with primary arterial operations (abdominal aortic aneurysm [open], aortobifemoral bypass, carotid endarterectomy, and infrainguinal bypass). Procedure codes were crossed by diagnosis code for DVT and PE diagnoses. Next the researchers subselected the population that was associated with VTE, including VTE discharges.
The incidence of VTE was 0.34% of 73,545 patients undergoing abdominal aortic aneurysm repair, 0.06% of 372,465 patients undergoing carotid endarterectomy, 0.27% of 50,415 patients undergoing aortobifemoral bypass, and 0.31% of 253,234 patients undergoing bypass graft.
"We then created risk families to capture the relatively common perioperative events," said Dr. Mureebe. The risk families included intestinal (ileus, small-bowel obstruction), pulmonary (aspiration, bronchitis, pneumonia, lobar pneumonia), urinary complications (urinary tract infection not otherwise specified, indwelling urinary catheter), infectious complications (postoperative infection, postoperative abscess, intra-abdominal infection, stitch abscess, subabscess, wound complications, septicemia, infection due to vascular device, and systemic inflammatory response syndrome), and cardiac (acute myocardial infarction, acute coronary occlusion without MI).
Potential confounders included age at admission, sex, a history of DVT/PE, and a history of a coagulopathy (clotting defect, thrombocytosis, heparin-induced thrombocytopenia, antithrombin deficiency, and mutations [factor V Leiden, prothrombin gene]). Logistic regression was used to assess the association between VTE and risk families. The model was adjusted for age and sex.
In all, 755,536 weighted procedures were identified. VTEs were found in 1,445 diagnoses, for an overall prevalence of 0.19%. "Interestingly, each family of complications was associated with a different risk of VTE," said Dr. Mureebe. The risk of intestinal family complications was 0.62%. Pulmonary, urinary, and infectious family risk rates were 1.2%, 0.66%, and 1.46%, respectively. "Cardiac fell out of all analyses and was not associated – at least in this dataset – with the development of VTEs."
Confounders were more strongly associated with VTEs, Dr. Mureebe noted. A history of VTE was associated with a 2.2% increased risk, and a history of coagulopathy was associated with a 1.68% increased risk.
"So, in addition to discrete risk families having increased risk, there’s also a different profile dependent upon the actual surgical procedure."
For example, in carotid endarterectomy – which is associated with an overall low risk of VTEs – "we really see a large contribution from these potential risk families," she said.
Dr. Mureebe did not report whether she had any relevant financial disclosures.
ORLANDO – Researchers have identified risk groups of common perioperative conditions that indicate an increased risk for venous thrombotic events during arterial reconstruction procedures in an analysis of a large administrative database.
The findings could lead to more aggressive venous thrombotic event (VTE) prophylaxis strategies for patients with those "risk families," Dr. Leila Mureebe said at the annual meeting of the American Venous Forum.
Infectious and pulmonary risk families were more commonly associated with VTE. Urinary and intestinal risk families were associated with a lower – although still important – risk of VTEs, said Dr. Mureebe, a vascular surgeon at Duke University in Durham, N.C.
Rates of deep vein thrombosis (DVT) and pulmonary embolism (PE) after common vascular procedures are poorly defined. However, determining the true incidence and/or prevalence would be impractical, she noted.
The researchers used administrative data from the National Inpatient Sample (NIS) to identify patients at increased risk of VTE by identifying associated pre- and postoperative factors. The NIS captures discharges by procedure, and is designed to approximate a 20% sample of U.S. community hospitals. All discharges from sampled hospitals are included in the NIS database, which contains clinical and resource-use information (typically included in a discharge abstract).
This study included all discharges during 2000-2008 with primary arterial operations (abdominal aortic aneurysm [open], aortobifemoral bypass, carotid endarterectomy, and infrainguinal bypass). Procedure codes were crossed by diagnosis code for DVT and PE diagnoses. Next the researchers subselected the population that was associated with VTE, including VTE discharges.
The incidence of VTE was 0.34% of 73,545 patients undergoing abdominal aortic aneurysm repair, 0.06% of 372,465 patients undergoing carotid endarterectomy, 0.27% of 50,415 patients undergoing aortobifemoral bypass, and 0.31% of 253,234 patients undergoing bypass graft.
"We then created risk families to capture the relatively common perioperative events," said Dr. Mureebe. The risk families included intestinal (ileus, small-bowel obstruction), pulmonary (aspiration, bronchitis, pneumonia, lobar pneumonia), urinary complications (urinary tract infection not otherwise specified, indwelling urinary catheter), infectious complications (postoperative infection, postoperative abscess, intra-abdominal infection, stitch abscess, subabscess, wound complications, septicemia, infection due to vascular device, and systemic inflammatory response syndrome), and cardiac (acute myocardial infarction, acute coronary occlusion without MI).
Potential confounders included age at admission, sex, a history of DVT/PE, and a history of a coagulopathy (clotting defect, thrombocytosis, heparin-induced thrombocytopenia, antithrombin deficiency, and mutations [factor V Leiden, prothrombin gene]). Logistic regression was used to assess the association between VTE and risk families. The model was adjusted for age and sex.
In all, 755,536 weighted procedures were identified. VTEs were found in 1,445 diagnoses, for an overall prevalence of 0.19%. "Interestingly, each family of complications was associated with a different risk of VTE," said Dr. Mureebe. The risk of intestinal family complications was 0.62%. Pulmonary, urinary, and infectious family risk rates were 1.2%, 0.66%, and 1.46%, respectively. "Cardiac fell out of all analyses and was not associated – at least in this dataset – with the development of VTEs."
Confounders were more strongly associated with VTEs, Dr. Mureebe noted. A history of VTE was associated with a 2.2% increased risk, and a history of coagulopathy was associated with a 1.68% increased risk.
"So, in addition to discrete risk families having increased risk, there’s also a different profile dependent upon the actual surgical procedure."
For example, in carotid endarterectomy – which is associated with an overall low risk of VTEs – "we really see a large contribution from these potential risk families," she said.
Dr. Mureebe did not report whether she had any relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN VENOUS FORUM