User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Medicare proposes direct payments to PAs, telehealth expansion
It also intends to change the approach to payments for office visits and for coaching programs for diabetes prevention.

The Centers for Medicare & Medicaid Services recently posted its proposed 2022 physician fee schedule. Running to more than 1,700 pages, the draft rule contains myriad other changes in how the giant federal health program pays for medical care, including revisions to its approach to evaluation and management (E/M) services, which represent many office visits. In addition, Medicare is seeking to increase participation in a program intended to prevent people from developing diabetes.
Physician groups posted quick complaints about a proposed 3.75% reduction to the conversion factor because of budget neutrality requirements. The cut reinstates a reduction Congress prevented in late 2020.
In a statement, Anders Gilberg, senior vice president of government affairs for the Medical Group Management Association, called the draft rule a “mixed bag for physician practices.” Mr. Gilberg said the MGMA will seek congressional intervention to avert the cut for services in 2022.
In keeping with a provision Congress included in a massive spending bill enacted in December, Medicare will let PAs directly bill, as nurse practitioners already can. In a press release, CMS on July 13 described this as a move likely to expand access to care and reduce administrative burden. In 2020, the American Academy of PAs praised the inclusion in the spending bill of the provision allowing its members to directly bill Medicare.
In the draft rule, CMS also intends to remove certain geographic restrictions regarding use of telehealth services for diagnosis, evaluation, and treatment of mental health disorders. CMS also is proposing to allow payment to eligible clinicians for certain mental health and behavioral health services to patients via audio-only telephone calls. These services would include counseling and therapy services provided through opioid treatment programs.
“These changes would be particularly helpful for those in areas with poor broadband infrastructure and among people with Medicare who are not capable of, or do not consent to the use of, devices that permit a two-way, audio/video interaction for their health care visits,” CMS said in a statement.
Slimmer Medicare enrollees, bigger payments for coaches?
CMS is seeking to draw more participants to the Medicare Diabetes Prevention Program (MDPP). This program includes organizations that provide structured, coach-led sessions in community and health care settings to help people lose weight and exercise more. During the COVID-19 public health emergency, CMS waived an enrollment fee for new suppliers of services in MDPP. CMS now is proposing to waive this fee for all organizations that submit an application to enroll in Medicare as an MDPP supplier on or after Jan. 1, 2022.
Another proposed change in MDPP services is a restructuring of payments so that organizations involved in coaching would receive larger payments when their participants reach milestones for attendance and for becoming slimmer.
“We propose to increase performance payments for MDPP beneficiary achievement of the 5% weight-loss goal, as well as continued attendance during each core maintenance interval,” CMS said in a statement.
Medicare remains engaged in a review of its payments for E/M services. In the draft rule, CMS is proposing a number of refinements to current policies for split, or shared, E/M visits, critical care services, and services furnished by teaching physicians involving residents. The intention of these changes is to “better reflect the current practice of medicine, the evolving role of nonphysician practitioners as members of the medical team, and to clarify conditions of payment that must be met to bill Medicare for these services,” CMS said.
A version of this article first appeared on Medscape.com.
It also intends to change the approach to payments for office visits and for coaching programs for diabetes prevention.
The Centers for Medicare & Medicaid Services recently posted its proposed 2022 physician fee schedule. Running to more than 1,700 pages, the draft rule contains myriad other changes in how the giant federal health program pays for medical care, including revisions to its approach to evaluation and management (E/M) services, which represent many office visits. In addition, Medicare is seeking to increase participation in a program intended to prevent people from developing diabetes.
Physician groups posted quick complaints about a proposed 3.75% reduction to the conversion factor because of budget neutrality requirements. The cut reinstates a reduction Congress prevented in late 2020.
In a statement, Anders Gilberg, senior vice president of government affairs for the Medical Group Management Association, called the draft rule a “mixed bag for physician practices.” Mr. Gilberg said the MGMA will seek congressional intervention to avert the cut for services in 2022.
In keeping with a provision Congress included in a massive spending bill enacted in December, Medicare will let PAs directly bill, as nurse practitioners already can. In a press release, CMS on July 13 described this as a move likely to expand access to care and reduce administrative burden. In 2020, the American Academy of PAs praised the inclusion in the spending bill of the provision allowing its members to directly bill Medicare.
In the draft rule, CMS also intends to remove certain geographic restrictions regarding use of telehealth services for diagnosis, evaluation, and treatment of mental health disorders. CMS also is proposing to allow payment to eligible clinicians for certain mental health and behavioral health services to patients via audio-only telephone calls. These services would include counseling and therapy services provided through opioid treatment programs.
“These changes would be particularly helpful for those in areas with poor broadband infrastructure and among people with Medicare who are not capable of, or do not consent to the use of, devices that permit a two-way, audio/video interaction for their health care visits,” CMS said in a statement.
Slimmer Medicare enrollees, bigger payments for coaches?
CMS is seeking to draw more participants to the Medicare Diabetes Prevention Program (MDPP). This program includes organizations that provide structured, coach-led sessions in community and health care settings to help people lose weight and exercise more. During the COVID-19 public health emergency, CMS waived an enrollment fee for new suppliers of services in MDPP. CMS now is proposing to waive this fee for all organizations that submit an application to enroll in Medicare as an MDPP supplier on or after Jan. 1, 2022.
Another proposed change in MDPP services is a restructuring of payments so that organizations involved in coaching would receive larger payments when their participants reach milestones for attendance and for becoming slimmer.
“We propose to increase performance payments for MDPP beneficiary achievement of the 5% weight-loss goal, as well as continued attendance during each core maintenance interval,” CMS said in a statement.
Medicare remains engaged in a review of its payments for E/M services. In the draft rule, CMS is proposing a number of refinements to current policies for split, or shared, E/M visits, critical care services, and services furnished by teaching physicians involving residents. The intention of these changes is to “better reflect the current practice of medicine, the evolving role of nonphysician practitioners as members of the medical team, and to clarify conditions of payment that must be met to bill Medicare for these services,” CMS said.
A version of this article first appeared on Medscape.com.
It also intends to change the approach to payments for office visits and for coaching programs for diabetes prevention.
The Centers for Medicare & Medicaid Services recently posted its proposed 2022 physician fee schedule. Running to more than 1,700 pages, the draft rule contains myriad other changes in how the giant federal health program pays for medical care, including revisions to its approach to evaluation and management (E/M) services, which represent many office visits. In addition, Medicare is seeking to increase participation in a program intended to prevent people from developing diabetes.
Physician groups posted quick complaints about a proposed 3.75% reduction to the conversion factor because of budget neutrality requirements. The cut reinstates a reduction Congress prevented in late 2020.
In a statement, Anders Gilberg, senior vice president of government affairs for the Medical Group Management Association, called the draft rule a “mixed bag for physician practices.” Mr. Gilberg said the MGMA will seek congressional intervention to avert the cut for services in 2022.
In keeping with a provision Congress included in a massive spending bill enacted in December, Medicare will let PAs directly bill, as nurse practitioners already can. In a press release, CMS on July 13 described this as a move likely to expand access to care and reduce administrative burden. In 2020, the American Academy of PAs praised the inclusion in the spending bill of the provision allowing its members to directly bill Medicare.
In the draft rule, CMS also intends to remove certain geographic restrictions regarding use of telehealth services for diagnosis, evaluation, and treatment of mental health disorders. CMS also is proposing to allow payment to eligible clinicians for certain mental health and behavioral health services to patients via audio-only telephone calls. These services would include counseling and therapy services provided through opioid treatment programs.
“These changes would be particularly helpful for those in areas with poor broadband infrastructure and among people with Medicare who are not capable of, or do not consent to the use of, devices that permit a two-way, audio/video interaction for their health care visits,” CMS said in a statement.
Slimmer Medicare enrollees, bigger payments for coaches?
CMS is seeking to draw more participants to the Medicare Diabetes Prevention Program (MDPP). This program includes organizations that provide structured, coach-led sessions in community and health care settings to help people lose weight and exercise more. During the COVID-19 public health emergency, CMS waived an enrollment fee for new suppliers of services in MDPP. CMS now is proposing to waive this fee for all organizations that submit an application to enroll in Medicare as an MDPP supplier on or after Jan. 1, 2022.
Another proposed change in MDPP services is a restructuring of payments so that organizations involved in coaching would receive larger payments when their participants reach milestones for attendance and for becoming slimmer.
“We propose to increase performance payments for MDPP beneficiary achievement of the 5% weight-loss goal, as well as continued attendance during each core maintenance interval,” CMS said in a statement.
Medicare remains engaged in a review of its payments for E/M services. In the draft rule, CMS is proposing a number of refinements to current policies for split, or shared, E/M visits, critical care services, and services furnished by teaching physicians involving residents. The intention of these changes is to “better reflect the current practice of medicine, the evolving role of nonphysician practitioners as members of the medical team, and to clarify conditions of payment that must be met to bill Medicare for these services,” CMS said.
A version of this article first appeared on Medscape.com.
New agents for youth-onset type 2 diabetes ‘finally in sight’
There are limited treatment options for children and youth with type 2 diabetes, but a few novel therapies beyond metformin are on the horizon, experts said at the annual scientific sessions of the American Diabetes Association.
“Type 2 diabetes in youth only emerged as a well-recognized pediatric medical problem in the 1990s and the first decade of the 21st century,” session chair Kenneth C. Copeland, MD, said in an interview.
“Fortunately, a number of clinical trials of antidiabetic pharmacologic agents in diabetic youth have now been completed, demonstrating both safety and efficacy, and at long last, a ... variety of agents are finally in sight,” he noted.
Type 2 diabetes in youth is profoundly different from type 2 diabetes in adults, added Dr. Copeland, pediatrics professor emeritus, University of Oklahoma, Oklahoma City. In youth, its course is typically aggressive and refractive to treatment.
Concerted efforts at lifestyle intervention are important but insufficient, and a response to metformin, even when initiated at diagnosis, is often short lived, he added.
Because of the rapid glycemic deterioration that is typical of type 2 diabetes in youth and leads to the full array of diabetic complications, early aggressive pharmacologic treatment is indicated.
“We all look forward to this next decade ushering in new treatment options, spanning the spectrum from obesity prevention to complex pharmacologic intervention,” Dr. Copeland summarized.
Increasing prevalence of T2D in youth, limited therapies
Rates of type 2 diabetes in youth continue to increase, especially among non-White groups, and most of these individuals have less than optimal diabetes control, Elvira Isganaitis, MD, MPH, a pediatric endocrinologist at the Joslin Diabetes Center and assistant professor of pediatrics at Harvard Medical School, both in Boston, told the meeting.

Although the Food and Drug Administration has approved more than 25 drugs to treat type 2 diabetes in adults, “unfortunately,” metformin is the only oral medication approved to treat the disease in a pediatric population, “and a majority of youth either do not respond to it or do not tolerate it,” she said in an interview.
Dr. Copeland observed that “the TODAY study demonstrated conclusively that, despite an often dramatic initial improvement in glycemic control upon initiation of pharmacologic and lifestyle intervention, this initial response was followed by a rapid deterioration of beta-cell function and glycemic failure, indicating that additional pharmacologic agents were sorely needed for this population.”
The RISE study also showed that, compared with adults, youth had more rapid beta-cell deterioration despite treatment.
Until the June 2019 FDA approval of the injectable glucagonlike peptide–1 receptor agonist liraglutide (Victoza, Novo Nordisk) for children 10 years or older, “except for insulin, metformin was the only antidiabetic medication available for use in youth, severely limiting treatment options,” he added.
Liraglutide ‘a huge breakthrough,’ other options on the horizon
The FDA approval of liraglutide was “a huge breakthrough” as the first noninsulin drug for pediatric type 2 diabetes since metformin was approved for pediatric use in 2000, Dr. Isganaitis said.
The ELLIPSE study, on which the approval was based, showed liraglutide was effective at lowering hemoglobin A1c and was generally well tolerated, although it was associated with a higher incidence of gastrointestinal symptoms.
In December 2020, the FDA also approved liraglutide (Saxenda) for the treatment of obesity in youth age 12 and older (at a dose of 3 mg as opposed to the 1.8-mg dose of liraglutide [Victoza]), “which is wonderful news considering that the majority of pediatric patients with type 2 diabetes also have obesity,” Dr. Isganaitis added.
“The results of studies of liraglutide on glycemia in diabetic youth are impressive, with both an additional benefit of weight loss and without unacceptable identified risks or side effects,” Dr. Copeland concurred.
Waiting in the wings
Dr. Isganaitis reported that a few phase 3 clinical trials of other therapies for pediatric patients with type 2 diabetes are in the wings.
The 24-week phase 3 T2GO clinical trial of the sodium-glucose cotransporter 2 inhibitor dapagliflozin (AstraZeneca) versus placebo in 72 patients with type 2 diabetes aged 10-24 years was completed in April 2020, and the data are being analyzed.
An AstraZeneca-sponsored phase 3 trial of the safety and efficacy of a weekly injection of the GLP-1 receptor agonist exenatide in 10- to 17-year-olds with type 2 diabetes (n = 82) has also been completed and data are being analyzed.
A Takeda-sponsored phase 3 pediatric study of the dipeptidyl peptidase–4 inhibitor alogliptin in 10- to 17-year-olds with type 2 diabetes (n = 150) is estimated to be completed by February 2022.
And the phase 3 DINAMO trial, sponsored by Boehringer Ingelheim, which is evaluating the efficacy and safety of the SGLT2 inhibitor empagliflozin (10 mg/25 mg) versus the DPP-4 inhibitor linagliptin (5 mg) versus placebo over 26 weeks in 10- to 17-year-olds with type 2 diabetes (estimated 186 participants), is expected to be completed in May 2023.
“I hope that these medications will demonstrate efficacy and allow pediatric patients with type 2 diabetes to have more treatment options,” Dr. Isganaitis concluded.
Type 2 diabetes more aggressive than type 1 diabetes in kids
According to Dr. Isganaitis, “there is a widely held misconception among the general public and even among some physicians that type 2 diabetes is somehow less worrisome or ‘milder’ than a diagnosis of type 1 diabetes.”
However, the risk of complications and severe morbidity is higher with a diagnosis of type 2 diabetes versus type 1 diabetes in a child, so “this condition needs to be managed intensively with a multidisciplinary team including pediatric endocrinology, nutrition [support], diabetes educators, and mental health support,” she emphasized.
Many people also believe that “type 2 diabetes in kids is a ‘lifestyle disease,’ ” she continued, “but in fact, there is a strong role for genetics.”
The ADA Presidents’ Select Abstract “paints a picture of youth-onset type 2 diabetes as a disease intermediate in extremity between monogenic diabetes [caused by mutations in a single gene] and type 2 diabetes [caused by multiple genes and lifestyle factors such as obesity], in which genetic variants in both insulin secretion and insulin response pathways are implicated.”
Along the same lines, Dr. Isganaitis presented an oral abstract at the meeting that showed that, among youth with newly diagnosed type 2 diabetes, those whose mothers had diabetes had faster disease progression and earlier onset of diabetes complications.
Dr. Isganaitis has reported no relevant financial relationships. Dr. Copeland has reported serving on data monitoring committees for Boehringer Ingelheim and Novo Nordisk, and on an advisory committee for a research study for Daiichi Sankyo.
A version of this article first appeared on Medscape.com.
There are limited treatment options for children and youth with type 2 diabetes, but a few novel therapies beyond metformin are on the horizon, experts said at the annual scientific sessions of the American Diabetes Association.
“Type 2 diabetes in youth only emerged as a well-recognized pediatric medical problem in the 1990s and the first decade of the 21st century,” session chair Kenneth C. Copeland, MD, said in an interview.
“Fortunately, a number of clinical trials of antidiabetic pharmacologic agents in diabetic youth have now been completed, demonstrating both safety and efficacy, and at long last, a ... variety of agents are finally in sight,” he noted.
Type 2 diabetes in youth is profoundly different from type 2 diabetes in adults, added Dr. Copeland, pediatrics professor emeritus, University of Oklahoma, Oklahoma City. In youth, its course is typically aggressive and refractive to treatment.
Concerted efforts at lifestyle intervention are important but insufficient, and a response to metformin, even when initiated at diagnosis, is often short lived, he added.
Because of the rapid glycemic deterioration that is typical of type 2 diabetes in youth and leads to the full array of diabetic complications, early aggressive pharmacologic treatment is indicated.
“We all look forward to this next decade ushering in new treatment options, spanning the spectrum from obesity prevention to complex pharmacologic intervention,” Dr. Copeland summarized.
Increasing prevalence of T2D in youth, limited therapies
Rates of type 2 diabetes in youth continue to increase, especially among non-White groups, and most of these individuals have less than optimal diabetes control, Elvira Isganaitis, MD, MPH, a pediatric endocrinologist at the Joslin Diabetes Center and assistant professor of pediatrics at Harvard Medical School, both in Boston, told the meeting.
Although the Food and Drug Administration has approved more than 25 drugs to treat type 2 diabetes in adults, “unfortunately,” metformin is the only oral medication approved to treat the disease in a pediatric population, “and a majority of youth either do not respond to it or do not tolerate it,” she said in an interview.
Dr. Copeland observed that “the TODAY study demonstrated conclusively that, despite an often dramatic initial improvement in glycemic control upon initiation of pharmacologic and lifestyle intervention, this initial response was followed by a rapid deterioration of beta-cell function and glycemic failure, indicating that additional pharmacologic agents were sorely needed for this population.”
The RISE study also showed that, compared with adults, youth had more rapid beta-cell deterioration despite treatment.
Until the June 2019 FDA approval of the injectable glucagonlike peptide–1 receptor agonist liraglutide (Victoza, Novo Nordisk) for children 10 years or older, “except for insulin, metformin was the only antidiabetic medication available for use in youth, severely limiting treatment options,” he added.
Liraglutide ‘a huge breakthrough,’ other options on the horizon
The FDA approval of liraglutide was “a huge breakthrough” as the first noninsulin drug for pediatric type 2 diabetes since metformin was approved for pediatric use in 2000, Dr. Isganaitis said.
The ELLIPSE study, on which the approval was based, showed liraglutide was effective at lowering hemoglobin A1c and was generally well tolerated, although it was associated with a higher incidence of gastrointestinal symptoms.
In December 2020, the FDA also approved liraglutide (Saxenda) for the treatment of obesity in youth age 12 and older (at a dose of 3 mg as opposed to the 1.8-mg dose of liraglutide [Victoza]), “which is wonderful news considering that the majority of pediatric patients with type 2 diabetes also have obesity,” Dr. Isganaitis added.
“The results of studies of liraglutide on glycemia in diabetic youth are impressive, with both an additional benefit of weight loss and without unacceptable identified risks or side effects,” Dr. Copeland concurred.
Waiting in the wings
Dr. Isganaitis reported that a few phase 3 clinical trials of other therapies for pediatric patients with type 2 diabetes are in the wings.
The 24-week phase 3 T2GO clinical trial of the sodium-glucose cotransporter 2 inhibitor dapagliflozin (AstraZeneca) versus placebo in 72 patients with type 2 diabetes aged 10-24 years was completed in April 2020, and the data are being analyzed.
An AstraZeneca-sponsored phase 3 trial of the safety and efficacy of a weekly injection of the GLP-1 receptor agonist exenatide in 10- to 17-year-olds with type 2 diabetes (n = 82) has also been completed and data are being analyzed.
A Takeda-sponsored phase 3 pediatric study of the dipeptidyl peptidase–4 inhibitor alogliptin in 10- to 17-year-olds with type 2 diabetes (n = 150) is estimated to be completed by February 2022.
And the phase 3 DINAMO trial, sponsored by Boehringer Ingelheim, which is evaluating the efficacy and safety of the SGLT2 inhibitor empagliflozin (10 mg/25 mg) versus the DPP-4 inhibitor linagliptin (5 mg) versus placebo over 26 weeks in 10- to 17-year-olds with type 2 diabetes (estimated 186 participants), is expected to be completed in May 2023.
“I hope that these medications will demonstrate efficacy and allow pediatric patients with type 2 diabetes to have more treatment options,” Dr. Isganaitis concluded.
Type 2 diabetes more aggressive than type 1 diabetes in kids
According to Dr. Isganaitis, “there is a widely held misconception among the general public and even among some physicians that type 2 diabetes is somehow less worrisome or ‘milder’ than a diagnosis of type 1 diabetes.”
However, the risk of complications and severe morbidity is higher with a diagnosis of type 2 diabetes versus type 1 diabetes in a child, so “this condition needs to be managed intensively with a multidisciplinary team including pediatric endocrinology, nutrition [support], diabetes educators, and mental health support,” she emphasized.
Many people also believe that “type 2 diabetes in kids is a ‘lifestyle disease,’ ” she continued, “but in fact, there is a strong role for genetics.”
The ADA Presidents’ Select Abstract “paints a picture of youth-onset type 2 diabetes as a disease intermediate in extremity between monogenic diabetes [caused by mutations in a single gene] and type 2 diabetes [caused by multiple genes and lifestyle factors such as obesity], in which genetic variants in both insulin secretion and insulin response pathways are implicated.”
Along the same lines, Dr. Isganaitis presented an oral abstract at the meeting that showed that, among youth with newly diagnosed type 2 diabetes, those whose mothers had diabetes had faster disease progression and earlier onset of diabetes complications.
Dr. Isganaitis has reported no relevant financial relationships. Dr. Copeland has reported serving on data monitoring committees for Boehringer Ingelheim and Novo Nordisk, and on an advisory committee for a research study for Daiichi Sankyo.
A version of this article first appeared on Medscape.com.
There are limited treatment options for children and youth with type 2 diabetes, but a few novel therapies beyond metformin are on the horizon, experts said at the annual scientific sessions of the American Diabetes Association.
“Type 2 diabetes in youth only emerged as a well-recognized pediatric medical problem in the 1990s and the first decade of the 21st century,” session chair Kenneth C. Copeland, MD, said in an interview.
“Fortunately, a number of clinical trials of antidiabetic pharmacologic agents in diabetic youth have now been completed, demonstrating both safety and efficacy, and at long last, a ... variety of agents are finally in sight,” he noted.
Type 2 diabetes in youth is profoundly different from type 2 diabetes in adults, added Dr. Copeland, pediatrics professor emeritus, University of Oklahoma, Oklahoma City. In youth, its course is typically aggressive and refractive to treatment.
Concerted efforts at lifestyle intervention are important but insufficient, and a response to metformin, even when initiated at diagnosis, is often short lived, he added.
Because of the rapid glycemic deterioration that is typical of type 2 diabetes in youth and leads to the full array of diabetic complications, early aggressive pharmacologic treatment is indicated.
“We all look forward to this next decade ushering in new treatment options, spanning the spectrum from obesity prevention to complex pharmacologic intervention,” Dr. Copeland summarized.
Increasing prevalence of T2D in youth, limited therapies
Rates of type 2 diabetes in youth continue to increase, especially among non-White groups, and most of these individuals have less than optimal diabetes control, Elvira Isganaitis, MD, MPH, a pediatric endocrinologist at the Joslin Diabetes Center and assistant professor of pediatrics at Harvard Medical School, both in Boston, told the meeting.
Although the Food and Drug Administration has approved more than 25 drugs to treat type 2 diabetes in adults, “unfortunately,” metformin is the only oral medication approved to treat the disease in a pediatric population, “and a majority of youth either do not respond to it or do not tolerate it,” she said in an interview.
Dr. Copeland observed that “the TODAY study demonstrated conclusively that, despite an often dramatic initial improvement in glycemic control upon initiation of pharmacologic and lifestyle intervention, this initial response was followed by a rapid deterioration of beta-cell function and glycemic failure, indicating that additional pharmacologic agents were sorely needed for this population.”
The RISE study also showed that, compared with adults, youth had more rapid beta-cell deterioration despite treatment.
Until the June 2019 FDA approval of the injectable glucagonlike peptide–1 receptor agonist liraglutide (Victoza, Novo Nordisk) for children 10 years or older, “except for insulin, metformin was the only antidiabetic medication available for use in youth, severely limiting treatment options,” he added.
Liraglutide ‘a huge breakthrough,’ other options on the horizon
The FDA approval of liraglutide was “a huge breakthrough” as the first noninsulin drug for pediatric type 2 diabetes since metformin was approved for pediatric use in 2000, Dr. Isganaitis said.
The ELLIPSE study, on which the approval was based, showed liraglutide was effective at lowering hemoglobin A1c and was generally well tolerated, although it was associated with a higher incidence of gastrointestinal symptoms.
In December 2020, the FDA also approved liraglutide (Saxenda) for the treatment of obesity in youth age 12 and older (at a dose of 3 mg as opposed to the 1.8-mg dose of liraglutide [Victoza]), “which is wonderful news considering that the majority of pediatric patients with type 2 diabetes also have obesity,” Dr. Isganaitis added.
“The results of studies of liraglutide on glycemia in diabetic youth are impressive, with both an additional benefit of weight loss and without unacceptable identified risks or side effects,” Dr. Copeland concurred.
Waiting in the wings
Dr. Isganaitis reported that a few phase 3 clinical trials of other therapies for pediatric patients with type 2 diabetes are in the wings.
The 24-week phase 3 T2GO clinical trial of the sodium-glucose cotransporter 2 inhibitor dapagliflozin (AstraZeneca) versus placebo in 72 patients with type 2 diabetes aged 10-24 years was completed in April 2020, and the data are being analyzed.
An AstraZeneca-sponsored phase 3 trial of the safety and efficacy of a weekly injection of the GLP-1 receptor agonist exenatide in 10- to 17-year-olds with type 2 diabetes (n = 82) has also been completed and data are being analyzed.
A Takeda-sponsored phase 3 pediatric study of the dipeptidyl peptidase–4 inhibitor alogliptin in 10- to 17-year-olds with type 2 diabetes (n = 150) is estimated to be completed by February 2022.
And the phase 3 DINAMO trial, sponsored by Boehringer Ingelheim, which is evaluating the efficacy and safety of the SGLT2 inhibitor empagliflozin (10 mg/25 mg) versus the DPP-4 inhibitor linagliptin (5 mg) versus placebo over 26 weeks in 10- to 17-year-olds with type 2 diabetes (estimated 186 participants), is expected to be completed in May 2023.
“I hope that these medications will demonstrate efficacy and allow pediatric patients with type 2 diabetes to have more treatment options,” Dr. Isganaitis concluded.
Type 2 diabetes more aggressive than type 1 diabetes in kids
According to Dr. Isganaitis, “there is a widely held misconception among the general public and even among some physicians that type 2 diabetes is somehow less worrisome or ‘milder’ than a diagnosis of type 1 diabetes.”
However, the risk of complications and severe morbidity is higher with a diagnosis of type 2 diabetes versus type 1 diabetes in a child, so “this condition needs to be managed intensively with a multidisciplinary team including pediatric endocrinology, nutrition [support], diabetes educators, and mental health support,” she emphasized.
Many people also believe that “type 2 diabetes in kids is a ‘lifestyle disease,’ ” she continued, “but in fact, there is a strong role for genetics.”
The ADA Presidents’ Select Abstract “paints a picture of youth-onset type 2 diabetes as a disease intermediate in extremity between monogenic diabetes [caused by mutations in a single gene] and type 2 diabetes [caused by multiple genes and lifestyle factors such as obesity], in which genetic variants in both insulin secretion and insulin response pathways are implicated.”
Along the same lines, Dr. Isganaitis presented an oral abstract at the meeting that showed that, among youth with newly diagnosed type 2 diabetes, those whose mothers had diabetes had faster disease progression and earlier onset of diabetes complications.
Dr. Isganaitis has reported no relevant financial relationships. Dr. Copeland has reported serving on data monitoring committees for Boehringer Ingelheim and Novo Nordisk, and on an advisory committee for a research study for Daiichi Sankyo.
A version of this article first appeared on Medscape.com.
Cancer mortality continues to drop in females as breast cancer reversal looms
Overall cancer mortality in females continues to decrease in the United States, but “previous declining trends in death rates slowed” for breast cancer in recent years, according to an annual report by several national organizations.
The analysis of long-term trends in cancer death rates shows that a decline of 1.4% per year from 2001 to 2016 accelerated to 2.1% per year in 2016-2018, the American Cancer Society, Centers for Disease Control and Prevention, National Cancer Institute, and the North American Association of Central Cancer Registries said.
Decreases in overall cancer mortality were seen in females of all races and ethnic groups over the most recent 5-year period included in the report, 2014-2018, varying from –1.6% per year in both non-Hispanic Blacks and Whites to –0.9% for non-Hispanic American Indians/Alaska Natives (AI/ANs), Farhad Islami, MD, PhD, of the American Cancer Society, Atlanta, and associates said in the Journal of the National Cancer Institute.
Over those 5 years, death rates fell for 14 of the 20 most common cancers in females; increased for liver, uterus, brain, pancreas, and soft tissue including heart; and remained stable for cancers of the oral cavity/pharynx, they reported.
Breast cancer was among those that declined, but the rate of that decline has been slowing. Mortality declined by an average of 2.3% per year in 2003-2007, by 1.6% a year in 2007-2014, and by just 1.0% annually during 2014-2018, based on data from the National Center for Health Statistics’ National Vital Statistics System.
Mortality from all cancers in 2014-2018 was 133.5 deaths per 100,000 standard population, with the racial/ethnic gap ranging from 85.4 per 100,000 (non-Hispanic Asian/Pacific Islander) to 154.9 (non-Hispanic Black), Dr. Islami and associates said.
Melanoma had the largest decline in mortality over that period among the 20 most common cancers in females, falling by an average of 4.4% per year, with lung cancer next at 4.3%. Among those with increased death rates, uterine cancer saw the largest rise at 2.0% a year, the research team said.
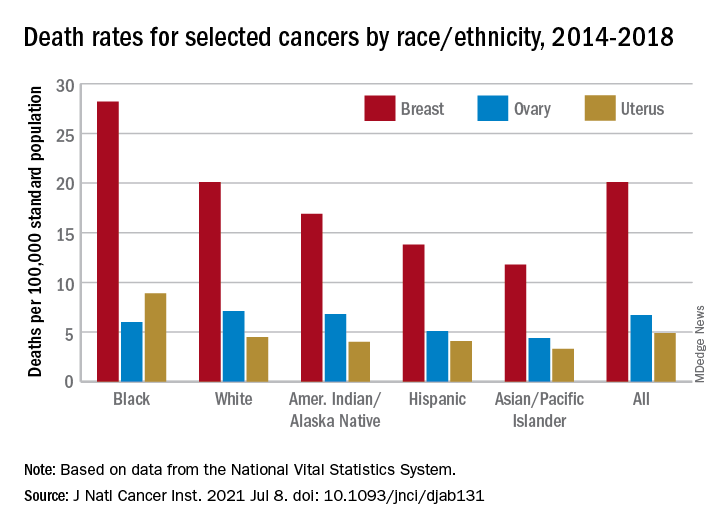
The deaths caused by cancer of the uterus were most common in non-Hispanic Black females, 8.9 per 100,000 population, followed by non-Hispanic White (4.5), Hispanic (4.1), non-Hispanic AI/AN (4.0), and non-Hispanic Asian/Pacific Islander (3.3), they reported.
“Long-term increasing trends in uterine cancer death rates parallel trends in incidence, although death rates are increasing at a somewhat faster rate. Increasing uterine cancer incidence has been attributed to increasing obesity prevalence and decreased use of combined hormone replacement therapy,” Dr. Islami and associates pointed out.
Breast cancer deaths also were most common among Blacks in 2014-2018, occurring at a rate of 28.2 per 100,000, as were deaths from cancer of the cervix (3.4 per 100,000), while ovarian cancers deaths were highest in White females (7.1 per 100,000), the researchers noted.
The continuing racial and ethnic disparity “largely reflects a combination of multiple intertwined factors” of tumor biology, diagnosis, treatment, and systemic discrimination, they wrote, adding that Black persons “are more likely to have a higher exposure to some cancer risk factors and limited access to healthy food, safe places for physical activity, and evidence-based cancer preventive services.”
The report was funded by the four participating groups. Six of the 12 investigators are employees of the American Cancer Society whose salaries are solely paid by the society; the other authors had no conflicts of interest to disclose.
Overall cancer mortality in females continues to decrease in the United States, but “previous declining trends in death rates slowed” for breast cancer in recent years, according to an annual report by several national organizations.
The analysis of long-term trends in cancer death rates shows that a decline of 1.4% per year from 2001 to 2016 accelerated to 2.1% per year in 2016-2018, the American Cancer Society, Centers for Disease Control and Prevention, National Cancer Institute, and the North American Association of Central Cancer Registries said.
Decreases in overall cancer mortality were seen in females of all races and ethnic groups over the most recent 5-year period included in the report, 2014-2018, varying from –1.6% per year in both non-Hispanic Blacks and Whites to –0.9% for non-Hispanic American Indians/Alaska Natives (AI/ANs), Farhad Islami, MD, PhD, of the American Cancer Society, Atlanta, and associates said in the Journal of the National Cancer Institute.
Over those 5 years, death rates fell for 14 of the 20 most common cancers in females; increased for liver, uterus, brain, pancreas, and soft tissue including heart; and remained stable for cancers of the oral cavity/pharynx, they reported.
Breast cancer was among those that declined, but the rate of that decline has been slowing. Mortality declined by an average of 2.3% per year in 2003-2007, by 1.6% a year in 2007-2014, and by just 1.0% annually during 2014-2018, based on data from the National Center for Health Statistics’ National Vital Statistics System.
Mortality from all cancers in 2014-2018 was 133.5 deaths per 100,000 standard population, with the racial/ethnic gap ranging from 85.4 per 100,000 (non-Hispanic Asian/Pacific Islander) to 154.9 (non-Hispanic Black), Dr. Islami and associates said.
Melanoma had the largest decline in mortality over that period among the 20 most common cancers in females, falling by an average of 4.4% per year, with lung cancer next at 4.3%. Among those with increased death rates, uterine cancer saw the largest rise at 2.0% a year, the research team said.
The deaths caused by cancer of the uterus were most common in non-Hispanic Black females, 8.9 per 100,000 population, followed by non-Hispanic White (4.5), Hispanic (4.1), non-Hispanic AI/AN (4.0), and non-Hispanic Asian/Pacific Islander (3.3), they reported.
“Long-term increasing trends in uterine cancer death rates parallel trends in incidence, although death rates are increasing at a somewhat faster rate. Increasing uterine cancer incidence has been attributed to increasing obesity prevalence and decreased use of combined hormone replacement therapy,” Dr. Islami and associates pointed out.
Breast cancer deaths also were most common among Blacks in 2014-2018, occurring at a rate of 28.2 per 100,000, as were deaths from cancer of the cervix (3.4 per 100,000), while ovarian cancers deaths were highest in White females (7.1 per 100,000), the researchers noted.
The continuing racial and ethnic disparity “largely reflects a combination of multiple intertwined factors” of tumor biology, diagnosis, treatment, and systemic discrimination, they wrote, adding that Black persons “are more likely to have a higher exposure to some cancer risk factors and limited access to healthy food, safe places for physical activity, and evidence-based cancer preventive services.”
The report was funded by the four participating groups. Six of the 12 investigators are employees of the American Cancer Society whose salaries are solely paid by the society; the other authors had no conflicts of interest to disclose.
Overall cancer mortality in females continues to decrease in the United States, but “previous declining trends in death rates slowed” for breast cancer in recent years, according to an annual report by several national organizations.
The analysis of long-term trends in cancer death rates shows that a decline of 1.4% per year from 2001 to 2016 accelerated to 2.1% per year in 2016-2018, the American Cancer Society, Centers for Disease Control and Prevention, National Cancer Institute, and the North American Association of Central Cancer Registries said.
Decreases in overall cancer mortality were seen in females of all races and ethnic groups over the most recent 5-year period included in the report, 2014-2018, varying from –1.6% per year in both non-Hispanic Blacks and Whites to –0.9% for non-Hispanic American Indians/Alaska Natives (AI/ANs), Farhad Islami, MD, PhD, of the American Cancer Society, Atlanta, and associates said in the Journal of the National Cancer Institute.
Over those 5 years, death rates fell for 14 of the 20 most common cancers in females; increased for liver, uterus, brain, pancreas, and soft tissue including heart; and remained stable for cancers of the oral cavity/pharynx, they reported.
Breast cancer was among those that declined, but the rate of that decline has been slowing. Mortality declined by an average of 2.3% per year in 2003-2007, by 1.6% a year in 2007-2014, and by just 1.0% annually during 2014-2018, based on data from the National Center for Health Statistics’ National Vital Statistics System.
Mortality from all cancers in 2014-2018 was 133.5 deaths per 100,000 standard population, with the racial/ethnic gap ranging from 85.4 per 100,000 (non-Hispanic Asian/Pacific Islander) to 154.9 (non-Hispanic Black), Dr. Islami and associates said.
Melanoma had the largest decline in mortality over that period among the 20 most common cancers in females, falling by an average of 4.4% per year, with lung cancer next at 4.3%. Among those with increased death rates, uterine cancer saw the largest rise at 2.0% a year, the research team said.
The deaths caused by cancer of the uterus were most common in non-Hispanic Black females, 8.9 per 100,000 population, followed by non-Hispanic White (4.5), Hispanic (4.1), non-Hispanic AI/AN (4.0), and non-Hispanic Asian/Pacific Islander (3.3), they reported.
“Long-term increasing trends in uterine cancer death rates parallel trends in incidence, although death rates are increasing at a somewhat faster rate. Increasing uterine cancer incidence has been attributed to increasing obesity prevalence and decreased use of combined hormone replacement therapy,” Dr. Islami and associates pointed out.
Breast cancer deaths also were most common among Blacks in 2014-2018, occurring at a rate of 28.2 per 100,000, as were deaths from cancer of the cervix (3.4 per 100,000), while ovarian cancers deaths were highest in White females (7.1 per 100,000), the researchers noted.
The continuing racial and ethnic disparity “largely reflects a combination of multiple intertwined factors” of tumor biology, diagnosis, treatment, and systemic discrimination, they wrote, adding that Black persons “are more likely to have a higher exposure to some cancer risk factors and limited access to healthy food, safe places for physical activity, and evidence-based cancer preventive services.”
The report was funded by the four participating groups. Six of the 12 investigators are employees of the American Cancer Society whose salaries are solely paid by the society; the other authors had no conflicts of interest to disclose.
FROM THE JOURNAL OF THE NATIONAL CANCER INSTITUTE
Rising rates of T1D in children: Is COVID to blame?
In early 2020, the COVID-19 pandemic changed everything about life as we know it, with widespread shutdowns across the globe. The U.S. health care system quickly adapted, pivoting to telehealth visits when able and proactively managing outpatient conditions to prevent overwhelming hospital resources and utilization. Meanwhile, at my practice, the typical rate of about one new-onset pediatric type 1 diabetes (T1D) case per week increased to about two per week.

However, the new diabetes cases continued to accumulate, and I saw more patients being diagnosed who did not have a known family history of autoimmunity. I began to ask friends at other centers whether they were noticing the same trend.
One colleague documented a 36% increase in her large center compared with the previous year. Another noted a 40% rise at his children’s hospital. We observed that there was often a respiratory illness reported several weeks before presenting with T1D. Sometimes the child was known to be COVID-positive. Sometimes the child had not been tested. Sometimes we suspected that COVID had been a preceding illness and then found negative SARS-CoV-2 antibodies – but we were not certain whether the result was meaningful given the time lapsed since infection.
Soon, reports emerged of large increases in severe diabetic ketoacidosis (DKA) and hyperglycemic hyperosmolar state at initial presentation, a trend reported in other countries.
Is COVID-19 a trigger for T1D?
There is known precedent for increased risk for T1D after viral infections in patients who are already genetically susceptible. Mechanisms of immune-mediated islet cell failure would make sense following SARS-CoV-2 infection; direct islet toxicity was noted with SARS-CoV-1 and has been suspected with SARS-CoV-2 but not proven. Some have suggested that hypercoagulability with COVID-19 may lead to ischemic damage to the pancreas.
With multiple potential pathways for islet damage, increases in insulin-dependent diabetes would logically follow. Still, whether this is the case remains unclear. There is not yet definitive evidence that there is uptake of SARS-CoV-2 via receptors in the pancreatic beta cells.
Our current understanding of T1D pathogenesis is that susceptible individuals develop autoimmunity in response to an environmental trigger, with beta-cell failure developing over months to years. Perhaps vulnerable patients with genetic risk for pancreatic autoimmunity were stressed by SARS-CoV-2 infection and were diagnosed earlier than they might have been, showing some lead-time bias. Adult patients with COVID-19 demonstrated hyperglycemia that has been reversible in some cases, like the stress hyperglycemia seen with other infections and surgery in response to proinflammatory states.
The true question seems to be whether there is a unique type of diabetes related to direct viral toxicity. Do newly diagnosed patients have measurable traditional antibodies, like anti-glutamic acid decarboxylase or anti-islet cell antibodies? Is there proof of preceding SARS-CoV-2 infection? In the new cases that I thought were unusual at first glance, I found typical pancreatic autoimmunity and negative SARS-CoV-2 antibodies. The small cohorts reported thus far have had similar findings.
A stronger case can be made for the risk of developing diabetes (types 1 and 2) with rapid weight gain. Another marked pattern that pediatric endocrinologists have observed has been increased weight gain in children with closed schools, decreased activity, and more social isolation. I have seen weight change as great as 100 lb in a teen over the past year; 30- to 50-lb weight increases over the course of the pandemic have been common. Considering the “accelerator hypothesis” of faster onset of type 2 diabetes with rapid weight gain, implications for hastening of T1D with weight gain have also been considered. The full impact of these dramatic weight changes will take time to understand.
The true story may not emerge for years
Anecdotes and theoretical concerns may give us pause, but they are far from scientific truth. Efforts are underway to explore this perceived trend with international registries, including the CoviDIAB Registry as well as T1D Exchange. The true story may not emerge until years have passed to see the cumulative fallout of COVID-19. Regardless, these troubling observations should be considered as pandemic safeguards continue to loosen.
While pediatric mortality from COVID-19 has been relatively low (though sadly not zero), some have placed too little focus on possible morbidity. Long-term effects like long COVID and neuropsychiatric sequelae are becoming evident in all populations, including children. If a lifelong illness like diabetes can be directly linked to COVID-19, protecting children from infection with measures like masks becomes all the more crucial until vaccines are more readily available. Despite our rapid progress with understanding COVID-19 disease, there is still much left to learn.
A version of this article first appeared on Medscape.com.
In early 2020, the COVID-19 pandemic changed everything about life as we know it, with widespread shutdowns across the globe. The U.S. health care system quickly adapted, pivoting to telehealth visits when able and proactively managing outpatient conditions to prevent overwhelming hospital resources and utilization. Meanwhile, at my practice, the typical rate of about one new-onset pediatric type 1 diabetes (T1D) case per week increased to about two per week.
However, the new diabetes cases continued to accumulate, and I saw more patients being diagnosed who did not have a known family history of autoimmunity. I began to ask friends at other centers whether they were noticing the same trend.
One colleague documented a 36% increase in her large center compared with the previous year. Another noted a 40% rise at his children’s hospital. We observed that there was often a respiratory illness reported several weeks before presenting with T1D. Sometimes the child was known to be COVID-positive. Sometimes the child had not been tested. Sometimes we suspected that COVID had been a preceding illness and then found negative SARS-CoV-2 antibodies – but we were not certain whether the result was meaningful given the time lapsed since infection.
Soon, reports emerged of large increases in severe diabetic ketoacidosis (DKA) and hyperglycemic hyperosmolar state at initial presentation, a trend reported in other countries.
Is COVID-19 a trigger for T1D?
There is known precedent for increased risk for T1D after viral infections in patients who are already genetically susceptible. Mechanisms of immune-mediated islet cell failure would make sense following SARS-CoV-2 infection; direct islet toxicity was noted with SARS-CoV-1 and has been suspected with SARS-CoV-2 but not proven. Some have suggested that hypercoagulability with COVID-19 may lead to ischemic damage to the pancreas.
With multiple potential pathways for islet damage, increases in insulin-dependent diabetes would logically follow. Still, whether this is the case remains unclear. There is not yet definitive evidence that there is uptake of SARS-CoV-2 via receptors in the pancreatic beta cells.
Our current understanding of T1D pathogenesis is that susceptible individuals develop autoimmunity in response to an environmental trigger, with beta-cell failure developing over months to years. Perhaps vulnerable patients with genetic risk for pancreatic autoimmunity were stressed by SARS-CoV-2 infection and were diagnosed earlier than they might have been, showing some lead-time bias. Adult patients with COVID-19 demonstrated hyperglycemia that has been reversible in some cases, like the stress hyperglycemia seen with other infections and surgery in response to proinflammatory states.
The true question seems to be whether there is a unique type of diabetes related to direct viral toxicity. Do newly diagnosed patients have measurable traditional antibodies, like anti-glutamic acid decarboxylase or anti-islet cell antibodies? Is there proof of preceding SARS-CoV-2 infection? In the new cases that I thought were unusual at first glance, I found typical pancreatic autoimmunity and negative SARS-CoV-2 antibodies. The small cohorts reported thus far have had similar findings.
A stronger case can be made for the risk of developing diabetes (types 1 and 2) with rapid weight gain. Another marked pattern that pediatric endocrinologists have observed has been increased weight gain in children with closed schools, decreased activity, and more social isolation. I have seen weight change as great as 100 lb in a teen over the past year; 30- to 50-lb weight increases over the course of the pandemic have been common. Considering the “accelerator hypothesis” of faster onset of type 2 diabetes with rapid weight gain, implications for hastening of T1D with weight gain have also been considered. The full impact of these dramatic weight changes will take time to understand.
The true story may not emerge for years
Anecdotes and theoretical concerns may give us pause, but they are far from scientific truth. Efforts are underway to explore this perceived trend with international registries, including the CoviDIAB Registry as well as T1D Exchange. The true story may not emerge until years have passed to see the cumulative fallout of COVID-19. Regardless, these troubling observations should be considered as pandemic safeguards continue to loosen.
While pediatric mortality from COVID-19 has been relatively low (though sadly not zero), some have placed too little focus on possible morbidity. Long-term effects like long COVID and neuropsychiatric sequelae are becoming evident in all populations, including children. If a lifelong illness like diabetes can be directly linked to COVID-19, protecting children from infection with measures like masks becomes all the more crucial until vaccines are more readily available. Despite our rapid progress with understanding COVID-19 disease, there is still much left to learn.
A version of this article first appeared on Medscape.com.
In early 2020, the COVID-19 pandemic changed everything about life as we know it, with widespread shutdowns across the globe. The U.S. health care system quickly adapted, pivoting to telehealth visits when able and proactively managing outpatient conditions to prevent overwhelming hospital resources and utilization. Meanwhile, at my practice, the typical rate of about one new-onset pediatric type 1 diabetes (T1D) case per week increased to about two per week.
However, the new diabetes cases continued to accumulate, and I saw more patients being diagnosed who did not have a known family history of autoimmunity. I began to ask friends at other centers whether they were noticing the same trend.
One colleague documented a 36% increase in her large center compared with the previous year. Another noted a 40% rise at his children’s hospital. We observed that there was often a respiratory illness reported several weeks before presenting with T1D. Sometimes the child was known to be COVID-positive. Sometimes the child had not been tested. Sometimes we suspected that COVID had been a preceding illness and then found negative SARS-CoV-2 antibodies – but we were not certain whether the result was meaningful given the time lapsed since infection.
Soon, reports emerged of large increases in severe diabetic ketoacidosis (DKA) and hyperglycemic hyperosmolar state at initial presentation, a trend reported in other countries.
Is COVID-19 a trigger for T1D?
There is known precedent for increased risk for T1D after viral infections in patients who are already genetically susceptible. Mechanisms of immune-mediated islet cell failure would make sense following SARS-CoV-2 infection; direct islet toxicity was noted with SARS-CoV-1 and has been suspected with SARS-CoV-2 but not proven. Some have suggested that hypercoagulability with COVID-19 may lead to ischemic damage to the pancreas.
With multiple potential pathways for islet damage, increases in insulin-dependent diabetes would logically follow. Still, whether this is the case remains unclear. There is not yet definitive evidence that there is uptake of SARS-CoV-2 via receptors in the pancreatic beta cells.
Our current understanding of T1D pathogenesis is that susceptible individuals develop autoimmunity in response to an environmental trigger, with beta-cell failure developing over months to years. Perhaps vulnerable patients with genetic risk for pancreatic autoimmunity were stressed by SARS-CoV-2 infection and were diagnosed earlier than they might have been, showing some lead-time bias. Adult patients with COVID-19 demonstrated hyperglycemia that has been reversible in some cases, like the stress hyperglycemia seen with other infections and surgery in response to proinflammatory states.
The true question seems to be whether there is a unique type of diabetes related to direct viral toxicity. Do newly diagnosed patients have measurable traditional antibodies, like anti-glutamic acid decarboxylase or anti-islet cell antibodies? Is there proof of preceding SARS-CoV-2 infection? In the new cases that I thought were unusual at first glance, I found typical pancreatic autoimmunity and negative SARS-CoV-2 antibodies. The small cohorts reported thus far have had similar findings.
A stronger case can be made for the risk of developing diabetes (types 1 and 2) with rapid weight gain. Another marked pattern that pediatric endocrinologists have observed has been increased weight gain in children with closed schools, decreased activity, and more social isolation. I have seen weight change as great as 100 lb in a teen over the past year; 30- to 50-lb weight increases over the course of the pandemic have been common. Considering the “accelerator hypothesis” of faster onset of type 2 diabetes with rapid weight gain, implications for hastening of T1D with weight gain have also been considered. The full impact of these dramatic weight changes will take time to understand.
The true story may not emerge for years
Anecdotes and theoretical concerns may give us pause, but they are far from scientific truth. Efforts are underway to explore this perceived trend with international registries, including the CoviDIAB Registry as well as T1D Exchange. The true story may not emerge until years have passed to see the cumulative fallout of COVID-19. Regardless, these troubling observations should be considered as pandemic safeguards continue to loosen.
While pediatric mortality from COVID-19 has been relatively low (though sadly not zero), some have placed too little focus on possible morbidity. Long-term effects like long COVID and neuropsychiatric sequelae are becoming evident in all populations, including children. If a lifelong illness like diabetes can be directly linked to COVID-19, protecting children from infection with measures like masks becomes all the more crucial until vaccines are more readily available. Despite our rapid progress with understanding COVID-19 disease, there is still much left to learn.
A version of this article first appeared on Medscape.com.
Good survival, outcomes with TARE for HCC in practice
Patients with hepatocellular carcinoma (HCC) can be offered transarterial radioembolization (TARE) as a safe and effective first-line treatment or adjunct to other locoregional therapies, authors of a large multicenter study reported.
Among 422 patients with HCC treated with TARE in eight European countries, the median overall survival was 16.5 months, with fewer than 10% of patients experiencing grade 3 or greater adverse events, reported Frank Kolligs, MD, from Helios Hospital Berlin-Buch.
“This exploratory study evaluated factors that can influence the application and outcome of transarterial radioembolization in clinical practice. TARE is generally applied according to guideline recommendations, and randomized, controlled trials are needed to confirm the effect of personalized dosimetry on the effectiveness of TARE,” he said in an oral abstract presented at the meeting sponsored by the European Association for the Study of the Liver.
Intriguingly, the investigators found evidence suggesting that patients whose treatments were planned using a partition model had better survival outcomes than those patients who treatments were based on calculated body surface area or measured BSA (mBSA), but this finding will need to be explored in more detail, Dr. Kolligs said.
The partition model incorporates variables such as tumor volume and liver volume, shunt fractions, the ratio of radiation uptake between tumor and normal tissues, vascular anatomy and other factors to estimate the optimal dose.
Study design
Dr. Kolligs and colleagues looked at prospective data from the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) Registry for SIR-Spheres Therapy to evaluate the real-world clinical application of TARE with yttrium Y-90 resin microspheres in Europe, clinical outcomes, safety, and quality of life.
They selected data from centers with a minimum of 10 cases performed in the previous 12 months and at least 40 total cases overall.
The patients included adults 18 years and older scheduled for treatment with Y-90 resin microspheres for primary or metastatic liver tumors, with no specific exclusion criteria. The patients were followed for at least 24 months at recommended intervals of every 3 months. The first patient was enrolled in January 2015, and the last follow-up visit was in December 2019. A total of 422 registry patients had a diagnosis of HCC and were included in the study.
The median age was 68 years (range, 60-74), 80.8% were male, 70.9% had cirrhosis, 14.5% had ascites, and 8.5% had extrahepatic disease. About 32% of patients had one tumor nodule, 33% had two to five nodules, and the remainder had either more than five or an uncountable number.
In all, 14% of patients had Barcelona Clinic Liver Cancer stage A disease, 51.4% had stage B, 33.6% had stage C, and 0.9% stage D.
About one-third of patients had portal vein occlusion. Tumors were in both left and right lobes in 35.5%, the left lobe alone in 12.1%, and the right lobe alone in 52.4%.
Half of all patients (50.2%) received TARE as first-line therapy, 44.8% had it following surgery (17.1%), ablation (14.7%), and/or transarterial chemoembolization (; 23%). In addition, 9.7% of patients received systemic therapy prior to TARE, primarily with sorafenib (Nexavar).
Treatment intent was palliative for 57.3% of patients, and tumor downsizing/downstaging in 32.5% (remainder unspecified).
Survival and prognostic factors
As noted before, median overall survival was 16.5 months. Median progression-free survival was 6.1 months, and median hepatic PFS was 6.7 months.
Factors prognostic for better overall survival included hepatitis B or C virus as the cirrhosis cause versus alcohol (hazard ratio for death, 0.51 for each; P = .0060 for HBV and P = .0007 for HCV); unilobar versus bilobar tumors (HR, 0.67; P = .0422 for left-lobe; HR 0.55; P < .0001 for right); prior surgery (HR, 0.67; P = .0258); prior ablation (HR, 0.65; P = .0394); and curative versus palliative intent (HR, 0.53; P < .0001).
Factors associated with worse overall survival were presence of ascites (HR 1.75, P = .001); presence of extrahepatic disease before TARE (HR, 1.81, P = .0037); tumor burden greater than 5 nodules (HR, 1.67; P = .0073); main portal vein occlusion (HR, 2.14; P = .0064); lobar portal vein occlusion (HR, 1.77; P = .0083); total bilirubin greater than 1.5 mg/dL (HR, 1.69; P = .0094); albumin-bilirubin grade A2 (HR, 1.66; P = .0005); ALB1 grade A3 (HR, 3.92; P < .0001); and BSA/mBSA versus partition-model dosimetry (HR, 1.89; P < .0001).
The safety analysis showed that 36.7% of patients had at least one adverse event, but only 7.1% had at least one grade 3 or greater event.
Grade 3 or greater events were abdominal pain (nine patients), fatigue (six), nausea (three), radioembolization-induced liver disease (three), vomiting (two), and GI ulceration (one). Fifteen additional patients had other unspecified events.
The investigators acknowledged broad inclusion criteria, relatively high rates of loss to follow-up, and differences in national guidelines and local standards of practice as potential limitations to their findings.
In the question-and-answer following the presentation, session comoderator María Varela, MD, PhD, a pathologist in the liver unit at the Hospital Universitario Central de Asturia, Oviedo, Spain, questioned why about one-third of patients received TARE for downstaging, but only 13 underwent subsequent surgical resection.
“We don’t have a detailed analysis of this subgroup of patients who received curative intent as yet, ” Dr. Kolligs said.
Pierre Nahon, MD, from the University of Paris and Hôpital Jean Verdier in Bondy, France, commented that, among this heterogenous population, one of the best indications for TARE is probably localized HCC with adjacent portal vein thrombosis.
He asked whether the investigators had examined overall survival among patients with localized unilobar HCC with adjacent small portal vein thrombosis.
“We find that patients with portal vein occlusion have a worse prognosis in the total group,” Dr. Kolligs replied. “To look into the question whether partial thrombosis with a small tumor might benefit is an interesting question, and we should look into that, but I don’t have any data on that yet.”
Another audience member asked: “According to your data, which patients are the best candidates for radioembolization?”
“According to these data, the best candidates are of course patients with good liver function, ascites should ideally not be present, and what is probably is important is that we identify or include patients without extrahepatic disease,” he said.
The study was sponsored by CIRSE. Dr. Kolligs disclosed speaking activities and consulting for several companies. Dr. Varela disclosed speaking for several companies and advisory board activity for Bayer. Dr. Nahon disclosed honoraria and consulting fees from several companies.
Patients with hepatocellular carcinoma (HCC) can be offered transarterial radioembolization (TARE) as a safe and effective first-line treatment or adjunct to other locoregional therapies, authors of a large multicenter study reported.
Among 422 patients with HCC treated with TARE in eight European countries, the median overall survival was 16.5 months, with fewer than 10% of patients experiencing grade 3 or greater adverse events, reported Frank Kolligs, MD, from Helios Hospital Berlin-Buch.
“This exploratory study evaluated factors that can influence the application and outcome of transarterial radioembolization in clinical practice. TARE is generally applied according to guideline recommendations, and randomized, controlled trials are needed to confirm the effect of personalized dosimetry on the effectiveness of TARE,” he said in an oral abstract presented at the meeting sponsored by the European Association for the Study of the Liver.
Intriguingly, the investigators found evidence suggesting that patients whose treatments were planned using a partition model had better survival outcomes than those patients who treatments were based on calculated body surface area or measured BSA (mBSA), but this finding will need to be explored in more detail, Dr. Kolligs said.
The partition model incorporates variables such as tumor volume and liver volume, shunt fractions, the ratio of radiation uptake between tumor and normal tissues, vascular anatomy and other factors to estimate the optimal dose.
Study design
Dr. Kolligs and colleagues looked at prospective data from the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) Registry for SIR-Spheres Therapy to evaluate the real-world clinical application of TARE with yttrium Y-90 resin microspheres in Europe, clinical outcomes, safety, and quality of life.
They selected data from centers with a minimum of 10 cases performed in the previous 12 months and at least 40 total cases overall.
The patients included adults 18 years and older scheduled for treatment with Y-90 resin microspheres for primary or metastatic liver tumors, with no specific exclusion criteria. The patients were followed for at least 24 months at recommended intervals of every 3 months. The first patient was enrolled in January 2015, and the last follow-up visit was in December 2019. A total of 422 registry patients had a diagnosis of HCC and were included in the study.
The median age was 68 years (range, 60-74), 80.8% were male, 70.9% had cirrhosis, 14.5% had ascites, and 8.5% had extrahepatic disease. About 32% of patients had one tumor nodule, 33% had two to five nodules, and the remainder had either more than five or an uncountable number.
In all, 14% of patients had Barcelona Clinic Liver Cancer stage A disease, 51.4% had stage B, 33.6% had stage C, and 0.9% stage D.
About one-third of patients had portal vein occlusion. Tumors were in both left and right lobes in 35.5%, the left lobe alone in 12.1%, and the right lobe alone in 52.4%.
Half of all patients (50.2%) received TARE as first-line therapy, 44.8% had it following surgery (17.1%), ablation (14.7%), and/or transarterial chemoembolization (; 23%). In addition, 9.7% of patients received systemic therapy prior to TARE, primarily with sorafenib (Nexavar).
Treatment intent was palliative for 57.3% of patients, and tumor downsizing/downstaging in 32.5% (remainder unspecified).
Survival and prognostic factors
As noted before, median overall survival was 16.5 months. Median progression-free survival was 6.1 months, and median hepatic PFS was 6.7 months.
Factors prognostic for better overall survival included hepatitis B or C virus as the cirrhosis cause versus alcohol (hazard ratio for death, 0.51 for each; P = .0060 for HBV and P = .0007 for HCV); unilobar versus bilobar tumors (HR, 0.67; P = .0422 for left-lobe; HR 0.55; P < .0001 for right); prior surgery (HR, 0.67; P = .0258); prior ablation (HR, 0.65; P = .0394); and curative versus palliative intent (HR, 0.53; P < .0001).
Factors associated with worse overall survival were presence of ascites (HR 1.75, P = .001); presence of extrahepatic disease before TARE (HR, 1.81, P = .0037); tumor burden greater than 5 nodules (HR, 1.67; P = .0073); main portal vein occlusion (HR, 2.14; P = .0064); lobar portal vein occlusion (HR, 1.77; P = .0083); total bilirubin greater than 1.5 mg/dL (HR, 1.69; P = .0094); albumin-bilirubin grade A2 (HR, 1.66; P = .0005); ALB1 grade A3 (HR, 3.92; P < .0001); and BSA/mBSA versus partition-model dosimetry (HR, 1.89; P < .0001).
The safety analysis showed that 36.7% of patients had at least one adverse event, but only 7.1% had at least one grade 3 or greater event.
Grade 3 or greater events were abdominal pain (nine patients), fatigue (six), nausea (three), radioembolization-induced liver disease (three), vomiting (two), and GI ulceration (one). Fifteen additional patients had other unspecified events.
The investigators acknowledged broad inclusion criteria, relatively high rates of loss to follow-up, and differences in national guidelines and local standards of practice as potential limitations to their findings.
In the question-and-answer following the presentation, session comoderator María Varela, MD, PhD, a pathologist in the liver unit at the Hospital Universitario Central de Asturia, Oviedo, Spain, questioned why about one-third of patients received TARE for downstaging, but only 13 underwent subsequent surgical resection.
“We don’t have a detailed analysis of this subgroup of patients who received curative intent as yet, ” Dr. Kolligs said.
Pierre Nahon, MD, from the University of Paris and Hôpital Jean Verdier in Bondy, France, commented that, among this heterogenous population, one of the best indications for TARE is probably localized HCC with adjacent portal vein thrombosis.
He asked whether the investigators had examined overall survival among patients with localized unilobar HCC with adjacent small portal vein thrombosis.
“We find that patients with portal vein occlusion have a worse prognosis in the total group,” Dr. Kolligs replied. “To look into the question whether partial thrombosis with a small tumor might benefit is an interesting question, and we should look into that, but I don’t have any data on that yet.”
Another audience member asked: “According to your data, which patients are the best candidates for radioembolization?”
“According to these data, the best candidates are of course patients with good liver function, ascites should ideally not be present, and what is probably is important is that we identify or include patients without extrahepatic disease,” he said.
The study was sponsored by CIRSE. Dr. Kolligs disclosed speaking activities and consulting for several companies. Dr. Varela disclosed speaking for several companies and advisory board activity for Bayer. Dr. Nahon disclosed honoraria and consulting fees from several companies.
Patients with hepatocellular carcinoma (HCC) can be offered transarterial radioembolization (TARE) as a safe and effective first-line treatment or adjunct to other locoregional therapies, authors of a large multicenter study reported.
Among 422 patients with HCC treated with TARE in eight European countries, the median overall survival was 16.5 months, with fewer than 10% of patients experiencing grade 3 or greater adverse events, reported Frank Kolligs, MD, from Helios Hospital Berlin-Buch.
“This exploratory study evaluated factors that can influence the application and outcome of transarterial radioembolization in clinical practice. TARE is generally applied according to guideline recommendations, and randomized, controlled trials are needed to confirm the effect of personalized dosimetry on the effectiveness of TARE,” he said in an oral abstract presented at the meeting sponsored by the European Association for the Study of the Liver.
Intriguingly, the investigators found evidence suggesting that patients whose treatments were planned using a partition model had better survival outcomes than those patients who treatments were based on calculated body surface area or measured BSA (mBSA), but this finding will need to be explored in more detail, Dr. Kolligs said.
The partition model incorporates variables such as tumor volume and liver volume, shunt fractions, the ratio of radiation uptake between tumor and normal tissues, vascular anatomy and other factors to estimate the optimal dose.
Study design
Dr. Kolligs and colleagues looked at prospective data from the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) Registry for SIR-Spheres Therapy to evaluate the real-world clinical application of TARE with yttrium Y-90 resin microspheres in Europe, clinical outcomes, safety, and quality of life.
They selected data from centers with a minimum of 10 cases performed in the previous 12 months and at least 40 total cases overall.
The patients included adults 18 years and older scheduled for treatment with Y-90 resin microspheres for primary or metastatic liver tumors, with no specific exclusion criteria. The patients were followed for at least 24 months at recommended intervals of every 3 months. The first patient was enrolled in January 2015, and the last follow-up visit was in December 2019. A total of 422 registry patients had a diagnosis of HCC and were included in the study.
The median age was 68 years (range, 60-74), 80.8% were male, 70.9% had cirrhosis, 14.5% had ascites, and 8.5% had extrahepatic disease. About 32% of patients had one tumor nodule, 33% had two to five nodules, and the remainder had either more than five or an uncountable number.
In all, 14% of patients had Barcelona Clinic Liver Cancer stage A disease, 51.4% had stage B, 33.6% had stage C, and 0.9% stage D.
About one-third of patients had portal vein occlusion. Tumors were in both left and right lobes in 35.5%, the left lobe alone in 12.1%, and the right lobe alone in 52.4%.
Half of all patients (50.2%) received TARE as first-line therapy, 44.8% had it following surgery (17.1%), ablation (14.7%), and/or transarterial chemoembolization (; 23%). In addition, 9.7% of patients received systemic therapy prior to TARE, primarily with sorafenib (Nexavar).
Treatment intent was palliative for 57.3% of patients, and tumor downsizing/downstaging in 32.5% (remainder unspecified).
Survival and prognostic factors
As noted before, median overall survival was 16.5 months. Median progression-free survival was 6.1 months, and median hepatic PFS was 6.7 months.
Factors prognostic for better overall survival included hepatitis B or C virus as the cirrhosis cause versus alcohol (hazard ratio for death, 0.51 for each; P = .0060 for HBV and P = .0007 for HCV); unilobar versus bilobar tumors (HR, 0.67; P = .0422 for left-lobe; HR 0.55; P < .0001 for right); prior surgery (HR, 0.67; P = .0258); prior ablation (HR, 0.65; P = .0394); and curative versus palliative intent (HR, 0.53; P < .0001).
Factors associated with worse overall survival were presence of ascites (HR 1.75, P = .001); presence of extrahepatic disease before TARE (HR, 1.81, P = .0037); tumor burden greater than 5 nodules (HR, 1.67; P = .0073); main portal vein occlusion (HR, 2.14; P = .0064); lobar portal vein occlusion (HR, 1.77; P = .0083); total bilirubin greater than 1.5 mg/dL (HR, 1.69; P = .0094); albumin-bilirubin grade A2 (HR, 1.66; P = .0005); ALB1 grade A3 (HR, 3.92; P < .0001); and BSA/mBSA versus partition-model dosimetry (HR, 1.89; P < .0001).
The safety analysis showed that 36.7% of patients had at least one adverse event, but only 7.1% had at least one grade 3 or greater event.
Grade 3 or greater events were abdominal pain (nine patients), fatigue (six), nausea (three), radioembolization-induced liver disease (three), vomiting (two), and GI ulceration (one). Fifteen additional patients had other unspecified events.
The investigators acknowledged broad inclusion criteria, relatively high rates of loss to follow-up, and differences in national guidelines and local standards of practice as potential limitations to their findings.
In the question-and-answer following the presentation, session comoderator María Varela, MD, PhD, a pathologist in the liver unit at the Hospital Universitario Central de Asturia, Oviedo, Spain, questioned why about one-third of patients received TARE for downstaging, but only 13 underwent subsequent surgical resection.
“We don’t have a detailed analysis of this subgroup of patients who received curative intent as yet, ” Dr. Kolligs said.
Pierre Nahon, MD, from the University of Paris and Hôpital Jean Verdier in Bondy, France, commented that, among this heterogenous population, one of the best indications for TARE is probably localized HCC with adjacent portal vein thrombosis.
He asked whether the investigators had examined overall survival among patients with localized unilobar HCC with adjacent small portal vein thrombosis.
“We find that patients with portal vein occlusion have a worse prognosis in the total group,” Dr. Kolligs replied. “To look into the question whether partial thrombosis with a small tumor might benefit is an interesting question, and we should look into that, but I don’t have any data on that yet.”
Another audience member asked: “According to your data, which patients are the best candidates for radioembolization?”
“According to these data, the best candidates are of course patients with good liver function, ascites should ideally not be present, and what is probably is important is that we identify or include patients without extrahepatic disease,” he said.
The study was sponsored by CIRSE. Dr. Kolligs disclosed speaking activities and consulting for several companies. Dr. Varela disclosed speaking for several companies and advisory board activity for Bayer. Dr. Nahon disclosed honoraria and consulting fees from several companies.
FROM ILC 2021
PPIs could be bad news for oral cancer therapies
A substantial proportion of patients with cancer use proton pump inhibitors (PPIs), and up to one-third of these patients are also using oral cancer treatments that could be adversely affected by concomitant PPI use, according to a cross-sectional analysis.
Amit Patel, MD, a gastroenterologist with Duke University, Durham, N.C., was not involved in the study but commented on it in an interview. The “sobering” study findings highlight the need for “clinicians to carefully and regularly assess the indications and need for PPI, which are often overutilized, and consider ‘deprescribing’ based on clinical guidance,” he explained.
Previous research indicates the use of PPIs can lower the bioavailability and efficacy of oral cancer treatments, such as tyrosine kinase inhibitors (TKIs) and checkpoint inhibitors. In the current study, published in JAMA Network Open, researchers sought to identify how many patients with cancer were taking treatments at risk for altered efficacy from PPI use and what factors were associated with use of PPIs.
The study findings
Jean-Luc Raoul, MD, and colleagues, analyzed physician-reported medical data of 566 women and 306 men with cancer from four comprehensive cancer centers in France, with a median age of 63 years. A total of 229 patients in the study (26.3%) were taking PPIs.
Most patients (71.1%) were using PPIs on a regular basis; reasons included epigastric pain (50.0%), retrosternal pain (14.0%), proven esophageal or gastric ulcer (8.0%), or gastroprotection (15.0%).
Factors associated with PPI use in this cohort included older age (odds ratio, 1.02; P <.001), Eastern Cooperative Oncology Group performance status (PS) (PS 1: OR, 1.92; PS 2: OR, 2.51; PS 3: OR, 2.33; P <.001), receipt of hormone therapy (OR, 0.59; P =.01), metastatic stage (P =.03), and tumor site (P =.045).
Older age and PS are particularly important characteristics, explained Dr. Patel. “Unfortunately, older patients with cancer and/or poor PS are more likely to have medical interactions that may result in their being prescribed PPI medications, often for indications that may not justify their use, and/or for indefinite durations.”
He noted that clinicians who are considering prescribing PPI medications should carefully address the indications for PPIs in the clinical scenario, the evidence supporting PPI use for the indication, ratio of benefits and risks, and potential alternatives to PPI use to mitigate potential issues with other therapies.
Approximately 29% of patients who took drugs whose efficacy might be affected by PPI use were also taking other medications, including capecitabine (n = 5), sunitinib (n = 5), cabozantinib (n = 2), pazopanib (n = 1), gefitinib (n = 1), erlotinib (n = 1), and sorafenib (n = 1). Another 39 out of 90 patients (25.6%) taking PPIs were also receiving checkpoint inhibitors. Of the 20 patients who took TKIs and PPIs, a total of 16 reported long-term PPI use. The most common reason for long-term use of PPIs was related to epigastric pain (n = 11).
Since this study was based on physician-reported data, the analysis was limited by the lack of data for all patients seen by each participating physician. In spite of this limitation, the investigators reported no sources of major bias and suggested the study’s prospective nature and relatively large-sized cohorts strengthened the analysis.
PPI use and cancer care
Although issues exist with PPIs in respect to cancer therapies, there are some strategies which may help reduce possible negative effects, Dr. Patel said. “When PPI medications are prescribed, they should be used at the lowest effective dose for the shortest necessary duration, and their use should be regularly reevaluated for dose reduction and/or potential discontinuation.”
Dr. Patel noted that, based on the indication for PPIs, alternatives to PPIs should be considered in the setting of potential drug-drug interactions that may affect the efficacy of oral cancer therapies. “For example, for intermittent typical reflux symptoms such as heartburn, over-the-counter antacids may be considered, along with reflux lifestyle medications,” he explained.
Likewise, the study authors stated in their research letter that “PPIs should be actively identified and substituted” in certain cases. The authors added that antacids are also the best option for patients taking checkpoint inhibitors.
“For those patients who absolutely must take TKI and PPI, clinicians can also consider staggering the dosing schedule, such as taking the TKI in the morning at least 2 hours before PPI and/or with an acidic beverage,” added Dr. Patel.
Although the findings from this study raise potential concerns, Dr. Patel stated further clinical investigations are needed to help the medical community better understand the specific effects of PPIs on the efficacy of various chemotherapeutic agents and to also help develop better management options for patients in these settings.
The authors reported relationships with Bayer, Merck, Transgene, and others. Dr. Patel has no relevant conflicts of interest to report.
A substantial proportion of patients with cancer use proton pump inhibitors (PPIs), and up to one-third of these patients are also using oral cancer treatments that could be adversely affected by concomitant PPI use, according to a cross-sectional analysis.
Amit Patel, MD, a gastroenterologist with Duke University, Durham, N.C., was not involved in the study but commented on it in an interview. The “sobering” study findings highlight the need for “clinicians to carefully and regularly assess the indications and need for PPI, which are often overutilized, and consider ‘deprescribing’ based on clinical guidance,” he explained.
Previous research indicates the use of PPIs can lower the bioavailability and efficacy of oral cancer treatments, such as tyrosine kinase inhibitors (TKIs) and checkpoint inhibitors. In the current study, published in JAMA Network Open, researchers sought to identify how many patients with cancer were taking treatments at risk for altered efficacy from PPI use and what factors were associated with use of PPIs.
The study findings
Jean-Luc Raoul, MD, and colleagues, analyzed physician-reported medical data of 566 women and 306 men with cancer from four comprehensive cancer centers in France, with a median age of 63 years. A total of 229 patients in the study (26.3%) were taking PPIs.
Most patients (71.1%) were using PPIs on a regular basis; reasons included epigastric pain (50.0%), retrosternal pain (14.0%), proven esophageal or gastric ulcer (8.0%), or gastroprotection (15.0%).
Factors associated with PPI use in this cohort included older age (odds ratio, 1.02; P <.001), Eastern Cooperative Oncology Group performance status (PS) (PS 1: OR, 1.92; PS 2: OR, 2.51; PS 3: OR, 2.33; P <.001), receipt of hormone therapy (OR, 0.59; P =.01), metastatic stage (P =.03), and tumor site (P =.045).
Older age and PS are particularly important characteristics, explained Dr. Patel. “Unfortunately, older patients with cancer and/or poor PS are more likely to have medical interactions that may result in their being prescribed PPI medications, often for indications that may not justify their use, and/or for indefinite durations.”
He noted that clinicians who are considering prescribing PPI medications should carefully address the indications for PPIs in the clinical scenario, the evidence supporting PPI use for the indication, ratio of benefits and risks, and potential alternatives to PPI use to mitigate potential issues with other therapies.
Approximately 29% of patients who took drugs whose efficacy might be affected by PPI use were also taking other medications, including capecitabine (n = 5), sunitinib (n = 5), cabozantinib (n = 2), pazopanib (n = 1), gefitinib (n = 1), erlotinib (n = 1), and sorafenib (n = 1). Another 39 out of 90 patients (25.6%) taking PPIs were also receiving checkpoint inhibitors. Of the 20 patients who took TKIs and PPIs, a total of 16 reported long-term PPI use. The most common reason for long-term use of PPIs was related to epigastric pain (n = 11).
Since this study was based on physician-reported data, the analysis was limited by the lack of data for all patients seen by each participating physician. In spite of this limitation, the investigators reported no sources of major bias and suggested the study’s prospective nature and relatively large-sized cohorts strengthened the analysis.
PPI use and cancer care
Although issues exist with PPIs in respect to cancer therapies, there are some strategies which may help reduce possible negative effects, Dr. Patel said. “When PPI medications are prescribed, they should be used at the lowest effective dose for the shortest necessary duration, and their use should be regularly reevaluated for dose reduction and/or potential discontinuation.”
Dr. Patel noted that, based on the indication for PPIs, alternatives to PPIs should be considered in the setting of potential drug-drug interactions that may affect the efficacy of oral cancer therapies. “For example, for intermittent typical reflux symptoms such as heartburn, over-the-counter antacids may be considered, along with reflux lifestyle medications,” he explained.
Likewise, the study authors stated in their research letter that “PPIs should be actively identified and substituted” in certain cases. The authors added that antacids are also the best option for patients taking checkpoint inhibitors.
“For those patients who absolutely must take TKI and PPI, clinicians can also consider staggering the dosing schedule, such as taking the TKI in the morning at least 2 hours before PPI and/or with an acidic beverage,” added Dr. Patel.
Although the findings from this study raise potential concerns, Dr. Patel stated further clinical investigations are needed to help the medical community better understand the specific effects of PPIs on the efficacy of various chemotherapeutic agents and to also help develop better management options for patients in these settings.
The authors reported relationships with Bayer, Merck, Transgene, and others. Dr. Patel has no relevant conflicts of interest to report.
A substantial proportion of patients with cancer use proton pump inhibitors (PPIs), and up to one-third of these patients are also using oral cancer treatments that could be adversely affected by concomitant PPI use, according to a cross-sectional analysis.
Amit Patel, MD, a gastroenterologist with Duke University, Durham, N.C., was not involved in the study but commented on it in an interview. The “sobering” study findings highlight the need for “clinicians to carefully and regularly assess the indications and need for PPI, which are often overutilized, and consider ‘deprescribing’ based on clinical guidance,” he explained.
Previous research indicates the use of PPIs can lower the bioavailability and efficacy of oral cancer treatments, such as tyrosine kinase inhibitors (TKIs) and checkpoint inhibitors. In the current study, published in JAMA Network Open, researchers sought to identify how many patients with cancer were taking treatments at risk for altered efficacy from PPI use and what factors were associated with use of PPIs.
The study findings
Jean-Luc Raoul, MD, and colleagues, analyzed physician-reported medical data of 566 women and 306 men with cancer from four comprehensive cancer centers in France, with a median age of 63 years. A total of 229 patients in the study (26.3%) were taking PPIs.
Most patients (71.1%) were using PPIs on a regular basis; reasons included epigastric pain (50.0%), retrosternal pain (14.0%), proven esophageal or gastric ulcer (8.0%), or gastroprotection (15.0%).
Factors associated with PPI use in this cohort included older age (odds ratio, 1.02; P <.001), Eastern Cooperative Oncology Group performance status (PS) (PS 1: OR, 1.92; PS 2: OR, 2.51; PS 3: OR, 2.33; P <.001), receipt of hormone therapy (OR, 0.59; P =.01), metastatic stage (P =.03), and tumor site (P =.045).
Older age and PS are particularly important characteristics, explained Dr. Patel. “Unfortunately, older patients with cancer and/or poor PS are more likely to have medical interactions that may result in their being prescribed PPI medications, often for indications that may not justify their use, and/or for indefinite durations.”
He noted that clinicians who are considering prescribing PPI medications should carefully address the indications for PPIs in the clinical scenario, the evidence supporting PPI use for the indication, ratio of benefits and risks, and potential alternatives to PPI use to mitigate potential issues with other therapies.
Approximately 29% of patients who took drugs whose efficacy might be affected by PPI use were also taking other medications, including capecitabine (n = 5), sunitinib (n = 5), cabozantinib (n = 2), pazopanib (n = 1), gefitinib (n = 1), erlotinib (n = 1), and sorafenib (n = 1). Another 39 out of 90 patients (25.6%) taking PPIs were also receiving checkpoint inhibitors. Of the 20 patients who took TKIs and PPIs, a total of 16 reported long-term PPI use. The most common reason for long-term use of PPIs was related to epigastric pain (n = 11).
Since this study was based on physician-reported data, the analysis was limited by the lack of data for all patients seen by each participating physician. In spite of this limitation, the investigators reported no sources of major bias and suggested the study’s prospective nature and relatively large-sized cohorts strengthened the analysis.
PPI use and cancer care
Although issues exist with PPIs in respect to cancer therapies, there are some strategies which may help reduce possible negative effects, Dr. Patel said. “When PPI medications are prescribed, they should be used at the lowest effective dose for the shortest necessary duration, and their use should be regularly reevaluated for dose reduction and/or potential discontinuation.”
Dr. Patel noted that, based on the indication for PPIs, alternatives to PPIs should be considered in the setting of potential drug-drug interactions that may affect the efficacy of oral cancer therapies. “For example, for intermittent typical reflux symptoms such as heartburn, over-the-counter antacids may be considered, along with reflux lifestyle medications,” he explained.
Likewise, the study authors stated in their research letter that “PPIs should be actively identified and substituted” in certain cases. The authors added that antacids are also the best option for patients taking checkpoint inhibitors.
“For those patients who absolutely must take TKI and PPI, clinicians can also consider staggering the dosing schedule, such as taking the TKI in the morning at least 2 hours before PPI and/or with an acidic beverage,” added Dr. Patel.
Although the findings from this study raise potential concerns, Dr. Patel stated further clinical investigations are needed to help the medical community better understand the specific effects of PPIs on the efficacy of various chemotherapeutic agents and to also help develop better management options for patients in these settings.
The authors reported relationships with Bayer, Merck, Transgene, and others. Dr. Patel has no relevant conflicts of interest to report.
FROM JAMA NETWORK OPEN
Respiratory infection– and asthma-prone children
Some children are more susceptible to viral and bacterial respiratory infections in the first few years of life than others. However, the factors contributing to this susceptibility are incompletely understood. The pathogenesis, development, severity, and clinical outcomes of respiratory infections are largely dependent on the resident composition of the nasopharyngeal microbiome and immune defense.1

Respiratory infections caused by bacteria and/or viruses are a leading cause of death in children in the United States and worldwide. The well-recognized, predominant causative bacteria are Streptococcus pneumoniae (pneumococcus), nontypeable Haemophilus influenzae (Hflu), and Moraxella catarrhalis (Mcat). Respiratory infections caused by these pathogens result in considerable morbidity, mortality, and account for high health care costs. The clinical and laboratory group that I lead in Rochester, N.Y., has been studying acute otitis media (AOM) etiology, epidemiology, pathogenesis, prevention, and treatment for over 3 decades. Our research findings are likely applicable and generalizable to understanding the pathogenesis and immune response to other infectious diseases induced by pneumococcus, Hflu, and Mcat since they are also key pathogens causing sinusitis and lung infections.
Previous immunologic analysis of children with AOM by our group provided clarity in differences between infection-prone children manifest as otitis prone (OP; often referred to in our publications as stringently defined OP because of the stringent diagnostic requirement of tympanocentesis-proven etiology of infection) and non-OP children. We showed that about 90% of OP children have deficient immune responses following nasopharyngeal colonization and AOM, demonstrated by inadequate innate responses and adaptive immune responses.2 Many of these children also showed an increased propensity to viral upper respiratory infection and 30% fail to produce protective antibody responses after injection of routine pediatric vaccines.3,4
In this column, I want to share new information regarding differences in the nasopharyngeal microbiome of children who are respiratory infection prone versus those who are non–respiratory infection prone and children with asthma versus those who do not exhibit that clinical phenotype. We performed a retrospective analysis of clinical samples collected from 358 children, aged 6 months to 5 years, from our prospectively enrolled cohort in Rochester, N.Y., to determine associations between AOM and other childhood respiratory illnesses and nasopharyngeal microbiota. In order to define subgroups of children within the cohort, we used a statistical method called unsupervised clustering analysis to see if relatively unique groups of children could be discerned. The overall cohort successfully clustered into two groups, showing marked differences in the prevalence of respiratory infections and asthma.5 We termed the two clinical phenotypes infection and asthma prone (n = 99, 28% of the children) and non–infection and asthma prone (n = 259, 72% of the children). Infection- and asthma-prone children were significantly more likely to experience recurrent AOM, influenza, sinusitis, pneumonia, asthma, and allergic rhinitis, compared with non–infection- and asthma-prone children (Figure).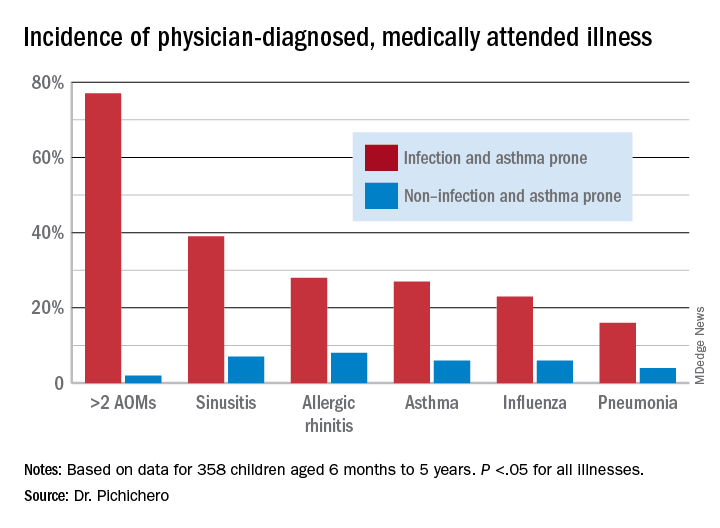
The two groups did not experience significantly different rates of eczema, food allergy, skin infections, urinary tract infections, or acute gastroenteritis, suggesting a common thread involving the respiratory tract that did not cross over to the gastrointestinal, skin, or urinary tract. We found that age at first nasopharyngeal colonization with any of the three bacterial respiratory pathogens (pneumococcus, Hflu, or Mcat) was significantly associated with the respiratory infection– and asthma-prone clinical phenotype. Specifically, respiratory infection– and asthma-prone children experienced colonization at a significantly earlier age than nonprone children did for all three bacteria. In an analysis of individual conditions, early Mcat colonization significantly associated with pneumonia, sinusitis, and asthma susceptibility; Hflu with pneumonia, sinusitis, influenza, and allergic rhinitis; and pneumococcus with sinusitis.
Since early colonization with the three bacterial respiratory pathogens was strongly associated with respiratory illnesses and asthma, nasopharyngeal microbiome analysis was performed on an available subset of samples. Bacterial diversity trended lower in infection- and asthma-prone children, consistent with dysbiosis in the respiratory infection– and asthma-prone clinical phenotype. Nine different bacteria genera were found to be differentially abundant when comparing respiratory infection– and asthma-prone and nonprone children, pointing the way to possible interventions to make the respiratory infection– and asthma-prone child nasopharyngeal microbiome more like the nonprone child.
As I have written previously in this column, recent accumulating data have shed light on the importance of the human microbiome in modulating immune homeostasis and disease susceptibility.6 My group is working toward generating new knowledge for the long-term goal of identifying new therapeutic strategies to facilitate a protective, diverse nasopharyngeal microbiome (with appropriately tuned intranasal probiotics) to prevent respiratory pathogen colonization and/or subsequent progression to respiratory infection and asthma. Also, vaccines directed against colonization-enhancing members of the microbiome may provide a means to indirectly control respiratory pathogen nasopharyngeal colonization.
Dr. Pichichero is a specialist in pediatric infectious diseases and director of the Research Institute at Rochester (N.Y.) General Hospital. He has no conflicts to declare. Contact him at [email protected]
References
1. Man WH et al. Nat Rev Microbiol. 2017;15(5):259-70.
2. Pichichero ME. J Infect. 2020;80(6):614-22.
3. Ren D et al. Clin Infect Dis. 2019;68(9):1566-74.
4. Pichichero ME et al. Pediatr Infect Dis J. 2013;32(11):1163-8.
5. Chapman T et al. PLoS One. 2020 Dec 11;15(12).
6. Blaser MJ. The microbiome revolution. J Clin Invest. 2014;124:4162-5.
Some children are more susceptible to viral and bacterial respiratory infections in the first few years of life than others. However, the factors contributing to this susceptibility are incompletely understood. The pathogenesis, development, severity, and clinical outcomes of respiratory infections are largely dependent on the resident composition of the nasopharyngeal microbiome and immune defense.1
Respiratory infections caused by bacteria and/or viruses are a leading cause of death in children in the United States and worldwide. The well-recognized, predominant causative bacteria are Streptococcus pneumoniae (pneumococcus), nontypeable Haemophilus influenzae (Hflu), and Moraxella catarrhalis (Mcat). Respiratory infections caused by these pathogens result in considerable morbidity, mortality, and account for high health care costs. The clinical and laboratory group that I lead in Rochester, N.Y., has been studying acute otitis media (AOM) etiology, epidemiology, pathogenesis, prevention, and treatment for over 3 decades. Our research findings are likely applicable and generalizable to understanding the pathogenesis and immune response to other infectious diseases induced by pneumococcus, Hflu, and Mcat since they are also key pathogens causing sinusitis and lung infections.
Previous immunologic analysis of children with AOM by our group provided clarity in differences between infection-prone children manifest as otitis prone (OP; often referred to in our publications as stringently defined OP because of the stringent diagnostic requirement of tympanocentesis-proven etiology of infection) and non-OP children. We showed that about 90% of OP children have deficient immune responses following nasopharyngeal colonization and AOM, demonstrated by inadequate innate responses and adaptive immune responses.2 Many of these children also showed an increased propensity to viral upper respiratory infection and 30% fail to produce protective antibody responses after injection of routine pediatric vaccines.3,4
In this column, I want to share new information regarding differences in the nasopharyngeal microbiome of children who are respiratory infection prone versus those who are non–respiratory infection prone and children with asthma versus those who do not exhibit that clinical phenotype. We performed a retrospective analysis of clinical samples collected from 358 children, aged 6 months to 5 years, from our prospectively enrolled cohort in Rochester, N.Y., to determine associations between AOM and other childhood respiratory illnesses and nasopharyngeal microbiota. In order to define subgroups of children within the cohort, we used a statistical method called unsupervised clustering analysis to see if relatively unique groups of children could be discerned. The overall cohort successfully clustered into two groups, showing marked differences in the prevalence of respiratory infections and asthma.5 We termed the two clinical phenotypes infection and asthma prone (n = 99, 28% of the children) and non–infection and asthma prone (n = 259, 72% of the children). Infection- and asthma-prone children were significantly more likely to experience recurrent AOM, influenza, sinusitis, pneumonia, asthma, and allergic rhinitis, compared with non–infection- and asthma-prone children (Figure).
The two groups did not experience significantly different rates of eczema, food allergy, skin infections, urinary tract infections, or acute gastroenteritis, suggesting a common thread involving the respiratory tract that did not cross over to the gastrointestinal, skin, or urinary tract. We found that age at first nasopharyngeal colonization with any of the three bacterial respiratory pathogens (pneumococcus, Hflu, or Mcat) was significantly associated with the respiratory infection– and asthma-prone clinical phenotype. Specifically, respiratory infection– and asthma-prone children experienced colonization at a significantly earlier age than nonprone children did for all three bacteria. In an analysis of individual conditions, early Mcat colonization significantly associated with pneumonia, sinusitis, and asthma susceptibility; Hflu with pneumonia, sinusitis, influenza, and allergic rhinitis; and pneumococcus with sinusitis.
Since early colonization with the three bacterial respiratory pathogens was strongly associated with respiratory illnesses and asthma, nasopharyngeal microbiome analysis was performed on an available subset of samples. Bacterial diversity trended lower in infection- and asthma-prone children, consistent with dysbiosis in the respiratory infection– and asthma-prone clinical phenotype. Nine different bacteria genera were found to be differentially abundant when comparing respiratory infection– and asthma-prone and nonprone children, pointing the way to possible interventions to make the respiratory infection– and asthma-prone child nasopharyngeal microbiome more like the nonprone child.
As I have written previously in this column, recent accumulating data have shed light on the importance of the human microbiome in modulating immune homeostasis and disease susceptibility.6 My group is working toward generating new knowledge for the long-term goal of identifying new therapeutic strategies to facilitate a protective, diverse nasopharyngeal microbiome (with appropriately tuned intranasal probiotics) to prevent respiratory pathogen colonization and/or subsequent progression to respiratory infection and asthma. Also, vaccines directed against colonization-enhancing members of the microbiome may provide a means to indirectly control respiratory pathogen nasopharyngeal colonization.
Dr. Pichichero is a specialist in pediatric infectious diseases and director of the Research Institute at Rochester (N.Y.) General Hospital. He has no conflicts to declare. Contact him at [email protected]
References
1. Man WH et al. Nat Rev Microbiol. 2017;15(5):259-70.
2. Pichichero ME. J Infect. 2020;80(6):614-22.
3. Ren D et al. Clin Infect Dis. 2019;68(9):1566-74.
4. Pichichero ME et al. Pediatr Infect Dis J. 2013;32(11):1163-8.
5. Chapman T et al. PLoS One. 2020 Dec 11;15(12).
6. Blaser MJ. The microbiome revolution. J Clin Invest. 2014;124:4162-5.
Some children are more susceptible to viral and bacterial respiratory infections in the first few years of life than others. However, the factors contributing to this susceptibility are incompletely understood. The pathogenesis, development, severity, and clinical outcomes of respiratory infections are largely dependent on the resident composition of the nasopharyngeal microbiome and immune defense.1
Respiratory infections caused by bacteria and/or viruses are a leading cause of death in children in the United States and worldwide. The well-recognized, predominant causative bacteria are Streptococcus pneumoniae (pneumococcus), nontypeable Haemophilus influenzae (Hflu), and Moraxella catarrhalis (Mcat). Respiratory infections caused by these pathogens result in considerable morbidity, mortality, and account for high health care costs. The clinical and laboratory group that I lead in Rochester, N.Y., has been studying acute otitis media (AOM) etiology, epidemiology, pathogenesis, prevention, and treatment for over 3 decades. Our research findings are likely applicable and generalizable to understanding the pathogenesis and immune response to other infectious diseases induced by pneumococcus, Hflu, and Mcat since they are also key pathogens causing sinusitis and lung infections.
Previous immunologic analysis of children with AOM by our group provided clarity in differences between infection-prone children manifest as otitis prone (OP; often referred to in our publications as stringently defined OP because of the stringent diagnostic requirement of tympanocentesis-proven etiology of infection) and non-OP children. We showed that about 90% of OP children have deficient immune responses following nasopharyngeal colonization and AOM, demonstrated by inadequate innate responses and adaptive immune responses.2 Many of these children also showed an increased propensity to viral upper respiratory infection and 30% fail to produce protective antibody responses after injection of routine pediatric vaccines.3,4
In this column, I want to share new information regarding differences in the nasopharyngeal microbiome of children who are respiratory infection prone versus those who are non–respiratory infection prone and children with asthma versus those who do not exhibit that clinical phenotype. We performed a retrospective analysis of clinical samples collected from 358 children, aged 6 months to 5 years, from our prospectively enrolled cohort in Rochester, N.Y., to determine associations between AOM and other childhood respiratory illnesses and nasopharyngeal microbiota. In order to define subgroups of children within the cohort, we used a statistical method called unsupervised clustering analysis to see if relatively unique groups of children could be discerned. The overall cohort successfully clustered into two groups, showing marked differences in the prevalence of respiratory infections and asthma.5 We termed the two clinical phenotypes infection and asthma prone (n = 99, 28% of the children) and non–infection and asthma prone (n = 259, 72% of the children). Infection- and asthma-prone children were significantly more likely to experience recurrent AOM, influenza, sinusitis, pneumonia, asthma, and allergic rhinitis, compared with non–infection- and asthma-prone children (Figure).
The two groups did not experience significantly different rates of eczema, food allergy, skin infections, urinary tract infections, or acute gastroenteritis, suggesting a common thread involving the respiratory tract that did not cross over to the gastrointestinal, skin, or urinary tract. We found that age at first nasopharyngeal colonization with any of the three bacterial respiratory pathogens (pneumococcus, Hflu, or Mcat) was significantly associated with the respiratory infection– and asthma-prone clinical phenotype. Specifically, respiratory infection– and asthma-prone children experienced colonization at a significantly earlier age than nonprone children did for all three bacteria. In an analysis of individual conditions, early Mcat colonization significantly associated with pneumonia, sinusitis, and asthma susceptibility; Hflu with pneumonia, sinusitis, influenza, and allergic rhinitis; and pneumococcus with sinusitis.
Since early colonization with the three bacterial respiratory pathogens was strongly associated with respiratory illnesses and asthma, nasopharyngeal microbiome analysis was performed on an available subset of samples. Bacterial diversity trended lower in infection- and asthma-prone children, consistent with dysbiosis in the respiratory infection– and asthma-prone clinical phenotype. Nine different bacteria genera were found to be differentially abundant when comparing respiratory infection– and asthma-prone and nonprone children, pointing the way to possible interventions to make the respiratory infection– and asthma-prone child nasopharyngeal microbiome more like the nonprone child.
As I have written previously in this column, recent accumulating data have shed light on the importance of the human microbiome in modulating immune homeostasis and disease susceptibility.6 My group is working toward generating new knowledge for the long-term goal of identifying new therapeutic strategies to facilitate a protective, diverse nasopharyngeal microbiome (with appropriately tuned intranasal probiotics) to prevent respiratory pathogen colonization and/or subsequent progression to respiratory infection and asthma. Also, vaccines directed against colonization-enhancing members of the microbiome may provide a means to indirectly control respiratory pathogen nasopharyngeal colonization.
Dr. Pichichero is a specialist in pediatric infectious diseases and director of the Research Institute at Rochester (N.Y.) General Hospital. He has no conflicts to declare. Contact him at [email protected]
References
1. Man WH et al. Nat Rev Microbiol. 2017;15(5):259-70.
2. Pichichero ME. J Infect. 2020;80(6):614-22.
3. Ren D et al. Clin Infect Dis. 2019;68(9):1566-74.
4. Pichichero ME et al. Pediatr Infect Dis J. 2013;32(11):1163-8.
5. Chapman T et al. PLoS One. 2020 Dec 11;15(12).
6. Blaser MJ. The microbiome revolution. J Clin Invest. 2014;124:4162-5.
South Asian ancestry associated with twice the risk of heart disease
according to the results of a new study.
These findings confirm previous reports and practice guidelines that identify South Asian ancestry as a risk enhancer for atherosclerotic cardiovascular disease (ASCVD), suggesting that earlier heart disease screening and prevention is warranted in this patient population, lead author Aniruddh P. Patel, MD, research fellow at the Center for Genomic Medicine, Massachusetts General Hospital, Boston, and colleagues said.
“Previous studies in multiple countries have estimated a 1.7- to 4-fold higher risk of ASCVD among South Asian individuals, compared with other ancestries, but have important potential limitations,” Dr. Patel and colleagues wrote in the paper on their prospective cohort study, published in Circulation.
The INTERHEART case-control study, for example, which assessed risk factors for acute myocardial infarction among more than 15,000 cases from 52 countries, is now 2 decades old, and “may not reflect recent advances in cardiovascular disease prevention,” the investigators wrote.
Most studies in the area have been small and retrospective, they added, and have not adequately assessed emerging risk factors, such as prediabetes, which appear to play a relatively greater role in the development of heart disease among South Asians.
Methods and results
To address this knowledge gap, Dr. Patel and colleagues analyzed data from the UK Biobank prospective cohort study, including 449,349 middle-aged participants of European ancestry and 8,124 similarly aged participants of South Asian descent who did not have heart disease upon enrollment. Respective rates of incident ASCVD (i.e., MI, ischemic stroke, or coronary revascularization) were analyzed in the context of a variety of lifestyle, anthropometric, and clinical factors.
After a median follow-up of 11.1 years, individuals of South Asian descent had an incident ASCVD rate of 6.8%, compared with 4.4% for individuals of European descent, representing twice the relative risk (adjusted hazard ratio, 2.03; 95% CI, 1.86-2.22; P < .001). Even after accounting for all covariates, risk of ASCVD remained 45% higher for South Asian individuals (aHR, 1.45; 95% CI, 1.28-1.65; P < .001). This elevation in risk was not captured by existing risk calculators, including the American College of Cardiology/American Heart Association Pooled Cohort Equations, or the QRISK3 equations.
The findings were “largely consistent across a range of age, sex, and clinical subgroups,” and “confirm and extend previous reports that hypertension, diabetes, and central adiposity are the leading associations in this observed disparity,” the investigators wrote.
Two diabetes subtypes are more prevalent in South Asians
Hypertension, diabetes, and central adiposity do not fully explain South Asians’ higher risk for ASCVD, wrote Namratha R. Kandula, MD, of Northwestern University Medical Center, Chicago, and Alka M. Kanaya, MD, of the University of California, San Francisco, in an accompanying editorial published in Circulation.
Some of the undetected risk may stem from unique diabetes disease factors, Dr. Kandula and Dr. Kanaya added.
“Newer data have demonstrated distinct subtypes of type 2 diabetes, with South Asians having a higher prevalence of both a severe insulin resistant with obesity subtype and a less recognized severe insulin deficient subtype,” they wrote. “Importantly, both of these more prevalent diabetes subtypes in South Asians were associated with a higher incidence of coronary artery calcium, a marker of subclinical atherosclerosis and strong predictor of future ASCVD, compared to other diabetes subtypes.”
Diabetes rate is higher for South Asians in the U.S.
Although the present study was conducted in the United Kingdom, the findings likely apply to individuals of South Asian ancestry living in the United States, according to principal author Amit V. Khera, MD, associate director of the precision medicine unit at the Center for Genomic Medicine, Massachusetts General Hospital.
“There are already more than 5 million individuals of South Asian ancestry in the U.S. and this represents one of the fastest-growing ethnic subgroups,” Dr. Khera said in an interview. “As in our study of individuals in the U.K., South Asians in the U.S. suffer from diabetes at much higher rates – 23% versus 12% – and this often occurs even in the absence of obesity.”
Dr. Khera noted that the 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease identify South Asian ancestry as a risk-enhancing factor, calling this a “stopgap measure.” More work is needed, he said, in the research arena and in the clinic.
Zero South Asians included in studies used to develop risk estimator
“I think the first step is to simply acknowledge that the risk estimators we use in clinical practice have important limitations when it comes to diverse patient populations,” Dr. Khera said in an interview. “We saw this in our study, where – despite a more than doubling of risk – the predicted risk based on the equations used in primary care showed no difference. This risk estimator was developed based on legacy cohort studies, in [which] zero South Asians were included. Despite important differences across race/ethnicity, the current state-of-the-art in the U.S. is to use one equation for Black individuals and another for all other ethnicities.”
Experts suggest steps for reducing heart disease risk
While risk modeling remains suboptimal, Dr. Khera suggested that clinicians can take immediate steps to reduce the risk of heart disease among individuals with South Asian ancestry.
“Despite all of the uncertainty – we still don’t have a complete understanding of why the risk is so high – there are still several things primary care doctors can do for their patients,” Dr. Khera said.
Foremost, he recommended lifestyle and dietary counseling.
“Dietary counseling is particularly effective if put in the context of cultural norms,” Dr. Khera said. “Many South Asians consider fruit juices or white rice to be healthy, when they lead to rapid spikes in blood sugar.”
Dr. Khera also advised earlier heart disease screening, such as coronary calcium scanning “sometime between age 40-50 years,” noting that positive test results may motivate patients to start or adhere to medications, such as cholesterol-lowering therapies. If necessary, clinicians can also refer to heart centers for South Asian patients, which are becoming increasingly common.

According to Cheryl A.M. Anderson, PhD, chair of the AHA’s Council on Epidemiology and Prevention, and professor and dean of the Herbert Wertheim School of Public Health and Human Longevity Science at the University of California, San Diego, the current study suggests that heart disease management strategies for South Asian patients may be lacking.
“We have had a tradition of preventing or trying to treat heart disease in a fashion that doesn’t yet account for the increased risk that might be prevalent in those of South Asian ancestry,” Dr. Anderson said in an interview.
She suggested that improving associated risk-analysis tools could be beneficial, although the tools themselves, in the context of race or ethnicity, may present their own risks.
“We want to be mindful of potential adverse implications from having everything linked to one’s ancestry, which I think this tool doesn’t do,” Dr. Anderson said, referring to the AHA/ACC Pooled Cohort Equations. “But in sort of the bigger picture of things, we always want to expand and refine our toolkit.”
According to Rajesh Dash, MD, PhD, associate professor, cardiologist, and director of the South Asian Translational Heart Initiative (SSATHI) Prevention Clinic and CardioClick Telemedicine Clinic at Stanford (Calif.) HealthCare, the science supports more active risk mitigation strategies for South Asian patients, and the AHA and the ACC “are the two entities that need to lead the way.”
“Certainly the American Heart Association and the American College of Cardiology should be taking a more active leadership role in this,” Dr. Dash said in an interview.
In 2018, the AHA issued a scientific statement about the elevated risk of ASCVD among South Asian individuals, “but it did not rise to the level of specific recommendations, and did not necessarily go as far as to incorporate new screening parameters for that population,” Dr. Dash said. He also noted that the most recent AHA/ACC guideline identifies South Asian ancestry as a risk-enhancing feature, a statement similarly lacking in actionable value.
“That does not definitively lead someone like a primary care physician to a decision to start a statin, or to be more aggressive with a diagnostic workup, like a stress test, for instance, for a patient who they otherwise would not have done one in had they not been South Asian,” Dr. Dash said.
The steps taken by the AHA and the ACC are “a healthy step forward,” he noted, “but not nearly the degree of attention or vigilance that is required, as well as the level of action that is required to change the narrative for the population.”
At the SSATHI Prevention Clinic, Dr. Dash and colleagues aren’t waiting for the narrative to change, and are already taking a more aggressive approach.
The clinic has an average patient age of 41 years, “easily 15 years younger than the average age in most cardiology clinics,” Dr. Dash said, based on the fact that approximately two-thirds of heart attacks in South Asian individuals occur under the age of 55. “We have to look earlier.”
The SSATHI Prevention Clinic screens for both traditional and emerging risk factors, and Dr. Dash suggested that primary care doctors should do the same.
“If you have a South Asian patient as a primary care physician, you should be aggressively looking for risk factors, traditional ones to start, like elevated cholesterol, hypertension, diabetes, or – and I would argue strongly – prediabetes or insulin resistance.”
Dr. Dash also recommended looking into family history, and considering screening for inflammatory biomarkers, the latter of which are commonly elevated at an earlier age among South Asian individuals, and may have a relatively greater prognostic impact.
To encourage broader implementation of this kind of approach, Dr. Dash called for more large-scale studies. Ideally, these would be randomized clinical trials, but, realistically, real-world datasets may be the answer.
The study was supported by the National Heart, Lung, and Blood Institute; the Broad Institute at MIT and Harvard; the National Human Genome Research Institute; and others. The investigators disclosed relationships with IBM Research, Sanofi, Amgen, and others. Dr. Dash disclosed relationships with HealthPals and AstraZeneca. Dr. Anderson reported no relevant conflicts of interest.
according to the results of a new study.
These findings confirm previous reports and practice guidelines that identify South Asian ancestry as a risk enhancer for atherosclerotic cardiovascular disease (ASCVD), suggesting that earlier heart disease screening and prevention is warranted in this patient population, lead author Aniruddh P. Patel, MD, research fellow at the Center for Genomic Medicine, Massachusetts General Hospital, Boston, and colleagues said.
“Previous studies in multiple countries have estimated a 1.7- to 4-fold higher risk of ASCVD among South Asian individuals, compared with other ancestries, but have important potential limitations,” Dr. Patel and colleagues wrote in the paper on their prospective cohort study, published in Circulation.
The INTERHEART case-control study, for example, which assessed risk factors for acute myocardial infarction among more than 15,000 cases from 52 countries, is now 2 decades old, and “may not reflect recent advances in cardiovascular disease prevention,” the investigators wrote.
Most studies in the area have been small and retrospective, they added, and have not adequately assessed emerging risk factors, such as prediabetes, which appear to play a relatively greater role in the development of heart disease among South Asians.
Methods and results
To address this knowledge gap, Dr. Patel and colleagues analyzed data from the UK Biobank prospective cohort study, including 449,349 middle-aged participants of European ancestry and 8,124 similarly aged participants of South Asian descent who did not have heart disease upon enrollment. Respective rates of incident ASCVD (i.e., MI, ischemic stroke, or coronary revascularization) were analyzed in the context of a variety of lifestyle, anthropometric, and clinical factors.
After a median follow-up of 11.1 years, individuals of South Asian descent had an incident ASCVD rate of 6.8%, compared with 4.4% for individuals of European descent, representing twice the relative risk (adjusted hazard ratio, 2.03; 95% CI, 1.86-2.22; P < .001). Even after accounting for all covariates, risk of ASCVD remained 45% higher for South Asian individuals (aHR, 1.45; 95% CI, 1.28-1.65; P < .001). This elevation in risk was not captured by existing risk calculators, including the American College of Cardiology/American Heart Association Pooled Cohort Equations, or the QRISK3 equations.
The findings were “largely consistent across a range of age, sex, and clinical subgroups,” and “confirm and extend previous reports that hypertension, diabetes, and central adiposity are the leading associations in this observed disparity,” the investigators wrote.
Two diabetes subtypes are more prevalent in South Asians
Hypertension, diabetes, and central adiposity do not fully explain South Asians’ higher risk for ASCVD, wrote Namratha R. Kandula, MD, of Northwestern University Medical Center, Chicago, and Alka M. Kanaya, MD, of the University of California, San Francisco, in an accompanying editorial published in Circulation.
Some of the undetected risk may stem from unique diabetes disease factors, Dr. Kandula and Dr. Kanaya added.
“Newer data have demonstrated distinct subtypes of type 2 diabetes, with South Asians having a higher prevalence of both a severe insulin resistant with obesity subtype and a less recognized severe insulin deficient subtype,” they wrote. “Importantly, both of these more prevalent diabetes subtypes in South Asians were associated with a higher incidence of coronary artery calcium, a marker of subclinical atherosclerosis and strong predictor of future ASCVD, compared to other diabetes subtypes.”
Diabetes rate is higher for South Asians in the U.S.
Although the present study was conducted in the United Kingdom, the findings likely apply to individuals of South Asian ancestry living in the United States, according to principal author Amit V. Khera, MD, associate director of the precision medicine unit at the Center for Genomic Medicine, Massachusetts General Hospital.
“There are already more than 5 million individuals of South Asian ancestry in the U.S. and this represents one of the fastest-growing ethnic subgroups,” Dr. Khera said in an interview. “As in our study of individuals in the U.K., South Asians in the U.S. suffer from diabetes at much higher rates – 23% versus 12% – and this often occurs even in the absence of obesity.”
Dr. Khera noted that the 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease identify South Asian ancestry as a risk-enhancing factor, calling this a “stopgap measure.” More work is needed, he said, in the research arena and in the clinic.
Zero South Asians included in studies used to develop risk estimator
“I think the first step is to simply acknowledge that the risk estimators we use in clinical practice have important limitations when it comes to diverse patient populations,” Dr. Khera said in an interview. “We saw this in our study, where – despite a more than doubling of risk – the predicted risk based on the equations used in primary care showed no difference. This risk estimator was developed based on legacy cohort studies, in [which] zero South Asians were included. Despite important differences across race/ethnicity, the current state-of-the-art in the U.S. is to use one equation for Black individuals and another for all other ethnicities.”
Experts suggest steps for reducing heart disease risk
While risk modeling remains suboptimal, Dr. Khera suggested that clinicians can take immediate steps to reduce the risk of heart disease among individuals with South Asian ancestry.
“Despite all of the uncertainty – we still don’t have a complete understanding of why the risk is so high – there are still several things primary care doctors can do for their patients,” Dr. Khera said.
Foremost, he recommended lifestyle and dietary counseling.
“Dietary counseling is particularly effective if put in the context of cultural norms,” Dr. Khera said. “Many South Asians consider fruit juices or white rice to be healthy, when they lead to rapid spikes in blood sugar.”
Dr. Khera also advised earlier heart disease screening, such as coronary calcium scanning “sometime between age 40-50 years,” noting that positive test results may motivate patients to start or adhere to medications, such as cholesterol-lowering therapies. If necessary, clinicians can also refer to heart centers for South Asian patients, which are becoming increasingly common.
According to Cheryl A.M. Anderson, PhD, chair of the AHA’s Council on Epidemiology and Prevention, and professor and dean of the Herbert Wertheim School of Public Health and Human Longevity Science at the University of California, San Diego, the current study suggests that heart disease management strategies for South Asian patients may be lacking.
“We have had a tradition of preventing or trying to treat heart disease in a fashion that doesn’t yet account for the increased risk that might be prevalent in those of South Asian ancestry,” Dr. Anderson said in an interview.
She suggested that improving associated risk-analysis tools could be beneficial, although the tools themselves, in the context of race or ethnicity, may present their own risks.
“We want to be mindful of potential adverse implications from having everything linked to one’s ancestry, which I think this tool doesn’t do,” Dr. Anderson said, referring to the AHA/ACC Pooled Cohort Equations. “But in sort of the bigger picture of things, we always want to expand and refine our toolkit.”
According to Rajesh Dash, MD, PhD, associate professor, cardiologist, and director of the South Asian Translational Heart Initiative (SSATHI) Prevention Clinic and CardioClick Telemedicine Clinic at Stanford (Calif.) HealthCare, the science supports more active risk mitigation strategies for South Asian patients, and the AHA and the ACC “are the two entities that need to lead the way.”
“Certainly the American Heart Association and the American College of Cardiology should be taking a more active leadership role in this,” Dr. Dash said in an interview.
In 2018, the AHA issued a scientific statement about the elevated risk of ASCVD among South Asian individuals, “but it did not rise to the level of specific recommendations, and did not necessarily go as far as to incorporate new screening parameters for that population,” Dr. Dash said. He also noted that the most recent AHA/ACC guideline identifies South Asian ancestry as a risk-enhancing feature, a statement similarly lacking in actionable value.
“That does not definitively lead someone like a primary care physician to a decision to start a statin, or to be more aggressive with a diagnostic workup, like a stress test, for instance, for a patient who they otherwise would not have done one in had they not been South Asian,” Dr. Dash said.
The steps taken by the AHA and the ACC are “a healthy step forward,” he noted, “but not nearly the degree of attention or vigilance that is required, as well as the level of action that is required to change the narrative for the population.”
At the SSATHI Prevention Clinic, Dr. Dash and colleagues aren’t waiting for the narrative to change, and are already taking a more aggressive approach.
The clinic has an average patient age of 41 years, “easily 15 years younger than the average age in most cardiology clinics,” Dr. Dash said, based on the fact that approximately two-thirds of heart attacks in South Asian individuals occur under the age of 55. “We have to look earlier.”
The SSATHI Prevention Clinic screens for both traditional and emerging risk factors, and Dr. Dash suggested that primary care doctors should do the same.
“If you have a South Asian patient as a primary care physician, you should be aggressively looking for risk factors, traditional ones to start, like elevated cholesterol, hypertension, diabetes, or – and I would argue strongly – prediabetes or insulin resistance.”
Dr. Dash also recommended looking into family history, and considering screening for inflammatory biomarkers, the latter of which are commonly elevated at an earlier age among South Asian individuals, and may have a relatively greater prognostic impact.
To encourage broader implementation of this kind of approach, Dr. Dash called for more large-scale studies. Ideally, these would be randomized clinical trials, but, realistically, real-world datasets may be the answer.
The study was supported by the National Heart, Lung, and Blood Institute; the Broad Institute at MIT and Harvard; the National Human Genome Research Institute; and others. The investigators disclosed relationships with IBM Research, Sanofi, Amgen, and others. Dr. Dash disclosed relationships with HealthPals and AstraZeneca. Dr. Anderson reported no relevant conflicts of interest.
according to the results of a new study.
These findings confirm previous reports and practice guidelines that identify South Asian ancestry as a risk enhancer for atherosclerotic cardiovascular disease (ASCVD), suggesting that earlier heart disease screening and prevention is warranted in this patient population, lead author Aniruddh P. Patel, MD, research fellow at the Center for Genomic Medicine, Massachusetts General Hospital, Boston, and colleagues said.
“Previous studies in multiple countries have estimated a 1.7- to 4-fold higher risk of ASCVD among South Asian individuals, compared with other ancestries, but have important potential limitations,” Dr. Patel and colleagues wrote in the paper on their prospective cohort study, published in Circulation.
The INTERHEART case-control study, for example, which assessed risk factors for acute myocardial infarction among more than 15,000 cases from 52 countries, is now 2 decades old, and “may not reflect recent advances in cardiovascular disease prevention,” the investigators wrote.
Most studies in the area have been small and retrospective, they added, and have not adequately assessed emerging risk factors, such as prediabetes, which appear to play a relatively greater role in the development of heart disease among South Asians.
Methods and results
To address this knowledge gap, Dr. Patel and colleagues analyzed data from the UK Biobank prospective cohort study, including 449,349 middle-aged participants of European ancestry and 8,124 similarly aged participants of South Asian descent who did not have heart disease upon enrollment. Respective rates of incident ASCVD (i.e., MI, ischemic stroke, or coronary revascularization) were analyzed in the context of a variety of lifestyle, anthropometric, and clinical factors.
After a median follow-up of 11.1 years, individuals of South Asian descent had an incident ASCVD rate of 6.8%, compared with 4.4% for individuals of European descent, representing twice the relative risk (adjusted hazard ratio, 2.03; 95% CI, 1.86-2.22; P < .001). Even after accounting for all covariates, risk of ASCVD remained 45% higher for South Asian individuals (aHR, 1.45; 95% CI, 1.28-1.65; P < .001). This elevation in risk was not captured by existing risk calculators, including the American College of Cardiology/American Heart Association Pooled Cohort Equations, or the QRISK3 equations.
The findings were “largely consistent across a range of age, sex, and clinical subgroups,” and “confirm and extend previous reports that hypertension, diabetes, and central adiposity are the leading associations in this observed disparity,” the investigators wrote.
Two diabetes subtypes are more prevalent in South Asians
Hypertension, diabetes, and central adiposity do not fully explain South Asians’ higher risk for ASCVD, wrote Namratha R. Kandula, MD, of Northwestern University Medical Center, Chicago, and Alka M. Kanaya, MD, of the University of California, San Francisco, in an accompanying editorial published in Circulation.
Some of the undetected risk may stem from unique diabetes disease factors, Dr. Kandula and Dr. Kanaya added.
“Newer data have demonstrated distinct subtypes of type 2 diabetes, with South Asians having a higher prevalence of both a severe insulin resistant with obesity subtype and a less recognized severe insulin deficient subtype,” they wrote. “Importantly, both of these more prevalent diabetes subtypes in South Asians were associated with a higher incidence of coronary artery calcium, a marker of subclinical atherosclerosis and strong predictor of future ASCVD, compared to other diabetes subtypes.”
Diabetes rate is higher for South Asians in the U.S.
Although the present study was conducted in the United Kingdom, the findings likely apply to individuals of South Asian ancestry living in the United States, according to principal author Amit V. Khera, MD, associate director of the precision medicine unit at the Center for Genomic Medicine, Massachusetts General Hospital.
“There are already more than 5 million individuals of South Asian ancestry in the U.S. and this represents one of the fastest-growing ethnic subgroups,” Dr. Khera said in an interview. “As in our study of individuals in the U.K., South Asians in the U.S. suffer from diabetes at much higher rates – 23% versus 12% – and this often occurs even in the absence of obesity.”
Dr. Khera noted that the 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease identify South Asian ancestry as a risk-enhancing factor, calling this a “stopgap measure.” More work is needed, he said, in the research arena and in the clinic.
Zero South Asians included in studies used to develop risk estimator
“I think the first step is to simply acknowledge that the risk estimators we use in clinical practice have important limitations when it comes to diverse patient populations,” Dr. Khera said in an interview. “We saw this in our study, where – despite a more than doubling of risk – the predicted risk based on the equations used in primary care showed no difference. This risk estimator was developed based on legacy cohort studies, in [which] zero South Asians were included. Despite important differences across race/ethnicity, the current state-of-the-art in the U.S. is to use one equation for Black individuals and another for all other ethnicities.”
Experts suggest steps for reducing heart disease risk
While risk modeling remains suboptimal, Dr. Khera suggested that clinicians can take immediate steps to reduce the risk of heart disease among individuals with South Asian ancestry.
“Despite all of the uncertainty – we still don’t have a complete understanding of why the risk is so high – there are still several things primary care doctors can do for their patients,” Dr. Khera said.
Foremost, he recommended lifestyle and dietary counseling.
“Dietary counseling is particularly effective if put in the context of cultural norms,” Dr. Khera said. “Many South Asians consider fruit juices or white rice to be healthy, when they lead to rapid spikes in blood sugar.”
Dr. Khera also advised earlier heart disease screening, such as coronary calcium scanning “sometime between age 40-50 years,” noting that positive test results may motivate patients to start or adhere to medications, such as cholesterol-lowering therapies. If necessary, clinicians can also refer to heart centers for South Asian patients, which are becoming increasingly common.
According to Cheryl A.M. Anderson, PhD, chair of the AHA’s Council on Epidemiology and Prevention, and professor and dean of the Herbert Wertheim School of Public Health and Human Longevity Science at the University of California, San Diego, the current study suggests that heart disease management strategies for South Asian patients may be lacking.
“We have had a tradition of preventing or trying to treat heart disease in a fashion that doesn’t yet account for the increased risk that might be prevalent in those of South Asian ancestry,” Dr. Anderson said in an interview.
She suggested that improving associated risk-analysis tools could be beneficial, although the tools themselves, in the context of race or ethnicity, may present their own risks.
“We want to be mindful of potential adverse implications from having everything linked to one’s ancestry, which I think this tool doesn’t do,” Dr. Anderson said, referring to the AHA/ACC Pooled Cohort Equations. “But in sort of the bigger picture of things, we always want to expand and refine our toolkit.”
According to Rajesh Dash, MD, PhD, associate professor, cardiologist, and director of the South Asian Translational Heart Initiative (SSATHI) Prevention Clinic and CardioClick Telemedicine Clinic at Stanford (Calif.) HealthCare, the science supports more active risk mitigation strategies for South Asian patients, and the AHA and the ACC “are the two entities that need to lead the way.”
“Certainly the American Heart Association and the American College of Cardiology should be taking a more active leadership role in this,” Dr. Dash said in an interview.
In 2018, the AHA issued a scientific statement about the elevated risk of ASCVD among South Asian individuals, “but it did not rise to the level of specific recommendations, and did not necessarily go as far as to incorporate new screening parameters for that population,” Dr. Dash said. He also noted that the most recent AHA/ACC guideline identifies South Asian ancestry as a risk-enhancing feature, a statement similarly lacking in actionable value.
“That does not definitively lead someone like a primary care physician to a decision to start a statin, or to be more aggressive with a diagnostic workup, like a stress test, for instance, for a patient who they otherwise would not have done one in had they not been South Asian,” Dr. Dash said.
The steps taken by the AHA and the ACC are “a healthy step forward,” he noted, “but not nearly the degree of attention or vigilance that is required, as well as the level of action that is required to change the narrative for the population.”
At the SSATHI Prevention Clinic, Dr. Dash and colleagues aren’t waiting for the narrative to change, and are already taking a more aggressive approach.
The clinic has an average patient age of 41 years, “easily 15 years younger than the average age in most cardiology clinics,” Dr. Dash said, based on the fact that approximately two-thirds of heart attacks in South Asian individuals occur under the age of 55. “We have to look earlier.”
The SSATHI Prevention Clinic screens for both traditional and emerging risk factors, and Dr. Dash suggested that primary care doctors should do the same.
“If you have a South Asian patient as a primary care physician, you should be aggressively looking for risk factors, traditional ones to start, like elevated cholesterol, hypertension, diabetes, or – and I would argue strongly – prediabetes or insulin resistance.”
Dr. Dash also recommended looking into family history, and considering screening for inflammatory biomarkers, the latter of which are commonly elevated at an earlier age among South Asian individuals, and may have a relatively greater prognostic impact.
To encourage broader implementation of this kind of approach, Dr. Dash called for more large-scale studies. Ideally, these would be randomized clinical trials, but, realistically, real-world datasets may be the answer.
The study was supported by the National Heart, Lung, and Blood Institute; the Broad Institute at MIT and Harvard; the National Human Genome Research Institute; and others. The investigators disclosed relationships with IBM Research, Sanofi, Amgen, and others. Dr. Dash disclosed relationships with HealthPals and AstraZeneca. Dr. Anderson reported no relevant conflicts of interest.
FROM CIRCULATION
New drug, finerenone, approved for slowing kidney disease in diabetes
The U.S. Food and Drug Administration approved finerenone (Kerendia), the first agent from a new class of nonsteroidal mineralocorticoid receptor antagonists (MRAs), on July 9 for treating patients with chronic kidney disease (CKD) associated with type 2 diabetes.
Janani Rangaswami, MD, a nephrologist not involved with finerenone’s development, hailed the action as a “welcome addition to therapies in the cardiorenal space.”
She also highlighted that until more evidence accumulates, finerenone will take a back seat to two more established renal-protective drug classes for patients with type 2 diabetes, the renin-angiotensin system inhibitors (RASIs), and the sodium-glucose cotransporter 2 (SGLT2) inhibitors.
RASIs, which include angiotensin-converting enzyme inhibitors and angiotensin receptor blockers, remain first-line treatments for slowing the progression of CKD in patients with type 2 diabetes. The efficacy and safety of these agents are well-established. The trial that led to the FDA’s decision to approve finerenone, FIDELIO-DKD, compared it against placebo in more than 5,700 patients with type 2 diabetes who were all already taking a maximum-tolerated dose of an RASI.
Scant data on combining finerenone with an SGLT2 inhibitor
Two agents in the SGLT2 inhibitor class, approved initially for type 2 diabetes, received additional FDA approvals for slowing kidney disease: Canagliflozin (Invokana), which was approved in September 2019 on the basis of the CREDENCE trial, and dapagliflozin (Forxiga/Farxiga), which was approved in April 2021 on the basis of DAPA-CKD. Nephrologists now speak of this drug class as “practice changing.”
When FIDELIO-DKD enrolled patients from September 2015 to June 2018, it was still early days for use of SGLT2 inhibitors for patients with type 2 diabetes; hence, fewer than 5% of enrolled patients received an SGLT2 inhibitor, making it impossible to say how well finerenone works when taken along with one of these drugs.
“The big question that persists is the incremental benefit [from finerenone] on top of an SGLT2 inhibitor,” commented Dr. Rangaswami, director of the cardiorenal program at George Washington University, Washington, and chair-elect of the Council on the Kidney in Cardiovascular Disease of the American Heart Association.
“It is hard to extrapolate incremental benefit from existing finerenone trial data given the low background use of SGLT2 inhibitors [in FIDELIO-DKD],” she said in an interview.
George Bakris, MD, lead investigator for FIDELIO-DKD, agrees.
SGLT2 inhibitors are a ‘must’ for CKD
An SGLT2 inhibitor “must be used, period,” for patients with type 2 diabetes and CKD. “The evidence is very strong,” said Dr. Bakris, speaking in June 2021 during a session of the virtual annual Congress of the European Renal Association and European Dialysis and Transplant Association.
Because of inadequate evidence on how finerenone works when administered in addition to an SGLT2 inhibitor, for the time being, the combination must be considered investigational, he added.
Study results “need to show that combination therapy [with an SGLT2 inhibitor and finerenone] is better” than an SGLT2 inhibitor alone, said Dr. Bakris, professor of medicine and director of the Comprehensive Hypertension Center of the University of Chicago.
During his June talk, Dr. Bakris predicted that by 2023, enough data will exist from patients treated with both an SGLT2 inhibitor and finerenone to allow an evidence-based approach to combination treatment.
Finerenone’s approval makes it an immediate choice for patients with type 2 diabetes and CKD secondary to polycystic kidney disease, a group who are not candidates for an SGLT2 inhibitor, said Dr. Rangaswami.
But “if a patient is eligible for an SGLT2 inhibitor, I would not stop that in favor of starting finerenone” on the basis of current knowledge, she noted.
‘Not your mother’s spironolactone’
Although finerenone is classified an MRA, the class that also includes the steroidal agents spironolactone and eplerenone, the nonsteroidal structure of finerenone means “it has nothing to do with spironolactone. It’s a different molecule with different chemistry,” Dr. Bakris said in his June talk.
Although the risk for hyperkalemia has been a limiting factor and a deterrent to routine use of steroidal MRAs for preventing progression of CKD, hyperkalemia is much less of a problem with finerenone.
Main results from FIDELIO-DKD, published in late 2020, showed that the percentage of patients receiving finerenone who permanently stopped taking the drug because of hyperkalemia was 2.3%, higher than the 0.9% rate among patients in the trial who received placebo but about a third of the rate of patients treated with spironolactone in a historical cohort.
“You need to pay attention” to the potential development of hyperkalemia in patients taking finerenone, “but it is not a major issue,” Dr. Bakris said. “Finerenone is not your mother’s spironolactone,” he declared.
FIDELIO-DKD’s primary outcome, a combination of several adverse renal events, showed that treatment with finerenone cut this endpoint by a significant 18% compared with placebo. The study’s main secondary endpoint showed that finerenone cut the incidence of combined cardiovascular disease events by a significant 14% compared with placebo. Adverse events were similar in the finerenone and placebo arms.
Finerenone also shows promise for reducing CVD events
Bayer, the company that developed and will market finerenone, announced in May 2021 topline results from a companion trial, FIGARO-DKD. That trial also enrolled patients with type 2 diabetes and CKD, but a primary endpoint of that trial combined the rates of cardiovascular death and nonfatal cardiovascular disease events. The results from this trial showed a significant difference in favor of finerenone compared with placebo.
“Given the common pathways that progression of CKD and cardiovascular disease share with respect to [moderating] inflammation and [slowing development of] fibrosis, it is not surprising that a signal for benefit was seen at the different ends of the cardiorenal spectrum,” Dr. Rangaswami said.
FIDELIO-DKD and FIGARO-DKD were sponsored by Bayer, the company that markets finerenone (Kerendia). Dr. Bakris has been a consultant to and has received research funding from Bayer and from numerous other companies. Dr. Rangaswami has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration approved finerenone (Kerendia), the first agent from a new class of nonsteroidal mineralocorticoid receptor antagonists (MRAs), on July 9 for treating patients with chronic kidney disease (CKD) associated with type 2 diabetes.
Janani Rangaswami, MD, a nephrologist not involved with finerenone’s development, hailed the action as a “welcome addition to therapies in the cardiorenal space.”
She also highlighted that until more evidence accumulates, finerenone will take a back seat to two more established renal-protective drug classes for patients with type 2 diabetes, the renin-angiotensin system inhibitors (RASIs), and the sodium-glucose cotransporter 2 (SGLT2) inhibitors.
RASIs, which include angiotensin-converting enzyme inhibitors and angiotensin receptor blockers, remain first-line treatments for slowing the progression of CKD in patients with type 2 diabetes. The efficacy and safety of these agents are well-established. The trial that led to the FDA’s decision to approve finerenone, FIDELIO-DKD, compared it against placebo in more than 5,700 patients with type 2 diabetes who were all already taking a maximum-tolerated dose of an RASI.
Scant data on combining finerenone with an SGLT2 inhibitor
Two agents in the SGLT2 inhibitor class, approved initially for type 2 diabetes, received additional FDA approvals for slowing kidney disease: Canagliflozin (Invokana), which was approved in September 2019 on the basis of the CREDENCE trial, and dapagliflozin (Forxiga/Farxiga), which was approved in April 2021 on the basis of DAPA-CKD. Nephrologists now speak of this drug class as “practice changing.”
When FIDELIO-DKD enrolled patients from September 2015 to June 2018, it was still early days for use of SGLT2 inhibitors for patients with type 2 diabetes; hence, fewer than 5% of enrolled patients received an SGLT2 inhibitor, making it impossible to say how well finerenone works when taken along with one of these drugs.
“The big question that persists is the incremental benefit [from finerenone] on top of an SGLT2 inhibitor,” commented Dr. Rangaswami, director of the cardiorenal program at George Washington University, Washington, and chair-elect of the Council on the Kidney in Cardiovascular Disease of the American Heart Association.
“It is hard to extrapolate incremental benefit from existing finerenone trial data given the low background use of SGLT2 inhibitors [in FIDELIO-DKD],” she said in an interview.
George Bakris, MD, lead investigator for FIDELIO-DKD, agrees.
SGLT2 inhibitors are a ‘must’ for CKD
An SGLT2 inhibitor “must be used, period,” for patients with type 2 diabetes and CKD. “The evidence is very strong,” said Dr. Bakris, speaking in June 2021 during a session of the virtual annual Congress of the European Renal Association and European Dialysis and Transplant Association.
Because of inadequate evidence on how finerenone works when administered in addition to an SGLT2 inhibitor, for the time being, the combination must be considered investigational, he added.
Study results “need to show that combination therapy [with an SGLT2 inhibitor and finerenone] is better” than an SGLT2 inhibitor alone, said Dr. Bakris, professor of medicine and director of the Comprehensive Hypertension Center of the University of Chicago.
During his June talk, Dr. Bakris predicted that by 2023, enough data will exist from patients treated with both an SGLT2 inhibitor and finerenone to allow an evidence-based approach to combination treatment.
Finerenone’s approval makes it an immediate choice for patients with type 2 diabetes and CKD secondary to polycystic kidney disease, a group who are not candidates for an SGLT2 inhibitor, said Dr. Rangaswami.
But “if a patient is eligible for an SGLT2 inhibitor, I would not stop that in favor of starting finerenone” on the basis of current knowledge, she noted.
‘Not your mother’s spironolactone’
Although finerenone is classified an MRA, the class that also includes the steroidal agents spironolactone and eplerenone, the nonsteroidal structure of finerenone means “it has nothing to do with spironolactone. It’s a different molecule with different chemistry,” Dr. Bakris said in his June talk.
Although the risk for hyperkalemia has been a limiting factor and a deterrent to routine use of steroidal MRAs for preventing progression of CKD, hyperkalemia is much less of a problem with finerenone.
Main results from FIDELIO-DKD, published in late 2020, showed that the percentage of patients receiving finerenone who permanently stopped taking the drug because of hyperkalemia was 2.3%, higher than the 0.9% rate among patients in the trial who received placebo but about a third of the rate of patients treated with spironolactone in a historical cohort.
“You need to pay attention” to the potential development of hyperkalemia in patients taking finerenone, “but it is not a major issue,” Dr. Bakris said. “Finerenone is not your mother’s spironolactone,” he declared.
FIDELIO-DKD’s primary outcome, a combination of several adverse renal events, showed that treatment with finerenone cut this endpoint by a significant 18% compared with placebo. The study’s main secondary endpoint showed that finerenone cut the incidence of combined cardiovascular disease events by a significant 14% compared with placebo. Adverse events were similar in the finerenone and placebo arms.
Finerenone also shows promise for reducing CVD events
Bayer, the company that developed and will market finerenone, announced in May 2021 topline results from a companion trial, FIGARO-DKD. That trial also enrolled patients with type 2 diabetes and CKD, but a primary endpoint of that trial combined the rates of cardiovascular death and nonfatal cardiovascular disease events. The results from this trial showed a significant difference in favor of finerenone compared with placebo.
“Given the common pathways that progression of CKD and cardiovascular disease share with respect to [moderating] inflammation and [slowing development of] fibrosis, it is not surprising that a signal for benefit was seen at the different ends of the cardiorenal spectrum,” Dr. Rangaswami said.
FIDELIO-DKD and FIGARO-DKD were sponsored by Bayer, the company that markets finerenone (Kerendia). Dr. Bakris has been a consultant to and has received research funding from Bayer and from numerous other companies. Dr. Rangaswami has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration approved finerenone (Kerendia), the first agent from a new class of nonsteroidal mineralocorticoid receptor antagonists (MRAs), on July 9 for treating patients with chronic kidney disease (CKD) associated with type 2 diabetes.
Janani Rangaswami, MD, a nephrologist not involved with finerenone’s development, hailed the action as a “welcome addition to therapies in the cardiorenal space.”
She also highlighted that until more evidence accumulates, finerenone will take a back seat to two more established renal-protective drug classes for patients with type 2 diabetes, the renin-angiotensin system inhibitors (RASIs), and the sodium-glucose cotransporter 2 (SGLT2) inhibitors.
RASIs, which include angiotensin-converting enzyme inhibitors and angiotensin receptor blockers, remain first-line treatments for slowing the progression of CKD in patients with type 2 diabetes. The efficacy and safety of these agents are well-established. The trial that led to the FDA’s decision to approve finerenone, FIDELIO-DKD, compared it against placebo in more than 5,700 patients with type 2 diabetes who were all already taking a maximum-tolerated dose of an RASI.
Scant data on combining finerenone with an SGLT2 inhibitor
Two agents in the SGLT2 inhibitor class, approved initially for type 2 diabetes, received additional FDA approvals for slowing kidney disease: Canagliflozin (Invokana), which was approved in September 2019 on the basis of the CREDENCE trial, and dapagliflozin (Forxiga/Farxiga), which was approved in April 2021 on the basis of DAPA-CKD. Nephrologists now speak of this drug class as “practice changing.”
When FIDELIO-DKD enrolled patients from September 2015 to June 2018, it was still early days for use of SGLT2 inhibitors for patients with type 2 diabetes; hence, fewer than 5% of enrolled patients received an SGLT2 inhibitor, making it impossible to say how well finerenone works when taken along with one of these drugs.
“The big question that persists is the incremental benefit [from finerenone] on top of an SGLT2 inhibitor,” commented Dr. Rangaswami, director of the cardiorenal program at George Washington University, Washington, and chair-elect of the Council on the Kidney in Cardiovascular Disease of the American Heart Association.
“It is hard to extrapolate incremental benefit from existing finerenone trial data given the low background use of SGLT2 inhibitors [in FIDELIO-DKD],” she said in an interview.
George Bakris, MD, lead investigator for FIDELIO-DKD, agrees.
SGLT2 inhibitors are a ‘must’ for CKD
An SGLT2 inhibitor “must be used, period,” for patients with type 2 diabetes and CKD. “The evidence is very strong,” said Dr. Bakris, speaking in June 2021 during a session of the virtual annual Congress of the European Renal Association and European Dialysis and Transplant Association.
Because of inadequate evidence on how finerenone works when administered in addition to an SGLT2 inhibitor, for the time being, the combination must be considered investigational, he added.
Study results “need to show that combination therapy [with an SGLT2 inhibitor and finerenone] is better” than an SGLT2 inhibitor alone, said Dr. Bakris, professor of medicine and director of the Comprehensive Hypertension Center of the University of Chicago.
During his June talk, Dr. Bakris predicted that by 2023, enough data will exist from patients treated with both an SGLT2 inhibitor and finerenone to allow an evidence-based approach to combination treatment.
Finerenone’s approval makes it an immediate choice for patients with type 2 diabetes and CKD secondary to polycystic kidney disease, a group who are not candidates for an SGLT2 inhibitor, said Dr. Rangaswami.
But “if a patient is eligible for an SGLT2 inhibitor, I would not stop that in favor of starting finerenone” on the basis of current knowledge, she noted.
‘Not your mother’s spironolactone’
Although finerenone is classified an MRA, the class that also includes the steroidal agents spironolactone and eplerenone, the nonsteroidal structure of finerenone means “it has nothing to do with spironolactone. It’s a different molecule with different chemistry,” Dr. Bakris said in his June talk.
Although the risk for hyperkalemia has been a limiting factor and a deterrent to routine use of steroidal MRAs for preventing progression of CKD, hyperkalemia is much less of a problem with finerenone.
Main results from FIDELIO-DKD, published in late 2020, showed that the percentage of patients receiving finerenone who permanently stopped taking the drug because of hyperkalemia was 2.3%, higher than the 0.9% rate among patients in the trial who received placebo but about a third of the rate of patients treated with spironolactone in a historical cohort.
“You need to pay attention” to the potential development of hyperkalemia in patients taking finerenone, “but it is not a major issue,” Dr. Bakris said. “Finerenone is not your mother’s spironolactone,” he declared.
FIDELIO-DKD’s primary outcome, a combination of several adverse renal events, showed that treatment with finerenone cut this endpoint by a significant 18% compared with placebo. The study’s main secondary endpoint showed that finerenone cut the incidence of combined cardiovascular disease events by a significant 14% compared with placebo. Adverse events were similar in the finerenone and placebo arms.
Finerenone also shows promise for reducing CVD events
Bayer, the company that developed and will market finerenone, announced in May 2021 topline results from a companion trial, FIGARO-DKD. That trial also enrolled patients with type 2 diabetes and CKD, but a primary endpoint of that trial combined the rates of cardiovascular death and nonfatal cardiovascular disease events. The results from this trial showed a significant difference in favor of finerenone compared with placebo.
“Given the common pathways that progression of CKD and cardiovascular disease share with respect to [moderating] inflammation and [slowing development of] fibrosis, it is not surprising that a signal for benefit was seen at the different ends of the cardiorenal spectrum,” Dr. Rangaswami said.
FIDELIO-DKD and FIGARO-DKD were sponsored by Bayer, the company that markets finerenone (Kerendia). Dr. Bakris has been a consultant to and has received research funding from Bayer and from numerous other companies. Dr. Rangaswami has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Malpractice claims from the COVID-19 pandemic: More questions than answers
Editor’s note: This article has been provided by The Doctors Company, the exclusively endorsed medical malpractice carrier for the Society of Hospital Medicine.
The pandemic has raised pressing questions around preventive measures, vaccines, and safe treatment, but it has also obscured one key lingering uncertainty for medical professionals: Where are all the medical malpractice claims?
A variety of factors create a cloud of uncertainty around when, if ever, we will see the claims we expected from care provided just before the pandemic, much less claims deriving from care during the pandemic of both COVID-19 and non–COVID-19 patients.
Malpractice claims take time to surface
We won’t know until 2022 or later whether there will be an increase in claims related to the pandemic. When a medical error occurs, it’s not like an automobile accident. Everybody nearby knows when there’s been an automobile accident because they hear screeching tires, a loud crash, and then sirens. But when a medical error occurs, generally speaking, neither the doctor nor the patient immediately knows that something is amiss. It can take months or years for people to realize that something untoward has occurred.
Claims from medical errors that occurred before the pandemic bring additional uncertainties. In 2020, we saw fewer than expected overall claims filed from events occurring 18-24 months before the pandemic. In total, 20% fewer claims were filed than in 2019. This may have had to do with courts shutting down, people being reluctant to meet with attorneys to discuss a claim, and/or lawyers working from home. We may see these claims filed later than expected, or maybe we won’t see them at all.
But without a doubt, pandemic-related claims will be filed. The pandemic’s impact on physicians increases the risk of claims. Burnout is a major cause of medical errors, and a recent study found that out of 60 countries, U.S. health care providers showed the highest rates of burnout. We’re concerned about the stress affecting physicians’ performance – not just the physical stress of the demands put on them while treating COVID-19 patients, but all of the worry. For instance, a lot of doctors at the start of this pandemic stayed at hotels because they didn’t want to bring the virus home to their families – if they got exposed. Those sorts of stressors from life disruptions, on top of the stress of treating COVID-19 patients and the stress of treating non–COVID-19 patients within overtaxed health care systems, contribute to the possibilities for error.
Immunity protections are not fail-safe
And while health care providers have medical liability protections during the pandemic, these protections may not prevent claims. Health care provider pandemic-related liability laws vary from state to state, and they will be tested in the courts as to whether they’re constitutional. For example, there is pending legislation in New York state that would repeal the provider protections created there at the start of the pandemic. Further, some expert witnesses will couch their statements in terms of what it takes to get around one of these statutes. Therefore, physicians do have reason for concern, even in states with strong liability protections.
The following case example, which is one of about 40 COVID-19–related claims made against our members so far, is a poster child for why these protections are necessary: A quadriplegic patient with COVID-19 had reached the point of organ failure before he reached the ED. There was really nothing medical science could do for him at that point, in terms of a chance at recovery. Therefore, the patient’s physician and conservator placed him in assisted living for palliative care. This was a sad but reasonable decision during a pandemic, with hospital beds needed for patients with a shot at surviving. Following that patient’s death, the physician is being sued.
Defending claims regarding treatment vs. regarding infection control
We are very confident in our ability to protect our members against claims where they are being sued over the treatment of the disease. Claims arising out of treatment are not concerning to us because there is no cure for COVID-19 – one can only treat the symptoms as the virus runs its course.
On the other hand, suits harder to defend would be those that revolve around transmitting the disease because providers didn’t follow guidelines from the Centers for Disease Control and Prevention or there wasn’t enough personal protective equipment. That’s why we stress the importance of following CDC guidelines, and why we’ve taken proactive steps to communicate with the entire medical community throughout the pandemic as part of our commitment to serve those who provide care.
Mr. White is chief operating officer at The Doctors Company. The guidelines suggested here are not rules, do not constitute legal advice, and do not ensure a successful outcome. The ultimate decision regarding the appropriateness of any treatment must be made by each health care provider considering the circumstances of the individual situation and in accordance with the laws of the jurisdiction in which the care is rendered.
Editor’s note: This article has been provided by The Doctors Company, the exclusively endorsed medical malpractice carrier for the Society of Hospital Medicine.
The pandemic has raised pressing questions around preventive measures, vaccines, and safe treatment, but it has also obscured one key lingering uncertainty for medical professionals: Where are all the medical malpractice claims?
A variety of factors create a cloud of uncertainty around when, if ever, we will see the claims we expected from care provided just before the pandemic, much less claims deriving from care during the pandemic of both COVID-19 and non–COVID-19 patients.
Malpractice claims take time to surface
We won’t know until 2022 or later whether there will be an increase in claims related to the pandemic. When a medical error occurs, it’s not like an automobile accident. Everybody nearby knows when there’s been an automobile accident because they hear screeching tires, a loud crash, and then sirens. But when a medical error occurs, generally speaking, neither the doctor nor the patient immediately knows that something is amiss. It can take months or years for people to realize that something untoward has occurred.
Claims from medical errors that occurred before the pandemic bring additional uncertainties. In 2020, we saw fewer than expected overall claims filed from events occurring 18-24 months before the pandemic. In total, 20% fewer claims were filed than in 2019. This may have had to do with courts shutting down, people being reluctant to meet with attorneys to discuss a claim, and/or lawyers working from home. We may see these claims filed later than expected, or maybe we won’t see them at all.
But without a doubt, pandemic-related claims will be filed. The pandemic’s impact on physicians increases the risk of claims. Burnout is a major cause of medical errors, and a recent study found that out of 60 countries, U.S. health care providers showed the highest rates of burnout. We’re concerned about the stress affecting physicians’ performance – not just the physical stress of the demands put on them while treating COVID-19 patients, but all of the worry. For instance, a lot of doctors at the start of this pandemic stayed at hotels because they didn’t want to bring the virus home to their families – if they got exposed. Those sorts of stressors from life disruptions, on top of the stress of treating COVID-19 patients and the stress of treating non–COVID-19 patients within overtaxed health care systems, contribute to the possibilities for error.
Immunity protections are not fail-safe
And while health care providers have medical liability protections during the pandemic, these protections may not prevent claims. Health care provider pandemic-related liability laws vary from state to state, and they will be tested in the courts as to whether they’re constitutional. For example, there is pending legislation in New York state that would repeal the provider protections created there at the start of the pandemic. Further, some expert witnesses will couch their statements in terms of what it takes to get around one of these statutes. Therefore, physicians do have reason for concern, even in states with strong liability protections.
The following case example, which is one of about 40 COVID-19–related claims made against our members so far, is a poster child for why these protections are necessary: A quadriplegic patient with COVID-19 had reached the point of organ failure before he reached the ED. There was really nothing medical science could do for him at that point, in terms of a chance at recovery. Therefore, the patient’s physician and conservator placed him in assisted living for palliative care. This was a sad but reasonable decision during a pandemic, with hospital beds needed for patients with a shot at surviving. Following that patient’s death, the physician is being sued.
Defending claims regarding treatment vs. regarding infection control
We are very confident in our ability to protect our members against claims where they are being sued over the treatment of the disease. Claims arising out of treatment are not concerning to us because there is no cure for COVID-19 – one can only treat the symptoms as the virus runs its course.
On the other hand, suits harder to defend would be those that revolve around transmitting the disease because providers didn’t follow guidelines from the Centers for Disease Control and Prevention or there wasn’t enough personal protective equipment. That’s why we stress the importance of following CDC guidelines, and why we’ve taken proactive steps to communicate with the entire medical community throughout the pandemic as part of our commitment to serve those who provide care.
Mr. White is chief operating officer at The Doctors Company. The guidelines suggested here are not rules, do not constitute legal advice, and do not ensure a successful outcome. The ultimate decision regarding the appropriateness of any treatment must be made by each health care provider considering the circumstances of the individual situation and in accordance with the laws of the jurisdiction in which the care is rendered.
Editor’s note: This article has been provided by The Doctors Company, the exclusively endorsed medical malpractice carrier for the Society of Hospital Medicine.
The pandemic has raised pressing questions around preventive measures, vaccines, and safe treatment, but it has also obscured one key lingering uncertainty for medical professionals: Where are all the medical malpractice claims?
A variety of factors create a cloud of uncertainty around when, if ever, we will see the claims we expected from care provided just before the pandemic, much less claims deriving from care during the pandemic of both COVID-19 and non–COVID-19 patients.
Malpractice claims take time to surface
We won’t know until 2022 or later whether there will be an increase in claims related to the pandemic. When a medical error occurs, it’s not like an automobile accident. Everybody nearby knows when there’s been an automobile accident because they hear screeching tires, a loud crash, and then sirens. But when a medical error occurs, generally speaking, neither the doctor nor the patient immediately knows that something is amiss. It can take months or years for people to realize that something untoward has occurred.
Claims from medical errors that occurred before the pandemic bring additional uncertainties. In 2020, we saw fewer than expected overall claims filed from events occurring 18-24 months before the pandemic. In total, 20% fewer claims were filed than in 2019. This may have had to do with courts shutting down, people being reluctant to meet with attorneys to discuss a claim, and/or lawyers working from home. We may see these claims filed later than expected, or maybe we won’t see them at all.
But without a doubt, pandemic-related claims will be filed. The pandemic’s impact on physicians increases the risk of claims. Burnout is a major cause of medical errors, and a recent study found that out of 60 countries, U.S. health care providers showed the highest rates of burnout. We’re concerned about the stress affecting physicians’ performance – not just the physical stress of the demands put on them while treating COVID-19 patients, but all of the worry. For instance, a lot of doctors at the start of this pandemic stayed at hotels because they didn’t want to bring the virus home to their families – if they got exposed. Those sorts of stressors from life disruptions, on top of the stress of treating COVID-19 patients and the stress of treating non–COVID-19 patients within overtaxed health care systems, contribute to the possibilities for error.
Immunity protections are not fail-safe
And while health care providers have medical liability protections during the pandemic, these protections may not prevent claims. Health care provider pandemic-related liability laws vary from state to state, and they will be tested in the courts as to whether they’re constitutional. For example, there is pending legislation in New York state that would repeal the provider protections created there at the start of the pandemic. Further, some expert witnesses will couch their statements in terms of what it takes to get around one of these statutes. Therefore, physicians do have reason for concern, even in states with strong liability protections.
The following case example, which is one of about 40 COVID-19–related claims made against our members so far, is a poster child for why these protections are necessary: A quadriplegic patient with COVID-19 had reached the point of organ failure before he reached the ED. There was really nothing medical science could do for him at that point, in terms of a chance at recovery. Therefore, the patient’s physician and conservator placed him in assisted living for palliative care. This was a sad but reasonable decision during a pandemic, with hospital beds needed for patients with a shot at surviving. Following that patient’s death, the physician is being sued.
Defending claims regarding treatment vs. regarding infection control
We are very confident in our ability to protect our members against claims where they are being sued over the treatment of the disease. Claims arising out of treatment are not concerning to us because there is no cure for COVID-19 – one can only treat the symptoms as the virus runs its course.
On the other hand, suits harder to defend would be those that revolve around transmitting the disease because providers didn’t follow guidelines from the Centers for Disease Control and Prevention or there wasn’t enough personal protective equipment. That’s why we stress the importance of following CDC guidelines, and why we’ve taken proactive steps to communicate with the entire medical community throughout the pandemic as part of our commitment to serve those who provide care.
Mr. White is chief operating officer at The Doctors Company. The guidelines suggested here are not rules, do not constitute legal advice, and do not ensure a successful outcome. The ultimate decision regarding the appropriateness of any treatment must be made by each health care provider considering the circumstances of the individual situation and in accordance with the laws of the jurisdiction in which the care is rendered.