User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Low threshold to biopsy atypical lesions may ID vulvar melanoma early, experts say
Having a low threshold to biopsy atypical pigmented lesions on the vulva may identify melanoma early, according to a lecture at virtual conference on diseases of the vulva and vagina, hosted by the International Society for the Study of Vulvovaginal Disease.
Pigmented brown or black vulvar lesions occur in approximately 10% of women, and they may be normal and benign.
“Often we will see a pigmented lesion on the vulva and think that there is nothing to worry about,” said Melissa Mauskar, MD.
Lesions could be angiokeratomas, petechiae, purpura, melanosis, and nevi, for example. Seborrheic keratoses can mimic melanoma. “If it looks odd, don’t be afraid to biopsy it,” said Dr. Mauskar, assistant professor of dermatology and obstetrics and gynecology at the University of Texas Southwestern Medical Center in Dallas.
Characteristics of melanoma, covered by the mnemonic ABCDE, include asymmetry, borders that are irregular, coloring that is uneven, diameter greater than 7 mm, and evolution over time.
When biopsying a lesion because of concerns about melanoma, the goal is to remove the whole lesion at once, Dr. Mauskar said.
In a recent U.S. population-based study of more than 1,800 patients with malignant melanoma of the vulva or vagina (including 1,400 patients with vulvar melanoma and 463 patients with vaginal melanoma), median disease-specific survival was 99 months for vulvar melanoma and 19 months for vaginal melanoma.
Patients with vaginal melanoma were more likely than patients with vulvar melanoma to have nodular lesions. The American Joint Committee on Cancer staging system predicts vulvar melanoma outcomes, the researchers found. In addition, lymph node status and mitotic rate were important predictors of survival.
A wide local excision is the mainstay of therapy for melanoma. Other therapeutic advances are “changing the survival curves for these patients, especially when we can find things early,” Dr. Mauskar said.
Photographing lesions can help doctors monitor them over time, she added.
It is important for dermatologists to include the vulva in skin exams and for gynecologists to have a low threshold to biopsy atypical pigmented lesions, Dr. Mauskar said. “Having a very low threshold for biopsy ... will increase our chances of finding these lesions when they are more at the superficial spreading phase as opposed to the nodular phase,” she said.
Capturing the depth of a tumor within the confines of a biopsy may help accurately stage malignant melanoma, Jason Reutter, MD, a pathologist in Hickory, N.C., said in a separate presentation. He suggested trying to get around the lesion with a punch biopsy if possible. A shave biopsy may be advantageous for larger macular lesions. To diagnose one melanoma, doctors may have to biopsy many lesions, Dr. Reutter noted.
At one institution, the number of skin biopsies needed to diagnose skin cancer ranged from 2.82 to 6.55, depending on the type of clinician, according to a recent study. The number of biopsies needed to detect one melanoma was greater – between 14 and 54 – depending on type of clinician.
For larger lesions, scouting biopsies of different areas may be the best approach, Dr. Reutter said.
Dr. Mauskar and Dr. Reutter had no relevant financial conflicts of interest.
Having a low threshold to biopsy atypical pigmented lesions on the vulva may identify melanoma early, according to a lecture at virtual conference on diseases of the vulva and vagina, hosted by the International Society for the Study of Vulvovaginal Disease.
Pigmented brown or black vulvar lesions occur in approximately 10% of women, and they may be normal and benign.
“Often we will see a pigmented lesion on the vulva and think that there is nothing to worry about,” said Melissa Mauskar, MD.
Lesions could be angiokeratomas, petechiae, purpura, melanosis, and nevi, for example. Seborrheic keratoses can mimic melanoma. “If it looks odd, don’t be afraid to biopsy it,” said Dr. Mauskar, assistant professor of dermatology and obstetrics and gynecology at the University of Texas Southwestern Medical Center in Dallas.
Characteristics of melanoma, covered by the mnemonic ABCDE, include asymmetry, borders that are irregular, coloring that is uneven, diameter greater than 7 mm, and evolution over time.
When biopsying a lesion because of concerns about melanoma, the goal is to remove the whole lesion at once, Dr. Mauskar said.
In a recent U.S. population-based study of more than 1,800 patients with malignant melanoma of the vulva or vagina (including 1,400 patients with vulvar melanoma and 463 patients with vaginal melanoma), median disease-specific survival was 99 months for vulvar melanoma and 19 months for vaginal melanoma.
Patients with vaginal melanoma were more likely than patients with vulvar melanoma to have nodular lesions. The American Joint Committee on Cancer staging system predicts vulvar melanoma outcomes, the researchers found. In addition, lymph node status and mitotic rate were important predictors of survival.
A wide local excision is the mainstay of therapy for melanoma. Other therapeutic advances are “changing the survival curves for these patients, especially when we can find things early,” Dr. Mauskar said.
Photographing lesions can help doctors monitor them over time, she added.
It is important for dermatologists to include the vulva in skin exams and for gynecologists to have a low threshold to biopsy atypical pigmented lesions, Dr. Mauskar said. “Having a very low threshold for biopsy ... will increase our chances of finding these lesions when they are more at the superficial spreading phase as opposed to the nodular phase,” she said.
Capturing the depth of a tumor within the confines of a biopsy may help accurately stage malignant melanoma, Jason Reutter, MD, a pathologist in Hickory, N.C., said in a separate presentation. He suggested trying to get around the lesion with a punch biopsy if possible. A shave biopsy may be advantageous for larger macular lesions. To diagnose one melanoma, doctors may have to biopsy many lesions, Dr. Reutter noted.
At one institution, the number of skin biopsies needed to diagnose skin cancer ranged from 2.82 to 6.55, depending on the type of clinician, according to a recent study. The number of biopsies needed to detect one melanoma was greater – between 14 and 54 – depending on type of clinician.
For larger lesions, scouting biopsies of different areas may be the best approach, Dr. Reutter said.
Dr. Mauskar and Dr. Reutter had no relevant financial conflicts of interest.
Having a low threshold to biopsy atypical pigmented lesions on the vulva may identify melanoma early, according to a lecture at virtual conference on diseases of the vulva and vagina, hosted by the International Society for the Study of Vulvovaginal Disease.
Pigmented brown or black vulvar lesions occur in approximately 10% of women, and they may be normal and benign.
“Often we will see a pigmented lesion on the vulva and think that there is nothing to worry about,” said Melissa Mauskar, MD.
Lesions could be angiokeratomas, petechiae, purpura, melanosis, and nevi, for example. Seborrheic keratoses can mimic melanoma. “If it looks odd, don’t be afraid to biopsy it,” said Dr. Mauskar, assistant professor of dermatology and obstetrics and gynecology at the University of Texas Southwestern Medical Center in Dallas.
Characteristics of melanoma, covered by the mnemonic ABCDE, include asymmetry, borders that are irregular, coloring that is uneven, diameter greater than 7 mm, and evolution over time.
When biopsying a lesion because of concerns about melanoma, the goal is to remove the whole lesion at once, Dr. Mauskar said.
In a recent U.S. population-based study of more than 1,800 patients with malignant melanoma of the vulva or vagina (including 1,400 patients with vulvar melanoma and 463 patients with vaginal melanoma), median disease-specific survival was 99 months for vulvar melanoma and 19 months for vaginal melanoma.
Patients with vaginal melanoma were more likely than patients with vulvar melanoma to have nodular lesions. The American Joint Committee on Cancer staging system predicts vulvar melanoma outcomes, the researchers found. In addition, lymph node status and mitotic rate were important predictors of survival.
A wide local excision is the mainstay of therapy for melanoma. Other therapeutic advances are “changing the survival curves for these patients, especially when we can find things early,” Dr. Mauskar said.
Photographing lesions can help doctors monitor them over time, she added.
It is important for dermatologists to include the vulva in skin exams and for gynecologists to have a low threshold to biopsy atypical pigmented lesions, Dr. Mauskar said. “Having a very low threshold for biopsy ... will increase our chances of finding these lesions when they are more at the superficial spreading phase as opposed to the nodular phase,” she said.
Capturing the depth of a tumor within the confines of a biopsy may help accurately stage malignant melanoma, Jason Reutter, MD, a pathologist in Hickory, N.C., said in a separate presentation. He suggested trying to get around the lesion with a punch biopsy if possible. A shave biopsy may be advantageous for larger macular lesions. To diagnose one melanoma, doctors may have to biopsy many lesions, Dr. Reutter noted.
At one institution, the number of skin biopsies needed to diagnose skin cancer ranged from 2.82 to 6.55, depending on the type of clinician, according to a recent study. The number of biopsies needed to detect one melanoma was greater – between 14 and 54 – depending on type of clinician.
For larger lesions, scouting biopsies of different areas may be the best approach, Dr. Reutter said.
Dr. Mauskar and Dr. Reutter had no relevant financial conflicts of interest.
FROM A CONFERENCE ON DISEASES OF THE VULVA AND VAGINA
Poor image quality may limit televulvology care
Seeing patients with vulvar problems via telemedicine can lead to efficient and successful care, but there are challenges and limitations with this approach, doctors are finding.
Image quality is one key factor that determines whether a clinician can assess and manage a condition remotely, said Aruna Venkatesan, MD, chief of dermatology and director of the genital dermatology clinic at Santa Clara Valley Medical Center in San Jose, Calif. Other issues may be especially relevant to televulvology, including privacy concerns.
“Who is helping with the positioning? Who is the photographer? Is the patient comfortable with having photos taken of this part of their body and submitted, even if they know it is submitted securely? Because they might not be,” Dr. Venkatesan said in a lecture at a virtual conference on diseases of the vulva and vagina, hosted by the International Society for the Study of Vulvovaginal Disease.
When quality photographs from referring providers are available, Dr. Venkatesan has conducted virtual new consultations. “But sometimes I will do a virtual telemedicine visit as the first visit and then figure out, okay, this isn’t really sufficient. I need to see them in person.”
Melissa Mauskar, MD, assistant professor of dermatology and obstetrics and gynecology at the University of Texas Southwestern Medical Center, Dallas, described a case early on during the COVID-19 pandemic that illustrates a limitation of virtual visits.
A patient sent in a photograph that appeared to show lichen sclerosus. “There looked like some classic lichen sclerosus changes,” Dr. Mauskar said during a discussion at the meeting. “But she was having a lot of pain, and after a week, her pain still was not better.”
Dr. Mauskar brought the patient into the office and ultimately diagnosed a squamous cell carcinoma. “What I thought was a normal erosion was actually an ulcerated plaque,” she said.
Like Dr. Venkatesan, Dr. Mauskar has found that image quality can be uneven. Photographs may be out of focus. Video visits have been a mixed bag. Some are successful. Other times, Dr. Mauskar has to tell the patient she needs to see her in the office.
Certain clinical scenarios require a vaginal exam, Dr. Venkatesan noted. Although some type of assessment may be possible if a patient is with a primary care provider during the telemedicine visit, the examination may not be equivalent. Doctors also should anticipate where a patient might go to have a biopsy if one is necessary.
Another telemedicine caveat pertains to patient counseling. When using store-and-forward telemedicine systems, advising patients in a written report can be challenging. “Is there an easy way ... to counsel patients how to apply their topical medications?” Dr. Venkatesan said.
Excellent care is possible
Vulvology is a small part of Dr. Venkatesan’s general dermatology practice, which has used telemedicine extensively since the pandemic.
In recent years, Dr. Venkatesan’s clinic began encouraging providers in their health system to submit photographs with referrals. “That has really paid off now because we have been able to help provide a lot of excellent quality care for patients without them having to come in,” she said. “We may be able to say: ‘These are excellent photos. We know what this patient has. We can manage it. They don’t need to come see us in person.’ ” That could be the case for certain types of acne, eczema, and psoriasis.
In other cases, they may be able to provide initial advice remotely but still want to see the patient. For a patient with severe acne, “I may be able to tell the referring doctor: ‘Please start the patient on these three medicines. It will take 2 months for those medicines to start working and then we will plan to have an in-person dermatology visit.’ ” In this case, telemedicine essentially replaces one in-person visit.
If photographs are poor, the differential diagnosis is broad, a procedure is required, the doctor needs to touch the lesion, or more involved history taking or counseling are required, the patient may need to go into the office.
Beyond its public health advantages during a pandemic, telemedicine can improve access for patients who live far away, lack transportation, or are unable to take time off from work. It also can decrease patient wait times. “Once we started doing some telemedicine work … we went from having a 5-month wait time for patients to see us in person to a 72-hour wait time for providing some care for patients if they had good photos as part of their referral,” Dr. Venkatesan said.
Telemedicine has been used in inpatient and outpatient dermatology settings. Primary care providers who consult with dermatologists using a store-and-forward telemedicine system may improve their dermatology knowledge and feel more confident in their ability to diagnose and manage dermatologic conditions, research indicates.
In obstetrics and gynecology, telemedicine may play a role in preconception, contraception, and medical abortion care, prenatal visits, well-woman exams, mental health, and pre- and postoperative counseling, a recent review suggests.
Image quality is key
“Quality of the image is so critical for being able to provide good care, especially in such a visual exam field as dermatology,” Dr. Venkatesan said.
To that end, doctors have offered recommendations on how to photograph skin conditions. A guide shared by the mobile telehealth system company ClickMedix suggests focusing on the area of importance, capturing the extent of involvement, and including involved and uninvolved areas.
Good lighting and checking the image resolution can help, Dr. Venkatesan offered. Nevertheless, patients may have difficulty photographing themselves. If a patient is with their primary care doctor, “we are much more likely to be able to get good quality photos,” she said.
Dr. Venkatesan is a paid consultant for DirectDerm, a store-and-forward teledermatology company. Dr. Mauskar had no relevant disclosures.
Seeing patients with vulvar problems via telemedicine can lead to efficient and successful care, but there are challenges and limitations with this approach, doctors are finding.
Image quality is one key factor that determines whether a clinician can assess and manage a condition remotely, said Aruna Venkatesan, MD, chief of dermatology and director of the genital dermatology clinic at Santa Clara Valley Medical Center in San Jose, Calif. Other issues may be especially relevant to televulvology, including privacy concerns.
“Who is helping with the positioning? Who is the photographer? Is the patient comfortable with having photos taken of this part of their body and submitted, even if they know it is submitted securely? Because they might not be,” Dr. Venkatesan said in a lecture at a virtual conference on diseases of the vulva and vagina, hosted by the International Society for the Study of Vulvovaginal Disease.
When quality photographs from referring providers are available, Dr. Venkatesan has conducted virtual new consultations. “But sometimes I will do a virtual telemedicine visit as the first visit and then figure out, okay, this isn’t really sufficient. I need to see them in person.”
Melissa Mauskar, MD, assistant professor of dermatology and obstetrics and gynecology at the University of Texas Southwestern Medical Center, Dallas, described a case early on during the COVID-19 pandemic that illustrates a limitation of virtual visits.
A patient sent in a photograph that appeared to show lichen sclerosus. “There looked like some classic lichen sclerosus changes,” Dr. Mauskar said during a discussion at the meeting. “But she was having a lot of pain, and after a week, her pain still was not better.”
Dr. Mauskar brought the patient into the office and ultimately diagnosed a squamous cell carcinoma. “What I thought was a normal erosion was actually an ulcerated plaque,” she said.
Like Dr. Venkatesan, Dr. Mauskar has found that image quality can be uneven. Photographs may be out of focus. Video visits have been a mixed bag. Some are successful. Other times, Dr. Mauskar has to tell the patient she needs to see her in the office.
Certain clinical scenarios require a vaginal exam, Dr. Venkatesan noted. Although some type of assessment may be possible if a patient is with a primary care provider during the telemedicine visit, the examination may not be equivalent. Doctors also should anticipate where a patient might go to have a biopsy if one is necessary.
Another telemedicine caveat pertains to patient counseling. When using store-and-forward telemedicine systems, advising patients in a written report can be challenging. “Is there an easy way ... to counsel patients how to apply their topical medications?” Dr. Venkatesan said.
Excellent care is possible
Vulvology is a small part of Dr. Venkatesan’s general dermatology practice, which has used telemedicine extensively since the pandemic.
In recent years, Dr. Venkatesan’s clinic began encouraging providers in their health system to submit photographs with referrals. “That has really paid off now because we have been able to help provide a lot of excellent quality care for patients without them having to come in,” she said. “We may be able to say: ‘These are excellent photos. We know what this patient has. We can manage it. They don’t need to come see us in person.’ ” That could be the case for certain types of acne, eczema, and psoriasis.
In other cases, they may be able to provide initial advice remotely but still want to see the patient. For a patient with severe acne, “I may be able to tell the referring doctor: ‘Please start the patient on these three medicines. It will take 2 months for those medicines to start working and then we will plan to have an in-person dermatology visit.’ ” In this case, telemedicine essentially replaces one in-person visit.
If photographs are poor, the differential diagnosis is broad, a procedure is required, the doctor needs to touch the lesion, or more involved history taking or counseling are required, the patient may need to go into the office.
Beyond its public health advantages during a pandemic, telemedicine can improve access for patients who live far away, lack transportation, or are unable to take time off from work. It also can decrease patient wait times. “Once we started doing some telemedicine work … we went from having a 5-month wait time for patients to see us in person to a 72-hour wait time for providing some care for patients if they had good photos as part of their referral,” Dr. Venkatesan said.
Telemedicine has been used in inpatient and outpatient dermatology settings. Primary care providers who consult with dermatologists using a store-and-forward telemedicine system may improve their dermatology knowledge and feel more confident in their ability to diagnose and manage dermatologic conditions, research indicates.
In obstetrics and gynecology, telemedicine may play a role in preconception, contraception, and medical abortion care, prenatal visits, well-woman exams, mental health, and pre- and postoperative counseling, a recent review suggests.
Image quality is key
“Quality of the image is so critical for being able to provide good care, especially in such a visual exam field as dermatology,” Dr. Venkatesan said.
To that end, doctors have offered recommendations on how to photograph skin conditions. A guide shared by the mobile telehealth system company ClickMedix suggests focusing on the area of importance, capturing the extent of involvement, and including involved and uninvolved areas.
Good lighting and checking the image resolution can help, Dr. Venkatesan offered. Nevertheless, patients may have difficulty photographing themselves. If a patient is with their primary care doctor, “we are much more likely to be able to get good quality photos,” she said.
Dr. Venkatesan is a paid consultant for DirectDerm, a store-and-forward teledermatology company. Dr. Mauskar had no relevant disclosures.
Seeing patients with vulvar problems via telemedicine can lead to efficient and successful care, but there are challenges and limitations with this approach, doctors are finding.
Image quality is one key factor that determines whether a clinician can assess and manage a condition remotely, said Aruna Venkatesan, MD, chief of dermatology and director of the genital dermatology clinic at Santa Clara Valley Medical Center in San Jose, Calif. Other issues may be especially relevant to televulvology, including privacy concerns.
“Who is helping with the positioning? Who is the photographer? Is the patient comfortable with having photos taken of this part of their body and submitted, even if they know it is submitted securely? Because they might not be,” Dr. Venkatesan said in a lecture at a virtual conference on diseases of the vulva and vagina, hosted by the International Society for the Study of Vulvovaginal Disease.
When quality photographs from referring providers are available, Dr. Venkatesan has conducted virtual new consultations. “But sometimes I will do a virtual telemedicine visit as the first visit and then figure out, okay, this isn’t really sufficient. I need to see them in person.”
Melissa Mauskar, MD, assistant professor of dermatology and obstetrics and gynecology at the University of Texas Southwestern Medical Center, Dallas, described a case early on during the COVID-19 pandemic that illustrates a limitation of virtual visits.
A patient sent in a photograph that appeared to show lichen sclerosus. “There looked like some classic lichen sclerosus changes,” Dr. Mauskar said during a discussion at the meeting. “But she was having a lot of pain, and after a week, her pain still was not better.”
Dr. Mauskar brought the patient into the office and ultimately diagnosed a squamous cell carcinoma. “What I thought was a normal erosion was actually an ulcerated plaque,” she said.
Like Dr. Venkatesan, Dr. Mauskar has found that image quality can be uneven. Photographs may be out of focus. Video visits have been a mixed bag. Some are successful. Other times, Dr. Mauskar has to tell the patient she needs to see her in the office.
Certain clinical scenarios require a vaginal exam, Dr. Venkatesan noted. Although some type of assessment may be possible if a patient is with a primary care provider during the telemedicine visit, the examination may not be equivalent. Doctors also should anticipate where a patient might go to have a biopsy if one is necessary.
Another telemedicine caveat pertains to patient counseling. When using store-and-forward telemedicine systems, advising patients in a written report can be challenging. “Is there an easy way ... to counsel patients how to apply their topical medications?” Dr. Venkatesan said.
Excellent care is possible
Vulvology is a small part of Dr. Venkatesan’s general dermatology practice, which has used telemedicine extensively since the pandemic.
In recent years, Dr. Venkatesan’s clinic began encouraging providers in their health system to submit photographs with referrals. “That has really paid off now because we have been able to help provide a lot of excellent quality care for patients without them having to come in,” she said. “We may be able to say: ‘These are excellent photos. We know what this patient has. We can manage it. They don’t need to come see us in person.’ ” That could be the case for certain types of acne, eczema, and psoriasis.
In other cases, they may be able to provide initial advice remotely but still want to see the patient. For a patient with severe acne, “I may be able to tell the referring doctor: ‘Please start the patient on these three medicines. It will take 2 months for those medicines to start working and then we will plan to have an in-person dermatology visit.’ ” In this case, telemedicine essentially replaces one in-person visit.
If photographs are poor, the differential diagnosis is broad, a procedure is required, the doctor needs to touch the lesion, or more involved history taking or counseling are required, the patient may need to go into the office.
Beyond its public health advantages during a pandemic, telemedicine can improve access for patients who live far away, lack transportation, or are unable to take time off from work. It also can decrease patient wait times. “Once we started doing some telemedicine work … we went from having a 5-month wait time for patients to see us in person to a 72-hour wait time for providing some care for patients if they had good photos as part of their referral,” Dr. Venkatesan said.
Telemedicine has been used in inpatient and outpatient dermatology settings. Primary care providers who consult with dermatologists using a store-and-forward telemedicine system may improve their dermatology knowledge and feel more confident in their ability to diagnose and manage dermatologic conditions, research indicates.
In obstetrics and gynecology, telemedicine may play a role in preconception, contraception, and medical abortion care, prenatal visits, well-woman exams, mental health, and pre- and postoperative counseling, a recent review suggests.
Image quality is key
“Quality of the image is so critical for being able to provide good care, especially in such a visual exam field as dermatology,” Dr. Venkatesan said.
To that end, doctors have offered recommendations on how to photograph skin conditions. A guide shared by the mobile telehealth system company ClickMedix suggests focusing on the area of importance, capturing the extent of involvement, and including involved and uninvolved areas.
Good lighting and checking the image resolution can help, Dr. Venkatesan offered. Nevertheless, patients may have difficulty photographing themselves. If a patient is with their primary care doctor, “we are much more likely to be able to get good quality photos,” she said.
Dr. Venkatesan is a paid consultant for DirectDerm, a store-and-forward teledermatology company. Dr. Mauskar had no relevant disclosures.
FROM THE ISSVD BIENNIAL CONFERENCE
Chronic inflammatory diseases vary widely in CHD risk
Not all chronic systemic inflammatory diseases are equal enhancers of atherosclerotic cardiovascular disease risk, according to a large case-control study.
Current AHA/American College of Cardiology guidelines cite three chronic inflammatory diseases as atherosclerotic cardiovascular disease risk enhancers: rheumatoid arthritis, psoriasis, and HIV infection. But this study of those three diseases, along with three others marked by elevated high sensitivity C-reactive protein (systemic sclerosis, inflammatory bowel disease, and systemic lupus erythematosus [SLE]), showed that chronic inflammatory diseases are not monolithic in terms of their associated risk of incident coronary heart disease (CHD).
Indeed, two of the six inflammatory diseases – psoriasis and inflammatory bowel disease – turned out to be not at all associated with increased cardiovascular risk in the 37,117-patient study. The highest-risk disease was SLE, not specifically mentioned in the guidelines, Arjun Sinha, MD, a cardiology fellow at Northwestern University, Chicago, noted in his presentation at the virtual American Heart Association scientific sessions.
The study included 18,129 patients with one of the six chronic inflammatory diseases and 18,988 matched controls, none with CHD at baseline. All regularly received outpatient care at Northwestern during 2000-2019. There were 1,011 incident CHD events during a median of 3.5 years of follow-up.
In a Cox proportional hazards analysis adjusted for demographics, insurance status, hypertension, diabetes, current smoking, total cholesterol, and estimated glomerular filtration rate, here’s how the chronic inflammatory diseases stacked up in terms of incident CHD and MI risks:
- SLE: hazard ratio for CHD, 2.85; for MI, 4.76.
- Systemic sclerosis: HR for CHD, 2.14; for MI, 3.19.
- HIV: HR for CHD, 1.38; for MI, 1.69.
- Rheumatoid arthritis: HR for CHD, 1.22; for MI, 1.45.
- Psoriasis: no significant increase.
- Inflammatory bowel disease: no significant increase.
In an exploratory analysis, Dr. Sinha and coinvestigators evaluated the risk of incident CHD stratified by disease severity. For lack of standardized disease severity scales, the investigators relied upon tertiles of CD4 T cell count in the HIV group and CRP in the others. The HR for new-onset CHD in the more than 5,000 patients with psoriasis didn’t vary by CRP tertile. However, there was a nonsignificant trend for greater disease severity, as reflected by CRP tertile, to be associated with increased incident CHD risk in the HIV and inflammatory bowel disease groups.
In contrast, patients with rheumatoid arthritis or systemic sclerosis who were in the top CRP tertile had a significantly greater risk of developing CHD than that of controls, with HRs of 2.11 in the rheumatoid arthritis group and 4.59 with systemic sclerosis, although patients in the other two tertiles weren’t at significantly increased risk. But all three tertiles of CRP in patients with SLE were associated with significantly increased CHD risk: 3.17-fold in the lowest tertile of lupus severity, 5.38-fold in the middle tertile, and 4.04-fold in the top tertile for inflammation.
These findings could be used in clinical practice to fine-tune atherosclerotic cardiovascular disease risk assessment based upon chronic inflammatory disease type and severity. That’s information which in turn can help guide the timing and intensity of preventive therapy for patients with each disease type.
But studying the association between chronic systemic inflammatory diseases and CHD risk can be useful in additional ways, according to Dr. Sinha. These inflammatory diseases can serve as models of atherosclerosis that shed light on the non–lipid-related mechanisms involved in cardiovascular disease.
“The gradient in risk may be hypothesis-generating with respect to which specific inflammatory pathways may contribute to CHD,” he explained.
Each of these six chronic inflammatory diseases is characterized by a different form of major immune dysfunction, Dr. Sinha continued. A case in point is SLE, the inflammatory disease associated with the highest risk of CHD and MI. Lupus is characterized by a form of neutrophil dysfunction marked by increased formation and reduced degradation of neutrophil extracellular traps, or NETs, as well as by an increase in autoreactive B cells and dysfunctional CD4+ T helper cells. The increase in NETs of of particular interest because NETs have also been shown to contribute to the development of atherosclerosis, endothelial dysfunction, plaque erosion, and thrombosis.
In another exploratory analysis, Dr. Sinha and coworkers found that SLE patients with a neutrophil count above the median level were twice as likely to develop CHD than were those with a neutrophil count below the median.
A better understanding of the upstream pathways linking NET formation in SLE and atherosclerosis could lead to development of new or repurposed medications that target immune dysfunction in order to curb atherosclerosis, said Dr. Sinha, whose study won the AHA’s Samuel A. Levine Early Career Clinical Investigator Award.
He reported having no financial conflicts regarding his study.
Not all chronic systemic inflammatory diseases are equal enhancers of atherosclerotic cardiovascular disease risk, according to a large case-control study.
Current AHA/American College of Cardiology guidelines cite three chronic inflammatory diseases as atherosclerotic cardiovascular disease risk enhancers: rheumatoid arthritis, psoriasis, and HIV infection. But this study of those three diseases, along with three others marked by elevated high sensitivity C-reactive protein (systemic sclerosis, inflammatory bowel disease, and systemic lupus erythematosus [SLE]), showed that chronic inflammatory diseases are not monolithic in terms of their associated risk of incident coronary heart disease (CHD).
Indeed, two of the six inflammatory diseases – psoriasis and inflammatory bowel disease – turned out to be not at all associated with increased cardiovascular risk in the 37,117-patient study. The highest-risk disease was SLE, not specifically mentioned in the guidelines, Arjun Sinha, MD, a cardiology fellow at Northwestern University, Chicago, noted in his presentation at the virtual American Heart Association scientific sessions.
The study included 18,129 patients with one of the six chronic inflammatory diseases and 18,988 matched controls, none with CHD at baseline. All regularly received outpatient care at Northwestern during 2000-2019. There were 1,011 incident CHD events during a median of 3.5 years of follow-up.
In a Cox proportional hazards analysis adjusted for demographics, insurance status, hypertension, diabetes, current smoking, total cholesterol, and estimated glomerular filtration rate, here’s how the chronic inflammatory diseases stacked up in terms of incident CHD and MI risks:
- SLE: hazard ratio for CHD, 2.85; for MI, 4.76.
- Systemic sclerosis: HR for CHD, 2.14; for MI, 3.19.
- HIV: HR for CHD, 1.38; for MI, 1.69.
- Rheumatoid arthritis: HR for CHD, 1.22; for MI, 1.45.
- Psoriasis: no significant increase.
- Inflammatory bowel disease: no significant increase.
In an exploratory analysis, Dr. Sinha and coinvestigators evaluated the risk of incident CHD stratified by disease severity. For lack of standardized disease severity scales, the investigators relied upon tertiles of CD4 T cell count in the HIV group and CRP in the others. The HR for new-onset CHD in the more than 5,000 patients with psoriasis didn’t vary by CRP tertile. However, there was a nonsignificant trend for greater disease severity, as reflected by CRP tertile, to be associated with increased incident CHD risk in the HIV and inflammatory bowel disease groups.
In contrast, patients with rheumatoid arthritis or systemic sclerosis who were in the top CRP tertile had a significantly greater risk of developing CHD than that of controls, with HRs of 2.11 in the rheumatoid arthritis group and 4.59 with systemic sclerosis, although patients in the other two tertiles weren’t at significantly increased risk. But all three tertiles of CRP in patients with SLE were associated with significantly increased CHD risk: 3.17-fold in the lowest tertile of lupus severity, 5.38-fold in the middle tertile, and 4.04-fold in the top tertile for inflammation.
These findings could be used in clinical practice to fine-tune atherosclerotic cardiovascular disease risk assessment based upon chronic inflammatory disease type and severity. That’s information which in turn can help guide the timing and intensity of preventive therapy for patients with each disease type.
But studying the association between chronic systemic inflammatory diseases and CHD risk can be useful in additional ways, according to Dr. Sinha. These inflammatory diseases can serve as models of atherosclerosis that shed light on the non–lipid-related mechanisms involved in cardiovascular disease.
“The gradient in risk may be hypothesis-generating with respect to which specific inflammatory pathways may contribute to CHD,” he explained.
Each of these six chronic inflammatory diseases is characterized by a different form of major immune dysfunction, Dr. Sinha continued. A case in point is SLE, the inflammatory disease associated with the highest risk of CHD and MI. Lupus is characterized by a form of neutrophil dysfunction marked by increased formation and reduced degradation of neutrophil extracellular traps, or NETs, as well as by an increase in autoreactive B cells and dysfunctional CD4+ T helper cells. The increase in NETs of of particular interest because NETs have also been shown to contribute to the development of atherosclerosis, endothelial dysfunction, plaque erosion, and thrombosis.
In another exploratory analysis, Dr. Sinha and coworkers found that SLE patients with a neutrophil count above the median level were twice as likely to develop CHD than were those with a neutrophil count below the median.
A better understanding of the upstream pathways linking NET formation in SLE and atherosclerosis could lead to development of new or repurposed medications that target immune dysfunction in order to curb atherosclerosis, said Dr. Sinha, whose study won the AHA’s Samuel A. Levine Early Career Clinical Investigator Award.
He reported having no financial conflicts regarding his study.
Not all chronic systemic inflammatory diseases are equal enhancers of atherosclerotic cardiovascular disease risk, according to a large case-control study.
Current AHA/American College of Cardiology guidelines cite three chronic inflammatory diseases as atherosclerotic cardiovascular disease risk enhancers: rheumatoid arthritis, psoriasis, and HIV infection. But this study of those three diseases, along with three others marked by elevated high sensitivity C-reactive protein (systemic sclerosis, inflammatory bowel disease, and systemic lupus erythematosus [SLE]), showed that chronic inflammatory diseases are not monolithic in terms of their associated risk of incident coronary heart disease (CHD).
Indeed, two of the six inflammatory diseases – psoriasis and inflammatory bowel disease – turned out to be not at all associated with increased cardiovascular risk in the 37,117-patient study. The highest-risk disease was SLE, not specifically mentioned in the guidelines, Arjun Sinha, MD, a cardiology fellow at Northwestern University, Chicago, noted in his presentation at the virtual American Heart Association scientific sessions.
The study included 18,129 patients with one of the six chronic inflammatory diseases and 18,988 matched controls, none with CHD at baseline. All regularly received outpatient care at Northwestern during 2000-2019. There were 1,011 incident CHD events during a median of 3.5 years of follow-up.
In a Cox proportional hazards analysis adjusted for demographics, insurance status, hypertension, diabetes, current smoking, total cholesterol, and estimated glomerular filtration rate, here’s how the chronic inflammatory diseases stacked up in terms of incident CHD and MI risks:
- SLE: hazard ratio for CHD, 2.85; for MI, 4.76.
- Systemic sclerosis: HR for CHD, 2.14; for MI, 3.19.
- HIV: HR for CHD, 1.38; for MI, 1.69.
- Rheumatoid arthritis: HR for CHD, 1.22; for MI, 1.45.
- Psoriasis: no significant increase.
- Inflammatory bowel disease: no significant increase.
In an exploratory analysis, Dr. Sinha and coinvestigators evaluated the risk of incident CHD stratified by disease severity. For lack of standardized disease severity scales, the investigators relied upon tertiles of CD4 T cell count in the HIV group and CRP in the others. The HR for new-onset CHD in the more than 5,000 patients with psoriasis didn’t vary by CRP tertile. However, there was a nonsignificant trend for greater disease severity, as reflected by CRP tertile, to be associated with increased incident CHD risk in the HIV and inflammatory bowel disease groups.
In contrast, patients with rheumatoid arthritis or systemic sclerosis who were in the top CRP tertile had a significantly greater risk of developing CHD than that of controls, with HRs of 2.11 in the rheumatoid arthritis group and 4.59 with systemic sclerosis, although patients in the other two tertiles weren’t at significantly increased risk. But all three tertiles of CRP in patients with SLE were associated with significantly increased CHD risk: 3.17-fold in the lowest tertile of lupus severity, 5.38-fold in the middle tertile, and 4.04-fold in the top tertile for inflammation.
These findings could be used in clinical practice to fine-tune atherosclerotic cardiovascular disease risk assessment based upon chronic inflammatory disease type and severity. That’s information which in turn can help guide the timing and intensity of preventive therapy for patients with each disease type.
But studying the association between chronic systemic inflammatory diseases and CHD risk can be useful in additional ways, according to Dr. Sinha. These inflammatory diseases can serve as models of atherosclerosis that shed light on the non–lipid-related mechanisms involved in cardiovascular disease.
“The gradient in risk may be hypothesis-generating with respect to which specific inflammatory pathways may contribute to CHD,” he explained.
Each of these six chronic inflammatory diseases is characterized by a different form of major immune dysfunction, Dr. Sinha continued. A case in point is SLE, the inflammatory disease associated with the highest risk of CHD and MI. Lupus is characterized by a form of neutrophil dysfunction marked by increased formation and reduced degradation of neutrophil extracellular traps, or NETs, as well as by an increase in autoreactive B cells and dysfunctional CD4+ T helper cells. The increase in NETs of of particular interest because NETs have also been shown to contribute to the development of atherosclerosis, endothelial dysfunction, plaque erosion, and thrombosis.
In another exploratory analysis, Dr. Sinha and coworkers found that SLE patients with a neutrophil count above the median level were twice as likely to develop CHD than were those with a neutrophil count below the median.
A better understanding of the upstream pathways linking NET formation in SLE and atherosclerosis could lead to development of new or repurposed medications that target immune dysfunction in order to curb atherosclerosis, said Dr. Sinha, whose study won the AHA’s Samuel A. Levine Early Career Clinical Investigator Award.
He reported having no financial conflicts regarding his study.
FROM AHA 2020
Empagliflozin favorably reshaped left ventricles in HFrEF patients
Treatment with the SGLT2 inhibitor empagliflozin led to significant reductions in both left ventricular end systolic and diastolic volumes in two independent randomized studies of patients with heart failure with reduced ejection fraction.
These results provide important new evidence that one way a drug from this class exerts its beneficial effects on cardiovascular outcomes in these patients is by producing favorable left-ventricular remodeling.
One of the two studies involved only patients with heart failure with reduced ejection fraction (HFrEF) with diabetes and examined treatment impact after 36 weeks. The second study focused exclusively on HFrEF patients without diabetes and followed patients for 6 months. Both studies also generated additional significant evidence of favorable left-ventricular effects.
“The results of these two new trials are incredibly important, as they tell cardiologists one of the mechanisms by which SGLT2 [sodium glucose co-transporter 2] inhibitors reduce heart failure hospitalizations and cardiovascular death,” said Mark C. Petrie, MBChB, professor at the Institute of Cardiovascular & Medical Sciences at the University of Glasgow, and principal investigator for one of the two studies.
“Many cardiologists want to know mechanisms as well as clinical benefit. These remodeling data showing that these drugs reduce the size of abnormally large hearts [and] are also very important for patients,” Dr. Petrie said in an interview. “There have been more than 50 publications on potential mechanisms of benefit of SGLT2 inhibitors in HFrEF, but these are the first randomized, mechanistic data.”
Mechanistic clues follow large cardiovascular outcome trials
Results from a large randomized trial, EMPEROR-Reduced, recently showed that treatment with empagliflozin (Jardiance) on top of standard HFrEF treatment led to significant benefits in patients with or without type 2 diabetes (T2D), compared with placebo, for major cardiovascular and renal endpoints, including the combination of cardiovascular death or hospitalization for heart failure. And results from a second large randomized trial, DAPA-HF, showed similar results with a different drug from the same class, dapagliflozin (Farxiga), in an earlier report.
But while these reports led to quick uptake of these two drugs for the treatment of patients with HFrEF, the means by which these agents exert their HFrEF benefits have been unclear.
“Our study identifies why this drug [empagliflozin] is effective – because it improves heart function, something that has not been understood until now,” Carlos G. Santos-Gallego, MD, lead investigator for the second new report, said in a written statement. “Many doctors are afraid of prescribing a drug they do not understand, and our findings will help clinicians feel more comfortable giving this to patients once approved.”
On the strength of the DAPA-HF results, dapagliflozin received a revised U.S. label in May 2020 that added the indication for treating patients with HFrEF regardless of the whether patients also have T2D, the original indication for prescribing the drug. Many experts anticipate that a similar addition to the label for empagliflozin will soon occur.
EMPA-TROPISM examines patients with no T2D
The single-center study reported by Dr. Santos-Gallego randomized 84 patients with HFrEF and no diabetes to standard treatment with empagliflozin or placebo and measured several parameters in 80 patients who completed the planned 6 months of treatment. The primary endpoints were the changes in both left ventricular end systolic and diastolic volume from baseline in the empagliflozin-treated patients compared with patients on placebo, measured by cardiac MR.
The results showed an average reduction of end systolic volume of 26.6 mL from baseline compared with a small rise in the placebo patients, and an average drop in end diastolic volume of 25.1 mL from baseline compared again with a small increase in the controls. Both differences were statistically significant, reported the senior author of the study, Juan J. Badimon, PhD, in a talk at the virtual scientific sessions of the American Heart Association. Concurrently, the results were published online in the Journal of the American College of Cardiology.
Results from the EMPA-TROPISM study also showed several other significant benefits from empagliflozin treatment, both to left ventricular shape and function as well as to other measures of patient well being. The drug regimen led to an increase in left ventricular ejection fraction, a decrease in left ventricular mass, reduced myocardial fibrosis and aortic stiffness, increased peak oxygen consumption, an increased distance traveled in a 6-minute walk test, and improved quality of life, said Dr. Badimon, professor of medicine and director of the Atherothrombosis Research Unit at the Cardiovascular Institute at the Icahn School of Medicine at Mount Sinai in New York.
SUGAR-DM-HF enrolled only T2D patients
The second study, SUGAR-DM-HF, randomized 105 patients with HFrEF and T2D to treatment with empagliflozin or placebo at any of 15 centers in Scotland, with 92 patients completing the full 36 weeks on treatment. One of the study’s two primary endpoints was the change in left ventricular end systolic volume index, which dropped by an average of 7.9 mL/m2 in patients who received empagliflozin and by 1.5 mL/m2 in the controls, a significant average between-group difference of 6.0 mL/m2, reported Matthew M.Y. Lee, MBChB, at the same meeting.
However, the second primary endpoint, change in left ventricular global longitudinal strain, showed no significant difference in effect on empagliflozin compared with placebo, said Dr. Lee, a cardiologist at the University of Glasgow. Concurrently with his report the results appeared in an article published online in Circulation.
The results also showed a significant drop in left ventricular end diastolic volume index from baseline compared with the control patients, with an average between-group difference in the reduction from baseline of 8.2 mL/m2.
“Reverse cardiac remodeling is a mechanism by which SGLT2 inhibitors reduce heart failure hospitalizations and cardiovascular mortality,” Dr. Lee concluded during his presentation at the meeting.
Although the findings from both studies together provide strong evidence for an effect by empagliflozin on left ventricular shape and function, neither study provides much insight into how this drug exerts these effects. The authors of both studies agreed on several potential explanations, including reductions in cardiac preload and afterload that could reduce left ventricular stretch and volume; a change triggered in myocardial energetics that switches from a metabolism mostly dependent on glucose to one more geared to using fatty acids, ketone bodies, and branched chain amino acids; and a possible drug-induced reduction in oxidative stress and inflammation.
SUGAR-DM-HF was sponsored by a grant from Boehringer Ingelheim, the company that along with Eli Lilly markets empagliflozin (Jardiance). Dr. Lee had no disclosures. Dr. Petrie has been a consultant to Boehringer Ingelheim and Eli Lilly and to several other companies. EMPA-TROPISM was sponsored by a grant from Boehringer Ingelheim. Dr. Badimon and Dr. Santos-Gallego had no disclosures.
Treatment with the SGLT2 inhibitor empagliflozin led to significant reductions in both left ventricular end systolic and diastolic volumes in two independent randomized studies of patients with heart failure with reduced ejection fraction.
These results provide important new evidence that one way a drug from this class exerts its beneficial effects on cardiovascular outcomes in these patients is by producing favorable left-ventricular remodeling.
One of the two studies involved only patients with heart failure with reduced ejection fraction (HFrEF) with diabetes and examined treatment impact after 36 weeks. The second study focused exclusively on HFrEF patients without diabetes and followed patients for 6 months. Both studies also generated additional significant evidence of favorable left-ventricular effects.
“The results of these two new trials are incredibly important, as they tell cardiologists one of the mechanisms by which SGLT2 [sodium glucose co-transporter 2] inhibitors reduce heart failure hospitalizations and cardiovascular death,” said Mark C. Petrie, MBChB, professor at the Institute of Cardiovascular & Medical Sciences at the University of Glasgow, and principal investigator for one of the two studies.
“Many cardiologists want to know mechanisms as well as clinical benefit. These remodeling data showing that these drugs reduce the size of abnormally large hearts [and] are also very important for patients,” Dr. Petrie said in an interview. “There have been more than 50 publications on potential mechanisms of benefit of SGLT2 inhibitors in HFrEF, but these are the first randomized, mechanistic data.”
Mechanistic clues follow large cardiovascular outcome trials
Results from a large randomized trial, EMPEROR-Reduced, recently showed that treatment with empagliflozin (Jardiance) on top of standard HFrEF treatment led to significant benefits in patients with or without type 2 diabetes (T2D), compared with placebo, for major cardiovascular and renal endpoints, including the combination of cardiovascular death or hospitalization for heart failure. And results from a second large randomized trial, DAPA-HF, showed similar results with a different drug from the same class, dapagliflozin (Farxiga), in an earlier report.
But while these reports led to quick uptake of these two drugs for the treatment of patients with HFrEF, the means by which these agents exert their HFrEF benefits have been unclear.
“Our study identifies why this drug [empagliflozin] is effective – because it improves heart function, something that has not been understood until now,” Carlos G. Santos-Gallego, MD, lead investigator for the second new report, said in a written statement. “Many doctors are afraid of prescribing a drug they do not understand, and our findings will help clinicians feel more comfortable giving this to patients once approved.”
On the strength of the DAPA-HF results, dapagliflozin received a revised U.S. label in May 2020 that added the indication for treating patients with HFrEF regardless of the whether patients also have T2D, the original indication for prescribing the drug. Many experts anticipate that a similar addition to the label for empagliflozin will soon occur.
EMPA-TROPISM examines patients with no T2D
The single-center study reported by Dr. Santos-Gallego randomized 84 patients with HFrEF and no diabetes to standard treatment with empagliflozin or placebo and measured several parameters in 80 patients who completed the planned 6 months of treatment. The primary endpoints were the changes in both left ventricular end systolic and diastolic volume from baseline in the empagliflozin-treated patients compared with patients on placebo, measured by cardiac MR.
The results showed an average reduction of end systolic volume of 26.6 mL from baseline compared with a small rise in the placebo patients, and an average drop in end diastolic volume of 25.1 mL from baseline compared again with a small increase in the controls. Both differences were statistically significant, reported the senior author of the study, Juan J. Badimon, PhD, in a talk at the virtual scientific sessions of the American Heart Association. Concurrently, the results were published online in the Journal of the American College of Cardiology.
Results from the EMPA-TROPISM study also showed several other significant benefits from empagliflozin treatment, both to left ventricular shape and function as well as to other measures of patient well being. The drug regimen led to an increase in left ventricular ejection fraction, a decrease in left ventricular mass, reduced myocardial fibrosis and aortic stiffness, increased peak oxygen consumption, an increased distance traveled in a 6-minute walk test, and improved quality of life, said Dr. Badimon, professor of medicine and director of the Atherothrombosis Research Unit at the Cardiovascular Institute at the Icahn School of Medicine at Mount Sinai in New York.
SUGAR-DM-HF enrolled only T2D patients
The second study, SUGAR-DM-HF, randomized 105 patients with HFrEF and T2D to treatment with empagliflozin or placebo at any of 15 centers in Scotland, with 92 patients completing the full 36 weeks on treatment. One of the study’s two primary endpoints was the change in left ventricular end systolic volume index, which dropped by an average of 7.9 mL/m2 in patients who received empagliflozin and by 1.5 mL/m2 in the controls, a significant average between-group difference of 6.0 mL/m2, reported Matthew M.Y. Lee, MBChB, at the same meeting.
However, the second primary endpoint, change in left ventricular global longitudinal strain, showed no significant difference in effect on empagliflozin compared with placebo, said Dr. Lee, a cardiologist at the University of Glasgow. Concurrently with his report the results appeared in an article published online in Circulation.
The results also showed a significant drop in left ventricular end diastolic volume index from baseline compared with the control patients, with an average between-group difference in the reduction from baseline of 8.2 mL/m2.
“Reverse cardiac remodeling is a mechanism by which SGLT2 inhibitors reduce heart failure hospitalizations and cardiovascular mortality,” Dr. Lee concluded during his presentation at the meeting.
Although the findings from both studies together provide strong evidence for an effect by empagliflozin on left ventricular shape and function, neither study provides much insight into how this drug exerts these effects. The authors of both studies agreed on several potential explanations, including reductions in cardiac preload and afterload that could reduce left ventricular stretch and volume; a change triggered in myocardial energetics that switches from a metabolism mostly dependent on glucose to one more geared to using fatty acids, ketone bodies, and branched chain amino acids; and a possible drug-induced reduction in oxidative stress and inflammation.
SUGAR-DM-HF was sponsored by a grant from Boehringer Ingelheim, the company that along with Eli Lilly markets empagliflozin (Jardiance). Dr. Lee had no disclosures. Dr. Petrie has been a consultant to Boehringer Ingelheim and Eli Lilly and to several other companies. EMPA-TROPISM was sponsored by a grant from Boehringer Ingelheim. Dr. Badimon and Dr. Santos-Gallego had no disclosures.
Treatment with the SGLT2 inhibitor empagliflozin led to significant reductions in both left ventricular end systolic and diastolic volumes in two independent randomized studies of patients with heart failure with reduced ejection fraction.
These results provide important new evidence that one way a drug from this class exerts its beneficial effects on cardiovascular outcomes in these patients is by producing favorable left-ventricular remodeling.
One of the two studies involved only patients with heart failure with reduced ejection fraction (HFrEF) with diabetes and examined treatment impact after 36 weeks. The second study focused exclusively on HFrEF patients without diabetes and followed patients for 6 months. Both studies also generated additional significant evidence of favorable left-ventricular effects.
“The results of these two new trials are incredibly important, as they tell cardiologists one of the mechanisms by which SGLT2 [sodium glucose co-transporter 2] inhibitors reduce heart failure hospitalizations and cardiovascular death,” said Mark C. Petrie, MBChB, professor at the Institute of Cardiovascular & Medical Sciences at the University of Glasgow, and principal investigator for one of the two studies.
“Many cardiologists want to know mechanisms as well as clinical benefit. These remodeling data showing that these drugs reduce the size of abnormally large hearts [and] are also very important for patients,” Dr. Petrie said in an interview. “There have been more than 50 publications on potential mechanisms of benefit of SGLT2 inhibitors in HFrEF, but these are the first randomized, mechanistic data.”
Mechanistic clues follow large cardiovascular outcome trials
Results from a large randomized trial, EMPEROR-Reduced, recently showed that treatment with empagliflozin (Jardiance) on top of standard HFrEF treatment led to significant benefits in patients with or without type 2 diabetes (T2D), compared with placebo, for major cardiovascular and renal endpoints, including the combination of cardiovascular death or hospitalization for heart failure. And results from a second large randomized trial, DAPA-HF, showed similar results with a different drug from the same class, dapagliflozin (Farxiga), in an earlier report.
But while these reports led to quick uptake of these two drugs for the treatment of patients with HFrEF, the means by which these agents exert their HFrEF benefits have been unclear.
“Our study identifies why this drug [empagliflozin] is effective – because it improves heart function, something that has not been understood until now,” Carlos G. Santos-Gallego, MD, lead investigator for the second new report, said in a written statement. “Many doctors are afraid of prescribing a drug they do not understand, and our findings will help clinicians feel more comfortable giving this to patients once approved.”
On the strength of the DAPA-HF results, dapagliflozin received a revised U.S. label in May 2020 that added the indication for treating patients with HFrEF regardless of the whether patients also have T2D, the original indication for prescribing the drug. Many experts anticipate that a similar addition to the label for empagliflozin will soon occur.
EMPA-TROPISM examines patients with no T2D
The single-center study reported by Dr. Santos-Gallego randomized 84 patients with HFrEF and no diabetes to standard treatment with empagliflozin or placebo and measured several parameters in 80 patients who completed the planned 6 months of treatment. The primary endpoints were the changes in both left ventricular end systolic and diastolic volume from baseline in the empagliflozin-treated patients compared with patients on placebo, measured by cardiac MR.
The results showed an average reduction of end systolic volume of 26.6 mL from baseline compared with a small rise in the placebo patients, and an average drop in end diastolic volume of 25.1 mL from baseline compared again with a small increase in the controls. Both differences were statistically significant, reported the senior author of the study, Juan J. Badimon, PhD, in a talk at the virtual scientific sessions of the American Heart Association. Concurrently, the results were published online in the Journal of the American College of Cardiology.
Results from the EMPA-TROPISM study also showed several other significant benefits from empagliflozin treatment, both to left ventricular shape and function as well as to other measures of patient well being. The drug regimen led to an increase in left ventricular ejection fraction, a decrease in left ventricular mass, reduced myocardial fibrosis and aortic stiffness, increased peak oxygen consumption, an increased distance traveled in a 6-minute walk test, and improved quality of life, said Dr. Badimon, professor of medicine and director of the Atherothrombosis Research Unit at the Cardiovascular Institute at the Icahn School of Medicine at Mount Sinai in New York.
SUGAR-DM-HF enrolled only T2D patients
The second study, SUGAR-DM-HF, randomized 105 patients with HFrEF and T2D to treatment with empagliflozin or placebo at any of 15 centers in Scotland, with 92 patients completing the full 36 weeks on treatment. One of the study’s two primary endpoints was the change in left ventricular end systolic volume index, which dropped by an average of 7.9 mL/m2 in patients who received empagliflozin and by 1.5 mL/m2 in the controls, a significant average between-group difference of 6.0 mL/m2, reported Matthew M.Y. Lee, MBChB, at the same meeting.
However, the second primary endpoint, change in left ventricular global longitudinal strain, showed no significant difference in effect on empagliflozin compared with placebo, said Dr. Lee, a cardiologist at the University of Glasgow. Concurrently with his report the results appeared in an article published online in Circulation.
The results also showed a significant drop in left ventricular end diastolic volume index from baseline compared with the control patients, with an average between-group difference in the reduction from baseline of 8.2 mL/m2.
“Reverse cardiac remodeling is a mechanism by which SGLT2 inhibitors reduce heart failure hospitalizations and cardiovascular mortality,” Dr. Lee concluded during his presentation at the meeting.
Although the findings from both studies together provide strong evidence for an effect by empagliflozin on left ventricular shape and function, neither study provides much insight into how this drug exerts these effects. The authors of both studies agreed on several potential explanations, including reductions in cardiac preload and afterload that could reduce left ventricular stretch and volume; a change triggered in myocardial energetics that switches from a metabolism mostly dependent on glucose to one more geared to using fatty acids, ketone bodies, and branched chain amino acids; and a possible drug-induced reduction in oxidative stress and inflammation.
SUGAR-DM-HF was sponsored by a grant from Boehringer Ingelheim, the company that along with Eli Lilly markets empagliflozin (Jardiance). Dr. Lee had no disclosures. Dr. Petrie has been a consultant to Boehringer Ingelheim and Eli Lilly and to several other companies. EMPA-TROPISM was sponsored by a grant from Boehringer Ingelheim. Dr. Badimon and Dr. Santos-Gallego had no disclosures.
FROM AHA 2020
Don’t miss cardiovascular risk factors in transgender patients
Cardiovascular disease risk is elevated among transgender individuals seeking gender-affirming hormone therapy, according to a retrospective study in 427 patients.

The transgender population often experiences socioeconomic and health disparities, including reduced access to care, Kara J. Denby, MD, said in an interview.
Previous research suggests that the use of gender-affirming hormone therapy (GAHT) may place transgender persons at increased cardiovascular risk, she said.
To identify the potential risk for transgender individuals, the researchers identified baseline cardiovascular risk in patients who had not yet undergone GAHT. Study participants were enrolled in a multidisciplinary transgender program, and the researchers collected data on demographics, medical history, vitals, medications, and laboratory results. The average age of the participants was 26 years, 172 identified as men, 236 as women, and 20 as nonbinary.
Overall, 55% of the participants had a chronic medical condition at baseline. Of these, 74 patients had hypertension, 41 had hyperlipidemia, 2 had a history of stroke, 7 had coronary artery disease, and 4 had chronic obstructive pulmonary disease.
For all patients who did not have documented atherosclerotic cardiovascular disease, their American College of Cardiology/American Heart Association ASCVD and QRISK3 risk scores were calculated. “The incidence of undiagnosed hypertension and hyperlipidemia was 6.8% and 11.3% respectively, and of these cases, only 64% and 24% were on appropriate therapies,” noted Dr. Denby of the Cleveland (Ohio) Clinic.
She reported the results Nov. 13 in a presentation at the at the virtual American Heart Association scientific sessions.
The findings were limited by the observational nature of the study.
However, the results suggest that transgender patients “appear to be at higher risk than their age-matched historical cohorts regardless of gender,” said Dr. Denby. More research is needed, but cardiovascular disease–prevention efforts may be inadequate in the transgender population given the elevated risk observed in this study, she concluded.
Growing transgender population is medically underserved
The transgender population is growing in the United States and internationally, said Dr. Denby. “This group has a history of being marginalized as a result of their transgender status with socioeconomic and health repercussions,” she said. “It is well known that transgender patients are less likely to have access to health care or utilize health care for a variety of reasons, including stigma and fear of mistreatment. This often leads transgender individuals to present to care late in disease processes which makes their disease harder to treat and often leads to emergent medical conditions,” she added.
“Transgender men and women are at high risk for cardiovascular disease and often aren’t screened at recommended intervals because of decreased health care use compared to their cisgender counterparts,” she said. “This may lead to untreated diseases that make them even more likely to suffer poor health outcomes.”
The current study is important because there are “almost no prior data regarding the cardiovascular health status of this population prior to gender-affirming care,” Dr. Denby emphasized. “There are data that gay, lesbian, and bisexual individuals are at higher risk for poor cardiovascular outcomes, but the same data are lacking in the transgender group,” she said.
“As transgender individuals have frequent physician visits while on hormonal therapy, this seems like the opportune time to screen for cardiovascular risk factors and treat previously undiagnosed diseases that can lead to poor health outcomes in the future,” Dr. Denby explained. “If we are able to intervene at an earlier age, perhaps we can help prevent poor health outcomes down the road,” she said.
Additional research can inform practice
Dr. Denby said she was not surprised by the findings. “This is a very high-risk population that often doesn’t follow closely in the health care system,” she said. “These data are very important in thinking holistically about transgender patients.” Clinicians can “use the opportunities we have when they present for gender-affirming care to optimize their overall health status, promote long-term health, and reduce the risks associated with hormonal therapy and gender-affirming surgeries,” she noted. “We hope to use this information to change our practice at the Cleveland Clinic and nationally as well. Transgender patients should be screened and aggressively treated for cardiovascular disease and risk factors,” she said.
Key barriers to overcome include determining the best way to reach out to transgender individuals and then making them feel comfortable in the clinical setting, Dr. Denby said. “This means that we must set up clinics that are approachable and safe for all comers. The lack of laws in many states that protect this vulnerable population also contributes to lack of access to care,” she added.
“We hope to continue research in this arena about how to effectively screen and treat transgender patients as they present to care, not only in the transgender clinic, but also to primary care providers (ob.gyn., internal medicine, family medicine, pediatrics) who also care for this population” since no specific guidelines currently exist to direct the screening for cardiovascular patients in particular, she said.
Findings offer foundation for LGBTQ cardiovascular studies
“This [study] provides us with a good rationale for why we should be considering cardiovascular health in transgender adults,” Billy A. Caceres, PhD, RN, of Columbia University School of Nursing, New York, said in an interview. “It is largely descriptive, but I think that that’s a good step in terms of at least understanding the magnitude of this problem. In addition, I think that what this abstract might do is help lead to future research that examines potentially the associations between not only gender-affirming hormone therapies but other potential social determinants like discrimination or poverty on the cardiovascular health of transgender people,” he noted.
Dr. Caceres served as chair of the writing group for the recent American Heart Association Scientific Statement: LGBTQ Heart Health published in Circulation. He had no financial conflicts to disclose.
The study received no outside funding. Dr. Denby had no financial conflicts to disclose.
SOURCE: Denby KJ et al. AHA 2020, Presentation P2274.
Cardiovascular disease risk is elevated among transgender individuals seeking gender-affirming hormone therapy, according to a retrospective study in 427 patients.
The transgender population often experiences socioeconomic and health disparities, including reduced access to care, Kara J. Denby, MD, said in an interview.
Previous research suggests that the use of gender-affirming hormone therapy (GAHT) may place transgender persons at increased cardiovascular risk, she said.
To identify the potential risk for transgender individuals, the researchers identified baseline cardiovascular risk in patients who had not yet undergone GAHT. Study participants were enrolled in a multidisciplinary transgender program, and the researchers collected data on demographics, medical history, vitals, medications, and laboratory results. The average age of the participants was 26 years, 172 identified as men, 236 as women, and 20 as nonbinary.
Overall, 55% of the participants had a chronic medical condition at baseline. Of these, 74 patients had hypertension, 41 had hyperlipidemia, 2 had a history of stroke, 7 had coronary artery disease, and 4 had chronic obstructive pulmonary disease.
For all patients who did not have documented atherosclerotic cardiovascular disease, their American College of Cardiology/American Heart Association ASCVD and QRISK3 risk scores were calculated. “The incidence of undiagnosed hypertension and hyperlipidemia was 6.8% and 11.3% respectively, and of these cases, only 64% and 24% were on appropriate therapies,” noted Dr. Denby of the Cleveland (Ohio) Clinic.
She reported the results Nov. 13 in a presentation at the at the virtual American Heart Association scientific sessions.
The findings were limited by the observational nature of the study.
However, the results suggest that transgender patients “appear to be at higher risk than their age-matched historical cohorts regardless of gender,” said Dr. Denby. More research is needed, but cardiovascular disease–prevention efforts may be inadequate in the transgender population given the elevated risk observed in this study, she concluded.
Growing transgender population is medically underserved
The transgender population is growing in the United States and internationally, said Dr. Denby. “This group has a history of being marginalized as a result of their transgender status with socioeconomic and health repercussions,” she said. “It is well known that transgender patients are less likely to have access to health care or utilize health care for a variety of reasons, including stigma and fear of mistreatment. This often leads transgender individuals to present to care late in disease processes which makes their disease harder to treat and often leads to emergent medical conditions,” she added.
“Transgender men and women are at high risk for cardiovascular disease and often aren’t screened at recommended intervals because of decreased health care use compared to their cisgender counterparts,” she said. “This may lead to untreated diseases that make them even more likely to suffer poor health outcomes.”
The current study is important because there are “almost no prior data regarding the cardiovascular health status of this population prior to gender-affirming care,” Dr. Denby emphasized. “There are data that gay, lesbian, and bisexual individuals are at higher risk for poor cardiovascular outcomes, but the same data are lacking in the transgender group,” she said.
“As transgender individuals have frequent physician visits while on hormonal therapy, this seems like the opportune time to screen for cardiovascular risk factors and treat previously undiagnosed diseases that can lead to poor health outcomes in the future,” Dr. Denby explained. “If we are able to intervene at an earlier age, perhaps we can help prevent poor health outcomes down the road,” she said.
Additional research can inform practice
Dr. Denby said she was not surprised by the findings. “This is a very high-risk population that often doesn’t follow closely in the health care system,” she said. “These data are very important in thinking holistically about transgender patients.” Clinicians can “use the opportunities we have when they present for gender-affirming care to optimize their overall health status, promote long-term health, and reduce the risks associated with hormonal therapy and gender-affirming surgeries,” she noted. “We hope to use this information to change our practice at the Cleveland Clinic and nationally as well. Transgender patients should be screened and aggressively treated for cardiovascular disease and risk factors,” she said.
Key barriers to overcome include determining the best way to reach out to transgender individuals and then making them feel comfortable in the clinical setting, Dr. Denby said. “This means that we must set up clinics that are approachable and safe for all comers. The lack of laws in many states that protect this vulnerable population also contributes to lack of access to care,” she added.
“We hope to continue research in this arena about how to effectively screen and treat transgender patients as they present to care, not only in the transgender clinic, but also to primary care providers (ob.gyn., internal medicine, family medicine, pediatrics) who also care for this population” since no specific guidelines currently exist to direct the screening for cardiovascular patients in particular, she said.
Findings offer foundation for LGBTQ cardiovascular studies
“This [study] provides us with a good rationale for why we should be considering cardiovascular health in transgender adults,” Billy A. Caceres, PhD, RN, of Columbia University School of Nursing, New York, said in an interview. “It is largely descriptive, but I think that that’s a good step in terms of at least understanding the magnitude of this problem. In addition, I think that what this abstract might do is help lead to future research that examines potentially the associations between not only gender-affirming hormone therapies but other potential social determinants like discrimination or poverty on the cardiovascular health of transgender people,” he noted.
Dr. Caceres served as chair of the writing group for the recent American Heart Association Scientific Statement: LGBTQ Heart Health published in Circulation. He had no financial conflicts to disclose.
The study received no outside funding. Dr. Denby had no financial conflicts to disclose.
SOURCE: Denby KJ et al. AHA 2020, Presentation P2274.
Cardiovascular disease risk is elevated among transgender individuals seeking gender-affirming hormone therapy, according to a retrospective study in 427 patients.
The transgender population often experiences socioeconomic and health disparities, including reduced access to care, Kara J. Denby, MD, said in an interview.
Previous research suggests that the use of gender-affirming hormone therapy (GAHT) may place transgender persons at increased cardiovascular risk, she said.
To identify the potential risk for transgender individuals, the researchers identified baseline cardiovascular risk in patients who had not yet undergone GAHT. Study participants were enrolled in a multidisciplinary transgender program, and the researchers collected data on demographics, medical history, vitals, medications, and laboratory results. The average age of the participants was 26 years, 172 identified as men, 236 as women, and 20 as nonbinary.
Overall, 55% of the participants had a chronic medical condition at baseline. Of these, 74 patients had hypertension, 41 had hyperlipidemia, 2 had a history of stroke, 7 had coronary artery disease, and 4 had chronic obstructive pulmonary disease.
For all patients who did not have documented atherosclerotic cardiovascular disease, their American College of Cardiology/American Heart Association ASCVD and QRISK3 risk scores were calculated. “The incidence of undiagnosed hypertension and hyperlipidemia was 6.8% and 11.3% respectively, and of these cases, only 64% and 24% were on appropriate therapies,” noted Dr. Denby of the Cleveland (Ohio) Clinic.
She reported the results Nov. 13 in a presentation at the at the virtual American Heart Association scientific sessions.
The findings were limited by the observational nature of the study.
However, the results suggest that transgender patients “appear to be at higher risk than their age-matched historical cohorts regardless of gender,” said Dr. Denby. More research is needed, but cardiovascular disease–prevention efforts may be inadequate in the transgender population given the elevated risk observed in this study, she concluded.
Growing transgender population is medically underserved
The transgender population is growing in the United States and internationally, said Dr. Denby. “This group has a history of being marginalized as a result of their transgender status with socioeconomic and health repercussions,” she said. “It is well known that transgender patients are less likely to have access to health care or utilize health care for a variety of reasons, including stigma and fear of mistreatment. This often leads transgender individuals to present to care late in disease processes which makes their disease harder to treat and often leads to emergent medical conditions,” she added.
“Transgender men and women are at high risk for cardiovascular disease and often aren’t screened at recommended intervals because of decreased health care use compared to their cisgender counterparts,” she said. “This may lead to untreated diseases that make them even more likely to suffer poor health outcomes.”
The current study is important because there are “almost no prior data regarding the cardiovascular health status of this population prior to gender-affirming care,” Dr. Denby emphasized. “There are data that gay, lesbian, and bisexual individuals are at higher risk for poor cardiovascular outcomes, but the same data are lacking in the transgender group,” she said.
“As transgender individuals have frequent physician visits while on hormonal therapy, this seems like the opportune time to screen for cardiovascular risk factors and treat previously undiagnosed diseases that can lead to poor health outcomes in the future,” Dr. Denby explained. “If we are able to intervene at an earlier age, perhaps we can help prevent poor health outcomes down the road,” she said.
Additional research can inform practice
Dr. Denby said she was not surprised by the findings. “This is a very high-risk population that often doesn’t follow closely in the health care system,” she said. “These data are very important in thinking holistically about transgender patients.” Clinicians can “use the opportunities we have when they present for gender-affirming care to optimize their overall health status, promote long-term health, and reduce the risks associated with hormonal therapy and gender-affirming surgeries,” she noted. “We hope to use this information to change our practice at the Cleveland Clinic and nationally as well. Transgender patients should be screened and aggressively treated for cardiovascular disease and risk factors,” she said.
Key barriers to overcome include determining the best way to reach out to transgender individuals and then making them feel comfortable in the clinical setting, Dr. Denby said. “This means that we must set up clinics that are approachable and safe for all comers. The lack of laws in many states that protect this vulnerable population also contributes to lack of access to care,” she added.
“We hope to continue research in this arena about how to effectively screen and treat transgender patients as they present to care, not only in the transgender clinic, but also to primary care providers (ob.gyn., internal medicine, family medicine, pediatrics) who also care for this population” since no specific guidelines currently exist to direct the screening for cardiovascular patients in particular, she said.
Findings offer foundation for LGBTQ cardiovascular studies
“This [study] provides us with a good rationale for why we should be considering cardiovascular health in transgender adults,” Billy A. Caceres, PhD, RN, of Columbia University School of Nursing, New York, said in an interview. “It is largely descriptive, but I think that that’s a good step in terms of at least understanding the magnitude of this problem. In addition, I think that what this abstract might do is help lead to future research that examines potentially the associations between not only gender-affirming hormone therapies but other potential social determinants like discrimination or poverty on the cardiovascular health of transgender people,” he noted.
Dr. Caceres served as chair of the writing group for the recent American Heart Association Scientific Statement: LGBTQ Heart Health published in Circulation. He had no financial conflicts to disclose.
The study received no outside funding. Dr. Denby had no financial conflicts to disclose.
SOURCE: Denby KJ et al. AHA 2020, Presentation P2274.
FROM AHA 2020
Major breakthrough? Average 10% weight loss with semaglutide
In a phase 3 trial where all participants received intensive behavior therapy, investigational 2.4-mg once-weekly subcutaneous semaglutide (Novo Nordisk) resulted in a 10.3% greater average weight loss than placebo over a period of 68 weeks.
If approved, this medication could be a “potential major breakthrough” in obesity management, the investigators suggested. But other experts urged caution, as cost and uptake are important considerations.
‘Potential weight loss that patients would be happy with’
Thomas A. Wadden, PhD, presented results from the study of 611 adults with overweight or obesity but no diabetes at the virtual ObesityWeek® Interactive 2020 meeting.
“Perhaps even more impressive was the finding that 75% of patients lost 10% or more of baseline body weight,” said Dr. Wadden, of the department of psychiatry at the University of Pennsylvania, Philadelphia.
Moreover, in this trial of semaglutide, a glucagonlike peptide–1 (GLP-1) receptor agonist that is approved for treating type 2 diabetes at a weekly subcutaneous dose of 1 mg, but is being investigated at the higher dose for weight loss – 55% of patients lost ≥15% of their initial weight, and 36% lost ≥20% of their initial weight.
“These large categorical weight losses – particularly of 15% and 20% of initial weight – are potentially a major breakthrough in the management of obesity,” Dr. Wadden said in an interview.
Weight losses of this size, he added, “should confer greater improvements in cardiometabolic risk factors (such as hypertension, sleep apnea, and type 2 diabetes) as compared with losses of 5%-10% achieved with current behavioral or pharmacological approaches.” And patients are generally not satisfied with losses of less than 10% of initial weight when participating in intensive behavior programs or taking weight-loss medications.
Now, “the larger categorical weight losses will mean that a greater number of patients with obesity will be able to achieve a weight loss with which they are ... happy,” Dr. Wadden said in an interview.
According to Louis J. Aronne, MD, Weill Professor of Metabolic Research, Weill Cornell Medicine, New York, who is an investigator for another trial of semaglutide: “Even though it has the same mechanism of action [as liraglutide], the weight loss is two or more times greater [with semaglutide]. In my opinion, it’s really going to be a major advance in the treatment of obesity.”
In the discussion that followed the virtual presentation, one attendee asked about potential weight regain if a patient stopped taking the drug. Based on experience with another subcutaneous injectable GLP-1 receptor agonist, liraglutide (Saxenda), already approved for obesity, it may be that taking medicine for chronic overweight may become like taking a statin for elevated cholesterol, said Dr. Wadden.
Novo Nordisk has now completed the four trials in the STEP (Semaglutide Treatment Effect in People With Obesity) global phase 3 clinical development program, and plans to file applications with the Food and Drug Administration later this year and with the European Medicines Agency in early 2021 for review of semaglutide 2.4 mg for weight management.
“Fundamental issues need to be figured out”
Invited to comment, Scott Kahan, MD, said: “This is impressive data, confirming that semaglutide, particularly when used in concert with evidence-based counseling, is a highly effective agent for obesity management.”
However, “the real question, though, is what comes next,” stressed Dr. Kahan, director of the National Center for Weight and Wellness, Washington, DC.
“Will it be approved by the U.S. FDA? I believe so,” he said in an interview. “Yet we already have several effective obesity medications approved over the past decade – all of which are rarely used and therefore make little impact for patients in the real world.”
“Will there be insurance coverage, and therefore practical access for those who could most benefit?” he continued. “Will prescribers counsel their patients about obesity management, including the use of effective medications? Will patients utilize available options?”
“These and other fundamental issues must be figured out before we anoint any treatment option as a meaningful step forward, let alone a transformative development,” according to Dr. Kahan.
Similarly, Irl B. Hirsch, MD, stressed that, should this medication be approved for weight loss, cost would be a major factor in its uptake.
“I’m old enough to recall when we started using lovastatin in the late 1980s,” Dr. Hirsch, professor of medicine, University of Washington Medicine Diabetes Institute, Seattle, said in an interview.
“We used it without the type of evidence of statin use we have today. A pill, but in those days the statins were expensive. But over time, the evidence for statins grew and over the next 15 years it was quite clear that for both primary prevention (for those with diabetes) and secondary intervention these drugs needed to be used by millions of people. These recommendations became easier once the drugs became generic.
“Will the same thing happen for GLP-1 agonists? The problem is we need both ‘hard-outcome data’ [such as 3-point major adverse cardiovascular events] and more reasonable cost before we see this expanding to an entire population.
“In the future perhaps we could have a biosimilar GLP-1 agonist that would be more affordable than what we pay now, but even before that we need agreement from our reimbursement thought leaders that our society should reimburse these agents.
“My thinking now is the cost-benefit could be favorable, but this is all dependent on what happens to the cost of the drugs over time,” he said.
Additive effect of intensive behavior therapy plus medication
Dr. Wadden explained that intensive behavioral therapy “provides 14 or more counseling sessions in 6 months to modify diet and physical activity, through the patients’ use of behavioral strategies (such as keeping daily food and activity diaries).”
Such programs typically produce mean weight loss of 5%-8% of initial weight; less frequent (e.g., monthly) programs typically produce weight loss of only 1%-3%.
Prior studies suggest that intensive behavioral therapy and medication have additive effects. To investigate this, Dr. Wadden and colleagues randomized 611 adults (81% women) who were a mean age of 46 years and had a mean body mass index of 38 kg/m2.
All participants received 30 intensive behavior therapy sessions provided by a registered dietitian (or other qualified provider), which typically lasted 20-30 minutes and were given weekly for 12 weeks, every other week for the next 12 weeks, and then monthly.
The dietitian gave participants behavioral strategies to help them adhere to diet and physical activity goals.
During the first 8 weeks, participants were provided with a 1,000-1,200 kcal/day meal replacement diet that included liquid shakes, meal bars, and prepared entrees designed to facilitate a large initial weight loss.
They then transitioned to a diet of conventional foods (of their choosing), with a goal of 1,200-1,800 kcal/day based on body weight.
The physical activity goal was 100 minutes/week of walking or other aerobic activity in the first month, building up to 200 minutes/week by month 6.
‘More effective than current FDA-approved weight-loss medications’
At week 68, mean body weight decreased from baseline by 16.0% in the semaglutide group versus 5.7% in the placebo group (P < .0001).
In this trial, where all participants received extensive intensive behavior therapy, more participants had weight loss ≥5%, ≥10%, ≥15%, and ≥20% of their initial weight with semaglutide versus placebo (87% vs. 48%; 75% vs. 27%; 56% vs. 13%; 36% vs. 4%, respectively; all P < .0001).
From baseline to week 68, the proportion of participants with prediabetes decreased from 48% to 7% in the semaglutide group and from 53% to 26% in the placebo group.
Patients who received semaglutide had greater improvements in lipids, too.
Although the weight loss was 10.3% (10.6 kg) greater with semaglutide, Dr. Wadden noted, “additional studies have shown this net benefit to be as great as 11%-12%, which would make semaglutide 2.4 mg more effective than current [FDA-approved] weight-loss medications.”
“Naltrexone-bupropion (Contrave) with lifestyle counseling, for example,” he continued, “produces a loss that is 5 kg greater than lifestyle counseling plus placebo, liraglutide 3.0 mg (Saxenda) a loss 5.3 kg greater than placebo, and phentermine-topiramate (Qsymia) a loss that is 8.8 kg greater than placebo.”
Semaglutide was well tolerated. Gastrointestinal adverse events, the most common type, occurred in 83% of patients in the semaglutide group and 63% of patients in the placebo group.
Nausea, as well as constipation and diarrhea, are common in medications that increase GLP-1 levels, Dr. Wadden noted. Side effects can be managed by slowly increasing the medication dose over 4 months.
Dr. Wadden expects that, if approved, semaglutide 2.4 mg subcutaneous once-weekly will be recommended as an adjunct to a reduced calorie diet and increased physical activity. Additional studies suggest that monthly counseling should be sufficient to obtain similar weight losses as those seen in the current trial, which had more intensive counseling.
As well as being approved as a weekly subcutaneous injectable treatment for type 2 diabetes, semaglutide is also approved as an once-daily oral agent for the same indication (Rybelsus, Novo Nordisk) in doses of 7 mg and 14 mg to improve glycemic control along with diet and exercise. It is the first GLP-1 agonist available in tablet form.
Dr. Wadden serves on scientific advisory boards for Novo Nordisk and WW (formerly Weight Watchers), and has received grant support, on behalf of the University of Pennsylvania, from Novo Nordisk. Dr. Aronne is an investigator in a long-term trial of semaglutide and has served on scientific advisory boards for Novo Nordisk in the past. He also has other industry relationships that are not related to semaglutide.
A version of this article originally appeared on Medscape.com.
In a phase 3 trial where all participants received intensive behavior therapy, investigational 2.4-mg once-weekly subcutaneous semaglutide (Novo Nordisk) resulted in a 10.3% greater average weight loss than placebo over a period of 68 weeks.
If approved, this medication could be a “potential major breakthrough” in obesity management, the investigators suggested. But other experts urged caution, as cost and uptake are important considerations.
‘Potential weight loss that patients would be happy with’
Thomas A. Wadden, PhD, presented results from the study of 611 adults with overweight or obesity but no diabetes at the virtual ObesityWeek® Interactive 2020 meeting.
“Perhaps even more impressive was the finding that 75% of patients lost 10% or more of baseline body weight,” said Dr. Wadden, of the department of psychiatry at the University of Pennsylvania, Philadelphia.
Moreover, in this trial of semaglutide, a glucagonlike peptide–1 (GLP-1) receptor agonist that is approved for treating type 2 diabetes at a weekly subcutaneous dose of 1 mg, but is being investigated at the higher dose for weight loss – 55% of patients lost ≥15% of their initial weight, and 36% lost ≥20% of their initial weight.
“These large categorical weight losses – particularly of 15% and 20% of initial weight – are potentially a major breakthrough in the management of obesity,” Dr. Wadden said in an interview.
Weight losses of this size, he added, “should confer greater improvements in cardiometabolic risk factors (such as hypertension, sleep apnea, and type 2 diabetes) as compared with losses of 5%-10% achieved with current behavioral or pharmacological approaches.” And patients are generally not satisfied with losses of less than 10% of initial weight when participating in intensive behavior programs or taking weight-loss medications.
Now, “the larger categorical weight losses will mean that a greater number of patients with obesity will be able to achieve a weight loss with which they are ... happy,” Dr. Wadden said in an interview.
According to Louis J. Aronne, MD, Weill Professor of Metabolic Research, Weill Cornell Medicine, New York, who is an investigator for another trial of semaglutide: “Even though it has the same mechanism of action [as liraglutide], the weight loss is two or more times greater [with semaglutide]. In my opinion, it’s really going to be a major advance in the treatment of obesity.”
In the discussion that followed the virtual presentation, one attendee asked about potential weight regain if a patient stopped taking the drug. Based on experience with another subcutaneous injectable GLP-1 receptor agonist, liraglutide (Saxenda), already approved for obesity, it may be that taking medicine for chronic overweight may become like taking a statin for elevated cholesterol, said Dr. Wadden.
Novo Nordisk has now completed the four trials in the STEP (Semaglutide Treatment Effect in People With Obesity) global phase 3 clinical development program, and plans to file applications with the Food and Drug Administration later this year and with the European Medicines Agency in early 2021 for review of semaglutide 2.4 mg for weight management.
“Fundamental issues need to be figured out”
Invited to comment, Scott Kahan, MD, said: “This is impressive data, confirming that semaglutide, particularly when used in concert with evidence-based counseling, is a highly effective agent for obesity management.”
However, “the real question, though, is what comes next,” stressed Dr. Kahan, director of the National Center for Weight and Wellness, Washington, DC.
“Will it be approved by the U.S. FDA? I believe so,” he said in an interview. “Yet we already have several effective obesity medications approved over the past decade – all of which are rarely used and therefore make little impact for patients in the real world.”
“Will there be insurance coverage, and therefore practical access for those who could most benefit?” he continued. “Will prescribers counsel their patients about obesity management, including the use of effective medications? Will patients utilize available options?”
“These and other fundamental issues must be figured out before we anoint any treatment option as a meaningful step forward, let alone a transformative development,” according to Dr. Kahan.
Similarly, Irl B. Hirsch, MD, stressed that, should this medication be approved for weight loss, cost would be a major factor in its uptake.
“I’m old enough to recall when we started using lovastatin in the late 1980s,” Dr. Hirsch, professor of medicine, University of Washington Medicine Diabetes Institute, Seattle, said in an interview.
“We used it without the type of evidence of statin use we have today. A pill, but in those days the statins were expensive. But over time, the evidence for statins grew and over the next 15 years it was quite clear that for both primary prevention (for those with diabetes) and secondary intervention these drugs needed to be used by millions of people. These recommendations became easier once the drugs became generic.
“Will the same thing happen for GLP-1 agonists? The problem is we need both ‘hard-outcome data’ [such as 3-point major adverse cardiovascular events] and more reasonable cost before we see this expanding to an entire population.
“In the future perhaps we could have a biosimilar GLP-1 agonist that would be more affordable than what we pay now, but even before that we need agreement from our reimbursement thought leaders that our society should reimburse these agents.
“My thinking now is the cost-benefit could be favorable, but this is all dependent on what happens to the cost of the drugs over time,” he said.
Additive effect of intensive behavior therapy plus medication
Dr. Wadden explained that intensive behavioral therapy “provides 14 or more counseling sessions in 6 months to modify diet and physical activity, through the patients’ use of behavioral strategies (such as keeping daily food and activity diaries).”
Such programs typically produce mean weight loss of 5%-8% of initial weight; less frequent (e.g., monthly) programs typically produce weight loss of only 1%-3%.
Prior studies suggest that intensive behavioral therapy and medication have additive effects. To investigate this, Dr. Wadden and colleagues randomized 611 adults (81% women) who were a mean age of 46 years and had a mean body mass index of 38 kg/m2.
All participants received 30 intensive behavior therapy sessions provided by a registered dietitian (or other qualified provider), which typically lasted 20-30 minutes and were given weekly for 12 weeks, every other week for the next 12 weeks, and then monthly.
The dietitian gave participants behavioral strategies to help them adhere to diet and physical activity goals.
During the first 8 weeks, participants were provided with a 1,000-1,200 kcal/day meal replacement diet that included liquid shakes, meal bars, and prepared entrees designed to facilitate a large initial weight loss.
They then transitioned to a diet of conventional foods (of their choosing), with a goal of 1,200-1,800 kcal/day based on body weight.
The physical activity goal was 100 minutes/week of walking or other aerobic activity in the first month, building up to 200 minutes/week by month 6.
‘More effective than current FDA-approved weight-loss medications’
At week 68, mean body weight decreased from baseline by 16.0% in the semaglutide group versus 5.7% in the placebo group (P < .0001).
In this trial, where all participants received extensive intensive behavior therapy, more participants had weight loss ≥5%, ≥10%, ≥15%, and ≥20% of their initial weight with semaglutide versus placebo (87% vs. 48%; 75% vs. 27%; 56% vs. 13%; 36% vs. 4%, respectively; all P < .0001).
From baseline to week 68, the proportion of participants with prediabetes decreased from 48% to 7% in the semaglutide group and from 53% to 26% in the placebo group.
Patients who received semaglutide had greater improvements in lipids, too.
Although the weight loss was 10.3% (10.6 kg) greater with semaglutide, Dr. Wadden noted, “additional studies have shown this net benefit to be as great as 11%-12%, which would make semaglutide 2.4 mg more effective than current [FDA-approved] weight-loss medications.”
“Naltrexone-bupropion (Contrave) with lifestyle counseling, for example,” he continued, “produces a loss that is 5 kg greater than lifestyle counseling plus placebo, liraglutide 3.0 mg (Saxenda) a loss 5.3 kg greater than placebo, and phentermine-topiramate (Qsymia) a loss that is 8.8 kg greater than placebo.”
Semaglutide was well tolerated. Gastrointestinal adverse events, the most common type, occurred in 83% of patients in the semaglutide group and 63% of patients in the placebo group.
Nausea, as well as constipation and diarrhea, are common in medications that increase GLP-1 levels, Dr. Wadden noted. Side effects can be managed by slowly increasing the medication dose over 4 months.
Dr. Wadden expects that, if approved, semaglutide 2.4 mg subcutaneous once-weekly will be recommended as an adjunct to a reduced calorie diet and increased physical activity. Additional studies suggest that monthly counseling should be sufficient to obtain similar weight losses as those seen in the current trial, which had more intensive counseling.
As well as being approved as a weekly subcutaneous injectable treatment for type 2 diabetes, semaglutide is also approved as an once-daily oral agent for the same indication (Rybelsus, Novo Nordisk) in doses of 7 mg and 14 mg to improve glycemic control along with diet and exercise. It is the first GLP-1 agonist available in tablet form.
Dr. Wadden serves on scientific advisory boards for Novo Nordisk and WW (formerly Weight Watchers), and has received grant support, on behalf of the University of Pennsylvania, from Novo Nordisk. Dr. Aronne is an investigator in a long-term trial of semaglutide and has served on scientific advisory boards for Novo Nordisk in the past. He also has other industry relationships that are not related to semaglutide.
A version of this article originally appeared on Medscape.com.
In a phase 3 trial where all participants received intensive behavior therapy, investigational 2.4-mg once-weekly subcutaneous semaglutide (Novo Nordisk) resulted in a 10.3% greater average weight loss than placebo over a period of 68 weeks.
If approved, this medication could be a “potential major breakthrough” in obesity management, the investigators suggested. But other experts urged caution, as cost and uptake are important considerations.
‘Potential weight loss that patients would be happy with’
Thomas A. Wadden, PhD, presented results from the study of 611 adults with overweight or obesity but no diabetes at the virtual ObesityWeek® Interactive 2020 meeting.
“Perhaps even more impressive was the finding that 75% of patients lost 10% or more of baseline body weight,” said Dr. Wadden, of the department of psychiatry at the University of Pennsylvania, Philadelphia.
Moreover, in this trial of semaglutide, a glucagonlike peptide–1 (GLP-1) receptor agonist that is approved for treating type 2 diabetes at a weekly subcutaneous dose of 1 mg, but is being investigated at the higher dose for weight loss – 55% of patients lost ≥15% of their initial weight, and 36% lost ≥20% of their initial weight.
“These large categorical weight losses – particularly of 15% and 20% of initial weight – are potentially a major breakthrough in the management of obesity,” Dr. Wadden said in an interview.
Weight losses of this size, he added, “should confer greater improvements in cardiometabolic risk factors (such as hypertension, sleep apnea, and type 2 diabetes) as compared with losses of 5%-10% achieved with current behavioral or pharmacological approaches.” And patients are generally not satisfied with losses of less than 10% of initial weight when participating in intensive behavior programs or taking weight-loss medications.
Now, “the larger categorical weight losses will mean that a greater number of patients with obesity will be able to achieve a weight loss with which they are ... happy,” Dr. Wadden said in an interview.
According to Louis J. Aronne, MD, Weill Professor of Metabolic Research, Weill Cornell Medicine, New York, who is an investigator for another trial of semaglutide: “Even though it has the same mechanism of action [as liraglutide], the weight loss is two or more times greater [with semaglutide]. In my opinion, it’s really going to be a major advance in the treatment of obesity.”
In the discussion that followed the virtual presentation, one attendee asked about potential weight regain if a patient stopped taking the drug. Based on experience with another subcutaneous injectable GLP-1 receptor agonist, liraglutide (Saxenda), already approved for obesity, it may be that taking medicine for chronic overweight may become like taking a statin for elevated cholesterol, said Dr. Wadden.
Novo Nordisk has now completed the four trials in the STEP (Semaglutide Treatment Effect in People With Obesity) global phase 3 clinical development program, and plans to file applications with the Food and Drug Administration later this year and with the European Medicines Agency in early 2021 for review of semaglutide 2.4 mg for weight management.
“Fundamental issues need to be figured out”
Invited to comment, Scott Kahan, MD, said: “This is impressive data, confirming that semaglutide, particularly when used in concert with evidence-based counseling, is a highly effective agent for obesity management.”
However, “the real question, though, is what comes next,” stressed Dr. Kahan, director of the National Center for Weight and Wellness, Washington, DC.
“Will it be approved by the U.S. FDA? I believe so,” he said in an interview. “Yet we already have several effective obesity medications approved over the past decade – all of which are rarely used and therefore make little impact for patients in the real world.”
“Will there be insurance coverage, and therefore practical access for those who could most benefit?” he continued. “Will prescribers counsel their patients about obesity management, including the use of effective medications? Will patients utilize available options?”
“These and other fundamental issues must be figured out before we anoint any treatment option as a meaningful step forward, let alone a transformative development,” according to Dr. Kahan.
Similarly, Irl B. Hirsch, MD, stressed that, should this medication be approved for weight loss, cost would be a major factor in its uptake.
“I’m old enough to recall when we started using lovastatin in the late 1980s,” Dr. Hirsch, professor of medicine, University of Washington Medicine Diabetes Institute, Seattle, said in an interview.
“We used it without the type of evidence of statin use we have today. A pill, but in those days the statins were expensive. But over time, the evidence for statins grew and over the next 15 years it was quite clear that for both primary prevention (for those with diabetes) and secondary intervention these drugs needed to be used by millions of people. These recommendations became easier once the drugs became generic.
“Will the same thing happen for GLP-1 agonists? The problem is we need both ‘hard-outcome data’ [such as 3-point major adverse cardiovascular events] and more reasonable cost before we see this expanding to an entire population.
“In the future perhaps we could have a biosimilar GLP-1 agonist that would be more affordable than what we pay now, but even before that we need agreement from our reimbursement thought leaders that our society should reimburse these agents.
“My thinking now is the cost-benefit could be favorable, but this is all dependent on what happens to the cost of the drugs over time,” he said.
Additive effect of intensive behavior therapy plus medication
Dr. Wadden explained that intensive behavioral therapy “provides 14 or more counseling sessions in 6 months to modify diet and physical activity, through the patients’ use of behavioral strategies (such as keeping daily food and activity diaries).”
Such programs typically produce mean weight loss of 5%-8% of initial weight; less frequent (e.g., monthly) programs typically produce weight loss of only 1%-3%.
Prior studies suggest that intensive behavioral therapy and medication have additive effects. To investigate this, Dr. Wadden and colleagues randomized 611 adults (81% women) who were a mean age of 46 years and had a mean body mass index of 38 kg/m2.
All participants received 30 intensive behavior therapy sessions provided by a registered dietitian (or other qualified provider), which typically lasted 20-30 minutes and were given weekly for 12 weeks, every other week for the next 12 weeks, and then monthly.
The dietitian gave participants behavioral strategies to help them adhere to diet and physical activity goals.
During the first 8 weeks, participants were provided with a 1,000-1,200 kcal/day meal replacement diet that included liquid shakes, meal bars, and prepared entrees designed to facilitate a large initial weight loss.
They then transitioned to a diet of conventional foods (of their choosing), with a goal of 1,200-1,800 kcal/day based on body weight.
The physical activity goal was 100 minutes/week of walking or other aerobic activity in the first month, building up to 200 minutes/week by month 6.
‘More effective than current FDA-approved weight-loss medications’
At week 68, mean body weight decreased from baseline by 16.0% in the semaglutide group versus 5.7% in the placebo group (P < .0001).
In this trial, where all participants received extensive intensive behavior therapy, more participants had weight loss ≥5%, ≥10%, ≥15%, and ≥20% of their initial weight with semaglutide versus placebo (87% vs. 48%; 75% vs. 27%; 56% vs. 13%; 36% vs. 4%, respectively; all P < .0001).
From baseline to week 68, the proportion of participants with prediabetes decreased from 48% to 7% in the semaglutide group and from 53% to 26% in the placebo group.
Patients who received semaglutide had greater improvements in lipids, too.
Although the weight loss was 10.3% (10.6 kg) greater with semaglutide, Dr. Wadden noted, “additional studies have shown this net benefit to be as great as 11%-12%, which would make semaglutide 2.4 mg more effective than current [FDA-approved] weight-loss medications.”
“Naltrexone-bupropion (Contrave) with lifestyle counseling, for example,” he continued, “produces a loss that is 5 kg greater than lifestyle counseling plus placebo, liraglutide 3.0 mg (Saxenda) a loss 5.3 kg greater than placebo, and phentermine-topiramate (Qsymia) a loss that is 8.8 kg greater than placebo.”
Semaglutide was well tolerated. Gastrointestinal adverse events, the most common type, occurred in 83% of patients in the semaglutide group and 63% of patients in the placebo group.
Nausea, as well as constipation and diarrhea, are common in medications that increase GLP-1 levels, Dr. Wadden noted. Side effects can be managed by slowly increasing the medication dose over 4 months.
Dr. Wadden expects that, if approved, semaglutide 2.4 mg subcutaneous once-weekly will be recommended as an adjunct to a reduced calorie diet and increased physical activity. Additional studies suggest that monthly counseling should be sufficient to obtain similar weight losses as those seen in the current trial, which had more intensive counseling.
As well as being approved as a weekly subcutaneous injectable treatment for type 2 diabetes, semaglutide is also approved as an once-daily oral agent for the same indication (Rybelsus, Novo Nordisk) in doses of 7 mg and 14 mg to improve glycemic control along with diet and exercise. It is the first GLP-1 agonist available in tablet form.
Dr. Wadden serves on scientific advisory boards for Novo Nordisk and WW (formerly Weight Watchers), and has received grant support, on behalf of the University of Pennsylvania, from Novo Nordisk. Dr. Aronne is an investigator in a long-term trial of semaglutide and has served on scientific advisory boards for Novo Nordisk in the past. He also has other industry relationships that are not related to semaglutide.
A version of this article originally appeared on Medscape.com.
Semaglutide shows promise in NASH phase 2 study
according to a phase 2, double-blind, randomized, placebo-controlled trial published in the New England Journal of Medicine and presented at the 2020 American Association for the Study of Liver Diseases (AASLD) meeting.
“This bodes well for further study of semaglutide and is supported further by marked improvements in weight, glycemic control and lipid profile,” commented the study’s senior author Philip N. Newsome, PhD, FRCPE, of the University of Birmingham (England), in an interview.
The highest daily dose (0.4 mg) of the glucagonlike peptide-1 (GLP-1) receptor agonist, semaglutide, which is approved for the treatment of type 2 diabetes, led to levels of NASH resolution “which are higher than any previously demonstrated,” noted Dr. Newsome. “This was also accompanied by improvement in noninvasive markers of liver fibrosis and also less fibrosis progression, compared to placebo.”
“I think this represents an exciting advance and will, if confirmed in further studies, mark a step-change in our management of patients with NASH,” he added.
The multicenter study, conducted at 143 sites in 16 countries, included 320 patients, aged 18-75 years, with or without type 2 diabetes, who had histologic evidence of NASH and stage 1-3 liver fibrosis.
They were randomized in a 3:3:3:1:1:1 ratio to receive once-daily subcutaneous semaglutide at a dose of 0.1, 0.2, or 0.4 mg, or placebo for 72 weeks.
The primary endpoint was resolution of NASH and no worsening of fibrosis, with a secondary endpoint being improvement of fibrosis by at least one stage without worsening of NASH.
The study found 40% of patients in the 0.1-mg semaglutide group, 36% in the 0.2-mg group, and 59% in the 0.4-mg group achieved NASH resolution with no worsening of fibrosis, compared with 17% of the placebo group (odds ratio, 6.87; P < .001 for the highest semaglutide dose). However, the treatment did not lead to significant between-group differences in the secondary endpoint, which occurred in 43% of patients on the highest semaglutide dose compared to 33% in the placebo group (OR, 1.42; P = .48).
Treatment with semaglutide also resulted in dose-dependent reductions in body weight, as well as in glycated hemoglobin levels. Bodyweight was reduced by a mean of 5% in the 0.1-mg semaglutide group, followed by mean reductions of 9% and 13% in the 0.2-mg and 0.4-mg groups respectively. This compared to a mean reduction of 1% in the placebo group.
Similarly, glycated hemoglobin levels among patients with type 2 diabetes dropped by 0.63, 1.07, and 1.15 percentage points in the 0.1-mg, 0.2-mg, and 0.4-mg semaglutide groups respectively, compared with a drop of 0.01 percentage point in the placebo group.
“The fact that the percentage of patients who had an improvement in fibrosis stage was not significantly higher with semaglutide than with placebo – despite a greater benefit with respect to NASH resolution and dose-dependent weight loss – was unexpected, given that previous studies have suggested that resolution of NASH and improvements in activity scores for the components of nonalcoholic fatty liver disease are associated with regression of fibrosis,” wrote the authors. “However, the temporal association among NASH resolution, weight loss, and improvement in fibrosis stage is not fully understood. It is possible that the current trial was not of sufficient duration for improvements in fibrosis stage to become apparent.”
The authors also noted that the safety profile of semaglutide was “consistent with that observed in patients with type 2 diabetes in other trials and with the known effects of GLP-1 receptor agonists,” with gastrointestinal disorders being the most commonly reported.
Nausea, constipation, and vomiting were reported more often in the 0.4-mg semaglutide group than in the placebo group (nausea, 42% vs. 11%; constipation, 22% vs. 12%; and vomiting, 15% vs. 2%).
The overall incidence of benign, malignant, or unspecified neoplasms was 15% in the treatment groups versus 8% in the placebo group.
Rowen K. Zetterman, MD, who was not involved with the study, noted that “treatment of NASH is currently limited, and no therapies have yet been approved by the Food and Drug Administration.”
The findings are “important but not yet exciting,” added Dr. Zetterman, who is professor emeritus of internal medicine and associate vice chancellor for strategic planning for the University of Nebraska Medical Center, Omaha.
“Though reversal of liver fibrosis was not noted, the resolution of hepatic inflammation and liver cell injury by semaglutide suggests it may be slowing disease progression,” said Dr. Zetterman, who also serves on the editorial advisory board of Internal Medicine News. This “warrants additional studies where longer treatment with semaglutide may prove reversal of fibrosis and/or prevention of progression to cirrhosis.”
The study was sponsored by Novo Nordisk. Dr. Newsome reported disclosures related to Novo Nordisk during the conduct of the study, and to Boehringer Ingelheim, Bristol-Myers Squibb, Echosens, Gilead, Pfizer, Pharmaxis, and Poxel. Several of the other study authors reported receiving fees and grants from various pharmaceutical companies, including Novo Nordisk One author reported pending patents for the use of semaglutide. Dr. Zetterman had no relevant disclosures.
SOURCE: Newsome PN et al. N Engl J Med. 2020 Nov 13. doi: 10.1056/NEJMoa2028395.
according to a phase 2, double-blind, randomized, placebo-controlled trial published in the New England Journal of Medicine and presented at the 2020 American Association for the Study of Liver Diseases (AASLD) meeting.
“This bodes well for further study of semaglutide and is supported further by marked improvements in weight, glycemic control and lipid profile,” commented the study’s senior author Philip N. Newsome, PhD, FRCPE, of the University of Birmingham (England), in an interview.
The highest daily dose (0.4 mg) of the glucagonlike peptide-1 (GLP-1) receptor agonist, semaglutide, which is approved for the treatment of type 2 diabetes, led to levels of NASH resolution “which are higher than any previously demonstrated,” noted Dr. Newsome. “This was also accompanied by improvement in noninvasive markers of liver fibrosis and also less fibrosis progression, compared to placebo.”
“I think this represents an exciting advance and will, if confirmed in further studies, mark a step-change in our management of patients with NASH,” he added.
The multicenter study, conducted at 143 sites in 16 countries, included 320 patients, aged 18-75 years, with or without type 2 diabetes, who had histologic evidence of NASH and stage 1-3 liver fibrosis.
They were randomized in a 3:3:3:1:1:1 ratio to receive once-daily subcutaneous semaglutide at a dose of 0.1, 0.2, or 0.4 mg, or placebo for 72 weeks.
The primary endpoint was resolution of NASH and no worsening of fibrosis, with a secondary endpoint being improvement of fibrosis by at least one stage without worsening of NASH.
The study found 40% of patients in the 0.1-mg semaglutide group, 36% in the 0.2-mg group, and 59% in the 0.4-mg group achieved NASH resolution with no worsening of fibrosis, compared with 17% of the placebo group (odds ratio, 6.87; P < .001 for the highest semaglutide dose). However, the treatment did not lead to significant between-group differences in the secondary endpoint, which occurred in 43% of patients on the highest semaglutide dose compared to 33% in the placebo group (OR, 1.42; P = .48).
Treatment with semaglutide also resulted in dose-dependent reductions in body weight, as well as in glycated hemoglobin levels. Bodyweight was reduced by a mean of 5% in the 0.1-mg semaglutide group, followed by mean reductions of 9% and 13% in the 0.2-mg and 0.4-mg groups respectively. This compared to a mean reduction of 1% in the placebo group.
Similarly, glycated hemoglobin levels among patients with type 2 diabetes dropped by 0.63, 1.07, and 1.15 percentage points in the 0.1-mg, 0.2-mg, and 0.4-mg semaglutide groups respectively, compared with a drop of 0.01 percentage point in the placebo group.
“The fact that the percentage of patients who had an improvement in fibrosis stage was not significantly higher with semaglutide than with placebo – despite a greater benefit with respect to NASH resolution and dose-dependent weight loss – was unexpected, given that previous studies have suggested that resolution of NASH and improvements in activity scores for the components of nonalcoholic fatty liver disease are associated with regression of fibrosis,” wrote the authors. “However, the temporal association among NASH resolution, weight loss, and improvement in fibrosis stage is not fully understood. It is possible that the current trial was not of sufficient duration for improvements in fibrosis stage to become apparent.”
The authors also noted that the safety profile of semaglutide was “consistent with that observed in patients with type 2 diabetes in other trials and with the known effects of GLP-1 receptor agonists,” with gastrointestinal disorders being the most commonly reported.
Nausea, constipation, and vomiting were reported more often in the 0.4-mg semaglutide group than in the placebo group (nausea, 42% vs. 11%; constipation, 22% vs. 12%; and vomiting, 15% vs. 2%).
The overall incidence of benign, malignant, or unspecified neoplasms was 15% in the treatment groups versus 8% in the placebo group.
Rowen K. Zetterman, MD, who was not involved with the study, noted that “treatment of NASH is currently limited, and no therapies have yet been approved by the Food and Drug Administration.”
The findings are “important but not yet exciting,” added Dr. Zetterman, who is professor emeritus of internal medicine and associate vice chancellor for strategic planning for the University of Nebraska Medical Center, Omaha.
“Though reversal of liver fibrosis was not noted, the resolution of hepatic inflammation and liver cell injury by semaglutide suggests it may be slowing disease progression,” said Dr. Zetterman, who also serves on the editorial advisory board of Internal Medicine News. This “warrants additional studies where longer treatment with semaglutide may prove reversal of fibrosis and/or prevention of progression to cirrhosis.”
The study was sponsored by Novo Nordisk. Dr. Newsome reported disclosures related to Novo Nordisk during the conduct of the study, and to Boehringer Ingelheim, Bristol-Myers Squibb, Echosens, Gilead, Pfizer, Pharmaxis, and Poxel. Several of the other study authors reported receiving fees and grants from various pharmaceutical companies, including Novo Nordisk One author reported pending patents for the use of semaglutide. Dr. Zetterman had no relevant disclosures.
SOURCE: Newsome PN et al. N Engl J Med. 2020 Nov 13. doi: 10.1056/NEJMoa2028395.
according to a phase 2, double-blind, randomized, placebo-controlled trial published in the New England Journal of Medicine and presented at the 2020 American Association for the Study of Liver Diseases (AASLD) meeting.
“This bodes well for further study of semaglutide and is supported further by marked improvements in weight, glycemic control and lipid profile,” commented the study’s senior author Philip N. Newsome, PhD, FRCPE, of the University of Birmingham (England), in an interview.
The highest daily dose (0.4 mg) of the glucagonlike peptide-1 (GLP-1) receptor agonist, semaglutide, which is approved for the treatment of type 2 diabetes, led to levels of NASH resolution “which are higher than any previously demonstrated,” noted Dr. Newsome. “This was also accompanied by improvement in noninvasive markers of liver fibrosis and also less fibrosis progression, compared to placebo.”
“I think this represents an exciting advance and will, if confirmed in further studies, mark a step-change in our management of patients with NASH,” he added.
The multicenter study, conducted at 143 sites in 16 countries, included 320 patients, aged 18-75 years, with or without type 2 diabetes, who had histologic evidence of NASH and stage 1-3 liver fibrosis.
They were randomized in a 3:3:3:1:1:1 ratio to receive once-daily subcutaneous semaglutide at a dose of 0.1, 0.2, or 0.4 mg, or placebo for 72 weeks.
The primary endpoint was resolution of NASH and no worsening of fibrosis, with a secondary endpoint being improvement of fibrosis by at least one stage without worsening of NASH.
The study found 40% of patients in the 0.1-mg semaglutide group, 36% in the 0.2-mg group, and 59% in the 0.4-mg group achieved NASH resolution with no worsening of fibrosis, compared with 17% of the placebo group (odds ratio, 6.87; P < .001 for the highest semaglutide dose). However, the treatment did not lead to significant between-group differences in the secondary endpoint, which occurred in 43% of patients on the highest semaglutide dose compared to 33% in the placebo group (OR, 1.42; P = .48).
Treatment with semaglutide also resulted in dose-dependent reductions in body weight, as well as in glycated hemoglobin levels. Bodyweight was reduced by a mean of 5% in the 0.1-mg semaglutide group, followed by mean reductions of 9% and 13% in the 0.2-mg and 0.4-mg groups respectively. This compared to a mean reduction of 1% in the placebo group.
Similarly, glycated hemoglobin levels among patients with type 2 diabetes dropped by 0.63, 1.07, and 1.15 percentage points in the 0.1-mg, 0.2-mg, and 0.4-mg semaglutide groups respectively, compared with a drop of 0.01 percentage point in the placebo group.
“The fact that the percentage of patients who had an improvement in fibrosis stage was not significantly higher with semaglutide than with placebo – despite a greater benefit with respect to NASH resolution and dose-dependent weight loss – was unexpected, given that previous studies have suggested that resolution of NASH and improvements in activity scores for the components of nonalcoholic fatty liver disease are associated with regression of fibrosis,” wrote the authors. “However, the temporal association among NASH resolution, weight loss, and improvement in fibrosis stage is not fully understood. It is possible that the current trial was not of sufficient duration for improvements in fibrosis stage to become apparent.”
The authors also noted that the safety profile of semaglutide was “consistent with that observed in patients with type 2 diabetes in other trials and with the known effects of GLP-1 receptor agonists,” with gastrointestinal disorders being the most commonly reported.
Nausea, constipation, and vomiting were reported more often in the 0.4-mg semaglutide group than in the placebo group (nausea, 42% vs. 11%; constipation, 22% vs. 12%; and vomiting, 15% vs. 2%).
The overall incidence of benign, malignant, or unspecified neoplasms was 15% in the treatment groups versus 8% in the placebo group.
Rowen K. Zetterman, MD, who was not involved with the study, noted that “treatment of NASH is currently limited, and no therapies have yet been approved by the Food and Drug Administration.”
The findings are “important but not yet exciting,” added Dr. Zetterman, who is professor emeritus of internal medicine and associate vice chancellor for strategic planning for the University of Nebraska Medical Center, Omaha.
“Though reversal of liver fibrosis was not noted, the resolution of hepatic inflammation and liver cell injury by semaglutide suggests it may be slowing disease progression,” said Dr. Zetterman, who also serves on the editorial advisory board of Internal Medicine News. This “warrants additional studies where longer treatment with semaglutide may prove reversal of fibrosis and/or prevention of progression to cirrhosis.”
The study was sponsored by Novo Nordisk. Dr. Newsome reported disclosures related to Novo Nordisk during the conduct of the study, and to Boehringer Ingelheim, Bristol-Myers Squibb, Echosens, Gilead, Pfizer, Pharmaxis, and Poxel. Several of the other study authors reported receiving fees and grants from various pharmaceutical companies, including Novo Nordisk One author reported pending patents for the use of semaglutide. Dr. Zetterman had no relevant disclosures.
SOURCE: Newsome PN et al. N Engl J Med. 2020 Nov 13. doi: 10.1056/NEJMoa2028395.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Lipid profiles distinguish obese and nonobese NAFLD patients
Both obese and nonobese individuals can develop nonalcoholic fatty liver disease (NAFLD), and lipid profiles were effective predictors in both groups, based on data from a cross-sectional study of 361 individuals.

Given the strong association between obesity and NAFLD, previous research on lipidomic profiles have focused on obese White patients, wrote Youngae Jung, MD, of the Korea Basic Science Institute, Seoul, and colleagues.
“However, there are insufficient data on circulating lipidomics of nonobese NAFLD patients,” they added.
In a study published in Alimentary Pharmacology and Therapeutics, the researchers identified 295 adults with NAFLD and 66 controls. Overall, 130 participants were nonobese (body mass index <25 kg/m2) and 231 were obese (BMI, 25 or higher). The nonobese group included 51 patients with NAFL, 31 with nonalcoholic steatohepatitis , and 48 controls; the obese group included 106 patients with NAFL, 107 with NASH, and 18 controls.
Lipid profiles show predictive promise
Overall, changes in diacylglycerol (DAG) and triacylglycerol (TAG) appeared in both obese and nonobese patients with increases from NAFL to NASH, the researchers noted.
“Levels of DAGs with relatively short chains and a low degree of desaturation significantly increased in NAFL versus no NAFLD, regardless of obesity,” the researchers said. “In contrast, levels of DAGs with relatively long chains and a high degree of desaturation significantly decreased in NASH versus NAFL in the obese group, which was not observed in the nonobese group,” they noted.
In addition, saturated sphingomyelin (SM) species were significantly associated with visceral adiposity in nonobese NAFLD patients, but not in obese NAFLD patients, and SM levels were significantly associated with both systemic and adipose tissue insulin resistance.
The researchers identified five potential lipid metabolites for nonobese subjects and seven potential lipids for obese subjects that included DAGs, TAGs, and SMs that were distinct between NAFL and NASH patients in order to predict the histologic severity of NAFLD. Overall, these metabolite combinations were effective predictors of NAFLD/NASH in nonobese and obese patients. The areas under the receiver operator characteristic curve were 0.916 versus 0.813 for NAFLD versus non-NAFLD in nonobese patients, and 0.967 versus 0.812 for NAFLD versus non-NAFLD in the obese patients.
More BMI groups may yield more information
The key study limitation was the cross-sectional study design, the researchers noted. In addition, dividing patients into only two groups based on BMI may not reveal any distinct biology among lean NAFLD patients, who were included with overweight patients in the nonobese group.
However, the results were strengthened by the large amount of data and the confirmed diagnoses of NASH and fibrosis by an expert liver pathologist, they added.
“Therefore, our findings provide new insights that aid in the understanding of pathophysiological mechanisms responsible for the development and severity of nonobese NAFLD, which are relevant to precision medicine and personalized therapy based on various phenotypes of NAFLD,” they concluded.
Validation needed in other populations
“Liver biopsy remains the gold standard for diagnosing NAFLD/NASH but has its own limitations and risks, so many researchers in this field are looking for a noninvasive alternative to help with diagnosis,” Zachary Henry, MD, of the University of Virginia, Charlottesville, said in an interview. “Imaging methods such as transient elastography and MR-elastography have been introduced and many biochemical markers have been evaluated, yet all have their limitations. In the current study, the authors report a high diagnostic accuracy for evaluating NAFLD using lipidomic profiles, which could introduce a new noninvasive measurement of NAFLD.”
Dr. Henry said that he was not surprised by the study findings. However, “I believe they are important as they define a lipid profile that shows differences between patients with NASH versus patients with NAFLD versus patients without NAFLD,” he said. “NAFLD is a disease of disordered lipid metabolism in hepatocytes, and although it stands to reason there would be differences in lipid profiles, it is interesting to see the changes between DAGs and TAGs especially as disease progresses from NAFLD to NASH.
“Clinically, I do not think this really changes practice right now since it needs to be validated in other populations of NAFLD. However, it certainly adds to a growing armamentarium of noninvasive testing. Hopefully, we are able to combine some of these noninvasive tests in the future to better predict NAFLD and NASH as well as outcomes such as cirrhosis and hepatocellular carcinoma,” he said.
“I think these lipidomic profiles need to be validated in non-Korean populations of patients with NAFLD to determine if these changes are ubiquitous to everyone or if a different profile exists based upon different genetics and environment,” Dr. Henry added. “As the authors note in their paper, there have been previously published differences between populations of NAFLD in Asia as compared to Western countries and it is unclear how, if at all, these lipidomic profiles relate to those differences.”
The study was funded by the Korea Basic Science Institute, the Korea Health Industry Department Institute, and the National Research Foundation of Korea. The researchers had no financial conflicts to disclose. Dr. Henry had no financial conflicts to disclose.
SOURCE: Jung Y et al. Aliment Pharmacol Ther. 2020 Sep 6. doi: 10.1111/apt.16066.
Both obese and nonobese individuals can develop nonalcoholic fatty liver disease (NAFLD), and lipid profiles were effective predictors in both groups, based on data from a cross-sectional study of 361 individuals.
Given the strong association between obesity and NAFLD, previous research on lipidomic profiles have focused on obese White patients, wrote Youngae Jung, MD, of the Korea Basic Science Institute, Seoul, and colleagues.
“However, there are insufficient data on circulating lipidomics of nonobese NAFLD patients,” they added.
In a study published in Alimentary Pharmacology and Therapeutics, the researchers identified 295 adults with NAFLD and 66 controls. Overall, 130 participants were nonobese (body mass index <25 kg/m2) and 231 were obese (BMI, 25 or higher). The nonobese group included 51 patients with NAFL, 31 with nonalcoholic steatohepatitis , and 48 controls; the obese group included 106 patients with NAFL, 107 with NASH, and 18 controls.
Lipid profiles show predictive promise
Overall, changes in diacylglycerol (DAG) and triacylglycerol (TAG) appeared in both obese and nonobese patients with increases from NAFL to NASH, the researchers noted.
“Levels of DAGs with relatively short chains and a low degree of desaturation significantly increased in NAFL versus no NAFLD, regardless of obesity,” the researchers said. “In contrast, levels of DAGs with relatively long chains and a high degree of desaturation significantly decreased in NASH versus NAFL in the obese group, which was not observed in the nonobese group,” they noted.
In addition, saturated sphingomyelin (SM) species were significantly associated with visceral adiposity in nonobese NAFLD patients, but not in obese NAFLD patients, and SM levels were significantly associated with both systemic and adipose tissue insulin resistance.
The researchers identified five potential lipid metabolites for nonobese subjects and seven potential lipids for obese subjects that included DAGs, TAGs, and SMs that were distinct between NAFL and NASH patients in order to predict the histologic severity of NAFLD. Overall, these metabolite combinations were effective predictors of NAFLD/NASH in nonobese and obese patients. The areas under the receiver operator characteristic curve were 0.916 versus 0.813 for NAFLD versus non-NAFLD in nonobese patients, and 0.967 versus 0.812 for NAFLD versus non-NAFLD in the obese patients.
More BMI groups may yield more information
The key study limitation was the cross-sectional study design, the researchers noted. In addition, dividing patients into only two groups based on BMI may not reveal any distinct biology among lean NAFLD patients, who were included with overweight patients in the nonobese group.
However, the results were strengthened by the large amount of data and the confirmed diagnoses of NASH and fibrosis by an expert liver pathologist, they added.
“Therefore, our findings provide new insights that aid in the understanding of pathophysiological mechanisms responsible for the development and severity of nonobese NAFLD, which are relevant to precision medicine and personalized therapy based on various phenotypes of NAFLD,” they concluded.
Validation needed in other populations
“Liver biopsy remains the gold standard for diagnosing NAFLD/NASH but has its own limitations and risks, so many researchers in this field are looking for a noninvasive alternative to help with diagnosis,” Zachary Henry, MD, of the University of Virginia, Charlottesville, said in an interview. “Imaging methods such as transient elastography and MR-elastography have been introduced and many biochemical markers have been evaluated, yet all have their limitations. In the current study, the authors report a high diagnostic accuracy for evaluating NAFLD using lipidomic profiles, which could introduce a new noninvasive measurement of NAFLD.”
Dr. Henry said that he was not surprised by the study findings. However, “I believe they are important as they define a lipid profile that shows differences between patients with NASH versus patients with NAFLD versus patients without NAFLD,” he said. “NAFLD is a disease of disordered lipid metabolism in hepatocytes, and although it stands to reason there would be differences in lipid profiles, it is interesting to see the changes between DAGs and TAGs especially as disease progresses from NAFLD to NASH.
“Clinically, I do not think this really changes practice right now since it needs to be validated in other populations of NAFLD. However, it certainly adds to a growing armamentarium of noninvasive testing. Hopefully, we are able to combine some of these noninvasive tests in the future to better predict NAFLD and NASH as well as outcomes such as cirrhosis and hepatocellular carcinoma,” he said.
“I think these lipidomic profiles need to be validated in non-Korean populations of patients with NAFLD to determine if these changes are ubiquitous to everyone or if a different profile exists based upon different genetics and environment,” Dr. Henry added. “As the authors note in their paper, there have been previously published differences between populations of NAFLD in Asia as compared to Western countries and it is unclear how, if at all, these lipidomic profiles relate to those differences.”
The study was funded by the Korea Basic Science Institute, the Korea Health Industry Department Institute, and the National Research Foundation of Korea. The researchers had no financial conflicts to disclose. Dr. Henry had no financial conflicts to disclose.
SOURCE: Jung Y et al. Aliment Pharmacol Ther. 2020 Sep 6. doi: 10.1111/apt.16066.
Both obese and nonobese individuals can develop nonalcoholic fatty liver disease (NAFLD), and lipid profiles were effective predictors in both groups, based on data from a cross-sectional study of 361 individuals.
Given the strong association between obesity and NAFLD, previous research on lipidomic profiles have focused on obese White patients, wrote Youngae Jung, MD, of the Korea Basic Science Institute, Seoul, and colleagues.
“However, there are insufficient data on circulating lipidomics of nonobese NAFLD patients,” they added.
In a study published in Alimentary Pharmacology and Therapeutics, the researchers identified 295 adults with NAFLD and 66 controls. Overall, 130 participants were nonobese (body mass index <25 kg/m2) and 231 were obese (BMI, 25 or higher). The nonobese group included 51 patients with NAFL, 31 with nonalcoholic steatohepatitis , and 48 controls; the obese group included 106 patients with NAFL, 107 with NASH, and 18 controls.
Lipid profiles show predictive promise
Overall, changes in diacylglycerol (DAG) and triacylglycerol (TAG) appeared in both obese and nonobese patients with increases from NAFL to NASH, the researchers noted.
“Levels of DAGs with relatively short chains and a low degree of desaturation significantly increased in NAFL versus no NAFLD, regardless of obesity,” the researchers said. “In contrast, levels of DAGs with relatively long chains and a high degree of desaturation significantly decreased in NASH versus NAFL in the obese group, which was not observed in the nonobese group,” they noted.
In addition, saturated sphingomyelin (SM) species were significantly associated with visceral adiposity in nonobese NAFLD patients, but not in obese NAFLD patients, and SM levels were significantly associated with both systemic and adipose tissue insulin resistance.
The researchers identified five potential lipid metabolites for nonobese subjects and seven potential lipids for obese subjects that included DAGs, TAGs, and SMs that were distinct between NAFL and NASH patients in order to predict the histologic severity of NAFLD. Overall, these metabolite combinations were effective predictors of NAFLD/NASH in nonobese and obese patients. The areas under the receiver operator characteristic curve were 0.916 versus 0.813 for NAFLD versus non-NAFLD in nonobese patients, and 0.967 versus 0.812 for NAFLD versus non-NAFLD in the obese patients.
More BMI groups may yield more information
The key study limitation was the cross-sectional study design, the researchers noted. In addition, dividing patients into only two groups based on BMI may not reveal any distinct biology among lean NAFLD patients, who were included with overweight patients in the nonobese group.
However, the results were strengthened by the large amount of data and the confirmed diagnoses of NASH and fibrosis by an expert liver pathologist, they added.
“Therefore, our findings provide new insights that aid in the understanding of pathophysiological mechanisms responsible for the development and severity of nonobese NAFLD, which are relevant to precision medicine and personalized therapy based on various phenotypes of NAFLD,” they concluded.
Validation needed in other populations
“Liver biopsy remains the gold standard for diagnosing NAFLD/NASH but has its own limitations and risks, so many researchers in this field are looking for a noninvasive alternative to help with diagnosis,” Zachary Henry, MD, of the University of Virginia, Charlottesville, said in an interview. “Imaging methods such as transient elastography and MR-elastography have been introduced and many biochemical markers have been evaluated, yet all have their limitations. In the current study, the authors report a high diagnostic accuracy for evaluating NAFLD using lipidomic profiles, which could introduce a new noninvasive measurement of NAFLD.”
Dr. Henry said that he was not surprised by the study findings. However, “I believe they are important as they define a lipid profile that shows differences between patients with NASH versus patients with NAFLD versus patients without NAFLD,” he said. “NAFLD is a disease of disordered lipid metabolism in hepatocytes, and although it stands to reason there would be differences in lipid profiles, it is interesting to see the changes between DAGs and TAGs especially as disease progresses from NAFLD to NASH.
“Clinically, I do not think this really changes practice right now since it needs to be validated in other populations of NAFLD. However, it certainly adds to a growing armamentarium of noninvasive testing. Hopefully, we are able to combine some of these noninvasive tests in the future to better predict NAFLD and NASH as well as outcomes such as cirrhosis and hepatocellular carcinoma,” he said.
“I think these lipidomic profiles need to be validated in non-Korean populations of patients with NAFLD to determine if these changes are ubiquitous to everyone or if a different profile exists based upon different genetics and environment,” Dr. Henry added. “As the authors note in their paper, there have been previously published differences between populations of NAFLD in Asia as compared to Western countries and it is unclear how, if at all, these lipidomic profiles relate to those differences.”
The study was funded by the Korea Basic Science Institute, the Korea Health Industry Department Institute, and the National Research Foundation of Korea. The researchers had no financial conflicts to disclose. Dr. Henry had no financial conflicts to disclose.
SOURCE: Jung Y et al. Aliment Pharmacol Ther. 2020 Sep 6. doi: 10.1111/apt.16066.
FROM ALIMENTARY PHARMACOLOGY & THERAPEUTICS
Poverty raises depression risk in patients with cystic fibrosis
Poor people with chronic illness have greater difficulty managing their disease than do their better-off counterparts, and a new study confirms this reality for patients with cystic fibrosis.
and anxiety symptoms, according to a new cross-sectional study. The data were drawn from the Cystic Fibrosis Foundation’s Success with Therapies Research Consortium.
“Assessing the special challenges that individuals with lower SES face, including financial barriers, is essential to understand how we can address the unique combinations of adherence barriers. In other chronic disorders, financial barriers or lower socioeconomic status is associated with nonadherence, but this relationship has not been well established in cystic fibrosis,” said Kimberly Dickinson, MD, MPH, of Johns Hopkins University, Baltimore, during her presentation of the results at the virtual North American Cystic Fibrosis Conference.

“I’ve always thought that my patients in the poorer population were doing worse, and I think this demonstrates that that’s true,” said Robert Giusti, MD, in an interview. Dr. Giusti is a clinical professor of pediatrics at the New York University and director of the Pediatric Cystic Fibrosis Center in New York. He was not involved in the study.
“These are very pertinent issues, especially if you think about the pandemic, and some of the issues related to mental health. It just highlights the importance of socioeconomic status and screening for some of the known risk factors so that we can develop interventions or programs to provide equitable care to all of our cystic fibrosis patients,” said Ryan Perkins, MD, who moderated the session where the study was presented. He is a pediatric and adult pulmonary fellow at Boston Children’s Hospital and Brigham and Women’s Hospital, also in Boston.
The researchers looked retrospectively at 1 year’s worth of pharmacy refill receipts and number of times prescriptions were refilled versus the number of times prescribed, then calculated medicinal possession ratios. This was cross-referenced with annual household income and insurance status of patients with CF at 12 pediatric and 9 adult CF care centers, for a total of 376 patients (128 pediatric and 248 adult).
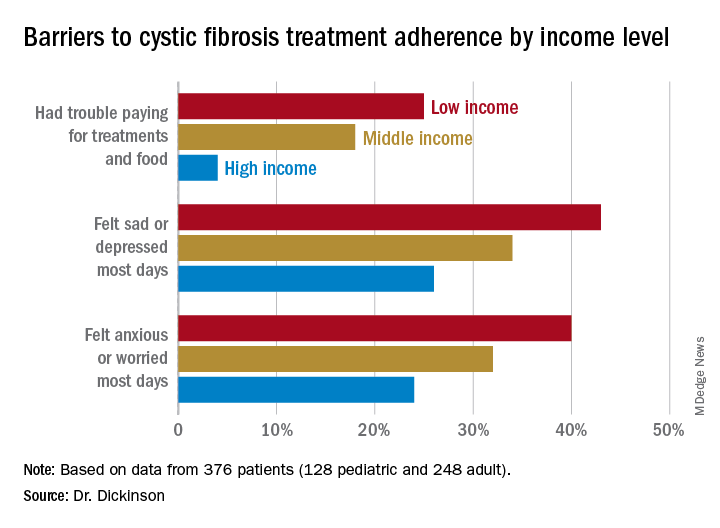
In this population, 32% of participants had public or no insurance, 68% had private or military insurance. The public/no insurance group was more likely than the private/military insurance group to report having trouble paying for treatments, food, or critical expenses related to CF care (23.3% vs. 12.1%, respectively); feeling symptoms on most days of depression (42.5% vs. 31.3%) or anxiety (40.0% vs. 28.5%); and experiencing conflict or stress with loved ones over treatments (30.0% vs. 20.3%) (P < .05 for all).
In all, 35% had a household income less than $40,000 per year, 33% between $44,000 and $100,000, and 32% higher than $100,000. The low-income group had a lower composite medication possession ratio (0.41) than the middle- (0.44) or high-income (0.52) groups, were more likely to have trouble paying for treatments, food, or treatment-related expenses (25%, 18%, 4%, respectively); were more likely most days to report symptoms of depression (43%, 34%, 26%) or anxiety (40%, 32%, 24%), and to have concerns about whether treatments were effective (42%, 27%, 29%). They were more likely to not be able to maintain a daily schedule or routine for treatments (28%, 22%, 14%).
The study showed that adherence barriers and suboptimal adherence are issues that cross all socioeconomic categories, though they were more problematic in the lowest bracket. Greater anxiety and depression among lower income individuals and those with private or no insurance was a key finding, according to Dr. Dickinson. “It highlights the importance of screening for mental health comorbidities that may impact non-adherence,” she said.
The study received funding from the Cystic Fibrosis Foundation. Dr. Dickinson, Dr. Giusti, and Dr. Perkins have no relevant financial disclosures.
Poor people with chronic illness have greater difficulty managing their disease than do their better-off counterparts, and a new study confirms this reality for patients with cystic fibrosis.
and anxiety symptoms, according to a new cross-sectional study. The data were drawn from the Cystic Fibrosis Foundation’s Success with Therapies Research Consortium.
“Assessing the special challenges that individuals with lower SES face, including financial barriers, is essential to understand how we can address the unique combinations of adherence barriers. In other chronic disorders, financial barriers or lower socioeconomic status is associated with nonadherence, but this relationship has not been well established in cystic fibrosis,” said Kimberly Dickinson, MD, MPH, of Johns Hopkins University, Baltimore, during her presentation of the results at the virtual North American Cystic Fibrosis Conference.
“I’ve always thought that my patients in the poorer population were doing worse, and I think this demonstrates that that’s true,” said Robert Giusti, MD, in an interview. Dr. Giusti is a clinical professor of pediatrics at the New York University and director of the Pediatric Cystic Fibrosis Center in New York. He was not involved in the study.
“These are very pertinent issues, especially if you think about the pandemic, and some of the issues related to mental health. It just highlights the importance of socioeconomic status and screening for some of the known risk factors so that we can develop interventions or programs to provide equitable care to all of our cystic fibrosis patients,” said Ryan Perkins, MD, who moderated the session where the study was presented. He is a pediatric and adult pulmonary fellow at Boston Children’s Hospital and Brigham and Women’s Hospital, also in Boston.
The researchers looked retrospectively at 1 year’s worth of pharmacy refill receipts and number of times prescriptions were refilled versus the number of times prescribed, then calculated medicinal possession ratios. This was cross-referenced with annual household income and insurance status of patients with CF at 12 pediatric and 9 adult CF care centers, for a total of 376 patients (128 pediatric and 248 adult).
In this population, 32% of participants had public or no insurance, 68% had private or military insurance. The public/no insurance group was more likely than the private/military insurance group to report having trouble paying for treatments, food, or critical expenses related to CF care (23.3% vs. 12.1%, respectively); feeling symptoms on most days of depression (42.5% vs. 31.3%) or anxiety (40.0% vs. 28.5%); and experiencing conflict or stress with loved ones over treatments (30.0% vs. 20.3%) (P < .05 for all).
In all, 35% had a household income less than $40,000 per year, 33% between $44,000 and $100,000, and 32% higher than $100,000. The low-income group had a lower composite medication possession ratio (0.41) than the middle- (0.44) or high-income (0.52) groups, were more likely to have trouble paying for treatments, food, or treatment-related expenses (25%, 18%, 4%, respectively); were more likely most days to report symptoms of depression (43%, 34%, 26%) or anxiety (40%, 32%, 24%), and to have concerns about whether treatments were effective (42%, 27%, 29%). They were more likely to not be able to maintain a daily schedule or routine for treatments (28%, 22%, 14%).
The study showed that adherence barriers and suboptimal adherence are issues that cross all socioeconomic categories, though they were more problematic in the lowest bracket. Greater anxiety and depression among lower income individuals and those with private or no insurance was a key finding, according to Dr. Dickinson. “It highlights the importance of screening for mental health comorbidities that may impact non-adherence,” she said.
The study received funding from the Cystic Fibrosis Foundation. Dr. Dickinson, Dr. Giusti, and Dr. Perkins have no relevant financial disclosures.
Poor people with chronic illness have greater difficulty managing their disease than do their better-off counterparts, and a new study confirms this reality for patients with cystic fibrosis.
and anxiety symptoms, according to a new cross-sectional study. The data were drawn from the Cystic Fibrosis Foundation’s Success with Therapies Research Consortium.
“Assessing the special challenges that individuals with lower SES face, including financial barriers, is essential to understand how we can address the unique combinations of adherence barriers. In other chronic disorders, financial barriers or lower socioeconomic status is associated with nonadherence, but this relationship has not been well established in cystic fibrosis,” said Kimberly Dickinson, MD, MPH, of Johns Hopkins University, Baltimore, during her presentation of the results at the virtual North American Cystic Fibrosis Conference.
“I’ve always thought that my patients in the poorer population were doing worse, and I think this demonstrates that that’s true,” said Robert Giusti, MD, in an interview. Dr. Giusti is a clinical professor of pediatrics at the New York University and director of the Pediatric Cystic Fibrosis Center in New York. He was not involved in the study.
“These are very pertinent issues, especially if you think about the pandemic, and some of the issues related to mental health. It just highlights the importance of socioeconomic status and screening for some of the known risk factors so that we can develop interventions or programs to provide equitable care to all of our cystic fibrosis patients,” said Ryan Perkins, MD, who moderated the session where the study was presented. He is a pediatric and adult pulmonary fellow at Boston Children’s Hospital and Brigham and Women’s Hospital, also in Boston.
The researchers looked retrospectively at 1 year’s worth of pharmacy refill receipts and number of times prescriptions were refilled versus the number of times prescribed, then calculated medicinal possession ratios. This was cross-referenced with annual household income and insurance status of patients with CF at 12 pediatric and 9 adult CF care centers, for a total of 376 patients (128 pediatric and 248 adult).
In this population, 32% of participants had public or no insurance, 68% had private or military insurance. The public/no insurance group was more likely than the private/military insurance group to report having trouble paying for treatments, food, or critical expenses related to CF care (23.3% vs. 12.1%, respectively); feeling symptoms on most days of depression (42.5% vs. 31.3%) or anxiety (40.0% vs. 28.5%); and experiencing conflict or stress with loved ones over treatments (30.0% vs. 20.3%) (P < .05 for all).
In all, 35% had a household income less than $40,000 per year, 33% between $44,000 and $100,000, and 32% higher than $100,000. The low-income group had a lower composite medication possession ratio (0.41) than the middle- (0.44) or high-income (0.52) groups, were more likely to have trouble paying for treatments, food, or treatment-related expenses (25%, 18%, 4%, respectively); were more likely most days to report symptoms of depression (43%, 34%, 26%) or anxiety (40%, 32%, 24%), and to have concerns about whether treatments were effective (42%, 27%, 29%). They were more likely to not be able to maintain a daily schedule or routine for treatments (28%, 22%, 14%).
The study showed that adherence barriers and suboptimal adherence are issues that cross all socioeconomic categories, though they were more problematic in the lowest bracket. Greater anxiety and depression among lower income individuals and those with private or no insurance was a key finding, according to Dr. Dickinson. “It highlights the importance of screening for mental health comorbidities that may impact non-adherence,” she said.
The study received funding from the Cystic Fibrosis Foundation. Dr. Dickinson, Dr. Giusti, and Dr. Perkins have no relevant financial disclosures.
FROM NACFC 2020
.
What happened to melanoma care during COVID-19 sequestration
Initial evidence suggests that the , Rebecca I. Hartman, MD, MPH, said at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medication Education.

This is not what National Comprehensive Cancer Network officials expected when they issued short-term recommendations on how to manage cutaneous melanoma during the first wave of the COVID-19 pandemic. Those recommendations for restriction of care, which Dr. Hartman characterized as “pretty significant changes from how we typically practice melanoma care in the U.S.,” came at a time when there was justifiable concern that the first COVID-19 surge would strain the U.S. health care system beyond the breaking point.
The rationale given for the NCCN recommendations was that most time-to-treat studies have shown no adverse patient outcomes for 90-day delays in treatment, even for thicker melanomas. But those studies, all retrospective, have been called into question. And the first real-world data on the impact of care restrictions during the lockdown, reported by Italian dermatologists, highlights adverse effects with potentially far-reaching consequences, noted Dr. Hartman, director of melanoma epidemiology at Brigham and Women’s Hospital and a dermatologist, Harvard University, Boston.
Analysis of the impact of lockdown-induced delays in melanoma care is not merely an academic exercise, she added. While everyone hopes that the spring 2020 COVID-19 shelter-in-place was a once-in-a-lifetime event, there’s no guarantee that will be the case. Moreover, the lockdown provides a natural experiment addressing the possible consequences of melanoma care delays on patient outcomes, a topic that for ethical reasons could never be addressed in a randomized trial.
The short-term NCCN recommendations included the use of excisional biopsies for melanoma diagnosis whenever possible; and delay of up to 3 months for wide local excision of in situ melanoma, any invasive melanoma with negative margins, and even T1 melanomas with positive margins provided the bulk of the lesion had been excised. The guidance also suggested delaying sentinel lymph node biopsy (SLNB), along with increased use of neoadjuvant therapy in patients with clinically palpable regional lymph nodes in order to delay surgery for up to 8 weeks. Single-agent systemic therapy at the least-frequent dosing was advised in order to minimize toxicity and reduce the need for additional health care resources: for example, nivolumab (Opdivo) at 480 mg every 4 weeks instead of every 2 weeks, and pembrolizumab (Keytruda) at 400 mg every 6 weeks, rather than every 3 weeks.
So, that’s what the NCCN recommended. Here’s what actually happened during shelter-in-place as captured in Dr. Hartman’s survey of 18 U.S. members of the Melanoma Prevention Working Group, all practicing dermatology in centers particularly hard-hit in the first wave of the pandemic: In-person new melanoma patient visits plunged from an average of 4.83 per week per provider to 0.83 per week. Telemedicine visits with new melanoma patients went from zero prepandemic to 0.67 visits per week per provider, which doesn’t come close to making up for the drop in in-person visits. Interestingly, two respondents reported turning to gene-expression profile testing for patient prognostication because of delays in SLNB.
Wide local excision was delayed by an average of 6 weeks in roughly one-third of melanoma patients with early tumor stage disease, regardless of margin status. For patients with stage T1b disease, wide local excision was typically performed on time during shelter-in-place; however, SLNB was delayed by an average of 5 weeks in 22% of patients with positive margins and 28% of those with negative margins. In contrast, 80% of patients with more advanced T2-T4 melanoma underwent on-schedule definitive management with wide local excision and SLNB, Dr. Hartman reported.
Critics have taken issue with the NCCN’s conclusion that most time-to-treatment studies show no harm arising from 90-day treatment delays. A review of the relevant published literature by Dr. Hartman’s Harvard colleagues, published in July, found that the evidence is mixed. “There is insufficient evidence to definitively conclude that delayed wide resection after gross removal of the primary melanoma is without harm,” they concluded in the review.
Spanish dermatologists performed a modeling study in order to estimate the potential impact of COVID-19 lockdowns on 5- and 10-year survival of melanoma patients. Using the growth rate of a random sample of 1,000 melanomas to model estimates of tumor thickness after various delays, coupled with American Joint Committee on Cancer survival data for different T stages, they estimated that 5-year survival would be reduced from 94.2% to 92.3% with a 90-day delay in diagnosis, and that 10-year survival would drop from 90.0% to 87.6%.
But that’s merely modeling. Francesco Ricci, MD, PhD, and colleagues from the melanoma unit at the Istituto Dermopatico dell’Immacolata, Rome, have provided a first look at the real-world impact of the lockdown. In the prelockdown period of January through March 9th, 2020, the referral center averaged 2.3 new melanoma diagnoses per day. During the Rome lockdown, from March 10th through May 3rd, this figure dropped to a mean of 0.6 melanoma diagnoses per day. Postlockdown, from May 4th to June 6th, the average climbed to 1.3 per day. The rate of newly diagnosed nodular melanoma was 5.5-fold greater postlockdown, compared with prelockdown; the rate of ulcerated melanoma was 4.9-fold greater.
“We can hypothesize that this may have been due to delays in diagnosis and care,” Dr. Hartman commented. “This is important because we know that nodular melanoma as well as ulceration tend to have a worse prognosis in terms of mortality.”
The mean Breslow thickness of newly diagnosed melanomas was 0.88 mm prelockdown, 0.66 mm during lockdown, and 1.96 mm postlockdown. The investigators speculated that the reduced Breslow thickness of melanomas diagnosed during lockdown might be explained by a greater willingness of more health-conscious people to defy the shelter-in-place instructions because of their concern about a suspicious skin lesion. “Though it is way too early to gauge the consequences of such diagnostic delay, should this issue be neglected, dermatologists and their patients may pay a higher price later with increased morbidity, mortality, and financial burden,” according to the investigators.
Dr. Hartman observed that it will be important to learn whether similar experiences occurred elsewhere during lockdown.

Another speaker, John M. Kirkwood, MD, said he has seen several melanoma patients referred from outside centers who had delays of up to 3 months in sentinel lymph node management of T2 and T3 tumors during lockdown who now have widespread metastatic disease.
“Now, is that anecdotal? I don’t know, it’s just worrisome to me,” commented Dr. Kirkwood, professor of medicine, dermatology, and translational science at the University of Pittsburgh.
Merrick Ross, MD, professor of surgical oncology at M.D. Anderson Cancer Center, Houston, recalled, “There was a period of time [during the lockdown] when we weren’t allowed to do certain elective procedures, if you want to call cancer surgery elective.”

“It’s too soon to talk about outcomes because a lot of patients are still in the process of being treated after what I would consider a significant delay in diagnosis,” the surgeon added.
An audience member asked if there will be an opportunity to see data on the damage done by delaying melanoma management as compared to lives saved through the lockdown for COVID-19. Dr. Ross replied that M.D. Anderson is in the midst of an institution-wide study analyzing the delay in diagnosis of a range of cancers.
“In our melanoma center it is absolutely clear, although we’re still collecting data, that the median tumor thickness is much higher since the lockdown,” Dr. Ross commented.
Dr. Hartman said she and her coinvestigators in the Melanoma Prevention Working Group are attempting to tally up the damage done via the lockdown by delaying melanoma diagnosis and treatment. But she agreed with the questioner that the most important thing is overall net lives saved through shelter-in-place.
“I’m sure that, separately, nondermatologists – perhaps infectious disease doctors and internists – are looking at how many lives were saved by the lockdown policy. So I do think all that data will come out,” Dr. Hartman predicted.
She reported having no financial conflicts regarding her presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
SOURCE: Hartman, R. Cutaneous malignancies forum.
Initial evidence suggests that the , Rebecca I. Hartman, MD, MPH, said at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medication Education.
This is not what National Comprehensive Cancer Network officials expected when they issued short-term recommendations on how to manage cutaneous melanoma during the first wave of the COVID-19 pandemic. Those recommendations for restriction of care, which Dr. Hartman characterized as “pretty significant changes from how we typically practice melanoma care in the U.S.,” came at a time when there was justifiable concern that the first COVID-19 surge would strain the U.S. health care system beyond the breaking point.
The rationale given for the NCCN recommendations was that most time-to-treat studies have shown no adverse patient outcomes for 90-day delays in treatment, even for thicker melanomas. But those studies, all retrospective, have been called into question. And the first real-world data on the impact of care restrictions during the lockdown, reported by Italian dermatologists, highlights adverse effects with potentially far-reaching consequences, noted Dr. Hartman, director of melanoma epidemiology at Brigham and Women’s Hospital and a dermatologist, Harvard University, Boston.
Analysis of the impact of lockdown-induced delays in melanoma care is not merely an academic exercise, she added. While everyone hopes that the spring 2020 COVID-19 shelter-in-place was a once-in-a-lifetime event, there’s no guarantee that will be the case. Moreover, the lockdown provides a natural experiment addressing the possible consequences of melanoma care delays on patient outcomes, a topic that for ethical reasons could never be addressed in a randomized trial.
The short-term NCCN recommendations included the use of excisional biopsies for melanoma diagnosis whenever possible; and delay of up to 3 months for wide local excision of in situ melanoma, any invasive melanoma with negative margins, and even T1 melanomas with positive margins provided the bulk of the lesion had been excised. The guidance also suggested delaying sentinel lymph node biopsy (SLNB), along with increased use of neoadjuvant therapy in patients with clinically palpable regional lymph nodes in order to delay surgery for up to 8 weeks. Single-agent systemic therapy at the least-frequent dosing was advised in order to minimize toxicity and reduce the need for additional health care resources: for example, nivolumab (Opdivo) at 480 mg every 4 weeks instead of every 2 weeks, and pembrolizumab (Keytruda) at 400 mg every 6 weeks, rather than every 3 weeks.
So, that’s what the NCCN recommended. Here’s what actually happened during shelter-in-place as captured in Dr. Hartman’s survey of 18 U.S. members of the Melanoma Prevention Working Group, all practicing dermatology in centers particularly hard-hit in the first wave of the pandemic: In-person new melanoma patient visits plunged from an average of 4.83 per week per provider to 0.83 per week. Telemedicine visits with new melanoma patients went from zero prepandemic to 0.67 visits per week per provider, which doesn’t come close to making up for the drop in in-person visits. Interestingly, two respondents reported turning to gene-expression profile testing for patient prognostication because of delays in SLNB.
Wide local excision was delayed by an average of 6 weeks in roughly one-third of melanoma patients with early tumor stage disease, regardless of margin status. For patients with stage T1b disease, wide local excision was typically performed on time during shelter-in-place; however, SLNB was delayed by an average of 5 weeks in 22% of patients with positive margins and 28% of those with negative margins. In contrast, 80% of patients with more advanced T2-T4 melanoma underwent on-schedule definitive management with wide local excision and SLNB, Dr. Hartman reported.
Critics have taken issue with the NCCN’s conclusion that most time-to-treatment studies show no harm arising from 90-day treatment delays. A review of the relevant published literature by Dr. Hartman’s Harvard colleagues, published in July, found that the evidence is mixed. “There is insufficient evidence to definitively conclude that delayed wide resection after gross removal of the primary melanoma is without harm,” they concluded in the review.
Spanish dermatologists performed a modeling study in order to estimate the potential impact of COVID-19 lockdowns on 5- and 10-year survival of melanoma patients. Using the growth rate of a random sample of 1,000 melanomas to model estimates of tumor thickness after various delays, coupled with American Joint Committee on Cancer survival data for different T stages, they estimated that 5-year survival would be reduced from 94.2% to 92.3% with a 90-day delay in diagnosis, and that 10-year survival would drop from 90.0% to 87.6%.
But that’s merely modeling. Francesco Ricci, MD, PhD, and colleagues from the melanoma unit at the Istituto Dermopatico dell’Immacolata, Rome, have provided a first look at the real-world impact of the lockdown. In the prelockdown period of January through March 9th, 2020, the referral center averaged 2.3 new melanoma diagnoses per day. During the Rome lockdown, from March 10th through May 3rd, this figure dropped to a mean of 0.6 melanoma diagnoses per day. Postlockdown, from May 4th to June 6th, the average climbed to 1.3 per day. The rate of newly diagnosed nodular melanoma was 5.5-fold greater postlockdown, compared with prelockdown; the rate of ulcerated melanoma was 4.9-fold greater.
“We can hypothesize that this may have been due to delays in diagnosis and care,” Dr. Hartman commented. “This is important because we know that nodular melanoma as well as ulceration tend to have a worse prognosis in terms of mortality.”
The mean Breslow thickness of newly diagnosed melanomas was 0.88 mm prelockdown, 0.66 mm during lockdown, and 1.96 mm postlockdown. The investigators speculated that the reduced Breslow thickness of melanomas diagnosed during lockdown might be explained by a greater willingness of more health-conscious people to defy the shelter-in-place instructions because of their concern about a suspicious skin lesion. “Though it is way too early to gauge the consequences of such diagnostic delay, should this issue be neglected, dermatologists and their patients may pay a higher price later with increased morbidity, mortality, and financial burden,” according to the investigators.
Dr. Hartman observed that it will be important to learn whether similar experiences occurred elsewhere during lockdown.
Another speaker, John M. Kirkwood, MD, said he has seen several melanoma patients referred from outside centers who had delays of up to 3 months in sentinel lymph node management of T2 and T3 tumors during lockdown who now have widespread metastatic disease.
“Now, is that anecdotal? I don’t know, it’s just worrisome to me,” commented Dr. Kirkwood, professor of medicine, dermatology, and translational science at the University of Pittsburgh.
Merrick Ross, MD, professor of surgical oncology at M.D. Anderson Cancer Center, Houston, recalled, “There was a period of time [during the lockdown] when we weren’t allowed to do certain elective procedures, if you want to call cancer surgery elective.”
“It’s too soon to talk about outcomes because a lot of patients are still in the process of being treated after what I would consider a significant delay in diagnosis,” the surgeon added.
An audience member asked if there will be an opportunity to see data on the damage done by delaying melanoma management as compared to lives saved through the lockdown for COVID-19. Dr. Ross replied that M.D. Anderson is in the midst of an institution-wide study analyzing the delay in diagnosis of a range of cancers.
“In our melanoma center it is absolutely clear, although we’re still collecting data, that the median tumor thickness is much higher since the lockdown,” Dr. Ross commented.
Dr. Hartman said she and her coinvestigators in the Melanoma Prevention Working Group are attempting to tally up the damage done via the lockdown by delaying melanoma diagnosis and treatment. But she agreed with the questioner that the most important thing is overall net lives saved through shelter-in-place.
“I’m sure that, separately, nondermatologists – perhaps infectious disease doctors and internists – are looking at how many lives were saved by the lockdown policy. So I do think all that data will come out,” Dr. Hartman predicted.
She reported having no financial conflicts regarding her presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
SOURCE: Hartman, R. Cutaneous malignancies forum.
Initial evidence suggests that the , Rebecca I. Hartman, MD, MPH, said at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medication Education.
This is not what National Comprehensive Cancer Network officials expected when they issued short-term recommendations on how to manage cutaneous melanoma during the first wave of the COVID-19 pandemic. Those recommendations for restriction of care, which Dr. Hartman characterized as “pretty significant changes from how we typically practice melanoma care in the U.S.,” came at a time when there was justifiable concern that the first COVID-19 surge would strain the U.S. health care system beyond the breaking point.
The rationale given for the NCCN recommendations was that most time-to-treat studies have shown no adverse patient outcomes for 90-day delays in treatment, even for thicker melanomas. But those studies, all retrospective, have been called into question. And the first real-world data on the impact of care restrictions during the lockdown, reported by Italian dermatologists, highlights adverse effects with potentially far-reaching consequences, noted Dr. Hartman, director of melanoma epidemiology at Brigham and Women’s Hospital and a dermatologist, Harvard University, Boston.
Analysis of the impact of lockdown-induced delays in melanoma care is not merely an academic exercise, she added. While everyone hopes that the spring 2020 COVID-19 shelter-in-place was a once-in-a-lifetime event, there’s no guarantee that will be the case. Moreover, the lockdown provides a natural experiment addressing the possible consequences of melanoma care delays on patient outcomes, a topic that for ethical reasons could never be addressed in a randomized trial.
The short-term NCCN recommendations included the use of excisional biopsies for melanoma diagnosis whenever possible; and delay of up to 3 months for wide local excision of in situ melanoma, any invasive melanoma with negative margins, and even T1 melanomas with positive margins provided the bulk of the lesion had been excised. The guidance also suggested delaying sentinel lymph node biopsy (SLNB), along with increased use of neoadjuvant therapy in patients with clinically palpable regional lymph nodes in order to delay surgery for up to 8 weeks. Single-agent systemic therapy at the least-frequent dosing was advised in order to minimize toxicity and reduce the need for additional health care resources: for example, nivolumab (Opdivo) at 480 mg every 4 weeks instead of every 2 weeks, and pembrolizumab (Keytruda) at 400 mg every 6 weeks, rather than every 3 weeks.
So, that’s what the NCCN recommended. Here’s what actually happened during shelter-in-place as captured in Dr. Hartman’s survey of 18 U.S. members of the Melanoma Prevention Working Group, all practicing dermatology in centers particularly hard-hit in the first wave of the pandemic: In-person new melanoma patient visits plunged from an average of 4.83 per week per provider to 0.83 per week. Telemedicine visits with new melanoma patients went from zero prepandemic to 0.67 visits per week per provider, which doesn’t come close to making up for the drop in in-person visits. Interestingly, two respondents reported turning to gene-expression profile testing for patient prognostication because of delays in SLNB.
Wide local excision was delayed by an average of 6 weeks in roughly one-third of melanoma patients with early tumor stage disease, regardless of margin status. For patients with stage T1b disease, wide local excision was typically performed on time during shelter-in-place; however, SLNB was delayed by an average of 5 weeks in 22% of patients with positive margins and 28% of those with negative margins. In contrast, 80% of patients with more advanced T2-T4 melanoma underwent on-schedule definitive management with wide local excision and SLNB, Dr. Hartman reported.
Critics have taken issue with the NCCN’s conclusion that most time-to-treatment studies show no harm arising from 90-day treatment delays. A review of the relevant published literature by Dr. Hartman’s Harvard colleagues, published in July, found that the evidence is mixed. “There is insufficient evidence to definitively conclude that delayed wide resection after gross removal of the primary melanoma is without harm,” they concluded in the review.
Spanish dermatologists performed a modeling study in order to estimate the potential impact of COVID-19 lockdowns on 5- and 10-year survival of melanoma patients. Using the growth rate of a random sample of 1,000 melanomas to model estimates of tumor thickness after various delays, coupled with American Joint Committee on Cancer survival data for different T stages, they estimated that 5-year survival would be reduced from 94.2% to 92.3% with a 90-day delay in diagnosis, and that 10-year survival would drop from 90.0% to 87.6%.
But that’s merely modeling. Francesco Ricci, MD, PhD, and colleagues from the melanoma unit at the Istituto Dermopatico dell’Immacolata, Rome, have provided a first look at the real-world impact of the lockdown. In the prelockdown period of January through March 9th, 2020, the referral center averaged 2.3 new melanoma diagnoses per day. During the Rome lockdown, from March 10th through May 3rd, this figure dropped to a mean of 0.6 melanoma diagnoses per day. Postlockdown, from May 4th to June 6th, the average climbed to 1.3 per day. The rate of newly diagnosed nodular melanoma was 5.5-fold greater postlockdown, compared with prelockdown; the rate of ulcerated melanoma was 4.9-fold greater.
“We can hypothesize that this may have been due to delays in diagnosis and care,” Dr. Hartman commented. “This is important because we know that nodular melanoma as well as ulceration tend to have a worse prognosis in terms of mortality.”
The mean Breslow thickness of newly diagnosed melanomas was 0.88 mm prelockdown, 0.66 mm during lockdown, and 1.96 mm postlockdown. The investigators speculated that the reduced Breslow thickness of melanomas diagnosed during lockdown might be explained by a greater willingness of more health-conscious people to defy the shelter-in-place instructions because of their concern about a suspicious skin lesion. “Though it is way too early to gauge the consequences of such diagnostic delay, should this issue be neglected, dermatologists and their patients may pay a higher price later with increased morbidity, mortality, and financial burden,” according to the investigators.
Dr. Hartman observed that it will be important to learn whether similar experiences occurred elsewhere during lockdown.
Another speaker, John M. Kirkwood, MD, said he has seen several melanoma patients referred from outside centers who had delays of up to 3 months in sentinel lymph node management of T2 and T3 tumors during lockdown who now have widespread metastatic disease.
“Now, is that anecdotal? I don’t know, it’s just worrisome to me,” commented Dr. Kirkwood, professor of medicine, dermatology, and translational science at the University of Pittsburgh.
Merrick Ross, MD, professor of surgical oncology at M.D. Anderson Cancer Center, Houston, recalled, “There was a period of time [during the lockdown] when we weren’t allowed to do certain elective procedures, if you want to call cancer surgery elective.”
“It’s too soon to talk about outcomes because a lot of patients are still in the process of being treated after what I would consider a significant delay in diagnosis,” the surgeon added.
An audience member asked if there will be an opportunity to see data on the damage done by delaying melanoma management as compared to lives saved through the lockdown for COVID-19. Dr. Ross replied that M.D. Anderson is in the midst of an institution-wide study analyzing the delay in diagnosis of a range of cancers.
“In our melanoma center it is absolutely clear, although we’re still collecting data, that the median tumor thickness is much higher since the lockdown,” Dr. Ross commented.
Dr. Hartman said she and her coinvestigators in the Melanoma Prevention Working Group are attempting to tally up the damage done via the lockdown by delaying melanoma diagnosis and treatment. But she agreed with the questioner that the most important thing is overall net lives saved through shelter-in-place.
“I’m sure that, separately, nondermatologists – perhaps infectious disease doctors and internists – are looking at how many lives were saved by the lockdown policy. So I do think all that data will come out,” Dr. Hartman predicted.
She reported having no financial conflicts regarding her presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
SOURCE: Hartman, R. Cutaneous malignancies forum.
REPORTING FROM THE CUTANEOUS MALIGNANCIES FORUM