User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Enhanced recovery program improves outcomes after cesarean delivery
according to recent research published in Obstetrics & Gynecology.

Luciana Mullman, MPH, of Saint Barnabas Medical Center in Livingston, N.J., and colleagues used a pre-post study design to evaluate the effectiveness of ERAS at a tertiary care institution after implementing the program for patients undergoing scheduled or emergent cesarean delivery between December 2018 and August 2019. The researchers compared the rates of opioid use, length of stay, and costs of care for patients undergoing cesarean section after ERAS was implemented with those outcomes for cesarean deliveries at the center prior to ERAS between January 2018 and December 2018.
The ERAS program
ERAS was described in the study as incorporating a preoperative strategy, intraoperative management and postoperative care for cesarean delivery. The preoperative strategy consisted of a patient guidebook and a personal meeting for patient education on what to expect for preoperative and postoperative experiences as well as instructions leading up to the surgery.
For intraoperative management, intravenous opioids were minimized and replaced with neuraxial opioids when appropriate. The patient’s body temperature was monitored and controlled during the intraoperative pathway, and fluid balance was maintained. To prevent postoperative nausea and vomiting, IV ondansetron at a dose of 4 mg was started at the beginning of the cesarean delivery. When the cesarean delivery was complete, an anesthesiologist administered transversus abdominis plane blocks with 0.3% ropivacaine 30 mL on each side before the patient moved to the recovery area.
Postoperatively, the patient’s catheter was removed in the recovery room, and then transferred to postpartum floors if appropriate based on patient status. Patients began resuming a clear liquid diet 1 hour after cesarean delivery and a regular diet 6 hours after delivery. At 6 hours after surgery, the patient was out of bed and moving; walks around the nursing unit were scheduled three times per day at minimum. For pain, patients were given a 1,000-mg acetaminophen tablet every 8 hours, a 600-mg ibuprofen tablet every 6 hours, and dextromethorphan 30 mg/mL every 8 hours, with oral oxycodone 5 mg administered after physician evaluation for breakthrough pain.
Overall, there were 3,679 cesarean deliveries in the study, which included 2,171 deliveries prior to ERAS implementation and 1,508 cesarean deliveries after implementation. Patients with a scheduled cesarean delivery prior to ERAS implementation received no consistent educational program for anticipating cesarean delivery. After implementation, those patients with scheduled cesarean delivery received the full preoperative, intraoperative, and postoperative pathway, while emergent cesarean cases included the intraoperative management and postoperative care, but did not contain the preoperative component.
Improved outcomes after ERAS
The researchers found a significant decrease in the use of opioids after implementing ERAS at the center, with 24% of patients receiving opioids after ERAS, compared with 84% of patients prior to ERAS (odds ratio, 16.8; 95% confidence interval, 14.3-19.9; P < .001). These reductions in opioid use from the pre- and postimplementation periods were similar for patients with scheduled cesarean deliveries (85% vs. 27%; OR, 14.9; 95% CI, 12.2-18.3; P < .001) and emergent cesarean deliveries (83% vs. 19%; OR, 21.4; 95% CI, 16.1-28.7; P < .001).
There was also a significant reduction in total morphine milligram equivalents (MME) for patients who received opioids after ERAS (median, 15.0 MME), compared with before (median, 56.5 MME) implementing ERAS (mean relative change, 0.32; 95% CI, 0.28-0.35; P < .001). These results also were significant among both scheduled (median 59.9 vs. 15.0 MME; mean relative change, 0.31; 95% CI, 0.27-0.36; P < .001) and emergent (median 56.5 vs. 15.0 MME; mean relative change, 0.95; 95% CI, 0.89-1.01; P < .001) cesarean deliveries.
The overall length of stay after cesarean delivery significantly decreased after ERAS from an average of 3.2 days to 2.7 days (mean relative change, 0.82, 95% CI, 0.80-0.83; P < .001), and was significant in both scheduled (3.2 vs. 2.7 days; mean relative change, 0.83; 95% CI, 0.81-0.85; P < .001) and emergent (3.1 vs. 2.5 days; mean relative change, 0.80; 95% CI, 0.77-0.82; P < .001) groups. While the number of patients discharged within 2 days increased from 9% to 49% after ERAS implementation, there was no significant difference overall or in either group regarding 30-day readmission. The researchers also noted the median direct costs of cesarean delivery decreased by $349 per case after starting ERAS (mean relative change, 0.93; 95% CI, 0.91-0.95).
ERAS implementation lagging in obstetrics
In an interview, Iris Krishna, MD, MPH, a maternal-fetal medicine specialist at Emory University, Atlanta, said the ERAS approach has been used successfully in other surgical specialties but has “lagged” in obstetrics. “To date, there has been less attention in improving perioperative outcomes for women undergoing cesarean delivery, the most common abdominal surgery for women.”
Dr. Krishna said this study shows ERAS can be used in obstetrics to improve outcomes after cesarean section without increasing readmission rates. “Overall, this study demonstrates that ERAS can be successfully implemented for cesarean delivery as it has been for a variety of surgical specialties. ERAS for cesarean delivery can improve the quality of patient care while reducing health care costs.”
Women in the postpartum and postoperative period could benefit from ERAS as they recover from surgery and adjust to becoming a new mother, Dr. Krishna noted. “The goal of ERAS is to help patients return to physiological functioning as quickly as possible. Improving postoperative recovery can help with mother-infant bonding and breastfeeding.
“Implementation of a standardized approach for cesarean delivery has the potential to reduce health disparities and the disproportionately high rates of maternal morbidity and mortality in the United States,” she added. “ERAS for cesarean delivery also has the potential to address the opioid epidemic amongst reproductive-age women by improving postcesarean pain management and reducing opioid prescribing.”
Dr. Krishna also explained that an ERAS program would be feasible to implement in most centers. “It will require a shift of some elements of care from the inpatient to outpatient setting, but theoretically feasible as pregnant women frequently undergo many clinic visits during their pregnancy course.
“Education on ERAS for cesarean delivery can be implemented into prenatal care visits. ERAS implementation will also require a multidisciplinary team approach that includes obstetrics, anesthesia, nursing, pharmacy, pediatrics – all key stakeholders that will need to ‘buy in’ or be willing to support the protocol to ensure its success. As in this study, it would be helpful for hospitals to have an ERAS coordinator to champion and ensure compliance of protocol.”
Dr. Miller reported that he has received payments from the Coventus Professional Liability Insurance: Risk Management Committee and the New Jersey Board of Medical Examiners. The other authors reported no relevant conflicts of interest. Dr. Krishna reported no relevant conflicts of interest.
SOURCE: Mullman L et al. Obstet Gynecol. 2020 Oct. doi: 10.1097/AOG.0000000000004023.
according to recent research published in Obstetrics & Gynecology.
Luciana Mullman, MPH, of Saint Barnabas Medical Center in Livingston, N.J., and colleagues used a pre-post study design to evaluate the effectiveness of ERAS at a tertiary care institution after implementing the program for patients undergoing scheduled or emergent cesarean delivery between December 2018 and August 2019. The researchers compared the rates of opioid use, length of stay, and costs of care for patients undergoing cesarean section after ERAS was implemented with those outcomes for cesarean deliveries at the center prior to ERAS between January 2018 and December 2018.
The ERAS program
ERAS was described in the study as incorporating a preoperative strategy, intraoperative management and postoperative care for cesarean delivery. The preoperative strategy consisted of a patient guidebook and a personal meeting for patient education on what to expect for preoperative and postoperative experiences as well as instructions leading up to the surgery.
For intraoperative management, intravenous opioids were minimized and replaced with neuraxial opioids when appropriate. The patient’s body temperature was monitored and controlled during the intraoperative pathway, and fluid balance was maintained. To prevent postoperative nausea and vomiting, IV ondansetron at a dose of 4 mg was started at the beginning of the cesarean delivery. When the cesarean delivery was complete, an anesthesiologist administered transversus abdominis plane blocks with 0.3% ropivacaine 30 mL on each side before the patient moved to the recovery area.
Postoperatively, the patient’s catheter was removed in the recovery room, and then transferred to postpartum floors if appropriate based on patient status. Patients began resuming a clear liquid diet 1 hour after cesarean delivery and a regular diet 6 hours after delivery. At 6 hours after surgery, the patient was out of bed and moving; walks around the nursing unit were scheduled three times per day at minimum. For pain, patients were given a 1,000-mg acetaminophen tablet every 8 hours, a 600-mg ibuprofen tablet every 6 hours, and dextromethorphan 30 mg/mL every 8 hours, with oral oxycodone 5 mg administered after physician evaluation for breakthrough pain.
Overall, there were 3,679 cesarean deliveries in the study, which included 2,171 deliveries prior to ERAS implementation and 1,508 cesarean deliveries after implementation. Patients with a scheduled cesarean delivery prior to ERAS implementation received no consistent educational program for anticipating cesarean delivery. After implementation, those patients with scheduled cesarean delivery received the full preoperative, intraoperative, and postoperative pathway, while emergent cesarean cases included the intraoperative management and postoperative care, but did not contain the preoperative component.
Improved outcomes after ERAS
The researchers found a significant decrease in the use of opioids after implementing ERAS at the center, with 24% of patients receiving opioids after ERAS, compared with 84% of patients prior to ERAS (odds ratio, 16.8; 95% confidence interval, 14.3-19.9; P < .001). These reductions in opioid use from the pre- and postimplementation periods were similar for patients with scheduled cesarean deliveries (85% vs. 27%; OR, 14.9; 95% CI, 12.2-18.3; P < .001) and emergent cesarean deliveries (83% vs. 19%; OR, 21.4; 95% CI, 16.1-28.7; P < .001).
There was also a significant reduction in total morphine milligram equivalents (MME) for patients who received opioids after ERAS (median, 15.0 MME), compared with before (median, 56.5 MME) implementing ERAS (mean relative change, 0.32; 95% CI, 0.28-0.35; P < .001). These results also were significant among both scheduled (median 59.9 vs. 15.0 MME; mean relative change, 0.31; 95% CI, 0.27-0.36; P < .001) and emergent (median 56.5 vs. 15.0 MME; mean relative change, 0.95; 95% CI, 0.89-1.01; P < .001) cesarean deliveries.
The overall length of stay after cesarean delivery significantly decreased after ERAS from an average of 3.2 days to 2.7 days (mean relative change, 0.82, 95% CI, 0.80-0.83; P < .001), and was significant in both scheduled (3.2 vs. 2.7 days; mean relative change, 0.83; 95% CI, 0.81-0.85; P < .001) and emergent (3.1 vs. 2.5 days; mean relative change, 0.80; 95% CI, 0.77-0.82; P < .001) groups. While the number of patients discharged within 2 days increased from 9% to 49% after ERAS implementation, there was no significant difference overall or in either group regarding 30-day readmission. The researchers also noted the median direct costs of cesarean delivery decreased by $349 per case after starting ERAS (mean relative change, 0.93; 95% CI, 0.91-0.95).
ERAS implementation lagging in obstetrics
In an interview, Iris Krishna, MD, MPH, a maternal-fetal medicine specialist at Emory University, Atlanta, said the ERAS approach has been used successfully in other surgical specialties but has “lagged” in obstetrics. “To date, there has been less attention in improving perioperative outcomes for women undergoing cesarean delivery, the most common abdominal surgery for women.”
Dr. Krishna said this study shows ERAS can be used in obstetrics to improve outcomes after cesarean section without increasing readmission rates. “Overall, this study demonstrates that ERAS can be successfully implemented for cesarean delivery as it has been for a variety of surgical specialties. ERAS for cesarean delivery can improve the quality of patient care while reducing health care costs.”
Women in the postpartum and postoperative period could benefit from ERAS as they recover from surgery and adjust to becoming a new mother, Dr. Krishna noted. “The goal of ERAS is to help patients return to physiological functioning as quickly as possible. Improving postoperative recovery can help with mother-infant bonding and breastfeeding.
“Implementation of a standardized approach for cesarean delivery has the potential to reduce health disparities and the disproportionately high rates of maternal morbidity and mortality in the United States,” she added. “ERAS for cesarean delivery also has the potential to address the opioid epidemic amongst reproductive-age women by improving postcesarean pain management and reducing opioid prescribing.”
Dr. Krishna also explained that an ERAS program would be feasible to implement in most centers. “It will require a shift of some elements of care from the inpatient to outpatient setting, but theoretically feasible as pregnant women frequently undergo many clinic visits during their pregnancy course.
“Education on ERAS for cesarean delivery can be implemented into prenatal care visits. ERAS implementation will also require a multidisciplinary team approach that includes obstetrics, anesthesia, nursing, pharmacy, pediatrics – all key stakeholders that will need to ‘buy in’ or be willing to support the protocol to ensure its success. As in this study, it would be helpful for hospitals to have an ERAS coordinator to champion and ensure compliance of protocol.”
Dr. Miller reported that he has received payments from the Coventus Professional Liability Insurance: Risk Management Committee and the New Jersey Board of Medical Examiners. The other authors reported no relevant conflicts of interest. Dr. Krishna reported no relevant conflicts of interest.
SOURCE: Mullman L et al. Obstet Gynecol. 2020 Oct. doi: 10.1097/AOG.0000000000004023.
according to recent research published in Obstetrics & Gynecology.
Luciana Mullman, MPH, of Saint Barnabas Medical Center in Livingston, N.J., and colleagues used a pre-post study design to evaluate the effectiveness of ERAS at a tertiary care institution after implementing the program for patients undergoing scheduled or emergent cesarean delivery between December 2018 and August 2019. The researchers compared the rates of opioid use, length of stay, and costs of care for patients undergoing cesarean section after ERAS was implemented with those outcomes for cesarean deliveries at the center prior to ERAS between January 2018 and December 2018.
The ERAS program
ERAS was described in the study as incorporating a preoperative strategy, intraoperative management and postoperative care for cesarean delivery. The preoperative strategy consisted of a patient guidebook and a personal meeting for patient education on what to expect for preoperative and postoperative experiences as well as instructions leading up to the surgery.
For intraoperative management, intravenous opioids were minimized and replaced with neuraxial opioids when appropriate. The patient’s body temperature was monitored and controlled during the intraoperative pathway, and fluid balance was maintained. To prevent postoperative nausea and vomiting, IV ondansetron at a dose of 4 mg was started at the beginning of the cesarean delivery. When the cesarean delivery was complete, an anesthesiologist administered transversus abdominis plane blocks with 0.3% ropivacaine 30 mL on each side before the patient moved to the recovery area.
Postoperatively, the patient’s catheter was removed in the recovery room, and then transferred to postpartum floors if appropriate based on patient status. Patients began resuming a clear liquid diet 1 hour after cesarean delivery and a regular diet 6 hours after delivery. At 6 hours after surgery, the patient was out of bed and moving; walks around the nursing unit were scheduled three times per day at minimum. For pain, patients were given a 1,000-mg acetaminophen tablet every 8 hours, a 600-mg ibuprofen tablet every 6 hours, and dextromethorphan 30 mg/mL every 8 hours, with oral oxycodone 5 mg administered after physician evaluation for breakthrough pain.
Overall, there were 3,679 cesarean deliveries in the study, which included 2,171 deliveries prior to ERAS implementation and 1,508 cesarean deliveries after implementation. Patients with a scheduled cesarean delivery prior to ERAS implementation received no consistent educational program for anticipating cesarean delivery. After implementation, those patients with scheduled cesarean delivery received the full preoperative, intraoperative, and postoperative pathway, while emergent cesarean cases included the intraoperative management and postoperative care, but did not contain the preoperative component.
Improved outcomes after ERAS
The researchers found a significant decrease in the use of opioids after implementing ERAS at the center, with 24% of patients receiving opioids after ERAS, compared with 84% of patients prior to ERAS (odds ratio, 16.8; 95% confidence interval, 14.3-19.9; P < .001). These reductions in opioid use from the pre- and postimplementation periods were similar for patients with scheduled cesarean deliveries (85% vs. 27%; OR, 14.9; 95% CI, 12.2-18.3; P < .001) and emergent cesarean deliveries (83% vs. 19%; OR, 21.4; 95% CI, 16.1-28.7; P < .001).
There was also a significant reduction in total morphine milligram equivalents (MME) for patients who received opioids after ERAS (median, 15.0 MME), compared with before (median, 56.5 MME) implementing ERAS (mean relative change, 0.32; 95% CI, 0.28-0.35; P < .001). These results also were significant among both scheduled (median 59.9 vs. 15.0 MME; mean relative change, 0.31; 95% CI, 0.27-0.36; P < .001) and emergent (median 56.5 vs. 15.0 MME; mean relative change, 0.95; 95% CI, 0.89-1.01; P < .001) cesarean deliveries.
The overall length of stay after cesarean delivery significantly decreased after ERAS from an average of 3.2 days to 2.7 days (mean relative change, 0.82, 95% CI, 0.80-0.83; P < .001), and was significant in both scheduled (3.2 vs. 2.7 days; mean relative change, 0.83; 95% CI, 0.81-0.85; P < .001) and emergent (3.1 vs. 2.5 days; mean relative change, 0.80; 95% CI, 0.77-0.82; P < .001) groups. While the number of patients discharged within 2 days increased from 9% to 49% after ERAS implementation, there was no significant difference overall or in either group regarding 30-day readmission. The researchers also noted the median direct costs of cesarean delivery decreased by $349 per case after starting ERAS (mean relative change, 0.93; 95% CI, 0.91-0.95).
ERAS implementation lagging in obstetrics
In an interview, Iris Krishna, MD, MPH, a maternal-fetal medicine specialist at Emory University, Atlanta, said the ERAS approach has been used successfully in other surgical specialties but has “lagged” in obstetrics. “To date, there has been less attention in improving perioperative outcomes for women undergoing cesarean delivery, the most common abdominal surgery for women.”
Dr. Krishna said this study shows ERAS can be used in obstetrics to improve outcomes after cesarean section without increasing readmission rates. “Overall, this study demonstrates that ERAS can be successfully implemented for cesarean delivery as it has been for a variety of surgical specialties. ERAS for cesarean delivery can improve the quality of patient care while reducing health care costs.”
Women in the postpartum and postoperative period could benefit from ERAS as they recover from surgery and adjust to becoming a new mother, Dr. Krishna noted. “The goal of ERAS is to help patients return to physiological functioning as quickly as possible. Improving postoperative recovery can help with mother-infant bonding and breastfeeding.
“Implementation of a standardized approach for cesarean delivery has the potential to reduce health disparities and the disproportionately high rates of maternal morbidity and mortality in the United States,” she added. “ERAS for cesarean delivery also has the potential to address the opioid epidemic amongst reproductive-age women by improving postcesarean pain management and reducing opioid prescribing.”
Dr. Krishna also explained that an ERAS program would be feasible to implement in most centers. “It will require a shift of some elements of care from the inpatient to outpatient setting, but theoretically feasible as pregnant women frequently undergo many clinic visits during their pregnancy course.
“Education on ERAS for cesarean delivery can be implemented into prenatal care visits. ERAS implementation will also require a multidisciplinary team approach that includes obstetrics, anesthesia, nursing, pharmacy, pediatrics – all key stakeholders that will need to ‘buy in’ or be willing to support the protocol to ensure its success. As in this study, it would be helpful for hospitals to have an ERAS coordinator to champion and ensure compliance of protocol.”
Dr. Miller reported that he has received payments from the Coventus Professional Liability Insurance: Risk Management Committee and the New Jersey Board of Medical Examiners. The other authors reported no relevant conflicts of interest. Dr. Krishna reported no relevant conflicts of interest.
SOURCE: Mullman L et al. Obstet Gynecol. 2020 Oct. doi: 10.1097/AOG.0000000000004023.
FROM OBSTETRICS & GYNECOLOGY
Full-time, part-time, FTE: Know the differences
The wholesale to them. While rules vary from state to state, some generalizations can be made.

Even the definitions of full-time and part-time vary. For instance, under the Affordable Care Act (ACA), full time means working at least 30 hours per week. Under the Families First Coronavirus Response Act (FFCRA), it is 40 hours.
Full-time equivalent (FTE) is a concept designed to document a part-time workforce in terms of full-time employment, by taking the total hours worked by all part-time employees and dividing by the full-time schedule. Of course, the ACA and the Paycheck Protection Program (PPP) calculate that number differently: The ACA requires you to total all the hours worked by part-time employees per month, and divide by 120. For the PPP, you divide the total part-time hours per week by 40, and round to the nearest tenth. (You can also use a simplified method that assigns a 1.0 for employees who work 40 hours or more per week and 0.5 for those who work fewer; whichever method you choose, you must apply it consistently on all PPP forms.)
FTEs are important for the purposes of the ACA because employers with 50 or more full-timers plus FTEs must offer health coverage to their full-timers and dependents. But most private practitioners need an accurate FTE total to deal with the PPP: If staffing levels weren’t maintained after you received a PPP loan, your loan forgiveness amount may be reduced. Staffing levels are determined by comparing the average number of full-timers plus FTEs during the “covered period” to either the period from Feb. 15 through June 30, 2019, or Jan. 1 through Feb. 28, 2020.
The PPP aside, FTEs have created confusion over when an employee is entitled to overtime pay. Under federal law, overtime is due whenever an employee works more than 40 hours per week; up to 40 hours, the regular wage is paid. (There are exemptions, and a few states use a daily number.) For example, if a part-timer receiving $900 per week for a 30-hour workweek works more than 30 hours, the hours from 30 to 40 would be compensated at their normal wage of $30 per hour ($900 ÷ 30). If the employee worked more than 40 hours, you would pay overtime (in this case $45 per hour, $30 x 1.5) for the hours in excess of 40.
To address a few other employment questions that I am frequently asked:
Under the FFCRA, you must provide both full- and part-time employees with emergency paid sick leave (EPSL) if they’re unable to work from your office or their home because of illness attributable to COVID-19, quarantine, or caring for a sick family member or child whose school is closed. Full-time employees are entitled to up to 80 hours of EPSL, and part-timers an average of what they work every 2 weeks. Some states have their own laws independent from the FFCRA. Check your state or local laws.
- Some states require you to provide meal and rest breaks to both full- and part-time employees. In California, for example, employers must provide a 30-minute meal break after no more than 5 hours of work, unless the total workday is less than 6 hours and both employers and employees consent to waive breaks. California also requires rest breaks after every 4 hours worked. Check the laws in your state.
- You must include part-time employees in a 401(k) retirement plan if they work at least 1,000 hours in a year, which is about 20 hours per week. That rule is changing in 2021 to 500 hours for employees older than 21. There are state-run retirement programs in California, Connecticut, New Jersey, Washington, and Oregon, among other states. Check your state law for details.
- If you offer paid vacations to full-time employees, you do not have to do the same for part-timers. (In fact, there is no requirement in most states to offer vacation time at all.) My office does offer it to part-time employees on a pro rata basis, as do many others in my area. Again, check your state law.
As always, consult with your attorney if it’s not clear which rules apply in your specific situation.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. He has no relevant disclosures related to the topic of this column. Write to him at [email protected].
The wholesale to them. While rules vary from state to state, some generalizations can be made.
Even the definitions of full-time and part-time vary. For instance, under the Affordable Care Act (ACA), full time means working at least 30 hours per week. Under the Families First Coronavirus Response Act (FFCRA), it is 40 hours.
Full-time equivalent (FTE) is a concept designed to document a part-time workforce in terms of full-time employment, by taking the total hours worked by all part-time employees and dividing by the full-time schedule. Of course, the ACA and the Paycheck Protection Program (PPP) calculate that number differently: The ACA requires you to total all the hours worked by part-time employees per month, and divide by 120. For the PPP, you divide the total part-time hours per week by 40, and round to the nearest tenth. (You can also use a simplified method that assigns a 1.0 for employees who work 40 hours or more per week and 0.5 for those who work fewer; whichever method you choose, you must apply it consistently on all PPP forms.)
FTEs are important for the purposes of the ACA because employers with 50 or more full-timers plus FTEs must offer health coverage to their full-timers and dependents. But most private practitioners need an accurate FTE total to deal with the PPP: If staffing levels weren’t maintained after you received a PPP loan, your loan forgiveness amount may be reduced. Staffing levels are determined by comparing the average number of full-timers plus FTEs during the “covered period” to either the period from Feb. 15 through June 30, 2019, or Jan. 1 through Feb. 28, 2020.
The PPP aside, FTEs have created confusion over when an employee is entitled to overtime pay. Under federal law, overtime is due whenever an employee works more than 40 hours per week; up to 40 hours, the regular wage is paid. (There are exemptions, and a few states use a daily number.) For example, if a part-timer receiving $900 per week for a 30-hour workweek works more than 30 hours, the hours from 30 to 40 would be compensated at their normal wage of $30 per hour ($900 ÷ 30). If the employee worked more than 40 hours, you would pay overtime (in this case $45 per hour, $30 x 1.5) for the hours in excess of 40.
To address a few other employment questions that I am frequently asked:
Under the FFCRA, you must provide both full- and part-time employees with emergency paid sick leave (EPSL) if they’re unable to work from your office or their home because of illness attributable to COVID-19, quarantine, or caring for a sick family member or child whose school is closed. Full-time employees are entitled to up to 80 hours of EPSL, and part-timers an average of what they work every 2 weeks. Some states have their own laws independent from the FFCRA. Check your state or local laws.
- Some states require you to provide meal and rest breaks to both full- and part-time employees. In California, for example, employers must provide a 30-minute meal break after no more than 5 hours of work, unless the total workday is less than 6 hours and both employers and employees consent to waive breaks. California also requires rest breaks after every 4 hours worked. Check the laws in your state.
- You must include part-time employees in a 401(k) retirement plan if they work at least 1,000 hours in a year, which is about 20 hours per week. That rule is changing in 2021 to 500 hours for employees older than 21. There are state-run retirement programs in California, Connecticut, New Jersey, Washington, and Oregon, among other states. Check your state law for details.
- If you offer paid vacations to full-time employees, you do not have to do the same for part-timers. (In fact, there is no requirement in most states to offer vacation time at all.) My office does offer it to part-time employees on a pro rata basis, as do many others in my area. Again, check your state law.
As always, consult with your attorney if it’s not clear which rules apply in your specific situation.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. He has no relevant disclosures related to the topic of this column. Write to him at [email protected].
The wholesale to them. While rules vary from state to state, some generalizations can be made.
Even the definitions of full-time and part-time vary. For instance, under the Affordable Care Act (ACA), full time means working at least 30 hours per week. Under the Families First Coronavirus Response Act (FFCRA), it is 40 hours.
Full-time equivalent (FTE) is a concept designed to document a part-time workforce in terms of full-time employment, by taking the total hours worked by all part-time employees and dividing by the full-time schedule. Of course, the ACA and the Paycheck Protection Program (PPP) calculate that number differently: The ACA requires you to total all the hours worked by part-time employees per month, and divide by 120. For the PPP, you divide the total part-time hours per week by 40, and round to the nearest tenth. (You can also use a simplified method that assigns a 1.0 for employees who work 40 hours or more per week and 0.5 for those who work fewer; whichever method you choose, you must apply it consistently on all PPP forms.)
FTEs are important for the purposes of the ACA because employers with 50 or more full-timers plus FTEs must offer health coverage to their full-timers and dependents. But most private practitioners need an accurate FTE total to deal with the PPP: If staffing levels weren’t maintained after you received a PPP loan, your loan forgiveness amount may be reduced. Staffing levels are determined by comparing the average number of full-timers plus FTEs during the “covered period” to either the period from Feb. 15 through June 30, 2019, or Jan. 1 through Feb. 28, 2020.
The PPP aside, FTEs have created confusion over when an employee is entitled to overtime pay. Under federal law, overtime is due whenever an employee works more than 40 hours per week; up to 40 hours, the regular wage is paid. (There are exemptions, and a few states use a daily number.) For example, if a part-timer receiving $900 per week for a 30-hour workweek works more than 30 hours, the hours from 30 to 40 would be compensated at their normal wage of $30 per hour ($900 ÷ 30). If the employee worked more than 40 hours, you would pay overtime (in this case $45 per hour, $30 x 1.5) for the hours in excess of 40.
To address a few other employment questions that I am frequently asked:
Under the FFCRA, you must provide both full- and part-time employees with emergency paid sick leave (EPSL) if they’re unable to work from your office or their home because of illness attributable to COVID-19, quarantine, or caring for a sick family member or child whose school is closed. Full-time employees are entitled to up to 80 hours of EPSL, and part-timers an average of what they work every 2 weeks. Some states have their own laws independent from the FFCRA. Check your state or local laws.
- Some states require you to provide meal and rest breaks to both full- and part-time employees. In California, for example, employers must provide a 30-minute meal break after no more than 5 hours of work, unless the total workday is less than 6 hours and both employers and employees consent to waive breaks. California also requires rest breaks after every 4 hours worked. Check the laws in your state.
- You must include part-time employees in a 401(k) retirement plan if they work at least 1,000 hours in a year, which is about 20 hours per week. That rule is changing in 2021 to 500 hours for employees older than 21. There are state-run retirement programs in California, Connecticut, New Jersey, Washington, and Oregon, among other states. Check your state law for details.
- If you offer paid vacations to full-time employees, you do not have to do the same for part-timers. (In fact, there is no requirement in most states to offer vacation time at all.) My office does offer it to part-time employees on a pro rata basis, as do many others in my area. Again, check your state law.
As always, consult with your attorney if it’s not clear which rules apply in your specific situation.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. He has no relevant disclosures related to the topic of this column. Write to him at [email protected].

Alcohol problems linked to legal performance-enhancement products
Adolescent alcohol use among boys was prospectively associated with use of legal performance-enhancing substances in young adulthood, based on prospective cohort data from more than 12,000 individuals, wrote Kyle T. Ganson, PhD, MSW, of the University of Toronto, and colleagues.

In addition, legal use of performance-enhancing substances (PES) among young men was associated with increased risk of alcohol use problems.
Although previous studies have shown a range of adverse effects associated with the use of anabolic-androgenic steroid derivatives (defined as illegal PES), the possible adverse effects of legal PES (defined in this report as protein powders, creatine monohydrate, dehydroepiandrostenedione, and amino acids) have not been well studied, the researchers wrote.
In a study published in Pediatrics, the researchers reviewed data from 12,133 young adults aged 18-26 years who were part of the National Longitudinal Study of Adolescent to Adult Health from 1994 to 2008.
Overall, 16% of young men and 1% of young women reported using legal PES in the past year. Among men, legal PES use was prospectively associated with increased risk of a range of alcohol-related problem behaviors including binge drinking (adjusted odds ratio, 1.35), injurious and risky behaviors (aOR, 1.78), legal problems (aOR, 1.52), reduced activities and socializing (aOR, 1.91), and problems with emotional or physical health (aOR, 1.44).
Legal PES use among young adult women was associated with an increased risk of emotional or physical health problems (aOR, 3.00).
Adolescent impact
Between adolescence and young adulthood (an average of 7 years’ follow-up), alcohol use was prospectively associated with legal PES use in young men (OR, 1.39), but neither cigarette smoking nor marijuana use in adolescence was associated with later use of legal PES. Among young women, no type of adolescent substance use was prospectively associated with later use of legal PES.
“To date, legal PES have not been largely considered as part of the spectrum of substances used among adolescents, have not been subject to the same regulatory scrutiny as other substances known to be linked to subsequent substance use and are freely available over the counter to adolescents,” Dr. Ganson and associates noted.
“Clearly, the robust reciprocal temporal relationship between substance use and legal PES suggests that each may serve as a gateway for the other,” they wrote.
The study findings were limited by several factors including the inability to identify outcomes associated with variable PES components, incomplete data collection on several drinking-related risk behaviors, and inability to analyze prospective use of illegal or other substances associated with use of legal PES, the researchers wrote.
However, “these results provide further evidence in support of the gateway theory and prospective health risk behaviors associated with legal PES and substance use,” they wrote.
The data may inform policy on the additional regulation of legal PES use in minors. In the meantime, “it is important for medical providers and clinicians to assess problematic alcohol use and drinking-related risk behaviors among young adult men who have previously used legal PES,” Dr. Ganson and associates concluded.
Challenges to clinicians
An important point to recognize is that PES is a misleading term, Steven Cuff, MD, of the Ohio State University, Columbus, and Michele LaBotz, MD, of Tufts University, Boston, wrote in an accompanying editorial. “Most legal supplements marketed for athletic performance enhancement are ineffective at increasing muscle mass or athletic performance beyond what can be achieved through appropriate nutrition and training,” they emphasized. The current study findings suggest that “legal PES should be integrated into the gateway hypothesis regarding patterns and progression of substance use through adolescence and early adulthood,” and support discouragement of any PES use among adolescents and young adults.
Even legal PES can be dangerous because of the lack of oversight of dietary supplements by the Food and Drug Administration. “There is widespread evidence that many over-the-counter dietary supplements lack stated ingredients, contain unlabeled ingredients (including potential allergens), or are contaminated with impurities or illegal or dangerous substances, such as steroids and stimulants,” the editorialists emphasized.
In addition, the association found in the study between muscle dysphoria and both PES use and substance use disorders, notably alcohol-related morbidity, highlights the need for a proactive approach by pediatricians to minimize the risk, they noted.
“For pediatricians uncomfortable with initiating discussions on PES use with their patients, an American Academy of Pediatrics–supported role-play simulation is available,” they concluded.
The study is important because “PES use is ubiquitous among adolescents and young adults,” Dr. LaBotz said in an interview. “Although it is widely believed that PES use serves as a likely ‘gateway’ to use of anabolic steroids and other substances, this is one of the very few studies that explores this relationship. Their findings that alcohol use appears to correlate with subsequent use of PES, and that PES use appears to correlate with future alcohol-related issues, suggest that this is not a simple linear progression of problematic behavior.”
Dr. LaBotz added that she was not surprised by the study findings, and emphasized that pediatric health care providers should be aware of the association between PES and alcohol use. “PES screening should be incorporated into screening done for alcohol and other substance use. This appears to be particularly true for athletes and other subpopulations who are at higher risk for problematic alcohol use.”
She said much of PES use is driven by the desire by young men for a muscular appearance, but more research is needed on young women. “In the past, this was a goal primarily associated with males, but females have become increasingly interested in achieving muscularity as well, which suggests an increasing risk of PES use among females as compared to earlier reports. We need updated data on patterns, prevalence and consequences of PES use in females.”
In addition, “although preparticipation physical examination forms include screening questions for PES use among athletes, further information is needed on how to incorporate PES into substance use screening that is performed in a general pediatric population, such as including athletes and nonathletes,” Dr. LaBotz said.
The study was supported by the National Institutes of Health and by grants to one of the coauthors from the Pediatric Scientist Development Program funded by the American Academy of Pediatrics and the American Pediatric Society, as well as the American Heart Association Career Development Award. The researchers had no financial conflicts to disclose. Dr. Cuff and Dr. LaBotz had no financial conflicts to disclose.
SOURCE: Ganson KT et al. Pediatrics. 2020 Sep. doi: 10.1542/peds.2020-0409.
Adolescent alcohol use among boys was prospectively associated with use of legal performance-enhancing substances in young adulthood, based on prospective cohort data from more than 12,000 individuals, wrote Kyle T. Ganson, PhD, MSW, of the University of Toronto, and colleagues.
In addition, legal use of performance-enhancing substances (PES) among young men was associated with increased risk of alcohol use problems.
Although previous studies have shown a range of adverse effects associated with the use of anabolic-androgenic steroid derivatives (defined as illegal PES), the possible adverse effects of legal PES (defined in this report as protein powders, creatine monohydrate, dehydroepiandrostenedione, and amino acids) have not been well studied, the researchers wrote.
In a study published in Pediatrics, the researchers reviewed data from 12,133 young adults aged 18-26 years who were part of the National Longitudinal Study of Adolescent to Adult Health from 1994 to 2008.
Overall, 16% of young men and 1% of young women reported using legal PES in the past year. Among men, legal PES use was prospectively associated with increased risk of a range of alcohol-related problem behaviors including binge drinking (adjusted odds ratio, 1.35), injurious and risky behaviors (aOR, 1.78), legal problems (aOR, 1.52), reduced activities and socializing (aOR, 1.91), and problems with emotional or physical health (aOR, 1.44).
Legal PES use among young adult women was associated with an increased risk of emotional or physical health problems (aOR, 3.00).
Adolescent impact
Between adolescence and young adulthood (an average of 7 years’ follow-up), alcohol use was prospectively associated with legal PES use in young men (OR, 1.39), but neither cigarette smoking nor marijuana use in adolescence was associated with later use of legal PES. Among young women, no type of adolescent substance use was prospectively associated with later use of legal PES.
“To date, legal PES have not been largely considered as part of the spectrum of substances used among adolescents, have not been subject to the same regulatory scrutiny as other substances known to be linked to subsequent substance use and are freely available over the counter to adolescents,” Dr. Ganson and associates noted.
“Clearly, the robust reciprocal temporal relationship between substance use and legal PES suggests that each may serve as a gateway for the other,” they wrote.
The study findings were limited by several factors including the inability to identify outcomes associated with variable PES components, incomplete data collection on several drinking-related risk behaviors, and inability to analyze prospective use of illegal or other substances associated with use of legal PES, the researchers wrote.
However, “these results provide further evidence in support of the gateway theory and prospective health risk behaviors associated with legal PES and substance use,” they wrote.
The data may inform policy on the additional regulation of legal PES use in minors. In the meantime, “it is important for medical providers and clinicians to assess problematic alcohol use and drinking-related risk behaviors among young adult men who have previously used legal PES,” Dr. Ganson and associates concluded.
Challenges to clinicians
An important point to recognize is that PES is a misleading term, Steven Cuff, MD, of the Ohio State University, Columbus, and Michele LaBotz, MD, of Tufts University, Boston, wrote in an accompanying editorial. “Most legal supplements marketed for athletic performance enhancement are ineffective at increasing muscle mass or athletic performance beyond what can be achieved through appropriate nutrition and training,” they emphasized. The current study findings suggest that “legal PES should be integrated into the gateway hypothesis regarding patterns and progression of substance use through adolescence and early adulthood,” and support discouragement of any PES use among adolescents and young adults.
Even legal PES can be dangerous because of the lack of oversight of dietary supplements by the Food and Drug Administration. “There is widespread evidence that many over-the-counter dietary supplements lack stated ingredients, contain unlabeled ingredients (including potential allergens), or are contaminated with impurities or illegal or dangerous substances, such as steroids and stimulants,” the editorialists emphasized.
In addition, the association found in the study between muscle dysphoria and both PES use and substance use disorders, notably alcohol-related morbidity, highlights the need for a proactive approach by pediatricians to minimize the risk, they noted.
“For pediatricians uncomfortable with initiating discussions on PES use with their patients, an American Academy of Pediatrics–supported role-play simulation is available,” they concluded.
The study is important because “PES use is ubiquitous among adolescents and young adults,” Dr. LaBotz said in an interview. “Although it is widely believed that PES use serves as a likely ‘gateway’ to use of anabolic steroids and other substances, this is one of the very few studies that explores this relationship. Their findings that alcohol use appears to correlate with subsequent use of PES, and that PES use appears to correlate with future alcohol-related issues, suggest that this is not a simple linear progression of problematic behavior.”
Dr. LaBotz added that she was not surprised by the study findings, and emphasized that pediatric health care providers should be aware of the association between PES and alcohol use. “PES screening should be incorporated into screening done for alcohol and other substance use. This appears to be particularly true for athletes and other subpopulations who are at higher risk for problematic alcohol use.”
She said much of PES use is driven by the desire by young men for a muscular appearance, but more research is needed on young women. “In the past, this was a goal primarily associated with males, but females have become increasingly interested in achieving muscularity as well, which suggests an increasing risk of PES use among females as compared to earlier reports. We need updated data on patterns, prevalence and consequences of PES use in females.”
In addition, “although preparticipation physical examination forms include screening questions for PES use among athletes, further information is needed on how to incorporate PES into substance use screening that is performed in a general pediatric population, such as including athletes and nonathletes,” Dr. LaBotz said.
The study was supported by the National Institutes of Health and by grants to one of the coauthors from the Pediatric Scientist Development Program funded by the American Academy of Pediatrics and the American Pediatric Society, as well as the American Heart Association Career Development Award. The researchers had no financial conflicts to disclose. Dr. Cuff and Dr. LaBotz had no financial conflicts to disclose.
SOURCE: Ganson KT et al. Pediatrics. 2020 Sep. doi: 10.1542/peds.2020-0409.
Adolescent alcohol use among boys was prospectively associated with use of legal performance-enhancing substances in young adulthood, based on prospective cohort data from more than 12,000 individuals, wrote Kyle T. Ganson, PhD, MSW, of the University of Toronto, and colleagues.
In addition, legal use of performance-enhancing substances (PES) among young men was associated with increased risk of alcohol use problems.
Although previous studies have shown a range of adverse effects associated with the use of anabolic-androgenic steroid derivatives (defined as illegal PES), the possible adverse effects of legal PES (defined in this report as protein powders, creatine monohydrate, dehydroepiandrostenedione, and amino acids) have not been well studied, the researchers wrote.
In a study published in Pediatrics, the researchers reviewed data from 12,133 young adults aged 18-26 years who were part of the National Longitudinal Study of Adolescent to Adult Health from 1994 to 2008.
Overall, 16% of young men and 1% of young women reported using legal PES in the past year. Among men, legal PES use was prospectively associated with increased risk of a range of alcohol-related problem behaviors including binge drinking (adjusted odds ratio, 1.35), injurious and risky behaviors (aOR, 1.78), legal problems (aOR, 1.52), reduced activities and socializing (aOR, 1.91), and problems with emotional or physical health (aOR, 1.44).
Legal PES use among young adult women was associated with an increased risk of emotional or physical health problems (aOR, 3.00).
Adolescent impact
Between adolescence and young adulthood (an average of 7 years’ follow-up), alcohol use was prospectively associated with legal PES use in young men (OR, 1.39), but neither cigarette smoking nor marijuana use in adolescence was associated with later use of legal PES. Among young women, no type of adolescent substance use was prospectively associated with later use of legal PES.
“To date, legal PES have not been largely considered as part of the spectrum of substances used among adolescents, have not been subject to the same regulatory scrutiny as other substances known to be linked to subsequent substance use and are freely available over the counter to adolescents,” Dr. Ganson and associates noted.
“Clearly, the robust reciprocal temporal relationship between substance use and legal PES suggests that each may serve as a gateway for the other,” they wrote.
The study findings were limited by several factors including the inability to identify outcomes associated with variable PES components, incomplete data collection on several drinking-related risk behaviors, and inability to analyze prospective use of illegal or other substances associated with use of legal PES, the researchers wrote.
However, “these results provide further evidence in support of the gateway theory and prospective health risk behaviors associated with legal PES and substance use,” they wrote.
The data may inform policy on the additional regulation of legal PES use in minors. In the meantime, “it is important for medical providers and clinicians to assess problematic alcohol use and drinking-related risk behaviors among young adult men who have previously used legal PES,” Dr. Ganson and associates concluded.
Challenges to clinicians
An important point to recognize is that PES is a misleading term, Steven Cuff, MD, of the Ohio State University, Columbus, and Michele LaBotz, MD, of Tufts University, Boston, wrote in an accompanying editorial. “Most legal supplements marketed for athletic performance enhancement are ineffective at increasing muscle mass or athletic performance beyond what can be achieved through appropriate nutrition and training,” they emphasized. The current study findings suggest that “legal PES should be integrated into the gateway hypothesis regarding patterns and progression of substance use through adolescence and early adulthood,” and support discouragement of any PES use among adolescents and young adults.
Even legal PES can be dangerous because of the lack of oversight of dietary supplements by the Food and Drug Administration. “There is widespread evidence that many over-the-counter dietary supplements lack stated ingredients, contain unlabeled ingredients (including potential allergens), or are contaminated with impurities or illegal or dangerous substances, such as steroids and stimulants,” the editorialists emphasized.
In addition, the association found in the study between muscle dysphoria and both PES use and substance use disorders, notably alcohol-related morbidity, highlights the need for a proactive approach by pediatricians to minimize the risk, they noted.
“For pediatricians uncomfortable with initiating discussions on PES use with their patients, an American Academy of Pediatrics–supported role-play simulation is available,” they concluded.
The study is important because “PES use is ubiquitous among adolescents and young adults,” Dr. LaBotz said in an interview. “Although it is widely believed that PES use serves as a likely ‘gateway’ to use of anabolic steroids and other substances, this is one of the very few studies that explores this relationship. Their findings that alcohol use appears to correlate with subsequent use of PES, and that PES use appears to correlate with future alcohol-related issues, suggest that this is not a simple linear progression of problematic behavior.”
Dr. LaBotz added that she was not surprised by the study findings, and emphasized that pediatric health care providers should be aware of the association between PES and alcohol use. “PES screening should be incorporated into screening done for alcohol and other substance use. This appears to be particularly true for athletes and other subpopulations who are at higher risk for problematic alcohol use.”
She said much of PES use is driven by the desire by young men for a muscular appearance, but more research is needed on young women. “In the past, this was a goal primarily associated with males, but females have become increasingly interested in achieving muscularity as well, which suggests an increasing risk of PES use among females as compared to earlier reports. We need updated data on patterns, prevalence and consequences of PES use in females.”
In addition, “although preparticipation physical examination forms include screening questions for PES use among athletes, further information is needed on how to incorporate PES into substance use screening that is performed in a general pediatric population, such as including athletes and nonathletes,” Dr. LaBotz said.
The study was supported by the National Institutes of Health and by grants to one of the coauthors from the Pediatric Scientist Development Program funded by the American Academy of Pediatrics and the American Pediatric Society, as well as the American Heart Association Career Development Award. The researchers had no financial conflicts to disclose. Dr. Cuff and Dr. LaBotz had no financial conflicts to disclose.
SOURCE: Ganson KT et al. Pediatrics. 2020 Sep. doi: 10.1542/peds.2020-0409.
FROM PEDIATRICS
LSD microdosing to boost attention: Too soon to tell?
Microdosing with lysergic acid diethylamide (LSD) is associated with improved mood and increased attention, early research suggests. However, at least one expert believes it’s far too soon to tell and warns against endorsing patient microdosing.
In a dose-finding exploratory study, three low doses of LSD were compared with placebo in healthy volunteers who were all recreational drug users. Adjusted results showed that the highest dose boosted attention and mood, although participants were aware of psychedelic effects, prompting researchers to conclude the results demonstrated “selective, beneficial effects.”
“The majority of participants have improved attention,” study investigator Nadia Hutten, PhD, Department of Neuropsychology and Psychopharmacology, Maastricht University, the Netherlands, told Medscape Medical News.
“So we think that patients with attention deficits might have more beneficial effects,” she added, noting her team plans to study LSD microdosing in patients with attention deficit hyperactivity disorder.
The study was presented at the 33rd European College of Neuropsychopharmacology (ECNP) Congress, which was held online this year because of the COVID-19 pandemic.
Growing interest
Over the past 10 years there has been growing interest in psychedelic microdosing, which is defined as a dose that aims to enhance mood and/or performance but does not affect perception.
However, there has been considerable debate over what constitutes a “microdose.” One tenth of a “full” psychedelic dose is typically suggested, but users report a much wider dose range in practice, suggesting potential “individual variation in response to low doses,” the researchers note.
In the current dose-finding study, the researchers explored whether the effects of LSD on cognition and subjective measures differed between individuals.
The study included 24 healthy recreational drug users and compared the acute effects of 5 mcg, 20 mcg, and 20 mcg LSD with placebo on a computer-based psychomotor vigilance task (PVT) that measured attention and on a Digit Symbol Substitution Test (DSST).
Participants also completed the 72-item Profile of Mood States (POMS) questionnaire, a visual analog scale (VAS) on mood, and the 94-item 5-Dimensional Altered States of Consciousness Rating scales (5D-ASC).
Unadjusted results showed that the 20-mcg LSD dose significantly reduced correct substitutions on the DSST vs placebo (P < .05), but had no effect on attentional lapses on the PCT or on positive mood on the POMS.
Correcting the DSST score for the number of total responses revealed no dose effect of LSD. This suggested that participants were no less accurate when under the influence of LSD, even though they encoded fewer digits, the researchers note.
Participants also reported that both the 10-mcg and 20-mcg dose of LSD increased subjective experiences on the VAS and alternated states of consciousness on the 5D-ASC compared with placebo.
After stratifying the results by dose and participant, the effect of LSD differed between individuals. For example, both the 5-mcg and 20-mcg doses were associated with improvement in attention on the PVT (P < .05), but not the 10-mcg dose.
These results also indicated that the 20-mcg dose was associated with a significant increase in the correct number of substitutions on the DSST and with a significant increase in positive mood on the POMS (P < .05 for both outcomes).
The findings suggest that future studies in patient populations with impaired attention are needed, “including biological parameters involved in LSD receptor-binding and metabolism, in order to understand the inter-individual variation in response to LSD,” the investigators note.
In an educational session at the meeting, the study’s lead researcher, Kim Kuypers, PhD, associate professor at Maastricht University, said research shows individuals are already self-medicating with psychedelic microdosing to treat a wide range of mental health problems, and rated it as significantly more effective than conventional therapy at alleviating symptoms and improving quality of life.
Nevertheless, Kuypers noted there have been fewer than 20 published placebo-controlled studies examining psychedelic microdosing in humans – and much of the current evidence is anecdotal.
However, there is some clinical research suggesting that low-dose LSD is associated with improved mood and cognitive performance and that it also has an effect on resting-state amygdala functional connectivity and acutely increases brain-derived neurotrophic factor plasma levels.
Furthermore, said Kuypers, the evidence in healthy volunteers thus far suggests microdosing is “safe.”
Jumping ahead of the science?
Commenting on the study for Medscape Medical News, Jeffrey A. Lieberman, MD, professor and chair of psychiatry at Columbia University, New York City, said he “gives the investigators credit for doing such a study” but does not believe anything can be gleaned from the findings.
He said he is also concerned that the resurgence of psychedelic research is not congruent with “the methodologic rigor and scientific thinking that accompanies treatment development in other disease areas.”
Lieberman, who is also psychiatrist-in-chief at the NewYork–Presbyterian Hospital Columbia Medical Center and was not involved with the study, added that some of the research is also being conducted in individuals who are “true believers and not sufficiently dispassionate and objective.”
“ But because these are such notorious and interesting compounds, they have attracted a lot of peripheral interest to promote and to disseminate; and the risk is that it will be done in the wrong way and there may be consequences,” he said.
Moreover, Lieberman noted that the psychedelic drugs may be used in practice ahead of strong evidence of safety and efficacy. As an example, he pointed to ketamine, a drug that was identified as a treatment for people with depression who had not responded to standard treatments, he noted.
“But before you knew it, there were clinics being opened up all over the place by anesthesiologists or other people that were trying to make a quick buck,” he said.
“That was alarming because they were stretching the criteria for whom the treatment was appropriate; there were no protocols for dosing, for frequency of administration, and there was inadequate psychiatric follow-up,” Lieberman added.
Preliminary but promising
He agreed with Kuypers that cases of microdosing with psychedelics are largely anecdotal.
“So in that context, when these investigators tried to put it to a test, which is commendable, the results in no way tell you whether it’s good, bad, or indifferent,” Lieberman said. In fact, the results are “disappointing in terms of suggesting any beneficial effect.”
Lieberman said more and larger studies are needed in order to determine whether LSD microdosing is beneficial.
In response to Lieberman’s comments, Kuypers told Medscape Medical News that the investigators tried to base their placebo-controlled research on previous anecdotal research.
She emphasized that the “whole field is still in its infancy,” including research on the use of “full” doses of psychedelics.
“I sometimes think that the message is too positive. We should never forget to communicate that not a lot of research has been done.” In addition, she agreed that researchers should “keep a balanced message.”
“All the data to date is preliminary, in my view, but promising,” she stressed, “and the evidence is growing.”
The study received financial support from the Beckley Foundation. The study authors and Lieberman have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Microdosing with lysergic acid diethylamide (LSD) is associated with improved mood and increased attention, early research suggests. However, at least one expert believes it’s far too soon to tell and warns against endorsing patient microdosing.
In a dose-finding exploratory study, three low doses of LSD were compared with placebo in healthy volunteers who were all recreational drug users. Adjusted results showed that the highest dose boosted attention and mood, although participants were aware of psychedelic effects, prompting researchers to conclude the results demonstrated “selective, beneficial effects.”
“The majority of participants have improved attention,” study investigator Nadia Hutten, PhD, Department of Neuropsychology and Psychopharmacology, Maastricht University, the Netherlands, told Medscape Medical News.
“So we think that patients with attention deficits might have more beneficial effects,” she added, noting her team plans to study LSD microdosing in patients with attention deficit hyperactivity disorder.
The study was presented at the 33rd European College of Neuropsychopharmacology (ECNP) Congress, which was held online this year because of the COVID-19 pandemic.
Growing interest
Over the past 10 years there has been growing interest in psychedelic microdosing, which is defined as a dose that aims to enhance mood and/or performance but does not affect perception.
However, there has been considerable debate over what constitutes a “microdose.” One tenth of a “full” psychedelic dose is typically suggested, but users report a much wider dose range in practice, suggesting potential “individual variation in response to low doses,” the researchers note.
In the current dose-finding study, the researchers explored whether the effects of LSD on cognition and subjective measures differed between individuals.
The study included 24 healthy recreational drug users and compared the acute effects of 5 mcg, 20 mcg, and 20 mcg LSD with placebo on a computer-based psychomotor vigilance task (PVT) that measured attention and on a Digit Symbol Substitution Test (DSST).
Participants also completed the 72-item Profile of Mood States (POMS) questionnaire, a visual analog scale (VAS) on mood, and the 94-item 5-Dimensional Altered States of Consciousness Rating scales (5D-ASC).
Unadjusted results showed that the 20-mcg LSD dose significantly reduced correct substitutions on the DSST vs placebo (P < .05), but had no effect on attentional lapses on the PCT or on positive mood on the POMS.
Correcting the DSST score for the number of total responses revealed no dose effect of LSD. This suggested that participants were no less accurate when under the influence of LSD, even though they encoded fewer digits, the researchers note.
Participants also reported that both the 10-mcg and 20-mcg dose of LSD increased subjective experiences on the VAS and alternated states of consciousness on the 5D-ASC compared with placebo.
After stratifying the results by dose and participant, the effect of LSD differed between individuals. For example, both the 5-mcg and 20-mcg doses were associated with improvement in attention on the PVT (P < .05), but not the 10-mcg dose.
These results also indicated that the 20-mcg dose was associated with a significant increase in the correct number of substitutions on the DSST and with a significant increase in positive mood on the POMS (P < .05 for both outcomes).
The findings suggest that future studies in patient populations with impaired attention are needed, “including biological parameters involved in LSD receptor-binding and metabolism, in order to understand the inter-individual variation in response to LSD,” the investigators note.
In an educational session at the meeting, the study’s lead researcher, Kim Kuypers, PhD, associate professor at Maastricht University, said research shows individuals are already self-medicating with psychedelic microdosing to treat a wide range of mental health problems, and rated it as significantly more effective than conventional therapy at alleviating symptoms and improving quality of life.
Nevertheless, Kuypers noted there have been fewer than 20 published placebo-controlled studies examining psychedelic microdosing in humans – and much of the current evidence is anecdotal.
However, there is some clinical research suggesting that low-dose LSD is associated with improved mood and cognitive performance and that it also has an effect on resting-state amygdala functional connectivity and acutely increases brain-derived neurotrophic factor plasma levels.
Furthermore, said Kuypers, the evidence in healthy volunteers thus far suggests microdosing is “safe.”
Jumping ahead of the science?
Commenting on the study for Medscape Medical News, Jeffrey A. Lieberman, MD, professor and chair of psychiatry at Columbia University, New York City, said he “gives the investigators credit for doing such a study” but does not believe anything can be gleaned from the findings.
He said he is also concerned that the resurgence of psychedelic research is not congruent with “the methodologic rigor and scientific thinking that accompanies treatment development in other disease areas.”
Lieberman, who is also psychiatrist-in-chief at the NewYork–Presbyterian Hospital Columbia Medical Center and was not involved with the study, added that some of the research is also being conducted in individuals who are “true believers and not sufficiently dispassionate and objective.”
“ But because these are such notorious and interesting compounds, they have attracted a lot of peripheral interest to promote and to disseminate; and the risk is that it will be done in the wrong way and there may be consequences,” he said.
Moreover, Lieberman noted that the psychedelic drugs may be used in practice ahead of strong evidence of safety and efficacy. As an example, he pointed to ketamine, a drug that was identified as a treatment for people with depression who had not responded to standard treatments, he noted.
“But before you knew it, there were clinics being opened up all over the place by anesthesiologists or other people that were trying to make a quick buck,” he said.
“That was alarming because they were stretching the criteria for whom the treatment was appropriate; there were no protocols for dosing, for frequency of administration, and there was inadequate psychiatric follow-up,” Lieberman added.
Preliminary but promising
He agreed with Kuypers that cases of microdosing with psychedelics are largely anecdotal.
“So in that context, when these investigators tried to put it to a test, which is commendable, the results in no way tell you whether it’s good, bad, or indifferent,” Lieberman said. In fact, the results are “disappointing in terms of suggesting any beneficial effect.”
Lieberman said more and larger studies are needed in order to determine whether LSD microdosing is beneficial.
In response to Lieberman’s comments, Kuypers told Medscape Medical News that the investigators tried to base their placebo-controlled research on previous anecdotal research.
She emphasized that the “whole field is still in its infancy,” including research on the use of “full” doses of psychedelics.
“I sometimes think that the message is too positive. We should never forget to communicate that not a lot of research has been done.” In addition, she agreed that researchers should “keep a balanced message.”
“All the data to date is preliminary, in my view, but promising,” she stressed, “and the evidence is growing.”
The study received financial support from the Beckley Foundation. The study authors and Lieberman have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Microdosing with lysergic acid diethylamide (LSD) is associated with improved mood and increased attention, early research suggests. However, at least one expert believes it’s far too soon to tell and warns against endorsing patient microdosing.
In a dose-finding exploratory study, three low doses of LSD were compared with placebo in healthy volunteers who were all recreational drug users. Adjusted results showed that the highest dose boosted attention and mood, although participants were aware of psychedelic effects, prompting researchers to conclude the results demonstrated “selective, beneficial effects.”
“The majority of participants have improved attention,” study investigator Nadia Hutten, PhD, Department of Neuropsychology and Psychopharmacology, Maastricht University, the Netherlands, told Medscape Medical News.
“So we think that patients with attention deficits might have more beneficial effects,” she added, noting her team plans to study LSD microdosing in patients with attention deficit hyperactivity disorder.
The study was presented at the 33rd European College of Neuropsychopharmacology (ECNP) Congress, which was held online this year because of the COVID-19 pandemic.
Growing interest
Over the past 10 years there has been growing interest in psychedelic microdosing, which is defined as a dose that aims to enhance mood and/or performance but does not affect perception.
However, there has been considerable debate over what constitutes a “microdose.” One tenth of a “full” psychedelic dose is typically suggested, but users report a much wider dose range in practice, suggesting potential “individual variation in response to low doses,” the researchers note.
In the current dose-finding study, the researchers explored whether the effects of LSD on cognition and subjective measures differed between individuals.
The study included 24 healthy recreational drug users and compared the acute effects of 5 mcg, 20 mcg, and 20 mcg LSD with placebo on a computer-based psychomotor vigilance task (PVT) that measured attention and on a Digit Symbol Substitution Test (DSST).
Participants also completed the 72-item Profile of Mood States (POMS) questionnaire, a visual analog scale (VAS) on mood, and the 94-item 5-Dimensional Altered States of Consciousness Rating scales (5D-ASC).
Unadjusted results showed that the 20-mcg LSD dose significantly reduced correct substitutions on the DSST vs placebo (P < .05), but had no effect on attentional lapses on the PCT or on positive mood on the POMS.
Correcting the DSST score for the number of total responses revealed no dose effect of LSD. This suggested that participants were no less accurate when under the influence of LSD, even though they encoded fewer digits, the researchers note.
Participants also reported that both the 10-mcg and 20-mcg dose of LSD increased subjective experiences on the VAS and alternated states of consciousness on the 5D-ASC compared with placebo.
After stratifying the results by dose and participant, the effect of LSD differed between individuals. For example, both the 5-mcg and 20-mcg doses were associated with improvement in attention on the PVT (P < .05), but not the 10-mcg dose.
These results also indicated that the 20-mcg dose was associated with a significant increase in the correct number of substitutions on the DSST and with a significant increase in positive mood on the POMS (P < .05 for both outcomes).
The findings suggest that future studies in patient populations with impaired attention are needed, “including biological parameters involved in LSD receptor-binding and metabolism, in order to understand the inter-individual variation in response to LSD,” the investigators note.
In an educational session at the meeting, the study’s lead researcher, Kim Kuypers, PhD, associate professor at Maastricht University, said research shows individuals are already self-medicating with psychedelic microdosing to treat a wide range of mental health problems, and rated it as significantly more effective than conventional therapy at alleviating symptoms and improving quality of life.
Nevertheless, Kuypers noted there have been fewer than 20 published placebo-controlled studies examining psychedelic microdosing in humans – and much of the current evidence is anecdotal.
However, there is some clinical research suggesting that low-dose LSD is associated with improved mood and cognitive performance and that it also has an effect on resting-state amygdala functional connectivity and acutely increases brain-derived neurotrophic factor plasma levels.
Furthermore, said Kuypers, the evidence in healthy volunteers thus far suggests microdosing is “safe.”
Jumping ahead of the science?
Commenting on the study for Medscape Medical News, Jeffrey A. Lieberman, MD, professor and chair of psychiatry at Columbia University, New York City, said he “gives the investigators credit for doing such a study” but does not believe anything can be gleaned from the findings.
He said he is also concerned that the resurgence of psychedelic research is not congruent with “the methodologic rigor and scientific thinking that accompanies treatment development in other disease areas.”
Lieberman, who is also psychiatrist-in-chief at the NewYork–Presbyterian Hospital Columbia Medical Center and was not involved with the study, added that some of the research is also being conducted in individuals who are “true believers and not sufficiently dispassionate and objective.”
“ But because these are such notorious and interesting compounds, they have attracted a lot of peripheral interest to promote and to disseminate; and the risk is that it will be done in the wrong way and there may be consequences,” he said.
Moreover, Lieberman noted that the psychedelic drugs may be used in practice ahead of strong evidence of safety and efficacy. As an example, he pointed to ketamine, a drug that was identified as a treatment for people with depression who had not responded to standard treatments, he noted.
“But before you knew it, there were clinics being opened up all over the place by anesthesiologists or other people that were trying to make a quick buck,” he said.
“That was alarming because they were stretching the criteria for whom the treatment was appropriate; there were no protocols for dosing, for frequency of administration, and there was inadequate psychiatric follow-up,” Lieberman added.
Preliminary but promising
He agreed with Kuypers that cases of microdosing with psychedelics are largely anecdotal.
“So in that context, when these investigators tried to put it to a test, which is commendable, the results in no way tell you whether it’s good, bad, or indifferent,” Lieberman said. In fact, the results are “disappointing in terms of suggesting any beneficial effect.”
Lieberman said more and larger studies are needed in order to determine whether LSD microdosing is beneficial.
In response to Lieberman’s comments, Kuypers told Medscape Medical News that the investigators tried to base their placebo-controlled research on previous anecdotal research.
She emphasized that the “whole field is still in its infancy,” including research on the use of “full” doses of psychedelics.
“I sometimes think that the message is too positive. We should never forget to communicate that not a lot of research has been done.” In addition, she agreed that researchers should “keep a balanced message.”
“All the data to date is preliminary, in my view, but promising,” she stressed, “and the evidence is growing.”
The study received financial support from the Beckley Foundation. The study authors and Lieberman have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
COVID-19 vaccine hesitancy ‘somewhat understandable,’ expert says
“I worry that vaccines are going to be sold like magic powder that we sprinkle across the land and make the virus go away,” Paul Offit, MD, said at the virtual American Academy of Pediatrics (AAP) 2020 National Conference. “That’s not true.”
according to Dr. Offit, director of the Vaccine Education Center and an attending physician in the Division of Infectious Diseases at Children’s Hospital of Philadelphia.
“I think we can get a vaccine that’s 75%-80% effective at preventing mild to moderate disease, but that means one of every four people can still get moderate to severe disease,” Dr. Offit continued.
And that’s if there is high uptake of the vaccine, which may not be the case. Recent polls have suggested there is considerable concern about the pending vaccines.
“It’s somewhat understandable,” Dr. Offitt acknowledged, especially given the “frightening” language used to describe vaccine development. Terms such as “warp speed” may suggest that haste might trump safety considerations. Before COVID-19, the fastest vaccine ever developed was for mumps, he said, with the virus isolated in 1963 and a commercial product available in 1967.
Addressing hesitancy in clinics
In a wide-ranging livestream plenary presentation, Dr. Offit, coinventor of a rotavirus vaccine, shed light on SARS-CoV-2 vaccine development and his impressions of vaccine hesitancy among patients and families. He also offered advice for how to reassure those skeptical of the safety and efficacy of any SARS-COV-2 vaccine, given the accelerated development process.
With more than 180 different vaccines in various stages of investigation, Dr. Offit called the effort to develop COVID-19 vaccines “unprecedented.” Part of that is a result of governments relieving pharmaceutical companies of much of the typical financial risk – which often climbs to hundreds of millions of dollars – by underwriting the costs of vaccine development to battle the pandemic-inducing virus, he said.
But this very swiftness is also stoking antivaccine sentiment. Dr. Offit, part of vaccine advisory groups for the National Institutes of Health and U.S. Food and Drug Administration, cited recent research reporting nearly half of American adults definitely or probably would not get a COVID-19 vaccine if it were available today.
“One way you convince skeptics is with data presented in a clear, compassionate, and compelling way,” he said.
“The other group is vaccine cynics, who are basically conspiracy theorists who believe pharmaceutical companies control the world, the government, the medical establishment. I think there’s no talking them down from this.”
Numerous strategies are being used in COVID-19 vaccine development, he noted, including messenger RNA, DNA, viral vectors, purified protein, and whole killed virus. Dr. Offit believes any candidates approved for distribution will likely be in the range of 75% effective at preventing mild to moderate symptoms.
But clinicians should be ready to face immediate questions of safety. “Even if this vaccination is given to 20,000 [trial participants] safely, that’s not 20 million,” Dr. Offit said. “Anyone could reasonably ask questions about if it causes rare, serious side effects.
“The good news is, there are systems in place,” such as adverse event reporting systems, to identify rare events, even those that occur in one in a million vaccine recipients. Reminding patients of that continued surveillance can be reassuring.
Another reassuring point is that COVID-19 vaccine trial participants have included people from many diverse populations, he said. But children, notably absent so far, should be added to trials immediately, Dr. Offit contends.
“This is going to be important when you consider strategies to get children universally back into school,” he said, which is a “critical issue” from both learning and wellness standpoints. “It breaks my heart that we’ve been unable to do this when other countries have.”
Transparency will be paramount
While presenting data transparently to patients is key in helping them accept COVID-19 vaccination, Dr. Offit said, he also believes “telling stories” can be just as effective, if not more so. When the varicella vaccine was approved in 1995, he said, the “uptake the first few years was pretty miserable” until public service messaging emphasized that some children die from chickenpox.
“Fear works,” he said. “You always worry about pushback of something being oversold, but hopefully we’re scared enough about this virus” to convince people that vaccination is wise. “I do think personal stories carry weight on both sides,” Dr. Offit said.
Mark Sawyer, MD, of University of California San Diego School of Medicine and Rady Children’s Hospital in San Diego, California, said Offit’s presentation offered important takeaways for clinicians about how to broach the topic of COVID-19 vaccination with patients and families.
“We need to communicate clearly and transparently to patients about what we do and don’t know” about the vaccines, Dr. Sawyer said in an interview. “We will know if they have common side effects, but we will not know about very rare side effects until we have used the vaccines for a while.
“We will know how well the vaccine works over the short-term, but we won’t know over the long term,” added Dr. Sawyer, a member of the AAP Committee on Infectious Diseases.
“We can reassure the community that SARS-CoV-2 vaccines are being evaluated in trials in the same way and with the same thoroughness as other vaccines have been,” he said. “That should give people confidence that shortcuts are not being taken with regard to safety and effectiveness evaluations.”
Dr. Offit and Dr. Sawyer have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
“I worry that vaccines are going to be sold like magic powder that we sprinkle across the land and make the virus go away,” Paul Offit, MD, said at the virtual American Academy of Pediatrics (AAP) 2020 National Conference. “That’s not true.”
according to Dr. Offit, director of the Vaccine Education Center and an attending physician in the Division of Infectious Diseases at Children’s Hospital of Philadelphia.
“I think we can get a vaccine that’s 75%-80% effective at preventing mild to moderate disease, but that means one of every four people can still get moderate to severe disease,” Dr. Offit continued.
And that’s if there is high uptake of the vaccine, which may not be the case. Recent polls have suggested there is considerable concern about the pending vaccines.
“It’s somewhat understandable,” Dr. Offitt acknowledged, especially given the “frightening” language used to describe vaccine development. Terms such as “warp speed” may suggest that haste might trump safety considerations. Before COVID-19, the fastest vaccine ever developed was for mumps, he said, with the virus isolated in 1963 and a commercial product available in 1967.
Addressing hesitancy in clinics
In a wide-ranging livestream plenary presentation, Dr. Offit, coinventor of a rotavirus vaccine, shed light on SARS-CoV-2 vaccine development and his impressions of vaccine hesitancy among patients and families. He also offered advice for how to reassure those skeptical of the safety and efficacy of any SARS-COV-2 vaccine, given the accelerated development process.
With more than 180 different vaccines in various stages of investigation, Dr. Offit called the effort to develop COVID-19 vaccines “unprecedented.” Part of that is a result of governments relieving pharmaceutical companies of much of the typical financial risk – which often climbs to hundreds of millions of dollars – by underwriting the costs of vaccine development to battle the pandemic-inducing virus, he said.
But this very swiftness is also stoking antivaccine sentiment. Dr. Offit, part of vaccine advisory groups for the National Institutes of Health and U.S. Food and Drug Administration, cited recent research reporting nearly half of American adults definitely or probably would not get a COVID-19 vaccine if it were available today.
“One way you convince skeptics is with data presented in a clear, compassionate, and compelling way,” he said.
“The other group is vaccine cynics, who are basically conspiracy theorists who believe pharmaceutical companies control the world, the government, the medical establishment. I think there’s no talking them down from this.”
Numerous strategies are being used in COVID-19 vaccine development, he noted, including messenger RNA, DNA, viral vectors, purified protein, and whole killed virus. Dr. Offit believes any candidates approved for distribution will likely be in the range of 75% effective at preventing mild to moderate symptoms.
But clinicians should be ready to face immediate questions of safety. “Even if this vaccination is given to 20,000 [trial participants] safely, that’s not 20 million,” Dr. Offit said. “Anyone could reasonably ask questions about if it causes rare, serious side effects.
“The good news is, there are systems in place,” such as adverse event reporting systems, to identify rare events, even those that occur in one in a million vaccine recipients. Reminding patients of that continued surveillance can be reassuring.
Another reassuring point is that COVID-19 vaccine trial participants have included people from many diverse populations, he said. But children, notably absent so far, should be added to trials immediately, Dr. Offit contends.
“This is going to be important when you consider strategies to get children universally back into school,” he said, which is a “critical issue” from both learning and wellness standpoints. “It breaks my heart that we’ve been unable to do this when other countries have.”
Transparency will be paramount
While presenting data transparently to patients is key in helping them accept COVID-19 vaccination, Dr. Offit said, he also believes “telling stories” can be just as effective, if not more so. When the varicella vaccine was approved in 1995, he said, the “uptake the first few years was pretty miserable” until public service messaging emphasized that some children die from chickenpox.
“Fear works,” he said. “You always worry about pushback of something being oversold, but hopefully we’re scared enough about this virus” to convince people that vaccination is wise. “I do think personal stories carry weight on both sides,” Dr. Offit said.
Mark Sawyer, MD, of University of California San Diego School of Medicine and Rady Children’s Hospital in San Diego, California, said Offit’s presentation offered important takeaways for clinicians about how to broach the topic of COVID-19 vaccination with patients and families.
“We need to communicate clearly and transparently to patients about what we do and don’t know” about the vaccines, Dr. Sawyer said in an interview. “We will know if they have common side effects, but we will not know about very rare side effects until we have used the vaccines for a while.
“We will know how well the vaccine works over the short-term, but we won’t know over the long term,” added Dr. Sawyer, a member of the AAP Committee on Infectious Diseases.
“We can reassure the community that SARS-CoV-2 vaccines are being evaluated in trials in the same way and with the same thoroughness as other vaccines have been,” he said. “That should give people confidence that shortcuts are not being taken with regard to safety and effectiveness evaluations.”
Dr. Offit and Dr. Sawyer have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
“I worry that vaccines are going to be sold like magic powder that we sprinkle across the land and make the virus go away,” Paul Offit, MD, said at the virtual American Academy of Pediatrics (AAP) 2020 National Conference. “That’s not true.”
according to Dr. Offit, director of the Vaccine Education Center and an attending physician in the Division of Infectious Diseases at Children’s Hospital of Philadelphia.
“I think we can get a vaccine that’s 75%-80% effective at preventing mild to moderate disease, but that means one of every four people can still get moderate to severe disease,” Dr. Offit continued.
And that’s if there is high uptake of the vaccine, which may not be the case. Recent polls have suggested there is considerable concern about the pending vaccines.
“It’s somewhat understandable,” Dr. Offitt acknowledged, especially given the “frightening” language used to describe vaccine development. Terms such as “warp speed” may suggest that haste might trump safety considerations. Before COVID-19, the fastest vaccine ever developed was for mumps, he said, with the virus isolated in 1963 and a commercial product available in 1967.
Addressing hesitancy in clinics
In a wide-ranging livestream plenary presentation, Dr. Offit, coinventor of a rotavirus vaccine, shed light on SARS-CoV-2 vaccine development and his impressions of vaccine hesitancy among patients and families. He also offered advice for how to reassure those skeptical of the safety and efficacy of any SARS-COV-2 vaccine, given the accelerated development process.
With more than 180 different vaccines in various stages of investigation, Dr. Offit called the effort to develop COVID-19 vaccines “unprecedented.” Part of that is a result of governments relieving pharmaceutical companies of much of the typical financial risk – which often climbs to hundreds of millions of dollars – by underwriting the costs of vaccine development to battle the pandemic-inducing virus, he said.
But this very swiftness is also stoking antivaccine sentiment. Dr. Offit, part of vaccine advisory groups for the National Institutes of Health and U.S. Food and Drug Administration, cited recent research reporting nearly half of American adults definitely or probably would not get a COVID-19 vaccine if it were available today.
“One way you convince skeptics is with data presented in a clear, compassionate, and compelling way,” he said.
“The other group is vaccine cynics, who are basically conspiracy theorists who believe pharmaceutical companies control the world, the government, the medical establishment. I think there’s no talking them down from this.”
Numerous strategies are being used in COVID-19 vaccine development, he noted, including messenger RNA, DNA, viral vectors, purified protein, and whole killed virus. Dr. Offit believes any candidates approved for distribution will likely be in the range of 75% effective at preventing mild to moderate symptoms.
But clinicians should be ready to face immediate questions of safety. “Even if this vaccination is given to 20,000 [trial participants] safely, that’s not 20 million,” Dr. Offit said. “Anyone could reasonably ask questions about if it causes rare, serious side effects.
“The good news is, there are systems in place,” such as adverse event reporting systems, to identify rare events, even those that occur in one in a million vaccine recipients. Reminding patients of that continued surveillance can be reassuring.
Another reassuring point is that COVID-19 vaccine trial participants have included people from many diverse populations, he said. But children, notably absent so far, should be added to trials immediately, Dr. Offit contends.
“This is going to be important when you consider strategies to get children universally back into school,” he said, which is a “critical issue” from both learning and wellness standpoints. “It breaks my heart that we’ve been unable to do this when other countries have.”
Transparency will be paramount
While presenting data transparently to patients is key in helping them accept COVID-19 vaccination, Dr. Offit said, he also believes “telling stories” can be just as effective, if not more so. When the varicella vaccine was approved in 1995, he said, the “uptake the first few years was pretty miserable” until public service messaging emphasized that some children die from chickenpox.
“Fear works,” he said. “You always worry about pushback of something being oversold, but hopefully we’re scared enough about this virus” to convince people that vaccination is wise. “I do think personal stories carry weight on both sides,” Dr. Offit said.
Mark Sawyer, MD, of University of California San Diego School of Medicine and Rady Children’s Hospital in San Diego, California, said Offit’s presentation offered important takeaways for clinicians about how to broach the topic of COVID-19 vaccination with patients and families.
“We need to communicate clearly and transparently to patients about what we do and don’t know” about the vaccines, Dr. Sawyer said in an interview. “We will know if they have common side effects, but we will not know about very rare side effects until we have used the vaccines for a while.
“We will know how well the vaccine works over the short-term, but we won’t know over the long term,” added Dr. Sawyer, a member of the AAP Committee on Infectious Diseases.
“We can reassure the community that SARS-CoV-2 vaccines are being evaluated in trials in the same way and with the same thoroughness as other vaccines have been,” he said. “That should give people confidence that shortcuts are not being taken with regard to safety and effectiveness evaluations.”
Dr. Offit and Dr. Sawyer have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
COVID-19 and the superspreaders: Teens
Although cases of COVID-19 in children is reported to be low, we are seeing a surge in Wisconsin with a 27.6% positivity rate reported on Sept. 27. Numerous other states across the country are reporting similar jumps of 10% or more.

According to the Wisconsin Department of Health Services as of Sept. 20, 2020, there were 10,644 cumulative cases in persons aged less than 18 years. This rise in cases is consistent with a return to school and sports. This cumulative case load amounts to 836.7/100, 000 cases. This population may not experience the level of illness seen in the older populations with hospitalization rates of only 3% under the age of 9 years and 13% of those age 10- 19-years, yet exposing older family and members of the community is driving the death rates. The combined influenza and COVID-19 season may greatly impact hospitalization rates of young and old. Additionally, we may see a surge in pediatric cancer rates and autoimmune diseases secondary to these trends.
I believe the overall number of adolescents with COVID-19 is underreported. Teens admit to a lack of understanding of symptoms. Many do not realize they have COVID-19 until someone points out the symptoms they describe such as a loss of taste or smell are COVID-19 symptoms. Others report they do not report symptoms to prevent quarantine. Additionally, others endorse ridicule from peers if they have tested positive and contract tracing identifies others potentially exposed and forced to sit out of sports because of quarantine. They have been bullied into amnesia when contract tracers call to prevent identifying others at school or in the community. All these behaviors proliferate the spread of disease within the community and will continue to drive both exposures and death rates.
Teens in high schools require increased education of the symptoms of COVID-19, promotion of the flu vaccine, and knowledge of the impact they can have on preventing the spread of viruses.
Ms. Thew is the medical director of the department of adolescent medicine at Children’s Wisconsin in Milwaukee. She is a member of the Pediatric News editorial advisory board. She said she had no relevant financial disclosures. Email her at [email protected].
Reference
COVID-19: Wisconsin Cases, Wisconsin Department of Health Services. Accessed 2020 Sep 27.
Although cases of COVID-19 in children is reported to be low, we are seeing a surge in Wisconsin with a 27.6% positivity rate reported on Sept. 27. Numerous other states across the country are reporting similar jumps of 10% or more.
According to the Wisconsin Department of Health Services as of Sept. 20, 2020, there were 10,644 cumulative cases in persons aged less than 18 years. This rise in cases is consistent with a return to school and sports. This cumulative case load amounts to 836.7/100, 000 cases. This population may not experience the level of illness seen in the older populations with hospitalization rates of only 3% under the age of 9 years and 13% of those age 10- 19-years, yet exposing older family and members of the community is driving the death rates. The combined influenza and COVID-19 season may greatly impact hospitalization rates of young and old. Additionally, we may see a surge in pediatric cancer rates and autoimmune diseases secondary to these trends.
I believe the overall number of adolescents with COVID-19 is underreported. Teens admit to a lack of understanding of symptoms. Many do not realize they have COVID-19 until someone points out the symptoms they describe such as a loss of taste or smell are COVID-19 symptoms. Others report they do not report symptoms to prevent quarantine. Additionally, others endorse ridicule from peers if they have tested positive and contract tracing identifies others potentially exposed and forced to sit out of sports because of quarantine. They have been bullied into amnesia when contract tracers call to prevent identifying others at school or in the community. All these behaviors proliferate the spread of disease within the community and will continue to drive both exposures and death rates.
Teens in high schools require increased education of the symptoms of COVID-19, promotion of the flu vaccine, and knowledge of the impact they can have on preventing the spread of viruses.
Ms. Thew is the medical director of the department of adolescent medicine at Children’s Wisconsin in Milwaukee. She is a member of the Pediatric News editorial advisory board. She said she had no relevant financial disclosures. Email her at [email protected].
Reference
COVID-19: Wisconsin Cases, Wisconsin Department of Health Services. Accessed 2020 Sep 27.
Although cases of COVID-19 in children is reported to be low, we are seeing a surge in Wisconsin with a 27.6% positivity rate reported on Sept. 27. Numerous other states across the country are reporting similar jumps of 10% or more.
According to the Wisconsin Department of Health Services as of Sept. 20, 2020, there were 10,644 cumulative cases in persons aged less than 18 years. This rise in cases is consistent with a return to school and sports. This cumulative case load amounts to 836.7/100, 000 cases. This population may not experience the level of illness seen in the older populations with hospitalization rates of only 3% under the age of 9 years and 13% of those age 10- 19-years, yet exposing older family and members of the community is driving the death rates. The combined influenza and COVID-19 season may greatly impact hospitalization rates of young and old. Additionally, we may see a surge in pediatric cancer rates and autoimmune diseases secondary to these trends.
I believe the overall number of adolescents with COVID-19 is underreported. Teens admit to a lack of understanding of symptoms. Many do not realize they have COVID-19 until someone points out the symptoms they describe such as a loss of taste or smell are COVID-19 symptoms. Others report they do not report symptoms to prevent quarantine. Additionally, others endorse ridicule from peers if they have tested positive and contract tracing identifies others potentially exposed and forced to sit out of sports because of quarantine. They have been bullied into amnesia when contract tracers call to prevent identifying others at school or in the community. All these behaviors proliferate the spread of disease within the community and will continue to drive both exposures and death rates.
Teens in high schools require increased education of the symptoms of COVID-19, promotion of the flu vaccine, and knowledge of the impact they can have on preventing the spread of viruses.
Ms. Thew is the medical director of the department of adolescent medicine at Children’s Wisconsin in Milwaukee. She is a member of the Pediatric News editorial advisory board. She said she had no relevant financial disclosures. Email her at [email protected].
Reference
COVID-19: Wisconsin Cases, Wisconsin Department of Health Services. Accessed 2020 Sep 27.
Pediatric fractures shift during pandemic
Pediatric fractures dropped by 2.5-fold during the early months of the COVID-19 pandemic, but more breaks happened at home and on bicycles, and younger kids were more affected, new research indicates.
The study of 1,745 patients also found that those with distal radius torus fractures were more likely to receive a Velcro splint during the pandemic. Experts said this key trend points toward widespread shifts to streamline treatment, which should persist after the pandemic.
“We expected to see a drop in fracture volume, but what was a bit unexpected was the proportional rise in at-home injuries, which we weren’t immediately aware of,” said senior author Apurva Shah, MD, MBA, of Children’s Hospital of Philadelphia (CHOP) and the University of Pennsylvania in Philadelphia.
“As time went on, it became more apparent that trampoline and bicycle injuries were on the rise, but at the beginning of the pandemic, we didn’t intuitively expect that,” he added.
“Whenever there’s a major shift in how the world is working, we want to understand how that impacts child safety,” Dr. Shah said in an interview. “The message to get out to parents is that it’s obviously difficult to supervise kids while working from home” during the pandemic “and that supervision obviously is not always working as well as intended.”
Joshua T. Bram, a medical student, presented the study at the virtual American Academy of Pediatrics (AAP) 2020 National Conference.
Dr. Bram, Dr. Shah, and colleagues compared patients with acute fractures who presented at CHOP between March and April 2020 with those who presented during the same months in 2018 and 2019.
Overall, the number of patients with pediatric fractures who presented to CHOP fell to an average of just under 10 per day, compared with more than 22 per day in prior years (P < .001). In addition, the age of the patients fell from an average of 9.4 years to 7.5 years (P < .001), with fewer adolescents affected in 2020.
“I think when you cancel a 14-year-old’s baseball season” because of the pandemic, “unfortunately, that lost outdoor time might be substituted with time on a screen,” he explained. “But canceling a 6-year-old’s soccer season might mean substituting that with more time outside on bikes or on a trampoline.”
As noted, because of the pandemic, a higher proportion of pediatric fractures occurred at home (57.8% vs. 32.5%; P < .001) or on bicycles (18.3% vs. 8.2%; P < .001), but there were fewer organized sports–related (7.2% vs. 26.0%; P < .001) or playground-related injuries (5.2% vs. 9.0%; P < .001).
In the study period this year, the researchers saw no increase in the amount of time between injury and presentation. However, data suggest that, in more recent months, “kids are presenting with fractures late, with sometimes great consequences,” Dr. Shah said.
“What has changed is that a lot of adults have lost their jobs, and as a consequence, a lot of children have lost their access to private insurance,” he said. “But fracture is really a major injury, and this is a reminder for pediatricians and primary care physicians to recognize that families are going through these changes and that delays in care can really be detrimental to children.”
Velcro splints more common
A potential upside to shifts seen during the pandemic, Dr. Shah said, is the finding that distal radius torus fractures were more likely to be treated with a Velcro splint than in previous years (44.2% vs. 25.9%; P = .010).
“This is hitting on something important – that sometimes it’s crisis that forces us as physicians to evolve,” he said. “This is something I think is here to stay.
“Although research had already been there suggesting a close equivalent between splints and casting, culturally, a lot of surgeons hadn’t made that shift when historically the gold standard had been casting,” Dr. Shah added. “But with the pandemic, the shift to minimize contact with the health care system to keep families safe in their COVID bubble helped [usage of] splints take off.
“I suspect – and we’ll only know when we’re on the other side of this – when physicians see good results in splints in their own patients, they’re going to adopt those strategies more permanently,” he said.
Benjamin Shore, MD, MPH, of Boston Children’s Hospital, agreed with Dr. Shah’s prediction that fracture care will be more streamlined after the pandemic. Dr. Shore, who wasn’t involved in the study, said not only are more orthopedic providers treating patients with Velcro splints and bivalve casts, but they are also monitoring patients via telehealth.
“All of these are great examples of innovation, and one of the unique parts of the pandemic is it created a lot of rapid change across healthcare because it caused us to scrutinize the ways we practice and make a change,” Dr. Shore said in an interview.
“It wasn’t a very fancy study, but it’s very important in terms of demonstrating a change in practice,” Dr. Shore said. “The research here basically validated what many of us are seeing and hopefully will help us in future pandemics – which hopefully won’t happen – to tell families what to be proactive about.”
Dr. Shah and Dr. Shore agreed that, because fewer fractures are occurring in kids during the pandemic, there is an opportunity to redeploy orthopedic providers to other clinical areas on the basis of volume and need.
Dr. Shah and Dr. Shore have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Pediatric fractures dropped by 2.5-fold during the early months of the COVID-19 pandemic, but more breaks happened at home and on bicycles, and younger kids were more affected, new research indicates.
The study of 1,745 patients also found that those with distal radius torus fractures were more likely to receive a Velcro splint during the pandemic. Experts said this key trend points toward widespread shifts to streamline treatment, which should persist after the pandemic.
“We expected to see a drop in fracture volume, but what was a bit unexpected was the proportional rise in at-home injuries, which we weren’t immediately aware of,” said senior author Apurva Shah, MD, MBA, of Children’s Hospital of Philadelphia (CHOP) and the University of Pennsylvania in Philadelphia.
“As time went on, it became more apparent that trampoline and bicycle injuries were on the rise, but at the beginning of the pandemic, we didn’t intuitively expect that,” he added.
“Whenever there’s a major shift in how the world is working, we want to understand how that impacts child safety,” Dr. Shah said in an interview. “The message to get out to parents is that it’s obviously difficult to supervise kids while working from home” during the pandemic “and that supervision obviously is not always working as well as intended.”
Joshua T. Bram, a medical student, presented the study at the virtual American Academy of Pediatrics (AAP) 2020 National Conference.
Dr. Bram, Dr. Shah, and colleagues compared patients with acute fractures who presented at CHOP between March and April 2020 with those who presented during the same months in 2018 and 2019.
Overall, the number of patients with pediatric fractures who presented to CHOP fell to an average of just under 10 per day, compared with more than 22 per day in prior years (P < .001). In addition, the age of the patients fell from an average of 9.4 years to 7.5 years (P < .001), with fewer adolescents affected in 2020.
“I think when you cancel a 14-year-old’s baseball season” because of the pandemic, “unfortunately, that lost outdoor time might be substituted with time on a screen,” he explained. “But canceling a 6-year-old’s soccer season might mean substituting that with more time outside on bikes or on a trampoline.”
As noted, because of the pandemic, a higher proportion of pediatric fractures occurred at home (57.8% vs. 32.5%; P < .001) or on bicycles (18.3% vs. 8.2%; P < .001), but there were fewer organized sports–related (7.2% vs. 26.0%; P < .001) or playground-related injuries (5.2% vs. 9.0%; P < .001).
In the study period this year, the researchers saw no increase in the amount of time between injury and presentation. However, data suggest that, in more recent months, “kids are presenting with fractures late, with sometimes great consequences,” Dr. Shah said.
“What has changed is that a lot of adults have lost their jobs, and as a consequence, a lot of children have lost their access to private insurance,” he said. “But fracture is really a major injury, and this is a reminder for pediatricians and primary care physicians to recognize that families are going through these changes and that delays in care can really be detrimental to children.”
Velcro splints more common
A potential upside to shifts seen during the pandemic, Dr. Shah said, is the finding that distal radius torus fractures were more likely to be treated with a Velcro splint than in previous years (44.2% vs. 25.9%; P = .010).
“This is hitting on something important – that sometimes it’s crisis that forces us as physicians to evolve,” he said. “This is something I think is here to stay.
“Although research had already been there suggesting a close equivalent between splints and casting, culturally, a lot of surgeons hadn’t made that shift when historically the gold standard had been casting,” Dr. Shah added. “But with the pandemic, the shift to minimize contact with the health care system to keep families safe in their COVID bubble helped [usage of] splints take off.
“I suspect – and we’ll only know when we’re on the other side of this – when physicians see good results in splints in their own patients, they’re going to adopt those strategies more permanently,” he said.
Benjamin Shore, MD, MPH, of Boston Children’s Hospital, agreed with Dr. Shah’s prediction that fracture care will be more streamlined after the pandemic. Dr. Shore, who wasn’t involved in the study, said not only are more orthopedic providers treating patients with Velcro splints and bivalve casts, but they are also monitoring patients via telehealth.
“All of these are great examples of innovation, and one of the unique parts of the pandemic is it created a lot of rapid change across healthcare because it caused us to scrutinize the ways we practice and make a change,” Dr. Shore said in an interview.
“It wasn’t a very fancy study, but it’s very important in terms of demonstrating a change in practice,” Dr. Shore said. “The research here basically validated what many of us are seeing and hopefully will help us in future pandemics – which hopefully won’t happen – to tell families what to be proactive about.”
Dr. Shah and Dr. Shore agreed that, because fewer fractures are occurring in kids during the pandemic, there is an opportunity to redeploy orthopedic providers to other clinical areas on the basis of volume and need.
Dr. Shah and Dr. Shore have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Pediatric fractures dropped by 2.5-fold during the early months of the COVID-19 pandemic, but more breaks happened at home and on bicycles, and younger kids were more affected, new research indicates.
The study of 1,745 patients also found that those with distal radius torus fractures were more likely to receive a Velcro splint during the pandemic. Experts said this key trend points toward widespread shifts to streamline treatment, which should persist after the pandemic.
“We expected to see a drop in fracture volume, but what was a bit unexpected was the proportional rise in at-home injuries, which we weren’t immediately aware of,” said senior author Apurva Shah, MD, MBA, of Children’s Hospital of Philadelphia (CHOP) and the University of Pennsylvania in Philadelphia.
“As time went on, it became more apparent that trampoline and bicycle injuries were on the rise, but at the beginning of the pandemic, we didn’t intuitively expect that,” he added.
“Whenever there’s a major shift in how the world is working, we want to understand how that impacts child safety,” Dr. Shah said in an interview. “The message to get out to parents is that it’s obviously difficult to supervise kids while working from home” during the pandemic “and that supervision obviously is not always working as well as intended.”
Joshua T. Bram, a medical student, presented the study at the virtual American Academy of Pediatrics (AAP) 2020 National Conference.
Dr. Bram, Dr. Shah, and colleagues compared patients with acute fractures who presented at CHOP between March and April 2020 with those who presented during the same months in 2018 and 2019.
Overall, the number of patients with pediatric fractures who presented to CHOP fell to an average of just under 10 per day, compared with more than 22 per day in prior years (P < .001). In addition, the age of the patients fell from an average of 9.4 years to 7.5 years (P < .001), with fewer adolescents affected in 2020.
“I think when you cancel a 14-year-old’s baseball season” because of the pandemic, “unfortunately, that lost outdoor time might be substituted with time on a screen,” he explained. “But canceling a 6-year-old’s soccer season might mean substituting that with more time outside on bikes or on a trampoline.”
As noted, because of the pandemic, a higher proportion of pediatric fractures occurred at home (57.8% vs. 32.5%; P < .001) or on bicycles (18.3% vs. 8.2%; P < .001), but there were fewer organized sports–related (7.2% vs. 26.0%; P < .001) or playground-related injuries (5.2% vs. 9.0%; P < .001).
In the study period this year, the researchers saw no increase in the amount of time between injury and presentation. However, data suggest that, in more recent months, “kids are presenting with fractures late, with sometimes great consequences,” Dr. Shah said.
“What has changed is that a lot of adults have lost their jobs, and as a consequence, a lot of children have lost their access to private insurance,” he said. “But fracture is really a major injury, and this is a reminder for pediatricians and primary care physicians to recognize that families are going through these changes and that delays in care can really be detrimental to children.”
Velcro splints more common
A potential upside to shifts seen during the pandemic, Dr. Shah said, is the finding that distal radius torus fractures were more likely to be treated with a Velcro splint than in previous years (44.2% vs. 25.9%; P = .010).
“This is hitting on something important – that sometimes it’s crisis that forces us as physicians to evolve,” he said. “This is something I think is here to stay.
“Although research had already been there suggesting a close equivalent between splints and casting, culturally, a lot of surgeons hadn’t made that shift when historically the gold standard had been casting,” Dr. Shah added. “But with the pandemic, the shift to minimize contact with the health care system to keep families safe in their COVID bubble helped [usage of] splints take off.
“I suspect – and we’ll only know when we’re on the other side of this – when physicians see good results in splints in their own patients, they’re going to adopt those strategies more permanently,” he said.
Benjamin Shore, MD, MPH, of Boston Children’s Hospital, agreed with Dr. Shah’s prediction that fracture care will be more streamlined after the pandemic. Dr. Shore, who wasn’t involved in the study, said not only are more orthopedic providers treating patients with Velcro splints and bivalve casts, but they are also monitoring patients via telehealth.
“All of these are great examples of innovation, and one of the unique parts of the pandemic is it created a lot of rapid change across healthcare because it caused us to scrutinize the ways we practice and make a change,” Dr. Shore said in an interview.
“It wasn’t a very fancy study, but it’s very important in terms of demonstrating a change in practice,” Dr. Shore said. “The research here basically validated what many of us are seeing and hopefully will help us in future pandemics – which hopefully won’t happen – to tell families what to be proactive about.”
Dr. Shah and Dr. Shore agreed that, because fewer fractures are occurring in kids during the pandemic, there is an opportunity to redeploy orthopedic providers to other clinical areas on the basis of volume and need.
Dr. Shah and Dr. Shore have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Teen affective disorders raise risk for midlife acute MI
in a Swedish national registry study presented at the virtual annual congress of the European Society of Cardiology.

The association was mediated in part by poor stress resilience and lack of physical fitness among these teenagers with an affective disorder, reported Cecilia Bergh, PhD, of Obrero (Sweden) University.
Her study was made possible by Sweden’s comprehensive national health care registries coupled with the Nordic nation’s compulsory conscription for military service. The mandatory conscription evaluation during the study years included a semistructured interview with a psychologist to assess stress resilience through questions about coping with everyday life, a medical history and physical examination, and a cardiovascular fitness test using a bicycle ergometer.
The study included 238,013 males born in 1952-1956. They were aged 18-19 years when they underwent their conscription examination, at which time 34,503 of them either received or already had a diagnosis of depression or anxiety. During follow-up from 1987 to 2010, a first acute MI occurred in 5,891 of the men. The risk was increased 51% among those with an earlier teen diagnosis of depression or anxiety.
In a Cox regression analysis adjusted for levels of adolescent cardiovascular risk factors, including blood pressure, body mass index, and systemic inflammation, as well as additional potential confounders, such as cognitive function, parental socioeconomic index, and a summary disease score, the midlife MI risk associated with adolescent depression or anxiety was attenuated, but still significant, with a 24% increase. Upon further statistical adjustment incorporating adolescent stress resilience and cardiovascular fitness, the increased risk of acute MI in midlife associated with adolescent depression or anxiety was further attenuated yet remained significant, at 18%.
Dr. Bergh shared her thoughts on preventing this increased risk of acute MI at a relatively young age: “Effective prevention might focus on behavior, lifestyle, and psychosocial stress in early life. If a healthy lifestyle is encouraged as early as possible in childhood and adolescence, it is more likely to persist into adulthood and to improve longterm health. So look for signs of stress, depression, or anxiety that is beyond normal teenager behavior and a persistent problem. Teenagers with poor well-being could benefit from additional support to encourage exercise and also to develop strategies to deal with stress.”
She reported having no financial conflicts regarding her study, conducted free of commercial support.
SOURCE: Bergh C et al. ESC 2020, Abstract 90524.
in a Swedish national registry study presented at the virtual annual congress of the European Society of Cardiology.
The association was mediated in part by poor stress resilience and lack of physical fitness among these teenagers with an affective disorder, reported Cecilia Bergh, PhD, of Obrero (Sweden) University.
Her study was made possible by Sweden’s comprehensive national health care registries coupled with the Nordic nation’s compulsory conscription for military service. The mandatory conscription evaluation during the study years included a semistructured interview with a psychologist to assess stress resilience through questions about coping with everyday life, a medical history and physical examination, and a cardiovascular fitness test using a bicycle ergometer.
The study included 238,013 males born in 1952-1956. They were aged 18-19 years when they underwent their conscription examination, at which time 34,503 of them either received or already had a diagnosis of depression or anxiety. During follow-up from 1987 to 2010, a first acute MI occurred in 5,891 of the men. The risk was increased 51% among those with an earlier teen diagnosis of depression or anxiety.
In a Cox regression analysis adjusted for levels of adolescent cardiovascular risk factors, including blood pressure, body mass index, and systemic inflammation, as well as additional potential confounders, such as cognitive function, parental socioeconomic index, and a summary disease score, the midlife MI risk associated with adolescent depression or anxiety was attenuated, but still significant, with a 24% increase. Upon further statistical adjustment incorporating adolescent stress resilience and cardiovascular fitness, the increased risk of acute MI in midlife associated with adolescent depression or anxiety was further attenuated yet remained significant, at 18%.
Dr. Bergh shared her thoughts on preventing this increased risk of acute MI at a relatively young age: “Effective prevention might focus on behavior, lifestyle, and psychosocial stress in early life. If a healthy lifestyle is encouraged as early as possible in childhood and adolescence, it is more likely to persist into adulthood and to improve longterm health. So look for signs of stress, depression, or anxiety that is beyond normal teenager behavior and a persistent problem. Teenagers with poor well-being could benefit from additional support to encourage exercise and also to develop strategies to deal with stress.”
She reported having no financial conflicts regarding her study, conducted free of commercial support.
SOURCE: Bergh C et al. ESC 2020, Abstract 90524.
in a Swedish national registry study presented at the virtual annual congress of the European Society of Cardiology.
The association was mediated in part by poor stress resilience and lack of physical fitness among these teenagers with an affective disorder, reported Cecilia Bergh, PhD, of Obrero (Sweden) University.
Her study was made possible by Sweden’s comprehensive national health care registries coupled with the Nordic nation’s compulsory conscription for military service. The mandatory conscription evaluation during the study years included a semistructured interview with a psychologist to assess stress resilience through questions about coping with everyday life, a medical history and physical examination, and a cardiovascular fitness test using a bicycle ergometer.
The study included 238,013 males born in 1952-1956. They were aged 18-19 years when they underwent their conscription examination, at which time 34,503 of them either received or already had a diagnosis of depression or anxiety. During follow-up from 1987 to 2010, a first acute MI occurred in 5,891 of the men. The risk was increased 51% among those with an earlier teen diagnosis of depression or anxiety.
In a Cox regression analysis adjusted for levels of adolescent cardiovascular risk factors, including blood pressure, body mass index, and systemic inflammation, as well as additional potential confounders, such as cognitive function, parental socioeconomic index, and a summary disease score, the midlife MI risk associated with adolescent depression or anxiety was attenuated, but still significant, with a 24% increase. Upon further statistical adjustment incorporating adolescent stress resilience and cardiovascular fitness, the increased risk of acute MI in midlife associated with adolescent depression or anxiety was further attenuated yet remained significant, at 18%.
Dr. Bergh shared her thoughts on preventing this increased risk of acute MI at a relatively young age: “Effective prevention might focus on behavior, lifestyle, and psychosocial stress in early life. If a healthy lifestyle is encouraged as early as possible in childhood and adolescence, it is more likely to persist into adulthood and to improve longterm health. So look for signs of stress, depression, or anxiety that is beyond normal teenager behavior and a persistent problem. Teenagers with poor well-being could benefit from additional support to encourage exercise and also to develop strategies to deal with stress.”
She reported having no financial conflicts regarding her study, conducted free of commercial support.
SOURCE: Bergh C et al. ESC 2020, Abstract 90524.
FROM ESC CONGRESS 2020
One measure of child COVID-19 may be trending downward
After increasing for several weeks, the proportion of new COVID-19 cases occurring in children has dropped for the second week in a row, according to data in a new report from the American Academy of Pediatrics and the Children’s Hospital Association.
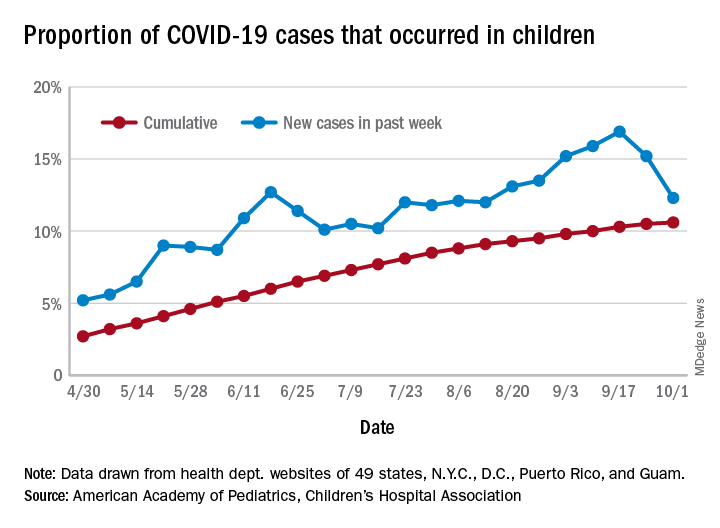
COVID-19 cases in children accounted for 12.3% of all new cases in the United States for the week ending Oct. 1, down from 15.2% the previous week. That measure had reached its highest point, 16.9%, just one week earlier (Sept. 17), the AAP and the CHA said in their weekly COVID-19 report.
based on data from the health departments of 49 states (New York does not provide ages on its website), as well as the District of Columbia, New York City, Puerto Rico, and Guam.
The child COVID-19 rate for the United States was 874 per 100,000 children as of Oct. 1, and that figure has doubled since the end of July. At the state level, the highest rates can be found in Tennessee (2,031.4 per 100,000), North Dakota (2,029.6), and South Carolina (2,002.6), with the lowest rates in Vermont (168.9), Maine (229.1), and New Hampshire (268.3), the AAP/CHA report shows.
The children of Wyoming make up the largest share, 22.4%, of any state’s COVID-19 cases, followed by North Dakota and Tennessee, both at 18.3%. New Jersey is lower than any other state at 3.9%, although New York City is a slightly lower 3.6%, the AAP and CHA said.
“The data are limited because the states differ in how they report the data, and it is unknown how many children have been infected but not tested. It is unclear how much of the increase in child cases is due to increased testing capacity,” the AAP said in an earlier statement.
After increasing for several weeks, the proportion of new COVID-19 cases occurring in children has dropped for the second week in a row, according to data in a new report from the American Academy of Pediatrics and the Children’s Hospital Association.
COVID-19 cases in children accounted for 12.3% of all new cases in the United States for the week ending Oct. 1, down from 15.2% the previous week. That measure had reached its highest point, 16.9%, just one week earlier (Sept. 17), the AAP and the CHA said in their weekly COVID-19 report.
based on data from the health departments of 49 states (New York does not provide ages on its website), as well as the District of Columbia, New York City, Puerto Rico, and Guam.
The child COVID-19 rate for the United States was 874 per 100,000 children as of Oct. 1, and that figure has doubled since the end of July. At the state level, the highest rates can be found in Tennessee (2,031.4 per 100,000), North Dakota (2,029.6), and South Carolina (2,002.6), with the lowest rates in Vermont (168.9), Maine (229.1), and New Hampshire (268.3), the AAP/CHA report shows.
The children of Wyoming make up the largest share, 22.4%, of any state’s COVID-19 cases, followed by North Dakota and Tennessee, both at 18.3%. New Jersey is lower than any other state at 3.9%, although New York City is a slightly lower 3.6%, the AAP and CHA said.
“The data are limited because the states differ in how they report the data, and it is unknown how many children have been infected but not tested. It is unclear how much of the increase in child cases is due to increased testing capacity,” the AAP said in an earlier statement.
After increasing for several weeks, the proportion of new COVID-19 cases occurring in children has dropped for the second week in a row, according to data in a new report from the American Academy of Pediatrics and the Children’s Hospital Association.
COVID-19 cases in children accounted for 12.3% of all new cases in the United States for the week ending Oct. 1, down from 15.2% the previous week. That measure had reached its highest point, 16.9%, just one week earlier (Sept. 17), the AAP and the CHA said in their weekly COVID-19 report.
based on data from the health departments of 49 states (New York does not provide ages on its website), as well as the District of Columbia, New York City, Puerto Rico, and Guam.
The child COVID-19 rate for the United States was 874 per 100,000 children as of Oct. 1, and that figure has doubled since the end of July. At the state level, the highest rates can be found in Tennessee (2,031.4 per 100,000), North Dakota (2,029.6), and South Carolina (2,002.6), with the lowest rates in Vermont (168.9), Maine (229.1), and New Hampshire (268.3), the AAP/CHA report shows.
The children of Wyoming make up the largest share, 22.4%, of any state’s COVID-19 cases, followed by North Dakota and Tennessee, both at 18.3%. New Jersey is lower than any other state at 3.9%, although New York City is a slightly lower 3.6%, the AAP and CHA said.
“The data are limited because the states differ in how they report the data, and it is unknown how many children have been infected but not tested. It is unclear how much of the increase in child cases is due to increased testing capacity,” the AAP said in an earlier statement.
How ObGyns can best work with radiologists to optimize screening for patients with dense breasts
If your ObGyn practices are anything like ours, every time there is news coverage of a study regarding mammography or about efforts to pass a breast density inform law, your phone rings with patient calls. In fact, every density inform law enacted in the United States, except for in Illinois, directs patients to their referring provider—generally their ObGyn—to discuss the screening and risk implications of dense breast tissue.
The steady increased awareness of breast density means that we, as ObGyns and other primary care providers (PCPs), have additional responsibilities in managing the breast health of our patients. This includes guiding discussions with patients about what breast density means and whether supplemental screening beyond mammography might be beneficial.
As members of the Medical Advisory Board for DenseBreast-info.org (an online educational resource dedicated to providing breast density information to patients and health care professionals), we are aware of the growing body of evidence demonstrating improved detection of early breast cancer using supplemental screening in dense breasts. However, we know that there is confusion among clinicians about how and when to facilitate tailored screening for women with dense breasts or other breast cancer risk factors. Here we answer 6 questions focusing on how to navigate patient discussions around the topic and the best way to collaborate with radiologists to improve breast care for patients.
Play an active role
1. What role should ObGyns and PCPs play in women’s breast health?
Elizabeth Etkin-Kramer, MD: I am a firm believer that ObGyns and all women’s health providers should be able to assess their patients’ risk of breast cancer and explain the process for managing this risk with their patients. This explanation includes the clinical implications of breast density and when supplemental screening should be employed. It is also important for providers to know when to offer genetic testing and when a patient’s personal or family history indicates supplemental screening with breast magnetic resonance imaging (MRI).
DaCarla M. Albright, MD: I absolutely agree that PCPs, ObGyns, and family practitioners should spend the time to be educated about breast density and supplemental screening options. While the exact role providers play in managing patients’ breast health may vary depending on the practice type or location, the need for knowledge and comfort when talking with patients to help them make informed decisions is critical. Breast health and screening, including the importance of breast density, happen to be a particular interest of mine. I have participated in educational webinars, invited lectures, and breast cancer awareness media events on this topic in the past.
Continue to: Join forces with imaging centers...
Join forces with imaging centers
2. How can ObGyns and radiologists collaborate most effectively to use screening results to personalize breast care for patients?
Dr. Etkin-Kramer: It is important to have a close relationship with the radiologists that read our patients’ mammograms. We need to be able to easily contact the radiologist and quickly get clarification on a patient’s report or discuss next steps. Imaging centers should consider running outreach programs to educate their referring providers on how to risk assess, with this assessment inclusive of breast density. Dinner lectures or grand round meetings are effective to facilitate communication between the radiology community and the ObGyn community. Finally, as we all know, supplemental screening is often subject to copays and deductibles per insurance coverage. If advocacy groups, who are working to eliminate these types of costs, cannot get insurers to waive these payments, we need a less expensive self-pay option.
Dr. Albright: I definitely have and encourage an open line of communication between my practice and breast radiology, as well as our breast surgeons and cancer center to set up consultations as needed. We also invite our radiologists as guests to monthly practice meetings or grand rounds within our department to further improve access and open communication, as this environment is one in which greater provider education on density and adjunctive screening can be achieved.
Know when to refer a high-risk patient
3. Most ObGyns routinely collect family history and perform formal risk assessment. What do you need to know about referring patients to a high-risk program?
Dr. Etkin-Kramer: It is important as ObGyns to be knowledgeable about breast and ovarian cancer risk assessment and genetic testing for cancer susceptibility genes. Our patients expect that of us. I am comfortable doing risk assessment in my office, but I sometimes refer to other specialists in the community if the patient needs additional counseling. For risk assessment, I look at family and personal history, breast density, and other factors that might lead me to believe the patient might carry a hereditary cancer susceptibility gene, including Ashkenazi Jewish ancestry.1 When indicated, I check lifetime as well as short-term (5- to 10-year) risk, usually using Breast Cancer Surveillance Consortium (BCSC) or Tyrer-Cuzick/International Breast Cancer Intervention Study (IBIS) models, as these include breast density.
I discuss risk-reducing medications. The US Preventive Services Task Force recommends these agents if my patient’s 5-year risk of breast cancer is 1.67% or greater, and I strongly recommend chemoprevention when the patient’s 5-year BCSC risk exceeds 3%, provided likely benefits exceed risks.2,3 I discuss adding screening breast MRI if lifetime risk by Tyrer-Cuzick exceeds 20%. (Note that Gail and BCSC models are not recommended to be used to determine risk for purposes of supplemental screening with MRI as they do not consider paternal family history nor age of relatives at diagnosis.)
Dr. Albright: ObGyns should be able to ascertain a pertinent history and identify patients at risk for breast cancer based on their personal history, family history, and breast imaging/biopsy history, if relevant. We also need to improve our discussions of supplemental screening for patients who have heterogeneously dense or extremely dense breast tissue. I sense that some ObGyns may rely heavily on the radiologist to suggest supplemental screening, but patients actually look to ObGyns as their providers to have this knowledge and give them direction.
Since I practice at a large academic medical center, I have the opportunity to refer patients to our Breast Cancer Genetics Program because I may be limited on time for counseling in the office and do not want to miss salient details. With all of the information I have ascertained about the patient, I am able to determine and encourage appropriate screening and assure insurance coverage for adjunctive breast MRI when appropriate.
Continue to: Consider how you order patients’ screening to reduce barriers and cost...
Consider how you order patients’ screening to reduce barriers and cost
4. How would you suggest reducing barriers when referring patients for supplemental screening, such as MRI for high-risk women or ultrasound for those with dense breasts? Would you prefer it if such screening could be performed without additional script/referral? How does insurance coverage factor in?
Dr. Etkin-Kramer: I would love for a screening mammogram with possible ultrasound, on one script, to be the norm. One of the centers that I work with accepts a script written this way. Further, when a patient receives screening at a freestanding facility as opposed to a hospital, the fee for the supplemental screening may be lower because they do not add on a facility fee.
Dr. Albright: We have an order in our electronic health record that allows for screening mammography but adds on diagnostic mammography/bilateral ultrasonography, if indicated by imaging. I am mostly ordering that option now for all of my screening patients; rarely have I had issues with insurance accepting that script. As for when ordering an MRI, I always try to ensure that I have done the patient’s personal risk assessment and included that lifetime breast cancer risk on the order. If the risk is 20% or higher, I typically do not have any insurance coverage issues. If I am ordering MRI as supplemental screening, I typically order the “Fast MRI” protocol that our center offers. This order incurs a $299 out-of-pocket cost for the patient. Any patient with heterogeneously or extremely dense breasts on mammography should have this option, but it requires patient education, discussion with the provider, and an additional cost. I definitely think that insurers need to consider covering supplemental screening, since breast density is reportable in a majority of the US states and will soon be the national standard.
Pearls for guiding patients
5. How do you discuss breast density and the need for supplemental screening with your patients?
Dr. Etkin-Kramer: I strongly feel that my patients need to know when a screening test has limited ability to do its job. This is the case with dense breasts. Visuals help; when discussing breast density, I like the images supplied by DenseBreast-info.org (FIGURE). I explain the two implications of dense tissue:
- First, dense tissue makes it harder to visualize cancers in the breast—the denser the breasts, the less likely the radiologist can pick up a cancer, so mammographic sensitivity for extremely dense breasts can be as low as 25% to 50%.
- Second, high breast density adds to the risk of developing breast cancer. I explain that supplemental screening will pick up additional cancers in women with dense breasts. For example, breast ultrasound will pick up about 2-3/1000 additional breast cancers per year and MRI or molecular breast imaging (MBI) will pick up much more, perhaps 10/1000.
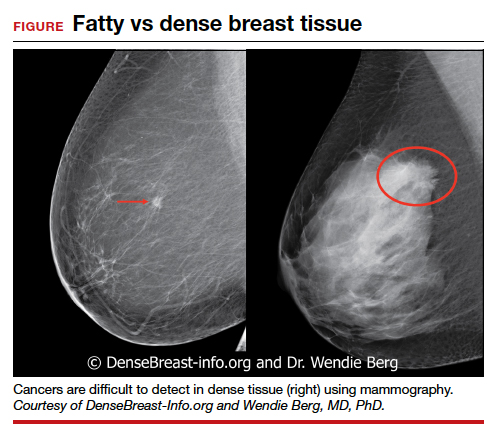
MRI is more invasive than an ultrasound and uses gadolinium, and MBI has more radiation. Supplemental screening is not endorsed by ACOG’s most recent Committee Opinion from 2017; 4 however, patients may choose to have it done. This is where shared-decision making is important.
I strongly recommend that all women’s health care providers complete the CME course on the DenseBreast-info.org website. “ Breast Density: Why It Matters ” is a certified educational program for referring physicians that helps health care professionals learn about breast density, its associated risks, and how best to guide patients regarding breast cancer screening.
Continue to: Dr. Albright...
Dr. Albright: When I discuss breast density, I make sure that patients understand that their mammogram determines the density of their breast tissue. I review that in the higher density categories (heterogeneously dense or extremely dense), there is a higher risk of missing cancer, and that these categories are also associated with a higher risk of breast cancer. I also discuss the potential need for supplemental screening, for which my institution primarily offers Fast MRI. However, we can offer breast ultrasonography instead as an option, especially for those concerned about gadolinium exposure. Our center offers either of these supplemental screenings at a cost of $299. I also review the lack of coverage for supplemental screening by some insurance carriers, as both providers and patients may need to advocate for insurer coverage of adjunct studies.
Educational resources
6. What reference materials, illustrations, or other tools do you use to educate your patients?
Dr. Etkin-Kramer: I frequently use handouts printed from the DenseBreast-info.org website, and there is now a brand new patient fact sheet that I have just started using. I also have an example of breast density categories from fatty replaced to extremely dense on my computer, and I am putting it on a new smart board.
Dr. Albright: The extensive resources available at DenseBreast-info.org can improve both patient and provider knowledge of these important issues, so I suggest patients visit that website, and I use many of the images and visuals to help explain breast density. I even use the materials from the website for educating my resident trainees on breast health and screening. ●
Nearly 16,000 children (up to age 19 years) face cancer-related treatment every year.1 For girls and young women, undergoing chest radiotherapy puts them at higher risk for secondary breast cancer. In fact, they have a 30% chance of developing such cancer by age 50—a risk that is similar to women with a BRCA1 mutation.2 Therefore, current recommendations for breast cancer screening among those who have undergone childhood chest radiation (≥20 Gy) are to begin annual mammography, with adjunct magnetic resonance imaging (MRI), at age 25 years (or 8 years after chest radiotherapy).3
To determine the benefits and risks of these recommendations, as well as of similar strategies, Yeh and colleagues performed simulation modeling using data from the Childhood Cancer Survivor Study and two CISNET (Cancer Intervention and Surveillance Modeling Network) models.4 For their study they targeted a cohort of female childhood cancer survivors having undergone chest radiotherapy and evaluated breast cancer screening with the following strategies:
- mammography plus MRI, starting at ages 25, 30, or 35 years and continuing to age 74
- MRI alone, starting at ages 25, 30, or 35 years and continuing to age 74.
They found that both strategies reduced the risk of breast cancer in the targeted cohort but that screening beginning at the earliest ages prevented most deaths. No screening at all was associated with a 10% to 11% lifetime risk of breast cancer, but mammography plus MRI beginning at age 25 reduced that risk by 56% to 71% depending on the model. Screening with MRI alone reduced mortality risk by 56% to 62%. When considering cost per quality adjusted life-year gained, the researchers found that screening beginning at age 30 to be the most cost-effective.4
Yeh and colleagues addressed concerns with mammography and radiation. Although they said the associated amount of radiation exposure is small, the use of mammography in women younger than age 30 is controversial—and not recommended by the American Cancer Society or the National Comprehensive Cancer Network.5,6
Bottom line. Yeh and colleagues conclude that MRI screening, with or without mammography, beginning between the ages of 25 and 30 should be emphasized in screening guidelines. They note the importance of insurance coverage for MRI in those at risk for breast cancer due to childhood radiation exposure.4
References
- National Cancer Institute. How common is cancer in children? https://www.cancer.gov/types/childhood-cancers/child-adolescentcancers-fact-sheet#how-common-is-cancer-in-children. Accessed September 25, 2020.
- Moskowitz CS, Chou JF, Wolden SL, et al. Breast cancer after chest radiation therapy for childhood cancer. J Clin Oncol. 2014;32:2217- 2223.
- Children’s Oncology Group. Long-term follow-up guidelines for survivors of childhood, adolescent, and young adult cancers. http:// www.survivorshipguidelines.org/pdf/2018/COG_LTFU_Guidelines_v5.pdf. Accessed September 25, 2020.
- Yeh JM, Lowry KP, Schechter CB, et al. Clinical benefits, harms, and cost-effectiveness of breast cancer screening for survivors of childhood cancer treated with chest radiation. Ann Intern Med. 2020;173:331-341.
- Saslow D, Boetes C, Burke W, et al; American Cancer Society Breast Cancer Advisory Group. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007;57:75-89.
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Breast cancer screening and diagnosis version 1.2019. https://www.nccn.org/professionals/physician_gls/default.aspx. Accessed September 25, 2020.
- Bharucha PP, Chiu KE, Francois FM, et al. Genetic testing and screening recommendations for patients with hereditary breast cancer. RadioGraphics. 2020;40:913-936.
- Freedman AN, Yu B, Gail MH, et al. Benefit/risk assessment for breast cancer chemoprevention with raloxifene or tamoxifen for women age 50 years or older. J Clin Oncol. 2011;29:2327-2333.
- Pruthi S, Heisey RE, Bevers TB. Chemoprevention for breast cancer. Ann Surg Oncol. 2015;22:3230-3235.
- American College of Obstetricians and Gynecologists. Committee opinion no. 625: management of women with dense breasts diagnosed by mammography [published correction appears in Obstet Gynecol. 2016;127:166]. Obstet Gynecol. 2015;125(3):750-751.
If your ObGyn practices are anything like ours, every time there is news coverage of a study regarding mammography or about efforts to pass a breast density inform law, your phone rings with patient calls. In fact, every density inform law enacted in the United States, except for in Illinois, directs patients to their referring provider—generally their ObGyn—to discuss the screening and risk implications of dense breast tissue.
The steady increased awareness of breast density means that we, as ObGyns and other primary care providers (PCPs), have additional responsibilities in managing the breast health of our patients. This includes guiding discussions with patients about what breast density means and whether supplemental screening beyond mammography might be beneficial.
As members of the Medical Advisory Board for DenseBreast-info.org (an online educational resource dedicated to providing breast density information to patients and health care professionals), we are aware of the growing body of evidence demonstrating improved detection of early breast cancer using supplemental screening in dense breasts. However, we know that there is confusion among clinicians about how and when to facilitate tailored screening for women with dense breasts or other breast cancer risk factors. Here we answer 6 questions focusing on how to navigate patient discussions around the topic and the best way to collaborate with radiologists to improve breast care for patients.
Play an active role
1. What role should ObGyns and PCPs play in women’s breast health?
Elizabeth Etkin-Kramer, MD: I am a firm believer that ObGyns and all women’s health providers should be able to assess their patients’ risk of breast cancer and explain the process for managing this risk with their patients. This explanation includes the clinical implications of breast density and when supplemental screening should be employed. It is also important for providers to know when to offer genetic testing and when a patient’s personal or family history indicates supplemental screening with breast magnetic resonance imaging (MRI).
DaCarla M. Albright, MD: I absolutely agree that PCPs, ObGyns, and family practitioners should spend the time to be educated about breast density and supplemental screening options. While the exact role providers play in managing patients’ breast health may vary depending on the practice type or location, the need for knowledge and comfort when talking with patients to help them make informed decisions is critical. Breast health and screening, including the importance of breast density, happen to be a particular interest of mine. I have participated in educational webinars, invited lectures, and breast cancer awareness media events on this topic in the past.
Continue to: Join forces with imaging centers...
Join forces with imaging centers
2. How can ObGyns and radiologists collaborate most effectively to use screening results to personalize breast care for patients?
Dr. Etkin-Kramer: It is important to have a close relationship with the radiologists that read our patients’ mammograms. We need to be able to easily contact the radiologist and quickly get clarification on a patient’s report or discuss next steps. Imaging centers should consider running outreach programs to educate their referring providers on how to risk assess, with this assessment inclusive of breast density. Dinner lectures or grand round meetings are effective to facilitate communication between the radiology community and the ObGyn community. Finally, as we all know, supplemental screening is often subject to copays and deductibles per insurance coverage. If advocacy groups, who are working to eliminate these types of costs, cannot get insurers to waive these payments, we need a less expensive self-pay option.
Dr. Albright: I definitely have and encourage an open line of communication between my practice and breast radiology, as well as our breast surgeons and cancer center to set up consultations as needed. We also invite our radiologists as guests to monthly practice meetings or grand rounds within our department to further improve access and open communication, as this environment is one in which greater provider education on density and adjunctive screening can be achieved.
Know when to refer a high-risk patient
3. Most ObGyns routinely collect family history and perform formal risk assessment. What do you need to know about referring patients to a high-risk program?
Dr. Etkin-Kramer: It is important as ObGyns to be knowledgeable about breast and ovarian cancer risk assessment and genetic testing for cancer susceptibility genes. Our patients expect that of us. I am comfortable doing risk assessment in my office, but I sometimes refer to other specialists in the community if the patient needs additional counseling. For risk assessment, I look at family and personal history, breast density, and other factors that might lead me to believe the patient might carry a hereditary cancer susceptibility gene, including Ashkenazi Jewish ancestry.1 When indicated, I check lifetime as well as short-term (5- to 10-year) risk, usually using Breast Cancer Surveillance Consortium (BCSC) or Tyrer-Cuzick/International Breast Cancer Intervention Study (IBIS) models, as these include breast density.
I discuss risk-reducing medications. The US Preventive Services Task Force recommends these agents if my patient’s 5-year risk of breast cancer is 1.67% or greater, and I strongly recommend chemoprevention when the patient’s 5-year BCSC risk exceeds 3%, provided likely benefits exceed risks.2,3 I discuss adding screening breast MRI if lifetime risk by Tyrer-Cuzick exceeds 20%. (Note that Gail and BCSC models are not recommended to be used to determine risk for purposes of supplemental screening with MRI as they do not consider paternal family history nor age of relatives at diagnosis.)
Dr. Albright: ObGyns should be able to ascertain a pertinent history and identify patients at risk for breast cancer based on their personal history, family history, and breast imaging/biopsy history, if relevant. We also need to improve our discussions of supplemental screening for patients who have heterogeneously dense or extremely dense breast tissue. I sense that some ObGyns may rely heavily on the radiologist to suggest supplemental screening, but patients actually look to ObGyns as their providers to have this knowledge and give them direction.
Since I practice at a large academic medical center, I have the opportunity to refer patients to our Breast Cancer Genetics Program because I may be limited on time for counseling in the office and do not want to miss salient details. With all of the information I have ascertained about the patient, I am able to determine and encourage appropriate screening and assure insurance coverage for adjunctive breast MRI when appropriate.
Continue to: Consider how you order patients’ screening to reduce barriers and cost...
Consider how you order patients’ screening to reduce barriers and cost
4. How would you suggest reducing barriers when referring patients for supplemental screening, such as MRI for high-risk women or ultrasound for those with dense breasts? Would you prefer it if such screening could be performed without additional script/referral? How does insurance coverage factor in?
Dr. Etkin-Kramer: I would love for a screening mammogram with possible ultrasound, on one script, to be the norm. One of the centers that I work with accepts a script written this way. Further, when a patient receives screening at a freestanding facility as opposed to a hospital, the fee for the supplemental screening may be lower because they do not add on a facility fee.
Dr. Albright: We have an order in our electronic health record that allows for screening mammography but adds on diagnostic mammography/bilateral ultrasonography, if indicated by imaging. I am mostly ordering that option now for all of my screening patients; rarely have I had issues with insurance accepting that script. As for when ordering an MRI, I always try to ensure that I have done the patient’s personal risk assessment and included that lifetime breast cancer risk on the order. If the risk is 20% or higher, I typically do not have any insurance coverage issues. If I am ordering MRI as supplemental screening, I typically order the “Fast MRI” protocol that our center offers. This order incurs a $299 out-of-pocket cost for the patient. Any patient with heterogeneously or extremely dense breasts on mammography should have this option, but it requires patient education, discussion with the provider, and an additional cost. I definitely think that insurers need to consider covering supplemental screening, since breast density is reportable in a majority of the US states and will soon be the national standard.
Pearls for guiding patients
5. How do you discuss breast density and the need for supplemental screening with your patients?
Dr. Etkin-Kramer: I strongly feel that my patients need to know when a screening test has limited ability to do its job. This is the case with dense breasts. Visuals help; when discussing breast density, I like the images supplied by DenseBreast-info.org (FIGURE). I explain the two implications of dense tissue:
- First, dense tissue makes it harder to visualize cancers in the breast—the denser the breasts, the less likely the radiologist can pick up a cancer, so mammographic sensitivity for extremely dense breasts can be as low as 25% to 50%.
- Second, high breast density adds to the risk of developing breast cancer. I explain that supplemental screening will pick up additional cancers in women with dense breasts. For example, breast ultrasound will pick up about 2-3/1000 additional breast cancers per year and MRI or molecular breast imaging (MBI) will pick up much more, perhaps 10/1000.
MRI is more invasive than an ultrasound and uses gadolinium, and MBI has more radiation. Supplemental screening is not endorsed by ACOG’s most recent Committee Opinion from 2017; 4 however, patients may choose to have it done. This is where shared-decision making is important.
I strongly recommend that all women’s health care providers complete the CME course on the DenseBreast-info.org website. “ Breast Density: Why It Matters ” is a certified educational program for referring physicians that helps health care professionals learn about breast density, its associated risks, and how best to guide patients regarding breast cancer screening.
Continue to: Dr. Albright...
Dr. Albright: When I discuss breast density, I make sure that patients understand that their mammogram determines the density of their breast tissue. I review that in the higher density categories (heterogeneously dense or extremely dense), there is a higher risk of missing cancer, and that these categories are also associated with a higher risk of breast cancer. I also discuss the potential need for supplemental screening, for which my institution primarily offers Fast MRI. However, we can offer breast ultrasonography instead as an option, especially for those concerned about gadolinium exposure. Our center offers either of these supplemental screenings at a cost of $299. I also review the lack of coverage for supplemental screening by some insurance carriers, as both providers and patients may need to advocate for insurer coverage of adjunct studies.
Educational resources
6. What reference materials, illustrations, or other tools do you use to educate your patients?
Dr. Etkin-Kramer: I frequently use handouts printed from the DenseBreast-info.org website, and there is now a brand new patient fact sheet that I have just started using. I also have an example of breast density categories from fatty replaced to extremely dense on my computer, and I am putting it on a new smart board.
Dr. Albright: The extensive resources available at DenseBreast-info.org can improve both patient and provider knowledge of these important issues, so I suggest patients visit that website, and I use many of the images and visuals to help explain breast density. I even use the materials from the website for educating my resident trainees on breast health and screening. ●
Nearly 16,000 children (up to age 19 years) face cancer-related treatment every year.1 For girls and young women, undergoing chest radiotherapy puts them at higher risk for secondary breast cancer. In fact, they have a 30% chance of developing such cancer by age 50—a risk that is similar to women with a BRCA1 mutation.2 Therefore, current recommendations for breast cancer screening among those who have undergone childhood chest radiation (≥20 Gy) are to begin annual mammography, with adjunct magnetic resonance imaging (MRI), at age 25 years (or 8 years after chest radiotherapy).3
To determine the benefits and risks of these recommendations, as well as of similar strategies, Yeh and colleagues performed simulation modeling using data from the Childhood Cancer Survivor Study and two CISNET (Cancer Intervention and Surveillance Modeling Network) models.4 For their study they targeted a cohort of female childhood cancer survivors having undergone chest radiotherapy and evaluated breast cancer screening with the following strategies:
- mammography plus MRI, starting at ages 25, 30, or 35 years and continuing to age 74
- MRI alone, starting at ages 25, 30, or 35 years and continuing to age 74.
They found that both strategies reduced the risk of breast cancer in the targeted cohort but that screening beginning at the earliest ages prevented most deaths. No screening at all was associated with a 10% to 11% lifetime risk of breast cancer, but mammography plus MRI beginning at age 25 reduced that risk by 56% to 71% depending on the model. Screening with MRI alone reduced mortality risk by 56% to 62%. When considering cost per quality adjusted life-year gained, the researchers found that screening beginning at age 30 to be the most cost-effective.4
Yeh and colleagues addressed concerns with mammography and radiation. Although they said the associated amount of radiation exposure is small, the use of mammography in women younger than age 30 is controversial—and not recommended by the American Cancer Society or the National Comprehensive Cancer Network.5,6
Bottom line. Yeh and colleagues conclude that MRI screening, with or without mammography, beginning between the ages of 25 and 30 should be emphasized in screening guidelines. They note the importance of insurance coverage for MRI in those at risk for breast cancer due to childhood radiation exposure.4
References
- National Cancer Institute. How common is cancer in children? https://www.cancer.gov/types/childhood-cancers/child-adolescentcancers-fact-sheet#how-common-is-cancer-in-children. Accessed September 25, 2020.
- Moskowitz CS, Chou JF, Wolden SL, et al. Breast cancer after chest radiation therapy for childhood cancer. J Clin Oncol. 2014;32:2217- 2223.
- Children’s Oncology Group. Long-term follow-up guidelines for survivors of childhood, adolescent, and young adult cancers. http:// www.survivorshipguidelines.org/pdf/2018/COG_LTFU_Guidelines_v5.pdf. Accessed September 25, 2020.
- Yeh JM, Lowry KP, Schechter CB, et al. Clinical benefits, harms, and cost-effectiveness of breast cancer screening for survivors of childhood cancer treated with chest radiation. Ann Intern Med. 2020;173:331-341.
- Saslow D, Boetes C, Burke W, et al; American Cancer Society Breast Cancer Advisory Group. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007;57:75-89.
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Breast cancer screening and diagnosis version 1.2019. https://www.nccn.org/professionals/physician_gls/default.aspx. Accessed September 25, 2020.
If your ObGyn practices are anything like ours, every time there is news coverage of a study regarding mammography or about efforts to pass a breast density inform law, your phone rings with patient calls. In fact, every density inform law enacted in the United States, except for in Illinois, directs patients to their referring provider—generally their ObGyn—to discuss the screening and risk implications of dense breast tissue.
The steady increased awareness of breast density means that we, as ObGyns and other primary care providers (PCPs), have additional responsibilities in managing the breast health of our patients. This includes guiding discussions with patients about what breast density means and whether supplemental screening beyond mammography might be beneficial.
As members of the Medical Advisory Board for DenseBreast-info.org (an online educational resource dedicated to providing breast density information to patients and health care professionals), we are aware of the growing body of evidence demonstrating improved detection of early breast cancer using supplemental screening in dense breasts. However, we know that there is confusion among clinicians about how and when to facilitate tailored screening for women with dense breasts or other breast cancer risk factors. Here we answer 6 questions focusing on how to navigate patient discussions around the topic and the best way to collaborate with radiologists to improve breast care for patients.
Play an active role
1. What role should ObGyns and PCPs play in women’s breast health?
Elizabeth Etkin-Kramer, MD: I am a firm believer that ObGyns and all women’s health providers should be able to assess their patients’ risk of breast cancer and explain the process for managing this risk with their patients. This explanation includes the clinical implications of breast density and when supplemental screening should be employed. It is also important for providers to know when to offer genetic testing and when a patient’s personal or family history indicates supplemental screening with breast magnetic resonance imaging (MRI).
DaCarla M. Albright, MD: I absolutely agree that PCPs, ObGyns, and family practitioners should spend the time to be educated about breast density and supplemental screening options. While the exact role providers play in managing patients’ breast health may vary depending on the practice type or location, the need for knowledge and comfort when talking with patients to help them make informed decisions is critical. Breast health and screening, including the importance of breast density, happen to be a particular interest of mine. I have participated in educational webinars, invited lectures, and breast cancer awareness media events on this topic in the past.
Continue to: Join forces with imaging centers...
Join forces with imaging centers
2. How can ObGyns and radiologists collaborate most effectively to use screening results to personalize breast care for patients?
Dr. Etkin-Kramer: It is important to have a close relationship with the radiologists that read our patients’ mammograms. We need to be able to easily contact the radiologist and quickly get clarification on a patient’s report or discuss next steps. Imaging centers should consider running outreach programs to educate their referring providers on how to risk assess, with this assessment inclusive of breast density. Dinner lectures or grand round meetings are effective to facilitate communication between the radiology community and the ObGyn community. Finally, as we all know, supplemental screening is often subject to copays and deductibles per insurance coverage. If advocacy groups, who are working to eliminate these types of costs, cannot get insurers to waive these payments, we need a less expensive self-pay option.
Dr. Albright: I definitely have and encourage an open line of communication between my practice and breast radiology, as well as our breast surgeons and cancer center to set up consultations as needed. We also invite our radiologists as guests to monthly practice meetings or grand rounds within our department to further improve access and open communication, as this environment is one in which greater provider education on density and adjunctive screening can be achieved.
Know when to refer a high-risk patient
3. Most ObGyns routinely collect family history and perform formal risk assessment. What do you need to know about referring patients to a high-risk program?
Dr. Etkin-Kramer: It is important as ObGyns to be knowledgeable about breast and ovarian cancer risk assessment and genetic testing for cancer susceptibility genes. Our patients expect that of us. I am comfortable doing risk assessment in my office, but I sometimes refer to other specialists in the community if the patient needs additional counseling. For risk assessment, I look at family and personal history, breast density, and other factors that might lead me to believe the patient might carry a hereditary cancer susceptibility gene, including Ashkenazi Jewish ancestry.1 When indicated, I check lifetime as well as short-term (5- to 10-year) risk, usually using Breast Cancer Surveillance Consortium (BCSC) or Tyrer-Cuzick/International Breast Cancer Intervention Study (IBIS) models, as these include breast density.
I discuss risk-reducing medications. The US Preventive Services Task Force recommends these agents if my patient’s 5-year risk of breast cancer is 1.67% or greater, and I strongly recommend chemoprevention when the patient’s 5-year BCSC risk exceeds 3%, provided likely benefits exceed risks.2,3 I discuss adding screening breast MRI if lifetime risk by Tyrer-Cuzick exceeds 20%. (Note that Gail and BCSC models are not recommended to be used to determine risk for purposes of supplemental screening with MRI as they do not consider paternal family history nor age of relatives at diagnosis.)
Dr. Albright: ObGyns should be able to ascertain a pertinent history and identify patients at risk for breast cancer based on their personal history, family history, and breast imaging/biopsy history, if relevant. We also need to improve our discussions of supplemental screening for patients who have heterogeneously dense or extremely dense breast tissue. I sense that some ObGyns may rely heavily on the radiologist to suggest supplemental screening, but patients actually look to ObGyns as their providers to have this knowledge and give them direction.
Since I practice at a large academic medical center, I have the opportunity to refer patients to our Breast Cancer Genetics Program because I may be limited on time for counseling in the office and do not want to miss salient details. With all of the information I have ascertained about the patient, I am able to determine and encourage appropriate screening and assure insurance coverage for adjunctive breast MRI when appropriate.
Continue to: Consider how you order patients’ screening to reduce barriers and cost...
Consider how you order patients’ screening to reduce barriers and cost
4. How would you suggest reducing barriers when referring patients for supplemental screening, such as MRI for high-risk women or ultrasound for those with dense breasts? Would you prefer it if such screening could be performed without additional script/referral? How does insurance coverage factor in?
Dr. Etkin-Kramer: I would love for a screening mammogram with possible ultrasound, on one script, to be the norm. One of the centers that I work with accepts a script written this way. Further, when a patient receives screening at a freestanding facility as opposed to a hospital, the fee for the supplemental screening may be lower because they do not add on a facility fee.
Dr. Albright: We have an order in our electronic health record that allows for screening mammography but adds on diagnostic mammography/bilateral ultrasonography, if indicated by imaging. I am mostly ordering that option now for all of my screening patients; rarely have I had issues with insurance accepting that script. As for when ordering an MRI, I always try to ensure that I have done the patient’s personal risk assessment and included that lifetime breast cancer risk on the order. If the risk is 20% or higher, I typically do not have any insurance coverage issues. If I am ordering MRI as supplemental screening, I typically order the “Fast MRI” protocol that our center offers. This order incurs a $299 out-of-pocket cost for the patient. Any patient with heterogeneously or extremely dense breasts on mammography should have this option, but it requires patient education, discussion with the provider, and an additional cost. I definitely think that insurers need to consider covering supplemental screening, since breast density is reportable in a majority of the US states and will soon be the national standard.
Pearls for guiding patients
5. How do you discuss breast density and the need for supplemental screening with your patients?
Dr. Etkin-Kramer: I strongly feel that my patients need to know when a screening test has limited ability to do its job. This is the case with dense breasts. Visuals help; when discussing breast density, I like the images supplied by DenseBreast-info.org (FIGURE). I explain the two implications of dense tissue:
- First, dense tissue makes it harder to visualize cancers in the breast—the denser the breasts, the less likely the radiologist can pick up a cancer, so mammographic sensitivity for extremely dense breasts can be as low as 25% to 50%.
- Second, high breast density adds to the risk of developing breast cancer. I explain that supplemental screening will pick up additional cancers in women with dense breasts. For example, breast ultrasound will pick up about 2-3/1000 additional breast cancers per year and MRI or molecular breast imaging (MBI) will pick up much more, perhaps 10/1000.
MRI is more invasive than an ultrasound and uses gadolinium, and MBI has more radiation. Supplemental screening is not endorsed by ACOG’s most recent Committee Opinion from 2017; 4 however, patients may choose to have it done. This is where shared-decision making is important.
I strongly recommend that all women’s health care providers complete the CME course on the DenseBreast-info.org website. “ Breast Density: Why It Matters ” is a certified educational program for referring physicians that helps health care professionals learn about breast density, its associated risks, and how best to guide patients regarding breast cancer screening.
Continue to: Dr. Albright...
Dr. Albright: When I discuss breast density, I make sure that patients understand that their mammogram determines the density of their breast tissue. I review that in the higher density categories (heterogeneously dense or extremely dense), there is a higher risk of missing cancer, and that these categories are also associated with a higher risk of breast cancer. I also discuss the potential need for supplemental screening, for which my institution primarily offers Fast MRI. However, we can offer breast ultrasonography instead as an option, especially for those concerned about gadolinium exposure. Our center offers either of these supplemental screenings at a cost of $299. I also review the lack of coverage for supplemental screening by some insurance carriers, as both providers and patients may need to advocate for insurer coverage of adjunct studies.
Educational resources
6. What reference materials, illustrations, or other tools do you use to educate your patients?
Dr. Etkin-Kramer: I frequently use handouts printed from the DenseBreast-info.org website, and there is now a brand new patient fact sheet that I have just started using. I also have an example of breast density categories from fatty replaced to extremely dense on my computer, and I am putting it on a new smart board.
Dr. Albright: The extensive resources available at DenseBreast-info.org can improve both patient and provider knowledge of these important issues, so I suggest patients visit that website, and I use many of the images and visuals to help explain breast density. I even use the materials from the website for educating my resident trainees on breast health and screening. ●
Nearly 16,000 children (up to age 19 years) face cancer-related treatment every year.1 For girls and young women, undergoing chest radiotherapy puts them at higher risk for secondary breast cancer. In fact, they have a 30% chance of developing such cancer by age 50—a risk that is similar to women with a BRCA1 mutation.2 Therefore, current recommendations for breast cancer screening among those who have undergone childhood chest radiation (≥20 Gy) are to begin annual mammography, with adjunct magnetic resonance imaging (MRI), at age 25 years (or 8 years after chest radiotherapy).3
To determine the benefits and risks of these recommendations, as well as of similar strategies, Yeh and colleagues performed simulation modeling using data from the Childhood Cancer Survivor Study and two CISNET (Cancer Intervention and Surveillance Modeling Network) models.4 For their study they targeted a cohort of female childhood cancer survivors having undergone chest radiotherapy and evaluated breast cancer screening with the following strategies:
- mammography plus MRI, starting at ages 25, 30, or 35 years and continuing to age 74
- MRI alone, starting at ages 25, 30, or 35 years and continuing to age 74.
They found that both strategies reduced the risk of breast cancer in the targeted cohort but that screening beginning at the earliest ages prevented most deaths. No screening at all was associated with a 10% to 11% lifetime risk of breast cancer, but mammography plus MRI beginning at age 25 reduced that risk by 56% to 71% depending on the model. Screening with MRI alone reduced mortality risk by 56% to 62%. When considering cost per quality adjusted life-year gained, the researchers found that screening beginning at age 30 to be the most cost-effective.4
Yeh and colleagues addressed concerns with mammography and radiation. Although they said the associated amount of radiation exposure is small, the use of mammography in women younger than age 30 is controversial—and not recommended by the American Cancer Society or the National Comprehensive Cancer Network.5,6
Bottom line. Yeh and colleagues conclude that MRI screening, with or without mammography, beginning between the ages of 25 and 30 should be emphasized in screening guidelines. They note the importance of insurance coverage for MRI in those at risk for breast cancer due to childhood radiation exposure.4
References
- National Cancer Institute. How common is cancer in children? https://www.cancer.gov/types/childhood-cancers/child-adolescentcancers-fact-sheet#how-common-is-cancer-in-children. Accessed September 25, 2020.
- Moskowitz CS, Chou JF, Wolden SL, et al. Breast cancer after chest radiation therapy for childhood cancer. J Clin Oncol. 2014;32:2217- 2223.
- Children’s Oncology Group. Long-term follow-up guidelines for survivors of childhood, adolescent, and young adult cancers. http:// www.survivorshipguidelines.org/pdf/2018/COG_LTFU_Guidelines_v5.pdf. Accessed September 25, 2020.
- Yeh JM, Lowry KP, Schechter CB, et al. Clinical benefits, harms, and cost-effectiveness of breast cancer screening for survivors of childhood cancer treated with chest radiation. Ann Intern Med. 2020;173:331-341.
- Saslow D, Boetes C, Burke W, et al; American Cancer Society Breast Cancer Advisory Group. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007;57:75-89.
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Breast cancer screening and diagnosis version 1.2019. https://www.nccn.org/professionals/physician_gls/default.aspx. Accessed September 25, 2020.
- Bharucha PP, Chiu KE, Francois FM, et al. Genetic testing and screening recommendations for patients with hereditary breast cancer. RadioGraphics. 2020;40:913-936.
- Freedman AN, Yu B, Gail MH, et al. Benefit/risk assessment for breast cancer chemoprevention with raloxifene or tamoxifen for women age 50 years or older. J Clin Oncol. 2011;29:2327-2333.
- Pruthi S, Heisey RE, Bevers TB. Chemoprevention for breast cancer. Ann Surg Oncol. 2015;22:3230-3235.
- American College of Obstetricians and Gynecologists. Committee opinion no. 625: management of women with dense breasts diagnosed by mammography [published correction appears in Obstet Gynecol. 2016;127:166]. Obstet Gynecol. 2015;125(3):750-751.
- Bharucha PP, Chiu KE, Francois FM, et al. Genetic testing and screening recommendations for patients with hereditary breast cancer. RadioGraphics. 2020;40:913-936.
- Freedman AN, Yu B, Gail MH, et al. Benefit/risk assessment for breast cancer chemoprevention with raloxifene or tamoxifen for women age 50 years or older. J Clin Oncol. 2011;29:2327-2333.
- Pruthi S, Heisey RE, Bevers TB. Chemoprevention for breast cancer. Ann Surg Oncol. 2015;22:3230-3235.
- American College of Obstetricians and Gynecologists. Committee opinion no. 625: management of women with dense breasts diagnosed by mammography [published correction appears in Obstet Gynecol. 2016;127:166]. Obstet Gynecol. 2015;125(3):750-751.