User login
ID Practitioner is an independent news source that provides infectious disease specialists with timely and relevant news and commentary about clinical developments and the impact of health care policy on the infectious disease specialist’s practice. Specialty focus topics include antimicrobial resistance, emerging infections, global ID, hepatitis, HIV, hospital-acquired infections, immunizations and vaccines, influenza, mycoses, pediatric infections, and STIs. Infectious Diseases News is owned by Frontline Medical Communications.
sofosbuvir
ritonavir with dasabuvir
discount
support path
program
ritonavir
greedy
ledipasvir
assistance
viekira pak
vpak
advocacy
needy
protest
abbvie
paritaprevir
ombitasvir
direct-acting antivirals
dasabuvir
gilead
fake-ovir
support
v pak
oasis
harvoni
section[contains(@class, 'footer-nav-section-wrapper')]
div[contains(@class, 'pane-pub-article-idp')]
div[contains(@class, 'pane-medstat-latest-articles-articles-section')]
div[contains(@class, 'pane-pub-home-idp')]
div[contains(@class, 'pane-pub-topic-idp')]
Anaplasmosis quadruples in New York state
Anaplasmosis prevalence in New York state nearly quadrupled statewide from 2010 to 2018, new research suggests, increasing by more than eightfold in the region surrounding Albany, the state capital. The proportion of ticks carrying Anaplasma phagocytophilum, the bacterium that causes the tick-borne disease, also increased during the study period.
Although not as well-recognized as Lyme disease, anaplasmosis is one of the most common tickborne diseases in the United States. The bacterial disease is primarily transmitted to humans by the bites of blacklegged ticks infected with A. phagocytophilum, and often causes fever, headache, muscle aches, and chills. If treatment is delayed – or if a patient has underlying medical conditions – anaplasmosis can lead to difficulty breathing, bleeding problems, organ failure, and even death.
Since anaplasmosis become a nationally notifiable disease in 1999, cases have increased 16-fold in the United States, from 351 cases in 2000 to a high of 5,762 cases in 2017, according to data from the Centers for Disease Control and Prevention. Just eight states – Vermont, Maine, Rhode Island, Minnesota, Massachusetts, Wisconsin, New Hampshire, and New York – make up 90% of reported cases.
“While Lyme disease remains the most common tick-borne illness reported in New York state, anaplasmosis continues to account for a growing proportion of our tick-borne disease cases each year,” Melissa Prusinski, a research scientist at the New York State Department of Health and author of the study, told this news organization in an email. “It is critically important to investigate the environmental and epidemiological drivers facilitating this increase to better understand why and how risk for this serious illness is increasing.” The results were published in Emerging Infectious Diseases.
For the study, investigators analyzed human anaplasmosis cases reported to the New York State Department of Health from 2010-2018. They also included data from tick collection and pathogen testing in order to determine whether the prevalence of A. phagocytophilum in ticks increased along with cases. All New York State counties were included in the study, apart from the five boroughs of New York City: Manhattan, Brooklyn, the Bronx, Queens, and Staten Island.
There were 5,146 reported anaplasmosis cases in New York, with annual case numbers peaking at 1,112 in 2017. Researchers reported a dip in cases in 2018, a trend that was also seen nationally. Anaplasmosis incidence surged in the area surrounding Albany, increasing 8.4-fold from 4.3 cases per 100,000 people in 2010 to 36.3 cases per 100,000 persons in 2018.
Ms. Prusinski noted that the rapid increase in and around this inland hot spot is unlike the gradual spread of Lyme disease and other tick-borne illnesses like babesiosis, which spreads from coastal areas both northward and westward across New York. The research team also found that the incidence of ticks infected with A. phagocytophilum nearly doubled statewide and increased fourfold – from 2.9% to 12% – between 2010 and 2018 in the Albany area.
This increase in cases could be the result, at least in part, of more robust testing efforts over time, said Susan Elias, PhD, of the Vector-Borne Disease Laboratory at the Maine Medical Center Research Institute in Scarborough. She was not involved with the recently published study. “The more you look for something, the more you find,” she said. For example, she added, a 602% surge in anaplasmosis cases in Maine from 2013-2017 occurred alongside a 10-fold increase in use of tick-borne disease panels that test for multiple pathogens.
Ms. Prusinski agreed that increased testing at least partially explains the surge of cases in New York, but she did not have data on how many tick-borne disease panels were used to diagnose cases in the state.
Proliferation of A. phagocytophilum in tick populations could also partially explain this dramatic increase in cases. With the suburbanization of America, “we have basically laid out a buffet” for ticks, Dr. Elias said. Patches of forest and yards create edge habitats where ticks, and the small mammals they feed on, thrive. “Then, once you have a large expanding blacklegged tick population, it makes it easier for the pathogens and carriers to amplify,” she added.
While the study did not differentiate between a variant of A. phagocytophilum associated with small mammals that causes illness and another found in white-tailed deer that is nonpathogenic, Ms. Prusinski suspects that the infectious variant is likely more prevalent and is circulating in animals and ticks in and around Albany. Research is ongoing to see if this could help explain the spread of disease in this anaplasmosis hotspot.
“The unique geographic pattern of anaplasmosis spread in New York state and elsewhere leads to many further questions about the vector ecology and epidemiology of this emerging tick-borne illness,” Ms. Prusinski added. “Learning all we can about this dynamic disease system will help us better identify at-risk populations and may lead to novel ways to prevent anaplasmosis.”
Dr. Elias and Ms. Prusinski disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Anaplasmosis prevalence in New York state nearly quadrupled statewide from 2010 to 2018, new research suggests, increasing by more than eightfold in the region surrounding Albany, the state capital. The proportion of ticks carrying Anaplasma phagocytophilum, the bacterium that causes the tick-borne disease, also increased during the study period.
Although not as well-recognized as Lyme disease, anaplasmosis is one of the most common tickborne diseases in the United States. The bacterial disease is primarily transmitted to humans by the bites of blacklegged ticks infected with A. phagocytophilum, and often causes fever, headache, muscle aches, and chills. If treatment is delayed – or if a patient has underlying medical conditions – anaplasmosis can lead to difficulty breathing, bleeding problems, organ failure, and even death.
Since anaplasmosis become a nationally notifiable disease in 1999, cases have increased 16-fold in the United States, from 351 cases in 2000 to a high of 5,762 cases in 2017, according to data from the Centers for Disease Control and Prevention. Just eight states – Vermont, Maine, Rhode Island, Minnesota, Massachusetts, Wisconsin, New Hampshire, and New York – make up 90% of reported cases.
“While Lyme disease remains the most common tick-borne illness reported in New York state, anaplasmosis continues to account for a growing proportion of our tick-borne disease cases each year,” Melissa Prusinski, a research scientist at the New York State Department of Health and author of the study, told this news organization in an email. “It is critically important to investigate the environmental and epidemiological drivers facilitating this increase to better understand why and how risk for this serious illness is increasing.” The results were published in Emerging Infectious Diseases.
For the study, investigators analyzed human anaplasmosis cases reported to the New York State Department of Health from 2010-2018. They also included data from tick collection and pathogen testing in order to determine whether the prevalence of A. phagocytophilum in ticks increased along with cases. All New York State counties were included in the study, apart from the five boroughs of New York City: Manhattan, Brooklyn, the Bronx, Queens, and Staten Island.
There were 5,146 reported anaplasmosis cases in New York, with annual case numbers peaking at 1,112 in 2017. Researchers reported a dip in cases in 2018, a trend that was also seen nationally. Anaplasmosis incidence surged in the area surrounding Albany, increasing 8.4-fold from 4.3 cases per 100,000 people in 2010 to 36.3 cases per 100,000 persons in 2018.
Ms. Prusinski noted that the rapid increase in and around this inland hot spot is unlike the gradual spread of Lyme disease and other tick-borne illnesses like babesiosis, which spreads from coastal areas both northward and westward across New York. The research team also found that the incidence of ticks infected with A. phagocytophilum nearly doubled statewide and increased fourfold – from 2.9% to 12% – between 2010 and 2018 in the Albany area.
This increase in cases could be the result, at least in part, of more robust testing efforts over time, said Susan Elias, PhD, of the Vector-Borne Disease Laboratory at the Maine Medical Center Research Institute in Scarborough. She was not involved with the recently published study. “The more you look for something, the more you find,” she said. For example, she added, a 602% surge in anaplasmosis cases in Maine from 2013-2017 occurred alongside a 10-fold increase in use of tick-borne disease panels that test for multiple pathogens.
Ms. Prusinski agreed that increased testing at least partially explains the surge of cases in New York, but she did not have data on how many tick-borne disease panels were used to diagnose cases in the state.
Proliferation of A. phagocytophilum in tick populations could also partially explain this dramatic increase in cases. With the suburbanization of America, “we have basically laid out a buffet” for ticks, Dr. Elias said. Patches of forest and yards create edge habitats where ticks, and the small mammals they feed on, thrive. “Then, once you have a large expanding blacklegged tick population, it makes it easier for the pathogens and carriers to amplify,” she added.
While the study did not differentiate between a variant of A. phagocytophilum associated with small mammals that causes illness and another found in white-tailed deer that is nonpathogenic, Ms. Prusinski suspects that the infectious variant is likely more prevalent and is circulating in animals and ticks in and around Albany. Research is ongoing to see if this could help explain the spread of disease in this anaplasmosis hotspot.
“The unique geographic pattern of anaplasmosis spread in New York state and elsewhere leads to many further questions about the vector ecology and epidemiology of this emerging tick-borne illness,” Ms. Prusinski added. “Learning all we can about this dynamic disease system will help us better identify at-risk populations and may lead to novel ways to prevent anaplasmosis.”
Dr. Elias and Ms. Prusinski disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Anaplasmosis prevalence in New York state nearly quadrupled statewide from 2010 to 2018, new research suggests, increasing by more than eightfold in the region surrounding Albany, the state capital. The proportion of ticks carrying Anaplasma phagocytophilum, the bacterium that causes the tick-borne disease, also increased during the study period.
Although not as well-recognized as Lyme disease, anaplasmosis is one of the most common tickborne diseases in the United States. The bacterial disease is primarily transmitted to humans by the bites of blacklegged ticks infected with A. phagocytophilum, and often causes fever, headache, muscle aches, and chills. If treatment is delayed – or if a patient has underlying medical conditions – anaplasmosis can lead to difficulty breathing, bleeding problems, organ failure, and even death.
Since anaplasmosis become a nationally notifiable disease in 1999, cases have increased 16-fold in the United States, from 351 cases in 2000 to a high of 5,762 cases in 2017, according to data from the Centers for Disease Control and Prevention. Just eight states – Vermont, Maine, Rhode Island, Minnesota, Massachusetts, Wisconsin, New Hampshire, and New York – make up 90% of reported cases.
“While Lyme disease remains the most common tick-borne illness reported in New York state, anaplasmosis continues to account for a growing proportion of our tick-borne disease cases each year,” Melissa Prusinski, a research scientist at the New York State Department of Health and author of the study, told this news organization in an email. “It is critically important to investigate the environmental and epidemiological drivers facilitating this increase to better understand why and how risk for this serious illness is increasing.” The results were published in Emerging Infectious Diseases.
For the study, investigators analyzed human anaplasmosis cases reported to the New York State Department of Health from 2010-2018. They also included data from tick collection and pathogen testing in order to determine whether the prevalence of A. phagocytophilum in ticks increased along with cases. All New York State counties were included in the study, apart from the five boroughs of New York City: Manhattan, Brooklyn, the Bronx, Queens, and Staten Island.
There were 5,146 reported anaplasmosis cases in New York, with annual case numbers peaking at 1,112 in 2017. Researchers reported a dip in cases in 2018, a trend that was also seen nationally. Anaplasmosis incidence surged in the area surrounding Albany, increasing 8.4-fold from 4.3 cases per 100,000 people in 2010 to 36.3 cases per 100,000 persons in 2018.
Ms. Prusinski noted that the rapid increase in and around this inland hot spot is unlike the gradual spread of Lyme disease and other tick-borne illnesses like babesiosis, which spreads from coastal areas both northward and westward across New York. The research team also found that the incidence of ticks infected with A. phagocytophilum nearly doubled statewide and increased fourfold – from 2.9% to 12% – between 2010 and 2018 in the Albany area.
This increase in cases could be the result, at least in part, of more robust testing efforts over time, said Susan Elias, PhD, of the Vector-Borne Disease Laboratory at the Maine Medical Center Research Institute in Scarborough. She was not involved with the recently published study. “The more you look for something, the more you find,” she said. For example, she added, a 602% surge in anaplasmosis cases in Maine from 2013-2017 occurred alongside a 10-fold increase in use of tick-borne disease panels that test for multiple pathogens.
Ms. Prusinski agreed that increased testing at least partially explains the surge of cases in New York, but she did not have data on how many tick-borne disease panels were used to diagnose cases in the state.
Proliferation of A. phagocytophilum in tick populations could also partially explain this dramatic increase in cases. With the suburbanization of America, “we have basically laid out a buffet” for ticks, Dr. Elias said. Patches of forest and yards create edge habitats where ticks, and the small mammals they feed on, thrive. “Then, once you have a large expanding blacklegged tick population, it makes it easier for the pathogens and carriers to amplify,” she added.
While the study did not differentiate between a variant of A. phagocytophilum associated with small mammals that causes illness and another found in white-tailed deer that is nonpathogenic, Ms. Prusinski suspects that the infectious variant is likely more prevalent and is circulating in animals and ticks in and around Albany. Research is ongoing to see if this could help explain the spread of disease in this anaplasmosis hotspot.
“The unique geographic pattern of anaplasmosis spread in New York state and elsewhere leads to many further questions about the vector ecology and epidemiology of this emerging tick-borne illness,” Ms. Prusinski added. “Learning all we can about this dynamic disease system will help us better identify at-risk populations and may lead to novel ways to prevent anaplasmosis.”
Dr. Elias and Ms. Prusinski disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Surge of new child COVID cases continues for 6th consecutive week
The current COVID-19 surge has brought new cases in children to their highest level since February, according to a new report.
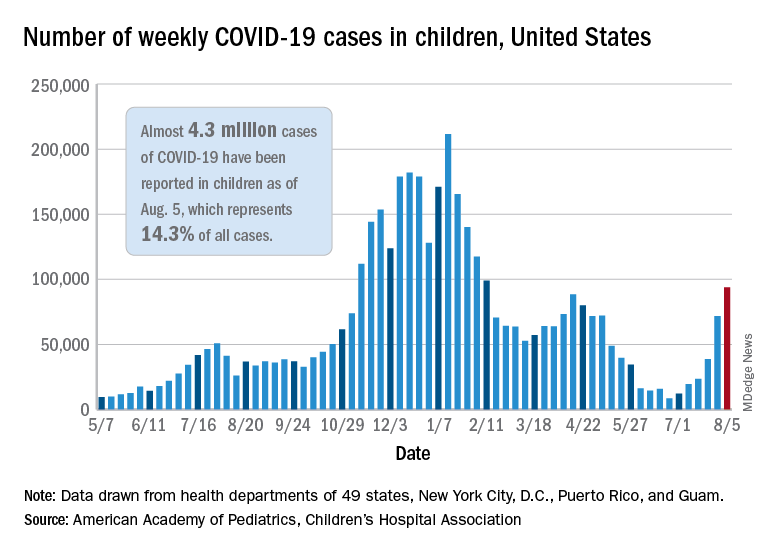
New pediatric cases rose for the 6th straight week, with almost 94,000 reported for the week ending Aug. 5.
That weekly total was up by 31% over the previous week and by over 1,000% since late June, when the new-case figure was at its lowest point (8,447) since early in the pandemic, the American Academy of Pediatrics and the Children’s Hospital Association said. COVID-related deaths – 13 for the week – were also higher than at any time since March 2021.
Almost 4.3 million children have been infected with SARS-CoV-2, which is 14.3% of all cases reported in 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam. Children represented 15.0% of the new cases reported in those jurisdictions during the week ending Aug. 5, the AAP and CHA said in their weekly report.
Another measure that has been trending upward recently is vaccine initiation among 12- to 15-year-olds, although the latest weekly total is still well below the high of 1.4 million seen in May. First-time vaccinations reached almost 411,000 for the week of Aug. 3-9, marking the fourth consecutive increase in that age group, the Centers for Disease Control and Prevention said on its COVID Data Tracker. Vaccinations also increased, although more modestly, for 16- and 17-year-olds in the most recent week.
Cumulative figures for children aged 12-17 show that almost 10.4 million have received at least one dose and that 7.7 million are fully vaccinated as of Aug. 9. By age group, 42.2% of those aged 12-15 have received at least one dose, and 30.4% have completed the vaccine regimen. Among those aged 16-17 years, 52.2% have gotten their first dose, and 41.4% are fully vaccinated, according to the COVID Data Tracker.
Looking at vaccination rates on the state level shows that only 20% of children aged 12-17 in Wyoming and 21% in Mississippi have gotten at least one dose as of Aug. 4, while Massachusetts is up to 68% and Vermont reports 70%. Rates for full vaccination range from 11% in Mississippi and Alabama to 61% in Vermont, based on an AAP analysis of CDC data, which is not available for Idaho.
The current COVID-19 surge has brought new cases in children to their highest level since February, according to a new report.
New pediatric cases rose for the 6th straight week, with almost 94,000 reported for the week ending Aug. 5.
That weekly total was up by 31% over the previous week and by over 1,000% since late June, when the new-case figure was at its lowest point (8,447) since early in the pandemic, the American Academy of Pediatrics and the Children’s Hospital Association said. COVID-related deaths – 13 for the week – were also higher than at any time since March 2021.
Almost 4.3 million children have been infected with SARS-CoV-2, which is 14.3% of all cases reported in 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam. Children represented 15.0% of the new cases reported in those jurisdictions during the week ending Aug. 5, the AAP and CHA said in their weekly report.
Another measure that has been trending upward recently is vaccine initiation among 12- to 15-year-olds, although the latest weekly total is still well below the high of 1.4 million seen in May. First-time vaccinations reached almost 411,000 for the week of Aug. 3-9, marking the fourth consecutive increase in that age group, the Centers for Disease Control and Prevention said on its COVID Data Tracker. Vaccinations also increased, although more modestly, for 16- and 17-year-olds in the most recent week.
Cumulative figures for children aged 12-17 show that almost 10.4 million have received at least one dose and that 7.7 million are fully vaccinated as of Aug. 9. By age group, 42.2% of those aged 12-15 have received at least one dose, and 30.4% have completed the vaccine regimen. Among those aged 16-17 years, 52.2% have gotten their first dose, and 41.4% are fully vaccinated, according to the COVID Data Tracker.
Looking at vaccination rates on the state level shows that only 20% of children aged 12-17 in Wyoming and 21% in Mississippi have gotten at least one dose as of Aug. 4, while Massachusetts is up to 68% and Vermont reports 70%. Rates for full vaccination range from 11% in Mississippi and Alabama to 61% in Vermont, based on an AAP analysis of CDC data, which is not available for Idaho.
The current COVID-19 surge has brought new cases in children to their highest level since February, according to a new report.
New pediatric cases rose for the 6th straight week, with almost 94,000 reported for the week ending Aug. 5.
That weekly total was up by 31% over the previous week and by over 1,000% since late June, when the new-case figure was at its lowest point (8,447) since early in the pandemic, the American Academy of Pediatrics and the Children’s Hospital Association said. COVID-related deaths – 13 for the week – were also higher than at any time since March 2021.
Almost 4.3 million children have been infected with SARS-CoV-2, which is 14.3% of all cases reported in 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam. Children represented 15.0% of the new cases reported in those jurisdictions during the week ending Aug. 5, the AAP and CHA said in their weekly report.
Another measure that has been trending upward recently is vaccine initiation among 12- to 15-year-olds, although the latest weekly total is still well below the high of 1.4 million seen in May. First-time vaccinations reached almost 411,000 for the week of Aug. 3-9, marking the fourth consecutive increase in that age group, the Centers for Disease Control and Prevention said on its COVID Data Tracker. Vaccinations also increased, although more modestly, for 16- and 17-year-olds in the most recent week.
Cumulative figures for children aged 12-17 show that almost 10.4 million have received at least one dose and that 7.7 million are fully vaccinated as of Aug. 9. By age group, 42.2% of those aged 12-15 have received at least one dose, and 30.4% have completed the vaccine regimen. Among those aged 16-17 years, 52.2% have gotten their first dose, and 41.4% are fully vaccinated, according to the COVID Data Tracker.
Looking at vaccination rates on the state level shows that only 20% of children aged 12-17 in Wyoming and 21% in Mississippi have gotten at least one dose as of Aug. 4, while Massachusetts is up to 68% and Vermont reports 70%. Rates for full vaccination range from 11% in Mississippi and Alabama to 61% in Vermont, based on an AAP analysis of CDC data, which is not available for Idaho.
Achieving a ‘new sexual-health paradigm’ means expanding STI care
A vital aspect of expanding access and care for sexually transmitted infections (STIs) in the United States is broadening responsibility for this care across the health care system and other community resources, according to an article published online July 6 in Clinical Infectious Diseases. This expansion and decentralization of care are central to adopting the “new sexual health paradigm” recommended by a National Academies report that was published in March.
“STIs represent a sizable, longstanding, and growing public health challenge,” write Vincent Guilamo-Ramos, PhD, MPH, dean and professor at the Duke University School of Nursing and director of the Center for Latino Adolescent and Family Health (CLAFH) at Duke University, both in Durham, N.C., and his colleagues. Yet the limitations on the current STI workforce and limited federal funding and support for STI prevention and care mean it will take clinicians of all types from across the health care spectrum to meet the challenge, they explain.
“For too long, STI prevention and treatment has been perceived as the sole responsibility of a narrow workforce of specialized STI and HIV service providers,” Dr. Guilamo-Ramos and his coauthor, Marco Thimm-Kaiser, MPH, associate in research at Duke University and epidemiologist at CLAFH, wrote in an email.
“However, the resources allocated to this STI specialty workforce have diminished over time, along with decreasing investments in the broader U.S. public health infrastructure,” they continued. “At the same time – and in part due to this underinvestment – STI rates have soared, reaching a record high for the sixth year in a row in 2019.”
Those factors led to the National Academies report, which recommends moving “away from the traditional, disease-focused perspective on STIs in favor of a holistic perspective of sexual health as an integral component of overall health and well-being,” Dr. Guilamo-Ramos and Mr. Thimm-Kaiser wrote to this news organization.
In their article, the authors review the limitations in the STI workforce, the implications of those limitations for the broader health care industry, and what it will take for STI and HIV specialists as well as regulators to ensure it’s possible to achieve the paradigm shift recommended by the National Academies.
Currently, the biggest limitation is access to care, said Laura Mercer, MD, MBA, of the department of obstetrics and gynecology and the ob.gyn. clerkship director at the University of Arizona, Phoenix. Dr. Mercer, who was not involved with the National Academies report or the analysis of it, said in an interview that it’s essential to emphasize “sexual health as a core element of routine primary and preventative care” to ensure it becomes more accessible to patients without the need to seek out specialty care.
Dr. Guilamo-Ramos and his colleagues drive home the importance of such a shift by noting that more than 200 million Americans live in counties with no practicing infectious disease physicians. The disparities are greatest in Southern states, which account for 40% of all reported STIs. The workforce shortage has continued to worsen alongside the deterioration of the clinical infrastructure supporting STI specialty services, the authors write.
Hence the need to expand accountability for care not only to primary-care physicians but also to nurses, pharmacists, physician assistants, nurse practitioners, and behavioral health practitioners. Doing so also requires normalizing sexual health services across health care professions.
“Prevention is a crucial first step” to this, Dr. Mercer said. “This is particularly important as we recall that almost half of new sexually transmitted infections occur in teenagers. Destigmatizing sexual health and sexual health education will also help encourage patients of all ages to request and accept testing.”
Further, with primary care practitioners managing most STI testing and treatment, subspecialists can focus primarily on complex or refractory cases, she added. Ways to help broaden care include developing point-of-care testing for STIs and improving the accuracy of existing testing, she said.
“The goal is to make routine sexual health services accessible in a wide range of settings, such as in primary care, at pharmacies, and in community-based settings, and to draw on a broader workforce for delivery of sexual health services,” Dr. Guilamo-Ramos and Mr. Thimm-Kaiser said in an interview.
Kevin Ault, MD, professor of obstetrics and gynecology and director of clinical and translational research at the University of Kansas Medical Center in Kansas City, said that many medical organizations, such as the American College of Obstetricians and Gynecologists, have long advocated incorporating sexual health into routine preventive care. He also noted that pharmacists have already become proactive in preventing STIs and could continue to do so.
“Vaccines for hepatitis and human papillomavirus are commonly available at pharmacies,” Dr. Ault said. He was not involved in the article by Dr. Guilamo-Ramos and colleagues or the original report. “Pharmacists could also fill a gap by administering injectable medications such as penicillin. States would have to approve changes in policy, but many states have already done this for expedited partner therapy.”
Dr. Guilamo-Ramos and Mr. Thimm-Kaiser noted similar barriers that must be removed to broaden delivery of STI services.
“Unfortunately, too many highly trained health care providers who are well-positioned for the delivery of sexual health services face regulatory or administrative barriers to practice to the full scope of their training,” they wrote. “These barriers can have a particularly negative impact in medically underserved communities, where physician shortages are common and where novel, decentralized health care service delivery models that draw on nonphysician providers may hold the greatest promise.”
As more diverse health care practitioners take on these roles, ID and HIV specialists can provide their expertise in developing training and technical assistance to support generalists, Dr. Guilamo-Ramos and Mr. Thimm-Kaiser wrote. They can also aid in aligning “clinical training curricula, licensing criteria, and practice guidelines with routine delivery of sexual health services.”
Dr. Guilamo-Ramos and his coauthors offer specific recommendations for professional training, licensing, and practice guidelines to help overcome the “insufficient knowledge, inadequate training, and absence of explicit protocols” that currently impede delivery of STI services in general practice settings.
Although the paradigm shift recommended by the National Academies is ambitious, it’s also necessary, and “none of the recommendations are out of reach,” Dr. Guilamo-Ramos and Mr. Thimm-Kaiser said in an interview. They pointed out how the COVID-19 pandemic has highlighted how underresourced the health care workforce and infrastructure are and how great health care disparities are.
“There is momentum toward rebuilding the nation’s health and public health system in a more effective and efficient way,” they said, and many of the STI report’s recommendations “overlap with priorities for the broader health and public health system moving forward.”
Dr. Mercer also believes the recommendations are realistic, “but only the beginning,” she told this news organization. “Comprehensive sexual education to expand knowledge about STI prevention and public health campaigns to help destigmatize sexual health care in general will remain crucial,” she said.
Sexual education, expanded access, and destigmatizing sexual care are particularly important for reaching the populations most in need of care, such as adolescents and young adults, as well as ethnic, racial, sexual, and gender-minority youth.
“It cannot be overstated how important of a priority population adolescents and young adults are,” Dr. Guilamo-Ramos and Mr. Thimm-Kaiser wrote. They noted that those aged 15-24 account for half of all STIs each year but represent only a quarter of the sexually active population. “Targeted efforts for STI prevention and treatment among adolescents and young adults are therefore essential for an overall successful strategy to address STIs and sexual health in the United States.”
The National Academies report was supported by the Centers for Disease Control and Prevention and the National Association of County and City Health Officials. Dr. Mercer, Dr. Ault, and Mr. Thimm-Kaiser have disclosed no relevant financial relationships. Dr. Guilamo-Ramos has received grants and personal fees from ViiV Health care.
A version of this article first appeared on Medscape.com.
A vital aspect of expanding access and care for sexually transmitted infections (STIs) in the United States is broadening responsibility for this care across the health care system and other community resources, according to an article published online July 6 in Clinical Infectious Diseases. This expansion and decentralization of care are central to adopting the “new sexual health paradigm” recommended by a National Academies report that was published in March.
“STIs represent a sizable, longstanding, and growing public health challenge,” write Vincent Guilamo-Ramos, PhD, MPH, dean and professor at the Duke University School of Nursing and director of the Center for Latino Adolescent and Family Health (CLAFH) at Duke University, both in Durham, N.C., and his colleagues. Yet the limitations on the current STI workforce and limited federal funding and support for STI prevention and care mean it will take clinicians of all types from across the health care spectrum to meet the challenge, they explain.
“For too long, STI prevention and treatment has been perceived as the sole responsibility of a narrow workforce of specialized STI and HIV service providers,” Dr. Guilamo-Ramos and his coauthor, Marco Thimm-Kaiser, MPH, associate in research at Duke University and epidemiologist at CLAFH, wrote in an email.
“However, the resources allocated to this STI specialty workforce have diminished over time, along with decreasing investments in the broader U.S. public health infrastructure,” they continued. “At the same time – and in part due to this underinvestment – STI rates have soared, reaching a record high for the sixth year in a row in 2019.”
Those factors led to the National Academies report, which recommends moving “away from the traditional, disease-focused perspective on STIs in favor of a holistic perspective of sexual health as an integral component of overall health and well-being,” Dr. Guilamo-Ramos and Mr. Thimm-Kaiser wrote to this news organization.
In their article, the authors review the limitations in the STI workforce, the implications of those limitations for the broader health care industry, and what it will take for STI and HIV specialists as well as regulators to ensure it’s possible to achieve the paradigm shift recommended by the National Academies.
Currently, the biggest limitation is access to care, said Laura Mercer, MD, MBA, of the department of obstetrics and gynecology and the ob.gyn. clerkship director at the University of Arizona, Phoenix. Dr. Mercer, who was not involved with the National Academies report or the analysis of it, said in an interview that it’s essential to emphasize “sexual health as a core element of routine primary and preventative care” to ensure it becomes more accessible to patients without the need to seek out specialty care.
Dr. Guilamo-Ramos and his colleagues drive home the importance of such a shift by noting that more than 200 million Americans live in counties with no practicing infectious disease physicians. The disparities are greatest in Southern states, which account for 40% of all reported STIs. The workforce shortage has continued to worsen alongside the deterioration of the clinical infrastructure supporting STI specialty services, the authors write.
Hence the need to expand accountability for care not only to primary-care physicians but also to nurses, pharmacists, physician assistants, nurse practitioners, and behavioral health practitioners. Doing so also requires normalizing sexual health services across health care professions.
“Prevention is a crucial first step” to this, Dr. Mercer said. “This is particularly important as we recall that almost half of new sexually transmitted infections occur in teenagers. Destigmatizing sexual health and sexual health education will also help encourage patients of all ages to request and accept testing.”
Further, with primary care practitioners managing most STI testing and treatment, subspecialists can focus primarily on complex or refractory cases, she added. Ways to help broaden care include developing point-of-care testing for STIs and improving the accuracy of existing testing, she said.
“The goal is to make routine sexual health services accessible in a wide range of settings, such as in primary care, at pharmacies, and in community-based settings, and to draw on a broader workforce for delivery of sexual health services,” Dr. Guilamo-Ramos and Mr. Thimm-Kaiser said in an interview.
Kevin Ault, MD, professor of obstetrics and gynecology and director of clinical and translational research at the University of Kansas Medical Center in Kansas City, said that many medical organizations, such as the American College of Obstetricians and Gynecologists, have long advocated incorporating sexual health into routine preventive care. He also noted that pharmacists have already become proactive in preventing STIs and could continue to do so.
“Vaccines for hepatitis and human papillomavirus are commonly available at pharmacies,” Dr. Ault said. He was not involved in the article by Dr. Guilamo-Ramos and colleagues or the original report. “Pharmacists could also fill a gap by administering injectable medications such as penicillin. States would have to approve changes in policy, but many states have already done this for expedited partner therapy.”
Dr. Guilamo-Ramos and Mr. Thimm-Kaiser noted similar barriers that must be removed to broaden delivery of STI services.
“Unfortunately, too many highly trained health care providers who are well-positioned for the delivery of sexual health services face regulatory or administrative barriers to practice to the full scope of their training,” they wrote. “These barriers can have a particularly negative impact in medically underserved communities, where physician shortages are common and where novel, decentralized health care service delivery models that draw on nonphysician providers may hold the greatest promise.”
As more diverse health care practitioners take on these roles, ID and HIV specialists can provide their expertise in developing training and technical assistance to support generalists, Dr. Guilamo-Ramos and Mr. Thimm-Kaiser wrote. They can also aid in aligning “clinical training curricula, licensing criteria, and practice guidelines with routine delivery of sexual health services.”
Dr. Guilamo-Ramos and his coauthors offer specific recommendations for professional training, licensing, and practice guidelines to help overcome the “insufficient knowledge, inadequate training, and absence of explicit protocols” that currently impede delivery of STI services in general practice settings.
Although the paradigm shift recommended by the National Academies is ambitious, it’s also necessary, and “none of the recommendations are out of reach,” Dr. Guilamo-Ramos and Mr. Thimm-Kaiser said in an interview. They pointed out how the COVID-19 pandemic has highlighted how underresourced the health care workforce and infrastructure are and how great health care disparities are.
“There is momentum toward rebuilding the nation’s health and public health system in a more effective and efficient way,” they said, and many of the STI report’s recommendations “overlap with priorities for the broader health and public health system moving forward.”
Dr. Mercer also believes the recommendations are realistic, “but only the beginning,” she told this news organization. “Comprehensive sexual education to expand knowledge about STI prevention and public health campaigns to help destigmatize sexual health care in general will remain crucial,” she said.
Sexual education, expanded access, and destigmatizing sexual care are particularly important for reaching the populations most in need of care, such as adolescents and young adults, as well as ethnic, racial, sexual, and gender-minority youth.
“It cannot be overstated how important of a priority population adolescents and young adults are,” Dr. Guilamo-Ramos and Mr. Thimm-Kaiser wrote. They noted that those aged 15-24 account for half of all STIs each year but represent only a quarter of the sexually active population. “Targeted efforts for STI prevention and treatment among adolescents and young adults are therefore essential for an overall successful strategy to address STIs and sexual health in the United States.”
The National Academies report was supported by the Centers for Disease Control and Prevention and the National Association of County and City Health Officials. Dr. Mercer, Dr. Ault, and Mr. Thimm-Kaiser have disclosed no relevant financial relationships. Dr. Guilamo-Ramos has received grants and personal fees from ViiV Health care.
A version of this article first appeared on Medscape.com.
A vital aspect of expanding access and care for sexually transmitted infections (STIs) in the United States is broadening responsibility for this care across the health care system and other community resources, according to an article published online July 6 in Clinical Infectious Diseases. This expansion and decentralization of care are central to adopting the “new sexual health paradigm” recommended by a National Academies report that was published in March.
“STIs represent a sizable, longstanding, and growing public health challenge,” write Vincent Guilamo-Ramos, PhD, MPH, dean and professor at the Duke University School of Nursing and director of the Center for Latino Adolescent and Family Health (CLAFH) at Duke University, both in Durham, N.C., and his colleagues. Yet the limitations on the current STI workforce and limited federal funding and support for STI prevention and care mean it will take clinicians of all types from across the health care spectrum to meet the challenge, they explain.
“For too long, STI prevention and treatment has been perceived as the sole responsibility of a narrow workforce of specialized STI and HIV service providers,” Dr. Guilamo-Ramos and his coauthor, Marco Thimm-Kaiser, MPH, associate in research at Duke University and epidemiologist at CLAFH, wrote in an email.
“However, the resources allocated to this STI specialty workforce have diminished over time, along with decreasing investments in the broader U.S. public health infrastructure,” they continued. “At the same time – and in part due to this underinvestment – STI rates have soared, reaching a record high for the sixth year in a row in 2019.”
Those factors led to the National Academies report, which recommends moving “away from the traditional, disease-focused perspective on STIs in favor of a holistic perspective of sexual health as an integral component of overall health and well-being,” Dr. Guilamo-Ramos and Mr. Thimm-Kaiser wrote to this news organization.
In their article, the authors review the limitations in the STI workforce, the implications of those limitations for the broader health care industry, and what it will take for STI and HIV specialists as well as regulators to ensure it’s possible to achieve the paradigm shift recommended by the National Academies.
Currently, the biggest limitation is access to care, said Laura Mercer, MD, MBA, of the department of obstetrics and gynecology and the ob.gyn. clerkship director at the University of Arizona, Phoenix. Dr. Mercer, who was not involved with the National Academies report or the analysis of it, said in an interview that it’s essential to emphasize “sexual health as a core element of routine primary and preventative care” to ensure it becomes more accessible to patients without the need to seek out specialty care.
Dr. Guilamo-Ramos and his colleagues drive home the importance of such a shift by noting that more than 200 million Americans live in counties with no practicing infectious disease physicians. The disparities are greatest in Southern states, which account for 40% of all reported STIs. The workforce shortage has continued to worsen alongside the deterioration of the clinical infrastructure supporting STI specialty services, the authors write.
Hence the need to expand accountability for care not only to primary-care physicians but also to nurses, pharmacists, physician assistants, nurse practitioners, and behavioral health practitioners. Doing so also requires normalizing sexual health services across health care professions.
“Prevention is a crucial first step” to this, Dr. Mercer said. “This is particularly important as we recall that almost half of new sexually transmitted infections occur in teenagers. Destigmatizing sexual health and sexual health education will also help encourage patients of all ages to request and accept testing.”
Further, with primary care practitioners managing most STI testing and treatment, subspecialists can focus primarily on complex or refractory cases, she added. Ways to help broaden care include developing point-of-care testing for STIs and improving the accuracy of existing testing, she said.
“The goal is to make routine sexual health services accessible in a wide range of settings, such as in primary care, at pharmacies, and in community-based settings, and to draw on a broader workforce for delivery of sexual health services,” Dr. Guilamo-Ramos and Mr. Thimm-Kaiser said in an interview.
Kevin Ault, MD, professor of obstetrics and gynecology and director of clinical and translational research at the University of Kansas Medical Center in Kansas City, said that many medical organizations, such as the American College of Obstetricians and Gynecologists, have long advocated incorporating sexual health into routine preventive care. He also noted that pharmacists have already become proactive in preventing STIs and could continue to do so.
“Vaccines for hepatitis and human papillomavirus are commonly available at pharmacies,” Dr. Ault said. He was not involved in the article by Dr. Guilamo-Ramos and colleagues or the original report. “Pharmacists could also fill a gap by administering injectable medications such as penicillin. States would have to approve changes in policy, but many states have already done this for expedited partner therapy.”
Dr. Guilamo-Ramos and Mr. Thimm-Kaiser noted similar barriers that must be removed to broaden delivery of STI services.
“Unfortunately, too many highly trained health care providers who are well-positioned for the delivery of sexual health services face regulatory or administrative barriers to practice to the full scope of their training,” they wrote. “These barriers can have a particularly negative impact in medically underserved communities, where physician shortages are common and where novel, decentralized health care service delivery models that draw on nonphysician providers may hold the greatest promise.”
As more diverse health care practitioners take on these roles, ID and HIV specialists can provide their expertise in developing training and technical assistance to support generalists, Dr. Guilamo-Ramos and Mr. Thimm-Kaiser wrote. They can also aid in aligning “clinical training curricula, licensing criteria, and practice guidelines with routine delivery of sexual health services.”
Dr. Guilamo-Ramos and his coauthors offer specific recommendations for professional training, licensing, and practice guidelines to help overcome the “insufficient knowledge, inadequate training, and absence of explicit protocols” that currently impede delivery of STI services in general practice settings.
Although the paradigm shift recommended by the National Academies is ambitious, it’s also necessary, and “none of the recommendations are out of reach,” Dr. Guilamo-Ramos and Mr. Thimm-Kaiser said in an interview. They pointed out how the COVID-19 pandemic has highlighted how underresourced the health care workforce and infrastructure are and how great health care disparities are.
“There is momentum toward rebuilding the nation’s health and public health system in a more effective and efficient way,” they said, and many of the STI report’s recommendations “overlap with priorities for the broader health and public health system moving forward.”
Dr. Mercer also believes the recommendations are realistic, “but only the beginning,” she told this news organization. “Comprehensive sexual education to expand knowledge about STI prevention and public health campaigns to help destigmatize sexual health care in general will remain crucial,” she said.
Sexual education, expanded access, and destigmatizing sexual care are particularly important for reaching the populations most in need of care, such as adolescents and young adults, as well as ethnic, racial, sexual, and gender-minority youth.
“It cannot be overstated how important of a priority population adolescents and young adults are,” Dr. Guilamo-Ramos and Mr. Thimm-Kaiser wrote. They noted that those aged 15-24 account for half of all STIs each year but represent only a quarter of the sexually active population. “Targeted efforts for STI prevention and treatment among adolescents and young adults are therefore essential for an overall successful strategy to address STIs and sexual health in the United States.”
The National Academies report was supported by the Centers for Disease Control and Prevention and the National Association of County and City Health Officials. Dr. Mercer, Dr. Ault, and Mr. Thimm-Kaiser have disclosed no relevant financial relationships. Dr. Guilamo-Ramos has received grants and personal fees from ViiV Health care.
A version of this article first appeared on Medscape.com.
Patients with diabetes more likely to be hospitalized, especially with foot infection
People with diabetes are at increased risk of hospitalization for infection, as well as infection-related mortality, shows a large U.S. study that suggests the risk is even higher in younger and Black individuals.
Michael Fang, PhD, Johns Hopkins University, Baltimore, and colleagues studied more than 12,000 participants in a community cohort study who were followed for an average of 24 years, between 1987-1989 and 2019.
Participants with diabetes faced a 67% increase risk of infection-related hospitalization, compared with those without diabetes.
Of particular note, the risk of hospitalization with foot infection was almost sixfold higher for people with diabetes than those without.
The research, published in Diabetologia on August 4, also suggests that diabetes may be associated with a 72% increased risk of infection-related mortality, although the absolute numbers were small.
Dr. Fang explained to this news organization that they focused on infection-related hospitalization and mortality “because these are comprehensively tracked in administrative data and ... are the most severe types of outcomes.”
However, this is probably just the tip of the iceberg, as people with diabetes are “likely at increased risk for milder infection too,” which can have a “significant adverse impact on people’s well-being and quality of life.”
As a result of their findings, the authors call for “broader guidance on infection prevention and management” in people with diabetes. To achieve this, Dr. Fang said, “we need to better understand why diabetes is associated with an increased risk of infection-related complications.”
“One likely factor is glycemic control: Emerging research suggests patients with diabetes with better glycemic control may be at significantly lower risk of infection-related complications.”
He continued that, in younger patients, a factor for worse outcomes could be that “diabetes tends to be more aggressive when it emerges early in life,” while in Black patients “there is research highlighting Black-White differences in glycemic control, access to care, and beliefs around vaccines.”
Overall, their findings – coupled with recent data showing that diabetes is an important risk factor for adverse outcomes with COVID-19 infection – paint “a common picture,” Dr. Fang said.
“People with diabetes are much more susceptible to infection-related complications, including COVID-related hospitalization and mortality,” which suggests people with diabetes “may need to be especially cautious.”
Adds to existing literature; amputations begin with infections
Robert A. Gabbay, MD, PhD, chief scientific and medical officer for the American Diabetes Association (ADA), said the study “does add to the existing literature by having followed a larger number of people over time and linking them to serious complications from infections.”
“Sadly, we have seen this play out in real-time during the COVID-19 pandemic.”
“One of the sobering bits of data is the significant health disparities that exist in Black Americans and the fact that foot infections remain a significant problem,” he said in an interview.
“Given that amputation rates for [Black Americans] are three times higher than White Americans, amputations begin with infections,” Dr. Gabbay added, noting the ADA “has been taking a strong stand to prevent amputations and address the inequities in health that exist.”
Jamie Hartmann-Boyce, PhD, from the University of Oxford, U.K., who was not involved in the study, commented that diabetes is a “well-known risk factor for worse outcomes from all kinds of infection,” which is why they “are prioritized for flu vaccination every year.”
She told this news organization that the current study “further confirms that people with diabetes are more likely to be hospitalized for infection of any type and most markedly for foot infection.”
“These new data further highlight the need for public health interventions to prevent type 2 diabetes, and for preventive health care in people with diabetes, including access to diabetes medications and support and to vaccinations to prevent infection,” added Dr. Hartmann-Boyce, who is a senior research fellow in health behaviors.
Diabetes is thought to be associated with susceptibility to infection via mechanisms such as impaired neutrophil functioning and humoral immune responses, and studies have shown a link with both common and rare infections.
However, the authors point out that “most” of those included “small clinical populations and were cross-sectional or had short follow-up.”
Guidelines for diabetes management, they note, also “pay less attention” to infectious diseases than they do to the prevention of micro- and macrovascular complications.
ARIC data mined for infections in those with diabetes
The team analyzed data from the ongoing U.S. community-based Atherosclerosis Risk in Communities (ARIC) study.
The National Heart, Lung, and Blood Institute–sponsored cohort was comprised of adults aged 45-64 years from four U.S. communities, recruited between 1987 and 1989 for clinical examinations, medical interviews, and laboratory tests, repeated over five more visits up to 2018-2019.
For the current analysis, the team included 12,739 individuals with a mean age of 54.5 years, of whom 54.3% were female and 24.7% were Black.
Patients were defined as having diabetes if their baseline fasting blood glucose was greater than or equal to 7 mmol/L, or nonfasting glucose was greater than or equal to 11.1 mmol/l, they self-reported a diagnosis of diabetes by a physician, or they were taking glucose-lowering medication at the first study visit. The researchers weren’t able to distinguish between type 1 and type 2 diabetes.
In total, 1,485 individuals had diabetes at baseline. They were more likely to be older, Black, have a low socioeconomic status, and have worse cardiometabolic health than participants without diabetes.
Over an average follow-up of 23.8 years, there were 4,229 incident hospitalizations for infection, at an overall rate of 15.9 per 1,000 person-years.
Individuals with diabetes at baseline had a higher rate of hospitalizations than those without, at 25.4 per 1,000 person-years versus 15.2 per 1,000 person-years.
After taking into account sociodemographic characteristics, socioeconomic status, and cardiometabolic risk factors, this equated to a hazard ratio for hospitalization with any infection of 1.67 (P < .001).
The risk of hospitalization for any infection was significantly higher for younger patients with diabetes, defined as aged less than 55 years (P = .005), and for Black patients (P < .001).
While the increased risk was generally consistent across infection types, it was markedly increased for foot infection, at a hazard ratio of 5.99 (P < .001).
Overall, there were few deaths due to infection in the study, at just 362. The risk of infection mortality was nevertheless significantly increased in people with diabetes, at an adjusted hazard ratio of 1.72 (P < .001).
Dr. Fang has reported being supported by a grant from the National Institutes of Health/National Heart, Lung, and Blood Institute. Dr. Selvin has reported being supported by grants from the National Institutes of Health/National Heart, Lung, and Blood Institute and National Institutes of Health/National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Selvin is an associate editor for Diabetologia and had no role in the peer review of the manuscript.
A version of this article first appeared on Medscape.com.
People with diabetes are at increased risk of hospitalization for infection, as well as infection-related mortality, shows a large U.S. study that suggests the risk is even higher in younger and Black individuals.
Michael Fang, PhD, Johns Hopkins University, Baltimore, and colleagues studied more than 12,000 participants in a community cohort study who were followed for an average of 24 years, between 1987-1989 and 2019.
Participants with diabetes faced a 67% increase risk of infection-related hospitalization, compared with those without diabetes.
Of particular note, the risk of hospitalization with foot infection was almost sixfold higher for people with diabetes than those without.
The research, published in Diabetologia on August 4, also suggests that diabetes may be associated with a 72% increased risk of infection-related mortality, although the absolute numbers were small.
Dr. Fang explained to this news organization that they focused on infection-related hospitalization and mortality “because these are comprehensively tracked in administrative data and ... are the most severe types of outcomes.”
However, this is probably just the tip of the iceberg, as people with diabetes are “likely at increased risk for milder infection too,” which can have a “significant adverse impact on people’s well-being and quality of life.”
As a result of their findings, the authors call for “broader guidance on infection prevention and management” in people with diabetes. To achieve this, Dr. Fang said, “we need to better understand why diabetes is associated with an increased risk of infection-related complications.”
“One likely factor is glycemic control: Emerging research suggests patients with diabetes with better glycemic control may be at significantly lower risk of infection-related complications.”
He continued that, in younger patients, a factor for worse outcomes could be that “diabetes tends to be more aggressive when it emerges early in life,” while in Black patients “there is research highlighting Black-White differences in glycemic control, access to care, and beliefs around vaccines.”
Overall, their findings – coupled with recent data showing that diabetes is an important risk factor for adverse outcomes with COVID-19 infection – paint “a common picture,” Dr. Fang said.
“People with diabetes are much more susceptible to infection-related complications, including COVID-related hospitalization and mortality,” which suggests people with diabetes “may need to be especially cautious.”
Adds to existing literature; amputations begin with infections
Robert A. Gabbay, MD, PhD, chief scientific and medical officer for the American Diabetes Association (ADA), said the study “does add to the existing literature by having followed a larger number of people over time and linking them to serious complications from infections.”
“Sadly, we have seen this play out in real-time during the COVID-19 pandemic.”
“One of the sobering bits of data is the significant health disparities that exist in Black Americans and the fact that foot infections remain a significant problem,” he said in an interview.
“Given that amputation rates for [Black Americans] are three times higher than White Americans, amputations begin with infections,” Dr. Gabbay added, noting the ADA “has been taking a strong stand to prevent amputations and address the inequities in health that exist.”
Jamie Hartmann-Boyce, PhD, from the University of Oxford, U.K., who was not involved in the study, commented that diabetes is a “well-known risk factor for worse outcomes from all kinds of infection,” which is why they “are prioritized for flu vaccination every year.”
She told this news organization that the current study “further confirms that people with diabetes are more likely to be hospitalized for infection of any type and most markedly for foot infection.”
“These new data further highlight the need for public health interventions to prevent type 2 diabetes, and for preventive health care in people with diabetes, including access to diabetes medications and support and to vaccinations to prevent infection,” added Dr. Hartmann-Boyce, who is a senior research fellow in health behaviors.
Diabetes is thought to be associated with susceptibility to infection via mechanisms such as impaired neutrophil functioning and humoral immune responses, and studies have shown a link with both common and rare infections.
However, the authors point out that “most” of those included “small clinical populations and were cross-sectional or had short follow-up.”
Guidelines for diabetes management, they note, also “pay less attention” to infectious diseases than they do to the prevention of micro- and macrovascular complications.
ARIC data mined for infections in those with diabetes
The team analyzed data from the ongoing U.S. community-based Atherosclerosis Risk in Communities (ARIC) study.
The National Heart, Lung, and Blood Institute–sponsored cohort was comprised of adults aged 45-64 years from four U.S. communities, recruited between 1987 and 1989 for clinical examinations, medical interviews, and laboratory tests, repeated over five more visits up to 2018-2019.
For the current analysis, the team included 12,739 individuals with a mean age of 54.5 years, of whom 54.3% were female and 24.7% were Black.
Patients were defined as having diabetes if their baseline fasting blood glucose was greater than or equal to 7 mmol/L, or nonfasting glucose was greater than or equal to 11.1 mmol/l, they self-reported a diagnosis of diabetes by a physician, or they were taking glucose-lowering medication at the first study visit. The researchers weren’t able to distinguish between type 1 and type 2 diabetes.
In total, 1,485 individuals had diabetes at baseline. They were more likely to be older, Black, have a low socioeconomic status, and have worse cardiometabolic health than participants without diabetes.
Over an average follow-up of 23.8 years, there were 4,229 incident hospitalizations for infection, at an overall rate of 15.9 per 1,000 person-years.
Individuals with diabetes at baseline had a higher rate of hospitalizations than those without, at 25.4 per 1,000 person-years versus 15.2 per 1,000 person-years.
After taking into account sociodemographic characteristics, socioeconomic status, and cardiometabolic risk factors, this equated to a hazard ratio for hospitalization with any infection of 1.67 (P < .001).
The risk of hospitalization for any infection was significantly higher for younger patients with diabetes, defined as aged less than 55 years (P = .005), and for Black patients (P < .001).
While the increased risk was generally consistent across infection types, it was markedly increased for foot infection, at a hazard ratio of 5.99 (P < .001).
Overall, there were few deaths due to infection in the study, at just 362. The risk of infection mortality was nevertheless significantly increased in people with diabetes, at an adjusted hazard ratio of 1.72 (P < .001).
Dr. Fang has reported being supported by a grant from the National Institutes of Health/National Heart, Lung, and Blood Institute. Dr. Selvin has reported being supported by grants from the National Institutes of Health/National Heart, Lung, and Blood Institute and National Institutes of Health/National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Selvin is an associate editor for Diabetologia and had no role in the peer review of the manuscript.
A version of this article first appeared on Medscape.com.
People with diabetes are at increased risk of hospitalization for infection, as well as infection-related mortality, shows a large U.S. study that suggests the risk is even higher in younger and Black individuals.
Michael Fang, PhD, Johns Hopkins University, Baltimore, and colleagues studied more than 12,000 participants in a community cohort study who were followed for an average of 24 years, between 1987-1989 and 2019.
Participants with diabetes faced a 67% increase risk of infection-related hospitalization, compared with those without diabetes.
Of particular note, the risk of hospitalization with foot infection was almost sixfold higher for people with diabetes than those without.
The research, published in Diabetologia on August 4, also suggests that diabetes may be associated with a 72% increased risk of infection-related mortality, although the absolute numbers were small.
Dr. Fang explained to this news organization that they focused on infection-related hospitalization and mortality “because these are comprehensively tracked in administrative data and ... are the most severe types of outcomes.”
However, this is probably just the tip of the iceberg, as people with diabetes are “likely at increased risk for milder infection too,” which can have a “significant adverse impact on people’s well-being and quality of life.”
As a result of their findings, the authors call for “broader guidance on infection prevention and management” in people with diabetes. To achieve this, Dr. Fang said, “we need to better understand why diabetes is associated with an increased risk of infection-related complications.”
“One likely factor is glycemic control: Emerging research suggests patients with diabetes with better glycemic control may be at significantly lower risk of infection-related complications.”
He continued that, in younger patients, a factor for worse outcomes could be that “diabetes tends to be more aggressive when it emerges early in life,” while in Black patients “there is research highlighting Black-White differences in glycemic control, access to care, and beliefs around vaccines.”
Overall, their findings – coupled with recent data showing that diabetes is an important risk factor for adverse outcomes with COVID-19 infection – paint “a common picture,” Dr. Fang said.
“People with diabetes are much more susceptible to infection-related complications, including COVID-related hospitalization and mortality,” which suggests people with diabetes “may need to be especially cautious.”
Adds to existing literature; amputations begin with infections
Robert A. Gabbay, MD, PhD, chief scientific and medical officer for the American Diabetes Association (ADA), said the study “does add to the existing literature by having followed a larger number of people over time and linking them to serious complications from infections.”
“Sadly, we have seen this play out in real-time during the COVID-19 pandemic.”
“One of the sobering bits of data is the significant health disparities that exist in Black Americans and the fact that foot infections remain a significant problem,” he said in an interview.
“Given that amputation rates for [Black Americans] are three times higher than White Americans, amputations begin with infections,” Dr. Gabbay added, noting the ADA “has been taking a strong stand to prevent amputations and address the inequities in health that exist.”
Jamie Hartmann-Boyce, PhD, from the University of Oxford, U.K., who was not involved in the study, commented that diabetes is a “well-known risk factor for worse outcomes from all kinds of infection,” which is why they “are prioritized for flu vaccination every year.”
She told this news organization that the current study “further confirms that people with diabetes are more likely to be hospitalized for infection of any type and most markedly for foot infection.”
“These new data further highlight the need for public health interventions to prevent type 2 diabetes, and for preventive health care in people with diabetes, including access to diabetes medications and support and to vaccinations to prevent infection,” added Dr. Hartmann-Boyce, who is a senior research fellow in health behaviors.
Diabetes is thought to be associated with susceptibility to infection via mechanisms such as impaired neutrophil functioning and humoral immune responses, and studies have shown a link with both common and rare infections.
However, the authors point out that “most” of those included “small clinical populations and were cross-sectional or had short follow-up.”
Guidelines for diabetes management, they note, also “pay less attention” to infectious diseases than they do to the prevention of micro- and macrovascular complications.
ARIC data mined for infections in those with diabetes
The team analyzed data from the ongoing U.S. community-based Atherosclerosis Risk in Communities (ARIC) study.
The National Heart, Lung, and Blood Institute–sponsored cohort was comprised of adults aged 45-64 years from four U.S. communities, recruited between 1987 and 1989 for clinical examinations, medical interviews, and laboratory tests, repeated over five more visits up to 2018-2019.
For the current analysis, the team included 12,739 individuals with a mean age of 54.5 years, of whom 54.3% were female and 24.7% were Black.
Patients were defined as having diabetes if their baseline fasting blood glucose was greater than or equal to 7 mmol/L, or nonfasting glucose was greater than or equal to 11.1 mmol/l, they self-reported a diagnosis of diabetes by a physician, or they were taking glucose-lowering medication at the first study visit. The researchers weren’t able to distinguish between type 1 and type 2 diabetes.
In total, 1,485 individuals had diabetes at baseline. They were more likely to be older, Black, have a low socioeconomic status, and have worse cardiometabolic health than participants without diabetes.
Over an average follow-up of 23.8 years, there were 4,229 incident hospitalizations for infection, at an overall rate of 15.9 per 1,000 person-years.
Individuals with diabetes at baseline had a higher rate of hospitalizations than those without, at 25.4 per 1,000 person-years versus 15.2 per 1,000 person-years.
After taking into account sociodemographic characteristics, socioeconomic status, and cardiometabolic risk factors, this equated to a hazard ratio for hospitalization with any infection of 1.67 (P < .001).
The risk of hospitalization for any infection was significantly higher for younger patients with diabetes, defined as aged less than 55 years (P = .005), and for Black patients (P < .001).
While the increased risk was generally consistent across infection types, it was markedly increased for foot infection, at a hazard ratio of 5.99 (P < .001).
Overall, there were few deaths due to infection in the study, at just 362. The risk of infection mortality was nevertheless significantly increased in people with diabetes, at an adjusted hazard ratio of 1.72 (P < .001).
Dr. Fang has reported being supported by a grant from the National Institutes of Health/National Heart, Lung, and Blood Institute. Dr. Selvin has reported being supported by grants from the National Institutes of Health/National Heart, Lung, and Blood Institute and National Institutes of Health/National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Selvin is an associate editor for Diabetologia and had no role in the peer review of the manuscript.
A version of this article first appeared on Medscape.com.
New-AFib risk may not rise with light drinking, may fall with wine
Alcoholic drinks are in the news again, served with a twist. A large cohort study saw a familiar J-shaped curve detailing risk for new atrial fibrillation (AFib) in which the risk rose steadily with greater number of drinks per week, except at the lowest levels of alcohol intake.

There, the curve turned the other way. Light drinkers overall showed no higher AFib risk than nondrinkers, and the risk was lowest at any degree of alcohol intake up to 56 g per week.
On closer analysis of risk patterns, the type of alcoholic beverage mattered.
Alcohol content per drink was defined by standards in the United Kingdom, where the cohort was based.
The risk of AFib also didn’t climb at low intake levels of white wine or with “very low” use of liquor or spirits. But it went up consistently at any level of beer or cider consumption, and to be sure, “high intake of any beverage was associated with greater AF[ib] risk,” notes a report on the study published July 27, 2021, in JACC: Clinical Electrophysiology.
The results, based on more than 400,000 adults in the community, “raise the possibility that, for current consumers, drinking red or white wine could potentially be a safer alternative to other types of alcoholic beverages with respect to AF[ib] risk,” the report proposes.
The J-shaped risk curve for new AFib by degree of alcohol consumption follows the pattern sometimes seen for cardiovascular risk in general. But the intake level at which AFib risk is flat or reduced “is at a far lower dose of alcohol than what we’ve seen for cardiovascular disease,” lead author Samuel J. Tu, BHlthMedSc, said in an interview.
“That being said, even with the threshold sitting quite low, it still tells us that cutting down on alcohol is a good thing and perhaps one of the best things for our heart,” said Mr. Tu, University of Adelaide and Royal Adelaide Hospital, who also presented the findings at the Heart Rhythm Society 2021 Scientific Sessions, held in Boston and virtually.
How much alcohol is in a drink?
In a caution for anyone looking to beer, wine, or liquor to protect against AFib, or at least not cause it, the weekly number of drinks associated with the lowest AFib risk may be fewer than expected. That bottom of 56 g per week works out to one drink a day or less for British and only four or fewer per week for Americans, according to the study’s internationally varying definitions for the alcohol content of one drink.
For example, a drink was considered to have 8 g of alcohol in the United Kingdom, 14 g in the United States and some other countries, and up to 20 g in Austria. Those numbers came from definitions used by the respective national health agencies, such as the National Health Service in the United Kingdom and Centers for Disease Control and Prevention in the United States, Mr. Tu explained.
“They all defined standard drinks slightly differently. But wherever we looked, the threshold we found was far lower than what our governments recommend” based on what is known about alcohol and overall cardiovascular risk, he said.
First to show a hint of protection
The current study “is especially noteworthy because it’s the really the first to demonstrate any hint that there could be a protective effect from any particular amount of alcohol in regard to atrial fibrillation,” Gregory M. Marcus, MD, MAS, University of California, San Francisco, said in an interview. “The J-shaped association fits with what’s been observed with myocardial infarction and overall mortality, and hasn’t previously been seen in the setting of atrial fibrillation.”
Quite interestingly, “it appeared to be the wine drinkers, rather than those who consumed other types of alcohol, that enjoyed this benefit,” said Dr. Marcus, who was not involved in the research but co-authored an accompanying editorial with UCSF colleague Thomas A. Dewland, MD.
“It’s important to recognize the overwhelming evidence that alcohol in general increases the risk for atrial fibrillation,” he said. But “perhaps there’s something in wine that is anti-inflammatory that has some beneficial effect that maybe overwhelms the proarrhythmic aspect.”
The current study “opens the door to the question as to whether there is a small amount of alcohol, perhaps in the form of wine, where there are some benefits that outweigh the risks of atrial fibrillation.”
Still, the findings are observational and “clearly prone to confounding,” Dr. Marcus said. “We need to be very cautious in inferring causality.”
For example, it’s possible that “there is something about individuals that are able to drink alcohol on a regular basis and in small amounts that is the actual causal factor in reducing atrial fibrillation episodes.”
The analysis was based on 403,281 participants in the UK Biobank registry, a prospective cohort study in the United Kingdom, who were aged 40-69 when recruited from 2006 to 2010; it excluded anyone with a history of AFib or who was a former drinker. About 52% were women, the report noted.
Their median alcohol consumption was eight U.K. drinks per week, with 5.5% reporting they had never consumed alcohol. About 21,300 incident cases of AFib or atrial flutter were documented over almost 4.5 million person-years, or a median follow-up of 11.4 years.
The hazard ratio for incident AFib among those with a weekly alcohol consumption corresponding to 1-7 U.K. drinks, compared with intake of less than 1 U.K. drink per week, was 0.95 (95% confidence interval, 0.91-1.00). Within that range of 1-7 drinks, the absolute lowest AFib risk on the J curve was at 5 per week.
No increased risk of new AFib was seen in association with weekly U.K. drink levels of 10 for red wine, 8 for white wine, and 3 for spirits.
Compared with weekly intake of less than 1 U.K. drink per week, red wine intake at 1-7 per week showed an HR for AFib of 0.94 (95% CI, 0.91-0.97). Indeed, at no observed consumption level was red wine associated with a significant increase in AFib risk. White wine until the highest observed level of intake, above 28 U.K. drinks per week, at which point the HR for AFib was 1.48 (98% CI 1.19-1.86). The curve for spirit intake followed a similar but steeper curve, its HR risk reaching 1.61 (95% CI, 1.34-1.93) at intake levels beyond 28 U.K. drinks per week.
Consumption of beer or cider showed a linear association with AFib risk, which was elevated at all recorded intake levels, including 8-14 U.K. drinks per week (HR, 1.11; 95% CI 1.06-1.17) and up to 28 or more per week (HR, 1.35; 95% CI, 1.26-1.45).
The analysis is hypothesis generating at best, Dr. Marcus emphasized. “Ultimately, a randomized trial would be the only way to be fairly certain if there is indeed a causal protective relationship between red wine, in low amounts, and atrial fib.”
The message for patients, proposed Dr. Dewland and Dr. Marcus, is that alcohol abstinence is best for secondary AFib prevention, “especially if alcohol is a personal trigger for acute AF[ib] episodes,” and that for primary AFib prevention, “continued consumption of some alcohol may be reasonable, but the exact threshold is unclear and is likely a very low amount.”
Mr. Tu has disclosed no relevant financial relationships. Disclosures for the other authors are in the report. Dr. Marcus disclosed receiving research funding from Baylis Medical; consulting for Johnson & Johnson and InCarda; and holding equity interest in InCarda. Dr. Dewland reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Alcoholic drinks are in the news again, served with a twist. A large cohort study saw a familiar J-shaped curve detailing risk for new atrial fibrillation (AFib) in which the risk rose steadily with greater number of drinks per week, except at the lowest levels of alcohol intake.
There, the curve turned the other way. Light drinkers overall showed no higher AFib risk than nondrinkers, and the risk was lowest at any degree of alcohol intake up to 56 g per week.
On closer analysis of risk patterns, the type of alcoholic beverage mattered.
Alcohol content per drink was defined by standards in the United Kingdom, where the cohort was based.
The risk of AFib also didn’t climb at low intake levels of white wine or with “very low” use of liquor or spirits. But it went up consistently at any level of beer or cider consumption, and to be sure, “high intake of any beverage was associated with greater AF[ib] risk,” notes a report on the study published July 27, 2021, in JACC: Clinical Electrophysiology.
The results, based on more than 400,000 adults in the community, “raise the possibility that, for current consumers, drinking red or white wine could potentially be a safer alternative to other types of alcoholic beverages with respect to AF[ib] risk,” the report proposes.
The J-shaped risk curve for new AFib by degree of alcohol consumption follows the pattern sometimes seen for cardiovascular risk in general. But the intake level at which AFib risk is flat or reduced “is at a far lower dose of alcohol than what we’ve seen for cardiovascular disease,” lead author Samuel J. Tu, BHlthMedSc, said in an interview.
“That being said, even with the threshold sitting quite low, it still tells us that cutting down on alcohol is a good thing and perhaps one of the best things for our heart,” said Mr. Tu, University of Adelaide and Royal Adelaide Hospital, who also presented the findings at the Heart Rhythm Society 2021 Scientific Sessions, held in Boston and virtually.
How much alcohol is in a drink?
In a caution for anyone looking to beer, wine, or liquor to protect against AFib, or at least not cause it, the weekly number of drinks associated with the lowest AFib risk may be fewer than expected. That bottom of 56 g per week works out to one drink a day or less for British and only four or fewer per week for Americans, according to the study’s internationally varying definitions for the alcohol content of one drink.
For example, a drink was considered to have 8 g of alcohol in the United Kingdom, 14 g in the United States and some other countries, and up to 20 g in Austria. Those numbers came from definitions used by the respective national health agencies, such as the National Health Service in the United Kingdom and Centers for Disease Control and Prevention in the United States, Mr. Tu explained.
“They all defined standard drinks slightly differently. But wherever we looked, the threshold we found was far lower than what our governments recommend” based on what is known about alcohol and overall cardiovascular risk, he said.
First to show a hint of protection
The current study “is especially noteworthy because it’s the really the first to demonstrate any hint that there could be a protective effect from any particular amount of alcohol in regard to atrial fibrillation,” Gregory M. Marcus, MD, MAS, University of California, San Francisco, said in an interview. “The J-shaped association fits with what’s been observed with myocardial infarction and overall mortality, and hasn’t previously been seen in the setting of atrial fibrillation.”
Quite interestingly, “it appeared to be the wine drinkers, rather than those who consumed other types of alcohol, that enjoyed this benefit,” said Dr. Marcus, who was not involved in the research but co-authored an accompanying editorial with UCSF colleague Thomas A. Dewland, MD.
“It’s important to recognize the overwhelming evidence that alcohol in general increases the risk for atrial fibrillation,” he said. But “perhaps there’s something in wine that is anti-inflammatory that has some beneficial effect that maybe overwhelms the proarrhythmic aspect.”
The current study “opens the door to the question as to whether there is a small amount of alcohol, perhaps in the form of wine, where there are some benefits that outweigh the risks of atrial fibrillation.”
Still, the findings are observational and “clearly prone to confounding,” Dr. Marcus said. “We need to be very cautious in inferring causality.”
For example, it’s possible that “there is something about individuals that are able to drink alcohol on a regular basis and in small amounts that is the actual causal factor in reducing atrial fibrillation episodes.”
The analysis was based on 403,281 participants in the UK Biobank registry, a prospective cohort study in the United Kingdom, who were aged 40-69 when recruited from 2006 to 2010; it excluded anyone with a history of AFib or who was a former drinker. About 52% were women, the report noted.
Their median alcohol consumption was eight U.K. drinks per week, with 5.5% reporting they had never consumed alcohol. About 21,300 incident cases of AFib or atrial flutter were documented over almost 4.5 million person-years, or a median follow-up of 11.4 years.
The hazard ratio for incident AFib among those with a weekly alcohol consumption corresponding to 1-7 U.K. drinks, compared with intake of less than 1 U.K. drink per week, was 0.95 (95% confidence interval, 0.91-1.00). Within that range of 1-7 drinks, the absolute lowest AFib risk on the J curve was at 5 per week.
No increased risk of new AFib was seen in association with weekly U.K. drink levels of 10 for red wine, 8 for white wine, and 3 for spirits.
Compared with weekly intake of less than 1 U.K. drink per week, red wine intake at 1-7 per week showed an HR for AFib of 0.94 (95% CI, 0.91-0.97). Indeed, at no observed consumption level was red wine associated with a significant increase in AFib risk. White wine until the highest observed level of intake, above 28 U.K. drinks per week, at which point the HR for AFib was 1.48 (98% CI 1.19-1.86). The curve for spirit intake followed a similar but steeper curve, its HR risk reaching 1.61 (95% CI, 1.34-1.93) at intake levels beyond 28 U.K. drinks per week.
Consumption of beer or cider showed a linear association with AFib risk, which was elevated at all recorded intake levels, including 8-14 U.K. drinks per week (HR, 1.11; 95% CI 1.06-1.17) and up to 28 or more per week (HR, 1.35; 95% CI, 1.26-1.45).
The analysis is hypothesis generating at best, Dr. Marcus emphasized. “Ultimately, a randomized trial would be the only way to be fairly certain if there is indeed a causal protective relationship between red wine, in low amounts, and atrial fib.”
The message for patients, proposed Dr. Dewland and Dr. Marcus, is that alcohol abstinence is best for secondary AFib prevention, “especially if alcohol is a personal trigger for acute AF[ib] episodes,” and that for primary AFib prevention, “continued consumption of some alcohol may be reasonable, but the exact threshold is unclear and is likely a very low amount.”
Mr. Tu has disclosed no relevant financial relationships. Disclosures for the other authors are in the report. Dr. Marcus disclosed receiving research funding from Baylis Medical; consulting for Johnson & Johnson and InCarda; and holding equity interest in InCarda. Dr. Dewland reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Alcoholic drinks are in the news again, served with a twist. A large cohort study saw a familiar J-shaped curve detailing risk for new atrial fibrillation (AFib) in which the risk rose steadily with greater number of drinks per week, except at the lowest levels of alcohol intake.
There, the curve turned the other way. Light drinkers overall showed no higher AFib risk than nondrinkers, and the risk was lowest at any degree of alcohol intake up to 56 g per week.
On closer analysis of risk patterns, the type of alcoholic beverage mattered.
Alcohol content per drink was defined by standards in the United Kingdom, where the cohort was based.
The risk of AFib also didn’t climb at low intake levels of white wine or with “very low” use of liquor or spirits. But it went up consistently at any level of beer or cider consumption, and to be sure, “high intake of any beverage was associated with greater AF[ib] risk,” notes a report on the study published July 27, 2021, in JACC: Clinical Electrophysiology.
The results, based on more than 400,000 adults in the community, “raise the possibility that, for current consumers, drinking red or white wine could potentially be a safer alternative to other types of alcoholic beverages with respect to AF[ib] risk,” the report proposes.
The J-shaped risk curve for new AFib by degree of alcohol consumption follows the pattern sometimes seen for cardiovascular risk in general. But the intake level at which AFib risk is flat or reduced “is at a far lower dose of alcohol than what we’ve seen for cardiovascular disease,” lead author Samuel J. Tu, BHlthMedSc, said in an interview.
“That being said, even with the threshold sitting quite low, it still tells us that cutting down on alcohol is a good thing and perhaps one of the best things for our heart,” said Mr. Tu, University of Adelaide and Royal Adelaide Hospital, who also presented the findings at the Heart Rhythm Society 2021 Scientific Sessions, held in Boston and virtually.
How much alcohol is in a drink?
In a caution for anyone looking to beer, wine, or liquor to protect against AFib, or at least not cause it, the weekly number of drinks associated with the lowest AFib risk may be fewer than expected. That bottom of 56 g per week works out to one drink a day or less for British and only four or fewer per week for Americans, according to the study’s internationally varying definitions for the alcohol content of one drink.
For example, a drink was considered to have 8 g of alcohol in the United Kingdom, 14 g in the United States and some other countries, and up to 20 g in Austria. Those numbers came from definitions used by the respective national health agencies, such as the National Health Service in the United Kingdom and Centers for Disease Control and Prevention in the United States, Mr. Tu explained.
“They all defined standard drinks slightly differently. But wherever we looked, the threshold we found was far lower than what our governments recommend” based on what is known about alcohol and overall cardiovascular risk, he said.
First to show a hint of protection
The current study “is especially noteworthy because it’s the really the first to demonstrate any hint that there could be a protective effect from any particular amount of alcohol in regard to atrial fibrillation,” Gregory M. Marcus, MD, MAS, University of California, San Francisco, said in an interview. “The J-shaped association fits with what’s been observed with myocardial infarction and overall mortality, and hasn’t previously been seen in the setting of atrial fibrillation.”
Quite interestingly, “it appeared to be the wine drinkers, rather than those who consumed other types of alcohol, that enjoyed this benefit,” said Dr. Marcus, who was not involved in the research but co-authored an accompanying editorial with UCSF colleague Thomas A. Dewland, MD.
“It’s important to recognize the overwhelming evidence that alcohol in general increases the risk for atrial fibrillation,” he said. But “perhaps there’s something in wine that is anti-inflammatory that has some beneficial effect that maybe overwhelms the proarrhythmic aspect.”
The current study “opens the door to the question as to whether there is a small amount of alcohol, perhaps in the form of wine, where there are some benefits that outweigh the risks of atrial fibrillation.”
Still, the findings are observational and “clearly prone to confounding,” Dr. Marcus said. “We need to be very cautious in inferring causality.”
For example, it’s possible that “there is something about individuals that are able to drink alcohol on a regular basis and in small amounts that is the actual causal factor in reducing atrial fibrillation episodes.”
The analysis was based on 403,281 participants in the UK Biobank registry, a prospective cohort study in the United Kingdom, who were aged 40-69 when recruited from 2006 to 2010; it excluded anyone with a history of AFib or who was a former drinker. About 52% were women, the report noted.
Their median alcohol consumption was eight U.K. drinks per week, with 5.5% reporting they had never consumed alcohol. About 21,300 incident cases of AFib or atrial flutter were documented over almost 4.5 million person-years, or a median follow-up of 11.4 years.
The hazard ratio for incident AFib among those with a weekly alcohol consumption corresponding to 1-7 U.K. drinks, compared with intake of less than 1 U.K. drink per week, was 0.95 (95% confidence interval, 0.91-1.00). Within that range of 1-7 drinks, the absolute lowest AFib risk on the J curve was at 5 per week.
No increased risk of new AFib was seen in association with weekly U.K. drink levels of 10 for red wine, 8 for white wine, and 3 for spirits.
Compared with weekly intake of less than 1 U.K. drink per week, red wine intake at 1-7 per week showed an HR for AFib of 0.94 (95% CI, 0.91-0.97). Indeed, at no observed consumption level was red wine associated with a significant increase in AFib risk. White wine until the highest observed level of intake, above 28 U.K. drinks per week, at which point the HR for AFib was 1.48 (98% CI 1.19-1.86). The curve for spirit intake followed a similar but steeper curve, its HR risk reaching 1.61 (95% CI, 1.34-1.93) at intake levels beyond 28 U.K. drinks per week.
Consumption of beer or cider showed a linear association with AFib risk, which was elevated at all recorded intake levels, including 8-14 U.K. drinks per week (HR, 1.11; 95% CI 1.06-1.17) and up to 28 or more per week (HR, 1.35; 95% CI, 1.26-1.45).
The analysis is hypothesis generating at best, Dr. Marcus emphasized. “Ultimately, a randomized trial would be the only way to be fairly certain if there is indeed a causal protective relationship between red wine, in low amounts, and atrial fib.”
The message for patients, proposed Dr. Dewland and Dr. Marcus, is that alcohol abstinence is best for secondary AFib prevention, “especially if alcohol is a personal trigger for acute AF[ib] episodes,” and that for primary AFib prevention, “continued consumption of some alcohol may be reasonable, but the exact threshold is unclear and is likely a very low amount.”
Mr. Tu has disclosed no relevant financial relationships. Disclosures for the other authors are in the report. Dr. Marcus disclosed receiving research funding from Baylis Medical; consulting for Johnson & Johnson and InCarda; and holding equity interest in InCarda. Dr. Dewland reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Exposure to marijuana smoke linked to increased risk of respiratory infections in children
Exposure to secondhand marijuana smoke is more strongly associated with viral respiratory infections in children, compared with children who were exposed to tobacco smoke and those with no smoke exposure, new research shows.
“The findings of this study are interesting and pleasantly raise further questions,” said Kristen Miller, MD, attending physician in the division of pulmonary and sleep medicine at Children’s Hospital of Philadelphia, who was not involved in the study. “Given the robust literature regarding secondhand smoke exposure and the current landscape surrounding marijuana, this is a timely study to evaluate the prevalence of marijuana use and the associated effects of marijuana exposure among children.”
Prior research has linked primary marijuana use with respiratory effects. A 2020 study associated cannabis use with an increased risk of severe bronchitis, lung hyperinflation, and increased central airway resistance. However, according to the Centers for Disease Control and Prevention, there are still a lot of unanswered questions surrounding secondhand marijuana smoke exposure and its effects.
“If kids are exposed to enough secondhand smoke, regardless of what the substance is, they’re going to have some negative health outcomes with it,” study author Adam Johnson, MD, of Wake Forest University, Winston-Salem, N.C., said in an interview.
The study, published in Pediatric Research, looked at rates of reported ED and urgent care visits and specific illnesses – such as otitis media, viral respiratory infections, and asthma exacerbations – among children with marijuana exposure and tobacco exposure.
For the study, Dr. Johnson and colleagues surveyed 1,500 parents and caregivers who went to an academic children’s hospital between Dec. 1, 2015, and July 30, 2017. Researchers found that children exposed to marijuana smoke had higher rates of ED visits at 2.21 within the past 12 months, compared with those exposed to tobacco smoke (2.14 within the past 12 months) and those with no smoke exposure (1.94 within the past 12 months). However, the difference in these visits were not statistically significant.
Researchers saw that children exposed to secondhand marijuana smoke saw a 30% increase in viral respiratory infections, compared with those who were not exposed to tobacco or marijuana smoke, Dr. Johnson said. Caregivers who smoked marijuana reported a rate of 1.31 viral infections in their children within the last year. Meanwhile those who smoked tobacco reported a rate of 1.00 infections within the last 12 months and caregivers who did not smoke reported 1.04 infections within the year.
“It suggests that components in marijuana smoke may depress the body’s immune responses to viral infections in children,” Dr. Miller said in an interview.
When it came to otitis media episodes, children exposed to marijuana had a rate of 0.96 episodes within the past 12 months. Children experiencing secondhand tobacco smoke had a rate of 0.83 episodes and those with no smoke exposure had 0.75 episodes within the past 12 months. Researchers did not note this difference as statistically significant.
When it came to asthma exacerbations, children exposed to marijuana smoke also had statistically insignificantly higher rates of exacerbations, compared with those exposed to tobacco smoke and those not exposed to smoke.
“I think it was surprising that the survey results found that marijuana seemed to be more strongly associated with the viral respiratory infections than tobacco,” Dr. Johnson said. “We know that secondhand tobacco smoke exposure in kids does lead to things like otitis media or ear infections, asthma attacks, and other processes, including colds. It was interesting that we didn’t find that association [in the new study], but we found that with marijuana.”
Dr. Johnson said the findings are especially concerning with increases in the acceptance and accessibility of marijuana as it becomes legalized in many states.
A 2015 study examined the effect of secondhand marijuana smoke exposure. Researchers found that exposure to secondhand marijuana smoke can increase heart rate, have mild to moderate sedative effects and can produce detectable cannabinoid levels in blood and urine. However, another study published in 2012 found that low to moderate primary marijuana use is less harmful to users’ lungs than tobacco exposure.
Dr. Miller added that little is known about how exposure to marijuana smoke can affect the innate responses to pathogens and there is a need to “study this in more detail” to figure out if secondhand marijuana smoke is a risk factor for either an increase in respiratory virus infections or their severity.
“These questions could have considerable implications for the health of our children and public health measures regarding marijuana use,” she explained. “As documented marijuana use increases, health care providers need to be aware of the effects of marijuana use and exposure.”
Neither Dr. Johnson nor Dr. Miller has any relevant financial disclosures.
Exposure to secondhand marijuana smoke is more strongly associated with viral respiratory infections in children, compared with children who were exposed to tobacco smoke and those with no smoke exposure, new research shows.
“The findings of this study are interesting and pleasantly raise further questions,” said Kristen Miller, MD, attending physician in the division of pulmonary and sleep medicine at Children’s Hospital of Philadelphia, who was not involved in the study. “Given the robust literature regarding secondhand smoke exposure and the current landscape surrounding marijuana, this is a timely study to evaluate the prevalence of marijuana use and the associated effects of marijuana exposure among children.”
Prior research has linked primary marijuana use with respiratory effects. A 2020 study associated cannabis use with an increased risk of severe bronchitis, lung hyperinflation, and increased central airway resistance. However, according to the Centers for Disease Control and Prevention, there are still a lot of unanswered questions surrounding secondhand marijuana smoke exposure and its effects.
“If kids are exposed to enough secondhand smoke, regardless of what the substance is, they’re going to have some negative health outcomes with it,” study author Adam Johnson, MD, of Wake Forest University, Winston-Salem, N.C., said in an interview.
The study, published in Pediatric Research, looked at rates of reported ED and urgent care visits and specific illnesses – such as otitis media, viral respiratory infections, and asthma exacerbations – among children with marijuana exposure and tobacco exposure.
For the study, Dr. Johnson and colleagues surveyed 1,500 parents and caregivers who went to an academic children’s hospital between Dec. 1, 2015, and July 30, 2017. Researchers found that children exposed to marijuana smoke had higher rates of ED visits at 2.21 within the past 12 months, compared with those exposed to tobacco smoke (2.14 within the past 12 months) and those with no smoke exposure (1.94 within the past 12 months). However, the difference in these visits were not statistically significant.
Researchers saw that children exposed to secondhand marijuana smoke saw a 30% increase in viral respiratory infections, compared with those who were not exposed to tobacco or marijuana smoke, Dr. Johnson said. Caregivers who smoked marijuana reported a rate of 1.31 viral infections in their children within the last year. Meanwhile those who smoked tobacco reported a rate of 1.00 infections within the last 12 months and caregivers who did not smoke reported 1.04 infections within the year.
“It suggests that components in marijuana smoke may depress the body’s immune responses to viral infections in children,” Dr. Miller said in an interview.
When it came to otitis media episodes, children exposed to marijuana had a rate of 0.96 episodes within the past 12 months. Children experiencing secondhand tobacco smoke had a rate of 0.83 episodes and those with no smoke exposure had 0.75 episodes within the past 12 months. Researchers did not note this difference as statistically significant.
When it came to asthma exacerbations, children exposed to marijuana smoke also had statistically insignificantly higher rates of exacerbations, compared with those exposed to tobacco smoke and those not exposed to smoke.
“I think it was surprising that the survey results found that marijuana seemed to be more strongly associated with the viral respiratory infections than tobacco,” Dr. Johnson said. “We know that secondhand tobacco smoke exposure in kids does lead to things like otitis media or ear infections, asthma attacks, and other processes, including colds. It was interesting that we didn’t find that association [in the new study], but we found that with marijuana.”
Dr. Johnson said the findings are especially concerning with increases in the acceptance and accessibility of marijuana as it becomes legalized in many states.
A 2015 study examined the effect of secondhand marijuana smoke exposure. Researchers found that exposure to secondhand marijuana smoke can increase heart rate, have mild to moderate sedative effects and can produce detectable cannabinoid levels in blood and urine. However, another study published in 2012 found that low to moderate primary marijuana use is less harmful to users’ lungs than tobacco exposure.
Dr. Miller added that little is known about how exposure to marijuana smoke can affect the innate responses to pathogens and there is a need to “study this in more detail” to figure out if secondhand marijuana smoke is a risk factor for either an increase in respiratory virus infections or their severity.
“These questions could have considerable implications for the health of our children and public health measures regarding marijuana use,” she explained. “As documented marijuana use increases, health care providers need to be aware of the effects of marijuana use and exposure.”
Neither Dr. Johnson nor Dr. Miller has any relevant financial disclosures.
Exposure to secondhand marijuana smoke is more strongly associated with viral respiratory infections in children, compared with children who were exposed to tobacco smoke and those with no smoke exposure, new research shows.
“The findings of this study are interesting and pleasantly raise further questions,” said Kristen Miller, MD, attending physician in the division of pulmonary and sleep medicine at Children’s Hospital of Philadelphia, who was not involved in the study. “Given the robust literature regarding secondhand smoke exposure and the current landscape surrounding marijuana, this is a timely study to evaluate the prevalence of marijuana use and the associated effects of marijuana exposure among children.”
Prior research has linked primary marijuana use with respiratory effects. A 2020 study associated cannabis use with an increased risk of severe bronchitis, lung hyperinflation, and increased central airway resistance. However, according to the Centers for Disease Control and Prevention, there are still a lot of unanswered questions surrounding secondhand marijuana smoke exposure and its effects.
“If kids are exposed to enough secondhand smoke, regardless of what the substance is, they’re going to have some negative health outcomes with it,” study author Adam Johnson, MD, of Wake Forest University, Winston-Salem, N.C., said in an interview.
The study, published in Pediatric Research, looked at rates of reported ED and urgent care visits and specific illnesses – such as otitis media, viral respiratory infections, and asthma exacerbations – among children with marijuana exposure and tobacco exposure.
For the study, Dr. Johnson and colleagues surveyed 1,500 parents and caregivers who went to an academic children’s hospital between Dec. 1, 2015, and July 30, 2017. Researchers found that children exposed to marijuana smoke had higher rates of ED visits at 2.21 within the past 12 months, compared with those exposed to tobacco smoke (2.14 within the past 12 months) and those with no smoke exposure (1.94 within the past 12 months). However, the difference in these visits were not statistically significant.
Researchers saw that children exposed to secondhand marijuana smoke saw a 30% increase in viral respiratory infections, compared with those who were not exposed to tobacco or marijuana smoke, Dr. Johnson said. Caregivers who smoked marijuana reported a rate of 1.31 viral infections in their children within the last year. Meanwhile those who smoked tobacco reported a rate of 1.00 infections within the last 12 months and caregivers who did not smoke reported 1.04 infections within the year.
“It suggests that components in marijuana smoke may depress the body’s immune responses to viral infections in children,” Dr. Miller said in an interview.
When it came to otitis media episodes, children exposed to marijuana had a rate of 0.96 episodes within the past 12 months. Children experiencing secondhand tobacco smoke had a rate of 0.83 episodes and those with no smoke exposure had 0.75 episodes within the past 12 months. Researchers did not note this difference as statistically significant.
When it came to asthma exacerbations, children exposed to marijuana smoke also had statistically insignificantly higher rates of exacerbations, compared with those exposed to tobacco smoke and those not exposed to smoke.
“I think it was surprising that the survey results found that marijuana seemed to be more strongly associated with the viral respiratory infections than tobacco,” Dr. Johnson said. “We know that secondhand tobacco smoke exposure in kids does lead to things like otitis media or ear infections, asthma attacks, and other processes, including colds. It was interesting that we didn’t find that association [in the new study], but we found that with marijuana.”
Dr. Johnson said the findings are especially concerning with increases in the acceptance and accessibility of marijuana as it becomes legalized in many states.
A 2015 study examined the effect of secondhand marijuana smoke exposure. Researchers found that exposure to secondhand marijuana smoke can increase heart rate, have mild to moderate sedative effects and can produce detectable cannabinoid levels in blood and urine. However, another study published in 2012 found that low to moderate primary marijuana use is less harmful to users’ lungs than tobacco exposure.
Dr. Miller added that little is known about how exposure to marijuana smoke can affect the innate responses to pathogens and there is a need to “study this in more detail” to figure out if secondhand marijuana smoke is a risk factor for either an increase in respiratory virus infections or their severity.
“These questions could have considerable implications for the health of our children and public health measures regarding marijuana use,” she explained. “As documented marijuana use increases, health care providers need to be aware of the effects of marijuana use and exposure.”
Neither Dr. Johnson nor Dr. Miller has any relevant financial disclosures.
FROM PEDIATRIC RESEARCH
CDC: Vaccination may cut risk of COVID reinfection in half
The Centers for Disease Control and Prevention has recommended that everyone get a COVID-19 vaccine, even if they’ve had the virus before. Yet many skeptics have held off getting the shots, believing that immunity generated by their previous infection will protect them if they should encounter the virus again.
A new study published in the CDC’s Morbidity and Mortality Weekly Report pokes holes in this notion. It shows people who have recovered from COVID-19 but haven’t been vaccinated have more than double the risk of testing positive for the virus again, compared with someone who was vaccinated after an initial infection.
The study looked at 738 Kentucky residents who had an initial bout of COVID-19 in 2020. About 250 of them tested positive for COVID-19 a second time between May and July of 2021, when the Delta variant became dominant in the United States.
The study matched each person who’d been reinfected with two people of the same sex and roughly the same age who had caught their initial COVID infection within the same week. The researchers then cross-matched those cases with data from Kentucky’s Immunization Registry.
They found that those who were unvaccinated had more than double the risk of being reinfected during the Delta wave. Partial vaccination appeared to have no significant impact on the risk of reinfection.
Among those who were reinfected, 20% were fully vaccinated, while 34% of those who did not get reinfected were fully vaccinated.
The study is observational, meaning it can’t show cause and effect; and the researchers had no information on the severity of the infections. Alyson Cavanaugh, PhD, a member of the CDC’s Epidemic Intelligence Service who led the study, said it is possible that some of the people who tested positive a second time had asymptomatic infections that were picked up through routine screening.
Still, the study backs up previous research and suggests that vaccination offers important additional protection.
“Our laboratory studies have shown that there’s an added benefit of vaccine for people who’ve had previous COVID-19. This is a real-world, epidemiologic study that found that among people who’d previously already had COVID-19, those who were vaccinated had lower odds of being reinfected,” Dr. Cavanaugh said.
“If you have had COVID-19 before, please still get vaccinated,” said CDC Director Rochelle Walensky, MD, in a written media statement. “This study shows you are twice as likely to get infected again if you are unvaccinated. Getting the vaccine is the best way to protect yourself and others around you, especially as the more contagious Delta variant spreads around the country.”
In a White House COVID-19 Response Team briefing in May, Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Disease, explained why vaccines create stronger immunity than infection. He highlighted new research showing that two doses of an mRNA vaccine produce levels of neutralizing antibodies that are up to 10 times higher than the levels found in the blood of people who’ve recovered from COVID-19. Vaccines also enhance B cells and T cells in people who’ve recovered from COVID-19, which broadens the spectrum of protection and helps to fend off variants.
The study has some important limitations, which the authors acknowledged. The first is that second infections weren’t confirmed with genetic sequencing, so the researchers couldn’t definitively tell if a person tested positive a second time because they caught a new virus, or if they were somehow still shedding virus from their first infection. Given that the tests were at least 5 months apart, though, the researchers think reinfection is the most likely explanation.
Another bias in the study could have something to do with vaccination. Vaccinated people may have been less likely to be tested for COVID-19 after their vaccines, so the association or reinfection with a lack of vaccination may be overestimated.
Also, people who were vaccinated at federal sites or in another state were not logged in the state’s immunization registry, which may have skewed the data.
A version of this article first appeared on Medscape.com.
The Centers for Disease Control and Prevention has recommended that everyone get a COVID-19 vaccine, even if they’ve had the virus before. Yet many skeptics have held off getting the shots, believing that immunity generated by their previous infection will protect them if they should encounter the virus again.
A new study published in the CDC’s Morbidity and Mortality Weekly Report pokes holes in this notion. It shows people who have recovered from COVID-19 but haven’t been vaccinated have more than double the risk of testing positive for the virus again, compared with someone who was vaccinated after an initial infection.
The study looked at 738 Kentucky residents who had an initial bout of COVID-19 in 2020. About 250 of them tested positive for COVID-19 a second time between May and July of 2021, when the Delta variant became dominant in the United States.
The study matched each person who’d been reinfected with two people of the same sex and roughly the same age who had caught their initial COVID infection within the same week. The researchers then cross-matched those cases with data from Kentucky’s Immunization Registry.
They found that those who were unvaccinated had more than double the risk of being reinfected during the Delta wave. Partial vaccination appeared to have no significant impact on the risk of reinfection.
Among those who were reinfected, 20% were fully vaccinated, while 34% of those who did not get reinfected were fully vaccinated.
The study is observational, meaning it can’t show cause and effect; and the researchers had no information on the severity of the infections. Alyson Cavanaugh, PhD, a member of the CDC’s Epidemic Intelligence Service who led the study, said it is possible that some of the people who tested positive a second time had asymptomatic infections that were picked up through routine screening.
Still, the study backs up previous research and suggests that vaccination offers important additional protection.
“Our laboratory studies have shown that there’s an added benefit of vaccine for people who’ve had previous COVID-19. This is a real-world, epidemiologic study that found that among people who’d previously already had COVID-19, those who were vaccinated had lower odds of being reinfected,” Dr. Cavanaugh said.
“If you have had COVID-19 before, please still get vaccinated,” said CDC Director Rochelle Walensky, MD, in a written media statement. “This study shows you are twice as likely to get infected again if you are unvaccinated. Getting the vaccine is the best way to protect yourself and others around you, especially as the more contagious Delta variant spreads around the country.”
In a White House COVID-19 Response Team briefing in May, Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Disease, explained why vaccines create stronger immunity than infection. He highlighted new research showing that two doses of an mRNA vaccine produce levels of neutralizing antibodies that are up to 10 times higher than the levels found in the blood of people who’ve recovered from COVID-19. Vaccines also enhance B cells and T cells in people who’ve recovered from COVID-19, which broadens the spectrum of protection and helps to fend off variants.
The study has some important limitations, which the authors acknowledged. The first is that second infections weren’t confirmed with genetic sequencing, so the researchers couldn’t definitively tell if a person tested positive a second time because they caught a new virus, or if they were somehow still shedding virus from their first infection. Given that the tests were at least 5 months apart, though, the researchers think reinfection is the most likely explanation.
Another bias in the study could have something to do with vaccination. Vaccinated people may have been less likely to be tested for COVID-19 after their vaccines, so the association or reinfection with a lack of vaccination may be overestimated.
Also, people who were vaccinated at federal sites or in another state were not logged in the state’s immunization registry, which may have skewed the data.
A version of this article first appeared on Medscape.com.
The Centers for Disease Control and Prevention has recommended that everyone get a COVID-19 vaccine, even if they’ve had the virus before. Yet many skeptics have held off getting the shots, believing that immunity generated by their previous infection will protect them if they should encounter the virus again.
A new study published in the CDC’s Morbidity and Mortality Weekly Report pokes holes in this notion. It shows people who have recovered from COVID-19 but haven’t been vaccinated have more than double the risk of testing positive for the virus again, compared with someone who was vaccinated after an initial infection.
The study looked at 738 Kentucky residents who had an initial bout of COVID-19 in 2020. About 250 of them tested positive for COVID-19 a second time between May and July of 2021, when the Delta variant became dominant in the United States.
The study matched each person who’d been reinfected with two people of the same sex and roughly the same age who had caught their initial COVID infection within the same week. The researchers then cross-matched those cases with data from Kentucky’s Immunization Registry.
They found that those who were unvaccinated had more than double the risk of being reinfected during the Delta wave. Partial vaccination appeared to have no significant impact on the risk of reinfection.
Among those who were reinfected, 20% were fully vaccinated, while 34% of those who did not get reinfected were fully vaccinated.
The study is observational, meaning it can’t show cause and effect; and the researchers had no information on the severity of the infections. Alyson Cavanaugh, PhD, a member of the CDC’s Epidemic Intelligence Service who led the study, said it is possible that some of the people who tested positive a second time had asymptomatic infections that were picked up through routine screening.
Still, the study backs up previous research and suggests that vaccination offers important additional protection.
“Our laboratory studies have shown that there’s an added benefit of vaccine for people who’ve had previous COVID-19. This is a real-world, epidemiologic study that found that among people who’d previously already had COVID-19, those who were vaccinated had lower odds of being reinfected,” Dr. Cavanaugh said.
“If you have had COVID-19 before, please still get vaccinated,” said CDC Director Rochelle Walensky, MD, in a written media statement. “This study shows you are twice as likely to get infected again if you are unvaccinated. Getting the vaccine is the best way to protect yourself and others around you, especially as the more contagious Delta variant spreads around the country.”
In a White House COVID-19 Response Team briefing in May, Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Disease, explained why vaccines create stronger immunity than infection. He highlighted new research showing that two doses of an mRNA vaccine produce levels of neutralizing antibodies that are up to 10 times higher than the levels found in the blood of people who’ve recovered from COVID-19. Vaccines also enhance B cells and T cells in people who’ve recovered from COVID-19, which broadens the spectrum of protection and helps to fend off variants.
The study has some important limitations, which the authors acknowledged. The first is that second infections weren’t confirmed with genetic sequencing, so the researchers couldn’t definitively tell if a person tested positive a second time because they caught a new virus, or if they were somehow still shedding virus from their first infection. Given that the tests were at least 5 months apart, though, the researchers think reinfection is the most likely explanation.
Another bias in the study could have something to do with vaccination. Vaccinated people may have been less likely to be tested for COVID-19 after their vaccines, so the association or reinfection with a lack of vaccination may be overestimated.
Also, people who were vaccinated at federal sites or in another state were not logged in the state’s immunization registry, which may have skewed the data.
A version of this article first appeared on Medscape.com.
What is the real risk of smart phones in medicine?
Over the 10 years we’ve been writing this column, we have often found inspiration for topics while traveling – especially while flying. This is not just because of the idle time spent in the air, but instead because of the many ways that air travel and health care experiences are similar. Both industries focus heavily on safety, are tightly regulated, and employ highly trained individuals.

Consumers may recognize the similarities as well – health care and air travel are both well-known for long waits, uncertainty, and implicit risk. Both sectors are also notorious drivers of innovation, constantly leveraging new technologies in pursuit of better outcomes and experiences. Occasionally, however, advancements in technology can present unforeseen challenges and even compromise safety, with the potential to produce unexpected consequences.
A familiar reminder of this potential was provided to us at the commencement of a recent flight, when we were instructed to turn off our personal electronic devices or flip them into “airplane mode.” This same admonishment is often given to patients and visitors in health care settings – everywhere from clinic waiting rooms to intensive care units – though the reason for this is typically left vague. This got us thinking. More importantly, what other emerging technologies have the potential to create issues we may not have anticipated?
Mayo Clinic findings on radio communication used by mobile phones
Once our flight landed, we did some research to answer our initial question about personal communication technology and its ability to interfere with sensitive electronic devices. Specifically, we wanted to know whether radio communication used by mobile phones could affect the operation of medical equipment, potentially leading to dire consequences for patients. Spoiler alert: There is very little evidence that this can occur. In fact, a well-documented study performed by the Mayo Clinic in 2007 found interference in 0 out of 300 tests performed. To quote the authors, “the incidence of clinically important interference was 0%.”
We could find no other studies since 2007 that strongly contradict Mayo’s findings, except for several anecdotal reports and articles that postulate the theoretical possibility.
This is confirmed by the American Heart Association, who maintains a list of devices that may interfere with ICDs and pacemakers on their website. According to the AHA, “wireless transmissions from the antennae of phones available in the United States are a very small risk to ICDs and even less of a risk for pacemakers.” And in case you’re wondering, the story is quite similar for airplanes as well.
The latest publication from NASA’s Aviation Safety Reporting System (ASRS) documents incidents related to personal electronic devices during air travel. Most involve smoke production – or even small fires – caused by malfunctioning phone batteries during charging. Only a few entries reference wireless interference, and these were all minor and unconfirmed events. As with health care environments, airplanes don’t appear to face significant risks from radio interference. But that doesn’t mean personal electronics are completely harmless to patients.
Smartphones’ risks to patient with cardiac devices
On May 13 of 2021, the FDA issued a warning to cardiac patients about their smart phones and smart watches. Many current personal electronic devices and accessories are equipped with strong magnets, such as those contained in the “MagSafe” connector on the iPhone 12, that can deactivate pacemakers and implanted cardiac defibrillators. These medical devices are designed to be manipulated by magnets for diagnostic and therapeutic purposes, but strong magnetic fields can disable them unintentionally, leading to catastrophic results.
Apple and other manufacturers have acknowledged this risk and recommend that smartphones and other devices be kept at least 6 inches from cardiac devices. Given the ubiquity of offending products, it is also imperative that we warn our patients about this risk to their physical wellbeing.
Dr. Notte is a family physician and chief medical officer of Abington (Pa.) Hospital–Jefferson Health. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington Hospital–Jefferson Health. They have no conflicts related to the content of this piece.
Over the 10 years we’ve been writing this column, we have often found inspiration for topics while traveling – especially while flying. This is not just because of the idle time spent in the air, but instead because of the many ways that air travel and health care experiences are similar. Both industries focus heavily on safety, are tightly regulated, and employ highly trained individuals.
Consumers may recognize the similarities as well – health care and air travel are both well-known for long waits, uncertainty, and implicit risk. Both sectors are also notorious drivers of innovation, constantly leveraging new technologies in pursuit of better outcomes and experiences. Occasionally, however, advancements in technology can present unforeseen challenges and even compromise safety, with the potential to produce unexpected consequences.
A familiar reminder of this potential was provided to us at the commencement of a recent flight, when we were instructed to turn off our personal electronic devices or flip them into “airplane mode.” This same admonishment is often given to patients and visitors in health care settings – everywhere from clinic waiting rooms to intensive care units – though the reason for this is typically left vague. This got us thinking. More importantly, what other emerging technologies have the potential to create issues we may not have anticipated?
Mayo Clinic findings on radio communication used by mobile phones
Once our flight landed, we did some research to answer our initial question about personal communication technology and its ability to interfere with sensitive electronic devices. Specifically, we wanted to know whether radio communication used by mobile phones could affect the operation of medical equipment, potentially leading to dire consequences for patients. Spoiler alert: There is very little evidence that this can occur. In fact, a well-documented study performed by the Mayo Clinic in 2007 found interference in 0 out of 300 tests performed. To quote the authors, “the incidence of clinically important interference was 0%.”
We could find no other studies since 2007 that strongly contradict Mayo’s findings, except for several anecdotal reports and articles that postulate the theoretical possibility.
This is confirmed by the American Heart Association, who maintains a list of devices that may interfere with ICDs and pacemakers on their website. According to the AHA, “wireless transmissions from the antennae of phones available in the United States are a very small risk to ICDs and even less of a risk for pacemakers.” And in case you’re wondering, the story is quite similar for airplanes as well.
The latest publication from NASA’s Aviation Safety Reporting System (ASRS) documents incidents related to personal electronic devices during air travel. Most involve smoke production – or even small fires – caused by malfunctioning phone batteries during charging. Only a few entries reference wireless interference, and these were all minor and unconfirmed events. As with health care environments, airplanes don’t appear to face significant risks from radio interference. But that doesn’t mean personal electronics are completely harmless to patients.
Smartphones’ risks to patient with cardiac devices
On May 13 of 2021, the FDA issued a warning to cardiac patients about their smart phones and smart watches. Many current personal electronic devices and accessories are equipped with strong magnets, such as those contained in the “MagSafe” connector on the iPhone 12, that can deactivate pacemakers and implanted cardiac defibrillators. These medical devices are designed to be manipulated by magnets for diagnostic and therapeutic purposes, but strong magnetic fields can disable them unintentionally, leading to catastrophic results.
Apple and other manufacturers have acknowledged this risk and recommend that smartphones and other devices be kept at least 6 inches from cardiac devices. Given the ubiquity of offending products, it is also imperative that we warn our patients about this risk to their physical wellbeing.
Dr. Notte is a family physician and chief medical officer of Abington (Pa.) Hospital–Jefferson Health. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington Hospital–Jefferson Health. They have no conflicts related to the content of this piece.
Over the 10 years we’ve been writing this column, we have often found inspiration for topics while traveling – especially while flying. This is not just because of the idle time spent in the air, but instead because of the many ways that air travel and health care experiences are similar. Both industries focus heavily on safety, are tightly regulated, and employ highly trained individuals.
Consumers may recognize the similarities as well – health care and air travel are both well-known for long waits, uncertainty, and implicit risk. Both sectors are also notorious drivers of innovation, constantly leveraging new technologies in pursuit of better outcomes and experiences. Occasionally, however, advancements in technology can present unforeseen challenges and even compromise safety, with the potential to produce unexpected consequences.
A familiar reminder of this potential was provided to us at the commencement of a recent flight, when we were instructed to turn off our personal electronic devices or flip them into “airplane mode.” This same admonishment is often given to patients and visitors in health care settings – everywhere from clinic waiting rooms to intensive care units – though the reason for this is typically left vague. This got us thinking. More importantly, what other emerging technologies have the potential to create issues we may not have anticipated?
Mayo Clinic findings on radio communication used by mobile phones
Once our flight landed, we did some research to answer our initial question about personal communication technology and its ability to interfere with sensitive electronic devices. Specifically, we wanted to know whether radio communication used by mobile phones could affect the operation of medical equipment, potentially leading to dire consequences for patients. Spoiler alert: There is very little evidence that this can occur. In fact, a well-documented study performed by the Mayo Clinic in 2007 found interference in 0 out of 300 tests performed. To quote the authors, “the incidence of clinically important interference was 0%.”
We could find no other studies since 2007 that strongly contradict Mayo’s findings, except for several anecdotal reports and articles that postulate the theoretical possibility.
This is confirmed by the American Heart Association, who maintains a list of devices that may interfere with ICDs and pacemakers on their website. According to the AHA, “wireless transmissions from the antennae of phones available in the United States are a very small risk to ICDs and even less of a risk for pacemakers.” And in case you’re wondering, the story is quite similar for airplanes as well.
The latest publication from NASA’s Aviation Safety Reporting System (ASRS) documents incidents related to personal electronic devices during air travel. Most involve smoke production – or even small fires – caused by malfunctioning phone batteries during charging. Only a few entries reference wireless interference, and these were all minor and unconfirmed events. As with health care environments, airplanes don’t appear to face significant risks from radio interference. But that doesn’t mean personal electronics are completely harmless to patients.
Smartphones’ risks to patient with cardiac devices
On May 13 of 2021, the FDA issued a warning to cardiac patients about their smart phones and smart watches. Many current personal electronic devices and accessories are equipped with strong magnets, such as those contained in the “MagSafe” connector on the iPhone 12, that can deactivate pacemakers and implanted cardiac defibrillators. These medical devices are designed to be manipulated by magnets for diagnostic and therapeutic purposes, but strong magnetic fields can disable them unintentionally, leading to catastrophic results.
Apple and other manufacturers have acknowledged this risk and recommend that smartphones and other devices be kept at least 6 inches from cardiac devices. Given the ubiquity of offending products, it is also imperative that we warn our patients about this risk to their physical wellbeing.
Dr. Notte is a family physician and chief medical officer of Abington (Pa.) Hospital–Jefferson Health. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington Hospital–Jefferson Health. They have no conflicts related to the content of this piece.
Injectable monoclonal antibodies prevent COVID-19 in trial
according to results of a randomized, double-blind, placebo-controlled clinical trial published online August 4, 2021, in the New England Journal of Medicine.
The cocktail of the monoclonal antibodies casirivimab and imdevimab (REGEN-COV, Regeneron Pharmaceuticals) reduced participants’ relative risk of infection by 72%, compared with placebo within the first week. After the first week, risk reduction increased to 93%.
“Long after you would be exposed by your household, there is an enduring effect that prevents you from community spread,” said David Wohl, MD, professor of medicine in the division of infectious diseases at the University of North Carolina at Chapel Hill, who was a site investigator for the trial but not a study author.
Participants were enrolled within 96 hours after someone in their household tested positive for SARS-CoV-2. Participants were randomly assigned to receive 1,200 mg of REGEN-COV subcutaneously or a placebo. Based on serologic testing, study participants showed no evidence of current or previous SARS-CoV-2 infection. The median age of participants was 42.9, but 45% were male teenagers (ages 12-17).
In the group that received REGEN-COV, 11 out of 753 participants developed symptomatic COVID-19, compared with 59 out of 752 participants who received placebo. The relative risk reduction for the study’s 4-week period was 81.4% (P < .001). Of the participants that did develop a SARS-CoV-2 infection, those that received REGEN-COV were less likely to be symptomatic. Asymptomatic infections developed in 25 participants who received REGEN-COV versus 48 in the placebo group. The relative risk of developing any SARS-CoV-2 infection, symptomatic or asymptomatic, was reduced by 66.4% with REGEN-COV (P < .001).
Among the patients who were symptomatic, symptoms subsided within a median of 1.2 weeks for the group that received REGEN-COV, 2 weeks earlier than the placebo group. These patients also had a shorter duration of a high viral load (>104 copies/mL). Few adverse events were reported in the treatment or placebo groups. Monoclonal antibodies “seem to be incredibly safe,” Dr. Wohl said.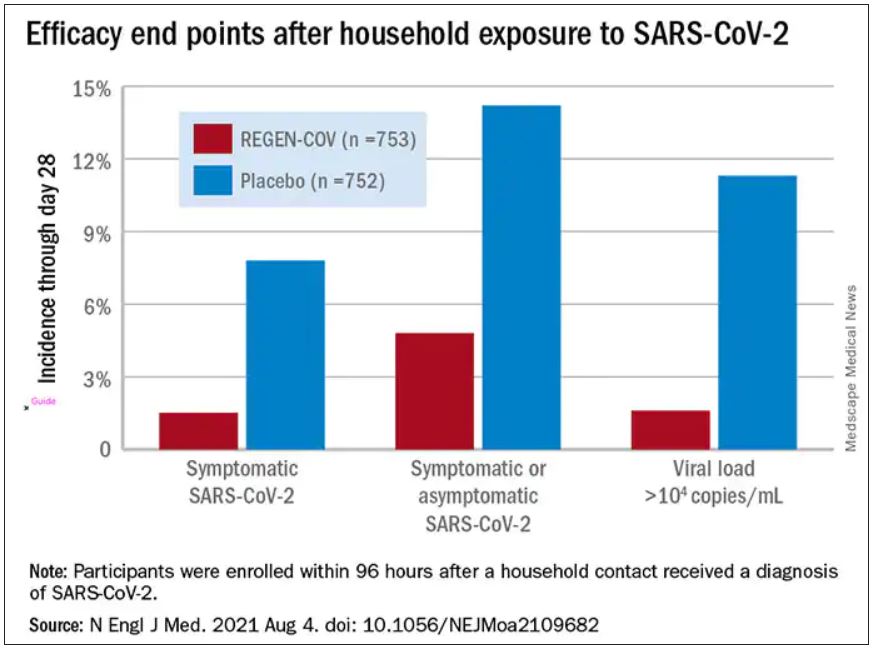
“These monoclonal antibodies have proven they can reduce the viral replication in the nose,” said study author Myron Cohen, MD, an infectious disease specialist and professor of epidemiology at the University of North Carolina.
The Food and Drug Administration first granted REGEN-COV emergency use authorization (EUA) in November 2020 for use in patients with mild or moderate COVID-19 who were also at high risk for progressing to severe COVID-19. At that time, the cocktail of monoclonal antibodies was delivered by a single intravenous infusion.
In January, Regeneron first announced the success of this trial of the subcutaneous injection for exposed household contacts based on early results, and in June of 2021, the FDA expanded the EUA to include a subcutaneous delivery when IV is not feasible. On July 30, the EUA was expanded again to include prophylactic use in exposed patients based on these trial results.
The U.S. government has purchased approximately 1.5 million doses of REGEN-COV from Regeneron and has agreed to make the treatments free of charge to patients.
But despite being free, available, and backed by promising data, monoclonal antibodies as a therapeutic answer to COVID-19 still hasn’t really taken off. “The problem is, it first requires knowledge and awareness,” Dr. Wohl said. “A lot [of people] don’t know this exists. To be honest, vaccination has taken up all the oxygen in the room.”
Dr. Cohen agreed. One reason for the slow uptake may be because the drug supply is owned by the government and not a pharmaceutical company. There hasn’t been a typical marketing push to make physicians and consumers aware. Additionally, “the logistics are daunting,” Dr. Cohen said. The office spaces where many physicians care for patients “often aren’t appropriate for patients who think they have SARS-CoV-2.”
“Right now, there’s not a mechanism” to administer the drug to people who could benefit from it, Dr. Wohl said. Eligible patients are either immunocompromised and unlikely to mount a sufficient immune response with vaccination, or not fully vaccinated. They should have been exposed to an infected individual or have a high likelihood of exposure due to where they live, such as in a prison or nursing home. Local doctors are unlikely to be the primary administrators of the drug, Dr. Wohl added. “How do we operationalize this for people who fit the criteria?”
There’s also an issue of timing. REGEN-COV is most effective when given early, Dr. Cohen said. “[Monoclonal antibodies] really only work well in the replication phase.” Many patients who would be eligible delay care until they’ve had symptoms for several days, when REGEN-COV would no longer have the desired effect.
Eventually, Dr. Wohl suspects demand will increase when people realize REGEN-COV can help those with COVID-19 and those who have been exposed. But before then, “we do have to think about how to integrate this into a workflow people can access without being confused.”
The trial was done before there was widespread vaccination, so it’s unclear what the results mean for people who have been vaccinated. Dr. Cohen and Dr. Wohl said there are ongoing conversations about whether monoclonal antibodies could be complementary to vaccination and if there’s potential for continued monthly use of these therapies.
Cohen and Wohl reported no relevant financial relationships. The trial was supported by Regeneron Pharmaceuticals, F. Hoffmann–La Roche, the National Institute of Allergy and Infectious Diseases, NIH, and the COVID-19 Prevention Network.
A version of this article first appeared on Medscape.com.
according to results of a randomized, double-blind, placebo-controlled clinical trial published online August 4, 2021, in the New England Journal of Medicine.
The cocktail of the monoclonal antibodies casirivimab and imdevimab (REGEN-COV, Regeneron Pharmaceuticals) reduced participants’ relative risk of infection by 72%, compared with placebo within the first week. After the first week, risk reduction increased to 93%.
“Long after you would be exposed by your household, there is an enduring effect that prevents you from community spread,” said David Wohl, MD, professor of medicine in the division of infectious diseases at the University of North Carolina at Chapel Hill, who was a site investigator for the trial but not a study author.
Participants were enrolled within 96 hours after someone in their household tested positive for SARS-CoV-2. Participants were randomly assigned to receive 1,200 mg of REGEN-COV subcutaneously or a placebo. Based on serologic testing, study participants showed no evidence of current or previous SARS-CoV-2 infection. The median age of participants was 42.9, but 45% were male teenagers (ages 12-17).
In the group that received REGEN-COV, 11 out of 753 participants developed symptomatic COVID-19, compared with 59 out of 752 participants who received placebo. The relative risk reduction for the study’s 4-week period was 81.4% (P < .001). Of the participants that did develop a SARS-CoV-2 infection, those that received REGEN-COV were less likely to be symptomatic. Asymptomatic infections developed in 25 participants who received REGEN-COV versus 48 in the placebo group. The relative risk of developing any SARS-CoV-2 infection, symptomatic or asymptomatic, was reduced by 66.4% with REGEN-COV (P < .001).
Among the patients who were symptomatic, symptoms subsided within a median of 1.2 weeks for the group that received REGEN-COV, 2 weeks earlier than the placebo group. These patients also had a shorter duration of a high viral load (>104 copies/mL). Few adverse events were reported in the treatment or placebo groups. Monoclonal antibodies “seem to be incredibly safe,” Dr. Wohl said.
“These monoclonal antibodies have proven they can reduce the viral replication in the nose,” said study author Myron Cohen, MD, an infectious disease specialist and professor of epidemiology at the University of North Carolina.
The Food and Drug Administration first granted REGEN-COV emergency use authorization (EUA) in November 2020 for use in patients with mild or moderate COVID-19 who were also at high risk for progressing to severe COVID-19. At that time, the cocktail of monoclonal antibodies was delivered by a single intravenous infusion.
In January, Regeneron first announced the success of this trial of the subcutaneous injection for exposed household contacts based on early results, and in June of 2021, the FDA expanded the EUA to include a subcutaneous delivery when IV is not feasible. On July 30, the EUA was expanded again to include prophylactic use in exposed patients based on these trial results.
The U.S. government has purchased approximately 1.5 million doses of REGEN-COV from Regeneron and has agreed to make the treatments free of charge to patients.
But despite being free, available, and backed by promising data, monoclonal antibodies as a therapeutic answer to COVID-19 still hasn’t really taken off. “The problem is, it first requires knowledge and awareness,” Dr. Wohl said. “A lot [of people] don’t know this exists. To be honest, vaccination has taken up all the oxygen in the room.”
Dr. Cohen agreed. One reason for the slow uptake may be because the drug supply is owned by the government and not a pharmaceutical company. There hasn’t been a typical marketing push to make physicians and consumers aware. Additionally, “the logistics are daunting,” Dr. Cohen said. The office spaces where many physicians care for patients “often aren’t appropriate for patients who think they have SARS-CoV-2.”
“Right now, there’s not a mechanism” to administer the drug to people who could benefit from it, Dr. Wohl said. Eligible patients are either immunocompromised and unlikely to mount a sufficient immune response with vaccination, or not fully vaccinated. They should have been exposed to an infected individual or have a high likelihood of exposure due to where they live, such as in a prison or nursing home. Local doctors are unlikely to be the primary administrators of the drug, Dr. Wohl added. “How do we operationalize this for people who fit the criteria?”
There’s also an issue of timing. REGEN-COV is most effective when given early, Dr. Cohen said. “[Monoclonal antibodies] really only work well in the replication phase.” Many patients who would be eligible delay care until they’ve had symptoms for several days, when REGEN-COV would no longer have the desired effect.
Eventually, Dr. Wohl suspects demand will increase when people realize REGEN-COV can help those with COVID-19 and those who have been exposed. But before then, “we do have to think about how to integrate this into a workflow people can access without being confused.”
The trial was done before there was widespread vaccination, so it’s unclear what the results mean for people who have been vaccinated. Dr. Cohen and Dr. Wohl said there are ongoing conversations about whether monoclonal antibodies could be complementary to vaccination and if there’s potential for continued monthly use of these therapies.
Cohen and Wohl reported no relevant financial relationships. The trial was supported by Regeneron Pharmaceuticals, F. Hoffmann–La Roche, the National Institute of Allergy and Infectious Diseases, NIH, and the COVID-19 Prevention Network.
A version of this article first appeared on Medscape.com.
according to results of a randomized, double-blind, placebo-controlled clinical trial published online August 4, 2021, in the New England Journal of Medicine.
The cocktail of the monoclonal antibodies casirivimab and imdevimab (REGEN-COV, Regeneron Pharmaceuticals) reduced participants’ relative risk of infection by 72%, compared with placebo within the first week. After the first week, risk reduction increased to 93%.
“Long after you would be exposed by your household, there is an enduring effect that prevents you from community spread,” said David Wohl, MD, professor of medicine in the division of infectious diseases at the University of North Carolina at Chapel Hill, who was a site investigator for the trial but not a study author.
Participants were enrolled within 96 hours after someone in their household tested positive for SARS-CoV-2. Participants were randomly assigned to receive 1,200 mg of REGEN-COV subcutaneously or a placebo. Based on serologic testing, study participants showed no evidence of current or previous SARS-CoV-2 infection. The median age of participants was 42.9, but 45% were male teenagers (ages 12-17).
In the group that received REGEN-COV, 11 out of 753 participants developed symptomatic COVID-19, compared with 59 out of 752 participants who received placebo. The relative risk reduction for the study’s 4-week period was 81.4% (P < .001). Of the participants that did develop a SARS-CoV-2 infection, those that received REGEN-COV were less likely to be symptomatic. Asymptomatic infections developed in 25 participants who received REGEN-COV versus 48 in the placebo group. The relative risk of developing any SARS-CoV-2 infection, symptomatic or asymptomatic, was reduced by 66.4% with REGEN-COV (P < .001).
Among the patients who were symptomatic, symptoms subsided within a median of 1.2 weeks for the group that received REGEN-COV, 2 weeks earlier than the placebo group. These patients also had a shorter duration of a high viral load (>104 copies/mL). Few adverse events were reported in the treatment or placebo groups. Monoclonal antibodies “seem to be incredibly safe,” Dr. Wohl said.
“These monoclonal antibodies have proven they can reduce the viral replication in the nose,” said study author Myron Cohen, MD, an infectious disease specialist and professor of epidemiology at the University of North Carolina.
The Food and Drug Administration first granted REGEN-COV emergency use authorization (EUA) in November 2020 for use in patients with mild or moderate COVID-19 who were also at high risk for progressing to severe COVID-19. At that time, the cocktail of monoclonal antibodies was delivered by a single intravenous infusion.
In January, Regeneron first announced the success of this trial of the subcutaneous injection for exposed household contacts based on early results, and in June of 2021, the FDA expanded the EUA to include a subcutaneous delivery when IV is not feasible. On July 30, the EUA was expanded again to include prophylactic use in exposed patients based on these trial results.
The U.S. government has purchased approximately 1.5 million doses of REGEN-COV from Regeneron and has agreed to make the treatments free of charge to patients.
But despite being free, available, and backed by promising data, monoclonal antibodies as a therapeutic answer to COVID-19 still hasn’t really taken off. “The problem is, it first requires knowledge and awareness,” Dr. Wohl said. “A lot [of people] don’t know this exists. To be honest, vaccination has taken up all the oxygen in the room.”
Dr. Cohen agreed. One reason for the slow uptake may be because the drug supply is owned by the government and not a pharmaceutical company. There hasn’t been a typical marketing push to make physicians and consumers aware. Additionally, “the logistics are daunting,” Dr. Cohen said. The office spaces where many physicians care for patients “often aren’t appropriate for patients who think they have SARS-CoV-2.”
“Right now, there’s not a mechanism” to administer the drug to people who could benefit from it, Dr. Wohl said. Eligible patients are either immunocompromised and unlikely to mount a sufficient immune response with vaccination, or not fully vaccinated. They should have been exposed to an infected individual or have a high likelihood of exposure due to where they live, such as in a prison or nursing home. Local doctors are unlikely to be the primary administrators of the drug, Dr. Wohl added. “How do we operationalize this for people who fit the criteria?”
There’s also an issue of timing. REGEN-COV is most effective when given early, Dr. Cohen said. “[Monoclonal antibodies] really only work well in the replication phase.” Many patients who would be eligible delay care until they’ve had symptoms for several days, when REGEN-COV would no longer have the desired effect.
Eventually, Dr. Wohl suspects demand will increase when people realize REGEN-COV can help those with COVID-19 and those who have been exposed. But before then, “we do have to think about how to integrate this into a workflow people can access without being confused.”
The trial was done before there was widespread vaccination, so it’s unclear what the results mean for people who have been vaccinated. Dr. Cohen and Dr. Wohl said there are ongoing conversations about whether monoclonal antibodies could be complementary to vaccination and if there’s potential for continued monthly use of these therapies.
Cohen and Wohl reported no relevant financial relationships. The trial was supported by Regeneron Pharmaceuticals, F. Hoffmann–La Roche, the National Institute of Allergy and Infectious Diseases, NIH, and the COVID-19 Prevention Network.
A version of this article first appeared on Medscape.com.
Moderna says boosters may be needed after 6 months
Moderna says neutralizing antibodies generated by its COVID-19 vaccine against three variants of the virus that causes the disease waned substantially 6 months after the second dose.
Because of this, the company expects an increase in breakthrough infections with a need for boosters before winter.
In an experiment, a 50-mg dose of the vaccine, given as a third shot, boosted levels of antibodies in 20 previously vaccinated people by 32 times against the Beta variant, by 44 times against the Gamma variant, and by 42 times against Delta.
The new data was presented in an earnings call to investors and is based on a small study that hasn’t yet been published in medical literature.
The company also said its vaccine remained highly effective at preventing severe COVID outcomes through 6 months.
Last week, Pfizer released early data suggesting a similar drop in protection from its vaccine. The company also showed a third dose substantially boosted protection, including against the Delta variant.
The new results come just 1 day after the World Health Organization implored wealthy nations to hold off on third doses until more of the world’s population could get a first dose.
More than 80% of the 4 billion vaccine doses given around the world have been distributed to high-income countries.
A version of this article first appeared on WebMD.com.
Moderna says neutralizing antibodies generated by its COVID-19 vaccine against three variants of the virus that causes the disease waned substantially 6 months after the second dose.
Because of this, the company expects an increase in breakthrough infections with a need for boosters before winter.
In an experiment, a 50-mg dose of the vaccine, given as a third shot, boosted levels of antibodies in 20 previously vaccinated people by 32 times against the Beta variant, by 44 times against the Gamma variant, and by 42 times against Delta.
The new data was presented in an earnings call to investors and is based on a small study that hasn’t yet been published in medical literature.
The company also said its vaccine remained highly effective at preventing severe COVID outcomes through 6 months.
Last week, Pfizer released early data suggesting a similar drop in protection from its vaccine. The company also showed a third dose substantially boosted protection, including against the Delta variant.
The new results come just 1 day after the World Health Organization implored wealthy nations to hold off on third doses until more of the world’s population could get a first dose.
More than 80% of the 4 billion vaccine doses given around the world have been distributed to high-income countries.
A version of this article first appeared on WebMD.com.
Moderna says neutralizing antibodies generated by its COVID-19 vaccine against three variants of the virus that causes the disease waned substantially 6 months after the second dose.
Because of this, the company expects an increase in breakthrough infections with a need for boosters before winter.
In an experiment, a 50-mg dose of the vaccine, given as a third shot, boosted levels of antibodies in 20 previously vaccinated people by 32 times against the Beta variant, by 44 times against the Gamma variant, and by 42 times against Delta.
The new data was presented in an earnings call to investors and is based on a small study that hasn’t yet been published in medical literature.
The company also said its vaccine remained highly effective at preventing severe COVID outcomes through 6 months.
Last week, Pfizer released early data suggesting a similar drop in protection from its vaccine. The company also showed a third dose substantially boosted protection, including against the Delta variant.
The new results come just 1 day after the World Health Organization implored wealthy nations to hold off on third doses until more of the world’s population could get a first dose.
More than 80% of the 4 billion vaccine doses given around the world have been distributed to high-income countries.
A version of this article first appeared on WebMD.com.