User login
Analysis: Don’t want a vaccine? Be prepared to pay more for insurance
America’s COVID-19 vaccination rate is around 60% for ages 12 and up. That’s not enough to reach so-called herd immunity, and in states like Missouri – where a number of counties have vaccination rates under 25% – hospitals are overwhelmed by serious outbreaks of the more contagious delta variant.
The vaccine resisters offer all kinds of reasons for refusing the free shots and for ignoring efforts to nudge them to get inoculated. Campaigns urging Americans to get vaccinated for their health, for their grandparents, for their neighbors, or to get free doughnuts or a free joint haven’t done the trick. States have even held lotteries with a chance to win millions or a college scholarship.
And yet there are still huge numbers of unvaccinated people. Federal, state, and municipal governments as well as private businesses continue to largely avoid mandates for their employees out of fears they will provoke a backlash.
So, how about an economic argument? Get a COVID shot to protect your wallet.
Getting hospitalized with COVID in the United States typically generates huge bills. Those submitted by COVID patients to the NPR-Kaiser Health News “Bill of the Month” project include a $17,000 bill for a brief hospital stay in Marietta, Ga., (reduced to about $4,000 for an uninsured patient under a “charity care” policy); a $104,000 bill for a 14-day hospitalization in Miami for an uninsured man; and a bill for possibly hundreds of thousands for a 2-week hospital stay – some of it on a ventilator – for a foreign tourist in Hawaii whose travel health insurance contained a “pandemic exclusion.”
Even though insurance companies negotiate lower prices and cover much of the cost of care, an over-$1,000 out-of-pocket bill for a deductible – plus more for copays and possibly some out-of-network care – should be a pretty scary incentive.
In 2020, before COVID vaccines, most major private insurers waived patient payments – from coinsurance to deductibles – for COVID treatment. But many, if not most, have allowed that policy to lapse. Aetna, for example, ended that policy Feb. 28; UnitedHealthcare began rolling back its waivers late last year and ended them by the end of March.
More than 97% of hospitalized patients last month were unvaccinated. Though the vaccines will not necessarily prevent you from catching the coronavirus, they are highly effective at assuring you will have a milder case and are kept out of the hospital.
For this reason, there’s logic behind insurers’ waiver rollback: Why should patients be kept financially unharmed from what is now a preventable hospitalization, thanks to a vaccine that the government paid for and made available free of charge? It is now in many drugstores, it’s popping up at highway rest stops and bus stops, and it can be delivered and administered at home in parts of the country.
A harsher society might impose tough penalties on people who refuse vaccinations and contract the virus. Recently, the National Football League decreed that teams will forfeit a game canceled because of a COVID outbreak among unvaccinated players – and neither team’s players will be paid.
But insurers could try to do more, like penalizing the unvaccinated. And there is precedent. Already, some policies won’t cover treatment necessitated by what insurance companies deem risky behavior, such as scuba diving and rock climbing.
The Affordable Care Act allows insurers to charge smokers up to 50% more than what nonsmokers pay for some health plans. Four-fifths of states follow that protocol, though most employer-based plans do not do so. In 49 states, people caught driving without auto insurance face fines, confiscation of their car, loss of their license, and even jail. And reckless drivers pay more for insurance.
The logic behind the policies is that the offenders’ behavior can hurt others and costs society a lot of money. If a person decides not to get vaccinated and contracts a bad case of COVID, they are not only exposing others in their workplace or neighborhoods; the tens or hundreds of thousands spent on their care could mean higher premiums for others as well in their insurance plans next year. What’s more, outbreaks in low-vaccination regions could help breed more vaccine-resistant variants that affect everyone.
Yes, we often cover people whose habits may have contributed to their illness – insurance regularly pays for drug and alcohol rehab and cancer treatment for smokers.
That’s one reason, perhaps, that insurers too have so far favored carrots, not sticks, to get people vaccinated. Some private insurers are offering people who get vaccinated a credit toward their medical premiums, or gift cards and sweepstakes prizes, according to America’s Health Insurance Plans, an industry organization.
Tough love might be easier if the Food and Drug Administration gives vaccines full approval, rather than the current emergency use authorization. Even so, taxpayer-financed plans like Medicaid and Medicare must treat everyone the same and would encounter a lengthy process to secure federal waivers to experiment with incentives, according to Larry Levitt, executive vice president of Kaiser Family Foundation. These programs cannot charge different rates to different patients in a state.
KFF polling shows such incentives are of limited value, anyway. Many holdouts say they will be vaccinated only if required to do so by their employers.
But what if the financial cost of not getting vaccinated were just too high? If patients thought about the price they might need to pay for their own care, maybe they would reconsider remaining unprotected.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
America’s COVID-19 vaccination rate is around 60% for ages 12 and up. That’s not enough to reach so-called herd immunity, and in states like Missouri – where a number of counties have vaccination rates under 25% – hospitals are overwhelmed by serious outbreaks of the more contagious delta variant.
The vaccine resisters offer all kinds of reasons for refusing the free shots and for ignoring efforts to nudge them to get inoculated. Campaigns urging Americans to get vaccinated for their health, for their grandparents, for their neighbors, or to get free doughnuts or a free joint haven’t done the trick. States have even held lotteries with a chance to win millions or a college scholarship.
And yet there are still huge numbers of unvaccinated people. Federal, state, and municipal governments as well as private businesses continue to largely avoid mandates for their employees out of fears they will provoke a backlash.
So, how about an economic argument? Get a COVID shot to protect your wallet.
Getting hospitalized with COVID in the United States typically generates huge bills. Those submitted by COVID patients to the NPR-Kaiser Health News “Bill of the Month” project include a $17,000 bill for a brief hospital stay in Marietta, Ga., (reduced to about $4,000 for an uninsured patient under a “charity care” policy); a $104,000 bill for a 14-day hospitalization in Miami for an uninsured man; and a bill for possibly hundreds of thousands for a 2-week hospital stay – some of it on a ventilator – for a foreign tourist in Hawaii whose travel health insurance contained a “pandemic exclusion.”
Even though insurance companies negotiate lower prices and cover much of the cost of care, an over-$1,000 out-of-pocket bill for a deductible – plus more for copays and possibly some out-of-network care – should be a pretty scary incentive.
In 2020, before COVID vaccines, most major private insurers waived patient payments – from coinsurance to deductibles – for COVID treatment. But many, if not most, have allowed that policy to lapse. Aetna, for example, ended that policy Feb. 28; UnitedHealthcare began rolling back its waivers late last year and ended them by the end of March.
More than 97% of hospitalized patients last month were unvaccinated. Though the vaccines will not necessarily prevent you from catching the coronavirus, they are highly effective at assuring you will have a milder case and are kept out of the hospital.
For this reason, there’s logic behind insurers’ waiver rollback: Why should patients be kept financially unharmed from what is now a preventable hospitalization, thanks to a vaccine that the government paid for and made available free of charge? It is now in many drugstores, it’s popping up at highway rest stops and bus stops, and it can be delivered and administered at home in parts of the country.
A harsher society might impose tough penalties on people who refuse vaccinations and contract the virus. Recently, the National Football League decreed that teams will forfeit a game canceled because of a COVID outbreak among unvaccinated players – and neither team’s players will be paid.
But insurers could try to do more, like penalizing the unvaccinated. And there is precedent. Already, some policies won’t cover treatment necessitated by what insurance companies deem risky behavior, such as scuba diving and rock climbing.
The Affordable Care Act allows insurers to charge smokers up to 50% more than what nonsmokers pay for some health plans. Four-fifths of states follow that protocol, though most employer-based plans do not do so. In 49 states, people caught driving without auto insurance face fines, confiscation of their car, loss of their license, and even jail. And reckless drivers pay more for insurance.
The logic behind the policies is that the offenders’ behavior can hurt others and costs society a lot of money. If a person decides not to get vaccinated and contracts a bad case of COVID, they are not only exposing others in their workplace or neighborhoods; the tens or hundreds of thousands spent on their care could mean higher premiums for others as well in their insurance plans next year. What’s more, outbreaks in low-vaccination regions could help breed more vaccine-resistant variants that affect everyone.
Yes, we often cover people whose habits may have contributed to their illness – insurance regularly pays for drug and alcohol rehab and cancer treatment for smokers.
That’s one reason, perhaps, that insurers too have so far favored carrots, not sticks, to get people vaccinated. Some private insurers are offering people who get vaccinated a credit toward their medical premiums, or gift cards and sweepstakes prizes, according to America’s Health Insurance Plans, an industry organization.
Tough love might be easier if the Food and Drug Administration gives vaccines full approval, rather than the current emergency use authorization. Even so, taxpayer-financed plans like Medicaid and Medicare must treat everyone the same and would encounter a lengthy process to secure federal waivers to experiment with incentives, according to Larry Levitt, executive vice president of Kaiser Family Foundation. These programs cannot charge different rates to different patients in a state.
KFF polling shows such incentives are of limited value, anyway. Many holdouts say they will be vaccinated only if required to do so by their employers.
But what if the financial cost of not getting vaccinated were just too high? If patients thought about the price they might need to pay for their own care, maybe they would reconsider remaining unprotected.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
America’s COVID-19 vaccination rate is around 60% for ages 12 and up. That’s not enough to reach so-called herd immunity, and in states like Missouri – where a number of counties have vaccination rates under 25% – hospitals are overwhelmed by serious outbreaks of the more contagious delta variant.
The vaccine resisters offer all kinds of reasons for refusing the free shots and for ignoring efforts to nudge them to get inoculated. Campaigns urging Americans to get vaccinated for their health, for their grandparents, for their neighbors, or to get free doughnuts or a free joint haven’t done the trick. States have even held lotteries with a chance to win millions or a college scholarship.
And yet there are still huge numbers of unvaccinated people. Federal, state, and municipal governments as well as private businesses continue to largely avoid mandates for their employees out of fears they will provoke a backlash.
So, how about an economic argument? Get a COVID shot to protect your wallet.
Getting hospitalized with COVID in the United States typically generates huge bills. Those submitted by COVID patients to the NPR-Kaiser Health News “Bill of the Month” project include a $17,000 bill for a brief hospital stay in Marietta, Ga., (reduced to about $4,000 for an uninsured patient under a “charity care” policy); a $104,000 bill for a 14-day hospitalization in Miami for an uninsured man; and a bill for possibly hundreds of thousands for a 2-week hospital stay – some of it on a ventilator – for a foreign tourist in Hawaii whose travel health insurance contained a “pandemic exclusion.”
Even though insurance companies negotiate lower prices and cover much of the cost of care, an over-$1,000 out-of-pocket bill for a deductible – plus more for copays and possibly some out-of-network care – should be a pretty scary incentive.
In 2020, before COVID vaccines, most major private insurers waived patient payments – from coinsurance to deductibles – for COVID treatment. But many, if not most, have allowed that policy to lapse. Aetna, for example, ended that policy Feb. 28; UnitedHealthcare began rolling back its waivers late last year and ended them by the end of March.
More than 97% of hospitalized patients last month were unvaccinated. Though the vaccines will not necessarily prevent you from catching the coronavirus, they are highly effective at assuring you will have a milder case and are kept out of the hospital.
For this reason, there’s logic behind insurers’ waiver rollback: Why should patients be kept financially unharmed from what is now a preventable hospitalization, thanks to a vaccine that the government paid for and made available free of charge? It is now in many drugstores, it’s popping up at highway rest stops and bus stops, and it can be delivered and administered at home in parts of the country.
A harsher society might impose tough penalties on people who refuse vaccinations and contract the virus. Recently, the National Football League decreed that teams will forfeit a game canceled because of a COVID outbreak among unvaccinated players – and neither team’s players will be paid.
But insurers could try to do more, like penalizing the unvaccinated. And there is precedent. Already, some policies won’t cover treatment necessitated by what insurance companies deem risky behavior, such as scuba diving and rock climbing.
The Affordable Care Act allows insurers to charge smokers up to 50% more than what nonsmokers pay for some health plans. Four-fifths of states follow that protocol, though most employer-based plans do not do so. In 49 states, people caught driving without auto insurance face fines, confiscation of their car, loss of their license, and even jail. And reckless drivers pay more for insurance.
The logic behind the policies is that the offenders’ behavior can hurt others and costs society a lot of money. If a person decides not to get vaccinated and contracts a bad case of COVID, they are not only exposing others in their workplace or neighborhoods; the tens or hundreds of thousands spent on their care could mean higher premiums for others as well in their insurance plans next year. What’s more, outbreaks in low-vaccination regions could help breed more vaccine-resistant variants that affect everyone.
Yes, we often cover people whose habits may have contributed to their illness – insurance regularly pays for drug and alcohol rehab and cancer treatment for smokers.
That’s one reason, perhaps, that insurers too have so far favored carrots, not sticks, to get people vaccinated. Some private insurers are offering people who get vaccinated a credit toward their medical premiums, or gift cards and sweepstakes prizes, according to America’s Health Insurance Plans, an industry organization.
Tough love might be easier if the Food and Drug Administration gives vaccines full approval, rather than the current emergency use authorization. Even so, taxpayer-financed plans like Medicaid and Medicare must treat everyone the same and would encounter a lengthy process to secure federal waivers to experiment with incentives, according to Larry Levitt, executive vice president of Kaiser Family Foundation. These programs cannot charge different rates to different patients in a state.
KFF polling shows such incentives are of limited value, anyway. Many holdouts say they will be vaccinated only if required to do so by their employers.
But what if the financial cost of not getting vaccinated were just too high? If patients thought about the price they might need to pay for their own care, maybe they would reconsider remaining unprotected.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
FDA panel balks at TriGuard 3 cerebral embolic device for TAVR
A Food and Drug Administration advisory panel struggled to muster support for marketing clearance of the TriGuard 3 (Keystone Heart) device for use during transcatheter aortic valve replacement (TAVR).
The Circulatory Systems Devices Panel of the Medical Devices Advisory Committee took no vote when it met Aug. 3, but weighed evidence for a proposed indication for the device “to minimize the risk of cerebral damage by deflecting embolic debris away from the cerebral circulation” during TAVR.
“While this device may deflect some debris, the data would suggest it may also create issues,” said Keith B. Allen, MD, director of surgical research at the Mid America Heart & Lung Surgeons, Kansas City, Mo. “I am really concerned that our desire and the emotion that surrounds preventing stroke are not being supported by the data.”
TriGuard 3 received CE Mark in Europe in March 2020. It was submitted for 510(k) clearance and seeks to prove substantial equivalence to the predicate Sentinel device (Claret Medical), currently the only approved embolic protection device in the United States.
The device is designed to cover all three major aortic vessels (innominate, left carotid, and left subclavian arteries) and is delivered transfemorally through an 8F sheath, whereas the Sentinel is positioned within the branch vessels, doesn’t cover the left subclavian artery, and is introduced through the radial or brachial artery via a 6F sheath.
TriGuard 3 faced an uphill battle, however, after failing to meet the primary composite efficacy endpoint in the REFLECT phase 2 trial (P = .857), with numeric trends showing higher all-cause mortality or any stroke at 30 days (9.8% vs. 6.7%) than pooled control subjects without embolic protection.
Rates for other components of the endpoint also trended higher with the device: National Institutes of Stroke Stroke Scale score worsening 2-5 days after the procedure, cerebral ischemic lesions on MRI 2-5 days after the procedure, and total cerebral ischemic lesion volume.
The Sentinel device was approved in 2017 after it failed to meet its primary efficacy endpoint of new brain lesion volume on MRI, but death and stroke rates favored the device over control, the panel pointed out.
The sponsor provided additional analyses in the per treatment (PT) population, defined as those with complete three-vessel coverage in at least two of three procedural time points. Compared with pooled control subjects, most of the imaging endpoints favored the TriGuard 3 device, but clinical neurologic event rates continued to favor the control group.
“The data used to demonstrate efficacy are all based on the PT subpopulation of the whole population, and those have to be considered promissory data,” said John Hirshfeld, MD, emeritus professor, University of Pennsylvania, Philadelphia. “This is the group where everything went well and for us to decide that’s achievable in the general population is speculative.”
Safety data
The REFLECT trial did meet its primary safety endpoint, with a 30-day major adverse cardiovascular event rate of 15.9%, compared with a performance goal of 34.4% (P < .0001).
Although prespecified, panel members pushed back, saying that the performance goal was unacceptably high, with several members remarking they’d never heard of a trial adding 9% as a “fudge factor” to a 25% historic control rate to get to the 34% performance target.
Keystone health officials noted that REFLECT was not designed to demonstrate a significant difference in the rate of primary safety events, compared with control. Instead, its purpose was to demonstrate that TriGuard 3 did not increase the risk associated with a TAVR procedure.
The TriGuard 3 device was successfully placed and retrieved in 100% of patients, but complete coverage was not uniform, with 72% of 157 as-treated patients having complete three-vessel coverage post TAVR but 15% having no coverage.
Panel members also expressed concern over device interference during TAVR, which was reported in nearly 10% of all TriGuard patients.
The TriGuard 3 group had 11 major vascular complications, 2 directly related to the device, and 3 stage 3 acute kidney injuries, whereas neither complication occurred in the control group.
Throughout the 9-hour hearing, the panel wrestled with what was described as a highly select patient group and small patient numbers that made it difficult to interpret observed differences. The trial involved 157 TriGuard 3 patients (including 41 from the roll-in phase) and 119 control subjects pooled from phase 2 of the trial (n = 57) and from phase 1 using the early-stage TriGuard HDH device (n = 57).
Pieter Stella, MD, PhD, Utrecht (the Netherlands) Medical Center, also presented “real-world” evidence from 75 patients in the Netherlands using the latest iteration of the device available in Europe with updates to the crimper and additional training materials to prevent the device from torquing during delivery. No strokes were reported, one patient had a transient ischemic attack (TIA), and two patients had a dissection, which resolved without sequelae.
Ralph Brindis, MD, MPH, professor of medicine, University of California, San Francisco, countered that there were only three experienced operators from a single center and that the stroke incidence was physician reported, “not data we can really embrace.”
There was much debate over why enrollment in phase 2 of the RHYTHM trial was temporarily paused in February 2019, briefly restarted, and then prematurely stopped in April 2019.
FDA officials said the study was paused at the recommendation of the data monitoring committee (DMC) because rates of safety events were different between patients and control subjects and operational errors called into question the accuracy of the data being reviewed. Ultimately, both the DMC and FDA recommended study suspension.
During the public hearing, TAVR pioneer Alain Cribier, MD, University of Rouen’s Charles Nicolle Hospital, Mont-Saint-Aignan, France, said the TriGuard 3 is of interest because it can be used with minimal need for manipulation and complete coverage of the cerebral vessels that is achieved by diverting rather than capturing debris. “The rapid and exponential growth of TAVR procedures demands safe TAVR interventions and the use of cerebral protection devices is a step in this direction.”

Others took a dim view. “Given that the Sentinel device has not demonstrated benefit on clinical outcomes, there is significant concern about similar devices, such as the TriGuard 3, providing clinical benefit,” Rita Redberg, MD, Sanket Dhruva, MD, and Robin Ji, University of California, San Francisco, wrote in a letter submitted to the panel.
Commenting further, they added: “With the results from the REFLECT II trial demonstrating no evidence for clinical outcome benefit in TAVR patients, and numerically higher rates for stroke risk, mortality, bleeding risk, and other dangerous adverse complications among those treated, it is concerning and dangerous for patient safety that the TriGUARD 3 cerebral embolic protection device is being considered for FDA 510(k) clearance.”
The FDA panel members reported no financial relationships.
A version of this article first appeared on Medscape.com.
A Food and Drug Administration advisory panel struggled to muster support for marketing clearance of the TriGuard 3 (Keystone Heart) device for use during transcatheter aortic valve replacement (TAVR).
The Circulatory Systems Devices Panel of the Medical Devices Advisory Committee took no vote when it met Aug. 3, but weighed evidence for a proposed indication for the device “to minimize the risk of cerebral damage by deflecting embolic debris away from the cerebral circulation” during TAVR.
“While this device may deflect some debris, the data would suggest it may also create issues,” said Keith B. Allen, MD, director of surgical research at the Mid America Heart & Lung Surgeons, Kansas City, Mo. “I am really concerned that our desire and the emotion that surrounds preventing stroke are not being supported by the data.”
TriGuard 3 received CE Mark in Europe in March 2020. It was submitted for 510(k) clearance and seeks to prove substantial equivalence to the predicate Sentinel device (Claret Medical), currently the only approved embolic protection device in the United States.
The device is designed to cover all three major aortic vessels (innominate, left carotid, and left subclavian arteries) and is delivered transfemorally through an 8F sheath, whereas the Sentinel is positioned within the branch vessels, doesn’t cover the left subclavian artery, and is introduced through the radial or brachial artery via a 6F sheath.
TriGuard 3 faced an uphill battle, however, after failing to meet the primary composite efficacy endpoint in the REFLECT phase 2 trial (P = .857), with numeric trends showing higher all-cause mortality or any stroke at 30 days (9.8% vs. 6.7%) than pooled control subjects without embolic protection.
Rates for other components of the endpoint also trended higher with the device: National Institutes of Stroke Stroke Scale score worsening 2-5 days after the procedure, cerebral ischemic lesions on MRI 2-5 days after the procedure, and total cerebral ischemic lesion volume.
The Sentinel device was approved in 2017 after it failed to meet its primary efficacy endpoint of new brain lesion volume on MRI, but death and stroke rates favored the device over control, the panel pointed out.
The sponsor provided additional analyses in the per treatment (PT) population, defined as those with complete three-vessel coverage in at least two of three procedural time points. Compared with pooled control subjects, most of the imaging endpoints favored the TriGuard 3 device, but clinical neurologic event rates continued to favor the control group.
“The data used to demonstrate efficacy are all based on the PT subpopulation of the whole population, and those have to be considered promissory data,” said John Hirshfeld, MD, emeritus professor, University of Pennsylvania, Philadelphia. “This is the group where everything went well and for us to decide that’s achievable in the general population is speculative.”
Safety data
The REFLECT trial did meet its primary safety endpoint, with a 30-day major adverse cardiovascular event rate of 15.9%, compared with a performance goal of 34.4% (P < .0001).
Although prespecified, panel members pushed back, saying that the performance goal was unacceptably high, with several members remarking they’d never heard of a trial adding 9% as a “fudge factor” to a 25% historic control rate to get to the 34% performance target.
Keystone health officials noted that REFLECT was not designed to demonstrate a significant difference in the rate of primary safety events, compared with control. Instead, its purpose was to demonstrate that TriGuard 3 did not increase the risk associated with a TAVR procedure.
The TriGuard 3 device was successfully placed and retrieved in 100% of patients, but complete coverage was not uniform, with 72% of 157 as-treated patients having complete three-vessel coverage post TAVR but 15% having no coverage.
Panel members also expressed concern over device interference during TAVR, which was reported in nearly 10% of all TriGuard patients.
The TriGuard 3 group had 11 major vascular complications, 2 directly related to the device, and 3 stage 3 acute kidney injuries, whereas neither complication occurred in the control group.
Throughout the 9-hour hearing, the panel wrestled with what was described as a highly select patient group and small patient numbers that made it difficult to interpret observed differences. The trial involved 157 TriGuard 3 patients (including 41 from the roll-in phase) and 119 control subjects pooled from phase 2 of the trial (n = 57) and from phase 1 using the early-stage TriGuard HDH device (n = 57).
Pieter Stella, MD, PhD, Utrecht (the Netherlands) Medical Center, also presented “real-world” evidence from 75 patients in the Netherlands using the latest iteration of the device available in Europe with updates to the crimper and additional training materials to prevent the device from torquing during delivery. No strokes were reported, one patient had a transient ischemic attack (TIA), and two patients had a dissection, which resolved without sequelae.
Ralph Brindis, MD, MPH, professor of medicine, University of California, San Francisco, countered that there were only three experienced operators from a single center and that the stroke incidence was physician reported, “not data we can really embrace.”
There was much debate over why enrollment in phase 2 of the RHYTHM trial was temporarily paused in February 2019, briefly restarted, and then prematurely stopped in April 2019.
FDA officials said the study was paused at the recommendation of the data monitoring committee (DMC) because rates of safety events were different between patients and control subjects and operational errors called into question the accuracy of the data being reviewed. Ultimately, both the DMC and FDA recommended study suspension.
During the public hearing, TAVR pioneer Alain Cribier, MD, University of Rouen’s Charles Nicolle Hospital, Mont-Saint-Aignan, France, said the TriGuard 3 is of interest because it can be used with minimal need for manipulation and complete coverage of the cerebral vessels that is achieved by diverting rather than capturing debris. “The rapid and exponential growth of TAVR procedures demands safe TAVR interventions and the use of cerebral protection devices is a step in this direction.”
Others took a dim view. “Given that the Sentinel device has not demonstrated benefit on clinical outcomes, there is significant concern about similar devices, such as the TriGuard 3, providing clinical benefit,” Rita Redberg, MD, Sanket Dhruva, MD, and Robin Ji, University of California, San Francisco, wrote in a letter submitted to the panel.
Commenting further, they added: “With the results from the REFLECT II trial demonstrating no evidence for clinical outcome benefit in TAVR patients, and numerically higher rates for stroke risk, mortality, bleeding risk, and other dangerous adverse complications among those treated, it is concerning and dangerous for patient safety that the TriGUARD 3 cerebral embolic protection device is being considered for FDA 510(k) clearance.”
The FDA panel members reported no financial relationships.
A version of this article first appeared on Medscape.com.
A Food and Drug Administration advisory panel struggled to muster support for marketing clearance of the TriGuard 3 (Keystone Heart) device for use during transcatheter aortic valve replacement (TAVR).
The Circulatory Systems Devices Panel of the Medical Devices Advisory Committee took no vote when it met Aug. 3, but weighed evidence for a proposed indication for the device “to minimize the risk of cerebral damage by deflecting embolic debris away from the cerebral circulation” during TAVR.
“While this device may deflect some debris, the data would suggest it may also create issues,” said Keith B. Allen, MD, director of surgical research at the Mid America Heart & Lung Surgeons, Kansas City, Mo. “I am really concerned that our desire and the emotion that surrounds preventing stroke are not being supported by the data.”
TriGuard 3 received CE Mark in Europe in March 2020. It was submitted for 510(k) clearance and seeks to prove substantial equivalence to the predicate Sentinel device (Claret Medical), currently the only approved embolic protection device in the United States.
The device is designed to cover all three major aortic vessels (innominate, left carotid, and left subclavian arteries) and is delivered transfemorally through an 8F sheath, whereas the Sentinel is positioned within the branch vessels, doesn’t cover the left subclavian artery, and is introduced through the radial or brachial artery via a 6F sheath.
TriGuard 3 faced an uphill battle, however, after failing to meet the primary composite efficacy endpoint in the REFLECT phase 2 trial (P = .857), with numeric trends showing higher all-cause mortality or any stroke at 30 days (9.8% vs. 6.7%) than pooled control subjects without embolic protection.
Rates for other components of the endpoint also trended higher with the device: National Institutes of Stroke Stroke Scale score worsening 2-5 days after the procedure, cerebral ischemic lesions on MRI 2-5 days after the procedure, and total cerebral ischemic lesion volume.
The Sentinel device was approved in 2017 after it failed to meet its primary efficacy endpoint of new brain lesion volume on MRI, but death and stroke rates favored the device over control, the panel pointed out.
The sponsor provided additional analyses in the per treatment (PT) population, defined as those with complete three-vessel coverage in at least two of three procedural time points. Compared with pooled control subjects, most of the imaging endpoints favored the TriGuard 3 device, but clinical neurologic event rates continued to favor the control group.
“The data used to demonstrate efficacy are all based on the PT subpopulation of the whole population, and those have to be considered promissory data,” said John Hirshfeld, MD, emeritus professor, University of Pennsylvania, Philadelphia. “This is the group where everything went well and for us to decide that’s achievable in the general population is speculative.”
Safety data
The REFLECT trial did meet its primary safety endpoint, with a 30-day major adverse cardiovascular event rate of 15.9%, compared with a performance goal of 34.4% (P < .0001).
Although prespecified, panel members pushed back, saying that the performance goal was unacceptably high, with several members remarking they’d never heard of a trial adding 9% as a “fudge factor” to a 25% historic control rate to get to the 34% performance target.
Keystone health officials noted that REFLECT was not designed to demonstrate a significant difference in the rate of primary safety events, compared with control. Instead, its purpose was to demonstrate that TriGuard 3 did not increase the risk associated with a TAVR procedure.
The TriGuard 3 device was successfully placed and retrieved in 100% of patients, but complete coverage was not uniform, with 72% of 157 as-treated patients having complete three-vessel coverage post TAVR but 15% having no coverage.
Panel members also expressed concern over device interference during TAVR, which was reported in nearly 10% of all TriGuard patients.
The TriGuard 3 group had 11 major vascular complications, 2 directly related to the device, and 3 stage 3 acute kidney injuries, whereas neither complication occurred in the control group.
Throughout the 9-hour hearing, the panel wrestled with what was described as a highly select patient group and small patient numbers that made it difficult to interpret observed differences. The trial involved 157 TriGuard 3 patients (including 41 from the roll-in phase) and 119 control subjects pooled from phase 2 of the trial (n = 57) and from phase 1 using the early-stage TriGuard HDH device (n = 57).
Pieter Stella, MD, PhD, Utrecht (the Netherlands) Medical Center, also presented “real-world” evidence from 75 patients in the Netherlands using the latest iteration of the device available in Europe with updates to the crimper and additional training materials to prevent the device from torquing during delivery. No strokes were reported, one patient had a transient ischemic attack (TIA), and two patients had a dissection, which resolved without sequelae.
Ralph Brindis, MD, MPH, professor of medicine, University of California, San Francisco, countered that there were only three experienced operators from a single center and that the stroke incidence was physician reported, “not data we can really embrace.”
There was much debate over why enrollment in phase 2 of the RHYTHM trial was temporarily paused in February 2019, briefly restarted, and then prematurely stopped in April 2019.
FDA officials said the study was paused at the recommendation of the data monitoring committee (DMC) because rates of safety events were different between patients and control subjects and operational errors called into question the accuracy of the data being reviewed. Ultimately, both the DMC and FDA recommended study suspension.
During the public hearing, TAVR pioneer Alain Cribier, MD, University of Rouen’s Charles Nicolle Hospital, Mont-Saint-Aignan, France, said the TriGuard 3 is of interest because it can be used with minimal need for manipulation and complete coverage of the cerebral vessels that is achieved by diverting rather than capturing debris. “The rapid and exponential growth of TAVR procedures demands safe TAVR interventions and the use of cerebral protection devices is a step in this direction.”
Others took a dim view. “Given that the Sentinel device has not demonstrated benefit on clinical outcomes, there is significant concern about similar devices, such as the TriGuard 3, providing clinical benefit,” Rita Redberg, MD, Sanket Dhruva, MD, and Robin Ji, University of California, San Francisco, wrote in a letter submitted to the panel.
Commenting further, they added: “With the results from the REFLECT II trial demonstrating no evidence for clinical outcome benefit in TAVR patients, and numerically higher rates for stroke risk, mortality, bleeding risk, and other dangerous adverse complications among those treated, it is concerning and dangerous for patient safety that the TriGUARD 3 cerebral embolic protection device is being considered for FDA 510(k) clearance.”
The FDA panel members reported no financial relationships.
A version of this article first appeared on Medscape.com.
Androgenetic alopecia fuels negative emotions and poor quality of life
and meta-analysis of 41 studies.
“Hair loss affects self-image, causes trichodynia, and plays a role in emotions and social activity, which may be associated with psychiatric problems and impaired health-related quality of life,” wrote Chun-Hsien Huang, MD, of Chang Gung Memorial Hospital, Linkou, Taiwan, and colleagues. However, systematic reviews of the associations between androgenetic alopecia (AGA) and health-related quality of life (HRQOL) are lacking, they said.
In a study published in JAMA Dermatology, the researchers reviewed data from a total of 7,995 AGA patients in 41 studies. The studies included 11 tools for HRQOL assessment and 29 tools for psychological assessment. Of these, the Dermatology Life Quality Index (DLQI) and the Hair-Specific Skindex-29 were used to assess quality of life, and the Center for Epidemiologic Studies Depression Scale (CES-D) was used for psychological assessment in the meta-analysis.
Overall, 27 studies identified 18 factors associated with HRQOL; those with an inverse effect were higher self-rated hair loss severity, lower VAS score, and higher educational level. Of note, neither physician-rated hair loss severity nor treatment response were factors in HRQOL, the researchers said.
The pooled DLQI score across studies was 8.16, and subgroup analysis showed no differences in HRQOL between men and women or between patients from European vs. Asian countries. However, five studies showed significant differences in HRQOL between men and women when different assessment tools were used, which emphasized the need for more studies to examine the association of AGA with HRQOL by sex, the researchers said.
The meta-analysis of the Hair-Specific Skindex-29 scores showed pooled averages of 21.95 for symptom dimension, 18.52 in function dimension, and 29.22 in emotion dimension. Of these, the emotion dimension scores indicated moderate emotional impairment.
The average pooled score on the CES-D in the meta-analysis was 14.98, indicating no association between AGA and depression, the researchers said. However, “depression accounts for only a part of the emotion dimension,” they said. “Therefore, emotion dimension could be impaired even if no depressive symptoms were noted.”
The pooled DLQI scores for AGA (8.16) were higher than scores for other skin conditions including alopecia areata (6.3), contact dermatitis (7.35), and acne vulgaris (7.45), but lower than the pooled scores for vitiligo (9.11), urticaria (9.8), psoriasis (10.53), and atopic dermatitis (11.2), the researchers noted. “However, additional head-to-head studies are needed for direct comparisons of HRQOL in patients with various dermatoses,” they said.
The study findings were limited by the cross-sectional design of many of the included studies, and the limited number of assessment tools included in the analysis, the researchers noted. Other limitations were the lack of specific domain scores and the inclusion of only three studies from China, they said.
However, the results are consistent with findings from previous studies, and suggest that patients with AGA may benefit from psychological and psychosocial support, the researchers said.
Quality of life issues deserve attention
“Studies of the quality-of-life impact of various conditions are becoming more common in the medical literature,” Jamie B. MacKelfresh, MD, associate professor of dermatology, Emory University, Atlanta, said in an interview.
“Androgenetic alopecia is the most common type of hair loss in men and women,” she noted. “Hair loss can be labeled as a cosmetic concern, so it is important that providers understand the significant quality-of-life impact androgenetic alopecia has on the many people with this diagnosis,” she emphasized.
Dr. MacKelfresh, who was asked to comment on the study, said she was surprised that the subgroup analysis of the DLQI showed no significant difference between men and women. “This surprised me because a number of past studies have highlighted the relatively greater quality-of-life impact of hair loss on women compared to men,” she noted.
However, she added, “I was not surprised to see that androgenetic alopecia has a significant quality-of-life impact on many patients, and that physician objective assessments of the hair loss do not always correlate with the amount of quality-of-life impact,” said Dr. MacKelfresh. “In the patients I see, I find hair loss very often has a significant quality-of-life impact on patients, regardless of gender, and the amount of quality-of-life impact definitely does not always correlate with the objective amount of hair loss,” she noted.
A takeaway message for clinicians is to be aware that androgenetic alopecia frequently has a significant impact on patients, “particularly in the emotional dimension,” and can affect both men and women, Dr. MacKelfresh said. “Objective assessments of hair loss severity by providers may not accurately predict the degree of quality-of-life impact a patient may experience; therefore providers should include quality-of-life questions as part of their standard evaluation of patients with androgenetic alopecia,” she said. In addition to treating the hair loss, providers can help these patients by guiding them to psychological support resources, she emphasized.
More research is needed to assess the impact of androgenetic alopecia on “men, women, and the non-binary gender population,” as well as the relationship between self-esteem and hair loss, she said. “Finally, it would be helpful to understand what interventions can best help improve androgenetic alopecia patients’ quality of life,” she noted.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. MacKelfresh had no financial conflicts to disclose.
and meta-analysis of 41 studies.
“Hair loss affects self-image, causes trichodynia, and plays a role in emotions and social activity, which may be associated with psychiatric problems and impaired health-related quality of life,” wrote Chun-Hsien Huang, MD, of Chang Gung Memorial Hospital, Linkou, Taiwan, and colleagues. However, systematic reviews of the associations between androgenetic alopecia (AGA) and health-related quality of life (HRQOL) are lacking, they said.
In a study published in JAMA Dermatology, the researchers reviewed data from a total of 7,995 AGA patients in 41 studies. The studies included 11 tools for HRQOL assessment and 29 tools for psychological assessment. Of these, the Dermatology Life Quality Index (DLQI) and the Hair-Specific Skindex-29 were used to assess quality of life, and the Center for Epidemiologic Studies Depression Scale (CES-D) was used for psychological assessment in the meta-analysis.
Overall, 27 studies identified 18 factors associated with HRQOL; those with an inverse effect were higher self-rated hair loss severity, lower VAS score, and higher educational level. Of note, neither physician-rated hair loss severity nor treatment response were factors in HRQOL, the researchers said.
The pooled DLQI score across studies was 8.16, and subgroup analysis showed no differences in HRQOL between men and women or between patients from European vs. Asian countries. However, five studies showed significant differences in HRQOL between men and women when different assessment tools were used, which emphasized the need for more studies to examine the association of AGA with HRQOL by sex, the researchers said.
The meta-analysis of the Hair-Specific Skindex-29 scores showed pooled averages of 21.95 for symptom dimension, 18.52 in function dimension, and 29.22 in emotion dimension. Of these, the emotion dimension scores indicated moderate emotional impairment.
The average pooled score on the CES-D in the meta-analysis was 14.98, indicating no association between AGA and depression, the researchers said. However, “depression accounts for only a part of the emotion dimension,” they said. “Therefore, emotion dimension could be impaired even if no depressive symptoms were noted.”
The pooled DLQI scores for AGA (8.16) were higher than scores for other skin conditions including alopecia areata (6.3), contact dermatitis (7.35), and acne vulgaris (7.45), but lower than the pooled scores for vitiligo (9.11), urticaria (9.8), psoriasis (10.53), and atopic dermatitis (11.2), the researchers noted. “However, additional head-to-head studies are needed for direct comparisons of HRQOL in patients with various dermatoses,” they said.
The study findings were limited by the cross-sectional design of many of the included studies, and the limited number of assessment tools included in the analysis, the researchers noted. Other limitations were the lack of specific domain scores and the inclusion of only three studies from China, they said.
However, the results are consistent with findings from previous studies, and suggest that patients with AGA may benefit from psychological and psychosocial support, the researchers said.
Quality of life issues deserve attention
“Studies of the quality-of-life impact of various conditions are becoming more common in the medical literature,” Jamie B. MacKelfresh, MD, associate professor of dermatology, Emory University, Atlanta, said in an interview.
“Androgenetic alopecia is the most common type of hair loss in men and women,” she noted. “Hair loss can be labeled as a cosmetic concern, so it is important that providers understand the significant quality-of-life impact androgenetic alopecia has on the many people with this diagnosis,” she emphasized.
Dr. MacKelfresh, who was asked to comment on the study, said she was surprised that the subgroup analysis of the DLQI showed no significant difference between men and women. “This surprised me because a number of past studies have highlighted the relatively greater quality-of-life impact of hair loss on women compared to men,” she noted.
However, she added, “I was not surprised to see that androgenetic alopecia has a significant quality-of-life impact on many patients, and that physician objective assessments of the hair loss do not always correlate with the amount of quality-of-life impact,” said Dr. MacKelfresh. “In the patients I see, I find hair loss very often has a significant quality-of-life impact on patients, regardless of gender, and the amount of quality-of-life impact definitely does not always correlate with the objective amount of hair loss,” she noted.
A takeaway message for clinicians is to be aware that androgenetic alopecia frequently has a significant impact on patients, “particularly in the emotional dimension,” and can affect both men and women, Dr. MacKelfresh said. “Objective assessments of hair loss severity by providers may not accurately predict the degree of quality-of-life impact a patient may experience; therefore providers should include quality-of-life questions as part of their standard evaluation of patients with androgenetic alopecia,” she said. In addition to treating the hair loss, providers can help these patients by guiding them to psychological support resources, she emphasized.
More research is needed to assess the impact of androgenetic alopecia on “men, women, and the non-binary gender population,” as well as the relationship between self-esteem and hair loss, she said. “Finally, it would be helpful to understand what interventions can best help improve androgenetic alopecia patients’ quality of life,” she noted.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. MacKelfresh had no financial conflicts to disclose.
and meta-analysis of 41 studies.
“Hair loss affects self-image, causes trichodynia, and plays a role in emotions and social activity, which may be associated with psychiatric problems and impaired health-related quality of life,” wrote Chun-Hsien Huang, MD, of Chang Gung Memorial Hospital, Linkou, Taiwan, and colleagues. However, systematic reviews of the associations between androgenetic alopecia (AGA) and health-related quality of life (HRQOL) are lacking, they said.
In a study published in JAMA Dermatology, the researchers reviewed data from a total of 7,995 AGA patients in 41 studies. The studies included 11 tools for HRQOL assessment and 29 tools for psychological assessment. Of these, the Dermatology Life Quality Index (DLQI) and the Hair-Specific Skindex-29 were used to assess quality of life, and the Center for Epidemiologic Studies Depression Scale (CES-D) was used for psychological assessment in the meta-analysis.
Overall, 27 studies identified 18 factors associated with HRQOL; those with an inverse effect were higher self-rated hair loss severity, lower VAS score, and higher educational level. Of note, neither physician-rated hair loss severity nor treatment response were factors in HRQOL, the researchers said.
The pooled DLQI score across studies was 8.16, and subgroup analysis showed no differences in HRQOL between men and women or between patients from European vs. Asian countries. However, five studies showed significant differences in HRQOL between men and women when different assessment tools were used, which emphasized the need for more studies to examine the association of AGA with HRQOL by sex, the researchers said.
The meta-analysis of the Hair-Specific Skindex-29 scores showed pooled averages of 21.95 for symptom dimension, 18.52 in function dimension, and 29.22 in emotion dimension. Of these, the emotion dimension scores indicated moderate emotional impairment.
The average pooled score on the CES-D in the meta-analysis was 14.98, indicating no association between AGA and depression, the researchers said. However, “depression accounts for only a part of the emotion dimension,” they said. “Therefore, emotion dimension could be impaired even if no depressive symptoms were noted.”
The pooled DLQI scores for AGA (8.16) were higher than scores for other skin conditions including alopecia areata (6.3), contact dermatitis (7.35), and acne vulgaris (7.45), but lower than the pooled scores for vitiligo (9.11), urticaria (9.8), psoriasis (10.53), and atopic dermatitis (11.2), the researchers noted. “However, additional head-to-head studies are needed for direct comparisons of HRQOL in patients with various dermatoses,” they said.
The study findings were limited by the cross-sectional design of many of the included studies, and the limited number of assessment tools included in the analysis, the researchers noted. Other limitations were the lack of specific domain scores and the inclusion of only three studies from China, they said.
However, the results are consistent with findings from previous studies, and suggest that patients with AGA may benefit from psychological and psychosocial support, the researchers said.
Quality of life issues deserve attention
“Studies of the quality-of-life impact of various conditions are becoming more common in the medical literature,” Jamie B. MacKelfresh, MD, associate professor of dermatology, Emory University, Atlanta, said in an interview.
“Androgenetic alopecia is the most common type of hair loss in men and women,” she noted. “Hair loss can be labeled as a cosmetic concern, so it is important that providers understand the significant quality-of-life impact androgenetic alopecia has on the many people with this diagnosis,” she emphasized.
Dr. MacKelfresh, who was asked to comment on the study, said she was surprised that the subgroup analysis of the DLQI showed no significant difference between men and women. “This surprised me because a number of past studies have highlighted the relatively greater quality-of-life impact of hair loss on women compared to men,” she noted.
However, she added, “I was not surprised to see that androgenetic alopecia has a significant quality-of-life impact on many patients, and that physician objective assessments of the hair loss do not always correlate with the amount of quality-of-life impact,” said Dr. MacKelfresh. “In the patients I see, I find hair loss very often has a significant quality-of-life impact on patients, regardless of gender, and the amount of quality-of-life impact definitely does not always correlate with the objective amount of hair loss,” she noted.
A takeaway message for clinicians is to be aware that androgenetic alopecia frequently has a significant impact on patients, “particularly in the emotional dimension,” and can affect both men and women, Dr. MacKelfresh said. “Objective assessments of hair loss severity by providers may not accurately predict the degree of quality-of-life impact a patient may experience; therefore providers should include quality-of-life questions as part of their standard evaluation of patients with androgenetic alopecia,” she said. In addition to treating the hair loss, providers can help these patients by guiding them to psychological support resources, she emphasized.
More research is needed to assess the impact of androgenetic alopecia on “men, women, and the non-binary gender population,” as well as the relationship between self-esteem and hair loss, she said. “Finally, it would be helpful to understand what interventions can best help improve androgenetic alopecia patients’ quality of life,” she noted.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. MacKelfresh had no financial conflicts to disclose.
FROM JAMA DERMATOLOGY
Graying of hair: Could it be reversed?
as hair pigment goes through its natural progression of senescence.

However, the recent publication that is a collaboration between the department of psychiatry at Columbia University, New York; and the departments of dermatology at the University College Dublin, University of Miami, and the University of Manchester (England); and the Monasterium Laboratory in Münster, Germany, demonstrates a quantitative mapping of human hair graying – and its reversal – in relation to stress.
In the study, hair color of single strands of hair from seven healthy females and seven healthy males, whose mean age was 35 years (range, 9-65 years), were analyzed. In addition to hair pigment analysis, study subjects documented the stress they were experiencing each week in diaries. Using either high resolution image scanners, electron microscopy, and/or hair shaft proteomics, the investigators were able to evaluate loss of pigment within fragments small enough to have grown over one hour.

When changes in hair color were noted, variations in up to 300 proteins were documented, including an up-regulation of the fatty acid synthesis and metabolism machinery in graying. Recent studies also corroborate that fatty acid synthesis by fatty acid synthase and “transport by CPT1A ... are sufficient drivers of cell senescence, and that fatty acid metabolism regulates melanocyte aging biology” the authors wrote.
Molecularly, the investigators found that gray hairs up-regulate proteins associated with energy metabolism, mitochondria, and antioxidant defenses. The graying correlated with stress was also reversible, “at least temporarily,” based on their retrospective analysis and analysis over the 2.5-year recruitment period, the investigators wrote. Specifically, they found that graying hair “may be acutely triggered by stressful life experiences, the removal of which can trigger reversal.” From the data, they also developed a mathematical model to predict what might happen to human hair over time.

Through this study, proof-of-concept evidence is provided indicating that biobehavioral factors are linked to human hair graying dynamics. Future analysis with larger sample sizes and incorporating neuroendocrine markers may further support these correlations. This is an interesting study that elucidates the mechanisms responsible for how stress and other life exposures manifest in human biology, and, if we as human beings effectively manage that stress, how it may both reverse the negative impact and outcomes affecting our body and health.
The study was supported by the Wharton Fund and grants from the National Institutes of Health.
Dr. Wesley and Dr. Lily Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at [email protected]. They have no relevant disclosures.
as hair pigment goes through its natural progression of senescence.
However, the recent publication that is a collaboration between the department of psychiatry at Columbia University, New York; and the departments of dermatology at the University College Dublin, University of Miami, and the University of Manchester (England); and the Monasterium Laboratory in Münster, Germany, demonstrates a quantitative mapping of human hair graying – and its reversal – in relation to stress.
In the study, hair color of single strands of hair from seven healthy females and seven healthy males, whose mean age was 35 years (range, 9-65 years), were analyzed. In addition to hair pigment analysis, study subjects documented the stress they were experiencing each week in diaries. Using either high resolution image scanners, electron microscopy, and/or hair shaft proteomics, the investigators were able to evaluate loss of pigment within fragments small enough to have grown over one hour.
When changes in hair color were noted, variations in up to 300 proteins were documented, including an up-regulation of the fatty acid synthesis and metabolism machinery in graying. Recent studies also corroborate that fatty acid synthesis by fatty acid synthase and “transport by CPT1A ... are sufficient drivers of cell senescence, and that fatty acid metabolism regulates melanocyte aging biology” the authors wrote.
Molecularly, the investigators found that gray hairs up-regulate proteins associated with energy metabolism, mitochondria, and antioxidant defenses. The graying correlated with stress was also reversible, “at least temporarily,” based on their retrospective analysis and analysis over the 2.5-year recruitment period, the investigators wrote. Specifically, they found that graying hair “may be acutely triggered by stressful life experiences, the removal of which can trigger reversal.” From the data, they also developed a mathematical model to predict what might happen to human hair over time.
Through this study, proof-of-concept evidence is provided indicating that biobehavioral factors are linked to human hair graying dynamics. Future analysis with larger sample sizes and incorporating neuroendocrine markers may further support these correlations. This is an interesting study that elucidates the mechanisms responsible for how stress and other life exposures manifest in human biology, and, if we as human beings effectively manage that stress, how it may both reverse the negative impact and outcomes affecting our body and health.
The study was supported by the Wharton Fund and grants from the National Institutes of Health.
Dr. Wesley and Dr. Lily Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at [email protected]. They have no relevant disclosures.
as hair pigment goes through its natural progression of senescence.
However, the recent publication that is a collaboration between the department of psychiatry at Columbia University, New York; and the departments of dermatology at the University College Dublin, University of Miami, and the University of Manchester (England); and the Monasterium Laboratory in Münster, Germany, demonstrates a quantitative mapping of human hair graying – and its reversal – in relation to stress.
In the study, hair color of single strands of hair from seven healthy females and seven healthy males, whose mean age was 35 years (range, 9-65 years), were analyzed. In addition to hair pigment analysis, study subjects documented the stress they were experiencing each week in diaries. Using either high resolution image scanners, electron microscopy, and/or hair shaft proteomics, the investigators were able to evaluate loss of pigment within fragments small enough to have grown over one hour.
When changes in hair color were noted, variations in up to 300 proteins were documented, including an up-regulation of the fatty acid synthesis and metabolism machinery in graying. Recent studies also corroborate that fatty acid synthesis by fatty acid synthase and “transport by CPT1A ... are sufficient drivers of cell senescence, and that fatty acid metabolism regulates melanocyte aging biology” the authors wrote.
Molecularly, the investigators found that gray hairs up-regulate proteins associated with energy metabolism, mitochondria, and antioxidant defenses. The graying correlated with stress was also reversible, “at least temporarily,” based on their retrospective analysis and analysis over the 2.5-year recruitment period, the investigators wrote. Specifically, they found that graying hair “may be acutely triggered by stressful life experiences, the removal of which can trigger reversal.” From the data, they also developed a mathematical model to predict what might happen to human hair over time.
Through this study, proof-of-concept evidence is provided indicating that biobehavioral factors are linked to human hair graying dynamics. Future analysis with larger sample sizes and incorporating neuroendocrine markers may further support these correlations. This is an interesting study that elucidates the mechanisms responsible for how stress and other life exposures manifest in human biology, and, if we as human beings effectively manage that stress, how it may both reverse the negative impact and outcomes affecting our body and health.
The study was supported by the Wharton Fund and grants from the National Institutes of Health.
Dr. Wesley and Dr. Lily Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at [email protected]. They have no relevant disclosures.
Summer campers spread COVID at home, follow-up finds
In a report published online in The New England Journal of Medicine, researchers found that campers spread COVID to household members after returning home – but transmission was more likely from some than others. Distancing and masking helped reduce the risk.
Victoria T. Chu, MD, MPH, with the Centers for Disease Control and Prevention, Atlanta, and colleagues with the agency and the Georgia Department of Health followed up with 224 camp attendees, aged 7 to 19 years, who had evidence of SARS-CoV-2 infection on laboratory testing.
These index patients – 88% of whom had symptoms – had 526 household contacts, mainly parents and siblings. Of 377 household contacts who underwent testing, 46 (12%) tested positive. Another two cases in household contacts were identified using clinical and epidemiologic criteria.
Family members hospitalized
Of the 41 adult household contacts who were infected, four (about 10%) were hospitalized. Their hospital stays ranged from 5 to 11 days. Of the seven infected household contacts who were younger than 18 years, none were hospitalized.
The four hospitalized adults were parents and grandparents aged 45 to 80 years, Dr. Chu said. Two of the four had underlying conditions. None of the household contacts died.
In an adjusted analysis, campers who had practiced physical distancing were less likely to transmit the virus at home, compared with those who had not practiced physical distancing (adjusted odds ratio, 0.4). Household members who had had close or direct contact with the index patients were more than 5 times more likely to become infected, compared with family members with minimal or no contact, analyses showed.
“This retrospective study showed that the efficient transmission of SARS-CoV-2 from school-age children and adolescents to household members led to the hospitalization of adults with secondary cases of COVID-19,” the researchers write. “In households in which transmission occurred, half the household contacts were infected.”
The secondary attack rates in this report may be an underestimate because testing was voluntary and participants reported the results themselves, the authors note. It is possible that infected household contacts spread the virus further, but this study did not address that question, Dr. Chu said.
For the study, investigators interviewed all camp attendees and their parents or guardians by phone between July 17, 2020 and Aug. 24, 2020, to collect information about demographic and clinical characteristics, SARS-CoV-2 testing, and preventive measures. The researchers’ analysis excluded households in which illness onset in a household contact occurred before or less than 2 days after a camper became sick.
About a third of the index patients began to have symptoms while still at camp. These campers may have been less infectious by the time they got home, compared with those whose symptoms started after they returned.
Two-thirds of the index patients adopted physical distancing at home, which “probably reduced the transmission of SARS-CoV-2 in the household,” Dr. Chu and colleagues wrote.
“Children who have had a known COVID-19 exposure should quarantine and obtain testing if they develop symptoms within the 14 days of returning home,” Dr. Chu advised. “If a child develops COVID-19, the child should be cared for and monitored using the proper combination of physical distancing, isolation when feasible, and mask use to prevent household transmission as much as possible. In addition, any person over the age of 12 is now eligible for vaccination in the United States. If eligible, children attending camp and their family members should get vaccinated to protect themselves and others, as vaccinations are our most effective public health prevention strategy.”
Mitigation can help
Another report regarding four overnight camps in Maine – in which three campers tested positive after they arrived last summer – shows that “aggressive mitigation strategies can be effective” in limiting transmission of the virus, William T. Basco Jr., MD, writes in a commentary for this news organization.
This summer, a range of factors, including vaccination rates at the camp, may influence transmission dynamics, Dr. Chu said in an interview. In July, the Associated Press reported outbreaks tied to summer camps in several states.
“Transmission dynamics will probably vary from summer camp to summer camp depending on many factors, such as vaccination rates of camp attendees, the mitigation measures in place, and the number of individual introductions during camp,” Dr. Chu said. “We would expect that a camp with a low vaccination rate among attendees and no enforcement of mitigation measures” still may experience a large outbreak.
“On the other hand, a large proportion of vaccinated individuals and appropriate implementation of multiple mitigation measures, such as wearing masks, may be quite effective at keeping their transmission rates low,” Dr. Chu added. “For camps with younger children who are not currently eligible for vaccination, implementing layered prevention strategies (e.g., mask use, physical distancing, and encouraging outdoor activities when feasible) is important to prevent transmission.”
Although COVID-19 transmission from children to adults, potentially leading to hospitalization, is not a new phenomenon, “data on the extent of transmission driven by children and adolescents in different settings are still quite sparse,” Dr. Chu said. “A better understanding of their impact on household and community transmission to help guide public health recommendations is particularly important, as most children are still not eligible for vaccination, and in-person schools will be reopening this fall.”
A version of this article first appeared on Medscape.com.
In a report published online in The New England Journal of Medicine, researchers found that campers spread COVID to household members after returning home – but transmission was more likely from some than others. Distancing and masking helped reduce the risk.
Victoria T. Chu, MD, MPH, with the Centers for Disease Control and Prevention, Atlanta, and colleagues with the agency and the Georgia Department of Health followed up with 224 camp attendees, aged 7 to 19 years, who had evidence of SARS-CoV-2 infection on laboratory testing.
These index patients – 88% of whom had symptoms – had 526 household contacts, mainly parents and siblings. Of 377 household contacts who underwent testing, 46 (12%) tested positive. Another two cases in household contacts were identified using clinical and epidemiologic criteria.
Family members hospitalized
Of the 41 adult household contacts who were infected, four (about 10%) were hospitalized. Their hospital stays ranged from 5 to 11 days. Of the seven infected household contacts who were younger than 18 years, none were hospitalized.
The four hospitalized adults were parents and grandparents aged 45 to 80 years, Dr. Chu said. Two of the four had underlying conditions. None of the household contacts died.
In an adjusted analysis, campers who had practiced physical distancing were less likely to transmit the virus at home, compared with those who had not practiced physical distancing (adjusted odds ratio, 0.4). Household members who had had close or direct contact with the index patients were more than 5 times more likely to become infected, compared with family members with minimal or no contact, analyses showed.
“This retrospective study showed that the efficient transmission of SARS-CoV-2 from school-age children and adolescents to household members led to the hospitalization of adults with secondary cases of COVID-19,” the researchers write. “In households in which transmission occurred, half the household contacts were infected.”
The secondary attack rates in this report may be an underestimate because testing was voluntary and participants reported the results themselves, the authors note. It is possible that infected household contacts spread the virus further, but this study did not address that question, Dr. Chu said.
For the study, investigators interviewed all camp attendees and their parents or guardians by phone between July 17, 2020 and Aug. 24, 2020, to collect information about demographic and clinical characteristics, SARS-CoV-2 testing, and preventive measures. The researchers’ analysis excluded households in which illness onset in a household contact occurred before or less than 2 days after a camper became sick.
About a third of the index patients began to have symptoms while still at camp. These campers may have been less infectious by the time they got home, compared with those whose symptoms started after they returned.
Two-thirds of the index patients adopted physical distancing at home, which “probably reduced the transmission of SARS-CoV-2 in the household,” Dr. Chu and colleagues wrote.
“Children who have had a known COVID-19 exposure should quarantine and obtain testing if they develop symptoms within the 14 days of returning home,” Dr. Chu advised. “If a child develops COVID-19, the child should be cared for and monitored using the proper combination of physical distancing, isolation when feasible, and mask use to prevent household transmission as much as possible. In addition, any person over the age of 12 is now eligible for vaccination in the United States. If eligible, children attending camp and their family members should get vaccinated to protect themselves and others, as vaccinations are our most effective public health prevention strategy.”
Mitigation can help
Another report regarding four overnight camps in Maine – in which three campers tested positive after they arrived last summer – shows that “aggressive mitigation strategies can be effective” in limiting transmission of the virus, William T. Basco Jr., MD, writes in a commentary for this news organization.
This summer, a range of factors, including vaccination rates at the camp, may influence transmission dynamics, Dr. Chu said in an interview. In July, the Associated Press reported outbreaks tied to summer camps in several states.
“Transmission dynamics will probably vary from summer camp to summer camp depending on many factors, such as vaccination rates of camp attendees, the mitigation measures in place, and the number of individual introductions during camp,” Dr. Chu said. “We would expect that a camp with a low vaccination rate among attendees and no enforcement of mitigation measures” still may experience a large outbreak.
“On the other hand, a large proportion of vaccinated individuals and appropriate implementation of multiple mitigation measures, such as wearing masks, may be quite effective at keeping their transmission rates low,” Dr. Chu added. “For camps with younger children who are not currently eligible for vaccination, implementing layered prevention strategies (e.g., mask use, physical distancing, and encouraging outdoor activities when feasible) is important to prevent transmission.”
Although COVID-19 transmission from children to adults, potentially leading to hospitalization, is not a new phenomenon, “data on the extent of transmission driven by children and adolescents in different settings are still quite sparse,” Dr. Chu said. “A better understanding of their impact on household and community transmission to help guide public health recommendations is particularly important, as most children are still not eligible for vaccination, and in-person schools will be reopening this fall.”
A version of this article first appeared on Medscape.com.
In a report published online in The New England Journal of Medicine, researchers found that campers spread COVID to household members after returning home – but transmission was more likely from some than others. Distancing and masking helped reduce the risk.
Victoria T. Chu, MD, MPH, with the Centers for Disease Control and Prevention, Atlanta, and colleagues with the agency and the Georgia Department of Health followed up with 224 camp attendees, aged 7 to 19 years, who had evidence of SARS-CoV-2 infection on laboratory testing.
These index patients – 88% of whom had symptoms – had 526 household contacts, mainly parents and siblings. Of 377 household contacts who underwent testing, 46 (12%) tested positive. Another two cases in household contacts were identified using clinical and epidemiologic criteria.
Family members hospitalized
Of the 41 adult household contacts who were infected, four (about 10%) were hospitalized. Their hospital stays ranged from 5 to 11 days. Of the seven infected household contacts who were younger than 18 years, none were hospitalized.
The four hospitalized adults were parents and grandparents aged 45 to 80 years, Dr. Chu said. Two of the four had underlying conditions. None of the household contacts died.
In an adjusted analysis, campers who had practiced physical distancing were less likely to transmit the virus at home, compared with those who had not practiced physical distancing (adjusted odds ratio, 0.4). Household members who had had close or direct contact with the index patients were more than 5 times more likely to become infected, compared with family members with minimal or no contact, analyses showed.
“This retrospective study showed that the efficient transmission of SARS-CoV-2 from school-age children and adolescents to household members led to the hospitalization of adults with secondary cases of COVID-19,” the researchers write. “In households in which transmission occurred, half the household contacts were infected.”
The secondary attack rates in this report may be an underestimate because testing was voluntary and participants reported the results themselves, the authors note. It is possible that infected household contacts spread the virus further, but this study did not address that question, Dr. Chu said.
For the study, investigators interviewed all camp attendees and their parents or guardians by phone between July 17, 2020 and Aug. 24, 2020, to collect information about demographic and clinical characteristics, SARS-CoV-2 testing, and preventive measures. The researchers’ analysis excluded households in which illness onset in a household contact occurred before or less than 2 days after a camper became sick.
About a third of the index patients began to have symptoms while still at camp. These campers may have been less infectious by the time they got home, compared with those whose symptoms started after they returned.
Two-thirds of the index patients adopted physical distancing at home, which “probably reduced the transmission of SARS-CoV-2 in the household,” Dr. Chu and colleagues wrote.
“Children who have had a known COVID-19 exposure should quarantine and obtain testing if they develop symptoms within the 14 days of returning home,” Dr. Chu advised. “If a child develops COVID-19, the child should be cared for and monitored using the proper combination of physical distancing, isolation when feasible, and mask use to prevent household transmission as much as possible. In addition, any person over the age of 12 is now eligible for vaccination in the United States. If eligible, children attending camp and their family members should get vaccinated to protect themselves and others, as vaccinations are our most effective public health prevention strategy.”
Mitigation can help
Another report regarding four overnight camps in Maine – in which three campers tested positive after they arrived last summer – shows that “aggressive mitigation strategies can be effective” in limiting transmission of the virus, William T. Basco Jr., MD, writes in a commentary for this news organization.
This summer, a range of factors, including vaccination rates at the camp, may influence transmission dynamics, Dr. Chu said in an interview. In July, the Associated Press reported outbreaks tied to summer camps in several states.
“Transmission dynamics will probably vary from summer camp to summer camp depending on many factors, such as vaccination rates of camp attendees, the mitigation measures in place, and the number of individual introductions during camp,” Dr. Chu said. “We would expect that a camp with a low vaccination rate among attendees and no enforcement of mitigation measures” still may experience a large outbreak.
“On the other hand, a large proportion of vaccinated individuals and appropriate implementation of multiple mitigation measures, such as wearing masks, may be quite effective at keeping their transmission rates low,” Dr. Chu added. “For camps with younger children who are not currently eligible for vaccination, implementing layered prevention strategies (e.g., mask use, physical distancing, and encouraging outdoor activities when feasible) is important to prevent transmission.”
Although COVID-19 transmission from children to adults, potentially leading to hospitalization, is not a new phenomenon, “data on the extent of transmission driven by children and adolescents in different settings are still quite sparse,” Dr. Chu said. “A better understanding of their impact on household and community transmission to help guide public health recommendations is particularly important, as most children are still not eligible for vaccination, and in-person schools will be reopening this fall.”
A version of this article first appeared on Medscape.com.
IBD risk rises with higher ultraprocessed food intake
Individuals who consumed more ultraprocessed foods had a significantly increased risk of developing inflammatory bowel disease (IBD) than those who consumed less, according to data from more than 100,000 adults.

“Diet alters the microbiome and modifies the intestinal immune response and so could play a role in the pathogenesis of IBD,” Neeraj Narula, MD, of McMaster University, Hamilton, Ont., and colleagues wrote. Although previous studies have investigated the impact of dietary risk factors on IBD, an association with ultraprocessed foods (defined as foods containing additives and preservatives) in particular has not been examined, they wrote.
In a study published in BMJ, the researchers examined data from 116,087 adults aged 35-70 years from 21 countries between 2003 and 2016 who were part of the large Prospective Urban Rural Epidemiology (PURE) Cohort. Participants completed baseline food frequency questionnaires and were followed at least every 3 years; the median follow-up time was 9.7 years. The primary outcome was the development of Crohn’s disease or ulcerative colitis. In this study, ultraprocessed food included all packaged and formulated foods and beverages that contained food additives, artificial flavors or colors, or other chemical ingredients.
The categories of ultraprocessed foods included processed meat, cold breakfast cereal, various sauces, soft drinks, and fruit drinks, and refined sweetened foods such as candy, chocolate, jam, jelly, and brownies.
Overall, 467 participants developed IBD, including 90 with Crohn’s disease and 377 with ulcerative colitis.
After controlling for confounding factors, the investigators found that increased consumption of ultraprocessed foods was significantly associated with an increased risk of incident IBD. Compared with individuals who consumed less than 1 serving per day of ultraprocessed foods, the hazard ratio was 1.82 for those who consumed 5 or more servings and 1.67 for those who consumed 1-4 servings daily (P = .006).
“The pattern of increased ultraprocessed food intake and higher risk of IBD persisted within each of the regions examined, and effect estimates were generally similar, with overlapping confidence intervals and no significant heterogeneity,” the researchers noted.
The risk of IBD increased among individuals who consumed 1 serving per week or more of processed meat, compared with those who consumed less than 1 serving per week, and the risk increased with the amount consumed (HR, 2.07 for 1 or more servings per day). Similarly, IBD risk was higher among individuals who consumed 100 g/day or more of refined sweetened foods compared with no intake of these foods (HR, 2.58).
Individuals who consumed at least one serving of fried foods per day had the highest risk of IBD (HR, 3.02), the researchers noted. The reason for the association is uncertain, but may occur not only because many fried foods are also processed but also because the action of frying food and the processing of oil, as well as type and quality of oil, might modify the nutrients.
In the subgroup analysis, higher consumption of salty snacks and soft drinks also was associated with higher risk for IBD. However, the researchers found no association between increased risk of IBD and consumption of white meat, unprocessed red meat, dairy, starchy foods, and fruit/vegetables/legumes.
The study findings were limited by several factors including the relatively small number of individuals with Crohn’s disease, potential lack of generalizability to those who develop IBD in childhood or young adulthood, and possible confounding from unmeasured variables. The study also did not account for dietary changes over time, the investigators reported. However, the longitudinal design allowed them “to focus on people with incident IBD and to use medical record review and central adjudication to validate a sample of the diagnoses.”
The results suggest that the way food is processed or ultraprocessed, rather than the food itself, may be what confers the risk for IBD, given the lack of association between IBD and other food categories such as unprocessed red meat and dairy, the researchers concluded.
Next steps: Pin down driving factors
“There is significant interest in the apparent increase in the incidence and prevalence of IBD, particularly in previously low incidence areas,” Edward L. Barnes, MD, MPH, of the University of North Carolina at Chapel Hill said in an interview.

“Many research groups and clinicians suspect that environmental exposures, including dietary exposures, may play a critical role in these trends,” said Dr. Barnes. “This study utilized a large, multinational prospective cohort design to assess the influence of diet on the risk of developing IBD,” which is particularly important considering the potential for processed foods and food additives to impact the gastrointestinal tract.
“The strong associations demonstrated by the authors were impressive, particularly given that the authors performed multiple subanalyses, including evaluations by participant age and evaluations of particular food groups/types [e.g., processed meat, soft drinks, and refined sweet foods],” he noted. Dr. Barnes also found the lack of association with intake of white meat and unprocessed red meat interesting. “In my opinion, these subanalyses strengthen the overall associations demonstrated by the authors given their prospective study design and their attention to evaluating all potential associations that may be driving the relationships present in this cohort.
“At this point, the take-home message for clinicians treating patients with Crohn’s disease and ulcerative colitis should be that this association exists,” said Dr. Barnes. “One question that remains is whether the same risk factors that are present for developing disease also influence the disease course, given that the primary outcome of this study was the development of IBD. Given that much of our data with regard to the interplay between diet and IBD are still emerging, physicians treating patients with IBD can make patients aware of these associations and the potential benefit of limiting ultraprocessed foods in their diet.”
For these important results to become actionable, “further research is likely necessary to identify the factors that are driving this association,” Dr. Barnes explained. “This would likely build on prior animal models that have demonstrated an association between food additives such as emulsifiers and changes in the gastrointestinal tract that could ultimately lead to increased inflammation and the development of IBD.” Such information about specific drivers “would then allow clinicians to determine which population would benefit most from dietary changes/recommendations.”
The overall PURE study was supported by the Population Health Research Institute, Hamilton Health Sciences Research Institute, Canadian Institutes of Health Research, Heart and Stroke Foundation of Ontario, CIHR’s Strategy for Patient Oriented Research through the Ontario SPOR Support Unit, and the Ontario Ministry of Health and Long-term Care. PURE also was supported in part by unrestricted grants from several pharmaceutical companies, notably AstraZeneca, Sanofi-Aventis, Boehringer Ingelheim, Servier, and GlaxoSmithKline. The researchers had no relevant financial conflicts to disclose. Dr. Barnes disclosed serving as a consultant for AbbVie, Gilead, Pfizer, Takeda, and Target RWE.
Individuals who consumed more ultraprocessed foods had a significantly increased risk of developing inflammatory bowel disease (IBD) than those who consumed less, according to data from more than 100,000 adults.
“Diet alters the microbiome and modifies the intestinal immune response and so could play a role in the pathogenesis of IBD,” Neeraj Narula, MD, of McMaster University, Hamilton, Ont., and colleagues wrote. Although previous studies have investigated the impact of dietary risk factors on IBD, an association with ultraprocessed foods (defined as foods containing additives and preservatives) in particular has not been examined, they wrote.
In a study published in BMJ, the researchers examined data from 116,087 adults aged 35-70 years from 21 countries between 2003 and 2016 who were part of the large Prospective Urban Rural Epidemiology (PURE) Cohort. Participants completed baseline food frequency questionnaires and were followed at least every 3 years; the median follow-up time was 9.7 years. The primary outcome was the development of Crohn’s disease or ulcerative colitis. In this study, ultraprocessed food included all packaged and formulated foods and beverages that contained food additives, artificial flavors or colors, or other chemical ingredients.
The categories of ultraprocessed foods included processed meat, cold breakfast cereal, various sauces, soft drinks, and fruit drinks, and refined sweetened foods such as candy, chocolate, jam, jelly, and brownies.
Overall, 467 participants developed IBD, including 90 with Crohn’s disease and 377 with ulcerative colitis.
After controlling for confounding factors, the investigators found that increased consumption of ultraprocessed foods was significantly associated with an increased risk of incident IBD. Compared with individuals who consumed less than 1 serving per day of ultraprocessed foods, the hazard ratio was 1.82 for those who consumed 5 or more servings and 1.67 for those who consumed 1-4 servings daily (P = .006).
“The pattern of increased ultraprocessed food intake and higher risk of IBD persisted within each of the regions examined, and effect estimates were generally similar, with overlapping confidence intervals and no significant heterogeneity,” the researchers noted.
The risk of IBD increased among individuals who consumed 1 serving per week or more of processed meat, compared with those who consumed less than 1 serving per week, and the risk increased with the amount consumed (HR, 2.07 for 1 or more servings per day). Similarly, IBD risk was higher among individuals who consumed 100 g/day or more of refined sweetened foods compared with no intake of these foods (HR, 2.58).
Individuals who consumed at least one serving of fried foods per day had the highest risk of IBD (HR, 3.02), the researchers noted. The reason for the association is uncertain, but may occur not only because many fried foods are also processed but also because the action of frying food and the processing of oil, as well as type and quality of oil, might modify the nutrients.
In the subgroup analysis, higher consumption of salty snacks and soft drinks also was associated with higher risk for IBD. However, the researchers found no association between increased risk of IBD and consumption of white meat, unprocessed red meat, dairy, starchy foods, and fruit/vegetables/legumes.
The study findings were limited by several factors including the relatively small number of individuals with Crohn’s disease, potential lack of generalizability to those who develop IBD in childhood or young adulthood, and possible confounding from unmeasured variables. The study also did not account for dietary changes over time, the investigators reported. However, the longitudinal design allowed them “to focus on people with incident IBD and to use medical record review and central adjudication to validate a sample of the diagnoses.”
The results suggest that the way food is processed or ultraprocessed, rather than the food itself, may be what confers the risk for IBD, given the lack of association between IBD and other food categories such as unprocessed red meat and dairy, the researchers concluded.
Next steps: Pin down driving factors
“There is significant interest in the apparent increase in the incidence and prevalence of IBD, particularly in previously low incidence areas,” Edward L. Barnes, MD, MPH, of the University of North Carolina at Chapel Hill said in an interview.
“Many research groups and clinicians suspect that environmental exposures, including dietary exposures, may play a critical role in these trends,” said Dr. Barnes. “This study utilized a large, multinational prospective cohort design to assess the influence of diet on the risk of developing IBD,” which is particularly important considering the potential for processed foods and food additives to impact the gastrointestinal tract.
“The strong associations demonstrated by the authors were impressive, particularly given that the authors performed multiple subanalyses, including evaluations by participant age and evaluations of particular food groups/types [e.g., processed meat, soft drinks, and refined sweet foods],” he noted. Dr. Barnes also found the lack of association with intake of white meat and unprocessed red meat interesting. “In my opinion, these subanalyses strengthen the overall associations demonstrated by the authors given their prospective study design and their attention to evaluating all potential associations that may be driving the relationships present in this cohort.
“At this point, the take-home message for clinicians treating patients with Crohn’s disease and ulcerative colitis should be that this association exists,” said Dr. Barnes. “One question that remains is whether the same risk factors that are present for developing disease also influence the disease course, given that the primary outcome of this study was the development of IBD. Given that much of our data with regard to the interplay between diet and IBD are still emerging, physicians treating patients with IBD can make patients aware of these associations and the potential benefit of limiting ultraprocessed foods in their diet.”
For these important results to become actionable, “further research is likely necessary to identify the factors that are driving this association,” Dr. Barnes explained. “This would likely build on prior animal models that have demonstrated an association between food additives such as emulsifiers and changes in the gastrointestinal tract that could ultimately lead to increased inflammation and the development of IBD.” Such information about specific drivers “would then allow clinicians to determine which population would benefit most from dietary changes/recommendations.”
The overall PURE study was supported by the Population Health Research Institute, Hamilton Health Sciences Research Institute, Canadian Institutes of Health Research, Heart and Stroke Foundation of Ontario, CIHR’s Strategy for Patient Oriented Research through the Ontario SPOR Support Unit, and the Ontario Ministry of Health and Long-term Care. PURE also was supported in part by unrestricted grants from several pharmaceutical companies, notably AstraZeneca, Sanofi-Aventis, Boehringer Ingelheim, Servier, and GlaxoSmithKline. The researchers had no relevant financial conflicts to disclose. Dr. Barnes disclosed serving as a consultant for AbbVie, Gilead, Pfizer, Takeda, and Target RWE.
Individuals who consumed more ultraprocessed foods had a significantly increased risk of developing inflammatory bowel disease (IBD) than those who consumed less, according to data from more than 100,000 adults.
“Diet alters the microbiome and modifies the intestinal immune response and so could play a role in the pathogenesis of IBD,” Neeraj Narula, MD, of McMaster University, Hamilton, Ont., and colleagues wrote. Although previous studies have investigated the impact of dietary risk factors on IBD, an association with ultraprocessed foods (defined as foods containing additives and preservatives) in particular has not been examined, they wrote.
In a study published in BMJ, the researchers examined data from 116,087 adults aged 35-70 years from 21 countries between 2003 and 2016 who were part of the large Prospective Urban Rural Epidemiology (PURE) Cohort. Participants completed baseline food frequency questionnaires and were followed at least every 3 years; the median follow-up time was 9.7 years. The primary outcome was the development of Crohn’s disease or ulcerative colitis. In this study, ultraprocessed food included all packaged and formulated foods and beverages that contained food additives, artificial flavors or colors, or other chemical ingredients.
The categories of ultraprocessed foods included processed meat, cold breakfast cereal, various sauces, soft drinks, and fruit drinks, and refined sweetened foods such as candy, chocolate, jam, jelly, and brownies.
Overall, 467 participants developed IBD, including 90 with Crohn’s disease and 377 with ulcerative colitis.
After controlling for confounding factors, the investigators found that increased consumption of ultraprocessed foods was significantly associated with an increased risk of incident IBD. Compared with individuals who consumed less than 1 serving per day of ultraprocessed foods, the hazard ratio was 1.82 for those who consumed 5 or more servings and 1.67 for those who consumed 1-4 servings daily (P = .006).
“The pattern of increased ultraprocessed food intake and higher risk of IBD persisted within each of the regions examined, and effect estimates were generally similar, with overlapping confidence intervals and no significant heterogeneity,” the researchers noted.
The risk of IBD increased among individuals who consumed 1 serving per week or more of processed meat, compared with those who consumed less than 1 serving per week, and the risk increased with the amount consumed (HR, 2.07 for 1 or more servings per day). Similarly, IBD risk was higher among individuals who consumed 100 g/day or more of refined sweetened foods compared with no intake of these foods (HR, 2.58).
Individuals who consumed at least one serving of fried foods per day had the highest risk of IBD (HR, 3.02), the researchers noted. The reason for the association is uncertain, but may occur not only because many fried foods are also processed but also because the action of frying food and the processing of oil, as well as type and quality of oil, might modify the nutrients.
In the subgroup analysis, higher consumption of salty snacks and soft drinks also was associated with higher risk for IBD. However, the researchers found no association between increased risk of IBD and consumption of white meat, unprocessed red meat, dairy, starchy foods, and fruit/vegetables/legumes.
The study findings were limited by several factors including the relatively small number of individuals with Crohn’s disease, potential lack of generalizability to those who develop IBD in childhood or young adulthood, and possible confounding from unmeasured variables. The study also did not account for dietary changes over time, the investigators reported. However, the longitudinal design allowed them “to focus on people with incident IBD and to use medical record review and central adjudication to validate a sample of the diagnoses.”
The results suggest that the way food is processed or ultraprocessed, rather than the food itself, may be what confers the risk for IBD, given the lack of association between IBD and other food categories such as unprocessed red meat and dairy, the researchers concluded.
Next steps: Pin down driving factors
“There is significant interest in the apparent increase in the incidence and prevalence of IBD, particularly in previously low incidence areas,” Edward L. Barnes, MD, MPH, of the University of North Carolina at Chapel Hill said in an interview.
“Many research groups and clinicians suspect that environmental exposures, including dietary exposures, may play a critical role in these trends,” said Dr. Barnes. “This study utilized a large, multinational prospective cohort design to assess the influence of diet on the risk of developing IBD,” which is particularly important considering the potential for processed foods and food additives to impact the gastrointestinal tract.
“The strong associations demonstrated by the authors were impressive, particularly given that the authors performed multiple subanalyses, including evaluations by participant age and evaluations of particular food groups/types [e.g., processed meat, soft drinks, and refined sweet foods],” he noted. Dr. Barnes also found the lack of association with intake of white meat and unprocessed red meat interesting. “In my opinion, these subanalyses strengthen the overall associations demonstrated by the authors given their prospective study design and their attention to evaluating all potential associations that may be driving the relationships present in this cohort.
“At this point, the take-home message for clinicians treating patients with Crohn’s disease and ulcerative colitis should be that this association exists,” said Dr. Barnes. “One question that remains is whether the same risk factors that are present for developing disease also influence the disease course, given that the primary outcome of this study was the development of IBD. Given that much of our data with regard to the interplay between diet and IBD are still emerging, physicians treating patients with IBD can make patients aware of these associations and the potential benefit of limiting ultraprocessed foods in their diet.”
For these important results to become actionable, “further research is likely necessary to identify the factors that are driving this association,” Dr. Barnes explained. “This would likely build on prior animal models that have demonstrated an association between food additives such as emulsifiers and changes in the gastrointestinal tract that could ultimately lead to increased inflammation and the development of IBD.” Such information about specific drivers “would then allow clinicians to determine which population would benefit most from dietary changes/recommendations.”
The overall PURE study was supported by the Population Health Research Institute, Hamilton Health Sciences Research Institute, Canadian Institutes of Health Research, Heart and Stroke Foundation of Ontario, CIHR’s Strategy for Patient Oriented Research through the Ontario SPOR Support Unit, and the Ontario Ministry of Health and Long-term Care. PURE also was supported in part by unrestricted grants from several pharmaceutical companies, notably AstraZeneca, Sanofi-Aventis, Boehringer Ingelheim, Servier, and GlaxoSmithKline. The researchers had no relevant financial conflicts to disclose. Dr. Barnes disclosed serving as a consultant for AbbVie, Gilead, Pfizer, Takeda, and Target RWE.
FROM THE BMJ
Long COVID symptoms rare but real in some kids
School-aged children with SARS-CoV-2 infection had only a few mild symptoms and typically recovered in 6 days, with more than 98% recovering in 8 weeks, a large U.K. study of smartphone data reassuringly reports.
In a small proportion (4.4%), however, COVID-19 symptoms such as fatigue, headache, or loss of smell persisted beyond a month, highlighting the need for ongoing pediatric care, according to Erika Molteni, PhD, a research fellow at King’s College, London, and colleagues.
The results, published online in The Lancet Child & Adolescent Health, also indicated that some children who had non-COVID infections were also susceptible to prolonged symptoms. “Our data highlight that other illnesses, such as colds and flu, can also have prolonged symptoms in children and it is important to consider this when planning for pediatric health services during the pandemic and beyond,” Michael Absoud, PhD, a senior coauthor and a King’s College consultant and senior lecturer, said in a news release. “All children who have persistent symptoms – from any illness – need timely multidisciplinary support linked with education, to enable them to find their individual pathway to recovery.”
Using a “citizen science” approach, the study extracted data from a smartphone app for tracking COVID symptoms in the ZOE COVID Study. The researchers looked at 258,790 children aged 5-17 years whose details were reported by adult proxies such as parents and carers from March 24, 2020, to Feb. 22, 2021. Of these, 75,529 had undergone a valid SARS-CoV-2 test.
The study also assessed symptoms in a randomly selected, age- and sex-matched cohort of 1,734 children in the app database who tested negative for COVID-19 but may have had other illnesses such as colds or flu.
In the 1,734 children testing positive for COVID-19 (approximately 50% each boys and girls), the most common symptoms were headache (62.2%) and fatigue (55.0%). More than 10% of the entire cohort had underlying asthma, but other comorbidities were very rare.
To assess the effect of age, the children were assessed in two groups: 5-11 years (n = 588) and 12-17 years (n = 1,146).
While unable to cross-check app reporting against actual medical records, the study suggested that illness lasted longer in COVID-positive than COVID-negative children, with a median of 6 days (interquartile range, 3-11) versus 3 days (IQR, 2-7). Furthermore, illness duration was positively associated with age: older children (median, 7 days; IQR, 3-12) versus younger children (median, 5 days; IQR, 2-9).
In 77 (4.4%) of the 1,734 COVID-positive children, illness persisted for at least 28 days, again more often in older than younger children: 5.1% of older children versus 3.1% of younger children (P = .046).
In addition, those with COVID-19 were more likely than children with non-COVID illness to be sick for more than 4 weeks: 4.4% versus 0.9%. At 4 weeks, however, the few children with other illnesses tended to have more symptoms, exhibiting a median of five symptoms versus two symptoms in the COVID-positive group.

“I tend to agree with the U.K. findings. COVID-19 in most school-age children is asymptomatic or a brief, self-limiting illness,” Sindhu Mohandas, MD, a pediatric infectious disease specialist at the Children’s Hospital Los Angeles, said in an interview. “The few children who need hospitalization have also mostly fully recovered by the time they are seen for their first outpatient clinic follow-up visit.”
Dr. Mohandas, who was not involved in the U.K. study, added that in her experience a small percentage, particularly adolescents, have some lingering symptoms after infection including fatigue, loss of appetite, and changes in smell and taste. “Identifying children with persistent illness and providing support and multidisciplinary care based on their symptomatology can make a positive impact on patients and their families.”
Recent research has suggested that long symptoms can persist for 3 months in 6% of children with COVID-19. And data from China have indicated that the prevalence of coinfection may be higher than in older patients.
In an accompanying comment, Dana Mahr, PhD, and Bruno J. Strasser, PhD, researchers in the faculty of science at the University of Geneva, said the app-based study “illustrates the potential and challenges of what has been called citizenship science,” in which projects rely on data input from nonscientists.
But while potentially democratizing participation in medical research, this subjective approach has the inherent bias of self-reporting (and in the case of the current study, proxy reporting), and can introduce potential conflicts of interest owing to the politicization of certain diseases.
In the case of the current study, Dr. Mahr and Dr. Strasser argued that, since the COVID-19 test result is known to participants, a pediatrician using objective criteria is better positioned to control for reporting biases than a parent asking a child about symptoms. “Entering data on a smartphone app is not equivalent to discussing with a pediatrician or health care worker who can answer further questions and concerns of participants, an especially important factor for underserved communities,” they wrote. “Citizen science will continue to require a close interaction with professional medical researchers to turn unique illness experiences into research data.”
This study was funded by Zoe Limited, the U.K. Government Department of Health and Social Care, Wellcome Trust, the U.K. Engineering and Physical Sciences Research Council, the U.K. Research and Innovation London Medical Imaging and Artificial Intelligence Centre for Value Based Healthcare, the U.K. National Institute for Health Research, the U.K. Medical Research Council, the British Heart Foundation, and the Alzheimer’s Society. Several study authors have disclosed support from various research-funding agencies and Zoe Limited supported all aspects of building and running the symptom-tracking application. Dr. Mahr and Dr. Strasser declared no competing interests. Dr. Mohandas disclosed no competing interests with regard to her comments.
School-aged children with SARS-CoV-2 infection had only a few mild symptoms and typically recovered in 6 days, with more than 98% recovering in 8 weeks, a large U.K. study of smartphone data reassuringly reports.
In a small proportion (4.4%), however, COVID-19 symptoms such as fatigue, headache, or loss of smell persisted beyond a month, highlighting the need for ongoing pediatric care, according to Erika Molteni, PhD, a research fellow at King’s College, London, and colleagues.
The results, published online in The Lancet Child & Adolescent Health, also indicated that some children who had non-COVID infections were also susceptible to prolonged symptoms. “Our data highlight that other illnesses, such as colds and flu, can also have prolonged symptoms in children and it is important to consider this when planning for pediatric health services during the pandemic and beyond,” Michael Absoud, PhD, a senior coauthor and a King’s College consultant and senior lecturer, said in a news release. “All children who have persistent symptoms – from any illness – need timely multidisciplinary support linked with education, to enable them to find their individual pathway to recovery.”
Using a “citizen science” approach, the study extracted data from a smartphone app for tracking COVID symptoms in the ZOE COVID Study. The researchers looked at 258,790 children aged 5-17 years whose details were reported by adult proxies such as parents and carers from March 24, 2020, to Feb. 22, 2021. Of these, 75,529 had undergone a valid SARS-CoV-2 test.
The study also assessed symptoms in a randomly selected, age- and sex-matched cohort of 1,734 children in the app database who tested negative for COVID-19 but may have had other illnesses such as colds or flu.
In the 1,734 children testing positive for COVID-19 (approximately 50% each boys and girls), the most common symptoms were headache (62.2%) and fatigue (55.0%). More than 10% of the entire cohort had underlying asthma, but other comorbidities were very rare.
To assess the effect of age, the children were assessed in two groups: 5-11 years (n = 588) and 12-17 years (n = 1,146).
While unable to cross-check app reporting against actual medical records, the study suggested that illness lasted longer in COVID-positive than COVID-negative children, with a median of 6 days (interquartile range, 3-11) versus 3 days (IQR, 2-7). Furthermore, illness duration was positively associated with age: older children (median, 7 days; IQR, 3-12) versus younger children (median, 5 days; IQR, 2-9).
In 77 (4.4%) of the 1,734 COVID-positive children, illness persisted for at least 28 days, again more often in older than younger children: 5.1% of older children versus 3.1% of younger children (P = .046).
In addition, those with COVID-19 were more likely than children with non-COVID illness to be sick for more than 4 weeks: 4.4% versus 0.9%. At 4 weeks, however, the few children with other illnesses tended to have more symptoms, exhibiting a median of five symptoms versus two symptoms in the COVID-positive group.
“I tend to agree with the U.K. findings. COVID-19 in most school-age children is asymptomatic or a brief, self-limiting illness,” Sindhu Mohandas, MD, a pediatric infectious disease specialist at the Children’s Hospital Los Angeles, said in an interview. “The few children who need hospitalization have also mostly fully recovered by the time they are seen for their first outpatient clinic follow-up visit.”
Dr. Mohandas, who was not involved in the U.K. study, added that in her experience a small percentage, particularly adolescents, have some lingering symptoms after infection including fatigue, loss of appetite, and changes in smell and taste. “Identifying children with persistent illness and providing support and multidisciplinary care based on their symptomatology can make a positive impact on patients and their families.”
Recent research has suggested that long symptoms can persist for 3 months in 6% of children with COVID-19. And data from China have indicated that the prevalence of coinfection may be higher than in older patients.
In an accompanying comment, Dana Mahr, PhD, and Bruno J. Strasser, PhD, researchers in the faculty of science at the University of Geneva, said the app-based study “illustrates the potential and challenges of what has been called citizenship science,” in which projects rely on data input from nonscientists.
But while potentially democratizing participation in medical research, this subjective approach has the inherent bias of self-reporting (and in the case of the current study, proxy reporting), and can introduce potential conflicts of interest owing to the politicization of certain diseases.
In the case of the current study, Dr. Mahr and Dr. Strasser argued that, since the COVID-19 test result is known to participants, a pediatrician using objective criteria is better positioned to control for reporting biases than a parent asking a child about symptoms. “Entering data on a smartphone app is not equivalent to discussing with a pediatrician or health care worker who can answer further questions and concerns of participants, an especially important factor for underserved communities,” they wrote. “Citizen science will continue to require a close interaction with professional medical researchers to turn unique illness experiences into research data.”
This study was funded by Zoe Limited, the U.K. Government Department of Health and Social Care, Wellcome Trust, the U.K. Engineering and Physical Sciences Research Council, the U.K. Research and Innovation London Medical Imaging and Artificial Intelligence Centre for Value Based Healthcare, the U.K. National Institute for Health Research, the U.K. Medical Research Council, the British Heart Foundation, and the Alzheimer’s Society. Several study authors have disclosed support from various research-funding agencies and Zoe Limited supported all aspects of building and running the symptom-tracking application. Dr. Mahr and Dr. Strasser declared no competing interests. Dr. Mohandas disclosed no competing interests with regard to her comments.
School-aged children with SARS-CoV-2 infection had only a few mild symptoms and typically recovered in 6 days, with more than 98% recovering in 8 weeks, a large U.K. study of smartphone data reassuringly reports.
In a small proportion (4.4%), however, COVID-19 symptoms such as fatigue, headache, or loss of smell persisted beyond a month, highlighting the need for ongoing pediatric care, according to Erika Molteni, PhD, a research fellow at King’s College, London, and colleagues.
The results, published online in The Lancet Child & Adolescent Health, also indicated that some children who had non-COVID infections were also susceptible to prolonged symptoms. “Our data highlight that other illnesses, such as colds and flu, can also have prolonged symptoms in children and it is important to consider this when planning for pediatric health services during the pandemic and beyond,” Michael Absoud, PhD, a senior coauthor and a King’s College consultant and senior lecturer, said in a news release. “All children who have persistent symptoms – from any illness – need timely multidisciplinary support linked with education, to enable them to find their individual pathway to recovery.”
Using a “citizen science” approach, the study extracted data from a smartphone app for tracking COVID symptoms in the ZOE COVID Study. The researchers looked at 258,790 children aged 5-17 years whose details were reported by adult proxies such as parents and carers from March 24, 2020, to Feb. 22, 2021. Of these, 75,529 had undergone a valid SARS-CoV-2 test.
The study also assessed symptoms in a randomly selected, age- and sex-matched cohort of 1,734 children in the app database who tested negative for COVID-19 but may have had other illnesses such as colds or flu.
In the 1,734 children testing positive for COVID-19 (approximately 50% each boys and girls), the most common symptoms were headache (62.2%) and fatigue (55.0%). More than 10% of the entire cohort had underlying asthma, but other comorbidities were very rare.
To assess the effect of age, the children were assessed in two groups: 5-11 years (n = 588) and 12-17 years (n = 1,146).
While unable to cross-check app reporting against actual medical records, the study suggested that illness lasted longer in COVID-positive than COVID-negative children, with a median of 6 days (interquartile range, 3-11) versus 3 days (IQR, 2-7). Furthermore, illness duration was positively associated with age: older children (median, 7 days; IQR, 3-12) versus younger children (median, 5 days; IQR, 2-9).
In 77 (4.4%) of the 1,734 COVID-positive children, illness persisted for at least 28 days, again more often in older than younger children: 5.1% of older children versus 3.1% of younger children (P = .046).
In addition, those with COVID-19 were more likely than children with non-COVID illness to be sick for more than 4 weeks: 4.4% versus 0.9%. At 4 weeks, however, the few children with other illnesses tended to have more symptoms, exhibiting a median of five symptoms versus two symptoms in the COVID-positive group.
“I tend to agree with the U.K. findings. COVID-19 in most school-age children is asymptomatic or a brief, self-limiting illness,” Sindhu Mohandas, MD, a pediatric infectious disease specialist at the Children’s Hospital Los Angeles, said in an interview. “The few children who need hospitalization have also mostly fully recovered by the time they are seen for their first outpatient clinic follow-up visit.”
Dr. Mohandas, who was not involved in the U.K. study, added that in her experience a small percentage, particularly adolescents, have some lingering symptoms after infection including fatigue, loss of appetite, and changes in smell and taste. “Identifying children with persistent illness and providing support and multidisciplinary care based on their symptomatology can make a positive impact on patients and their families.”
Recent research has suggested that long symptoms can persist for 3 months in 6% of children with COVID-19. And data from China have indicated that the prevalence of coinfection may be higher than in older patients.
In an accompanying comment, Dana Mahr, PhD, and Bruno J. Strasser, PhD, researchers in the faculty of science at the University of Geneva, said the app-based study “illustrates the potential and challenges of what has been called citizenship science,” in which projects rely on data input from nonscientists.
But while potentially democratizing participation in medical research, this subjective approach has the inherent bias of self-reporting (and in the case of the current study, proxy reporting), and can introduce potential conflicts of interest owing to the politicization of certain diseases.
In the case of the current study, Dr. Mahr and Dr. Strasser argued that, since the COVID-19 test result is known to participants, a pediatrician using objective criteria is better positioned to control for reporting biases than a parent asking a child about symptoms. “Entering data on a smartphone app is not equivalent to discussing with a pediatrician or health care worker who can answer further questions and concerns of participants, an especially important factor for underserved communities,” they wrote. “Citizen science will continue to require a close interaction with professional medical researchers to turn unique illness experiences into research data.”
This study was funded by Zoe Limited, the U.K. Government Department of Health and Social Care, Wellcome Trust, the U.K. Engineering and Physical Sciences Research Council, the U.K. Research and Innovation London Medical Imaging and Artificial Intelligence Centre for Value Based Healthcare, the U.K. National Institute for Health Research, the U.K. Medical Research Council, the British Heart Foundation, and the Alzheimer’s Society. Several study authors have disclosed support from various research-funding agencies and Zoe Limited supported all aspects of building and running the symptom-tracking application. Dr. Mahr and Dr. Strasser declared no competing interests. Dr. Mohandas disclosed no competing interests with regard to her comments.
FROM THE LANCET CHILD & ADOLESCENT HEALTH
Pruritic welts

The patient’s history and the classic morphology of raised plaques was consistent with chronic spontaneous urticaria. Erythema may be subtle or not visible in patients with skin of color.
Individual urticarial lesions last less than 24 hours with itching and burning. Angioedema also occurs, and manifests as a deeper edema with itching, burning, and pain. Symptoms typically last for 2 to 3 days and involve the eyelids, lips, and tongue.
Chronic urticaria (CU) is defined as episodes of spontaneous wheals or angioedema lasting for more than 6 weeks and is subdivided into chronic spontaneous urticaria or inducible urticaria (if there is a known cause). Triggers include infection, emotional stressors, or medications (eg, angiotensin-converting enzyme inhibitors, nonsteroidal anti-inflammatory drugs). Autoimmunity is seen in one-third of CU patients.1
Only a limited routine-diagnostic work-up is necessary for CU and it may include a complete blood count with differential and erythrocyte sedimentation rate and C-reactive protein testing. Further diagnostic testing is based on history and may include functional autoantibodies, thyroid stimulating hormone, and thyroid autoantibodies.
The initial step in treatment involves identification and elimination of triggers. If this is not possible, first-line therapy includes second-generation antihistamines. If symptoms persist beyond 2 weeks, the dose of the antihistamine is increased up to 4-fold. Patients should be counseled that the lowest necessary dose needs to be taken habitually to prevent urticaria. If symptoms persist, omalizumab, a recombinant humanized IgG monoclonal antibody against serum IgE, cyclosporine, or montelukast, may be added. Leukotriene-receptor antagonists such as montelukast were previously second-line therapy, but they have had mixed results in randomized controlled trials. With a much lower cost than omalizumab, leukotriene-receptor antagonists are a reasonable alternative for patients who are refractory to antihistamines.1
This patient was given high-dose nonsedating antihistamines; she experienced sedation and inadequate relief. A prior authorization was successfully obtained, and she was prescribed omalizumab.
Image courtesy of Kriti Mishra, MD, Department of Dermatology, University of New Mexico School of Medicine, Albuquerque. Text courtesy of Kriti Mishra, MD, and Daniel Stulberg, MD, FAAFP, Department of Family and Community Medicine, University of New Mexico School of Medicine, Albuquerque.
1. Antia C, Baquerizo K, Korman A, et al. Urticaria: a comprehensive review: treatment of chronic urticaria, special populations, and disease outcomes. J Am Acad Dermatol. 2018;79:617-633. doi: 10.1016/j.jaad.2018.01.023
The patient’s history and the classic morphology of raised plaques was consistent with chronic spontaneous urticaria. Erythema may be subtle or not visible in patients with skin of color.
Individual urticarial lesions last less than 24 hours with itching and burning. Angioedema also occurs, and manifests as a deeper edema with itching, burning, and pain. Symptoms typically last for 2 to 3 days and involve the eyelids, lips, and tongue.
Chronic urticaria (CU) is defined as episodes of spontaneous wheals or angioedema lasting for more than 6 weeks and is subdivided into chronic spontaneous urticaria or inducible urticaria (if there is a known cause). Triggers include infection, emotional stressors, or medications (eg, angiotensin-converting enzyme inhibitors, nonsteroidal anti-inflammatory drugs). Autoimmunity is seen in one-third of CU patients.1
Only a limited routine-diagnostic work-up is necessary for CU and it may include a complete blood count with differential and erythrocyte sedimentation rate and C-reactive protein testing. Further diagnostic testing is based on history and may include functional autoantibodies, thyroid stimulating hormone, and thyroid autoantibodies.
The initial step in treatment involves identification and elimination of triggers. If this is not possible, first-line therapy includes second-generation antihistamines. If symptoms persist beyond 2 weeks, the dose of the antihistamine is increased up to 4-fold. Patients should be counseled that the lowest necessary dose needs to be taken habitually to prevent urticaria. If symptoms persist, omalizumab, a recombinant humanized IgG monoclonal antibody against serum IgE, cyclosporine, or montelukast, may be added. Leukotriene-receptor antagonists such as montelukast were previously second-line therapy, but they have had mixed results in randomized controlled trials. With a much lower cost than omalizumab, leukotriene-receptor antagonists are a reasonable alternative for patients who are refractory to antihistamines.1
This patient was given high-dose nonsedating antihistamines; she experienced sedation and inadequate relief. A prior authorization was successfully obtained, and she was prescribed omalizumab.
Image courtesy of Kriti Mishra, MD, Department of Dermatology, University of New Mexico School of Medicine, Albuquerque. Text courtesy of Kriti Mishra, MD, and Daniel Stulberg, MD, FAAFP, Department of Family and Community Medicine, University of New Mexico School of Medicine, Albuquerque.
The patient’s history and the classic morphology of raised plaques was consistent with chronic spontaneous urticaria. Erythema may be subtle or not visible in patients with skin of color.
Individual urticarial lesions last less than 24 hours with itching and burning. Angioedema also occurs, and manifests as a deeper edema with itching, burning, and pain. Symptoms typically last for 2 to 3 days and involve the eyelids, lips, and tongue.
Chronic urticaria (CU) is defined as episodes of spontaneous wheals or angioedema lasting for more than 6 weeks and is subdivided into chronic spontaneous urticaria or inducible urticaria (if there is a known cause). Triggers include infection, emotional stressors, or medications (eg, angiotensin-converting enzyme inhibitors, nonsteroidal anti-inflammatory drugs). Autoimmunity is seen in one-third of CU patients.1
Only a limited routine-diagnostic work-up is necessary for CU and it may include a complete blood count with differential and erythrocyte sedimentation rate and C-reactive protein testing. Further diagnostic testing is based on history and may include functional autoantibodies, thyroid stimulating hormone, and thyroid autoantibodies.
The initial step in treatment involves identification and elimination of triggers. If this is not possible, first-line therapy includes second-generation antihistamines. If symptoms persist beyond 2 weeks, the dose of the antihistamine is increased up to 4-fold. Patients should be counseled that the lowest necessary dose needs to be taken habitually to prevent urticaria. If symptoms persist, omalizumab, a recombinant humanized IgG monoclonal antibody against serum IgE, cyclosporine, or montelukast, may be added. Leukotriene-receptor antagonists such as montelukast were previously second-line therapy, but they have had mixed results in randomized controlled trials. With a much lower cost than omalizumab, leukotriene-receptor antagonists are a reasonable alternative for patients who are refractory to antihistamines.1
This patient was given high-dose nonsedating antihistamines; she experienced sedation and inadequate relief. A prior authorization was successfully obtained, and she was prescribed omalizumab.
Image courtesy of Kriti Mishra, MD, Department of Dermatology, University of New Mexico School of Medicine, Albuquerque. Text courtesy of Kriti Mishra, MD, and Daniel Stulberg, MD, FAAFP, Department of Family and Community Medicine, University of New Mexico School of Medicine, Albuquerque.
1. Antia C, Baquerizo K, Korman A, et al. Urticaria: a comprehensive review: treatment of chronic urticaria, special populations, and disease outcomes. J Am Acad Dermatol. 2018;79:617-633. doi: 10.1016/j.jaad.2018.01.023
1. Antia C, Baquerizo K, Korman A, et al. Urticaria: a comprehensive review: treatment of chronic urticaria, special populations, and disease outcomes. J Am Acad Dermatol. 2018;79:617-633. doi: 10.1016/j.jaad.2018.01.023

Isolated Scrotal Granular Parakeratosis: An Atypical Clinical Presentation
To the Editor:
Granular parakeratosis is a rare condition with an unclear etiology that results from a myriad of factors, including exposure to irritants, friction, moisture, and heat. The diagnosis is made based on a distinct histologic reaction pattern that may be protective against the triggers. We present a case of isolated scrotal granular parakeratosis in a patient with compensatory hyperhidrosis after endoscopic thoracic sympathectomy.
A 52-year-old man presented with a 5-year history of a recurrent rash affecting the scrotum. He experienced monthly flares that were exacerbated by inguinal hyperhidrosis. His symptoms included a burning sensation and pruritus followed by superficial desquamation, with gradual yet temporary improvement. His medical history was remarkable for primary axillary and palmoplantar hyperhidrosis, with compensatory inguinal hyperhidrosis after endoscopic thoracic sympathectomy 8 years prior to presentation.
Physical examination revealed a well-demarcated, scaly, erythematous plaque affecting the scrotal skin with sparing of the median raphe, penis, and inguinal folds (Figure 1). There were no other lesions noted in the axillary region or other skin folds.

Prior treatments prescribed by other providers included topical pimecrolimus, antifungal creams, topical corticosteroids, zinc oxide ointment, and daily application of an over-the-counter medicated powder with no resolution.
A punch biopsy performed at the current presentation showed psoriasiform hyperplasia of the epidermis with only a focally diminished granular layer. There was overlying thick parakeratosis and retention of keratohyalin granules (Figure 2). Grocott-Gomori methenamine- silver staining was negative for fungal elements in the sections examined. Clinical history, morphology of the eruption, and histologic features were consistent with granular parakeratosis.
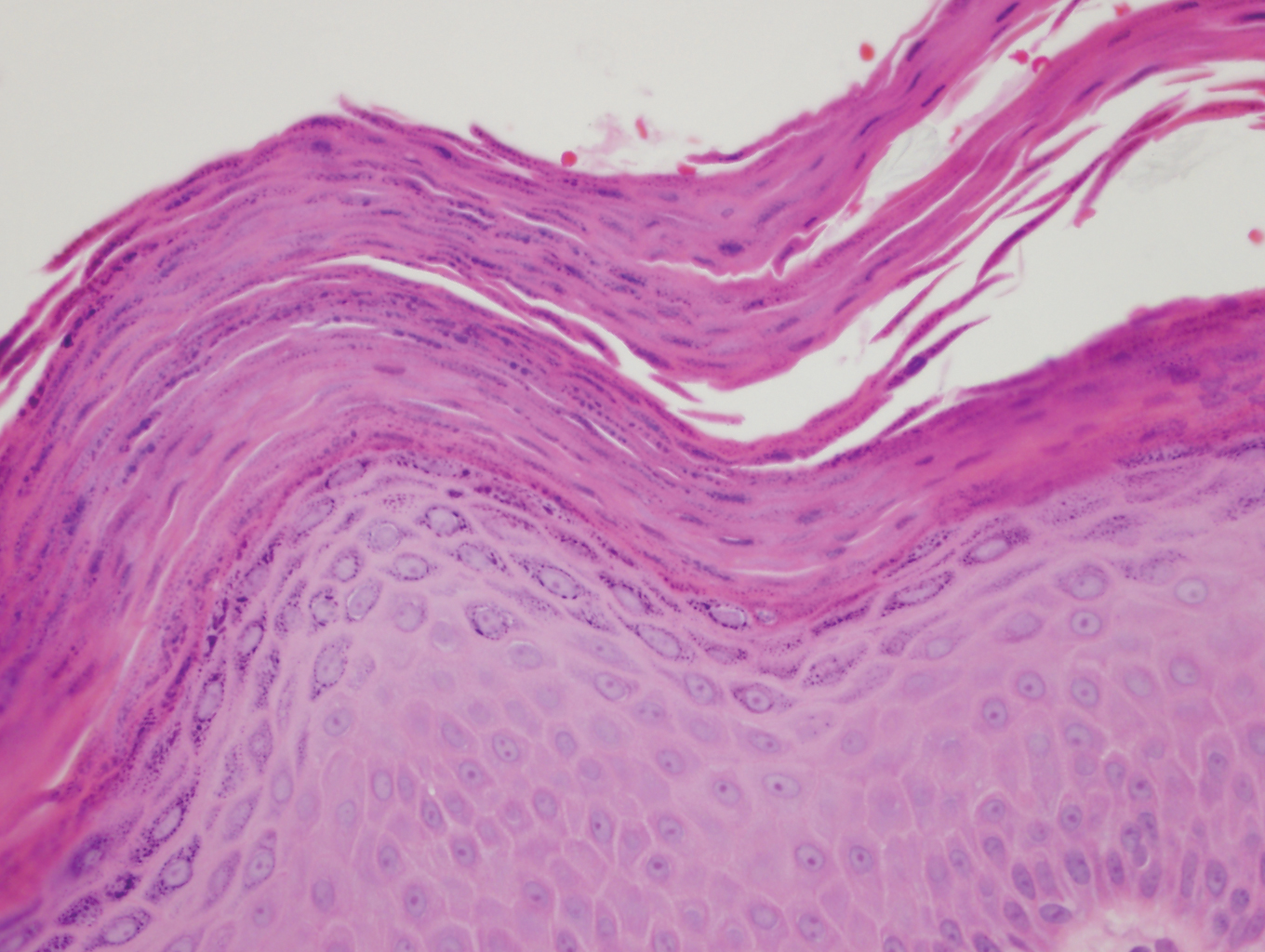
Since the first reported incident of granular parakeratosis of the axilla in 1991,1 granular parakeratosis has been reported in other intertriginous areas, including the inframammary folds, inguinal folds, genitalia, perianal skin, and beneath the abdominal pannus.2 One case study in 1998 reported a patient with isolated involvement of the inguinal region3; however, this presentation is rare.4 This condition has been reported in both sexes and all age groups, including children.5
Granular parakeratosis classically presents as erythematous to brown hyperkeratotic papules that coalesce into plaques.6 It is thought to be a reactive inflammatory condition secondary to aggravating factors such as exposure to heat,7 moisture, and friction; skin occlusion; repeated washing; irritation from external agents; antiperspirants; and use of depilatory creams.8 Histopathology is characteristic and consists of retained nuclei and keratohyalin granules within the stratum corneum, beneath which there is a retained stratum granulosum. Epidermal changes may be varied and include atrophy or hyperplasia.
Murine models have postulated that granular parakeratosis may result from a deficiency in caspase 14, a protease vital to the formation of a well-functioning skin barrier.9 A cornified envelope often is noted in granular parakeratotic cells with no defects in desmosomes and cell membranes, suggesting that the pathogenesis lies within processing of profilaggrin to filaggrin, resulting in a failure to degrade keratohyalin granules and aggregation of keratin filaments.10 Granular parakeratosis is not known to be associated with other medical conditions, but it has been observed in patients receiving chemotherapy for breast11 and ovarian12 carcinomas. In infants with atopic dermatitis, granular parakeratosis was reported in 5 out of 7 cases.6 In our patient with secondary inguinal hyperhidrosis after thoracic sympathectomy, granular parakeratosis may be reactive to excess sweating and friction in the scrotal area.
Granular parakeratosis follows a waxing and waning pattern that may spontaneously resolve without any treatment; it also can follow a protracted course, as in a case with associated facial papules that persisted for 20 years.13 Topical corticosteroids alone or in combination with topical antifungal agents have been used for the treatment of granular parakeratosis with the goal of accelerating resolution.2,14 However, the efficacy of these therapeutic interventions is limited, and no controlled trials are underway. Topical vitamin D analogues15,16 and topical retinoids17 also have been reported with successful outcomes. Spontaneous resolution also has been observed in 2 different cases after previously being unresponsive to topical treatment.18,19 Treatment with Clostridium botulinum toxin A resulted in complete remission of the disease observed at 6-month follow-up. The pharmacologic action of the neurotoxin disrupts the stimulation of eccrine sweat glands, resulting in decreased sweating, a known exacerbating factor of granular parakeratosis.20
In summary, our case represents a unique clinical presentation of granular parakeratosis with classic histopathologic features. A high index of suspicion and a biopsy are vital to arriving at the correct diagnosis.
- Northcutt AD, Nelson DM, Tschen JA. Axillary granular parakeratosis. J Am Acad Dermatol. 1991;24:541-544.
- Burford C. Granular parakeratosis of multiple intertriginous areas. Australas J Dermatol. 2008;49:35-38.
- Mehregan DA, Thomas JE, Mehregan DR. Intertriginous granular parakeratosis. J Am Acad Dermatol. 1998;39:495-496.
- Leclerc-Mercier S, Prost-Squarcioni C, Hamel-Teillac D, et al. A case of congenital granular parakeratosis. Am J Dermatopathol. 2011;33:531-533.
- Scheinfeld NS, Mones J. Granular parakeratosis: pathologic and clinical correlation of 18 cases of granular parakeratosis. J Am Acad Dermatol. 2005;52:863-867.
- Akkaya AD, Oram Y, Aydin O. Infantile granular parakeratosis: cytologic examination of superficial scrapings as an aid to diagnosis. Pediatr Dermatol. 2015;32:392-396.
- Rodríguez G. Axillary granular parakeratosis [in Spanish]. Biomedica. 2002;22:519-523.
- Samrao A, Reis M, Niedt G, et al. Granular parakeratosis: response to calcipotriene and brief review of current therapeutic options. Skinmed. 2010;8:357-359.
- Hoste E, Denecker G, Gilbert B, et al. Caspase-14-deficient mice are more prone to the development of parakeratosis. J Invest Dermatol. 2013;133:742-750.
- Metze D, Rutten A. Granular parakeratosis—a unique acquired disorder of keratinization. J Cutan Pathol. 1999;26:339-352.
- Wallace CA, Pichardo RO, Yosipovitch G, et al. Granular parakeratosis: a case report and literature review. J Cutan Pathol. 2003;30:332-335.
- Jaconelli L, Doebelin B, Kanitakis J, et al. Granular parakeratosis in a patient treated with liposomal doxorubicin for ovarian carcinoma. J Am Acad Dermatol. 2008;58(5 suppl 1):S84-S87.
- Reddy IS, Swarnalata G, Mody T. Intertriginous granular parakeratosis persisting for 20 years. Indian J Dermatol Venereol Leprol. 2008;74:405-407.
- Dearden C, al-Nakib W, Andries K, et al. Drug resistant rhinoviruses from the nose of experimentally treated volunteers. Arch Virol. 1989;109:71-81.
- Patel U, Patel T, Skinner RB Jr. Resolution of granular parakeratosis with topical calcitriol. Arch Dermatol. 2011;147:997-998.
- Contreras ME, Gottfried LC, Bang RH, et al. Axillary intertriginous granular parakeratosis responsive to topical calcipotriene and ammonium lactate. Int J Dermatol. 2003;42:382-383.
- Brown SK, Heilman ER. Granular parakeratosis: resolution with topical tretinoin. J Am Acad Dermatol. 2002;47(5 suppl):S279-S280.
- Compton AK, Jackson JM. Isotretinoin as a treatment for axillary granular parakeratosis. Cutis. 2007;80:55-56.
- Webster CG, Resnik KS, Webster GF. Axillary granular parakeratosis: response to isotretinoin. J Am Acad Dermatol. 1997; 37:789-790.
- Ravitskiy L, Heymann WR. Botulinum toxin-induced resolution of axillary granular parakeratosis. Skinmed. 2005;4:118-120.
To the Editor:
Granular parakeratosis is a rare condition with an unclear etiology that results from a myriad of factors, including exposure to irritants, friction, moisture, and heat. The diagnosis is made based on a distinct histologic reaction pattern that may be protective against the triggers. We present a case of isolated scrotal granular parakeratosis in a patient with compensatory hyperhidrosis after endoscopic thoracic sympathectomy.
A 52-year-old man presented with a 5-year history of a recurrent rash affecting the scrotum. He experienced monthly flares that were exacerbated by inguinal hyperhidrosis. His symptoms included a burning sensation and pruritus followed by superficial desquamation, with gradual yet temporary improvement. His medical history was remarkable for primary axillary and palmoplantar hyperhidrosis, with compensatory inguinal hyperhidrosis after endoscopic thoracic sympathectomy 8 years prior to presentation.
Physical examination revealed a well-demarcated, scaly, erythematous plaque affecting the scrotal skin with sparing of the median raphe, penis, and inguinal folds (Figure 1). There were no other lesions noted in the axillary region or other skin folds.
Prior treatments prescribed by other providers included topical pimecrolimus, antifungal creams, topical corticosteroids, zinc oxide ointment, and daily application of an over-the-counter medicated powder with no resolution.
A punch biopsy performed at the current presentation showed psoriasiform hyperplasia of the epidermis with only a focally diminished granular layer. There was overlying thick parakeratosis and retention of keratohyalin granules (Figure 2). Grocott-Gomori methenamine- silver staining was negative for fungal elements in the sections examined. Clinical history, morphology of the eruption, and histologic features were consistent with granular parakeratosis.
Since the first reported incident of granular parakeratosis of the axilla in 1991,1 granular parakeratosis has been reported in other intertriginous areas, including the inframammary folds, inguinal folds, genitalia, perianal skin, and beneath the abdominal pannus.2 One case study in 1998 reported a patient with isolated involvement of the inguinal region3; however, this presentation is rare.4 This condition has been reported in both sexes and all age groups, including children.5
Granular parakeratosis classically presents as erythematous to brown hyperkeratotic papules that coalesce into plaques.6 It is thought to be a reactive inflammatory condition secondary to aggravating factors such as exposure to heat,7 moisture, and friction; skin occlusion; repeated washing; irritation from external agents; antiperspirants; and use of depilatory creams.8 Histopathology is characteristic and consists of retained nuclei and keratohyalin granules within the stratum corneum, beneath which there is a retained stratum granulosum. Epidermal changes may be varied and include atrophy or hyperplasia.
Murine models have postulated that granular parakeratosis may result from a deficiency in caspase 14, a protease vital to the formation of a well-functioning skin barrier.9 A cornified envelope often is noted in granular parakeratotic cells with no defects in desmosomes and cell membranes, suggesting that the pathogenesis lies within processing of profilaggrin to filaggrin, resulting in a failure to degrade keratohyalin granules and aggregation of keratin filaments.10 Granular parakeratosis is not known to be associated with other medical conditions, but it has been observed in patients receiving chemotherapy for breast11 and ovarian12 carcinomas. In infants with atopic dermatitis, granular parakeratosis was reported in 5 out of 7 cases.6 In our patient with secondary inguinal hyperhidrosis after thoracic sympathectomy, granular parakeratosis may be reactive to excess sweating and friction in the scrotal area.
Granular parakeratosis follows a waxing and waning pattern that may spontaneously resolve without any treatment; it also can follow a protracted course, as in a case with associated facial papules that persisted for 20 years.13 Topical corticosteroids alone or in combination with topical antifungal agents have been used for the treatment of granular parakeratosis with the goal of accelerating resolution.2,14 However, the efficacy of these therapeutic interventions is limited, and no controlled trials are underway. Topical vitamin D analogues15,16 and topical retinoids17 also have been reported with successful outcomes. Spontaneous resolution also has been observed in 2 different cases after previously being unresponsive to topical treatment.18,19 Treatment with Clostridium botulinum toxin A resulted in complete remission of the disease observed at 6-month follow-up. The pharmacologic action of the neurotoxin disrupts the stimulation of eccrine sweat glands, resulting in decreased sweating, a known exacerbating factor of granular parakeratosis.20
In summary, our case represents a unique clinical presentation of granular parakeratosis with classic histopathologic features. A high index of suspicion and a biopsy are vital to arriving at the correct diagnosis.
To the Editor:
Granular parakeratosis is a rare condition with an unclear etiology that results from a myriad of factors, including exposure to irritants, friction, moisture, and heat. The diagnosis is made based on a distinct histologic reaction pattern that may be protective against the triggers. We present a case of isolated scrotal granular parakeratosis in a patient with compensatory hyperhidrosis after endoscopic thoracic sympathectomy.
A 52-year-old man presented with a 5-year history of a recurrent rash affecting the scrotum. He experienced monthly flares that were exacerbated by inguinal hyperhidrosis. His symptoms included a burning sensation and pruritus followed by superficial desquamation, with gradual yet temporary improvement. His medical history was remarkable for primary axillary and palmoplantar hyperhidrosis, with compensatory inguinal hyperhidrosis after endoscopic thoracic sympathectomy 8 years prior to presentation.
Physical examination revealed a well-demarcated, scaly, erythematous plaque affecting the scrotal skin with sparing of the median raphe, penis, and inguinal folds (Figure 1). There were no other lesions noted in the axillary region or other skin folds.
Prior treatments prescribed by other providers included topical pimecrolimus, antifungal creams, topical corticosteroids, zinc oxide ointment, and daily application of an over-the-counter medicated powder with no resolution.
A punch biopsy performed at the current presentation showed psoriasiform hyperplasia of the epidermis with only a focally diminished granular layer. There was overlying thick parakeratosis and retention of keratohyalin granules (Figure 2). Grocott-Gomori methenamine- silver staining was negative for fungal elements in the sections examined. Clinical history, morphology of the eruption, and histologic features were consistent with granular parakeratosis.
Since the first reported incident of granular parakeratosis of the axilla in 1991,1 granular parakeratosis has been reported in other intertriginous areas, including the inframammary folds, inguinal folds, genitalia, perianal skin, and beneath the abdominal pannus.2 One case study in 1998 reported a patient with isolated involvement of the inguinal region3; however, this presentation is rare.4 This condition has been reported in both sexes and all age groups, including children.5
Granular parakeratosis classically presents as erythematous to brown hyperkeratotic papules that coalesce into plaques.6 It is thought to be a reactive inflammatory condition secondary to aggravating factors such as exposure to heat,7 moisture, and friction; skin occlusion; repeated washing; irritation from external agents; antiperspirants; and use of depilatory creams.8 Histopathology is characteristic and consists of retained nuclei and keratohyalin granules within the stratum corneum, beneath which there is a retained stratum granulosum. Epidermal changes may be varied and include atrophy or hyperplasia.
Murine models have postulated that granular parakeratosis may result from a deficiency in caspase 14, a protease vital to the formation of a well-functioning skin barrier.9 A cornified envelope often is noted in granular parakeratotic cells with no defects in desmosomes and cell membranes, suggesting that the pathogenesis lies within processing of profilaggrin to filaggrin, resulting in a failure to degrade keratohyalin granules and aggregation of keratin filaments.10 Granular parakeratosis is not known to be associated with other medical conditions, but it has been observed in patients receiving chemotherapy for breast11 and ovarian12 carcinomas. In infants with atopic dermatitis, granular parakeratosis was reported in 5 out of 7 cases.6 In our patient with secondary inguinal hyperhidrosis after thoracic sympathectomy, granular parakeratosis may be reactive to excess sweating and friction in the scrotal area.
Granular parakeratosis follows a waxing and waning pattern that may spontaneously resolve without any treatment; it also can follow a protracted course, as in a case with associated facial papules that persisted for 20 years.13 Topical corticosteroids alone or in combination with topical antifungal agents have been used for the treatment of granular parakeratosis with the goal of accelerating resolution.2,14 However, the efficacy of these therapeutic interventions is limited, and no controlled trials are underway. Topical vitamin D analogues15,16 and topical retinoids17 also have been reported with successful outcomes. Spontaneous resolution also has been observed in 2 different cases after previously being unresponsive to topical treatment.18,19 Treatment with Clostridium botulinum toxin A resulted in complete remission of the disease observed at 6-month follow-up. The pharmacologic action of the neurotoxin disrupts the stimulation of eccrine sweat glands, resulting in decreased sweating, a known exacerbating factor of granular parakeratosis.20
In summary, our case represents a unique clinical presentation of granular parakeratosis with classic histopathologic features. A high index of suspicion and a biopsy are vital to arriving at the correct diagnosis.
- Northcutt AD, Nelson DM, Tschen JA. Axillary granular parakeratosis. J Am Acad Dermatol. 1991;24:541-544.
- Burford C. Granular parakeratosis of multiple intertriginous areas. Australas J Dermatol. 2008;49:35-38.
- Mehregan DA, Thomas JE, Mehregan DR. Intertriginous granular parakeratosis. J Am Acad Dermatol. 1998;39:495-496.
- Leclerc-Mercier S, Prost-Squarcioni C, Hamel-Teillac D, et al. A case of congenital granular parakeratosis. Am J Dermatopathol. 2011;33:531-533.
- Scheinfeld NS, Mones J. Granular parakeratosis: pathologic and clinical correlation of 18 cases of granular parakeratosis. J Am Acad Dermatol. 2005;52:863-867.
- Akkaya AD, Oram Y, Aydin O. Infantile granular parakeratosis: cytologic examination of superficial scrapings as an aid to diagnosis. Pediatr Dermatol. 2015;32:392-396.
- Rodríguez G. Axillary granular parakeratosis [in Spanish]. Biomedica. 2002;22:519-523.
- Samrao A, Reis M, Niedt G, et al. Granular parakeratosis: response to calcipotriene and brief review of current therapeutic options. Skinmed. 2010;8:357-359.
- Hoste E, Denecker G, Gilbert B, et al. Caspase-14-deficient mice are more prone to the development of parakeratosis. J Invest Dermatol. 2013;133:742-750.
- Metze D, Rutten A. Granular parakeratosis—a unique acquired disorder of keratinization. J Cutan Pathol. 1999;26:339-352.
- Wallace CA, Pichardo RO, Yosipovitch G, et al. Granular parakeratosis: a case report and literature review. J Cutan Pathol. 2003;30:332-335.
- Jaconelli L, Doebelin B, Kanitakis J, et al. Granular parakeratosis in a patient treated with liposomal doxorubicin for ovarian carcinoma. J Am Acad Dermatol. 2008;58(5 suppl 1):S84-S87.
- Reddy IS, Swarnalata G, Mody T. Intertriginous granular parakeratosis persisting for 20 years. Indian J Dermatol Venereol Leprol. 2008;74:405-407.
- Dearden C, al-Nakib W, Andries K, et al. Drug resistant rhinoviruses from the nose of experimentally treated volunteers. Arch Virol. 1989;109:71-81.
- Patel U, Patel T, Skinner RB Jr. Resolution of granular parakeratosis with topical calcitriol. Arch Dermatol. 2011;147:997-998.
- Contreras ME, Gottfried LC, Bang RH, et al. Axillary intertriginous granular parakeratosis responsive to topical calcipotriene and ammonium lactate. Int J Dermatol. 2003;42:382-383.
- Brown SK, Heilman ER. Granular parakeratosis: resolution with topical tretinoin. J Am Acad Dermatol. 2002;47(5 suppl):S279-S280.
- Compton AK, Jackson JM. Isotretinoin as a treatment for axillary granular parakeratosis. Cutis. 2007;80:55-56.
- Webster CG, Resnik KS, Webster GF. Axillary granular parakeratosis: response to isotretinoin. J Am Acad Dermatol. 1997; 37:789-790.
- Ravitskiy L, Heymann WR. Botulinum toxin-induced resolution of axillary granular parakeratosis. Skinmed. 2005;4:118-120.
- Northcutt AD, Nelson DM, Tschen JA. Axillary granular parakeratosis. J Am Acad Dermatol. 1991;24:541-544.
- Burford C. Granular parakeratosis of multiple intertriginous areas. Australas J Dermatol. 2008;49:35-38.
- Mehregan DA, Thomas JE, Mehregan DR. Intertriginous granular parakeratosis. J Am Acad Dermatol. 1998;39:495-496.
- Leclerc-Mercier S, Prost-Squarcioni C, Hamel-Teillac D, et al. A case of congenital granular parakeratosis. Am J Dermatopathol. 2011;33:531-533.
- Scheinfeld NS, Mones J. Granular parakeratosis: pathologic and clinical correlation of 18 cases of granular parakeratosis. J Am Acad Dermatol. 2005;52:863-867.
- Akkaya AD, Oram Y, Aydin O. Infantile granular parakeratosis: cytologic examination of superficial scrapings as an aid to diagnosis. Pediatr Dermatol. 2015;32:392-396.
- Rodríguez G. Axillary granular parakeratosis [in Spanish]. Biomedica. 2002;22:519-523.
- Samrao A, Reis M, Niedt G, et al. Granular parakeratosis: response to calcipotriene and brief review of current therapeutic options. Skinmed. 2010;8:357-359.
- Hoste E, Denecker G, Gilbert B, et al. Caspase-14-deficient mice are more prone to the development of parakeratosis. J Invest Dermatol. 2013;133:742-750.
- Metze D, Rutten A. Granular parakeratosis—a unique acquired disorder of keratinization. J Cutan Pathol. 1999;26:339-352.
- Wallace CA, Pichardo RO, Yosipovitch G, et al. Granular parakeratosis: a case report and literature review. J Cutan Pathol. 2003;30:332-335.
- Jaconelli L, Doebelin B, Kanitakis J, et al. Granular parakeratosis in a patient treated with liposomal doxorubicin for ovarian carcinoma. J Am Acad Dermatol. 2008;58(5 suppl 1):S84-S87.
- Reddy IS, Swarnalata G, Mody T. Intertriginous granular parakeratosis persisting for 20 years. Indian J Dermatol Venereol Leprol. 2008;74:405-407.
- Dearden C, al-Nakib W, Andries K, et al. Drug resistant rhinoviruses from the nose of experimentally treated volunteers. Arch Virol. 1989;109:71-81.
- Patel U, Patel T, Skinner RB Jr. Resolution of granular parakeratosis with topical calcitriol. Arch Dermatol. 2011;147:997-998.
- Contreras ME, Gottfried LC, Bang RH, et al. Axillary intertriginous granular parakeratosis responsive to topical calcipotriene and ammonium lactate. Int J Dermatol. 2003;42:382-383.
- Brown SK, Heilman ER. Granular parakeratosis: resolution with topical tretinoin. J Am Acad Dermatol. 2002;47(5 suppl):S279-S280.
- Compton AK, Jackson JM. Isotretinoin as a treatment for axillary granular parakeratosis. Cutis. 2007;80:55-56.
- Webster CG, Resnik KS, Webster GF. Axillary granular parakeratosis: response to isotretinoin. J Am Acad Dermatol. 1997; 37:789-790.
- Ravitskiy L, Heymann WR. Botulinum toxin-induced resolution of axillary granular parakeratosis. Skinmed. 2005;4:118-120.
Practice Points
- Granular parakeratosis can occur in response to triggers such as irritants, friction, hyperhidrosis, and heat.
- Granular parakeratosis can have an atypical presentation; therefore, a high index of suspicion and punch biopsy are vital to arrive at the correct diagnosis.
- Classic histopathology demonstrates retained nuclei and keratohyalin granules within the stratum corneum beneath which there is a retained stratum granulosum.

Please interrupt me, but don't heat your fish
Bother me, I’m working
Although some of us have been comfortably functioning in a virtual work environment, others are now trickling back into the office. And you know what that means? People come to your desk to show you pictures of their cat or tell you about their kid’s birthday party. You may sneer at the interruption, but a study shows you actually like it.

A team of researchers at the University of Cincinnati surveyed 111 full-time employees twice a day for 3 weeks about their work experience. They asked about mental exhaustion, workplace interruptions, sense of belonging, and overall job satisfaction. They found that employees had a higher sense of belonging and job satisfaction when interrupted with a social versus work interruption.
“Interruptions can actually benefit individuals from an interpersonal perspective – people feel like they belong when others come and talk to them or ask them questions, even while being distracted from their tasks,” said Heather C. Vough, senior investigator and a former university faculty member.
Chitchatting at work is often seen as a distraction, but this study suggests that it’s not like heating up fish in the breakroom microwave.
So the next time someone hits you with the “Hey, do you have a sec?,” do yourself a favor and enjoy the interruption.
A smorgasbord of science
It’s probably difficult to recruit patients for some medical trials. Try this new drug and potentially get all sorts of interesting and unpleasant side effects. Pass. We suggest the approach a group of researchers from the University of Kansas took for a recent study into weight gain: Invite a bunch of 20-something adults to an all-you-can-eat buffet. They’ll be beating down your door in no time.

Their study, published in Appetite, focused on hyperpalatable food – the sort of food you can keep eating – and compared it with high-energy-dense food and ultra processed food. The test patients had their body composition measured, were let loose on the buffet, and were measured again a year later.
The patients who favored salty/carbohydrate-filled hyperpalatable food (such as pretzels or popcorn) were much more likely to gain weight, compared with those who focused on salty/fat-filled food of any variety. As a matter of fact, those who stuck to fatty food during the buffet had no change in weight over the 1-year study period. The researchers noted that those who ate the carb-filled food tended more toward hedonic eating, or the act of eating simply for pleasure.
The study is no doubt helpful in the long battle against obesity and overeating, but it’s also a very helpful guide to getting the most bang for your buck at the buffet. Stay away from the cheap salty snack food. Go for the steak and seafood. Get your money’s worth. In the long run you won’t even gain any weight. No promises about tomorrow though.
There’s a cheat code for that
For a large percentage of kids and young adults, and maybe even older adults (we don’t judge), a storm warning means a cozy night in playing video games. Staying inside is probably the safest bet when there’s a storm, and the weatherman never says to avoid playing video games when there’s lightning.

Maybe he should, though, since a man from Tennessee reportedly got struck by lightning through his game controller. Emergency crews determined that lightning either hit the man’s house or struck near it and went through the controller. The type of console was not revealed, even though some people may want to know the specifics before playing during the next storm.
Luckily, the man was not seriously hurt and did not need to go to the hospital. This is apparently not unheard of, as a professional gamer was shocked through a wired controller last year, causing burns on her hands and a broken controller.
This might be our cue to do less electrical types of activities during thunderstorms, like knitting or reading by candlelight.
Freeze, squeeze, and enjoy … cramping
As you were ingesting last week’s installment of the never-ending buffet that is LOTME, you probably wondered: What’s going on? Where’s the latest bodily insult being perpetuated by the gang over at TikTok?

Have no fear, good readers. We would never make you go 2 straight weeks without serving up some hyperpalatable TikTok tidbits.
Our bodily insult du jour is frozen honey, and it’s exploding all over TikTok … and a few other places. “The hashtag ‘#FrozenHoney’ has been viewed nearly 600 million times, and the hashtag ‘#FrozenHoneyChallenge’ has been viewed more than 80 million times,” NBC News recently reported.
After a few hours in the freezer, honey can be squeezed out of a plastic bottle as a semisolid, toothpastelike goo – it’s stiff enough to rise out of a container that’s pointed straight up – and bitten off in large chunks. And therein lies the problem.
Some people are overdoing it. “Honey is great, but having it in small amounts to sweeten is really a healthy relationship with food, and using it to get a lot of followers and a lot of attention and having it in excess amounts is crazy,” Kristin Kirkpatrick, a registered dietitian at the Cleveland Clinic, told NBC.
Besides the possible weight gain from eating massive amounts of sugar, experts warned that “gobbling up bottles of frozen honey” could lead to stomach cramping, bloating, and diarrhea. Some TikTokers, NBC noted, said that they “were running for the bathroom.”
As we said, it’s a trend that is exploding.
Be sure to tune in next week, when we learn how TikTokers use ground meat as a skin moisturizer.
Bother me, I’m working
Although some of us have been comfortably functioning in a virtual work environment, others are now trickling back into the office. And you know what that means? People come to your desk to show you pictures of their cat or tell you about their kid’s birthday party. You may sneer at the interruption, but a study shows you actually like it.
A team of researchers at the University of Cincinnati surveyed 111 full-time employees twice a day for 3 weeks about their work experience. They asked about mental exhaustion, workplace interruptions, sense of belonging, and overall job satisfaction. They found that employees had a higher sense of belonging and job satisfaction when interrupted with a social versus work interruption.
“Interruptions can actually benefit individuals from an interpersonal perspective – people feel like they belong when others come and talk to them or ask them questions, even while being distracted from their tasks,” said Heather C. Vough, senior investigator and a former university faculty member.
Chitchatting at work is often seen as a distraction, but this study suggests that it’s not like heating up fish in the breakroom microwave.
So the next time someone hits you with the “Hey, do you have a sec?,” do yourself a favor and enjoy the interruption.
A smorgasbord of science
It’s probably difficult to recruit patients for some medical trials. Try this new drug and potentially get all sorts of interesting and unpleasant side effects. Pass. We suggest the approach a group of researchers from the University of Kansas took for a recent study into weight gain: Invite a bunch of 20-something adults to an all-you-can-eat buffet. They’ll be beating down your door in no time.
Their study, published in Appetite, focused on hyperpalatable food – the sort of food you can keep eating – and compared it with high-energy-dense food and ultra processed food. The test patients had their body composition measured, were let loose on the buffet, and were measured again a year later.
The patients who favored salty/carbohydrate-filled hyperpalatable food (such as pretzels or popcorn) were much more likely to gain weight, compared with those who focused on salty/fat-filled food of any variety. As a matter of fact, those who stuck to fatty food during the buffet had no change in weight over the 1-year study period. The researchers noted that those who ate the carb-filled food tended more toward hedonic eating, or the act of eating simply for pleasure.
The study is no doubt helpful in the long battle against obesity and overeating, but it’s also a very helpful guide to getting the most bang for your buck at the buffet. Stay away from the cheap salty snack food. Go for the steak and seafood. Get your money’s worth. In the long run you won’t even gain any weight. No promises about tomorrow though.
There’s a cheat code for that
For a large percentage of kids and young adults, and maybe even older adults (we don’t judge), a storm warning means a cozy night in playing video games. Staying inside is probably the safest bet when there’s a storm, and the weatherman never says to avoid playing video games when there’s lightning.
Maybe he should, though, since a man from Tennessee reportedly got struck by lightning through his game controller. Emergency crews determined that lightning either hit the man’s house or struck near it and went through the controller. The type of console was not revealed, even though some people may want to know the specifics before playing during the next storm.
Luckily, the man was not seriously hurt and did not need to go to the hospital. This is apparently not unheard of, as a professional gamer was shocked through a wired controller last year, causing burns on her hands and a broken controller.
This might be our cue to do less electrical types of activities during thunderstorms, like knitting or reading by candlelight.
Freeze, squeeze, and enjoy … cramping
As you were ingesting last week’s installment of the never-ending buffet that is LOTME, you probably wondered: What’s going on? Where’s the latest bodily insult being perpetuated by the gang over at TikTok?
Have no fear, good readers. We would never make you go 2 straight weeks without serving up some hyperpalatable TikTok tidbits.
Our bodily insult du jour is frozen honey, and it’s exploding all over TikTok … and a few other places. “The hashtag ‘#FrozenHoney’ has been viewed nearly 600 million times, and the hashtag ‘#FrozenHoneyChallenge’ has been viewed more than 80 million times,” NBC News recently reported.
After a few hours in the freezer, honey can be squeezed out of a plastic bottle as a semisolid, toothpastelike goo – it’s stiff enough to rise out of a container that’s pointed straight up – and bitten off in large chunks. And therein lies the problem.
Some people are overdoing it. “Honey is great, but having it in small amounts to sweeten is really a healthy relationship with food, and using it to get a lot of followers and a lot of attention and having it in excess amounts is crazy,” Kristin Kirkpatrick, a registered dietitian at the Cleveland Clinic, told NBC.
Besides the possible weight gain from eating massive amounts of sugar, experts warned that “gobbling up bottles of frozen honey” could lead to stomach cramping, bloating, and diarrhea. Some TikTokers, NBC noted, said that they “were running for the bathroom.”
As we said, it’s a trend that is exploding.
Be sure to tune in next week, when we learn how TikTokers use ground meat as a skin moisturizer.
Bother me, I’m working
Although some of us have been comfortably functioning in a virtual work environment, others are now trickling back into the office. And you know what that means? People come to your desk to show you pictures of their cat or tell you about their kid’s birthday party. You may sneer at the interruption, but a study shows you actually like it.
A team of researchers at the University of Cincinnati surveyed 111 full-time employees twice a day for 3 weeks about their work experience. They asked about mental exhaustion, workplace interruptions, sense of belonging, and overall job satisfaction. They found that employees had a higher sense of belonging and job satisfaction when interrupted with a social versus work interruption.
“Interruptions can actually benefit individuals from an interpersonal perspective – people feel like they belong when others come and talk to them or ask them questions, even while being distracted from their tasks,” said Heather C. Vough, senior investigator and a former university faculty member.
Chitchatting at work is often seen as a distraction, but this study suggests that it’s not like heating up fish in the breakroom microwave.
So the next time someone hits you with the “Hey, do you have a sec?,” do yourself a favor and enjoy the interruption.
A smorgasbord of science
It’s probably difficult to recruit patients for some medical trials. Try this new drug and potentially get all sorts of interesting and unpleasant side effects. Pass. We suggest the approach a group of researchers from the University of Kansas took for a recent study into weight gain: Invite a bunch of 20-something adults to an all-you-can-eat buffet. They’ll be beating down your door in no time.
Their study, published in Appetite, focused on hyperpalatable food – the sort of food you can keep eating – and compared it with high-energy-dense food and ultra processed food. The test patients had their body composition measured, were let loose on the buffet, and were measured again a year later.
The patients who favored salty/carbohydrate-filled hyperpalatable food (such as pretzels or popcorn) were much more likely to gain weight, compared with those who focused on salty/fat-filled food of any variety. As a matter of fact, those who stuck to fatty food during the buffet had no change in weight over the 1-year study period. The researchers noted that those who ate the carb-filled food tended more toward hedonic eating, or the act of eating simply for pleasure.
The study is no doubt helpful in the long battle against obesity and overeating, but it’s also a very helpful guide to getting the most bang for your buck at the buffet. Stay away from the cheap salty snack food. Go for the steak and seafood. Get your money’s worth. In the long run you won’t even gain any weight. No promises about tomorrow though.
There’s a cheat code for that
For a large percentage of kids and young adults, and maybe even older adults (we don’t judge), a storm warning means a cozy night in playing video games. Staying inside is probably the safest bet when there’s a storm, and the weatherman never says to avoid playing video games when there’s lightning.
Maybe he should, though, since a man from Tennessee reportedly got struck by lightning through his game controller. Emergency crews determined that lightning either hit the man’s house or struck near it and went through the controller. The type of console was not revealed, even though some people may want to know the specifics before playing during the next storm.
Luckily, the man was not seriously hurt and did not need to go to the hospital. This is apparently not unheard of, as a professional gamer was shocked through a wired controller last year, causing burns on her hands and a broken controller.
This might be our cue to do less electrical types of activities during thunderstorms, like knitting or reading by candlelight.
Freeze, squeeze, and enjoy … cramping
As you were ingesting last week’s installment of the never-ending buffet that is LOTME, you probably wondered: What’s going on? Where’s the latest bodily insult being perpetuated by the gang over at TikTok?
Have no fear, good readers. We would never make you go 2 straight weeks without serving up some hyperpalatable TikTok tidbits.
Our bodily insult du jour is frozen honey, and it’s exploding all over TikTok … and a few other places. “The hashtag ‘#FrozenHoney’ has been viewed nearly 600 million times, and the hashtag ‘#FrozenHoneyChallenge’ has been viewed more than 80 million times,” NBC News recently reported.
After a few hours in the freezer, honey can be squeezed out of a plastic bottle as a semisolid, toothpastelike goo – it’s stiff enough to rise out of a container that’s pointed straight up – and bitten off in large chunks. And therein lies the problem.
Some people are overdoing it. “Honey is great, but having it in small amounts to sweeten is really a healthy relationship with food, and using it to get a lot of followers and a lot of attention and having it in excess amounts is crazy,” Kristin Kirkpatrick, a registered dietitian at the Cleveland Clinic, told NBC.
Besides the possible weight gain from eating massive amounts of sugar, experts warned that “gobbling up bottles of frozen honey” could lead to stomach cramping, bloating, and diarrhea. Some TikTokers, NBC noted, said that they “were running for the bathroom.”
As we said, it’s a trend that is exploding.
Be sure to tune in next week, when we learn how TikTokers use ground meat as a skin moisturizer.