User login
Tai chi as good as working out to shrink waistline

Results of a randomized controlled trial published online May 31 in Annals of Internal Medicine show that people who have a tough time with some kinds of aerobic exercise may gain similar benefits from tai chi.
The study is “very impressive,” said Bavani Nadeswaran, MD, of the University of California Irvine’s Susan Samueli Integrative Health Institute, who was not involved in the study.
Many people have arthritis or back pain, “and aerobic exercise can be hard on them,” she said. “The good thing about exercises like tai chi and yoga is that they are low-impact.” That means that people who can’t run or get access to a pool for swimming have a viable alternative.
The study included nearly 550 adults ages 50 and up in Hong Kong who were randomly assigned to engage in tai chi, aerobic exercise with strength training, or no exercise program for 12 weeks. All had waistlines greater than 35.4 inches for men and 31.5 inches for women.
The tai chi program involved three 1-hour weekly sessions of the practice, led by an instructor. Those who took part in the aerobic exercise group engaged three times each week in an exercise program of brisk tai chi and strength training, also led by an instructor.
The researchers measured changes in waistline size, cholesterol levels, and weight for about 9 months. Those who didn’t exercise had little change in their average waistline. Compared to the group that didn’t exercise, the average waistline of people in the two exercise groups declined more: by 0.7 inches more with tai chi, and 0.5 inches more with brisk walking and strength training.
Both exercise groups also had greater drops in body weight and triglyceride (a type of fat found in the blood) levels, and larger increases in high-density lipoprotein cholesterol, the “good” cholesterol, compared to the no-exercise group. All of these improvements lasted about 9 months with tai chi. But improvements in cholesterol levels did not last as long in those in the brisk-walking program.
The researchers also looked at the effects on blood pressure and blood sugar, but they found no differences between the groups.
The findings don’t necessarily mean that people with larger waistlines should dispense with their current exercise programs and turn to tai chi, said study author Parco Siu, PhD, head of the Division of Kinesiology at the University of Hong Kong’s School of Public Health. They show that tai chi is a good option if a person prefers it.
“This is good news for middle-aged and older adults who may be averse to conventional exercise,” he said in an email. But “certainly it is no problem for people to keep regularly participating in conventional exercise.”
Tai chi may also be a good choice for people without larger waistlines because practicing this form of exercise is a way to follow advice from the World Health Organization on physical activity, said Dr. Siu, though the study did not address this question.
Dr. Siu and the other researchers noted several limits to the study, including that all the people who took part were in China, so how the practice would affect people in different regions is not clear. Also, almost a third of those who began the study dropped out before it ended, and they tended to have a higher body weight than those who remained to the end. The authors said this high dropout rate could mean that some people had negative experiences during their exercise programs.
Next steps, said Dr. Siu, include further assessing how tai chi affects things such as blood sugar and blood pressure. Other, early-stage studies also show tai chi having some positive effects on mood and cognition, he said, pointing to a need for more research.
UC Irvine’s Dr. Nadeswaran agreed. The work opens the door, she said, to taking a long-term look at how practicing tai chi might affect a person’s risk of dying from heart disease or another cause. Her team’s work involves evaluating tai chi’s effects on several conditions, including metabolic syndrome and even the aftermath of COVID-19.
While researchers pursue these questions, tai chi is accessible in many ways. Dr. Siu noted the availability of classes in this “meditation in motion” practice at community centers and fitness clubs. For people who can’t yet rejoin activities in the real world, Dr. Nadeswaran said virtual tai chi classes also are available.
A version of this article first appeared on WebMD.com.
Results of a randomized controlled trial published online May 31 in Annals of Internal Medicine show that people who have a tough time with some kinds of aerobic exercise may gain similar benefits from tai chi.
The study is “very impressive,” said Bavani Nadeswaran, MD, of the University of California Irvine’s Susan Samueli Integrative Health Institute, who was not involved in the study.
Many people have arthritis or back pain, “and aerobic exercise can be hard on them,” she said. “The good thing about exercises like tai chi and yoga is that they are low-impact.” That means that people who can’t run or get access to a pool for swimming have a viable alternative.
The study included nearly 550 adults ages 50 and up in Hong Kong who were randomly assigned to engage in tai chi, aerobic exercise with strength training, or no exercise program for 12 weeks. All had waistlines greater than 35.4 inches for men and 31.5 inches for women.
The tai chi program involved three 1-hour weekly sessions of the practice, led by an instructor. Those who took part in the aerobic exercise group engaged three times each week in an exercise program of brisk tai chi and strength training, also led by an instructor.
The researchers measured changes in waistline size, cholesterol levels, and weight for about 9 months. Those who didn’t exercise had little change in their average waistline. Compared to the group that didn’t exercise, the average waistline of people in the two exercise groups declined more: by 0.7 inches more with tai chi, and 0.5 inches more with brisk walking and strength training.
Both exercise groups also had greater drops in body weight and triglyceride (a type of fat found in the blood) levels, and larger increases in high-density lipoprotein cholesterol, the “good” cholesterol, compared to the no-exercise group. All of these improvements lasted about 9 months with tai chi. But improvements in cholesterol levels did not last as long in those in the brisk-walking program.
The researchers also looked at the effects on blood pressure and blood sugar, but they found no differences between the groups.
The findings don’t necessarily mean that people with larger waistlines should dispense with their current exercise programs and turn to tai chi, said study author Parco Siu, PhD, head of the Division of Kinesiology at the University of Hong Kong’s School of Public Health. They show that tai chi is a good option if a person prefers it.
“This is good news for middle-aged and older adults who may be averse to conventional exercise,” he said in an email. But “certainly it is no problem for people to keep regularly participating in conventional exercise.”
Tai chi may also be a good choice for people without larger waistlines because practicing this form of exercise is a way to follow advice from the World Health Organization on physical activity, said Dr. Siu, though the study did not address this question.
Dr. Siu and the other researchers noted several limits to the study, including that all the people who took part were in China, so how the practice would affect people in different regions is not clear. Also, almost a third of those who began the study dropped out before it ended, and they tended to have a higher body weight than those who remained to the end. The authors said this high dropout rate could mean that some people had negative experiences during their exercise programs.
Next steps, said Dr. Siu, include further assessing how tai chi affects things such as blood sugar and blood pressure. Other, early-stage studies also show tai chi having some positive effects on mood and cognition, he said, pointing to a need for more research.
UC Irvine’s Dr. Nadeswaran agreed. The work opens the door, she said, to taking a long-term look at how practicing tai chi might affect a person’s risk of dying from heart disease or another cause. Her team’s work involves evaluating tai chi’s effects on several conditions, including metabolic syndrome and even the aftermath of COVID-19.
While researchers pursue these questions, tai chi is accessible in many ways. Dr. Siu noted the availability of classes in this “meditation in motion” practice at community centers and fitness clubs. For people who can’t yet rejoin activities in the real world, Dr. Nadeswaran said virtual tai chi classes also are available.
A version of this article first appeared on WebMD.com.
Results of a randomized controlled trial published online May 31 in Annals of Internal Medicine show that people who have a tough time with some kinds of aerobic exercise may gain similar benefits from tai chi.
The study is “very impressive,” said Bavani Nadeswaran, MD, of the University of California Irvine’s Susan Samueli Integrative Health Institute, who was not involved in the study.
Many people have arthritis or back pain, “and aerobic exercise can be hard on them,” she said. “The good thing about exercises like tai chi and yoga is that they are low-impact.” That means that people who can’t run or get access to a pool for swimming have a viable alternative.
The study included nearly 550 adults ages 50 and up in Hong Kong who were randomly assigned to engage in tai chi, aerobic exercise with strength training, or no exercise program for 12 weeks. All had waistlines greater than 35.4 inches for men and 31.5 inches for women.
The tai chi program involved three 1-hour weekly sessions of the practice, led by an instructor. Those who took part in the aerobic exercise group engaged three times each week in an exercise program of brisk tai chi and strength training, also led by an instructor.
The researchers measured changes in waistline size, cholesterol levels, and weight for about 9 months. Those who didn’t exercise had little change in their average waistline. Compared to the group that didn’t exercise, the average waistline of people in the two exercise groups declined more: by 0.7 inches more with tai chi, and 0.5 inches more with brisk walking and strength training.
Both exercise groups also had greater drops in body weight and triglyceride (a type of fat found in the blood) levels, and larger increases in high-density lipoprotein cholesterol, the “good” cholesterol, compared to the no-exercise group. All of these improvements lasted about 9 months with tai chi. But improvements in cholesterol levels did not last as long in those in the brisk-walking program.
The researchers also looked at the effects on blood pressure and blood sugar, but they found no differences between the groups.
The findings don’t necessarily mean that people with larger waistlines should dispense with their current exercise programs and turn to tai chi, said study author Parco Siu, PhD, head of the Division of Kinesiology at the University of Hong Kong’s School of Public Health. They show that tai chi is a good option if a person prefers it.
“This is good news for middle-aged and older adults who may be averse to conventional exercise,” he said in an email. But “certainly it is no problem for people to keep regularly participating in conventional exercise.”
Tai chi may also be a good choice for people without larger waistlines because practicing this form of exercise is a way to follow advice from the World Health Organization on physical activity, said Dr. Siu, though the study did not address this question.
Dr. Siu and the other researchers noted several limits to the study, including that all the people who took part were in China, so how the practice would affect people in different regions is not clear. Also, almost a third of those who began the study dropped out before it ended, and they tended to have a higher body weight than those who remained to the end. The authors said this high dropout rate could mean that some people had negative experiences during their exercise programs.
Next steps, said Dr. Siu, include further assessing how tai chi affects things such as blood sugar and blood pressure. Other, early-stage studies also show tai chi having some positive effects on mood and cognition, he said, pointing to a need for more research.
UC Irvine’s Dr. Nadeswaran agreed. The work opens the door, she said, to taking a long-term look at how practicing tai chi might affect a person’s risk of dying from heart disease or another cause. Her team’s work involves evaluating tai chi’s effects on several conditions, including metabolic syndrome and even the aftermath of COVID-19.
While researchers pursue these questions, tai chi is accessible in many ways. Dr. Siu noted the availability of classes in this “meditation in motion” practice at community centers and fitness clubs. For people who can’t yet rejoin activities in the real world, Dr. Nadeswaran said virtual tai chi classes also are available.
A version of this article first appeared on WebMD.com.
'Exciting': Olaparib benefit also in early BRCA+ breast cancer
New clinical data show that the PARP inhibitor olaparib (Lynparza, AstraZeneca/Merck) also has a place in the treatment of early stage breast cancer with BRCA mutations, in addition to its already established role in the treatment of metastatic disease.
It’s a notable outcome given that at least 5% of all breast cancers are associated with BRCA1 or BRCA2 mutations, said first author Andrew Tutt, MBChB, PhD, head of the division of breast cancer research at the Institute of Cancer Research and Guy’s Hospital, King’s College London.
The new results come from the phase 3 OlympiA trial, which involved nearly 2,000 women and showed that 1 year of adjuvant treatment with olaparib improved invasive and distant disease-free survival when used following adjuvant or neoadjuvant chemotherapy in patients with germline BRCA-mutated (gBRCAm) high-risk HER2-negative early breast cancer.
The study was highlighted at a press briefing ahead of the American Society of Clinical Oncology (ASCO) Annual Meeting, where the data will be presented during a plenary session. The study will also be published simultaneously in The New England Journal of Medicine.
The “exciting findings” highlight the importance of genetic testing in appropriate patients to identify those who might benefit from this treatment, and could open the door to additional trials of adjuvant PARP inhibitor in other BRCA1- and BRCA2-associated cancers, ASCO President Lori J. Pierce, MD, said during the press briefing.
“I think the implications are ... one, it’s an early stage disease, and two, it’s a reminder that when you see a patient in clinic and you’re taking a history that you query them for family history,” Dr. Pierce said in an interview. “You try to find out which of these patients could have a mutation so we [can] refer them for testing, and if they have a mutation this will be a therapy that they would be able to get and will likely benefit from.”
Improved IDFS and DDFS
The double-blind OlympiA trial enrolled 1,836 patients with gBRCAm and HER2-negative stage II-III breast cancer, including triple-negative or hormone receptor–positive disease with high risk of recurrence after completion of primary local treatment and adjuvant or neoadjuvant chemotherapy. Patients were randomized 1:1 to receive 1 year of continuous oral olaparib at a dose of 300 mg twice daily or placebo.
“Compared with placebo, patients receiving olaparib had a 42% reduction in the risk of the following events: local recurrence of breast cancer, metastatic recurrence of breast cancer, other new cancers, or death due to any cause,” Dr. Tutt said, describing the factors comprising the study’s primary endpoint of invasive disease-free survival (IDSF).
The hazard ratio for IDSF with olaparib versus placebo at a median follow-up of 2.5 years was 0.58, prompting the independent data monitoring committee to recommend unblinding the study at the time of the interim analysis.
At 3 years, 85.9% of patients in the olaparib group and 77.1% in the placebo group were alive and free from invasive disease, for a difference of 8.8%, Dr. Tutt said.
For the secondary endpoint of distant disease-free survival (DDFS), defined as the absence of metastatic breast cancer, new cancer, and death due to any cause, a highly statistically significant 43% reduction was observed with olaparib versus placebo (hazard ratio [HR], 0.57). The survival curves separated early and remained separated, with 3-year DDFS of 87.5% and 80.4%, for a 7.1% difference between the treatment and placebo group, he said.
“The secondary endpoint of overall survival is inevitably immature,” he added, noting that fewer deaths were nonetheless reported with olaparib at 3 years (3-year overall survival 92.0% vs. 88.3%; HR, 0.68), although the difference did not reach statistical significance.
Adverse events observed in the trial were limited and manageable, and were consistent with known effects and product labeling, he said.
Grade 3 adverse events that occurred in more than 10% of patients receiving olaparib were anemia (8.7%), neutropenia (4.8%), leukopenia (3.0%), and fatigue (1.8%). Serious adverse events and adverse events of special interest, including myelodysplastic syndrome/acute myeloid leukemia, new primary malignancy, and pneumonitis, were not increased with olaparib; they occurred in 8.7% vs. 8.4% and 2.6% vs. 4.6% of patients in the treatment and placebo groups, respectively.
Future implications
The findings have important implications for the future of breast cancer treatment, Dr. Tutt said.
Olaparib was already approved for use in the metastatic setting for gBRCAm HER2-negative breast cancer in 2018 on the basis of data from the pivotal OlympiAD trial, led by Mark E. Robson, MD, and colleagues.
In the high-risk early breast cancer setting, however, recurrence rates can be high even after chemotherapy, and novel adjuvant treatments have been lacking, Dr. Tutt said.
The latest findings from OlympiA appear to represent “a major advance for the subset of patients who have inherited BRCA1 and BRCA2 mutations,” Dr. Robson said in an interview.
“The absolute differences – even with relatively short follow-up – in invasive disease-free survival are impressive, and even though overall survival is not yet statistically significant, one surely would be hopeful that with further follow-up a difference would emerge,” he said.
There was some suggestion, even in the OlympiAD trial, that the earlier patients with metastatic disease were treated with PARP inhibition, the more benefit they received, so it’s not surprising that research has moved into the early stage disease setting, he noted.
Future directions may include looking at different drug combinations as investigators did with some success in the BROCADE3 trial of the PARP inhibitor veliparib plus carboplatin and paclitaxel in metastatic gBRCAmut HER2-negative breast cancer – particularly if concerns about worsening myelosuppression when combining a PARP inhibitor and chemotherapy are attenuated with newer PARP inhibitors, he said.
“But for now, using [olaparib] after completion of conventional chemotherapy is the approach that makes the most sense,” he added.
Dr. Robson also noted that some smaller studies show “fairly dramatic pathologic complete response rates” with preoperative PARP inhibitor therapy. He said that “the idea of giving therapy even before surgery, perhaps as a de-escalation approach, is something that would be worth studying in the future.”
For now, it will be important to keep a close eye on whether there is any worsening of rates of second malignancies, especially leukemia, over time in the OlympiA trial participants.
“That was not seen in either the OlympiAD or EMBRACA study [another phase 3 study looking at PARP inhibition in advanced gBRCAmut HER2-negative breast cancer] in the metastatic setting, but obviously [the early breast cancer] population will be at risk for a longer period of time and we will need to see what the data are,” he said. “So far the results are all very encouraging, and this could lead to a new paradigm where we’re basically testing all women with breast cancer at the time of diagnosis to figure out whether or not this is an appropriate adjuvant treatment for them.”
The OlympiA trial was funded by the National Cancer Institute and AstraZeneca. Dr. Tutt has reported multiple relationships with companies including Inbiomotion, Medscape, Prime Oncology, Artios, AstraZeneca, Merck Serono, Pfizer, Merck KGaA, Roche/Genentech, Breast Cancer Now Charity, and Cancer Research UK. Dr. Robson has reported being an investigator for clinical trials of PARP inhibitors and receiving research grants (to his institution) from AstraZeneca, Merck, and Pfizer.
A version of this article first appeared on Medscape.com.
New clinical data show that the PARP inhibitor olaparib (Lynparza, AstraZeneca/Merck) also has a place in the treatment of early stage breast cancer with BRCA mutations, in addition to its already established role in the treatment of metastatic disease.
It’s a notable outcome given that at least 5% of all breast cancers are associated with BRCA1 or BRCA2 mutations, said first author Andrew Tutt, MBChB, PhD, head of the division of breast cancer research at the Institute of Cancer Research and Guy’s Hospital, King’s College London.
The new results come from the phase 3 OlympiA trial, which involved nearly 2,000 women and showed that 1 year of adjuvant treatment with olaparib improved invasive and distant disease-free survival when used following adjuvant or neoadjuvant chemotherapy in patients with germline BRCA-mutated (gBRCAm) high-risk HER2-negative early breast cancer.
The study was highlighted at a press briefing ahead of the American Society of Clinical Oncology (ASCO) Annual Meeting, where the data will be presented during a plenary session. The study will also be published simultaneously in The New England Journal of Medicine.
The “exciting findings” highlight the importance of genetic testing in appropriate patients to identify those who might benefit from this treatment, and could open the door to additional trials of adjuvant PARP inhibitor in other BRCA1- and BRCA2-associated cancers, ASCO President Lori J. Pierce, MD, said during the press briefing.
“I think the implications are ... one, it’s an early stage disease, and two, it’s a reminder that when you see a patient in clinic and you’re taking a history that you query them for family history,” Dr. Pierce said in an interview. “You try to find out which of these patients could have a mutation so we [can] refer them for testing, and if they have a mutation this will be a therapy that they would be able to get and will likely benefit from.”
Improved IDFS and DDFS
The double-blind OlympiA trial enrolled 1,836 patients with gBRCAm and HER2-negative stage II-III breast cancer, including triple-negative or hormone receptor–positive disease with high risk of recurrence after completion of primary local treatment and adjuvant or neoadjuvant chemotherapy. Patients were randomized 1:1 to receive 1 year of continuous oral olaparib at a dose of 300 mg twice daily or placebo.
“Compared with placebo, patients receiving olaparib had a 42% reduction in the risk of the following events: local recurrence of breast cancer, metastatic recurrence of breast cancer, other new cancers, or death due to any cause,” Dr. Tutt said, describing the factors comprising the study’s primary endpoint of invasive disease-free survival (IDSF).
The hazard ratio for IDSF with olaparib versus placebo at a median follow-up of 2.5 years was 0.58, prompting the independent data monitoring committee to recommend unblinding the study at the time of the interim analysis.
At 3 years, 85.9% of patients in the olaparib group and 77.1% in the placebo group were alive and free from invasive disease, for a difference of 8.8%, Dr. Tutt said.
For the secondary endpoint of distant disease-free survival (DDFS), defined as the absence of metastatic breast cancer, new cancer, and death due to any cause, a highly statistically significant 43% reduction was observed with olaparib versus placebo (hazard ratio [HR], 0.57). The survival curves separated early and remained separated, with 3-year DDFS of 87.5% and 80.4%, for a 7.1% difference between the treatment and placebo group, he said.
“The secondary endpoint of overall survival is inevitably immature,” he added, noting that fewer deaths were nonetheless reported with olaparib at 3 years (3-year overall survival 92.0% vs. 88.3%; HR, 0.68), although the difference did not reach statistical significance.
Adverse events observed in the trial were limited and manageable, and were consistent with known effects and product labeling, he said.
Grade 3 adverse events that occurred in more than 10% of patients receiving olaparib were anemia (8.7%), neutropenia (4.8%), leukopenia (3.0%), and fatigue (1.8%). Serious adverse events and adverse events of special interest, including myelodysplastic syndrome/acute myeloid leukemia, new primary malignancy, and pneumonitis, were not increased with olaparib; they occurred in 8.7% vs. 8.4% and 2.6% vs. 4.6% of patients in the treatment and placebo groups, respectively.
Future implications
The findings have important implications for the future of breast cancer treatment, Dr. Tutt said.
Olaparib was already approved for use in the metastatic setting for gBRCAm HER2-negative breast cancer in 2018 on the basis of data from the pivotal OlympiAD trial, led by Mark E. Robson, MD, and colleagues.
In the high-risk early breast cancer setting, however, recurrence rates can be high even after chemotherapy, and novel adjuvant treatments have been lacking, Dr. Tutt said.
The latest findings from OlympiA appear to represent “a major advance for the subset of patients who have inherited BRCA1 and BRCA2 mutations,” Dr. Robson said in an interview.
“The absolute differences – even with relatively short follow-up – in invasive disease-free survival are impressive, and even though overall survival is not yet statistically significant, one surely would be hopeful that with further follow-up a difference would emerge,” he said.
There was some suggestion, even in the OlympiAD trial, that the earlier patients with metastatic disease were treated with PARP inhibition, the more benefit they received, so it’s not surprising that research has moved into the early stage disease setting, he noted.
Future directions may include looking at different drug combinations as investigators did with some success in the BROCADE3 trial of the PARP inhibitor veliparib plus carboplatin and paclitaxel in metastatic gBRCAmut HER2-negative breast cancer – particularly if concerns about worsening myelosuppression when combining a PARP inhibitor and chemotherapy are attenuated with newer PARP inhibitors, he said.
“But for now, using [olaparib] after completion of conventional chemotherapy is the approach that makes the most sense,” he added.
Dr. Robson also noted that some smaller studies show “fairly dramatic pathologic complete response rates” with preoperative PARP inhibitor therapy. He said that “the idea of giving therapy even before surgery, perhaps as a de-escalation approach, is something that would be worth studying in the future.”
For now, it will be important to keep a close eye on whether there is any worsening of rates of second malignancies, especially leukemia, over time in the OlympiA trial participants.
“That was not seen in either the OlympiAD or EMBRACA study [another phase 3 study looking at PARP inhibition in advanced gBRCAmut HER2-negative breast cancer] in the metastatic setting, but obviously [the early breast cancer] population will be at risk for a longer period of time and we will need to see what the data are,” he said. “So far the results are all very encouraging, and this could lead to a new paradigm where we’re basically testing all women with breast cancer at the time of diagnosis to figure out whether or not this is an appropriate adjuvant treatment for them.”
The OlympiA trial was funded by the National Cancer Institute and AstraZeneca. Dr. Tutt has reported multiple relationships with companies including Inbiomotion, Medscape, Prime Oncology, Artios, AstraZeneca, Merck Serono, Pfizer, Merck KGaA, Roche/Genentech, Breast Cancer Now Charity, and Cancer Research UK. Dr. Robson has reported being an investigator for clinical trials of PARP inhibitors and receiving research grants (to his institution) from AstraZeneca, Merck, and Pfizer.
A version of this article first appeared on Medscape.com.
New clinical data show that the PARP inhibitor olaparib (Lynparza, AstraZeneca/Merck) also has a place in the treatment of early stage breast cancer with BRCA mutations, in addition to its already established role in the treatment of metastatic disease.
It’s a notable outcome given that at least 5% of all breast cancers are associated with BRCA1 or BRCA2 mutations, said first author Andrew Tutt, MBChB, PhD, head of the division of breast cancer research at the Institute of Cancer Research and Guy’s Hospital, King’s College London.
The new results come from the phase 3 OlympiA trial, which involved nearly 2,000 women and showed that 1 year of adjuvant treatment with olaparib improved invasive and distant disease-free survival when used following adjuvant or neoadjuvant chemotherapy in patients with germline BRCA-mutated (gBRCAm) high-risk HER2-negative early breast cancer.
The study was highlighted at a press briefing ahead of the American Society of Clinical Oncology (ASCO) Annual Meeting, where the data will be presented during a plenary session. The study will also be published simultaneously in The New England Journal of Medicine.
The “exciting findings” highlight the importance of genetic testing in appropriate patients to identify those who might benefit from this treatment, and could open the door to additional trials of adjuvant PARP inhibitor in other BRCA1- and BRCA2-associated cancers, ASCO President Lori J. Pierce, MD, said during the press briefing.
“I think the implications are ... one, it’s an early stage disease, and two, it’s a reminder that when you see a patient in clinic and you’re taking a history that you query them for family history,” Dr. Pierce said in an interview. “You try to find out which of these patients could have a mutation so we [can] refer them for testing, and if they have a mutation this will be a therapy that they would be able to get and will likely benefit from.”
Improved IDFS and DDFS
The double-blind OlympiA trial enrolled 1,836 patients with gBRCAm and HER2-negative stage II-III breast cancer, including triple-negative or hormone receptor–positive disease with high risk of recurrence after completion of primary local treatment and adjuvant or neoadjuvant chemotherapy. Patients were randomized 1:1 to receive 1 year of continuous oral olaparib at a dose of 300 mg twice daily or placebo.
“Compared with placebo, patients receiving olaparib had a 42% reduction in the risk of the following events: local recurrence of breast cancer, metastatic recurrence of breast cancer, other new cancers, or death due to any cause,” Dr. Tutt said, describing the factors comprising the study’s primary endpoint of invasive disease-free survival (IDSF).
The hazard ratio for IDSF with olaparib versus placebo at a median follow-up of 2.5 years was 0.58, prompting the independent data monitoring committee to recommend unblinding the study at the time of the interim analysis.
At 3 years, 85.9% of patients in the olaparib group and 77.1% in the placebo group were alive and free from invasive disease, for a difference of 8.8%, Dr. Tutt said.
For the secondary endpoint of distant disease-free survival (DDFS), defined as the absence of metastatic breast cancer, new cancer, and death due to any cause, a highly statistically significant 43% reduction was observed with olaparib versus placebo (hazard ratio [HR], 0.57). The survival curves separated early and remained separated, with 3-year DDFS of 87.5% and 80.4%, for a 7.1% difference between the treatment and placebo group, he said.
“The secondary endpoint of overall survival is inevitably immature,” he added, noting that fewer deaths were nonetheless reported with olaparib at 3 years (3-year overall survival 92.0% vs. 88.3%; HR, 0.68), although the difference did not reach statistical significance.
Adverse events observed in the trial were limited and manageable, and were consistent with known effects and product labeling, he said.
Grade 3 adverse events that occurred in more than 10% of patients receiving olaparib were anemia (8.7%), neutropenia (4.8%), leukopenia (3.0%), and fatigue (1.8%). Serious adverse events and adverse events of special interest, including myelodysplastic syndrome/acute myeloid leukemia, new primary malignancy, and pneumonitis, were not increased with olaparib; they occurred in 8.7% vs. 8.4% and 2.6% vs. 4.6% of patients in the treatment and placebo groups, respectively.
Future implications
The findings have important implications for the future of breast cancer treatment, Dr. Tutt said.
Olaparib was already approved for use in the metastatic setting for gBRCAm HER2-negative breast cancer in 2018 on the basis of data from the pivotal OlympiAD trial, led by Mark E. Robson, MD, and colleagues.
In the high-risk early breast cancer setting, however, recurrence rates can be high even after chemotherapy, and novel adjuvant treatments have been lacking, Dr. Tutt said.
The latest findings from OlympiA appear to represent “a major advance for the subset of patients who have inherited BRCA1 and BRCA2 mutations,” Dr. Robson said in an interview.
“The absolute differences – even with relatively short follow-up – in invasive disease-free survival are impressive, and even though overall survival is not yet statistically significant, one surely would be hopeful that with further follow-up a difference would emerge,” he said.
There was some suggestion, even in the OlympiAD trial, that the earlier patients with metastatic disease were treated with PARP inhibition, the more benefit they received, so it’s not surprising that research has moved into the early stage disease setting, he noted.
Future directions may include looking at different drug combinations as investigators did with some success in the BROCADE3 trial of the PARP inhibitor veliparib plus carboplatin and paclitaxel in metastatic gBRCAmut HER2-negative breast cancer – particularly if concerns about worsening myelosuppression when combining a PARP inhibitor and chemotherapy are attenuated with newer PARP inhibitors, he said.
“But for now, using [olaparib] after completion of conventional chemotherapy is the approach that makes the most sense,” he added.
Dr. Robson also noted that some smaller studies show “fairly dramatic pathologic complete response rates” with preoperative PARP inhibitor therapy. He said that “the idea of giving therapy even before surgery, perhaps as a de-escalation approach, is something that would be worth studying in the future.”
For now, it will be important to keep a close eye on whether there is any worsening of rates of second malignancies, especially leukemia, over time in the OlympiA trial participants.
“That was not seen in either the OlympiAD or EMBRACA study [another phase 3 study looking at PARP inhibition in advanced gBRCAmut HER2-negative breast cancer] in the metastatic setting, but obviously [the early breast cancer] population will be at risk for a longer period of time and we will need to see what the data are,” he said. “So far the results are all very encouraging, and this could lead to a new paradigm where we’re basically testing all women with breast cancer at the time of diagnosis to figure out whether or not this is an appropriate adjuvant treatment for them.”
The OlympiA trial was funded by the National Cancer Institute and AstraZeneca. Dr. Tutt has reported multiple relationships with companies including Inbiomotion, Medscape, Prime Oncology, Artios, AstraZeneca, Merck Serono, Pfizer, Merck KGaA, Roche/Genentech, Breast Cancer Now Charity, and Cancer Research UK. Dr. Robson has reported being an investigator for clinical trials of PARP inhibitors and receiving research grants (to his institution) from AstraZeneca, Merck, and Pfizer.
A version of this article first appeared on Medscape.com.
Mavacamten boosts quality of life in patients with hypertrophic cardiomyopathy
Of patients with symptomatic, obstructive hypertrophic cardiomyopathy treated with the investigational oral agent mavacamten, more than twice as many, compared with placebo, had a very large improvement from baseline in their summary quality of life score after 30 weeks of treatment in a pivotal trial with 194 patients evaluable for this endpoint.

The trial’s health-related quality of life assessment, the Kansas City Cardiomyopathy Questionnaire (KCCQ), also showed an average improvement of more than 9 points, compared with placebo, in summary KCCQ scores among 98 mavacamten-treated patients, and a nearly 15-point improvement from baseline that represents a “moderate to large” improvement in overall health-related quality of life, John A. Spertus, MD, said at the annual scientific sessions of the American College of Cardiology.
Largest drug benefit ever seen in KCCQ
The 9-point average incremental improvement on mavacamten, a selective cardiac myosin inhibitor, compared with placebo-treated patients, is “the largest drug-mediated benefit we’ve ever observed on the KCCQ,” said Dr. Spertus, who spearheaded development of the KCCQ. Concurrently with his report the results also appeared online in the Lancet.
“Given the strength of the data, I’d reach for this drug early” to treat patients with obstructive hypertrophic cardiomyopathy (HCM), added Dr. Spertus, a professor and cardiovascular outcomes researcher at the University of Missouri–Kansas City and clinical director of outcomes research at Saint Luke’s Mid America Heart Institute, also in Kansas City.
No available treatment for obstructive HCM has had “as vigorous an assessment of impact on health status,” and the study that supplied the data he and his associates analyzed, EXPLORER-HCM, is “the largest trial ever done” in patients with HCM, he added.
Management guidelines for HCM released last year by the ACC and American Heart Association named beta-blockers “first-line” medical therapy for the disorder, with the calcium channel blockers verapamil or diltiazem named as “reasonable alternatives” to beta-blockers. However, these commonly used agents have “limited” evidence supporting health-status benefits in patients with HCM, Dr. Spertus and coauthors wrote in their report.
Longer follow-up needed
“This is an important study,” commented Matthew W. Martinez, MD, director of sports cardiology and a HCM specialist at Morristown (N.J.) Medical Center. But “given the longevity of HCM we need follow-up that goes beyond 30 weeks,” he said as designated discussant for the report.

EXPLORER-HCM randomized 251 patients with symptomatic obstructive HCM at 68 centers in 13 countries during 2018-2019. The 30-week trial’s primary outcome was a composite to assess clinical response, compared with baseline, that included a 1.5-mL/kg per min or greater increase in peak oxygen consumption (pVO2) and at least one New York Heart Association (NYHA) functional class reduction; or a 3.0 mL/kg per min or greater improvement in pVO2 and no worsening of NYHA class.
Patients averaged about 59 years of age, about 60% were men, and their pVO2 at entry averaged about 20 mL/kg per min. About 73% were in NYHA functional class II, with the remainder in functional class III. Patients received mavacamten as a once-daily oral dose that gradually up-titrated during the trial to reach targeted reductions in each patient’s plasma levels of the drug and in their left ventricular outflow tract gradient.
The results showed that, after 30 weeks on treatment, the primary endpoint was reached by 37% of 123 patients on mavacamten and by 17% of 128 patients on placebo, a significant difference in an intention-to-treat analysis. About 70% of patients completed their KCCQ after 30 weeks, which meant that fewer patients were in the quality of life analyses, according to the report that was published in The Lancet .
Based on these results the drug is now under consideration for approval by the Food and Drug Administration, with a decision expected by early 2022.
Benefit fades quickly when mavacamten stops
More detailed analysis of quality of life findings in the new report also showed that, while average KCCQ scores (both overall summary score and clinical summary score) steadily improved with mavacamten treatment, compared with control patients, through 18 weeks on treatment, the scores then roughly plateaued out to 30 weeks. This was followed by a sharp reversal back down to baseline levels and similar to control patients 8 weeks after stopping mavacamten, suggesting that the drug’s benefit quickly fades off treatment and hence must be taken chronically.
The responder analysis showed that 9% of patients on mavacamten had a worsening in their KCCQ overall summary scores by more than 5 points after 30 weeks, compared with 23% of the control patients. In contrast, a very large improvement in KCCQ score, defined as a rise of at least 20 points from baseline after 30 weeks, occurred in 36% of those who received mavacamten and in 15% of the controls. The between-group difference indicates a number needed to treat with mavacamten of roughly five to produce one additional patient with a very large improvement in KCCQ overall summary score, Dr. Spertus noted.
By design, all patients enrolled in EXPLORER-HCM had a left ventricular ejection fraction of at least 55%. During treatment, seven of the mavacamten-treated patients and two in the control arm had a transient decrease in their left ventricular ejection fraction to below 50%, although this later normalized in all affected patients. “An initial criticism” of the trial was that a significant percentage of mavacamten patients “developed left ventricular dysfunction” noted Dr. Martinez, but Dr. Spertus highlighted the poor apparent correlation between this phenomenon and quality of life self-assessment. Six of the seven patients on mavacamten who had a transient drop in their left ventricular ejection fraction had very large improvements in their KCCQ summary scores, Dr. Spertus reported.
Hypertrophic cardiomyopathy is a myocardial disorder characterized by primary left ventricular hypertrophy. Although a complex disease, HCM is broadly defined by pathologically enhanced cardiac actin-myosin interactions that result in hypercontractility, diastolic abnormalities, and dynamic left ventricular outflow tract obstruction. Mavacamten is a first-in-class, small-molecule, selective allosteric inhibitor of cardiac myosin ATPase developed to target the underlying pathophysiology of HCM by reducing actin-myosin cross-bridge formation, thereby reducing contractility and improving myocardial energetics.
EXPLORER-HCM was sponsored by MyoKardia, the company developing mavacamten and a subsidiary of Bristol-Myers Squibb. Dr. Spertus has been a consultant to MyoKardia, as well as to Abbott, Amgen, Bayer, Janssen, Merck, and Novartis. He has received research support from Abbott Vascular, and he holds the copyright for the KCCQ. Dr. Martinez has been a consultant to and received honoraria from Bristol-Myers Squibb.
Of patients with symptomatic, obstructive hypertrophic cardiomyopathy treated with the investigational oral agent mavacamten, more than twice as many, compared with placebo, had a very large improvement from baseline in their summary quality of life score after 30 weeks of treatment in a pivotal trial with 194 patients evaluable for this endpoint.
The trial’s health-related quality of life assessment, the Kansas City Cardiomyopathy Questionnaire (KCCQ), also showed an average improvement of more than 9 points, compared with placebo, in summary KCCQ scores among 98 mavacamten-treated patients, and a nearly 15-point improvement from baseline that represents a “moderate to large” improvement in overall health-related quality of life, John A. Spertus, MD, said at the annual scientific sessions of the American College of Cardiology.
Largest drug benefit ever seen in KCCQ
The 9-point average incremental improvement on mavacamten, a selective cardiac myosin inhibitor, compared with placebo-treated patients, is “the largest drug-mediated benefit we’ve ever observed on the KCCQ,” said Dr. Spertus, who spearheaded development of the KCCQ. Concurrently with his report the results also appeared online in the Lancet.
“Given the strength of the data, I’d reach for this drug early” to treat patients with obstructive hypertrophic cardiomyopathy (HCM), added Dr. Spertus, a professor and cardiovascular outcomes researcher at the University of Missouri–Kansas City and clinical director of outcomes research at Saint Luke’s Mid America Heart Institute, also in Kansas City.
No available treatment for obstructive HCM has had “as vigorous an assessment of impact on health status,” and the study that supplied the data he and his associates analyzed, EXPLORER-HCM, is “the largest trial ever done” in patients with HCM, he added.
Management guidelines for HCM released last year by the ACC and American Heart Association named beta-blockers “first-line” medical therapy for the disorder, with the calcium channel blockers verapamil or diltiazem named as “reasonable alternatives” to beta-blockers. However, these commonly used agents have “limited” evidence supporting health-status benefits in patients with HCM, Dr. Spertus and coauthors wrote in their report.
Longer follow-up needed
“This is an important study,” commented Matthew W. Martinez, MD, director of sports cardiology and a HCM specialist at Morristown (N.J.) Medical Center. But “given the longevity of HCM we need follow-up that goes beyond 30 weeks,” he said as designated discussant for the report.
EXPLORER-HCM randomized 251 patients with symptomatic obstructive HCM at 68 centers in 13 countries during 2018-2019. The 30-week trial’s primary outcome was a composite to assess clinical response, compared with baseline, that included a 1.5-mL/kg per min or greater increase in peak oxygen consumption (pVO2) and at least one New York Heart Association (NYHA) functional class reduction; or a 3.0 mL/kg per min or greater improvement in pVO2 and no worsening of NYHA class.
Patients averaged about 59 years of age, about 60% were men, and their pVO2 at entry averaged about 20 mL/kg per min. About 73% were in NYHA functional class II, with the remainder in functional class III. Patients received mavacamten as a once-daily oral dose that gradually up-titrated during the trial to reach targeted reductions in each patient’s plasma levels of the drug and in their left ventricular outflow tract gradient.
The results showed that, after 30 weeks on treatment, the primary endpoint was reached by 37% of 123 patients on mavacamten and by 17% of 128 patients on placebo, a significant difference in an intention-to-treat analysis. About 70% of patients completed their KCCQ after 30 weeks, which meant that fewer patients were in the quality of life analyses, according to the report that was published in The Lancet .
Based on these results the drug is now under consideration for approval by the Food and Drug Administration, with a decision expected by early 2022.
Benefit fades quickly when mavacamten stops
More detailed analysis of quality of life findings in the new report also showed that, while average KCCQ scores (both overall summary score and clinical summary score) steadily improved with mavacamten treatment, compared with control patients, through 18 weeks on treatment, the scores then roughly plateaued out to 30 weeks. This was followed by a sharp reversal back down to baseline levels and similar to control patients 8 weeks after stopping mavacamten, suggesting that the drug’s benefit quickly fades off treatment and hence must be taken chronically.
The responder analysis showed that 9% of patients on mavacamten had a worsening in their KCCQ overall summary scores by more than 5 points after 30 weeks, compared with 23% of the control patients. In contrast, a very large improvement in KCCQ score, defined as a rise of at least 20 points from baseline after 30 weeks, occurred in 36% of those who received mavacamten and in 15% of the controls. The between-group difference indicates a number needed to treat with mavacamten of roughly five to produce one additional patient with a very large improvement in KCCQ overall summary score, Dr. Spertus noted.
By design, all patients enrolled in EXPLORER-HCM had a left ventricular ejection fraction of at least 55%. During treatment, seven of the mavacamten-treated patients and two in the control arm had a transient decrease in their left ventricular ejection fraction to below 50%, although this later normalized in all affected patients. “An initial criticism” of the trial was that a significant percentage of mavacamten patients “developed left ventricular dysfunction” noted Dr. Martinez, but Dr. Spertus highlighted the poor apparent correlation between this phenomenon and quality of life self-assessment. Six of the seven patients on mavacamten who had a transient drop in their left ventricular ejection fraction had very large improvements in their KCCQ summary scores, Dr. Spertus reported.
Hypertrophic cardiomyopathy is a myocardial disorder characterized by primary left ventricular hypertrophy. Although a complex disease, HCM is broadly defined by pathologically enhanced cardiac actin-myosin interactions that result in hypercontractility, diastolic abnormalities, and dynamic left ventricular outflow tract obstruction. Mavacamten is a first-in-class, small-molecule, selective allosteric inhibitor of cardiac myosin ATPase developed to target the underlying pathophysiology of HCM by reducing actin-myosin cross-bridge formation, thereby reducing contractility and improving myocardial energetics.
EXPLORER-HCM was sponsored by MyoKardia, the company developing mavacamten and a subsidiary of Bristol-Myers Squibb. Dr. Spertus has been a consultant to MyoKardia, as well as to Abbott, Amgen, Bayer, Janssen, Merck, and Novartis. He has received research support from Abbott Vascular, and he holds the copyright for the KCCQ. Dr. Martinez has been a consultant to and received honoraria from Bristol-Myers Squibb.
Of patients with symptomatic, obstructive hypertrophic cardiomyopathy treated with the investigational oral agent mavacamten, more than twice as many, compared with placebo, had a very large improvement from baseline in their summary quality of life score after 30 weeks of treatment in a pivotal trial with 194 patients evaluable for this endpoint.
The trial’s health-related quality of life assessment, the Kansas City Cardiomyopathy Questionnaire (KCCQ), also showed an average improvement of more than 9 points, compared with placebo, in summary KCCQ scores among 98 mavacamten-treated patients, and a nearly 15-point improvement from baseline that represents a “moderate to large” improvement in overall health-related quality of life, John A. Spertus, MD, said at the annual scientific sessions of the American College of Cardiology.
Largest drug benefit ever seen in KCCQ
The 9-point average incremental improvement on mavacamten, a selective cardiac myosin inhibitor, compared with placebo-treated patients, is “the largest drug-mediated benefit we’ve ever observed on the KCCQ,” said Dr. Spertus, who spearheaded development of the KCCQ. Concurrently with his report the results also appeared online in the Lancet.
“Given the strength of the data, I’d reach for this drug early” to treat patients with obstructive hypertrophic cardiomyopathy (HCM), added Dr. Spertus, a professor and cardiovascular outcomes researcher at the University of Missouri–Kansas City and clinical director of outcomes research at Saint Luke’s Mid America Heart Institute, also in Kansas City.
No available treatment for obstructive HCM has had “as vigorous an assessment of impact on health status,” and the study that supplied the data he and his associates analyzed, EXPLORER-HCM, is “the largest trial ever done” in patients with HCM, he added.
Management guidelines for HCM released last year by the ACC and American Heart Association named beta-blockers “first-line” medical therapy for the disorder, with the calcium channel blockers verapamil or diltiazem named as “reasonable alternatives” to beta-blockers. However, these commonly used agents have “limited” evidence supporting health-status benefits in patients with HCM, Dr. Spertus and coauthors wrote in their report.
Longer follow-up needed
“This is an important study,” commented Matthew W. Martinez, MD, director of sports cardiology and a HCM specialist at Morristown (N.J.) Medical Center. But “given the longevity of HCM we need follow-up that goes beyond 30 weeks,” he said as designated discussant for the report.
EXPLORER-HCM randomized 251 patients with symptomatic obstructive HCM at 68 centers in 13 countries during 2018-2019. The 30-week trial’s primary outcome was a composite to assess clinical response, compared with baseline, that included a 1.5-mL/kg per min or greater increase in peak oxygen consumption (pVO2) and at least one New York Heart Association (NYHA) functional class reduction; or a 3.0 mL/kg per min or greater improvement in pVO2 and no worsening of NYHA class.
Patients averaged about 59 years of age, about 60% were men, and their pVO2 at entry averaged about 20 mL/kg per min. About 73% were in NYHA functional class II, with the remainder in functional class III. Patients received mavacamten as a once-daily oral dose that gradually up-titrated during the trial to reach targeted reductions in each patient’s plasma levels of the drug and in their left ventricular outflow tract gradient.
The results showed that, after 30 weeks on treatment, the primary endpoint was reached by 37% of 123 patients on mavacamten and by 17% of 128 patients on placebo, a significant difference in an intention-to-treat analysis. About 70% of patients completed their KCCQ after 30 weeks, which meant that fewer patients were in the quality of life analyses, according to the report that was published in The Lancet .
Based on these results the drug is now under consideration for approval by the Food and Drug Administration, with a decision expected by early 2022.
Benefit fades quickly when mavacamten stops
More detailed analysis of quality of life findings in the new report also showed that, while average KCCQ scores (both overall summary score and clinical summary score) steadily improved with mavacamten treatment, compared with control patients, through 18 weeks on treatment, the scores then roughly plateaued out to 30 weeks. This was followed by a sharp reversal back down to baseline levels and similar to control patients 8 weeks after stopping mavacamten, suggesting that the drug’s benefit quickly fades off treatment and hence must be taken chronically.
The responder analysis showed that 9% of patients on mavacamten had a worsening in their KCCQ overall summary scores by more than 5 points after 30 weeks, compared with 23% of the control patients. In contrast, a very large improvement in KCCQ score, defined as a rise of at least 20 points from baseline after 30 weeks, occurred in 36% of those who received mavacamten and in 15% of the controls. The between-group difference indicates a number needed to treat with mavacamten of roughly five to produce one additional patient with a very large improvement in KCCQ overall summary score, Dr. Spertus noted.
By design, all patients enrolled in EXPLORER-HCM had a left ventricular ejection fraction of at least 55%. During treatment, seven of the mavacamten-treated patients and two in the control arm had a transient decrease in their left ventricular ejection fraction to below 50%, although this later normalized in all affected patients. “An initial criticism” of the trial was that a significant percentage of mavacamten patients “developed left ventricular dysfunction” noted Dr. Martinez, but Dr. Spertus highlighted the poor apparent correlation between this phenomenon and quality of life self-assessment. Six of the seven patients on mavacamten who had a transient drop in their left ventricular ejection fraction had very large improvements in their KCCQ summary scores, Dr. Spertus reported.
Hypertrophic cardiomyopathy is a myocardial disorder characterized by primary left ventricular hypertrophy. Although a complex disease, HCM is broadly defined by pathologically enhanced cardiac actin-myosin interactions that result in hypercontractility, diastolic abnormalities, and dynamic left ventricular outflow tract obstruction. Mavacamten is a first-in-class, small-molecule, selective allosteric inhibitor of cardiac myosin ATPase developed to target the underlying pathophysiology of HCM by reducing actin-myosin cross-bridge formation, thereby reducing contractility and improving myocardial energetics.
EXPLORER-HCM was sponsored by MyoKardia, the company developing mavacamten and a subsidiary of Bristol-Myers Squibb. Dr. Spertus has been a consultant to MyoKardia, as well as to Abbott, Amgen, Bayer, Janssen, Merck, and Novartis. He has received research support from Abbott Vascular, and he holds the copyright for the KCCQ. Dr. Martinez has been a consultant to and received honoraria from Bristol-Myers Squibb.
FROM ACC 2021
Nintedanib slows interstitial lung disease in RA patients
Subgroup analysis from INBUILD trial finds results similar to overall study cohort
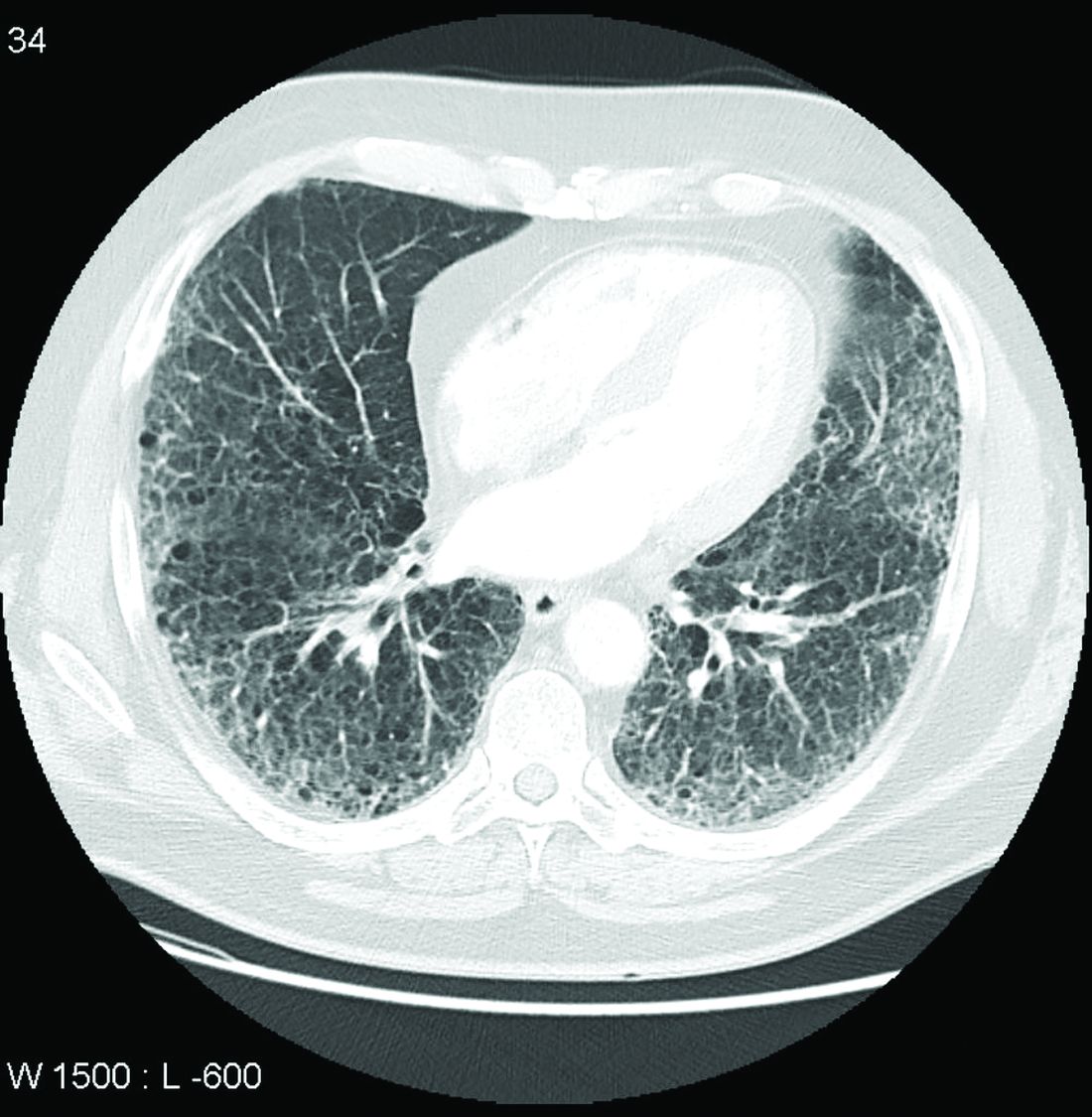
In a new subgroup analysis of a previously published multinational trial, the preservation of lung function with nintedanib (Ofev) was about the same in patients with interstitial lung disease related to rheumatoid arthritis (RA-ILD) as it was in patients with other etiologies, according to data presented at the annual European Congress of Rheumatology.

“There was no significant heterogeneity across any of several characteristics we evaluated,” reported Clive Kelly, MBBS, of the Institute of Cellular Medicine at Newcastle University (England).
The INBUILD trial, which enrolled more than 600 patients in 15 countries with a range of fibrosing lung diseases, was published almost 2 years ago. On the primary endpoint of rate of decline in forced vital capacity (FVC), the medians were –80.8 mL per year among those randomized to nintedanib and –187.8 mL per year (P < .001) on placebo.
The INBUILD study provided evidence that fibrosing lung diseases have a common pathobiologic mechanism that can be slowed by targeting intracellular kinases. Nintedanib inhibits several growth factor receptors as well as nonreceptor tyrosine kinases, but its exact mechanism for slowing fibrosing lung diseases remains unclear. Initially approved for, nintedanib received approvals from the FDA for systemic sclerosis–associated ILD in 2019 and for chronic fibrosing ILD with progressive phenotypes in 2020 after being initially approved for the treatment of idiopathic pulmonary fibrosis in 2014.
When asked for comment, Paul F. Dellaripa, MD, an associate professor of medicine in the division of rheumatology, immunology, and allergy at Harvard Medical School, Boston, indicated these data are helpful in considering strategies for RA patients with ILD, but he encouraged collaboration between joint and lung specialists.
“Antifibrotic agents for patients with progressive ILD in autoimmune diseases like RA is a welcome addition to our care of this challenging complication,” said Dr. Dellaripa, who has published frequently on the diagnosis and treatment of lung diseases associated with RA. Yet, treatment must be individualized, he added.
“It will be incumbent for rheumatologists to incorporate lung health as a critical part of patient care and work closely with pulmonologists to consider when to institute antifibrotic therapy in patients with ILD,” he said.
Details of subanalysis
In the RA-ILD subpopulation of 89 patients, there was no further decline in FVC from 24 weeks after randomization to the end of 52 weeks for those on nintedanib, but the decline remained steady over the full course of follow-up among those in the placebo group. At 52 weeks, the decline in the placebo group reached –200 mL at the end of 52 weeks. As a result, the between-group relative reduction in FVC at 52 weeks of 116.7 mL favoring nintedanib over placebo (P < .037) slightly exceeded the 107-mL reduction (P < .001) observed in the overall INBUILD study population.
Among other subgroups the investigators evaluated, outcomes with nintedanib did not differ when patients were split into groups with higher or lower baseline levels of high-sensitivity C-reactive protein, regardless of whether the groups were defined by levels above and below 1 mg/L or 3 mg/L. The same was true for those who were taking nonbiologic disease-modifying antirheumatic drugs or glucocorticoids.
However, for these latter analyses, Dr. Kelly conceded that the differences were based on small numbers of patients and so cannot be considered conclusive.
The adverse event most closely associated with nintedanib in the RA-ILD population was diarrhea, just as in the overall study, and it was more than twice as frequent in the RA-ILD patients receiving the active therapy, compared with placebo (54.8% vs. 25.5%). Nausea was also more common (21.4% vs. 10.6%), and so was decreased appetite (11.9% vs. 2.1%) and weight reduction (9.5% vs. 2.1%).
Lung-related adverse events, such as bronchiolitis (21.4% vs. 17.0%) and dyspnea (11.9% vs. 10.6%), were only slightly more frequent in the nintedanib group. Nasopharyngitis (7.1% vs. 12.8%) was less common. Side effects leading to treatment discontinuation were higher on nintedanib (19.0% vs. 12.8%)
The RA-ILD subgroup represented 13.4% of those randomized in INBUILD. The mean time since diagnosis of RA was about 10 years. More than 60% were smokers or former smokers. At baseline, the mean FVC of predicted was 71%. More than 85% had a usual interstitial pneumonia (UIP) radiologic pattern.
Acute exacerbations and death were not evaluated in the RA-ILD subpopulation, but these were secondary endpoints in the published INBUILD study according to the presence or absence of a UIP-like fibrotic pattern. For the combined endpoint of acute exacerbation of ILD or death, the protection associated with nintedanib approached statistical significance for the population overall (odds ratio, 0.68; 95% confidence interval, 0.46-1.01) and reached significance for those with a UIP pattern (OR, 0.61; 95% CI, 0.38-0.98).
Nintedanib led to lower death rates at 52 weeks in the overall population (8.1% vs. 11.5% with placebo) and in the group with a UIP pattern (9.7% vs. 15.0% with placebo).
Dr. Kelly has financial relationships with multiple pharmaceutical companies, including Boehringer Ingelheim, which provided funding for INBUILD and this subpopulation analysis. Dr. Dellaripa reported financial relationships with Bristol-Myers Squibb and Genentech.
Subgroup analysis from INBUILD trial finds results similar to overall study cohort
Subgroup analysis from INBUILD trial finds results similar to overall study cohort
In a new subgroup analysis of a previously published multinational trial, the preservation of lung function with nintedanib (Ofev) was about the same in patients with interstitial lung disease related to rheumatoid arthritis (RA-ILD) as it was in patients with other etiologies, according to data presented at the annual European Congress of Rheumatology.
“There was no significant heterogeneity across any of several characteristics we evaluated,” reported Clive Kelly, MBBS, of the Institute of Cellular Medicine at Newcastle University (England).
The INBUILD trial, which enrolled more than 600 patients in 15 countries with a range of fibrosing lung diseases, was published almost 2 years ago. On the primary endpoint of rate of decline in forced vital capacity (FVC), the medians were –80.8 mL per year among those randomized to nintedanib and –187.8 mL per year (P < .001) on placebo.
The INBUILD study provided evidence that fibrosing lung diseases have a common pathobiologic mechanism that can be slowed by targeting intracellular kinases. Nintedanib inhibits several growth factor receptors as well as nonreceptor tyrosine kinases, but its exact mechanism for slowing fibrosing lung diseases remains unclear. Initially approved for, nintedanib received approvals from the FDA for systemic sclerosis–associated ILD in 2019 and for chronic fibrosing ILD with progressive phenotypes in 2020 after being initially approved for the treatment of idiopathic pulmonary fibrosis in 2014.
When asked for comment, Paul F. Dellaripa, MD, an associate professor of medicine in the division of rheumatology, immunology, and allergy at Harvard Medical School, Boston, indicated these data are helpful in considering strategies for RA patients with ILD, but he encouraged collaboration between joint and lung specialists.
“Antifibrotic agents for patients with progressive ILD in autoimmune diseases like RA is a welcome addition to our care of this challenging complication,” said Dr. Dellaripa, who has published frequently on the diagnosis and treatment of lung diseases associated with RA. Yet, treatment must be individualized, he added.
“It will be incumbent for rheumatologists to incorporate lung health as a critical part of patient care and work closely with pulmonologists to consider when to institute antifibrotic therapy in patients with ILD,” he said.
Details of subanalysis
In the RA-ILD subpopulation of 89 patients, there was no further decline in FVC from 24 weeks after randomization to the end of 52 weeks for those on nintedanib, but the decline remained steady over the full course of follow-up among those in the placebo group. At 52 weeks, the decline in the placebo group reached –200 mL at the end of 52 weeks. As a result, the between-group relative reduction in FVC at 52 weeks of 116.7 mL favoring nintedanib over placebo (P < .037) slightly exceeded the 107-mL reduction (P < .001) observed in the overall INBUILD study population.
Among other subgroups the investigators evaluated, outcomes with nintedanib did not differ when patients were split into groups with higher or lower baseline levels of high-sensitivity C-reactive protein, regardless of whether the groups were defined by levels above and below 1 mg/L or 3 mg/L. The same was true for those who were taking nonbiologic disease-modifying antirheumatic drugs or glucocorticoids.
However, for these latter analyses, Dr. Kelly conceded that the differences were based on small numbers of patients and so cannot be considered conclusive.
The adverse event most closely associated with nintedanib in the RA-ILD population was diarrhea, just as in the overall study, and it was more than twice as frequent in the RA-ILD patients receiving the active therapy, compared with placebo (54.8% vs. 25.5%). Nausea was also more common (21.4% vs. 10.6%), and so was decreased appetite (11.9% vs. 2.1%) and weight reduction (9.5% vs. 2.1%).
Lung-related adverse events, such as bronchiolitis (21.4% vs. 17.0%) and dyspnea (11.9% vs. 10.6%), were only slightly more frequent in the nintedanib group. Nasopharyngitis (7.1% vs. 12.8%) was less common. Side effects leading to treatment discontinuation were higher on nintedanib (19.0% vs. 12.8%)
The RA-ILD subgroup represented 13.4% of those randomized in INBUILD. The mean time since diagnosis of RA was about 10 years. More than 60% were smokers or former smokers. At baseline, the mean FVC of predicted was 71%. More than 85% had a usual interstitial pneumonia (UIP) radiologic pattern.
Acute exacerbations and death were not evaluated in the RA-ILD subpopulation, but these were secondary endpoints in the published INBUILD study according to the presence or absence of a UIP-like fibrotic pattern. For the combined endpoint of acute exacerbation of ILD or death, the protection associated with nintedanib approached statistical significance for the population overall (odds ratio, 0.68; 95% confidence interval, 0.46-1.01) and reached significance for those with a UIP pattern (OR, 0.61; 95% CI, 0.38-0.98).
Nintedanib led to lower death rates at 52 weeks in the overall population (8.1% vs. 11.5% with placebo) and in the group with a UIP pattern (9.7% vs. 15.0% with placebo).
Dr. Kelly has financial relationships with multiple pharmaceutical companies, including Boehringer Ingelheim, which provided funding for INBUILD and this subpopulation analysis. Dr. Dellaripa reported financial relationships with Bristol-Myers Squibb and Genentech.
In a new subgroup analysis of a previously published multinational trial, the preservation of lung function with nintedanib (Ofev) was about the same in patients with interstitial lung disease related to rheumatoid arthritis (RA-ILD) as it was in patients with other etiologies, according to data presented at the annual European Congress of Rheumatology.
“There was no significant heterogeneity across any of several characteristics we evaluated,” reported Clive Kelly, MBBS, of the Institute of Cellular Medicine at Newcastle University (England).
The INBUILD trial, which enrolled more than 600 patients in 15 countries with a range of fibrosing lung diseases, was published almost 2 years ago. On the primary endpoint of rate of decline in forced vital capacity (FVC), the medians were –80.8 mL per year among those randomized to nintedanib and –187.8 mL per year (P < .001) on placebo.
The INBUILD study provided evidence that fibrosing lung diseases have a common pathobiologic mechanism that can be slowed by targeting intracellular kinases. Nintedanib inhibits several growth factor receptors as well as nonreceptor tyrosine kinases, but its exact mechanism for slowing fibrosing lung diseases remains unclear. Initially approved for, nintedanib received approvals from the FDA for systemic sclerosis–associated ILD in 2019 and for chronic fibrosing ILD with progressive phenotypes in 2020 after being initially approved for the treatment of idiopathic pulmonary fibrosis in 2014.
When asked for comment, Paul F. Dellaripa, MD, an associate professor of medicine in the division of rheumatology, immunology, and allergy at Harvard Medical School, Boston, indicated these data are helpful in considering strategies for RA patients with ILD, but he encouraged collaboration between joint and lung specialists.
“Antifibrotic agents for patients with progressive ILD in autoimmune diseases like RA is a welcome addition to our care of this challenging complication,” said Dr. Dellaripa, who has published frequently on the diagnosis and treatment of lung diseases associated with RA. Yet, treatment must be individualized, he added.
“It will be incumbent for rheumatologists to incorporate lung health as a critical part of patient care and work closely with pulmonologists to consider when to institute antifibrotic therapy in patients with ILD,” he said.
Details of subanalysis
In the RA-ILD subpopulation of 89 patients, there was no further decline in FVC from 24 weeks after randomization to the end of 52 weeks for those on nintedanib, but the decline remained steady over the full course of follow-up among those in the placebo group. At 52 weeks, the decline in the placebo group reached –200 mL at the end of 52 weeks. As a result, the between-group relative reduction in FVC at 52 weeks of 116.7 mL favoring nintedanib over placebo (P < .037) slightly exceeded the 107-mL reduction (P < .001) observed in the overall INBUILD study population.
Among other subgroups the investigators evaluated, outcomes with nintedanib did not differ when patients were split into groups with higher or lower baseline levels of high-sensitivity C-reactive protein, regardless of whether the groups were defined by levels above and below 1 mg/L or 3 mg/L. The same was true for those who were taking nonbiologic disease-modifying antirheumatic drugs or glucocorticoids.
However, for these latter analyses, Dr. Kelly conceded that the differences were based on small numbers of patients and so cannot be considered conclusive.
The adverse event most closely associated with nintedanib in the RA-ILD population was diarrhea, just as in the overall study, and it was more than twice as frequent in the RA-ILD patients receiving the active therapy, compared with placebo (54.8% vs. 25.5%). Nausea was also more common (21.4% vs. 10.6%), and so was decreased appetite (11.9% vs. 2.1%) and weight reduction (9.5% vs. 2.1%).
Lung-related adverse events, such as bronchiolitis (21.4% vs. 17.0%) and dyspnea (11.9% vs. 10.6%), were only slightly more frequent in the nintedanib group. Nasopharyngitis (7.1% vs. 12.8%) was less common. Side effects leading to treatment discontinuation were higher on nintedanib (19.0% vs. 12.8%)
The RA-ILD subgroup represented 13.4% of those randomized in INBUILD. The mean time since diagnosis of RA was about 10 years. More than 60% were smokers or former smokers. At baseline, the mean FVC of predicted was 71%. More than 85% had a usual interstitial pneumonia (UIP) radiologic pattern.
Acute exacerbations and death were not evaluated in the RA-ILD subpopulation, but these were secondary endpoints in the published INBUILD study according to the presence or absence of a UIP-like fibrotic pattern. For the combined endpoint of acute exacerbation of ILD or death, the protection associated with nintedanib approached statistical significance for the population overall (odds ratio, 0.68; 95% confidence interval, 0.46-1.01) and reached significance for those with a UIP pattern (OR, 0.61; 95% CI, 0.38-0.98).
Nintedanib led to lower death rates at 52 weeks in the overall population (8.1% vs. 11.5% with placebo) and in the group with a UIP pattern (9.7% vs. 15.0% with placebo).
Dr. Kelly has financial relationships with multiple pharmaceutical companies, including Boehringer Ingelheim, which provided funding for INBUILD and this subpopulation analysis. Dr. Dellaripa reported financial relationships with Bristol-Myers Squibb and Genentech.
FROM THE EULAR 2021 CONGRESS
Medical licensing questions continue to violate ADA
With the COVID-19 pandemic, already high rates of suicide, depression, and burnout among physicians became even more acute. Yet, 3 years after the Federation of State Medical Boards issued recommendations on what questions about mental health status license applications should – or mostly should not – include, only North Carolina fully complies with all four recommendations, and most states comply with two or fewer, a study of state medical board applications has found (JAMA. 2021 May 18;325[19];2017-8).

Questions about mental health history or “its hypothetical effect on competency,” violate the Americans with Disabilities Act, the study authors stated. In a research letter to JAMA, the authors also reported that five state boards do not comply with any of the FSMB recommendations. Twenty-four states comply with three of the four recommendations.
Overall, the mean consistency score was 2.1, which means state medical licensing applications typically run afoul of the Americans With Disabilities Act when it comes to mental health history of applicants.
“No one should ever wonder, ‘Will I lose my job, or should I get help?’ ” said co–senior author Jessica A. Gold, MD, MS, a psychiatrist at Washington University in St. Louis. “This should absolutely never be a question on someone’s mind. And the fact that it is, in medicine, is a problem that needs to be solved. I hope that people are beginning to see that, and we can make a change to get people the help they need before it is too late.”
High rates of depression, suicide
She noted that before COVID-19, physicians already had higher rates of depression, burnout, and suicide than the general population. “Over COVID-19, it has become clear that the mental health of physicians has become additionally compounded,” Dr. Gold said.
One study found that physicians had a 44% higher rate of suicide (PLoS One. 2019 Dec;14[12]:e0226361), but they’re notoriously reluctant to seek out mental health care. A 2017 study reported that 40% of physicians would be reluctant to seek mental health care because of concerns about their licensure (Mayo Clin Proc. 2017;92[10]:1486-93).
As the pandemic went on, Dr. Gold and her colleagues decided to study whether state boards had improved their compliance with the FSMB recommendations issued in 2018. Those recommendations include these four limitations regarding questions about mental health conditions on license applications:
- Include only when they result in impairment.
- Include only when the mental health conditions are current – that is, when they’ve occurred within the past 2 years.
- Provide safe haven nonreporting – that is, allow physicians to not report previously diagnosed and treated mental health conditions if they’re being monitored and are in good standing with a physician health program.
- Include supportive or nonjudgmental language about seeking mental health care.
The study considered board applications that had questions about mental health status as consistent with the first three recommendations. Seventeen states complied.
Thirty-nine state boards complied with the first recommendation regarding impairment; 41 with the second recommendation about near-term history; 25 with safe-haven nonreporting. Only eight states were consistent with the recommendation on supportive language.
The ADA limits inquiries about an applicant’s impairment to only current conditions. In a 2017 study, only 21 state boards had limited questions to current impairment. “This is a significant improvement, but this still means the rest of the states are violating an actual law,” Dr. Gold said. “Another plus is that 17 states asked no questions at all that could require mental health disclosure. This, too is significant because it highlights change in thinking.”
But still, the fact that five states didn’t comply with any recommendation and only one followed all of them is “utterly unacceptable,” Dr. Gold said. “Instead, we should have universal adoption of FSMB recommendations.”
Time to remove stigma
Michael F. Myers, MD, a clinical psychiatrist at the State University of New York, Brooklyn, said removing the stigma of seeking help for mental health conditions is especially important for physicians. He’s written several books about physician mental health, including his latest, “Becoming a Doctor’s Doctor: A Memoir.”

“I would say at least 15% of the families that I interviewed who lost a physician loved one to suicide have said the doctor was petrified of going for professional help because of fears of what this could do to their medical license,” he said. “It is extremely important that those licensing questions will be either brought up to speed, or – the ones that are clearly violating the ADA – that they be removed.”
Applications for hospital privileges can also run afoul of the same ADA standard, Dr. Myers added. “Physicians have told me that when they go to get medical privileges at a medical center, they get asked all kinds of questions that are outdated, that are intrusive, that violate the ADA,” he said.
Credentialing is another area that Dr. Gold and her colleagues are interested in studying, she said. “Sometimes the licensing applications can be fine, but then the hospital someone is applying to work at can ask the same illegal questions anyway,” she said. “So it doesn’t matter that the state fixed the problem because the hospital asked them anyway. You feel your job is at risk in the same way, so you still don’t get help.”
Dr. Gold and Dr. Myers have no relevant financial relationships to disclose.
With the COVID-19 pandemic, already high rates of suicide, depression, and burnout among physicians became even more acute. Yet, 3 years after the Federation of State Medical Boards issued recommendations on what questions about mental health status license applications should – or mostly should not – include, only North Carolina fully complies with all four recommendations, and most states comply with two or fewer, a study of state medical board applications has found (JAMA. 2021 May 18;325[19];2017-8).
Questions about mental health history or “its hypothetical effect on competency,” violate the Americans with Disabilities Act, the study authors stated. In a research letter to JAMA, the authors also reported that five state boards do not comply with any of the FSMB recommendations. Twenty-four states comply with three of the four recommendations.
Overall, the mean consistency score was 2.1, which means state medical licensing applications typically run afoul of the Americans With Disabilities Act when it comes to mental health history of applicants.
“No one should ever wonder, ‘Will I lose my job, or should I get help?’ ” said co–senior author Jessica A. Gold, MD, MS, a psychiatrist at Washington University in St. Louis. “This should absolutely never be a question on someone’s mind. And the fact that it is, in medicine, is a problem that needs to be solved. I hope that people are beginning to see that, and we can make a change to get people the help they need before it is too late.”
High rates of depression, suicide
She noted that before COVID-19, physicians already had higher rates of depression, burnout, and suicide than the general population. “Over COVID-19, it has become clear that the mental health of physicians has become additionally compounded,” Dr. Gold said.
One study found that physicians had a 44% higher rate of suicide (PLoS One. 2019 Dec;14[12]:e0226361), but they’re notoriously reluctant to seek out mental health care. A 2017 study reported that 40% of physicians would be reluctant to seek mental health care because of concerns about their licensure (Mayo Clin Proc. 2017;92[10]:1486-93).
As the pandemic went on, Dr. Gold and her colleagues decided to study whether state boards had improved their compliance with the FSMB recommendations issued in 2018. Those recommendations include these four limitations regarding questions about mental health conditions on license applications:
- Include only when they result in impairment.
- Include only when the mental health conditions are current – that is, when they’ve occurred within the past 2 years.
- Provide safe haven nonreporting – that is, allow physicians to not report previously diagnosed and treated mental health conditions if they’re being monitored and are in good standing with a physician health program.
- Include supportive or nonjudgmental language about seeking mental health care.
The study considered board applications that had questions about mental health status as consistent with the first three recommendations. Seventeen states complied.
Thirty-nine state boards complied with the first recommendation regarding impairment; 41 with the second recommendation about near-term history; 25 with safe-haven nonreporting. Only eight states were consistent with the recommendation on supportive language.
The ADA limits inquiries about an applicant’s impairment to only current conditions. In a 2017 study, only 21 state boards had limited questions to current impairment. “This is a significant improvement, but this still means the rest of the states are violating an actual law,” Dr. Gold said. “Another plus is that 17 states asked no questions at all that could require mental health disclosure. This, too is significant because it highlights change in thinking.”
But still, the fact that five states didn’t comply with any recommendation and only one followed all of them is “utterly unacceptable,” Dr. Gold said. “Instead, we should have universal adoption of FSMB recommendations.”
Time to remove stigma
Michael F. Myers, MD, a clinical psychiatrist at the State University of New York, Brooklyn, said removing the stigma of seeking help for mental health conditions is especially important for physicians. He’s written several books about physician mental health, including his latest, “Becoming a Doctor’s Doctor: A Memoir.”
“I would say at least 15% of the families that I interviewed who lost a physician loved one to suicide have said the doctor was petrified of going for professional help because of fears of what this could do to their medical license,” he said. “It is extremely important that those licensing questions will be either brought up to speed, or – the ones that are clearly violating the ADA – that they be removed.”
Applications for hospital privileges can also run afoul of the same ADA standard, Dr. Myers added. “Physicians have told me that when they go to get medical privileges at a medical center, they get asked all kinds of questions that are outdated, that are intrusive, that violate the ADA,” he said.
Credentialing is another area that Dr. Gold and her colleagues are interested in studying, she said. “Sometimes the licensing applications can be fine, but then the hospital someone is applying to work at can ask the same illegal questions anyway,” she said. “So it doesn’t matter that the state fixed the problem because the hospital asked them anyway. You feel your job is at risk in the same way, so you still don’t get help.”
Dr. Gold and Dr. Myers have no relevant financial relationships to disclose.
With the COVID-19 pandemic, already high rates of suicide, depression, and burnout among physicians became even more acute. Yet, 3 years after the Federation of State Medical Boards issued recommendations on what questions about mental health status license applications should – or mostly should not – include, only North Carolina fully complies with all four recommendations, and most states comply with two or fewer, a study of state medical board applications has found (JAMA. 2021 May 18;325[19];2017-8).
Questions about mental health history or “its hypothetical effect on competency,” violate the Americans with Disabilities Act, the study authors stated. In a research letter to JAMA, the authors also reported that five state boards do not comply with any of the FSMB recommendations. Twenty-four states comply with three of the four recommendations.
Overall, the mean consistency score was 2.1, which means state medical licensing applications typically run afoul of the Americans With Disabilities Act when it comes to mental health history of applicants.
“No one should ever wonder, ‘Will I lose my job, or should I get help?’ ” said co–senior author Jessica A. Gold, MD, MS, a psychiatrist at Washington University in St. Louis. “This should absolutely never be a question on someone’s mind. And the fact that it is, in medicine, is a problem that needs to be solved. I hope that people are beginning to see that, and we can make a change to get people the help they need before it is too late.”
High rates of depression, suicide
She noted that before COVID-19, physicians already had higher rates of depression, burnout, and suicide than the general population. “Over COVID-19, it has become clear that the mental health of physicians has become additionally compounded,” Dr. Gold said.
One study found that physicians had a 44% higher rate of suicide (PLoS One. 2019 Dec;14[12]:e0226361), but they’re notoriously reluctant to seek out mental health care. A 2017 study reported that 40% of physicians would be reluctant to seek mental health care because of concerns about their licensure (Mayo Clin Proc. 2017;92[10]:1486-93).
As the pandemic went on, Dr. Gold and her colleagues decided to study whether state boards had improved their compliance with the FSMB recommendations issued in 2018. Those recommendations include these four limitations regarding questions about mental health conditions on license applications:
- Include only when they result in impairment.
- Include only when the mental health conditions are current – that is, when they’ve occurred within the past 2 years.
- Provide safe haven nonreporting – that is, allow physicians to not report previously diagnosed and treated mental health conditions if they’re being monitored and are in good standing with a physician health program.
- Include supportive or nonjudgmental language about seeking mental health care.
The study considered board applications that had questions about mental health status as consistent with the first three recommendations. Seventeen states complied.
Thirty-nine state boards complied with the first recommendation regarding impairment; 41 with the second recommendation about near-term history; 25 with safe-haven nonreporting. Only eight states were consistent with the recommendation on supportive language.
The ADA limits inquiries about an applicant’s impairment to only current conditions. In a 2017 study, only 21 state boards had limited questions to current impairment. “This is a significant improvement, but this still means the rest of the states are violating an actual law,” Dr. Gold said. “Another plus is that 17 states asked no questions at all that could require mental health disclosure. This, too is significant because it highlights change in thinking.”
But still, the fact that five states didn’t comply with any recommendation and only one followed all of them is “utterly unacceptable,” Dr. Gold said. “Instead, we should have universal adoption of FSMB recommendations.”
Time to remove stigma
Michael F. Myers, MD, a clinical psychiatrist at the State University of New York, Brooklyn, said removing the stigma of seeking help for mental health conditions is especially important for physicians. He’s written several books about physician mental health, including his latest, “Becoming a Doctor’s Doctor: A Memoir.”
“I would say at least 15% of the families that I interviewed who lost a physician loved one to suicide have said the doctor was petrified of going for professional help because of fears of what this could do to their medical license,” he said. “It is extremely important that those licensing questions will be either brought up to speed, or – the ones that are clearly violating the ADA – that they be removed.”
Applications for hospital privileges can also run afoul of the same ADA standard, Dr. Myers added. “Physicians have told me that when they go to get medical privileges at a medical center, they get asked all kinds of questions that are outdated, that are intrusive, that violate the ADA,” he said.
Credentialing is another area that Dr. Gold and her colleagues are interested in studying, she said. “Sometimes the licensing applications can be fine, but then the hospital someone is applying to work at can ask the same illegal questions anyway,” she said. “So it doesn’t matter that the state fixed the problem because the hospital asked them anyway. You feel your job is at risk in the same way, so you still don’t get help.”
Dr. Gold and Dr. Myers have no relevant financial relationships to disclose.
FROM JAMA
IL-6 levels predict distant breast cancer recurrence
The inflammatory cytokine interleukin 6 may be a biomarker for distant recurrence of breast cancer among patients treated for stage II-III HER2-negative disease, investigators have found.
In a case-control study of 498 women with breast cancer treated with surgery and adjuvant chemotherapy, as well as endocrine therapy for women with estrogen receptor (ER)–positive tumors, those with higher serum levels of IL-6 at diagnosis had a significantly greater risk for disease recurrence than women with lower levels of the cytokine, Joseph A. Sparano, MD, from the Albert Einstein College of Medicine and Montefiore Medical Center, New York, and colleagues reported.
“This analysis provides level 1B evidence indicating that higher levels of the cytokine IL-6 at diagnosis are associated with a significantly higher distant recurrence risk in high-risk stage II-III breast cancer despite optimal adjuvant systemic therapy,” they wrote in a study presented in a poster discussion session at the American Society of Clinical Oncology Annual Meeting.(Abstract 520)
In an interview, Dr. Sparano said that their findings first need to be validated in a larger study.
“When validated, I think the other key issue is to try to understand what the best cut point for identifying high risk is, “ he said.
If further studies confirm that higher IL-6 levels are prognostic for worse outcomes, it might be possible to use levels of the cytokine as a biomarker to predict for therapies targeting the IL-6/Janus kinase/STAT3 pathway.
“There are trials ongoing testing IL-6 antibodies in combination chemotherapy, and this could be a rational biomarker to identify which patients would be more likely to benefit from that approach,” he said.
Systemic inflammation
Systemic inflammation is suspected as a contributing factor to cancer progression and disease recurrence, Dr. Sparano and colleagues noted.
To test their hypothesis that inflammatory cytokines and/or chemokines could be associated with distant recurrence, they conducted a case-control study with 249 matched pairs of patients enrolled in a phase 3 trial of adjuvant chemotherapy for lymph-node positive and high-risk lymph-node negative breast cancer (NCT00433511).
The patients all had surgery and adjuvant chemotherapy with doxorubicin, cyclophosphamide, and paclitaxel with or without bevacizumab, and endocrine therapy for patients whose tumors were ER positive.
They used propensity score matching to pair each patient with distant recurrence to one without, with covariates including post versus premenopausal or perimenopausal status, estrogen and/or progesterone receptor positivity, tumor size (less than 2 cm, greater than 2-5 cm, or greater than 5 cm) nodal status, and grade.
The only biomarker that met the prespecified boundary for statistical significance (P < .0014) was IL-6, with a hazard ratio for distant recurrence of 1.37 (P = .0006).
The median and mean values for IL-6 were 0.95 and 7.5 pg/mL, respectively
Other substances associated with distant recurrence (with a two-sided P value < .05) were macrophage-derived chemokine/CCL22 (HR, 1.90; P = .0098), IL-17A, a T-helper cell inflammatory cytokine (HR, 1.36; P = .0052), and the cytokine vascular endothelial growth factor A (VEGF-A, HR, 1.13; P = 0.037).
There was no statistical interaction between VEGF-A levels and the benefit of bevacizumab.
Prognostic value, not clinical utility
“This is a nice abstract. It looks at inflammatory cytokines and provides evidence that inflammatory cytokines, particularly IL-6, could have a prognostic role in predicting risk of recurrence in HER2-negative disease, and the team did a very nice job in multivariate analysis looking at different factors,” said Aditya Bardia, MD, MPH, from the Mass General Cancer Center in Boston, the invited discussant for the study.*
In an interview, Dr. Bardia said that the finding “provides prognostic value, but does not provide clinical utility. It’s unclear if we used this assay and it identified that a patient was at high risk of recurrence whether we could change that. Is there any intervention that could be done to potentially alter the course of disease, alter the natural history? That’s unknown.”
He agreed with Dr. Sparano and colleagues that validation of the finding was still needed, ideally in a prospective or retrospective cohort study.
The study was supported by grants from the National Cancer Institute, Komen Foundation, and Breast Cancer Research Foundation. Dr. Sparano disclosed relationships with multiple companies. Dr. Bardia disclosed a consulting or advisory role and research funding to his institution from multiple companies.
*Correction, 6/4/21: An earlier version of this article misstated Dr. Bardia's name.
The inflammatory cytokine interleukin 6 may be a biomarker for distant recurrence of breast cancer among patients treated for stage II-III HER2-negative disease, investigators have found.
In a case-control study of 498 women with breast cancer treated with surgery and adjuvant chemotherapy, as well as endocrine therapy for women with estrogen receptor (ER)–positive tumors, those with higher serum levels of IL-6 at diagnosis had a significantly greater risk for disease recurrence than women with lower levels of the cytokine, Joseph A. Sparano, MD, from the Albert Einstein College of Medicine and Montefiore Medical Center, New York, and colleagues reported.
“This analysis provides level 1B evidence indicating that higher levels of the cytokine IL-6 at diagnosis are associated with a significantly higher distant recurrence risk in high-risk stage II-III breast cancer despite optimal adjuvant systemic therapy,” they wrote in a study presented in a poster discussion session at the American Society of Clinical Oncology Annual Meeting.(Abstract 520)
In an interview, Dr. Sparano said that their findings first need to be validated in a larger study.
“When validated, I think the other key issue is to try to understand what the best cut point for identifying high risk is, “ he said.
If further studies confirm that higher IL-6 levels are prognostic for worse outcomes, it might be possible to use levels of the cytokine as a biomarker to predict for therapies targeting the IL-6/Janus kinase/STAT3 pathway.
“There are trials ongoing testing IL-6 antibodies in combination chemotherapy, and this could be a rational biomarker to identify which patients would be more likely to benefit from that approach,” he said.
Systemic inflammation
Systemic inflammation is suspected as a contributing factor to cancer progression and disease recurrence, Dr. Sparano and colleagues noted.
To test their hypothesis that inflammatory cytokines and/or chemokines could be associated with distant recurrence, they conducted a case-control study with 249 matched pairs of patients enrolled in a phase 3 trial of adjuvant chemotherapy for lymph-node positive and high-risk lymph-node negative breast cancer (NCT00433511).
The patients all had surgery and adjuvant chemotherapy with doxorubicin, cyclophosphamide, and paclitaxel with or without bevacizumab, and endocrine therapy for patients whose tumors were ER positive.
They used propensity score matching to pair each patient with distant recurrence to one without, with covariates including post versus premenopausal or perimenopausal status, estrogen and/or progesterone receptor positivity, tumor size (less than 2 cm, greater than 2-5 cm, or greater than 5 cm) nodal status, and grade.
The only biomarker that met the prespecified boundary for statistical significance (P < .0014) was IL-6, with a hazard ratio for distant recurrence of 1.37 (P = .0006).
The median and mean values for IL-6 were 0.95 and 7.5 pg/mL, respectively
Other substances associated with distant recurrence (with a two-sided P value < .05) were macrophage-derived chemokine/CCL22 (HR, 1.90; P = .0098), IL-17A, a T-helper cell inflammatory cytokine (HR, 1.36; P = .0052), and the cytokine vascular endothelial growth factor A (VEGF-A, HR, 1.13; P = 0.037).
There was no statistical interaction between VEGF-A levels and the benefit of bevacizumab.
Prognostic value, not clinical utility
“This is a nice abstract. It looks at inflammatory cytokines and provides evidence that inflammatory cytokines, particularly IL-6, could have a prognostic role in predicting risk of recurrence in HER2-negative disease, and the team did a very nice job in multivariate analysis looking at different factors,” said Aditya Bardia, MD, MPH, from the Mass General Cancer Center in Boston, the invited discussant for the study.*
In an interview, Dr. Bardia said that the finding “provides prognostic value, but does not provide clinical utility. It’s unclear if we used this assay and it identified that a patient was at high risk of recurrence whether we could change that. Is there any intervention that could be done to potentially alter the course of disease, alter the natural history? That’s unknown.”
He agreed with Dr. Sparano and colleagues that validation of the finding was still needed, ideally in a prospective or retrospective cohort study.
The study was supported by grants from the National Cancer Institute, Komen Foundation, and Breast Cancer Research Foundation. Dr. Sparano disclosed relationships with multiple companies. Dr. Bardia disclosed a consulting or advisory role and research funding to his institution from multiple companies.
*Correction, 6/4/21: An earlier version of this article misstated Dr. Bardia's name.
The inflammatory cytokine interleukin 6 may be a biomarker for distant recurrence of breast cancer among patients treated for stage II-III HER2-negative disease, investigators have found.
In a case-control study of 498 women with breast cancer treated with surgery and adjuvant chemotherapy, as well as endocrine therapy for women with estrogen receptor (ER)–positive tumors, those with higher serum levels of IL-6 at diagnosis had a significantly greater risk for disease recurrence than women with lower levels of the cytokine, Joseph A. Sparano, MD, from the Albert Einstein College of Medicine and Montefiore Medical Center, New York, and colleagues reported.
“This analysis provides level 1B evidence indicating that higher levels of the cytokine IL-6 at diagnosis are associated with a significantly higher distant recurrence risk in high-risk stage II-III breast cancer despite optimal adjuvant systemic therapy,” they wrote in a study presented in a poster discussion session at the American Society of Clinical Oncology Annual Meeting.(Abstract 520)
In an interview, Dr. Sparano said that their findings first need to be validated in a larger study.
“When validated, I think the other key issue is to try to understand what the best cut point for identifying high risk is, “ he said.
If further studies confirm that higher IL-6 levels are prognostic for worse outcomes, it might be possible to use levels of the cytokine as a biomarker to predict for therapies targeting the IL-6/Janus kinase/STAT3 pathway.
“There are trials ongoing testing IL-6 antibodies in combination chemotherapy, and this could be a rational biomarker to identify which patients would be more likely to benefit from that approach,” he said.
Systemic inflammation
Systemic inflammation is suspected as a contributing factor to cancer progression and disease recurrence, Dr. Sparano and colleagues noted.
To test their hypothesis that inflammatory cytokines and/or chemokines could be associated with distant recurrence, they conducted a case-control study with 249 matched pairs of patients enrolled in a phase 3 trial of adjuvant chemotherapy for lymph-node positive and high-risk lymph-node negative breast cancer (NCT00433511).
The patients all had surgery and adjuvant chemotherapy with doxorubicin, cyclophosphamide, and paclitaxel with or without bevacizumab, and endocrine therapy for patients whose tumors were ER positive.
They used propensity score matching to pair each patient with distant recurrence to one without, with covariates including post versus premenopausal or perimenopausal status, estrogen and/or progesterone receptor positivity, tumor size (less than 2 cm, greater than 2-5 cm, or greater than 5 cm) nodal status, and grade.
The only biomarker that met the prespecified boundary for statistical significance (P < .0014) was IL-6, with a hazard ratio for distant recurrence of 1.37 (P = .0006).
The median and mean values for IL-6 were 0.95 and 7.5 pg/mL, respectively
Other substances associated with distant recurrence (with a two-sided P value < .05) were macrophage-derived chemokine/CCL22 (HR, 1.90; P = .0098), IL-17A, a T-helper cell inflammatory cytokine (HR, 1.36; P = .0052), and the cytokine vascular endothelial growth factor A (VEGF-A, HR, 1.13; P = 0.037).
There was no statistical interaction between VEGF-A levels and the benefit of bevacizumab.
Prognostic value, not clinical utility
“This is a nice abstract. It looks at inflammatory cytokines and provides evidence that inflammatory cytokines, particularly IL-6, could have a prognostic role in predicting risk of recurrence in HER2-negative disease, and the team did a very nice job in multivariate analysis looking at different factors,” said Aditya Bardia, MD, MPH, from the Mass General Cancer Center in Boston, the invited discussant for the study.*
In an interview, Dr. Bardia said that the finding “provides prognostic value, but does not provide clinical utility. It’s unclear if we used this assay and it identified that a patient was at high risk of recurrence whether we could change that. Is there any intervention that could be done to potentially alter the course of disease, alter the natural history? That’s unknown.”
He agreed with Dr. Sparano and colleagues that validation of the finding was still needed, ideally in a prospective or retrospective cohort study.
The study was supported by grants from the National Cancer Institute, Komen Foundation, and Breast Cancer Research Foundation. Dr. Sparano disclosed relationships with multiple companies. Dr. Bardia disclosed a consulting or advisory role and research funding to his institution from multiple companies.
*Correction, 6/4/21: An earlier version of this article misstated Dr. Bardia's name.
FROM ASCO 2021
A1c below prediabetes cutoff linked to subclinical atherosclerosis
, according to an analysis of data on almost 4,000 middle-aged individuals.

“If one looks at the incidence of generalized subclinical atherosclerosis, we are not talking small numbers,” senior study author Valentin Fuster, MD, PhD, said in an interview. “We are talking about between 45% and 82% of this middle-age population that already has atherosclerotic disease subclinically.
“Actually,” he added, “the disease was extensive in 5%-30% of these individuals of middle age.”
The study included 3,973 participants from the Progression of Early Subclinical Atherosclerosis study who did not have diabetes. A1c showed an association with the prevalence and multiterritorial extent of subclinical atherosclerosis as measured by two-dimensional ultrasound and coronary artery calcium score (CACS; P < .001). For example, those with A1c above 6.1% (133 participants) had a 33.1% rate of generalized subclinical atherosclerosis, compared with 4.9% for those with A1c below 4.8% (243), the lowest-score group in the study.
Patients in the subprediabetes band, between 5.0% and 5.5%, had significantly higher rates of generalized subclinical atherosclerosis than did the lowest-score group: 8% in the 4.9%-5.0% group (375 participants); 9.9% in the 5.1%-5.2% range (687); 10.3% in the 5.3%-5.4% group (928); and 11.5% in the 5.5%-5.6% group (842).
Those in the 5.1%-5.2% and 5/3%-5.4% A1c groups had a 27% greater chance of having subclinical atherosclerosis, while those in the 5.5%-5.6% group had a 36% greater risk, according to an odds ratio analysis adjusted for established cardiovascular risk factors. The risks were even higher for patients with prediabetes, the researchers reported in the Journal of the American College of Cardiology.
A call for earlier intervention
Notably, the study found that fasting plasma glucose testing did not yield a similar association between A1c and atherosclerosis.
“The message is that we all talk about people when they are close to the development of cardiovascular events, and here we are talking about people who we should pay attention to much earlier,” said Dr. Fuster, physician-in-chief at Icahn School of Medicine at Mount Sinai in New York and director of the National Center for Cardiovascular Investigation in Madrid, where the observational study originated said. “People should be sensitized to HbA1c much more than they would’ve been in the past, and I think this study actually validates that.”
Christie Ballantyne, MD, noted in an interview that these findings support the utility of A1c for predicting CVD risk.

“I think more and more we should be ordering a HbA1c” during routine physical exams, Dr. Ballantyne said. “You don’t have to be obese to get it; there are lots of people, maybe they’re slightly overweight. It’s a reasonable test to be getting when you get to middle age and older to get an idea for assessing for both developing diabetes and also the presence of atherosclerosis and the risk for having cardiovascular events.”
Dr. Ballantyne, chief of cardiology at Baylor College of Medicine and director of cardiovascular disease prevention at Methodist DeBakey Heart Center in Houston, coauthored an editorial comment on the study.
Clinicians typically start to manage CVD and diabetes risk “late in the process,” Dr. Ballantyne said. This study suggested that earlier use of antidiabetes therapies, namely peptide-1 agonists and semisynthetic glucagon-like peptide-2 inhibitors, may be warranted in patients with intermediate risk of CVD.
“It’s just more data for the rationale that, perhaps we could end up doing trials to show we can take high-risk people and prevent them from getting both heart disease and diabetes,” Dr. Ballantyne added. “Could we start a little earlier with better precision?”
These finding don’t yet call for a change in how cardiologists and endocrinologists manage patients on the cusp of prediabetes, said Paul S. Jellinger, MD, of Hollywood, Fla., and a professor at the University of Miami. “The endpoint of subclinical atherosclerosis does not necessarily translate into the harder endpoint of CVD events, although there is certainly reason to believe it does,” he said in an interview, noting that he’s often used CACS to stratify atherosclerotic CVD risk in patients.

“I will now consider extending that assessment to patients with lower A1c levels,” he said.
If future studies validate this finding, he said, “serious consideration will have to be made for treating the very large numbers of patients with A1c levels in the prediabetic range and below with antidiabetic agents that have ASCVD prevention properties while lowering A1c. We have those agents today.”
The Progression of Early Subclinical Atherosclerosis study received funding from the National Center for Cardiovascular Investigation in Madrid, Santander Bank, and the Carlos III Health Institute in Madrid. Dr. Fuster had no disclosures. Dr. Ballantyne disclosed receiving research funding through his institution from Abbott Diagnostic, Akcea, Amgen, Esperion, Ionis, Novartis, Regeneron, and Roche Diagnostic; and has served as a consultant for Abbott Diagnostics, Althera, Amarin, Amgen, Arrowhead, AstraZeneca, Corvidia, Denka Seiken, Esperion, Genentech, Gilead, Matinas BioPharma, New Amsterdam, Novartis, Novo Nordisk, Pfizer, Regeneron, Roche Diagnostic and Sanofi-Synthélabo.
Dr. Jellinger had no disclosures.
, according to an analysis of data on almost 4,000 middle-aged individuals.
“If one looks at the incidence of generalized subclinical atherosclerosis, we are not talking small numbers,” senior study author Valentin Fuster, MD, PhD, said in an interview. “We are talking about between 45% and 82% of this middle-age population that already has atherosclerotic disease subclinically.
“Actually,” he added, “the disease was extensive in 5%-30% of these individuals of middle age.”
The study included 3,973 participants from the Progression of Early Subclinical Atherosclerosis study who did not have diabetes. A1c showed an association with the prevalence and multiterritorial extent of subclinical atherosclerosis as measured by two-dimensional ultrasound and coronary artery calcium score (CACS; P < .001). For example, those with A1c above 6.1% (133 participants) had a 33.1% rate of generalized subclinical atherosclerosis, compared with 4.9% for those with A1c below 4.8% (243), the lowest-score group in the study.
Patients in the subprediabetes band, between 5.0% and 5.5%, had significantly higher rates of generalized subclinical atherosclerosis than did the lowest-score group: 8% in the 4.9%-5.0% group (375 participants); 9.9% in the 5.1%-5.2% range (687); 10.3% in the 5.3%-5.4% group (928); and 11.5% in the 5.5%-5.6% group (842).
Those in the 5.1%-5.2% and 5/3%-5.4% A1c groups had a 27% greater chance of having subclinical atherosclerosis, while those in the 5.5%-5.6% group had a 36% greater risk, according to an odds ratio analysis adjusted for established cardiovascular risk factors. The risks were even higher for patients with prediabetes, the researchers reported in the Journal of the American College of Cardiology.
A call for earlier intervention
Notably, the study found that fasting plasma glucose testing did not yield a similar association between A1c and atherosclerosis.
“The message is that we all talk about people when they are close to the development of cardiovascular events, and here we are talking about people who we should pay attention to much earlier,” said Dr. Fuster, physician-in-chief at Icahn School of Medicine at Mount Sinai in New York and director of the National Center for Cardiovascular Investigation in Madrid, where the observational study originated said. “People should be sensitized to HbA1c much more than they would’ve been in the past, and I think this study actually validates that.”
Christie Ballantyne, MD, noted in an interview that these findings support the utility of A1c for predicting CVD risk.
“I think more and more we should be ordering a HbA1c” during routine physical exams, Dr. Ballantyne said. “You don’t have to be obese to get it; there are lots of people, maybe they’re slightly overweight. It’s a reasonable test to be getting when you get to middle age and older to get an idea for assessing for both developing diabetes and also the presence of atherosclerosis and the risk for having cardiovascular events.”
Dr. Ballantyne, chief of cardiology at Baylor College of Medicine and director of cardiovascular disease prevention at Methodist DeBakey Heart Center in Houston, coauthored an editorial comment on the study.
Clinicians typically start to manage CVD and diabetes risk “late in the process,” Dr. Ballantyne said. This study suggested that earlier use of antidiabetes therapies, namely peptide-1 agonists and semisynthetic glucagon-like peptide-2 inhibitors, may be warranted in patients with intermediate risk of CVD.
“It’s just more data for the rationale that, perhaps we could end up doing trials to show we can take high-risk people and prevent them from getting both heart disease and diabetes,” Dr. Ballantyne added. “Could we start a little earlier with better precision?”
These finding don’t yet call for a change in how cardiologists and endocrinologists manage patients on the cusp of prediabetes, said Paul S. Jellinger, MD, of Hollywood, Fla., and a professor at the University of Miami. “The endpoint of subclinical atherosclerosis does not necessarily translate into the harder endpoint of CVD events, although there is certainly reason to believe it does,” he said in an interview, noting that he’s often used CACS to stratify atherosclerotic CVD risk in patients.
“I will now consider extending that assessment to patients with lower A1c levels,” he said.
If future studies validate this finding, he said, “serious consideration will have to be made for treating the very large numbers of patients with A1c levels in the prediabetic range and below with antidiabetic agents that have ASCVD prevention properties while lowering A1c. We have those agents today.”
The Progression of Early Subclinical Atherosclerosis study received funding from the National Center for Cardiovascular Investigation in Madrid, Santander Bank, and the Carlos III Health Institute in Madrid. Dr. Fuster had no disclosures. Dr. Ballantyne disclosed receiving research funding through his institution from Abbott Diagnostic, Akcea, Amgen, Esperion, Ionis, Novartis, Regeneron, and Roche Diagnostic; and has served as a consultant for Abbott Diagnostics, Althera, Amarin, Amgen, Arrowhead, AstraZeneca, Corvidia, Denka Seiken, Esperion, Genentech, Gilead, Matinas BioPharma, New Amsterdam, Novartis, Novo Nordisk, Pfizer, Regeneron, Roche Diagnostic and Sanofi-Synthélabo.
Dr. Jellinger had no disclosures.
, according to an analysis of data on almost 4,000 middle-aged individuals.
“If one looks at the incidence of generalized subclinical atherosclerosis, we are not talking small numbers,” senior study author Valentin Fuster, MD, PhD, said in an interview. “We are talking about between 45% and 82% of this middle-age population that already has atherosclerotic disease subclinically.
“Actually,” he added, “the disease was extensive in 5%-30% of these individuals of middle age.”
The study included 3,973 participants from the Progression of Early Subclinical Atherosclerosis study who did not have diabetes. A1c showed an association with the prevalence and multiterritorial extent of subclinical atherosclerosis as measured by two-dimensional ultrasound and coronary artery calcium score (CACS; P < .001). For example, those with A1c above 6.1% (133 participants) had a 33.1% rate of generalized subclinical atherosclerosis, compared with 4.9% for those with A1c below 4.8% (243), the lowest-score group in the study.
Patients in the subprediabetes band, between 5.0% and 5.5%, had significantly higher rates of generalized subclinical atherosclerosis than did the lowest-score group: 8% in the 4.9%-5.0% group (375 participants); 9.9% in the 5.1%-5.2% range (687); 10.3% in the 5.3%-5.4% group (928); and 11.5% in the 5.5%-5.6% group (842).
Those in the 5.1%-5.2% and 5/3%-5.4% A1c groups had a 27% greater chance of having subclinical atherosclerosis, while those in the 5.5%-5.6% group had a 36% greater risk, according to an odds ratio analysis adjusted for established cardiovascular risk factors. The risks were even higher for patients with prediabetes, the researchers reported in the Journal of the American College of Cardiology.
A call for earlier intervention
Notably, the study found that fasting plasma glucose testing did not yield a similar association between A1c and atherosclerosis.
“The message is that we all talk about people when they are close to the development of cardiovascular events, and here we are talking about people who we should pay attention to much earlier,” said Dr. Fuster, physician-in-chief at Icahn School of Medicine at Mount Sinai in New York and director of the National Center for Cardiovascular Investigation in Madrid, where the observational study originated said. “People should be sensitized to HbA1c much more than they would’ve been in the past, and I think this study actually validates that.”
Christie Ballantyne, MD, noted in an interview that these findings support the utility of A1c for predicting CVD risk.
“I think more and more we should be ordering a HbA1c” during routine physical exams, Dr. Ballantyne said. “You don’t have to be obese to get it; there are lots of people, maybe they’re slightly overweight. It’s a reasonable test to be getting when you get to middle age and older to get an idea for assessing for both developing diabetes and also the presence of atherosclerosis and the risk for having cardiovascular events.”
Dr. Ballantyne, chief of cardiology at Baylor College of Medicine and director of cardiovascular disease prevention at Methodist DeBakey Heart Center in Houston, coauthored an editorial comment on the study.
Clinicians typically start to manage CVD and diabetes risk “late in the process,” Dr. Ballantyne said. This study suggested that earlier use of antidiabetes therapies, namely peptide-1 agonists and semisynthetic glucagon-like peptide-2 inhibitors, may be warranted in patients with intermediate risk of CVD.
“It’s just more data for the rationale that, perhaps we could end up doing trials to show we can take high-risk people and prevent them from getting both heart disease and diabetes,” Dr. Ballantyne added. “Could we start a little earlier with better precision?”
These finding don’t yet call for a change in how cardiologists and endocrinologists manage patients on the cusp of prediabetes, said Paul S. Jellinger, MD, of Hollywood, Fla., and a professor at the University of Miami. “The endpoint of subclinical atherosclerosis does not necessarily translate into the harder endpoint of CVD events, although there is certainly reason to believe it does,” he said in an interview, noting that he’s often used CACS to stratify atherosclerotic CVD risk in patients.
“I will now consider extending that assessment to patients with lower A1c levels,” he said.
If future studies validate this finding, he said, “serious consideration will have to be made for treating the very large numbers of patients with A1c levels in the prediabetic range and below with antidiabetic agents that have ASCVD prevention properties while lowering A1c. We have those agents today.”
The Progression of Early Subclinical Atherosclerosis study received funding from the National Center for Cardiovascular Investigation in Madrid, Santander Bank, and the Carlos III Health Institute in Madrid. Dr. Fuster had no disclosures. Dr. Ballantyne disclosed receiving research funding through his institution from Abbott Diagnostic, Akcea, Amgen, Esperion, Ionis, Novartis, Regeneron, and Roche Diagnostic; and has served as a consultant for Abbott Diagnostics, Althera, Amarin, Amgen, Arrowhead, AstraZeneca, Corvidia, Denka Seiken, Esperion, Genentech, Gilead, Matinas BioPharma, New Amsterdam, Novartis, Novo Nordisk, Pfizer, Regeneron, Roche Diagnostic and Sanofi-Synthélabo.
Dr. Jellinger had no disclosures.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Medtronic yanks Heartware VAD, calls for halt to new implants
Medtronic has stopped the sale of its Heartware Ventricular Assist Device (HVAD) system and is advising that physicians cease implanting the device because problems with an internal pump can lead to death or serious injuries.
“There is an increased risk of neurological adverse events and mortality associated with the internal pump,” the U.S. Food and Drug Administration announced today.
There is also a potential for the internal pump to stop, and there may be delay or failure to restart. “Both problems may lead to death or serious injuries,” the agency said.
Between January 2009 and April 22, 2021, Medtronic received a total of 106 complaints involving delay or failure to restart with the HVAD pump. Of these, 26 complaints involved HVAD devices operating under normal conditions (dual stator mode) and 80 involved devices operating in a back-up mode (single stator mode) that allows for continued pump function if electrical continuity between the pump and controller is interrupted.
Of the 26 complaints that occurred under normal conditions, four resulted in patient death and five led to urgent explant. Of the 80 complaints that occurred in single stator mode, 10 deaths and eight explants were reported to Medtronic, according to an urgent medical device communication letter issued by the company today.
“Considering these findings and given the availability of alternative devices such as the Abbott HeartMate 3, Medtronic has made the decision to stop the distribution and sale of the HVAD System,” the letter says. “Medtronic advises that there be no further implantations of the HVAD System.”
Medtronic undertook a previous recall of the Heartware HVAD system in February, focusing on batteries, power, datalink cables, and other peripheral equipment, because of the “risk of wear and tear of the connector plugs (power sources, data cable, and alarm adapter), which could cause damage to the controller port metal pins (for example, bent pins).” The FDA deemed that recall Class I, the most serious category of safety alert, in April.
The company noted that patients who currently have an HVAD implant “may require support for many years,” and that it is moving as quickly as possible to create a plan to guide the ongoing support for patients, caregivers, and health care professionals.
In response to the restart failure issue and evolving data about neurologic risks associated with the HVAD pump, Medtronic said it engaged an Independent Practitioner Quality Panel (IPQP), composed of cardiologists, surgeons, and VAD coordinators, to advise on recommendations for appropriate patient management. Based on information collected to date and IPQP input, Medtronic is recommending that physicians continue following best clinical practices and manage patients implanted with the HVAD pump according to the recommendations in the Instructions for Use (IFU).
“Prophylactic explant of the HVAD™ device is not recommended, as risks associated with explantation may outweigh the potential benefits,” the letter says. “The decision regarding explant and exchange of the HVAD™ pump should be made by physicians on a case-by-case basis, considering the patient’s clinical condition and surgical risks. If a physician determines that pump exchange is appropriate, we recommend exchanging to an alternative commercial LVAD.”
For patients in urgent need of an LVAD, Medtronic said physicians should use an alternative commercial LVAD or, if one is not available, that “a Patient Information form is required to be completed by you and your patient to acknowledge the risks of an HVAD implant prior to implanting your HVAD inventory.”
Today’s letter also provides recommendations on blood pressure management goals and anticoagulation. For any other questions or concerns, physicians should contact the Medtronic Office of Medical Affairs at: [email protected].
Medtronic issued another urgent letter in December 2020, warning physicians that a subset of HVAD devices included an internal pump component from three specific lots that increased the risk for restart failure. At that time, the company had not been able to pinpoint a root cause of the pump restart failure.
Consistent with the December 2020 notice, the rate of failure among pumps outside of the subset of three specific lots currently remains at about 0.4%, according to today’s notice.
Although Medtronic has identified the root cause and mitigations for pumps within the three specific lots, it has not been able to identify a root cause of the other restart failures reported with the HVAD pumps, the company said.
A version of this article first appeared on Medscape.com.
Medtronic has stopped the sale of its Heartware Ventricular Assist Device (HVAD) system and is advising that physicians cease implanting the device because problems with an internal pump can lead to death or serious injuries.
“There is an increased risk of neurological adverse events and mortality associated with the internal pump,” the U.S. Food and Drug Administration announced today.
There is also a potential for the internal pump to stop, and there may be delay or failure to restart. “Both problems may lead to death or serious injuries,” the agency said.
Between January 2009 and April 22, 2021, Medtronic received a total of 106 complaints involving delay or failure to restart with the HVAD pump. Of these, 26 complaints involved HVAD devices operating under normal conditions (dual stator mode) and 80 involved devices operating in a back-up mode (single stator mode) that allows for continued pump function if electrical continuity between the pump and controller is interrupted.
Of the 26 complaints that occurred under normal conditions, four resulted in patient death and five led to urgent explant. Of the 80 complaints that occurred in single stator mode, 10 deaths and eight explants were reported to Medtronic, according to an urgent medical device communication letter issued by the company today.
“Considering these findings and given the availability of alternative devices such as the Abbott HeartMate 3, Medtronic has made the decision to stop the distribution and sale of the HVAD System,” the letter says. “Medtronic advises that there be no further implantations of the HVAD System.”
Medtronic undertook a previous recall of the Heartware HVAD system in February, focusing on batteries, power, datalink cables, and other peripheral equipment, because of the “risk of wear and tear of the connector plugs (power sources, data cable, and alarm adapter), which could cause damage to the controller port metal pins (for example, bent pins).” The FDA deemed that recall Class I, the most serious category of safety alert, in April.
The company noted that patients who currently have an HVAD implant “may require support for many years,” and that it is moving as quickly as possible to create a plan to guide the ongoing support for patients, caregivers, and health care professionals.
In response to the restart failure issue and evolving data about neurologic risks associated with the HVAD pump, Medtronic said it engaged an Independent Practitioner Quality Panel (IPQP), composed of cardiologists, surgeons, and VAD coordinators, to advise on recommendations for appropriate patient management. Based on information collected to date and IPQP input, Medtronic is recommending that physicians continue following best clinical practices and manage patients implanted with the HVAD pump according to the recommendations in the Instructions for Use (IFU).
“Prophylactic explant of the HVAD™ device is not recommended, as risks associated with explantation may outweigh the potential benefits,” the letter says. “The decision regarding explant and exchange of the HVAD™ pump should be made by physicians on a case-by-case basis, considering the patient’s clinical condition and surgical risks. If a physician determines that pump exchange is appropriate, we recommend exchanging to an alternative commercial LVAD.”
For patients in urgent need of an LVAD, Medtronic said physicians should use an alternative commercial LVAD or, if one is not available, that “a Patient Information form is required to be completed by you and your patient to acknowledge the risks of an HVAD implant prior to implanting your HVAD inventory.”
Today’s letter also provides recommendations on blood pressure management goals and anticoagulation. For any other questions or concerns, physicians should contact the Medtronic Office of Medical Affairs at: [email protected].
Medtronic issued another urgent letter in December 2020, warning physicians that a subset of HVAD devices included an internal pump component from three specific lots that increased the risk for restart failure. At that time, the company had not been able to pinpoint a root cause of the pump restart failure.
Consistent with the December 2020 notice, the rate of failure among pumps outside of the subset of three specific lots currently remains at about 0.4%, according to today’s notice.
Although Medtronic has identified the root cause and mitigations for pumps within the three specific lots, it has not been able to identify a root cause of the other restart failures reported with the HVAD pumps, the company said.
A version of this article first appeared on Medscape.com.
Medtronic has stopped the sale of its Heartware Ventricular Assist Device (HVAD) system and is advising that physicians cease implanting the device because problems with an internal pump can lead to death or serious injuries.
“There is an increased risk of neurological adverse events and mortality associated with the internal pump,” the U.S. Food and Drug Administration announced today.
There is also a potential for the internal pump to stop, and there may be delay or failure to restart. “Both problems may lead to death or serious injuries,” the agency said.
Between January 2009 and April 22, 2021, Medtronic received a total of 106 complaints involving delay or failure to restart with the HVAD pump. Of these, 26 complaints involved HVAD devices operating under normal conditions (dual stator mode) and 80 involved devices operating in a back-up mode (single stator mode) that allows for continued pump function if electrical continuity between the pump and controller is interrupted.
Of the 26 complaints that occurred under normal conditions, four resulted in patient death and five led to urgent explant. Of the 80 complaints that occurred in single stator mode, 10 deaths and eight explants were reported to Medtronic, according to an urgent medical device communication letter issued by the company today.
“Considering these findings and given the availability of alternative devices such as the Abbott HeartMate 3, Medtronic has made the decision to stop the distribution and sale of the HVAD System,” the letter says. “Medtronic advises that there be no further implantations of the HVAD System.”
Medtronic undertook a previous recall of the Heartware HVAD system in February, focusing on batteries, power, datalink cables, and other peripheral equipment, because of the “risk of wear and tear of the connector plugs (power sources, data cable, and alarm adapter), which could cause damage to the controller port metal pins (for example, bent pins).” The FDA deemed that recall Class I, the most serious category of safety alert, in April.
The company noted that patients who currently have an HVAD implant “may require support for many years,” and that it is moving as quickly as possible to create a plan to guide the ongoing support for patients, caregivers, and health care professionals.
In response to the restart failure issue and evolving data about neurologic risks associated with the HVAD pump, Medtronic said it engaged an Independent Practitioner Quality Panel (IPQP), composed of cardiologists, surgeons, and VAD coordinators, to advise on recommendations for appropriate patient management. Based on information collected to date and IPQP input, Medtronic is recommending that physicians continue following best clinical practices and manage patients implanted with the HVAD pump according to the recommendations in the Instructions for Use (IFU).
“Prophylactic explant of the HVAD™ device is not recommended, as risks associated with explantation may outweigh the potential benefits,” the letter says. “The decision regarding explant and exchange of the HVAD™ pump should be made by physicians on a case-by-case basis, considering the patient’s clinical condition and surgical risks. If a physician determines that pump exchange is appropriate, we recommend exchanging to an alternative commercial LVAD.”
For patients in urgent need of an LVAD, Medtronic said physicians should use an alternative commercial LVAD or, if one is not available, that “a Patient Information form is required to be completed by you and your patient to acknowledge the risks of an HVAD implant prior to implanting your HVAD inventory.”
Today’s letter also provides recommendations on blood pressure management goals and anticoagulation. For any other questions or concerns, physicians should contact the Medtronic Office of Medical Affairs at: [email protected].
Medtronic issued another urgent letter in December 2020, warning physicians that a subset of HVAD devices included an internal pump component from three specific lots that increased the risk for restart failure. At that time, the company had not been able to pinpoint a root cause of the pump restart failure.
Consistent with the December 2020 notice, the rate of failure among pumps outside of the subset of three specific lots currently remains at about 0.4%, according to today’s notice.
Although Medtronic has identified the root cause and mitigations for pumps within the three specific lots, it has not been able to identify a root cause of the other restart failures reported with the HVAD pumps, the company said.
A version of this article first appeared on Medscape.com.
NCAA athletes: ECG abnormalities persist after COVID-19
College athletes who have recently recovered from COVID-19 infection show cardiac abnormalities on electrocardiography.
In a small study of ECGs on National Collegiate Athletic Association Division II athletes, those who had been infected with COVID-19 had a prolonged PR interval, compared with matched athletes who had not been infected.
The study was presented at the 2021 Virtual American College of Sports Medicine Annual Meeting & World Congresses.
“The NCAA was requiring athletes to have an ECG for return to play after noting there could be some myocardial abnormalities following COVID-19 infection,” lead author Frank Wyatt, EdD, a sports physiologist and professor at Midwestern State University in Wichita Falls, Tex., told this news organization.
“Our head athletic trainer asked me if I could do ECGs on our COVID-19–recovered athletes, and I decided to do a matched pair–design study to see how our infected and noninfected athletes compared,” Dr. Wyatt said.
Research in the general population has suggested that COVID-19 can cause damage not only to the lungs, but also to the myocardium, he said. “Recent literature suggests COVID-19 is actually infusing itself into the cells of the myocardium and killing those cells, much the way it did in the lung, and possibly kidney and liver, so it’s going after those organs as well, not just the lungs.”
Dr. Wyatt presented results of ECGs that were done in seven COVID-infected athletes and in seven controls, who were free of infection.
The athletes’ recovery from COVID-19 infection was documented after two negative tests.
All subjects were matched by sport, gender, ethnicity, and anthropometry. Investigators obtained ECG recordings 2-4 weeks after the infected athletes had their recovery documented.
Study participants engaged in football, basketball, soccer, and volleyball, and Dr. Wyatt and associates were blinded as to their infected or control status.
Participants self-reported their ethnicity. Most were White or African American.
The main abnormality found was a prolonged PR interval. In the athletes who were recovered from COVID-19, the mean PR interval was 183.6 milliseconds (± 32.4 ms), compared with 141.7 ms (± 22.7 ms) among the controls.
Baseline ECGs for all young athletes?
Dr. Wyatt said he would like to see ECGs done at baseline as part of the physical exam NCAA athletes have to undergo at the start of each season. But that would be expensive.
“It has been suggested that they all need to have ECGs for baseline information, but they don’t do it because of money. If we had that baseline data on these athletes it would really give us a better picture of whether there was damage or not,” he said. “At our small university, if I wasn’t available to do these ECGs, our athletic department would then have to go to the cardiologist to do them, and that is tremendously expensive. It has also been suggested that high school athletes get ECGs as a preliminary test when they start their season, and I think that is warranted as well as for the NCAA athletes, but because of the expense, they’re not doing it.”
Dr. Wyatt has continued to do ECGs on athletes who have survived COVID-19 and to date has ECG data on 70 athletes. He plans further comparisons between the infected and noninfected athletes.
“We want to see if we can solidify the results we presented at ACSM. We had small numbers, so our follow up is to see if we can statistically show in a more robust manner whether or not there was widespread abnormality in the athletes who got infected. They were only 2-4 weeks post infected, and I don’t know what the long-term effects are going to be,” he said.
May be an important finding
“This may be an important finding, but needs many more athletes, as there were only seven in each group,” commented Curt J. Daniels, MD, director of the sports cardiology program and professor at Ohio State University Wexner Medical Center, Columbus.
“Plus, it will need some imaging correlate and recovery ECGs to see if this effect of PR interval prolongation correlates with myocardial changes and whether it persists or resolves,” added Dr. Daniels, who was not part of the study. “But I do find this interesting. ... I agree we are looking for any ECG sign that might help tell us who needs a cardiac MRI. The Big Ten COVID-19 Cardiac Registry has 1,597 ECGs on post COVID athletes we are analyzing, but preliminarily did not see any changes.”
Dr. Wyatt and Dr. Daniels reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
College athletes who have recently recovered from COVID-19 infection show cardiac abnormalities on electrocardiography.
In a small study of ECGs on National Collegiate Athletic Association Division II athletes, those who had been infected with COVID-19 had a prolonged PR interval, compared with matched athletes who had not been infected.
The study was presented at the 2021 Virtual American College of Sports Medicine Annual Meeting & World Congresses.
“The NCAA was requiring athletes to have an ECG for return to play after noting there could be some myocardial abnormalities following COVID-19 infection,” lead author Frank Wyatt, EdD, a sports physiologist and professor at Midwestern State University in Wichita Falls, Tex., told this news organization.
“Our head athletic trainer asked me if I could do ECGs on our COVID-19–recovered athletes, and I decided to do a matched pair–design study to see how our infected and noninfected athletes compared,” Dr. Wyatt said.
Research in the general population has suggested that COVID-19 can cause damage not only to the lungs, but also to the myocardium, he said. “Recent literature suggests COVID-19 is actually infusing itself into the cells of the myocardium and killing those cells, much the way it did in the lung, and possibly kidney and liver, so it’s going after those organs as well, not just the lungs.”
Dr. Wyatt presented results of ECGs that were done in seven COVID-infected athletes and in seven controls, who were free of infection.
The athletes’ recovery from COVID-19 infection was documented after two negative tests.
All subjects were matched by sport, gender, ethnicity, and anthropometry. Investigators obtained ECG recordings 2-4 weeks after the infected athletes had their recovery documented.
Study participants engaged in football, basketball, soccer, and volleyball, and Dr. Wyatt and associates were blinded as to their infected or control status.
Participants self-reported their ethnicity. Most were White or African American.
The main abnormality found was a prolonged PR interval. In the athletes who were recovered from COVID-19, the mean PR interval was 183.6 milliseconds (± 32.4 ms), compared with 141.7 ms (± 22.7 ms) among the controls.
Baseline ECGs for all young athletes?
Dr. Wyatt said he would like to see ECGs done at baseline as part of the physical exam NCAA athletes have to undergo at the start of each season. But that would be expensive.
“It has been suggested that they all need to have ECGs for baseline information, but they don’t do it because of money. If we had that baseline data on these athletes it would really give us a better picture of whether there was damage or not,” he said. “At our small university, if I wasn’t available to do these ECGs, our athletic department would then have to go to the cardiologist to do them, and that is tremendously expensive. It has also been suggested that high school athletes get ECGs as a preliminary test when they start their season, and I think that is warranted as well as for the NCAA athletes, but because of the expense, they’re not doing it.”
Dr. Wyatt has continued to do ECGs on athletes who have survived COVID-19 and to date has ECG data on 70 athletes. He plans further comparisons between the infected and noninfected athletes.
“We want to see if we can solidify the results we presented at ACSM. We had small numbers, so our follow up is to see if we can statistically show in a more robust manner whether or not there was widespread abnormality in the athletes who got infected. They were only 2-4 weeks post infected, and I don’t know what the long-term effects are going to be,” he said.
May be an important finding
“This may be an important finding, but needs many more athletes, as there were only seven in each group,” commented Curt J. Daniels, MD, director of the sports cardiology program and professor at Ohio State University Wexner Medical Center, Columbus.
“Plus, it will need some imaging correlate and recovery ECGs to see if this effect of PR interval prolongation correlates with myocardial changes and whether it persists or resolves,” added Dr. Daniels, who was not part of the study. “But I do find this interesting. ... I agree we are looking for any ECG sign that might help tell us who needs a cardiac MRI. The Big Ten COVID-19 Cardiac Registry has 1,597 ECGs on post COVID athletes we are analyzing, but preliminarily did not see any changes.”
Dr. Wyatt and Dr. Daniels reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
College athletes who have recently recovered from COVID-19 infection show cardiac abnormalities on electrocardiography.
In a small study of ECGs on National Collegiate Athletic Association Division II athletes, those who had been infected with COVID-19 had a prolonged PR interval, compared with matched athletes who had not been infected.
The study was presented at the 2021 Virtual American College of Sports Medicine Annual Meeting & World Congresses.
“The NCAA was requiring athletes to have an ECG for return to play after noting there could be some myocardial abnormalities following COVID-19 infection,” lead author Frank Wyatt, EdD, a sports physiologist and professor at Midwestern State University in Wichita Falls, Tex., told this news organization.
“Our head athletic trainer asked me if I could do ECGs on our COVID-19–recovered athletes, and I decided to do a matched pair–design study to see how our infected and noninfected athletes compared,” Dr. Wyatt said.
Research in the general population has suggested that COVID-19 can cause damage not only to the lungs, but also to the myocardium, he said. “Recent literature suggests COVID-19 is actually infusing itself into the cells of the myocardium and killing those cells, much the way it did in the lung, and possibly kidney and liver, so it’s going after those organs as well, not just the lungs.”
Dr. Wyatt presented results of ECGs that were done in seven COVID-infected athletes and in seven controls, who were free of infection.
The athletes’ recovery from COVID-19 infection was documented after two negative tests.
All subjects were matched by sport, gender, ethnicity, and anthropometry. Investigators obtained ECG recordings 2-4 weeks after the infected athletes had their recovery documented.
Study participants engaged in football, basketball, soccer, and volleyball, and Dr. Wyatt and associates were blinded as to their infected or control status.
Participants self-reported their ethnicity. Most were White or African American.
The main abnormality found was a prolonged PR interval. In the athletes who were recovered from COVID-19, the mean PR interval was 183.6 milliseconds (± 32.4 ms), compared with 141.7 ms (± 22.7 ms) among the controls.
Baseline ECGs for all young athletes?
Dr. Wyatt said he would like to see ECGs done at baseline as part of the physical exam NCAA athletes have to undergo at the start of each season. But that would be expensive.
“It has been suggested that they all need to have ECGs for baseline information, but they don’t do it because of money. If we had that baseline data on these athletes it would really give us a better picture of whether there was damage or not,” he said. “At our small university, if I wasn’t available to do these ECGs, our athletic department would then have to go to the cardiologist to do them, and that is tremendously expensive. It has also been suggested that high school athletes get ECGs as a preliminary test when they start their season, and I think that is warranted as well as for the NCAA athletes, but because of the expense, they’re not doing it.”
Dr. Wyatt has continued to do ECGs on athletes who have survived COVID-19 and to date has ECG data on 70 athletes. He plans further comparisons between the infected and noninfected athletes.
“We want to see if we can solidify the results we presented at ACSM. We had small numbers, so our follow up is to see if we can statistically show in a more robust manner whether or not there was widespread abnormality in the athletes who got infected. They were only 2-4 weeks post infected, and I don’t know what the long-term effects are going to be,” he said.
May be an important finding
“This may be an important finding, but needs many more athletes, as there were only seven in each group,” commented Curt J. Daniels, MD, director of the sports cardiology program and professor at Ohio State University Wexner Medical Center, Columbus.
“Plus, it will need some imaging correlate and recovery ECGs to see if this effect of PR interval prolongation correlates with myocardial changes and whether it persists or resolves,” added Dr. Daniels, who was not part of the study. “But I do find this interesting. ... I agree we are looking for any ECG sign that might help tell us who needs a cardiac MRI. The Big Ten COVID-19 Cardiac Registry has 1,597 ECGs on post COVID athletes we are analyzing, but preliminarily did not see any changes.”
Dr. Wyatt and Dr. Daniels reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Intersection of trauma and race in pregnancy calls for more study
Black patients experienced more moderate to severe violent trauma during pregnancy than did non-Black patients at a single Baltimore institution, according to a small retrospective cohort study presented in a poster at the 2021 virtual meeting of the American College of Obstetricians and Gynecologists.
“Trauma is the leading nonobstetric cause of death in pregnant women,” and Black communities are at a disproportionately greater risk of trauma, Rebecca H. Jessel, MD, of Icahn School of Medicine at Mount Sinai in New York, and associates wrote in their poster.
The study’s findings raise research questions that need more exploration, according to Neel Shah, MD, assistant professor of obstetrics, gynecology, and reproductive biology at Harvard Medical School, Boston, and founding director of the Delivery Decisions Initiative at Harvard’s Ariadne Labs.
“This is an interesting study that opens a line of inquiry into how trauma may impact the pregnancies of those who are Black differently,” Dr. Shah, who was not involved in the research, said in an interview. “The observed disparity is consistent with the racial inequities in outcomes we see across obstetric outcomes and requires further research into the causes and solutions.”
The researchers retrospectively reviewed all pregnant patients treated between 2015 and 2018 at the University of Maryland’s R Adams Cowley Shock Trauma Center in Baltimore. In addition to maternal demographics, details about the delivery, and perinatal outcomes, the researchers noted whether the trauma was violent, such as assault, or nonviolent, such as motor vehicle accidents. Moderate to severe trauma was defined as an injury severity score of at least 9.
Among 3,536 women aged 15-49 treated at the shock trauma center, 62 were pregnant, and 71% of these women were Black. Nineteen percent were White patients, 5% were Asian patients, and 5% were of a different race/ethnicity. Black patients were, on average, 27 years old at the time of the trauma. Non-Black patients were, on average, 25 years old. The average gestational age at the time of trauma was 25 weeks, 3 days in Black women and 23 weeks, 4 days in non-Black women.
The most common cause of trauma was a car accident, implicated in 56% of the trauma cases. Assault was the next most common cause of trauma, making up nearly a quarter (23%) of cases. The other injuries came from accidents (16%) or inhalation (5%). The average injury severity score was 4.7, with a mild injury for 76% of patients and a moderate to severe injury in 24%.
The researchers then compared the mechanisms and severity of injuries between Black and non-Black patients. The severity of trauma was similar between the two groups: Seventy-five percent of Black patients and 78% of non-Black patients had mild trauma with injury severity scores below 9. However, assault or another violent form of trauma was more likely to occur to Black patients than to non-Black patients. More than a quarter (27%) of Black patients experienced violent trauma, compared to 11% of non-Black patients.
“It is very notable that among pregnant people who experience trauma, obstetric complications leading to preterm delivery were observed much more often for those who are Black,” Dr. Shah said. “A case series to understand the underlying causes could be very valuable.”
Black patients delivered an average 59 days (8 weeks, 3 days) after the trauma compared to an average 83 days (11 weeks, 6 days) for non-Black patients, but the difference was not statistically significant. However, preterm birth was more likely in non-Black patients (83%) than in Black patients (78%). A similar proportion of deliveries were preterm in Black (57%) and non-Black (56%) patients.
Though the poster did not show the data, the researchers wrote that Black women who experienced moderate to severe trauma after 24 weeks’ gestational age either had a preterm birth or a fetal demise.
Though the study findings warrant deeper investigation, the study has substantial limitations.
“It is challenging to generalize from this study because the sample size is small and it is from a single institution,” Dr. Shah said. “It does not appear to be adequately powered to draw statistically significant conclusions. In particular, the data are not adequate to support the authors’ statement that Black people are more likely to experience the forms of described trauma generally.”
The authors and Dr. Shah reported no disclosures.
Black patients experienced more moderate to severe violent trauma during pregnancy than did non-Black patients at a single Baltimore institution, according to a small retrospective cohort study presented in a poster at the 2021 virtual meeting of the American College of Obstetricians and Gynecologists.
“Trauma is the leading nonobstetric cause of death in pregnant women,” and Black communities are at a disproportionately greater risk of trauma, Rebecca H. Jessel, MD, of Icahn School of Medicine at Mount Sinai in New York, and associates wrote in their poster.
The study’s findings raise research questions that need more exploration, according to Neel Shah, MD, assistant professor of obstetrics, gynecology, and reproductive biology at Harvard Medical School, Boston, and founding director of the Delivery Decisions Initiative at Harvard’s Ariadne Labs.
“This is an interesting study that opens a line of inquiry into how trauma may impact the pregnancies of those who are Black differently,” Dr. Shah, who was not involved in the research, said in an interview. “The observed disparity is consistent with the racial inequities in outcomes we see across obstetric outcomes and requires further research into the causes and solutions.”
The researchers retrospectively reviewed all pregnant patients treated between 2015 and 2018 at the University of Maryland’s R Adams Cowley Shock Trauma Center in Baltimore. In addition to maternal demographics, details about the delivery, and perinatal outcomes, the researchers noted whether the trauma was violent, such as assault, or nonviolent, such as motor vehicle accidents. Moderate to severe trauma was defined as an injury severity score of at least 9.
Among 3,536 women aged 15-49 treated at the shock trauma center, 62 were pregnant, and 71% of these women were Black. Nineteen percent were White patients, 5% were Asian patients, and 5% were of a different race/ethnicity. Black patients were, on average, 27 years old at the time of the trauma. Non-Black patients were, on average, 25 years old. The average gestational age at the time of trauma was 25 weeks, 3 days in Black women and 23 weeks, 4 days in non-Black women.
The most common cause of trauma was a car accident, implicated in 56% of the trauma cases. Assault was the next most common cause of trauma, making up nearly a quarter (23%) of cases. The other injuries came from accidents (16%) or inhalation (5%). The average injury severity score was 4.7, with a mild injury for 76% of patients and a moderate to severe injury in 24%.
The researchers then compared the mechanisms and severity of injuries between Black and non-Black patients. The severity of trauma was similar between the two groups: Seventy-five percent of Black patients and 78% of non-Black patients had mild trauma with injury severity scores below 9. However, assault or another violent form of trauma was more likely to occur to Black patients than to non-Black patients. More than a quarter (27%) of Black patients experienced violent trauma, compared to 11% of non-Black patients.
“It is very notable that among pregnant people who experience trauma, obstetric complications leading to preterm delivery were observed much more often for those who are Black,” Dr. Shah said. “A case series to understand the underlying causes could be very valuable.”
Black patients delivered an average 59 days (8 weeks, 3 days) after the trauma compared to an average 83 days (11 weeks, 6 days) for non-Black patients, but the difference was not statistically significant. However, preterm birth was more likely in non-Black patients (83%) than in Black patients (78%). A similar proportion of deliveries were preterm in Black (57%) and non-Black (56%) patients.
Though the poster did not show the data, the researchers wrote that Black women who experienced moderate to severe trauma after 24 weeks’ gestational age either had a preterm birth or a fetal demise.
Though the study findings warrant deeper investigation, the study has substantial limitations.
“It is challenging to generalize from this study because the sample size is small and it is from a single institution,” Dr. Shah said. “It does not appear to be adequately powered to draw statistically significant conclusions. In particular, the data are not adequate to support the authors’ statement that Black people are more likely to experience the forms of described trauma generally.”
The authors and Dr. Shah reported no disclosures.
Black patients experienced more moderate to severe violent trauma during pregnancy than did non-Black patients at a single Baltimore institution, according to a small retrospective cohort study presented in a poster at the 2021 virtual meeting of the American College of Obstetricians and Gynecologists.
“Trauma is the leading nonobstetric cause of death in pregnant women,” and Black communities are at a disproportionately greater risk of trauma, Rebecca H. Jessel, MD, of Icahn School of Medicine at Mount Sinai in New York, and associates wrote in their poster.
The study’s findings raise research questions that need more exploration, according to Neel Shah, MD, assistant professor of obstetrics, gynecology, and reproductive biology at Harvard Medical School, Boston, and founding director of the Delivery Decisions Initiative at Harvard’s Ariadne Labs.
“This is an interesting study that opens a line of inquiry into how trauma may impact the pregnancies of those who are Black differently,” Dr. Shah, who was not involved in the research, said in an interview. “The observed disparity is consistent with the racial inequities in outcomes we see across obstetric outcomes and requires further research into the causes and solutions.”
The researchers retrospectively reviewed all pregnant patients treated between 2015 and 2018 at the University of Maryland’s R Adams Cowley Shock Trauma Center in Baltimore. In addition to maternal demographics, details about the delivery, and perinatal outcomes, the researchers noted whether the trauma was violent, such as assault, or nonviolent, such as motor vehicle accidents. Moderate to severe trauma was defined as an injury severity score of at least 9.
Among 3,536 women aged 15-49 treated at the shock trauma center, 62 were pregnant, and 71% of these women were Black. Nineteen percent were White patients, 5% were Asian patients, and 5% were of a different race/ethnicity. Black patients were, on average, 27 years old at the time of the trauma. Non-Black patients were, on average, 25 years old. The average gestational age at the time of trauma was 25 weeks, 3 days in Black women and 23 weeks, 4 days in non-Black women.
The most common cause of trauma was a car accident, implicated in 56% of the trauma cases. Assault was the next most common cause of trauma, making up nearly a quarter (23%) of cases. The other injuries came from accidents (16%) or inhalation (5%). The average injury severity score was 4.7, with a mild injury for 76% of patients and a moderate to severe injury in 24%.
The researchers then compared the mechanisms and severity of injuries between Black and non-Black patients. The severity of trauma was similar between the two groups: Seventy-five percent of Black patients and 78% of non-Black patients had mild trauma with injury severity scores below 9. However, assault or another violent form of trauma was more likely to occur to Black patients than to non-Black patients. More than a quarter (27%) of Black patients experienced violent trauma, compared to 11% of non-Black patients.
“It is very notable that among pregnant people who experience trauma, obstetric complications leading to preterm delivery were observed much more often for those who are Black,” Dr. Shah said. “A case series to understand the underlying causes could be very valuable.”
Black patients delivered an average 59 days (8 weeks, 3 days) after the trauma compared to an average 83 days (11 weeks, 6 days) for non-Black patients, but the difference was not statistically significant. However, preterm birth was more likely in non-Black patients (83%) than in Black patients (78%). A similar proportion of deliveries were preterm in Black (57%) and non-Black (56%) patients.
Though the poster did not show the data, the researchers wrote that Black women who experienced moderate to severe trauma after 24 weeks’ gestational age either had a preterm birth or a fetal demise.
Though the study findings warrant deeper investigation, the study has substantial limitations.
“It is challenging to generalize from this study because the sample size is small and it is from a single institution,” Dr. Shah said. “It does not appear to be adequately powered to draw statistically significant conclusions. In particular, the data are not adequate to support the authors’ statement that Black people are more likely to experience the forms of described trauma generally.”
The authors and Dr. Shah reported no disclosures.
FROM ACOG 2021