User login
Tinea Incognito in a Tattoo
To the Editor:
Tinea incognito occurs when superficial fungal infections fail to demonstrate typical clinical features in the setting of immune suppression caused by topical or systemic steroids.1,2 A case of tinea corporis obscured by an allergic tattoo reaction is presented.
A 52-year-old man presented for evaluation of a rash overlying a tattoo on the right calf of 3 weeks’ duration (Figure, A). The tattoo was placed 4 years prior to presentation. Within 6 months of the tattoo’s placement, pruritus, scaling, and edema developed in a 2-mm rim around the outer border and in the eyes of the elephant tattoo but not in the lettering portion of the tattoo, which was added by a different tattoo artist with a different red dye. A diagnosis of red dye tattoo allergic reaction was made. Daily treatment with tacrolimus ointment 0.1% and halobetasol propionate cream 0.05% under occlusion for 18 months provided only partial relief of incessant pruritus. Three months prior to presentation the tattoo reaction appeared to become worse with more pruritus and extension outside the bounds of the original tattoo.

Physical examination revealed the red rim of the tattoo was erythematous, edematous, and crusted. In addition, a 5×4-cm well-demarcated, erythematous, scaling patch was present overlying the elephant tattoo on the right calf and extending superiorly and laterally away from the tattoo. Scaling and maceration also were present in the web spaces between the fourth and fifth toes, and the toenails were yellowed, thickened, and dystrophic with signs of distal onycholysis. A potassium hydroxide preparation performed from the plaque on the right calf demonstrated septate fungal hyphae.
The diagnosis of tinea corporis secondary to tinea pedis overlying a red dye tattoo allergic reaction was made. Tacrolimus and halobetasol propionate were discontinued and treatment with ketoconazole cream 2% twice daily and oral terbinafine 250 mg once daily was started. The erythematous patch beyond the borders of the tattoo cleared within weeks, but the patient reported worsening of cracking, itching, and swelling overlying the red dye in the rim of the tattoo following discontinuation of topical anti-inflammatory drugs (Figure, B).
A potassium hydroxide preparation demonstrated that the expansible rash was tinea corporis disguised in its character by the coloration of the tattoo; the erythematous, edematous, pruritic tattoo allergic reaction at its rim; and suppression of the normal inflammatory response by daily use of a topical steroid and a calcineurin inhibitor. The latter effect (an immunocompromised district) impacts the classic exaggerated scaling, inflamed rim, and central clearing of tinea corporis present in individuals with a normal inflammatory response.2 Although tinea incognito is classically described on the ankles and lower legs of patients with stasis dermatitis chronically treated with topical steroids, it could occur anywhere in the setting of immunosuppression.3
An analysis of this case using Occam’s razor suggests that the association of this tattoo and tinea was not a coincidence. This guiding principle (heuristic) suggests that economy and succinctness in the logic of science is most likely to produce a correct medical diagnosis (eg, associated findings can be explained by identifying one underlying cause).4 The topical anti-inflammatory drugs increase the likelihood that the patient’s interdigital tinea would spread to this precise location symmetrically expanding in the outline of the tattoo.2
- Gathings RM, Abide JM, Brodell RT. An unusual inflammatory rash. JAMA Pediatr. 2014;168:185-186.
- Ruocco V, Brunetti G, Puca RV, et al. The immunocompromised district: a unifying concept for lymphoedematous, herpes-infected and otherwise damaged sites. J Eur Acad Dermatol Venereol. 2009;23:1364-1373.
- Romano C, Maritati E, Gianni C. Tinea incognito in Italy: a 15-year survey. Mycoses. 2006;49:383-387.
- Jefferys WH, Berger JO. Ockham’s razor and Bayesian analysis. American Scientist. 1992;80:64-72.
To the Editor:
Tinea incognito occurs when superficial fungal infections fail to demonstrate typical clinical features in the setting of immune suppression caused by topical or systemic steroids.1,2 A case of tinea corporis obscured by an allergic tattoo reaction is presented.
A 52-year-old man presented for evaluation of a rash overlying a tattoo on the right calf of 3 weeks’ duration (Figure, A). The tattoo was placed 4 years prior to presentation. Within 6 months of the tattoo’s placement, pruritus, scaling, and edema developed in a 2-mm rim around the outer border and in the eyes of the elephant tattoo but not in the lettering portion of the tattoo, which was added by a different tattoo artist with a different red dye. A diagnosis of red dye tattoo allergic reaction was made. Daily treatment with tacrolimus ointment 0.1% and halobetasol propionate cream 0.05% under occlusion for 18 months provided only partial relief of incessant pruritus. Three months prior to presentation the tattoo reaction appeared to become worse with more pruritus and extension outside the bounds of the original tattoo.
Physical examination revealed the red rim of the tattoo was erythematous, edematous, and crusted. In addition, a 5×4-cm well-demarcated, erythematous, scaling patch was present overlying the elephant tattoo on the right calf and extending superiorly and laterally away from the tattoo. Scaling and maceration also were present in the web spaces between the fourth and fifth toes, and the toenails were yellowed, thickened, and dystrophic with signs of distal onycholysis. A potassium hydroxide preparation performed from the plaque on the right calf demonstrated septate fungal hyphae.
The diagnosis of tinea corporis secondary to tinea pedis overlying a red dye tattoo allergic reaction was made. Tacrolimus and halobetasol propionate were discontinued and treatment with ketoconazole cream 2% twice daily and oral terbinafine 250 mg once daily was started. The erythematous patch beyond the borders of the tattoo cleared within weeks, but the patient reported worsening of cracking, itching, and swelling overlying the red dye in the rim of the tattoo following discontinuation of topical anti-inflammatory drugs (Figure, B).
A potassium hydroxide preparation demonstrated that the expansible rash was tinea corporis disguised in its character by the coloration of the tattoo; the erythematous, edematous, pruritic tattoo allergic reaction at its rim; and suppression of the normal inflammatory response by daily use of a topical steroid and a calcineurin inhibitor. The latter effect (an immunocompromised district) impacts the classic exaggerated scaling, inflamed rim, and central clearing of tinea corporis present in individuals with a normal inflammatory response.2 Although tinea incognito is classically described on the ankles and lower legs of patients with stasis dermatitis chronically treated with topical steroids, it could occur anywhere in the setting of immunosuppression.3
An analysis of this case using Occam’s razor suggests that the association of this tattoo and tinea was not a coincidence. This guiding principle (heuristic) suggests that economy and succinctness in the logic of science is most likely to produce a correct medical diagnosis (eg, associated findings can be explained by identifying one underlying cause).4 The topical anti-inflammatory drugs increase the likelihood that the patient’s interdigital tinea would spread to this precise location symmetrically expanding in the outline of the tattoo.2
To the Editor:
Tinea incognito occurs when superficial fungal infections fail to demonstrate typical clinical features in the setting of immune suppression caused by topical or systemic steroids.1,2 A case of tinea corporis obscured by an allergic tattoo reaction is presented.
A 52-year-old man presented for evaluation of a rash overlying a tattoo on the right calf of 3 weeks’ duration (Figure, A). The tattoo was placed 4 years prior to presentation. Within 6 months of the tattoo’s placement, pruritus, scaling, and edema developed in a 2-mm rim around the outer border and in the eyes of the elephant tattoo but not in the lettering portion of the tattoo, which was added by a different tattoo artist with a different red dye. A diagnosis of red dye tattoo allergic reaction was made. Daily treatment with tacrolimus ointment 0.1% and halobetasol propionate cream 0.05% under occlusion for 18 months provided only partial relief of incessant pruritus. Three months prior to presentation the tattoo reaction appeared to become worse with more pruritus and extension outside the bounds of the original tattoo.
Physical examination revealed the red rim of the tattoo was erythematous, edematous, and crusted. In addition, a 5×4-cm well-demarcated, erythematous, scaling patch was present overlying the elephant tattoo on the right calf and extending superiorly and laterally away from the tattoo. Scaling and maceration also were present in the web spaces between the fourth and fifth toes, and the toenails were yellowed, thickened, and dystrophic with signs of distal onycholysis. A potassium hydroxide preparation performed from the plaque on the right calf demonstrated septate fungal hyphae.
The diagnosis of tinea corporis secondary to tinea pedis overlying a red dye tattoo allergic reaction was made. Tacrolimus and halobetasol propionate were discontinued and treatment with ketoconazole cream 2% twice daily and oral terbinafine 250 mg once daily was started. The erythematous patch beyond the borders of the tattoo cleared within weeks, but the patient reported worsening of cracking, itching, and swelling overlying the red dye in the rim of the tattoo following discontinuation of topical anti-inflammatory drugs (Figure, B).
A potassium hydroxide preparation demonstrated that the expansible rash was tinea corporis disguised in its character by the coloration of the tattoo; the erythematous, edematous, pruritic tattoo allergic reaction at its rim; and suppression of the normal inflammatory response by daily use of a topical steroid and a calcineurin inhibitor. The latter effect (an immunocompromised district) impacts the classic exaggerated scaling, inflamed rim, and central clearing of tinea corporis present in individuals with a normal inflammatory response.2 Although tinea incognito is classically described on the ankles and lower legs of patients with stasis dermatitis chronically treated with topical steroids, it could occur anywhere in the setting of immunosuppression.3
An analysis of this case using Occam’s razor suggests that the association of this tattoo and tinea was not a coincidence. This guiding principle (heuristic) suggests that economy and succinctness in the logic of science is most likely to produce a correct medical diagnosis (eg, associated findings can be explained by identifying one underlying cause).4 The topical anti-inflammatory drugs increase the likelihood that the patient’s interdigital tinea would spread to this precise location symmetrically expanding in the outline of the tattoo.2
- Gathings RM, Abide JM, Brodell RT. An unusual inflammatory rash. JAMA Pediatr. 2014;168:185-186.
- Ruocco V, Brunetti G, Puca RV, et al. The immunocompromised district: a unifying concept for lymphoedematous, herpes-infected and otherwise damaged sites. J Eur Acad Dermatol Venereol. 2009;23:1364-1373.
- Romano C, Maritati E, Gianni C. Tinea incognito in Italy: a 15-year survey. Mycoses. 2006;49:383-387.
- Jefferys WH, Berger JO. Ockham’s razor and Bayesian analysis. American Scientist. 1992;80:64-72.
- Gathings RM, Abide JM, Brodell RT. An unusual inflammatory rash. JAMA Pediatr. 2014;168:185-186.
- Ruocco V, Brunetti G, Puca RV, et al. The immunocompromised district: a unifying concept for lymphoedematous, herpes-infected and otherwise damaged sites. J Eur Acad Dermatol Venereol. 2009;23:1364-1373.
- Romano C, Maritati E, Gianni C. Tinea incognito in Italy: a 15-year survey. Mycoses. 2006;49:383-387.
- Jefferys WH, Berger JO. Ockham’s razor and Bayesian analysis. American Scientist. 1992;80:64-72.
Practice Points
- Health care providers should have a low threshold to perform a potassium hydroxide preparation when the possibility of a superficial fungal infection is considered.
- Tinea incognito occurs when a superficial fungal infection has unusual clinical features in the setting of local immune suppression.

Dr Jame Abraham's top ASCO selections in breast cancer
Jame Abraham, MD, FACP, an Editor on The Journal of Community and Supportive Oncology, shares his top selections in breast cancer from this year's annual meeting of the American Society of Clinical Oncology in Chicago.
1001 Efficacy of sacituzumab govitecan (anti-Trop-2-SN-38 antibody-drug conjugate) for treatment-refractory hormone-receptor positive (HR+)/HER2- metastatic breast cancer (mBC) (Aditya Bardia et al). The study drug was well tolerated and produced objective responses in this heavily pretreated population, with an overall response rate of 31% at 6 months and a clinical benefit rate of 48%.
LBA1 TAILORx: Phase III trial of chemoendocrine therapy versus endocrine therapy alone in hormone receptor-positive, HER2-negative, node-negative breast cancer and an intermediate prognosis 21-gene recurrence score (Joseph A Sparano et al)
506 PERSEPHONE: 6 versus 12 months (m) of adjuvant trastuzumab in patients (pts) with HER2 positive (+) early breast cancer (EBC): randomised phase 3 non-inferiority trial with definitive 4-year (yr) disease-free survival (DFS) results (Helena Margaret Earl et al). Six months of trastuzumab was found to be noninferior to 12 months, although cardiac events were reduced in the 6-month group compared with the 12-month group (4% vs 8% of patients, respectively, ended treatment because of cardiotoxicity).
In addition, Dr David Henry, the Editor-in-Chief of JCSO, also selected:
500 Adjuvant denosumab in early breast cancer: disease-free survival analysis of postmenopausal patients in the ABCSG-18 trial (Michael Gnant et al). In this double-blind placebo controlled trial, disease-free survival in the denosumab group was 89% at 5 years and 80% at 8 years, compared with 87% and 77%, respectively, for placebo.
Jame Abraham, MD, FACP, an Editor on The Journal of Community and Supportive Oncology, shares his top selections in breast cancer from this year's annual meeting of the American Society of Clinical Oncology in Chicago.
1001 Efficacy of sacituzumab govitecan (anti-Trop-2-SN-38 antibody-drug conjugate) for treatment-refractory hormone-receptor positive (HR+)/HER2- metastatic breast cancer (mBC) (Aditya Bardia et al). The study drug was well tolerated and produced objective responses in this heavily pretreated population, with an overall response rate of 31% at 6 months and a clinical benefit rate of 48%.
LBA1 TAILORx: Phase III trial of chemoendocrine therapy versus endocrine therapy alone in hormone receptor-positive, HER2-negative, node-negative breast cancer and an intermediate prognosis 21-gene recurrence score (Joseph A Sparano et al)
506 PERSEPHONE: 6 versus 12 months (m) of adjuvant trastuzumab in patients (pts) with HER2 positive (+) early breast cancer (EBC): randomised phase 3 non-inferiority trial with definitive 4-year (yr) disease-free survival (DFS) results (Helena Margaret Earl et al). Six months of trastuzumab was found to be noninferior to 12 months, although cardiac events were reduced in the 6-month group compared with the 12-month group (4% vs 8% of patients, respectively, ended treatment because of cardiotoxicity).
In addition, Dr David Henry, the Editor-in-Chief of JCSO, also selected:
500 Adjuvant denosumab in early breast cancer: disease-free survival analysis of postmenopausal patients in the ABCSG-18 trial (Michael Gnant et al). In this double-blind placebo controlled trial, disease-free survival in the denosumab group was 89% at 5 years and 80% at 8 years, compared with 87% and 77%, respectively, for placebo.
Jame Abraham, MD, FACP, an Editor on The Journal of Community and Supportive Oncology, shares his top selections in breast cancer from this year's annual meeting of the American Society of Clinical Oncology in Chicago.
1001 Efficacy of sacituzumab govitecan (anti-Trop-2-SN-38 antibody-drug conjugate) for treatment-refractory hormone-receptor positive (HR+)/HER2- metastatic breast cancer (mBC) (Aditya Bardia et al). The study drug was well tolerated and produced objective responses in this heavily pretreated population, with an overall response rate of 31% at 6 months and a clinical benefit rate of 48%.
LBA1 TAILORx: Phase III trial of chemoendocrine therapy versus endocrine therapy alone in hormone receptor-positive, HER2-negative, node-negative breast cancer and an intermediate prognosis 21-gene recurrence score (Joseph A Sparano et al)
506 PERSEPHONE: 6 versus 12 months (m) of adjuvant trastuzumab in patients (pts) with HER2 positive (+) early breast cancer (EBC): randomised phase 3 non-inferiority trial with definitive 4-year (yr) disease-free survival (DFS) results (Helena Margaret Earl et al). Six months of trastuzumab was found to be noninferior to 12 months, although cardiac events were reduced in the 6-month group compared with the 12-month group (4% vs 8% of patients, respectively, ended treatment because of cardiotoxicity).
In addition, Dr David Henry, the Editor-in-Chief of JCSO, also selected:
500 Adjuvant denosumab in early breast cancer: disease-free survival analysis of postmenopausal patients in the ABCSG-18 trial (Michael Gnant et al). In this double-blind placebo controlled trial, disease-free survival in the denosumab group was 89% at 5 years and 80% at 8 years, compared with 87% and 77%, respectively, for placebo.
AAN Publishes Practice Guideline on DMTs for MS
LOS ANGELES—Clinicians must engage in an ongoing dialogue with patients with multiple sclerosis (MS) regarding treatment decisions throughout the disease course, according to a new practice guideline from the American Academy of Ne
When considering therapy for a patient with MS, clinicians must take into account the patient’s preferences regarding safety, route of administration, lifestyle, cost, efficacy, common adverse events, and tolerability, the guideline says.
The guideline—which includes 30 recommendations related to starting, switching, and stopping DMTs—“emphasizes that you need to have that discussion with patients, but it does not say for an individual which drug you should take,” said guideline author Ruth Ann Marrie, MD, PhD, Professor of Neurology and Community Health Sciences at the University of Manitoba in Winnipeg. “It provides information about the available therapies so that each clinician–patient dyad can use information specific to that patient to make the best decision for that particular scenario.”

The guideline was presented at the 70th Annual Meeting of the AAN and published in the April 24 issue of Neurology. It was endorsed by the MS Association of America and the National MS Society.
Therapeutic Advances
Neurologists have “little evidence to decide which drug to use at what time,” said lead guideline author Alexander Rae-Grant, MD, Professor of Neurology at the Cleveland Clinic.
The previous AAN clinical practice guideline on DMTs in MS, published in 2002, reviewed the injectable medications that were approved for MS at the time, such as interferon beta-1b, interferon beta-1a, and glatiramer acetate. Since then, “the treatment landscape has changed considerably … with more than 17 medications currently approved and widely prescribed for treating MS in the United States,” the authors said. “As a result, clinicians and people with MS may now choose from several medications with differing mechanisms of action, risk profiles, and monitoring requirements.” Clinicians must balance the potential therapeutic benefits and risks of a medication and the long-term risk of MS-related morbidity.

Since the 2002 guideline was published, studies have evaluated the treatment of patients with a first episode of demyelination, Dr. Rae-Grant said. “We now know that treating earlier is better, in terms of reducing the number of new relapses,” which reduces the risk of further brain injury, he said.
For people with highly active MS, clinicians should prescribe alemtuzumab, fingolimod, or natalizumab (Level B recommendation), according to the guideline. In addition, the guideline discusses pregnancy planning, setting realistic treatment expectations, and managing the risk of progressive multifocal leukoencephalopathy (PML). It mentions off-label options and support programs for people who are unable to afford approved DMTs.
Methods and Limitations
To assess evidence for starting, switching, and stopping DMTs for MS and develop relevant recommendations, the guideline authors surveyed peer-reviewed research articles, systematic reviews, and abstracts that they identified searching MEDLINE, CENTRAL, and EMBASE through November 2016. They selected 20 Cochrane reviews and 73 articles for data extraction and rated the studies using the AAN therapeutic classification of evidence scheme. The authors made recommendations using a modified Delphi process.
The guideline largely is based on trial data, which may limit the generalizability of the results to real-world populations, the authors noted. In addition, they anticipate that new research in the rapidly changing field of MS treatment will necessitate updates to the recommendations.
Future studies of DMTs for MS should address gaps in knowledge about long-term outcomes, safety in patients with comorbidities, predictive markers for patient response to treatment, treatment strategies for the initial management of MS, DMT use in pregnant women, and outcomes after stopping DMTs, according to the guideline. Neurologists also need evidence about the effect of DMTs on measures that are important to patients, but are not standard trial outcomes, such as cognition, fatigue, urinary urgency, pain, and visual function.
Navigating a Complex Landscape
The recommendations and systematic review of the evidence “reflect the complexity of MS management in the current treatment era,” said Tanuja Chitnis, MD, of Partners MS Center at Brigham and Women’s Hospital in Boston, and colleagues, in an accompanying editorial. “These statements serve as guidelines for MS patient care; however, they do not replace the clinician–patient relationship on which the most informed decision rests.”
The summary of more than 50 trials “provides a useful scale that can inform clinical decisions,” Dr. Chitnis and colleagues said. Certain drugs that were found to have limited evidence in the systematic review nevertheless “are in common clinical use … based on scientific principles and clinical acumen,” they said. In addition, the guideline reviews the evidence for combination therapies that rarely are used in clinical practice, which “may confuse the casual reader,” the editorialists noted.
“The experienced MS clinician … is needed to help guide patients through this complex landscape,” Dr. Chitnis and colleagues said. “The revised AAN guidelines are a starting point for the use of the multiple treatments now available for MS; however, further work is needed to further refine the choices appropriate for the individual patient.”
—Jake Remaly
Suggested Reading
Chitnis T, Giovannoni G, Trojano M. Complexity of MS management in the current treatment era. Neurology. 2018;90(17):761-762.
Corboy JR, Weinshenker BG, Wingerchuk DM. Comment on 2018 American Academy of Neurology guidelines on disease-modifying therapies in MS. Neurology. 2018 Apr 23 [Epub ahead of print].
Rae-Grant A, Day GS, Marrie RA, et al. Comprehensive systematic review summary: Disease-modifying therapies for adults with multiple sclerosis. Neurology. 2018;90(17):789-800.
Rae-Grant A, Day GS, Marrie RA, et al. Practice guideline recommendations summary: Disease-modifying therapies for adults with multiple sclerosis. Neurology. 2018;90(17):777-788.
LOS ANGELES—Clinicians must engage in an ongoing dialogue with patients with multiple sclerosis (MS) regarding treatment decisions throughout the disease course, according to a new practice guideline from the American Academy of Ne
When considering therapy for a patient with MS, clinicians must take into account the patient’s preferences regarding safety, route of administration, lifestyle, cost, efficacy, common adverse events, and tolerability, the guideline says.
The guideline—which includes 30 recommendations related to starting, switching, and stopping DMTs—“emphasizes that you need to have that discussion with patients, but it does not say for an individual which drug you should take,” said guideline author Ruth Ann Marrie, MD, PhD, Professor of Neurology and Community Health Sciences at the University of Manitoba in Winnipeg. “It provides information about the available therapies so that each clinician–patient dyad can use information specific to that patient to make the best decision for that particular scenario.”
The guideline was presented at the 70th Annual Meeting of the AAN and published in the April 24 issue of Neurology. It was endorsed by the MS Association of America and the National MS Society.
Therapeutic Advances
Neurologists have “little evidence to decide which drug to use at what time,” said lead guideline author Alexander Rae-Grant, MD, Professor of Neurology at the Cleveland Clinic.
The previous AAN clinical practice guideline on DMTs in MS, published in 2002, reviewed the injectable medications that were approved for MS at the time, such as interferon beta-1b, interferon beta-1a, and glatiramer acetate. Since then, “the treatment landscape has changed considerably … with more than 17 medications currently approved and widely prescribed for treating MS in the United States,” the authors said. “As a result, clinicians and people with MS may now choose from several medications with differing mechanisms of action, risk profiles, and monitoring requirements.” Clinicians must balance the potential therapeutic benefits and risks of a medication and the long-term risk of MS-related morbidity.
Since the 2002 guideline was published, studies have evaluated the treatment of patients with a first episode of demyelination, Dr. Rae-Grant said. “We now know that treating earlier is better, in terms of reducing the number of new relapses,” which reduces the risk of further brain injury, he said.
For people with highly active MS, clinicians should prescribe alemtuzumab, fingolimod, or natalizumab (Level B recommendation), according to the guideline. In addition, the guideline discusses pregnancy planning, setting realistic treatment expectations, and managing the risk of progressive multifocal leukoencephalopathy (PML). It mentions off-label options and support programs for people who are unable to afford approved DMTs.
Methods and Limitations
To assess evidence for starting, switching, and stopping DMTs for MS and develop relevant recommendations, the guideline authors surveyed peer-reviewed research articles, systematic reviews, and abstracts that they identified searching MEDLINE, CENTRAL, and EMBASE through November 2016. They selected 20 Cochrane reviews and 73 articles for data extraction and rated the studies using the AAN therapeutic classification of evidence scheme. The authors made recommendations using a modified Delphi process.
The guideline largely is based on trial data, which may limit the generalizability of the results to real-world populations, the authors noted. In addition, they anticipate that new research in the rapidly changing field of MS treatment will necessitate updates to the recommendations.
Future studies of DMTs for MS should address gaps in knowledge about long-term outcomes, safety in patients with comorbidities, predictive markers for patient response to treatment, treatment strategies for the initial management of MS, DMT use in pregnant women, and outcomes after stopping DMTs, according to the guideline. Neurologists also need evidence about the effect of DMTs on measures that are important to patients, but are not standard trial outcomes, such as cognition, fatigue, urinary urgency, pain, and visual function.
Navigating a Complex Landscape
The recommendations and systematic review of the evidence “reflect the complexity of MS management in the current treatment era,” said Tanuja Chitnis, MD, of Partners MS Center at Brigham and Women’s Hospital in Boston, and colleagues, in an accompanying editorial. “These statements serve as guidelines for MS patient care; however, they do not replace the clinician–patient relationship on which the most informed decision rests.”
The summary of more than 50 trials “provides a useful scale that can inform clinical decisions,” Dr. Chitnis and colleagues said. Certain drugs that were found to have limited evidence in the systematic review nevertheless “are in common clinical use … based on scientific principles and clinical acumen,” they said. In addition, the guideline reviews the evidence for combination therapies that rarely are used in clinical practice, which “may confuse the casual reader,” the editorialists noted.
“The experienced MS clinician … is needed to help guide patients through this complex landscape,” Dr. Chitnis and colleagues said. “The revised AAN guidelines are a starting point for the use of the multiple treatments now available for MS; however, further work is needed to further refine the choices appropriate for the individual patient.”
—Jake Remaly
Suggested Reading
Chitnis T, Giovannoni G, Trojano M. Complexity of MS management in the current treatment era. Neurology. 2018;90(17):761-762.
Corboy JR, Weinshenker BG, Wingerchuk DM. Comment on 2018 American Academy of Neurology guidelines on disease-modifying therapies in MS. Neurology. 2018 Apr 23 [Epub ahead of print].
Rae-Grant A, Day GS, Marrie RA, et al. Comprehensive systematic review summary: Disease-modifying therapies for adults with multiple sclerosis. Neurology. 2018;90(17):789-800.
Rae-Grant A, Day GS, Marrie RA, et al. Practice guideline recommendations summary: Disease-modifying therapies for adults with multiple sclerosis. Neurology. 2018;90(17):777-788.
LOS ANGELES—Clinicians must engage in an ongoing dialogue with patients with multiple sclerosis (MS) regarding treatment decisions throughout the disease course, according to a new practice guideline from the American Academy of Ne
When considering therapy for a patient with MS, clinicians must take into account the patient’s preferences regarding safety, route of administration, lifestyle, cost, efficacy, common adverse events, and tolerability, the guideline says.
The guideline—which includes 30 recommendations related to starting, switching, and stopping DMTs—“emphasizes that you need to have that discussion with patients, but it does not say for an individual which drug you should take,” said guideline author Ruth Ann Marrie, MD, PhD, Professor of Neurology and Community Health Sciences at the University of Manitoba in Winnipeg. “It provides information about the available therapies so that each clinician–patient dyad can use information specific to that patient to make the best decision for that particular scenario.”
The guideline was presented at the 70th Annual Meeting of the AAN and published in the April 24 issue of Neurology. It was endorsed by the MS Association of America and the National MS Society.
Therapeutic Advances
Neurologists have “little evidence to decide which drug to use at what time,” said lead guideline author Alexander Rae-Grant, MD, Professor of Neurology at the Cleveland Clinic.
The previous AAN clinical practice guideline on DMTs in MS, published in 2002, reviewed the injectable medications that were approved for MS at the time, such as interferon beta-1b, interferon beta-1a, and glatiramer acetate. Since then, “the treatment landscape has changed considerably … with more than 17 medications currently approved and widely prescribed for treating MS in the United States,” the authors said. “As a result, clinicians and people with MS may now choose from several medications with differing mechanisms of action, risk profiles, and monitoring requirements.” Clinicians must balance the potential therapeutic benefits and risks of a medication and the long-term risk of MS-related morbidity.
Since the 2002 guideline was published, studies have evaluated the treatment of patients with a first episode of demyelination, Dr. Rae-Grant said. “We now know that treating earlier is better, in terms of reducing the number of new relapses,” which reduces the risk of further brain injury, he said.
For people with highly active MS, clinicians should prescribe alemtuzumab, fingolimod, or natalizumab (Level B recommendation), according to the guideline. In addition, the guideline discusses pregnancy planning, setting realistic treatment expectations, and managing the risk of progressive multifocal leukoencephalopathy (PML). It mentions off-label options and support programs for people who are unable to afford approved DMTs.
Methods and Limitations
To assess evidence for starting, switching, and stopping DMTs for MS and develop relevant recommendations, the guideline authors surveyed peer-reviewed research articles, systematic reviews, and abstracts that they identified searching MEDLINE, CENTRAL, and EMBASE through November 2016. They selected 20 Cochrane reviews and 73 articles for data extraction and rated the studies using the AAN therapeutic classification of evidence scheme. The authors made recommendations using a modified Delphi process.
The guideline largely is based on trial data, which may limit the generalizability of the results to real-world populations, the authors noted. In addition, they anticipate that new research in the rapidly changing field of MS treatment will necessitate updates to the recommendations.
Future studies of DMTs for MS should address gaps in knowledge about long-term outcomes, safety in patients with comorbidities, predictive markers for patient response to treatment, treatment strategies for the initial management of MS, DMT use in pregnant women, and outcomes after stopping DMTs, according to the guideline. Neurologists also need evidence about the effect of DMTs on measures that are important to patients, but are not standard trial outcomes, such as cognition, fatigue, urinary urgency, pain, and visual function.
Navigating a Complex Landscape
The recommendations and systematic review of the evidence “reflect the complexity of MS management in the current treatment era,” said Tanuja Chitnis, MD, of Partners MS Center at Brigham and Women’s Hospital in Boston, and colleagues, in an accompanying editorial. “These statements serve as guidelines for MS patient care; however, they do not replace the clinician–patient relationship on which the most informed decision rests.”
The summary of more than 50 trials “provides a useful scale that can inform clinical decisions,” Dr. Chitnis and colleagues said. Certain drugs that were found to have limited evidence in the systematic review nevertheless “are in common clinical use … based on scientific principles and clinical acumen,” they said. In addition, the guideline reviews the evidence for combination therapies that rarely are used in clinical practice, which “may confuse the casual reader,” the editorialists noted.
“The experienced MS clinician … is needed to help guide patients through this complex landscape,” Dr. Chitnis and colleagues said. “The revised AAN guidelines are a starting point for the use of the multiple treatments now available for MS; however, further work is needed to further refine the choices appropriate for the individual patient.”
—Jake Remaly
Suggested Reading
Chitnis T, Giovannoni G, Trojano M. Complexity of MS management in the current treatment era. Neurology. 2018;90(17):761-762.
Corboy JR, Weinshenker BG, Wingerchuk DM. Comment on 2018 American Academy of Neurology guidelines on disease-modifying therapies in MS. Neurology. 2018 Apr 23 [Epub ahead of print].
Rae-Grant A, Day GS, Marrie RA, et al. Comprehensive systematic review summary: Disease-modifying therapies for adults with multiple sclerosis. Neurology. 2018;90(17):789-800.
Rae-Grant A, Day GS, Marrie RA, et al. Practice guideline recommendations summary: Disease-modifying therapies for adults with multiple sclerosis. Neurology. 2018;90(17):777-788.
Eye-opening findings cast spondyloarthritis in new light, expert says
SANDESTIN, FLA. – Recent findings have led to eye-opening results in the axial spondyloarthritis (SpA) field, including a surprisingly high number of patients with inflammatory back pain who don’t progress to the disease, healthy people who develop SpA-like details on imaging, and significant gender differences in the efficacy of biologic therapy, said Arthur Kavanaugh, MD, professor of medicine at the University of California, San Diego.
The findings could lead clinicians to see the disease differently and consult with patients in new ways, he said.

Just over 20% of the patients progressed to SpA within 5 years, and about 30% over 15 years. But after 5 years, the condition resolved in over 30% of patients – and after 15 years, it resolved in almost half.
In about 5% of patients, symptoms persisted but the condition remained unidentified.
“A lot of people with inflammatory back pain, it doesn’t continue to be an issue – this goes out a decade and a half,” Dr. Kavanaugh said. “I was surprised with this. I would have guess that over this many years, more people would have developed ankylosing spondylitis, but they don’t.”
He said that clinicians should cite this information in their discussions with patients. They should review their case and evaluate spinal symptoms, but let them know that the condition might not progress and might not be permanent.
“I would use this information and say, ‘Well you’re having inflammatory back pain, but let’s go review things,’ ” he said. “ ‘If you don’t have the true spondyloarthropathy or ankylosing spondylitis now, there’s a chance that this will go away. It’s almost 50-50, or we still don’t know what it is even if you’re having some symptoms (after 15 years).’ ”
Other important findings underscore the need for a complete clinical picture rather than just findings on imaging for an axial SpA diagnosis, Dr. Kavanaugh said. Researchers examined MRI images of new military recruits who were healthy with no back pain (Rheumatology [Oxford]. 2018 Mar 1;57[3]:508-13). They found that 23% of them at baseline – and 37% after strenuous training – had MRI findings that would qualify as positive for spondyloarthritis by Assessment of Spondyloarthritis international Society criteria. But they wouldn’t meet the definition of disease.
More recent findings showed similar results in imaging of healthy runners and hockey players (Arthritis Rheumatol. 2018 May;70[5]:736-45), with 30%-40% of them having MRI findings that would be considered positive on ASAS, Dr. Kavanaugh said.
“These were just people who were out stressing their joints,” he said. “We were super excited at the start of having MRI because now we can look and evaluate the activity within a joint. But I think, like everything, we have to take it with a little bit of caution. Just in and of itself, without the clinical picture, it does not diagnose axial spondyloarthropathy.”
In another recent study, women with axial SpA were found to have significantly lower responses over time than men with axial SpA (J Rheumatol. 2018 Feb;45[2]:195-201). Dr. Kavanaugh said that there might be some selection bias because of the higher male prevalence of disease but said the findings were noteworthy, especially in light of findings in animal models suggesting gender differences in disease expression and response to treatment.
“I think this is fascinating,” he said. “I think there’s a lot more to come for this.”
Dr. Kavanaugh reported financial relationships with AbbVie, Amgen, AstraZeneca, Bristol-Myers Squibb, Celgene, Gilead, Genentech, Novartis, Pfizer, and other companies.
SANDESTIN, FLA. – Recent findings have led to eye-opening results in the axial spondyloarthritis (SpA) field, including a surprisingly high number of patients with inflammatory back pain who don’t progress to the disease, healthy people who develop SpA-like details on imaging, and significant gender differences in the efficacy of biologic therapy, said Arthur Kavanaugh, MD, professor of medicine at the University of California, San Diego.
The findings could lead clinicians to see the disease differently and consult with patients in new ways, he said.
Just over 20% of the patients progressed to SpA within 5 years, and about 30% over 15 years. But after 5 years, the condition resolved in over 30% of patients – and after 15 years, it resolved in almost half.
In about 5% of patients, symptoms persisted but the condition remained unidentified.
“A lot of people with inflammatory back pain, it doesn’t continue to be an issue – this goes out a decade and a half,” Dr. Kavanaugh said. “I was surprised with this. I would have guess that over this many years, more people would have developed ankylosing spondylitis, but they don’t.”
He said that clinicians should cite this information in their discussions with patients. They should review their case and evaluate spinal symptoms, but let them know that the condition might not progress and might not be permanent.
“I would use this information and say, ‘Well you’re having inflammatory back pain, but let’s go review things,’ ” he said. “ ‘If you don’t have the true spondyloarthropathy or ankylosing spondylitis now, there’s a chance that this will go away. It’s almost 50-50, or we still don’t know what it is even if you’re having some symptoms (after 15 years).’ ”
Other important findings underscore the need for a complete clinical picture rather than just findings on imaging for an axial SpA diagnosis, Dr. Kavanaugh said. Researchers examined MRI images of new military recruits who were healthy with no back pain (Rheumatology [Oxford]. 2018 Mar 1;57[3]:508-13). They found that 23% of them at baseline – and 37% after strenuous training – had MRI findings that would qualify as positive for spondyloarthritis by Assessment of Spondyloarthritis international Society criteria. But they wouldn’t meet the definition of disease.
More recent findings showed similar results in imaging of healthy runners and hockey players (Arthritis Rheumatol. 2018 May;70[5]:736-45), with 30%-40% of them having MRI findings that would be considered positive on ASAS, Dr. Kavanaugh said.
“These were just people who were out stressing their joints,” he said. “We were super excited at the start of having MRI because now we can look and evaluate the activity within a joint. But I think, like everything, we have to take it with a little bit of caution. Just in and of itself, without the clinical picture, it does not diagnose axial spondyloarthropathy.”
In another recent study, women with axial SpA were found to have significantly lower responses over time than men with axial SpA (J Rheumatol. 2018 Feb;45[2]:195-201). Dr. Kavanaugh said that there might be some selection bias because of the higher male prevalence of disease but said the findings were noteworthy, especially in light of findings in animal models suggesting gender differences in disease expression and response to treatment.
“I think this is fascinating,” he said. “I think there’s a lot more to come for this.”
Dr. Kavanaugh reported financial relationships with AbbVie, Amgen, AstraZeneca, Bristol-Myers Squibb, Celgene, Gilead, Genentech, Novartis, Pfizer, and other companies.
SANDESTIN, FLA. – Recent findings have led to eye-opening results in the axial spondyloarthritis (SpA) field, including a surprisingly high number of patients with inflammatory back pain who don’t progress to the disease, healthy people who develop SpA-like details on imaging, and significant gender differences in the efficacy of biologic therapy, said Arthur Kavanaugh, MD, professor of medicine at the University of California, San Diego.
The findings could lead clinicians to see the disease differently and consult with patients in new ways, he said.
Just over 20% of the patients progressed to SpA within 5 years, and about 30% over 15 years. But after 5 years, the condition resolved in over 30% of patients – and after 15 years, it resolved in almost half.
In about 5% of patients, symptoms persisted but the condition remained unidentified.
“A lot of people with inflammatory back pain, it doesn’t continue to be an issue – this goes out a decade and a half,” Dr. Kavanaugh said. “I was surprised with this. I would have guess that over this many years, more people would have developed ankylosing spondylitis, but they don’t.”
He said that clinicians should cite this information in their discussions with patients. They should review their case and evaluate spinal symptoms, but let them know that the condition might not progress and might not be permanent.
“I would use this information and say, ‘Well you’re having inflammatory back pain, but let’s go review things,’ ” he said. “ ‘If you don’t have the true spondyloarthropathy or ankylosing spondylitis now, there’s a chance that this will go away. It’s almost 50-50, or we still don’t know what it is even if you’re having some symptoms (after 15 years).’ ”
Other important findings underscore the need for a complete clinical picture rather than just findings on imaging for an axial SpA diagnosis, Dr. Kavanaugh said. Researchers examined MRI images of new military recruits who were healthy with no back pain (Rheumatology [Oxford]. 2018 Mar 1;57[3]:508-13). They found that 23% of them at baseline – and 37% after strenuous training – had MRI findings that would qualify as positive for spondyloarthritis by Assessment of Spondyloarthritis international Society criteria. But they wouldn’t meet the definition of disease.
More recent findings showed similar results in imaging of healthy runners and hockey players (Arthritis Rheumatol. 2018 May;70[5]:736-45), with 30%-40% of them having MRI findings that would be considered positive on ASAS, Dr. Kavanaugh said.
“These were just people who were out stressing their joints,” he said. “We were super excited at the start of having MRI because now we can look and evaluate the activity within a joint. But I think, like everything, we have to take it with a little bit of caution. Just in and of itself, without the clinical picture, it does not diagnose axial spondyloarthropathy.”
In another recent study, women with axial SpA were found to have significantly lower responses over time than men with axial SpA (J Rheumatol. 2018 Feb;45[2]:195-201). Dr. Kavanaugh said that there might be some selection bias because of the higher male prevalence of disease but said the findings were noteworthy, especially in light of findings in animal models suggesting gender differences in disease expression and response to treatment.
“I think this is fascinating,” he said. “I think there’s a lot more to come for this.”
Dr. Kavanaugh reported financial relationships with AbbVie, Amgen, AstraZeneca, Bristol-Myers Squibb, Celgene, Gilead, Genentech, Novartis, Pfizer, and other companies.
EXPERT ANALYSIS FROM CCR 18
Can a Finger Displacement Test Help Assess Parkinson’s Disease Dementia?
LOS ANGELES—A simple test of finger displacement may distinguish between Parkinson’s disease dementia and Alzheimer’s disease and help neurologists assess the progression of dementia in Parkinson’s disease, according to a study presented at the 70th Annual Meeting of the American Academy of Neurology.
Parkinson’s disease dementia is one of the most disabling nonmotor complications of Parkinson’s disease, but “there is no simple bedside test available that can measure the progression of dementia,” said Aman Deep, MD, a neurology resident at the University of Tennessee Health Science Center in Memphis, and colleagues.

To study the clinical utility of finger displacement in patients with dementia, Dr. Deep and colleagues examined 56 patients with Parkinson’s disease dementia and 35 patients with Alzheimer’s disease. The patients pointed their index fingers toward a grid ruler. After maintaining the pointing position for 15 seconds, patients were asked to close their eyes for another 15 seconds while maintaining the same position. A positive result was downward index finger displacement of 5 cm or greater while patients had their eyes closed.
The patients with Parkinson’s disease dementia (42 male; mean age, 75) had a mean Parkinson’s disease duration of 9.1 years, a mean dementia duration of 3.1 years, and a mean Unified Parkinson’s Disease Rating Scale score of 37. The group’s mean Mini-Mental State Examination (MMSE) score was 17.5. Fifty-three patients out of 56 (95%) exhibited bilateral downward drift of 5 cm or greater, and three patients exhibited less than 5 cm of downward drift. The mean bilateral downward finger drift was 6.8 cm for the group.
Among patients with Alzheimer’s disease (21 male; mean age, 77.4), the mean dementia duration was 3.9 years. The group’s mean MMSE score was 17.8. In the Alzheimer’s disease group, only one patient had minimal drift, and the group’s mean bilateral downward drift was 0.2 cm.
According to the researchers, the finger displacement test has a sensitivity of 100% and a specificity of 92.1%. “Downward finger displacement, especially bilateral downward displacement, may signal extensive disruption of subcortical–cortical circuits,” Dr. Deep and colleagues said. “The simple and inexpensive bedside test of finger displacement may be used to help distinguish Parkinson’s disease dementia from Alzheimer’s disease.”
—Jake Remaly
Suggested Reading
Lieberman A, Deep A, Shi J, et al. Downward finger displacement distinguishes Parkinson disease dementia from Alzheimer disease. Int J Neurosci. 2018;128(2):151-154.
LOS ANGELES—A simple test of finger displacement may distinguish between Parkinson’s disease dementia and Alzheimer’s disease and help neurologists assess the progression of dementia in Parkinson’s disease, according to a study presented at the 70th Annual Meeting of the American Academy of Neurology.
Parkinson’s disease dementia is one of the most disabling nonmotor complications of Parkinson’s disease, but “there is no simple bedside test available that can measure the progression of dementia,” said Aman Deep, MD, a neurology resident at the University of Tennessee Health Science Center in Memphis, and colleagues.
To study the clinical utility of finger displacement in patients with dementia, Dr. Deep and colleagues examined 56 patients with Parkinson’s disease dementia and 35 patients with Alzheimer’s disease. The patients pointed their index fingers toward a grid ruler. After maintaining the pointing position for 15 seconds, patients were asked to close their eyes for another 15 seconds while maintaining the same position. A positive result was downward index finger displacement of 5 cm or greater while patients had their eyes closed.
The patients with Parkinson’s disease dementia (42 male; mean age, 75) had a mean Parkinson’s disease duration of 9.1 years, a mean dementia duration of 3.1 years, and a mean Unified Parkinson’s Disease Rating Scale score of 37. The group’s mean Mini-Mental State Examination (MMSE) score was 17.5. Fifty-three patients out of 56 (95%) exhibited bilateral downward drift of 5 cm or greater, and three patients exhibited less than 5 cm of downward drift. The mean bilateral downward finger drift was 6.8 cm for the group.
Among patients with Alzheimer’s disease (21 male; mean age, 77.4), the mean dementia duration was 3.9 years. The group’s mean MMSE score was 17.8. In the Alzheimer’s disease group, only one patient had minimal drift, and the group’s mean bilateral downward drift was 0.2 cm.
According to the researchers, the finger displacement test has a sensitivity of 100% and a specificity of 92.1%. “Downward finger displacement, especially bilateral downward displacement, may signal extensive disruption of subcortical–cortical circuits,” Dr. Deep and colleagues said. “The simple and inexpensive bedside test of finger displacement may be used to help distinguish Parkinson’s disease dementia from Alzheimer’s disease.”
—Jake Remaly
Suggested Reading
Lieberman A, Deep A, Shi J, et al. Downward finger displacement distinguishes Parkinson disease dementia from Alzheimer disease. Int J Neurosci. 2018;128(2):151-154.
LOS ANGELES—A simple test of finger displacement may distinguish between Parkinson’s disease dementia and Alzheimer’s disease and help neurologists assess the progression of dementia in Parkinson’s disease, according to a study presented at the 70th Annual Meeting of the American Academy of Neurology.
Parkinson’s disease dementia is one of the most disabling nonmotor complications of Parkinson’s disease, but “there is no simple bedside test available that can measure the progression of dementia,” said Aman Deep, MD, a neurology resident at the University of Tennessee Health Science Center in Memphis, and colleagues.
To study the clinical utility of finger displacement in patients with dementia, Dr. Deep and colleagues examined 56 patients with Parkinson’s disease dementia and 35 patients with Alzheimer’s disease. The patients pointed their index fingers toward a grid ruler. After maintaining the pointing position for 15 seconds, patients were asked to close their eyes for another 15 seconds while maintaining the same position. A positive result was downward index finger displacement of 5 cm or greater while patients had their eyes closed.
The patients with Parkinson’s disease dementia (42 male; mean age, 75) had a mean Parkinson’s disease duration of 9.1 years, a mean dementia duration of 3.1 years, and a mean Unified Parkinson’s Disease Rating Scale score of 37. The group’s mean Mini-Mental State Examination (MMSE) score was 17.5. Fifty-three patients out of 56 (95%) exhibited bilateral downward drift of 5 cm or greater, and three patients exhibited less than 5 cm of downward drift. The mean bilateral downward finger drift was 6.8 cm for the group.
Among patients with Alzheimer’s disease (21 male; mean age, 77.4), the mean dementia duration was 3.9 years. The group’s mean MMSE score was 17.8. In the Alzheimer’s disease group, only one patient had minimal drift, and the group’s mean bilateral downward drift was 0.2 cm.
According to the researchers, the finger displacement test has a sensitivity of 100% and a specificity of 92.1%. “Downward finger displacement, especially bilateral downward displacement, may signal extensive disruption of subcortical–cortical circuits,” Dr. Deep and colleagues said. “The simple and inexpensive bedside test of finger displacement may be used to help distinguish Parkinson’s disease dementia from Alzheimer’s disease.”
—Jake Remaly
Suggested Reading
Lieberman A, Deep A, Shi J, et al. Downward finger displacement distinguishes Parkinson disease dementia from Alzheimer disease. Int J Neurosci. 2018;128(2):151-154.
Kawasaki disease: New info to enhance our index of suspicion
Most U.S. mainland pediatric practitioners will see only one or two cases of Kawasaki disease (KD) in their careers, but no one wants to miss even one case.
Making the diagnosis as early as possible is important to reduce the chance of sequelae, particularly the coronary artery aneurysms that will eventually lead to 5% of overall acute coronary syndromes in adults. And because there is no “KD test,” or sometimes incomplete KD. And there are some new data that complicate this. Despite the recently updated 2017 guideline,1 most cases end up being confirmed and managed by regional “experts.” But nearly all of the approximately 6,000 KD cases/year in U.S. children younger than 5 years old start out with one or more primary care, urgent care, or ED visits.
This means that every clinician in the trenches not only needs a high index of suspicion but also needs to be at least a partial expert, too. What raises our index of suspicion? Classic data tell us we need 5 consecutive days of fever plus four or five other principal clinical findings for a KD diagnosis. The principal findings are:
1. Eyes: Bilateral bulbar nonexudative conjunctival injection.
2. Mouth: Erythema of oral/pharyngeal mucosa or cracked lips or strawberry tongue or oral mucositis.
3. Rash.
4. Hands or feet findings: Swelling/erythema or later periungual desquamation.
5. Cervical adenopathy greater than 1.4 cm, usually unilateral.
Other factors that have classically increased suspicion are winter/early spring presentation in North America, male gender (1.5:1 ratio to females), and Asian (particularly Japanese) ancestry. The importance of genetics was initially based on epidemiology (Japan/Asian risk) but lately has been further associated with six gene polymorphisms. However, molecular genetic testing is not currently a practical tool.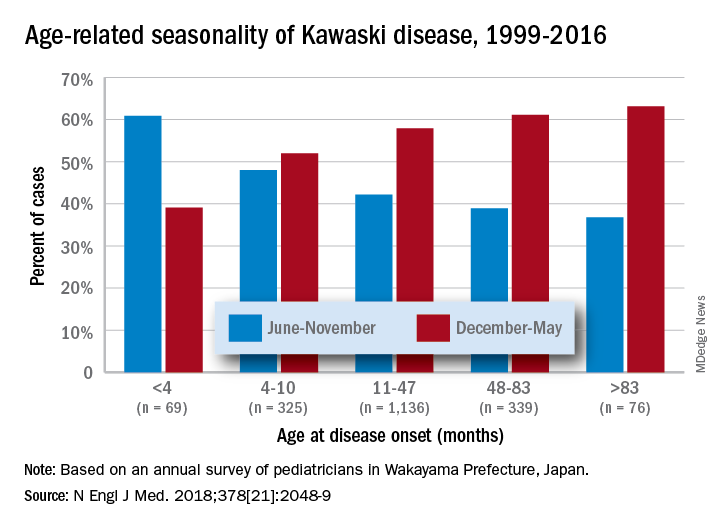
Clinical scenarios that also should raise suspicion include less-than-6-month-old infants with prolonged fever/irritability (may be the only clinical manifestations of KD) and children over 4 years old who more often may have incomplete KD. Both groups have higher prevalence of coronary artery abnormalities. Other high suspicion scenarios include prolonged fever with unexplained/culture-negative shock, or antibiotic treatment failure for cervical adenitis or retro/parapharyngeal phlegmon. Consultation with or referral to a regional KD expert may be needed.
Fuzzy KD math
Current guidelines list an exception to the 5-day fever requirement in that only 4 days of fever are needed with four or more principal clinical features, particularly when hand and feet findings exist. Some call this the “4X4 exception.” Then there is a sub-caveat: “Experienced clinicians who have treated many patients with KD may establish the diagnosis with 3 days of fever in rare cases.”1
Incomplete KD
This is another exception, which seems to be a more frequent diagnosis in the past decade. Incomplete KD requires the 5 days of fever duration plus an elevated C-reactive protein or erythrocyte sedimentation rate. But one needs only two or three of the five principal clinical KD criteria plus three or more of six other laboratory findings (anemia, low albumin, leukocytosis, thrombocytosis, pyuria, or elevated alanine aminotransferase). Incomplete KD can be confirmed by an abnormal echocardiogram – usually not until after 7 days of KD symptoms.1
New KD nuances
In a recent report on 20 years of data from Japan (n = 1,945 KD cases), more granularity on age, seasonal epidemiology, and outcome were seen.2 There was an inverse correlation of male predominance to age, i.e. as age groups got older, there was a gradual shift to female predominance by 7 years of age. The winter/spring predominance (60% of overall cases) did not hold true in younger age groups where summer/fall was the peak season (65% of cases).

With the goal of not missing any KD and diagnosing as early as possible to limit sequelae, we all need to be relative experts and keep alert for clinical scenarios that warrant our raising our index of suspicion. But now the seasonality trends appear blurred in the youngest cases and the male predominance is blurred in the oldest cases. And remember that fever and irritability for longer than 7 days in young infants may be the only clue to KD.
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics, Kansas City, Mo. He said he had no relevant financial disclosures. Email him at [email protected].
References
1. Circulation. 2017 Mar 29. doi: 10.1161/CIR.0000000000000484
2. N Engl J Med. 2018 May 24. doi: 10.1056/NEJMc1804312.
Most U.S. mainland pediatric practitioners will see only one or two cases of Kawasaki disease (KD) in their careers, but no one wants to miss even one case.
Making the diagnosis as early as possible is important to reduce the chance of sequelae, particularly the coronary artery aneurysms that will eventually lead to 5% of overall acute coronary syndromes in adults. And because there is no “KD test,” or sometimes incomplete KD. And there are some new data that complicate this. Despite the recently updated 2017 guideline,1 most cases end up being confirmed and managed by regional “experts.” But nearly all of the approximately 6,000 KD cases/year in U.S. children younger than 5 years old start out with one or more primary care, urgent care, or ED visits.
This means that every clinician in the trenches not only needs a high index of suspicion but also needs to be at least a partial expert, too. What raises our index of suspicion? Classic data tell us we need 5 consecutive days of fever plus four or five other principal clinical findings for a KD diagnosis. The principal findings are:
1. Eyes: Bilateral bulbar nonexudative conjunctival injection.
2. Mouth: Erythema of oral/pharyngeal mucosa or cracked lips or strawberry tongue or oral mucositis.
3. Rash.
4. Hands or feet findings: Swelling/erythema or later periungual desquamation.
5. Cervical adenopathy greater than 1.4 cm, usually unilateral.
Other factors that have classically increased suspicion are winter/early spring presentation in North America, male gender (1.5:1 ratio to females), and Asian (particularly Japanese) ancestry. The importance of genetics was initially based on epidemiology (Japan/Asian risk) but lately has been further associated with six gene polymorphisms. However, molecular genetic testing is not currently a practical tool.
Clinical scenarios that also should raise suspicion include less-than-6-month-old infants with prolonged fever/irritability (may be the only clinical manifestations of KD) and children over 4 years old who more often may have incomplete KD. Both groups have higher prevalence of coronary artery abnormalities. Other high suspicion scenarios include prolonged fever with unexplained/culture-negative shock, or antibiotic treatment failure for cervical adenitis or retro/parapharyngeal phlegmon. Consultation with or referral to a regional KD expert may be needed.
Fuzzy KD math
Current guidelines list an exception to the 5-day fever requirement in that only 4 days of fever are needed with four or more principal clinical features, particularly when hand and feet findings exist. Some call this the “4X4 exception.” Then there is a sub-caveat: “Experienced clinicians who have treated many patients with KD may establish the diagnosis with 3 days of fever in rare cases.”1
Incomplete KD
This is another exception, which seems to be a more frequent diagnosis in the past decade. Incomplete KD requires the 5 days of fever duration plus an elevated C-reactive protein or erythrocyte sedimentation rate. But one needs only two or three of the five principal clinical KD criteria plus three or more of six other laboratory findings (anemia, low albumin, leukocytosis, thrombocytosis, pyuria, or elevated alanine aminotransferase). Incomplete KD can be confirmed by an abnormal echocardiogram – usually not until after 7 days of KD symptoms.1
New KD nuances
In a recent report on 20 years of data from Japan (n = 1,945 KD cases), more granularity on age, seasonal epidemiology, and outcome were seen.2 There was an inverse correlation of male predominance to age, i.e. as age groups got older, there was a gradual shift to female predominance by 7 years of age. The winter/spring predominance (60% of overall cases) did not hold true in younger age groups where summer/fall was the peak season (65% of cases).
With the goal of not missing any KD and diagnosing as early as possible to limit sequelae, we all need to be relative experts and keep alert for clinical scenarios that warrant our raising our index of suspicion. But now the seasonality trends appear blurred in the youngest cases and the male predominance is blurred in the oldest cases. And remember that fever and irritability for longer than 7 days in young infants may be the only clue to KD.
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics, Kansas City, Mo. He said he had no relevant financial disclosures. Email him at [email protected].
References
1. Circulation. 2017 Mar 29. doi: 10.1161/CIR.0000000000000484
2. N Engl J Med. 2018 May 24. doi: 10.1056/NEJMc1804312.
Most U.S. mainland pediatric practitioners will see only one or two cases of Kawasaki disease (KD) in their careers, but no one wants to miss even one case.
Making the diagnosis as early as possible is important to reduce the chance of sequelae, particularly the coronary artery aneurysms that will eventually lead to 5% of overall acute coronary syndromes in adults. And because there is no “KD test,” or sometimes incomplete KD. And there are some new data that complicate this. Despite the recently updated 2017 guideline,1 most cases end up being confirmed and managed by regional “experts.” But nearly all of the approximately 6,000 KD cases/year in U.S. children younger than 5 years old start out with one or more primary care, urgent care, or ED visits.
This means that every clinician in the trenches not only needs a high index of suspicion but also needs to be at least a partial expert, too. What raises our index of suspicion? Classic data tell us we need 5 consecutive days of fever plus four or five other principal clinical findings for a KD diagnosis. The principal findings are:
1. Eyes: Bilateral bulbar nonexudative conjunctival injection.
2. Mouth: Erythema of oral/pharyngeal mucosa or cracked lips or strawberry tongue or oral mucositis.
3. Rash.
4. Hands or feet findings: Swelling/erythema or later periungual desquamation.
5. Cervical adenopathy greater than 1.4 cm, usually unilateral.
Other factors that have classically increased suspicion are winter/early spring presentation in North America, male gender (1.5:1 ratio to females), and Asian (particularly Japanese) ancestry. The importance of genetics was initially based on epidemiology (Japan/Asian risk) but lately has been further associated with six gene polymorphisms. However, molecular genetic testing is not currently a practical tool.
Clinical scenarios that also should raise suspicion include less-than-6-month-old infants with prolonged fever/irritability (may be the only clinical manifestations of KD) and children over 4 years old who more often may have incomplete KD. Both groups have higher prevalence of coronary artery abnormalities. Other high suspicion scenarios include prolonged fever with unexplained/culture-negative shock, or antibiotic treatment failure for cervical adenitis or retro/parapharyngeal phlegmon. Consultation with or referral to a regional KD expert may be needed.
Fuzzy KD math
Current guidelines list an exception to the 5-day fever requirement in that only 4 days of fever are needed with four or more principal clinical features, particularly when hand and feet findings exist. Some call this the “4X4 exception.” Then there is a sub-caveat: “Experienced clinicians who have treated many patients with KD may establish the diagnosis with 3 days of fever in rare cases.”1
Incomplete KD
This is another exception, which seems to be a more frequent diagnosis in the past decade. Incomplete KD requires the 5 days of fever duration plus an elevated C-reactive protein or erythrocyte sedimentation rate. But one needs only two or three of the five principal clinical KD criteria plus three or more of six other laboratory findings (anemia, low albumin, leukocytosis, thrombocytosis, pyuria, or elevated alanine aminotransferase). Incomplete KD can be confirmed by an abnormal echocardiogram – usually not until after 7 days of KD symptoms.1
New KD nuances
In a recent report on 20 years of data from Japan (n = 1,945 KD cases), more granularity on age, seasonal epidemiology, and outcome were seen.2 There was an inverse correlation of male predominance to age, i.e. as age groups got older, there was a gradual shift to female predominance by 7 years of age. The winter/spring predominance (60% of overall cases) did not hold true in younger age groups where summer/fall was the peak season (65% of cases).
With the goal of not missing any KD and diagnosing as early as possible to limit sequelae, we all need to be relative experts and keep alert for clinical scenarios that warrant our raising our index of suspicion. But now the seasonality trends appear blurred in the youngest cases and the male predominance is blurred in the oldest cases. And remember that fever and irritability for longer than 7 days in young infants may be the only clue to KD.
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics, Kansas City, Mo. He said he had no relevant financial disclosures. Email him at [email protected].
References
1. Circulation. 2017 Mar 29. doi: 10.1161/CIR.0000000000000484
2. N Engl J Med. 2018 May 24. doi: 10.1056/NEJMc1804312.
Simple bedside tool effectively detected sepsis in the ED
SAN DIEGO – The product of compared with the quick Sequential Organ Failure Assessment prompt, a small, single-center study showed.
“We know a lot about the pathophysiology of sepsis, but we don’t have great ways of identifying septic patients at an early stage,” lead study author David Lynch, MD, said in an interview at an international conference of the American Thoracic Society.
He noted that screening tools such as the quick Sequential Organ Failure Assessment and Systemic Inflammatory Response Syndrome criteria have a sensitivity of about 70% in detecting sepsis. “Over the last 10-15 years we’ve been able to find ways of improving outcomes in patients whom we confirm are septic with early antibiotics and fluids,” said Dr. Lynch, a second-year resident in the division of pulmonary and critical care medicine within the department of medicine at the University of North Carolina at Chapel Hill. “We know that in sepsis, systemic vascular resistance is decreased and cardiac output is increased. We tried to come up with a way of estimating cardiac output at the bedside by multiplying heart rate with pulse pressure, with the pulse pressure being the surrogate for stroke volume, which you can measure easily.”
In a cross-sectional, observational study, Dr. Lynch, senior author Thomas Bice, MD, and their associates reviewed the records of 116 patients who were admitted directly to the University of North Carolina’s medical ICU (MICU) from the UNC ED between Jan. 5, 2016, and June 30, 2017. The primary outcome of interest was culture-positive sepsis, and the primary exposure was the product of pulse pressure and heart rate. Patients were determined to be positive for sepsis if an infection was suspected (such as if blood cultures were drawn and antibiotics were started), the admitting physician suspected sepsis, and cultures were subsequently positive.
The average age of all patients was 53 years, 51% were female, the mortality rate was 12%, and the median length of stay was 4 days. A total of 25 of the 116 patients (22%) were positive for sepsis. The researchers observed that the pulse pressure multiplied by the heart rate was significantly higher in the culture-positive sepsis group, compared with controls (6,710 vs. 3,741, respectively; P less than .001).
Dr. Lynch and his associates found that, as a continuous variable, pulse pressure multiplied by the heart rate accurately classified 90% of sepsis cases (area under the receiver operator curve, 0.96; P less than .001). When using 5,000 as a cutoff, pulse pressure multiplied by the heart rate had a sensitivity of 100% and a specificity of 89% in detecting culture-positive sepsis. “We were surprised by how high the sensitivity was,” Dr. Lynch said. “The question is, will this translate to a larger cohort? And, would this be transferable to all patients in the ED, as opposed to the sicker patients who are going to the MICU?”
He and his associates plan to confirm the study’s results in a broader population of patients. “We don’t yet understand at what point in time this would be most applicable,” he added. “We looked at the first set of vitals when they came into the ED. We’d like to know if that applies to the second, third and fourth set of vitals, and whether it would be most useful to have an average of those.”
The study was supported in part by a grant from the National Institutes of Health. Dr. Lynch reported having no financial disclosures.
SAN DIEGO – The product of compared with the quick Sequential Organ Failure Assessment prompt, a small, single-center study showed.
“We know a lot about the pathophysiology of sepsis, but we don’t have great ways of identifying septic patients at an early stage,” lead study author David Lynch, MD, said in an interview at an international conference of the American Thoracic Society.
He noted that screening tools such as the quick Sequential Organ Failure Assessment and Systemic Inflammatory Response Syndrome criteria have a sensitivity of about 70% in detecting sepsis. “Over the last 10-15 years we’ve been able to find ways of improving outcomes in patients whom we confirm are septic with early antibiotics and fluids,” said Dr. Lynch, a second-year resident in the division of pulmonary and critical care medicine within the department of medicine at the University of North Carolina at Chapel Hill. “We know that in sepsis, systemic vascular resistance is decreased and cardiac output is increased. We tried to come up with a way of estimating cardiac output at the bedside by multiplying heart rate with pulse pressure, with the pulse pressure being the surrogate for stroke volume, which you can measure easily.”
In a cross-sectional, observational study, Dr. Lynch, senior author Thomas Bice, MD, and their associates reviewed the records of 116 patients who were admitted directly to the University of North Carolina’s medical ICU (MICU) from the UNC ED between Jan. 5, 2016, and June 30, 2017. The primary outcome of interest was culture-positive sepsis, and the primary exposure was the product of pulse pressure and heart rate. Patients were determined to be positive for sepsis if an infection was suspected (such as if blood cultures were drawn and antibiotics were started), the admitting physician suspected sepsis, and cultures were subsequently positive.
The average age of all patients was 53 years, 51% were female, the mortality rate was 12%, and the median length of stay was 4 days. A total of 25 of the 116 patients (22%) were positive for sepsis. The researchers observed that the pulse pressure multiplied by the heart rate was significantly higher in the culture-positive sepsis group, compared with controls (6,710 vs. 3,741, respectively; P less than .001).
Dr. Lynch and his associates found that, as a continuous variable, pulse pressure multiplied by the heart rate accurately classified 90% of sepsis cases (area under the receiver operator curve, 0.96; P less than .001). When using 5,000 as a cutoff, pulse pressure multiplied by the heart rate had a sensitivity of 100% and a specificity of 89% in detecting culture-positive sepsis. “We were surprised by how high the sensitivity was,” Dr. Lynch said. “The question is, will this translate to a larger cohort? And, would this be transferable to all patients in the ED, as opposed to the sicker patients who are going to the MICU?”
He and his associates plan to confirm the study’s results in a broader population of patients. “We don’t yet understand at what point in time this would be most applicable,” he added. “We looked at the first set of vitals when they came into the ED. We’d like to know if that applies to the second, third and fourth set of vitals, and whether it would be most useful to have an average of those.”
The study was supported in part by a grant from the National Institutes of Health. Dr. Lynch reported having no financial disclosures.
SAN DIEGO – The product of compared with the quick Sequential Organ Failure Assessment prompt, a small, single-center study showed.
“We know a lot about the pathophysiology of sepsis, but we don’t have great ways of identifying septic patients at an early stage,” lead study author David Lynch, MD, said in an interview at an international conference of the American Thoracic Society.
He noted that screening tools such as the quick Sequential Organ Failure Assessment and Systemic Inflammatory Response Syndrome criteria have a sensitivity of about 70% in detecting sepsis. “Over the last 10-15 years we’ve been able to find ways of improving outcomes in patients whom we confirm are septic with early antibiotics and fluids,” said Dr. Lynch, a second-year resident in the division of pulmonary and critical care medicine within the department of medicine at the University of North Carolina at Chapel Hill. “We know that in sepsis, systemic vascular resistance is decreased and cardiac output is increased. We tried to come up with a way of estimating cardiac output at the bedside by multiplying heart rate with pulse pressure, with the pulse pressure being the surrogate for stroke volume, which you can measure easily.”
In a cross-sectional, observational study, Dr. Lynch, senior author Thomas Bice, MD, and their associates reviewed the records of 116 patients who were admitted directly to the University of North Carolina’s medical ICU (MICU) from the UNC ED between Jan. 5, 2016, and June 30, 2017. The primary outcome of interest was culture-positive sepsis, and the primary exposure was the product of pulse pressure and heart rate. Patients were determined to be positive for sepsis if an infection was suspected (such as if blood cultures were drawn and antibiotics were started), the admitting physician suspected sepsis, and cultures were subsequently positive.
The average age of all patients was 53 years, 51% were female, the mortality rate was 12%, and the median length of stay was 4 days. A total of 25 of the 116 patients (22%) were positive for sepsis. The researchers observed that the pulse pressure multiplied by the heart rate was significantly higher in the culture-positive sepsis group, compared with controls (6,710 vs. 3,741, respectively; P less than .001).
Dr. Lynch and his associates found that, as a continuous variable, pulse pressure multiplied by the heart rate accurately classified 90% of sepsis cases (area under the receiver operator curve, 0.96; P less than .001). When using 5,000 as a cutoff, pulse pressure multiplied by the heart rate had a sensitivity of 100% and a specificity of 89% in detecting culture-positive sepsis. “We were surprised by how high the sensitivity was,” Dr. Lynch said. “The question is, will this translate to a larger cohort? And, would this be transferable to all patients in the ED, as opposed to the sicker patients who are going to the MICU?”
He and his associates plan to confirm the study’s results in a broader population of patients. “We don’t yet understand at what point in time this would be most applicable,” he added. “We looked at the first set of vitals when they came into the ED. We’d like to know if that applies to the second, third and fourth set of vitals, and whether it would be most useful to have an average of those.”
The study was supported in part by a grant from the National Institutes of Health. Dr. Lynch reported having no financial disclosures.
REPORTING FROM ATS 2018
Key clinical point: A simple calculation of pulse pressure multiplied by heart rate at ED triage could lead to earlier implementation of lifesaving interventions in septic patients.
Major finding: When using 5,000 as a cutoff, pulse pressure multiplied by heart rate had a sensitivity of 100% and a specificity of 89% in detecting culture-positive sepsis.
Study details: A cross-sectional, observational study of 116 medical ICU patients who were admitted directly from an ED.
Disclosures: The study was supported in part by a grant from the National Institutes of Health. Dr. Lynch reported having no financial disclosures.
Patient adjustments needed for closed-loop insulin delivery
TORONTO – Closed-loop insulin delivery is expected to become the standard of care in type 1 diabetes mellitus (T1DM), but there are multiple barriers that patients need to overcome.
“Many people who are potentially going to be using closed-loop systems are enthusiastic but have unrealistic expectations of how the systems are going to perform, and there are many barriers to uptake and optimal use that we still haven’t quite figured out,” said Korey K. Hood, PhD, a professor in the departments of pediatrics and psychiatry & behavioral sciences at Stanford (Calif.) University.
In a session dedicated to all aspects of closed-loop automated insulin delivery at the Pediatric Academic Societies annual meeting, Dr. Hood offered comments on patient and family factors important to the uptake and use of closed-loop technologies. His research at Stanford is focused on understanding the psychosocial aspects of diabetes management and how these factors contribute to disease outcomes.
Closed-loop insulin delivery refers to technologies that combine automated glucose monitoring (AGM) with an algorithm to determine insulin needs and an insulin delivery device. Sometimes called an “artificial pancreas” or “bionic pancreas,” closed-loop insulin delivery is considered a significant advance in the management of T1DM, relegating daily finger sticks and nighttime hypoglycemia to things of the past.
In a recent meta-analysis of randomized clinical trials, use of any automated device added nearly 2.5 hours of time in near normoglycemia over 24 hours in patients with TIDM, compared with any other type of insulin-based treatment (BMJ. 2018. doi: 10.1136/bmj.k1310). The benefit was primarily based on better glucose control in the overnight period.
In September 2016, the Food and Drug Administration approved the MiniMed 670G Insulin Pump System (Medtronic), the first hybrid automated insulin delivery device for T1DM and the only one approved in the United States. The system is intended for subcutaneous continuous glucose monitoring (CGM) and continuous delivery of basal insulin and administration of insulin for the management of T1DM in persons 14 years of age and older.
Barriers from different perspectives
Barriers to uptake and use are common for the devices that are components of closed-loop systems. In a survey of 1,503 adults with TIDM, Dr. Hood’s group found a wide range of barriers to adoption of CGM or insulin pumps that could potentially also impact use of closed-loop systems (Diabetes Care. 2017;40:181-7). Some were nonmodifiable, like costs, but most were modifiable.
“Many people talk about the hassle of wearing devices. They don’t like having multiple devices on their bodies. They don’t always like the way that they look, and so these are things that we can have some kind of impact on and need to be paying attention to,” he said.
“The younger participants indicated a lot more barriers to using devices, and as they got older, they indicated fewer barriers. But what was also interesting is that the younger participants also indicated a lot more diabetes distress. As time went on, that was less of a factor in whether or not people were using diabetes devices,” reported Dr. Hood.
Not surprisingly, he added, was that younger participants had more favorable views of technology in general. “But they had less favorable views of diabetes technology [than older participants], so they’re really not crazy about using these devices.”
Dr. Hood’s group has also studied whether patient-reported barriers to CGM use align with what clinicians perceive to be patient-related barriers (Diabetes Sci Technol. 2017;11[3]484-92). Similar to the patients, clinicians most frequently endorsed the perception that patients dislike having the device on their body. However, other things they felt their patients worried about were the alarms on the device and the difficulty in understanding its features, neither of which patients considered a primary barrier to CGM or insulin pump adoption.
“So, we need to be cautious and mindful as we move forward that there are mismatches between the patient-reported and clinician-reported barriers,” said Dr. Hood. “Our response, often, is to teach and to provide some kind of education, when that’s not necessarily what the patient is asking for.”
Would you use it?
In 2017, a group of investigators conducted a qualitative study of 284 participants, ranging in age from 8 to 86 years, with T1DM. The researchers used structured interviews or focus groups to explore expectations, desired features, potential benefits, and perceived burdens of automated insulin delivery systems (Diabetes Care. 2017;40[11]:1453-61).
“We were interested in children, adolescents, and adults with type 1, and then also the partners of the adults and the parents of the youth,” he explained.
“The findings revealed three themes identified as pressing for the uptake of automated insulin delivery: considerations of trust and control, system features, and concerns and barriers to adoption.
“For children, the areas of most concern revolved around specific social situations. Adolescents, on the other hand, were more concerned about the physical features of the device, the wearability, the discreetness of using it, and the comfort,” said Dr. Hood.
Adults and parents were much more interested in device accuracy, safety, adaptability, and algorithm quality. “For the kids and teens, not surprisingly, this wasn’t high on their list,” he added.
A clear indication of the unrealistic expectations surrounding this technology came from a 2018 study of almost 200 family members, which found that “reducing the constant concerns about diabetes, relieving family stress, and improving overall family relationships” were the three major areas the participants hoped would be helped with automated insulin delivery (Diabetes Technol Ther. 2018;20[3]:222-8).
“If we come up with a device that does this, then I think we will have fixed everything!” Dr. Hood said, adding that it really highlights the “very high hopes and expectations” of what closed-loop systems should deliver.
Device readiness is another area researchers have studied in the run-up to closed-loop systems. “The idea that everybody’s going to be ready to start in the same way, I think, is going to set us up for some failures,” he noted, adding that, in general, parents are much more enthusiastic about this than pediatric patients.
“Individuals who had been using diabetes devices – and some had already been in closed-loop studies – They had more realistic expectations of what these systems are going to be, because they knew that it wasn’t going to be a complete fix. Whereas others with more limited experience with component devices and these systems had much higher expectations and reported a fair amount of dissatisfaction at the end of the study because it didn’t do everything that they wanted it to do.”
Waves of uptake
“Ultimately, a closed-loop system is going to be judged by whether it can increase time on target and reduce cognitive burden,” said Dr. Hood. He finished his talk with some projections about the future of closed-loop systems. “I think we’re going to probably to have different waves, or types, of closed-loop users.”
The first wave will be the group that’s already “sold” on the idea, which might encompass about 15% of patients. The second wave, which might represent about 30% of the relevant patient population, will be those who are sold on the idea and will likely use it but will have high expectations of the system’s ease of use and effectiveness and thus are highly likely to discontinue its use if those expectations are not met.
“The third wave will be those who might use a closed-loop system but might be unaware of them currently and will need a fair amount of education.” And, finally, the fourth group are unlikely to ever use closed-loop insulin delivery. “They are a group that feels burned by previous generations of systems, and I think that they may not perceive benefit,” Dr. Hood suggested.
“But all of this is to say that I do think that a tailored experience, and one that is focused on different profiles, can optimize both the uptake and the use of these systems.”
Dr. Hood reported receiving grant/research support from Dexcom and being a consultant for Lilly Innovation Center, J&J Diabetes Institute, and Bigfoot Biomedical.
TORONTO – Closed-loop insulin delivery is expected to become the standard of care in type 1 diabetes mellitus (T1DM), but there are multiple barriers that patients need to overcome.
“Many people who are potentially going to be using closed-loop systems are enthusiastic but have unrealistic expectations of how the systems are going to perform, and there are many barriers to uptake and optimal use that we still haven’t quite figured out,” said Korey K. Hood, PhD, a professor in the departments of pediatrics and psychiatry & behavioral sciences at Stanford (Calif.) University.
In a session dedicated to all aspects of closed-loop automated insulin delivery at the Pediatric Academic Societies annual meeting, Dr. Hood offered comments on patient and family factors important to the uptake and use of closed-loop technologies. His research at Stanford is focused on understanding the psychosocial aspects of diabetes management and how these factors contribute to disease outcomes.
Closed-loop insulin delivery refers to technologies that combine automated glucose monitoring (AGM) with an algorithm to determine insulin needs and an insulin delivery device. Sometimes called an “artificial pancreas” or “bionic pancreas,” closed-loop insulin delivery is considered a significant advance in the management of T1DM, relegating daily finger sticks and nighttime hypoglycemia to things of the past.
In a recent meta-analysis of randomized clinical trials, use of any automated device added nearly 2.5 hours of time in near normoglycemia over 24 hours in patients with TIDM, compared with any other type of insulin-based treatment (BMJ. 2018. doi: 10.1136/bmj.k1310). The benefit was primarily based on better glucose control in the overnight period.
In September 2016, the Food and Drug Administration approved the MiniMed 670G Insulin Pump System (Medtronic), the first hybrid automated insulin delivery device for T1DM and the only one approved in the United States. The system is intended for subcutaneous continuous glucose monitoring (CGM) and continuous delivery of basal insulin and administration of insulin for the management of T1DM in persons 14 years of age and older.
Barriers from different perspectives
Barriers to uptake and use are common for the devices that are components of closed-loop systems. In a survey of 1,503 adults with TIDM, Dr. Hood’s group found a wide range of barriers to adoption of CGM or insulin pumps that could potentially also impact use of closed-loop systems (Diabetes Care. 2017;40:181-7). Some were nonmodifiable, like costs, but most were modifiable.
“Many people talk about the hassle of wearing devices. They don’t like having multiple devices on their bodies. They don’t always like the way that they look, and so these are things that we can have some kind of impact on and need to be paying attention to,” he said.
“The younger participants indicated a lot more barriers to using devices, and as they got older, they indicated fewer barriers. But what was also interesting is that the younger participants also indicated a lot more diabetes distress. As time went on, that was less of a factor in whether or not people were using diabetes devices,” reported Dr. Hood.
Not surprisingly, he added, was that younger participants had more favorable views of technology in general. “But they had less favorable views of diabetes technology [than older participants], so they’re really not crazy about using these devices.”
Dr. Hood’s group has also studied whether patient-reported barriers to CGM use align with what clinicians perceive to be patient-related barriers (Diabetes Sci Technol. 2017;11[3]484-92). Similar to the patients, clinicians most frequently endorsed the perception that patients dislike having the device on their body. However, other things they felt their patients worried about were the alarms on the device and the difficulty in understanding its features, neither of which patients considered a primary barrier to CGM or insulin pump adoption.
“So, we need to be cautious and mindful as we move forward that there are mismatches between the patient-reported and clinician-reported barriers,” said Dr. Hood. “Our response, often, is to teach and to provide some kind of education, when that’s not necessarily what the patient is asking for.”
Would you use it?
In 2017, a group of investigators conducted a qualitative study of 284 participants, ranging in age from 8 to 86 years, with T1DM. The researchers used structured interviews or focus groups to explore expectations, desired features, potential benefits, and perceived burdens of automated insulin delivery systems (Diabetes Care. 2017;40[11]:1453-61).
“We were interested in children, adolescents, and adults with type 1, and then also the partners of the adults and the parents of the youth,” he explained.
“The findings revealed three themes identified as pressing for the uptake of automated insulin delivery: considerations of trust and control, system features, and concerns and barriers to adoption.
“For children, the areas of most concern revolved around specific social situations. Adolescents, on the other hand, were more concerned about the physical features of the device, the wearability, the discreetness of using it, and the comfort,” said Dr. Hood.
Adults and parents were much more interested in device accuracy, safety, adaptability, and algorithm quality. “For the kids and teens, not surprisingly, this wasn’t high on their list,” he added.
A clear indication of the unrealistic expectations surrounding this technology came from a 2018 study of almost 200 family members, which found that “reducing the constant concerns about diabetes, relieving family stress, and improving overall family relationships” were the three major areas the participants hoped would be helped with automated insulin delivery (Diabetes Technol Ther. 2018;20[3]:222-8).
“If we come up with a device that does this, then I think we will have fixed everything!” Dr. Hood said, adding that it really highlights the “very high hopes and expectations” of what closed-loop systems should deliver.
Device readiness is another area researchers have studied in the run-up to closed-loop systems. “The idea that everybody’s going to be ready to start in the same way, I think, is going to set us up for some failures,” he noted, adding that, in general, parents are much more enthusiastic about this than pediatric patients.
“Individuals who had been using diabetes devices – and some had already been in closed-loop studies – They had more realistic expectations of what these systems are going to be, because they knew that it wasn’t going to be a complete fix. Whereas others with more limited experience with component devices and these systems had much higher expectations and reported a fair amount of dissatisfaction at the end of the study because it didn’t do everything that they wanted it to do.”
Waves of uptake
“Ultimately, a closed-loop system is going to be judged by whether it can increase time on target and reduce cognitive burden,” said Dr. Hood. He finished his talk with some projections about the future of closed-loop systems. “I think we’re going to probably to have different waves, or types, of closed-loop users.”
The first wave will be the group that’s already “sold” on the idea, which might encompass about 15% of patients. The second wave, which might represent about 30% of the relevant patient population, will be those who are sold on the idea and will likely use it but will have high expectations of the system’s ease of use and effectiveness and thus are highly likely to discontinue its use if those expectations are not met.
“The third wave will be those who might use a closed-loop system but might be unaware of them currently and will need a fair amount of education.” And, finally, the fourth group are unlikely to ever use closed-loop insulin delivery. “They are a group that feels burned by previous generations of systems, and I think that they may not perceive benefit,” Dr. Hood suggested.
“But all of this is to say that I do think that a tailored experience, and one that is focused on different profiles, can optimize both the uptake and the use of these systems.”
Dr. Hood reported receiving grant/research support from Dexcom and being a consultant for Lilly Innovation Center, J&J Diabetes Institute, and Bigfoot Biomedical.
TORONTO – Closed-loop insulin delivery is expected to become the standard of care in type 1 diabetes mellitus (T1DM), but there are multiple barriers that patients need to overcome.
“Many people who are potentially going to be using closed-loop systems are enthusiastic but have unrealistic expectations of how the systems are going to perform, and there are many barriers to uptake and optimal use that we still haven’t quite figured out,” said Korey K. Hood, PhD, a professor in the departments of pediatrics and psychiatry & behavioral sciences at Stanford (Calif.) University.
In a session dedicated to all aspects of closed-loop automated insulin delivery at the Pediatric Academic Societies annual meeting, Dr. Hood offered comments on patient and family factors important to the uptake and use of closed-loop technologies. His research at Stanford is focused on understanding the psychosocial aspects of diabetes management and how these factors contribute to disease outcomes.
Closed-loop insulin delivery refers to technologies that combine automated glucose monitoring (AGM) with an algorithm to determine insulin needs and an insulin delivery device. Sometimes called an “artificial pancreas” or “bionic pancreas,” closed-loop insulin delivery is considered a significant advance in the management of T1DM, relegating daily finger sticks and nighttime hypoglycemia to things of the past.
In a recent meta-analysis of randomized clinical trials, use of any automated device added nearly 2.5 hours of time in near normoglycemia over 24 hours in patients with TIDM, compared with any other type of insulin-based treatment (BMJ. 2018. doi: 10.1136/bmj.k1310). The benefit was primarily based on better glucose control in the overnight period.
In September 2016, the Food and Drug Administration approved the MiniMed 670G Insulin Pump System (Medtronic), the first hybrid automated insulin delivery device for T1DM and the only one approved in the United States. The system is intended for subcutaneous continuous glucose monitoring (CGM) and continuous delivery of basal insulin and administration of insulin for the management of T1DM in persons 14 years of age and older.
Barriers from different perspectives
Barriers to uptake and use are common for the devices that are components of closed-loop systems. In a survey of 1,503 adults with TIDM, Dr. Hood’s group found a wide range of barriers to adoption of CGM or insulin pumps that could potentially also impact use of closed-loop systems (Diabetes Care. 2017;40:181-7). Some were nonmodifiable, like costs, but most were modifiable.
“Many people talk about the hassle of wearing devices. They don’t like having multiple devices on their bodies. They don’t always like the way that they look, and so these are things that we can have some kind of impact on and need to be paying attention to,” he said.
“The younger participants indicated a lot more barriers to using devices, and as they got older, they indicated fewer barriers. But what was also interesting is that the younger participants also indicated a lot more diabetes distress. As time went on, that was less of a factor in whether or not people were using diabetes devices,” reported Dr. Hood.
Not surprisingly, he added, was that younger participants had more favorable views of technology in general. “But they had less favorable views of diabetes technology [than older participants], so they’re really not crazy about using these devices.”
Dr. Hood’s group has also studied whether patient-reported barriers to CGM use align with what clinicians perceive to be patient-related barriers (Diabetes Sci Technol. 2017;11[3]484-92). Similar to the patients, clinicians most frequently endorsed the perception that patients dislike having the device on their body. However, other things they felt their patients worried about were the alarms on the device and the difficulty in understanding its features, neither of which patients considered a primary barrier to CGM or insulin pump adoption.
“So, we need to be cautious and mindful as we move forward that there are mismatches between the patient-reported and clinician-reported barriers,” said Dr. Hood. “Our response, often, is to teach and to provide some kind of education, when that’s not necessarily what the patient is asking for.”
Would you use it?
In 2017, a group of investigators conducted a qualitative study of 284 participants, ranging in age from 8 to 86 years, with T1DM. The researchers used structured interviews or focus groups to explore expectations, desired features, potential benefits, and perceived burdens of automated insulin delivery systems (Diabetes Care. 2017;40[11]:1453-61).
“We were interested in children, adolescents, and adults with type 1, and then also the partners of the adults and the parents of the youth,” he explained.
“The findings revealed three themes identified as pressing for the uptake of automated insulin delivery: considerations of trust and control, system features, and concerns and barriers to adoption.
“For children, the areas of most concern revolved around specific social situations. Adolescents, on the other hand, were more concerned about the physical features of the device, the wearability, the discreetness of using it, and the comfort,” said Dr. Hood.
Adults and parents were much more interested in device accuracy, safety, adaptability, and algorithm quality. “For the kids and teens, not surprisingly, this wasn’t high on their list,” he added.
A clear indication of the unrealistic expectations surrounding this technology came from a 2018 study of almost 200 family members, which found that “reducing the constant concerns about diabetes, relieving family stress, and improving overall family relationships” were the three major areas the participants hoped would be helped with automated insulin delivery (Diabetes Technol Ther. 2018;20[3]:222-8).
“If we come up with a device that does this, then I think we will have fixed everything!” Dr. Hood said, adding that it really highlights the “very high hopes and expectations” of what closed-loop systems should deliver.
Device readiness is another area researchers have studied in the run-up to closed-loop systems. “The idea that everybody’s going to be ready to start in the same way, I think, is going to set us up for some failures,” he noted, adding that, in general, parents are much more enthusiastic about this than pediatric patients.
“Individuals who had been using diabetes devices – and some had already been in closed-loop studies – They had more realistic expectations of what these systems are going to be, because they knew that it wasn’t going to be a complete fix. Whereas others with more limited experience with component devices and these systems had much higher expectations and reported a fair amount of dissatisfaction at the end of the study because it didn’t do everything that they wanted it to do.”
Waves of uptake
“Ultimately, a closed-loop system is going to be judged by whether it can increase time on target and reduce cognitive burden,” said Dr. Hood. He finished his talk with some projections about the future of closed-loop systems. “I think we’re going to probably to have different waves, or types, of closed-loop users.”
The first wave will be the group that’s already “sold” on the idea, which might encompass about 15% of patients. The second wave, which might represent about 30% of the relevant patient population, will be those who are sold on the idea and will likely use it but will have high expectations of the system’s ease of use and effectiveness and thus are highly likely to discontinue its use if those expectations are not met.
“The third wave will be those who might use a closed-loop system but might be unaware of them currently and will need a fair amount of education.” And, finally, the fourth group are unlikely to ever use closed-loop insulin delivery. “They are a group that feels burned by previous generations of systems, and I think that they may not perceive benefit,” Dr. Hood suggested.
“But all of this is to say that I do think that a tailored experience, and one that is focused on different profiles, can optimize both the uptake and the use of these systems.”
Dr. Hood reported receiving grant/research support from Dexcom and being a consultant for Lilly Innovation Center, J&J Diabetes Institute, and Bigfoot Biomedical.
EXPERT ANALYSIS FROM PAS 2018
Testosterone therapy tied to kidney stone risk
SAN FRANCISCO – , according to an analysis of more than 50,000 men with low testosterone.
When researchers compared hypogonadal men to age- and comorbidity-matched controls, they found a statistically significantly higher number of clinical diagnoses of a kidney stone, or of patients undergoing a kidney stone–related procedure.
The new study is the first large-scale analysis of the question in humans, according to Tyler McClintock, MD, who presented the findings at a poster session at the annual meeting of the American Urological Association. Dr. McClintock is a urology resident at Brigham and Women’s Hospital and Harvard Medical School in Boston.
Dr. McClintock and his colleagues analyzed data from the Military Health System Data Repository (MDR). The MDR includes beneficiaries of the TRICARE program for service members, retirees, and their families. They looked at 26,586 men aged 40-64 years who had been diagnosed with low testosterone and who had received continuous testosterone replacement therapy between April 2006 and March 2014. The researchers compared them to 26,586 controls with low testosterone who did not receive testosterone replacement therapy.
Stone events were significantly higher in the treatment group. There were 67 extracorporeal shock wave lithotripsy procedures in the treatment group, compared with 51 among controls. Similar trends were seen with ureteroscopy with lithotripsy (75 vs. 46) and clinical diagnoses of kidney stone (1,059 vs. 794).
The researchers also broke down stone events by type of testosterone replacement therapy. A total of 5.4% of patients who received pellets (9 of 167) experienced an event (P = .27), compared with 5.1% of those who received injections (218 of 4,259; P = .004) and 3.5% of those who received it topically (655 of 18,895; P less than .0001).
At 2 years, Dr. McClintock reported that there were significantly more kidney stone events in the testosterone-treated group than in the untreated group (659 and 482, respectively; P less than .001). Two years after starting testosterone replacement therapy, significantly more of the treatment group had experienced a stone episode, compared with the matched controls during the same time period (3.9% and 3%, respectively; P less than .001).
Dr. McClintock said the study is convincing in part because it used data from TRICARE, which sets a lower testosterone level even than AUA guidelines for determining if a patient is eligible for testosterone therapy.
“It would suggest that those are the real low testosterone patients, not necessarily men who heard an ad or went to a test center,” noted Patrick Shepherd Lowry, MD, associate professor of urology at Scott & White Medical Center, Temple, Texas, who attended the presentation but was not involved in the study. “It’s preliminary, but it’s very interesting. It hasn’t been shown before.”
The Department of Defense funded the study. Dr. McClintock reported having no relevant financial disclosures.
SOURCE: McClintock T. AUA Annual Meeting. Abstract MP13-19.
SAN FRANCISCO – , according to an analysis of more than 50,000 men with low testosterone.
When researchers compared hypogonadal men to age- and comorbidity-matched controls, they found a statistically significantly higher number of clinical diagnoses of a kidney stone, or of patients undergoing a kidney stone–related procedure.
The new study is the first large-scale analysis of the question in humans, according to Tyler McClintock, MD, who presented the findings at a poster session at the annual meeting of the American Urological Association. Dr. McClintock is a urology resident at Brigham and Women’s Hospital and Harvard Medical School in Boston.
Dr. McClintock and his colleagues analyzed data from the Military Health System Data Repository (MDR). The MDR includes beneficiaries of the TRICARE program for service members, retirees, and their families. They looked at 26,586 men aged 40-64 years who had been diagnosed with low testosterone and who had received continuous testosterone replacement therapy between April 2006 and March 2014. The researchers compared them to 26,586 controls with low testosterone who did not receive testosterone replacement therapy.
Stone events were significantly higher in the treatment group. There were 67 extracorporeal shock wave lithotripsy procedures in the treatment group, compared with 51 among controls. Similar trends were seen with ureteroscopy with lithotripsy (75 vs. 46) and clinical diagnoses of kidney stone (1,059 vs. 794).
The researchers also broke down stone events by type of testosterone replacement therapy. A total of 5.4% of patients who received pellets (9 of 167) experienced an event (P = .27), compared with 5.1% of those who received injections (218 of 4,259; P = .004) and 3.5% of those who received it topically (655 of 18,895; P less than .0001).
At 2 years, Dr. McClintock reported that there were significantly more kidney stone events in the testosterone-treated group than in the untreated group (659 and 482, respectively; P less than .001). Two years after starting testosterone replacement therapy, significantly more of the treatment group had experienced a stone episode, compared with the matched controls during the same time period (3.9% and 3%, respectively; P less than .001).
Dr. McClintock said the study is convincing in part because it used data from TRICARE, which sets a lower testosterone level even than AUA guidelines for determining if a patient is eligible for testosterone therapy.
“It would suggest that those are the real low testosterone patients, not necessarily men who heard an ad or went to a test center,” noted Patrick Shepherd Lowry, MD, associate professor of urology at Scott & White Medical Center, Temple, Texas, who attended the presentation but was not involved in the study. “It’s preliminary, but it’s very interesting. It hasn’t been shown before.”
The Department of Defense funded the study. Dr. McClintock reported having no relevant financial disclosures.
SOURCE: McClintock T. AUA Annual Meeting. Abstract MP13-19.
SAN FRANCISCO – , according to an analysis of more than 50,000 men with low testosterone.
When researchers compared hypogonadal men to age- and comorbidity-matched controls, they found a statistically significantly higher number of clinical diagnoses of a kidney stone, or of patients undergoing a kidney stone–related procedure.
The new study is the first large-scale analysis of the question in humans, according to Tyler McClintock, MD, who presented the findings at a poster session at the annual meeting of the American Urological Association. Dr. McClintock is a urology resident at Brigham and Women’s Hospital and Harvard Medical School in Boston.
Dr. McClintock and his colleagues analyzed data from the Military Health System Data Repository (MDR). The MDR includes beneficiaries of the TRICARE program for service members, retirees, and their families. They looked at 26,586 men aged 40-64 years who had been diagnosed with low testosterone and who had received continuous testosterone replacement therapy between April 2006 and March 2014. The researchers compared them to 26,586 controls with low testosterone who did not receive testosterone replacement therapy.
Stone events were significantly higher in the treatment group. There were 67 extracorporeal shock wave lithotripsy procedures in the treatment group, compared with 51 among controls. Similar trends were seen with ureteroscopy with lithotripsy (75 vs. 46) and clinical diagnoses of kidney stone (1,059 vs. 794).
The researchers also broke down stone events by type of testosterone replacement therapy. A total of 5.4% of patients who received pellets (9 of 167) experienced an event (P = .27), compared with 5.1% of those who received injections (218 of 4,259; P = .004) and 3.5% of those who received it topically (655 of 18,895; P less than .0001).
At 2 years, Dr. McClintock reported that there were significantly more kidney stone events in the testosterone-treated group than in the untreated group (659 and 482, respectively; P less than .001). Two years after starting testosterone replacement therapy, significantly more of the treatment group had experienced a stone episode, compared with the matched controls during the same time period (3.9% and 3%, respectively; P less than .001).
Dr. McClintock said the study is convincing in part because it used data from TRICARE, which sets a lower testosterone level even than AUA guidelines for determining if a patient is eligible for testosterone therapy.
“It would suggest that those are the real low testosterone patients, not necessarily men who heard an ad or went to a test center,” noted Patrick Shepherd Lowry, MD, associate professor of urology at Scott & White Medical Center, Temple, Texas, who attended the presentation but was not involved in the study. “It’s preliminary, but it’s very interesting. It hasn’t been shown before.”
The Department of Defense funded the study. Dr. McClintock reported having no relevant financial disclosures.
SOURCE: McClintock T. AUA Annual Meeting. Abstract MP13-19.
REPORTING FROM THE AUA ANNUAL MEETING
Key clinical point: Kidney stone risk may be a factor when considering testosterone replacement therapy.
Major finding: In untreated men, 482 kidney stone events occurred, compared with 659 in those receiving testosterone.
Study details: A case-control analysis of 26,586 treated men and 26,586 matched controls.
Disclosures: The Department of Defense funded the study. Dr. McClintock reported having no relevant financial disclosures.
Source: McClintock T. AUA Annual Meeting. Abstract MP13-19.
Do Cardiovascular Risk Factors Contribute to Brain Atrophy in MS?
LOS ANGELES—Hypertension and heart disease may contribute to advanced central and white matter atrophy in patients with multiple sclerosis (MS) over five years, according to a study presented at the 70th Annual Meeting of the American Academy of Neurology.
The findings suggest that management of cardiovascular comorbidities in MS may improve overall long-term disease outcomes, said Dejan Jakimovski, MD, a clinical research fellow at the Buffalo Neuroimaging Analysis Center at the University at Buffalo, New York, and colleagues.

Cardiovascular diseases and risk factors are more common in patients with MS, compared with healthy individuals, and cross-sectional studies have linked smoking, hypertension, hyperlipidemia, and heart disease to lesion burden and brain atrophy, the researchers said.
To determine the influence of cardiovascular diseases over five years in a larger number of patients with MS, Dr. Jakimovski and colleagues examined data from 194 patients with MS in a prospective study of cardiovascular, environmental, and genetic risk factors in MS (CEG-MS). Patients in the study underwent clinical evaluation and completed questionnaires about cardiovascular risk factors (ie, hypertension, hyperlipidemia, heart disease, smoking, diabetes, and obesity or overweight status). The researchers assessed T2 and T1 lesion volumes and volumes of whole brain, gray matter, white matter, cortex, and lateral ventricles using 3-T MRI. They used analysis of covariance adjusted for age, sex, and disease duration to detect significant differences between patients with and without cardiovascular risk factors.
The 194 patients with MS (73.7% female; mean age, 46.7) had an average disease duration of 13.6 years, a median baseline Expanded Disability Status Scale (EDSS) score of 2.5, and a median EDSS at follow-up of 3. Mean BMI was 27.6, 14.9% had hypertension, and 9.8% had heart disease.
At baseline, patients with hypertension had larger lateral ventricular volume, compared with patients without hypertension (66.1 mL vs 49.9 mL). Over the follow-up period, the percentage lateral ventricular volume change was significantly greater in patients with hypertension, compared with patients without hypertension (24.5% vs 14.1%). Over the follow-up period, patients with a diagnosis of heart disease had greater white matter volume loss, compared with those without heart disease (–4.2% vs –0.7%).
Hyperlipidemia, diabetes, smoking, and obesity or overweight status
—Jake Remaly
LOS ANGELES—Hypertension and heart disease may contribute to advanced central and white matter atrophy in patients with multiple sclerosis (MS) over five years, according to a study presented at the 70th Annual Meeting of the American Academy of Neurology.
The findings suggest that management of cardiovascular comorbidities in MS may improve overall long-term disease outcomes, said Dejan Jakimovski, MD, a clinical research fellow at the Buffalo Neuroimaging Analysis Center at the University at Buffalo, New York, and colleagues.
Cardiovascular diseases and risk factors are more common in patients with MS, compared with healthy individuals, and cross-sectional studies have linked smoking, hypertension, hyperlipidemia, and heart disease to lesion burden and brain atrophy, the researchers said.
To determine the influence of cardiovascular diseases over five years in a larger number of patients with MS, Dr. Jakimovski and colleagues examined data from 194 patients with MS in a prospective study of cardiovascular, environmental, and genetic risk factors in MS (CEG-MS). Patients in the study underwent clinical evaluation and completed questionnaires about cardiovascular risk factors (ie, hypertension, hyperlipidemia, heart disease, smoking, diabetes, and obesity or overweight status). The researchers assessed T2 and T1 lesion volumes and volumes of whole brain, gray matter, white matter, cortex, and lateral ventricles using 3-T MRI. They used analysis of covariance adjusted for age, sex, and disease duration to detect significant differences between patients with and without cardiovascular risk factors.
The 194 patients with MS (73.7% female; mean age, 46.7) had an average disease duration of 13.6 years, a median baseline Expanded Disability Status Scale (EDSS) score of 2.5, and a median EDSS at follow-up of 3. Mean BMI was 27.6, 14.9% had hypertension, and 9.8% had heart disease.
At baseline, patients with hypertension had larger lateral ventricular volume, compared with patients without hypertension (66.1 mL vs 49.9 mL). Over the follow-up period, the percentage lateral ventricular volume change was significantly greater in patients with hypertension, compared with patients without hypertension (24.5% vs 14.1%). Over the follow-up period, patients with a diagnosis of heart disease had greater white matter volume loss, compared with those without heart disease (–4.2% vs –0.7%).
Hyperlipidemia, diabetes, smoking, and obesity or overweight status
—Jake Remaly
LOS ANGELES—Hypertension and heart disease may contribute to advanced central and white matter atrophy in patients with multiple sclerosis (MS) over five years, according to a study presented at the 70th Annual Meeting of the American Academy of Neurology.
The findings suggest that management of cardiovascular comorbidities in MS may improve overall long-term disease outcomes, said Dejan Jakimovski, MD, a clinical research fellow at the Buffalo Neuroimaging Analysis Center at the University at Buffalo, New York, and colleagues.
Cardiovascular diseases and risk factors are more common in patients with MS, compared with healthy individuals, and cross-sectional studies have linked smoking, hypertension, hyperlipidemia, and heart disease to lesion burden and brain atrophy, the researchers said.
To determine the influence of cardiovascular diseases over five years in a larger number of patients with MS, Dr. Jakimovski and colleagues examined data from 194 patients with MS in a prospective study of cardiovascular, environmental, and genetic risk factors in MS (CEG-MS). Patients in the study underwent clinical evaluation and completed questionnaires about cardiovascular risk factors (ie, hypertension, hyperlipidemia, heart disease, smoking, diabetes, and obesity or overweight status). The researchers assessed T2 and T1 lesion volumes and volumes of whole brain, gray matter, white matter, cortex, and lateral ventricles using 3-T MRI. They used analysis of covariance adjusted for age, sex, and disease duration to detect significant differences between patients with and without cardiovascular risk factors.
The 194 patients with MS (73.7% female; mean age, 46.7) had an average disease duration of 13.6 years, a median baseline Expanded Disability Status Scale (EDSS) score of 2.5, and a median EDSS at follow-up of 3. Mean BMI was 27.6, 14.9% had hypertension, and 9.8% had heart disease.
At baseline, patients with hypertension had larger lateral ventricular volume, compared with patients without hypertension (66.1 mL vs 49.9 mL). Over the follow-up period, the percentage lateral ventricular volume change was significantly greater in patients with hypertension, compared with patients without hypertension (24.5% vs 14.1%). Over the follow-up period, patients with a diagnosis of heart disease had greater white matter volume loss, compared with those without heart disease (–4.2% vs –0.7%).
Hyperlipidemia, diabetes, smoking, and obesity or overweight status
—Jake Remaly