User login
FDA grants priority review to gilteritinib for R/R AML

The US Food and Drug Administration (FDA) has granted priority review to gilteritinib for the treatment of adult patients with relapsed or refractory (R/R) acute myeloid leukemia (AML) who have a FLT3 mutation.
At present, no FLT3-targeting agents are approved for the treatment of R/R FLT3-mutation-positive AML, according to Astellas, the developer of the drug.
The FDA previously granted gilteritinib orphan drug designation and fast track designation.
The European Commission (EC) also granted gilteritinib orphan designation and the Japan Ministry of Health, Labor and Welfare (MHLW) did likewise.
Gilteritinib has demonstrated inhibitory activity against FLT3 internal tandem duplication (ITD) and FLT tyrosine kinase domain (TKD) mutation. These 2 FLT3 mutations are present in approximately 1/3 of AML patients.
The priority review for the new drug application is based on the ongoing phase 3 ADMIRAL trial.
The FDA aims to take action on a priority review application within 6 months of receiving it, rather than the standard 10 months.
The agency grants priority review to applications for products that may provide significant improvements in the treatment, diagnosis, or prevention of serious conditions.
The goal date for a decision by the FDA is the end of November.
This open-label multicenter randomized study compares gilteritinib with salvage chemotherapy in adult patients with FLT3 mutations who are refractory to or have relapsed after first-line AML therapy.
The study has enrolled 371 patients with FLT3 mutations present in bone marrow or whole blood, as determined by a central lab.
Patients were randomized in a 2:1 ratio to receive gilteritinib (120 mg) or salvage chemotherapy.
Salvage chemotherapy could consist of low-dose cytarabine, azacitidine, MEC (mitoxantrone, etoposide, cytarabine) induction chemotherapy, or FLAG-IDA (fludarabine, cytarabine, and granulocyte colony-stimulating factor [G-CSF] with idarubicin) induction chemotherapy.
The primary endpoints of the study are overall survival and complete remission or complete remission with partial hematologic recovery.
Secondary endpoints include event-free survival, complete remission rate, leukemia-free survival, duration of remission, transplantation rate, fatigue inventory, among other outcomes.
The study is estimated to be completed in October for its primary endpoint and February 2020 for the entire study.
The US Food and Drug Administration (FDA) has granted priority review to gilteritinib for the treatment of adult patients with relapsed or refractory (R/R) acute myeloid leukemia (AML) who have a FLT3 mutation.
At present, no FLT3-targeting agents are approved for the treatment of R/R FLT3-mutation-positive AML, according to Astellas, the developer of the drug.
The FDA previously granted gilteritinib orphan drug designation and fast track designation.
The European Commission (EC) also granted gilteritinib orphan designation and the Japan Ministry of Health, Labor and Welfare (MHLW) did likewise.
Gilteritinib has demonstrated inhibitory activity against FLT3 internal tandem duplication (ITD) and FLT tyrosine kinase domain (TKD) mutation. These 2 FLT3 mutations are present in approximately 1/3 of AML patients.
The priority review for the new drug application is based on the ongoing phase 3 ADMIRAL trial.
The FDA aims to take action on a priority review application within 6 months of receiving it, rather than the standard 10 months.
The agency grants priority review to applications for products that may provide significant improvements in the treatment, diagnosis, or prevention of serious conditions.
The goal date for a decision by the FDA is the end of November.
This open-label multicenter randomized study compares gilteritinib with salvage chemotherapy in adult patients with FLT3 mutations who are refractory to or have relapsed after first-line AML therapy.
The study has enrolled 371 patients with FLT3 mutations present in bone marrow or whole blood, as determined by a central lab.
Patients were randomized in a 2:1 ratio to receive gilteritinib (120 mg) or salvage chemotherapy.
Salvage chemotherapy could consist of low-dose cytarabine, azacitidine, MEC (mitoxantrone, etoposide, cytarabine) induction chemotherapy, or FLAG-IDA (fludarabine, cytarabine, and granulocyte colony-stimulating factor [G-CSF] with idarubicin) induction chemotherapy.
The primary endpoints of the study are overall survival and complete remission or complete remission with partial hematologic recovery.
Secondary endpoints include event-free survival, complete remission rate, leukemia-free survival, duration of remission, transplantation rate, fatigue inventory, among other outcomes.
The study is estimated to be completed in October for its primary endpoint and February 2020 for the entire study.
The US Food and Drug Administration (FDA) has granted priority review to gilteritinib for the treatment of adult patients with relapsed or refractory (R/R) acute myeloid leukemia (AML) who have a FLT3 mutation.
At present, no FLT3-targeting agents are approved for the treatment of R/R FLT3-mutation-positive AML, according to Astellas, the developer of the drug.
The FDA previously granted gilteritinib orphan drug designation and fast track designation.
The European Commission (EC) also granted gilteritinib orphan designation and the Japan Ministry of Health, Labor and Welfare (MHLW) did likewise.
Gilteritinib has demonstrated inhibitory activity against FLT3 internal tandem duplication (ITD) and FLT tyrosine kinase domain (TKD) mutation. These 2 FLT3 mutations are present in approximately 1/3 of AML patients.
The priority review for the new drug application is based on the ongoing phase 3 ADMIRAL trial.
The FDA aims to take action on a priority review application within 6 months of receiving it, rather than the standard 10 months.
The agency grants priority review to applications for products that may provide significant improvements in the treatment, diagnosis, or prevention of serious conditions.
The goal date for a decision by the FDA is the end of November.
This open-label multicenter randomized study compares gilteritinib with salvage chemotherapy in adult patients with FLT3 mutations who are refractory to or have relapsed after first-line AML therapy.
The study has enrolled 371 patients with FLT3 mutations present in bone marrow or whole blood, as determined by a central lab.
Patients were randomized in a 2:1 ratio to receive gilteritinib (120 mg) or salvage chemotherapy.
Salvage chemotherapy could consist of low-dose cytarabine, azacitidine, MEC (mitoxantrone, etoposide, cytarabine) induction chemotherapy, or FLAG-IDA (fludarabine, cytarabine, and granulocyte colony-stimulating factor [G-CSF] with idarubicin) induction chemotherapy.
The primary endpoints of the study are overall survival and complete remission or complete remission with partial hematologic recovery.
Secondary endpoints include event-free survival, complete remission rate, leukemia-free survival, duration of remission, transplantation rate, fatigue inventory, among other outcomes.
The study is estimated to be completed in October for its primary endpoint and February 2020 for the entire study.
Inpatient Portals: The Questions that Remain
Personal health records (PHRs) are a broad group of applications “through which individuals can access, manage, and share their health information,” and are intended as a means to increase consumer health awareness, activation, safety, and self-efficacy.1 Patient portals—PHRs that are tethered to an electronic health record (EHR)—have expanded over the past decade, driven in part by the “Meaningful Use” EHR Incentive Program of the Centers for Medicare and Medicaid Services.2 This has been particularly true in the outpatient setting. Unfortunately, despite increased adoption and a large number of research studies, it is not clear whether outpatient portal use is associated with improved clinical outcomes.3
Both the use of portals in the inpatient setting and the research thereof are at a more nascent stage. In this issue of the Journal of Hospital Medicine, Kelly et al.4 provide a systematic review of the existing research on the implementation of inpatient portals. The authors identified 17 studies and categorized the papers’ findings into the following 3 themes: design, use and usability, and impact. Most of the studies elicited feedback from patients, caregivers, and/or providers – sometimes in multiple phases as portals were redesigned – allowing the authors to offer the following recommendations for inpatient portal design: portals should present timely information, include the care plan in ways patients can understand, and facilitate identification and communication with the care team.4 Most of the included studies focused on portal design and use, thereby limiting knowledge regarding impact on the outcomes portals are intended to target. All findings should be interpreted with caution, as many of the included studies were small and qualitative, most of them used convenience samples and subject-reported outcomes, and all were conducted at a single center. Many sites also used customized portals, thus limiting generalizability.
Participants often found portals to be useful, but this finding is of uncertain value in the absence of robust evidence on outcomes. In addition, providers included in the reviewed studies expressed concerns that have not yet been well studied, such as the potential impact of portals on workload and on patient anxiety. Some studies reported that provider concerns lessened following a portal rollout, but few studies evaluated physician input on features such as direct communication and test result reporting in active use. The outpatient portal literature suggests potential harm related to how results are delivered, thus placing importance on conducting additional inpatient studies. Patients value online access to their health information5 and in previous literature have indicated a preference for immediate access to results even if abnormal results would then be given without explanation.6 However, in a recent study, even normal findings delivered without context were a cause of negative emotions and increased calls to physicians.7 This effect could be more pronounced in inpatient settings, given the large volume of tests and abnormal results, the rapidly evolving treatment plans, and generally higher acuity and medical uncertainty.
This review and other current literature highlight challenges for vendors and hospitals. Vendors must ensure that patient health information is contextualized and delivered in a manner that meets individual learning styles.8 Patients and caregivers need clinical decision support to process today’s large amount of data, just as providers do. We must be careful not to implement patient portals in ways that increase cognitive load and generate anxiety and confusion. Hospitals have infrastructural challenges if portals are to be successful. Care provider information must be accurately registered in the EHR to route patient-to-provider communications, a difficult task across frequent handoffs and staffing changes.
We now have the beginnings of an informed vision for inpatient portal design. Future research and industry directions include greater exploration of recognized concerns and how to best reconcile these concerns with the benefits of portals espoused by consumer health advocates and experienced by patients, caregivers, and providers in the reviewed studies. Specifically, we need a better understanding of how best to incorporate inpatient portals into routine care delivery in ways that are useful to both patients and providers. We also need a better understanding of why patients opt out of portal use. Most of the studies to date report on the set of patients who decided to use the portals, leaving a knowledge gap in design and use implications for patients who opted out. Studies should include comparisons of patient outcomes between users and nonusers. Although inpatient portals show promise, many questions remain.
Disclosures
The authors declare no conflicts of interest.
1. Markle Foundation. Connecting Americans to their healthcare. Working group on policies for electronic information sharing between doctors and patients final report. https://www.markle.org/sites/default/files/CnctAmerHC_fullreport.pdf. Accessed February 18, 2018.
2. Centers for Medicare and Medicaid Services. Electronic health records (EHR) incentive programs. https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/index.html?redirect=/EHRIncentivePrograms. Accessed February 18, 2018.
3. Kruse CS, Bolton K, Freriks G. The effect of patient portals on quality outcomes and its implications to meaningful use: a systematic review. J Med Internet Res. 2015;17(2):e44-e48. DOI:10.2196/jmir.3171. PubMed
4. Kelly MM, Coller RJ, Hoonakker PLT. Inpatient portals for hospitalized patients and caregivers: a systematic review. J Hosp Med. 2018;13(5):405-412.Published online first December 20, 2017. PubMed
5. Peacock S, Reddy A, Leveille SG, et al. Patient portals and personal health information online: perception, access, and use by US adults. J Am Med Inform Assoc. 2017;24(e1):e173-e177. DOI:10.1093/jamia/ocw095. PubMed
6. Johnson AJ, Easterling D, Nelson R, Chen MY, Frankel RM. Access to radiologic reports via a patient portal: clinical simulations to investigate patient preferences. JACR. 2012;9(4):256-263. DOI:10.1016/j.jacr.2011.12.023. PubMed
7. Giardina TD, Baldwin J, Nystrom DT, Sittig DF, Singh H. Patient perceptions of receiving test results via online portals: a mixed-methods study. J Am Med Inform Assoc. 2018;25(4)440-446. DOI:10.1093/jamia/ocx140. PubMed
8. Dalal AK, Bates DW, Collins S. Opportunities and challenges for improving the patient experience in the acute and post–acute care setting using patient portals: the patient’s perspective. J Hosp Med. 2017;12(12):1012-1016. DOI:10.12788/jhm.2860. PubMed
Personal health records (PHRs) are a broad group of applications “through which individuals can access, manage, and share their health information,” and are intended as a means to increase consumer health awareness, activation, safety, and self-efficacy.1 Patient portals—PHRs that are tethered to an electronic health record (EHR)—have expanded over the past decade, driven in part by the “Meaningful Use” EHR Incentive Program of the Centers for Medicare and Medicaid Services.2 This has been particularly true in the outpatient setting. Unfortunately, despite increased adoption and a large number of research studies, it is not clear whether outpatient portal use is associated with improved clinical outcomes.3
Both the use of portals in the inpatient setting and the research thereof are at a more nascent stage. In this issue of the Journal of Hospital Medicine, Kelly et al.4 provide a systematic review of the existing research on the implementation of inpatient portals. The authors identified 17 studies and categorized the papers’ findings into the following 3 themes: design, use and usability, and impact. Most of the studies elicited feedback from patients, caregivers, and/or providers – sometimes in multiple phases as portals were redesigned – allowing the authors to offer the following recommendations for inpatient portal design: portals should present timely information, include the care plan in ways patients can understand, and facilitate identification and communication with the care team.4 Most of the included studies focused on portal design and use, thereby limiting knowledge regarding impact on the outcomes portals are intended to target. All findings should be interpreted with caution, as many of the included studies were small and qualitative, most of them used convenience samples and subject-reported outcomes, and all were conducted at a single center. Many sites also used customized portals, thus limiting generalizability.
Participants often found portals to be useful, but this finding is of uncertain value in the absence of robust evidence on outcomes. In addition, providers included in the reviewed studies expressed concerns that have not yet been well studied, such as the potential impact of portals on workload and on patient anxiety. Some studies reported that provider concerns lessened following a portal rollout, but few studies evaluated physician input on features such as direct communication and test result reporting in active use. The outpatient portal literature suggests potential harm related to how results are delivered, thus placing importance on conducting additional inpatient studies. Patients value online access to their health information5 and in previous literature have indicated a preference for immediate access to results even if abnormal results would then be given without explanation.6 However, in a recent study, even normal findings delivered without context were a cause of negative emotions and increased calls to physicians.7 This effect could be more pronounced in inpatient settings, given the large volume of tests and abnormal results, the rapidly evolving treatment plans, and generally higher acuity and medical uncertainty.
This review and other current literature highlight challenges for vendors and hospitals. Vendors must ensure that patient health information is contextualized and delivered in a manner that meets individual learning styles.8 Patients and caregivers need clinical decision support to process today’s large amount of data, just as providers do. We must be careful not to implement patient portals in ways that increase cognitive load and generate anxiety and confusion. Hospitals have infrastructural challenges if portals are to be successful. Care provider information must be accurately registered in the EHR to route patient-to-provider communications, a difficult task across frequent handoffs and staffing changes.
We now have the beginnings of an informed vision for inpatient portal design. Future research and industry directions include greater exploration of recognized concerns and how to best reconcile these concerns with the benefits of portals espoused by consumer health advocates and experienced by patients, caregivers, and providers in the reviewed studies. Specifically, we need a better understanding of how best to incorporate inpatient portals into routine care delivery in ways that are useful to both patients and providers. We also need a better understanding of why patients opt out of portal use. Most of the studies to date report on the set of patients who decided to use the portals, leaving a knowledge gap in design and use implications for patients who opted out. Studies should include comparisons of patient outcomes between users and nonusers. Although inpatient portals show promise, many questions remain.
Disclosures
The authors declare no conflicts of interest.
Personal health records (PHRs) are a broad group of applications “through which individuals can access, manage, and share their health information,” and are intended as a means to increase consumer health awareness, activation, safety, and self-efficacy.1 Patient portals—PHRs that are tethered to an electronic health record (EHR)—have expanded over the past decade, driven in part by the “Meaningful Use” EHR Incentive Program of the Centers for Medicare and Medicaid Services.2 This has been particularly true in the outpatient setting. Unfortunately, despite increased adoption and a large number of research studies, it is not clear whether outpatient portal use is associated with improved clinical outcomes.3
Both the use of portals in the inpatient setting and the research thereof are at a more nascent stage. In this issue of the Journal of Hospital Medicine, Kelly et al.4 provide a systematic review of the existing research on the implementation of inpatient portals. The authors identified 17 studies and categorized the papers’ findings into the following 3 themes: design, use and usability, and impact. Most of the studies elicited feedback from patients, caregivers, and/or providers – sometimes in multiple phases as portals were redesigned – allowing the authors to offer the following recommendations for inpatient portal design: portals should present timely information, include the care plan in ways patients can understand, and facilitate identification and communication with the care team.4 Most of the included studies focused on portal design and use, thereby limiting knowledge regarding impact on the outcomes portals are intended to target. All findings should be interpreted with caution, as many of the included studies were small and qualitative, most of them used convenience samples and subject-reported outcomes, and all were conducted at a single center. Many sites also used customized portals, thus limiting generalizability.
Participants often found portals to be useful, but this finding is of uncertain value in the absence of robust evidence on outcomes. In addition, providers included in the reviewed studies expressed concerns that have not yet been well studied, such as the potential impact of portals on workload and on patient anxiety. Some studies reported that provider concerns lessened following a portal rollout, but few studies evaluated physician input on features such as direct communication and test result reporting in active use. The outpatient portal literature suggests potential harm related to how results are delivered, thus placing importance on conducting additional inpatient studies. Patients value online access to their health information5 and in previous literature have indicated a preference for immediate access to results even if abnormal results would then be given without explanation.6 However, in a recent study, even normal findings delivered without context were a cause of negative emotions and increased calls to physicians.7 This effect could be more pronounced in inpatient settings, given the large volume of tests and abnormal results, the rapidly evolving treatment plans, and generally higher acuity and medical uncertainty.
This review and other current literature highlight challenges for vendors and hospitals. Vendors must ensure that patient health information is contextualized and delivered in a manner that meets individual learning styles.8 Patients and caregivers need clinical decision support to process today’s large amount of data, just as providers do. We must be careful not to implement patient portals in ways that increase cognitive load and generate anxiety and confusion. Hospitals have infrastructural challenges if portals are to be successful. Care provider information must be accurately registered in the EHR to route patient-to-provider communications, a difficult task across frequent handoffs and staffing changes.
We now have the beginnings of an informed vision for inpatient portal design. Future research and industry directions include greater exploration of recognized concerns and how to best reconcile these concerns with the benefits of portals espoused by consumer health advocates and experienced by patients, caregivers, and providers in the reviewed studies. Specifically, we need a better understanding of how best to incorporate inpatient portals into routine care delivery in ways that are useful to both patients and providers. We also need a better understanding of why patients opt out of portal use. Most of the studies to date report on the set of patients who decided to use the portals, leaving a knowledge gap in design and use implications for patients who opted out. Studies should include comparisons of patient outcomes between users and nonusers. Although inpatient portals show promise, many questions remain.
Disclosures
The authors declare no conflicts of interest.
1. Markle Foundation. Connecting Americans to their healthcare. Working group on policies for electronic information sharing between doctors and patients final report. https://www.markle.org/sites/default/files/CnctAmerHC_fullreport.pdf. Accessed February 18, 2018.
2. Centers for Medicare and Medicaid Services. Electronic health records (EHR) incentive programs. https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/index.html?redirect=/EHRIncentivePrograms. Accessed February 18, 2018.
3. Kruse CS, Bolton K, Freriks G. The effect of patient portals on quality outcomes and its implications to meaningful use: a systematic review. J Med Internet Res. 2015;17(2):e44-e48. DOI:10.2196/jmir.3171. PubMed
4. Kelly MM, Coller RJ, Hoonakker PLT. Inpatient portals for hospitalized patients and caregivers: a systematic review. J Hosp Med. 2018;13(5):405-412.Published online first December 20, 2017. PubMed
5. Peacock S, Reddy A, Leveille SG, et al. Patient portals and personal health information online: perception, access, and use by US adults. J Am Med Inform Assoc. 2017;24(e1):e173-e177. DOI:10.1093/jamia/ocw095. PubMed
6. Johnson AJ, Easterling D, Nelson R, Chen MY, Frankel RM. Access to radiologic reports via a patient portal: clinical simulations to investigate patient preferences. JACR. 2012;9(4):256-263. DOI:10.1016/j.jacr.2011.12.023. PubMed
7. Giardina TD, Baldwin J, Nystrom DT, Sittig DF, Singh H. Patient perceptions of receiving test results via online portals: a mixed-methods study. J Am Med Inform Assoc. 2018;25(4)440-446. DOI:10.1093/jamia/ocx140. PubMed
8. Dalal AK, Bates DW, Collins S. Opportunities and challenges for improving the patient experience in the acute and post–acute care setting using patient portals: the patient’s perspective. J Hosp Med. 2017;12(12):1012-1016. DOI:10.12788/jhm.2860. PubMed
1. Markle Foundation. Connecting Americans to their healthcare. Working group on policies for electronic information sharing between doctors and patients final report. https://www.markle.org/sites/default/files/CnctAmerHC_fullreport.pdf. Accessed February 18, 2018.
2. Centers for Medicare and Medicaid Services. Electronic health records (EHR) incentive programs. https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/index.html?redirect=/EHRIncentivePrograms. Accessed February 18, 2018.
3. Kruse CS, Bolton K, Freriks G. The effect of patient portals on quality outcomes and its implications to meaningful use: a systematic review. J Med Internet Res. 2015;17(2):e44-e48. DOI:10.2196/jmir.3171. PubMed
4. Kelly MM, Coller RJ, Hoonakker PLT. Inpatient portals for hospitalized patients and caregivers: a systematic review. J Hosp Med. 2018;13(5):405-412.Published online first December 20, 2017. PubMed
5. Peacock S, Reddy A, Leveille SG, et al. Patient portals and personal health information online: perception, access, and use by US adults. J Am Med Inform Assoc. 2017;24(e1):e173-e177. DOI:10.1093/jamia/ocw095. PubMed
6. Johnson AJ, Easterling D, Nelson R, Chen MY, Frankel RM. Access to radiologic reports via a patient portal: clinical simulations to investigate patient preferences. JACR. 2012;9(4):256-263. DOI:10.1016/j.jacr.2011.12.023. PubMed
7. Giardina TD, Baldwin J, Nystrom DT, Sittig DF, Singh H. Patient perceptions of receiving test results via online portals: a mixed-methods study. J Am Med Inform Assoc. 2018;25(4)440-446. DOI:10.1093/jamia/ocx140. PubMed
8. Dalal AK, Bates DW, Collins S. Opportunities and challenges for improving the patient experience in the acute and post–acute care setting using patient portals: the patient’s perspective. J Hosp Med. 2017;12(12):1012-1016. DOI:10.12788/jhm.2860. PubMed
© 2018 Society of Hospital Medicine
Is it Time to Re-Examine the Physical Exam?
“Am I supposed to have such a hard time feeling the kidneys?” “I think I’m doing it wrong,” echoed another classmate. The frustration of these first-year students, who were already overwhelmed by the three pages of physical exam techniques that they were responsible for, became increasingly visible as they palpated the abdomens of their standardized patients. Then, they asked the dreaded question: “How often do you do this on real patients?”
When we teach first-year medical students the physical exam, these students are already aware that they have never observed physicians perform these maneuvers in their own medical care. “How come I’ve never seen my doctor do this before?” is a common question that we are often asked. We as faculty struggle with demonstrating and defending techniques that we hardly ever use given their variable utility in daily clinical practice. However, students are told that they must be familiar with the various “tools” in the repertoire, and they are led to believe that these skills will be a fundamental part of their future practice as physicians. Of course, when they begin their clerkships, the truth is revealed: the currency on the wards revolves around the computer. The experienced and passionate clinicians who may astonish them with the bedside exam are the exception and are hardly the rule.
In this issue of Journal of Hospital Medicine, Bergl et al.1 found that when medical students rotated on their internal medicine clerkship, patients were rarely examined during attending rounds and were even examined less often when these rounds were not at the bedside. Although the students themselves consistently incorporated the physical exam into patient assessments and presentations, neither their findings nor those of the residents were ever validated by the attending physician or by others. Notably, the physical exam did not influence clinical decision making as much as one might expect.
These findings should not come as a surprise. The current generation of residents and junior attendings today are more accustomed to emphasizing labs, imaging studies, pathology reports, and other data within the electronic health record (EHR) and with formulating initial plans before having met the patient.2 Physicians become uneasy when asked to decide without the reassurance of daily lab results, as if the information in the EHR is highly fundamental to patient care. Caring for the “iPatient” often trumps revisiting and reexamining the real patient.3 Medical teams are also bombarded with increasing demands for their attention and time and are pushed to expedite patient discharges while constantly responding to documentation queries in the EHR. Emphasis on patient throughput, quality metrics, and multidisciplinary communication is essential to provide effective patient care but often feels at odds with opportunities for bedside teaching.
Although discussions on these obstacles have increased in recent years, time-motion studies spanning decades and even preceding the duty-hours era have consistently shown that physicians reserve little time for physical examination and direct patient care.4 In other words, the challenges in bringing physicians to the bedside might have less to do with environmental barriers than we think.
Much of what we teach about physical diagnosis is imperfect,5 and the routine annual exam might well be eliminated given its low yield.6 Nevertheless, we cannot discount the importance of the physical exam in fostering the bond between the patient and the healthcare provider, particularly in patients with acute illnesses, and in making the interaction meaningful to the practitioner.
Many of us can easily recall embarrassing examples of obvious physical exam findings that were critical and overlooked with consequences – the missed incarcerated hernia in a patient labeled with gastritis and vomiting, or the patient with chest pain who had to undergo catheterization because the shingles rash was missed. The confidence in normal findings that might save a patient from unnecessary lab tests, imaging, or consultation is often not discussed. The burden is on us to retire maneuvers that have outlived their usefulness and to demonstrate to students the hazards and consequences of poor examination skills. We must also further what we know and understand about the physical exam as Osler, Laennec, and others before us once did. Point-of-care ultrasound is only one example of how innovation can bring trainees to the bedside, excite learners, engage patients, and affect care in a meaningful way while enhancing the nonultrasound-based skills of practitioners.7
It is promising that the students in this study consistently examined their patients each day. As future physicians, they can be very enthusiastic learners eager to apply the physical exam skills they have recently acquired during their early years of training. However, this excitement can taper off if not actively encouraged and reinforced, especially if role models are unintentionally sending the message that the physical exam does not matter or emphasizing exam maneuvers that do not serve a meaningful purpose. New technology will hopefully help us develop novel exam skills. If we can advance what we can diagnose at the bedside, students will remain motivated to improve and learn exam skills that truly affect patient-care decisions. After all, one day, they too will serve as role models for the next generation of physicians and hopefully will be the ones taking care of us at the bedside.
Disclosures
The authors declare no conflicts of interest.
1. Bergl PA, Taylor AC, Klumb J, et al. Teaching physical examination to medical students on inpatient medicine reams: A prospective mixed-methods descriptive study. J Hosp Med. 2018;13:399-402. PubMed
2. Chi J, Verghese A. Clinical education and the electronic health record: the flipped patient. JAMA. 2010;312(22):2331-2332. DOI: 10.1001/jama.2014.12820. PubMed
2. Verghese A. Culture shock—patient as icon, icon as patient. N Engl J Med. 2008;359(26):2748-2751. DOI: 10.1056/NEJMp0807461 PubMed
3. Czernik Z, Lin CT. A piece of my mind. Time at the bedside (Computing). JAMA. 2016;315(22):2399-2400. DOI: 10.1001/jama.2016.1722 PubMed
5. Jauhar S. The demise of the physical exam. N Engl J Med. 2006;354(6):548-551. DOI: 10.1056/NEJMp068013 PubMed
6. Mehrotra A, Prochazka A. Improving value in health care--against the annual physical. N Engl J Med. 2015;373(16):1485-1487. DOI: 10.1056/NEJMp1507485 PubMed
7. Kugler J. Price and the evolution of the physical examination. JAMA Cardiol. 2018. DOI: 10.1001/jamacardio.2018.0002. [Epub ahead of print] PubMed
“Am I supposed to have such a hard time feeling the kidneys?” “I think I’m doing it wrong,” echoed another classmate. The frustration of these first-year students, who were already overwhelmed by the three pages of physical exam techniques that they were responsible for, became increasingly visible as they palpated the abdomens of their standardized patients. Then, they asked the dreaded question: “How often do you do this on real patients?”
When we teach first-year medical students the physical exam, these students are already aware that they have never observed physicians perform these maneuvers in their own medical care. “How come I’ve never seen my doctor do this before?” is a common question that we are often asked. We as faculty struggle with demonstrating and defending techniques that we hardly ever use given their variable utility in daily clinical practice. However, students are told that they must be familiar with the various “tools” in the repertoire, and they are led to believe that these skills will be a fundamental part of their future practice as physicians. Of course, when they begin their clerkships, the truth is revealed: the currency on the wards revolves around the computer. The experienced and passionate clinicians who may astonish them with the bedside exam are the exception and are hardly the rule.
In this issue of Journal of Hospital Medicine, Bergl et al.1 found that when medical students rotated on their internal medicine clerkship, patients were rarely examined during attending rounds and were even examined less often when these rounds were not at the bedside. Although the students themselves consistently incorporated the physical exam into patient assessments and presentations, neither their findings nor those of the residents were ever validated by the attending physician or by others. Notably, the physical exam did not influence clinical decision making as much as one might expect.
These findings should not come as a surprise. The current generation of residents and junior attendings today are more accustomed to emphasizing labs, imaging studies, pathology reports, and other data within the electronic health record (EHR) and with formulating initial plans before having met the patient.2 Physicians become uneasy when asked to decide without the reassurance of daily lab results, as if the information in the EHR is highly fundamental to patient care. Caring for the “iPatient” often trumps revisiting and reexamining the real patient.3 Medical teams are also bombarded with increasing demands for their attention and time and are pushed to expedite patient discharges while constantly responding to documentation queries in the EHR. Emphasis on patient throughput, quality metrics, and multidisciplinary communication is essential to provide effective patient care but often feels at odds with opportunities for bedside teaching.
Although discussions on these obstacles have increased in recent years, time-motion studies spanning decades and even preceding the duty-hours era have consistently shown that physicians reserve little time for physical examination and direct patient care.4 In other words, the challenges in bringing physicians to the bedside might have less to do with environmental barriers than we think.
Much of what we teach about physical diagnosis is imperfect,5 and the routine annual exam might well be eliminated given its low yield.6 Nevertheless, we cannot discount the importance of the physical exam in fostering the bond between the patient and the healthcare provider, particularly in patients with acute illnesses, and in making the interaction meaningful to the practitioner.
Many of us can easily recall embarrassing examples of obvious physical exam findings that were critical and overlooked with consequences – the missed incarcerated hernia in a patient labeled with gastritis and vomiting, or the patient with chest pain who had to undergo catheterization because the shingles rash was missed. The confidence in normal findings that might save a patient from unnecessary lab tests, imaging, or consultation is often not discussed. The burden is on us to retire maneuvers that have outlived their usefulness and to demonstrate to students the hazards and consequences of poor examination skills. We must also further what we know and understand about the physical exam as Osler, Laennec, and others before us once did. Point-of-care ultrasound is only one example of how innovation can bring trainees to the bedside, excite learners, engage patients, and affect care in a meaningful way while enhancing the nonultrasound-based skills of practitioners.7
It is promising that the students in this study consistently examined their patients each day. As future physicians, they can be very enthusiastic learners eager to apply the physical exam skills they have recently acquired during their early years of training. However, this excitement can taper off if not actively encouraged and reinforced, especially if role models are unintentionally sending the message that the physical exam does not matter or emphasizing exam maneuvers that do not serve a meaningful purpose. New technology will hopefully help us develop novel exam skills. If we can advance what we can diagnose at the bedside, students will remain motivated to improve and learn exam skills that truly affect patient-care decisions. After all, one day, they too will serve as role models for the next generation of physicians and hopefully will be the ones taking care of us at the bedside.
Disclosures
The authors declare no conflicts of interest.
“Am I supposed to have such a hard time feeling the kidneys?” “I think I’m doing it wrong,” echoed another classmate. The frustration of these first-year students, who were already overwhelmed by the three pages of physical exam techniques that they were responsible for, became increasingly visible as they palpated the abdomens of their standardized patients. Then, they asked the dreaded question: “How often do you do this on real patients?”
When we teach first-year medical students the physical exam, these students are already aware that they have never observed physicians perform these maneuvers in their own medical care. “How come I’ve never seen my doctor do this before?” is a common question that we are often asked. We as faculty struggle with demonstrating and defending techniques that we hardly ever use given their variable utility in daily clinical practice. However, students are told that they must be familiar with the various “tools” in the repertoire, and they are led to believe that these skills will be a fundamental part of their future practice as physicians. Of course, when they begin their clerkships, the truth is revealed: the currency on the wards revolves around the computer. The experienced and passionate clinicians who may astonish them with the bedside exam are the exception and are hardly the rule.
In this issue of Journal of Hospital Medicine, Bergl et al.1 found that when medical students rotated on their internal medicine clerkship, patients were rarely examined during attending rounds and were even examined less often when these rounds were not at the bedside. Although the students themselves consistently incorporated the physical exam into patient assessments and presentations, neither their findings nor those of the residents were ever validated by the attending physician or by others. Notably, the physical exam did not influence clinical decision making as much as one might expect.
These findings should not come as a surprise. The current generation of residents and junior attendings today are more accustomed to emphasizing labs, imaging studies, pathology reports, and other data within the electronic health record (EHR) and with formulating initial plans before having met the patient.2 Physicians become uneasy when asked to decide without the reassurance of daily lab results, as if the information in the EHR is highly fundamental to patient care. Caring for the “iPatient” often trumps revisiting and reexamining the real patient.3 Medical teams are also bombarded with increasing demands for their attention and time and are pushed to expedite patient discharges while constantly responding to documentation queries in the EHR. Emphasis on patient throughput, quality metrics, and multidisciplinary communication is essential to provide effective patient care but often feels at odds with opportunities for bedside teaching.
Although discussions on these obstacles have increased in recent years, time-motion studies spanning decades and even preceding the duty-hours era have consistently shown that physicians reserve little time for physical examination and direct patient care.4 In other words, the challenges in bringing physicians to the bedside might have less to do with environmental barriers than we think.
Much of what we teach about physical diagnosis is imperfect,5 and the routine annual exam might well be eliminated given its low yield.6 Nevertheless, we cannot discount the importance of the physical exam in fostering the bond between the patient and the healthcare provider, particularly in patients with acute illnesses, and in making the interaction meaningful to the practitioner.
Many of us can easily recall embarrassing examples of obvious physical exam findings that were critical and overlooked with consequences – the missed incarcerated hernia in a patient labeled with gastritis and vomiting, or the patient with chest pain who had to undergo catheterization because the shingles rash was missed. The confidence in normal findings that might save a patient from unnecessary lab tests, imaging, or consultation is often not discussed. The burden is on us to retire maneuvers that have outlived their usefulness and to demonstrate to students the hazards and consequences of poor examination skills. We must also further what we know and understand about the physical exam as Osler, Laennec, and others before us once did. Point-of-care ultrasound is only one example of how innovation can bring trainees to the bedside, excite learners, engage patients, and affect care in a meaningful way while enhancing the nonultrasound-based skills of practitioners.7
It is promising that the students in this study consistently examined their patients each day. As future physicians, they can be very enthusiastic learners eager to apply the physical exam skills they have recently acquired during their early years of training. However, this excitement can taper off if not actively encouraged and reinforced, especially if role models are unintentionally sending the message that the physical exam does not matter or emphasizing exam maneuvers that do not serve a meaningful purpose. New technology will hopefully help us develop novel exam skills. If we can advance what we can diagnose at the bedside, students will remain motivated to improve and learn exam skills that truly affect patient-care decisions. After all, one day, they too will serve as role models for the next generation of physicians and hopefully will be the ones taking care of us at the bedside.
Disclosures
The authors declare no conflicts of interest.
1. Bergl PA, Taylor AC, Klumb J, et al. Teaching physical examination to medical students on inpatient medicine reams: A prospective mixed-methods descriptive study. J Hosp Med. 2018;13:399-402. PubMed
2. Chi J, Verghese A. Clinical education and the electronic health record: the flipped patient. JAMA. 2010;312(22):2331-2332. DOI: 10.1001/jama.2014.12820. PubMed
2. Verghese A. Culture shock—patient as icon, icon as patient. N Engl J Med. 2008;359(26):2748-2751. DOI: 10.1056/NEJMp0807461 PubMed
3. Czernik Z, Lin CT. A piece of my mind. Time at the bedside (Computing). JAMA. 2016;315(22):2399-2400. DOI: 10.1001/jama.2016.1722 PubMed
5. Jauhar S. The demise of the physical exam. N Engl J Med. 2006;354(6):548-551. DOI: 10.1056/NEJMp068013 PubMed
6. Mehrotra A, Prochazka A. Improving value in health care--against the annual physical. N Engl J Med. 2015;373(16):1485-1487. DOI: 10.1056/NEJMp1507485 PubMed
7. Kugler J. Price and the evolution of the physical examination. JAMA Cardiol. 2018. DOI: 10.1001/jamacardio.2018.0002. [Epub ahead of print] PubMed
1. Bergl PA, Taylor AC, Klumb J, et al. Teaching physical examination to medical students on inpatient medicine reams: A prospective mixed-methods descriptive study. J Hosp Med. 2018;13:399-402. PubMed
2. Chi J, Verghese A. Clinical education and the electronic health record: the flipped patient. JAMA. 2010;312(22):2331-2332. DOI: 10.1001/jama.2014.12820. PubMed
2. Verghese A. Culture shock—patient as icon, icon as patient. N Engl J Med. 2008;359(26):2748-2751. DOI: 10.1056/NEJMp0807461 PubMed
3. Czernik Z, Lin CT. A piece of my mind. Time at the bedside (Computing). JAMA. 2016;315(22):2399-2400. DOI: 10.1001/jama.2016.1722 PubMed
5. Jauhar S. The demise of the physical exam. N Engl J Med. 2006;354(6):548-551. DOI: 10.1056/NEJMp068013 PubMed
6. Mehrotra A, Prochazka A. Improving value in health care--against the annual physical. N Engl J Med. 2015;373(16):1485-1487. DOI: 10.1056/NEJMp1507485 PubMed
7. Kugler J. Price and the evolution of the physical examination. JAMA Cardiol. 2018. DOI: 10.1001/jamacardio.2018.0002. [Epub ahead of print] PubMed
©2018 Society of Hospital Medicine
Faculty Development for Hospitalists: A Call to Arms
Over the past two decades, the field of hospital medicine has gone from relative obscurity to a viable career pathway for approximately 50,000 physicians in this country.1 A subset of hospitalists pursue careers in academic medicine, which is a pathway that traditionally includes education and scholarship in addition to patient care. While the academic career pathway is well paved in many clinical specialties, it is still relatively underdeveloped for academic hospitalists, and thus what defines career success for this group is even less clear.
In this issue of the Journal of Hospital Medicine, Cumbler et al. performed a qualitative analysis to explore how early career academic hospitalists self-define and perceive their career success.2 Drawing on interviews with 17 early-career hospitalists at 3 academic medical centers, the authors created a theoretical framework organized around a traditional conceptual model of career success that is divided into intrinsic and extrinsic motivating factors. They found that early-career academic hospitalists, (clinician-educators in first 2-5 years), defined their career success almost exclusively around factors intrinsic to their day-to-day job. These factors included such things as excitement about their daily work, developing proficiency in the delivery of high-quality clinical care, and passion for doing work that is meaningful to them. In addition to these immediate job satisfiers, many hospitalists emphasized long-term career success factors such as becoming an expert in a particular domain of hospital medicine and gaining respect and recognition within their local or national environment. Surprisingly, compensation and career advancement through promotion, two traditional external career success factors, were not uniformly valued.
These findings come at a critical time for our field in which early-career faculty outnumber mid- and late-career faculty by an order of magnitude. Indeed, how to develop, promote, sustain, and retain young hospitalists is a topic on the minds of most hospital medicine group directors. Putting aside the impact of hospitalist turnover on productivity, patient care outcomes, and morale within an individual hospital medicine group, we agree with the authors that understanding and cultivating career success for academic hospitalists is imperative for the future of our field. For this reason, we launched a formal faculty development program at Penn this year, which focuses on supporting the growth of hospitalists in their first two years on faculty. The findings of this study provide interesting new perspectives and encourage us to continue our focus on early-career academic hospitalists. We laud the previous efforts in this area and hope that the paper by Cumbler et al. encourages and inspires other programs to start or accelerate their hospitalist faculty development efforts.3-5
However, some findings from this study are somewhat perplexing or even a bit discouraging for those who are invested in faculty development in academia. For example, the authors raise the possibility that there may be a disconnect in the minds of early-career hospitalists as it pertains to their thoughts on career success. On the one hand, the hospitalists interviewed in this study are happy doing their clinical work and cite this as a primary driver of their career success. On the other hand, they equate career success with things such as developing expertise within a particular domain of hospital medicine, acquiring leadership roles, collaborating academically with other specialties or professions, or developing new innovations. Presumably this is part of the reason that they selected a job in an academic setting as opposed to a community setting. However, in order to achieve these goals, one must devote time and effort to purposefully developing them. Therefore, identifying and developing mentors who can assist early-career hospitalists with identifying, articulating, and developing strategies to achieve both their short- and long-term career goals is critical. One mentor–mentee conversation may reveal that an individual hospitalist values being an excellent clinician and has little interest in developing a niche within hospital medicine; another may reveal a lack of awareness of available professional development resources; still another may uncover a lack of realism regarding the time or skills it takes to achieve a particular career goal. These realities highlight an imperative for our field to develop robust and sustainable mentorship programs for not only early-career hospitalists but also some mid-career hospitalists whose careers may not yet be fully developed. Indeed, one of the biggest challenges that have emerged in our experience with a faculty development program at Penn is creating meaningful mentorship and career development advice for mid-career hospitalists (late assistant or early associate professors who are typically 5-10 years into their careers).
We found it interesting that the hospitalists interviewed did not mention three of the four pillars of career satisfaction outlined in the white paper on Hospitalist Career Satisfaction from the Society for Hospital Medicine: workload schedule, autonomy control, and community/environment.6 Perhaps this is because hospitalists, like many other professionals, recognize that feeling satisfied in one’s career is not the same as feeling successful. Satisfaction in one’s career refers to the foundational needs that one requires in order to feel content, whereas success is more often equated with achievement, even if that achievement is simply the acquisition of one’s goals for themselves. The reality is that given the constant growth and change within teaching hospitals, and therefore academic hospital medicine groups, tending to the satisfiers for hospitalists (eg, schedule and workload) often takes a front seat to assisting faculty in achieving their individual career potential. We assert that despite the inherent difficulty, academic hospital medicine group leaders need to focus their attention on both the satisfaction and career success of their early-career faculty.
Finally, this paper raises many interesting questions
In conclusion, the findings of Cumbler et al. should promote unrest among leaders of academic hospital medicine groups and their departments of medicine. While it is inspiring to see so many early-career hospitalists focused on their daily happiness at work, we are unsure about whether they have the knowledge, tools, and guidance to achieve their self-professed academic goals, which many equate with career success. Given the continued growth of the hospital medicine workforce, we view this important new work as a national call to arms for the purposeful development of academic hospitalist faculty development programs.
Disclosures
Dr. Myers and Dr. Greysen have nothing to disclose.
1. Wachter RM, Goldman L. Zero to 50,000-The 20th anniversary of the hospitalist. N Engl J Med. 2016;375(11):1009-1011. PubMed
2. Cumbler E, Yirdaw E, Kneeland P, et al. What is career success for academic hospitalists? A qualitative analysis of early-career faculty perspectives. J Hosp Med. 2018;13(5):372-377. doi: 10.12788/jhm.2924. Published online first January 31, 2018. PubMed
3. Nagarur A, O’Neill RM, Lawton D, Greenwald JL. Supporting faculty development in hospital medicine: design and implementation of a personalized structured mentoring program. J Hosp Med. 2018;13(2):96-99. PubMed
4. Sehgal NL, Sharpe BA, Auerbach AA, Wachter RM. Investing in the future: building an academic hospitalist faculty development program. J Hosp Med. 2011;6(3):161-166. PubMed
5. Howell E, Kravet S, Kisuule F, Wright SM. An innovative approach to supporting hospitalist physicians towards academic success. J Hosp Med. 2008;3(4):314-318. PubMed
6. Society of Hospital Medicine Career Satisfaction Taskforce: A Challenge for a new Specialty. A White paper on hospitalist career satisfaction. http://dev.hospitalmedicine.org/Web/Media_Center/shm_white_papers.aspx . Accessed February 9, 2018.
Over the past two decades, the field of hospital medicine has gone from relative obscurity to a viable career pathway for approximately 50,000 physicians in this country.1 A subset of hospitalists pursue careers in academic medicine, which is a pathway that traditionally includes education and scholarship in addition to patient care. While the academic career pathway is well paved in many clinical specialties, it is still relatively underdeveloped for academic hospitalists, and thus what defines career success for this group is even less clear.
In this issue of the Journal of Hospital Medicine, Cumbler et al. performed a qualitative analysis to explore how early career academic hospitalists self-define and perceive their career success.2 Drawing on interviews with 17 early-career hospitalists at 3 academic medical centers, the authors created a theoretical framework organized around a traditional conceptual model of career success that is divided into intrinsic and extrinsic motivating factors. They found that early-career academic hospitalists, (clinician-educators in first 2-5 years), defined their career success almost exclusively around factors intrinsic to their day-to-day job. These factors included such things as excitement about their daily work, developing proficiency in the delivery of high-quality clinical care, and passion for doing work that is meaningful to them. In addition to these immediate job satisfiers, many hospitalists emphasized long-term career success factors such as becoming an expert in a particular domain of hospital medicine and gaining respect and recognition within their local or national environment. Surprisingly, compensation and career advancement through promotion, two traditional external career success factors, were not uniformly valued.
These findings come at a critical time for our field in which early-career faculty outnumber mid- and late-career faculty by an order of magnitude. Indeed, how to develop, promote, sustain, and retain young hospitalists is a topic on the minds of most hospital medicine group directors. Putting aside the impact of hospitalist turnover on productivity, patient care outcomes, and morale within an individual hospital medicine group, we agree with the authors that understanding and cultivating career success for academic hospitalists is imperative for the future of our field. For this reason, we launched a formal faculty development program at Penn this year, which focuses on supporting the growth of hospitalists in their first two years on faculty. The findings of this study provide interesting new perspectives and encourage us to continue our focus on early-career academic hospitalists. We laud the previous efforts in this area and hope that the paper by Cumbler et al. encourages and inspires other programs to start or accelerate their hospitalist faculty development efforts.3-5
However, some findings from this study are somewhat perplexing or even a bit discouraging for those who are invested in faculty development in academia. For example, the authors raise the possibility that there may be a disconnect in the minds of early-career hospitalists as it pertains to their thoughts on career success. On the one hand, the hospitalists interviewed in this study are happy doing their clinical work and cite this as a primary driver of their career success. On the other hand, they equate career success with things such as developing expertise within a particular domain of hospital medicine, acquiring leadership roles, collaborating academically with other specialties or professions, or developing new innovations. Presumably this is part of the reason that they selected a job in an academic setting as opposed to a community setting. However, in order to achieve these goals, one must devote time and effort to purposefully developing them. Therefore, identifying and developing mentors who can assist early-career hospitalists with identifying, articulating, and developing strategies to achieve both their short- and long-term career goals is critical. One mentor–mentee conversation may reveal that an individual hospitalist values being an excellent clinician and has little interest in developing a niche within hospital medicine; another may reveal a lack of awareness of available professional development resources; still another may uncover a lack of realism regarding the time or skills it takes to achieve a particular career goal. These realities highlight an imperative for our field to develop robust and sustainable mentorship programs for not only early-career hospitalists but also some mid-career hospitalists whose careers may not yet be fully developed. Indeed, one of the biggest challenges that have emerged in our experience with a faculty development program at Penn is creating meaningful mentorship and career development advice for mid-career hospitalists (late assistant or early associate professors who are typically 5-10 years into their careers).
We found it interesting that the hospitalists interviewed did not mention three of the four pillars of career satisfaction outlined in the white paper on Hospitalist Career Satisfaction from the Society for Hospital Medicine: workload schedule, autonomy control, and community/environment.6 Perhaps this is because hospitalists, like many other professionals, recognize that feeling satisfied in one’s career is not the same as feeling successful. Satisfaction in one’s career refers to the foundational needs that one requires in order to feel content, whereas success is more often equated with achievement, even if that achievement is simply the acquisition of one’s goals for themselves. The reality is that given the constant growth and change within teaching hospitals, and therefore academic hospital medicine groups, tending to the satisfiers for hospitalists (eg, schedule and workload) often takes a front seat to assisting faculty in achieving their individual career potential. We assert that despite the inherent difficulty, academic hospital medicine group leaders need to focus their attention on both the satisfaction and career success of their early-career faculty.
Finally, this paper raises many interesting questions
In conclusion, the findings of Cumbler et al. should promote unrest among leaders of academic hospital medicine groups and their departments of medicine. While it is inspiring to see so many early-career hospitalists focused on their daily happiness at work, we are unsure about whether they have the knowledge, tools, and guidance to achieve their self-professed academic goals, which many equate with career success. Given the continued growth of the hospital medicine workforce, we view this important new work as a national call to arms for the purposeful development of academic hospitalist faculty development programs.
Disclosures
Dr. Myers and Dr. Greysen have nothing to disclose.
Over the past two decades, the field of hospital medicine has gone from relative obscurity to a viable career pathway for approximately 50,000 physicians in this country.1 A subset of hospitalists pursue careers in academic medicine, which is a pathway that traditionally includes education and scholarship in addition to patient care. While the academic career pathway is well paved in many clinical specialties, it is still relatively underdeveloped for academic hospitalists, and thus what defines career success for this group is even less clear.
In this issue of the Journal of Hospital Medicine, Cumbler et al. performed a qualitative analysis to explore how early career academic hospitalists self-define and perceive their career success.2 Drawing on interviews with 17 early-career hospitalists at 3 academic medical centers, the authors created a theoretical framework organized around a traditional conceptual model of career success that is divided into intrinsic and extrinsic motivating factors. They found that early-career academic hospitalists, (clinician-educators in first 2-5 years), defined their career success almost exclusively around factors intrinsic to their day-to-day job. These factors included such things as excitement about their daily work, developing proficiency in the delivery of high-quality clinical care, and passion for doing work that is meaningful to them. In addition to these immediate job satisfiers, many hospitalists emphasized long-term career success factors such as becoming an expert in a particular domain of hospital medicine and gaining respect and recognition within their local or national environment. Surprisingly, compensation and career advancement through promotion, two traditional external career success factors, were not uniformly valued.
These findings come at a critical time for our field in which early-career faculty outnumber mid- and late-career faculty by an order of magnitude. Indeed, how to develop, promote, sustain, and retain young hospitalists is a topic on the minds of most hospital medicine group directors. Putting aside the impact of hospitalist turnover on productivity, patient care outcomes, and morale within an individual hospital medicine group, we agree with the authors that understanding and cultivating career success for academic hospitalists is imperative for the future of our field. For this reason, we launched a formal faculty development program at Penn this year, which focuses on supporting the growth of hospitalists in their first two years on faculty. The findings of this study provide interesting new perspectives and encourage us to continue our focus on early-career academic hospitalists. We laud the previous efforts in this area and hope that the paper by Cumbler et al. encourages and inspires other programs to start or accelerate their hospitalist faculty development efforts.3-5
However, some findings from this study are somewhat perplexing or even a bit discouraging for those who are invested in faculty development in academia. For example, the authors raise the possibility that there may be a disconnect in the minds of early-career hospitalists as it pertains to their thoughts on career success. On the one hand, the hospitalists interviewed in this study are happy doing their clinical work and cite this as a primary driver of their career success. On the other hand, they equate career success with things such as developing expertise within a particular domain of hospital medicine, acquiring leadership roles, collaborating academically with other specialties or professions, or developing new innovations. Presumably this is part of the reason that they selected a job in an academic setting as opposed to a community setting. However, in order to achieve these goals, one must devote time and effort to purposefully developing them. Therefore, identifying and developing mentors who can assist early-career hospitalists with identifying, articulating, and developing strategies to achieve both their short- and long-term career goals is critical. One mentor–mentee conversation may reveal that an individual hospitalist values being an excellent clinician and has little interest in developing a niche within hospital medicine; another may reveal a lack of awareness of available professional development resources; still another may uncover a lack of realism regarding the time or skills it takes to achieve a particular career goal. These realities highlight an imperative for our field to develop robust and sustainable mentorship programs for not only early-career hospitalists but also some mid-career hospitalists whose careers may not yet be fully developed. Indeed, one of the biggest challenges that have emerged in our experience with a faculty development program at Penn is creating meaningful mentorship and career development advice for mid-career hospitalists (late assistant or early associate professors who are typically 5-10 years into their careers).
We found it interesting that the hospitalists interviewed did not mention three of the four pillars of career satisfaction outlined in the white paper on Hospitalist Career Satisfaction from the Society for Hospital Medicine: workload schedule, autonomy control, and community/environment.6 Perhaps this is because hospitalists, like many other professionals, recognize that feeling satisfied in one’s career is not the same as feeling successful. Satisfaction in one’s career refers to the foundational needs that one requires in order to feel content, whereas success is more often equated with achievement, even if that achievement is simply the acquisition of one’s goals for themselves. The reality is that given the constant growth and change within teaching hospitals, and therefore academic hospital medicine groups, tending to the satisfiers for hospitalists (eg, schedule and workload) often takes a front seat to assisting faculty in achieving their individual career potential. We assert that despite the inherent difficulty, academic hospital medicine group leaders need to focus their attention on both the satisfaction and career success of their early-career faculty.
Finally, this paper raises many interesting questions
In conclusion, the findings of Cumbler et al. should promote unrest among leaders of academic hospital medicine groups and their departments of medicine. While it is inspiring to see so many early-career hospitalists focused on their daily happiness at work, we are unsure about whether they have the knowledge, tools, and guidance to achieve their self-professed academic goals, which many equate with career success. Given the continued growth of the hospital medicine workforce, we view this important new work as a national call to arms for the purposeful development of academic hospitalist faculty development programs.
Disclosures
Dr. Myers and Dr. Greysen have nothing to disclose.
1. Wachter RM, Goldman L. Zero to 50,000-The 20th anniversary of the hospitalist. N Engl J Med. 2016;375(11):1009-1011. PubMed
2. Cumbler E, Yirdaw E, Kneeland P, et al. What is career success for academic hospitalists? A qualitative analysis of early-career faculty perspectives. J Hosp Med. 2018;13(5):372-377. doi: 10.12788/jhm.2924. Published online first January 31, 2018. PubMed
3. Nagarur A, O’Neill RM, Lawton D, Greenwald JL. Supporting faculty development in hospital medicine: design and implementation of a personalized structured mentoring program. J Hosp Med. 2018;13(2):96-99. PubMed
4. Sehgal NL, Sharpe BA, Auerbach AA, Wachter RM. Investing in the future: building an academic hospitalist faculty development program. J Hosp Med. 2011;6(3):161-166. PubMed
5. Howell E, Kravet S, Kisuule F, Wright SM. An innovative approach to supporting hospitalist physicians towards academic success. J Hosp Med. 2008;3(4):314-318. PubMed
6. Society of Hospital Medicine Career Satisfaction Taskforce: A Challenge for a new Specialty. A White paper on hospitalist career satisfaction. http://dev.hospitalmedicine.org/Web/Media_Center/shm_white_papers.aspx . Accessed February 9, 2018.
1. Wachter RM, Goldman L. Zero to 50,000-The 20th anniversary of the hospitalist. N Engl J Med. 2016;375(11):1009-1011. PubMed
2. Cumbler E, Yirdaw E, Kneeland P, et al. What is career success for academic hospitalists? A qualitative analysis of early-career faculty perspectives. J Hosp Med. 2018;13(5):372-377. doi: 10.12788/jhm.2924. Published online first January 31, 2018. PubMed
3. Nagarur A, O’Neill RM, Lawton D, Greenwald JL. Supporting faculty development in hospital medicine: design and implementation of a personalized structured mentoring program. J Hosp Med. 2018;13(2):96-99. PubMed
4. Sehgal NL, Sharpe BA, Auerbach AA, Wachter RM. Investing in the future: building an academic hospitalist faculty development program. J Hosp Med. 2011;6(3):161-166. PubMed
5. Howell E, Kravet S, Kisuule F, Wright SM. An innovative approach to supporting hospitalist physicians towards academic success. J Hosp Med. 2008;3(4):314-318. PubMed
6. Society of Hospital Medicine Career Satisfaction Taskforce: A Challenge for a new Specialty. A White paper on hospitalist career satisfaction. http://dev.hospitalmedicine.org/Web/Media_Center/shm_white_papers.aspx . Accessed February 9, 2018.
©2018 Society of Hospital Medicine
Teaching Physical Examination to Medical Students on Inpatient Medicine Teams: A Prospective, Mixed-Methods Descriptive Study
1Medical College of Wisconsin Affiliated Hospitals, Milwaukee, Wisconsin. At the time of this study, Dr. Bergl was with the Division of General Internal Medicine, Medical College of Wisconsin, Milwaukee, Wisconsin. 2Medical College of Wisconsin, Milwaukee, Wisconsin.Physical examination (PE) is a core clinical skill in undergraduate medical education.1 Although the optimal approach to teaching clinical skills is debated, robust preclinical curricula should generally be followed by iterative skill development during clinical rotations.2,3
The internal medicine rotation represents a critical time to enhance PE skills. Diagnostic decision making and PE are highly prioritized competencies for the internal medicine clerkship,4 and students will likely utilize many core examination skills1,2 during this time. Bedside teaching of PE during the internal medicine service also provides an opportunity for students to receive feedback based on direct observation,5 a sine qua non of competency-based assessment.
Unfortunately, current internal medicine training environments limit opportunities for workplace-based instruction in PE. Recent studies suggest diminishing time spent on bedside patient care and teaching, with computer-based “indirect patient care” dominating much of the clinical workday of internal medicine services.6-8 However, the literature does not delineate how often medical students are enhancing their PE skills during clinical rotations or describe how the educational environment may influence PE teaching.
We aimed to describe the content and context of PE instruction during the internal medicine clerkship workflow. Specifically, we sought to explore what strategies physician team members used to teach PE to students. We also sought to describe factors in the inpatient learning environment that might explain why physical examination (PE) instruction occurs infrequently.
METHODS
We conducted a prospective mixed-methods study using time motion analysis, checklists on clinical teaching, and daily open-ended observations written by a trained observer from June through August 2015 at a single academic medical center. Subjects were recruited from internal medicine teaching teams and were allowed to opt out. Teaching teams had 2 formats: (1) traditional team with an attending physician (hospitalist or general internist), a senior resident, 2 interns, a fourth-year medical student, and 2 third-year students or (2) hospitalist team in which a third-year student works directly with a hospitalist and advanced practitioner. The proposal was submitted to the Medical College of Wisconsin Institutional Review Board and deemed exempt from further review.
All observations were carried out by a single investigator (A.T.), who was a second-year medical student at the time. To train this observer and to pilot the data collection instruments, our lead investigator (P.B.) directly supervised our observer on 4 separate occasions, totaling over 12 hours of mentored co-observation. Immediately after each training session, both investigators (A.T. and P.B.) debriefed to compare notes, to review checklists on recorded observations, and to discuss areas of uncertainty. During the training period, formal metrics of agreement (eg, kappa coefficients) were not gathered, as data collection instruments were still being refined.
Observation periods were centered on third-year medical students and their interactions with patients and members of the teaching team. Observed activities included pre-rounding, teaching rounds with the attending physician, and new patient admissions during call days. Observations generally occurred between the hours of 7 AM and 6 PM, and we limited periods of observation to 3 consecutive hours to minimize observer fatigue. Observation periods were selected to maximize the number of subjects and teams observed, to adequately capture pre-rounding and new admissions activities, and to account for variations in rounding styles throughout the call cycle. Teams were excluded if a member of the study team was an attending physician on the clinical team or if any member of the patient care team had opted out of the study.
Data were collected on paper checklists that included idealized bedside teaching activities around PE. Teaching activities were identified through a review of relevant literature9,10 and were further informed by our senior investigator’s own experience with faculty development in this area11 and team members’ attendance at bedside teaching workshops. At the end of each day, our observer also wrote brief observations that summarized factors affecting bedside teaching of PE. Checklist data were transferred to an Excel file (Microsoft), and written observations were imported into NVivo 10 (QRS International, Melbourne, Australia) for coding and analysis.
Checklist data were analyzed using simple descriptive statistics. We compared time spent on various types of rounding using ANOVA, and we used a Student two-tailed t-test to compare the amount of time students spent examining patients on pre-rounds versus new admissions. To ascertain differences in the frequency of PE teaching activities by location, we used chi-squared tests. Statistical analysis was performed using embedded statistics functions in Microsoft Excel. A P value of <.05 was used as the cut-off for significance.
We analyzed the written observations using conventional qualitative content analysis. Two investigators (A.T. and P.B.) reviewed the written comments and used open coding to devise a preliminary inductive coding scheme. Codes were refined iteratively, and a schema of categories and nodes was outlined in a codebook that was periodically reviewed by the entire research team. The coding investigators met regularly to ensure consistency in coding, and a third team member remained available to reconcile significant disagreements in code definitions.
RESULTS
Eighty-one subjects participated in the study: 21 were attending physicians, 12 residents, 21 interns, 11 senior medical students, and 26 junior medical students. We observed 16 distinct inpatient teaching teams and 329 unique patient-related events (discussions and/or patient-clinician encounters), with most events being observed during attending rounds (269/329, or 82%). There were 123 encounters at the bedside, averaging 7 minutes; 43 encounters occurred in the hallway, averaging 8 minutes each; and 163 encounters occurred in a workroom and averaged 7 minutes per patient discussion. We also observed 28 student-patient encounters during pre-round activities and 30 student-patient encounters during new admissions.
Teaching and Direct Observation
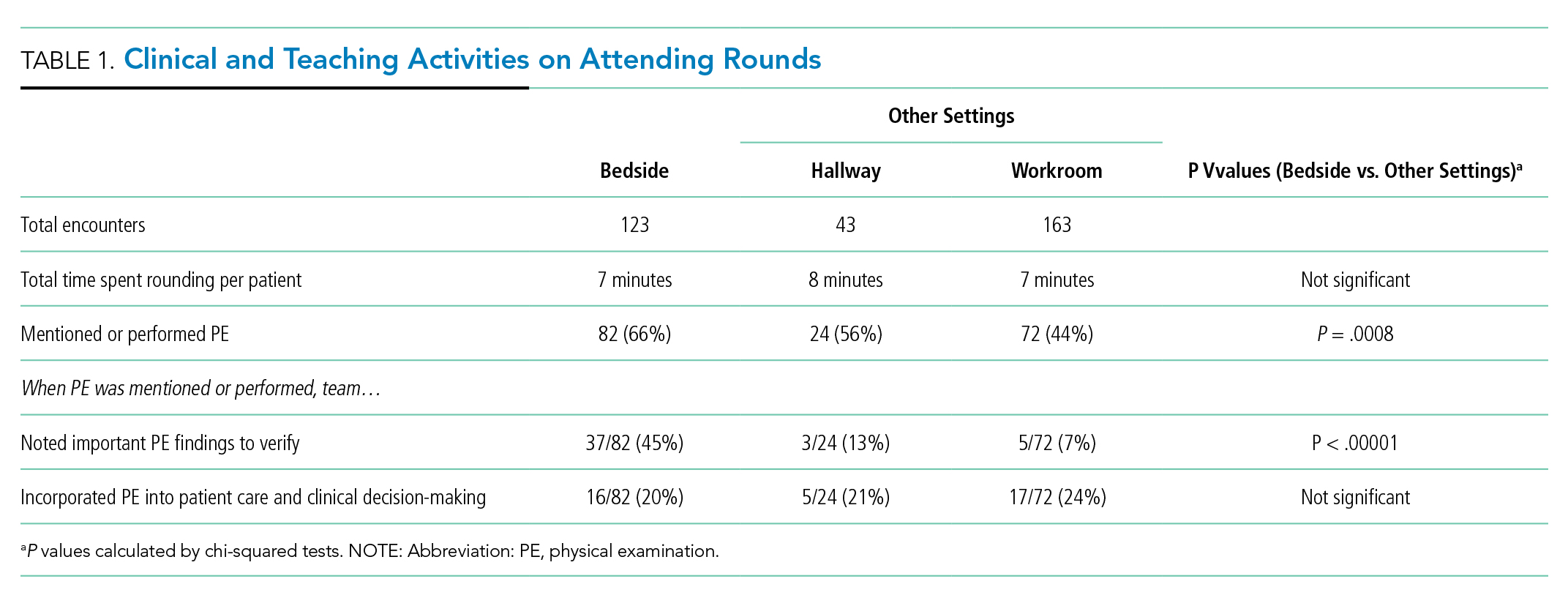
During 28 pre-rounding encounters, students usually examined the patient (26 out of 28 instances, 93%) but were observed only 4 times doing so (out of 26 instances, or 15%). During 30 new patient admissions, students examined 27 patients (90%) and had their PE observed 6 times (out of 27 instances, or 22%). There were no significant differences in frequency of these activities (P > .05, chi-squared) between pre-rounds or new admissions.
Observations on Teaching Strategies
In the written observations, we categorized various methods being used to teach PE. Bedside teaching of PE most often involved teachers simply describing or discussing physical findings (42 mentions in observations) or verifying a student’s reported findings (15 mentions). Teachers were also observed to use bedside teaching to contextualize findings (13 mentions), such as relating the quality of bowel sounds to the patient’s constipation or to discuss expected pupillary light reflexes in a neurologically intact patient. Less commonly, attending physicians narrated steps in their PE technique (9 mentions). Students were infrequently encouraged to practice a specific PE skill again (7 mentions) or allowed to re-examine and reconsider their initial interpretations (5 mentions).
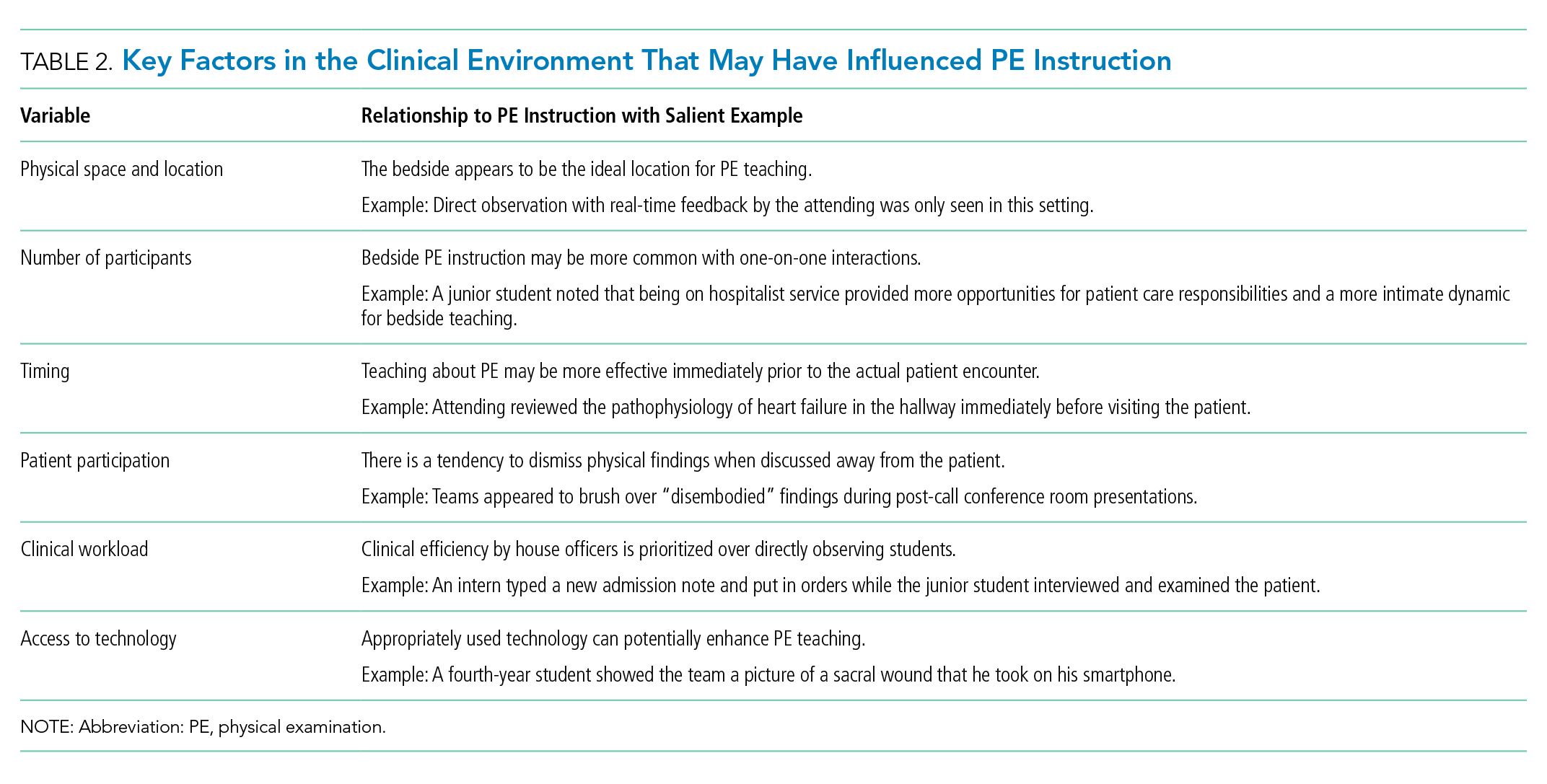
DISCUSSION
This observational study of clinical teaching on internal medicine teaching services demonstrates that PE teaching is most likely to occur during bedside rounding. However, even in bedside encounters, most PE instruction is limited to physician team members pointing out significant findings. Although physical findings were mentioned for the majority of patients seen on rounds, attending physicians infrequently verified students’ or residents’ findings, demonstrated technique, or incorporated PE into clinical decision making. We witnessed an alarming dearth of direct observation of students and almost no real-time feedback in performing and teaching PE. Thus, students rarely had opportunities to engage in higher-order learning activities related to PE on the internal medicine rotation.
We posit that the learning environment influenced PE instruction on the internal medicine rotation. To optimize inpatient teaching of PE, attending physicians need to consider the factors we identified in Table 2. Such teaching may be effective with a more limited number of participants and without distraction from technology. Time constraints are one of the major perceived barriers to bedside teaching of PE, and our data support this concern, as teams spent an average of only 7 minutes on each bedside encounter. However, many of the strategies observed to be used in real-time PE instruction, such as validating the learners’ findings or examining patients as a team, naturally fit into clinical routines and generally do not require extra thought or preparation.
One of the key strengths of our study is the use of direct observation of students and their teachers. This study is unique in its exclusive focus on PE and its description of factors affecting PE teaching activities on an internal medicine service. This observational, descriptive study also has obvious limitations. The study was conducted at a single institution during a limited time period. Moreover, the study period June through August, which was chosen based on our observer’s availability, includes the transition to a new academic year (July 1, 2015) when medical students and residents were becoming acclimated to their new roles. Additionally, the data were collected by a single researcher, and observer bias may affect the results of qualitative analysis of journal entries.
In conclusion, this study highlights the infrequency of applied PE skills in the daily clinical and educational workflow of internal medicine teaching teams. These findings may reflect a more widespread problem in clinical education, and replication of our findings at other teaching centers could galvanize faculty development around bedside PE teaching.
Disclosures
Dr. Bergl has nothing to disclose. Ms. Taylor reports grant support from the Cohen Endowment for Medical Student Research at the Medical College of Wisconsin during the conduct of the study. Mrs. Klumb, Ms. Quirk, Dr. Muntz, and Dr. Fletcher have nothing to disclose.
Funding
This work was funded in part by the Cohen Endowment for Medical Student Research at the Medical College of Wisconsin.
1. Corbett E, Berkow R, Bernstein L, et al on behalf of the AAMC Task Force on the Preclerkship Clinical Skills Education of Medical Students. Recommendations for clinical skills curricula for undergraduate medical education. Achieving excellence in basic clinical method through clinical skills education: The medical school clinical skills curriculum. Association of American Medical Colleges; 2008. https://www.aamc.org/download/130608/data/clinicalskills_oct09.qxd.pdf.pdf. Accessed July 12, 2017.
2. Gowda D, Blatt B, Fink MJ, Kosowicz LY, Baecker A, Silvestri RC. A core physical exam for medical students: Results of a national survey. Acad Med. 2014;89(3):436-442. PubMed
3. Uchida T, Farnan JM, Schwartz JE, Heiman HL. Teaching the physical examination: A longitudinal strategy for tomorrow’s physicians. Acad Med. 2014;89(3):373-375. PubMed
4. Fazio S, De Fer T, Goroll A . Core Medicine Clerkship Curriculum Guide: A resource for teachers and learners. Clerkship Directors in Internal Medicine and Society of General Internal Medicine; 2006. http://www.im.org/d/do/2285/. Accessed July 12, 2017.
5. Gonzalo J, Heist B, Duffy B, et al. Content and timing of feedback and reflection: A multi-center qualitative study of experienced bedside teachers. BMC Med Educ. 2014;(14):212. doi: 10.1186/1472-6920-14-212. PubMed
6. Stickrath C, Noble M, Prochazka A, et al. Attending rounds in the current era: What is and is not happening. JAMA Intern Med. 2013;173(12):1084-1089. PubMed
7. Block L, Habicht R, Wu AW, et al. In the wake of the 2003 and 2011 duty hours regulations, how do internal medicine interns spend their time? J Gen Intern Med. 2013;28(8):1042-1047. PubMed
8. Wenger N, Méan M, Castioni J, Marques-Vidal P, Waeber G, Garnier A. Allocation of internal medicine resident time in a Swiss Hospital: A time and motion study of day and evening shifts. Ann Intern Med. 2017;166(8):579-586. PubMed
9. Ramani S. Twelve tips for excellent physical examination teaching. Med Teach. 2008;30(9-10):851-856. PubMed
10. Gonzalo JD, Heist BS, Duffy BL, et al. The art of bedside rounds: A multi-center qualitative study of strategies used by experienced bedside teachers. J Gen Intern Med. 2013;28(3):412-420. PubMed
11. Janicik RW, Fletcher KE. Teaching at the bedside: A new model. Med Teach. 2003;25(2):127-130. PubMed
1Medical College of Wisconsin Affiliated Hospitals, Milwaukee, Wisconsin. At the time of this study, Dr. Bergl was with the Division of General Internal Medicine, Medical College of Wisconsin, Milwaukee, Wisconsin. 2Medical College of Wisconsin, Milwaukee, Wisconsin.Physical examination (PE) is a core clinical skill in undergraduate medical education.1 Although the optimal approach to teaching clinical skills is debated, robust preclinical curricula should generally be followed by iterative skill development during clinical rotations.2,3
The internal medicine rotation represents a critical time to enhance PE skills. Diagnostic decision making and PE are highly prioritized competencies for the internal medicine clerkship,4 and students will likely utilize many core examination skills1,2 during this time. Bedside teaching of PE during the internal medicine service also provides an opportunity for students to receive feedback based on direct observation,5 a sine qua non of competency-based assessment.
Unfortunately, current internal medicine training environments limit opportunities for workplace-based instruction in PE. Recent studies suggest diminishing time spent on bedside patient care and teaching, with computer-based “indirect patient care” dominating much of the clinical workday of internal medicine services.6-8 However, the literature does not delineate how often medical students are enhancing their PE skills during clinical rotations or describe how the educational environment may influence PE teaching.
We aimed to describe the content and context of PE instruction during the internal medicine clerkship workflow. Specifically, we sought to explore what strategies physician team members used to teach PE to students. We also sought to describe factors in the inpatient learning environment that might explain why physical examination (PE) instruction occurs infrequently.
METHODS
We conducted a prospective mixed-methods study using time motion analysis, checklists on clinical teaching, and daily open-ended observations written by a trained observer from June through August 2015 at a single academic medical center. Subjects were recruited from internal medicine teaching teams and were allowed to opt out. Teaching teams had 2 formats: (1) traditional team with an attending physician (hospitalist or general internist), a senior resident, 2 interns, a fourth-year medical student, and 2 third-year students or (2) hospitalist team in which a third-year student works directly with a hospitalist and advanced practitioner. The proposal was submitted to the Medical College of Wisconsin Institutional Review Board and deemed exempt from further review.
All observations were carried out by a single investigator (A.T.), who was a second-year medical student at the time. To train this observer and to pilot the data collection instruments, our lead investigator (P.B.) directly supervised our observer on 4 separate occasions, totaling over 12 hours of mentored co-observation. Immediately after each training session, both investigators (A.T. and P.B.) debriefed to compare notes, to review checklists on recorded observations, and to discuss areas of uncertainty. During the training period, formal metrics of agreement (eg, kappa coefficients) were not gathered, as data collection instruments were still being refined.
Observation periods were centered on third-year medical students and their interactions with patients and members of the teaching team. Observed activities included pre-rounding, teaching rounds with the attending physician, and new patient admissions during call days. Observations generally occurred between the hours of 7 AM and 6 PM, and we limited periods of observation to 3 consecutive hours to minimize observer fatigue. Observation periods were selected to maximize the number of subjects and teams observed, to adequately capture pre-rounding and new admissions activities, and to account for variations in rounding styles throughout the call cycle. Teams were excluded if a member of the study team was an attending physician on the clinical team or if any member of the patient care team had opted out of the study.
Data were collected on paper checklists that included idealized bedside teaching activities around PE. Teaching activities were identified through a review of relevant literature9,10 and were further informed by our senior investigator’s own experience with faculty development in this area11 and team members’ attendance at bedside teaching workshops. At the end of each day, our observer also wrote brief observations that summarized factors affecting bedside teaching of PE. Checklist data were transferred to an Excel file (Microsoft), and written observations were imported into NVivo 10 (QRS International, Melbourne, Australia) for coding and analysis.
Checklist data were analyzed using simple descriptive statistics. We compared time spent on various types of rounding using ANOVA, and we used a Student two-tailed t-test to compare the amount of time students spent examining patients on pre-rounds versus new admissions. To ascertain differences in the frequency of PE teaching activities by location, we used chi-squared tests. Statistical analysis was performed using embedded statistics functions in Microsoft Excel. A P value of <.05 was used as the cut-off for significance.
We analyzed the written observations using conventional qualitative content analysis. Two investigators (A.T. and P.B.) reviewed the written comments and used open coding to devise a preliminary inductive coding scheme. Codes were refined iteratively, and a schema of categories and nodes was outlined in a codebook that was periodically reviewed by the entire research team. The coding investigators met regularly to ensure consistency in coding, and a third team member remained available to reconcile significant disagreements in code definitions.
RESULTS
Eighty-one subjects participated in the study: 21 were attending physicians, 12 residents, 21 interns, 11 senior medical students, and 26 junior medical students. We observed 16 distinct inpatient teaching teams and 329 unique patient-related events (discussions and/or patient-clinician encounters), with most events being observed during attending rounds (269/329, or 82%). There were 123 encounters at the bedside, averaging 7 minutes; 43 encounters occurred in the hallway, averaging 8 minutes each; and 163 encounters occurred in a workroom and averaged 7 minutes per patient discussion. We also observed 28 student-patient encounters during pre-round activities and 30 student-patient encounters during new admissions.
Teaching and Direct Observation
During 28 pre-rounding encounters, students usually examined the patient (26 out of 28 instances, 93%) but were observed only 4 times doing so (out of 26 instances, or 15%). During 30 new patient admissions, students examined 27 patients (90%) and had their PE observed 6 times (out of 27 instances, or 22%). There were no significant differences in frequency of these activities (P > .05, chi-squared) between pre-rounds or new admissions.
Observations on Teaching Strategies
In the written observations, we categorized various methods being used to teach PE. Bedside teaching of PE most often involved teachers simply describing or discussing physical findings (42 mentions in observations) or verifying a student’s reported findings (15 mentions). Teachers were also observed to use bedside teaching to contextualize findings (13 mentions), such as relating the quality of bowel sounds to the patient’s constipation or to discuss expected pupillary light reflexes in a neurologically intact patient. Less commonly, attending physicians narrated steps in their PE technique (9 mentions). Students were infrequently encouraged to practice a specific PE skill again (7 mentions) or allowed to re-examine and reconsider their initial interpretations (5 mentions).
DISCUSSION
This observational study of clinical teaching on internal medicine teaching services demonstrates that PE teaching is most likely to occur during bedside rounding. However, even in bedside encounters, most PE instruction is limited to physician team members pointing out significant findings. Although physical findings were mentioned for the majority of patients seen on rounds, attending physicians infrequently verified students’ or residents’ findings, demonstrated technique, or incorporated PE into clinical decision making. We witnessed an alarming dearth of direct observation of students and almost no real-time feedback in performing and teaching PE. Thus, students rarely had opportunities to engage in higher-order learning activities related to PE on the internal medicine rotation.
We posit that the learning environment influenced PE instruction on the internal medicine rotation. To optimize inpatient teaching of PE, attending physicians need to consider the factors we identified in Table 2. Such teaching may be effective with a more limited number of participants and without distraction from technology. Time constraints are one of the major perceived barriers to bedside teaching of PE, and our data support this concern, as teams spent an average of only 7 minutes on each bedside encounter. However, many of the strategies observed to be used in real-time PE instruction, such as validating the learners’ findings or examining patients as a team, naturally fit into clinical routines and generally do not require extra thought or preparation.
One of the key strengths of our study is the use of direct observation of students and their teachers. This study is unique in its exclusive focus on PE and its description of factors affecting PE teaching activities on an internal medicine service. This observational, descriptive study also has obvious limitations. The study was conducted at a single institution during a limited time period. Moreover, the study period June through August, which was chosen based on our observer’s availability, includes the transition to a new academic year (July 1, 2015) when medical students and residents were becoming acclimated to their new roles. Additionally, the data were collected by a single researcher, and observer bias may affect the results of qualitative analysis of journal entries.
In conclusion, this study highlights the infrequency of applied PE skills in the daily clinical and educational workflow of internal medicine teaching teams. These findings may reflect a more widespread problem in clinical education, and replication of our findings at other teaching centers could galvanize faculty development around bedside PE teaching.
Disclosures
Dr. Bergl has nothing to disclose. Ms. Taylor reports grant support from the Cohen Endowment for Medical Student Research at the Medical College of Wisconsin during the conduct of the study. Mrs. Klumb, Ms. Quirk, Dr. Muntz, and Dr. Fletcher have nothing to disclose.
Funding
This work was funded in part by the Cohen Endowment for Medical Student Research at the Medical College of Wisconsin.
1Medical College of Wisconsin Affiliated Hospitals, Milwaukee, Wisconsin. At the time of this study, Dr. Bergl was with the Division of General Internal Medicine, Medical College of Wisconsin, Milwaukee, Wisconsin. 2Medical College of Wisconsin, Milwaukee, Wisconsin.Physical examination (PE) is a core clinical skill in undergraduate medical education.1 Although the optimal approach to teaching clinical skills is debated, robust preclinical curricula should generally be followed by iterative skill development during clinical rotations.2,3
The internal medicine rotation represents a critical time to enhance PE skills. Diagnostic decision making and PE are highly prioritized competencies for the internal medicine clerkship,4 and students will likely utilize many core examination skills1,2 during this time. Bedside teaching of PE during the internal medicine service also provides an opportunity for students to receive feedback based on direct observation,5 a sine qua non of competency-based assessment.
Unfortunately, current internal medicine training environments limit opportunities for workplace-based instruction in PE. Recent studies suggest diminishing time spent on bedside patient care and teaching, with computer-based “indirect patient care” dominating much of the clinical workday of internal medicine services.6-8 However, the literature does not delineate how often medical students are enhancing their PE skills during clinical rotations or describe how the educational environment may influence PE teaching.
We aimed to describe the content and context of PE instruction during the internal medicine clerkship workflow. Specifically, we sought to explore what strategies physician team members used to teach PE to students. We also sought to describe factors in the inpatient learning environment that might explain why physical examination (PE) instruction occurs infrequently.
METHODS
We conducted a prospective mixed-methods study using time motion analysis, checklists on clinical teaching, and daily open-ended observations written by a trained observer from June through August 2015 at a single academic medical center. Subjects were recruited from internal medicine teaching teams and were allowed to opt out. Teaching teams had 2 formats: (1) traditional team with an attending physician (hospitalist or general internist), a senior resident, 2 interns, a fourth-year medical student, and 2 third-year students or (2) hospitalist team in which a third-year student works directly with a hospitalist and advanced practitioner. The proposal was submitted to the Medical College of Wisconsin Institutional Review Board and deemed exempt from further review.
All observations were carried out by a single investigator (A.T.), who was a second-year medical student at the time. To train this observer and to pilot the data collection instruments, our lead investigator (P.B.) directly supervised our observer on 4 separate occasions, totaling over 12 hours of mentored co-observation. Immediately after each training session, both investigators (A.T. and P.B.) debriefed to compare notes, to review checklists on recorded observations, and to discuss areas of uncertainty. During the training period, formal metrics of agreement (eg, kappa coefficients) were not gathered, as data collection instruments were still being refined.
Observation periods were centered on third-year medical students and their interactions with patients and members of the teaching team. Observed activities included pre-rounding, teaching rounds with the attending physician, and new patient admissions during call days. Observations generally occurred between the hours of 7 AM and 6 PM, and we limited periods of observation to 3 consecutive hours to minimize observer fatigue. Observation periods were selected to maximize the number of subjects and teams observed, to adequately capture pre-rounding and new admissions activities, and to account for variations in rounding styles throughout the call cycle. Teams were excluded if a member of the study team was an attending physician on the clinical team or if any member of the patient care team had opted out of the study.
Data were collected on paper checklists that included idealized bedside teaching activities around PE. Teaching activities were identified through a review of relevant literature9,10 and were further informed by our senior investigator’s own experience with faculty development in this area11 and team members’ attendance at bedside teaching workshops. At the end of each day, our observer also wrote brief observations that summarized factors affecting bedside teaching of PE. Checklist data were transferred to an Excel file (Microsoft), and written observations were imported into NVivo 10 (QRS International, Melbourne, Australia) for coding and analysis.
Checklist data were analyzed using simple descriptive statistics. We compared time spent on various types of rounding using ANOVA, and we used a Student two-tailed t-test to compare the amount of time students spent examining patients on pre-rounds versus new admissions. To ascertain differences in the frequency of PE teaching activities by location, we used chi-squared tests. Statistical analysis was performed using embedded statistics functions in Microsoft Excel. A P value of <.05 was used as the cut-off for significance.
We analyzed the written observations using conventional qualitative content analysis. Two investigators (A.T. and P.B.) reviewed the written comments and used open coding to devise a preliminary inductive coding scheme. Codes were refined iteratively, and a schema of categories and nodes was outlined in a codebook that was periodically reviewed by the entire research team. The coding investigators met regularly to ensure consistency in coding, and a third team member remained available to reconcile significant disagreements in code definitions.
RESULTS
Eighty-one subjects participated in the study: 21 were attending physicians, 12 residents, 21 interns, 11 senior medical students, and 26 junior medical students. We observed 16 distinct inpatient teaching teams and 329 unique patient-related events (discussions and/or patient-clinician encounters), with most events being observed during attending rounds (269/329, or 82%). There were 123 encounters at the bedside, averaging 7 minutes; 43 encounters occurred in the hallway, averaging 8 minutes each; and 163 encounters occurred in a workroom and averaged 7 minutes per patient discussion. We also observed 28 student-patient encounters during pre-round activities and 30 student-patient encounters during new admissions.
Teaching and Direct Observation
During 28 pre-rounding encounters, students usually examined the patient (26 out of 28 instances, 93%) but were observed only 4 times doing so (out of 26 instances, or 15%). During 30 new patient admissions, students examined 27 patients (90%) and had their PE observed 6 times (out of 27 instances, or 22%). There were no significant differences in frequency of these activities (P > .05, chi-squared) between pre-rounds or new admissions.
Observations on Teaching Strategies
In the written observations, we categorized various methods being used to teach PE. Bedside teaching of PE most often involved teachers simply describing or discussing physical findings (42 mentions in observations) or verifying a student’s reported findings (15 mentions). Teachers were also observed to use bedside teaching to contextualize findings (13 mentions), such as relating the quality of bowel sounds to the patient’s constipation or to discuss expected pupillary light reflexes in a neurologically intact patient. Less commonly, attending physicians narrated steps in their PE technique (9 mentions). Students were infrequently encouraged to practice a specific PE skill again (7 mentions) or allowed to re-examine and reconsider their initial interpretations (5 mentions).
DISCUSSION
This observational study of clinical teaching on internal medicine teaching services demonstrates that PE teaching is most likely to occur during bedside rounding. However, even in bedside encounters, most PE instruction is limited to physician team members pointing out significant findings. Although physical findings were mentioned for the majority of patients seen on rounds, attending physicians infrequently verified students’ or residents’ findings, demonstrated technique, or incorporated PE into clinical decision making. We witnessed an alarming dearth of direct observation of students and almost no real-time feedback in performing and teaching PE. Thus, students rarely had opportunities to engage in higher-order learning activities related to PE on the internal medicine rotation.
We posit that the learning environment influenced PE instruction on the internal medicine rotation. To optimize inpatient teaching of PE, attending physicians need to consider the factors we identified in Table 2. Such teaching may be effective with a more limited number of participants and without distraction from technology. Time constraints are one of the major perceived barriers to bedside teaching of PE, and our data support this concern, as teams spent an average of only 7 minutes on each bedside encounter. However, many of the strategies observed to be used in real-time PE instruction, such as validating the learners’ findings or examining patients as a team, naturally fit into clinical routines and generally do not require extra thought or preparation.
One of the key strengths of our study is the use of direct observation of students and their teachers. This study is unique in its exclusive focus on PE and its description of factors affecting PE teaching activities on an internal medicine service. This observational, descriptive study also has obvious limitations. The study was conducted at a single institution during a limited time period. Moreover, the study period June through August, which was chosen based on our observer’s availability, includes the transition to a new academic year (July 1, 2015) when medical students and residents were becoming acclimated to their new roles. Additionally, the data were collected by a single researcher, and observer bias may affect the results of qualitative analysis of journal entries.
In conclusion, this study highlights the infrequency of applied PE skills in the daily clinical and educational workflow of internal medicine teaching teams. These findings may reflect a more widespread problem in clinical education, and replication of our findings at other teaching centers could galvanize faculty development around bedside PE teaching.
Disclosures
Dr. Bergl has nothing to disclose. Ms. Taylor reports grant support from the Cohen Endowment for Medical Student Research at the Medical College of Wisconsin during the conduct of the study. Mrs. Klumb, Ms. Quirk, Dr. Muntz, and Dr. Fletcher have nothing to disclose.
Funding
This work was funded in part by the Cohen Endowment for Medical Student Research at the Medical College of Wisconsin.
1. Corbett E, Berkow R, Bernstein L, et al on behalf of the AAMC Task Force on the Preclerkship Clinical Skills Education of Medical Students. Recommendations for clinical skills curricula for undergraduate medical education. Achieving excellence in basic clinical method through clinical skills education: The medical school clinical skills curriculum. Association of American Medical Colleges; 2008. https://www.aamc.org/download/130608/data/clinicalskills_oct09.qxd.pdf.pdf. Accessed July 12, 2017.
2. Gowda D, Blatt B, Fink MJ, Kosowicz LY, Baecker A, Silvestri RC. A core physical exam for medical students: Results of a national survey. Acad Med. 2014;89(3):436-442. PubMed
3. Uchida T, Farnan JM, Schwartz JE, Heiman HL. Teaching the physical examination: A longitudinal strategy for tomorrow’s physicians. Acad Med. 2014;89(3):373-375. PubMed
4. Fazio S, De Fer T, Goroll A . Core Medicine Clerkship Curriculum Guide: A resource for teachers and learners. Clerkship Directors in Internal Medicine and Society of General Internal Medicine; 2006. http://www.im.org/d/do/2285/. Accessed July 12, 2017.
5. Gonzalo J, Heist B, Duffy B, et al. Content and timing of feedback and reflection: A multi-center qualitative study of experienced bedside teachers. BMC Med Educ. 2014;(14):212. doi: 10.1186/1472-6920-14-212. PubMed
6. Stickrath C, Noble M, Prochazka A, et al. Attending rounds in the current era: What is and is not happening. JAMA Intern Med. 2013;173(12):1084-1089. PubMed
7. Block L, Habicht R, Wu AW, et al. In the wake of the 2003 and 2011 duty hours regulations, how do internal medicine interns spend their time? J Gen Intern Med. 2013;28(8):1042-1047. PubMed
8. Wenger N, Méan M, Castioni J, Marques-Vidal P, Waeber G, Garnier A. Allocation of internal medicine resident time in a Swiss Hospital: A time and motion study of day and evening shifts. Ann Intern Med. 2017;166(8):579-586. PubMed
9. Ramani S. Twelve tips for excellent physical examination teaching. Med Teach. 2008;30(9-10):851-856. PubMed
10. Gonzalo JD, Heist BS, Duffy BL, et al. The art of bedside rounds: A multi-center qualitative study of strategies used by experienced bedside teachers. J Gen Intern Med. 2013;28(3):412-420. PubMed
11. Janicik RW, Fletcher KE. Teaching at the bedside: A new model. Med Teach. 2003;25(2):127-130. PubMed
1. Corbett E, Berkow R, Bernstein L, et al on behalf of the AAMC Task Force on the Preclerkship Clinical Skills Education of Medical Students. Recommendations for clinical skills curricula for undergraduate medical education. Achieving excellence in basic clinical method through clinical skills education: The medical school clinical skills curriculum. Association of American Medical Colleges; 2008. https://www.aamc.org/download/130608/data/clinicalskills_oct09.qxd.pdf.pdf. Accessed July 12, 2017.
2. Gowda D, Blatt B, Fink MJ, Kosowicz LY, Baecker A, Silvestri RC. A core physical exam for medical students: Results of a national survey. Acad Med. 2014;89(3):436-442. PubMed
3. Uchida T, Farnan JM, Schwartz JE, Heiman HL. Teaching the physical examination: A longitudinal strategy for tomorrow’s physicians. Acad Med. 2014;89(3):373-375. PubMed
4. Fazio S, De Fer T, Goroll A . Core Medicine Clerkship Curriculum Guide: A resource for teachers and learners. Clerkship Directors in Internal Medicine and Society of General Internal Medicine; 2006. http://www.im.org/d/do/2285/. Accessed July 12, 2017.
5. Gonzalo J, Heist B, Duffy B, et al. Content and timing of feedback and reflection: A multi-center qualitative study of experienced bedside teachers. BMC Med Educ. 2014;(14):212. doi: 10.1186/1472-6920-14-212. PubMed
6. Stickrath C, Noble M, Prochazka A, et al. Attending rounds in the current era: What is and is not happening. JAMA Intern Med. 2013;173(12):1084-1089. PubMed
7. Block L, Habicht R, Wu AW, et al. In the wake of the 2003 and 2011 duty hours regulations, how do internal medicine interns spend their time? J Gen Intern Med. 2013;28(8):1042-1047. PubMed
8. Wenger N, Méan M, Castioni J, Marques-Vidal P, Waeber G, Garnier A. Allocation of internal medicine resident time in a Swiss Hospital: A time and motion study of day and evening shifts. Ann Intern Med. 2017;166(8):579-586. PubMed
9. Ramani S. Twelve tips for excellent physical examination teaching. Med Teach. 2008;30(9-10):851-856. PubMed
10. Gonzalo JD, Heist BS, Duffy BL, et al. The art of bedside rounds: A multi-center qualitative study of strategies used by experienced bedside teachers. J Gen Intern Med. 2013;28(3):412-420. PubMed
11. Janicik RW, Fletcher KE. Teaching at the bedside: A new model. Med Teach. 2003;25(2):127-130. PubMed
© 2018 Society of Hospital Medicine
Regular skin exams reduced advanced KCs in posttransplant patients
ORLANDO – Annual skin exams reduced the rate of advanced keratinocyte carcinoma (KC) after solid organ transplant by 34%, according to a review of 10,198 transplant patients in Ontario, Canada.
Transplant patients have a far higher risk of KC than the general public because of immunosuppression: A quarter of patients are affected within 5 years. Transplant guidelines have recommended annual skin exams.

Other studies have reported adherence rates of up to 50%, but the numbers were based largely on patient self-report. Instead, the Ontario study used billing codes and other administrative data to get an idea of how many patients actually followed through.
“I would be surprised if other jurisdictions have significantly better rates of adherence,” said lead investigator An-Wen Chan, MD, of the division of dermatology at the University of Toronto and director of a transplant dermatology clinic at the University Health Network.
Part of the problem is that there’s just not a lot of evidence that annual screenings improve KC outcomes, he noted.
To help plug that evidence gap, Dr. Chan and his team reviewed transplant cases in Ontario going back to the mid-1990s; 62% of the patients had kidney transplants, 24% had liver transplants, and the rest had heart or lung transplants. The patients were all aged over 18 years; 60% were white, 15% Asian, 4% black, and the rest unknown. About two-thirds were men.
Adherence to annual dermatology checkups at least 75% of the time was associated with a marked reduction in the development of advanced KC, defined as lesions greater than 2 cm and requiring reconstruction and lymphadenectomy (adjusted hazard ratio, 0.66; 95% CI, 0.48-0.92).
Increasing age at transplant, white race, male sex, and past history of skin cancer were among the factors that were associated with increased risk. There was a trend toward increased risk with liver, lung, and heart transplants, as opposed to kidney transplants. Results were adjusted for demographic, transplant, and other variables.
In short, “adherence to annual dermatology assessments ... reduced KC-related morbidity and death. The highest risk patients were not necessarily the ones that saw their dermatologist annually,” Dr. Chan said.
Rates of adherence varied across transplant sites. It’s probably less of a problem at the University of Toronto, where Dr. Chan is embedded with the transplant team and where he can educate patients and providers on the importance of annual screening and help ensure that it’s done.
“We have a rigorous skin referral policy in place and really target transplant patients to be seen within a year. Having a dermatologist dedicated to transplant dermatology really helps,” he said. The next step is to define the optimal frequency of posttransplant skin cancer screening and to address barriers to screening.
There was no industry funding for the work, and Dr. Chan had no relevant disclosures.
SOURCE: Chan A et al. IID 2018, Abstract 522.
ORLANDO – Annual skin exams reduced the rate of advanced keratinocyte carcinoma (KC) after solid organ transplant by 34%, according to a review of 10,198 transplant patients in Ontario, Canada.
Transplant patients have a far higher risk of KC than the general public because of immunosuppression: A quarter of patients are affected within 5 years. Transplant guidelines have recommended annual skin exams.
Other studies have reported adherence rates of up to 50%, but the numbers were based largely on patient self-report. Instead, the Ontario study used billing codes and other administrative data to get an idea of how many patients actually followed through.
“I would be surprised if other jurisdictions have significantly better rates of adherence,” said lead investigator An-Wen Chan, MD, of the division of dermatology at the University of Toronto and director of a transplant dermatology clinic at the University Health Network.
Part of the problem is that there’s just not a lot of evidence that annual screenings improve KC outcomes, he noted.
To help plug that evidence gap, Dr. Chan and his team reviewed transplant cases in Ontario going back to the mid-1990s; 62% of the patients had kidney transplants, 24% had liver transplants, and the rest had heart or lung transplants. The patients were all aged over 18 years; 60% were white, 15% Asian, 4% black, and the rest unknown. About two-thirds were men.
Adherence to annual dermatology checkups at least 75% of the time was associated with a marked reduction in the development of advanced KC, defined as lesions greater than 2 cm and requiring reconstruction and lymphadenectomy (adjusted hazard ratio, 0.66; 95% CI, 0.48-0.92).
Increasing age at transplant, white race, male sex, and past history of skin cancer were among the factors that were associated with increased risk. There was a trend toward increased risk with liver, lung, and heart transplants, as opposed to kidney transplants. Results were adjusted for demographic, transplant, and other variables.
In short, “adherence to annual dermatology assessments ... reduced KC-related morbidity and death. The highest risk patients were not necessarily the ones that saw their dermatologist annually,” Dr. Chan said.
Rates of adherence varied across transplant sites. It’s probably less of a problem at the University of Toronto, where Dr. Chan is embedded with the transplant team and where he can educate patients and providers on the importance of annual screening and help ensure that it’s done.
“We have a rigorous skin referral policy in place and really target transplant patients to be seen within a year. Having a dermatologist dedicated to transplant dermatology really helps,” he said. The next step is to define the optimal frequency of posttransplant skin cancer screening and to address barriers to screening.
There was no industry funding for the work, and Dr. Chan had no relevant disclosures.
SOURCE: Chan A et al. IID 2018, Abstract 522.
ORLANDO – Annual skin exams reduced the rate of advanced keratinocyte carcinoma (KC) after solid organ transplant by 34%, according to a review of 10,198 transplant patients in Ontario, Canada.
Transplant patients have a far higher risk of KC than the general public because of immunosuppression: A quarter of patients are affected within 5 years. Transplant guidelines have recommended annual skin exams.
Other studies have reported adherence rates of up to 50%, but the numbers were based largely on patient self-report. Instead, the Ontario study used billing codes and other administrative data to get an idea of how many patients actually followed through.
“I would be surprised if other jurisdictions have significantly better rates of adherence,” said lead investigator An-Wen Chan, MD, of the division of dermatology at the University of Toronto and director of a transplant dermatology clinic at the University Health Network.
Part of the problem is that there’s just not a lot of evidence that annual screenings improve KC outcomes, he noted.
To help plug that evidence gap, Dr. Chan and his team reviewed transplant cases in Ontario going back to the mid-1990s; 62% of the patients had kidney transplants, 24% had liver transplants, and the rest had heart or lung transplants. The patients were all aged over 18 years; 60% were white, 15% Asian, 4% black, and the rest unknown. About two-thirds were men.
Adherence to annual dermatology checkups at least 75% of the time was associated with a marked reduction in the development of advanced KC, defined as lesions greater than 2 cm and requiring reconstruction and lymphadenectomy (adjusted hazard ratio, 0.66; 95% CI, 0.48-0.92).
Increasing age at transplant, white race, male sex, and past history of skin cancer were among the factors that were associated with increased risk. There was a trend toward increased risk with liver, lung, and heart transplants, as opposed to kidney transplants. Results were adjusted for demographic, transplant, and other variables.
In short, “adherence to annual dermatology assessments ... reduced KC-related morbidity and death. The highest risk patients were not necessarily the ones that saw their dermatologist annually,” Dr. Chan said.
Rates of adherence varied across transplant sites. It’s probably less of a problem at the University of Toronto, where Dr. Chan is embedded with the transplant team and where he can educate patients and providers on the importance of annual screening and help ensure that it’s done.
“We have a rigorous skin referral policy in place and really target transplant patients to be seen within a year. Having a dermatologist dedicated to transplant dermatology really helps,” he said. The next step is to define the optimal frequency of posttransplant skin cancer screening and to address barriers to screening.
There was no industry funding for the work, and Dr. Chan had no relevant disclosures.
SOURCE: Chan A et al. IID 2018, Abstract 522.
REPORTING FROM IID 2018
Key clinical point: Transplant patients need help to ensure they get annual dermatology checkups.
Major finding: Just 2.1% of the patients in the review had annual exams, and less than half saw a dermatologist even once during an average of 5-years follow-up.
Study details: A review of 10,198 solid organ transplant cases.
Disclosures: There was no industry funding, and the lead investigator had no disclosures.
Source: Chan A et al. IID 2018, Abstract 522
Epilepsy: Past, Present, and Future
Vijay M. Thadani,
Dr. Thadani is Professor of Neurology, Geisel School of Medicine at Dartmouth, Dartmouth-Hitchcock Medical Center in Lebanon, New Hampshire. He reports no conflict of interest.
As Neurology Reviews celebrates its 25th anniversary, we take this opportunity to look back and to look ahead in the area of epilepsy care and research. Epilepsy is a disease whose earliest descriptions date back to Egypt and Mesopotamia 3,000 years ago. A modern understanding of epilepsy as an electrical disorder of the brain dates back perhaps 150 years. The last 25 years have seen considerable progress in diagnosis and treatment, but in the Western world, the prevalence of epilepsy has held steady at around 1%, and a quarter of those patients have seizures that are not controlled, in spite of appropriate therapy.

While generalized and focal seizures remain the cornerstones of classification, the most recent theoretical advance is the network concept of epilepsy. By definition, a network must have nodes and connections. In generalized forms of epilepsy, these are recognized to be diffuse groupings of neurons and the fiber tracts that connect them. They are widely distributed and conducive to the rapid and bilateral spread of electrical abnormalities throughout the brain. In focal epilepsies, the abnormal electrical activity in the network is more constrained by traditional anatomic landmarks, but this does not preclude the possibility of secondary generalization. The elucidation of such networks by intracranial EEG and fMRI studies is a major triumph of the last 25 years.
All network activities, and therefore all forms of epilepsy, are ultimately based on the electrical behavior of individual neurons. At the cellular level, the last 25 years have seen enormous progress in the understanding of normal and abnormal electrical activity, and that progress is rooted in genetics. Genetic studies, correlated with electrophysiologic ones, have identified many mutations in ion channels that are responsible for various epilepsy syndromes. Examples of this are mutations in Na+ channels that lead to Dravet syndrome and mutations in GABA receptor subunits that are responsible for juvenile myoclonic epilepsy.
The mechanistic understanding of seizures and epilepsy has also been greatly enhanced in the last three decades by structural and developmental studies closely tied to genetics. Various forms of epilepsy are caused by aberrant neurogenesis and neuronal migration, leading to dysplastic cortex that has abnormal electrical activity and connectivity. The recent elucidation of the mTOR pathway, for example, has shown us how neuronal development and migration are controlled through several genetic steps, and mutations there can lead to tuberous sclerosis and related disorders that are accompanied by epilepsy.
Treatment
From the time that epilepsy was first recognized as a disease of the brain, treatment emphasized the control of seizures and not much else. A century after the introduction of bromide, there were, by 1967, perhaps half a dozen effective drugs available, including phenobarbital, phenytoin, and carbamazepine. Between 1967 and 1993, no new drugs for epilepsy were marketed in the USA, but the next 25 years saw a dramatic improvement. The years from 1993 to 2018 saw the introduction of perhaps 15 new drugs, most recently brivaracetam. However, in spite of this huge effort, at the expense of billions of dollars, each new drug makes less than 5% of previously refractory patients seizure-free.
Surgery
The idea of treating medically refractory epilepsy by surgical removal of the epileptic focus or network goes back more than a century, but advances in the last 25 years have been based on the revolution in imaging brought about by MRI. The easy and noninvasive identification of mesial temporal sclerosis and focal cortical dysplasias has enabled thousands of patients to become seizure-free. Complete control of seizures is obtained in only 50% to 75% of patients who undergo surgery, hardly better than a century ago, but advanced imaging and electrographic techniques have made surgery possible for many patients who previously would not have been candidates.
Looking Ahead
As they say, it is difficult to make predictions, especially about the future, but one can anticipate not only the identification of more gene mutations that cause epilepsy, but their correction with CRISPR/Cas9 and related technologies. Likewise, we can anticipate new antiepileptic drugs, but whether they will be broad-spectrum blockbusters like the cannabis derivatives are thought to be, or designer molecules tailored to specific types of seizures and epilepsy remains to be seen. In tuberous sclerosis, for example, drugs like tacrolimus that inhibit the mTOR pathway not only suppress abnormal cell proliferation, but also help with seizure control. Likewise, a small minority of epilepsies, now recognized to be autoimmune, will be treated with targeted immune suppression. A major goal is the discovery of drugs that will prevent the development of epilepsy or cure it in its early stages, as opposed to merely controlling the seizures.
Imaging of epileptic foci and networks of seizure spread will continue to improve with higher field strength MRI scans. EEG, MRI, and fMRI will probably coalesce, and PET scans will play a larger role. Combined images will guide epilepsy surgeons with regard to the boundaries of resections. The nature of EEG recording will also change. Until recently, owing to the properties of available amplifiers, we have looked at electrical oscillations between 1 Hz and 70 Hz. However, much higher frequencies are increasingly recognized as important in defining the epileptogenic zone and network. Epilepsy surgery that takes high-frequency oscillations into account will optimize the removal of epileptogenic lesions and the disruption of epileptic networks, while minimizing injury to normal brain functions.
Resective surgery may itself be rendered obsolete by cerebral stimulation, now in its infancy. Implanted devices such as Neuropace have shown promise in detecting seizures and delivering a counter-shock to abort them. Biologic stimulation is also on the horizon. In animal models, transplantation of GABA-producing cells has cured epilepsy, and optogenetic techniques may soon make it possible to activate particular classes of neurons that can turn off epileptic activity.
One can also anticipate a shift in treatment away from the exclusive emphasis on seizure control. We increasingly recognize that epilepsy is much more than seizures, and that patients with epilepsy may also have depression, impaired memory, and anxiety related to their illness. In the long run, the psychosocial problems of patients with epilepsy cannot be separated from social problems as a whole. Will, for example, the new, and doubtless expensive, treatments for epilepsy be made available to all who need them, or will we be obliged to work in a two-tier system? As health care providers, we can be cautiously optimistic regarding the medical aspects of epilepsy, but we will have to think in quite unanticipated ways to ensure equitable outcomes.
Vijay M. Thadani,
Dr. Thadani is Professor of Neurology, Geisel School of Medicine at Dartmouth, Dartmouth-Hitchcock Medical Center in Lebanon, New Hampshire. He reports no conflict of interest.
As Neurology Reviews celebrates its 25th anniversary, we take this opportunity to look back and to look ahead in the area of epilepsy care and research. Epilepsy is a disease whose earliest descriptions date back to Egypt and Mesopotamia 3,000 years ago. A modern understanding of epilepsy as an electrical disorder of the brain dates back perhaps 150 years. The last 25 years have seen considerable progress in diagnosis and treatment, but in the Western world, the prevalence of epilepsy has held steady at around 1%, and a quarter of those patients have seizures that are not controlled, in spite of appropriate therapy.
While generalized and focal seizures remain the cornerstones of classification, the most recent theoretical advance is the network concept of epilepsy. By definition, a network must have nodes and connections. In generalized forms of epilepsy, these are recognized to be diffuse groupings of neurons and the fiber tracts that connect them. They are widely distributed and conducive to the rapid and bilateral spread of electrical abnormalities throughout the brain. In focal epilepsies, the abnormal electrical activity in the network is more constrained by traditional anatomic landmarks, but this does not preclude the possibility of secondary generalization. The elucidation of such networks by intracranial EEG and fMRI studies is a major triumph of the last 25 years.
All network activities, and therefore all forms of epilepsy, are ultimately based on the electrical behavior of individual neurons. At the cellular level, the last 25 years have seen enormous progress in the understanding of normal and abnormal electrical activity, and that progress is rooted in genetics. Genetic studies, correlated with electrophysiologic ones, have identified many mutations in ion channels that are responsible for various epilepsy syndromes. Examples of this are mutations in Na+ channels that lead to Dravet syndrome and mutations in GABA receptor subunits that are responsible for juvenile myoclonic epilepsy.
The mechanistic understanding of seizures and epilepsy has also been greatly enhanced in the last three decades by structural and developmental studies closely tied to genetics. Various forms of epilepsy are caused by aberrant neurogenesis and neuronal migration, leading to dysplastic cortex that has abnormal electrical activity and connectivity. The recent elucidation of the mTOR pathway, for example, has shown us how neuronal development and migration are controlled through several genetic steps, and mutations there can lead to tuberous sclerosis and related disorders that are accompanied by epilepsy.
Treatment
From the time that epilepsy was first recognized as a disease of the brain, treatment emphasized the control of seizures and not much else. A century after the introduction of bromide, there were, by 1967, perhaps half a dozen effective drugs available, including phenobarbital, phenytoin, and carbamazepine. Between 1967 and 1993, no new drugs for epilepsy were marketed in the USA, but the next 25 years saw a dramatic improvement. The years from 1993 to 2018 saw the introduction of perhaps 15 new drugs, most recently brivaracetam. However, in spite of this huge effort, at the expense of billions of dollars, each new drug makes less than 5% of previously refractory patients seizure-free.
Surgery
The idea of treating medically refractory epilepsy by surgical removal of the epileptic focus or network goes back more than a century, but advances in the last 25 years have been based on the revolution in imaging brought about by MRI. The easy and noninvasive identification of mesial temporal sclerosis and focal cortical dysplasias has enabled thousands of patients to become seizure-free. Complete control of seizures is obtained in only 50% to 75% of patients who undergo surgery, hardly better than a century ago, but advanced imaging and electrographic techniques have made surgery possible for many patients who previously would not have been candidates.
Looking Ahead
As they say, it is difficult to make predictions, especially about the future, but one can anticipate not only the identification of more gene mutations that cause epilepsy, but their correction with CRISPR/Cas9 and related technologies. Likewise, we can anticipate new antiepileptic drugs, but whether they will be broad-spectrum blockbusters like the cannabis derivatives are thought to be, or designer molecules tailored to specific types of seizures and epilepsy remains to be seen. In tuberous sclerosis, for example, drugs like tacrolimus that inhibit the mTOR pathway not only suppress abnormal cell proliferation, but also help with seizure control. Likewise, a small minority of epilepsies, now recognized to be autoimmune, will be treated with targeted immune suppression. A major goal is the discovery of drugs that will prevent the development of epilepsy or cure it in its early stages, as opposed to merely controlling the seizures.
Imaging of epileptic foci and networks of seizure spread will continue to improve with higher field strength MRI scans. EEG, MRI, and fMRI will probably coalesce, and PET scans will play a larger role. Combined images will guide epilepsy surgeons with regard to the boundaries of resections. The nature of EEG recording will also change. Until recently, owing to the properties of available amplifiers, we have looked at electrical oscillations between 1 Hz and 70 Hz. However, much higher frequencies are increasingly recognized as important in defining the epileptogenic zone and network. Epilepsy surgery that takes high-frequency oscillations into account will optimize the removal of epileptogenic lesions and the disruption of epileptic networks, while minimizing injury to normal brain functions.
Resective surgery may itself be rendered obsolete by cerebral stimulation, now in its infancy. Implanted devices such as Neuropace have shown promise in detecting seizures and delivering a counter-shock to abort them. Biologic stimulation is also on the horizon. In animal models, transplantation of GABA-producing cells has cured epilepsy, and optogenetic techniques may soon make it possible to activate particular classes of neurons that can turn off epileptic activity.
One can also anticipate a shift in treatment away from the exclusive emphasis on seizure control. We increasingly recognize that epilepsy is much more than seizures, and that patients with epilepsy may also have depression, impaired memory, and anxiety related to their illness. In the long run, the psychosocial problems of patients with epilepsy cannot be separated from social problems as a whole. Will, for example, the new, and doubtless expensive, treatments for epilepsy be made available to all who need them, or will we be obliged to work in a two-tier system? As health care providers, we can be cautiously optimistic regarding the medical aspects of epilepsy, but we will have to think in quite unanticipated ways to ensure equitable outcomes.
Vijay M. Thadani,
Dr. Thadani is Professor of Neurology, Geisel School of Medicine at Dartmouth, Dartmouth-Hitchcock Medical Center in Lebanon, New Hampshire. He reports no conflict of interest.
As Neurology Reviews celebrates its 25th anniversary, we take this opportunity to look back and to look ahead in the area of epilepsy care and research. Epilepsy is a disease whose earliest descriptions date back to Egypt and Mesopotamia 3,000 years ago. A modern understanding of epilepsy as an electrical disorder of the brain dates back perhaps 150 years. The last 25 years have seen considerable progress in diagnosis and treatment, but in the Western world, the prevalence of epilepsy has held steady at around 1%, and a quarter of those patients have seizures that are not controlled, in spite of appropriate therapy.
While generalized and focal seizures remain the cornerstones of classification, the most recent theoretical advance is the network concept of epilepsy. By definition, a network must have nodes and connections. In generalized forms of epilepsy, these are recognized to be diffuse groupings of neurons and the fiber tracts that connect them. They are widely distributed and conducive to the rapid and bilateral spread of electrical abnormalities throughout the brain. In focal epilepsies, the abnormal electrical activity in the network is more constrained by traditional anatomic landmarks, but this does not preclude the possibility of secondary generalization. The elucidation of such networks by intracranial EEG and fMRI studies is a major triumph of the last 25 years.
All network activities, and therefore all forms of epilepsy, are ultimately based on the electrical behavior of individual neurons. At the cellular level, the last 25 years have seen enormous progress in the understanding of normal and abnormal electrical activity, and that progress is rooted in genetics. Genetic studies, correlated with electrophysiologic ones, have identified many mutations in ion channels that are responsible for various epilepsy syndromes. Examples of this are mutations in Na+ channels that lead to Dravet syndrome and mutations in GABA receptor subunits that are responsible for juvenile myoclonic epilepsy.
The mechanistic understanding of seizures and epilepsy has also been greatly enhanced in the last three decades by structural and developmental studies closely tied to genetics. Various forms of epilepsy are caused by aberrant neurogenesis and neuronal migration, leading to dysplastic cortex that has abnormal electrical activity and connectivity. The recent elucidation of the mTOR pathway, for example, has shown us how neuronal development and migration are controlled through several genetic steps, and mutations there can lead to tuberous sclerosis and related disorders that are accompanied by epilepsy.
Treatment
From the time that epilepsy was first recognized as a disease of the brain, treatment emphasized the control of seizures and not much else. A century after the introduction of bromide, there were, by 1967, perhaps half a dozen effective drugs available, including phenobarbital, phenytoin, and carbamazepine. Between 1967 and 1993, no new drugs for epilepsy were marketed in the USA, but the next 25 years saw a dramatic improvement. The years from 1993 to 2018 saw the introduction of perhaps 15 new drugs, most recently brivaracetam. However, in spite of this huge effort, at the expense of billions of dollars, each new drug makes less than 5% of previously refractory patients seizure-free.
Surgery
The idea of treating medically refractory epilepsy by surgical removal of the epileptic focus or network goes back more than a century, but advances in the last 25 years have been based on the revolution in imaging brought about by MRI. The easy and noninvasive identification of mesial temporal sclerosis and focal cortical dysplasias has enabled thousands of patients to become seizure-free. Complete control of seizures is obtained in only 50% to 75% of patients who undergo surgery, hardly better than a century ago, but advanced imaging and electrographic techniques have made surgery possible for many patients who previously would not have been candidates.
Looking Ahead
As they say, it is difficult to make predictions, especially about the future, but one can anticipate not only the identification of more gene mutations that cause epilepsy, but their correction with CRISPR/Cas9 and related technologies. Likewise, we can anticipate new antiepileptic drugs, but whether they will be broad-spectrum blockbusters like the cannabis derivatives are thought to be, or designer molecules tailored to specific types of seizures and epilepsy remains to be seen. In tuberous sclerosis, for example, drugs like tacrolimus that inhibit the mTOR pathway not only suppress abnormal cell proliferation, but also help with seizure control. Likewise, a small minority of epilepsies, now recognized to be autoimmune, will be treated with targeted immune suppression. A major goal is the discovery of drugs that will prevent the development of epilepsy or cure it in its early stages, as opposed to merely controlling the seizures.
Imaging of epileptic foci and networks of seizure spread will continue to improve with higher field strength MRI scans. EEG, MRI, and fMRI will probably coalesce, and PET scans will play a larger role. Combined images will guide epilepsy surgeons with regard to the boundaries of resections. The nature of EEG recording will also change. Until recently, owing to the properties of available amplifiers, we have looked at electrical oscillations between 1 Hz and 70 Hz. However, much higher frequencies are increasingly recognized as important in defining the epileptogenic zone and network. Epilepsy surgery that takes high-frequency oscillations into account will optimize the removal of epileptogenic lesions and the disruption of epileptic networks, while minimizing injury to normal brain functions.
Resective surgery may itself be rendered obsolete by cerebral stimulation, now in its infancy. Implanted devices such as Neuropace have shown promise in detecting seizures and delivering a counter-shock to abort them. Biologic stimulation is also on the horizon. In animal models, transplantation of GABA-producing cells has cured epilepsy, and optogenetic techniques may soon make it possible to activate particular classes of neurons that can turn off epileptic activity.
One can also anticipate a shift in treatment away from the exclusive emphasis on seizure control. We increasingly recognize that epilepsy is much more than seizures, and that patients with epilepsy may also have depression, impaired memory, and anxiety related to their illness. In the long run, the psychosocial problems of patients with epilepsy cannot be separated from social problems as a whole. Will, for example, the new, and doubtless expensive, treatments for epilepsy be made available to all who need them, or will we be obliged to work in a two-tier system? As health care providers, we can be cautiously optimistic regarding the medical aspects of epilepsy, but we will have to think in quite unanticipated ways to ensure equitable outcomes.
Staging System Classifies Nearly All Patients With Lewy Body Synucleinopathy
LOS ANGELES—The Unified Staging System for Lewy Body Disorders (USSLB) enables the categorization of almost all brains with Lewy body synucleinopathy, according to research described at the 70th Annual Meeting of the American Academy of Neurology. The USSLB’s stages correlate significantly with motor and nonmotor findings. “Wider use of the USSLB would help standardize research in synucleinopathies,” said Charles H. Adler, MD, PhD, Professor of Neurology at Mayo Clinic in Scottsdale, Arizona.

Investigators have developed several neuropathologic staging systems for Lewy body disorders, but many focus on specific diseases, such as Parkinson’s disease or dementia with Lewy bodies. They thus do not allow the classification of all patients with Lewy body disorders. In addition, the literature contains few data about how well these systems’ stages correlate with clinical and pathologic findings.
The Emergence of the USSLB
Dr. Adler and colleagues proposed the USSLB in research published in Acta Neuropathologica in 2009. Their goal was to enable the classification of patients with Lewy body disorders, regardless of their specific diagnoses. The USSLB includes four stages. Stage I denotes pathology limited to the olfactory bulb. Stage IIa denotes predominantly brainstem involvement. Stage IIb refers to pathology predominantly in the limbic system, rather than the brainstem. Stage III denotes pathology in the brainstem and limbic system. Stage IV represents neocortical pathology.
To examine the correlation between patients’ motor and nonmotor findings, including cognitive measures, and the extent of Lewy-type synucleinopathy, as categorized by the USSLB, Dr. Adler and others examined data from the Arizona Study of Aging and Neurodegenerative Disorders (AZSAND). That study includes participants in the Banner Sun Health Research Institute brain and body donation program. Participants undergo annual clinical exams that include movement testing, cognitive testing, sleep and autonomic questionnaires, and a smell test.
The investigators searched the AZSAND database for patients who presented from January 1997 through December 2015. They identified 641 autopsies. Clinical data and information on Lewy-type synucleinopathy were available for 280 of the cases. The population included cases with Lewy bodies and those with synuclein pathology within the neuropil and fibers. The population’s mean age at death was 83. Greater severity of synucleinopathy was associated with younger age at death.
Braak Staging Could Not Characterize Some Patients
The researchers classified 8.6% of cases as Stage I, 15.4% as Stage IIa, 13.6% as Stage IIb, 31.8% as Stage III, and 30.7% as Stage IV. Cognition was normal in 25.7% of the cases, 8.6% had mild cognitive impairment, and 65.7% had dementia.
Multiple measures of motor parkinsonism and cognitive impairment, as well as of hyposmia and probable REM sleep behavior disorder, correlated significantly with increasing USSLB stage. A few clinical features had no correlation with USSLB stage.
Dr. Adler and colleagues also applied the Braak staging criteria to the cases. To classify all cases, the investigators added an olfactory-bulb-only stage to the Braak criteria. Of the initial cohort, 70 cases could not be assigned a Braak stage. When the researchers removed cases with Alzheimer’s disease, 21% of cases could not be staged.
—Erik Greb
LOS ANGELES—The Unified Staging System for Lewy Body Disorders (USSLB) enables the categorization of almost all brains with Lewy body synucleinopathy, according to research described at the 70th Annual Meeting of the American Academy of Neurology. The USSLB’s stages correlate significantly with motor and nonmotor findings. “Wider use of the USSLB would help standardize research in synucleinopathies,” said Charles H. Adler, MD, PhD, Professor of Neurology at Mayo Clinic in Scottsdale, Arizona.
Investigators have developed several neuropathologic staging systems for Lewy body disorders, but many focus on specific diseases, such as Parkinson’s disease or dementia with Lewy bodies. They thus do not allow the classification of all patients with Lewy body disorders. In addition, the literature contains few data about how well these systems’ stages correlate with clinical and pathologic findings.
The Emergence of the USSLB
Dr. Adler and colleagues proposed the USSLB in research published in Acta Neuropathologica in 2009. Their goal was to enable the classification of patients with Lewy body disorders, regardless of their specific diagnoses. The USSLB includes four stages. Stage I denotes pathology limited to the olfactory bulb. Stage IIa denotes predominantly brainstem involvement. Stage IIb refers to pathology predominantly in the limbic system, rather than the brainstem. Stage III denotes pathology in the brainstem and limbic system. Stage IV represents neocortical pathology.
To examine the correlation between patients’ motor and nonmotor findings, including cognitive measures, and the extent of Lewy-type synucleinopathy, as categorized by the USSLB, Dr. Adler and others examined data from the Arizona Study of Aging and Neurodegenerative Disorders (AZSAND). That study includes participants in the Banner Sun Health Research Institute brain and body donation program. Participants undergo annual clinical exams that include movement testing, cognitive testing, sleep and autonomic questionnaires, and a smell test.
The investigators searched the AZSAND database for patients who presented from January 1997 through December 2015. They identified 641 autopsies. Clinical data and information on Lewy-type synucleinopathy were available for 280 of the cases. The population included cases with Lewy bodies and those with synuclein pathology within the neuropil and fibers. The population’s mean age at death was 83. Greater severity of synucleinopathy was associated with younger age at death.
Braak Staging Could Not Characterize Some Patients
The researchers classified 8.6% of cases as Stage I, 15.4% as Stage IIa, 13.6% as Stage IIb, 31.8% as Stage III, and 30.7% as Stage IV. Cognition was normal in 25.7% of the cases, 8.6% had mild cognitive impairment, and 65.7% had dementia.
Multiple measures of motor parkinsonism and cognitive impairment, as well as of hyposmia and probable REM sleep behavior disorder, correlated significantly with increasing USSLB stage. A few clinical features had no correlation with USSLB stage.
Dr. Adler and colleagues also applied the Braak staging criteria to the cases. To classify all cases, the investigators added an olfactory-bulb-only stage to the Braak criteria. Of the initial cohort, 70 cases could not be assigned a Braak stage. When the researchers removed cases with Alzheimer’s disease, 21% of cases could not be staged.
—Erik Greb
LOS ANGELES—The Unified Staging System for Lewy Body Disorders (USSLB) enables the categorization of almost all brains with Lewy body synucleinopathy, according to research described at the 70th Annual Meeting of the American Academy of Neurology. The USSLB’s stages correlate significantly with motor and nonmotor findings. “Wider use of the USSLB would help standardize research in synucleinopathies,” said Charles H. Adler, MD, PhD, Professor of Neurology at Mayo Clinic in Scottsdale, Arizona.
Investigators have developed several neuropathologic staging systems for Lewy body disorders, but many focus on specific diseases, such as Parkinson’s disease or dementia with Lewy bodies. They thus do not allow the classification of all patients with Lewy body disorders. In addition, the literature contains few data about how well these systems’ stages correlate with clinical and pathologic findings.
The Emergence of the USSLB
Dr. Adler and colleagues proposed the USSLB in research published in Acta Neuropathologica in 2009. Their goal was to enable the classification of patients with Lewy body disorders, regardless of their specific diagnoses. The USSLB includes four stages. Stage I denotes pathology limited to the olfactory bulb. Stage IIa denotes predominantly brainstem involvement. Stage IIb refers to pathology predominantly in the limbic system, rather than the brainstem. Stage III denotes pathology in the brainstem and limbic system. Stage IV represents neocortical pathology.
To examine the correlation between patients’ motor and nonmotor findings, including cognitive measures, and the extent of Lewy-type synucleinopathy, as categorized by the USSLB, Dr. Adler and others examined data from the Arizona Study of Aging and Neurodegenerative Disorders (AZSAND). That study includes participants in the Banner Sun Health Research Institute brain and body donation program. Participants undergo annual clinical exams that include movement testing, cognitive testing, sleep and autonomic questionnaires, and a smell test.
The investigators searched the AZSAND database for patients who presented from January 1997 through December 2015. They identified 641 autopsies. Clinical data and information on Lewy-type synucleinopathy were available for 280 of the cases. The population included cases with Lewy bodies and those with synuclein pathology within the neuropil and fibers. The population’s mean age at death was 83. Greater severity of synucleinopathy was associated with younger age at death.
Braak Staging Could Not Characterize Some Patients
The researchers classified 8.6% of cases as Stage I, 15.4% as Stage IIa, 13.6% as Stage IIb, 31.8% as Stage III, and 30.7% as Stage IV. Cognition was normal in 25.7% of the cases, 8.6% had mild cognitive impairment, and 65.7% had dementia.
Multiple measures of motor parkinsonism and cognitive impairment, as well as of hyposmia and probable REM sleep behavior disorder, correlated significantly with increasing USSLB stage. A few clinical features had no correlation with USSLB stage.
Dr. Adler and colleagues also applied the Braak staging criteria to the cases. To classify all cases, the investigators added an olfactory-bulb-only stage to the Braak criteria. Of the initial cohort, 70 cases could not be assigned a Braak stage. When the researchers removed cases with Alzheimer’s disease, 21% of cases could not be staged.
—Erik Greb
Ad hoc PCI dominates in elderly
ORLANDO – Ad hoc percutaneous coronary intervention is performed nearly six times more frequently than planned PCI in older patients undergoing elective PCI for stable coronary artery disease, according to a national study of Medicare claims data for 2009-2014.
The data showed no evident downside to ad hoc PCI in patients over age 65. Indeed, the ad hoc PCI strategy was associated with a significantly lower adjusted risk of in-hospital bleeding, compared with non–ad hoc PCI. The two approaches didn’t differ significantly in terms of in-hospital acute kidney injury or mortality, Kamil F. Faridi, MD, reported at the annual meeting of the American College of Cardiology.
In the past, concern had been voiced that ad hoc PCI – that is, PCI performed during the same session as diagnostic coronary angiography – doesn’t allow time for optimization of medical therapy prior to intervention, which might in theory result in worse outcomes. But such was not the case in a study of 169,434 patients age 65 years and up who underwent PCI for stable CAD with no evidence of acute coronary syndrome.
Moreover, ad hoc PCI offers several distinct advantages: a single vascular access, shorter net time in hospital, and lower cost, noted Dr. Faridi, of Beth Israel Deaconess Medical Center in Boston.
The proportion of elective PCIs that were performed on an ad hoc basis rose during the study years, from 77% in 2009 to 85% in 2014.
Patients who underwent ad hoc PCI were more likely to have angina symptoms before intervention. They were less likely to have peripheral vascular disease, heart failure, chronic kidney disease, complex lesion anatomy, or multivessel PCI than were patients who had planned PCI. Non–ad hoc PCI was more likely to occur at high-volume centers.
The in-hospital bleeding rate was 2.9% in the ad hoc PCI group, significantly lower than the 3.8% rate in the planned PCI patients. In an analysis adjusted for potential confounders, this translated to a 14% relative risk reduction. In-hospital acute kidney injury occurred in 8.0% of the ad hoc PCI group and 9.2% of the planned PCI group. The in-hospital mortality rate was 0.4% with ad hoc and 0.5% with planned PCI.
Dr. Faridi’s study was supported by the ACC National Cardiovascular Data Registry. He reported having no financial conflicts.
SOURCE: Faridi KF. ACC 2018, Abstract 1306-468/468
ORLANDO – Ad hoc percutaneous coronary intervention is performed nearly six times more frequently than planned PCI in older patients undergoing elective PCI for stable coronary artery disease, according to a national study of Medicare claims data for 2009-2014.
The data showed no evident downside to ad hoc PCI in patients over age 65. Indeed, the ad hoc PCI strategy was associated with a significantly lower adjusted risk of in-hospital bleeding, compared with non–ad hoc PCI. The two approaches didn’t differ significantly in terms of in-hospital acute kidney injury or mortality, Kamil F. Faridi, MD, reported at the annual meeting of the American College of Cardiology.
In the past, concern had been voiced that ad hoc PCI – that is, PCI performed during the same session as diagnostic coronary angiography – doesn’t allow time for optimization of medical therapy prior to intervention, which might in theory result in worse outcomes. But such was not the case in a study of 169,434 patients age 65 years and up who underwent PCI for stable CAD with no evidence of acute coronary syndrome.
Moreover, ad hoc PCI offers several distinct advantages: a single vascular access, shorter net time in hospital, and lower cost, noted Dr. Faridi, of Beth Israel Deaconess Medical Center in Boston.
The proportion of elective PCIs that were performed on an ad hoc basis rose during the study years, from 77% in 2009 to 85% in 2014.
Patients who underwent ad hoc PCI were more likely to have angina symptoms before intervention. They were less likely to have peripheral vascular disease, heart failure, chronic kidney disease, complex lesion anatomy, or multivessel PCI than were patients who had planned PCI. Non–ad hoc PCI was more likely to occur at high-volume centers.
The in-hospital bleeding rate was 2.9% in the ad hoc PCI group, significantly lower than the 3.8% rate in the planned PCI patients. In an analysis adjusted for potential confounders, this translated to a 14% relative risk reduction. In-hospital acute kidney injury occurred in 8.0% of the ad hoc PCI group and 9.2% of the planned PCI group. The in-hospital mortality rate was 0.4% with ad hoc and 0.5% with planned PCI.
Dr. Faridi’s study was supported by the ACC National Cardiovascular Data Registry. He reported having no financial conflicts.
SOURCE: Faridi KF. ACC 2018, Abstract 1306-468/468
ORLANDO – Ad hoc percutaneous coronary intervention is performed nearly six times more frequently than planned PCI in older patients undergoing elective PCI for stable coronary artery disease, according to a national study of Medicare claims data for 2009-2014.
The data showed no evident downside to ad hoc PCI in patients over age 65. Indeed, the ad hoc PCI strategy was associated with a significantly lower adjusted risk of in-hospital bleeding, compared with non–ad hoc PCI. The two approaches didn’t differ significantly in terms of in-hospital acute kidney injury or mortality, Kamil F. Faridi, MD, reported at the annual meeting of the American College of Cardiology.
In the past, concern had been voiced that ad hoc PCI – that is, PCI performed during the same session as diagnostic coronary angiography – doesn’t allow time for optimization of medical therapy prior to intervention, which might in theory result in worse outcomes. But such was not the case in a study of 169,434 patients age 65 years and up who underwent PCI for stable CAD with no evidence of acute coronary syndrome.
Moreover, ad hoc PCI offers several distinct advantages: a single vascular access, shorter net time in hospital, and lower cost, noted Dr. Faridi, of Beth Israel Deaconess Medical Center in Boston.
The proportion of elective PCIs that were performed on an ad hoc basis rose during the study years, from 77% in 2009 to 85% in 2014.
Patients who underwent ad hoc PCI were more likely to have angina symptoms before intervention. They were less likely to have peripheral vascular disease, heart failure, chronic kidney disease, complex lesion anatomy, or multivessel PCI than were patients who had planned PCI. Non–ad hoc PCI was more likely to occur at high-volume centers.
The in-hospital bleeding rate was 2.9% in the ad hoc PCI group, significantly lower than the 3.8% rate in the planned PCI patients. In an analysis adjusted for potential confounders, this translated to a 14% relative risk reduction. In-hospital acute kidney injury occurred in 8.0% of the ad hoc PCI group and 9.2% of the planned PCI group. The in-hospital mortality rate was 0.4% with ad hoc and 0.5% with planned PCI.
Dr. Faridi’s study was supported by the ACC National Cardiovascular Data Registry. He reported having no financial conflicts.
SOURCE: Faridi KF. ACC 2018, Abstract 1306-468/468
REPORTING FROM ACC 2018
Key clinical point: Ad hoc PCI in older patients has a lower bleeding risk than non–ad hoc PCI.
Major finding: Older patients undergoing ad hoc PCI for stable CAD were 14% less likely to experience significant in-hospital bleeding than were those undergoing planned PCI.
Study details: This was a retrospective study of nearly 170,000 patients age 65 years or older who underwent elective PCI for stable CAD.
Disclosures: The study was supported by the ACC National Cardiovascular Data Registry. The presenter reported having no financial conflicts.
Source: Faridi KF. ACC 2018, Abstract 1306-468/468
Positivity Rates in Oropharyngeal and Nonoropharyngeal Head and Neck Cancer in the VA
Head and neck cancer (HNC) continues to be a major health issue with an estimated 51,540 cases in the US in 2018, making it the eighth most common cancer among men with an estimated 4% of all new cancer diagnoses.1 Over the past decade, human papillomavirus (HPV) has emerged as a major prognostic factor for survival in squamous cell carcinomas of the oropharynx. Patients who are HPV-positive (HPV+) have a much higher survival rate than patients who have HPV-negative (HPV-) cancers of the oropharynx. The 8th edition of the American Joint Committee on Cancer (AJCC) staging manual has 2 distinct stagings for HPV+ and HPV- oropharyngeal tumors using p16-positivity (p16+) as a surrogate marker.2
Squamous cell carcinomas of the oropharynx that are HPV+ have about half the risk of death of HPV- tumors, are highly responsive to treatment, and are more often seen in younger and healthier patients with little to no tobacco use.2,3 As such, there also is a movement to de-escalate HPV+ oropharyngeal cancers with multiple trials by either replacing cytotoxic chemotherapy with a targeted agent (cisplatin vs cetuximab in RTOG 1016) or reducing the radiation dose (ECOG 1308, NRG HN002, Quarterback, and OPTIMA trials).3
The focus of many epidemiologic studies has been in the HNC general population. A recent epidemiologic analysis of the HNC general population found a p16 positivity rate of 60% in oropharyngeal squamous cell carcinomas (OPSCC) and 10% in nonoropharyngeal squamous cell carcinomas (NOPSCC).4 There has been a lack of studies focusing on the US Department of Veterans Administration (VA) population. The VA HNC population consists mostly of older white male smokers; whereas the rise of OPSCC in the general population consists primarily of males aged < 60 years often with little or no tobacco use.5 Furthermore, the importance of p16 positivity in NOPSCC also may be prognostic.6 Population data on this subset in the VA are lacking as well.This study’s purpose is to analyze the p16 positivity rate in both the OPSCC and NOPSCC in the VA population. Elucidation of epidemiologic factors that are associated with these groups may bring to light important differences between the VA and general HNC populations.
Methods
A review of the Kansas City VA Medical Center database for patients with HNC was performed from 2011 to 2017. The review consisted of 183 patient records (second primaries were scored separately), and 123 were deemed eligible for the study. Epidemiologic data were collected, including site, OPSCC vs NOPSCC, age, race, education level, tobacco use, alcohol use, TNM stage, and marital status (Table). 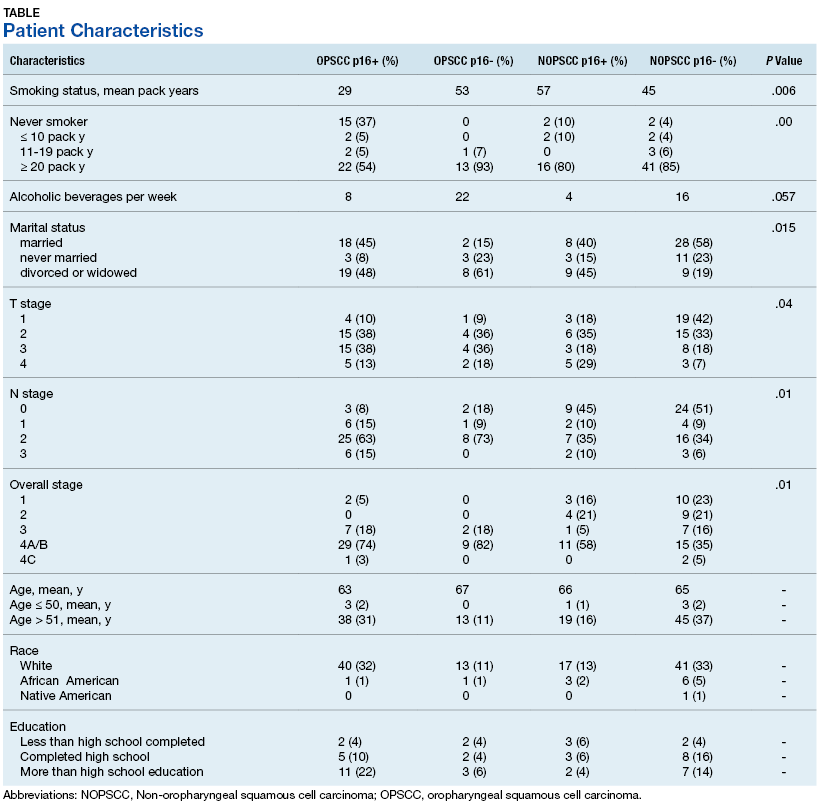
Results
The NOPSCC p16+ group had the greatest mean pack-year use (57). The lowest was in the OPSCC p16+ group (29). The OPSCC p16+ group had 37% never smokers compared with ≤ 10% for the other groups. Both the OPSCC and NOPSCC p16- groups had much more alcohol use per week than that of the p16+ groups. The differences in marital status included a lower rate of never married individuals in the p16+ group and a higher rate of marriage in the NOPSCC p16- group. The T stage distribution within the OPSCC groups was similar, but NOPSCC groups saw more T1 lesions in the NOPSCC p16- group (42% p16- vs 18% p16+). Conversely, more T4 lesions were found in the NOPSCC p16+ patients (7% p16- vs 29% p16+).
Discussion
The overall HPV positivity rate in the general population of patients with HNC has been reported as between 57% and 72% for OPSCC and between 1.3% and 7% for NOPSCC.6 One study, however, examined the p16 positivity rate in NOPSCC patients enrolled in major trials (RTOG 0129, 0234, and 0522 studies) and found that up to 19.3% of NOPSCC patients had p16 positivity.6 Even with the near 20% rate in those aforementioned trials that are above the reported norm, the current study found that nearly 30% of its VA population had p16+ NOPSCC. It has been shown that regardless of site, HPV-driven head and neck tumors share a similar gene expression and DNA methylation profiles (nonkeratinizing, basaloid histopathologic features, and lack of TP53 or CDKN2A alterations).5 p16+ NOPSCC has a different immune microenvironment with less lymphocyte infiltration, and there is some debate in the literature about the effects on tumor outcomes for NOPSCC cancer.5
In the aforementioned RTOG trials, p16- NOPSCC had worse outcomes compared with those of p16+ NOPSCC.6 This result is in contrast to the Danish Head and Neck Cancer Group (DAHANCA) and the combined Johns Hopkins University (JHU) and University of California, San Francisco (UCSF) data that found no difference between p16+ NOPSCC or p16- NOPSCC.7,8 In regards to race, this study did not find any differences. Another UCSF and JHU study showed lower p16+ rates in African American patients with OPSCC, but no distinction between race in the NOPSCC group. This result is consistent with the data in the current study as the distribution of race was no different among the 4 groups; however, this study's cohort was 90% white, 10% African American, and only < 1% Native American.4 This study's cohort population also was consistent with HPV-positive tumors presenting with earlier T, but higher N staging.9
Smoking is known to decrease survival in HPV-positive HNC, with the RTOG 0129 study separating head and neck tumors into low, medium, and high risk, based on HPV status, smoking, and stage.10 Although the average smoking pack-years in the current study’s OPC p16+ group was high at 29 pack-years, there was still a significant number of nonsmokers in that same group (37%). The University of Michigan conducted a study that had a similar profile of patients with an average age of 56.5 and 32.4% never smokers in their p16+ OPSCC cohort; thus, the VA p16+ OPSCC group in this study may be similar to the general population's p16+ OPSCC group.11 Nonmonogamous relationships also have been shown to be a risk factor for HPV positivity, and there was a difference in marital status (assuming it was a surrogate for monogamy) between the 4 groups; however, in contrast, the p16+ group in the current study had a high number of married patients, 45% in OPC p16+ group, and may not have been a good surrogate for monogamy in this VA population.
Limitations
Limitations of this study include all the caveats that come with a retrospective study, such as confounding variables, unbalanced groups, and selection bias. A detailed sexual history was not included, although it is well known that sexual activity is linked with oral HPV positivity.12 Human papillomavirus positivity based on p16 immunohistochemical analysis also was used as a surrogate marker for HPV instead of DNA in situ hybridization. The data also may be skewed due to the study patient’s being predominantly white and male: Both groups have a higher predilection for HPV-driven HNCs.13
Conclusion
The proportion of p16+ VA OPSCC cases was similar to that of the general population at 75% with 37% never smokers, but the percentage in NOPSCC was higher at 29% with only 10% never smokers. The p16+ NOPSCC also presented with more T4 lesions and a higher overall stage compared with p16- NOPSCC. Further studies are needed to compare these subgroups in the VA and in the general HNC populations.
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7-30.
2. Lydiatt WM, Patel SG, O’Sullivan B, et al. Head and neck cancers major changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J Clin. 2017;67(2):122-137.
3. Mirghani H, Blanchard P. Treatment de-escalation for HPV-driven oropharyngeal cancer: where do we stand? Clin Transl Radiat Oncol. 2017;8:4-11.
4. D’Souza G, Westra WH, Wang SJ, et al. Differences in the prevalence of human papillomavirus (HPV) in head and neck squamous cell cancers by sex, race, anatomic tumor site, and HPV detection method. JAMA Oncol. 2017;3(2):169-177.
5. Chakravarthy A, Henderson S, Thirdborough SM, et al. Human papillomavirus drives tumor development throughout the head and neck: improved prognosis is associated with an immune response largely restricted to the oropharynx. J Clin Oncol. 2016;34(34):4132-4141.
6. Chung CH, Zhang Q, Kong CS, et al. p16 protein expression and human papillomavirus status as prognostic biomarkers of nonoropharyngeal head and neck squamous cell carcinoma. J Clin Oncol. 2014;32(35):3930-3938.
7. Lassen P, Primdahl H, Johansen J, et al; Danish Head and Neck Cancer Group (DAHANCA). Impact of HPV-associated p16-expression on radiotherapy outcome in advanced oropharynx and non-oropharynx cancer. Radiother Oncol. 2014;113(3):310-316.
8. Fakhry C, Westra WH, Wang SJ, et al. The prognostic role of sex, race, and human papillomavirus in oropharyngeal and nonoropharyngeal head and neck squamous cell cancer. Cancer. 2017;123(9):1566-1575.
9. Elrefaey S, Massaro MA, Chiocca S, Chiesa F, Ansarin M. HPV in oropharyngeal cancer: the basics to know in clinical practice. Acta Otorhinolaryngol Ital. 2014;34(5):299-309.
10. Ang KK, Harris J, Wheeler R, et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med. 2010;363(1):24-35.
11. Maxwell, JH, Kumar B, Feng FY, et al. Tobacco use in HPV-positive advanced oropharynx cancer patients related to increased risk of distant metastases and tumor recurrence. Clin Cancer Res. 2010;16(4):1226-1235.
12. Gillison ML, Broutian T, Pickard RK, et al. Prevalence of oral HPV infection in the United States, 2009-2010. JAMA. 2012;307(7):693-703.
13. Benson E, Li R, Eisele D, Fakhry C. The clinical impact of HPV tumor status upon head and neck squamous cell carcinomas. Oral Oncol. 2014;50(6):565-574.
Head and neck cancer (HNC) continues to be a major health issue with an estimated 51,540 cases in the US in 2018, making it the eighth most common cancer among men with an estimated 4% of all new cancer diagnoses.1 Over the past decade, human papillomavirus (HPV) has emerged as a major prognostic factor for survival in squamous cell carcinomas of the oropharynx. Patients who are HPV-positive (HPV+) have a much higher survival rate than patients who have HPV-negative (HPV-) cancers of the oropharynx. The 8th edition of the American Joint Committee on Cancer (AJCC) staging manual has 2 distinct stagings for HPV+ and HPV- oropharyngeal tumors using p16-positivity (p16+) as a surrogate marker.2
Squamous cell carcinomas of the oropharynx that are HPV+ have about half the risk of death of HPV- tumors, are highly responsive to treatment, and are more often seen in younger and healthier patients with little to no tobacco use.2,3 As such, there also is a movement to de-escalate HPV+ oropharyngeal cancers with multiple trials by either replacing cytotoxic chemotherapy with a targeted agent (cisplatin vs cetuximab in RTOG 1016) or reducing the radiation dose (ECOG 1308, NRG HN002, Quarterback, and OPTIMA trials).3
The focus of many epidemiologic studies has been in the HNC general population. A recent epidemiologic analysis of the HNC general population found a p16 positivity rate of 60% in oropharyngeal squamous cell carcinomas (OPSCC) and 10% in nonoropharyngeal squamous cell carcinomas (NOPSCC).4 There has been a lack of studies focusing on the US Department of Veterans Administration (VA) population. The VA HNC population consists mostly of older white male smokers; whereas the rise of OPSCC in the general population consists primarily of males aged < 60 years often with little or no tobacco use.5 Furthermore, the importance of p16 positivity in NOPSCC also may be prognostic.6 Population data on this subset in the VA are lacking as well.This study’s purpose is to analyze the p16 positivity rate in both the OPSCC and NOPSCC in the VA population. Elucidation of epidemiologic factors that are associated with these groups may bring to light important differences between the VA and general HNC populations.
Methods
A review of the Kansas City VA Medical Center database for patients with HNC was performed from 2011 to 2017. The review consisted of 183 patient records (second primaries were scored separately), and 123 were deemed eligible for the study. Epidemiologic data were collected, including site, OPSCC vs NOPSCC, age, race, education level, tobacco use, alcohol use, TNM stage, and marital status (Table).
Results
The NOPSCC p16+ group had the greatest mean pack-year use (57). The lowest was in the OPSCC p16+ group (29). The OPSCC p16+ group had 37% never smokers compared with ≤ 10% for the other groups. Both the OPSCC and NOPSCC p16- groups had much more alcohol use per week than that of the p16+ groups. The differences in marital status included a lower rate of never married individuals in the p16+ group and a higher rate of marriage in the NOPSCC p16- group. The T stage distribution within the OPSCC groups was similar, but NOPSCC groups saw more T1 lesions in the NOPSCC p16- group (42% p16- vs 18% p16+). Conversely, more T4 lesions were found in the NOPSCC p16+ patients (7% p16- vs 29% p16+).
Discussion
The overall HPV positivity rate in the general population of patients with HNC has been reported as between 57% and 72% for OPSCC and between 1.3% and 7% for NOPSCC.6 One study, however, examined the p16 positivity rate in NOPSCC patients enrolled in major trials (RTOG 0129, 0234, and 0522 studies) and found that up to 19.3% of NOPSCC patients had p16 positivity.6 Even with the near 20% rate in those aforementioned trials that are above the reported norm, the current study found that nearly 30% of its VA population had p16+ NOPSCC. It has been shown that regardless of site, HPV-driven head and neck tumors share a similar gene expression and DNA methylation profiles (nonkeratinizing, basaloid histopathologic features, and lack of TP53 or CDKN2A alterations).5 p16+ NOPSCC has a different immune microenvironment with less lymphocyte infiltration, and there is some debate in the literature about the effects on tumor outcomes for NOPSCC cancer.5
In the aforementioned RTOG trials, p16- NOPSCC had worse outcomes compared with those of p16+ NOPSCC.6 This result is in contrast to the Danish Head and Neck Cancer Group (DAHANCA) and the combined Johns Hopkins University (JHU) and University of California, San Francisco (UCSF) data that found no difference between p16+ NOPSCC or p16- NOPSCC.7,8 In regards to race, this study did not find any differences. Another UCSF and JHU study showed lower p16+ rates in African American patients with OPSCC, but no distinction between race in the NOPSCC group. This result is consistent with the data in the current study as the distribution of race was no different among the 4 groups; however, this study's cohort was 90% white, 10% African American, and only < 1% Native American.4 This study's cohort population also was consistent with HPV-positive tumors presenting with earlier T, but higher N staging.9
Smoking is known to decrease survival in HPV-positive HNC, with the RTOG 0129 study separating head and neck tumors into low, medium, and high risk, based on HPV status, smoking, and stage.10 Although the average smoking pack-years in the current study’s OPC p16+ group was high at 29 pack-years, there was still a significant number of nonsmokers in that same group (37%). The University of Michigan conducted a study that had a similar profile of patients with an average age of 56.5 and 32.4% never smokers in their p16+ OPSCC cohort; thus, the VA p16+ OPSCC group in this study may be similar to the general population's p16+ OPSCC group.11 Nonmonogamous relationships also have been shown to be a risk factor for HPV positivity, and there was a difference in marital status (assuming it was a surrogate for monogamy) between the 4 groups; however, in contrast, the p16+ group in the current study had a high number of married patients, 45% in OPC p16+ group, and may not have been a good surrogate for monogamy in this VA population.
Limitations
Limitations of this study include all the caveats that come with a retrospective study, such as confounding variables, unbalanced groups, and selection bias. A detailed sexual history was not included, although it is well known that sexual activity is linked with oral HPV positivity.12 Human papillomavirus positivity based on p16 immunohistochemical analysis also was used as a surrogate marker for HPV instead of DNA in situ hybridization. The data also may be skewed due to the study patient’s being predominantly white and male: Both groups have a higher predilection for HPV-driven HNCs.13
Conclusion
The proportion of p16+ VA OPSCC cases was similar to that of the general population at 75% with 37% never smokers, but the percentage in NOPSCC was higher at 29% with only 10% never smokers. The p16+ NOPSCC also presented with more T4 lesions and a higher overall stage compared with p16- NOPSCC. Further studies are needed to compare these subgroups in the VA and in the general HNC populations.
Head and neck cancer (HNC) continues to be a major health issue with an estimated 51,540 cases in the US in 2018, making it the eighth most common cancer among men with an estimated 4% of all new cancer diagnoses.1 Over the past decade, human papillomavirus (HPV) has emerged as a major prognostic factor for survival in squamous cell carcinomas of the oropharynx. Patients who are HPV-positive (HPV+) have a much higher survival rate than patients who have HPV-negative (HPV-) cancers of the oropharynx. The 8th edition of the American Joint Committee on Cancer (AJCC) staging manual has 2 distinct stagings for HPV+ and HPV- oropharyngeal tumors using p16-positivity (p16+) as a surrogate marker.2
Squamous cell carcinomas of the oropharynx that are HPV+ have about half the risk of death of HPV- tumors, are highly responsive to treatment, and are more often seen in younger and healthier patients with little to no tobacco use.2,3 As such, there also is a movement to de-escalate HPV+ oropharyngeal cancers with multiple trials by either replacing cytotoxic chemotherapy with a targeted agent (cisplatin vs cetuximab in RTOG 1016) or reducing the radiation dose (ECOG 1308, NRG HN002, Quarterback, and OPTIMA trials).3
The focus of many epidemiologic studies has been in the HNC general population. A recent epidemiologic analysis of the HNC general population found a p16 positivity rate of 60% in oropharyngeal squamous cell carcinomas (OPSCC) and 10% in nonoropharyngeal squamous cell carcinomas (NOPSCC).4 There has been a lack of studies focusing on the US Department of Veterans Administration (VA) population. The VA HNC population consists mostly of older white male smokers; whereas the rise of OPSCC in the general population consists primarily of males aged < 60 years often with little or no tobacco use.5 Furthermore, the importance of p16 positivity in NOPSCC also may be prognostic.6 Population data on this subset in the VA are lacking as well.This study’s purpose is to analyze the p16 positivity rate in both the OPSCC and NOPSCC in the VA population. Elucidation of epidemiologic factors that are associated with these groups may bring to light important differences between the VA and general HNC populations.
Methods
A review of the Kansas City VA Medical Center database for patients with HNC was performed from 2011 to 2017. The review consisted of 183 patient records (second primaries were scored separately), and 123 were deemed eligible for the study. Epidemiologic data were collected, including site, OPSCC vs NOPSCC, age, race, education level, tobacco use, alcohol use, TNM stage, and marital status (Table).
Results
The NOPSCC p16+ group had the greatest mean pack-year use (57). The lowest was in the OPSCC p16+ group (29). The OPSCC p16+ group had 37% never smokers compared with ≤ 10% for the other groups. Both the OPSCC and NOPSCC p16- groups had much more alcohol use per week than that of the p16+ groups. The differences in marital status included a lower rate of never married individuals in the p16+ group and a higher rate of marriage in the NOPSCC p16- group. The T stage distribution within the OPSCC groups was similar, but NOPSCC groups saw more T1 lesions in the NOPSCC p16- group (42% p16- vs 18% p16+). Conversely, more T4 lesions were found in the NOPSCC p16+ patients (7% p16- vs 29% p16+).
Discussion
The overall HPV positivity rate in the general population of patients with HNC has been reported as between 57% and 72% for OPSCC and between 1.3% and 7% for NOPSCC.6 One study, however, examined the p16 positivity rate in NOPSCC patients enrolled in major trials (RTOG 0129, 0234, and 0522 studies) and found that up to 19.3% of NOPSCC patients had p16 positivity.6 Even with the near 20% rate in those aforementioned trials that are above the reported norm, the current study found that nearly 30% of its VA population had p16+ NOPSCC. It has been shown that regardless of site, HPV-driven head and neck tumors share a similar gene expression and DNA methylation profiles (nonkeratinizing, basaloid histopathologic features, and lack of TP53 or CDKN2A alterations).5 p16+ NOPSCC has a different immune microenvironment with less lymphocyte infiltration, and there is some debate in the literature about the effects on tumor outcomes for NOPSCC cancer.5
In the aforementioned RTOG trials, p16- NOPSCC had worse outcomes compared with those of p16+ NOPSCC.6 This result is in contrast to the Danish Head and Neck Cancer Group (DAHANCA) and the combined Johns Hopkins University (JHU) and University of California, San Francisco (UCSF) data that found no difference between p16+ NOPSCC or p16- NOPSCC.7,8 In regards to race, this study did not find any differences. Another UCSF and JHU study showed lower p16+ rates in African American patients with OPSCC, but no distinction between race in the NOPSCC group. This result is consistent with the data in the current study as the distribution of race was no different among the 4 groups; however, this study's cohort was 90% white, 10% African American, and only < 1% Native American.4 This study's cohort population also was consistent with HPV-positive tumors presenting with earlier T, but higher N staging.9
Smoking is known to decrease survival in HPV-positive HNC, with the RTOG 0129 study separating head and neck tumors into low, medium, and high risk, based on HPV status, smoking, and stage.10 Although the average smoking pack-years in the current study’s OPC p16+ group was high at 29 pack-years, there was still a significant number of nonsmokers in that same group (37%). The University of Michigan conducted a study that had a similar profile of patients with an average age of 56.5 and 32.4% never smokers in their p16+ OPSCC cohort; thus, the VA p16+ OPSCC group in this study may be similar to the general population's p16+ OPSCC group.11 Nonmonogamous relationships also have been shown to be a risk factor for HPV positivity, and there was a difference in marital status (assuming it was a surrogate for monogamy) between the 4 groups; however, in contrast, the p16+ group in the current study had a high number of married patients, 45% in OPC p16+ group, and may not have been a good surrogate for monogamy in this VA population.
Limitations
Limitations of this study include all the caveats that come with a retrospective study, such as confounding variables, unbalanced groups, and selection bias. A detailed sexual history was not included, although it is well known that sexual activity is linked with oral HPV positivity.12 Human papillomavirus positivity based on p16 immunohistochemical analysis also was used as a surrogate marker for HPV instead of DNA in situ hybridization. The data also may be skewed due to the study patient’s being predominantly white and male: Both groups have a higher predilection for HPV-driven HNCs.13
Conclusion
The proportion of p16+ VA OPSCC cases was similar to that of the general population at 75% with 37% never smokers, but the percentage in NOPSCC was higher at 29% with only 10% never smokers. The p16+ NOPSCC also presented with more T4 lesions and a higher overall stage compared with p16- NOPSCC. Further studies are needed to compare these subgroups in the VA and in the general HNC populations.
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7-30.
2. Lydiatt WM, Patel SG, O’Sullivan B, et al. Head and neck cancers major changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J Clin. 2017;67(2):122-137.
3. Mirghani H, Blanchard P. Treatment de-escalation for HPV-driven oropharyngeal cancer: where do we stand? Clin Transl Radiat Oncol. 2017;8:4-11.
4. D’Souza G, Westra WH, Wang SJ, et al. Differences in the prevalence of human papillomavirus (HPV) in head and neck squamous cell cancers by sex, race, anatomic tumor site, and HPV detection method. JAMA Oncol. 2017;3(2):169-177.
5. Chakravarthy A, Henderson S, Thirdborough SM, et al. Human papillomavirus drives tumor development throughout the head and neck: improved prognosis is associated with an immune response largely restricted to the oropharynx. J Clin Oncol. 2016;34(34):4132-4141.
6. Chung CH, Zhang Q, Kong CS, et al. p16 protein expression and human papillomavirus status as prognostic biomarkers of nonoropharyngeal head and neck squamous cell carcinoma. J Clin Oncol. 2014;32(35):3930-3938.
7. Lassen P, Primdahl H, Johansen J, et al; Danish Head and Neck Cancer Group (DAHANCA). Impact of HPV-associated p16-expression on radiotherapy outcome in advanced oropharynx and non-oropharynx cancer. Radiother Oncol. 2014;113(3):310-316.
8. Fakhry C, Westra WH, Wang SJ, et al. The prognostic role of sex, race, and human papillomavirus in oropharyngeal and nonoropharyngeal head and neck squamous cell cancer. Cancer. 2017;123(9):1566-1575.
9. Elrefaey S, Massaro MA, Chiocca S, Chiesa F, Ansarin M. HPV in oropharyngeal cancer: the basics to know in clinical practice. Acta Otorhinolaryngol Ital. 2014;34(5):299-309.
10. Ang KK, Harris J, Wheeler R, et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med. 2010;363(1):24-35.
11. Maxwell, JH, Kumar B, Feng FY, et al. Tobacco use in HPV-positive advanced oropharynx cancer patients related to increased risk of distant metastases and tumor recurrence. Clin Cancer Res. 2010;16(4):1226-1235.
12. Gillison ML, Broutian T, Pickard RK, et al. Prevalence of oral HPV infection in the United States, 2009-2010. JAMA. 2012;307(7):693-703.
13. Benson E, Li R, Eisele D, Fakhry C. The clinical impact of HPV tumor status upon head and neck squamous cell carcinomas. Oral Oncol. 2014;50(6):565-574.
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7-30.
2. Lydiatt WM, Patel SG, O’Sullivan B, et al. Head and neck cancers major changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J Clin. 2017;67(2):122-137.
3. Mirghani H, Blanchard P. Treatment de-escalation for HPV-driven oropharyngeal cancer: where do we stand? Clin Transl Radiat Oncol. 2017;8:4-11.
4. D’Souza G, Westra WH, Wang SJ, et al. Differences in the prevalence of human papillomavirus (HPV) in head and neck squamous cell cancers by sex, race, anatomic tumor site, and HPV detection method. JAMA Oncol. 2017;3(2):169-177.
5. Chakravarthy A, Henderson S, Thirdborough SM, et al. Human papillomavirus drives tumor development throughout the head and neck: improved prognosis is associated with an immune response largely restricted to the oropharynx. J Clin Oncol. 2016;34(34):4132-4141.
6. Chung CH, Zhang Q, Kong CS, et al. p16 protein expression and human papillomavirus status as prognostic biomarkers of nonoropharyngeal head and neck squamous cell carcinoma. J Clin Oncol. 2014;32(35):3930-3938.
7. Lassen P, Primdahl H, Johansen J, et al; Danish Head and Neck Cancer Group (DAHANCA). Impact of HPV-associated p16-expression on radiotherapy outcome in advanced oropharynx and non-oropharynx cancer. Radiother Oncol. 2014;113(3):310-316.
8. Fakhry C, Westra WH, Wang SJ, et al. The prognostic role of sex, race, and human papillomavirus in oropharyngeal and nonoropharyngeal head and neck squamous cell cancer. Cancer. 2017;123(9):1566-1575.
9. Elrefaey S, Massaro MA, Chiocca S, Chiesa F, Ansarin M. HPV in oropharyngeal cancer: the basics to know in clinical practice. Acta Otorhinolaryngol Ital. 2014;34(5):299-309.
10. Ang KK, Harris J, Wheeler R, et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med. 2010;363(1):24-35.
11. Maxwell, JH, Kumar B, Feng FY, et al. Tobacco use in HPV-positive advanced oropharynx cancer patients related to increased risk of distant metastases and tumor recurrence. Clin Cancer Res. 2010;16(4):1226-1235.
12. Gillison ML, Broutian T, Pickard RK, et al. Prevalence of oral HPV infection in the United States, 2009-2010. JAMA. 2012;307(7):693-703.
13. Benson E, Li R, Eisele D, Fakhry C. The clinical impact of HPV tumor status upon head and neck squamous cell carcinomas. Oral Oncol. 2014;50(6):565-574.