User login
CDC’s Fitzgerald resigns amid tobacco stock brouhaha
Brenda Fitzgerald, MD, director of the Centers for Disease Control and Prevention, resigned Jan. 31 after reports surfaced on the public affairs website Politico that she purchased shares of Japan Tobacco about 1 month after becoming the agency’s director.
Dr. Fitzgerald, an ob.gyn., also bought stock in Merck & Co., Bayer, and Humana after joining the Trump Administration in July 2017, according to the report. Financial disclosure records confirm that she sold the tobacco stock in October and “all of her stock holdings above $1,000 by Nov. 21, more than 4 months after she became CDC director,” according to the Politico report.
According to a spokesperson for the Health and Human Services department, “This morning Secretary Azar accepted Dr. Brenda Fitzgerald’s resignation as Director of the Centers for Disease Control and Prevention.
“Dr. Fitzgerald owns certain complex financial interests that have imposed a broad recusal limiting her ability to complete all of her duties as the CDC Director. Due to the nature of these financial interests, Dr. Fitzgerald could not divest from them in a definitive time period. After advising Secretary Azar of both the status of the financial interests and the scope of her recusal, Dr. Fitzgerald tendered, and the Secretary accepted, her resignation. The Secretary thanks Dr. Brenda Fitzgerald for her service and wishes her the best in all her endeavors,” according to a report on CNBC.
Brenda Fitzgerald, MD, director of the Centers for Disease Control and Prevention, resigned Jan. 31 after reports surfaced on the public affairs website Politico that she purchased shares of Japan Tobacco about 1 month after becoming the agency’s director.
Dr. Fitzgerald, an ob.gyn., also bought stock in Merck & Co., Bayer, and Humana after joining the Trump Administration in July 2017, according to the report. Financial disclosure records confirm that she sold the tobacco stock in October and “all of her stock holdings above $1,000 by Nov. 21, more than 4 months after she became CDC director,” according to the Politico report.
According to a spokesperson for the Health and Human Services department, “This morning Secretary Azar accepted Dr. Brenda Fitzgerald’s resignation as Director of the Centers for Disease Control and Prevention.
“Dr. Fitzgerald owns certain complex financial interests that have imposed a broad recusal limiting her ability to complete all of her duties as the CDC Director. Due to the nature of these financial interests, Dr. Fitzgerald could not divest from them in a definitive time period. After advising Secretary Azar of both the status of the financial interests and the scope of her recusal, Dr. Fitzgerald tendered, and the Secretary accepted, her resignation. The Secretary thanks Dr. Brenda Fitzgerald for her service and wishes her the best in all her endeavors,” according to a report on CNBC.
Brenda Fitzgerald, MD, director of the Centers for Disease Control and Prevention, resigned Jan. 31 after reports surfaced on the public affairs website Politico that she purchased shares of Japan Tobacco about 1 month after becoming the agency’s director.
Dr. Fitzgerald, an ob.gyn., also bought stock in Merck & Co., Bayer, and Humana after joining the Trump Administration in July 2017, according to the report. Financial disclosure records confirm that she sold the tobacco stock in October and “all of her stock holdings above $1,000 by Nov. 21, more than 4 months after she became CDC director,” according to the Politico report.
According to a spokesperson for the Health and Human Services department, “This morning Secretary Azar accepted Dr. Brenda Fitzgerald’s resignation as Director of the Centers for Disease Control and Prevention.
“Dr. Fitzgerald owns certain complex financial interests that have imposed a broad recusal limiting her ability to complete all of her duties as the CDC Director. Due to the nature of these financial interests, Dr. Fitzgerald could not divest from them in a definitive time period. After advising Secretary Azar of both the status of the financial interests and the scope of her recusal, Dr. Fitzgerald tendered, and the Secretary accepted, her resignation. The Secretary thanks Dr. Brenda Fitzgerald for her service and wishes her the best in all her endeavors,” according to a report on CNBC.
2018 Update on fertility
Clinicians always should consider endometriosis in the diagnostic work-up of an infertility patient. But the diagnosis of endometriosis is often difficult, and management is complex. In this Update, we summarize international consensus documents on endometriosis with the aim of enhancing clinicians’ ability to make evidence-based decisions. In addition, we explore the interesting results of a large hysterosalpingography trial in which 2 different contrast mediums were used. Finally, we urge all clinicians to adapt the new standardized lexicon of infertility and fertility care terms that comprise the recently revised international glossary.
Endometriosis and infertility: The knowns and unknowns
Johnson NP, Hummelshoj L, Adamson GD, et al; World Endometriosis Society Sao Paulo Consortium. World Endometriosis Society consensus on the classification of endometriosis. Hum Reprod. 2017;32(2):315-324.
Johnson NP, Hummelshoj L; World Endometriosis Society Montpellier Consortium. Consensus on current management of endometriosis. Hum Reprod. 2013;28(6):1552-1568.
Rogers PA, Adamson GD, Al-Jefout M, et al; WES/WERF Consortium for Research Priorities in Endometriosis. Research priorities for endometriosis. Reprod Sci. 2017;24(2):202-226.
Endometriosis is defined as "a disease characterized by the presence of endometrium-like epithelium and stroma outside the endometrium and myometrium. Intrapelvic endometriosis can be located superficially on the peritoneum (peritoneal endometriosis), can extend 5 mm or more beneath the peritoneum (deep endometriosis) or can be present as an ovarian endometriotic cyst (endometrioma)."1 Always consider endometriosis in the infertile patient.
Although many professional societies and numerous Cochrane Database Systematic Reviews have provided guidelines on endometriosis, controversy and uncertainty remain. The World Endometriosis Society (WES) and the World Endometriosis Research Foundation (WERF), however, have now published several consensus documents that assess the global literature and professional organization guidelines in a structured, consensus-driven process.2-4 These WES and WERF documents consolidate known information and can be used to inform the clinician in making evidence-linked diagnostic and treatment decisions. Recommendations offered in this discussion are based on those documents.
Establishing the diagnosis can be difficult
Diagnosis of endometriosis is often difficult and is delayed an average of 7 years from onset of symptoms. These include severe dysmenorrhea, deep dyspareunia, chronic pelvic pain, ovulation pain, cyclical or perimenstrual symptoms (bowel or bladder associated) with or without abnormal bleeding, chronic fatigue, and infertility. A major difficulty is that the predictive value of any one symptom or set of symptoms remains uncertain, as each of these symptoms can have other causes, and a significant proportion of affected women are asymptomatic.
For a definitive diagnosis of endometriosis, visual inspection of the pelvis at laparoscopy is the gold standard investigation, unless disease is visible in the vagina or elsewhere. Positive histology confirms the diagnosis of endometriosis; negative histology does not exclude it. Whether histology should be obtained if peritoneal disease alone is present is controversial: visual inspection usually is adequate, but histologic confirmation of at least one lesion is ideal. In cases of ovarian endometrioma (>4 cm in diameter) and in deeply infiltrating disease, histology should be obtained to identify endometriosis and to exclude rare instances of malignancy.
Compared with laparoscopy, transvaginal ultrasonography (TVUS) has no value in diagnosing peritoneal endometriosis, but it is a useful tool for both making and excluding the diagnosis of an ovarian endometrioma. TVUS may have a role in the diagnosis of disease involving the bladder or rectum.
At present, evidence is insufficient to indicate that magnetic resonance imaging (MRI) is useful for diagnosing or excluding endometriosis compared with laparoscopy. MRI should be reserved for when ultrasound results are equivocal in cases of rectovaginal or bladder endometriosis.
Serum cancer antigen 125 (CA 125) levels may be elevated in endometriosis. However, measuring serum CA 125 levels has no value as a diagnostic tool.
No fertility benefit with ovarian suppression
More than 2 dozen randomized controlled trials (RCTs) provide strong evidence that there is no fertility benefit from ovarian suppression. The drug costs and delayed time to pregnancy mean that ovarian suppression with oral contraceptives, other progestational agents, or gonadotropin-releasing hormone (GnRH) agonists before fertility treatment is not indicated, with the possible exception of using it prior to in vitro fertilization (IVF).
Ovarian suppression also has been suggested as beneficial in conjunction with surgery. However, at least 16 RCTs have failed to show fertility improvement when ovarian suppression is given either preoperatively or postoperatively. Again, the delay in attempting pregnancy, drug costs, and adverse effects render ovarian suppression not appropriate.
While ovarian suppression has not been shown to increase pregnancy rates, ovarian stimulation (OS) likely does, especially when combined with intrauterine insemination (IUI).5
Laparoscopy: Appropriate for selected patients
A major decision for clinicians and patients dealing with infertility is whether to perform a laparoscopy, both for diagnostic and for treatment reasons. Currently, data are insufficient to recommend laparoscopic surgery prior to OS/IUI unless there is a history of evidence of anatomic disease and/or the patient has sufficient pain to justify the physical, emotional, financial, and time costs of laparoscopy. Laparoscopy therefore can be considered as possibly appropriate in younger women (<37 years of age) with short duration of infertility (<4 years), normal male factor, normal or treatable uterus, normal or treatable ovulation disorder, and limited prior treatment.
It is important to consider what disease might be found and how much of an increase in fertility can be obtained by treatment, so that the number needed to treat (NNT) can be used as an estimate of the potential value of laparoscopy in a given patient. A patient also should have no contraindications to laparoscopy and accept 9 to 15 months of attempting pregnancy before undergoing IVF treatment.
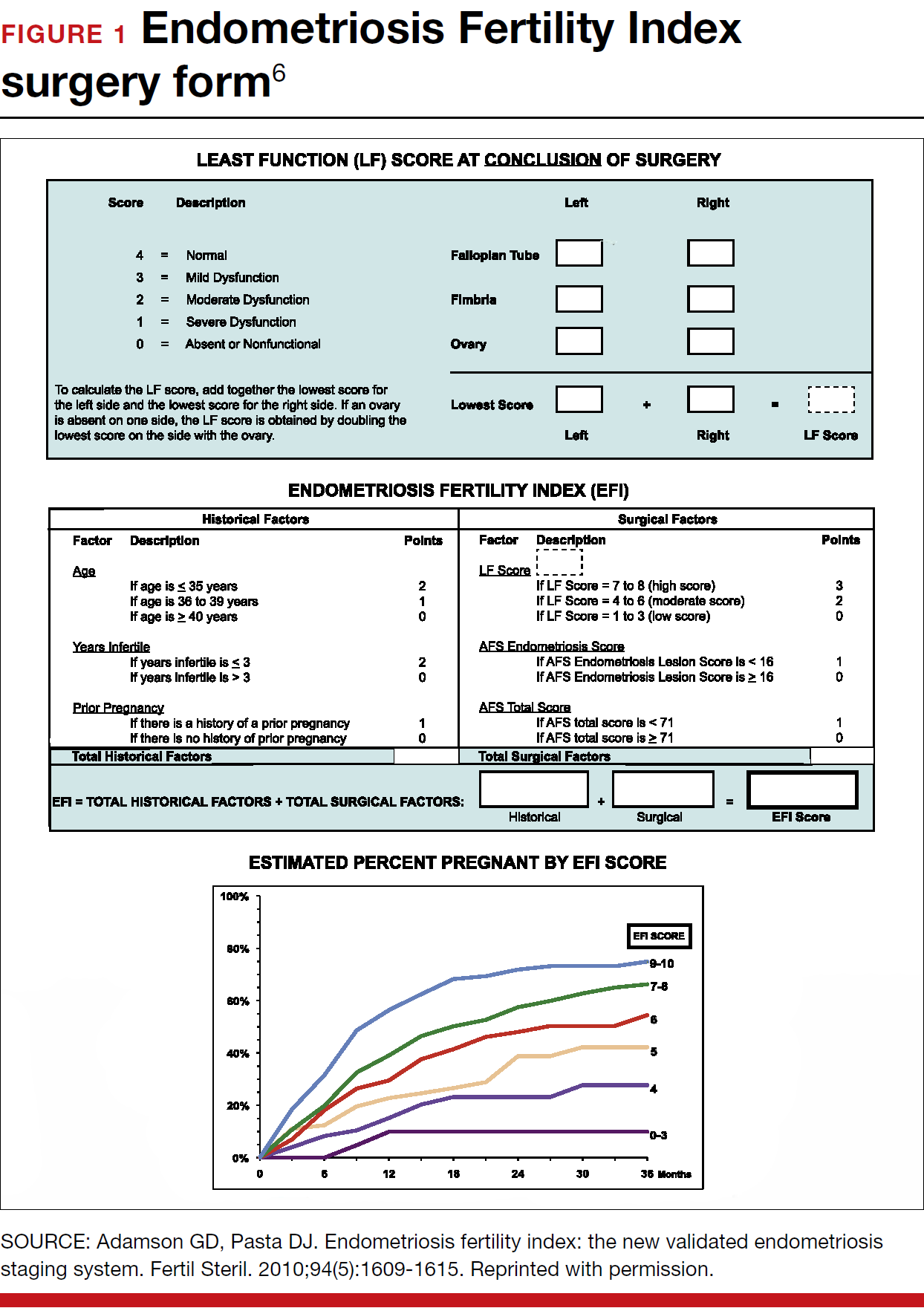
When laparoscopy is performed for minimal to mild disease, the odds ratio for pregnancy is 1.66 with treatment. It is important to remove all visible disease without injuring healthy tissue. When disease is moderate to severe, there is often severe anatomic distortion and a very low background pregnancy rate. Numerous uncontrolled trials show benefit of operative laparoscopy, especially for invasive, adhesive, and cystic endometriosis. However, repeat surgery is rarely indicated. After surgery, the Endometriosis Fertility Index (EFI) can be used to determine prognosis and plan management (FIGURE 1).6 An easy-to-use electronic EFI calculator is available online at www.endometriosisefi.com.
Management of endometriomas
Endometriomas are often operated on because of pain. Initial pain relief occurs in 60% to 100% of patients, but cysts recur following stripping about 10% of the time, and drainage without stripping, about 20%. With recurrence, pain is present about 75% of the time.
Pregnancy rates following endometrioma treatment depend on patient age and the status of the pelvis following operative intervention. This can be determined from the EFI. Often, the dilemma with endometriomas is how aggressive to be in removing them. The principles involved are to remove all the cyst wall if possible, but absolutely to minimize ovarian tissue damage, because reduced ovarian reserve is a possible major negative consequence of ovarian surgery.
Recommendations
While endometriosis is often a cause of infertility, often infertile patients do not have endometriosis. A careful history, physical examination, and ultrasonography, and possibly other imaging studies, are prerequisites to careful clinical judgment in diagnosing and treating infertile patients who might or do have endometriosis.
When pelvic pain is present, initially nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives (OCs), progestational agents, or an intrauterine device can be helpful. These ovarian suppression medications do not increase fertility, however, and should be stopped in any patient who desires to get pregnant.
When pelvic and male fertility factors appear reasonably normal (even if minimal or mild endometriosis is suspected), treatment with clomiphene 100 mg on cycle days 3 through 7 and IUI for 3 to 6 cycles is an effective first step. However, if the patient has persistent pain and/or infertility without other significant infertility factors, then diagnostic laparoscopy with intraoperative treatment of disease is indicated.
Surgery well performed is effective treatment for all stages of endometriosis and endometriomas, both for infertility and for pain. Repeat surgery, however, is rarely indicated because of limited results, so it is important to obtain the best possible result on the first surgery. Surgery is indicated for large endometriomas (>4 cm). Endometriosis has almost no effect on the IVF live birth rate unless ovarian reserve has been reduced by endometriomas or surgery, so endometriosis surgery should be performed by skilled and experienced surgeons.
Endometriosis is a complex disease that can cause infertility. Its diagnosis and management are frequently difficult, requiring knowledge, experience, and good medical judgment and surgical skills. However, if evidence-linked principles are followed, effective treatment plans and good outcomes can be obtained for most patients.
Read about why oil-based contrast may be better than water-based contrast with HSG.
Oil-based contrast medium use in hysterosalpingography is associated with higher pregnancy rates compared with water-based contrast
Dreyer K, van Rijswijk J, Mijatovic V, et al. Oil-based or water-based contrast for hysterosalpingography in infertile women. N Engl J Med. 2017;376(21):2043-2052.
Hysterosalpingography (HSG) to assess tubal patency has been a mainstay of infertility diagnosis for decades. Some, but not all, studies also have suggested that pregnancy rates are higher after this tubal flushing procedure, especially if performed with oil contrast.7,8 A recent multicenter, randomized, controlled trial by Dreyer and colleagues that compared ongoing pregnancy rates and other outcomes among women who had HSG with oil contrast versus with water contrast provides additional valuable information.9
Trial details
In this study, 1,294 infertile women in 27 academic, teaching and nonteaching hospitals were screened for trial eligibility; 1,119 women provided written informed consent. Of these, 557 women were randomly assigned to HSG with oil contrast and 562 to water contrast. The women had spontaneous menstrual cycles, had been attempting pregnancy for at least 1 year, and had indications for HSG.
Exclusion criteria were known endocrine disorders, fewer than 8 menstrual cycles per year, a high risk of tubal disease, iodine allergy, and a total motile sperm count after sperm wash of less than 3 million/mL in the male partner (or a total motile sperm count of less than 1 million/mL when an analysis after sperm wash was not performed).
Just prior to undergoing HSG, the women were randomly assigned to receive either oil contrast or water contrast medium. (The trial was not blinded to participants or caregivers.) HSG was performed according to local protocols using cervical vacuum cup, metal cannula (hysterophore), or balloon catheter and approximately 5 to 10 mL of contrast medium.
After HSG, couples received expectant management when the predicted likelihood of pregnancy within 12 months, based on the prognostic model of Hunault, was 30% or greater.10 IUI was offered for pregnancy likelihood less than 30%, mild male infertility, or failure after a period of expectant management. IUI with or without mild ovarian stimulation (2-3 follicles) with clomiphene or gonadotropins was initiated after a minimum of 2 months of expectant management after HSG.
The primary outcome measure was ongoing pregnancy, defined as a positive fetal heartbeat on ultrasonographic examination after 12 weeks of gestation, with the first day of the last menstrual cycle for the pregnancy within 6 months after randomization. Secondary outcome measures were clinical pregnancy, live birth, miscarriage, ectopic pregnancy, time to pregnancy, and pain scores after HSG. All data were analyzed according to intention-to-treat.
Pregnancy rates increased with oil-contrast HSG
The baseline characteristics of the 2 groups were similar. HSG showed bilateral tubal patency in 477 of 554 women (86.1%) in the oil contrast group and in 491 of 554 women (88.6%) who received the water contrast (rate ratio, 0.97; 95% confidence interval [CI], 0.93-1.02). Bilateral tubal occlusion occurred in 9 women in the oil group (1.6%) and in 13 in the water group (2.3%) (relative risk, 0.69; 95% CI, 0.30-1.61).
A total of 58.3% of the women assigned to oil contrast and 57.2% of those assigned to water contrast received expectant management. Similar percentages of women in the oil group and in the water group underwent IUI (39.7% and 41.0%, respectively), IVF or intracytoplasmic sperm injection (ICSI) (2.3% and 2.2%), laparoscopy (6.2% in each group), and hysteroscopy (4.4% and 4.2%).
Ongoing pregnancy occurred in 220 of 554 women (39.7%) in the oil contrast group and in 161 of 554 women (29.1%) in the water contrast group (rate ratio, 1.37; 95% CI, 1.16-1.61; P<.001). The median time to the onset of pregnancy in the oil group was 2.7 months (interquartile range, 1.5-4.7) (FIGURE 2), while in the water group it was 3.1 months (interquartile range, 1.6-4.8) (P = .44).
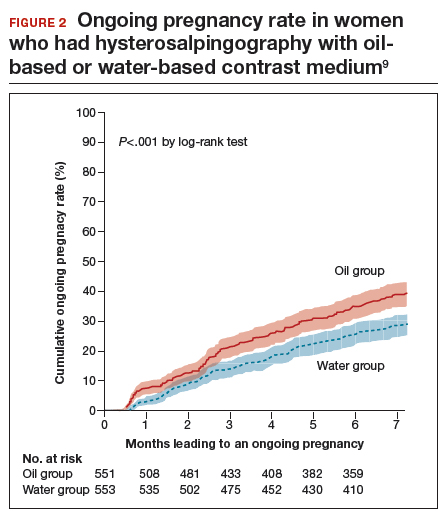
While the proportion of women getting pregnant with or without the different interventions was similar in both groups, the live birth rate was 38.8% in the oil group versus 28.1% in the water group (rate ratio, 1.38; 95% CI, 1.17-1.64; P<.001). Three of 554 women (0.5%) assigned to oil contrast and 4 of 554 women (0.7%) in the water contrast group had an adverse event during the trial period. Three women (1.4%), all in the oil group, delivered a child with a congenital anomaly.
Why this study is important
This is the largest and best methodologic study on this clinical issue. It showed higher pregnancy and live birth rates within 6 months of HSG performed with oil compared with water. Although the study was not blinded, the group similarities and objective outcomes support minimal bias. Importantly, these results can be generalized only to women with similar inclusion characteristics.
It is unclear why oil HSG might enhance fertility. Suggested mechanisms include flushing of debris and/or mucous plugs or an effect on peritoneal macrophages or endometrial receptivity. Since HSG is minimally invasive and inexpensive, and the 10% increase in pregnancy rates corresponds to an NNT of 10, it is reasonable to consider, although formal cost-effectiveness data are lacking.
Concerns include the rare theoretical risk of intravasation with subsequent allergic reaction or fat embolism. Three infants in the oil group and none in the water group had congenital anomalies. This is likely due to chance, since this rate is not higher than that in the general population and no other data suggest an increased risk. Comparison of these results with other new techniques, such as sonohysterography (saline infusion sonogram), awaits further studies.
Recommendation
HSG with oil contrast should be considered a potential therapeutic as well as diagnostic intervention in selected patients.
HSG is an important diagnostic test for most infertility patients. The fact that a therapeutic benefit probably also is associated with oil-based HSG increases the clinical indications for this test.
Read about new definitions of infertility terminology you should know.
Infertility glossary is newly updated
Zegers-Hochchild F, Adamson GD, Dyer S, et al. The International Glossary on Infertility and Fertility Care, 2017. Fertil Steril. 2017;108(3):393-406.
Terms and definitions used in infertility and fertility care frequently have had different meanings for different stakeholders, especially on a global basis. This can result in misunderstandings and inappropriate interpretation and comparison of published information and research. To help address these issues, international fertility organizations recently developed an updated glossary on infertilityterminology.
The consensus process for updating the glossary
The International Glossary on Infertility and Fertility Care, 2017, was recently published simultaneously in Fertility and Sterility and Human Reproduction. This is the second revision; the first glossary was published in 2006 and revised in 2009. This revision's 25 lead experts began work in 2014. Their teams of professionals interacted by electronic mail, at international and regional society meetings, and at 2 consultations held in Geneva, Switzerland. This glossary represents consensus agreement reached on 283 evidence-driven terms and definitions.
The work was led by the International Committee for Monitoring Assisted Reproductive Technologies in partnership with the American Society for Reproductive Medicine, European Society of Human Reproduction and Embryology, International Federation of Fertility Societies, March of Dimes, African Fertility Society, Groupe Inter-africain d'Etude de Recherche et d'Application sur la Fertilité, Asian Pacific Initiative on Reproduction, Middle East Fertility Society, Red Latinoamericana de Reproducción Asistida, and the International Federation of Gynecology and Obstetrics.
All together, 108 international professional experts (clinicians, basic scientists, epidemiologists, and social scientists), along with national and regional representatives of infertile persons, participated in the development of this evidence-base driven glossary. As such, these definitions now set the standard for international communication among clinicians, scientists, and policymakers.
Definition of infertility is broadened
The definitions take account of ethics, human rights, cultural sensitivities, ethnic minorities, and gender equality. For example, the first modification included broadening the concept of infertility to be an "impairment of individuals" in their capacity to reproduce, irrespective of whether the individual has a partner. (See “Broadened definition of infertility” below). Reproductive rights are individual human rights and do not depend on a relationship with another individual. The revised definition also reinforces the concept of infertility as a disease that can generate an impairment of function.
Infertility: A disease characterized by the failure to establish a clinical pregnancy after 12 months of regular, unprotected sexual intercourse or due to an impairment of a person’s capacity to reproduce either as an individual or with his/her partner. Fertility interventions may be initiated in less than 1 year based on medical, sexual and reproductive history, age, physical findings and diagnostic testing. Infertility is a disease, which generates disability as an impairment of function.
Reference
- Zegers-Hochchild F, Adamson GD, Dyer S, et al. The International Glossary on Infertility and Fertility Care, 2017. Fertil Steril. 2017;108(3):393–406
New--and changed--definitions
Certain terms need to be consistent with those used currently internationally, for example, at which gestational age a miscarriage/abortion becomes a stillbirth.
Some terms are confusing, such as subfertility, which does not define a different or less severe fertility status than infertility, does not exist before infertility is diagnosed, and should not be confused with sterility, which is a permanent state of infertility. The term subfertility therefore is redundant and has been removed and replaced by infertility (See “Some terms with an important new definition” below).
- Clinical pregnancy
- Conception (removed from glossary)
- Diminished ovarian reserve
- Fertility care
- Hypospermia (replaces oligospermia)
- Ovarian reserve
- Pregnancy
- Preimplantation genetic testing
- Spontaneous abortion/miscarriage
- Subfertility (should be used interchangeably with infertility)
Reference
- Zegers-Hochchild F, Adamson GD, Dyer S, et al. The International Glossary on Infertility and Fertility Care, 2017. Fertil Steril. 2017;108(3):393–406.
In a different context, the term conception, and its derivatives such as conceiving or conceived, was removed because it cannot be described biologically during the process of reproduction. Instead, terms such as fertilization, implantation, pregnancy, and live birth should be used.
Important male terms also changed: oligospermia is a term for low semen volume that is now replaced by hypospermia to avoid confusion with oligozoospermia, which is low concentration of spermatozoa in the ejaculate below the lower reference limit. When reporting results, the reference criteria should be specified.
Lastly, owing to the lack of standardization in determining the burden of infertility, and to better ensure comparability of prevalence data published globally, this glossary includes definitions for terms frequently used in epidemiology and public health. Examples include voluntary and involuntary childlessness, primary and secondary infertility, fertility care, fecundity, and fecundability, among others.
Getting the word out
The glossary has been approved by all of the participating organizations who are assisting in its distribution. It is being presented at national and international meetings and is used in The FIGO Fertility Toolbox (www.fertilitytool.com). It is hoped that all professionals and other stakeholders will begin to use its terminology globally to provide quality care and ensure consistency in registering specific fertility care interventions and more accurate reporting of their outcomes.
The language we use determines our individual and collective understanding of the scientific and clinical care of our patients. This glossary provides an essential and comprehensive standardization of terms and definitions essential to quality reproductive health care.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Zegers-Hochchild F, Adamson GD, Dyer S, et al. The International Glossary on Infertility and Fertility Care, 2017. Fertil Steril. 2017;108(3):393–406.
- Johnson NP, Hummelshoj L; World Endometriosis Society Montpellier Consortium. Consensus on current management of endometriosis. Hum Reprod. 2013;28(6):1552–1568.
- Rogers PA, Adamson GD, Al-Jefout M, et al; WES/WERF Consortium for Research Priorities in Endometriosis. Research priorities for endometriosis. Reprod Sci. 2017;24(2):202–226.
- Johnson NP, Hummelshoj L, Adamson GD, et al; World Endometriosis Society Sao Paulo Consortium. World Endometriosis Society consensus on the classification of endometriosis. Hum Reprod. 2017;32(2):315–324.
- Practice Committee of the American Society for Reproductive Medicine. Endometriosis and infertility: a committee opinion. Fertil Steril. 2012;98(3):591–598.
- Adamson GD, Pasta DJ. Endometriosis fertility index: the new, validated endometriosis staging system. Fertil Steril. 2010;94(5):1609–1615.
- Weir WC, Weir DR. Therapeutic value of salpingograms in infertility. Fertil Steril. 1951;2(6);514–522.
- Johnson NP, Farquhar CM, Hadden WE, Suckling J, Yu Y, Sadler L. The FLUSH trial—flushing with lipiodol for unexplained (and endometriosis-related) subfertility by hysterosalpingography: a randomized trial. Hum Reprod. 2004;19(9):2043–2051.
- Dreyer K, van Rijswijk J, Mijatovic V, et al. Oil-based or water-based contrast for hysterosalpingography in infertile women. N Engl J Med. 2017;376(21):2043–2052.
- Van der Steeg JW, Steures P, Eijkemans MJ, et al; Collaborative Effort for Clinical Evaluation in Reproductive Medicine. Pregnancy is predictable: a large-scale prospective external validation of the prediction of spontaneous pregnancy in sub-fertile couples. Hum Reprod. 2007;22(2):536–542.

Dr. Adamson is Founder and CEO of Advanced Reproductive Care, Inc (ARC Fertility); Clinical Professor, ACF, at Stanford University School of Medicine; and Associate Clinical Professor at the University of California, San Francisco. He is also Medical Director, Palo Alto Medical Foundation Fertility Physicians of Northern California in Palo Alto and San Jose.

Dr. Abusief is a Board-Certified Specialist in Reproductive Endocrinology and Infertility and Chair, Department of Reproductive Endocrinology and Infertility at Palo Alto Medical Foundation Fertility Physicians of Northern California.
Dr. Adamson reports being a consultant to AbbVie, Bayer, Ferring, Guerbet, Hernest, and Merck, and that he has equity in ARC Fertility. Dr. Abusief reports no financial relationships relevant to this article.
Dr. Adamson is Founder and CEO of Advanced Reproductive Care, Inc (ARC Fertility); Clinical Professor, ACF, at Stanford University School of Medicine; and Associate Clinical Professor at the University of California, San Francisco. He is also Medical Director, Palo Alto Medical Foundation Fertility Physicians of Northern California in Palo Alto and San Jose.
Dr. Abusief is a Board-Certified Specialist in Reproductive Endocrinology and Infertility and Chair, Department of Reproductive Endocrinology and Infertility at Palo Alto Medical Foundation Fertility Physicians of Northern California.
Dr. Adamson reports being a consultant to AbbVie, Bayer, Ferring, Guerbet, Hernest, and Merck, and that he has equity in ARC Fertility. Dr. Abusief reports no financial relationships relevant to this article.
Dr. Adamson is Founder and CEO of Advanced Reproductive Care, Inc (ARC Fertility); Clinical Professor, ACF, at Stanford University School of Medicine; and Associate Clinical Professor at the University of California, San Francisco. He is also Medical Director, Palo Alto Medical Foundation Fertility Physicians of Northern California in Palo Alto and San Jose.
Dr. Abusief is a Board-Certified Specialist in Reproductive Endocrinology and Infertility and Chair, Department of Reproductive Endocrinology and Infertility at Palo Alto Medical Foundation Fertility Physicians of Northern California.
Dr. Adamson reports being a consultant to AbbVie, Bayer, Ferring, Guerbet, Hernest, and Merck, and that he has equity in ARC Fertility. Dr. Abusief reports no financial relationships relevant to this article.
Clinicians always should consider endometriosis in the diagnostic work-up of an infertility patient. But the diagnosis of endometriosis is often difficult, and management is complex. In this Update, we summarize international consensus documents on endometriosis with the aim of enhancing clinicians’ ability to make evidence-based decisions. In addition, we explore the interesting results of a large hysterosalpingography trial in which 2 different contrast mediums were used. Finally, we urge all clinicians to adapt the new standardized lexicon of infertility and fertility care terms that comprise the recently revised international glossary.
Endometriosis and infertility: The knowns and unknowns
Johnson NP, Hummelshoj L, Adamson GD, et al; World Endometriosis Society Sao Paulo Consortium. World Endometriosis Society consensus on the classification of endometriosis. Hum Reprod. 2017;32(2):315-324.
Johnson NP, Hummelshoj L; World Endometriosis Society Montpellier Consortium. Consensus on current management of endometriosis. Hum Reprod. 2013;28(6):1552-1568.
Rogers PA, Adamson GD, Al-Jefout M, et al; WES/WERF Consortium for Research Priorities in Endometriosis. Research priorities for endometriosis. Reprod Sci. 2017;24(2):202-226.
Endometriosis is defined as "a disease characterized by the presence of endometrium-like epithelium and stroma outside the endometrium and myometrium. Intrapelvic endometriosis can be located superficially on the peritoneum (peritoneal endometriosis), can extend 5 mm or more beneath the peritoneum (deep endometriosis) or can be present as an ovarian endometriotic cyst (endometrioma)."1 Always consider endometriosis in the infertile patient.
Although many professional societies and numerous Cochrane Database Systematic Reviews have provided guidelines on endometriosis, controversy and uncertainty remain. The World Endometriosis Society (WES) and the World Endometriosis Research Foundation (WERF), however, have now published several consensus documents that assess the global literature and professional organization guidelines in a structured, consensus-driven process.2-4 These WES and WERF documents consolidate known information and can be used to inform the clinician in making evidence-linked diagnostic and treatment decisions. Recommendations offered in this discussion are based on those documents.
Establishing the diagnosis can be difficult
Diagnosis of endometriosis is often difficult and is delayed an average of 7 years from onset of symptoms. These include severe dysmenorrhea, deep dyspareunia, chronic pelvic pain, ovulation pain, cyclical or perimenstrual symptoms (bowel or bladder associated) with or without abnormal bleeding, chronic fatigue, and infertility. A major difficulty is that the predictive value of any one symptom or set of symptoms remains uncertain, as each of these symptoms can have other causes, and a significant proportion of affected women are asymptomatic.
For a definitive diagnosis of endometriosis, visual inspection of the pelvis at laparoscopy is the gold standard investigation, unless disease is visible in the vagina or elsewhere. Positive histology confirms the diagnosis of endometriosis; negative histology does not exclude it. Whether histology should be obtained if peritoneal disease alone is present is controversial: visual inspection usually is adequate, but histologic confirmation of at least one lesion is ideal. In cases of ovarian endometrioma (>4 cm in diameter) and in deeply infiltrating disease, histology should be obtained to identify endometriosis and to exclude rare instances of malignancy.
Compared with laparoscopy, transvaginal ultrasonography (TVUS) has no value in diagnosing peritoneal endometriosis, but it is a useful tool for both making and excluding the diagnosis of an ovarian endometrioma. TVUS may have a role in the diagnosis of disease involving the bladder or rectum.
At present, evidence is insufficient to indicate that magnetic resonance imaging (MRI) is useful for diagnosing or excluding endometriosis compared with laparoscopy. MRI should be reserved for when ultrasound results are equivocal in cases of rectovaginal or bladder endometriosis.
Serum cancer antigen 125 (CA 125) levels may be elevated in endometriosis. However, measuring serum CA 125 levels has no value as a diagnostic tool.
No fertility benefit with ovarian suppression
More than 2 dozen randomized controlled trials (RCTs) provide strong evidence that there is no fertility benefit from ovarian suppression. The drug costs and delayed time to pregnancy mean that ovarian suppression with oral contraceptives, other progestational agents, or gonadotropin-releasing hormone (GnRH) agonists before fertility treatment is not indicated, with the possible exception of using it prior to in vitro fertilization (IVF).
Ovarian suppression also has been suggested as beneficial in conjunction with surgery. However, at least 16 RCTs have failed to show fertility improvement when ovarian suppression is given either preoperatively or postoperatively. Again, the delay in attempting pregnancy, drug costs, and adverse effects render ovarian suppression not appropriate.
While ovarian suppression has not been shown to increase pregnancy rates, ovarian stimulation (OS) likely does, especially when combined with intrauterine insemination (IUI).5
Laparoscopy: Appropriate for selected patients
A major decision for clinicians and patients dealing with infertility is whether to perform a laparoscopy, both for diagnostic and for treatment reasons. Currently, data are insufficient to recommend laparoscopic surgery prior to OS/IUI unless there is a history of evidence of anatomic disease and/or the patient has sufficient pain to justify the physical, emotional, financial, and time costs of laparoscopy. Laparoscopy therefore can be considered as possibly appropriate in younger women (<37 years of age) with short duration of infertility (<4 years), normal male factor, normal or treatable uterus, normal or treatable ovulation disorder, and limited prior treatment.
It is important to consider what disease might be found and how much of an increase in fertility can be obtained by treatment, so that the number needed to treat (NNT) can be used as an estimate of the potential value of laparoscopy in a given patient. A patient also should have no contraindications to laparoscopy and accept 9 to 15 months of attempting pregnancy before undergoing IVF treatment.
When laparoscopy is performed for minimal to mild disease, the odds ratio for pregnancy is 1.66 with treatment. It is important to remove all visible disease without injuring healthy tissue. When disease is moderate to severe, there is often severe anatomic distortion and a very low background pregnancy rate. Numerous uncontrolled trials show benefit of operative laparoscopy, especially for invasive, adhesive, and cystic endometriosis. However, repeat surgery is rarely indicated. After surgery, the Endometriosis Fertility Index (EFI) can be used to determine prognosis and plan management (FIGURE 1).6 An easy-to-use electronic EFI calculator is available online at www.endometriosisefi.com.
Management of endometriomas
Endometriomas are often operated on because of pain. Initial pain relief occurs in 60% to 100% of patients, but cysts recur following stripping about 10% of the time, and drainage without stripping, about 20%. With recurrence, pain is present about 75% of the time.
Pregnancy rates following endometrioma treatment depend on patient age and the status of the pelvis following operative intervention. This can be determined from the EFI. Often, the dilemma with endometriomas is how aggressive to be in removing them. The principles involved are to remove all the cyst wall if possible, but absolutely to minimize ovarian tissue damage, because reduced ovarian reserve is a possible major negative consequence of ovarian surgery.
Recommendations
While endometriosis is often a cause of infertility, often infertile patients do not have endometriosis. A careful history, physical examination, and ultrasonography, and possibly other imaging studies, are prerequisites to careful clinical judgment in diagnosing and treating infertile patients who might or do have endometriosis.
When pelvic pain is present, initially nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives (OCs), progestational agents, or an intrauterine device can be helpful. These ovarian suppression medications do not increase fertility, however, and should be stopped in any patient who desires to get pregnant.
When pelvic and male fertility factors appear reasonably normal (even if minimal or mild endometriosis is suspected), treatment with clomiphene 100 mg on cycle days 3 through 7 and IUI for 3 to 6 cycles is an effective first step. However, if the patient has persistent pain and/or infertility without other significant infertility factors, then diagnostic laparoscopy with intraoperative treatment of disease is indicated.
Surgery well performed is effective treatment for all stages of endometriosis and endometriomas, both for infertility and for pain. Repeat surgery, however, is rarely indicated because of limited results, so it is important to obtain the best possible result on the first surgery. Surgery is indicated for large endometriomas (>4 cm). Endometriosis has almost no effect on the IVF live birth rate unless ovarian reserve has been reduced by endometriomas or surgery, so endometriosis surgery should be performed by skilled and experienced surgeons.
Endometriosis is a complex disease that can cause infertility. Its diagnosis and management are frequently difficult, requiring knowledge, experience, and good medical judgment and surgical skills. However, if evidence-linked principles are followed, effective treatment plans and good outcomes can be obtained for most patients.
Read about why oil-based contrast may be better than water-based contrast with HSG.
Oil-based contrast medium use in hysterosalpingography is associated with higher pregnancy rates compared with water-based contrast
Dreyer K, van Rijswijk J, Mijatovic V, et al. Oil-based or water-based contrast for hysterosalpingography in infertile women. N Engl J Med. 2017;376(21):2043-2052.
Hysterosalpingography (HSG) to assess tubal patency has been a mainstay of infertility diagnosis for decades. Some, but not all, studies also have suggested that pregnancy rates are higher after this tubal flushing procedure, especially if performed with oil contrast.7,8 A recent multicenter, randomized, controlled trial by Dreyer and colleagues that compared ongoing pregnancy rates and other outcomes among women who had HSG with oil contrast versus with water contrast provides additional valuable information.9
Trial details
In this study, 1,294 infertile women in 27 academic, teaching and nonteaching hospitals were screened for trial eligibility; 1,119 women provided written informed consent. Of these, 557 women were randomly assigned to HSG with oil contrast and 562 to water contrast. The women had spontaneous menstrual cycles, had been attempting pregnancy for at least 1 year, and had indications for HSG.
Exclusion criteria were known endocrine disorders, fewer than 8 menstrual cycles per year, a high risk of tubal disease, iodine allergy, and a total motile sperm count after sperm wash of less than 3 million/mL in the male partner (or a total motile sperm count of less than 1 million/mL when an analysis after sperm wash was not performed).
Just prior to undergoing HSG, the women were randomly assigned to receive either oil contrast or water contrast medium. (The trial was not blinded to participants or caregivers.) HSG was performed according to local protocols using cervical vacuum cup, metal cannula (hysterophore), or balloon catheter and approximately 5 to 10 mL of contrast medium.
After HSG, couples received expectant management when the predicted likelihood of pregnancy within 12 months, based on the prognostic model of Hunault, was 30% or greater.10 IUI was offered for pregnancy likelihood less than 30%, mild male infertility, or failure after a period of expectant management. IUI with or without mild ovarian stimulation (2-3 follicles) with clomiphene or gonadotropins was initiated after a minimum of 2 months of expectant management after HSG.
The primary outcome measure was ongoing pregnancy, defined as a positive fetal heartbeat on ultrasonographic examination after 12 weeks of gestation, with the first day of the last menstrual cycle for the pregnancy within 6 months after randomization. Secondary outcome measures were clinical pregnancy, live birth, miscarriage, ectopic pregnancy, time to pregnancy, and pain scores after HSG. All data were analyzed according to intention-to-treat.
Pregnancy rates increased with oil-contrast HSG
The baseline characteristics of the 2 groups were similar. HSG showed bilateral tubal patency in 477 of 554 women (86.1%) in the oil contrast group and in 491 of 554 women (88.6%) who received the water contrast (rate ratio, 0.97; 95% confidence interval [CI], 0.93-1.02). Bilateral tubal occlusion occurred in 9 women in the oil group (1.6%) and in 13 in the water group (2.3%) (relative risk, 0.69; 95% CI, 0.30-1.61).
A total of 58.3% of the women assigned to oil contrast and 57.2% of those assigned to water contrast received expectant management. Similar percentages of women in the oil group and in the water group underwent IUI (39.7% and 41.0%, respectively), IVF or intracytoplasmic sperm injection (ICSI) (2.3% and 2.2%), laparoscopy (6.2% in each group), and hysteroscopy (4.4% and 4.2%).
Ongoing pregnancy occurred in 220 of 554 women (39.7%) in the oil contrast group and in 161 of 554 women (29.1%) in the water contrast group (rate ratio, 1.37; 95% CI, 1.16-1.61; P<.001). The median time to the onset of pregnancy in the oil group was 2.7 months (interquartile range, 1.5-4.7) (FIGURE 2), while in the water group it was 3.1 months (interquartile range, 1.6-4.8) (P = .44).
While the proportion of women getting pregnant with or without the different interventions was similar in both groups, the live birth rate was 38.8% in the oil group versus 28.1% in the water group (rate ratio, 1.38; 95% CI, 1.17-1.64; P<.001). Three of 554 women (0.5%) assigned to oil contrast and 4 of 554 women (0.7%) in the water contrast group had an adverse event during the trial period. Three women (1.4%), all in the oil group, delivered a child with a congenital anomaly.
Why this study is important
This is the largest and best methodologic study on this clinical issue. It showed higher pregnancy and live birth rates within 6 months of HSG performed with oil compared with water. Although the study was not blinded, the group similarities and objective outcomes support minimal bias. Importantly, these results can be generalized only to women with similar inclusion characteristics.
It is unclear why oil HSG might enhance fertility. Suggested mechanisms include flushing of debris and/or mucous plugs or an effect on peritoneal macrophages or endometrial receptivity. Since HSG is minimally invasive and inexpensive, and the 10% increase in pregnancy rates corresponds to an NNT of 10, it is reasonable to consider, although formal cost-effectiveness data are lacking.
Concerns include the rare theoretical risk of intravasation with subsequent allergic reaction or fat embolism. Three infants in the oil group and none in the water group had congenital anomalies. This is likely due to chance, since this rate is not higher than that in the general population and no other data suggest an increased risk. Comparison of these results with other new techniques, such as sonohysterography (saline infusion sonogram), awaits further studies.
Recommendation
HSG with oil contrast should be considered a potential therapeutic as well as diagnostic intervention in selected patients.
HSG is an important diagnostic test for most infertility patients. The fact that a therapeutic benefit probably also is associated with oil-based HSG increases the clinical indications for this test.
Read about new definitions of infertility terminology you should know.
Infertility glossary is newly updated
Zegers-Hochchild F, Adamson GD, Dyer S, et al. The International Glossary on Infertility and Fertility Care, 2017. Fertil Steril. 2017;108(3):393-406.
Terms and definitions used in infertility and fertility care frequently have had different meanings for different stakeholders, especially on a global basis. This can result in misunderstandings and inappropriate interpretation and comparison of published information and research. To help address these issues, international fertility organizations recently developed an updated glossary on infertilityterminology.
The consensus process for updating the glossary
The International Glossary on Infertility and Fertility Care, 2017, was recently published simultaneously in Fertility and Sterility and Human Reproduction. This is the second revision; the first glossary was published in 2006 and revised in 2009. This revision's 25 lead experts began work in 2014. Their teams of professionals interacted by electronic mail, at international and regional society meetings, and at 2 consultations held in Geneva, Switzerland. This glossary represents consensus agreement reached on 283 evidence-driven terms and definitions.
The work was led by the International Committee for Monitoring Assisted Reproductive Technologies in partnership with the American Society for Reproductive Medicine, European Society of Human Reproduction and Embryology, International Federation of Fertility Societies, March of Dimes, African Fertility Society, Groupe Inter-africain d'Etude de Recherche et d'Application sur la Fertilité, Asian Pacific Initiative on Reproduction, Middle East Fertility Society, Red Latinoamericana de Reproducción Asistida, and the International Federation of Gynecology and Obstetrics.
All together, 108 international professional experts (clinicians, basic scientists, epidemiologists, and social scientists), along with national and regional representatives of infertile persons, participated in the development of this evidence-base driven glossary. As such, these definitions now set the standard for international communication among clinicians, scientists, and policymakers.
Definition of infertility is broadened
The definitions take account of ethics, human rights, cultural sensitivities, ethnic minorities, and gender equality. For example, the first modification included broadening the concept of infertility to be an "impairment of individuals" in their capacity to reproduce, irrespective of whether the individual has a partner. (See “Broadened definition of infertility” below). Reproductive rights are individual human rights and do not depend on a relationship with another individual. The revised definition also reinforces the concept of infertility as a disease that can generate an impairment of function.
Infertility: A disease characterized by the failure to establish a clinical pregnancy after 12 months of regular, unprotected sexual intercourse or due to an impairment of a person’s capacity to reproduce either as an individual or with his/her partner. Fertility interventions may be initiated in less than 1 year based on medical, sexual and reproductive history, age, physical findings and diagnostic testing. Infertility is a disease, which generates disability as an impairment of function.
Reference
- Zegers-Hochchild F, Adamson GD, Dyer S, et al. The International Glossary on Infertility and Fertility Care, 2017. Fertil Steril. 2017;108(3):393–406
New--and changed--definitions
Certain terms need to be consistent with those used currently internationally, for example, at which gestational age a miscarriage/abortion becomes a stillbirth.
Some terms are confusing, such as subfertility, which does not define a different or less severe fertility status than infertility, does not exist before infertility is diagnosed, and should not be confused with sterility, which is a permanent state of infertility. The term subfertility therefore is redundant and has been removed and replaced by infertility (See “Some terms with an important new definition” below).
- Clinical pregnancy
- Conception (removed from glossary)
- Diminished ovarian reserve
- Fertility care
- Hypospermia (replaces oligospermia)
- Ovarian reserve
- Pregnancy
- Preimplantation genetic testing
- Spontaneous abortion/miscarriage
- Subfertility (should be used interchangeably with infertility)
Reference
- Zegers-Hochchild F, Adamson GD, Dyer S, et al. The International Glossary on Infertility and Fertility Care, 2017. Fertil Steril. 2017;108(3):393–406.
In a different context, the term conception, and its derivatives such as conceiving or conceived, was removed because it cannot be described biologically during the process of reproduction. Instead, terms such as fertilization, implantation, pregnancy, and live birth should be used.
Important male terms also changed: oligospermia is a term for low semen volume that is now replaced by hypospermia to avoid confusion with oligozoospermia, which is low concentration of spermatozoa in the ejaculate below the lower reference limit. When reporting results, the reference criteria should be specified.
Lastly, owing to the lack of standardization in determining the burden of infertility, and to better ensure comparability of prevalence data published globally, this glossary includes definitions for terms frequently used in epidemiology and public health. Examples include voluntary and involuntary childlessness, primary and secondary infertility, fertility care, fecundity, and fecundability, among others.
Getting the word out
The glossary has been approved by all of the participating organizations who are assisting in its distribution. It is being presented at national and international meetings and is used in The FIGO Fertility Toolbox (www.fertilitytool.com). It is hoped that all professionals and other stakeholders will begin to use its terminology globally to provide quality care and ensure consistency in registering specific fertility care interventions and more accurate reporting of their outcomes.
The language we use determines our individual and collective understanding of the scientific and clinical care of our patients. This glossary provides an essential and comprehensive standardization of terms and definitions essential to quality reproductive health care.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Clinicians always should consider endometriosis in the diagnostic work-up of an infertility patient. But the diagnosis of endometriosis is often difficult, and management is complex. In this Update, we summarize international consensus documents on endometriosis with the aim of enhancing clinicians’ ability to make evidence-based decisions. In addition, we explore the interesting results of a large hysterosalpingography trial in which 2 different contrast mediums were used. Finally, we urge all clinicians to adapt the new standardized lexicon of infertility and fertility care terms that comprise the recently revised international glossary.
Endometriosis and infertility: The knowns and unknowns
Johnson NP, Hummelshoj L, Adamson GD, et al; World Endometriosis Society Sao Paulo Consortium. World Endometriosis Society consensus on the classification of endometriosis. Hum Reprod. 2017;32(2):315-324.
Johnson NP, Hummelshoj L; World Endometriosis Society Montpellier Consortium. Consensus on current management of endometriosis. Hum Reprod. 2013;28(6):1552-1568.
Rogers PA, Adamson GD, Al-Jefout M, et al; WES/WERF Consortium for Research Priorities in Endometriosis. Research priorities for endometriosis. Reprod Sci. 2017;24(2):202-226.
Endometriosis is defined as "a disease characterized by the presence of endometrium-like epithelium and stroma outside the endometrium and myometrium. Intrapelvic endometriosis can be located superficially on the peritoneum (peritoneal endometriosis), can extend 5 mm or more beneath the peritoneum (deep endometriosis) or can be present as an ovarian endometriotic cyst (endometrioma)."1 Always consider endometriosis in the infertile patient.
Although many professional societies and numerous Cochrane Database Systematic Reviews have provided guidelines on endometriosis, controversy and uncertainty remain. The World Endometriosis Society (WES) and the World Endometriosis Research Foundation (WERF), however, have now published several consensus documents that assess the global literature and professional organization guidelines in a structured, consensus-driven process.2-4 These WES and WERF documents consolidate known information and can be used to inform the clinician in making evidence-linked diagnostic and treatment decisions. Recommendations offered in this discussion are based on those documents.
Establishing the diagnosis can be difficult
Diagnosis of endometriosis is often difficult and is delayed an average of 7 years from onset of symptoms. These include severe dysmenorrhea, deep dyspareunia, chronic pelvic pain, ovulation pain, cyclical or perimenstrual symptoms (bowel or bladder associated) with or without abnormal bleeding, chronic fatigue, and infertility. A major difficulty is that the predictive value of any one symptom or set of symptoms remains uncertain, as each of these symptoms can have other causes, and a significant proportion of affected women are asymptomatic.
For a definitive diagnosis of endometriosis, visual inspection of the pelvis at laparoscopy is the gold standard investigation, unless disease is visible in the vagina or elsewhere. Positive histology confirms the diagnosis of endometriosis; negative histology does not exclude it. Whether histology should be obtained if peritoneal disease alone is present is controversial: visual inspection usually is adequate, but histologic confirmation of at least one lesion is ideal. In cases of ovarian endometrioma (>4 cm in diameter) and in deeply infiltrating disease, histology should be obtained to identify endometriosis and to exclude rare instances of malignancy.
Compared with laparoscopy, transvaginal ultrasonography (TVUS) has no value in diagnosing peritoneal endometriosis, but it is a useful tool for both making and excluding the diagnosis of an ovarian endometrioma. TVUS may have a role in the diagnosis of disease involving the bladder or rectum.
At present, evidence is insufficient to indicate that magnetic resonance imaging (MRI) is useful for diagnosing or excluding endometriosis compared with laparoscopy. MRI should be reserved for when ultrasound results are equivocal in cases of rectovaginal or bladder endometriosis.
Serum cancer antigen 125 (CA 125) levels may be elevated in endometriosis. However, measuring serum CA 125 levels has no value as a diagnostic tool.
No fertility benefit with ovarian suppression
More than 2 dozen randomized controlled trials (RCTs) provide strong evidence that there is no fertility benefit from ovarian suppression. The drug costs and delayed time to pregnancy mean that ovarian suppression with oral contraceptives, other progestational agents, or gonadotropin-releasing hormone (GnRH) agonists before fertility treatment is not indicated, with the possible exception of using it prior to in vitro fertilization (IVF).
Ovarian suppression also has been suggested as beneficial in conjunction with surgery. However, at least 16 RCTs have failed to show fertility improvement when ovarian suppression is given either preoperatively or postoperatively. Again, the delay in attempting pregnancy, drug costs, and adverse effects render ovarian suppression not appropriate.
While ovarian suppression has not been shown to increase pregnancy rates, ovarian stimulation (OS) likely does, especially when combined with intrauterine insemination (IUI).5
Laparoscopy: Appropriate for selected patients
A major decision for clinicians and patients dealing with infertility is whether to perform a laparoscopy, both for diagnostic and for treatment reasons. Currently, data are insufficient to recommend laparoscopic surgery prior to OS/IUI unless there is a history of evidence of anatomic disease and/or the patient has sufficient pain to justify the physical, emotional, financial, and time costs of laparoscopy. Laparoscopy therefore can be considered as possibly appropriate in younger women (<37 years of age) with short duration of infertility (<4 years), normal male factor, normal or treatable uterus, normal or treatable ovulation disorder, and limited prior treatment.
It is important to consider what disease might be found and how much of an increase in fertility can be obtained by treatment, so that the number needed to treat (NNT) can be used as an estimate of the potential value of laparoscopy in a given patient. A patient also should have no contraindications to laparoscopy and accept 9 to 15 months of attempting pregnancy before undergoing IVF treatment.
When laparoscopy is performed for minimal to mild disease, the odds ratio for pregnancy is 1.66 with treatment. It is important to remove all visible disease without injuring healthy tissue. When disease is moderate to severe, there is often severe anatomic distortion and a very low background pregnancy rate. Numerous uncontrolled trials show benefit of operative laparoscopy, especially for invasive, adhesive, and cystic endometriosis. However, repeat surgery is rarely indicated. After surgery, the Endometriosis Fertility Index (EFI) can be used to determine prognosis and plan management (FIGURE 1).6 An easy-to-use electronic EFI calculator is available online at www.endometriosisefi.com.
Management of endometriomas
Endometriomas are often operated on because of pain. Initial pain relief occurs in 60% to 100% of patients, but cysts recur following stripping about 10% of the time, and drainage without stripping, about 20%. With recurrence, pain is present about 75% of the time.
Pregnancy rates following endometrioma treatment depend on patient age and the status of the pelvis following operative intervention. This can be determined from the EFI. Often, the dilemma with endometriomas is how aggressive to be in removing them. The principles involved are to remove all the cyst wall if possible, but absolutely to minimize ovarian tissue damage, because reduced ovarian reserve is a possible major negative consequence of ovarian surgery.
Recommendations
While endometriosis is often a cause of infertility, often infertile patients do not have endometriosis. A careful history, physical examination, and ultrasonography, and possibly other imaging studies, are prerequisites to careful clinical judgment in diagnosing and treating infertile patients who might or do have endometriosis.
When pelvic pain is present, initially nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives (OCs), progestational agents, or an intrauterine device can be helpful. These ovarian suppression medications do not increase fertility, however, and should be stopped in any patient who desires to get pregnant.
When pelvic and male fertility factors appear reasonably normal (even if minimal or mild endometriosis is suspected), treatment with clomiphene 100 mg on cycle days 3 through 7 and IUI for 3 to 6 cycles is an effective first step. However, if the patient has persistent pain and/or infertility without other significant infertility factors, then diagnostic laparoscopy with intraoperative treatment of disease is indicated.
Surgery well performed is effective treatment for all stages of endometriosis and endometriomas, both for infertility and for pain. Repeat surgery, however, is rarely indicated because of limited results, so it is important to obtain the best possible result on the first surgery. Surgery is indicated for large endometriomas (>4 cm). Endometriosis has almost no effect on the IVF live birth rate unless ovarian reserve has been reduced by endometriomas or surgery, so endometriosis surgery should be performed by skilled and experienced surgeons.
Endometriosis is a complex disease that can cause infertility. Its diagnosis and management are frequently difficult, requiring knowledge, experience, and good medical judgment and surgical skills. However, if evidence-linked principles are followed, effective treatment plans and good outcomes can be obtained for most patients.
Read about why oil-based contrast may be better than water-based contrast with HSG.
Oil-based contrast medium use in hysterosalpingography is associated with higher pregnancy rates compared with water-based contrast
Dreyer K, van Rijswijk J, Mijatovic V, et al. Oil-based or water-based contrast for hysterosalpingography in infertile women. N Engl J Med. 2017;376(21):2043-2052.
Hysterosalpingography (HSG) to assess tubal patency has been a mainstay of infertility diagnosis for decades. Some, but not all, studies also have suggested that pregnancy rates are higher after this tubal flushing procedure, especially if performed with oil contrast.7,8 A recent multicenter, randomized, controlled trial by Dreyer and colleagues that compared ongoing pregnancy rates and other outcomes among women who had HSG with oil contrast versus with water contrast provides additional valuable information.9
Trial details
In this study, 1,294 infertile women in 27 academic, teaching and nonteaching hospitals were screened for trial eligibility; 1,119 women provided written informed consent. Of these, 557 women were randomly assigned to HSG with oil contrast and 562 to water contrast. The women had spontaneous menstrual cycles, had been attempting pregnancy for at least 1 year, and had indications for HSG.
Exclusion criteria were known endocrine disorders, fewer than 8 menstrual cycles per year, a high risk of tubal disease, iodine allergy, and a total motile sperm count after sperm wash of less than 3 million/mL in the male partner (or a total motile sperm count of less than 1 million/mL when an analysis after sperm wash was not performed).
Just prior to undergoing HSG, the women were randomly assigned to receive either oil contrast or water contrast medium. (The trial was not blinded to participants or caregivers.) HSG was performed according to local protocols using cervical vacuum cup, metal cannula (hysterophore), or balloon catheter and approximately 5 to 10 mL of contrast medium.
After HSG, couples received expectant management when the predicted likelihood of pregnancy within 12 months, based on the prognostic model of Hunault, was 30% or greater.10 IUI was offered for pregnancy likelihood less than 30%, mild male infertility, or failure after a period of expectant management. IUI with or without mild ovarian stimulation (2-3 follicles) with clomiphene or gonadotropins was initiated after a minimum of 2 months of expectant management after HSG.
The primary outcome measure was ongoing pregnancy, defined as a positive fetal heartbeat on ultrasonographic examination after 12 weeks of gestation, with the first day of the last menstrual cycle for the pregnancy within 6 months after randomization. Secondary outcome measures were clinical pregnancy, live birth, miscarriage, ectopic pregnancy, time to pregnancy, and pain scores after HSG. All data were analyzed according to intention-to-treat.
Pregnancy rates increased with oil-contrast HSG
The baseline characteristics of the 2 groups were similar. HSG showed bilateral tubal patency in 477 of 554 women (86.1%) in the oil contrast group and in 491 of 554 women (88.6%) who received the water contrast (rate ratio, 0.97; 95% confidence interval [CI], 0.93-1.02). Bilateral tubal occlusion occurred in 9 women in the oil group (1.6%) and in 13 in the water group (2.3%) (relative risk, 0.69; 95% CI, 0.30-1.61).
A total of 58.3% of the women assigned to oil contrast and 57.2% of those assigned to water contrast received expectant management. Similar percentages of women in the oil group and in the water group underwent IUI (39.7% and 41.0%, respectively), IVF or intracytoplasmic sperm injection (ICSI) (2.3% and 2.2%), laparoscopy (6.2% in each group), and hysteroscopy (4.4% and 4.2%).
Ongoing pregnancy occurred in 220 of 554 women (39.7%) in the oil contrast group and in 161 of 554 women (29.1%) in the water contrast group (rate ratio, 1.37; 95% CI, 1.16-1.61; P<.001). The median time to the onset of pregnancy in the oil group was 2.7 months (interquartile range, 1.5-4.7) (FIGURE 2), while in the water group it was 3.1 months (interquartile range, 1.6-4.8) (P = .44).
While the proportion of women getting pregnant with or without the different interventions was similar in both groups, the live birth rate was 38.8% in the oil group versus 28.1% in the water group (rate ratio, 1.38; 95% CI, 1.17-1.64; P<.001). Three of 554 women (0.5%) assigned to oil contrast and 4 of 554 women (0.7%) in the water contrast group had an adverse event during the trial period. Three women (1.4%), all in the oil group, delivered a child with a congenital anomaly.
Why this study is important
This is the largest and best methodologic study on this clinical issue. It showed higher pregnancy and live birth rates within 6 months of HSG performed with oil compared with water. Although the study was not blinded, the group similarities and objective outcomes support minimal bias. Importantly, these results can be generalized only to women with similar inclusion characteristics.
It is unclear why oil HSG might enhance fertility. Suggested mechanisms include flushing of debris and/or mucous plugs or an effect on peritoneal macrophages or endometrial receptivity. Since HSG is minimally invasive and inexpensive, and the 10% increase in pregnancy rates corresponds to an NNT of 10, it is reasonable to consider, although formal cost-effectiveness data are lacking.
Concerns include the rare theoretical risk of intravasation with subsequent allergic reaction or fat embolism. Three infants in the oil group and none in the water group had congenital anomalies. This is likely due to chance, since this rate is not higher than that in the general population and no other data suggest an increased risk. Comparison of these results with other new techniques, such as sonohysterography (saline infusion sonogram), awaits further studies.
Recommendation
HSG with oil contrast should be considered a potential therapeutic as well as diagnostic intervention in selected patients.
HSG is an important diagnostic test for most infertility patients. The fact that a therapeutic benefit probably also is associated with oil-based HSG increases the clinical indications for this test.
Read about new definitions of infertility terminology you should know.
Infertility glossary is newly updated
Zegers-Hochchild F, Adamson GD, Dyer S, et al. The International Glossary on Infertility and Fertility Care, 2017. Fertil Steril. 2017;108(3):393-406.
Terms and definitions used in infertility and fertility care frequently have had different meanings for different stakeholders, especially on a global basis. This can result in misunderstandings and inappropriate interpretation and comparison of published information and research. To help address these issues, international fertility organizations recently developed an updated glossary on infertilityterminology.
The consensus process for updating the glossary
The International Glossary on Infertility and Fertility Care, 2017, was recently published simultaneously in Fertility and Sterility and Human Reproduction. This is the second revision; the first glossary was published in 2006 and revised in 2009. This revision's 25 lead experts began work in 2014. Their teams of professionals interacted by electronic mail, at international and regional society meetings, and at 2 consultations held in Geneva, Switzerland. This glossary represents consensus agreement reached on 283 evidence-driven terms and definitions.
The work was led by the International Committee for Monitoring Assisted Reproductive Technologies in partnership with the American Society for Reproductive Medicine, European Society of Human Reproduction and Embryology, International Federation of Fertility Societies, March of Dimes, African Fertility Society, Groupe Inter-africain d'Etude de Recherche et d'Application sur la Fertilité, Asian Pacific Initiative on Reproduction, Middle East Fertility Society, Red Latinoamericana de Reproducción Asistida, and the International Federation of Gynecology and Obstetrics.
All together, 108 international professional experts (clinicians, basic scientists, epidemiologists, and social scientists), along with national and regional representatives of infertile persons, participated in the development of this evidence-base driven glossary. As such, these definitions now set the standard for international communication among clinicians, scientists, and policymakers.
Definition of infertility is broadened
The definitions take account of ethics, human rights, cultural sensitivities, ethnic minorities, and gender equality. For example, the first modification included broadening the concept of infertility to be an "impairment of individuals" in their capacity to reproduce, irrespective of whether the individual has a partner. (See “Broadened definition of infertility” below). Reproductive rights are individual human rights and do not depend on a relationship with another individual. The revised definition also reinforces the concept of infertility as a disease that can generate an impairment of function.
Infertility: A disease characterized by the failure to establish a clinical pregnancy after 12 months of regular, unprotected sexual intercourse or due to an impairment of a person’s capacity to reproduce either as an individual or with his/her partner. Fertility interventions may be initiated in less than 1 year based on medical, sexual and reproductive history, age, physical findings and diagnostic testing. Infertility is a disease, which generates disability as an impairment of function.
Reference
- Zegers-Hochchild F, Adamson GD, Dyer S, et al. The International Glossary on Infertility and Fertility Care, 2017. Fertil Steril. 2017;108(3):393–406
New--and changed--definitions
Certain terms need to be consistent with those used currently internationally, for example, at which gestational age a miscarriage/abortion becomes a stillbirth.
Some terms are confusing, such as subfertility, which does not define a different or less severe fertility status than infertility, does not exist before infertility is diagnosed, and should not be confused with sterility, which is a permanent state of infertility. The term subfertility therefore is redundant and has been removed and replaced by infertility (See “Some terms with an important new definition” below).
- Clinical pregnancy
- Conception (removed from glossary)
- Diminished ovarian reserve
- Fertility care
- Hypospermia (replaces oligospermia)
- Ovarian reserve
- Pregnancy
- Preimplantation genetic testing
- Spontaneous abortion/miscarriage
- Subfertility (should be used interchangeably with infertility)
Reference
- Zegers-Hochchild F, Adamson GD, Dyer S, et al. The International Glossary on Infertility and Fertility Care, 2017. Fertil Steril. 2017;108(3):393–406.
In a different context, the term conception, and its derivatives such as conceiving or conceived, was removed because it cannot be described biologically during the process of reproduction. Instead, terms such as fertilization, implantation, pregnancy, and live birth should be used.
Important male terms also changed: oligospermia is a term for low semen volume that is now replaced by hypospermia to avoid confusion with oligozoospermia, which is low concentration of spermatozoa in the ejaculate below the lower reference limit. When reporting results, the reference criteria should be specified.
Lastly, owing to the lack of standardization in determining the burden of infertility, and to better ensure comparability of prevalence data published globally, this glossary includes definitions for terms frequently used in epidemiology and public health. Examples include voluntary and involuntary childlessness, primary and secondary infertility, fertility care, fecundity, and fecundability, among others.
Getting the word out
The glossary has been approved by all of the participating organizations who are assisting in its distribution. It is being presented at national and international meetings and is used in The FIGO Fertility Toolbox (www.fertilitytool.com). It is hoped that all professionals and other stakeholders will begin to use its terminology globally to provide quality care and ensure consistency in registering specific fertility care interventions and more accurate reporting of their outcomes.
The language we use determines our individual and collective understanding of the scientific and clinical care of our patients. This glossary provides an essential and comprehensive standardization of terms and definitions essential to quality reproductive health care.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Zegers-Hochchild F, Adamson GD, Dyer S, et al. The International Glossary on Infertility and Fertility Care, 2017. Fertil Steril. 2017;108(3):393–406.
- Johnson NP, Hummelshoj L; World Endometriosis Society Montpellier Consortium. Consensus on current management of endometriosis. Hum Reprod. 2013;28(6):1552–1568.
- Rogers PA, Adamson GD, Al-Jefout M, et al; WES/WERF Consortium for Research Priorities in Endometriosis. Research priorities for endometriosis. Reprod Sci. 2017;24(2):202–226.
- Johnson NP, Hummelshoj L, Adamson GD, et al; World Endometriosis Society Sao Paulo Consortium. World Endometriosis Society consensus on the classification of endometriosis. Hum Reprod. 2017;32(2):315–324.
- Practice Committee of the American Society for Reproductive Medicine. Endometriosis and infertility: a committee opinion. Fertil Steril. 2012;98(3):591–598.
- Adamson GD, Pasta DJ. Endometriosis fertility index: the new, validated endometriosis staging system. Fertil Steril. 2010;94(5):1609–1615.
- Weir WC, Weir DR. Therapeutic value of salpingograms in infertility. Fertil Steril. 1951;2(6);514–522.
- Johnson NP, Farquhar CM, Hadden WE, Suckling J, Yu Y, Sadler L. The FLUSH trial—flushing with lipiodol for unexplained (and endometriosis-related) subfertility by hysterosalpingography: a randomized trial. Hum Reprod. 2004;19(9):2043–2051.
- Dreyer K, van Rijswijk J, Mijatovic V, et al. Oil-based or water-based contrast for hysterosalpingography in infertile women. N Engl J Med. 2017;376(21):2043–2052.
- Van der Steeg JW, Steures P, Eijkemans MJ, et al; Collaborative Effort for Clinical Evaluation in Reproductive Medicine. Pregnancy is predictable: a large-scale prospective external validation of the prediction of spontaneous pregnancy in sub-fertile couples. Hum Reprod. 2007;22(2):536–542.
- Zegers-Hochchild F, Adamson GD, Dyer S, et al. The International Glossary on Infertility and Fertility Care, 2017. Fertil Steril. 2017;108(3):393–406.
- Johnson NP, Hummelshoj L; World Endometriosis Society Montpellier Consortium. Consensus on current management of endometriosis. Hum Reprod. 2013;28(6):1552–1568.
- Rogers PA, Adamson GD, Al-Jefout M, et al; WES/WERF Consortium for Research Priorities in Endometriosis. Research priorities for endometriosis. Reprod Sci. 2017;24(2):202–226.
- Johnson NP, Hummelshoj L, Adamson GD, et al; World Endometriosis Society Sao Paulo Consortium. World Endometriosis Society consensus on the classification of endometriosis. Hum Reprod. 2017;32(2):315–324.
- Practice Committee of the American Society for Reproductive Medicine. Endometriosis and infertility: a committee opinion. Fertil Steril. 2012;98(3):591–598.
- Adamson GD, Pasta DJ. Endometriosis fertility index: the new, validated endometriosis staging system. Fertil Steril. 2010;94(5):1609–1615.
- Weir WC, Weir DR. Therapeutic value of salpingograms in infertility. Fertil Steril. 1951;2(6);514–522.
- Johnson NP, Farquhar CM, Hadden WE, Suckling J, Yu Y, Sadler L. The FLUSH trial—flushing with lipiodol for unexplained (and endometriosis-related) subfertility by hysterosalpingography: a randomized trial. Hum Reprod. 2004;19(9):2043–2051.
- Dreyer K, van Rijswijk J, Mijatovic V, et al. Oil-based or water-based contrast for hysterosalpingography in infertile women. N Engl J Med. 2017;376(21):2043–2052.
- Van der Steeg JW, Steures P, Eijkemans MJ, et al; Collaborative Effort for Clinical Evaluation in Reproductive Medicine. Pregnancy is predictable: a large-scale prospective external validation of the prediction of spontaneous pregnancy in sub-fertile couples. Hum Reprod. 2007;22(2):536–542.
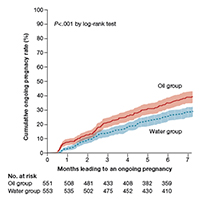
Health care gets little attention in State of the Union address
President Trump reaffirmed his campaign promise to lower prescription drug prices during his first State of the Union address – but gave no details on how he plans to do so.
“One of my greatest priorities is to reduce the price of prescription drugs,” President Trump said in his Jan. 30 address to a joint session of Congress. “In many other countries, these drugs cost far less than what we pay in the United States, and it is very, very unfair. That is why I have directed my administration to make fixing the injustice of high drug prices one of my top priorities for the year.”

His words followed the confirmation of Alex Azar as Health & Human Services secretary. Mr. Azar’s nomination was criticized by some who questioned whether the former president of Eli Lilly’s U.S. operations could be effective at tackling the surging prices of pharmaceuticals.
President Trump also expressed his support for allowing terminally ill patients to access experimental drugs prior to Food and Drug Administration approval, the so-called right to try.
“We also believe that patients with terminal conditions, terminal illness, should have access to experimental treatment immediately that could potentially save their lives,” he said. “People who are terminally ill should not have to go from country to country to seek a cure. I want to give them a chance right here at home. It’s time for the Congress to give these wonderful incredible Americans the right to try.”
The Senate passed a right to try bill (S. 204) in 2017 by unanimous consent, but the House has yet to act upon it.
President Trump reaffirmed his commitment to fighting the opioid epidemic and made a loose connection between it and his overall platform for immigration reform, saying that “these reforms will also support our response to the terrible crisis of opioid and drug addiction.”
As far as addressing the epidemic itself, Mr. Trump said that his administration “is committed to fighting the drug epidemic and helping get treatment for those in need, for those who have been so terribly hurt. The struggle will be long and it will be difficult, but, as Americans always do, in the end we will succeed. We will prevail.”
The president also commended Congress for effectively eliminating the Affordable Care Act’s individual mandate that required people to have health insurance or suffer a financial penalty.

President Trump reaffirmed his campaign promise to lower prescription drug prices during his first State of the Union address – but gave no details on how he plans to do so.
“One of my greatest priorities is to reduce the price of prescription drugs,” President Trump said in his Jan. 30 address to a joint session of Congress. “In many other countries, these drugs cost far less than what we pay in the United States, and it is very, very unfair. That is why I have directed my administration to make fixing the injustice of high drug prices one of my top priorities for the year.”
His words followed the confirmation of Alex Azar as Health & Human Services secretary. Mr. Azar’s nomination was criticized by some who questioned whether the former president of Eli Lilly’s U.S. operations could be effective at tackling the surging prices of pharmaceuticals.
President Trump also expressed his support for allowing terminally ill patients to access experimental drugs prior to Food and Drug Administration approval, the so-called right to try.
“We also believe that patients with terminal conditions, terminal illness, should have access to experimental treatment immediately that could potentially save their lives,” he said. “People who are terminally ill should not have to go from country to country to seek a cure. I want to give them a chance right here at home. It’s time for the Congress to give these wonderful incredible Americans the right to try.”
The Senate passed a right to try bill (S. 204) in 2017 by unanimous consent, but the House has yet to act upon it.
President Trump reaffirmed his commitment to fighting the opioid epidemic and made a loose connection between it and his overall platform for immigration reform, saying that “these reforms will also support our response to the terrible crisis of opioid and drug addiction.”
As far as addressing the epidemic itself, Mr. Trump said that his administration “is committed to fighting the drug epidemic and helping get treatment for those in need, for those who have been so terribly hurt. The struggle will be long and it will be difficult, but, as Americans always do, in the end we will succeed. We will prevail.”
The president also commended Congress for effectively eliminating the Affordable Care Act’s individual mandate that required people to have health insurance or suffer a financial penalty.
President Trump reaffirmed his campaign promise to lower prescription drug prices during his first State of the Union address – but gave no details on how he plans to do so.
“One of my greatest priorities is to reduce the price of prescription drugs,” President Trump said in his Jan. 30 address to a joint session of Congress. “In many other countries, these drugs cost far less than what we pay in the United States, and it is very, very unfair. That is why I have directed my administration to make fixing the injustice of high drug prices one of my top priorities for the year.”
His words followed the confirmation of Alex Azar as Health & Human Services secretary. Mr. Azar’s nomination was criticized by some who questioned whether the former president of Eli Lilly’s U.S. operations could be effective at tackling the surging prices of pharmaceuticals.
President Trump also expressed his support for allowing terminally ill patients to access experimental drugs prior to Food and Drug Administration approval, the so-called right to try.
“We also believe that patients with terminal conditions, terminal illness, should have access to experimental treatment immediately that could potentially save their lives,” he said. “People who are terminally ill should not have to go from country to country to seek a cure. I want to give them a chance right here at home. It’s time for the Congress to give these wonderful incredible Americans the right to try.”
The Senate passed a right to try bill (S. 204) in 2017 by unanimous consent, but the House has yet to act upon it.
President Trump reaffirmed his commitment to fighting the opioid epidemic and made a loose connection between it and his overall platform for immigration reform, saying that “these reforms will also support our response to the terrible crisis of opioid and drug addiction.”
As far as addressing the epidemic itself, Mr. Trump said that his administration “is committed to fighting the drug epidemic and helping get treatment for those in need, for those who have been so terribly hurt. The struggle will be long and it will be difficult, but, as Americans always do, in the end we will succeed. We will prevail.”
The president also commended Congress for effectively eliminating the Affordable Care Act’s individual mandate that required people to have health insurance or suffer a financial penalty.
Study finds rising use of newer DMTs in pediatric-onset MS
Newer disease-modifying therapies are often used in patients with pediatric-onset MS, and they appear to have short-term side effect profiles similar to those observed in adults, a study of data from multiple clinics demonstrated.
“There are limited studies of MS treatments in pediatric-onset MS (onset before 18 years) as the main trials used to approve disease-modifying therapies [DMTs] are performed in adults,” lead study author Kristen Krysko, MD, said in an interview prior to a meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis in San Diego. “This makes it difficult to treat children with MS as there is limited high-quality evidence for safety and effectiveness of treatments.”

DMTs considered to be “newer” include dimethyl fumarate (Tecfidera), fingolimod (Gilenya), teriflunomide (Aubagio), natalizumab (Tysabri), rituximab (Rituxan), ocrelizumab (Ocrevus), alemtuzumab (Lemtrada), and daclizumab (Zinbryta). DMTs were classified as injectable (glatiramer acetate, beta-interferons), oral (dimethyl fumarate, fingolimod, teriflunomide) or intravenous (natalizumab, rituximab, alemtuzumab, ocrelizumab).
Dr. Krysko, a multiple sclerosis clinical research fellow at the University of California, San Francisco, and her associates reported findings from 749 pediatric patients with MS and 274 with clinically-isolated syndrome whose data had been entered into the network as of August 2017 and who were followed for a mean of 3.3 years. The majority of patients were female (65%) with a mean age at disease onset of 12.9 years. Over time, the researchers observed increasing overall and first-line use of newer oral and intravenous DMTs in those younger than and older than 12 years of age at the start of a DMT (P less than .001).
Of the 618 patients who received a DMT before 18 years of age, 259 (42%) received a newer DMT and 104 (17%) received a newer DMT as first-line therapy. Dimethyl fumarate was the newer DMT used most often (ever in 100, as a first-line therapy in 36), followed by natalizumab (ever in 101, as a first-line therapy in 30), rituximab (ever in 57, as a first-line therapy in 22), fingolimod (ever in 37, as a first-line therapy in 14), daclizumab (ever in 5, as a first-line therapy in none), and teriflunomide (ever in 3, as a first-line therapy in 2).
The overall side effect profiles of newer DMTs were not different from those reported with the same agents in adults. Specifically, the number of side effects was greatest for dimethyl fumarate (37.7 per 100 person-years), followed by rituximab (20.1 per 100 person-years), natalizumab (15.7 per 100 person-years), and daclizumab (9.6 per 100 person-years).
“We found that newer medications are being prescribed more often in children with MS over time,” Dr. Krysko said. “Even children who were quite young (younger than 12 years old) received newer MS treatments in some cases, although older children (12 years and older) were more likely to receive newer treatments than were the very young children. We did not find new safety concerns with these medications compared to adults.”
She acknowledged certain limitations of the study, including the “likely underestimate” of side effects and the lack of access to laboratory results of children while on these medications. “Thus, further investigation of the safety of these newer medications in children is needed,” she said.
The National MS Society funded the study. Dr. Krysko disclosed that she is funded by the society as a Sylvia Lawry Physician Fellow.
Newer disease-modifying therapies are often used in patients with pediatric-onset MS, and they appear to have short-term side effect profiles similar to those observed in adults, a study of data from multiple clinics demonstrated.
“There are limited studies of MS treatments in pediatric-onset MS (onset before 18 years) as the main trials used to approve disease-modifying therapies [DMTs] are performed in adults,” lead study author Kristen Krysko, MD, said in an interview prior to a meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis in San Diego. “This makes it difficult to treat children with MS as there is limited high-quality evidence for safety and effectiveness of treatments.”
DMTs considered to be “newer” include dimethyl fumarate (Tecfidera), fingolimod (Gilenya), teriflunomide (Aubagio), natalizumab (Tysabri), rituximab (Rituxan), ocrelizumab (Ocrevus), alemtuzumab (Lemtrada), and daclizumab (Zinbryta). DMTs were classified as injectable (glatiramer acetate, beta-interferons), oral (dimethyl fumarate, fingolimod, teriflunomide) or intravenous (natalizumab, rituximab, alemtuzumab, ocrelizumab).
Dr. Krysko, a multiple sclerosis clinical research fellow at the University of California, San Francisco, and her associates reported findings from 749 pediatric patients with MS and 274 with clinically-isolated syndrome whose data had been entered into the network as of August 2017 and who were followed for a mean of 3.3 years. The majority of patients were female (65%) with a mean age at disease onset of 12.9 years. Over time, the researchers observed increasing overall and first-line use of newer oral and intravenous DMTs in those younger than and older than 12 years of age at the start of a DMT (P less than .001).
Of the 618 patients who received a DMT before 18 years of age, 259 (42%) received a newer DMT and 104 (17%) received a newer DMT as first-line therapy. Dimethyl fumarate was the newer DMT used most often (ever in 100, as a first-line therapy in 36), followed by natalizumab (ever in 101, as a first-line therapy in 30), rituximab (ever in 57, as a first-line therapy in 22), fingolimod (ever in 37, as a first-line therapy in 14), daclizumab (ever in 5, as a first-line therapy in none), and teriflunomide (ever in 3, as a first-line therapy in 2).
The overall side effect profiles of newer DMTs were not different from those reported with the same agents in adults. Specifically, the number of side effects was greatest for dimethyl fumarate (37.7 per 100 person-years), followed by rituximab (20.1 per 100 person-years), natalizumab (15.7 per 100 person-years), and daclizumab (9.6 per 100 person-years).
“We found that newer medications are being prescribed more often in children with MS over time,” Dr. Krysko said. “Even children who were quite young (younger than 12 years old) received newer MS treatments in some cases, although older children (12 years and older) were more likely to receive newer treatments than were the very young children. We did not find new safety concerns with these medications compared to adults.”
She acknowledged certain limitations of the study, including the “likely underestimate” of side effects and the lack of access to laboratory results of children while on these medications. “Thus, further investigation of the safety of these newer medications in children is needed,” she said.
The National MS Society funded the study. Dr. Krysko disclosed that she is funded by the society as a Sylvia Lawry Physician Fellow.
Newer disease-modifying therapies are often used in patients with pediatric-onset MS, and they appear to have short-term side effect profiles similar to those observed in adults, a study of data from multiple clinics demonstrated.
“There are limited studies of MS treatments in pediatric-onset MS (onset before 18 years) as the main trials used to approve disease-modifying therapies [DMTs] are performed in adults,” lead study author Kristen Krysko, MD, said in an interview prior to a meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis in San Diego. “This makes it difficult to treat children with MS as there is limited high-quality evidence for safety and effectiveness of treatments.”
DMTs considered to be “newer” include dimethyl fumarate (Tecfidera), fingolimod (Gilenya), teriflunomide (Aubagio), natalizumab (Tysabri), rituximab (Rituxan), ocrelizumab (Ocrevus), alemtuzumab (Lemtrada), and daclizumab (Zinbryta). DMTs were classified as injectable (glatiramer acetate, beta-interferons), oral (dimethyl fumarate, fingolimod, teriflunomide) or intravenous (natalizumab, rituximab, alemtuzumab, ocrelizumab).
Dr. Krysko, a multiple sclerosis clinical research fellow at the University of California, San Francisco, and her associates reported findings from 749 pediatric patients with MS and 274 with clinically-isolated syndrome whose data had been entered into the network as of August 2017 and who were followed for a mean of 3.3 years. The majority of patients were female (65%) with a mean age at disease onset of 12.9 years. Over time, the researchers observed increasing overall and first-line use of newer oral and intravenous DMTs in those younger than and older than 12 years of age at the start of a DMT (P less than .001).
Of the 618 patients who received a DMT before 18 years of age, 259 (42%) received a newer DMT and 104 (17%) received a newer DMT as first-line therapy. Dimethyl fumarate was the newer DMT used most often (ever in 100, as a first-line therapy in 36), followed by natalizumab (ever in 101, as a first-line therapy in 30), rituximab (ever in 57, as a first-line therapy in 22), fingolimod (ever in 37, as a first-line therapy in 14), daclizumab (ever in 5, as a first-line therapy in none), and teriflunomide (ever in 3, as a first-line therapy in 2).
The overall side effect profiles of newer DMTs were not different from those reported with the same agents in adults. Specifically, the number of side effects was greatest for dimethyl fumarate (37.7 per 100 person-years), followed by rituximab (20.1 per 100 person-years), natalizumab (15.7 per 100 person-years), and daclizumab (9.6 per 100 person-years).
“We found that newer medications are being prescribed more often in children with MS over time,” Dr. Krysko said. “Even children who were quite young (younger than 12 years old) received newer MS treatments in some cases, although older children (12 years and older) were more likely to receive newer treatments than were the very young children. We did not find new safety concerns with these medications compared to adults.”
She acknowledged certain limitations of the study, including the “likely underestimate” of side effects and the lack of access to laboratory results of children while on these medications. “Thus, further investigation of the safety of these newer medications in children is needed,” she said.
The National MS Society funded the study. Dr. Krysko disclosed that she is funded by the society as a Sylvia Lawry Physician Fellow.
FROM ACTRIMS FORUM 2018
Key clinical point: Newer DMTs are often used in individuals with pediatric MS.
Major finding: Among pediatric MS patients, the first agent used was a newer DMT in 17% of cases.
Study details: A retrospective review of prospectively collected data on 1,023 pediatric patients with MS.
Disclosures: The National MS Society funded the study. Dr. Krysko disclosed that she is funded by the society as a Sylvia Lawry Physician Fellow.
Source: Krysko K et al. ACTRIMS Forum 2018 Poster 68.
What makes a quality “quality measure”?
The future of health care is value-based care. If Value equals Quality divided by Cost, then a defined, validated way to measure Quality is paramount to that equation. (Fortunately, Cost comes with convenient measurement units called dollars.) Payers now are asking health care providers to shift from a fee-for-service to a value-based reimbursement structure to encourage providers to deliver the best care at the lowest cost. Providers who can embrace this data-driven paradigm will succeed in this new environment.
So how do we define high-quality care? What makes a good quality measure? How do you actually measure what happens in a clinical encounter that impacts health outcomes?
To answer these questions, organizations have constructed standardized clinical quality measures. Clinical quality measures facilitate value-based care by providing a metric on which to measure a patient’s quality of care. They can be used 1) to decrease the overuse, underuse, and misuse of health care services and 2) to measure patient engagement and satisfaction with care.
What are quality measures?
The Academy of Medicine (formerly named the Institute of Medicine) defines health care quality as “the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge.”1
Clearly defined components and terminology. From a quantitative standpoint, quality measures must have a clearly defined numerator and denominator and appropriate inclusions, exclusions, and exceptions. These components need to be expressed clearly in terms of publicly available terminologies, such as ICD (International Classification of Diseases) codes or SNOMED CT (Systematized Nomenclature of Medicine—Clinical Terms) terms. A measure that asks if “antihypertensive meds” have been given will not nearly be as specific as one that asks if “labetalol IV, or hydralazine IV, or nifedipine SL” has been administered. The decision to tie the data elements in a measure to administrative data, such as ICD codes, or to clinical data, such as SNOMED CT, also affects how these measures can be calculated.
Moving targets. The target of the measure also must carefully be considered. Quality measures can be used to evaluate care across the full range of health care settings—from individual providers, to care teams, to hospitals and hospital systems, to health plans. While some measures easily can be assigned to a specific provider, others are not as straightforward. For example, who gets assigned the cesarean delivery when a midwife turns the case over to an obstetrician?
Timeframe in outcomes measurement. The data infrastructure is currently set up to support measurement of immediate events, 30-day or 90-day episodes, and health insurance plan member years. Longer-term outcomes, such as over 5- and 10- year periods, are out of reach for most measures. To obtain an accurate view of the impact of medical interventions or disease conditions, however, it will be important to follow patients over time. For example, to know the failure rate of intrauterine systems, sterilization, or hormonal contraceptives, it is important to be able to track pregnancy occurrence during use of these methods for longer than 90 days. Failures can occur years after a method is initiated.
Another example is to create a performance measure focused on the overall improvement in quality of life and costs related to different treatments for abnormal uterine bleeding. How does the patient experience vary over time between treatment with hormonal contraception, endometrial ablation, or hysterectomy? Which option is most “valuable” over time when the patient experience and the cost are assessed for more than a 90-day episode? These important questions need to be answered as we maneuver into a value-based health system.
Risk adjustment. Quality measures also may need to be risk adjusted. The “My patients are sicker” refrain must be accounted for with full transparency and based on the best available data. Quality measures can be adjusted using an Observed/Expected factor, which helps to account for complicated cases.2
Clearly, social and behavioral determinants of health also play a role in these adjustments, but it can be more challenging to acquire the data elements needed for those types of adjustments. Including these data enables us to evaluate health disparities between populations, both demographically and socioeconomically.3 This is important for future development of minority inclusive quality measures. Some racial and ethnic minority populations have poorer health outcomes from preventable and treatable diseases. Evidence shows that these groups have differences in access to health care, quality of care, and health measures, including life expectancy and maternal mortality. Access to clinical data through quality measures allows for these health disparities to be brought into quantifiable perspective and assists in the development of future incentive programs to combat health inequalities and provide improved delivery of care.
Read about how to develop quality measures
Developing quality measures
Quality measures generally fall into 4 broad categories: structure, process, outcome, and patient experience (TABLE).4,5 Quality measure development begins with an assessment of the evidence, which is usually derived from clinical guidelines that link a particular process, structure, or outcome with improved patient health or experience of care. For example, the American College of Obstetricians and Gynecologists (ACOG) has developed a clinical practice guideline for screening, diagnosing, and managing gestational diabetes. The guideline addresses drug therapies, such as insulin, and alternative treatments, such as nutrition therapy. Much like the process for creating the guideline itself, translating the guideline into a quality measure requires a thoughtful, transparent, and well-defined process.
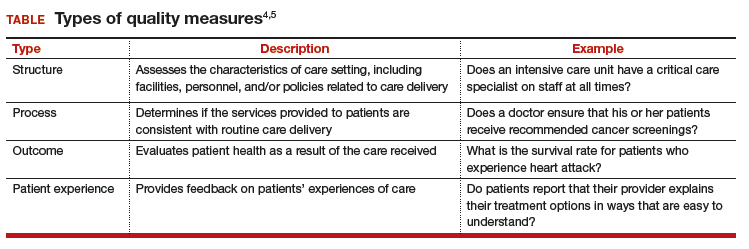
Role of the quality measure steward. Coordinating the process of translating evidence-based guidelines into quality measures requires a measure steward. Measure stewards usually are government agencies, nonprofit organizations, and/or for-profit companies. During the development process, the steward usually reaches out to additional stakeholders for feedback and consensus. Development process steps include:
- evaluation of the evidence, including the clinical practice guideline(s)
- consensus on the best measurement approach (consider the feasibility of the measurement and how it will be collected)
- development of detailed measure specifications (that is, what will be measured and how)
- feedback on the specifications from stakeholders, including professional societies and patient advocates
- testing of the measure logic and clinical validity against clinical data
- final approval by the measure steward.
Endorsement of quality measures. After a quality measure is developed, it is often endorsed by government agencies, professional societies, and/or consumer groups. Endorsement is a consensus-based process in which stakeholders evaluate a proposed measure based on established standards. Generally, stakeholders include health care professionals, consumers, payers, hospitals, health plans, and government agencies.
Evaluation of quality measures includes these important considerations:
- Are the necessary data fields available in a typical electronic health record (EHR) system?
- What is the data quality for those data fields?
- Can the measure be calculated reliably across different data sets or EHRs?
- Does the measure address one of the National Academy of Medicine quality properties? According to the academy, quality in the context of clinical care can be defined in terms of properties of effectiveness, equity, safety, efficiency, patient centeredness, and timeliness.1
Read about ACOG’s role in developing quality measures
ACOG’s role in developing quality measures
In October 2016, the Centers for Medicare and Medicaid Services released the final Medicare Access and CHIP Reauthorization Act of 2015 (MACRA). Under this rule, the Merit-based Incentive Payment System (MIPS) was created, which was intended to drive “value” rather than “volume” in payment incentives. Measures are critical to defining value-based care. However, the law has limited or no impact on providers who do not care for Medicare patients.
Clinicians eligible to participate in MACRA must bill more than $90,000 a year in Medicare Part B allowed charges and provide care for more than 200 Medicare patients per year.6 This means that the MIPS largely overlooks ObGyns, as the bulk of our patients are insured either by private insurance or by Medicaid. However, maternity care spending is a significant part of both Medicaid and private insurers’ outlay, and both payers are actively considering using value-based financial models that will need to be fed by quality metrics. ACOG wants to be at the forefront of measure development for quality metrics that affect members and has committed resources to formation of a measure development team.
ACOG wants providers to be in control of how their practices are evaluated. For this reason, ACOG is focusing on measures that are based on clinical data entered by providers into an EHR at the point of care. At the same time, ACOG is cognizant of not increasing the documentation burden for providers. Understanding the quality of the data, as opposed to the quality of care, will be a fundamental task for the maternity care registry that ACOG is launching in 2018.
What can ObGyns do?
Quality measures are about more than just money. Public reporting of these measures on government and payer websites may influence public perception of a practice.7 The focus on patient-centered care means that patients have a voice in their care, financially as well as literally, so expect to see increased scrutiny of provider performance by patients as well as payers. One way to measure patient experience of treatments, symptoms, and quality of life is through patient-reported outcome measures (PROMs). Assessing PROMs in routine care ensures that information only the patient can provide is collected and analyzed, thus further enhancing the delivery of care and evaluating how that care is impacting the lives of your patients.
The transition from fee-for-service to a value-based system will not happen overnight, but it will happen. This transition—from being paid for the quantity of documentation to the quality of documentation—will require some change management, rethinking of workflows, and better documentation tools (such as apps instead of EHR customization).
Many in the medical profession are actively exploring these changes and new developments. These changes are too important to leave to administrators, coders, scribes, app developers, and policy makers. Someone in your practice, hospital, or health system is working on these issues today. Tomorrow, you need to be at the table. The voices of practicing ObGyns are critical as we work to address the current challenging environment in which we spend more per capita than any other nation with far inferior results. Measures that matter to us and to our patients will help us provide better and more cost-effective care that payers and patients value.8
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- National Academy of Sciences. Crossing the quality chasm: the IOM Health Care Quality Initiative. http://www.nationalacademies.org/hmd/Global/News%20Announcements/Crossing-the-Quality-Chasm-The-IOM-Health-Care-Quality-Initiative.aspx. Updated January 2, 2018. Accessed January 11, 2018.
- Agency for Healthcare Research and Quality. Selecting quality and resource use measures: a decision guide for community quality collaboratives. Part 2. Introduction to measures of quality (continued). https://www.ahrq.gov/professionals/quality-patient-safety/quality-resources/tools/perfmeasguide/perfmeaspt2a.html. Reviewed 2014. Accessed December 12, 2017.
- Thomas SB, Fine MJ, Ibrahim SA. Health disparities: the importance of culture and health communication. Am J Public Health. 2004;94(12):2050.
- Agency for Healthcare Research and Quality. Types of quality measures. https://www.ahrq.gov/professionals/quality-patient-safety/talkingquality/create/types.html. Reviewed 2011. Accessed December 12, 2017.
- Agency for Healthcare Research and Quality. Understanding quality measurement. https://www.ahrq.gov/professionals/quality-patient-safety/quality-resources/tools/chtoolbx/understand/index.html. Reviewed November 2017. Accessed December 12, 2017.
- Centers for Medicare and Medicaid Services. Quality payment program. https://www.cms.gov/Medicare/Quality-Payment-Program/resource-library/QPP-Year-2-Final-Rule-Fact-Sheet.pdf. Published December 2017. Accessed December 12, 2017.
- Howell EA, Zeitlin J, Hebert PL, Balbierz, A, Egorova N. Association between hospital-level obstetric quality indicators and maternal and neonatal morbidity. JAMA. 2014;312(15):1531–1541.
- Tooker J. The importance of measuring quality and performance in healthcare. MedGenMed. 2005;7(2):49.

Ms. Gomez is Health Information Technology Analyst for the American College of Obstetricians and Gynecologists, Washington, DC.

Dr. Hasley is Chief Medical Information Officer for the American College of Obstetricians and Gynecologists.

Dr. Ramey is Senior Director for Health Information Technology for the American College of Obstetricians and Gynecologists.

Mr. Currigan is Officer for Quality and Safety for the American College of Obstetricians and Gynecologists.

Dr. Levy is Vice President for Health Policy for the American College of Obstetricians and Gynecologists.
The authors report no financial relationships relevant to this article.
Ms. Gomez is Health Information Technology Analyst for the American College of Obstetricians and Gynecologists, Washington, DC.
Dr. Hasley is Chief Medical Information Officer for the American College of Obstetricians and Gynecologists.
Dr. Ramey is Senior Director for Health Information Technology for the American College of Obstetricians and Gynecologists.
Mr. Currigan is Officer for Quality and Safety for the American College of Obstetricians and Gynecologists.
Dr. Levy is Vice President for Health Policy for the American College of Obstetricians and Gynecologists.
The authors report no financial relationships relevant to this article.
Ms. Gomez is Health Information Technology Analyst for the American College of Obstetricians and Gynecologists, Washington, DC.
Dr. Hasley is Chief Medical Information Officer for the American College of Obstetricians and Gynecologists.
Dr. Ramey is Senior Director for Health Information Technology for the American College of Obstetricians and Gynecologists.
Mr. Currigan is Officer for Quality and Safety for the American College of Obstetricians and Gynecologists.
Dr. Levy is Vice President for Health Policy for the American College of Obstetricians and Gynecologists.
The authors report no financial relationships relevant to this article.
The future of health care is value-based care. If Value equals Quality divided by Cost, then a defined, validated way to measure Quality is paramount to that equation. (Fortunately, Cost comes with convenient measurement units called dollars.) Payers now are asking health care providers to shift from a fee-for-service to a value-based reimbursement structure to encourage providers to deliver the best care at the lowest cost. Providers who can embrace this data-driven paradigm will succeed in this new environment.
So how do we define high-quality care? What makes a good quality measure? How do you actually measure what happens in a clinical encounter that impacts health outcomes?
To answer these questions, organizations have constructed standardized clinical quality measures. Clinical quality measures facilitate value-based care by providing a metric on which to measure a patient’s quality of care. They can be used 1) to decrease the overuse, underuse, and misuse of health care services and 2) to measure patient engagement and satisfaction with care.
What are quality measures?
The Academy of Medicine (formerly named the Institute of Medicine) defines health care quality as “the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge.”1
Clearly defined components and terminology. From a quantitative standpoint, quality measures must have a clearly defined numerator and denominator and appropriate inclusions, exclusions, and exceptions. These components need to be expressed clearly in terms of publicly available terminologies, such as ICD (International Classification of Diseases) codes or SNOMED CT (Systematized Nomenclature of Medicine—Clinical Terms) terms. A measure that asks if “antihypertensive meds” have been given will not nearly be as specific as one that asks if “labetalol IV, or hydralazine IV, or nifedipine SL” has been administered. The decision to tie the data elements in a measure to administrative data, such as ICD codes, or to clinical data, such as SNOMED CT, also affects how these measures can be calculated.
Moving targets. The target of the measure also must carefully be considered. Quality measures can be used to evaluate care across the full range of health care settings—from individual providers, to care teams, to hospitals and hospital systems, to health plans. While some measures easily can be assigned to a specific provider, others are not as straightforward. For example, who gets assigned the cesarean delivery when a midwife turns the case over to an obstetrician?
Timeframe in outcomes measurement. The data infrastructure is currently set up to support measurement of immediate events, 30-day or 90-day episodes, and health insurance plan member years. Longer-term outcomes, such as over 5- and 10- year periods, are out of reach for most measures. To obtain an accurate view of the impact of medical interventions or disease conditions, however, it will be important to follow patients over time. For example, to know the failure rate of intrauterine systems, sterilization, or hormonal contraceptives, it is important to be able to track pregnancy occurrence during use of these methods for longer than 90 days. Failures can occur years after a method is initiated.
Another example is to create a performance measure focused on the overall improvement in quality of life and costs related to different treatments for abnormal uterine bleeding. How does the patient experience vary over time between treatment with hormonal contraception, endometrial ablation, or hysterectomy? Which option is most “valuable” over time when the patient experience and the cost are assessed for more than a 90-day episode? These important questions need to be answered as we maneuver into a value-based health system.
Risk adjustment. Quality measures also may need to be risk adjusted. The “My patients are sicker” refrain must be accounted for with full transparency and based on the best available data. Quality measures can be adjusted using an Observed/Expected factor, which helps to account for complicated cases.2
Clearly, social and behavioral determinants of health also play a role in these adjustments, but it can be more challenging to acquire the data elements needed for those types of adjustments. Including these data enables us to evaluate health disparities between populations, both demographically and socioeconomically.3 This is important for future development of minority inclusive quality measures. Some racial and ethnic minority populations have poorer health outcomes from preventable and treatable diseases. Evidence shows that these groups have differences in access to health care, quality of care, and health measures, including life expectancy and maternal mortality. Access to clinical data through quality measures allows for these health disparities to be brought into quantifiable perspective and assists in the development of future incentive programs to combat health inequalities and provide improved delivery of care.
Read about how to develop quality measures
Developing quality measures
Quality measures generally fall into 4 broad categories: structure, process, outcome, and patient experience (TABLE).4,5 Quality measure development begins with an assessment of the evidence, which is usually derived from clinical guidelines that link a particular process, structure, or outcome with improved patient health or experience of care. For example, the American College of Obstetricians and Gynecologists (ACOG) has developed a clinical practice guideline for screening, diagnosing, and managing gestational diabetes. The guideline addresses drug therapies, such as insulin, and alternative treatments, such as nutrition therapy. Much like the process for creating the guideline itself, translating the guideline into a quality measure requires a thoughtful, transparent, and well-defined process.
Role of the quality measure steward. Coordinating the process of translating evidence-based guidelines into quality measures requires a measure steward. Measure stewards usually are government agencies, nonprofit organizations, and/or for-profit companies. During the development process, the steward usually reaches out to additional stakeholders for feedback and consensus. Development process steps include:
- evaluation of the evidence, including the clinical practice guideline(s)
- consensus on the best measurement approach (consider the feasibility of the measurement and how it will be collected)
- development of detailed measure specifications (that is, what will be measured and how)
- feedback on the specifications from stakeholders, including professional societies and patient advocates
- testing of the measure logic and clinical validity against clinical data
- final approval by the measure steward.
Endorsement of quality measures. After a quality measure is developed, it is often endorsed by government agencies, professional societies, and/or consumer groups. Endorsement is a consensus-based process in which stakeholders evaluate a proposed measure based on established standards. Generally, stakeholders include health care professionals, consumers, payers, hospitals, health plans, and government agencies.
Evaluation of quality measures includes these important considerations:
- Are the necessary data fields available in a typical electronic health record (EHR) system?
- What is the data quality for those data fields?
- Can the measure be calculated reliably across different data sets or EHRs?
- Does the measure address one of the National Academy of Medicine quality properties? According to the academy, quality in the context of clinical care can be defined in terms of properties of effectiveness, equity, safety, efficiency, patient centeredness, and timeliness.1
Read about ACOG’s role in developing quality measures
ACOG’s role in developing quality measures
In October 2016, the Centers for Medicare and Medicaid Services released the final Medicare Access and CHIP Reauthorization Act of 2015 (MACRA). Under this rule, the Merit-based Incentive Payment System (MIPS) was created, which was intended to drive “value” rather than “volume” in payment incentives. Measures are critical to defining value-based care. However, the law has limited or no impact on providers who do not care for Medicare patients.
Clinicians eligible to participate in MACRA must bill more than $90,000 a year in Medicare Part B allowed charges and provide care for more than 200 Medicare patients per year.6 This means that the MIPS largely overlooks ObGyns, as the bulk of our patients are insured either by private insurance or by Medicaid. However, maternity care spending is a significant part of both Medicaid and private insurers’ outlay, and both payers are actively considering using value-based financial models that will need to be fed by quality metrics. ACOG wants to be at the forefront of measure development for quality metrics that affect members and has committed resources to formation of a measure development team.
ACOG wants providers to be in control of how their practices are evaluated. For this reason, ACOG is focusing on measures that are based on clinical data entered by providers into an EHR at the point of care. At the same time, ACOG is cognizant of not increasing the documentation burden for providers. Understanding the quality of the data, as opposed to the quality of care, will be a fundamental task for the maternity care registry that ACOG is launching in 2018.
What can ObGyns do?
Quality measures are about more than just money. Public reporting of these measures on government and payer websites may influence public perception of a practice.7 The focus on patient-centered care means that patients have a voice in their care, financially as well as literally, so expect to see increased scrutiny of provider performance by patients as well as payers. One way to measure patient experience of treatments, symptoms, and quality of life is through patient-reported outcome measures (PROMs). Assessing PROMs in routine care ensures that information only the patient can provide is collected and analyzed, thus further enhancing the delivery of care and evaluating how that care is impacting the lives of your patients.
The transition from fee-for-service to a value-based system will not happen overnight, but it will happen. This transition—from being paid for the quantity of documentation to the quality of documentation—will require some change management, rethinking of workflows, and better documentation tools (such as apps instead of EHR customization).
Many in the medical profession are actively exploring these changes and new developments. These changes are too important to leave to administrators, coders, scribes, app developers, and policy makers. Someone in your practice, hospital, or health system is working on these issues today. Tomorrow, you need to be at the table. The voices of practicing ObGyns are critical as we work to address the current challenging environment in which we spend more per capita than any other nation with far inferior results. Measures that matter to us and to our patients will help us provide better and more cost-effective care that payers and patients value.8
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
The future of health care is value-based care. If Value equals Quality divided by Cost, then a defined, validated way to measure Quality is paramount to that equation. (Fortunately, Cost comes with convenient measurement units called dollars.) Payers now are asking health care providers to shift from a fee-for-service to a value-based reimbursement structure to encourage providers to deliver the best care at the lowest cost. Providers who can embrace this data-driven paradigm will succeed in this new environment.
So how do we define high-quality care? What makes a good quality measure? How do you actually measure what happens in a clinical encounter that impacts health outcomes?
To answer these questions, organizations have constructed standardized clinical quality measures. Clinical quality measures facilitate value-based care by providing a metric on which to measure a patient’s quality of care. They can be used 1) to decrease the overuse, underuse, and misuse of health care services and 2) to measure patient engagement and satisfaction with care.
What are quality measures?
The Academy of Medicine (formerly named the Institute of Medicine) defines health care quality as “the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge.”1
Clearly defined components and terminology. From a quantitative standpoint, quality measures must have a clearly defined numerator and denominator and appropriate inclusions, exclusions, and exceptions. These components need to be expressed clearly in terms of publicly available terminologies, such as ICD (International Classification of Diseases) codes or SNOMED CT (Systematized Nomenclature of Medicine—Clinical Terms) terms. A measure that asks if “antihypertensive meds” have been given will not nearly be as specific as one that asks if “labetalol IV, or hydralazine IV, or nifedipine SL” has been administered. The decision to tie the data elements in a measure to administrative data, such as ICD codes, or to clinical data, such as SNOMED CT, also affects how these measures can be calculated.
Moving targets. The target of the measure also must carefully be considered. Quality measures can be used to evaluate care across the full range of health care settings—from individual providers, to care teams, to hospitals and hospital systems, to health plans. While some measures easily can be assigned to a specific provider, others are not as straightforward. For example, who gets assigned the cesarean delivery when a midwife turns the case over to an obstetrician?
Timeframe in outcomes measurement. The data infrastructure is currently set up to support measurement of immediate events, 30-day or 90-day episodes, and health insurance plan member years. Longer-term outcomes, such as over 5- and 10- year periods, are out of reach for most measures. To obtain an accurate view of the impact of medical interventions or disease conditions, however, it will be important to follow patients over time. For example, to know the failure rate of intrauterine systems, sterilization, or hormonal contraceptives, it is important to be able to track pregnancy occurrence during use of these methods for longer than 90 days. Failures can occur years after a method is initiated.
Another example is to create a performance measure focused on the overall improvement in quality of life and costs related to different treatments for abnormal uterine bleeding. How does the patient experience vary over time between treatment with hormonal contraception, endometrial ablation, or hysterectomy? Which option is most “valuable” over time when the patient experience and the cost are assessed for more than a 90-day episode? These important questions need to be answered as we maneuver into a value-based health system.
Risk adjustment. Quality measures also may need to be risk adjusted. The “My patients are sicker” refrain must be accounted for with full transparency and based on the best available data. Quality measures can be adjusted using an Observed/Expected factor, which helps to account for complicated cases.2
Clearly, social and behavioral determinants of health also play a role in these adjustments, but it can be more challenging to acquire the data elements needed for those types of adjustments. Including these data enables us to evaluate health disparities between populations, both demographically and socioeconomically.3 This is important for future development of minority inclusive quality measures. Some racial and ethnic minority populations have poorer health outcomes from preventable and treatable diseases. Evidence shows that these groups have differences in access to health care, quality of care, and health measures, including life expectancy and maternal mortality. Access to clinical data through quality measures allows for these health disparities to be brought into quantifiable perspective and assists in the development of future incentive programs to combat health inequalities and provide improved delivery of care.
Read about how to develop quality measures
Developing quality measures
Quality measures generally fall into 4 broad categories: structure, process, outcome, and patient experience (TABLE).4,5 Quality measure development begins with an assessment of the evidence, which is usually derived from clinical guidelines that link a particular process, structure, or outcome with improved patient health or experience of care. For example, the American College of Obstetricians and Gynecologists (ACOG) has developed a clinical practice guideline for screening, diagnosing, and managing gestational diabetes. The guideline addresses drug therapies, such as insulin, and alternative treatments, such as nutrition therapy. Much like the process for creating the guideline itself, translating the guideline into a quality measure requires a thoughtful, transparent, and well-defined process.
Role of the quality measure steward. Coordinating the process of translating evidence-based guidelines into quality measures requires a measure steward. Measure stewards usually are government agencies, nonprofit organizations, and/or for-profit companies. During the development process, the steward usually reaches out to additional stakeholders for feedback and consensus. Development process steps include:
- evaluation of the evidence, including the clinical practice guideline(s)
- consensus on the best measurement approach (consider the feasibility of the measurement and how it will be collected)
- development of detailed measure specifications (that is, what will be measured and how)
- feedback on the specifications from stakeholders, including professional societies and patient advocates
- testing of the measure logic and clinical validity against clinical data
- final approval by the measure steward.
Endorsement of quality measures. After a quality measure is developed, it is often endorsed by government agencies, professional societies, and/or consumer groups. Endorsement is a consensus-based process in which stakeholders evaluate a proposed measure based on established standards. Generally, stakeholders include health care professionals, consumers, payers, hospitals, health plans, and government agencies.
Evaluation of quality measures includes these important considerations:
- Are the necessary data fields available in a typical electronic health record (EHR) system?
- What is the data quality for those data fields?
- Can the measure be calculated reliably across different data sets or EHRs?
- Does the measure address one of the National Academy of Medicine quality properties? According to the academy, quality in the context of clinical care can be defined in terms of properties of effectiveness, equity, safety, efficiency, patient centeredness, and timeliness.1
Read about ACOG’s role in developing quality measures
ACOG’s role in developing quality measures
In October 2016, the Centers for Medicare and Medicaid Services released the final Medicare Access and CHIP Reauthorization Act of 2015 (MACRA). Under this rule, the Merit-based Incentive Payment System (MIPS) was created, which was intended to drive “value” rather than “volume” in payment incentives. Measures are critical to defining value-based care. However, the law has limited or no impact on providers who do not care for Medicare patients.
Clinicians eligible to participate in MACRA must bill more than $90,000 a year in Medicare Part B allowed charges and provide care for more than 200 Medicare patients per year.6 This means that the MIPS largely overlooks ObGyns, as the bulk of our patients are insured either by private insurance or by Medicaid. However, maternity care spending is a significant part of both Medicaid and private insurers’ outlay, and both payers are actively considering using value-based financial models that will need to be fed by quality metrics. ACOG wants to be at the forefront of measure development for quality metrics that affect members and has committed resources to formation of a measure development team.
ACOG wants providers to be in control of how their practices are evaluated. For this reason, ACOG is focusing on measures that are based on clinical data entered by providers into an EHR at the point of care. At the same time, ACOG is cognizant of not increasing the documentation burden for providers. Understanding the quality of the data, as opposed to the quality of care, will be a fundamental task for the maternity care registry that ACOG is launching in 2018.
What can ObGyns do?
Quality measures are about more than just money. Public reporting of these measures on government and payer websites may influence public perception of a practice.7 The focus on patient-centered care means that patients have a voice in their care, financially as well as literally, so expect to see increased scrutiny of provider performance by patients as well as payers. One way to measure patient experience of treatments, symptoms, and quality of life is through patient-reported outcome measures (PROMs). Assessing PROMs in routine care ensures that information only the patient can provide is collected and analyzed, thus further enhancing the delivery of care and evaluating how that care is impacting the lives of your patients.
The transition from fee-for-service to a value-based system will not happen overnight, but it will happen. This transition—from being paid for the quantity of documentation to the quality of documentation—will require some change management, rethinking of workflows, and better documentation tools (such as apps instead of EHR customization).
Many in the medical profession are actively exploring these changes and new developments. These changes are too important to leave to administrators, coders, scribes, app developers, and policy makers. Someone in your practice, hospital, or health system is working on these issues today. Tomorrow, you need to be at the table. The voices of practicing ObGyns are critical as we work to address the current challenging environment in which we spend more per capita than any other nation with far inferior results. Measures that matter to us and to our patients will help us provide better and more cost-effective care that payers and patients value.8
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- National Academy of Sciences. Crossing the quality chasm: the IOM Health Care Quality Initiative. http://www.nationalacademies.org/hmd/Global/News%20Announcements/Crossing-the-Quality-Chasm-The-IOM-Health-Care-Quality-Initiative.aspx. Updated January 2, 2018. Accessed January 11, 2018.
- Agency for Healthcare Research and Quality. Selecting quality and resource use measures: a decision guide for community quality collaboratives. Part 2. Introduction to measures of quality (continued). https://www.ahrq.gov/professionals/quality-patient-safety/quality-resources/tools/perfmeasguide/perfmeaspt2a.html. Reviewed 2014. Accessed December 12, 2017.
- Thomas SB, Fine MJ, Ibrahim SA. Health disparities: the importance of culture and health communication. Am J Public Health. 2004;94(12):2050.
- Agency for Healthcare Research and Quality. Types of quality measures. https://www.ahrq.gov/professionals/quality-patient-safety/talkingquality/create/types.html. Reviewed 2011. Accessed December 12, 2017.
- Agency for Healthcare Research and Quality. Understanding quality measurement. https://www.ahrq.gov/professionals/quality-patient-safety/quality-resources/tools/chtoolbx/understand/index.html. Reviewed November 2017. Accessed December 12, 2017.
- Centers for Medicare and Medicaid Services. Quality payment program. https://www.cms.gov/Medicare/Quality-Payment-Program/resource-library/QPP-Year-2-Final-Rule-Fact-Sheet.pdf. Published December 2017. Accessed December 12, 2017.
- Howell EA, Zeitlin J, Hebert PL, Balbierz, A, Egorova N. Association between hospital-level obstetric quality indicators and maternal and neonatal morbidity. JAMA. 2014;312(15):1531–1541.
- Tooker J. The importance of measuring quality and performance in healthcare. MedGenMed. 2005;7(2):49.
- National Academy of Sciences. Crossing the quality chasm: the IOM Health Care Quality Initiative. http://www.nationalacademies.org/hmd/Global/News%20Announcements/Crossing-the-Quality-Chasm-The-IOM-Health-Care-Quality-Initiative.aspx. Updated January 2, 2018. Accessed January 11, 2018.
- Agency for Healthcare Research and Quality. Selecting quality and resource use measures: a decision guide for community quality collaboratives. Part 2. Introduction to measures of quality (continued). https://www.ahrq.gov/professionals/quality-patient-safety/quality-resources/tools/perfmeasguide/perfmeaspt2a.html. Reviewed 2014. Accessed December 12, 2017.
- Thomas SB, Fine MJ, Ibrahim SA. Health disparities: the importance of culture and health communication. Am J Public Health. 2004;94(12):2050.
- Agency for Healthcare Research and Quality. Types of quality measures. https://www.ahrq.gov/professionals/quality-patient-safety/talkingquality/create/types.html. Reviewed 2011. Accessed December 12, 2017.
- Agency for Healthcare Research and Quality. Understanding quality measurement. https://www.ahrq.gov/professionals/quality-patient-safety/quality-resources/tools/chtoolbx/understand/index.html. Reviewed November 2017. Accessed December 12, 2017.
- Centers for Medicare and Medicaid Services. Quality payment program. https://www.cms.gov/Medicare/Quality-Payment-Program/resource-library/QPP-Year-2-Final-Rule-Fact-Sheet.pdf. Published December 2017. Accessed December 12, 2017.
- Howell EA, Zeitlin J, Hebert PL, Balbierz, A, Egorova N. Association between hospital-level obstetric quality indicators and maternal and neonatal morbidity. JAMA. 2014;312(15):1531–1541.
- Tooker J. The importance of measuring quality and performance in healthcare. MedGenMed. 2005;7(2):49.
Read all parts of this series
PART 1 Value-based payment: What does it mean and how can ObGyns get out ahead
PART 2 What makes a “quality” quality measure?
PART 3 The role of patient-reported outcomes in women’s health
PART 4 It costs what?! How we can educate residents and students on how much things cost

COPD in Primary Care: Key Consideration for Optimized Management

Contents
Introduction
Barbara P. Yawn, MD, MSc, FAAFP
Dyspnea and Hyperinflation in Chronic Obstructive Pulmonary Disease: Impact on Physical Activity
Nathaniel Marchetti, DO, and Alan Kaplan, MD
Anxiety and Depression in Chronic Obstructive Pulmonary Disease: Recognition and Management
Abebaw Mengistu Yohannes, PhD; Alan Kaplan, MD; and Nicola A. Hanania, MD, MS
Considerations for Optimal Inhaler Device Selection in Chronic Obstructive Pulmonary Disease
Rajiv Dhand, MD; Tricia Cavanaugh, MD; and Neil Skolnik, MD
Treatment Options for Stable Chronic Obstructive Pulmonary Disease: Current Recommendations and Unmet Needs
Barbara Yawn, DM, MSc, FAAFP; and Victor Kim, MD
Contents
Introduction
Barbara P. Yawn, MD, MSc, FAAFP
Dyspnea and Hyperinflation in Chronic Obstructive Pulmonary Disease: Impact on Physical Activity
Nathaniel Marchetti, DO, and Alan Kaplan, MD
Anxiety and Depression in Chronic Obstructive Pulmonary Disease: Recognition and Management
Abebaw Mengistu Yohannes, PhD; Alan Kaplan, MD; and Nicola A. Hanania, MD, MS
Considerations for Optimal Inhaler Device Selection in Chronic Obstructive Pulmonary Disease
Rajiv Dhand, MD; Tricia Cavanaugh, MD; and Neil Skolnik, MD
Treatment Options for Stable Chronic Obstructive Pulmonary Disease: Current Recommendations and Unmet Needs
Barbara Yawn, DM, MSc, FAAFP; and Victor Kim, MD
Contents
Introduction
Barbara P. Yawn, MD, MSc, FAAFP
Dyspnea and Hyperinflation in Chronic Obstructive Pulmonary Disease: Impact on Physical Activity
Nathaniel Marchetti, DO, and Alan Kaplan, MD
Anxiety and Depression in Chronic Obstructive Pulmonary Disease: Recognition and Management
Abebaw Mengistu Yohannes, PhD; Alan Kaplan, MD; and Nicola A. Hanania, MD, MS
Considerations for Optimal Inhaler Device Selection in Chronic Obstructive Pulmonary Disease
Rajiv Dhand, MD; Tricia Cavanaugh, MD; and Neil Skolnik, MD
Treatment Options for Stable Chronic Obstructive Pulmonary Disease: Current Recommendations and Unmet Needs
Barbara Yawn, DM, MSc, FAAFP; and Victor Kim, MD

3 cases of chronic pelvic pain managed with nonsurgical, nonopioid therapies
Chronic pelvic pain (CPP) is defined as noncyclic pain in the pelvis, anterior abdominal wall, back, or buttocks that has been present for at least 6 months and is severe enough to cause functional disability or require medical care.1 CPP is very common, with an estimated prevalence of 15% to 20%. It accounts for 20% of gynecology visits and 15% of hysterectomies in the United States, and it is believed to account for $2.8 billion in direct health care spending annually.2–5
Caring for patients with CPP can be very challenging. They often arrive at your office frustrated, having seen multiple providers or having undergone multiple surgeries. They may come to you whether you are a general ObGyn or subspecialize in maternal-fetal medicine, oncology, reproductive endocrinology, urogynecology, or adolescent gynecology. From interactions with other providers or their own family members, these patients may have received the message—either subtly or overtly—that their pain is “all in their head.” As such, some patients may resist any implication that their pain does not have an anatomic source. It is therefore critical to have appropriate tools for evaluating and managing the complex problem of CPP.
Perform a thorough and thoughtful assessment
Chronic pelvic pain often presents as a constellation of symptoms with contributions from multiple sources, as opposed to a single disease entity. Occasionally there is a single cause of pain, such as a large endometrioma or degenerating fibroid, where surgery can be curative. But more commonly the pain arises from multiple organ systems. In such cases, surgery may be unnecessary and, often, can worsen pain.
Thoughtful evaluation is critical in the CPP population. Take a thorough patient history to determine the characteristics of pain (cyclic or constant, widespread or localized), exacerbating factors, sleep disturbances, fatigue, and current coping strategies. Focus a comprehensive physical examination on identifying the maneuvers that reproduce the patient’s pain, and include an examination of the pelvic floor muscles.6 In most cases, pelvic ultrasonography provides adequate evaluation for anatomic sources of pain.
Chronic pain does not behave like acute injury or postsurgical pain. Continuous peripheral pain signals for a prolonged period can lead to changes in how the brain processes pain; specifically, the brain can begin to amplify pain signals. This “central pain amplification” is characterized clinically by widespread pain, fatigue, sleep disturbances, memory difficulties, and somatic symptoms. Central pain amplification occurs in many chronic pain conditions, including fibromyalgia, interstitial cystitis, irritable bowel syndrome, low back pain, chronic headaches, and temporomandibular joint disorder.7,8 Recent clinical and functional magnetic resonance imaging (MRI) studies demonstrate central pain amplification in many patients with CPP.9–12 Notably, these findings are independent of the presence or severity of endometriosis.
In this article we discuss many therapies that have not been specifically studied in patients with CPP, and treatment efficacy is extrapolated from other conditions with chronic pain amplification, such as fibromyalgia or interstitial cystitis. Additionally, many treatments for conditions associated with central pain amplification are used off-label, that is, the US Food and Drug Administration (FDA) has not approved the medication for treatment of these specific conditions. This should be disclosed to patients during counseling.
Discuss treatment expectations with patients
Educating patients regarding the pathophysiology of chronic pain and setting reasonable expectations is the cornerstone of providing patient-centered care for this complex condition. We start most of our discussions about treatment options by telling patients that while we may not cure their pain, we will provide them with medical, surgical, and behavioral strategies that will reduce their pain, improve their function, and enhance their quality of life.
Surprisingly, most patients say that a cure is not their goal. They just want to feel better so they can return to work or activities, fully participate in family life, or not feel exhausted all the time. As such, a multimodal treatment plan is generally the best strategy for achieving a satisfactory improvement in symptoms.
Read about treating a case of continued pain after endometriosis treatment.
CASE 1 Patient’s pain continues after endometriosis excision
A 32-year-old woman (G1P1) reports having CPP for 8 years. She underwent excision of stage 1 endometriosis last year, which resulted in a modest improvement in pain for 6 months. Her pain is worse during menses, at the end of the day, and with vaginal intercourse (both during and lasting for 1 to 2 days after). On examination, you find diffuse pelvic floor tenderness but no adnexal masses or rectovaginal nodularity on palpation.
What treatment options would you consider for this patient?
Multimodal treatment often needed to manage CPP symptoms
The patient described in Case 1 may benefit from a combination of therapies that include analgesics, hormone suppression agents, and physical therapy (PT) (TABLE).
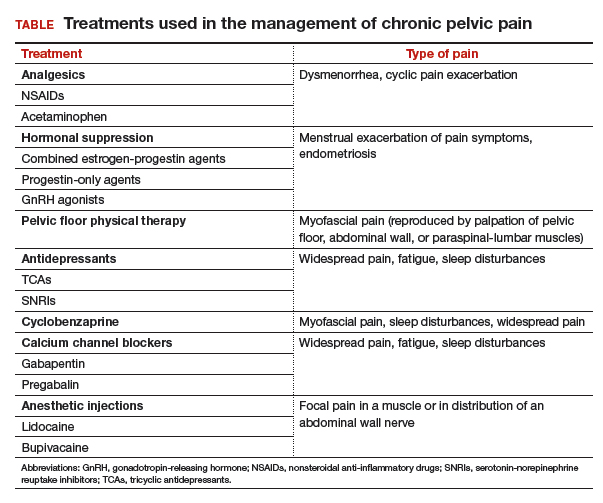
Analgesics
Nonsteroidal anti-inflammatory drugs (NSAIDs), including ibuprofen and naproxen, work by inhibiting cyclooxygenase enzyme, which decreases assembly of peripheral prostaglandins and thromboxane. In a large Cochrane review, NSAIDs were associated with moderate or excellent pain relief for approximately 50% of patients with dysmenorrhea, and they have been shown to reduce menstrual flow due to decreased production of uterine prostaglandins.13 There is little evidence for use of NSAIDs in chronic pain conditions.
Acetaminophen’s mechanism of action is unclear, but the drug likely inhibits central prostaglandin synthesis, and it works synergistically with other analgesics.
Opioids act on μ and δ opioid receptors in the central and peripheral nervous systems as well as in the gastrointestinal system. No evidence supports opioid use in CPP or other chronic pain conditions. Long-term opioid use is associated with a multitude of adverse effects, risk for dependence, and the induction of opioid-induced hyperalgesia (in which patients develop greater sensitivity to pain stimuli).
Analgesics, specifically NSAIDs, can be considered for use in patients with dysmenorrhea, cyclic pain exacerbation, or a suspected inflammatory component of pain. Best practices include scheduling NSAID use before the onset of menses and continuing the drugs on a scheduled basis throughout. NSAIDs should be used for a brief period, and regular use on an empty stomach should be avoided.
Hormone suppression
Many types of hormone suppression therapy are available, including combined estrogen-progestin medications, progestin-only medications, and gonadotropin-releasing hormone (GnRH) agonists and antagonists.
Combined estrogen-progestin medications include oral contraceptive pills (OCPs), vaginal rings, and transdermal patches. Combined estrogen-progestin methods cause atrophy of eutopic and ectopic endometrium and suppress GnRH.
Progestin-only methods include oral formulations, the levonorgestrel intrauterine device, intramuscular and subcuticular injections, and subdermal implants. Progestin-only methods lead to atrophy of eutopic and ectopic endometrium.
A GnRH agonist, leuprolide depot works by downregulating luteinizing hormone and follicle stimulating hormone release from the pituitary, causing suppression of ovarian follicular development and ovulation, leading to a hypoestrogenic state.
Combined estrogen-progestin formulations and progestin-only options are often considered first-line therapy for dysmenorrhea and endometriosis.13 Continuous administration, with the goal of inducing amenorrhea, is effective in the treatment of dysmenorrhea. Several randomized controlled trials have shown that different types of hormone suppression agents are, essentially, equally effective.13–15 Treatment recommendations therefore should focus on adverse effects, cost, and patient preference. GnRH agonists and norethindrone are not FDA approved for the treatment of endometriosis.
It may be appropriate to consider use of hormone suppression therapy in patients with menstrual exacerbation of pain symptoms, including those with a history of endometriosis. We generally advise patients that the goal is amenorrhea and that achieving it often involves a process of trying different formulations to find the best fit. Remember that GnRH agonists are dependent on a functional hypothalamic-pituitary-ovarian axis, and they are unlikely to be effective in women with suspected residual endometriosis who have had a bilateral oophorectomy.
Physical therapy
For CPP, PT typically targets musculoskeletal dysfunction in the pelvic floor, abdominal wall, hips, and back. Interventions include muscle control, mobilization, and biofeedback. Pelvic PT has been shown to improve pain and dyspareunia in patients with CPP, coccydynia, and vestibulodynia.16–18 One large study found a significant, patient-directed decrease in pain medication use after pelvic floor PT.19 Pelvic PT for patients with interstitial cystitis and pelvic floor tenderness resulted in improved pain and bladder symptoms.20
Pelvic PT can be considered for patients with pain reproducible with palpation of the pelvic floor, abdominal wall, paraspinal-lumbar muscles, or sacroiliac joints. Best practices include referral to a therapist who has specialized training in CPP, including pelvic floor therapy. It is important to clearly list the indication for referral, as many of these therapists also treat stress urinary incontinence. The wrong exercises can result in increased hypercontractility of pelvic floor muscles, which can worsen pelvic pain.
It is also critical to clarify expectations with your patient at the time of PT referral. Specifically, advise patients that when beginning therapy, it is common to experience a temporary increase in discomfort of the pelvic muscles. Inform patients also to expect that their therapist will perform internal manipulation of the pelvic floor muscles through the vagina, as this can be surprising for some patients. Finally, counsel patients that their adherence to daily home exercises improves their chance of a durable, long-term successful response.21
CASE 1 Treatment recommendations
For treatment of this patient’s CPP, consider scheduled naproxen therapy during menses, continuous OCPs, and referral for pelvic floor PT.
Read about treating a case of pain, sleep disturbance, and depression.
CASE 2 Patient with long-standing CPP, multiple diagnoses, and sleep problems
A 30-year-old woman (G2P2) reports having had CPP for 17 years. She is amenorrheic with continuous OCP treatment. She had experienced some improvement with pelvic PT. The patient reports that she has daily pain with intermittent pain flares and that she is exhausted and has poor sleep quality, which she attributes to pain. She has been diagnosed with interstitial cystitis, irritable bowel syndrome, and temporomandibular joint disorder. She has a history of depression, which she feels is well controlled with bupropion. Physical examination reveals that the patient has diffuse but mild pain in the pelvic floor and abdominal wall muscles.
What further pain management options can you offer for this patient?
Managing pain, sleep disturbance, and depression
This patient has been living with CPP for many years, and she has sleep difficulties that might be exacerbating pain or result from pain (or both). She is already on continuous OCPs and has had some relief with pelvic PT. Other options that may help with her multiple issues include antidepressants, cyclobenzaprine, and calcium channel blockers.
Antidepressants
Several classes of antidepressants have been used in the treatment of chronic pain conditions, specifically, tricyclic antidepressants (TCAs) and serotonin-norepinephrine reuptake inhibitors (SNRIs). Commonly used TCAs include amitriptyline, nortriptyline, desipramine, and doxepin. Commonly used SNRIs are duloxetine and milnacipran. Both TCAs and SNRIs increase the availability of norepinephrine and serotonin, which are thought to act on the descending pain inhibitory systems to decrease pain sensitivity. Of note, most selective serotonin reuptake inhibitors (SSRIs) at typical doses do not exert a significant enough impact on norepinephrine to be useful for chronic pain.22
Evidence is limited on the use of antidepressants for treating CPP. Amitriptyline is the most extensively studied antidepressant. Amitriptyline treatment resulted in modest pain improvement in patients with CPP and fibromyalgia.23,24 Bothersome anticholinergic effects, including fatigue, dry mouth, and constipation, often are reported with TCAs. Adverse effects tend to be less with nortriptyline or desipramine compared with amitriptyline, but possibly at the expense of efficacy.
While SNRIs have not yet been studied in CPP, several investigations have shown that they improve pain and quality of life in fibromyalgia patients.22,25
Antidepressant therapy may be appropriate for patients with suspected central pain amplification, widespread pain, and sleep disturbances. Best practices include patient education and careful discussion of this option with your patient. We suggest that clinicians explain that antidepressant medications alter the function of neurotransmitters, which modulate pain signals. While neurotransmitters also are involved in mood modulation, this is not the therapeutic goal in this circumstance. In addition, the doses used for the effective treatment of chronic pain are significantly lower than those needed to treat depression effectively.
Patients often need to hear that you believe that their pain is real and is not a manifestation of depression or another mood disorder. If you suspect that the patient also has untreated depression, address this as its own issue and use medications that have greater efficacy for mood symptoms.
Because many antidepressants can cause sedation, they are best taken before bedtime. Also, slow dose titration over several weeks will reduce the chance of bothersome adverse effects. Counsel patients that efficacy is not generally seen until at goal dose for several weeks. Be aware of interactions with other medications that can cause serotonin syndrome.
Cyclobenzaprine
Cyclobenzaprine is a muscle relaxant that also has activity in the central nervous system. The drug’s precise mechanism of action is not known, but it appears to potentiate norepinephrine and bind to serotonin receptors. Thus, it also likely has some TCA-like activity.
Cyclobenzaprine has not been studied in patients with CPP. In fibromyalgia patients, however, it produced significant improvements in pain, sleep, fatigue, and tenderness.26,27 In our anecdotal experience with CPP patients, cyclobenzaprine has been one of the most impactful therapies. It hits the “chronic pain triad,” meaning that it helps with myofascial pain, neuropathic pain, and sleep disturbances.
Cyclobenzaprine treatment may be considered for patients with myofascial pain, sleep disturbances, and clinical symptoms of central pain amplification. Best practices include starting with low (5 mg) scheduled doses at bedtime and slowly titrating the dose. Drowsiness is a very common side effect, so we try to use that to the patient’s advantage to help with sleep quality.
Notably, sleep disturbances are highly prevalent in patients with chronic pain.28 The relationship appears to be bidirectional, meaning that chronic pain negatively impacts sleep quality, and poor sleep quality causes amplified perception of pain.28–30 Interventions that improve sleep quality have been associated with improvements in pain, coping, mood, and functional status.31 Helping a patient to improve her sleep generally requires a multifaceted approach. It always involves “sleep hygiene” or a behavioral component, and pharmacologic assistance may be considered when improved sleep hygiene does not provide adequately improved sleep quality.
Calcium channel blockers
Gabapentin and pregabalin are calcium channel blockers that inhibit the reuptake of glutamate, norepinephrine, and substance P, which helps to decrease pain sensitivity. They also act as membrane stabilizers, reducing hyperexcitability of peripheral and central nerves. Studies have shown that in patients with CPP, gabapentin resulted in improved pain and mood symptoms with few adverse effects.23,32 Patients with fibromyalgia had improvements in pain, sleep, quality of life, fatigue, and anxiety with both gabapentin and pregabalin.33
It is appropriate to consider use of gabapentin or pregabalin in patients with central pain amplification and sleep disturbances. Best practices include starting with a low dose at bedtime. Traditionally, gabapentin is given in 3 equal doses throughout the day. In our experience, patients report less daytime drowsiness and better sleep quality if two-thirds of the daily dose is given at night, with the remaining daily dose broken up into 2 smaller daytime doses. Slow titration over several weeks will reduce risk of bothersome adverse effects. Patients should be counseled that efficacy is not generally seen until treatment is at goal dose for several weeks.
CASE 2 Treatment recommendations
For this patient with daily pelvic pain, multiple diagnoses that have a pain component, and poor sleep quality, consider a treatment plan that includes scheduled cyclobenzaprine, improved sleep hygiene, and, if needed, gabapentin.
Read about treating a case of focal pain.
CASE 3 Cesarean delivery, hysterectomy, and continued pelvic pain
A 38-year-old woman (G2P2) has had CPP for the past 10 years. She developed persistent left lower-quadrant pain after cesarean delivery of her son. She had a hysterectomy 2 years ago for CPP, after which her pain worsened. She describes daily pain with intermittent flares. On examination, the patient has focal left lower-quadrant pain lateral to the left apex of her Pfannenstiel incision.
What treatment approach would be appropriate for this patient?
Focal pain requires a precisely targeted treatment
This patient with focal left lower-quadrant pain is a candidate for anesthetic trigger point injections in the affected area near her Pfannenstiel incision.
Anesthetic injections
Consider the presence of trigger points and peripheral neuropathy in patients with focal abdominal wall pain. Trigger points are focal, palpable nodules within muscles. They are markedly painful to palpation and are associated with referred pain, motor dysfunction, and occasionally autonomic symptoms. They frequently are seen in abdominal wall or pelvic floor muscles in patients with CPP and are caused by abnormal neuromuscular depolarization.
The ilioinguinal, iliohypogastric, and genitofemoral nerves are in close proximity to Pfannenstiel and laparoscopic port site incisions. These nerves may be injured directly during surgery, but they also may be compressed by postoperative scarring.
Anesthetics, such as lidocaine and bupivacaine, which act as sodium channel blockers, can be injected into this area, and improvement often substantially outlasts the anesthetic’s duration of action. While these drugs’ mechanism of action is not clear, theories include altered function of sodium channels on sensory nerves with repeated anesthetic exposure, dry needling that occurs during injection, hydrodissection of tight connective tissue bands surrounding neuromuscular bundles, or depletion of substance P and neuropeptides as a result of injection.34,35
In several studies, patients with CPP reported decreased pain with lidocaine injections in pelvic floor or abdominal wall trigger points.36–38 Patients with fibromyalgia reported improvement in pain and a decreased need for NSAIDs with bupivacaine trigger point injections.39 While abdominal wall nerve blocks have not been extensively studied in patients with chronic neuropathic pain following gynecologic surgery, they have been shown to substantially improve chronic neuropathic pain following inguinal hernia repair.40
Anesthetic injections appropriately may be considered in patients with focal pain in a muscle or in the distribution of abdominal wall nerves, palpation of which reproduces pain symptoms. Patients with diffuse pain are less likely to benefit from anesthetic injections. Best practices include careful examination with attention to areas of prior abdominal incisions.
Our practice is to inject each affected area with a mix of 9 mL of 1% lidocaine and 1 mL of sodium bicarbonate. If a patient reports at least 24 hours of improvement, we repeat the injection in 2 to 4 weeks. The goal is for the patient to experience a progressively longer duration of benefit with subsequent injections. We perform repeat injections shortly after pain begins to recur at that site. The patient should eventually graduate from receiving regular injections and may return for a remedial injection if pain recurs.
CASE 3 Treatment recommendations
For this patient with persistent focal left-lower quadrant pain and a defined trigger point near her Pfannenstiel incision, consider anesthetic injection in the left lower quadrant.
Work toward realistic symptom improvement
Remember that living with chronic pain is exhausting, and empathy with a patient-centered approach is the most important ingredient for patient improvement and satisfaction. Discuss realistic expectations with patients. Remind them that there is no magic bullet for the complex problem of CPP, and that chronic conditions generally do not improve overnight. Focus on improving the patient’s function and quality of life, and applaud symptom improvement rather than focusing on complete pain resolution.
As these visits often require a good deal of patient education, budget more appointment time if feasible. We find that scheduling frequent return visits (approximately every 3 to 4 months) allows timely treatment follow-up so that changes may be made if needed. If you have maximized your available treatment options, referring the patient to a specialist with additional training in CPP is a sensible next step.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Howard FM. Chronic pelvic pain. Obstet Gynecol. 2003;101(3):594–611.
- Mathias SD, Kuppermann M, Liberman RF, Lipschutz RC, Steege JF. Chronic pelvic pain: prevalence, health-related uality of life, and economic correlates. Obstet Gynecol. 1996;87(3):321–327.
- Gelbaya TA, El-Halwagy HE. Focus on primary care: chronic pelvic pain in women. Obstet Gynecol Surv. 2001;56(12):757–764.
- Broder MS, Kanouse DE, Mittman BS, Bernstein SJ. The appropriateness of recommendations for hysterectomy. Obstet Gynecol. 2000;95(2):199–205.
- Whiteman MK, Hillis SD, Jamieson DJ, et al. Inpatient hysterectomy surveillance in the United States, 2000–2004. Am J Obstet Gynecol. 2008;198(1):34.e1–34.e7.
- Steege JF, Siedhoff MT. Chronic pelvic pain. Obstet Gynecol. 2014;124(3):616–629.
- Williams DA, Clauw DJ. Understanding fibromyalgia: lessons from the broader pain research community. J Pain. 2009;10(8):777–791.
- Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011;152(3 suppl):S2–S15.
- Brawn J, Morotti M, Zondervan KT, Becker CM, Vincent K. Central changes associated with chronic pelvic pain and endometriosis. Hum Reprod Update. 2014;20(5):737–747.
- As-Sanie S, Harris RE, Harte SE, Tu FF, Neshewat G, Clauw DJ. Increased pressure pain sensitivity in women with chronic pelvic pain. Obstet Gynecol. 2013;122(5):1047–1055.
- As-Sanie S, Kim J, Schmidt-Wilcke T, et al. Functional connectivity is associated with altered brain chemistry in women with endometriosis-associated chronic pelvic pain. J Pain. 2016;17(1):1–13.
- As-Sanie S, Harris RE, Napadow V, et al. Changes in regional gray matter volume in women with chronic pelvic pain: a voxel-based morphometry study. Pain. 2012;153(5):1006–1014.
- Marjoribanks J, Ayeleke RO, Farquhar C, Proctor M. Nonsteroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database Syst Rev. 2015;(7):CD001751.
- Falcone T, Lebovic DI. Clinical management of endometriosis. Obstet Gynecol. 2011;118(3):691–705.
- Brown J, Pan A, Hart RJ. Gonadotrophin-releasing hormone analogues for pain associated with endometriosis. Cochrane Database Syst Rev. 2010;(12):CD008475.
- Zoorob D, South M, Karram M, et al. A pilot randomized trial of levator injections versus physical therapy for treatment of pelvic floor myalgia and sexual pain. Int Urogynecol J. 2015;26(6):845–852.
- Scott KM, Fisher LW, Bernstein IH, Bradley MH. The treatment of chronic coccydynia and postcoccygectomy pain with pelvic floor physical therapy. PM R. 2017;9(4):367–376.
- Goldfinger C, Pukall CF, Thibault-Gagnon S, McLean L, Chamberlain S. Effectiveness of cognitive-behavioral therapy and physical therapy for provoked vestibulodynia: a randomized pilot study. J Sex Med. 2016;13(1):88–94.
- Anderson RU, Harvey RH, Wise D, Nevin Smith J, Nathanson BH, Sawyer T. Chronic pelvic pain syndrome: reduction of medication use after pelvic floor physical therapy with an internal myofascial trigger point wand. Appl Psychophysiol Biofeedback. 2015;40(1):45–52.
- FitzGerald MP, Payne CK, Lukacz ES, et al. Randomized multicenter clinical trial of myofascial physical therapy in women with interstitial cystitis/painful bladder syndrome and pelvic floor tenderness. J Urol. 2012;187(6):2113–2118.
- FitzGerald MP, Kotarinos R. Rehabilitation of the short pelvic floor. II: Treatment of the patient with the short pelvic floor. Int Urogynecol J Pelvic Floor Dysfunct. 2003;14(4):269–275.
- Arnold LM. Duloxetine and other antidepressants in the treatment of patients with fibromyalgia. Pain Med. 2007;8(suppl 2):S63–S74.
- Sator-Katzenschlager SM, Scharbert G, Kress HG, et al. Chronic pelvic pain treated with gabapentin and amitriptyline: a randomized controlled pilot study. Wien Klin Wochenschr. 2005;117(21–22):761–78.
- Moore RA, Derry S, Aldington D, Cole P, Wiffen PJ. Amitriptyline for neuropathic pain and fibromyalgia in adults. Cochrane Database Syst Rev. 2012;12:CD008242.
- Gendreau RM, Thorn MD, Gendreau JF, et al. Efficacy of milnacipran in patients with fibromyalgia. J Rheumatol. 2005;32(10):1975–1985.
- Tofferi JK, Jackson JL, O’Malley PG. Treatment of fibromyalgia with cyclobenzaprine: a meta-analysis. Arthritis Rheum. 2004;51(1):9–13.
- Moldofsky H, Harris HW, Archambault WT, Kwong T, Lederman S. Effects of bedtime very low dose cyclobenzaprine on symptoms and sleep physiology in patients with fibromyalgia syndrome: a double-blind randomized placebo-controlled study. J Rheumatol. 2011;38(12):2653–2463.
- Cheatle MD, Foster S, Pinkett A, Lesneski M, Qu D, Dhingra L. Assessing and managing sleep disturbance in patients with chronic pain. Sleep Med Clin. 2016;11(4):531–541.
- Larson RA, Carter JR. Total sleep deprivation and pain perception during cold noxious stimuli in humans. Scand J Pain. 2016;13:12–16.
- Generaal E, Vogelzangs N, Penninx BW, Dekker J. Insomnia, sleep duration, depressive symptoms, and the onset of chronic multisite musculoskeletal pain [published online ahead of print January 1, 2017]. Sleep. doi:10.1093/sleep/zsw030.
- Gerhart JI, Burns JW, Post KM, et al. Relationships between sleep quality and pain-related factors for people with chronic low back pain: tests of reciprocal and time of day effects. Ann Behav Med. 2017;51(3):365–375.
- Lewis SC, Bhattacharya S, Wu O, et al. Gabapentin for the management of chronic pelvic pain in women (GaPP1): a pilot randomised controlled trial. PLoS One. 2016;11(4):e0153037.
- Häuser W, Bernardy K, Uçeyler N, Sommer C. Treatment of fibromyalgia syndrome with gabapentin and pregabalin—a meta-analysis of randomized controlled trials. Pain. 2009;145(1–2):69–81.
- Scott NA, Guo B, Barton PM, Gerwin RD. Trigger point injections for chronic non-malignant musculoskeletal pain: a systematic review. Pain Med. 2009;10(1):54–69.
- Hameroff SR, Crago BR, Blitt CD, Womble J, Kanel J. Comparison of bupivacaine, etidocaine, and saline for trigger-point therapy. Anesth Analg. 1981;60(10):752–755.
- Montenegro ML, Braz CA, Rosa-e-Silva JC, Candido-dos-Reis FJ, Nogueira AA, Poli-Neto OB. Anaesthetic injection versus ischemic compression for the pain relief of abdominal wall trigger points in women with chronic pelvic pain. BMC Anesthesiol. 2015;15:175.
- Kim DS, Jeong TY, Kim YK, Chang WH, Yoon JG, Lee SC. Usefulness of a myofascial trigger point injection for groin pain in patients with chronic prostatitis/chronic pelvic pain syndrome: a pilot study. Arch Phys Med Rehabil. 2013;94(5):930–936.
- Huang QM, Liu L. Wet needling of myofascial trigger points in abdominal muscles for treatment of primary dysmenorrhoea. Acupunct Med. 2014;32(4):346–349.
- Affaitati G, Fabrizio A, Savini A, et al. A randomized, controlled study comparing a lidocaine patch, a placebo patch, and anesthetic injection for treatment of trigger points in patients with myofascial pain syndrome: evaluation of pain and somatic pain thresholds. Clin Ther. 2009;31(4):705–720.
- Thomassen I, van Suijlekom JA, van de Gaag A, Ponten JE, Nienhuijs SW. Ultrasound-guided ilioinguinal/iliohypogastric nerve blocks for chronic pain after inguinal hernia repair. Hernia. 2013;17(3):329–332.

Dr. Till is Assistant Professor, Minimally Invasive Gynecologic Surgery, Department of Obstetrics and Gynecology, University of Michigan, Ann Arbor.

Dr. As-Sanie is Associate Professor and Director, Minimally Invasive Gynecologic Surgery, Department of Obstetrics and Gynecology, University of Michigan, Ann Arbor.
Dr. Till reports no financial relationships relevant to this article. Dr. As-Sanie reports that she is a consultant to AbbVie.
Dr. Till is Assistant Professor, Minimally Invasive Gynecologic Surgery, Department of Obstetrics and Gynecology, University of Michigan, Ann Arbor.
Dr. As-Sanie is Associate Professor and Director, Minimally Invasive Gynecologic Surgery, Department of Obstetrics and Gynecology, University of Michigan, Ann Arbor.
Dr. Till reports no financial relationships relevant to this article. Dr. As-Sanie reports that she is a consultant to AbbVie.
Dr. Till is Assistant Professor, Minimally Invasive Gynecologic Surgery, Department of Obstetrics and Gynecology, University of Michigan, Ann Arbor.
Dr. As-Sanie is Associate Professor and Director, Minimally Invasive Gynecologic Surgery, Department of Obstetrics and Gynecology, University of Michigan, Ann Arbor.
Dr. Till reports no financial relationships relevant to this article. Dr. As-Sanie reports that she is a consultant to AbbVie.
Chronic pelvic pain (CPP) is defined as noncyclic pain in the pelvis, anterior abdominal wall, back, or buttocks that has been present for at least 6 months and is severe enough to cause functional disability or require medical care.1 CPP is very common, with an estimated prevalence of 15% to 20%. It accounts for 20% of gynecology visits and 15% of hysterectomies in the United States, and it is believed to account for $2.8 billion in direct health care spending annually.2–5
Caring for patients with CPP can be very challenging. They often arrive at your office frustrated, having seen multiple providers or having undergone multiple surgeries. They may come to you whether you are a general ObGyn or subspecialize in maternal-fetal medicine, oncology, reproductive endocrinology, urogynecology, or adolescent gynecology. From interactions with other providers or their own family members, these patients may have received the message—either subtly or overtly—that their pain is “all in their head.” As such, some patients may resist any implication that their pain does not have an anatomic source. It is therefore critical to have appropriate tools for evaluating and managing the complex problem of CPP.
Perform a thorough and thoughtful assessment
Chronic pelvic pain often presents as a constellation of symptoms with contributions from multiple sources, as opposed to a single disease entity. Occasionally there is a single cause of pain, such as a large endometrioma or degenerating fibroid, where surgery can be curative. But more commonly the pain arises from multiple organ systems. In such cases, surgery may be unnecessary and, often, can worsen pain.
Thoughtful evaluation is critical in the CPP population. Take a thorough patient history to determine the characteristics of pain (cyclic or constant, widespread or localized), exacerbating factors, sleep disturbances, fatigue, and current coping strategies. Focus a comprehensive physical examination on identifying the maneuvers that reproduce the patient’s pain, and include an examination of the pelvic floor muscles.6 In most cases, pelvic ultrasonography provides adequate evaluation for anatomic sources of pain.
Chronic pain does not behave like acute injury or postsurgical pain. Continuous peripheral pain signals for a prolonged period can lead to changes in how the brain processes pain; specifically, the brain can begin to amplify pain signals. This “central pain amplification” is characterized clinically by widespread pain, fatigue, sleep disturbances, memory difficulties, and somatic symptoms. Central pain amplification occurs in many chronic pain conditions, including fibromyalgia, interstitial cystitis, irritable bowel syndrome, low back pain, chronic headaches, and temporomandibular joint disorder.7,8 Recent clinical and functional magnetic resonance imaging (MRI) studies demonstrate central pain amplification in many patients with CPP.9–12 Notably, these findings are independent of the presence or severity of endometriosis.
In this article we discuss many therapies that have not been specifically studied in patients with CPP, and treatment efficacy is extrapolated from other conditions with chronic pain amplification, such as fibromyalgia or interstitial cystitis. Additionally, many treatments for conditions associated with central pain amplification are used off-label, that is, the US Food and Drug Administration (FDA) has not approved the medication for treatment of these specific conditions. This should be disclosed to patients during counseling.
Discuss treatment expectations with patients
Educating patients regarding the pathophysiology of chronic pain and setting reasonable expectations is the cornerstone of providing patient-centered care for this complex condition. We start most of our discussions about treatment options by telling patients that while we may not cure their pain, we will provide them with medical, surgical, and behavioral strategies that will reduce their pain, improve their function, and enhance their quality of life.
Surprisingly, most patients say that a cure is not their goal. They just want to feel better so they can return to work or activities, fully participate in family life, or not feel exhausted all the time. As such, a multimodal treatment plan is generally the best strategy for achieving a satisfactory improvement in symptoms.
Read about treating a case of continued pain after endometriosis treatment.
CASE 1 Patient’s pain continues after endometriosis excision
A 32-year-old woman (G1P1) reports having CPP for 8 years. She underwent excision of stage 1 endometriosis last year, which resulted in a modest improvement in pain for 6 months. Her pain is worse during menses, at the end of the day, and with vaginal intercourse (both during and lasting for 1 to 2 days after). On examination, you find diffuse pelvic floor tenderness but no adnexal masses or rectovaginal nodularity on palpation.
What treatment options would you consider for this patient?
Multimodal treatment often needed to manage CPP symptoms
The patient described in Case 1 may benefit from a combination of therapies that include analgesics, hormone suppression agents, and physical therapy (PT) (TABLE).
Analgesics
Nonsteroidal anti-inflammatory drugs (NSAIDs), including ibuprofen and naproxen, work by inhibiting cyclooxygenase enzyme, which decreases assembly of peripheral prostaglandins and thromboxane. In a large Cochrane review, NSAIDs were associated with moderate or excellent pain relief for approximately 50% of patients with dysmenorrhea, and they have been shown to reduce menstrual flow due to decreased production of uterine prostaglandins.13 There is little evidence for use of NSAIDs in chronic pain conditions.
Acetaminophen’s mechanism of action is unclear, but the drug likely inhibits central prostaglandin synthesis, and it works synergistically with other analgesics.
Opioids act on μ and δ opioid receptors in the central and peripheral nervous systems as well as in the gastrointestinal system. No evidence supports opioid use in CPP or other chronic pain conditions. Long-term opioid use is associated with a multitude of adverse effects, risk for dependence, and the induction of opioid-induced hyperalgesia (in which patients develop greater sensitivity to pain stimuli).
Analgesics, specifically NSAIDs, can be considered for use in patients with dysmenorrhea, cyclic pain exacerbation, or a suspected inflammatory component of pain. Best practices include scheduling NSAID use before the onset of menses and continuing the drugs on a scheduled basis throughout. NSAIDs should be used for a brief period, and regular use on an empty stomach should be avoided.
Hormone suppression
Many types of hormone suppression therapy are available, including combined estrogen-progestin medications, progestin-only medications, and gonadotropin-releasing hormone (GnRH) agonists and antagonists.
Combined estrogen-progestin medications include oral contraceptive pills (OCPs), vaginal rings, and transdermal patches. Combined estrogen-progestin methods cause atrophy of eutopic and ectopic endometrium and suppress GnRH.
Progestin-only methods include oral formulations, the levonorgestrel intrauterine device, intramuscular and subcuticular injections, and subdermal implants. Progestin-only methods lead to atrophy of eutopic and ectopic endometrium.
A GnRH agonist, leuprolide depot works by downregulating luteinizing hormone and follicle stimulating hormone release from the pituitary, causing suppression of ovarian follicular development and ovulation, leading to a hypoestrogenic state.
Combined estrogen-progestin formulations and progestin-only options are often considered first-line therapy for dysmenorrhea and endometriosis.13 Continuous administration, with the goal of inducing amenorrhea, is effective in the treatment of dysmenorrhea. Several randomized controlled trials have shown that different types of hormone suppression agents are, essentially, equally effective.13–15 Treatment recommendations therefore should focus on adverse effects, cost, and patient preference. GnRH agonists and norethindrone are not FDA approved for the treatment of endometriosis.
It may be appropriate to consider use of hormone suppression therapy in patients with menstrual exacerbation of pain symptoms, including those with a history of endometriosis. We generally advise patients that the goal is amenorrhea and that achieving it often involves a process of trying different formulations to find the best fit. Remember that GnRH agonists are dependent on a functional hypothalamic-pituitary-ovarian axis, and they are unlikely to be effective in women with suspected residual endometriosis who have had a bilateral oophorectomy.
Physical therapy
For CPP, PT typically targets musculoskeletal dysfunction in the pelvic floor, abdominal wall, hips, and back. Interventions include muscle control, mobilization, and biofeedback. Pelvic PT has been shown to improve pain and dyspareunia in patients with CPP, coccydynia, and vestibulodynia.16–18 One large study found a significant, patient-directed decrease in pain medication use after pelvic floor PT.19 Pelvic PT for patients with interstitial cystitis and pelvic floor tenderness resulted in improved pain and bladder symptoms.20
Pelvic PT can be considered for patients with pain reproducible with palpation of the pelvic floor, abdominal wall, paraspinal-lumbar muscles, or sacroiliac joints. Best practices include referral to a therapist who has specialized training in CPP, including pelvic floor therapy. It is important to clearly list the indication for referral, as many of these therapists also treat stress urinary incontinence. The wrong exercises can result in increased hypercontractility of pelvic floor muscles, which can worsen pelvic pain.
It is also critical to clarify expectations with your patient at the time of PT referral. Specifically, advise patients that when beginning therapy, it is common to experience a temporary increase in discomfort of the pelvic muscles. Inform patients also to expect that their therapist will perform internal manipulation of the pelvic floor muscles through the vagina, as this can be surprising for some patients. Finally, counsel patients that their adherence to daily home exercises improves their chance of a durable, long-term successful response.21
CASE 1 Treatment recommendations
For treatment of this patient’s CPP, consider scheduled naproxen therapy during menses, continuous OCPs, and referral for pelvic floor PT.
Read about treating a case of pain, sleep disturbance, and depression.
CASE 2 Patient with long-standing CPP, multiple diagnoses, and sleep problems
A 30-year-old woman (G2P2) reports having had CPP for 17 years. She is amenorrheic with continuous OCP treatment. She had experienced some improvement with pelvic PT. The patient reports that she has daily pain with intermittent pain flares and that she is exhausted and has poor sleep quality, which she attributes to pain. She has been diagnosed with interstitial cystitis, irritable bowel syndrome, and temporomandibular joint disorder. She has a history of depression, which she feels is well controlled with bupropion. Physical examination reveals that the patient has diffuse but mild pain in the pelvic floor and abdominal wall muscles.
What further pain management options can you offer for this patient?
Managing pain, sleep disturbance, and depression
This patient has been living with CPP for many years, and she has sleep difficulties that might be exacerbating pain or result from pain (or both). She is already on continuous OCPs and has had some relief with pelvic PT. Other options that may help with her multiple issues include antidepressants, cyclobenzaprine, and calcium channel blockers.
Antidepressants
Several classes of antidepressants have been used in the treatment of chronic pain conditions, specifically, tricyclic antidepressants (TCAs) and serotonin-norepinephrine reuptake inhibitors (SNRIs). Commonly used TCAs include amitriptyline, nortriptyline, desipramine, and doxepin. Commonly used SNRIs are duloxetine and milnacipran. Both TCAs and SNRIs increase the availability of norepinephrine and serotonin, which are thought to act on the descending pain inhibitory systems to decrease pain sensitivity. Of note, most selective serotonin reuptake inhibitors (SSRIs) at typical doses do not exert a significant enough impact on norepinephrine to be useful for chronic pain.22
Evidence is limited on the use of antidepressants for treating CPP. Amitriptyline is the most extensively studied antidepressant. Amitriptyline treatment resulted in modest pain improvement in patients with CPP and fibromyalgia.23,24 Bothersome anticholinergic effects, including fatigue, dry mouth, and constipation, often are reported with TCAs. Adverse effects tend to be less with nortriptyline or desipramine compared with amitriptyline, but possibly at the expense of efficacy.
While SNRIs have not yet been studied in CPP, several investigations have shown that they improve pain and quality of life in fibromyalgia patients.22,25
Antidepressant therapy may be appropriate for patients with suspected central pain amplification, widespread pain, and sleep disturbances. Best practices include patient education and careful discussion of this option with your patient. We suggest that clinicians explain that antidepressant medications alter the function of neurotransmitters, which modulate pain signals. While neurotransmitters also are involved in mood modulation, this is not the therapeutic goal in this circumstance. In addition, the doses used for the effective treatment of chronic pain are significantly lower than those needed to treat depression effectively.
Patients often need to hear that you believe that their pain is real and is not a manifestation of depression or another mood disorder. If you suspect that the patient also has untreated depression, address this as its own issue and use medications that have greater efficacy for mood symptoms.
Because many antidepressants can cause sedation, they are best taken before bedtime. Also, slow dose titration over several weeks will reduce the chance of bothersome adverse effects. Counsel patients that efficacy is not generally seen until at goal dose for several weeks. Be aware of interactions with other medications that can cause serotonin syndrome.
Cyclobenzaprine
Cyclobenzaprine is a muscle relaxant that also has activity in the central nervous system. The drug’s precise mechanism of action is not known, but it appears to potentiate norepinephrine and bind to serotonin receptors. Thus, it also likely has some TCA-like activity.
Cyclobenzaprine has not been studied in patients with CPP. In fibromyalgia patients, however, it produced significant improvements in pain, sleep, fatigue, and tenderness.26,27 In our anecdotal experience with CPP patients, cyclobenzaprine has been one of the most impactful therapies. It hits the “chronic pain triad,” meaning that it helps with myofascial pain, neuropathic pain, and sleep disturbances.
Cyclobenzaprine treatment may be considered for patients with myofascial pain, sleep disturbances, and clinical symptoms of central pain amplification. Best practices include starting with low (5 mg) scheduled doses at bedtime and slowly titrating the dose. Drowsiness is a very common side effect, so we try to use that to the patient’s advantage to help with sleep quality.
Notably, sleep disturbances are highly prevalent in patients with chronic pain.28 The relationship appears to be bidirectional, meaning that chronic pain negatively impacts sleep quality, and poor sleep quality causes amplified perception of pain.28–30 Interventions that improve sleep quality have been associated with improvements in pain, coping, mood, and functional status.31 Helping a patient to improve her sleep generally requires a multifaceted approach. It always involves “sleep hygiene” or a behavioral component, and pharmacologic assistance may be considered when improved sleep hygiene does not provide adequately improved sleep quality.
Calcium channel blockers
Gabapentin and pregabalin are calcium channel blockers that inhibit the reuptake of glutamate, norepinephrine, and substance P, which helps to decrease pain sensitivity. They also act as membrane stabilizers, reducing hyperexcitability of peripheral and central nerves. Studies have shown that in patients with CPP, gabapentin resulted in improved pain and mood symptoms with few adverse effects.23,32 Patients with fibromyalgia had improvements in pain, sleep, quality of life, fatigue, and anxiety with both gabapentin and pregabalin.33
It is appropriate to consider use of gabapentin or pregabalin in patients with central pain amplification and sleep disturbances. Best practices include starting with a low dose at bedtime. Traditionally, gabapentin is given in 3 equal doses throughout the day. In our experience, patients report less daytime drowsiness and better sleep quality if two-thirds of the daily dose is given at night, with the remaining daily dose broken up into 2 smaller daytime doses. Slow titration over several weeks will reduce risk of bothersome adverse effects. Patients should be counseled that efficacy is not generally seen until treatment is at goal dose for several weeks.
CASE 2 Treatment recommendations
For this patient with daily pelvic pain, multiple diagnoses that have a pain component, and poor sleep quality, consider a treatment plan that includes scheduled cyclobenzaprine, improved sleep hygiene, and, if needed, gabapentin.
Read about treating a case of focal pain.
CASE 3 Cesarean delivery, hysterectomy, and continued pelvic pain
A 38-year-old woman (G2P2) has had CPP for the past 10 years. She developed persistent left lower-quadrant pain after cesarean delivery of her son. She had a hysterectomy 2 years ago for CPP, after which her pain worsened. She describes daily pain with intermittent flares. On examination, the patient has focal left lower-quadrant pain lateral to the left apex of her Pfannenstiel incision.
What treatment approach would be appropriate for this patient?
Focal pain requires a precisely targeted treatment
This patient with focal left lower-quadrant pain is a candidate for anesthetic trigger point injections in the affected area near her Pfannenstiel incision.
Anesthetic injections
Consider the presence of trigger points and peripheral neuropathy in patients with focal abdominal wall pain. Trigger points are focal, palpable nodules within muscles. They are markedly painful to palpation and are associated with referred pain, motor dysfunction, and occasionally autonomic symptoms. They frequently are seen in abdominal wall or pelvic floor muscles in patients with CPP and are caused by abnormal neuromuscular depolarization.
The ilioinguinal, iliohypogastric, and genitofemoral nerves are in close proximity to Pfannenstiel and laparoscopic port site incisions. These nerves may be injured directly during surgery, but they also may be compressed by postoperative scarring.
Anesthetics, such as lidocaine and bupivacaine, which act as sodium channel blockers, can be injected into this area, and improvement often substantially outlasts the anesthetic’s duration of action. While these drugs’ mechanism of action is not clear, theories include altered function of sodium channels on sensory nerves with repeated anesthetic exposure, dry needling that occurs during injection, hydrodissection of tight connective tissue bands surrounding neuromuscular bundles, or depletion of substance P and neuropeptides as a result of injection.34,35
In several studies, patients with CPP reported decreased pain with lidocaine injections in pelvic floor or abdominal wall trigger points.36–38 Patients with fibromyalgia reported improvement in pain and a decreased need for NSAIDs with bupivacaine trigger point injections.39 While abdominal wall nerve blocks have not been extensively studied in patients with chronic neuropathic pain following gynecologic surgery, they have been shown to substantially improve chronic neuropathic pain following inguinal hernia repair.40
Anesthetic injections appropriately may be considered in patients with focal pain in a muscle or in the distribution of abdominal wall nerves, palpation of which reproduces pain symptoms. Patients with diffuse pain are less likely to benefit from anesthetic injections. Best practices include careful examination with attention to areas of prior abdominal incisions.
Our practice is to inject each affected area with a mix of 9 mL of 1% lidocaine and 1 mL of sodium bicarbonate. If a patient reports at least 24 hours of improvement, we repeat the injection in 2 to 4 weeks. The goal is for the patient to experience a progressively longer duration of benefit with subsequent injections. We perform repeat injections shortly after pain begins to recur at that site. The patient should eventually graduate from receiving regular injections and may return for a remedial injection if pain recurs.
CASE 3 Treatment recommendations
For this patient with persistent focal left-lower quadrant pain and a defined trigger point near her Pfannenstiel incision, consider anesthetic injection in the left lower quadrant.
Work toward realistic symptom improvement
Remember that living with chronic pain is exhausting, and empathy with a patient-centered approach is the most important ingredient for patient improvement and satisfaction. Discuss realistic expectations with patients. Remind them that there is no magic bullet for the complex problem of CPP, and that chronic conditions generally do not improve overnight. Focus on improving the patient’s function and quality of life, and applaud symptom improvement rather than focusing on complete pain resolution.
As these visits often require a good deal of patient education, budget more appointment time if feasible. We find that scheduling frequent return visits (approximately every 3 to 4 months) allows timely treatment follow-up so that changes may be made if needed. If you have maximized your available treatment options, referring the patient to a specialist with additional training in CPP is a sensible next step.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Chronic pelvic pain (CPP) is defined as noncyclic pain in the pelvis, anterior abdominal wall, back, or buttocks that has been present for at least 6 months and is severe enough to cause functional disability or require medical care.1 CPP is very common, with an estimated prevalence of 15% to 20%. It accounts for 20% of gynecology visits and 15% of hysterectomies in the United States, and it is believed to account for $2.8 billion in direct health care spending annually.2–5
Caring for patients with CPP can be very challenging. They often arrive at your office frustrated, having seen multiple providers or having undergone multiple surgeries. They may come to you whether you are a general ObGyn or subspecialize in maternal-fetal medicine, oncology, reproductive endocrinology, urogynecology, or adolescent gynecology. From interactions with other providers or their own family members, these patients may have received the message—either subtly or overtly—that their pain is “all in their head.” As such, some patients may resist any implication that their pain does not have an anatomic source. It is therefore critical to have appropriate tools for evaluating and managing the complex problem of CPP.
Perform a thorough and thoughtful assessment
Chronic pelvic pain often presents as a constellation of symptoms with contributions from multiple sources, as opposed to a single disease entity. Occasionally there is a single cause of pain, such as a large endometrioma or degenerating fibroid, where surgery can be curative. But more commonly the pain arises from multiple organ systems. In such cases, surgery may be unnecessary and, often, can worsen pain.
Thoughtful evaluation is critical in the CPP population. Take a thorough patient history to determine the characteristics of pain (cyclic or constant, widespread or localized), exacerbating factors, sleep disturbances, fatigue, and current coping strategies. Focus a comprehensive physical examination on identifying the maneuvers that reproduce the patient’s pain, and include an examination of the pelvic floor muscles.6 In most cases, pelvic ultrasonography provides adequate evaluation for anatomic sources of pain.
Chronic pain does not behave like acute injury or postsurgical pain. Continuous peripheral pain signals for a prolonged period can lead to changes in how the brain processes pain; specifically, the brain can begin to amplify pain signals. This “central pain amplification” is characterized clinically by widespread pain, fatigue, sleep disturbances, memory difficulties, and somatic symptoms. Central pain amplification occurs in many chronic pain conditions, including fibromyalgia, interstitial cystitis, irritable bowel syndrome, low back pain, chronic headaches, and temporomandibular joint disorder.7,8 Recent clinical and functional magnetic resonance imaging (MRI) studies demonstrate central pain amplification in many patients with CPP.9–12 Notably, these findings are independent of the presence or severity of endometriosis.
In this article we discuss many therapies that have not been specifically studied in patients with CPP, and treatment efficacy is extrapolated from other conditions with chronic pain amplification, such as fibromyalgia or interstitial cystitis. Additionally, many treatments for conditions associated with central pain amplification are used off-label, that is, the US Food and Drug Administration (FDA) has not approved the medication for treatment of these specific conditions. This should be disclosed to patients during counseling.
Discuss treatment expectations with patients
Educating patients regarding the pathophysiology of chronic pain and setting reasonable expectations is the cornerstone of providing patient-centered care for this complex condition. We start most of our discussions about treatment options by telling patients that while we may not cure their pain, we will provide them with medical, surgical, and behavioral strategies that will reduce their pain, improve their function, and enhance their quality of life.
Surprisingly, most patients say that a cure is not their goal. They just want to feel better so they can return to work or activities, fully participate in family life, or not feel exhausted all the time. As such, a multimodal treatment plan is generally the best strategy for achieving a satisfactory improvement in symptoms.
Read about treating a case of continued pain after endometriosis treatment.
CASE 1 Patient’s pain continues after endometriosis excision
A 32-year-old woman (G1P1) reports having CPP for 8 years. She underwent excision of stage 1 endometriosis last year, which resulted in a modest improvement in pain for 6 months. Her pain is worse during menses, at the end of the day, and with vaginal intercourse (both during and lasting for 1 to 2 days after). On examination, you find diffuse pelvic floor tenderness but no adnexal masses or rectovaginal nodularity on palpation.
What treatment options would you consider for this patient?
Multimodal treatment often needed to manage CPP symptoms
The patient described in Case 1 may benefit from a combination of therapies that include analgesics, hormone suppression agents, and physical therapy (PT) (TABLE).
Analgesics
Nonsteroidal anti-inflammatory drugs (NSAIDs), including ibuprofen and naproxen, work by inhibiting cyclooxygenase enzyme, which decreases assembly of peripheral prostaglandins and thromboxane. In a large Cochrane review, NSAIDs were associated with moderate or excellent pain relief for approximately 50% of patients with dysmenorrhea, and they have been shown to reduce menstrual flow due to decreased production of uterine prostaglandins.13 There is little evidence for use of NSAIDs in chronic pain conditions.
Acetaminophen’s mechanism of action is unclear, but the drug likely inhibits central prostaglandin synthesis, and it works synergistically with other analgesics.
Opioids act on μ and δ opioid receptors in the central and peripheral nervous systems as well as in the gastrointestinal system. No evidence supports opioid use in CPP or other chronic pain conditions. Long-term opioid use is associated with a multitude of adverse effects, risk for dependence, and the induction of opioid-induced hyperalgesia (in which patients develop greater sensitivity to pain stimuli).
Analgesics, specifically NSAIDs, can be considered for use in patients with dysmenorrhea, cyclic pain exacerbation, or a suspected inflammatory component of pain. Best practices include scheduling NSAID use before the onset of menses and continuing the drugs on a scheduled basis throughout. NSAIDs should be used for a brief period, and regular use on an empty stomach should be avoided.
Hormone suppression
Many types of hormone suppression therapy are available, including combined estrogen-progestin medications, progestin-only medications, and gonadotropin-releasing hormone (GnRH) agonists and antagonists.
Combined estrogen-progestin medications include oral contraceptive pills (OCPs), vaginal rings, and transdermal patches. Combined estrogen-progestin methods cause atrophy of eutopic and ectopic endometrium and suppress GnRH.
Progestin-only methods include oral formulations, the levonorgestrel intrauterine device, intramuscular and subcuticular injections, and subdermal implants. Progestin-only methods lead to atrophy of eutopic and ectopic endometrium.
A GnRH agonist, leuprolide depot works by downregulating luteinizing hormone and follicle stimulating hormone release from the pituitary, causing suppression of ovarian follicular development and ovulation, leading to a hypoestrogenic state.
Combined estrogen-progestin formulations and progestin-only options are often considered first-line therapy for dysmenorrhea and endometriosis.13 Continuous administration, with the goal of inducing amenorrhea, is effective in the treatment of dysmenorrhea. Several randomized controlled trials have shown that different types of hormone suppression agents are, essentially, equally effective.13–15 Treatment recommendations therefore should focus on adverse effects, cost, and patient preference. GnRH agonists and norethindrone are not FDA approved for the treatment of endometriosis.
It may be appropriate to consider use of hormone suppression therapy in patients with menstrual exacerbation of pain symptoms, including those with a history of endometriosis. We generally advise patients that the goal is amenorrhea and that achieving it often involves a process of trying different formulations to find the best fit. Remember that GnRH agonists are dependent on a functional hypothalamic-pituitary-ovarian axis, and they are unlikely to be effective in women with suspected residual endometriosis who have had a bilateral oophorectomy.
Physical therapy
For CPP, PT typically targets musculoskeletal dysfunction in the pelvic floor, abdominal wall, hips, and back. Interventions include muscle control, mobilization, and biofeedback. Pelvic PT has been shown to improve pain and dyspareunia in patients with CPP, coccydynia, and vestibulodynia.16–18 One large study found a significant, patient-directed decrease in pain medication use after pelvic floor PT.19 Pelvic PT for patients with interstitial cystitis and pelvic floor tenderness resulted in improved pain and bladder symptoms.20
Pelvic PT can be considered for patients with pain reproducible with palpation of the pelvic floor, abdominal wall, paraspinal-lumbar muscles, or sacroiliac joints. Best practices include referral to a therapist who has specialized training in CPP, including pelvic floor therapy. It is important to clearly list the indication for referral, as many of these therapists also treat stress urinary incontinence. The wrong exercises can result in increased hypercontractility of pelvic floor muscles, which can worsen pelvic pain.
It is also critical to clarify expectations with your patient at the time of PT referral. Specifically, advise patients that when beginning therapy, it is common to experience a temporary increase in discomfort of the pelvic muscles. Inform patients also to expect that their therapist will perform internal manipulation of the pelvic floor muscles through the vagina, as this can be surprising for some patients. Finally, counsel patients that their adherence to daily home exercises improves their chance of a durable, long-term successful response.21
CASE 1 Treatment recommendations
For treatment of this patient’s CPP, consider scheduled naproxen therapy during menses, continuous OCPs, and referral for pelvic floor PT.
Read about treating a case of pain, sleep disturbance, and depression.
CASE 2 Patient with long-standing CPP, multiple diagnoses, and sleep problems
A 30-year-old woman (G2P2) reports having had CPP for 17 years. She is amenorrheic with continuous OCP treatment. She had experienced some improvement with pelvic PT. The patient reports that she has daily pain with intermittent pain flares and that she is exhausted and has poor sleep quality, which she attributes to pain. She has been diagnosed with interstitial cystitis, irritable bowel syndrome, and temporomandibular joint disorder. She has a history of depression, which she feels is well controlled with bupropion. Physical examination reveals that the patient has diffuse but mild pain in the pelvic floor and abdominal wall muscles.
What further pain management options can you offer for this patient?
Managing pain, sleep disturbance, and depression
This patient has been living with CPP for many years, and she has sleep difficulties that might be exacerbating pain or result from pain (or both). She is already on continuous OCPs and has had some relief with pelvic PT. Other options that may help with her multiple issues include antidepressants, cyclobenzaprine, and calcium channel blockers.
Antidepressants
Several classes of antidepressants have been used in the treatment of chronic pain conditions, specifically, tricyclic antidepressants (TCAs) and serotonin-norepinephrine reuptake inhibitors (SNRIs). Commonly used TCAs include amitriptyline, nortriptyline, desipramine, and doxepin. Commonly used SNRIs are duloxetine and milnacipran. Both TCAs and SNRIs increase the availability of norepinephrine and serotonin, which are thought to act on the descending pain inhibitory systems to decrease pain sensitivity. Of note, most selective serotonin reuptake inhibitors (SSRIs) at typical doses do not exert a significant enough impact on norepinephrine to be useful for chronic pain.22
Evidence is limited on the use of antidepressants for treating CPP. Amitriptyline is the most extensively studied antidepressant. Amitriptyline treatment resulted in modest pain improvement in patients with CPP and fibromyalgia.23,24 Bothersome anticholinergic effects, including fatigue, dry mouth, and constipation, often are reported with TCAs. Adverse effects tend to be less with nortriptyline or desipramine compared with amitriptyline, but possibly at the expense of efficacy.
While SNRIs have not yet been studied in CPP, several investigations have shown that they improve pain and quality of life in fibromyalgia patients.22,25
Antidepressant therapy may be appropriate for patients with suspected central pain amplification, widespread pain, and sleep disturbances. Best practices include patient education and careful discussion of this option with your patient. We suggest that clinicians explain that antidepressant medications alter the function of neurotransmitters, which modulate pain signals. While neurotransmitters also are involved in mood modulation, this is not the therapeutic goal in this circumstance. In addition, the doses used for the effective treatment of chronic pain are significantly lower than those needed to treat depression effectively.
Patients often need to hear that you believe that their pain is real and is not a manifestation of depression or another mood disorder. If you suspect that the patient also has untreated depression, address this as its own issue and use medications that have greater efficacy for mood symptoms.
Because many antidepressants can cause sedation, they are best taken before bedtime. Also, slow dose titration over several weeks will reduce the chance of bothersome adverse effects. Counsel patients that efficacy is not generally seen until at goal dose for several weeks. Be aware of interactions with other medications that can cause serotonin syndrome.
Cyclobenzaprine
Cyclobenzaprine is a muscle relaxant that also has activity in the central nervous system. The drug’s precise mechanism of action is not known, but it appears to potentiate norepinephrine and bind to serotonin receptors. Thus, it also likely has some TCA-like activity.
Cyclobenzaprine has not been studied in patients with CPP. In fibromyalgia patients, however, it produced significant improvements in pain, sleep, fatigue, and tenderness.26,27 In our anecdotal experience with CPP patients, cyclobenzaprine has been one of the most impactful therapies. It hits the “chronic pain triad,” meaning that it helps with myofascial pain, neuropathic pain, and sleep disturbances.
Cyclobenzaprine treatment may be considered for patients with myofascial pain, sleep disturbances, and clinical symptoms of central pain amplification. Best practices include starting with low (5 mg) scheduled doses at bedtime and slowly titrating the dose. Drowsiness is a very common side effect, so we try to use that to the patient’s advantage to help with sleep quality.
Notably, sleep disturbances are highly prevalent in patients with chronic pain.28 The relationship appears to be bidirectional, meaning that chronic pain negatively impacts sleep quality, and poor sleep quality causes amplified perception of pain.28–30 Interventions that improve sleep quality have been associated with improvements in pain, coping, mood, and functional status.31 Helping a patient to improve her sleep generally requires a multifaceted approach. It always involves “sleep hygiene” or a behavioral component, and pharmacologic assistance may be considered when improved sleep hygiene does not provide adequately improved sleep quality.
Calcium channel blockers
Gabapentin and pregabalin are calcium channel blockers that inhibit the reuptake of glutamate, norepinephrine, and substance P, which helps to decrease pain sensitivity. They also act as membrane stabilizers, reducing hyperexcitability of peripheral and central nerves. Studies have shown that in patients with CPP, gabapentin resulted in improved pain and mood symptoms with few adverse effects.23,32 Patients with fibromyalgia had improvements in pain, sleep, quality of life, fatigue, and anxiety with both gabapentin and pregabalin.33
It is appropriate to consider use of gabapentin or pregabalin in patients with central pain amplification and sleep disturbances. Best practices include starting with a low dose at bedtime. Traditionally, gabapentin is given in 3 equal doses throughout the day. In our experience, patients report less daytime drowsiness and better sleep quality if two-thirds of the daily dose is given at night, with the remaining daily dose broken up into 2 smaller daytime doses. Slow titration over several weeks will reduce risk of bothersome adverse effects. Patients should be counseled that efficacy is not generally seen until treatment is at goal dose for several weeks.
CASE 2 Treatment recommendations
For this patient with daily pelvic pain, multiple diagnoses that have a pain component, and poor sleep quality, consider a treatment plan that includes scheduled cyclobenzaprine, improved sleep hygiene, and, if needed, gabapentin.
Read about treating a case of focal pain.
CASE 3 Cesarean delivery, hysterectomy, and continued pelvic pain
A 38-year-old woman (G2P2) has had CPP for the past 10 years. She developed persistent left lower-quadrant pain after cesarean delivery of her son. She had a hysterectomy 2 years ago for CPP, after which her pain worsened. She describes daily pain with intermittent flares. On examination, the patient has focal left lower-quadrant pain lateral to the left apex of her Pfannenstiel incision.
What treatment approach would be appropriate for this patient?
Focal pain requires a precisely targeted treatment
This patient with focal left lower-quadrant pain is a candidate for anesthetic trigger point injections in the affected area near her Pfannenstiel incision.
Anesthetic injections
Consider the presence of trigger points and peripheral neuropathy in patients with focal abdominal wall pain. Trigger points are focal, palpable nodules within muscles. They are markedly painful to palpation and are associated with referred pain, motor dysfunction, and occasionally autonomic symptoms. They frequently are seen in abdominal wall or pelvic floor muscles in patients with CPP and are caused by abnormal neuromuscular depolarization.
The ilioinguinal, iliohypogastric, and genitofemoral nerves are in close proximity to Pfannenstiel and laparoscopic port site incisions. These nerves may be injured directly during surgery, but they also may be compressed by postoperative scarring.
Anesthetics, such as lidocaine and bupivacaine, which act as sodium channel blockers, can be injected into this area, and improvement often substantially outlasts the anesthetic’s duration of action. While these drugs’ mechanism of action is not clear, theories include altered function of sodium channels on sensory nerves with repeated anesthetic exposure, dry needling that occurs during injection, hydrodissection of tight connective tissue bands surrounding neuromuscular bundles, or depletion of substance P and neuropeptides as a result of injection.34,35
In several studies, patients with CPP reported decreased pain with lidocaine injections in pelvic floor or abdominal wall trigger points.36–38 Patients with fibromyalgia reported improvement in pain and a decreased need for NSAIDs with bupivacaine trigger point injections.39 While abdominal wall nerve blocks have not been extensively studied in patients with chronic neuropathic pain following gynecologic surgery, they have been shown to substantially improve chronic neuropathic pain following inguinal hernia repair.40
Anesthetic injections appropriately may be considered in patients with focal pain in a muscle or in the distribution of abdominal wall nerves, palpation of which reproduces pain symptoms. Patients with diffuse pain are less likely to benefit from anesthetic injections. Best practices include careful examination with attention to areas of prior abdominal incisions.
Our practice is to inject each affected area with a mix of 9 mL of 1% lidocaine and 1 mL of sodium bicarbonate. If a patient reports at least 24 hours of improvement, we repeat the injection in 2 to 4 weeks. The goal is for the patient to experience a progressively longer duration of benefit with subsequent injections. We perform repeat injections shortly after pain begins to recur at that site. The patient should eventually graduate from receiving regular injections and may return for a remedial injection if pain recurs.
CASE 3 Treatment recommendations
For this patient with persistent focal left-lower quadrant pain and a defined trigger point near her Pfannenstiel incision, consider anesthetic injection in the left lower quadrant.
Work toward realistic symptom improvement
Remember that living with chronic pain is exhausting, and empathy with a patient-centered approach is the most important ingredient for patient improvement and satisfaction. Discuss realistic expectations with patients. Remind them that there is no magic bullet for the complex problem of CPP, and that chronic conditions generally do not improve overnight. Focus on improving the patient’s function and quality of life, and applaud symptom improvement rather than focusing on complete pain resolution.
As these visits often require a good deal of patient education, budget more appointment time if feasible. We find that scheduling frequent return visits (approximately every 3 to 4 months) allows timely treatment follow-up so that changes may be made if needed. If you have maximized your available treatment options, referring the patient to a specialist with additional training in CPP is a sensible next step.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Howard FM. Chronic pelvic pain. Obstet Gynecol. 2003;101(3):594–611.
- Mathias SD, Kuppermann M, Liberman RF, Lipschutz RC, Steege JF. Chronic pelvic pain: prevalence, health-related uality of life, and economic correlates. Obstet Gynecol. 1996;87(3):321–327.
- Gelbaya TA, El-Halwagy HE. Focus on primary care: chronic pelvic pain in women. Obstet Gynecol Surv. 2001;56(12):757–764.
- Broder MS, Kanouse DE, Mittman BS, Bernstein SJ. The appropriateness of recommendations for hysterectomy. Obstet Gynecol. 2000;95(2):199–205.
- Whiteman MK, Hillis SD, Jamieson DJ, et al. Inpatient hysterectomy surveillance in the United States, 2000–2004. Am J Obstet Gynecol. 2008;198(1):34.e1–34.e7.
- Steege JF, Siedhoff MT. Chronic pelvic pain. Obstet Gynecol. 2014;124(3):616–629.
- Williams DA, Clauw DJ. Understanding fibromyalgia: lessons from the broader pain research community. J Pain. 2009;10(8):777–791.
- Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011;152(3 suppl):S2–S15.
- Brawn J, Morotti M, Zondervan KT, Becker CM, Vincent K. Central changes associated with chronic pelvic pain and endometriosis. Hum Reprod Update. 2014;20(5):737–747.
- As-Sanie S, Harris RE, Harte SE, Tu FF, Neshewat G, Clauw DJ. Increased pressure pain sensitivity in women with chronic pelvic pain. Obstet Gynecol. 2013;122(5):1047–1055.
- As-Sanie S, Kim J, Schmidt-Wilcke T, et al. Functional connectivity is associated with altered brain chemistry in women with endometriosis-associated chronic pelvic pain. J Pain. 2016;17(1):1–13.
- As-Sanie S, Harris RE, Napadow V, et al. Changes in regional gray matter volume in women with chronic pelvic pain: a voxel-based morphometry study. Pain. 2012;153(5):1006–1014.
- Marjoribanks J, Ayeleke RO, Farquhar C, Proctor M. Nonsteroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database Syst Rev. 2015;(7):CD001751.
- Falcone T, Lebovic DI. Clinical management of endometriosis. Obstet Gynecol. 2011;118(3):691–705.
- Brown J, Pan A, Hart RJ. Gonadotrophin-releasing hormone analogues for pain associated with endometriosis. Cochrane Database Syst Rev. 2010;(12):CD008475.
- Zoorob D, South M, Karram M, et al. A pilot randomized trial of levator injections versus physical therapy for treatment of pelvic floor myalgia and sexual pain. Int Urogynecol J. 2015;26(6):845–852.
- Scott KM, Fisher LW, Bernstein IH, Bradley MH. The treatment of chronic coccydynia and postcoccygectomy pain with pelvic floor physical therapy. PM R. 2017;9(4):367–376.
- Goldfinger C, Pukall CF, Thibault-Gagnon S, McLean L, Chamberlain S. Effectiveness of cognitive-behavioral therapy and physical therapy for provoked vestibulodynia: a randomized pilot study. J Sex Med. 2016;13(1):88–94.
- Anderson RU, Harvey RH, Wise D, Nevin Smith J, Nathanson BH, Sawyer T. Chronic pelvic pain syndrome: reduction of medication use after pelvic floor physical therapy with an internal myofascial trigger point wand. Appl Psychophysiol Biofeedback. 2015;40(1):45–52.
- FitzGerald MP, Payne CK, Lukacz ES, et al. Randomized multicenter clinical trial of myofascial physical therapy in women with interstitial cystitis/painful bladder syndrome and pelvic floor tenderness. J Urol. 2012;187(6):2113–2118.
- FitzGerald MP, Kotarinos R. Rehabilitation of the short pelvic floor. II: Treatment of the patient with the short pelvic floor. Int Urogynecol J Pelvic Floor Dysfunct. 2003;14(4):269–275.
- Arnold LM. Duloxetine and other antidepressants in the treatment of patients with fibromyalgia. Pain Med. 2007;8(suppl 2):S63–S74.
- Sator-Katzenschlager SM, Scharbert G, Kress HG, et al. Chronic pelvic pain treated with gabapentin and amitriptyline: a randomized controlled pilot study. Wien Klin Wochenschr. 2005;117(21–22):761–78.
- Moore RA, Derry S, Aldington D, Cole P, Wiffen PJ. Amitriptyline for neuropathic pain and fibromyalgia in adults. Cochrane Database Syst Rev. 2012;12:CD008242.
- Gendreau RM, Thorn MD, Gendreau JF, et al. Efficacy of milnacipran in patients with fibromyalgia. J Rheumatol. 2005;32(10):1975–1985.
- Tofferi JK, Jackson JL, O’Malley PG. Treatment of fibromyalgia with cyclobenzaprine: a meta-analysis. Arthritis Rheum. 2004;51(1):9–13.
- Moldofsky H, Harris HW, Archambault WT, Kwong T, Lederman S. Effects of bedtime very low dose cyclobenzaprine on symptoms and sleep physiology in patients with fibromyalgia syndrome: a double-blind randomized placebo-controlled study. J Rheumatol. 2011;38(12):2653–2463.
- Cheatle MD, Foster S, Pinkett A, Lesneski M, Qu D, Dhingra L. Assessing and managing sleep disturbance in patients with chronic pain. Sleep Med Clin. 2016;11(4):531–541.
- Larson RA, Carter JR. Total sleep deprivation and pain perception during cold noxious stimuli in humans. Scand J Pain. 2016;13:12–16.
- Generaal E, Vogelzangs N, Penninx BW, Dekker J. Insomnia, sleep duration, depressive symptoms, and the onset of chronic multisite musculoskeletal pain [published online ahead of print January 1, 2017]. Sleep. doi:10.1093/sleep/zsw030.
- Gerhart JI, Burns JW, Post KM, et al. Relationships between sleep quality and pain-related factors for people with chronic low back pain: tests of reciprocal and time of day effects. Ann Behav Med. 2017;51(3):365–375.
- Lewis SC, Bhattacharya S, Wu O, et al. Gabapentin for the management of chronic pelvic pain in women (GaPP1): a pilot randomised controlled trial. PLoS One. 2016;11(4):e0153037.
- Häuser W, Bernardy K, Uçeyler N, Sommer C. Treatment of fibromyalgia syndrome with gabapentin and pregabalin—a meta-analysis of randomized controlled trials. Pain. 2009;145(1–2):69–81.
- Scott NA, Guo B, Barton PM, Gerwin RD. Trigger point injections for chronic non-malignant musculoskeletal pain: a systematic review. Pain Med. 2009;10(1):54–69.
- Hameroff SR, Crago BR, Blitt CD, Womble J, Kanel J. Comparison of bupivacaine, etidocaine, and saline for trigger-point therapy. Anesth Analg. 1981;60(10):752–755.
- Montenegro ML, Braz CA, Rosa-e-Silva JC, Candido-dos-Reis FJ, Nogueira AA, Poli-Neto OB. Anaesthetic injection versus ischemic compression for the pain relief of abdominal wall trigger points in women with chronic pelvic pain. BMC Anesthesiol. 2015;15:175.
- Kim DS, Jeong TY, Kim YK, Chang WH, Yoon JG, Lee SC. Usefulness of a myofascial trigger point injection for groin pain in patients with chronic prostatitis/chronic pelvic pain syndrome: a pilot study. Arch Phys Med Rehabil. 2013;94(5):930–936.
- Huang QM, Liu L. Wet needling of myofascial trigger points in abdominal muscles for treatment of primary dysmenorrhoea. Acupunct Med. 2014;32(4):346–349.
- Affaitati G, Fabrizio A, Savini A, et al. A randomized, controlled study comparing a lidocaine patch, a placebo patch, and anesthetic injection for treatment of trigger points in patients with myofascial pain syndrome: evaluation of pain and somatic pain thresholds. Clin Ther. 2009;31(4):705–720.
- Thomassen I, van Suijlekom JA, van de Gaag A, Ponten JE, Nienhuijs SW. Ultrasound-guided ilioinguinal/iliohypogastric nerve blocks for chronic pain after inguinal hernia repair. Hernia. 2013;17(3):329–332.
- Howard FM. Chronic pelvic pain. Obstet Gynecol. 2003;101(3):594–611.
- Mathias SD, Kuppermann M, Liberman RF, Lipschutz RC, Steege JF. Chronic pelvic pain: prevalence, health-related uality of life, and economic correlates. Obstet Gynecol. 1996;87(3):321–327.
- Gelbaya TA, El-Halwagy HE. Focus on primary care: chronic pelvic pain in women. Obstet Gynecol Surv. 2001;56(12):757–764.
- Broder MS, Kanouse DE, Mittman BS, Bernstein SJ. The appropriateness of recommendations for hysterectomy. Obstet Gynecol. 2000;95(2):199–205.
- Whiteman MK, Hillis SD, Jamieson DJ, et al. Inpatient hysterectomy surveillance in the United States, 2000–2004. Am J Obstet Gynecol. 2008;198(1):34.e1–34.e7.
- Steege JF, Siedhoff MT. Chronic pelvic pain. Obstet Gynecol. 2014;124(3):616–629.
- Williams DA, Clauw DJ. Understanding fibromyalgia: lessons from the broader pain research community. J Pain. 2009;10(8):777–791.
- Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011;152(3 suppl):S2–S15.
- Brawn J, Morotti M, Zondervan KT, Becker CM, Vincent K. Central changes associated with chronic pelvic pain and endometriosis. Hum Reprod Update. 2014;20(5):737–747.
- As-Sanie S, Harris RE, Harte SE, Tu FF, Neshewat G, Clauw DJ. Increased pressure pain sensitivity in women with chronic pelvic pain. Obstet Gynecol. 2013;122(5):1047–1055.
- As-Sanie S, Kim J, Schmidt-Wilcke T, et al. Functional connectivity is associated with altered brain chemistry in women with endometriosis-associated chronic pelvic pain. J Pain. 2016;17(1):1–13.
- As-Sanie S, Harris RE, Napadow V, et al. Changes in regional gray matter volume in women with chronic pelvic pain: a voxel-based morphometry study. Pain. 2012;153(5):1006–1014.
- Marjoribanks J, Ayeleke RO, Farquhar C, Proctor M. Nonsteroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database Syst Rev. 2015;(7):CD001751.
- Falcone T, Lebovic DI. Clinical management of endometriosis. Obstet Gynecol. 2011;118(3):691–705.
- Brown J, Pan A, Hart RJ. Gonadotrophin-releasing hormone analogues for pain associated with endometriosis. Cochrane Database Syst Rev. 2010;(12):CD008475.
- Zoorob D, South M, Karram M, et al. A pilot randomized trial of levator injections versus physical therapy for treatment of pelvic floor myalgia and sexual pain. Int Urogynecol J. 2015;26(6):845–852.
- Scott KM, Fisher LW, Bernstein IH, Bradley MH. The treatment of chronic coccydynia and postcoccygectomy pain with pelvic floor physical therapy. PM R. 2017;9(4):367–376.
- Goldfinger C, Pukall CF, Thibault-Gagnon S, McLean L, Chamberlain S. Effectiveness of cognitive-behavioral therapy and physical therapy for provoked vestibulodynia: a randomized pilot study. J Sex Med. 2016;13(1):88–94.
- Anderson RU, Harvey RH, Wise D, Nevin Smith J, Nathanson BH, Sawyer T. Chronic pelvic pain syndrome: reduction of medication use after pelvic floor physical therapy with an internal myofascial trigger point wand. Appl Psychophysiol Biofeedback. 2015;40(1):45–52.
- FitzGerald MP, Payne CK, Lukacz ES, et al. Randomized multicenter clinical trial of myofascial physical therapy in women with interstitial cystitis/painful bladder syndrome and pelvic floor tenderness. J Urol. 2012;187(6):2113–2118.
- FitzGerald MP, Kotarinos R. Rehabilitation of the short pelvic floor. II: Treatment of the patient with the short pelvic floor. Int Urogynecol J Pelvic Floor Dysfunct. 2003;14(4):269–275.
- Arnold LM. Duloxetine and other antidepressants in the treatment of patients with fibromyalgia. Pain Med. 2007;8(suppl 2):S63–S74.
- Sator-Katzenschlager SM, Scharbert G, Kress HG, et al. Chronic pelvic pain treated with gabapentin and amitriptyline: a randomized controlled pilot study. Wien Klin Wochenschr. 2005;117(21–22):761–78.
- Moore RA, Derry S, Aldington D, Cole P, Wiffen PJ. Amitriptyline for neuropathic pain and fibromyalgia in adults. Cochrane Database Syst Rev. 2012;12:CD008242.
- Gendreau RM, Thorn MD, Gendreau JF, et al. Efficacy of milnacipran in patients with fibromyalgia. J Rheumatol. 2005;32(10):1975–1985.
- Tofferi JK, Jackson JL, O’Malley PG. Treatment of fibromyalgia with cyclobenzaprine: a meta-analysis. Arthritis Rheum. 2004;51(1):9–13.
- Moldofsky H, Harris HW, Archambault WT, Kwong T, Lederman S. Effects of bedtime very low dose cyclobenzaprine on symptoms and sleep physiology in patients with fibromyalgia syndrome: a double-blind randomized placebo-controlled study. J Rheumatol. 2011;38(12):2653–2463.
- Cheatle MD, Foster S, Pinkett A, Lesneski M, Qu D, Dhingra L. Assessing and managing sleep disturbance in patients with chronic pain. Sleep Med Clin. 2016;11(4):531–541.
- Larson RA, Carter JR. Total sleep deprivation and pain perception during cold noxious stimuli in humans. Scand J Pain. 2016;13:12–16.
- Generaal E, Vogelzangs N, Penninx BW, Dekker J. Insomnia, sleep duration, depressive symptoms, and the onset of chronic multisite musculoskeletal pain [published online ahead of print January 1, 2017]. Sleep. doi:10.1093/sleep/zsw030.
- Gerhart JI, Burns JW, Post KM, et al. Relationships between sleep quality and pain-related factors for people with chronic low back pain: tests of reciprocal and time of day effects. Ann Behav Med. 2017;51(3):365–375.
- Lewis SC, Bhattacharya S, Wu O, et al. Gabapentin for the management of chronic pelvic pain in women (GaPP1): a pilot randomised controlled trial. PLoS One. 2016;11(4):e0153037.
- Häuser W, Bernardy K, Uçeyler N, Sommer C. Treatment of fibromyalgia syndrome with gabapentin and pregabalin—a meta-analysis of randomized controlled trials. Pain. 2009;145(1–2):69–81.
- Scott NA, Guo B, Barton PM, Gerwin RD. Trigger point injections for chronic non-malignant musculoskeletal pain: a systematic review. Pain Med. 2009;10(1):54–69.
- Hameroff SR, Crago BR, Blitt CD, Womble J, Kanel J. Comparison of bupivacaine, etidocaine, and saline for trigger-point therapy. Anesth Analg. 1981;60(10):752–755.
- Montenegro ML, Braz CA, Rosa-e-Silva JC, Candido-dos-Reis FJ, Nogueira AA, Poli-Neto OB. Anaesthetic injection versus ischemic compression for the pain relief of abdominal wall trigger points in women with chronic pelvic pain. BMC Anesthesiol. 2015;15:175.
- Kim DS, Jeong TY, Kim YK, Chang WH, Yoon JG, Lee SC. Usefulness of a myofascial trigger point injection for groin pain in patients with chronic prostatitis/chronic pelvic pain syndrome: a pilot study. Arch Phys Med Rehabil. 2013;94(5):930–936.
- Huang QM, Liu L. Wet needling of myofascial trigger points in abdominal muscles for treatment of primary dysmenorrhoea. Acupunct Med. 2014;32(4):346–349.
- Affaitati G, Fabrizio A, Savini A, et al. A randomized, controlled study comparing a lidocaine patch, a placebo patch, and anesthetic injection for treatment of trigger points in patients with myofascial pain syndrome: evaluation of pain and somatic pain thresholds. Clin Ther. 2009;31(4):705–720.
- Thomassen I, van Suijlekom JA, van de Gaag A, Ponten JE, Nienhuijs SW. Ultrasound-guided ilioinguinal/iliohypogastric nerve blocks for chronic pain after inguinal hernia repair. Hernia. 2013;17(3):329–332.

Introduction
More than 13 million people in the United States have been diagnosed with chronic obstructive pulmonary disease (COPD),1 a complex, heterogeneous respiratory condition characterized by persistent, and usually progressive, airflow limitation.2,3 The prevalence of COPD is rising: It has been declared the third leading cause of death in the United States,4 and the World Health Organization has predicted that it will become the third leading cause of death worldwide by 2030.5 This increase is driven by an aging population, and tobacco smoking, which is the primary risk factor for COPD in high-income countries.6
Symptoms of COPD, as well as the severity of these symptoms, can vary, but patients typically present with dyspnea, chronic cough, and sputum production.2 These symptoms are often underreported by patients with COPD,2 but have a significant impact on patients’ day-to-day lives, adversely affecting their quality of life and their ability to engage in physical activity, further contributing to disease progression.7,8
Comorbidities are common in patients with COPD, and can pose significant challenges to the diagnosis and management of the condition. Some of these comorbidities, such as lung cancer and ischemic heart disease, share a common etiologic pathway with COPD—smoking; while others, such as anxiety and depression, appear to be unrelated to COPD pathogenesis, although they may share a systemic inflammatory basis, and are highly prevalent in patients with COPD.9
Primary care physicians are the key point of contact for most patients with COPD,10 and play a critical role in diagnosis, drug and device selection, and long-term disease management of COPD and associated comorbidities. A number of pharmacologic and nonpharmacologic treatment options are available to manage COPD symptoms, which can confer considerable benefits to patients. Selection of pharmacologic treatment should be based on an individual patient’s symptom burden and their exacerbation history, and it is important that physicians are aware of when therapy should be escalated, and indeed stopped if no longer required.2
Proper device selection is an important part of choosing treatments for patients with COPD. A variety of inhaler devices are available for COPD medications, and it is important that devices are matched to patients’ needs and preferences based on device characteristics and individual patient capabilities.
The aim of this supplement is to provide readers with an introduction to 4 key topics critical to the effective management of COPD in primary care, highlighting best practices to optimize patient care and outcomes. In the first article, Dr. Marchetti and Dr. Kaplan review physical activity in COPD, discussing its inter-relationship with dyspnea and hyperinflation, and its importance in modifying disease progression.
The second article examines anxiety and depression in COPD. Prof. Yohannes, Dr. Kaplan, and Dr. Hanania review the prevalence, mechanisms, and impact of the 2 often overlooked and undertreated psychologic comorbidities in patients with COPD. The authors provide guidance on how anxiety and depression can be detected and managed in patients with COPD in a primary care setting.
The third article is authored by Dr. Dhand, Dr. Cavanaugh, and Dr. Skolnik, and reviews the device options available for COPD pharmacologic therapy. It summarizes the key features of each respective inhaler device, discusses considerations for patient-device matching, and emphasizes the importance of training in correct device use.
Finally, Dr. Victor Kim and I assess different COPD treatment options in the supplement’s fourth article. We review the latest updates in recommendations from both the Global Initiative for Chronic Obstructive Lung Disease (GOLD) and the COPD Foundation, discuss the importance of personalized treatment goals for patients, and review how to address current unmet needs in patient management.
- Ford ES, Croft JB, Mannino DM, Wheaton AG, Zhang X, Giles WH. COPD surveillance—United States, 1999-2011. Chest. 2013;144(1):284-305.
- Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report. GOLD Executive Summary. Am J Respir Crit Care Med. 2017;195(5):557-582.
- Barrecheguren M, Miravitlles M. COPD heterogeneity: implications for management. Multidiscip Respir Med. 2016;11:14.
- National Center for Health Statistics (US). Health, United States, 2015: With Special Feature on Racial and Ethnic Health Disparities. Hyattsville, MD; National Center for Health Statistics: 2016.
- World Health Organization. World Health Statistics 2008. http://www.who.int/whosis/whostat/EN_WHS08_Full.pdf?ua=1. Accessed August 2017.
- Waatevik M, Skorge TD, Omenaas E, Bakke PS, Gulsvik A, Johannessen A. Increased prevalence of chronic obstructive pulmonary disease in a general population. Respir Med. 2013;107(7):1037-1045.
- O’Donnell DE, Gebke KB. Activity restriction in mild COPD: a challenging clinical problem. Int J Chron Obstruct Pulmon Dis. 2014;9:577-588.
- Miravitlles M, Ribera A. Understanding the impact of symptoms on the burden of COPD. Respir Res. 2017;18(1):67.
- Hillas G, Perlikos F, Tsiligianni I, Tzanakis N. Managing comorbidities in COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:95-109.
- Foster JA, Yawn BP, Maziar A, Jenkins T, Rennard SI, Casebeer L. Enhancing COPD management in primary care settings. MedGenMed. 2007;9(3):24.
More than 13 million people in the United States have been diagnosed with chronic obstructive pulmonary disease (COPD),1 a complex, heterogeneous respiratory condition characterized by persistent, and usually progressive, airflow limitation.2,3 The prevalence of COPD is rising: It has been declared the third leading cause of death in the United States,4 and the World Health Organization has predicted that it will become the third leading cause of death worldwide by 2030.5 This increase is driven by an aging population, and tobacco smoking, which is the primary risk factor for COPD in high-income countries.6
Symptoms of COPD, as well as the severity of these symptoms, can vary, but patients typically present with dyspnea, chronic cough, and sputum production.2 These symptoms are often underreported by patients with COPD,2 but have a significant impact on patients’ day-to-day lives, adversely affecting their quality of life and their ability to engage in physical activity, further contributing to disease progression.7,8
Comorbidities are common in patients with COPD, and can pose significant challenges to the diagnosis and management of the condition. Some of these comorbidities, such as lung cancer and ischemic heart disease, share a common etiologic pathway with COPD—smoking; while others, such as anxiety and depression, appear to be unrelated to COPD pathogenesis, although they may share a systemic inflammatory basis, and are highly prevalent in patients with COPD.9
Primary care physicians are the key point of contact for most patients with COPD,10 and play a critical role in diagnosis, drug and device selection, and long-term disease management of COPD and associated comorbidities. A number of pharmacologic and nonpharmacologic treatment options are available to manage COPD symptoms, which can confer considerable benefits to patients. Selection of pharmacologic treatment should be based on an individual patient’s symptom burden and their exacerbation history, and it is important that physicians are aware of when therapy should be escalated, and indeed stopped if no longer required.2
Proper device selection is an important part of choosing treatments for patients with COPD. A variety of inhaler devices are available for COPD medications, and it is important that devices are matched to patients’ needs and preferences based on device characteristics and individual patient capabilities.
The aim of this supplement is to provide readers with an introduction to 4 key topics critical to the effective management of COPD in primary care, highlighting best practices to optimize patient care and outcomes. In the first article, Dr. Marchetti and Dr. Kaplan review physical activity in COPD, discussing its inter-relationship with dyspnea and hyperinflation, and its importance in modifying disease progression.
The second article examines anxiety and depression in COPD. Prof. Yohannes, Dr. Kaplan, and Dr. Hanania review the prevalence, mechanisms, and impact of the 2 often overlooked and undertreated psychologic comorbidities in patients with COPD. The authors provide guidance on how anxiety and depression can be detected and managed in patients with COPD in a primary care setting.
The third article is authored by Dr. Dhand, Dr. Cavanaugh, and Dr. Skolnik, and reviews the device options available for COPD pharmacologic therapy. It summarizes the key features of each respective inhaler device, discusses considerations for patient-device matching, and emphasizes the importance of training in correct device use.
Finally, Dr. Victor Kim and I assess different COPD treatment options in the supplement’s fourth article. We review the latest updates in recommendations from both the Global Initiative for Chronic Obstructive Lung Disease (GOLD) and the COPD Foundation, discuss the importance of personalized treatment goals for patients, and review how to address current unmet needs in patient management.
More than 13 million people in the United States have been diagnosed with chronic obstructive pulmonary disease (COPD),1 a complex, heterogeneous respiratory condition characterized by persistent, and usually progressive, airflow limitation.2,3 The prevalence of COPD is rising: It has been declared the third leading cause of death in the United States,4 and the World Health Organization has predicted that it will become the third leading cause of death worldwide by 2030.5 This increase is driven by an aging population, and tobacco smoking, which is the primary risk factor for COPD in high-income countries.6
Symptoms of COPD, as well as the severity of these symptoms, can vary, but patients typically present with dyspnea, chronic cough, and sputum production.2 These symptoms are often underreported by patients with COPD,2 but have a significant impact on patients’ day-to-day lives, adversely affecting their quality of life and their ability to engage in physical activity, further contributing to disease progression.7,8
Comorbidities are common in patients with COPD, and can pose significant challenges to the diagnosis and management of the condition. Some of these comorbidities, such as lung cancer and ischemic heart disease, share a common etiologic pathway with COPD—smoking; while others, such as anxiety and depression, appear to be unrelated to COPD pathogenesis, although they may share a systemic inflammatory basis, and are highly prevalent in patients with COPD.9
Primary care physicians are the key point of contact for most patients with COPD,10 and play a critical role in diagnosis, drug and device selection, and long-term disease management of COPD and associated comorbidities. A number of pharmacologic and nonpharmacologic treatment options are available to manage COPD symptoms, which can confer considerable benefits to patients. Selection of pharmacologic treatment should be based on an individual patient’s symptom burden and their exacerbation history, and it is important that physicians are aware of when therapy should be escalated, and indeed stopped if no longer required.2
Proper device selection is an important part of choosing treatments for patients with COPD. A variety of inhaler devices are available for COPD medications, and it is important that devices are matched to patients’ needs and preferences based on device characteristics and individual patient capabilities.
The aim of this supplement is to provide readers with an introduction to 4 key topics critical to the effective management of COPD in primary care, highlighting best practices to optimize patient care and outcomes. In the first article, Dr. Marchetti and Dr. Kaplan review physical activity in COPD, discussing its inter-relationship with dyspnea and hyperinflation, and its importance in modifying disease progression.
The second article examines anxiety and depression in COPD. Prof. Yohannes, Dr. Kaplan, and Dr. Hanania review the prevalence, mechanisms, and impact of the 2 often overlooked and undertreated psychologic comorbidities in patients with COPD. The authors provide guidance on how anxiety and depression can be detected and managed in patients with COPD in a primary care setting.
The third article is authored by Dr. Dhand, Dr. Cavanaugh, and Dr. Skolnik, and reviews the device options available for COPD pharmacologic therapy. It summarizes the key features of each respective inhaler device, discusses considerations for patient-device matching, and emphasizes the importance of training in correct device use.
Finally, Dr. Victor Kim and I assess different COPD treatment options in the supplement’s fourth article. We review the latest updates in recommendations from both the Global Initiative for Chronic Obstructive Lung Disease (GOLD) and the COPD Foundation, discuss the importance of personalized treatment goals for patients, and review how to address current unmet needs in patient management.
- Ford ES, Croft JB, Mannino DM, Wheaton AG, Zhang X, Giles WH. COPD surveillance—United States, 1999-2011. Chest. 2013;144(1):284-305.
- Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report. GOLD Executive Summary. Am J Respir Crit Care Med. 2017;195(5):557-582.
- Barrecheguren M, Miravitlles M. COPD heterogeneity: implications for management. Multidiscip Respir Med. 2016;11:14.
- National Center for Health Statistics (US). Health, United States, 2015: With Special Feature on Racial and Ethnic Health Disparities. Hyattsville, MD; National Center for Health Statistics: 2016.
- World Health Organization. World Health Statistics 2008. http://www.who.int/whosis/whostat/EN_WHS08_Full.pdf?ua=1. Accessed August 2017.
- Waatevik M, Skorge TD, Omenaas E, Bakke PS, Gulsvik A, Johannessen A. Increased prevalence of chronic obstructive pulmonary disease in a general population. Respir Med. 2013;107(7):1037-1045.
- O’Donnell DE, Gebke KB. Activity restriction in mild COPD: a challenging clinical problem. Int J Chron Obstruct Pulmon Dis. 2014;9:577-588.
- Miravitlles M, Ribera A. Understanding the impact of symptoms on the burden of COPD. Respir Res. 2017;18(1):67.
- Hillas G, Perlikos F, Tsiligianni I, Tzanakis N. Managing comorbidities in COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:95-109.
- Foster JA, Yawn BP, Maziar A, Jenkins T, Rennard SI, Casebeer L. Enhancing COPD management in primary care settings. MedGenMed. 2007;9(3):24.
- Ford ES, Croft JB, Mannino DM, Wheaton AG, Zhang X, Giles WH. COPD surveillance—United States, 1999-2011. Chest. 2013;144(1):284-305.
- Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report. GOLD Executive Summary. Am J Respir Crit Care Med. 2017;195(5):557-582.
- Barrecheguren M, Miravitlles M. COPD heterogeneity: implications for management. Multidiscip Respir Med. 2016;11:14.
- National Center for Health Statistics (US). Health, United States, 2015: With Special Feature on Racial and Ethnic Health Disparities. Hyattsville, MD; National Center for Health Statistics: 2016.
- World Health Organization. World Health Statistics 2008. http://www.who.int/whosis/whostat/EN_WHS08_Full.pdf?ua=1. Accessed August 2017.
- Waatevik M, Skorge TD, Omenaas E, Bakke PS, Gulsvik A, Johannessen A. Increased prevalence of chronic obstructive pulmonary disease in a general population. Respir Med. 2013;107(7):1037-1045.
- O’Donnell DE, Gebke KB. Activity restriction in mild COPD: a challenging clinical problem. Int J Chron Obstruct Pulmon Dis. 2014;9:577-588.
- Miravitlles M, Ribera A. Understanding the impact of symptoms on the burden of COPD. Respir Res. 2017;18(1):67.
- Hillas G, Perlikos F, Tsiligianni I, Tzanakis N. Managing comorbidities in COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:95-109.
- Foster JA, Yawn BP, Maziar A, Jenkins T, Rennard SI, Casebeer L. Enhancing COPD management in primary care settings. MedGenMed. 2007;9(3):24.
Dyspnea and Hyperinflation in Chronic Obstructive Pulmonary Disease: Impact on Physical Activity
Introduction
Dyspnea, the sensation of difficult or labored breathing, is the most common symptom in chronic obstructive pulmonary disease (COPD) and the primary symptom that limits physical activity in more advanced disease.1 According to the American Thoracic Society, dyspnea may be measured according to 3 domains2:
- what breathing feels like for the patient
- how distressed the patient feels when breathing
- how dyspnea affects functional ability, employment, health-related quality of life, or health status.

As disease severity increases, breathlessness becomes more disabling at lower activity levels. These changes further impact the quality of life of patients, and can lead to anxiety and depression.11
Physical inactivity is often considered to be a major contributor to the progression of COPD,6 and is linked to hospitalizations and increased all-cause mortality.12 There is therefore a need to recognize symptoms early and treat them accordingly.
CASE STUDY:
KD, a 64-year-old woman, presented to her primary care physician’s office for a routine visit. Upon assessment, KD revealed that she used to enjoy going on walks with her neighbor, but she cannot walk up the hills in her neighborhood anymore without feeling “incredibly breathless.” She has become increasingly concerned that she is “having trouble getting a full breath.” KD informed her doctor that these symptoms had worsened since her last visit, and so she had stopped going on neighborhood walks. She was diagnosed with COPD 4 years ago, and is currently using a long-acting muscarinic antagonist (LAMA) bronchodilator. KD has a 40 pack-year smoking history, and has previously been advised to stop smoking, but has relapsed several times. She has a medical history of hypertension and depression, and a notable family history of emphysema, breast cancer, and diabetes.
The relationship between lung hyperinflation and dyspnea in COPD
In COPD, pathologic changes give rise to physiologic abnormalities such as mucus hypersecretion and ciliary dysfunction, gas exchange abnormalities, pulmonary hypertension, and airflow limitation and lung hyperinflation.13 Lung hyperinflation, an increase in resting functional residual volume above a normal level, represents a mechanical link between the characteristic expiratory airflow impairment, dyspnea, and physical activity limitation in COPD.1
 healthy individuals and (B) patients with COPD.")
Although patients can compensate for several of the negative consequences of hyperinflation (eg, altering the chest wall due to overdistended lungs), such compensatory mechanisms are unable to cope with large increases in ventilation, such as those that occur during exercise.1 Air trapping, together with ineffectiveness of respiratory muscle function, leads to increased ventilation requirements and dynamic pulmonary hyperinflation, resulting in dyspnea.1
Patients with COPD describe a sensation of “air hunger,” reporting “unsatisfied” or “unrewarded” inhalation, “shallow breathing,” and a feeling that they “cannot get a deep breath,”18 whereas, in fact, they are limited in their ability to fully exhale. Verbal descriptors (eg, “air hunger” or “chest tightness”) are important tools in understanding a patient’s experience with dyspnea, and a patient’s choice of descriptor may be related to dyspnea severity, and the level of distress that dyspnea causes a given patient.19 Air hunger in turn encourages faster breathing, leading to further shortness of breath and more dynamic hyperinflation.1,20
To deflate the lungs of patients with COPD, physiologic, pharmacologic, and possibly surgical interventions are required:
- Controlled breathing techniques (eg, purse-lipped breathing) that encourage slow and deep breathing can correct abnormal chest wall motion, decrease the work of breathing, increase breathing efficiency, and improve the distribution of ventilation to empty the lungs.21
- Bronchodilators can help to achieve lung deflation by improving ventilatory mechanics, as shown by increases in inspiratory capacity and vital capacity.22
- Lung volume reduction surgery can also be considered to treat severe hyperinflation in emphysematous patients5; bronchoscopic interventions that lower lung volumes are also in development.23
The impact of lung hyperinflation and dyspnea on physical activity in COPD
 percentage of predicted FEV1 and (B) dyspnea level.")
Dyspnea and hyperinflation are closely interrelated with physical activity limitation,16,29,30 and so can be viewed as significant contributors to patient disability. During an acute exacerbation, patients with COPD will experience worsening airway obstruction, dynamic hyperinflation, and dyspnea.31 Patients with a greater number of comorbid conditions may also have greater shortness of breath.32 In addition, patients with COPD and hyperinflation perform less physical activity than individuals without hyperinflation, regardless of COPD severity, as assessed using the 2007 Global Initiative for Chronic Obstructive Lung Disease (GOLD) staging (stage I, mild; stage II, moderate; stage III, severe; stage IV, very severe) and BODE (Body-mass index, airflow Obstruction, Dyspnea, and Exercise) index.33 These patients also exhibit increases in dyspnea perception during commonly performed ADLs, which may limit physical activity and worsen lung hyperinflation.33 More limited physical activity also contributes to higher dyspnea scores during ADLs.8
Furthermore, the ability to perform typical ADLs may be significantly altered or eliminated altogether in patients with COPD.11 Leisure activities are often the first to be dropped by patients, as they generally require greater effort than simpler tasks, and are not critical to daily life.11 Eventually, these activities become progressively more difficult, and most patients with moderate or severe COPD can struggle to complete even the most basic daily activities.11
In addition to the morbidity burden and impact on ADLs, lower levels of physical activity in patients with COPD have also been shown to increase the risk of mortality and exacerbations, and elevate the risk of comorbidities such as heart disease and metabolic disease.34 In light of these observations, improving exercise capacity should be a key goal in COPD management.
Assessment and measurement of dyspnea and hyperinflation
Reducing hyperinflation and dyspnea is essential for improving physical activity endurance and overall physical activity in patients with COPD; therefore, measuring the degree of impairment is important.22 Clinicians should be aware that some patients may have relief of dyspnea due to improvements in hyperinflation, despite relatively mild changes in FEV1.35 Lung volume measures, including total lung capacity, residual volume and functional residual capacity, are valuable tools in the assessment of lung hyperinflation in COPD, and therefore constitute a key component of pulmonary function testing.36 However, expanded pulmonary function testing may be required for patients with severe dyspnea that does not correspond to spirometric findings, or cases in which diagnosis is uncertain.37
Lung volumes are evaluated primarily by body plethysmography, during which a patient sits inside an airtight “body box” equipped to measure pressure and volume changes.14,38 Helium dilution and nitrogen washing can also be used to measure functional residual capacity in patients with COPD,14 but body plethysmography is considered to be a more accurate method of lung volume evaluation in patients with severe airflow obstruction.14,38 Radiographic techniques can also be used, but due to a lack of standardization, they are not typically utilized in clinical practice.14 Measurement of IC may complement other lung volume measures as part of assessment of hyperinflation.16 This can be measured using either spirometry or body plethysmography.39,40
In addition to evaluating hyperinflation, ADLs, physical activity, exercise capacity, and dyspnea should all be assessed in patients with COPD in primary care. It is known that patients may self-limit ADLs to avoid symptoms of COPD; in doing so, worsening symptoms may be underappreciated, and subsequently underreported, by the patient. Thus, it is essential that physicians ask patients with COPD, as well as individuals at risk of COPD, questions about changes in their physical activity or ability to perform common tasks. There are a number of methods to measure functional performance, but for a simple assessment of ADLs, clinicians can ask the patient or caregiver questions related to basic daily tasks.11 In early COPD, patients who experience mild dyspnea during exercise should be able to perform most productive activities. Patients with stable COPD and moderate dyspnea during exercise should be able to carry out most of the higher functioning ADLs, whereas patients with severe COPD may struggle to complete basic ADLs without assistance.11 It should be noted, however, that patients may experience dyspnea with fairly routine activities, and even reduce physical activity at relatively early stages of airflow limitation.41,42

Other tests may be useful in assessing the impact of an intervention, be it pharmacologic or nonpharmacologic, on dyspnea severity. For example, increases in the 6-minute-walk distance (6MWD) have been shown to correlate with improvements in dyspnea.46 The 6MWD has also been shown to be an important predictor of hospitalization and mortality in patients with COPD.47 However, it is important to note that improvements in 6MWD show only a very weak correlation with patient-reported outcomes,48 and may be a less sensitive measure for patients with less disability than those with more profound functional limitation.49 Moreover, 6MWD can be affected by a patient’s psychologic motivation,6,50 as well as other comorbidities observed in patients with COPD, such as osteoporosis, heart failure, and peripheral vascular disease.46,51 Although not used for COPD diagnosis or evaluation of dyspnea or physical activity limitation, a chest X-ray can also be a useful tool for excluding alternative diagnoses, as well as for detecting significant comorbidities in patients with COPD, such as concomitant respiratory, cardiac, and skeletal diseases.5
Management of dyspnea and hyperinflation in primary care

Pulmonary rehabilitation is a tailored intervention that encompasses exercise training, education, and self-management support for people with chronic respiratory disease, based on detailed assessment of their exercise capacity and symptoms.52 Pulmonary rehabilitation is as important as medication in COPD management, providing a cost-effective intervention with minimal adverse effects.53 Moreover, pulmonary rehabilitation has been shown to benefit patients with mild to severe dyspnea (as classified according to the Medical Research Council dyspnea scale), demonstrating the value of successful execution of these programs in patients with COPD, irrespective of disease severity.54 Although the most significant improvements in patient quality of life are observed when a multimodality approach is used, exercise and proper pulmonary rehabilitation programs have been shown to improve quality of life more than medication alone.5,55 Notably, there are few supporting data for the use of supplemental oxygen in patients experiencing dyspnea without hypoxemia. Oxygen supplementation is only of minimal benefit to relieving the sensation of dyspnea.56,57
The relationship between the impact of pulmonary rehabilitation in patients with COPD and frailty scores has also been evaluated. Frailty scores are calculated based on an individual’s level of physical activity, and other key criteria that are indicative of their ability to self-manage their medical condition.58 These scores are particularly relevant in the context of COPD, given the high prevalence of the condition in older people.58 Although frailty is a strong independent predictor of noncompletion of pulmonary rehabilitation, completion of a pulmonary rehabilitation program in patients who are frail has been shown to reverse their frailty in the short term.58 It is therefore important that physicians guide and encourage these patients for the duration of a pulmonary rehabilitation program, from initiation through to completion, to ensure that those who are likely to derive the greatest benefit from pulmonary rehabilitation are supported to do so.
In addition to pulmonary rehabilitation, other nonpharmacologic interventions have emerged in recent years that may help to relieve dyspnea in patients with COPD. Airway clearance devices, such as acapella (Smiths Medical; Minneapolis, MN), Flutter (Allergan; Dublin, Ireland), Lung Flute (Medical Acoustics; Buffalo, NY), Quake (Thayer Medical; Tucson, AZ), and Aerobika (Monaghan Medical; Plattsburgh, NY) promote the clearance of sputum through the application of positive expiratory pressure, possibly allowing medicines to penetrate the lungs more effectively, and improving diffuse airflow obstruction.59-61 Incorporating an airway clearance device into a bronchodilator therapy regimen has been shown to improve dyspnea scores, both before and after exercise, compared with bronchodilator therapy combined with a nonfunctional control device in patients with severe COPD.59 In addition, noninvasive forms of ventilation, such as continuous positive airway pressure and bi-level positive airway pressure (BiPAP), have been shown to effectively reduce dyspnea in patients with COPD.62,63 In a 24-month study in patients with severe COPD, resting dyspnea improved significantly in patients using the BiPAP Auto-Trak (Philips Respironics, Best, The Netherlands) in conjunction with their regular bronchodilator therapy, compared with those receiving long-term oxygen therapy in addition to their typical therapeutic regimen.63 Further studies are required to establish the impact of these devices in the management of dyspnea and other symptoms of COPD.
These nonpharmacologic interventions can be supplemented with pharmacologic treatments to help patients achieve their treatment goals of improved dyspnea and increased exercise performance. Bronchodilators, which form the basis of various COPD treatment options, include5:
- short-acting muscarinic antagonists (SAMAs), such as ipratropium
- short-acting β2-agonists (SABAs), such as albuterol, levalbuterol, and terbutaline
- SAMA/SABA combinations
- LAMAs, such as aclidinium, glycopyrrolate, tiotropium, and umeclidinium
- long-acting β 2-agonists (LABAs), such as arformoterol, indacaterol, formoterol, olodaterol, salmeterol, and vilanterol
- LAMA/LABA combinations (umeclidinium/vilanterol, tiotropium/olodaterol, glycopyrrolate/formoterol, glycopyrrolate/indacaterol)
Inhaled corticosteroids can also be used in a fixed-dose combination with a LABA, which can be combined with a LAMA, in select patients5; however, these combination products may have minimal value in treating dyspnea unless asthma is concomitantly present.5,64 Further discussion of the different treatment options available for patients with COPD can be found in the final article of this supplement.
In addition to improving quality of life, long-acting bronchodilators, such as LAMAs, LABAs, and LAMA/LABA combinations, increase expiratory flow, reduce dynamic hyperinflation, and improve exercise capacity of patients.65-67 As disease severity worsens, physicians may opt for long-acting bronchodilator options that have twice-daily dosing, which may confer a benefit in improving night-time symptom control.68
As well as active pharmacologic and nonpharmacologic interventions, physicians should always encourage smoking cessation in patients with COPD, as this has the greatest capacity to influence the natural course of the disease.5 It is essential that health care providers continually deliver smoking cessation messages to patients with COPD; patients can also be supported to stop smoking by using nicotine replacement therapy, pharmacologic interventions, attending smoking cessation programs, and counseling.5
Lung volume reduction surgery may also be considered as a strategy for the management of dyspnea in severe, refractory COPD.69 Similarly, nonsurgical bronchoscopic interventions are being developed that look to achieve similar results to lung volume reduction surgery, including endobronchial one-way valves, lung volume reduction coils, airway bypasses, adhesives, and vapor therapy.23
CASE STUDY:
The primary care physician assessed KD’s dyspnea using the CAT and ordered a chest X-ray to identify any significant comorbidities, such as concomitant respiratory, skeletal, or cardiac diseases. As KD’s CAT score was 17, and her symptoms were uncontrolled on LAMA monotherapy, her physician prescribed a long-acting LAMA/LABA combination, along with pulmonary rehabilitation. The physician also counseled KD on the importance of smoking cessation, and referred her to a local smoking cessation program.
Conclusions
Dyspnea, the most common symptom of COPD and the primary consequence of the condition’s characteristic lung hyperinflation, is a heavy burden on the lives of patients. The impact of dyspnea is perhaps most apparent in the context of physical activity, with activity limitation observed frequently in patients with COPD, regardless of disease stage. This can affect patients’ quality of life significantly, and has long-term consequences on disease progression. Improving dyspnea and increasing exercise endurance should therefore be a key goal for COPD management, which should encompass both nonpharmacologic interventions, such as pulmonary rehabilitation, and pharmacologic interventions, such as use of bronchodilator therapy.
- O’Donnell DE. Hyperinflation, dyspnea, and exercise intolerance in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2006;3(2):180-184.
- Parshall MB, Schwartzstein RM, Adams L, et al; American Thoracic Society Committee on Dyspnea. An official American Thoracic Society statement: update on the mechanisms, assessment, and management of dyspnea. Am J Respir Crit Care Med. 2012;185(4):435-452.
- Kessler R, Partridge MR, Miravitlles M, et al. Symptom variability in patients with severe COPD: a pan-European cross-sectional study. Eur Respir J. 2011;37(2):264-272.
- Agusti A, Hedner J, Marin J, Barbé F, Cazzola M, Rennard S. Night-time symptoms: a forgotten dimension of COPD. Eur Respir Rev. 2011;20(121):183-194.
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of COPD. 2017. http://gold.copd.org/gold-2017-global-strategy-diagnosis-management-prevention-copd. Accessed November 27, 2017.
- O’Donnell DE, Gebke KB. Activity restriction in mild COPD: a challenging clinical problem. Int J Chron Obstruct Pulmon Dis. 2014;9:577-588.
- Elbehairy AF, Ciavaglia CE, Webb KA, et al; Canadian Respiratory Research Network. Pulmonary gas exchange abnormalities in mild chronic obstructive pulmonary disease. Implications for dyspnea and exercise intolerance. Am J Respir Crit Care Med. 2015;191(12):1384-1394.
- Barriga S, Rodrigues F, Bárbara C. Factors that influence physical activity in the daily life of male patients with chronic obstructive pulmonary disease. Rev Port Pneumol. 2014;20(3):131-137.
- Pitta F, Troosters T, Spruit MA, Probst VS, Decramer M, Gosselink R. Characteristics of physical activities in daily life in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(9):972-977.
- Haas F, Salazar-Schicci J, Axen K. Desensitization to dyspnoea in chronic obstructive pulmonary disease. In: Casaburi R, Petty TL, eds. Principles and Practice of Pulmonary Rehabilitation. Philadelphia, PA: W.B. Saunders; 1993:241-251.
- Belfer MH, Reardon JZ. Improving exercise tolerance and quality of life in patients with chronic obstructive pulmonary disease. J Am Osteopath Assoc. 2009;109(5):268-278.
- Troosters T, van der Molen T, Polkey M, et al. Improving physical activity in COPD: towards a new paradigm. Respir Res. 2013;14:115.
- Celli BR, MacNee W; ATS/ERS Task Force. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23(6):932-946.
- Gagnon P, Guenette JA, Langer D, et al. Pathogenesis of hyperinflation in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2014;9:187-201.
- Ferguson GT. Why does the lung hyperinflate? Proc Am Thorac Soc. 2006;3(2):176-179.
- O’Donnell DE, Revill SM, Webb KA. Dynamic hyperinflation and exercise intolerance in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;164(5):770-777.
- Dubé BP, Guerder A, Morelot-Panzini C, Laveneziana P. The clinical relevance of the emphysema-hyperinflated phenotype in COPD. COPD Res Pract. 2016;2:1.
- Scano G, Stendardi L, Grazzini M. Understanding dyspnoea by its language. Eur Respir J. 2005;25(2):380-385.
- Chowienczyk S, Javadzadeh S, Booth S, Farquhar M. Association of descriptors of breathlessness with diagnosis and self-reported severity of breathlessness in patients with advanced chronic obstructive pulmonary disease or cancer. J Pain Symptom Manage. 2016;52(2):259-264.
- Thomas M, Decramer M, O’Donnell DE. No room to breathe: the importance of lung hyperinflation in COPD. Prim Care Respir J. 2013;22(1):101-111.
- Gosselink R. Controlled breathing and dyspnea in patients with chronic obstructive pulmonary disease (COPD). J Rehabil Res Dev. 2003;40(5 Suppl 2):25-33.
- O’Donnell DE, Webb KA, Neder JA. Lung hyperinflation in COPD: applying physiology to clinical practice. COPD Res Pract. 2015;1:4.
- Browning RF, Parrish S, Sarkar S, et al. Bronchoscopic interventions for severe COPD. J Thorac Dis. 2014;6(Suppl 4):S407-S415.
- Nishimura K, Izumi T, Tsukino M, Oga T. Dyspnea is a better predictor of 5-year survival than airway obstruction in patients with COPD. Chest. 2002;121(5):1434-1440.
- Fletcher CM, Elmes PC, Fairbairn AS, Wood CH. The significance of respiratory symptoms and the diagnosis of chronic bronchitis in a working population. Br Med J. 1959;2(5147):257-266.
- O’Donnell DE, Lam M, Webb KA. Spirometric correlates of improvement in exercise performance after anticholinergic therapy in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1999;160(2):542-549.
- Light RW. Mechanics of respiration. In: George RB, ed. Chest Medicine: Essentials of Pulmonary and Critical Care Medicine. Philadelphia, PA: Lippincott Williams & Wilkins; 2005:24-38.
- Casanova C, Cote C, de Torres JP, et al. Inspiratory-to-total lung capacity ratio predicts mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(6):591-597.
- O’Donnell DE, Guenette JA, Maltais F, Webb KA. Decline of resting inspiratory capacity in COPD: the impact on breathing pattern, dyspnea, and ventilatory capacity during exercise. Chest. 2012;141(3):753-762.
- O’Donnell DE, Laveneziana P. Dyspnea and activity limitation in COPD: mechanical factors. COPD. 2007;4(3):225-236.
- Holland AE. Physiotherapy management of acute exacerbations of chronic obstructive pulmonary disease. J Physiother. 2014;60(4):181-188.
- Barr RG, Bluemke DA, Ahmed FS, et al. Percent emphysema, airflow obstruction, and impaired left ventricular filling. N Engl J Med. 2010;362(3):217-227.
- Garcia-Rio F, Lores V, Mediano O, et al. Daily physical activity in patients with chronic obstructive pulmonary disease is mainly associated with dynamic hyperinflation. Am J Respir Crit Care Med. 2009;180(6):506-512.
- Di Marco F, Santus P, Sotgiu G, Blasi F, Centanni S. Does improving exercise capacity and daily activity represent the holistic perspective of a new COPD approach? COPD. 2015;12(5):575-581.
- Newton MF, O’Donnell DE, Forkert L. Response of lung volumes to inhaled salbutamol in a large population of patients with severe hyperinflation. Chest. 2002;121(4):1042-1050.
- Bailey KL. The importance of the assessment of pulmonary function in COPD. Med Clin North Am. 2012;96(4):745-752.
- Burkhardt R, Pankow W. The diagnosis of chronic obstructive pulmonary disease. Dtsch Arztebl Int. 2014;111(49):834-845, quiz 846.
- O’Donnell CR, Bankier AA, Stiebellehner L, Reilly JJ, Brown R, Loring SH. Comparison of plethysmographic and helium dilution lung volumes: which is best for COPD? Chest. 2010;137(5):1108-1115.
- Criée CP, Sorichter S, Smith HJ, et al; Working Group for Body Plethysmography of the German Society for Pneumology and Respiratory Care. Body plethysmography—its principles and clinical use. Respir Med. 2011;105(7):959-971.
- Lutfi MF. The physiological basis and clinical significance of lung volume measurements. Multidiscip Respir Med. 2017;12:3.
- Lahaije AJ, van Helvoort HA, Dekhuijzen PN, Vercoulen JH, Heijdra YF. Resting and ADL-induced dynamic hyperinflation explain physical inactivity in COPD better than FEV1. Respir Med. 2013;107(6):834-840.
- Troosters T, Sciurba F, Battaglia S, et al. Physical inactivity in patients with COPD, a controlled multi-center pilot-study. Respir Med. 2010;104(7):1005-1011.
- Calverley PMA, Georgopoulos D. Symptoms and signs of COPD. In: Siafakas NM, ed. Management of Chronic Obstructive Pulmonary Disease: European Respiratory Society Journals; 2006.
- Cave AJ, Atkinson L, Tsiligianni IG, Kaplan AG. Assessment of COPD wellness tools for use in primary care: an IPCRG initiative. Int J Chron Obstruct Pulmon Dis. 2012;7:447-456.
- Cazzola M, Hanania NA, MacNee W, Rüdell K, Hackford C, Tamimi N. A review of the most common patient-reported outcomes in COPD—revisiting current knowledge and estimating future challenges. Int J Chron Obstruct Pulmon Dis. 2015;10:725-738.
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111-117.
- Polkey MI, Spruit MA, Edwards LD, et al; Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) Study Investigators. Six-minute-walk test in chronic obstructive pulmonary disease: minimal clinically important difference for death or hospitalization. Am J Respir Crit Care Med. 2013;187(4):382-386.
- Puhan MA, Mador MJ, Held U, Goldstein R, Guyatt GH, Schünemann HJ. Interpretation of treatment changes in 6-minute walk distance in patients with COPD. Eur Respir J. 2008;32(3):637-643.
- Holland AE, Hill CJ, Rasekaba T, Lee A, Naughton MT, McDonald CF. Updating the minimal important difference for six-minute walk distance in patients with chronic obstructive pulmonary disease. Arch Phys Med Rehabil. 2010;91(2):221-225.
- Grant A, Moore L. Pulmonary rehabilitation. In: Blackler L, Jones C, Mooney C, eds. Managing Chronic Obstructive Pulmonary Disease. West Sussex, England: John Wiley & Sons; 2007.
- Crisafulli E, Gorgone P, Vagaggini B, et al. Efficacy of standard rehabilitation in COPD outpatients with comorbidities. Eur Respir J. 2010;36(5):1042-1048.
- Spruit MA, Singh SJ, Garvey C, et al; ATS/ERS Task Force on Pulmonary Rehabilitation. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13-e64.
- Ries AL, Bauldoff GS, Carlin BW, et al. Pulmonary Rehabilitation: Joint ACCP/AACVPR Evidence-Based Clinical Practice Guidelines. Chest. 2007;131(5 Suppl):4S-42S.
- Evans RA, Singh SJ, Collier R, Williams JE, Morgan MD. Pulmonary rehabilitation is successful for COPD irrespective of MRC dyspnoea grade. Respir Med. 2009;103(7):1070-1075.
- McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015;(2):CD003793.
- Stoller JK, Panos RJ, Krachman S, Doherty DE, Make B; Long-term Oxygen Treatment Trial Research Group. Oxygen therapy for patients with COPD: current evidence and the long-term oxygen treatment trial. Chest. 2010;138(1):179-187.
- Ekström M, Ahmadi Z, Bornefalk-Hermansson A, Abernethy A, Currow D. Oxygen for breathlessness in patients with chronic obstructive pulmonary disease who do not qualify for home oxygen therapy. Cochrane Database Syst Rev. 2016;11:CD006429.
- Maddocks M, Kon SS, Canavan JL, et al. Physical frailty and pulmonary rehabilitation in COPD: a prospective cohort study. Thorax. 2016;71(11):988-995.
- Wolkove N, Kamel H, Rotaple M, Baltzan MA Jr. Use of a mucus clearance device enhances the bronchodilator response in patients with stable COPD. Chest. 2002;121(3):702-707.
- Chatburn RL. High-frequency assisted airway clearance. Respir Care. 2007;52(9):1224-1235; discussion 1235-1227.
- Clini E. Positive expiratory pressure techniques in respiratory patients: old evidence and new insights. Breathe. 2009;6(2):153-159.
- Petrof BJ, Legaré M, Goldberg P, Milic-Emili J, Gottfried SB. Continuous positive airway pressure reduces work of breathing and dyspnea during weaning from mechanical ventilation in severe chronic obstructive pulmonary disease. Am Rev Respir Dis. 1990;141(2):281-289.
- Clini E, Sturani C, Rossi A, et al; Rehabilitation and Chronic Care Study Group; Italian Association of Hospital Pulmonologists (AIPO). The Italian multicentre study on noninvasive ventilation in chronic obstructive pulmonary disease patients. Eur Respir J. 2002;20(3):529-538.
- Bourbeau J, Rouleau MY, Boucher S. Randomised controlled trial of inhaled corticosteroids in patients with chronic obstructive pulmonary disease. Thorax. 1998;53(6):477-482.
- Berton DC, Reis M, Siqueira AC, et al. Effects of tiotropium and formoterol on dynamic hyperinflation and exercise endurance in COPD. Respir Med. 2010;104(9):1288-1296.
- O’Donnell DE, Flüge T, Gerken F, et al. Effects of tiotropium on lung hyperinflation, dyspnoea and exercise tolerance in COPD. Eur Respir J. 2004;23(6):832-840.
- O’Donnell DE, Sciurba F, Celli B, et al. Effect of fluticasone propionate/salmeterol on lung hyperinflation and exercise endurance in COPD. Chest. 2006;130(3):647-656.
- Blasi F, Canonica GW, Miravitlles M. Is aclidinium alone or combined with a LABA a rational choice for symptomatic COPD patients [published correction appears in Respir Res. 2017;18(1):35]. Respir Res. 2017;18(1):19.
- Shah AA, D’Amico TA. Lung volume reduction surgery for the management of refractory dyspnea in chronic obstructive pulmonary disease. Curr Opin Support Palliat Care. 2009;3(2):107-111.
Introduction
Dyspnea, the sensation of difficult or labored breathing, is the most common symptom in chronic obstructive pulmonary disease (COPD) and the primary symptom that limits physical activity in more advanced disease.1 According to the American Thoracic Society, dyspnea may be measured according to 3 domains2:
- what breathing feels like for the patient
- how distressed the patient feels when breathing
- how dyspnea affects functional ability, employment, health-related quality of life, or health status.
As disease severity increases, breathlessness becomes more disabling at lower activity levels. These changes further impact the quality of life of patients, and can lead to anxiety and depression.11
Physical inactivity is often considered to be a major contributor to the progression of COPD,6 and is linked to hospitalizations and increased all-cause mortality.12 There is therefore a need to recognize symptoms early and treat them accordingly.
CASE STUDY:
KD, a 64-year-old woman, presented to her primary care physician’s office for a routine visit. Upon assessment, KD revealed that she used to enjoy going on walks with her neighbor, but she cannot walk up the hills in her neighborhood anymore without feeling “incredibly breathless.” She has become increasingly concerned that she is “having trouble getting a full breath.” KD informed her doctor that these symptoms had worsened since her last visit, and so she had stopped going on neighborhood walks. She was diagnosed with COPD 4 years ago, and is currently using a long-acting muscarinic antagonist (LAMA) bronchodilator. KD has a 40 pack-year smoking history, and has previously been advised to stop smoking, but has relapsed several times. She has a medical history of hypertension and depression, and a notable family history of emphysema, breast cancer, and diabetes.
The relationship between lung hyperinflation and dyspnea in COPD
In COPD, pathologic changes give rise to physiologic abnormalities such as mucus hypersecretion and ciliary dysfunction, gas exchange abnormalities, pulmonary hypertension, and airflow limitation and lung hyperinflation.13 Lung hyperinflation, an increase in resting functional residual volume above a normal level, represents a mechanical link between the characteristic expiratory airflow impairment, dyspnea, and physical activity limitation in COPD.1
Although patients can compensate for several of the negative consequences of hyperinflation (eg, altering the chest wall due to overdistended lungs), such compensatory mechanisms are unable to cope with large increases in ventilation, such as those that occur during exercise.1 Air trapping, together with ineffectiveness of respiratory muscle function, leads to increased ventilation requirements and dynamic pulmonary hyperinflation, resulting in dyspnea.1
Patients with COPD describe a sensation of “air hunger,” reporting “unsatisfied” or “unrewarded” inhalation, “shallow breathing,” and a feeling that they “cannot get a deep breath,”18 whereas, in fact, they are limited in their ability to fully exhale. Verbal descriptors (eg, “air hunger” or “chest tightness”) are important tools in understanding a patient’s experience with dyspnea, and a patient’s choice of descriptor may be related to dyspnea severity, and the level of distress that dyspnea causes a given patient.19 Air hunger in turn encourages faster breathing, leading to further shortness of breath and more dynamic hyperinflation.1,20
To deflate the lungs of patients with COPD, physiologic, pharmacologic, and possibly surgical interventions are required:
- Controlled breathing techniques (eg, purse-lipped breathing) that encourage slow and deep breathing can correct abnormal chest wall motion, decrease the work of breathing, increase breathing efficiency, and improve the distribution of ventilation to empty the lungs.21
- Bronchodilators can help to achieve lung deflation by improving ventilatory mechanics, as shown by increases in inspiratory capacity and vital capacity.22
- Lung volume reduction surgery can also be considered to treat severe hyperinflation in emphysematous patients5; bronchoscopic interventions that lower lung volumes are also in development.23
The impact of lung hyperinflation and dyspnea on physical activity in COPD
Dyspnea and hyperinflation are closely interrelated with physical activity limitation,16,29,30 and so can be viewed as significant contributors to patient disability. During an acute exacerbation, patients with COPD will experience worsening airway obstruction, dynamic hyperinflation, and dyspnea.31 Patients with a greater number of comorbid conditions may also have greater shortness of breath.32 In addition, patients with COPD and hyperinflation perform less physical activity than individuals without hyperinflation, regardless of COPD severity, as assessed using the 2007 Global Initiative for Chronic Obstructive Lung Disease (GOLD) staging (stage I, mild; stage II, moderate; stage III, severe; stage IV, very severe) and BODE (Body-mass index, airflow Obstruction, Dyspnea, and Exercise) index.33 These patients also exhibit increases in dyspnea perception during commonly performed ADLs, which may limit physical activity and worsen lung hyperinflation.33 More limited physical activity also contributes to higher dyspnea scores during ADLs.8
Furthermore, the ability to perform typical ADLs may be significantly altered or eliminated altogether in patients with COPD.11 Leisure activities are often the first to be dropped by patients, as they generally require greater effort than simpler tasks, and are not critical to daily life.11 Eventually, these activities become progressively more difficult, and most patients with moderate or severe COPD can struggle to complete even the most basic daily activities.11
In addition to the morbidity burden and impact on ADLs, lower levels of physical activity in patients with COPD have also been shown to increase the risk of mortality and exacerbations, and elevate the risk of comorbidities such as heart disease and metabolic disease.34 In light of these observations, improving exercise capacity should be a key goal in COPD management.
Assessment and measurement of dyspnea and hyperinflation
Reducing hyperinflation and dyspnea is essential for improving physical activity endurance and overall physical activity in patients with COPD; therefore, measuring the degree of impairment is important.22 Clinicians should be aware that some patients may have relief of dyspnea due to improvements in hyperinflation, despite relatively mild changes in FEV1.35 Lung volume measures, including total lung capacity, residual volume and functional residual capacity, are valuable tools in the assessment of lung hyperinflation in COPD, and therefore constitute a key component of pulmonary function testing.36 However, expanded pulmonary function testing may be required for patients with severe dyspnea that does not correspond to spirometric findings, or cases in which diagnosis is uncertain.37
Lung volumes are evaluated primarily by body plethysmography, during which a patient sits inside an airtight “body box” equipped to measure pressure and volume changes.14,38 Helium dilution and nitrogen washing can also be used to measure functional residual capacity in patients with COPD,14 but body plethysmography is considered to be a more accurate method of lung volume evaluation in patients with severe airflow obstruction.14,38 Radiographic techniques can also be used, but due to a lack of standardization, they are not typically utilized in clinical practice.14 Measurement of IC may complement other lung volume measures as part of assessment of hyperinflation.16 This can be measured using either spirometry or body plethysmography.39,40
In addition to evaluating hyperinflation, ADLs, physical activity, exercise capacity, and dyspnea should all be assessed in patients with COPD in primary care. It is known that patients may self-limit ADLs to avoid symptoms of COPD; in doing so, worsening symptoms may be underappreciated, and subsequently underreported, by the patient. Thus, it is essential that physicians ask patients with COPD, as well as individuals at risk of COPD, questions about changes in their physical activity or ability to perform common tasks. There are a number of methods to measure functional performance, but for a simple assessment of ADLs, clinicians can ask the patient or caregiver questions related to basic daily tasks.11 In early COPD, patients who experience mild dyspnea during exercise should be able to perform most productive activities. Patients with stable COPD and moderate dyspnea during exercise should be able to carry out most of the higher functioning ADLs, whereas patients with severe COPD may struggle to complete basic ADLs without assistance.11 It should be noted, however, that patients may experience dyspnea with fairly routine activities, and even reduce physical activity at relatively early stages of airflow limitation.41,42
Other tests may be useful in assessing the impact of an intervention, be it pharmacologic or nonpharmacologic, on dyspnea severity. For example, increases in the 6-minute-walk distance (6MWD) have been shown to correlate with improvements in dyspnea.46 The 6MWD has also been shown to be an important predictor of hospitalization and mortality in patients with COPD.47 However, it is important to note that improvements in 6MWD show only a very weak correlation with patient-reported outcomes,48 and may be a less sensitive measure for patients with less disability than those with more profound functional limitation.49 Moreover, 6MWD can be affected by a patient’s psychologic motivation,6,50 as well as other comorbidities observed in patients with COPD, such as osteoporosis, heart failure, and peripheral vascular disease.46,51 Although not used for COPD diagnosis or evaluation of dyspnea or physical activity limitation, a chest X-ray can also be a useful tool for excluding alternative diagnoses, as well as for detecting significant comorbidities in patients with COPD, such as concomitant respiratory, cardiac, and skeletal diseases.5
Management of dyspnea and hyperinflation in primary care
Pulmonary rehabilitation is a tailored intervention that encompasses exercise training, education, and self-management support for people with chronic respiratory disease, based on detailed assessment of their exercise capacity and symptoms.52 Pulmonary rehabilitation is as important as medication in COPD management, providing a cost-effective intervention with minimal adverse effects.53 Moreover, pulmonary rehabilitation has been shown to benefit patients with mild to severe dyspnea (as classified according to the Medical Research Council dyspnea scale), demonstrating the value of successful execution of these programs in patients with COPD, irrespective of disease severity.54 Although the most significant improvements in patient quality of life are observed when a multimodality approach is used, exercise and proper pulmonary rehabilitation programs have been shown to improve quality of life more than medication alone.5,55 Notably, there are few supporting data for the use of supplemental oxygen in patients experiencing dyspnea without hypoxemia. Oxygen supplementation is only of minimal benefit to relieving the sensation of dyspnea.56,57
The relationship between the impact of pulmonary rehabilitation in patients with COPD and frailty scores has also been evaluated. Frailty scores are calculated based on an individual’s level of physical activity, and other key criteria that are indicative of their ability to self-manage their medical condition.58 These scores are particularly relevant in the context of COPD, given the high prevalence of the condition in older people.58 Although frailty is a strong independent predictor of noncompletion of pulmonary rehabilitation, completion of a pulmonary rehabilitation program in patients who are frail has been shown to reverse their frailty in the short term.58 It is therefore important that physicians guide and encourage these patients for the duration of a pulmonary rehabilitation program, from initiation through to completion, to ensure that those who are likely to derive the greatest benefit from pulmonary rehabilitation are supported to do so.
In addition to pulmonary rehabilitation, other nonpharmacologic interventions have emerged in recent years that may help to relieve dyspnea in patients with COPD. Airway clearance devices, such as acapella (Smiths Medical; Minneapolis, MN), Flutter (Allergan; Dublin, Ireland), Lung Flute (Medical Acoustics; Buffalo, NY), Quake (Thayer Medical; Tucson, AZ), and Aerobika (Monaghan Medical; Plattsburgh, NY) promote the clearance of sputum through the application of positive expiratory pressure, possibly allowing medicines to penetrate the lungs more effectively, and improving diffuse airflow obstruction.59-61 Incorporating an airway clearance device into a bronchodilator therapy regimen has been shown to improve dyspnea scores, both before and after exercise, compared with bronchodilator therapy combined with a nonfunctional control device in patients with severe COPD.59 In addition, noninvasive forms of ventilation, such as continuous positive airway pressure and bi-level positive airway pressure (BiPAP), have been shown to effectively reduce dyspnea in patients with COPD.62,63 In a 24-month study in patients with severe COPD, resting dyspnea improved significantly in patients using the BiPAP Auto-Trak (Philips Respironics, Best, The Netherlands) in conjunction with their regular bronchodilator therapy, compared with those receiving long-term oxygen therapy in addition to their typical therapeutic regimen.63 Further studies are required to establish the impact of these devices in the management of dyspnea and other symptoms of COPD.
These nonpharmacologic interventions can be supplemented with pharmacologic treatments to help patients achieve their treatment goals of improved dyspnea and increased exercise performance. Bronchodilators, which form the basis of various COPD treatment options, include5:
- short-acting muscarinic antagonists (SAMAs), such as ipratropium
- short-acting β2-agonists (SABAs), such as albuterol, levalbuterol, and terbutaline
- SAMA/SABA combinations
- LAMAs, such as aclidinium, glycopyrrolate, tiotropium, and umeclidinium
- long-acting β 2-agonists (LABAs), such as arformoterol, indacaterol, formoterol, olodaterol, salmeterol, and vilanterol
- LAMA/LABA combinations (umeclidinium/vilanterol, tiotropium/olodaterol, glycopyrrolate/formoterol, glycopyrrolate/indacaterol)
Inhaled corticosteroids can also be used in a fixed-dose combination with a LABA, which can be combined with a LAMA, in select patients5; however, these combination products may have minimal value in treating dyspnea unless asthma is concomitantly present.5,64 Further discussion of the different treatment options available for patients with COPD can be found in the final article of this supplement.
In addition to improving quality of life, long-acting bronchodilators, such as LAMAs, LABAs, and LAMA/LABA combinations, increase expiratory flow, reduce dynamic hyperinflation, and improve exercise capacity of patients.65-67 As disease severity worsens, physicians may opt for long-acting bronchodilator options that have twice-daily dosing, which may confer a benefit in improving night-time symptom control.68
As well as active pharmacologic and nonpharmacologic interventions, physicians should always encourage smoking cessation in patients with COPD, as this has the greatest capacity to influence the natural course of the disease.5 It is essential that health care providers continually deliver smoking cessation messages to patients with COPD; patients can also be supported to stop smoking by using nicotine replacement therapy, pharmacologic interventions, attending smoking cessation programs, and counseling.5
Lung volume reduction surgery may also be considered as a strategy for the management of dyspnea in severe, refractory COPD.69 Similarly, nonsurgical bronchoscopic interventions are being developed that look to achieve similar results to lung volume reduction surgery, including endobronchial one-way valves, lung volume reduction coils, airway bypasses, adhesives, and vapor therapy.23
CASE STUDY:
The primary care physician assessed KD’s dyspnea using the CAT and ordered a chest X-ray to identify any significant comorbidities, such as concomitant respiratory, skeletal, or cardiac diseases. As KD’s CAT score was 17, and her symptoms were uncontrolled on LAMA monotherapy, her physician prescribed a long-acting LAMA/LABA combination, along with pulmonary rehabilitation. The physician also counseled KD on the importance of smoking cessation, and referred her to a local smoking cessation program.
Conclusions
Dyspnea, the most common symptom of COPD and the primary consequence of the condition’s characteristic lung hyperinflation, is a heavy burden on the lives of patients. The impact of dyspnea is perhaps most apparent in the context of physical activity, with activity limitation observed frequently in patients with COPD, regardless of disease stage. This can affect patients’ quality of life significantly, and has long-term consequences on disease progression. Improving dyspnea and increasing exercise endurance should therefore be a key goal for COPD management, which should encompass both nonpharmacologic interventions, such as pulmonary rehabilitation, and pharmacologic interventions, such as use of bronchodilator therapy.
Introduction
Dyspnea, the sensation of difficult or labored breathing, is the most common symptom in chronic obstructive pulmonary disease (COPD) and the primary symptom that limits physical activity in more advanced disease.1 According to the American Thoracic Society, dyspnea may be measured according to 3 domains2:
- what breathing feels like for the patient
- how distressed the patient feels when breathing
- how dyspnea affects functional ability, employment, health-related quality of life, or health status.
As disease severity increases, breathlessness becomes more disabling at lower activity levels. These changes further impact the quality of life of patients, and can lead to anxiety and depression.11
Physical inactivity is often considered to be a major contributor to the progression of COPD,6 and is linked to hospitalizations and increased all-cause mortality.12 There is therefore a need to recognize symptoms early and treat them accordingly.
CASE STUDY:
KD, a 64-year-old woman, presented to her primary care physician’s office for a routine visit. Upon assessment, KD revealed that she used to enjoy going on walks with her neighbor, but she cannot walk up the hills in her neighborhood anymore without feeling “incredibly breathless.” She has become increasingly concerned that she is “having trouble getting a full breath.” KD informed her doctor that these symptoms had worsened since her last visit, and so she had stopped going on neighborhood walks. She was diagnosed with COPD 4 years ago, and is currently using a long-acting muscarinic antagonist (LAMA) bronchodilator. KD has a 40 pack-year smoking history, and has previously been advised to stop smoking, but has relapsed several times. She has a medical history of hypertension and depression, and a notable family history of emphysema, breast cancer, and diabetes.
The relationship between lung hyperinflation and dyspnea in COPD
In COPD, pathologic changes give rise to physiologic abnormalities such as mucus hypersecretion and ciliary dysfunction, gas exchange abnormalities, pulmonary hypertension, and airflow limitation and lung hyperinflation.13 Lung hyperinflation, an increase in resting functional residual volume above a normal level, represents a mechanical link between the characteristic expiratory airflow impairment, dyspnea, and physical activity limitation in COPD.1
Although patients can compensate for several of the negative consequences of hyperinflation (eg, altering the chest wall due to overdistended lungs), such compensatory mechanisms are unable to cope with large increases in ventilation, such as those that occur during exercise.1 Air trapping, together with ineffectiveness of respiratory muscle function, leads to increased ventilation requirements and dynamic pulmonary hyperinflation, resulting in dyspnea.1
Patients with COPD describe a sensation of “air hunger,” reporting “unsatisfied” or “unrewarded” inhalation, “shallow breathing,” and a feeling that they “cannot get a deep breath,”18 whereas, in fact, they are limited in their ability to fully exhale. Verbal descriptors (eg, “air hunger” or “chest tightness”) are important tools in understanding a patient’s experience with dyspnea, and a patient’s choice of descriptor may be related to dyspnea severity, and the level of distress that dyspnea causes a given patient.19 Air hunger in turn encourages faster breathing, leading to further shortness of breath and more dynamic hyperinflation.1,20
To deflate the lungs of patients with COPD, physiologic, pharmacologic, and possibly surgical interventions are required:
- Controlled breathing techniques (eg, purse-lipped breathing) that encourage slow and deep breathing can correct abnormal chest wall motion, decrease the work of breathing, increase breathing efficiency, and improve the distribution of ventilation to empty the lungs.21
- Bronchodilators can help to achieve lung deflation by improving ventilatory mechanics, as shown by increases in inspiratory capacity and vital capacity.22
- Lung volume reduction surgery can also be considered to treat severe hyperinflation in emphysematous patients5; bronchoscopic interventions that lower lung volumes are also in development.23
The impact of lung hyperinflation and dyspnea on physical activity in COPD
Dyspnea and hyperinflation are closely interrelated with physical activity limitation,16,29,30 and so can be viewed as significant contributors to patient disability. During an acute exacerbation, patients with COPD will experience worsening airway obstruction, dynamic hyperinflation, and dyspnea.31 Patients with a greater number of comorbid conditions may also have greater shortness of breath.32 In addition, patients with COPD and hyperinflation perform less physical activity than individuals without hyperinflation, regardless of COPD severity, as assessed using the 2007 Global Initiative for Chronic Obstructive Lung Disease (GOLD) staging (stage I, mild; stage II, moderate; stage III, severe; stage IV, very severe) and BODE (Body-mass index, airflow Obstruction, Dyspnea, and Exercise) index.33 These patients also exhibit increases in dyspnea perception during commonly performed ADLs, which may limit physical activity and worsen lung hyperinflation.33 More limited physical activity also contributes to higher dyspnea scores during ADLs.8
Furthermore, the ability to perform typical ADLs may be significantly altered or eliminated altogether in patients with COPD.11 Leisure activities are often the first to be dropped by patients, as they generally require greater effort than simpler tasks, and are not critical to daily life.11 Eventually, these activities become progressively more difficult, and most patients with moderate or severe COPD can struggle to complete even the most basic daily activities.11
In addition to the morbidity burden and impact on ADLs, lower levels of physical activity in patients with COPD have also been shown to increase the risk of mortality and exacerbations, and elevate the risk of comorbidities such as heart disease and metabolic disease.34 In light of these observations, improving exercise capacity should be a key goal in COPD management.
Assessment and measurement of dyspnea and hyperinflation
Reducing hyperinflation and dyspnea is essential for improving physical activity endurance and overall physical activity in patients with COPD; therefore, measuring the degree of impairment is important.22 Clinicians should be aware that some patients may have relief of dyspnea due to improvements in hyperinflation, despite relatively mild changes in FEV1.35 Lung volume measures, including total lung capacity, residual volume and functional residual capacity, are valuable tools in the assessment of lung hyperinflation in COPD, and therefore constitute a key component of pulmonary function testing.36 However, expanded pulmonary function testing may be required for patients with severe dyspnea that does not correspond to spirometric findings, or cases in which diagnosis is uncertain.37
Lung volumes are evaluated primarily by body plethysmography, during which a patient sits inside an airtight “body box” equipped to measure pressure and volume changes.14,38 Helium dilution and nitrogen washing can also be used to measure functional residual capacity in patients with COPD,14 but body plethysmography is considered to be a more accurate method of lung volume evaluation in patients with severe airflow obstruction.14,38 Radiographic techniques can also be used, but due to a lack of standardization, they are not typically utilized in clinical practice.14 Measurement of IC may complement other lung volume measures as part of assessment of hyperinflation.16 This can be measured using either spirometry or body plethysmography.39,40
In addition to evaluating hyperinflation, ADLs, physical activity, exercise capacity, and dyspnea should all be assessed in patients with COPD in primary care. It is known that patients may self-limit ADLs to avoid symptoms of COPD; in doing so, worsening symptoms may be underappreciated, and subsequently underreported, by the patient. Thus, it is essential that physicians ask patients with COPD, as well as individuals at risk of COPD, questions about changes in their physical activity or ability to perform common tasks. There are a number of methods to measure functional performance, but for a simple assessment of ADLs, clinicians can ask the patient or caregiver questions related to basic daily tasks.11 In early COPD, patients who experience mild dyspnea during exercise should be able to perform most productive activities. Patients with stable COPD and moderate dyspnea during exercise should be able to carry out most of the higher functioning ADLs, whereas patients with severe COPD may struggle to complete basic ADLs without assistance.11 It should be noted, however, that patients may experience dyspnea with fairly routine activities, and even reduce physical activity at relatively early stages of airflow limitation.41,42
Other tests may be useful in assessing the impact of an intervention, be it pharmacologic or nonpharmacologic, on dyspnea severity. For example, increases in the 6-minute-walk distance (6MWD) have been shown to correlate with improvements in dyspnea.46 The 6MWD has also been shown to be an important predictor of hospitalization and mortality in patients with COPD.47 However, it is important to note that improvements in 6MWD show only a very weak correlation with patient-reported outcomes,48 and may be a less sensitive measure for patients with less disability than those with more profound functional limitation.49 Moreover, 6MWD can be affected by a patient’s psychologic motivation,6,50 as well as other comorbidities observed in patients with COPD, such as osteoporosis, heart failure, and peripheral vascular disease.46,51 Although not used for COPD diagnosis or evaluation of dyspnea or physical activity limitation, a chest X-ray can also be a useful tool for excluding alternative diagnoses, as well as for detecting significant comorbidities in patients with COPD, such as concomitant respiratory, cardiac, and skeletal diseases.5
Management of dyspnea and hyperinflation in primary care
Pulmonary rehabilitation is a tailored intervention that encompasses exercise training, education, and self-management support for people with chronic respiratory disease, based on detailed assessment of their exercise capacity and symptoms.52 Pulmonary rehabilitation is as important as medication in COPD management, providing a cost-effective intervention with minimal adverse effects.53 Moreover, pulmonary rehabilitation has been shown to benefit patients with mild to severe dyspnea (as classified according to the Medical Research Council dyspnea scale), demonstrating the value of successful execution of these programs in patients with COPD, irrespective of disease severity.54 Although the most significant improvements in patient quality of life are observed when a multimodality approach is used, exercise and proper pulmonary rehabilitation programs have been shown to improve quality of life more than medication alone.5,55 Notably, there are few supporting data for the use of supplemental oxygen in patients experiencing dyspnea without hypoxemia. Oxygen supplementation is only of minimal benefit to relieving the sensation of dyspnea.56,57
The relationship between the impact of pulmonary rehabilitation in patients with COPD and frailty scores has also been evaluated. Frailty scores are calculated based on an individual’s level of physical activity, and other key criteria that are indicative of their ability to self-manage their medical condition.58 These scores are particularly relevant in the context of COPD, given the high prevalence of the condition in older people.58 Although frailty is a strong independent predictor of noncompletion of pulmonary rehabilitation, completion of a pulmonary rehabilitation program in patients who are frail has been shown to reverse their frailty in the short term.58 It is therefore important that physicians guide and encourage these patients for the duration of a pulmonary rehabilitation program, from initiation through to completion, to ensure that those who are likely to derive the greatest benefit from pulmonary rehabilitation are supported to do so.
In addition to pulmonary rehabilitation, other nonpharmacologic interventions have emerged in recent years that may help to relieve dyspnea in patients with COPD. Airway clearance devices, such as acapella (Smiths Medical; Minneapolis, MN), Flutter (Allergan; Dublin, Ireland), Lung Flute (Medical Acoustics; Buffalo, NY), Quake (Thayer Medical; Tucson, AZ), and Aerobika (Monaghan Medical; Plattsburgh, NY) promote the clearance of sputum through the application of positive expiratory pressure, possibly allowing medicines to penetrate the lungs more effectively, and improving diffuse airflow obstruction.59-61 Incorporating an airway clearance device into a bronchodilator therapy regimen has been shown to improve dyspnea scores, both before and after exercise, compared with bronchodilator therapy combined with a nonfunctional control device in patients with severe COPD.59 In addition, noninvasive forms of ventilation, such as continuous positive airway pressure and bi-level positive airway pressure (BiPAP), have been shown to effectively reduce dyspnea in patients with COPD.62,63 In a 24-month study in patients with severe COPD, resting dyspnea improved significantly in patients using the BiPAP Auto-Trak (Philips Respironics, Best, The Netherlands) in conjunction with their regular bronchodilator therapy, compared with those receiving long-term oxygen therapy in addition to their typical therapeutic regimen.63 Further studies are required to establish the impact of these devices in the management of dyspnea and other symptoms of COPD.
These nonpharmacologic interventions can be supplemented with pharmacologic treatments to help patients achieve their treatment goals of improved dyspnea and increased exercise performance. Bronchodilators, which form the basis of various COPD treatment options, include5:
- short-acting muscarinic antagonists (SAMAs), such as ipratropium
- short-acting β2-agonists (SABAs), such as albuterol, levalbuterol, and terbutaline
- SAMA/SABA combinations
- LAMAs, such as aclidinium, glycopyrrolate, tiotropium, and umeclidinium
- long-acting β 2-agonists (LABAs), such as arformoterol, indacaterol, formoterol, olodaterol, salmeterol, and vilanterol
- LAMA/LABA combinations (umeclidinium/vilanterol, tiotropium/olodaterol, glycopyrrolate/formoterol, glycopyrrolate/indacaterol)
Inhaled corticosteroids can also be used in a fixed-dose combination with a LABA, which can be combined with a LAMA, in select patients5; however, these combination products may have minimal value in treating dyspnea unless asthma is concomitantly present.5,64 Further discussion of the different treatment options available for patients with COPD can be found in the final article of this supplement.
In addition to improving quality of life, long-acting bronchodilators, such as LAMAs, LABAs, and LAMA/LABA combinations, increase expiratory flow, reduce dynamic hyperinflation, and improve exercise capacity of patients.65-67 As disease severity worsens, physicians may opt for long-acting bronchodilator options that have twice-daily dosing, which may confer a benefit in improving night-time symptom control.68
As well as active pharmacologic and nonpharmacologic interventions, physicians should always encourage smoking cessation in patients with COPD, as this has the greatest capacity to influence the natural course of the disease.5 It is essential that health care providers continually deliver smoking cessation messages to patients with COPD; patients can also be supported to stop smoking by using nicotine replacement therapy, pharmacologic interventions, attending smoking cessation programs, and counseling.5
Lung volume reduction surgery may also be considered as a strategy for the management of dyspnea in severe, refractory COPD.69 Similarly, nonsurgical bronchoscopic interventions are being developed that look to achieve similar results to lung volume reduction surgery, including endobronchial one-way valves, lung volume reduction coils, airway bypasses, adhesives, and vapor therapy.23
CASE STUDY:
The primary care physician assessed KD’s dyspnea using the CAT and ordered a chest X-ray to identify any significant comorbidities, such as concomitant respiratory, skeletal, or cardiac diseases. As KD’s CAT score was 17, and her symptoms were uncontrolled on LAMA monotherapy, her physician prescribed a long-acting LAMA/LABA combination, along with pulmonary rehabilitation. The physician also counseled KD on the importance of smoking cessation, and referred her to a local smoking cessation program.
Conclusions
Dyspnea, the most common symptom of COPD and the primary consequence of the condition’s characteristic lung hyperinflation, is a heavy burden on the lives of patients. The impact of dyspnea is perhaps most apparent in the context of physical activity, with activity limitation observed frequently in patients with COPD, regardless of disease stage. This can affect patients’ quality of life significantly, and has long-term consequences on disease progression. Improving dyspnea and increasing exercise endurance should therefore be a key goal for COPD management, which should encompass both nonpharmacologic interventions, such as pulmonary rehabilitation, and pharmacologic interventions, such as use of bronchodilator therapy.
- O’Donnell DE. Hyperinflation, dyspnea, and exercise intolerance in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2006;3(2):180-184.
- Parshall MB, Schwartzstein RM, Adams L, et al; American Thoracic Society Committee on Dyspnea. An official American Thoracic Society statement: update on the mechanisms, assessment, and management of dyspnea. Am J Respir Crit Care Med. 2012;185(4):435-452.
- Kessler R, Partridge MR, Miravitlles M, et al. Symptom variability in patients with severe COPD: a pan-European cross-sectional study. Eur Respir J. 2011;37(2):264-272.
- Agusti A, Hedner J, Marin J, Barbé F, Cazzola M, Rennard S. Night-time symptoms: a forgotten dimension of COPD. Eur Respir Rev. 2011;20(121):183-194.
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of COPD. 2017. http://gold.copd.org/gold-2017-global-strategy-diagnosis-management-prevention-copd. Accessed November 27, 2017.
- O’Donnell DE, Gebke KB. Activity restriction in mild COPD: a challenging clinical problem. Int J Chron Obstruct Pulmon Dis. 2014;9:577-588.
- Elbehairy AF, Ciavaglia CE, Webb KA, et al; Canadian Respiratory Research Network. Pulmonary gas exchange abnormalities in mild chronic obstructive pulmonary disease. Implications for dyspnea and exercise intolerance. Am J Respir Crit Care Med. 2015;191(12):1384-1394.
- Barriga S, Rodrigues F, Bárbara C. Factors that influence physical activity in the daily life of male patients with chronic obstructive pulmonary disease. Rev Port Pneumol. 2014;20(3):131-137.
- Pitta F, Troosters T, Spruit MA, Probst VS, Decramer M, Gosselink R. Characteristics of physical activities in daily life in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(9):972-977.
- Haas F, Salazar-Schicci J, Axen K. Desensitization to dyspnoea in chronic obstructive pulmonary disease. In: Casaburi R, Petty TL, eds. Principles and Practice of Pulmonary Rehabilitation. Philadelphia, PA: W.B. Saunders; 1993:241-251.
- Belfer MH, Reardon JZ. Improving exercise tolerance and quality of life in patients with chronic obstructive pulmonary disease. J Am Osteopath Assoc. 2009;109(5):268-278.
- Troosters T, van der Molen T, Polkey M, et al. Improving physical activity in COPD: towards a new paradigm. Respir Res. 2013;14:115.
- Celli BR, MacNee W; ATS/ERS Task Force. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23(6):932-946.
- Gagnon P, Guenette JA, Langer D, et al. Pathogenesis of hyperinflation in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2014;9:187-201.
- Ferguson GT. Why does the lung hyperinflate? Proc Am Thorac Soc. 2006;3(2):176-179.
- O’Donnell DE, Revill SM, Webb KA. Dynamic hyperinflation and exercise intolerance in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;164(5):770-777.
- Dubé BP, Guerder A, Morelot-Panzini C, Laveneziana P. The clinical relevance of the emphysema-hyperinflated phenotype in COPD. COPD Res Pract. 2016;2:1.
- Scano G, Stendardi L, Grazzini M. Understanding dyspnoea by its language. Eur Respir J. 2005;25(2):380-385.
- Chowienczyk S, Javadzadeh S, Booth S, Farquhar M. Association of descriptors of breathlessness with diagnosis and self-reported severity of breathlessness in patients with advanced chronic obstructive pulmonary disease or cancer. J Pain Symptom Manage. 2016;52(2):259-264.
- Thomas M, Decramer M, O’Donnell DE. No room to breathe: the importance of lung hyperinflation in COPD. Prim Care Respir J. 2013;22(1):101-111.
- Gosselink R. Controlled breathing and dyspnea in patients with chronic obstructive pulmonary disease (COPD). J Rehabil Res Dev. 2003;40(5 Suppl 2):25-33.
- O’Donnell DE, Webb KA, Neder JA. Lung hyperinflation in COPD: applying physiology to clinical practice. COPD Res Pract. 2015;1:4.
- Browning RF, Parrish S, Sarkar S, et al. Bronchoscopic interventions for severe COPD. J Thorac Dis. 2014;6(Suppl 4):S407-S415.
- Nishimura K, Izumi T, Tsukino M, Oga T. Dyspnea is a better predictor of 5-year survival than airway obstruction in patients with COPD. Chest. 2002;121(5):1434-1440.
- Fletcher CM, Elmes PC, Fairbairn AS, Wood CH. The significance of respiratory symptoms and the diagnosis of chronic bronchitis in a working population. Br Med J. 1959;2(5147):257-266.
- O’Donnell DE, Lam M, Webb KA. Spirometric correlates of improvement in exercise performance after anticholinergic therapy in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1999;160(2):542-549.
- Light RW. Mechanics of respiration. In: George RB, ed. Chest Medicine: Essentials of Pulmonary and Critical Care Medicine. Philadelphia, PA: Lippincott Williams & Wilkins; 2005:24-38.
- Casanova C, Cote C, de Torres JP, et al. Inspiratory-to-total lung capacity ratio predicts mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(6):591-597.
- O’Donnell DE, Guenette JA, Maltais F, Webb KA. Decline of resting inspiratory capacity in COPD: the impact on breathing pattern, dyspnea, and ventilatory capacity during exercise. Chest. 2012;141(3):753-762.
- O’Donnell DE, Laveneziana P. Dyspnea and activity limitation in COPD: mechanical factors. COPD. 2007;4(3):225-236.
- Holland AE. Physiotherapy management of acute exacerbations of chronic obstructive pulmonary disease. J Physiother. 2014;60(4):181-188.
- Barr RG, Bluemke DA, Ahmed FS, et al. Percent emphysema, airflow obstruction, and impaired left ventricular filling. N Engl J Med. 2010;362(3):217-227.
- Garcia-Rio F, Lores V, Mediano O, et al. Daily physical activity in patients with chronic obstructive pulmonary disease is mainly associated with dynamic hyperinflation. Am J Respir Crit Care Med. 2009;180(6):506-512.
- Di Marco F, Santus P, Sotgiu G, Blasi F, Centanni S. Does improving exercise capacity and daily activity represent the holistic perspective of a new COPD approach? COPD. 2015;12(5):575-581.
- Newton MF, O’Donnell DE, Forkert L. Response of lung volumes to inhaled salbutamol in a large population of patients with severe hyperinflation. Chest. 2002;121(4):1042-1050.
- Bailey KL. The importance of the assessment of pulmonary function in COPD. Med Clin North Am. 2012;96(4):745-752.
- Burkhardt R, Pankow W. The diagnosis of chronic obstructive pulmonary disease. Dtsch Arztebl Int. 2014;111(49):834-845, quiz 846.
- O’Donnell CR, Bankier AA, Stiebellehner L, Reilly JJ, Brown R, Loring SH. Comparison of plethysmographic and helium dilution lung volumes: which is best for COPD? Chest. 2010;137(5):1108-1115.
- Criée CP, Sorichter S, Smith HJ, et al; Working Group for Body Plethysmography of the German Society for Pneumology and Respiratory Care. Body plethysmography—its principles and clinical use. Respir Med. 2011;105(7):959-971.
- Lutfi MF. The physiological basis and clinical significance of lung volume measurements. Multidiscip Respir Med. 2017;12:3.
- Lahaije AJ, van Helvoort HA, Dekhuijzen PN, Vercoulen JH, Heijdra YF. Resting and ADL-induced dynamic hyperinflation explain physical inactivity in COPD better than FEV1. Respir Med. 2013;107(6):834-840.
- Troosters T, Sciurba F, Battaglia S, et al. Physical inactivity in patients with COPD, a controlled multi-center pilot-study. Respir Med. 2010;104(7):1005-1011.
- Calverley PMA, Georgopoulos D. Symptoms and signs of COPD. In: Siafakas NM, ed. Management of Chronic Obstructive Pulmonary Disease: European Respiratory Society Journals; 2006.
- Cave AJ, Atkinson L, Tsiligianni IG, Kaplan AG. Assessment of COPD wellness tools for use in primary care: an IPCRG initiative. Int J Chron Obstruct Pulmon Dis. 2012;7:447-456.
- Cazzola M, Hanania NA, MacNee W, Rüdell K, Hackford C, Tamimi N. A review of the most common patient-reported outcomes in COPD—revisiting current knowledge and estimating future challenges. Int J Chron Obstruct Pulmon Dis. 2015;10:725-738.
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111-117.
- Polkey MI, Spruit MA, Edwards LD, et al; Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) Study Investigators. Six-minute-walk test in chronic obstructive pulmonary disease: minimal clinically important difference for death or hospitalization. Am J Respir Crit Care Med. 2013;187(4):382-386.
- Puhan MA, Mador MJ, Held U, Goldstein R, Guyatt GH, Schünemann HJ. Interpretation of treatment changes in 6-minute walk distance in patients with COPD. Eur Respir J. 2008;32(3):637-643.
- Holland AE, Hill CJ, Rasekaba T, Lee A, Naughton MT, McDonald CF. Updating the minimal important difference for six-minute walk distance in patients with chronic obstructive pulmonary disease. Arch Phys Med Rehabil. 2010;91(2):221-225.
- Grant A, Moore L. Pulmonary rehabilitation. In: Blackler L, Jones C, Mooney C, eds. Managing Chronic Obstructive Pulmonary Disease. West Sussex, England: John Wiley & Sons; 2007.
- Crisafulli E, Gorgone P, Vagaggini B, et al. Efficacy of standard rehabilitation in COPD outpatients with comorbidities. Eur Respir J. 2010;36(5):1042-1048.
- Spruit MA, Singh SJ, Garvey C, et al; ATS/ERS Task Force on Pulmonary Rehabilitation. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13-e64.
- Ries AL, Bauldoff GS, Carlin BW, et al. Pulmonary Rehabilitation: Joint ACCP/AACVPR Evidence-Based Clinical Practice Guidelines. Chest. 2007;131(5 Suppl):4S-42S.
- Evans RA, Singh SJ, Collier R, Williams JE, Morgan MD. Pulmonary rehabilitation is successful for COPD irrespective of MRC dyspnoea grade. Respir Med. 2009;103(7):1070-1075.
- McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015;(2):CD003793.
- Stoller JK, Panos RJ, Krachman S, Doherty DE, Make B; Long-term Oxygen Treatment Trial Research Group. Oxygen therapy for patients with COPD: current evidence and the long-term oxygen treatment trial. Chest. 2010;138(1):179-187.
- Ekström M, Ahmadi Z, Bornefalk-Hermansson A, Abernethy A, Currow D. Oxygen for breathlessness in patients with chronic obstructive pulmonary disease who do not qualify for home oxygen therapy. Cochrane Database Syst Rev. 2016;11:CD006429.
- Maddocks M, Kon SS, Canavan JL, et al. Physical frailty and pulmonary rehabilitation in COPD: a prospective cohort study. Thorax. 2016;71(11):988-995.
- Wolkove N, Kamel H, Rotaple M, Baltzan MA Jr. Use of a mucus clearance device enhances the bronchodilator response in patients with stable COPD. Chest. 2002;121(3):702-707.
- Chatburn RL. High-frequency assisted airway clearance. Respir Care. 2007;52(9):1224-1235; discussion 1235-1227.
- Clini E. Positive expiratory pressure techniques in respiratory patients: old evidence and new insights. Breathe. 2009;6(2):153-159.
- Petrof BJ, Legaré M, Goldberg P, Milic-Emili J, Gottfried SB. Continuous positive airway pressure reduces work of breathing and dyspnea during weaning from mechanical ventilation in severe chronic obstructive pulmonary disease. Am Rev Respir Dis. 1990;141(2):281-289.
- Clini E, Sturani C, Rossi A, et al; Rehabilitation and Chronic Care Study Group; Italian Association of Hospital Pulmonologists (AIPO). The Italian multicentre study on noninvasive ventilation in chronic obstructive pulmonary disease patients. Eur Respir J. 2002;20(3):529-538.
- Bourbeau J, Rouleau MY, Boucher S. Randomised controlled trial of inhaled corticosteroids in patients with chronic obstructive pulmonary disease. Thorax. 1998;53(6):477-482.
- Berton DC, Reis M, Siqueira AC, et al. Effects of tiotropium and formoterol on dynamic hyperinflation and exercise endurance in COPD. Respir Med. 2010;104(9):1288-1296.
- O’Donnell DE, Flüge T, Gerken F, et al. Effects of tiotropium on lung hyperinflation, dyspnoea and exercise tolerance in COPD. Eur Respir J. 2004;23(6):832-840.
- O’Donnell DE, Sciurba F, Celli B, et al. Effect of fluticasone propionate/salmeterol on lung hyperinflation and exercise endurance in COPD. Chest. 2006;130(3):647-656.
- Blasi F, Canonica GW, Miravitlles M. Is aclidinium alone or combined with a LABA a rational choice for symptomatic COPD patients [published correction appears in Respir Res. 2017;18(1):35]. Respir Res. 2017;18(1):19.
- Shah AA, D’Amico TA. Lung volume reduction surgery for the management of refractory dyspnea in chronic obstructive pulmonary disease. Curr Opin Support Palliat Care. 2009;3(2):107-111.
- O’Donnell DE. Hyperinflation, dyspnea, and exercise intolerance in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2006;3(2):180-184.
- Parshall MB, Schwartzstein RM, Adams L, et al; American Thoracic Society Committee on Dyspnea. An official American Thoracic Society statement: update on the mechanisms, assessment, and management of dyspnea. Am J Respir Crit Care Med. 2012;185(4):435-452.
- Kessler R, Partridge MR, Miravitlles M, et al. Symptom variability in patients with severe COPD: a pan-European cross-sectional study. Eur Respir J. 2011;37(2):264-272.
- Agusti A, Hedner J, Marin J, Barbé F, Cazzola M, Rennard S. Night-time symptoms: a forgotten dimension of COPD. Eur Respir Rev. 2011;20(121):183-194.
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of COPD. 2017. http://gold.copd.org/gold-2017-global-strategy-diagnosis-management-prevention-copd. Accessed November 27, 2017.
- O’Donnell DE, Gebke KB. Activity restriction in mild COPD: a challenging clinical problem. Int J Chron Obstruct Pulmon Dis. 2014;9:577-588.
- Elbehairy AF, Ciavaglia CE, Webb KA, et al; Canadian Respiratory Research Network. Pulmonary gas exchange abnormalities in mild chronic obstructive pulmonary disease. Implications for dyspnea and exercise intolerance. Am J Respir Crit Care Med. 2015;191(12):1384-1394.
- Barriga S, Rodrigues F, Bárbara C. Factors that influence physical activity in the daily life of male patients with chronic obstructive pulmonary disease. Rev Port Pneumol. 2014;20(3):131-137.
- Pitta F, Troosters T, Spruit MA, Probst VS, Decramer M, Gosselink R. Characteristics of physical activities in daily life in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(9):972-977.
- Haas F, Salazar-Schicci J, Axen K. Desensitization to dyspnoea in chronic obstructive pulmonary disease. In: Casaburi R, Petty TL, eds. Principles and Practice of Pulmonary Rehabilitation. Philadelphia, PA: W.B. Saunders; 1993:241-251.
- Belfer MH, Reardon JZ. Improving exercise tolerance and quality of life in patients with chronic obstructive pulmonary disease. J Am Osteopath Assoc. 2009;109(5):268-278.
- Troosters T, van der Molen T, Polkey M, et al. Improving physical activity in COPD: towards a new paradigm. Respir Res. 2013;14:115.
- Celli BR, MacNee W; ATS/ERS Task Force. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23(6):932-946.
- Gagnon P, Guenette JA, Langer D, et al. Pathogenesis of hyperinflation in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2014;9:187-201.
- Ferguson GT. Why does the lung hyperinflate? Proc Am Thorac Soc. 2006;3(2):176-179.
- O’Donnell DE, Revill SM, Webb KA. Dynamic hyperinflation and exercise intolerance in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;164(5):770-777.
- Dubé BP, Guerder A, Morelot-Panzini C, Laveneziana P. The clinical relevance of the emphysema-hyperinflated phenotype in COPD. COPD Res Pract. 2016;2:1.
- Scano G, Stendardi L, Grazzini M. Understanding dyspnoea by its language. Eur Respir J. 2005;25(2):380-385.
- Chowienczyk S, Javadzadeh S, Booth S, Farquhar M. Association of descriptors of breathlessness with diagnosis and self-reported severity of breathlessness in patients with advanced chronic obstructive pulmonary disease or cancer. J Pain Symptom Manage. 2016;52(2):259-264.
- Thomas M, Decramer M, O’Donnell DE. No room to breathe: the importance of lung hyperinflation in COPD. Prim Care Respir J. 2013;22(1):101-111.
- Gosselink R. Controlled breathing and dyspnea in patients with chronic obstructive pulmonary disease (COPD). J Rehabil Res Dev. 2003;40(5 Suppl 2):25-33.
- O’Donnell DE, Webb KA, Neder JA. Lung hyperinflation in COPD: applying physiology to clinical practice. COPD Res Pract. 2015;1:4.
- Browning RF, Parrish S, Sarkar S, et al. Bronchoscopic interventions for severe COPD. J Thorac Dis. 2014;6(Suppl 4):S407-S415.
- Nishimura K, Izumi T, Tsukino M, Oga T. Dyspnea is a better predictor of 5-year survival than airway obstruction in patients with COPD. Chest. 2002;121(5):1434-1440.
- Fletcher CM, Elmes PC, Fairbairn AS, Wood CH. The significance of respiratory symptoms and the diagnosis of chronic bronchitis in a working population. Br Med J. 1959;2(5147):257-266.
- O’Donnell DE, Lam M, Webb KA. Spirometric correlates of improvement in exercise performance after anticholinergic therapy in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1999;160(2):542-549.
- Light RW. Mechanics of respiration. In: George RB, ed. Chest Medicine: Essentials of Pulmonary and Critical Care Medicine. Philadelphia, PA: Lippincott Williams & Wilkins; 2005:24-38.
- Casanova C, Cote C, de Torres JP, et al. Inspiratory-to-total lung capacity ratio predicts mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(6):591-597.
- O’Donnell DE, Guenette JA, Maltais F, Webb KA. Decline of resting inspiratory capacity in COPD: the impact on breathing pattern, dyspnea, and ventilatory capacity during exercise. Chest. 2012;141(3):753-762.
- O’Donnell DE, Laveneziana P. Dyspnea and activity limitation in COPD: mechanical factors. COPD. 2007;4(3):225-236.
- Holland AE. Physiotherapy management of acute exacerbations of chronic obstructive pulmonary disease. J Physiother. 2014;60(4):181-188.
- Barr RG, Bluemke DA, Ahmed FS, et al. Percent emphysema, airflow obstruction, and impaired left ventricular filling. N Engl J Med. 2010;362(3):217-227.
- Garcia-Rio F, Lores V, Mediano O, et al. Daily physical activity in patients with chronic obstructive pulmonary disease is mainly associated with dynamic hyperinflation. Am J Respir Crit Care Med. 2009;180(6):506-512.
- Di Marco F, Santus P, Sotgiu G, Blasi F, Centanni S. Does improving exercise capacity and daily activity represent the holistic perspective of a new COPD approach? COPD. 2015;12(5):575-581.
- Newton MF, O’Donnell DE, Forkert L. Response of lung volumes to inhaled salbutamol in a large population of patients with severe hyperinflation. Chest. 2002;121(4):1042-1050.
- Bailey KL. The importance of the assessment of pulmonary function in COPD. Med Clin North Am. 2012;96(4):745-752.
- Burkhardt R, Pankow W. The diagnosis of chronic obstructive pulmonary disease. Dtsch Arztebl Int. 2014;111(49):834-845, quiz 846.
- O’Donnell CR, Bankier AA, Stiebellehner L, Reilly JJ, Brown R, Loring SH. Comparison of plethysmographic and helium dilution lung volumes: which is best for COPD? Chest. 2010;137(5):1108-1115.
- Criée CP, Sorichter S, Smith HJ, et al; Working Group for Body Plethysmography of the German Society for Pneumology and Respiratory Care. Body plethysmography—its principles and clinical use. Respir Med. 2011;105(7):959-971.
- Lutfi MF. The physiological basis and clinical significance of lung volume measurements. Multidiscip Respir Med. 2017;12:3.
- Lahaije AJ, van Helvoort HA, Dekhuijzen PN, Vercoulen JH, Heijdra YF. Resting and ADL-induced dynamic hyperinflation explain physical inactivity in COPD better than FEV1. Respir Med. 2013;107(6):834-840.
- Troosters T, Sciurba F, Battaglia S, et al. Physical inactivity in patients with COPD, a controlled multi-center pilot-study. Respir Med. 2010;104(7):1005-1011.
- Calverley PMA, Georgopoulos D. Symptoms and signs of COPD. In: Siafakas NM, ed. Management of Chronic Obstructive Pulmonary Disease: European Respiratory Society Journals; 2006.
- Cave AJ, Atkinson L, Tsiligianni IG, Kaplan AG. Assessment of COPD wellness tools for use in primary care: an IPCRG initiative. Int J Chron Obstruct Pulmon Dis. 2012;7:447-456.
- Cazzola M, Hanania NA, MacNee W, Rüdell K, Hackford C, Tamimi N. A review of the most common patient-reported outcomes in COPD—revisiting current knowledge and estimating future challenges. Int J Chron Obstruct Pulmon Dis. 2015;10:725-738.
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111-117.
- Polkey MI, Spruit MA, Edwards LD, et al; Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) Study Investigators. Six-minute-walk test in chronic obstructive pulmonary disease: minimal clinically important difference for death or hospitalization. Am J Respir Crit Care Med. 2013;187(4):382-386.
- Puhan MA, Mador MJ, Held U, Goldstein R, Guyatt GH, Schünemann HJ. Interpretation of treatment changes in 6-minute walk distance in patients with COPD. Eur Respir J. 2008;32(3):637-643.
- Holland AE, Hill CJ, Rasekaba T, Lee A, Naughton MT, McDonald CF. Updating the minimal important difference for six-minute walk distance in patients with chronic obstructive pulmonary disease. Arch Phys Med Rehabil. 2010;91(2):221-225.
- Grant A, Moore L. Pulmonary rehabilitation. In: Blackler L, Jones C, Mooney C, eds. Managing Chronic Obstructive Pulmonary Disease. West Sussex, England: John Wiley & Sons; 2007.
- Crisafulli E, Gorgone P, Vagaggini B, et al. Efficacy of standard rehabilitation in COPD outpatients with comorbidities. Eur Respir J. 2010;36(5):1042-1048.
- Spruit MA, Singh SJ, Garvey C, et al; ATS/ERS Task Force on Pulmonary Rehabilitation. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13-e64.
- Ries AL, Bauldoff GS, Carlin BW, et al. Pulmonary Rehabilitation: Joint ACCP/AACVPR Evidence-Based Clinical Practice Guidelines. Chest. 2007;131(5 Suppl):4S-42S.
- Evans RA, Singh SJ, Collier R, Williams JE, Morgan MD. Pulmonary rehabilitation is successful for COPD irrespective of MRC dyspnoea grade. Respir Med. 2009;103(7):1070-1075.
- McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015;(2):CD003793.
- Stoller JK, Panos RJ, Krachman S, Doherty DE, Make B; Long-term Oxygen Treatment Trial Research Group. Oxygen therapy for patients with COPD: current evidence and the long-term oxygen treatment trial. Chest. 2010;138(1):179-187.
- Ekström M, Ahmadi Z, Bornefalk-Hermansson A, Abernethy A, Currow D. Oxygen for breathlessness in patients with chronic obstructive pulmonary disease who do not qualify for home oxygen therapy. Cochrane Database Syst Rev. 2016;11:CD006429.
- Maddocks M, Kon SS, Canavan JL, et al. Physical frailty and pulmonary rehabilitation in COPD: a prospective cohort study. Thorax. 2016;71(11):988-995.
- Wolkove N, Kamel H, Rotaple M, Baltzan MA Jr. Use of a mucus clearance device enhances the bronchodilator response in patients with stable COPD. Chest. 2002;121(3):702-707.
- Chatburn RL. High-frequency assisted airway clearance. Respir Care. 2007;52(9):1224-1235; discussion 1235-1227.
- Clini E. Positive expiratory pressure techniques in respiratory patients: old evidence and new insights. Breathe. 2009;6(2):153-159.
- Petrof BJ, Legaré M, Goldberg P, Milic-Emili J, Gottfried SB. Continuous positive airway pressure reduces work of breathing and dyspnea during weaning from mechanical ventilation in severe chronic obstructive pulmonary disease. Am Rev Respir Dis. 1990;141(2):281-289.
- Clini E, Sturani C, Rossi A, et al; Rehabilitation and Chronic Care Study Group; Italian Association of Hospital Pulmonologists (AIPO). The Italian multicentre study on noninvasive ventilation in chronic obstructive pulmonary disease patients. Eur Respir J. 2002;20(3):529-538.
- Bourbeau J, Rouleau MY, Boucher S. Randomised controlled trial of inhaled corticosteroids in patients with chronic obstructive pulmonary disease. Thorax. 1998;53(6):477-482.
- Berton DC, Reis M, Siqueira AC, et al. Effects of tiotropium and formoterol on dynamic hyperinflation and exercise endurance in COPD. Respir Med. 2010;104(9):1288-1296.
- O’Donnell DE, Flüge T, Gerken F, et al. Effects of tiotropium on lung hyperinflation, dyspnoea and exercise tolerance in COPD. Eur Respir J. 2004;23(6):832-840.
- O’Donnell DE, Sciurba F, Celli B, et al. Effect of fluticasone propionate/salmeterol on lung hyperinflation and exercise endurance in COPD. Chest. 2006;130(3):647-656.
- Blasi F, Canonica GW, Miravitlles M. Is aclidinium alone or combined with a LABA a rational choice for symptomatic COPD patients [published correction appears in Respir Res. 2017;18(1):35]. Respir Res. 2017;18(1):19.
- Shah AA, D’Amico TA. Lung volume reduction surgery for the management of refractory dyspnea in chronic obstructive pulmonary disease. Curr Opin Support Palliat Care. 2009;3(2):107-111.

Anxiety and Depression in Chronic Obstructive Pulmonary Disease: Recognition and Management
Introduction
Anxiety and depression are common in patients with chronic obstructive pulmonary disease (COPD), occurring more frequently than in the general population1-4 or patients with other chronic diseases such as hypertension, diabetes, cancer, or musculoskeletal disorders.5,6 Their presence is associated with worse outcomes of COPD, and increased morbidity, mortality, disability, and health care expenditure.6-8 In spite of this, both anxiety and depression are frequently overlooked and undertreated in patients with COPD,9 and symptoms of anxiety and depression can overlap significantly, as well as overlap with COPD symptoms.7,10
Comorbid depressive disorders that may occur in patients with COPD include major depressive disorder, dysthymias (chronic depressive symptoms of mild severity), and minor depression.11 Depressive disorders are characterized by feelings of sadness, emptiness, and/or irritability, along with cognitive and somatic symptoms, which have a detrimental effect on the patient’s ability to function.11 Anxiety disorders include generalized anxiety disorder (GAD), phobias, and panic disorders.11 The main features of anxiety disorders, such as excessive fear and anxiety, may be accompanied by behavioral disturbances related to these symptoms, such as panic attacks and avoidance.11,12
The reported prevalence of depression in COPD varies widely between studies, owing to differences in sampling methods and degrees of illness severity used in assessment of depression6; rates have been reported to range from 10% to 42% in patients with stable COPD,6,13 and from 10% to 86% in patients with acute COPD exacerbation.14 Individuals with severe COPD are twice as likely to develop depression than patients with mild COPD.10
Prevalence rates for clinical anxiety in COPD range from 13% to 46% in outpatients and 10% to 55% among inpatients. GAD, panic disorders, and specific phobias are reported most frequently.15 Patients with COPD are 85% more likely to develop anxiety disorders compared with matched controls without COPD,4 and panic disorder is reported with a prevalence that is up to 10-fold higher than in the general population.16
Global prevalence rates of anxiety and depression are 1.8- and 1.4-fold higher in women than men, respectively17; the same gender difference is observed in patients with COPD.6 The higher prevalence rates of anxiety and depression in women are thought to be a result of sex differences in brain structure, function, and stress responses, as well as differences in exposure to reproductive hormones, social constraints, and experiences between women and men.18 However, psychologic comorbidity is an issue for both men and women with COPD, so it is important that clinicians are vigilant in recognizing anxiety and depression in both sexes, and are careful not to underestimate the burden in the male patient population.
It is also important to note that depression and anxiety often occur simultaneously in patients with COPD, with prevalence estimates of 26% to 43%.9,19,20 COPD patients with both depression and anxiety are at a heightened risk of suicidal ideation, increased physical disability, and chronic depressive symptoms versus those with either disorder alone.10,15 It is therefore important that comorbid anxiety and depression is not overlooked in patients with COPD.
Ensuring that anxiety and depression are recognized and treated effectively in patients with COPD is essential for optimizing outcomes. Primary care practitioners are well placed to diagnose anxiety and depression, and to ensure these conditions are suitably managed alongside treatments of COPD.
Potential mechanisms of anxiety and depression in COPD
Growing evidence suggests that the relationship between mood disorders—particularly depression—and COPD is bidirectional, meaning that mood disorders adversely impact prognosis in COPD, whereas COPD increases the risk of developing depression.21 For example, in a study of
60 stable patients with COPD, elevated dyspnea and reduced exercise capacity were the predominant mechanisms leading to anxiety and depression symptoms associated with the condition.22 In addition, the risk of new-onset depression was increased in COPD patients with moderate-to-severe dyspnea in a 3-year follow-up study.23 Conversely, depression has been shown to be a significant risk factor for disabling dyspnea (modified Medical Research Council score ≥2) in patients with COPD.24
COPD can lead to feelings of hopelessness, social isolation, reduced physical functioning, and sedentary lifestyle, all of which are associated with an increased level of depressive symptoms.25 Similarly, inadequate social support increases the risk of anxiety in patients with COPD.26 Therefore, ensuring that patients with COPD have high-quality support is very important for reducing anxiety and depressive symptoms.27
The exact mechanisms for the association between mood disorders and COPD remain unclear.7,10 Research to date indicates that the relationship between depression and impaired pulmonary function may be partly mediated by chronic inflammation7,10; systemic inflammation has been associated with other comorbidities of COPD (eg, muscle wasting and osteoporosis),28 and emerging data appear to show that proinflammatory cytokines partly mediate the association between depressive symptoms and pulmonary function.29 Smoking and hypoxemia may also influence the prevalence of depression in COPD, but symptom severity and impaired quality of life remain the most important determinants.6,30
Clinical studies have demonstrated that a number of patient-related factors, including female gender, younger age, current smoking, greater severity of airflow limitation, and lower socioeconomic status, are associated with a higher prevalence and/or increased risk of depression and/or anxiety in COPD.3,4,30,31 Frequent episodes of rehospitalization, and comorbidities such as hypertension, arthritis, cancer, and heart disease, have been found to increase the risk of anxiety and depression in patients with COPD.3,32 Risk of anxiety has been shown to increase with greater dyspnea severity.4 Pain, a frequently overlooked symptom in COPD, has been shown to be associated with symptoms of both anxiety and depression in patients with COPD.33 This is driven by worsened quality of life and sleep quality, decreased physical activity, and an increased fear of movement that occur as a result of pain.34
The impact of anxiety and depression in COPD
Comorbid anxiety and depression have a significant detrimental impact on morbidity and mortality in patients with COPD. Both disorders have been associated with an increased risk of death in COPD.13,35-37 Indeed, of 12 comorbidities proposed to be predictors of mortality in a cohort of 187 female outpatients with COPD, anxiety was associated with the highest risk of death.35,36
In addition, patients with COPD and anxiety and/or depression have a higher risk of COPD exacerbations,4,8,23,36,38-40 hospitalization,41,42 rehospitalization,14,36,43 longer hospital stays,37,41,44 and mortality after exacerbations,14,36,41 compared with patients without these comorbidities. Patients with COPD who have elevated anxiety symptoms also often experience their first hospitalization earlier in the natural course of COPD than those without anxiety.36
Psychologic comorbidities are also associated with worse lung function, dyspnea, and respiratory symptom burden in patients with COPD.37,40 Patients with COPD and anxiety are more likely to experience greater dyspnea at an earlier stage of disease than those without anxiety.36 Persistent smoking at 6 months after hospitalization for an acute exacerbation of COPD is also more likely to be seen in patients with depression.37
Patient-centered outcomes are worse in COPD patients with mood disorders. Both anxiety and depression have been shown to correlate with significantly reduced health-related quality of life (HRQoL), poorer physical health status, functional limitations, and reduced exercise capacity.4,23,37,40,45 The presence of either anxiety or depression at baseline has been shown to correlate with reduced HRQoL at 1-year follow-up, but depression appears to be the stronger predictor of low future HRQoL than anxiety.45
Additionally, mood disorders—particularly depression—reduce physical activity in patients with COPD.46,47 Emotional responses to COPD symptoms, such as dyspnea, can further decrease activity and worsen deconditioning, resulting in a downward spiral of reduced inactivity, social isolation, fear, anxiety, and depression.48
COPD patients with any comorbidity exhibit lower rates of medication adherence than those without comorbidities.49-51 Clinical studies have demonstrated that anxiety and depression are significant predictors of poor adherence to COPD interventions, including pulmonary rehabilitation (PR).51-55 Nonadherence to COPD therapies is associated with poor clinical outcomes, including higher hospitalization rates and increased emergency department visits, and increased costs.56,57 Health care expenditure, in terms of both specific COPD-related costs and general “all-cause” costs, is significantly higher in COPD patients with anxiety and/or depression than in those without.8
Diagnosis of anxiety and depression in patients with COPD
The underdiagnosis and undertreatment of anxiety and depression in this population is common and can adversely affect patient outcomes.6,7,9,10,58 Hence, it is crucial that anxiety and depression are identified and more effectively managed in clinical practice.10
Primary care practitioners are the main point of contact for many patients with COPD,6,59,60 and so can play a key role in screening for and early identification of anxiety and depression. However, detection of mood disorders by primary care practitioners is challenging for several reasons. These include the lack of a standardized approach in diagnosis, and inadequate knowledge or confidence in assessing psychological status (particularly given the number of strategies available for screening patients for mood disorders),6 as well as factors associated with time constraints, such as competing agendas, duration of visits, and high patient load.6,61 Furthermore, system-level barriers, such as lack of electronic medical records and adequate health insurance, as well as any communication gaps between primary care and mental health care, may hinder the detection and management of anxiety and depression.6 In addition, patients themselves may have a limited understanding of these comorbidities, or may be hesitant to discuss symptoms of anxiety or depression with their primary care practitioner owing to stigma around mental illness.6
Patients with COPD should be screened and assessed for anxiety and depression, and the United States Preventive Services Task Force recommends that clinicians screen for depression in all adults.6,62 There are several validated screening tools suitable for clinical use:
- Anxiety Inventory for Respiratory (AIR) Disease scale: a brief, easy-to-use tool for screening and measuring anxiety in COPD.63,64 It is a self-administered scale, and takes approximately 2 minutes to complete. The AIR scale is responsive to PR.64
- COPD Anxiety Questionnaire (CAF): a reliable tool for early identification of COPD-related anxiety.65
- Primary Care Evaluation of Mental Disorders (PRIME-MD) Patient Health Questionnaire (PHQ; available at: http://www.phqscreeners.com/select-screener/): the PRIME-MD comprises 26 yes/no questions on the 5 most common psychiatric disorders, including depression and anxiety.66,67 This is not a diagnostic tool, but a high number of positive responses from a patient in any given module indicates that they require further clinical evaluation.
- PHQ-2 and PHQ-9 (Table 1; PHQ-9 available at http://www.phqscreeners.com/select-screener/): widely-used self-administered 2- and 9-item versions of the PRIME-MD, specific to depression; similarly, the 3-item PHQ-3 is available for anxiety assessment (Table 2).6,67,68 In a study investigating tools used by family physicians in England to assess depression, over 75% used PHQ-9.69


- Hospital Anxiety and Depression Scale (HADS) and General Health Questionnaire-version 20 (GHQ-20): both can be used to screen for psychologic distress in patients with COPD.71
- The Beck Anxiety Inventory (BAI) and Beck Depression Inventory (BDI): two 21-item self-report questionnaires that are widely used in the United States to evaluate anxiety and depression.72


In addition to specific anxiety and depression questionnaires (Tables 1 and 2), more general COPD assessments tools, such as the COPD Assessment Test and the COPD Clinical Questionnaire, also incorporate questions that may be indicative of symptoms of these comorbidities in patients with COPD.73
Management of anxiety and depression in COPD
Even though anxiety and depression are among the most common and burdensome comorbid conditions in COPD, less than one-third of patients with these comorbidities receive effective intervention.6,10 Primary care providers have an excellent opportunity to impact this care gap.

As in non-COPD patients, comorbid depression and anxiety may be treated with nonpharmacologic and/or pharmacologic interventions (Figure 1).76
Nonpharmacologic interventions
Evidence to date suggests that nonpharmacologic interventions such as behavioral therapy are as effective as antidepressants, and may be preferred by patients with mood disorders.12
Cognitive behavioral therapy (CBT), which is typically administered by psychologists/psychiatrists, may be effective in treating COPD-related anxiety and depression, especially in conjunction with exercise and education.12,76,77 Individualized or group CBT is the treatment of choice for addressing thinking patterns that contribute to anxiety and depression to change a patient’s behavior and emotional state.76 PR programs involve several components, including aerobic exercise, lung function training, and psycho-education.62,76 PR is suitable for most patients with COPD, and provides multiple benefits, including reduced hospitalizations in patients who have had a recent exacerbation, and improved dyspnea, exercise tolerance, and health status in patients with stable disease,62 as well as clinically and statistically significant improvements in depression and anxiety, irrespective of age.7,78,79 Exercise-based forms of PR appear to be the most effective for reducing mood symptoms,12,76 and incorporating psychotherapy may also improve psychologic outcomes.80 Stress reduction (relaxation) therapy aims to reduce anxiety-related physiologic changes, and includes a variety of techniques (eg, breathing exercises, sequential muscle relaxation, hypnosis, mindfulness meditation), some of which may be included in PR or used alongside other treatments (eg, CBT).76 Limited data indicate that such therapy may be beneficial for reducing anxiety and depression, as well as respiratory symptoms and dyspnea, in patients with COPD.12,76
Self-management techniques improve clinical outcomes in patients with COPD, but data on the management of depression or anxiety are inconclusive.7,12 A minimal, home-based, nurse-led, psycho-educational intervention was designed to encourage more open-ended, descriptive discussions of thoughts, emotions, behaviors, and bodily sensations in patients with COPD.81 The intervention, which involved nurses attending a 1-hour face-to-face session in the patients’ homes with a 15-minute telephone “booster” session 2 weeks later, helped patients with advanced COPD to self-manage their condition and provide relief from anxiety.81,82 However, it should be noted that there is currently a lack of high-quality data evaluating psychologic interventions in the COPD population.83
In addition, it is important that caregivers are supported in the management of patients with COPD and comorbid anxiety and/or depression; areas in which caregivers can be assisted in their role may include disease education and counseling, where appropriate.84
Given that smoking cessation is a key recommendation for patients with COPD,44,62 practitioners should be aware that patients with comorbid depression and anxiety may experience greater difficulty in smoking cessation, and worsened mood during nicotine withdrawal.44 Clinicians should therefore carefully monitor current smokers with COPD and comorbid depression/anxiety (using the tools described previously63,68,70,71) when they are attempting to quit smoking.
Pharmacologic interventions
Pharmacologic therapy of anxiety and depression has so far only been investigated in patients with COPD in small studies.76 However, the available evidence does not indicate that COPD patients with anxiety and depression should be managed any differently from individuals without COPD.62 As such, pharmacologic interventions are particularly important for patients with acute or severe anxiety or depression.
Antidepressant agents are categorized according to their mechanism of action, and most commonly include selective serotonin-reuptake inhibitors (SSRIs), selective norepinephrine-reuptake inhibitors, bupropion (a norepinephrine- and dopamine-reuptake inhibitor; also approved for smoking cessation85), and mirtazapine (a norepinephrine and serotonin modulator), among others.86 SSRIs are the current firstline drug treatment for depression, and have been shown to significantly improve depression and anxiety in patients with COPD in some, but not all, trials published to date.76 However, it is important to note that a diagnosis of bipolar disorder must be ruled out before initiating standard antidepressant therapy.87 In addition to antidepressants, atypical antipsychotics have also been shown to be useful for treating anxiety, either as monotherapy or combination therapy, and possibly as an adjunctive therapy for the management of depression.88,89
Primary care practitioners can refer to existing guidelines on the management of anxiety and depression in patients with COPD,86,90 while taking certain factors into consideration. Any pharmacologic management strategy for the treatment of COPD may increase the risk of drug–drug or drug–disease interactions.76 For example, it is important to avoid medications that cause respiratory depression (eg, benzodiazepines [unless used with extreme caution], particularly in patients who are already CO2 retainers) or sedation; chosen drugs should have minimal other adverse effects.76 Moreover, SSRIs may also be associated with troublesome adverse effects during treatment initiation, such as gastrointestinal upset, headache, tremor, psychomotor activation, and sedation76; in addition, dry mouth is an adverse effect associated with both SSRI treatment and several inhaled therapies, so may be particularly problematic in patients with COPD.91,92 Currently, data are particularly scarce for the management of anxiety in patients with COPD, with inconclusive or contradictory findings reported for SSRIs, azapirones (including buspirone), and tricyclic antidepressants.76
In addition to monitoring adherence to COPD therapies, primary care practitioners should carefully monitor patients treated with antidepressants and anxiolytics for adherence. A meta-analysis of 18,245 individuals with chronic diseases showed that depressed patients had a 76% significantly higher risk of nonadherence to medication compared with those without depressive symptoms.93
Targeting dyspnea is key to the management of anxiety and depression in COPD, as breathlessness is frequently associated with the onset of both comorbidities.21,22 Therapeutic approaches to alleviating dyspnea include PR, optimizing respiratory mechanics and muscle function (with bronchodilator therapy), and reducing central neural drive to respiratory muscles with supplemental oxygen or opioid medication.94
Although bronchodilator therapy for COPD has not been shown to have significant direct effects on depression or anxiety,95 it can be assumed that the beneficial effects on dyspnea are likely to alleviate associated emotional and mood symptoms.
Further research into effective screening, diagnosis, and management of comorbid anxiety and depressive disorders in COPD is warranted, including evaluation of a broad range of nonpharmacologic and drug-based interventions, alone and in combination.76
Conclusions
Anxiety and depression are common, yet frequently overlooked, comorbidities in COPD. The impact of these psychologic comorbidities is significant; their consequences are evident in morbidity and mortality data, as well as in patient-reported outcomes. As key points of contact for patients with COPD, it is essential that primary care practitioners are vigilant in monitoring for anxiety and depression in their patients with COPD, making the most of the available tools that can support them in doing so, and maintain an ongoing line of communication with other members of the multidisciplinary team. Treatment of anxiety and depression in COPD should adopt a holistic approach that incorporates both nonpharmacologic and pharmacologic interventions. However, the impact of effective screening, diagnosis, and management of anxiety and depression on COPD burden in patients requires further investigation.
- Chaudhary SC, Nanda S, Tripathi A, et al. Prevalence of psychiatric comorbidities in chronic obstructive pulmonary disease patients. Lung India. 2016;33(2):174-178.
- Zhang MW, Ho RC, Cheung MW, Fu E, Mak A. Prevalence of depressive symptoms in patients with chronic obstructive pulmonary disease: a systematic review, meta-analysis and meta-regression. Gen Hosp Psychiatry. 2011;33(3):217-223.
- Tsai TY, Livneh H, Lu MC, Tsai PY, Chen PC, Sung FC. Increased risk and related factors of depression among patients with COPD: a population-based cohort study. BMC Public Health. 2013;13:976.
- Eisner MD, Blanc PD, Yelin EH, et al. Influence of anxiety on health outcomes in COPD. Thorax. 2010;65(3):229-234.
- Marsh S, Guck TP. Anxiety and depression: easing the burden in COPD patients. J Fam Pract. 2016;65(4):246-256.
- Maurer J, Rebbapragada V, Borson S, et al; ACCP Workshop Panel on Anxiety and Depression in COPD. Anxiety and depression in COPD: current understanding, unanswered questions, and research needs. Chest. 2008;134(4 Suppl):43S-56S.
- Pumar MI, Gray CR, Walsh JR, Yang IA, Rolls TA, Ward DL. Anxiety and depression—important psychological comorbidities of COPD. J Thorac Dis. 2014;6(11):1615-1631.
- Dalal AA, Shah M, Lunacsek O, Hanania NA. Clinical and economic burden of depression/anxiety in chronic obstructive pulmonary disease patients within a managed care population. COPD. 2011;8(4):293-299.
- Kunik ME, Roundy K, Veazey C, et al. Surprisingly high prevalence of anxiety and depression in chronic breathing disorders. Chest. 2005;127(4):1205-1211.
- Yohannes AM, Alexopoulos GS. Depression and anxiety in patients with COPD. Eur Respir Rev. 2014;23(133):345-349.
- American Psychiatric Association. Depressive Disorders. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA: American Psychiatric Association; 2013.
- Panagioti M, Scott C, Blakemore A, Coventry PA. Overview of the prevalence, impact, and management of depression and anxiety in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2014;9:1289-1306.
- Laforest L, Roche N, Devouassoux G, et al. Frequency of comorbidities in chronic obstructive pulmonary disease, and impact on all-cause mortality: a population-based cohort study. Respir Med. 2016;117:33-39.
- Lecheler L, Richter M, Franzen DP, et al. The frequent and underrecognised co-occurrence of acute exacerbated COPD and depression warrants screening: a systematic review. Eur Respir Rev. 2017;26(144):pii: 170026.
- Willgoss TG, Yohannes AM. Anxiety disorders in patients with COPD: a systematic review. Respir Care. 2013;58(5):858-866.
- Livermore N, Sharpe L, McKenzie D. Panic attacks and panic disorder in chronic obstructive pulmonary disease: a cognitive behavioral perspective. Respir Med. 2010;104(9):1246-1253.
- World Health Organization. Depression and other common mental disorders: global health estimates. Geneva, Switzerland; World Health Organization: 2017.
- Altemus M, Sarvaiya N, Neill Epperson C. Sex differences in anxiety and depression clinical perspectives. Front Neuroendocrinol. 2014;35(3):320-330.
- Biswas D, Mukherjee S, Chakroborty R, et al. Occurrence of anxiety and depression among stable COPD patients and its impact on functional capability. J Clin Diagn Res. 2017;11(2):OC24-OC27.
- Yohannes AM, Baldwin RC, Connolly MJ. Depression and anxiety in elderly outpatients with chronic obstructive pulmonary disease: prevalence, and validation of the BASDEC screening questionnaire. Int J Geriatr Psychiatry. 2000;15(12):1090-1096.
- Atlantis E, Fahey P, Cochrane B, Smith S. Bidirectional associations between clinically relevant depression or anxiety and COPD: a systematic review and meta-analysis. Chest. 2013;144(3):766-777.
- Tetikkurt C, Ozdemir I, Tetikkurt S, Yilmaz N, Ertan T, Bayar N. Anxiety and depression in COPD patients and correlation with sputum and BAL cytology. Multidiscip Respir Med. 2011;6(4):226-231.
- Yohannes AM, Müllerová H, Hanania NA, et al. Long-term course of depression trajectories in patients with COPD: a 3-year follow-up analysis of the evaluation of COPD longitudinally to identify predictive surrogate endpoints cohort. Chest. 2016;149(4):916-926.
- Sundh J, Ekström M. Persistent disabling breathlessness in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2016;11:2805-2812.
- Kirkil G, Deveci F, Deveci SE, Atmaca M. Anxiety and depression symptoms in patients with chronic obstructive pulmonary disease. Bulletin Clin Psychopharmacol. 2015;25(2):151-161.
- Fuller-Thomson E, Lacombe-Duncan A. Understanding the association between chronic obstructive pulmonary disease and current anxiety: a population-based study. COPD. 2016;13(5):622-631.
- Yohannes AM. Is it quality or quantity of social support needed for patients with chronic medical illness? J Psychosom Res. 2013;74(2):87-88.
- Fabbri LM, Luppi F, Beghe B, Rabe KF. The multiple components of COPD. In: Hanania NA, Sharafkhaneh A, eds. COPD: a guide to diagnosis and clinical management. Humana Press; 2010.
- Lu Y, Feng L, Feng L, Nyunt MS, Yap KB, Ng TP. Systemic inflammation, depression and obstructive pulmonary function: a population-based study. Respir Res. 2013;14:53.
- Hanania NA, Müllerova H, Locantore NW, et al. Determinants of depression in the ECLIPSE chronic obstructive pulmonary disease cohort. Am J Respir Crit Care Med. 2011;183(5):604-611.
- Zhang Q, Liao J, Liao X, et al. Disease knowledge level is a noteworthy risk factor of anxiety and depression in patients with chronic obstructive pulmonary disease: a cross-sectional study. BMC Pulm Med. 2014;14:92.
- Jose AK, Chelangara DP, Shaji KS. Factors associated with anxiety and depression in chronic obstructive pulmonary disease. Int J Res Med Sci. 2016;4(4):1074-1079.
- van Dam van Isselt EF, Groenewegen-Sipkema KH, Spruit-van Eijk M, et al. Pain in patients with COPD: a systematic review and meta-analysis. BMJ Open. 2014;4(9):e005898.
- Lee AL, Harrison SL, Goldstein RS, Brooks D. Pain and its clinical associations in individuals with COPD: a systematic review. Chest. 2015;147(5):1246-1258.
- Divo M, Cote C, de Torres JP, et al; BODE Collaborative Group. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(2):155-161.
- Hillas G, Perlikos F, Tsiligianni I, Tzanakis N. Managing comorbidities in COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:95-109.
- Ng TP, Niti M, Tan WC, Cao Z, Ong KC, Eng P. Depressive symptoms and chronic obstructive pulmonary disease: effect on mortality, hospital readmission, symptom burden, functional status, and quality of life. Arch Intern Med. 2007;167(1):60-67.
- Montserrat-Capdevila J, Godoy P, Marsal JR, et al. Overview of the impact of depression and anxiety in chronic obstructive pulmonary disease. Lung. 2017;195(1):77-85.
- Laurin C, Moullec G, Bacon SL, Lavoie KL. Impact of anxiety and depression on chronic obstructive pulmonary disease exacerbation risk. Am J Respir Crit Care Med. 2012;185(9):918-923.
- Martinez Rivera C, Costan Galicia J, Alcázar Navarrete B, et al. Factors associated with depression in COPD: a multicenter study. Lung. 2016;194(3):335-343.
- Pooler A, Beech R. Examining the relationship between anxiety and depression and exacerbations of COPD which result in hospital admission: a systematic review. Int J Chron Obstruct Pulmon Dis. 2014;9:315-330.
- Dahlén I, Janson C. Anxiety and depression are related to the outcome of emergency treatment in patients with obstructive pulmonary disease. Chest. 2002;122(5):1633-1637.
- Gudmundsson G, Gislason T, Janson C, et al. Risk factors for rehospitalisation in COPD: role of health status, anxiety and depression. Eur Respir J. 2005;26(3):414-419.
- Mikkelsen RL, Middelboe T, Pisinger C, Stage KB. Anxiety and depression in patients with chronic obstructive pulmonary disease (COPD). A review. Nord J Psychiatry. 2004;58(1):65-70.
- Blakemore A, Dickens C, Guthrie E, et al. Depression and anxiety predict health-related quality of life in chronic obstructive pulmonary disease: systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2014;9:501-512.
- Dueñas-Espín I, Demeyer H, Gimeno-Santos E, et al. Depression symptoms reduce physical activity in COPD patients: a prospective multicenter study. Int J Chron Obstruct Pulmon Dis. 2016;11:1287-1295.
- Lee SH, Kim KU, Lee H, Kim YS, Lee MK, Park HK. Factors associated with low-level physical activity in elderly patients with chronic obstructive pulmonary disease [published online ahead of print June 7, 2017]. Korean J Intern Med. 2017;doi: 10.3904/kjim.2016.090.
- Hill K, Geist R, Goldstein RS, Lacasse Y. Anxiety and depression in end-stage COPD. Eur Respir J. 2008;31(3):667-677.
- George J, Kong DC, Thoman R, Stewart K. Factors associated with medication nonadherence in patients with COPD. Chest. 2005;128(5):3198-3204.
- Morrison D, Agur K, Mercer S, Eiras A, González-Montalvo JI, Gruffydd-Jones K. Managing multimorbidity in primary care in patients with chronic respiratory conditions. NPJ Prim Care Respir Med. 2016;26:16043.
- Khdour MR, Hawwa AF, Kidney JC, Smyth BM, McElnay JC. Potential risk factors for medication non-adherence in patients with chronic obstructive pulmonary disease (COPD). Eur J Clin Pharmacol. 2012;68(10):1365-1373.
- Busch AM, Scott-Sheldon LA, Pierce J, et al. Depressed mood predicts pulmonary rehabilitation completion among women, but not men. Respir Med. 2014;108(7):1007-1013.
- Heerema-Poelman A, Stuive I, Wempe JB. Adherence to a maintenance exercise program 1 year after pulmonary rehabilitation: what are the predictors of dropout? J Cardiopulm Rehabil Prev. 2013;33(6):419-426.
- DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherence. Arch Intern Med. 2000;160(14):2101-2107.
- Fan VS, Giardino ND, Blough DK, Kaplan RM, Ramsey SD; Nett Research Group. Costs of pulmonary rehabilitation and predictors of adherence in the National Emphysema Treatment Trial. COPD. 2008;5(2):105-116.
- Bourbeau J, Bartlett SJ. Patient adherence in COPD. Thorax. 2008;63(9):831-838.
- van Boven JF, Chavannes NH, van der Molen T, Rutten-van Mölken MP, Postma MJ, Vegter S. Clinical and economic impact of non-adherence in COPD: a systematic review. Respir Med. 2014;108(1):103-113.
- Dury R. COPD and emotional distress: not always noticed and therefore untreated. Br J Community Nurs. 2016;21(3):138-141.
- Price D, Crockett A, Arne M, et al. Spirometry in primary care case-identification, diagnosis and management of COPD. Prim Care Respir J. 2009;18(3):216-223.
- van Boven JF, Ryan D, Eakin MN, Canonica GW, Barot A, Foster JM; Respiratory Effectiveness Group. Enhancing respiratory medication adherence: the role of health care professionals and cost-effectiveness considerations. J Allergy Clin Immunol Pract. 2016;4(5):835-846.
- Wittchen HU, Mühlig S, Beesdo K. Mental disorders in primary care. Dialogues Clin Neurosci. 2003;5(2):115-128.
- Global Initiative for Chronic Obstructive Lung Disease. GOLD 2017 Global Strategy for the Diagnosis, Management and Prevention of COPD. http://goldcopd.org/gold-2017-global-strategy-diagnosis-management-prevention-copd. Accessed June 2017.
- Willgoss TG, Goldbart J, Fatoye F, Yohannes AM. The development and validation of the anxiety inventory for respiratory disease. Chest. 2013;144(5):1587-1596.
- Yohannes AM, Dryden S, Hanania NA. The responsiveness of the anxiety inventory for respiratory disease scale following pulmonary rehabilitation. Chest. 2016;150(1):188-195.
- Kühl K, Kuhn C, Kenn K, Rief W. [The COPD-Anxiety-Questionnaire (CAF): a new instrument to assess illness specific anxiety in COPD patients]. Psychother Psychosom Med Psychol. 2011;61(1):e1-e9. German.
- Tamburrino MB, Lynch DJ, Nagel RW, Smith MK. Primary care evaluation of mental disorders (PRIME-MD) screening for minor depressive disorder in primary care. Prim Care Companion J Clin Psychiatry. 2009;11(6):339-343.
- Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA. 1999;282(18):1737-1744.
- Arroll B, Goodyear-Smith F, Crengle S, et al. Validation of PHQ-2 and PHQ-9 to screen for major depression in the primary care population. Ann Fam Med. 2010;8(4):348-353.
- Yohannes AM, Hann M, Sibbald B. The management of depressive symptoms in patients with COPD: a postal survey of general practitioners. Prim Health Care Res Dev. 2011;12(3):237-244.
- Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092-1097.
- Bratås O, Grønning K, Forbord T. Psychometric properties of the Hospital Anxiety and Depression Scale and The General Health Questionnaire-20 in COPD inpatients. Scand J Caring Sci. 2014;28(2):413-420.
- Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995;33(3):335-343.
- Sundh J, Ställberg B, Lisspers K, Kämpe M, Janson C, Montgomery S. Comparison of the COPD Assessment Test (CAT) and the Clinical COPD Questionnaire (CCQ) in a clinical population. COPD. 2016;13(1):57-65.
- Cantor L, Jacobson R. COPD: How to manage comorbid depression and anxiety. Curr Psychiatry. 2003;2(11):45-54.
- Yohannes AM. Palliative care provision for patients with chronic obstructive pulmonary disease. Health Qual Life Outcomes. 2007;5:17.
- Tselebis A, Pachi A, Ilias I, et al. Strategies to improve anxiety and depression in patients with COPD: a mental health perspective. Neuropsychiatr Dis Treat. 2016;12:297-328.
- Doyle C, Bhar S, Fearn M, et al. The impact of telephone-delivered cognitive behaviour therapy and befriending on mood disorders in people with chronic obstructive pulmonary disease: a randomized controlled trial. Br J Health Psychol. 2017;22(3):542-556.
- Alsaraireh FA, Aloush SA. Does pulmonary rehabilitation alleviate depression in older patients with chronic obstructive pulmonary disease. Saudi Med J. 2017;38(5):491-496.
- Bennett D, Bowen B, McCarthy P, Subramaniam A, O’Connor M, Henry MT. Outcomes of pulmonary rehabilitation for COPD in older patients: a comparative study. COPD. 2017;14(2):170-175.
- Smith SM, Sonego S, Ketcheson L, Larson JL. A review of the effectiveness of psychological interventions used for anxiety and depression in chronic obstructive pulmonary disease. BMJ Open Respir Res. 2014;1(1):e000042.
- Bove DG, Overgaard D, Lomborg K, Lindhardt BØ, Midtgaard J. Efficacy of a minimal home-based psychoeducative intervention versus usual care for managing anxiety and dyspnoea in patients with severe chronic obstructive pulmonary disease: a randomised controlled trial protocol. BMJ Open. 2015;5(7):e008031.
- Bove DG, Lomborg K, Jensen AK, Overgaard D, Lindhardt BØ, Midtgaard J. Efficacy of a minimal home-based psychoeducative intervention in patients with advanced COPD: a randomised controlled trial. Respir Med. 2016;121:109-116.
- Usmani ZA, Carson KV, Heslop K, Esterman AJ, De Soyza A, Smith BJ. Psychological therapies for the treatment of anxiety disorders in chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2017;3: CD010673. doi:10.002/14651858.CD010673.pub2.
- Cafarella P, Effing T, Frith P. An evaluation of the needs of carers of people with COPD. EurResp J. 2012;40(Suppl 56).
- Zyban [package insert]. Research Triangle Park, NC: GlaxoSmithKline; 2017. Available at: https://www.gsksource.com/pharma/content/dam/GlaxoSmithKline/US/en/Prescribing_Information/Zyban/pdf/ZYBAN-PI-MG.PDF. Accessed June 2017.
- Gelenberg AJ, Freeman MP, Markowitz JC, et al. Practice guideline for the treatment of patients with major depressive disorder. Am J Psychiatry. 2010;167(10):1.
- Pary R, Matuschka PR, Lewis S, Lippmann S. Managing bipolar depression. Psychiatry (Edgmont). 2006;3(2):30-41.
- Blier P. Atypical antipsychotics for mood and anxiety disorders: safe and effective adjuncts? J Psychiatry Neurosci. 2005;30(4):232-233.
- Vulink NC, Figee M, Denys D. Review of atypical antipsychotics in anxiety. Eur Neuropsychopharmacol. 2011;21(6):429-449.
- Locke AB, Kirst N, Shultz CG. Diagnosis and management of generalized anxiety disorder and panic disorder in adults. Am Fam Physician. 2015;91(9):617-624.
- Kew KM, Dias S, Cates CJ. Long-acting inhaled therapy (beta-agonists, anticholinergics and steroids) for COPD: a network meta-analysis. Cochrane Database Syst Rev. 2014;(3):CD010844. doi:10.1002/14651858.CD010844.pub2.
- Scully C. Drug effects on salivary glands: dry mouth. Oral Dis. 2003;9(4):165-176.
- Grenard JL, Munjas BA, Adams JL, et al. Depression and medication adherence in the treatment of chronic diseases in the United States: a meta-analysis. J Gen Intern Med. 2011;26(10):1175-1182.
- O’Donnell DE, Webb KA, Harle I, Neder JA. Pharmacological management of breathlessness in COPD: recent advances and hopes for the future. Expert Rev Respir Med. 2016;10(7):823-834.
- Hyun MK, Lee NR, Jang EJ, Yim JJ, Lee CH. Effect of inhaled drugs on anxiety and depression in patients with chronic obstructive pulmonary disease: a prospective observational study. Int J Chron Obstruct Pulmon Dis. 2016;11:747-754.
Introduction
Anxiety and depression are common in patients with chronic obstructive pulmonary disease (COPD), occurring more frequently than in the general population1-4 or patients with other chronic diseases such as hypertension, diabetes, cancer, or musculoskeletal disorders.5,6 Their presence is associated with worse outcomes of COPD, and increased morbidity, mortality, disability, and health care expenditure.6-8 In spite of this, both anxiety and depression are frequently overlooked and undertreated in patients with COPD,9 and symptoms of anxiety and depression can overlap significantly, as well as overlap with COPD symptoms.7,10
Comorbid depressive disorders that may occur in patients with COPD include major depressive disorder, dysthymias (chronic depressive symptoms of mild severity), and minor depression.11 Depressive disorders are characterized by feelings of sadness, emptiness, and/or irritability, along with cognitive and somatic symptoms, which have a detrimental effect on the patient’s ability to function.11 Anxiety disorders include generalized anxiety disorder (GAD), phobias, and panic disorders.11 The main features of anxiety disorders, such as excessive fear and anxiety, may be accompanied by behavioral disturbances related to these symptoms, such as panic attacks and avoidance.11,12
The reported prevalence of depression in COPD varies widely between studies, owing to differences in sampling methods and degrees of illness severity used in assessment of depression6; rates have been reported to range from 10% to 42% in patients with stable COPD,6,13 and from 10% to 86% in patients with acute COPD exacerbation.14 Individuals with severe COPD are twice as likely to develop depression than patients with mild COPD.10
Prevalence rates for clinical anxiety in COPD range from 13% to 46% in outpatients and 10% to 55% among inpatients. GAD, panic disorders, and specific phobias are reported most frequently.15 Patients with COPD are 85% more likely to develop anxiety disorders compared with matched controls without COPD,4 and panic disorder is reported with a prevalence that is up to 10-fold higher than in the general population.16
Global prevalence rates of anxiety and depression are 1.8- and 1.4-fold higher in women than men, respectively17; the same gender difference is observed in patients with COPD.6 The higher prevalence rates of anxiety and depression in women are thought to be a result of sex differences in brain structure, function, and stress responses, as well as differences in exposure to reproductive hormones, social constraints, and experiences between women and men.18 However, psychologic comorbidity is an issue for both men and women with COPD, so it is important that clinicians are vigilant in recognizing anxiety and depression in both sexes, and are careful not to underestimate the burden in the male patient population.
It is also important to note that depression and anxiety often occur simultaneously in patients with COPD, with prevalence estimates of 26% to 43%.9,19,20 COPD patients with both depression and anxiety are at a heightened risk of suicidal ideation, increased physical disability, and chronic depressive symptoms versus those with either disorder alone.10,15 It is therefore important that comorbid anxiety and depression is not overlooked in patients with COPD.
Ensuring that anxiety and depression are recognized and treated effectively in patients with COPD is essential for optimizing outcomes. Primary care practitioners are well placed to diagnose anxiety and depression, and to ensure these conditions are suitably managed alongside treatments of COPD.
Potential mechanisms of anxiety and depression in COPD
Growing evidence suggests that the relationship between mood disorders—particularly depression—and COPD is bidirectional, meaning that mood disorders adversely impact prognosis in COPD, whereas COPD increases the risk of developing depression.21 For example, in a study of
60 stable patients with COPD, elevated dyspnea and reduced exercise capacity were the predominant mechanisms leading to anxiety and depression symptoms associated with the condition.22 In addition, the risk of new-onset depression was increased in COPD patients with moderate-to-severe dyspnea in a 3-year follow-up study.23 Conversely, depression has been shown to be a significant risk factor for disabling dyspnea (modified Medical Research Council score ≥2) in patients with COPD.24
COPD can lead to feelings of hopelessness, social isolation, reduced physical functioning, and sedentary lifestyle, all of which are associated with an increased level of depressive symptoms.25 Similarly, inadequate social support increases the risk of anxiety in patients with COPD.26 Therefore, ensuring that patients with COPD have high-quality support is very important for reducing anxiety and depressive symptoms.27
The exact mechanisms for the association between mood disorders and COPD remain unclear.7,10 Research to date indicates that the relationship between depression and impaired pulmonary function may be partly mediated by chronic inflammation7,10; systemic inflammation has been associated with other comorbidities of COPD (eg, muscle wasting and osteoporosis),28 and emerging data appear to show that proinflammatory cytokines partly mediate the association between depressive symptoms and pulmonary function.29 Smoking and hypoxemia may also influence the prevalence of depression in COPD, but symptom severity and impaired quality of life remain the most important determinants.6,30
Clinical studies have demonstrated that a number of patient-related factors, including female gender, younger age, current smoking, greater severity of airflow limitation, and lower socioeconomic status, are associated with a higher prevalence and/or increased risk of depression and/or anxiety in COPD.3,4,30,31 Frequent episodes of rehospitalization, and comorbidities such as hypertension, arthritis, cancer, and heart disease, have been found to increase the risk of anxiety and depression in patients with COPD.3,32 Risk of anxiety has been shown to increase with greater dyspnea severity.4 Pain, a frequently overlooked symptom in COPD, has been shown to be associated with symptoms of both anxiety and depression in patients with COPD.33 This is driven by worsened quality of life and sleep quality, decreased physical activity, and an increased fear of movement that occur as a result of pain.34
The impact of anxiety and depression in COPD
Comorbid anxiety and depression have a significant detrimental impact on morbidity and mortality in patients with COPD. Both disorders have been associated with an increased risk of death in COPD.13,35-37 Indeed, of 12 comorbidities proposed to be predictors of mortality in a cohort of 187 female outpatients with COPD, anxiety was associated with the highest risk of death.35,36
In addition, patients with COPD and anxiety and/or depression have a higher risk of COPD exacerbations,4,8,23,36,38-40 hospitalization,41,42 rehospitalization,14,36,43 longer hospital stays,37,41,44 and mortality after exacerbations,14,36,41 compared with patients without these comorbidities. Patients with COPD who have elevated anxiety symptoms also often experience their first hospitalization earlier in the natural course of COPD than those without anxiety.36
Psychologic comorbidities are also associated with worse lung function, dyspnea, and respiratory symptom burden in patients with COPD.37,40 Patients with COPD and anxiety are more likely to experience greater dyspnea at an earlier stage of disease than those without anxiety.36 Persistent smoking at 6 months after hospitalization for an acute exacerbation of COPD is also more likely to be seen in patients with depression.37
Patient-centered outcomes are worse in COPD patients with mood disorders. Both anxiety and depression have been shown to correlate with significantly reduced health-related quality of life (HRQoL), poorer physical health status, functional limitations, and reduced exercise capacity.4,23,37,40,45 The presence of either anxiety or depression at baseline has been shown to correlate with reduced HRQoL at 1-year follow-up, but depression appears to be the stronger predictor of low future HRQoL than anxiety.45
Additionally, mood disorders—particularly depression—reduce physical activity in patients with COPD.46,47 Emotional responses to COPD symptoms, such as dyspnea, can further decrease activity and worsen deconditioning, resulting in a downward spiral of reduced inactivity, social isolation, fear, anxiety, and depression.48
COPD patients with any comorbidity exhibit lower rates of medication adherence than those without comorbidities.49-51 Clinical studies have demonstrated that anxiety and depression are significant predictors of poor adherence to COPD interventions, including pulmonary rehabilitation (PR).51-55 Nonadherence to COPD therapies is associated with poor clinical outcomes, including higher hospitalization rates and increased emergency department visits, and increased costs.56,57 Health care expenditure, in terms of both specific COPD-related costs and general “all-cause” costs, is significantly higher in COPD patients with anxiety and/or depression than in those without.8
Diagnosis of anxiety and depression in patients with COPD
The underdiagnosis and undertreatment of anxiety and depression in this population is common and can adversely affect patient outcomes.6,7,9,10,58 Hence, it is crucial that anxiety and depression are identified and more effectively managed in clinical practice.10
Primary care practitioners are the main point of contact for many patients with COPD,6,59,60 and so can play a key role in screening for and early identification of anxiety and depression. However, detection of mood disorders by primary care practitioners is challenging for several reasons. These include the lack of a standardized approach in diagnosis, and inadequate knowledge or confidence in assessing psychological status (particularly given the number of strategies available for screening patients for mood disorders),6 as well as factors associated with time constraints, such as competing agendas, duration of visits, and high patient load.6,61 Furthermore, system-level barriers, such as lack of electronic medical records and adequate health insurance, as well as any communication gaps between primary care and mental health care, may hinder the detection and management of anxiety and depression.6 In addition, patients themselves may have a limited understanding of these comorbidities, or may be hesitant to discuss symptoms of anxiety or depression with their primary care practitioner owing to stigma around mental illness.6
Patients with COPD should be screened and assessed for anxiety and depression, and the United States Preventive Services Task Force recommends that clinicians screen for depression in all adults.6,62 There are several validated screening tools suitable for clinical use:
- Anxiety Inventory for Respiratory (AIR) Disease scale: a brief, easy-to-use tool for screening and measuring anxiety in COPD.63,64 It is a self-administered scale, and takes approximately 2 minutes to complete. The AIR scale is responsive to PR.64
- COPD Anxiety Questionnaire (CAF): a reliable tool for early identification of COPD-related anxiety.65
- Primary Care Evaluation of Mental Disorders (PRIME-MD) Patient Health Questionnaire (PHQ; available at: http://www.phqscreeners.com/select-screener/): the PRIME-MD comprises 26 yes/no questions on the 5 most common psychiatric disorders, including depression and anxiety.66,67 This is not a diagnostic tool, but a high number of positive responses from a patient in any given module indicates that they require further clinical evaluation.
- PHQ-2 and PHQ-9 (Table 1; PHQ-9 available at http://www.phqscreeners.com/select-screener/): widely-used self-administered 2- and 9-item versions of the PRIME-MD, specific to depression; similarly, the 3-item PHQ-3 is available for anxiety assessment (Table 2).6,67,68 In a study investigating tools used by family physicians in England to assess depression, over 75% used PHQ-9.69
-
- Hospital Anxiety and Depression Scale (HADS) and General Health Questionnaire-version 20 (GHQ-20): both can be used to screen for psychologic distress in patients with COPD.71
- The Beck Anxiety Inventory (BAI) and Beck Depression Inventory (BDI): two 21-item self-report questionnaires that are widely used in the United States to evaluate anxiety and depression.72
In addition to specific anxiety and depression questionnaires (Tables 1 and 2), more general COPD assessments tools, such as the COPD Assessment Test and the COPD Clinical Questionnaire, also incorporate questions that may be indicative of symptoms of these comorbidities in patients with COPD.73
Management of anxiety and depression in COPD
Even though anxiety and depression are among the most common and burdensome comorbid conditions in COPD, less than one-third of patients with these comorbidities receive effective intervention.6,10 Primary care providers have an excellent opportunity to impact this care gap.
As in non-COPD patients, comorbid depression and anxiety may be treated with nonpharmacologic and/or pharmacologic interventions (Figure 1).76
Nonpharmacologic interventions
Evidence to date suggests that nonpharmacologic interventions such as behavioral therapy are as effective as antidepressants, and may be preferred by patients with mood disorders.12
Cognitive behavioral therapy (CBT), which is typically administered by psychologists/psychiatrists, may be effective in treating COPD-related anxiety and depression, especially in conjunction with exercise and education.12,76,77 Individualized or group CBT is the treatment of choice for addressing thinking patterns that contribute to anxiety and depression to change a patient’s behavior and emotional state.76 PR programs involve several components, including aerobic exercise, lung function training, and psycho-education.62,76 PR is suitable for most patients with COPD, and provides multiple benefits, including reduced hospitalizations in patients who have had a recent exacerbation, and improved dyspnea, exercise tolerance, and health status in patients with stable disease,62 as well as clinically and statistically significant improvements in depression and anxiety, irrespective of age.7,78,79 Exercise-based forms of PR appear to be the most effective for reducing mood symptoms,12,76 and incorporating psychotherapy may also improve psychologic outcomes.80 Stress reduction (relaxation) therapy aims to reduce anxiety-related physiologic changes, and includes a variety of techniques (eg, breathing exercises, sequential muscle relaxation, hypnosis, mindfulness meditation), some of which may be included in PR or used alongside other treatments (eg, CBT).76 Limited data indicate that such therapy may be beneficial for reducing anxiety and depression, as well as respiratory symptoms and dyspnea, in patients with COPD.12,76
Self-management techniques improve clinical outcomes in patients with COPD, but data on the management of depression or anxiety are inconclusive.7,12 A minimal, home-based, nurse-led, psycho-educational intervention was designed to encourage more open-ended, descriptive discussions of thoughts, emotions, behaviors, and bodily sensations in patients with COPD.81 The intervention, which involved nurses attending a 1-hour face-to-face session in the patients’ homes with a 15-minute telephone “booster” session 2 weeks later, helped patients with advanced COPD to self-manage their condition and provide relief from anxiety.81,82 However, it should be noted that there is currently a lack of high-quality data evaluating psychologic interventions in the COPD population.83
In addition, it is important that caregivers are supported in the management of patients with COPD and comorbid anxiety and/or depression; areas in which caregivers can be assisted in their role may include disease education and counseling, where appropriate.84
Given that smoking cessation is a key recommendation for patients with COPD,44,62 practitioners should be aware that patients with comorbid depression and anxiety may experience greater difficulty in smoking cessation, and worsened mood during nicotine withdrawal.44 Clinicians should therefore carefully monitor current smokers with COPD and comorbid depression/anxiety (using the tools described previously63,68,70,71) when they are attempting to quit smoking.
Pharmacologic interventions
Pharmacologic therapy of anxiety and depression has so far only been investigated in patients with COPD in small studies.76 However, the available evidence does not indicate that COPD patients with anxiety and depression should be managed any differently from individuals without COPD.62 As such, pharmacologic interventions are particularly important for patients with acute or severe anxiety or depression.
Antidepressant agents are categorized according to their mechanism of action, and most commonly include selective serotonin-reuptake inhibitors (SSRIs), selective norepinephrine-reuptake inhibitors, bupropion (a norepinephrine- and dopamine-reuptake inhibitor; also approved for smoking cessation85), and mirtazapine (a norepinephrine and serotonin modulator), among others.86 SSRIs are the current firstline drug treatment for depression, and have been shown to significantly improve depression and anxiety in patients with COPD in some, but not all, trials published to date.76 However, it is important to note that a diagnosis of bipolar disorder must be ruled out before initiating standard antidepressant therapy.87 In addition to antidepressants, atypical antipsychotics have also been shown to be useful for treating anxiety, either as monotherapy or combination therapy, and possibly as an adjunctive therapy for the management of depression.88,89
Primary care practitioners can refer to existing guidelines on the management of anxiety and depression in patients with COPD,86,90 while taking certain factors into consideration. Any pharmacologic management strategy for the treatment of COPD may increase the risk of drug–drug or drug–disease interactions.76 For example, it is important to avoid medications that cause respiratory depression (eg, benzodiazepines [unless used with extreme caution], particularly in patients who are already CO2 retainers) or sedation; chosen drugs should have minimal other adverse effects.76 Moreover, SSRIs may also be associated with troublesome adverse effects during treatment initiation, such as gastrointestinal upset, headache, tremor, psychomotor activation, and sedation76; in addition, dry mouth is an adverse effect associated with both SSRI treatment and several inhaled therapies, so may be particularly problematic in patients with COPD.91,92 Currently, data are particularly scarce for the management of anxiety in patients with COPD, with inconclusive or contradictory findings reported for SSRIs, azapirones (including buspirone), and tricyclic antidepressants.76
In addition to monitoring adherence to COPD therapies, primary care practitioners should carefully monitor patients treated with antidepressants and anxiolytics for adherence. A meta-analysis of 18,245 individuals with chronic diseases showed that depressed patients had a 76% significantly higher risk of nonadherence to medication compared with those without depressive symptoms.93
Targeting dyspnea is key to the management of anxiety and depression in COPD, as breathlessness is frequently associated with the onset of both comorbidities.21,22 Therapeutic approaches to alleviating dyspnea include PR, optimizing respiratory mechanics and muscle function (with bronchodilator therapy), and reducing central neural drive to respiratory muscles with supplemental oxygen or opioid medication.94
Although bronchodilator therapy for COPD has not been shown to have significant direct effects on depression or anxiety,95 it can be assumed that the beneficial effects on dyspnea are likely to alleviate associated emotional and mood symptoms.
Further research into effective screening, diagnosis, and management of comorbid anxiety and depressive disorders in COPD is warranted, including evaluation of a broad range of nonpharmacologic and drug-based interventions, alone and in combination.76
Conclusions
Anxiety and depression are common, yet frequently overlooked, comorbidities in COPD. The impact of these psychologic comorbidities is significant; their consequences are evident in morbidity and mortality data, as well as in patient-reported outcomes. As key points of contact for patients with COPD, it is essential that primary care practitioners are vigilant in monitoring for anxiety and depression in their patients with COPD, making the most of the available tools that can support them in doing so, and maintain an ongoing line of communication with other members of the multidisciplinary team. Treatment of anxiety and depression in COPD should adopt a holistic approach that incorporates both nonpharmacologic and pharmacologic interventions. However, the impact of effective screening, diagnosis, and management of anxiety and depression on COPD burden in patients requires further investigation.
Introduction
Anxiety and depression are common in patients with chronic obstructive pulmonary disease (COPD), occurring more frequently than in the general population1-4 or patients with other chronic diseases such as hypertension, diabetes, cancer, or musculoskeletal disorders.5,6 Their presence is associated with worse outcomes of COPD, and increased morbidity, mortality, disability, and health care expenditure.6-8 In spite of this, both anxiety and depression are frequently overlooked and undertreated in patients with COPD,9 and symptoms of anxiety and depression can overlap significantly, as well as overlap with COPD symptoms.7,10
Comorbid depressive disorders that may occur in patients with COPD include major depressive disorder, dysthymias (chronic depressive symptoms of mild severity), and minor depression.11 Depressive disorders are characterized by feelings of sadness, emptiness, and/or irritability, along with cognitive and somatic symptoms, which have a detrimental effect on the patient’s ability to function.11 Anxiety disorders include generalized anxiety disorder (GAD), phobias, and panic disorders.11 The main features of anxiety disorders, such as excessive fear and anxiety, may be accompanied by behavioral disturbances related to these symptoms, such as panic attacks and avoidance.11,12
The reported prevalence of depression in COPD varies widely between studies, owing to differences in sampling methods and degrees of illness severity used in assessment of depression6; rates have been reported to range from 10% to 42% in patients with stable COPD,6,13 and from 10% to 86% in patients with acute COPD exacerbation.14 Individuals with severe COPD are twice as likely to develop depression than patients with mild COPD.10
Prevalence rates for clinical anxiety in COPD range from 13% to 46% in outpatients and 10% to 55% among inpatients. GAD, panic disorders, and specific phobias are reported most frequently.15 Patients with COPD are 85% more likely to develop anxiety disorders compared with matched controls without COPD,4 and panic disorder is reported with a prevalence that is up to 10-fold higher than in the general population.16
Global prevalence rates of anxiety and depression are 1.8- and 1.4-fold higher in women than men, respectively17; the same gender difference is observed in patients with COPD.6 The higher prevalence rates of anxiety and depression in women are thought to be a result of sex differences in brain structure, function, and stress responses, as well as differences in exposure to reproductive hormones, social constraints, and experiences between women and men.18 However, psychologic comorbidity is an issue for both men and women with COPD, so it is important that clinicians are vigilant in recognizing anxiety and depression in both sexes, and are careful not to underestimate the burden in the male patient population.
It is also important to note that depression and anxiety often occur simultaneously in patients with COPD, with prevalence estimates of 26% to 43%.9,19,20 COPD patients with both depression and anxiety are at a heightened risk of suicidal ideation, increased physical disability, and chronic depressive symptoms versus those with either disorder alone.10,15 It is therefore important that comorbid anxiety and depression is not overlooked in patients with COPD.
Ensuring that anxiety and depression are recognized and treated effectively in patients with COPD is essential for optimizing outcomes. Primary care practitioners are well placed to diagnose anxiety and depression, and to ensure these conditions are suitably managed alongside treatments of COPD.
Potential mechanisms of anxiety and depression in COPD
Growing evidence suggests that the relationship between mood disorders—particularly depression—and COPD is bidirectional, meaning that mood disorders adversely impact prognosis in COPD, whereas COPD increases the risk of developing depression.21 For example, in a study of
60 stable patients with COPD, elevated dyspnea and reduced exercise capacity were the predominant mechanisms leading to anxiety and depression symptoms associated with the condition.22 In addition, the risk of new-onset depression was increased in COPD patients with moderate-to-severe dyspnea in a 3-year follow-up study.23 Conversely, depression has been shown to be a significant risk factor for disabling dyspnea (modified Medical Research Council score ≥2) in patients with COPD.24
COPD can lead to feelings of hopelessness, social isolation, reduced physical functioning, and sedentary lifestyle, all of which are associated with an increased level of depressive symptoms.25 Similarly, inadequate social support increases the risk of anxiety in patients with COPD.26 Therefore, ensuring that patients with COPD have high-quality support is very important for reducing anxiety and depressive symptoms.27
The exact mechanisms for the association between mood disorders and COPD remain unclear.7,10 Research to date indicates that the relationship between depression and impaired pulmonary function may be partly mediated by chronic inflammation7,10; systemic inflammation has been associated with other comorbidities of COPD (eg, muscle wasting and osteoporosis),28 and emerging data appear to show that proinflammatory cytokines partly mediate the association between depressive symptoms and pulmonary function.29 Smoking and hypoxemia may also influence the prevalence of depression in COPD, but symptom severity and impaired quality of life remain the most important determinants.6,30
Clinical studies have demonstrated that a number of patient-related factors, including female gender, younger age, current smoking, greater severity of airflow limitation, and lower socioeconomic status, are associated with a higher prevalence and/or increased risk of depression and/or anxiety in COPD.3,4,30,31 Frequent episodes of rehospitalization, and comorbidities such as hypertension, arthritis, cancer, and heart disease, have been found to increase the risk of anxiety and depression in patients with COPD.3,32 Risk of anxiety has been shown to increase with greater dyspnea severity.4 Pain, a frequently overlooked symptom in COPD, has been shown to be associated with symptoms of both anxiety and depression in patients with COPD.33 This is driven by worsened quality of life and sleep quality, decreased physical activity, and an increased fear of movement that occur as a result of pain.34
The impact of anxiety and depression in COPD
Comorbid anxiety and depression have a significant detrimental impact on morbidity and mortality in patients with COPD. Both disorders have been associated with an increased risk of death in COPD.13,35-37 Indeed, of 12 comorbidities proposed to be predictors of mortality in a cohort of 187 female outpatients with COPD, anxiety was associated with the highest risk of death.35,36
In addition, patients with COPD and anxiety and/or depression have a higher risk of COPD exacerbations,4,8,23,36,38-40 hospitalization,41,42 rehospitalization,14,36,43 longer hospital stays,37,41,44 and mortality after exacerbations,14,36,41 compared with patients without these comorbidities. Patients with COPD who have elevated anxiety symptoms also often experience their first hospitalization earlier in the natural course of COPD than those without anxiety.36
Psychologic comorbidities are also associated with worse lung function, dyspnea, and respiratory symptom burden in patients with COPD.37,40 Patients with COPD and anxiety are more likely to experience greater dyspnea at an earlier stage of disease than those without anxiety.36 Persistent smoking at 6 months after hospitalization for an acute exacerbation of COPD is also more likely to be seen in patients with depression.37
Patient-centered outcomes are worse in COPD patients with mood disorders. Both anxiety and depression have been shown to correlate with significantly reduced health-related quality of life (HRQoL), poorer physical health status, functional limitations, and reduced exercise capacity.4,23,37,40,45 The presence of either anxiety or depression at baseline has been shown to correlate with reduced HRQoL at 1-year follow-up, but depression appears to be the stronger predictor of low future HRQoL than anxiety.45
Additionally, mood disorders—particularly depression—reduce physical activity in patients with COPD.46,47 Emotional responses to COPD symptoms, such as dyspnea, can further decrease activity and worsen deconditioning, resulting in a downward spiral of reduced inactivity, social isolation, fear, anxiety, and depression.48
COPD patients with any comorbidity exhibit lower rates of medication adherence than those without comorbidities.49-51 Clinical studies have demonstrated that anxiety and depression are significant predictors of poor adherence to COPD interventions, including pulmonary rehabilitation (PR).51-55 Nonadherence to COPD therapies is associated with poor clinical outcomes, including higher hospitalization rates and increased emergency department visits, and increased costs.56,57 Health care expenditure, in terms of both specific COPD-related costs and general “all-cause” costs, is significantly higher in COPD patients with anxiety and/or depression than in those without.8
Diagnosis of anxiety and depression in patients with COPD
The underdiagnosis and undertreatment of anxiety and depression in this population is common and can adversely affect patient outcomes.6,7,9,10,58 Hence, it is crucial that anxiety and depression are identified and more effectively managed in clinical practice.10
Primary care practitioners are the main point of contact for many patients with COPD,6,59,60 and so can play a key role in screening for and early identification of anxiety and depression. However, detection of mood disorders by primary care practitioners is challenging for several reasons. These include the lack of a standardized approach in diagnosis, and inadequate knowledge or confidence in assessing psychological status (particularly given the number of strategies available for screening patients for mood disorders),6 as well as factors associated with time constraints, such as competing agendas, duration of visits, and high patient load.6,61 Furthermore, system-level barriers, such as lack of electronic medical records and adequate health insurance, as well as any communication gaps between primary care and mental health care, may hinder the detection and management of anxiety and depression.6 In addition, patients themselves may have a limited understanding of these comorbidities, or may be hesitant to discuss symptoms of anxiety or depression with their primary care practitioner owing to stigma around mental illness.6
Patients with COPD should be screened and assessed for anxiety and depression, and the United States Preventive Services Task Force recommends that clinicians screen for depression in all adults.6,62 There are several validated screening tools suitable for clinical use:
- Anxiety Inventory for Respiratory (AIR) Disease scale: a brief, easy-to-use tool for screening and measuring anxiety in COPD.63,64 It is a self-administered scale, and takes approximately 2 minutes to complete. The AIR scale is responsive to PR.64
- COPD Anxiety Questionnaire (CAF): a reliable tool for early identification of COPD-related anxiety.65
- Primary Care Evaluation of Mental Disorders (PRIME-MD) Patient Health Questionnaire (PHQ; available at: http://www.phqscreeners.com/select-screener/): the PRIME-MD comprises 26 yes/no questions on the 5 most common psychiatric disorders, including depression and anxiety.66,67 This is not a diagnostic tool, but a high number of positive responses from a patient in any given module indicates that they require further clinical evaluation.
- PHQ-2 and PHQ-9 (Table 1; PHQ-9 available at http://www.phqscreeners.com/select-screener/): widely-used self-administered 2- and 9-item versions of the PRIME-MD, specific to depression; similarly, the 3-item PHQ-3 is available for anxiety assessment (Table 2).6,67,68 In a study investigating tools used by family physicians in England to assess depression, over 75% used PHQ-9.69
-
- Hospital Anxiety and Depression Scale (HADS) and General Health Questionnaire-version 20 (GHQ-20): both can be used to screen for psychologic distress in patients with COPD.71
- The Beck Anxiety Inventory (BAI) and Beck Depression Inventory (BDI): two 21-item self-report questionnaires that are widely used in the United States to evaluate anxiety and depression.72
In addition to specific anxiety and depression questionnaires (Tables 1 and 2), more general COPD assessments tools, such as the COPD Assessment Test and the COPD Clinical Questionnaire, also incorporate questions that may be indicative of symptoms of these comorbidities in patients with COPD.73
Management of anxiety and depression in COPD
Even though anxiety and depression are among the most common and burdensome comorbid conditions in COPD, less than one-third of patients with these comorbidities receive effective intervention.6,10 Primary care providers have an excellent opportunity to impact this care gap.
As in non-COPD patients, comorbid depression and anxiety may be treated with nonpharmacologic and/or pharmacologic interventions (Figure 1).76
Nonpharmacologic interventions
Evidence to date suggests that nonpharmacologic interventions such as behavioral therapy are as effective as antidepressants, and may be preferred by patients with mood disorders.12
Cognitive behavioral therapy (CBT), which is typically administered by psychologists/psychiatrists, may be effective in treating COPD-related anxiety and depression, especially in conjunction with exercise and education.12,76,77 Individualized or group CBT is the treatment of choice for addressing thinking patterns that contribute to anxiety and depression to change a patient’s behavior and emotional state.76 PR programs involve several components, including aerobic exercise, lung function training, and psycho-education.62,76 PR is suitable for most patients with COPD, and provides multiple benefits, including reduced hospitalizations in patients who have had a recent exacerbation, and improved dyspnea, exercise tolerance, and health status in patients with stable disease,62 as well as clinically and statistically significant improvements in depression and anxiety, irrespective of age.7,78,79 Exercise-based forms of PR appear to be the most effective for reducing mood symptoms,12,76 and incorporating psychotherapy may also improve psychologic outcomes.80 Stress reduction (relaxation) therapy aims to reduce anxiety-related physiologic changes, and includes a variety of techniques (eg, breathing exercises, sequential muscle relaxation, hypnosis, mindfulness meditation), some of which may be included in PR or used alongside other treatments (eg, CBT).76 Limited data indicate that such therapy may be beneficial for reducing anxiety and depression, as well as respiratory symptoms and dyspnea, in patients with COPD.12,76
Self-management techniques improve clinical outcomes in patients with COPD, but data on the management of depression or anxiety are inconclusive.7,12 A minimal, home-based, nurse-led, psycho-educational intervention was designed to encourage more open-ended, descriptive discussions of thoughts, emotions, behaviors, and bodily sensations in patients with COPD.81 The intervention, which involved nurses attending a 1-hour face-to-face session in the patients’ homes with a 15-minute telephone “booster” session 2 weeks later, helped patients with advanced COPD to self-manage their condition and provide relief from anxiety.81,82 However, it should be noted that there is currently a lack of high-quality data evaluating psychologic interventions in the COPD population.83
In addition, it is important that caregivers are supported in the management of patients with COPD and comorbid anxiety and/or depression; areas in which caregivers can be assisted in their role may include disease education and counseling, where appropriate.84
Given that smoking cessation is a key recommendation for patients with COPD,44,62 practitioners should be aware that patients with comorbid depression and anxiety may experience greater difficulty in smoking cessation, and worsened mood during nicotine withdrawal.44 Clinicians should therefore carefully monitor current smokers with COPD and comorbid depression/anxiety (using the tools described previously63,68,70,71) when they are attempting to quit smoking.
Pharmacologic interventions
Pharmacologic therapy of anxiety and depression has so far only been investigated in patients with COPD in small studies.76 However, the available evidence does not indicate that COPD patients with anxiety and depression should be managed any differently from individuals without COPD.62 As such, pharmacologic interventions are particularly important for patients with acute or severe anxiety or depression.
Antidepressant agents are categorized according to their mechanism of action, and most commonly include selective serotonin-reuptake inhibitors (SSRIs), selective norepinephrine-reuptake inhibitors, bupropion (a norepinephrine- and dopamine-reuptake inhibitor; also approved for smoking cessation85), and mirtazapine (a norepinephrine and serotonin modulator), among others.86 SSRIs are the current firstline drug treatment for depression, and have been shown to significantly improve depression and anxiety in patients with COPD in some, but not all, trials published to date.76 However, it is important to note that a diagnosis of bipolar disorder must be ruled out before initiating standard antidepressant therapy.87 In addition to antidepressants, atypical antipsychotics have also been shown to be useful for treating anxiety, either as monotherapy or combination therapy, and possibly as an adjunctive therapy for the management of depression.88,89
Primary care practitioners can refer to existing guidelines on the management of anxiety and depression in patients with COPD,86,90 while taking certain factors into consideration. Any pharmacologic management strategy for the treatment of COPD may increase the risk of drug–drug or drug–disease interactions.76 For example, it is important to avoid medications that cause respiratory depression (eg, benzodiazepines [unless used with extreme caution], particularly in patients who are already CO2 retainers) or sedation; chosen drugs should have minimal other adverse effects.76 Moreover, SSRIs may also be associated with troublesome adverse effects during treatment initiation, such as gastrointestinal upset, headache, tremor, psychomotor activation, and sedation76; in addition, dry mouth is an adverse effect associated with both SSRI treatment and several inhaled therapies, so may be particularly problematic in patients with COPD.91,92 Currently, data are particularly scarce for the management of anxiety in patients with COPD, with inconclusive or contradictory findings reported for SSRIs, azapirones (including buspirone), and tricyclic antidepressants.76
In addition to monitoring adherence to COPD therapies, primary care practitioners should carefully monitor patients treated with antidepressants and anxiolytics for adherence. A meta-analysis of 18,245 individuals with chronic diseases showed that depressed patients had a 76% significantly higher risk of nonadherence to medication compared with those without depressive symptoms.93
Targeting dyspnea is key to the management of anxiety and depression in COPD, as breathlessness is frequently associated with the onset of both comorbidities.21,22 Therapeutic approaches to alleviating dyspnea include PR, optimizing respiratory mechanics and muscle function (with bronchodilator therapy), and reducing central neural drive to respiratory muscles with supplemental oxygen or opioid medication.94
Although bronchodilator therapy for COPD has not been shown to have significant direct effects on depression or anxiety,95 it can be assumed that the beneficial effects on dyspnea are likely to alleviate associated emotional and mood symptoms.
Further research into effective screening, diagnosis, and management of comorbid anxiety and depressive disorders in COPD is warranted, including evaluation of a broad range of nonpharmacologic and drug-based interventions, alone and in combination.76
Conclusions
Anxiety and depression are common, yet frequently overlooked, comorbidities in COPD. The impact of these psychologic comorbidities is significant; their consequences are evident in morbidity and mortality data, as well as in patient-reported outcomes. As key points of contact for patients with COPD, it is essential that primary care practitioners are vigilant in monitoring for anxiety and depression in their patients with COPD, making the most of the available tools that can support them in doing so, and maintain an ongoing line of communication with other members of the multidisciplinary team. Treatment of anxiety and depression in COPD should adopt a holistic approach that incorporates both nonpharmacologic and pharmacologic interventions. However, the impact of effective screening, diagnosis, and management of anxiety and depression on COPD burden in patients requires further investigation.
- Chaudhary SC, Nanda S, Tripathi A, et al. Prevalence of psychiatric comorbidities in chronic obstructive pulmonary disease patients. Lung India. 2016;33(2):174-178.
- Zhang MW, Ho RC, Cheung MW, Fu E, Mak A. Prevalence of depressive symptoms in patients with chronic obstructive pulmonary disease: a systematic review, meta-analysis and meta-regression. Gen Hosp Psychiatry. 2011;33(3):217-223.
- Tsai TY, Livneh H, Lu MC, Tsai PY, Chen PC, Sung FC. Increased risk and related factors of depression among patients with COPD: a population-based cohort study. BMC Public Health. 2013;13:976.
- Eisner MD, Blanc PD, Yelin EH, et al. Influence of anxiety on health outcomes in COPD. Thorax. 2010;65(3):229-234.
- Marsh S, Guck TP. Anxiety and depression: easing the burden in COPD patients. J Fam Pract. 2016;65(4):246-256.
- Maurer J, Rebbapragada V, Borson S, et al; ACCP Workshop Panel on Anxiety and Depression in COPD. Anxiety and depression in COPD: current understanding, unanswered questions, and research needs. Chest. 2008;134(4 Suppl):43S-56S.
- Pumar MI, Gray CR, Walsh JR, Yang IA, Rolls TA, Ward DL. Anxiety and depression—important psychological comorbidities of COPD. J Thorac Dis. 2014;6(11):1615-1631.
- Dalal AA, Shah M, Lunacsek O, Hanania NA. Clinical and economic burden of depression/anxiety in chronic obstructive pulmonary disease patients within a managed care population. COPD. 2011;8(4):293-299.
- Kunik ME, Roundy K, Veazey C, et al. Surprisingly high prevalence of anxiety and depression in chronic breathing disorders. Chest. 2005;127(4):1205-1211.
- Yohannes AM, Alexopoulos GS. Depression and anxiety in patients with COPD. Eur Respir Rev. 2014;23(133):345-349.
- American Psychiatric Association. Depressive Disorders. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA: American Psychiatric Association; 2013.
- Panagioti M, Scott C, Blakemore A, Coventry PA. Overview of the prevalence, impact, and management of depression and anxiety in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2014;9:1289-1306.
- Laforest L, Roche N, Devouassoux G, et al. Frequency of comorbidities in chronic obstructive pulmonary disease, and impact on all-cause mortality: a population-based cohort study. Respir Med. 2016;117:33-39.
- Lecheler L, Richter M, Franzen DP, et al. The frequent and underrecognised co-occurrence of acute exacerbated COPD and depression warrants screening: a systematic review. Eur Respir Rev. 2017;26(144):pii: 170026.
- Willgoss TG, Yohannes AM. Anxiety disorders in patients with COPD: a systematic review. Respir Care. 2013;58(5):858-866.
- Livermore N, Sharpe L, McKenzie D. Panic attacks and panic disorder in chronic obstructive pulmonary disease: a cognitive behavioral perspective. Respir Med. 2010;104(9):1246-1253.
- World Health Organization. Depression and other common mental disorders: global health estimates. Geneva, Switzerland; World Health Organization: 2017.
- Altemus M, Sarvaiya N, Neill Epperson C. Sex differences in anxiety and depression clinical perspectives. Front Neuroendocrinol. 2014;35(3):320-330.
- Biswas D, Mukherjee S, Chakroborty R, et al. Occurrence of anxiety and depression among stable COPD patients and its impact on functional capability. J Clin Diagn Res. 2017;11(2):OC24-OC27.
- Yohannes AM, Baldwin RC, Connolly MJ. Depression and anxiety in elderly outpatients with chronic obstructive pulmonary disease: prevalence, and validation of the BASDEC screening questionnaire. Int J Geriatr Psychiatry. 2000;15(12):1090-1096.
- Atlantis E, Fahey P, Cochrane B, Smith S. Bidirectional associations between clinically relevant depression or anxiety and COPD: a systematic review and meta-analysis. Chest. 2013;144(3):766-777.
- Tetikkurt C, Ozdemir I, Tetikkurt S, Yilmaz N, Ertan T, Bayar N. Anxiety and depression in COPD patients and correlation with sputum and BAL cytology. Multidiscip Respir Med. 2011;6(4):226-231.
- Yohannes AM, Müllerová H, Hanania NA, et al. Long-term course of depression trajectories in patients with COPD: a 3-year follow-up analysis of the evaluation of COPD longitudinally to identify predictive surrogate endpoints cohort. Chest. 2016;149(4):916-926.
- Sundh J, Ekström M. Persistent disabling breathlessness in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2016;11:2805-2812.
- Kirkil G, Deveci F, Deveci SE, Atmaca M. Anxiety and depression symptoms in patients with chronic obstructive pulmonary disease. Bulletin Clin Psychopharmacol. 2015;25(2):151-161.
- Fuller-Thomson E, Lacombe-Duncan A. Understanding the association between chronic obstructive pulmonary disease and current anxiety: a population-based study. COPD. 2016;13(5):622-631.
- Yohannes AM. Is it quality or quantity of social support needed for patients with chronic medical illness? J Psychosom Res. 2013;74(2):87-88.
- Fabbri LM, Luppi F, Beghe B, Rabe KF. The multiple components of COPD. In: Hanania NA, Sharafkhaneh A, eds. COPD: a guide to diagnosis and clinical management. Humana Press; 2010.
- Lu Y, Feng L, Feng L, Nyunt MS, Yap KB, Ng TP. Systemic inflammation, depression and obstructive pulmonary function: a population-based study. Respir Res. 2013;14:53.
- Hanania NA, Müllerova H, Locantore NW, et al. Determinants of depression in the ECLIPSE chronic obstructive pulmonary disease cohort. Am J Respir Crit Care Med. 2011;183(5):604-611.
- Zhang Q, Liao J, Liao X, et al. Disease knowledge level is a noteworthy risk factor of anxiety and depression in patients with chronic obstructive pulmonary disease: a cross-sectional study. BMC Pulm Med. 2014;14:92.
- Jose AK, Chelangara DP, Shaji KS. Factors associated with anxiety and depression in chronic obstructive pulmonary disease. Int J Res Med Sci. 2016;4(4):1074-1079.
- van Dam van Isselt EF, Groenewegen-Sipkema KH, Spruit-van Eijk M, et al. Pain in patients with COPD: a systematic review and meta-analysis. BMJ Open. 2014;4(9):e005898.
- Lee AL, Harrison SL, Goldstein RS, Brooks D. Pain and its clinical associations in individuals with COPD: a systematic review. Chest. 2015;147(5):1246-1258.
- Divo M, Cote C, de Torres JP, et al; BODE Collaborative Group. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(2):155-161.
- Hillas G, Perlikos F, Tsiligianni I, Tzanakis N. Managing comorbidities in COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:95-109.
- Ng TP, Niti M, Tan WC, Cao Z, Ong KC, Eng P. Depressive symptoms and chronic obstructive pulmonary disease: effect on mortality, hospital readmission, symptom burden, functional status, and quality of life. Arch Intern Med. 2007;167(1):60-67.
- Montserrat-Capdevila J, Godoy P, Marsal JR, et al. Overview of the impact of depression and anxiety in chronic obstructive pulmonary disease. Lung. 2017;195(1):77-85.
- Laurin C, Moullec G, Bacon SL, Lavoie KL. Impact of anxiety and depression on chronic obstructive pulmonary disease exacerbation risk. Am J Respir Crit Care Med. 2012;185(9):918-923.
- Martinez Rivera C, Costan Galicia J, Alcázar Navarrete B, et al. Factors associated with depression in COPD: a multicenter study. Lung. 2016;194(3):335-343.
- Pooler A, Beech R. Examining the relationship between anxiety and depression and exacerbations of COPD which result in hospital admission: a systematic review. Int J Chron Obstruct Pulmon Dis. 2014;9:315-330.
- Dahlén I, Janson C. Anxiety and depression are related to the outcome of emergency treatment in patients with obstructive pulmonary disease. Chest. 2002;122(5):1633-1637.
- Gudmundsson G, Gislason T, Janson C, et al. Risk factors for rehospitalisation in COPD: role of health status, anxiety and depression. Eur Respir J. 2005;26(3):414-419.
- Mikkelsen RL, Middelboe T, Pisinger C, Stage KB. Anxiety and depression in patients with chronic obstructive pulmonary disease (COPD). A review. Nord J Psychiatry. 2004;58(1):65-70.
- Blakemore A, Dickens C, Guthrie E, et al. Depression and anxiety predict health-related quality of life in chronic obstructive pulmonary disease: systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2014;9:501-512.
- Dueñas-Espín I, Demeyer H, Gimeno-Santos E, et al. Depression symptoms reduce physical activity in COPD patients: a prospective multicenter study. Int J Chron Obstruct Pulmon Dis. 2016;11:1287-1295.
- Lee SH, Kim KU, Lee H, Kim YS, Lee MK, Park HK. Factors associated with low-level physical activity in elderly patients with chronic obstructive pulmonary disease [published online ahead of print June 7, 2017]. Korean J Intern Med. 2017;doi: 10.3904/kjim.2016.090.
- Hill K, Geist R, Goldstein RS, Lacasse Y. Anxiety and depression in end-stage COPD. Eur Respir J. 2008;31(3):667-677.
- George J, Kong DC, Thoman R, Stewart K. Factors associated with medication nonadherence in patients with COPD. Chest. 2005;128(5):3198-3204.
- Morrison D, Agur K, Mercer S, Eiras A, González-Montalvo JI, Gruffydd-Jones K. Managing multimorbidity in primary care in patients with chronic respiratory conditions. NPJ Prim Care Respir Med. 2016;26:16043.
- Khdour MR, Hawwa AF, Kidney JC, Smyth BM, McElnay JC. Potential risk factors for medication non-adherence in patients with chronic obstructive pulmonary disease (COPD). Eur J Clin Pharmacol. 2012;68(10):1365-1373.
- Busch AM, Scott-Sheldon LA, Pierce J, et al. Depressed mood predicts pulmonary rehabilitation completion among women, but not men. Respir Med. 2014;108(7):1007-1013.
- Heerema-Poelman A, Stuive I, Wempe JB. Adherence to a maintenance exercise program 1 year after pulmonary rehabilitation: what are the predictors of dropout? J Cardiopulm Rehabil Prev. 2013;33(6):419-426.
- DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherence. Arch Intern Med. 2000;160(14):2101-2107.
- Fan VS, Giardino ND, Blough DK, Kaplan RM, Ramsey SD; Nett Research Group. Costs of pulmonary rehabilitation and predictors of adherence in the National Emphysema Treatment Trial. COPD. 2008;5(2):105-116.
- Bourbeau J, Bartlett SJ. Patient adherence in COPD. Thorax. 2008;63(9):831-838.
- van Boven JF, Chavannes NH, van der Molen T, Rutten-van Mölken MP, Postma MJ, Vegter S. Clinical and economic impact of non-adherence in COPD: a systematic review. Respir Med. 2014;108(1):103-113.
- Dury R. COPD and emotional distress: not always noticed and therefore untreated. Br J Community Nurs. 2016;21(3):138-141.
- Price D, Crockett A, Arne M, et al. Spirometry in primary care case-identification, diagnosis and management of COPD. Prim Care Respir J. 2009;18(3):216-223.
- van Boven JF, Ryan D, Eakin MN, Canonica GW, Barot A, Foster JM; Respiratory Effectiveness Group. Enhancing respiratory medication adherence: the role of health care professionals and cost-effectiveness considerations. J Allergy Clin Immunol Pract. 2016;4(5):835-846.
- Wittchen HU, Mühlig S, Beesdo K. Mental disorders in primary care. Dialogues Clin Neurosci. 2003;5(2):115-128.
- Global Initiative for Chronic Obstructive Lung Disease. GOLD 2017 Global Strategy for the Diagnosis, Management and Prevention of COPD. http://goldcopd.org/gold-2017-global-strategy-diagnosis-management-prevention-copd. Accessed June 2017.
- Willgoss TG, Goldbart J, Fatoye F, Yohannes AM. The development and validation of the anxiety inventory for respiratory disease. Chest. 2013;144(5):1587-1596.
- Yohannes AM, Dryden S, Hanania NA. The responsiveness of the anxiety inventory for respiratory disease scale following pulmonary rehabilitation. Chest. 2016;150(1):188-195.
- Kühl K, Kuhn C, Kenn K, Rief W. [The COPD-Anxiety-Questionnaire (CAF): a new instrument to assess illness specific anxiety in COPD patients]. Psychother Psychosom Med Psychol. 2011;61(1):e1-e9. German.
- Tamburrino MB, Lynch DJ, Nagel RW, Smith MK. Primary care evaluation of mental disorders (PRIME-MD) screening for minor depressive disorder in primary care. Prim Care Companion J Clin Psychiatry. 2009;11(6):339-343.
- Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA. 1999;282(18):1737-1744.
- Arroll B, Goodyear-Smith F, Crengle S, et al. Validation of PHQ-2 and PHQ-9 to screen for major depression in the primary care population. Ann Fam Med. 2010;8(4):348-353.
- Yohannes AM, Hann M, Sibbald B. The management of depressive symptoms in patients with COPD: a postal survey of general practitioners. Prim Health Care Res Dev. 2011;12(3):237-244.
- Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092-1097.
- Bratås O, Grønning K, Forbord T. Psychometric properties of the Hospital Anxiety and Depression Scale and The General Health Questionnaire-20 in COPD inpatients. Scand J Caring Sci. 2014;28(2):413-420.
- Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995;33(3):335-343.
- Sundh J, Ställberg B, Lisspers K, Kämpe M, Janson C, Montgomery S. Comparison of the COPD Assessment Test (CAT) and the Clinical COPD Questionnaire (CCQ) in a clinical population. COPD. 2016;13(1):57-65.
- Cantor L, Jacobson R. COPD: How to manage comorbid depression and anxiety. Curr Psychiatry. 2003;2(11):45-54.
- Yohannes AM. Palliative care provision for patients with chronic obstructive pulmonary disease. Health Qual Life Outcomes. 2007;5:17.
- Tselebis A, Pachi A, Ilias I, et al. Strategies to improve anxiety and depression in patients with COPD: a mental health perspective. Neuropsychiatr Dis Treat. 2016;12:297-328.
- Doyle C, Bhar S, Fearn M, et al. The impact of telephone-delivered cognitive behaviour therapy and befriending on mood disorders in people with chronic obstructive pulmonary disease: a randomized controlled trial. Br J Health Psychol. 2017;22(3):542-556.
- Alsaraireh FA, Aloush SA. Does pulmonary rehabilitation alleviate depression in older patients with chronic obstructive pulmonary disease. Saudi Med J. 2017;38(5):491-496.
- Bennett D, Bowen B, McCarthy P, Subramaniam A, O’Connor M, Henry MT. Outcomes of pulmonary rehabilitation for COPD in older patients: a comparative study. COPD. 2017;14(2):170-175.
- Smith SM, Sonego S, Ketcheson L, Larson JL. A review of the effectiveness of psychological interventions used for anxiety and depression in chronic obstructive pulmonary disease. BMJ Open Respir Res. 2014;1(1):e000042.
- Bove DG, Overgaard D, Lomborg K, Lindhardt BØ, Midtgaard J. Efficacy of a minimal home-based psychoeducative intervention versus usual care for managing anxiety and dyspnoea in patients with severe chronic obstructive pulmonary disease: a randomised controlled trial protocol. BMJ Open. 2015;5(7):e008031.
- Bove DG, Lomborg K, Jensen AK, Overgaard D, Lindhardt BØ, Midtgaard J. Efficacy of a minimal home-based psychoeducative intervention in patients with advanced COPD: a randomised controlled trial. Respir Med. 2016;121:109-116.
- Usmani ZA, Carson KV, Heslop K, Esterman AJ, De Soyza A, Smith BJ. Psychological therapies for the treatment of anxiety disorders in chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2017;3: CD010673. doi:10.002/14651858.CD010673.pub2.
- Cafarella P, Effing T, Frith P. An evaluation of the needs of carers of people with COPD. EurResp J. 2012;40(Suppl 56).
- Zyban [package insert]. Research Triangle Park, NC: GlaxoSmithKline; 2017. Available at: https://www.gsksource.com/pharma/content/dam/GlaxoSmithKline/US/en/Prescribing_Information/Zyban/pdf/ZYBAN-PI-MG.PDF. Accessed June 2017.
- Gelenberg AJ, Freeman MP, Markowitz JC, et al. Practice guideline for the treatment of patients with major depressive disorder. Am J Psychiatry. 2010;167(10):1.
- Pary R, Matuschka PR, Lewis S, Lippmann S. Managing bipolar depression. Psychiatry (Edgmont). 2006;3(2):30-41.
- Blier P. Atypical antipsychotics for mood and anxiety disorders: safe and effective adjuncts? J Psychiatry Neurosci. 2005;30(4):232-233.
- Vulink NC, Figee M, Denys D. Review of atypical antipsychotics in anxiety. Eur Neuropsychopharmacol. 2011;21(6):429-449.
- Locke AB, Kirst N, Shultz CG. Diagnosis and management of generalized anxiety disorder and panic disorder in adults. Am Fam Physician. 2015;91(9):617-624.
- Kew KM, Dias S, Cates CJ. Long-acting inhaled therapy (beta-agonists, anticholinergics and steroids) for COPD: a network meta-analysis. Cochrane Database Syst Rev. 2014;(3):CD010844. doi:10.1002/14651858.CD010844.pub2.
- Scully C. Drug effects on salivary glands: dry mouth. Oral Dis. 2003;9(4):165-176.
- Grenard JL, Munjas BA, Adams JL, et al. Depression and medication adherence in the treatment of chronic diseases in the United States: a meta-analysis. J Gen Intern Med. 2011;26(10):1175-1182.
- O’Donnell DE, Webb KA, Harle I, Neder JA. Pharmacological management of breathlessness in COPD: recent advances and hopes for the future. Expert Rev Respir Med. 2016;10(7):823-834.
- Hyun MK, Lee NR, Jang EJ, Yim JJ, Lee CH. Effect of inhaled drugs on anxiety and depression in patients with chronic obstructive pulmonary disease: a prospective observational study. Int J Chron Obstruct Pulmon Dis. 2016;11:747-754.
- Chaudhary SC, Nanda S, Tripathi A, et al. Prevalence of psychiatric comorbidities in chronic obstructive pulmonary disease patients. Lung India. 2016;33(2):174-178.
- Zhang MW, Ho RC, Cheung MW, Fu E, Mak A. Prevalence of depressive symptoms in patients with chronic obstructive pulmonary disease: a systematic review, meta-analysis and meta-regression. Gen Hosp Psychiatry. 2011;33(3):217-223.
- Tsai TY, Livneh H, Lu MC, Tsai PY, Chen PC, Sung FC. Increased risk and related factors of depression among patients with COPD: a population-based cohort study. BMC Public Health. 2013;13:976.
- Eisner MD, Blanc PD, Yelin EH, et al. Influence of anxiety on health outcomes in COPD. Thorax. 2010;65(3):229-234.
- Marsh S, Guck TP. Anxiety and depression: easing the burden in COPD patients. J Fam Pract. 2016;65(4):246-256.
- Maurer J, Rebbapragada V, Borson S, et al; ACCP Workshop Panel on Anxiety and Depression in COPD. Anxiety and depression in COPD: current understanding, unanswered questions, and research needs. Chest. 2008;134(4 Suppl):43S-56S.
- Pumar MI, Gray CR, Walsh JR, Yang IA, Rolls TA, Ward DL. Anxiety and depression—important psychological comorbidities of COPD. J Thorac Dis. 2014;6(11):1615-1631.
- Dalal AA, Shah M, Lunacsek O, Hanania NA. Clinical and economic burden of depression/anxiety in chronic obstructive pulmonary disease patients within a managed care population. COPD. 2011;8(4):293-299.
- Kunik ME, Roundy K, Veazey C, et al. Surprisingly high prevalence of anxiety and depression in chronic breathing disorders. Chest. 2005;127(4):1205-1211.
- Yohannes AM, Alexopoulos GS. Depression and anxiety in patients with COPD. Eur Respir Rev. 2014;23(133):345-349.
- American Psychiatric Association. Depressive Disorders. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA: American Psychiatric Association; 2013.
- Panagioti M, Scott C, Blakemore A, Coventry PA. Overview of the prevalence, impact, and management of depression and anxiety in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2014;9:1289-1306.
- Laforest L, Roche N, Devouassoux G, et al. Frequency of comorbidities in chronic obstructive pulmonary disease, and impact on all-cause mortality: a population-based cohort study. Respir Med. 2016;117:33-39.
- Lecheler L, Richter M, Franzen DP, et al. The frequent and underrecognised co-occurrence of acute exacerbated COPD and depression warrants screening: a systematic review. Eur Respir Rev. 2017;26(144):pii: 170026.
- Willgoss TG, Yohannes AM. Anxiety disorders in patients with COPD: a systematic review. Respir Care. 2013;58(5):858-866.
- Livermore N, Sharpe L, McKenzie D. Panic attacks and panic disorder in chronic obstructive pulmonary disease: a cognitive behavioral perspective. Respir Med. 2010;104(9):1246-1253.
- World Health Organization. Depression and other common mental disorders: global health estimates. Geneva, Switzerland; World Health Organization: 2017.
- Altemus M, Sarvaiya N, Neill Epperson C. Sex differences in anxiety and depression clinical perspectives. Front Neuroendocrinol. 2014;35(3):320-330.
- Biswas D, Mukherjee S, Chakroborty R, et al. Occurrence of anxiety and depression among stable COPD patients and its impact on functional capability. J Clin Diagn Res. 2017;11(2):OC24-OC27.
- Yohannes AM, Baldwin RC, Connolly MJ. Depression and anxiety in elderly outpatients with chronic obstructive pulmonary disease: prevalence, and validation of the BASDEC screening questionnaire. Int J Geriatr Psychiatry. 2000;15(12):1090-1096.
- Atlantis E, Fahey P, Cochrane B, Smith S. Bidirectional associations between clinically relevant depression or anxiety and COPD: a systematic review and meta-analysis. Chest. 2013;144(3):766-777.
- Tetikkurt C, Ozdemir I, Tetikkurt S, Yilmaz N, Ertan T, Bayar N. Anxiety and depression in COPD patients and correlation with sputum and BAL cytology. Multidiscip Respir Med. 2011;6(4):226-231.
- Yohannes AM, Müllerová H, Hanania NA, et al. Long-term course of depression trajectories in patients with COPD: a 3-year follow-up analysis of the evaluation of COPD longitudinally to identify predictive surrogate endpoints cohort. Chest. 2016;149(4):916-926.
- Sundh J, Ekström M. Persistent disabling breathlessness in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2016;11:2805-2812.
- Kirkil G, Deveci F, Deveci SE, Atmaca M. Anxiety and depression symptoms in patients with chronic obstructive pulmonary disease. Bulletin Clin Psychopharmacol. 2015;25(2):151-161.
- Fuller-Thomson E, Lacombe-Duncan A. Understanding the association between chronic obstructive pulmonary disease and current anxiety: a population-based study. COPD. 2016;13(5):622-631.
- Yohannes AM. Is it quality or quantity of social support needed for patients with chronic medical illness? J Psychosom Res. 2013;74(2):87-88.
- Fabbri LM, Luppi F, Beghe B, Rabe KF. The multiple components of COPD. In: Hanania NA, Sharafkhaneh A, eds. COPD: a guide to diagnosis and clinical management. Humana Press; 2010.
- Lu Y, Feng L, Feng L, Nyunt MS, Yap KB, Ng TP. Systemic inflammation, depression and obstructive pulmonary function: a population-based study. Respir Res. 2013;14:53.
- Hanania NA, Müllerova H, Locantore NW, et al. Determinants of depression in the ECLIPSE chronic obstructive pulmonary disease cohort. Am J Respir Crit Care Med. 2011;183(5):604-611.
- Zhang Q, Liao J, Liao X, et al. Disease knowledge level is a noteworthy risk factor of anxiety and depression in patients with chronic obstructive pulmonary disease: a cross-sectional study. BMC Pulm Med. 2014;14:92.
- Jose AK, Chelangara DP, Shaji KS. Factors associated with anxiety and depression in chronic obstructive pulmonary disease. Int J Res Med Sci. 2016;4(4):1074-1079.
- van Dam van Isselt EF, Groenewegen-Sipkema KH, Spruit-van Eijk M, et al. Pain in patients with COPD: a systematic review and meta-analysis. BMJ Open. 2014;4(9):e005898.
- Lee AL, Harrison SL, Goldstein RS, Brooks D. Pain and its clinical associations in individuals with COPD: a systematic review. Chest. 2015;147(5):1246-1258.
- Divo M, Cote C, de Torres JP, et al; BODE Collaborative Group. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(2):155-161.
- Hillas G, Perlikos F, Tsiligianni I, Tzanakis N. Managing comorbidities in COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:95-109.
- Ng TP, Niti M, Tan WC, Cao Z, Ong KC, Eng P. Depressive symptoms and chronic obstructive pulmonary disease: effect on mortality, hospital readmission, symptom burden, functional status, and quality of life. Arch Intern Med. 2007;167(1):60-67.
- Montserrat-Capdevila J, Godoy P, Marsal JR, et al. Overview of the impact of depression and anxiety in chronic obstructive pulmonary disease. Lung. 2017;195(1):77-85.
- Laurin C, Moullec G, Bacon SL, Lavoie KL. Impact of anxiety and depression on chronic obstructive pulmonary disease exacerbation risk. Am J Respir Crit Care Med. 2012;185(9):918-923.
- Martinez Rivera C, Costan Galicia J, Alcázar Navarrete B, et al. Factors associated with depression in COPD: a multicenter study. Lung. 2016;194(3):335-343.
- Pooler A, Beech R. Examining the relationship between anxiety and depression and exacerbations of COPD which result in hospital admission: a systematic review. Int J Chron Obstruct Pulmon Dis. 2014;9:315-330.
- Dahlén I, Janson C. Anxiety and depression are related to the outcome of emergency treatment in patients with obstructive pulmonary disease. Chest. 2002;122(5):1633-1637.
- Gudmundsson G, Gislason T, Janson C, et al. Risk factors for rehospitalisation in COPD: role of health status, anxiety and depression. Eur Respir J. 2005;26(3):414-419.
- Mikkelsen RL, Middelboe T, Pisinger C, Stage KB. Anxiety and depression in patients with chronic obstructive pulmonary disease (COPD). A review. Nord J Psychiatry. 2004;58(1):65-70.
- Blakemore A, Dickens C, Guthrie E, et al. Depression and anxiety predict health-related quality of life in chronic obstructive pulmonary disease: systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2014;9:501-512.
- Dueñas-Espín I, Demeyer H, Gimeno-Santos E, et al. Depression symptoms reduce physical activity in COPD patients: a prospective multicenter study. Int J Chron Obstruct Pulmon Dis. 2016;11:1287-1295.
- Lee SH, Kim KU, Lee H, Kim YS, Lee MK, Park HK. Factors associated with low-level physical activity in elderly patients with chronic obstructive pulmonary disease [published online ahead of print June 7, 2017]. Korean J Intern Med. 2017;doi: 10.3904/kjim.2016.090.
- Hill K, Geist R, Goldstein RS, Lacasse Y. Anxiety and depression in end-stage COPD. Eur Respir J. 2008;31(3):667-677.
- George J, Kong DC, Thoman R, Stewart K. Factors associated with medication nonadherence in patients with COPD. Chest. 2005;128(5):3198-3204.
- Morrison D, Agur K, Mercer S, Eiras A, González-Montalvo JI, Gruffydd-Jones K. Managing multimorbidity in primary care in patients with chronic respiratory conditions. NPJ Prim Care Respir Med. 2016;26:16043.
- Khdour MR, Hawwa AF, Kidney JC, Smyth BM, McElnay JC. Potential risk factors for medication non-adherence in patients with chronic obstructive pulmonary disease (COPD). Eur J Clin Pharmacol. 2012;68(10):1365-1373.
- Busch AM, Scott-Sheldon LA, Pierce J, et al. Depressed mood predicts pulmonary rehabilitation completion among women, but not men. Respir Med. 2014;108(7):1007-1013.
- Heerema-Poelman A, Stuive I, Wempe JB. Adherence to a maintenance exercise program 1 year after pulmonary rehabilitation: what are the predictors of dropout? J Cardiopulm Rehabil Prev. 2013;33(6):419-426.
- DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherence. Arch Intern Med. 2000;160(14):2101-2107.
- Fan VS, Giardino ND, Blough DK, Kaplan RM, Ramsey SD; Nett Research Group. Costs of pulmonary rehabilitation and predictors of adherence in the National Emphysema Treatment Trial. COPD. 2008;5(2):105-116.
- Bourbeau J, Bartlett SJ. Patient adherence in COPD. Thorax. 2008;63(9):831-838.
- van Boven JF, Chavannes NH, van der Molen T, Rutten-van Mölken MP, Postma MJ, Vegter S. Clinical and economic impact of non-adherence in COPD: a systematic review. Respir Med. 2014;108(1):103-113.
- Dury R. COPD and emotional distress: not always noticed and therefore untreated. Br J Community Nurs. 2016;21(3):138-141.
- Price D, Crockett A, Arne M, et al. Spirometry in primary care case-identification, diagnosis and management of COPD. Prim Care Respir J. 2009;18(3):216-223.
- van Boven JF, Ryan D, Eakin MN, Canonica GW, Barot A, Foster JM; Respiratory Effectiveness Group. Enhancing respiratory medication adherence: the role of health care professionals and cost-effectiveness considerations. J Allergy Clin Immunol Pract. 2016;4(5):835-846.
- Wittchen HU, Mühlig S, Beesdo K. Mental disorders in primary care. Dialogues Clin Neurosci. 2003;5(2):115-128.
- Global Initiative for Chronic Obstructive Lung Disease. GOLD 2017 Global Strategy for the Diagnosis, Management and Prevention of COPD. http://goldcopd.org/gold-2017-global-strategy-diagnosis-management-prevention-copd. Accessed June 2017.
- Willgoss TG, Goldbart J, Fatoye F, Yohannes AM. The development and validation of the anxiety inventory for respiratory disease. Chest. 2013;144(5):1587-1596.
- Yohannes AM, Dryden S, Hanania NA. The responsiveness of the anxiety inventory for respiratory disease scale following pulmonary rehabilitation. Chest. 2016;150(1):188-195.
- Kühl K, Kuhn C, Kenn K, Rief W. [The COPD-Anxiety-Questionnaire (CAF): a new instrument to assess illness specific anxiety in COPD patients]. Psychother Psychosom Med Psychol. 2011;61(1):e1-e9. German.
- Tamburrino MB, Lynch DJ, Nagel RW, Smith MK. Primary care evaluation of mental disorders (PRIME-MD) screening for minor depressive disorder in primary care. Prim Care Companion J Clin Psychiatry. 2009;11(6):339-343.
- Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA. 1999;282(18):1737-1744.
- Arroll B, Goodyear-Smith F, Crengle S, et al. Validation of PHQ-2 and PHQ-9 to screen for major depression in the primary care population. Ann Fam Med. 2010;8(4):348-353.
- Yohannes AM, Hann M, Sibbald B. The management of depressive symptoms in patients with COPD: a postal survey of general practitioners. Prim Health Care Res Dev. 2011;12(3):237-244.
- Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092-1097.
- Bratås O, Grønning K, Forbord T. Psychometric properties of the Hospital Anxiety and Depression Scale and The General Health Questionnaire-20 in COPD inpatients. Scand J Caring Sci. 2014;28(2):413-420.
- Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995;33(3):335-343.
- Sundh J, Ställberg B, Lisspers K, Kämpe M, Janson C, Montgomery S. Comparison of the COPD Assessment Test (CAT) and the Clinical COPD Questionnaire (CCQ) in a clinical population. COPD. 2016;13(1):57-65.
- Cantor L, Jacobson R. COPD: How to manage comorbid depression and anxiety. Curr Psychiatry. 2003;2(11):45-54.
- Yohannes AM. Palliative care provision for patients with chronic obstructive pulmonary disease. Health Qual Life Outcomes. 2007;5:17.
- Tselebis A, Pachi A, Ilias I, et al. Strategies to improve anxiety and depression in patients with COPD: a mental health perspective. Neuropsychiatr Dis Treat. 2016;12:297-328.
- Doyle C, Bhar S, Fearn M, et al. The impact of telephone-delivered cognitive behaviour therapy and befriending on mood disorders in people with chronic obstructive pulmonary disease: a randomized controlled trial. Br J Health Psychol. 2017;22(3):542-556.
- Alsaraireh FA, Aloush SA. Does pulmonary rehabilitation alleviate depression in older patients with chronic obstructive pulmonary disease. Saudi Med J. 2017;38(5):491-496.
- Bennett D, Bowen B, McCarthy P, Subramaniam A, O’Connor M, Henry MT. Outcomes of pulmonary rehabilitation for COPD in older patients: a comparative study. COPD. 2017;14(2):170-175.
- Smith SM, Sonego S, Ketcheson L, Larson JL. A review of the effectiveness of psychological interventions used for anxiety and depression in chronic obstructive pulmonary disease. BMJ Open Respir Res. 2014;1(1):e000042.
- Bove DG, Overgaard D, Lomborg K, Lindhardt BØ, Midtgaard J. Efficacy of a minimal home-based psychoeducative intervention versus usual care for managing anxiety and dyspnoea in patients with severe chronic obstructive pulmonary disease: a randomised controlled trial protocol. BMJ Open. 2015;5(7):e008031.
- Bove DG, Lomborg K, Jensen AK, Overgaard D, Lindhardt BØ, Midtgaard J. Efficacy of a minimal home-based psychoeducative intervention in patients with advanced COPD: a randomised controlled trial. Respir Med. 2016;121:109-116.
- Usmani ZA, Carson KV, Heslop K, Esterman AJ, De Soyza A, Smith BJ. Psychological therapies for the treatment of anxiety disorders in chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2017;3: CD010673. doi:10.002/14651858.CD010673.pub2.
- Cafarella P, Effing T, Frith P. An evaluation of the needs of carers of people with COPD. EurResp J. 2012;40(Suppl 56).
- Zyban [package insert]. Research Triangle Park, NC: GlaxoSmithKline; 2017. Available at: https://www.gsksource.com/pharma/content/dam/GlaxoSmithKline/US/en/Prescribing_Information/Zyban/pdf/ZYBAN-PI-MG.PDF. Accessed June 2017.
- Gelenberg AJ, Freeman MP, Markowitz JC, et al. Practice guideline for the treatment of patients with major depressive disorder. Am J Psychiatry. 2010;167(10):1.
- Pary R, Matuschka PR, Lewis S, Lippmann S. Managing bipolar depression. Psychiatry (Edgmont). 2006;3(2):30-41.
- Blier P. Atypical antipsychotics for mood and anxiety disorders: safe and effective adjuncts? J Psychiatry Neurosci. 2005;30(4):232-233.
- Vulink NC, Figee M, Denys D. Review of atypical antipsychotics in anxiety. Eur Neuropsychopharmacol. 2011;21(6):429-449.
- Locke AB, Kirst N, Shultz CG. Diagnosis and management of generalized anxiety disorder and panic disorder in adults. Am Fam Physician. 2015;91(9):617-624.
- Kew KM, Dias S, Cates CJ. Long-acting inhaled therapy (beta-agonists, anticholinergics and steroids) for COPD: a network meta-analysis. Cochrane Database Syst Rev. 2014;(3):CD010844. doi:10.1002/14651858.CD010844.pub2.
- Scully C. Drug effects on salivary glands: dry mouth. Oral Dis. 2003;9(4):165-176.
- Grenard JL, Munjas BA, Adams JL, et al. Depression and medication adherence in the treatment of chronic diseases in the United States: a meta-analysis. J Gen Intern Med. 2011;26(10):1175-1182.
- O’Donnell DE, Webb KA, Harle I, Neder JA. Pharmacological management of breathlessness in COPD: recent advances and hopes for the future. Expert Rev Respir Med. 2016;10(7):823-834.
- Hyun MK, Lee NR, Jang EJ, Yim JJ, Lee CH. Effect of inhaled drugs on anxiety and depression in patients with chronic obstructive pulmonary disease: a prospective observational study. Int J Chron Obstruct Pulmon Dis. 2016;11:747-754.
