User login
Risk Factors Associated With Multidrug-Resistant Pneumonia in Nonhospitalized Patients
Successful treatment of pneumonia depends on timely diagnosis and administration of antibiotics. Multidrug-resistant organisms (MDROs) complicate antibiotic therapies by rendering some antibiotic agents ineffective. Inappropriate initial therapy has been associated with a more than 2-fold increase in the risk of mortality.1 Because culture results are not available immediately, clinicians prescribe antibiotics empirically and must rely on guidelines and knowledge of risk factors associated with MDRO infection to make these selections.
Treatment guidelines exist for hospital-acquired and ventilator-associated pneumonia (HAP/VAP) and community-acquired pneumonia (CAP) to assist with empiric antibiotic selection. For HAP/VAP, 2 to 3 antibiotics with a broad-spectrum of activity are used due to increased prevalence of MDROs in hospitals, whereastreatment of CAP involves more narrow coverage because bacteria that cause this infection typically have fewer antibiotic resistances.2,3 The HAP/VAP guidelines stratify the risk of pneumonia due to the presence of a MDRO acquired during a hospitalization. However, neither the CAP nor HAP/VAP guidelines offer risk-stratification guidance for nonhospitalized patients who develop pneumonia but who may have become colonized with a MDRO during a previous hospitalization or from another exposure to a health care facility.
Health care-associated pneumonia (HCAP) was first described in the 2005 American Thoracic Society and the Infectious Diseases Society of America (ATS/IDSA) nosocomial pneumonia guidelines and was associated with criteria intended to aid clinician identification of nonhospitalized patients at risk for MDRO pneumonia, which warranted empiric broad-spectrum antibiotic therapy.2 According to these guidelines, patients were classified as having HCAP if they had been hospitalized for at least 48 hours in the past 90 days, admitted from a nursing home, received recent intravenous antibiotics, had hemodialysis in the past 30 days, had a history of home infusion therapy or wound care, received intravenous chemotherapy, or had a family member with MDRO colonization.
Since publication of the 2005 guidelines, HCAP has been criticized as being a poor predictor of MDRO infection. A 2014 meta-analysis of 24 studies investigated the discriminating ability of HCAP and reported that the specificity and sensitivity for MDRO infections was 71.2% and 53.7%, respectively.3 In 2016, the ATS/IDSA guidelines were updated to remove HCAP due to the risk of antibiotic overprescribing.4
Literature Review
Although criteria previously defining a patient as having HCAP have been shown to be a poor discriminator of MDRO pneumonia as a whole, MDRO infections still pose a threat to nonhospitalized patients who have exposure to the health care system. A literature review was performed to identify independent HCAP risk factors that may increase the risk of MDRO pneumonia infecting a nonhospitalized patient needing empiric broad-spectrum antibiotic therapy. All included studies were prospective or retrospective observational cohort studies that performed logistic regression analyses to assess the association between MDRO isolation and the previously defined HCAP risk factors (Table 1). 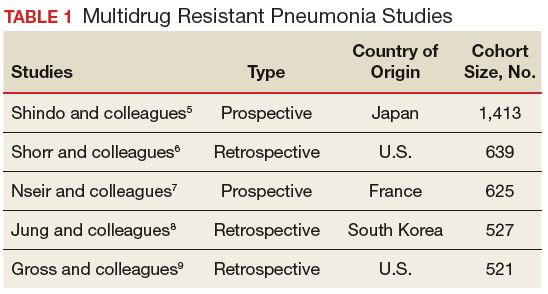
Five studies examined the risk of MDRO infection in patients with a previous hospital admission of 2 days or more in the past 90 days. Shindo and colleagues found a significant increase in MDRO infections by about 2-fold (adjusted odds ratio [AOR], 2.1; 95% confidence interval [CI], 1.2-3.4).5 Shorr and colleagues found a 4-fold increase in likelihood of identifying a MDRO in HCAP (AOR, 4.2; 95% CI, 2.9-6.3).6 Nseir and colleagues and Jung and colleagues found similar results (AOR 3.9, 95% CI 1.7-8.8; AOR 2.7, 95% CI 1.3-5.5, respectively).7,8 Conflicting results were reported by Gross and colleagues who did not find a significant relationship between previous hospitalization and MDRO isolation (AOR 1.2, 95% CI, 0.5-3.2).9
In patients with pneumonia admitted from a nursing home, MDRO infection risk also was evaluated in these 5 studies. Shorr and colleagues, Nseir and colleagues, and Gross and colleagues found significant AORs of 2.7 (95% CI 1.7-4.3), 2.0 (95% CI 1.1-3.7), and 4.2 (95% CI 1.6-11.3), respectively.6,7,9 Shindo and colleagues (AOR 1.1; 95% CI, 0.6-2.0) and Jung and colleagues (AOR 1.9, 95% CI, 0.5-6.9) found this risk factor not significant.5
Receipt of antibiotics within the previous 90 days was assessed in 3 studies. Shindo and colleagues, Nseir and colleagues, and Gross and colleagues all found significant AORs of 2.5 (95% CI 1.2-4.0), 2.3 (95% CI 1.2-4.3), and 2.9 (95% CI 1.1-7.5), respectively.5,7,9 Antibiotic therapy within the previous 90 days is an established risk factor for MDRO pneumonia, and the 2016 ATS/IDSA guidelines consider this a risk factor for HAP and VAP, including pneumonia caused by methicillin resistant Staphylococcus aureus and Pseudomonas aeruginosa.4
The impact of hemodialysis in the previous month on acquisition of MDRO pneumonia was investigated in 4 studies. Shindo and colleagues, Jung and colleagues, and Gross and colleagues concluded that this risk factor was not significantly related to MDRO infection, reporting AORs of 2.2 (95% CI 0.5-9.7), 2.8 (95% CI 0.9-9.2) and 0.7 (95% CI 0.1-5.1), respectively.5,8,9 Shorr and colleagues, however, found a significant AOR of 2.1 (95% CI 1.0-4.3).6
Shindo and colleagues investigated the impact of home infusion therapy on acquisition of pneumonia due to a MDRO and reported a nonsignificant AOR of 0.8 (95% CI 0.4-1.8).5 Gross and colleagues also found a nonsignificant AOR of 0 (P = .1).9 In the Shindo and colleagues study, resistance was found in 107 of 679 patients who did not receive infusion therapy, and 12 of 55 patients who were receiving infusion therapy.5 Gross and colleagues reported that home-infusion therapy was received by 0 of 20 patients with MDRO infection and 4 of the 501 patients without MDRO infection.9
Shindo and colleagues reported that home wound care was not found to be significantly related to MDRO pneumonia as well as did Gross and colleagues: AORs of 3.8 (0.8-18.4) and 1.4 (95% CI 0.5-4.4), respectively.5,9 Jung and colleagues examined IV chemotherapy in the past 30 days, and found this to not significantly impact the odds of MDRO isolation (AOR = 0.62, 95% CI 0.2-1.8).8 No data were available reflecting the risk of a family member with a MDRO.
Limitations
The variables on which logistic regression were performed differed among the studies. Therefore, results cannot be averaged or compared quantitatively, as AORs varied, depending on the variables included. In addition, data were drawn from multiple geographic locations that may impact MDRO prevalence within each patient population. Finally, this review examines the utility of the risk factors formerly included in HCAP. However, other risk factors for MDRO pneumonia outlined by the ATS/IDSA guidelines still should be considered when evaluating patient risk. The 2016 guidelines recommend local incidence of resistant strains be considered when initiating empiric therapy. Review of medical records for previous positive cultures and duration of current hospitalization also should be considered. Although the 2016 ATS/IDSA HAP guidelines are not intended for immunosuppressed patients, this risk factor also may be taken into account.
Conclusion
Review and synthesis of published literature found previous hospital admission (of ≥ 2 days in the past 90 days), admission from a nursing home, and IV antibiotic therapy in the last 90 days to be independent risk factors for identification of MDRO pneumonia in previously nonhospitalized patients (Table 2). Additionally, although no data were found to support this risk factor, existence of an in-home (close contact) source of MDROs would provide ample opportunity for transmission, so evaluation of known exposure to MDROs from contacts should be considered. When choosing empiric antibiotic therapy for patients admitted to the hospital for treatment of pneumonia, consideration of patient history and risk factors that may contribute to infection with a MDRO are recommended. 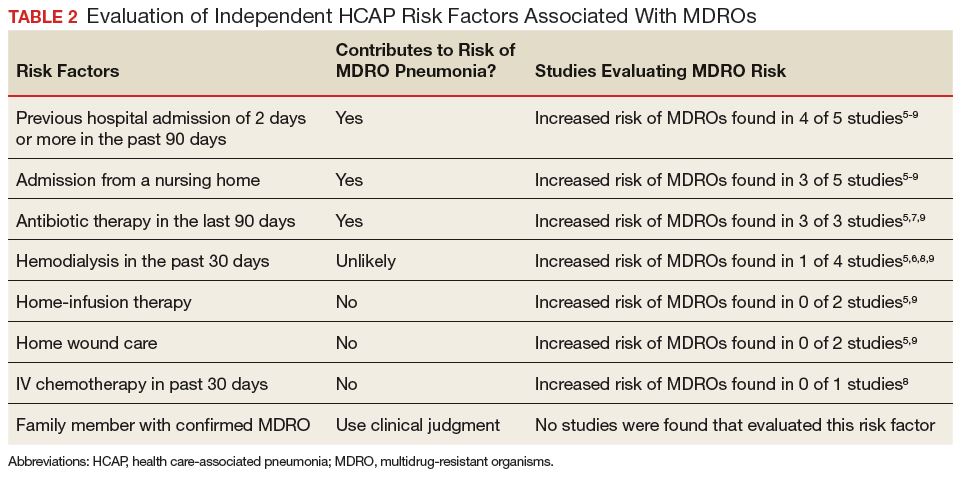
1. Kollef MH, Sherman G, Ward S, Fraser VJ. Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients. Chest. 1999;115(2):462-474.
2. American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388-416.
3. Chalmers JD, Rother C, Salih W, Ewig S. Healthcare-associated pneumonia does not accurately identify potentially resistant pathogens: a systematic review and meta-analysis. Clin Infect Dis. 2014;58(3):330-339.
4. Kalil AC, Metersky ML, Klompas M, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63(5):e61-e111.
5. Shindo Y, Ito R, Kobayashi D, et al. Risk factors for drug-resistant pathogens in community-acquired and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2013;188(8):985-995.
6. Shorr AF, Zilberberg MD, Micek ST, Kollef MH. Prediction of infection due to antibiotic-resistant bacteria by select risk factors for health care–associated pneumonia. Arch Intern Med. 2008;168(20):2205-2210.
7. Nseir S, Grailles G, Soury-Lavergne A, Minacori F, Alves I, Durocher A. Accuracy of American Thoracic Society/Infectious Diseases Society of America criteria in predicting infection or colonization with multidrug-resistant bacteria at intensive-care unit admission. Clin Microbiol Infect. 2010;16(7):902-908.
8. Jung JY, Park MS, Kim YS, et al. Healthcare-associated pneumonia among hospitalized patients in a Korean tertiary hospital. BMC Infectious Diseases. 2011;11:61.
9. Gross AE, Van Schooneveld TC, Olsen KM, et al. Epidemiology and predictors of multidrug-resistant community-acquired and health care-associated pneumonia. Antimicrob Agents Chemother. 2014;58(9):5262-5268.
Successful treatment of pneumonia depends on timely diagnosis and administration of antibiotics. Multidrug-resistant organisms (MDROs) complicate antibiotic therapies by rendering some antibiotic agents ineffective. Inappropriate initial therapy has been associated with a more than 2-fold increase in the risk of mortality.1 Because culture results are not available immediately, clinicians prescribe antibiotics empirically and must rely on guidelines and knowledge of risk factors associated with MDRO infection to make these selections.
Treatment guidelines exist for hospital-acquired and ventilator-associated pneumonia (HAP/VAP) and community-acquired pneumonia (CAP) to assist with empiric antibiotic selection. For HAP/VAP, 2 to 3 antibiotics with a broad-spectrum of activity are used due to increased prevalence of MDROs in hospitals, whereastreatment of CAP involves more narrow coverage because bacteria that cause this infection typically have fewer antibiotic resistances.2,3 The HAP/VAP guidelines stratify the risk of pneumonia due to the presence of a MDRO acquired during a hospitalization. However, neither the CAP nor HAP/VAP guidelines offer risk-stratification guidance for nonhospitalized patients who develop pneumonia but who may have become colonized with a MDRO during a previous hospitalization or from another exposure to a health care facility.
Health care-associated pneumonia (HCAP) was first described in the 2005 American Thoracic Society and the Infectious Diseases Society of America (ATS/IDSA) nosocomial pneumonia guidelines and was associated with criteria intended to aid clinician identification of nonhospitalized patients at risk for MDRO pneumonia, which warranted empiric broad-spectrum antibiotic therapy.2 According to these guidelines, patients were classified as having HCAP if they had been hospitalized for at least 48 hours in the past 90 days, admitted from a nursing home, received recent intravenous antibiotics, had hemodialysis in the past 30 days, had a history of home infusion therapy or wound care, received intravenous chemotherapy, or had a family member with MDRO colonization.
Since publication of the 2005 guidelines, HCAP has been criticized as being a poor predictor of MDRO infection. A 2014 meta-analysis of 24 studies investigated the discriminating ability of HCAP and reported that the specificity and sensitivity for MDRO infections was 71.2% and 53.7%, respectively.3 In 2016, the ATS/IDSA guidelines were updated to remove HCAP due to the risk of antibiotic overprescribing.4
Literature Review
Although criteria previously defining a patient as having HCAP have been shown to be a poor discriminator of MDRO pneumonia as a whole, MDRO infections still pose a threat to nonhospitalized patients who have exposure to the health care system. A literature review was performed to identify independent HCAP risk factors that may increase the risk of MDRO pneumonia infecting a nonhospitalized patient needing empiric broad-spectrum antibiotic therapy. All included studies were prospective or retrospective observational cohort studies that performed logistic regression analyses to assess the association between MDRO isolation and the previously defined HCAP risk factors (Table 1).
Five studies examined the risk of MDRO infection in patients with a previous hospital admission of 2 days or more in the past 90 days. Shindo and colleagues found a significant increase in MDRO infections by about 2-fold (adjusted odds ratio [AOR], 2.1; 95% confidence interval [CI], 1.2-3.4).5 Shorr and colleagues found a 4-fold increase in likelihood of identifying a MDRO in HCAP (AOR, 4.2; 95% CI, 2.9-6.3).6 Nseir and colleagues and Jung and colleagues found similar results (AOR 3.9, 95% CI 1.7-8.8; AOR 2.7, 95% CI 1.3-5.5, respectively).7,8 Conflicting results were reported by Gross and colleagues who did not find a significant relationship between previous hospitalization and MDRO isolation (AOR 1.2, 95% CI, 0.5-3.2).9
In patients with pneumonia admitted from a nursing home, MDRO infection risk also was evaluated in these 5 studies. Shorr and colleagues, Nseir and colleagues, and Gross and colleagues found significant AORs of 2.7 (95% CI 1.7-4.3), 2.0 (95% CI 1.1-3.7), and 4.2 (95% CI 1.6-11.3), respectively.6,7,9 Shindo and colleagues (AOR 1.1; 95% CI, 0.6-2.0) and Jung and colleagues (AOR 1.9, 95% CI, 0.5-6.9) found this risk factor not significant.5
Receipt of antibiotics within the previous 90 days was assessed in 3 studies. Shindo and colleagues, Nseir and colleagues, and Gross and colleagues all found significant AORs of 2.5 (95% CI 1.2-4.0), 2.3 (95% CI 1.2-4.3), and 2.9 (95% CI 1.1-7.5), respectively.5,7,9 Antibiotic therapy within the previous 90 days is an established risk factor for MDRO pneumonia, and the 2016 ATS/IDSA guidelines consider this a risk factor for HAP and VAP, including pneumonia caused by methicillin resistant Staphylococcus aureus and Pseudomonas aeruginosa.4
The impact of hemodialysis in the previous month on acquisition of MDRO pneumonia was investigated in 4 studies. Shindo and colleagues, Jung and colleagues, and Gross and colleagues concluded that this risk factor was not significantly related to MDRO infection, reporting AORs of 2.2 (95% CI 0.5-9.7), 2.8 (95% CI 0.9-9.2) and 0.7 (95% CI 0.1-5.1), respectively.5,8,9 Shorr and colleagues, however, found a significant AOR of 2.1 (95% CI 1.0-4.3).6
Shindo and colleagues investigated the impact of home infusion therapy on acquisition of pneumonia due to a MDRO and reported a nonsignificant AOR of 0.8 (95% CI 0.4-1.8).5 Gross and colleagues also found a nonsignificant AOR of 0 (P = .1).9 In the Shindo and colleagues study, resistance was found in 107 of 679 patients who did not receive infusion therapy, and 12 of 55 patients who were receiving infusion therapy.5 Gross and colleagues reported that home-infusion therapy was received by 0 of 20 patients with MDRO infection and 4 of the 501 patients without MDRO infection.9
Shindo and colleagues reported that home wound care was not found to be significantly related to MDRO pneumonia as well as did Gross and colleagues: AORs of 3.8 (0.8-18.4) and 1.4 (95% CI 0.5-4.4), respectively.5,9 Jung and colleagues examined IV chemotherapy in the past 30 days, and found this to not significantly impact the odds of MDRO isolation (AOR = 0.62, 95% CI 0.2-1.8).8 No data were available reflecting the risk of a family member with a MDRO.
Limitations
The variables on which logistic regression were performed differed among the studies. Therefore, results cannot be averaged or compared quantitatively, as AORs varied, depending on the variables included. In addition, data were drawn from multiple geographic locations that may impact MDRO prevalence within each patient population. Finally, this review examines the utility of the risk factors formerly included in HCAP. However, other risk factors for MDRO pneumonia outlined by the ATS/IDSA guidelines still should be considered when evaluating patient risk. The 2016 guidelines recommend local incidence of resistant strains be considered when initiating empiric therapy. Review of medical records for previous positive cultures and duration of current hospitalization also should be considered. Although the 2016 ATS/IDSA HAP guidelines are not intended for immunosuppressed patients, this risk factor also may be taken into account.
Conclusion
Review and synthesis of published literature found previous hospital admission (of ≥ 2 days in the past 90 days), admission from a nursing home, and IV antibiotic therapy in the last 90 days to be independent risk factors for identification of MDRO pneumonia in previously nonhospitalized patients (Table 2). Additionally, although no data were found to support this risk factor, existence of an in-home (close contact) source of MDROs would provide ample opportunity for transmission, so evaluation of known exposure to MDROs from contacts should be considered. When choosing empiric antibiotic therapy for patients admitted to the hospital for treatment of pneumonia, consideration of patient history and risk factors that may contribute to infection with a MDRO are recommended.
Successful treatment of pneumonia depends on timely diagnosis and administration of antibiotics. Multidrug-resistant organisms (MDROs) complicate antibiotic therapies by rendering some antibiotic agents ineffective. Inappropriate initial therapy has been associated with a more than 2-fold increase in the risk of mortality.1 Because culture results are not available immediately, clinicians prescribe antibiotics empirically and must rely on guidelines and knowledge of risk factors associated with MDRO infection to make these selections.
Treatment guidelines exist for hospital-acquired and ventilator-associated pneumonia (HAP/VAP) and community-acquired pneumonia (CAP) to assist with empiric antibiotic selection. For HAP/VAP, 2 to 3 antibiotics with a broad-spectrum of activity are used due to increased prevalence of MDROs in hospitals, whereastreatment of CAP involves more narrow coverage because bacteria that cause this infection typically have fewer antibiotic resistances.2,3 The HAP/VAP guidelines stratify the risk of pneumonia due to the presence of a MDRO acquired during a hospitalization. However, neither the CAP nor HAP/VAP guidelines offer risk-stratification guidance for nonhospitalized patients who develop pneumonia but who may have become colonized with a MDRO during a previous hospitalization or from another exposure to a health care facility.
Health care-associated pneumonia (HCAP) was first described in the 2005 American Thoracic Society and the Infectious Diseases Society of America (ATS/IDSA) nosocomial pneumonia guidelines and was associated with criteria intended to aid clinician identification of nonhospitalized patients at risk for MDRO pneumonia, which warranted empiric broad-spectrum antibiotic therapy.2 According to these guidelines, patients were classified as having HCAP if they had been hospitalized for at least 48 hours in the past 90 days, admitted from a nursing home, received recent intravenous antibiotics, had hemodialysis in the past 30 days, had a history of home infusion therapy or wound care, received intravenous chemotherapy, or had a family member with MDRO colonization.
Since publication of the 2005 guidelines, HCAP has been criticized as being a poor predictor of MDRO infection. A 2014 meta-analysis of 24 studies investigated the discriminating ability of HCAP and reported that the specificity and sensitivity for MDRO infections was 71.2% and 53.7%, respectively.3 In 2016, the ATS/IDSA guidelines were updated to remove HCAP due to the risk of antibiotic overprescribing.4
Literature Review
Although criteria previously defining a patient as having HCAP have been shown to be a poor discriminator of MDRO pneumonia as a whole, MDRO infections still pose a threat to nonhospitalized patients who have exposure to the health care system. A literature review was performed to identify independent HCAP risk factors that may increase the risk of MDRO pneumonia infecting a nonhospitalized patient needing empiric broad-spectrum antibiotic therapy. All included studies were prospective or retrospective observational cohort studies that performed logistic regression analyses to assess the association between MDRO isolation and the previously defined HCAP risk factors (Table 1).
Five studies examined the risk of MDRO infection in patients with a previous hospital admission of 2 days or more in the past 90 days. Shindo and colleagues found a significant increase in MDRO infections by about 2-fold (adjusted odds ratio [AOR], 2.1; 95% confidence interval [CI], 1.2-3.4).5 Shorr and colleagues found a 4-fold increase in likelihood of identifying a MDRO in HCAP (AOR, 4.2; 95% CI, 2.9-6.3).6 Nseir and colleagues and Jung and colleagues found similar results (AOR 3.9, 95% CI 1.7-8.8; AOR 2.7, 95% CI 1.3-5.5, respectively).7,8 Conflicting results were reported by Gross and colleagues who did not find a significant relationship between previous hospitalization and MDRO isolation (AOR 1.2, 95% CI, 0.5-3.2).9
In patients with pneumonia admitted from a nursing home, MDRO infection risk also was evaluated in these 5 studies. Shorr and colleagues, Nseir and colleagues, and Gross and colleagues found significant AORs of 2.7 (95% CI 1.7-4.3), 2.0 (95% CI 1.1-3.7), and 4.2 (95% CI 1.6-11.3), respectively.6,7,9 Shindo and colleagues (AOR 1.1; 95% CI, 0.6-2.0) and Jung and colleagues (AOR 1.9, 95% CI, 0.5-6.9) found this risk factor not significant.5
Receipt of antibiotics within the previous 90 days was assessed in 3 studies. Shindo and colleagues, Nseir and colleagues, and Gross and colleagues all found significant AORs of 2.5 (95% CI 1.2-4.0), 2.3 (95% CI 1.2-4.3), and 2.9 (95% CI 1.1-7.5), respectively.5,7,9 Antibiotic therapy within the previous 90 days is an established risk factor for MDRO pneumonia, and the 2016 ATS/IDSA guidelines consider this a risk factor for HAP and VAP, including pneumonia caused by methicillin resistant Staphylococcus aureus and Pseudomonas aeruginosa.4
The impact of hemodialysis in the previous month on acquisition of MDRO pneumonia was investigated in 4 studies. Shindo and colleagues, Jung and colleagues, and Gross and colleagues concluded that this risk factor was not significantly related to MDRO infection, reporting AORs of 2.2 (95% CI 0.5-9.7), 2.8 (95% CI 0.9-9.2) and 0.7 (95% CI 0.1-5.1), respectively.5,8,9 Shorr and colleagues, however, found a significant AOR of 2.1 (95% CI 1.0-4.3).6
Shindo and colleagues investigated the impact of home infusion therapy on acquisition of pneumonia due to a MDRO and reported a nonsignificant AOR of 0.8 (95% CI 0.4-1.8).5 Gross and colleagues also found a nonsignificant AOR of 0 (P = .1).9 In the Shindo and colleagues study, resistance was found in 107 of 679 patients who did not receive infusion therapy, and 12 of 55 patients who were receiving infusion therapy.5 Gross and colleagues reported that home-infusion therapy was received by 0 of 20 patients with MDRO infection and 4 of the 501 patients without MDRO infection.9
Shindo and colleagues reported that home wound care was not found to be significantly related to MDRO pneumonia as well as did Gross and colleagues: AORs of 3.8 (0.8-18.4) and 1.4 (95% CI 0.5-4.4), respectively.5,9 Jung and colleagues examined IV chemotherapy in the past 30 days, and found this to not significantly impact the odds of MDRO isolation (AOR = 0.62, 95% CI 0.2-1.8).8 No data were available reflecting the risk of a family member with a MDRO.
Limitations
The variables on which logistic regression were performed differed among the studies. Therefore, results cannot be averaged or compared quantitatively, as AORs varied, depending on the variables included. In addition, data were drawn from multiple geographic locations that may impact MDRO prevalence within each patient population. Finally, this review examines the utility of the risk factors formerly included in HCAP. However, other risk factors for MDRO pneumonia outlined by the ATS/IDSA guidelines still should be considered when evaluating patient risk. The 2016 guidelines recommend local incidence of resistant strains be considered when initiating empiric therapy. Review of medical records for previous positive cultures and duration of current hospitalization also should be considered. Although the 2016 ATS/IDSA HAP guidelines are not intended for immunosuppressed patients, this risk factor also may be taken into account.
Conclusion
Review and synthesis of published literature found previous hospital admission (of ≥ 2 days in the past 90 days), admission from a nursing home, and IV antibiotic therapy in the last 90 days to be independent risk factors for identification of MDRO pneumonia in previously nonhospitalized patients (Table 2). Additionally, although no data were found to support this risk factor, existence of an in-home (close contact) source of MDROs would provide ample opportunity for transmission, so evaluation of known exposure to MDROs from contacts should be considered. When choosing empiric antibiotic therapy for patients admitted to the hospital for treatment of pneumonia, consideration of patient history and risk factors that may contribute to infection with a MDRO are recommended.
1. Kollef MH, Sherman G, Ward S, Fraser VJ. Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients. Chest. 1999;115(2):462-474.
2. American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388-416.
3. Chalmers JD, Rother C, Salih W, Ewig S. Healthcare-associated pneumonia does not accurately identify potentially resistant pathogens: a systematic review and meta-analysis. Clin Infect Dis. 2014;58(3):330-339.
4. Kalil AC, Metersky ML, Klompas M, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63(5):e61-e111.
5. Shindo Y, Ito R, Kobayashi D, et al. Risk factors for drug-resistant pathogens in community-acquired and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2013;188(8):985-995.
6. Shorr AF, Zilberberg MD, Micek ST, Kollef MH. Prediction of infection due to antibiotic-resistant bacteria by select risk factors for health care–associated pneumonia. Arch Intern Med. 2008;168(20):2205-2210.
7. Nseir S, Grailles G, Soury-Lavergne A, Minacori F, Alves I, Durocher A. Accuracy of American Thoracic Society/Infectious Diseases Society of America criteria in predicting infection or colonization with multidrug-resistant bacteria at intensive-care unit admission. Clin Microbiol Infect. 2010;16(7):902-908.
8. Jung JY, Park MS, Kim YS, et al. Healthcare-associated pneumonia among hospitalized patients in a Korean tertiary hospital. BMC Infectious Diseases. 2011;11:61.
9. Gross AE, Van Schooneveld TC, Olsen KM, et al. Epidemiology and predictors of multidrug-resistant community-acquired and health care-associated pneumonia. Antimicrob Agents Chemother. 2014;58(9):5262-5268.
1. Kollef MH, Sherman G, Ward S, Fraser VJ. Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients. Chest. 1999;115(2):462-474.
2. American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388-416.
3. Chalmers JD, Rother C, Salih W, Ewig S. Healthcare-associated pneumonia does not accurately identify potentially resistant pathogens: a systematic review and meta-analysis. Clin Infect Dis. 2014;58(3):330-339.
4. Kalil AC, Metersky ML, Klompas M, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63(5):e61-e111.
5. Shindo Y, Ito R, Kobayashi D, et al. Risk factors for drug-resistant pathogens in community-acquired and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2013;188(8):985-995.
6. Shorr AF, Zilberberg MD, Micek ST, Kollef MH. Prediction of infection due to antibiotic-resistant bacteria by select risk factors for health care–associated pneumonia. Arch Intern Med. 2008;168(20):2205-2210.
7. Nseir S, Grailles G, Soury-Lavergne A, Minacori F, Alves I, Durocher A. Accuracy of American Thoracic Society/Infectious Diseases Society of America criteria in predicting infection or colonization with multidrug-resistant bacteria at intensive-care unit admission. Clin Microbiol Infect. 2010;16(7):902-908.
8. Jung JY, Park MS, Kim YS, et al. Healthcare-associated pneumonia among hospitalized patients in a Korean tertiary hospital. BMC Infectious Diseases. 2011;11:61.
9. Gross AE, Van Schooneveld TC, Olsen KM, et al. Epidemiology and predictors of multidrug-resistant community-acquired and health care-associated pneumonia. Antimicrob Agents Chemother. 2014;58(9):5262-5268.
Real-world data show risk of major bleeding, stroke with NOACs

LOS ANGELES—A real-world analysis has quantified the risks of stroke and major bleeding in patients with non-valvular atrial fibrillation (NVAF) starting treatment with novel oral anticoagulants (NOACs).
The data showed that patients receiving dabigatran had a significantly lower rate of major bleeding but a similar rate of stroke as patients receiving rivaroxaban.
Rates of stroke and major bleeding were not significantly different in patients receiving dabigatran and those receiving apixaban.
These findings were presented at the International Stroke Conference 2018 (abstract 100). This research was supported by Boehringer Ingelheim, makers of dabigatran. The researchers are employed by, or have received payments from, the company.
“With an increasing number of the 2.7 million Americans living with atrial fibrillation being treated with NOACs, real-world analyses like this that compare their effectiveness and safety are important,” said lead investigator Todd C. Villines, MD, of Walter Reed National Military Medical Center in Bethesda, Maryland.
“As a researcher and treating physician, I hope that this large-scale, US practice-based comparison will provide additional insight on available NOAC therapies . . . .”
In this retrospective, observational study, Dr Villines and his colleagues assessed the safety and effectiveness of NOACs in NVAF patients treated through the US Department of Defense Military Health System.
The researchers analyzed data from patients newly initiating treatment with apixaban, dabigatran, or rivaroxaban.
The team examined 2 cohorts. One resulted in 12,763 propensity-score-matched patients receiving dabigatran (150 mg bid) or rivaroxaban (20 mg daily). The other resulted in 4802 propensity-score- matched patients receiving dabigatran (150 mg bid) or apixaban (5 mg bid).
The primary outcomes in this study were the risk of major bleeding and stroke.
Dabigatran-treated patients had a significantly lower rate of major bleeding than rivaroxaban-treated patients—2.08% (266/12,763) and 2.53% (323/12,763), respectively (hazard ratio [HR]=0.82; 95% confidence interval [CI], 0.70-0.97; P=0.0182).
However, rates of stroke were not significantly different in the dabigatran and rivaroxaban groups—0.60% (77/12,763) and 0.78% (100/12,763), respectively (HR=0.77; 95% CI 0.57-1.04; P=0.0844).
Likewise, there was no significant difference in stroke rates for patients receiving dabigatran and apixaban—0.44% (21/4802) and 0.35% (17/4802), respectively (HR=1.26; 95% CI, 0.66-2.39; P=0.4892].
And there was no significant difference in major bleeding—1.60% (77/4802) and 1.21% (58/4802), respectively (HR=1.37; 95% CI, 0.97-1.94; P=0.0702).
The researchers said limitations of this study include the potential for residual confounding as an observational, on-treatment study. In addition, the study included data from electronic health records, which may not have been optimal to identify baseline risk and outcomes. Finally, there were limited dabigatran users available for matching with apixaban users. ![]()
LOS ANGELES—A real-world analysis has quantified the risks of stroke and major bleeding in patients with non-valvular atrial fibrillation (NVAF) starting treatment with novel oral anticoagulants (NOACs).
The data showed that patients receiving dabigatran had a significantly lower rate of major bleeding but a similar rate of stroke as patients receiving rivaroxaban.
Rates of stroke and major bleeding were not significantly different in patients receiving dabigatran and those receiving apixaban.
These findings were presented at the International Stroke Conference 2018 (abstract 100). This research was supported by Boehringer Ingelheim, makers of dabigatran. The researchers are employed by, or have received payments from, the company.
“With an increasing number of the 2.7 million Americans living with atrial fibrillation being treated with NOACs, real-world analyses like this that compare their effectiveness and safety are important,” said lead investigator Todd C. Villines, MD, of Walter Reed National Military Medical Center in Bethesda, Maryland.
“As a researcher and treating physician, I hope that this large-scale, US practice-based comparison will provide additional insight on available NOAC therapies . . . .”
In this retrospective, observational study, Dr Villines and his colleagues assessed the safety and effectiveness of NOACs in NVAF patients treated through the US Department of Defense Military Health System.
The researchers analyzed data from patients newly initiating treatment with apixaban, dabigatran, or rivaroxaban.
The team examined 2 cohorts. One resulted in 12,763 propensity-score-matched patients receiving dabigatran (150 mg bid) or rivaroxaban (20 mg daily). The other resulted in 4802 propensity-score- matched patients receiving dabigatran (150 mg bid) or apixaban (5 mg bid).
The primary outcomes in this study were the risk of major bleeding and stroke.
Dabigatran-treated patients had a significantly lower rate of major bleeding than rivaroxaban-treated patients—2.08% (266/12,763) and 2.53% (323/12,763), respectively (hazard ratio [HR]=0.82; 95% confidence interval [CI], 0.70-0.97; P=0.0182).
However, rates of stroke were not significantly different in the dabigatran and rivaroxaban groups—0.60% (77/12,763) and 0.78% (100/12,763), respectively (HR=0.77; 95% CI 0.57-1.04; P=0.0844).
Likewise, there was no significant difference in stroke rates for patients receiving dabigatran and apixaban—0.44% (21/4802) and 0.35% (17/4802), respectively (HR=1.26; 95% CI, 0.66-2.39; P=0.4892].
And there was no significant difference in major bleeding—1.60% (77/4802) and 1.21% (58/4802), respectively (HR=1.37; 95% CI, 0.97-1.94; P=0.0702).
The researchers said limitations of this study include the potential for residual confounding as an observational, on-treatment study. In addition, the study included data from electronic health records, which may not have been optimal to identify baseline risk and outcomes. Finally, there were limited dabigatran users available for matching with apixaban users. ![]()
LOS ANGELES—A real-world analysis has quantified the risks of stroke and major bleeding in patients with non-valvular atrial fibrillation (NVAF) starting treatment with novel oral anticoagulants (NOACs).
The data showed that patients receiving dabigatran had a significantly lower rate of major bleeding but a similar rate of stroke as patients receiving rivaroxaban.
Rates of stroke and major bleeding were not significantly different in patients receiving dabigatran and those receiving apixaban.
These findings were presented at the International Stroke Conference 2018 (abstract 100). This research was supported by Boehringer Ingelheim, makers of dabigatran. The researchers are employed by, or have received payments from, the company.
“With an increasing number of the 2.7 million Americans living with atrial fibrillation being treated with NOACs, real-world analyses like this that compare their effectiveness and safety are important,” said lead investigator Todd C. Villines, MD, of Walter Reed National Military Medical Center in Bethesda, Maryland.
“As a researcher and treating physician, I hope that this large-scale, US practice-based comparison will provide additional insight on available NOAC therapies . . . .”
In this retrospective, observational study, Dr Villines and his colleagues assessed the safety and effectiveness of NOACs in NVAF patients treated through the US Department of Defense Military Health System.
The researchers analyzed data from patients newly initiating treatment with apixaban, dabigatran, or rivaroxaban.
The team examined 2 cohorts. One resulted in 12,763 propensity-score-matched patients receiving dabigatran (150 mg bid) or rivaroxaban (20 mg daily). The other resulted in 4802 propensity-score- matched patients receiving dabigatran (150 mg bid) or apixaban (5 mg bid).
The primary outcomes in this study were the risk of major bleeding and stroke.
Dabigatran-treated patients had a significantly lower rate of major bleeding than rivaroxaban-treated patients—2.08% (266/12,763) and 2.53% (323/12,763), respectively (hazard ratio [HR]=0.82; 95% confidence interval [CI], 0.70-0.97; P=0.0182).
However, rates of stroke were not significantly different in the dabigatran and rivaroxaban groups—0.60% (77/12,763) and 0.78% (100/12,763), respectively (HR=0.77; 95% CI 0.57-1.04; P=0.0844).
Likewise, there was no significant difference in stroke rates for patients receiving dabigatran and apixaban—0.44% (21/4802) and 0.35% (17/4802), respectively (HR=1.26; 95% CI, 0.66-2.39; P=0.4892].
And there was no significant difference in major bleeding—1.60% (77/4802) and 1.21% (58/4802), respectively (HR=1.37; 95% CI, 0.97-1.94; P=0.0702).
The researchers said limitations of this study include the potential for residual confounding as an observational, on-treatment study. In addition, the study included data from electronic health records, which may not have been optimal to identify baseline risk and outcomes. Finally, there were limited dabigatran users available for matching with apixaban users. ![]()
T-cell therapy produces durable responses in rel/ref HL

Engineered T cells can produce durable responses in patients with Epstein Barr virus–positive (EBV+), relapsed/refractory Hodgkin lymphoma (HL), according to research published in the Journal of Clinical Oncology.
These T cells, known as DNRII-LSTs, produced responses in 4 of the 8 patients studied.
This included 3 complete responses (CRs), the longest of which has exceeded 7 years.
What’s more, these responses were achieved without the use of lymphodepleting chemotherapy.
“While the study is small, its findings are incredibly encouraging for our [patients’] families and for the cancer field,” said study author Catherine M. Bollard, MD, MBChB, of Children’s National Health System in Washington, DC.
To engineer the DNRII-LSTs, Dr Bollard and her colleagues forced expression of a dominant-negative TGF-beta receptor type 2 (DNRII) on LMP-specific T cells (LSTs), which are T cells directed to the EBV latency-associated antigens LMP-1 and LMP-2.
The goal of forcing DNRII expression was to enable the LSTs to resist the hostile tumor environment so they could seek out and kill the tumor cells.
Dr Bollard and her colleagues administered DNRII-LSTs to 8 patients with EBV+ HL. The patients ranged in age from 27 to 47.
Seven of the 8 patients had active disease at the time of DNRII-LST infusion. Two patients had stage IVB HL, 1 had stage IIIB, and 2 had stage IIB. Four patients had nodular-sclerosing HL.
Six patients had relapsed twice. The remaining 2 patients had relapsed 3 and 4 times, respectively. All patients had previously received an autologous stem cell transplant and a range of multi-agent chemotherapy regimens (eg, ABVD, R-ICE, and MOPP).
For this study, the patients received 2 to 12 infusions of DNRII-LSTs, at doses ranging from 2 × 107 to 1.5 × 108 cells/m2.
Results
The researchers found that autologous DNRII-LSTs (given to 7 patients) did not cause autoimmunity, and donor-derived DNRII-LSTs (n=1) did not induce graft-vs-host disease.
The team also noted there were no toxicities resulting from cytokine release syndrome.
Four patients achieved a response to treatment—3 CRs and a partial response.
All complete responders are still in CR, but the partial responder progressed at 19 months and ultimately died of sepsis (2 years after the first dose of DNRII-LSTs).
The other 4 patients had stable disease (SD) for 4 months to 13 months after treatment with DNRII-LSTs.
One patient with SD died of disease progression 2 years after receiving DNRII-LSTs, and another died of transplant complications less than 2 years after the last dose of DNRII-LSTs.
One patient with SD went on to receive additional therapy and is still alive more than 6 years after receiving DNRII-LSTs (currently receiving nivolumab). Another SD patient went on to receive additional therapy, achieved a CR, and is still alive.
One of the patients who achieved a CR to DNRII-LSTs remains in CR more than 7 years after the last dose. Another patient’s CR has exceeded 2 years, and another’s has exceeded 5 years.
All 3 of these patients received doses of 2 × 107 cells/m2. The patients with the longest and shortest CRs each received 2 infusions of DNRII-LSTs. The patient with the CR exceeding 5 years received 12 infusions.
“These results come 18 years after this revolutionary approach was first conceptualized,” Dr Bollard said. “I started work in this area in 2000. At that time, the oncology community had little enthusiasm for the use of T-cell therapies to treat cancer.”
“Even then, when T-cell therapy was in its relative infancy, some research institutions began to see more than 90% complete responses and cure rates in some settings. This most recent study points to the potential of specialized T cells to fight even more types of immune-evading tumors.” ![]()
Engineered T cells can produce durable responses in patients with Epstein Barr virus–positive (EBV+), relapsed/refractory Hodgkin lymphoma (HL), according to research published in the Journal of Clinical Oncology.
These T cells, known as DNRII-LSTs, produced responses in 4 of the 8 patients studied.
This included 3 complete responses (CRs), the longest of which has exceeded 7 years.
What’s more, these responses were achieved without the use of lymphodepleting chemotherapy.
“While the study is small, its findings are incredibly encouraging for our [patients’] families and for the cancer field,” said study author Catherine M. Bollard, MD, MBChB, of Children’s National Health System in Washington, DC.
To engineer the DNRII-LSTs, Dr Bollard and her colleagues forced expression of a dominant-negative TGF-beta receptor type 2 (DNRII) on LMP-specific T cells (LSTs), which are T cells directed to the EBV latency-associated antigens LMP-1 and LMP-2.
The goal of forcing DNRII expression was to enable the LSTs to resist the hostile tumor environment so they could seek out and kill the tumor cells.
Dr Bollard and her colleagues administered DNRII-LSTs to 8 patients with EBV+ HL. The patients ranged in age from 27 to 47.
Seven of the 8 patients had active disease at the time of DNRII-LST infusion. Two patients had stage IVB HL, 1 had stage IIIB, and 2 had stage IIB. Four patients had nodular-sclerosing HL.
Six patients had relapsed twice. The remaining 2 patients had relapsed 3 and 4 times, respectively. All patients had previously received an autologous stem cell transplant and a range of multi-agent chemotherapy regimens (eg, ABVD, R-ICE, and MOPP).
For this study, the patients received 2 to 12 infusions of DNRII-LSTs, at doses ranging from 2 × 107 to 1.5 × 108 cells/m2.
Results
The researchers found that autologous DNRII-LSTs (given to 7 patients) did not cause autoimmunity, and donor-derived DNRII-LSTs (n=1) did not induce graft-vs-host disease.
The team also noted there were no toxicities resulting from cytokine release syndrome.
Four patients achieved a response to treatment—3 CRs and a partial response.
All complete responders are still in CR, but the partial responder progressed at 19 months and ultimately died of sepsis (2 years after the first dose of DNRII-LSTs).
The other 4 patients had stable disease (SD) for 4 months to 13 months after treatment with DNRII-LSTs.
One patient with SD died of disease progression 2 years after receiving DNRII-LSTs, and another died of transplant complications less than 2 years after the last dose of DNRII-LSTs.
One patient with SD went on to receive additional therapy and is still alive more than 6 years after receiving DNRII-LSTs (currently receiving nivolumab). Another SD patient went on to receive additional therapy, achieved a CR, and is still alive.
One of the patients who achieved a CR to DNRII-LSTs remains in CR more than 7 years after the last dose. Another patient’s CR has exceeded 2 years, and another’s has exceeded 5 years.
All 3 of these patients received doses of 2 × 107 cells/m2. The patients with the longest and shortest CRs each received 2 infusions of DNRII-LSTs. The patient with the CR exceeding 5 years received 12 infusions.
“These results come 18 years after this revolutionary approach was first conceptualized,” Dr Bollard said. “I started work in this area in 2000. At that time, the oncology community had little enthusiasm for the use of T-cell therapies to treat cancer.”
“Even then, when T-cell therapy was in its relative infancy, some research institutions began to see more than 90% complete responses and cure rates in some settings. This most recent study points to the potential of specialized T cells to fight even more types of immune-evading tumors.” ![]()
Engineered T cells can produce durable responses in patients with Epstein Barr virus–positive (EBV+), relapsed/refractory Hodgkin lymphoma (HL), according to research published in the Journal of Clinical Oncology.
These T cells, known as DNRII-LSTs, produced responses in 4 of the 8 patients studied.
This included 3 complete responses (CRs), the longest of which has exceeded 7 years.
What’s more, these responses were achieved without the use of lymphodepleting chemotherapy.
“While the study is small, its findings are incredibly encouraging for our [patients’] families and for the cancer field,” said study author Catherine M. Bollard, MD, MBChB, of Children’s National Health System in Washington, DC.
To engineer the DNRII-LSTs, Dr Bollard and her colleagues forced expression of a dominant-negative TGF-beta receptor type 2 (DNRII) on LMP-specific T cells (LSTs), which are T cells directed to the EBV latency-associated antigens LMP-1 and LMP-2.
The goal of forcing DNRII expression was to enable the LSTs to resist the hostile tumor environment so they could seek out and kill the tumor cells.
Dr Bollard and her colleagues administered DNRII-LSTs to 8 patients with EBV+ HL. The patients ranged in age from 27 to 47.
Seven of the 8 patients had active disease at the time of DNRII-LST infusion. Two patients had stage IVB HL, 1 had stage IIIB, and 2 had stage IIB. Four patients had nodular-sclerosing HL.
Six patients had relapsed twice. The remaining 2 patients had relapsed 3 and 4 times, respectively. All patients had previously received an autologous stem cell transplant and a range of multi-agent chemotherapy regimens (eg, ABVD, R-ICE, and MOPP).
For this study, the patients received 2 to 12 infusions of DNRII-LSTs, at doses ranging from 2 × 107 to 1.5 × 108 cells/m2.
Results
The researchers found that autologous DNRII-LSTs (given to 7 patients) did not cause autoimmunity, and donor-derived DNRII-LSTs (n=1) did not induce graft-vs-host disease.
The team also noted there were no toxicities resulting from cytokine release syndrome.
Four patients achieved a response to treatment—3 CRs and a partial response.
All complete responders are still in CR, but the partial responder progressed at 19 months and ultimately died of sepsis (2 years after the first dose of DNRII-LSTs).
The other 4 patients had stable disease (SD) for 4 months to 13 months after treatment with DNRII-LSTs.
One patient with SD died of disease progression 2 years after receiving DNRII-LSTs, and another died of transplant complications less than 2 years after the last dose of DNRII-LSTs.
One patient with SD went on to receive additional therapy and is still alive more than 6 years after receiving DNRII-LSTs (currently receiving nivolumab). Another SD patient went on to receive additional therapy, achieved a CR, and is still alive.
One of the patients who achieved a CR to DNRII-LSTs remains in CR more than 7 years after the last dose. Another patient’s CR has exceeded 2 years, and another’s has exceeded 5 years.
All 3 of these patients received doses of 2 × 107 cells/m2. The patients with the longest and shortest CRs each received 2 infusions of DNRII-LSTs. The patient with the CR exceeding 5 years received 12 infusions.
“These results come 18 years after this revolutionary approach was first conceptualized,” Dr Bollard said. “I started work in this area in 2000. At that time, the oncology community had little enthusiasm for the use of T-cell therapies to treat cancer.”
“Even then, when T-cell therapy was in its relative infancy, some research institutions began to see more than 90% complete responses and cure rates in some settings. This most recent study points to the potential of specialized T cells to fight even more types of immune-evading tumors.” ![]()
Treatment costs threaten cancer program growth

Treatment costs are the greatest threat to the growth of cancer programs, according to a survey of nearly 300 cancer program administrators and providers.
Sixty-eight percent of survey respondents said treatment costs were among the biggest threats to future cancer program growth at their organization.
Other top threats to growth included physician alignment around services and program goals—cited by 47% of respondents—and changes in healthcare coverage—cited by 46%.
This survey—the “2017 Trending Now in Cancer Care Survey”—was conducted by the Association of Community Cancer Centers (ACCC) and Advisory Board’s Oncology Roundtable. It was supported by Pfizer Oncology.
The survey was distributed via email on July 24, 2017. Respondents included 293 cancer program administrators and providers from 209 institutions. They submitted responses over 6 weeks.
Respondents identified the following “biggest threats” to cancer program growth:
- Cost of drugs and/or new treatment modalities—68%
- Physician alignment around services and program goals—47%
- Changes in healthcare coverage—46%
- Cuts to fee-for-service reimbursement—44%
- Shifting reimbursement to value-based care—43%
- Marketplace competition—35%
- Workforce planning (eg, managing staff shortages)—34%
- Network strategy and integration—33%
- Site of care policies issued by private payers—27%
- Access to capital—26%
- Quality reporting requirements—22%
- Health information technology—21%
- Other—6%.
When asked to identify their greatest opportunities for cost savings, respondents overwhelmingly pointed toward clinical standardization (63%) and drugs (62%).
Other opportunities included:
- Supplies—28%
- Capital expenses (eg, imaging technology)—24%
- Non-clinical staff (eg, billing and coding specialists)—22%
- Technology maintenance—20%
- Clinical staff—16%
- Retail pharmacy—14%
- Clinical research—10%
- Support services (eg, acupuncture)—9%
- Other—4%.
Respondents also said the investments most likely to yield a return for their cancer program were:
- Increasing the number of sub-specialists (eg, breast surgeons)—59%
- Marketing—41%
- Specialty pharmacy—36%
- Increasing the number of general oncology physicians—34%
- Screening services (eg, mobile screening unit)—29%
- Capital investments—24%
- Clinical research—16%
- Support services—15%
- Retail pharmacy—14%
- Building upgrades—14%.
More details on the “2017 Trending Now in Cancer Care Survey” can be found on the ACCC website. ![]()
Treatment costs are the greatest threat to the growth of cancer programs, according to a survey of nearly 300 cancer program administrators and providers.
Sixty-eight percent of survey respondents said treatment costs were among the biggest threats to future cancer program growth at their organization.
Other top threats to growth included physician alignment around services and program goals—cited by 47% of respondents—and changes in healthcare coverage—cited by 46%.
This survey—the “2017 Trending Now in Cancer Care Survey”—was conducted by the Association of Community Cancer Centers (ACCC) and Advisory Board’s Oncology Roundtable. It was supported by Pfizer Oncology.
The survey was distributed via email on July 24, 2017. Respondents included 293 cancer program administrators and providers from 209 institutions. They submitted responses over 6 weeks.
Respondents identified the following “biggest threats” to cancer program growth:
- Cost of drugs and/or new treatment modalities—68%
- Physician alignment around services and program goals—47%
- Changes in healthcare coverage—46%
- Cuts to fee-for-service reimbursement—44%
- Shifting reimbursement to value-based care—43%
- Marketplace competition—35%
- Workforce planning (eg, managing staff shortages)—34%
- Network strategy and integration—33%
- Site of care policies issued by private payers—27%
- Access to capital—26%
- Quality reporting requirements—22%
- Health information technology—21%
- Other—6%.
When asked to identify their greatest opportunities for cost savings, respondents overwhelmingly pointed toward clinical standardization (63%) and drugs (62%).
Other opportunities included:
- Supplies—28%
- Capital expenses (eg, imaging technology)—24%
- Non-clinical staff (eg, billing and coding specialists)—22%
- Technology maintenance—20%
- Clinical staff—16%
- Retail pharmacy—14%
- Clinical research—10%
- Support services (eg, acupuncture)—9%
- Other—4%.
Respondents also said the investments most likely to yield a return for their cancer program were:
- Increasing the number of sub-specialists (eg, breast surgeons)—59%
- Marketing—41%
- Specialty pharmacy—36%
- Increasing the number of general oncology physicians—34%
- Screening services (eg, mobile screening unit)—29%
- Capital investments—24%
- Clinical research—16%
- Support services—15%
- Retail pharmacy—14%
- Building upgrades—14%.
More details on the “2017 Trending Now in Cancer Care Survey” can be found on the ACCC website. ![]()
Treatment costs are the greatest threat to the growth of cancer programs, according to a survey of nearly 300 cancer program administrators and providers.
Sixty-eight percent of survey respondents said treatment costs were among the biggest threats to future cancer program growth at their organization.
Other top threats to growth included physician alignment around services and program goals—cited by 47% of respondents—and changes in healthcare coverage—cited by 46%.
This survey—the “2017 Trending Now in Cancer Care Survey”—was conducted by the Association of Community Cancer Centers (ACCC) and Advisory Board’s Oncology Roundtable. It was supported by Pfizer Oncology.
The survey was distributed via email on July 24, 2017. Respondents included 293 cancer program administrators and providers from 209 institutions. They submitted responses over 6 weeks.
Respondents identified the following “biggest threats” to cancer program growth:
- Cost of drugs and/or new treatment modalities—68%
- Physician alignment around services and program goals—47%
- Changes in healthcare coverage—46%
- Cuts to fee-for-service reimbursement—44%
- Shifting reimbursement to value-based care—43%
- Marketplace competition—35%
- Workforce planning (eg, managing staff shortages)—34%
- Network strategy and integration—33%
- Site of care policies issued by private payers—27%
- Access to capital—26%
- Quality reporting requirements—22%
- Health information technology—21%
- Other—6%.
When asked to identify their greatest opportunities for cost savings, respondents overwhelmingly pointed toward clinical standardization (63%) and drugs (62%).
Other opportunities included:
- Supplies—28%
- Capital expenses (eg, imaging technology)—24%
- Non-clinical staff (eg, billing and coding specialists)—22%
- Technology maintenance—20%
- Clinical staff—16%
- Retail pharmacy—14%
- Clinical research—10%
- Support services (eg, acupuncture)—9%
- Other—4%.
Respondents also said the investments most likely to yield a return for their cancer program were:
- Increasing the number of sub-specialists (eg, breast surgeons)—59%
- Marketing—41%
- Specialty pharmacy—36%
- Increasing the number of general oncology physicians—34%
- Screening services (eg, mobile screening unit)—29%
- Capital investments—24%
- Clinical research—16%
- Support services—15%
- Retail pharmacy—14%
- Building upgrades—14%.
More details on the “2017 Trending Now in Cancer Care Survey” can be found on the ACCC website. ![]()
VIDEO: Practice changers out of ASH 2017
ATLANTA – There were a lot of new data presented during the annual meeting of the American Society of Hematology. But what findings could actually change the way you practice?
Robert A. Brodsky, MD, director of the division of hematology at Johns Hopkins University in Baltimore and the moderator for the late-breaking abstract session at ASH, highlighted results from two studies.
Data from the MURANO trial showed robust results for a combination of venetoclax and rituximab in patients with relapsed/refractory chronic lymphocytic leukemia (CLL). At a median follow-up of 23.8 months, median progression-free survival -had not been reached in patients randomized to venetoclax/rituximab, while patients who received bendamustine plus rituximab had a median PFS of 17 months.
The based on the data presented, Dr. Brodsky said.
Another “enormously exciting and practice-changing” finding is that direct oral anticoagulants can be used safely in patients with cancer, Dr. Brodsky said in an interview.
In a randomized, open-label study, 12 months of daily treatment with edoxaban was noninferior to standard subcutaneous therapy with dalteparin for treatment of venous thromboembolism in cancer patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ATLANTA – There were a lot of new data presented during the annual meeting of the American Society of Hematology. But what findings could actually change the way you practice?
Robert A. Brodsky, MD, director of the division of hematology at Johns Hopkins University in Baltimore and the moderator for the late-breaking abstract session at ASH, highlighted results from two studies.
Data from the MURANO trial showed robust results for a combination of venetoclax and rituximab in patients with relapsed/refractory chronic lymphocytic leukemia (CLL). At a median follow-up of 23.8 months, median progression-free survival -had not been reached in patients randomized to venetoclax/rituximab, while patients who received bendamustine plus rituximab had a median PFS of 17 months.
The based on the data presented, Dr. Brodsky said.
Another “enormously exciting and practice-changing” finding is that direct oral anticoagulants can be used safely in patients with cancer, Dr. Brodsky said in an interview.
In a randomized, open-label study, 12 months of daily treatment with edoxaban was noninferior to standard subcutaneous therapy with dalteparin for treatment of venous thromboembolism in cancer patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ATLANTA – There were a lot of new data presented during the annual meeting of the American Society of Hematology. But what findings could actually change the way you practice?
Robert A. Brodsky, MD, director of the division of hematology at Johns Hopkins University in Baltimore and the moderator for the late-breaking abstract session at ASH, highlighted results from two studies.
Data from the MURANO trial showed robust results for a combination of venetoclax and rituximab in patients with relapsed/refractory chronic lymphocytic leukemia (CLL). At a median follow-up of 23.8 months, median progression-free survival -had not been reached in patients randomized to venetoclax/rituximab, while patients who received bendamustine plus rituximab had a median PFS of 17 months.
The based on the data presented, Dr. Brodsky said.
Another “enormously exciting and practice-changing” finding is that direct oral anticoagulants can be used safely in patients with cancer, Dr. Brodsky said in an interview.
In a randomized, open-label study, 12 months of daily treatment with edoxaban was noninferior to standard subcutaneous therapy with dalteparin for treatment of venous thromboembolism in cancer patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
REPORTING FROM ASH 2017
CLL drug in limited supply outside U.S.
Ofatumumab (Arzerra), a monoclonal antibody treatment for chronic lymphocytic leukemia, will soon be available outside the United States through compassionate use programs only. The drug will continue to be widely available in the United States.
Novartis announced in January that it would begin limiting the availability of the drug outside of the United States and would work with regulatory authorities to set up compassionate use programs for patients who are currently being treated with the drug. Patients who use these programs will receive the drug for free.
The decision was driven by the surge in CLL drugs that have become available over the last 5 years, according to Novartis.
The decision to pull the drug from international markets will not affect its use in ongoing clinical trials, particularly two phase 3 studies in relapsing multiple sclerosis and indolent non-Hodgkin lymphoma.
Ofatumumab (Arzerra), a monoclonal antibody treatment for chronic lymphocytic leukemia, will soon be available outside the United States through compassionate use programs only. The drug will continue to be widely available in the United States.
Novartis announced in January that it would begin limiting the availability of the drug outside of the United States and would work with regulatory authorities to set up compassionate use programs for patients who are currently being treated with the drug. Patients who use these programs will receive the drug for free.
The decision was driven by the surge in CLL drugs that have become available over the last 5 years, according to Novartis.
The decision to pull the drug from international markets will not affect its use in ongoing clinical trials, particularly two phase 3 studies in relapsing multiple sclerosis and indolent non-Hodgkin lymphoma.
Ofatumumab (Arzerra), a monoclonal antibody treatment for chronic lymphocytic leukemia, will soon be available outside the United States through compassionate use programs only. The drug will continue to be widely available in the United States.
Novartis announced in January that it would begin limiting the availability of the drug outside of the United States and would work with regulatory authorities to set up compassionate use programs for patients who are currently being treated with the drug. Patients who use these programs will receive the drug for free.
The decision was driven by the surge in CLL drugs that have become available over the last 5 years, according to Novartis.
The decision to pull the drug from international markets will not affect its use in ongoing clinical trials, particularly two phase 3 studies in relapsing multiple sclerosis and indolent non-Hodgkin lymphoma.
Emergent colectomies for ulcerative colitis declining
LAS VEGAS – , a large database analysis has shown.
“Despite advances in medical therapy for ulcerative colitis (UC), many patients still need surgery,” Ryan C. Ungaro, MD, said at the Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association. “Prior epidemiologic studies have demonstrated a decline in colectomy rates over time, particularly comparing the pre- and postbiologic eras, but less is known about rates of emergent colectomy over time,” he said. In particular, he continued, data on UC colectomy and ileal pouch anal anastomosis (IPAA) surgery rates in the United States are limited.
In an effort to examine UC emergent colectomy rates and IPAA over time, Dr. Ungaro, of the division of gastroenterology at the Icahn School of Medicine at Mount Sinai, New York, and his associates analyzed data from the U.S. Nationwide Inpatient Sample from 2000 through 2014. They defined emergent colectomy cases as admission through the emergency department and used the ICD-9-CM code for subtotal colectomy (45.8) as the outcome variable, and defined a second cohort of UC patients admitted electively with an outcome variable of ICD-9-CM code for IPAA (45.95). To evaluate temporal trends of colectomy and IPAA, the researchers used joinpoint regression analysis with calculation of annual percentage change.

They also observed disparities in IPAA surgery rates based on race and insurance type. Specifically, whites had higher rates of elective IPAA during the study period, compared with black or Hispanic patients (P less than .01), while patients with private insurance had higher rates of elective IPAA, compared with those insured by Medicare or Medicaid (P less than .01). Dr. Ungaro acknowledged certain limitations of the study, including the fact that the Nationwide Inpatient Sample relies on administrative codes, “which may increase risk of misclassification bias,” he said. They were also unable to track individual patients across time and lacked data on medication use and disease severity.
“There has been a significant decline in emergency colectomy for ulcerative colitis in the United States,” Dr. Ungaro concluded. “We expect that this is due to more effective inpatient care. However, the overall need for surgery in UC appears to be stable given unchanged IPAA rates. This suggests a limited impact on overall surgery rates with a shift from emergent to elective procedures.” He reported having no relevant financial disclosures.
*This story was updated on 3/26.
SOURCE: Ungaro RC et al. Crohn’s & Colitis Congress, Clinical Abstract 23.
LAS VEGAS – , a large database analysis has shown.
“Despite advances in medical therapy for ulcerative colitis (UC), many patients still need surgery,” Ryan C. Ungaro, MD, said at the Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association. “Prior epidemiologic studies have demonstrated a decline in colectomy rates over time, particularly comparing the pre- and postbiologic eras, but less is known about rates of emergent colectomy over time,” he said. In particular, he continued, data on UC colectomy and ileal pouch anal anastomosis (IPAA) surgery rates in the United States are limited.
In an effort to examine UC emergent colectomy rates and IPAA over time, Dr. Ungaro, of the division of gastroenterology at the Icahn School of Medicine at Mount Sinai, New York, and his associates analyzed data from the U.S. Nationwide Inpatient Sample from 2000 through 2014. They defined emergent colectomy cases as admission through the emergency department and used the ICD-9-CM code for subtotal colectomy (45.8) as the outcome variable, and defined a second cohort of UC patients admitted electively with an outcome variable of ICD-9-CM code for IPAA (45.95). To evaluate temporal trends of colectomy and IPAA, the researchers used joinpoint regression analysis with calculation of annual percentage change.
They also observed disparities in IPAA surgery rates based on race and insurance type. Specifically, whites had higher rates of elective IPAA during the study period, compared with black or Hispanic patients (P less than .01), while patients with private insurance had higher rates of elective IPAA, compared with those insured by Medicare or Medicaid (P less than .01). Dr. Ungaro acknowledged certain limitations of the study, including the fact that the Nationwide Inpatient Sample relies on administrative codes, “which may increase risk of misclassification bias,” he said. They were also unable to track individual patients across time and lacked data on medication use and disease severity.
“There has been a significant decline in emergency colectomy for ulcerative colitis in the United States,” Dr. Ungaro concluded. “We expect that this is due to more effective inpatient care. However, the overall need for surgery in UC appears to be stable given unchanged IPAA rates. This suggests a limited impact on overall surgery rates with a shift from emergent to elective procedures.” He reported having no relevant financial disclosures.
*This story was updated on 3/26.
SOURCE: Ungaro RC et al. Crohn’s & Colitis Congress, Clinical Abstract 23.
LAS VEGAS – , a large database analysis has shown.
“Despite advances in medical therapy for ulcerative colitis (UC), many patients still need surgery,” Ryan C. Ungaro, MD, said at the Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association. “Prior epidemiologic studies have demonstrated a decline in colectomy rates over time, particularly comparing the pre- and postbiologic eras, but less is known about rates of emergent colectomy over time,” he said. In particular, he continued, data on UC colectomy and ileal pouch anal anastomosis (IPAA) surgery rates in the United States are limited.
In an effort to examine UC emergent colectomy rates and IPAA over time, Dr. Ungaro, of the division of gastroenterology at the Icahn School of Medicine at Mount Sinai, New York, and his associates analyzed data from the U.S. Nationwide Inpatient Sample from 2000 through 2014. They defined emergent colectomy cases as admission through the emergency department and used the ICD-9-CM code for subtotal colectomy (45.8) as the outcome variable, and defined a second cohort of UC patients admitted electively with an outcome variable of ICD-9-CM code for IPAA (45.95). To evaluate temporal trends of colectomy and IPAA, the researchers used joinpoint regression analysis with calculation of annual percentage change.
They also observed disparities in IPAA surgery rates based on race and insurance type. Specifically, whites had higher rates of elective IPAA during the study period, compared with black or Hispanic patients (P less than .01), while patients with private insurance had higher rates of elective IPAA, compared with those insured by Medicare or Medicaid (P less than .01). Dr. Ungaro acknowledged certain limitations of the study, including the fact that the Nationwide Inpatient Sample relies on administrative codes, “which may increase risk of misclassification bias,” he said. They were also unable to track individual patients across time and lacked data on medication use and disease severity.
“There has been a significant decline in emergency colectomy for ulcerative colitis in the United States,” Dr. Ungaro concluded. “We expect that this is due to more effective inpatient care. However, the overall need for surgery in UC appears to be stable given unchanged IPAA rates. This suggests a limited impact on overall surgery rates with a shift from emergent to elective procedures.” He reported having no relevant financial disclosures.
*This story was updated on 3/26.
SOURCE: Ungaro RC et al. Crohn’s & Colitis Congress, Clinical Abstract 23.
REPORTING FROM THE CROHN’S & COLITIS CONGRESS
Key clinical point: There has been a significant decline in emergent ulcerative colitis colectomies in the United States.
Major finding: Between 2000 and 2014, the colectomy rate among patients emergently admitted to the hospital declined more than 7% annually (P less than .05).
Study details: An analysis of 470,720 hospital admissions from the Nationwide Inpatient Sample.
Disclosures: Dr. Ungaro reported having no financial disclosures.
Source: Ungaro RC et al. Crohn’s & Colitis Congress, Clinical Abstract 23.
Shorter walk test predicts IPF outcomes
, based on data from 179 adults. The findings were presented at the CHEST annual meeting.
The 6-minute test is often used to evaluate functional capacity in IPF patients, but is not always practical in a busy clinic setting, according to Flavia S. Nunes, MD, of Inova Fairfax Hospital in Falls Church, VA, and colleagues.
“Among the clinical and physiologic predictors associated with survival in IPF, the 6MWT has been increasingly used over the past 5 years as a secondary endpoint in the efficacy analyses of potential therapies for IPF. Validation of shorter time of walking might make the test more feasible to be applied in routine clinical care,” she said.
To determine the predictive value of the first minute of the 6-minute test, the researchers reviewed data from 142 men and 37 women at a tertiary referral center between May 2010 and February 2017. The average age of the patients was 68 years, the average body mass index was 28.3 kg/m2, and 27% used oxygen supplementation during the walk test.
Overall, the mean distance for the 6-minute test was 372 m, and the average distance for the 1-minute test was 65 m. Study participants who achieved a 6-minute walk distance greater than 372 m were defined as high walkers, and those with a 6-minute walk distance less than 372 m were defined as low walkers. A strong correlation appeared between the 6-minute distance and 1-minute distance in terms of predicting survival, and 1-year transplant-free survival was significantly better in high walkers than in low walkers (27 months vs. 22 months; P = .015).
Dr. Nunes said she was not surprised by the results, in part because previous research has shown a strong correlation among 2-minute, 6-minute, and 12-minute walking tests.
Although more research is needed to validate the findings, the results suggest that the 1-minute test might be a practical substitute for the 6-minute test by providing similar prognostic information more quickly and easily than the 6-minute test, the researchers said.
“It is important for clinicians to know that the time chosen to assess exercise tolerance by walking tests might not be critical,” said Dr. Nunes. “Shorter walks are not only less time consuming, and easier for both patients and clinicians, but are also reproducible and discriminatory of survival.
“We need to validate the test performance characteristics and prognostic value of distance walked in a 1MWT compared to the standard 6MWT in an independent cohort of patients with IPF,” Dr. Nunes noted. “Additionally, the evaluation of alternate instruction, for example changing the wording from ‘walk as far’ to ‘walk as fast’ might facilitate a better effort, and a greater distance with improved reproducibility. Other novel parameters and modifications to the 6MWT or 1MWT might further improve the utility of these tests in the management of IPF and other patients,” she added.
The researchers had no financial conflicts to disclose.

, based on data from 179 adults. The findings were presented at the CHEST annual meeting.
The 6-minute test is often used to evaluate functional capacity in IPF patients, but is not always practical in a busy clinic setting, according to Flavia S. Nunes, MD, of Inova Fairfax Hospital in Falls Church, VA, and colleagues.
“Among the clinical and physiologic predictors associated with survival in IPF, the 6MWT has been increasingly used over the past 5 years as a secondary endpoint in the efficacy analyses of potential therapies for IPF. Validation of shorter time of walking might make the test more feasible to be applied in routine clinical care,” she said.
To determine the predictive value of the first minute of the 6-minute test, the researchers reviewed data from 142 men and 37 women at a tertiary referral center between May 2010 and February 2017. The average age of the patients was 68 years, the average body mass index was 28.3 kg/m2, and 27% used oxygen supplementation during the walk test.
Overall, the mean distance for the 6-minute test was 372 m, and the average distance for the 1-minute test was 65 m. Study participants who achieved a 6-minute walk distance greater than 372 m were defined as high walkers, and those with a 6-minute walk distance less than 372 m were defined as low walkers. A strong correlation appeared between the 6-minute distance and 1-minute distance in terms of predicting survival, and 1-year transplant-free survival was significantly better in high walkers than in low walkers (27 months vs. 22 months; P = .015).
Dr. Nunes said she was not surprised by the results, in part because previous research has shown a strong correlation among 2-minute, 6-minute, and 12-minute walking tests.
Although more research is needed to validate the findings, the results suggest that the 1-minute test might be a practical substitute for the 6-minute test by providing similar prognostic information more quickly and easily than the 6-minute test, the researchers said.
“It is important for clinicians to know that the time chosen to assess exercise tolerance by walking tests might not be critical,” said Dr. Nunes. “Shorter walks are not only less time consuming, and easier for both patients and clinicians, but are also reproducible and discriminatory of survival.
“We need to validate the test performance characteristics and prognostic value of distance walked in a 1MWT compared to the standard 6MWT in an independent cohort of patients with IPF,” Dr. Nunes noted. “Additionally, the evaluation of alternate instruction, for example changing the wording from ‘walk as far’ to ‘walk as fast’ might facilitate a better effort, and a greater distance with improved reproducibility. Other novel parameters and modifications to the 6MWT or 1MWT might further improve the utility of these tests in the management of IPF and other patients,” she added.
The researchers had no financial conflicts to disclose.
, based on data from 179 adults. The findings were presented at the CHEST annual meeting.
The 6-minute test is often used to evaluate functional capacity in IPF patients, but is not always practical in a busy clinic setting, according to Flavia S. Nunes, MD, of Inova Fairfax Hospital in Falls Church, VA, and colleagues.
“Among the clinical and physiologic predictors associated with survival in IPF, the 6MWT has been increasingly used over the past 5 years as a secondary endpoint in the efficacy analyses of potential therapies for IPF. Validation of shorter time of walking might make the test more feasible to be applied in routine clinical care,” she said.
To determine the predictive value of the first minute of the 6-minute test, the researchers reviewed data from 142 men and 37 women at a tertiary referral center between May 2010 and February 2017. The average age of the patients was 68 years, the average body mass index was 28.3 kg/m2, and 27% used oxygen supplementation during the walk test.
Overall, the mean distance for the 6-minute test was 372 m, and the average distance for the 1-minute test was 65 m. Study participants who achieved a 6-minute walk distance greater than 372 m were defined as high walkers, and those with a 6-minute walk distance less than 372 m were defined as low walkers. A strong correlation appeared between the 6-minute distance and 1-minute distance in terms of predicting survival, and 1-year transplant-free survival was significantly better in high walkers than in low walkers (27 months vs. 22 months; P = .015).
Dr. Nunes said she was not surprised by the results, in part because previous research has shown a strong correlation among 2-minute, 6-minute, and 12-minute walking tests.
Although more research is needed to validate the findings, the results suggest that the 1-minute test might be a practical substitute for the 6-minute test by providing similar prognostic information more quickly and easily than the 6-minute test, the researchers said.
“It is important for clinicians to know that the time chosen to assess exercise tolerance by walking tests might not be critical,” said Dr. Nunes. “Shorter walks are not only less time consuming, and easier for both patients and clinicians, but are also reproducible and discriminatory of survival.
“We need to validate the test performance characteristics and prognostic value of distance walked in a 1MWT compared to the standard 6MWT in an independent cohort of patients with IPF,” Dr. Nunes noted. “Additionally, the evaluation of alternate instruction, for example changing the wording from ‘walk as far’ to ‘walk as fast’ might facilitate a better effort, and a greater distance with improved reproducibility. Other novel parameters and modifications to the 6MWT or 1MWT might further improve the utility of these tests in the management of IPF and other patients,” she added.
The researchers had no financial conflicts to disclose.
FROM CHEST 2017
2017 GI thought leaders
Trainee and early-career members made an impact in the GI field this past year, especially through contributing to and engaging in various collaborations via the American Gastroenterological Association’s member-only online discussion forum – the AGA Community.
We’re proud to announce that the title of 2017 top contributor is held by an early-career member: Meet Dmitriy Kedrin, MD, PhD, of Elliot Hospital in Manchester, N.H., and find out a little more about how the AGA Community is an important part of his routine in this brief Q&A session.
Thanks for being such an active member of the AGA Community! Why do you contribute?
“I think it is important for GI docs to be a part of a larger community, stay informed on the latest guidelines, research publications, and approaches to difficult cases, where more than one road can be taken. I feel that it is a great forum for someone like me, a relatively junior gastroenterologist.”
Why do you enjoy being part of the AGA Community?
“I find the case discussions informative. I learn a great deal about current trends and opinions on important topics in the GI world.”
What do you like to do in your free time?
“I bake bread and run a gastroenterology literature review podcast called ‘GI Pearls.’ ”
What’s your approach to handling a difficult patient case you come across in your practice?
“I often seek advice of other clinicians, some with more expertise in a particular area. I also go to the literature and try to learn more that way, to help expand my differential as well as figure out the best therapeutic approach.”
Was there a conversation in the AGA Community in 2017 that was your favorite?
“Oh, there were several. I recall a patient case where there were several thought leaders in the field who had a disagreement about the best approach to treatment. The work-life balance conversation was also very good. I also enjoyed reading about different opinions regarding the values of clinical versus observational trials that happened a while back.”
Here are other trainee and early-career members who made the list of top contributors in the AGA Community last year:
- Avinash Ketwaroo, MD
- Hüseyin Bozkurt, MD
- Peter Liang, MD, MPH
- Fola May, MD, PhD
- Richa Shukla, MD
- Arthur Beyder, MD, PhD
- Shazia Siddique, MD
- Brigid Boland, MD
Check the achievements section of your AGA Community profile to see whether you made the list. We look forward to seeing you all in the forum in 2018!
Trainee and early-career members made an impact in the GI field this past year, especially through contributing to and engaging in various collaborations via the American Gastroenterological Association’s member-only online discussion forum – the AGA Community.
We’re proud to announce that the title of 2017 top contributor is held by an early-career member: Meet Dmitriy Kedrin, MD, PhD, of Elliot Hospital in Manchester, N.H., and find out a little more about how the AGA Community is an important part of his routine in this brief Q&A session.
Thanks for being such an active member of the AGA Community! Why do you contribute?
“I think it is important for GI docs to be a part of a larger community, stay informed on the latest guidelines, research publications, and approaches to difficult cases, where more than one road can be taken. I feel that it is a great forum for someone like me, a relatively junior gastroenterologist.”
Why do you enjoy being part of the AGA Community?
“I find the case discussions informative. I learn a great deal about current trends and opinions on important topics in the GI world.”
What do you like to do in your free time?
“I bake bread and run a gastroenterology literature review podcast called ‘GI Pearls.’ ”
What’s your approach to handling a difficult patient case you come across in your practice?
“I often seek advice of other clinicians, some with more expertise in a particular area. I also go to the literature and try to learn more that way, to help expand my differential as well as figure out the best therapeutic approach.”
Was there a conversation in the AGA Community in 2017 that was your favorite?
“Oh, there were several. I recall a patient case where there were several thought leaders in the field who had a disagreement about the best approach to treatment. The work-life balance conversation was also very good. I also enjoyed reading about different opinions regarding the values of clinical versus observational trials that happened a while back.”
Here are other trainee and early-career members who made the list of top contributors in the AGA Community last year:
- Avinash Ketwaroo, MD
- Hüseyin Bozkurt, MD
- Peter Liang, MD, MPH
- Fola May, MD, PhD
- Richa Shukla, MD
- Arthur Beyder, MD, PhD
- Shazia Siddique, MD
- Brigid Boland, MD
Check the achievements section of your AGA Community profile to see whether you made the list. We look forward to seeing you all in the forum in 2018!
Trainee and early-career members made an impact in the GI field this past year, especially through contributing to and engaging in various collaborations via the American Gastroenterological Association’s member-only online discussion forum – the AGA Community.
We’re proud to announce that the title of 2017 top contributor is held by an early-career member: Meet Dmitriy Kedrin, MD, PhD, of Elliot Hospital in Manchester, N.H., and find out a little more about how the AGA Community is an important part of his routine in this brief Q&A session.
Thanks for being such an active member of the AGA Community! Why do you contribute?
“I think it is important for GI docs to be a part of a larger community, stay informed on the latest guidelines, research publications, and approaches to difficult cases, where more than one road can be taken. I feel that it is a great forum for someone like me, a relatively junior gastroenterologist.”
Why do you enjoy being part of the AGA Community?
“I find the case discussions informative. I learn a great deal about current trends and opinions on important topics in the GI world.”
What do you like to do in your free time?
“I bake bread and run a gastroenterology literature review podcast called ‘GI Pearls.’ ”
What’s your approach to handling a difficult patient case you come across in your practice?
“I often seek advice of other clinicians, some with more expertise in a particular area. I also go to the literature and try to learn more that way, to help expand my differential as well as figure out the best therapeutic approach.”
Was there a conversation in the AGA Community in 2017 that was your favorite?
“Oh, there were several. I recall a patient case where there were several thought leaders in the field who had a disagreement about the best approach to treatment. The work-life balance conversation was also very good. I also enjoyed reading about different opinions regarding the values of clinical versus observational trials that happened a while back.”
Here are other trainee and early-career members who made the list of top contributors in the AGA Community last year:
- Avinash Ketwaroo, MD
- Hüseyin Bozkurt, MD
- Peter Liang, MD, MPH
- Fola May, MD, PhD
- Richa Shukla, MD
- Arthur Beyder, MD, PhD
- Shazia Siddique, MD
- Brigid Boland, MD
Check the achievements section of your AGA Community profile to see whether you made the list. We look forward to seeing you all in the forum in 2018!
Nutrition early in life has long-term effects on neurodevelopment
Nutrition within the first 1,000 days of childhood are pivotal in a child’s neurodevelopment and lifelong health, according to an American Academy of Pediatrics policy statement.
“Healthy, normal neurodevelopment is a complex process involving cellular and structural changes in the brain that proceed in a specified sequence,” wrote Sara Jane Schwarzenberg, MD and Michael K. Georgieff, MD, both of the University of Minnesota Masonic Children’s Hospital, Minneapolis, and the AAP Committee on Nutrition. “Changes that are too rapid or too slow in one part of the brain may result in the failure of crucial pathway connections to other parts of the brain. Timing is crucial; once a particular developmental sequence fails, it may not be possible to retrieve all the lost function,” the investigators and committee noted in a report published in Pediatrics (Pediatrics. 2018; 141[2]:e20173716).
The importance of macronutrients was highlighted in a study of rural Guatemalan children during 1969-1989 who received high-calorie or low-calorie protein supplements. Children who received the high-calorie/high protein supplements before age 2 years had higher test scores, better reading and vocabulary skills, and faster information processing abilities, compared with their low-calorie/low-protein counterparts.
Like the low-calorie/low-protein Guatemalans, there are many populations that lack access to high-quality macronutrient sources or have access to only low-quality macronutrients. In the United States in 2015, 16.6% of households (6.4 million) were food insecure. This was even more pronounced in households with incomes below the poverty line, with 36.8% being food insecure, according to studies from the Department of Agriculture.
Food insecurity is not limited to macronutrients but extends to micronutrients such as vitamins and minerals like zinc; iron; choline; folate; iodine; vitamins A, D, B6, and B12; and long-chain polyunsaturated fatty acids. A lack of any of these micronutrients in early childhood can lead to neurodevelopmental issues later in life, Dr. Schwarzenberg, Dr. Georgieff, and the committee emphasized. An important source of micronutrients is human milk, provided by breastfeeding. Studies have shown that breastfeeding of preterm and term infants improves cognitive performance, compared with infants who consume formula (J Pediatr. 2016;177:133-9.e1; Curr Opin Pediatr. 2016;28[4]:559-66).
Because proper consumption of macronutrients and micronutrients is so important, a number of government-sponsored programs exist that provide nutritional support to women, infants, and young children. The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) is one of the most important programs, helping 53% of children under the age of 1 year. The Supplemental Nutrition Assistance Program (SNAP) also supplies economic aid to buy nutritious foods; it kept approximately 4.9 million children out of poverty in 2012, the researchers said. SNAP Nutrition Education, a partnership between SNAP and the Department of Agriculture, gives SNAP participants and eligible nonparticipants skills and information to help them to make healthy food choices with limited money.
The article highlights some important information, but is not an exhaustive discussion of the AAP policy statement. To make the information from the policy statement more applicable, Dr. Schwarzenberg, Dr. Georgieff, and the committee provided 10 takeaway recommendations for pediatricians.
1. Be knowledgeable about breastfeeding and help breastfeeding mothers. The AAP recommends exclusive breastfeeding for the first 6 months of a child’s life and to continue breastfeeding with the addition of food for at least the first year of life, and even after that if the mother and child so desire.
2. Advocate at the local, state, and federal levels to preserve and strengthen nutritional and assistance programs focusing on prenatal and neonatal nutrition. This can help support proper neurodevelopment and minimize negative environmental factors.
3. Openly discuss proper nutritions effects on infant neurodevelopment with parents. Know which nutrients are at risk in the breastfed infant after 6 months, such as zinc, iron, and vitamin D. A good resource is “Pediatric Nutrition, 7th edition” (Itasca, Ill. American Academy of Pediatrics, 2014).
4. Convey that eating healthy is a positive choice, not just an avoidance of unhealthy foods.
5. Inform food pantries and soup kitchens that the food packages and meals they provide should have higher levels of macronutrients and micronutrients.
6. Encourage parents to make use of programs like WIC and SNAP, and advocate for removing barriers that parents face in enrolling or reenrolling in such programs.
7. Oppose changes in eligibility to assistance programs that would adversely affect children.
8. Anticipate neurodevelopmental issues with children and address the issue early. For example, educate yourself about which nutrients are at risk for deficiency and at what ages.
9. Work with obstetricians to encourage improvements in maternal diet, which will affect the micronutrients available for the developing fetus.
10. Become advocates in the “Hunger Community,” working to reduce hunger at the local level across the United States. A chart in the article lists organizations focused on hunger, such as Feeding America, 1,000 Days, Share Our Strength, and others.
There was no external funding for this research, and the authors had no relevant financial disclosures or potential conflicts of interest to report.
While you might not typically put chopped or blended, unsalted, boiled canned oysters on your usual list of recommended infant and toddler foods, maybe you should.
The AAP just published a new policy statement on advocacy to improve child nutrition in the first 1,000 days (from conception to age 2 years). The statement emphasizes the importance of nutrition to optimal brain development. Pediatricians are encouraged to be familiar with community services to support optimal nutrition such as the Special Supplemental Nutrition Program for Women, Infants, and Children, the Supplemental Nutrition Assistance Program, the Child and Adult Care Food Program, and food pantries and soup kitchens, but also to get beyond recommending a “good diet” to something more specific which is high in key nutrients important for brain development such as protein; zinc; iron; choline; folate; iodine; vitamins A, D, B6, and B12; and polyunsaturated fatty acids. That’s where the boiled oysters, a decent source of the listed nutrients and especially loaded with zinc, iron, and vitamin B12, come in. While not everyone is going to rush out to buy their baby such an unexpected (and for many, unfamiliar) food, the statement reminds pediatricians to recommend foods that are good sources of the nutrients that babies and toddlers need most. Other foods that fit the bill include oatmeal, meat and poultry, fish like salmon and tuna, eggs, tofu and soybeans, and other legumes and beans like chickpeas and lentils.
Natalie D. Muth, MD, is a pediatrician at Children’s Primary Care Medical Group in Carlsbad, Calif. She has no relevant financial disclosures.
While you might not typically put chopped or blended, unsalted, boiled canned oysters on your usual list of recommended infant and toddler foods, maybe you should.
The AAP just published a new policy statement on advocacy to improve child nutrition in the first 1,000 days (from conception to age 2 years). The statement emphasizes the importance of nutrition to optimal brain development. Pediatricians are encouraged to be familiar with community services to support optimal nutrition such as the Special Supplemental Nutrition Program for Women, Infants, and Children, the Supplemental Nutrition Assistance Program, the Child and Adult Care Food Program, and food pantries and soup kitchens, but also to get beyond recommending a “good diet” to something more specific which is high in key nutrients important for brain development such as protein; zinc; iron; choline; folate; iodine; vitamins A, D, B6, and B12; and polyunsaturated fatty acids. That’s where the boiled oysters, a decent source of the listed nutrients and especially loaded with zinc, iron, and vitamin B12, come in. While not everyone is going to rush out to buy their baby such an unexpected (and for many, unfamiliar) food, the statement reminds pediatricians to recommend foods that are good sources of the nutrients that babies and toddlers need most. Other foods that fit the bill include oatmeal, meat and poultry, fish like salmon and tuna, eggs, tofu and soybeans, and other legumes and beans like chickpeas and lentils.
Natalie D. Muth, MD, is a pediatrician at Children’s Primary Care Medical Group in Carlsbad, Calif. She has no relevant financial disclosures.
While you might not typically put chopped or blended, unsalted, boiled canned oysters on your usual list of recommended infant and toddler foods, maybe you should.
The AAP just published a new policy statement on advocacy to improve child nutrition in the first 1,000 days (from conception to age 2 years). The statement emphasizes the importance of nutrition to optimal brain development. Pediatricians are encouraged to be familiar with community services to support optimal nutrition such as the Special Supplemental Nutrition Program for Women, Infants, and Children, the Supplemental Nutrition Assistance Program, the Child and Adult Care Food Program, and food pantries and soup kitchens, but also to get beyond recommending a “good diet” to something more specific which is high in key nutrients important for brain development such as protein; zinc; iron; choline; folate; iodine; vitamins A, D, B6, and B12; and polyunsaturated fatty acids. That’s where the boiled oysters, a decent source of the listed nutrients and especially loaded with zinc, iron, and vitamin B12, come in. While not everyone is going to rush out to buy their baby such an unexpected (and for many, unfamiliar) food, the statement reminds pediatricians to recommend foods that are good sources of the nutrients that babies and toddlers need most. Other foods that fit the bill include oatmeal, meat and poultry, fish like salmon and tuna, eggs, tofu and soybeans, and other legumes and beans like chickpeas and lentils.
Natalie D. Muth, MD, is a pediatrician at Children’s Primary Care Medical Group in Carlsbad, Calif. She has no relevant financial disclosures.
Nutrition within the first 1,000 days of childhood are pivotal in a child’s neurodevelopment and lifelong health, according to an American Academy of Pediatrics policy statement.
“Healthy, normal neurodevelopment is a complex process involving cellular and structural changes in the brain that proceed in a specified sequence,” wrote Sara Jane Schwarzenberg, MD and Michael K. Georgieff, MD, both of the University of Minnesota Masonic Children’s Hospital, Minneapolis, and the AAP Committee on Nutrition. “Changes that are too rapid or too slow in one part of the brain may result in the failure of crucial pathway connections to other parts of the brain. Timing is crucial; once a particular developmental sequence fails, it may not be possible to retrieve all the lost function,” the investigators and committee noted in a report published in Pediatrics (Pediatrics. 2018; 141[2]:e20173716).
The importance of macronutrients was highlighted in a study of rural Guatemalan children during 1969-1989 who received high-calorie or low-calorie protein supplements. Children who received the high-calorie/high protein supplements before age 2 years had higher test scores, better reading and vocabulary skills, and faster information processing abilities, compared with their low-calorie/low-protein counterparts.
Like the low-calorie/low-protein Guatemalans, there are many populations that lack access to high-quality macronutrient sources or have access to only low-quality macronutrients. In the United States in 2015, 16.6% of households (6.4 million) were food insecure. This was even more pronounced in households with incomes below the poverty line, with 36.8% being food insecure, according to studies from the Department of Agriculture.
Food insecurity is not limited to macronutrients but extends to micronutrients such as vitamins and minerals like zinc; iron; choline; folate; iodine; vitamins A, D, B6, and B12; and long-chain polyunsaturated fatty acids. A lack of any of these micronutrients in early childhood can lead to neurodevelopmental issues later in life, Dr. Schwarzenberg, Dr. Georgieff, and the committee emphasized. An important source of micronutrients is human milk, provided by breastfeeding. Studies have shown that breastfeeding of preterm and term infants improves cognitive performance, compared with infants who consume formula (J Pediatr. 2016;177:133-9.e1; Curr Opin Pediatr. 2016;28[4]:559-66).
Because proper consumption of macronutrients and micronutrients is so important, a number of government-sponsored programs exist that provide nutritional support to women, infants, and young children. The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) is one of the most important programs, helping 53% of children under the age of 1 year. The Supplemental Nutrition Assistance Program (SNAP) also supplies economic aid to buy nutritious foods; it kept approximately 4.9 million children out of poverty in 2012, the researchers said. SNAP Nutrition Education, a partnership between SNAP and the Department of Agriculture, gives SNAP participants and eligible nonparticipants skills and information to help them to make healthy food choices with limited money.
The article highlights some important information, but is not an exhaustive discussion of the AAP policy statement. To make the information from the policy statement more applicable, Dr. Schwarzenberg, Dr. Georgieff, and the committee provided 10 takeaway recommendations for pediatricians.
1. Be knowledgeable about breastfeeding and help breastfeeding mothers. The AAP recommends exclusive breastfeeding for the first 6 months of a child’s life and to continue breastfeeding with the addition of food for at least the first year of life, and even after that if the mother and child so desire.
2. Advocate at the local, state, and federal levels to preserve and strengthen nutritional and assistance programs focusing on prenatal and neonatal nutrition. This can help support proper neurodevelopment and minimize negative environmental factors.
3. Openly discuss proper nutritions effects on infant neurodevelopment with parents. Know which nutrients are at risk in the breastfed infant after 6 months, such as zinc, iron, and vitamin D. A good resource is “Pediatric Nutrition, 7th edition” (Itasca, Ill. American Academy of Pediatrics, 2014).
4. Convey that eating healthy is a positive choice, not just an avoidance of unhealthy foods.
5. Inform food pantries and soup kitchens that the food packages and meals they provide should have higher levels of macronutrients and micronutrients.
6. Encourage parents to make use of programs like WIC and SNAP, and advocate for removing barriers that parents face in enrolling or reenrolling in such programs.
7. Oppose changes in eligibility to assistance programs that would adversely affect children.
8. Anticipate neurodevelopmental issues with children and address the issue early. For example, educate yourself about which nutrients are at risk for deficiency and at what ages.
9. Work with obstetricians to encourage improvements in maternal diet, which will affect the micronutrients available for the developing fetus.
10. Become advocates in the “Hunger Community,” working to reduce hunger at the local level across the United States. A chart in the article lists organizations focused on hunger, such as Feeding America, 1,000 Days, Share Our Strength, and others.
There was no external funding for this research, and the authors had no relevant financial disclosures or potential conflicts of interest to report.
Nutrition within the first 1,000 days of childhood are pivotal in a child’s neurodevelopment and lifelong health, according to an American Academy of Pediatrics policy statement.
“Healthy, normal neurodevelopment is a complex process involving cellular and structural changes in the brain that proceed in a specified sequence,” wrote Sara Jane Schwarzenberg, MD and Michael K. Georgieff, MD, both of the University of Minnesota Masonic Children’s Hospital, Minneapolis, and the AAP Committee on Nutrition. “Changes that are too rapid or too slow in one part of the brain may result in the failure of crucial pathway connections to other parts of the brain. Timing is crucial; once a particular developmental sequence fails, it may not be possible to retrieve all the lost function,” the investigators and committee noted in a report published in Pediatrics (Pediatrics. 2018; 141[2]:e20173716).
The importance of macronutrients was highlighted in a study of rural Guatemalan children during 1969-1989 who received high-calorie or low-calorie protein supplements. Children who received the high-calorie/high protein supplements before age 2 years had higher test scores, better reading and vocabulary skills, and faster information processing abilities, compared with their low-calorie/low-protein counterparts.
Like the low-calorie/low-protein Guatemalans, there are many populations that lack access to high-quality macronutrient sources or have access to only low-quality macronutrients. In the United States in 2015, 16.6% of households (6.4 million) were food insecure. This was even more pronounced in households with incomes below the poverty line, with 36.8% being food insecure, according to studies from the Department of Agriculture.
Food insecurity is not limited to macronutrients but extends to micronutrients such as vitamins and minerals like zinc; iron; choline; folate; iodine; vitamins A, D, B6, and B12; and long-chain polyunsaturated fatty acids. A lack of any of these micronutrients in early childhood can lead to neurodevelopmental issues later in life, Dr. Schwarzenberg, Dr. Georgieff, and the committee emphasized. An important source of micronutrients is human milk, provided by breastfeeding. Studies have shown that breastfeeding of preterm and term infants improves cognitive performance, compared with infants who consume formula (J Pediatr. 2016;177:133-9.e1; Curr Opin Pediatr. 2016;28[4]:559-66).
Because proper consumption of macronutrients and micronutrients is so important, a number of government-sponsored programs exist that provide nutritional support to women, infants, and young children. The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) is one of the most important programs, helping 53% of children under the age of 1 year. The Supplemental Nutrition Assistance Program (SNAP) also supplies economic aid to buy nutritious foods; it kept approximately 4.9 million children out of poverty in 2012, the researchers said. SNAP Nutrition Education, a partnership between SNAP and the Department of Agriculture, gives SNAP participants and eligible nonparticipants skills and information to help them to make healthy food choices with limited money.
The article highlights some important information, but is not an exhaustive discussion of the AAP policy statement. To make the information from the policy statement more applicable, Dr. Schwarzenberg, Dr. Georgieff, and the committee provided 10 takeaway recommendations for pediatricians.
1. Be knowledgeable about breastfeeding and help breastfeeding mothers. The AAP recommends exclusive breastfeeding for the first 6 months of a child’s life and to continue breastfeeding with the addition of food for at least the first year of life, and even after that if the mother and child so desire.
2. Advocate at the local, state, and federal levels to preserve and strengthen nutritional and assistance programs focusing on prenatal and neonatal nutrition. This can help support proper neurodevelopment and minimize negative environmental factors.
3. Openly discuss proper nutritions effects on infant neurodevelopment with parents. Know which nutrients are at risk in the breastfed infant after 6 months, such as zinc, iron, and vitamin D. A good resource is “Pediatric Nutrition, 7th edition” (Itasca, Ill. American Academy of Pediatrics, 2014).
4. Convey that eating healthy is a positive choice, not just an avoidance of unhealthy foods.
5. Inform food pantries and soup kitchens that the food packages and meals they provide should have higher levels of macronutrients and micronutrients.
6. Encourage parents to make use of programs like WIC and SNAP, and advocate for removing barriers that parents face in enrolling or reenrolling in such programs.
7. Oppose changes in eligibility to assistance programs that would adversely affect children.
8. Anticipate neurodevelopmental issues with children and address the issue early. For example, educate yourself about which nutrients are at risk for deficiency and at what ages.
9. Work with obstetricians to encourage improvements in maternal diet, which will affect the micronutrients available for the developing fetus.
10. Become advocates in the “Hunger Community,” working to reduce hunger at the local level across the United States. A chart in the article lists organizations focused on hunger, such as Feeding America, 1,000 Days, Share Our Strength, and others.
There was no external funding for this research, and the authors had no relevant financial disclosures or potential conflicts of interest to report.
FROM PEDIATRICS