User login
Together Since Birth
A 51-year-old Hispanic man presents for evaluation of a lesion he was born with. It grew as he did and was never more than a cosmetic problem until recently, when it became enlarged and sensitive. His family members convinced him to have it evaluated by primary care, who referred him to dermatology.
The patient denies any health problems other than type 2 diabetes, which is adequately controlled. His dark skin almost always tans, rather than burns, with sun exposure.
EXAMINATION
The lesion is hard to miss, measuring 1.8 cm x 5.5 mm and located prominently in the upper left nasolabial fold. It is quite firm, brownish red, hair-bearing, and round, with fine mammilations on the surface. It sits on a base only slightly smaller than the lesion’s surface. The rest of the patient’s skin is unremarkable.

Given that the lesion has changed and is quite sizeable, it is excised with a curving elliptiform incision along relaxed skin tension lines, paralleling the nasolabial fold, and sent for pathologic examination.
What is the diagnosis?
DISCUSSION
The pathology report confirmed the benign nature of this congenital melanocytic nevus (CMN). CMNs are hamartomatous lesions that form when collections of melanocytes (normal pigment cells) congregate in one location. These cells migrate during the embryonal stage of development—but some never make it to their final destination.
While CMNs are almost always benign, the history of change in this case made excision compelling. Given the lesion’s likely extension well under the surface of the skin, a shave removal would not suffice—and would leave a noticeable scar.
Despite their low potential for malignancy, CMNs—like any lesion removed from the body—must be sent for pathologic examination. The general rule is: the larger the congenital lesion, the greater the malignant potential.
Remember, too, that not all skin cancers are melanomas. Virtually any cell in the skin (sweat glands, neural tissue, sebaceous glands, smooth muscle, and even hair follicles) can undergo malignant transformation, so microscopic examination is mandatory for all removed lesions, except tiny tags or warts.
Interestingly, CMNs are more common on patients with lighter skin. However, besides the case patient, there were also several family members reporting a history of similar lesions. They were all thrilled with the patient’s cosmetic outcome—and more so with the benign report.
TAKE-HOME LEARNING POINTS
- Congenital melanocytic nevi (CMNs) are collections of melanocytes in one area.
- CMNs have little malignant potential, but morphology (eg, color, shape, symptoms) or size may dictate the need for removal or biopsy.
- Deep shave or excision are the best options for removal; patient age, lesion location, potential for scarring, and surgical ability of the provider influence choice.
- Since melanocytes can end up in other extracutaneous locations, primary melanomas can develop almost anywhere—including the lungs, the gut, or even the eyes.
A 51-year-old Hispanic man presents for evaluation of a lesion he was born with. It grew as he did and was never more than a cosmetic problem until recently, when it became enlarged and sensitive. His family members convinced him to have it evaluated by primary care, who referred him to dermatology.
The patient denies any health problems other than type 2 diabetes, which is adequately controlled. His dark skin almost always tans, rather than burns, with sun exposure.
EXAMINATION
The lesion is hard to miss, measuring 1.8 cm x 5.5 mm and located prominently in the upper left nasolabial fold. It is quite firm, brownish red, hair-bearing, and round, with fine mammilations on the surface. It sits on a base only slightly smaller than the lesion’s surface. The rest of the patient’s skin is unremarkable.
Given that the lesion has changed and is quite sizeable, it is excised with a curving elliptiform incision along relaxed skin tension lines, paralleling the nasolabial fold, and sent for pathologic examination.
What is the diagnosis?
DISCUSSION
The pathology report confirmed the benign nature of this congenital melanocytic nevus (CMN). CMNs are hamartomatous lesions that form when collections of melanocytes (normal pigment cells) congregate in one location. These cells migrate during the embryonal stage of development—but some never make it to their final destination.
While CMNs are almost always benign, the history of change in this case made excision compelling. Given the lesion’s likely extension well under the surface of the skin, a shave removal would not suffice—and would leave a noticeable scar.
Despite their low potential for malignancy, CMNs—like any lesion removed from the body—must be sent for pathologic examination. The general rule is: the larger the congenital lesion, the greater the malignant potential.
Remember, too, that not all skin cancers are melanomas. Virtually any cell in the skin (sweat glands, neural tissue, sebaceous glands, smooth muscle, and even hair follicles) can undergo malignant transformation, so microscopic examination is mandatory for all removed lesions, except tiny tags or warts.
Interestingly, CMNs are more common on patients with lighter skin. However, besides the case patient, there were also several family members reporting a history of similar lesions. They were all thrilled with the patient’s cosmetic outcome—and more so with the benign report.
TAKE-HOME LEARNING POINTS
- Congenital melanocytic nevi (CMNs) are collections of melanocytes in one area.
- CMNs have little malignant potential, but morphology (eg, color, shape, symptoms) or size may dictate the need for removal or biopsy.
- Deep shave or excision are the best options for removal; patient age, lesion location, potential for scarring, and surgical ability of the provider influence choice.
- Since melanocytes can end up in other extracutaneous locations, primary melanomas can develop almost anywhere—including the lungs, the gut, or even the eyes.
A 51-year-old Hispanic man presents for evaluation of a lesion he was born with. It grew as he did and was never more than a cosmetic problem until recently, when it became enlarged and sensitive. His family members convinced him to have it evaluated by primary care, who referred him to dermatology.
The patient denies any health problems other than type 2 diabetes, which is adequately controlled. His dark skin almost always tans, rather than burns, with sun exposure.
EXAMINATION
The lesion is hard to miss, measuring 1.8 cm x 5.5 mm and located prominently in the upper left nasolabial fold. It is quite firm, brownish red, hair-bearing, and round, with fine mammilations on the surface. It sits on a base only slightly smaller than the lesion’s surface. The rest of the patient’s skin is unremarkable.
Given that the lesion has changed and is quite sizeable, it is excised with a curving elliptiform incision along relaxed skin tension lines, paralleling the nasolabial fold, and sent for pathologic examination.
What is the diagnosis?
DISCUSSION
The pathology report confirmed the benign nature of this congenital melanocytic nevus (CMN). CMNs are hamartomatous lesions that form when collections of melanocytes (normal pigment cells) congregate in one location. These cells migrate during the embryonal stage of development—but some never make it to their final destination.
While CMNs are almost always benign, the history of change in this case made excision compelling. Given the lesion’s likely extension well under the surface of the skin, a shave removal would not suffice—and would leave a noticeable scar.
Despite their low potential for malignancy, CMNs—like any lesion removed from the body—must be sent for pathologic examination. The general rule is: the larger the congenital lesion, the greater the malignant potential.
Remember, too, that not all skin cancers are melanomas. Virtually any cell in the skin (sweat glands, neural tissue, sebaceous glands, smooth muscle, and even hair follicles) can undergo malignant transformation, so microscopic examination is mandatory for all removed lesions, except tiny tags or warts.
Interestingly, CMNs are more common on patients with lighter skin. However, besides the case patient, there were also several family members reporting a history of similar lesions. They were all thrilled with the patient’s cosmetic outcome—and more so with the benign report.
TAKE-HOME LEARNING POINTS
- Congenital melanocytic nevi (CMNs) are collections of melanocytes in one area.
- CMNs have little malignant potential, but morphology (eg, color, shape, symptoms) or size may dictate the need for removal or biopsy.
- Deep shave or excision are the best options for removal; patient age, lesion location, potential for scarring, and surgical ability of the provider influence choice.
- Since melanocytes can end up in other extracutaneous locations, primary melanomas can develop almost anywhere—including the lungs, the gut, or even the eyes.
Gene therapy seems safe, effective in hemophilia B

The gene therapy SPK-9001 has produced positive results in a phase 1/2 trial of adults with hemophilia B, according to researchers.
SPK-9001 produced sustained factor IX (FIX) activity and allowed all 10 patients in this study to stop FIX prophylaxis.
Eight patients had no further FIX treatment after SPK-9001, and 9 patients had 0 bleeds.
There were no serious adverse events, and none of the patients had thrombotic events or developed FIX inhibitors.
“A one-time therapy sufficient to prevent bleeding without further medical intervention is the ideal treatment goal for patients with hemophilia,” said Lindsey A. George, MD, a hematologist at Children’s Hospital of Philadelphia in Pennsylvania.
“This cohort of 10 patients all safely experienced sustained clinical benefit after one infusion.”
Dr George and her colleagues reported these results in NEJM. The trial was sponsored by Spark Therapeutics and Pfizer.
SPK-9001 is an investigational vector that contains a bio-engineered adeno-associated virus capsid and a codon-optimized, high-activity human FIX gene enabling endogenous production of FIX.
The researchers tested SPK-9001 in 10 males with hemophilia B.
With a cumulative follow-up of 492 weeks, the mean steady-state FIX activity was 34% of normal (range, 14% to 81%) after a single administration of SPK-9001.
The annualized bleeding rate was reduced 97%, from a mean rate of 11.1 events per year before SPK-9001 administration to 0.4 events per year after (P=0.02).
Nine patients had 0 bleeds after SPK-9001, and 1 patient had 4 bleeds.
Use of FIX treatment was reduced 99% during this study, from a mean dose of 2908 IU/kg (range, 0 to 8090) before SPK-9001 to a mean dose of 49.3 IU/kg (range, 0 to 376) after SPK-9001 (P=0.004).
Two patients did receive FIX treatment after SPK-9001, but none of the patients received FIX prophylaxis.
The researchers noted that the patient who required FIX treatment for bleeding (4 events) had significant baseline joint damage. However, this patient still used 91% less FIX than before he received SPK-9001.
There were a total of 40 adverse events in this study, but none were serious. There were no deaths, no thrombotic events, and no cases of inhibitor development.
The only adverse events thought to be related to SPK-9001 were asymptomatic and transient increases in liver enzymes in 2 patients. These events resolved with a tapering dose of oral corticosteroids.
“People who live with hemophilia face a life-long need for vigilant monitoring and recurrent factor concentrate infusions to prevent spontaneous, potentially life-threatening bleeds and to protect their joints,” said study author Katherine High, MD, president and head of Research and Development at Spark Therapeutics.
“The data suggest a one-time infusion of SPK-9001 has the potential to safely sustain factor IX coagulant activity level that may result in the termination of baseline prophylaxis factor infusions, significantly reduce bleeding, and nearly eliminate the need for exogenous factor IX concentrate infusions.” ![]()
The gene therapy SPK-9001 has produced positive results in a phase 1/2 trial of adults with hemophilia B, according to researchers.
SPK-9001 produced sustained factor IX (FIX) activity and allowed all 10 patients in this study to stop FIX prophylaxis.
Eight patients had no further FIX treatment after SPK-9001, and 9 patients had 0 bleeds.
There were no serious adverse events, and none of the patients had thrombotic events or developed FIX inhibitors.
“A one-time therapy sufficient to prevent bleeding without further medical intervention is the ideal treatment goal for patients with hemophilia,” said Lindsey A. George, MD, a hematologist at Children’s Hospital of Philadelphia in Pennsylvania.
“This cohort of 10 patients all safely experienced sustained clinical benefit after one infusion.”
Dr George and her colleagues reported these results in NEJM. The trial was sponsored by Spark Therapeutics and Pfizer.
SPK-9001 is an investigational vector that contains a bio-engineered adeno-associated virus capsid and a codon-optimized, high-activity human FIX gene enabling endogenous production of FIX.
The researchers tested SPK-9001 in 10 males with hemophilia B.
With a cumulative follow-up of 492 weeks, the mean steady-state FIX activity was 34% of normal (range, 14% to 81%) after a single administration of SPK-9001.
The annualized bleeding rate was reduced 97%, from a mean rate of 11.1 events per year before SPK-9001 administration to 0.4 events per year after (P=0.02).
Nine patients had 0 bleeds after SPK-9001, and 1 patient had 4 bleeds.
Use of FIX treatment was reduced 99% during this study, from a mean dose of 2908 IU/kg (range, 0 to 8090) before SPK-9001 to a mean dose of 49.3 IU/kg (range, 0 to 376) after SPK-9001 (P=0.004).
Two patients did receive FIX treatment after SPK-9001, but none of the patients received FIX prophylaxis.
The researchers noted that the patient who required FIX treatment for bleeding (4 events) had significant baseline joint damage. However, this patient still used 91% less FIX than before he received SPK-9001.
There were a total of 40 adverse events in this study, but none were serious. There were no deaths, no thrombotic events, and no cases of inhibitor development.
The only adverse events thought to be related to SPK-9001 were asymptomatic and transient increases in liver enzymes in 2 patients. These events resolved with a tapering dose of oral corticosteroids.
“People who live with hemophilia face a life-long need for vigilant monitoring and recurrent factor concentrate infusions to prevent spontaneous, potentially life-threatening bleeds and to protect their joints,” said study author Katherine High, MD, president and head of Research and Development at Spark Therapeutics.
“The data suggest a one-time infusion of SPK-9001 has the potential to safely sustain factor IX coagulant activity level that may result in the termination of baseline prophylaxis factor infusions, significantly reduce bleeding, and nearly eliminate the need for exogenous factor IX concentrate infusions.” ![]()
The gene therapy SPK-9001 has produced positive results in a phase 1/2 trial of adults with hemophilia B, according to researchers.
SPK-9001 produced sustained factor IX (FIX) activity and allowed all 10 patients in this study to stop FIX prophylaxis.
Eight patients had no further FIX treatment after SPK-9001, and 9 patients had 0 bleeds.
There were no serious adverse events, and none of the patients had thrombotic events or developed FIX inhibitors.
“A one-time therapy sufficient to prevent bleeding without further medical intervention is the ideal treatment goal for patients with hemophilia,” said Lindsey A. George, MD, a hematologist at Children’s Hospital of Philadelphia in Pennsylvania.
“This cohort of 10 patients all safely experienced sustained clinical benefit after one infusion.”
Dr George and her colleagues reported these results in NEJM. The trial was sponsored by Spark Therapeutics and Pfizer.
SPK-9001 is an investigational vector that contains a bio-engineered adeno-associated virus capsid and a codon-optimized, high-activity human FIX gene enabling endogenous production of FIX.
The researchers tested SPK-9001 in 10 males with hemophilia B.
With a cumulative follow-up of 492 weeks, the mean steady-state FIX activity was 34% of normal (range, 14% to 81%) after a single administration of SPK-9001.
The annualized bleeding rate was reduced 97%, from a mean rate of 11.1 events per year before SPK-9001 administration to 0.4 events per year after (P=0.02).
Nine patients had 0 bleeds after SPK-9001, and 1 patient had 4 bleeds.
Use of FIX treatment was reduced 99% during this study, from a mean dose of 2908 IU/kg (range, 0 to 8090) before SPK-9001 to a mean dose of 49.3 IU/kg (range, 0 to 376) after SPK-9001 (P=0.004).
Two patients did receive FIX treatment after SPK-9001, but none of the patients received FIX prophylaxis.
The researchers noted that the patient who required FIX treatment for bleeding (4 events) had significant baseline joint damage. However, this patient still used 91% less FIX than before he received SPK-9001.
There were a total of 40 adverse events in this study, but none were serious. There were no deaths, no thrombotic events, and no cases of inhibitor development.
The only adverse events thought to be related to SPK-9001 were asymptomatic and transient increases in liver enzymes in 2 patients. These events resolved with a tapering dose of oral corticosteroids.
“People who live with hemophilia face a life-long need for vigilant monitoring and recurrent factor concentrate infusions to prevent spontaneous, potentially life-threatening bleeds and to protect their joints,” said study author Katherine High, MD, president and head of Research and Development at Spark Therapeutics.
“The data suggest a one-time infusion of SPK-9001 has the potential to safely sustain factor IX coagulant activity level that may result in the termination of baseline prophylaxis factor infusions, significantly reduce bleeding, and nearly eliminate the need for exogenous factor IX concentrate infusions.” ![]()
FDA lifts partial hold on nivolumab trials

The US Food and Drug Administration (FDA) has lifted the partial clinical hold placed on 2 trials of the PD-1 immune checkpoint inhibitor nivolumab (Opdivo).
In these trials, CheckMate-039 (CA209 -039) and CA204142, researchers are investigating nivolumab-based combinations in patients with relapsed or refractory multiple myeloma (MM).
The partial clinical hold on these trials was a result of risks identified in studies involving another anti-PD-1 agent, pembrolizumab.
Data from the pembrolizumab trials suggested that risks outweigh benefits when PD-1/PD-L1 treatment is given to MM patients in combination with dexamethasone and pomalidomide or lenalidomide.
In addition, there could be an unfavorable risk-benefit ratio for MM patients receiving PD-1/PD-L1 treatments alone or in other combinations.
Therefore, the FDA placed a partial hold on the following nivolumab trials:
- CheckMate-602: A randomized, phase 3 trial of combinations of nivolumab, elotuzumab, pomalidomide, and dexamethasone in relapsed and refractory MM
- CheckMate-039: A phase 1 study intended to establish the tolerability of nivolumab and the combination of nivolumab and daratumumab, with or without pomalidomide and dexamethasone, in patients with relapsed or refractory MM
- CA204142: A phase 2 study of elotuzumab in combination with pomalidomide and low-dose dexamethasone, and in combination with nivolumab, in patients with MM who relapsed after or were refractory to prior treatment with lenalidomide.
After consulting with Bristol-Myers Squibb, the FDA decided to lift the hold on CheckMate-039 (CA209 -039) and CA204142. These trials will continue with amended protocols.
The third trial, CheckMate-602, remains on partial clinical hold. Bristol-Myers Squibb said it is continuing to work with the FDA to determine next steps for this trial.
CheckMate-602 is not enrolling new patients. However, patients who are experiencing clinical benefit are continuing to receive treatment. ![]()
The US Food and Drug Administration (FDA) has lifted the partial clinical hold placed on 2 trials of the PD-1 immune checkpoint inhibitor nivolumab (Opdivo).
In these trials, CheckMate-039 (CA209 -039) and CA204142, researchers are investigating nivolumab-based combinations in patients with relapsed or refractory multiple myeloma (MM).
The partial clinical hold on these trials was a result of risks identified in studies involving another anti-PD-1 agent, pembrolizumab.
Data from the pembrolizumab trials suggested that risks outweigh benefits when PD-1/PD-L1 treatment is given to MM patients in combination with dexamethasone and pomalidomide or lenalidomide.
In addition, there could be an unfavorable risk-benefit ratio for MM patients receiving PD-1/PD-L1 treatments alone or in other combinations.
Therefore, the FDA placed a partial hold on the following nivolumab trials:
- CheckMate-602: A randomized, phase 3 trial of combinations of nivolumab, elotuzumab, pomalidomide, and dexamethasone in relapsed and refractory MM
- CheckMate-039: A phase 1 study intended to establish the tolerability of nivolumab and the combination of nivolumab and daratumumab, with or without pomalidomide and dexamethasone, in patients with relapsed or refractory MM
- CA204142: A phase 2 study of elotuzumab in combination with pomalidomide and low-dose dexamethasone, and in combination with nivolumab, in patients with MM who relapsed after or were refractory to prior treatment with lenalidomide.
After consulting with Bristol-Myers Squibb, the FDA decided to lift the hold on CheckMate-039 (CA209 -039) and CA204142. These trials will continue with amended protocols.
The third trial, CheckMate-602, remains on partial clinical hold. Bristol-Myers Squibb said it is continuing to work with the FDA to determine next steps for this trial.
CheckMate-602 is not enrolling new patients. However, patients who are experiencing clinical benefit are continuing to receive treatment. ![]()
The US Food and Drug Administration (FDA) has lifted the partial clinical hold placed on 2 trials of the PD-1 immune checkpoint inhibitor nivolumab (Opdivo).
In these trials, CheckMate-039 (CA209 -039) and CA204142, researchers are investigating nivolumab-based combinations in patients with relapsed or refractory multiple myeloma (MM).
The partial clinical hold on these trials was a result of risks identified in studies involving another anti-PD-1 agent, pembrolizumab.
Data from the pembrolizumab trials suggested that risks outweigh benefits when PD-1/PD-L1 treatment is given to MM patients in combination with dexamethasone and pomalidomide or lenalidomide.
In addition, there could be an unfavorable risk-benefit ratio for MM patients receiving PD-1/PD-L1 treatments alone or in other combinations.
Therefore, the FDA placed a partial hold on the following nivolumab trials:
- CheckMate-602: A randomized, phase 3 trial of combinations of nivolumab, elotuzumab, pomalidomide, and dexamethasone in relapsed and refractory MM
- CheckMate-039: A phase 1 study intended to establish the tolerability of nivolumab and the combination of nivolumab and daratumumab, with or without pomalidomide and dexamethasone, in patients with relapsed or refractory MM
- CA204142: A phase 2 study of elotuzumab in combination with pomalidomide and low-dose dexamethasone, and in combination with nivolumab, in patients with MM who relapsed after or were refractory to prior treatment with lenalidomide.
After consulting with Bristol-Myers Squibb, the FDA decided to lift the hold on CheckMate-039 (CA209 -039) and CA204142. These trials will continue with amended protocols.
The third trial, CheckMate-602, remains on partial clinical hold. Bristol-Myers Squibb said it is continuing to work with the FDA to determine next steps for this trial.
CheckMate-602 is not enrolling new patients. However, patients who are experiencing clinical benefit are continuing to receive treatment. ![]()
Company launches digital PCR test for monitoring CML

Bio-Rad Laboratories, Inc., has launched the QXDx BCR-ABL %IS Kit, a digital polymerase chain reaction (PCR) test that can monitor molecular response to therapy in patients with chronic myeloid leukemia (CML).
The kit has a CE-IVD mark and is available for in vitro diagnostic use in Europe, Hong Kong, and New Zealand.
The QXDx BCR-ABL %IS Kit uses Bio-Rad’s Droplet Digital PCR (ddPCR) technology to provide an absolute measure of BCR-ABL transcripts.
The kit measures BCR-ABL1 and ABL1 chromosomal transcripts in total RNA from whole blood of t(9;22)-positive CML patients expressing BCR-ABL1 fusion transcripts type e13a2 and/or e14a2.
The QXDx BCR-ABL %IS Kit measures the e13a2 and/or e14a2 transcripts of BCR-ABL1, normalized to the ABL1 endogenous control. The kit does not differentiate between e13a2 and e14a2 transcripts and does not monitor other rare fusion transcripts resulting from t(9;22).
The kit’s results are reported as percent reduction from a baseline of 100% on the International Scale (%IS) and on a log molecular reduction (MR) scale.
The kit is able to detect deep molecular response values of MR 4.7 (%IS 0.002) or MR 5.0 (%IS 0.001) in 2- or 4-well formats. This exceeds the typical limitations of reverse transcription quantitative PCR-based tests that are reliable down to MR 4.5 (%IS 0.0032).
Bio-Rad says the QXDx BCR-ABL %IS Kit delivers absolute quantitation, which eliminates the need for standard curves and minimizes variation between samples. The kit also provides scalable throughput, allowing for testing of 8 to 48 samples per run.
The QXDx BCR-ABL %IS Kit can be used with Bio-Rad’s QX200 AutoDG ddPCR Dx System or with the QX200 ddPCR Dx System. The QXDx BCR-ABL %IS Kit uses QuantaSoft Software v1.7 for data acquisition and output. ![]()
Bio-Rad Laboratories, Inc., has launched the QXDx BCR-ABL %IS Kit, a digital polymerase chain reaction (PCR) test that can monitor molecular response to therapy in patients with chronic myeloid leukemia (CML).
The kit has a CE-IVD mark and is available for in vitro diagnostic use in Europe, Hong Kong, and New Zealand.
The QXDx BCR-ABL %IS Kit uses Bio-Rad’s Droplet Digital PCR (ddPCR) technology to provide an absolute measure of BCR-ABL transcripts.
The kit measures BCR-ABL1 and ABL1 chromosomal transcripts in total RNA from whole blood of t(9;22)-positive CML patients expressing BCR-ABL1 fusion transcripts type e13a2 and/or e14a2.
The QXDx BCR-ABL %IS Kit measures the e13a2 and/or e14a2 transcripts of BCR-ABL1, normalized to the ABL1 endogenous control. The kit does not differentiate between e13a2 and e14a2 transcripts and does not monitor other rare fusion transcripts resulting from t(9;22).
The kit’s results are reported as percent reduction from a baseline of 100% on the International Scale (%IS) and on a log molecular reduction (MR) scale.
The kit is able to detect deep molecular response values of MR 4.7 (%IS 0.002) or MR 5.0 (%IS 0.001) in 2- or 4-well formats. This exceeds the typical limitations of reverse transcription quantitative PCR-based tests that are reliable down to MR 4.5 (%IS 0.0032).
Bio-Rad says the QXDx BCR-ABL %IS Kit delivers absolute quantitation, which eliminates the need for standard curves and minimizes variation between samples. The kit also provides scalable throughput, allowing for testing of 8 to 48 samples per run.
The QXDx BCR-ABL %IS Kit can be used with Bio-Rad’s QX200 AutoDG ddPCR Dx System or with the QX200 ddPCR Dx System. The QXDx BCR-ABL %IS Kit uses QuantaSoft Software v1.7 for data acquisition and output. ![]()
Bio-Rad Laboratories, Inc., has launched the QXDx BCR-ABL %IS Kit, a digital polymerase chain reaction (PCR) test that can monitor molecular response to therapy in patients with chronic myeloid leukemia (CML).
The kit has a CE-IVD mark and is available for in vitro diagnostic use in Europe, Hong Kong, and New Zealand.
The QXDx BCR-ABL %IS Kit uses Bio-Rad’s Droplet Digital PCR (ddPCR) technology to provide an absolute measure of BCR-ABL transcripts.
The kit measures BCR-ABL1 and ABL1 chromosomal transcripts in total RNA from whole blood of t(9;22)-positive CML patients expressing BCR-ABL1 fusion transcripts type e13a2 and/or e14a2.
The QXDx BCR-ABL %IS Kit measures the e13a2 and/or e14a2 transcripts of BCR-ABL1, normalized to the ABL1 endogenous control. The kit does not differentiate between e13a2 and e14a2 transcripts and does not monitor other rare fusion transcripts resulting from t(9;22).
The kit’s results are reported as percent reduction from a baseline of 100% on the International Scale (%IS) and on a log molecular reduction (MR) scale.
The kit is able to detect deep molecular response values of MR 4.7 (%IS 0.002) or MR 5.0 (%IS 0.001) in 2- or 4-well formats. This exceeds the typical limitations of reverse transcription quantitative PCR-based tests that are reliable down to MR 4.5 (%IS 0.0032).
Bio-Rad says the QXDx BCR-ABL %IS Kit delivers absolute quantitation, which eliminates the need for standard curves and minimizes variation between samples. The kit also provides scalable throughput, allowing for testing of 8 to 48 samples per run.
The QXDx BCR-ABL %IS Kit can be used with Bio-Rad’s QX200 AutoDG ddPCR Dx System or with the QX200 ddPCR Dx System. The QXDx BCR-ABL %IS Kit uses QuantaSoft Software v1.7 for data acquisition and output. ![]()
Growths and darkened skin

Based on the dark velvety skin on the patient’s neck, the FP diagnosed acanthosis nigricans accompanied by multiple skin tags (acrochordons). The patient told the physician that he wanted to have the skin tags removed and the darkened skin treated. Because both conditions are associated with obesity and diabetes, the FP recommended that the patient increase his weight loss efforts through improved diet and increased exercise.
The FP also explained that treatment options for the skin tags included cryotherapy, snip excisions, and electrosurgery. The patient did not want to wait for the skin tags to fall off after cryotherapy or electrosurgery, so he chose snip excisions for immediate results. The skin tags were pedunculated with narrow stalks, so the snip excisions were performed without anesthesia. Aluminum chloride was applied to stop the bleeding on some of the skin tags. The patient noted some stinging, but tolerated the treatment well.
For the acanthosis nigricans, the FP explained that there are no highly effective treatments. In addition to recommending weight loss, the FP prescribed topical tretinoin cream 0.025% to be applied to the darkened skin before bed (only after the cuts from the skin tag removals had healed). The FP told the patient that the treatment might be only partially beneficial (or might not work at all). Other treatment options for acanthosis nigricans (with limited effectiveness) include keratolytic agents (eg, salicylic acid, ammonium lactate) and topical vitamin D analogs. At follow-up one month later, the patient had not yet noticed any changes to the acanthosis nigricans, but he was satisfied with the results of the skin tag removal.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Smith AM. Skin tags. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013: 922-925.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
Based on the dark velvety skin on the patient’s neck, the FP diagnosed acanthosis nigricans accompanied by multiple skin tags (acrochordons). The patient told the physician that he wanted to have the skin tags removed and the darkened skin treated. Because both conditions are associated with obesity and diabetes, the FP recommended that the patient increase his weight loss efforts through improved diet and increased exercise.
The FP also explained that treatment options for the skin tags included cryotherapy, snip excisions, and electrosurgery. The patient did not want to wait for the skin tags to fall off after cryotherapy or electrosurgery, so he chose snip excisions for immediate results. The skin tags were pedunculated with narrow stalks, so the snip excisions were performed without anesthesia. Aluminum chloride was applied to stop the bleeding on some of the skin tags. The patient noted some stinging, but tolerated the treatment well.
For the acanthosis nigricans, the FP explained that there are no highly effective treatments. In addition to recommending weight loss, the FP prescribed topical tretinoin cream 0.025% to be applied to the darkened skin before bed (only after the cuts from the skin tag removals had healed). The FP told the patient that the treatment might be only partially beneficial (or might not work at all). Other treatment options for acanthosis nigricans (with limited effectiveness) include keratolytic agents (eg, salicylic acid, ammonium lactate) and topical vitamin D analogs. At follow-up one month later, the patient had not yet noticed any changes to the acanthosis nigricans, but he was satisfied with the results of the skin tag removal.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Smith AM. Skin tags. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013: 922-925.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
Based on the dark velvety skin on the patient’s neck, the FP diagnosed acanthosis nigricans accompanied by multiple skin tags (acrochordons). The patient told the physician that he wanted to have the skin tags removed and the darkened skin treated. Because both conditions are associated with obesity and diabetes, the FP recommended that the patient increase his weight loss efforts through improved diet and increased exercise.
The FP also explained that treatment options for the skin tags included cryotherapy, snip excisions, and electrosurgery. The patient did not want to wait for the skin tags to fall off after cryotherapy or electrosurgery, so he chose snip excisions for immediate results. The skin tags were pedunculated with narrow stalks, so the snip excisions were performed without anesthesia. Aluminum chloride was applied to stop the bleeding on some of the skin tags. The patient noted some stinging, but tolerated the treatment well.
For the acanthosis nigricans, the FP explained that there are no highly effective treatments. In addition to recommending weight loss, the FP prescribed topical tretinoin cream 0.025% to be applied to the darkened skin before bed (only after the cuts from the skin tag removals had healed). The FP told the patient that the treatment might be only partially beneficial (or might not work at all). Other treatment options for acanthosis nigricans (with limited effectiveness) include keratolytic agents (eg, salicylic acid, ammonium lactate) and topical vitamin D analogs. At follow-up one month later, the patient had not yet noticed any changes to the acanthosis nigricans, but he was satisfied with the results of the skin tag removal.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Smith AM. Skin tags. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013: 922-925.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com

¿No hablás español? Help Is Here
According to the 2015 US Census Bureau, more than 60 million individuals—about 19% of Americans—reported speaking a language other than English at home, and more than 25 million reported their English-speaking ability as less than “very well.” The top five non-English languages spoken at home were Spanish, French, Chinese, Tagalog, and Vietnamese, encompassing 72% of non-English speakers. 1,2
In the health care sector, translator services are essential for providing accurate and culturally competent care. Current options for translator services include face-to-face interpreters, phone-based translator services, and translator apps on mobile devices. In settings where face-to-face interpreters or phone-based translator services are not available, translator apps may be a reasonable alternative.
THREE TYPES OF TRANSLATOR APPS
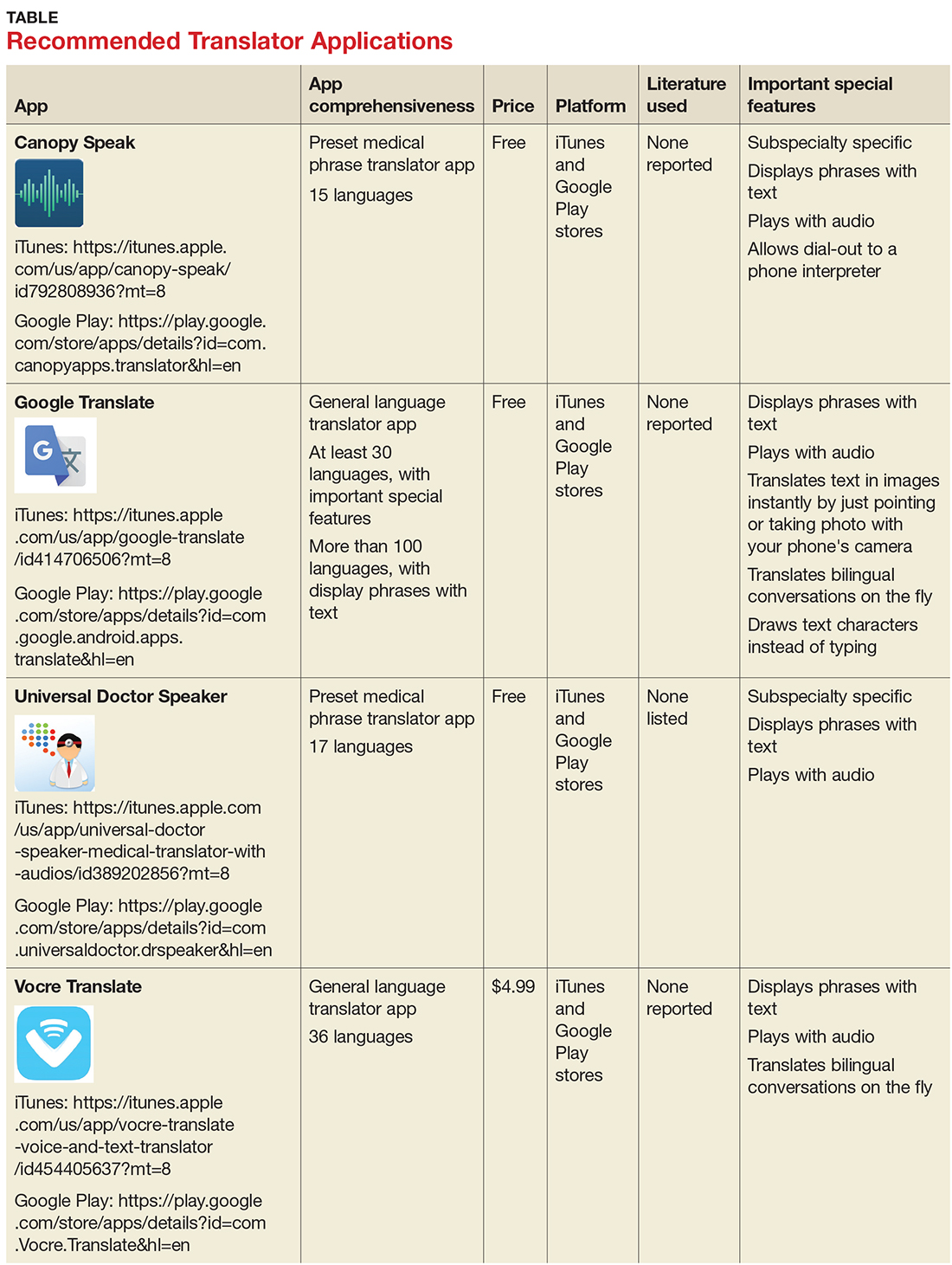
Preset medical phrase translator apps require the user to search for or find a question or statement in order to facilitate a conversation. With these types of apps, a health care provider can choose fully conjugated sentences, which then can be played or read back to the patient in the chosen translated language. Within this group of apps, Canopy Speak and Universal Doctor Speaker are highly accessible, since both apps are available from the Apple iTunes and Google Play stores and both are free.
Medical dictionary apps require the user to search for a medical term in one language to receive a translation in another language. These apps are less practical, but they can help providers find and define specific terms in a given language.
General language translator apps require the user to enter a term, statement, or question in one language and then provide a translation in another language. Google Translate and Vocre Translate are examples.
Recommended apps
My colleagues, Dr. Amrin Khander and Dr. Sara Farag, and I identified and evaluated medical translator apps that are available from the Apple iTunes and Google Play stores, to aid clinicians in using such apps during clinical encounters with non-English speakers.3
The top recommended translator apps are listed in the table, evaluated with criteria from a shortened version of the APPLICATIONS scoring system: app comprehensiveness, price, platform, literature use, and important special features.4 We hope these tools will help you enhance communication with your patients who have limited English proficiency.
1. United States Census Bureau. Detailed language spoken at home and ability to speak English for the population 5 years and over: 2009–2013. www.census.gov/data/tables/2013/demo/2009-2013-lang-tables.html. Accessed November 1, 2017.
2. United States Census Bureau. U.S. and world population clock. www.census.gov/popclock/?intcmp=home_pop. Accessed November 1, 2017.
3. Khander A, Farag S, Chen KT. Identification and rating of medical translator mobile applications using the APPLICATIONS scoring system [abstract 321]. Obstet Gynecol. 2017;129(5 suppl):101S.
4. Chyjek K, Farag S, Chen KT. Rating pregnancy wheel applications using the APPLICATIONS scoring system. Obstet Gynecol. 2015;125(6):1478-1483.
According to the 2015 US Census Bureau, more than 60 million individuals—about 19% of Americans—reported speaking a language other than English at home, and more than 25 million reported their English-speaking ability as less than “very well.” The top five non-English languages spoken at home were Spanish, French, Chinese, Tagalog, and Vietnamese, encompassing 72% of non-English speakers. 1,2
In the health care sector, translator services are essential for providing accurate and culturally competent care. Current options for translator services include face-to-face interpreters, phone-based translator services, and translator apps on mobile devices. In settings where face-to-face interpreters or phone-based translator services are not available, translator apps may be a reasonable alternative.
THREE TYPES OF TRANSLATOR APPS
Preset medical phrase translator apps require the user to search for or find a question or statement in order to facilitate a conversation. With these types of apps, a health care provider can choose fully conjugated sentences, which then can be played or read back to the patient in the chosen translated language. Within this group of apps, Canopy Speak and Universal Doctor Speaker are highly accessible, since both apps are available from the Apple iTunes and Google Play stores and both are free.
Medical dictionary apps require the user to search for a medical term in one language to receive a translation in another language. These apps are less practical, but they can help providers find and define specific terms in a given language.
General language translator apps require the user to enter a term, statement, or question in one language and then provide a translation in another language. Google Translate and Vocre Translate are examples.
Recommended apps
My colleagues, Dr. Amrin Khander and Dr. Sara Farag, and I identified and evaluated medical translator apps that are available from the Apple iTunes and Google Play stores, to aid clinicians in using such apps during clinical encounters with non-English speakers.3
The top recommended translator apps are listed in the table, evaluated with criteria from a shortened version of the APPLICATIONS scoring system: app comprehensiveness, price, platform, literature use, and important special features.4 We hope these tools will help you enhance communication with your patients who have limited English proficiency.
According to the 2015 US Census Bureau, more than 60 million individuals—about 19% of Americans—reported speaking a language other than English at home, and more than 25 million reported their English-speaking ability as less than “very well.” The top five non-English languages spoken at home were Spanish, French, Chinese, Tagalog, and Vietnamese, encompassing 72% of non-English speakers. 1,2
In the health care sector, translator services are essential for providing accurate and culturally competent care. Current options for translator services include face-to-face interpreters, phone-based translator services, and translator apps on mobile devices. In settings where face-to-face interpreters or phone-based translator services are not available, translator apps may be a reasonable alternative.
THREE TYPES OF TRANSLATOR APPS
Preset medical phrase translator apps require the user to search for or find a question or statement in order to facilitate a conversation. With these types of apps, a health care provider can choose fully conjugated sentences, which then can be played or read back to the patient in the chosen translated language. Within this group of apps, Canopy Speak and Universal Doctor Speaker are highly accessible, since both apps are available from the Apple iTunes and Google Play stores and both are free.
Medical dictionary apps require the user to search for a medical term in one language to receive a translation in another language. These apps are less practical, but they can help providers find and define specific terms in a given language.
General language translator apps require the user to enter a term, statement, or question in one language and then provide a translation in another language. Google Translate and Vocre Translate are examples.
Recommended apps
My colleagues, Dr. Amrin Khander and Dr. Sara Farag, and I identified and evaluated medical translator apps that are available from the Apple iTunes and Google Play stores, to aid clinicians in using such apps during clinical encounters with non-English speakers.3
The top recommended translator apps are listed in the table, evaluated with criteria from a shortened version of the APPLICATIONS scoring system: app comprehensiveness, price, platform, literature use, and important special features.4 We hope these tools will help you enhance communication with your patients who have limited English proficiency.
1. United States Census Bureau. Detailed language spoken at home and ability to speak English for the population 5 years and over: 2009–2013. www.census.gov/data/tables/2013/demo/2009-2013-lang-tables.html. Accessed November 1, 2017.
2. United States Census Bureau. U.S. and world population clock. www.census.gov/popclock/?intcmp=home_pop. Accessed November 1, 2017.
3. Khander A, Farag S, Chen KT. Identification and rating of medical translator mobile applications using the APPLICATIONS scoring system [abstract 321]. Obstet Gynecol. 2017;129(5 suppl):101S.
4. Chyjek K, Farag S, Chen KT. Rating pregnancy wheel applications using the APPLICATIONS scoring system. Obstet Gynecol. 2015;125(6):1478-1483.
1. United States Census Bureau. Detailed language spoken at home and ability to speak English for the population 5 years and over: 2009–2013. www.census.gov/data/tables/2013/demo/2009-2013-lang-tables.html. Accessed November 1, 2017.
2. United States Census Bureau. U.S. and world population clock. www.census.gov/popclock/?intcmp=home_pop. Accessed November 1, 2017.
3. Khander A, Farag S, Chen KT. Identification and rating of medical translator mobile applications using the APPLICATIONS scoring system [abstract 321]. Obstet Gynecol. 2017;129(5 suppl):101S.
4. Chyjek K, Farag S, Chen KT. Rating pregnancy wheel applications using the APPLICATIONS scoring system. Obstet Gynecol. 2015;125(6):1478-1483.
FDA recommends voluntary recall of Limbrel
The Food and Drug Administration announced on Dec. 4 that it recommends the voluntary recall of Limbrel, a medical food product in capsule form that is currently marketed to “manage the metabolic processes associated with osteoarthritis.”
![]()
The FDA’s ongoing investigation at this point considers the product to be an unapproved new drug rather than a medical food product. However, the agency does not have mandatory recall authority. It has recommended the recall to the product’s manufacturer, Primus Pharmaceuticals, on the basis of the risk of liver injury and hypersensitivity pneumonitis associated with continued use of the product.
The agency had received 194 adverse event reports as of Nov. 21, of which it found a likely association of the events with Limbrel in at least 30 cases, and continues to evaluate reports, which consumers can submit through MedWatch. The FDA is currently testing samples of the product and has advised consumers to cease taking it, though the manufacturer has declined thus far to recall it.
The safety alert advises that “health care providers who are aware that their patients are taking Limbrel should advise them to immediately stop taking the product.”
The Food and Drug Administration announced on Dec. 4 that it recommends the voluntary recall of Limbrel, a medical food product in capsule form that is currently marketed to “manage the metabolic processes associated with osteoarthritis.”
![]()
The FDA’s ongoing investigation at this point considers the product to be an unapproved new drug rather than a medical food product. However, the agency does not have mandatory recall authority. It has recommended the recall to the product’s manufacturer, Primus Pharmaceuticals, on the basis of the risk of liver injury and hypersensitivity pneumonitis associated with continued use of the product.
The agency had received 194 adverse event reports as of Nov. 21, of which it found a likely association of the events with Limbrel in at least 30 cases, and continues to evaluate reports, which consumers can submit through MedWatch. The FDA is currently testing samples of the product and has advised consumers to cease taking it, though the manufacturer has declined thus far to recall it.
The safety alert advises that “health care providers who are aware that their patients are taking Limbrel should advise them to immediately stop taking the product.”
The Food and Drug Administration announced on Dec. 4 that it recommends the voluntary recall of Limbrel, a medical food product in capsule form that is currently marketed to “manage the metabolic processes associated with osteoarthritis.”
![]()
The FDA’s ongoing investigation at this point considers the product to be an unapproved new drug rather than a medical food product. However, the agency does not have mandatory recall authority. It has recommended the recall to the product’s manufacturer, Primus Pharmaceuticals, on the basis of the risk of liver injury and hypersensitivity pneumonitis associated with continued use of the product.
The agency had received 194 adverse event reports as of Nov. 21, of which it found a likely association of the events with Limbrel in at least 30 cases, and continues to evaluate reports, which consumers can submit through MedWatch. The FDA is currently testing samples of the product and has advised consumers to cease taking it, though the manufacturer has declined thus far to recall it.
The safety alert advises that “health care providers who are aware that their patients are taking Limbrel should advise them to immediately stop taking the product.”
Newer hormonal contraception formulations linked to breast cancer risk*
The risk of developing breast cancer is about 20% higher among women who are current or recent users of hormonal contraceptives, compared with women who never used them, according to a prospective cohort study that included current contraception formulations.

Lina S. Mørch, PhD, of the University of Copenhagen, and colleagues conducted a nationwide, prospective cohort study of 1,797,932 women in Denmark who were aged 15-49 years between 1995 and 2012. The risk of developing breast cancer among all women currently using or who had recently used hormonal contraception correlated to a relative risk (RR) of 1.20 (95% confidence interval [CI], 1.14-1.26). The report was published in the New England Journal of Medicine.
The risk of breast cancer was heavily associated with the length of time during which the women had taken hormonal contraceptives. Women with less than a year of exposure had the lowest risk elevation (RR 1.09, 95% CI, 0.96-1.23), while women with more than 10 years of exposure faced the greatest increase in risk (RR 1.38, 95% CI, 1.26-1.51, P = .002).
The increased risk persisted even after women had stopped taking contraceptives. Researchers found that contraception use of less than a year (RR 1.01, 95% CI, 0.88-1.15), between 1 year and 5 years (RR 1.07, 95% CI, 0.94-1.20), and between 5 years and 10 years (RR 1.30, 95% CI, 1.06-1.58) correlated to increased risks of breast cancer 5-10 years after cessation of use. The number of events in women who had used hormonal contraceptive for more than 10 years was too small to accurately determine risks and was not reported in the study.
The combinations and formulations of oral contraceptives had little effect on breast cancer risk elevation, the researchers found. Triphasic and monophasic formulations containing levonorgestrel had similar relative risk levels of 1.21 (95% CI, 1.04-1.41) and 1.45 (95% CI, 1.26-1.67), respectively (P = .07). The relative risk was similar for intrauterine devices containing levonorgestrel (RR 1.21, 95% CI, 1.11-1.33).
The difference in risk between current and recent users of hormonal contraception and women who never took it was 13 (CI, 10-16) per 100,000 person-years, which translates into an one extra breast cancer diagnosis for every 7,690 women using hormonal contraception for 1 year.
“The estimated number of additional breast cancers that were associated with hormonal contraception did not include extra cases diagnosed after the discontinuation of long-term use. Even so, the estimated number of additional breast cancers among premenopausal women that were attributable to hormonal contraception is likely to be low,” the researchers wrote. “This risk should be weighed against important benefits of hormonal contraceptives such as good contraceptive efficacy and reduced risks of ovarian, endometrial, and perhaps colorectal cancer (at least for combined oral contraceptives that were commonly used in the 1970s and 1980s).
”Dr. Mørch and a coauthor received grant support from the Novo Nordisk Foundation and became employed by Novo Nordisk Foundation after the study was accepted for publication. No other relevant disclosures were reported.
Source: Mørch L. et al. N Engl J Med 2017;377(23):2228-39.
*12/7/2017: The headline for this story has been corrected to reflect an association between contraception and breast cancer risk.
The association between increased breast cancer risk and hormonal contraceptives is well documented but the research by Mørch et al. offers several factors for physicians to consider when prescribing hormonal contraceptives.
Mørch et al. found a 20% total increase in breast cancer in women but that finding is not consistent across age groups. As seen in the study, breast cancer risk was more than five times higher in women in their 40s than in women in their 30s, with an overall increase in breast cancer risk of 13 women per 100,000 women. The increased risk of breast cancer was much less pronounced in women under 35, at only 2 women per 100,000 women. For women in their 40s, hormonal contraceptives not only increase their cancer risk, but they can suffer uncommon adverse side effects such as myocardial infarction and stroke as well. Older women should consider using alternative methods of contraception, such as nonhormonal long-acting, reversible contraceptives.
But the breast cancer risk needs to be balanced against the benefits, including the association between oral contraceptives and substantial reductions in the risk of ovarian, endometrial, and colorectal cancers later in life.
Ultimately, the need for contraceptives that do not increase breast cancer risk is evident.
David J. Hunter , MBBS, ScD, is from the University of Oxford, England. He reported having no relevant financial disclosures. These comments are adapted from an editorial (N Engl J Med. 2017;377[23]:2276-7).
The association between increased breast cancer risk and hormonal contraceptives is well documented but the research by Mørch et al. offers several factors for physicians to consider when prescribing hormonal contraceptives.
Mørch et al. found a 20% total increase in breast cancer in women but that finding is not consistent across age groups. As seen in the study, breast cancer risk was more than five times higher in women in their 40s than in women in their 30s, with an overall increase in breast cancer risk of 13 women per 100,000 women. The increased risk of breast cancer was much less pronounced in women under 35, at only 2 women per 100,000 women. For women in their 40s, hormonal contraceptives not only increase their cancer risk, but they can suffer uncommon adverse side effects such as myocardial infarction and stroke as well. Older women should consider using alternative methods of contraception, such as nonhormonal long-acting, reversible contraceptives.
But the breast cancer risk needs to be balanced against the benefits, including the association between oral contraceptives and substantial reductions in the risk of ovarian, endometrial, and colorectal cancers later in life.
Ultimately, the need for contraceptives that do not increase breast cancer risk is evident.
David J. Hunter , MBBS, ScD, is from the University of Oxford, England. He reported having no relevant financial disclosures. These comments are adapted from an editorial (N Engl J Med. 2017;377[23]:2276-7).
The association between increased breast cancer risk and hormonal contraceptives is well documented but the research by Mørch et al. offers several factors for physicians to consider when prescribing hormonal contraceptives.
Mørch et al. found a 20% total increase in breast cancer in women but that finding is not consistent across age groups. As seen in the study, breast cancer risk was more than five times higher in women in their 40s than in women in their 30s, with an overall increase in breast cancer risk of 13 women per 100,000 women. The increased risk of breast cancer was much less pronounced in women under 35, at only 2 women per 100,000 women. For women in their 40s, hormonal contraceptives not only increase their cancer risk, but they can suffer uncommon adverse side effects such as myocardial infarction and stroke as well. Older women should consider using alternative methods of contraception, such as nonhormonal long-acting, reversible contraceptives.
But the breast cancer risk needs to be balanced against the benefits, including the association between oral contraceptives and substantial reductions in the risk of ovarian, endometrial, and colorectal cancers later in life.
Ultimately, the need for contraceptives that do not increase breast cancer risk is evident.
David J. Hunter , MBBS, ScD, is from the University of Oxford, England. He reported having no relevant financial disclosures. These comments are adapted from an editorial (N Engl J Med. 2017;377[23]:2276-7).
The risk of developing breast cancer is about 20% higher among women who are current or recent users of hormonal contraceptives, compared with women who never used them, according to a prospective cohort study that included current contraception formulations.
Lina S. Mørch, PhD, of the University of Copenhagen, and colleagues conducted a nationwide, prospective cohort study of 1,797,932 women in Denmark who were aged 15-49 years between 1995 and 2012. The risk of developing breast cancer among all women currently using or who had recently used hormonal contraception correlated to a relative risk (RR) of 1.20 (95% confidence interval [CI], 1.14-1.26). The report was published in the New England Journal of Medicine.
The risk of breast cancer was heavily associated with the length of time during which the women had taken hormonal contraceptives. Women with less than a year of exposure had the lowest risk elevation (RR 1.09, 95% CI, 0.96-1.23), while women with more than 10 years of exposure faced the greatest increase in risk (RR 1.38, 95% CI, 1.26-1.51, P = .002).
The increased risk persisted even after women had stopped taking contraceptives. Researchers found that contraception use of less than a year (RR 1.01, 95% CI, 0.88-1.15), between 1 year and 5 years (RR 1.07, 95% CI, 0.94-1.20), and between 5 years and 10 years (RR 1.30, 95% CI, 1.06-1.58) correlated to increased risks of breast cancer 5-10 years after cessation of use. The number of events in women who had used hormonal contraceptive for more than 10 years was too small to accurately determine risks and was not reported in the study.
The combinations and formulations of oral contraceptives had little effect on breast cancer risk elevation, the researchers found. Triphasic and monophasic formulations containing levonorgestrel had similar relative risk levels of 1.21 (95% CI, 1.04-1.41) and 1.45 (95% CI, 1.26-1.67), respectively (P = .07). The relative risk was similar for intrauterine devices containing levonorgestrel (RR 1.21, 95% CI, 1.11-1.33).
The difference in risk between current and recent users of hormonal contraception and women who never took it was 13 (CI, 10-16) per 100,000 person-years, which translates into an one extra breast cancer diagnosis for every 7,690 women using hormonal contraception for 1 year.
“The estimated number of additional breast cancers that were associated with hormonal contraception did not include extra cases diagnosed after the discontinuation of long-term use. Even so, the estimated number of additional breast cancers among premenopausal women that were attributable to hormonal contraception is likely to be low,” the researchers wrote. “This risk should be weighed against important benefits of hormonal contraceptives such as good contraceptive efficacy and reduced risks of ovarian, endometrial, and perhaps colorectal cancer (at least for combined oral contraceptives that were commonly used in the 1970s and 1980s).
”Dr. Mørch and a coauthor received grant support from the Novo Nordisk Foundation and became employed by Novo Nordisk Foundation after the study was accepted for publication. No other relevant disclosures were reported.
Source: Mørch L. et al. N Engl J Med 2017;377(23):2228-39.
*12/7/2017: The headline for this story has been corrected to reflect an association between contraception and breast cancer risk.
The risk of developing breast cancer is about 20% higher among women who are current or recent users of hormonal contraceptives, compared with women who never used them, according to a prospective cohort study that included current contraception formulations.
Lina S. Mørch, PhD, of the University of Copenhagen, and colleagues conducted a nationwide, prospective cohort study of 1,797,932 women in Denmark who were aged 15-49 years between 1995 and 2012. The risk of developing breast cancer among all women currently using or who had recently used hormonal contraception correlated to a relative risk (RR) of 1.20 (95% confidence interval [CI], 1.14-1.26). The report was published in the New England Journal of Medicine.
The risk of breast cancer was heavily associated with the length of time during which the women had taken hormonal contraceptives. Women with less than a year of exposure had the lowest risk elevation (RR 1.09, 95% CI, 0.96-1.23), while women with more than 10 years of exposure faced the greatest increase in risk (RR 1.38, 95% CI, 1.26-1.51, P = .002).
The increased risk persisted even after women had stopped taking contraceptives. Researchers found that contraception use of less than a year (RR 1.01, 95% CI, 0.88-1.15), between 1 year and 5 years (RR 1.07, 95% CI, 0.94-1.20), and between 5 years and 10 years (RR 1.30, 95% CI, 1.06-1.58) correlated to increased risks of breast cancer 5-10 years after cessation of use. The number of events in women who had used hormonal contraceptive for more than 10 years was too small to accurately determine risks and was not reported in the study.
The combinations and formulations of oral contraceptives had little effect on breast cancer risk elevation, the researchers found. Triphasic and monophasic formulations containing levonorgestrel had similar relative risk levels of 1.21 (95% CI, 1.04-1.41) and 1.45 (95% CI, 1.26-1.67), respectively (P = .07). The relative risk was similar for intrauterine devices containing levonorgestrel (RR 1.21, 95% CI, 1.11-1.33).
The difference in risk between current and recent users of hormonal contraception and women who never took it was 13 (CI, 10-16) per 100,000 person-years, which translates into an one extra breast cancer diagnosis for every 7,690 women using hormonal contraception for 1 year.
“The estimated number of additional breast cancers that were associated with hormonal contraception did not include extra cases diagnosed after the discontinuation of long-term use. Even so, the estimated number of additional breast cancers among premenopausal women that were attributable to hormonal contraception is likely to be low,” the researchers wrote. “This risk should be weighed against important benefits of hormonal contraceptives such as good contraceptive efficacy and reduced risks of ovarian, endometrial, and perhaps colorectal cancer (at least for combined oral contraceptives that were commonly used in the 1970s and 1980s).
”Dr. Mørch and a coauthor received grant support from the Novo Nordisk Foundation and became employed by Novo Nordisk Foundation after the study was accepted for publication. No other relevant disclosures were reported.
Source: Mørch L. et al. N Engl J Med 2017;377(23):2228-39.
*12/7/2017: The headline for this story has been corrected to reflect an association between contraception and breast cancer risk.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point:
Major finding: The relative risk of breast cancer was 1.20 for current and recent users of hormonal contraception, compared with women who never used hormonal contraception (95% CI 1.14-1.26).
Data source: Nationwide, prospective cohort study of 1,797,932 women in Denmark aged 15-49 years between 1995 and 2012.
Disclosures: Dr. Mørch and a coauthor received grant support from the Novo Nordisk Foundation and became employed by Novo Nordisk Foundation after the study was accepted for publication. No other relevant disclosures were reported.
Source: Mørch L et al. N Engl J Med 2017;377(23):2228-39.
Gene therapy found promising in patients with hemophilia B
, according to results of a recent phase 1-2a study including 10 men with hemophilia B.
The treatment, known as SPK-9001, prevented bleeding and virtually eliminated the need for exogenous factors, said authors of the study, published online Dec. 6 in the New England Journal of Medicine.
The 10 men enrolled in the study had factor IX coagulation activity 2% or less of normal value. Within a week of treatment with SPK-9001, patients exhibited vector-derived factor IX coagulant activity, according to Dr. George and her colleagues.
For all participants, the mean vector-derived factor IX coagulant activity was 33.7% of normal value, they noted in the report.
Moreover, the bleeding rate was significantly reduced over follow-up, which ranged from 28 to 78 weeks. Annualized bleeding rate was 11.1 events per year before treatment and 0.4 events per year afterward (P = .02), with 9 of 10 patients experiencing no bleeds over the follow-up period, they reported.
Factor use also dropped substantially, from a mean dose of 2,908 IU/kg before vector administration to 49.3 IU/kg afterward, the researchers said, noting that 8 of 10 patients used no factor at all.
No serious adverse events were observed during vector infusion or afterward, but the long-term safety of adeno-associated viral gene transfer will require further study, the researchers said. “However, to date, no genotoxic or gene-silencing events have been noted in human participants, including those who have been followed since the first [adeno-associated virus] trials were reported in 1998,” Dr. George and her colleagues wrote.
Spark Therapeutics and Pfizer funded the study. Dr. George reported support from Spark Therapeutics for the study, and personal fees from Pfizer outside the submitted work. Some of the authors are employees of Spark or had other financial relationships with Spark and/or Pfizer.
The positive results seen in this trial of the adeno-associated viral vector SPK-9001 represent “an important milestone for the community of patients with hemophilia B and their caregivers and advocates, who now are within touching distance of having an ideal cure for this terrible disease,” Matthew Porteus, MD, PhD, wrote in an editorial.
To reduce spontaneous bleed risk in patients with hemophilia, the current standard of care is transitioning from prophylactic intravenous infusions of clotting factor multiple times per week to longer-acting agents that can be given every 7-10 days.
However, an “ideal therapy” according to Dr. Porteus, would be one that can be delivered once with minimal toxicity and last a lifetime, and be affordable for patients anywhere in the world.
“Gene therapy in which a sufficient number of cells are modified by the delivery of a gene with prolonged or even permanent expression to produce the missing clotting factor has the potential to be such an ideal therapy for hemophilia,” he wrote.
The findings regarding SPK-9001 are “striking” but are limited due to short follow-up, he said, although investigators have started a longer-term study to better investigate safety and efficacy.
Future research on hemophilia gene therapy should focus on broadening the number of patients who could benefit from it, including children, patients with preexisting antibodies, and the 80% of hemophilia patients with hemophilia A, he added.
Dr. Porteus is with the department of pediatrics at Stanford (Calif.) University. These comments are derived from his editorial (N Engl J Med. 2017;377[23]2274-5). Dr. Porteus reported receiving personal fees from CRISPR Therapeutics outside of his submitted editorial.
The positive results seen in this trial of the adeno-associated viral vector SPK-9001 represent “an important milestone for the community of patients with hemophilia B and their caregivers and advocates, who now are within touching distance of having an ideal cure for this terrible disease,” Matthew Porteus, MD, PhD, wrote in an editorial.
To reduce spontaneous bleed risk in patients with hemophilia, the current standard of care is transitioning from prophylactic intravenous infusions of clotting factor multiple times per week to longer-acting agents that can be given every 7-10 days.
However, an “ideal therapy” according to Dr. Porteus, would be one that can be delivered once with minimal toxicity and last a lifetime, and be affordable for patients anywhere in the world.
“Gene therapy in which a sufficient number of cells are modified by the delivery of a gene with prolonged or even permanent expression to produce the missing clotting factor has the potential to be such an ideal therapy for hemophilia,” he wrote.
The findings regarding SPK-9001 are “striking” but are limited due to short follow-up, he said, although investigators have started a longer-term study to better investigate safety and efficacy.
Future research on hemophilia gene therapy should focus on broadening the number of patients who could benefit from it, including children, patients with preexisting antibodies, and the 80% of hemophilia patients with hemophilia A, he added.
Dr. Porteus is with the department of pediatrics at Stanford (Calif.) University. These comments are derived from his editorial (N Engl J Med. 2017;377[23]2274-5). Dr. Porteus reported receiving personal fees from CRISPR Therapeutics outside of his submitted editorial.
The positive results seen in this trial of the adeno-associated viral vector SPK-9001 represent “an important milestone for the community of patients with hemophilia B and their caregivers and advocates, who now are within touching distance of having an ideal cure for this terrible disease,” Matthew Porteus, MD, PhD, wrote in an editorial.
To reduce spontaneous bleed risk in patients with hemophilia, the current standard of care is transitioning from prophylactic intravenous infusions of clotting factor multiple times per week to longer-acting agents that can be given every 7-10 days.
However, an “ideal therapy” according to Dr. Porteus, would be one that can be delivered once with minimal toxicity and last a lifetime, and be affordable for patients anywhere in the world.
“Gene therapy in which a sufficient number of cells are modified by the delivery of a gene with prolonged or even permanent expression to produce the missing clotting factor has the potential to be such an ideal therapy for hemophilia,” he wrote.
The findings regarding SPK-9001 are “striking” but are limited due to short follow-up, he said, although investigators have started a longer-term study to better investigate safety and efficacy.
Future research on hemophilia gene therapy should focus on broadening the number of patients who could benefit from it, including children, patients with preexisting antibodies, and the 80% of hemophilia patients with hemophilia A, he added.
Dr. Porteus is with the department of pediatrics at Stanford (Calif.) University. These comments are derived from his editorial (N Engl J Med. 2017;377[23]2274-5). Dr. Porteus reported receiving personal fees from CRISPR Therapeutics outside of his submitted editorial.
, according to results of a recent phase 1-2a study including 10 men with hemophilia B.
The treatment, known as SPK-9001, prevented bleeding and virtually eliminated the need for exogenous factors, said authors of the study, published online Dec. 6 in the New England Journal of Medicine.
The 10 men enrolled in the study had factor IX coagulation activity 2% or less of normal value. Within a week of treatment with SPK-9001, patients exhibited vector-derived factor IX coagulant activity, according to Dr. George and her colleagues.
For all participants, the mean vector-derived factor IX coagulant activity was 33.7% of normal value, they noted in the report.
Moreover, the bleeding rate was significantly reduced over follow-up, which ranged from 28 to 78 weeks. Annualized bleeding rate was 11.1 events per year before treatment and 0.4 events per year afterward (P = .02), with 9 of 10 patients experiencing no bleeds over the follow-up period, they reported.
Factor use also dropped substantially, from a mean dose of 2,908 IU/kg before vector administration to 49.3 IU/kg afterward, the researchers said, noting that 8 of 10 patients used no factor at all.
No serious adverse events were observed during vector infusion or afterward, but the long-term safety of adeno-associated viral gene transfer will require further study, the researchers said. “However, to date, no genotoxic or gene-silencing events have been noted in human participants, including those who have been followed since the first [adeno-associated virus] trials were reported in 1998,” Dr. George and her colleagues wrote.
Spark Therapeutics and Pfizer funded the study. Dr. George reported support from Spark Therapeutics for the study, and personal fees from Pfizer outside the submitted work. Some of the authors are employees of Spark or had other financial relationships with Spark and/or Pfizer.
, according to results of a recent phase 1-2a study including 10 men with hemophilia B.
The treatment, known as SPK-9001, prevented bleeding and virtually eliminated the need for exogenous factors, said authors of the study, published online Dec. 6 in the New England Journal of Medicine.
The 10 men enrolled in the study had factor IX coagulation activity 2% or less of normal value. Within a week of treatment with SPK-9001, patients exhibited vector-derived factor IX coagulant activity, according to Dr. George and her colleagues.
For all participants, the mean vector-derived factor IX coagulant activity was 33.7% of normal value, they noted in the report.
Moreover, the bleeding rate was significantly reduced over follow-up, which ranged from 28 to 78 weeks. Annualized bleeding rate was 11.1 events per year before treatment and 0.4 events per year afterward (P = .02), with 9 of 10 patients experiencing no bleeds over the follow-up period, they reported.
Factor use also dropped substantially, from a mean dose of 2,908 IU/kg before vector administration to 49.3 IU/kg afterward, the researchers said, noting that 8 of 10 patients used no factor at all.
No serious adverse events were observed during vector infusion or afterward, but the long-term safety of adeno-associated viral gene transfer will require further study, the researchers said. “However, to date, no genotoxic or gene-silencing events have been noted in human participants, including those who have been followed since the first [adeno-associated virus] trials were reported in 1998,” Dr. George and her colleagues wrote.
Spark Therapeutics and Pfizer funded the study. Dr. George reported support from Spark Therapeutics for the study, and personal fees from Pfizer outside the submitted work. Some of the authors are employees of Spark or had other financial relationships with Spark and/or Pfizer.
FROM NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: A single intravenous dose of the adeno-associated viral vector SPK-9001 produced sustained expression of factor IX coagulant activity, virtually eliminating bleeding and use of clotting factors in patients with hemophilia B.
Major finding: A mean functional clotting-factor activity of 33.7% of the normal value (median, 29.8% of the normal value) was achieved among study participants.
Data source: An open-label, nonrandomized, multicenter phase 1-2a study including 10 men with hemophilia B and factor IX coagulant activity 2% or less of normal value.
Disclosures: Spark Therapeutics and Pfizer funded the study. Lead author Lindsey A. George, MD, reported support from Spark Therapeutics for the study, and personal fees from Pfizer outside the submitted work. Full author disclosures were published on the New England Journal of Medicine website.
Pharmacomechanical thrombolysis does not reduce post-thrombotic syndrome risk
In patients with acute proximal deep vein thrombosis who were undergoing anticoagulation, adding pharmacomechanical catheter-directed thrombolysis did not reduce risk of the post-thrombotic syndrome, according to results of a phase 3, randomized, controlled trial.
Moreover, addition of pharmacomechanical thrombolysis increased risk of major bleeding risk, investigators wrote in a report published online Dec. 6 in the New England Journal of Medicine.
“Our trial, for uncertain reasons, did not confirm these findings,” wrote Suresh Vedantham, MD of Washington University, St. Louis, and his coauthors.
Post-thrombotic syndrome is associated with chronic limb swelling and pain, and can lead to leg ulcers, impaired quality of life, and major disability. About half of patients with proximal deep vein thrombosis (DVT) will develop the post-thrombotic syndrome within 2 years, despite use of anticoagulation therapy, Dr. Vedantham and his colleagues noted.
Pharmacomechanical thrombosis is the catheter-directed delivery of a fibrinolytic agent into the thrombus, along with aspiration or maceration of the thrombus. The goal of the treatment is to reduce the burden of thrombus, which in turn might reduce risk of the post-thrombotic syndrome.
However, in their randomized trial known as ATTRACT, which included 692 patients with an acute proximal DVT, rates of post-thrombotic syndrome between 6 to 24 months after intervention were 47% in the pharmacomechanical thrombolysis group and 48% in the control group (risk ratio, 0.96; 95% CI, 0.82-1.11; P = .56), according to the report (N Engl J Med. 2017;377:2240-52). Control group patients received no procedural intervention.
Major bleeds within 10 days of the intervention were 1.7% and 0.3% for the pharmacomechanical thrombolysis and control groups, respectively (P = .049).
By contrast, in the CAVENT trial, catheter-directed thrombolysis reduced the risk of the post-thrombotic syndrome over 5 years of follow-up (Lancet Haematol. 2016;3[2]:e64-71). Dr. Vedantham and his coauthors suggested that factors potentially explaining the difference in outcomes include the number of patients enrolled (692 in ATTRACT, versus 209 in CAVENT), or the greater use of mechanical therapies in ATTRACT versus longer recombinant tissue plasminogen activator infusions in CAVENT.
The study was supported by multiple sources, including the National Heart, Lung and Blood Institute (NHLBI), Boston Scientific, Covidien (now Medtronic), Genentech, and others. Dr. Vedantham reported receiving grant support from Cook Medical and Volcano. Some of the other authors reported financial ties to Abbott Vascular, Boston Scientific, Medtronic, and other pharmaceutical and device companies.
In patients with acute proximal deep vein thrombosis who were undergoing anticoagulation, adding pharmacomechanical catheter-directed thrombolysis did not reduce risk of the post-thrombotic syndrome, according to results of a phase 3, randomized, controlled trial.
Moreover, addition of pharmacomechanical thrombolysis increased risk of major bleeding risk, investigators wrote in a report published online Dec. 6 in the New England Journal of Medicine.
“Our trial, for uncertain reasons, did not confirm these findings,” wrote Suresh Vedantham, MD of Washington University, St. Louis, and his coauthors.
Post-thrombotic syndrome is associated with chronic limb swelling and pain, and can lead to leg ulcers, impaired quality of life, and major disability. About half of patients with proximal deep vein thrombosis (DVT) will develop the post-thrombotic syndrome within 2 years, despite use of anticoagulation therapy, Dr. Vedantham and his colleagues noted.
Pharmacomechanical thrombosis is the catheter-directed delivery of a fibrinolytic agent into the thrombus, along with aspiration or maceration of the thrombus. The goal of the treatment is to reduce the burden of thrombus, which in turn might reduce risk of the post-thrombotic syndrome.
However, in their randomized trial known as ATTRACT, which included 692 patients with an acute proximal DVT, rates of post-thrombotic syndrome between 6 to 24 months after intervention were 47% in the pharmacomechanical thrombolysis group and 48% in the control group (risk ratio, 0.96; 95% CI, 0.82-1.11; P = .56), according to the report (N Engl J Med. 2017;377:2240-52). Control group patients received no procedural intervention.
Major bleeds within 10 days of the intervention were 1.7% and 0.3% for the pharmacomechanical thrombolysis and control groups, respectively (P = .049).
By contrast, in the CAVENT trial, catheter-directed thrombolysis reduced the risk of the post-thrombotic syndrome over 5 years of follow-up (Lancet Haematol. 2016;3[2]:e64-71). Dr. Vedantham and his coauthors suggested that factors potentially explaining the difference in outcomes include the number of patients enrolled (692 in ATTRACT, versus 209 in CAVENT), or the greater use of mechanical therapies in ATTRACT versus longer recombinant tissue plasminogen activator infusions in CAVENT.
The study was supported by multiple sources, including the National Heart, Lung and Blood Institute (NHLBI), Boston Scientific, Covidien (now Medtronic), Genentech, and others. Dr. Vedantham reported receiving grant support from Cook Medical and Volcano. Some of the other authors reported financial ties to Abbott Vascular, Boston Scientific, Medtronic, and other pharmaceutical and device companies.
In patients with acute proximal deep vein thrombosis who were undergoing anticoagulation, adding pharmacomechanical catheter-directed thrombolysis did not reduce risk of the post-thrombotic syndrome, according to results of a phase 3, randomized, controlled trial.
Moreover, addition of pharmacomechanical thrombolysis increased risk of major bleeding risk, investigators wrote in a report published online Dec. 6 in the New England Journal of Medicine.
“Our trial, for uncertain reasons, did not confirm these findings,” wrote Suresh Vedantham, MD of Washington University, St. Louis, and his coauthors.
Post-thrombotic syndrome is associated with chronic limb swelling and pain, and can lead to leg ulcers, impaired quality of life, and major disability. About half of patients with proximal deep vein thrombosis (DVT) will develop the post-thrombotic syndrome within 2 years, despite use of anticoagulation therapy, Dr. Vedantham and his colleagues noted.
Pharmacomechanical thrombosis is the catheter-directed delivery of a fibrinolytic agent into the thrombus, along with aspiration or maceration of the thrombus. The goal of the treatment is to reduce the burden of thrombus, which in turn might reduce risk of the post-thrombotic syndrome.
However, in their randomized trial known as ATTRACT, which included 692 patients with an acute proximal DVT, rates of post-thrombotic syndrome between 6 to 24 months after intervention were 47% in the pharmacomechanical thrombolysis group and 48% in the control group (risk ratio, 0.96; 95% CI, 0.82-1.11; P = .56), according to the report (N Engl J Med. 2017;377:2240-52). Control group patients received no procedural intervention.
Major bleeds within 10 days of the intervention were 1.7% and 0.3% for the pharmacomechanical thrombolysis and control groups, respectively (P = .049).
By contrast, in the CAVENT trial, catheter-directed thrombolysis reduced the risk of the post-thrombotic syndrome over 5 years of follow-up (Lancet Haematol. 2016;3[2]:e64-71). Dr. Vedantham and his coauthors suggested that factors potentially explaining the difference in outcomes include the number of patients enrolled (692 in ATTRACT, versus 209 in CAVENT), or the greater use of mechanical therapies in ATTRACT versus longer recombinant tissue plasminogen activator infusions in CAVENT.
The study was supported by multiple sources, including the National Heart, Lung and Blood Institute (NHLBI), Boston Scientific, Covidien (now Medtronic), Genentech, and others. Dr. Vedantham reported receiving grant support from Cook Medical and Volcano. Some of the other authors reported financial ties to Abbott Vascular, Boston Scientific, Medtronic, and other pharmaceutical and device companies.
FROM NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point:
Major finding: Rates of post-thrombotic syndrome were 47% in the pharmacomechanical thrombolysis group, and 48% in the control group (risk ratio, 0.96; 95% CI, 0.82-1.11; P = .56).
Data source: A phase 3, multicenter, randomized, open-label, assessor-blinded, controlled clinical trial, including 692 patients with acute proximal deep vein thrombosis.
Disclosures: The study was supported by multiple sources, including the National Heart, Lung and Blood Institute (NHLBI), Boston Scientific, Covidien (now Medtronic), Genentech, and others. First author Suresh Vedantham, MD, reported receiving grant support from Cook Medical and Volcano. Some of the other authors reported financial ties to Abbott Vascular, Boston Scientific, Medtronic, and other pharmaceutical and device companies.