User login
ASCO platelet transfusion guidelines updated
A lot has happened in oncology since the American Society of Clinical Oncology (ASCO) first issued its guidelines on platelet transfusion for patients with cancer in 2001, noted the authors of the updated recommendations.
“The expense of platelet transfusions, coupled with potential adverse effects such as febrile and allergic reactions, transfusion-related acute lung injury, and bacterial contamination point to the importance of evidence-based transfusion practice,” wrote Charles A Schiffer, MD, of Wayne State Michigan, Detroit, and his colleagues in the updated guidelines.
Many of the original recommendations remain unchanged, but there are updated evidence-based recommendations in five key areas.
For example, regarding platelet transfusion thresholds in the setting of hematologic stem-cell transplantation in adults, the guidelines incorporate evidence from randomized clinical trials showing that among adults who have received autologous hematologic stem-cell transplantation, bleeding rates with decreased use of platelets are similar whether patients are treated prophylactically or at the first sign of bleeding, “and this approach may be used in experienced centers,” wrote Dr. Schiffer and his colleagues (J Clin Oncol. 2017 Nov 28. doi: 10.1200/JCO.2017.76.1734).
The authors caution, however, that the recommendation applies to adults only.
Other updated recommendations include:
• Rhesus D alloimmunization from platelet transfusions to RhD-negative patients can be prevented through either exclusive use of platelet products from RhD-negative donors or immunoprophylaxis. The guidelines note that there is a low rate of RhD alloimmunization in cancer patients in general, but state that prevention may be used in girls and in women of child-bearing age who are being treated with curative intent.
• For patients with acute myeloid leukemia, receiving induction chemotherapy, the use of leukoreduced platelet and red blood cell products can reduce the likelihood that patients will develop alloantibody-mediated refractory reactions to plate transfusions.
“It is therefore appropriate to provide leukoreduced blood products to patients with [acute myeloid leukemia] from the time of diagnosis to ameliorate this important clinical problem,” the investigators wrote.
They noted that leukoreduction to prevent alloimmunization might benefit patients with other leukemia histologies and with other types of cancer who are undergoing chemotherapy, but added that there is a lack of evidence to support this as a recommendation outside of acute myeloid leukemia.
To reduce the risk of bleeding due to thrombocytopenia in patients with solid tumors who are undergoing chemotherapy, the panelists recommend transfusing patients when their platelet levels fall below 10 x 109 per liter. It is appropriate to give platelet transfusions to patients with higher levels when there is active localized bleeding, they stated.
The guideline authors also recommend that when refractoriness to platelet infusions is suspected, clinicians should perform platelet counts from 10 to 60 minutes after the transfusion is completed. A refractoriness determination should be made only after two or more infusions of ABO-compatible units that have been stored for less than 72 hours result in poor increments, they advised.
The guideline development process is supported by ASCO. Dr. Schiffer and six other guideline authors disclosed consulting or advisory roles, research funding, honoraria and/or fees with various pharmaceutical companies or other corporate entities.
A lot has happened in oncology since the American Society of Clinical Oncology (ASCO) first issued its guidelines on platelet transfusion for patients with cancer in 2001, noted the authors of the updated recommendations.
“The expense of platelet transfusions, coupled with potential adverse effects such as febrile and allergic reactions, transfusion-related acute lung injury, and bacterial contamination point to the importance of evidence-based transfusion practice,” wrote Charles A Schiffer, MD, of Wayne State Michigan, Detroit, and his colleagues in the updated guidelines.
Many of the original recommendations remain unchanged, but there are updated evidence-based recommendations in five key areas.
For example, regarding platelet transfusion thresholds in the setting of hematologic stem-cell transplantation in adults, the guidelines incorporate evidence from randomized clinical trials showing that among adults who have received autologous hematologic stem-cell transplantation, bleeding rates with decreased use of platelets are similar whether patients are treated prophylactically or at the first sign of bleeding, “and this approach may be used in experienced centers,” wrote Dr. Schiffer and his colleagues (J Clin Oncol. 2017 Nov 28. doi: 10.1200/JCO.2017.76.1734).
The authors caution, however, that the recommendation applies to adults only.
Other updated recommendations include:
• Rhesus D alloimmunization from platelet transfusions to RhD-negative patients can be prevented through either exclusive use of platelet products from RhD-negative donors or immunoprophylaxis. The guidelines note that there is a low rate of RhD alloimmunization in cancer patients in general, but state that prevention may be used in girls and in women of child-bearing age who are being treated with curative intent.
• For patients with acute myeloid leukemia, receiving induction chemotherapy, the use of leukoreduced platelet and red blood cell products can reduce the likelihood that patients will develop alloantibody-mediated refractory reactions to plate transfusions.
“It is therefore appropriate to provide leukoreduced blood products to patients with [acute myeloid leukemia] from the time of diagnosis to ameliorate this important clinical problem,” the investigators wrote.
They noted that leukoreduction to prevent alloimmunization might benefit patients with other leukemia histologies and with other types of cancer who are undergoing chemotherapy, but added that there is a lack of evidence to support this as a recommendation outside of acute myeloid leukemia.
To reduce the risk of bleeding due to thrombocytopenia in patients with solid tumors who are undergoing chemotherapy, the panelists recommend transfusing patients when their platelet levels fall below 10 x 109 per liter. It is appropriate to give platelet transfusions to patients with higher levels when there is active localized bleeding, they stated.
The guideline authors also recommend that when refractoriness to platelet infusions is suspected, clinicians should perform platelet counts from 10 to 60 minutes after the transfusion is completed. A refractoriness determination should be made only after two or more infusions of ABO-compatible units that have been stored for less than 72 hours result in poor increments, they advised.
The guideline development process is supported by ASCO. Dr. Schiffer and six other guideline authors disclosed consulting or advisory roles, research funding, honoraria and/or fees with various pharmaceutical companies or other corporate entities.
A lot has happened in oncology since the American Society of Clinical Oncology (ASCO) first issued its guidelines on platelet transfusion for patients with cancer in 2001, noted the authors of the updated recommendations.
“The expense of platelet transfusions, coupled with potential adverse effects such as febrile and allergic reactions, transfusion-related acute lung injury, and bacterial contamination point to the importance of evidence-based transfusion practice,” wrote Charles A Schiffer, MD, of Wayne State Michigan, Detroit, and his colleagues in the updated guidelines.
Many of the original recommendations remain unchanged, but there are updated evidence-based recommendations in five key areas.
For example, regarding platelet transfusion thresholds in the setting of hematologic stem-cell transplantation in adults, the guidelines incorporate evidence from randomized clinical trials showing that among adults who have received autologous hematologic stem-cell transplantation, bleeding rates with decreased use of platelets are similar whether patients are treated prophylactically or at the first sign of bleeding, “and this approach may be used in experienced centers,” wrote Dr. Schiffer and his colleagues (J Clin Oncol. 2017 Nov 28. doi: 10.1200/JCO.2017.76.1734).
The authors caution, however, that the recommendation applies to adults only.
Other updated recommendations include:
• Rhesus D alloimmunization from platelet transfusions to RhD-negative patients can be prevented through either exclusive use of platelet products from RhD-negative donors or immunoprophylaxis. The guidelines note that there is a low rate of RhD alloimmunization in cancer patients in general, but state that prevention may be used in girls and in women of child-bearing age who are being treated with curative intent.
• For patients with acute myeloid leukemia, receiving induction chemotherapy, the use of leukoreduced platelet and red blood cell products can reduce the likelihood that patients will develop alloantibody-mediated refractory reactions to plate transfusions.
“It is therefore appropriate to provide leukoreduced blood products to patients with [acute myeloid leukemia] from the time of diagnosis to ameliorate this important clinical problem,” the investigators wrote.
They noted that leukoreduction to prevent alloimmunization might benefit patients with other leukemia histologies and with other types of cancer who are undergoing chemotherapy, but added that there is a lack of evidence to support this as a recommendation outside of acute myeloid leukemia.
To reduce the risk of bleeding due to thrombocytopenia in patients with solid tumors who are undergoing chemotherapy, the panelists recommend transfusing patients when their platelet levels fall below 10 x 109 per liter. It is appropriate to give platelet transfusions to patients with higher levels when there is active localized bleeding, they stated.
The guideline authors also recommend that when refractoriness to platelet infusions is suspected, clinicians should perform platelet counts from 10 to 60 minutes after the transfusion is completed. A refractoriness determination should be made only after two or more infusions of ABO-compatible units that have been stored for less than 72 hours result in poor increments, they advised.
The guideline development process is supported by ASCO. Dr. Schiffer and six other guideline authors disclosed consulting or advisory roles, research funding, honoraria and/or fees with various pharmaceutical companies or other corporate entities.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Myth of the Month: MONA for acute treatment of chest pain?
A 66-year-old man presents with substernal chest pressure and dyspnea that has been present for 45 minutes. He has nausea. Vital signs: blood pressure, 110/60; pulse, 100; oxygen saturation, 92%. Neck: elevated jugular venous pressure. Chest: clear. Cardiac: normal S1 S2, no murmurs. ECG: ST elevation in 2, 3, and aVF leads.
Which of these treatments do you recommend?
A. Morphine, oxygen, nitroglycerin, and aspirin (ASA).
B. Oxygen, morphine, ASA.
C. ASA.
In this patient, I think the correct approach would be to just give aspirin. Nitroglycerin would be problematic, as it appears that this patient might be having a right ventricular infarct, and lowering right-sided filling pressures with nitroglycerin may lead to severe hypotension.
There is controversy over the safety of routine morphine use for patients with chest pain.
Trip J. Meine, MD, and colleagues found that use of morphine either alone or in combination with nitroglycerin for patients presenting with non–ST-elevation acute coronary syndrome (NSTE-ACS) was associated with higher mortality.1 Cian P. McCarthy, MD, and colleagues found the same results, with morphine use associated with larger infarct size, a longer hospital stay, and a trend toward increased mortality in invasively managed NSTE-ACS patients.2 Suzanne de Waha and colleagues found that morphine use in patients with ST-segment elevation MIs had larger infarct size and less reperfusion success, as measured by cardiac MRI.3
Not all recent studies show a detrimental effect of morphine. Etienne Puymirat et al. reviewed in-hospital complications (death, nonfatal re-MI, stroke, stent thrombosis, and bleeding) and 1-year survival according to prehospital morphine use in 2,438 ST-elevation MI (STEMI) patients from the French Registry of Acute ST-elevation and non–ST-elevation Myocardial Infarction (FAST-MI).4 They found no increase in in-hospital complications or 1-year mortality.
The practice of using supplemental oxygen to treat all patients with MI became standard nearly a century ago, after oxygen was found in 1900 to relieve angina, and led to clinical improvement in four MI patients in a 1930 case series.5,6
It was not studied in a controlled trial until 1976, when J.M. Rawles, MD, and colleagues randomized 157 patients with MI to 24 hours of oxygen at 8 L/min or to ambient air. They found no difference in mortality between the groups, but they did find a higher burden of MI in the intervention arm receiving supplemental oxygen, as measured by mean serum aspartate aminotransferase levels.7
The topic was not addressed again in a significant randomized trial until this century. Most notably, two recent studies again demonstrated no benefit of supplemental oxygen in normoxemic patients with MI.
In the AVOID trial in 2015, Dion Stub, MD, PhD, and colleagues randomized 441 patients with STEMI to oxygen at 8 L/min – from diagnosis in an ambulance until after cardiac catheterization – or to ambient air. They found no difference in death at 6 months, but did find an increased rate of in-hospital recurrent MIs, with 0.9% of the control group and 5.5% of the oxygen intervention arm suffering recurrence (P = .006).8 They also showed a larger area of myocardial infarct in the oxygen group, as measured by peak creatine kinase levels and cardiac MRI at 6 months.
Proposed mechanisms of increased myocardial injury from hyperoxia include increased coronary vascular resistance resulting in decreased myocardial perfusion, and increased reperfusion injury from formation of free radicals.9

Where does all this leave us in the treatment of suspected MI?
Morphine should only be used when the patient has pain, and is probably best reserved for severe pain, as the safety of its use is not clear. While hypoxemia is a common consequence of MI – and may correlate with worse outcomes – treatment with supplemental oxygen in the absence of hypoxemia is not supported by current evidence, and may carry risk of harm. Nitroglycerin should be avoided in patients with right ventricular infarcts, and in patients who present with hypotension.
Dr. Tubbesing is a senior resident in medicine at the University of Washington, Seattle. Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at [email protected].
References
1. Am Heart J. 2005 Jun;149(6):1043-9.
2. J Interv Cardiol. 2017 Nov 22. doi: 10.1111/joic.12464.
3. Clin Res Cardiol. 2015 Sep;104(9):727-34.
4. Eur Heart J. 2016 Apr 1;37(13):1063-71.
5. BMJ. 1900 Dec 1;2(2083):1568.
6. JAMA. 1930 May 3;94(18):1363-5.
7. Br Med J. 1976 May 8;1(6018):1121-3.
8. Circulation. 2015 Jun 16;131(24):2143-50.
9. Cochrane Database Syst Rev. 2016 Dec 19;12:CD007160.
10. N Engl J Med. 2017 Sep 28;377(13):1240-9.
A 66-year-old man presents with substernal chest pressure and dyspnea that has been present for 45 minutes. He has nausea. Vital signs: blood pressure, 110/60; pulse, 100; oxygen saturation, 92%. Neck: elevated jugular venous pressure. Chest: clear. Cardiac: normal S1 S2, no murmurs. ECG: ST elevation in 2, 3, and aVF leads.
Which of these treatments do you recommend?
A. Morphine, oxygen, nitroglycerin, and aspirin (ASA).
B. Oxygen, morphine, ASA.
C. ASA.
In this patient, I think the correct approach would be to just give aspirin. Nitroglycerin would be problematic, as it appears that this patient might be having a right ventricular infarct, and lowering right-sided filling pressures with nitroglycerin may lead to severe hypotension.
There is controversy over the safety of routine morphine use for patients with chest pain.
Trip J. Meine, MD, and colleagues found that use of morphine either alone or in combination with nitroglycerin for patients presenting with non–ST-elevation acute coronary syndrome (NSTE-ACS) was associated with higher mortality.1 Cian P. McCarthy, MD, and colleagues found the same results, with morphine use associated with larger infarct size, a longer hospital stay, and a trend toward increased mortality in invasively managed NSTE-ACS patients.2 Suzanne de Waha and colleagues found that morphine use in patients with ST-segment elevation MIs had larger infarct size and less reperfusion success, as measured by cardiac MRI.3
Not all recent studies show a detrimental effect of morphine. Etienne Puymirat et al. reviewed in-hospital complications (death, nonfatal re-MI, stroke, stent thrombosis, and bleeding) and 1-year survival according to prehospital morphine use in 2,438 ST-elevation MI (STEMI) patients from the French Registry of Acute ST-elevation and non–ST-elevation Myocardial Infarction (FAST-MI).4 They found no increase in in-hospital complications or 1-year mortality.
The practice of using supplemental oxygen to treat all patients with MI became standard nearly a century ago, after oxygen was found in 1900 to relieve angina, and led to clinical improvement in four MI patients in a 1930 case series.5,6
It was not studied in a controlled trial until 1976, when J.M. Rawles, MD, and colleagues randomized 157 patients with MI to 24 hours of oxygen at 8 L/min or to ambient air. They found no difference in mortality between the groups, but they did find a higher burden of MI in the intervention arm receiving supplemental oxygen, as measured by mean serum aspartate aminotransferase levels.7
The topic was not addressed again in a significant randomized trial until this century. Most notably, two recent studies again demonstrated no benefit of supplemental oxygen in normoxemic patients with MI.
In the AVOID trial in 2015, Dion Stub, MD, PhD, and colleagues randomized 441 patients with STEMI to oxygen at 8 L/min – from diagnosis in an ambulance until after cardiac catheterization – or to ambient air. They found no difference in death at 6 months, but did find an increased rate of in-hospital recurrent MIs, with 0.9% of the control group and 5.5% of the oxygen intervention arm suffering recurrence (P = .006).8 They also showed a larger area of myocardial infarct in the oxygen group, as measured by peak creatine kinase levels and cardiac MRI at 6 months.
Proposed mechanisms of increased myocardial injury from hyperoxia include increased coronary vascular resistance resulting in decreased myocardial perfusion, and increased reperfusion injury from formation of free radicals.9
Where does all this leave us in the treatment of suspected MI?
Morphine should only be used when the patient has pain, and is probably best reserved for severe pain, as the safety of its use is not clear. While hypoxemia is a common consequence of MI – and may correlate with worse outcomes – treatment with supplemental oxygen in the absence of hypoxemia is not supported by current evidence, and may carry risk of harm. Nitroglycerin should be avoided in patients with right ventricular infarcts, and in patients who present with hypotension.
Dr. Tubbesing is a senior resident in medicine at the University of Washington, Seattle. Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at [email protected].
References
1. Am Heart J. 2005 Jun;149(6):1043-9.
2. J Interv Cardiol. 2017 Nov 22. doi: 10.1111/joic.12464.
3. Clin Res Cardiol. 2015 Sep;104(9):727-34.
4. Eur Heart J. 2016 Apr 1;37(13):1063-71.
5. BMJ. 1900 Dec 1;2(2083):1568.
6. JAMA. 1930 May 3;94(18):1363-5.
7. Br Med J. 1976 May 8;1(6018):1121-3.
8. Circulation. 2015 Jun 16;131(24):2143-50.
9. Cochrane Database Syst Rev. 2016 Dec 19;12:CD007160.
10. N Engl J Med. 2017 Sep 28;377(13):1240-9.
A 66-year-old man presents with substernal chest pressure and dyspnea that has been present for 45 minutes. He has nausea. Vital signs: blood pressure, 110/60; pulse, 100; oxygen saturation, 92%. Neck: elevated jugular venous pressure. Chest: clear. Cardiac: normal S1 S2, no murmurs. ECG: ST elevation in 2, 3, and aVF leads.
Which of these treatments do you recommend?
A. Morphine, oxygen, nitroglycerin, and aspirin (ASA).
B. Oxygen, morphine, ASA.
C. ASA.
In this patient, I think the correct approach would be to just give aspirin. Nitroglycerin would be problematic, as it appears that this patient might be having a right ventricular infarct, and lowering right-sided filling pressures with nitroglycerin may lead to severe hypotension.
There is controversy over the safety of routine morphine use for patients with chest pain.
Trip J. Meine, MD, and colleagues found that use of morphine either alone or in combination with nitroglycerin for patients presenting with non–ST-elevation acute coronary syndrome (NSTE-ACS) was associated with higher mortality.1 Cian P. McCarthy, MD, and colleagues found the same results, with morphine use associated with larger infarct size, a longer hospital stay, and a trend toward increased mortality in invasively managed NSTE-ACS patients.2 Suzanne de Waha and colleagues found that morphine use in patients with ST-segment elevation MIs had larger infarct size and less reperfusion success, as measured by cardiac MRI.3
Not all recent studies show a detrimental effect of morphine. Etienne Puymirat et al. reviewed in-hospital complications (death, nonfatal re-MI, stroke, stent thrombosis, and bleeding) and 1-year survival according to prehospital morphine use in 2,438 ST-elevation MI (STEMI) patients from the French Registry of Acute ST-elevation and non–ST-elevation Myocardial Infarction (FAST-MI).4 They found no increase in in-hospital complications or 1-year mortality.
The practice of using supplemental oxygen to treat all patients with MI became standard nearly a century ago, after oxygen was found in 1900 to relieve angina, and led to clinical improvement in four MI patients in a 1930 case series.5,6
It was not studied in a controlled trial until 1976, when J.M. Rawles, MD, and colleagues randomized 157 patients with MI to 24 hours of oxygen at 8 L/min or to ambient air. They found no difference in mortality between the groups, but they did find a higher burden of MI in the intervention arm receiving supplemental oxygen, as measured by mean serum aspartate aminotransferase levels.7
The topic was not addressed again in a significant randomized trial until this century. Most notably, two recent studies again demonstrated no benefit of supplemental oxygen in normoxemic patients with MI.
In the AVOID trial in 2015, Dion Stub, MD, PhD, and colleagues randomized 441 patients with STEMI to oxygen at 8 L/min – from diagnosis in an ambulance until after cardiac catheterization – or to ambient air. They found no difference in death at 6 months, but did find an increased rate of in-hospital recurrent MIs, with 0.9% of the control group and 5.5% of the oxygen intervention arm suffering recurrence (P = .006).8 They also showed a larger area of myocardial infarct in the oxygen group, as measured by peak creatine kinase levels and cardiac MRI at 6 months.
Proposed mechanisms of increased myocardial injury from hyperoxia include increased coronary vascular resistance resulting in decreased myocardial perfusion, and increased reperfusion injury from formation of free radicals.9
Where does all this leave us in the treatment of suspected MI?
Morphine should only be used when the patient has pain, and is probably best reserved for severe pain, as the safety of its use is not clear. While hypoxemia is a common consequence of MI – and may correlate with worse outcomes – treatment with supplemental oxygen in the absence of hypoxemia is not supported by current evidence, and may carry risk of harm. Nitroglycerin should be avoided in patients with right ventricular infarcts, and in patients who present with hypotension.
Dr. Tubbesing is a senior resident in medicine at the University of Washington, Seattle. Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at [email protected].
References
1. Am Heart J. 2005 Jun;149(6):1043-9.
2. J Interv Cardiol. 2017 Nov 22. doi: 10.1111/joic.12464.
3. Clin Res Cardiol. 2015 Sep;104(9):727-34.
4. Eur Heart J. 2016 Apr 1;37(13):1063-71.
5. BMJ. 1900 Dec 1;2(2083):1568.
6. JAMA. 1930 May 3;94(18):1363-5.
7. Br Med J. 1976 May 8;1(6018):1121-3.
8. Circulation. 2015 Jun 16;131(24):2143-50.
9. Cochrane Database Syst Rev. 2016 Dec 19;12:CD007160.
10. N Engl J Med. 2017 Sep 28;377(13):1240-9.

Genital Ulcers and Swelling in an Adolescent Girl
The Diagnosis: Epstein-Barr Virus
Physical examination revealed bilateral 1-cm ulcerated lesions on the labia minora with vulvar edema (Figure). She had a palpable liver edge but no splenomegaly, oral ulcers or lesions, conjunctivitis or scleral icterus, or cervical or inguinal lymphadenopathy. A detailed genitourinary examination was performed under anesthesia, but the hymen was not commented on. Inflammatory markers were elevated with a C-reactive protein level of 16.4 mg/L (reference range, 0.08-3.1 mg/mL), erythrocyte sedimentation rate of39 mm/h (reference range, 0-20 mm/h), white blood cell count of 7.1×109/L (reference range, 4.5-11.0×109/L) with 57% neutrophils and 30% lymphocytes, an alanine aminotransferase level of 41 U/L (reference range, 10-40 U/L), and an aspartate aminotransferase level of 126 U/L (reference range, 10-30 U/L).

Bacterial and fungal cultures of vulvar tissue were negative as well as blood and urine cultures. Serological tests for herpes simplex virus (HSV), syphilis, and cytomegalovirus were negative, and urine testing for gonorrhea and chlamydia were negative. Serologies for Epstein-Barr virus (EBV) all were strongly positive with an EBV viral capsid antigen (VCA) IgM greater than 160 U/mL, early antigen IgG of 68 U/mL, and EBV VCA IgG of 456 U/mL. Two years after the initial presentation, repeat EBV serologies were obtained, showing a strongly positive EBV VCA IgG (>8.0 antibody index; reference range, 0-0.8), and a negative EBV VCA IgM.
Infectious etiologies of genital ulcers in a sexually active female include HSV, syphilis, lymphogranuloma venereum, and chancroid. Herpes simplex virus often is the assumed etiology of genital ulcers, especially in sexually active patients, and misdiagnosis in the setting of negative HSV testing may be high. Less common infectious causes such as mumps and cytomegalovirus also have been reported.1,2 Lichen planus and lichen sclerosus are noninfectious inflammatory causes, both of which may involve and be limited to the genitals. Autoimmune disorders include Crohn disease and Behçet disease, and vulvar ulcers with an eschar, consistent with aphthous major or complex apotheosis, has been used to describe patients with severe recurrent oral and genital ulcerations without other systemic manifestations of Behçet disease.3
Genital ulcers are an uncommon manifestation of EBV infection. The formation of genital ulcers in EBV infection has been hypothesized to be due to immune complex formation during the acute phase that becomes activated in the vasculature, leading to microthrombosis and eventually necrosis of the tissue.4 The mode of transmission for EBV-related acute genital ulcers has been postulated to be hematogenous spread in lymphocytes or EBV shedding in the urine with subsequent transfer to the genital mucosa.5
Epstein-Barr virus-related acute genital ulcers are self-limiting. The average healing time for the ulcers is 14 to 18 days.6,7 Antivirals are ineffective in treating this condition; however, supportive treatment with systemic glucocorticoids for associated swelling and pain medications could be considered. Our patient was treated symptomatically. Two weeks after debridement, granulation tissue was noted at the site and her pain and discomfort had resolved. This case illustrates an uncommon manifestation of EBV in a sexually inactive adolescent and is a reminder for the dermatologist of the diverse spectrum of illness caused by this common virus.
- Chanal J, Carlotti A, Laude H, et al. Lipschütz genital ulceration associated with mumps. Dermatology. 2010;221:292-295.
- Martin JM, Godoy R, Calduch L, et al. Lipschütz acute vulval ulcers associated with primary cytomegalovirus infection. Pediatr Dermatol. 2008;25:113-115.
- Huppert JS, Gerber MA, Deitch HR, et al. Vulvar ulcers in young females: a manifestation of aphthosis. J Pediatr Adolesc Gynecol. 2006;19:195-204.
- Sárdy M, Wollenberg A, Niedermeier A, et al. Genital ulcers associated with Epstein-Barr virus infection (ulcus vulvae acutum). Acta Derm Venereol. 2011;91:55-59.
- Di Lernia V, Mansouri Y. Epstein-Barr virus and skin manifestations in childhood. Int J Dermatol. 2013;52:1177-1184.
- Halvorsen JA, Brevig T, Aas T, et al. Genital ulcers as initial manifestation of Epstein-Barr virus infection: two new cases and a review of the literature. Acta Derm Venereol. 2006;86:439-442.
- Jerdan K, Aronson I, Hernandez C, et al. Genital ulcers associated with Epstein-Barr virus. Cutis. 2013;91:273-276.
The Diagnosis: Epstein-Barr Virus
Physical examination revealed bilateral 1-cm ulcerated lesions on the labia minora with vulvar edema (Figure). She had a palpable liver edge but no splenomegaly, oral ulcers or lesions, conjunctivitis or scleral icterus, or cervical or inguinal lymphadenopathy. A detailed genitourinary examination was performed under anesthesia, but the hymen was not commented on. Inflammatory markers were elevated with a C-reactive protein level of 16.4 mg/L (reference range, 0.08-3.1 mg/mL), erythrocyte sedimentation rate of39 mm/h (reference range, 0-20 mm/h), white blood cell count of 7.1×109/L (reference range, 4.5-11.0×109/L) with 57% neutrophils and 30% lymphocytes, an alanine aminotransferase level of 41 U/L (reference range, 10-40 U/L), and an aspartate aminotransferase level of 126 U/L (reference range, 10-30 U/L).
Bacterial and fungal cultures of vulvar tissue were negative as well as blood and urine cultures. Serological tests for herpes simplex virus (HSV), syphilis, and cytomegalovirus were negative, and urine testing for gonorrhea and chlamydia were negative. Serologies for Epstein-Barr virus (EBV) all were strongly positive with an EBV viral capsid antigen (VCA) IgM greater than 160 U/mL, early antigen IgG of 68 U/mL, and EBV VCA IgG of 456 U/mL. Two years after the initial presentation, repeat EBV serologies were obtained, showing a strongly positive EBV VCA IgG (>8.0 antibody index; reference range, 0-0.8), and a negative EBV VCA IgM.
Infectious etiologies of genital ulcers in a sexually active female include HSV, syphilis, lymphogranuloma venereum, and chancroid. Herpes simplex virus often is the assumed etiology of genital ulcers, especially in sexually active patients, and misdiagnosis in the setting of negative HSV testing may be high. Less common infectious causes such as mumps and cytomegalovirus also have been reported.1,2 Lichen planus and lichen sclerosus are noninfectious inflammatory causes, both of which may involve and be limited to the genitals. Autoimmune disorders include Crohn disease and Behçet disease, and vulvar ulcers with an eschar, consistent with aphthous major or complex apotheosis, has been used to describe patients with severe recurrent oral and genital ulcerations without other systemic manifestations of Behçet disease.3
Genital ulcers are an uncommon manifestation of EBV infection. The formation of genital ulcers in EBV infection has been hypothesized to be due to immune complex formation during the acute phase that becomes activated in the vasculature, leading to microthrombosis and eventually necrosis of the tissue.4 The mode of transmission for EBV-related acute genital ulcers has been postulated to be hematogenous spread in lymphocytes or EBV shedding in the urine with subsequent transfer to the genital mucosa.5
Epstein-Barr virus-related acute genital ulcers are self-limiting. The average healing time for the ulcers is 14 to 18 days.6,7 Antivirals are ineffective in treating this condition; however, supportive treatment with systemic glucocorticoids for associated swelling and pain medications could be considered. Our patient was treated symptomatically. Two weeks after debridement, granulation tissue was noted at the site and her pain and discomfort had resolved. This case illustrates an uncommon manifestation of EBV in a sexually inactive adolescent and is a reminder for the dermatologist of the diverse spectrum of illness caused by this common virus.
The Diagnosis: Epstein-Barr Virus
Physical examination revealed bilateral 1-cm ulcerated lesions on the labia minora with vulvar edema (Figure). She had a palpable liver edge but no splenomegaly, oral ulcers or lesions, conjunctivitis or scleral icterus, or cervical or inguinal lymphadenopathy. A detailed genitourinary examination was performed under anesthesia, but the hymen was not commented on. Inflammatory markers were elevated with a C-reactive protein level of 16.4 mg/L (reference range, 0.08-3.1 mg/mL), erythrocyte sedimentation rate of39 mm/h (reference range, 0-20 mm/h), white blood cell count of 7.1×109/L (reference range, 4.5-11.0×109/L) with 57% neutrophils and 30% lymphocytes, an alanine aminotransferase level of 41 U/L (reference range, 10-40 U/L), and an aspartate aminotransferase level of 126 U/L (reference range, 10-30 U/L).
Bacterial and fungal cultures of vulvar tissue were negative as well as blood and urine cultures. Serological tests for herpes simplex virus (HSV), syphilis, and cytomegalovirus were negative, and urine testing for gonorrhea and chlamydia were negative. Serologies for Epstein-Barr virus (EBV) all were strongly positive with an EBV viral capsid antigen (VCA) IgM greater than 160 U/mL, early antigen IgG of 68 U/mL, and EBV VCA IgG of 456 U/mL. Two years after the initial presentation, repeat EBV serologies were obtained, showing a strongly positive EBV VCA IgG (>8.0 antibody index; reference range, 0-0.8), and a negative EBV VCA IgM.
Infectious etiologies of genital ulcers in a sexually active female include HSV, syphilis, lymphogranuloma venereum, and chancroid. Herpes simplex virus often is the assumed etiology of genital ulcers, especially in sexually active patients, and misdiagnosis in the setting of negative HSV testing may be high. Less common infectious causes such as mumps and cytomegalovirus also have been reported.1,2 Lichen planus and lichen sclerosus are noninfectious inflammatory causes, both of which may involve and be limited to the genitals. Autoimmune disorders include Crohn disease and Behçet disease, and vulvar ulcers with an eschar, consistent with aphthous major or complex apotheosis, has been used to describe patients with severe recurrent oral and genital ulcerations without other systemic manifestations of Behçet disease.3
Genital ulcers are an uncommon manifestation of EBV infection. The formation of genital ulcers in EBV infection has been hypothesized to be due to immune complex formation during the acute phase that becomes activated in the vasculature, leading to microthrombosis and eventually necrosis of the tissue.4 The mode of transmission for EBV-related acute genital ulcers has been postulated to be hematogenous spread in lymphocytes or EBV shedding in the urine with subsequent transfer to the genital mucosa.5
Epstein-Barr virus-related acute genital ulcers are self-limiting. The average healing time for the ulcers is 14 to 18 days.6,7 Antivirals are ineffective in treating this condition; however, supportive treatment with systemic glucocorticoids for associated swelling and pain medications could be considered. Our patient was treated symptomatically. Two weeks after debridement, granulation tissue was noted at the site and her pain and discomfort had resolved. This case illustrates an uncommon manifestation of EBV in a sexually inactive adolescent and is a reminder for the dermatologist of the diverse spectrum of illness caused by this common virus.
- Chanal J, Carlotti A, Laude H, et al. Lipschütz genital ulceration associated with mumps. Dermatology. 2010;221:292-295.
- Martin JM, Godoy R, Calduch L, et al. Lipschütz acute vulval ulcers associated with primary cytomegalovirus infection. Pediatr Dermatol. 2008;25:113-115.
- Huppert JS, Gerber MA, Deitch HR, et al. Vulvar ulcers in young females: a manifestation of aphthosis. J Pediatr Adolesc Gynecol. 2006;19:195-204.
- Sárdy M, Wollenberg A, Niedermeier A, et al. Genital ulcers associated with Epstein-Barr virus infection (ulcus vulvae acutum). Acta Derm Venereol. 2011;91:55-59.
- Di Lernia V, Mansouri Y. Epstein-Barr virus and skin manifestations in childhood. Int J Dermatol. 2013;52:1177-1184.
- Halvorsen JA, Brevig T, Aas T, et al. Genital ulcers as initial manifestation of Epstein-Barr virus infection: two new cases and a review of the literature. Acta Derm Venereol. 2006;86:439-442.
- Jerdan K, Aronson I, Hernandez C, et al. Genital ulcers associated with Epstein-Barr virus. Cutis. 2013;91:273-276.
- Chanal J, Carlotti A, Laude H, et al. Lipschütz genital ulceration associated with mumps. Dermatology. 2010;221:292-295.
- Martin JM, Godoy R, Calduch L, et al. Lipschütz acute vulval ulcers associated with primary cytomegalovirus infection. Pediatr Dermatol. 2008;25:113-115.
- Huppert JS, Gerber MA, Deitch HR, et al. Vulvar ulcers in young females: a manifestation of aphthosis. J Pediatr Adolesc Gynecol. 2006;19:195-204.
- Sárdy M, Wollenberg A, Niedermeier A, et al. Genital ulcers associated with Epstein-Barr virus infection (ulcus vulvae acutum). Acta Derm Venereol. 2011;91:55-59.
- Di Lernia V, Mansouri Y. Epstein-Barr virus and skin manifestations in childhood. Int J Dermatol. 2013;52:1177-1184.
- Halvorsen JA, Brevig T, Aas T, et al. Genital ulcers as initial manifestation of Epstein-Barr virus infection: two new cases and a review of the literature. Acta Derm Venereol. 2006;86:439-442.
- Jerdan K, Aronson I, Hernandez C, et al. Genital ulcers associated with Epstein-Barr virus. Cutis. 2013;91:273-276.

A 14-year-old previously healthy, postmenarcheal adolescent girl with a family history of thyroid disease and rheumatoid arthritis presented with vulvar pain and swelling. Vulvar pruritus was noted 6 days prior, which worsened and became associated with vulvar swelling, yellow vaginal discharge, difficulty walking, and a fever (temperature, 39.3.2 °C). Her condition did not improve after a course of cephalexin and trimethoprim-sulfamethoxazole. She denied being sexually active or exposing foreign objects or chemicals to the vaginal area.

Helping patients process sexual harassment
Years ago, after the revelation of sexual predations of male members of the U.S. Navy upon their female underlings, the Navy announced a “zero tolerance” policy. I, then the chair of the American Psychiatric Association Committee on Women, was invited to address a meeting of top Naval officers. They seemed dismayed when I told them that zero tolerance was just the beginning. Declarations that certain behaviors are unacceptable are facile, flimsy, and ultimately disingenuous substitutes for the infinitely more difficult task of monitoring and policing forbidden behaviors and protecting potential and actual victims.
The United States, I pointed out, has a zero tolerance policy on murder but still has to maintain a large force of police officers, detectives, judges, and prison guards to enforce that policy. The Navy had to have a similar approach to sexual assaults. Judging from the recent reports of female members of the military, that hasn’t happened.

Clarity in the law
Unwanted physical intrusion by one adult on another is against the law in the United States. Then why do we need laws specifically banning rape? In addition to the fact that rape, unlike any other assault, can result in conception, sexual assault is recognized as a particularly and uniquely evil and damaging invasion and degradation.
Although there are cultural differences about responsibility for rape, and whether marriage obviates a woman’s right to refuse sexual contact, there is little or no dispute about the need to recognize rape as a distinct, degrading, and particularly heinous attack. It is, therefore, no surprise that people who are raped feel soiled, shamed, and degraded. Those feelings are exacerbated by centuries of shifting responsibility for sexual assault, whether forced intercourse or other unwanted sexual behavior, from the perpetrator onto the victim.
The shifting of blame has been rejected in theory, but it very much persists in actuality. Who among us does not wonder how the victim was dressed or why (s)he was on that street, at that party, in that man’s room? Other forms of harassment echo the motivations of rape – to demonstrate the unanswerable power to degrade – and result in similar psychological responses.
The recent media revelations have lumped physical assault together with unwanted touching, sexual acts undergone as a result of psychological coercion, unwanted exposure to perpetrators’ genitalia and masturbation, and offensive sexual requests and comments. All of those acts are wrong, but they are not equivalent. An elderly man in a wheelchair grabbing an adult woman’s buttocks is not in the same category as an adult man sexually assaulting an underage girl.
What is the genesis of all this misbehavior? It’s not just about sex; it’s about sex and power. For many men, bragging about sexual conquests and making derogatory remarks about women’s physical appearance demonstrate machismo – define maleness.
It is not surprising that such comments are called “locker room talk”; sports are macho displays as well. Physically violating sexual boundaries is just the talk put into action. And macho works. Last November, more than 40% of female voters in the United States voted for the candidate who reportedly cheated on at least one of his three wives, bragged about unwanted sexual assault, and has been credibly accused of many other illegal and/or inappropriate behaviors.
Where does it end?
What is going to be the result of all this hullabaloo? The list of convincingly accused perpetrators grows by the day. Sexism and sexual misbehavior are endemic in every sphere of human endeavor, up to and including, of course, the clergy, who are meant to be models and protectors of virtue. The scope of recent revelations may be unusual, but revelations about one sector or another have happened every few years: the military, clergy, Wall Street, Silicon Valley, academia. What would happen if all the sexual misbehavior were to be revealed, and the perpetrators removed from their leadership and management positions? Would we have a film industry, a financial industry, a legislature? I saw a headline somewhere: “He’s always indispensable; you never are.” The argument, or myth, of indispensability is a powerful protection for powerful individuals. The powerful are too powerful to tolerate mass expulsions. Already, Congress has resorted to the time-honored and demonstrably useless response: training. Others among the accused report that they are undergoing treatment of sex addiction, a diagnosis our profession has wisely discarded, and for which there was no effective treatment.
Sex, while not addictive, does have a role in sexual misbehavior. Through the ages, women’s reproductive hormones have been a focus of social and medical attention, as the source of unpleasant behaviors, and, in fact, psychopathology: premenstrual dysphoric disorder, postpartum depression. Little or no attention has been paid to the problematic psychosocial effects of male reproductive hormones. In addition to the offensive behaviors currently in the headlines, there is the behavior of adolescent males. Isn’t reckless driving related to the pubertal influx of testosterone (Neurosci Biobehav Rev. 2006;30[3]:319-45)? This gender discrepancy deserves scientific and social attention.
What can psychiatrists do to help women (and men) who are affected by sexual misbehavior? This is a difficult problem. What would help most victims, of any injustice, most would be to confront those responsible, and see them removed from positions of power and otherwise punished. However, the recent reports of seemingly swift and severe responses are misleading. The responsible journalists who have reported these cases have, in most cases, devoted months to finding victimized women, persuading them to go public, and corroborating their accounts. The perpetrators, even when complaints have been made, have gone unpunished, and often been promoted, for years or even decades. Women who complain often are subject to employer retaliation.
So a treating psychiatrist is left with less-than-satisfactory recommendations and responses. The most important intervention is to identify and counter the patient’s inaccurate and damaging assumptions: that she was responsible, that she should and could have refused to tolerate the misbehavior, that she has been left tainted, impure. Some social groups and families will have reinforced the latter feeling. The remainder of the psychiatric intervention will be focused on the patient’s particular symptoms – of posttraumatic stress, anxiety, or depression – and the relationship between her symptoms, history, and psychodynamics. Group therapy or other support by women who have faced similar abuse may be helpful. I’m afraid that we will continue to have many such patients to treat.
Dr. Stotland, past president of the American Psychiatric Association, is professor of psychiatry, and obstetrics and gynecology, at Rush Medical College, Chicago. She has written numerous articles and books, including “Cutting Edge Medicine: What Psychiatrists Need to Know” (American Psychiatric Association Publishing, 2002).
Years ago, after the revelation of sexual predations of male members of the U.S. Navy upon their female underlings, the Navy announced a “zero tolerance” policy. I, then the chair of the American Psychiatric Association Committee on Women, was invited to address a meeting of top Naval officers. They seemed dismayed when I told them that zero tolerance was just the beginning. Declarations that certain behaviors are unacceptable are facile, flimsy, and ultimately disingenuous substitutes for the infinitely more difficult task of monitoring and policing forbidden behaviors and protecting potential and actual victims.
The United States, I pointed out, has a zero tolerance policy on murder but still has to maintain a large force of police officers, detectives, judges, and prison guards to enforce that policy. The Navy had to have a similar approach to sexual assaults. Judging from the recent reports of female members of the military, that hasn’t happened.
Clarity in the law
Unwanted physical intrusion by one adult on another is against the law in the United States. Then why do we need laws specifically banning rape? In addition to the fact that rape, unlike any other assault, can result in conception, sexual assault is recognized as a particularly and uniquely evil and damaging invasion and degradation.
Although there are cultural differences about responsibility for rape, and whether marriage obviates a woman’s right to refuse sexual contact, there is little or no dispute about the need to recognize rape as a distinct, degrading, and particularly heinous attack. It is, therefore, no surprise that people who are raped feel soiled, shamed, and degraded. Those feelings are exacerbated by centuries of shifting responsibility for sexual assault, whether forced intercourse or other unwanted sexual behavior, from the perpetrator onto the victim.
The shifting of blame has been rejected in theory, but it very much persists in actuality. Who among us does not wonder how the victim was dressed or why (s)he was on that street, at that party, in that man’s room? Other forms of harassment echo the motivations of rape – to demonstrate the unanswerable power to degrade – and result in similar psychological responses.
The recent media revelations have lumped physical assault together with unwanted touching, sexual acts undergone as a result of psychological coercion, unwanted exposure to perpetrators’ genitalia and masturbation, and offensive sexual requests and comments. All of those acts are wrong, but they are not equivalent. An elderly man in a wheelchair grabbing an adult woman’s buttocks is not in the same category as an adult man sexually assaulting an underage girl.
What is the genesis of all this misbehavior? It’s not just about sex; it’s about sex and power. For many men, bragging about sexual conquests and making derogatory remarks about women’s physical appearance demonstrate machismo – define maleness.
It is not surprising that such comments are called “locker room talk”; sports are macho displays as well. Physically violating sexual boundaries is just the talk put into action. And macho works. Last November, more than 40% of female voters in the United States voted for the candidate who reportedly cheated on at least one of his three wives, bragged about unwanted sexual assault, and has been credibly accused of many other illegal and/or inappropriate behaviors.
Where does it end?
What is going to be the result of all this hullabaloo? The list of convincingly accused perpetrators grows by the day. Sexism and sexual misbehavior are endemic in every sphere of human endeavor, up to and including, of course, the clergy, who are meant to be models and protectors of virtue. The scope of recent revelations may be unusual, but revelations about one sector or another have happened every few years: the military, clergy, Wall Street, Silicon Valley, academia. What would happen if all the sexual misbehavior were to be revealed, and the perpetrators removed from their leadership and management positions? Would we have a film industry, a financial industry, a legislature? I saw a headline somewhere: “He’s always indispensable; you never are.” The argument, or myth, of indispensability is a powerful protection for powerful individuals. The powerful are too powerful to tolerate mass expulsions. Already, Congress has resorted to the time-honored and demonstrably useless response: training. Others among the accused report that they are undergoing treatment of sex addiction, a diagnosis our profession has wisely discarded, and for which there was no effective treatment.
Sex, while not addictive, does have a role in sexual misbehavior. Through the ages, women’s reproductive hormones have been a focus of social and medical attention, as the source of unpleasant behaviors, and, in fact, psychopathology: premenstrual dysphoric disorder, postpartum depression. Little or no attention has been paid to the problematic psychosocial effects of male reproductive hormones. In addition to the offensive behaviors currently in the headlines, there is the behavior of adolescent males. Isn’t reckless driving related to the pubertal influx of testosterone (Neurosci Biobehav Rev. 2006;30[3]:319-45)? This gender discrepancy deserves scientific and social attention.
What can psychiatrists do to help women (and men) who are affected by sexual misbehavior? This is a difficult problem. What would help most victims, of any injustice, most would be to confront those responsible, and see them removed from positions of power and otherwise punished. However, the recent reports of seemingly swift and severe responses are misleading. The responsible journalists who have reported these cases have, in most cases, devoted months to finding victimized women, persuading them to go public, and corroborating their accounts. The perpetrators, even when complaints have been made, have gone unpunished, and often been promoted, for years or even decades. Women who complain often are subject to employer retaliation.
So a treating psychiatrist is left with less-than-satisfactory recommendations and responses. The most important intervention is to identify and counter the patient’s inaccurate and damaging assumptions: that she was responsible, that she should and could have refused to tolerate the misbehavior, that she has been left tainted, impure. Some social groups and families will have reinforced the latter feeling. The remainder of the psychiatric intervention will be focused on the patient’s particular symptoms – of posttraumatic stress, anxiety, or depression – and the relationship between her symptoms, history, and psychodynamics. Group therapy or other support by women who have faced similar abuse may be helpful. I’m afraid that we will continue to have many such patients to treat.
Dr. Stotland, past president of the American Psychiatric Association, is professor of psychiatry, and obstetrics and gynecology, at Rush Medical College, Chicago. She has written numerous articles and books, including “Cutting Edge Medicine: What Psychiatrists Need to Know” (American Psychiatric Association Publishing, 2002).
Years ago, after the revelation of sexual predations of male members of the U.S. Navy upon their female underlings, the Navy announced a “zero tolerance” policy. I, then the chair of the American Psychiatric Association Committee on Women, was invited to address a meeting of top Naval officers. They seemed dismayed when I told them that zero tolerance was just the beginning. Declarations that certain behaviors are unacceptable are facile, flimsy, and ultimately disingenuous substitutes for the infinitely more difficult task of monitoring and policing forbidden behaviors and protecting potential and actual victims.
The United States, I pointed out, has a zero tolerance policy on murder but still has to maintain a large force of police officers, detectives, judges, and prison guards to enforce that policy. The Navy had to have a similar approach to sexual assaults. Judging from the recent reports of female members of the military, that hasn’t happened.
Clarity in the law
Unwanted physical intrusion by one adult on another is against the law in the United States. Then why do we need laws specifically banning rape? In addition to the fact that rape, unlike any other assault, can result in conception, sexual assault is recognized as a particularly and uniquely evil and damaging invasion and degradation.
Although there are cultural differences about responsibility for rape, and whether marriage obviates a woman’s right to refuse sexual contact, there is little or no dispute about the need to recognize rape as a distinct, degrading, and particularly heinous attack. It is, therefore, no surprise that people who are raped feel soiled, shamed, and degraded. Those feelings are exacerbated by centuries of shifting responsibility for sexual assault, whether forced intercourse or other unwanted sexual behavior, from the perpetrator onto the victim.
The shifting of blame has been rejected in theory, but it very much persists in actuality. Who among us does not wonder how the victim was dressed or why (s)he was on that street, at that party, in that man’s room? Other forms of harassment echo the motivations of rape – to demonstrate the unanswerable power to degrade – and result in similar psychological responses.
The recent media revelations have lumped physical assault together with unwanted touching, sexual acts undergone as a result of psychological coercion, unwanted exposure to perpetrators’ genitalia and masturbation, and offensive sexual requests and comments. All of those acts are wrong, but they are not equivalent. An elderly man in a wheelchair grabbing an adult woman’s buttocks is not in the same category as an adult man sexually assaulting an underage girl.
What is the genesis of all this misbehavior? It’s not just about sex; it’s about sex and power. For many men, bragging about sexual conquests and making derogatory remarks about women’s physical appearance demonstrate machismo – define maleness.
It is not surprising that such comments are called “locker room talk”; sports are macho displays as well. Physically violating sexual boundaries is just the talk put into action. And macho works. Last November, more than 40% of female voters in the United States voted for the candidate who reportedly cheated on at least one of his three wives, bragged about unwanted sexual assault, and has been credibly accused of many other illegal and/or inappropriate behaviors.
Where does it end?
What is going to be the result of all this hullabaloo? The list of convincingly accused perpetrators grows by the day. Sexism and sexual misbehavior are endemic in every sphere of human endeavor, up to and including, of course, the clergy, who are meant to be models and protectors of virtue. The scope of recent revelations may be unusual, but revelations about one sector or another have happened every few years: the military, clergy, Wall Street, Silicon Valley, academia. What would happen if all the sexual misbehavior were to be revealed, and the perpetrators removed from their leadership and management positions? Would we have a film industry, a financial industry, a legislature? I saw a headline somewhere: “He’s always indispensable; you never are.” The argument, or myth, of indispensability is a powerful protection for powerful individuals. The powerful are too powerful to tolerate mass expulsions. Already, Congress has resorted to the time-honored and demonstrably useless response: training. Others among the accused report that they are undergoing treatment of sex addiction, a diagnosis our profession has wisely discarded, and for which there was no effective treatment.
Sex, while not addictive, does have a role in sexual misbehavior. Through the ages, women’s reproductive hormones have been a focus of social and medical attention, as the source of unpleasant behaviors, and, in fact, psychopathology: premenstrual dysphoric disorder, postpartum depression. Little or no attention has been paid to the problematic psychosocial effects of male reproductive hormones. In addition to the offensive behaviors currently in the headlines, there is the behavior of adolescent males. Isn’t reckless driving related to the pubertal influx of testosterone (Neurosci Biobehav Rev. 2006;30[3]:319-45)? This gender discrepancy deserves scientific and social attention.
What can psychiatrists do to help women (and men) who are affected by sexual misbehavior? This is a difficult problem. What would help most victims, of any injustice, most would be to confront those responsible, and see them removed from positions of power and otherwise punished. However, the recent reports of seemingly swift and severe responses are misleading. The responsible journalists who have reported these cases have, in most cases, devoted months to finding victimized women, persuading them to go public, and corroborating their accounts. The perpetrators, even when complaints have been made, have gone unpunished, and often been promoted, for years or even decades. Women who complain often are subject to employer retaliation.
So a treating psychiatrist is left with less-than-satisfactory recommendations and responses. The most important intervention is to identify and counter the patient’s inaccurate and damaging assumptions: that she was responsible, that she should and could have refused to tolerate the misbehavior, that she has been left tainted, impure. Some social groups and families will have reinforced the latter feeling. The remainder of the psychiatric intervention will be focused on the patient’s particular symptoms – of posttraumatic stress, anxiety, or depression – and the relationship between her symptoms, history, and psychodynamics. Group therapy or other support by women who have faced similar abuse may be helpful. I’m afraid that we will continue to have many such patients to treat.
Dr. Stotland, past president of the American Psychiatric Association, is professor of psychiatry, and obstetrics and gynecology, at Rush Medical College, Chicago. She has written numerous articles and books, including “Cutting Edge Medicine: What Psychiatrists Need to Know” (American Psychiatric Association Publishing, 2002).
Retinal changes may reflect brain changes in preclinical Alzheimer’s
BOSTON – Changes in the retina seem to mirror changes that begin to reshape the brain in preclinical Alzheimer’s disease.
Manifested as a reduction in volume in the retinal nerve fiber layer, these changes appear to track the aggregation of beta amyloid brain plaques well before cognitive problems arise – and can be easily measured with a piece of equipment already in many optometry offices, Peter J. Snyder, PhD, said at the Clinical Trials in Alzheimer’s Disease conference.

“If we are lucky enough to live past age 45, then it’s a given that we’re all going to develop some presbyopia. So we all have to go to the optometrist sometime, and that may become a point of entry for broad screening and to track changes over time, to keep an eye on at-risk patients, and to refer those with retinal changes that fit the preclinical AD profile to specialty care for more comprehensive diagnostic evaluations.”
The retina begins to form in the third week of embryologic life, arising from the neural tube cells that also form the brain and spinal cord. It makes sense then that very early neuronal changes in Alzheimer’s disease could be occurring in the retina as well, said Dr. Snyder, professor of neurology and surgery (ophthalmology) at Rhode Island Hospital and Brown University, Providence.
“The retina is really a protrusion of the brain, and it is part and parcel of the central nervous system. In terms of the neuronal structure, the retina develops in layers with very specific cell types that are neurochemically and physiologically the same as the nervous tissue in the brain. That’s why it is, potentially, literally a window that could let us see what’s happening in the brain in early Alzheimer’s disease.”
Other researchers have explored amyloid in the lens and retina as a possible early Alzheimer’s identification tool. But Dr. Snyder’s study is the first to demonstrate a longitudinal association between neuronal changes in the eye and amyloid burden in the brain among clinically normal subjects.
For 27 months, he followed 56 people who had normal cognition but were beginning to experience subjective memory complaints. All subjects had at least one parent with Alzheimer’s disease. Everyone underwent an amyloid PET scan at baseline. Of the cohort, 15 had PET imaging evidence of abnormal beta-amyloid protein aggregation in the neocortex. This group was deemed to have preclinical Alzheimer’s disease, while the remainder served as a control group.
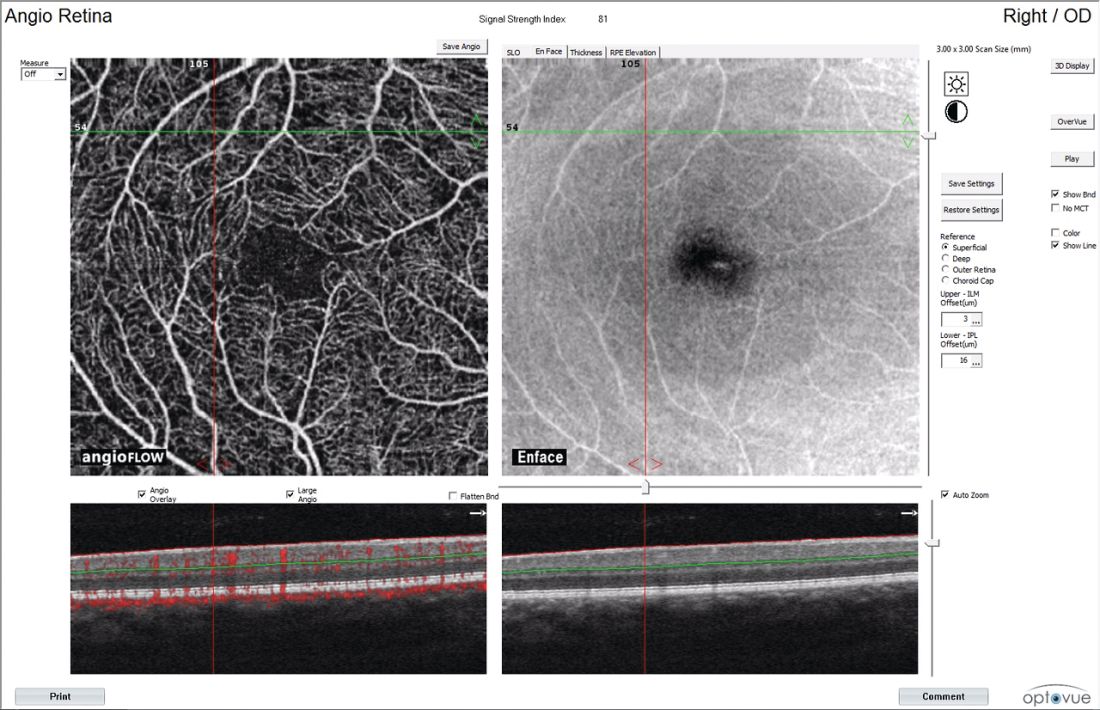
Dr. Snyder imaged each subject’s retinas twice – once at baseline and once at 27 months, when everyone underwent a second amyloid PET scan as well. He examined the retina with spectral domain optical coherence tomography, a relatively new method of imaging the retina.
These scanners are becoming increasingly more common in optometry practices, Dr. Snyder said. “Graduate optometrists tell me they would not want to be in a practice without one.” The scanners are typically used to detect retinal and ocular changes associated with diabetes, macular degeneration, glaucoma and multiple sclerosis.
Dr. Snyder used the scanner to examine the optic nerve head and macula at both baseline and 27 months in his cohort. He was looking for volumetric changes in several of the retinal layers: the peripapillary retinal nerve fiber layer (pRNFL), macular RNFL (mRNFL), ganglion cell layer (GCL), inner plexiform layer (IPL), outer nuclear layer (ONL), outer plexiform layer (OPL), and inner nuclear layer (INL). He also computed changes in total retinal volume.
Even at baseline, he found a significant difference between the groups. Among the amyloid-positive subjects, the inner plexiform layer was slightly larger in volume. “This seems a bit counterintuitive, but I think it suggests that there may be some inflammatory processes going on in this early stage and that we are catching that inflammation.”
Dr. Snyder noted that this finding has recently been replicated by an independent research group in Perth, Australia – with a much larger sample of participants – and will be reported at international conferences this coming year.
At 27 months, both the total retinal volume and the macular retinal nerve fiber layer volume were significantly lower in the preclinical AD group than in the control group. There was also a volume reduction in the peripapillary retinal nerve fiber layer, although the between-group difference was not statistically significant.
In a multivariate linear regression model that controlled for age and total amyloid burden, the mean volume change in the macular retinal nerve fiber layer accounted for about 10% of the variation in PET binding to brain amyloid by 27 months. Volume reductions in all the other layers appeared to be associated only with age, representing normal age-related changes in the eye.
Dr. Snyder said this volume loss in the retinal nerve fiber layer probably represents early demyelination and/or degeneration of the axons coursing from the cell bodies in the ganglion cell layer, which project to the optic nerve head.
“This finding in the retina appears analogous, and possibly directly related to, a similar loss of white matter that is readily observable in the early stages of Alzheimer’s disease. At the same time, patients are beginning to experience both cholinergic changes in the basal forebrain and the abnormal aggregation of fibrillar beta-amyloid plaques. I don’t know to what extent these changes are mechanistically dependent on each other, but they appear to also be happening, in the earliest stages of the disease course, in the retina.”
There is a lot of work left to be done before retinal scanning could be employed as a risk-assessment tool, however. With every new biomarker – and especially with imaging – the ability to measure change occurs far in advance of an understanding of what those changes mean, and how to judge them accurately.
“Every time we have a major advance in imaging, the technical engineering breakthroughs precede our detailed understanding of what we’re looking at and what to measure. This is where we are right now with retinal imaging. Biologically, it makes sense to be looking at this as a marker of risk in those who are clinically healthy, and maybe later as a marker of disease progression. But there is a lot of work to be done here yet.”
Dr. Snyder’s project was funded in part by a research award from Pfizer, with PET imaging supported in part by a grant from Avid Radiopharmaceuticals. He has no financial ties to the company, or other financial interest related to the study.
[email protected]
On Twitter @Alz_Gal
BOSTON – Changes in the retina seem to mirror changes that begin to reshape the brain in preclinical Alzheimer’s disease.
Manifested as a reduction in volume in the retinal nerve fiber layer, these changes appear to track the aggregation of beta amyloid brain plaques well before cognitive problems arise – and can be easily measured with a piece of equipment already in many optometry offices, Peter J. Snyder, PhD, said at the Clinical Trials in Alzheimer’s Disease conference.
“If we are lucky enough to live past age 45, then it’s a given that we’re all going to develop some presbyopia. So we all have to go to the optometrist sometime, and that may become a point of entry for broad screening and to track changes over time, to keep an eye on at-risk patients, and to refer those with retinal changes that fit the preclinical AD profile to specialty care for more comprehensive diagnostic evaluations.”
The retina begins to form in the third week of embryologic life, arising from the neural tube cells that also form the brain and spinal cord. It makes sense then that very early neuronal changes in Alzheimer’s disease could be occurring in the retina as well, said Dr. Snyder, professor of neurology and surgery (ophthalmology) at Rhode Island Hospital and Brown University, Providence.
“The retina is really a protrusion of the brain, and it is part and parcel of the central nervous system. In terms of the neuronal structure, the retina develops in layers with very specific cell types that are neurochemically and physiologically the same as the nervous tissue in the brain. That’s why it is, potentially, literally a window that could let us see what’s happening in the brain in early Alzheimer’s disease.”
Other researchers have explored amyloid in the lens and retina as a possible early Alzheimer’s identification tool. But Dr. Snyder’s study is the first to demonstrate a longitudinal association between neuronal changes in the eye and amyloid burden in the brain among clinically normal subjects.
For 27 months, he followed 56 people who had normal cognition but were beginning to experience subjective memory complaints. All subjects had at least one parent with Alzheimer’s disease. Everyone underwent an amyloid PET scan at baseline. Of the cohort, 15 had PET imaging evidence of abnormal beta-amyloid protein aggregation in the neocortex. This group was deemed to have preclinical Alzheimer’s disease, while the remainder served as a control group.
Dr. Snyder imaged each subject’s retinas twice – once at baseline and once at 27 months, when everyone underwent a second amyloid PET scan as well. He examined the retina with spectral domain optical coherence tomography, a relatively new method of imaging the retina.
These scanners are becoming increasingly more common in optometry practices, Dr. Snyder said. “Graduate optometrists tell me they would not want to be in a practice without one.” The scanners are typically used to detect retinal and ocular changes associated with diabetes, macular degeneration, glaucoma and multiple sclerosis.
Dr. Snyder used the scanner to examine the optic nerve head and macula at both baseline and 27 months in his cohort. He was looking for volumetric changes in several of the retinal layers: the peripapillary retinal nerve fiber layer (pRNFL), macular RNFL (mRNFL), ganglion cell layer (GCL), inner plexiform layer (IPL), outer nuclear layer (ONL), outer plexiform layer (OPL), and inner nuclear layer (INL). He also computed changes in total retinal volume.
Even at baseline, he found a significant difference between the groups. Among the amyloid-positive subjects, the inner plexiform layer was slightly larger in volume. “This seems a bit counterintuitive, but I think it suggests that there may be some inflammatory processes going on in this early stage and that we are catching that inflammation.”
Dr. Snyder noted that this finding has recently been replicated by an independent research group in Perth, Australia – with a much larger sample of participants – and will be reported at international conferences this coming year.
At 27 months, both the total retinal volume and the macular retinal nerve fiber layer volume were significantly lower in the preclinical AD group than in the control group. There was also a volume reduction in the peripapillary retinal nerve fiber layer, although the between-group difference was not statistically significant.
In a multivariate linear regression model that controlled for age and total amyloid burden, the mean volume change in the macular retinal nerve fiber layer accounted for about 10% of the variation in PET binding to brain amyloid by 27 months. Volume reductions in all the other layers appeared to be associated only with age, representing normal age-related changes in the eye.
Dr. Snyder said this volume loss in the retinal nerve fiber layer probably represents early demyelination and/or degeneration of the axons coursing from the cell bodies in the ganglion cell layer, which project to the optic nerve head.
“This finding in the retina appears analogous, and possibly directly related to, a similar loss of white matter that is readily observable in the early stages of Alzheimer’s disease. At the same time, patients are beginning to experience both cholinergic changes in the basal forebrain and the abnormal aggregation of fibrillar beta-amyloid plaques. I don’t know to what extent these changes are mechanistically dependent on each other, but they appear to also be happening, in the earliest stages of the disease course, in the retina.”
There is a lot of work left to be done before retinal scanning could be employed as a risk-assessment tool, however. With every new biomarker – and especially with imaging – the ability to measure change occurs far in advance of an understanding of what those changes mean, and how to judge them accurately.
“Every time we have a major advance in imaging, the technical engineering breakthroughs precede our detailed understanding of what we’re looking at and what to measure. This is where we are right now with retinal imaging. Biologically, it makes sense to be looking at this as a marker of risk in those who are clinically healthy, and maybe later as a marker of disease progression. But there is a lot of work to be done here yet.”
Dr. Snyder’s project was funded in part by a research award from Pfizer, with PET imaging supported in part by a grant from Avid Radiopharmaceuticals. He has no financial ties to the company, or other financial interest related to the study.
[email protected]
On Twitter @Alz_Gal
BOSTON – Changes in the retina seem to mirror changes that begin to reshape the brain in preclinical Alzheimer’s disease.
Manifested as a reduction in volume in the retinal nerve fiber layer, these changes appear to track the aggregation of beta amyloid brain plaques well before cognitive problems arise – and can be easily measured with a piece of equipment already in many optometry offices, Peter J. Snyder, PhD, said at the Clinical Trials in Alzheimer’s Disease conference.
“If we are lucky enough to live past age 45, then it’s a given that we’re all going to develop some presbyopia. So we all have to go to the optometrist sometime, and that may become a point of entry for broad screening and to track changes over time, to keep an eye on at-risk patients, and to refer those with retinal changes that fit the preclinical AD profile to specialty care for more comprehensive diagnostic evaluations.”
The retina begins to form in the third week of embryologic life, arising from the neural tube cells that also form the brain and spinal cord. It makes sense then that very early neuronal changes in Alzheimer’s disease could be occurring in the retina as well, said Dr. Snyder, professor of neurology and surgery (ophthalmology) at Rhode Island Hospital and Brown University, Providence.
“The retina is really a protrusion of the brain, and it is part and parcel of the central nervous system. In terms of the neuronal structure, the retina develops in layers with very specific cell types that are neurochemically and physiologically the same as the nervous tissue in the brain. That’s why it is, potentially, literally a window that could let us see what’s happening in the brain in early Alzheimer’s disease.”
Other researchers have explored amyloid in the lens and retina as a possible early Alzheimer’s identification tool. But Dr. Snyder’s study is the first to demonstrate a longitudinal association between neuronal changes in the eye and amyloid burden in the brain among clinically normal subjects.
For 27 months, he followed 56 people who had normal cognition but were beginning to experience subjective memory complaints. All subjects had at least one parent with Alzheimer’s disease. Everyone underwent an amyloid PET scan at baseline. Of the cohort, 15 had PET imaging evidence of abnormal beta-amyloid protein aggregation in the neocortex. This group was deemed to have preclinical Alzheimer’s disease, while the remainder served as a control group.
Dr. Snyder imaged each subject’s retinas twice – once at baseline and once at 27 months, when everyone underwent a second amyloid PET scan as well. He examined the retina with spectral domain optical coherence tomography, a relatively new method of imaging the retina.
These scanners are becoming increasingly more common in optometry practices, Dr. Snyder said. “Graduate optometrists tell me they would not want to be in a practice without one.” The scanners are typically used to detect retinal and ocular changes associated with diabetes, macular degeneration, glaucoma and multiple sclerosis.
Dr. Snyder used the scanner to examine the optic nerve head and macula at both baseline and 27 months in his cohort. He was looking for volumetric changes in several of the retinal layers: the peripapillary retinal nerve fiber layer (pRNFL), macular RNFL (mRNFL), ganglion cell layer (GCL), inner plexiform layer (IPL), outer nuclear layer (ONL), outer plexiform layer (OPL), and inner nuclear layer (INL). He also computed changes in total retinal volume.
Even at baseline, he found a significant difference between the groups. Among the amyloid-positive subjects, the inner plexiform layer was slightly larger in volume. “This seems a bit counterintuitive, but I think it suggests that there may be some inflammatory processes going on in this early stage and that we are catching that inflammation.”
Dr. Snyder noted that this finding has recently been replicated by an independent research group in Perth, Australia – with a much larger sample of participants – and will be reported at international conferences this coming year.
At 27 months, both the total retinal volume and the macular retinal nerve fiber layer volume were significantly lower in the preclinical AD group than in the control group. There was also a volume reduction in the peripapillary retinal nerve fiber layer, although the between-group difference was not statistically significant.
In a multivariate linear regression model that controlled for age and total amyloid burden, the mean volume change in the macular retinal nerve fiber layer accounted for about 10% of the variation in PET binding to brain amyloid by 27 months. Volume reductions in all the other layers appeared to be associated only with age, representing normal age-related changes in the eye.
Dr. Snyder said this volume loss in the retinal nerve fiber layer probably represents early demyelination and/or degeneration of the axons coursing from the cell bodies in the ganglion cell layer, which project to the optic nerve head.
“This finding in the retina appears analogous, and possibly directly related to, a similar loss of white matter that is readily observable in the early stages of Alzheimer’s disease. At the same time, patients are beginning to experience both cholinergic changes in the basal forebrain and the abnormal aggregation of fibrillar beta-amyloid plaques. I don’t know to what extent these changes are mechanistically dependent on each other, but they appear to also be happening, in the earliest stages of the disease course, in the retina.”
There is a lot of work left to be done before retinal scanning could be employed as a risk-assessment tool, however. With every new biomarker – and especially with imaging – the ability to measure change occurs far in advance of an understanding of what those changes mean, and how to judge them accurately.
“Every time we have a major advance in imaging, the technical engineering breakthroughs precede our detailed understanding of what we’re looking at and what to measure. This is where we are right now with retinal imaging. Biologically, it makes sense to be looking at this as a marker of risk in those who are clinically healthy, and maybe later as a marker of disease progression. But there is a lot of work to be done here yet.”
Dr. Snyder’s project was funded in part by a research award from Pfizer, with PET imaging supported in part by a grant from Avid Radiopharmaceuticals. He has no financial ties to the company, or other financial interest related to the study.
[email protected]
On Twitter @Alz_Gal
AT CTAD
Key clinical point: Retinal scans might eventually be an easy, noninvasive, and inexpensive way to tag people who may be at elevated risk for Alzheimer’s disease.
Major finding: At 27 months, both the total retinal volume and the macular retinal nerve fiber layer volume were significantly lower in 15 patients in the preclinical AD group than in the 41 patients in the control group.
Data source: A follow-up study of 56 people who had at least one parent with Alzheimer’s disease and were beginning to experience subjective memory complaints.
Disclosures: Dr. Snyder’s project was funded in part by a research award from Pfizer, with PET imaging supported in part by a grant from Avid Radiopharmaceuticals. He has no financial ties to the company, or other financial interest related to the study.
Swarm and suspicion leadership
During your career, you serve as staff member and leader to many different professional groups. Some are collaborative, collegial, and supportive. Others are competitive, antagonistic, or even combative. What are the benefits and downsides of each of these cultures and what can you do, as a hospitalist leader, to influence the character of your workplace?

The field of “game theory” provides insights into the distinction. The first questions to ask are “What is the game you are playing?” and then “Who is the competition?” In a “winner-takes-all” scenario, such as a sporting event, each team seeks strategic advantage over the other team. In baseball terms, the winner gets more points when at bat and denies more points when on the field. However, when competing as a team, winning together requires collaboration to build strategy, execute plays, and reach victory. You compete against the other team and collaborate within your own team.
Scientists who study negotiation strategies and conflict resolution find that collaborative groups spend less time countering one another and, instead, investing that same effort into building constructive outcomes, a force multiplier.
In the winner-takes-all model, the baseball team that gets “outs,” makes plays, and advances team members to home plate, wins. If there is contest within the team, players invest that same effort into seeking their own gain at the expense of others. Benefits derived from shared effort are shunned in favor of benefits accrued to one player over the other. It is a distinction between “I won” versus “We won.”
Hospital medicine is not a win/lose sport, yet over the years, hospitalists have shared with me that their institution or group at times feels like a competitive field with winners and losers. If this distinction is placed on a continuum, what factors encourage a more collaborative environment and what factors do the opposite, toward the adversarial side of the continuum? It makes a substantive difference in the interactions and accomplishments that a group achieves.
My colleagues and I at Harvard study leaders in times of crisis. A crisis makes apparent what is often more subtle during routine times. Our study of leaders in the wake of the Boston Marathon bombings was among our most revealing.
During most crises, an operational leader is designated to oversee the whole of the response. This is an individual with organizational authority and subject-matter expertise appropriate to the situation at hand. In Boston, however, there were so many different jurisdictions – federal, state, and local – and so many different agencies, that no one leader stood above the others. They worked in a remarkably collaborative fashion. While the bombings themselves were tragic, the response itself was a success: All who survived the initial blasts lived, a function of remarkable emergency care, distribution to hospitals, and good medical care. The perpetrators were caught in 102 hours, and “Boston Strong” reflected a genuine city resilience.
These leaders worked together in ways that we had rarely seen before. What we discovered was a phenomenon we call “swarm leadership,” inspired by the ways ants, bees, and termites engage in collective work and decision making. These creatures have clear lines of communication and structures for judgment calls, often about food sources, nesting locations, and threats.
There are five principles of swarm leadership:
- Unity of mission – In Boston, that was to “save lives,” and it motivated and activated the whole of the response.
- Generosity of spirit and action – Across the community, people were eager to assist in the response.
- Everyone stayed in their own lanes of responsibility and helped others succeed in theirs – There were law enforcement, medical, and resilience activities and the theme across the leaders was “how can I help make you a success?”
- No ego and no blame – There was a level of emotional intelligence and maturity among the leaders.
- A foundation of trusting relations – These leaders had known one another for years and, though the decisions were tough, they were confident in the motives and actions of the others.
While the discovery emerged from our crisis research, the findings equally apply to other, more routine work and interactions. Conduct your own assessment. Have you worked in groups in which these principles of swarm leadership characterized the experience? People were focused on a shared mission: They were available to assist one another; accomplished their work in ways that were respectful and supportive of their different responsibilities; did not claim undue credit or swipe at each another; and knew one another well enough to trust the others’ actions and motives.
The flip side of this continuum of collaboration and competition we term “suspicion leadership.” This is characterized by selfish ambitions; narcissistic actions; grabs for authority and resources; credit taking for the good and accusations for the bad; and an environment of mistrust and back stabbing.
Leaders influence the tone and tenor of their own group’s interactions as well as interactions among different working groups. As role models, if they articulate and demonstrate a mission that others can rally around, they forge that critical unity of mission. By contrast, suspicion leaders make it clear that “it is all about me and my priorities.” There is much work to be done, and swarm leaders ensure that people have the resources, autonomy, and support necessary to get the job done. On the other end, the work environment is burdened by the uncertainties about who does what and who is responsible. Swarm leaders are focused on “we” and suspicion leaders are caught up on “me.” There is no trust when people are suspicious of one another. Much can be accomplished when people believe in themselves, their colleagues, and the reasons that bring them together.
As a hospitalist leader, you influence where on this continuum your group will lie. It is your choice to be a role model for the principles of swarm, encouraging the same among others. When those principles become the beacons by which you work and relate, you will find an environment that inspires people to be and to do their best.
In the next column, how to build trust within your teams.
Dr. Marcus is director, Program on Health Care Negotiation and Conflict Resolution, at the Harvard T.H. Chan School of Public Health, in Boston.
During your career, you serve as staff member and leader to many different professional groups. Some are collaborative, collegial, and supportive. Others are competitive, antagonistic, or even combative. What are the benefits and downsides of each of these cultures and what can you do, as a hospitalist leader, to influence the character of your workplace?
The field of “game theory” provides insights into the distinction. The first questions to ask are “What is the game you are playing?” and then “Who is the competition?” In a “winner-takes-all” scenario, such as a sporting event, each team seeks strategic advantage over the other team. In baseball terms, the winner gets more points when at bat and denies more points when on the field. However, when competing as a team, winning together requires collaboration to build strategy, execute plays, and reach victory. You compete against the other team and collaborate within your own team.
Scientists who study negotiation strategies and conflict resolution find that collaborative groups spend less time countering one another and, instead, investing that same effort into building constructive outcomes, a force multiplier.
In the winner-takes-all model, the baseball team that gets “outs,” makes plays, and advances team members to home plate, wins. If there is contest within the team, players invest that same effort into seeking their own gain at the expense of others. Benefits derived from shared effort are shunned in favor of benefits accrued to one player over the other. It is a distinction between “I won” versus “We won.”
Hospital medicine is not a win/lose sport, yet over the years, hospitalists have shared with me that their institution or group at times feels like a competitive field with winners and losers. If this distinction is placed on a continuum, what factors encourage a more collaborative environment and what factors do the opposite, toward the adversarial side of the continuum? It makes a substantive difference in the interactions and accomplishments that a group achieves.
My colleagues and I at Harvard study leaders in times of crisis. A crisis makes apparent what is often more subtle during routine times. Our study of leaders in the wake of the Boston Marathon bombings was among our most revealing.
During most crises, an operational leader is designated to oversee the whole of the response. This is an individual with organizational authority and subject-matter expertise appropriate to the situation at hand. In Boston, however, there were so many different jurisdictions – federal, state, and local – and so many different agencies, that no one leader stood above the others. They worked in a remarkably collaborative fashion. While the bombings themselves were tragic, the response itself was a success: All who survived the initial blasts lived, a function of remarkable emergency care, distribution to hospitals, and good medical care. The perpetrators were caught in 102 hours, and “Boston Strong” reflected a genuine city resilience.
These leaders worked together in ways that we had rarely seen before. What we discovered was a phenomenon we call “swarm leadership,” inspired by the ways ants, bees, and termites engage in collective work and decision making. These creatures have clear lines of communication and structures for judgment calls, often about food sources, nesting locations, and threats.
There are five principles of swarm leadership:
- Unity of mission – In Boston, that was to “save lives,” and it motivated and activated the whole of the response.
- Generosity of spirit and action – Across the community, people were eager to assist in the response.
- Everyone stayed in their own lanes of responsibility and helped others succeed in theirs – There were law enforcement, medical, and resilience activities and the theme across the leaders was “how can I help make you a success?”
- No ego and no blame – There was a level of emotional intelligence and maturity among the leaders.
- A foundation of trusting relations – These leaders had known one another for years and, though the decisions were tough, they were confident in the motives and actions of the others.
While the discovery emerged from our crisis research, the findings equally apply to other, more routine work and interactions. Conduct your own assessment. Have you worked in groups in which these principles of swarm leadership characterized the experience? People were focused on a shared mission: They were available to assist one another; accomplished their work in ways that were respectful and supportive of their different responsibilities; did not claim undue credit or swipe at each another; and knew one another well enough to trust the others’ actions and motives.
The flip side of this continuum of collaboration and competition we term “suspicion leadership.” This is characterized by selfish ambitions; narcissistic actions; grabs for authority and resources; credit taking for the good and accusations for the bad; and an environment of mistrust and back stabbing.
Leaders influence the tone and tenor of their own group’s interactions as well as interactions among different working groups. As role models, if they articulate and demonstrate a mission that others can rally around, they forge that critical unity of mission. By contrast, suspicion leaders make it clear that “it is all about me and my priorities.” There is much work to be done, and swarm leaders ensure that people have the resources, autonomy, and support necessary to get the job done. On the other end, the work environment is burdened by the uncertainties about who does what and who is responsible. Swarm leaders are focused on “we” and suspicion leaders are caught up on “me.” There is no trust when people are suspicious of one another. Much can be accomplished when people believe in themselves, their colleagues, and the reasons that bring them together.
As a hospitalist leader, you influence where on this continuum your group will lie. It is your choice to be a role model for the principles of swarm, encouraging the same among others. When those principles become the beacons by which you work and relate, you will find an environment that inspires people to be and to do their best.
In the next column, how to build trust within your teams.
Dr. Marcus is director, Program on Health Care Negotiation and Conflict Resolution, at the Harvard T.H. Chan School of Public Health, in Boston.
During your career, you serve as staff member and leader to many different professional groups. Some are collaborative, collegial, and supportive. Others are competitive, antagonistic, or even combative. What are the benefits and downsides of each of these cultures and what can you do, as a hospitalist leader, to influence the character of your workplace?
The field of “game theory” provides insights into the distinction. The first questions to ask are “What is the game you are playing?” and then “Who is the competition?” In a “winner-takes-all” scenario, such as a sporting event, each team seeks strategic advantage over the other team. In baseball terms, the winner gets more points when at bat and denies more points when on the field. However, when competing as a team, winning together requires collaboration to build strategy, execute plays, and reach victory. You compete against the other team and collaborate within your own team.
Scientists who study negotiation strategies and conflict resolution find that collaborative groups spend less time countering one another and, instead, investing that same effort into building constructive outcomes, a force multiplier.
In the winner-takes-all model, the baseball team that gets “outs,” makes plays, and advances team members to home plate, wins. If there is contest within the team, players invest that same effort into seeking their own gain at the expense of others. Benefits derived from shared effort are shunned in favor of benefits accrued to one player over the other. It is a distinction between “I won” versus “We won.”
Hospital medicine is not a win/lose sport, yet over the years, hospitalists have shared with me that their institution or group at times feels like a competitive field with winners and losers. If this distinction is placed on a continuum, what factors encourage a more collaborative environment and what factors do the opposite, toward the adversarial side of the continuum? It makes a substantive difference in the interactions and accomplishments that a group achieves.
My colleagues and I at Harvard study leaders in times of crisis. A crisis makes apparent what is often more subtle during routine times. Our study of leaders in the wake of the Boston Marathon bombings was among our most revealing.
During most crises, an operational leader is designated to oversee the whole of the response. This is an individual with organizational authority and subject-matter expertise appropriate to the situation at hand. In Boston, however, there were so many different jurisdictions – federal, state, and local – and so many different agencies, that no one leader stood above the others. They worked in a remarkably collaborative fashion. While the bombings themselves were tragic, the response itself was a success: All who survived the initial blasts lived, a function of remarkable emergency care, distribution to hospitals, and good medical care. The perpetrators were caught in 102 hours, and “Boston Strong” reflected a genuine city resilience.
These leaders worked together in ways that we had rarely seen before. What we discovered was a phenomenon we call “swarm leadership,” inspired by the ways ants, bees, and termites engage in collective work and decision making. These creatures have clear lines of communication and structures for judgment calls, often about food sources, nesting locations, and threats.
There are five principles of swarm leadership:
- Unity of mission – In Boston, that was to “save lives,” and it motivated and activated the whole of the response.
- Generosity of spirit and action – Across the community, people were eager to assist in the response.
- Everyone stayed in their own lanes of responsibility and helped others succeed in theirs – There were law enforcement, medical, and resilience activities and the theme across the leaders was “how can I help make you a success?”
- No ego and no blame – There was a level of emotional intelligence and maturity among the leaders.
- A foundation of trusting relations – These leaders had known one another for years and, though the decisions were tough, they were confident in the motives and actions of the others.
While the discovery emerged from our crisis research, the findings equally apply to other, more routine work and interactions. Conduct your own assessment. Have you worked in groups in which these principles of swarm leadership characterized the experience? People were focused on a shared mission: They were available to assist one another; accomplished their work in ways that were respectful and supportive of their different responsibilities; did not claim undue credit or swipe at each another; and knew one another well enough to trust the others’ actions and motives.
The flip side of this continuum of collaboration and competition we term “suspicion leadership.” This is characterized by selfish ambitions; narcissistic actions; grabs for authority and resources; credit taking for the good and accusations for the bad; and an environment of mistrust and back stabbing.
Leaders influence the tone and tenor of their own group’s interactions as well as interactions among different working groups. As role models, if they articulate and demonstrate a mission that others can rally around, they forge that critical unity of mission. By contrast, suspicion leaders make it clear that “it is all about me and my priorities.” There is much work to be done, and swarm leaders ensure that people have the resources, autonomy, and support necessary to get the job done. On the other end, the work environment is burdened by the uncertainties about who does what and who is responsible. Swarm leaders are focused on “we” and suspicion leaders are caught up on “me.” There is no trust when people are suspicious of one another. Much can be accomplished when people believe in themselves, their colleagues, and the reasons that bring them together.
As a hospitalist leader, you influence where on this continuum your group will lie. It is your choice to be a role model for the principles of swarm, encouraging the same among others. When those principles become the beacons by which you work and relate, you will find an environment that inspires people to be and to do their best.
In the next column, how to build trust within your teams.
Dr. Marcus is director, Program on Health Care Negotiation and Conflict Resolution, at the Harvard T.H. Chan School of Public Health, in Boston.
Urge PAs to Join New SVS Section
SVS members, please remember to urge your physician assistants -- and other PAs you know who work in a vascular setting -- to apply to become charter members of the new SVS section created for them. The first step is becoming an affiliate member of the SVS. For our new charter PA members, SVS is waiving the application fee. For more information, email [email protected] or call the SVS Membership Department at 312-334-2313.
We welcome nurses and nurse practitioners as well. Please consider becoming a part of the Society for Vascular Nursing, which makes its management home at SVS.
SVS members, please remember to urge your physician assistants -- and other PAs you know who work in a vascular setting -- to apply to become charter members of the new SVS section created for them. The first step is becoming an affiliate member of the SVS. For our new charter PA members, SVS is waiving the application fee. For more information, email [email protected] or call the SVS Membership Department at 312-334-2313.
We welcome nurses and nurse practitioners as well. Please consider becoming a part of the Society for Vascular Nursing, which makes its management home at SVS.
SVS members, please remember to urge your physician assistants -- and other PAs you know who work in a vascular setting -- to apply to become charter members of the new SVS section created for them. The first step is becoming an affiliate member of the SVS. For our new charter PA members, SVS is waiving the application fee. For more information, email [email protected] or call the SVS Membership Department at 312-334-2313.
We welcome nurses and nurse practitioners as well. Please consider becoming a part of the Society for Vascular Nursing, which makes its management home at SVS.
With CHIP in limbo, here are five takeaways on the congressional impasse
Two months past its deadline, Congress has yet to fund the Children’s Health Insurance Program, leaving several states scrambling for cash.
Lawmakers grappling with the failed repeal of the Affordable Care Act allowed authorization of the program to lapse on Sept. 30. Although CHIP has always had broad bipartisan support, the House and Senate cannot agree on how to continue federal funding. And the Trump administration has been mostly silent on the issue.
CHIP benefits 9 million children nationwide and 370,000 pregnant women a year. It helps lower- and middle-income families who otherwise earn too much to be eligible for Medicaid. Like Medicaid, CHIP is paid for with state and federal funds, but the federal government covers close to 90% of the cost.
To keep the program going, states with unspent federal CHIP money have seen their excess sent to a handful of states running low on funds. But that is a bureaucratic Band-Aid; some large states are warning families they may not be able to rely on CHIP for much longer.
All told, the CMS has given out $1.2 billion in redistribution dollars since October. To keep the program going would cost the federal government $8.5 billion over 5 years, the Congressional Budget Office estimates.
Dec. 2 marked the 25th anniversary of Pennsylvania approving the original CHIP program, which served as a model for the national law, established in 1997. Since then, CHIP has been left in the fiscal lurch only once before. In 2007, CHIP went several weeks without funding authorization from Congress.
Here’s a quick look at what the shortfall may mean to daily life.
1. Are any kids hurting because Congress has failed to fund CHIP?
No. But states such as California will run out of money within weeks. That state alone accounts for nearly 15% of all children benefiting from CHIP. Without federal money, state programs could freeze enrollment or suspend operation.
2. What are states doing since Congress missed the deadline?
Most states are doing little except looking for other unspent federal funds or asking the federal government to send some unspent funds from other states. But some, such as Colorado, are sending warning letters to beneficiaries to tell them that the program could soon end and to look for alternatives. This could mean exploring the ACA marketplace for coverage or researching if a child qualifies for Medicaid.
Colorado said it has only enough CHIP funding to last through January and then the program, without federal dollars, will end.
Arizona officials announced Nov. 30 that it will use Medicaid funding to fill in the shortage of CHIP dollars to extend the life of its CHIP program.
Virginia officials plan to send out a similar notice to parents of CHIP members by early December.
Minnesota is keeping CHIP alive by paying the federal share with state funds.
In Oregon, Democratic Gov. Kate Brown recently said that she is ready to spend $35 million in state funds to keep CHIP running through December.
Nevada announced on Nov. 30 it had been approved for extra funding from the Centers for Medicare & Medicaid Services – nearly $5.7 million – which could keep CHIP alive through December and possibly January.
California, which leads the nation in CHIP enrollment, has received the lion’s share of CMS redistribution funds since October: nearly $692 million.
“Approximately 98% of the 1.3 million population now covered using CHIP funding would continue to receive coverage under the Medicaid program because of a legal obligation to cover them through September 2019,” said California Medicaid/CHIP spokesman Tony Cava. “If CHIP is not reauthorized, the governor and Legislature would need to deliberate on how best to address the population no longer eligible for federal CHIP funding.”
3. When is Congress likely to act?
Not sure. CHIP reauthorization could be included in an appropriations bill that Congress must pass to fund the government into 2018. (Congress now has funded the government through Dec. 8.) A “continuing resolution” bill would have to be approved by then to avert a government shutdown.
4. If CHIP is so popular among Republicans and Democrats, what’s the problem?
There is little debate about its worth and value, but the momentum on CHIP was lost amid disagreements over the Affordable Care Act. The House did extend authorization with a vote – mostly along party lines – on Nov. 3. The Senate itself has yet to vote. The Senate Finance Committee on Oct. 3 approved a bipartisan bill to extend the program for 5 years.
The sticking point is not whether to keep CHIP running but how to raise the cash needed. The House agreed to charge higher premiums to wealthier Medicare beneficiaries, cut money from the ACA’s preventive health fund and shorten the grace period for ACA enrollees who fail to make monthly premium payments.
Like the House bill, the Senate committee bill eliminated an ACA provision to increase CHIP matching funds – to states – by 23%. The increased funding would continue through fiscal year 2019 and fall to 11.5 percent in fiscal year 2020. It would be cut entirely in the following fiscal year.
5. How does CHIP differ based on where you live?
CHIP income eligibility levels vary by state. About 90% of children who qualify are from families earning 200% of poverty or less ($40,840 for a family of three). CHIP covers children up to age 19. But states have the option to cover pregnant women, and 18 states plus the District of Columbia do so.
Some states call CHIP by different names. For example, it is known as Hoosier Healthwise in Indiana, PeachCare for Kids in Georgia and KidsCare in Arizona.
KHN’s coverage of children’s health care issues is supported in part by the Heising-Simons Foundation. Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Two months past its deadline, Congress has yet to fund the Children’s Health Insurance Program, leaving several states scrambling for cash.
Lawmakers grappling with the failed repeal of the Affordable Care Act allowed authorization of the program to lapse on Sept. 30. Although CHIP has always had broad bipartisan support, the House and Senate cannot agree on how to continue federal funding. And the Trump administration has been mostly silent on the issue.
CHIP benefits 9 million children nationwide and 370,000 pregnant women a year. It helps lower- and middle-income families who otherwise earn too much to be eligible for Medicaid. Like Medicaid, CHIP is paid for with state and federal funds, but the federal government covers close to 90% of the cost.
To keep the program going, states with unspent federal CHIP money have seen their excess sent to a handful of states running low on funds. But that is a bureaucratic Band-Aid; some large states are warning families they may not be able to rely on CHIP for much longer.
All told, the CMS has given out $1.2 billion in redistribution dollars since October. To keep the program going would cost the federal government $8.5 billion over 5 years, the Congressional Budget Office estimates.
Dec. 2 marked the 25th anniversary of Pennsylvania approving the original CHIP program, which served as a model for the national law, established in 1997. Since then, CHIP has been left in the fiscal lurch only once before. In 2007, CHIP went several weeks without funding authorization from Congress.
Here’s a quick look at what the shortfall may mean to daily life.
1. Are any kids hurting because Congress has failed to fund CHIP?
No. But states such as California will run out of money within weeks. That state alone accounts for nearly 15% of all children benefiting from CHIP. Without federal money, state programs could freeze enrollment or suspend operation.
2. What are states doing since Congress missed the deadline?
Most states are doing little except looking for other unspent federal funds or asking the federal government to send some unspent funds from other states. But some, such as Colorado, are sending warning letters to beneficiaries to tell them that the program could soon end and to look for alternatives. This could mean exploring the ACA marketplace for coverage or researching if a child qualifies for Medicaid.
Colorado said it has only enough CHIP funding to last through January and then the program, without federal dollars, will end.
Arizona officials announced Nov. 30 that it will use Medicaid funding to fill in the shortage of CHIP dollars to extend the life of its CHIP program.
Virginia officials plan to send out a similar notice to parents of CHIP members by early December.
Minnesota is keeping CHIP alive by paying the federal share with state funds.
In Oregon, Democratic Gov. Kate Brown recently said that she is ready to spend $35 million in state funds to keep CHIP running through December.
Nevada announced on Nov. 30 it had been approved for extra funding from the Centers for Medicare & Medicaid Services – nearly $5.7 million – which could keep CHIP alive through December and possibly January.
California, which leads the nation in CHIP enrollment, has received the lion’s share of CMS redistribution funds since October: nearly $692 million.
“Approximately 98% of the 1.3 million population now covered using CHIP funding would continue to receive coverage under the Medicaid program because of a legal obligation to cover them through September 2019,” said California Medicaid/CHIP spokesman Tony Cava. “If CHIP is not reauthorized, the governor and Legislature would need to deliberate on how best to address the population no longer eligible for federal CHIP funding.”
3. When is Congress likely to act?
Not sure. CHIP reauthorization could be included in an appropriations bill that Congress must pass to fund the government into 2018. (Congress now has funded the government through Dec. 8.) A “continuing resolution” bill would have to be approved by then to avert a government shutdown.
4. If CHIP is so popular among Republicans and Democrats, what’s the problem?
There is little debate about its worth and value, but the momentum on CHIP was lost amid disagreements over the Affordable Care Act. The House did extend authorization with a vote – mostly along party lines – on Nov. 3. The Senate itself has yet to vote. The Senate Finance Committee on Oct. 3 approved a bipartisan bill to extend the program for 5 years.
The sticking point is not whether to keep CHIP running but how to raise the cash needed. The House agreed to charge higher premiums to wealthier Medicare beneficiaries, cut money from the ACA’s preventive health fund and shorten the grace period for ACA enrollees who fail to make monthly premium payments.
Like the House bill, the Senate committee bill eliminated an ACA provision to increase CHIP matching funds – to states – by 23%. The increased funding would continue through fiscal year 2019 and fall to 11.5 percent in fiscal year 2020. It would be cut entirely in the following fiscal year.
5. How does CHIP differ based on where you live?
CHIP income eligibility levels vary by state. About 90% of children who qualify are from families earning 200% of poverty or less ($40,840 for a family of three). CHIP covers children up to age 19. But states have the option to cover pregnant women, and 18 states plus the District of Columbia do so.
Some states call CHIP by different names. For example, it is known as Hoosier Healthwise in Indiana, PeachCare for Kids in Georgia and KidsCare in Arizona.
KHN’s coverage of children’s health care issues is supported in part by the Heising-Simons Foundation. Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Two months past its deadline, Congress has yet to fund the Children’s Health Insurance Program, leaving several states scrambling for cash.
Lawmakers grappling with the failed repeal of the Affordable Care Act allowed authorization of the program to lapse on Sept. 30. Although CHIP has always had broad bipartisan support, the House and Senate cannot agree on how to continue federal funding. And the Trump administration has been mostly silent on the issue.
CHIP benefits 9 million children nationwide and 370,000 pregnant women a year. It helps lower- and middle-income families who otherwise earn too much to be eligible for Medicaid. Like Medicaid, CHIP is paid for with state and federal funds, but the federal government covers close to 90% of the cost.
To keep the program going, states with unspent federal CHIP money have seen their excess sent to a handful of states running low on funds. But that is a bureaucratic Band-Aid; some large states are warning families they may not be able to rely on CHIP for much longer.
All told, the CMS has given out $1.2 billion in redistribution dollars since October. To keep the program going would cost the federal government $8.5 billion over 5 years, the Congressional Budget Office estimates.
Dec. 2 marked the 25th anniversary of Pennsylvania approving the original CHIP program, which served as a model for the national law, established in 1997. Since then, CHIP has been left in the fiscal lurch only once before. In 2007, CHIP went several weeks without funding authorization from Congress.
Here’s a quick look at what the shortfall may mean to daily life.
1. Are any kids hurting because Congress has failed to fund CHIP?
No. But states such as California will run out of money within weeks. That state alone accounts for nearly 15% of all children benefiting from CHIP. Without federal money, state programs could freeze enrollment or suspend operation.
2. What are states doing since Congress missed the deadline?
Most states are doing little except looking for other unspent federal funds or asking the federal government to send some unspent funds from other states. But some, such as Colorado, are sending warning letters to beneficiaries to tell them that the program could soon end and to look for alternatives. This could mean exploring the ACA marketplace for coverage or researching if a child qualifies for Medicaid.
Colorado said it has only enough CHIP funding to last through January and then the program, without federal dollars, will end.
Arizona officials announced Nov. 30 that it will use Medicaid funding to fill in the shortage of CHIP dollars to extend the life of its CHIP program.
Virginia officials plan to send out a similar notice to parents of CHIP members by early December.
Minnesota is keeping CHIP alive by paying the federal share with state funds.
In Oregon, Democratic Gov. Kate Brown recently said that she is ready to spend $35 million in state funds to keep CHIP running through December.
Nevada announced on Nov. 30 it had been approved for extra funding from the Centers for Medicare & Medicaid Services – nearly $5.7 million – which could keep CHIP alive through December and possibly January.
California, which leads the nation in CHIP enrollment, has received the lion’s share of CMS redistribution funds since October: nearly $692 million.
“Approximately 98% of the 1.3 million population now covered using CHIP funding would continue to receive coverage under the Medicaid program because of a legal obligation to cover them through September 2019,” said California Medicaid/CHIP spokesman Tony Cava. “If CHIP is not reauthorized, the governor and Legislature would need to deliberate on how best to address the population no longer eligible for federal CHIP funding.”
3. When is Congress likely to act?
Not sure. CHIP reauthorization could be included in an appropriations bill that Congress must pass to fund the government into 2018. (Congress now has funded the government through Dec. 8.) A “continuing resolution” bill would have to be approved by then to avert a government shutdown.
4. If CHIP is so popular among Republicans and Democrats, what’s the problem?
There is little debate about its worth and value, but the momentum on CHIP was lost amid disagreements over the Affordable Care Act. The House did extend authorization with a vote – mostly along party lines – on Nov. 3. The Senate itself has yet to vote. The Senate Finance Committee on Oct. 3 approved a bipartisan bill to extend the program for 5 years.
The sticking point is not whether to keep CHIP running but how to raise the cash needed. The House agreed to charge higher premiums to wealthier Medicare beneficiaries, cut money from the ACA’s preventive health fund and shorten the grace period for ACA enrollees who fail to make monthly premium payments.
Like the House bill, the Senate committee bill eliminated an ACA provision to increase CHIP matching funds – to states – by 23%. The increased funding would continue through fiscal year 2019 and fall to 11.5 percent in fiscal year 2020. It would be cut entirely in the following fiscal year.
5. How does CHIP differ based on where you live?
CHIP income eligibility levels vary by state. About 90% of children who qualify are from families earning 200% of poverty or less ($40,840 for a family of three). CHIP covers children up to age 19. But states have the option to cover pregnant women, and 18 states plus the District of Columbia do so.
Some states call CHIP by different names. For example, it is known as Hoosier Healthwise in Indiana, PeachCare for Kids in Georgia and KidsCare in Arizona.
KHN’s coverage of children’s health care issues is supported in part by the Heising-Simons Foundation. Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
ASCO larynx-preservation guidelines reflect important practice changes
The latest edition of the clinical practice guideline on larynx preservation strategies for the treatment of laryngeal cancer from the American Society of Clinical Oncology (ASCO) emphasizes that larynx preservation in patients with early stage disease does not compromise survival compared with total laryngectomy.
“The nuances of treatment selection, assessments of pretreatment voice and swallowing, and public awareness of new organ-preservation treatment and decision making have increased to the point that careful and individualized discussion with patients and families with the multidisciplinary treatment team is a critical element of modern care,” wrote Arlene A. Forastiere, MD, of Johns Hopkins Medicine in Baltimore, and her colleagues. The report was published in the Journal of Clinical Oncology.
Changes since the last guideline on the subject, issued in 2006, include evidence-based support for the use of endoscopic resection in patients with limited stage (T1 and T2) disease, and as an initial total laryngectomy therapy both in patients with stage T4a disease, and in those with severe laryngeal dysfunction prior to treatment.
Also new since the last guideline are recommendations for the use of positron-emission tomography imaging for evaluating the status of regional nodes after treatment, as well as guidance on the best techniques for evaluating voice and swallowing function.
While the initial recommendation that all patients with T1 and T2 laryngeal cancer should be treated with the intent to preserve the larynx has not changed, there is a new recommendation (1.3) stating that surgery may be more effective than radiotherapy for initial larynx preservation therapy, although this recommendation is based on retrospective data and may be affected by patient selection factors, the authors acknowledged. The new recommendation also notes that in an experienced operator’s hands, endoscopic resections can have outcomes that are equal to or better than those with open partial laryngectomy.
The initial recommendation stating that “[e]very effort should be made to avoid combining surgery with radiation therapy because functional outcomes may be compromised by combined-modality therapy; single-modality treatment is effective for limited-stage, invasive cancer of the larynx” remains unchanged.
There is also an updated recommendation that tumor-free margins should be the goal when surgery with larynx preservation intent is performed (1.4).
“Surgery that anticipates the need for postoperative [radiation therapy] to treat close or involved tumor margins or widespread dysplasia is not an acceptable treatment approach,” the guideline authors noted.
There are two other new recommendations including the opinion, based on evidence of benefits vs. harms, that total laryngectomy rather than larynx preservation may be associated with better survival and quality of life in patients with extensive T3 lesions, large T4 lesions, or in those who have poor pretreatment laryngeal function.
The third new recommendation is that “[a]s part of a comprehensive pretreatment evaluation, all patients should undergo a baseline assessment of voice and swallowing function, voice (use and requirements), and counseling with regard to the potential effect of treatment options on voice, swallowing, and quality of life.”
Among the updated recommendations are the following:
• An emphasis on the importance of considering a multiplicity of factors when choosing therapy for patients with limited-stage disease (1.7).
• The option of specialized organ-preservation procedures for a small number of patients with T3 or T4 primary site disease (2.4).
• A strong recommendation for the use of concurrent chemoradiotherapy compared with radiotherapy alone or sequential therapy (2.5).
• Elective neck dissection is not required for patients with clinically involved regional cervical nodes treated with definitive radiotherapy of chemoradiotherapy who have complete clinical, radiologic, and metabolic imaging (3.3).
• “Selection of therapy for an individual patient requires assessment by the multidisciplinary team as well as consideration of voice and swallowing function; patient comorbidity, psychosocial situation, and preferences; and local therapeutic expertise” (4.2).
The guideline development process was supported by ASCO. Dr, Forastiere disclosed employment and stock ownership in NantHealth. Many of her coauthors disclosed institutional funding, consultation/advising, travel support and expenses, honoraria, and or patents/royalties with multiple entities.
The latest edition of the clinical practice guideline on larynx preservation strategies for the treatment of laryngeal cancer from the American Society of Clinical Oncology (ASCO) emphasizes that larynx preservation in patients with early stage disease does not compromise survival compared with total laryngectomy.
“The nuances of treatment selection, assessments of pretreatment voice and swallowing, and public awareness of new organ-preservation treatment and decision making have increased to the point that careful and individualized discussion with patients and families with the multidisciplinary treatment team is a critical element of modern care,” wrote Arlene A. Forastiere, MD, of Johns Hopkins Medicine in Baltimore, and her colleagues. The report was published in the Journal of Clinical Oncology.
Changes since the last guideline on the subject, issued in 2006, include evidence-based support for the use of endoscopic resection in patients with limited stage (T1 and T2) disease, and as an initial total laryngectomy therapy both in patients with stage T4a disease, and in those with severe laryngeal dysfunction prior to treatment.
Also new since the last guideline are recommendations for the use of positron-emission tomography imaging for evaluating the status of regional nodes after treatment, as well as guidance on the best techniques for evaluating voice and swallowing function.
While the initial recommendation that all patients with T1 and T2 laryngeal cancer should be treated with the intent to preserve the larynx has not changed, there is a new recommendation (1.3) stating that surgery may be more effective than radiotherapy for initial larynx preservation therapy, although this recommendation is based on retrospective data and may be affected by patient selection factors, the authors acknowledged. The new recommendation also notes that in an experienced operator’s hands, endoscopic resections can have outcomes that are equal to or better than those with open partial laryngectomy.
The initial recommendation stating that “[e]very effort should be made to avoid combining surgery with radiation therapy because functional outcomes may be compromised by combined-modality therapy; single-modality treatment is effective for limited-stage, invasive cancer of the larynx” remains unchanged.
There is also an updated recommendation that tumor-free margins should be the goal when surgery with larynx preservation intent is performed (1.4).
“Surgery that anticipates the need for postoperative [radiation therapy] to treat close or involved tumor margins or widespread dysplasia is not an acceptable treatment approach,” the guideline authors noted.
There are two other new recommendations including the opinion, based on evidence of benefits vs. harms, that total laryngectomy rather than larynx preservation may be associated with better survival and quality of life in patients with extensive T3 lesions, large T4 lesions, or in those who have poor pretreatment laryngeal function.
The third new recommendation is that “[a]s part of a comprehensive pretreatment evaluation, all patients should undergo a baseline assessment of voice and swallowing function, voice (use and requirements), and counseling with regard to the potential effect of treatment options on voice, swallowing, and quality of life.”
Among the updated recommendations are the following:
• An emphasis on the importance of considering a multiplicity of factors when choosing therapy for patients with limited-stage disease (1.7).
• The option of specialized organ-preservation procedures for a small number of patients with T3 or T4 primary site disease (2.4).
• A strong recommendation for the use of concurrent chemoradiotherapy compared with radiotherapy alone or sequential therapy (2.5).
• Elective neck dissection is not required for patients with clinically involved regional cervical nodes treated with definitive radiotherapy of chemoradiotherapy who have complete clinical, radiologic, and metabolic imaging (3.3).
• “Selection of therapy for an individual patient requires assessment by the multidisciplinary team as well as consideration of voice and swallowing function; patient comorbidity, psychosocial situation, and preferences; and local therapeutic expertise” (4.2).
The guideline development process was supported by ASCO. Dr, Forastiere disclosed employment and stock ownership in NantHealth. Many of her coauthors disclosed institutional funding, consultation/advising, travel support and expenses, honoraria, and or patents/royalties with multiple entities.
The latest edition of the clinical practice guideline on larynx preservation strategies for the treatment of laryngeal cancer from the American Society of Clinical Oncology (ASCO) emphasizes that larynx preservation in patients with early stage disease does not compromise survival compared with total laryngectomy.
“The nuances of treatment selection, assessments of pretreatment voice and swallowing, and public awareness of new organ-preservation treatment and decision making have increased to the point that careful and individualized discussion with patients and families with the multidisciplinary treatment team is a critical element of modern care,” wrote Arlene A. Forastiere, MD, of Johns Hopkins Medicine in Baltimore, and her colleagues. The report was published in the Journal of Clinical Oncology.
Changes since the last guideline on the subject, issued in 2006, include evidence-based support for the use of endoscopic resection in patients with limited stage (T1 and T2) disease, and as an initial total laryngectomy therapy both in patients with stage T4a disease, and in those with severe laryngeal dysfunction prior to treatment.
Also new since the last guideline are recommendations for the use of positron-emission tomography imaging for evaluating the status of regional nodes after treatment, as well as guidance on the best techniques for evaluating voice and swallowing function.
While the initial recommendation that all patients with T1 and T2 laryngeal cancer should be treated with the intent to preserve the larynx has not changed, there is a new recommendation (1.3) stating that surgery may be more effective than radiotherapy for initial larynx preservation therapy, although this recommendation is based on retrospective data and may be affected by patient selection factors, the authors acknowledged. The new recommendation also notes that in an experienced operator’s hands, endoscopic resections can have outcomes that are equal to or better than those with open partial laryngectomy.
The initial recommendation stating that “[e]very effort should be made to avoid combining surgery with radiation therapy because functional outcomes may be compromised by combined-modality therapy; single-modality treatment is effective for limited-stage, invasive cancer of the larynx” remains unchanged.
There is also an updated recommendation that tumor-free margins should be the goal when surgery with larynx preservation intent is performed (1.4).
“Surgery that anticipates the need for postoperative [radiation therapy] to treat close or involved tumor margins or widespread dysplasia is not an acceptable treatment approach,” the guideline authors noted.
There are two other new recommendations including the opinion, based on evidence of benefits vs. harms, that total laryngectomy rather than larynx preservation may be associated with better survival and quality of life in patients with extensive T3 lesions, large T4 lesions, or in those who have poor pretreatment laryngeal function.
The third new recommendation is that “[a]s part of a comprehensive pretreatment evaluation, all patients should undergo a baseline assessment of voice and swallowing function, voice (use and requirements), and counseling with regard to the potential effect of treatment options on voice, swallowing, and quality of life.”
Among the updated recommendations are the following:
• An emphasis on the importance of considering a multiplicity of factors when choosing therapy for patients with limited-stage disease (1.7).
• The option of specialized organ-preservation procedures for a small number of patients with T3 or T4 primary site disease (2.4).
• A strong recommendation for the use of concurrent chemoradiotherapy compared with radiotherapy alone or sequential therapy (2.5).
• Elective neck dissection is not required for patients with clinically involved regional cervical nodes treated with definitive radiotherapy of chemoradiotherapy who have complete clinical, radiologic, and metabolic imaging (3.3).
• “Selection of therapy for an individual patient requires assessment by the multidisciplinary team as well as consideration of voice and swallowing function; patient comorbidity, psychosocial situation, and preferences; and local therapeutic expertise” (4.2).
The guideline development process was supported by ASCO. Dr, Forastiere disclosed employment and stock ownership in NantHealth. Many of her coauthors disclosed institutional funding, consultation/advising, travel support and expenses, honoraria, and or patents/royalties with multiple entities.
FROM JCO
Sjögren-Larsson Syndrome: Definitive Diagnosis on Magnetic Resonance Spectroscopy
Sjögren-Larsson syndrome (SLS) is a rare autosomal-recessive neurocutaneous disorder comprising a triad of ichthyosis, mental retardation, and spastic diplegia or quadriplegia.1 The disorder was first described by Sjögren and Larsson2 in 1957. Early reports of SLS were mainly in white patients, with a particularly high prevalence of 8.3 cases per 100,000 individuals in the county of Västerbotten in Sweden.3 Reports of SLS in Asian and Indian populations are rare.4,5 We report a case of SLS in an Indian boy.
Case Report
A 12-year-old Indian boy born to nonconsanguineous parents after a full-term pregnancy with normal vaginal delivery presented with generalized dry scaly skin that had been present since 2 months of age. He had a history of delayed milestones (ie, facial recognition, sitting without support at 3 years of age), inability to walk, dysarthria, mental retardation). He had never attended school due to subnormal intellectual functioning. He had a single episode of a tonic-clonic seizure at 4 years of age but was not on any regular antiepileptic medication. There was a history of similar skin lesions in one male sibling of the patient and in 2 maternal uncles. None of them survived beyond early childhood, but detailed information regarding the cutaneous and neurologic manifestations in these family members was not available.
Cutaneous examination revealed lamellarlike ichthyosis on the dorsal aspects of the arms and legs (Figure 1A). Ichthyosis with lichenification was present on the neck, axillae, cubital and popliteal fossae, and abdomen (Figure 1B). The palms and soles showed keratoderma. Neurologic examination of the arms revealed mild rigidity and brisk reflexes. Examination of the legs showed marked rigidity, brisk knee jerks, ankle clonus, extensor plantar reflexes, flexion deformity with contractures, and scissor gait. A Goddard (Seguin) formboard test was performed and indicated a mental age of 4 years. The patient’s IQ was in the range of 25 to 30, indicating a severe degree of subnormality in intellectual functioning. The clinical presentation suggested a diagnosis of SLS.

A skin biopsy from the ichthyotic lesion showed hyperkeratosis, acanthosis, and papillomatosis with sparse superficial perivascular lymphocytic infiltrate, thus confirming the diagnosis of lamellar ichthyosis. Fundus examination was normal. Magnetic resonance imaging (MRI) of the brain revealed confluent symmetrical signal abnormalities along the body of the lateral ventricles, white matter in the perioccipital horn, and in deep white matter of centrum semiovale (Figure 2). Magnetic resonance spectroscopy revealed a narrow lipid peak at approximately 1.3 ppm in the region of signal abnormality (Figure 3). Thus, the diagnosis of SLS was confirmed. Measurement of fatty aldehyde dehydrogenase (FALDH) activity and genetic analysis were not performed due to unavailability.
The patient was treated with topical emollients for the ichthyosis. To reduce his dietary intake of long-chain fatty acids and increase the intake of omega-3 and omega-6 fatty acids, the patient’s parents were advised to use canola, mustard, and/or coconut oil for cooking for the patient, and skim milk was recommended instead of whole milk. Neurodevelopmental techniques in the form of stretching exercises were given to maintain his range of movements. Gutter splints were given to maintain the knees in extension for physiological standing and to prevent osteoporosis. Subsequently, the patient also underwent a multilevel soft-tissue release (hip and knee joints) to relieve the contractures. These measures resulted in considerable improvement and the patient was able to walk with support.
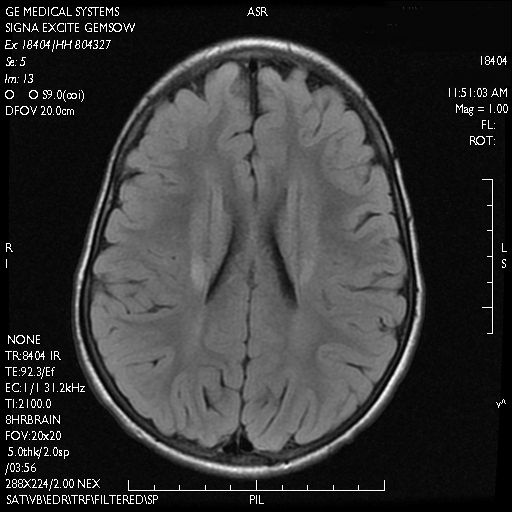
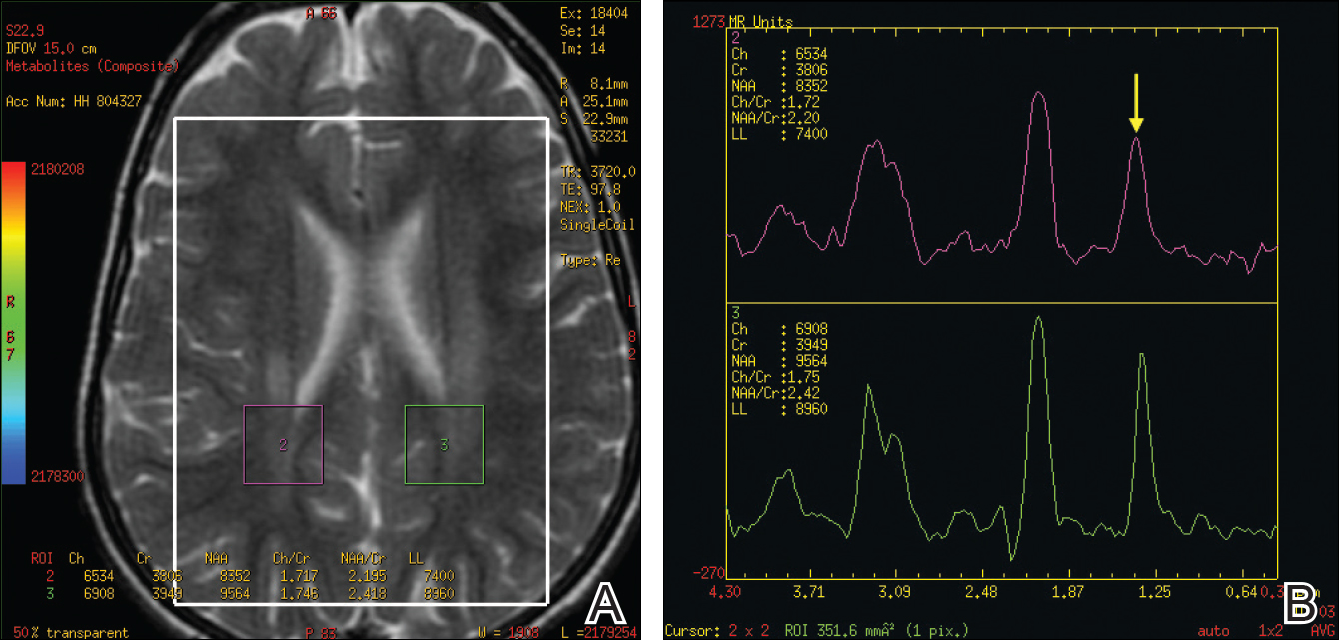
Comment
Presentation
The characteristic clinical features of SLS begin to develop during the intranatal period and infancy.1,6 Pathologic skin involvement can be detected as early as week 23 of gestation. Preterm births associated with SLS have commonly been described.3 Ichthyosis often is evident at birth, but collodion membrane is uncommon. Severe pruritus is a marked feature unlike most other types of ichthyosis. The ichthyosis often is generalized with prominent involvement of the flexural areas and nape of the neck, varying from fine furfuraceous to larger lamellarlike scales. Velvety orange or brown lichenification often is a predominant feature in the flexures of the arms, legs, neck, and mid abdomen. Mental retardation, developmental delay, and spasticity usually become apparent at 1 to 2 years of age and subsequently are nonprogressive.6,7 However, patients rarely have been described with normal intellectual functioning.7 Spasticity often is more severe in the lower limbs and may lead to contractures, kyphoscoliosis, hip dislocation, and short stature. Delayed speech and dysarthria are common. Parafoveal glistening white dots on the retina are a pathognomonic feature and typically appear in the first 2 years of life; however, they are seen in approximately 30% of patients and increase slightly in number with age.6,8 There may be associated decreased visual acuity, photophobia, myopia, and astigmatism. Other clinical features include enamel hypoplasia, metaphyseal dysplasia, and epilepsy.1,6
Gene Mutations
Sjögren-Larsson syndrome is caused by mutation in the aldehyde dehydrogenase 3 family member A2 gene, ALDH3A2 (17p11.2), which codes for FALDH.1,6,7 The ALDH3A2 gene is 11 exons long and gives rise to 2 protein isoforms that differ in their carboxy-terminal domains; the major isoform, composed of 485 amino acids, localizes to the endoplasmic reticulum. The minor protein isoform (FALDHv) is composed of 508 amino acids, possesses a longer carboxy-terminal, and appears to be targeted to the peroxisome. Several mutations have been reported throughout the ALDH3A2 gene, including missense mutations (most common [38% of cases of SLS6]), deletions, insertions, splicing errors, and complex rearrangements. Although several of these mutations are private, several common mutations may be indicative of founder effects (ie, shared ancestry), consanguinity, or recurrent mutational events (mutation hotspots).6,7 Despite the wide spectrum of mutations, there is very little phenotypic variation, with consistently severe cutaneous and neurological involvement occurring in a majority of patients.7 However, Lossos et al9 described remarkable phenotypic variation in 6 siblings of an Arab family and suggested that additional unknown genetic or environmental factors may compensate for the biochemical defect.
Lipid Metabolism
Fatty aldehyde dehydrogenase is expressed in almost all cells and tissues and catalyzes the oxidation of fatty aldehydes to fatty acids (eFigure 1). It also is a part of the fatty alcohol:NAD oxidoreductase (FAO) enzyme complex, which catalyzes fatty alcohol oxidation to fatty acid. Fatty aldehyde dehydrogenase deficiency leads to accumulation of long-chain alcohols (eg, hexadecanol, octadecanol, octadecenol) and diversion of fatty alcohol into alternate biosynthetic pathways such as wax esters and 1-O-alkyl-2,3-diacylglycerol.10 Other lipids that are increased are illustrated in eFigure 2. Accumulation of these lipids, toxic effects of abnormal lipids (especially fatty aldehydes and Schiff base protein-lipid adducts), and lack of essential lipids (eg, polyunsaturated fatty acids, ceramides 1 and 6, triglycerides) are responsible for the classical cutaneous, neurologic, and ophthalmologic features of SLS.

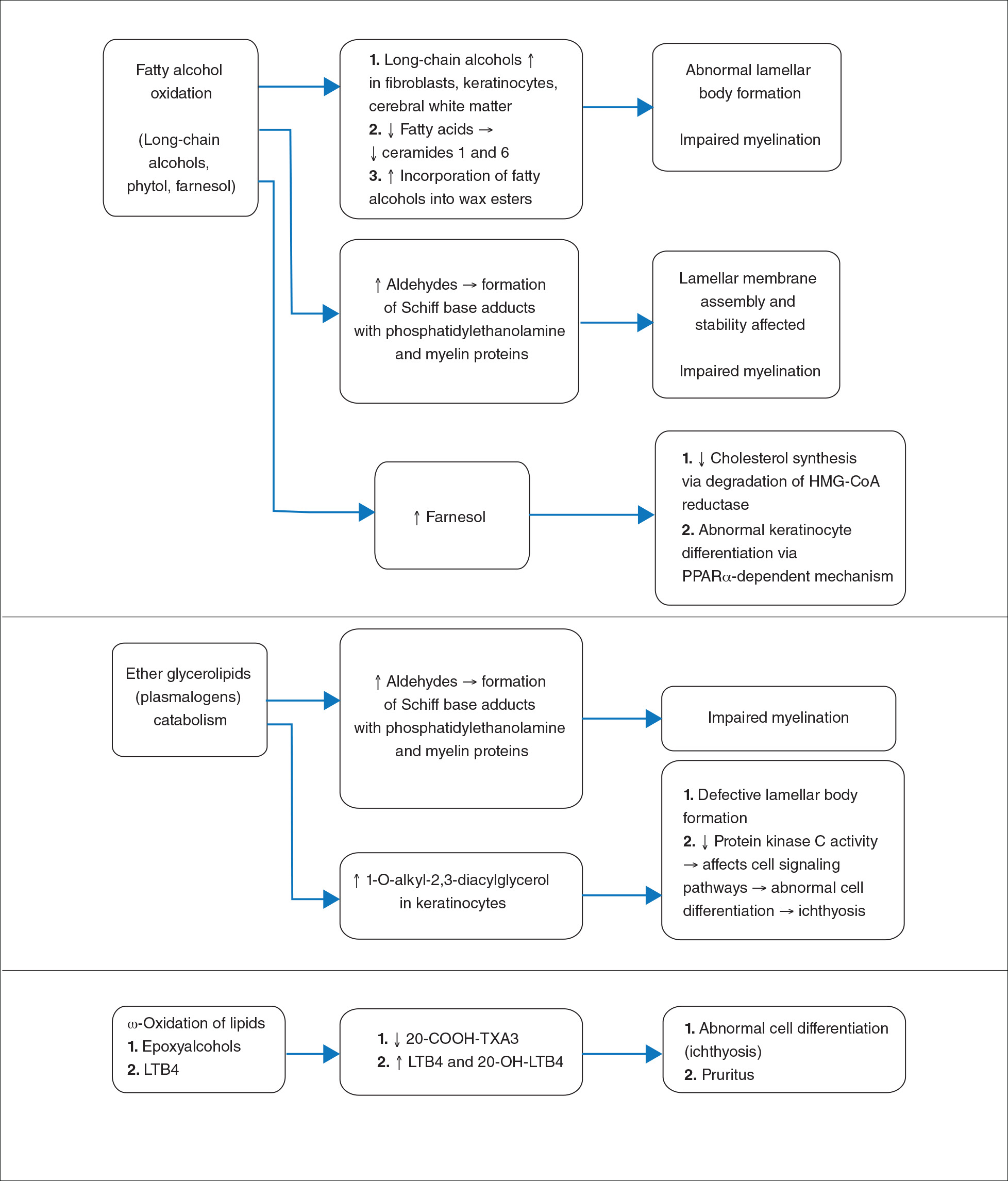
Histopathology
The epidermal permeability barrier is critically dependent on the appropriate lipid composition of the multilamellar stratum corneum intercellular membranes, an equimolar ratio of cholesterol, ceramides, and fatty acids. Histopathology of the skin in SLS generally shows hyperkeratosis, papillomatosis, acanthosis, and a mildly thickened granular layer. Ultrastructural studies of the skin reveal misshapen/empty lamellar bodies, abnormal cytoplasmic lamellar inclusions in the granular keratinocytes, lipid droplets in the stratum corneum with decreased lamellar bilayers, and lamellar/nonlamellar phase separation in the stratum corneum interstitium.11 These findings indicate that lipid metabolism dysfunction in SLS results in marked impairment in formation and secretion of lamellar bodies in the epidermis and consequent disorganization of the stratum corneum lamellar membranes. The resulting disruption of the skin barrier function leads to increased transepidermal water loss, resulting in ichthyosis.11,12 Another proposed mechanism for ichthyosis in SLS is disruption of the normal epidermal differentiation resulting from abnormal lipid metabolites (eFigure 2). Also, increased leukotriene B4 (LTB4) and 20-hydroxy-leukotriene B4 (20-OH-LTB4)(eFigure 1) may be responsible for the considerable pruritus seen in SLS.10
Neurologic Findings
Neurologic changes in SLS result from delayed and deficient myelination. Neuropathological studies have shown ballooning of myelin sheaths, extensive loss of myelin, axonal damage, and astrogliosis. The presence of lipoid material positive for periodic acid–Schiff that stains light rather than dark pink, dense distribution of round/ellipsoid bodies in the white matter of the cerebrum and brainstem positive for periodic acid–Schiff, and proliferation of perivascular macrophages containing lipofuscinlike pigments also have been described.13 Possibly, in the absence of FALDH, metabolism of plasmalogens (a major component of myelin) results in increased fatty aldehydes, which are either diverted to fatty alcohols or form adducts with phosphatidylethanolamine and myelin basic proteins (eFigure 1). Magnetic resonance imaging of the brain usually shows hypomyelination involving the periventricular white matter extending from the frontal to the occipital area.7,14 Mild ventricular enlargement may be an additional feature.14
A useful application of MRI is the proton magnetic resonance spectroscopy, which quantifies the brain metabolites noninvasively, displaying them as a spectrum on a graph. The spectrum comprises a set of resonances/peaks distributed along an x-axis. The resonances of these metabolites are obtained after suppressing the large signals from water protons. Proton magnetic resonance spectroscopy of the normal brain shows 3 prominent peaks: (1) N-acetylaspartate (NAA) at 2.02 ppm, (2) creatine at 3.02 ppm, and (3) choline at 3.22 ppm. In SLS, cerebral proton MRI spectroscopy reveals a characteristic abnormal, prominent, and narrow lipid peak at 1.3 ppm (corresponding to hexadecanol and octadecanol) and may offer a quantitative parameter for monitoring the effects of therapeutic interventions.7,14,15 The most intense lipid peaks are located in the periventricular regions in the anterior and posterior trigones. An abnormal but much smaller peak may be seen at 0.8 to 0.9 ppm, corresponding to phytol.14 Gradual emergence of these changes occurs in the first 2 years of life and then remains stable.15 Proton magnetic resonance spectroscopy also can be used for screening of SLS heterozygotes.16 Lipid peaks have been described in other disorders of lipid metabolism, but they are less intense, broader, and disappear on longer echo time sequences.14
Besides the characteristic parafoveal glistening white dots the retina, optical coherence tomography shows focal hyperreflectivitity in the perifoveal ganglion cell layer and inner plexiform layer of the retina as well as cystoid foveal degeneration.17 The intraretinal deposition of lipid metabolites probably leads to Müller cell degeneration with subsequent formation of cystoid spaces and atrophic changes in the fovea.
Measurement of FALDH or FAO activity in cultured skin fibroblasts and leukocytes using flurometric or gas chromatography mass spectrometry assays is a reliable biochemical test in cases of SLS as well as in heterozygotes.17 A decrease in FALDH/FAO activity also can be demonstrated by histochemical staining in skin biopsy.11 Pathologic urinary excretion of LTB4 and 20-OH-LTB4 also is a biochemical marker of SLS. Mutation analysis for a specific gene defect is diagnostic in cases of SLS as well as in heterozygotes. Prenatal diagnosis of SLS is possible by assessing FALDH activity or gene defects in cultured chorionic villus fibroblasts and amniocytes.18,19
Differential Diagnosis
The differential diagnosis of SLS includes congenital ichthyosiform erythroderma with neurological signs (Tay syndrome, Conradi-Hünermann-Happle syndrome) and neurocutaneous disorders such as neutral lipid storage disease and multiple sulfatase deficiency; however, the nature of the ichthyosis, presence of spastic diplegia/tetraplegia, characteristic parafoveal glistening white dots on the retina, and MRI and proton magnetic resonance spectroscopy findings help to easily differentiate SLS from these disorders.
Treatment
Treatment of SLS mainly is palliative. Ichthyosis can be treated with topical keratolytics, emollients, calcipotriol, and oral retinoids (acitretin).6 Zileuton, a 5-lipoxygenase inhibitor, inhibits synthesis of LTB4 and cysteinyl leukotrienes, thereby reducing the severity of pruritus and also has been shown to improve the speed of information processing.18 Similarly, montelukast, a leuko-triene antagonist, is helpful in relieving the agonizing pruritus.19 Experimental studies have shown that bezafibrate, a peroxisome proliferator-activated receptor α agonist, induces FALDH activity in fibroblasts of SLS patients that still have some residual FALDH activity, but further research is required to determine whether SLS patients could benefit from treatment.20 Physiotherapy helps in relieving the spasticity to some extent, such as in our case. Dietary intervention with reduced fat intake (up to 30% of total daily calorific requirement) and supplementation with omega-3 and omega-6 fatty acids has shown variable results in anecdotal reports.21-23 Gene therapy using recombinant adeno-associated virus 2 vectors to restore FALDH has been projected as a future treatment option.24 Despite lack of effective treatment options, most patients of SLS survive well into adulthood.
Conclusion
Because ichthyosis is one of the earliest and prominent symptoms of SLS, a dermatologist can play an important role in early diagnosis. Any child with the classical pattern of ichthyosis should be thoroughly examined for early neurologic signs and investigated to rule out SLS. Proton magnetic resonance spectroscopy serves as a useful adjunct in the diagnosis of SLS by confirming the accumulation of abnormal lipids in the periventricular white matter, especially when specific enzyme analysis and genetic analysis are not available in resource-restricted settings.
- Judge MR, McLean WHI, Munro CS. Disorders of keratinization. In: Burns T, Breathnach S, Cox N, eds. Rook’s Textbook of Dermatology. 7th ed. West Sussex, United Kingdom: Wiley & Sons; 2004:34.37-34.39.
- Sjögren T, Larsson T. Oligophrenia in association with congenital ichthyosis and spastic disorders. Acta Psychiatr Neurol Scand. 1957;32:1-113.
- Jagell S, Gustavson KH, Holmgren G. Sjögren-Larsson syndrome in Sweden. a clinical, genetic and epidemiological study. Clin Genet. 1981;19:233-256.
- Sood M, Trehan A, Dinakaran J, et al. Sjögren-Larsson syndrome. Indian J Pediatr. 2002;69:193-194.
- Uppal M, Srinivas CR, Thowfeeq KT. Sjögren-Larsson syndrome: report of two cases. Indian J Dermatol Venereol Leprol. 2004;70:110-111.
- Rizzo WB. Sjögren-Larsson syndrome: molecular genetics and biochemical pathogenesis of fatty aldehyde dehydrogenase deficiency. Mol Genet Metab. 2007;90:1-9.
- Willemsen MA, Ijlst L, Steijlen PM, et al. Clinical, biochemical and molecular genetic characteristics of 19 patients with the Sjögren-Larsson syndrome. Brain. 2001;124(pt 7):1426-1437.
- Willemsen MA, Cruysberg JR, Rotteveel JJ, et al. Juvenile macular dystrophy associated with deficient activity of fatty aldehyde dehydrogenase in Sjögren-Larsson syndrome. Am J Ophthalmol. 2000;130:782-789.
- Lossos A, Khoury M, Rizzo WB, et al. Phenotypic variability among adult siblings with Sjögren-Larsson syndrome. Arch Neurol. 2006;63:278-280.
- Rizzo WB, Craft DA, Somer T, et al. Abnormal fatty alcohol metabolism in cultured keratinocytes from patients with Sjögren-Larsson syndrome. J Lipid Res. 2008;49:410-419.
- Rizzo WB, S’Aulis D, Jennings MA, et al. Ichthyosis in Sjögren-Larsson syndrome reflects defective barrier function due to abnormal lamellar body structure and secretion. Arch Dermatol Res. 2010;302:443-451.
- Rizzo WB. The role of fatty aldehyde dehydrogenase in epidermal structure and function. Dermatoendocrinol. 2011;2:91-99.
- Yamaguchi K, Handa T. Sjögren-Larsson syndrome: postmortem brain abnormalities. Pediatr Neurol. 1998;18:338-341.
- Mano T, Ono J, Kaminaga T, et al. Proton MR spectroscopy of Sjögren-Larsson’s Syndrome. Am J Neuroradiol. 1999;20:1671-1673.
- Willemsen MA, van der Graf M, van der Knaap MS, et al. MR imaging and proton MR spectroscopic studies in Sjögren-Larsson syndrome: characterization of the leukoencephalopathy. Am J Neuroradiol. 2004;25:649-657.
- Kaminaga T, Mano T, Ono J, et al. Proton magnetic resonance spectroscopy of Sjögren-Larsson Syndrome. Magn Reson Med. 2001;45:1112-1115.
- Fuijkschot J, Cruysberg JR, Willemsen MA, et al. Subclinical changes in the juvenile crystalline macular dystrophy in Sjögren-Larsson syndrome detected by optical coherence tomography. Ophthalmology. 2008;115:870-875.
- Willemsen MA, Lutt MA, Steijlen PM, et al. Clinical and biochemical effects of zileuton in patients with the Sjögren-Larsson syndrome. Eur J Pediatr. 2001;160:711-717.
- Pirgon O, Aydin K, Atabek ME. Proton magnetic resonance spectroscopy findings and clinical effects of montelukast sodium in a case with Sjögren-Larsson syndrome. J Child Neurol. 2006;21:1092-1095.
- Gloerich J, Ijlst L, Wanders RJ, et al. Bezafibrate induces FALDH in human fibroblasts; implications for Sjögren-Larsson syndrome Mol Genet Metab. 2006;89:111-115.
- Auada MP, Taube MB, Collares EF, et al. Sjögren-Larsson syndrome: biochemical defects and follow up in three cases. Eur J Dermatol. 2002;12:263-266.
- Taube B, Billeaud C, Labreze C, et al. Sjögren-Larsson syndrome: early diagnosis, dietary management and biochemical studies in two cases. Dermatology. 1999;198:340-345.
- Rizzo WB. Genetics and prospective therapeutic targets for Sjögren-Larsson Syndrome. Expert Opin Orphan Drugs. 2016;4:395-406.
- Haug S, Braun-Falco M. Restoration of fatty aldehyde dehydrogenase deficiency in Sjögren-Larsson syndrome. Gene Ther. 2006;13:1021-1026.
Sjögren-Larsson syndrome (SLS) is a rare autosomal-recessive neurocutaneous disorder comprising a triad of ichthyosis, mental retardation, and spastic diplegia or quadriplegia.1 The disorder was first described by Sjögren and Larsson2 in 1957. Early reports of SLS were mainly in white patients, with a particularly high prevalence of 8.3 cases per 100,000 individuals in the county of Västerbotten in Sweden.3 Reports of SLS in Asian and Indian populations are rare.4,5 We report a case of SLS in an Indian boy.
Case Report
A 12-year-old Indian boy born to nonconsanguineous parents after a full-term pregnancy with normal vaginal delivery presented with generalized dry scaly skin that had been present since 2 months of age. He had a history of delayed milestones (ie, facial recognition, sitting without support at 3 years of age), inability to walk, dysarthria, mental retardation). He had never attended school due to subnormal intellectual functioning. He had a single episode of a tonic-clonic seizure at 4 years of age but was not on any regular antiepileptic medication. There was a history of similar skin lesions in one male sibling of the patient and in 2 maternal uncles. None of them survived beyond early childhood, but detailed information regarding the cutaneous and neurologic manifestations in these family members was not available.
Cutaneous examination revealed lamellarlike ichthyosis on the dorsal aspects of the arms and legs (Figure 1A). Ichthyosis with lichenification was present on the neck, axillae, cubital and popliteal fossae, and abdomen (Figure 1B). The palms and soles showed keratoderma. Neurologic examination of the arms revealed mild rigidity and brisk reflexes. Examination of the legs showed marked rigidity, brisk knee jerks, ankle clonus, extensor plantar reflexes, flexion deformity with contractures, and scissor gait. A Goddard (Seguin) formboard test was performed and indicated a mental age of 4 years. The patient’s IQ was in the range of 25 to 30, indicating a severe degree of subnormality in intellectual functioning. The clinical presentation suggested a diagnosis of SLS.
A skin biopsy from the ichthyotic lesion showed hyperkeratosis, acanthosis, and papillomatosis with sparse superficial perivascular lymphocytic infiltrate, thus confirming the diagnosis of lamellar ichthyosis. Fundus examination was normal. Magnetic resonance imaging (MRI) of the brain revealed confluent symmetrical signal abnormalities along the body of the lateral ventricles, white matter in the perioccipital horn, and in deep white matter of centrum semiovale (Figure 2). Magnetic resonance spectroscopy revealed a narrow lipid peak at approximately 1.3 ppm in the region of signal abnormality (Figure 3). Thus, the diagnosis of SLS was confirmed. Measurement of fatty aldehyde dehydrogenase (FALDH) activity and genetic analysis were not performed due to unavailability.
The patient was treated with topical emollients for the ichthyosis. To reduce his dietary intake of long-chain fatty acids and increase the intake of omega-3 and omega-6 fatty acids, the patient’s parents were advised to use canola, mustard, and/or coconut oil for cooking for the patient, and skim milk was recommended instead of whole milk. Neurodevelopmental techniques in the form of stretching exercises were given to maintain his range of movements. Gutter splints were given to maintain the knees in extension for physiological standing and to prevent osteoporosis. Subsequently, the patient also underwent a multilevel soft-tissue release (hip and knee joints) to relieve the contractures. These measures resulted in considerable improvement and the patient was able to walk with support.
Comment
Presentation
The characteristic clinical features of SLS begin to develop during the intranatal period and infancy.1,6 Pathologic skin involvement can be detected as early as week 23 of gestation. Preterm births associated with SLS have commonly been described.3 Ichthyosis often is evident at birth, but collodion membrane is uncommon. Severe pruritus is a marked feature unlike most other types of ichthyosis. The ichthyosis often is generalized with prominent involvement of the flexural areas and nape of the neck, varying from fine furfuraceous to larger lamellarlike scales. Velvety orange or brown lichenification often is a predominant feature in the flexures of the arms, legs, neck, and mid abdomen. Mental retardation, developmental delay, and spasticity usually become apparent at 1 to 2 years of age and subsequently are nonprogressive.6,7 However, patients rarely have been described with normal intellectual functioning.7 Spasticity often is more severe in the lower limbs and may lead to contractures, kyphoscoliosis, hip dislocation, and short stature. Delayed speech and dysarthria are common. Parafoveal glistening white dots on the retina are a pathognomonic feature and typically appear in the first 2 years of life; however, they are seen in approximately 30% of patients and increase slightly in number with age.6,8 There may be associated decreased visual acuity, photophobia, myopia, and astigmatism. Other clinical features include enamel hypoplasia, metaphyseal dysplasia, and epilepsy.1,6
Gene Mutations
Sjögren-Larsson syndrome is caused by mutation in the aldehyde dehydrogenase 3 family member A2 gene, ALDH3A2 (17p11.2), which codes for FALDH.1,6,7 The ALDH3A2 gene is 11 exons long and gives rise to 2 protein isoforms that differ in their carboxy-terminal domains; the major isoform, composed of 485 amino acids, localizes to the endoplasmic reticulum. The minor protein isoform (FALDHv) is composed of 508 amino acids, possesses a longer carboxy-terminal, and appears to be targeted to the peroxisome. Several mutations have been reported throughout the ALDH3A2 gene, including missense mutations (most common [38% of cases of SLS6]), deletions, insertions, splicing errors, and complex rearrangements. Although several of these mutations are private, several common mutations may be indicative of founder effects (ie, shared ancestry), consanguinity, or recurrent mutational events (mutation hotspots).6,7 Despite the wide spectrum of mutations, there is very little phenotypic variation, with consistently severe cutaneous and neurological involvement occurring in a majority of patients.7 However, Lossos et al9 described remarkable phenotypic variation in 6 siblings of an Arab family and suggested that additional unknown genetic or environmental factors may compensate for the biochemical defect.
Lipid Metabolism
Fatty aldehyde dehydrogenase is expressed in almost all cells and tissues and catalyzes the oxidation of fatty aldehydes to fatty acids (eFigure 1). It also is a part of the fatty alcohol:NAD oxidoreductase (FAO) enzyme complex, which catalyzes fatty alcohol oxidation to fatty acid. Fatty aldehyde dehydrogenase deficiency leads to accumulation of long-chain alcohols (eg, hexadecanol, octadecanol, octadecenol) and diversion of fatty alcohol into alternate biosynthetic pathways such as wax esters and 1-O-alkyl-2,3-diacylglycerol.10 Other lipids that are increased are illustrated in eFigure 2. Accumulation of these lipids, toxic effects of abnormal lipids (especially fatty aldehydes and Schiff base protein-lipid adducts), and lack of essential lipids (eg, polyunsaturated fatty acids, ceramides 1 and 6, triglycerides) are responsible for the classical cutaneous, neurologic, and ophthalmologic features of SLS.
Histopathology
The epidermal permeability barrier is critically dependent on the appropriate lipid composition of the multilamellar stratum corneum intercellular membranes, an equimolar ratio of cholesterol, ceramides, and fatty acids. Histopathology of the skin in SLS generally shows hyperkeratosis, papillomatosis, acanthosis, and a mildly thickened granular layer. Ultrastructural studies of the skin reveal misshapen/empty lamellar bodies, abnormal cytoplasmic lamellar inclusions in the granular keratinocytes, lipid droplets in the stratum corneum with decreased lamellar bilayers, and lamellar/nonlamellar phase separation in the stratum corneum interstitium.11 These findings indicate that lipid metabolism dysfunction in SLS results in marked impairment in formation and secretion of lamellar bodies in the epidermis and consequent disorganization of the stratum corneum lamellar membranes. The resulting disruption of the skin barrier function leads to increased transepidermal water loss, resulting in ichthyosis.11,12 Another proposed mechanism for ichthyosis in SLS is disruption of the normal epidermal differentiation resulting from abnormal lipid metabolites (eFigure 2). Also, increased leukotriene B4 (LTB4) and 20-hydroxy-leukotriene B4 (20-OH-LTB4)(eFigure 1) may be responsible for the considerable pruritus seen in SLS.10
Neurologic Findings
Neurologic changes in SLS result from delayed and deficient myelination. Neuropathological studies have shown ballooning of myelin sheaths, extensive loss of myelin, axonal damage, and astrogliosis. The presence of lipoid material positive for periodic acid–Schiff that stains light rather than dark pink, dense distribution of round/ellipsoid bodies in the white matter of the cerebrum and brainstem positive for periodic acid–Schiff, and proliferation of perivascular macrophages containing lipofuscinlike pigments also have been described.13 Possibly, in the absence of FALDH, metabolism of plasmalogens (a major component of myelin) results in increased fatty aldehydes, which are either diverted to fatty alcohols or form adducts with phosphatidylethanolamine and myelin basic proteins (eFigure 1). Magnetic resonance imaging of the brain usually shows hypomyelination involving the periventricular white matter extending from the frontal to the occipital area.7,14 Mild ventricular enlargement may be an additional feature.14
A useful application of MRI is the proton magnetic resonance spectroscopy, which quantifies the brain metabolites noninvasively, displaying them as a spectrum on a graph. The spectrum comprises a set of resonances/peaks distributed along an x-axis. The resonances of these metabolites are obtained after suppressing the large signals from water protons. Proton magnetic resonance spectroscopy of the normal brain shows 3 prominent peaks: (1) N-acetylaspartate (NAA) at 2.02 ppm, (2) creatine at 3.02 ppm, and (3) choline at 3.22 ppm. In SLS, cerebral proton MRI spectroscopy reveals a characteristic abnormal, prominent, and narrow lipid peak at 1.3 ppm (corresponding to hexadecanol and octadecanol) and may offer a quantitative parameter for monitoring the effects of therapeutic interventions.7,14,15 The most intense lipid peaks are located in the periventricular regions in the anterior and posterior trigones. An abnormal but much smaller peak may be seen at 0.8 to 0.9 ppm, corresponding to phytol.14 Gradual emergence of these changes occurs in the first 2 years of life and then remains stable.15 Proton magnetic resonance spectroscopy also can be used for screening of SLS heterozygotes.16 Lipid peaks have been described in other disorders of lipid metabolism, but they are less intense, broader, and disappear on longer echo time sequences.14
Besides the characteristic parafoveal glistening white dots the retina, optical coherence tomography shows focal hyperreflectivitity in the perifoveal ganglion cell layer and inner plexiform layer of the retina as well as cystoid foveal degeneration.17 The intraretinal deposition of lipid metabolites probably leads to Müller cell degeneration with subsequent formation of cystoid spaces and atrophic changes in the fovea.
Measurement of FALDH or FAO activity in cultured skin fibroblasts and leukocytes using flurometric or gas chromatography mass spectrometry assays is a reliable biochemical test in cases of SLS as well as in heterozygotes.17 A decrease in FALDH/FAO activity also can be demonstrated by histochemical staining in skin biopsy.11 Pathologic urinary excretion of LTB4 and 20-OH-LTB4 also is a biochemical marker of SLS. Mutation analysis for a specific gene defect is diagnostic in cases of SLS as well as in heterozygotes. Prenatal diagnosis of SLS is possible by assessing FALDH activity or gene defects in cultured chorionic villus fibroblasts and amniocytes.18,19
Differential Diagnosis
The differential diagnosis of SLS includes congenital ichthyosiform erythroderma with neurological signs (Tay syndrome, Conradi-Hünermann-Happle syndrome) and neurocutaneous disorders such as neutral lipid storage disease and multiple sulfatase deficiency; however, the nature of the ichthyosis, presence of spastic diplegia/tetraplegia, characteristic parafoveal glistening white dots on the retina, and MRI and proton magnetic resonance spectroscopy findings help to easily differentiate SLS from these disorders.
Treatment
Treatment of SLS mainly is palliative. Ichthyosis can be treated with topical keratolytics, emollients, calcipotriol, and oral retinoids (acitretin).6 Zileuton, a 5-lipoxygenase inhibitor, inhibits synthesis of LTB4 and cysteinyl leukotrienes, thereby reducing the severity of pruritus and also has been shown to improve the speed of information processing.18 Similarly, montelukast, a leuko-triene antagonist, is helpful in relieving the agonizing pruritus.19 Experimental studies have shown that bezafibrate, a peroxisome proliferator-activated receptor α agonist, induces FALDH activity in fibroblasts of SLS patients that still have some residual FALDH activity, but further research is required to determine whether SLS patients could benefit from treatment.20 Physiotherapy helps in relieving the spasticity to some extent, such as in our case. Dietary intervention with reduced fat intake (up to 30% of total daily calorific requirement) and supplementation with omega-3 and omega-6 fatty acids has shown variable results in anecdotal reports.21-23 Gene therapy using recombinant adeno-associated virus 2 vectors to restore FALDH has been projected as a future treatment option.24 Despite lack of effective treatment options, most patients of SLS survive well into adulthood.
Conclusion
Because ichthyosis is one of the earliest and prominent symptoms of SLS, a dermatologist can play an important role in early diagnosis. Any child with the classical pattern of ichthyosis should be thoroughly examined for early neurologic signs and investigated to rule out SLS. Proton magnetic resonance spectroscopy serves as a useful adjunct in the diagnosis of SLS by confirming the accumulation of abnormal lipids in the periventricular white matter, especially when specific enzyme analysis and genetic analysis are not available in resource-restricted settings.
Sjögren-Larsson syndrome (SLS) is a rare autosomal-recessive neurocutaneous disorder comprising a triad of ichthyosis, mental retardation, and spastic diplegia or quadriplegia.1 The disorder was first described by Sjögren and Larsson2 in 1957. Early reports of SLS were mainly in white patients, with a particularly high prevalence of 8.3 cases per 100,000 individuals in the county of Västerbotten in Sweden.3 Reports of SLS in Asian and Indian populations are rare.4,5 We report a case of SLS in an Indian boy.
Case Report
A 12-year-old Indian boy born to nonconsanguineous parents after a full-term pregnancy with normal vaginal delivery presented with generalized dry scaly skin that had been present since 2 months of age. He had a history of delayed milestones (ie, facial recognition, sitting without support at 3 years of age), inability to walk, dysarthria, mental retardation). He had never attended school due to subnormal intellectual functioning. He had a single episode of a tonic-clonic seizure at 4 years of age but was not on any regular antiepileptic medication. There was a history of similar skin lesions in one male sibling of the patient and in 2 maternal uncles. None of them survived beyond early childhood, but detailed information regarding the cutaneous and neurologic manifestations in these family members was not available.
Cutaneous examination revealed lamellarlike ichthyosis on the dorsal aspects of the arms and legs (Figure 1A). Ichthyosis with lichenification was present on the neck, axillae, cubital and popliteal fossae, and abdomen (Figure 1B). The palms and soles showed keratoderma. Neurologic examination of the arms revealed mild rigidity and brisk reflexes. Examination of the legs showed marked rigidity, brisk knee jerks, ankle clonus, extensor plantar reflexes, flexion deformity with contractures, and scissor gait. A Goddard (Seguin) formboard test was performed and indicated a mental age of 4 years. The patient’s IQ was in the range of 25 to 30, indicating a severe degree of subnormality in intellectual functioning. The clinical presentation suggested a diagnosis of SLS.
A skin biopsy from the ichthyotic lesion showed hyperkeratosis, acanthosis, and papillomatosis with sparse superficial perivascular lymphocytic infiltrate, thus confirming the diagnosis of lamellar ichthyosis. Fundus examination was normal. Magnetic resonance imaging (MRI) of the brain revealed confluent symmetrical signal abnormalities along the body of the lateral ventricles, white matter in the perioccipital horn, and in deep white matter of centrum semiovale (Figure 2). Magnetic resonance spectroscopy revealed a narrow lipid peak at approximately 1.3 ppm in the region of signal abnormality (Figure 3). Thus, the diagnosis of SLS was confirmed. Measurement of fatty aldehyde dehydrogenase (FALDH) activity and genetic analysis were not performed due to unavailability.
The patient was treated with topical emollients for the ichthyosis. To reduce his dietary intake of long-chain fatty acids and increase the intake of omega-3 and omega-6 fatty acids, the patient’s parents were advised to use canola, mustard, and/or coconut oil for cooking for the patient, and skim milk was recommended instead of whole milk. Neurodevelopmental techniques in the form of stretching exercises were given to maintain his range of movements. Gutter splints were given to maintain the knees in extension for physiological standing and to prevent osteoporosis. Subsequently, the patient also underwent a multilevel soft-tissue release (hip and knee joints) to relieve the contractures. These measures resulted in considerable improvement and the patient was able to walk with support.
Comment
Presentation
The characteristic clinical features of SLS begin to develop during the intranatal period and infancy.1,6 Pathologic skin involvement can be detected as early as week 23 of gestation. Preterm births associated with SLS have commonly been described.3 Ichthyosis often is evident at birth, but collodion membrane is uncommon. Severe pruritus is a marked feature unlike most other types of ichthyosis. The ichthyosis often is generalized with prominent involvement of the flexural areas and nape of the neck, varying from fine furfuraceous to larger lamellarlike scales. Velvety orange or brown lichenification often is a predominant feature in the flexures of the arms, legs, neck, and mid abdomen. Mental retardation, developmental delay, and spasticity usually become apparent at 1 to 2 years of age and subsequently are nonprogressive.6,7 However, patients rarely have been described with normal intellectual functioning.7 Spasticity often is more severe in the lower limbs and may lead to contractures, kyphoscoliosis, hip dislocation, and short stature. Delayed speech and dysarthria are common. Parafoveal glistening white dots on the retina are a pathognomonic feature and typically appear in the first 2 years of life; however, they are seen in approximately 30% of patients and increase slightly in number with age.6,8 There may be associated decreased visual acuity, photophobia, myopia, and astigmatism. Other clinical features include enamel hypoplasia, metaphyseal dysplasia, and epilepsy.1,6
Gene Mutations
Sjögren-Larsson syndrome is caused by mutation in the aldehyde dehydrogenase 3 family member A2 gene, ALDH3A2 (17p11.2), which codes for FALDH.1,6,7 The ALDH3A2 gene is 11 exons long and gives rise to 2 protein isoforms that differ in their carboxy-terminal domains; the major isoform, composed of 485 amino acids, localizes to the endoplasmic reticulum. The minor protein isoform (FALDHv) is composed of 508 amino acids, possesses a longer carboxy-terminal, and appears to be targeted to the peroxisome. Several mutations have been reported throughout the ALDH3A2 gene, including missense mutations (most common [38% of cases of SLS6]), deletions, insertions, splicing errors, and complex rearrangements. Although several of these mutations are private, several common mutations may be indicative of founder effects (ie, shared ancestry), consanguinity, or recurrent mutational events (mutation hotspots).6,7 Despite the wide spectrum of mutations, there is very little phenotypic variation, with consistently severe cutaneous and neurological involvement occurring in a majority of patients.7 However, Lossos et al9 described remarkable phenotypic variation in 6 siblings of an Arab family and suggested that additional unknown genetic or environmental factors may compensate for the biochemical defect.
Lipid Metabolism
Fatty aldehyde dehydrogenase is expressed in almost all cells and tissues and catalyzes the oxidation of fatty aldehydes to fatty acids (eFigure 1). It also is a part of the fatty alcohol:NAD oxidoreductase (FAO) enzyme complex, which catalyzes fatty alcohol oxidation to fatty acid. Fatty aldehyde dehydrogenase deficiency leads to accumulation of long-chain alcohols (eg, hexadecanol, octadecanol, octadecenol) and diversion of fatty alcohol into alternate biosynthetic pathways such as wax esters and 1-O-alkyl-2,3-diacylglycerol.10 Other lipids that are increased are illustrated in eFigure 2. Accumulation of these lipids, toxic effects of abnormal lipids (especially fatty aldehydes and Schiff base protein-lipid adducts), and lack of essential lipids (eg, polyunsaturated fatty acids, ceramides 1 and 6, triglycerides) are responsible for the classical cutaneous, neurologic, and ophthalmologic features of SLS.
Histopathology
The epidermal permeability barrier is critically dependent on the appropriate lipid composition of the multilamellar stratum corneum intercellular membranes, an equimolar ratio of cholesterol, ceramides, and fatty acids. Histopathology of the skin in SLS generally shows hyperkeratosis, papillomatosis, acanthosis, and a mildly thickened granular layer. Ultrastructural studies of the skin reveal misshapen/empty lamellar bodies, abnormal cytoplasmic lamellar inclusions in the granular keratinocytes, lipid droplets in the stratum corneum with decreased lamellar bilayers, and lamellar/nonlamellar phase separation in the stratum corneum interstitium.11 These findings indicate that lipid metabolism dysfunction in SLS results in marked impairment in formation and secretion of lamellar bodies in the epidermis and consequent disorganization of the stratum corneum lamellar membranes. The resulting disruption of the skin barrier function leads to increased transepidermal water loss, resulting in ichthyosis.11,12 Another proposed mechanism for ichthyosis in SLS is disruption of the normal epidermal differentiation resulting from abnormal lipid metabolites (eFigure 2). Also, increased leukotriene B4 (LTB4) and 20-hydroxy-leukotriene B4 (20-OH-LTB4)(eFigure 1) may be responsible for the considerable pruritus seen in SLS.10
Neurologic Findings
Neurologic changes in SLS result from delayed and deficient myelination. Neuropathological studies have shown ballooning of myelin sheaths, extensive loss of myelin, axonal damage, and astrogliosis. The presence of lipoid material positive for periodic acid–Schiff that stains light rather than dark pink, dense distribution of round/ellipsoid bodies in the white matter of the cerebrum and brainstem positive for periodic acid–Schiff, and proliferation of perivascular macrophages containing lipofuscinlike pigments also have been described.13 Possibly, in the absence of FALDH, metabolism of plasmalogens (a major component of myelin) results in increased fatty aldehydes, which are either diverted to fatty alcohols or form adducts with phosphatidylethanolamine and myelin basic proteins (eFigure 1). Magnetic resonance imaging of the brain usually shows hypomyelination involving the periventricular white matter extending from the frontal to the occipital area.7,14 Mild ventricular enlargement may be an additional feature.14
A useful application of MRI is the proton magnetic resonance spectroscopy, which quantifies the brain metabolites noninvasively, displaying them as a spectrum on a graph. The spectrum comprises a set of resonances/peaks distributed along an x-axis. The resonances of these metabolites are obtained after suppressing the large signals from water protons. Proton magnetic resonance spectroscopy of the normal brain shows 3 prominent peaks: (1) N-acetylaspartate (NAA) at 2.02 ppm, (2) creatine at 3.02 ppm, and (3) choline at 3.22 ppm. In SLS, cerebral proton MRI spectroscopy reveals a characteristic abnormal, prominent, and narrow lipid peak at 1.3 ppm (corresponding to hexadecanol and octadecanol) and may offer a quantitative parameter for monitoring the effects of therapeutic interventions.7,14,15 The most intense lipid peaks are located in the periventricular regions in the anterior and posterior trigones. An abnormal but much smaller peak may be seen at 0.8 to 0.9 ppm, corresponding to phytol.14 Gradual emergence of these changes occurs in the first 2 years of life and then remains stable.15 Proton magnetic resonance spectroscopy also can be used for screening of SLS heterozygotes.16 Lipid peaks have been described in other disorders of lipid metabolism, but they are less intense, broader, and disappear on longer echo time sequences.14
Besides the characteristic parafoveal glistening white dots the retina, optical coherence tomography shows focal hyperreflectivitity in the perifoveal ganglion cell layer and inner plexiform layer of the retina as well as cystoid foveal degeneration.17 The intraretinal deposition of lipid metabolites probably leads to Müller cell degeneration with subsequent formation of cystoid spaces and atrophic changes in the fovea.
Measurement of FALDH or FAO activity in cultured skin fibroblasts and leukocytes using flurometric or gas chromatography mass spectrometry assays is a reliable biochemical test in cases of SLS as well as in heterozygotes.17 A decrease in FALDH/FAO activity also can be demonstrated by histochemical staining in skin biopsy.11 Pathologic urinary excretion of LTB4 and 20-OH-LTB4 also is a biochemical marker of SLS. Mutation analysis for a specific gene defect is diagnostic in cases of SLS as well as in heterozygotes. Prenatal diagnosis of SLS is possible by assessing FALDH activity or gene defects in cultured chorionic villus fibroblasts and amniocytes.18,19
Differential Diagnosis
The differential diagnosis of SLS includes congenital ichthyosiform erythroderma with neurological signs (Tay syndrome, Conradi-Hünermann-Happle syndrome) and neurocutaneous disorders such as neutral lipid storage disease and multiple sulfatase deficiency; however, the nature of the ichthyosis, presence of spastic diplegia/tetraplegia, characteristic parafoveal glistening white dots on the retina, and MRI and proton magnetic resonance spectroscopy findings help to easily differentiate SLS from these disorders.
Treatment
Treatment of SLS mainly is palliative. Ichthyosis can be treated with topical keratolytics, emollients, calcipotriol, and oral retinoids (acitretin).6 Zileuton, a 5-lipoxygenase inhibitor, inhibits synthesis of LTB4 and cysteinyl leukotrienes, thereby reducing the severity of pruritus and also has been shown to improve the speed of information processing.18 Similarly, montelukast, a leuko-triene antagonist, is helpful in relieving the agonizing pruritus.19 Experimental studies have shown that bezafibrate, a peroxisome proliferator-activated receptor α agonist, induces FALDH activity in fibroblasts of SLS patients that still have some residual FALDH activity, but further research is required to determine whether SLS patients could benefit from treatment.20 Physiotherapy helps in relieving the spasticity to some extent, such as in our case. Dietary intervention with reduced fat intake (up to 30% of total daily calorific requirement) and supplementation with omega-3 and omega-6 fatty acids has shown variable results in anecdotal reports.21-23 Gene therapy using recombinant adeno-associated virus 2 vectors to restore FALDH has been projected as a future treatment option.24 Despite lack of effective treatment options, most patients of SLS survive well into adulthood.
Conclusion
Because ichthyosis is one of the earliest and prominent symptoms of SLS, a dermatologist can play an important role in early diagnosis. Any child with the classical pattern of ichthyosis should be thoroughly examined for early neurologic signs and investigated to rule out SLS. Proton magnetic resonance spectroscopy serves as a useful adjunct in the diagnosis of SLS by confirming the accumulation of abnormal lipids in the periventricular white matter, especially when specific enzyme analysis and genetic analysis are not available in resource-restricted settings.
- Judge MR, McLean WHI, Munro CS. Disorders of keratinization. In: Burns T, Breathnach S, Cox N, eds. Rook’s Textbook of Dermatology. 7th ed. West Sussex, United Kingdom: Wiley & Sons; 2004:34.37-34.39.
- Sjögren T, Larsson T. Oligophrenia in association with congenital ichthyosis and spastic disorders. Acta Psychiatr Neurol Scand. 1957;32:1-113.
- Jagell S, Gustavson KH, Holmgren G. Sjögren-Larsson syndrome in Sweden. a clinical, genetic and epidemiological study. Clin Genet. 1981;19:233-256.
- Sood M, Trehan A, Dinakaran J, et al. Sjögren-Larsson syndrome. Indian J Pediatr. 2002;69:193-194.
- Uppal M, Srinivas CR, Thowfeeq KT. Sjögren-Larsson syndrome: report of two cases. Indian J Dermatol Venereol Leprol. 2004;70:110-111.
- Rizzo WB. Sjögren-Larsson syndrome: molecular genetics and biochemical pathogenesis of fatty aldehyde dehydrogenase deficiency. Mol Genet Metab. 2007;90:1-9.
- Willemsen MA, Ijlst L, Steijlen PM, et al. Clinical, biochemical and molecular genetic characteristics of 19 patients with the Sjögren-Larsson syndrome. Brain. 2001;124(pt 7):1426-1437.
- Willemsen MA, Cruysberg JR, Rotteveel JJ, et al. Juvenile macular dystrophy associated with deficient activity of fatty aldehyde dehydrogenase in Sjögren-Larsson syndrome. Am J Ophthalmol. 2000;130:782-789.
- Lossos A, Khoury M, Rizzo WB, et al. Phenotypic variability among adult siblings with Sjögren-Larsson syndrome. Arch Neurol. 2006;63:278-280.
- Rizzo WB, Craft DA, Somer T, et al. Abnormal fatty alcohol metabolism in cultured keratinocytes from patients with Sjögren-Larsson syndrome. J Lipid Res. 2008;49:410-419.
- Rizzo WB, S’Aulis D, Jennings MA, et al. Ichthyosis in Sjögren-Larsson syndrome reflects defective barrier function due to abnormal lamellar body structure and secretion. Arch Dermatol Res. 2010;302:443-451.
- Rizzo WB. The role of fatty aldehyde dehydrogenase in epidermal structure and function. Dermatoendocrinol. 2011;2:91-99.
- Yamaguchi K, Handa T. Sjögren-Larsson syndrome: postmortem brain abnormalities. Pediatr Neurol. 1998;18:338-341.
- Mano T, Ono J, Kaminaga T, et al. Proton MR spectroscopy of Sjögren-Larsson’s Syndrome. Am J Neuroradiol. 1999;20:1671-1673.
- Willemsen MA, van der Graf M, van der Knaap MS, et al. MR imaging and proton MR spectroscopic studies in Sjögren-Larsson syndrome: characterization of the leukoencephalopathy. Am J Neuroradiol. 2004;25:649-657.
- Kaminaga T, Mano T, Ono J, et al. Proton magnetic resonance spectroscopy of Sjögren-Larsson Syndrome. Magn Reson Med. 2001;45:1112-1115.
- Fuijkschot J, Cruysberg JR, Willemsen MA, et al. Subclinical changes in the juvenile crystalline macular dystrophy in Sjögren-Larsson syndrome detected by optical coherence tomography. Ophthalmology. 2008;115:870-875.
- Willemsen MA, Lutt MA, Steijlen PM, et al. Clinical and biochemical effects of zileuton in patients with the Sjögren-Larsson syndrome. Eur J Pediatr. 2001;160:711-717.
- Pirgon O, Aydin K, Atabek ME. Proton magnetic resonance spectroscopy findings and clinical effects of montelukast sodium in a case with Sjögren-Larsson syndrome. J Child Neurol. 2006;21:1092-1095.
- Gloerich J, Ijlst L, Wanders RJ, et al. Bezafibrate induces FALDH in human fibroblasts; implications for Sjögren-Larsson syndrome Mol Genet Metab. 2006;89:111-115.
- Auada MP, Taube MB, Collares EF, et al. Sjögren-Larsson syndrome: biochemical defects and follow up in three cases. Eur J Dermatol. 2002;12:263-266.
- Taube B, Billeaud C, Labreze C, et al. Sjögren-Larsson syndrome: early diagnosis, dietary management and biochemical studies in two cases. Dermatology. 1999;198:340-345.
- Rizzo WB. Genetics and prospective therapeutic targets for Sjögren-Larsson Syndrome. Expert Opin Orphan Drugs. 2016;4:395-406.
- Haug S, Braun-Falco M. Restoration of fatty aldehyde dehydrogenase deficiency in Sjögren-Larsson syndrome. Gene Ther. 2006;13:1021-1026.
- Judge MR, McLean WHI, Munro CS. Disorders of keratinization. In: Burns T, Breathnach S, Cox N, eds. Rook’s Textbook of Dermatology. 7th ed. West Sussex, United Kingdom: Wiley & Sons; 2004:34.37-34.39.
- Sjögren T, Larsson T. Oligophrenia in association with congenital ichthyosis and spastic disorders. Acta Psychiatr Neurol Scand. 1957;32:1-113.
- Jagell S, Gustavson KH, Holmgren G. Sjögren-Larsson syndrome in Sweden. a clinical, genetic and epidemiological study. Clin Genet. 1981;19:233-256.
- Sood M, Trehan A, Dinakaran J, et al. Sjögren-Larsson syndrome. Indian J Pediatr. 2002;69:193-194.
- Uppal M, Srinivas CR, Thowfeeq KT. Sjögren-Larsson syndrome: report of two cases. Indian J Dermatol Venereol Leprol. 2004;70:110-111.
- Rizzo WB. Sjögren-Larsson syndrome: molecular genetics and biochemical pathogenesis of fatty aldehyde dehydrogenase deficiency. Mol Genet Metab. 2007;90:1-9.
- Willemsen MA, Ijlst L, Steijlen PM, et al. Clinical, biochemical and molecular genetic characteristics of 19 patients with the Sjögren-Larsson syndrome. Brain. 2001;124(pt 7):1426-1437.
- Willemsen MA, Cruysberg JR, Rotteveel JJ, et al. Juvenile macular dystrophy associated with deficient activity of fatty aldehyde dehydrogenase in Sjögren-Larsson syndrome. Am J Ophthalmol. 2000;130:782-789.
- Lossos A, Khoury M, Rizzo WB, et al. Phenotypic variability among adult siblings with Sjögren-Larsson syndrome. Arch Neurol. 2006;63:278-280.
- Rizzo WB, Craft DA, Somer T, et al. Abnormal fatty alcohol metabolism in cultured keratinocytes from patients with Sjögren-Larsson syndrome. J Lipid Res. 2008;49:410-419.
- Rizzo WB, S’Aulis D, Jennings MA, et al. Ichthyosis in Sjögren-Larsson syndrome reflects defective barrier function due to abnormal lamellar body structure and secretion. Arch Dermatol Res. 2010;302:443-451.
- Rizzo WB. The role of fatty aldehyde dehydrogenase in epidermal structure and function. Dermatoendocrinol. 2011;2:91-99.
- Yamaguchi K, Handa T. Sjögren-Larsson syndrome: postmortem brain abnormalities. Pediatr Neurol. 1998;18:338-341.
- Mano T, Ono J, Kaminaga T, et al. Proton MR spectroscopy of Sjögren-Larsson’s Syndrome. Am J Neuroradiol. 1999;20:1671-1673.
- Willemsen MA, van der Graf M, van der Knaap MS, et al. MR imaging and proton MR spectroscopic studies in Sjögren-Larsson syndrome: characterization of the leukoencephalopathy. Am J Neuroradiol. 2004;25:649-657.
- Kaminaga T, Mano T, Ono J, et al. Proton magnetic resonance spectroscopy of Sjögren-Larsson Syndrome. Magn Reson Med. 2001;45:1112-1115.
- Fuijkschot J, Cruysberg JR, Willemsen MA, et al. Subclinical changes in the juvenile crystalline macular dystrophy in Sjögren-Larsson syndrome detected by optical coherence tomography. Ophthalmology. 2008;115:870-875.
- Willemsen MA, Lutt MA, Steijlen PM, et al. Clinical and biochemical effects of zileuton in patients with the Sjögren-Larsson syndrome. Eur J Pediatr. 2001;160:711-717.
- Pirgon O, Aydin K, Atabek ME. Proton magnetic resonance spectroscopy findings and clinical effects of montelukast sodium in a case with Sjögren-Larsson syndrome. J Child Neurol. 2006;21:1092-1095.
- Gloerich J, Ijlst L, Wanders RJ, et al. Bezafibrate induces FALDH in human fibroblasts; implications for Sjögren-Larsson syndrome Mol Genet Metab. 2006;89:111-115.
- Auada MP, Taube MB, Collares EF, et al. Sjögren-Larsson syndrome: biochemical defects and follow up in three cases. Eur J Dermatol. 2002;12:263-266.
- Taube B, Billeaud C, Labreze C, et al. Sjögren-Larsson syndrome: early diagnosis, dietary management and biochemical studies in two cases. Dermatology. 1999;198:340-345.
- Rizzo WB. Genetics and prospective therapeutic targets for Sjögren-Larsson Syndrome. Expert Opin Orphan Drugs. 2016;4:395-406.
- Haug S, Braun-Falco M. Restoration of fatty aldehyde dehydrogenase deficiency in Sjögren-Larsson syndrome. Gene Ther. 2006;13:1021-1026.
Practice Points
- Sjögren-Larsson syndrome (SLS) is characterized by a clinical triad of ichthyosis, mental retardation, and spastic diplegia or quadriplegia.
- A characteristic lipid peak at 1.3 ppm on magnetic resonance spectroscopy is diagnostic of SLS.
