User login
Light therapy offers brighter future for scar patients
Current treatment with available light-based devices, notably ablative fractional resurfacing, can greatly improve quality of life for patients struggling with scars, according to Kristen Kelly, MD, of the University of California, Irvine.
Using multiple devices, and combining devices with other therapies, are among the strategies that can improve pain and function in these patients, she said in a presentation at Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar.

Dr. Kelly recommends “a CO2 laser or an Er:YAG [erbium-doped YAG],” as AFR options for scar treatment. The Er:YAG is less painful, but may cause bleeding, she noted.
Tips for a scar treatment protocol with AFR include low density and treating the entire scar plus a 1-2 mm rim, Dr. Kelly said. AFR treatment of scars can start in some cases soon after an injury, but it depends on the cause of the scar and treatment timing is controversial, especially for burn scars, she said. Dr. Kelly outlined a plan of treatment every 2-3 months, with the option of adding triamcinolone suspension immediately after the AFR treatment, she noted.
Other medications used after AFR to improve results include 5-fluorouracil, bimatoprost, and poly-L-lactic acid. However, “you should only consider this for medications that you would safely inject into the skin or bloodstream,” she emphasized.
Combining AFR with other devices can improve results, depending on the type of scar, said Dr. Kelly. Atrophic scars may be treated with AFR or NAFR, while red atrophic scars may improve with a combination AFR or NAFR and a pulsed dye laser, she said. For red hypertrophic scars, consider a combination of AFR plus a steroid combined with a pulsed dye laser, she added.
When embarking on a scar treatment plan, be sure to define goals and remind patients that scars can be “improved but not removed,” said Dr. Kelly. “Laser therapy is often not monotherapy,” she added. A surgical revision, such as a Z-plasty, and the use of physical and occupational therapy also can improve results and improve quality of life for patients, she said.
Dr. Kelly disclosed relationships with multiple companies including Allergan, MundiPharma, Syneron Candela, Light Sciences Oncology, Novartis, Sciton, and ThermiRF.
SDEF and this news organization are owned by the same parent company.
Current treatment with available light-based devices, notably ablative fractional resurfacing, can greatly improve quality of life for patients struggling with scars, according to Kristen Kelly, MD, of the University of California, Irvine.
Using multiple devices, and combining devices with other therapies, are among the strategies that can improve pain and function in these patients, she said in a presentation at Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar.
Dr. Kelly recommends “a CO2 laser or an Er:YAG [erbium-doped YAG],” as AFR options for scar treatment. The Er:YAG is less painful, but may cause bleeding, she noted.
Tips for a scar treatment protocol with AFR include low density and treating the entire scar plus a 1-2 mm rim, Dr. Kelly said. AFR treatment of scars can start in some cases soon after an injury, but it depends on the cause of the scar and treatment timing is controversial, especially for burn scars, she said. Dr. Kelly outlined a plan of treatment every 2-3 months, with the option of adding triamcinolone suspension immediately after the AFR treatment, she noted.
Other medications used after AFR to improve results include 5-fluorouracil, bimatoprost, and poly-L-lactic acid. However, “you should only consider this for medications that you would safely inject into the skin or bloodstream,” she emphasized.
Combining AFR with other devices can improve results, depending on the type of scar, said Dr. Kelly. Atrophic scars may be treated with AFR or NAFR, while red atrophic scars may improve with a combination AFR or NAFR and a pulsed dye laser, she said. For red hypertrophic scars, consider a combination of AFR plus a steroid combined with a pulsed dye laser, she added.
When embarking on a scar treatment plan, be sure to define goals and remind patients that scars can be “improved but not removed,” said Dr. Kelly. “Laser therapy is often not monotherapy,” she added. A surgical revision, such as a Z-plasty, and the use of physical and occupational therapy also can improve results and improve quality of life for patients, she said.
Dr. Kelly disclosed relationships with multiple companies including Allergan, MundiPharma, Syneron Candela, Light Sciences Oncology, Novartis, Sciton, and ThermiRF.
SDEF and this news organization are owned by the same parent company.
Current treatment with available light-based devices, notably ablative fractional resurfacing, can greatly improve quality of life for patients struggling with scars, according to Kristen Kelly, MD, of the University of California, Irvine.
Using multiple devices, and combining devices with other therapies, are among the strategies that can improve pain and function in these patients, she said in a presentation at Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar.
Dr. Kelly recommends “a CO2 laser or an Er:YAG [erbium-doped YAG],” as AFR options for scar treatment. The Er:YAG is less painful, but may cause bleeding, she noted.
Tips for a scar treatment protocol with AFR include low density and treating the entire scar plus a 1-2 mm rim, Dr. Kelly said. AFR treatment of scars can start in some cases soon after an injury, but it depends on the cause of the scar and treatment timing is controversial, especially for burn scars, she said. Dr. Kelly outlined a plan of treatment every 2-3 months, with the option of adding triamcinolone suspension immediately after the AFR treatment, she noted.
Other medications used after AFR to improve results include 5-fluorouracil, bimatoprost, and poly-L-lactic acid. However, “you should only consider this for medications that you would safely inject into the skin or bloodstream,” she emphasized.
Combining AFR with other devices can improve results, depending on the type of scar, said Dr. Kelly. Atrophic scars may be treated with AFR or NAFR, while red atrophic scars may improve with a combination AFR or NAFR and a pulsed dye laser, she said. For red hypertrophic scars, consider a combination of AFR plus a steroid combined with a pulsed dye laser, she added.
When embarking on a scar treatment plan, be sure to define goals and remind patients that scars can be “improved but not removed,” said Dr. Kelly. “Laser therapy is often not monotherapy,” she added. A surgical revision, such as a Z-plasty, and the use of physical and occupational therapy also can improve results and improve quality of life for patients, she said.
Dr. Kelly disclosed relationships with multiple companies including Allergan, MundiPharma, Syneron Candela, Light Sciences Oncology, Novartis, Sciton, and ThermiRF.
SDEF and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM SDEF LAS VEGAS DERMATOLOGY SEMINAR
Shorter Length of Stay May Be Better for Some PE Patients
Discharging patients with low-risk pulmonary embolism (PE) sooner not only saves money, but it could be saving their lives, according to a study of 6,746 VHA patients with PE.
Of the patients, 1,918 were low-risk, and of those, 688 had a short length of stay (LOS) (2 days or less). While adverse events associated with PE (recurrent venous thromboembolism, major bleeding, and death) were similar, patients with short LOS had fewer hospital-acquired complications (1.5% vs 13.3%) and bacterial pneumonias (5.9% vs 11.7%). Patients in the long LOS cohort had a higher number of pharmacy visits per patient (12.2 vs 9.4) and surgeries for placement of the inferior vena cava filter.
The researchers note that PE is associated with a “substantial burden” of health care utilization and associated costs. The annual cost per patient for an initial episode of PE ranges from $13,000 to $31,000; with recurrent episodes, the cost can be $11,014-$14,722 per year. In this study, inpatient costs for short LOS were half those of the longer LOS costs ($2,164 vs $5,100). Total costs were $9,056 for short LOS vs $12,544.
But they also note that since patients with low-risk PE can be identified using the validated risk stratification tools, an opportunity exists to select patients who can be safely treated without a traditional hospital admission. The researchers cite estimates that, in fact, up to 50% of PE patients can be treated safely as outpatients. Although this is common practice in Europe, U.S. physicians have been less willing to adopt the strategy, they add.
Risk stratification, the researchers conclude, is “of utmost importance”: Reducing the LOS among low-risk PE patients may substantially reduce the disease’s clinical and economic burden.
Discharging patients with low-risk pulmonary embolism (PE) sooner not only saves money, but it could be saving their lives, according to a study of 6,746 VHA patients with PE.
Of the patients, 1,918 were low-risk, and of those, 688 had a short length of stay (LOS) (2 days or less). While adverse events associated with PE (recurrent venous thromboembolism, major bleeding, and death) were similar, patients with short LOS had fewer hospital-acquired complications (1.5% vs 13.3%) and bacterial pneumonias (5.9% vs 11.7%). Patients in the long LOS cohort had a higher number of pharmacy visits per patient (12.2 vs 9.4) and surgeries for placement of the inferior vena cava filter.
The researchers note that PE is associated with a “substantial burden” of health care utilization and associated costs. The annual cost per patient for an initial episode of PE ranges from $13,000 to $31,000; with recurrent episodes, the cost can be $11,014-$14,722 per year. In this study, inpatient costs for short LOS were half those of the longer LOS costs ($2,164 vs $5,100). Total costs were $9,056 for short LOS vs $12,544.
But they also note that since patients with low-risk PE can be identified using the validated risk stratification tools, an opportunity exists to select patients who can be safely treated without a traditional hospital admission. The researchers cite estimates that, in fact, up to 50% of PE patients can be treated safely as outpatients. Although this is common practice in Europe, U.S. physicians have been less willing to adopt the strategy, they add.
Risk stratification, the researchers conclude, is “of utmost importance”: Reducing the LOS among low-risk PE patients may substantially reduce the disease’s clinical and economic burden.
Discharging patients with low-risk pulmonary embolism (PE) sooner not only saves money, but it could be saving their lives, according to a study of 6,746 VHA patients with PE.
Of the patients, 1,918 were low-risk, and of those, 688 had a short length of stay (LOS) (2 days or less). While adverse events associated with PE (recurrent venous thromboembolism, major bleeding, and death) were similar, patients with short LOS had fewer hospital-acquired complications (1.5% vs 13.3%) and bacterial pneumonias (5.9% vs 11.7%). Patients in the long LOS cohort had a higher number of pharmacy visits per patient (12.2 vs 9.4) and surgeries for placement of the inferior vena cava filter.
The researchers note that PE is associated with a “substantial burden” of health care utilization and associated costs. The annual cost per patient for an initial episode of PE ranges from $13,000 to $31,000; with recurrent episodes, the cost can be $11,014-$14,722 per year. In this study, inpatient costs for short LOS were half those of the longer LOS costs ($2,164 vs $5,100). Total costs were $9,056 for short LOS vs $12,544.
But they also note that since patients with low-risk PE can be identified using the validated risk stratification tools, an opportunity exists to select patients who can be safely treated without a traditional hospital admission. The researchers cite estimates that, in fact, up to 50% of PE patients can be treated safely as outpatients. Although this is common practice in Europe, U.S. physicians have been less willing to adopt the strategy, they add.
Risk stratification, the researchers conclude, is “of utmost importance”: Reducing the LOS among low-risk PE patients may substantially reduce the disease’s clinical and economic burden.
Study reveals predictor of early mortality in AML
New research has shown an increased risk of early death in patients with acute myeloid leukemia (AML) who have high levels of indoleamine 2,3 dioxygenase-1 (IDO-1), an enzyme known to suppress the immune system.
Researchers quantified IDO-1 expression in diagnostic samples from patients with AML and discovered that high levels of IDO-1 were significantly associated with induction failure and poor overall survival (OS).
Ravindra Kolhe, MD, PhD, of the Medical College of Georgia at Augusta University, and his colleagues recounted these findings in Scientific Reports.
The researchers reviewed data from 40 AML patients. They had a median age at diagnosis of 60 (range, 27–89), 60% were female, and 55% were self-reported as Caucasian.
Most patients (72.5%) received standard anthracycline and cytarabine as induction, 10% received hypomethylating agents, and 17.5% were untreated or had unknown treatment status.
Fifteen percent of patients underwent allogeneic hematopoietic stem cell transplant (allo-HSCT) at the time of first complete remission.
Half of all patients achieved remission, and half of those patients (n=10, 25%) had a subsequent relapse. The median OS was 283 days (range, 32–1941). Twenty percent of patients (n=8) were still alive at the time of data analysis.
IDO-1 analysis
“We wanted to look at what makes this leukemia so aggressive that initial induction chemotherapy is not working,” Dr Kolhe said. “Early relapse tends to predict early mortality in these patients, and one of the things we looked at was IDO.”
The researchers extracted IDO-1 mRNA from diagnostic bone marrow samples from 29 of the patients but assessed IDO-1 protein expression in all 40 patients via immunohistochemistry.
The team quantified IDO-1 expression using a “composite IDO-1 score.” They used a cut-off point of 0.45 and divided patients’ samples into 2 groups: high (≥0.45) and low (<0.45) IDO-1 score.
The researchers compared IDO-1 results across 4 survival groups, which included patients surviving:
- Less than 6 months
- More than 6 months to 1 year
- More than 1 year to less than 5 years
- Beyond 5 years.
The team found a direct correlation between poor OS and higher composite IDO-1 score (P=0.0005).
“The patients who died at 6 months had a high expression of IDO, while the blasts produced relatively little IDO in the patients who lived 5 years or more,” Dr Kolhe said.
Independent predictor
The researchers conducted a univariate analysis and identified several factors that were significantly associated with poor OS, including:
- Higher IDO-1 mRNA (P=0.005)
- Higher composite IDO-1 score (P<0.0001)
- Higher age (P=0.0018)
- Male gender (P=0.019)
- High-risk cytogenetics (P=0.002)
- Not undergoing allo-HSCT (P=0.0005).
In a multivariate analysis including the above variables, the researchers found that a higher composite IDO-1 score (P=0.007) and not undergoing allo-HSCT (P=0.007) were significantly associated with poor OS.
The team also found that patients who failed induction had a higher composite IDO-1 score (P=0.01).
“Most of the time, we don’t know why patients are not responding to chemotherapy,” Dr Kolhe noted. “But when the researchers adjusted for other risk factors for AML, like increased age and severe anemia, IDO levels were a standout. Right now, we know it’s high in patients who die at 6 months, and we show that it’s an independent indicator if you adjust for other known variables.”
Dr Kolhe said these results suggest IDO-1 expression should be measured when the diagnostic bone marrow biopsy is performed. This may help identify AML patients who could benefit from receiving an IDO inhibitor along with standard therapy.
Researchers are currently conducting a phase 1/2 trial of the IDO inhibitor indoximod in combination with idarubicin and cytarabine in patients with newly diagnosed AML (NCT02835729). ![]()
New research has shown an increased risk of early death in patients with acute myeloid leukemia (AML) who have high levels of indoleamine 2,3 dioxygenase-1 (IDO-1), an enzyme known to suppress the immune system.
Researchers quantified IDO-1 expression in diagnostic samples from patients with AML and discovered that high levels of IDO-1 were significantly associated with induction failure and poor overall survival (OS).
Ravindra Kolhe, MD, PhD, of the Medical College of Georgia at Augusta University, and his colleagues recounted these findings in Scientific Reports.
The researchers reviewed data from 40 AML patients. They had a median age at diagnosis of 60 (range, 27–89), 60% were female, and 55% were self-reported as Caucasian.
Most patients (72.5%) received standard anthracycline and cytarabine as induction, 10% received hypomethylating agents, and 17.5% were untreated or had unknown treatment status.
Fifteen percent of patients underwent allogeneic hematopoietic stem cell transplant (allo-HSCT) at the time of first complete remission.
Half of all patients achieved remission, and half of those patients (n=10, 25%) had a subsequent relapse. The median OS was 283 days (range, 32–1941). Twenty percent of patients (n=8) were still alive at the time of data analysis.
IDO-1 analysis
“We wanted to look at what makes this leukemia so aggressive that initial induction chemotherapy is not working,” Dr Kolhe said. “Early relapse tends to predict early mortality in these patients, and one of the things we looked at was IDO.”
The researchers extracted IDO-1 mRNA from diagnostic bone marrow samples from 29 of the patients but assessed IDO-1 protein expression in all 40 patients via immunohistochemistry.
The team quantified IDO-1 expression using a “composite IDO-1 score.” They used a cut-off point of 0.45 and divided patients’ samples into 2 groups: high (≥0.45) and low (<0.45) IDO-1 score.
The researchers compared IDO-1 results across 4 survival groups, which included patients surviving:
- Less than 6 months
- More than 6 months to 1 year
- More than 1 year to less than 5 years
- Beyond 5 years.
The team found a direct correlation between poor OS and higher composite IDO-1 score (P=0.0005).
“The patients who died at 6 months had a high expression of IDO, while the blasts produced relatively little IDO in the patients who lived 5 years or more,” Dr Kolhe said.
Independent predictor
The researchers conducted a univariate analysis and identified several factors that were significantly associated with poor OS, including:
- Higher IDO-1 mRNA (P=0.005)
- Higher composite IDO-1 score (P<0.0001)
- Higher age (P=0.0018)
- Male gender (P=0.019)
- High-risk cytogenetics (P=0.002)
- Not undergoing allo-HSCT (P=0.0005).
In a multivariate analysis including the above variables, the researchers found that a higher composite IDO-1 score (P=0.007) and not undergoing allo-HSCT (P=0.007) were significantly associated with poor OS.
The team also found that patients who failed induction had a higher composite IDO-1 score (P=0.01).
“Most of the time, we don’t know why patients are not responding to chemotherapy,” Dr Kolhe noted. “But when the researchers adjusted for other risk factors for AML, like increased age and severe anemia, IDO levels were a standout. Right now, we know it’s high in patients who die at 6 months, and we show that it’s an independent indicator if you adjust for other known variables.”
Dr Kolhe said these results suggest IDO-1 expression should be measured when the diagnostic bone marrow biopsy is performed. This may help identify AML patients who could benefit from receiving an IDO inhibitor along with standard therapy.
Researchers are currently conducting a phase 1/2 trial of the IDO inhibitor indoximod in combination with idarubicin and cytarabine in patients with newly diagnosed AML (NCT02835729). ![]()
New research has shown an increased risk of early death in patients with acute myeloid leukemia (AML) who have high levels of indoleamine 2,3 dioxygenase-1 (IDO-1), an enzyme known to suppress the immune system.
Researchers quantified IDO-1 expression in diagnostic samples from patients with AML and discovered that high levels of IDO-1 were significantly associated with induction failure and poor overall survival (OS).
Ravindra Kolhe, MD, PhD, of the Medical College of Georgia at Augusta University, and his colleagues recounted these findings in Scientific Reports.
The researchers reviewed data from 40 AML patients. They had a median age at diagnosis of 60 (range, 27–89), 60% were female, and 55% were self-reported as Caucasian.
Most patients (72.5%) received standard anthracycline and cytarabine as induction, 10% received hypomethylating agents, and 17.5% were untreated or had unknown treatment status.
Fifteen percent of patients underwent allogeneic hematopoietic stem cell transplant (allo-HSCT) at the time of first complete remission.
Half of all patients achieved remission, and half of those patients (n=10, 25%) had a subsequent relapse. The median OS was 283 days (range, 32–1941). Twenty percent of patients (n=8) were still alive at the time of data analysis.
IDO-1 analysis
“We wanted to look at what makes this leukemia so aggressive that initial induction chemotherapy is not working,” Dr Kolhe said. “Early relapse tends to predict early mortality in these patients, and one of the things we looked at was IDO.”
The researchers extracted IDO-1 mRNA from diagnostic bone marrow samples from 29 of the patients but assessed IDO-1 protein expression in all 40 patients via immunohistochemistry.
The team quantified IDO-1 expression using a “composite IDO-1 score.” They used a cut-off point of 0.45 and divided patients’ samples into 2 groups: high (≥0.45) and low (<0.45) IDO-1 score.
The researchers compared IDO-1 results across 4 survival groups, which included patients surviving:
- Less than 6 months
- More than 6 months to 1 year
- More than 1 year to less than 5 years
- Beyond 5 years.
The team found a direct correlation between poor OS and higher composite IDO-1 score (P=0.0005).
“The patients who died at 6 months had a high expression of IDO, while the blasts produced relatively little IDO in the patients who lived 5 years or more,” Dr Kolhe said.
Independent predictor
The researchers conducted a univariate analysis and identified several factors that were significantly associated with poor OS, including:
- Higher IDO-1 mRNA (P=0.005)
- Higher composite IDO-1 score (P<0.0001)
- Higher age (P=0.0018)
- Male gender (P=0.019)
- High-risk cytogenetics (P=0.002)
- Not undergoing allo-HSCT (P=0.0005).
In a multivariate analysis including the above variables, the researchers found that a higher composite IDO-1 score (P=0.007) and not undergoing allo-HSCT (P=0.007) were significantly associated with poor OS.
The team also found that patients who failed induction had a higher composite IDO-1 score (P=0.01).
“Most of the time, we don’t know why patients are not responding to chemotherapy,” Dr Kolhe noted. “But when the researchers adjusted for other risk factors for AML, like increased age and severe anemia, IDO levels were a standout. Right now, we know it’s high in patients who die at 6 months, and we show that it’s an independent indicator if you adjust for other known variables.”
Dr Kolhe said these results suggest IDO-1 expression should be measured when the diagnostic bone marrow biopsy is performed. This may help identify AML patients who could benefit from receiving an IDO inhibitor along with standard therapy.
Researchers are currently conducting a phase 1/2 trial of the IDO inhibitor indoximod in combination with idarubicin and cytarabine in patients with newly diagnosed AML (NCT02835729). ![]()
Thoughts, emotions linked to opioid use in SCD

Results of a small study suggest that negative thoughts and emotions may increase opioid use in patients with sickle cell disease (SCD).
Researchers analyzed data from daily electronic patient diaries and found that patients were more likely to use short-acting opioids both when they experienced increased pain and “catastrophic” thoughts about that pain.
In fact, pain catastrophizing led to an increased use of short-acting opioids even when patients reported low levels of pain.
In addition, patients were more likely to use long-acting opioids when they experienced negative emotions.
The researchers noted that this study wasn’t designed to show that negative emotions or thinking cause an increase in opioid use. It was only designed to determine if there was an association.
Patrick Finan, PhD, of Johns Hopkins University School of Medicine in Baltimore, Maryland, and his colleagues described this study in The Journal of Pain.
The researchers enrolled 85 adults with SCD in this study. Patients were asked to fill out electronic diaries on a handheld personal computer every evening for 90 days.
The final analysis included only 45 patients, as these were the subjects who filled out the diary more than 25% of the time and had taken opioid pills at least once during the study period.
The patients had an average age of 37, and 71% were female. Most (93%) were African American, and 7% were classified as “other” or did not report their race.
At the start of the study, the patients reported on the dosage and type of opioid pill they were prescribed for long-acting and short-acting use. The daily diary collected data on the number of long-acting and short-acting opioid pills taken per day.
Patients rated their daily pain level on a scale of 0 to 10, with 0 being no pain and 10 being the worst pain imaginable.
Patients also rated positive emotions—including happy, calm, and cheerful—and negative emotions—including lonely, sad, anxious, and tired—on a scale of 0 to 10, with 0 being no emotion and 10 being the most intense emotion. The scores were converted to a 0-to-100 scale for the data analysis.
Separately, the researchers measured negative thinking using a Pain Catastrophizing Scale to rate “rumination,” or focus on pain, helplessness, and magnification of a current pain situation.
Results
Negative emotions were significantly associated with increased levels of long-acting opioids (P=0.001). The opioid dosage increased by 3.4 morphine milligram equivalents for every 10-point increase in negative emotions.
On the other hand, patients’ daily pain level, positive emotions, and negative thinking through catastrophizing did not significantly affect the amount of long-acting opioids taken.
“When someone is prescribed a daily, long-acting opioid, it is typically supposed to be at a fixed dose, and their pain level or emotions shouldn’t dictate whether they take more of this prescription or not,” Dr Finan said.
“Although we can’t prove misuse of the medication in our study, these data suggest that physicians and patients should clearly communicate about how patients should be taking their daily, long-acting opioids in order to minimize the potential for misuse.”
The researchers also found a significant association with short-acting opioid use and daily pain levels (P=0.006) as well as negative thinking by catastrophizing (P<0.001).
For every 10-point increase on the pain scale, the amount of short-acting opioids increased by 1.8 morphine milligram equivalents, and for every 10-point increase on the catastrophizing scale, pain medicine dosage increased by 2.5 morphine milligram equivalents.
Positive and negative emotions had no significant effect on the use of short-acting opioids.
“When pain was reported as low, sickle cell disease patients reported higher opioid use if they catastrophized, or focused their thinking on their pain, than if they didn’t,” Dr Finan said. “When pain levels were higher, negative thinking played less of a role in influencing opioid use.”
Dr Finan cautioned that studies such as this have some weaknesses, including the fact that self-reports are always uncertain, and the study only included 1 time point per day, although a person’s mood may fluctuate throughout the day based on life events and experiences.
For future studies, Dr Finan wants to use smartphone technology that can assess moods randomly throughout the day.
“Once we have a more intensive study to track mood variations throughout the day,” Dr Finan said, “then we can determine when it will be appropriate to send messages through text to intervene and affect patient behavior.” ![]()
Results of a small study suggest that negative thoughts and emotions may increase opioid use in patients with sickle cell disease (SCD).
Researchers analyzed data from daily electronic patient diaries and found that patients were more likely to use short-acting opioids both when they experienced increased pain and “catastrophic” thoughts about that pain.
In fact, pain catastrophizing led to an increased use of short-acting opioids even when patients reported low levels of pain.
In addition, patients were more likely to use long-acting opioids when they experienced negative emotions.
The researchers noted that this study wasn’t designed to show that negative emotions or thinking cause an increase in opioid use. It was only designed to determine if there was an association.
Patrick Finan, PhD, of Johns Hopkins University School of Medicine in Baltimore, Maryland, and his colleagues described this study in The Journal of Pain.
The researchers enrolled 85 adults with SCD in this study. Patients were asked to fill out electronic diaries on a handheld personal computer every evening for 90 days.
The final analysis included only 45 patients, as these were the subjects who filled out the diary more than 25% of the time and had taken opioid pills at least once during the study period.
The patients had an average age of 37, and 71% were female. Most (93%) were African American, and 7% were classified as “other” or did not report their race.
At the start of the study, the patients reported on the dosage and type of opioid pill they were prescribed for long-acting and short-acting use. The daily diary collected data on the number of long-acting and short-acting opioid pills taken per day.
Patients rated their daily pain level on a scale of 0 to 10, with 0 being no pain and 10 being the worst pain imaginable.
Patients also rated positive emotions—including happy, calm, and cheerful—and negative emotions—including lonely, sad, anxious, and tired—on a scale of 0 to 10, with 0 being no emotion and 10 being the most intense emotion. The scores were converted to a 0-to-100 scale for the data analysis.
Separately, the researchers measured negative thinking using a Pain Catastrophizing Scale to rate “rumination,” or focus on pain, helplessness, and magnification of a current pain situation.
Results
Negative emotions were significantly associated with increased levels of long-acting opioids (P=0.001). The opioid dosage increased by 3.4 morphine milligram equivalents for every 10-point increase in negative emotions.
On the other hand, patients’ daily pain level, positive emotions, and negative thinking through catastrophizing did not significantly affect the amount of long-acting opioids taken.
“When someone is prescribed a daily, long-acting opioid, it is typically supposed to be at a fixed dose, and their pain level or emotions shouldn’t dictate whether they take more of this prescription or not,” Dr Finan said.
“Although we can’t prove misuse of the medication in our study, these data suggest that physicians and patients should clearly communicate about how patients should be taking their daily, long-acting opioids in order to minimize the potential for misuse.”
The researchers also found a significant association with short-acting opioid use and daily pain levels (P=0.006) as well as negative thinking by catastrophizing (P<0.001).
For every 10-point increase on the pain scale, the amount of short-acting opioids increased by 1.8 morphine milligram equivalents, and for every 10-point increase on the catastrophizing scale, pain medicine dosage increased by 2.5 morphine milligram equivalents.
Positive and negative emotions had no significant effect on the use of short-acting opioids.
“When pain was reported as low, sickle cell disease patients reported higher opioid use if they catastrophized, or focused their thinking on their pain, than if they didn’t,” Dr Finan said. “When pain levels were higher, negative thinking played less of a role in influencing opioid use.”
Dr Finan cautioned that studies such as this have some weaknesses, including the fact that self-reports are always uncertain, and the study only included 1 time point per day, although a person’s mood may fluctuate throughout the day based on life events and experiences.
For future studies, Dr Finan wants to use smartphone technology that can assess moods randomly throughout the day.
“Once we have a more intensive study to track mood variations throughout the day,” Dr Finan said, “then we can determine when it will be appropriate to send messages through text to intervene and affect patient behavior.” ![]()
Results of a small study suggest that negative thoughts and emotions may increase opioid use in patients with sickle cell disease (SCD).
Researchers analyzed data from daily electronic patient diaries and found that patients were more likely to use short-acting opioids both when they experienced increased pain and “catastrophic” thoughts about that pain.
In fact, pain catastrophizing led to an increased use of short-acting opioids even when patients reported low levels of pain.
In addition, patients were more likely to use long-acting opioids when they experienced negative emotions.
The researchers noted that this study wasn’t designed to show that negative emotions or thinking cause an increase in opioid use. It was only designed to determine if there was an association.
Patrick Finan, PhD, of Johns Hopkins University School of Medicine in Baltimore, Maryland, and his colleagues described this study in The Journal of Pain.
The researchers enrolled 85 adults with SCD in this study. Patients were asked to fill out electronic diaries on a handheld personal computer every evening for 90 days.
The final analysis included only 45 patients, as these were the subjects who filled out the diary more than 25% of the time and had taken opioid pills at least once during the study period.
The patients had an average age of 37, and 71% were female. Most (93%) were African American, and 7% were classified as “other” or did not report their race.
At the start of the study, the patients reported on the dosage and type of opioid pill they were prescribed for long-acting and short-acting use. The daily diary collected data on the number of long-acting and short-acting opioid pills taken per day.
Patients rated their daily pain level on a scale of 0 to 10, with 0 being no pain and 10 being the worst pain imaginable.
Patients also rated positive emotions—including happy, calm, and cheerful—and negative emotions—including lonely, sad, anxious, and tired—on a scale of 0 to 10, with 0 being no emotion and 10 being the most intense emotion. The scores were converted to a 0-to-100 scale for the data analysis.
Separately, the researchers measured negative thinking using a Pain Catastrophizing Scale to rate “rumination,” or focus on pain, helplessness, and magnification of a current pain situation.
Results
Negative emotions were significantly associated with increased levels of long-acting opioids (P=0.001). The opioid dosage increased by 3.4 morphine milligram equivalents for every 10-point increase in negative emotions.
On the other hand, patients’ daily pain level, positive emotions, and negative thinking through catastrophizing did not significantly affect the amount of long-acting opioids taken.
“When someone is prescribed a daily, long-acting opioid, it is typically supposed to be at a fixed dose, and their pain level or emotions shouldn’t dictate whether they take more of this prescription or not,” Dr Finan said.
“Although we can’t prove misuse of the medication in our study, these data suggest that physicians and patients should clearly communicate about how patients should be taking their daily, long-acting opioids in order to minimize the potential for misuse.”
The researchers also found a significant association with short-acting opioid use and daily pain levels (P=0.006) as well as negative thinking by catastrophizing (P<0.001).
For every 10-point increase on the pain scale, the amount of short-acting opioids increased by 1.8 morphine milligram equivalents, and for every 10-point increase on the catastrophizing scale, pain medicine dosage increased by 2.5 morphine milligram equivalents.
Positive and negative emotions had no significant effect on the use of short-acting opioids.
“When pain was reported as low, sickle cell disease patients reported higher opioid use if they catastrophized, or focused their thinking on their pain, than if they didn’t,” Dr Finan said. “When pain levels were higher, negative thinking played less of a role in influencing opioid use.”
Dr Finan cautioned that studies such as this have some weaknesses, including the fact that self-reports are always uncertain, and the study only included 1 time point per day, although a person’s mood may fluctuate throughout the day based on life events and experiences.
For future studies, Dr Finan wants to use smartphone technology that can assess moods randomly throughout the day.
“Once we have a more intensive study to track mood variations throughout the day,” Dr Finan said, “then we can determine when it will be appropriate to send messages through text to intervene and affect patient behavior.” ![]()
Authors’ contributions to studies often unclear

Although many scientific journals try to provide details about authors’ contributions to a publication by requiring explicit statements, contribution statements get much less attention than authorship order, according to research published in Science Advances.
Researchers surveyed more than 6000 corresponding authors of studies published in recent years and found they consider contribution statements helpful for understanding the specific skills individual authors bring to a study.
However, the respondents said they still use author order for deciphering which authors did how much of the work and deserve most of the credit.
“The lack of uniformity and detail in contribution statements leaves open the door for varied interpretations, which could be why only a minority of respondents found them more useful than author order,” said Henry Sauermann, PhD, of ESMT Berlin in Germany.
Dr Sauermann and his colleagues also examined the relationship between author order and contribution statements on more than 12,000 published articles.
The contribution statements studied did include information about the types of work contributed by each author. However, multiple authors could be listed under the same contributions, and the statements had little information about the level of effort for each author.
The statements also said little about how important a particular contribution was for project success.
Still, Dr Sauermann and his colleagues noted that author order has its own problems.
“When we talked to scientists, many think that there are certain norms, and they know how to interpret author order,” Dr Sauermann said. “But when you really push, it’s not clear at all, at least not at the level of detail we need.”
That’s further complicated by the fact that conventions of author order vary depending on the research field.
This work also revealed a difference of opinion between junior and senior researchers, with the former caring more strongly about contribution statements and how they are discussed and crafted.
“When we read open-ended responses to our survey questions, we got the impression of a really divided community,” Dr Sauermann said. “Some believe that forcing more detail in contribution statements is great, and some are concerned that it could really hurt teamwork and collaboration. It’s not that everyone is lukewarm; many really care.”
That level of interest could pave the way for more discussion, which is something Dr Sauermann said is ultimately needed for the scientific and research community to move forward and add more clarity to the process.
“This is not going to get any easier,” Dr Sauermann said. “It’s going to get harder as how we perform research changes and as teams get bigger and more diverse.” ![]()
Although many scientific journals try to provide details about authors’ contributions to a publication by requiring explicit statements, contribution statements get much less attention than authorship order, according to research published in Science Advances.
Researchers surveyed more than 6000 corresponding authors of studies published in recent years and found they consider contribution statements helpful for understanding the specific skills individual authors bring to a study.
However, the respondents said they still use author order for deciphering which authors did how much of the work and deserve most of the credit.
“The lack of uniformity and detail in contribution statements leaves open the door for varied interpretations, which could be why only a minority of respondents found them more useful than author order,” said Henry Sauermann, PhD, of ESMT Berlin in Germany.
Dr Sauermann and his colleagues also examined the relationship between author order and contribution statements on more than 12,000 published articles.
The contribution statements studied did include information about the types of work contributed by each author. However, multiple authors could be listed under the same contributions, and the statements had little information about the level of effort for each author.
The statements also said little about how important a particular contribution was for project success.
Still, Dr Sauermann and his colleagues noted that author order has its own problems.
“When we talked to scientists, many think that there are certain norms, and they know how to interpret author order,” Dr Sauermann said. “But when you really push, it’s not clear at all, at least not at the level of detail we need.”
That’s further complicated by the fact that conventions of author order vary depending on the research field.
This work also revealed a difference of opinion between junior and senior researchers, with the former caring more strongly about contribution statements and how they are discussed and crafted.
“When we read open-ended responses to our survey questions, we got the impression of a really divided community,” Dr Sauermann said. “Some believe that forcing more detail in contribution statements is great, and some are concerned that it could really hurt teamwork and collaboration. It’s not that everyone is lukewarm; many really care.”
That level of interest could pave the way for more discussion, which is something Dr Sauermann said is ultimately needed for the scientific and research community to move forward and add more clarity to the process.
“This is not going to get any easier,” Dr Sauermann said. “It’s going to get harder as how we perform research changes and as teams get bigger and more diverse.” ![]()
Although many scientific journals try to provide details about authors’ contributions to a publication by requiring explicit statements, contribution statements get much less attention than authorship order, according to research published in Science Advances.
Researchers surveyed more than 6000 corresponding authors of studies published in recent years and found they consider contribution statements helpful for understanding the specific skills individual authors bring to a study.
However, the respondents said they still use author order for deciphering which authors did how much of the work and deserve most of the credit.
“The lack of uniformity and detail in contribution statements leaves open the door for varied interpretations, which could be why only a minority of respondents found them more useful than author order,” said Henry Sauermann, PhD, of ESMT Berlin in Germany.
Dr Sauermann and his colleagues also examined the relationship between author order and contribution statements on more than 12,000 published articles.
The contribution statements studied did include information about the types of work contributed by each author. However, multiple authors could be listed under the same contributions, and the statements had little information about the level of effort for each author.
The statements also said little about how important a particular contribution was for project success.
Still, Dr Sauermann and his colleagues noted that author order has its own problems.
“When we talked to scientists, many think that there are certain norms, and they know how to interpret author order,” Dr Sauermann said. “But when you really push, it’s not clear at all, at least not at the level of detail we need.”
That’s further complicated by the fact that conventions of author order vary depending on the research field.
This work also revealed a difference of opinion between junior and senior researchers, with the former caring more strongly about contribution statements and how they are discussed and crafted.
“When we read open-ended responses to our survey questions, we got the impression of a really divided community,” Dr Sauermann said. “Some believe that forcing more detail in contribution statements is great, and some are concerned that it could really hurt teamwork and collaboration. It’s not that everyone is lukewarm; many really care.”
That level of interest could pave the way for more discussion, which is something Dr Sauermann said is ultimately needed for the scientific and research community to move forward and add more clarity to the process.
“This is not going to get any easier,” Dr Sauermann said. “It’s going to get harder as how we perform research changes and as teams get bigger and more diverse.” ![]()
Rare epidermotropic MZL yields to rituximab
Epidermotropic marginal zone lymphoma (MZL), a rare cutaneous B-cell lymphoma identified in only eight patients to date, appears to be responsive to rituximab, according to authors of a case report.
A 69-year-old man who presented with a generalized papulosquamous eruption that was eventually diagnosed as epidermotropic MZL achieved a near total remission within 3 months of receiving four total weekly rituximab infusions, reported Cynthia M. Magro, MD, from Cornell University, New York, and her colleagues from the University of Arizona, Tucson (JAAD Case Rep. 2017 Sep 23;3[6]:474-6).
“Epidermotropic MZL represents a distinctive nosologic B-cell lymphoma that should be considered a diagnostic possibility in older men who present with an unexplained papulosquamous eruption resembling pityriasis rosea,” the researchers wrote.
“Epidermotropism refers to a state of abnormal colonization of the epidermis by leukocytes, which often reflects a clonal T-cell or monocyte dyscrasia. Epidermotropism is a distinctive pattern of passive migration into epithelial structures that is not otherwise attributable to the normal function of innate and adaptive immunity,” the researchers explained.
They described the case of the aforementioned patient, who presented with asymptomatic indurated, red-to-brown papules and plaques on his chest, abdomen, back, and buttocks, which gave the clinical impression of pityriasis rosea or a similarly appearing drug reaction.
Histopathologic examination of two biopsied lesions “demonstrated a dense superficial lymphocytic infiltrate that expanded and effaced the papillary and superficial reticular dermis.”
After epidermotropic MZL was diagnosed, the patient was evaluated for systemic disease with a bone marrow biopsy, which revealed a low-grade B-cell lymphoproliferative disorder, and with a PET scan showing lymphomatous infiltration of the spleen. The patient was treated with four weekly infusions of rituximab 375 mg/m2.
“Within 3 months, he experienced marked regression of his cutaneous disease. Repeat radiographic imaging found an interval decrease in the size of his spleen, signifying an objective response. Since achieving near total clinical remission, the patient remains under the close observation of medical oncology services,” the researchers wrote.
The investigators noted that if histopathology is the only method used to diagnosis the condition, epidermotropic MZL could be mistaken for a T-cell lymphoproliferative disorder, such as mycosis fungoides, because of the similar architecture at low resolution.
“In these settings, immunohistochemical staining for B-cell markers represents an indispensable diagnostic test,” they wrote.
The researchers reported having no conflicts of interest.
Epidermotropic marginal zone lymphoma (MZL), a rare cutaneous B-cell lymphoma identified in only eight patients to date, appears to be responsive to rituximab, according to authors of a case report.
A 69-year-old man who presented with a generalized papulosquamous eruption that was eventually diagnosed as epidermotropic MZL achieved a near total remission within 3 months of receiving four total weekly rituximab infusions, reported Cynthia M. Magro, MD, from Cornell University, New York, and her colleagues from the University of Arizona, Tucson (JAAD Case Rep. 2017 Sep 23;3[6]:474-6).
“Epidermotropic MZL represents a distinctive nosologic B-cell lymphoma that should be considered a diagnostic possibility in older men who present with an unexplained papulosquamous eruption resembling pityriasis rosea,” the researchers wrote.
“Epidermotropism refers to a state of abnormal colonization of the epidermis by leukocytes, which often reflects a clonal T-cell or monocyte dyscrasia. Epidermotropism is a distinctive pattern of passive migration into epithelial structures that is not otherwise attributable to the normal function of innate and adaptive immunity,” the researchers explained.
They described the case of the aforementioned patient, who presented with asymptomatic indurated, red-to-brown papules and plaques on his chest, abdomen, back, and buttocks, which gave the clinical impression of pityriasis rosea or a similarly appearing drug reaction.
Histopathologic examination of two biopsied lesions “demonstrated a dense superficial lymphocytic infiltrate that expanded and effaced the papillary and superficial reticular dermis.”
After epidermotropic MZL was diagnosed, the patient was evaluated for systemic disease with a bone marrow biopsy, which revealed a low-grade B-cell lymphoproliferative disorder, and with a PET scan showing lymphomatous infiltration of the spleen. The patient was treated with four weekly infusions of rituximab 375 mg/m2.
“Within 3 months, he experienced marked regression of his cutaneous disease. Repeat radiographic imaging found an interval decrease in the size of his spleen, signifying an objective response. Since achieving near total clinical remission, the patient remains under the close observation of medical oncology services,” the researchers wrote.
The investigators noted that if histopathology is the only method used to diagnosis the condition, epidermotropic MZL could be mistaken for a T-cell lymphoproliferative disorder, such as mycosis fungoides, because of the similar architecture at low resolution.
“In these settings, immunohistochemical staining for B-cell markers represents an indispensable diagnostic test,” they wrote.
The researchers reported having no conflicts of interest.
Epidermotropic marginal zone lymphoma (MZL), a rare cutaneous B-cell lymphoma identified in only eight patients to date, appears to be responsive to rituximab, according to authors of a case report.
A 69-year-old man who presented with a generalized papulosquamous eruption that was eventually diagnosed as epidermotropic MZL achieved a near total remission within 3 months of receiving four total weekly rituximab infusions, reported Cynthia M. Magro, MD, from Cornell University, New York, and her colleagues from the University of Arizona, Tucson (JAAD Case Rep. 2017 Sep 23;3[6]:474-6).
“Epidermotropic MZL represents a distinctive nosologic B-cell lymphoma that should be considered a diagnostic possibility in older men who present with an unexplained papulosquamous eruption resembling pityriasis rosea,” the researchers wrote.
“Epidermotropism refers to a state of abnormal colonization of the epidermis by leukocytes, which often reflects a clonal T-cell or monocyte dyscrasia. Epidermotropism is a distinctive pattern of passive migration into epithelial structures that is not otherwise attributable to the normal function of innate and adaptive immunity,” the researchers explained.
They described the case of the aforementioned patient, who presented with asymptomatic indurated, red-to-brown papules and plaques on his chest, abdomen, back, and buttocks, which gave the clinical impression of pityriasis rosea or a similarly appearing drug reaction.
Histopathologic examination of two biopsied lesions “demonstrated a dense superficial lymphocytic infiltrate that expanded and effaced the papillary and superficial reticular dermis.”
After epidermotropic MZL was diagnosed, the patient was evaluated for systemic disease with a bone marrow biopsy, which revealed a low-grade B-cell lymphoproliferative disorder, and with a PET scan showing lymphomatous infiltration of the spleen. The patient was treated with four weekly infusions of rituximab 375 mg/m2.
“Within 3 months, he experienced marked regression of his cutaneous disease. Repeat radiographic imaging found an interval decrease in the size of his spleen, signifying an objective response. Since achieving near total clinical remission, the patient remains under the close observation of medical oncology services,” the researchers wrote.
The investigators noted that if histopathology is the only method used to diagnosis the condition, epidermotropic MZL could be mistaken for a T-cell lymphoproliferative disorder, such as mycosis fungoides, because of the similar architecture at low resolution.
“In these settings, immunohistochemical staining for B-cell markers represents an indispensable diagnostic test,” they wrote.
The researchers reported having no conflicts of interest.
FROM JAAD CASE REPORTS
Key clinical point: Epidermotropic marginal zone lymphoma, a very rare B-cell disorder, can be effectively treated with rituximab.
Major finding: A patient with epidermotropic MZL had a near complete response to rituximab within 3 months.
Data source: Case study of a 69-year-old man presenting with an otherwise asymptomatic diffuse dermatologic eruption.
Disclosures: The researchers reported no conflicts of interest.
Sneak Peek: The Hospital Leader blog – Nov. 2017
What we expect and what we get from work
Are American workers becoming happier with less? An interesting article in the Wall Street Journal reported on the findings of a recent survey of U.S. workers by the Conference Board, a research organization. Although the survey wasn’t specific to health care, much less to hospitalists, I see some parallels that might cause many of us to stop and think more carefully about what we expect from our work.

American workers today tend to have less job security and fewer employer-paid benefits than they did in previous generations. A companion graphic in the WSJ reported that, while in 1973 only 6% of Americans said they worked too many hours and 7% said they had trouble completing their work in the time allotted, by 2016 26% said they often worked more than 48 hours a week and half said they work during their free time at least periodically. Two-thirds of Americans now say they need to spend at least half of their day working at high speeds or meeting tight deadlines.
Yet, despite these trends, the Conference Board found that overall, U.S. workers are more satisfied with their jobs than they have been in the past. The WSJ article posits that workers are happier at work because they have adjusted to lower expectations of the employer-employee relationship. In addition, workers have more flexibility today to change jobs or companies to find the right fit or pursue advancement, and often have more influence over when, where, and how they do their jobs than ever before. Many are working as temps or independent contractors, or in similar “contingent” arrangements. Finally, more employers are offering a wider array of tools to aid with work-life balance, such as paid medical and family leave.
So what does all this have to do with hospitalists?
Read the full post at hospitalleader.org.
Also on The Hospital Leader…
- 95% of inpatient providers would get an F on this exam by Brad Flansbaum, DO, MPH, MHM
- When it comes to health care violence, silence isn’t an option by Danielle Scheurer, MD, MSCR, SFHM,
- How do we keep our providers safe? by Tracy Cardin, ACNP-BC, SFHM
- We have a voice. It’s time we use it #DoctorsSpeakOut by Vineet Arora, MD, MAPP, MHM
What we expect and what we get from work
Are American workers becoming happier with less? An interesting article in the Wall Street Journal reported on the findings of a recent survey of U.S. workers by the Conference Board, a research organization. Although the survey wasn’t specific to health care, much less to hospitalists, I see some parallels that might cause many of us to stop and think more carefully about what we expect from our work.
American workers today tend to have less job security and fewer employer-paid benefits than they did in previous generations. A companion graphic in the WSJ reported that, while in 1973 only 6% of Americans said they worked too many hours and 7% said they had trouble completing their work in the time allotted, by 2016 26% said they often worked more than 48 hours a week and half said they work during their free time at least periodically. Two-thirds of Americans now say they need to spend at least half of their day working at high speeds or meeting tight deadlines.
Yet, despite these trends, the Conference Board found that overall, U.S. workers are more satisfied with their jobs than they have been in the past. The WSJ article posits that workers are happier at work because they have adjusted to lower expectations of the employer-employee relationship. In addition, workers have more flexibility today to change jobs or companies to find the right fit or pursue advancement, and often have more influence over when, where, and how they do their jobs than ever before. Many are working as temps or independent contractors, or in similar “contingent” arrangements. Finally, more employers are offering a wider array of tools to aid with work-life balance, such as paid medical and family leave.
So what does all this have to do with hospitalists?
Read the full post at hospitalleader.org.
Also on The Hospital Leader…
- 95% of inpatient providers would get an F on this exam by Brad Flansbaum, DO, MPH, MHM
- When it comes to health care violence, silence isn’t an option by Danielle Scheurer, MD, MSCR, SFHM,
- How do we keep our providers safe? by Tracy Cardin, ACNP-BC, SFHM
- We have a voice. It’s time we use it #DoctorsSpeakOut by Vineet Arora, MD, MAPP, MHM
What we expect and what we get from work
Are American workers becoming happier with less? An interesting article in the Wall Street Journal reported on the findings of a recent survey of U.S. workers by the Conference Board, a research organization. Although the survey wasn’t specific to health care, much less to hospitalists, I see some parallels that might cause many of us to stop and think more carefully about what we expect from our work.
American workers today tend to have less job security and fewer employer-paid benefits than they did in previous generations. A companion graphic in the WSJ reported that, while in 1973 only 6% of Americans said they worked too many hours and 7% said they had trouble completing their work in the time allotted, by 2016 26% said they often worked more than 48 hours a week and half said they work during their free time at least periodically. Two-thirds of Americans now say they need to spend at least half of their day working at high speeds or meeting tight deadlines.
Yet, despite these trends, the Conference Board found that overall, U.S. workers are more satisfied with their jobs than they have been in the past. The WSJ article posits that workers are happier at work because they have adjusted to lower expectations of the employer-employee relationship. In addition, workers have more flexibility today to change jobs or companies to find the right fit or pursue advancement, and often have more influence over when, where, and how they do their jobs than ever before. Many are working as temps or independent contractors, or in similar “contingent” arrangements. Finally, more employers are offering a wider array of tools to aid with work-life balance, such as paid medical and family leave.
So what does all this have to do with hospitalists?
Read the full post at hospitalleader.org.
Also on The Hospital Leader…
- 95% of inpatient providers would get an F on this exam by Brad Flansbaum, DO, MPH, MHM
- When it comes to health care violence, silence isn’t an option by Danielle Scheurer, MD, MSCR, SFHM,
- How do we keep our providers safe? by Tracy Cardin, ACNP-BC, SFHM
- We have a voice. It’s time we use it #DoctorsSpeakOut by Vineet Arora, MD, MAPP, MHM
VIDEO: Study supports close follow-up of patients with high-risk adenomas plus serrated polyps
The simultaneous colonoscopic presence of serrated polyps and high-risk adenomas led to a fivefold increase in the odds of metachronous high-risk adenomas in a large population-based registry study reported in Gastroenterology (2017. doi: 10.1053/j.gastro.2017.09.011).
The data “support the recommendation that individuals with large and high-risk serrated lesions require closer surveillance,” said Joseph C. Anderson, MD, of White River Junction Department of Veterans Affairs Medical Center, Vt., with his associates. When discounting size and histology, the presence of serrated polyps alone was not associated with an increased risk for metachronous high-risk adenoma, they also reported. Although serrated polyps are important precursors of colorectal cancer, relevant longitudinal surveillance data are sparse. Therefore, the investigators studied 5,433 adults who underwent index and follow-up colonoscopies a median of 4.9 years apart and were tracked in the population-based New Hampshire Colonoscopy Registry. The cohort had a median age of 61 years and half of individuals were male.
SOURCE: AMERICAN GASTROENTEROLOGICAL ASSOCIATION
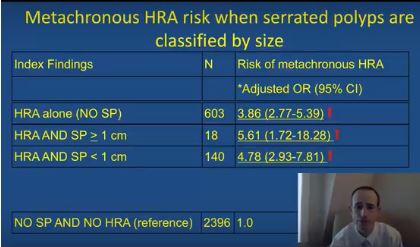
After adjusting for age, sex, smoking status, body mass index, and median interval between colonoscopies, individuals were at significantly increased risk of metachronous high-risk adenoma if their baseline colonoscopy showed high-risk adenoma and synchronous serrated polyps (odds ratio, 5.6; 95% confidence interval, 1.7-18.3), high-risk adenoma with synchronous sessile serrated adenomas (or polyps) or traditional serrated adenomas (OR, 16.0; 95% CI, 7.0-37.0), or high-risk adenoma alone (OR, 3.9; 95% CI, 2.8-5.4), vs. participants with no findings.
The researchers also found that the index presence of large (at least 1-cm) serrated polyps greatly increased the likelihood of finding large metachronous serrated polyps on subsequent colonoscopy (OR, 14.0; 95% CI, 5.0-40.9). “This has clinical relevance, since previous studies have demonstrated an increased risk for colorectal cancer in individuals with large serrated polyps,” the researchers wrote. “However, this increased risk may occur over a protracted time period of 10 years or more, and addressing variation in serrated polyp detection rates and completeness of resection may be more effective than a shorter surveillance interval at reducing risk in these individuals.”
The index presence of sessile serrated adenomas or polyps, or traditional serrated adenomas, also predicted the subsequent development of large serrated polyps (OR, 9.7; 95% CI, 3.6-25.9). The study did not examine polyp location or morphology (flat versus polypoid), but the association might be related to right-sided or flat lesions, which colonoscopists are more likely to miss or to incompletely excise than more defined polypoid lesions, the researchers commented. “Additional research is needed to further clarify the associations between index patient characteristics, polyp location, size, endoscopic appearance and histology, and the metachronous risk of advanced lesions and colorectal cancer in order to refine current surveillance recommendations for individuals undergoing colonoscopy,” they commented.
The study spanned January 2004 to June 2015, and awareness about the importance of serrated polyps rose during this period, they also noted.
The National Cancer Institute and the Norris Cotton Cancer Center provided funding. The researchers reported having no conflicts of interest.
The simultaneous colonoscopic presence of serrated polyps and high-risk adenomas led to a fivefold increase in the odds of metachronous high-risk adenomas in a large population-based registry study reported in Gastroenterology (2017. doi: 10.1053/j.gastro.2017.09.011).
The data “support the recommendation that individuals with large and high-risk serrated lesions require closer surveillance,” said Joseph C. Anderson, MD, of White River Junction Department of Veterans Affairs Medical Center, Vt., with his associates. When discounting size and histology, the presence of serrated polyps alone was not associated with an increased risk for metachronous high-risk adenoma, they also reported. Although serrated polyps are important precursors of colorectal cancer, relevant longitudinal surveillance data are sparse. Therefore, the investigators studied 5,433 adults who underwent index and follow-up colonoscopies a median of 4.9 years apart and were tracked in the population-based New Hampshire Colonoscopy Registry. The cohort had a median age of 61 years and half of individuals were male.
SOURCE: AMERICAN GASTROENTEROLOGICAL ASSOCIATION
After adjusting for age, sex, smoking status, body mass index, and median interval between colonoscopies, individuals were at significantly increased risk of metachronous high-risk adenoma if their baseline colonoscopy showed high-risk adenoma and synchronous serrated polyps (odds ratio, 5.6; 95% confidence interval, 1.7-18.3), high-risk adenoma with synchronous sessile serrated adenomas (or polyps) or traditional serrated adenomas (OR, 16.0; 95% CI, 7.0-37.0), or high-risk adenoma alone (OR, 3.9; 95% CI, 2.8-5.4), vs. participants with no findings.
The researchers also found that the index presence of large (at least 1-cm) serrated polyps greatly increased the likelihood of finding large metachronous serrated polyps on subsequent colonoscopy (OR, 14.0; 95% CI, 5.0-40.9). “This has clinical relevance, since previous studies have demonstrated an increased risk for colorectal cancer in individuals with large serrated polyps,” the researchers wrote. “However, this increased risk may occur over a protracted time period of 10 years or more, and addressing variation in serrated polyp detection rates and completeness of resection may be more effective than a shorter surveillance interval at reducing risk in these individuals.”
The index presence of sessile serrated adenomas or polyps, or traditional serrated adenomas, also predicted the subsequent development of large serrated polyps (OR, 9.7; 95% CI, 3.6-25.9). The study did not examine polyp location or morphology (flat versus polypoid), but the association might be related to right-sided or flat lesions, which colonoscopists are more likely to miss or to incompletely excise than more defined polypoid lesions, the researchers commented. “Additional research is needed to further clarify the associations between index patient characteristics, polyp location, size, endoscopic appearance and histology, and the metachronous risk of advanced lesions and colorectal cancer in order to refine current surveillance recommendations for individuals undergoing colonoscopy,” they commented.
The study spanned January 2004 to June 2015, and awareness about the importance of serrated polyps rose during this period, they also noted.
The National Cancer Institute and the Norris Cotton Cancer Center provided funding. The researchers reported having no conflicts of interest.
The simultaneous colonoscopic presence of serrated polyps and high-risk adenomas led to a fivefold increase in the odds of metachronous high-risk adenomas in a large population-based registry study reported in Gastroenterology (2017. doi: 10.1053/j.gastro.2017.09.011).
The data “support the recommendation that individuals with large and high-risk serrated lesions require closer surveillance,” said Joseph C. Anderson, MD, of White River Junction Department of Veterans Affairs Medical Center, Vt., with his associates. When discounting size and histology, the presence of serrated polyps alone was not associated with an increased risk for metachronous high-risk adenoma, they also reported. Although serrated polyps are important precursors of colorectal cancer, relevant longitudinal surveillance data are sparse. Therefore, the investigators studied 5,433 adults who underwent index and follow-up colonoscopies a median of 4.9 years apart and were tracked in the population-based New Hampshire Colonoscopy Registry. The cohort had a median age of 61 years and half of individuals were male.
SOURCE: AMERICAN GASTROENTEROLOGICAL ASSOCIATION
After adjusting for age, sex, smoking status, body mass index, and median interval between colonoscopies, individuals were at significantly increased risk of metachronous high-risk adenoma if their baseline colonoscopy showed high-risk adenoma and synchronous serrated polyps (odds ratio, 5.6; 95% confidence interval, 1.7-18.3), high-risk adenoma with synchronous sessile serrated adenomas (or polyps) or traditional serrated adenomas (OR, 16.0; 95% CI, 7.0-37.0), or high-risk adenoma alone (OR, 3.9; 95% CI, 2.8-5.4), vs. participants with no findings.
The researchers also found that the index presence of large (at least 1-cm) serrated polyps greatly increased the likelihood of finding large metachronous serrated polyps on subsequent colonoscopy (OR, 14.0; 95% CI, 5.0-40.9). “This has clinical relevance, since previous studies have demonstrated an increased risk for colorectal cancer in individuals with large serrated polyps,” the researchers wrote. “However, this increased risk may occur over a protracted time period of 10 years or more, and addressing variation in serrated polyp detection rates and completeness of resection may be more effective than a shorter surveillance interval at reducing risk in these individuals.”
The index presence of sessile serrated adenomas or polyps, or traditional serrated adenomas, also predicted the subsequent development of large serrated polyps (OR, 9.7; 95% CI, 3.6-25.9). The study did not examine polyp location or morphology (flat versus polypoid), but the association might be related to right-sided or flat lesions, which colonoscopists are more likely to miss or to incompletely excise than more defined polypoid lesions, the researchers commented. “Additional research is needed to further clarify the associations between index patient characteristics, polyp location, size, endoscopic appearance and histology, and the metachronous risk of advanced lesions and colorectal cancer in order to refine current surveillance recommendations for individuals undergoing colonoscopy,” they commented.
The study spanned January 2004 to June 2015, and awareness about the importance of serrated polyps rose during this period, they also noted.
The National Cancer Institute and the Norris Cotton Cancer Center provided funding. The researchers reported having no conflicts of interest.
FROM GASTROENTEROLOGY
Key clinical point: High-risk adenomas and the synchronous presence of serrated polyps significantly increased the risk of metachronous high-risk adenomas.
Major finding: Compared with individuals with unremarkable colonoscopies, the odds ratio was 5.6 after adjusting for age, sex, smoking status, body mass index, and median interval between colonoscopies.
Data source: Analyses of index and follow-up colonoscopies of 5,433 individuals from a population-based surveillance registry.
Disclosures: The National Cancer Institute and the Norris Cotton Cancer Center provided funding. The researchers reported having no conflicts of interest.
Upfront chemotherapy yields excellent survival in patients with MZLs
For patients with advanced or recurrent marginal zone lymphomas (MZL) typically treated with radiotherapy, antibiotics, single-agent therapy, or observation, upfront chemotherapy was associated with high rates of both failure-free and overall survival at 10 years.
A retrospective analysis of data on 44 patients with either extranodal MZL (MALT), splenic MZL (SMZL), or nodal MZL (NMZL) treated with either the standard of care (for early-stage MALT) or with chemotherapy plus rituximab (for patients with advanced MALT, SMZL, or NMZL) showed a projected 10-year failure-free survival rate of 80%, and an overall survival rate of 100%, reported José L. Ortega, MD, of the University of Puerto Rico in San Juan, and his colleagues (Clin Lymphoma Myeloma Leuk. 2017 Sep 23. pii: S2152-2650[17]30632-8. doi: 10.1016/j.clml.2017.09.014).
“Although the watch and wait modality is still the most-used strategy for patients with advanced MZLs, with chemotherapy traditionally reserved for relapsed or advanced symptomatic disease, our data suggest that upfront chemotherapy is very effective for patients with advanced MALT, SMZL, and NMZL. However, it was not possible to definitely exclude that a less-aggressive approach such as single-agent rituximab could yield similar results,” the investigators wrote.
The standard of care for patients with localized MALT has traditionally been either antibiotic therapy for gastric MALT, or radiotherapy when antibiotics are not feasible. There is no standard of care, however, for either SMZL or NMZL, which are typically managed with either observation or single-agent rituximab, the investigators stated.
To see whether upfront chemotherapy with either FND-R (fludarabine, mitoxantrone, dexamethasone, and rituximab) or CHOP-R (cyclophosphamide, doxorubicin, vincristine, prednisone, and rituximab) could improve outcomes in patients with advanced or recurrent MZLs, the investigators conducted a retrospective study of outcomes for 44 patients treated at their institution.
Group 1 comprised 22 patients with early-stage MALT treated with either radiotherapy or antibiotics, with or without surgery. Group 2 comprised 9 patients with advanced MALT, 9 with SMZL, and 4 with NMZL. Patients in this group underwent upfront chemotherapy with either FND-R (14 patients) or CHOP-R (8 patients). In addition, 16 patients in group 2 received maintenance rituximab.
All patients in each group had complete remissions. Two patients in group 1 had relapses (one at 70 months and one at 75 months) of stage I MALT that had previously been treated with radiotherapy. Both patients underwent salvage FND-R, and remained disease free at 27 and 39 months after relapse. There were no relapses in group 2.
The investigators deemed long-term toxicities to be “acceptable,” with most adverse effects in group 2 being hematologic in origin, including grade 3 or 4 neutropenia in 70%, thrombocytopenia in 22%, and anemia in 17%. Nonhematologic adverse events were mostly grade 1 or 2. There were no second malignancies reported at the most recent follow-up.
The investigators noted that the high complete remission rate and durable remissions with FND-R suggest that it has excellent activity against MZL, and that the long failure-free survival suggests the possibility of cure. They acknowledged, however, that their impressions were based on retrospective data and a small sample size, and that larger clinical trials are needed to confirm their results.
The investigators reported having no conflicts of interest.
For patients with advanced or recurrent marginal zone lymphomas (MZL) typically treated with radiotherapy, antibiotics, single-agent therapy, or observation, upfront chemotherapy was associated with high rates of both failure-free and overall survival at 10 years.
A retrospective analysis of data on 44 patients with either extranodal MZL (MALT), splenic MZL (SMZL), or nodal MZL (NMZL) treated with either the standard of care (for early-stage MALT) or with chemotherapy plus rituximab (for patients with advanced MALT, SMZL, or NMZL) showed a projected 10-year failure-free survival rate of 80%, and an overall survival rate of 100%, reported José L. Ortega, MD, of the University of Puerto Rico in San Juan, and his colleagues (Clin Lymphoma Myeloma Leuk. 2017 Sep 23. pii: S2152-2650[17]30632-8. doi: 10.1016/j.clml.2017.09.014).
“Although the watch and wait modality is still the most-used strategy for patients with advanced MZLs, with chemotherapy traditionally reserved for relapsed or advanced symptomatic disease, our data suggest that upfront chemotherapy is very effective for patients with advanced MALT, SMZL, and NMZL. However, it was not possible to definitely exclude that a less-aggressive approach such as single-agent rituximab could yield similar results,” the investigators wrote.
The standard of care for patients with localized MALT has traditionally been either antibiotic therapy for gastric MALT, or radiotherapy when antibiotics are not feasible. There is no standard of care, however, for either SMZL or NMZL, which are typically managed with either observation or single-agent rituximab, the investigators stated.
To see whether upfront chemotherapy with either FND-R (fludarabine, mitoxantrone, dexamethasone, and rituximab) or CHOP-R (cyclophosphamide, doxorubicin, vincristine, prednisone, and rituximab) could improve outcomes in patients with advanced or recurrent MZLs, the investigators conducted a retrospective study of outcomes for 44 patients treated at their institution.
Group 1 comprised 22 patients with early-stage MALT treated with either radiotherapy or antibiotics, with or without surgery. Group 2 comprised 9 patients with advanced MALT, 9 with SMZL, and 4 with NMZL. Patients in this group underwent upfront chemotherapy with either FND-R (14 patients) or CHOP-R (8 patients). In addition, 16 patients in group 2 received maintenance rituximab.
All patients in each group had complete remissions. Two patients in group 1 had relapses (one at 70 months and one at 75 months) of stage I MALT that had previously been treated with radiotherapy. Both patients underwent salvage FND-R, and remained disease free at 27 and 39 months after relapse. There were no relapses in group 2.
The investigators deemed long-term toxicities to be “acceptable,” with most adverse effects in group 2 being hematologic in origin, including grade 3 or 4 neutropenia in 70%, thrombocytopenia in 22%, and anemia in 17%. Nonhematologic adverse events were mostly grade 1 or 2. There were no second malignancies reported at the most recent follow-up.
The investigators noted that the high complete remission rate and durable remissions with FND-R suggest that it has excellent activity against MZL, and that the long failure-free survival suggests the possibility of cure. They acknowledged, however, that their impressions were based on retrospective data and a small sample size, and that larger clinical trials are needed to confirm their results.
The investigators reported having no conflicts of interest.
For patients with advanced or recurrent marginal zone lymphomas (MZL) typically treated with radiotherapy, antibiotics, single-agent therapy, or observation, upfront chemotherapy was associated with high rates of both failure-free and overall survival at 10 years.
A retrospective analysis of data on 44 patients with either extranodal MZL (MALT), splenic MZL (SMZL), or nodal MZL (NMZL) treated with either the standard of care (for early-stage MALT) or with chemotherapy plus rituximab (for patients with advanced MALT, SMZL, or NMZL) showed a projected 10-year failure-free survival rate of 80%, and an overall survival rate of 100%, reported José L. Ortega, MD, of the University of Puerto Rico in San Juan, and his colleagues (Clin Lymphoma Myeloma Leuk. 2017 Sep 23. pii: S2152-2650[17]30632-8. doi: 10.1016/j.clml.2017.09.014).
“Although the watch and wait modality is still the most-used strategy for patients with advanced MZLs, with chemotherapy traditionally reserved for relapsed or advanced symptomatic disease, our data suggest that upfront chemotherapy is very effective for patients with advanced MALT, SMZL, and NMZL. However, it was not possible to definitely exclude that a less-aggressive approach such as single-agent rituximab could yield similar results,” the investigators wrote.
The standard of care for patients with localized MALT has traditionally been either antibiotic therapy for gastric MALT, or radiotherapy when antibiotics are not feasible. There is no standard of care, however, for either SMZL or NMZL, which are typically managed with either observation or single-agent rituximab, the investigators stated.
To see whether upfront chemotherapy with either FND-R (fludarabine, mitoxantrone, dexamethasone, and rituximab) or CHOP-R (cyclophosphamide, doxorubicin, vincristine, prednisone, and rituximab) could improve outcomes in patients with advanced or recurrent MZLs, the investigators conducted a retrospective study of outcomes for 44 patients treated at their institution.
Group 1 comprised 22 patients with early-stage MALT treated with either radiotherapy or antibiotics, with or without surgery. Group 2 comprised 9 patients with advanced MALT, 9 with SMZL, and 4 with NMZL. Patients in this group underwent upfront chemotherapy with either FND-R (14 patients) or CHOP-R (8 patients). In addition, 16 patients in group 2 received maintenance rituximab.
All patients in each group had complete remissions. Two patients in group 1 had relapses (one at 70 months and one at 75 months) of stage I MALT that had previously been treated with radiotherapy. Both patients underwent salvage FND-R, and remained disease free at 27 and 39 months after relapse. There were no relapses in group 2.
The investigators deemed long-term toxicities to be “acceptable,” with most adverse effects in group 2 being hematologic in origin, including grade 3 or 4 neutropenia in 70%, thrombocytopenia in 22%, and anemia in 17%. Nonhematologic adverse events were mostly grade 1 or 2. There were no second malignancies reported at the most recent follow-up.
The investigators noted that the high complete remission rate and durable remissions with FND-R suggest that it has excellent activity against MZL, and that the long failure-free survival suggests the possibility of cure. They acknowledged, however, that their impressions were based on retrospective data and a small sample size, and that larger clinical trials are needed to confirm their results.
The investigators reported having no conflicts of interest.
FROM CLINICAL LYMPHOMA, MYELOMA & LEUKEMIA
Key clinical point:
Major finding: The 10-year projected failure-free survival rate was 80%, and the overall survival rate was 100%.
Data source: Retrospective single-center study of 44 patients with marginal zone lymphomas.
Disclosures: The investigators reported having no conflicts of interest.
Marginal zone lymphoma treatment studies to be presented at ASH
Findings from several studies on marginal zone lymphoma (MZL) will be presented during oral and poster sessions at the annual meeting of the American Society of Hematology, with a focus on evaluating combination treatment approaches.
Some of the MZL treatment–related studies include the assessment of chlorambucil plus rituximab in patients with extranodal marginal zone B-cell lymphoma of mucosa associated lymphoid tissue, the combination of bendamustine with rituximab for first-line treatment of splenic MZL, and the safety and progression-free survival associated with lenalidomide and rituximab in previously untreated patients with MZL.
Other studies consider how to approach refractory disease. One study looks at the use of ibrutinib in patients with relapsed/refractory MZL, and researchers will also present findings from a systematic literature review of the efficacy and safety of various treatments among patients with relapsed/refractory MZL.
Abstract 1506: IELSG-38: A Phase II Study of Chlorambucil in Combination with Rituximab Followed by Maintenance Therapy with Subcutaneous Rituximab in Patients with Extranodal Marginal Zone B-Cell Lymphoma of Mucosa Associated Lymphoid Tissue (MALT) .
Abstract 4062: Bendamustine in Combination with Rituximab as First-Line Treatment of Splenic Marginal Zone Lymphoma (BRISMA). Results of the IELSG-36 Phase II Study.
Abstract 3026: Ibrutinib Therapy in Patients with Relapsed/Refractory Marginal Zone Lymphoma: Analysis by Prior Rituximab Treatment and Baseline Mutations.
Abstract 4040: Safety and Activity of Lenalidomide and Rituximab in Previously Untreated Marginal Zone Lymphoma: Subgroup Analysis and Long-Term Follow-Up of an Open-Label Phase II Trial.
Abstract 2783: Systematic Literature Review of the Clinical Efficacy and Safety of Treatments in the Relapsed/Refractory Setting for Patients with Follicular Lymphoma or Marginal Zone Lymphoma.
Findings from several studies on marginal zone lymphoma (MZL) will be presented during oral and poster sessions at the annual meeting of the American Society of Hematology, with a focus on evaluating combination treatment approaches.
Some of the MZL treatment–related studies include the assessment of chlorambucil plus rituximab in patients with extranodal marginal zone B-cell lymphoma of mucosa associated lymphoid tissue, the combination of bendamustine with rituximab for first-line treatment of splenic MZL, and the safety and progression-free survival associated with lenalidomide and rituximab in previously untreated patients with MZL.
Other studies consider how to approach refractory disease. One study looks at the use of ibrutinib in patients with relapsed/refractory MZL, and researchers will also present findings from a systematic literature review of the efficacy and safety of various treatments among patients with relapsed/refractory MZL.
Abstract 1506: IELSG-38: A Phase II Study of Chlorambucil in Combination with Rituximab Followed by Maintenance Therapy with Subcutaneous Rituximab in Patients with Extranodal Marginal Zone B-Cell Lymphoma of Mucosa Associated Lymphoid Tissue (MALT) .
Abstract 4062: Bendamustine in Combination with Rituximab as First-Line Treatment of Splenic Marginal Zone Lymphoma (BRISMA). Results of the IELSG-36 Phase II Study.
Abstract 3026: Ibrutinib Therapy in Patients with Relapsed/Refractory Marginal Zone Lymphoma: Analysis by Prior Rituximab Treatment and Baseline Mutations.
Abstract 4040: Safety and Activity of Lenalidomide and Rituximab in Previously Untreated Marginal Zone Lymphoma: Subgroup Analysis and Long-Term Follow-Up of an Open-Label Phase II Trial.
Abstract 2783: Systematic Literature Review of the Clinical Efficacy and Safety of Treatments in the Relapsed/Refractory Setting for Patients with Follicular Lymphoma or Marginal Zone Lymphoma.
Findings from several studies on marginal zone lymphoma (MZL) will be presented during oral and poster sessions at the annual meeting of the American Society of Hematology, with a focus on evaluating combination treatment approaches.
Some of the MZL treatment–related studies include the assessment of chlorambucil plus rituximab in patients with extranodal marginal zone B-cell lymphoma of mucosa associated lymphoid tissue, the combination of bendamustine with rituximab for first-line treatment of splenic MZL, and the safety and progression-free survival associated with lenalidomide and rituximab in previously untreated patients with MZL.
Other studies consider how to approach refractory disease. One study looks at the use of ibrutinib in patients with relapsed/refractory MZL, and researchers will also present findings from a systematic literature review of the efficacy and safety of various treatments among patients with relapsed/refractory MZL.
Abstract 1506: IELSG-38: A Phase II Study of Chlorambucil in Combination with Rituximab Followed by Maintenance Therapy with Subcutaneous Rituximab in Patients with Extranodal Marginal Zone B-Cell Lymphoma of Mucosa Associated Lymphoid Tissue (MALT) .
Abstract 4062: Bendamustine in Combination with Rituximab as First-Line Treatment of Splenic Marginal Zone Lymphoma (BRISMA). Results of the IELSG-36 Phase II Study.
Abstract 3026: Ibrutinib Therapy in Patients with Relapsed/Refractory Marginal Zone Lymphoma: Analysis by Prior Rituximab Treatment and Baseline Mutations.
Abstract 4040: Safety and Activity of Lenalidomide and Rituximab in Previously Untreated Marginal Zone Lymphoma: Subgroup Analysis and Long-Term Follow-Up of an Open-Label Phase II Trial.
Abstract 2783: Systematic Literature Review of the Clinical Efficacy and Safety of Treatments in the Relapsed/Refractory Setting for Patients with Follicular Lymphoma or Marginal Zone Lymphoma.
FROM ASH 2017