User login
DoD Offers ‘Drug Take Back’ Program
Unwanted, unused, and expired prescription drugs are a major contributor to prescription drug abuse, according to the Office of National Drug Control Policy. And nearly one third of suicide attempts among veterans involve prescription medicines. But a change in the rules at the Drug Enforcement Administration now allows military treatment facilities to accept and dispose of those unused medications. The Department of Defense was the first federal agency to put the “Drug Take Back” program into effect nationwide for its beneficiaries.
Military treatment facility pharmacies can accept legal prescription and over-the-counter bottled pills, tablets and capsules, ointments, creams, lotions, powders, and liquid medicines that are no more than 4 ounces. (Pet medicines are included.)
Patients can take the drugs to their faculty or send them by mail in a special envelope available at some military treatment facility pharmacies.
Bringing back the drugs not only helps the environment by reducing the amount of drugs that can filter through water supplies and landfills, but it also cuts down on the risk of accidental or intentional drug misuse. “DoD and the [Military Health System] are committed to reducing the risk of prescription and over-the-counter drug abuse in the military community, supporting the nation’s efforts to reduce opioid abuse,” said Dr. George Jones, chief of the Defense Health Agency’s Pharmacy Operations Division, in a news report on health.mil.
Unwanted, unused, and expired prescription drugs are a major contributor to prescription drug abuse, according to the Office of National Drug Control Policy. And nearly one third of suicide attempts among veterans involve prescription medicines. But a change in the rules at the Drug Enforcement Administration now allows military treatment facilities to accept and dispose of those unused medications. The Department of Defense was the first federal agency to put the “Drug Take Back” program into effect nationwide for its beneficiaries.
Military treatment facility pharmacies can accept legal prescription and over-the-counter bottled pills, tablets and capsules, ointments, creams, lotions, powders, and liquid medicines that are no more than 4 ounces. (Pet medicines are included.)
Patients can take the drugs to their faculty or send them by mail in a special envelope available at some military treatment facility pharmacies.
Bringing back the drugs not only helps the environment by reducing the amount of drugs that can filter through water supplies and landfills, but it also cuts down on the risk of accidental or intentional drug misuse. “DoD and the [Military Health System] are committed to reducing the risk of prescription and over-the-counter drug abuse in the military community, supporting the nation’s efforts to reduce opioid abuse,” said Dr. George Jones, chief of the Defense Health Agency’s Pharmacy Operations Division, in a news report on health.mil.
Unwanted, unused, and expired prescription drugs are a major contributor to prescription drug abuse, according to the Office of National Drug Control Policy. And nearly one third of suicide attempts among veterans involve prescription medicines. But a change in the rules at the Drug Enforcement Administration now allows military treatment facilities to accept and dispose of those unused medications. The Department of Defense was the first federal agency to put the “Drug Take Back” program into effect nationwide for its beneficiaries.
Military treatment facility pharmacies can accept legal prescription and over-the-counter bottled pills, tablets and capsules, ointments, creams, lotions, powders, and liquid medicines that are no more than 4 ounces. (Pet medicines are included.)
Patients can take the drugs to their faculty or send them by mail in a special envelope available at some military treatment facility pharmacies.
Bringing back the drugs not only helps the environment by reducing the amount of drugs that can filter through water supplies and landfills, but it also cuts down on the risk of accidental or intentional drug misuse. “DoD and the [Military Health System] are committed to reducing the risk of prescription and over-the-counter drug abuse in the military community, supporting the nation’s efforts to reduce opioid abuse,” said Dr. George Jones, chief of the Defense Health Agency’s Pharmacy Operations Division, in a news report on health.mil.
Allergic Rhinitis
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

Inherited Thrombophilia Testing
The Things We Do for No Reason (TWDFNR) series reviews practices which have become common parts of hospital care but which may provide little value to our patients. Practices reviewed in the TWDFNR series do not represent black and white conclusions or clinical practice standards, but are meant as a starting place for research and active discussions among hospitalists and patients. We invite you to be part of that discussion. https://www.choosingwisely.org/
Inherited thrombophilia refers to a genetic condition that predisposes to an increased risk of venous thromboembolism (VTE). This disorder is prevalent in approximately 7% of the population and includes mutations such as factor V Leiden, prothrombin 20210, protein C deficiency, protein S deficiency, antithrombin deficiency, and methylene tetrahydrofolate reductase. The relative risk of VTE is 3‐ to 20‐fold greater in patients with inherited thrombophilia compared with the general population. Is testing for inherited thrombophilia recommended? The available evidence suggests that testing for inherited thrombophilia is not recommended in most clinical settings. In patients without a personal history of VTE, thrombophilia results do not change management, as there is no evidence to support thromboprophylaxis in this setting. In patients with a personal history of provoked or unprovoked VTE, inpatient testing is not indicated, as results do not influence management, testing is not cost‐effective, and a positive test result may lead to unnecessary patient anxiety or may result in unnecessary involvement of consultants. Testing in hospitalized patients has even more limitations because many thrombophilia tests are inaccurate in the setting of acute VTE and/or anticoagulation.
CASE PRESENTATION
A 23‐year‐old man presents to the emergency room with pleuritic chest pain and new oxygen requirement of 2 L nasal cannula. He has a history of unprovoked lower extremity deep venous thrombosis (DVT) diagnosed at age 20 and completed 3 months of systemic anticoagulation without complications. He reports no family history of clotting disorders or venous thromboembolism (VTE) and no reversible risk factors for VTE such as prolonged immobility, recent surgery, or high‐risk medications. A computed tomogram pulmonary embolism protocol shows multiple right lower lobe, segmental pulmonary emboli. Anticoagulation is initiated, and the patient is admitted to the hospital. Will inpatient inherited thrombophilia testing impact management for this case?
WHY MAY INHERITED THROMBOPHILIA TESTING PROVE HELPFUL?
The annual incidence rate of a first VTE event is estimated as 117 per 100,000 individuals per year.[1] The most common presentations are symptomatic DVT of the leg (annual incidence approximately 48 per 100,000 people), or a pulmonary embolism (annual incidence approximately 69 per 100,000 people).[1] Pulmonary embolism results in death in up to 30% of untreated patients and 2.5% of patients who receive systemic anticoagulation.[2] Principal in the pathogenesis of VTE are factors described by Virchow's triad: venous stasis, endothelial injury, and systemic hypercoagulability. By identifying a mutation in 1 or more of the factors in the clotting pathway, an evaluation for inherited thrombophilia theoretically may unearth factors that drive systemic hypercoagulability and inform decision making so as to prevent future events.
Inherited thrombophilia refers to a genetic condition that predisposes to an increased risk of VTE.[3] Approximately 7% of the general population has inherited thrombophilia, which includes factor V Leiden (FVL) mutation, prothrombin 20210 mutation (PT20210), protein C deficiency, protein S deficiency, antithrombin III (ATIII) deficiency, and methylene tetrahydrofolate reductase mutation (MTHFR).[4] Of note, the definition does not include acquired etiologies, such as antiphospholipid antibody syndrome. Depending on the underlying condition and expression of the genetic abnormality, the relative risk of VTE in patients with inherited thrombophilia is 3‐ to 20‐fold greater than that of the general population.[5] Therefore, it is logical to consider that testing for inherited thrombophilia might be clinically useful. However, the evidence for doing so is very limited.
DOES INHERITED THROMBOPHILIA TESTING CHANGE MANAGEMENT?
An inherited thrombophilia evaluation is unlikely to affect management in most clinical settings. There is no current evidence to support primary prophylaxis[6] nor is there evidence that management of patients with recurrent VTE should be altered in the setting of inherited thrombophilia.
To date, no prospective trials have evaluated the efficacy of anticoagulant use for primary prevention of VTE in patients with inherited thrombophilia.[6] Given the limited evidence for thromboprophylaxis and risks of anticoagulation, primary prevention for patients with inherited thrombophilia that remain asymptomatic is not recommended by the current American College of Chest Physicians guidelines.[7, 8]
Similarly, in patients with a first VTE or recurrent VTE, diagnosis of inherited thrombophilia is often not associated with recurrent events, which suggests that other nongenetic factors may be just as important, if not more important, in determining the risk of recurrence.[9] Although no randomized controlled or controlled clinical trials have evaluated the effects of testing for inherited thrombophilia on recurrent VTE,[10, 11] several prospective studies have assessed risk factors for recurrence. Data from these studies suggest that recurrence rates after unprovoked VTE are only weakly correlated with inherited thrombophilia status.[12, 13] Rather, it is postulated that patients with recurrent VTE may exhibit a prothrombotic tendency regardless of underlying genetic predisposition. In this case, decisions regarding anticoagulation do not vary by thrombophilia status. Instead, thrombophilia testing may divert attention away from the management of more prevalent, potentially modifiable risk factors such as immobility, oral contraceptive use, or malignancy, all of which are associated with recurrent VTE.[14] These provoking factors are the most important determinants of the chance of VTE recurrence as well as the most significant factors to take into account when deciding duration of anticoagulation.
Christiansen et al. performed a prospective study evaluating the association between recurrent VTE and thrombophilia status. After following 474 patients with confirmed first episode VTE for a mean of 7.3 years, no statistically significant risk of VTE was found for patients with FVL (hazard ratio [HR]: 1.2, 95% confidence interval [CI]: 0.7‐1.9), PT20210 (HR: 0.7, 95% CI: 0.3‐2.0), or an anticoagulant (protein C, protein S or ATIII) deficiency (HR: 1.8, 95% CI: 0.9‐3.7).[15] Although unexplained VTE was statistically associated with VTE recurrence, heritable thrombophilia status was not.
In a systematic review and meta‐analysis investigating the association of FVL and PT20210 with recurrent VTE, Ho and colleagues found a statistically significant risk of recurrent VTE in patients with inherited thrombophilia due to FVL (odds ratio [OR]: 1.41, 95% CI: 1.14‐1.75) and PT20210 (OR: 1.72, 95% CI: 1.27‐2.31), and reported that at most, only up to 1 in 6 recurrent VTEs may be attributable to these mutations.[16] Based on this relatively modest effect, the authors question the utility of testing for inherited thrombophilia, as thrombophilia status is unlikely to warrant a change in type or duration of treatment.
Regardless of whether an underlying inherited thrombophilia is identified, patients with history of recurrent VTE are often candidates for long‐term anticoagulation. Testing for inherited thrombophilia in patients with prior VTE events will therefore not influence decisions regarding clinical management. Additionally, such testing may be confounded by ongoing disease or treatment (Table 1). For example, protein C, protein S antigen, and ATIII levels are low in the setting of acute VTE.[17, 18] Likewise, protein C and S (vitamin Kdependent proteins) will be low in the setting of anticoagulation with warfarin.[19] Moreover, ATIII activity and antigen levels are low in the setting of heparin use.[20] Lack of provider awareness regarding these interactions may have important negative consequences, including a spurious diagnosis of thrombophilia,[21, 22] unnecessary hematology consultation, and psychological distress to patients in the form of ongoing unwarranted testing or apprehension regarding recurrence.[23]
| Acute VTE | Anticoagulation With Warfarin | Anticoagulation With NOACs | Anticoagulation With Heparin/LMWH | |
|---|---|---|---|---|
| ||||
| FVL/PT20210/MTHFR gene mutations | No Impact | No Impact | No Impact | No Impact |
| Protein C* | Decreased | Decreased | No impact | No impact |
| Protein S* | Decreased | Decreased | No impact | No impact |
| ATIII activity | Decreased | Slight increase | Slight increase | Decreased |
| ATIII antigen | Decreased | Slight increase | Slight increase | Decreased |
Additionally, this expensive evaluation has estimated direct costs of $1100 to $2400 per thrombophilia panel based on estimation of charges billed by a large commercial laboratory.[24, 25] In 2014, over 280,000 claims were submitted under Medicare Part B across all care settings for a thrombophilia analysis including FVL, PT20210, and MTHFR gene mutations,[24] which would equate to between $300 million to $672 million.[26] Unfortunately, there have been no large‐scale trials to assess cost‐effectiveness. However, the Evaluation of Genomic Applications in Practice and Prevention (EGAPP) Working Group stated that cost‐effectiveness modeling studies in this area require updating with current VTE risk estimates but are suggestive that routine FVL/PT20210 testing is not cost‐effective.[27]
ARE THERE CIRCUMSTANCES IN WHICH INPATIENT INHERITED THROMBOPHILIA TESTING PROVES BENEFICIAL?
The evidence for when to test for inherited thrombophilia is very limited and is often based on individualized risk. The current EGAPP guidelines acknowledge this limitation, specifically noting that there is a paucity of data evaluating management or prophylaxis of patients with homozygous or compound heterozygous FVL or P20210 mutation, and a lack of data surrounding whether or not knowledge of thrombophilia mutation should affect anticoagulation treatment.[27] This is why an individualized approach is deemed necessary. For example, the decision to prescribe hormone replacement therapy in women with a family history of inherited thrombophilia may be better informed by testing prior to treatment. Similarly, pregnant women with a family history or personal history of VTE may also benefit from inherited thrombophilia testing, as this may influence antepartum or postpartum management.[28, 29] The National Institute for Health and Clinical Excellence (NICE) guidelines recommend consideration of testing for hereditary thrombophilia in patients with unprovoked VTE and a first‐degree relative with VTE, if stopping anticoagulation treatment is planned; however, these recommendations are based solely on Guideline Development Group's experience and opinion.[30] Regardless, testing for inherited thrombophilia has significant potential consequences. Patients at risk should meet with an outpatient hematologist and/or a genetic counselor, if available, to determine the risks and benefits of testing.
WHAT DO GUIDELINES SAY ABOUT INHERITED THROMBOPHILIA TESTING?
The most recent NICE guidelines recommend against offering inherited thrombophilia testing to patients presenting with a provoked VTE in any clinical setting.[30] In patients diagnosed with unprovoked VTE, testing should not be considered unless a first degree relative with a history of VTE exists.[30] The NICE guidelines also recommend against routinely offering thrombophilia testing to asymptomatic first‐degree relatives of patients with a history of VTE or known inherited thrombophilia. This recommendation is reflected in the American Society of Hematology's Choosing Wisely recommendations since 2013.[31] Further, The American College of Medical Genetics and Genomics' Choosing Wisely recommendations from 2015 state that MTHFR mutations should never be included in any thrombophilia workup, as recent meta‐analyses have disproven an association between the presence of these variants and venous thromboembolism.[32]
The EGAPP Working Group recommends against routine testing for FVL or PT20210 in patients who present with an idiopathic VTE, as longer‐term anticoagulation offers similar benefits to patients with or without these mutations.[27] EGAPP also recommends against testing asymptomatic adult family members of patients with VTE and/or an FVL or PT20210 mutation for the purpose of considering primary prophylactic anticoagulation. In these circumstances, it is felt that the potential risks of thrombophilia testing outweigh any potential benefits.
HOW SHOULD HOSPITALISTS APPROACH TESTING OF INHERITED THROMBOPHILIA?
The providers in our case presentation are challenged with determining whether inpatient thrombophilia evaluation will add value to the evaluation of patients with unprovoked VTE. The available evidence suggests that clinicians should avoid ordering thrombophilia testing for hospitalized patients with unprovoked VTE because (1) many thrombophilia tests are inaccurate in the setting of acute VTE and/or anticoagulation, (2) results of testing often do not influence management, (3) testing is not cost‐effective, (4) a positive test result may lead to unnecessary patient anxiety, and (5) testing may result in inappropriately prolonged anticoagulation courses or unnecessary involvement of inpatient consultants. For these reasons, the patient in our case presentation should not be tested for inherited thrombophilia. In patients with personal or family histories of recurrent thromboembolism, modifiable clinical risk factors should be addressed, as these are more likely to influence treatment decisions compared to genetic testing. Finally, patients may be referred to an outpatient hematologist or geneticist for individualized discussions of risks and benefits of testing for inherited thrombophilia.
CONCLUSION
Inpatient evaluation for inherited thrombophilia for VTE is not clinically useful, cost‐effective, or reliable in the setting of VTE. The result of such testing does not affect management of acute primary or recurrent VTE. Testing should only be considered using an individualized approach in the outpatient setting with appropriate genetic counseling.
Disclosure: Christopher M. Petrilli, MD, and Lauren Heidemann, MD, contributed equally to this work. The authors report no conflicts of interest.
Do you think this is a low‐value practice? Is this truly a Thing We Do for No Reason? Share what you do in your practice and join in the conversation online by retweeting it on Twitter (#TWDFNR) and liking it on Facebook. We invite you to propose ideas for other Things We Do for No Reason topics by emailing [email protected].
- , , , , , . Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25‐year population‐based study. Arch Intern Med. 1998;158(6):585–593.
- , , , et al. The clinical course of pulmonary embolism. N Engl J Med. 1992;326(19):1240–1245.
- , . Hereditary thrombophilia. Thromb J. 2006;4:15.
- , , , . Deep‐vein thrombosis. Lancet. 1999;353(9151):479–485.
- , , , et al. A risk assessment model for the identification of hospitalized medical patients at risk for venous thromboembolism: the Padua Prediction Score. J Thromb Haemost. 2010;8(11):2450–2457.
- , , , et al. VTE, thrombophilia, antithrombotic therapy, and pregnancy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines. Chest. 2012;141(2 suppl):e691S–e736S.
- , . Testing for inherited thrombophilia and consequences for antithrombotic prophylaxis in patients with venous thromboembolism and their relatives. A review of the Guidelines from Scientific Societies and Working Groups. Thromb Haemost. 2013;110(4):697–705.
- , , , et al. Prevention of VTE in nonsurgical patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines. Chest. 2012;141(2 suppl):e195S–e226S.
- , , , et al. Predictive value of factor V Leiden and prothrombin G20210A in adults with venous thromboembolism and in family members of those with a mutation: a systematic review. JAMA. 2009;301(23):2472–2485.
- , , , . Thrombophilia testing for prevention of recurrent venous thromboembolism. Cochrane Database Syst Rev. 2009;(1):CD007069.
- , , , . Thrombophilia testing for prevention of recurrent venous thromboembolism. Cochrane Database Syst Rev. 2012;12:CD007069.
- , , , . Incidence of recurrent venous thromboembolism in relation to clinical and thrombophilic risk factors: prospective cohort study. Lancet. 2003;362(9383):523–526.
- , , , et al. Influence of thrombophilia on risk of recurrent venous thromboembolism while on warfarin: results from a randomized trial. Blood. 2008;112(12):4432–4436.
- , . Testing for thrombophilia: an evidence‐based approach. Postgrad Med J. 2006;82(973):699–704.
- , , , , . Thrombophilia, clinical factors, and recurrent venous thrombotic events. JAMA. 2005;293(19):2352–2361.
- , , , . Risk of recurrent venous thromboembolism in patients with common thrombophilia: a systematic review. Arch Intern Med. 2006;166(7):729–736.
- , , , . Relationship between protein C antigen and anticoagulant activity during oral anticoagulation and in selected disease states. J Clin Invest. 1986;77(2):416–425.
- , . Inherited antithrombin deficiency: a review. Haemophilia. 2008;14(6):1229–1239.
- , , , . Decline of proteins C and S and factors II, VII, IX and X during the initiation of warfarin therapy. Thromb Res. 1987;45(6):783–790.
- . Thrombophilia: common questions on laboratory assessment and management. Hematology Am Soc Hematol Educ Program. 2007:127–135.
- , , . Activated protein C resistance testing for factor V Leiden. Am J Hematol. 2014;89(12):1147–1150.
- , . Quantitation of human protein S in the plasma of normal and warfarin‐treated individuals by radioimmunoassay. Thromb Res. 1984;36(6):527–535.
- , , , . Social aspects of genetic testing for factor V Leiden mutation in healthy individuals and their importance for daily practice. Thromb Res. 2004;113(1):7–12.
- , . Hypercoagulability: clinical assessment and treatment. South Med J. 2001;94(10):1013–1020.
- , , . An evaluation of thrombophilia screening in an urban tertiary care medical center: A “real world” experience. Am J Clin Pathol. 2006;126(1):120–127.
- CodeMap. Available at: https://www.codemap.com. Accessed January 18, 2016.
- Evaluation of Genomic Applications in Practice and Prevention (EGAPP) Working Group. Recommendations from the EGAPP Working Group: routine testing for Factor V Leiden (R506Q) and prothrombin (20210G>A) mutations in adults with a history of idiopathic venous thromboembolism and their adult family members. Genet Med. 2011;13(1):67–76.
- , , , et al. Safety of withholding heparin in pregnant women with a history of venous thromboembolism. Recurrence of Clot in This Pregnancy Study Group. N Engl J Med. 2000;343(20):1439–1444.
- , , , et al. Frequency of pregnancy‐related venous thromboembolism in anticoagulant factor‐deficient women: implications for prophylaxis. Ann Intern Med. 1996;125(12):955–960.
- , , , ; Guideline Development Group. Management of venous thromboembolic diseases and the role of thrombophilia testing: summary of NICE guidance. BMJ. 2012;344:e3979.
- American Society of Hematology. Ten things physicians and patients should question. Choosing Wisely website. Available at: http://www.choosingwisely.org/societies/american‐society‐of‐hematology. Published December 4, 2013. Accessed January 18, 2016.
- American College of Medical Genetics and Genomics. Five Things patients and providers should question. Choosing Wisely website. Available at: http://www.choosingwisely.org/societies/american‐college‐of‐medical‐genetics‐and‐genomics. Published July 10, 2015. Accessed March 13, 2016.
The Things We Do for No Reason (TWDFNR) series reviews practices which have become common parts of hospital care but which may provide little value to our patients. Practices reviewed in the TWDFNR series do not represent black and white conclusions or clinical practice standards, but are meant as a starting place for research and active discussions among hospitalists and patients. We invite you to be part of that discussion. https://www.choosingwisely.org/
Inherited thrombophilia refers to a genetic condition that predisposes to an increased risk of venous thromboembolism (VTE). This disorder is prevalent in approximately 7% of the population and includes mutations such as factor V Leiden, prothrombin 20210, protein C deficiency, protein S deficiency, antithrombin deficiency, and methylene tetrahydrofolate reductase. The relative risk of VTE is 3‐ to 20‐fold greater in patients with inherited thrombophilia compared with the general population. Is testing for inherited thrombophilia recommended? The available evidence suggests that testing for inherited thrombophilia is not recommended in most clinical settings. In patients without a personal history of VTE, thrombophilia results do not change management, as there is no evidence to support thromboprophylaxis in this setting. In patients with a personal history of provoked or unprovoked VTE, inpatient testing is not indicated, as results do not influence management, testing is not cost‐effective, and a positive test result may lead to unnecessary patient anxiety or may result in unnecessary involvement of consultants. Testing in hospitalized patients has even more limitations because many thrombophilia tests are inaccurate in the setting of acute VTE and/or anticoagulation.
CASE PRESENTATION
A 23‐year‐old man presents to the emergency room with pleuritic chest pain and new oxygen requirement of 2 L nasal cannula. He has a history of unprovoked lower extremity deep venous thrombosis (DVT) diagnosed at age 20 and completed 3 months of systemic anticoagulation without complications. He reports no family history of clotting disorders or venous thromboembolism (VTE) and no reversible risk factors for VTE such as prolonged immobility, recent surgery, or high‐risk medications. A computed tomogram pulmonary embolism protocol shows multiple right lower lobe, segmental pulmonary emboli. Anticoagulation is initiated, and the patient is admitted to the hospital. Will inpatient inherited thrombophilia testing impact management for this case?
WHY MAY INHERITED THROMBOPHILIA TESTING PROVE HELPFUL?
The annual incidence rate of a first VTE event is estimated as 117 per 100,000 individuals per year.[1] The most common presentations are symptomatic DVT of the leg (annual incidence approximately 48 per 100,000 people), or a pulmonary embolism (annual incidence approximately 69 per 100,000 people).[1] Pulmonary embolism results in death in up to 30% of untreated patients and 2.5% of patients who receive systemic anticoagulation.[2] Principal in the pathogenesis of VTE are factors described by Virchow's triad: venous stasis, endothelial injury, and systemic hypercoagulability. By identifying a mutation in 1 or more of the factors in the clotting pathway, an evaluation for inherited thrombophilia theoretically may unearth factors that drive systemic hypercoagulability and inform decision making so as to prevent future events.
Inherited thrombophilia refers to a genetic condition that predisposes to an increased risk of VTE.[3] Approximately 7% of the general population has inherited thrombophilia, which includes factor V Leiden (FVL) mutation, prothrombin 20210 mutation (PT20210), protein C deficiency, protein S deficiency, antithrombin III (ATIII) deficiency, and methylene tetrahydrofolate reductase mutation (MTHFR).[4] Of note, the definition does not include acquired etiologies, such as antiphospholipid antibody syndrome. Depending on the underlying condition and expression of the genetic abnormality, the relative risk of VTE in patients with inherited thrombophilia is 3‐ to 20‐fold greater than that of the general population.[5] Therefore, it is logical to consider that testing for inherited thrombophilia might be clinically useful. However, the evidence for doing so is very limited.
DOES INHERITED THROMBOPHILIA TESTING CHANGE MANAGEMENT?
An inherited thrombophilia evaluation is unlikely to affect management in most clinical settings. There is no current evidence to support primary prophylaxis[6] nor is there evidence that management of patients with recurrent VTE should be altered in the setting of inherited thrombophilia.
To date, no prospective trials have evaluated the efficacy of anticoagulant use for primary prevention of VTE in patients with inherited thrombophilia.[6] Given the limited evidence for thromboprophylaxis and risks of anticoagulation, primary prevention for patients with inherited thrombophilia that remain asymptomatic is not recommended by the current American College of Chest Physicians guidelines.[7, 8]
Similarly, in patients with a first VTE or recurrent VTE, diagnosis of inherited thrombophilia is often not associated with recurrent events, which suggests that other nongenetic factors may be just as important, if not more important, in determining the risk of recurrence.[9] Although no randomized controlled or controlled clinical trials have evaluated the effects of testing for inherited thrombophilia on recurrent VTE,[10, 11] several prospective studies have assessed risk factors for recurrence. Data from these studies suggest that recurrence rates after unprovoked VTE are only weakly correlated with inherited thrombophilia status.[12, 13] Rather, it is postulated that patients with recurrent VTE may exhibit a prothrombotic tendency regardless of underlying genetic predisposition. In this case, decisions regarding anticoagulation do not vary by thrombophilia status. Instead, thrombophilia testing may divert attention away from the management of more prevalent, potentially modifiable risk factors such as immobility, oral contraceptive use, or malignancy, all of which are associated with recurrent VTE.[14] These provoking factors are the most important determinants of the chance of VTE recurrence as well as the most significant factors to take into account when deciding duration of anticoagulation.
Christiansen et al. performed a prospective study evaluating the association between recurrent VTE and thrombophilia status. After following 474 patients with confirmed first episode VTE for a mean of 7.3 years, no statistically significant risk of VTE was found for patients with FVL (hazard ratio [HR]: 1.2, 95% confidence interval [CI]: 0.7‐1.9), PT20210 (HR: 0.7, 95% CI: 0.3‐2.0), or an anticoagulant (protein C, protein S or ATIII) deficiency (HR: 1.8, 95% CI: 0.9‐3.7).[15] Although unexplained VTE was statistically associated with VTE recurrence, heritable thrombophilia status was not.
In a systematic review and meta‐analysis investigating the association of FVL and PT20210 with recurrent VTE, Ho and colleagues found a statistically significant risk of recurrent VTE in patients with inherited thrombophilia due to FVL (odds ratio [OR]: 1.41, 95% CI: 1.14‐1.75) and PT20210 (OR: 1.72, 95% CI: 1.27‐2.31), and reported that at most, only up to 1 in 6 recurrent VTEs may be attributable to these mutations.[16] Based on this relatively modest effect, the authors question the utility of testing for inherited thrombophilia, as thrombophilia status is unlikely to warrant a change in type or duration of treatment.
Regardless of whether an underlying inherited thrombophilia is identified, patients with history of recurrent VTE are often candidates for long‐term anticoagulation. Testing for inherited thrombophilia in patients with prior VTE events will therefore not influence decisions regarding clinical management. Additionally, such testing may be confounded by ongoing disease or treatment (Table 1). For example, protein C, protein S antigen, and ATIII levels are low in the setting of acute VTE.[17, 18] Likewise, protein C and S (vitamin Kdependent proteins) will be low in the setting of anticoagulation with warfarin.[19] Moreover, ATIII activity and antigen levels are low in the setting of heparin use.[20] Lack of provider awareness regarding these interactions may have important negative consequences, including a spurious diagnosis of thrombophilia,[21, 22] unnecessary hematology consultation, and psychological distress to patients in the form of ongoing unwarranted testing or apprehension regarding recurrence.[23]
| Acute VTE | Anticoagulation With Warfarin | Anticoagulation With NOACs | Anticoagulation With Heparin/LMWH | |
|---|---|---|---|---|
| ||||
| FVL/PT20210/MTHFR gene mutations | No Impact | No Impact | No Impact | No Impact |
| Protein C* | Decreased | Decreased | No impact | No impact |
| Protein S* | Decreased | Decreased | No impact | No impact |
| ATIII activity | Decreased | Slight increase | Slight increase | Decreased |
| ATIII antigen | Decreased | Slight increase | Slight increase | Decreased |
Additionally, this expensive evaluation has estimated direct costs of $1100 to $2400 per thrombophilia panel based on estimation of charges billed by a large commercial laboratory.[24, 25] In 2014, over 280,000 claims were submitted under Medicare Part B across all care settings for a thrombophilia analysis including FVL, PT20210, and MTHFR gene mutations,[24] which would equate to between $300 million to $672 million.[26] Unfortunately, there have been no large‐scale trials to assess cost‐effectiveness. However, the Evaluation of Genomic Applications in Practice and Prevention (EGAPP) Working Group stated that cost‐effectiveness modeling studies in this area require updating with current VTE risk estimates but are suggestive that routine FVL/PT20210 testing is not cost‐effective.[27]
ARE THERE CIRCUMSTANCES IN WHICH INPATIENT INHERITED THROMBOPHILIA TESTING PROVES BENEFICIAL?
The evidence for when to test for inherited thrombophilia is very limited and is often based on individualized risk. The current EGAPP guidelines acknowledge this limitation, specifically noting that there is a paucity of data evaluating management or prophylaxis of patients with homozygous or compound heterozygous FVL or P20210 mutation, and a lack of data surrounding whether or not knowledge of thrombophilia mutation should affect anticoagulation treatment.[27] This is why an individualized approach is deemed necessary. For example, the decision to prescribe hormone replacement therapy in women with a family history of inherited thrombophilia may be better informed by testing prior to treatment. Similarly, pregnant women with a family history or personal history of VTE may also benefit from inherited thrombophilia testing, as this may influence antepartum or postpartum management.[28, 29] The National Institute for Health and Clinical Excellence (NICE) guidelines recommend consideration of testing for hereditary thrombophilia in patients with unprovoked VTE and a first‐degree relative with VTE, if stopping anticoagulation treatment is planned; however, these recommendations are based solely on Guideline Development Group's experience and opinion.[30] Regardless, testing for inherited thrombophilia has significant potential consequences. Patients at risk should meet with an outpatient hematologist and/or a genetic counselor, if available, to determine the risks and benefits of testing.
WHAT DO GUIDELINES SAY ABOUT INHERITED THROMBOPHILIA TESTING?
The most recent NICE guidelines recommend against offering inherited thrombophilia testing to patients presenting with a provoked VTE in any clinical setting.[30] In patients diagnosed with unprovoked VTE, testing should not be considered unless a first degree relative with a history of VTE exists.[30] The NICE guidelines also recommend against routinely offering thrombophilia testing to asymptomatic first‐degree relatives of patients with a history of VTE or known inherited thrombophilia. This recommendation is reflected in the American Society of Hematology's Choosing Wisely recommendations since 2013.[31] Further, The American College of Medical Genetics and Genomics' Choosing Wisely recommendations from 2015 state that MTHFR mutations should never be included in any thrombophilia workup, as recent meta‐analyses have disproven an association between the presence of these variants and venous thromboembolism.[32]
The EGAPP Working Group recommends against routine testing for FVL or PT20210 in patients who present with an idiopathic VTE, as longer‐term anticoagulation offers similar benefits to patients with or without these mutations.[27] EGAPP also recommends against testing asymptomatic adult family members of patients with VTE and/or an FVL or PT20210 mutation for the purpose of considering primary prophylactic anticoagulation. In these circumstances, it is felt that the potential risks of thrombophilia testing outweigh any potential benefits.
HOW SHOULD HOSPITALISTS APPROACH TESTING OF INHERITED THROMBOPHILIA?
The providers in our case presentation are challenged with determining whether inpatient thrombophilia evaluation will add value to the evaluation of patients with unprovoked VTE. The available evidence suggests that clinicians should avoid ordering thrombophilia testing for hospitalized patients with unprovoked VTE because (1) many thrombophilia tests are inaccurate in the setting of acute VTE and/or anticoagulation, (2) results of testing often do not influence management, (3) testing is not cost‐effective, (4) a positive test result may lead to unnecessary patient anxiety, and (5) testing may result in inappropriately prolonged anticoagulation courses or unnecessary involvement of inpatient consultants. For these reasons, the patient in our case presentation should not be tested for inherited thrombophilia. In patients with personal or family histories of recurrent thromboembolism, modifiable clinical risk factors should be addressed, as these are more likely to influence treatment decisions compared to genetic testing. Finally, patients may be referred to an outpatient hematologist or geneticist for individualized discussions of risks and benefits of testing for inherited thrombophilia.
CONCLUSION
Inpatient evaluation for inherited thrombophilia for VTE is not clinically useful, cost‐effective, or reliable in the setting of VTE. The result of such testing does not affect management of acute primary or recurrent VTE. Testing should only be considered using an individualized approach in the outpatient setting with appropriate genetic counseling.
Disclosure: Christopher M. Petrilli, MD, and Lauren Heidemann, MD, contributed equally to this work. The authors report no conflicts of interest.
Do you think this is a low‐value practice? Is this truly a Thing We Do for No Reason? Share what you do in your practice and join in the conversation online by retweeting it on Twitter (#TWDFNR) and liking it on Facebook. We invite you to propose ideas for other Things We Do for No Reason topics by emailing [email protected].
The Things We Do for No Reason (TWDFNR) series reviews practices which have become common parts of hospital care but which may provide little value to our patients. Practices reviewed in the TWDFNR series do not represent black and white conclusions or clinical practice standards, but are meant as a starting place for research and active discussions among hospitalists and patients. We invite you to be part of that discussion. https://www.choosingwisely.org/
Inherited thrombophilia refers to a genetic condition that predisposes to an increased risk of venous thromboembolism (VTE). This disorder is prevalent in approximately 7% of the population and includes mutations such as factor V Leiden, prothrombin 20210, protein C deficiency, protein S deficiency, antithrombin deficiency, and methylene tetrahydrofolate reductase. The relative risk of VTE is 3‐ to 20‐fold greater in patients with inherited thrombophilia compared with the general population. Is testing for inherited thrombophilia recommended? The available evidence suggests that testing for inherited thrombophilia is not recommended in most clinical settings. In patients without a personal history of VTE, thrombophilia results do not change management, as there is no evidence to support thromboprophylaxis in this setting. In patients with a personal history of provoked or unprovoked VTE, inpatient testing is not indicated, as results do not influence management, testing is not cost‐effective, and a positive test result may lead to unnecessary patient anxiety or may result in unnecessary involvement of consultants. Testing in hospitalized patients has even more limitations because many thrombophilia tests are inaccurate in the setting of acute VTE and/or anticoagulation.
CASE PRESENTATION
A 23‐year‐old man presents to the emergency room with pleuritic chest pain and new oxygen requirement of 2 L nasal cannula. He has a history of unprovoked lower extremity deep venous thrombosis (DVT) diagnosed at age 20 and completed 3 months of systemic anticoagulation without complications. He reports no family history of clotting disorders or venous thromboembolism (VTE) and no reversible risk factors for VTE such as prolonged immobility, recent surgery, or high‐risk medications. A computed tomogram pulmonary embolism protocol shows multiple right lower lobe, segmental pulmonary emboli. Anticoagulation is initiated, and the patient is admitted to the hospital. Will inpatient inherited thrombophilia testing impact management for this case?
WHY MAY INHERITED THROMBOPHILIA TESTING PROVE HELPFUL?
The annual incidence rate of a first VTE event is estimated as 117 per 100,000 individuals per year.[1] The most common presentations are symptomatic DVT of the leg (annual incidence approximately 48 per 100,000 people), or a pulmonary embolism (annual incidence approximately 69 per 100,000 people).[1] Pulmonary embolism results in death in up to 30% of untreated patients and 2.5% of patients who receive systemic anticoagulation.[2] Principal in the pathogenesis of VTE are factors described by Virchow's triad: venous stasis, endothelial injury, and systemic hypercoagulability. By identifying a mutation in 1 or more of the factors in the clotting pathway, an evaluation for inherited thrombophilia theoretically may unearth factors that drive systemic hypercoagulability and inform decision making so as to prevent future events.
Inherited thrombophilia refers to a genetic condition that predisposes to an increased risk of VTE.[3] Approximately 7% of the general population has inherited thrombophilia, which includes factor V Leiden (FVL) mutation, prothrombin 20210 mutation (PT20210), protein C deficiency, protein S deficiency, antithrombin III (ATIII) deficiency, and methylene tetrahydrofolate reductase mutation (MTHFR).[4] Of note, the definition does not include acquired etiologies, such as antiphospholipid antibody syndrome. Depending on the underlying condition and expression of the genetic abnormality, the relative risk of VTE in patients with inherited thrombophilia is 3‐ to 20‐fold greater than that of the general population.[5] Therefore, it is logical to consider that testing for inherited thrombophilia might be clinically useful. However, the evidence for doing so is very limited.
DOES INHERITED THROMBOPHILIA TESTING CHANGE MANAGEMENT?
An inherited thrombophilia evaluation is unlikely to affect management in most clinical settings. There is no current evidence to support primary prophylaxis[6] nor is there evidence that management of patients with recurrent VTE should be altered in the setting of inherited thrombophilia.
To date, no prospective trials have evaluated the efficacy of anticoagulant use for primary prevention of VTE in patients with inherited thrombophilia.[6] Given the limited evidence for thromboprophylaxis and risks of anticoagulation, primary prevention for patients with inherited thrombophilia that remain asymptomatic is not recommended by the current American College of Chest Physicians guidelines.[7, 8]
Similarly, in patients with a first VTE or recurrent VTE, diagnosis of inherited thrombophilia is often not associated with recurrent events, which suggests that other nongenetic factors may be just as important, if not more important, in determining the risk of recurrence.[9] Although no randomized controlled or controlled clinical trials have evaluated the effects of testing for inherited thrombophilia on recurrent VTE,[10, 11] several prospective studies have assessed risk factors for recurrence. Data from these studies suggest that recurrence rates after unprovoked VTE are only weakly correlated with inherited thrombophilia status.[12, 13] Rather, it is postulated that patients with recurrent VTE may exhibit a prothrombotic tendency regardless of underlying genetic predisposition. In this case, decisions regarding anticoagulation do not vary by thrombophilia status. Instead, thrombophilia testing may divert attention away from the management of more prevalent, potentially modifiable risk factors such as immobility, oral contraceptive use, or malignancy, all of which are associated with recurrent VTE.[14] These provoking factors are the most important determinants of the chance of VTE recurrence as well as the most significant factors to take into account when deciding duration of anticoagulation.
Christiansen et al. performed a prospective study evaluating the association between recurrent VTE and thrombophilia status. After following 474 patients with confirmed first episode VTE for a mean of 7.3 years, no statistically significant risk of VTE was found for patients with FVL (hazard ratio [HR]: 1.2, 95% confidence interval [CI]: 0.7‐1.9), PT20210 (HR: 0.7, 95% CI: 0.3‐2.0), or an anticoagulant (protein C, protein S or ATIII) deficiency (HR: 1.8, 95% CI: 0.9‐3.7).[15] Although unexplained VTE was statistically associated with VTE recurrence, heritable thrombophilia status was not.
In a systematic review and meta‐analysis investigating the association of FVL and PT20210 with recurrent VTE, Ho and colleagues found a statistically significant risk of recurrent VTE in patients with inherited thrombophilia due to FVL (odds ratio [OR]: 1.41, 95% CI: 1.14‐1.75) and PT20210 (OR: 1.72, 95% CI: 1.27‐2.31), and reported that at most, only up to 1 in 6 recurrent VTEs may be attributable to these mutations.[16] Based on this relatively modest effect, the authors question the utility of testing for inherited thrombophilia, as thrombophilia status is unlikely to warrant a change in type or duration of treatment.
Regardless of whether an underlying inherited thrombophilia is identified, patients with history of recurrent VTE are often candidates for long‐term anticoagulation. Testing for inherited thrombophilia in patients with prior VTE events will therefore not influence decisions regarding clinical management. Additionally, such testing may be confounded by ongoing disease or treatment (Table 1). For example, protein C, protein S antigen, and ATIII levels are low in the setting of acute VTE.[17, 18] Likewise, protein C and S (vitamin Kdependent proteins) will be low in the setting of anticoagulation with warfarin.[19] Moreover, ATIII activity and antigen levels are low in the setting of heparin use.[20] Lack of provider awareness regarding these interactions may have important negative consequences, including a spurious diagnosis of thrombophilia,[21, 22] unnecessary hematology consultation, and psychological distress to patients in the form of ongoing unwarranted testing or apprehension regarding recurrence.[23]
| Acute VTE | Anticoagulation With Warfarin | Anticoagulation With NOACs | Anticoagulation With Heparin/LMWH | |
|---|---|---|---|---|
| ||||
| FVL/PT20210/MTHFR gene mutations | No Impact | No Impact | No Impact | No Impact |
| Protein C* | Decreased | Decreased | No impact | No impact |
| Protein S* | Decreased | Decreased | No impact | No impact |
| ATIII activity | Decreased | Slight increase | Slight increase | Decreased |
| ATIII antigen | Decreased | Slight increase | Slight increase | Decreased |
Additionally, this expensive evaluation has estimated direct costs of $1100 to $2400 per thrombophilia panel based on estimation of charges billed by a large commercial laboratory.[24, 25] In 2014, over 280,000 claims were submitted under Medicare Part B across all care settings for a thrombophilia analysis including FVL, PT20210, and MTHFR gene mutations,[24] which would equate to between $300 million to $672 million.[26] Unfortunately, there have been no large‐scale trials to assess cost‐effectiveness. However, the Evaluation of Genomic Applications in Practice and Prevention (EGAPP) Working Group stated that cost‐effectiveness modeling studies in this area require updating with current VTE risk estimates but are suggestive that routine FVL/PT20210 testing is not cost‐effective.[27]
ARE THERE CIRCUMSTANCES IN WHICH INPATIENT INHERITED THROMBOPHILIA TESTING PROVES BENEFICIAL?
The evidence for when to test for inherited thrombophilia is very limited and is often based on individualized risk. The current EGAPP guidelines acknowledge this limitation, specifically noting that there is a paucity of data evaluating management or prophylaxis of patients with homozygous or compound heterozygous FVL or P20210 mutation, and a lack of data surrounding whether or not knowledge of thrombophilia mutation should affect anticoagulation treatment.[27] This is why an individualized approach is deemed necessary. For example, the decision to prescribe hormone replacement therapy in women with a family history of inherited thrombophilia may be better informed by testing prior to treatment. Similarly, pregnant women with a family history or personal history of VTE may also benefit from inherited thrombophilia testing, as this may influence antepartum or postpartum management.[28, 29] The National Institute for Health and Clinical Excellence (NICE) guidelines recommend consideration of testing for hereditary thrombophilia in patients with unprovoked VTE and a first‐degree relative with VTE, if stopping anticoagulation treatment is planned; however, these recommendations are based solely on Guideline Development Group's experience and opinion.[30] Regardless, testing for inherited thrombophilia has significant potential consequences. Patients at risk should meet with an outpatient hematologist and/or a genetic counselor, if available, to determine the risks and benefits of testing.
WHAT DO GUIDELINES SAY ABOUT INHERITED THROMBOPHILIA TESTING?
The most recent NICE guidelines recommend against offering inherited thrombophilia testing to patients presenting with a provoked VTE in any clinical setting.[30] In patients diagnosed with unprovoked VTE, testing should not be considered unless a first degree relative with a history of VTE exists.[30] The NICE guidelines also recommend against routinely offering thrombophilia testing to asymptomatic first‐degree relatives of patients with a history of VTE or known inherited thrombophilia. This recommendation is reflected in the American Society of Hematology's Choosing Wisely recommendations since 2013.[31] Further, The American College of Medical Genetics and Genomics' Choosing Wisely recommendations from 2015 state that MTHFR mutations should never be included in any thrombophilia workup, as recent meta‐analyses have disproven an association between the presence of these variants and venous thromboembolism.[32]
The EGAPP Working Group recommends against routine testing for FVL or PT20210 in patients who present with an idiopathic VTE, as longer‐term anticoagulation offers similar benefits to patients with or without these mutations.[27] EGAPP also recommends against testing asymptomatic adult family members of patients with VTE and/or an FVL or PT20210 mutation for the purpose of considering primary prophylactic anticoagulation. In these circumstances, it is felt that the potential risks of thrombophilia testing outweigh any potential benefits.
HOW SHOULD HOSPITALISTS APPROACH TESTING OF INHERITED THROMBOPHILIA?
The providers in our case presentation are challenged with determining whether inpatient thrombophilia evaluation will add value to the evaluation of patients with unprovoked VTE. The available evidence suggests that clinicians should avoid ordering thrombophilia testing for hospitalized patients with unprovoked VTE because (1) many thrombophilia tests are inaccurate in the setting of acute VTE and/or anticoagulation, (2) results of testing often do not influence management, (3) testing is not cost‐effective, (4) a positive test result may lead to unnecessary patient anxiety, and (5) testing may result in inappropriately prolonged anticoagulation courses or unnecessary involvement of inpatient consultants. For these reasons, the patient in our case presentation should not be tested for inherited thrombophilia. In patients with personal or family histories of recurrent thromboembolism, modifiable clinical risk factors should be addressed, as these are more likely to influence treatment decisions compared to genetic testing. Finally, patients may be referred to an outpatient hematologist or geneticist for individualized discussions of risks and benefits of testing for inherited thrombophilia.
CONCLUSION
Inpatient evaluation for inherited thrombophilia for VTE is not clinically useful, cost‐effective, or reliable in the setting of VTE. The result of such testing does not affect management of acute primary or recurrent VTE. Testing should only be considered using an individualized approach in the outpatient setting with appropriate genetic counseling.
Disclosure: Christopher M. Petrilli, MD, and Lauren Heidemann, MD, contributed equally to this work. The authors report no conflicts of interest.
Do you think this is a low‐value practice? Is this truly a Thing We Do for No Reason? Share what you do in your practice and join in the conversation online by retweeting it on Twitter (#TWDFNR) and liking it on Facebook. We invite you to propose ideas for other Things We Do for No Reason topics by emailing [email protected].
- , , , , , . Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25‐year population‐based study. Arch Intern Med. 1998;158(6):585–593.
- , , , et al. The clinical course of pulmonary embolism. N Engl J Med. 1992;326(19):1240–1245.
- , . Hereditary thrombophilia. Thromb J. 2006;4:15.
- , , , . Deep‐vein thrombosis. Lancet. 1999;353(9151):479–485.
- , , , et al. A risk assessment model for the identification of hospitalized medical patients at risk for venous thromboembolism: the Padua Prediction Score. J Thromb Haemost. 2010;8(11):2450–2457.
- , , , et al. VTE, thrombophilia, antithrombotic therapy, and pregnancy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines. Chest. 2012;141(2 suppl):e691S–e736S.
- , . Testing for inherited thrombophilia and consequences for antithrombotic prophylaxis in patients with venous thromboembolism and their relatives. A review of the Guidelines from Scientific Societies and Working Groups. Thromb Haemost. 2013;110(4):697–705.
- , , , et al. Prevention of VTE in nonsurgical patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines. Chest. 2012;141(2 suppl):e195S–e226S.
- , , , et al. Predictive value of factor V Leiden and prothrombin G20210A in adults with venous thromboembolism and in family members of those with a mutation: a systematic review. JAMA. 2009;301(23):2472–2485.
- , , , . Thrombophilia testing for prevention of recurrent venous thromboembolism. Cochrane Database Syst Rev. 2009;(1):CD007069.
- , , , . Thrombophilia testing for prevention of recurrent venous thromboembolism. Cochrane Database Syst Rev. 2012;12:CD007069.
- , , , . Incidence of recurrent venous thromboembolism in relation to clinical and thrombophilic risk factors: prospective cohort study. Lancet. 2003;362(9383):523–526.
- , , , et al. Influence of thrombophilia on risk of recurrent venous thromboembolism while on warfarin: results from a randomized trial. Blood. 2008;112(12):4432–4436.
- , . Testing for thrombophilia: an evidence‐based approach. Postgrad Med J. 2006;82(973):699–704.
- , , , , . Thrombophilia, clinical factors, and recurrent venous thrombotic events. JAMA. 2005;293(19):2352–2361.
- , , , . Risk of recurrent venous thromboembolism in patients with common thrombophilia: a systematic review. Arch Intern Med. 2006;166(7):729–736.
- , , , . Relationship between protein C antigen and anticoagulant activity during oral anticoagulation and in selected disease states. J Clin Invest. 1986;77(2):416–425.
- , . Inherited antithrombin deficiency: a review. Haemophilia. 2008;14(6):1229–1239.
- , , , . Decline of proteins C and S and factors II, VII, IX and X during the initiation of warfarin therapy. Thromb Res. 1987;45(6):783–790.
- . Thrombophilia: common questions on laboratory assessment and management. Hematology Am Soc Hematol Educ Program. 2007:127–135.
- , , . Activated protein C resistance testing for factor V Leiden. Am J Hematol. 2014;89(12):1147–1150.
- , . Quantitation of human protein S in the plasma of normal and warfarin‐treated individuals by radioimmunoassay. Thromb Res. 1984;36(6):527–535.
- , , , . Social aspects of genetic testing for factor V Leiden mutation in healthy individuals and their importance for daily practice. Thromb Res. 2004;113(1):7–12.
- , . Hypercoagulability: clinical assessment and treatment. South Med J. 2001;94(10):1013–1020.
- , , . An evaluation of thrombophilia screening in an urban tertiary care medical center: A “real world” experience. Am J Clin Pathol. 2006;126(1):120–127.
- CodeMap. Available at: https://www.codemap.com. Accessed January 18, 2016.
- Evaluation of Genomic Applications in Practice and Prevention (EGAPP) Working Group. Recommendations from the EGAPP Working Group: routine testing for Factor V Leiden (R506Q) and prothrombin (20210G>A) mutations in adults with a history of idiopathic venous thromboembolism and their adult family members. Genet Med. 2011;13(1):67–76.
- , , , et al. Safety of withholding heparin in pregnant women with a history of venous thromboembolism. Recurrence of Clot in This Pregnancy Study Group. N Engl J Med. 2000;343(20):1439–1444.
- , , , et al. Frequency of pregnancy‐related venous thromboembolism in anticoagulant factor‐deficient women: implications for prophylaxis. Ann Intern Med. 1996;125(12):955–960.
- , , , ; Guideline Development Group. Management of venous thromboembolic diseases and the role of thrombophilia testing: summary of NICE guidance. BMJ. 2012;344:e3979.
- American Society of Hematology. Ten things physicians and patients should question. Choosing Wisely website. Available at: http://www.choosingwisely.org/societies/american‐society‐of‐hematology. Published December 4, 2013. Accessed January 18, 2016.
- American College of Medical Genetics and Genomics. Five Things patients and providers should question. Choosing Wisely website. Available at: http://www.choosingwisely.org/societies/american‐college‐of‐medical‐genetics‐and‐genomics. Published July 10, 2015. Accessed March 13, 2016.
- , , , , , . Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25‐year population‐based study. Arch Intern Med. 1998;158(6):585–593.
- , , , et al. The clinical course of pulmonary embolism. N Engl J Med. 1992;326(19):1240–1245.
- , . Hereditary thrombophilia. Thromb J. 2006;4:15.
- , , , . Deep‐vein thrombosis. Lancet. 1999;353(9151):479–485.
- , , , et al. A risk assessment model for the identification of hospitalized medical patients at risk for venous thromboembolism: the Padua Prediction Score. J Thromb Haemost. 2010;8(11):2450–2457.
- , , , et al. VTE, thrombophilia, antithrombotic therapy, and pregnancy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines. Chest. 2012;141(2 suppl):e691S–e736S.
- , . Testing for inherited thrombophilia and consequences for antithrombotic prophylaxis in patients with venous thromboembolism and their relatives. A review of the Guidelines from Scientific Societies and Working Groups. Thromb Haemost. 2013;110(4):697–705.
- , , , et al. Prevention of VTE in nonsurgical patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines. Chest. 2012;141(2 suppl):e195S–e226S.
- , , , et al. Predictive value of factor V Leiden and prothrombin G20210A in adults with venous thromboembolism and in family members of those with a mutation: a systematic review. JAMA. 2009;301(23):2472–2485.
- , , , . Thrombophilia testing for prevention of recurrent venous thromboembolism. Cochrane Database Syst Rev. 2009;(1):CD007069.
- , , , . Thrombophilia testing for prevention of recurrent venous thromboembolism. Cochrane Database Syst Rev. 2012;12:CD007069.
- , , , . Incidence of recurrent venous thromboembolism in relation to clinical and thrombophilic risk factors: prospective cohort study. Lancet. 2003;362(9383):523–526.
- , , , et al. Influence of thrombophilia on risk of recurrent venous thromboembolism while on warfarin: results from a randomized trial. Blood. 2008;112(12):4432–4436.
- , . Testing for thrombophilia: an evidence‐based approach. Postgrad Med J. 2006;82(973):699–704.
- , , , , . Thrombophilia, clinical factors, and recurrent venous thrombotic events. JAMA. 2005;293(19):2352–2361.
- , , , . Risk of recurrent venous thromboembolism in patients with common thrombophilia: a systematic review. Arch Intern Med. 2006;166(7):729–736.
- , , , . Relationship between protein C antigen and anticoagulant activity during oral anticoagulation and in selected disease states. J Clin Invest. 1986;77(2):416–425.
- , . Inherited antithrombin deficiency: a review. Haemophilia. 2008;14(6):1229–1239.
- , , , . Decline of proteins C and S and factors II, VII, IX and X during the initiation of warfarin therapy. Thromb Res. 1987;45(6):783–790.
- . Thrombophilia: common questions on laboratory assessment and management. Hematology Am Soc Hematol Educ Program. 2007:127–135.
- , , . Activated protein C resistance testing for factor V Leiden. Am J Hematol. 2014;89(12):1147–1150.
- , . Quantitation of human protein S in the plasma of normal and warfarin‐treated individuals by radioimmunoassay. Thromb Res. 1984;36(6):527–535.
- , , , . Social aspects of genetic testing for factor V Leiden mutation in healthy individuals and their importance for daily practice. Thromb Res. 2004;113(1):7–12.
- , . Hypercoagulability: clinical assessment and treatment. South Med J. 2001;94(10):1013–1020.
- , , . An evaluation of thrombophilia screening in an urban tertiary care medical center: A “real world” experience. Am J Clin Pathol. 2006;126(1):120–127.
- CodeMap. Available at: https://www.codemap.com. Accessed January 18, 2016.
- Evaluation of Genomic Applications in Practice and Prevention (EGAPP) Working Group. Recommendations from the EGAPP Working Group: routine testing for Factor V Leiden (R506Q) and prothrombin (20210G>A) mutations in adults with a history of idiopathic venous thromboembolism and their adult family members. Genet Med. 2011;13(1):67–76.
- , , , et al. Safety of withholding heparin in pregnant women with a history of venous thromboembolism. Recurrence of Clot in This Pregnancy Study Group. N Engl J Med. 2000;343(20):1439–1444.
- , , , et al. Frequency of pregnancy‐related venous thromboembolism in anticoagulant factor‐deficient women: implications for prophylaxis. Ann Intern Med. 1996;125(12):955–960.
- , , , ; Guideline Development Group. Management of venous thromboembolic diseases and the role of thrombophilia testing: summary of NICE guidance. BMJ. 2012;344:e3979.
- American Society of Hematology. Ten things physicians and patients should question. Choosing Wisely website. Available at: http://www.choosingwisely.org/societies/american‐society‐of‐hematology. Published December 4, 2013. Accessed January 18, 2016.
- American College of Medical Genetics and Genomics. Five Things patients and providers should question. Choosing Wisely website. Available at: http://www.choosingwisely.org/societies/american‐college‐of‐medical‐genetics‐and‐genomics. Published July 10, 2015. Accessed March 13, 2016.
© 2016 Society of Hospital Medicine
New mechanical ventilation guidelines unveiled
LOS ANGELES – Acutely hospitalized patients who have been on mechanical ventilation for more than 24 hours, are at high risk for extubation failure, and have passed a spontaneous breathing trial should be extubated to noninvasive ventilation.
The recommendation comes from new clinical practice guidelines from the American College of Chest Physicians and the American Thoracic Society. Moderate-quality evidence suggests that early extubation and a switch to noninvasive ventilation reduces ventilator-related and ICU-related complications, including infections and injury to the lungs and other organs. Extubation also cuts costs by reducing ICU stays.

At the annual meeting of the American College of Chest Physicians, one of the six project cochairs, Daniel R. Ouellette, MD, said that the guidelines were intended to address “new territory” from the evidence-based guidelines for weaning and discontinuing ventilator support that were published in 2001. That effort, chaired by Neil R. MacIntyre, MD, “was a landmark article that helped us learn about the steps that we needed to take to liberate patients from mechanical ventilation,” said Dr. Ouellette of the Henry Ford Hospital Department of Pulmonary and Critical Care Medicine, Detroit. “We hope that this guideline lives up to the importance of that one. We wanted to look over new information and give new recommendations about things that haven’t been addressed in the past.”
Six recommendations from the guideline panel include:
We suggest that the initial spontaneous breathing trial be conducted with inspiratory pressure augmentation rather than T-piece or continuous positive airway pressure. The committee wrote that conducting the initial spontaneous breathing trial with pressure augmentation was more likely to be successful, produced a higher rate of extubation success, and was associated with a trend towards lower intensive care unit mortality.
We suggest protocols attempting to minimize sedation. The committee found that sedation protocols reduced ICU length of stay. However, the protocols did not appear to decrease time on the ventilator or reduce short-term mortality. The authors could not recommend one protocol over another but said the burden of providing sedation by any of the protocols was “very low.”
We suggest protocolized rehabilitation directed toward early mobilization. The committee wrote that patients receiving the intervention spent less time on the ventilator and were more likely to be able to walk when they left the hospital. However, their mortality rate appeared unchanged. The authors noted the exercises created additional work for ICU staff that might have come at the expense of other care priorities.
We suggest managing patients with a ventilator liberation protocol. The committee said that patients managed by protocol spent on average 25 fewer hours on mechanical ventilation and were discharged from the ICU a day early. However, their mortality rate appeared unchanged.
We suggest performing a cuff leak test in patients who meet extubation criteria and are deemed at high risk for postextubation stridor. The committee suggested that the test should be used only in patients with a high risk of stridor (abnormal breathing caused by blockage of windpipe) after extubation. Although patients passing the test had lower stridor and reintubation rates, the authors wrote that a high percentage of patients who failed the test could be successfully extubated.
For patients who failed the cuff leak test but are otherwise ready for extubation, we suggest administering systemic steroids at least 4 hours before extubation. The committee said that clinical judgment should take priority over test results, and systemic steroids should be administered to these patients at least 4 hours before extubation. The authors added that the short duration of the steroid therapy was likely to improve success rates without resulting in adverse events.
In a prepared statement, Timothy Girard, MD, of the department of medicine at the University of Pittsburgh and a lead author of the guidelines said the committee hoped the guidelines would help reduce variations in practice that do not benefit patients. “We are not prescribing a specific approach to care for every patient every time,” he said. “But we are trying to summarize the available evidence in as clear and succinct a way as possible so that clinicians know how it applies to most patients.”
Dr. Ouellette disclosed that he has received a research grant from Cardeas Pharma for health care–associated pneumonia.
Daniel R. Ouellette, MD, FCCP, comments: Liberation from mechanical ventilation is one of the most important goals in taking care of critically ill patients receiving mechanical ventilation in the ICU. Patients who have a prolonged ventilator course are at risk for many complications and so physicians who work in the intensive care unit must work carefully to liberate patients from the ventilator at the earliest possible moment. That has to be done in a safe fashion so criteria to ensure that this can be done safely are important as well.
Patients often have medical illness that requires sedation, and it is often necessary to sedate patients so that they can tolerate being on mechanical ventilation; however, we know that oversedation can lead to failure to liberate patients from mechanical ventilation expeditiously. Therefore, one of our recommendations’ suggestions is to design protocols for sedation that focus on minimizing sedation so that patients can be extubated expeditiously.
All of the recommendations ultimately focused on a team approach to liberation from mechanical ventilation, because involvement of team members is always important. However, there are a couple of our recommendations that are particularly important in terms of their implications for the team approach and those include recommendations about using protocols to liberate patients from ventilators, in general, and also to use sedation protocols to minimize sedations.
We began to look at developing this topic, because we had initially published guidelines on [liberation from mechanical ventilation] in 2001. We knew that there was much new information that had emerged since the 2001 guidelines. For that reason we began to think about an update. With the initial inception of this project, we reached out to the American Thoracic Society so as to develop a collaborative effort since this was a topic that interested both societies. This collaboration was at all levels at CHEST and it involved not only the guidelines organization, but also the leadership of both societies and, of course, the panel that was ultimately constructed to address these issues was made up of members from both societies. The entire process [of developing the new guideline] took nearly 3 years.
When one develops a guideline, one makes an effort to make a guideline as comprehensive and globally applicable as possible. I think the practices in Europe are very similar to practices in North America in terms of mechanical ventilation. Several of our panelists are European and some of the important work that we reviewed came from centers in Europe. It’s my opinion that our guideline will be broadly applicable in both North America and Europe, but there may be regional or local differences. Nevertheless, we recognize in different regions in the world, there are different resource allocations for medical treatment, there are different cultural precepts, and there are other factors that implicate medical problems.
Certainly the European Respiratory Society and other European organizations developed guidelines on related topics ... one of the important caveats when CHEST decides to develop a guideline is that we are not reproducing the work that has been done elsewhere and so this guideline represents a project that fills a gap that previously had not been filled.
All guidelines that CHEST develops are living guidelines … it’s hard to envision exactly how often a guideline will be updated. We know that there will be certain areas of our guideline that will stand the test of time, but there will be other areas that will need to be updated, some sooner than others.
The original CHEST guideline on liberation from mechanical ventilation was a very important document that appeared in 2001 and changed the practice of medicine and the practice of managing patients on mechanical ventilation. Nevertheless, the guideline was somewhat limited in scope, because there was only so much information available. … Our goal in developing this guideline was to address some of practitioners’ questions that had emerged in the last decade by looking at newly available data.
[In formulating these guidelines], we purposely chose six new questions that were not directly related to any of the questions [that has been answered] in the previous guideline.
Daniel R. Ouellette, MD, FCCP, comments: Liberation from mechanical ventilation is one of the most important goals in taking care of critically ill patients receiving mechanical ventilation in the ICU. Patients who have a prolonged ventilator course are at risk for many complications and so physicians who work in the intensive care unit must work carefully to liberate patients from the ventilator at the earliest possible moment. That has to be done in a safe fashion so criteria to ensure that this can be done safely are important as well.
Patients often have medical illness that requires sedation, and it is often necessary to sedate patients so that they can tolerate being on mechanical ventilation; however, we know that oversedation can lead to failure to liberate patients from mechanical ventilation expeditiously. Therefore, one of our recommendations’ suggestions is to design protocols for sedation that focus on minimizing sedation so that patients can be extubated expeditiously.
All of the recommendations ultimately focused on a team approach to liberation from mechanical ventilation, because involvement of team members is always important. However, there are a couple of our recommendations that are particularly important in terms of their implications for the team approach and those include recommendations about using protocols to liberate patients from ventilators, in general, and also to use sedation protocols to minimize sedations.
We began to look at developing this topic, because we had initially published guidelines on [liberation from mechanical ventilation] in 2001. We knew that there was much new information that had emerged since the 2001 guidelines. For that reason we began to think about an update. With the initial inception of this project, we reached out to the American Thoracic Society so as to develop a collaborative effort since this was a topic that interested both societies. This collaboration was at all levels at CHEST and it involved not only the guidelines organization, but also the leadership of both societies and, of course, the panel that was ultimately constructed to address these issues was made up of members from both societies. The entire process [of developing the new guideline] took nearly 3 years.
When one develops a guideline, one makes an effort to make a guideline as comprehensive and globally applicable as possible. I think the practices in Europe are very similar to practices in North America in terms of mechanical ventilation. Several of our panelists are European and some of the important work that we reviewed came from centers in Europe. It’s my opinion that our guideline will be broadly applicable in both North America and Europe, but there may be regional or local differences. Nevertheless, we recognize in different regions in the world, there are different resource allocations for medical treatment, there are different cultural precepts, and there are other factors that implicate medical problems.
Certainly the European Respiratory Society and other European organizations developed guidelines on related topics ... one of the important caveats when CHEST decides to develop a guideline is that we are not reproducing the work that has been done elsewhere and so this guideline represents a project that fills a gap that previously had not been filled.
All guidelines that CHEST develops are living guidelines … it’s hard to envision exactly how often a guideline will be updated. We know that there will be certain areas of our guideline that will stand the test of time, but there will be other areas that will need to be updated, some sooner than others.
The original CHEST guideline on liberation from mechanical ventilation was a very important document that appeared in 2001 and changed the practice of medicine and the practice of managing patients on mechanical ventilation. Nevertheless, the guideline was somewhat limited in scope, because there was only so much information available. … Our goal in developing this guideline was to address some of practitioners’ questions that had emerged in the last decade by looking at newly available data.
[In formulating these guidelines], we purposely chose six new questions that were not directly related to any of the questions [that has been answered] in the previous guideline.
Daniel R. Ouellette, MD, FCCP, comments: Liberation from mechanical ventilation is one of the most important goals in taking care of critically ill patients receiving mechanical ventilation in the ICU. Patients who have a prolonged ventilator course are at risk for many complications and so physicians who work in the intensive care unit must work carefully to liberate patients from the ventilator at the earliest possible moment. That has to be done in a safe fashion so criteria to ensure that this can be done safely are important as well.
Patients often have medical illness that requires sedation, and it is often necessary to sedate patients so that they can tolerate being on mechanical ventilation; however, we know that oversedation can lead to failure to liberate patients from mechanical ventilation expeditiously. Therefore, one of our recommendations’ suggestions is to design protocols for sedation that focus on minimizing sedation so that patients can be extubated expeditiously.
All of the recommendations ultimately focused on a team approach to liberation from mechanical ventilation, because involvement of team members is always important. However, there are a couple of our recommendations that are particularly important in terms of their implications for the team approach and those include recommendations about using protocols to liberate patients from ventilators, in general, and also to use sedation protocols to minimize sedations.
We began to look at developing this topic, because we had initially published guidelines on [liberation from mechanical ventilation] in 2001. We knew that there was much new information that had emerged since the 2001 guidelines. For that reason we began to think about an update. With the initial inception of this project, we reached out to the American Thoracic Society so as to develop a collaborative effort since this was a topic that interested both societies. This collaboration was at all levels at CHEST and it involved not only the guidelines organization, but also the leadership of both societies and, of course, the panel that was ultimately constructed to address these issues was made up of members from both societies. The entire process [of developing the new guideline] took nearly 3 years.
When one develops a guideline, one makes an effort to make a guideline as comprehensive and globally applicable as possible. I think the practices in Europe are very similar to practices in North America in terms of mechanical ventilation. Several of our panelists are European and some of the important work that we reviewed came from centers in Europe. It’s my opinion that our guideline will be broadly applicable in both North America and Europe, but there may be regional or local differences. Nevertheless, we recognize in different regions in the world, there are different resource allocations for medical treatment, there are different cultural precepts, and there are other factors that implicate medical problems.
Certainly the European Respiratory Society and other European organizations developed guidelines on related topics ... one of the important caveats when CHEST decides to develop a guideline is that we are not reproducing the work that has been done elsewhere and so this guideline represents a project that fills a gap that previously had not been filled.
All guidelines that CHEST develops are living guidelines … it’s hard to envision exactly how often a guideline will be updated. We know that there will be certain areas of our guideline that will stand the test of time, but there will be other areas that will need to be updated, some sooner than others.
The original CHEST guideline on liberation from mechanical ventilation was a very important document that appeared in 2001 and changed the practice of medicine and the practice of managing patients on mechanical ventilation. Nevertheless, the guideline was somewhat limited in scope, because there was only so much information available. … Our goal in developing this guideline was to address some of practitioners’ questions that had emerged in the last decade by looking at newly available data.
[In formulating these guidelines], we purposely chose six new questions that were not directly related to any of the questions [that has been answered] in the previous guideline.
LOS ANGELES – Acutely hospitalized patients who have been on mechanical ventilation for more than 24 hours, are at high risk for extubation failure, and have passed a spontaneous breathing trial should be extubated to noninvasive ventilation.
The recommendation comes from new clinical practice guidelines from the American College of Chest Physicians and the American Thoracic Society. Moderate-quality evidence suggests that early extubation and a switch to noninvasive ventilation reduces ventilator-related and ICU-related complications, including infections and injury to the lungs and other organs. Extubation also cuts costs by reducing ICU stays.
At the annual meeting of the American College of Chest Physicians, one of the six project cochairs, Daniel R. Ouellette, MD, said that the guidelines were intended to address “new territory” from the evidence-based guidelines for weaning and discontinuing ventilator support that were published in 2001. That effort, chaired by Neil R. MacIntyre, MD, “was a landmark article that helped us learn about the steps that we needed to take to liberate patients from mechanical ventilation,” said Dr. Ouellette of the Henry Ford Hospital Department of Pulmonary and Critical Care Medicine, Detroit. “We hope that this guideline lives up to the importance of that one. We wanted to look over new information and give new recommendations about things that haven’t been addressed in the past.”
Six recommendations from the guideline panel include:
We suggest that the initial spontaneous breathing trial be conducted with inspiratory pressure augmentation rather than T-piece or continuous positive airway pressure. The committee wrote that conducting the initial spontaneous breathing trial with pressure augmentation was more likely to be successful, produced a higher rate of extubation success, and was associated with a trend towards lower intensive care unit mortality.
We suggest protocols attempting to minimize sedation. The committee found that sedation protocols reduced ICU length of stay. However, the protocols did not appear to decrease time on the ventilator or reduce short-term mortality. The authors could not recommend one protocol over another but said the burden of providing sedation by any of the protocols was “very low.”
We suggest protocolized rehabilitation directed toward early mobilization. The committee wrote that patients receiving the intervention spent less time on the ventilator and were more likely to be able to walk when they left the hospital. However, their mortality rate appeared unchanged. The authors noted the exercises created additional work for ICU staff that might have come at the expense of other care priorities.
We suggest managing patients with a ventilator liberation protocol. The committee said that patients managed by protocol spent on average 25 fewer hours on mechanical ventilation and were discharged from the ICU a day early. However, their mortality rate appeared unchanged.
We suggest performing a cuff leak test in patients who meet extubation criteria and are deemed at high risk for postextubation stridor. The committee suggested that the test should be used only in patients with a high risk of stridor (abnormal breathing caused by blockage of windpipe) after extubation. Although patients passing the test had lower stridor and reintubation rates, the authors wrote that a high percentage of patients who failed the test could be successfully extubated.
For patients who failed the cuff leak test but are otherwise ready for extubation, we suggest administering systemic steroids at least 4 hours before extubation. The committee said that clinical judgment should take priority over test results, and systemic steroids should be administered to these patients at least 4 hours before extubation. The authors added that the short duration of the steroid therapy was likely to improve success rates without resulting in adverse events.
In a prepared statement, Timothy Girard, MD, of the department of medicine at the University of Pittsburgh and a lead author of the guidelines said the committee hoped the guidelines would help reduce variations in practice that do not benefit patients. “We are not prescribing a specific approach to care for every patient every time,” he said. “But we are trying to summarize the available evidence in as clear and succinct a way as possible so that clinicians know how it applies to most patients.”
Dr. Ouellette disclosed that he has received a research grant from Cardeas Pharma for health care–associated pneumonia.
LOS ANGELES – Acutely hospitalized patients who have been on mechanical ventilation for more than 24 hours, are at high risk for extubation failure, and have passed a spontaneous breathing trial should be extubated to noninvasive ventilation.
The recommendation comes from new clinical practice guidelines from the American College of Chest Physicians and the American Thoracic Society. Moderate-quality evidence suggests that early extubation and a switch to noninvasive ventilation reduces ventilator-related and ICU-related complications, including infections and injury to the lungs and other organs. Extubation also cuts costs by reducing ICU stays.
At the annual meeting of the American College of Chest Physicians, one of the six project cochairs, Daniel R. Ouellette, MD, said that the guidelines were intended to address “new territory” from the evidence-based guidelines for weaning and discontinuing ventilator support that were published in 2001. That effort, chaired by Neil R. MacIntyre, MD, “was a landmark article that helped us learn about the steps that we needed to take to liberate patients from mechanical ventilation,” said Dr. Ouellette of the Henry Ford Hospital Department of Pulmonary and Critical Care Medicine, Detroit. “We hope that this guideline lives up to the importance of that one. We wanted to look over new information and give new recommendations about things that haven’t been addressed in the past.”
Six recommendations from the guideline panel include:
We suggest that the initial spontaneous breathing trial be conducted with inspiratory pressure augmentation rather than T-piece or continuous positive airway pressure. The committee wrote that conducting the initial spontaneous breathing trial with pressure augmentation was more likely to be successful, produced a higher rate of extubation success, and was associated with a trend towards lower intensive care unit mortality.
We suggest protocols attempting to minimize sedation. The committee found that sedation protocols reduced ICU length of stay. However, the protocols did not appear to decrease time on the ventilator or reduce short-term mortality. The authors could not recommend one protocol over another but said the burden of providing sedation by any of the protocols was “very low.”
We suggest protocolized rehabilitation directed toward early mobilization. The committee wrote that patients receiving the intervention spent less time on the ventilator and were more likely to be able to walk when they left the hospital. However, their mortality rate appeared unchanged. The authors noted the exercises created additional work for ICU staff that might have come at the expense of other care priorities.
We suggest managing patients with a ventilator liberation protocol. The committee said that patients managed by protocol spent on average 25 fewer hours on mechanical ventilation and were discharged from the ICU a day early. However, their mortality rate appeared unchanged.
We suggest performing a cuff leak test in patients who meet extubation criteria and are deemed at high risk for postextubation stridor. The committee suggested that the test should be used only in patients with a high risk of stridor (abnormal breathing caused by blockage of windpipe) after extubation. Although patients passing the test had lower stridor and reintubation rates, the authors wrote that a high percentage of patients who failed the test could be successfully extubated.
For patients who failed the cuff leak test but are otherwise ready for extubation, we suggest administering systemic steroids at least 4 hours before extubation. The committee said that clinical judgment should take priority over test results, and systemic steroids should be administered to these patients at least 4 hours before extubation. The authors added that the short duration of the steroid therapy was likely to improve success rates without resulting in adverse events.
In a prepared statement, Timothy Girard, MD, of the department of medicine at the University of Pittsburgh and a lead author of the guidelines said the committee hoped the guidelines would help reduce variations in practice that do not benefit patients. “We are not prescribing a specific approach to care for every patient every time,” he said. “But we are trying to summarize the available evidence in as clear and succinct a way as possible so that clinicians know how it applies to most patients.”
Dr. Ouellette disclosed that he has received a research grant from Cardeas Pharma for health care–associated pneumonia.
AT CHEST 2016
Doctors have at least seven APM options in 2017
Physicians will have several options to choose from when it comes to advanced alternative payment models (APMs) in 2017.
In an Oct. 25 release, the Centers for Medicare & Medicaid Services announced seven models that will be considered advanced APMs in 2017, including the new Oncology Care Model with two-sided risk. Other advanced APM choices will include:
• Comprehensive Primary Care Plus (CPC+).
• Comprehensive ESRD Care Model (Large Dialysis Organization [LDO] arrangement).
• Comprehensive ESRD Care Model (non-LDO arrangement).
• Medicare Shared Savings Program Accountable Care Organizations (ACOs) – Track 2.
• Medicare Shared Savings Program ACOs – Track 3.
• Next Generation ACO Model.

For the 2017 performance year, CMS estimates that 70,000-120,000 clinicians will participate in an advanced APM. In 2018, more than 125,000 clinicians will likely participate, according to CMS. The agency plans to reopen applications for new practices in the Comprehensive Primary Care Plus (CPC+) model and the Next Generation ACO model for the 2018 performance year.
Other models available for the 2018 performance year will include:
• ACO – Track 1+.
• New voluntary bundled payment model.
• Comprehensive Care for Joint Replacement Payment Model (Certified Electronic Health Record Technology [CEHRT] track).
• Advancing Care Coordination through Episode Payment Models – Track 1 (CEHRT).
For performance years 2017 and 2018, participation requirements will apply only to Medicare payments and physicians who treat Medicare patients. Starting in 2019, clinicians may also meet an alternative standard for advanced APMs that will include non-Medicare payments and patients.
“With these new opportunities, CMS expects that by the 2018 performance period, 25% of clinicians in the Quality Payment Program will earn incentive payments by being a part of these advanced models,” Patrick Conway, MD, CMS deputy administrator said in a statement. “Thanks to MACRA and the Innovation Center, we’re striving to see more Medicare patients benefit from better care when they visit their doctor for a knee replacement, receive cancer treatment, or have a coordinated care team manage their complex conditions.”
CMS is accepting feedback from physicians on the Quality Payment Program final rule until Dec. 17. Doctors can submit their comments and suggestions electronically through the CMS e-Regulation website.
[email protected]
On Twitter @legal_med
Physicians will have several options to choose from when it comes to advanced alternative payment models (APMs) in 2017.
In an Oct. 25 release, the Centers for Medicare & Medicaid Services announced seven models that will be considered advanced APMs in 2017, including the new Oncology Care Model with two-sided risk. Other advanced APM choices will include:
• Comprehensive Primary Care Plus (CPC+).
• Comprehensive ESRD Care Model (Large Dialysis Organization [LDO] arrangement).
• Comprehensive ESRD Care Model (non-LDO arrangement).
• Medicare Shared Savings Program Accountable Care Organizations (ACOs) – Track 2.
• Medicare Shared Savings Program ACOs – Track 3.
• Next Generation ACO Model.
For the 2017 performance year, CMS estimates that 70,000-120,000 clinicians will participate in an advanced APM. In 2018, more than 125,000 clinicians will likely participate, according to CMS. The agency plans to reopen applications for new practices in the Comprehensive Primary Care Plus (CPC+) model and the Next Generation ACO model for the 2018 performance year.
Other models available for the 2018 performance year will include:
• ACO – Track 1+.
• New voluntary bundled payment model.
• Comprehensive Care for Joint Replacement Payment Model (Certified Electronic Health Record Technology [CEHRT] track).
• Advancing Care Coordination through Episode Payment Models – Track 1 (CEHRT).
For performance years 2017 and 2018, participation requirements will apply only to Medicare payments and physicians who treat Medicare patients. Starting in 2019, clinicians may also meet an alternative standard for advanced APMs that will include non-Medicare payments and patients.
“With these new opportunities, CMS expects that by the 2018 performance period, 25% of clinicians in the Quality Payment Program will earn incentive payments by being a part of these advanced models,” Patrick Conway, MD, CMS deputy administrator said in a statement. “Thanks to MACRA and the Innovation Center, we’re striving to see more Medicare patients benefit from better care when they visit their doctor for a knee replacement, receive cancer treatment, or have a coordinated care team manage their complex conditions.”
CMS is accepting feedback from physicians on the Quality Payment Program final rule until Dec. 17. Doctors can submit their comments and suggestions electronically through the CMS e-Regulation website.
[email protected]
On Twitter @legal_med
Physicians will have several options to choose from when it comes to advanced alternative payment models (APMs) in 2017.
In an Oct. 25 release, the Centers for Medicare & Medicaid Services announced seven models that will be considered advanced APMs in 2017, including the new Oncology Care Model with two-sided risk. Other advanced APM choices will include:
• Comprehensive Primary Care Plus (CPC+).
• Comprehensive ESRD Care Model (Large Dialysis Organization [LDO] arrangement).
• Comprehensive ESRD Care Model (non-LDO arrangement).
• Medicare Shared Savings Program Accountable Care Organizations (ACOs) – Track 2.
• Medicare Shared Savings Program ACOs – Track 3.
• Next Generation ACO Model.
For the 2017 performance year, CMS estimates that 70,000-120,000 clinicians will participate in an advanced APM. In 2018, more than 125,000 clinicians will likely participate, according to CMS. The agency plans to reopen applications for new practices in the Comprehensive Primary Care Plus (CPC+) model and the Next Generation ACO model for the 2018 performance year.
Other models available for the 2018 performance year will include:
• ACO – Track 1+.
• New voluntary bundled payment model.
• Comprehensive Care for Joint Replacement Payment Model (Certified Electronic Health Record Technology [CEHRT] track).
• Advancing Care Coordination through Episode Payment Models – Track 1 (CEHRT).
For performance years 2017 and 2018, participation requirements will apply only to Medicare payments and physicians who treat Medicare patients. Starting in 2019, clinicians may also meet an alternative standard for advanced APMs that will include non-Medicare payments and patients.
“With these new opportunities, CMS expects that by the 2018 performance period, 25% of clinicians in the Quality Payment Program will earn incentive payments by being a part of these advanced models,” Patrick Conway, MD, CMS deputy administrator said in a statement. “Thanks to MACRA and the Innovation Center, we’re striving to see more Medicare patients benefit from better care when they visit their doctor for a knee replacement, receive cancer treatment, or have a coordinated care team manage their complex conditions.”
CMS is accepting feedback from physicians on the Quality Payment Program final rule until Dec. 17. Doctors can submit their comments and suggestions electronically through the CMS e-Regulation website.
[email protected]
On Twitter @legal_med
Risk tool labels 59%-81% of adults as prediabetic
A Web-based risk test endorsed by the American Medical Association, the American Diabetes Association, and the Centers for Disease Control and Prevention would label 59%-81% of adults as prediabetic if it were applied to the general U.S. population, according to a Research Letter to the Editor published online Oct. 3 in JAMA Internal Medicine.
The test is intended to evaluate the risk for prediabetes of any adult patient, and it advises those it identifies as prediabetic to see their physicians for confirmatory blood glucose testing. But given the results of their study, labeling this many people as prediabetic constitutes overmedicalization and could have the unintended consequence of diluting access to health care for people who actually have type 2 diabetes and other chronic conditions, said Saeid Shahraz, MD, PhD, of the Predictive Analytics and Comparative Effectiveness Center, Tufts Medical Center, Boston, and his associates.
The investigators assessed how many people this test would classify as prediabetic by analyzing data for a nationally representative sample of 10,175 adults who participated in the National Health and Nutrition Examination Survey in 2013-2014. They extracted the same information from participant responses to the NHANES survey that is elicited by the Web-based test: age, sex, history of gestational diabetes, first-degree relatives with diabetes, hypertension, physical activity level, and weight.
Among Americans aged 40 years and older, this test would classify an estimated 73.3 million, or 58.7%, as prediabetic; among those aged 60 years and older, it would classify 80.8% as prediabetic. The test also would advise all those people to see their physicians and undergo blood glucose testing for confirmation, Dr. Shahraz and his associates said (JAMA Intern Med. 2016 Oct 3. doi: 10.1001/jamainternmed.2016.5919).
This would be “premature” for many reasons. Intensive lifestyle modifications are not known to be beneficial for such patients, even those who are found to have impaired glucose tolerance. And there is no direct evidence that preventing type 2 diabetes actually reduces the risk for diabetes-related complications. Moreover, the natural progression from prediabetes to type 2 diabetes is likely to be slow, which calls into question the need for any intervention, particularly for older patients likely to die from competing causes, the researchers noted.
“A valid method to examine for prediabetes should avoid unnecessary medicalization by labeling a disease predecessor as a medical condition and seek to concentrate on people at highest risk to allow for efficient distribution of limited health care resources,” they added.
A Web-based risk test endorsed by the American Medical Association, the American Diabetes Association, and the Centers for Disease Control and Prevention would label 59%-81% of adults as prediabetic if it were applied to the general U.S. population, according to a Research Letter to the Editor published online Oct. 3 in JAMA Internal Medicine.
The test is intended to evaluate the risk for prediabetes of any adult patient, and it advises those it identifies as prediabetic to see their physicians for confirmatory blood glucose testing. But given the results of their study, labeling this many people as prediabetic constitutes overmedicalization and could have the unintended consequence of diluting access to health care for people who actually have type 2 diabetes and other chronic conditions, said Saeid Shahraz, MD, PhD, of the Predictive Analytics and Comparative Effectiveness Center, Tufts Medical Center, Boston, and his associates.
The investigators assessed how many people this test would classify as prediabetic by analyzing data for a nationally representative sample of 10,175 adults who participated in the National Health and Nutrition Examination Survey in 2013-2014. They extracted the same information from participant responses to the NHANES survey that is elicited by the Web-based test: age, sex, history of gestational diabetes, first-degree relatives with diabetes, hypertension, physical activity level, and weight.
Among Americans aged 40 years and older, this test would classify an estimated 73.3 million, or 58.7%, as prediabetic; among those aged 60 years and older, it would classify 80.8% as prediabetic. The test also would advise all those people to see their physicians and undergo blood glucose testing for confirmation, Dr. Shahraz and his associates said (JAMA Intern Med. 2016 Oct 3. doi: 10.1001/jamainternmed.2016.5919).
This would be “premature” for many reasons. Intensive lifestyle modifications are not known to be beneficial for such patients, even those who are found to have impaired glucose tolerance. And there is no direct evidence that preventing type 2 diabetes actually reduces the risk for diabetes-related complications. Moreover, the natural progression from prediabetes to type 2 diabetes is likely to be slow, which calls into question the need for any intervention, particularly for older patients likely to die from competing causes, the researchers noted.
“A valid method to examine for prediabetes should avoid unnecessary medicalization by labeling a disease predecessor as a medical condition and seek to concentrate on people at highest risk to allow for efficient distribution of limited health care resources,” they added.
A Web-based risk test endorsed by the American Medical Association, the American Diabetes Association, and the Centers for Disease Control and Prevention would label 59%-81% of adults as prediabetic if it were applied to the general U.S. population, according to a Research Letter to the Editor published online Oct. 3 in JAMA Internal Medicine.
The test is intended to evaluate the risk for prediabetes of any adult patient, and it advises those it identifies as prediabetic to see their physicians for confirmatory blood glucose testing. But given the results of their study, labeling this many people as prediabetic constitutes overmedicalization and could have the unintended consequence of diluting access to health care for people who actually have type 2 diabetes and other chronic conditions, said Saeid Shahraz, MD, PhD, of the Predictive Analytics and Comparative Effectiveness Center, Tufts Medical Center, Boston, and his associates.
The investigators assessed how many people this test would classify as prediabetic by analyzing data for a nationally representative sample of 10,175 adults who participated in the National Health and Nutrition Examination Survey in 2013-2014. They extracted the same information from participant responses to the NHANES survey that is elicited by the Web-based test: age, sex, history of gestational diabetes, first-degree relatives with diabetes, hypertension, physical activity level, and weight.
Among Americans aged 40 years and older, this test would classify an estimated 73.3 million, or 58.7%, as prediabetic; among those aged 60 years and older, it would classify 80.8% as prediabetic. The test also would advise all those people to see their physicians and undergo blood glucose testing for confirmation, Dr. Shahraz and his associates said (JAMA Intern Med. 2016 Oct 3. doi: 10.1001/jamainternmed.2016.5919).
This would be “premature” for many reasons. Intensive lifestyle modifications are not known to be beneficial for such patients, even those who are found to have impaired glucose tolerance. And there is no direct evidence that preventing type 2 diabetes actually reduces the risk for diabetes-related complications. Moreover, the natural progression from prediabetes to type 2 diabetes is likely to be slow, which calls into question the need for any intervention, particularly for older patients likely to die from competing causes, the researchers noted.
“A valid method to examine for prediabetes should avoid unnecessary medicalization by labeling a disease predecessor as a medical condition and seek to concentrate on people at highest risk to allow for efficient distribution of limited health care resources,” they added.
FROM JAMA INTERNAL MEDICINE
Key clinical point:
Major finding: Among Americans aged 40 years and older, this test would classify 58.7%, as prediabetic, and among those aged 60 years and older, it would classify 80.8% as prediabetic.
Data source: An analysis of NHANES data for 10,175 adults in 2013-2014.
Disclosures: This study was supported by the National Institute of Diabetes and Digestive Diseases and the National Institutes of Health Office of Dietary Supplements. Dr. Shahraz and his associates reported having no relevant financial disclosures.
Oral bacterium linked to poor esophageal cancer survival
Fusobacterium nucleatum, a component of the human microbiome, appears to be associated with shorter survival in esophageal cancer, according to new findings.
F. nucleatum, generally found in the oral cavity and associated with periodontal disease, may have a potential role as a prognostic biomarker, and it might also contribute to aggressive tumor behavior via activation of chemokines, the study authors suggest (Clin Cancer Res. 2016 Oct. doi: 10.1158/1078-0432.CCR-16-1786).
They add that this is “the first study to provide the evidence for the relationship between F. nucleatum and poor prognosis in esophageal cancer.”
An assessment of F. nucleatum DNA in esophageal cancer tissues by qPCR assay showed that levels were higher in malignant tissue than in paired adjacent nontumor tissues (P = .021). The relative F. nucleatum DNA levels were also measured in samples from 325 esophageal cancer cases.
Within those samples, F. nucleatum was detected in 74 (23%) of 325 cases. F. nucleatum positivity was not associated with most clinicopathologic features including patient sex, year of surgery, preoperative performance status, smoking history, alcohol history, comorbidity, tumor location, histology, tumor size, or preoperative therapy (all P greater than .05). However, it was associated with tumor stage (P = .016), T stage (P less than .01), and N stage (P = .039).
There were a total of 112 deaths among the 325 esophageal cancer patients, with 75 specific to the disease. The median follow-up time for censored patients was 2.6 years.
Patients positive for F. nucleatum had significantly shorter cancer-specific survival (logrank P = .0039) and overall survival (logrank P = .046) as compared with those who were F. nucleatum negative. In an analysis of F. nucleatum DNA status by Cox regression analysis, patients who were positive had significantly higher cancer-specific mortality as compared with those who were negative (hazard ratio, 2.01; P = .0068). After the analysis was adjusted for clinical, pathologic, and epidemiologic features, F. nucleatum positivity was associated with significantly higher cancer-specific mortality (multivariate HR, 1.78; P = .032), and similar findings were observed for overall mortality.
Dr. Yamamura and his team had also hypothesized that F. nucleatum might contribute to aggressive tumor behavior by activation of chemokines, and they were able to confirm that the presence or absence of F. nucleatum was significantly associated with CCL20 expression status, which was identified as the most upregulated chemokine.
*This article was updated 10/26/2016.
Fusobacterium nucleatum, a component of the human microbiome, appears to be associated with shorter survival in esophageal cancer, according to new findings.
F. nucleatum, generally found in the oral cavity and associated with periodontal disease, may have a potential role as a prognostic biomarker, and it might also contribute to aggressive tumor behavior via activation of chemokines, the study authors suggest (Clin Cancer Res. 2016 Oct. doi: 10.1158/1078-0432.CCR-16-1786).
They add that this is “the first study to provide the evidence for the relationship between F. nucleatum and poor prognosis in esophageal cancer.”
An assessment of F. nucleatum DNA in esophageal cancer tissues by qPCR assay showed that levels were higher in malignant tissue than in paired adjacent nontumor tissues (P = .021). The relative F. nucleatum DNA levels were also measured in samples from 325 esophageal cancer cases.
Within those samples, F. nucleatum was detected in 74 (23%) of 325 cases. F. nucleatum positivity was not associated with most clinicopathologic features including patient sex, year of surgery, preoperative performance status, smoking history, alcohol history, comorbidity, tumor location, histology, tumor size, or preoperative therapy (all P greater than .05). However, it was associated with tumor stage (P = .016), T stage (P less than .01), and N stage (P = .039).
There were a total of 112 deaths among the 325 esophageal cancer patients, with 75 specific to the disease. The median follow-up time for censored patients was 2.6 years.
Patients positive for F. nucleatum had significantly shorter cancer-specific survival (logrank P = .0039) and overall survival (logrank P = .046) as compared with those who were F. nucleatum negative. In an analysis of F. nucleatum DNA status by Cox regression analysis, patients who were positive had significantly higher cancer-specific mortality as compared with those who were negative (hazard ratio, 2.01; P = .0068). After the analysis was adjusted for clinical, pathologic, and epidemiologic features, F. nucleatum positivity was associated with significantly higher cancer-specific mortality (multivariate HR, 1.78; P = .032), and similar findings were observed for overall mortality.
Dr. Yamamura and his team had also hypothesized that F. nucleatum might contribute to aggressive tumor behavior by activation of chemokines, and they were able to confirm that the presence or absence of F. nucleatum was significantly associated with CCL20 expression status, which was identified as the most upregulated chemokine.
*This article was updated 10/26/2016.
Fusobacterium nucleatum, a component of the human microbiome, appears to be associated with shorter survival in esophageal cancer, according to new findings.
F. nucleatum, generally found in the oral cavity and associated with periodontal disease, may have a potential role as a prognostic biomarker, and it might also contribute to aggressive tumor behavior via activation of chemokines, the study authors suggest (Clin Cancer Res. 2016 Oct. doi: 10.1158/1078-0432.CCR-16-1786).
They add that this is “the first study to provide the evidence for the relationship between F. nucleatum and poor prognosis in esophageal cancer.”
An assessment of F. nucleatum DNA in esophageal cancer tissues by qPCR assay showed that levels were higher in malignant tissue than in paired adjacent nontumor tissues (P = .021). The relative F. nucleatum DNA levels were also measured in samples from 325 esophageal cancer cases.
Within those samples, F. nucleatum was detected in 74 (23%) of 325 cases. F. nucleatum positivity was not associated with most clinicopathologic features including patient sex, year of surgery, preoperative performance status, smoking history, alcohol history, comorbidity, tumor location, histology, tumor size, or preoperative therapy (all P greater than .05). However, it was associated with tumor stage (P = .016), T stage (P less than .01), and N stage (P = .039).
There were a total of 112 deaths among the 325 esophageal cancer patients, with 75 specific to the disease. The median follow-up time for censored patients was 2.6 years.
Patients positive for F. nucleatum had significantly shorter cancer-specific survival (logrank P = .0039) and overall survival (logrank P = .046) as compared with those who were F. nucleatum negative. In an analysis of F. nucleatum DNA status by Cox regression analysis, patients who were positive had significantly higher cancer-specific mortality as compared with those who were negative (hazard ratio, 2.01; P = .0068). After the analysis was adjusted for clinical, pathologic, and epidemiologic features, F. nucleatum positivity was associated with significantly higher cancer-specific mortality (multivariate HR, 1.78; P = .032), and similar findings were observed for overall mortality.
Dr. Yamamura and his team had also hypothesized that F. nucleatum might contribute to aggressive tumor behavior by activation of chemokines, and they were able to confirm that the presence or absence of F. nucleatum was significantly associated with CCL20 expression status, which was identified as the most upregulated chemokine.
*This article was updated 10/26/2016.
FROM CLINICAL CANCER RESEARCH
Key clinical point: F. nucleatum present in esophageal cancer tissue is associated with poorer prognosis.
Major finding: Patients positive for F. nucleatum had significantly shorter cancer-specific survival (logrank P = .0039) and OS (logrank P = .046).
Data source: Tissue samples from 325 patients with esophageal cancer.
Disclosures: This study was supported in part by the SGH Foundation. The authors have no disclosures.
How to Increase Patient Adherence to Therapy
How do we increase patient adherence to therapy? This question fascinates me. As dermatologists, we will see thousands of patients over the course of our careers, most with treatable conditions that will improve with therapy and others with chronic or genetic conditions that will at least be made more tolerable with therapy. Only 50% of patients with a chronic condition are adherent to therapy.1 Why some patients adhere to treatment and others do not can be difficult to understand. The emotional makeup, culture, family background, socioeconomic status, and motivation of each person is unique, which leads to complexity. This column is not meant to answer a question that is both complex and broad; rather, it is meant to survey and summarize the literature on this topic.
Education
Health literacy is defined as cognitive and social skills that determine the motivation and ability of individuals to gain access to, understand, and use information in ways that promote and maintain good health.2 Greater health literacy leads to improved compliance and health outcomes.3,4 When we take the time to educate patients about their condition, it improves health literacy, treatment compliance, and patient safety and satisfaction, factors that ultimately are linked to better health outcomes.3-8
There are many practical ways of educating patients. Interestingly, one meta-analysis found that no single strategy is more effective than another.6 This analysis found that "[c]omprehensive interventions combining cognitive, behavioral, and affective components were more effective than single-focus interventions."6 The Centers for Disease Control and Prevention (CDC) website is an excellent source of information on how to educate patients and increase patient treatment compliance.2 The CDC website offers a free tool kit on how to design educational information to your target audience, resources for children, a database of health-related educational images, an electronic textbook on teaching patients with low literacy skills, a summary of evidence-based ideas on how to improve patient adherence to medications used long-term, and more.2
Facilitating Adherence
The World Health Organization (WHO) emphasizes 5 dimensions of patient adherence: health system, socioeconomic, condition-related, therapy-related, and patient-related factors.9 Becker and Maiman5 summarized it eloquently when they wrote that we must take "clinically appropriate steps to reduce the cost, complexity, duration, and amount of behavioral change required by the regimen and increasing the regimen's convenience through 'tailoring' and other approaches." It is a broad ultimatum that will require creativity and persistence on the part of the dermatology community.
Some common patient-related factors associated with nonadherence to treatment are lack of information and skills as they pertain to self-management, difficulty with motivation and self-efficacy, and lack of support for behavioral changes.9 It is interesting that low socioeconomic status has not been consistently shown to portend low treatment adherence. It has been shown that children, especially adolescents, and elderly patients tend to be the least adherent.9-11
Dermatologists Take Action
As dermatologists, the WHO encourages us (physicians) to promote optimism, provide enthusiasm, and encourage maintenance of healthy behaviors.9 Comprehensive interventions that have had a positive impact on patient adherence to therapy for diseases such as diabetes mellitus, asthma, and hypertension may serve as motivating examples.9 Some specific dermatologic conditions that will benefit from increased patient adherence include acne, vesiculobullous disease, psoriasis, and atopic dermatitis. We can lend support to efforts to reduce the cost of dermatologic medications and be aware of the populations most at risk for low adherence to treatment.9-12
Final Thoughts
As we work to increase patient adherence to therapy in dermatology, we will help improve health literacy, patient safety, and patient satisfaction. These factors are ultimately linked to better health outcomes. The CDC and WHO websites are excellent sources of information on practical methods for doing so.2,9
- Haynes RB, McDonald H, Garg AX, et al. Interventions for helping patients to follow prescriptions for medications. Cochrane Database Syst Rev. 2002:CD000011.
- Centers for Disease Control and Prevention. Health literacy. http://www.cdc.gov/healthliteracy/index.html. Updated January 13, 2016. Accessed September 23, 2016.
- Berkman ND, Sheridan SL, Donahue KE, et al. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155:97-107.
- Pignone MP, DeWalt DA. Literacy and health outcomes: is adherence the missing link? J Gen Intern Med. 2006;21:896-897.
- Becker MH, Maiman LA. Strategies for enhancing patient compliance. J Community Health. 1980;6:113-135.
- Roter DL, Hall JA, Merisca R, et al. Effectiveness of interventions to improve patient compliance: a meta-analysis. Med Care. 1998;36:1138-1161.
- Renzi C, Abeni D, Picardi A, et al. Factors associated with patient satisfaction with care among dermatological outpatients. Br J Dermatol. 2001;145:617-623.
- Stewart MA. Effective physician-patient communication and health outcomes: a review. CMAJ. 1995;152:1423-1433.
- World Health Organization. Adherence to long-term therapies: evidence for action. http://www.who.int/chp/knowledge/publications/adherence_full_report.pdf. Posted 2003. Accessed September 23, 2016.
- Lee IA, Maibach HI. Pharmionics in dermatology: a review of topical medication adherence. Am J Clin Dermatol. 2006;7:231-236.
- Burkhart P, Dunbar-Jacob J. Adherence research in the pediatric and adolescent populations: a decade in review. In: Hayman L, Mahon M, Turner R, eds. Chronic Illness in Children: An Evidence-Based Approach. New York, NY: Springer Publishing Company; 2002:199-229.
- Rosenberg ME, Rosenberg SP. Changes in retail prices of prescription dermatologic drugs from 2009 to 2015. JAMA Dermatol. 2016;152:158-163.
How do we increase patient adherence to therapy? This question fascinates me. As dermatologists, we will see thousands of patients over the course of our careers, most with treatable conditions that will improve with therapy and others with chronic or genetic conditions that will at least be made more tolerable with therapy. Only 50% of patients with a chronic condition are adherent to therapy.1 Why some patients adhere to treatment and others do not can be difficult to understand. The emotional makeup, culture, family background, socioeconomic status, and motivation of each person is unique, which leads to complexity. This column is not meant to answer a question that is both complex and broad; rather, it is meant to survey and summarize the literature on this topic.
Education
Health literacy is defined as cognitive and social skills that determine the motivation and ability of individuals to gain access to, understand, and use information in ways that promote and maintain good health.2 Greater health literacy leads to improved compliance and health outcomes.3,4 When we take the time to educate patients about their condition, it improves health literacy, treatment compliance, and patient safety and satisfaction, factors that ultimately are linked to better health outcomes.3-8
There are many practical ways of educating patients. Interestingly, one meta-analysis found that no single strategy is more effective than another.6 This analysis found that "[c]omprehensive interventions combining cognitive, behavioral, and affective components were more effective than single-focus interventions."6 The Centers for Disease Control and Prevention (CDC) website is an excellent source of information on how to educate patients and increase patient treatment compliance.2 The CDC website offers a free tool kit on how to design educational information to your target audience, resources for children, a database of health-related educational images, an electronic textbook on teaching patients with low literacy skills, a summary of evidence-based ideas on how to improve patient adherence to medications used long-term, and more.2
Facilitating Adherence
The World Health Organization (WHO) emphasizes 5 dimensions of patient adherence: health system, socioeconomic, condition-related, therapy-related, and patient-related factors.9 Becker and Maiman5 summarized it eloquently when they wrote that we must take "clinically appropriate steps to reduce the cost, complexity, duration, and amount of behavioral change required by the regimen and increasing the regimen's convenience through 'tailoring' and other approaches." It is a broad ultimatum that will require creativity and persistence on the part of the dermatology community.
Some common patient-related factors associated with nonadherence to treatment are lack of information and skills as they pertain to self-management, difficulty with motivation and self-efficacy, and lack of support for behavioral changes.9 It is interesting that low socioeconomic status has not been consistently shown to portend low treatment adherence. It has been shown that children, especially adolescents, and elderly patients tend to be the least adherent.9-11
Dermatologists Take Action
As dermatologists, the WHO encourages us (physicians) to promote optimism, provide enthusiasm, and encourage maintenance of healthy behaviors.9 Comprehensive interventions that have had a positive impact on patient adherence to therapy for diseases such as diabetes mellitus, asthma, and hypertension may serve as motivating examples.9 Some specific dermatologic conditions that will benefit from increased patient adherence include acne, vesiculobullous disease, psoriasis, and atopic dermatitis. We can lend support to efforts to reduce the cost of dermatologic medications and be aware of the populations most at risk for low adherence to treatment.9-12
Final Thoughts
As we work to increase patient adherence to therapy in dermatology, we will help improve health literacy, patient safety, and patient satisfaction. These factors are ultimately linked to better health outcomes. The CDC and WHO websites are excellent sources of information on practical methods for doing so.2,9
How do we increase patient adherence to therapy? This question fascinates me. As dermatologists, we will see thousands of patients over the course of our careers, most with treatable conditions that will improve with therapy and others with chronic or genetic conditions that will at least be made more tolerable with therapy. Only 50% of patients with a chronic condition are adherent to therapy.1 Why some patients adhere to treatment and others do not can be difficult to understand. The emotional makeup, culture, family background, socioeconomic status, and motivation of each person is unique, which leads to complexity. This column is not meant to answer a question that is both complex and broad; rather, it is meant to survey and summarize the literature on this topic.
Education
Health literacy is defined as cognitive and social skills that determine the motivation and ability of individuals to gain access to, understand, and use information in ways that promote and maintain good health.2 Greater health literacy leads to improved compliance and health outcomes.3,4 When we take the time to educate patients about their condition, it improves health literacy, treatment compliance, and patient safety and satisfaction, factors that ultimately are linked to better health outcomes.3-8
There are many practical ways of educating patients. Interestingly, one meta-analysis found that no single strategy is more effective than another.6 This analysis found that "[c]omprehensive interventions combining cognitive, behavioral, and affective components were more effective than single-focus interventions."6 The Centers for Disease Control and Prevention (CDC) website is an excellent source of information on how to educate patients and increase patient treatment compliance.2 The CDC website offers a free tool kit on how to design educational information to your target audience, resources for children, a database of health-related educational images, an electronic textbook on teaching patients with low literacy skills, a summary of evidence-based ideas on how to improve patient adherence to medications used long-term, and more.2
Facilitating Adherence
The World Health Organization (WHO) emphasizes 5 dimensions of patient adherence: health system, socioeconomic, condition-related, therapy-related, and patient-related factors.9 Becker and Maiman5 summarized it eloquently when they wrote that we must take "clinically appropriate steps to reduce the cost, complexity, duration, and amount of behavioral change required by the regimen and increasing the regimen's convenience through 'tailoring' and other approaches." It is a broad ultimatum that will require creativity and persistence on the part of the dermatology community.
Some common patient-related factors associated with nonadherence to treatment are lack of information and skills as they pertain to self-management, difficulty with motivation and self-efficacy, and lack of support for behavioral changes.9 It is interesting that low socioeconomic status has not been consistently shown to portend low treatment adherence. It has been shown that children, especially adolescents, and elderly patients tend to be the least adherent.9-11
Dermatologists Take Action
As dermatologists, the WHO encourages us (physicians) to promote optimism, provide enthusiasm, and encourage maintenance of healthy behaviors.9 Comprehensive interventions that have had a positive impact on patient adherence to therapy for diseases such as diabetes mellitus, asthma, and hypertension may serve as motivating examples.9 Some specific dermatologic conditions that will benefit from increased patient adherence include acne, vesiculobullous disease, psoriasis, and atopic dermatitis. We can lend support to efforts to reduce the cost of dermatologic medications and be aware of the populations most at risk for low adherence to treatment.9-12
Final Thoughts
As we work to increase patient adherence to therapy in dermatology, we will help improve health literacy, patient safety, and patient satisfaction. These factors are ultimately linked to better health outcomes. The CDC and WHO websites are excellent sources of information on practical methods for doing so.2,9
- Haynes RB, McDonald H, Garg AX, et al. Interventions for helping patients to follow prescriptions for medications. Cochrane Database Syst Rev. 2002:CD000011.
- Centers for Disease Control and Prevention. Health literacy. http://www.cdc.gov/healthliteracy/index.html. Updated January 13, 2016. Accessed September 23, 2016.
- Berkman ND, Sheridan SL, Donahue KE, et al. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155:97-107.
- Pignone MP, DeWalt DA. Literacy and health outcomes: is adherence the missing link? J Gen Intern Med. 2006;21:896-897.
- Becker MH, Maiman LA. Strategies for enhancing patient compliance. J Community Health. 1980;6:113-135.
- Roter DL, Hall JA, Merisca R, et al. Effectiveness of interventions to improve patient compliance: a meta-analysis. Med Care. 1998;36:1138-1161.
- Renzi C, Abeni D, Picardi A, et al. Factors associated with patient satisfaction with care among dermatological outpatients. Br J Dermatol. 2001;145:617-623.
- Stewart MA. Effective physician-patient communication and health outcomes: a review. CMAJ. 1995;152:1423-1433.
- World Health Organization. Adherence to long-term therapies: evidence for action. http://www.who.int/chp/knowledge/publications/adherence_full_report.pdf. Posted 2003. Accessed September 23, 2016.
- Lee IA, Maibach HI. Pharmionics in dermatology: a review of topical medication adherence. Am J Clin Dermatol. 2006;7:231-236.
- Burkhart P, Dunbar-Jacob J. Adherence research in the pediatric and adolescent populations: a decade in review. In: Hayman L, Mahon M, Turner R, eds. Chronic Illness in Children: An Evidence-Based Approach. New York, NY: Springer Publishing Company; 2002:199-229.
- Rosenberg ME, Rosenberg SP. Changes in retail prices of prescription dermatologic drugs from 2009 to 2015. JAMA Dermatol. 2016;152:158-163.
- Haynes RB, McDonald H, Garg AX, et al. Interventions for helping patients to follow prescriptions for medications. Cochrane Database Syst Rev. 2002:CD000011.
- Centers for Disease Control and Prevention. Health literacy. http://www.cdc.gov/healthliteracy/index.html. Updated January 13, 2016. Accessed September 23, 2016.
- Berkman ND, Sheridan SL, Donahue KE, et al. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155:97-107.
- Pignone MP, DeWalt DA. Literacy and health outcomes: is adherence the missing link? J Gen Intern Med. 2006;21:896-897.
- Becker MH, Maiman LA. Strategies for enhancing patient compliance. J Community Health. 1980;6:113-135.
- Roter DL, Hall JA, Merisca R, et al. Effectiveness of interventions to improve patient compliance: a meta-analysis. Med Care. 1998;36:1138-1161.
- Renzi C, Abeni D, Picardi A, et al. Factors associated with patient satisfaction with care among dermatological outpatients. Br J Dermatol. 2001;145:617-623.
- Stewart MA. Effective physician-patient communication and health outcomes: a review. CMAJ. 1995;152:1423-1433.
- World Health Organization. Adherence to long-term therapies: evidence for action. http://www.who.int/chp/knowledge/publications/adherence_full_report.pdf. Posted 2003. Accessed September 23, 2016.
- Lee IA, Maibach HI. Pharmionics in dermatology: a review of topical medication adherence. Am J Clin Dermatol. 2006;7:231-236.
- Burkhart P, Dunbar-Jacob J. Adherence research in the pediatric and adolescent populations: a decade in review. In: Hayman L, Mahon M, Turner R, eds. Chronic Illness in Children: An Evidence-Based Approach. New York, NY: Springer Publishing Company; 2002:199-229.
- Rosenberg ME, Rosenberg SP. Changes in retail prices of prescription dermatologic drugs from 2009 to 2015. JAMA Dermatol. 2016;152:158-163.

Children on antipsychotics show more early weight gain than adults
VIENNA – Antipsychotic-naive children and adolescents are at greater risk for clinically significant weight gain during their first 6 months on a second-generation antipsychotic agent than adults, Covadonga M. Diaz-Caneja, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
She presented what she believes to be the first prospective observational study comparing weight gain between antipsychotic-naive children and adults during their first 6 months on second-generation antipsychotics. Weight gains were significantly greater with olanzapine (Zyprexa) than risperidone (Risperdal) or quetiapine (Seroquel) in both age groups, but the magnitude and trajectory of olanzapine-related weight gain was significantly more impressive in the pediatric patients.

The study included 226 pediatric patients with a mean age of 15.2 years and 135 adults, average age 39 years. All were antipsychotic naive when placed on one of the three second-generation antipsychotics at clinician discretion. Fifty percent of the youths and 60% of adults had a psychosis diagnosis. Sixty-four percent of the pediatric group and 55% of the adults were male.
Weight gain during the first 6 months of therapy was expressed as change in body mass index z score. An increase in BMI z score of 0.5 or more is considered clinically significant.
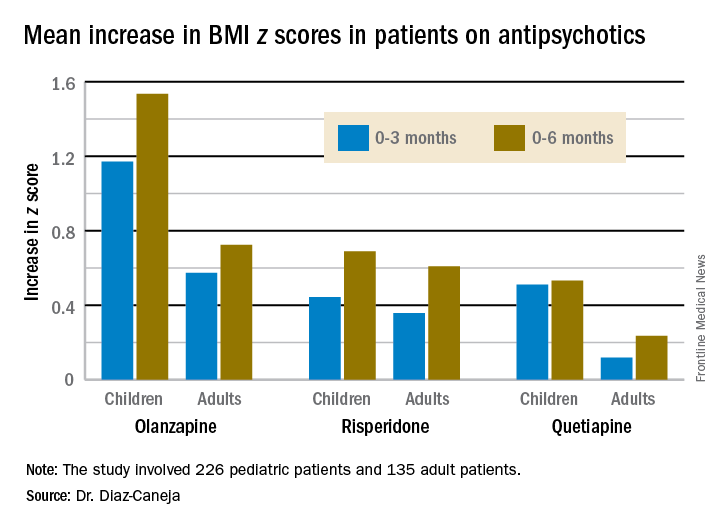
The least weight gain at 6 months occurred with quetiapine in both age groups. However, the BMI z score increased by 0.532 in the pediatric patients on the drug, more than twice the 0.236 increase in adults.
Risperidone was the only second-generation antipsychotic where the weight gain trajectories in pediatric and adult patients were not significantly different.
The study was funded by the Spanish Ministry of Economy and Competitiveness, and the European Commission. Dr. Diaz-Caneja reported having no financial conflicts of interest.
VIENNA – Antipsychotic-naive children and adolescents are at greater risk for clinically significant weight gain during their first 6 months on a second-generation antipsychotic agent than adults, Covadonga M. Diaz-Caneja, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
She presented what she believes to be the first prospective observational study comparing weight gain between antipsychotic-naive children and adults during their first 6 months on second-generation antipsychotics. Weight gains were significantly greater with olanzapine (Zyprexa) than risperidone (Risperdal) or quetiapine (Seroquel) in both age groups, but the magnitude and trajectory of olanzapine-related weight gain was significantly more impressive in the pediatric patients.
The study included 226 pediatric patients with a mean age of 15.2 years and 135 adults, average age 39 years. All were antipsychotic naive when placed on one of the three second-generation antipsychotics at clinician discretion. Fifty percent of the youths and 60% of adults had a psychosis diagnosis. Sixty-four percent of the pediatric group and 55% of the adults were male.
Weight gain during the first 6 months of therapy was expressed as change in body mass index z score. An increase in BMI z score of 0.5 or more is considered clinically significant.
The least weight gain at 6 months occurred with quetiapine in both age groups. However, the BMI z score increased by 0.532 in the pediatric patients on the drug, more than twice the 0.236 increase in adults.
Risperidone was the only second-generation antipsychotic where the weight gain trajectories in pediatric and adult patients were not significantly different.
The study was funded by the Spanish Ministry of Economy and Competitiveness, and the European Commission. Dr. Diaz-Caneja reported having no financial conflicts of interest.
VIENNA – Antipsychotic-naive children and adolescents are at greater risk for clinically significant weight gain during their first 6 months on a second-generation antipsychotic agent than adults, Covadonga M. Diaz-Caneja, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
She presented what she believes to be the first prospective observational study comparing weight gain between antipsychotic-naive children and adults during their first 6 months on second-generation antipsychotics. Weight gains were significantly greater with olanzapine (Zyprexa) than risperidone (Risperdal) or quetiapine (Seroquel) in both age groups, but the magnitude and trajectory of olanzapine-related weight gain was significantly more impressive in the pediatric patients.
The study included 226 pediatric patients with a mean age of 15.2 years and 135 adults, average age 39 years. All were antipsychotic naive when placed on one of the three second-generation antipsychotics at clinician discretion. Fifty percent of the youths and 60% of adults had a psychosis diagnosis. Sixty-four percent of the pediatric group and 55% of the adults were male.
Weight gain during the first 6 months of therapy was expressed as change in body mass index z score. An increase in BMI z score of 0.5 or more is considered clinically significant.
The least weight gain at 6 months occurred with quetiapine in both age groups. However, the BMI z score increased by 0.532 in the pediatric patients on the drug, more than twice the 0.236 increase in adults.
Risperidone was the only second-generation antipsychotic where the weight gain trajectories in pediatric and adult patients were not significantly different.
The study was funded by the Spanish Ministry of Economy and Competitiveness, and the European Commission. Dr. Diaz-Caneja reported having no financial conflicts of interest.
Key clinical point:
Major finding: The BMI z score increased by 1.535 in pediatric patients during their first 6 months on olanzapine – the most weight unfriendly of the second-generation antipsychotics – compared with 0.724 in adults.
Data source: This prospective, observational study examined weight gain in 361 antipsychotic-naive children, adolescents, and adults during their first 6 months on second-generation antipsychotic agents.
Disclosures: The study was funded by the Spanish Ministry of Economy and Competitiveness and the European Commission.
CEQUEL: Combo therapy a win in bipolar depression
VIENNA – Psychiatrists have received a welcome gift in the form of CEQUEL, a randomized trial that offers much needed guidance on how to proceed when quetiapine for bipolar depression isn’t achieving sufficient response, Eduard Vieta, MD, said at the annual congress of the European College of Neuropsychopharmacology.
The answer provided by CEQUEL is to add lamotrigine.
“Quetiapine is indicated for treatment of symptoms of bipolar depression, but many clinicians – including myself – are a bit underwhelmed about the practical results. In the clinical trials, quetiapine looks great, but when we use it in practice we’re not so happy with the results. The trials are consistently positive with a large effect size, whereas in clinical practice many patients respond only partially to quetiapine. The question has been what to do next,” observed Dr. Vieta, professor of psychiatry and head of the bipolar disorders program at the University of Barcelona.

Increasing the dose of quetiapine (Seroquel) above the recommended 300 mg/day in an effort to boost efficacy is problematic. Patients become extremely sedated. The CEQUEL (Comparative Evaluation of Quetiapine plus Lamotrigine) investigators decided to examine combination therapy with two drugs having completely different mechanisms of action.
A total of 202 patients with bipolar depression at 27 U.K. sites were placed on quetiapine and randomized double-blind to lamotrigine or placebo. Lamotrigine (Lamictal) was started at 25 mg/day and gradually increased to 200 mg daily. Because there is some limited evidence that folic acid is effective in unipolar depression, the investigators employed a 2x2 factorial design, further randomizing participants to 500 mcg/day of folic acid or placebo.
The primary endpoint was improvement in depressive symptoms at 12 weeks, with 52-week outcomes as a secondary endpoint. The group on combination therapy with quetiapine and lamotrigine showed significantly greater improvement both on mean depressive symptoms as measured with the Quick Inventory of Depressive Symptomatology-self report version 16 (QIDS-SR16), and on rates of remission at 12 and 52 weeks, compared with patients on quetiapine and placebo. The combination also reduced the risk of relapse in patients with bipolar I disorder with predominantly depressive symptoms.
Folic acid proved to be not only ineffective, it actually interfered with lamotrigine’s effectiveness. The mean reduction from baseline to 12 weeks on the QIDS-SR16 was 4.4 points in patients who received lamotrigine without folic acid, compared with a 0.12-point increase in those receiving lamotrigine plus folic acid (Lancet Psychiatry. 2016 Jan;3[1]:31-9).
Dr. Vieta wasn’t involved in CEQUEL, but he considers the study one of the highlights of the year in the field of affective disorders and urged his colleagues to consider lamotrigine/quetiapine combination therapy for bipolar depression.
“Quetiapine and lamotrigine are both now generic drugs. CEQUEL showed both are superior to quetiapine alone. It’s good news – a not-expensive treatment combining quetiapine with a drug, lamotrigine, that’s quite well tolerated,” he said.
CEQUEL was funded by the Medical Research Council. Dr. Vieta reported having no financial conflicts of interest.
VIENNA – Psychiatrists have received a welcome gift in the form of CEQUEL, a randomized trial that offers much needed guidance on how to proceed when quetiapine for bipolar depression isn’t achieving sufficient response, Eduard Vieta, MD, said at the annual congress of the European College of Neuropsychopharmacology.
The answer provided by CEQUEL is to add lamotrigine.
“Quetiapine is indicated for treatment of symptoms of bipolar depression, but many clinicians – including myself – are a bit underwhelmed about the practical results. In the clinical trials, quetiapine looks great, but when we use it in practice we’re not so happy with the results. The trials are consistently positive with a large effect size, whereas in clinical practice many patients respond only partially to quetiapine. The question has been what to do next,” observed Dr. Vieta, professor of psychiatry and head of the bipolar disorders program at the University of Barcelona.
Increasing the dose of quetiapine (Seroquel) above the recommended 300 mg/day in an effort to boost efficacy is problematic. Patients become extremely sedated. The CEQUEL (Comparative Evaluation of Quetiapine plus Lamotrigine) investigators decided to examine combination therapy with two drugs having completely different mechanisms of action.
A total of 202 patients with bipolar depression at 27 U.K. sites were placed on quetiapine and randomized double-blind to lamotrigine or placebo. Lamotrigine (Lamictal) was started at 25 mg/day and gradually increased to 200 mg daily. Because there is some limited evidence that folic acid is effective in unipolar depression, the investigators employed a 2x2 factorial design, further randomizing participants to 500 mcg/day of folic acid or placebo.
The primary endpoint was improvement in depressive symptoms at 12 weeks, with 52-week outcomes as a secondary endpoint. The group on combination therapy with quetiapine and lamotrigine showed significantly greater improvement both on mean depressive symptoms as measured with the Quick Inventory of Depressive Symptomatology-self report version 16 (QIDS-SR16), and on rates of remission at 12 and 52 weeks, compared with patients on quetiapine and placebo. The combination also reduced the risk of relapse in patients with bipolar I disorder with predominantly depressive symptoms.
Folic acid proved to be not only ineffective, it actually interfered with lamotrigine’s effectiveness. The mean reduction from baseline to 12 weeks on the QIDS-SR16 was 4.4 points in patients who received lamotrigine without folic acid, compared with a 0.12-point increase in those receiving lamotrigine plus folic acid (Lancet Psychiatry. 2016 Jan;3[1]:31-9).
Dr. Vieta wasn’t involved in CEQUEL, but he considers the study one of the highlights of the year in the field of affective disorders and urged his colleagues to consider lamotrigine/quetiapine combination therapy for bipolar depression.
“Quetiapine and lamotrigine are both now generic drugs. CEQUEL showed both are superior to quetiapine alone. It’s good news – a not-expensive treatment combining quetiapine with a drug, lamotrigine, that’s quite well tolerated,” he said.
CEQUEL was funded by the Medical Research Council. Dr. Vieta reported having no financial conflicts of interest.
VIENNA – Psychiatrists have received a welcome gift in the form of CEQUEL, a randomized trial that offers much needed guidance on how to proceed when quetiapine for bipolar depression isn’t achieving sufficient response, Eduard Vieta, MD, said at the annual congress of the European College of Neuropsychopharmacology.
The answer provided by CEQUEL is to add lamotrigine.
“Quetiapine is indicated for treatment of symptoms of bipolar depression, but many clinicians – including myself – are a bit underwhelmed about the practical results. In the clinical trials, quetiapine looks great, but when we use it in practice we’re not so happy with the results. The trials are consistently positive with a large effect size, whereas in clinical practice many patients respond only partially to quetiapine. The question has been what to do next,” observed Dr. Vieta, professor of psychiatry and head of the bipolar disorders program at the University of Barcelona.
Increasing the dose of quetiapine (Seroquel) above the recommended 300 mg/day in an effort to boost efficacy is problematic. Patients become extremely sedated. The CEQUEL (Comparative Evaluation of Quetiapine plus Lamotrigine) investigators decided to examine combination therapy with two drugs having completely different mechanisms of action.
A total of 202 patients with bipolar depression at 27 U.K. sites were placed on quetiapine and randomized double-blind to lamotrigine or placebo. Lamotrigine (Lamictal) was started at 25 mg/day and gradually increased to 200 mg daily. Because there is some limited evidence that folic acid is effective in unipolar depression, the investigators employed a 2x2 factorial design, further randomizing participants to 500 mcg/day of folic acid or placebo.
The primary endpoint was improvement in depressive symptoms at 12 weeks, with 52-week outcomes as a secondary endpoint. The group on combination therapy with quetiapine and lamotrigine showed significantly greater improvement both on mean depressive symptoms as measured with the Quick Inventory of Depressive Symptomatology-self report version 16 (QIDS-SR16), and on rates of remission at 12 and 52 weeks, compared with patients on quetiapine and placebo. The combination also reduced the risk of relapse in patients with bipolar I disorder with predominantly depressive symptoms.
Folic acid proved to be not only ineffective, it actually interfered with lamotrigine’s effectiveness. The mean reduction from baseline to 12 weeks on the QIDS-SR16 was 4.4 points in patients who received lamotrigine without folic acid, compared with a 0.12-point increase in those receiving lamotrigine plus folic acid (Lancet Psychiatry. 2016 Jan;3[1]:31-9).
Dr. Vieta wasn’t involved in CEQUEL, but he considers the study one of the highlights of the year in the field of affective disorders and urged his colleagues to consider lamotrigine/quetiapine combination therapy for bipolar depression.
“Quetiapine and lamotrigine are both now generic drugs. CEQUEL showed both are superior to quetiapine alone. It’s good news – a not-expensive treatment combining quetiapine with a drug, lamotrigine, that’s quite well tolerated,” he said.
CEQUEL was funded by the Medical Research Council. Dr. Vieta reported having no financial conflicts of interest.